CADTH Reimbursement Review
Ravulizumab (Ultomiris)
Sponsor: Alexion Pharma GmbH
Therapeutic area: Neuromyelitis optica spectrum disorder
This multi-part report includes:
Clinical Review
Pharmacoeconomic Review
Clinical Review
Abbreviations
AE
adverse event
AQP4
aquaporin 4
ARR
annualized relapse rate
C5
complement component 5
CDEC
Canadian Drug Expert Committee
CI
confidence interval
CNMSC
Canadian Network of Multiple Sclerosis Clinics
CNS
central nervous system
CSR
Clinical Study Report
EDSS
Expanded Disability Status Scale
GRADE
Grading of Recommendations Assessment, Development and Evaluation
HAI
Hauser Ambulation Index
HR
hazard ratio
HRQoL
health-related quality of life
Ig
immunoglobulin
IPTW
inverse probability of treatment weights
IST
immunosuppressive treatment
LS
least squares
MCID
minimally clinically important difference
MS
multiple sclerosis
NMA
network meta-analysis
NMOSD
neuromyelitis optica spectrum disorder
OR
odds ratio
PE
plasma exchange
PP
plasmapheresis
RCT
randomized controlled trial
SD
standard deviation
TSF
The Sumaira Foundation
VAS
visual analogue scale
Executive Summary
An overview of the submission details for the drug under review is provided in Table 1.
Table 1: Background Information of Application Submitted for Review
Item | Description |
|---|---|
Drug product | Ravulizumab (Ultomiris), 10 mg/mL and 100 mg/mL, concentrate for solution, IV infusion |
Sponsor | Alexion Pharma GmbH |
Indication | For the treatment of adult patients with anti-AQP4 antibody-positive NMOSD |
Reimbursement request | Per indication |
Health Canada approval status | NOC |
Health Canada review pathway | Standard |
NOC date | October 30, 2023 |
Recommended dose | Dosage according to body weight |
AQP4 = aquaporin-4; NMOSD = neuromyelitis optica spectrum disorder; NOC = Notice of Compliance.
Introduction
Neuromyelitis optica spectrum disorder (NMOSD) is a rare, inflammatory disease that affects the central nervous system (CNS), specifically the optic nerves and spinal cord, often leading to permanent blindness and paralysis.1-3 It is distinct from multiple sclerosis (MS) because of its association with serum aquaporin-4 (AQP4) immunoglobulin (Ig) G antibodies.4 Patients with NMOSD experience acute unpredictable attacks that can last from days to weeks and cause worsening symptoms.3 These attacks are recurrent, they occur in 80% to 90% of patients,5-7 and they can lead to permanent disabilities.3 The most common manifestation of an acute attack involves the inflammation of optic nerves (optic neuritis), which leads to eye pain and vision loss in 1 eye or both eyes. The clinical presentation also involves inflammation of the spinal cord (transverse myelitis), which can result in weakness or paralysis of the arms and legs, bladder or bowel control problems, sensory loss, and painful muscle spasms.1-3 NMOSD may involve brainstem syndromes, such as intractable nausea, vomiting, hiccups, facial nerve palsy, oculomotor dysfunction, and vertigo.8 Disease symptoms and cumulative damage associated with NMOSD are associated with poor health-related quality of life (HRQoL).9-11 At its worst, NMOSD can lead to fatal respiratory failure.2,12
Clinical deterioration in patients with NMOSD accumulates in a stepwise fashion after each attack and is often irreversible.1-3,13 Therefore, prevention of relapse is the key goal of therapy in the overall management of patients with NMOSD to minimize the amount of irreversible damage.5-7
NMOSD disproportionately affects females, with a reported 9:1 to 12:1 female-to-male ratio in patients with anti-AQP4 antibody-positive NMOSD.3,14 The reported mean age of disease onset is 40 years.15 Prevalence data for NMOSD in Canada are not available. The prevalence and incidence of neuromyelitis optica (NMO) range from 0.50 to 4.00 per 100,000 people and 0.053 to 0.40 per 100,000 people, respectively, and have been estimated in previous systematic reviews based on data from various countries.16 Regarding mortality, recent studies reported an NMOSD mortality rate from 3.3% to 7.0%.17-19 Other studies have estimated worldwide mortality rates for NMOSD that range from 9% to 32%, depending on age, relapse rate, and recovery from attacks.6,20
In Canada, NMOSD is diagnosed by a neurologist or physician who specializes in demyelinating disorders. Diagnostic criteria follow the 2015 consensus-based criteria developed by the International Panel for NMO Diagnosis.3 Diagnosis is based on clinical characteristics and anti-AQP4 antibody testing.2,3
Ravulizumab (Ultomiris) is a monoclonal antibody and a terminal complement inhibitor that binds to the complement protein C5 with high affinity and specificity, thereby inhibiting its cleavage to C5a (a proinflammatory anaphylatoxin) and C5b (the initiating subunit of the membrane attack complex [MAC or C5b-9]), and preventing the generation of MAC.21
Ravulizumab underwent standard review at Health Canada and received a Notice of Compliance on October 30, 2023. The relevant Health Canada indication is for the treatment of adult patients with anti-AQP4 antibody-positive NMOSD. The reimbursement request is fully aligned with the Health Canada indication. Ravulizumab is supplied as a 10 mg/mL or 100 mg/mL concentrate. The recommended ravulizumab IV maintenance dosing in adults (≥ 18 years of age) with NMOSD with a body weight of 40 kg or more is based on the patient’s body weight. Maintenance doses are administered every 8 weeks, starting 2 weeks after the loading dose.21 Ravulizumab should be administered by a qualified health care professional, per the product monograph.21
Ravulizumab was previously reviewed by CADTH “for the treatment of adult patients with paroxysmal nocturnal hemoglobinuria (PNH)” and received a reimburse recommendation from the CADTH Canadian Drug Expert Committee (CDEC) in March 2022.22 Ravulizumab was also previously reviewed by CADTH “for the treatment of adult and pediatric patients one month of age and older with atypical hemolytic uremic syndrome (aHUS) to inhibit complement-mediated thrombotic microangiopathy (TMA),” and received a recommendation for reimbursement with conditions from CDEC in March 2023.23 Also, ravulizumab was reviewed by CADTH “for the treatment of adult patients with anti-acetylcholine receptor (AChR) antibody-positive generalized myasthenia gravis (gMG),” and received a do not reimburse recommendation from CDEC in August 2023.24
The objective of this report was to perform a systematic review of the beneficial and harmful effects of ravulizumab for the treatment of adults with anti-AQP4 antibody-positive NMOSD.
Stakeholder Perspectives
The information in this section is a summary of input provided by the patient and clinician groups that responded to CADTH’s call for input and from clinical experts consulted by CADTH for the purpose of this review.
Patient Input
Two patient groups, MS Canada and The Sumaira Foundation (TSF), responded to CADTH’s call for patient input for the current review of ravulizumab.
MS Canada gathered information for this submission with a survey launched in 2023 that targeted people with NMOSD and their caregivers in Canada; there were 13 respondents. TSF gathered information through various surveys of patients and caregivers, patient narratives, focus groups, roundtables, discussions with key opinion leaders, ambassadors, TSF’s global medical advisory board, advisors, peer-reviewed medical literature, and TSF’s experience working in NMOSD communities.
The 2 patient groups indicated that NMOSD is more prevalent among women and that the disease is initiated with a severe attack and continues with subsequent devastating attacks that have a negative impact on vision, mobility, function, mental health, and the quality of life of patients. The disease has a tremendous impact on all aspects of patients' lives, including a negative effect on independence, their family and caregivers, community, employment, and social life.
The patient inputs stated that treatment for NMOSD involves IV steroids, IV Ig or plasmapheresis and/or plasma exchange, mofetil mycophenolate, and the off-label use of immunosuppressants to help prevent further attacks, with varying levels of therapeutic benefit that can partially manage the disease, worsening symptoms, and/or challenging side effects. There are some efficacious Health Canada–approved medications, such as eculizumab and satralizumab; however, access to these medications is very limited, and eculizumab is administered by infusion every 2 weeks, which can be onerous and disruptive to the lives of individuals living with NMOSD. According to patient inputs, patients need to have access to more treatment options that can prevent further attacks with less frequent infusion dosing and fewer side effects.
Ravulizumab is simply a more stable analogue of eculizumab that requires much less frequent dosing after initiation (every 8 weeks), which can improve treatment adherence.
Clinician Input
Input From Clinical Experts Consulted by CADTH
NMOSD is a rare and severe disease with a generally poor natural trajectory and an inherently high risk of relapse. Currently available therapies are often associated with an unacceptable harms profile and only provide suboptimal relapse prevention, resulting in the accumulation of irreversible neurologic disability, including paralysis and blindness. The clinical experts highlighted the unmet need for access to an effective treatment, which would make a huge difference in the lives of patients and their caregivers.
There are no formal treatment guidelines in Canada that specify which interventions should be used as first-line or second-line therapies. The clinical experts indicated that the treatment of individuals with NMOSD differs by province and territory, based on differential access to drugs. The primary goal of treatment for NMOSD is to prevent relapses, which, in turn, will prevent neurologic disability (including, but not limited to, paralysis and loss or impairment of vision) and mortality. There are many desirable downstream effects of early prevention and control of the disease; maintaining neurologic function will have a positive impact on a patient’s quality of life, decrease the risk of complications related to neurologic dysfunction, and, in turn, allow a patient to maintain independence, increase a patient’s ability to maintain employment, and reduce the burden on caregivers.
Oral glucocorticoids, azathioprine, mycophenolate mofetil, and rituximab are frequently used to prevent relapses in patients with NMOSD; however, many individuals with NMOSD have ongoing disease activity while receiving these treatments. Because the efficacy of corticosteroids is viewed as suboptimal, they are often used as adjunct therapy, adding to the harms profile. Although approved in Canada, satralizumab and eculizumab are rarely attainable for people living with NMOSD.
Access to ravulizumab is likely to cause a shift in the current treatment paradigm, as it addresses the underlying disease process of NMOSD with high efficacy. All individuals with anti-AQP4 antibody-positive NMOSD should be considered eligible to receive ravulizumab. The clinical experts emphasized that it would be inappropriate to recommend that patients try other treatments before initiating treatment with ravulizumab, as it is paramount to control the irreversible progression of NMOSD as early as possible.
Appropriate settings for the initiation and monitoring of treatment with ravulizumab are neurology clinics with professionals who have adequate expertise in NMOSD, such as neurologists with expertise or a subspecialty in MS or autoimmune neurology, and occasionally neuro-ophthalmology. Meningococcal vaccination should be mandatory in patients planning to receive this therapy.
Although the absence of relapse would be ideal, this may not be realistic because interindividual variations can be high. The severity of a relapse and the accumulation of disability are important factors to consider when determining response to therapy. Once stability is established, treatment response may be assessed every year. Patients may need to discontinue a treatment if they experience a severe relapse (e.g., require intubation and support on a ventilator), 2 or more relapses within 2 years (assessed on a case-by-case basis, depending on severity), or severe adverse events (AEs) while on treatment.
Clinician Group Input
One clinician group, the Canadian Network of Multiple Sclerosis Clinics (CNMSC) (authored by 1 clinician), responded to CADTH’s call for clinician group input. Clinician perspectives from the CNMSC were obtained through clinical experience, knowledge of the medical literature, and from clinicians across the country who specialize in this therapeutic area.
According to the clinician group, there is a variety of treatments available in Canada. Several therapies are, however, not specifically indicated for NMOSD. Other more efficacious therapies, such as monoclonal antibodies, have a Health Canada indication for NMOSD; however, access to these therapies is extremely limited due to their stringent funding coverage criteria. Failure of treatment, with even just 1 relapse, can lead to a profound, permanent disability, including blindness and paralysis.
Per the CNMSC, there is a large unmet need for high-efficacy, well-tolerated therapies for NMOSD in Canada that have a significant ability to prevent and/or reduce attacks. Use of some of the off-label therapies is limited because of many side effects and a lack of efficacy. Eculizumab is administered by IV infusion every 2 weeks, which is too onerous for some patients to tolerate. According to the clinician group, the best approach for patients is to use efficacious, safe, and tolerable therapy as soon after the first attack as possible to avoid all relapses, reduce the severity of attacks and the cumulative disability associated with them, and minimize AEs related to therapies. Ravulizumab would be the first therapy for patients with a confirmed diagnosis of NMOSD with a positive serum test for the anti-AQP4 antibody after their first relapse and/or attack, and for those who have severe AEs on first-line therapy.
According to the CNMSC, the prevention of a new attack, which includes vision loss, weakness, sensory impairment, or bladder and/or bowel dysfunction, is the outcome used to determine whether a patient is responding to treatment. The clinician group indicated that discontinuation of therapy should be considered for patients who have a new attack while on this therapy.
Drug Program Input
The drug programs provide input on each drug being reviewed through CADTH’s reimbursement review processes by identifying issues that may affect their ability to implement a recommendation. For the CADTH review of ravulizumab, the drug plans provided questions pertaining to the selection of comparators, criteria to determine eligibility, treatment algorithm for patients with NMOSD, and various considerations for the prescription, continuation, and discontinuation of therapy. These questions were addressed by the clinical experts consulted by CADTH for this review. Clinical expert responses have been included in the Drug Program Input section (Table 5).
Clinical Evidence
Systematic Review
Description of Studies
The 1 study was reviewed, CHAMPION-NMOSD (N = 58), was an externally placebo-controlled, open-label, phase III, multicenter trial designed to evaluate the efficacy and safety of ravulizumab in adults with anti-AQP4 antibody-positive NMOSD who had at least 1 relapse in the previous 12 months. The study had a single-arm treatment design and used the placebo group from the PREVENT (ECU-NMO-301) study as an external placebo comparator. The recent PREVENT study evaluated the efficacy and safety of eculizumab in preventing relapses in patients with anti-AQP4 antibody-positive NMOSD who had at least 2 relapses in the previous 12 months or 3 relapses in the previous 24 months, at least 1 of which occurred in the previous 12 months. Patients were randomly assigned in a 2:1 ratio to receive either eculizumab (n = 96) or a matching-administration placebo (n = 47) every 2 weeks.
The primary outcome in the study was time to first adjudicated on-trial relapse, which was defined as the new onset of neurologic symptoms or the worsening of existing neurologic symptoms, with an objective change on neurologic examination that persists for more than 24 hours confirmed by the treating physician. Neurologic signs and symptoms had to be attributed to NMOSD (e.g., not to other identifiable causes, such as an infection). On-trial relapses were independently reviewed by the relapse adjudication committee, which consisted of physicians who have particular expertise in NMOSD and who conduct independent reviews of all on-trial relapses.
Secondary outcomes in the study included function, measured by the Hauser Ambulation Index (HAI), which is a rating scale developed to assess mobility by evaluating the time and effort used by a patient to walk 8 m. The scale ranges from 0 to 9, with 0 being the best score (asymptomatic; fully ambulatory with no assistance) and 9 being the worst (uses a wheelchair; unable to transfer self independently). Function was also assessed using the Expanded Disability Status Scale (EDSS) score, an ordinal clinical rating scale that ranges from 0 (normal neurologic examination) to 10 (death) in half-point increments. The EDSS quantifies disability in the 7 Kurtzke functional systems (pyramidal, cerebellar, brainstem, sensory, bowel and bladder, visual, and cerebral); in conjunction with ambulation, disabilities are rated in the context of a standard neurologic examination, and these ratings are used together with observations and information concerning the patient’s mobility, gait, and use of assistive devices to assign a score.
Secondary outcomes in the study also included HRQoL, which was assessed using the EQ-5D questionnaire, a generic preference-based HRQoL instrument that consists of a visual analogue scale (VAS) and a composite index score of 5 dimensions: mobility, self-care, usual activities, pain/discomfort, and anxiety/depression. HRQoL was also assessed as an exploratory outcome using the ||||| |||| |||||| |||||| ||||||||||||||| ||||||||||||||||| ||||||||||||| |||||||| || |||||| ||||||| ||||| || ||||||| ||| ||| ||||| |||||||||||| ||| ||||| |||||||| || || ||||| ||||||||| |||| ||||||||| ||||||||| ||||||||| |||||| ||||||||| |||| ||||||||||| ||||||||| ||| ||||||||||| |||||| ||||| ||||||| ||||||| ||||||| |||||| ||||||| ||||||||| ||| |||||| |||||||||||| ||| ||||||||||||| |||| ||||||||||||| |||||||| || |||||||| |||||| ||| |||||| |||||| ||||||| |||| ||||| ||||||||||| |||||| |||||| |||||| ||| |||||||||| |||| |||||| ||||||| || |||||||||||||| |||||| |||||| ||| |||||||| || || ||||||||||| ||||||| ||||| ||| |||||||||||| |||||||||| ||||| ||||||||||||| |||||||||| ||||||||| |||||| |||||| ||| |||||| |||||||| ||| ||||||| ||||||||| ||||||||||||||||| ||| |||||||| ||| |||| |||||||||| ||||||| ||| ||||| |||||||| |||||| ||||||| ||| ||||||| ||| ||||| ||||||||||||| ||||| ||||||||| |||||| ||||||||||||||
Efficacy Results
NMOSD Attack or Relapse
The outcome of relapse was considered the preferred and most reliable end point by clinical experts. In patients with anti-AQP4 antibody-positive NMOSD, the use of ravulizumab was associated with a hazard ratio (HR) of 0.014 (95% confidence interval [CI], 0.000 to 0.103) versus placebo. The log-rank test yielded a significance level of P < 0.0001. The median analysis follow-up time was 73.50 weeks (range, 11.00 to 117.71 weeks) for the ravulizumab group and 36.00 weeks (range, 1.86 to 117.71 weeks) for the placebo arm. Throughout the study follow-up, no patients in the ravulizumab group reported a primary outcome event of adjudicated on-trial relapse, compared with 20 patients (42.6%) in the placebo group from the PREVENT study, yielding a relative relapse risk reduction of 98.6% (95% CI, 89.7% to 100.0%). Therefore, treatment with ravulizumab results in a clinically important reduction in the probability of having an NMOSD relapse, compared to placebo.
Results from sensitivity analyses, which aimed to assess whether any imbalances in observed baseline characteristics due to trial design could be sufficient to confound the observed treatment effect, were similar to those from the primary analysis. Results were also consistent across prespecified and posthoc subgroups.
Function
Treatment with ravulizumab likely results in a clinically important reduction in the proportion of patients who have a worsening of HAI score from baseline at the primary data cut-off, compared to placebo (odds ratio [OR] = 0.155; 95% CI, 0.031 to 0.771). The proportion of patients with a clinically important worsening from baseline through to the end of the study period in HAI score was 3.4% (2 of 58 patients) in the ravulizumab arm and 23.4% (11 of 47 patients) in the placebo arm.
The use of ravulizumab may result in a clinically important reduction in the proportion of patients who have worsening from baseline in EDSS score at the primary data cut-off, compared to placebo; however, the evidence is very uncertain, as the CI for difference between groups includes the possibility of no difference. The proportion of patients with a clinically important worsening from baseline through to the end of the study period in EDSS score was 10.3% (6 of 58 patients) in the ravulizumab arm and 23.4% (11 of 47 patients) in the placebo arm, yielding an OR of 0.332 (95% CI, 0.106 to 1.042).
Health-Related Quality of Life
Treatment with ravulizumab may result in a clinically important difference in HRQoL at the primary data cut-off, compared to placebo, as measured by the EQ-5D index score, the EQ-5D VAS score, and ||| ||||| |||||||| ||||||||| score; however, the evidence is very uncertain, as the CI for difference between groups includes the possibility of no difference. The mean change from baseline through to the end of the study period in EQ-5D index score was 0.01 (standard deviation [SD] = 0.152) in the ravulizumab arm and –0.04 (SD = 0.212) in the placebo arm, yielding a difference in least squares (LS) mean of 11.15 (95% CI, –0.32 to 22.62). For the EQ-5D VAS score, the mean change from baseline to the end of the study period was 2.6 (SD = 14.07) in the ravulizumab arm and 0.6 (SD = 16.39) in the placebo arm; the difference in LS mean was 13.38 (95% CI, 1.35 to 25.41). Finally, for the ||||| |||||||| ||||||||| |||||| ||| |||| |||||| |||| |||||||| || ||| || ||||| |||||| ||| ||||| |||||||| || ||| ||||||||||| ||| ||| |||| ||| |||||| || ||| ||||||| |||| || ||||||| || |||||||||| ||||||| ||||| ||| |||||||||
||||||||||| |||||| |||| ||| |||||| |||||||||||| ||||||||| |||||||||| || ||||| |||||| ||||||||| ||||| || ||| ||||||| |||| ||||||| |||||||| || |||||||| ||| |||| |||||| |||| |||||||| ||||||| ||| ||| || ||||| |||||| ||| |||| ||| |||||| || ||| ||||||||||| ||| ||| |||| ||| ||||||| || ||| ||||||| |||| || ||||||| || |||||||||| ||||||| ||||| ||| |||||||||
Visual Acuity
||| |||||||| || |||| ||||||||| ||||| ||| |||||| || ||||||||||| || |||| || ||| ||||||| |||| ||||||| |||||||| || |||||||| ||| |||| |||||| |||| |||||||| ||||||| ||| ||| || ||||| |||||| ||| |||||| ||| ||||||| || ||| ||||||||||| ||| ||| |||||| ||| ||||||| || ||| ||||||| |||| || ||||||| || |||||||||| ||||||| ||||| ||| |||||||| || || ||||||||| || ||| |||||||||||| ||||||||||| |||||||| || ||||||| ||| |||||||||||||| ||| |||| |||| ||||| ||| |||||||||||| |||||| |||| |||||||| || |||||||||| |||| ||| ||||||| || |||||||| || ||| ||||||||||| ||||| ||| |||| ||| |||| ||||| |||||| || |||||||| |||| |||||||| ||||||||| ||| ||||| ||||| || ||| ||||||| |||||||||| |||||| || ||||||||||| || ||||| || ||||| |||||| ||| || ||||||||||||||| |||||| |||||| || |||| ||||||||| |||| |||||||| |||| ||| ||||||||||| || ||| ||||||| || ||||||||||| ||||| ||||| ||| || |||||| |||| |||||||| || ||| ||||||||||| ||||| || ||||| || ||||| |||||| || || ||||||||||||||| |||||| ||||||| || |||| ||| |||||||| ||| ||| ||||||| ||||| |||||||||||||||| |||||||||
Health Care Resource Use
||| |||||| || ||||||||||| || |||||||||||||||| || |||| ||||||||| |||| |||||||| |||| ||| ||||||||||| || ||| ||||||| || ||||||||||| |||||||||| || || |||||||| ||||||| |||| |||||||||||| || ||| ||||||||||| |||||| |||||||| |||| |||||||| || |||| ||||||| ||||| || || |||||||| |||| ||||||||| |||||||||||||||| |||| ||| ||| || ||||||||| ||| ||||||||| || ||||| ||||||| || |||| ||| |||||||| ||| ||| ||||||| ||||| |||||||||||||||| |||||||||
Harms Results
A total of 93% of patients receiving ravulizumab reported at least 1 AE, and 19% of patients reported at least 1 serious AE, the most frequently reported of which were infections and infestations. However, ravulizumab appeared to be well tolerated; only 1 patient discontinued due to AEs, and the reason for withdrawal was infection. No deaths were reported in the study. Meningococcal infection was an AE of special interest. Two patients experienced meningococcal infection during the primary treatment period. No new meningococcal infections were reported during the long-term extension period.
The clinical experts indicated that the overall harms profile of ravulizumab in the CHAMPION-NMOSD study did not raise any particular safety signals, with the exception of meningococcal infections; as such, all patients should receive meningococcal vaccination before the start of ravulizumab therapy, per the product monograph.
Critical Appraisal
The CHAMPION-NMOSD study had a single-arm treatment design; the placebo group came from the PREVENT study as an external placebo comparator. This may have introduced a risk of bias leading to uncertainty about the estimates. The overall assessment suggests, however, that the 2 trials likely feature sufficient similarity to ensure a valid comparison, and that the differences observed in the patient populations might not substantially affect the results of the primary outcome of relapse prevention. According to the clinical experts consulted by CADTH, the differences observed in the number of historical relapses between groups is not expected to have a substantial impact on the risk of future relapses; in addition, the annualized relapse rate (ARR) in the previous 12 months and 24 months between treatment groups was consistent with the assumption that both groups were actually having a relatively similar evolution in terms of relapse frequency. Some level of uncertainty could be mitigated by the magnitude of the relapse risk reduction observed with ravulizumab treatment in the CHAMPION-NMOSD study, which was considered large and constant over time, and compensated for potential biases and the known variability in disease progression. In addition, results from sensitivity analyses of the primary outcome suggest that the findings are robust and statistically infer that imbalances in patient populations were not likely to have had a meaningful impact on the estimates.
Secondary efficacy outcomes of function, HRQoL, and visual acuity were assessed adequately using appropriate tools; however, no studies assessed their validity or reliability specifically in patients with NMOSD. Minimally clinically important differences (MCIDs) were established through clinical expert input, as none could be identified in the literature for this patient population. The thresholds used in the study for dichotomous outcome assessment (HAI and EDSS) were considered appropriate and consistent with clinical practice, according to the clinical experts. The clinical experts indicated that loss of function and loss of quality of life are cumulative over time, and that the magnitude of worsening depends on the severity of the relapse; therefore, measurement of these outcomes may be less sensitive to changes in the context of a clinical trial. The goal for patients receiving active treatment would be to maintain a stable status, while patients in the placebo group would be expected to have a worsening status based on natural disease trajectory; as follow-up only continues until a first on-trial relapse for ethical reasons (in the CHAMPION-NMOSD study, median follow-up time was 73.50 weeks for the ravulizumab group and 36.00 weeks for the placebo arm), assessment of these outcomes may lead to an underestimation of the active treatment effect over time.
Findings from the CHAMPION-NMOSD study can be considered generalizable to patients with NMOSD in Canada, as the study population was considered representative of patients in clinical practice; disability was consistent with what is expected in an NMOSD population. The primary outcome of relapse prevention is consistent with the treatment goals for patients with NMOSD in clinical practice, according to the clinical experts. Relapse assessment in the trial was performed in a manner similar to that in clinical practice. The clinical experts confirmed that follow-up duration was long enough for the trial to adequately capture relapses, considering the inherently high risk of relapse in patients with anti-AQP4 antibody-positive NMOSD.
GRADE Summary of Findings and Certainty of the Evidence
For nonrandomized comparative studies, such as a single-arm trial with an external control, CADTH follows the Grading of Recommendations, Assessment, Development, and Evaluations (GRADE) approach. The CADTH review team assessed study limitations (which refers to internal validity or risk of bias), inconsistency across studies, indirectness, imprecision of effects, and publication bias to present these important considerations. Because of the inherent risk of bias from the absence of randomization and differences in patient populations, the certainty of evidence of the single-arm trials started at low certainty, with opportunity for rating up.
When possible, certainty was rated in the context of the presence of an important (nontrivial) treatment effect; if this was not possible, certainty was rated in the context of the presence of any treatment effect (i.e., the clinical importance is unclear). In all cases, the target of the certainty of evidence assessment was based on the point estimate and where it was located relative to the threshold for a clinically important effect (when a threshold was available) or to the null.
The selection of outcomes for GRADE assessment was based on the sponsor’s Summary of Clinical Evidence, consultation with clinical experts, and input received from patient and clinician groups and public drug plans. The following list of outcomes was finalized in consultation with expert committee members:
NMOSD attack or relapse
function
HRQoL
visual acuity
health care resource use
harms.
Indirect Comparisons
Description of Network Meta-Analysis
The sponsor submitted indirect evidence in the form of a |||||||| |||, the objective of which was to determine the relative treatment effects between ravulizumab, ||||||||||| ||||||||||||| ||| |||||||||||| for the treatment of adults with anti-AQP4 antibody-positive NMOSD. Analyses were performed ||| |||||||||||||| ||||| || ||||| ||||||||| ||||||||| |||||||||||| ||||||||||| |||||||| ||| ||||| |||||||||||||||| |||||||| Outcomes of interest for evaluation included |||||||| ||||| || ||||| |||||||| |||||||||| ||||||| |||||||||| ||| |||||||||||||| ||||||| || |||| ||||||| ||||||||| ||| |||||||| |||||||||| |||||| ||||| ||||||| ||||||| ||||||||||| ||||||||||||| |||||||| |||||| |||||||||| ||||| ||||| |||||| |||||||| |||||| ||||| ||||| |||||| ||| ||||||| ||||| |||| |||||| ||||| ||||
Table 2: Summary of Findings for Ravulizumab vs. Placebo for Patients With Anti-AQP4 Antibody-Positive NMOSD in the CHAMPION-NMOSD Study (PREVENT Placebo Group as the External Control)
Outcome and follow-up | Patients (studies), n | Relative effect (95% CI) | Absolute effects | Certainty | What happens | ||
|---|---|---|---|---|---|---|---|
Placebo | New drug | Difference (95% CI) | |||||
NMOSD attack or relapse | |||||||
Patients with an adjudicated relapse during the primary treatment period Follow-up: primary analysis data cut-off | n = 58, ravulizumab n = 47, placebo (1 RCT) | RRR = 98.6 (89.7 to 100.0) | 426 per 1,000 patients | 0 per 1,000 patients | 426 fewer per 1,000 patients | Higha | Ravulizumab results in a clinically important reduction in the probability of having an NMOSD relapse at the primary data cut-off, compared to placebo |
Function | |||||||
Patients with clinically important worsening from baseline in HAI score Follow-up: Primary analysis data cut-off | n = 58, ravulizumab n = 47, placebo (1 RCT) | OR = 0.155 (0.031 to 0.771) | 234 per 1,000 patients | 34 per 1,000 patients | 200 fewer per 1,000 patients | Moderateb | Ravulizumab likely results in a clinically important reduction in the proportion of patients who have worsening from baseline in HAI score at the primary data cut-off, compared to placebo |
Patients with clinically important worsening from baseline in EDSS score Follow-up: primary analysis data cut-off | n = 58, ravulizumab n = 47, placebo (1 RCT) | OR = 0.332 (0.106 to 1.042) | 234 per 1,000 patients | 103 per 1,000 patients | 131 fewer per 1,000 patients | Very lowc | Ravulizumab may result in a clinically important reduction in the proportion of patients who have worsening from baseline in EDSS score at the primary data cut-off, compared to placebo; however, the evidence is very uncertain |
HRQoL | |||||||
Change from baseline in EQ-5D index score Follow-up: primary analysis data cut-off | n = 58, ravulizumab n = 47, placebo (1 RCT) | NR | Observed mean (SD): –0.043 (0.2115) LS mean (SE): 46.84 (4.229) | Observed mean (SD): 0.005 (0.1522) LS mean (SE): 57.99 (3.793) | LS mean difference: 11.15 (–0.32 to 22.62) | Very lowc | Ravulizumab may result in a clinically important difference in EQ-5D index score at the primary data cut-off, compared to placebo; however, the evidence is very uncertain |
Change from baseline in EQ-5D VAS score Follow-up: primary analysis data cut-off | n = 58, ravulizumab n = 47, placebo (1 RCT) | NR | Observed mean (SD): 0.6 (16.39) LS mean (SE): 45.61 (4.343) | Observed mean (SD): 2.6 (14.07) LS mean (SE): 58.99 (3.874) | LS mean difference: 13.38 (1.35 to 25.41) | Very lowc | Ravulizumab may result in a clinically important difference in EQ-5D VAS score at the primary data cut-off, compared to placebo; however, the evidence is very uncertain |
|||||| |||| |||||||| || ||||| |||||||| ||||||||| ||||| |||||||||||| ||||||| |||||||| |||| ||||||| | ||| ||| |||||||| |||||||| || |||| | || | |||||||| |||| ||||||||||| |||||||| | |||||||| |||| ||||||||||| |||||||| | ||| | |||| ||| | ||||||||||| ||| |||||| |||||||||||| ||||||||| |||||||||| || ||||| |||||||| ||||||||| ||||| || ||| ||||||| |||| ||||||| |||||||| || |||||||| |||||||| ||| |||||||| || |||| |||||||||| |
|||||| |||| |||||||| || ||||| |||||| ||||||||| ||||| |||||||||||| ||||||| |||||||| |||| ||||||| | ||| |||||||| |||||||| || |||| | || | |||||||| |||| ||||||||||| ||||||||| | |||||||| |||| ||||||||||| |||||||| | ||| | |||| || | ||||||||||| ||| ||| |||||| ||||||||||| ||||||||| |||||||||| || ||||| |||||| ||||||||| ||||| || ||| ||||||| |||| ||||||| |||||||| || |||||||| |||||||| ||| |||||||| || |||| |||||||||| |
Visual acuity | |||||||
|||||| |||| |||||||| || |||| |||||||||||| ||||||| |||||||| |||| ||||||| | ||| |||||||| |||||||| || |||| | || | |||||||| |||| |||||||||||| |||||||| | |||||||| |||| ||||| ||||||| |||||||| | ||| | |||| || | ||| |||||||| || |||| ||||||||| ||||| ||| |||||| || ||||||||||| || |||| || ||| ||||||| |||| ||||||| |||||||| || ||||||||| |
|||||||| |||| || |||||| |||| |||||| |||||||| || ||||| || ||||| |||||| |||||||||||| ||||||| |||||||| |||| ||||||| | ||| |||||||| |||||||| || |||| | || | || | ||||| ||| ||||| |||||||| | || | |||| ||| | ||| |||||||| || |||| ||||||||| ||||| ||| |||||| || ||||||||||| || ||||| |||||| |||| |||||||| |||| ||| ||||||||||| || ||| ||||||| || ||||||||||| ||||| |
|||||| |||| |||||||| || ||||||||||||||| |||||| |||||| |||||||||||| ||||||| |||||||| |||| ||||||| | ||| |||||||| |||||||| || |||| | || | || | |||||||| |||| ||||| |||| |||||| | || | |||| ||| | ||| |||||||| || |||| ||||||||| ||||| ||| |||||| || ||||||||||| || ||||||||||||||| |||||| |||||| |||| |||||||| |||| ||| ||||||||||| || ||| ||||||| || ||||||||||| ||||| |
Health care resource use | |||||||
|||||||| |||| ||||||||||||||| |||||||||||| ||||||| |||||||| |||| ||||||| | ||| |||||||| |||||||| || |||| | || | || | ||| ||| ||||| |||||||| | || | |||| ||| | ||| |||||||| || |||| ||||||||| ||||| ||| |||||| || ||||||||||| || |||||||||||||||| |||| |||||||| |||| ||| ||||||||||| || ||| ||||||| || ||||||||||| ||||| |
Harms | |||||||
Patients with AEs Follow-up: primary analysis data cut-off | n = 58, ravulizumab n = 47, placebo (1 RCT) | NR | NR | 931 per 1,000 patients | NA | Very low | The evidence is very uncertain about the effect of ravulizumab on AEs, compared with any comparator, in the absence of comparative data |
Patients with SAEs Follow-up: primary analysis data cut-off | n = 58, ravulizumab n = 47, placebo (1 RCT) | NR | NR | 190 per 1,000 patients | NA | Very low | The evidence is very uncertain about the effect of ravulizumab on SAEs, compared with any comparator, in the absence of comparative data |
AE = adverse event; AQP4 = antiaquaporin-4; CI = confidence interval; EDSS = Expanded Disability Status Scale; HAI = Hauser Ambulation Index; HRQoL = health-related quality of life; LS = least squares; NA = not applicable; NMOSD = neuromyelitis optica spectrum disorder; NR = not reported; OR = odds ratio; ||||||||||||||| |||||||||| |||||; RCT = randomized controlled trial; RRR = relative risk reduction; SAE = serious adverse event; SD = standard deviation; SE = standard error; VAS = visual analogue scale.
Note: Study limitations (which refer to internal validity or risk of bias), inconsistency across studies, indirectness, imprecision of effects, and publication bias were considered when assessing the certainty of the evidence. All serious concerns in these domains that led to the rating down of the level of certainty are documented in the table footnotes.
aRated up 2 levels due to the magnitude of relapse risk reduction observed with ravulizumab treatment in the CHAMPION-NMOSD study, which was large and constant over time, and compensated for potential biases and the known variability in disease progression.
bRated up 1 level due to the magnitude of effect observed with ravulizumab on preventing clinically important worsening from baseline in HAI score.
cRated down 1 level for serious imprecision because the CI for the difference between groups includes the possibility of no difference. MCID was established through clinical expert input.
Source: CHAMPION-NMOSD CSR.26 Details included in the table are from the sponsor’s Summary of Clinical Evidence.27
A total of |||||| |||||||| |||||| |||| |||||||| |||| ||| |||||||| |||| ||| ||| |||| ||||||||||||||| |||||||| ||||||||||| |||||||||| ||| ||||||||||| ||| |||||||||||| ||||| |||||||||||| ||| |||||||||||| |||||| ||||||||||| ||||||||||| |||||||| |||||||| |||||||||||| ||||||| ||||||||| |||||||| |||||||| ||| |||| ||||| |||| |||||||| |||| ||||||||| ||| |||||||| |||| |||||||||||||| ||| ||||||| ||| ||||||||| |||||||||| || |||||||||||
||| ||||| |||| || ||| ||||||| |||||| |||| |||| || ||||| ||||||||| |||||||| |||||| |||| ||||| |||||| ||| ||||||| ||||||||| ||||||||| ||||| |||||| ||| ||||||||| |||||| |||| |||||| |||| |||||| ||||||||| ||||||||||| ||| ||| ||| |||||||| || ||| |||||| ||| ||| ||||||||| || ||||||||| ||||||| ||| |||||||||| ||| |||| ||| || |||||||| |||||| |||| ||||| ||||| |||||| ||| |||||||
Efficacy Results
||||||||| |||||||| ||| |||||||||||||||| |||||||||||| || ||||| |||||||||||| || ||||| ||||||| |||||| |||||||||| || |||||||| || ||||||||||| || ||||||||||| ||||||| |||| |||||||| || |||| |||||| |||||||||| ||||||||||||||| |||||||||||||| ||| |||||||||||||||| ||| |||||||| ||||||||| |||||| || ||||||||||||||| ||| |||||||| || ||||||||| ||| ||||||| || |||||||||| ||||||||||||| ||| ||||||||| |||||||||||| ||||||||| |||||||| || ||||||||||||| |||| |||| |||||| || ||||||||||||| |||||||| |||||||| ||| |||||||||||||||| |||||||||||| || ||||| |||||||||||| || ||||| ||||||| |||||| |||||||||| || |||||||| || ||||||||||| || ||||||||||| ||||||| |||| |||||||| || |||| |||||| |||||||||| ||||||||||||||| |||||||||||||| ||| |||||||||||||||| ||| |||||||| ||||||||| |||||| || ||||||||||||||| ||| |||||||| || ||||||||| ||| ||||||| || |||||||||| ||||||||||||| ||| ||||||||| |||||||||||| ||||||||| |||||||| || ||||||||||||| |||| |||| |||||| |||||||||||||||||||||| |||||||| ||| |||||||||||||||| |||||||||||| || ||||| |||||||||||| || ||||| ||||||| |||||| |||||||||| || |||||||| || ||||||||||| || ||||||||||| ||||||| |||| |||||||| || |||| |||||| |||||||||| ||||||||||||||| |||||||||||||| ||| |||||||||||||||| ||| |||||||| ||||||||| |||||| || ||||||||||||||| ||| |||||||| || ||||||||| ||| ||||||| || |||||||||| ||||||||||||| ||| ||||||||| |||||||||||| ||||||||| |||||||| || ||||||||||||| |||| |||| |||||| |||||||||||||||||||||| |||||||| ||| |||||||||||||||| |||||||||||| || ||||| |||||||||||| || ||||| ||||||| |||||| |||||||||| || |||||||| || ||||||||||| || ||||||||||| ||||||| |||| |||||||| || |||| |||||| |||||||||| ||||||||||||||| |||||||||||||| ||| |||||||||||||||| ||| |||||||| ||||||||| |||||| || ||||||||||||||| ||| |||||||| || ||||||||| ||| ||||||| || |||||||||| ||||||||||||| ||| ||||||||| |||||||||||| ||||||||| |||||||| || ||||||||||||| |||| |||| |||||| |||||||||||||||||||||| |||||||| ||| |||||||||||||||| |||||||||||| || ||||| |||||||||||| || ||||| ||||||| |||||| |||||||||| || |||||||| || ||||||||||| || ||||||||||| ||||||| |||| |||||||| || |||| |||||| |||||||||| ||||||||||||||| |||||||||||||| ||| |||||||||||||||| ||| |||||||| ||||||||| |||||| || ||||||||||||||| ||| |||||||| || ||||||||| ||| ||||||| || |||||||||| ||||||||||||| ||| ||||||||| |||||||||||| ||||||||| |||||||| || ||||||||||||| |||| |||| |||||| |||||||||||||||||||||| |||||||| ||| |||||||||||||||| |||||||||||| || ||||| |||||||||||| || ||||| ||||||| |||||| |||||||||| || |||||||| || ||||||||||| || ||||||||||| ||||||| |||| |||||||| || |||| |||||| |||||||||| ||||||||||||||| |||||||||||||| ||| |||||||||||||||| ||| |||||||| ||||||||| |||||| || ||||||||||||||| ||| |||||||| || ||||||||| ||| ||||||| || |||||||||| ||||||||||||| ||| ||||||||| |||||||||||| ||||||||| |||||||| || ||||||||||||| |||| |||| |||||| |||||||||||||||||||||| |||||||| ||| |||||||||||||||| |||||||||||| || ||||| |||||||||||| || ||||| ||||||| |||||| |||||||||| || |||||||| || ||||||||||| || ||||||||||| ||||||| |||| |||||||| || |||| |||||| |||||||||| ||||||||||||||| |||||||||||||| ||| |||||||||||||||| ||| |||||||| ||||||||| |||||| || ||||||||||||||| ||| |||||||| || ||||||||| ||| ||||||| || |||||||||| ||||||||||||| ||| ||||||||| |||||||||||| ||||||||| |||||||| || ||||||||||||| |||| |||| |||||| |||||||||||||||||||||| |||||||| ||| |||||||||||||||| |||||||||||| || ||||| |||||||||||| || ||||| ||||||| |||||| |||||||||| || |||||||| || ||||||||||| || ||||||||||| ||||||| |||| |||||||| || |||| |||||| |||||||||| ||||||||||||||| |||||||||||||| ||| |||||||||||||||| ||| |||||||| ||||||||| |||||| || ||||||||||||||| ||| |||||||| || ||||||||| ||| ||||||| || |||||||||| ||||||||||||| ||| ||||||||| |||||||||||| ||||||||| |||||||| || ||||||||||||| |||| |||| |||||| || |||||||||||||
Harms Results
||||| |||| ||| |||||||| || ||| ||||||||| ||||
Critical Appraisal
The sponsor conducted a network meta-analysis (NMA) using |||||||| |||||||| ||||| ||||| ||||||| |||||| for all outcomes. This was a reasonable method to apply, given the availability of |||||||||| ||||||| |||| for only 2 of the included studies.
Comparisons in all NMAs were based on ||||| |||||| of trials and ||||| ||||||| of patients in each trial. The networks were linked to ravulizumab through |||||| ||||||| ||||| that was not part of the ||||||||||| trial. The validity of the ravulizumab comparative results relies entirely on the putative comparability of the |||||||| ||||||| || ||| ||||||||||| ||||| || ||||||||. The possibility of residual confounding exists when 2 nonrandomized groups ||||| ||||||||||| ||||||||| ||| ||| |||||||| |||||||| are being compared.
The sponsor’s decision to perform |||||||| NMAs based on the potential effect modifier of |||||||||| ||||||||||||||||| ||||||| was appropriate. The disadvantage of doing this was to create ||||| |||||||| |||| ||||| ||||||| || ||||||| There were other sources of heterogeneity that were not explored in the NMAs, and it is not clear if the homogeneity assumption is correct. These sources include the following:
The sponsor performed a quality assessment of the individual trials, but the results were not provided and no information was provided on how they used the results of the quality assessment in the NMA.
||||| ||||||||| ||| ||| |||| |||||| || |||||||| ||| ||||||| |||||||| || ||| ||||| |||||||| There could have been more residual effects from ||||| ||||||||| ||||||| || |||||||| ||| |||||||, compared to the other studies, because ||||||||| was not permitted in the 3 months before study start in the CHAMPION-NMOSD and PREVENT studies, whereas it was not permitted within |||||| of study start in the other trials.
The ||||||||| |||||||| |||||||| ||||||| ||| |||||| ||| ||| |||||||| || ||||||| ||||| |||| ||||||||. The randomized period in the N-MOmentum study ended at 197 days to limit exposure to placebo, whereas placebo was continued until the end of study || ||||| |||||| ||||| |||||||||.28 The |||||||||||| ||||||| |||||||| ||||| ||||||| |||| |||||| ||||||| |||||| ||||. The sponsor used |||||||||| ||||| |||||||| in their sensitivity analyses for the outcome of |||||||. The factors selected by the sponsor for adjustment in the |||||||||| ||||| were reasonable, but there was not enough information provided to assess the validity of the sensitivity analyses. Some analyses in the base-case results that favoured |||||||||||, no longer favoured ||||||||||| ||||| ||| ||| ||||||||||| |||||||| were performed for the |||| || ||||| ||||||| ||||. These included comparisons to |||||||||| ||||||||||||||||| ||||||||| ||||||||||| ||||||||| ||||||||||| ||||||| ||||||||| ||| |||||||||||| |||||||||||| ||||||| ||||||||||
Summary of NMA
Results of the sponsor’s NMA favoured ||||||||||| || |||| ||||||||||| |||||||| but the results were ||| |||||||||| |||||| ||| ||||||||| ||| |||| || |||||||| ||| ||||||| |||||||| ||||||||||| |||| |||||||||| || ||| |||||||||||||||| ||||||| ||||||| ||| ||| ||| ||| ||||||||||| ||||||| || ||| ||||||||||| ||||||| |||||||| ||||||| |||||||| ||||||||||| |||| |||||||||||| ||| ||| |||||||||||||||| ||||||| ||| ||||||||||| ||||||| ||| ||| ||| ||| ||||||||||| ||||||| |||||||| ||||||| |||||||| ||||||||||| |||| |||||||||||| || ||| ||||||||||| |||||||| ||||| |||||||| ||||| ||||||||| ||| ||||||||||| || |||||||| ||||||||||| ||||||| || ||||| ||||||| || ||||||||||||| ||||||| ||| ||||||| || ||| ||||||||| ||||||||||||||||||||| |||||||||| || |||||||||||| |||| ||||||||||| ||| ||| |||||||| ||| ||| || ||| ||||||| ||||||||| ||| ||||| ||||||| |||| ||||||||| || ||||||||| ||||||| ||||| |||| || ||||| ||||||||||| ||||||| ||| ||||||||||| ||| ||| || ||| ||||||||||| || ||| || ||| ||||| |||||||| ||| ||||| ||||||||||| ||| ||||| ||||| |||| || |||| ||| || ||| ||||||||||| ||| ||||||| || ||| ||||||| ||||||||| || ||||||||| || ||| |||||||| |||| || ||||| ||| ||||||||||
Conclusions
Findings from the CHAMPION-NMOSD study suggest that ravulizumab results in a clinically meaningful prevention of relapses, compared with placebo, in patients with anti-AQP4 antibody-positive NMOSD, which is paramount in preventing the accumulation of disability in patients. The use of a single-arm treatment design, with the placebo group from the PREVENT study as an external placebo comparator, may have introduced a risk of bias, leading to uncertainty surrounding the estimates. Overall assessment suggests, however, that the 2 trials likely feature sufficient similarity to ensure a valid comparison, and that the differences observed in patient populations might not meaningfully impact the risk of relapse, according to the clinical experts consulted by CADTH. Concern over this uncertainty was mitigated by the magnitude of relapse risk reduction observed with ravulizumab treatment in the CHAMPION-NMOSD study, which was considered large and constant over time, and compensated for potential biases and the known variability in disease progression. In addition, results from sensitivity analyses of the primary outcome suggest that the findings are robust, and statistically infer that imbalances in patient populations were not likely to have a substantial impact on the estimates. Ravulizumab may also have a clinically significant impact on function and HRQoL, although there is some uncertainty because of the noted limitations of the study design and the fact that statistical significance was not consistently reached or formally evaluated for all secondary end points. Maintaining function and HRQoL is very important to patients, according to the input received, but it may be difficult to observe changes in these outcomes in the context of a clinical trial, as loss of function and loss of quality of life are cumulative over time and related to the severity of the relapse. A high proportion of patients in the CHAMPION-NMOSD study experienced harms events, most notably related to infections and infestations; however, ravulizumab appeared to be well tolerated, especially considering that there were very few withdrawals due to AEs. The overall harms profile did not raise any particular safety signals, with the exception of meningococcal infections; per the product monograph, all patients should receive meningococcal vaccination before the start of ravulizumab therapy. Findings from the trial were considered generalizable to patients with NMOSD in Canada. Special consideration may be given to the fact that NMOSD is a rare and severe disease with a generally poor natural trajectory, and that there is, unfortunately, a limited number of effective therapeutic options, access to which is very limited and can be difficult across the country. Results from the NMA suggest that ravulizumab performs better || |||| |||||||| |||||||| || ||||| ||||||||||| ||| ||| |||||||||||||| || ||||||| |||| ||| ||||||||||| || ||| ||||| ||| || ||| ||||||||||| || ||| ||| ||| ||| |||| ||||| |||||| ||| ||||||||||
Introduction
The objective of this report is to review and critically appraise the evidence submitted by the sponsor on the beneficial and harmful effects of ravulizumab, (10 mg/mL and 100 mg/mL, concentrate for solution, IV infusion), in the treatment of patients with anti-AQP4 antibody-positive NMOSD.
Disease Background
The contents of this section have been informed by materials submitted by the sponsor and clinical expert input. The following information has been summarized and validated by the CADTH review team.
NMOSD is a rare, inflammatory disease that affects the CNS, specifically the optic nerves and spinal cord, often leading to permanent blindness and paralysis.1-3 It is distinct from MS because of its association with serum AQP4 IgG antibodies,4 which presents in 80% to 90% of patients with NMO and more than half of patients with NMOSD.30-32 Patients with NMOSD experience acute unpredictable attacks or relapses of CNS dysfunction that can last days to weeks and cause a worsening of symptoms.3 These attacks are recurrent; they occur in 80% to 90% of patients,5-7 are usually severe, and can lead to disabilities and permanent impairment.3 The most common manifestation of an acute attack is optic neuritis, which involves inflammation of the optic nerves that leads to eye pain and vision loss in 1 eye or both eyes. The clinical presentation also involves inflammation of the spinal cord (transverse myelitis), resulting in weakness or paralysis of the arms and legs, bladder or bowel control problems, sensory loss, and painful muscle spasms.1-3 NMOSD may involve brainstem syndromes such as intractable nausea, vomiting, hiccups, facial nerve palsy, oculomotor dysfunction, or vertigo.8 Disease symptoms and cumulative damage associated with NMOSD are associated with a poor HRQoL. In some instances, NMOSD can lead to fatal respiratory failure.9-11
Clinical deterioration and neurologic deficits in patients with NMOSD accumulate in a stepwise fashion after each inflammatory attack, and are often irreversible.1-3,13 As a result, prevention of relapse is the key goal of therapy and paramount in the overall management of patients with NMOSD to minimize the amount of irreversible damage, as 80% to 90% of patients with NMOSD experience relapses.5-7 The bulk of disability in patients with NMOSD is attributed to recurrent attacks; only 25% of long-term disability is related to the initial diagnostic attack, which highlights the importance of early effective treatment.33 Permanent visual disability was also more common in males than females. Overall, NMOSD is associated with an overwhelmingly high risk for permanent sequelae, regardless of age, ethnicity, or sex, that can result from a single attack.34
NMOSD disproportionately affects females, with a reported 9:1 to 12:1 female-to-male ratio in patients with anti-AQP4 antibody-positive NMOSD.3,14 The reported mean age at onset is 40 years.15 Prevalence data for NMOSD in the population in Canada are not available. The prevalence and incidence of NMO range from 0.50 to 4.00 per 100,000 people and 0.053 to 0.40 per 100,000 people, respectively, and have been estimated in previous systematic reviews based on data from various countries.16 It is not clear whether these estimates are representative of the population in Canada, given that the criteria for NMOSD are broader than those for NMO. Regarding mortality, recent studies have reported an NMOSD mortality rate of 3.3% to 7.0%.17-19 Other studies have estimated that worldwide mortality rates of NMOSD range from 9% to 32%, depending on age, relapse rate, and recovery from attacks.6,20
In Canada, NMOSD is diagnosed by a neurologist or physician who specializes in demyelinating disorders. Diagnostic criteria follow the 2015 consensus-based criteria developed by the International Panel for NMO Diagnosis.3 Diagnosis is based on clinical characteristics (e.g., optic neuritis, acute myelitis, area postrema syndrome, acute brainstem syndrome, symptomatic narcolepsy or acute diencephalic clinical syndrome with NMOSD-typical MRI lesions, or symptomatic cerebral syndrome with NMOSD-typical brain lesions), and anti-AQP4 antibody testing.2,3
Standards of Therapy
The contents of this section have been informed by materials submitted by the sponsor and clinical expert input. The following information has been summarized and validated by the CADTH review team.
The treatment goals of NMOSD are based on the acute management of attacks and the prevention of future attacks.2,12 Acute NMOSD attacks can be treated with IV methylprednisolone for 3 to 5 days.12,35,36 If resolution of the attack is not achieved or the patient’s condition worsens, then 5 to 7 rounds of plasma exchange is recommended.36
Considering the significant consequences of NMOSD attacks on patient morbidity and quality of life, avoidance of future attacks is paramount in preventing the accumulation of disability in patients and associated mortality. It should be noted that the occurrence of a relapse, however, does not automatically mean that there is treatment failure. The severity of the relapse, as well as subsequent recovery from the relapse, will have a significant impact on the decision of whether to escalate or switch therapy. Whether or not there are alternative options may also impact the decision to discontinue a particular treatment.
Prior to the 2019 Health Canada approval of eculizumab for the prevention of NMOSD, only off-label immunosuppressive treatments (ISTs) were available for the long-term management of patients with NMOSD in Canada. Off-label ISTs include rituximab, methotrexate, cyclosporine, tacrolimus, cyclophosphamide, and corticosteroids. The use of off-label ISTs is predominantly supported by evidence from observational and retrospective studies.12,35 In addition, Canadian clinicians noted that these treatments are associated with significant adverse effects, especially because preventive treatment for NMOSD must be used for the long-term.37
The value of eculizumab was recognized by CADTH with a positive reimbursement recommendation for patients who have had at least 2 relapses of NMOSD in the previous 12 months or 3 relapses in the previous 24 months, with at least 1 relapse in the previous 12 months.38 Although eculizumab provides clinical benefits for patients with NMOSD, a limitation of its use relates to the frequency of dosing — an IV infusion is required every 2 weeks — which places a considerable treatment-related burden on patients and caregivers.
Satralizumab, an interleukin-6 receptor antagonist, was recently approved by Health Canada as monotherapy or in combination with IST for the treatment of NMOSD in adults and adolescents who are anti-AQP4 seropositive.39 Satralizumab is administered by subcutaneous injection at week 0, week 2, and week 4, followed by maintenance doses every 4 weeks thereafter.39 CADTH issued a reimburse with condition recommendation for satralizumab for patients who are 12 years and older, are anti-AQP4 antibody-positive, have had at least 1 NMOSD relapse in the 12 months before initiation, despite an adequate trial of other preventive treatments, or who cannot tolerate other preventive treatments for NMOSD.40
Although CADTH provided positive recommendations for eculizumab (2020) and satralizumab (2021), clinician feedback states that both remain largely inaccessible to most patients with NMOSD in Canada.37
Drug Under Review
Key characteristics of ravulizumab are summarized in Table 4, along with other treatments available for NMOSD.
Ravulizumab is a terminal complement inhibitor that binds to the complement protein C5 with high affinity and specificity, thereby inhibiting its cleavage to C5a (a proinflammatory anaphylatoxin) and C5b (the initiating subunit of the membrane attack complex [MAC or C5b-9]), and thus preventing the generation of MAC.21 In patients with NMOSD, inhibition of terminal complement activation by ravulizumab limits astrocyte necrosis and damage to surrounding glial cells and neurons.21 In addition, complement inhibition may play a role in preventing the loss of blood-brain barrier integrity during neuroinflammatory processes.41
Ravulizumab is indicated for the treatment of adults with anti-AQP4 antibody-positive NMOSD. The reimbursement request is aligned with the Health Canada indication. The recommended ravulizumab IV maintenance dosing in adults (≥ 18 years) with NMOSD with a body weight of 40 kg or greater is based on the patient’s body weight, as shown in Table 3, with maintenance doses administered every 8 weeks, starting 2 weeks after the loading dose.21 Ravulizumab should be administered by a qualified health care professional, per the product monograph.21
Ravulizumab also has Health Canada indications for the treatment of patients with paroxysmal nocturnal hemoglobinuria, atypical hemolytic uremic syndrome, and antiacetylcholine receptor antibody-positive generalized myasthenia gravis.21
Table 3: Weight-Based Recommended Dosing Regimen of Ravulizumab
Indication | Body weight range (kg) | Loading dose (mg) | Maintenance dose (mg) |
|---|---|---|---|
NMOSD | ≥ 40 to < 60 | 2,400 | 3,000 |
≥ 60 to < 100 | 2,700 | 3,300 | |
≥ 100 | 3,000 | 3,600 |
NMOSD = neuromyelitis optica spectrum disorder.
Source: Ravulizumab product monograph.21
Table 4: Key Characteristics of Ravulizumab, Inebilizumab, Satralizumab, and Eculizumab
Characteristic | Ravulizumab (Ultomiris) | Inebilizumab (Uplizna) | Satralizumab (Enspyng) | Eculizumab (Soliris) |
|---|---|---|---|---|
Mechanism of action | Monoclonal antibody that specifically binds to the human terminal complement protein C5 | CD19-directed cytolytic antibody | Monoclonal antibody that blocks interleukin-6 receptors | Monoclonal antibody that specifically binds to the complement protein C5 |
Indicationa | For the treatment of adults with anti-AQP4 antibody-positive NMOSD | As monotherapy for the treatment of adults with NMOSD who are anti-AQP4 immunoglobulin G seropositive | As monotherapy or in combination with IST for the treatment of NMOSD in adults and adolescents who are anti-AQP4 seropositive | For the treatment of adults with anti-AQP4 antibody-positive NMOSD |
Route of administration | IV | IV | SC | IV |
Recommended dose | ≥ 40 to < 60 kg: 2,400 to 3,000 mg ≥ 60 to < 100 kg: 2,700 to 3,300 mg ≥ 100 kg: 3,000 to 3,600 mg | An initial 300 mg IV infusion, followed 2 weeks later by a second 300 mg IV infusion; subsequent doses (starting 6 months after the first infusion) are administered as single 300 mg infusions every 6 months | 120 mg at weeks 0, 2, and 4 for the first 3 administrations, followed by a maintenance dose of 120 mg every 4 weeks | 900 mg weekly for the first 4 weeks, followed by 1,200 mg for the fifth dose 1 week later, then 1,200 mg every 2 weeks thereafter |
Serious adverse effects or safety issues | Serious meningococcal infections | Infusion reactions Infections Reduction in Immunoglobulins Fetal risk | Infections Monitor liver enzymes and neutrophils | Serious or fatal meningococcal infections |
AQP4 = aquaporin-4; IST = immunosuppressive treatment; NMOSD = neuromyelitis optica spectrum disorder; SC = subcutaneous.
aHealth Canada–approved indication.
Sources: Ravulizumab,21 inebilizumab,42 satralizumab,39 eculizumab,43 product monographs.
Stakeholder Perspectives
Patient Group Input
This section was prepared by the CADTH review team based on the input provided by patient groups. The full original patient inputs received by CADTH have been included in the Stakeholder section of this report.
Two patient groups, MS Canada and The Sumaira Foundation (TSF), responded to CADTH’s call for patient input for the current review of ravulizumab for the treatment of adults with anti-AQP4 antibody-positive NMOSD.
MS Canada gathered information for this submission with a survey that ran from August 4, 2023, to August 14, 2023, and targeted patients living with NMOSD and their caregivers in Canada. The MS survey collected data from 13 respondents, most of them were female (83%), who ranged in age from 25 years to older than 65 years. TSF gathered information from various surveys of patients and caregivers, patient narratives, focus groups, roundtables, discussions with key opinion leaders, ambassadors, TSF’s global medical advisory board, advisors, peer-reviewed medical literature, and TSF’s experience working in the NMOSD communities.
The 2 patient groups indicated that NMOSD is more prevalent among women and that the disease is initiated with a severe attack and continues with subsequent devastating attacks that have a negative impact on vision, mobility, function, mental health, and quality of life of patients. The disease has a tremendous impact on all aspects of patients' lives, including a negative effect on independence, family and caregivers, community, employment, and social life.
The patient inputs stated that treatment for NMOSD includes IV steroids, IV immunoglobulin or plasmapheresis and/or plasma exchange, and mofetil mycophenolate, as well as the off-label use of immunosuppressants to help prevent further attacks, with various levels of therapeutic benefit. Symptoms such as neuropathy, pain, stiffness, muscle spasms, and bladder and bowel control problems can be managed with various medications and therapies. Many patients reported experiencing significant additional attacks and additional disability while cycling through off-label therapies, and others indicated that these therapies partially managed their disease but still involved a worsening of symptoms and/or challenging side effects.
According to patient inputs, there are some Health Canada–approved medications indicated for adults with NMOSD: AQP4 IgG, eculizumab, and satralizumab. Although patients reported that these medications were effective in managing their disease, access to these medications is very limited, and eculizumab is administered by infusion every 2 weeks, which can be onerous and disruptive to the lives of individuals living with NMOSD. According to patient inputs, patients need to have access to more treatment options that are able to prevent further attacks with less frequent infusion dosing and fewer side effects.
The 2 patient inputs agreed that ravulizumab is simply a more stable analogue of eculizumab, with a longer serum half-life, which therefore requires much less frequent dosing after initiation (every 8 weeks), which can improve treatment adherence.
According to the patient groups, ravulizumab is not yet available to patients with NMOSD outside the clinical trial settings; therefore, the patients had no direct experience with ravulizumab therapy. Patients with NMOSD who tried eculizumab had a positive experience, but indicated that they would prefer a less frequent infusion dosing schedule.
Clinician Input
Input From Clinical Experts Consulted by CADTH
All CADTH review teams include at least 1 clinical specialist with expertise in the diagnosis and management of the condition for which the drug is indicated. Clinical experts are a critical part of the review team and are involved in all phases of the review process (e.g., providing guidance on the development of the review protocol, assisting in the critical appraisal of clinical evidence, interpreting the clinical relevance of the results, and providing guidance on the potential place in therapy). The following input was provided by 2 clinical specialists with expertise in the diagnosis and management of NMOSD.
Unmet Needs
NMOSD is a rare and severe disease with a generally poor natural trajectory and inherently high risk of relapse, even at an early disease stage. The avoidance of relapses is paramount in preventing the accumulation of disability in patients, as any relapse could be a disabling 1 at any time in the disease trajectory. However, the clinical experts consulted by CADTH highlighted a significant unmet need, in that the available therapies only provide suboptimal treatment for relapses. Current first-line therapies, such as azathioprine and mycophenolate, are not considered particularly effective and, unfortunately, most people with NMOSD still have relapses despite their current treatment regimens. Suboptimal relapse prevention results in the accumulation of irreversible neurologic disability, including paralysis and blindness. The clinical experts emphasized that patients want, and need to be on, a therapy that prevents relapses, which cause the greatest disability associated with NMOSD. A treatment is needed that can have a benefit on their quality of life and improve both safety and the burden associated with getting treatment. The clinical experts agreed that having access to a more effective treatment would make a huge difference in the lives of patients and their caregivers. Current off-label therapies are often associated with an unacceptable harms profile, especially if used in conjunction with corticosteroids. Highly effective therapies exist, but access is very limited and difficult across the country.
Place in Therapy
In Canada, the clinical experts indicated that the treatment of individuals with NMOSD differs by province and territory, based on differential access to drugs. There are no formal treatment guidelines in Canada that specify which interventions should be used as first-line or second-line therapies. Treatment guidelines are still broad as a result of the inconsistent availability of treatment and the limited direct evidence related to the comparative efficacy of available treatments.
The treatment paradigm for NMOSD is related to 3 broad areas: prevention of relapses (disease modifying), treatment of acute relapses, and treatment of residual symptoms. Although it would be ideal, no single treatment covers all 3 areas. Disease-modifying or preventive treatment is of special interest because the goal of any intervention is to prevent relapses. Despite the best therapeutic measures at the time of relapse for acute therapy, recovery from relapses is often incomplete. Therefore, the prevention of relapses is of the upmost importance in the prevention of neurologic disability (including, but not limited to, paralysis, loss or impairment of vision) and mortality. There are many downstream desirable effects of the early prevention and control of the disease; maintaining neurologic function will have a positive impact on a patient’s quality of life, decrease the risk of complications related to neurologic dysfunction, and, in turn, help the patient maintain independence, increase the ability to maintain employment, and reduce the burden on caregivers.
Oral glucocorticoids, azathioprine, mycophenolate mofetil, and rituximab are frequently used to prevent relapses in patients with NMOSD. Rituximab is considered 1 of the most promising therapies for patients with NMOSD. However, its availability differs among provinces. When provinces have access to rituximab, it is generally used as a first-line therapy for patients with NMOSD. Although it is considered more effective than other off-label therapies, many individuals with NMOSD who are treated with rituximab still have ongoing disease activity. If rituximab is not available, treatments such as azathioprine and mycophenolate mofetil are classic immune suppressants that have been used for many years, but they are generally considered to be inferior to rituximab in preventing NMOSD relapses. As their efficacy is viewed as suboptimal, corticosteroids are often used as adjunct therapy, adding to the harms profile.
Although approved in Canada, satralizumab and eculizumab are rarely attainable for people living with NMOSD. They are either completely unavailable or only available with private insurance and/or coverage. Patients with NMOSD are often left with some level of disability after the first relapse, and almost certainly after any subsequent relapses, and are the least likely to have private coverage. In contrast to nonspecific immunosuppressants that modify the immune response, eculizumab and satralizumab more specifically target disease mechanism and pathophysiology. The clinical experts indicated that they would be used frequently in the first-line setting, due to their effectiveness for relapse prevention, if they were available. As such, access to ravulizumab is likely to cause a shift in the current treatment paradigm because it addresses the underlying disease process with high efficacy. It is paramount to control NMOSD progression as early as possible, as damage leading to disability (such as blindness, paralysis, and/or becoming wheelchair-dependent) may be irreversible. Therefore, the clinical experts emphasized that it would be inappropriate to recommend that patients try other treatments before initiating treatment with ravulizumab.
Patient Population
With the devastating impact of relapses on patients with NMOSD and the importance of preventing relapses to prevent significant disability, all individuals with anti-AQP4 antibody-positive NMOSD should be considered eligible to receive ravulizumab. With a realistic estimated incidence averaging 0.5 per 100,000 cases per year (details provided in the Disease Background section), NMOSD is considered a rare disease. Meningococcal vaccination should be mandatory in the patients planning to receive this therapy.
Assessing the Response Treatment
A clinically meaningful response to treatment is a reduction in relapses. The severity of a relapse and the accumulation of disability are important factors to consider when determining response to therapy. Although the absence of relapse would be ideal, this may not be realistic, considering high interindividual variations (e.g., some patients may have several relapses per year). In clinical practice, relapse assessment includes history and neurologic examination. Paraclinical investigations are not a routine part of clinical follow-up or assessment of treatment response, although they are sometimes used to adjudicate relapses or rule out other conditions. It would be reasonable to assess initial treatment response 3 months after the initial injection, then patients could be assessed every 6 months until stability is established, and then every year for patients with stable NMOSD.
Discontinuing Treatment
Patients may need to discontinue a treatment if they experience a severe relapse (e.g., requiring intubation and ventilator support), 2 or more relapses within 2 years (assessed on a case-by-case basis, depending on severity), or severe AEs while on treatment. If a person with NMOSD is completely dependent and bed-bound, treatment should be discontinued.
Prescribing Considerations
The appropriate settings for initiating and monitoring treatment with ravulizumab are neurology clinics with personnel who have adequate expertise in NMOSD, including neurologists with expertise or subspecialty in MS or autoimmune neurology, and occasionally neuro-ophthalmology.
Additional Considerations
Special consideration may be given to the fact that NMOSD is a rare and severe disease with a generally poor natural trajectory, and that there is, unfortunately, a limited number of effective therapeutic options, access to which is very limited and can be difficult across the country.
Clinician Group Input
This section was prepared by the CADTH review team based on the input provided by clinician groups. The full original clinician group input received by CADTH has been included in the Stakeholder section of this report.
One clinician group, the CNMSC, responded to CADTH’s call for clinician group input.
Clinician perspectives from the CNMSC were obtained through clinical experience, knowledge of the medical literature, and from clinicians across the country who specialize in this therapeutic area.
According to the clinician group, there is a variety of treatments available in Canada that are not specifically indicated for NMOSD, including corticosteroids, azathioprine, mycophenolate mofetil, and rituximab. Generally, azathioprine is perceived by specialists as the least efficacious of the currently available off-label options, while rituximab is perceived as the most efficacious. Recent evidence showed the efficacy of monoclonal antibodies, such as eculizumab, satralizumab, and inebilizumab, but access to these therapies is extremely limited due to their stringent funding coverage criteria. Failure of treatment, with even just 1 relapse, can lead to a profound, permanent disability, including blindness and paralysis.
Per the CNMSC, there is a large unmet need for high-efficacy, well-tolerated therapies for NMOSD in Canada that have a significant impact on preventing and/or reducing attacks. Use of some of the off-label therapies is limited by many side effects, and many patients continue to have attacks despite treatment with drugs such as azathioprine and mycophenolate, eculizumab and, to a lesser extent, rituximab. Also, eculizumab is administered by IV infusion every 2 weeks, which is too onerous for some patients to tolerate.
According to the clinician group, the best approach for patients is to use efficacious, safe, and tolerable therapy as soon as possible after the first attack to avoid all relapses, reduce the severity of attacks and the cumulative disability associated with them, and minimize AEs related to therapies. Ravulizumab would be the first therapy for patients with a confirmed diagnosis of NMOSD, for those with a positive serum test for the AQP4 antibody after their first relapse and/or attack, and for those who have severe AEs on first-line therapy.
According to the CNMSC, avoidance of a new attack, which could include vision loss, weakness, sensory impairment, or bladder and/or bowel dysfunction, is the outcome used to determine whether a patient is responding to treatment. The clinician group indicated that the discontinuation of therapy should be considered in patients who have a new attack on this therapy; however, the drug should be continued, despite serious side effects, when the benefits of continuation are thought to outweigh the risks.
The CNMSC stated that the treatment of patients with NMOSD should be assessed and managed by neurologists specialized in demyelinating diseases at a multiple sclerosis or demyelinating disease centre, and that ravulizumab can be administered in a hospital or private clinic.
Drug Program Input
The drug programs provide input on each drug being reviewed through CADTH’s reimbursement review processes by identifying issues that may impact their ability to implement a recommendation. The implementation questions and corresponding responses from the clinical experts consulted by CADTH are summarized in Table 5.
Table 5: Summary of Drug Plan Input and Clinical Expert Response
Drug program implementation questions | Clinical expert response |
|---|---|
Relevant comparators | |
Would any of the off-label preventive therapies for NMOSD (such as rituximab, azathioprine, mycophenolate, tacrolimus, cyclophosphamide, methotrexate, and corticosteroids) be considered an appropriate comparator? | The clinical experts suggested that azathioprine, mycophenolate, tacrolimus, cyclophosphamide, methotrexate, and corticosteroids should not be considered appropriate comparators, mainly due to the fact that they have different mechanisms of action and very limited effectiveness. Of the potential comparators listed, rituximab would be the closest to ravulizumab, according to the clinical experts; however, rituximab also has limited efficacy in preventing NMOSD relapses. |
Considerations for initiation of therapy | |
How should relapse be defined? Should the initial attack that leads to the diagnosis of NMOSD be considered a relapse for the purpose of the initiation criteria? | In clinical practice, the definition and assessment of relapses are based on a combination of patient-reported symptoms, clinical exam, clinical tools, and patient history. The clinical experts indicated that the initial attack that leads to the diagnosis of NMOSD should be considered a relapse for the purpose of the initiation criteria. |
Should patients be required to try (or rule out) off-label preventive therapies before accessing ravulizumab for NMOSD? | The clinical experts emphasized that patients should not be required to try off-label, less-effective therapies before being allowed to use an approved drug with high efficacy at preventing relapses. Any relapse could be a disabling relapse, even early in the disease trajectory; therefore, preventing all relapses is very important. |
What is the appropriate treatment sequence for satralizumab and ravulizumab? Should one be trialled in advance of the other? | The clinical experts indicated that currently there is no evidence to answer this question. |
Eculizumab is not funded publicly. Given the lack of availability, how should it be considered in the treatment algorithm? If patients fail eculizumab, would it be reasonable to try ravulizumab? Should a switch from eculizumab to ravulizumab be considered for patients who are responding to therapy with eculizumab? | The clinical experts mentioned that they do not use eculizumab and satralizumab due to very limited and difficult access, although they said they wish that the drugs could be used more routinely. The clinical experts indicated that patients with evidence of suboptimal response while on eculizumab would likely be switched to a drug with a different mechanism of action. However, patients with a good response on eculizumab may be switched to ravulizumab for convenience of administration. |
Is there evidence to support the use of ravulizumab in patients who do not respond to treatment with eculizumab and/or satralizumab? | The clinical experts indicated that, currently, there is no evidence in this patient population. |
The initiation criteria in the CDEC reimbursement recommendation for eculizumab for patients with NMOSD is as follows:
Although eculizumab is not publicly reimbursed for NMOSD, and an alignment in initiation criteria might not be necessary, is there evidence to align the initiation criteria for ravulizumab with that for eculizumab for patients with NMOSD? | Initiation criteria in the CDEC reimbursement recommendation for eculizumab are based on data from the eculizumab trial(s). The clinical experts suggested that initiation criteria in the CDEC reimbursement recommendation for ravulizumab should be based on data from the CHAMPION-NMOSD study. |
Considerations for continuation or renewal of therapy | |
How often are EDSS scores measured in clinical practice, and how frequently are these patients monitored? | The clinical experts indicated that EDSS scores are widely used in clinical practice, and routinely assessed in patients on a yearly basis. The clinical experts mentioned that for reimbursement purposes, it would be best to allow for more than 12 months to allow for delays that can occur in yearly appointments. |
Is EDSS score the appropriate tool to assess response to therapy? | The clinical experts highlighted that, although there are some limitations to the EDSS, it remains a part of the global evaluation of response to treatment. |
The renewal criteria in the CDEC reimbursement recommendation for eculizumab for patients with NMOSD is that the physician should measure and provide EDSS scores every 6 months after the initial authorization to determine if the continuation of eculizumab reimbursement should occur. Should consideration be given to aligning the renewal criteria for ravulizumab with those recommended for eculizumab? | The clinical experts highlighted that because assessment is performed yearly in clinical practice, an every-6-month requirement would add a substantial and unnecessary burden to patients, clinicians, and the health care system. The clinical experts strongly suggested yearly assessments. |
Considerations for discontinuation of therapy | |
The discontinuation criteria in the CDEC reimbursement recommendation for eculizumab for patients with NMOSD state that the reimbursement of eculizumab treatment should be discontinued if the patient’s EDSS score is 8 points or greater. Should consideration be given to aligning the discontinuation criteria of ravulizumab with those recommended for eculizumab? | Discontinuation criteria in the CDEC reimbursement recommendation for eculizumab are based on data from eculizumab trial(s). The clinical experts suggested that discontinuation criteria in the CDEC reimbursement recommendation for ravulizumab should be based on data from the CHAMPION-NMOSD study and experience from clinical practice. As such, patients in the CHAMPION-NMOSD study had an EDSS score ≤ 7. In clinical practice, however, some patients with an EDSS score above 7 are still considered to have some preservable function that could be taken away by the next relapse. Given that the EDSS has limitations in the assessment of function in patients with NMOSD, more flexibility would be required if this tool is used for discontinuation purposes. Therefore, the clinical experts suggested that ravulizumab treatment should be maintained as long as a patient’s EDSS score is ≤ 9 points. |
Should the relapse rate also be a consideration for discontinuation of therapy? | The clinical experts emphasized that a relapse, in itself, should not result in treatment discontinuation. Relapses are not all equal. The severity of the relapse and recovery from the relapse will have a significant impact on the decision of whether to escalate or switch therapies. Whether or not there are alternative options may also impact the decision to discontinue a particular treatment. |
Considerations for prescribing of therapy | |
Would ravulizumab be used in combination with satralizumab? Is there evidence to support other therapies in combination with ravulizumab (i.e., rituximab or inebilizumab)? | The clinical experts indicated that ravulizumab should be used as monotherapy, with the exception of the concomitant use of corticosteroids and/or other symptomatic therapies. There is no evidence with regard to combination therapies with ravulizumab and other drugs, such as rituximab or inebilizumab. |
As an accurate diagnosis of NMOSD is important to ensure appropriate prescribing, who should prescribe ravulizumab? Is it a neurologist, ophthalmologist, or someone else? How do patients living in remote areas access such specialties? | The clinical experts suggested that treatment should be supervised by a neurologist with expertise in this area (which may include autoimmune neurology and, occasionally, neuro-ophthalmology). Although NMOSD and MS are not the same disease, the populations and medications are similar, and people with NMOSD are often cared for in an MS clinic. Thus, the diagnosis could be confirmed by a neurologist associated with an MS clinic and treatment could be initiated and monitored by a neurologist associated with an MS clinic or similar subspecialty clinic with expertise in NMOSD. |
CDEC = CADTH Canadian Drug Expert Committee; EDSS = Expanded Disability Status Scale; MS = multiple sclerosis; NMOSD = neuromyelitis optica spectrum disorder.
Clinical Evidence
The objective of CADTH’s Clinical Review Report is to review and critically appraise the clinical evidence submitted by the sponsor on the beneficial and harmful effects of IV ravulizumab in the treatment of patients with anti-AQP4 antibody-positive NMOSD. The focus will be placed on comparing ravulizumab to relevant comparators and identifying gaps in the current evidence.
A summary of the clinical evidence included by the sponsor in the review of ravulizumab is presented in 2 sections, with CADTH’s critical appraisal of the evidence presented at the end of each section. The first section, the Systematic Review, includes pivotal studies and randomized controlled trials (RCTs) that were selected according to the sponsor’s systematic review protocol. CADTH’s assessment of the certainty of the evidence in this first section using the GRADE approach follows the critical appraisal of the evidence. The second section includes indirect evidence from the sponsor.
Included Studies
Clinical evidence from the following are included in the CADTH review and appraised in this document:
1 pivotal study or RCT identified in the systematic review
1 indirect treatment comparison.
Systematic Review
The contents of this section have been informed by materials submitted by the sponsor. The following information has been summarized and validated by the CADTH review team.
Description of Studies
One study was identified and included in the systematic review. The CHAMPION-NMOSD study (N = 58) is an externally placebo-controlled, open-label, phase III, multicenter trial designed to evaluate the efficacy and safety of ravulizumab in adults with anti-AQP4 antibody-positive NMOSD (at least 1 relapse in the previous 12 months). The primary outcome was time to first adjudicated on-trial relapse.
The study had a single-arm treatment design; the placebo group from the PREVENT study was used as an external placebo comparator. The PREVENT study evaluated the efficacy and safety of eculizumab in preventing relapses in patients with anti-AQP4 antibody-positive NMOSD and was conducted from 2014 to 2018 as a randomized, double-blind, time-to-event study. A total of 143 patients were randomly assigned in a 2:1 ratio to receive either eculizumab (n = 96) or a matching-administration placebo (n = 47) every 2 weeks.
The CHAMPION-NMOSD study is ongoing; results from the primary analysis based on the data cut-off date of March 15, 2022, are presented here. Results from a more recent data cut-off date of July 15, 2022, are also presented.
Characteristics of the included study are summarized in Table 6.
Table 6: Details of the Study Included in the Systematic Review (the CHAMPION-NMOSD Study)
Design and population | CHAMPION-NMOSD |
|---|---|
Study design | External placebo-controlled, open-label, phase III, multicenter trial |
Locations | This study was conducted at 36 sites that enrolled 58 patients in 11 countries (Australia, Canada, Denmark, Germany, Italy, Japan, the Republic of Korea, Poland, Spain, the UK, and the US) |
Patient enrolment dates | The CHAMPION-NMOSD study Start date: December 13, 2019 End date: Ongoing (primary analysis data cut-off was March 15, 2022; addendum data cut-off was July 15, 2022) External placebo control arm (from the PREVENT [ECU-NMO-301] study) Start date: April 11, 2014 End date: July 17, 2018 (study completion date of the last patient) |
Randomized (N) | A total of 58 patients were enrolled in the CHAMPION-NMOSD study (ravulizumab group) The external placebo group from the PREVENT study consisted of 47 patients |
Key inclusion criteria |
|
Key exclusion criteria |
|
Drugs | |
Intervention | During the primary treatment period, patients received ravulizumab through IV infusion. Dosing consisted of a loading dose (day 1) and maintenance doses (day 15 and once every 8 weeks thereafter). Dosages were based on the patient’s body weight: Loading dose:
Maintenance dose:
Patients received ravulizumab until the primary treatment period was triggered (when all patients had completed the study or discontinued before 50 weeks on the study) and they were able to enter the long-term extension period to continue ravulizumab for up to approximately 2 years. |
Comparator(s) | This study employs a single-arm treatment design; the placebo group from the PREVENT study was used as an external placebo comparator. Patients randomized to the placebo group in the PREVENT study received an eculizumab-matching placebo every 2 weeks until they experienced a relapse, discontinued the trial, or the trial ended. |
Study duration | |
Screening period | Up to 6 weeks |
Primary treatment period | Per protocol, the primary treatment period could be triggered if 2 patients had an adjudicated on-trial relapse and all patients had completed or discontinued the study by 26 weeks. If these criteria were not met, then the primary treatment period would end when all patients completed the study or discontinued before 50 weeks on the study. Because no patients had an adjudicated on-trial relapse during the study, the end of the primary treatment period was triggered when all patients completed at least 50 weeks on the study or discontinued. |
Long-term extension period | Up to 2 years. The long-term extension period started when all patients completed the end of the primary treatment visit within a 2 week time frame. Patients who enrolled in the long term extension period continued to receive ravulizumab for approximately 2 years, or until ravulizumab was approved for the studied indication and/or available in the country of the study site, whichever occurred first. |
Safety follow-up period | 8 weeks after the last dose of the study drug |
Outcomes | |
Primary end point | Time to first adjudicated on-trial relapse and relapse risk reduction. |
Secondary and exploratory end points | Secondary:
Exploratory:
|
Publication status | |
Publications | Publications : Pittock SJ, Barnett M, Bennett JL, et al. Ravulizumab in aquaporin-4-positive neuromyelitis optica spectrum disorder. Ann Neurol. 2023;93:1053-1068. Abstracts: Allen K, Pittock SJ, Levy M, et al. Sensitivity analysis using propensity score methods for primary efficacy outcome in the CHAMPION-NMOSD trial. Multiple Sclerosis Journal. 2022;28(3 Supplement):138-140. Pittock SJ, Barnett M, Bennett JL, et al. Efficacy and safety of ravulizumab in adults with anti-aquaporin-4 antibody-positive neuromyelitis optica spectrum disorder: outcomes from the phase 3 CHAMPION-NMOSD trial. Multiple Sclerosis Journal. 2022;28(3 Supplement):39-40. Pittock SJ, Barnett M, Bennett JL, et al. Efficacy subgroup analyses from the phase 3 CHAMPION-NMOSD trial in adults with antiaquaporin-4 antibody-positive neuromyelitis optica spectrum disorder. Multiple Sclerosis Journal. 2022;28(3 Supplement):136-137. Other: clinicaltrials.gov link: NCT04201262. |
ADA = antidrug antibody; AQP4 = antiaquaporin-4; ARR = annualized relapse rate; CSF = cerebrospinal fluid; C-SSRS = Columbia-Suicide Severity Rating Scale; ECG = electrocardiogram; EDSS = Expanded Disability Status Scale; HAI = Hauser Ambulation Index; Ig = immunoglobulin; NMO = neuromyelitis optica; NMOSD = neuromyelitis optica spectrum disorder; ||||||||| |||| |||||| ||||||; TEAE = treatment-emergent adverse event; TESAE = treatment-emergent serious adverse event; VAS = visual analogue scale.
Sources: ALXN1210-NMO-307 (CHAMPION-NMOSD) CSR,26 Pittock et al. (2023).44 Details included in the table are from the sponsor’s Summary of Clinical Evidence.27
The end of the primary treatment period was to be triggered when 2 patients had an adjudicated on-trial relapse and all patients had completed the study or discontinued before 26 weeks on the study. If 2 patients had not had an adjudicated on-trial relapse by the time all patients had completed the study or discontinued before 50 weeks on the study, the end of the primary treatment period was to be triggered at that time. After the primary treatment period, patients could continue to receive ravulizumab during the long-term extension period (which was part of the same study protocol) for up to approximately 2 years or until ravulizumab was approved and/or available in the country of the study site, whichever occurs first. Patients are to be followed for 8 weeks after the last dose of the study drug.
Figure 1: CHAMPION-NMOSD Study Design
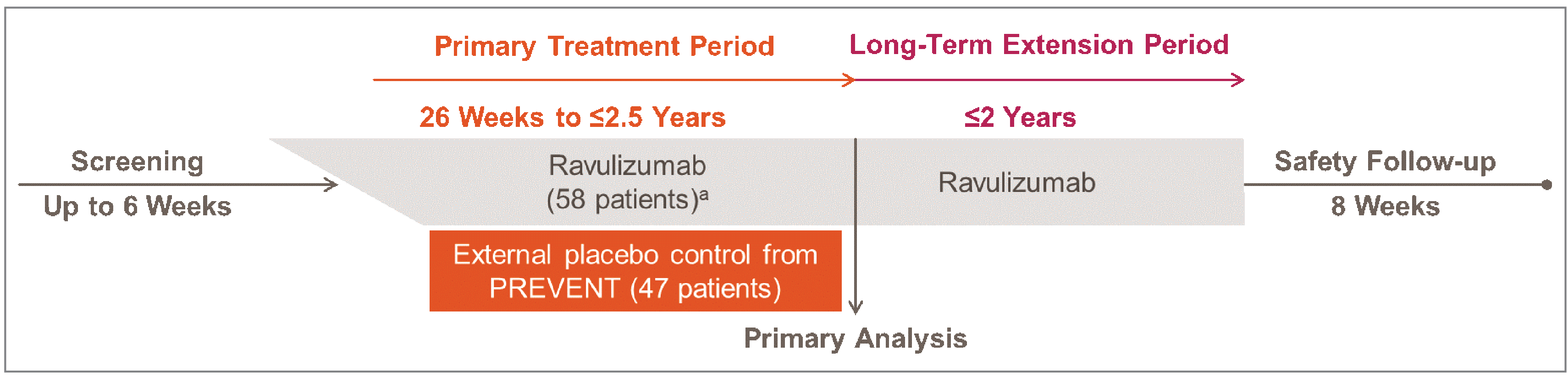
a All patients were vaccinated against Neisseria meningitidis in the 3 years before, or at the time of, ravulizumab initiation. Patients who initiate the study drug treatment less than 2 weeks after receiving a meningococcal vaccine must receive appropriate prophylactic antibiotics until 2 weeks after vaccination.
Source: CHAMPION-NMOSD 307 Study Design Deck.45
Populations
Inclusion and Exclusion Criteria
Patients were eligible for the trial if they had anti-AQP4 antibody-positive NMOSD, as defined by the 2015 international consensus diagnostic criteria, with at least 1 relapse in the prior 12 months and an EDSS score of 7 or less. Patients needed to be vaccinated against Neisseria meningitidis. Stable doses of background ISTs were permitted but not required. Patients were excluded from the trial if they participated in the PREVENT study, regardless of the study drug received, if they had active systemic bacterial, viral, or fungal infection within the prior 14 days, or if they received previous or current treatment with a complement inhibitor.
To ensure a valid comparison with the external placebo arm from PREVENT, constancy would need to be maintained by including a similar patient population and concomitant medications in CHAMPION-NMOSD. There were 2 main differences between trial designs, including using the most recently updated NMOSD diagnostic criteria in CHAMPION-NMOSD for facilitating enrolment of a population matching the current clinical practice. In addition, relapse inclusion criteria were broadened in CHAMPION-NMOSD to consider at least 1 attack in the last 12 months, which reflects clinical practice guideline recommendations that long-term treatment options should be initiated as soon as possible to prevent the occurrence of relapses and curtail the progressive accumulation of neurologic disability.3,12,35 In contrast, the criteria for PREVENT was ≥ 2 relapses in 12 months before screening or ≥ 3 relapses in 24 months before screening with at least 1 of the 3 relapses in 12 months before screening.
A comparison of the key elements of eligibility criteria between PREVENT and CHAMPION-NMOSD is presented as follows.
Table 7: Relevant Inclusion Criteria for the Patient Populations
CHAMPION-NMOSD (ravulizumab arm) | PREVENT (placebo arm) |
|---|---|
Adult patients with anti-AQP4 antibody-positive NMOSD (as defined by the 2015 international consensus diagnostic criteria) | Adult patients with anti-AQP4 antibody-positive NMO (defined by Wingerchuk 2006 criteria) or anti-AQP4 antibody-positive NMOSD (defined by Wingerchuk 2007 criteria) |
> 1 relapse in the prior 12 months | > 2 relapses in the prior 12 months; or 3 relapses in the prior 24 months, with > 1 relapse in the prior 12 months |
EDSS score ≤ 7 | EDSS score ≤ 7 |
Vaccinated against Neisseria meningitidis | No unresolved meningococcal disease |
Stable doses of background immunosuppressive therapies permitted but not required | Stable doses of background immunosuppressive therapies permitted but not required |
AQP4 = antiaquaporin-4; EDSS = Expanded Disability Status Scale; NMO = neuromyelitis optica; NMOSD = neuromyelitis optica spectrum disorder.
Note: Bolding indicates potential areas of differences between the studies.
Source: Details included in the table are from the sponsor’s Summary of Clinical Evidence.27
Interventions
The CHAMPION-NMOSD study was designed to evaluate the efficacy and safety of ravulizumab using placebo data from the PREVENT trial as an external control; the following rationale discussion points were provided by the sponsor to explain this decision:
The use of a placebo arm was considered unethical, as such a study would require administering placebo to patients and waiting for them to relapse for an efficacy demonstration when highly effective treatment with eculizumab is available, and approvals were anticipated for other products (i.e., satralizumab and inebilizumab) during the time frame that the clinical development of ravulizumab was planned. This is particularly unacceptable, considering the serious, irreversible, long-term impact of NMOSD attacks that can cause debilitating sequelae.
The use of an active comparator arm was not feasible. The rare nature of NMOSD made the conduct of a direct noninferiority comparison between ravulizumab and a reference therapy unfeasible due to the large number of patients (> 8,600 patients) required to adequately power such a comparison for a statistically significant efficacy demonstration.
Regulatory bodies (the European Medicines Agency and the FDA) were consulted regarding the use of the external placebo arm. The CHAMPION-NMOSD study meets almost all the criteria established by the FDA and the International Conference on Harmonization for identifying situations in which a single-arm trial with an external control group would be appropriate.
The ravulizumab mechanism of action (C5 inhibition) for NMOSD is well established. Ravulizumab was engineered by modifying the amino acid sequence of eculizumab to allow for a prolonged half-life, resulting in an extended dosing interval of 8 weeks while retaining the same mechanism of action as eculizumab in targeting the C5 epitope.
In the CHAMPION-NMOSD study, all patients received open-label ravulizumab during the primary treatment period. All doses, including the loading dose on day 1 and maintenance doses on day 15 and once every 8 weeks thereafter, were administered by IV infusion under the supervision of the investigator at the infusion centre. Dosages were based on the patient’s body weight. Patients received treatment until the primary treatment period was completed for all patients; therefore, the overall duration of treatment for each patient varied and was dependent on when they enrolled in the study.
Patients in the placebo arm of the PREVENT trial received matching-administration placebo to eculizumab every 2 weeks as IV infusions.44
Treatment with plasma exchange (PE) and/or plasmapheresis (PP) or IV Ig was allowed at the discretion of the treating physician, according to the protocol, to treat on-trial relapses. If PE and/or PP was administered, a supplemental dose of ravulizumab was to be administered in the 4 hours after each session of PE and/or PP was completed. If PE and/or PP was administered on a scheduled dosing visit, patients received the regularly scheduled dose of ravulizumab within 1 to 2 hours of completion. If IV Ig was administered, a ravulizumab supplemental dose was administered after the last dose of IV Ig in the series. A similar approach to the acute treatment of relapses was used during the PREVENT trial.44,46
Outcomes
A list of efficacy end points assessed in this Clinical Review Report is provided in Table 8, followed by descriptions of the outcome measures. Summarized end points are based on outcomes included in the sponsor’s Summary of Clinical Evidence as well as any outcomes identified as important to this review by the clinical experts consulted by CADTH and from stakeholder input from patient and clinician groups and public drug plans. Using the same considerations, the CADTH review team selected end points that were considered to be most relevant to CADTH’s expert committee deliberations and finalized this list of end points in consultation with members of the expert committee. All summarized efficacy end points were assessed using GRADE. Select notable harms outcomes considered important to CADTH’s expert committee deliberations were also assessed using GRADE.
Table 8: Outcomes Summarized From the CHAMPION-NMOSD Study
Outcome measure | Time point | CHAMPION-NMOSD |
|---|---|---|
NMOSD attack or relapse | ||
Time to first relapse | Primary analysis data cut-off (March 15, 2022) and addendum data cut-off (July 15, 2022) | Primary |
Relapse risk reduction | Primary | |
Annualized relapse rate (noncomparative) | Secondarya | |
Function | ||
Clinically important change from baseline in HAI score | Primary analysis data cut-off (March 15, 2022) | Secondarya |
Clinically important worsening from baseline in EDSS score | Secondarya | |
HRQoL | ||
Change from baseline in EQ-5D index score | Primary analysis data cut-off (March 15, 2022) | Secondarya |
Change from baseline in EQ-5D VAS score | Secondarya | |
|||||| |||| |||||||| || ||||| | Exploratory | |
Visual acuity | ||
|||||| |||| |||||||| || ||||| | Primary analysis data cut-off (March 15, 2022) | Exploratory |
|||||| |||| |||||||| || |||||| ||||||| ||||| ||||||| ||| ||||||||||||||| |||||| ||||||| | Exploratory | |
Health care resource use | ||
|||||||| || ||||||||||||||||||||||||||||||||| | Primary analysis data cut-off (March 15, 2022) | Exploratory |
Harms | ||
Incidence of AEs, SAEs, and AEs leading to study discontinuation | Addendum data cut-off (July 15, 2022) | Secondary |
AE = adverse event; EDSS = Expanded Disability Status Scale; HAI = Hauser Ambulation Index; HRQoL = health-related quality of life; NMOSD = neuromyelitis optica spectrum disorder; ||||||||| |||||| |||||||||| |||||; |||||||||| |||| |||||| ||||||| SAE = serious adverse event; VAS = visual analogue scale.
aStatistical testing for these end points was adjusted for multiple comparisons (e.g., hierarchal testing) using a closed testing procedure. If an end point did not achieve statistical significance (P > 0.05), subsequent end points in the prespecified order were considered to be not statistically significant and reported P values were considered nominal.
Source: CSR for CHAMPION-NMOSD study.26 Details included in the table are from the sponsor’s Summary of Clinical Evidence.27
NMOSD Attack or Relapse
The primary outcome in the CHAMPION-NMOSD study was time to first adjudicated on-trial relapse, which also included the assessment of relapse risk reduction. Considering the significant consequences of NMOSD attacks on patient morbidity and quality of life, avoidance of future attacks is paramount in preventing the accumulation of disability in patients and associated mortality.
On-trial relapse was defined as a new onset of neurologic symptoms or worsening of existing neurologic symptoms with an objective change on neurologic examination that persists for more than 24 hours, confirmed by the treating physician. Neurologic signs and symptoms must be attributed to NMOSD (e.g., not caused by other identifiable causes, such as an infection). In clinical practice, the determination of relapses is considered fairly objective, according to the clinical exerts consulted by CADTH; assessment is based on a combination of patient-reported symptoms, clinical exam, clinical tools, and patient history. On-trial relapses were independently reviewed by the relapse adjudication committee, which consisted of physicians who have particular expertise in NMOSD and who conduct independent reviews of all on-trial relapses.
Accurate identification of potential relapses is crucial for the scientific integrity of the study. The adjudication process and relapse definition used in the CHAMPION-NMOSD study were consistent with those used for the external placebo control group in the PREVENT study.
The adjudicated on-trial ARR was assessed as the first hierarchical secondary end point in the trial to account for patients who experienced more than 1 relapse during the primary treatment period. The ARR was computed as the total number of relapses divided by the person-time (in years) and was tested against a rate of 0.25 (1 relapse per 4 patient-years). This comparison was selected, as opposed to a comparison to the PREVENT placebo arm, because of differences in the design of the PREVENT and CHAMPION-NMOSD studies that resulted in different follow-up times for patients who experienced an on-trial relapse. In the PREVENT study, patients were followed for 6 weeks after a relapse; in the CHAMPION-NMOSD study, however, the design allowed for more follow-up time after an initial on-trial relapse, during which additional relapses were recorded. Published registry data support an ARR of 0.6 in patients with NMOSD on commonly used therapies, and a range of ARRs from 0.2 to 0.63 in patients on various first-line therapies has been reported for patients with NMOSD.47 The comparator rate of 0.25 was therefore chosen to represent a conservative ARR that may be seen in the NMOSD patient population.48
Function
Clinically important changes from baseline in ambulatory function, as measured by the HAI, was a second outcome in the trial. The HAI is a rating scale developed to assess mobility by evaluating the time and effort used by the patient to walk 8 m. The scale ranges from 0 to 9, with 0 being the best score (asymptomatic; fully ambulatory with no assistance) and 9 being the worst (uses a wheelchair; unable to transfer self independently). The HAI score was evaluated as a binary end point of clinically important change (clinically important worsening or no clinically important worsening) and was conditional on the baseline value. In the trial, clinically important worsening from baseline was defined as follows:
if the baseline HAI score was 0, then the increase had to be at least 2 points
if the baseline HAI score was greater than 0, then the increase had to be a minimum of 1 point.
The HAI is not routinely used in clinical practice. No MCID could be identified in the literature for patients with NMOSD.
Function was also assessed using the clinically important change from baseline in EDSS score, an ordinal clinical rating scale that ranges from 0 (normal neurologic examination) to 10 (death) in half-point increments. The EDSS quantifies disability in the 7 Kurtzke functional systems (pyramidal, cerebellar, brainstem, sensory, bowel and bladder, visual, and cerebral); in conjunction with ambulation, the disabilities are rated in the context of a standard neurologic examination. These ratings are used together with observations and information concerning the patient’s mobility, gait, and use of assistive devices to assign a score. The validity of this tool has been established and it is usually used as a gold standard for evaluating new scales. In the trial, clinically important worsening from baseline in EDSS score was defined as follows:
if the baseline EDSS score was 0, then the increase had to be at least 2 points
if the baseline EDSS score was 1 to 5, then the increase had to be at least 1 point
if the baseline EDSS score was greater than 5, then the increase had to be at least 0.5 points.
These selected thresholds were considered appropriate by the clinical experts consulted by CADTH, and they reflect the fact that EDSS becomes less sensitive at higher levels.
The EDSS is widely known and used in clinical practice. However, it is heavily dependent on ambulation, and not very sensitive to changes in nonambulatory symptoms, according to the clinical experts. This is the case for changes in vision, which are likely to not be captured, even when these changes may have a very significant impact.
Health-Related Quality of Life
HRQoL was assessed using the EQ-5D (secondary outcome) and ||||| |||||||||||| ||||||||| The EQ-5D is a generic preference-based HRQoL instrument, consisting of a VAS and a composite index score with 5 dimensions: mobility, self-care, usual activities, pain/discomfort, and anxiety/depression. No MCID has been identified in the literature for patients with NMOSD. ||| ||||| ||||||| ||||||||||||| |||||||| || |||||| ||||||| |||||| ||||||| ||||||| || |||| ||||| || ||||||| ||| ||| ||||| |||||||||||| ||| ||||| |||||||| || || ||||| ||||||||| |||| |||||||| ||||||||| ||||||||| |||||| ||||||||| |||| ||||||||||| ||||||||| ||| ||||||||||| |||||| ||||| ||||||| ||||||| ||||||| |||||| ||||||| ||||||||| ||| |||||| |||||||||||| ||| ||||||||||||| |||| |||||||||||| |||||||| || |||||||| |||||| ||| |||||| |||||| ||||||| |||| ||||| ||||||||||| |||||| |||||| |||||| ||| |||||||||| |||| |||||| ||||||| || |||||.
Visual Acuity
|||||| |||||| ||| |||||||| || || ||||||||||| ||||||| ||||| ||| |||||||||||| |||||||||| ||||| ||||||||||||| |||||||||| |||| |||||||| |||||| |||||| ||| |||||| |||||||| ||| ||||||| ||||||||| ||||||||||||||||| ||| |||||||| ||| |||| |||||||||| ||||||| ||| |||||| ||||||| |||||| ||||||| ||| ||||||| ||| ||||| |||||||||||| ||||| ||||||||| |||||| ||||||||||| ||| |||||||||||| |||| || |||||||| ||||||||| ||| || ||||| || |||||||| || ||||||||||| ||| |||| ||||| |||| ||||| || |||||||| |||| ||||||||||| ||||||||| ||| |||||| |||| |||||||| || |||||| ||||||| ||||| ||||||| ||| ||||||||||||||| |||||| |||||||.
Health Care Resource Use
Health care resource use included the |||||||||| || |||||||| ||||||||||||| || |||| || |||||||| || ||||||||||||||||. This was assessed as an exploratory, noncomparative outcome, as no data were reported for the external control group.
Harms
The safety analysis included AEs, SAEs, and AEs leading to study discontinuation.
Table 9: Summary of Outcome Measures and Their Measurement Properties
Outcome measure | Type | Conclusions about measurement properties | MID |
|---|---|---|---|
HAI | Used to evaluate gait and assess the time and effort used by the patient to walk 8 m. The scale ranges from 0 to 9, with 0 being the best score (asymptomatic; fully ambulatory with no assistance) and 9 being the worst (uses a wheelchair; unable to transfer self independently). | No studies of patients with NMOSD assessing validity or reliability were identified. Interrater reliability seems adequate (ICC = 0.96), as does test-retest reliability (ICC = 0.91)40,41 Criterion and construct validity are reported as excellent when correlated with other instruments that assess gait and ambulation.41-43 | None identified for patients with NMOSD or MS. |
EQ-5D | Generic preference-based HRQoL instrument, consisting of a VAS and a composite index score with 5 dimensions: mobility, self-care, usual activities, pain/discomfort, and anxiety/depression. | One systematic review31 that assessed the EQ-5D (9 studies) in patients with MS: Content validity: included certain domains, such as walking (mobility) and mood (anxiety/depression), that patients considered important to their quality of life; however, other critical domains (fatigue and cognition) were not included in the EQ-5D. Convergent validity of impairment (gait, speed, severity) was moderate (pooled correlation estimate = 0.35; 95% CI, 0.25 to 0.45). For activity limitations, the pooled correlation was 0.51 (95% CI, 0.45 to 0.57). When EQ-5D was compared against measures evaluating HRQoL, the correlation value was 0.56 (95% CI, 0.54 to 0.59). Discriminative validity was evaluated in 3 studies; the mobility item lacked discriminative ability. The EQ-5D was able to differentiate among all EDSS levels, except between EDSS levels 3 and 4. Test-retest reliability: The ICC for test-retest reliability of the EQ-5D was 0.81 (acceptable). | None identified for patients with NMOSD. An MID was reported for fatigue in only 1 study (of patients with MS),44 although this dimension is not included in the EQ-5D. |
EDSS | Ordinal clinical rating scale that ranges from 0 (normal neurologic examination) to 10 (death) in half-point increments. The Kurtzke functional systems (pyramidal, cerebellar, brainstem, sensory, bowel and bladder, visual, cerebral) and ambulation are rated in the context of a standard neurologic examination. These ratings are used in conjunction with observations and information concerning the patient’s mobility, gait, and use of assistive devices to assign an EDSS score. | Validity has been established, and EDSS is usually used as a gold standard for evaluating new scales.39 Reliability has low to moderate values, with interrater kappa values between 0.32 and 0.76 for EDSS and between 0.23 and 0.58 for the individual functional systems. For scores below 3.5, reliability is regarded as good.39 | No MID specific to NMOSD was found. Indirect estimates can be obtained from patients with MS; 1 study showed that a change of 1.5 points on a single score was considered enough deterioration from the patient perspective.28 This was in agreement with a second study, which stated that, from a baseline score of 0, a 1.5-point increase was important; from a baseline score of 1 to 5.5, a 1-point increase was considered important, and from a baseline score ≥ 6, a 0.5-point increase was considered important.29 |
||||| | |||||||||||| |||||||||| ||||| |||||||| |||||||||| |||| |||||||| |||||| |||||| ||| |||||| |||||||| ||| ||||||| | | || ||||||| || |||||||| || ||||||||||| ||| |||| ||||| |||| ||||| |||||| || |||||||| |||| ||||| || |||| | |||| ||||||||||| |
|||||| | ||||||| ||||||||||||| ||||||||||||| |||||||||| || ||||| |||||||| |||||||| |||||||||||| |||| ||||||||| |||||| ||||| ||||||| ||||||| ||||||||| |||||| |||||||||||| |||| |||||||||| ||| |||||| |||||||||||| ||||| |||| ||||||||||||| |||||||| || |||||||| |||||| |||| |||||||| ||||||||| ||||| ||||| |||||||| ||| |||||| |||||| |||| |||||| ||||||||| ||||| ||||| |||||||| ||||||| |||| ||||| ||||||||||| |||||| |||||| |||||| ||| |||||||||| |||| |||||| ||||||| || |||||| | || ||||||| || |||||||| |||| ||||| |||| ||||||||||| |||||||||| ||| |||| ||||||||| || |||||||| |||| || ||| |||||||||||| ||||||||||||| ||| |||||||||||||| ||||||||||||||||| ||| |||| |||||||| |||||| |||||| ||||||||||| ||||||||||| ||||| |||| ||| ||| ||||||||||| ||| |||||||| ||||| |||||||||||| ||||||| |||| ||| || ||||| ||| ||| |||||||| ||| ||||||| |||||| ||||||||||||||||| |||||||| ||||||||||| ||| ||| ||||| |||||||||| ||| ||| ||| ||||||||| ||||||| ||| ||| |||| |||| ||| ||||||||| || |||||| ||||||||| |||||||||||| ||||||| || || ||||||||| ||| |||||||||| |||||||| |||| ||||| ||||||||||| ||||||||||| ||||||| |||||||| |||| |||||||||||| ||| ||||| |||||||||| ||| |||||||||| | || ||| ||||||| |||| ||||| ||| |||||||| |||| |||||| |||||||| |||||||| |||| |||||||| |||| || ||| ||||||||| |||| ||| |||||||| |||||||||||| |||| ||||||||| |||||| |||||||||||| ||| ||| |||| ||| ||||| |||| |||||||| || ||| ||||||||| |||||| ||| ||| ||||| ||||||| |||| || ||||||||||||||| ||| |||||||| ||||||||||||||| |||| ||||||||| |||||||| |||||| |||||||||||| ||| ||| ||| |||||| ||| ||| ||| |||||||||||| ||| |
CI = confidence interval; EDSS = Expanded Disability Status Scale; HAI = Hauser Ambulation Index; HRQoL = health-related quality of life; ICC = intraclass correlation coefficient; MID = minimal important difference; MS = multiple sclerosis; mRS = Modified Rankin Scale; NMOSD = neuromyelitis optica spectrum disorder; |||||||||||||| |||||| |||||||||||| ||||| |||||; VAS = visual analogue scale.
Source: CADTH Clinical Review Report for Eculizumab (Soliris) 2020.38
Statistical Analysis
Primary End Point Analysis
The primary efficacy end point (time to first adjudicated on-trial relapse) was evaluated using the log-rank test, with the null hypothesis being no difference in the survival curves for the ravulizumab and placebo treatment groups. The alternative hypothesis is a difference between the 2 survival curves, with ravulizumab superior to placebo.
The primary end point was considered to have met its primary efficacy objective if a statistically significant difference (i.e., 2-sided P ≤ 0.05) is observed between the ravulizumab group and the placebo group for the primary end point of time to first adjudicated on-trial relapse. A Cox proportional hazards model that included treatment group as a factor was used for the HR and risk reduction. The Kaplan-Meier estimates of the proportion of patients with no adjudicated on-trial relapse is presented for various time points (e.g., week 26, week 50), with a 95% CI based on the complementary log-log transformation.
Key Sensitivity Analyses of the Primary End Point
Sensitivity analysis stratified by propensity score: A sensitivity analysis for the comparison of the treatment groups for the primary end point was conducted using propensity score strata. The propensity score is the probability of being assigned to the placebo arm, as opposed to the ravulizumab arm, and was estimated from a logistic regression that included observed baseline characteristics as predictors of the treatment assignment. |||||||||| ||||| ||| ||||||||| ||| |||| ||||||| ||| ||||||||||| |||| ||| ||||||| |||| |||| |||| ||||||| || |||||||||| || |||||||| || ||||||| || |||| || ||||||| ||||||||||| || ||||| || ||| ||||||| ||||||||| |||||| |||||| ||||| ||| |||| ||||||||| ||| |||||||||| ||||||| |||||||||||| ||||||| |||||| |||| |||||||||| ||||| |||||||||| ||||| |||||||.
Furthermore, stabilized inverse probability of treatment weights (IPTWs) were used in a weighted analysis of the primary end point. The IPTW is the weight defined as the inverse of the probability of being in the treatment group to which the patient was assigned. If a few patients have large weights, the resulting weighted estimator may have a large variance. To reduce the variance, these weights are stabilized by multiplying the IPTW by the marginal probability of receiving the given treatment.
Tipping point analysis (E-value): The E-value, constructed as a risk ratio, quantifies the level of confounding that could compensate the estimated treatment effect; the smallest E-value, of 1, represents no confounding. The E-value was calculated using the HR from the Cox proportional hazards model using both the unstratified model described for the primary analysis and the model |||||||||| ||||| |||||||||| ||||| |||||||.
Secondary End Point Analyses
The adjudicated on-trial ARR was presented with a 95% CI from a Poisson regression model in which the log of time in the study period was used as the offset variable and historical ARR for the 24 months before screening was a covariate in the model. The null hypothesis was that the mean adjudicated on-trial ARR is equal to 0.25 relapse/patient-year. The alternative hypothesis was that the mean adjudicated on-trial ARR is not equal to 0.25. This end point would be met if the adjudicated on-trial ARR was less than 0.25 (i.e., in favour of ravulizumab) and a 2-sided P value was less than 0.05. A sensitivity analysis comparing the ARR in the ravulizumab arm with the ARR in the placebo arm was performed using Poisson regression, with treatment group as a factor, the log of time as an offset variable, and adjustment for historical ARR for the 24 months before screening. |||||||||| ||||||||||| |||||||| |||| ||||||||| ||||||||| ||| |||||||||| ||||| ||||||| ||||||||| ||| |||||||| ||||||||||||| |||||| || ||||||||| ||| ||| ||||||| |||||||||.
For a clinically important change in HAI score, the null hypothesis was that the odds of a better outcome are the same in the ravulizumab and placebo arms. The alternative hypothesis was that there is a difference between treatment arms in the odds of a better outcome, and that ravulizumab has higher odds of a better outcome. Logistic regression was used to evaluate the effect of ravulizumab on reduction in clinical worsening. |||||||||| |||||||| || ||| |||||||||| ||||||||| |||||| || ||| ||| |||||||||| ||||||||| ||| |||||||||| ||||| |||||||.
For the EQ-5D and the EQ-5D VAS, the null hypothesis was that there is no difference in the distribution between the ravulizumab arm and the placebo arm. The alternative hypothesis was that there is a difference in the distribution between treatment arms, and that ravulizumab is superior to placebo. The change from baseline in the EQ-5D index score was analyzed using analysis of covariance (ANCOVA), in which the ranks of the change from baseline were the dependent variable, with treatment as a factor and the ranks of the baseline values as a covariate.
For the EDSS, the null hypothesis was that the odds of a worse outcome are the same in the ravulizumab and placebo arms. The alternative hypothesis was that there is a difference in the odds of a worse outcome between the treatment arms, and that the odds of a worse outcome are lower in the ravulizumab arm. The change from baseline in the EDSS score was categorized by clinically important worsening (no worsening, clinical worsening). This end point was analyzed using a logistic regression model that included treatment group, with baseline EDSS as a covariate.
Sample Size and Power Calculation
The sample size and power calculation assumptions for this study using the primary end point, time to first relapse, are as follows:
the log-rank test was used to compare ravulizumab and placebo
there were 47 patients in the placebo treatment group
power was 90% to detect a treatment difference
the 2-sided level of significance was 5%
the dropout rate was 2% to 10%
the relapse-free rate was 92% in the ravulizumab arm at 12 months
the relapse-free rate was 63% in the placebo arm at 12 months.
With these assumptions, a maximum sample size of approximately 55 patients in the ravulizumab treatment group provides at least 90% power to detect a treatment difference in time to first positively adjudicated relapse.
Statistical Testing
Both the primary and secondary efficacy analyses were conducted on the full analysis set. The CHAMPION-NMOSD analyses used aggregated data for outcome results from the PREVENT study and individual data for the propensity score analysis.
Type I error was controlled using a closed testing procedure. If the primary end point was statistically significant, the following secondary end points were evaluated in the following rank order:
adjudicated on-trial ARR
clinically important changes from baseline in ambulatory function, as measured by HAI score
change from baseline in EQ-5D index score
change from baseline in EQ-5D VAS score
clinically important worsening from baseline in EDSS score.
Hypothesis testing proceeded from the highest rank (the adjudicated on-trial ARR) to the lowest rank (EDSS score). CIs and P values were calculated for all secondary end points.
Baseline was defined as the last available assessment before treatment for all patients. The HAI, EQ-5D index score, EQ-5D VAS score, and the EDSS were evaluated as the change from baseline to the 6-week postrelapse period or the end of the primary treatment time point. For the external placebo arm, scores were evaluated for the 6-week postrelapse period for patients who had an on-trial relapse and for the end of the study for patients who did not have a relapse. For the treatment group, scores were evaluated for the 6 week postrelapse visit for the first observed on-trial relapse for patients who had an on-trial relapse and for the end of the primary treatment visit for patients who did not have a relapse.
Subgroup Analyses
The following prespecified subgroup analyses were performed for the full analysis set:
The assessment of the severity and type of relapse was conducted by treatment group in the subgroup of patients who had adjudicated on-trial relapses. The following subgroups were used —
region
age group (≥ 45 vs < 45 years)
sex
race
use of concomitant IST at baseline
prior rituximab use
propensity score strata
randomization stratification variable from the PREVENT study.
The assessment of visual acuity, colour vision, and confrontational visual fields was conducted in the subgroup of patients who had vision at baseline in at least 1 eye.
In addition, a posthoc analysis of the primary and all key secondary end points was conducted on the subgroup of patients who have had more than 1 historical relapse (i.e., patients who entered the trial after a second lifetime attack) and were using supportive IST for NMOSD before the most recent relapse.
Table 10: Statistical Analysis of Efficacy End Points in the CHAMPION-NMOSD Study
End point | Statistical model | Adjustment factors | Handling of missing data | Sensitivity analyses |
|---|---|---|---|---|
Time to first adjudicated on-trial relapse and relapse risk reduction | Time to first adjudicated on-trial relapse: log-rank test Relapse risk reduction: Cox proportional hazards model | To account for potential differences in baseline characteristics between the treatment group in the CHAMPION-NMOSD study and the external placebo arm from the PREVENT study, sensitivity analyses included a covariate adjustment methodology (propensity score methodology) The variables in the propensity score calculation included region, sex, age at first dose, background IST use, baseline EDSS score, and ARR in the 24 months before screening | Patients who did not have adjudicated ON-TRIAL RELAPSEs were censored and had a censor time based on the time from first dose to the end of the primary treatment period (or the end of the study for the placebo group) | ||||||||||| |||||||| |||||||||| || |||||||||| ||||| |||||| Sensitivity analysis using propensity scores in a weighted analysis |
Adjudicated on-trial ARR | Poisson regression model | Sensitivity analysis adjusted for historical ARR, historical ARR and propensity score strata, historical ARR and observed PREVENT randomization strata, and time since the last relapse before screening; the duration of COVID-19 infection was excluded | ||
Clinically important change from baseline in HAI | Logistic regression model | |||||||| ||||||||| |||| || |||||||||| ||| ||||||||||| ||||| || |||||||| |||||||| ||| |||| |||||||| ||||| ||||||||||| ||||||||| ||||| ||| || || |||| ||||||| |||||||||| ||| || ||||||||||||| |||||||||||| ||| |||||||| ||||| ||| || || |||| | ||||||||||| |||||||| ||||||||| ||| |||||||||| ||||| |||||| | |
Change from baseline in EQ-5D index score and EQ-5D VAS score | ANCOVA of the ranks | |||
Clinically important worsening from baseline in EDSS | Logistic regression model |
ANCOVA = analysis of covariance; ARR = annualized relapse rate; EDSS = Expanded Disability Status Scale; HAI = Hauser Ambulation Index; IST = immunosuppressive treatment; LOCF = last observation carried forward; NMOSD = neuromyelitis optica spectrum disorder; VAS = visual analogue scale.
Source: CSR for CHAMPION-NMOSD study (CSR Section 5.1.1.2, Statistical Analysis Plan Section 7.2.1.1).26 Details included in the table are from the sponsor’s Summary of Clinical Evidence.27
Analysis Populations
Table 11: Analysis Populations of the CHAMPION-NMOSD Study
Population | Definition | Application |
|---|---|---|
Full analysis set | All patients who received at least 1 dose of the study drug (ravulizumab or placebo) | Primary efficacy analysis, secondary efficacy analysis, and exploratory efficacy analysis |
Per-protocol set | Subset of the full analysis set population, excluding patients with major protocol deviations, which includes all patients who:
| Primary efficacy analysis and sensitivity analysis |
Safety analysis set | All patients who received at least 1 dose of the study drug (ravulizumab or placebo) | Safety analysis |
Pharmacokinetics and/or pharmacodynamics | Patients who received at least 1 dose of the study drug and who had at least 1 evaluable pharmacokinetic or pharmacodynamic result | Pharmacokinetic and pharmacodynamic analyses |
Source: CHAMPION-NMOSD CSR, Section 626 Details included in the table are from the sponsor’s Summary of Clinical Evidence.27
Results
Patient Disposition
Of the 78 screened patients, 20 (25.6%) were screen failures. The most common (≥ 5%) reason for a screen failure was not meeting the inclusion criteria of being anti-AQP4 antibody-positive at screening and having a diagnosis of NMOSD (n = 9; 11.5%). A total of 58 patients were treated with ravulizumab in the CHAMPION-NMOSD study. As of the clinical data cut-off date (March 15, 2022), 56 of the 58 patients completed the primary treatment period and 57 patients were reported to be continuing the study. This is consistent with the results from the PREVENT placebo group, in which 44 of 47 patients completed the study.
Table 12: Summary of Patient Disposition From the CHAMPION-NMOSD and PREVENT Studies
Variable category | PREVENT Placebo (N = 47) n (%) | CHAMPION-NMOSD Ravulizumab (N = 58) n (%) |
|---|---|---|
Treated | 47 | 58 |
Completed primary treatment period | NR | 56 (96.6) |
Discontinued primary treatment period | NR | 2 (3.4) |
Adverse event | NR | 2 (3.4) |
Continuing in or completed the study | 44 (93.6) | 57 (98.3) |
Discontinued the study | 3 (6.4) | 1 (1.7) |
Adverse event | 2 (4.3) | 1 (1.7) |
Withdrawal by patient | 1 (2.1) | 0 |
NR = not reported.
Sources: CHAMPION-NMOSD CSR,26 CADTH Clinical Review Report for Eculizumab (Soliris) 2020.38 Details included in the table are from the sponsor’s Summary of Clinical Evidence.27
Baseline Characteristics
The baseline demographic characteristics were similar in the 2 treatment groups and are outlined in Table 13. Patient age differed marginally, with patients in the ravulizumab group being slightly older than patients in the placebo group. NMOSD in itself is a severe disease with a generally poor natural trajectory; according to the clinical experts consulted by CADTH, the risk of relapse is considered high for any patient at any disease stage, regardless of demographic or disease characteristics.
Table 13: Summary of Baseline Characteristics From the CHAMPION-NMOSD Study (Safety Set) and the PREVENT Study
Variable | PREVENT Placebo (N = 47) | CHAMPION-NMOSD Ravulizumab (N = 58) |
|---|---|---|
Age category, n (%) | ||
< 45 years | 24 (51.1) | 25 (43.1) |
≥ 45 years | 23 (48.9) | 33 (56.9) |
Age category, n (%) | ||
18 to < 65 years | 44 (93.6) | 51 (87.9) |
≥ 65 years | 3 (6.4) | 7 (12.1) |
Sex, n (%) | ||
Male | 5 (10.6) | 6 (10.3) |
Female | 42 (89.4) | 52 (89.7) |
Ethnicity, n (%) | ||
Hispanic or Latino | 3 (6.4) | 9 (15.5) |
Not Hispanic and not Latino | 41 (87.2) | 45 (77.6) |
Not reported | 1 (2.1) | 4 (6.9) |
Unknown | 2 (4.3) | 0 (0.0) |
Race, n (%) | ||
Asian | 15 (31.9) | 21 (36.2) |
Black or African American | 8 (17.0) | 6 (10.3) |
White | 24 (51.1) | 29 (50.0) |
Unknown | 0 (0.0) | 2 (3.4) |
Japanese origin, n (%) | ||
Yes | 5 (10.6) | 9 (15.5) |
No | 42 (89.4) | 49 (84.5) |
Region,a n (%) | ||
Americas | 15 (31.9) | 21 (36.2) |
Europe | 19 (40.4) | 17 (29.3) |
Asia-Pacific | 13 (27.7) | 20 (34.5) |
Weight (kg), n | 47 | 58 |
Mean (SD) | 69.65 (16.441) | 69.85 (19.343) |
Median | 67.00 | 63.80 |
Range | 46.1 to 116.0 | 41.0 to 124.7 |
Height (cm), n | 47 | 56 |
Mean (SD) | 164.50 (8.147) | 161.86 (8.157) |
Median | 163.50 | 160.00 |
Range | 149.9 to 193.0 | 148.0 to 193.0 |
Body mass index (kg/m2), n | 47 | 56 |
Mean (SD) | 25.65 (5.240) | 26.68 (6.501) |
Median | 24.73 | 25.65 |
Range | 17.7 to 38.5 | 17.7 to 45.8 |
SD = standard deviation.
Note: The placebo group data were collected as part of the PREVENT study.
aAmericas: Argentina, Canada, and the US; Europe: Germany, Denmark, Spain, the UK, Croatia, Italy, Poland, Russia, and Turkey; Asia-Pacific: Australia, Hong Kong, Japan, the Republic of Korea, and Taiwan.
Source: CHAMPION-NMOSD CSR.26 Details included in the table are from the sponsor’s Summary of Clinical Evidence.27
Disease characteristics are outlined in Table 14. Patients in the ravulizumab group appeared to have a slightly better level of function, based on HAI and EDSS scores; a similar observation can be made for HRQoL, assessed by the EQ-5D index score and EQ-5D VAS. According to the clinical experts, differences in disease characteristics between the ravulizumab and placebo groups were not expected to meaningfully affect outcome results. Baseline EDSS, HAI, and EQ-5D scores in both groups were considered to be representative of disability in an NMOSD population.
Table 14: Summary of NMOSD Disease Characteristics From the CHAMPION-NMOSD Study (Safety Set) and the PREVENT Study
Variable | Statistic | PREVENT placebo (N = 47) | CHAMPTION-NMOSD ravulizumab (N = 58) |
|---|---|---|---|
Baseline HAI score | Mean (SD) | 2.1 (1.40) | 1.2 (1.42) |
Median | 2.0 | 1.0 | |
Range | 0 to 6 | 0 to 7 | |
Baseline EQ-5D Index Score | Mean (SD) | 0.680 (0.1961) | 0.766 (0.2203) |
Median | 0.706 | 0.815 | |
Range | 0.27 to 1.00 | 0.04 to 1.00 | |
Baseline EQ-5D VAS | Mean (SD) | 59.1 (20.39) | 73.6 (14.81) |
Median | 60.0 | 77.5 | |
Range | 0 to 95 | 30 to 97 | |
Baseline EDSS score | Mean (SD) | 4.26 (1.510) | 3.30 (1.584) |
Median | 4.00 | 3.25 | |
Range | 1.0 to 6.5 | 0.0 to 7.0 | |
Age at NMOSD initial clinical presentation (years) | Mean (SD) | 38.5 (14.98) | 42.3 (15.15) |
Median | 38.0 | 42.5 | |
Range | 12 to 73 | 16 to 73 | |
Age at NMOSD diagnosis (years) | Mean (SD) | 41.1 (14.36) | 44.2 (14.48) |
Median | 42.0 | 44.0 | |
Range | 14 to 73 | 17 to 73 | |
Time from initial clinical presentation to first IP dose (years) | Mean (SD) | 6.601 (6.5863) | 5.189 (6.3762) |
Median | 3.760 | 1.955 | |
Range | 0.51 to 29.10 | 0.19 to 24.49 | |
Time from NMOSD diagnosis to first IP dose (years) | Mean (SD) | 3.932 (4.4804) | 3.267 (4.3616) |
Median | 2.030 | 0.935 | |
Range | 0.23 to 23.78 | 0.08 to 24.13 | |
Time from initial clinical presentation to NMOSD diagnosis (months) | Mean (SD) | 32.067 (58.1952) | 23.093 (47.9133) |
Median | 9.510 | 1.960 | |
Range | 0.00 to 269.24 | 0.00 to 202.20 |
EDSS = Expanded Disability Status Scale; EQ-5D = European Quality of Life Health 5-dimension Questionnaire; HAI = Hauser Ambulation Index; IP = investigational product; max = maximum; min = minimum; NMOSD = neuromyelitis optica spectrum disorder; SD = standard deviation; VAS = visual analogue scale.
Note: The placebo group data were collected as part of the PREVENT study.
Details included in the table are from the sponsor’s Summary of Clinical Evidence.27
Source: CHAMPION-NMOSD CSR26
History of prior relapses is outlined in Table 15. Patients in the PREVENT placebo group had a mean of 6.3 (SD = 4.58) historical relapses; of these, 2.1 (SD = 0.78) relapses occurred in the 12 months before the study. This was higher than for patients in the ravulizumab group, who had a mean of 3.6 (SD = 4.00) historical relapses, of which 1.4 (SD = 0.68) were in the prior 12 months. According to the clinical experts consulted by CADTH, the history of prior relapse is not expected to have any impact on the risk of future relapses. As such, differences in NMOSD history for patients in the ravulizumab and placebo groups would not meaningfully affect results for the primary outcome of relapse prevention.
However, the clinical experts emphasized that the frequency and severity of prior attacks might be correlated with the likelihood of being incapacitated with future relapse. The mean (SD) ARR, which may inform the frequency of relapses, was 2.04 (1.533) in the ravulizumab group and 2.23 (1.088) in the placebo group in the prior 12 months, and 1.87 (1.594) in the ravulizumab group and 2.07 (1.037) in the placebo group in the prior 24 months. This was consistent with the assumption that both groups were having a relatively similar evolution in terms of relapse frequency, according to the clinical experts.
Table 15: History of Prior Relapses From the Studies Included in the Systematic Review (Safety Set)
Variable | Statistic | PREVENT placebo (N = 47) | CHAMPION-NMOSD ravulizumab (N = 58) |
|---|---|---|---|
Total number of historical relapses | Mean (SD) | 6.3 (4.58) | 3.6 (4.00) |
Median | 4.0 | 2.0 | |
Range | 2 to 20 | 1 to 22 | |
Number of relapses (within the 12 months before screening) | Mean (SD) | 2.1 (0.78) | 1.4 (0.68) |
Median | 2.0 | 1.0 | |
Range | 1 to 4 | 1 to 4 | |
Historical ARR (within the 12 months before screening) | Mean (SD) | 2.23 (1.088) | 2.04 (1.533) |
Median | 1.85 | 1.75 | |
Range | 0.9 to 6.4 | 0.9 to 6.9 | |
Number of relapses (within the 24 months before screening) | Mean (SD) | 3.2 (0.97) | 1.7 (0.87) |
Median | 3.0 | 1.5 | |
Range | 2 to 6 | 1 to 4 | |
Historical ARR (within the 24 months before screening) | Mean (SD) | 2.07 (1.037) | 1.87 (1.594) |
Median | 1.92 | 1.44 | |
Range | 1.0 to 6.4 | 0.5 to 6.9 |
ARR = annualized relapse rate; SD = standard deviation
Note: The placebo group data were collected as part of the PREVENT study.
Source: CHAMPION-NMOSD CSR.26 Details included in the table are from the sponsor’s Summary of Clinical Evidence.27
History of prior NMOSD therapies is outlined in Table 16. Most patients in both the ravulizumab (n = 50; 86.2%) and placebo (n = 45; 95.7%) groups had used supportive therapy for NMOSD before the study; the most common drugs were corticosteroids, rituximab, and azathioprine. According to the clinical experts, prior treatment is not expected to change the magnitude of response to future treatment. The only exception to this would be in the case of 2 drugs that have the same mechanism of action; however, no patient in the studies had received prior treatment with eculizumab.
Table 16: Supportive Therapy for Patients With NMOSD Prior to the Study Included in the Systematic Review (Safety Set) and the PREVENT Study
Therapy categorization | PREVENT placebo (N = 47) n (%) | CHAMPION-NMOSD ravulizumab (N = 58) n (%) |
|---|---|---|
Patients with any prior supportive therapy for NMOSD | 45 (95.7) | 50 (86.2) |
Azathioprine | 26 (55.3) | 13 (22.4) |
Cyclosporine and tacrolimus | 3 (6.4) | 1 (1.7) |
Corticosteroids | 30 (63.8) | 29 (50.0) |
Cyclophosphamide | 5 (10.6) | 0 (0.0) |
IV immunoglobulin | 2 (4.3) | 1 (1.7) |
Methotrexate | 5 (10.6) | 0 (0.0) |
Mitoxantrone and 2-CDA | 3 (6.4) | 1 (1.7) |
Mizoribine | 2 (4.3) | 0 (0.0) |
Mycophenolate mofetil | 15 (31.9) | 7 (12.1) |
Rituximab | 20 (42.6) | 21 (36.2) |
Satralizumab | 0 (0.0) | 1 (1.7) |
2-CDA = cladribine (2-chloro-deoxyadenosine); NMOSD = neuromyelitis optica spectrum disorder.
Source: CHAMPION-NMOSD CSR.26 Details included in the table are from the sponsor’s Summary of Clinical Evidence.27
A summary of baseline characteristics to support the posthoc subgroup analysis is provided in Table 17; patients were segregated by number of historical relapse and use of supportive IST. In the ravulizumab group, 42 of 58 (72.4%) patients had more than 1 historical relapse at trial entry. Of these patients, the majority (30 patients, or 71.4%) had used supportive ISTs before the most recent relapse. All patients in the PREVENT placebo arm had more than 1 historical relapse, in accordance with trial inclusion criteria definition.
Table 17: Summary of Historical Relapse and Supportive Therapy for the CHAMPION-NMOSD Study (Safety Set) and the PREVENT Study
Relapse and supportive therapy | PREVENT placebo (N = 47) n (%) | CHAMPION-NMOSD ravulizumab (N = 58) n (%) |
|---|---|---|
History of > 1 historical relapse | ||
Number of patients | 47 (100.0) | 42 (72.4) |
Use of supportive IST for NMOSD before the last relapse | ||
Yes | 39 (83.0) | 30 (71.4) |
No | 8 (17.0) | 12 (28.6) |
IST = immunosuppressive treatment; NMOSD = neuromyelitis optica spectrum disorder.
Note: The placebo group data were collected as part of the PREVENT study.
Source: Details included in the table are from the sponsor’s Summary of Clinical Evidence.27
Propensity scores were used to evaluate any differences in baseline characteristics between patients in the CHAMPION-NMOSD ravulizumab group and those in the PREVENT placebo group. The variables in the propensity score calculation included region, sex, age at first dose, background IST use, baseline EDSS score, and historical ARR in the 24 months before screening. Sensitivity analyses for the efficacy end points ||||||||||| || |||||||||| ||||| |||||| |||| ||||||||| || ||||||| ||||| |||||||| |||||||||| ||||||| ||||||||| |||||| ||| ||||||| |||||| ||||||||| |||| |||||||||| ||||||| || |||||||| |||||||| ||||||||| |||||||||||||| || |||||| |||||||||| |||||| ||||| || |||||||| || ||| ||||||||||| ||||| ||| ||||| || |||||||| || ||| ||||||| ||||| |||||||||||| ||||| |||| ||| ||||| ||| ||||||| ||||| ||||||||| |||| |||||||| |||||||| ||||||||||||||| |||||||| || ||| |||||||||| ||||| ||||||||||| ||||||| ||||||||||| || ||||||||| || ||| ||||||||||| ||||| |||| ||| ||||||| ||||||| ||||| |||| ||||||||||| ||||||| ||||||||| |||||| ||||||||| ||||||||||||||| |||| ||||| |||||||| |||||| ||| |||||||||| ||||| ||||||| ||| |||||||| || |||||||||| |||||||| || ||| |||||||||| ||||| ||||||||||| |||||||||||||| |||| |||||||||| |||||||| |||||||||| |||| ||||| |||||||||| |||| |||||||| |||||| |||||||.
As another approach to balance the baseline covariates between treatment groups and more closely match the patients between treatment groups, standardized IPTWs, derived from propensity scores, were applied in the summary of baseline characteristics. Following this method of weighting, the standardized mean difference for all covariates included in the propensity score calculation was less than ± 0.25, indicating that the objective of balancing the baseline characteristics between treatment groups was achieved. This method of weighting also balanced covariates not included in the propensity score calculation, including HAI score and EQ-5D index score.
Exposure to Study Treatments
Exposure to study treatment is outlined in Table 18. As of the data cut-off date (July 15, 2022), the median (range) study duration was 90.93 (13.7 to 135.1) weeks in the ravulizumab group, which represents an additional median study duration of 17.43 weeks from the last data cut-off date (March 15, 2022). The median (range) study duration during the primary treatment period was 73.50 (13.7 to 117.7) weeks. The majority (47 patients; 81.0%) of patients were followed for more than 18 months, with 14 (24.1%) patients followed for more than 24 months. The median (range) number of ravulizumab infusions was 13.0 (2 to 20). The follow-up duration was considered long enough for the trial to adequately capture relapses in the included population, according to the clinical experts.
Table 18: Summary of Patient Exposure From the Study Included in the Systematic Review
Variable | Statistic | CHAMPION-NMOSD ravulizumab (N = 58) |
|---|---|---|
Study duration (weeks)a | Mean (SD) | 92.54 (19.463) |
Median | 90.93 | |
Range | 13.7 to 135.1 | |
Total patient-years | 102.9 | |
Treatment duration (weeks)b | Mean (SD) | 88.20 (19.680) |
Median | 89.93 | |
Range | 2.0 to 131.1 | |
Total patient-years | 98.0 |
SD = standard deviation
Note: Study duration and treatment duration from the start of the primary treatment period through the data cut-off date (July 15, 2022) in the long term extension period are included.
aStudy duration = date of completion, discontinuation, last assessment (or death), or data cut-off – date of first study drug dose + 1.
bTreatment duration = date of last study drug dose – date of first study drug dose + 1.
Source: CHAMPION-NMOSD CSR.26 Details included in the table are from the sponsor’s Summary of Clinical Evidence.27
A summary of supportive therapies used at baseline and concomitantly throughout the study is outlined in Table 19. A greater percentage of patients in the placebo group than in the ravulizumab group were on ISTs (72.3% versus 48.3%); of these, 23.4% and 20.7% of patients, respectively, received corticosteroids. According to the clinical experts, the concomitant use of ISTs is not likely to introduce bias, as these do not impact disease trajectory. However, early aggressive rescue therapy with corticosteroids for an acute attack is expected to have a positive impact that will ultimately limit disability.
Patients on ISTs at baseline were required to remain on a stable dose of IST, within prespecified limits. Patients with changes in IST treatment during the study that were not allowed per protocol were excluded from the per-protocol set; 2 (3.4%) patients in the ravulizumab group and 1 (2.1%) patient in the placebo group had a concomitant important IST change that resulted in their exclusion from the per-protocol analyses.
Table 19: Summary of Supportive Therapy Used at Baseline in the CHAMPION-NMOSD and PREVENT Studies
IST categorization | PREVENT placebo (N = 47) n (%) | CHAMPION-NMOSD ravulizumab (N = 58) n (%) |
|---|---|---|
Any IST usage | 34 (72.3) | 28 (48.3) |
Steroids alone | 11 (23.4) | 12 (20.7) |
Azathioprine subgroup | 13 (27.7) | 7 (12.1) |
|||||||||||| ||||| | |||||| | |||||| |
||||||||||||||||||| | |||||| | |||||| |
Mycophenolate mofetil subgroup | 8 (17.0) | 6 (10.3) |
||||||||||||| ||||||| ||||| | |||||| | |||||| |
||||||||||||| |||||||||||||| | |||||| | |||||| |
Other ISTs | 2 (4.3) | 3 (5.2) |
||||| |||| ||||| | |||||| | |||||| |
||||| ||||||||||| | |||||| | |||||| |
No IST usage (monotherapy) | 13 (27.7) | 30 (51.7) |
IST = immunosuppressive treatment.
Note: The placebo group data were collected as part of the PREVENT study.
Source: CHAMPION-NMOSD CSR.26 Details included in the table are from the sponsor’s Summary of Clinical Evidence.27
Efficacy
Results of the primary and key secondary end points are presented for both the primary analysis (data cut-off date of March 15, 2022) and the latest addendum based on a data cut-off date of July 15, 2022. The median analysis follow-up time as of the July cut-off date was 90.93 weeks, which represents an additional median analysis follow-up of 17.43 weeks over that reported from the primary analysis period. Results for the remaining secondary end points are from the primary analysis, with the data cut-off date of March 15, 2022.
NMOSD Attack or Relapse
No patients in the ravulizumab group reported a primary outcome event of adjudicated on-trial relapse during the primary treatment period, compared with 20 patients (42.6%) in the placebo group from the PREVENT study. In the primary analysis, performed at the data cut-off date of March 15, 2022, the use of ravulizumab was associated with an HR of 0.014 (95% CI, 0.000 to 0.103) versus placebo. The log-rank test yielded a P < 0.0001. The median analysis follow-up time was 73.50 (95% CI, 11.00 to 117.71) weeks for the ravulizumab group and 36.00 (95% CI, 1.86 to 117.71) weeks for the placebo arm. The use of ravulizumab was associated with a relative relapse risk reduction of 98.6% (95% CI, 89.7% to 100.0%) compared with placebo.
Results of the analysis performed at the data cut-off date of July 15, 2022 (through the long-term extension period) were consistent with those from the primary analysis, with an HR of 0.013 (95% CI, 0.000 to 0.093; P < 0.0001) versus placebo. Median (range) follow-up was 90.0 (11.0 to 135.1) weeks for patients in the ravulizumab group (102.8 patient-years) and 36.0 (1.9 to 135.1) weeks for patients in the placebo group (48.6 patient-years). Kaplan-Meier survival curves are presented in Figure 2; the curves separate early, favouring ravulizumab, and remain separated throughout follow-up.
Figure 2: Kaplan-Meier Survival Estimates for Time to First Adjudicated On-Trial Relapse Through to the July 15, 2022 Data Cut-Off Date (Full Analysis Set)
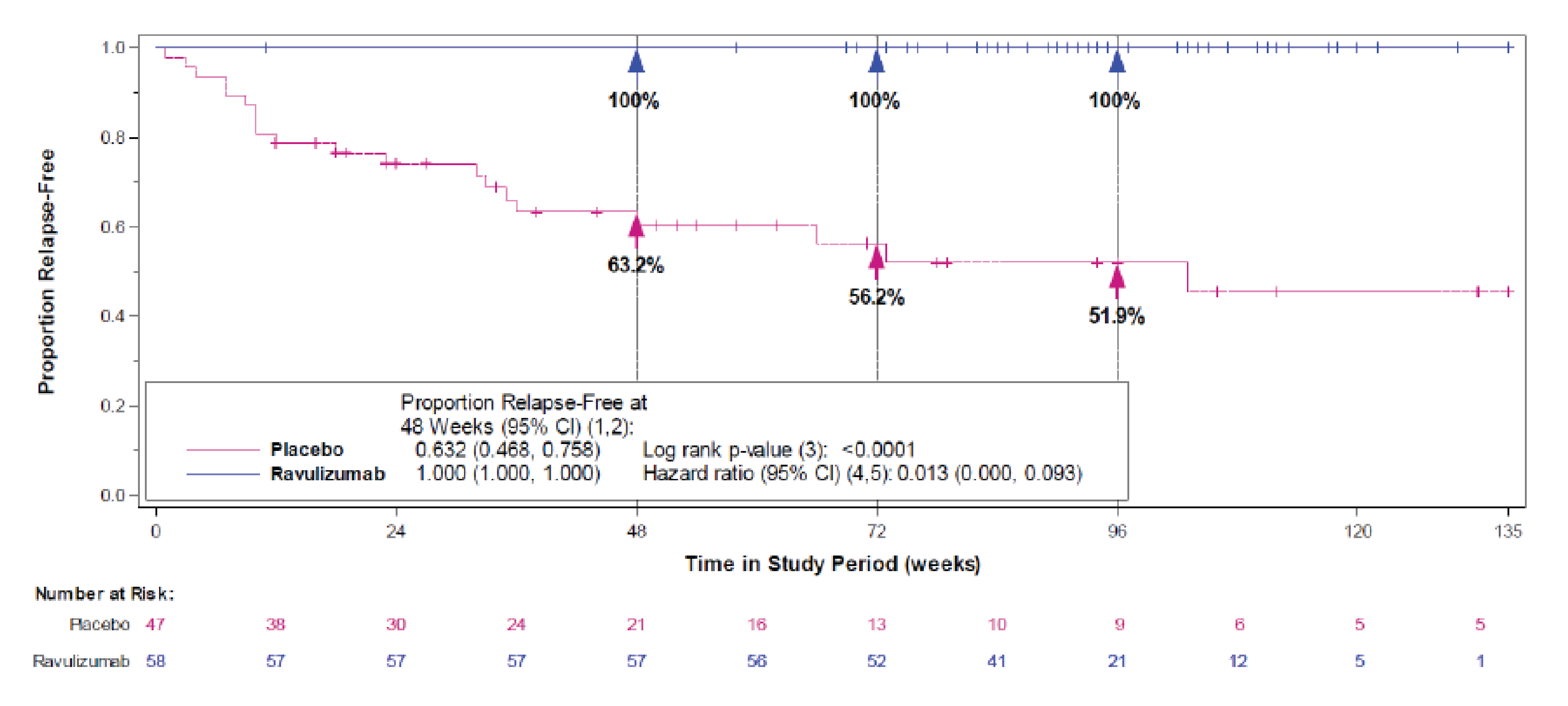
CI = confidence interval; HR = hazard ratio.
Notes: Analysis follow-up time from the start of the primary treatment period through the data cut-off date (July 15, 2022) in the long term extension period is included.
Patients who did not experience an adjudicated on-trial relapse were censored at the end of the study period. If a patient in the placebo group was followed longer than any of the patients in the ravulizumab arm, that patient was censored at the longest ravulizumab follow-up time.
(1) Based on the Kaplan-Meier product-limit method.
(2) Based on the complementary log-log transformation.
(3) Based on a log-rank test.
(4) Based on a Cox proportional hazards model, with Firth’s adjustment.
(5) Wald CI or profile likelihood confidence limits.
Source: CHAMPION-NMOSD CSR.26
Results from sensitivity analyses, which aim to assess whether any imbalances in observed baseline characteristics due to trial design could be sufficient to confound the observed treatment effect, were also consistent with those from the primary analysis. |||| ||||||||||| || |||||||||| |||||| ||| ||| || ||||||||||| ||| |||||||||| |||| || ||||| |||| || |||||| |||||| ||||||||| |||||| |||||||| using propensity scores in a weighted analysis, the use of ravulizumab was associated with an HR of 0.014 (95% CI, 0.000 to 0.101; P < 0.0001) versus placebo. The E-value of the upper confidence limit (8.45) indicates that only an unmeasured confounder that is associated with an 8.45 times greater risk of an adjudicated on-trial relapse and that occurs 8.45 times more in patients in the placebo group would result in a nonsignificant treatment effect.
Subgroup Analyses
Results from the prespecified subgroup analyses based on patient characteristics were consistent with those from the primary analysis, and are shown in Figure 3.
Figure 3: Prespecified Subgroup Analyses for Time to First Adjudicated On-Trial Relapse (Full Analysis Set)
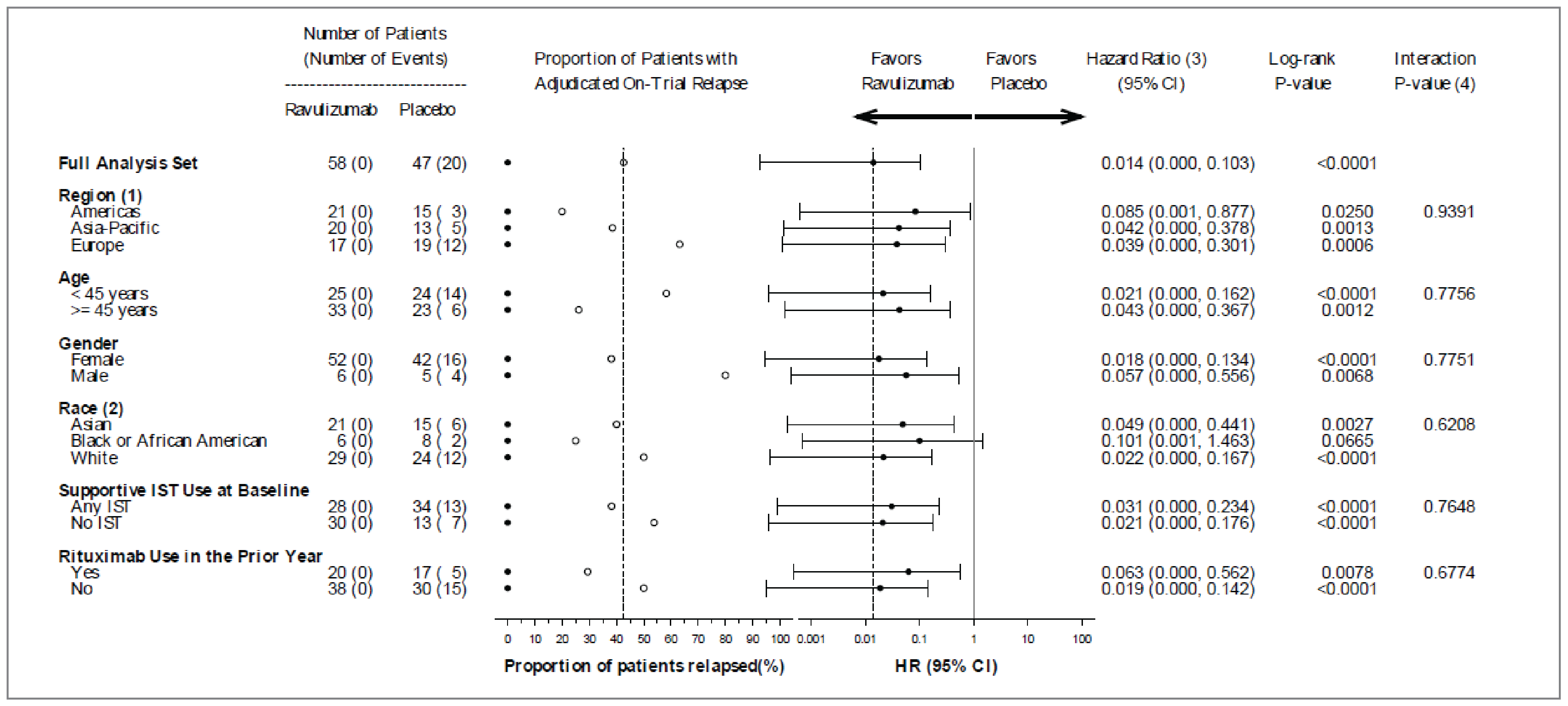
CI = confidence interval; HR = hazard ratio; IST = immunosuppressive treatment.
Notes: Dotted vertical lines show the overall placebo proportion with a relapse and the overall HR for the full analysis set; open circles represent placebo and closed circles represent ravulizumab.
(1) Americas: Argentina, Canada, and the US; Europe: Germany, Denmark, Spain, the UK, Croatia, Italy, Poland, Russia, and Turkey; Asia-Pacific: Australia, Hong Kong, Japan, the Republic of Korea, and Taiwan.
(2) Unknown race excluded from forest plot and interaction effect model.
(3) Based on a Cox proportional hazards model with treatment covariate. Firth’s adjustment with profile likelihood confidence limits applied.
(4) Based on a Cox proportional hazards model with interaction term.
Source: CHAMPION-NMOSD CSR.26
A posthoc subgroup analysis was conducted in patients with more than 1 historical relapse and who used supportive IST for NMOSD before the last historical relapse. Results for this subgroup were consistent with those from the primary analysis, yielding an HR of 0.024 (95% CI, 0.000 to 0.179; P < 0.0001) versus placebo. Kaplan-Meier survival curves are presented in Figure 4; the curves separate early, favouring ravulizumab, and remain separated throughout follow-up.
Function
The proportion of patients with clinically important worsening from baseline through the end of the study period in HAI score was 3.4% (2 of 58 patients) in the ravulizumab arm and 23.4% (11 of 47 patients) in the placebo arm. The use of ravulizumab was associated with an OR of 0.155 (95% CI, 0.031 to 0.771; P = 0.0228) versus placebo. The magnitude of the between-group difference was considered clinically meaningful by the clinical experts consulted by CADTH, and consistent with the level of efficacy observed with ravulizumab for relapse prevention.
Figure 4: Kaplan-Meier Survival Estimates for Time to First Adjudicated On-Trial Relapse (Patients Who Used Supportive IST for NMOSD Prior to the Last Historical Relapse [Full Analysis Set — Patients With > 1 Historical Relapse])
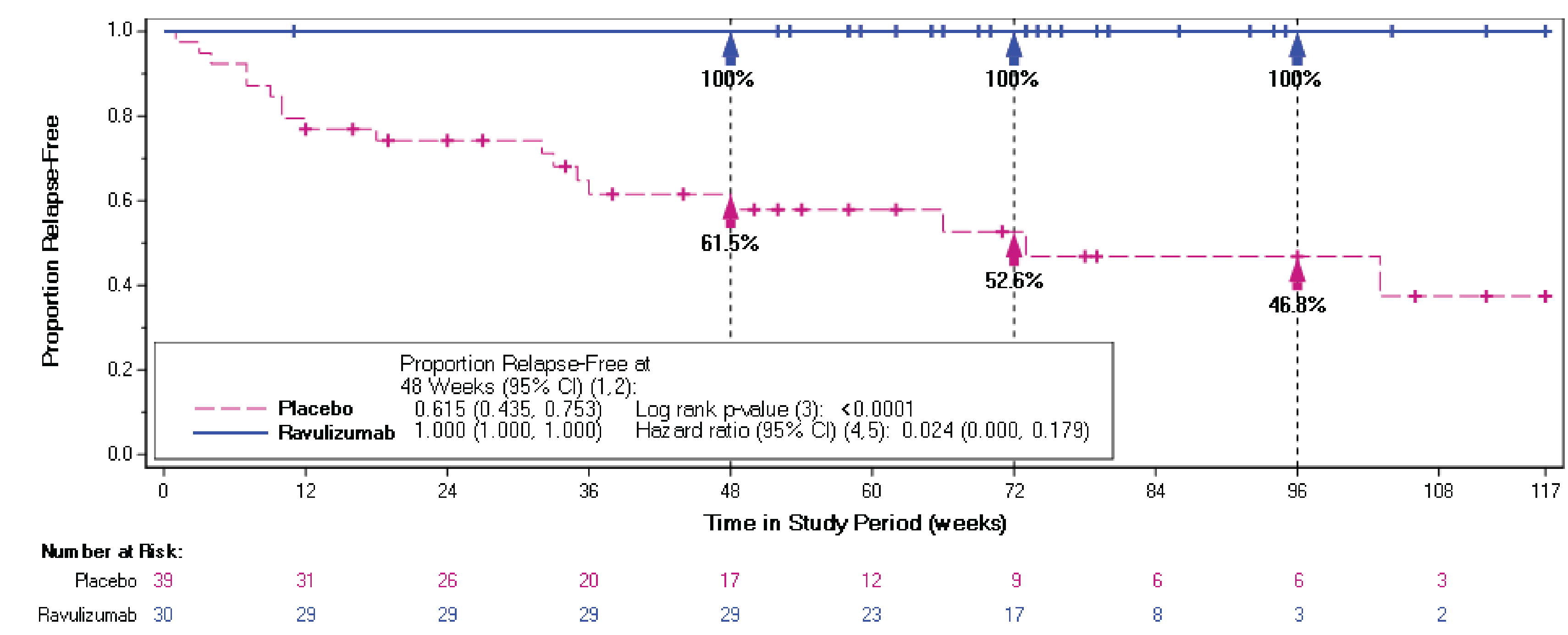
CI = confidence interval; HR = hazard ratio; IST = immunosuppressive treatment; NMOSD = neuromyelitis optica spectrum disorder.
Notes: The placebo group data were collected as part of the PREVENT trial.
Patients who did not experience an adjudicated on-trial relapse were censored at the earlier of the end of the study period and 35 days after a missed or > 35-day delayed dose due to the COVID-19 pandemic. If a patient in the placebo group was followed longer than any of the patients in the ravulizumab arm, that patient was censored at the longest ravulizumab follow-up time.
(1) Based on the Kaplan-Meier product-limit method.
(2) Based on the complementary log-log transformation.
(3) Based on the log-rank test.
(4) Based on a Cox proportional hazards model, with Firth’s adjustment if no relapses were observed in a treatment arm.
(5) Wald CI or profile likelihood confidence limits, if no relapses were observed in a treatment arm.
Source: CHAMPION-NMOSD CSR.26
The proportion of patients with clinically important worsening from baseline through the end of the study period in EDSS score was 10.3% (6 of 58 patients) in the ravulizumab arm and 23.4% (11 of 47 patients) in the placebo arm. The use of ravulizumab was associated with an OR of 0.332 (95% CI, 0.106 to 1.042) versus placebo. The magnitude of the between-group difference was considered clinically meaningful by the clinical experts.
Health-Related Quality of Life
The mean change from baseline through the end of the study period in EQ-5D index score was 0.01 (SD = 0.152) in the ravulizumab arm and –0.04 (SD = 0.212) in the placebo arm (P = 0.0567). The distribution for the change from baseline in EQ-5D index score showed that 86.0% of ravulizumab-treated patients and 72.2% of placebo-treated patients had changes that ranged from greater than –0.2 to less than 0.2, 6.8% of the ravulizumab-treated patients and 8.4% of the placebo-treated patients had an improvement of at least 0.2 points in EQ-5D index score, and 6.8% of the ravulizumab-treated patients and 18.9% of the placebo-treated patients had a worsening of at least 0.2 points in EQ-5D index score.
Table 20: Summary of Key Efficacy Results From the Studies Included in the Systematic Review (Through to the March 15, 2022 Data Cut-Off Date)
Efficacy results | PREVENT placebo (N = 47) | CHAMPION-NMOSD ravulizumab (N = 58) |
|---|---|---|
NMOSD attack or relapse | ||
Time to first adjudicated on-trial relapse | ||
Events, n (%) | 20 (42.6)a | 0 (0.0) |
Relapse-free time, weeks | ||
10th percentile | 7.71 | NA |
25th percentile | 23.71 | NA |
50th percentile | 103.41 | NA |
HR (95% CI) | 0.014 (0.000 to 0.103) | |
P value (log-rank test) | < 0.0001 | |
Estimated proportion of patients relapse-free at the following times, cumulative probability (95% CI): | ||
24 weeks | 0.740 (0.587 to 0.843) | 1.000 (1.000 to 1.000) |
48 weeks | 0.632 (0.468 to 0.758) | 1.000 (1.000 to 1.000) |
72 weeks | 0.562 (0.389 to 0.703) | 1.000 (1.000 to 1.000) |
96 weeks | 0.519 (0.341 to 0.670) | 1.000 (1.000 to 1.000) |
120 weeks | NA | NA |
144 weeks | NA | NA |
Percent relapse risk reduction (95% CI) | 98.6 (89.7 to 100.0) | |
||||||||||| ||||||||| |||||||||| || |||||||||| ||||| | ||
|| |||| ||| | ||||| ||||||| |||||| | |
||||| ||||||||| ||||| | ||||||| | |
Sensitivity analysis: using propensity scores in a weighted analysis | ||
HR (95% CI) | 0.014 (0.000 to 0.101) | |
P value (log-rank test) | < 0.0001 | |
E-value | ||
For estimate | 24.68 | |
For upper 95% CL | 8.45 | |
|||||||| ||||||||| ||||||||| |||||||||||| |||||||| ||| ||| |||| |||||||||| ||| ||| ||||| ||||| || |||| |||||||||| ||||||| | ||
|||||||| |||||||||| | ||||||||| | ||||||||| |
|||||||||| | ||||||||| | ||||||||| |
|| |||| || | ||||| ||||||| |||||| | |
|||| ||||||||| ||||| | ||||||| | |
||||||| ||||||| |||| ||||||||| |||| || | |||| |||||| |||||| | |
Adjudicated on-trial ARR (noncomparative data) | ||
Patients with a total relapse count of 0, n (%) | NA | 58 (100.00) |
Total number of relapses | NA | 0 |
Total number of patient-years in the study period | NA | 84.01 |
Unadjusted ARRc | ||
Rate | NA | 0.000 |
95% CI | NA | NA to NA |
Exact methodd | ||
95% CI | NA | NA to 0.044 |
P valuee | NA | < 0.0001 |
Adjusted ARRf | ||
Rate | NA | 0.000 |
Poisson model | ||
95% CI | NA | NA to NA |
P valuee | NA | NA |
Patient relapse rateg | ||
Mean (SD) | NA | 0.00 (0.000) |
Median (range) | NA | 0.00 (0.00 to 0.00) |
Function | ||
Clinically important changes from baseline in HAI score | ||
Baseline | ||
Mean (SD) | 2.1 (1.40) | 1.2 (1.42) |
Median (range) | 2.0 (0 to 6) | 1.0 (0 to 7) |
||| || ||||| |||||| | ||
|||| |||| | ||| |||||| | ||| |||||| |
|||||| ||||||| | ||| ||| || | ||| ||| || |
|||||| |||| |||||||| | ||
|||| |||| | ||| |||||| | |||| |||||| |
|||||| ||||||| | ||| |||| || | ||| |||| || |
Between-group comparison | ||
No clinically important worsening, n (%) | 36 (76.6) | 56 (96.6) |
Clinically important worsening, n (%) | 11 (23.4) | 2 (3.4) |
OR (95% CI) | 0.155 (0.031 to 0.771) | |
P valuee | 0.0228 | |
Clinically important worsening from baseline in EDSS score | ||
Baseline | ||
Mean (SD) | 4.26 (1.510) | 3.30 (1.584) |
Median (range) | 4.00 (1.0 to 6.5) | 3.25 (0.0 to 7.0) |
||| || ||||| |||||| | ||
|||| |||| | |||| ||||||| | |||| ||||||| |
|||||| ||||||| | |||| ||||| |||| | |||| ||||| |||| |
|||||| |||| |||||||| | ||
|||| |||| | |||| ||||||| | ||||| ||||||| |
|||||| ||||||| | |||| |||||| |||| | |||| |||||| |||| |
Between-group comparison | ||
No clinically important worsening, n (%) | 36 (76.6) | 52 (89.7) |
Clinically important worsening, n (%) | 11 (23.4) | 6 (10.3) |
OR (95% CI) | 0.332 (0.106 to 1.042) | |
P valuee,h,i | 0.0588 | |
HRQoL | ||
Change from baseline in EQ-5D index score | ||
Baseline | ||
Mean (SD) | 0.680 (0.1961) | 0.766 (0.2203) |
Median (range) | 0.706 (0.27 to 1.00) | 0.815 (0.04 to 1.00) |
End of study period | ||
Mean (SD) | 0.637 (0.2374) | 0.771 (0.2042) |
Median (range) | 0.687 (0.05 to 1.00) | 0.827 (0.08 to 1.00) |
Change from baseline | ||
Mean (SD) | –0.043 (0.2115) | 0.005 (0.1522) |
Median (range) | 0.000 (–0.67 to 0.41) | 0.000 (–0.33 to 0.50) |
P valuee | 0.0567 | |
Between-group comparison | ||
LS mean (SE) | 46.84 (4.229) | 57.99 (3.793) |
Difference in LS means (95% CI) | 11.15 (–0.32 to 22.62) | |
P valuee | 0.0567 | |
Change from baseline in EQ-5D VAS score | ||
Baseline | ||
Mean (SD) | 59.1 (20.39) | 73.6 (14.81) |
Median (range) | 60.0 (0 to 95) | 77.5 (30 to 97) |
End of study period | ||
Mean (SD) | 59.7 (20.87) | 76.2 (16.50) |
Median (range) | 60.0 (2 to 100) | 80.0 (13 to 98) |
Change from baseline | ||
Mean (SD) | 0.6 (16.39) | 2.6 (14.07) |
Median (range) | 0.0 (–28 to 40) | 0.5 (–45 to 40) |
P valuee,i | 0.0297 | |
Between-group comparison | ||
LS mean (SE) | 45.61 (4.343) | 58.99 (3.874) |
Difference in LS mean (95% CI) | 13.38 (1.35 to 25.41) | |
P valuee,i | 0.0297 | |
|||||| |||| |||||||| || ||||| |||||||| ||||||||| ||||| | ||
|||||||| | ||
|||| |||| | |||||| ||||||||| | |||||| |||||||| |
|||||| ||||||| | |||||| ||||||| |||||| | |||||| ||||||| |||||| |
||| || ||||| |||||| | ||
|||| |||| | |||||| ||||||||| | |||||| |||||||| |
|||||| ||||||| | |||||| ||||||| |||||| | |||||| ||||||| |||||| |
|||||| |||| |||||||| | ||
|||| |||| | ||||| |||||||| | ||||| |||||||| |
|||||| ||||||| | ||||| |||||||| |||||| | ||||| |||||||| |||||| |
||||||||| | |||||| | |
|||||| |||| |||||||| || ||||| |||||| ||||||||| ||||| | ||
|||||||| | ||
|||| |||| | |||||| ||||||||| | |||||| ||||||||| |
|||||| ||||||| | |||||| ||||||| |||||| | |||||| ||||||| |||||| |
||| || ||||| |||||| | ||
|||| |||| | |||||| ||||||||| | |||||| ||||||||| |
|||||| ||||||| | |||||| ||||||| |||||| | |||||| ||||||| |||||| |
|||||| |||| |||||||| | ||
|||| |||| | ||||| ||||||||| | ||||| |||||||| |
|||||| ||||||| | ||||| |||||||| |||||| | ||||| |||||||| |||||| |
||||||||| | |||||| | |
|||||| |||||| | ||
|||||| |||| |||||||| || |||| | ||
|||||||| | ||
|||| |||| | ||||| |||||||| | ||||| |||||||| |
|||||| ||||||| | ||||| |||||| ||||| | ||||| |||||| ||||| |
||| || ||||| |||||| | ||
|||| |||| | ||||| |||||||| | ||||| |||||||| |
|||||| ||||||| | ||||| |||||| ||||| | ||||| |||||| ||||| |
|||||| |||| |||||||| | ||
|||| |||| | |||||| |||||||| | |||||| |||||||| |
|||||| ||||||| | ||||| ||||||| ||||| | ||||| ||||||| ||||| |
||||||||| | |||||| | |
|||||| |||| |||||||| || ||||| || ||||| |||||| | ||
|||||||| ||||||||| | ||||||||| | ||||||||| |
|| |||||| |||| |||||||||| | || ||||| | |
|||||| |||| |||||||| || ||||||||||||||| |||||| |||||| | ||
|||||| |||| |||||||| | ||
|||| |||| | || | ||| |||||| |
|||||| ||||||| | ||| |||| || | |
|||||||||| |||||||| ||||||||||| | ||
|||||||||||||||| | ||
||||||||| | ||||||||| | || |||||| |
|||||||| || ||||| |||| |||| | |||| ||||||| | |
ARR = annualized relapse rate; CI = confidence interval; CL = confidence limit; EDSS = Expanded Disability Status Scale; HAI = Hauser Ambulation Index; HR = hazard ratio; HRQoL = health-related quality of life; LS = least squares; NA = not applicable; NMOSD = neuromyelitis optica spectrum disorder; OR = odds ratio; |||||||||||||||| |||||||||| ||||||; SD = standard deviation; SE = standard error; VAS = visual analogue scale.
Note: Summary statistics across all patients are presented.
aIn the PREVENT placebo arm, the overall treatment exposure was 51.5 patient-years and the median treatment duration was 41.29 weeks.
bBased on a Cox proportional hazards model, with Firth’s adjustment if no relapses observed in a treatment arm. Wald CI or profile likelihood confidence limits, if no relapses were observed in a treatment arm.
cCalculated as the total number of relapses during the study period for all patients divided by the total number of patient-years in the study period. CI, based on a Poisson regression, could not be estimated.
dUpper 95% CL using exact method is based on the chi-square distribution with 1 degree of freedom divided by patient-years; the lower CL is not defined for 0 relapses. The P value was based on the Poisson distribution with 0 relapses and patient-years.
eType I error was controlled using a closed testing procedure. If the primary end point was statistically significant, the following secondary end points were evaluated in the following rank order: adjudicated on-trial ARR; clinically important changes from baseline in ambulatory function, as measured by HAI; change from baseline in EQ-5D index score; change from baseline in EQ-5D VAS score; clinically important worsening from baseline in EDSS score.
fBased on a Poisson regression centred on the mean historical ARR in the 24 months before screening; P value tests the significance of the difference from 0.25 relapses/patient-year. The model results could not be estimated when the relapse rate was 0.
gThe number of relapses for each patient divided by the number of years in the study period for that patient.
hP value from the logistic regression model adjusted for baseline score.
iBecause statistical significance was not achieved for change from baseline in EQ-5D index score (P = 0.0567), all end points of lower rank in the hierarchy (i.e., EQ-5D VAS score, EDSS score) could not be evaluated for statistically significance.
jThe comparison has not been controlled for multiple comparisons.
Source: CHAMPION-NMOSD CSR, sections 5.1.1 and 5.1.2.26 Details included in the table are from the sponsor’s Summary of Clinical Evidence.27
The mean change from baseline through the end of the study period in EQ-5D VAS score was 2.6 (SD = 14.07) in the ravulizumab arm and 0.6 (SD = 16.39) in the placebo arm. Formal testing of this difference between groups cannot be interpreted because it would violate the prespecified testing procedure to control for multiple comparisons. The distribution for the change from baseline in EQ-5D VAS score showed that 70.6% of ravulizumab-treated patients and 55.3% of placebo-treated patients had changes that ranged from at least –14 to no more than 14, 20.6% of ravulizumab-treated patients and 21.2% of placebo-treated patients had an improvement of more than 14 points in EQ-5D VAS score, and 6.8% of ravulizumab-treated patients and 23.4% of placebo-treated patients had a worsening of more than 14 points in EQ-5D VAS score.
||| |||| |||||| |||| |||||||| ||||||| ||| ||| || ||||| |||||| || ||||| |||||||| ||||||||| |||||| |||||||| || || ||||||||||| |||||||| ||| ||||| ||| |||||| || ||| ||||||||||| ||| ||| |||| ||| |||||| || ||| ||||||| |||| ||| ||| ||||| |||||| ||||||||| |||||| ||| |||| |||||| |||| |||||||| ||||||| ||| ||| || ||||| |||||| ||| |||| ||| |||||| || ||| ||||||||||| ||| ||| |||| ||| ||||||| || ||| ||||||| ||||.
According to the clinical experts consulted by CADTH, the magnitude of the between-group difference for the EQ-5D index score, the EQ-5D VAS score, and the ||||| |||||||| ||||||||| ||||| can be considered clinically meaningful. Results for HRQoL was considered consistent with disease evolution in clinical practice, as illustrated by either a lack of change in the placebo group combined with an improved status in the ravulizumab group, or with a worsening status in the placebo group combined with stability in the ravulizumab group.
Visual Acuity
||| |||| |||||| |||| |||||||| ||||||| ||| ||| || ||||| |||||| || ||||| |||||||| || || ||||||||||| |||||||| ||| |||||| ||| ||||||| || ||| ||||||||||| ||| ||| |||||| ||| ||||||| || ||| ||||||| |||| ||| |||| |||| ||||| ||| || |||||| |||| |||||||| || ||| ||||||||||| ||||| || |||||||||| |||| ||| ||||||| || ||||||||| || ||| ||| ||||||| |||||| || |||||| || ||||| |||| |||||||||| || ||| || |||||||| |||| ||||||| ||||||||||| ||||| ||||||||| ||||| |||||||| |||||||| ||| ||| ||||||| ||| ||||| |||||| |||| || |||||||||| |||| ||| ||||| ||||||||||||| |||| |||||||| |||||||| || ||| ||||||| |||||| ||| || |||||||||||||| || ||||||| |||||||||| || |||||||| ||||||||| |||||| ||| || |||||| |||| |||||||| || ||| ||||||||||| ||||| || ||||| || ||||| |||||| || || ||||||||||||||| |||||| |||||| ||| |||| ||| |||||||| ||| ||| ||||||| |||||||.
Hospitalizations
|||| || || |||||||| ||||||| |||| |||||||||||| || ||| ||||||||||| |||||| ||||||| |||| |||||||| || |||| ||||||| ||||| || || |||||||| |||| ||||||||| |||||||||||||||| |||| ||| ||| || ||||||||| ||| ||||||||| || ||||| ||||||| ||||||||| ||||||| ||||||| ||||||||| || ||| |||||||| |||||||| |||| |||||| |||||||| |||||||| |||||| |||| |||||||| ||| |||||| ||||||||||||| ||||||||| ||| ||| |||||| |||| ||| ||||||| ||||| ||||||| |||||||||| || |||||||| ||||||||| || |||| ||| |||||||| ||| ||| ||||||| ||||||.
Harms
Results for the safety end points are from the addendum analysis with the data cut-off date of July 15, 2022, during the long-term extension period and are presented in Table 21. In the initial Clinical Study Report (data cut-off date of March 15, 2022), the safety analysis for the primary treatment period represents 84.1 patient-years of exposure to ravulizumab. The cumulative safety data provided in the addendum (data cut-off date of July 15, 2022) represents 102.9 patient-years of exposure to ravulizumab.
Adverse Events
In the CHAMPION-NMOSD study, 93.0% of patients receiving ravulizumab reported at least 1 AE. The most common treatment-emergent AEs included COVID-19 (34.5%), headache (31.0%), arthralgia (12.1%), backpain (12.1%), upper respiratory tract infection (10.3%), and urinary tract infection (10.3%).
Serious Adverse Events
Overall, 19.0% of patients receiving ravulizumab reported at least 1 serious AE. The most common serious AEs were infections and infestations and are outlined in Table 21.
Withdrawals Due to Adverse Events
One patient discontinued due to AEs; the reason for withdrawal from the study drug was infections (bronchitis, encephalitis meningococcal, and stenotrophomonas infection).
Mortality
No deaths were reported in the study.
Notable Harms
Meningococcal infection was the only AE of special interest. Two patients experienced meningococcal infection during the primary treatment period, and both recovered. One patient discontinued ravulizumab and the study during the primary treatment period and the other continued ravulizumab into the long-term extension period as of the cut-off date of July 15, 2022. No new meningococcal infections were reported during the long-term extension period.
Table 21: Summary of Harms Results From the CHAMPION-NMOSD Study
Patients, n (%) | CHAMPION-NMOSD ravulizumab (N = 58) |
|---|---|
Any AE | 54 (93.1) |
Most frequently reported AEs (≥ 10% of patients) | |
COVID-19 | 20 (34.5) |
Headache | 18 (31.0) |
Arthralgia | 7 (12.1) |
Back pain | 7 (12.1) |
Upper respiratory tract infection | 6 (10.3) |
Urinary tract infection | 6 (10.3) |
SAEs | 11 (19.0) |
Infections and infestations | 5 (8.6) |
Encephalitis meningococcal | 1 (1.7) |
Infection | 1 (1.7) |
Intervertebral discitis | 1 (1.7) |
Meningococcal sepsis | 1 (1.7) |
Pneumonia | 1 (1.7) |
Injury, poisoning, and procedural complications | 1 (1.7) |
Ankle fracturea | 1 (1.7) |
Musculoskeletal and connective tissue disorders | 1 (1.7) |
Spinal osteoarthritis | 1 (1.7) |
Neoplasms benign, malignant and unspecified (including cysts and polyps) | 1 (1.7) |
Invasive lobular breast carcinoma | 1 (1.7) |
Nervous system disorders | 1 (1.7) |
Neuromyelitis optica pseudorelapsea | 1 (1.7) |
Psychiatric disorders | 1 (1.7) |
Suicidal ideation | 1 (1.7) |
Respiratory, thoracic, and mediastinal disorders | 1 (1.7) |
Pulmonary embolisma | 1 (1.7) |
Vascular disorders | 1 (1.7) |
Deep vein thrombosisa | 1 (1.7) |
Withdrawal from study drug due to AEs | 1 (1.7) |
Bronchitis | 1 (1.7) |
Encephalitis meningococcal | 1 (1.7) |
Stenotrophomonas infection | 1 (1.7) |
Deaths | 0 (0.0) |
AEs of special interest | 2 (3.4) |
Meningococcal infection | 2 (3.4) |
AE = adverse event.
aReported as of the data cut-off date (July 15, 2022) during the long-term extension period, and new since the cut-off date for the initial CSR.
Source: CHAMPION-NMOSD CSR addendum.26 Details included in the table are from the sponsor’s Summary of Clinical Evidence.27
Critical Appraisal
Internal Validity
Study Design
The CHAMPION-NMOSD study had a single-arm treatment design, and used the placebo group from the PREVENT study as an external placebo comparator; this introduces a risk of bias, unlike an RCT design, because of the absence of randomization, allocation concealment, and blinding. The clinical experts and CADTH review team acknowledged that there is a rationale for this decision, in that the use of a placebo arm can be considered unethical when treatment options of expected similar efficacy are available. Also, because of the rare nature of NMOSD, the use of an active comparator arm may not be feasible; because of the large number of patients that the study would require, it is unlikely that such a comparison would be adequately powered for a statistically significant efficacy demonstration. In addition, ravulizumab has a known mechanism of action targeting the C5 epitope; the drug was engineered by modifying the amino acid sequence of eculizumab to allow for a prolonged half-life.
However, the comparison is only valid as long as the 2 trials have sufficient similarity, particularly in terms of patient characteristics and outcome assessment. A critical appraisal of these 2 issues follows. Although the overall assessment suggests that the comparison is likely valid, the choice of single-arm, externally controlled study design introduces uncertainty regarding the true effect of ravulizumab, which should be considered when interpreting the findings.
Uncertainty may, however, be mitigated in part by the magnitude of the relapse risk reduction with ravulizumab treatment observed in the CHAMPION-NMOSD study, which is large and constant over time, and compensated for potential biases and the known variability in disease progression. The clinical experts confirmed that the follow-up duration was long enough for the trial to adequately capture relapses in the included population; considering the inherently high risk of relapse in patients with anti-AQP4 antibody-positive NMOSD, those treated with ravulizumab in the CHAMPION-NMOSD study would likely have relapsed otherwise.
Patient Population
The use of the placebo group in the PREVENT study was considered appropriate by the clinical experts, in that the trial was performed relatively recently and there was no change in natural disease history, and there were only minor updates in diagnostic criteria, which happened between the time that the 2 studies were performed.
There were some differences in patient populations worth highlighting between the 2 trials. The most notable was in the number of historical relapses, which was higher in the placebo group than in the ravulizumab group. According to the clinical experts consulted by CADTH, the history of prior relapse is not expected to have a substantial impact on the risk of future relapses and, as such, this would not meaningfully affect results for the primary outcome of relapse prevention. However, the clinical experts highlighted that the frequency and severity of prior attacks might be correlated with the likelihood of being incapacitated with future relapse. The ARR, which is indicative of the frequency of relapses, was similar in both groups. This was consistent with the assumption that patients were having a relatively similar evolution in terms of relapse frequency, despite differences in the total number of historical relapses. Therefore, the comparison between the 2 study groups appears valid, considering disease trajectory and experience from clinical practice.
Interventions and Cointerventions
A greater percentage of patients in the placebo group than in the ravulizumab group were on ISTs; however, the concomitant use of ISTs is not likely to introduce bias, according to the clinical experts, as these do not impact disease trajectory. The use of corticosteroids was similar in both groups, which is important to assess, as early aggressive rescue therapy with corticosteroids for an acute attack is expected to have a positive impact by ultimately limiting disability.
Outcome Measures
The primary outcome in the CHAMPION-NMOSD study was relapse, which was considered the preferred and most reliable end point by clinical experts. The definition of relapse used was similar in both studies. According to the clinical experts, the determination of relapses is fairly objective; assessment is based on a combination of patient-reported symptoms, clinical exam, clinical tools, and patient history. Therefore, it is not expected that this outcome would have been subject to bias that pertains to the open-label, external control design.
Other efficacy outcomes (i.e., function, HRQoL and visual acuity) were assessed adequately using appropriate tools; however, no studies assessed their validity or reliability in patients with NMOSD specifically. MCIDs used for dichotomous outcome assessment (i.e., HAI and EDSS) were considered appropriate and consistent with clinical practice by the clinical experts, as no MCIDs could be identified in the literature for HAI, whereas MCIDs for EDSS have been established in patients with MS. Assessment of these outcomes implies some level of subjectivity from the patients and investigators; as such, it is possible that the knowledge of treatment received may have favoured ravulizumab.
Statistical Analysis
The CHAMPION-NMOSD study had sufficient power for the analysis of the primary outcome; statistical significance was also reached for the key secondary outcomes of ARR and ambulatory function measured by HAI. In line with the closed testing procedure used to control for type I error, other secondary outcomes were not considered to be statistically significant; indeed, because statistical significance was not achieved for change from baseline in EQ-5D score (||||||||), all end points of lower rank in the hierarchy (i.e., EQ-5D VAS score, EDSS score, |||||| ||| ||||) could not be evaluated for statistically significance.
The methods used for the primary analysis were appropriate for time-to-event outcomes (Cox proportional hazards model, with treatment group as a factor); the methods used for secondary outcome analyses were appropriate for both dichotomous data (logistic regression model) and continuous data (analysis of covariance). Only few patients discontinued the study. For the outcomes of function (HAI, EDSS) and HRQoL (EQ-5D), missing data were imputed using the last observation carried forward, which may favour placebo; because patients are expected to worsen due to the natural disease trajectory, especially in the placebo group, carrying forward the last available observation may overestimate the effect in the placebo group. However, this single imputation approach may also favour ravulizumab because such approaches tend to underestimate the variance of the estimated effect, which would artificially increase precision around the estimate and increase the likelihood of detecting a statistically significant difference.
A key concern when comparing a nonrandomized trial with an RCT is the issue of unmeasured confounding, which can lead to potential biases and influence trial results; based on the tipping point analysis results, the sponsor concluded that unmeasured confounders are unlikely to have an effect large enough to completely explain the large observed relative treatment effect in the external placebo-controlled CHAMPION-NMOSD study. The CADTH review team agrees with this assessment. The sensitivity analysis using propensity scores also showed that differences in patient characteristics between the ravulizumab group and the external placebo group as a result of different trial-level characteristics that were observed in the trial did not have a large confounding impact.
Subgroup analyses based on patient characteristics were specified a priori; however, the subgroup analysis of patients who have had more than 1 historical relapse and who were using supportive IST for NMOSD before the most recent relapse was conducted as a posthoc analysis.
External Validity
Patient Population
The inclusion and exclusion criteria were deemed clinically relevant and reasonable by CADTH’s clinical experts. More important, baseline patient characteristics, disease history, and prior use of NMOSD therapies were considered to be representative of the NMOSD population seen in clinical practice.
Treatment Regimen and Length of Follow-Up
The administration of ravulizumab in the CHAMPION-NMOSD study was in line with the Health Canada–recommended dosages for this indication and with what is expected to be used in the reimbursement population. The clinical experts confirmed that follow-up duration was of appropriate length.
Outcome Measures
The primary outcome of relapse prevention is consistent with the treatment goals of NMOSD in clinical practice, according to the clinical experts. Considering the significant consequences of NMOSD attacks on patient morbidity and quality of life, avoidance of future relapses is paramount in preventing the accumulation of disability in patients and associated mortality. Relapse assessment in the trial was similar to that performed in clinical practice.
Among the secondary outcome measures, the EDSS is the only tool that is currently used in clinical practice. The clinical experts mentioned the importance of interpreting results from the EDSS with a measure of visual acuity, as it is heavily dependent on ambulation and not very sensitive to changes in nonambulatory symptoms, such as changes in vision, which are likely to not be captured, even when they may have a very significant impact on a patient’s life.
Patient groups that provided input for this review identified the outcomes assessed and reported in the CHAMPION-NMOSD study as being important, with a focus on relapse prevention and maintaining or slowing the decline in vision, HRQoL, and function.
GRADE Summary of Findings and Certainty of the Evidence
Methods for Assessing the Certainty of the Evidence
For pivotal studies and RCTs identified in the sponsor’s systematic review, GRADE was used to assess the certainty of the evidence for outcomes considered to be most relevant to CADTH’s expert committee deliberations, and a final certainty rating was determined as outlined by the GRADE working group:49,50
High certainty: We are very confident that the true effect lies close to that of the estimate of the effect.
Moderate certainty: We are moderately confident in the effect estimate — The true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different. We use the word “likely” for evidence of moderate certainty (e.g., “X intervention likely results in Y outcome”).
Low certainty: Our confidence in the effect estimate is limited — The true effect may be substantially different from the estimate of the effect. We use the word “may” for evidence of low certainty (e.g., “X intervention may result in Y outcome”).
Very low certainty: We have very little confidence in the effect estimate — The true effect is likely to be substantially different from the estimate of effect. We describe evidence of very low certainty as “very uncertain.”
For nonrandomized comparative studies, such as a single-arm trial with an external control, CADTH followed the GRADE approach. The CADTH review team assessed study limitations (which refer to internal validity or risk of bias), inconsistency across studies, indirectness, imprecision of effects, and publication bias to present these important considerations. Because of the inherent risk of bias from the absence of randomization and differences in patient populations, the certainty of the evidence for single-arm trials starts at low certainty, with an opportunity for rating up.
When possible, certainty was rated in the context of the presence of an important (nontrivial) treatment effect; if this was not possible, certainty was rated in the context of the presence of any treatment effect (i.e., the clinical importance is unclear). In all cases, the target of the certainty of the evidence assessment was based on the point estimate and where it was located relative to the threshold for a clinically important effect (when a threshold was available) or to the null.
Results of GRADE Assessments
Table 2 presents the GRADE summary of findings for ravulizumab compared with placebo.
Indirect Evidence
The contents of this section have been informed by materials submitted by the sponsor. The following information has been summarized and validated by the CADTH review team.
Objectives for the Summary of Indirect Evidence
The objective of this section is to summarize and critically appraise the methods and findings of the indirect evidence submitted by the sponsor. The sponsor submitted indirect evidence in the form of an NMA that compared the effects of ravulizumab with key comparators in the context of adults with NMOSD who are anti-AQP4 antibody-positive.51
||||| ||||| ||| |||| || ||||| ||| ||||||||| ||| |||| |||||||| ||| ||||||| || ||||||||||| ||||||||||||| ||| |||||||||||| || |||||||| |||| ||||| ||| ||| |||||| ||| |||||||||||| |||||| |||| ||||| ||||||||| ||| || ||| ||||| |||| |||||||| ||||||||||| || |||| |||||||||.
Description of Indirect Comparison(s)
The sponsor conducted a systematic literature review in March 2023 to identify evidence for the NMA. A feasibility analysis was conducted to determine the comparability of the CHAMPION-NMOSD study with other studies, but focused on compatibility with the PREVENT study. The PREVENT study was also conducted by the sponsor and compared eculizumab to placebo in patients with NMOSD.44 |||| ||||||| || ||||| |||| |||||||| || ||| ||| ||| ||||| ||| ||||||||| |||| |||| |||||||| |||||||||||| ||||||||||| ||||||||||||| |||||||||||| ||| |||||||| ||| ||| |||||||| |||||||| || ||||||| |||| ||| |||||| ||||| ||||||||| |||||||| |||| |||||||||| || ||| |||| |||||||||||| ||||||||||| ||||||| |||| ||||||||||||||||| ||||||||| ||| ||||| |||||||||||||||| therapy.
Table 22: Study Selection Criteria and Methods for the NMA Submitted by the Sponsor
Characteristics | Indirect comparison |
|---|---|
Population | Adults with NMOSD who are anti-AQP4 antibody-positive |
Intervention | Ravulizumab |
Comparatora | ||||||||||||||||||||||||||||||||||||||||||| || |||| |||||||||| |||||||| |||||||||||| || |||||||||||| ||||||||| |||| ||||||||||| || |||||||| |||||||||| |
Outcomea | ||||||||||||| || ||||| |||||||||||||||||| ||||||| |||| ||||||||||||||||||||| ||||||| || ||||||||||||| |||||||||| |||||| ||||| |||||||||||||| |||||||||||||| |||||||||| ||||| ||||| |||||||||||||| |||||| ||||| ||||| ||||||||||||| ||||| |||| |||||| ||||||| |
Study designsb | ||||||||||||||| |||||| || || ||| || ||||||||| |||| |||||||| ||| || ||| ||||||||||||| || |||||||| |
Publication characteristics | ||||||||| ||||||| ||| ||| ||||||||||| ||||||||||| ||||||| ||||||| |||| ||| ||||||| ||| ||||||||||||||| |
Exclusion criteria | |||| |
Databases searched | ||||||||||||| ||||||||| |||| |||||||||||||||||||||||||||||| ||||||| |||||||| || |||||||||| |||||||||||| |||||||||||||||||||| ||||| ||||||| |||| |||||||||| ||||||||||||||||||||| ||||||| ||||||| || ||| ||||||||| ||| ||||||| ||||||||| ||||||||| ||| ||||||||| ||| |||||||| ||| |||||||| ||||||||| |||||||| ||||||||||||||||||| ||||||||| ||| ||||||||| ||| |||||||| || |||||||| ||||||||| |||||||| ||||||||||||||||||| ||||||| || ||||||||| |||| ||||||||||||||||||| ||||||| || ||||||||| |||| |||||||||| |
Selection process | ||| ||||||||||| |||||||||| ||||||| || |||||||||| ||||||||| ||| ||||||||| ||| |||| || |||| ||||||||||| || |||||||| |||||||| |
Data extraction process | ||| ||||||||||| |||||||||| ||||||| || |||||||||| ||||||||| |||| ||||||||||| || |||||||| |||||||| |
Quality assessment | |||||||| |||| || |||| |||| ||| |||||||| |||||| |
AQP4 = antiaquaporin-4; EDSS = Expanded Disability Status Scale; HAI = Hauser Ambulation Index; mRS = Modified Rankin Scale Score; NMOSD = neuromyelitis optica spectrum disorder; SF-36 = 36-Item Short Form Survey.
aNo restrictions around dosing for the intervention and comparators were used to limit the search results (i.e., all studies were included regardless of dosing schedule).
bNo restrictions around timing of the end point evaluation were used to limit the search results (i.e., all studies were included regardless of when end points were evaluated).
Source: Details included in the table are from the sponsor’s Summary of Clinical Evidence and the sponsor’s full NMA report.27,51
Network Meta-Analysis
Objectives
The objective was to obtain relative treatment effects between ravulizumab, ||||||||||| ||||||||||||| ||| |||||||||||| for the treatment of adults with anti-AQP4 antibody-positive NMOSD based on currently available clinical trial evidence obtained by means of an NMA. |||||||| |||| ||||||||| ||| |||||||||| |||||||| |||||||||||||| ||||| || ||||| ||||||||| ||||||||| |||||||||||| ||||||||||| |||||||| ||| ||||| |||||||||||||||| |||||||| |||||||| || |||||||| ||| |||||||||| |||||||| |||||||| ||||| || ||||| |||||||| |||||||||| ||||||| |||||||||| ||| |||||||||||||| ||||||| || |||| ||||||| ||||||||| ||| |||||||| |||||||||| |||||| ||||| ||||||| ||||||| ||||||||||| ||||||||||||| |||||||| |||||| |||||||||| ||||| ||||| |||||| |||||||| |||||| ||||| ||||| |||||| ||| ||||||| ||||| |||| |||||| ||||| ||||.
Study Selection Methods
||| ||||||| |||||||||||||||| |||||||||| |||||| || |||||| ||| |||| |||||||||| |||| || ||||| || |||||||| |||||||| ||||||| || ||||||| |||||||| ||| |||||||| ||||||| |||||||| || |||||||||| ||||||| ||| ||||||| |||||||| |||||||||| ||||||||||| ||| |||||||||| || ||| ||||||||| ||| ||||| |||| ||| |||||| |||| ||||||||| |||||||| ||||||||| ||| ||||||||| ||| |||||||| ||| |||||||| ||||||||| |||||||| ||||||||||| |||||||| ||||||||| ||| ||||||||| ||| |||||||| || |||||||| ||||||||| |||||||| ||||||||||| |||||||| ||||||| || ||||||||| |||| ||||||||||| ||| |||||||| ||||||| || ||||||||| |||| ||||||||||| || ||||||||| ||| || |||||||| |||||||||| || |||||| |||||||| ||||| |||||||| |||||||||||||||||||||||| ||| |||||||| ||| |||||||| || |||||||| ||| |||||||| |||||| |||| |||| |||| |||||||||| |||| |||||||| ||||||| ||||||| ||| ||| ||| |||||||| || ||| |||||| ||||||||||||| ||| ||||||||||| |||||||||| ||||||| || |||||||||| ||||||||| ||| ||||||||| ||| |||| |||||||||||| ||| |||||||| |||| || |||| |||| ||| |||| || |||||| ||||| |||||||| ||| ||||||| ||| ||| ||||| ||| |||| ||||||||||| ||| ||||||||||||||||| |||||||| ||| ||| |||||||||| |||||||||| |||||| ||| ||| ||| |||||||||| || Table 21 ||| |||||| |||||||||| |||| ||||| |||||||| |||| ||||| ||| |||| ||||| ||| ||||||| |||| |||||||||||| ||||||||||| ||||||||||||| || ||||||||||||| ||| |||||||| || |||||||| || ||| ||| |||| |||| || ||||| |||||||| |||||||||| ||||||| |||| ||| ||||| ||||||||| ||| ||||||| |||||||| |||| ||| |||||| ||| ||||||| || ||||| ||| || ||| ||||||||| |||| |||||||| ||| || ||| ||||||||||||| || |||||||||.
NMA Analysis Methods
||||||||||| |||||||||||||| ||||||| ||||||||||||||||||| |||||||||| |||| |||||||| |||||||||||||| || ||||||| ||| |||||||| ||| ||| ||||||||||||| || |||||||| |||| ||| |||||||| ||||||| ||| |||| |||||||||| ||||| ||| ||||||| || ||||||||||| |||||||||| || ||| |||||||||| || |||||| |||||||||| |||||||||||||| ||||||||||| || ||| |||||||||||| || |||||||| ||||||| ||||||||||||||| |||| |||||| ||| ||||||| ||||||||||| || |||||||| ||||||| |||| ||| |||| |||||||| ||||||||| ||||| |||||||| |||||| ||||||||||||| |||||||||| || ||||||| ||||||||||||| |||||||||||| ||| ||| |||||||||| || ||||| |||||||| ||| ||||||||||| ||||||||||| || ||| |||||||| ||||||||| ||||||| || |||||| ||||||||||| || ||||||| ||||||||| ||| |||||||||||| ||||||| |||| |||||||||| ||| |||| || ||||| ||||||||| ||| ||| ||||||||||| ||||||||||| ||| ||||||| ||||| ||||||| ||||||| ||||||||||||||| || |||||||| |||| ||||||||| || ||| |||||||| |||||| ||||||||||| || ||| |||||||| |||||| |||||||| |||| |||||||| ||| |||||||| ||||||| || ||| ||||||| ||||||||||||| |||| |||| ||||||| |||||||| |||||||||||| || ||||| ||||||||| ||| ||||||| || ||| ||||||||||| ||||| |||||||| |||| ||| |||||||||| ||||||| ||| |||||||||| ||||||| ||||||||||| |||||||||| ||| |||||| || |||||| ||||| || |||||||||| |||||||||| || |||||||| || |||||||||||||||||| ||||| || |||||||||||||||| |||||| ||| |||||||||| |||||||| |||||||||| || |||||||| || ||| || |||||||| |||| ||||| || ||| ||||||||||| |||||||.
NMA Methods
|||||||||| |||||||||||||| ||||||| ||||||||||||||||||| |||||||||| |||| |||||||| |||||||||||||| || ||||||| ||| |||||||| ||| ||| ||||||||||||| || |||||||| |||| ||| |||||||| ||||||| ||| |||| |||||||||| ||||| ||| ||||||| || ||||||||||| |||||||||| || ||| |||||||||| || |||||| |||||||||| |||||||||||||| ||||||||||| || ||| |||||||||||| || |||||||| ||||||| ||||||||||||||| |||| |||||| ||| ||||||| ||||||||||| || |||||||| ||||||| |||| ||| |||| |||||||| ||||||||| ||||| |||||||| |||||| ||||||||||||| |||||||||| || ||||||| ||||||||||||| |||||||||||| ||| ||| |||||||||| || ||||| |||||||| ||| ||||||||||| ||||||||||| || ||| |||||||| ||||||||| ||||||| || |||||| ||||||||||| || ||||||| ||||||||| ||| |||||||||||| ||||||| |||| |||||||||| ||| |||| || ||||| ||||||||| ||| ||| ||||||||||| ||||||||||| ||| ||||||| ||||| ||||||| ||||||| ||||||||||||||| || |||||||| |||| ||||||||| || ||| |||||||| |||||| ||||||||||| || ||| |||||||| |||||| |||||||| |||| |||||||| ||| |||||||| ||||||| || ||| ||||||| ||||||||||||| |||| |||| ||||||| |||||||| |||||||||||| || ||||| ||||||||| ||| ||||||| || ||| ||||||||||| ||||| |||||||| |||| ||| |||||||||| ||||||| ||| |||||||||| ||||||| ||||||||||| |||||||||| ||| |||||| || |||||| ||||| || |||||||||| |||||||||| || |||||||| || |||||||||||||||||| ||||| || |||||||||||||||| |||||| ||| |||||||||| |||||||| |||||||||| || |||||||| || ||| || |||||||| |||| ||||| || ||| ||||||||||| ||||||||||||||||| |||||||||||||| ||||||| ||||||||||||||||||| |||||||||| |||| |||||||| |||||||||||||| || ||||||| ||| |||||||| ||| ||| ||||||||||||| || |||||||| |||| ||| |||||||| ||||||| ||| |||| |||||||||| ||||| ||| ||||||| || ||||||||||| |||||||||| || ||| |||||||||| || |||||| |||||||||| |||||||||||||| ||||||||||| || ||| |||||||||||| || |||||||| ||||||| ||||||||||||||| |||| |||||| ||| ||||||| ||||||||||| || |||||||| ||||||| |||| ||| |||| |||||||| ||||||||| ||||| |||||||| |||||| ||||||||||||| |||||||||| || ||||||| ||||||||||||| |||||||||||| ||| ||| |||||||||| || ||||| |||||||| ||| ||||||||||| ||||||||||| || ||| |||||||| ||||||||| ||||||| || |||||| ||||||||||| || ||||||| ||||||||| ||| |||||||||||| ||||||| |||| |||||||||| ||| |||| || ||||| ||||||||| ||| ||| ||||||||||| ||||||||||| ||| ||||||| ||||| ||||||| ||||||| ||||||||||||||| || |||||||| |||| ||||||||| || ||| |||||||| |||||| ||||||||||| || ||| |||||||| |||||| |||||||| |||| |||||||| ||| |||||||| ||||||| || ||| ||||||| ||||||||||||| |||| |||| ||||||| |||||||| |||||||||||| || ||||| ||||||||| ||| ||||||| || ||| ||||||||||| ||||| |||||||| |||| ||| |||||||||| ||||||| ||| |||||||||| ||||||| ||||||||||| |||||||||| ||| |||||| || |||||| ||||| || |||||||||| |||||||||| || |||||||| || |||||||||||||||||| ||||| || |||||||||||||||| |||||| ||| |||||||||| |||||||| |||||||||.
Results of NMA
Summary of Included Studies
||||| ||||||| |||||||| |||||| |||| |||||||| |||| ||| |||||||| |||| ||| ||| |||| ||||||||||||||| |||||||| ||||||||||| |||||||||| ||| ||||||||||| ||| |||||||||||| ||||| |||||||||||| ||| |||||||||||| |||||| ||||||||||| ||||||||||| |||||||| |||||||| |||||||||||| ||||||| ||||||||| |||||||| |||||||| ||| |||| ||||| |||| |||||||| |||| ||||||||| ||| |||||||| |||| |||||||||||||| ||| ||||||| ||| ||||||||| |||||||||| || |||||||||||||||||||| |||||||| ||| ||| ||| |||| |||||| || |||| ||||| ||||||||| |||||||||| || ||||| ||||| |||||||| ||||||||| |||||||||| |||||||| || ||||||||||| || ||||| ||||| |||||||| ||||||||| |||||||||| |||||||| |||| |||||||||| |||| ||| || ||||| ||||| |||||||| ||||||||| |||||||||| |||||||| |||| || ||||||| |||||||||| |||||||||||| || |||||| ||| |||||||||| ||||||||||||||||||| |||||||| ||||||| |||| |||| |||||| ||| |||||||| ||||| ||||||||||||| ||||||||| |||||| ||| ||| ||||||| ||||| |||| ||| ||||||| ||||| || || |||||||| |||||||| |||||||| || |||||||||| ||||||||||||| |||| ||||| || ||||||| |||||||||||| ||||||||||| ||| ||||||| ||||||| |||||| |||||| |||||||||||||| ||| ||||||| |||||| |||||| || |||||||||| |||||||||| ||||| |||||||||| ||||| |||| || ||| ||||||| |||||| |||| |||| || ||||| ||| |||||| |||||||| |||||||| ||||| || |||||||| ||||||||| |||||| ||||| |||||||||||||||| |||||||||| || |||||| |||||||| |||| |||||||| || ||||||||| |||||| |||||||||| || |||||| |||||||| |||| |||||||| || |||||||||| |||||||| || ||| ||||| ||||||| ||| ||||||||||||| |||| |||||||||||| |||||| |||||||||||||| || ||||||||||||| ||| ||||||||| |||||||| |||||| |||| ||||| ||||| |||| |||| ||||||| ||||||||||| |||||||| || ||||||||| ||||| || ||| |||||| || |||||||| ||||||| ||||| |||||||||| ||| ||||||| |||||||| |||||||| |||||| ||||||||| ||||| ||| ||||||||||| ||| ||||||| |||||||| ||||||||| ||||| |||||| ||| ||||||||| |||||| |||| |||||| |||| |||||| ||||||||| ||||||||||| ||| ||| ||| |||||||| || ||| |||||| ||| ||| ||||||||| || ||||||||| ||||||| ||| |||||||||| ||||||||||| ||| ||| ||| ||||||||| || |||||||||||| ||| ||||||||||| ||| |||| ||| || |||||||| |||||| |||| ||||| ||||| |||||| ||| ||||||| |||| |||||||| ||||| |||||||| ||||| || ||| |||||||| |||||||||||| ||||||| |||||||| |||||||| |||| || ||||||| || ||| |||||||| ||||| |||||||| |||||||||| ||||||||| || |||||||| |||| || |||||||| || ||| |||||||| ||||| ||| |||| |||||||||| ||||||| |||| |||||| |||| ||||||| |||||| ||| ||||||||| ||||||||| ||| ||| |||||| || ||| |||||||| ||| ||||||| ||||||| |||||||| || ||| |||||||||||| ||| |||| |||||| |||||| |||||| || ||| |||||||||||| ||| |||||||| |||||| ||| ||||||| ||| ||||||||| |||||||||| |||||||| |||| |||| |||||| |||| ||||||| ||| ||| ||||| || ||| |||||||| ||||| || |||||||| |||||||||| ||||| ||||||||| ||||| |||||| |||| ||||| || |||||||| |||||| ||| ||||||||| ||||||||| ||| ||| |||||| || ||| |||||||| ||| ||||||| |||||||| |||||||| || ||| ||||| |||||||| ||||| |||| |||| ||||||||||| || ||| |||||||||| || |||||| |||||| ||||||||||| || ||| |||||||| |||| |||||||||| ||| |||||||||||| |||||| ||||| |||||||||||||| || |||||| |||||||| || ||| ||||| ||||||||.
||||||| || ||||||||
||||||||||||| || ||||| |||||| |||||||||| |||||||| |||||| ||||||||||| |||||||||| ||||||||||| ||| |||||||||||||||| |||| |||||||| ||| ||||||||||||| || |||| ||.
|| |||| || ||||| |||||||| |||| |||| || |||||||||| ||||||||| ||||| ||| ||||| |||||| ||||||||| ||||||| ||||| ||| |||||||| ||||||||| ||||||| ||||| ||||||||| |||| |||||||| |||||| ||| |||||| || ||| ||||| |||||||| ||||||||| ||||| ||| ||| |||||||| |||||| ||| |||||| || ||| ||||||||||||||||| ||||||| ||| ||||||||||| ||||||| |||||||| ||| |||||||| || |||||||||| ||| ||||||||| || ||| |||||||||| |||||||||||| ||| ||||| ||| ||| ||| ||||||||| ||| || ||||| |||||| |||| ||| ||| ||||||||| |||| ||||||||| ||| |||||||| ||| ||| ||||| ||||| || ||||||||| || ||||| ||||||||| ||||||||| |||| ||| |||||||||||| ||| |||||||||||| ||||||| ||| || |||||| |||||||| ||| ||| ||||||||| || ||| ||||||||.
Results of the Sponsor-Submitted NMA

Critical Appraisal of the NMA
The sponsor conducted an NMA using a |||||||| |||||||| ||||| ||||| ||||||| |||||| for all outcomes. This was a reasonable method to apply, given the availability of |||||||||| ||||||| |||| for only 2 of the included studies. The NMA was |||||||| ||||||||||| |||||||||| |||||| |||| ||||||||||||||||| |||||||||| |||||| || |||||||| |||||||||| |||||||||| ||| |||| ||||||||||| ||||| ||||||||| ||| ||||| || ||||||||||| ||||| |||||||| ||| ||| ||||||| ||||||||| ||||||||| |||| ||||||||||| ||||| ||||| || |||||||| || |||||| || |||||||| |||||| |||||||||| ||||||| |||||||||| ||| ||||||||| ||||| ||| |||||||| |||| || |||| |||| ||| ||||| ||| || ||||||||||| || ||| ||||||| ||| || ||||||||||| ||| |||||||| || || ||| ||||||| |||||||||| ||| |||||||||||| |||| ||| |||| ||| ||||||||| |||||||| |||| ||||||||||| ||||| ||| |||||||| |||||||| |||||||| ||| ||| || |||||||||||| || ||| ||| |||||||| || |||||| ||| |||||| ||||||||| || |||| ||||||||| || ||||| ||||| ||| ||| ||||||| ||||| || ||||||| || |||| ||| ||| ||||||| |||| |||||||||| ||||||||| ||||| ||||||||||| || ||| || |||||||||| || ||| |||||||| ||||| ||||||||||| |||| || ||||||||||| ||||||||||| |||| ||||||||| ||||||||||||| |||||||||| || |||| |||||||.
Comparisons in all NMAs were based on ||||| |||||| of trials and ||||| ||||||| of patients in each trial. The networks were linked to ravulizumab through |||||| ||||||| ||||| that was not part of the ||||||||||| trial. The validity of the ravulizumab comparative results relies entirely on the putative comparability of the |||||||| ||||||| || ||| ||||||||||| ||||| || ||||||||. The possibility of residual confounding exists when 2 nonrandomized groups ||||| ||||||||||| ||||||||| ||| ||| |||||||| |||||||| are being compared.
Comparisons for all outcomes were based on ||||| || |||||| |||||||| |||||||||||||| || ||| ||| |||||||| || ||||| ||| ||||||||| |||||||||| || |||||||| ||| |||||| ||||||||||| ||||||| ||| |||||||| ||| || |||||| ||||||.
The sponsor’s decision to perform ||||||| NMA analyses based on the potential effect modifier of |||||||||| ||||||||||||||||| ||||||| was appropriate. The disadvantage of doing this was to create ||||| |||||||| |||| ||||| ||||||| || ||||||. There were other sources of heterogeneity that were not explored in the NMA, and it is not clear if the homogeneity assumption is correct. These following sources were included:
The sponsor performed a quality assessment of the individual trials, but the results were not provided and no information was provided on how they used the results of the quality assessment in the NMA.
|||||||| |||| || |||||| || |||||| |||| ||||||||| |||||| ||| |||||||| |||||||| ||| ||||||| |||||||| |||| |||| |||||||| |||| ||| |||||||| |||| || ||| ||||| |||||||||||||| ||||||||| ||| ||| |||| |||||| || |||||||| ||| ||||||| |||||||| || ||| ||||| |||||||| || ||||||||| there could have been more residual effects from ||||| ||||||||| ||||||| || |||||||| ||| |||||||, compared to the other studies because ||||||||| was not permitted within 3 months of the start of the CHAMPION-NMOSD and PREVENT studies, whereas it was not permitted within |||||| of the start of the other trials.
The ||||||||| |||||||| ||| ||||||||| ||||| differed between the trials, and the handling of placebo usage also differed. The randomized period in the N-MOmentum study ended at 197 days to limit exposure to placebo, whereas placebo was continued until the end of study || ||||| |||||| ||||| |||||||||.28 The |||||||||||| ||||||| |||||||| ||||| ||||||| |||| |||||| ||||||| |||||| ||||.
The sponsor used a |||||||||| ||||| |||||||| in their sensitivity analyses for the outcome of |||||||. The factors selected by the sponsor for adjustment in the |||||||||| ||||| were reasonable, but there was not enough information provided to assess the validity of the sensitivity analyses. Some analyses in the base-case results that favoured ||||||||||| no longer favoured ||||||||||| ||||| ||| ||| ||||||||||| |||||||| were performed for the |||| || ||||| ||||||| ||||. These included comparisons to |||||||||| ||||||||||||||||| ||||||||| ||||||||||| ||||||||| ||||||||||| ||||||| ||||||||| ||| |||||||||||| |||||||||||| ||||||| |||||||||||.
Summary of NMA
Results of the sponsor’s NMA favoured ||||||||||| || |||| ||||||||||| |||||||| but the results were ||| |||||||||| |||||| ||| ||||||||| ||| |||| || |||||||| ||| ||||||| |||||||| ||||||||||| |||| |||||||||| || ||| |||||||||||||||| ||||||| ||||||| ||| ||| ||| ||| ||||||||||| ||||||| || ||| ||||||||||| ||||||| |||||||| ||||||| |||||||| ||||||||||| |||| |||||||||||| ||| ||| |||||||||||||||| ||||||| ||| ||||||||||| ||||||| ||| ||| ||| ||| ||||||||||| ||||||| |||||||| ||||||| |||||||| ||||||||||| |||| |||||||||||| || ||| ||||||||||| |||||||| ||||| |||||||| ||||| ||||||||| ||| ||||||||||| || |||||||| ||||||||||| ||||||| || ||||| ||||||| || ||||||||||||| ||||||| ||| ||||||| || ||| |||||||||| ||||||||||||||||||||| |||||||||| || |||||||||||| |||| ||||||||||| ||| ||| |||||||| ||| ||| || ||| ||||||| ||||||||| ||| ||||| ||||||| |||| ||||||||| || ||||||||| ||||||| ||||| |||| || ||||| ||||||||||| ||||||| ||| ||||||||||| ||| ||| || ||| ||||||||||| || ||| || ||| ||||| |||||||| ||| ||||| ||||||||||| ||| ||||| ||||| |||| || |||| ||| || ||| ||||||||||| ||| ||||||| || ||| ||||||| ||||||||| || ||||||||| || ||| |||||||| |||| || ||||| |||| |||||||||| ||||||| ||||||| |||| ||||||||||| |||||||| |||||| || |||| ||||||||| ||| ||| |||||||||||||| || ||||||| |||| ||| ||||||||||| || ||| ||||| ||| || ||| ||||||||||| || |||| ||| ||| ||| |||| ||||| |||||| ||| ||||||||||.
Discussion
Summary of Available Evidence
The 1 study was reviewed, CHAMPION-NMOSD (N = 58), was an externally placebo-controlled, open-label, phase III, multicenter trial designed to evaluate the efficacy and safety of ravulizumab in adults with anti-AQP4 antibody-positive NMOSD who had at least 1 relapse in the prior 12 months. The study had a single-arm treatment design; the placebo group from the PREVENT study was used as an external placebo comparator. The recent PREVENT study evaluated the efficacy and safety of eculizumab in the prevention of relapses in patients with anti-AQP4 antibody-positive NMOSD who had at least 2 relapses in the prior 12 months or 3 relapses in the prior 24 months, at least 1 of which occurring in the prior 12 months. Patients were randomly assigned in a 2:1 ratio to receive either eculizumab (n = 96) or a matching-administration placebo (n = 47) every 2 weeks. The primary outcome in both studies was time to first adjudicated on-trial relapse. The study population was considered representative of patients in clinical practice; disability was consistent with what is expected in an NMOSD population.
Interpretation of Results
Efficacy
The primary outcome in the CHAMPION-NMOSD study was adjudicated on-trial relapse, which was considered the preferred and most reliable end point by clinical experts. Avoidance of relapses is paramount in preventing the accumulation of disability in patients, as any relapse could be a disabling 1 at any time in the disease trajectory. No patient in the ravulizumab group reported a primary outcome event of adjudicated on-trial relapse during the study, compared with 42.6% of patients in the PREVENT placebo group. According to the clinical experts consulted by CADTH, the between-group difference was consistent with a high level of efficacy for ravulizumab and was considered clinically meaningful. NMOSD in itself is a severe disease with a generally poor natural trajectory and an inherently high risk of relapse at any disease stage; therefore, patients treated with ravulizumab would likely have relapsed otherwise over the duration of follow-up. Relapse definition and assessment were considered fairly objective and representative of clinical practice; therefore, it is not expected that this outcome would have been subject to bias related to the open-label design.
Results from additional analyses were supportive of the superiority of ravulizumab over placebo for relapse prevention. Two sensitivity analyses, ||| |||||||||| || |||||||||| ||||| and the other using propensity scores in a weighted analysis, suggest that imbalances in observed baseline characteristics due to trial design were not sufficient to substantially impact the observed treatment effect. In addition, an analysis of the primary outcome at a later date in the long term extension period confirms that the efficacy of ravulizumab was maintained over an extended period of time. |||||||| ||||||| ||||||||||| || |||||||| |||| ||||| || |||||||||| || ||||||||| |||||| |||||||| ||||| ||| ||| |||| |||| ||| |||||||||| ||||||| ||| ||| |||| |||||||||| ||| ||| ||||| ||||| || |||| |||||||||| |||||||| ||||||||| |||| ||||||||||| |||||||||| |||||||||| |||||| || |||| ||||||| |||||||||||.
Results also suggested benefits from ravulizumab on the secondary outcome of function and HRQoL. According to the clinical experts, the difference between ravulizumab and placebo was considered clinically meaningful for both the HAI and EDSS (assessing function), as well as for the EQ-5D index and VAS scores and for ||||| |||||||| ||||||||| ||||| |||||||||| |||||||. There is some uncertainty, however, as statistical significance was not reached for the EQ-5D index score and, because of this, results for EDSS and EQ-5D VAS could not be formally tested due to the prespecified statistical strategy to control for multiplicity. It should be noted, however, that the study was not powered to show a difference between treatment groups for any secondary outcome. Furthermore, ||||| |||||||| ||||||||| ||||| ||| ||| |||||||| || ||| ||||||| ||| |||||||| |||||||||||. The clinical experts indicated that loss of function and loss of quality of life are cumulative over time, and that the magnitude of worsening depends on the severity of the relapse. As a result, although maintaining function and HRQoL is very important to patients, according to the input received, it may be more difficult to observe changes in these outcomes in the context of a clinical trial, where patients in the placebo group are being followed only up to a first relapse for ethical reasons. Results were nevertheless considered consistent with disease evolution in clinical practice, in that patients receiving placebo tended to have a stable to worsening status, while patients receiving ravulizumab tended to have a stable to improved status.
||| ||||||| || |||||||||| |||||||| |||||| |||| |||||||| || |||||| |||||| ||| |||||||||| |||| ||| ||||||| || ||||||| || |||||||| ||| |||||||| |||||||||||| ||| |||| ||| |||| |||| |||| ||| |||||||| ||| |||||||| ||||||| ||||||||||| ||||| ||||||||| || |||||| |||| |||||||| ||| |||||||| |||||| || ||| ||||||||||| ||||| || ||||| || ||||| |||||| || || ||||||||||||||| |||||| |||||| ||| |||| ||| |||||||| ||| ||| ||||||| ||||||| |||| || |||||||||||||||| || |||||||||||||| |||| ||||||||||||||| || ||||| |||||||||||||||| |||| ||| ||| || |||||||| ||| ||||||||| || ||||| |||||||.
The CHAMPION-NMOSD study had a single-arm treatment design, and used the placebo group from the PREVENT study as an external placebo comparator. The clinical experts and CADTH review team acknowledged that there is a rationale behind this decision. The main differences observed between the studies included the number of historical relapses, which, according to the clinical experts, is not expected to have a substantial impact on the risk of future relapses and, therefore, would not meaningfully affect results for the primary outcome of relapse prevention. In addition, the ARR in the prior 12 months and 24 months between treatment groups were considered similar enough by the clinical experts to be consistent with the assumption that both groups were having a relatively similar evolution in terms of relapse frequency. The overall assessment suggests that the 2 trials are sufficiently similar and that the comparison between ravulizumab and placebo is likely valid, but that the external control design would introduce a risk of bias, leading to uncertainty regarding the true effect of ravulizumab. However, the magnitude of the relapse risk reduction with ravulizumab treatment observed in the CHAMPION-NMOSD study was considered large and constant over time, and compensated for potential biases and the known variability in disease progression. The estimated treatment effect of ravulizumab constitutes a precise estimate with narrow CIs, and the remaining level of uncertainty is not expected to be sufficient to change the primary conclusions from the study. Uncertainty would impact our confidence in the secondary outcome results; however, the role of secondary outcomes in the efficacy assessment of ravulizumab is not considered as important as relapse prevention, which is the ultimate treatment goal for patients with NMOSD in clinical practice.
The sponsor submitted indirect evidence in the form of an NMA that compared the effects of ravulizumab with key comparators in the context of adults with anti-AQP4 antibody-positive NMOSD. Results of the sponsor’s NMA favoured ||||||||||| || |||| ||||||||||| |||||||| ||| ||| ||||||| |||| ||| |||||||||| |||||| ||| ||||||||| ||| |||| || |||||||| ||| ||||||| |||||||| ||||||||||| |||| |||||||||| || ||| |||||||||||||||| ||||||| ||||||| ||| ||| ||| ||| ||||||||||| ||||||| || ||| ||||||||||| ||||||| |||||||| ||||||| |||||||| ||||||||||| |||| |||||||||||| ||| ||| |||||||||||||||| ||||||| ||| ||||||||||| ||||||| ||| ||| ||| ||| ||||||||||| ||||||| |||||||| ||||||| |||||||| ||||||||||| |||| |||||||||||| || ||| ||||||||||| |||||||| ||||| |||||||| ||||| ||||||||| ||| ||||||||||| || |||||||| ||||||||||| ||||||| || ||||| ||||||| || ||||||||||||| ||||||| ||| ||||||| || ||| ||||||||| ||||||||||||||||||||| |||||||||| || |||||||||||| |||| ||||||||||| ||| ||| |||||||| ||| ||| || ||| ||||||| ||||||||| ||| ||||| ||||||| |||| ||||||||| || ||||||||| ||||||| ||||| |||| || ||||| ||||||||||| ||||||| ||| ||||||||||| ||| ||| || ||| ||||||||||| || ||| || ||| ||||| |||||||| ||| ||||| ||||||||||| ||| ||||| ||||| |||| || |||| ||| || ||| ||||||||||| ||| ||||||| || ||| ||||||| |||||||||.
Harms
A high proportion of patients receiving ravulizumab in the CHAMPION-NMOSD study experienced at least 1 AE during the study follow-up period. SAEs were also relatively common with treatment; the most frequently reported SAEs involved infections and infestations. However, ravulizumab appeared to be well tolerated; only 1 patient discontinued treatment due to AEs. It should be noted that the reporting of subjective AEs may have been subject to bias (i.e., overestimated), due to the single-arm, open-label design of the study, in which patients and clinicians were aware that active treatment was being administered. No deaths were reported during the study. The clinical experts indicated that the overall harms profile of ravulizumab in the CHAMPION-NMOSD study did not raise any particular safety signals, with the exception of meningococcal infections; as such, all patients should receive meningococcal vaccination before the start of ravulizumab therapy, per the product monograph. No estimates of the relative risk of harms were performed in the sponsor-submitted NMA.
Other Considerations
Special consideration may be given to the fact that NMOSD is a rare and severe disease with a generally poor natural trajectory, and that there is, unfortunately, a limited number of effective therapeutic options, access to which is very limited and can be difficult across the country, according to patient and clinician group input, and also highlighted by the clinical experts consulted by CADTH.
Conclusion
The findings from the CHAMPION-NMOSD study suggest that ravulizumab results in the clinically meaningful prevention of relapses, compared to placebo, in patients with anti-AQP4 antibody-positive NMOSD, which is paramount in preventing the accumulation of disability in patients. The use of a single-arm treatment design, with the placebo group from the PREVENT study used as an external placebo comparator, may have introduced a risk of bias, leading to uncertainty surrounding the estimates. Overall assessment suggests, however, that the 2 trials likely feature sufficient similarity to ensure a valid comparison, and that differences observed in patient populations might not meaningfully impact the risk of relapse, according to the clinical experts consulted by CADTH. Concern over this uncertainty was mitigated by the magnitude of the relapse risk reduction with ravulizumab treatment observed in the CHAMPION-NMOSD study, which was considered large and constant over time, and compensated for potential biases and the known variability in disease progression. In addition, the sensitivity analyses of the primary outcome suggest that the findings are robust and statistically infer that imbalances in patient populations were not likely to have a substantial impact on the estimates. Ravulizumab may also have a clinically significant impact on function and HRQoL, although there is some uncertainty due to the noted limitations of the study design and the fact that statistical significance was not consistently reached or formally evaluated for all secondary end points. Maintaining function and HRQoL is very important to patients, according to the input received, but it may be more difficult to observe changes in these outcomes in the context of a clinical trial, as loss of function and loss of quality of life are cumulative over time and related to the severity of the relapse. A high proportion of patients in the CHAMPION-NMOSD study experienced harms events, most notably related to infections and infestations; however, ravulizumab appeared to be well tolerated, especially considering that there were very few withdrawals due to AEs. The overall harms profile did not raise any particular safety signals, with the exception of meningococcal infections; per the product monograph, all patients should receive meningococcal vaccination before the start of ravulizumab therapy. Findings from the trial were considered generalizable to the population of patients with NMOSD in Canada. Special consideration may be given to the fact that NMOSD is a rare and severe disease with a generally poor natural trajectory, and that there is, unfortunately, a limited number of effective therapeutic options, access to which is very limited and can be difficult across the country. Results from the NMA suggest that ravulizumab performs better || |||| |||||||| |||||||| || ||||| ||||||||||| ||| ||| |||||||||||||| || ||||||| |||| ||| ||||||||||| || ||| ||||| ||| || ||| ||||||||||| || ||| ||| ||| ||| |||| ||||| |||||| ||| ||||||||||.
References
1.Carnero Contentti E, Correale J. Neuromyelitis optica spectrum disorders: from pathophysiology to therapeutic strategies. J Neuroinflammation. 2021;18(1):208. PubMed
2.Wingerchuk DM, Lucchinetti CF. Neuromyelitis Optica Spectrum Disorder. N Engl J Med. 2022;387(7):631-639. PubMed
3.Wingerchuk DM, Banwell B, Bennett JL, et al. International consensus diagnostic criteria for neuromyelitis optica spectrum disorders. Neurology. 2015;85:177-189. PubMed
4.Lennon VA, Wingerchuk DM, Kryzer TJ, et al. A serum autoantibody marker of neuromyelitis optica: distinction from multiple sclerosis. Lancet. 2004;364(9451):2106-2112. PubMed
5.Jarius S, Ruprecht K, Wildemann B, et al. Contrasting disease patterns in seropositive and seronegative neuromyelitis optica: A multicentre study of 175 patients. J Neuroinflammation. 2012;9:14. PubMed
6.Kitley J, Leite MI, Nakashima I, et al. Prognostic factors and disease course in aquaporin-4 antibody-positive patients with neuromyelitis optica spectrum disorder from the United Kingdom and Japan. Brain. 2012;135(Pt 6):1834-1849. PubMed
7.Wingerchuk DM, Weinshenker BG. Neuromyelitis optica. Curr Treat Options Neurol. 2008;10(1):55-66. PubMed
8.Ajmera MR, Boscoe A, Mauskopf J, Candrilli SD, Levy M. Evaluation of comorbidities and health care resource use among patients with highly active neuromyelitis optica. J Neurol Sci. 2018;384:96-103. PubMed
9.Beekman J, Keisler A, Pedraza O, et al. Neuromyelitis optica spectrum disorder: Patient experience and quality of life. Neurol Neuroimmunol Neuroinflamm. 2019;6(4):e580. PubMed
10.Mealy MA, Boscoe A, Caro J, Levy M. Assessment of Patients with Neuromyelitis Optica Spectrum Disorder Using the EQ-5D. Int J MS Care. 2019;21(3):129-134. PubMed
11.Eaneff S, Wang V, Hanger M, et al. Patient perspectives on neuromyelitis optica spectrum disorders: Data from the PatientsLikeMe online community. Mult Scler Relat Disord. 2017;17:116-122. PubMed
12.Sellner J, Boggild M, Clanet M, et al. EFNS guidelines on diagnosis and management of neuromyelitis optica. Eur J Neurol. 2010;17(8):1019-1032. PubMed
13.Kawachi I, Lassmann H. Neurodegeneration in multiple sclerosis and neuromyelitis optica. J Neurol Neurosurg Psychiatry. 2017;88(2):137-145. PubMed
14.Papp V, Illes Z, Magyari M, et al. Nationwide prevalence and incidence study of neuromyelitis optica spectrum disorder in Denmark. Neurology. 2018;91(24):e2265-e2275. PubMed
15.Hor JY, Asgari N, Nakashima I, et al. Epidemiology of Neuromyelitis Optica Spectrum Disorder and Its Prevalence and Incidence Worldwide. Front Neurol. 2020;11:501. PubMed
16.Etemadifar M, Nasr Z, Khalili B, Taherioun M, Vosoughi R. Epidemiology of neuromyelitis optica in the world: a systematic review and meta-analysis. Mult Scler Int. 2015;2015:174720. PubMed
17.Mealy MA, Kessler RA, Rimler Z, et al. Mortality in neuromyelitis optica is strongly associated with African ancestry. Neurol Neuroimmunol Neuroinflamm. 2018;5(4):e468. PubMed
18.Jonsson DI, Sveinsson O, Hakim R, Brundin L. Epidemiology of NMOSD in Sweden from 1987 to 2013. Neurology. 2019;93(2):e181-e189. PubMed
19.Du Q, Shi Z, Chen H, et al. Mortality of neuromyelitis optica spectrum disorders in a Chinese population. Ann Clin Transl Neurol. 2021;8(7):1471-1479. PubMed
20.Collongues N, Marignier R, Jacob A, et al. Characterization of neuromyelitis optica and neuromyelitis optica spectrum disorder patients with a late onset. Mult Scler. 2014;20(8):1086-1094. PubMed
21.Ultomiris (ravulizumab for injection) 10 mg/mL & 100 mg/mL concentrate for solution for intravenous infusion [product monograph]. Mississauga (ON): Alexion Pharma Canada Corp.; 2023 Oct 30: https://pdf.hres.ca/dpd_pm/00073059.PDF. Accessed 2024 Nov 29.
22.CADTH reimbursement recommendation: ravulizumab (Ultomiris). Can J Health Technol. 2022;2(3). www.cadth.ca/sites/default/files/DRR/2022/SR0700%20Ultomiris%20-%20Final%20CADTH%20Rec.pdf. Accessed 2023 Nov 29.
23.CADTH reimbursement recommendation: ravulizumab (Ultomiris). Can J Health Technol. 2023;3(3). https://www.cadth.ca/sites/default/files/DRR/2023/SR0740%20Ultomiris%20-%20CADTH%20Final%20Recommendation%20Final.pdf. Accessed 2023 Nov 29.
24.CADTH reimbursement recommendation: ravulizumab (Ultomiris). Can J Health Technol. 2023;3(8). https://www.cadth.ca/sites/default/files/DRR/2023/SR0765Ultomiris%20-%20Confidential%20Final%20CADTH%20Recommendation%20August%2024%2C%202023%20revised.pdf. Accessed 2023 Nov 29.
25.Schwartz CE, Stark RB, Stucky BD. Response-shift effects in neuromyelitis optica spectrum disorder: a secondary analysis of clinical trial data. Qual Life Res. 2021;30(5):1267-1282. PubMed
26.Clinical Study Report: ALXN1210-NMO-307 (CHAMPION-NMOSD) Primary Analysis (data cut-off: 15 March 2022). In: Drug Reimbursement Review sponsor submission: Ultomiris (ravulizumab for injection) 10 mg/mL & 100 mg/mL concentrate for solution for intravenous infusion. Mississauga (ON): Alexion Pharma Canada Corp.; 2023 Aug 29. 2022.
27.Ultomiris (ravulizumab) For the treatment of adult patients with anti-aquaporin 4 (AQP4) antibody-positive neuromyelitis optica spectrum disorder (NMOSD): clinical summary [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Ultomiris (ravulizumab for injection) 10 mg/mL & 100 mg/mL concentrate for solution for intravenous infusion. Mississauga (ON): Alexion Pharma Canada Corp.; 2023 Aug 29.
28.Cree BAC, Bennett JL, Kim HJ, et al. Inebilizumab for the treatment of neuromyelitis optica spectrum disorder (N-MOmentum): a double-blind, randomised placebo-controlled phase 2/3 trial. Lancet. 2019;394(10206):1352-1363. PubMed
29.Traboulsee A, Greenberg BM, Bennett JL, et al. Safety and efficacy of satralizumab monotherapy in neuromyelitis optica spectrum disorder: a randomised, double-blind, multicentre, placebo-controlled phase 3 trial. Lancet Neurol. 2020;19(5):402-412. PubMed
30.Sato DK, Callegaro D, Lana-Peixoto MA, et al. Distinction between MOG antibody-positive and AQP4 antibody-positive NMO spectrum disorders. Neurology. 2014;82(6):474-481. PubMed
31.Cook LJ, Rose JW, Alvey JS, et al. Collaborative International Research in Clinical and Longitudinal Experience Study in NMOSD. Neurol Neuroimmunol Neuroinflamm. 2019;6(5):e583. PubMed
32.Liu J, Tan G, Li B, et al. Serum Aquaporin 4-Immunoglobulin G Titer and Neuromyelitis Optica Spectrum Disorder Activity and Severity: A Systematic Review and Meta-Analysis. Front Neurol. 2021;12:746959. PubMed
33.Palace J, Lin DY, Zeng D, et al. Outcome prediction models in AQP4-IgG positive neuromyelitis optica spectrum disorders. Brain. 2019;142(5):1310-1323. PubMed
34.Berthele A, Levy M, Wingerchuk DM, et al. A single relapse induces worsening of disability and health-related quality of life in patients with neuromyelitis optica spectrum disorder. Front Neurol. 2023;14:1099376. PubMed
35.Trebst C, Jarius S, Berthele A, et al. Update on the diagnosis and treatment of neuromyelitis optica: recommendations of the Neuromyelitis Optica Study Group (NEMOS). J Neurol. 2014;261(1):1-16. PubMed
36.Kimbrough DJ, Fujihara K, Jacob A, et al. Treatment of Neuromyelitis Optica: Review and Recommendations. Mult Scler Relat Disord. 2012;1(4):180-187. PubMed
37.Canadian Clinician Survey Report [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Ultomiris (ravulizumab for injection) 10 mg/mL & 100 mg/mL concentrate for solution for intravenous infusion. Mississauga (ON): Alexion Pharma Canada Corp.; 2023 Aug 29. 2023.
38.CADTH Common Drug Review Clinical Review Report: eculizumab (Soliris). Ottawa (ON): CADTH; 2020: https://www.cadth.ca/eculizumab-3. Accessed 2024 Nov 29.
39.Enspryng (satralizumab injection). In: Drug Reimbursement Review sponsor submission: Ultomiris (ravulizumab for injection) 10 mg/mL & 100 mg/mL concentrate for solution for intravenous infusion. Mississauga (ON): Alexion Pharma Canada Corp.; 2023 Aug 29.
40.CADTH Reimbursement recommendation: satralizumab (Enspryng). Ottawa (ON): CADTH; 2021: https://www.cadth.ca/sites/default/files/cdr/complete/SR0663%20Enspryng%20-%20CDEC%20Final%20Recommendation%20April%2023%2C%202021_for%20posting.pdf. Accessed 2024 Nov 29.
41.Alexander JJ. Blood-brain barrier (BBB) and the complement landscape. Mol Immunol. 2018;102:26-31. PubMed
42.Uplizna (inebilizumab-cdon) for injection. In: Drug Reimbursement Review sponsor submission: Ultomiris (ravulizumab for injection) 10 mg/mL & 100 mg/mL concentrate for solution for intravenous infusion. Mississauga (ON): Alexion Pharma Canada Corp.; 2023 Aug 29. 2022.
43.Soliris (eculizumab for injection). In: Drug Reimbursement Review sponsor submission: Ultomiris (ravulizumab for injection) 10 mg/mL & 100 mg/mL concentrate for solution for intravenous infusion. Mississauga (ON): Alexion Pharma Canada Corp.; 2023 Aug 29. Accessed 2019.
44.Pittock SJ, Barnett M, Bennett JL, et al. Ravulizumab in Aquaporin-4-Positive Neuromyelitis Optica Spectrum Disorder. Ann Neurol. 2023;93(6):1053-1068. PubMed
45.CHAMPION NMOSD 307 Study Design Deck [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Ultomiris (ravulizumab for injection) 10 mg/mL & 100 mg/mL concentrate for solution for intravenous infusion. Mississauga (ON): Alexion Pharma Canada Corp.; 2023 Aug 29.
46.Pittock SJ, Berthele A, Fujihara K, et al. Supplementary Appendix: Eculizumab in Aquaporin-4-Positive Neuromyelitis Optica Spectrum Disorder. N Engl J Med. 2019;381(7):614-625. PubMed
47.Stellmann JP, Krumbholz M, Friede T, et al. Immunotherapies in neuromyelitis optica spectrum disorder: efficacy and predictors of response. J Neurol Neurosurg Psychiatry. 2017;88(8):639-647. PubMed
48.Mealy MA, Wingerchuk DM, Palace J, Greenberg BM, Levy M. Comparison of relapse and treatment failure rates among patients with neuromyelitis optica: multicenter study of treatment efficacy. JAMA Neurol. 2014;71(3):324-330. PubMed
49.Balshem H, Helfand M, Schünemann HJ, et al. GRADE guidelines: 3. Rating the quality of evidence. J Clin Epidemiol. 2011;64(4):401-406. PubMed
50.Santesso N, Glenton C, Dahm P, et al. GRADE guidelines 26: informative statements to communicate the findings of systematic reviews of interventions. J Clin Epidemiol. 2020;119:126-135. PubMed
51.Network meta-analysis of ravulizumab, eculizumab, satralizumab and inebilizumab for the treatment of neuromyelitis optica spectrum disorder (NMOSD). In: Drug Reimbursement Review sponsor submission: Ultomiris (ravulizumab for injection) 10 mg/mL & 100 mg/mL concentrate for solution for intravenous infusion. Mississauga (ON): Alexion Pharma Canada Corp.; 2023 Aug 29.
52.Wingerchuk DM, Zhang I, Kielhorn A, et al. Network Meta-analysis of Food and Drug Administration-approved Treatment Options for Adults with Aquaporin-4 Immunoglobulin G-positive Neuromyelitis Optica Spectrum Disorder. Neurol Ther. 2022;11(1):123-135. PubMed
53.Evrenoglou T, White IR, Afach S, Mavridis D, Chaimani A. Network meta-analysis of rare events using penalized likelihood regression. Stat Med. 2022;41(26):5203-5219. PubMed
54.Heinze G, Schemper M. A solution to the problem of monotone likelihood in Cox regression. Biometrics. 2001;57(1):114-119. PubMed
55.Lin DY, Dai L, Cheng G, Sailer MO. On confidence intervals for the hazard ratio in randomized clinical trials. Biometrics. 2016;72(4):1098-1102. PubMed
Pharmacoeconomic Review
Abbreviations
AE
adverse event
AQP4
antiaquaporin-4
BIA
budget impact analysis
EDSS
expanded disability status scale
HR
hazard ratio
ICER
incremental cost-effectiveness ratio
IST
immunosuppressive therapy
LY
life-year
NMA
network meta-analysis
NMOSD
neuromyelitis optica spectrum disorder
QALY
quality-adjusted life-year
WTP
willingness to pay
Executive Summary
The executive summary comprises 2 tables (Table 1 and Table 2) and a conclusion.
Item | Description |
|---|---|
Drug product | Ravulizumab (Ultomiris), 10 mg/mL and 100 mg/mL concentrate for solution for IV infusion |
Submitted price | Ravulizumab 300 mg, vial: $7,282.15 1,100 mg, vial: $26,701.20 |
Indication | For the treatment of adults with anti-AQP4 antibody-positive NMOSD |
Health Canada approval status | NOC |
Health Canada review pathway | Standard review |
NOC date | October 30, 2023 |
Reimbursement request | Per indication |
Sponsor | Alexion Pharma GmbH |
Submission history | Previously reviewed: Yes Indication: Paroxysmal nocturnal hemoglobinuria Recommendation date: February 11, 2022 Recommendation: Reimburse with clinical criteria and/or conditions Indication: Atypical hemolytic uremic syndrome Recommendation date: February 17, 2023 Recommendation: Reimburse with clinical criteria and/or conditions Indication: AChR antibody-positive generalized myasthenia gravis Recommendation date: August 8, 2023 Recommendation: Do not reimburse |
AChR = acetylcholine receptor; AQP4 = antiaquaporin-4; NOC = Notice of Compliance; NMOSD = neuromyelitis optica spectrum disorder.
Table 2: Summary of Economic Evaluation
Component | Description |
|---|---|
Type of economic evaluation | Cost-utility analysis Markov model |
Target population | Adults with anti-AQP4 antibody-positive NMOSD |
Treatment | Ravulizumab |
Comparators | Eculizumab Satralizumab ISTs (steroids and nonsteroidal immunosuppressive therapy) |
Perspective | Canadian publicly funded health care payer |
Outcomes | QALYs, LYs |
Time horizon | Lifetime (53 years) |
Key data source | The CHAMPION-NMOSD study and the sponsor-conducted NMA to inform the comparative clinical efficacy of eculizumab, satralizumab, and ISTs. |
Submitted results |
|
Key limitations |
|
CADTH reanalysis results |
|
AQP4 = antiaquaporin-4; ICER = incremental cost-effectiveness ratio; IST = immunosuppressive therapy; LY = life-year; NMA = the network meta-analysis; NMOSD = neuromyelitis optica spectrum disorder; QALY = quality-adjusted life-year.
Conclusions
Based on the CADTH clinical review of the CHAMPION-NMOSD trial, treatment with ravulizumab (Ultomiris) resulted in a clinically meaningful decrease in the number of relapses, compared to placebo, in adults with anti-antiaquaporin-4 (AQP4) antibody–positive neuromyelitis optica spectrum disorder (NMOSD) (0% versus 43%, respectively). The indirect comparison of ravulizumab, eculizumab, satralizumab, and immunosuppressive therapy (IST) was subject to several limitations ||||||||| ||||| ||||||||||| ||| ||| ||| |||||||| ||||| |||| ||||||||| ||||||||| These limitations resulted in uncertain estimates of the relative clinical effectiveness of ravulizumab, leading to further uncertainty regarding the predicted costs and quality-adjusted life-year (QALYs) estimated by the model.
CADTH identified limitations of the sponsor’s submitted economic evaluation that could not be addressed through reanalysis, including uncertainty regarding the long-term clinical effectiveness of ravulizumab. In the sponsor’s base case, the cost-effectiveness frontier was represented by steroids and nonsteroidal ISTs, satralizumab, and ravulizumab. The incremental cost-effectiveness ratio (ICER) of ravulizumab compared to satralizumab was $2,386,625 per QALY gained (incremental costs = $11,261,849; incremental QALYs = 4.72). The probability of being cost-effective at a $50,000 per QALY gained threshold was 0%. A reduction in the price of ravulizumab of at least 73% (reducing the unit price of a 300 mg vial of ravulizumab from $7,282 to $1,966, and reducing annual costs from $567,618 to $414,361 per patient) would be necessary for ravulizumab to be considered cost-effective at a $50,000 per QALY gained threshold compared to satralizumab. In the economic analysis, treatment with ravulizumab was associated with increased costs and increased QALYs compared to treatment with satralizumab. The high ICER should be contextualized by the clinical uncertainty in the network meta-analysis (NMA), in addition to the potential underestimation of mortality for patients receiving ravulizumab and the potential overestimation of longer-term clinical effects and health care resource use. These limitations could not be resolved through reanalysis and contribute additional uncertainty to the estimate of incremental effectiveness. The estimated cost increase among patients treated with ravulizumab compared to satralizumab was entirely driven by the drug acquisition cost of ravulizumab. Finally, because the CHAMPION-NMOSD study only included patients receiving first-line treatment, the cost-effectiveness of ravulizumab as a second-line or subsequent-line treatment is unknown. Because of the high degree of uncertainty associated with these limitations, a further price reduction may be warranted.
Stakeholder Input Relevant to the Economic Review
This section is a summary of the feedback received from the patient groups, registered clinicians, and drug plans that participated in the CADTH review process.
Two patient groups provided input for this review: Multiple Sclerosis Canada and the Sumaira Foundation. Patient input was based on surveys of patients with NMOSD and their caregivers. The input noted that treatment options for these patients include off-label therapies, such as rituximab, mofetil mycophenolate, oral prednisone or methylprednisolone, and azathioprine, as well as eculizumab and satralizumab. However, patient input noted that eculizumab and satralizumab have limited access. Patient feedback emphasized that the need to prevent further attacks is paramount for patients. Patient feedback indicated that NMOSD has a significant impact on many aspects of daily life, including independence, family, relationships, and employment. Patients also indicated that they consider it important to have options regarding the administration route and the frequency of administration of therapies. No patient had experience with the drug under review.
Clinician input was received from Canadian Network of Multiple Sclerosis Clinics. Clinician input emphasized that treatment goals are to prevent NMOSD attacks and to reduce the severity of the attacks, reducing the cumulative disability associated with attacks and minimizing the adverse events (AEs) related to therapies. Clinician feedback noted the limited access to eculizumab and satralizumab because of their stringent funding coverage criteria. The clinician input indicated that the proposed place of ravulizumab in therapy would be similar to that of eculizumab (they share a similar mechanism of action), but with a less onerous administration schedule for patients (i.e., administration every 8 weeks with ravulizumab instead of every 2 weeks with eculizumab).
The drug plan input indicated issues with accessibility to eculizumab and satralizumab, and noted that many therapies for NMOSD are off-label. It also noted that the appropriate treatment algorithm for this population is unclear and that there is uncertainty regarding treatment sequence and switching criteria. The drug plan input also raised the question of whether patients should be required to rule out off-label therapies before accessing ravulizumab. The drug plan feedback indicated that Expanded Disability Status Scale (EDSS) scores might be required for the clinical assessment and monitoring of therapeutic response. Thus, clarification may be required on the use of EDSS scores in clinical practice and their appropriateness to assess response to therapy. The plans also noted that the IV administration of ravulizumab requires access to infusion clinics; however, ravulizumab’s less frequent infusions (every 8 weeks) may provide an advantage to the health care system and reduce treatment burden for patients and caregivers. Finally, the drug plans expressed concerns regarding the anticipated budget impact of ravulizumab, and noted that both eculizumab and satralizumab have completed price negotiations for NMOSD without reaching a price agreement.
Several of these concerns were addressed in the sponsor’s model:
The sponsor’s submitted model accounted for NMOSD relapses and long-term disability.
Loss of productivity was included in a scenario analysis.
CADTH was unable to address the following concerns raised from stakeholder input:
The comparators of interest in the model were not aligned with patient, physician, or drug plan input. CADTH accepted a request from the sponsor to exclude rituximab from the economic evaluation due to a lack of available comparative efficacy evidence.
Economic Review
The current review is for ravulizumab (Ultomiris) for adults with anti-AQP4 antibody-positive NMOSD.1
Economic Evaluation
Summary of Sponsor’s Economic Evaluation
Overview
The sponsor submitted a cost-utility analysis of ravulizumab compared with eculizumab, satralizumab, and ISTs. The model population included adults with anti-AQP4 antibody-positive NMOSD, which is aligned with the proposed Health Canada indication.
Ravulizumab is available as 300 mg and 1,100 mg vials for IV administration, at a concentration of 10 mg/mL. The submitted price was $7,282.15 and $ 26,701.20 per 300 mg and 1,100 mg vial, respectively. For the indicated population, the recommended dosage for treatment is between 2,400 mg and 3,000 mg, depending on the patient’s weight, followed by a maintenance dose between 3,000 mg and 3,600 mg every 8 weeks starting 2 weeks after the induction dose. At the submitted price, for a patient with an average weight of 69.85 kg, the maintenance dose will cost $1,425 per day and $520,674 per year.
A total of 3 alternative treatments to ravulizumab were considered in the economic evaluation: eculizumab, satralizumab, and ISTs. ISTs consisted of a basket of steroids and nonsteroidal immunosuppressive therapies, including azathioprine, mycophenolate mofetil, cyclosporine, tacrolimus, methotrexate, cyclophosphamide, and prednisone. The annual per-patient cost of maintenance eculizumab was $694,231, whereas the annual per-patient cost of maintenance satralizumab and ISTs was $122,850 and $251, respectively.
Modelled outcomes included life-years (LYs) and QALYs. Costs were estimated from the perspective of the Canadian public health care payer. Model outputs were generated over a lifetime horizon of 53 years. Costs and outcomes were discounted at a rate of 1.5%.
Model Structure
The sponsor submitted a Markov model that tracked a hypothetical cohort of patients across health states defined by a sequence of NMOSD relapses, with or without long-term NMOSD-related disability (Figure 1). The sponsor assumed that patients could have a maximum of 20 relapses during the model time horizon, resulting in a model with 42 mutually exclusive health states. In addition, the model tracked patients’ EDSS scores, which are assumed to increase every time patients experience a relapse. Meanwhile, patients who did not experience an NMOSD relapse (had stable disease) would remain in their current health state, resulting in no change in EDSS score. Patients entered the model in the relapse-free health state without long-term NMOSD-related disability. Patients could remain in the relapse-free health state, experience a relapse without long-term disability, or experience a relapse with long-term disability. With each relapse, patients have a fixed risk of entering health states with long-term disability. In addition to this risk, an EDSS score to 5.5 or greater would lead a patient to transition to long-term disability health states. Patients were assumed to remain on treatment for the entire model time horizon (i.e., no treatment discontinuation). Throughout the model time horizon, patients were subject to an all-cause mortality risk. The cycle length of the model was 30 days.
Model Inputs
All data summarizing baseline characteristics of the cohort were obtained from the CHAMPION-NMOSD trial. This was an external placebo-controlled, phase III trial that evaluated the efficacy and safety of ravulizumab in adults with anti-AQP4 antibody-positive NMOSD. Data of interest included mean baseline age (47 years), sex (90% female), baseline EDSS score, and mean weight at baseline (69.85 kg).2
Estimates of relative efficacy for the time to first adjudicated relapse were obtained from an NMA submitted by the sponsor.3 The NMA estimated the hazard ratio (HR) of ravulizumab, |||||||||| ||| |||||||||||| |||||||| || |||| ||||| |||| |||| ||| |||||||||||||| |||||||||||||| ||||||| |||||||||| || ||||||||| ||| |||||||||| ||||||||||||| || |||||||| |||||. The model relied on treatment-specific survival functions to predict the risk of NMSOD relapses. For ISTs, parametric survival curves were fitted to the time to first relapse obtained from PREVENT trial data.4 Independent parametric models were fit using the exponential, log-logistic, log-normal, Weibull, Gompertz, gamma, and generalized gamma distributions. Based on the sponsor’s assessment of model fit statistics, the submitted base case assumed an exponential distribution for IST. To generate the survival curves for the remaining treatments, the estimates of relative efficacy obtained from the NMA were applied to the IST reference curve. The sponsor assumed that the risk of relapse obtained from time to first relapse outcome would be applied to all subsequent relapse events.
The model included health states that accounted for NMOSD relapses with and without long-term NMOSD-related disability. Patients can transition to long-term disability health states based on a fixed risk at each relapse, which was obtained from a study that defined long-term disability as “patients who experienced disability as defined by loss of vision and/or ambulation.”6 In addition to this risk, an EDSS score to 5.5 or greater would also lead a patient to transition to long-term disability health states.
Mortality was assumed to be treatment-dependent. The mortality rate for patients receiving ISTs was obtained from sources in the literature.7 Mortality estimates for patients on treatment with ravulizumab, eculizumab, or satralizumab were derived by applying the mortality HRs. These mortality HRs were calculated taking into consideration the ||||||||| || ||| |||| || |||||||| |||||||| |||| ||| ||||||||| |||| The sponsor’s model assumed that lowering the risk of a relapse would reduce the mortality observed in patients with NMOSD. The mortality of patients receiving ravulizumab, eculizumab, or satralizumab was calculated to be not lower than the general population mortality from the Statistics Canada life tables published in January 2022.8 Patients who experienced long-term disability were assumed to have an increased mortality risk, which was applied to the mortality rate for patients without long-term disability; values were obtained from literature.9 The incidence of serious AEs was obtained from the CHAMPION-NMOSD (ravulizumab), PREVENT (eculizumab versus placebo), and SAKuraStar (satralizumab versus placebo) studies and incorporated into the model with an associated cost and disutility.2,4,5 Specific AEs considered in the model included: lower respiratory infection, pneumonia, bronchitis, sepsis, urinary tract infection, skin infection, infectious pleural effusion, suicidal ideation, fracture (rib, pubis, hip), neutrophil decrease (grade ≥ 3), and triglyceride increase (grade ≥ 3). The sponsor assumed patients receiving ISTs would not experience AEs. Health-related quality of life (HRQoL) was captured in the model by combining health state utilities with disutilities associated with NMOSD relapses and AEs. The health state utility value for the relapse-free state was obtained from the indirect measurement of patient preferences using EQ-5D, and was calculated using the CHAMPION-NMOSD and PREVENT trial data.2,4 A one-time utility decrement per relapse without long-term disability was obtained from PREVENT trial4 and applied for 50 days, whereas a one-time utility decrement per relapse with long-term disability was obtained from literature.10 The sponsor also applied age-specific and sex-specific population norm utilities (for a Canadian population) for age at each model cycle; values were obtained from literature.11 Values for AE-specific disutilities were sourced from literature.12
The sponsor’s submission considered costs associated with the acquisition, administration, vaccination, and monitoring of treatment, as well as costs associated with the management of AEs. Treatment acquisition costs were estimated from the application of treatment prices to the dosing schedule for each alternative treatment considered in the model. Although the price of ravulizumab reflected the sponsor’s submitted price,1 the price of eculizumab was provided by the sponsor;1 for the other alternative therapies, costs were sourced from the Ontario Drug Benefit Formulary13 and a previously published CADTH review.14 Dosing for eculizumab and satralizumab were established from the recommended dosage listed in the relevant product monographs; off-label dosing information for drugs considered to be ISTs were obtained from a range of sources in the published literature. Ravulizumab and eculizumab were assumed to have administration costs covered by the sponsor, satralizumab (which is self-administered by the patient) was assumed to have administration costs only in the first cycle, and ISTs were assumed to have no administration costs. The sponsor assumed that vaccination costs for patients receiving ravulizumab and eculizumab would be covered by the sponsor. Monitoring costs reflected the resource use associated with NMOSD relapses and all-cause health care resource use. The frequency of health care resource use was obtained from a study performed in the US,15 and unit costs were obtained from the Canadian Institute for Health Information,16 the Ontario Schedule of Benefits for Physician Services,17 Ontario Case Costing,1,8 and the literature. Costs to treat each AE were based on the Canadian Institute for Health Information,16 Ontario Case Costing,18 and the literature.
Summary of Sponsor’s Economic Evaluation Results
All analyses were run probabilistically (5,000 iterations for the base case and scenario analyses). The deterministic and probabilistic results were similar. The probabilistic findings are presented here.
Base-Case Results
In the sponsor’s base-case analysis, ravulizumab was more costly and more effective than satralizumab and ISTs, with an estimated cost of $15,387,892 and an estimated QALY gain of 18.90 for a patient over the 53-year horizon. Eculizumab was deemed more costly and less effective than ravulizumab, and it was dominated in the sequential analysis. In the sequential analysis, ravulizumab was associated with an ICER of $2,386,625 per QALY gained compared with satralizumab (incremental costs = $11,261,849; incremental QALYs = 4.72) (Table 3). Ravulizumab had a 0% probability of being cost-effective at willingness-to-pay (WTP) threshold of $50,000 per QALY.
Results were driven by the acquisition costs of ravulizumab (incremental costs compared with satralizumab = $11,648,295; incremental costs compared with ISTs = $15,064,783). Of the incremental QALYs gained, 99.5% was accrued after the CHAMPION-NMOSD study period (median follow-up [minimum to maximum], 73.5 weeks [14 to 118 weeks]), indicating that nearly all of the incremental benefits were generated through extrapolation beyond the available trial data. Ravulizumab resulted in a lower mean number of relapses (0.22) during the 53-year time horizon than eculizumab (0.99), satralizumab (3.38), and ISTs (7.55). Given that treatment options and the number of relapses were associated with mortality, ravulizumab resulted in an additional 11 LYs compared with ISTs and an additional 1 LY compared with satralizumab. At the end of the 53-year time horizon, approximately 3% of patients treated with ravulizumab remained alive.
Table 3: Summary of the Sponsor’s Economic Evaluation Results
Drug | Total costs ($) | Total QALYs | Sequential ICER ($/QALY) |
|---|---|---|---|
IST | 671,598 | 5.74 | Reference |
Satralizumab | 4,126,043 | 14.18 | 409,419 |
Ravulizumab | 15,387,892 | 18.90 | 2,386,625 |
Dominated treatments | |||
Eculizumab | 20,469,168 | 17.70 | Dominated by ravulizumab |
ICER = incremental cost-effectiveness ratio; IST = immunosuppressant therapy; QALY = quality-adjusted life-year.
Source: Sponsor’s pharmacoeconomic submission.1
Sensitivity and Scenario Analyses Results
The sponsor undertook scenario analyses with various parameters, including time horizon, discount rate, perspective, consideration of administration and vaccination costs, consideration of treatment discontinuation, increasing HRs for successive relapses, consideration of different NMA populations (|||||||||||| ||| ||||||||||| |||||||), and adjustment of NMA results using propensity scores. Shortening the time horizon had the greatest impact, with a sequential ICER of $3,959,395 per QALY gained, compared with satralizumab, over a 20-year time horizon. Additionally, changing the NMA population to ||||||||||| ||||||| |||||||||||||||) resulted in a sequential ICER of $3,221,750 per QALY gained, compared with satralizumab.
The sponsor conducted a scenario analysis from a societal perspective that included additional costs associated with productivity loss. In this analysis, the ICER per QALY gained was $2,318,555 relative to satralizumab. Overall, these ICERs were similar to the sponsor’s base case that used a health care payer perspective.
CADTH Appraisal of the Sponsor’s Economic Evaluation
CADTH identified several key limitations to the sponsor’s analysis that have notable implications for the economic analysis:
The comparative efficacy of ravulizumab is highly uncertain. In the absence of head-to-head comparative evidence for ravulizumab, eculizumab, satralizumab, and ISTs, the sponsor estimated comparative effectiveness using an NMA. CADTH’s clinical review team noted several methodological limitations of the NMA, ||||||||| ||||||||||| || ||| ||| |||||||| |||| ||||| ||||||| |||||| || |||||| ||| ||||| ||||||| || |||||||| || |||| |||||| ||| |||||||| |||| |||||| || ||||||||||| ||||||||||||| ||||||| ||||| |||| ||| ||| |||| || ||| ||||||||||| |||||| ||| |||||||||| ||| |||||||| || ||| ||||||||||| ||||||||||| ||||||| |||||| |||||||| || ||| |||||||| ||||||||||||| || ||| |||||||| ||||||| || ||| ||||||||||| ||||| || ||||||||||||||| || ||||||||| ||| ||||||| |||||||||| ||||||| |||| ||| ||||||||| ||| || ||||||||||| ||| |||||||| || ||| |||| |||| ||| ||||||| || ||| ||||||| |||||||||| || ||| |||| ||||||| || ||| ||||||||| ||| |||||||| ||||||||||| || |||| ||||||| ||||||||||| ||| ||| ||||||| |||| ||| ||||||||||| ||||||| ||||||| |||| ||||||||||| || |||| |||||||| ||||||||| |||||| |||| ||| ||||||||||| || ||| |||| ||| ||| |||||||||||||| || ||||||| |||| ||| ||||||||||| || ||| ||||| ||| || ||| ||||||||||| || |||| ||||. Therefore, substantial uncertainty remains concerning the clinical efficacy of ravulizumab compared to eculizumab, satralizumab, and ISTs.
CADTH was unable to address this issue due to limitations of the indirect comparison. The impact this limitation has on the magnitude of the cost-effectiveness results is unknown.
The long-term efficacy of ravulizumab is unknown. The efficacy and safety of ravulizumab in adults with anti-AQP4 antibody-positive NMOSD was assessed in the CHAMPION-NMOSD study, an externally placebo-controlled, open-label, phase III study. The CHAMPION-NMOSD study had a single-arm treatment design, and used the placebo group from the PREVENT study as an external placebo comparator. During the CHAMPION-NMOSD study (median follow-up was 91 weeks at the July 2022 cut-off date in the ravulizumab group), no patients receiving ravulizumab reported an adjudicated on-trial relapse, whereas 42.6% of patients in the PREVENT placebo group did. The lack of relapses observed in the CHAMPION-NMOSD study was extrapolated to the lifetime horizon (53 years) in the submitted model, resulting in almost no patients experiencing a relapse while on ravulizumab treatment (average of 0.2 relapses over 53 years). This implies that ravulizumab is a curative treatment for NMOSD. However, the long-term benefit of ravulizumab in comparison with eculizumab, satralizumab, and ISTs is unknown, given the short-term follow-up periods in the trials. Clinical expert feedback solicited by CADTH for this review did not support the conclusion that ravulizumab is curative, but the clinical experts could not estimate relapse rates beyond the trial period. Given that the majority of the incremental QALYs (99%) predicted by the sponsor’s model were derived from extrapolated findings rather than observed benefit, the lack of long-term data and the lack of consideration of the potential waning of effectiveness introduces considerable uncertainty into the analysis.
In addition, the decrease in the odds of a NMOSD relapse was used to adjust the mortality rate for patients receiving ravulizumab, eculizumab, or satralizumab, as noted in the previous limitation. This contributes to an overestimation of ravulizumab benefits throughout the model time horizon, resulting in ravulizumab having the same mortality rate as the general population.
CADTH was unable to address this limitation due to a lack of long-term clinical data. CADTH explored the impact of incorporating the waning of treatment effect after the trial maximum follow-up (135 weeks) as a scenario analysis.
The estimated mortality rate for ravulizumab, eculizumab, and satralizumab lacks face validity. The sponsor assumed that the decrease in the risk of a NMOSD relapse resulted in a decrease in the mortality rate for patients receiving ravulizumab, eculizumab, or satralizumab. Thus, the sponsor calculated the morality rate for each treatment group by applying a mortality HR to the general population mortality. This mortality HR was calculated using the relapse HR from the NMA. This approach resulted in a mortality rate that was lower than that in the general population for a substantial age group of patients receiving ravulizumab, eculizumab, or satralizumab. For instance, patients 80 years and younger who were treated with ravulizumab had a mortality rate below that of the general population. Because the sponsor also assumed that the mortality rate for patients with NMOSD would be capped at the mortality rate of the general population to prevent unrealistic scenarios, the mortality rate for patients treated with ravulizumab, eculizumab, or satralizumab resulted in a mortality rate that was the same as in the general population for the majority of the period that patients are followed in the model, which lacks face validity, according to feedback from the clinical experts consulted for this review.
CADTH was unable to address this limitation, which overestimates the effectiveness of ravulizumab, eculizumab, and satralizumab. However, the magnitude of its impact on the cost-effectiveness results is unknown.
The model structure does not reflect clinical practice. The model submitted by the sponsor assumed that patients would remain on the same treatment for the entire time horizon (no treatment discontinuation) and only accounted for 1 line of treatment. Feedback from clinical experts consulted by CADTH and international treatment guidelines indicated that, in clinical practice, patients with NMOSD who do not respond (i.e., patients who experience a severe relapse with a relevant functional deficit or impairment despite sufficient dosing and time to expect full action) to current therapy generally switch to a drug with a different mechanism of action.19 The assumption that patients would continue to receive their treatment indefinitely, the assumption of a sustained treatment benefit, and the assumption that the mortality rate would be equal to that in the general population all imply that patients treated with ravulizumab would be virtually cured for the 53-year time horizon, with the same life expectancy as general population, which lacks face validity.
The function available in the sponsor’s submitted model to change the treatment duration only accounted for changes in treatment costs, not utilities. As a consequence, any estimated changes in treatment duration lack face validity. CADTH was unable to address this limitation associated with the model structure.
The duration of utility decrement per relapse is uncertain. The sponsor applied a one-time utility decrement per relapse without long-term disability. This one-time disutility was assumed to occur during the first 50 days after the relapse event, based on analysis of the HRQoL data from the CHAMPION-NMOSD and PREVENT studies. Feedback from the experts consulted by CADTH for this review indicated that the impact of a relapse on a patient’s HRQoL depends on the relapse severity and can generally last from a month to a year.
CADTH explored the impact of increasing the duration of the disutility associated to relapses to 180 days in a scenario analysis.
Additionally, the following key assumptions were made by the sponsor and have been appraised by CADTH (refer to Table 4).
Table 4: Key Assumptions of the Submitted Economic Evaluation (Not Noted as Limitations to the Submission)
Sponsor’s key assumption | CADTH comment |
|---|---|
Use of EDSS as a measure of disability. | Appropriate, as the EDSS is routinely used in clinical practice. However, the EDSS has some limitations; according to the clinical experts consulted by CADTH, it becomes less sensitive at higher levels, it is heavily dependent on ambulation, and it is not very sensitive to changes in nonambulatory symptoms, such as changes in vision, which are not likely to be captured, even when they have a very significant impact on a patient’s life. |
EDSS score was assumed to permanently increase by 0.39 points (based on PREVENT trial data) with each relapse. | Inappropriate. The EDSS score is measured on an ordinal scale with 0.5 increments, so an increase of 0.39 points in EDSS score for each relapse would not reflect actual EDSS scores for patients. |
EDSS is assumed to decrease after a relapse. | Appropriate. Based on feedback from clinical experts, most patients will experience a decrease in their EDSS score after a relapse. However, some patients might maintain the same EDSS score, depending on the severity of the relapse. |
EDSS = Expanded Disability Status Scale.
CADTH Reanalyses of the Economic Evaluation
Base-Case Results
CADTH was unable to address the uncertainty in the comparative clinical data and the long-term effectiveness of ravulizumab. Given these limitations, CADTH was unable to provide a more reliable estimate of the cost-effectiveness of ravulizumab. Based on the sponsor’s results (Table 3), ravulizumab is more costly and more effective than satralizumab, with an ICER of $2,386,625 per QALY gained. The probability that ravulizumab is cost-effective compared to satralizumab at a WTP threshold of $50,000 per QALY was 0%. A detailed breakdown of the disaggregated results is available in Table 8 in Appendix 3.
CADTH indicates that the assumptions used by the sponsor to calculate of the mortality rate resulted in the mortality rate for ravulizumab being same as that for the general population because of the capping rules applied in the model (i.e., values were capped if they were below those for general population mortality) and ||| ||| ||||||| || ||| |||||||||||, implying that patients with NMOSD treated with ravulizumab were virtually cured and that NMOSD no longer had any impact on the mortality rate. Ravulizumab was associated with an increase in health care system costs of $11,261,849, compared with satralizumab. Of this increase in cost, $11,648,295 (> 100%) was due to drug acquisition costs, with some projected cost savings from background therapies and relapse care.
Scenario Analysis Results
CADTH undertook price reduction analyses based on the sponsor’s base case and sponsor’s base-case results. The sponsor’s base case suggests that a 93% reduction in the price of ravulizumab would be required to achieve cost-effectiveness at a WTP threshold of $50,000 per QALY gained compared to ISTs (Table 9 in Appendix 4). When compared to satralizumab in a pairwise analysis (using the sponsor’s indirect treatment comparison), a 73% price reduction is required to achieve cost-effectiveness at this threshold (Table 10 in Appendix 4); however, due to the identified uncertainty in the indirect treatment comparison, a greater price reduction may be required.
CADTH conducted an additional analysis based on the corrected sponsor’s base-case results to explore alternative assumptions regarding the duration of disutility after a relapse (increasing it to 180 days). There was no evidence to quantify the most likely rate at which treatment effectiveness may wane. Accordingly, CADTH performed a scenario analysis that incorporated an instantaneous treatment waning effect, which started after the maximum trial duration (135 weeks) in the model. The treatment waning scenario reflects the maximum possible value of the ICER if treatment effectiveness decreases over time. If there is an increase in the duration of disutility after a relapse, the ICER for ravulizumab is similar to the sponsor’s base case ($2,098,221 per QALY gained) (Table 10 in Appendix 4). If ravulizumab ceases to be more effective than ISTs after the end of the trial’s maximum follow-up time, the ICER for ravulizumab increases to $23,799,556 (incremental QALYs = 0.33; incremental costs = $7,807,511) compared with the sponsor’s base case. In this analysis, the total QALYs gained with ravulizumab decreases from 19.1 to 6.3 over the 53-year time horizon.
Issues for Consideration
The pan-Canadian Pharmaceutical Alliance (pCPA) concluded negotiations with a letter of intent for satralizumab for the treatment of NMOSD. The sponsor-submitted model is based on the publicly available price of satralizumab, which may be different than the confidential price and may influence the results of the cost-effectiveness and budget impact analyses (BIA).
Overall Conclusions
Based on the CADTH clinical review of the CHAMPION-NMOSD trial, evidence shows that treatment with ravulizumab resulted in a clinically meaningful decrease in the number of relapses, compared to the placebo external comparator, in adults with anti-AQP4 antibody-positive NMOSD (0% versus 43%). The indirect comparison between ravulizumab and eculizumab, satralizumab, and ISTs was subject to several limitations, which resulted in uncertainty for estimates of the relative clinical effectiveness of ravulizumab, as well as for the costs and QALYs estimated by the model, given that these estimates were used to inform the transition probabilities in the model. CADTH notes that both the CHAMPION-NMOSD study and the submitted NMA evaluated ravulizumab as a first-line treatment only; therefore, its efficacy and safety as a second-line or later-line treatment for NMOSD represents a gap in the evidence.
CADTH identified additional limitations of the sponsor’s submitted economic evaluation that could not be addressed through reanalysis, including uncertainty regarding the long-term effectiveness of ravulizumab. Given these limitations, CADTH was unable to provide a more reliable estimate of the cost-effectiveness of ravulizumab relative to currently available treatment options. In the sponsor’s base case, the ICER of ravulizumab versus satralizumab was $2,386,625 per QALY gained (incremental costs = $11,261,849; incremental QALYs = 4.72). The probability of being cost-effective at a $50,000 per QALY gained threshold was 0%. A reduction in the price of ravulizumab of at least 73% would be necessary for ravulizumab to be considered cost-effective at a $50,000 per QALY gained threshold compared to satralizumab. A 73% price reduction would reduce the unit price of a 300 mg vial of ravulizumab from $7,282 to $1,966, which would reduce annual costs from $567,618 to $414,361. CADTH identified key considerations regarding the magnitude of the long-term benefit of ravulizumab. The lack of relapses observed in the CHAMPION-NMOSD study (median follow-up of 21 months) was extrapolated to a lifetime horizon (53 years) in the submitted model, resulting in almost no patients experiencing a relapse while on ravulizumab treatment (average of 0.02 relapses in 53 years). This implies that ravulizumab is functionally curative for NMOSD (i.e., results in 0 relapses over a patient’s lifetime). In addition, the sponsor’s modelling assumptions resulted in patients treated with ravulizumab having the same mortality rate as the general population, and the assumption that ravulizumab would not be discontinued contributed to the overestimation of ravulizumab benefits throughout the model time horizon. CADTH conducted a scenario analysis in which the treatment effects of ravulizumab are equal to those of ISTs after the trial’s maximum follow-up, which resulted in decreased incremental and total QALYs and costs and an ICER of $23,799,556 per QALYs gained. Based on this analysis, the true ICER may lie between $2,386,625 and $23,799,556 per QALY gained.
In the economic analysis, treatment with ravulizumab was associated with increased costs and increased QALYs compared to treatment with satralizumab. The magnitude of these changes in cost and effectiveness are difficult to quantify. First, the NMA used to produce survival estimates in the model was informed by trials with ||||| ||||||||||| ||| ||| ||| ||||||||| ||||| |||| ||||||||| ||||||||. Second, the pharmacoeconomic model functionally assumes that ravulizumab is a curative treatment, based on the results of the CHAMPION-NMOSD trial. CADTH could not validate this assumption, but the scenario analysis suggested that it is highly influential on the ICER. Third, as a consequence of the uncertainty in the model’s transition probabilities (due to both the NMA and the curative assumption), estimates of total health care system costs associated with ravulizumab treatment are also uncertain. The estimated cost increase is entirely driven by the comparatively high drug acquisition cost of ravulizumab. Finally, the cost-effectiveness of ravulizumab as a second-line or subsequent-line treatment is unknown. Because of these limitations, a further price reduction may be warranted.
References
1.Pharmacoeconomic evaluation [internal sponsor's report]. Drug Reimbursement Review sponsor submission: Ultromiris (ravulizumab), 10 mg/mL & 100 mg/mL concentrate for solution for intravenous infusion. [internal sponsor's report].Mississauga (ON): Alexion Pharma GmbH; 2023 Aug 29.
2.Pittock SJ, Barnett M, Bennett JL, et al. Ravulizumab in Aquaporin-4-Positive Neuromyelitis Optica Spectrum Disorder. Ann Neurol. 2023;93(6):1053-1068. PubMed
3.PrecisionHeor. Network meta-analysis of ravulizumab, eculizumab, satralizumab and inebilizumab for the treatment of neuromyelitis optica spectrum disorder (NMOSD) - Technical Report. [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Ultomiris (ravulizumab for injection) 10 mg/mL & 100 mg/mL concentrate for solution for intravenous infusion. Mississauga (ON): Alexion Pharma Canada Corp.; 2023 Aug 29. 2023.
4.Pittock SJ, Berthele A, Fujihara K, et al. Eculizumab in Aquaporin-4-Positive Neuromyelitis Optica Spectrum Disorder. N Engl J Med. 2019;381(7):614-625. PubMed
5.Traboulsee A, Greenberg BM, Bennett JL, et al. Safety and efficacy of satralizumab monotherapy in neuromyelitis optica spectrum disorder: a randomised, double-blind, multicentre, placebo-controlled phase 3 trial. Lancet Neurol. 2020;19(5):402-412. PubMed
6.Seok JM, Cho EB, Lee HL, et al. Clinical characteristics of disabling attacks at onset in patients with neuromyelitis optica spectrum disorder. J Neurol Sci. 2016;368:209-213. PubMed
7.Eagle N. QOL associations with disability in Oxford AQP4 NMOSD cohort (1796). AAN Enterprises; 2021.
8.Statistics Canada. Table 13-10-0114-01, Life expectancy and other elements of the complete life table, three-year estimates, Canada, all provinces except Prince Edward Island, based on data for the years 2018-2020. 2022; https://www150.statcan.gc.ca/t1/tbl1/en/tv.action?pid=1310011401. Accessed 2023 Sep 7.
9.Buzzell A, Chamberlain JD, Eriks-Hoogland I, et al. All-cause and cause-specific mortality following non-traumatic spinal cord injury: evidence from a population-based cohort study in Switzerland. Spinal cord. 2020;58(2):157-164. PubMed
10.Hughes DA, Bourke S, Jones A, et al. Health utilities and costs for neuromyelitis optica spectrum disorder. Orphanet J Rare Dis. 2022;17(1):159. PubMed
11.Guertin JR, Feeny D, Tarride JE. Age- and sex-specific Canadian utility norms, based on the 2013-2014 Canadian Community Health Survey. CMAJ. 2018;190(6):E155-E161. PubMed
12.Sullivan PW, Ghushchyan V. Preference-Based EQ-5D index scores for chronic conditions in the United States. Med Decis Making. 2006;26(4):410-420. PubMed
13.Ontario Ministry of Health. Ontario Drug Benefit (ODB) Formulary Comparative Drug Index. 2023; https://www.formulary.health.gov.on.ca/formulary/. Accessed 2023 Aug 2.
14.CADTH Reinbursement recommendation: satralizumab (Enspryng). Ottawa (ON): CADTH; 2021: https://www.cadth.ca/sites/default/files/cdr/complete/SR0663%20Enspryng%20-%20CDEC%20Final%20Recommendation%20April%2023%2C%202021_for%20posting.pdf. Accessed 2023 Sep 7.
15.Royston M, Kielhorn A, Weycker D, et al. Neuromyelitis Optica Spectrum Disorder: Clinical Burden and Cost of Relapses and Disease-Related Care in US Clinical Practice. Neurol. 2021;10(2):767-783. PubMed
16.Canadian Institute for Health Information. Patient Cost Estimator. 2020; https://www.cihi.ca/en/patient-cost-estimator. Accessed 2023 Sep 7.
17.Ontario Ministry of Health. Schedule of Benefits. Physician Services Under the Health Insurance Act. 2023; https://www.health.gov.on.ca/en/pro/programs/ohip/sob/physserv/sob_master.pdf. Accessed 2023 Sep 7.
18.Ontario Case Costing. Ontario Case Costing Analysis Tool. 2023; https://www.ontario.ca/data/ontario-case-costing-initiative-occi. Accessed 2023 Sep 7.
19.Kümpfel T, Giglhuber K, Aktas O, et al. Update on the diagnosis and treatment of neuromyelitis optica spectrum disorders (NMOSD) - revised recommendations of the Neuromyelitis Optica Study Group (NEMOS). Part II: Attack therapy and long-term management. J Neurol. 2023. PubMed
Appendix 1: Cost Comparison Table
Note that this appendix has not been copy-edited.
The comparators presented in the following table have been deemed to be appropriate based on feedback from clinical expert(s) and drug plan. Comparators may be recommended (appropriate) practice or actual practice. Existing Product Listing Agreements are not reflected in the table and as such, the table may not represent the actual costs to public drug plans.
Table 5: CADTH Cost Comparison Table for NMOSD
Treatment | Strength / concentration | Form | Price | Recommended dosage | Daily cost | Annual cost |
|---|---|---|---|---|---|---|
Ravulizumab (Ultomiris) | 100 mg/mL | 300 mg Vial 1,100 mg Vial | $7,282.1500a $26,701.2000a | Loading Dose: 2,700 mg at week 0. Maintenance Dose: 3,300 mg every 8 weeks, administered 2 weeks after loading dose. | Year 1: $2,600.77 Year 2+: $1,430.42 | Year 1: $567,618 Year 2+: $522,104 |
Indicated for NMOSD | ||||||
Eculizumab (Soliris) | 10 mg / mL | 30 mL Vial | $6,675.3000b | Loading Dose: 900 mg weekly, for 4 weeks, then 1,200 mg in week 5. Maintenance Dose: 1,200 mg every 2 weeks. | Year 1: $4,768.07 Year 2+: $1,907.23 | Year 1: $722,839.63 Year 2+: $696,138.43 |
Satralizumab (Enspryng) | 10 mg / mL | 30 mL Vial | $9,450.0000c | Loading Dose: 120 mg at weeks 0, 2, and 4. Maintenance Dose: 120 mg every 4 weeks. | Year 1: $1,350.00 Year 2+: $337.50 | Year 1: $142,088 Year 2+: $123,188 |
NMOSD = neuromyelitis optica spectrum disorders.
Note: All prices do not include dispensing fees. Costs assume a body weight of 69.9 kg or a body surface area of 1.75m2 and include wastage of unused medication in vials.
aSponsor’s submitted price: $7,282.1500 per 300 mg vial.
bUnit price obtained from IQVIA Delta PA (accessed September 2023).
cUnit price obtained from the Ontario Exceptional Access Program (accessed October 2023).
Table 6: Cost Comparison Table for Off-Label Treatments for NMOSD
Treatment | Strength / concentration | Form | Price | Recommended dosage | Daily cost | Annual cost |
|---|---|---|---|---|---|---|
Rituximab (Truxima) | 100 mg / mL 500 mg / mL | 10 mL Vial Pack 50 mL Vial Pack | $297.0000 $1,485.0000 | Loading Dose: 1,000 mg at week 0 and 2. Maintenance Dose: 1,000 mg every 6 months (begins 6 months after initial dose). | Year 1: $24.41 Year 2+: $16.27 | Year 1: $8,910 Year 2+: $5,940 |
Usual Care | ||||||
Azathioprine (generic) | 50 mg | Tab | $0.2405 | 3 to 5 mg/kg daily | $0.96 | $351 |
Mycophenolate mofetil (generic) | 250 mg 500 mg | Tab | $0.3712 $0.7423 | 2000 mg daily | $2.97 | $1,084 |
Cyclosporine (generic) | 25 mg 50 mg 100 mg | Tab | $0.7870 $1.5350 $3.0720 | 150 mg per day | $4.61 | $1,681 |
Tacrolimus (generic) | 0.5 mg 1 mg 5 mg | Tab | $1.4775 $1.8900 $9.4650 | 1 to 3 mg per day | $3.78 | $1,380 |
Methotrexate (generic) | 2.5 mg | Tab | $0.2513 | 7.5 to 15 mg weekly | $1.13 | $59 |
Cyclophosphamide (generic) | 25 mg 50 mg | Tab | $0.3545 $0.4773 | 1,000 mg/m2 every 6 months | $16.71 | $33 |
Prednisone (generic) | 5 mg 50 mg | Tab | $0.0220 $0.1735 | 1 mg/kg daily | $0.31 | $112 |
Weighted annual cost of usual care | $251 | |||||
NMOSD = neuromyelitis optica spectrum disorders.
Note: All prices do not include dispensing fees. Costs assume a body weight of 69.9 kg or a body surface area of 1.75m2 and include wastage of unused medication in vials. All prices are from the Ontario Drug Benefit Formulary (accessed October 2023), unless otherwise indicated.
Appendix 2: Submission Quality
Note that this appendix has not been copy-edited.
Description | Yes/No | Comments |
|---|---|---|
Population is relevant, with no critical intervention missing, and no relevant outcome missing | Yes | No comments |
Model has been adequately programmed and has sufficient face validity | No | The calculations used to estimate mortality rate were considered inappropriate. Refer to limitations for details. |
Model structure is adequate for decision problem | No | The model assumed that patients would remain on the same treatment for the entire time horizon (no treatment discontinuation). Refer to limitations for details. |
Data incorporation into the model has been done adequately (e.g., parameters for probabilistic analysis) | Yes | No comments |
Parameter and structural uncertainty were adequately assessed; analyses were adequate to inform the decision problem | Yes | No comments |
The submission was well organized and complete; the information was easy to locate (clear and transparent reporting; technical documentation available in enough details) | No | It was unclear in the submitted pharmacoeconomic report how the mortality rates for active treatments were calculated. |
Appendix 3: Additional Information on the Submitted Economic Evaluation
Note that this appendix has not been copy-edited.
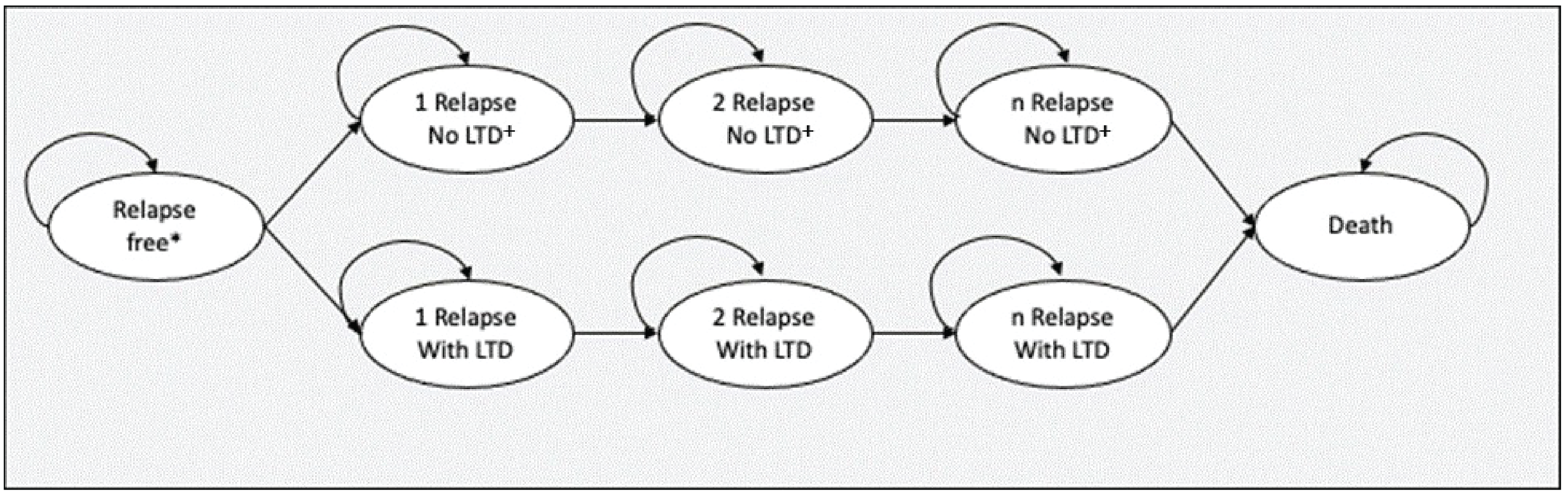
Detailed Results of the Sponsor’s Base Case
Table 8: Disaggregated Summary of CADTH’s Economic Evaluation Results
Treatment | Component | Value | Incremental (vs. reference) | Incremental (sequential) |
|---|---|---|---|---|
Discounted LYs | ||||
IST | Score < 3 | 0.00 | NA | NA |
Score 3 to 4 | 2.16 | NA | NA | |
Score 4 to 5 | 3.14 | NA | NA | |
Score 5 to 6 | 2.67 | NA | NA | |
Score 6 to 7 | 2.18 | NA | NA | |
Score 7 to 8 | 1.71 | NA | NA | |
Score ≥ 8 | 5.76 | NA | NA | |
Total | 17.62 | NA | NA | |
Satralizumab | Score < 3 | 0.00 | 0.00 | NA |
Score 3 to 4 | 8.18 | 6.01 | NA | |
Score 4 to 5 | 9.26 | 6.13 | NA | |
Score 5 to 6 | 5.33 | 2.65 | NA | |
Score 6 to 7 | 2.65 | 0.47 | NA | |
Score 7 to 8 | 1.20 | −0.51 | NA | |
Score ≥ 8 | 1.02 | −4.74 | NA | |
Total | 27.64 | 10.02 | NA | |
Ravulizumab | Score < 3 | 0.00 | 0.00 | 0.00 |
Score 3 to 4 | 25.17 | 23.01 | 16.99 | |
Score 4 to 5 | 3.34 | 0.20 | −5.92 | |
Score 5 to 6 | 0.17 | −2.51 | −5.16 | |
Score 6 to 7 | 0.01 | −2.18 | −2.64 | |
Score 7 to 8 | 0.00 | −1.71 | −1.20 | |
Score ≥ 8 | 0.00 | −5.76 | −1.02 | |
Total | 28.68 | 11.06 | 1.04 | |
Eculizumab | Score < 3 | 0.00 | 0.00 | 0.00 |
Score 3 to 4 | 17.99 | 15.83 | −7.18 | |
Score 4 to 5 | 8.23 | 5.09 | 4.89 | |
Score 5 to 6 | 1.89 | −0.78 | 1.73 | |
Score 6 to 7 | 0.41 | −1.77 | 0.41 | |
Score 7 to 8 | 0.10 | −1.60 | 0.10 | |
Score ≥ 8 | 0.05 | −5.71 | 0.05 | |
Total | 28.68 | 11.06 | 0.00 | |
Discounted QALYs | ||||
IST | Health states | 5.77 | NA | NA |
Relapses | −0.02 | NA | NA | |
Adverse events | 0.00 | NA | NA | |
Total | 5.74 | NA | NA | |
Satralizumab | Health states | 14.19 | 8.42 | NA |
Relapses | −0.01 | 0.01 | NA | |
Adverse events | −0.00 | 0.00 | NA | |
Total | 14.18 | 8.44 | NA | |
Ravulizumab | Health states | 18.90 | 13.13 | 4.71 |
Relapses | −0.00 | 0.02 | 0.01 | |
Adverse events | −0.00 | 0.00 | 0.00 | |
Total | 18.90 | 13.16 | 4.72 | |
Eculizumab | Health states | 17.71 | 11.94 | −1.19 |
Relapses | −0.00 | 0.02 | 0.00 | |
Adverse events | −0.00 | 0.00 | 0.00 | |
Total | 17.70 | 11.96 | -1.19 | |
Discounted costs ($) | ||||
IST | Acquisition | 4,422 | NA | NA |
Administration | 0 | NA | NA | |
Background | 622,385 | NA | NA | |
Relapses | 44,790 | NA | NA | |
AEs | 0 | NA | NA | |
Total | 671,598 | NA | NA | |
Satralizumab | Acquisition | 3,420,910 | 3,416,488 | NA |
Administration | 224 | 224 | NA | |
Background | 682,484 | 60,099 | NA | |
Relapses | 20,019 | −24,771 | NA | |
AEs | 2,405 | 2,405 | NA | |
Total | 4,126,043 | 3,454,445 | NA | |
Ravulizumab | Acquisition | 15,069,205 | 15,064,783 | 11,648,295 |
Administration | 0 | 0 | −224 | |
Background | 316,804 | −305,581 | −365,681 | |
Relapses | 1,304 | −43,486 | −18,715 | |
AEs | 579 | 579 | −1,827 | |
Total | 15,387,892 | 14,716,294 | 11,261,849 | |
Eculizumab | Acquisition | 20,015,488 | 20,011,066 | 4,946,283 |
Administration | 0 | 0 | $0 | |
Background | 445,969 | −176,416 | 129,166 | |
Relapses | 5,873 | −38,918 | 4,568 | |
AEs | 1,838 | 1,838 | 1,259 | |
Total | 20,469,168 | 19,797,571 | 5,081,277 | |
Treatment | ICER vs. reference ($) | Sequential ICER ($) | ||
IST | Ref. | Ref. | ||
Satralizumab | $409,419 | $409,419 vs ISTs | ||
Ravulizumab | $1,118,586 | $2,386,625 vs. satralizumab | ||
Dominated treatments | ||||
Eculizumab | $2,346,399 | Dominated by ravulizumab | ||
ICER = incremental cost-effectiveness ratio; LY = life-year; NA = not applicable; QALY = quality-adjusted life-year; Ref. = reference; vs. = versus.
Appendix 4: Additional Details on the CADTH Reanalyses and Sensitivity Analyses of the Economic Evaluation
Note that this appendix has not been copy-edited.
Scenario Analyses
Table 9: CADTH Price Reduction Analyses
Price reduction | ICERs for Ravulizumab vs. Comparators ($/QALY) |
|---|---|
No price reduction | WTP < $376,726: IST $376,726 < WTP < $2,386,625: satralizumab $2,386,625 < WTP: ravulizumab |
10% | WTP < $376,727: IST $376,727 < WTP < $2,066,750: satralizumab $2,066,750 < WTP: ravulizumab |
20% | WTP < $376,727: IST $376,727 < WTP < $1,747,516: satralizumab $1,747,516 < WTP: ravulizumab |
30% | WTP < $376,727: IST $376,727 < WTP < $1,428,281: satralizumab $1,428,281 < WTP: ravulizumab |
40% | WTP < $376,727: IST $376,727 < WTP < $1,109,04: satralizumab $1,109,047 < WTP: ravulizumab |
50% | WTP < $376,727: IST $376,727 < WTP < $789,812: satralizumab $789,812 < WTP: ravulizumab |
60% | WTP < $376,727: IST $376,727 < WTP < $470,578: satralizumab $470,578 < WTP: ravulizumab |
62% | WTP < $376,727: IST $376,727 < WTP < $406,730: satralizumab $406,730 < WTP: ravulizumab |
70% | WTP < $288,343: IST $288,343 < WTP: ravulizumab |
80% | WTP < $183,348: IST $183,348 < WTP: ravulizumab |
90% | WTP < $78,353: IST $78,353 < WTP: ravulizumab |
100% | — |
IST = immunosuppressant therapies; WTP = willingness-to-pay threshold.
Table 10: CADTH Pairwise Price Reduction Analyses
Price reduction | ICER for Ravulizumab vs. Satralizumab ($/QALY) |
|---|---|
No price reduction | $2,386,625 |
10% | $2,066,750 |
20% | $1,747,516 |
30% | $1,428,281 |
40% | $1,109,047 |
50% | $789,812 |
60% | $470,578 |
70% | $151,343 |
73.2% | $50,000 |
80% | Ravulizumab is dominant |
90% | Ravulizumab is dominant |
100% | Ravulizumab is dominant |
Stepped analysis | Comparator | Total costs ($) | Total QALYs | ICER ($/QALY) |
|---|---|---|---|---|
Sponsor’s base case | IST | 671,598 | 5.74 | Ref. |
Satralizumab | 4,126,043 | 14.18 | 409,419 | |
Ravulizumab | 15,387,892 | 18.90 | 2,386,625 | |
Dominated treatment | ||||
Eculizumab | 20,469,168 | 17.70 | Dominated by ravulizumab | |
CADTH scenario 1: disutility duration after relapses changed to 180 days. | IST | 669,576 | 4.65 | Ref. |
Satralizumab | 4,057,328 | 13.68 | 375,026 vs IST | |
Ravulizumab | 15,355,096 | 19.07 | 2,098,221 vs satralizumab | |
Dominated treatment | ||||
Eculizumab | 20,383,023 | 17.93 | Dominated by ravulizumab | |
CADTH scenario 2: starting waning of treatment effect after trial maximum follow-up (135 weeks). | IST | 669,576 | 4.72 | Ref. |
Satralizumab | 3,044,717 | 5.97 | 1,901,519 vs IST | |
Ravulizumab | 10,852,227 | 6.29 | 23,799,556 vs satralizumab | |
Dominated treatment | ||||
Eculizumab | 14,213,020 | 6.22 | Dominated by ravulizumab | |
ICER = incremental cost-effectiveness ratio; IST = immunosuppressive therapies; QALY = quality-adjusted life-year; Ref. = reference.
Note: All analyses were conducted deterministically.
Appendix 5: Submitted BIA and CADTH Appraisal
Note that this appendix has not been copy-edited.
Table 12: Summary of Key Takeaways
Key Takeaways of the BIA |
|---|
|
Summary of Sponsor’s BIA
The sponsor-submitted budget impact analysis (BIA) assessed the budgetary impact resulting from reimbursing ravulizumab for the treatment of adult patients with anti-AQP4 antibody-positive NMOSD. The BIA was conducted from the perspective of the Canadian public drug plans over a 3-year horizon (2024 to 2026) with 2023 as the base year using an epidemiological approach. The sponsor’s pan-Canadian estimates reflect the aggregated results from the provincial budgets (excluding Quebec), as well as the Non-Insured Health Benefits Program (NIHB). The analysis was performed using jurisdiction-specific values by summing up individual provincial results to obtain consolidated results. Key inputs to the BIA are documented in Table 13.
The following key assumptions were made by the sponsor:
As no epidemiological studies specific to NMOSD in Canada exist, the sponsor used the prevalence rate from a Hungarian study.
The sponsor assumed that patients treated received a full year of treatment and do not switch treatments midyear. The number of patients on each treatment is constant throughout the year.
Table 13: Summary of Key Model Parameters
Parameter | Sponsor’s estimate (reported as Year 1 / Year 2 / Year 3 if appropriate) |
|---|---|
Target Population | |
NMOSD prevalence Proportion of patients seropositive for anti-AQP4 antibodies Proportion of patients receiving treatment Proportion of patients who have public drug plan coverage | 1.91 per 100,000 73% 100% 50% |
Number of patients eligible for drug under review | 221 / 224 / 226 |
Market Uptake (3 years) | |
Uptake (reference scenario) Eculizumab Satralizumab Rituximab Usual Care | 0% / 0% / 0% 15% / 25% / 37% 77% / 70% / 60% 8% / 5% / 3% |
Uptake (new drug scenario) Ravulizumab Eculizumab Satralizumab Rituximab Usual Care | 9% / 17% / 25% 0% / 0% / 0% 10% / 20% / 28% 76% / 60% / 45% 5% / 3% / 2% |
Cost of treatment (per patient) | |
Cost of treatment over [per year]a Ravulizumab Eculizumab Satralizumab Rituximab Usual Care | $567,618 $736,190 $142,088 $13,505 $251 |
AQP4 = aquaporin-4 antibody; NMOSD = neuromyelitis optica spectrum disorder.
aCost of treatment for induction year. Maintenance costs of treatments may differ.
Summary of the Sponsor’s BIA Results
The sponsor’s base case reported that the reimbursement of ravulizumab for the treatment of adult patients with anti-AQP4 antibody-positive NMOSD would lead to an incremental budget impact of $9,692,067 in Year 1, $19,003,932 in Year 2, $27,262,665 in Year 3. The total 3-year incremental cost was $55,958,664. Sensitivity analyses were completed to (i) explore the range in prevalence for NMOSD, (ii) include alternative proportions of seropositivity rate for anti-AQP4 antibodies, (iii) reduce the patient population that would receive treatment based on the CHAMPION-NMOSD population and (iv) reduce the proportion of patients who have public drug plan coverage. The sensitivity analyses impacted the 3-year incremental budget impact, which varied from $14,648,865 to $117,190,919, with the range in prevalence for NMOSD driving the variation in the budget impact.
CADTH Appraisal of the Sponsor’s BIA
CADTH identified several key limitations to the sponsor’s analysis that have notable implications on the results of the BIA:
The market uptake of ravulizumab is underestimated: The sponsor’s submitted budget impact analysis indicated that ravulizumab would result in a market uptake of 9% in Year 1, 17% in Year 2 and 25% in Year 3. The report also indicated that satralizumab would capture 15% of the market in the reference scenario in Year 1, 25% in Year 2 and 37% in Year 3. In the new drug scenario, it was predicted that satralizumab would capture 10% of the market in Year 1, 20% in Year 2 and 28% in Year 3. However, CADTH obtained clinical expert feedback indicating that the market uptake of satralizumab is overestimated and does not align with clinical expectations. The feedback highlighted that access to satralizumab is limited and it is unreasonable to suggest that approximately one-third of the population would be on the treatment by Year 3. CADTH clinical expert feedback noted that the overestimated market shares would be split between ravulizumab and rituximab.
To address this limitation, CADTH undertook a reanalysis by revising the market shares for satralizumab, ravulizumab and rituximab in the reference and new drug scenario. Equal displacement of market share among ravulizumab and rituximab was assumed.
Additional limitations were identified, but were not considered to be key limitations. These limitations include: incorrect comparator pricing.
CADTH Reanalyses of the BIA
Table 14: CADTH Revisions to the Submitted BIA
Stepped analysis | Sponsor’s value or assumption | CADTH value or assumption |
|---|---|---|
Corrections to sponsor’s base case | ||
1. Incorrect comparator pricing | Rituximab unit costs: 100mg/10mL vial = $337.6135 500mg/mL vial = $1,688.0780 | Rituximab unit costs: 100mg/10mL vial = $297.000 500mg/mL vial = $1,485.0000 |
Changes to derive the CADTH base case | ||
1. Inappropriate market shares in reference and new drug scenario | Reference scenario: Ravulizumab: 0% / 0% / 0% Satralizumab: 15% / 25% / 37% Rituximab: 77% / 70% / 60% New drug scenario: Ravulizumab: 9% / 17% / 25% Satralizumab: 10% / 20% / 28% Rituximab: 76% / 60% / 45% | Reference scenario: Ravulizumab: 0% / 0% / 0% Satralizumab: 10% / 15% / 20% Rituximab: 82% / 80% / 77% New drug scenario: Ravulizumab: 12% / 22% / 29% Satralizumab: 5% / 10% / 20% Rituximab: 78% / 65% / 49% |
CADTH base case | Reanalysis 1 | |
BIA = budget impact analysis.
The results of the CADTH step-wise reanalysis are presented in summary format in Table 15 and a more detailed breakdown is presented in Table 16. Based on the CADTH base case, the budget impact associated with the reimbursement of ravulizumab in the indicated target population is expected to be $13,381,657 in Year 1, $24,956,594 in Year 2, $34,497,100 in Year 3, with a 3-year total of $72,835,350.
Table 15: Summary of the CADTH Reanalyses of the BIA
Stepped analysis | Three-year total |
|---|---|
Submitted base case | $55,958,664 |
Corrected base case | $56,053,798 |
CADTH base case (reanalysis 1) | $72,835,350 |
BIA = budget impact analysis.
Table 16: Detailed Breakdown of the CADTH Reanalyses of the BIA
Stepped analysis | Scenario | Year 0 (current situation) | Year 1 | Year 2 | Year 3 | Three-year total |
|---|---|---|---|---|---|---|
Submitted base case | Reference | $3,857,468 | $6,809,021 | $9,440,604 | $12,685,883 | $28,935,509 |
New drug | $3,857,468 | $16,501,088 | $28,444,536 | $39,948,549 | $84,894,172 | |
Budget impact | $0 | $9,692,067 | $19,003,932 | $27,262,665 | $55,958,664 | |
Corrected base case | Reference | $3,555,904 | $6,532,467 | $9,186,125 | $12,465,130 | $28,183,722 |
New drug | $3,555,904 | $16,228,125 | $28,226,411 | $39,782,984 | $84,237,520 | |
Budget impact | $0 | $9,695,658 | $19,040,286 | $27,317,853 | $56,053,798 | |
CADTH base case | Reference | $3,555,904 | $5,093,121 | $6,481,250 | $7,874,935 | $19,449,305 |
New drug | $3,555,904 | $18,474,777 | $31,437,844 | $42,372,035 | $92,284,656 | |
Budget impact | $0 | $13,381,657 | $24,956,594 | $34,497,100 | $72,835,350 | |
CADTH scenario analysis: 92.7% price reduction | Reference | $3,555,904 | $5,093,121 | $6,481,250 | $7,874,935 | $19,449,305 |
New drug | $3,555,904 | $4,515,076 | $6,652,274 | $9,890,372 | $21,057,722 | |
Budget impact | $0 | -$578,045 | $171,024 | $2,015,438 | $1,608,416 |
BIA = budget impact analysis
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up-to-date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
Redactions: Confidential information in this document may be redacted at the request of the sponsor in accordance with the CADTH Drug Reimbursement Review Confidentiality Guidelines
Stakeholder Input: The views expressed in each submission are those of the submitting organization or individual; not necessarily the views of CADTH or of other organizations. As such, they are independent of CADTH and do not necessarily represent or reflect the view of CADTH. No endorsement by CADTH is intended or should be inferred. By filing with CADTH, the submitting organization or individual agrees to the full disclosure of the information. CADTH does not edit the content of the submissions.
CADTH does use reasonable care to prevent disclosure of personal information in posted material; however, it is ultimately the submitter’s responsibility to ensure no identifying personal information or personal health information is included in the submission. The name of the submitting organization or individual and all conflict of interest information are included in the submission; however, the name of the author, including the name of an individual patient or caregiver submitting the patient input, are not posted.
Accessibility: CADTH is committed to treating people with disabilities in a way that respects their dignity and independence, supports them in accessing material in a timely manner, and provides a robust feedback process to support continuous improvement. All materials prepared by CADTH are available in an accessible format. Where materials provided to CADTH by a submitting organization or individual are not available in an accessible format, CADTH will provide a summary document upon request. More details on CADTH’s accessibility policies can be found here.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.