CADTH Reimbursement Review
Insulin icodec (Awiqli)
Sponsor: Novo Nordisk Canada Inc.
Therapeutic area: Diabetes mellitus, type 2
This multi-part report includes:
Clinical Review
Pharmacoeconomic Review
Clinical Review
Abbreviations
AE
adverse event
CDEC
Canadian Drug Expert Committee
CGM
continuous glucose monitoring
CI
confidence interval
CV
cardiovascular
DPP-4i
dipeptidyl peptidase 4 inhibitor
DTSQ
Diabetes Treatment Satisfaction Questionnaire
GLP-1 RA
glucagon-like peptide-1 receptor agonist
GRADE
Grading of Recommendations, Assessment, Development, and Evaluations
hemoglobin A1C
glycated hemoglobin
HRQoL
health-related quality of life
LS
least squares
LTE
long-term extension
MI
myocardial infarction
MID
minimal important difference
NMA
network meta-analysis
PYE
patient-years of exposure
RCT
randomized controlled trial
SAE
serious adverse event
SC
subcutaneous
SD
standard deviation
SE
standard error
SGLT2i
sodium-glucose cotransporter-2 inhibitor
SLR
systematic literature review
T2DM
type 2 diabetes mellitus
TRIM-D
Treatment-Related Impact Measure for Diabetes
Executive Summary
An overview of the submission details for the drug under review is provided in Table 1.
Table 1: Background Information of Application Submitted for Review
Item | Description |
|---|---|
Drug product | Insulin icodec (Awiqli), solution for once-weekly SC injection |
Sponsor | Novo Nordisk Canada Inc. |
Indication | The once-weekly treatment of adults with diabetes mellitus to improve glycemic control |
Reimbursement request | The once-weekly treatment of adults with type 2 diabetes mellitus to improve glycemic control |
Health Canada approval status | NOC |
Health Canada review pathway | Standard |
NOC date | March 12, 2024 |
Recommended dose | Dose of insulin icodec is individualized and titrated based on the patient’s needs to achieve their glycemic control goal. The prefilled FlexTouch pen delivers doses in 10-unit increments up to 700 units in a single injection; 1 mL of solution contains 700 units of insulin icodec (700 U/mL; equivalent to 26.8 mg insulin icodec). |
NOC = Notice of Compliance; SC = subcutaneous.
Source: Insulin icodec product monograph. Details included in the table are from the sponsor’s Summary of Clinical Evidence.1
Introduction
Type 2 diabetes mellitus (T2DM) is a chronic health condition that develops when the body is no longer able to use insulin efficiently or produce enough insulin to manage blood glucose levels within a normal range.2 This persistent hyperglycemia results in a constellation of symptoms and downstream impacts on the body.3 Diabetes Canada estimates that more than 4 million people living in Canada, representing approximately 10% of the population, live with diabetes mellitus in 2023, and that this will increase to more than 5 million (12%) by 2033.4 Approximately 90% of patients with diabetes specifically have T2DM.5 The prevalence of T2DM may be higher in racialized and minority groups4,5 such as Indigenous Peoples in Canada6 and South Asian or Black populations,7 compared to white populations. Indigenous Peoples in Canada are also at higher risk for diabetes-related complications.6,8
While T2DM does not directly result in death, it is associated with increased mortality from downstream ischemic heart disease, stroke, chronic liver disease, infections, and cancer of the liver, pancreas, breast, and female reproductive system.9 In Canada, diabetes mellitus is associated with a 20-fold increased risk of hospitalization for nontraumatic lower limb amputations, with an estimated 65% of lower limb amputations due to diabetes.10 Patients with T2DM may have lowered health-related quality of life (HRQoL) and social stigma associated with their condition.11-13
The main goals of treatment for patients with T2DM are to reduce the risk of long-term complications through control of glycemia and blood pressure, and cardiovascular (CV) risk reduction through control of lipids and hypertension.14 Management of T2DM is individualized and ideally combines lifestyle modifications (e.g., dietary modification, exercise, quitting smoking) with pharmacological interventions.14 As T2DM is a progressive condition, most patients will require pharmacological intervention eventually, and most commonly are first prescribed metformin. If a patient is unable to lower or maintain their glycated hemoglobin (hemoglobin A1C) or blood glucose levels with metformin treatment alone, additional therapies may be combined with continued metformin therapy, such as sulfonylureas, dipeptidyl peptidase-4 inhibitors (DPP-4is), sodium-glucose cotransporter-2 inhibitors (SGLT2is), glucagon-like peptide-1 receptor agonists (GLP-1 RAs), and insulin.14
According to Diabetes Canada treatment guidelines, insulin (in combination with metformin) should be initiated in a patient in whom fasting blood glucose levels and/or hemoglobin A1C are not at target on current antihyperglycemic drugs, or with symptomatic hyperglycemia and/or metabolic decompensation.14 Basal insulin should be initiated and titrated to achieve fasting blood glucose targets, and metformin should be continued unless contraindicated.14 Other antihyperglycemic drugs may also be used in combination with these therapies as needed, and therapy should be advanced if the patient’s hemoglobin A1C is not at target within 3 months to 6 months despite adequate titration of basal insulin and supports for lifestyle and other pharmacotherapeutic interventions.14 Basal insulins for treatment of T2DM can include long-acting or intermediate-acting insulins. Currently available long-acting insulins include insulin degludec (U100 or U200), insulin glargine (U100 or U300), and insulin detemir, while neutral protamine Hagedorn insulin is an intermediate-acting insulin. Insulin and its analogues work to lower blood glucose by stimulating peripheral glucose uptake and by inhibiting hepatic glucose production.15
Insulin icodec is a long-acting insulin which is administered subcutaneously on a once-weekly basis, in contrast to the currently available once-daily long-acting basal insulins (insulin degludec and insulin glargine).16 The Health Canada–approved indication is for the once-weekly treatment of adults with diabetes mellitus to improve glycemic control, and the reimbursement request is for adult patients with T2DM.
The objective of this report is to review and critically appraise the evidence submitted by the sponsor on the beneficial and harmful effects of insulin icodec once-weekly subcutaneous (SC) injection in the treatment of T2DM in adults.
Stakeholder Perspectives
The information in this section is a summary of input provided by the patient and clinician groups who responded to CADTH’s call for input and from the clinical expert consulted by CADTH for the purpose of this review.
Patient Input
Patient input was submitted for this CADTH review by Diabetes Canada, which fielded a self-directed questionnaire to people living with T2DM and their caregivers across Canada between October 3, 2023, and October 23, 2023, inquiring about respondents’ lived experiences with diabetes and with several questions pertaining to insulin icodec. Of the 21 respondents, 13 identified as living with T2DM and 1 identified as a caregiver, 93% (of 14 respondents for the question) were aged older than 55 years, 35% were aged 75 years to 84 years, and 71% reported living with T2DM for more than 10 years (of which 29% reported living with T2DM for more than 20 years).
Most respondents indicated that living with T2DM was preoccupying, inconvenient, and burdensome, with constant management requiring foresight and planning. A total of 24% (out of 20 respondents) reported experiencing hyperglycemia more than once per day and 10% reported experiencing it more than once per week. A total of 43% (out of 20 respondents) indicated they did not experience hypoglycemia or experienced it in the past but not currently, while 14% experienced it more than once per week; none reported experiencing hypoglycemia daily.
All respondents who provided data on diabetes-related drug use (n = 19) reported taking antihyperglycemic medication including long-, short-, and rapid-acting insulin, insulin icodec, and other noninsulin antihyperglycemic drugs, either as single-drug products or combined with metformin. A total of 5 of 18 (28%) respondents reported current insulin icodec use. A total of 61% (out of 18) respondents said they were very satisfied or satisfied with their medication; no respondents indicated dissatisfaction. Respondents indicated that ease of use, lack of side effects, and helping to lower hemoglobin A1C were aspects they liked about their medications.
When choosing a medication for diabetes management, several considerations were important to respondents including avoiding hypoglycemia and hyperglycemia, reducing the risk of heart problems, reducing high blood pressure, maintaining satisfactory blood glucose levels throughout the day, and avoiding yeast infections, urinary tract infections, fluid retention, or weight gain. Affordability was also highlighted as an important consideration. Improvements that respondents wished to see in a new treatment that are not currently being achieved with available therapies included fewer side effects, blood flow improvement to extremities, weight control, and better hemoglobin A1C results.
Clinician Input
Input From Clinical Expert Consulted by CADTH
The clinical expert consulted by CADTH indicated that treatment of T2DM must be individualized, provided in a culturally appropriate manner, and equitably and affordably accessible across Canada. Treatment goals for patients with T2DM include reducing symptoms of hyperglycemia, reducing risk of long-term complications through control of glycemia and blood pressure, and reducing CV risk through control of lipids and hypertension, through a combination of lifestyle modifications and pharmacotherapeutic approaches. The key unmet need highlighted by the clinical expert was a lack of widespread access to primary care and therefore lack of access to diabetes prevention, detection, and treatment. In particular, access to diabetes education and specialist care varies greatly across the country.
The clinical expert highlighted that insulin icodec would fit into the current paradigm for introduction of basal insulin in the management of T2DM. This includes patients who are not meeting glycemic targets despite lifestyle modification, and use of or intolerance or contraindication to metformin, GLP-1 RAs, and/or SGLT2 inhibitors. It may also be used as a first-line therapy in patients with T2DM who present with symptomatic hyperglycemia and/or metabolic decompensation with or without metformin. The clinical expert noted that insulin icodec may be preferred over daily basal insulins by some patients who are unable or unwilling to take daily basal insulin, or who would prefer a lower burden related to administration frequency.
The clinical expert consulted by CADTH noted that the timing of assessments varies substantially between physicians and between patients, but ideally a patient would be supported through phone and email to adjust dosing during the first 2 months to 3 months of insulin therapy, followed by an assessment of treatment suitability after 3 months to 6 months of therapy. Diabetes management is complex and individualized. As such, there are several factors a monitoring physician or nurse practitioner will assess with regard to insulin icodec, including: treatment acceptance, treatment adherence, hemoglobin A1C target achievement, time in range with continuous glucose monitoring (CGM) of more than 70%, time below range less than 4%, and no severe hypoglycemic episodes. A sign of positive response to insulin icodec would also be improved HRQoL, including but not limited to less diabetes distress and more treatment satisfaction. Factors influencing a decision to discontinue insulin icodec would include allergy, nonadherence, or diabetes remission or glycemic control improvement through weight loss or use of other antihyperglycemic drugs or bariatric surgery. The clinical expert stated that diagnosis, prescribing of therapies, and management of treatment for patients with T2DM may occur in primary care. The diagnosis of T2DM and the use of insulin icodec were described by the clinical expert to be uncomplicated and do not necessarily require specialist care. Additionally, there are limitations to access of specialist care due to the low number of endocrinologists in Canada and the high number of patients with T2DM.
Clinician Group Input
No clinician group feedback was received by the deadline for the call for input.
Drug Program Input
Input was obtained from the drug programs that participate in the CADTH reimbursement review process. The following were identified as key factors that could potentially impact the implementation of a CADTH recommendation for insulin icodec:
consideration for initiation of therapy
consideration for prescribing of therapy
care provision issues
system and economic issues.
The clinical expert consulted by CADTH provided advice on the potential implementation issues raised by the drug programs (refer to Table 5).
Clinical Evidence
Systematic Review
Description of Studies
Five active-controlled, multicentre randomized controlled trials (RCTs) were included in this review, all of which compared insulin icodec once weekly to once-daily basal insulins (insulin degludec and/or insulin glargine). Three of the included studies enrolled adult patients with T2DM who were insulin naive (ONWARDS 1, 3, and 5); of these, the ONWARDS 1 study was 52 weeks in duration, while the ONWARDS 3 and ONWARDS 5 studies were 26 weeks in duration. The ONWARDS 5 study additionally included the DoseGuide app to inform dosing choices in the insulin icodec arm. The remaining 2 included studies enrolled adult patients with T2DM who were insulin experienced. In the ONWARDS 2 study, patients were experienced with basal insulin, and in the ONWARDS 4 study, patients were experienced with basal and bolus insulin. Both of these studies were 26 weeks in duration. The ONWARDS 4 study additionally included insulin aspart (bolus) administered 2 times to 4 times per day before mealtimes. In all 5 studies, the primary outcome was an assessment of noninferiority of insulin icodec once weekly compared to the once-daily comparator for the outcome of change in hemoglobin A1C from baseline. In all but the ONWARDS 4 study, a secondary confirmatory analysis of superiority was also conducted for this outcome. Secondary outcomes varied between the studies and included percent time in range (3.9 mmol/L to 10.0 mmol/L blood glucose using CGM), time below range (< 3 mmol/L blood glucose using CGM), and time above range (> 10.0 mmol/L blood glucose using CGM) in the ONWARDS 1, 2, and 4 studies; change in body weight in all included studies; the number of clinically significant (level 2; < 3.0 mmol/L confirmed by blood glucose meter) or severe hypoglycemic episodes (level 3; any hypoglycemic event requiring active assistance of another person, for instance to administer corrective actions or receive medical care) in all studies; change in treatment satisfaction (measured via Diabetes Treatment Satisfaction Questionnaire [DTSQ] in which higher scores [ranging from 0 to 36] represent higher satisfaction with diabetes treatment) in the ONWARDS 5 and ONWARDS 2 studies (exploratory); and treatment compliance (measured via the Treatment-Related Impact Measure for Diabetes [TRIM-D] compliance domain, in which higher scores [ranging from 4 to 20] represent higher compliance with treatment) in the ONWARDS 5 study. All-cause mortality was a safety outcome in all trials. Additional outcomes of interest that were not reported include the long-term efficacy regarding CV death, nonfatal myocardial infarction (MI), nonfatal stroke, and other microvascular or macrovascular complications of T2DM.
At baseline, patients in the ONWARDS studies treatment arms had mean ages ranging from 58 years to 62 years, and 53% to 63% were male while 37% to 47% were female. Across all studies, the majority of patients were white (60% to 90%) followed by Asian (4% to 42%), Black or African American (2% to 5%), Other (< 1% to 4%), American Indian or Alaska Native (0 to < 1%), and Native Hawaiian or Other Pacific Islander (0 to < 1%). In the insulin-naive populations of the ONWARDS 1, 3, and 5 studies, the mean duration of diabetes was 11 years to 12 years and the mean hemoglobin A1C was 8.44% to 8.88% at baseline. In the insulin-experienced populations of the ONWARDS 2 and 4 studies, the mean duration of diabetes was 16 years to 18 years, and the mean hemoglobin A1C was 8.17% to 8.31% at baseline. Approximately 90% of patients were receiving metformin at baseline, and other common (> 15%) antihyperglycemic background medications included sulfonylureas, SGLT2is, DPP-4is, and GLP-1 RAs. Uncommon antihyperglycemic background medications included thiazolidinediones, alpha-glucosidase inhibitors, and glinides. In the ONWARDS 2 and 4 studies, insulin glargine U100 (approximately 41% to 50%) followed by insulin degludec (approximately 23% to 29%) were the most common basal insulins in use at screening; most patients in the ONWARDS 4 study were receiving basal insulin once daily and bolus insulin 3 times daily (approximately 75%).
Efficacy Results
Change in Hemoglobin A1C From Baseline
In the primary analyses for noninferiority among patients who were insulin naive (the ONWARDS 1, ONWARDS 3, and ONWARDS 5 studies), the between-group differences in mean change from baseline in hemoglobin A1C were –0.19% points (95% confidence interval [CI], –0.36% to –0.03%; P < 0.0001) in the ONWARDS 1 study at 52 weeks, –0.21% points (95% CI, –0.34% to –0.08%; P < 0.0001) in the ONWARDS 3 study at 26 weeks, and –0.38% points (95% CI, –0.66% to –0.09%; P < 0.0001) in the ONWARDS 5 study at 52 weeks, indicating that insulin icodec once weekly is noninferior to the once-daily comparator for the outcome of change in hemoglobin A1C from baseline in patients who were insulin naive. In the secondary analyses for superiority, the P values were 0.0210, 0.0016, and 0.0092, respectively, indicating that insulin icodec once weekly is superior to the once-daily comparator for the outcome of change in hemoglobin A1C from baseline in patients who were insulin naive.
In the primary analyses for noninferiority among patients who were insulin experienced (ONWARDS 2 and ONWARDS 4), the between-group differences in mean change from baseline in hemoglobin A1C was –0.22% points (95% CI, –0.37% to –0.08%; P < 0.0001) in the ONWARDS 2 study and 0.02% points (95% CI, –0.11% to 0.15%; P < 0.0001) for the ONWARDS 4 study, indicating that insulin icodec once weekly is noninferior to the once-daily comparator for the outcome of change in hemoglobin A1C from baseline in patients who were insulin experienced. In the ONWARDS 2 study, a secondary analysis for superiority was also conducted (P = 0.0028), indicating that insulin icodec once weekly is noninferior to the once-daily insulin glargine for the outcome of change in hemoglobin A1C from baseline in patients who were insulin experienced. No superiority analysis was conducted in the ONWARDS 4 study.
For each of the ONWARDS 1, 3, 5, 2, and 4 studies, a 2-dimensional tipping point sensitivity analysis was performed to evaluate the robustness of the assumptions regarding missing data; the results were consistent with the primary analysis for noninferiority of hemoglobin A1C.
Time in Range (3.9 mmol/L to 10.0 mmol/L)
In the ONWARDS 1 study from week 48 to week 52, the least squares (LS) mean time in glycemic range was 71.27% (standard error [SE] = 0.85) for insulin icodec and 67.00% (SE = 0.85) for insulin glargine, representing an estimated treatment difference of 4.27% points (95% CI, 1.92% to 6.62%; P = 0.0004). A 2-dimensional tipping point sensitivity analysis was conducted, which aligned with the primary analysis for time in range. This outcome was not assessed in the ONWARDS 3 or 5 studies.
In the ONWARDS 2 study from week 22 to week 26, the LS mean time in glycemic range between 3.9 mmol/L and 10.0 mmol/L was 62.34% (SE = 1.16) for the insulin icodec group and 59.93% (SE = 1.16) for the insulin degludec group. The estimated treatment difference between insulin icodec and insulin degludec was 2.41% (95% CI, –0.84% to 5.56%; P = 0.1461). In the ONWARDS 4 study from week 22 to week 26, the LS mean time in glycemic range between 3.9 mmol/L and 10.0 mmol/L was 66.75% (SE = 1.00) for the insulin icodec group and 66.46% (SE = 1.02) for the insulin glargine group. The estimated treatment difference between insulin icodec and insulin glargine was 0.29% (95% CI, –2.52% to 3.09%; P = 0.8406).
Time Spent at Less Than 3.0 mmol/L
In the ONWARDS 1 study from week 48 to week 52, the LS mean time in glycemic range below 3 mmol/L was 0.21% (SE = not reported) for insulin icodec and 0.16% for insulin glargine (SE = not reported), representing an estimated treatment ratio (insulin icodec:insulin glargine) of 1.27 (95% CI, 0.94 to 1.71; P = 0.1134). This outcome was not assessed in the ONWARDS 3 or 5 studies.
In the ONWARDS 2 study from week 22 to week 26, the LS mean time in glycemic range below 3.0 mmol/L was 0.33% in the insulin icodec group and 0.24% in the insulin degludec group. The estimated treatment ratio of insulin icodec and insulin degludec was 1.37 (95% CI, 0.92 to 2.04; P = 0.1180). In the ONWARDS 4 study from week 22 to week 26, the LS mean time in glycemic range below 3.0 mmol/L was 0.69% in the insulin icodec group and 0.58% in the insulin glargine group. The estimated treatment ratio of insulin icodec and insulin glargine was 1.20 (95% CI, 0.91 to 1.58; P = 0.2050).
Time Spent at Greater Than 10.0 mmol/L
In the ONWARDS 1 study from week 48 to week 52, the LS mean time in glycemic range above 10 mmol/L was 27.56% for insulin icodec and 32.13% for insulin glargine, representing an estimated treatment difference of –4.58% (95% CI, –6.99% to –2.17%; P = 0.0002). This outcome was not assessed in the ONWARDS 3 or 5 studies.
In the ONWARDS 2 study from week 22 to week 26, the LS mean time in glycemic range above 10 mmol/L was 36.34% (SE = 1.19) for insulin icodec and 39.28% (SE = 1.19) for insulin degludec, representing an estimated treatment difference of –2.93% (95% CI, –6.25% to 0.39%; P = 0.0833). In the ONWARDS 4 study from week 22 to week 26, the LS mean time in glycemic range above 10 mmol/L was 30.64% for insulin icodec (SE = 1.03) and 31.24% (SE = 1.04) for insulin glargine, representing an estimated treatment difference of –0.60% (95% CI, –3.47% to 2.28%; P = 0.6826).
Change in Body Weight
In the ONWARDS 1 (at 52 weeks), ONWARDS 3 (at 26 weeks), and ONWARDS 5 (at 52 weeks) studies, the between-group differences in change in body weight from baseline were 0.46 kg (95% CI, –0.12 kg to 1.04 kg; P = 0.1187), 0.46 kg (95% CI, –0.19 kg to 1.10 kg; P = 0.1657), and 0.83 kg (95% CI, –0.37 kg to 2.02 kg; P = 0.1747), respectively.
In the ONWARDS 2 (at 26 weeks) and ONWARDS 4 (at 26 weeks) studies, the between-group differences in change in body weight from baseline were 1.70 kg (95% CI, 0.76 kg to 2.63 kg; P = 0.0004) and 0.57 kg (95% CI, –0.39 kg to 1.54 kg; P = 0.2444), respectively.
Number of Level 2 or Level 3 Hypoglycemic Episodes
In the ONWARDS 1 study, a similar number of patients experienced level 2 hypoglycemic events in the 2 groups, but there were numerically more level 2 events in the insulin icodec group. There were 143 events in 48 patients (9.8%) in the insulin icodec group and 75 events occurring in 49 patients (10.0%) in the insulin glargine group. In the insulin icodec group, 3 of the 492 patients (0.6%) experienced 61 of the 143 clinically significant hypoglycemic events. The remaining patients in the insulin icodec group and all of the patients in the insulin glargine groups experienced between 1 episode and 5 episodes of level 2 hypoglycemic events. The estimated treatment ratio for level 2 events (insulin icodec:insulin glargine) was 1.67 (95% CI, 0.99 to 2.84; P = 0.0561). Severe (level 3) hypoglycemic events occurred in 1 patient (0.2%) in the insulin icodec group, and 3 patients (0.6%) in the insulin glargine group.
In the ONWARDS 3 study, there were 53 clinically significant events of hypoglycemia (level 2) reported in 26 patients (8.9%) in the insulin icodec group, and 23 events occurring in 17 patients (22.1%) in the insulin degludec group. In the insulin icodec group, 2 patients (0.7%) experienced 15 of the 53 clinically significant hypoglycemic events. The remaining patients in the insulin icodec group experienced between 1 episode and 4 episodes of level 2 hypoglycemic events. Patients in the insulin degludec group experienced between 1 episode and 3 episodes of level 2 hypoglycemic events. The estimated treatment ratio for level 2 events (insulin icodec:insulin degludec) was 2.09 (95% CI, 0.99 to 4.41; P = 0.0536). Severe hypoglycemic events occurred in zero patients in the insulin icodec group and 2 patients (0.7%) in the insulin degludec group.
In the ONWARDS 5 study, there were 104 clinically significant (level 2) hypoglycemic events that were reported in 64 patients (11.8%) in the insulin icodec group, and 81 events occurring in 45 patients (8.4%) in the once-daily analogues group. The estimated treatment ratio for level 2 events (insulin icodec:once-daily analogues) was 1.23 (95% CI, 0.77 to 1.98; P = 0.3928). Severe (level 3) hypoglycemic events occurred in zero patients in the insulin icodec group and 4 patients (0.7%) in the insulin glargine group.
In the ONWARDS 2 study, there were 113 clinically significant events of hypoglycemia (level 2) reported in 37 patients (14.1%) in the insulin icodec group, and 41 events occurring in 19 patients (7.2%) in the insulin degludec group. The estimated treatment ratio for level 2 events (insulin icodec:insulin degludec) was 1.98 (95% CI, 0.95 to 4.12; P = 0.0677). Severe hypoglycemic events occurred in zero patients in the insulin icodec group and 1 patient (0.4%) in the insulin degludec group.
In the ONWARDS 4 study, clinically significant events of hypoglycemia (level 2) were reported in 148 patients (50.9%) in the insulin icodec group, and 160 patients (55.0%) in the insulin glargine group. The estimated treatment ratio for level 2 events (insulin icodec:insulin glargine) was 0.99 (95% CI, 0.73 to 1.34; P = 0.9274). Severe (level 3) hypoglycemic events occurred in 4 patients (1.4%) in the insulin icodec group and 2 patients (0.7%) in the insulin glargine group.
Diabetes Treatment Satisfaction Questionnaire
This outcome was assessed only in the ONWARDS 5 and ONWARDS 2 studies.
In the ONWARDS 5 study, the observed mean DTSQ total score at baseline was 26.15 in the insulin icodec plus DoseGuide group and 26.77 in the once-daily analogues group. The estimated LS mean DTSQ total score at week 52 was 31.13 (SE = 0.25) in the insulin icodec group and 30.35 (SE = 0.25) in the once-daily analogues group, representing a LS mean change from baseline in DTSQ total satisfaction score of 4.68 (SE = 0.25) and 3.90 (SE = 0.25), respectively. The LS mean difference between groups was 0.78 (95% CI, 0.10 to 1.47; P = 0.0247).
In the ONWARDS 2 study, the observed mean DTSQ total score at baseline was 26.76 in the insulin icodec group and 26.69 in the insulin degludec group. The estimated LS mean DTSQ total score at week 26 was 30.95 (SE = 0.30) in the insulin icodec group and 29.69 (SE = 0.31) in the insulin degludec group, representing a LS mean change from baseline in DTSQ total satisfaction score of 4.22 (SE = 0.30) and 2.96 (SE = 0.31), respectively. The estimated LS mean treatment difference between insulin icodec and insulin degludec was 1.25 (95% CI, 0.41 to 2.10; P = 0.0036).
TRIM-D Compliance Domain
This outcome was assessed only in the ONWARDS 5 study. The estimated treatment difference was 3.04 (95% CI, 1.28 to 4.81; P = 0.0007) at 52 weeks.
CV Death
CV death was not measured as an outcome in the included trials.
Nonfatal MI
Nonfatal MI was not measured as an outcome in the included trials.
Nonfatal Stroke
Nonfatal stroke was not measured as an outcome in the included trials.
Other Microvascular and Macrovascular Complications of T2DM
Other microvascular and macrovascular complications of T2DM were not measured as outcomes in the included trials.
Harms Results
Adverse Events
The proportion of patients who had adverse events (AEs) was similar between the insulin icodec and once-daily insulin analogue comparator groups in all ONWARDS studies. The most common AEs were COVID-19, nasopharyngitis, diarrhea, and back pain. The majority of AEs were determined by the study investigators to be nonserious, mild to moderate in severity, unlikely related to trial products, and recovered or recovering by the end of the trial duration in each trial.
In the insulin-naive populations (ONWARDS 1, 3, and 5), 50% to 71% of patients across each treatment arm experienced at least 1 AE.
In the insulin-experienced populations (ONWARDS 2 and 4), 51% to 62% of patients across each treatment arm experienced at least 1 AE.
Serious Adverse Events
Serious AEs (SAEs) occurred in similar proportions across both the insulin icodec groups and the once-daily analogues groups in each trial.
In the insulin-naive populations (ONWARDS 1, 3, and 5), among patients treated with insulin icodec, 5.1% to 10.4% of patients had at least 1 SAE. In these same trials, among patients treated with the comparator once-daily analogues, 5.1% to 10.6% of patients had at least 1 SAE.
In the insulin-experienced populations (ONWARDS 2 and 4), among patients treated with insulin icodec or once-daily analogues, 7.6% to 8.4% and 6.1% to 8.6% had at least 1 SAE, respectively.
Reported SAEs included: cardiac disorders; infections and infestations; injury, poisoning, and procedural; vascular disorders; musculoskeletal and connective tissue disorders; neoplasms benign, malignant and unspecified nervous system disorders; eye disorders; reproductive system and breast disorders; respiratory, thoracic, and mediastinal disorders; blood and lymphatic system disorders; congenital, familial, and genetic disorders; gastrointestinal disorders; metabolism and nutrition disorders; and renal and urinary disorders. Each of these SAE categories occurred in 0% to less than 5% of patients. The most frequent category of SAE observed was cardiac disorders, which ranged from approximately 3% to 4% of patients in the included studies, followed by infections and infestations (in approximately 2% to 3% of patients). There was no 1 most common event observed.
Withdrawals Due to AEs
In the insulin-naive populations (ONWARDS 1, 3, and 5), permanent discontinuation of the study drug due to AE occurred in 0.7% to 1.2% of patients treated with insulin icodec, and 0.8% to 1.3% of patients treated with comparators (insulin glargine or insulin degludec). In the insulin-experienced populations (ONWARDS 2 and 4), permanent discontinuation of the study drug due to AE occurred in 1.0% to 1.9% of patients treated with insulin icodec, and 1.0% to 1.1% of patients treated with insulin degludec or insulin glargine. Temporary discontinuation was similarly uncommon, as were AEs leading to dose increases or dose decreases.
Mortality
In the ONWARDS 1 study, there were 6 (0.6%) patients with fatal outcomes, of which 4 (0.8%) patients died in the insulin icodec treatment group and 2 (0.4%) patients died in the insulin glargine treatment group. The events (of which some patients may have had multiple) included infections and infestations (n = 2) and 1 each of COVID-19, cardiac disorders (angina pectoris), postoperative infection, pancreatic neoplasm, glioblastoma, unknown cause, and acute coronary syndrome. The death due to unknown cause in the insulin glargine treatment group was judged by investigators as “possibly” related to the trial product.
In the ONWARDS 3 study, there were 2 patients (0.7%) in the insulin icodec group and 1 patient (0.3%) in the insulin degludec group with fatal outcomes. In the insulin icodec group, deaths were due to malignancy and an undetermined cause (n = 1 for each). In the insulin degludec group, death was due to acute MI (n = 1).
In the ONWARDS 5 study, there were 3 patients (0.6%) who died in the insulin icodec plus DoseGuide group, and 7 patients (1.3%) in the once-daily analogues group. In the insulin icodec plus DoseGuide group, deaths were due to an undetermined cause (n = 2) and malignancy (n = 1). In the once-daily analogues group, deaths were due to pulmonary causes (n = 2), undetermined causes (n = 2), malignancy, sudden cardiac death, and heart failure (n = 1 for each).
In the ONWARDS 2 study, there were 2 patients (0.8%) who died in the insulin icodec group and 2 patients (0.8%) who died in the insulin degludec group. In the insulin icodec group, deaths were due to infection (n = 2). In the insulin degludec group, deaths were due to CV procedures and malignancy (n = 1 for each).
In the ONWARDS 4 study, there were 2 patients (0.7%) in the insulin icodec group and 1 patient (0.3%) in the insulin glargine group who died. In the insulin icodec group, deaths were due to other CV causes and infection (including sepsis) (n = 1 for each). In the insulin glargine group, there was 1 instance of gastrointestinal bleeding which resulted in death.
Notable Harms
Prespecified notable harms included hypersensitivity, injection site reactions, hypoglycemia, and nocturnal hypoglycemia.
Events of hypersensitivity were reported among less than 7% patients during all ONWARDS studies and were similar between treatment groups in each trial. Serious events were rare.
Injection site reactions occurred among less than 9% of patients across all ONWARDS studies. In the ONWARDS 1 study, 6 patients (1.2%) experienced 6 events in the insulin icodec group compared to 12 patients (2.4%) experiencing 12 events in the insulin glargine group. All events were considered mild or moderate in severity. In the ONWARDS 3 study, 25 patients (8.5%) experienced 62 events in the insulin icodec group compared to 13 patients (4.4%) who experienced 22 events in the insulin degludec group. Of the 62 injection site reactions reported in the insulin icodec group, 24 events were reported by only 2 patients. No events were considered serious. In the ONWARDS 5 study, 5 patients (0.9%) experienced 6 events in the insulin icodec plus DoseGuide group compared to 7 patients (1.3%) who experienced 28 events in the once-daily insulin analogue group. No events of injection site reactions were considered serious. In the ONWARDS 2 study, 3 patients (1.1%) experienced 3 events in the insulin icodec group compared to 1 patient (0.4%) who experienced 1 event in the insulin degludec group. All events of injection site reactions were considered mild or moderate in severity. In the ONWARDS 4 study, 2 patients (0.7%) experienced 2 events in both the insulin icodec and insulin glargine groups. No events of injection site reactions were considered serious, and all were mild in severity.
Nocturnal Hypoglycemia
In the ONWARDS 1 study, level 1 nocturnal hypoglycemic events occurred in 67 patients (13.6%) in the insulin icodec group and 58 patients (11.8%) in the insulin glargine group. Clinically significant (level 2) nocturnal hypoglycemic events occurred in 9 patients (1.8%) in the insulin icodec group and 10 patients (2.0%) in the insulin glargine group, and severe (level 3) nocturnal hypoglycemic events occurred in zero patients and 1 patient (0.2%) in the insulin icodec and insulin glargine groups, respectively. The estimated treatment ratio between insulin icodec and insulin glargine for clinically significant (level 2) nocturnal hypoglycemic events was 0.92 (95% CI, 0.29 to 2.86; P = 0.8816). The estimated treatment ratio between insulin icodec and insulin glargine for clinically significant (level 2) or severe (level 3) nocturnal hypoglycemic events was 0.88 (95% CI, 0.29 to 2.64; P = 0.8189).
In the ONWARDS 3 study, level 1 nocturnal hypoglycemic events occurred in 24 patients (8.2%) in the insulin icodec group and 23 patients (7.8%) in the insulin degludec group. Clinically significant (level 2) nocturnal hypoglycemic events occurred in 1 patient (0.3%) in the insulin icodec group and 4 patients (1.4%) in the insulin degludec group. There were no severe (level 3) nocturnal hypoglycemic events in either treatment group. The estimated treatment ratio between insulin icodec and insulin degludec for clinically significant (level 2) nocturnal hypoglycemic events was 2.09 (95% CI, 0.99 to 4.41; P = 0.0536). The estimated treatment ratio between insulin icodec and insulin degludec for clinically significant (level 2) or severe (level 3) nocturnal hypoglycemic events was 1.82 (95% CI, 0.87 to 3.80; P = 0.1091).
In the ONWARDS 5 study, level 1 nocturnal hypoglycemic events occurred in 48 patients (8.9%) in the insulin icodec group and 46 patients (8.6%) in the once-daily analogues group. Clinically significant (level 2) nocturnal hypoglycemic events occurred in 11 patients (2.0%) in both treatment groups, and severe (level 3) nocturnal hypoglycemic events occurred in zero patients in the insulin icodec group and 1 patient (0.2%) in the once-daily analogues groups. The estimated treatment ratio between insulin icodec and once-daily analogues for clinically significant (level 2) or severe (level 3) nocturnal hypoglycemic events was 1.36 (95% CI, 0.82 to 2.27; P = 0.02396).
In the ONWARDS 2 study, level 1 nocturnal hypoglycemic events occurred in 60 patients (22.9%) in the insulin icodec group and 35 patients (13.3%) in the insulin degludec group. Clinically significant (level 2) nocturnal hypoglycemic events occurred in 16 patients (6.1%) in the insulin icodec group and 9 patients (3.4%) in the insulin degludec group. Severe (level 3) nocturnal hypoglycemic events occurred in zero patients in both treatment groups. The estimated treatment ratio between insulin icodec and insulin degludec for clinically significant (level 2) nocturnal hypoglycemic events was 1.98 (95% CI, 0.95 to 4.12; P = 0.0677). The estimated treatment ratio between insulin icodec and insulin degludec for clinically significant (level 2) or severe (level 3) nocturnal hypoglycemic events was 1.93 (95% CI, 0.93 to 4.02; P = 0.0782).
In the ONWARDS 4 study, level 1 nocturnal hypoglycemic events occurred in 108 patients (37.1%) in the insulin icodec group and 132 patients (45.4%) in the insulin glargine group. Clinically significant (level 2) nocturnal hypoglycemic events occurred in 54 patients (18.6%) in the insulin icodec group and 71 patients (24.4%) in the insulin glargine group, and severe (level 3) nocturnal hypoglycemic events occurred in zero patients and 1 patient (0.3%) in the insulin icodec and insulin glargine groups, respectively. The estimated treatment ratio between insulin icodec and insulin glargine for clinically significant (level 2) nocturnal hypoglycemic events was 0.74 (95% CI, 0.47 to 1.15; P = 0.1818). The estimated treatment ratio between insulin icodec and insulin glargine for clinically significant (level 2) or severe (level 3) nocturnal hypoglycemic events was 0.73 (95% CI, 0.47 to 1.14; P = 0.1694).
Critical Appraisal
All of the ONWARDS trials were randomized, active-controlled trials with adequate methodology related to randomization and allocation concealment, and there were no concerning between-arm imbalances in patient characteristics at baseline, nor in diabetes-related background medications. As such, the risk of bias arising from the randomization process is low in all trials. Each trial was adequately powered for the purpose of their primary hypotheses. The ONWARDS 1, ONWARDS 2, ONWARDS 4, and ONWARDS 5 studies were open-label trials, which is associated with a risk of bias in subjective and self-reported outcomes, while the ONWARDS 3 study was double-blinded with adequate blinding and concealment procedures including placebos matched in visual quality and administration methods to the active trial products.
The primary outcome in each trial was the change in hemoglobin A1C from baseline, and the noninferiority margin of 0.3% points was chosen based on established FDA guidance17 and previous trials of insulin products in the treatment of T2DM. Change in hemoglobin A1C from baseline was considered a clinically relevant outcome by the clinical expert consulted by CADTH. This outcome is considered acceptable by the FDA17 for trials of new antihyperglycemic therapies seeking a glycemic control indication, with the rationale being that it is a validated surrogate of microvascular disease risk reduction,17 and further it is currently recognized as the key surrogate marker for the development of long-term diabetes complications in people with type 1 diabetes mellitus or T2DM.18 The selection of this noninferiority margin was determined based on FDA guidance17 as previously described, and was considered clinically relevant as a threshold of minimal important difference (MID) according to the clinical expert consulted by CADTH. However, hemoglobin A1C is ultimately a surrogate biomarker, and there is evidence to suggest that hemoglobin A1C may not be appropriate as a surrogate outcome for downstream complications in diabetes mellitus trials due to poor associations with mortality,19,20 CV mortality,21 MI,19 heart failure,19 kidney injury,19 and stroke.19 Other limitations of hemoglobin A1C include a lack of information about acute glycemic events (i.e., hypo- or hyperglycemia) and insensitivity regarding day-to-day variations of glucose. As well, measurement of hemoglobin A1C can be confounded by other conditions such as anemia, hemoglobinopathies, iron deficiency, and pregnancy.18
Use of CGM allows for observation of time in and outside of range and daily glycemic variability,18 and the clinical expert consulted by CADTH indicated that this is of growing importance in clinical trials of glycemic control in patients with T2DM in addition to hemoglobin A1C.18 Time in range as measured by CGM is useful as a measure of short-term glycemic control,22 and there is good correlation between time in range and hemoglobin A1C.22 Time in range has been demonstrated to be associated with diabetic retinopathy23,24 and microalbuminuria23 but publications assessing this outcome as a surrogate for other diabetes-related complications (e.g., mortality, MI, and other major CV or renal events) were not identified.
The primary outcome in all trials was adjusted for multiple comparisons. Additionally, in the ONWARDS 1 study, the outcome of time in range (3.9 mmol/L to 10 mmol/L) was also adjusted for multiple comparisons. As the remaining outcomes were not adjusted for multiplicity, there is an increased risk of type I error (i.e., false-positive results) for statistically significant results for those outcomes.
Multiple imputation was used for all outcomes to account for missing data. Multiple imputation methods will not remove or reduce bias that occurs when missingness is not random, but the proportion of missing data in each case was low, so this was not considered cause for concern. Additionally, sensitivity analyses were conducted for the primary outcome which bolstered confidence in the primary analyses.
The study designs with respect to patient eligibility criteria and characteristics at baseline were appropriately reflective of the target population in Canada, with the exception that there is a notable lack of inclusion of Indigenous Peoples, who are at higher risk of developing T2DM and its complications.6,8 The selected comparators, medications at baseline among included patients, and concomitant mediations during the trials were considered by the consulted clinical expert to be appropriate and to reflect clinical practice in Canada.
The impact of insulin icodec on patients’ HRQoL was not measured in the ONWARDS trials. Although the DTSQ and TRIM-D compliance domain provide information about treatment satisfaction and compliance, they are not comprehensive measures of HRQoL. As such, the influence of insulin icodec on HRQoL as compared with insulin degludec or insulin glargine is not known. Additionally, there were no compliance data reported for the insulin-experienced populations.
There is a data gap regarding the long-term effect of insulin icodec versus daily insulins on outcomes such as CV death, nonfatal MI, nonfatal stroke, and long-term all-cause mortality beyond the duration of the included clinical trials. Additionally, the clinical trials did not evaluate any global HRQoL measures.
GRADE Summary of Findings and Certainty of the Evidence
The selection of outcomes for Grading of Recommendations, Assessment, Development, and Evaluations (GRADE) assessment was based on the sponsor’s Summary of Clinical Evidence, consultation with clinical experts, and input received from patient and clinician groups and public drug plans. The following list of outcomes was finalized in consultation with expert committee members:
outcomes related to blood glucose (percent change in hemoglobin A1C from baseline, percent time in range [3.9 mmol/L to 10.0 mmol/L], percent time spent below range, percent time spent above range)
mortality and morbidity (all-cause mortality, CV death, nonfatal MI, nonfatal stroke, microvascular and macrovascular complications of T2DM)
change in body weight from baseline
treatment satisfaction (DTSQ) and compliance (TRIM-D compliance domain)
proportion of patients with clinically significant or severe hypoglycemic events.
Table 2: Summary of Findings for Insulin Icodec Versus Daily Basal Insulinsa for Patients With T2DM — Patients Who Were Insulin Naive
Outcome and follow-up | Patients (studies) N | Effectb | Certainty | What happens |
|---|---|---|---|---|
Blood glucose outcomes | ||||
LS mean change in hemoglobin A1C from baseline, % (95% CI) Follow-up: 26 weeks (ONWARDS 3) 52 weeks (ONWARDS 1 and 5) | 2,657 (3 RCTs) | ONWARDS 1
ONWARDS 3
ONWARDS 5
| Moderatec | Insulin icodec likely results in little to no difference in change from baseline in hemoglobin A1C when compared with insulin glargine or insulin degludec. |
LS mean time in range (3.9 mmol/L to 10.0 mmol/L), % (95% CI) Follow-up: 52 weeks | 984 (1 RCT) | ONWARDS 1
| Moderated | Insulin icodec likely results in little to no difference in the percent time in range (3.9 mmol/L to 10.0 mmol/L) compared with insulin glargine. |
LS mean time spent < 3.0 mmol/L, % (95% CI) Follow-up: 52 weeks | 984 (1 RCT) | ONWARDS 1
| High | Insulin icodec results in little to no difference in the percent time spent < 3.0 mmol/L compared with insulin glargine. |
LS mean time spent > 10.0 mmol/L, % (95% CI) Follow-up: 52 weeks | 984 (1 RCT) | ONWARDS 1e
| Moderatef | Insulin icodec likely results in little to no difference in percent time spent > 10.0 mmol/L compared with insulin glargine. |
Mortality and morbidity | ||||
Patients who died, % (95% CI) Follow-up: 26 weeks (ONWARDS 3) 52 weeks (ONWARDS 1 and 5) | 2,657 (3 RCTs) | ONWARDS 1
ONWARDS 3
ONWARDS 5
| Very lowg | The evidence is very uncertain about the effect of insulin icodec on mortality when compared with insulin glargine or insulin degludec. |
Cardiovascular death | — | No data available | NA | There is no evidence for the effect of insulin icodec on cardiovascular death compared to insulin degludec or insulin glargine. |
Nonfatal MI | — | No data available | NA | There is no evidence for the effect of insulin icodec on nonfatal MI compared to insulin degludec or insulin glargine. |
Nonfatal stroke | — | No data available | NA | There is no evidence for the effect of insulin icodec on nonfatal stroke compared to insulin degludec or insulin glargine. |
Micro and macrovascular complications of T2DM | — | No data available | NA | There is no evidence for the effect of insulin icodec on the micro and macrovascular complication of T2DM when compared with insulin degludec or insulin glargine. |
Body weight | ||||
LS mean change in body weight from baseline (kg), mean (95% CI) Follow-up: 26 weeks (ONWARDS 3) 52 weeks (ONWARDS 1 and 5) | 2,657 (3 RCTs) | ONWARDS 1
ONWARDS 3
ONWARDS 5
| High | Insulin icodec results in little to no difference in change from baseline in body weight when compared with insulin glargine or insulin degludec. |
Treatment satisfaction and compliance | ||||
LS mean change in DTSQ score (0 [worst] to 36 [best]) from baseline (points), mean (95% CI) Follow-up: 52 weeks | 1,085 (1 RCT) | ONWARDS 5e
| Moderateh | Insulin icodec likely results in little to no difference in DTSQ score when compared with insulin glargine or insulin degludec. The clinical importance of the observed effect is uncertain. |
LS mean TRIM-D (0 [worst] to 100 [best]) compliance domain score (points), mean (95% CI) Follow-up: 52 weeks | 1,085 (1 RCT) | ONWARDS 5e
| Moderatei | Insulin icodec likely results in an increase in the TRIM-D compliance domain score when compared with insulin glargine or insulin degludec. The clinical importance of the increase is unclear. |
Hypoglycemia | ||||
Proportion of patients experiencing ≥ 1 clinically significant (level 2) or severe (level 3) hypoglycemia event, % (95% CI) Follow-up: 26 weeks (ONWARDS 3) 52 weeks (ONWARDS 1 and 5) | 2,657 (3 RCTs) | ONWARDS 1
ONWARDS 3
ONWARDS 5
| Moderatej | Insulin icodec likely results in little to no difference in the proportion of patients experiencing ≥ 1 level 2 or 3 hypoglycemia event when compared to insulin glargine or insulin degludec. |
CI = confidence interval; DTSQ = Diabetes Satisfaction Treatment Questionnaire; hemoglobin A1C = glycated hemoglobin; LS = least squares; MI = myocardial infarction; NA = not applicable; NR = not reported; RCT = randomized controlled trial; T2DM = type 2 diabetes mellitus; TRIM-D = Treatment-Related Impact Measure for Diabetes.
Note: Study limitations (which refers to internal validity or risk of bias), inconsistency across studies, indirectness, imprecision of effects, and publication bias were considered when assessing the certainty of the evidence. All serious concerns in these domains that led to the rating down a level of certainty are documented in the table footnotes.
aThe comparator for ONWARDS 1 was insulin glargine, the comparator for ONWARDS 3 was insulin degludec, and the comparators for ONWARDS 5 were insulin glargine and insulin degludec.
bAdditional information was requested from the sponsor to obtain 95% CIs for the LS mean estimates in each treatment group within the trials, and to obtain between-group differences with 95% CIs for hypoglycemia outcomes. This information was not necessarily part of the sponsor’s statistical analysis plan and is considered exploratory evidence.
cRated down 1 level for serious imprecision. The target of the certainty appraisal is little to no difference based on a threshold of 0.3% points for a clinically important between-group difference (the noninferiority margin). The 95% CI for all trials includes the potential for important benefit. There is high certainty that insulin icodec is noninferior to insulin glargine or insulin degludec with respect to change from baseline in hemoglobin A1C.
dRated down 1 level for serious imprecision. The CI for the percent time in range (3.9 mmol/L to 10.0 mmol/L) included a potential benefit (based on a threshold of importance of 5% provided by the clinical expert).
eIn the trial, statistical testing for this outcome was not adjusted for multiplicity. The results are considered as supportive evidence.
fRated down 1 level for serious imprecision. The CI for the percent time > 10.0 mmol/L included a potential benefit (based on a threshold of importance of 5% provided by the clinical expert).
gRated down 1 level for serious indirectness due to the short follow-up length in the trials, and –2 levels for very serious imprecision due to the small number of events.
hRated down 1 level for serious study limitations. The open-label design may bias reporting of subjective measures because patients were aware of the treatment they were receiving.
iRated down 1 level for serious imprecision. The CI for difference between groups in all trials included a potentially important increase (based on a threshold of importance of 3% provided by the clinical expert).
jRated down 1 level for serious imprecision. The CI for the proportion of patients experiencing level 2 or 3 hypoglycemia included potential harm (based on a threshold of importance of 3% provided by the clinical expert).
Sources: ONWARDS 1 Clinical Study Report,25 ONWARDS 3 Clinical Study Report,26 ONWARDS 5 Clinical Study Report,27 ONWARDS 2 Clinical Study Report,28 ONWARDS 4 Clinical Study Report,29 and additional information provided by the sponsor at CADTH request.30
Table 3: Summary of Findings for Insulin Icodec Versus Daily Basal Insulins for Patients With T2DM — Patients Who Were Insulin Experienceda
Outcome and follow-up | Patients (studies) N | Effectb | Certainty | What happens |
|---|---|---|---|---|
Blood glucose outcomes | ||||
LS mean change in hemoglobin A1C from baseline, % (95% CI) Follow-up: 26 weeks | 1,108 (2 RCTs) | ONWARDS 2
ONWARDS 4
| Moderatec | Insulin icodec likely results in little to no difference in change from baseline in hemoglobin A1C when compared with insulin glargine or insulin degludec. |
LS mean time in range (3.9 mmol/L to 10.0 mmol/L), % (95% CI) Follow-up: 26 weeks | 1,108 (2 RCTs) | ONWARDS 2
ONWARDS 4
| High | Insulin icodec results in little to no difference in the percent time in range (3.9 mmol/L to 10.0 mmol/L) when compared with insulin glargine or insulin degludec. |
LS mean time spent < 3.0 mmol/L, % (95% CI) Follow-up: 26 weeks | 1,108 (2 RCTs) | ONWARDS 2
ONWARDS 4
| High | Insulin icodec results in little to no difference in time spent < 3.0 mmol/L when compared with insulin glargine or insulin degludec. |
LS mean time spent > 10.0 mmol/L, % (95% CI) Follow-up: 26 weeks | 1,108 (2 RCTs) | ONWARDS 2
ONWARDS 4
| High | Insulin icodec results in little to no difference in the percent time spent > 10.0 mmol/L compared with insulin glargine or insulin degludec. |
Mortality and morbidity | ||||
Patients who died, % Follow-up: 26 weeks | 1,108 (2 RCTs) | ONWARDS 2
ONWARDS 4
| Very lowd | The evidence is very uncertain about the effect of insulin icodec on mortality when compared with insulin glargine or insulin degludec. |
Cardiovascular death | — | No data available | NA | There is no evidence for the effect of insulin icodec on cardiovascular death compared to insulin degludec or insulin glargine. |
Nonfatal MI | — | No data available | NA | There is no evidence for the effect of insulin icodec on nonfatal MI compared to insulin degludec or insulin glargine. |
Nonfatal stroke | — | No data available | NA | There is no evidence for the effect of insulin icodec on nonfatal stroke compared to insulin degludec or insulin glargine. |
Micro and macrovascular complications of T2DM | — | No data available | NA | There is no evidence for the effect of insulin icodec on micro and macrovascular complications of T2DM compared to insulin degludec or insulin glargine. |
Body weight | ||||
LS mean change in body weight from baseline (kg), mean (95% CI) Follow-up: 26 weeks | 1,108 (2 RCTs) | ONWARDS 2e
ONWARDS 4e
| High | Insulin icodec results in little to no difference in change from baseline in body weight when compared with insulin glargine or insulin degludec. |
Treatment satisfaction and compliance | ||||
LS mean change in DTSQ score (0 [worst] to 36 [best]) from baseline (points), mean (95% CI) Follow-up: 26 weeks | 526 (1 RCT) | ONWARDS 2e
| Moderatef | Insulin icodec likely results in little to no difference in DTSQ score when compared with insulin degludec. The clinical importance of the observed effect is uncertain. |
Treatment compliance | — | No data available | NA | There is no evidence for the effect of insulin icodec on treatment compliance compared to insulin degludec or insulin glargine. |
Hypoglycemia | ||||
Proportion of patients experiencing ≥ 1 clinically significant (level 2) or severe (level 3) hypoglycemia event, % (95% CI) Follow-up: 26 weeks | 526 (1 RCT) | ONWARDS 2e
| Moderateg | Among those previously treated with basal insulin only, insulin icodec likely results in an increase in the proportion of patients experiencing ≥ 1 level 2 or 3 hypoglycemic event when compared with insulin degludec. |
Proportion of patients experiencing ≥ 1 clinically significant (level 2) or severe (level 3) hypoglycemia event, % (95% CI) Follow-up: 26 weeks | 582 (1 RCT) | ONWARDS 4
| Lowh | Among those previously treated with basal and bolus insulin, insulin icodec may result in a decrease in the proportion of patients experiencing level 2 or 3 hypoglycemic events when compared with insulin glargine. |
CI = confidence interval; DTSQ = Diabetes Satisfaction Treatment Questionnaire; hemoglobin A1C = glycated hemoglobin; LS = least squares; MI = myocardial infarction; NA = not applicable; NR = not reported; RCT = randomized controlled trial; T2DM = type 2 diabetes mellitus.
Note: Study limitations (which refers to internal validity or risk of bias), inconsistency across studies, indirectness, imprecision of effects, and publication bias were considered when assessing the certainty of the evidence. All serious concerns in these domains that led to the rating down of the level of certainty are documented in the table footnotes.
aThe patient population for ONWARDS 2 was patients experienced with basal insulin, and the patient population for ONWARDS 4 was patients experienced with basal and bolus insulin.
bAdditional information was requested from the sponsor to obtain 95% CIs for the LS mean estimates in each treatment group within the trials, and to obtain between-group differences with 95% CIs for hypoglycemia outcomes. This information was not necessarily part of the sponsor’s statistical analysis plan and is considered exploratory evidence.
cRated down 1 level for serious imprecision. The target of the certainty appraisal is little to no difference based on a threshold of 0.3% points for a clinically important between-group difference (the noninferiority margin). The 95% CI for all trials includes the potential for important benefit. There is high certainty that insulin icodec is noninferior to insulin glargine or insulin degludec with respect to change from baseline in hemoglobin A1C.
dRated down 1 level for serious indirectness; the short follow-up length in the trials is insufficient to fully capture this outcome. –2 levels for very serious imprecision; there is a very small number of events captured.
eIn the trial, statistical testing for this outcome was not adjusted for multiplicity. The results are considered as supportive evidence.
fRated down 1 level for serious study limitations. The open-label design may bias reporting of subjective measures because patients were aware of the treatment they were receiving.
gRated down 1 level for serious imprecision. The target of the certainty appraisal is an increase based on a threshold for a clinically important between-group difference of 3% as informed by the clinical expert. The 95% CI includes the possibility of little to no difference.
hRated down 2 levels for very serious imprecision. The target of the certainty appraisal is a decrease based on a threshold for a clinically important between-group difference of 3% as informed by the clinical expert. The 95% CI includes the possibility of little to no difference and an increase.
Source: Details included in the table are from the sponsor’s Summary of Clinical Evidence, ONWARDS 2 Clinical Study Report,28 ONWARDS 4 Clinical Study Report,29 and additional information provided by the sponsor.3
Long-Term Extension Studies
Description of Studies
The sponsor submitted the long-term extension (LTE) phase of the ONWARDS 1 trial, which extended the original open-label trial design an additional 26 weeks to provide 78 weeks of data. Patients originally randomized to either insulin icodec or insulin glargine continued their treatment as per the protocol of the ONWARDS 1 study until the end of the LTE phase. Patient population, interventions, comparators, and trial design elements remained the same. The same efficacy and safety outcomes were also assessed using the same statistical methods with some exceptions; the efficacy outcomes were not controlled for multiplicity and there was no hierarchical testing procedure for the primary outcome.
Efficacy outcomes summarized by CADTH included change in hemoglobin A1C from baseline, change in body weight from baseline, proportion of patients with level 2 or 3 hypoglycemic events, as well as time spent in range (3.9 mmol/L to 10.0 mmol/L), time spent at less than 3.0 mmol/L, and time spent at greater than 10.0 mmol/L, all between weeks 74 and 78.
Efficacy Results
Briefly, similar to the 52-week mark of the ONWARDS 1 study, there was little to no difference between insulin icodec and insulin glargine in terms of change in hemoglobin A1C from baseline to week 78, change in body weight from baseline to week 78, or time spent at less than 3.0 mmol/L. Similar to the 52-week mark of the ONWARDS 1 study, insulin icodec was statistically favoured for time spent in range from 3.9 mmol/L to 10.0 mmol/L (treatment difference = 4.41; 95% CI, 1.92 to 6.90; P = 0.0005) and time spent at greater than 10.0 mmol/L (treatment difference = –4.65; 95% CI, –7.20 to –2.10; P = 0.0004) between weeks 74 and 78. The treatment ratio for level 2 or 3 hypoglycemic in the LTE phase was 1.63 (95% CI, 1.02 to 2.61).
Harms Results
Harms in the 2 study arms were broadly similar during the LTE phase of the study, with some exceptions. Patients in the insulin glargine arm had a numerically higher incidence of AEs requiring temporary discontinuation, although the proportion was low in each group (< 5%). There were a numerically higher proportion of patients in the insulin icodec arm who experienced level 1 hypoglycemic events (55.9% versus 48.2%). Level 2 events occurred in the same proportion of patients (12.4% in both arms) and level 3 hypoglycemic events were rare in both arms (1 patient [0.2%] in the insulin icodec arm and 5 patients [1.0%] in the insulin glargine arm). All-cause mortality was similar between treatment arms with 5 patients (1.0%) in the insulin icodec arm and 3 patients (0.6%) in the insulin glargine arm (1 additional death per group relative to the 52-week mark of ONWARDS 1).
Critical Appraisal
All appraisal points pertaining to the main phase of the ONWARDS 1 study also pertain here as this LTE was a continuation of the same study design, patients, and outcomes. In addition, the fact that all efficacy outcomes here are exploratory and not adjusted for multiplicity, resulting in an increased risk of type I error (false-positive conclusions) for statistically significant results, is an additional internal validity limitation. Regarding external validity, the LTE results are only applicable to patients who were insulin naive as this was the only patient population included in the ONWARDS 1 study, leaving a knowledge gap for these outcomes in patients who are insulin experienced. Data on all-cause mortality are only provided during the LTE phase and thus information on mortality beyond 78 weeks is lacking. The comparison was also based on a small number of events, limiting a conclusion as to which treatment may be favoured. Lastly, results on long-term treatment adherence or satisfaction and clinical outcomes such as microvascular and macrovascular complications (e.g., nonfatal MI, stroke) were not assessed.
Indirect Comparisons
A network meta-analysis (NMA) was submitted with the objectives of assessing the relative efficacy and safety of insulin icodec compared to other basal insulin analogues used by patients in Canada. Analyses were conducted for patients who were insulin naive, patients who were basal insulin experienced, and patients who were basal and bolus insulin experienced . Outcomes of interest appraised by CADTH were change in hemoglobin A1C, overall hypoglycemia, level 2 and 3 hypoglycemia, and nocturnal hypoglycemia. Relevant comparators were insulin glargine U100 and U300, insulin degludec U100 and U200, and insulin detemir.
Description of Studies
The literature search yielded a total of 8,760 citations which were screened at the title and abstract phase. Of these, 22 studies were considered for data extraction for the feasibility assessment of the NMA. For patients who were insulin naive, the NMAs contained 14 studies (11 phase III and IV studies, 1 phase II trial,31 and 2 studies with unreported trial phases). Trials were either open label (n = 13), or double blinded (n = 1). For the patients who were basal insulin experienced, there were a total of 5 unique trials contributing to the NMA. All trials were multicentre, open-label, phase III trials. For the patients who were basal and bolus insulin experienced, a total of 3 unique trials contributed to the NMA. Two studies were multicentre, multinational, open-label trials. One trial was a phase III study, and the phase was not reported for the other.
Efficacy Results
||| ||||||||||||| ||||||||| || || ||||| ||||||| |||||| ||| |||||||| ||| |||||| || ||| |||| |||||||| |||||||| || ||||||| |||||||| |||| ||||||| ||||||||| |||||||||| |||| |||| |||| ||||| |||||| || ||||||||| |||||||| ||| ||||| |||||||| ||| ||| ||||||| | |||||||||| ||||||||| ||||||| ||| ||| ||| ||||||||| ||||| |||| |||| || |||||| ||||||| |||||| ||| |||||||| ||| ||||||| |||||| || ||| |||| |||||||| |||||||| || ||||||| |||||||| |||| ||| |||| |||| ||||| ||||||| |||||||| |||||||| |||| ||| |||| |||| ||||| |||||| || |||||||| ||| ||||||| ||| |||| |||| ||||| |||||| || ||||||| |||||||||||| |||||||| || || |||||||||| ||| ||| ||||| |||||||| ||||||| | |||||||||| ||||||||| ||||||| ||||| ||| |||||||||||| |||||||| || |||| | |||||||||| ||||||| ||||||| |||||| ||| ||| ||||| |||||||||| ||| ||||| |||||||| || |||||| |||||||||||||| ||||| ||||||||||||||||||| ||||||||| ||||||| |||||| ||| |||||||| ||| |||||| |||| |||||||| || ||| |||||||| || ||||||| |||||||| |||| ||||||| || |||| |||| ||||| |||||| || |||||||| |||||||| ||| ||||| |||||||| ||| ||| ||||||| | |||||||||| ||||||||| ||||||| || ||| |||||||||| || ||||||| |||||| ||| ||||||| |||||||| |||| ||| ||||||| ||||||||||||| ||||||| |||||||| |||| ||| |||||||| ||||||| || |||| |||| |||| ||||| || ||||||| ||||| ||| |||||||||||| |||||||| || |||| | |||||||||| ||||||| ||||||| |||||| ||| ||| ||||| |||||||||| ||| ||| ||||| ||||||||| |||||||| || || ||||| |||| ||| |||||||||||||| ||||| | ||||| ||||||||||||||||||| ||||||||| ||| |||||||| |||| |||||| ||| ||| ||| |||||| |||||||||| || ||| |||||| ||||||||| |||||||| ||| ||| ||||||||||| |||| |||| ||||| || || ||||| || |||||| ||| ||||| ||| |||||||||||| |||||||| || |||| | |||||||||| ||||||| ||||||| |||||| ||| ||| |||||||||| ||| ||| |||||||| |||||||| || || ||||| |||| ||| ||||||||||.
Harms Results
No safety analysis was run beyond the NMAs for hypoglycemia outcomes.
Critical Appraisal
The systematic literature review (SLR) which informed the NMA did not specify which comorbidities were used for the exclusion criteria of “patients with comorbidities.” This could impact the generalizability of the NMA results and affect confidence in the transitivity assumption if patient populations with different comorbidities are included.32
With regards to the feasibility assessment in the NMA, the risk of bias appraisals was undertaken at the level of the trial, rather than at the level of the reported result (within each trial), ignoring that risk of bias can differ across outcomes within the same trial. Furthermore, the methods for appraising risk of bias were not reported. In addition, there was no discussion of how the treatment effect modifiers were chosen for the feasibility assessment, or how the assessment ensured that the list of treatment effect modifiers was comprehensive. There are also concerns with unmeasured treatment effect modifiers and heterogeneity across trials in treatment effect modifiers (e.g., a paucity of studies reported ethnicity and the ranges reported were wide). Overall, there remains uncertainty in the plausibility of the transitivity assumption underpinning the NMA.
Small treatment networks, particularly for the hypoglycemia outcomes and patients who were insulin experienced, necessitated the selection of fixed-effect models for most comparison outcomes as the SE was unstable to estimate with such a small network; however, these models do not account for between-study variance and this adds some uncertainty to the results. Furthermore, the submission did not contain any consistency assessments for the instances where there were closed loops in the network, which limits assessing the consistency of the results in the NMA with results from the individual trials.
In addition, in several analyses, the proportion of patients experiencing hypoglycemic events was much lower in the insulin icodec studies (ONWARDS trials) than the comparator studies. The submission raised the question whether the comparison was appropriate but did not adjust for these differences in any way or explore them in sensitivity analyses. For nearly all hypoglycemia outcome comparisons, the effect estimates were also affected by imprecision due to wide credible intervals, precluding any conclusions regarding which treatment in the comparison may be favoured.
Furthermore, the NMA is subject to some limitations in clinical meaningfulness. The clinical expert consulted by CADTH noted that while the results for hemoglobin A1C change from baseline across study populations may attain statistical significance, they overall do not provide an important clinical benefit. In addition, while the rationale for the NMA was to include insulin detemir and provide data for insulin icodec compared to insulin detemir, a lack of available results limited the outcomes for which insulin icodec could be compared to insulin detemir. Lastly the NMA is limited in its generalizability as the included studies primarily represent white patients younger than 70 years with relatively well-controlled diabetes, and the impact of insulin icodec on the long-term control of blood glucose and the long-term safety relative to daily insulin comparators remains unknown.
Studies Addressing Gaps in the Evidence From the Systematic Review
No studies were submitted addressing gaps in the evidence.
Conclusions
Based on evidence from 5 active-controlled RCTs which compared insulin icodec to insulin glargine and/or insulin degludec in adults with T2DM who were either insulin naive or insulin experienced, insulin icodec once-weekly injections were noninferior to the included once-daily basal insulin comparators for the change from baseline in hemoglobin A1C at week 26 or week 52 of treatment, and likely result in little to no difference in this outcome. Secondary analyses of superiority showed that insulin icodec is statistically superior compared with once-daily insulin analogues evaluated for this outcome, but the magnitude of the difference was not likely to be clinically important. Secondary and exploratory analyses of CGM outcomes (time in range, time above range, and time below range) and change in weight demonstrated that there is little to no difference associated with insulin icodec compared with insulin degludec or insulin glargine across the included studies.
Among patients who were insulin naive and insulin experienced, respectively, results of the ONWARDS 5 and ONWARDS 2 studies showed that insulin icodec likely results in little to no difference in treatment satisfaction per the DTSQ compared with insulin degludec or insulin glargine; in the absence of known MIDs, there is uncertainty in the clinical importance of the observed between-group difference, but all point estimates appeared small (0.78 points in ONWARDS 5 and 1.25 points in ONWARDS 2).
Treatment compliance was measured using the TRIM-D compliance domain only in patients who were insulin naive, and the results of the ONWARDS 5 study showed that insulin icodec likely results in increased compliance when compared to insulin degludec or insulin glargine; however, the clinical importance of the increase is uncertain. The effect of insulin icodec compared with daily insulins on treatment compliance among patients who were insulin experienced is not known.
The studies were generalizable to populations in Canada with T2DM and provided robust evidence versus key active comparators. Per the clinical expert consulted by CADTH, the uptake of insulin icodec is likely to be highest among eligible patients starting on basal insulin for the first time, and may also be preferred over daily basal insulins by patients who would prefer a lower burden of administration frequency.
The safety profile of insulin icodec was generally comparable to that of insulin glargine and degludec. In the insulin-naive populations, insulin icodec resulted in little to no difference in the proportion of patients experiencing hypoglycemia (level 2 or 3). In the insulin-experienced populations, the proportion of patients with level 2 or 3 hypoglycemic events was higher in the ONWARDS 2 study but lower in the ONWARDS 4 study in the insulin icodec treatment arms than the comparator arms. Additionally, there were more level 2 hypoglycemic events among patients treated with insulin icodec than the comparators in 4 of the 5 trials, although a few patients accounted for many events in the ONWARDS 1 and ONWARDS 3 studies. Evidence from the LTE was generally consistent with the results of the main trials. The NMA was inconclusive either due to substantial imprecision or inadequate evidence to make a comparison, or the results did not demonstrate clinically meaningful impact (in the case of hemoglobin A1C).
There is a data gap regarding long-term outcomes such as the downstream consequences of T2DM, including nonfatal CV events such as MI and stroke, CV deaths, and long-term all-cause mortality beyond the duration of the clinical trials. Additionally, there is a data gap regarding the effect of insulin icodec on patients’ HRQoL using more comprehensive global measures.
Introduction
The objective of this report is to review and critically appraise the evidence submitted by the sponsor on the beneficial and harmful effects of insulin icodec (Awiqli) once-weekly SC insulin injection in the treatment of T2DM in adults to improve glycemic control.
Disease Background
Contents within this section have been informed by materials submitted by the sponsor and clinical expert input. The following have been summarized and validated by the CADTH review team.
Diabetes mellitus is a chronic health condition affecting the body’s ability to convert sugar, or glucose, into energy. Insulin is released from beta cells in the pancreas when food is ingested, and under normal circumstances is involved in transferring glucose into cells to use as energy.2 T2DM develops when the body is no longer able to use insulin efficiently or produce enough insulin to manage blood glucose levels within a normal range.3 This persistent hyperglycemia results in a constellation of symptoms and downstream impacts on the body.3
Diagnosis of T2DM is made using blood tests and confirmed by a clinician. Diagnostic criteria are 1 of 3 results on a blood test:33
fasting blood glucose of 7.0 mmol/L or greater
hemoglobin A1C of 6.5% or greater
2-hour plasma glucose of 11.1 mmol/L or greater during an oral glucose tolerance test.
The vast majority of diabetes mellitus cases are T2DM, accounting for approximately 90% of patients.5 T2DM is more often diagnosed in adulthood with many being diagnosed after the age of 40;34,35 however, rates of diagnosis are increasing in younger ages.33 Diabetes Canada estimates that more than 4 million people living in Canada, representing approximately 10% of the population, will be diagnosed with diabetes mellitus in 2023, and that this will increase to more than 5 million (12%) by 2033.4
The prevalence of T2DM may be higher in racialized and minority groups.4,5 Indigenous Peoples in Canada have higher risk for diabetes and diabetes-related complications,6 and self-reported data from Ontario showed that the prevalence of T2DM was higher for South Asian (8.1%) and Black (8.5%) populations than white (4.2%) populations.7 Patients with COVID-19 are also at increased risk of developing T2DM, especially marginalized communities which are more likely to be impacted by the health, social, and economic effects caused by the pandemic.5 Insufficient access to primary care providers are also barriers which may impact T2DM prevention, diagnosis, and care.
While T2DM does not directly result in death, it is associated with increased mortality from ischemic heart disease, stroke, chronic liver disease, infections, and cancer of the liver, pancreas, breast, and female reproductive system.9 Similar associations are reported in patients living with undiagnosed diabetes, where age- and sex-standardized excess risk of all-cause mortality is at least as high as among persons with diagnosed T2DM, and approximately 2-fold higher compared with persons without diabetes.36
In addition to increased all-cause mortality, patients with poorly controlled T2DM are at increased risk of developing diabetes-related microvascular and macrovascular complications such as retinopathy, nephropathy, neuropathy, stroke, heart failure, MI, or other CV events.37 In Canada, diabetes mellitus is associated with a 20-times increased risk of hospitalization for nontraumatic lower limb amputations, with an estimated 65% of lower limb amputations due to diabetes.10
T2DM also has multifaceted impacts on patients’ HRQoL. Patients with T2DM may feel stigma from socially identifiable characteristics related to their condition, for example, insulin injections, blood glucose monitoring, dietary restrictions, having obesity, and experiences of hypoglycemic episodes.11 Of note, insulin injections and increased frequency of injections are associated with increased perceptions of burden.38,39 Hypoglycemia due to diabetes may result in both long- and short-term complications which can negatively impact patients’ HRQoL.13 A systematic review concluded that depression is associated with not only worse mental health, but also worse physical health in patients with diabetes mellitus; people living with both diabetes mellitus and depressive symptoms were less satisfied with their treatment, and worried more about the impact of diabetes in the future and about the social and vocational impact of diabetes.12
Risk factors for T2DM include age, overweight, lack of physical activity, and genetics.40 There is currently no cure for T2DM, but it is typically managed with a combination of nonpharmacological (i.e., weight management, nutrition, and physical activity) and pharmacological (i.e., noninsulin and insulin drugs) interventions.3
Standards of Therapy
Contents within this section have been informed by materials submitted by the sponsor and clinical expert input. The following have been summarized and validated by the CADTH review team.
The main goals of treatment for patients with T2DM are to reduce the risk of long-term complications through control of glycemia and blood pressure, and CV risk reduction through control of lipids and hypertension. Clinicians also aim to maintain or improve HRQoL for people living with T2DM41-45 and to reduce the symptoms of hyperglycemia.14 Treatment must be individualized, and it is recommended to combine lifestyle changes (e.g., dietary modification, exercise, quitting smoking) and pharmacological interventions as appropriate.14
Early intervention may include lifestyle modification alone, such as increased physical activity, dietary changes, and weight loss, or it may include these modifications in addition to pharmacotherapy, depending on the patient’s initial presentation.14 As T2DM is a progressive condition, eventually most patients will require pharmacological intervention. Metformin is a noninsulin antihyperglycemic drug and is usually the first pharmacological intervention that patients will be prescribed.14 If a patient is unable to lower or maintain their hemoglobin A1C or blood glucose levels with metformin treatment alone, additional therapies may be combined with continued metformin therapy, such as sulfonylureas, DPP-4is, SGLT2is, GLP-1 RAs, and insulin.14,46
According to Canadian diabetes treatment guidelines, insulin (in combination with metformin) should be initiated in the event of a patient in whom fasting glucose levels and/or hemoglobin A1C are not at target on current antihyperglycemic drugs, or with symptomatic hyperglycemia and/or metabolic decompensation.14 Basal insulin should be initiated and titrated to achieve fasting glucose targets, and metformin should be continued unless contraindicated. Other antihyperglycemic drugs may also be used in combination with these therapies as needed, and therapy should be advanced if the patient’s hemoglobin A1C is not at target within 3 months to 6 months despite adequate titration of basal insulin and supports for lifestyle and other pharmacotherapeutic interventions.14 Basal insulins for treatment of T2DM can include long-acting or intermediate-acting insulins.14 Currently available long-acting insulins include insulin degludec (U100 or U200), insulin glargine (U100 or U300), and insulin detemir, while neutral protamine Hagedorn insulin is an intermediate-acting insulin.14
For patients who require further treatment intensification beyond the use of basal insulin, a bolus (i.e., rapid-acting) insulin regimen may be added in a step-wise fashion, beginning with 1 mealtime injection per day followed by additional injections as recommended by a health care practitioner.14
Drug Under Review
Insulin icodec (Awiqli) is approved by Health Canada for the once-weekly treatment of adults with diabetes mellitus to improve glycemic control. The reimbursement request is for the once-weekly treatment of adults with T2DM to improve glycemic control. This drug has not been previously reviewed by CADTH. It is currently under review with the FDA, European Medicines Agency, and the Therapeutic Goods Administration (Australia).
Insulin icodec is recommended to be administered SC once weekly on any day of the week, but preferably on the same day each week.16 The dose of insulin icodec is to be titrated based on a patient’s metabolic needs, blood glucose monitoring results, and glycemic control goal.16 The recommended starting dose for patients with T2DM who are insulin naive is 70 units administered once weekly.16 Recommended doses for patients who switch from a daily basal insulin to insulin icodec are described separately in the Health Canada product monograph.16 Insulin icodec is not to be used in combination with other long-acting basal insulins.16
Insulin and insulin analogues work to lower blood glucose by stimulating peripheral glucose uptake, especially by skeletal muscle and fat, and by inhibiting hepatic glucose production.15 Insulin also inhibits lipolysis and proteolysis and enhances protein synthesis. Insulin icodec was developed by re-engineering the ultra-long basal insulin OI338.15 Three amino acids were changed and a C20 icosane fatty diacid chain was attached, resulting in molecular stability, reduced enzymatic degradation, strong reversible binding to albumin, and slow receptor-mediated clearance which allows for continuous insulin action.15 A depot of essentially inactive insulin icodec is formed in the circulation and interstitial compartment, from which insulin icodec is slowly and continuously released and binds specifically to the insulin receptor. Insulin icodec has a plasma half-life of 196 hours (approximately 8 days) while retaining the same biological properties as natural human insulin.15
Key characteristics of insulin icodec are summarized in Table 4 with other injectable long-acting insulin therapies available for the treatment of T2DM.
Table 4: Key Characteristics of Insulin Icodec and Relevant Comparators
Characteristic | Insulin icodec | Insulin glargine (Lantus, Basaglar, Semglee, Toujeo) | Insulin detemir (Levemir) | Insulin degludec (Tresiba) |
|---|---|---|---|---|
Mechanism of action | Insulin and its analogues lower blood glucose by stimulating peripheral glucose uptake, especially by skeletal muscle and fat, and by inhibiting hepatic glucose production. Insulin also inhibits lipolysis and proteolysis and enhances protein synthesis. | |||
Indicationa | Once-weekly treatment of adults with DM to improve glycemic control. | All except for Toujeo:
Toujeo:
|
|
|
Route of administration | SC | |||
Recommended dose |
| Lantus, Basaglar, Semglee (T2DM only):
Toujeo (T2DM only):
|
|
|
Serious adverse effects or safety issues |
|
Toujeo (in addition to the preceding):
|
|
|
DM = diabetes mellitus; GLP-1 = glucagon-like peptide-1; IM = intramuscular; OAD = oral antihyperglycemic drug; SC = subcutaneous; T1DM = type 1 diabetes mellitus; T2DM = type 2 diabetes mellitus.
aHealth Canada–approved indication.
Source: Product monographs for insulin icodec,16 Lantus,47 Basaglar,48 Semglee,49 Toujeo,50 Levemir,51 and Tresiba.52
Stakeholder Perspectives
Patient Group Input
This section was prepared by the CADTH review team based on the input provided by patient groups. The full original patient input received by CADTH have been included in the Stakeholder section of this report.
Patient input was submitted for this CADTH review by Diabetes Canada, which fielded a survey between October 3, 2023, and October 23, 2023, directed at people living with T2DM and their caregivers across Canada. The survey consisted of a self-directed questionnaire which inquired about respondents’ lived experiences with diabetes and contained several questions pertaining to insulin icodec. Of the 21 respondents, 13 identified as living with T2DM and 1 identified as a caregiver (the remainder did not self-identify whether they were a patient or a caregiver). A total of 93% (of 14 respondents for the question) were aged older than 55 years, 35% were aged 75 years to 84 years, and 71% reported living with T2DM for more than 10 years (of which 29% reported living with T2DM for more than 20 years). Respondents lived in Ontario, British Columbia, Prince Edward Island, Quebec, Manitoba, Alberta, and Nova Scotia. A total of 78% of respondents lived in urban or suburban areas and 79% identified as white, with 1 respondent identifying as being either South Asian, Southeast Asian, or Chinese.
Most respondents (n not specified) indicated that living with T2DM was preoccupying, inconvenient, and burdensome, with constant management requiring foresight and planning. Most respondents (n not specified) mentioned challenges in managing their blood glucose in relation to diet and food choices. A total of 24% (of 20 respondents) reported experiencing hyperglycemia more than once per day and 10% reported experiencing it more than once per week (3 respondents indicated no hyperglycemia or unknown). A total of 43% (of 20 respondents) indicated they did not experience hypoglycemia or experienced it in the past but not currently, while 14% experienced it more than once per week — none reported experiencing hypoglycemia daily.
All respondents who provided data on diabetes-related drug use (n = 19) reported taking antihyperglycemic medication (2 did not respond). Medications being taken included long-, short-, and rapid-acting insulin, insulin icodec, and other noninsulin antihyperglycemic drugs, either as single-drug products or combined with metformin. A total of 18 respondents also reported nonpharmacological interventions to manage their diabetes, with 50% reporting healthy eating and 28% reporting taking herbal remedies or over-the-counter supplements. A total of 5 of 18 (28%) respondents reported current insulin icodec use.
A total of 61% (of 18) respondents said they were very satisfied or satisfied with their medication; no respondents indicated dissatisfaction. Respondents indicated that ease of use, lack of side effects, and helping to lower hemoglobin A1C were aspects they liked about their medications. Quantity and/or timing of the dosing of different medications (e.g., number of pills or needles, managing weekly versus daily dosing), fluctuations to blood glucose levels, the need for antihyperglycemic medication, and medication cost were factors which respondents indicated they disliked.
When choosing a medication for diabetes management, several considerations were important to respondents including avoiding hypoglycemia and hyperglycemia, reducing the risk of heart problems, reducing high blood pressure, maintaining satisfactory blood glucose levels throughout the day, and avoiding yeast infections, urinary tract infections, fluid retention, or weight gain. Affordability was also highlighted as an important consideration. Improvements that respondents wished to see in a new treatment that are not currently being achieved with available therapies included fewer side effects, blood flow improvement to extremities, weight control, and better hemoglobin A1C results. A handful of respondents (n not specified) noted ways in which their daily life and overall quality of life would be different if a new treatment provided their desired improvements: reduced stress, staying healthy, reducing the number of medications, reducing insulin, reducing weight gain, better nutrition counselling, and improved mental health were highlighted.
Clinician Input
Input From Clinical Expert Consulted by CADTH
All CADTH review teams include at least 1 clinical specialist with expertise regarding the diagnosis and management of the condition for which the drug is indicated. Clinical experts are a critical part of the review team and are involved in all phases of the review process (e.g., providing guidance on the development of the review protocol, assisting in the critical appraisal of clinical evidence, interpreting the clinical relevance of the results, and providing guidance on the potential place in therapy). The following input was provided by 1 clinical specialist with expertise in the diagnosis and management of T2DM.
Unmet Needs
Treatment goals for patients with T2DM include reducing symptoms of hyperglycemia, reducing risk of long-term complications through control of glycemia and blood pressure, and reducing CV risk through control of lipids and hypertension, through a combination of lifestyle modifications and pharmacotherapeutic approaches. The clinical expert consulted by CADTH highlighted that treatment must be individualized, provided in a culturally appropriate manner, and equitably and affordably accessible across Canada. The bulk of care for patients with T2DM is provided in primary care but requires a multidisciplinary approach with nursing and nutrition services, and access to specialist care when required. The key unmet need highlighted by the clinical expert was a lack of widespread access to primary care and therefore lack of access to diabetes prevention, detection, and treatment. In particular, access to diabetes education and specialist care varies greatly across the country. Many medications and technologies for diabetes are not easily affordable and coverage on provincial formularies varies from province to province.
Place in Therapy
The clinical expert described that insulin icodec would be used in patients not meeting glycemic targets despite lifestyle modification, and use of or intolerance or contraindication to metformin, GLP-1 RAs, and/or SGLT2is. It may also be used as a first-line therapy in patients with T2DM who present with symptomatic hyperglycemia and/or metabolic decompensation with or without metformin.
The clinical expert highlighted that insulin icodec would fit into the current paradigm for introduction of basal insulin in the management of T2DM. Insulin icodec may be preferred by some patients who are unable or unwilling to take daily basal insulin, or who would prefer a lower burden related to administration frequency.
Patient Population
The clinical expert indicated that patients most suited for treatment with insulin icodec would be those with T2DM who are not meeting glycemic targets (hemoglobin A1C or blood glucose) despite lifestyle modification, with use of or intolerance or contraindication to metformin, GLP-1 RAs, and SGLT2is, or patients with T2DM with symptomatic hyperglycemia and/or metabolic decompensation with or without metformin. In the current treatment paradigm, these are the same patients who would be introducing a daily basal insulin to their diabetes management strategy. Patients who are unwilling or unable to take daily basal insulin, or who are reluctant to start insulin therapy due to concerns about the burden of daily injections, may be the most likely to benefit from insulin icodec compared to the daily basal insulin options.
Assessing the Response Treatment
The clinical expert consulted by CADTH noted that the timing of assessments varies substantially between monitoring clinicians and between patients, but ideally a patient would be supported through phone and email support to adjust dosing during the first 2 months to 3 months of insulin therapy, followed by an assessment of treatment suitability after 3 months to 6 months of therapy. Diabetes management is complex, individualized, and ideally holistic. As such, there are several factors a monitoring physician or nurse practitioner will assess with regards to insulin icodec, including: treatment acceptance, treatment adherence, hemoglobin A1C target achievement, time in range with CGM of more than 70%, time below range less than 4%, and no severe hypoglycemic episodes. A sign of positive response to insulin icodec would also be increased HRQoL, such as less diabetes distress and more treatment satisfaction.
Discontinuing Treatment
Factors influencing a decision to discontinue insulin icodec would include allergy, nonadherence, or diabetes remission or glycemic control improvement through weight loss or use of other antihyperglycemic drugs or bariatric surgery.
Prescribing Considerations
Diagnosis, prescribing, and management of treatment for patients with T2DM may occur in primary care. The diagnosis of T2DM and the use of insulin icodec were described by the clinical expert to be uncomplicated and do not necessarily require specialist care. There are limitations to access of specialist care due to the low number of endocrinologists in Canada and the high number of patients with T2DM.
Additional Considerations
According to the clinical expert, the use of sulfonylureas with insulin increases the risk of hypoglycemia, so combination of sulfonylureas with insulin icodec should likely be avoided.
Clinician Group Input
No clinician group feedback was received by the deadline of the call for input.
Drug Program Input
The drug programs provide input on each drug being reviewed through CADTH’s Reimbursement Review processes by identifying issues that may impact their ability to implement a recommendation. The implementation questions and corresponding responses from the clinical experts consulted by CADTH are summarized in Table 5.
Table 5: Summary of Drug Plan Input and Clinical Expert Response
Drug program implementation questions | Clinical expert response |
|---|---|
Considerations for initiation of therapy | |
Is insulin icodec appropriate for all patients with T2DM regardless of any previous medications tried or currently on? Studies included patients with and without prior insulin experience, as well as patients who were concurrently using noninsulin drugs. | The clinical expert consulted by CADTH indicated that insulin icodec would fall within the existing treatment paradigm for the introduction of basal insulins, which includes patients who are both insulin naive or insulin experienced, and patients who may or may not be on noninsulin antihyperglycemic drugs such as metformin or others. |
Considerations for prescribing of therapy | |
For patients with well-controlled blood glucose levels who need to switch back to once or twice-daily basal insulin from insulin icodec, could the weekly dose be divided by 7 to determine the daily basal insulin dose? | Yes, the clinical expert indicated that this is an appropriate way to estimate the dose. |
For patients who require multiple daily injections of rapid-acting insulin or regular insulin, will changing basal insulin from one daily to once weekly result in significant improvements in adherence or quality of life for most patients? | The clinical expert indicated that the response to this is only speculative, but hypothetically no, as the number of daily injections would only be reduced slightly. |
Are there any issues with combining this with short-acting insulins or noninsulin antihyperglycemic drugs for diabetes? Various medications were used in the study populations. | No, there were no issues flagged by the clinical expert. |
Care provision issues | |
How difficult will it be to treat a patient who intentionally or accidentally overdoses on insulin icodec? What might this management look like? | The clinical expert referred to an article by Pieber et al.,53 which tested intentional overdoses of insulin icodec and stated: “Double or triple doses of once-weekly icodec lead to a similar risk of hypoglycaemia compared with double or triple doses of once-daily glargine U100. During hypoglycaemia, comparable symptomatic and moderately greater endocrine responses are elicited by icodec vs glargine U100.” |
System and economic issues | |
Do you think there will there be a large number of patients who want to switch from a daily insulin to icodec for the dosing convenience? | The clinical expert consulted by CADTH speculated that most of the market would likely be patients who are newly starting basal insulin and are potentially reluctant to begin daily injections. Patients already stable on a daily regimen would be less likely to switch. |
T2DM = type 2 diabetes mellitus.
Clinical Evidence
The objective of CADTH’s Clinical Review Report is to review and critically appraise the clinical evidence submitted by the sponsor on the beneficial and harmful effects of insulin icodec once-weekly injection in the treatment of T2DM in adults. The focus will be placed on comparing insulin icodec to relevant comparators and identifying gaps in the current evidence.
A summary of the clinical evidence included by the sponsor in the review of insulin icodec is presented in 4 sections with CADTH’s critical appraisal of the evidence included at the end of each section. The first section, the systematic review, includes pivotal studies and RCTs that were selected according to the sponsor’s systematic review protocol. CADTH’s assessment of the certainty of the evidence in this first section using the GRADE approach follows the critical appraisal of the evidence. The second section includes sponsor-submitted LTE studies. The third section includes indirect evidence from the sponsor. The fourth section would include additional studies that were considered by the sponsor to address important gaps in the systematic review evidence; however, none were submitted for this review.
Included Studies
Clinical evidence from the following is included in the CADTH review and appraised in this document:
5 RCTs identified in systematic review
1 LTE study
1 indirect treatment comparison.
Systematic Review
Contents within this section have been informed by materials submitted by the sponsor. The following have been summarized and validated by the CADTH review team.
Description of Studies
Characteristics of the included studies are summarized in Table 6.
Table 6: Details of Studies Included in the Systematic Review
Studies | ONWARDS 1 | ONWARDS 3 | ONWARDS 5 | ONWARDS 2 | ONWARDS 4 |
|---|---|---|---|---|---|
Designs and populations | |||||
Study design | Phase III, open-label, active-controlled RCT | Phase III, double-blind active-controlled RCT | Phase III, open-label, active-controlled RCT | Phase III, open-label, active-controlled RCT | Phase III, open-label, active-controlled RCT |
Locations | 140 sites in 12 countries (Croatia, India, Israel, Italy, Japan, Mexico, Poland, Russia, Slovakia, Span, UK, US) | 89 sites in 11 countries (Argentina, Austria, Brazil, Canada, China, Czech Republic, Denmark, France, Mexico, Taiwan, US) | 176 sites in 7 countries (Canada, Germany, Greece, Hungary, Poland, Serbia, Türkiye, US) | 71 sites in 9 countries (Ukraine, Portugal, Poland, Republic of Korea, Japan, Germany, Bulgaria, South Africa, US) | 83 sites in 9 countries (Belgium, India, Italy, Japan, Mexico, Netherlands, Romania, Russia, US) |
Patient enrolment dates | FPFV: November 11, 2020 LPLV: December 1, 2022 | FPFV: March 24, 2021 LPLV: June 23, 2022 | FPFV: March 1, 2021 LPLV: August 29, 2022 | FPFV: March 5, 2021 LPLV: March 1, 2022 | FPFV: May 14, 2021 LPLV: June 16, 2022 |
Randomized (N) | N = 984 n = 491 in the insulin icodec group n = 492 in the insulin glargine group | N = 526 n = 263 in the insulin icodec group n = 263 in the insulin degludec group | N = 588 n = 294 in the insulin icodec group n = 294 in the q.d. analogues group (insulin degludec or insulin glargine) | N = 582 n = 291 in the insulin icodec group n = 291 in the insulin degludec group | N = 1,085 n = 542 in the insulin icodec group n = 543 in the insulin glargine group |
Key inclusion criteria |
|
|
| ||
Exclusion criteria |
|
|
| ||
Drugs | |||||
Intervention | Insulin icodec administered as a subcutaneous injection at a starting dose of 70 U once weekly. | Insulin icodec administered as a subcutaneous injection at a starting dose of 70 U once weeklyb (plus daily placebo). | Insulin icodec administered as a subcutaneous injection at a starting dose of 70 U once weekly (plus DoseGuide app). | Insulin icodec administered as a subcutaneous injection at a starting dose of 70 U once weekly. | Insulin icodec administered as a subcutaneous injection at a starting dose of 70 U once weekly, plus insulin aspart at a dose of 10 U, 2 to 4 times daily. |
Comparators | Insulin glargine administered as a subcutaneous injection at a starting dose of 10 U once daily. | Insulin degludec administered as a subcutaneous injection at a starting dose of 10 U once dailyb (plus weekly placebo). | Insulin degludec administered as a subcutaneous injection at a starting dose of 10 U once daily; or Insulin glargine administered as a subcutaneous injection at a dose of 10 units or 30 units once daily. | Insulin degludec administered as a subcutaneous injection at a starting dose of 10 U once daily. | Insulin glargine administered as a subcutaneous injection at a starting dose of 10 U once daily, plus insulin aspart at a dose of 10 U, 2 to 4 times daily. |
Study duration | |||||
Screening phase | 2 weeks | 2 weeks | 2 weeks | 2 weeks | 2 weeks |
Treatment phase | 52 weeks | 26 weeks | 52 weeks | 26 weeks | 26 weeks |
Long-term extension phase | 26 weeks | NA | NA | NA | NA |
Follow-up phase | 5 weeks | 5 weeks | 5 weeks | 5 weeks | 5 weeks |
Outcomes | |||||
Primary end point |
|
|
|
|
|
Secondary and exploratory end points | Secondary:
Exploratory:
| Secondary:
Exploratory:
| Secondary:
Exploratory:
| Secondary:
Exploratory:
| Secondary:
Exploratory:
|
Publication status | |||||
Publications | Rosenstock et al. (2023) Study IDs:
| Lingvay et al. (2023) Study IDs:
| Bajaj et al. (2023) Study IDs:
| Philis-Tsimikas et al. (2023) Study IDs:
| Mathieu et al. (2023) Study IDs:
|
BMI = body mass index; DPP = dipeptidyl peptidase; DTSQ = Diabetes Treatment Satisfaction Questionnaire; FPFV = first patient first visit; FPG = fasting plasma glucose; GLP-1 = glucagon-like peptide-1; hemoglobin A1C = glycated hemoglobin; LPLV = last patient last visit; NA = not applicable; q.d. = once a day; RCT = randomized controlled trial; SGLT2 = sodium-glucose cotransporter-2; T2DM = type 2 diabetes mellitus; TRIM-D = Treatment-Related Impact Measure for Diabetes.
aSimultaneous participation in a trial with the primary objective of evaluating an approved or nonapproved investigational medicinal product for prevention or treatment of COVID-19 disease or postinfectious conditions was allowed at the investigator’s discretion without discontinuing trial product.
bWeekly placebo in the intervention group or daily placebo in the comparator group of the ONWARDS 3 trial were administered to patients to maintain blinding.
Sources: ONWARDS 1 Clinical Study Report,25 ONWARDS 3 Clinical Study Report,26 ONWARDS 5 Clinical Study Report,27 ONWARDS 2 Clinical Study Report,28 and ONWARDS 4 Clinical Study Report.29 Details included in the table are from the sponsor’s Summary of Clinical Evidence.1
All 5 of the ONWARDS studies were multicentre, phase III RCTs comparing the efficacy and safety of insulin icodec to once-daily insulin analogues among patients with diabetes mellitus; all studies are open label, except the ONWARDS 3 study in which a double-blind, double-dummy design was used to compare insulin icodec to insulin degludec. The ONWARDS 1 through 5 studies randomized patients with T2DM; of these studies, the ONWARDS 1, ONWARDS 3, and ONWARDS 5 studies recruited patients who were insulin naive, while the ONWARDS 2 and ONWARDS 4 trials recruited patients who had previous experience with insulin. Specifically, the ONWARDS 2 trial enrolled patients who had previously received basal insulin, and the ONWARDS 4 trial enrolled patients with previous treatment with basal and bolus insulin. All studies consisted of a 2-week screening period followed by a main on-treatment phase (consisting of either 26 weeks or 52 weeks), and a follow-up phase of 5 weeks. The ONWARDS 1 trial also included a 26-week LTE phase. All patients were randomized at a 1:1 ratio to receive either insulin icodec or a once-daily basal insulin. Randomization was centrally conducted and adjudicated using an interactive web response system. In the ONWARDS 5 study, patients in the once-daily analogues treatment arm received either insulin degludec or insulin glargine as selected by the investigator before randomization per standard of care. No stratification was described in the ONWARDS 1, ONWARDS 2, ONWARDS 4, or ONWARDS 5 studies. However, in the ONWARDS 3 study, randomization was stratified by region and sulfonylurea or glinide use. Events for adjudication were evaluated by an independent external event adjudication committee in a blinded manner. All trials used a treat-to-target approach ensuring that patients received optimal titration of insulin to improve their hemoglobin A1C. Insulin titration was based on prebreakfast self-measured plasma glucose values. CGM was also employed in the ONWARDS 1, ONWARDS 2, and ONWARDS 4 trials based on patient preference to generate profiles for evaluating the glycemic control during the trial; the CGM data were blinded for both patients and the investigator to avoid influence on titration and the glycemic control.
Populations
Inclusion and Exclusion Criteria
Eligibility criteria were similar across the trials. Key inclusion criteria included adult patients (aged ≥ 18 years) diagnosed with T2DM a minimum of 180 days before baseline. All patients had to have a hemoglobin A1C from 7.0% to 11.0% (53.0 mmol/mol to approximately 96.7 mmol/mol) confirmed by central laboratory analysis. The ONWARDS 1, ONWARDS 3, and ONWARDS 5 trials specified inclusion of patients with T2DM who were naive to previous insulin therapy. The ONWARDS 2 and ONWARDS 4 trials included patients who were previously treated with basal insulin or basal and bolus insulin, respectively. Patients in the ONWARDS 2 and ONWARDS 4 trials had to have been treated with insulin with or without antihyperglycemic drug regimens at least 90 days before screening. Key exclusion criteria across the ONWARDS studies were also generally consistent. Exclusion criteria across the ONWARDS 1 to ONWARDS 5 studies specified patients with uncontrolled diabetes or other conditions, such as chronic heart failure or MI. Patients with any other safety concerns related to the trial product or unacceptable intolerability were also excluded.
Interventions
All patients who were insulin naive (ONWARDS 1, 3, and 5) were administered insulin icodec via SC injection at a dose of 70 U (700 units/mL) once weekly. Patients who were previously receiving insulin (ONWARDS 2 and 4) determined their weekly dose of insulin icodec by multiplying their daily basal insulin dose before randomization by 7. Patients switching from a daily insulin analogue treatment to insulin icodec were also required to have a 1-time dose which consisted of the total daily basal insulin dose before randomization multiplied by 7 plus an additional 50% of that dose.
In the ONWARDS 5 study, patients in the insulin icodec treatment arm also used an investigational device called the DoseGuide system. The DoseGuide system consists of the DoseGuide app for patients and the DoseGuide Portal for investigators, which are integrated with the DoseGuide Cloud, where dose recommendations are calculated. The system utilizes measurements from a blood glucose meter via Bluetooth, injection history, and prebreakfast fasting self-measured plasma glucose provided by the patient, and provides the patient with dosing recommendations through the app. Patients were trained on using the DoseGuide system by the investigators.
Comparators in the ONWARDS studies included insulin degludec or insulin glargine. Insulin degludec was administered to patients via SC injection at a concentration of 100 units/mL once daily. Insulin glargine was administered to patients via SC injection at a concentration of either 100 units/mL or 300 units/mL. Once-daily insulin analogues in all ONWARDS studies (degludec, glargine U100, or glargine U300), were initiated and titrated as per the local label and standard clinical practice. For patients enrolled in the ONWARDS 2 and ONWARDS 4 trials switching from a previous once-daily basal insulin, the dose of trial once-daily basal insulin was in accordance with the local label.
Patients’ doses of insulin could be adjusted during the treatment periods of the trials based on 3 prebreakfast values. In the ONWARDS 4 study, patients in the insulin icodec and comparator treatment groups were also administered insulin aspart at mealtimes. Insulin aspart was administered via SC injection (100 units/mL) 2 times to 4 times daily before consumption of food.
Any background medications taken during the trial were considered noninvestigational during the trial and were not provided by Novo Nordisk; patients purchased these medications themselves and were to take them as they were prescribed by their health care professional. Concomitant medications included any antihyperglycemic medication other than trial products that patients were receiving from screening until the end-of-trial visit. Until the end of treatment, only randomized trial products and pretrial noninsulin antihyperglycemic background medications were allowed, except for sulfonylureas and glinides which had to be discontinued (ONWARDS 1, 2, and 4) or reduced by approximately 50% (ONWARDS 3 and 5) at randomization; these medications could be discontinued at the discretion of the investigator if there were any safety concerns. If required, the investigators were also able to initiate antihyperglycemic medications before the end of the trial treatment period.
Outcomes
A list of efficacy end points assessed in this Clinical Review Report is provided in Table 7, followed by descriptions of the outcome measures. Summarized end points are based on outcomes included in the sponsor’s Summary of Clinical Evidence as well as any outcomes identified as important to this review according to the clinical expert consulted by CADTH and stakeholder input from patient and clinician groups and public drug plans. Using the same considerations, the CADTH review team selected end points that were considered to be most relevant to inform CADTH’s expert committee deliberations and finalized this list of end points in consultation with members of the expert committee. All summarized efficacy end points were assessed using GRADE. Select notable harms outcomes considered important for informing CADTH’s expert committee deliberations were also assessed using GRADE.
Table 7: Outcomes Summarized From the Studies Included in the Systematic Review
Outcome measure | ONWARDS 1 | ONWARDS 3 | ONWARDS 5 | ONWARDS 2 | ONWARDS 4 |
|---|---|---|---|---|---|
Change in hemoglobin A1C from baseline | Primarya At week 52 | Primarya At week 26 | Primarya At week 52 | Primarya At week 26 | Primary At week 26 |
Time in range (3.9 mmol/L to 10 mmol/L) | Secondarya At week 52 | NR | NR | Secondary At week 26 | Secondary At week 26 |
Time spent < 3.0 mmol/L | Secondary At week 52 | NR | NR | Secondary At week 26 | Secondary At week 26 |
Time spent > 10.0 mmol/L | Secondary At week 52 | NR | NR | Secondary At week 26 | Secondary At week 26 |
Change in body weight | Secondary At week 52 | Secondary At week 26 | Secondary At week 52 | Secondary At week 26 | Secondary At week 26 |
Number of level 2 or level 3 hypoglycemic episodes b | Secondary At week 52, 78, and 83 | Secondary At week 26 | Secondary At week 52 | Secondary At week 26 | Secondary At week 26 |
Change in DTSQ | NR | NR | Secondary At week 52 | Exploratory At week 26 | NR |
TRIM-D | NR | NR | Secondary At week 52 | NR | NR |
CV death | NR | NR | NR | NR | NR |
Nonfatal MI | NR | NR | NR | NR | NR |
Nonfatal stroke | NR | NR | NR | NR | NR |
All-cause mortality | Safety outcome | Safety outcome | Safety outcome | Safety outcome | Safety outcome |
Other microvascular and macrovascular complications of T2DM | NR | NR | NR | NR | NR |
BG = blood glucose; CV = cardiovascular; DTSQ = Diabetes Treatment Satisfaction Questionnaire; hemoglobin A1C = glycated hemoglobin; MI = myocardial infarction; NR = not reported; T2DM = type 2 diabetes mellitus; TRIM-D = Treatment-Related Impact Measure for Diabetes.
aStatistical testing for these end points was adjusted for multiple comparisons (e.g., hierarchal testing).
bLevel 2 hypoglycemic episodes are defined as “clinically significant” and level 3 as “severe.”
Source: ONWARDS 1 Clinical Study Report,25 ONWARDS 2 Clinical Study Report,28 ONWARDS 3 Clinical Study Report,26 ONWARDS 4 Clinical Study Report,29 and ONWARDS 5 Clinical Study Report.27 Details included in the table are from the sponsor’s Summary of Clinical Evidence.1
Change in Hemoglobin A1C From Baseline
This end point was calculated as the baseline value of hemoglobin A1C at week 0 subtracted from the hemoglobin A1C value at the last week of assessment. Testing for hemoglobin A1C was performed in a central laboratory. A noninferiority margin of 0.3% points was chosen based on the recommendation in the FDA guidance on developing drugs for the treatment of diabetes.17 The clinical expert consulted by CADTH agreed that this was a reasonable margin for the MID between groups.
Time in Range (3.9 mmol/L to 10.0 mmol/L)
Patients were equipped with CGM devices in the relevant trials in several 4-week intervals. In the ONWARDS 1 study, these were weeks 1 to 4, 22 to 26, 48 to 52, 74 to 78, and during follow-up from week 78 to 83. In the ONWARDS 2 study, these were weeks 0 to 4 and weeks 22 to 26. In the ONWARDS 4 study, these were weeks 0 to 4, weeks 22 to 26, and during follow-up from week 26 to 31. There was no CGM in the ONWARDS 3 or ONWARDS 5 studies. In the relevant trials (ONWARDS 1, 2, and 4), the system used was the Dexcom G6 and readings were blinded to both the patient and the investigator and were not used for dose titration or hypoglycemic episode reporting. The sensor and transmitter were fitted, verified, and uploaded by site staff on the patient during site visits and relevant training was the responsibility of the investigator or site staff.
This end point was calculated as 100 times the number of recorded measurements in the glycemic range of 3.9 mmol/L to 10.0 mmol/L, divided by the total number of measurements. International consensus criteria54 required that at least 70% of the planned CGM measurements during the last 4 weeks of treatment are available for end point data to be included in the analysis; the ONWARDS studies were in alignment with international consensus criteria for time in range. A 2019 International Consensus on Time in Range18 identified that a 5% increase in time in range is associated with clinically significant benefits for individuals with type 1 diabetes mellitus or T2DM, and based on this, a between-group difference of approximately 5% may be an appropriate threshold for a clinically important effect.
Time Spent Less Than 3.0 mmol/L
The measurement of blood glucose for the purpose of calculating this outcome was the same as for time in range (3.9 mmol/L to 10.0 mmol/L).
This end point was calculated as 100 times the number of recorded measurements below 3.0 mmol/L (54 mg/dL) divided by the total number of recorded measurements. Following international consensus criteria, it was required that at least 70% of the planned CGM measurements during the last 4 weeks of treatment be available for end point data to be included in the analysis. There was no MID identified in the literature, but the clinical expert consulted by CADTH indicated that a between-arm difference of approximately 1% may be an appropriate threshold for a clinically important effect, based on the fact that 1% of the day is equal to 15 minutes.18
Time Spent Greater Than 10.0 mmol/L
The measurement of blood glucose for the purpose of calculating this outcome was the same as for time in range (3.9 mmol/L to 10.0 mmol/L).
This end point was calculated as 100 times the number of recorded measurements above 10 mmol/L (180 mg/dL) divided by the total number of recorded measurements. Following international consensus criteria, it was required that at least 70% of the planned CGM measurements during the last 4 weeks of treatment be available for end point data to be included in the analysis. The clinical expert consulted by CADTH indicated that a between-group difference of approximately 5% may be an appropriate threshold for a clinically important effect, to align with the MID selected for time in range.18
Change in Body Weight
Body weight was measured by study investigators on predefined days in kilograms or pounds and recorded to 1 decimal place. In the ONWARDS 1, ONWARDS 3, ONWARDS 2, and ONWARDS 4 studies, it was specified in the protocol that weight should be measured without coat and shoes, wearing only light clothing, and assessed with the same equipment throughout the trial if possible. In the ONWARDS 5 study, this detail was not specified.
The body weight value at baseline (week 0) was subtracted from the body weight value measured at the last week of the main trial period (i.e., week 26 or week 52 as applicable). Based on clinical expert opinion, a threshold of clinical importance of 5 kg was selected by CADTH to assess the clinical importance of the results.
Number of Level 2 or Level 3 Hypoglycemic Episodes
Clinically significant (level 2) hypoglycemic events were defined as a reading of less than 3.0 mmol/L (54 mg/dL) confirmed by the trial-supplied blood glucose meter. Severe (level 3) hypoglycemic levels were defined as any event requiring assistance of another person to actively administer carbohydrates, glucagon, or take other corrective actions, whether or not plasma glucose could be recorded to confirm.
A count was conducted of all clinically significant hypoglycemic episodes (level 2) or severe hypoglycemic episodes (level 3) within the main trial time frame, and during the extension phase where appropriate (ONWARDS 1).
Patients were supplied a blood glucose meter including auxiliaries, which used test strips calibrated to plasma values. Patients were instructed to record their self-measured plasma glucose before breakfast daily throughout each of the trials (ONWARDS 1, 2, 3, 4, and 5). In the ONWARDS 4 study, patients were additionally instructed to measure their plasma glucose daily before lunch, before dinner, and at bedtime. These data were used to record relevant hypoglycemic events.
Diagnosis of hypoglycemic episodes included readings of fasting plasma glucose (where possible), neurologic examination after the event (for severe episodes in which readings of fasting plasma glucose were not possible), and patient recordings in an e-diary. Any event of plasma glucose recording under 3.9 mmol/L (70 mg/dL) on the trial-supplied blood glucose meter was to be recorded as a hypoglycemic event in the e-diary. In the event a patient was not able to fill in the e-diary, (e.g., in the case of hospitalization at the time of the episode), it could be reported by the patient retrospectively. If the event fulfilled the criteria for a SAE in addition to the previously mentioned criteria, then an AE form and safety information form were also to be completed.
A 3% between-group threshold of clinically important difference was suggested by the clinical expert consulted by CADTH.
Diabetes Treatment Satisfaction Questionnaire
The DTSQ was developed to assess patient satisfaction with diabetes treatment.55,56 The questionnaire consisted of 6 items which were scored on a scale of 0 to 6, with a total questionnaire score of 0 to 36. Higher scores indicated greater satisfaction with treatment. Patient’s scores in total treatment satisfaction from baseline were subtracted from their score at the final week of analysis. The DTSQ is widely used in the context of clinical trials, but publications on the validation of its psychometric properties in general or specifically for the English version were not identified. Further, it is unclear whether the ONWARDS trials used the Status(S) or the ChangeI version of the DTSQ, the latter of which may be more sensitive to change for patients closer to the ceiling level of satisfaction at baseline.57 No MID was identified in the literature and as this is not a measure used in clinical practice, the clinical expert consulted by CADTH did not provide a clinically informed threshold for a clinically important between-group difference in the change from baseline.
TRIM-D Compliance Domain
The TRIM-D measures patients’ perceptions of the impact of treatment on functioning and well-being.58 Only the compliance domain was reported. The questionnaire was scored with a total value ranging from 4 to 20. The questionnaire consisted of 4 items which were scored on a scale of 1 to 5 and the transformed to a 0 to 100 scale. In the compliance domain, higher scores indicated better compliance. The compliance domain of the TRIM-D was measured at the final week of analysis.
The TRIM-D has been demonstrated to be significantly responsive to change over time59 and demonstrated adequate internal consistency reliability and test-retest reliability.58 However, it is unknown whether these assessments of responsiveness and reliability are relevant to the compliance domain in isolation. No MID was identified in the literature and as this is not a measure used in clinical practice, the clinical expert consulted by CADTH did not provide a clinically informed threshold for a clinically important between-group difference in the change from baseline.
CV Death
This outcome was identified as an outcome of interest by the Canadian Drug Expert Committee (CDEC) presenters for patients with T2DM. However, it was not an outcome assessed in the included studies.
Nonfatal MI
This outcome was identified as an outcome of interest by the CDEC presenters for patients with T2DM. However, it was not an outcome assessed in the included studies.
Nonfatal Stroke
This outcome was identified as an outcome of interest by the CDEC presenters for patients with T2DM. However, it was not an outcome assessed in the included studies.
All-Cause Mortality
This outcome was identified as an outcome of interest by the CDEC presenters for patients with T2DM. It was assessed as a safety outcome (i.e., number of deaths).
Other Microvascular and Macrovascular Complications of T2DM
This outcome was identified as an outcome of interest for patients with T2DM. However, it was not an outcome assessed in the included studies.
Statistical Analysis
A summary of the statistical analyses conducted for each outcome is presented in Table 8.
Sample Size and Power Calculation
ONWARDS 1
Assumptions based on the NN1250-4252 trial,60 which compared insulin degludec 200 U/mL to insulin glargine 300 U/mL among patients with T2DM treated with basal insulin, were used to inform the sample size and power calculations. The sample size of the ONWARDS 1 study was determined based on FDA requirements to have a minimum of 300 patients completing 78 weeks of treatment with insulin icodec, as well as having sufficient marginal power for the confirmatory secondary hypothesis. Assuming 85% of patients would complete treatment, 353 patients per treatment group (i.e., 706 randomized patients) would be required.
The sample size calculation also considered the power for declaring noninferiority with a noninferiority margin of 0.3% points with respect to the primary end point, change in hemoglobin A1C from baseline to week 52, for the specified estimand and the full analysis set (primary analysis set). With 970 patients and the assumption of a mean treatment difference of 0.03% points, there would be 99% power for declaring noninferiority. Assuming 25% of patients will fail screening, approximately 1,293 patients had to be enrolled to randomize 485 patients to each treatment group.
Per assumptions from the NN1250-4252 trial,60 there would be 98% power to detect a true difference of 4% for time-in-target range (3.9 mmol/L to 10.0 mmol/L) from week 48 to 52.
ONWARDS 2
The sample size was calculated with the aim of having 90% power for declaring noninferiority with a noninferiority margin of 0.3% points with respect to change in hemoglobin A1C. Observations from recent studies with basal insulins (NN9068-418561 and NN9068-4229) were used to determine the power required and expected treatment difference for the primary end point. Therefore, based on the NN9068-4185 and NN9068-4229 studies, it was assumed that the ONWARDS 2 study would require 520 patients randomly assigned to the trial product to have 90% power to confirm noninferiority and detect a mean treatment difference of 0.015% points for the primary end point in the overall population. Assuming 25% of patients would be classified as screen failures, approximately 693 patients were required to be screened to achieve randomization of 520 patients. For the hypothesis of superiority of insulin icodec compared to insulin degludec in terms of change from baseline to week 26 in hemoglobin A1C, there would be 49% marginal power and also 49% combined power to detect if the true treatment difference in hemoglobin A1C was 0.18% points with the sample size of 520.
ONWARDS 3
The sample size was calculated with the aim of having 90% power for declaring noninferiority with a noninferiority margin of 0.3% points with respect to change in hemoglobin A1C. Observations from a study with basal insulin analogues in patients with T2DM (NN1250-3998,63 NN1250-3579,64 NN1250-3643,65 and NN1250-367266) were used to determine the number of patients and expected treatment difference in the primary end point for the ONWARDS 3 study. Therefore, there was an assumed mean treatment difference of 0.03% points for the primary end point in the overall population. A total of 580 patients were determined to be required to be randomly assigned to the trial product to have 90% power to confirm noninferiority. For the hypothesis of superiority of insulin icodec compared to insulin degludec in terms of change from baseline to week 26 in hemoglobin A1C there would be 50% marginal power and also 50% combined power to detect if the true treatment difference in hemoglobin A1C is 0.18% points with the sample size of 580.
ONWARDS 4
The sample size was calculated with the aim of having 90% power for declaring noninferiority with a noninferiority margin of 0.3% points with respect to change in hemoglobin A1C. Observations from studies with basal and bolus treatment (NN9068-418561 and NN1250-3582)67 were used to determine the number of patients required to be randomized and the expected treatment difference in the primary end point. Therefore, a total of 580 patients were required to be randomized to ensure 90% power for confirming noninferiority with an assumption of a mean treatment difference of 0.03% points for the primary end point in the overall population. A screen failure rate of 25% was expected, resulting in the need to screen approximately 774 patients to achieve 580 patients.
ONWARDS 5
The sample size was calculated with the aim of having 90% power for declaring noninferiority with a noninferiority margin of 0.3% points with respect to change in hemoglobin A1C. Assumptions for sample size and expected treatment difference for the primary end point in the ONWARDS 5 trial were based on observations from the CONFIRM study68 (a study that compared the real-world effectiveness of insulin degludec and insulin glargine U300 in patients who were insulin naive with T2DM in routine US clinical practice), market analytics on retention and switching from a basal insulin, phase III RCTs (NN1250,67 NN906861), and the Explorys database (a database of electronic medical records representing 39 integrated health care delivery networks in the US). Therefore, a treatment difference of 0.0% points in patients completing 52 weeks of treatment, and a treatment difference of 0.045% points in favour of basal insulin analogues for patients discontinuing randomized treatment before week 52 were expected. The investigators aimed for the trial to be powered to demonstrate noninferiority of insulin icodec used with DoseGuide versus once-daily basal insulin analogues. They also wanted the trial to have reasonable power to detect a treatment difference of 0.3% points in favour of insulin icodec used with DoseGuide in all randomized patients as being statistically significantly different from 0.0% points for the primary end point of change in hemoglobin A1C from baseline to week 52. A total of 1,092 patients were planned to be randomized to the trial to have 90% power to confirm noninferiority and to have 97% marginal power to detect a treatment difference of 0.3% points in favour of insulin icodec used with DoseGuide as being statistically significant different from 0.0% points. A screen failure rate of 9% was expected resulting in the need to screen approximately 1,200 patients to have 1,096 patients randomly assigned to the trial product.
Statistical Testing
The primary estimand for all ONWARDS studies was defined as the treatment difference in change in hemoglobin A1C from baseline to week 26 or week 52 between insulin icodec and once-daily insulin analogues for all randomized patients, regardless of adherence to randomized treatment and changes made to antihyperglycemic background medication. An intent-to-treat approach was used for assessment of the primary estimand.
For all trials, a noninferiority margin of 0.3% points was chosen based on the recommendation from the FDA guidance for industry on developing drugs for treatment of diabetes.17 This margin is also considered to provide sufficient assay sensitivity based on the following considerations.
ONWARDS 1, ONWARDS 3, ONWARDS 5 (insulin naive): The margin represents less than 50% of a suitable conservative estimate of insulin glargine’s treatment effect on hemoglobin A1C in a placebo-controlled trial (–0.85% points; 95% CI, −1.04% to −0.66%) in patients who were insulin naive.69 As only insulin glargine (not insulin degludec) has been compared to placebo in previous trials, the above-mentioned insulin glargine results were used as reference for consideration of the margin.
ONWARDS 2, ONWARDS 4 (insulin experienced): The treatment effect of insulin degludec relative to placebo among patients previously treated with basal insulin has not been investigated in trials. Among a similarly progressed patient population (previously treated with liraglutide) at 52 weeks, the between-group difference in change from baseline in hemoglobin A1C for patients randomized to insulin degludec versus placebo was 0.92% points (95% CI, −1.00% to −0.75%).70 A 0.30%-point noninferiority margin preserves less than 50% of this estimate of insulin degludec’s effect on hemoglobin A1C relative to placebo. The treatment effect of insulin glargine versus placebo in a basal and bolus insulin treated population is unknown.
In the ONWARDS 1 trial, a 2-sided hierarchical testing procedure was used to control the overall type I error at a 5% level. If the primary end point (noninferiority in glycemic control) was concluded, then confirmatory testing was conducted down the following hierarchy as long as the following confirmatory secondary hypothesis at a given stage was confirmed:
Insulin icodec is superior to insulin glargine in terms of time in range (3.9 mmol/L to 10.0 mmol/L) from week 48 to week 52.
Insulin icodec is superior to insulin glargine in terms of change from baseline to week 52 in hemoglobin A1C.
In the ONWARDS 2, ONWARDS 3, and ONWARDS 5 trials, a 2-sided hierarchical testing procedure was used to control the overall type I error at the 5% level. If noninferiority in glycemic control was demonstrated, then confirmatory testing was conducted to test superiority of insulin icodec (plus DoseGuide in ONWARDS 5) over insulin glargine (ONWARDS 2), insulin degludec (ONWARDS 3), or once-daily basal insulin analogues (ONWARDS 5) in terms of change from baseline in hemoglobin A1C at week 26 (ONWARDS 2 and 3) or week 52 (ONWARDS 5).
No hierarchical testing procedure was conducted in the ONWARDS 4 trial.
Table 8: Statistical Analysis of Efficacy End Points
End point | Statistical model | Adjustment factors | Handling of missing data | Sensitivity analyses |
|---|---|---|---|---|
All ONWARDS studies | ||||
Change in hemoglobin A1C | ANCOVA model | Randomized treatment, region, baseline value ONWARDS 3 also included treatment with SU or glinides (yes/no) as an adjustment factor ONWARDS 2 and 4 also included CGM device use (yes/no) as an adjustment factor | Multiple imputation | Two-dimensional tipping point analysis |
Time in range (3.9 mmol/L to 10.0 mmol/L) | ANCOVA model | Randomized treatment, region, baseline value ONWARDS 3 also included treatment with SU or glinides (yes/no) as an adjustment factor ONWARDS 2 and 4 also included CGM device use (yes/no) as an adjustment factor | Multiple imputation | Two-dimensional tipping point analysis |
Time spent > 10.0 mmol/L | ANCOVA model | Randomized treatment, region, baseline value ONWARDS 3 also included treatment with SU or glinides (yes/no) as an adjustment factor ONWARDS 2 and 4 also included CGM device use (yes/no) as an adjustment factor | Multiple imputation | None |
Time spent < 3.0 mmol/L | Negative binomial model with a log-link function and the logarithm of the total number of recorded measurements as an offset | Randomized treatment, region, baseline value ONWARDS 3 also included treatment with SU or glinides (yes/no) as an adjustment factor ONWARDS 2 and 4 also included CGM device use (yes/no) as an adjustment factor | Multiple imputation | None |
Change in FPG | ANCOVA model | Randomized treatment, region, baseline value ONWARDS 3 also included treatment with SU or glinides (yes/no) as an adjustment factor ONWARDS 2 and 4 also included CGM device use (yes/no) as an adjustment factor | Multiple imputation | None |
Change in body weight | ANCOVA model | Randomized treatment, region, baseline value ONWARDS 3 also included treatment with SU or glinides (yes/no) as an adjustment factor ONWARDS 2 and 4 also included CGM device use (yes/no) as an adjustment factor | Multiple imputation | None |
Number of clinically significant hypoglycemic episodes (level 2) (< 3.0 mmol/L [54 mg/dL] confirmed by BG meter) or severe hypoglycemic episodes (level 3) | Negative binomial model with log-link function and main on-treatment period as offset | Randomized treatment, region ONWARDS 3 also included treatment with SU or glinides (yes/no) as an adjustment factor. ONWARDS 2 and 4 also included CGM device use (yes/no) as an adjustment factor | Multiple imputation | None |
Achievement of hemoglobin A1C targetsa | Logistic regression model | Randomized treatment, region, baseline value ONWARDS 3 also included treatment with SU or glinides (yes/no) as an adjustment factor ONWARDS 2 and 4 also included CGM device use (yes/no) as an adjustment factor | Multiple imputation | None |
Mean weekly insulin dose | ANCOVA model | Randomized treatment, region, baseline value ONWARDS 3 also included treatment with SU or glinides (yes/no) as an adjustment factor ONWARDS 2 and 4 also included CGM device use (yes/no) as an adjustment factor | Multiple imputation | Two-dimensional tipping point analysis |
ONWARDS 2 and 5 | ||||
DTSQ | ANCOVA model | Randomized treatment, region, baseline DTSQ value | Multiple imputation | None |
ONWARDS 5 | ||||
Time from baseline to treatment discontinuation or intensification | Stratified log-rank test | Randomized treatment, region | None | None |
TRIM-D | ANCOVA model | Randomized treatment, region | Multiple imputation | None |
ANCOVA = analysis of covariance; BG = blood glucose; CGM: continuous glucose monitoring; DTSQ = Diabetes Treatment Satisfaction Questionnaire; FPG = fasting plasma glucose; hemoglobin A1C = glycated hemoglobin; SU = sulfonylurea; TRIM-D = Treatment-Related Impact Measure for Diabetes.
aAchievement of hemoglobin A1C targets was not a formal end point as part of the ONWARDS studies, although it was prespecified in the statistical analysis plans. This end point was considered to be informative to clinicians treating diabetes. The primary reason this was not included in the ONWARDS studies as a formal end point was to limit the number of end points to reduce biases related to multiplicity and to avoid regulatory guidelines surrounding the acceptance of exploratory end points for approval of new therapies in some countries.
Source: ONWARDS 1 protocol, ONWARDS 1 Clinical Study Report,25 ONWARDS 2 protocol, ONWARDS 2 Clinical Study Report,28 ONWARDS 3 protocol, ONWARDS 3 Clinical Study Report,26 ONWARDS 4 protocol, ONWARDS 4 Clinical Study Report, ONWARDS 5 protocol, and ONWARDS 5 Clinical Study Report.27 Details included in the table are from the sponsor’s Summary of Clinical Evidence.1
Analysis Populations
The definitions of the analysis sets were the same across all studies (refer to Table 9). In certain exceptional cases, patients or observations could be eliminated from the full analysis set; in these cases, the reasons for the exclusions were documented before unblinding.
No subgroup analyses were conducted.
Table 9: Analysis Populations of the ONWARDS Studies
Population | Definition | Application |
|---|---|---|
Full analysis set | All patients randomized. Patients were analyzed according to the randomized treatment. | Summary of patient disposition, protocol deviations, and baseline characteristics, and analysis of efficacy end points. |
Safety set | All patients randomly assigned to trial treatment and who took at least 1 dose of trial product. Patients were analyzed according to the treatment they actually received. | Analysis of study treatment duration, number of treatment injections, duration of exposure to study treatment, harms data, and prior and concomitant treatments. |
Source: ONWARDS 1 Clinical Study Report,25 ONWARDS 2 Clinical Study Report,28 ONWARDS 3 Clinical Study Report,26 ONWARDS 4 Clinical Study Report,29 and ONWARDS 5 Clinical Study Report.27 Details included in the table are from the sponsor’s Summary of Clinical Evidence.1
Results
Patient Disposition
Patient disposition of the ONWARDS 1, ONWARDS 3, and ONWARDS 5 studies is summarized in Table 10, and patient disposition of the ONWARDS 2 and ONWARDS 4 studies is summarized in Table 11. Patient disposition (e.g., percent who completed study, discontinuations) was generally balanced between the treatment arms of each trial. While permanent discontinuation of treatment (< 5%) or withdrawal from the trial (< 3%) was uncommon in most of the studies, approximately 10% of patients in each treatment group in the ONWARDS 5 study permanently discontinued the trial product, and approximately 9% of patients in each group withdrew from the trial. In the ONWARDS 4 study, across the treatment groups, 6% to 8% of patients discontinued the trial product and 8% to 9% of patients withdrew from the trial.
Table 10: Summary of Patient Disposition From ONWARDS 1, 3, and 5 — Patients With T2DM Who Were Insulin Naive
Patient disposition | ONWARDS 1 | ONWARDS 3 | ONWARDS 5 | |||
|---|---|---|---|---|---|---|
Insulin icodec | Insulin glargine | Insulin icodec | Insulin degludec | Insulin icodec | Once daily analoguesa | |
Screened, N | 1,192 | 737 | 1,250 | |||
Randomized, N | 492 | 492 | 294 | 294 | 542 | 543 |
Exposed, N (%) | 492 (100.0) | 492 (100.0) | 293 (99.7) | 294 (100.0) | 542 (100.0) | 538 (99.1) |
Permanent discontinuation from trial product, N (%) | 17 (3.5) | 12 (2.4) | 13 (4.4) | 11 (3.7) | 59 (10.9) | 50 (9.2) |
Permanent discontinuation from trial product and not withdrawn from trial during the treatment period | 7 (1.4) | 5 (1.0) | 7 (2.4) | 3 (1.0) | 20 (3.7) | 4 (0.7)b |
Adverse events | 4 (0.8) | 2 (0.4) | 2 (0.7) | 1 (0.3) | 3 (0.6) | 0 |
Hypoglycemic episode | 0 | 1 (0.2) | 0 | 0 | 3 (0.6) | 0 |
Protocol deviation | 0 | 0 | 1 (0.3) | 0 | 1 (0.2) | 0 |
Violation of the inclusion and/or exclusion criteria | 0 | 0 | 1 (0.3) | 0 | 0 | 0 |
Participation in another clinical trial | 0 | 0 | 0 | 0 | 1 (0.2) | 0 |
Switch to another basal insulin analogue | 0 | 0 | 0 | 0 | 0 | 0 |
Intensification to a basal-bolus regimen or continuous use of bolus insulin | 0 | 0 | 0 | 0 | 1 (0.2) | 0 |
Lack of efficacy | 1 (0.2) | 0 | 0 | 0 | 0 | 0 |
Lost to follow-up | 0 | 0 | 0 | 0 | 1 (0.2) | 0 |
Safety concern related to trial product or unacceptable intolerability | 0 | 0 | 0 | 0 | 0 | 0 |
Other | 2 (0.4) | 2 (0.4) | 4 (1.4) | 2 (0.7) | 11 (2.0) | 3 (0.6) |
Permanent discontinuation of trial product and withdrawn from trial during the treatment period | 10 (2.0) | 7 (1.4) | 6 (2.0) | 8 (2.7) | 39 (7.2) | 46 (8.5) |
Adverse events | 4 (0.8) | 2 (0.4) | 2 (0.7) | 1 (0.3) | 5 (0.9) | 11 (2.0) |
Hypoglycemic episode | 0 | 0 | 0 | 0 | 0 | 0 |
Protocol deviation | 0 | 0 | 0 | 1 (0.3) | 0 | 1 (0.2) |
Violation of the inclusion and/or exclusion criteria | 0 | 0 | 0 | 1 (0.3) | 0 | 1 (0.2) |
Participation in another clinical trial | 0 | 0 | 0 | 0 | 0 | 0 |
Switch to another basal insulin analogue | 0 | 0 | 0 | 0 | 0 | 0 |
Intensification to a basal-bolus regimen or continuous use of bolus insulin | 0 | 0 | 0 | 0 | 1 (0.2) | 0 |
Lack of efficacy | 0 | 0 | 0 | 0 | 0 | NR |
Lost to follow-up | 1 (0.2) | 0 | 0 | 1 (0.3) | 10 (1.8) | 14 (2.6) |
Pregnancy | 0 | 0 | 0 | 0 | 0 | 0 |
Site closure | 1 (0.2) | 0 | 0 | 0 | 0 | 0 |
Epidemic or pandemic | 0 | 0 | 0 | 0 | 0 | 0 |
Withdrawal of consent | 2 (0.4) | 5 (1.0) | 4 (1.4) | 3 (1.0) | 18 (3.3) | 16 (2.9) |
Safety concern related to trial product or unacceptable intolerability | 0 | 0 | 0 | 0 | 0 | 0 |
Other | 2 (0.4) | 0 | 0 | 2 (0.7) | 5 (0.9) | 4 (0.7) |
Withdrawn from trial, N (%) | 10 (2.0) | 7 (1.4) | 6 (2.0) | 8 (2.7) | 45 (8.3) | 50 (9.2) |
Withdrawal of consent by participant | 3 (0.6) | 5 (1.0) | 4 (1.4) | 4 (1.4) | 24 (4.4) | 20 (3.7) |
Lost to follow-up | 2 (0.4) | 0 | 0 | 1 (0.3) | 14 (2.6) | 19 (3.5) |
Investigator decision | 2 (0.4) | 0 | 0 | 2 (0.7) | 3 (0.6) | 5 (0.9) |
Death | 2 (0.4) | 2 (0.4) | 2 (0.7) | 1 (0.3) | 3 (0.6) | 6 (1.1) |
Site closure | 1 (0.2) | 0 | 0 | 0 | 1 (0.2) | 0 |
Epidemic or pandemic | 0 | 0 | 0 | 0 | 0 | 0 |
Completed week 26c of 52d visit, N (%) | 482 (98.0) | 482 (98.0) | 286 (97.3) | 290 (98.6) | 496 (91.5) | 496 (91.3) |
Completed week 26 of 52 visit without permanent discontinuation of trial product | 475 (96.5) | 479 (97.4) | 281 (95.6) | 283 (96.3) | 483 (89.1) | 493 (90.8) |
Completed week 26 of 52 visit after permanent discontinuation of trial product | 7 (1.4) | 3 (0.6) | 5 (1.7) | 7 (2.4) | 13 (2.4) | 3 (0.6) |
FAS, N (%) | 492 (100.0) | 492 (100.0) | 294 (100.0) | 294 (100.0) | 542 (100.0) | 543 (100.0) |
Safety, N (%) | 492 (100.0) | 492 (100.0) | 293 (99.7) | 294 (100.0) | 542 (100.0) | 538 (99.1) |
FAS = full analysis set; NR = not reported; T2DM = type 2 diabetes mellitus.
aOnce-daily basal insulin analogues: insulin degludec, insulin glargine (U100 and U300).
bOne patient was classified as “withdrawal of consent” but returned for follow-up and end-of-trial visit (n = 1).
cWeek 26 visit for ONWARDS 3.
dWeek 52 visit for ONWARDS 1 and ONWARDS 5.
Source: ONWARDS 1 Clinical Study Report,25 ONWARDS 3 Clinical Study Report,26 and ONWARDS 5 Clinical Study Report.27 Details included in the table are from the sponsor’s Summary of Clinical Evidence.1
Table 11: Summary of Patient Disposition From ONWARDS 2 and 4 — Patients With T2DM Who Were Basal or Bolus Insulin Experienced
Patient disposition | ONWARDS 2 | ONWARDS 4 | ||
|---|---|---|---|---|
Insulin icodec | Insulin glargine | Insulin icodec | Insulin degludec | |
Screened, N | 635 | 746 | ||
Randomized, N | 263 | 263 | 291 | 291 |
Exposed, N (%) | 262 (99.6) | 263 (100.0) | 291 (100.0) | 291 (100.0) |
Permanent discontinuation from trial product, N (%) | 7 (2.7) | 10 (3.8) | 17 (5.8) | 22 (7.6) |
Permanent discontinuation from trial product and not withdrawn from trial during the treatment period, N (%) | 4 (1.5) | 6 (2.3) | 2 (0.7) | 4 (1.4) |
Adverse events | 3 (1.1) | 1 (0.4) | 1 (0.3) | 2 (0.7) |
Hypoglycemic episode | 0 | 0 | 0 | 0 |
Protocol deviation | 0 | 1 (0.4) | 0 | 0 |
Violation of the inclusion and/or exclusion criteria | 0 | 1 (0.4) | 0 | 0 |
Participation in another clinical trial | 0 | 0 | 0 | 0 |
Lack of efficacy | 0 | 0 | 0 | 0 |
Lost to follow-up | 0 | 0 | 0 | 0 |
Safety concern related to trial product or unacceptable intolerability | 0 | 0 | 0 | 0 |
Other | 1 (0.4) | 4 (1.5) | 1 (0.3) | 2 (0.7) |
Permanent discontinuation of trial product and withdrawn from trial during the treatment period, N (%) | 3 (1.1) | 4 (1.5) | 15 (5.2) | 18 (6.2) |
Adverse events | 2 (0.8) | 2 (0.8) | 3 (1.0) | 1 (0.3) |
Hypoglycemic episode | 0 | 0 | 0 | 0 |
Protocol deviation | 1 (0.4) | 0 | 0 | 0 |
Violation of the inclusion and/or exclusion criteria | 1 (0.4) | 0 | 0 | 0 |
Intention of becoming pregnant | 0 | 0 | 0 | 0 |
Participation in another clinical trial | 0 | 0 | 0 | 0 |
Lack of efficacy | 0 | 0 | 0 | 0 |
Lost to follow-up | 0 | 0 | 3 (1.0) | 6 (2.1) |
Pregnancy | 0 | 0 | 0 | 0 |
Site closure | 0 | 0 | 0 | 0 |
Epidemic or pandemic | 0 | 0 | 0 | 0 |
Withdrawal of consent | 0 | 2 (0.8) | 6 (2.1) | 8 (2.7) |
Safety concern related to trial product or unacceptable intolerability | 0 | 0 | 0 | 0 |
Other | 0 | 0 | 3 (1.0) | 3 (1.0) |
Withdrawn from trial, N (%) | 3 (1.1) | 5 (1.9) | 16 (5.5) | 18 (6.2) |
Withdrawal of consent by participant | 0 | 3 (1.1) | 9 (3.1) | 10 (3.4) |
Lost to follow-up | 0 | 0 | 3 (1.0) | 6 (2.1) |
Investigator decision | 1 (0.4) | 0 | 2 (0.7) | 1 (0.3) |
Death | 2 (0.8) | 2 (0.8) | 2 (0.7) | 1 (0.3) |
Site closure | 0 | 0 | 0 | 0 |
Epidemic or pandemic | 0 | 0 | 0 | 0 |
Completed week 26 visit, N (%) | 260 (98.9) | 259 (98.5) | 280 (96.2) | 282 (96.9) |
Completed week 26 of 52 visit without permanent discontinuation of trial product | 256 (97.3) | 253 (96.2) | 274 (94.2) | 269 (92.4) |
Completed week 26 of 52 visit after permanent discontinuation of trial product | 4 (1.5) | 6 (2.3) | 6 (2.1) | 13 (4.5) |
FAS, N (%) | 263 (100.0) | 263 (100.0) | 291 (100.0) | 291 (100.0) |
Safety, N (%) | 262 (99.6) | 263 (100.0) | 291 (100.0) | 291 (100.0) |
FAS = full analysis set; T2DM = type 2 diabetes mellitus.
Source: ONWARDS 2 Clinical Study Report28 and ONWARDS 4 Clinical Study Report.29 Details included in the table are from the sponsor’s Summary of Clinical Evidence.1
Baseline Characteristics
Relevant baseline demographic and disease characteristics of patients randomized into the included trials are summarized for the insulin-naive populations (ONWARDS 1, 3, and 5) in Table 12 and for the insulin-experienced populations (ONWARDS 2 and 4) in Table 13.
In the insulin-naive populations (ONWARDS 1, 3, and 5), the mean age of patients in each treatment arm was approximately 58 years to 59 years, and a minority of patients were aged 75 years or older. More patients were male than female in each trial, and the percent male ranged from 54% to 63% across treatment arms. The ONWARDS 1 and ONWARDS 3 studies included sites in Asia, Europe, North America, and South America, while the ONWARDS 5 study included sites in Europe and North America only. No sites were located in Africa. The majority of patients were of white race in all trials; in the ONWARDS 1 and ONWARDS 3 studies, 61% to 68% of each treatment arm were white, while in the ONWARDS 5 study, 88% to 90% were white. In the ONWARDS 1 and ONWARDS 3 studies, the next most represented race was Asian at approximately 26% to 29%, followed by Black or African American, Other, and American Indian or Alaska Native. In the ONWARDS 5 study, the second most represented race was Black or African American (4.4% to 5.2%) followed by Asian (3.5% to 5.2%), while 0.2% to 0.4% were American Indian or Alaska Native, and 0.2% to 1.3% were Other. In each trial, more than half of patients had never smoked, while approximately one-quarter to one-third of patients were previous smokers, and the remainder (< 20%) were current smokers. On average, patients had between 11 years and 12 years of diabetes history and a mean hemoglobin A1C of 8.44% to 8.96% at baseline. Approximately 90% of patients were receiving metformin at baseline, and other common (> 15%) antihyperglycemic background medications included sulfonylureas, SGLT2is, DPP-4is, and GLP-1 RAs. Uncommon antihyperglycemic background medications included thiazolidinediones, alpha-glucosidase inhibitors, and glinides. There were no notable between-group differences in antihyperglycemic background medication at screening.
In the insulin-experienced populations (ONWARDS 2 and 4), the mean age of patients in each treatment arm was approximately 60 years to 62 years, and 3.4% to 7.2% were aged 75 years or older. The percentage who were male was 53% to 62% while 37% to 47% were female. Both studies included Asian, European, and North American sites; the ONWARDS 2 study also included African sites, while the ONWARDS 4 study also included South American sites. The racial distributions were similar to those described in the ONWARDS 1 and ONWARDS 3 studies, where the majority of patients were white (> 50% in each treatment arm), followed in sequence by Asian (32% to 42%), Black or African American (3% to 5%), and finally Other (0% to 2%) or American Indian or Alaska Native (0% to 1%). Similar to the insulin-naive populations, more than half of the patients had never smoked, while approximately one-quarter to one-third of patients were previous smokers, and fewer than 15% per treatment arm were current smokers. The mean duration of diabetes in each treatment arm ranged from 16 years to 18 years, and the mean hemoglobin A1C was 8.10% to 8.31%. Patients in the ONWARDS 2 and ONWARDS 4 studies received prior basal insulins, while patients in the ONWARDS 4 study also received basal and bolus insulins. Across both the ONWARDS 2 and ONWARDS 4 trials, most patients received once-daily regimens of basal insulins, most commonly insulin glargine U100 (43%), insulin degludec (26%), and insulin glargine U300 (18%), with few patients receiving neutral protamine Hagedorn insulin (5%) and insulin detemir (4%). In the ONWARDS 4 trial, the most commonly administered combination basal-bolus therapy was once-daily basal insulin with bolus insulin 3 times daily (75%) followed by once-daily basal insulin with twice-daily bolus insulin (20%).
Table 12: Summary of Baseline Characteristics in Insulin-Naive Populations — ONWARDS 1, 3, and 5 (FAS)
Characteristic | ONWARDS 1 | ONWARDS 3 | ONWARDS 5 | |||
|---|---|---|---|---|---|---|
Insulin icodec n = 492 | Insulin glargine n = 492 | Insulin icodec n = 294 | Insulin degludec n = 294 | Insulin icodec n = 542 | Once daily analogues n = 543 | |
Age, (years), mean (SD) | 59.06 (10.05) | 58.85 (9.85) | 57.70 (10.19) | 58.56 (9.74) | 59.15 (10.79) | 59.39 (10.15) |
18 to < 65 | 333 (67.7) | 332 (67.5) | 210 (71.4) | 201 (68.4) | 359 (66.2) | 363 (66.9) |
65 to < 75 | 134 (27.2) | 144 (29.3) | 74 (25.2) | 84 (28.6) | 150 (27.7) | 154 (28.4) |
≥ 75 | 25 (5.1) | 16 (3.3) | 10 (3.4) | 9 (3.1) | 33 (6.1) | 26 (4.8) |
Sex, n (%) | ||||||
Female | 197 (40.0) | 229 (46.5) | 109 (37.1) | 110 (37.4) | 233 (43.0) | 230 (42.4) |
Male | 295 (60.0) | 263 (53.5) | 185 (62.9) | 184 (62.6) | 309 (57.0) | 313 (57.6) |
Region, n (%) | ||||||
Africa | NA | NA | NA | NA | NA | NA |
Asia | 120 (24.4) | 132 (26.8) | 72 (24.5) | 73 (24.8) | 0 | 0 |
Europe | 245 (49.8) | 226 (45.9) | 71 (24.1) | 71 (24.1) | 286 (52.8) | 271 (49.9) |
North America | 108 (22.0) | 112 (22.8) | 75 (25.5) | 74 (25.2) | 256 (47.2) | 272 (50.1) |
South America | 19 (3.9) | 22 (4.5) | 76 (25.9) | 76 (25.9) | 0 | 0 |
Race, n (%) | ||||||
American Indian or Alaska Native | 2 (0.4) | 0 | 0 | 1 (0.3) | 2 (0.4) | 1 (0.2) |
Asian | 129 (26.2) | 145 (29.5) | 80 (27.2) | 85 (28.9) | 28 (5.2) | 19 (3.5) |
Black or African American | 10 (2.0) | 17 (3.5) | 9 (3.1) | 6 (2.0) | 24 (4.4) | 28 (5.2) |
Native Hawaiian or Other Pacific Islander | 2 (0.4) | 0 | NR | NR | 2 (0.4) | 1 (0.2) |
White | 333 (67.7) | 317 (64.4) | 179 (60.9) | 175 (59.5) | 478 (88.2) | 493 (90.8) |
Other | 16 (3.3) | 13 (2.6) | 11 (3.7) | 11 (3.7) | 7 (1.3) | 1 (0.2) |
Not reported | 0 | 0 | 15 (5.1) | 16 (5.4) | 1 (0.2) | 0 |
Smoking status, n (%) | ||||||
Current smoker | 89 (18.1) | 80 (16.3) | 43 (14.6) | 41 (13.9) | 103 (19.0) | 96 (17.7) |
Previous smoker | 126 (25.6) | 127 (25.8) | 90 (30.6) | 94 (32.0) | 164 (30.3) | 171 (31.5) |
Never smoked | 277 (56.3) | 285 (57.9) | 161 (54.8) | 159 (54.1) | 275 (50.7) | 276 (50.8) |
Antihyperglycemic background medication at screening, n (%) | ||||||
Metformin | 449 (91.3) | 436 (88.6) | 266 (90.5) | 264 (89.8) | 502 (92.6) | 496 (91.3) |
Sodium-glucose cotransporter-2 inhibitor | 187 (38.0) | 172 (35.0) | 119 (40.5) | 95 (32.3) | 234 (43.2) | 240 (44.2) |
Sulfonylurea | 219 (44.5) | 227 (46.1) | 132 (44.9) | 128 (43.5) | 209 (38.6) | 230 (42.4) |
Dipeptidyl peptidase-4 inhibitor | 178 (36.2) | 169 (34.3) | 76 (25.9) | 80 (27.2) | 160 (29.5) | 146 (26.9) |
Glucagon-like peptide-1 receptor agonist | 83 (16.9) | 92 (18.7) | 64 (21.8) | 48 (16.3) | 148 (27.3) | 158 (29.1) |
Thiazolidinedione | 25 (5.1) | 24 (4.9) | 26 (8.8) | 19 (6.5) | 22 (4.1) | 23 (4.2) |
Alpha-glucosidase inhibitor | 23 (4.7) | 22 (4.5) | 18 (6.1) | 20 (6.8) | 3 (0.6) | 3 (0.6) |
Glinide | 11 (2.2) | 15 (3.0) | 7 (2.4) | 4 (1.4) | 2 (0.4) | 11 (2.0) |
BMI (kg/m2), mean (SD) | 29.98 (4.78) | 30.13 (5.05) | 29.87 (5.23) | 29.24 (5.05) | 32.56 (6.99) | 32.95 (6.94) |
Duration of diabetes (years), mean (SD) | 11.62 (6.66) | 11.46 (6.75) | 11.15 (6.61) | 11.48 (6.54) | 11.86 (6.91) | 11.97 (7.60) |
Hemoglobin A1C (%), mean (SD) | 8.50 (0.99) | 8.44 (1.02) | 8.55 (1.11) | 8.48 (1.01) | 8.96 (1.62) | 8.88 (1.50) |
Hemoglobin A1C (mmol/mol), mean (SD) | 69.44 (10.86) | 68.79 (11.13) | 69.96 (12.19) | 69.23 (11.06) | 74.43 (17.73) | 73.60 (16.35) |
FPG (mmol/L), mean (SD) | 10.28 (2.72) | 10.31 (2.87) | 10.37 (3.01) | 9.78 (2.55) | 9.24 (3.00) | 9.60 (3.52) |
eGFR (mL/min/1.73 m2), mean (SD) | 86.05 (18.19) | 84.90 (19.58) | 91.17 (19.54) | 90.37 (18.33) | 88.11 (21.11) | 88.03 (20.31) |
BMI = body mass index; eGFR = estimated glomerular filtration rate; FAS = full analysis set; FPG = fasting plasma glucose; hemoglobin A1C = glycated hemoglobin NA = not applicable; NR = not reported; SD = standard deviation.
Source: ONWARDS 1 Clinical Study Report,25 ONWARDS 3 Clinical Study Report,26 and ONWARDS 5 Clinical Study Report.27 Details included in the table are from the sponsor’s Summary of Clinical Evidence.1
Table 13: Summary of Baseline Characteristics in Insulin-Experienced Populations — ONWARDS 2 and 4 (FAS)
Characteristic | ONWARDS 2 | ONWARDS 4 | ||
|---|---|---|---|---|
Insulin icodec n = 263 | Insulin degludec n = 263 | Insulin icodec n = 291 | Insulin glargine n = 291 | |
Age (years), mean (SD) | 62.35 (9.79) | 62.60 (8.42) | 59.67 (10.13) | 59.91 (9.92) |
18 to < 65 | 145 (55.1) | 149 (56.7) | 189 (64.9) | 184 (63.2) |
65 to < 75 | 99 (37.6) | 99 (37.6) | 92 (31.6) | 96 (33.0) |
≥ 75 | 19 (7.2) | 15 (5.7) | 10 (3.4) | 11 (3.8) |
Sex, n (%) | ||||
Female | 101 (38.4) | 123 (46.8) | 137 (47.1) | 141 (48.5) |
Male | 162 (61.6) | 140 (53.2) | 154 (52.9) | 150 (51.5) |
Region, n (%) | ||||
Africa | 25 (9.5) | 25 (9.5) | 0 | 0 |
Asia | 74 (28.1) | 96 (36.5) | 88 (30.2) | 90 (30.9) |
Europe | 86 (32.7) | 81 (30.8) | 96 (33.0) | 109 (37.5) |
North America | 78 (29.7) | 61 (23.2) | 74 (25.4) | 59 (20.3) |
South America | 0 | 0 | 33 (11.3) | 33 (11.3) |
Race, n (%) | ||||
American Indian or Alaska Native | 2 (0.8) | 0 | 0 | 1 (0.3) |
Asian | 86 (32.7) | 110 (41.8) | 95 (32.6) | 93 (32.0) |
Black Or African American | 11 (4.2) | 12 (4.6) | 13 (4.5) | 8 (2.7) |
Native Hawaiian or Other Pacific Islander | 0 | 0 | 0 | 0 |
White | 161 (61.2) | 137 (52.1) | 183 (62.9) | 187 (64.3) |
Other | 3 (1.1) | 4 (1.5) | 0 | 1 (0.3) |
Not reported | 0 | 0 | 0 | 1 (0.3) |
Smoking status, n (%) | ||||
Current smoker | 37 (14.1) | 36 (13.7) | 28 (9.6) | 39 (13.4) |
Previous smoker | 83 (31.6) | 90 (34.2) | 83 (28.5) | 64 (22.0) |
Never smoked | 143 (54.4) | 137 (52.1) | 180 (61.9) | 188 (64.6) |
Use of personal CGM or FGM, n (%) | ||||
Yes | 7 (2.7) | 16 (6.1) | 52 (17.9) | 50 (17.2) |
No | 256 (97.3) | 247 (93.9) | 239 (82.1) | 241 (82.8) |
Antihyperglycemic background medication at screening, n (%) | ||||
Metformin | 216 (82.1) | 224 (85.2) | 196 (67.4) | 189 (64.9) |
Sodium-glucose cotransporter-2 inhibitor | 89 (33.8) | 84 (31.9) | 82 (28.2) | 86 (29.6) |
Sulfonylurea | 60 (22.8) | 58 (22.1) | 28 (9.6) | 16 (5.5) |
Dipeptidyl peptidase-4 inhibitor | 61 (23.2) | 69 (26.2) | 47 (16.2) | 36 (12.4) |
Glucagon-like peptide-1 receptor agonist | 68 (25.9) | 69 (26.2) | 37 (12.7) | 34 (11.7) |
Thiazolidinedione | 14 (5.3) | 11 (4.2) | 12 (4.1) | 6 (2.1) |
Alpha-glucosidase inhibitor | 14 (5.3) | 14 (5.3) | 7 (2.4) | 11 (3.8) |
Glinide | 10 (3.8) | 9 (3.4) | 0 | 2 (0.7) |
Basal insulin q.d. at screening, n (%) | ||||
Insulin degludec | 75 (28.5) | 73 (27.8) | 73 (25.1) | 67 (23.0) |
Insulin detemir | 6 (2.3) | 6 (2.3) | 13 (4.5) | 15 (5.2) |
Insulin glargine U100 | 108 (41.1) | 103 (39.2) | 144 (49.5) | 129 (44.3) |
Insulin glargine U300 | 38 (14.4) | 43 (16.3) | 56 (19.2) | 67 (23.0) |
Isophane insulin | 20 (7.6) | 20 (7.6) | 3 (1.0) | 6 (2.1) |
Basal insulin b.i.d. at screening, n (%) | ||||
Insulin detemir | 2 (0.8) | 1 (0.4) | 0 | 2 (0.7) |
Insulin glargine U100 | 3 (1.1) | 5 (1.9) | 2 (0.7) | 3 (1.0) |
Insulin glargine U300 | 0 | 1 (0.4) | 0 | 0 |
Isophane insulin | 11 (4.2) | 11 (4.2) | 0 | 2 (0.7) |
Basal-bolus therapy at screening | ||||
Basal q.d. and bolus t.i.d. | NA | NA | 220 (75.6) | 217 (74.6) |
Basal q.d. and bolus b.i.d. | NA | NA | 60 (20.6) | 56 (19.2) |
Basal q.d. and bolus q.i.d. | NA | NA | 7 (2.4) | 5 (1.7) |
Basal b.i.d. and bolus t.i.d. | NA | NA | 2 (0.7) | 6 (2.1) |
Basal q.d. and bolus > q.i.d. | NA | NA | 2 (0.7) | 4 (1.4) |
Basal q.d. and bolus q.d. | NA | NA | 0 | 2 (0.7) |
Basal b.i.d. and bolus b.i.d. | NA | NA | 0 | 1 (0.3) |
BMI (kg/m2), mean (SD) | 29.52 (5.20) | 29.17 (4.89) | 30.55 (5.02) | 29.98 (5.02) |
Duration of diabetes (years), mean (SD) | 16.54 (8.36) | 16.93 (7.92) | 17.97 (9.09) | 16.33 (7.65) |
Hemoglobin A1C (%), mean (SD) | 8.17 (0.77) | 8.10 (0.77) | 8.29 (0.86) | 8.31 (0.90) |
Hemoglobin A1C (mmol/mol), mean (SD) | 65.76 (8.47) | 65.02 (8.46) | 67.11 (9.41) | 67.35 (9.79) |
FPG (mmol/L), mean (SD) | 8.45 (2.63) | 8.36 (2.27) | 9.24 (3.00) | 9.60 (3.52) |
eGFR (mL/min/1.73 m2), mean (SD) | 81.02 (18.81) | 80.23 (19.86) | 81.92 (20.48) | 81.88 (20.27) |
b.i.d. = twice a day; BMI = body mass index; CGM = continuous glucose monitoring; eGFR = estimated glomerular filtration rate; FAS = full analysis set; FGM = flash glucose monitoring; FPG = fasting plasma glucose; hemoglobin A1C = glycated hemoglobin; NA = not applicable; q.d. = once a day; q.i.d. = 4 times a day; SD = standard deviation; t.i.d. = 3 times a day.
Source: ONWARDS 2 Clinical Study Report28 and ONWARDS 4 Clinical Study Report.29 Details included in the table are from the sponsor’s Summary of Clinical Evidence.1
Exposure to Study Treatments
Exposure to study treatments is summarized in Table 14 (ONWARDS 1, 3, and 5) and Table 15 (ONWARDS 2 and 4).
Table 14: Exposure to Study Treatments for ONWARDS 1, 3, and 5 — Patients Who Were Insulin Naive
Exposure | ONWARDS 1 | ONWARDS 3 | ONWARDS 5 | |||
|---|---|---|---|---|---|---|
Insulin icodec n = 492 | Insulin glargine n = 492 | Insulin icodec n = 294 | Insulin degludec n = 294 | Insulin icodec plus DoseGuide n = 542 | Insulin degludec or glargine n = 543 | |
Study duration | 52 weeks | 26 weeks | 52 weeks | |||
Patient-years of exposurea | ||||||
Number of patients (SAS) | 492 | 492 | 293 | 294 | 542 | 538 |
Sum | 485.88 | 485.03 | 170.90 | 171.13 | 559.54 | 560.72 |
Mean (SD) | 0.99 (0.08) | 0.99 (0.11) | 0.58 (0.08) | 0.58 (0.07) | 1.03 (0.20) | 1.04 (0.20) |
Average weekly basal insulin dose during the last 2 weeks of treatment (U) | ||||||
Number of patientsb | 492 | 492 | 293 | 294 | 542 | 542 |
LS mean | 214.23 | 222.39 | 204.28 | 186.52 | 226.51 | 185.23 |
Treatment ratio (insulin icodec to comparator) (95% CI) | 0.96 (0.89 to 1.05) | 1.10 (0.98 to 1.22) | 1.22 (1.12 to 1.33) | |||
P valuec | 0.3701 | 0.0932 | < 0.0001 | |||
ANOVA = analysis of variance; CI = confidence interval; FAS = full analysis set; LS = least squares; SAS = safety analysis set; SD = standard deviation.
aOne patient-year of exposure = 365.25 days.
bReported from SAS in ONWARDS 3, and FAS in ONWARDS 1 and ONWARDS 5.
cP value: Two-sided P value for test of no treatment difference. No correction for multiplicity. The log-transformed response from week 50 to week 52 or week 24 to 26 is analyzed using an ANOVA model with treatment and region as fixed factors. Missing mean values from week 50 to week 52 or week 24 to 26 are imputed using multiple imputation based on values for participants from the comparator group who completed randomized treatment without initiation of bolus insulin for more than 2 weeks at any time before the week 52 visit. Each imputed dataset is analyzed separately, and estimates are combined using Rubin’s rules.
Source: ONWARDS 1 Clinical Study Report,25 ONWARDS 3 Clinical Study Report,26 and ONWARDS 5 Clinical Study Report.27
Table 15: Exposure to Study Treatments for ONWARDS 2 and 4 — Patients Who Were Insulin Experienced (FAS)
Exposure | ONWARDS 2 | ONWARDS 4 | ||
|---|---|---|---|---|
Insulin icodec n = 262 | Insulin degludec n = 263 | Insulin icodec n = 291 | Insulin glargine n = 291 | |
Study duration | 26 weeks | 26 weeks | ||
Patient-years of exposurea | ||||
Number of patients (SAS) | 262 | 263 | 291 | 291 |
Sum | 155.25 | 152.77 | 167.36 | 166.80 |
Mean (SD) | 0.59 (0.04) | 0.58 (0.08) | 0.58 (0.09) | 0.57 (0.10) |
Average weekly basal insulin dose during the last 2 weeks of treatment (U) | ||||
Number of patients (FAS) | 263 | 263 | 291 | 290 |
LS mean | 267.96 | 244.22 | 305.06 | 279.42 |
Treatment ratio (insulin icodec to comparator) (95% CI) | 1.10 (1.01 to 1.20) | 1.09 (1.01 to 1.18) | ||
P valueb | 0.0348 | 0.0286 | ||
Average weekly bolus insulin dose during the last 2 weeks of treatment (U) | ||||
Number of patients (FAS) | NA | 291 | 290 | |
LS mean | NA | 197.45 | 255.26 | |
Treatment ratio (insulin icodec to comparator) (95% CI) | NA | 0.77 (0.70 to 0.86) | ||
P valueb | NA | < 0.0001 | ||
ANOVA = analysis of variance; CI = confidence interval; FAS = full analysis set; LS = least squares; NA = not applicable; NR = not reported; SAS = safety analysis set; SD = standard deviation.
aOne patient-year of exposure = 365.25 days.
bP value: Two-sided P value for test of no treatment difference. No correction for multiplicity. The log-transformed response from week 50 to week 52 or week 24 to 26 is analyzed using an ANOVA model with treatment and region as fixed factors. Missing mean values from week 50 to week 52 or week 24 to 26 are imputed using multiple imputation based on values for participants from the comparator group who completed randomized treatment without initiation of bolus insulin for more than 2 weeks at any time before the week 52 visit. Each imputed dataset is analyzed separately, and estimates are combined using Rubin's rules.
Source: ONWARDS 2 Clinical Study Report28 and ONWARDS 4 Clinical Study Report.29
Efficacy
Key efficacy outcomes are summarized in Table 16 for insulin-naive populations (ONWARDS 1, 3, and 5), and in Table 17 for insulin-experienced populations (ONWARDS 2 and 4).
Change in Hemoglobin A1C From Baseline
Patients Who Were Insulin Naive (ONWARDS 1, ONWARDS 3, and ONWARDS 5)
In the primary analyses for noninferiority, the between-group differences in change from baseline in hemoglobin A1C was –0.19% points (95% CI, –0.36% to –0.03%; P < 0.0001) in the ONWARDS 1 study at 52 weeks, –0.21% points (95% CI, –0.34% to –0.08%; P < 0.0001) in the ONWARDS 3 study at 26 weeks, and –0.38% points (95% CI, –0.66% to –0.09%; P < 0.0001) in the ONWARDS 5 study at 52 weeks.
In each of the ONWARDS 1, ONWARDS 3, and ONWARDS 5 studies, a 2-dimensional tipping point sensitivity analysis was performed to evaluate the robustness of the assumptions regarding missing data; the results were consistent with the primary analysis for noninferiority of hemoglobin A1C and confirmed that insulin icodec was noninferior to the comparator in question.
In the secondary analyses for superiority, the P values were 0.0210, 0.0016, and 0.0092, respectively.
Insulin-Experienced Patients Who Were Insulin Experienced (ONWARDS 2 and ONWARDS 4)
In the primary analyses for noninferiority, estimated treatment difference of change from baseline in hemoglobin A1C was –0.22% points (95% CI, –0.37% to –0.08%; P < 0.0001) in the ONWARDS 2 study and 0.02% points (95% CI, –0.11% to 0.15%; P < 0.0001) for the ONWARDS 4 study.
For both the ONWARDS 2 and 4 studies, a 2-dimensional tipping point sensitivity analysis was performed to evaluate the robustness of the assumptions regarding missing data; the results were consistent with the primary analysis for noninferiority of hemoglobin A1C and confirmed that insulin icodec was noninferior to the comparator in question.
In the ONWARDS 2 study, a secondary analysis for superiority was also conducted (P = 0.0028). No superiority analysis was conducted in the ONWARDS 4 study.
Time in Range (3.9 mmol/L to 10.0 mmol/L)
Patients Who Were Insulin Naive (ONWARDS 1, ONWARDS 3, and ONWARDS 5)
In the ONWARDS 1 study from week 48 to week 52, the LS mean time in glycemic range was 71.27% (SE = 0.85) for insulin icodec and 67.00% (SE = 0.85) for insulin glargine, representing an estimated treatment difference of 4.27% points (95% CI, 1.92% to 6.62%; P = 0.0004). A 2-dimensional tipping point sensitivity analysis was conducted, which aligned with the primary analysis for time in range.
This outcome was not assessed in the ONWARDS 3 or ONWARDS 5 studies.
Patients Who Were Insulin Experienced (ONWARDS 2 and ONWARDS 4)
In the ONWARDS 2 study from week 22 to week 26, the LS mean time in glycemic range between 3.9 mmol/L and 10.0 mmol/L was 62.34% (SE = 1.16) for the insulin icodec group and 59.93% (SE = 1.16) for the insulin degludec group. The estimated treatment difference between insulin icodec and insulin degludec was 2.41% (95% CI, –0.84% to 5.56%; P = 0.1461).
In the ONWARDS 4 study from week 22 to week 26, the LS mean time in glycemic range between 3.9 mmol/L and 10.0 mmol/L was 66.75% (SE = 1.00) for the insulin icodec group and 66.46% (SE = 1.02) for the insulin glargine group. The estimated treatment difference between insulin icodec and insulin glargine was 0.29% (95% CI, –2.52% to 3.09%; P = 0.8406).
Time Spent Less Than 3.0 mmol/L
Patients Who Were Insulin Naive (ONWARDS 1, ONWARDS 3, and ONWARDS 5)
In the ONWARDS 1 study from week 48 to week 52, the LS mean time in glycemic range below 3 mmol/L was 0.21% (SE = not reported) for insulin icodec and 0.16% for insulin glargine (SE = not reported), representing an estimated treatment ratio (insulin icodec:insulin glargine) of 1.27 (95% CI, 0.94 to 1.71; P = 0.1134).
This outcome was not assessed in the ONWARDS 3 or 5 studies.
Patients Who Were Insulin Experienced (ONWARDS 2 and ONWARDS 4)
In the ONWARDS 2 study from week 22 to week 26, the LS mean time in glycemic range below 3.0 mmol/L was 0.33% in the insulin icodec group and 0.24% in the insulin degludec group. The estimated treatment ratio of insulin icodec and insulin degludec was 1.37 (95% CI, 0.92 to 2.04; P = 0.1180).
In the ONWARDS 4 study from week 22 to week 26, the LS mean time in glycemic range below 3.0 mmol/L was 0.69% in the insulin icodec group and 0.58% in the insulin glargine group. The estimated treatment ratio of insulin icodec and insulin glargine was 1.20 (95% CI, 0.91 to 1.58; P = 0.2050).
Time Spent Greater Than 10.0 mmol/L
Patients Who Were Insulin Naive (ONWARDS 1, ONWARDS 3, and ONWARDS 5)
In the ONWARDS 1 study from week 48 to week 52, the LS mean time in glycemic range above 10 mmol/L was 27.56% for insulin icodec and 32.13% for insulin glargine, representing an estimated treatment difference of –4.58% (95% CI, –6.99% to –2.17%; P = 0.0002).
This outcome was not assessed in the ONWARDS 3 or ONWARDS 5 studies.
Patients Who Were Insulin Experienced (ONWARDS 2 and ONWARDS 4)
In the ONWARDS 2 study from week 22 to week 26, the LS mean time in glycemic range above 10 mmol/L was 36.34% (SE = 1.19) for insulin icodec and 39.28% (SE = 1.19) for insulin degludec, representing an estimated treatment difference of –2.93% (95% CI, –6.25% to 0.39%; P = 0.0833).
In the ONWARDS 4 study from week 22 to week 26, the LS mean time in glycemic range above 10 mmol/L was 30.64% for insulin icodec (SE = 1.03) and 31.24% (SE = 1.04) for insulin glargine, representing an estimated treatment difference of –0.60% (95% CI, –3.47% to 2.28%; P = 0.6826).
Change in Body Weight
Patients Who Were Insulin Naive (ONWARDS 1, ONWARDS 3, and ONWARDS 5)
In the ONWARDS 1 study (at 52 weeks), ONWARDS 3 study (at 26 weeks), and ONWARDS 5 study (at 52 weeks), the between-group differences in change in body weight from baseline were 0.46 kg (95% CI, –0.12 kg to 1.04 kg; P = 0.1187), 0.46 kg (95% CI, –0.19 kg to 1.10 kg; P = 0.1657), and 0.83 kg (95% CI, –0.37 kg to 2.02 kg; P = 0.1747), respectively.
Patients Who Were Insulin Experienced (ONWARDS 2 and ONWARDS 4)
In the ONWARDS 2 study (at 26 weeks) and ONWARDS 4 study (at 26 weeks), the between-group differences in change in body weight from baseline were 1.70 kg (95% CI, 0.76 kg to 2.63 kg; P = 0.0004) and 0.57 kg (95% CI, –0.39 kg to 1.54 kg; P = 0.2444), respectively.
Number of Clinically Significant Level 2 or Level 3 Hypoglycemic Episodes
Patients Who Were Insulin Naive (ONWARDS 1, ONWARDS 3, and ONWARDS 5)
In the ONWARDS 1 study, a similar number of patients experienced level 2 hypoglycemic events in the 2 groups, but there were numerically more level 2 events in the insulin icodec group. There were 143 events in 48 patients (9.8%) in the insulin icodec group and 75 events occurring in 49 patients (10.0%) in the insulin glargine group. In the insulin icodec group, 3 of the 492 patients (0.6%) experienced 61 of the 143 clinically significant hypoglycemic events. The remaining patients in the insulin icodec group and all of the patients in the insulin glargine groups experienced between 1 and 5 episodes of level 2 hypoglycemic events. The estimated treatment ratio for level 2 events (insulin icodec:insulin glargine) was 1.67 (95% CI, 0.99 to 2.84; P = 0.0561). Severe (level 3) hypoglycemic events occurred in 1 patient (0.2%) in the insulin icodec group, and 3 patients (0.6%) in the insulin glargine group.
In the ONWARDS 3 study, there were 53 clinically significant events of hypoglycemia (level 2) reported in 26 patients (8.9%) in the insulin icodec group, and 23 events occurring in 17 patients (22.1%) in the insulin degludec group. In the insulin icodec group, 2 patients (0.7%) experienced 15 of the 53 clinically significant hypoglycemic events. The remaining patients in the insulin icodec group experienced between 1 and 4 episodes of level 2 hypoglycemic events. Patients in the insulin degludec group experienced between 1 and 3 episodes of level 2 hypoglycemic events. The estimated treatment ratio for level 2 events (insulin icodec:insulin degludec) was 2.09 (95% CI, 0.99 to 4.41; P = 0.0536). Severe hypoglycemic events occurred in zero patients in the insulin icodec group, and 2 patients (0.7%) in the insulin degludec group.
In the ONWARDS 5 study, there were 104 clinically significant (level 2) hypoglycemic events that were reported in 64 patients (11.8%) in the insulin icodec group, and 81 events occurring in 45 patients (8.4%) in the once-daily analogues group. The estimated treatment ratio for level 2 events (insulin icodec:once-daily analogues) was 1.23 (95% CI, 0.77 to 1.98; P = 0.3928). Severe (level 3) hypoglycemic events occurred in zero patients in the insulin icodec group, and 4 patients (0.7%) in the insulin glargine group.
Patients Who Were Insulin Naive (ONWARDS 2 and ONWARDS 4)
In the ONWARDS 2 study, there were 113 clinically significant events of hypoglycemia (level 2) reported in 37 patients (14.1%) in the insulin icodec group, and 41 events occurring in 19 patients (7.2%) in the insulin degludec group. The estimated treatment ratio for level 2 events (insulin icodec:insulin degludec) was 1.98 (95% CI, 0.95 to 4.12; P = 0.0677). Severe hypoglycemic events occurred in zero patients in the insulin icodec group, and 1 patient (0.4%) in the insulin degludec group.
In the ONWARDS 4 study, clinically significant events of hypoglycemia (level 2) were reported in 148 patients (50.9%) in the insulin icodec group, and 160 patients (55.0%) in the insulin glargine group. The estimated treatment ratio for level 2 events (insulin icodec/insulin glargine) was 0.99 (95% CI, 0.73 to 1.34; P = 0.9274). Severe (level 3) hypoglycemic events occurred in 4 patients (1.4%) in the insulin icodec group, and 2 patients (0.7%) in the insulin glargine group.
Diabetes Treatment Satisfaction Questionnaire
This outcome was assessed only in the ONWARDS 5 and ONWARDS 2 studies.
Patients Who Were Insulin Naive (ONWARDS 5)
In the ONWARDS 5 study, the observed mean DTSQ total score at baseline was 26.15 in the insulin icodec plus DoseGuide group and 26.77 in the once-daily analogues group. The estimated LS mean DTSQ total score at week 52 was 31.13 (SE = 0.25) in the insulin icodec group and 30.35 (SE = 0.25) in the once-daily analogues group, representing a LS mean change from baseline in DTSQ total satisfaction score of 4.68 (SE = 0.25) and 3.90 (SE = 0.25), respectively. The LS mean difference between groups was 0.78 (95% CI, 0.10 to 1.47; P = 0.0247).
Patients Who Were Insulin Experienced (ONWARDS 2)
In the ONWARDS 2 study, the observed mean DTSQ total score at baseline was 26.76 in the insulin icodec group and 26.69 in the insulin degludec group. The estimated LS mean DTSQ total score at week 26 was 30.95 (SE = 0.30) in the insulin icodec group and 29.69 (SE = 0.31) in the insulin degludec group, representing a LS mean change from baseline in DTSQ total satisfaction score of 4.22 (SE = 0.30) and 2.96 (SE = 0.31), respectively. The estimated LS mean treatment difference between insulin icodec and insulin degludec was 1.25 (95% CI, 0.41 to 2.10; P = 0.0036).
TRIM-D Compliance Domain
This outcome was assessed only in the ONWARDS 5 study. The estimated treatment difference was 3.04 (95% CI, 1.28 to 4.81; P = 0.0007) at 52 weeks.
CV Death
CV death was not measured as an outcome in the included trials.
Nonfatal MI
Nonfatal MI was not measured as an outcome in the included trials.
Nonfatal Stroke
Nonfatal stroke was not measured as an outcome in the included trials.
Other Microvascular and Macrovascular Complications of T2DM
Other microvascular and macrovascular complications of T2DM were not measured as outcomes in the included trials.
Table 16: Summary of Key Efficacy End Points for ONWARDS 1, 3, and 5 — Patients Who Were Insulin Naive
Outcome | ONWARDS 1 | ONWARDS 3 | ONWARDS 5 | |||
|---|---|---|---|---|---|---|
Insulin icodec n = 492 | Insulin glargine n = 492 | Insulin icodec n = 294 | Insulin degludec n = 294 | Insulin icodec n = 542 | Insulin degludec or glargine n = 543 | |
Change from baseline in hemoglobin A1C (% points) — FAS | ||||||
Primary | ||||||
Observed mean at baseline | 8.50 | 8.44 | 8.55 | 8.48 | 8.96 | 8.88 |
LS mean at week 26 of 52, estimate (SE) | 6.93 (0.06) | 7.12 (0.05) | 6.95 (0.05) | 7.16 (0.05) | 7.24 (0.09) | 7.61 (0.12) |
Change from baseline LS mean, estimate (SE) | –1.55 (0.06) | –1.35 (0.05) | –1.57 (0.05) | –1.36 (0.05) | –1.68 (0.09) | –1.31 (0.12) |
LS mean treatment difference of insulin icodec – insulin glargine or insulin degludec (95% CI) | –0.19 (–0.36 to –0.03) | –0.21 (–0.34 to –0.08) | –0.38 (–0.66 to –0.09) | |||
Noninferiority P value | < 0.0001a | < 0.0001a | < 0.0001a | |||
Secondary confirmatory | ||||||
Superiority P value | 0.0210a | 0.0016a | 0.0092a | |||
Time in range 3.9 mmol/L to 10.0 mmol/L (70 mg/dL to 180 mg/dL) (%) — FAS | ||||||
Complete cases, n (%) | 492 (100) | 492 (100) | NR | NR | ||
LS mean, % (SE) | 71.27 (0.85) | 67.00 (0.85) | NR | NR | ||
LS mean treatment difference of insulin icodec – insulin glargine (95% CI) | 4.27 (1.92 to 6.62) | NR | NR | |||
P value | 0.0004a | NR | NR | |||
Time spent < 3.0 mmol/L (54 mg/dL) (%) — FAS | ||||||
Complete cases, n (%) | 492 (100) | 492 (100) | NR | NR | ||
LS mean, % (SE) | 0.21 (NR) | 0.16 (NR) | NR | NR | ||
LS mean treatment difference of insulin icodec – insulin glargine (95% CI) | 1.27 (0.94 to 1.71) | NR | NR | |||
P value | 0.1134 | NR | NR | |||
Time spent > 10.0 mmol/L (180 mg/dL) (%) — FAS | ||||||
Complete cases, n (%) | 492 (100) | 492 (100) | NR | NR | ||
LS mean, % (SE) | 27.56 (0.87) | 32.13 (0.87) | NR | NR | ||
LS mean treatment difference of insulin icodec – insulin glargine (95% CI) | –4.58 (–6.99 to –2.17) | NR | NR | |||
P value | 0.0002 | NR | NR | |||
Change in body weight (kg) — FAS | ||||||
Complete cases, n (%) | 492 (100) | 492 (100) | 293 (99.7) | 294 (100) | 542 (100) | 542 (99.8) |
Observed mean at baseline | 85.17 | 84.31 | 85.78 | 83.24 | 93.21 | 94.37 |
LS mean at week 26 of 52 (SE) | 87.03 (0.21) | 86.57 (0.21) | 87.27 (0.22) | 86.82 (0.24) | 96.05 (0.37) | 95.22 (0.50) |
LS mean change from baseline (SE) | 2.29 (0.21) | 1.83 (0.21) | 2.77 (0.22) | 2.32 (0.24) | 2.28 (0.37) | 1.45 (0.50) |
LS mean treatment difference of insulin icodec – insulin glargine or insulin degludec (95% CI) | 0.46 (–0.12 to 1.04) | 0.46 (–0.19 to 1.10) | 0.83 (–0.37 to 2.02) | |||
P value | 0.1187 | 0.1657 | 0.1747 | |||
Number of level 2 or level 3 hypoglycemic episodesb — SAS | ||||||
Complete cases, n (%) | 492 (100) | 492 (100) | 293 (99.7) | 294 (100) | 542 (100) | 538 (99.1) |
Number of events | 144 | 78 | 53 | 25 | 104 | 81 |
Number of patients with event, n (%) | 48 (9.8) | 52 (10.6) | 26 (8.9) | 18 (6.1) | 64 (11.8) | 45 (8.4) |
Incidence rate, episodes per 100 PYEc | 29.64 | 16.08 | 31.01 | 14.61 | 18.61 | 14.56 |
Treatment difference of insulin icodec – insulin glargine or insulin degludec (95% CI) | 1.64 (0.98 to 2.75) | 1.82 (0.87 to 3.80) | 1.14 (0.70 to 1.87) | |||
P value | 0.0611 | 0.0111 | 0.6004 | |||
DTSQ — FAS | ||||||
Complete cases, n (%) | NR | NR | 513 (94.5) | 500 (92.1) | ||
Sum score for DTSQ, LS mean (SE) at week 52 | NR | NR | 31.13 (0.25) | 30.35 (0.25) | ||
Change from baseline, LS mean (SE) at week 52 | NR | NR | 4.68 (0.25) | 3.90 (0.25) | ||
Treatment difference of insulin icodec – insulin glargine or insulin degludec (95% CI) | NR | NR | 0.78 (0.10 to 1.47) | |||
P value | NR | NR | 0.0247 | |||
Treatment-Related Impact Measure for Diabetes compliance domain — FAS | ||||||
Complete cases, n (%) | NR | NR | 542 (100) | 543 (100) | ||
LS mean total score at week 52 (SE) | NR | NR | 90.42 (0.64) | 87.37 (0.64) | ||
LS mean treatment difference of insulin icodec – insulin glargine or insulin degludec (95% CI) | NR | NR | 3.04 (1.28 to 4.81) | |||
P value | NR | NR | 0.0007 | |||
BG = blood glucose; CI = confidence interval; DTSQ = Diabetes Treatment Satisfaction Questionnaire; FAS = full analysis set; hemoglobin A1C = glycated hemoglobin; LS = least squares; NR = not reported; PYE = patient-years of exposure; SAS = safety analysis set; SE = standard error.
aP value has been adjusted for multiple testing. P values not accompanied by this footnote are not adjusted for multiple testing.
bLevel 2 hypoglycemic episodes are defined as “clinically significant” episodes and level 3 hypoglycemic episodes are defined as “severe” episodes.
cOne PYE = 365.25 days.
Source: ONWARDS 1 Clinical Study Report,25 ONWARDS 3 Clinical Study Report,26 and ONWARDS 5 Clinical Study Report.27 Details included in the table are from the sponsor’s Summary of Clinical Evidence.1
Table 17: Summary of Key Efficacy End Points for ONWARDS 2 and 4 — Patients Who Were Insulin Experienced
Outcome | ONWARDS 2 | ONWARDS 4 | ||
|---|---|---|---|---|
Insulin icodec n = 263 | Insulin degludec n = 263 | Insulin icodec n = 291 | Insulin glargine n = 291 | |
Change from baseline in hemoglobin A1C (% points) — FAS | ||||
Primary | ||||
Observed mean at baseline | 8.17 | 8.10 | 8.29 | 8.31 |
LS mean at week 52 (SE) | 7.20 (0.05) | 7.42 (0.06) | 7.14 (0.05) | 7.12 (0.05) |
Change from baseline, LS mean (SE) | –0.93 (0.05) | –0.71 (0.06) | –1.16 (0.05) | –1.18 (0.05) |
LS mean treatment difference insulin icodec – insulin glargine (95% CI) | –0.22 (–0.37 to –0.08) | 0.02 (–0.11 to 0.15) | ||
Noninferiority P value | < 0.0001a | < 0.0001 | ||
Secondary confirmatory | ||||
Superiority P value | 0.0028 | NR | ||
Time in range 3.9 mmol/L to 10.0 mmol/L (70 mg/dL to 180 mg/dL) (%) — FAS | ||||
Complete cases, n (%) | 263 (100) | 263 (100) | 291 (100) | 291 (100) |
LS mean, % (SE) | 62.34 (1.16) | 59.93 (1.16) | 66.75 (1.00) | 66.46 (1.02) |
LS mean treatment difference of insulin icodec – insulin glargine or insulin degludec (95% CI) | 2.41 (–0.84 to 5.65) | 0.29 (–2.52 to 3.09) | ||
P value | 0.1461 | 0.8406 | ||
Time spent < 3.0 mmol/L (54 mg/dL) (%) — FAS | ||||
Complete cases, n (%) | 238 (91.5) | 239 (90.9) | 244 (83.8) | 237 (81.4) |
LS mean, % (SE) | 0.33 (NR) | 0.24 (NR) | 0.69 | 0.58 |
Treatment ratio of insulin icodec to insulin glargine or insulin degludec (95% CI) | 1.37 (0.92 to 2.04) | 1.20 (0.91 to 1.58) | ||
P value | 0.1180 | 0.2050 | ||
Time spent > 10.0 mmol/L (180 mg/dL) (%) — FAS | ||||
Complete cases, n (%) | 263 (100) | 263 (100) | 291 (100) | 291 (100) |
LS mean, % (SE) | 36.34 (1.19) | 39.28 (1.19) | 30.64 (1.03) | 31.24 (1.04) |
LS mean treatment difference of insulin icodec – insulin glargine or insulin degludec (95% CI) | –2.93 (–6.25 to 0.39) | –0.60 (–3.47 to 2.28) | ||
P value | 0.0833 | 0.6826 | ||
Change in body weight (kg) — FAS | ||||
Complete cases, n (%) | 263 (100) | 263 (100) | 291 (100) | 291 (100) |
Observed mean at baseline | 83.72 | 81.54 | 85.51 | 83.08 |
LS mean at week 26 (SE) | 84.03 (0.32) | 82.33 (0.36) | 87.03 (0.29) | 86.45 (0.40) |
LS mean change from baseline (SE) | 1.40 (0.32) | –0.30 (0.36) | 2.73 (0.29) | 2.16 (0.40) |
LS mean treatment difference of insulin icodec – insulin glargine or insulin degludec (95% CI) | 1.70 (0.76 to 2.63) | 0.57 (–0.39 to 1.54) | ||
P value | 0.0004 | 0.2444 | ||
Number of level 2 or level 3 hypoglycemic episodes (level 3)b — SAS | ||||
Complete cases, n (%) | 262 (99.6) | 263 (100) | 291 (100) | 291 (100) |
Number of events | 113 | 42 | 994 | 938 |
Number of patients with event, n (%) | 37 (14.1) | 19 (7.2) | 150 (51.5) | 162 (55.7) |
Incidence rate, episodes per 100 PYEc | 72.79 | 27.49 | 564.05 | 562.36 |
Treatment difference of insulin icodec – insulin glargine or insulin degludec (95% CI) | 1.93 (0.93 to 4.02) | 0.99 (0.73 to 1.33) | ||
P value | 0.0782 | 0.9270 | ||
DTSQ — FAS | ||||
Complete cases, n (%) | 263 (100) | 263 (100) | NR | NR |
Sum score for DTSQ, LS mean (SE) at week 26 | 30.95 (0.30) | 29.69 (0.31) | NR | NR |
Change from baseline, LS mean (SE) at week 26 | 4.22 (0.30) | 2.96 (0.31) | NR | NR |
LS mean treatment difference of insulin icodec – insulin glargine or insulin degludec (95% CI) | 1.25 (0.41 to 2.10) | NR | ||
P value | 0.0036 | NR | ||
Treatment-Related Impact Measure for Diabetes compliance domain — FAS | ||||
NR | NR | NR | NR | NR |
BG = blood glucose; CI = confidence interval; DTSQ = Diabetes Treatment Satisfaction Questionnaire; FAS = full analysis set; hemoglobin A1C = glycated hemoglobin; LS = least squares; NR = not reported; PYE = patient-years of exposure; SAS = safety analysis set; SE = standard error.
aP value has been adjusted for multiple testing. P values not accompanied by this footnote are not adjusted for multiple testing.
bLevel 2 hypoglycemic episodes are defined as “clinically significant” episodes and level 3 hypoglycemic episodes are defined as “severe” episodes.
cOne PYE = 365.25 days.
Source: ONWARDS 2 Clinical Study Report28 and ONWARDS 4 Clinical Study Report.29 Details included in the table are from the sponsor’s Summary of Clinical Evidence.1
Harms
Refer to Table 18 and Table 19 for harms data in the insulin-naive populations (ONWARDS 1, 3, and 5) and insulin-experienced populations (ONWARDS 2 and 4), respectively.
Adverse Events
The proportion of AEs was similar between the insulin icodec and once-daily insulin analogue comparator groups in all ONWARDS studies. The most common AEs were COVID-19, nasopharyngitis, diarrhea, and back pain. The majority of AEs were determined by the study investigators to be nonserious, mild to moderate in severity, unlikely related to trial products, and recovered or recovering by the end of the trial duration in each trial.
In the insulin-naive populations (ONWARDS 1, 3, and 5), 50% to 71% of patients across each treatment arm experienced at least 1 AE.
In the insulin-experienced populations (ONWARDS 2 and 4), 51% to 62% of patients across each treatment arm experienced at least 1 AE.
Serious AEs
SAEs occurred in similar proportions across both the insulin icodec groups and the once-daily analogues groups in each trial.
In the insulin-naive populations (ONWARDS 1, 3, and 5),among patients treated with insulin icodec, 5.1% to 10.4% of patients had at least 1 SAE. In these same trials, among patients treated with the comparator once-daily analogues, 5.1% to 10.6% of patients had at least 1 SAE.
In the insulin-experienced populations (ONWARDS 2 and 4), among patients treated with insulin icodec or once-daily analogues, 7.6% to 8.4% and 6.1% to 8.6% had at least 1 SAE, respectively.
Reported SAEs included: cardiac disorders; infections and infestations; injury, poisoning, and procedural; vascular disorders; musculoskeletal and connective tissue disorders; neoplasms benign, malignant and unspecified nervous system disorders; eye disorders; reproductive system and breast disorders; respiratory, thoracic, and mediastinal disorders; blood and lymphatic system disorders; congenital, familial, and genetic disorders; gastrointestinal disorders; and metabolism and nutrition disorders; renal and urinary disorders. Each of these SAE categories occurred in 0 to less than 5% of patients. The most frequent category of SAE observed was cardiac disorders, which ranged from approximately 3% to 4% of patients in the included studies, followed by infections and infestations (in approximately 2% to 3% of patients). There was no 1 most common event observed.
Withdrawals Due to AEs
In the insulin-naive populations (ONWARDS 1, 3, and 5), permanent discontinuation of the study drug due to AE occurred in 0.7% to 1.2% of patients treated with insulin icodec, and 0.8% to 1.3% of patients treated with comparators (insulin glargine or insulin degludec). In the insulin-experienced populations (ONWARDS 2 and 4), permanent discontinuation of the study drug due to AEs occurred in 1.0% to 1.9% of patients treated with insulin icodec, and 1.0 to 1.1% of patients treated with insulin degludec or insulin glargine. Temporary discontinuation was similarly uncommon, as were AEs leading to dose increases or dose decreases.
Mortality
In the ONWARDS 1 study, there were a total of 8 events in 6 (0.6%) patients with fatal outcomes, with 5 events in 4 (0.8%) patients in the insulin icodec treatment group and 3 events in 2 (0.4%) patients in the insulin glargine treatment group. The events included infections and infestations (n = 2) and 1 each of COVID-19, cardiac disorders (angina pectoris), postoperative infection, pancreatic neoplasm, glioblastoma, unknown cause, and acute coronary syndrome. The death due to unknown cause in the insulin glargine treatment group was judged by investigators as “possibly” related to the trial product.
In the ONWARDS 3 study, there were a total of 2 events occurring among 2 patients (0.7%) in the insulin icodec group, and 1 event in 1 patient (0.3%) in the insulin degludec group leading to fatal outcomes. In the insulin icodec group, deaths were due to malignancy and an undetermined cause (n = 1 for each). In the insulin degludec group, death was due to acute MI (n = 1).
In the ONWARDS 5 study, there were a total of 3 events occurring among 3 patients (0.6%) in the insulin icodec plus DoseGuide group, and 8 events in 7 patients (1.3%) in the once-daily analogues group leading to fatal outcomes. In the insulin icodec plus DoseGuide group, deaths were due to an undetermined cause (n = 2) and malignancy (n = 1). In the once-daily analogues group, deaths were due to pulmonary causes (n = 2), undetermined causes (n = 2), malignancy, sudden cardiac death, and heart failure (n = 1 for each).
In the ONWARDS 2 study, there were a total of 3 events in 2 patients (0.8%) in the insulin icodec group and 2 events in 2 patients (0.8%) in the insulin degludec group leading to fatal outcomes. In the insulin icodec group, deaths were due to infection (n = 2). In the insulin degludec group, deaths were due to CV procedures and malignancy (n = 1 for each).
In the ONWARDS 4 study, there were a total of 4 events in 2 patients (0.7%) in the insulin icodec group and 1 event in 1 patient (0.3%) in the insulin glargine group leading to fatal outcomes. In the insulin icodec group, deaths were due to other CV causes and infection (including sepsis) (n = 1 for each). In the insulin glargine group, there was 1 instance of gastrointestinal bleeding which resulted in death.
Notable Harms
Prespecified notable harms included hypersensitivity, injection site reactions, hypoglycemia, and nocturnal hypoglycemia.
Hypersensitivity
Events of hypersensitivity were reported among less than 7% patients during all ONWARDS studies.
In the ONWARDS 1 study, a total of 23 patients (4.7%) experienced 29 events of hypersensitivity in the insulin icodec group, compared to 32 patients (6.5%) who experienced 45 events in the insulin glargine group. No events were considered serious, and all events were considered moderate or mild in severity. In the ONWARDS 3 study, a total of 7 patients (2.4%) experienced 7 events of hypersensitivity in the insulin icodec group, compared to 13 patients (4.4%) who experienced 15 events in the insulin degludec group. No events were considered serious. In the ONWARDS 5 study, a total of 14 patients (2.6%) experienced 29 events of hypersensitivity in the insulin icodec plus DoseGuide group, compared to 14 patients (2.6%) who experienced 16 events in the once-daily insulin analogues group. One patient (0.2%) in the insulin icodec plus DoseGuide group experienced 1 event which was considered serious; no serious hypersensitivity events occurred in the once-daily insulin analogue comparator group.
In the ONWARDS 2 study, a total of 9 patients (3.4%) experienced 9 events of hypersensitivity in the insulin icodec group, compared to 5 patients (1.9%) who experienced 5 events in the insulin degludec group. One patient in each treatment group (0.4%) experienced 1 hypersensitivity event which was considered serious. In the ONWARDS 4 study, a total of 6 patients (2.1%) experienced 6 events of hypersensitivity in the insulin icodec group, compared to 7 patients (2.4%) who experienced 7 events in the insulin glargine group. No events were considered serious.
Injection Site Reactions
Injection site reactions occurred among less than 9% of patients across all ONWARDS studies.
In the ONWARDS 1 study, 6 patients (1.2%) experienced 6 events in the insulin icodec group compared to 12 patients (2.4%) experiencing 12 events in the insulin glargine group. All events were considered mild or moderate in severity. In the ONWARDS 3 study, 25 patients (8.5%) experienced 62 events in the insulin icodec group compared to 13 patients (4.4%) who experienced 22 events in the insulin degludec group. Of the 62 injection site reactions reported in the insulin icodec group, 24 events were reported by only 2 patients. No events were considered serious. In the ONWARDS 5 study, 5 patients (0.9%) experienced 6 events in the insulin icodec plus DoseGuide group compared to 7 patients (1.3%) who experienced 28 events in the once-daily insulin analogue group. No events of injection site reactions were considered serious.
In the ONWARDS 2 study, 3 patients (1.1%) experienced 3 events in the insulin icodec group compared to 1 patient (0.4%) who experienced 1 event in the insulin degludec group. All events of injection site reactions were considered mild or moderate in severity. In the ONWARDS 4 study, 2 patients (0.7%) experienced 2 events in both the insulin icodec and insulin glargine groups. No events of injection site reactions were considered serious, and all were mild in severity.
Hypoglycemia
In the ONWARDS 1 study, there was a greater proportion of level 1 hypoglycemic events in the insulin icodec group with a total of 232 patients (47.2%) compared to 191 patients (38.8%) in the insulin glargine group. There were similar proportions of patients who experienced level 2 events, but more level 2 events in total occurred in the insulin icodec group than the insulin glargine group, and a small number of patients experienced numerous level 2 events; level 3 events were rare in both groups (refer to hypoglycemia efficacy outcomes previously reported for additional detail on level 2 and 3 events).
In the ONWARDS 3 study, there was a greater proportion of level 1 hypoglycemic events in the insulin icodec group with a total of 145 patients (55.3%) compared to 118 patients (44.9%) in the insulin degludec group. More patients in the insulin icodec group experienced level 2 events, and there was a higher total number of level 2 events in the insulin icodec arm compared to the insulin degludec group, and a small number of patients experienced numerous level 2 events; level 3 events did not occur in the insulin icodec group and were rare in the insulin degludec group (refer to hypoglycemia efficacy outcomes previously reported for additional detail on level 2 and 3 events).
In the ONWARDS 5 study, there was a greater proportion of level 1 hypoglycemic events in the insulin icodec group with a total of 200 patients (36.9%) compared to 153 patients (28.4%) in the once-daily analogues group. There was a larger proportion of patients who experienced level 2 events and more total level 2 events in the insulin icodec group compared to the once-daily analogues group. Severe (level 3) events occurred in no patients in the insulin icodec group and were rare in the insulin glargine group (refer to hypoglycemia efficacy outcomes previously reported for additional detail on level 2 and 3 events).
In the ONWARDS 2 study, there was a greater proportion of level 1 hypoglycemic events in the insulin icodec group with a total of 145 patients (55.3%) compared to 118 patients (44.9%) in the insulin degludec group. There was a larger proportion of patients who experienced level 2 events and more total level 2 events in the insulin icodec group compared to the insulin degludec group. Severe hypoglycemic events occurred in zero patients in the insulin icodec group, and 1 patient (0.4%) in the insulin degludec group (refer to hypoglycemia efficacy outcomes previously reported for additional detail on level 2 and 3 events).
In the ONWARDS 4 study, level 1 hypoglycemic events occurred among 244 patients (83.8%) in the insulin icodec group compared to 251 patients (86.3%) in the insulin glargine group. There was a lower proportion of patients who experienced level 2 events and a lower total number of level 2 events in the insulin icodec group compared to the insulin glargine group. Level 3 events were rare in both groups (refer to hypoglycemia efficacy outcomes previously reported for additional detail on level 2 and 3 events).
Nocturnal Hypoglycemia
In the ONWARDS 1 study, level 1 nocturnal hypoglycemic events occurred in 67 patients (13.6%) in the insulin icodec group and 58 patients (11.8%) in the insulin glargine group. Clinically significant (level 2) nocturnal hypoglycemic events occurred in 9 patients (1.8%) in the insulin icodec group and 10 patients (2.0%) in the insulin glargine group, and severe (level 3) nocturnal hypoglycemic events occurred in zero patients and 1 patient (0.2%) in the insulin icodec and insulin glargine groups, respectively. The estimated treatment ratio between insulin icodec and insulin glargine for clinically significant (level 2) nocturnal hypoglycemic events was 0.92 (95% CI, 0.29 to 2.86; P = 0.8816). The estimated treatment ratio between insulin icodec and insulin glargine for clinically significant (level 2) or severe (level 3) nocturnal hypoglycemic events was 0.88 (95% CI, 0.29 to 2.64; P = 0.8189).
In the ONWARDS 3 study, level 1 nocturnal hypoglycemic events occurred in 24 patients (8.2%) in the insulin icodec group and 23 patients (7.8%) in the insulin degludec group. Clinically significant (level 2) nocturnal hypoglycemic events occurred in 1 patient (0.3%) in the insulin icodec group and 4 patients (1.4%) in the insulin degludec group. There were no severe (level 3) nocturnal hypoglycemic events in either treatment group. The estimated treatment ratio between insulin icodec and insulin degludec for clinically significant (level 2) nocturnal hypoglycemic events was 2.09 (95% CI, 0.99 to 4.41; P = 0.0536). The estimated treatment ratio between insulin icodec and insulin degludec for clinically significant (level 2) or severe (level 3) nocturnal hypoglycemic events was 1.82 (95% CI, 0.87 to 3.80; P = 0.1091).
In the ONWARDS 5 study, level 1 nocturnal hypoglycemic events occurred in 48 patients (8.9%) in the insulin icodec group and 46 patients (8.6%) in the once-daily analogues group. Clinically significant (level 2) nocturnal hypoglycemic events occurred in 11 patients (2.0%) in both treatment groups, and severe (level 3) nocturnal hypoglycemic events occurred in zero patients in the insulin icodec group and 1 patient (0.2%) in the once-daily analogues groups. The estimated treatment ratio between insulin icodec and once-daily analogues for clinically significant (level 2) or severe (level 3) nocturnal hypoglycemic events was 1.36 (95% CI, 0.82 to 2.27; P = 0.02396).
In the ONWARDS 2 study, level 1 nocturnal hypoglycemic events occurred in 60 patients (22.9%) in the insulin icodec group and 35 patients (13.3%) in the insulin degludec group. Clinically significant (level 2) nocturnal hypoglycemic events occurred in 16 patients (6.1%) in the insulin icodec group and 9 patients (3.4%) in the insulin degludec group. Severe (level 3) nocturnal hypoglycemic events occurred in zero patients in both treatment groups. The estimated treatment ratio between insulin icodec and insulin degludec for clinically significant (level 2) nocturnal hypoglycemic events was 1.98 (95% CI, 0.95 to 4.12; P = 0.0677). The estimated treatment ratio between insulin icodec and insulin degludec for clinically significant (level 2) or severe (level 3) nocturnal hypoglycemic events was 1.93 (95% CI, 0.93 to 4.02; P = 0.0782).
In the ONWARDS 4 study, level 1 nocturnal hypoglycemic events occurred in 108 patients (37.1%) in the insulin icodec group and 132 patients (45.4%) in the insulin glargine group. Clinically significant (level 2) nocturnal hypoglycemic events occurred in 54 patients (18.6%) in the insulin icodec group and 71 patients (24.4%) in the insulin glargine group, and severe (level 3) nocturnal hypoglycemic events occurred in zero patients and 1 patient (0.3%) in the insulin icodec and insulin glargine groups, respectively. The estimated treatment ratio between insulin icodec and insulin glargine for clinically significant (level 2) nocturnal hypoglycemic events was 0.74 (95% CI, 0.47 to 1.15; P = 0.1818). The estimated treatment ratio between insulin icodec and insulin glargine for clinically significant (level 2) or severe (level 3) nocturnal hypoglycemic events was 0.73 (95% CI, 0.47 to 1.14; P = 0.1694).
Table 18: Summary of Harms Results in ONWARDS 1, 3, and 5 — Patients Who Were Insulin Naive (SAS)
Adverse events | ONWARDS 1 | ONWARDS 3 | ONWARDS 5 | |||
|---|---|---|---|---|---|---|
Insulin icodec n = 492 | Insulin glargine n = 492 | Insulin icodec n = 293 | Insulin degludec n = 294 | Insulin icodec n = 542 | Once-daily analogues n = 538 | |
PYEa | 485.88 | 485.03 | 170.90 | 171.13 | 559.54 | 560.72 |
Most common adverse events, n (%)b | ||||||
≥ 1 adverse event | 351 (71.3) | 335 (68.1) | 177 (60.4) | 167 (56.8) | 279 (51.5) | 270 (50.2) |
COVID-19 | 49 (10.0) | 61 (12.4) | 25 (8.5) | 14 (4.8) | 43 (7.9) | 55 (10.2) |
Nasopharyngitis | 30 (6.1) | 34 (6.9) | 10 (3.4) | 12 (4.1) | 13 (2.4) | 11 (2.0) |
Diarrhea | 31 (6.3) | 21 (4.3) | 7 (2.4) | 7 (2.4) | 17 (3.1) | 5 (0.9) |
Back pain | 27 (5.5) | 24 (4.9) | 10 (3.4) | 7 (2.4) | 10 (1.8) | 8 (1.5) |
Influenza | 0 | 3 (0.6) | 16 (5.5) | 9 (3.1) | 6 (1.1) | 4 (0.7) |
Diabetic retinopathy | 3 (0.6) | 4 (0.8) | 15 (5.1) | 6 (2.0) | 12 (2.2) | 17 (3.2) |
SAEs, n (%) | ||||||
Patients with ≥ 1 SAE | 51 (10.4) | 49 (10.0) | 15 (5.1) | 15 (5.1) | 45 (8.3) | 57 (10.6) |
Adverse events leading to permanent discontinuation, n (%) | ||||||
Events | 6 (1.2) | 4 (0.8) | 2 (0.7) | 1 (0.3) | 6 (1.1) | 7 (1.3) |
Adverse events leading to temporary discontinuation, n (%) | ||||||
Events | 6 (1.2) | 15 (3.0) | 2 (0.7) | 2 (0.7) | 10 (1.8) | 20 (3.7) |
Adverse events leading to dose reduction, n (%) | ||||||
Events | 11 (2.2) | 20 (4.1) | 1 (0.3) | 4 (1.4) | 4 (0.7) | 2 (0.4) |
Adverse events leading to dose increase, n (%) | ||||||
Events | 12 (2.4) | 10 (2.0) | 1 (0.3) | 7 (2.4) | 10 (1.8) | 8 (1.5) |
Deaths, n (%) | ||||||
Patients who died | 4 (0.8) | 2 (0.4) | 2 (0.7) | 1 (0.3) | 3 (0.6) | 7 (1.3) |
PYE = patient-year of exposure; SAE = serious adverse event; SAS = safety analysis set.
a1 PYE = 365.25 days.
bMore than 5% in any treatment group.
Source: ONWARDS 1 Clinical Study Report,25 ONWARDS 3 Clinical Study Report,26 and ONWARDS 5 Clinical Study Report.27 Details included in the table are from the sponsor’s Summary of Clinical Evidence.1
Table 19: Summary of Harms Results in ONWARDS 2 and 4 — Patients Who Were Insulin Naive (SAS)
Adverse events | ONWARDS 2 | ONWARDS 4 | ||
|---|---|---|---|---|
Insulin icodec n = 262 | Insulin degludec n = 263 | Insulin icodec n = 291 | Insulin glargine n = 291 | |
PYEa | 155.25 | 152.77 | 167.36 | 166.80 |
Most common adverse events, n (%)b | ||||
≥ 1 adverse event | 161 (61.5) | 134 (51.0) | 171 (58.8) | 167 (57.4) |
Nasopharyngitis | 22 (8.4) | 10 (3.8) | 8 (2.7) | 12 (4.1) |
COVID-19 | 9 (3.4) | 7 (2.7) | 26 (8.9) | 23 (7.9) |
Diarrhea | 14 (5.3) | 9 (3.4) | 15 (5.2) | 9 (3.1) |
Back pain | 7 (2.7) | 11 (4.2) | 8 (2.7) | 11 (3.8) |
Influenza | 1 (0.4) | 4 (1.5) | 5 (1.7) | 8 (2.7) |
Diabetic retinopathy | 10 (3.8) | 16 (6.1) | 12 (4.1) | 15 (5.2) |
SAEs, n (%) | ||||
Patients with ≥ 1 SAE | 22 (8.4) | 16 (6.1) | 22 (7.6) | 25 (8.6) |
Adverse events leading to permanent discontinuation, n (%) | ||||
Events | 5 (1.9) | 3 (1.1) | 3 (1.0) | 3 (1.0) |
Adverse events leading to temporary discontinuation, n (%) | ||||
Events | 3 (1.1) | 7 (2.7) | 8 (2.7) | 5 (1.7) |
Adverse events leading to dose reduction, n (%) | ||||
Events | 4 (1.5) | 4 (1.5) | 5 (1.7) | 6 (2.1) |
Adverse events leading to dose increase, n (%) | ||||
Events | 3 (1.1) | 3 (1.1) | 4 (1.4) | 2 (0.7) |
Deaths, n (%) | ||||
Patients who died | 2 (0.8) | 2 (0.8) | 2 (0.7) | 1 (0.3) |
PYE = patient-years of exposure; SAE = serious adverse event; SAS = safety analysis set.
Note: Values are n (%) unless otherwise indicated.
aOne PYE = 365.25 days.
bMore than 5% in any treatment group.
Source: ONWARDS 2 Clinical Study Report28 and ONWARDS 4 Clinical Study Report.29 Details included in the table are from the sponsor’s Summary of Clinical Evidence.1
Critical Appraisal
Internal Validity
All of the ONWARDS trials were randomized, active-controlled trials with adequate methodology related to randomization and allocation concealment, and there were no concerning between-arm imbalances in patient characteristics at baseline, nor in diabetes-related background medications. As such, the risk of bias arising from the randomization process is low in all trials. Each trial was adequately powered for the purpose of their primary hypotheses. The ONWARDS 1, ONWARDS 2, ONWARDS 4, and ONWARDS 5 studies were open-label trials, while the ONWARDS 3 study was double-blinded with adequate blinding and concealment procedures including placebos matched in visual quality and administration methods to the active trial products.
There is an increased risk of bias associated with the open-label design of the ONWARDS 1, ONWARDS 2, ONWARDS 4 and ONWARDS 5 studies with respect to the measurement of the subjective outcomes due to the impact of knowledge of treatment assignment on both the patient (for self-reported outcomes) and the evaluating clinicians; however, this does not apply to objective measures such as the primary outcome (change in hemoglobin A1C from baseline), and other objective outcomes related to, for example, blood glucose monitoring. This may be a concern for subjective assessments, which in this case includes the DTSQ, TRIM-D, and subjective harms. As the intention of the DTSQ is to evaluate satisfaction with treatment and a key difference of the intervention versus comparators is the administration schedule, a blinded assessment of DTSQ with matched placebos would have been uninformative for this research question. The extent and direction of the potential bias could not be ascertained.
The intervention in each trial was insulin icodec; the comparator product was 1 or either of the once-daily insulins, insulin degludec or insulin glargine. Additionally, in the ONWARDS 5 study, patients in the insulin icodec arm used the DoseGuide app to inform dosage adjustments; however, there was no notable inconsistency in the results of the ONWARDS 5 study compared to the trials that did not use the DoseGuide app. The ONWARDS 4 study also differed from the other trials in that patients in both treatment groups also received insulin aspart after mealtimes (2 times to 4 times daily), but again there was no notable inconsistency in the results of the ONWARDS 4 study compared to other trials, and this trial feature was appropriate for the patient subpopulation recruited to the ONWARDS 4 study.
The primary outcome in each trial was the change in hemoglobin A1C from baseline, and the noninferiority margin of 0.3% points was chosen based on established FDA guidance17 and previous trials of insulin products in the treatment of T2DM. Change in hemoglobin A1C from baseline was considered a clinically relevant outcome by the clinical expert consulted by CADTH. This outcome is considered acceptable by the FDA17 for trials of new antihyperglycemic therapies seeking a glycemic control indication, the rationale being that it is a validated surrogate of microvascular disease risk reduction,17 and further it is currently recognized as the key surrogate marker for the development of long-term diabetes complications in people with type 1 diabetes mellitus or T2DM.18 The selection of this noninferiority margin was determined based on FDA guidance17 as previously described, and was considered clinically relevant as a threshold of MID according to the clinical expert consulted by CADTH. However, hemoglobin A1C is ultimately a surrogate biomarker, and there is evidence to suggest that hemoglobin A1C may not be appropriate as a surrogate outcome for downstream complications in diabetes trials due to poor associations with mortality,19,20 CV mortality,21 MI,19 heart failure,19 kidney injury,19 and stroke.19 Other limitations of hemoglobin A1C include a lack of information about acute glycemic events (i.e., hypoglycemia or hyperglycemia) and insensitivity regarding day-to-day variations of glucose, and measurement of hemoglobin A1C can be confounded by other conditions such as anemia, hemoglobinopathies, iron deficiency, and pregnancy.18
Use of CGM allows for observation of time in and outside of range and daily glycemic variability,18 and the clinical expert consulted by CADTH indicated that this is of growing importance in clinical trials of glycemic control in patients with T2DM in addition to hemoglobin A1C.18 Time in range as measured by CGM is a useful as a measure of short-term glycemic control,22 and there is good correlation between time in range and hemoglobin A1C.22 Time in range has been demonstrated to be associated with diabetic retinopathy23,24 and microalbuminuria23 but publications assessing this outcome as a surrogate for other diabetes-related complications (e.g., mortality, MI, and other major CV or renal events) were not identified.
The primary outcome in all trials was adjusted for multiple comparisons. Additionally, in the ONWARDS 1 study, the outcome of time in range (3.9 mmol/L to 10 mmol/L) was also adjusted for multiple comparisons. As the remaining outcomes were not adjusted for multiplicity, there is an increased risk of type I error (i.e., false-positive results) for statistically significant results for those outcomes.
In each trial, there were no obvious or substantial imbalances between groups with respect to treatment discontinuation. Notably, however, there was a higher rate of discontinuations in the ONWARDS 5 study overall (approximately 9% to 11% in each arm), compared to less than 5% in each arm in the other ONWARDS trials. The reason for the higher rate in the ONWARDS 5 study compared to other ONWARDS trials is unknown. In the ONWARDS 5 study, the most common reasons for permanent discontinuation were withdrawal of consent or loss to follow-up.
Multiple imputation was used for all outcomes to account for missing data. Multiple imputation methods will not remove or reduce bias that occurs when missingness is not random, but the proportion of missing data in each case was low, so this was not considered cause for concern. Additionally, sensitivity analyses were conducted for the primary outcome which bolstered confidence in the primary analyses.
External Validity
The study designs with respect to patient eligibility criteria and characteristics at baseline were appropriately reflective of the target population in Canada, with the exception that there is a notable lack of inclusion of Indigenous Peoples, who are at higher risk of T2DM and its complications.6,8 The selected comparators, medications at baseline among included patients, and concomitant mediations during the trials were considered by the consulted clinical expert to be appropriate and to reflect clinical practice in Canada.
The primary, secondary, and exploratory efficacy outcomes were considered appropriate for clinical trial evaluation in this population and the follow-up time was considered adequate, with the exception of all-cause mortality, for which a longer follow-up time would be necessary to compare between treatment arms. As is common in clinical trials, long-term clinical outcomes (i.e., microvascular and macrovascular complications of T2DM) relevant to T2DM were not directly measured due to the limited length of follow-up. Thus, the impact on these outcomes relative to the daily insulins is not known.
The impact of insulin icodec on patients’ HRQoL was not measured in the ONWARDS trials. Although the DTSQ and TRIM-D provide information about treatment satisfaction and compliance, they are not comprehensive measures of HRQoL. As such, the influence of insulin icodec on HRQoL as compared with insulin degludec or insulin glargine is not known. Additionally, there were no compliance data reported for the insulin-experienced populations.
The DoseGuide app used in the intervention arm of the ONWARDS 5 study is not publicly available to patients, so hypothetically could have impacted dosing decisions in a way that is less generalizable to clinical practice in Canada. However, this was not considered to be a major concern, in part because dosing of insulin icodec already differs from dosing of the daily insulins by design and, according to the clinical expert consulted by CADTH, typical practices around dosing adjustments for insulin icodec will be quickly evolving in the event of this therapy becoming available to patients with T2DM. Moreover, the results of the ONWARDS 5 study were aligned with those of the ONWARDS 1 and ONWARDS 3 studies, in which DoseGuide was not used.
GRADE Summary of Findings and Certainty of the Evidence
Methods for Assessing the Certainty of the Evidence
For pivotal studies and RCTs identified in the sponsor’s systematic review, GRADE was used to assess the certainty of the evidence for outcomes considered most relevant to inform CADTH’s expert committee deliberations, and a final certainty rating was determined as outlined by the GRADE Working Group.71,72
High certainty: We are very confident that the true effect lies close to that of the estimate of the effect.
Moderate certainty: We are moderately confident in the effect estimate — the true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different. We use the word “likely” for evidence of moderate certainty (e.g., “X intervention likely results in Y outcome”).
Low certainty: Our confidence in the effect estimate is limited — the true effect may be substantially different from the estimate of the effect. We use the word “may” for evidence of low certainty (e.g., “X intervention may result in Y outcome”).
Very low certainty: We have very little confidence in the effect estimate — the true effect is likely to be substantially different from the estimate of effect. We describe evidence of very low certainty as “very uncertain.”
Following the GRADE approach, evidence from RCTs started as high-certainty evidence and could be rated down for concerns related to study limitations (which refers to internal validity or risk of bias), inconsistency across studies, indirectness, imprecision of effects, and publication bias.
When possible, certainty was rated in the context of the presence of an important (nontrivial) treatment effect; if this was not possible, certainty was rated in the context of the presence of any treatment effect (i.e., the clinical importance is unclear). In all cases, the target of the certainty of evidence assessment was based on the point estimate and where it was located relative to the threshold for a clinically important effect (when a threshold was available) or to the null. The target of the certainty of evidence assessment was the presence or absence of important effect based on thresholds informed by the clinical expert consulted for this review.
For the insulin-naive population, findings from the ONWARDS 1, ONWARDS 3, and ONWARDS 5 studies were summarized narratively for the hemoglobin A1C, body weight, and hypoglycemia outcomes because these studies were similar in population, interventions, and outcome measures. For all other outcomes only 1 of the ONWARDS studies provided outcome data and as such each was assessed individually. For the insulin-experienced population, the ONWARDS 2 and ONWARDS 4 studies were summarized narratively for all outcomes with the exception of level 2 and 3 hypoglycemia as the point estimates for the between-group differences in the trials suggested different directions of effects. Although the study populations differed in their previous insulin treatment history (the ONWARDS 4 study was basal-bolus while the ONWARDS 2 study was basal only), there was an absence of notable heterogeneity in observed effects. Additional information was requested from the sponsor to obtain 95% CIs for the LS mean estimates in each treatment group within the trials, and to obtain between-group differences with 95% CI for hypoglycemia outcomes.
Results of GRADE Assessments in Table 2 present the GRADE summary of findings for insulin icodec versus insulin glargine or insulin degludec in patients with T2DM who were insulin naive. Table 3 presents the GRADE summary of findings for insulin icodec versus insulin degludec (ONWARDS 2) or insulin glargine (ONWARDS 4) in patients who were insulin experienced with T2DM.
Long-Term Extension Studies
Contents within this section have been informed by materials submitted by the sponsor. The following have been summarized and validated by the CADTH review team.
Description of Studies
One LTE of the ONWARDS 1 trial was included in the sponsor submission. The purpose of the 26-week extension phase was to continue to compare glycemic control and safety of insulin icodec versus insulin glargine among patients with T2DM who were previously insulin naive, with the primary focus of evaluating long-term safety data. The study design for the on-trial period and LTE phase are shown in Figure 1.
Figure 1: ONWARDS 1 Trial and LTE Study Design
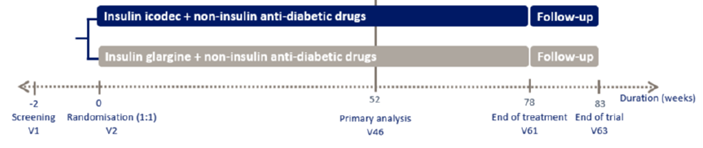
LTE = long-term extension; V = visit.
Source: Details included in the figure are from the sponsor’s ONWARDS 1 Clinical Trial Report.73
Populations
Eligibility criteria for the LTE study were the same as for the ONWARDS 1 trial and are described in the systematic review section of this report. Patient baseline characteristics for the ONWARDS trial overall are also described in the systematic review section of this report; specific baseline characteristics for the sample which completed the LTE phase were not provided in the submission.
Interventions
The experimental and control interventions during the LTE phase of the ONWARDS 1 study were the same as those assigned to patients during the main 52-week trial period. Briefly, patients initially randomized to receive insulin icodec or insulin glargine in the open-label ONWARDS 1 trial continued to receive the same treatment into the LTE phase; doses and administration are described in the systematic review section.
Outcomes
Outcomes during the LTE phase of ONWARDS 1 were assessed in the same manner as those assessed during the main trial phase and are described in the systematic review section of this report. The following efficacy outcomes were summarized by CADTH: change from baseline in hemoglobin A1C, time in range (3.9 mmol/L to 10.0 mmol/L), time spent at less than 3.0 mmol/L, time spent at greater than 10.0 mmol/L, change in body weight, and proportion of patients with level 2 or 3 hypoglycemic events.
Statistical Analysis
The statistical analyses used for the outcomes assessed during the LTE phase of the trial were similar to those used for the primary analyses, with the exception that there was no control for multiplicity of the efficacy outcomes. All efficacy end points apart from hypoglycemic events were assessed for a total of 78 weeks; hypoglycemic events were assessed for 83 weeks until the end of the follow-up period. Time in range (3.9 mmol/L to 10.0 mmol/L), time spent at less than 3.0 mmol/L, and time spent at greater than 10.0 mmol/L were reported as change from week 74 to week 78; all other outcomes were reported as changes from baseline.
Missing data for hemoglobin A1C and body weight were imputed using multiple imputation based on the change from last available value on treatment without initiation of bolus insulin for more than 2 weeks. Missing data for time-in-target range and time spent above or below range were imputed using multiple imputation from patients in the insulin glargine arm who completed their randomized insulin treatment.
Results
Patient Disposition
A summary of the patient disposition after the completion of the LTE phase of the ONWARDS 1 study is provided in Table 20. During the main phase of the ONWARDS 1 study, the majority of patients (98%) completed their final trial visit at week 52, and 97% of patients continued to complete their final week 78 visit. A total of 984 patients (492 patients in each arm) were randomized for the ONWARDS 1 study; 476 (97%) in the insulin icodec arm and 477 (97%) in the insulin glargine arm completed the LTE phase, respectively.
The rates and reasons for trial product discontinuation and trial withdrawal with or without trial product discontinuation were similar between treatment arms, with all withdrawals and/or discontinuations occurring in less than 6% of patients in each arm. Fewer than 1% of patients in each arm were lost to follow-up during the LTE phase. There were 2 discontinuation and withdrawals due to hypoglycemic episodes in the insulin glargine arm and none in the insulin icodec arm.
Patient disposition | Insulin icodec | Insulin glargine |
|---|---|---|
Screened, N | 1,192 | |
Randomized, N (%) | 492 (100.0) | 492 (100.0) |
Exposed, N (%) | 492 (100.0) | 492 (100.0) |
Completed study, N (%) | 476 (96.7) | 477 (97.0) |
Discontinued trial product, N (%) | 26 (5.3) | 20 (4.1) |
Permanently discontinued trial product and withdrew from trial during the treatment period | 18 (3.7) | 16 (3.3) |
Adverse events | 8 (1.6) | 5 (1.0) |
Hypoglycemic episode | 0 | 2 (0.4) |
Protocol deviation | 0 | 0 |
Violation of the inclusion and/or exclusion criteria | 0 | 0 |
Intention of becoming pregnant | 0 | 0 |
Participation in another clinical trial | 0 | 0 |
Lack of efficacy | 0 | 0 |
Lost to follow-up | 3 (0.6) | 1 (0.2) |
Pregnancy | 0 | 0 |
Site closure | 1 (0.2) | 0 |
Epidemic or pandemic | 0 | 0 |
Withdrawal of consent | 3 (0.6) | 6 (1.2) |
Safety concern related to trial product or unacceptable intolerability | 0 | 0 |
Other | 3 (0.6) | 2 (0.4) |
Withdrew from trial | 18 (3.7) | 17 (3.5) |
Withdrawal of consent by participant | 6 (1.2) | 8 (1.6) |
Lost to follow-up | 4 (0.8) | 4 (0.8) |
Investigator decision | 4 (0.8) | 1 (0.2) |
Death | 3 (0.6) | 4 (0.8) |
Site closure | 1 (0.2) | 0 |
Epidemic or pandemic | 0 | 0 |
Permanently discontinued trial product and did not withdraw from trial during the treatment period | 8 (1.6) | 4 (0.8) |
Adverse events | 4 (0.8) | 2 (0.4) |
Hypoglycemic episode | 0 | 0 |
Protocol deviation | 0 | 0 |
Violation of the inclusion and/or exclusion criteria | 0 | 0 |
Intention of becoming pregnant | 0 | 0 |
Participation in another clinical trial | 0 | 0 |
Lack of efficacy | 1 (0.2) | 0 |
Lost to follow-up | 0 | 0 |
Pregnancy | 0 | 0 |
Site closure | 0 | 0 |
Epidemic or pandemic | 0 | 0 |
Safety concern related to trial product or unacceptable intolerability | 0 | 0 |
Other | 3 (0.6) | 2 (0.4) |
Completed week 78 visit, n (%) | 476 (96.7) | 477 (97.0) |
Completed week 78 visit without permanent discontinuation of trial product | 466 (94.7) | 472 (95.9) |
Completed week 78 visit after permanent discontinuation of trial product | 10 (2.0) | 5 (1.0) |
FAS, N | 492 (100.0) | 492 (100.0) |
Safety, N | 492 (100.0) | 492 (100.0) |
FAS = full analysis set.
Source: ONWARDS 1 Clinical Trial Report — full report.73
Exposure to Study Treatments
The sum of exposure to study treatment was similar across the insulin icodec (765.50 patient-years of exposure [PYE]) and insulin glargine (766.76 PYE) groups. The mean exposure to study treatment was the same across the insulin icodec and insulin glargine treatment groups, with a mean of 1.56 PYE (standard deviation [SD] = 0.18) in the insulin icodec group and 1.56 PYE (SD = 0.20) in the insulin glargine group. The mean weekly basal insulin dose during the last 2 weeks of treatment (week 76 to week 78) was similar across the insulin icodec (223.81 U) and insulin glargine (234.35 U) treatment groups.
Efficacy
Full efficacy results are available in Table 21. Briefly, outcomes measured over the entire treatment period and reported as a change from baseline (body weight, hemoglobin A1C), were aligned with the results from the ONWARDS 1 study at the 52-week time point, with little to no difference between insulin icodec and insulin glargine reported at 78 weeks. For the time-in-range outcomes, which were measured between weeks 74 and weeks 78, similar to the 52-week mark of the ONWARDS 1 study, insulin icodec was statistically favoured for time spent between blood glucose levels of 3.9 mmol/L to 10.0 mmol/L (4.41%; 95% CI, 1.92% to 6.90%; P = 0.0005), and time spent with blood glucose levels greater 10.0 mmol/L (–4.65%; 95% CI, –7.20% to –2.10%; P = 0.0004). The incidence rate of level 2 or 3 hypoglycemic events was almost twice as high in the insulin icodec arm versus the insulin glargine arm (29.65 events per 100 PYE versus 15.78 episodes per 100 PYE, respectively), although these events occurred in similar proportions of patients (12.4% in the insulin icodec arm and 14.2% in the insulin glargine arm), suggesting repeat events in the same patients. The level 2 or level 3 hypoglycemia treatment ratio for insulin icodec relative to insulin glargine was (rate ratio = 1.63; 95% CI, 1.02 to 2.61).
Table 21: Summary of Efficacy Results From ONWARDS 1 LTE
Outcome | Insulin icodec | Insulin glargine |
|---|---|---|
Analyzed using FAS | ||
Analyzed, N | 492 | 492 |
Hemoglobin A1C change from baseline (% points) | ||
Complete cases, N (%) | 492 (100%) | 492 (100%) |
LS mean at week 78, estimate (SE) | 6.92 (0.04) | 7.03 (0.04) |
LS mean change from baseline, estimate (SE) | –1.55 (0.04) | –1.44 (0.04) |
Treatment difference (icodec – glargine), estimate (95% CI) | –0.11 (–0.22 to 0.00) | |
P valuea | 0.0506 | |
Time in range (3.9 mmol/L to 10.0 mmol/L) in week 74 to week 78 (% time) | ||
Complete cases, N (%) | 492 (100%) | 492 (100%) |
LS mean, estimate (SE) | 69.53 (0.90) | 64.94 (0.90) |
Treatment difference (icodec – glargine), estimate (95% CI) | 4.41 (1.92 to 6.90) | |
P valuea | 0.0005 | |
Time spent < 3.0 mmol/L in week 74 to week 78 (% time) | ||
Complete cases, N (%) | 428 (87%) | 432 (88%) |
LS mean, estimate (SE) | 0.26 (NR) | 0.22 (NR) |
Treatment ratio (icodec to glargine), estimate (95% CI) | 1.20 (0.89 to 1.61) | |
P valuea | 0.2346 | |
Time spent > 10.0 mmol/L in week 74 week 78 (% time) | ||
Complete cases, N (%) | 492 (100%) | 492 (100%) |
LS mean, estimate (SE) | 29.55 (0.92) | 34.20 (0.92) |
Treatment difference (icodec – glargine), estimate (95% CI) | –4.65 (–7.20 to –2.10) | |
P valuea | 0.0004 | |
Change in body weight from baseline (kg) | ||
Complete cases, N (%) | 492 (100%) | 492 (100%) |
LS mean at week 78, estimate (SE) | 86.95 (0.24) | 86.31 (0.24) |
LS mean change from baseline, estimate (SE) | 2.22 (0.24) | 1.58 (0.23) |
Treatment difference (icodec – glargine), estimate (95% CI) | 0.64 (–0.02 to 1.30) | |
P valuea | 0.0561 | |
Analyzed using SAS | ||
Analyzed, N | 492 | 492 |
Number of clinically significant hypoglycemic episodes (level 2) (< 3.0 mmol/L [54 mg/dL] confirmed by BG meter) or severe hypoglycemic episodes (level 3) — on-treatment periodb | ||
Complete cases, N (%) | 492 (100%) | 492 (100%) |
Number of events, n | 227 | 121 |
Number of patients with event | 61 (12.4) | 70 (14.2) |
Incidence rate, episodes per 100 PYEc | 29.65 | 15.78 |
Rate ratio of insulin icodec to insulin glargine (95% CI) | 1.63 (1.02 to 2.61) | |
P valuea | 0.0428 | |
BG = blood glucose; CI = confidence interval; FAS = full analysis set; hemoglobin A1C = glycated hemoglobin; LS = least squares; LTE = long-term extension; NR = not reported; PYE = patient-years of exposure; SAS = safety analysis set; SE = standard error.
aTwo-sided P value for test of no treatment difference. P value has not been adjusted for multiple testing.
bThe on-treatment period lasted from baseline to the end-of-trial visit at week 83, thus including the follow-up period.
cOne PYE = 365.25 days.
Source: ONWARDS 1 Clinical Trial Report.73
Harms
Complete details of harms can be found in Table 22. Briefly, harms accrued over the entire ONWARDS 1 trial and LTE phase in the 2 study arms were similar by the end of the LTE phase, with some exceptions. Patients in the insulin glargine arm had a numerically higher incidence of AEs requiring temporary discontinuation (4.9% versus 1.2%, respectively), and there were a numerically higher proportion of patients in the insulin icodec arm who experienced level 1 hypoglycemic events (55.9% versus 48.2%).
Mortality
There was a total of 14 events in 8 patients (0.8%) during the on-treatment period (from baseline to the end-of-trial visit at week 83) which had fatal outcomes. A total of 7 events occurred in 5 patients (1.0%) in the insulin icodec arm and 7 events occurred in 3 patients (0.6%) in the insulin glargine arm. This added up to 1 additional death in each treatment arm between the 52-week mark of the ONWARDS 1 study and the end of the LTE phase.
Notable Harms
Prespecified notable harms were the same as the ONWARDS 1 trial and included hypersensitivity, injection site reactions, hypoglycemia, and nocturnal hypoglycemia.
Hypersensitivity
The proportion of patients with 1 or more hypersensitivity events remained similar in both treatment arms (6.7% of patients in the insulin icodec arm versus 7.9% in the insulin glargine arm) at the end of the LTE phase relative to the 52-week mark of the ONWARDS 1 study. The proportion of patients with 1 or more systemic hypersensitivity events was the same between treatment arms at the end of the LTE phase (0.6% in both).
Injection Site Reactions
The proportion of patients with 1 or more injection site reactions was numerically similar between treatment arms (1.4% in the insulin icodec arm and 2.4% in the insulin glargine arm) by the end of the LTE phase.
Hypoglycemia
Hypoglycemic events were measured during the on-treatment period, lasting from baseline to the end-of-trial visit at week 83, which included the follow-up period. A numerically higher number of patients experienced level 1 hypoglycemic events (278 [56.5%] in the insulin icodec arm versus 239 patients [48.6%] in the insulin glargine arm). The same proportion of patients experienced level 2 hypoglycemic events (61 patients [12.4%] in the insulin icodec arm and 66 patients [12.4%] in the insulin glargine arm), while a numerically similar proportion of patients experienced level 3 hypoglycemic events (1 patient [0.2%] in the insulin icodec arm and 6 patients [1.2%] in the insulin glargine arm). Of note, a higher number of hypoglycemic episodes were recorded in a smaller number of patients, suggesting multiple repeat hypoglycemic events in both arms.
Nocturnal Hypoglycemia
Nocturnal hypoglycemia was also measured over the same time period as hypoglycemia, with similar proportions of patients experiencing all levels of nocturnal hypoglycemia in the 2 treatment arms. A total of 89 patients (18.1%) in the insulin icodec arm and 91 patients (18.5%) in the insulin glargine arm experienced level 1 nocturnal hypoglycemia; 9 patients (1.8%) in the insulin icodec arm and 15 patients (3.0%) in the insulin glargine arm experienced level 2 nocturnal hypoglycemia; and zero patients in the insulin icodec arm and 1 patient (0.2%) in the insulin glargine arm experienced level 3 nocturnal hypoglycemia. The estimated treatment ratio for level 2 or 3 nocturnal hypoglycemia was 0.54 (95% CI, 0.19 to 1.54), which was numerically less than the 52-week results of the ONWARDS 1 study although the CIs overlap with estimates from that time point.
CV Death
CV death was not measured as an outcome in the LTE phase.
Nonfatal MI
Nonfatal MI was not measured as an outcome in the LTE phase.
Nonfatal Stroke
Nonfatal stroke was not measured as an outcome in the LTE phase.
Other Microvascular and Macrovascular Complications of T2DM
Other microvascular and macrovascular complications of T2DM were not measured as outcomes in the LTE phase.
Table 22: Summary of Harms Results From ONWARDS 1 LTE — SAS
Adverse events | Insulin icodec n = 492 | Insulin glargine n = 492 |
|---|---|---|
Most common adverse events,a n (%) | ||
≥ 1 adverse event | 397 (80.7) | 389 (79.1) |
COVID-19 | 91 (18.5) | 104 (21.1) |
Back pain | 40 (8.1) | 32 (6.5) |
Diarrhea | 39 (7.9) | 26 (5.3) |
Nasopharyngitis | 38 (7.7) | 47 (9.6) |
Diabetic retinopathy | 36 (7.3) | 32 (6.5) |
Arthralgia | 30 (6.1) | 22 (4.5) |
URTI | 28 (5.7) | 22 (4.5) |
Pyrexia | 27 (5.5) | 23 (4.7) |
SAEs, n (%) | ||
Patients with ≥ 1 SAE | 64 (13.0) | 71 (14.4) |
Adverse events leading to permanent discontinuation, n (%) | ||
Patients with ≥ 1 event(s) | 9 (1.8) | 6 (1.2) |
Adverse events leading to temporary discontinuation, n (%) | ||
Patients with ≥ 1 event(s) | 6 (1.2) | 24 (4.9) |
Adverse events leading to dose reduction, n (%) | ||
Patients with ≥ 1 event(s) | 15 (3.0) | 25 (5.1) |
Adverse events leading to dose increase, n (%) | ||
Patients with ≥ 1 event(s) | 16 (3.3) | 16 (3.3) |
Deaths, n (%) | ||
Patients who died | 5 (1.0) | 3 (0.6) |
LTE = long-term extension; SAE = serious adverse event; SAS = safety analysis set; URTI = upper respiratory tract infection.
aCut-off for the most frequent adverse events was ≥ 5% of participants in either treatment group.
Source: Details included in the table are from the sponsor’s Summary of Clinical Evidence1 and the ONWARDS 1 LTE Clinical Study Report.73
Critical Appraisal
Internal Validity
All appraisal points pertaining to the main phase of the ONWARDS 1 study also pertain here as this LTE was a continuation of the same study design, patients, and outcomes. While there is a possibility of selection bias in the LTE phase since only patients who completed the ONWARDS 1 study moved on to the LTE phase, the overall proportion of patients who did not complete the study is small (< 3.0%) and the loss to follow-up was also low. There is 1 additional internal validity limitation which applies to the LTE phase of the study; all efficacy outcomes here are exploratory and not adjusted for multiplicity so there is an increased risk of type I error (false-positive conclusions) for statistically significant results.
External Validity
All appraisal points pertaining to the main phase of the ONWARDS 1 study also pertain here as this LTE was a continuation of the same patients, intervention, comparator, and outcomes. In addition to these, the LTE results are only applicable to patients who are insulin naive as this was the only patient population included in the ONWARDS 1 study. Overall, long-term results on the safety and efficacy outcomes assessed in this LTE remain lacking for patients who were insulin experienced. Furthermore, results on long-term (i.e., the length of the LTE phase and beyond) treatment adherence and satisfaction as well as clinical outcomes such as microvascular and macrovascular complications (e.g., nonfatal MI, stroke) were not assessed in the submission.
Indirect Evidence
Contents within this section have been informed by materials submitted by the sponsor. The following have been summarized and validated by the CADTH review team.
Objectives for the Summary of Indirect Evidence
A review of the indirect evidence was required as the pivotal trials and LTE phase conducted comparisons between insulin icodec relative to insulin glargine and insulin degludec, but not insulin detemir. An appraisal of the indirect treatment comparison was also necessary as these data were used to inform the pharmacoeconomic model.
Description of Indirect Comparison(s)
The submission consisted of an NMA. Outcomes were assessed at 26 weeks and 52 weeks.
Indirect Treatment Comparison Design
Objectives
The objective of the NMA was to assess the relative efficacy and safety of insulin icodec compared to other basal insulin analogues used by patients in Canada.
Study Selection Methods
A focused literature search of electronic databases was conducted to inform the NMA, as well as handsearching of conference proceedings, clinical trial registries, previous health technology assessment submissions plus searches of Google Scholar, International Network of Agencies for Health Technology Assessment, and the National Institute for Health Research Health Technology Assessment. The literature search was conducted on September 30, 2021, via the OVID platform to identify relevant evidence informing the efficacy and safety of insulin for T2DM. There was no mention of whether a protocol was registered in advance for this SLR. Details of the SLR are provided in Table 23.
The feasibility assessment was undertaken to explore the viability of doing the NMA for 2 time points (26 weeks and 52 weeks) and for 3 subgroups of interest (patients with T2DM who are insulin naive, patients with T2DM who are basal insulin experienced, and patients with T2DM who are basal and bolus insulin experienced). No minimum time frame for experience with the various insulins was specified in the submission. For the feasibility assessment, the following interventions were considered relevant: insulin icodec, insulin detemir, insulin degludec U100 and U200, insulin glargine U100 and U300, and biosimilar insulins. As part of the assessment, trials contributing data for each time point and each population were assessed for inclusion or exclusion in the NMA, preliminary evidence networks were constructed, and the trials were assessed for heterogeneity.
Study quality was assessed using the National Institute for Health and Care Excellence single technology appraisal user guide;74 each trial was appraised by answering the questions listed as the minimum criteria for assessing risk of bias and generalizability contained in the user guide.
Table 23: Study Selection Criteria and Methods for NMA Submitted by the Sponsor
Characteristics | SLR | Feasibility assessment |
|---|---|---|
Population | Patients with T2DM Subgroup populations of interest:
| |
Intervention | Long-acting insulins, either in monotherapy or combination therapy:
|
|
Comparator | Any of those listed in “intervention” | Any of those listed in “intervention” |
Outcome |
| The following outcomes were considered at 26, 52, and 78 weeks:
|
Study designs |
| |
Publication characteristics | English-language publications only were included. Conference abstracts were limited to those published in 2019 onwards. | |
Exclusion criteria | Population:
Interventions/comparators:
Study design:
| |
Databases searched | MEDLINE, incorporating:
The Cochrane Library, incorporating:
Conference proceedings:
Clinical trials registriesa:
Previous health technology assessment submissionsa:
Additional sourcesa:
| |
Selection process | A senior researcher carried out the searches. Results from the electronic database searches were downloaded into a bespoke database, which was used to manage citation screening. Duplicate citations were removed, and titles and abstracts of the remaining citations were screened by 2 reviewers (first pass), using the predefined eligibility criteria. Full publications of studies deemed potentially relevant at this stage were then obtained, and examined by 2 reviewers (second pass), and final inclusion and exclusion of citations was verified by the project lead. Disputes regarding eligibility were referred to a senior expert. | |
Data extraction process | On completion of the SLR, the sponsor reviewed the list of potentially relevant citations, and the final list of studies for data extraction were agreed. Relevant data from the included studies were extracted into a predesigned data extraction table in Microsoft Excel, which included data on study design, baseline characteristics, outcomes reported, results, and limitations. Data extraction was conducted by 1 reviewer and fully quality-checked by another reviewer. | |
Quality assessment | Included RCTs were assessed for bias using the National Institute for Health and Care Excellence STA user guide, evaluating 6 domains: selection bias (sequence generation and allocation concealment), performance bias (blinding of participants and personnel), detection bias (blinding of outcome assessors), and attrition bias (incomplete outcome data). | |
hemoglobin A1C = glycated hemoglobin; NMA = network meta-analysis; RCT = randomized controlled trial; SLR = systematic literature review; STA = single technology appraisal; T2DM = type 2 diabetes mellitus.
aReference lists of included studies and any identified SLRs were also scanned.
Source: Details included in the table are from the sponsor’s Summary of Clinical Evidence1 and indirect treatment comparison report.75
NMA Analysis Methods
Analyses were conducted for 3 subgroups: patients who were insulin naive, patients who were basal insulin experienced, and patients who were basal and bolus insulin experienced . The choice of an NMA methodology was justified by noting the lack of direct evidence for insulin icodec versus insulin detemir. Outcomes were assessed at the 26-week and 52-week mark, 4 weeks before and after each time point (data from the 78-week mark for the ONWARDS 1 study were not available at the time of analysis and no NMA was reported or summarized in the submission).
When constructing the NMA network, the doses of all daily basal insulin comparators were converted to weekly doses by multiplying each daily dose by 7, to match the once-weekly dosing of insulin icodec. In addition, once-daily and twice-daily doses of the same basal insulin were considered as a single treatment node (no studies were lost as a result of this). When daily doses were reported as doses per kilogram, these were converted to daily doses using the corresponding average patient weight from the study or, if not available, the average weight across all the studies in the corresponding analysis population.
The ONWARDS 5 trial, which contained 2 active comparators (the choice of which was assigned by the physician), was split into separate subgroups representing each treatment arm and contributed to the corresponding node. Because the dosing of insulin icodec was titrated using the DoseGuide app in the ONWARDS 5 study, this study was excluded from the NMA networks for the base-case analyses and the consequences of this exclusion tested by adding it back in a sensitivity analysis for each outcome.
Details of the analyses can be found in Table 24. Briefly, the NMA models were Bayesian fixed- and random-effects models run with vague, noninformative normal priors. For binomial outcomes, the possibility of rare events was handled by a continuity correction ( + 0.5). Studies with no events in both treatment arms were excluded from the analysis. A case where a continuous outcome was missing precision was resolved by imputing the average SD from the studies in the same network and tested by excluding this study in a sensitivity analysis. It was not clear from the submission whether this approach was preplanned or employed after initial analyses were done.
Preferred models were selected on the basis of deviance information criterion. The outputs of the NMAs were mean differences between insulin icodec and other comparators for the continuous outcomes, odds ratio for dichotomous outcomes, and associated 95% credible intervals.
Table 24: NMA Analysis Methods
Methods | Description |
|---|---|
Analysis methods | T2DM insulin-naive analysis population: No analysis was planned on the nocturnal hypoglycemia outcomes at 26 weeks as no data matching the definition used in the ONWARDS trials were available in any of the comparator studies; therefore, this end point was only assessed at 52 weeks. All NMAs were carried out using the entire ONWARDS 1, 3, and 5 populations. T2DM basal insulin-experienced population: All NMAs were carried out using the entire ONWARDS 2 population in the network. T2DM basal and bolus insulin-experienced population: All NMAs were carried out using the entire ONWARDS 4 population in the network. Models were fitted to the data via Bayesian Markov Chain Monte Carlo methods (Gibbs sampling) and implemented in WinBUGS, version 1.4.3. The models were run using 3 chains with different sets of initial values. For each analysis, an initial 20,000 iterations were run as a burn-in period to achieve convergence and then discarded. Autocorrelations between results from successive simulations were checked and a thinning factor was applied if needed. Results are based on a further 50,000 iterations. The magnitude of the Markov chain error was compared to the standard deviation of the posterior distributions to ensure this number of iterations was sufficient. NMAs for continuous outcomes were analyzed using a normal likelihood with an identity link function. Safety data were analyzed using a binomial likelihood with a logit link function. All models were implemented using both random and fixed effects. Indirect comparisons for networks restricted to only 2 studies and comparing 2 treatments using a common comparator were conducted using the Bucher method and run as additional sensitivity analyses. |
Priors | Vague noninformative normal priors were given in all models. The between-study standard deviation in the random-effects models were given a vague uniform prior distribution between 0 and 5 for all analyses except the ones on basal insulin dose. For the analyses on basal insulin dose, the between-study standard deviation in the random-effects models were given a vague uniform prior distribution between 0 and 100. |
Assessment of model fit | Model selection and assessment of model fit was based on total residual deviance and DIC. |
Assessment of consistency | Assessment of consistency was only possible for networks of patients who were insulin naive at 26 and 52 weeks of follow-up, as these were the only networks with loops (assessment results not provided in submission). |
Assessment of convergence | Convergence was assessed visually at the end of each simulation using the history trace plots, the smoothed Kernel posterior density plots, the autocorrelation plots, and the Brooks-Gelman-Rubin plots (not provided in submission). |
Outcomes | The end points considered in the NMAs and the CADTH appraisal were the following:
|
Follow-up time points | Outcomes were considered at 26, 52, and 78 weeks. Outcome selection was based on the availability in the ONWARDS trials to ensure comparisons of comparators with insulin icodec. All end points were assessed after 26 weeks of follow-up. Networks were built separately for assessment of end points after 52 weeks of follow-up where available. An additional network was constructed to assess end points after 78 weeks of follow-up; however, data were not available, and results are not reported for this time point. |
Construction of nodes | Once-daily and twice-daily regimens of the same treatment were combined into a single treatment node. Specifically, data regarding insulin detemir, which can be administered twice daily, were combined into a single node — this did not result in the exclusion of any studies. |
Sensitivity analyses | The following sensitivity analyses were conducted for each end point in each patient group: T2DM insulin-naive population (26 ± 4 weeks)
Insulin-naive population (52 ± 4 weeks)
T2DM basal insulin-experienced population (26 weeks)
T2DM basal and bolus insulin-experienced population (26 weeks) |
Subgroup analysis | No subgroup analyses were conducted within the 3 prespecified populations of interest |
Methods for pairwise meta-analysis | Not reported |
DIC = deviance information criterion; hemoglobin A1C = glycated hemoglobin; NMA = network meta-analysis; T2DM = type 2 diabetes mellitus.
Source: Details included in the table are from the sponsor’s Summary of Clinical Evidence1 and the sponsor’s insulin icodec indirect treatment comparison technical document.75
Results of NMA
Summary of Included Studies
The literature search yielded a total of 8,760 citations which were screened at the title and abstract phase. After full-text screening, a total of 402 publications were considered relevant for the review, along with an additional 28 publications included after handsearching. Of these, 22 studies were considered for data extraction for the feasibility assessment of the NMA.
||||||||||||| |||||||||| ||||| || ||| |||||| |||||| |||| ||||| |||||||| ||| |||| ||||||||||| || ||||| ||| |||| |||||||| |||| ||| ||||||||||| |||||||||| ||| || |||||| ||||||||| |||||||| ||||||||| || ||||| ||||||||| ||||||| |||||||||| |||| ||||| ||||||| |||||| ||||| |||||| ||||||||| |||||||| |||||| | | |||| ||| |||||||||| ||||| ||| ||||| | ||||||||| || |||||||| || | |||| ||| |||||||||| ||||| ||||| |||| || | ||||||||| || |||||||| ||| || | ||||| ||||| ||||||||||| || | |||| ||||||||| |||||| ||||| ||| |||| ||||||||| |||| ||||||||| |||||| |||||||| |||||| |||||||| | | ||| ||||||||| |||||| ||||| ||| |||| ||||||||| |||| | ||||||||| ||||||||| |||||| || | ||| ||| || || |||||||||| ||||||| ||| ||||||| |||||||| |||||| ||||| ||| ||||| | | ||| ||| || ||||||| |||||||| || ||| |||| ||||| || |||||||| || | ||| || | ||||||| || ||||||| |||| |||||||| |||| ||| ||| ||| | ||||| || || ||||||| |||| || ||| ||| ||||| ||| ||||||||| || ||||||| | ||| | |||||||| | ||| |||| |||||||| ||| ||||||||| ||| ||| |||||||| |||| || |||| || ||| ||||||||||| |||||||||| ||| || || ||||||| ||||| |||| || ||||| |||||| |||||||| ||| ||| | ||||| || ||||||| ||||||||||| ||||||||||||||||| ||| ||| ||||||| ||| ||| |||||| ||| ||||| |||||| |||||| |||| |||||| |||| ||||| || | |||| || |||||||||||||| || | ||||||| |||||||||||| |||||||||| ||||| |||| | ||||||| ||| || ||||||||| |||| || |||| ||| || ||||||| ||||||||||||| |||||||| ||| ||||||||||| || ||| ||||||||| |||||||||||||||| ||||| ||||||| |||| ||||| || ||||||||| |||| || |||| || || ||| ||| ||||| ||| ||||||| |||||||| |||| |||||||| |||| |||| ||||||||||||||||| ||||| ||||||| ||| |||||||||| |||||||||| || |||||||| ||||||| ||||||||||||||| |||||| ||||||||||||||||||| |||||||||||| ||| |||||||||| || |||||| |||||| |||||||| ||| |||| ||||||||||| || ||||| || |||| |||||||| |||| ||| ||||||||||| |||||||||| ||| || |||||| ||||||||| |||||||| ||||||||| || ||||| ||||||||| ||||||| |||||| ||||| |||||| | | ||| ||| |||||||||| ||||| ||| ||||| |||| || | ||||||||| || |||||||| || | |||| ||| |||||||||| ||||| |||| || | ||||||||| || |||||||| ||| || | ||||| ||||| ||||||||||| || | |||| ||| || ||||||| |||||||| || ||| |||| ||||| || |||||||| || | ||| |||||||||| ||||||||| ||||||| || ||||| |||| | ||||| || | |||||| |||||| |||||||||||| || ||| |||| ||| |||||| |||| ||||||||||||| |||||||||| ||||| ||| ||||||| |||| || ||| |||| ||||||| |||| |||||||||||||| ||||||| ||| ||| ||||||||| || ||| |||| |||| |||||||||||| |||||||||| ||||| |||| | ||||||| ||| || ||||||| |||| || |||| ||| || ||||||| |||||||||||||| | ||||||| ||| ||||||| |||| || |||| ||| || ||||||||| |||||||||| |||||||||||| ||| ||| ||||| ||| || ||||||| |||| || |||| ||| || |||||||||| |||||||||| || |||||||| ||||||| ||||||| |||||||| |||| ||| || | ||||||| ||| ||| |||| || ||||||| |||| || |||| || ||| || |||| |||||||||||||| | ||||||||||||||||| |||||||||||| ||| |||||||||| || |||||| |||||| |||||||| || |||| ||||||||||| || ||||| || |||| |||||||| |||| ||| ||||||||||| |||||||||| ||| || |||||| ||||||||| |||||||| ||||||||| || ||||| ||||||||| ||||||| |||||| | | ||| |||||||||| ||||| ||| ||||| | ||||||||| || |||||||| || | ||| |||||||||| ||||| ||||| |||| || | ||||||||| || |||||||| ||| || | ||||| ||||| ||||||||||| || | ||| |||||||||| || |||||||| || ||| ||||||| | |||||| ||||| ||| | ||||| || | |||||| |||||| |||||||||||| || ||| |||| ||| |||||||| ||||||||| ||| ||||||| | |||||| |||| ||||||||||||| |||||||||||||| |||||||||| ||||||| ||| ||||| ||| | ||||| ||| |||||| ||| ||| ||||| ||| ||| |||||||| ||| ||| |||||||||| |||||||||||| |||||||||| ||||| |||| | ||| || | ||||||| ||| || ||||||| |||| || |||| ||| ||||||||| |||||||||| ||||||||||| |||||||||||||||||||| ||||||||||||||| ||||||| || ||| ||||||||||| |||||||||| ||| || ||||| ||
Table 25| |||||||| ||| |||||||||| ||| ||||||||||| ||| ||||||||| |||||||||| || |||||||||||||| ||||| |||||||||||||||||||| ||| ||||| | ||||| ||||||||||||||||||| ||||||||||| ||| |||||||||| ||||||| |||| |||||||||| ||||||| |||| |||| ||||| |||||| ||||||| |||||||| ||| |||||||| ||| || |||||||| ||||||||| |||||| |||||||||| ||||||| |||||||| ||| ||| |||||||||| || || ||| ||| | |||||||||| || ||| || ||| |||||||| |||||||| ||| ||| |||||||| |||||||| |||| |||||| |||||||| |||||||||| ||||| ||||| || ||| ||||||||||| ||||||||||| |||| ||| ||||||| |||||| ||||||||||||| |||||||||| ||||| ||||||||||| ||||||||| |||||||| |||||||| ||| |||||||||||||||||| || ||||||||| |||| ||| |||||||||||
||||||||||||||| | ||||||||||| ||| |||||||| || ||||||||| |||||| ||||||||| |
|---|---|
||||||| |||||||| | ||||||| |||||| ||||| |||||||||||||||||||| ||| ||||| | ||||| ||||||||||||||||||| |||||||| |||| |||||||| ||||||||||| || ||||| |||||||| || ||| ||||| || ||| || ||||| |||||||| |||||||| |||||||| |||| ||||| |
||||||||| ||||||| | ||||||| |||||| ||||| |||||||||||||||||||| ||| ||||| | ||||| ||||||||||||||||||| |||||||| |||| |||||||| |||||||||| |
||||| ||||||||||| |||||||| | ||| |||||||| |
|||||| || ||||||||||| | || ||| ||||| || ||| |||||||||| |||| ||| ||||| |||| || ||| |||||||||| |||||| |||| |||||||||| |||| ||||| |||||||| || |||||| |||||| ||| |||| || |||||||| |||||||| ||||||||| ||||||| ||| ||||||| |||||| ||| || ||||| ||||||| ||||||||| |||| ||| ||||||| |||||| |||| |||||||| |||||||| |||| ||| |||||||| || ||||||| |||||| || ||| ||| |||||||| ||||| ||| || ||||||||| |||||| |||||||||| |||||||||| ||| |||||||||| ||| ||| ||||||| || ||| ||||| |||| ||| |||||| ||||| ||||||| || ||||| |||||||| || || |||| || ||||||||| |
||||||| |||||||| | ||| ||||||||| |||||||| ||| ||| | |||||||||| || ||| ||||||| |
||||||||||| || ||| |||||| | ||| ||||||||||| || | |||||||| |||||||||| ||||| ||| ||||||| |||||||||| ||||||| |||||| |||||||| |||| |||| |||| || ||| |||||||| ||| ||| |||||||||| || ||||| ||||||||| |||||||| ||| ||| ||||||||| ||||| ||||||| ||||||||||| ||| ||| |||||| |
|||||| || ||| ||||| |||||||||| | ||| ||| |||||||||| |||| ||||||| ||| |||||||| || ||||| || ||||||||| ||| ||| || ||||||| |
|||||||||| ||||||||| | ||| ||||||||| |
|||||||| ||||| ||||||| | ||| ||||||||| |
||||| |||||| | |||||||| || ||| |||||||||| ||| ||| ||||||||| |||||||||| |
||||||| ||||||||||| ||| |||||||| ||||||||||||||| | o ||||||| |||| |||||||||| ||||||| |||| ||||||| ||||||||| ||| ||| |||| |||||||| || |||||||| |||||| ||||||||| || |||||||| || ||||| |||||| |||||||| |||||| || |||| |||||||||||||| || |||| || |||||| || ||||||| ||||||||| || |||| ||||||||||| ||| ||||||||||||| |||||| |||| ||||| ||||||||||||| ||||||||| || ||||||| ||||||||||| || ||||||||||| |||| ||||||||||||||||| ||||||||| || ||||| |||||||| ||||||| |||| ||||||||||| |||||| || ||||||||||||| ||||||||||||||||| || ||| | |||||||| ||||||| |||| ||||||||||| |||||| || ||||||||||||||||| ||||||||||||||||| || ||| | |||||||| ||||||| |||| ||||||||||| |||||| || ||||| | ||||||||||||||||| ||||||||||||| ||||||||| || ||| || |||||||| ||||||| |||| ||||||||| ||||| || ||| ||||||||||||| ||||||||||||||||| || ||| | |||||||| ||||||| |||| ||||||| ||||| || ||||| ||||||||||| |||||||| ||||||||| || ||| | |||||||| ||||||| |||| ||||||||| ||||| || ||||| | ||||||||||||||||| ||||||||||||||||||| ||||||||| || ||||| |||||||| ||||||| |||| ||||||||||| ||||| || ||||||||||||| ||||||||||||||||| || ||| |||||||| ||||||| |||| ||||||||||| ||||| || ||||||||||||||||| |||||||| ||||||||| || ||| | |||||||| ||||||| |||| ||||||||||| ||||| || ||||| | ||||||||||||||||| |||||||||||||||| ||||||||| || ||||| |||||||| ||||||| |||| ||||||||||| || ||||||||||||| ||||||||||||||||| || ||| |||||||| ||||||| |||| ||||||||||| || ||||||||||||||||| ||||||||||||||||| || ||| | |||||||| ||||||| |||| |||||||||||| || ||||| | ||||||||||||||||| |||||||||||||||||||||| || ||| || |||||||| ||||||| |||| |||||||||||| || ||||||||||||| ||||||||||||||||| || ||| | |||||||| ||||||| |||| |||||||||||||| || ||||||||||||||||| ||||||||||||||||| || ||| | |||||||| ||||||| |||| |||||||||||||| || ||||| | ||||||||||||||||| |||||||||||||||| ||||||||||||||||| || ||| || |||||||| ||||||| |||| |||||||| ||||| || ||||||||||||| ||||||||||||||||| || ||| | |||||||| ||||||| |||| ||||||||| ||||| || ||||||||||||||||| ||||||||||||||||| || ||| | |||||||| ||||||| |||| ||||||||| ||||| || ||||| | ||||||||||||||||| ||||||||||||||||| |||||||||||| || ||| || |||||||| ||||||| |||| |||||||| || ||||||||||||| ||||||||||||||||| || ||| | |||||||| ||||||| |||| ||||||||| || ||||||||||||||||| ||||||||||||||||| || ||| | |||||||| ||||||| |||| |||||||| || ||||| | ||||||||||||||||| |||||||| |
||| | |||||||| ||||||||||| ||| | |||||||| ||||| ||||||| ||| | |||| | ||||||||| ||| | |||||| |||||| || |||||||||||||||| ||||||| |||||||| || |||| ||||| ||| |||| ||| ||||||||| ||||||| || |||||||| |||||||| ||| ||| ||||||||| ||||||||||||||||||||||||||||||||| ||||||||||||||||| |||||||| ||| ||| |||||||| ||| || |||||||| | ||| |||||||| ||||||| || ||| |||||||| ||| ||
Table 26| |||||||| |||||||| ||| ||||||| ||||||| |||||||| |||||||||||| ||||| ||||||| |||| ||||||| || || ||||| ||| ||| |||||||||| ||| ||| |||||| ||| |||||| || |||||||| ||||| |||| ||||||||||| || ||| ||| ||||||||| ||| || ||||| ||||||| |||||| ||| |||||||| ||| |||||| || ||| |||| |||||||| |||||||| || ||||||| |||||||| |||| ||||||| || |||| |||| ||||| ||||||| ||||||||| |||||||| ||| ||||| |||||||| ||| ||| ||||||| ||||| |||||||||| ||| ||| ||||||| | |||||||||| ||||||||| ||||||| ||||| ||| |||||||||||| |||||||| || |||| | |||||||||| || |||||| |||| |||||||| || ||| ||| ||| ||||| |||||||||||| ||| ||| ||| ||||||||||| ||| ||||||| || |||||| ||||||||||||| ||| ||| ||| ||||||||| ||||| |||| |||| || |||||| ||||||| |||||| ||| |||||||| ||| ||||||| |||||| || ||| |||| |||||||| |||||||| || ||||||| |||||||| |||| ||| |||| |||| ||||| ||||||| |||||||| |||||||| |||| ||| |||| |||| ||||| ||||||| |||||||| ||| ||||||| ||| |||| |||| ||||| ||||||| ||||||| |||||||||||| |||||||| ||| ||||| ||||||||| ||| ||| ||||||| ||||| |||||||||| ||| ||| ||||||||||| ||| ||| ||||||| | |||||||||| ||||||||| ||||||| ||||| ||| |||||||||||| |||||||| || |||| | |||||||||| ||||||| ||||||| |||||| ||| ||| |||||||||| ||| ||||||| ||||||||||||| |||||| ||||||||||||| || ||||||||| ||||||||||||| |
|||||||||| | ||| |||||| |||| |||||||| | ||||||| ||||||||||||| | |||||| ||||||||||||| | ||||||||| ||||||||||||| |
|---|---|---|---|---|
|||||| || |||| |||| | |||||| || |||| |||| | |||||| || |||| |||| | |||||| || |||| |||| | |
||||||| || || ||||| | ||||
||||| | |||||| |||||| | ||||| |||||| | ||||| |||||| | ||| |
| ||||||| | || | | | | | ||| |
|||||||| |||| | ||||| ||||||| ||||| | |||| |||||| ||||| | |||| |||||| ||||| | ||| |
|||||||| |||| | ||||| ||||||| ||||| | || | |||| |||||| ||||| | ||| |
|||||||| |||| | ||||| ||||||| ||||||| | |||| |||||| ||||| | |||| |||||| ||||| | ||| |
|||||||| |||| | ||||| ||||||| ||||| | |||| |||||| ||||| | || | ||| |
||||||| | ||||| ||||||| ||||||| | || | |||| |||||| ||||| | ||| |
||||||| || || ||||| | ||||
||||| | ||||| |||||| | ||||| |||||| | ||||| |||||| | ||||| |||||| |
| ||||||| | | | | | | | | |
|||||||| |||| | ||||| ||||||| |||||| | |||| |||||| ||||| | |||| |||||| ||||| | |||| |||||| ||||| |
|||||||| |||| | || | ||| | ||| | ||| |
|||||||| |||| | ||||| ||||||| |||||| | |||| |||||| ||||| | |||| |||||| |||||| | |||| |||||| ||||| |
|||||||| |||| | || | || | || | || |
||||||| | ||||| ||||||| |||||| | || | |||| |||||| ||||| | || |
||| | |||||||| ||||||||||| ||| | |||||||| ||||||||| || | |||| |||||| || | ||| |||||||||| ||| | ||||||| |||| ||||||||| || | ||| ||||||||| || | ||||||||| |||||||||||| |||||||||| ||||||||||| || |||||| |||||| ||||| || ||| ||||||||||| || ||| ||||||| |||||||||| || |||||||| ||| ||||||| ||| || ||| |||| || |||||||||| |||| || ||| || ||| |||||||||| |||||||||| |||| |||||||| || ||| ||| ||||||| ||| ||| |||||| |||||||||| || ||||||| || ||||| ||| |||||||| || | ||||||||||| ||||||||||||||||| ||||||| |||||||| || |||| ||||| ||| |||| ||| ||||||||| ||||||| || |||||||| |||||||| ||| ||| ||||||||| |||||||||||||| ||||| || ||| |||||| |||| ||||||||| || | ||||||||||| |||||||| || || ||||| ||||||||| ||| ||||| |||| ||||||| ||||||||| || ||||||||| ||||||| | || ||| ||| ||||||| ||| ||||||| || |||| ||||| ||| |||||||||||| |||||||| ||| | |||||||||| ||||||| ||||||| |||||| ||| ||| |||||||||||||||| ||||||| || ||||||| |||||||||||| || || |||||| ||||||||| ||||||| | ||||||||| ||| ||||||||| || ||| ||||||||| ||||||||||| ||| ||| ||||||| ||||||| || |||||| ||||||| |||||| |||| ||||||| |||||||| ||||| || || |||||| |||| ||||||| | ||| |||||||| || ||| ||||||||| ||||||| ||||||| || ||| ||||| ||||||||| ||| |||||||| ||||||||| |||| |||||||| ||| |||||||| ||| ||| ||||||| ||||||||| ||||| ||| |||||||||||| |||||||| || |||| | |||||||||| ||||||| ||||||| |||||| ||| ||| ||||||||||| ||||||||| ||| |||| |||| ||||||| | |||| ||| ||| ||||||| ||| ||||||||| || ||| |||||| ||||||||| || |||||| ||||||| |||||| ||| |||||| |||||||||||| || || |||||| |||||||||| ||| ||||||| |||||||| ||||| ||||| ||| ||| |||||||| || ||| |||| |||| ||||||| ||| ||| |||| || || |||||||| |||||| ||| ||||||||||| |||||||| ||||| ||||||| | ||| ||||||||| |||| ||||||| || ||||||||| || ||| ||||| ||||||| ||||||||||| || ||| ||||||||||| ||||||||| |||||||||| ||||| || |||||||||||| |||||||| || |||||||| || || ||||||||| |||| ||||| ||||||||||| ||| |||| |||||||||||||| ||||||||||||||||||| ||||||||||||||||| ||||||| || ||| ||| |||||||| ||| || ||||| ||
Table 27| |||||||| |||||||| ||| |||||||||||| |||||||| |||| |||||| |||| |||| | ||||||| |||| ||| ||| ||||||| ||||||||| ||| |||| |||||||||| |||| ||||||| |||||||| ||| ||||||||| ||||||| |||||| ||| |||||||| ||| |||||| |||| |||||||| || ||| |||||||| || ||||||| |||||||| |||| ||||||| || |||| |||| ||||| ||||||| |||||||| |||||||| ||| ||||||| ||||| |||||||||| ||| ||| ||||||| | |||||||||| ||||||||| ||||||| || ||| |||||||||| || ||||||| |||||| ||| ||||||| |||||||| |||| ||| ||||||| ||||||||||||| ||||||| |||||||| |||| ||| |||||||| ||||||| || |||| |||| |||| |||||| ||||||| ||||| ||| |||||||||||| |||||||| || |||| | |||||||||| ||||||| ||||||| |||||| ||| ||| ||||| |||||||||| ||| ||| ||||| ||||||||||
|||||||||| | ||| |||||| |||| |||||||| | ||||||| ||||||||||||| | |||||| |||||||||||| | ||||||||| ||||||||||||| |
|---|---|---|---|---|
|||||| || |||| |||| | |||||| || |||| |||| | |||||| || |||| |||| | |||||| || |||| |||| | |
||||| | ||||| |||||| | ||||| |||||| | ||||| |||||| | ||||| |||||| |
| ||||||| | | | | | | | | |
|||||||| |||| | ||||| ||||||| ||||| | ||| | ||| | ||| |
|||||||| |||| | ||||| ||||||| ||||| | ||| | ||| | ||| |
|||||||| |||| | ||||| ||||||| |||||| | |||| |||||| ||||| | |||| |||||| ||||| | |||| |||||| ||||| |
|||||||| |||| | ||||| ||||||| ||||| | |||| |||||| ||||| | |||| |||||| |||||| | |||| |||||| ||||| |
||||||| | || | || | || | || |
||| | |||||||| ||||||||||| ||| | |||||||| ||||||||| || | |||| |||||| || | ||| |||||||||| ||| | ||||||| |||| ||||||||| || | ||||||||| |||||||||||| |||||||||| ||||||||||| || |||||| ||||||||| |||||| || |||||| || ||| ||||||| ||| || | |||| || |||||||||| ||||||||||||| ||||||| |||||||| || |||| ||||| ||| |||| ||| ||||||||| ||||||| || |||||||| |||||||| ||| ||| ||||||||| ||||||||||||||||||||||| |||||||| ||||| ||| |||||||| |||| ||||||| | ||| ||| ||||||| |||||| |||||||| ||| ||| |||||||| ||||| ||| |||||| |||||||||| ||| ||||||| ||||||||| ||| |||||||||| || |||||||| |||||||||||| |||||| |||||||||||| ||| |||| ||| || ||| || |||| |||||| ||| ||||| |||| || |||||| || ||| ||||||| |||||| |||| |||||| ||| ||||||| |||||| |||||||||||||||| | ||||| ||||||||||||||||||| ||||||||||||||||| ||||||| || ||| ||| ||| || ||||| ||
Table 28| ||||| ||| |||||||| |||| |||||| ||| ||| ||| |||||| |||||||||| || ||| |||||| ||||||||| |||||||| ||| ||| ||||||||||| |||| |||| ||||| || || ||||| || |||||| ||| ||||| ||| |||||||||||| |||||||| || |||| | |||||||||| ||||||| ||||||| |||||| ||| ||||||| |||||||| |||| || |||| ||| ||| ||||||||| ||||| ||| |||| |||||||||||| |||||||| || |||| | |||||||||| ||||||| ||||||| |||||| ||| ||||||| ||||||| ||| |||||| |||| |||||||| || |||| ||||||||||| |||||||| ||| ||| |||| || ||||||| ||||||| || ||| ||||||| |||| ||| |||||
|||||||||| | ||| |||||| |||| |||||||| | ||||||| ||||||||||||| | |||||| |||||||||||| | ||||||||| ||||||||||||| |
|---|---|---|---|---|
|||||| || |||| |||| | |||||| || |||| |||| | |||||| || |||| |||| | |||||| || |||| |||| | |
||||| | ||||| |||||| | ||||| |||||| | ||||| |||||| | ||||| |||||| |
| ||||||| | | | | | | | | |
|||||||| |||| | |||| ||||||| ||||| | |||| |||||| ||||| | |||| |||||| |||||| | |||| |||||| ||||| |
|||||||| |||| | |||| ||||||| ||||| | |||| |||||| ||||| | |||| |||||| |||||| | |||| |||||| ||||| |
|||||||| |||| | || | || | || | || |
|||||||| |||| | || | || | || | || |
||||||| | ||||| ||||||| ||||| | ||| | ||| | ||| |
| |||||||||| ||||||||||| || |||||| ||||||||| |||||| || |||||| || ||| ||||||| ||| || | |||| || |||||||||| ||||||||||||| ||||||| |||||||| || |||| ||||| ||| |||| ||| ||||||||| ||||||| || |||||||| |||||||| ||| ||| ||||||||| |||||||||||
Critical Appraisal of NMA
The sponsor submitted an NMA with the objective of assessing the relative effectiveness and safety of insulin icodec relative to the daily basal insulin analogues used in clinical practice in Canada. It is not mentioned in the NMA whether this review was informed by a pre-established protocol; as such, the exact process for carrying out analyses is not known; specifically, whether sensitivities or adjustments in the NMA networks were the result of preplanned or post hoc analysis, or whether multiple analyses of the same data were conducted. The search was adequately comprehensive, including multiple electronic databases, conference proceedings, clinical trial registries, health technology assessment submissions, SLR or study reference lists, and grey literature. The search was conducted 2 years before the submission, allowing for a risk of bias due to missing evidence; however, the clinical expert was not aware of additional relevant studies published after the date last searched. Studies were selected by 2 reviewers who worked independently, limiting the potential for error and selection bias. A flow diagram of study selection was provided along with a list of excluded studies with rationale. The list of comparators was comprehensive per the clinical expert consulted by CADTH, and most of the outcomes, with the exception of basal insulin dose, were considered relevant for clinical practice. Data were extracted by 1 reviewer and checked by a second reviewer, reducing the risk of error and bias in the data extraction process. The assessment of risk of bias was conducted using the criteria listed for the National Institute for Health and Care Excellence single technology appraisal tool, which appears to include most domains that have empirically been linked to bias,82 with the exception of risk of bias in the selection of the reported result.83
The SLR is subject to a notable limitation, in that it excluded studies where the base population was patients with T2DM plus a coexisting condition, but did not provide additional information on the level of comorbidity burden for the patients included in the NMA. It therefore cannot be verified if there are differences across trials in the proportions of patients with various additional comorbidities; this could violate the transitivity assumption if specific comorbidities are considered treatment effect modifiers. This adds possible heterogeneity and thus increases the uncertainty in the NMA results.
With regards to the feasibility assessment, there are a couple of limitations. First, the risk of bias appraisals were undertaken at the level of the trial, rather than at the level of the reported result (within each trial). Undertaking risk of bias appraisals at the level of the trial ignores that risk of bias can differ across outcomes within the same trial. Furthermore, the methods for appraising risk of bias were not reported (i.e., number of reviewers involved and whether they worked independently). As such, the potential for error and bias in the appraisals is unknown. The risk of bias assessment itself noted unclear methods for randomization, treatment allocation concealment, and imbalances in dropouts between groups which, while affecting a minority of studies in the insulin-naive subgroup, affect the majority of studies in the other 2 study populations due to the small size of the network.
In addition, there was no discussion of how the treatment effect modifiers were chosen for the feasibility assessment, nor a discussion of how the assessment ensured that the list of treatment effect modifiers was comprehensive. To satisfy the transitivity assumption in an NMA, all of the included trials must be similar, on average, in all important factors other than the intervention comparison being made. To ascertain whether the assumption has been met, all treatment effect modifiers must be known, measured, and compared across potentially eligible trials.84 While the clinical expert CADTH consulted did not identify any missing treatment effect modifiers from the list in the submission, there are issues in measurement in that a paucity of studies reported ethnicity, and the ranges reported were wide. Overall, there remains uncertainty in the feasibility assessment which affects the confidence in the transitivity assumption underpinning the NMA.
An additional limitation is noted regarding the NMA networks for hypoglycemia across all populations as well as hemoglobin A1C in the insulin-experienced populations. While the submission provided a list of which studies contributed to each NMA, there were small networks containing as few as 2 studies for the basal and basal and bolus insulin-experienced populations. This necessitated the selection of fixed-effect models for most comparison outcomes as the SE was unstable to estimate with such a small network; however, these models do not account for between-study variances, and this adds some uncertainty to the results. Furthermore, the submission did not contain any consistency assessments for the instances where there were closed loops in the network, which limits assessing the consistency of the results in the NMA with results from the individual trials.
In addition, in several analyses, the proportion of patients experiencing hypoglycemic events was much lower in the insulin icodec studies (ONWARDS trials) than the comparator studies (hypoglycemia outcomes in patients who were insulin naive, in overall hypoglycemia and nocturnal hypoglycemia in patients who were basal insulin experienced, and severe hypoglycemia in patients who were basal and bolus insulin experienced). The submission raised the question whether the comparison was appropriate but did not explore it in any way. For the hypoglycemia outcomes, for nearly all comparisons, the effect estimates were affected by imprecision due to wide credible intervals, precluding any conclusions regarding which treatment in the comparison may be favoured.
The addition of the ONWARDS 5 study to the analyses changed the results for many outcomes, suggesting that 1 or more aspects of the design, population, intervention, outcome assessment, or comparators in the ONWARDS 5 study might not be comparable to the other studies in the NMA. The main differences between the ONWARDS 5 trial and other ONWARDS trials were the use of the DoseGuide app, which may have affected insulin titration, and the fact that the comparator arms were not randomized (the physician chose whether patients would receive insulin glargine or insulin degludec). These reasons suggest that it was reasonable to exclude this trial from the base-case NMA.
Apart from methodological limitations, the NMA is also subject to some limitations in clinical meaningfulness. The clinical expert consulted by CADTH noted that while the results for hemoglobin A1C change from baseline across study populations may attain statistical significance, they overall do not represent an important clinical benefit. In addition, while the rationale for the NMA was to include insulin detemir and provide data for insulin icodec compared to insulin detemir, results for insulin icodec relative to insulin detemir were not available at all for patients who were basal insulin experienced, and were only available for hemoglobin A1C and severe hypoglycemia in the other study populations. This limits the comparability of insulin icodec to insulin detemir.
Lastly, the NMA has some limitations in generalizability. While patient characteristics such as age range, hemoglobin A1C range, and ethnicity breakdown in the studies were typical of what would be seen in an RCT according to the clinical expert consulted by CADTH, these characteristics are likely not representative of all T2DM patients in all clinical settings. In particular, no studies included patients aged older than 70 years in higher hemoglobin A1C ranges, therefore older patients with T2DM or patients with less well-controlled T2DM are not represented. In addition, as there are no 52-week results for insulin-experienced populations, the impact of insulin icodec on the long-term control of blood glucose and the long-term safety relative to daily insulin comparators remains unknown. Outcomes that were important to this review, including time in range, change in body weight, treatment satisfaction, treatment compliance, all-cause mortality, CV mortality, and microvascular and macrovascular complications of T2DM, were not assessed in the NMA. Further, there was no evidence for the impact of insulin icodec on HRQoL relative to any comparator.
Studies Addressing Gaps in the Systematic Review Evidence
Contents within this section have been informed by materials submitted by the sponsor. The following have been summarized and validated by the CADTH review team.
No additional evidence was submitted by the sponsor.
Discussion
Summary of Available Evidence
Five active-controlled, multicentre RCTs were included in this review, all of which compared insulin icodec once weekly to once-daily basal insulins (insulin degludec and/or insulin glargine). Three of the included studies enrolled adult patients with T2DM who were insulin naive (ONWARDS 1, 3, and 5); of these, the ONWARDS 1 study included a primary analysis at 52 weeks in duration, while in the ONWARDS 3 and 5 studies, the primary analyses occurred at 26 weeks. The ONWARDS 5 study additionally included the DoseGuide app to inform dosing choices in the insulin icodec arm. The remaining 2 included studies enrolled adult patients with T2DM who were insulin experienced. In the ONWARDS 2 study, patients were experienced with basal insulin, and in the ONWARDS 4 study, patients were experienced with basal and bolus insulin. Both of these studies were 26 weeks in duration. The ONWARDS 4 study additionally included insulin aspart (bolus) administered 2 times to 4 times per day before mealtimes. In all 5 studies, the primary outcome was an assessment of noninferiority of insulin icodec once weekly compared to the once-daily comparator for the outcome of change in hemoglobin A1C from baseline. In all but the ONWARDS 4 study, a secondary confirmatory analysis of superiority was also conducted for this outcome. Secondary outcomes varied between the studies and included CGM assessments (time in range, time below range, and time above range) in the ONWARDS 1 and ONWARDS 2 studies, change in body weight in all included studies, the number of clinically significant or severe hypoglycemic episodes (level 2 or 3) in all studies, change in DTSQ in the ONWARDS 5 and ONWARDS 2 studies, and the TRIM-D compliance domain as a measure of treatment compliance in the ONWARDS 5 study. All-cause mortality was reported as a harm in all trials. Additional outcomes of interest that were not reported include the long-term efficacy regarding CV mortality, nonfatal MI, nonfatal stroke, and other microvascular or macrovascular complications of T2DM.
At baseline, patients in the insulin icodec arm of all ONWARDS studies had mean ages ranging from 58 years to 62 years, and 53% to 63% were male, while 37% to 47% were female. Across all studies, the majority of patients were white (60% to 90%) followed by Asian (4% to 42%), Black or African American (2% to 5%), Other (< 1% to 4%), American Indian or Alaska Native (0 to < 1%), and Native Hawaiian or Other Pacific Islander (0 to < 1%). In the insulin-naive populations of the ONWARDS 1, ONWARDS 3, and ONWARDS 5 studies, the mean duration of diabetes was 11 years to 12 years and the mean hemoglobin A1C was 8.44% to 8.88% at baseline. In the insulin-experienced populations of the ONWARDS 2 and ONWARDS 4 studies, the mean duration of diabetes was 16 years to 18 years, and the mean hemoglobin A1C was 8.17% to 8.31% at baseline. The majority (approximately 90%) of patients were receiving metformin as an antihyperglycemic background medication at baseline.
The ONWARDS 1 study also included a 26-week, active-controlled LTE in which patients continued on their initially assigned study treatment, with the primary goal of assessing longer-term safety outcomes at 78 weeks of follow-up.
A sponsor-submitted indirect treatment comparison was summarized and critically appraised, which consisted of NMAs in 3 distinct T2DM populations: patients who were insulin naive (n = 11 included studies), patients with basal insulin experience (n = 5 included studies), and patients experienced with basal and bolus insulin (n = 19 included studies). The outcomes assessed included change from baseline in hemoglobin A1C, mean weekly basal insulin dose, overall hypoglycemia (levels 2 and 3), proportion of severe (level 3) hypoglycemic events, and the proportion of nocturnal clinically significant (level 2) or severe (level 3) hypoglycemic events.
Interpretation of Results
Efficacy
Evidence from all 5 of the ONWARDS studies demonstrated that insulin icodec was noninferior to once-daily insulin degludec or insulin glargine for the outcome of change in hemoglobin A1C from baseline in adult patients with T2DM who were insulin naive or insulin experienced at week 26 (ONWARDS 3, 2, and 4) or week 52 (ONWARDS 1 and 5), and likely results in little to no clinically meaningful difference in this outcome compared with insulin glargine or insulin degludec. In all but the ONWARDS 4 study (where superiority was not tested), insulin icodec was considered statistically superior to insulin degludec or insulin glargine; however, the magnitude of benefit was not considered clinically important.
Among patients who were insulin naive or insulin experienced, evidence from the ONWARDS trials showed that insulin icodec results or in little to no difference in change in body weight, and results or likely results in little to no difference in time spent above or below range, compared with insulin degludec or insulin glargine. For change from baseline in hemoglobin A1C, time-in-range outcomes, and change in body weight, the results from the 78-week analysis of the ONWARDS 1 study in patients who were insulin naive were consistent with those from 52 weeks of follow-up.
Most outcomes, including the primary outcome, were objective measures and were not affected by serious concerns related to risk of bias. Interpretation of the subjective patient-reported measures (DTSQ and TRIM-D) was affected by a risk of bias in the measurement of the outcomes due to the open-label nature of the trials contributing results and a lack of established MIDs. As the intention of the DTSQ (and TRIM-D) is to evaluate satisfaction with treatment (and compliance) and a key difference of the intervention versus comparators is the administration schedule, a blinded assessment of DTSQ (and TRIM-D) with matched placebos would have been uninformative for this research question. Among both patients who were insulin naive or insulin experienced, respectively, results of the ONWARDS 5 and ONWARDS 2 studies showed that insulin icodec likely results in little to no difference in treatment satisfaction compared with insulin degludec or insulin glargine. In the absence of known MIDs, there is uncertainty in the clinical importance of the observed between-group difference, but all point estimates appeared small (0.78 points in ONWARDS 5 and 1.25 points in ONWARDS 2). Treatment compliance was measured only in patients who were insulin naive, and the results of the ONWARDS 5 study showed that insulin icodec likely results in increased compliance when compared to insulin degludec or insulin glargine; however, the clinical importance of the increase is uncertain. The effect of insulin icodec compared with daily insulins on treatment compliance among patients who are insulin experienced is not known.
With regards to hypoglycemia, insulin icodec likely results in little to no difference in the proportion of patients experiencing 1 or more level 2 or 3 hypoglycemia events when compared to insulin glargine or insulin degludec among the insulin-naive population, but the 2 studies conducted in patients who were insulin experienced (ONWARDS 2 and ONWARDS 4) suggested opposing directions of effect, both with limitations in certainty. As a result of this inconsistency between trials, it is difficult to reach a narrative conclusion regarding the effect of insulin icodec on level 2 or 3 hypoglycemic events among patients who were insulin experienced. The thresholds for minimally important clinical differences were selected by clinical expert input and may be subjective, so this observation may not be clinically meaningful.
The primary outcome of hemoglobin A1C and the associated noninferiority margin of 0.3% points is considered acceptable by the FDA17 for trials of new antihyperglycemic therapies seeking a glycemic control indication, and further it is currently recognized as the key surrogate marker for the development of long-term diabetes complications in people with type 1 diabetes mellitus or T2DM.18 However, hemoglobin A1C is ultimately a surrogate biomarker, and there is evidence to suggest that hemoglobin A1C may not be appropriate as a surrogate outcome for downstream complications in diabetes trials due to poor associations with mortality,19,20 CV mortality,21 MI,19 heart failure,19 kidney injury,19 and stroke.19 Other limitations of hemoglobin A1C include a lack of information about acute glycemic events (i.e., hypoglycemia or hyperglycemia) and insensitivity regarding day-to-day variations of glucose, and measurement of hemoglobin A1C can be confounded by other conditions such as anemia, hemoglobinopathies, iron deficiency, and pregnancy.18 Time in range as measured by CGM is useful as a measure of short-term glycemic control,22 and allows for observation of daily glycemic variability;18 the clinical expert consulted by CADTH indicated that this is of growing importance in clinical trials of glycemic control in patients with T2DM in addition to hemoglobin A1C. Time in range has been demonstrated to be associated with diabetic retinopathy23,24 and microalbuminuria23 but publications assessing this outcome as a surrogate for other diabetes-related complications (e.g., mortality, MI, and other major CV or renal events) were not identified.
The NMAs submitted by the sponsor showed that, among patients who were insulin naive, insulin icodec was favoured over insulin degludec U100 for change from baseline in hemoglobin A1C at 26 weeks; however, the point estimate did not suggest a clinically important effect. At 52 weeks, insulin icodec was favoured compared to insulin glargine U100, degludec U100, and detemir for change from baseline in hemoglobin A1C; however, the point estimate also did not suggest a clinically important effect. In the patients who were basal insulin experienced, analyses were only conducted at 26 weeks due to a lack of data for longer follow-up times. Results from the NMA showed that insulin icodec was favoured over insulin degludec U100 for change from baseline in hemoglobin A1C; however, the point estimate did not suggest a clinically important effect. In the comparison of insulin icodec and insulin degludec U100 for overall hypoglycemia, insulin degludec U100 was favoured; however, the magnitude of the difference is uncertain due to the absence of absolute effect estimates. For all other comparisons, there was insufficient evidence to show a difference between insulin icodec and the once-daily insulin analogues that were investigated. Across the NMAs, several effect estimates were affected by serious imprecision (i.e., wide credible intervals) particularly for hypoglycemia outcomes, precluding a conclusion as to which treatment may be favoured. The NMAs were also limited by small networks (few contributing studies) for patients who were insulin experienced and hypoglycemia outcomes, potential outcome definition differences, uncertainty around the comprehensiveness of the feasibility assessment for between-trial heterogeneity in treatment effect modifiers, and a paucity of data for ethnicity in the trials. Comparisons of insulin icodec to insulin detemir were not possible for several outcomes and populations. Specifically, comparisons in patients who were basal insulin experienced for any outcome lacked insulin detemir as a comparator, as well as overall and nocturnal hypoglycemia for patients who were insulin naive, and overall hypoglycemia, severe hypoglycemia, or nocturnal hypoglycemia for patients who were basal and bolus insulin experienced.
An important limitation of the included trials was that HRQoL was not measured, aside from the DTSQ and TRIM-D compliance domain; as such, the influence of insulin icodec on HRQoL compared with once-daily basal insulin analogues is not known. There is an absence of data regarding global HRQoL comparing insulin icodec to daily insulin analogues. There is also a data gap related to the long-term clinical outcomes such as nonfatal CV events (including MI or stroke), diabetes-related or CV-related deaths, and long-term all-cause mortality, which the CDEC presenters considered important.
Harms
Rates of AEs and SAEs were similar across treatment arms in each of the included trials. However, there were more events of level 1 hypoglycemia and more events of level 2 hypoglycemia among patients treated with insulin icodec, and a relatively small number of patients experienced numerous hypoglycemic events. Level 3 hypoglycemic events were rare in all treatment groups. Other notable harms such as injection site reactions and hypersensitivity events were rare, and all events were mild or moderate in severity. The proportions of patients experiencing nocturnal hypoglycemic events were similar between treatment groups in each trial; severe (level 3) nocturnal events were rare. In each treatment group, 1 to 6 patients died (< 1% in each group), and results were similar between insulin icodec and the comparator groups.
Conclusion
Based on evidence from 5 active-controlled RCTs which compared insulin icodec to insulin glargine and/or insulin degludec in adults with T2DM who were either insulin naive or insulin experienced, insulin icodec once-weekly injections were noninferior to the included once-daily basal insulin comparators for the change from baseline in hemoglobin A1C at week 26 or week 52 of treatment, and likely result in little to no difference in this outcome. Secondary analyses of superiority showed that insulin icodec is statistically superior compared with once-daily insulin analogues evaluated for this outcome, but the magnitude of the difference was not likely to be clinically important. Secondary and exploratory analyses of CGM outcomes (time in range, time above range, and time below range) and change in weight demonstrated that there is little to no difference associated with insulin icodec compared with insulin degludec or insulin glargine across the included studies. Among patients who were insulin naive or insulin experienced, respectively, results of the ONWARDS 5 and ONWARDS 2 studies showed that insulin icodec likely results in little to no difference in treatment satisfaction per the DTSQ compared with insulin degludec or insulin glargine; in the absence of known MIDs, there is uncertainty in the clinical importance of the observed between-group difference, but all point estimates appeared small (0.78 points in ONWARDS 5 and 1.25 points in ONWARDS 2). Treatment compliance was measured using the TRIM-D compliance domain only in patients who were insulin naive, and the results of the ONWARDS 5 study showed that insulin icodec likely results in increased compliance when compared to insulin degludec or insulin glargine; however, the clinical importance of the increase is uncertain. The effect of insulin icodec compared with daily insulins on treatment compliance among patients who were insulin experienced is not known. The studies were generalizable to populations in Canada with T2DM and provided robust evidence versus key active comparators. According to the clinical expert consulted by CADTH, the uptake of insulin icodec is likely to be highest among eligible patients starting on basal insulin for the first time, and may also be preferred over daily basal insulins by patients who would prefer a lower burden of administration frequency. The safety profile of insulin icodec was generally comparable to that of insulin glargine and degludec. In the insulin-naive populations, insulin icodec resulted in little to no difference in the proportion of patients experiencing hypoglycemia (level 2 or 3); in the insulin-experienced populations, the proportion of patients with level 2 or 3 hypoglycemic events was higher in the ONWARDS 2 study but lower in the ONWARDS 4 study in the insulin icodec treatment arms than the comparator arms. Additionally, there were more level 2 hypoglycemic events among patients treated with insulin icodec than the comparators in 4 of the 5 trials, although a few patients accounted for many events in the ONWARDS 1 and ONWARDS 3 studies. Evidence from the LTE was generally consistent with the results of the main trials. The NMA was inconclusive either due to substantial imprecision or inadequate evidence to make a comparison, or the results did not demonstrate clinically meaningful impact (in the case of hemoglobin A1C). There is a data gap regarding long-term outcomes such as the downstream consequences of T2DM, including nonfatal CV events such as MI and stroke, CV deaths, and long-term all-cause mortality beyond the duration of the clinical trials. Additionally, there is a data gap regarding the effect of insulin icodec on patients’ HRQoL using more comprehensive global measures.
References
1.Sponsor Summary of Clinical Evidence for insulin icodec (Brand Name TBD) for Type 2 Diabetes Mellitus. [internal sponsor's report] In: Drug Reimbursement Review sponsor submission: AWIQLI (insulin icodec), 700 units/mL, pre-filled pen for subcutaneous use. Mississauga, ON: Novo Nordisk Canada Inc; 2023 Jun.
2.CDC. What is diabetes? 2023; https://www.cdc.gov/diabetes/risk-factors/?CDC_AAref_Val=https://www.cdc.gov/diabetes/basics/risk-factors.html. Accessed by sponsor, no date provided.
3.Mayo Clinic. Type 2 diabetes. 2023; https://www.mayoclinic.org/diseases-conditions/type-2-diabetes/symptoms-causes/syc-20351193. Accessed 2023 May.
4.Diabetes Canada. Diabetes in Canada. https://www.diabetes.ca/advocacy—policies/advocacy-reports/national-and-provincial-backgrounders/diabetes-in-canada. Accessed 2023 May.
5.Framework for diabetes in Canada. Ottawa (ON): Public Health Agency of Canada; 2022: https://www.canada.ca/en/public-health/services/publications/diseases-conditions/framework-diabetes-canada.html. Accessed by sponsor, no date provided.
6.Crowshoe L, Dannenbaum D, Green M, Henderson R, Hayward MN, Toth E; Diabetes Canada Clinical Practice Guidelines Expert Committee. Type 2 diabetes and Indigenous peoples. Can J Diabetes. 2018;42(suppl 1):S296-S306.PubMed
7.Shah BR. Diabetes in visible minority populations in Ontario. Healthc Q. 2013;16(4):14-17.PubMed
8.Crowshoe L, Dannenbaum D, Green M, Henderson R, Hayward MN, Toth E; Diabetes Canada Clinical Practice Guidelines Expert Committee. Type 2 diabetes and Indigenous peoples. Can J Diabetes. 2018;42(suppl 1):S296-S306.PubMed
9.Bragg F, Holmes MV, Iona A, et al; China Kadoorie Biobank Collaborative Group. Association between diabetes and cause-specific mortality in rural and urban areas of China. JAMA. 2017;317(3):280-289.PubMed
10.Imam B, Miller WC, Finlayson HC, Eng JJ, Jarus T. Incidence of lower limb amputation in Canada. Can J Public Health. 2017;108(4):e374-e380.PubMed
11.Liu NF, Brown AS, Folias AE, et al. Stigma in people with type 1 or type 2 diabetes. Clin Diabetes. 2017;35(1):27-34.PubMed
12.Schram MT, Baan CA, Pouwer F. Depression and quality of life in patients with diabetes: a systematic review from the European depression in diabetes (EDID) research consortium. Curr Diabetes Rev. 2009;5(2):112-119.PubMed
13.Kalra S, Mukherjee JJ, Venkataraman S, et al. Hypoglycemia: The neglected complication. Indian J Endocrinol Metab. 2013;17(5):819-834.PubMed
14.Diabetes Canada Clinical Practice Guidelines Expert Committee. Diabetes Canada 2018 clinical practice guidelines for the prevention and management of diabetes in Canada. Can J Diabetes. 2018;42(suppl 1):S1-S325.
15.Kjeldsen TB, Hubálek F, Hjørringgaard CU, et al. Molecular engineering of insulin icodec, the first acylated insulin analog for once-weekly administration in humans. J Med Chem. 2021;64(13):8942-8950.PubMed
16.Awiqli (insulin icodec injection): 700 units/mL solution for subcutaneous injection in the FlexTouch pre-filled pen [product monograph]. Mississauga (ON): Novo Nordisk Canada Inc.; 2024 Mar 12.
17.Guidance for industry: diabetes mellitus: developing drugs and therapeutic biologics for treatment and prevention. Draft guidance. Silver Springs (MD): U.S. Food and Drug Administration (FDA); 2008: https://downloads.regulations.gov/FDA-2008-D-0118-0003/attachment_1.pdf. Accessed 2024 Jan 05.
18.Battelino T, Danne T, Bergenstal RM, et al. Clinical targets for continuous glucose monitoring data interpretation: recommendations from the international consensus on time in range. Diabetes Care. 2019;42(8):1593-1603.PubMed
19.Rivera PA, Rodríguez-Zúñiga MJM, Caballero-Alvarado J, Fiestas F. Glycated hemoglobin as a surrogate for evaluating the effectiveness of drugs in diabetes mellitus trials: a systematic review and trial-level meta-analysis. Int J Technol Assess Health Care. 2021;38(1):e12.PubMed
20.Baechle C, Scherler W, Lang A, Filla T, Kuss O. Is HbA1c a valid surrogate for mortality in type 2 diabetes? Evidence from a meta-analysis of randomized trials. Acta Diabetol. 2022;59(10):1257-1263.PubMed
21.Bejan-Angoulvant T, Cornu C, Archambault P, et al. Is HbA1c a valid surrogate for macrovascular and microvascular complications in type 2 diabetes? Diabetes Metab. 2015;41(3):195-201.PubMed
22.Vigersky RA, McMahon C. The relationship of hemoglobin A1C to time-in-range in patients with diabetes. Diabetes Technol Ther. 2019;21(2):81-85.PubMed
23.Beck RW, Bergenstal RM, Riddlesworth TD, et al. Validation of time in range as an outcome measure for diabetes clinical trials. Diabetes Care. 2019;42(3):400-405.PubMed
24.Lu J, Ma X, Zhou J, et al. Association of time in range, as assessed by continuous glucose monitoring, with diabetic retinopathy in type 2 diabetes. Diabetes Care. 2018;41(11):2370-2376.PubMed
25.Clinical Study Report: NN1436-4477, ONWARDS 1 – main part . A 78-week trial comparing the effect and safety of once weekly insulin icodec and once daily insulin glargine 100 units/mL, both in combination with non-insulin anti-diabetic treatment, in insulin naïve subjects with type 2 diabetes [internal sponsor's report]. Bagsvaerd (DK): Novo Nordisk; 2022 Jul 13.
26.Clinical Study Report: NN1436-4479, ONWARDS 3. A 26-week double blinded, multiregional trial comparing the effect and safety of once weekly insulin icodec and once daily insulin degludec 100 units/mL, both in combination with non-insulin anti-diabetic drugs, in insulin naïve subjects with type 2 diabetes [internal sponsor's report]. Bagsvaerd (DK): Novo Nordisk; 2022 Sep 07.
27.Clinical Study Report: NNN1436-4481, ONWARDS 5. Effectiveness and safety of once weekly insulin icodec used with DoseGuide versus once daily basal insulin analogues in an insulin naïve type 2 diabetes population in a clinical practice setting [internal sponsor's report]. Bagsvaerd (DK): Novo Nordisk; 2023 Oct 27.
28.Clinical Study Report: NN1436-4478, ONWARDS 2. A 26-week trial comparing the effect and safety of once weekly insulin icodec and once daily insulin degludec, both with or without non-insulin anti-diabetic drugs, in subjects with type 2 diabetes treated with basal insulin [internal sponsor's report]. Bagsvaerd (DK): Novo Nordisk; 2022 Jun 15.
29.Clinical Study Report: NN1436-4480, ONWARDS 4. A 26-week trial comparing the effect and safety of once weekly insulin icodec and once daily insulin glargine 100 units/mL, both in combination with bolus insulin with or without non-insulin anti-diabetic drugs, in subjects with type 2 diabetes on a basal-bolus regimen [internal sponsor's report]. Bagsvaerd (DK): Novo Nordisk; 2022 Sep 23.
30.Novo Nordisk response to December 5, 2023 CADTH request for additional information regarding insulin icodec review [internal additional sponsor's information]. Mississauga (ON): Novo Nordisk Canada Inc.; 2023 Dec 13 and 15.
31.Rosenstock J, Bajaj HS, Janež A, et al; NN1436-4383 Investigators. Once-weekly insulin for type 2 diabetes without previous insulin treatment. N Engl J Med. 2020;383(22):2107-2116.PubMed
32.Li T, Higgins JPT, Deeks JJ, eds. Chapter 5: collecting data. In: Higgins JPT, Thomas J, Chandler J, et al., eds. Cochrane Handbook for Systematic Reviews of Interventions version 6.4 (updated August 2023). Chichester (UK): Cochrane; 2023: https://training.cochrane.org/handbook. Accessed 2024 Jan 19.
33.Punthakee Z, Goldenberg R, Katz P; Diabetes Canada Clinical Practice Guidelines Expert Committee. Punthakee Z, Goldenberg R, Katz P. Definition, classification and diagnosis of diabetes, prediabetes and metabolic syndrome. Can J Diabetes. 2018;42(suppl 1):S10-S15.PubMed
34.International Diabetes Federation. IDF Diabetes Atlas. 2021; https://diabetesatlas.org/. Accessed by sponsor, no date provided.
35.Statista. Distribution of people registered with type 2 diabetes in England in 2020/21, by age. 2022; https://www.statista.com/statistics/387343/individuals-with-type-2-diabetes-by-age-in-england/. Accessed by sponsor, no date provided.
36.Röckl S, Brinks R, Baumert J, et al. All-cause mortality in adults with and without type 2 diabetes: findings from the national health monitoring in Germany. BMJ Open Diabetes Res Care. 2017;5(1):e000451.PubMed
37.Gregg EW, Menke A. Chapter 34: diabetes and disability. In: Cowie CC, Casagrande SS, Menke A, et al, eds. Diabetes in America. 3rd ed. Bethesda (MD): National Institute of Diabetes and Digestive and Kidney Diseases; 2018: https://www.ncbi.nlm.nih.gov/books/NBK567983/. Accessed by sponsor, no date provided.
38.McEwan P, Baker-Knight J, Ásbjörnsdóttir B, Yi Y, Fox A, Wyn R. Disutility of injectable therapies in obesity and type 2 diabetes mellitus: general population preferences in the UK, Canada, and China. Eur J Health Econ. 2023;24(2):187-196.PubMed
39.Vijan S, Hayward RA, Ronis DL, Hofer TP. Brief report: the burden of diabetes therapy: implications for the design of effective patient-centered treatment regimens. J Gen Intern Med. 2005;20(5):479-482.PubMed
40.CDC. Diabetes risk factors. 2022; https://www.cdc.gov/diabetes/risk-factors/?CDC_AAref_Val=https://www.cdc.gov/diabetes/basics/risk-factors.html. Accessed by sponsor, no date provided.
41.Araki E, Goto A, Kondo T, et al. Japanese clinical practice guideline for diabetes 2019. Diabetol Int. 2020;11(3):165-223.PubMed
42.Davies MJ, Aroda VR, Collins BS, et al. Management of hyperglycemia in type 2 diabetes, 2022. A consensus report by the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD). Diabetes Care. 2022;45(11):2753-2786.PubMed
43.Hur KY, Moon MK, Park JS, et al; Committee of Clinical Practice Guidelines, Korean Diabetes Association. 2021 Clinical Practice Guidelines for Diabetes Mellitus of the Korean Diabetes Association. Diabetes Metab J. 2021;45(4):461-481.PubMed
44.Lipscombe L, Butalia S, Dasgupta K, et al; Diabetes Canada Clinical Practice Guidelines Expert Committee. Pharmacologic glycemic management of type 2 diabetes in adults: 2020 update. Can J Diabetes. 2020;44(7):575-591.PubMed
45.McGibbon A, Adams L, Ingersoll K, Kader T, Tugwell B; Diabetes Canada Clinical Practice Guidelines Expert Committee. Glycemic management in adults with type 1 diabetes. Can J Diabetes. 2018;42(suppl 1):S80-S87.PubMed
46.Nathan DM, Buse JB, Davidson MB, et al; American Diabetes Association; European Association for Study of Diabetes. Medical management of hyperglycemia in type 2 diabetes: a consensus algorithm for the initiation and adjustment of therapy: a consensus statement of the American Diabetes Association and the European Association for the Study of Diabetes. Diabetes Care. 2009;32(1):193-203.PubMed
47.Lantus (insulin glargine injection (rDNA origin)): 100 U/mL solution for subcutaneous injection [product monograph]. Laval (QC): sanofi-aventis Canada Inc.; 2017 Oct 19.
48.Basaglar (insulin glargine (rDNA origin) injection): 100 U/mL solution for subcutaneous injection [product monograph]. Toronto (ON): Eli Lilly Canada Inc.; 2022 Aug 26. Accessed by sponsor.
49.Semglee (insulin glargine injection (rDNA origin)): 100 U/mL solution for subcutaneous injection [product monograph]. Etobicoke (ON): BGP Pharma ULC 2022 Apr 8.
50.Toujeo SoloSTAR (insulin glargine injection): 300 U/mL solution for subcutaneous injection in a disposable (prefilled) pen (1.5 mL); Toujeo DoubleSTAR (insulin glargine injection): 300 U/mL solution for subcutaneous injection in a disposable (prefilled) pen (3 mL) [product monograph]. Laval (QC): sanofi-aventis Canada Inc.; 2020 May 12.
51.Levemir (insulin detemir): 100 U/mL solution for subcutaneous inject in a Penfill cartridge; Levemir (insulin detemir): 100 U/mL solution for subcutaneous inject in a pre-filled FlexTouch disposable pen [product monograph]. Mississauga (ON): Novo Nordisk Canada Inc.; 2021 Aug 12: https://www.novonordisk.ca/content/dam/nncorp/ca/en/products/levemir-product-monograph.pdf. Accessed 2024 Jul 19.
52.Tresiba (insulin degludec injection): 100 U/mL solution for subcutaneous injection in a Penfill cartridge; Tresiba (insulin degludec injection): 100 U/mL or 200 U/m solution for subcutaneous injection in a the FlexTouch pre-filled pen [product monograph]. Mississauga (ON): Novo Nordisk Canada Inc.; 2022 Oct 27.
53.Pieber TR, Arfelt KN, Cailleteau R, et al. Hypoglycaemia frequency and physiological response after double or triple doses of once-weekly insulin icodec vs once-daily insulin glargine U100 in type 2 diabetes: a randomised crossover trial. Diabetologia. 2023;66(8):1413-1430.PubMed
54.Danne T, Nimri R, Battelino T, et al. International consensus on use of continuous glucose monitoring. Diabetes Care. 2017;40(12):1631-1640.PubMed
55.Saisho Y. Use of Diabetes Treatment Satisfaction Questionnaire in diabetes care: importance of patient-reported outcomes. Int J Environ Res Public Health. 2018;15(5):947.PubMed
56.Bradley C, Plowright R, Stewart J, Valentine J, Witthaus E. The Diabetes Treatment Satisfaction Questionnaire change version (DTSQc) evaluated in insulin glargine trials shows greater responsiveness to improvements than the original DTSQ. Health Qual Life Outcomes. 2007;5:57.PubMed
57.Howorka K, Pumprla J, Schlusche C, Wagner-Nosiska D, Schabmann A, Bradley C. Dealing with ceiling baseline treatment satisfaction level in patients with diabetes under flexible, functional insulin treatment: assessment of improvements in treatment satisfaction with a new insulin analogue. Qual Life Res. 2000;9(8):915-930.PubMed
58.Brod M, Hammer M, Christensen T, Lessard S, Bushnell DM. Understanding and assessing the impact of treatment in diabetes: the Treatment-Related Impact Measures for Diabetes and Devices (TRIM-Diabetes and TRIM-Diabetes Device). Health Qual Life Outcomes. 2009;7:83.PubMed
59.Brod M, Christensen T, Hammer M, Busk AK, Bushnell DM. Examining the ability to detect change using the TRIM-Diabetes and TRIM-Diabetes Device measures. Qual Life Res. 2011;20(9):1513-1518.PubMed
60.Philis-Tsimikas A, Klonoff DC, Khunti K, et al; CONCLUDE Study Group. Risk of hypoglycaemia with insulin degludec versus insulin glargine U300 in insulin-treated patients with type 2 diabetes: the randomised, head-to-head CONCLUDE trial. Diabetologia. 2020;63(4):698-710.PubMed
61.Billings LK, Doshi A, Gouet D, et al. Efficacy and safety of IDegLira versus basal-bolus insulin therapy in patients with type 2 diabetes uncontrolled on Metformin and basal insulin: the DUAL VII randomized clinical trial. Diabetes Care. 2018;41(5):1009-1016.PubMed
62.Galindo RJ, Moazzami B, Scioscia MF, et al. A randomized controlled trial comparing the efficacy and safety of IDegLira versus basal-bolus in patients with poorly controlled type 2 diabetes and very high HbA1c ≥9-15%: DUAL HIGH Trial. Diabetes Care. 2023;46(9):1640-1645.PubMed
63.Chaykin L, Bhargava A, de la Rosa R, et al. Effect of insulin degludec versus insulin glargine U100 on hypoglycemia in Hispanic patients with type 2 diabetes: results from the SWITCH 2 trial. Clin Diabetes. 2019;37(1):73-81.PubMed
64.Zinman B, Philis-Tsimikas A, Cariou B, et al; NN1250-3579 (BEGIN Once Long) Trial Investigators. Insulin degludec versus insulin glargine in insulin-naive patients with type 2 diabetes: a 1-year, randomized, treat-to-target trial (BEGIN Once Long). Diabetes Care. 2012;35(12):2464-2471.PubMed
65.Rodbard HW, Cariou B, Zinman B, et al; BEGIN Once Long trial investigators. Comparison of insulin degludec with insulin glargine in insulin-naive subjects with Type 2 diabetes: a 2-year randomized, treat-to-target trial. Diabet Med. 2013;30(11):1298-1304.PubMed
66.Gough SC, Bhargava A, Jain R, Mersebach H, Rasmussen S, Bergenstal RM. Low-volume insulin degludec 200 units/ml once daily improves glycemic control similarly to insulin glargine with a low risk of hypoglycemia in insulin-naive patients with type 2 diabetes: a 26-week, randomized, controlled, multinational, treat-to-target trial: the BEGIN LOW VOLUME trial. Diabetes Care. 2013;36(9):2536-2542.PubMed
67.Garber AJ, King AB, Del Prato S, et al; NN1250-3582 (BEGIN BB T2D) Trial Investigators. Insulin degludec, an ultra-longacting basal insulin, versus insulin glargine in basal-bolus treatment with mealtime insulin aspart in type 2 diabetes (BEGIN Basal-Bolus Type 2): a phase 3, randomised, open-label, treat-to-target non-inferiority trial. Lancet. 2012;379(9825):1498-1507.PubMed
68.Tibaldi J, Hadley-Brown M, Liebl A, et al. A comparative effectiveness study of degludec and insulin glargine 300 U/mL in insulin-naïve patients with type 2 diabetes. Diabetes Obes Metab. 2019;21(4):1001-1009.PubMed
69.Russell-Jones D, Vaag A, Schmitz O, et al; Liraglutide Effect and Action in Diabetes 5 (LEAD-5) met+SU Study Group. Liraglutide vs insulin glargine and placebo in combination with metformin and sulfonylurea therapy in type 2 diabetes mellitus (LEAD-5 met+SU): a randomised controlled trial. Diabetologia. 2009;52(10):2046-2055.PubMed
70.Aroda VR, Bailey TS, Cariou B, et al. Effect of adding insulin degludec to treatment in patients with type 2 diabetes inadequately controlled with metformin and liraglutide: a double-blind randomized controlled trial (BEGIN: ADD TO GLP-1 Study). Diabetes Obes Metab. 2016;18(7):663-670.PubMed
71.Balshem H, Helfand M, Schünemann HJ, et al. GRADE guidelines: 3. Rating the quality of evidence. J Clin Epidemiol. 2011;64(4):401-406.PubMed
72.Santesso N, Glenton C, Dahm P, et al; GRADE Working Group. GRADE guidelines 26: informative statements to communicate the findings of systematic reviews of interventions. J Clin Epidemiol. 2020;119:126-135.PubMed
73.Clinical Study Report: NN1436-4477, ONWARDS 1 – results from the complete trial. A 78-week trial comparing the effect and safety of once weekly insulin icodec and once daily insulin glargine 100 units/mL, both in combination with non-insulin anti-diabetic treatment, in insulin naïve subjects with type 2 diabetes [internal sponsor's report]. Bagsvaerd (DK): Novo Nordisk; 2023 Mar 17.
74.National Institute for Health and Care Excellence. Single technology appraisal and highly specialised technologies evaluation: user guide for company evidence submission template. (NICE process and methods PMG24) 2022; https://www.nice.org.uk/process/pmg24 Accessed 2024 Jan 19.
75.A systematic literature review and indirect treatment comparison of insulin icodec with other basal insulins in patients with type 2 diabetes, version 2. [internal sponsor's report] In: Drug Reimbursement Review sponsor submission: AWIQLI (insulin icodec), 700 units/mL, pre-filled pen for subcutaneous use. Mississauga, ON: Novo Nordisk Canada Inc; 2023 Sep 19.
76.Elisha B, Azar M, Taleb N, Bernard S, Iacobellis G, Rabasa-Lhoret R. Body composition and epicardial fat in type 2 diabetes patients following insulin detemir versus insulin glargine initiation. Horm Metab Res. 2016;48(1):42-47.PubMed
77.Riddle MC, Bolli GB, Ziemen M, Muehlen-Bartmer I, Bizet F, Home PD; EDITION 1 Study Investigators. New insulin glargine 300 units/mL versus glargine 100 units/mL in people with type 2 diabetes using basal and mealtime insulin: glucose control and hypoglycemia in a 6-month randomized controlled trial (EDITION 1). Diabetes Care. 2014;37(10):2755-2762.PubMed
78.Rosenstock J, Cheng A, Ritzel R, et al. More Similarities Than Differences Testing Insulin Glargine 300 Units/mL Versus Insulin Degludec 100 Units/mL in Insulin-Naive Type 2 Diabetes: The Randomized Head-to-Head BRIGHT Trial. Diabetes Care. 2018;41(10):2147-2154.PubMed
79.Pan C, Gross JL, Yang W, et al. A multinational, randomized, open-label, treat-to-target trial comparing insulin degludec and insulin glargine in insulin-naive patients with type 2 diabetes mellitus. Drugs R D. 2016;16(2):239-249.PubMed
80.Bolli GB, Riddle MC, Bergenstal RM, et al; on behalf of the EDITION 3 study investigators. New insulin glargine 300 U/ml compared with glargine 100 U/ml in insulin-naïve people with type 2 diabetes on oral glucose-lowering drugs: a randomized controlled trial (EDITION 3). Diabetes Obes Metab. 2015;17(4):386-394.PubMed
81.Rosenstock J, Davies M, Home PD, Larsen J, Koenen C, Schernthaner G. A randomised, 52-week, treat-to-target trial comparing insulin detemir with insulin glargine when administered as add-on to glucose-lowering drugs in insulin-naive people with type 2 diabetes. Diabetologia. 2008;51(3):408-416.PubMed
82.Higgins JPT, Savović J, Page MJ, Elbers RG, Sterne JAC. Chapter 8: assessing risk of bias in a randomized trial. In: Higgins JPT, Thomas J, Chandler J, et al., eds. Cochrane Handbook for Systematic Reviews of Interventions version 6.4 (updated August 2023). Chichester (UK): Cochrane; 2023: https://training.cochrane.org/handbook. Accessed 2024 Jan 29.
83.Single technology appraisal and highly specialised technologies evaluation: user guide for company evidence submission template. Supporting evidence: process and methods. London (UK): National Institute for Health and Care Excellence (NICE); 2022: https://www.nice.org.uk/process/pmg24/resources/single-technology-appraisal-and-highly-specialised-technologies-evaluation-user-guide-for-company-evidence-submission-template-pdf-72286715419333. Accessed 2024 Jan 29.
84.Dias S, Welton NJ, Sutton AJ, Ades AE. NICE DSU technical support document 2: a generalised linear modelling framework for pairwise and network meta-analysis of randomised controlled trials. Sheffield (UK): Decision Support Unit, ScHARR, University of Sheffield; 2011: https://www.sheffield.ac.uk/sites/default/files/2022-02/TSD2-General-meta-analysis-corrected-2Sep2016v2.pdf. Accessed by sponsor, no date provided.
Appendix 1: Detailed Outcome Data [Redacted]
Additional NMA Results [Redacted]
Information is this appendix were redacted based on the sponsor’s request.
Pharmacoeconomic Review
Abbreviations
BIA
budget impact analysis
CFB
change from baseline
DTSQ
Diabetes Treatment Satisfaction Questionnaire
hemoglobin A1C
glycated hemoglobin
HRQoL
health-related quality of life
ICER
incremental cost-effectiveness ratio
IHE-DCM
Institute of Health Economics Diabetes Cohort Model
NIAHA
noninsulin antihyperglycemic agent
NMA
network meta-analysis
QALY
quality-adjusted life-year
T2DM
type 2 diabetes mellitus
Executive Summary
The executive summary comprises 2 tables (Table 1 and Table 2) and a conclusion.
Item | Description |
|---|---|
Drug product | Insulin icodec (Awiqli), 700 units/mL solution for injection in a prefilled pen (1.5 mL, 3 mL) |
Indication | For the once-weekly treatment of adults with diabetes mellitus to improve glycemic control |
Health Canada approval status | Post NOC |
Health Canada review pathway | Standard review |
NOC date | March 12, 2024 |
Reimbursement request | For the once-weekly treatment of adults with type 2 diabetes mellitus to improve glycemic control |
Sponsor | Novo Nordisk Canada Inc. |
Submission history | Previously reviewed: No |
NOC = Notice of Compliance.
Table 2: Summary of Economic Evaluation
Component | Description |
|---|---|
Type of economic evaluation | Cost-utility analysis Markov cohort model |
Target population | Adult patients aged ≥ 18 years with T2DM who require insulin for glycemic control. Three populations are evaluated in separate analyses:
|
Treatment | Insulin icodec |
Submitted price | Insulin icodec, 700 units/mL, prefilled pen: $78.05 for 1,050 units (1.5 mL) and $156.10 for 2,100 units (3 mL) |
Comparators |
|
Perspective | Canadian publicly funded health care payer |
Outcomes | QALYs, LYs |
Time horizon | Lifetime (40 years) |
Key data sources |
|
Submitted results |
|
Key limitations |
|
CADTH reanalysis results |
|
CFB = change from baseline; hemoglobin A1C = glycated hemoglobin; ICER = incremental cost-effectiveness ratio; LY = life-year; NIAHA = noninsulin antihyperglycemic agent; NMA = network meta-analysis; QALY = quality-adjusted life-year; T2DM = type 2 diabetes mellitus; U = unit; vs. = versus.
Conclusions
Evidence from 5 active-controlled randomized controlled trials comparing insulin icodec to insulin glargine and/or insulin degludec in adults with type 2 diabetes mellitus (T2DM) suggests that once-weekly injections of insulin icodec were noninferior in change from baseline (CFB) in glycated hemoglobin (hemoglobin A1C) at week 26 or week 52. Secondary analyses of superiority suggest that, statistically, there may be a benefit associated with insulin icodec over the once-daily comparators for this outcome, but the clinical meaningfulness of this result is uncertain. The CADTH Clinical Review noted various limitations in the submitted network meta-analysis (NMA). Consequently, CADTH’s ability to draw conclusions regarding the long-term comparative efficacy and safety of insulin icodec relative to long-acting basal insulin analogues from the NMA is limited. This uncertainty is propagated into the submitted economic model given that the mean reductions in CFB in hemoglobin A1C and the annual event rate of severe hypoglycemia were used to generate transition probabilities extrapolating disease progression across the 40-year lifetime horizon.
In addition to limitations with the clinical evidence, CADTH identified several limitations with the sponsor’s economic submission. The main limitation was uncertainty regarding the impact of frequency of administration of injectable therapies on the health-related quality of life (HRQoL) of patients with T2DM. As part of the base-case reanalysis, CADTH excluded the utility decrements associated with once-weekly, once-daily, and multiple daily injections of insulin. This impact of treatment disutility was explored through scenario analysis.
In the 3 subgroups (insulin naive, basal insulin experienced, basal-bolus insulin experienced), insulin icodec was associated with higher costs (incremental costs: $7,599, $7,473, and $16,076, respectively) and quality-adjusted life-year (QALY) differences that trended close to zero (0.02, 0.01, and –0.02, respectively) indicating little to no additional benefit or harm. Higher costs were due to higher treatment acquisition costs and the small difference in QALYs was due to extrapolation of small hemoglobin A1C differences as estimated by the NMA. Differences in hemoglobin A1C from the NMA were not statistically significant, meaning that any estimation of incremental difference estimated by the model is highly uncertain. The only difference between the CADTH reanalysis and the sponsor’s is the removal of utility decrements associated with daily and weekly administration. There is likely a patient preference to receive weekly versus daily injections though the impact this has on patient HRQoL is uncertain. The impact on HRQoL submitted by the sponsor was deemed too large to meet expectations from a face validity perspective (weekly treatment administration having a larger impact on HRQoL than stroke for example).
To ensure cost-effectiveness, given the available clinical evidence, insulin icodec should be priced no more than the lowest-cost long-acting basal insulin analogue used to treat T2DM. A price premium may be warranted due to the lower administration burden associated with insulin icodec (once-weekly administration), although the size of this premium is highly uncertain.
Stakeholder Input Relevant to the Economic Review
This section is a summary of the feedback received from the patient groups and drug plans that participated in the CADTH review process. No registered clinician input was received for this review.
One patient group, Diabetes Canada, provided input through data collected from an online patient survey (n = 21) that was available from October 2, 2023, to October 23, 2023. All respondents were living in Canada and 5 among them were receiving treatment with insulin icodec. The most important outcomes for patients included delaying disease progression, with the ultimate objective of improving survival, improving glycemic control and reducing the risk of cardiovascular complications, and reducing high blood pressure. Overall, patients’ disease experience was influenced by the physical symptoms associated with T2DM (e.g., extreme fatigue, frequent urination, and unusual thirst) and the psychosocial effects associated with the disease (i.e., anxiety associated with disease progression and stress associated with the constant management of the disease). Regarding experience with current treatment options, respondents indicated that they currently receive insulin icodec, insulin glargine, as well as other long-acting, short-acting, and rapid-acting insulin analogues. Patients reported receiving additional treatment with sodium-glucose cotransporter-2 inhibitors, glucagon-like peptide-1 receptor agonists, dipeptidyl peptidase-4 inhibitors, thiazolidinediones, sulfonylureas, meglitinides, and metformin. Patients noted that their current antihyperglycemic therapies were better than previous treatments at meeting target fasting blood glucose levels, meeting target hemoglobin A1C, preventing vascular complications, and maintaining target weight. Patients who had experience with insulin icodec reported similar levels of satisfaction with the effect of treatment on improved clinical outcomes. Overall, patients with T2DM highlighted the desire for variably administered injectable therapies for glycemic control that may address their preferences and tolerance of therapy.
Participating drug plans were interested in understanding whether switching from daily to weekly administration of insulin injections may result in improvements in terms of adherence to medication and quality of life for patients with T2DM. Drug plans were further interested in clarifying how the administration of insulin degludec (U100 and U200) was incorporated in the model submitted by the sponsor, noting that its duration of action, which is often cited to be up to 42 hours, renders it the longest-acting basal insulin analogue currently available in Canada. Drug plans questioned whether and how patients treated with insulin icodec may switch back to a daily basal insulin analogues. Drug plans noted concerns regarding the anticipated budget impact associated with the reimbursement of insulin icodec, which may result in a substantial proportion of patients with T2DM expressing a preference to transition from daily to weekly insulin injections for dosing convenience. Finally, drug plans noted the presence of confidential negotiated prices for several comparators for the same indication.
Several of these concerns were addressed in the sponsor’s model.
The impact of disease and treatment on patient’s quality of life was captured with utility values.
Complications associated with T2DM were incorporated as disutilities within the analyses.
In addition, CADTH addressed some of these concerns as follows.
In light of concerns noted by participating drug plans regarding the potential for substantial market uptake, CADTH conducted a scenario analysis by increasing the projected market share of insulin icodec to explore the impact of uncertainty on the budget.
Economic Review
The current review is for insulin icodec (Awiqli) for adult patients with T2DM who require insulin for glycemic control.
Economic Evaluation
Summary of Sponsor’s Economic Evaluation
Overview
The sponsor submitted a cost-utility analysis of insulin icodec compared with long-acting basal insulin analogues.1 Aligned with the reimbursement request, the modelled population comprised adult patients with T2DM who require insulin for glycemic control. Three subpopulations are evaluated in separate analyses: patients with T2DM on noninsulin antihyperglycemic agents (NIAHAs) who are insulin naive (“T2DM insulin naive”); patients with T2DM with or without NIAHAs who have basal insulin experience (“T2DM basal switch”); and patients with T2DM with or without NIAHAs who have basal and bolus insulin experience (“T2DM basal and bolus switch”).1 The target population of the economic evaluation is consistent with the enrolled population in the ONWARDS trials.2-6
Insulin icodec is a long-lasting basal insulin analogue with a plasma half-life of approximately 8 days that is designed to be injected once a week. Insulin icodec is available as a 700 units/mL solution for injection in a prefilled pen.1 The recommended starting dose of insulin icodec in patients with T2DM who are insulin naive is 70 units administered once weekly.7 For patients with T2DM who have basal insulin experience switching to insulin icodec, the corresponding weekly dose of insulin icodec is the previous basal insulin dose multiplied by 7. A 1-time additional 50% insulin icodec dose is recommended for the week 1 dose.7 The dosage modelled for insulin icodec reflected the Health Canada dosing schedule. The submitted price for insulin icodec is $78.05 for 1 prefilled 1.5 mL pen and $156.10 for 1 prefilled 3 mL pen. At the recommended dose, and based on the number of yearly insulin units required, the annual per-patient drug acquisition cost of insulin icodec is $1,148 for patients who are insulin naive, $1,230 for patients who have basal insulin experience, and $1,956 for patients who have basal and bolus insulin experience.
The comparators for this analysis included: insulin glargine (U100 and U300), insulin degludec (U100 and U200), and insulin detemir.1 For patients who are insulin naive, the annual per-patient drug acquisition cost of long-acting basal insulin analogues ranged from $885 to $1,626. For patients who have basal insulin experience, the annual per-patient drug acquisition cost of long-acting basal insulin analogues ranged from $969 to $1,431. For patients who have basal and bolus insulin experience, the annual per-patient drug acquisition cost of long-acting basal insulin analogues ranged from $1,310 to $2,275.
The clinical outcomes modelled were CFB in hemoglobin A1C, severe hypoglycemic event rate, and weekly basal insulin dose.1 The economic outcomes of interest were QALYs and life-years. The economic evaluation was conducted over a lifetime time horizon (i.e., 40 years), from the perspective of the Canadian public health care payer. Costs and outcomes were discounted at 1.5% per annum.1
Model Structure
The sponsor submitted the Swedish Institute of Health Economics Diabetes Cohort Model (IHE-DCM)8,9 to evaluate the cost-effectiveness of insulin icodec relative to long-acting basal insulin analogues. The IHE-DCM is a cohort model that uses Markov health states to capture the microvascular complications (i.e., eye disease, lower extremity disease, and kidney disease) and macrovascular complications (i.e., ischemic heart disease, myocardial infarction, heart failure, and stroke) associated with T2DM, the incidence of hypoglycemic events, and the associated impact of complications and events on premature mortality resulting from T2DM (Figure 1).1 Due to the large number of health states and possible transitions within the model, CADTH accepted a deviation request that waived the requirement of a Markov trace for the IHE-DCM to allow for a model runtime that met submission requirements. Hence, the progression of the modelled cohort is inputted through a series of Visual Basic macros, which preclude examination of how patients transition between health states. Transitions between health states occur on a 1-year cycle length and patients accrue life-years, QALYs, and costs during each cycle.1
Model Inputs
Baseline patient characteristics were derived from the ONWARDS trials,2-6 multicentre, phase III, randomized trials comparing the efficacy and safety of insulin icodec to long-acting basal insulin analogues among patients with diabetes mellitus who require insulin for glycemic control (N = 3,765). The average patient in the insulin-naive T2DM-modelled cohort was 59 years old, had diabetes for a mean duration of 12 years, and was more likely to be male (58%). In the basal insulin–experienced T2DM-modelled cohort, the average patient was 63 years old, had diabetes for a mean duration of 17 years, and was more likely to be male (57%). Similarly, in the basal and bolus insulin–experienced T2DM-modelled cohort, the average patient was 60 years old, had diabetes for a mean duration of 17 years, and was more likely to be male (52%). These characteristics were derived from the enrolled patient population of the ONWARDS trials, assumed to reflect the patient population in Canada, and used to inform the age- and gender-specific distribution of the general population mortality risk.
Clinical efficacy and safety parameters used to characterize insulin icodec and long-acting basal insulin analogues were derived from a NMA conducted by the sponsor. The NMA results pertaining to CFB in hemoglobin A1C (at week 26) and proportion of patients with severe hypoglycemia (at week 52) were used to estimate comparative efficacy and safety, respectively. In the submitted IHE-DCM, treatment alternatives were defined in terms of their associated effects on risk factors (e.g., hemoglobin A1C, blood pressure, cholesterol, triglycerides, estimated glomerular filtration rate, and albumin-creatine ratio) and hypoglycemia. The sponsor applied the absolute treatment effect of insulin icodec and comparators on CFB in hemoglobin A1C at the start of the model and extrapolated its progression through time through annual simulations until the 40-year time horizon was reached. The development and progression of microvascular and macrovascular complications, as well as their impact on premature mortality, are modelled in parallel with biomarker changes using risk equations. The annual probability of major diabetes-related macrovascular complications was derived from risk equations based on the UK Prospective Diabetes Study,10 which is consistent with previous CADTH reports.11,12 Microvascular complications were divided into 3 groups (i.e., eye disease, lower extremity disease, and kidney disease) and modelled based on risk equations informed by previously published studies.13,14
Health state–specific utility values were derived from an analysis of EQ-5D data from 4,641 patients with T2DM in 5 European countries.15 QALYs are estimated based on a baseline utility value of 1.027 minus the total utility decrements resulting from microvascular and macrovascular complications, age, gender, and diabetes duration.15-18 In addition, a disutility was applied for each severe hypoglycemic event (–0.047).19 The decrement incurred from a complication occurring during a given cycle is assumed to persist throughout the lifetime horizon of the model. Given that the disutility values from CODE-2 data15 were derived using linear regression analysis, utility decrements accrued due to multiple complications were combined additively. The model included utility decrements corresponding to injection frequency, which were sourced from the study by McEwan et al.20 This vignette-based study elicited utilities associated with injection frequency (i.e., once-weekly, once-daily, and multiple daily injections) from members of the general population in Canada, the UK, and China (N = 310) to capture the administration-related disutility of more frequent injectable treatments.20 Participants were asked to evaluate vignettes describing the use of variably administered injectable therapies for glycemic control from the perspective of patients with T2DM, using the time trade-off methodology.20 The sponsor applied a utility decrement of –0.050 in patients treated with insulin icodec (representing the disutility associated with once-weekly injections) and a utility decrement of –0.107 in patients treated with long-acting basal insulin analogues (representing the disutility of once-daily injections). In the basal and bolus insulin–experienced cohort, the sponsor used a ratio approach to calculate the utility decrement of administering insulin icodec in combination with bolus insulin injections (–0.189) based on the utility decrement of administering once-daily basal insulin injections in combination with multiple daily bolus insulin injections (–0.203) (Table 10).
Costs captured in the model included those associated with drug acquisition, management of complications, management of severe hypoglycemic events, as well as needle costs.1 Drug acquisition costs for insulin icodec were based on the sponsor’s submitted price.1 The dosage modelled for insulin icodec is consistent with the recommended dose described in the overview section. The acquisition costs for long-acting basal insulin analogues were obtained from the Ontario Drug Benefit Formulary.21 The sponsor used a weighted cost for insulin glargine U100. NMA results on mean weekly basal insulin dose (at week 26) were used to calculate the annual drug acquisition cost for each treatment. The sponsor included needle costs in scenario analyses. For each microvascular and macrovascular complication, a direct cost associated with health care resource use for the first year and for each subsequent year was applied. Costs for complications were obtained from various sources,19,22,23 and inflated to reflect 2023 values. The cost per severe hypoglycemic event ($2,418) was sourced from the CADTH Therapeutic Review on new drugs for T2DM.19
Summary of Sponsor’s Economic Evaluation Results
The sponsor conducted the base case via a probabilistic sensitivity analysis with 1,000 simulations.1 The deterministic and probabilistic results were similar. The probabilistic findings are presented in the following.1
Base-Case Results
Results from the sponsor-submitted analysis can be found in Table 3. In the T2DM insulin-naive subpopulation, insulin icodec was associated with estimated costs of $131,014 and 9.57 QALYs over the 40-year model horizon. In sequential analysis, insulin icodec was associated with an incremental cost-effectiveness ratio (ICER) of $18,114 versus insulin glargine U100 (incremental costs: $7,558; incremental QALYs: 0.42). In the T2DM basal switch subpopulation, insulin icodec was associated with estimated costs of $113,313 and 8.6 QALYs over the 40-year model horizon. In sequential analysis, insulin icodec was associated with an ICER of $20,711 versus insulin glargine U100 (incremental costs: $7,473; incremental QALYs: 0.36). In the T2DM basal and bolus switch subpopulation, insulin icodec was associated with estimated costs of $153,509 and 8.6 QALYs over the 40-year model horizon. In sequential analysis, insulin icodec was associated with an ICER of $73,405 versus insulin glargine U100 (incremental costs: $16,076; incremental QALYs: 0.22).
The main driver for incremental QALYs was the impact of once-weekly versus once-daily treatment on HRQoL. This accounted for more than 95% of the QALY gain associated with insulin icodec versus other comparators. The main driver for incremental costs was treatment cost with very small differences in health care resource use to diabetes complications. The sponsor’s submitted analysis is based on the publicly available prices for all drug treatments. Additional results from the sponsor’s submitted economic evaluation base case are presented in Appendix 3.
Table 3: Summary of the Sponsor’s Economic Evaluation Results — Probabilistic
Drug | Total costs ($) | Total QALYs | Sequential ICER ($/QALY) |
|---|---|---|---|
Sponsor base case, insulin naive | |||
Insulin glargine U100 | 123,456 | 9.150 | Reference |
Insulin icodec | 131,014 | 9.567 | 18,114 |
Dominated treatments | |||
Insulin glargine U300 | 128,237 | 9.149 | Extendedly dominated |
Insulin detemir | 141,323 | 9.096 | Dominated |
Insulin degludec U200 | 136,653 | 9.124 | Dominated |
Insulin degludec U100 | 135,050 | 9.110 | Dominated |
Sponsor base case, basal insulin experienced | |||
Insulin glargine U100 | 105,840 | 8.230 | Reference |
Insulin icodec | 113,313 | 8.591 | 20,711 |
Dominated treatments | |||
Insulin glargine U300 | 110,271 | 8.235 | Extendedly dominated |
Insulin detemir | 121,347 | 8.184 | Dominated |
Insulin degludec U200 | 117,358 | 8.231 | Dominated |
Insulin degludec U100 | 116,454 | 8.188 | Dominated |
Sponsor base case, basal-bolus insulin experienced | |||
Insulin glargine U100 | 137,433 | 8.386 | Reference |
Insulin icodec | 153,509 | 8.605 | 73,405 |
Dominated treatments | |||
Insulin glargine U300 | 143,745 | 8.391 | Extendedly dominated |
Insulin detemir | 162,549 | 8.311 | Dominated |
Insulin degludec U200 | 156,747 | 8.348 | Dominated |
Insulin degludec U100 | 155,216 | 8.315 | Dominated |
ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year.
Source: Sponsor’s pharmacoeconomic submission.1
Sensitivity and Scenario Analysis Results
The sponsor assessed several model parameters and assumptions in probabilistic scenario analyses (conducted with 600 probabilistic iterations) which included: applying a shorter lifetime horizon of 20 years; excluding treatment intensification; excluding hypoglycemia events, using the cost of Semglee for the cost of insulin glargine, including needle costs; and assuming alternative estimates for utility decrements associated with injectable therapies. In all scenarios and across the insulin-naive, basal insulin–experienced, and basal and bolus insulin–experienced subpopulations, the cost-effectiveness frontier included insulin glargine U100 and insulin icodec. The most influential parameters were alternative assumptions regarding injection-related disutilities, the cost of insulin glargine, and the inclusion of needle costs.
When using the cost of Semglee for insulin glargine U100, the ICER of insulin icodec (relative to insulin glargine U100) increased to $29,543, $33,508, and $103,569 per QALY gained in the insulin-naive, basal insulin–experienced, and basal and bolus insulin–experienced subpopulations, respectively. When using alternative injection-related disutilities, the ICER increased to $24,949, $29,702, and $111,860 per QALY gained in the insulin-naive, basal insulin–experienced, and basal and bolus insulin–experienced subpopulations, respectively. All other scenarios resulted in ICERs ranging between $2,988 and $19,146 (insulin naive), $3,792 and $22,120 (basal insulin experienced), and $42,642 and $74,623 (basal-bolus insulin experienced) per QALY gained. No scenario analysis was conducted using a perspective other than the health care payer.
CADTH Appraisal of the Sponsor’s Economic Evaluation
CADTH identified several key limitations to the sponsor’s analysis that have notable implications on the economic analysis.
Impact of insulin icodec on quality of life of patients with T2DM is highly uncertain: The sponsor modelled HRQoL by applying a utility decrement of –0.050 among patients treated with insulin icodec (representing the disutility associated with once-weekly injections) and a utility decrement of –0.107 among patients treated with long-acting basal insulin analogues (representing the disutility of once-daily injections). As a result, in the sponsor’s base case, 96% to 100% of incremental QALY gains realized by treatment with insulin icodec (relative to insulin glargine U100) across T2DM subgroups are due to utility decrements associated with injection frequency.
The sponsor used a vignette-based study to elicit utilities associated with injection frequency, whereby general population respondents from Canada (N = 100) were asked to evaluate vignettes describing the use of variably administered injectable therapies for glycemic control from the perspective of patients with T2DM. The vignettes included in the study concentrated on aspects of injection frequency without offering a broader context of the lived experience of patients with T2DM, which may have led general population respondents to overemphasize the significance of minor attributes of the disease without accounting for other facets of health and well-being.24-26 The study also required extensive health state descriptions to communicate medical and pharmacological details to participants from the general population,20 which may have hindered a thorough comprehension of the health condition and the administration of treatment. Some respondents valued the experience of administering injectable therapies (irrespective of frequency) as equal to death (utility = 0). This heightens concerns about the reliability of utility values elicited from general population respondents, whose limited understanding of the disease may lead them to underestimate the HRQoL of patients with T2DM who administer injectable therapies.
The utility decrements derived from the vignette-based study have questionable face validity. For instance, the estimated utility decrement associated with once-daily insulin injections (–0.107) is greater than the decrement associated with severe visual loss (–0.050), stroke (–0.052), and symptomatic neuropathy (–0.084) according to the sponsor-submitted analysis. Hence, the submitted pharmacoeconomic model assumes that, for patients with T2DM, once-daily insulin injections would have a greater impact on HRQoL than severe visual loss and stroke combined. In fact, the administration of once-daily insulin injections was assumed to have a more detrimental impact on patient HRQoL than any other diabetic complication included in the model, with the exception of end-stage renal disease and lower extremity amputation.
Results from the vignette-based study show wide confidence intervals for each health state, demonstrating a large variability in the answers given (Figure 2) with responses ranging from no impact on health (utility = 1) to maximum impact on health (utility = 0). The study only gives utility scores for each health state rather than analyzing the uncertainty around mean differences between health states. Thus, no assessment of uncertainty between health states could be made.
The sponsor used the Diabetes Treatment Satisfaction Questionnaire (DTSQ) to assess patient satisfaction with treatment. As noted in the CADTH Clinical Review, a statistically significant difference in CFB DTSQ scores was observed between insulin icodec and insulin degludec (difference = 1.25; 95% confidence interval, 0.41 to 2.10; P = 0.0036). Given that the DTSQ is not used in clinical practice, it is unknown whether the estimated difference between treatments is clinically meaningful. It is uncertain whether a 1-point difference in a 36-item questionnaire amounts to a meaningful change in patient satisfaction between treatments. DTSQ results are not limited to a specific medication, but rather capture the overall satisfaction with the treatment of diabetes, which may include satisfaction with clinical consultation and interaction with health care professionals.27 DTSQ does not assess patient HRQoL.27 It has been reported that higher DTSQ scores do not translate into higher HRQoL for patients with diabetes.28
Given the aforementioned limitations, it is unknown to what extent frequency of injectable therapies may impact HRQoL. Clinical expert feedback noted that an injectable therapy with reduced administration frequency may be associated with greater patient satisfaction. However, there is uncertainty regarding the potential association between treatment satisfaction and improved HRQoL for patients with T2DM. As per the CADTH guidelines on economic evaluations, researchers should use health preferences obtained from an indirect method of measurement that is based on a generic classification system (such as EQ-5D). In the absence of such estimation, the magnitude of benefit that may be experienced by patients with T2DM who receive fewer injections of insulin icodec compared with alternative insulin options, remains highly uncertain.
CADTH conducted a reanalysis that removed the disutility associated with variably administered insulin therapies.
CADTH explored the impact of uncertainty in the magnitude of HRQoL benefit associated with injectable therapies in a scenario analysis that included frequency-related disutilities from a study by Boye et al. (2011).29 In it, patients with T2DM (N = 151) in Scotland completed interviews to assess the utility of hypothetical health states describing variable injection frequency (i.e., daily versus weekly). CADTH applied a disutility of –0.039 among patients treated with once-weekly injections and a disutility of –0.062 among patients receiving once-daily or multiple daily injections. Although these values are lower than the ones chosen by the sponsor, they are still high relative to other disutilities used in the model and therefore likely represent an upper limit of what the potential impact on HRQoL may be.
Impact of insulin icodec on CFB in hemoglobin A1C and severe hypoglycemic event rate is uncertain: Clinical efficacy and safety parameters used to characterize insulin icodec and long-acting basal insulin analogues were derived from an NMA conducted by the sponsor. The NMA results pertaining to CFB in hemoglobin A1C (at week 26) and proportion of patients with severe hypoglycemia (at week 52) were used to estimate comparative efficacy and safety, respectively.
As noted in the CADTH Clinical Review, the submitted NMA was subject to several limitations. Given that no adjustments were undertaken to mitigate heterogeneity between study and patient characteristics, the NMA did not satisfy the transitivity assumption, requiring that all known effect modifiers be known and measured.30 Hence, variability among included studies may have biased comparisons between treatments. Moreover, the presence of small networks (as few as 2 studies per network) required estimation through fixed-effect models, which do not account for between-study variance, thereby heightening the level of uncertainty associated with the NMA results. The CADTH Clinical Review additionally noted that, in several analyses, the proportion of patients experiencing severe hypoglycemic events was substantially lower in the ONWARDS trials than in the comparator studies, which rendered comparisons less robust and led to imprecise relative effect estimates for the hypoglycemia outcomes. The sponsor raised concerns about the appropriateness of the comparisons but did not undertake any adjustments to account for the differences. This contributed to the overall instability in the networks for hypoglycemia and introduced further uncertainty regarding the magnitude of the effect estimates. Moreover, owing to the limited duration of assessment across studies included in the NMA, the impact of insulin icodec on long-term glycemic control and long-term prevention of hypoglycemic events, relative to long-acting basal insulin comparators, remains unknown.
Regarding CFB in hemoglobin A1C, CADTH notes that the NMA results show wide credible intervals, which often included the potential for no significant difference between insulin icodec and long-acting basal insulin analogues. Numerical differences in change from hemoglobin A1C between insulin icodec and long-acting basal insulin analogues did not appear to be clinically meaningful according to clinical expert feedback. Moreover, while CFB in hemoglobin A1C was considered an appropriate selection for primary outcome based on discussion with the clinical expert consulted by CADTH, it is ultimately a surrogate biomarker of disease and does not directly speak to the critical downstream outcomes of T2DM. In light of these limitations, CADTH’s ability to draw conclusions regarding the efficacy and safety results derived from the NMA is limited. This uncertainty is propagated into the submitted economic model given that the mean reductions in CFB in hemoglobin A1C and the annual event rate of severe hypoglycemia were used to generate transition probabilities extrapolating disease progression across the 40-year lifetime horizon. Where it is expected that no differences in efficacy and safety exist between injectable basal insulin therapies, insulin icodec would be strictly dominated by the comparator with the lowest cost per insulin unit.
CADTH conducted a scenario analysis by assuming equivalence across insulin therapies.
Estimated weekly basal insulin dose for insulin icodec and long-acting basal insulin analogues is uncertain: The sponsor used the NMA results based on absolute mean weekly basal insulin dose (at week 26) to calculate the annual drug acquisition cost for each treatment. Absolute mean weekly doses estimated for insulin icodec tended to be the lowest among therapies considered, which reduced the annual drug acquisition cost of insulin icodec relative to long-acting basal insulin comparators.
The NMA results show wide credible intervals, which often included the potential for no significant dose differences between insulin icodec and long-acting basal insulin analogues. When including the ONWARDS 5 study in the insulin-naive network, the magnitude of the differences changed substantially for all treatments and the direction of effects was reversed for the comparisons with insulin glargine U100, insulin degludec U100, and insulin degludec U200. That is, when including the ONWARDS 5 study, the weekly insulin dose for insulin icodec was higher (not lower) than that of most comparators. This limitation remained unaddressed despite the uncertainty associated with the magnitude and direction of relative dose differences between insulin icodec and comparators. Additionally, the NMA results are subject to the limitations such as presence of unknown and unmeasured effect modifiers, and limited duration of assessment. These limitations preclude CADTH’s ability to draw any conclusions from the mean weekly basal insulin doses derived from the NMA. Furthermore, the sponsor did not adequately incorporate the parameter uncertainty associated with mean weekly insulin doses in probabilistic analysis. Rather than inputting the estimations and standard errors of mean weekly doses derived from the NMA, the sponsor opted to use estimated doses to calculate annual drug acquisition costs per treatment, whose mean values were set to fluctuate by 10% in probabilistic analysis.
Finally, although the NMA-derived doses may be numerically different between treatments, it is uncertain whether mean doses received by patients with T2DM in real-world clinical practice will reflect the doses estimated from the NMA. Given the studies included in the NMA excluded patients aged older than 70 years and those with higher hemoglobin A1C ranges, the results are not generalizable to the broader patient population with T2DM. Clinical expert feedback noted that it is unreasonable to assume that different long-acting insulin injectables require different doses to be effective, especially when considering that doses are individualized and titrated according to patient metabolic needs and glycemic control targets.31
CADTH conducted a scenario analysis by assuming equivalence across insulin therapies.
Submitted model lacked transparency: Due to the large number of health states and possible transitions within the model, CADTH accepted a deviation request that waived the requirement of a Markov trace for the IHE-DCM. However, the lack of a Markov trace precludes a robust examination of how patients transition between health states.
CADTH was unable to address this limitation due to the structure and programming of the submitted model.
Additionally, the following key assumptions were made by the sponsor and have been appraised by CADTH (refer to Table 4).
CADTH Reanalysis of the Economic Evaluation
Base-Case Results
CADTH’s reanalysis addressed 1 limitation within the economic model. The CADTH base case was derived by excluding the disutility associated with variably administered insulin therapies from the base case, in consultation with clinical experts. This change is summarized in Table 5.
In the T2DM insulin-naive subpopulation, insulin icodec was associated with estimated costs of $131,014 and 12.36 QALYs over the 40-year model horizon (Table 6). In sequential analysis, insulin icodec was associated with an ICER of $435,800 per QALY gained relative to insulin glargine U100 (incremental costs: $7,559; incremental QALYs: 0.02). In the T2DM basal insulin–experienced subpopulation, insulin icodec was associated with estimated costs of $113,313 and 11.17 QALYs over the 40-year model horizon. In sequential analysis, insulin icodec was associated with an ICER of $937,280 per QALY gained relative to insulin glargine U100 (incremental costs: $7,473; incremental QALYs: 0.01). In the CADTH base case for the T2DM basal and bolus insulin–experienced subpopulation, insulin icodec was associated with estimated costs of $153,509 and 11.73 QALYs over the 40-year model horizon. Insulin icodec was dominated (produced lower QALYs and higher costs) by insulin glargine U100.
Table 4: Key Assumptions of the Submitted Economic Evaluation
Sponsor’s key assumption | CADTH comment |
|---|---|
If insulin degludec U200 was absent from any NMA analyses, the sponsor considered it to be equivalent to insulin degludec U100 when the latter was available. Moreover, in instances where data for any other comparator were missing from the T2DM basal-experienced population in the NMA analyses, it was assumed that the ratio of the missing comparator to insulin icodec in the T2DM basal and bolus insulin–experienced population could be applied to the T2DM basal insulin–experienced population (and vice versa). | Acceptable, owing to the lack of available data for some therapies in certain NMAs. |
The treatment intensification step for the insulin-naive and basal insulin–experienced population was assumed to be treatment with basal and bolus insulin once patients reached the threshold of 8% hemoglobin A1C. For the basal and bolus insulin–experienced population, the sponsor assumed that treatment intensification would be dose increase. | Reasonable. CADTH acknowledges the difficulty in defining treatment intensification steps for patients with T2DM as intensification in clinical practice is typically individualized and based on patient-specific factors and requirements. The submitted model simplified this complexity by targeting a hemoglobin A1C level < 8%, which constitutes a commonly accepted goal of standard therapy for patients with T2DM.32 Hence, it is reasonable that treatment intensification would be warranted above that threshold. |
hemoglobin A1C = glycated hemoglobin; NMA = network meta-analysis; T2DM = type 2 diabetes mellitus.
CADTH’s estimated ICER was higher than the sponsor’s base-case value, driven by the exclusion of injection-related disutilities. Consistent with the sponsor’s analysis, the CADTH reanalysis estimates that the near entirety (98% to 100%) of incremental QALYs was accrued in the post-trial period of the model on the basis of extrapolation. The CADTH base case is based on publicly available prices of the comparator treatments. The detailed breakdown of the disaggregated results is available in Appendix 4.
Table 5: CADTH Revisions to the Submitted Economic Evaluation
Stepped analysis | Sponsor’s value or assumption | CADTH value or assumption |
|---|---|---|
Changes to derive the CADTH base case | ||
1. Impact of insulin icodec on quality of life of patients with T2DM is highly uncertain. | Included the disutilities associated with variably administered insulin therapies. | Excluded the disutility associated with variably administered insulin therapies. |
CADTH base case | Reanalysis 1 | |
hemoglobin A1C = glycated hemoglobin; T2DM = type 2 diabetes mellitus.
Table 6: Summary of the CADTH Reanalysis Results — Probabilistic
Drug | Total costs ($) | Total QALYs | Sequential ICER ($/QALY) |
|---|---|---|---|
CADTH base case, insulin naive | |||
Insulin glargine U100 | 123,456 | 12.35 | Reference |
Insulin icodec | 131,014 | 12.36 | 435,800 |
Dominated treatments | |||
Insulin glargine U300 | 128,237 | 12.35 | Extendedly dominated by insulin glargine U100 and insulin icodec |
Insulin degludec U100 | 135,050 | 12.30 | Dominated by insulin glargine U100 |
Insulin degludec U200 | 136,653 | 12.32 | Dominated by insulin glargine U100 |
Insulin detemir | 141,323 | 12.30 | Dominated by insulin glargine U100 |
CADTH base case, basal insulin experienced | |||
Insulin glargine U100 | 105,840 | 11.16 | Reference |
Insulin icodec | 113,313 | 11.17 | 937,280 |
Dominated treatments | |||
Insulin glargine U300 | 110,271 | 11.16 | Extendedly dominated by insulin glargine U100 and insulin icodec |
Insulin degludec U100 | 116,454 | 11.12 | Dominated by insulin glargine U100 |
Insulin degludec U200 | 117,358 | 11.15 | Dominated by insulin glargine U100 |
Insulin detemir | 121,347 | 11.11 | Dominated by insulin glargine U100 |
CADTH base case, basal-bolus insulin experienced | |||
Insulin glargine U100 | 137,433 | 11.75 | Reference |
Insulin glargine U300 | 143,745 | 11.76 | 1,122,703 |
Dominated treatments | |||
Insulin icodec | 153,509 | 11.73 | Dominated by insulin glargine U100 |
Insulin degludec U100 | 155,216 | 11.67 | Dominated by insulin glargine U100 |
Insulin degludec U200 | 156,747 | 11.71 | Dominated by insulin glargine U100 |
Insulin detemir | 162,549 | 11.66 | Dominated by insulin glargine U100 |
ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year.
Scenario Analysis Results
CADTH undertook price reduction analyses based on the sponsor’s results and CADTH’s base case. Results of the CADTH base case for the insulin-naive subpopulation suggested a price reduction of 24% would be required for insulin icodec to be cost-effective relative to insulin glargine U100 at a willingness-to-pay threshold of $50,000 per QALY gained (Table 14). In addition, a price reduction of 22% would be required for insulin icodec to be cost-effective in the basal insulin–experienced subpopulation (Table 15). In the basal and bolus insulin–experienced subpopulation, a price reduction of 34% would be required for insulin icodec to become an optimal therapeutic option on the cost-effectiveness frontier. These analyses are based on small differences in clinical benefit extrapolated from the NMA and are therefore uncertain given the large credible intervals. To ensure cost-effectiveness, insulin icodec should be priced no more than the lowest-cost comparator.
CADTH conducted a scenario analysis by assuming efficacy, safety, and mean weekly insulin dose parity across all therapies considered to explore the impact of uncertainty associated with the NMA-derived estimates. In this scenario, insulin glargine U100 was the only optimal therapy on the cost-effectiveness frontier across subpopulations. That is, when assuming parity in effectiveness and dose parameters, the therapy with the lowest cost per insulin unit is optimal.
CADTH conducted an additional scenario analysis by adopting alternative injection-related disutility estimates. In this scenario, the ICER of insulin icodec (relative to insulin glargine U100) decreased to $92,141 per QALY gained (incremental costs: $7,551; incremental QALYs: 0.08) in the insulin-naive subpopulation, and $113,686 per QALY gained (incremental costs: $7,395; incremental QALYs: 0.07) in the basal insulin–experienced subpopulation. In the basal and bolus insulin–experienced subpopulation, adopting alternative disutility estimates rendered insulin icodec more effective than insulin glargine U100, thereby joining the cost-effectiveness frontier with an ICER of $418,224 per QALY gained (incremental costs: $16,085; incremental QALYs: 0.04). This analysis still assumes a large reduction in HRQoL due to daily injection administration and therefore may overestimate the impact of once-weekly injections.
Issues for Consideration
Participating drug plans noted concerns regarding the anticipated budget impact associated with the reimbursement of insulin icodec, which may result in a substantial proportion of patients with T2DM expressing a preference to transition from once-daily to once-weekly insulin injections for dosing convenience. CADTH acknowledges that the introduction of an insulin product that may reduce the injection burden on patients with T2DM has the potential to shift the treatment landscape. While there is insufficient evidence to suggest that improved convenience may result in improved patient HRQoL, convenience alone may be sufficient for patients with T2DM to express a preference for once-weekly over once-daily insulin injections.
Insulin icodec has potential benefits in reducing the environmental impact of long-acting basal insulin products by decreasing the use of single-use medical supplies. As a result of weekly administration, it is expected that insulin icodec will be associated with a reduction in the number of needle tips and in the number of prefilled syringes required by patients.
The pan-Canadian Pharmaceutical Alliance (pCPA) concluded negotiations with letters of intent for insulin glargine (Semglee, Toujeo, Basaglar) for the treatment of type 1 and 2 diabetes mellitus.33-35 As such, insulin glargine products have confidential negotiated prices, and are currently funded by jurisdictional drug formularies.36,37
The pCPA concluded negotiations with a letter of intent for insulin degludec (Tresiba) for the treatment of type 1 and 2 diabetes mellitus.38 As such, insulin degludec has a confidential negotiated price, and is currently funded by jurisdictional drug formularies.39,40
Overall Conclusions
Evidence from 5 active-controlled, randomized controlled trials comparing insulin icodec to insulin glargine and/or insulin degludec in adults with T2DM suggest that once-weekly injections of insulin icodec were noninferior in CFB in hemoglobin A1C at week 26 or week 52. Secondary analyses of superiority suggest that, statistically, there may be a benefit associated with insulin icodec over the once-daily comparators for this outcome, but the clinical meaningfulness of this result is uncertain. The CADTH Clinical Review noted various limitations in the submitted NMA. Consequently, CADTH’s ability to draw conclusions regarding the long-term comparative efficacy and safety of insulin icodec relative to long-acting basal insulin analogues from the NMA is limited. This uncertainty is propagated into the submitted economic model given that the mean reductions in CFB in hemoglobin A1C and the annual event rate of severe hypoglycemia were used to generate transition probabilities extrapolating disease progression across the 40-year lifetime horizon.
In addition to limitations with the clinical evidence, CADTH identified several limitations with the sponsor’s economic submission. The main limitation was uncertainty regarding the impact of variably administered injectable therapies on the HRQoL of patients with T2DM. As part of the base-case reanalysis, CADTH excluded the utility decrements associated with once-weekly, once-daily, and multiple daily injections of insulin, and explored the impact of this through scenario analysis.
In the 3 subgroups (insulin naive, basal insulin experienced, and basal and bolus insulin experienced), insulin icodec was associated with higher costs (incremental costs: $7,599, $7,473, and $16,076, respectively) and QALY differences that trended close to 0 (0.02, 0.01, and –0.02, respectively). Higher costs were due to higher treatment acquisition costs and the small difference in QALYs was due to extrapolation of small hemoglobin A1C differences as estimated by the NMA. However, differences in hemoglobin A1C from the NMA were not statistically significant, meaning that any estimation of incremental difference estimated by the model is highly uncertain. The only difference between the CADTH reanalysis and the sponsor’s is the removal of utility decrements associated with daily and weekly administration. There is likely a patient preference to receive weekly versus daily injections, though the impact this has on patient HRQoL is uncertain. The impact on HRQoL submitted by the sponsor was highly uncertain and deemed too large to meet expectations from a face validity perspective (weekly treatment administration having a larger impact on HRQoL than stroke, for example). The cost-effectiveness of insulin icodec was sensitive to equivalence assumptions, as well as to the adoption of alternative injection-related disutilities. When assuming efficacy, safety, and dose parity across all therapies considered, insulin glargine U100 (the comparator with the lowest cost per insulin unit) was the only optimal therapy across subpopulation analyses. When applying alternative injection-related disutilities, the ICER of insulin icodec (relative to insulin glargine U100) decreased to $92,141 and $113,686 per QALY gained in the insulin-naive and basal insulin–experienced subpopulations, respectively. In the basal and bolus insulin–experienced subpopulation, adopting alternative disutility estimates rendered insulin icodec more effective than insulin glargine U100, joining the cost-effectiveness frontier with an ICER of $418,224 per QALY gained.
Given the limitations with the indirect comparisons of efficacy, safety, and dose between insulin icodec and long-acting basal insulin analogues, there remains considerable uncertainty in the cost-effectiveness results. To ensure cost-effectiveness, insulin icodec should be priced no more than the lowest-cost insulin alternative used to treat T2DM. A price premium may be warranted due to the lower administration burden associated with insulin icodec (once-weekly administration) though the size of this premium is highly uncertain.
References
1.Pharmacoeconomic evaluation. [internal sponsor's report] In: Drug Reimbursement Review sponsor submission: Awiqli (insulin icodec), 700 units/mL, pre-filled pen for subcutaneous use. Mississauga, ON: Novo Nordisk Canada Inc; 2023 Oct 18.
2.Clinical Study Report: NN1436-4477, ONWARDS 1. A 78-week trial comparing the effect and safety of once weekly insulin icodec and once daily insulin glargine 100 units/mL, both in combination with non-insulin anti-diabetic treatment, in insulin naïve subjects with type 2 diabetes [internal sponsor's report]. Bagsvaerd (DK): Novo Nordisk; 2022 Jul 13.
3.Clinical Study Report: NN1436-4478, ONWARDS 2. A 26-week trial comparing the effect and safety of once weekly insulin icodec and once daily insulin degludec, both with or without non-insulin anti-diabetic drugs, in subjects with type 2 diabetes treated with basal insulin [internal sponsor's report]. Bagsvaerd (DK): Novo Nordisk; 202 Jun 15.
4.Clinical Study Report: NN1436-4479, ONWARDS 3. A 26-week double blinded, multiregional trial comparing the effect and safety of once weekly insulin icodec and once daily insulin degludec 100 units/mL, both in combination with non-insulin anti-diabetic drugs, in insulin naïve subjects with type 2 diabetes [internal sponsor's report]. Bagsvaerd (DK): Novo Nordisk; 2022 Sep 7.
5.Clinical Study Report: NN1436-4480, ONWARDS 4. A 26-week trial comparing the effect and safety of once weekly insulin icodec and once daily insulin glargine 100 units/mL, both in combination with bolus insulin with or without non-insulin anti-diabetic drugs, in subjects with type 2 diabetes on a basal-bolus regimen [internal sponsor's report]. Bagsvaerd (DK): Novo Nordisk; 2022 Sep 23.
6.Clinical Study Report: NN1436-4481, ONWARDS 5. Effectiveness and safety of once weekly insulin icodec used with doseguide versus once daily basal insulin analogues in an insulin naïve type 2 diabetes population in a clinical practice setting [internal sponsor's report]. Bagsvaerd (DK): Novo Nordisk; 2022 Oct 27.
7.Awiqli (insulin icodec injection): 700 units/mL solution for subcutaneous injection in the FlexTouch pre-filled pen [product monograph]. Mississauga (ON): Novo Nordisk Canada Inc; 2024 Mar 12.
8.Nilsson K, Persson S, Fridhammar A. Technical report: the IHE Diabetes Cohort Model, version 4.4.2. Lund (SE): The Swedish institute for Health Economics (IHE); 2021.
9.Willis M, Fridhammar A, Gundgaard J, Nilsson A, Johansen P. Comparing the cohort and micro-simulation modeling approaches in cost-effectiveness modeling of type 2 diabetes mellitus: a case study of the IHE Diabetes Cohort Model and the Economics and Health Outcomes Model of T2DM. PharmacoEconomics. 2020;38(9):953-969.PubMed
10.Hayes AJ, Leal J, Gray AM, Holman RR, Clarke PM. UKPDS outcomes model 2: a new version of a model to simulate lifetime health outcomes of patients with type 2 diabetes mellitus using data from the 30 year United Kingdom Prospective Diabetes Study: UKPDS 82. Diabetologia. 2013;56(9):1925-1933.PubMed
11.Drug Reimbursement Review clinical and pharmacoeconomic reports: semaglutide (Rybelsus). Can J Health Technol. 2021;1(9). https://www.cda-amc.ca/sites/default/files/pdf/TR0012_T2D_Science_Report.pdf. Accessed May 10, 2024.
12.Drug Reimbursement Review pharmacoeconomic report: insulin degludec and liraglutide injection (Xultophy). Ottawa (ON): CADTH; 2019: https://www.cda-amc.ca/sites/default/files/pdf/TR0012_T2D_Science_Report.pdf. Accessed 2024 May 10.
13.Eastman RC, Javitt JC, Herman WH, et al. Model of complications of NIDDM. I. Model construction and assumptions. Diabetes Care. 1997;20(5):725-734.PubMed
14.Bagust A, Hopkinson PK, Maier W, Currie CJ. An economic model of the long-term health care burden of Type II diabetes. Diabetologia. 2001;44(12):2140-2155.PubMed
15.Bagust A, Beale S. Modelling EuroQol health-related utility values for diabetic complications from CODE-2 data. Health Econ. 2005;14(3):217-230.PubMed
16.New drugs for type 2 diabetes: second-line therapy - science report. (CADTH therapeutic review vol.4, no.1b). Ottawa (ON): CADTH; 2017: https://cadth.ca/sites/default/files/pdf/TR0012_T2D_Science_Report.pdf. Accessed 2019 Apr 26.
17.Fenwick EK, Xie J, Ratcliffe J, et al. The impact of diabetic retinopathy and diabetic macular edema on health-related quality of life in type 1 and type 2 diabetes. Invest Ophthalmol Vis Sci. 2012;53(2):677-684.PubMed
18.Fleurence RL, Hollenbeak CS. Rates and probabilities in economic modelling: transformation, translation and appropriate application. PharmacoEconomics. 2007;25(1):3-6.PubMed
19.New drugs for type 2 diabetes: second-line therapy – science report. (CADTH therapeutic review vol.4, no.1b). Ottawa (ON): CADTH; 2017: https://www.cadth.ca/sites/default/files/pdf/TR0012_T2D_Science_Report.pdf. Accessed 2023 Jul.
20.McEwan P, Baker-Knight J, Ásbjörnsdóttir B, Yi Y, Fox A, Wyn R. Disutility of injectable therapies in obesity and type 2 diabetes mellitus: general population preferences in the UK, Canada, and China. Eur J Health Econ. 2023;24(2):187-196.PubMed
21.Ontario Ministry of Health, Ontario Ministry of Long-Term Care. Ontario drug benefit formulary/comparative drug index. 2023; https://www.formulary.health.gov.on.ca/formulary/. Accessed 2023 Apr.
22.O’Brien JA, Patrick AR, Caro JJ. Cost of managing complications resulting from type 2 diabetes mellitus in Canada. BMC Health Serv Res. 2003;3(1):7.PubMed
23.Ward A, Alvarez P, Vo L, Martin S. Direct medical costs of complications of diabetes in the United States: estimates for event-year and annual state costs (USD 2012). J Med Econ. 2014;17(3):176-183.PubMed
24.Matza LS, Stewart KD, Lloyd AJ, Rowen D, Brazier JE. Vignette-Based Utilities: Usefulness, Limitations, and Methodological Recommendations. Value Health. 2021;24(6):812-821.PubMed
25.Takumoto Y, Sasahara Y, Narimatsu H, Murata T, Akazawa M. Health state utility values for metastatic pancreatic cancer using a composite time trade-off based on the vignette-based approach in Japan. Health Econ Rev. 2022;12(1):63.PubMed
26.Boye KS, Matza LS, Stewart KD, et al. Patient preferences and health state utilities associated with dulaglutide and semaglutide injection devices among patients with type 2 diabetes in Italy. J Med Econ. 2019;22(8):806-813.PubMed
27.Saisho Y. Use of Diabetes Treatment Satisfaction Questionnaire in diabetes care: importance of patient-reported outcomes. Int J Environ Res Public Health. 2018;15(5):947.PubMed
28.Bradley C, Speight J. Patient perceptions of diabetes and diabetes therapy: assessing quality of life. Diabetes Metab Res Rev. 2002;18(suppl 3):S64-S69.PubMed
29.Boye KS, Matza LS, Walter KN, Van Brunt K, Palsgrove AC, Tynan A. Utilities and disutilities for attributes of injectable treatments for type 2 diabetes. Eur J Health Econ. 2011;12(3):219-230.PubMed
30.Dias S, Welton NJ, Sutton AJ, Ades AE. NICE DSU technical support document 2: a generalised linear modelling framework for pairwise and network meta-analysis of randomised controlled trials. Sheffield (UK): Decision Support Unit, ScHARR, University of Sheffield; 2014: https://www.ncbi.nlm.nih.gov/books/NBK310366/. Accessed 2024 Jan 05.
31.Insulin prescription. Toronto (ON): Diabetes Canada; 2022: https://www.diabetes.ca/DiabetesCanadaWebsite/media/Managing-My-Diabetes/Tools%20and%20Resources/Insulin_Prescription_03_22.pdf. Accessed 2024 Jan 02.
32.Chew EY, Ambrosius WT, Davis MD, et al; ACCORD Study Group; ACCORD Eye Study Group. Effects of medical therapies on retinopathy progression in type 2 diabetes. N Engl J Med. 2010;363(3):233-244.PubMed
33.pan-Canadian Pharmaceutical Alliance. Semglee (insulin glargine). 2022; https://www.pcpacanada.ca/negotiation/21887. Accessed 2024 Jan 11.
34.pan-Canadian Pharmaceutical Alliance. Toujeo (insulin glargine injection). 2018; https://www.pcpacanada.ca/negotiation/21049. Accessed 2024 Jan 11.
35.pan-Canadian Pharmaceutical Alliance. Basaglar (insulin glargine). 2017; https://www.pcpacanada.ca/negotiation/20930. Accessed 2024 Jan 11.
36.Ontario Ministry of Health, Ontario Ministry of Long-Term Care. Ontario drug benefit formulary/comparative drug index: insulin glargine. 2023; https://www.formulary.health.gov.on.ca/formulary/results.xhtml?q=insulin%2Bglargine&type=1. Accessed 2024 Jan 11.
37.Alberta Interactive Drug Benefit List. Insulin glargine. 2023; https://idbl.ab.bluecross.ca/idbl/drugsList;jsessionid=H5P5QiVKFCQpG3Nh2CeE7zuHRwJE3GmfN9vHHHrQ8yB4vsCbwjCd!500427592?searchTerm=insulin+glargine&category=&genericName=&ptc=&mfgCode=. Accessed 2024 Jan 11.
38.pan-Canadian Pharmaceutical Alliance. Tresiba (insulin degludec). 2018; https://www.pcpacanada.ca/negotiation/21002. Accessed 2024 Jan 11.
39.Manitoba Health. Drug Formulary lookup - search results: Insulin degludec. 2024; https://web22.gov.mb.ca/eFormulary/searchResults.aspx?query=insulin%20degludec&type=basic. Accessed 2024 Jan 11.
40.Ontario Ministry of Health, Ontario Ministry of Long-Term Care. Ontario drug benefit formulary/comparative drug index: insulin degludec. 2023; https://www.formulary.health.gov.on.ca/formulary/results.xhtml?q=insulin%2Bdegludec&type=1. Accessed 2024 Jan 11.
41.Budget Impact Analysis. [internal sponsor's report] In: Drug Reimbursement Review sponsor submission: Awiqli (insulin icodec), 700 units/mL, pre-filled pen for subcutaneous use. Mississauga, ON: Novo Nordisk Canada Inc; 2023 Oct 18.
42.Framework for diabetes in Canada. Ottawa (ON): Public Health Agency of Canada; 2022: https://www.canada.ca/en/public-health/services/publications/diseases-conditions/framework-diabetes-canada.html. Accessed 2023 Sep.
Appendix 1: Cost Comparison Table
Note that this appendix has not been copy-edited.
The comparators presented in the following table have been deemed to be appropriate based on feedback from clinical experts and drug plan. Comparators may be recommended (appropriate) practice or actual practice. Existing Product Listing Agreements are not reflected in the table and as such, the table may not represent the actual costs to public drug plans.
Table 7: CADTH Cost Comparison Table for Long-Acting Basal Insulin Products Used to Treat Patients With T2DM Requiring Basal Insulin for Glycemic Control
Treatment | Strength | Form | Price ($) | Recommended dosage | Daily cost ($)a | Annual cost ($) |
|---|---|---|---|---|---|---|
Insulin icodec (Awiqli) | 700 U/mL | 1.5 mL prefilled pen (1,050 U per package) 3 mL prefilled pen (2,100 U per package) | 78.0400b 156.0900b | Starting dose is 70 U once weekly. Maintenance dose is titrated according to the metabolic needs of the patient and the glycemic control target.c,d,e | 2.97 to 3.72 | 1,085 to 1,356 |
Insulin degludec (Tresiba) | 100 U/mL | 3 × 5 mL cartridge (1,500 U per package) 5 × 3 mL prefilled pen (1,500 U per package) | 111.5000 111.5000 | Starting dose is 10 U once daily. Maintenance dose is titrated according to the metabolic needs of the patient and the glycemic control target.c,d,f | 2.97 to 3.72 | 1,085 to 1,357 |
200 U/mL | 3 × 3 mL prefilled pen (1,800 U per package) | 133.8000 | ||||
Insulin detemir (Levemir) | 100 U/mL | 5 × 3 mL cartridge (1,500 U per package) 5 × 3 mL prefilled pen (1,500 U per package) | 110.4100 111.5000 | 2.97 to 3.72g | 1,085 to 1,357 | |
Insulin glargine (Basaglar) | 100 U/mL | 5 × 3 mL cartridge (1,500 U per package) 5 × 3 mL prefilled pen (1,500 U per package) | 76.1100 76.1100 | 2.03 to 2.54 | 741 to 926 | |
Insulin glargine (Lantus) | 100 U/mL | 10 mL vial 5 × 3 mL cartridge (1,500 U per package) 5 × 3 mL prefilled pen (1,500 U per package) | 61.6900 92.8500 92.8500 | 2.48 to 3.10g | 904 to 1,130 | |
Insulin glargine (Semglee) | 100 U/mL | 3 mL prefilled pen (300 U per package) | 12.7668 | 1.70 to 2.13 | 621 to 777 | |
Insulin glargine (Toujeo) | 300 U/mL | 1.5 mL prefilled pen (450 U per package) 3 mL prefilled pen (900 U per package) | 26.4333 52.8666 | Starting dose is 0.2 U per kg of body weight once daily. Maintenance dose is titrated according to the metabolic needs of the patient and the glycemic control target.c,d,f | 2.35 to 2.94 | 858 to 1,072 |
T2DM = type 2 diabetes mellitus; U = unit.
Note: All prices are from the Ontario Drug Benefit Formulary (accessed January 2024), unless otherwise indicated, and do not include dispensing fees.
aCosts calculated assuming a maintenance dose of 40 to 50 units of insulin per day.31
bThe sponsor initially submitted prices of $78.0500 for the 1.5 mL prefilled pen and $156.1000 for the 3 mL prefilled pen, but later revised them to $78.0400 and $156.0900 respectively. CADTH acknowledges the sponsor's omission of a revised pharmacoeconomic model or updated pricing and distribution document to reflect the adjusted price. However, due to the minimal disparity between the initially submitted and revised prices, CADTH concludes that this difference is unlikely to affect the assessment of cost-effectiveness.
cRecommended dosage is based on the corresponding product monographs.
dAccording to Diabetes Canada insulin titration recommendations for patients with type 2 diabetes mellitus, the target fasting blood glucose is 4 to 7 mmol/L, and most patients will require 40 to 50 units of insulin per day to achieve target, however there is no maximum dose.31
eIn basal insulin–experienced patients, the weekly dose is the previous basal insulin dose multiplied by 7. A 1-time additional 50% dose is recommended in week 1.
fBasal insulin–experienced patients may require adjustment of dose and timing of administration to achieve glycemic target.
gAssuming the cost per insulin unit in the prefilled pen.
Table 8: CADTH Cost Comparison Table for Rapid- and Long-Acting Insulin Products Used to Treat Patients With T2DM Requiring Basal and Bolus Insulin for Glycemic Control
Treatment | Strength | Form | Price ($) | Recommended dosage | Daily cost ($)a | Annual cost ($) |
|---|---|---|---|---|---|---|
Insulin icodec (Awiqli) | 700 U/mL | 1.5 mL prefilled pen (1,050 U per package) 3 mL prefilled pen (2,100 U per package) | 78.0400b 156.0900b | Starting dose is 70 U once weekly. Maintenance dose is titrated according to the metabolic needs of the patient and the glycemic control target.c,d,e | 2.97 to 3.72 | 1,085 to 1,356 |
Long-acting insulin analogues (Basal) | ||||||
Insulin degludec (Tresiba) | 100 U/mL | 3 × 5 mL cartridge (1,500 U per package) 5 × 3 mL prefilled pen (1,500 U per package) | 111.5000 111.5000 | Starting dose is 10 U once daily. Maintenance dose is titrated according to the metabolic needs of the patient and the glycemic control target.c,d,f | 2.97 to 3.72 | 1,085 to 1,357 |
200 U/mL | 3 × 3 mL prefilled pen (1,800 U per package) | 133.8000 | ||||
Insulin detemir (Levemir) | 100 U/mL | 5 × 3 mL cartridge (1,500 U per package) 5 × 3 mL prefilled pen (1,500 U per package) | 110.4100 111.5000 | 2.97 to 3.72g | 1,085 to 1,357 | |
Insulin glargine (Basaglar) | 100 U/mL | 5 × 3 mL cartridge (1,500 U per package) 5 × 3 mL prefilled pen (1,500 U per package) | 76.1100 76.1100 | 2.03 to 2.54 | 741 to 926 | |
Insulin glargine (Lantus) | 100 U/mL | 10 mL vial 5 × 3 mL cartridge (1,500 U per package) 5 × 3 mL prefilled pen (1,500 U per package) | 61.6900 92.8500 92.8500 | 2.48 to 3.10g | 904 to 1,130 | |
Insulin glargine (Semglee) | 100 U/mL | 3 mL prefilled pen (300 U per package) | 12.7668 | 1.70 to 2.13 | 621 to 777 | |
Insulin glargine (Toujeo) | 300 U/mL | 1.5 mL prefilled pen (450 U per package) 3 mL prefilled pen (900 U per package) | 26.4333 52.8666 | Starting dose is 0.2 U per kg of body weight once daily. Maintenance dose is titrated according to the metabolic needs of the patient and the glycemic control target.c,d,f | 2.35 to 2.94 | 858 to 1,072 |
Rapid-acting insulin analogues (Bolus) | ||||||
Insulin aspart (Trurapi) | 100 U/mL | 10 mL vial 5 × 3 mL cartridge (1,500 U per package) 5 × 3 mL prefilled pen (1,500 U per package) | 22.6430 45.0000 45.0000 | Dosage is individualized and determined, based on the treating physician’s advice, in accordance with the needs of the patient. Bolus insulin should be added before or after meals.h | 0.36 to 0.45g | 131 to 164 |
Insulin glulisine (Apidra) | 100 U/mL | 10 mL vial 5 × 3 mL cartridge (1,500 U per package) 5 × 3 mL prefilled pen (1,500 U per package) | 26.5800 52.6500 53.1500 | 0.43 to 0.53g | 155 to 194 | |
Insulin lispro (Admelog) | 100 U/mL | 10 mL vial 5 × 3 mL cartridge (1,500 U per package) 5 × 3 mL prefilled pen (1,500 U per package) | 22.7000 45.0000 45.0000 | 0.36 to 0.45g | 131 to 164 | |
Regular human insulin (Humulin R) | 100 U/mL | 10 mL vial 5 × 3 mL cartridge (1,500 U per package) | 27.1900 53.3500 | 0.33 to 0.41 | 119 to 149 | |
Regular human insulin (Novolin ge Toronto) | 100 U/mL | 10 mL vial 5 × 3 mL cartridge (1,500 U per package) | 24.2800 47.6800 | 0.29 to 0.36 | 106 to 133 | |
Basal + bolus insulin analogues | ||||||
Insulin icodec + bolus insulin analogues | 3.25 to 4.25 | 1,184 to 1,551 | ||||
Insulin degludec (Tresiba) + bolus insulin analogues | 3.25 to 4.25 | 1,184 to 1,551 | ||||
Insulin detemir (Levemir) + bolus insulin analogues | 3.25 to 4.25 | 1,184 to 1,551 | ||||
Insulin glargine (Basaglar) + bolus insulin analogues | 2.30 to 3.07 | 840 to 1,121 | ||||
Insulin glargine (Lantus) + bolus insulin analogues | 2.75 to 3.63 | 1,003 to 1,324 | ||||
Insulin glargine (Semglee) + bolus insulin analogues | 1.97 to 2.66 | 720 to 971 | ||||
Insulin glargine (Toujeo) + bolus insulin analogues | 2.62 to 3.47 | 957 to 1,267 | ||||
T2DM = type 2 diabetes mellitus; U = unit.
Note: All prices are from the Ontario Drug Benefit Formulary (accessed January 2024), unless otherwise indicated, and do not include dispensing fees.
aCosts calculated assuming a maintenance dose of 40 to 50 units of insulin per day.31
bThe sponsor initially submitted prices of $78.0500 for the 1.5 mL prefilled pen and $156.1000 for the 3 mL prefilled pen, but later revised them to $78.0400 and $156.0900 respectively. CADTH acknowledges the sponsor's omission of a revised pharmacoeconomic model or updated pricing and distribution document to reflect the adjusted price. However, due to the minimal disparity between the initially submitted and revised prices, CADTH concludes that this difference is unlikely to affect the assessment of cost-effectiveness.
cRecommended dosage is based on the corresponding product monographs.
dAccording to Diabetes Canada insulin titration recommendations for patients with type 2 diabetes mellitus, the target fasting blood glucose is 4 to 7 mmol/L, and most patients will require 40 to 50 units of insulin per day to achieve target, however there is no maximum dose.31
eIn basal insulin–experienced patients, the weekly dose is the previous basal insulin dose multiplied by 7. A 1-time additional 50% dose is recommended in week 1.
fBasal insulin–experienced patients may require adjustment of dose and timing of administration to achieve glycemic target.
gAssuming the cost per insulin unit in the prefilled pen.
hAccording to Diabetes Canada insulin titration recommendations for patients with type 2 diabetes mellitus requiring basal + bolus insulin, current basal insulin users should maintain the basal dose and add bolus insulin with each meal at a dose equivalent to 10% of the basal dose.31 Hence, when calculating daily cost for bolus insulin, 12 units of bolus insulin per day were calculated among patients assumed to receive 40 units of basal insulin per day, while 15 units of bolus insulin per day were calculated among patients assumed to receive 50 units of basal insulin per day.
Appendix 2: Submission Quality
Note that this appendix has not been copy-edited.
Description | Yes/No | Comments |
|---|---|---|
Population is relevant, with no critical intervention missing, and no relevant outcome missing | Yes | No comment. |
Model has been adequately programmed and has sufficient face validity | Yes | No comment. |
Model structure is adequate for decision problem | Yes | No comment. |
Data incorporation into the model has been done adequately (e.g., parameters for probabilistic analysis) | Yes | No comment. |
Parameter and structural uncertainty were adequately assessed; analyses were adequate to inform the decision problem | No | The sponsor did not adequately incorporate the parameter uncertainty associated with mean weekly insulin doses in probabilistic analysis. Rather than inputting the punctual estimations and standard errors of mean weekly doses derived from the NMA, the sponsor opted to use estimated doses to calculate annual drug acquisition costs per treatment, whose mean values were set to fluctuate by 10% in probabilistic analysis. |
The submission was well organized and complete; the information was easy to locate (clear and transparent reporting; technical documentation available in enough details) | Yes | No comment. |
Appendix 3: Additional Information on the Submitted Economic Evaluation
Note that this appendix has not been copy-edited.
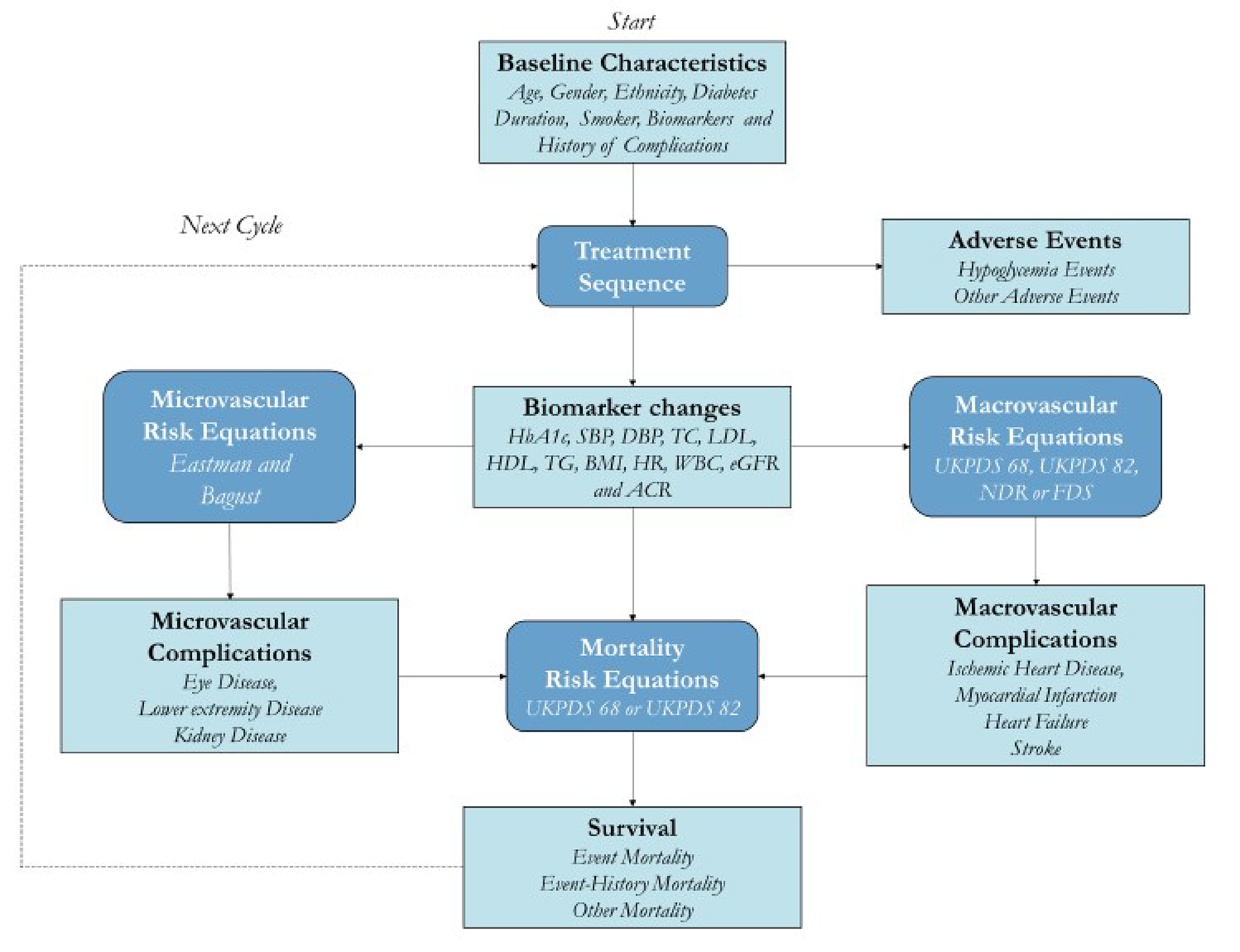
hemoglobin A1C = glycated hemoglobin; ACR = urinary albumin-creatine ratio; BMI = body mass index; DBP = diastolic blood pressure; eGFR = estimated glomerular filtration rate; FDS = Fremantle Diabetes Study; HDL = high-density lipoprotein; HR = heart rate; IHE-DCM = Swedish Institute of Health Economics Diabetes Cohort Model; LDL = low-density lipoprotein; NDR = National Diabetes Registry; SBP = systolic blood pressure; TC = total cholesterol; TG = triglycerides; UKPDS = UK Prospective Diabetes Study; WBC = white blood cell.
Source: Sponsor’s Pharmacoeconomic Submission.1
Table 10: Injection-Related Utility Values and Decrements
Parameter | Utility Value | Utility Decrement |
|---|---|---|
Living with controlled T2D | 0.872 | NA |
Once-weekly insulin injection | 0.822 | −0.050 |
Once-daily insulin injection | 0.765 | −0.107 |
Multiple daily insulin injections: Once-daily basal insulin + bolus insulin injections | 0.669 | −0.203 |
Multiple daily insulin injections: Once-weekly insulin icodec + bolus insulin injections | 0.683a | −0.189 |
NA = not applicable; T2D = type 2 diabetes.
aEstimated based on a ratio approach and clinical expert opinion in Canada.
Source: McEwan et al.20
Figure 2: Utility Values in Obesity and T2DB in Canada
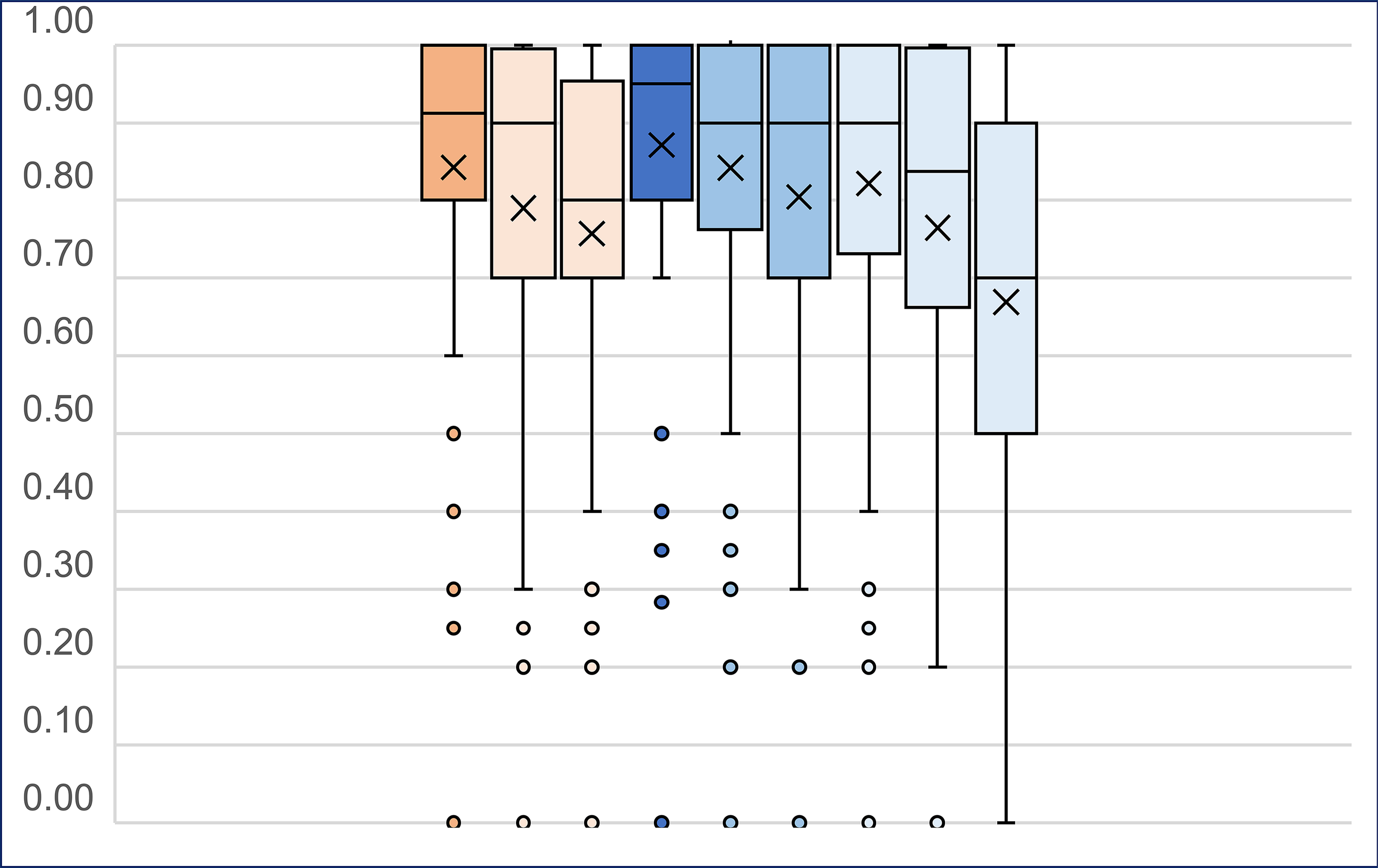
BB = basal bolus; GLP-1 RA = glucagon-like peptide-1 receptor agonist; q.d. = once a day; q.w. = every week; T2DB = type 2 diabetes.
Note: This figure is presented in the vignette-based study that included utility values in obesity and T2DB. Only the results for injection-related utilities in T2DB are relevant to the economic analysis. Order of presentation: obesity anchor state, GLP-1 RA q.w., GLP-1 RA q.d., T2DM anchor state, GLP-1 RA q.w., GLP-1 RA q.d., insulin q.w., insulin q.d., insulin BB.
Source: McEwan P et al. Eur J Health Econ. 2023;24(2):187 to 196. Copyright 2023 by the authors. Reprinted in accordance with Creative Commons Attribution 4.0 International License (CC BY 4.0): https://creativecommons.org/licenses/by/4.0/20
Detailed Results of the Sponsor’s Base Case
Table 11: Disaggregated Summary of the Sponsor’s Economic Evaluation Results — Insulin Naive
Parameter | Insulin icodec | Insulin glargine | Incremental |
|---|---|---|---|
Discounted life-years | |||
Total | 16.98 | 16.97 | 0.01 |
Discounted QALYs | |||
Total | 9.57 | 9.15 | 0.42a |
Disutility Due to Diabetes Treatment | −2.80 | −3.20 | 0.40 |
Disutility Due to Diabetes-Related Complications | −5.07 | −5.07 | < 0.01 |
Discounted costs ($) | |||
Total | 131,014 | 123,456 | 7,559 |
Diabetes Treatment | 35,311 | 27,018 | 8,292 |
Diabetes-Related Complications | 95,704 | 96,438 | −734 |
ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year.
Note: The cost-effectiveness frontier was constituted by insulin glargine U100 and insulin icodec (representing the optimal therapies). Dominated treatments are not presented in this table.
aIncremental QALYs are attributed to extension in life-years and differences in disutility.
Table 12: Disaggregated Summary of the Sponsor’s Economic Evaluation Results — Basal Insulin Experienced
Parameter | Insulin icodec | Insulin glargine | Incremental |
|---|---|---|---|
Discounted LYs | |||
Total | 15.60 | 15.60 | 0.01 |
Discounted QALYs | |||
Total | 8.59 | 8.23 | 0.36a |
Disutility Due to Diabetes Treatment | −2.57 | −2.93 | 0.35 |
Disutility Due to Diabetes-Related Complications | −4.85 | −4.86 | < 0.01 |
Discounted costs ($) | |||
Total | 113,313 | 105,840 | 7,473 |
Diabetes Treatment | 32,703 | 24,943 | 7,760 |
Diabetes-Related Complications | 80,610 | 80,897 | −287 |
ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year.
Note: The cost-effectiveness frontier was constituted by insulin glargine U100 and insulin icodec (representing the optimal therapies). Dominated treatments are not presented in this table.
aIncremental QALYs are attributed to extension in life-years and differences in disutility.
Table 13: Disaggregated Summary of the Sponsor’s Economic Evaluation Results — Basal-Bolus Insulin Experienced
Parameter | Insulin icodec | Insulin glargine | Incremental |
|---|---|---|---|
Discounted LYs | |||
Total | 16.60 | 16.62 | −0.02 |
Discounted QALYs | |||
Total | 8.60 | 8.39 | 0.22a |
Disutility Due to Diabetes Treatment | −3.13 | −3.37 | 0.24 |
Disutility Due to Diabetes-Related Complications | −5.32 | −5.31 | < 0.01 |
Discounted costs ($) | |||
Total | 153,509 | 137,433 | 16,076 |
Diabetes Treatment | 52,581 | 37,357 | 15,224 |
Diabetes-Related Complications | 100,928 | 100,076 | 852 |
ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year.
Note: The cost-effectiveness frontier was constituted by insulin glargine U100 and insulin icodec (representing the optimal therapies). Dominated treatments are not presented in this table.
aIncremental QALYs are attributed to extension in life-years and differences in disutility.
Table 14: CADTH Price Reduction Analyses — Insulin Naive
Analysis | Unit drug cost ($) | ICERs ($/QALY) | |
|---|---|---|---|
Price reduction | Price per 1.5 mL prefilled pen | Sponsor base case | CADTH reanalysis |
No price reduction | 78.05 | 23,137 (vs. insulin glargine U100) | 576,917 (vs. insulin glargine U100) |
10% | 70.25 | 14,064 (vs. insulin glargine U100) | 350,690 (vs. insulin glargine U100) |
20% | 62.44 | 5,264 (vs. insulin glargine U100) | 131,261 (vs. insulin glargine U100) |
30% | 54.64 | Dominant | Dominant |
ICER = incremental cost-effectiveness ratio; U = unit; vs. = versus.
Table 15: CADTH Price Reduction Analyses — Basal Insulin Experienced
Analysis | Unit drug cost ($) | ICERs ($/QALY) | |
|---|---|---|---|
Price reduction | Price per 1.5 mL prefilled pen | Sponsor base case | CADTH reanalysis |
No price reduction | 78.05 | 14,493 (vs. insulin glargine U100) | 686,446 (vs. insulin glargine U100) |
10% | 70.25 | 8,130 (vs. insulin glargine U100) | 385,062 (vs. insulin glargine U100) |
20% | 62.44 | 1,957 (vs. insulin glargine U100) | 92,674 (vs. insulin glargine U100) |
30% | 54.64 | Dominant | Dominant |
ICER = incremental cost-effectiveness ratio; U = unit; vs. = versus.
Table 16: CADTH Price Reduction Analyses — Basal-Bolus Insulin Experienced
Analysis | Unit drug cost ($) | ICERs ($/QALY) | |
|---|---|---|---|
Price reduction | Price per 1.5 mL prefilled pen | Sponsor base case | CADTH reanalysis |
No price reduction | 78.05 | 77,748 (vs. insulin glargine U100) | Dominated by insulin glargine U100. |
10% | 70.25 | 50,479 (vs. insulin glargine U100) | Dominated by insulin glargine U100. |
20% | 62.44 | 29,193 (vs. insulin glargine U100) | Dominated by insulin glargine U100. |
30% | 54.64 | 7,907 (vs. insulin glargine U100) | Dominated by insulin glargine U100. |
40% | 46.83 | Dominant | Insulin icodec is the reference treatment. |
50% | 39.03 | Dominant | Insulin icodec is the reference treatment. |
60% | 31.22 | Dominant | Insulin icodec is the reference treatment. |
70% | 23.42 | Dominant | Insulin icodec is the reference treatment. |
80% | 15.61 | Dominant | Insulin icodec is the reference treatment. |
90% | 7.81 | Dominant | Insulin icodec is the reference treatment. |
ICER = incremental cost-effectiveness ratio; U = unit; vs. = versus.
Note: At the 30% price reduction, insulin icodec is dominated by insulin glargine U100; that is, insulin icodec is more costly and less effective than insulin glargine U100. Insulin icodec joins the cost-effectiveness frontier at the 33.8% price reduction (as the reference treatment), thus becoming the least costly and least effective therapeutic option on the frontier. Insulin glargine U100 and insulin glargine U300 are also on the frontier representing optimal therapies; however, they have higher costs and higher effectiveness relative to insulin icodec.
Appendix 4: Additional Details on the CADTH Reanalyses and Sensitivity Analyses of the Economic Evaluation
Note that this appendix has not been copy-edited.
Detailed Results of CADTH Base Case
Table 17: Disaggregated Summary of CADTH’s Economic Evaluation Results — Insulin Naive
Parameter | Insulin icodec | Insulin glargine | Incremental |
|---|---|---|---|
Discounted LYs | |||
Total | 16.98 | 16.97 | 0.01 |
Discounted QALYs | |||
Total | 12.36 | 12.35 | 0.02a |
Disutility Due to Diabetes Treatment | 0.00 | 0.00 | 0.00 |
Disutility Due to Diabetes-Related Complications | −5.07 | −5.07 | < 0.01 |
Discounted costs ($) | |||
Total | 131,014 | 123,456 | 7,559 |
Diabetes Treatment | 35,311 | 27,018 | 8,292 |
Diabetes-related complications | 95,704 | 96,438 | −734 |
ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year.
aIncremental QALYs are attributed to extension in life-years and differences in disutility.
Note: The cost-effectiveness frontier was constituted by insulin glargine U100 and insulin icodec (representing the optimal therapies). Dominated treatments are not presented in this table.
Table 18: Disaggregated Summary of CADTH’s Economic Evaluation Results — Basal Insulin Experienced
Parameter | Insulin icodec | Insulin glargine | Incremental |
|---|---|---|---|
Discounted LYs | |||
Total | 15.60 | 15.60 | 0.01 |
Discounted QALYs | |||
Total | 11.17 | 11.16 | 0.01a |
Disutility Due to Diabetes Treatment | 0.00 | 0.00 | 0.00 |
Disutility Due to Diabetes-Related Complications | −4.85 | −4.86 | < 0.01 |
Discounted costs ($) | |||
Total | 113,313 | 105,840 | 7,473 |
Diabetes Treatment | 32,703 | 24,943 | 7,760 |
Diabetes-Related Complications | 80,610 | 80,897 | −287 |
ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year.
Note: The cost-effectiveness frontier was constituted by insulin glargine U100 and insulin icodec (representing the optimal therapies). Dominated treatments are not presented in this table.
aIncremental QALYs are attributed to extension in life-years and differences in disutility.
Table 19: Disaggregated Summary of CADTH’s Economic Evaluation Results — Basal-Bolus Insulin Experienced
Parameter | Insulin icodec | Insulin glargine | Incremental |
|---|---|---|---|
Discounted LYs | |||
Total | 16.60 | 16.62 | −0.02 |
Discounted QALYs | |||
Total | 11.73 | 11.75 | −0.02a |
Disutility Due to Diabetes Treatment | 0.00 | 0.00 | 0.00 |
Disutility Due to Diabetes-Related Complications | −5.32 | −5.31 | < 0.01 |
Discounted costs ($) | |||
Total | 153,509 | 137,433 | 16,076 |
Diabetes Treatment | 52,581 | 37,357 | 15,224 |
Diabetes-Related Complications | 100,928 | 100,076 | 852 |
ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year.
Note: The cost-effectiveness frontier was constituted by insulin glargine U100 and insulin glargine U300 (representing the optimal therapies). Insulin icodec was strictly dominated by insulin glargine U100.
aIncremental QALYs are attributed to extension in life-years and differences in disutility.
Scenario Analyses
Table 20: Scenario Analysis of CADTH’s Economic Evaluation Results — Insulin Naive
Stepped analysis | Drug | Total costs ($) | Total QALYs | ICER ($/QALY) |
|---|---|---|---|---|
CADTH base case (probabilistic) | Insulin glargine U100 | 123,456 | 12.35 | Reference |
Insulin icodec | 131,014 | 12.36 | 435,800 | |
Scenario analysis 1: Efficacy, safety, and dose equivalence across treatments | Insulin Glargine U100 | 121,593 | 12.35 | Reference |
Insulin Icodec | 129,381 | 12.35 | Dominated by insulin glargine U100. | |
Scenario analysis 2: Alternative injection-related disutilities | Insulin Glargine U100 | 123,182 | 11.27 | Reference |
Insulin Icodec | 130,732 | 11.35 | 92,141 |
ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year.
Note: all other comparators considered in the analysis were either dominated (generated lower QALYs and lower costs) or extendedly dominated
Table 21: Scenario Analysis of CADTH’s Economic Evaluation Results — Basal Insulin Experienced
Stepped analysis | Drug | Total costs ($) | Total QALYs | ICER ($/QALY) |
|---|---|---|---|---|
CADTH base case (probabilistic) | Insulin glargine U100 | 105,840 | 11.16 | Reference |
Insulin icodec | 113,313 | 11.17 | 937,280 | |
Scenario analysis 1: Efficacy, safety, and dose equivalence across treatments | Insulin Glargine U100 | 105,943 | 11.17 | Reference |
Insulin Icodec | 113,212 | 11.17 | Dominated by insulin glargine U100 (produces equivalent number of QALYs at a higher cost). | |
Scenario analysis 2: Alternative injection-related disutilities | Insulin Glargine U100 | 103,951 | 10.11 | Reference |
Insulin Icodec | 111,345 | 10.17 | 113,686 |
ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year.
Note: all other comparators considered in the analysis were either dominated (generated lower QALYs and lower costs) or extendedly dominated
Table 22: Scenario Analysis of CADTH’s Economic Evaluation Results — Basal-Bolus Insulin Experienced
Stepped analysis | Drug | Total costs ($) | Total QALYs | ICER ($/QALY) |
|---|---|---|---|---|
CADTH base case (probabilistic) | Insulin glargine U100 | 137,433 | 11.75 | Reference |
Insulin glargine U300 | 143,745 | 11.76 | 1,122,703 | |
Scenario analysis 1: Efficacy, safety, and dose equivalence across treatments | Insulin Glargine U100 | 140,474 | 11.73 | Reference |
Insulin Icodec | 152,206 | 11.73 | Dominated by insulin glargine U100 (produces equivalent number of QALYs at a higher cost). | |
Scenario analysis 2: Alternative injection-related disutilities | Insulin Glargine U100 | 137,145 | 10.73 | Reference |
Insulin Icodec | 153,230 | 10.77 | 418,224 |
ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year.
Note: all other comparators considered in the analysis were either dominated (generated lower QALYs and lower costs) or extendedly dominated
Appendix 5: Submitted BIA and CADTH Appraisal
Note that this appendix has not been copy-edited.
Table 23: Summary of Key Take-Aways
Key Take-Aways of the BIA |
|---|
• CADTH identified the following limitations in the sponsor’s base case: the estimated basal insulin dose for insulin icodec and long-acting basal insulin analogues is uncertain; the proportion of claims assumed to originate from patients with type 1 diabetes (T1D) is overestimated; the projected market uptake of insulin icodec is uncertain. • CADTH conducted reanalyses of the BIA by adopting average daily doses calculated from RWE and using published estimates to inform the proportion of claims that are likely to be generated by patients with T1D. • Based on the CADTH base case, the estimated budget impact associated with the reimbursement of insulin icodec as treatment for adult patients with T2D requiring glycemic control is expected to be $650,056 in Year 1, $4,288,283 in Year 2, and $10,317,977 in Year 3, for a 3-year budgetary impact of $15,256,316. • CADTH conducted a scenario analysis to address remaining uncertainty. If the projected market share of insulin icodec is assumed to be 10%, 20%, and 30% in Years 1, 2, and 3, respectively, the 3-year budget impact associated with reimbursing insulin icodec is expected to be $41,043,671. |
Summary of Sponsor’s BIA
The sponsor submitted a budget impact analysis (BIA) to estimate the incremental three-year budget impact of reimbursing insulin icodec for the treatment of adult patients with T2DM who require insulin for glycemic control, as per its reimbursement request. The analysis was performed from the perspective of the Canadian public drug plans. The sponsor estimated the budget impact by comparing 2 scenarios: a reference scenario that estimated the total costs associated with long-acting basal insulin analogues for the treatment of adult patients with T2DM who require insulin for glycemic control; and a new drug scenario, where insulin icodec is funded. The comparators for this analysis included: insulin glargine (U100 and U300), insulin degludec (U100 and U200), and insulin detemir. The sponsor estimated total drug costs using a claims-based approach, leveraging historical claims data for the basal analogue market from IQVIA PharmaStat. Drug acquisition costs were the only costs considered in the base case model. The dosing modelled for insulin icodec reflected the product monograph. Key inputs to the BIA are documented in Table 24.
Key assumptions made by the sponsor include:
Distribution of insulin-naive (52%), basal insulin–experienced (29%), and basal and bolus insulin–experienced (19%) patients was derived from the IQVIA LRx database as well as forecasting based on internal research conducted by the sponsor, and assumed to be reflective of the patient population with T2DM in Canada.
Mean daily insulin dose for insulin icodec and long-acting basal insulin analogues was obtained from an NMA conducted by the sponsor and assumed to be reflective of the real-world dosing received by patients with T2DM in Canada.
15% of claims were assumed to be generated from patients with type 1 diabetes (T1D) and removed from the BIA model.
Basal analogue insulin market is expected to expand by 20% over the following 3 years as patients currently treated with SGLT-2i and GLP-1 RA agents begin progressing, thus requiring insulin treatment.
Uptake for insulin icodec in the new drug scenario was assumed to be 1%, 7%, and 14% in Year 1, 2, and 3, respectively. Insulin icodec was assumed to displace all other therapeutic options equally.
Table 24: Summary of Key Model Parameters
Parameter | Sponsor’s estimate (reported as Year 1 / Year 2 / Year 3 if appropriate) |
|---|---|
pan-Canadian claim estimation | |
Historical claims data for the basal analogue market41 | NA |
% of claims assumed to be used in patients with T1D | 15% |
Forecasted claims for the basal analogue market (standardized for a 30-day supply) | 2,044,150 / 2,196,900 / 2,383,784 |
Market uptake (3 years) | |
Uptake (reference scenario) Insulin glargine U100 (Basaglar) Insulin glargine U100 (Lantus) Insulin glargine U100 (Semglee) Insulin glargine U300 (Toujeo) Insulin degludec U100 and U200 (Tresiba) Insulin detemir U100 (Levemir) | 40.1% / 38.9% / 37.8% 3.2% / 2.3% / 1.4% 0.9% / 0.5% / 0.2% 11.5% / 12.4% / 13.2% 42.0% / 44.9% / 47.2% 2.3% / 0.9% /0.2% |
Uptake (new drug scenario) Insulin icodec Insulin glargine U100 (Basaglar) Insulin glargine U100 (Lantus) Insulin glargine U100 (Semglee) Insulin glargine U300 (Toujeo) Insulin degludec U100 and U200 (Tresiba) Insulin detemir U100 (Levemir) | 1.1% / 6.5% / 14.4% 39.7% / 36.4% / 32.4% 3.2% / 2.1% / 1.2% 0.9% / 0.5% / 0.1% 11.4% / 11.6% / 11.3% 41.5% / 42.0% / 40.4% 2.3% / 0.9% / 0.2% |
Cost of treatment | |
Cost of treatment (per standardized 30-day claim)a Insulin icodec Insulin glargine U100 (Basaglar) Insulin glargine U100 (Lantus) Insulin glargine U100 (Semglee) Insulin glargine U300 (Toujeo) Insulin degludec U100 and U200 (Tresiba) Insulin detemir U100 (Levemir) | $109 $75 $91 $62 $100 $113 $139 |
NA = not applicable; T1D = type 1 diabetes.
aWeighted average costs per standardized claim for each comparator in Ontario.
Summary of the Sponsor’s BIA Results
Results of the sponsor’s base-case BIA suggest that the incremental expenditures associated with the reimbursement of insulin icodec for the treatment of adult patients with T2DM who require insulin for glycemic control, as per its reimbursement request, would be $292,877 in year 1, $1,882,089 in year 2, and $4,385,909 in year 3, for a 3-year cumulative total of $6,560,875.
CADTH Appraisal of the Sponsor’s BIA
CADTH identified several key limitations to the sponsor’s analysis that have notable implications on the results of the BIA:
Estimated basal insulin dose for insulin icodec and long-acting basal insulin analogues is uncertain: The sponsor used the NMA results on absolute mean weekly basal insulin dose (at week 26) to calculate the drug acquisition cost for each treatment. Absolute mean weekly doses estimated for insulin icodec tended to be the lowest among therapies considered, which reduced drug acquisition cost of insulin icodec relative to long-acting basal insulin comparators. CADTH notes that the NMA results show wide credible intervals, which often included the potential for no significant dose differences between insulin icodec and long-acting basal insulin analogues. CADTH additionally notes that the NMA results are subject to the limitations described in the critical appraisal of the pharmacoeconomic submission, including presence of unknown and unmeasured effect modifiers. As such, CADTH’s ability to draw any conclusions from the basal insulin doses derived from the NMA is limited.
CADTH conducted a reanalysis by adopting average daily doses calculated from real-world evidence (RWE), which was procured by the sponsor. Data from IQVIA’s TSA and LRx datasets were used to compare the total insulin units used and patient counts in the previous year, from which, an average daily dose was calculated for each comparator. A weighted average based on the comparators’ market shares and RWE doses was used to estimate the dose for insulin icodec.
Proportion of claims assumed to originate from patients with type 1 diabetes (T1D) is overestimated: The sponsor removed 15% of claims from the BIA model, assuming that these were likely generated from patients with T1D. The sponsor states that this assumption was based on internal estimates. CADTH notes that, according to the Public Health Agency of Canada (PHAC), 9% of diabetes cases among adults living in Canada are estimated to be type 1,42 thus suggesting that the corresponding proportion of claims are likely to be generated by patients with T1D.
CADTH conducted a reanalysis by adopting published estimates to inform the proportion of claims that are likely to be generated by patients with T1D.
CADTH conducted a scenario analysis assuming that 15.7% of claims are likely to be originated from patients with T1D. The sponsor provided additional information regarding their internal estimate, which was derived from the: the total number of basal insulin patients (approximately 1.4 million),41 and the total number of patients with T1D receiving basal and bolus insulin (222,081).3
Projected market uptake of insulin icodec is uncertain. The sponsor assumed that insulin icodec would have a market share of 1%, 7% and 14% in Years 1, 2, and 3, respectively. Clinical expert feedback indicated that the anticipated adoption in the market seemed plausible, though subject to uncertainty. Participating drug plans acknowledged the likelihood of a substantial proportion of patients with T2DM indicating a preference to transition from once-daily to once-weekly insulin injections for the purpose of dosing convenience. CADTH acknowledges that the introduction of an insulin product that may reduce the injection burden on patients with T2DM has the potential to shift the prescribing landscape.
CADTH conducted a scenario analysis by adjusting the projected market share of insulin icodec to 10%, 20%, and 30% in Years 1, 2, and 3, respectively, to explore the impact of uncertainty on the budget.
CADTH Reanalyses of the BIA
CADTH revised the sponsor’s submitted analyses by adopting average daily doses calculated from RWE and using published estimates to inform the proportion of claims that are likely to be generated by patients with T1D. The changes made to derive the CADTH base case are described in Table 25.
Table 25: CADTH Revisions to the Submitted Budget Impact Analysis
Stepped analysis | Sponsor’s value or assumption | CADTH value or assumption |
|---|---|---|
Changes to derive the CADTH base case | ||
1. Estimated basal insulin dose for insulin icodec and long-acting basal insulin analogues is uncertain. | NMA results were used to derive daily doses across insulin therapies.
| RWE was used to derive daily doses across insulin therapies.
|
2. Proportion of claims assumed to originate from patients with T1D is overestimated. | 15% | 9% |
CADTH base case | Reanalyses 1 + 2 | |
NMA = network meta-analysis; RWE = real-world evidence; T1D = type 1 diabetes.
The results of the CADTH stepwise reanalysis are presented in summary format in Table 26 and a more detailed breakdown is presented in Table 27. In the CADTH base case, the 3-year budget impact of reimbursing insulin icodec as treatment for adult patients with T2DM requiring glycemic control is expected to be $15,256,316 (Year 1: $650,056; Year 2: $4,288,283; Year 3: $10,317,977).
Table 26: Summary of the CADTH Reanalyses of the BIA
Stepped analysis | Three-year total |
|---|---|
Submitted base case | 6,560,875 |
CADTH reanalysis 1 | 14,250,405 |
CADTH reanalysis 2 | 7,023,995 |
CADTH base case (Reanalyses 1 + 2) | 15,256,316 |
BIA = budget impact analysis.
CADTH conducted additional scenario analyses to explore remaining uncertainty associated with the potential budget impact, using the CADTH base case. Results are provided in Table 27.
Assuming the projected market share of insulin icodec to be 10%, 20%, and 30% in Years 1, 2, and 3, respectively.
Assuming 15.7% of claims are likely to be generated by patients with T1D.
Table 27: Detailed Breakdown of the CADTH Reanalyses of the BIA
Stepped analysis | Scenario | Year 0 (current situation) | Year 1 | Year 2 | Year 3 | Three-year total |
|---|---|---|---|---|---|---|
Submitted base case | Reference | 181,461,368 | 194,408,377 | 209,733,233 | 228,690,812 | 632,832,421 |
New drug | 181,461,368 | 194,701,254 | 211,615,322 | 233,076,720 | 639,393,296 | |
Budget impact | 0 | 292,877 | 1,882,089 | 4,385,909 | 6,560,875 | |
CADTH base case | Reference | 194,400,574 | 204,701,755 | 224,637,980 | 248,580,147 | 677,919,882 |
New drug | 194,400,574 | 205,351,811 | 228,926,263 | 258,898,125 | 693,176,198 | |
Budget impact | 0 | 650,056 | 4,288,283 | 10,317,977 | 15,256,316 | |
CADTH scenario analysis 1: Increased market uptake for insulin icodec | Reference | 194,400,574 | 204,701,755 | 224,637,980 | 248,580,147 | 677,919,882 |
New drug | 194,400,574 | 210,892,763 | 237,934,980 | 270,135,810 | 718,963,554 | |
Budget impact | 0 | 6,191,008 | 13,297,000 | 21,555,663 | 41,043,671 | |
CADTH scenario analysis 2: Assuming 15.7% of patients have T1D | Reference | 180,087,564 | 189,630,307 | 208,098,700 | 230,278,093 | 628,007,100 |
New drug | 180,087,564 | 190,232,501 | 212,071,252 | 239,836,395 | 642,140,148 | |
Budget impact | 0 | 602,195 | 3,972,552 | 9,558,302 | 14,133,049 |
BIA = budget impact analysis.
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up-to-date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third-party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec