CADTH Reimbursement Review
Dupilumab (Dupixent)
Sponsor: sanofi-aventis Canada Inc.
Therapeutic area: Atopic dermatitis, pediatrics
This multi-part report includes:
Clinical Review
Pharmacoeconomic Review
Stakeholder Input
Clinical Review
Abbreviations
AE
adverse event
ANCOVA
analysis of covariance
BSA
body surface area
CDLQI
Children’s Dermatology Life Quality Index
CI
confidence interval
DB
double blind
DFI
Dermatitis Family Impact
EASI
Eczema Area and Severity Index
EASI-50
50% reduction in Eczema Area and Severity Index score
EASI-75
75% reduction in Eczema Area and Severity Index score
EASI-90
90% reduction in Eczema Area and Severity Index score
FAS
full analysis set
HRQoL
health-related quality of life
IDQOL
Infants’ Dermatitis Quality of Life Index
IGA
Investigator’s Global Assessment
IL
interleukin
ITC
indirect treatment comparison
LSM
least squares mean
LTE
long-term extension
mFAS
modified full analysis set
MID
minimal important difference
NRS
numeric rating scale
POEM
Patient-Oriented Eczema Measure
RCT
randomized controlled trial
SAE
serious adverse event
SAS
safety analysis set
SC
subcutaneous
SCORAD
Scoring Atopic Dermatitis
SD
standard deviation
TCI
topical calcineurin inhibitor
TCS
topical corticosteroid
TEAE
treatment-emergent adverse event
WOCF
worst observation carried forward
Executive Summary
An overview of the submission details for the drug under review is provided in Table 1.
Table 1: Background Information of Application Submitted for Review
Item | Description |
|---|---|
Information on drug submitted for review | |
Drug product | Dupilumab (Dupixent), 200 mg single-use syringe (200 mg per 1.14 mL) and 300 mg single-use syringe (300 mg per 2 mL), subcutaneous injection |
Sponsor | sanofi-aventis Canada Inc. |
Indication | For the treatment of patients aged 6 months and older with moderate-to-severe atopic dermatitis whose disease is not adequately controlled with topical prescription therapies or when those therapies are not advisable. Dupilumab can be used with or without topical corticosteroids. |
Reimbursement request | For the treatment of patients aged 6 months to younger than 12 years with moderate-to-severe atopic dermatitis whose disease is not adequately controlled with topical prescription therapies or when those therapies are not advisable. |
Health Canada approval status | NOC |
Health Canada review pathway | Standard |
NOC date | April 14, 2023 |
Recommended dose | Patients aged 6 months to 5 years with atopic dermatitis:
Patients aged 6 years to 17 years with atopic dermatitis:
|
NOC = Notice of Compliance; q.2.w. = every 2 weeks; q.4.w. = every 4 weeks.
Source: Sponsor’s submission package for review of dupilumab, dupilumab product monograph, and sponsor’s Summary of Clinical Evidence.1-3
Introduction
Disease Background
Atopic dermatitis is a chronic, relapsing, inflammatory skin condition characterized by intense itching, red and swollen skin, papules, excoriation, rash, and serous exudation.4,5 In pediatric patients, atopic dermatitis tends to present in the face, extensor extremities, and cheeks. Itching leads to frequent scratching and may result in skin infections and thickening of the skin.4,6 Atopic dermatitis is estimated to affect 15% to 20% of children globally.7,8 In Canada, the lifetime prevalence of atopic dermatitis is up to 17% of the population.9 Pediatric patients with atopic dermatitis experience substantial symptom burden, poor sleep quality, reduced health-related quality of life (HRQoL), and frequent comorbidities.10-20 Patients with atopic dermatitis are at an increased risk of developing other atopic diseases such as asthma, food allergy, allergic rhinitis, conjunctivitis or rhinoconjunctivitis,11-14,21 attention-deficit/hyperactivity disorder, and autism spectrum disorder.4,14,15 The care required for these pediatric patients can be time-consuming and interferes with day-to-day activities,22 leading to increased feelings of caregiver anxiety, depression, worry, and helplessness.23 Managing atopic dermatitis adds a substantial financial burden on health care systems, society, and families.22,24-30 The most commonly used instruments in clinical trials to measure severity are the Investigator’s Global Assessment (IGA), Eczema Area and Severity Index (EASI), Physician’s Global Assessment, body surface area (BSA) affected, and Scoring Atopic Dermatitis (SCORAD).31
According to the clinical experts consulted by CADTH, the goals of treatment for pediatric patients with moderate-to-severe atopic dermatitis are to reduce symptom severity and improve HRQoL with minimal adverse effects as well as reduce caregiver burden. While there is no cure for atopic dermatitis, several therapeutic options are available. The treatment paradigm consists of education regarding general skin care and identifying and avoiding triggers.32 Treatments include moisturizers and topical anti-inflammatory drugs; however, these are noted as being time-consuming to administer and can have side effects, which can lead to low compliance and refractory disease. Phototherapy and systemic immunosuppressants (off-label use) are occasionally used in patients with severe disease who do not respond to topical therapy or in addition to topical therapy, though use of the latter is uncommon in patients aged younger than 5 years and rare in patients aged younger than 2 years, and these therapies have significant limitations and intolerable adverse effects.32
Dupilumab (Dupixent) is a recombinant human immunoglobulin G4 monoclonal antibody and is indicated for the treatment of patients aged 6 months and older with moderate-to-severe atopic dermatitis whose disease is not adequately controlled with topical prescription therapies or when those therapies are not advisable, and can be used with or without topical corticosteroids (TCSs).1 For patients aged 6 months to 11 years, the drug is available as prefilled syringes containing either 200 mg or 300 mg dupilumab for subcutaneous (SC) injection with age-based and weight-based dosing (Table 1).1 Dupilumab was previously reviewed by CADTH for the treatment of patients aged 12 years and older with moderate-to-severe atopic dermatitis whose disease is not adequately controlled with topical prescription therapies or when those therapies are not advisable, and received a recommendation from the CADTH Canadian Drug Expert Committee to be reimbursed with clinical criteria and conditions.33 Currently, the sponsor has requested reimbursement be expanded to include younger patients.2
The objective of this report is to review and critically appraise the evidence submitted by the sponsor on the beneficial and harmful effects of dupilumab, 200 mg or 300 mg, for SC injection in the treatment of patients aged 6 months to younger than 12 years with moderate-to-severe atopic dermatitis whose disease is not adequately controlled with topical prescription therapies or when those therapies are not advisable.
Stakeholder Perspectives
The information in this section is a summary of input provided by the patient and clinician groups who responded to CADTH’s call for input and from clinical experts consulted by CADTH for the purpose of this review.
Patient Input
CADTH received input from 3 patient groups: the Eczema Society of Canada and a joint input from the Canadian Skin Patient Alliance and Eczéma Québec. The inputs were provided for a previous CADTH submission for dupilumab in 2021, where the indication was for patients aged 6 years to 11 years with moderate-to-severe atopic dermatitis. No new patient input was received for the current review of dupilumab.
According to the patient groups, the symptoms of atopic dermatitis negatively affect individuals and their families and interfere with sleep, contribute to missed school and activities, psychosocial issues, and result in an increased risk of mental health problems. The groups stated that quality of life, access to care, and disease management are concerns that are associated with significant psychosocial, educational, financial, and occupational burden. The authors of the joint input stated that the complex, time-consuming skin treatment routines and other associated burdens make managing the disease very challenging and exhausting. Furthermore, comorbidities associated with pediatric atopic dermatitis require multidisciplinary management and screening to manage the disease. Patients seek a treatment that safely and effectively manages symptoms, reduce flares, and improves the quality of life of both patients and caregivers.
Clinician Input
Input From Clinical Experts Consulted by CADTH
The clinical experts explained that current topical treatments for atopic dermatitis do not work for all patients, can be burdensome and have low adherence, can have side effects, and some are expensive and not covered by insurance plans. Likewise, systemic immunosuppressants are associated with numerous adverse effects, are poorly tolerated, and require regular blood monitoring. Phototherapy can be inaccessible to patients and is often not feasible for young children.
According to the experts, dupilumab would be used as a second-line therapy after failure of an adequate trial with topical therapies (e.g., TCSs, topical calcineurin inhibitors [TCIs]), but before systemic immunosuppressants due to their poor safety profile. Both experts believed that it would be inappropriate to require either phototherapy or systemic immunosuppressant failure in patients aged younger than 12 years before being eligible for dupilumab.
Both clinical experts indicated that patients who could receive dupilumab would be identified based on clinician examination and judgment, taking into account disease severity and inadequate response to topical therapies. They also stated that patients with severe disease that is refractory to topical therapy and has a major impact on their HRQoL are most in need of effective treatment.
The experts indicated that outcomes used in clinical trials can help to gauge treatment response but are not typically used in clinical practice, except when required by a health insurer. Instead, patient assessments are usually a combination of discussion with the patient and caregiver and examination of the skin. It was noted that patients receiving dupilumab can have a delayed response and that it would be reasonable to assess patients for response to treatment approximately 3 months to 6 months after initiating treatment with dupilumab then every 6 months thereafter.
According to the experts, discontinuation of dupilumab should be considered if there is a lack of response to treatment (e.g., no improvement in rash, itch, or HRQoL) or there are intolerable adverse effects. One clinician added that patients often continue to use topical treatments alongside dupilumab, and that would not be a reason to discontinue treatment. Although it is possible to outgrow childhood atopic dermatitis, both experts explained that this is less likely for patients with severe disease, other atopic comorbidities, or persistent and generalized atopic dermatitis. It was suggested that a trial of increasing the time between injections once disease control is achieved with the plan to stop dupilumab altogether could be an option discussed and decided on between the treating physician, patient, and caregiver, though stopping the drug should not be forced.
The experts agreed that a specialist (i.e., dermatologist) would prescribe dupilumab, and it would be initiated in a hospital or community clinical setting. In situations where there is limited access to a dermatologist or pediatric dermatologist, the experts suggested that a general pediatrician, allergist, immunologist, or a physician with training in atopic dermatitis could prescribe the drug.
Clinician Group Input
Clinician group input was provided by the Canadian Dermatology Association. The input provided was largely aligned with that of the clinical experts consulted by CADTH. According to the clinician group input, patients can experience long wait times before seeing a specialist while their atopic dermatitis remains poorly controlled. They also noted that most dermatologists in Canada are not trained in, nor are comfortable, managing pediatric safety laboratory results in the context of systemic immunosuppression. It was highlighted in the input that dupilumab is the only systemic treatment for atopic dermatitis indicated for this age group and does not carry the same risk profile as traditional immunosuppressants. The clinician group stated that an ideal treatment would have a proven safety record in this age group and would also be able to reduce symptoms and improve sleep, concentration at school, and the overall quality of life for both patients and caregivers. It was also emphasized that a trial of systemic immunosuppression should not be a prerequisite for dupilumab coverage in patients aged 6 months to 5 years. The authors of the input highlighted remote Indigenous communities as being vulnerable groups in which individuals with poorly controlled atopic dermatitis tend to be at higher risk for chronic skin diseases and secondary infections and that dupilumab can be a good option for patients in these communities.
Drug Program Input
The drug programs requested input from the clinical experts regarding whether the initiation criteria should reflect the different trial inclusion criteria (specifically, moderate versus severe disease), how an adequate trial of topical prescription therapies is defined, if reimbursement criteria for this population (younger than 12 years) should be aligned with the current criteria for patients aged 12 years and older, and who would prescribe the drug.
The clinical experts stated that it would be reasonable to expect that dupilumab would work similarly in patients with moderate atopic dermatitis as those with severe atopic dermatitis who are aged 6 years to younger than 12 years, based on results from age groups younger and older that included patients with moderate disease. They also noted that the literature supports consideration of dupilumab treatment for some patients with moderate atopic dermatitis and an EASI score less than 16 with severe lesions that are not widespread or are localized to special areas (e.g., hands, feet, scalp).34,35 According to the experts, an adequate trial of topical prescription therapies would include TCSs or TCIs once or twice daily for at least 4 weeks and a patient who continues to experience persistent moderate-to-severe dermatitis that substantially impacts their quality of life is considered to have inadequately controlled disease. Both clinical experts agreed that patients aged 6 months to younger than 12 years should not be required to try systemic immunosuppressants or phototherapy before accessing dupilumab. Furthermore, if they have initiated and are responding to dupilumab before becoming 12 years old, they should be allowed to continue using dupilumab without having to try other therapies once reaching the age of 12 years. In general, the clinical experts felt that the continuation criteria issued by the CADTH Canadian Drug Expert Committee for dupilumab for patients aged 12 years and older were acceptable for patients aged 6 months to younger than 12 years. They noted that although some patients may not experience a 75% reduction in Eczema Area and Severity Index score (EASI-75), they still show a meaningful improvement from baseline, and felt this should not preclude patients from continuing dupilumab. Lastly, the experts agreed that a specialist (i.e., dermatologist) would prescribe dupilumab and in situations where access to dermatologists or pediatric dermatologists is limited, a general pediatrician, allergist, immunologist, physician with training in atopic dermatitis, or family physician in conjunction with a specialist could do so.
Clinical Evidence
Pivotal Studies and Randomized Controlled Trial Evidence
Description of Studies
Two phase III, double-blind (DB) randomized controlled trials (RCTs) (the LIBERTY AD PRESCHOOL part B trial, N = 162, and LIBERTY AD PEDS trial, N = 367) assessed whether dupilumab with TCSs reduced a patient’s IGA score to 0 or 1 compared to placebo with TCSs after 16 weeks of treatment in patients aged 6 months to younger than 6 years with moderate-to-severe atopic dermatitis (LIBERTY AD PRESCHOOL trial) or aged 6 years to younger than 12 years with severe atopic dermatitis (LIBERTY AD PEDS trial). Patients enrolled in both studies had disease that was not adequately controlled with topical prescription therapies. Key secondary outcomes included the proportion of patients with an EASI-75, percent change from baseline in EASI score, and percent change from baseline in weekly average of daily worst itch numeric rating scale (NRS) score at week 16. In both studies, HRQoL outcomes were assessed as other secondary outcomes, and included the Dermatitis Family Impact (DFI) questionnaire, Children’s Dermatology Life Quality Index (CDLQI), and Infants’ Dermatitis Quality of Life Index (IDQOL), the last of which was only assessed in the LIBERTY AD PRESCHOOL trial.
The IGA is a 5-point scale that provides a global clinical assessment of atopic dermatitis severity ranging from 0 (clear) to 4 (severe atopic dermatitis). A decrease in score relates to an improvement in signs and symptoms. The EASI is a tool used in clinical trials to assess the severity and extent of atopic dermatitis. For this scale, 4 disease characteristics of atopic dermatitis (erythema, thickness, scratching, and lichenification) are assessed for severity by the investigator on a scale of 0 (absent) to 3 (severe), and the scores are added together for each of the 4 body regions (head, arms, trunk, and legs). The area affected by atopic dermatitis is assessed as a percentage by each body region and is converted to a score of 0 to 6, where the area is expressed as 0 (none), 1 (1% to 9%), 2 (10% to 29%), 3 (30% to 49%), 4 (50% to 69%), 5 (70% to 89%), or 6 (90% to 100%). Each of the body area scores are multiplied by the area affected. Therefore, the total EASI score ranges from 0 points to 72 points, with a higher score indicating worse disease severity. The itch NRS is a tool that patients use to report the intensity of their itch with a daily recall period. Patients rate their overall (average) and maximum intensity of itch experienced during the previous 24 hours, based on a scale of 0 (no itch) to 10 (worst itch imaginable). The DFI is an atopic dermatitis-specific, self-administered, 10-item questionnaire designed to assess the impact of disease on the quality of life of families of children affected by disease based on a 1-week recall. Responses are scored on a 4-point Likert scale (from 0 to 3) and the total score ranges from 0 to 30, with higher scores indicating greater impairment in family quality of life. The CDLQI is a questionnaire completed by the child (aged 3 years to 16 years) designed to measure the impact of any skin disease on the quality of life with a recall period of 7 days. It consists of 10 questions asking about the impact of a skin disease on the life of the affected child, including symptoms, embarrassment, friendships, clothes, playing, sports, bullying, sleep, and impact of treatment. Each response is rated on a 4-point Likert scale (from 0 to 3) and the total score ranges from 0 to 30, with higher scores indicating a greater degree of impairment in HRQoL. The IDQOL is a questionnaire designed to measure the impact of the skin disease on the quality of life of infants and preschool children aged younger than 4 years. It consists of 10 questions that examine the impact of the disease on the life of the affected child and includes, but is not limited to mood, sleep, and daily activities. Each question is rated on a 4-point Likert scale (from 0 to 3) and the total score ranges from 0 to 30, with higher scores indicating worse quality of life.
Overall, baseline patient characteristics were balanced among treatment groups in both trials. In the LIBERTY AD PRESCHOOL trial, the mean age of patients was 3.8 years, there were fewer females (38.9%) than males (61.1%), and the mean EASI score of patients was 34.1. In the LIBERTY AD PEDS trial, the mean age of patients was 8.5 years, males and females were evenly balanced, and the mean EASI score of patients was ||||.
Efficacy Results
Key efficacy and safety results are summarized in Table 2.
For the primary efficacy end point, there was a larger proportion of patients in the dupilumab group who experienced an IGA score of 0 or 1 compared to the placebo group at week 16 with a between-treatment group difference of 23.8% (95% confidence interval [CI], 13.27% to 34.37%; P < 0.0001) in the LIBERTY AD PRESCHOOL trial. Results were similar in the LIBERTY AD PEDS trial with a larger proportion of patients in both dupilumab groups (every 4 weeks and every 2 weeks) who experienced an IGA score of 0 or 1 compared to the placebo group at week 16 with between-treatment group differences of 21.4% (95% CI, 11.36% to 31.45%; P < 0.0001) and 18.1% (95% CI, 8.28% to 27.97%; P < 0.0001), respectively.
In the LIBERTY AD PRESCHOOL trial, a larger proportion of patients in the dupilumab group experienced EASI-75 compared to the placebo group at week 16 with a between-treatment group difference of 42.3% (95% CI, 29.47% to 55.16%; P < 0.0001). Similarly, there was a larger percent change from baseline to week 16 EASI score observed in the dupilumab group compared to the placebo group, with a between-treatment group least squares mean (LSM) difference of –50.4% (95% CI, –62.38% to –38.40%; P < 0.0001). Results for the proportion of patients experiencing a 90% reduction in Eczema Area and Severity Index score (EASI-90) at week 16 also favoured treatment with dupilumab. In the LIBERTY AD PEDS trial, a larger proportion of patients in both dupilumab groups, every 4 weeks and every 2 weeks, experienced an EASI-75 score compared to the placebo group at week 16 with between-treatment group differences of 42.8% (95% CI, 31.54% to 54.15%; P < 0.0001) and 40.4% (95% CI, 28.95% to 51.82%; P < 0.0001), respectively. Likewise, there was a larger percent change from baseline to week 16 EASI score observed in both dupilumab groups, every 4 weeks and every 2 weeks, compared to the placebo group with between-group LSM differences of –33.4% (95% CI, ||||||| || |||||||; P < 0.0001) and –29.8% (95% CI, ||||||| || |||||||; P < 0.0001), respectively. Results for the proportion of patients experiencing EASI-90 at week 16 also favoured treatment with dupilumab.
In the LIBERTY AD PRESCHOOL trial, for the itch NRS score, a larger percent change from baseline to week 16 was observed in the dupilumab group compared to the placebo group with a between-group LSM difference of –47.1% (95% CI, –59.47% to –34.79%; P < 0.0001). Results for the proportion of patients experiencing an improvement of at least 4 points in itch NRS score from baseline to week 16 also favoured treatment with dupilumab. In the LIBERTY AD PEDS trial, a larger percent change from baseline to week 16 was observed for the itch NRS score in both the dupilumab every 4 weeks and every 2 weeks groups compared to the placebo group with between-group LSM differences versus placebo of –28.6% (95% CI, ||||||| || |||||||; P < 0.0001) and –31.0% (95% CI, ||||||| || |||||||; P < 0.0001), respectively. Results for the proportion of patients experiencing an improvement of at least 4 points in itch NRS score from baseline to week 16 also favoured treatment with dupilumab.
In the LIBERTY AD PRESCHOOL trial, a larger change from baseline to week 16 in the DFI score was observed in the dupilumab group compared to the placebo group with a between-group LSM difference of –7.80 (95% CI, –9.79 to –5.81; P < 0.0001). In the LIBERTY AD PEDS trial, a larger change from baseline to week 16 in the DFI score was observed in both the dupilumab every 4 weeks and every 2 weeks groups compared to the placebo group with between-group LSM differences versus placebo of –3.98 (95% CI, ||||| || |||||) and –4.11 (95% CI, ||||| || |||||), respectively.
In the LIBERTY AD PRESCHOOL trial, a larger change from baseline to week 16 in the CDLQI score was observed in the dupilumab group compared to the placebo group with a between-group LSM difference of –7.5 (95% CI, –10.29 to –4.75; P < 0.0001). In the LIBERTY AD PEDS trial, a larger change from baseline to week 16 in the CDLQI score was observed in both the dupilumab every 4 weeks and every 2 weeks groups compared to the placebo group with between-group LSM differences versus placebo of –4.2 (95% CI, ||||| || |||||; P < 0.0001) and –4.3 (95% CI, ||||| || |||||; P < 0.0001), respectively.
In the LIBERTY AD PRESCHOOL trial, a larger change from baseline to week 16 in the IDQOL score was observed in the dupilumab group compared to the placebo group with a between-group LSM difference of –8.96 (95% CI, –11.71 to –6.20; P < 0.0001). This was not an outcome in the LIBERTY AD PEDS trial.
Harms Results
During the 16-week treatment period, more than half of patients in any treatment group for either trial experienced at least 1 treatment-emergent adverse event (TEAE). In the LIBERTY AD PRESCHOOL trial, 63.9% of patients in the dupilumab group and 74.4% of patients in the placebo group reported a TEAE with the most frequently reported events being atopic dermatitis (13.3% dupilumab and 32.1% placebo), nasopharyngitis (8.4% dupilumab and 9.0% placebo), and upper respiratory tract infection (6.0% dupilumab and 7.7% placebo). In the LIBERTY AD PEDS trial, 65.0% of patients in the dupilumab every 4 weeks group, 67.2% of patients in the dupilumab every 2 weeks group, and 73.3% of patients in the placebo group reported a TEAE with the most frequently reported events also being nasopharyngitis (12.5% dupilumab every 4 weeks, 6.6% dupilumab every 2 weeks, and 6.7% placebo), upper respiratory tract infection (10.8% dupilumab every 4 weeks, 8.2% dupilumab every 2 weeks, and 10.0% placebo), and atopic dermatitis (6.7% dupilumab every 4 weeks, 8.2% dupilumab every 2 weeks, and 14.2% placebo).
In the LIBERTY AD PRESCHOOL trial, there were 4 serious adverse events (SAEs) reported in the placebo group and 0 in the dupilumab group. In the LIBERTY AD PEDS trial, there were 2 SAEs reported in the dupilumab every 4 weeks group, 0 in the dupilumab every 2 weeks group, and 2 in the placebo group. No SAE was reported by more than 1 patient per trial.
In the LIBERTY AD PRESCHOOL trial, 2 patients stopped treatment due to adverse events (AEs) due to atopic dermatitis (dupilumab group) and nightmare (placebo group). In the LIBERTY AD PEDS trial, 4 patients stopped treatment due to AEs: 2 due to food allergy and bacterial conjunctivitis (both patients were in the dupilumab every 2 weeks group) and 2 due to atopic dermatitis and asthma (both patients were in the placebo group).
There were no patient deaths in either trial.
Notable Harms
There were no reports of anaphylactic reaction in either trial.
There were no reports of hypersensitivity in the LIBERTY AD PRESCHOOL trial. In the LIBERTY AD PEDS trial, no treatment-related events of hypersensitivity or anaphylaxis occurred during the study.
There were no reports of helminthic infection in the LIBERTY AD PRESCHOOL trial. In the LIBERTY AD PEDS trial, | ||||||| || |||| of the dupilumab every 4 weeks and placebo groups reported a helminthic infection and || |||||||| in the dupilumab every 2 weeks group.
In the LIBERTY AD PRESCHOOL trial, 3 patients in the dupilumab group and 0 patients in the placebo group reported conjunctivitis. In the LIBERTY AD PEDS trial, 5 patients, 7 patients, and 3 patients in the dupilumab every 4 weeks, dupilumab every 2 weeks, and placebo groups, respectively, reported conjunctivitis.
In the LIBERTY AD PRESCHOOL trial, 2 patients in the dupilumab group and 0 patients in the placebo group reported blepharitis. In the LIBERTY AD PEDS trial, blepharitis was reported by | ||||||| and | |||||||| in the dupilumab every 2 weeks and placebo groups, respectively, and || |||||||| in the dupilumab every 4 weeks group.
In the LIBERTY AD PRESCHOOL trial, 1 patient in the dupilumab group and 0 patients in the placebo group reported keratitis. In the LIBERTY AD PEDS trial, | ||||||| in the dupilumab every 2 weeks group reported keratitis and || |||||||| in either the dupilumab every 4 weeks or placebo groups.
In the LIBERTY AD PRESCHOOL trial, 2 patients in the dupilumab group and 0 patients in the placebo group reported eosinophilia. In the LIBERTY AD PEDS trial, 1 patient in the dupilumab every 2 weeks group reported eosinophilia and no patients in either the dupilumab every 4 weeks or placebo groups.
Facial erythema was not captured in either trial.
Injection site pain was not captured in the LIBERTY AD PRESCHOOL trial. In the LIBERTY AD PEDS trial, 3 patients, 2 patients, and 3 patients in the dupilumab every 4 weeks, dupilumab every 2 weeks, and placebo groups, respectively, reported injection site pain.
Table 2: Summary of Key Results From Pivotal Studies and RCT Evidence
Outcome | LIBERTY AD PRESCHOOL | LIBERTY AD PEDS | |||
|---|---|---|---|---|---|
Dupilumab 200 mg or 300 mg q.4.w. + TCS N = 83 | Placebo + TCS N = 79 | Dupilumab 300 mg q.4.w. + TCS N = 122 | Dupilumab 100 mg or 200 mg q.2.w. + TCS N = 122 | Placebo + TCS N = 123 | |
Primary outcome: Proportion of patients with IGA 0 to 1 at week 16 — FAS | |||||
Proportion of patients with IGA 0 to 1 at week 16, n (%) | 23 (27.7) | 3 (3.9) | 40 (32.8) | 36 (29.5) | 14 (11.4) |
Difference vs. placebo (95% CI) | 23.8 (13.27 to 34.37) | Reference | 21.4 (11.36 to 31.45) | 18.1 (8.28 to 27.97) | Reference |
P value | < 0.0001a,b | Reference | < 0.0001a,c | 0.0004a,c | Reference |
Secondary: Proportion of patients with EASI-75 at week 16 — FAS | |||||
Proportion of patients with EASI-75 at week 16, n (%) | 44 (53.0) | 8 (10.7) | 85 (69.7) | 82 (67.2) | 33 (26.8) |
Difference vs. placebo (95% CI) | 42.3 (29.47 to 55.16) | Reference | 42.8 (31.54 to 54.15) | 40.4 (28.95 to 51.82) | Reference |
P value | < 0.0001a,b | Reference | < 0.0001a,c | < 0.0001a,c | Reference |
Secondary outcome: Percent change in EASI from baseline to week 16 — FAS | |||||
Baseline mean (SD) | 35.13 (13.89) | 33.07 (12.18) | 37.35 (12.45) | 37.29 (10.86) | 38.96 (12.01) |
LSM percent change (SE) | –70.0 (4.85) | –19.6 (5.13) | –82.1 (2.37) | –78.4 (2.35) | –48.6 (2.46) |
LSM difference vs. placebo (95% CI) | –50.4 (–62.38 to –38.40)d | Reference | –33.4 |||||||| ||||||)e | –29.8 (||||||| ||||||)e | Reference |
P value | < 0.0001a,d | Reference | < 0.0001a,e | < 0.0001a,e | Reference |
Secondary outcome: Proportion of patients with EASI-90 at week 16 — FAS | |||||
Patients with EASI-90 at week 16, n (%) | 21 (25.3) | 2 (2.8) | 51 (41.8) | 37 (30.3) | 9 (7.3) |
Difference vs. placebo (95% CI) | 22.5 (12.37 to 32.60) | Reference | 34.5 (24.60 to 44.37) | 23.0 (13.65 to 32.38) | Reference |
P value | 0.0001a,b | Reference | < 0.0001a,c | < 0.0001a,c | Reference |
Secondary outcome: Percent change from baseline to week 16 in weekly average of daily worst itch NRS score at week 16 — FAS | |||||
Baseline mean (SD) | 7.51 (1.32) | 7.63 (1.49) | 7.81 (1.58) | 7.78 (1.52) | 7.73 (1.54) |
LSM percent change (SE) | –49.4 (5.03) | –2.2 (5.22) | –54.6 (2.89) | –57.0 (2.77) | –25.9 (2.90) |
LSM difference vs. placebo (95% CI) | –47.1 (–59.47 to –34.79)d | Reference | –28.6 |||||||| ||||||)e | –31.0 |||||||| ||||||)e | Reference |
P value | < 0.0001a,d | Reference | < 0.0001a,e | < 0.0001a,e | Reference |
Secondary outcome: Proportion of patients with improvement (reduction) of weekly average of daily worst itch NRS score ≥ 4 from baseline at week 16 — FAS | |||||
Patients with reduction of NRS from baseline ≥ 4 at week 16, n of N1f (%) | 40 of 83 (48.1) | 7 of 78 (8.9) | 61 of 120 (50.8) | 70 of 120 (58.3) | 15 of 122 (12.3) |
Difference vs. placebo (95% CI) | 39.2 (26.18 to 52.27) | Reference | 38.5 (|||||| |||||) | 46.0 (|||||| |||||) | Reference |
P value | < 0.0001a,b | Reference | < 0.0001a,c | < 0.0001a,c | Reference |
Secondary outcome: Change from baseline to week 16 in DFI — FAS | |||||
Baseline mean (SD) | 17.20 (5.99) | 17.58 (7.24) | 16.92 (8.65) | 14.91 (7.05) | 15.05 (7.54) |
LSM change (SE) | –10.48 (0.81) | –2.68 (0.84) | –10.75 (0.48) | –10.89 (0.47) | –6.77 (0.50) |
LSM difference vs. placebo (95% CI) | –7.80 (–9.79 to –5.81)d | Reference | –3.98 ||||||| |||||)e | –4.11 ||||||| |||||)e | Reference |
P value | < 0.0001a,d | Reference | < 0.0001e | < 0.0001e | Reference |
Secondary outcome: Change from baseline to week 16 in CDLQI — FAS | |||||
Baseline mean (SD) | 17.5 (5.48) | 17.7 (6.25) | 16.2 (7.85) | 14.5 (6.78) | 14.6 (7.41) |
LSM change (SE) | –10.0 (1.56) | –2.5 (1.66) | –10.6 (0.47) | –10.7 (0.46) | –6.4 (0.51) |
LSM difference vs. placebo (95% CI) | –7.5 (–10.29 to –4.75)d | Reference | –4.2 ||||||| |||||)e | –4.3 ||||||| |||||)e | Reference |
P value | < 0.0001a,d | Reference | < 0.0001a,e | < 0.0001a,e | Reference |
Secondary outcome: Change from baseline to week 16 in IDQOL — FAS | |||||
Baseline mean (SD) | 17.37 (5.41) | 17.10 (5.37) | NA | NA | NA |
LSM change (SE) | –10.91 (1.16) | –1.95 (1.08) | NA | NA | NA |
LSM difference vs. placebo (95% CI) | –8.96 (–11.71 to –6.20)d | Reference | NA | NA | NA |
P value | < 0.0001a,d | Reference | NA | NA | NA |
Harms, n (%) — SAS | |||||
Patients with ≥ 1 TEAE | 53 (63.9) | 58 (74.4) | 78 (65.0) | 82 (67.2) | 88 (73.3) |
Patients with ≥ 1 SAE | 0 (0.0) | 4 (5.1) | 2 (1.7) | 0 (0.0) | 2 (1.7) |
Patients who stopped treatment due to AE | 1 (1.2) | 1 (1.3) | 0 (0.0) | 2 (1.6) | 2 (1.7) |
Deaths | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) |
Notable harms, n (%) — SAS | |||||
Anaphylactic reaction | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) |
Hypersensitivity | 0 (0.0) | 1 (1.3) | 0 (0.0) | 0 (0.0) | 0 (0.0) |
Helminthic infection | 0 (0.0) | 0 (0.0) | | ||||| | ||| | | ||||| |
Conjunctivitis | 3 (3.6) | 0 (0.0) | 5 (4.2) | 7 (5.7) | 3 (2.5) |
Blepharitis | 2 (2.4) | 0 (0.0) | ||| | | ||||| | | ||||| |
Keratitis | 1 (1.2) | 0 (0.0) | 0 (0.0) | 1 (0.8) | 0 (0.0) |
Eosinophilia | 2 (2.4) | 0 (0.0) | 0 (0.0) | 1 (0.8) | 0 (0.0) |
Facial erythema | NR | NR | NR | NR | NR |
Injection site pain | NR | NR | 3 (2.5) | 2 (1.6) | 3 (2.5) |
AE = adverse event; CDLQI = Children’s Dermatology Life Quality Index; CI = confidence interval; DFI = Dermatitis Family Impact; EASI = Eczema Area and Severity Index; EASI-75 = 75% reduction in Eczema Area and Severity Index score; EASI-90 = 90% reduction in Eczema Area and Severity Index score; FAS = full analysis set; IDQOL = Infants’ Dermatitis Quality of Life Index; IGA = Investigator’s Global Assessment; LSM = least squares mean; NA = not applicable; NR = not reported; NRS = numeric rating scale; q.2.w. = every 2 weeks; q.4.w. = every 4 weeks; RCT = randomized controlled trial; SAE = serious adverse event; SAS = safety analysis set; SD = standard deviation; SE = standard error; TCS = topical corticosteroid; TEAE = treatment-emergent adverse event.
aP value has been adjusted for multiple testing.
bP values were derived by Cochran-Mantel-Haenszel test stratified by region (North America, Europe), baseline disease severity (IGA 3, IGA 4), and baseline body mass (5 kg to less than 15 kg, 15 kg to less than 30 kg). The stratum (Europe region, baseline weight less than 15 kg, IGA 3) was combined with the stratum (Europe region, baseline weight at least 15 kg, IGA 3) as the former had only 2 patients.
cP values were derived by Cochran-Mantel-Haenszel test stratified by region (North America, Europe) and baseline body mass (less than 30 kg, at least 30 kg).
dThe CI and P value were based on treatment difference (dupilumab vs. placebo) of the LSM percent change using an analysis of covariance model with baseline measurement as covariate and the treatment, randomization strata (North America, Europe), baseline disease severity (IGA 3, IGA 4), and baseline body mass (5 kg to less than 15 kg, 15 kg to less than 30 kg) as fixed factors.
eThe CI and P value were based on treatment difference (dupilumab vs. placebo) of the LSM percent change using an analysis of covariance model with baseline measurement as covariate and the treatment, randomization strata (North America, Europe), and baseline body mass (less than 30 kg, at least 30 kg) as fixed factors.
fN1 is the number of patients with baseline NRS score of at least 4.
Source: Sponsor’s Summary of Clinical Evidence, LIBERTY AD PRESCHOOL Clinical Study Report, and LIBERTY AD PEDS Clinical Study Report.3,36,37 (Note: Details from the table have been taken from the sponsor’s Summary of Clinical Evidence.)
Critical Appraisal
In both pivotal trials, the few differences in baseline patient characteristics were mostly small, could have been due to chance, and the clinical experts did not think they were likely to change treatment outcomes. In the LIBERTY AD PEDS trial, 68 patients may have been unblinded to their treatment assignment, but the trial enrolled additional patients and included a modified full analysis set (mFAS) for supportive analyses to mitigate the issue. In both trials, fewer patients in the dupilumab groups used rescue treatment compared to the placebo groups and the difference could impact how some outcomes (e.g., harms, HRQoL) are interpreted, though the direction of bias is not clear. Additionally, there was a lack of validity and reliability evidence for the itch NRS, and no minimal important differences (MIDs) for the IGA, DFI, or IDQOL scores for the patient population identified from the literature.
Although the LIBERTY AD PEDS trial included only patients with severe atopic dermatitis, the clinical experts were of the opinion that the results would likely be generalizable to those with moderate disease given the evidence for age groups both younger and older than that in the trial (i.e., aged 6 years to younger than 11 years). The experts suggested that, in practice, a patient with moderate atopic dermatitis and an EASI score less than 16 may be eligible for dupilumab if, for example, they have severe lesions, but low percent BSA affected or have lesions localized to special areas (e.g., hands, feet, scalp). This is supported by the literature showing that patients with moderate atopic dermatitis can have an EASI score as low as 6.34,35 In the trials, patients who used rescue treatment were considered nonresponders, which the clinical experts stated was inconsistent with clinical practice. As per the clinical experts, non-TCS topical therapies would be acceptable add-on treatment while receiving dupilumab and a short course (< 8 weeks) of systemic therapies could be permitted without having to discontinue dupilumab. Although the trial outcomes addressed most of the treatment goals and patients’ needs from the stakeholder input, it is unclear if dupilumab injections every 2 weeks or every 4 weeks meet the need for a simpler treatment, particularly if patients or their caregivers are uncomfortable with administering the injection and the injections must be given in a clinic or if patients are especially afraid of needles.
Long-Term Extension Studies
Study 1434 is an ongoing, global, open-label, single-group, long-term extension (LTE) study of patients aged 6 months to younger than 18 years with atopic dermatitis with the aim to assess the long-term safety and efficacy of dupilumab.38,39 Patients who participated in the parent (pivotal) trials were eligible to enrol in Study 1434; 180 patients were from the LIBERTY AD PRESCHOOL trial and 368 patients were from the LIBERTY AD PEDS trial. The primary outcome was the incidence rate (events per patient-year) of TEAEs. Results presented were based on a prespecified second-step analysis conducted on data from patients aged 6 years to younger than 12 years (data cut-off date July 22, 2019) and from a third-step analysis conducted on data from patients aged 6 months to younger than 6 years (data cut-off date July 31, 2021).
Efficacy Results
At the time of this CADTH review, Study 1434 was still ongoing and no patients had completed the 260-week assessment. However, early findings from baseline, 4, 16, 28, 52, and 104 weeks of primary and secondary efficacy end points indicated that treatment effects were maintained with continued dupilumab use.
Harms Results
No new safety signals arose during the course of the Study 1434 and early safety results indicated that the drug was generally well tolerated with an acceptable safety profile.
Critical Appraisal
The limited availability of long-term data (i.e., mature data), open-label design, lack of control arm, and absence of formal statistical hypothesis testing were key constraints that limit the interpretation of the long-term efficacy and safety of study outcomes for treatment with dupilumab.
Indirect Comparisons
No indirect evidence was available.
Studies Addressing Gaps in the Pivotal and RCT Evidence
PEDISTAD, an observational study, was submitted by the sponsor to address gaps in the RCT evidence comparing dupilumab to other systemic treatments, such as methotrexate or cyclosporine, for patients aged younger than 12 years with moderate-to-severe atopic dermatitis whose disease is not adequately controlled with topical therapies or when those therapies are not medically advisable.3 PEDISTAD is an ongoing, international, longitudinal, 5-year, prospective study initiated on September 28, 2018, aiming to examine the impact of systemic treatments on disease severity, safety, and treatment discontinuation in this patient population. Patients were eligible to enrol if they were currently receiving systemic treatment for atopic dermatitis, UV therapy, immunosuppressants, or were currently on topical treatment and would be candidates for systemic treatment. All analyses were descriptive, with no comparisons performed between different systemic treatment cohorts.
Efficacy Results
Based on findings from a 2-year interim analysis in the sponsor’s Summary of Clinical Evidence, there appeared to be greater numerical improvements in the EASI total score, percent BSA affected by atopic dermatitis, Patient-Oriented Eczema Measure (POEM) score, and combined CDLQI or IDQOL score among the patients receiving dupilumab compared to methotrexate or cyclosporine.
Harms Results
Patients receiving dupilumab had a lower discontinuation rate and reported fewer AEs than those treated with methotrexate or cyclosporine.
Critical Appraisal
Based on the limited available data and how they were presented, it was not possible to determine if the treatment groups were adequately similar enough to be compared to 1 another. Additionally, available data were limited to the 2-year interim results, which prevent long-term conclusions from being drawn for any outcome. There was a potential increased risk of uncontrolled confounding and selection bias in the study, no formal comparison between study groups was considered, and there was no information regarding how many patients had been lost to follow-up, nor how many patients were censored. The study included a small number of patients living in Canada and it is unclear how representative the preliminary results are to the population of pediatric patients with atopic dermatitis living in Canada.
Conclusions
Currently dupilumab is available for patients aged 12 years and older with moderate-to-severe atopic dermatitis whose condition is not adequately controlled with prescription topical therapy or when those treatments are not advisable. There are few treatments available for patients who are aged 6 months to younger than 12 years and often these treatments, such as systemic immunosuppressants or phototherapy, are not recommended, used off-label, are inappropriate or inaccessible, and are therefore not preferred in this patient population. Evidence from 2 phase III trials demonstrated that dupilumab in combination with TCS was clinically significantly more effective at improving all disease-related symptoms, including itching, disease severity, and also significantly improving HRQoL compared to TCS alone during 16 weeks of treatment. The treatment effect of dupilumab was likely maintained, though conclusions of long-term efficacy and safety are limited by the number of patients with long-term data at this time and the lack of long-term comparative evidence. No direct or indirect evidence was available on comparative effectiveness of dupilumab versus any alternative therapies including systemic therapies (such as cyclosporine, methotrexate, azathioprine, mycophenolate mofetil), and the ongoing observational study could not fill the evidence gaps of dupilumab treatment efficacy and safety versus other drugs for atopic dermatitis. The indication for dupilumab notes that the drug would be for patients in whom topical prescription therapies are not advisable; however, whether such patients were enrolled and the efficacy of dupilumab in this patient population were unclear. Finally, the Health Canada–approved indication for dupilumab is for the treatment of patients aged 6 months and older with moderate-to-severe atopic dermatitis, though there is no evidence available for patients with moderate atopic dermatitis who are aged 6 years to 12 years, and the magnitude of treatment effect of dupilumab in this patient population is unknown due to lack of data.
Introduction
The objective of this report is to review and critically appraise the evidence submitted by the sponsor on the beneficial and harmful effects of the use of dupilumab 200 mg single-use syringe (200 mg per 1.14 mL) and 300 mg single-use syringe (300 mg per 2 mL) for SC injection in the treatment of moderate-to-severe atopic dermatitis in patients aged 6 months to younger than 12 years whose disease is not adequately controlled with topical prescription therapies or when those therapies are not advisable.
Disease Background
Contents within this section have been informed by materials submitted by the sponsor and clinical expert input. The following have been summarized and validated by the CADTH review team.
Atopic dermatitis is a chronic, relapsing, inflammatory skin condition characterized by intense itching, red and swollen skin, papules, excoriation, and serous exudation.4,5 In pediatric patients, atopic dermatitis tends to present at different sites than in adult patients, such as the face, extensor extremities, and cheeks and lesions are more often associated with oozing.4,6
Multiple factors, including genetic mutations, environmental triggers, immune dysregulation, and microbial imbalance, can contribute to the development of atopic dermatitis.40-45 Environmental triggers activate type 2 immune response characterized by interleukin (IL)-4, IL-5, and IL-13 signalling and, in turn, result in an inflammatory reaction and itching.41-43 Family history of atopic dermatitis can be a significant risk factor for the development of disease and onset in early infancy or childhood can persist into adulthood in severe cases.46-48 Other risk factors include starting complementary food after the age of 6 months, skin problems in the first few months of life, and elevated blood eosinophils (defined as at least 5% of total leukocytes) at 4 weeks of age.48,49 Males younger than 2 years are also at an increased risk of developing atopic dermatitis.50
Though many children will outgrow the condition by the age of 6 years to 12 years, disease severity and a family history of asthma are factors significantly associated with disease that persists into later childhood.10 It is common for children with atopic dermatitis to develop other allergic disorders that share the same type 2 inflammatory response pathophysiology that underlies atopic dermatitis; this process is referred to as the “atopic march.”4,8,51 The prevalence of these comorbidities is generally high and ranges from 12% to 38% for asthma and wheezing,11-14,51 8% to 24% for food allergy,11,12,51 and 31% to 58% for allergic rhinitis or conjunctivitis.12,14 Greater severity of atopic dermatitis is associated with a higher prevalence of coexisting type 2 inflammatory diseases.51
It has been estimated that atopic dermatitis affects 15% to 20% of children globally.7,8 In Canada, the lifetime prevalence of atopic dermatitis is up to 17% of the population and there is evidence to suggest that the prevalence has increased during the past 30 years.9
Pediatric patients with atopic dermatitis experience substantial symptom burden with frequent comorbidities and reduced HRQoL.10-20 Patients can suffer from itchy lesions4 leading to serious infections and are at an increased risk of developing other atopic diseases,11-14,21 attention-deficit/hyperactivity disorder, autism spectrum disorder,14 and suffer from social stigma and bullying.22 Pediatric patients with moderate-to-severe atopic dermatitis experience chronic and severe itch affecting daily functioning, HRQoL, sleep, mental health, and wellbeing.4,16,27,52-56
There are no specific diagnostic tests for atopic dermatitis,4,6 though the clinical experts noted that there are several diagnostic criteria used for research purposes.57-59 The most commonly used instruments in clinical trials to measure severity are the IGA, EASI, Physician’s Global Assessment, BSA, and SCORAD.
The care required for pediatric patients with atopic dermatitis can be time-consuming and interferes with day-to-day activities,22 leading to increased caregiver feelings of anxiety, depression, worry, helplessness,23 suboptimal sleep quality, and chronic exhaustion.22,60 Additionally, atopic dermatitis management adds a substantial financial burden on the health care system and society,24,25,27-30 and incurs indirect social and financial costs to patients and caregivers due to school22 and work absenteeism.26
Standards of Therapy
Contents within this section have been informed by materials submitted by the sponsor and clinical expert input. The following have been summarized and validated by the CADTH review team.
According to the clinical experts consulted by CADTH, the goals of treatment for pediatric patients with moderate-to-severe atopic dermatitis are to reduce symptom severity (e.g., itch, impact on sleep) and improve HRQoL with minimal adverse effects as well as reduce caregiver burden.
It is recommended that initial management of atopic dermatitis starts with education about the condition along with consistent, liberal use of emollients throughout the day.32 Management also includes identifying and avoiding triggers that cause disease flares (e.g., hypersensitivity reaction to topical therapies, low humidity environments, stress, irritants, allergens) and using dilute bleach baths and wet wraps containing low-to-medium-potency TCS, though the clinical experts indicated that the latter 2 are not used for most patients.32 The clinical experts consulted by CADTH stated that most patients with moderate-to-severe atopic dermatitis are managed with prescription topical anti-inflammatory treatments such as medium-to-high-potency TCSs and TCIs. The experts noted that topical crisaborole is less commonly used among these patients and is indicated for mild-to-moderate atopic dermatitis.61 Topical treatments can have adverse effects, are time-consuming for patients and their caregivers, tend to have low compliance, which can contribute to refractory disease, and not all patients respond to them.32 As per 1 clinical expert, TCIs are expensive and not always covered by insurance, limiting the available options.
The experts stated that pediatric patients with severe disease who do not respond to topical therapies, or in addition to topical therapies, may receive UV B phototherapy or off-label systemic immunosuppressants (e.g., cyclosporine, methotrexate, azathioprine, or mycophenolate mofetil), though these both have significant limitations.32 Phototherapy can be effective for some patients and does not carry the same risks as immunosuppressants; however, it is noted in the literature and by the clinical experts that patients must be independent enough to stand unattended for the session, phototherapy is associated with skin cancer (low risk), and it can be time-consuming requiring repeated weekly visits, which is not always practical for a chronic condition.32
Although immunosuppressants can be used in pediatric patients with severe atopic dermatitis, the clinical experts expressed that their use is uncommon in patients aged younger than 5 years and rare in patients younger than 2 years. According to the literature, cyclosporine (3 mg/kg/day to 5 mg/kg/day in 2 divided doses) is given for 2 months to 4 months, after which it can be tapered over a number of months and discontinued once the patient improves and remains stable.32 Intermittent maintenance therapy may be necessary to prevent relapses.32 Methotrexate (0.5 mg/kg) is given once weekly to a maximum of 25 mg/week.32 Systemic corticosteroids are avoided in these patients but can be reserved for when there are no other available treatments, as a bridge to other treatments, for immediate treatment of acute flares, and for patients with very severe disease.32 Mycophenolate mofetil and azathioprine have been used to treat children with atopic dermatitis, but the evidence is very limited and of low quality.32 Systemic immunosuppressants can lead to an incomplete response in some patients and these drugs are not recommended for long-term use.3 Moreover, the clinicians stated that the drugs are associated with significant and intolerable adverse effects, such as cytopenia, increased risk of infection, hepatotoxicity, and renal damage and require regular bloodwork that is burdensome to patients.
Drug Under Review
Key characteristics of dupilumab are summarized in Table 3, along with other treatments available for moderate-to-severe atopic dermatitis.
Dupilumab is indicated for the treatment of patients aged 6 months and older with moderate-to-severe atopic dermatitis whose disease is not adequately controlled with topical prescription therapies or when those therapies are not advisable, and can be used with or without TCS.1 For patients aged 6 months to 11 years, the drug is available as prefilled syringes containing either 200 mg (200 mg per 1.14 mL) or 300 mg (300 mg per 2 mL) dupilumab for SC injection with age and weight-based dosing.1 According to the product monograph, patients aged 6 months to 5 years with atopic dermatitis who are 5 kg to less than 15 kg receive 200 mg every 4 weeks and those who are 15 kg to less than 30 kg receive 300 mg every 4 weeks.1 Patients aged 6 years to 17 years with atopic dermatitis who are 15 kg to less than 30 kg initially receive 600 mg (two 300 mg injections) and then 300 mg every 4 weeks as maintenance, those who are 30 kg to less than 60 kg initially receive 400 mg (two 200 mg injections) and then 200 mg every 2 weeks as maintenance, and those 60 kg or greater initially receive 600 mg (two 300 mg injections) and then 300 mg every 2 weeks as maintenance.1
Dupilumab is a recombinant human immunoglobulin G4 monoclonal antibody that inhibits IL-4 and IL-13 signalling, which is involved in type 2 inflammatory responses and atopic conditions.1
Dupilumab underwent a standard review by Health Canada and was issued a Notice of Compliance on April 14, 2023.2 Previously, dupilumab was reviewed by CADTH for the treatment of patients aged 12 years and older with moderate-to-severe atopic dermatitis whose disease is not adequately controlled with topical prescription therapies or when those therapies are not advisable.33 The CADTH Canadian Drug Expert Committee recommended that dupilumab be reimbursed with clinical criteria and/or conditions for patients aged 12 years and older with moderate-to-severe atopic dermatitis.33 Currently, the sponsor has requested reimbursement be expanded to include the treatment of patients aged 6 months to younger than 12 years with moderate-to-severe atopic dermatitis whose disease is not adequately controlled with topical prescription therapies or when those therapies are not advisable.2
Table 3: Key Characteristics of Dupilumab, Methotrexate, Cyclosporine, Azathioprine, and Mycophenolate Mofetil
Characteristic | Dupilumab | Methotrexate | Cyclosporine | Azathioprine | Mycophenolate mofetil |
|---|---|---|---|---|---|
Mechanism of action | Inhibits IL-4 and IL-13 signalling | Immunosuppressant | Immunosuppressant Inhibits IL-2 and T-cell activation | Immunosuppressant Suppresses T-cell effects | Immunosuppressant Inhibits purine synthesis, reduces lymphocyte proliferation, reduces B-cell antibody formation |
Indicationa | Moderate-to-severe atopic dermatitis in patients aged ≥ 6 months whose disease is not adequately controlled with prescription topical therapies, with or without TCS | None for atopic dermatitis Various neoplasia Psoriasis and/or psoriatic arthritis Rheumatoid arthritis | None for atopic dermatitis Prevention of transplant rejection Psoriasis Rheumatoid arthritis Nephrotic syndrome | None for atopic dermatitis Prevention of transplant rejection (renal) Rheumatoid arthritis | None for atopic dermatitis Prevention of transplant rejection (renal, cardiac, or hepatic) |
Route of administration | SC | Oral SC | Oral IV | Oral | Oral IV |
Recommended dose | Patients aged 6 months to 5 years:
Patients aged 6 years to 17 years:
| Varies with indication | Varies with indication | Renal transplant: 3 mg/kg/day to 5 mg/kg/day initial, 1 mg/kg/day to 3 mg/kg/day maintenance. Rheumatoid arthritis: 1 mg/kg/day (50 mg to 100 mg) initial, dose increments of 0.5 mg/kg/day up to a maximum of 2.5 mg/kg/day maintenance | Pediatric patients: 1g orally twice a day |
Serious adverse effects or safety issues | No serious adverse effects | Malignant lymphomas, vomiting, diarrhea, stomatitis, hepatotoxicity, bone marrow depression, interstitial pneumonitis, dermatological reactions | Malignancies, hypertension, hepatotoxicity, infection, neurotoxicity, nephrotoxicity | Carcinogenic, mutagenic, leukopenia, thrombocytopenia, infection, nausea, vomiting, macrocytic anemia, bone marrow depression, hepatoxicity | Infection, lymphoma, malignancies, somnolence, dizziness, pure red cell aplasia |
Other | None | Safety and effectiveness in pediatric patients have not been established | Not recommended in children for nontransplant indications | Safety and effectiveness in pediatric patients have not been established | None |
IL = interleukin; q.2.w. = every 2 weeks; q.4.w. = every 4 weeks; SC = subcutaneous; TCS = topical corticosteroid.
aHealth Canada–approved indication.
Source: Product monographs for dupilumab, methotrexate, cyclosporine, azathioprine, and mycophenolate mofetil.1,62-65
Stakeholder Perspectives
Patient Group Input
This section was prepared by the CADTH review team based on the input provided by 3 patient groups. The full original patient input received by CADTH has been included in the stakeholder section at the end of this report.
Three patient groups responded to CADTH’s call for patient input: Eczema Society of Canada and a joint input from Canadian Skin Patient Alliance and Eczéma Québec. The inputs were provided for a previous CADTH submission for dupilumab in 2021, where the indication was for patients aged 6 years to 11 years with moderate-to-severe atopic dermatitis. No new input was received for the current review of dupilumab.
Eczema Society of Canada is a registered Canadian charity dedicated to improving the lives of Canadians living with eczema. Canadian Skin Patient Alliance is a national nonprofit organization dedicated to advocating, educating, and supporting Canadians living with diseases that affect skin, hair, and nails. Eczéma Québec is a patient advisory committee and registered nonprofit organization with the goal of building resources and establishing knowledge translation tools to improve education and raise awareness and health outcomes of patients with atopic dermatitis and health care practitioners. Eczema Society of Canada gathered information for this submission via written questionnaires, surveys, and interviews. Eczema Society of Canada survey data included 1,035 respondents providing their experience about the impact of atopic dermatitis on their quality of life and 299 respondents about systemic treatments for atopic dermatitis and reports on patient experience for those aged 17 years and younger. Canadian Skin Patient Alliance and Eczéma Québec collaborated to hold discussions and one-on-one interviews with patients with atopic dermatitis and caregivers by reaching them through social media platforms, newsletters, and emails.
Based on the input from the 3 patient groups, chronic itch and pain negatively affect individuals and their families, though the impact varies depending on disease severity. Eczema Society of Canada input indicated that 70% of survey respondents with moderate-to-severe atopic dermatitis suffer from interrupted sleep, with 18% having poor sleep for more than 14 nights per month. Survey results indicated that 69% of caregivers reported experiencing anxiety, 25% of them reported experiencing depression due to managing a child with atopic dermatitis, and 41% indicated they feel like a failure when they cannot control their child’s flares. Parents of children with atopic dermatitis reported feeling exhausted and helpless dealing with extra daily burdens.
According to the patient groups, itching is consistently rated as the most bothersome symptom resulting in uncontrollable scratching and damaged skin, which leads to children feeling embarrassment and shame due to visible blood stains, skin rash crusting, bleeding, and scabbing. Furthermore, periods of flares add more burden and contribute to missed school and activities, social isolation, bullying, psychosocial issues, an increased risk of mental health problems, and suicidal ideation. Additionally, the authors of the joint input stated that quality of life, access to care, and disease management are all areas of concern for patients and their caregivers and are associated with significant psychosocial, educational, financial, and occupational burdens. They indicated that comorbidities associated with pediatric atopic dermatitis, such as food allergies, asthma, allergic rhinoconjunctivitis, eosinophilic esophagitis, learning disabilities, and mental health issues, require multidisciplinary management and screening to address these problems, yet many patients reported not having been recommended for screening.
The patient groups indicated that for many living with atopic dermatitis, frequent moisturizing, trigger avoidance, and the use of topical treatments work well to control flares. For others with more severe symptoms, phototherapy and systemic therapies, including corticosteroids and off-label systemic immunosuppressants, which are not indicated for pediatric patients, are used to manage their disease. These treatments raised significant safety concerns among patients and caregivers, have limited long-term benefits, can result in rebound flares after stopping (e.g., corticosteroids), and can be challenging to access (e.g., phototherapy clinics). The authors of the joint input stated that the complex, time-consuming skin maintenance and treatment routines and other associated burdens make managing the disease very challenging and exhausting. According to the patient groups, there is a need for new treatment options that safely and effectively manage itch, redness, and inflammation, reduce flares, and improve HRQoL.
Clinician Input
Input From Clinical Experts Consulted by CADTH
All CADTH review teams include at least 1 clinical specialist with expertise regarding the diagnosis and management of the condition for which the drug is indicated. Clinical experts are a critical part of the review team and are involved in all phases of the review process (e.g., assisting in the critical appraisal of clinical evidence, interpreting the clinical relevance of the results, and providing guidance on the potential place in therapy). The following input was provided by 2 clinical specialists with expertise in the diagnosis and management of moderate-to-severe atopic dermatitis.
Unmet Needs
The clinical experts consulted by CADTH explained that the currently available therapies have limitations that hinder effective management in pediatric patients with moderate-to-severe atopic dermatitis. They stated that not all patients respond to topical anti-inflammatory treatment, which 1 clinical expert stated was the safest option available for most patients. It was noted that topical treatments can be time-consuming and have low adherence, TCSs can have side effects, and TCIs are often expensive and not covered by insurance plans. The clinical experts stated that phototherapy is often not feasible for young children who must stand still and unattended in the phototherapy booth, it is associated with causing skin cancer (low risk), and requires repeated administration, but can only be used for a few months at a time, which is not ideal for treating a chronic disease. Lastly, the experts described the limitations with systemic immunosuppressants (e.g., methotrexate, cyclosporine, azathioprine, and mycophenolate mofetil), including numerous adverse effects, poor tolerance resulting in an incomplete response, and regular blood monitoring requirements that are burdensome for patients. The clinical experts added that while systemic immunosuppressants are currently prescribed for pediatric patients with severe atopic dermatitis, they are seldomly used in those aged younger than 5 years and rarely used in those younger than 2 years.
Place in Therapy
Dupilumab targets the underlying disease process and, according to the clinical experts, would be used as a second-line therapy after failure of an adequate trial with topical therapies (e.g., TCS, TCI), but before systemic immunosuppressants due to their poor safety profile. Both experts believed that for pediatric patients aged younger than 12 years, it would be inappropriate to require treatment failure of either phototherapy or systemic immunosuppressants before becoming eligible for dupilumab. The clinicians expect dupilumab to be used with or without topical treatments.
Patient Population
One expert stated that misdiagnosing atopic dermatitis is unlikely, particularly in children. Both clinical experts indicated that patients suitable for treatment with dupilumab would be identified through clinician examination and judgment, taking into account disease severity and inadequate response to topical therapies. As per 1 of the experts, these patients would have an IGA score of 3 or 4, EASI score of 16 or greater, and have 10% or greater BSA affected; however, these assessment tools are not routinely used in clinical practice. The experts agreed that patients with severe atopic dermatitis, whose disease is refractory to topical therapies and has a major impact on their HRQoL, are most in need of effective treatment.
Assessing the Response to Treatment
One clinical expert stated that patients are usually assessed through a combination of verbal discussion with the patient and their caregivers about treatment response (e.g., symptom improvement, better HRQoL) as well as physical exam of the affected areas. It was suggested that there are likely small differences among physicians in assessments of response to treatment. The experts indicated that instruments used in clinical trials, such as the IGA, EASI, itch NRS, and CDLQI, can help to gauge treatment response but are not typically used in clinical practice, except when required by a health insurer. One clinician added that of the listed instruments, the IGA is a simple and somewhat reliable measure that can be used in a clinical setting. It was noted that patients receiving dupilumab can have a delayed response and that it would be reasonable to assess patients for response to treatment approximately 3 months to 6 months after initiating treatment with dupilumab then every 6 months thereafter.
Discontinuing Treatment
According to the experts, discontinuation of dupilumab should be considered if there is a lack of response to treatment (e.g., no improvement in rash, itch, or HRQoL) or there are intolerable adverse effects. One clinician added that patients often continue to use topical treatments alongside dupilumab, and it would not be a reason for discontinuing treatment. Severe conjunctivitis was noted as being a reason some patients may stop treatment temporarily or permanently; however, the experts indicated that adverse effects may be transient or mild, and patients often continue to receive treatment.
Although it is possible to outgrow childhood atopic dermatitis, both experts explained that it is less likely for patients with severe disease, with other atopic comorbidities, or with persistent and generalized atopic dermatitis, and these patients may require ongoing treatment. At this time, it is unclear if a pediatric patient who has been treated with dupilumab should stop the drug to assess sustained disease remission without it, nevertheless, the experts suggested that a trial of increasing the time between injections (e.g., every 6 weeks as opposed to every 4 weeks) once disease control is achieved with the plan to stop dupilumab altogether could be an option discussed and decided on between the treating physician, patient, and caregiver, though stopping the drug should not be forced.
Prescribing Considerations
It was suggested that dupilumab be initiated in a hospital or community clinical setting and both experts agreed that a specialist (i.e., dermatologist who has experience with the instruments [e.g., EASI] required to access dupilumab) would prescribe the drug. It was noted that there may be limited access to pediatric dermatologists and general dermatologists may hesitate to prescribe dupilumab in children. In those instances, the clinical experts suggested that a general pediatrician, allergist, immunologist, or a physician with training in atopic dermatitis could prescribe the drug. The experts stated that some pediatric patients do not tolerate injectable medications, but techniques can be used to reduce the pain and anxiety around treatment.
Clinician Group Input
This section was prepared by the CADTH review team based on the input provided by 1 clinician group. The full original clinician group input received by CADTH has been included in the stakeholder section at the end of this report.
Clinician group input was provided by 1 group, the Canadian Dermatology Association, which advocates for continuing medical education for its members, supports patient care, and provides public education on several aspects of skin care.
According to the clinician group, the current treatment paradigm for atopic dermatitis in children aged 6 months to 11 years starts with education regarding general measures such as bathing practices and moisturizer use. The most common first-line therapies for atopic dermatitis are TCSs, TCIs, and topical phosphodiesterase type 4 inhibitors (e.g., crisaborole). Phototherapy or off-label systemic drugs such as short courses of prednisone and longer courses of methotrexate or cyclosporine are used occasionally.
The clinician group input provided insight into Eczema Society of Canada’s 2017 quality of life survey report for moderate-to-severe atopic dermatitis in children. According to this survey, issues include long wait times to access specialists and inadequate disease control among these patients. Furthermore, those with severe atopic dermatitis report failing topical steroids, moisturizers, oral antihistamines, TCIs, and even systemic steroids. Given the many different treatments and the regimented care involved with atopic dermatitis, caregivers find these treatments to be very challenging and described experiencing sleep loss, anxiety, stress, financial burden, and lack of support.
Eczema Society of Canada’s 2021 survey, also highlighted in the clinician group input, described how severe atopic dermatitis has a significant impact on children’s quality of life and affects their mood, school performance, and concentration. It was noted that there are many unavoidable external factors such as weather, stress, and exercise that can severely trigger itch and, in turn, affect patients’ quality of sleep.
The clinician group stated that an ideal treatment would have a proven safety record in this age group and would also be able to reduce itching and improve sleep, concentration at school, and the overall quality of life for both patients and caregivers.
It was stated in the input that recurrent courses of oral steroids for pediatric patients could lead to many short- and long-term adverse effects and that traditional systemic immunosuppressants, such as methotrexate and cyclosporine, are associated with a significant risk of cytopenias, multiorgan impairment (liver, renal), and increased risk of infection in young children. The clinician group also indicated that most dermatologists in Canada are not trained in, nor comfortable, managing pediatric safety laboratory tests in the context of systemic immunosuppression. According to the clinician group input, dupilumab is the only systemic treatment for atopic dermatitis indicated for this age group and does not carry the same profile risks as traditional immunosuppressants and thus, it is considered the treatment of choice for patients with moderate-to-severe disease requiring a systemic therapy.
The clinician group was of the opinion that any patient with moderate-to-severe atopic dermatitis who has experienced topical therapy failure with recurrent courses of oral steroids, and whose quality of life (and that of their caregiver) is significantly impacted, could potentially benefit from dupilumab. The group indicated that patients least suitable would include those with mild atopic dermatitis and those well-controlled with topical therapy.
According to the input, outcomes used in clinical practice to assess a clinically meaningful response would be measured at monthly intervals then every 4 months to 6 months and include a reduction in EASI scores and itching, improvements in skin appearance, quality of life, mental health, and outlook. As per the clinician group, factors to consider when deciding to discontinue therapy would include inability to achieve a clinically meaningful response 3 months to 4 months after initiating treatment or intolerance to dupilumab. The group stated that a dermatologist would be required to diagnose atopic dermatitis and prescribe dupilumab. It was also emphasized that systemic immunosuppressants (e.g., methotrexate, cyclosporine) should not be a prerequisite for dupilumab coverage in patients aged 6 months to 5 years due to the significant harms associated with their use and the limited number of pediatric dermatologists trained in managing pediatric immunosuppression.
The clinician group input highlighted remote Indigenous communities as being vulnerable groups in which individuals with poorly controlled atopic dermatitis tend to be at higher risk for chronic skin diseases and secondary infections due to environmental factors, low income, and the many barriers to accessing proper health care services and resources. The authors of the input suggested that dupilumab can be a better, straightforward option as a safe and efficacious treatment for children in these communities which can help control atopic dermatitis and decrease comorbid skin conditions associated with this disease.
Drug Program Input
The drug programs provide input on each drug being reviewed through CADTH’s reimbursement review processes by identifying issues that may impact their ability to implement a recommendation. The implementation questions and corresponding responses from the clinical experts consulted by CADTH are summarized in Table 4.
Table 4: Summary of Drug Plan Input and Clinical Expert Response
Drug program implementation questions | Clinical expert response |
|---|---|
Considerations for initiation of therapy | |
The reimbursement request is for treatment of patients aged 6 months to < 12 years with moderate-to-severe atopic dermatitis. The pivotal trials focused on 2 separate age groups with different disease severity. LIBERTY AD PRESCHOOL Part B trial:
LIBERTY AD PEDS trial:
Should there be different initiation criteria for the 2 age groups, based on the inclusion criteria for the 2 trials? | The clinical experts stated that it would be reasonable to expect that dupilumab would work similarly in patients with moderate atopic dermatitis as those with severe atopic dermatitis who are aged 6 years to < 12 years, based on results from age groups both younger and older that included patients with moderate atopic dermatitis. The clinical experts suggest that initiation criteria should include the full moderate-to-severe range of severity for both age groups. The experts also noted that, in practice, patients with moderate disease can have an EASI score of < 16 (which is supported by the literature)34,35 and could also be considered for dupilumab. They noted that these assessments consider different aspects of the disease, for example, the IGA focuses on lesion severity while the EASI varies more with BSA. The experts explained that assessments performed in clinic can consist of a balance of the severity of the lesions and how widespread the disease is. They described situations in which a patient may have a low EASI score, but could be considered for dupilumab:
|
The reimbursement request is for disease not adequately controlled with topical prescription therapies or when those therapies are not advisable, as per the Health Canada–approved indication. What would be considered an adequate trial of topical prescription therapies? | The clinical experts stated that an adequate trial of topical prescription therapies would include TCSs or TCIs once or twice daily for at least 4 weeks. Mild TCSs (class VI to VII) would be used on the face while moderate (class III to V) or higher would be used on the body. According to the experts, a patient who continues to experience persistent, moderate or severe dermatitis that substantially impacts their quality of life would be considered to have inadequately controlled disease. |
Consider alignment with dupilumab for patients aged ≥ 12 years, where possible. For example:
If reimbursement criteria are recommended for patients aged 6 months to < 12 years and they do not align with CDEC-recommended initiation criteria for those aged ≥ 12 years (which require the use of at least 1 systemic immunosuppressant), implementation advice will be required on transitioning patients when they become 12 years old. | Both clinical experts agreed that patients 6 months to < 12 years should not be required to try systemic immunosuppressants or phototherapy before accessing dupilumab. They also stated that the age of 12 years is not a clinically meaningful threshold and should not necessitate changes in clinical management. The experts agreed that once reaching the age of 12 years, patients should not be required to try phototherapy or other systemic immunosuppressants, and that if they have initiated and are responding to dupilumab before the age of 12 years, they should be allowed to continue using dupilumab after that. Given that atopic dermatitis can change over time, the experts noted that a patient (at any age) and their caregiver can discuss with their physician if it is appropriate to stop dupilumab and see if the condition can be managed with topical therapies alone. If the patient experiences residual and persistent disease after stopping, the experts recommended that the patient restart dupilumab. The clinical experts stated that patients between 6 months and 12 years who stop dupilumab should not be required to meet the initiation criteria again before restarting treatment if they are aged < 12 years. Likewise, patients who stop dupilumab before the age of 12 years should not be required to meet the initiation criteria (including not having to try phototherapy or systemic immunosuppressants) before restarting treatment after the age of 12 years. |
Considerations for continuation or renewal of therapy | |
Consider alignment with dupilumab for at least 12 years of age. For example:
Patients who are being treated with dupilumab based on any criteria recommended for the population aged 6 months to < 12 years may not meet the initiation criteria for those aged ≥ 12 years. How should these patients be assessed upon becoming 12 years old (e.g., using baseline values at initiation of treatment against renewal criteria for age > 12 years)? | The clinical experts stated that proof of maintenance of disease control would be an important criterion for continuing therapy and, in general, the listed continuation criteria were acceptable for patients aged 6 months to < 12 years. However, they were less certain if experiencing EASI-75 would be appropriate or reasonable for all patients. They noted that some patients show meaningful improvement, but may not experience a 75% improvement, which should not preclude them from continuing dupilumab. One expert also suggested that an initial authorization period of 6 months to 12 months would be reasonable considering that atopic dermatitis is a chronic disease and dupilumab is expected to be a relatively long-term treatment. As noted previously, the clinical experts stated that once a patient becomes 12 years old, they should not be required to try phototherapy or other systemic immunosuppressants to access dupilumab. One of the implementation considerations from the previous CDEC recommendation for dupilumab in patients aged ≥ 12 years defined moderate-to-severe atopic dermatitis based on the trials as, “an EASI score of 16 points or higher, or an Investigator’s (Physician’s) Global Assessment score of 3 or 4,” which the clinical experts felt was a reasonable definition. Furthermore, the clinical experts stated that continuation criteria should allow clinicians the same flexibility to use either the IGA or EASI. |
Considerations for prescribing of therapy | |
Is alignment with the following criteria appropriate?
In specific circumstances where in some jurisdictions, there is limited access to specialists (dermatologist, allergist, clinical immunologist, or pediatrician who has expertise in the management of moderate-to-severe atopic dermatitis), could a family physician in conjunction with a specialist prescribe dupilumab? | The clinical experts agreed that a specialist (i.e., dermatologist who has experience with the instruments [e.g., EASI] required to access dupilumab) would prescribe the drug. It was noted that there may be limited access to pediatric dermatologists and general dermatologists may hesitate to prescribe dupilumab in children. However, it was noted that in those instances, a general pediatrician, allergist, immunologist, a physician with training in atopic dermatitis, or a family physician in conjunction with a specialist could prescribe the drug. |
Generalizability | |
The LIBERTY AD PEDS trial (patients aged 6 years to < 12 years) only included patients with severe atopic dermatitis. Would patients with moderate atopic dermatitis within this age group be considered eligible for reimbursement? | Both clinical experts noted that the distinction between moderate and severe atopic dermatitis is not well defined and likely varies among physicians. Although there are a lack of data for dupilumab in patients with moderate disease aged 6 years to 12 years, the experts expect that dupilumab would likely work in these patients similarly to patients with severe disease. They also noted that the magnitude of benefit may appear to be greater in patients with severe atopic dermatitis due to them having a larger range for improvement compared to patients with moderate atopic dermatitis. |
BSA = body surface area; CDEC = CADTH Canadian Drug Expert Committee; EASI = Eczema Area and Severity Index; EASI-75 = 75% reduction in the Eczema Area and Severity Index score; IGA = Investigator’s Global Assessment; TCI = topical calcineurin inhibitor; TCS = topical corticosteroid.
Clinical Evidence
The objective of CADTH’s Clinical Review Report is to review and critically appraise the clinical evidence submitted by the sponsor on the beneficial and harmful effects of dupilumab 200 mg (200 mg per 1.14 mL) and 300 mg (300 mg per 2 mL) single-use syringes for SC injection in the treatment of moderate-to-severe atopic dermatitis in patients aged 6 months to younger than 12 years whose disease is not adequately controlled with topical prescription therapies or when those therapies are not advisable. The focus will be placed on comparing dupilumab to placebo and identifying gaps in the current evidence.
A summary of the clinical evidence included by the sponsor in the review of dupilumab is presented in 4 sections, and CADTH’s critical appraisal of the evidence is included after each section. The first section, the systematic review, includes 2 pivotal studies and RCTs that were selected according to the sponsor’s systematic review protocol. The second section includes 1 sponsor-submitted LTE study. The third section includes a feasibility assessment from the sponsor addressing the lack of indirect evidence. The fourth section includes an additional observational study that was considered by the sponsor to address important gaps in the pivotal and RCT evidence.
Included Studies
Clinical evidence from the following are included in the CADTH review and appraised in this document:
2 pivotal studies and RCT evidence
1 LTE study
1 feasibility assessment for conducting an indirect treatment comparison (ITC)
1 observational study to address gaps in the RCT evidence.
Pivotal Studies and RCT Evidence
Contents within this section have been informed by materials submitted by the sponsor. The following have been summarized and validated by the CADTH review team.
Description of Studies
Two phase III, DB, randomized, placebo-controlled trials (LIBERTY AD PRESCHOOL part B and LIBERTY AD PEDS) met the inclusion criteria for the sponsor’s systematic review. Characteristics of the LIBERTY AD PRESCHOOL part B and LIBERTY AD PEDS trials are summarized in Table 5 and the study designs are shown in Figure 1 and Figure 2, respectively.
The LIBERTY AD PRESCHOOL trial consisted of 2 parts. Part A (N = 40) was an open-label, single ascending dose, sequential cohort study investigating the pharmacokinetic, safety, and efficacy of a single dose of dupilumab in pediatric patients with severe atopic dermatitis (children aged 6 months to < 6 years). Data from part A were used to inform the dose regimen for part B, but results for the former are not presented in this CADTH review. Patients who enrolled in part A of the study were not eligible to participate in part B. Part B (N = 162; referred to as the LIBERTY AD PRESCHOOL trial in this report) was a double-blind RCT and its primary and secondary objectives were to investigate the efficacy and safety of dupilumab when administered concomitantly with TCS in patients aged 6 months to younger than 6 years with moderate-to-severe atopic dermatitis. The LIBERTY AD PRESCHOOL trial consisted of 3 periods: an 8-week screening period (including 2 weeks of TCS standardization), 16-week treatment period, and 12-week follow-up period (for patients who did not enter the LTE). During the screening period, systemic treatments for atopic dermatitis were washed out, as applicable, according to the eligibility requirements and starting on day –14, all patients initiated a standardized low-potency TCS treatment regimen. Low-potency TCS was to be applied once daily to areas with active lesions. Once a patient experienced an IGA score of 2 or less, TCS frequency was to be decreased to 3 times per week, and then stopped once lesions were clear (IGA 0). If lesions returned, treatment with low-potency TCS was to be reinstituted with the same step-down approach. For lesions persisting or worsening under daily treatment with low-potency TCS, patients could be treated with medium-potency or high-potency TCS; super-potent or very high-potency steroids were not allowed even for rescue.
Patients who met the eligibility criteria underwent baseline assessments. Patients were randomized in a 1:1 ratio stratified by baseline body mass (5 kg to < 15 kg, 15 kg to < 30 kg), baseline disease severity (IGA 3, IGA 4), and region (North America, Europe, Japan, China). The number of patients with moderate atopic dermatitis (IGA 3) was capped at approximately 40 patients. Patients received 1 of the following treatment regimens: dupilumab every 4 weeks with TCS (body mass 5 kg to < 15 kg, 200 mg; body mass 15 kg to < 30 kg, 300 mg) or placebo with TCS. The primary outcome was the proportion of patients with an IGA score of either 0 or 1 at week 16. Patients were enrolled starting June 30, 2017, and the data cut-off date was September 16, 2021.
The LIBERTY AD PEDS trial (N = 367) was a double-blind RCT and its primary and secondary objectives were to demonstrate the efficacy and safety of dupilumab administered concomitantly with TCS in patients aged 6 years to younger than 12 years with severe atopic dermatitis. The study was conducted at 61 sites with 3 sites in Canada. The study consisted of 3 periods: an 11-week screening period (including 2 weeks of TCS standardization), 16-week treatment period, and 12-week follow-up (for patients who did not enter the LTE). TCS usage was standardized according to the following guidelines. Medium-potency TCS was applied once daily to areas with active lesions. Once a patient experienced an IGA score of 2 or less, the frequency of medium-potency TCS was reduced to 3 times per week and then stopped once lesions were clear (IGA 0). If lesions returned, treatment with medium-potency TCS was to be reinstituted with the same step-down approach. If there were signs of local or systemic TCS toxicity with medium-potency TCS, then patients were switched to low-potency steroids. For lesions persisting or worsening under daily treatment with medium-potency TCS, patients were treated with high-potency TCS; super-potent or very high-potency steroids were not allowed even for rescue.
Patients who met the eligibility criteria (N = 367) were randomized in a 1:1:1 ratio stratified by baseline body mass (< 30 kg, ≥ 30 kg) and region (North America, Europe) to dupilumab every 4 weeks with TCS (all patients regardless of body mass: 600 mg initial dose followed by 300 mg every 4 weeks), dupilumab every 2 weeks with TCS (body mass 15 kg to < 30 kg, 200 mg initial dose followed by 100 mg every 2 weeks; body mass ≥ 30 kg, 400 mg initial dose followed by 200 mg every 2 weeks), or matching placebo with TCS. The primary outcome was the proportion of patients with IGA 0 or 1 at week 16. Patients were enrolled starting November 17, 2017, and the data cut-off date was June 28, 2019.
In both trials, patients could enter a long-term safety study and receive open-label dupilumab.
Table 5: Details of Pivotal Studies Identified by the Sponsor
Trial characteristic | LIBERTY AD PRESCHOOL | LIBERTY AD PEDS |
|---|---|---|
Designs and populations | ||
Study design | Phase III, DB, placebo-controlled RCT | Phase III, DB, placebo-controlled RCT |
Locations | 31 sites (including Germany, Poland, UK, US) | 61 sites (including Canada [3 sites], Czech Republic, Germany, Poland, UK, US) |
Patient enrolment dates | Start date: June 30, 2020 (Part B) End date: September 16, 2021 | Start date: November 17, 2017 End date: June 28, 2019 |
Randomized (N) | N = 162
| N = 367
|
Inclusion criteria |
|
|
Exclusion criteria |
|
|
Drugs | ||
Intervention | Dupilumab SC q.4.w. + TCS:
| Dupilumab SC q.2.w. + TCS:
Dupilumab SC q.4.w. + TCS:
|
Comparator | Placebo SC q.4.w. + TCS:
| Placebo SC + TCS:
|
Study duration | ||
Screening phase | 6 weeks | 9 weeks |
Run-in phase | 2 weeks | 2 weeks |
Treatment phase | 16 weeks | 16 weeks |
Follow-up phase | 12 weeks (patients may enter LTE, up to 272 weeks) | 12 weeks (patients may enter LTE, up to 272 weeks) |
Outcomes | ||
Primary end point | Proportion of patients with an IGA score of either 0 or 1 at week 16 | Proportion of patients with an IGA score of either 0 or 1 at week 16 |
Secondary and exploratory end points | Secondary:
Exploratory:
Safety:
| Secondary:
Exploratory:
Safety:
|
Publication status | ||
Publications | Paller et al. (2022)66 | Paller et al. (2020)67 |
BSA = body surface area; CDLQI = Children’s Dermatology Life Quality Index; CGIC = Caregiver Global Impression of Change; CGID = Caregiver Global Impression of Disease; CNSQ = Caregiver-Reported Nasal Symptom Questionnaire; DB = double blind; DFI = Dermatitis Family Impact; EASI = Eczema Area and Severity Index; EASI-50 = 50% reduction in Eczema Area and Severity Index score; EASI-75 = 75% reduction in Eczema Area and Severity Index score; EASI-90 = 90% reduction in Eczema Area and Severity Index score; GISS = Global Individual Signs Score; IDQOL = Infants’ Dermatitis Quality of Life Index; IFN = interferon gamma; IGA = Investigator’s Global Assessment; IgE = immunoglobulin E; LTE = long-term extension; NRS = numeric rating scale; PASQ = Pediatric Asthma Symptom Questionnaire; PGIC = Patient Global Impression of Change; PGID = Patient Global Impression of Disease; POEM = Patient-Oriented Eczema Measure; PROMIS = Patient-Reported Outcomes Measurement Information System; q.2.w. = every 2 weeks; q.4.w. = every 4 weeks; RCT = randomized controlled trial; SAE = serious adverse event; SC = subcutaneous; SCORAD = Scoring Atopic Dermatitis; SCORAD-50 = 50% reduction in Scoring Atopic Dermatitis score from baseline; SCORAD-75 = 75% reduction in Scoring Atopic Dermatitis score from baseline; SCORAD-90 = 90% reduction in Scoring Atopic Dermatitis score from baseline; TCI = topical calcineurin inhibitor; TCS = topical corticosteroid; TEAE = treatment-emergent adverse event; VAS = visual analogue scale.
Note: Two additional reports were included: Paller et al. and Paller et al.66,67
aInadequate response was defined as inability to achieve and/or maintain remission and low disease activity despite daily treatment with medium- to high-potency TCS (with or without TCI) used for at least 28 days. Patients who have received systemic atopic dermatitis treatment within 6 months before the trial were also considered inadequate responders to topical treatments.
Source: Sponsor’s Summary of Clinical Evidence, LIBERTY AD PRESCHOOL Clinical Study Report, and LIBERTY AD PEDS Clinical Study Report.3,36,37 (Note: Details from the table have been taken from the sponsor’s Summary of Clinical Evidence.)
Figure 1: Study Design for LIBERTY AD PRESCHOOL Trial

LTE = long-term extension; Std = standardization; TCS = topical corticosteroid.
Note: The length of the screening period, including TCS Std, was not fixed but did not exceed 56 days. The length of the TCS Std period was fixed at 14 days. Moisturizers were to be applied at least twice daily during the 7 consecutive days before randomization (not including the day of randomization) and were to be used throughout the trial. At least 11 of the 14 total applications of moisturizers before randomization must have been applied for the patient to remain eligible for the trial.
Source: LIBERTY AD PRESCHOOL Clinical Study Report.37
Figure 2: Study Design for LIBERTY AD PEDS Trial
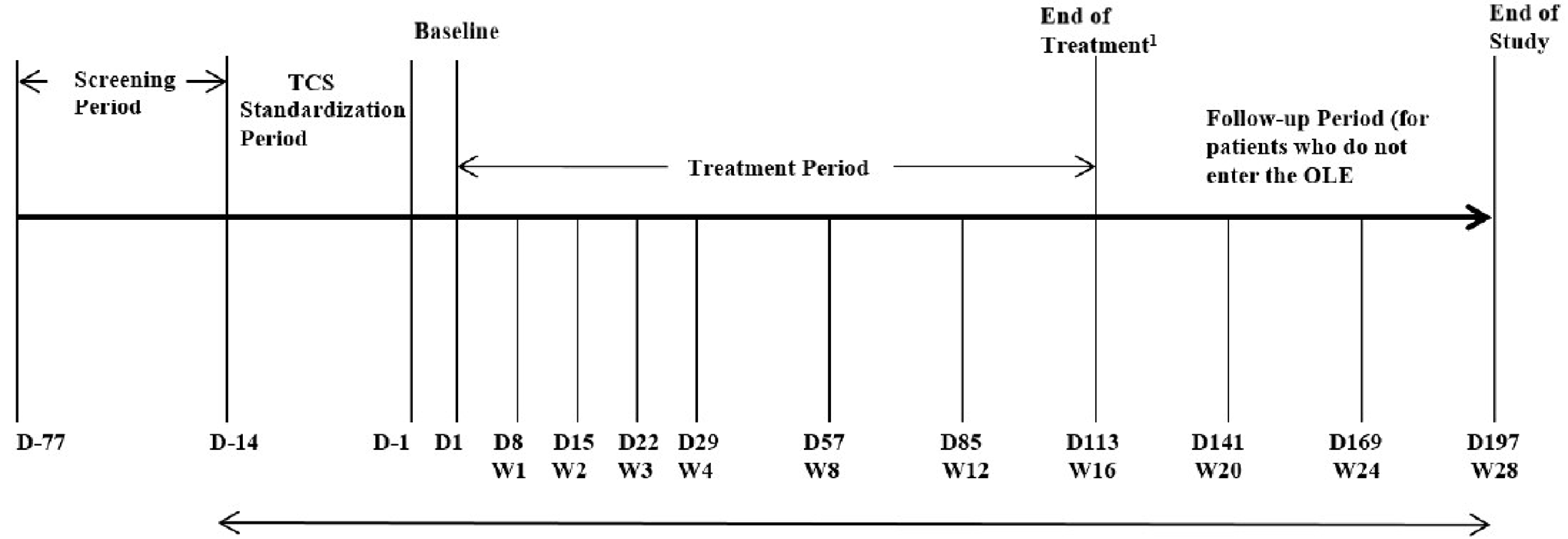
D = study day; LTE = long-term extension; OLE = open-label extension; TCS = topical corticosteroid; W = study week.
Note: The length of the screening period was not fixed, but the screening period and TCS standardization did not exceed 77 days. The length of the TCS standardization period was fixed at 14 days.
1 For patients who entered the OLE, week 16 was the end of the trial.
Source: LIBERTY AD PEDS Clinical Study Report.36
Populations
Inclusion and Exclusion Criteria
The LIBERTY AD PRESCHOOL trial included patients aged 6 months to younger than 6 years with moderate-to-severe atopic dermatitis that could not be adequately controlled with topical medications. At screening, patients must have had an IGA score of at least 3, EASI score of at least 16, and at least 10% BSA affected. Patient must have applied at least 11 out of 14 applications of a topical emollient during the 7 consecutive days before the baseline visit, and at least 11 out of 14 daily applications of low-potency TCS during the 2-week TCS standardization period leading up to the baseline visit. Patients were excluded if they had prior treatment with dupilumab, history of important side effects with low-potency TCS, or treatment with TCI or crisaborole within 2 weeks before baseline visit.
The LIBERTY AD PEDS trial included patients aged 6 years to younger than 12 years with severe atopic dermatitis that could not be adequately controlled with topical medications. At screening, patients must have had an IGA score of 4, EASI score of at least 21, and at least 15% BSA affected. Patients must have applied a stable dose of topical emollient twice daily during the 7 consecutive days before the baseline visit. Patients were excluded if they had prior treatment with dupilumab, history of important side effects with medium-potency TCS, or treatment with TCI or crisaborole within 2 weeks before baseline visit.
The key differences between the trials were the age groups and that the LIBERTY AD PEDS trial included patients with severe atopic dermatitis.
Interventions
In the LIBERTY AD PRESCHOOL trial, patients were randomized to either dupilumab every 4 weeks with TCS (fixed dose by body mass stratum of 200 mg every 4 weeks for patients 5 kg to < 15 kg; 300 mg every 4 weeks for patients 15 kg to < 30 kg) or matching placebo every 4 weeks with TCS. The assigned study drug was available in a single-use, prefilled glass syringe in doses of either 200 mg (175 mg per mL) or 300 mg (150 mg per mL) and was administered by SC injection by the investigator. Low-potency TCS treatment included hydrocortisone acetate 1% cream; if there was known hypersensitivity to hydrocortisone 1% or hydrocortisone acetate 1% cream or if neither was available, alclometasone dipropionate 0.05% cream or desonide 0.05% cream could be used.
In the LIBERTY AD PEDS trial, patients were randomized to dupilumab every 2 weeks with TCS (body mass-tiered dosing of 100 mg every 2 weeks with 200 mg initial dose for patients 15 kg to < 30 kg; 200 mg every 2 weeks with 400 mg initial dose for patients ≥ 30 kg), dupilumab every 4 weeks with TCS (300 mg every 4 weeks with 600 mg initial dose regardless of body mass), or matching placebo with TCS. Dupilumab was available in the same formats as described in the LIBERTY AD PRESCHOOL trial. Patients and caregivers could be trained to prepare and administer the study drug outside the study site during weeks in which no in-clinic visit was scheduled (for patients receiving treatment every 2 weeks) or they could have clinic staff administer the study drug in the clinic. Low-potency TCS treatment included hydrocortisone acetate 1% cream and medium-potency TCS treatment included triamcinolone acetonide 0.1% cream, fluocinolone acetonide 0.025% cream, or clobetasone butyrate 0.05%.
Rescue treatment for worsening atopic dermatitis was permitted at the discretion of the investigator and only after day 14 of the trial. Investigators were required to perform an IGA assessment before starting rescue treatment and initiate it only in patients who either had an IGA score of 4 or had intolerable symptoms. Efficacy and safety assessments were to be conducted before rescue treatment was administered. For the efficacy responder analysis, rescue treatment use was adjudicated by a blinded committee and patients who received rescue treatment were considered treatment failures. Investigators were encouraged to consider initial rescue with topical treatment and to escalate to systemic medications only for patients who did not respond adequately after at least 7 days of topical treatment. For the LIBERTY AD PRESCHOOL trial, rescue treatment included the medium-potency steroids triamcinolone acetonide 0.1% ointment, triamcinolone acetonide 0.1% cream, fluticasone propionate 0.05% cream, or fluocinolone acetonide 0.025% ointment and high-potency steroids mometasone furoate 0.1% ointment or triamcinolone acetonide 0.5% ointment. TCIs and crisaborole could also be used for rescue. For the LIBERTY AD PEDS trial, rescue treatment with high-potency steroids included mometasone furoate 0.1% ointment. Very high-potency steroids were prohibited in both trials. Patients could continue study treatment if rescue consisted of topical medications, but those who received systemic corticosteroids or systemic nonsteroid immunosuppressive drugs were discontinued permanently from the study drug.
Outcomes
A list of efficacy end points assessed in this clinical review report are provided in Table 6 and are further described in Table 7. Summarized end points are based on those included in the sponsor’s Summary of Clinical Evidence as well as any identified as important to this review according to stakeholders, for example the clinical experts, clinician groups, or patient group.
Table 6: Outcomes Summarized From Pivotal Studies Identified by the Sponsor
Outcome measure | Time point | LIBERTY AD PRESCHOOL | LIBERTY AD PEDS |
|---|---|---|---|
Proportion of patients with an IGA score of either 0 or 1 | At week 16 | Primarya | Primarya |
Proportion of patients with EASI-75 | At week 16 | Key secondarya | Key secondarya |
Percent change in EASI score | From baseline to week 16 | Key secondarya | Key secondarya |
Percent change in weekly average of daily worst itch NRS score | From baseline to week 16 | Key secondarya | Key secondarya |
Proportion of patients with improvement (reduction) of weekly average of daily worst itch NRS score ≥ 4 from baseline | At week 16 | Secondarya | Secondarya |
Proportion of patients with improvement (reduction) of weekly average of daily worst itch NRS score ≥ 3 from baseline | At week 16 | Secondarya | Secondarya |
Proportion of patients with EASI-50 | At week 16 | Secondarya | Secondarya |
Proportion of patients with EASI-90 | At week 16 | Secondarya | Secondarya |
Change in percent BSA affected by atopic dermatitis | From baseline to week 16 | Secondarya | Secondary |
Change in POEM | From baseline to week 16 | Secondarya | Secondarya |
Percent change in SCORAD | From baseline to week 16 | Secondarya | Secondarya |
Change in sleep quality NRS | From baseline to week 16 | Secondarya | NA |
Change in skin pain NRS | From baseline to week 16 | Secondarya | NA |
Change in DFI | From baseline to week 16 | Secondarya | Secondary |
Change in CDLQI (patients aged ≥ 4 years) and IDQOL (patients aged < 4 years) | From baseline to week 16 | Secondarya | Secondarya |
Change in IDQOL (patients aged < 4 years) | From baseline to week 16 | Secondarya | NA |
BSA = body surface area; CDLQI = Children’s Dermatology Life Quality Index; DFI = Dermatitis Family Impact; EASI = Eczema Area and Severity Index; EASI-50 = 50% reduction in Eczema Area and Severity Index score; EASI-75 = 75% reduction in Eczema Area and Severity Index score; EASI-90 = 90% reduction in Eczema Area and Severity Index score; IDQOL = Infants’ Dermatitis Quality of Life Index; IGA = Investigator’s Global Assessment; NA = not applicable; NRS = numeric rating scale; POEM = Patient-Oriented Eczema Measure; SCORAD = Scoring Atopic Dermatitis.
aStatistical testing for these end points was adjusted for multiple comparisons (e.g., hierarchal testing).
Source: LIBERTY AD PRESCHOOL Clinical Study Report and LIBERTY AD PEDS Clinical Study Report.36,37
Table 7: Summary of Outcome Measures and Their Measurement Properties
Outcome measure | Type | Conclusions about measurement properties | MID |
|---|---|---|---|
IGA | An investigator-completed 5-point scale that provides a global clinical assessment of atopic dermatitis severity ranging from 0 (clear) to 4 (severe) based on erythema and papulation or infiltration. A decrease in score indicates an improvement in symptoms.68,69 | No information on the validity, reliability, or responsiveness in pediatric patients with atopic dermatitis was identified. However, studies involving adult patients found this instrument to be adequately valid70 and reliable.71 | None identified. |
EASI | A scale used in clinical trials to assess the severity and extent of atopic dermatitis.72-75 Four disease characteristics (erythema, thickness, scratching, and lichenification) are assessed by the investigator and rated on a scale of 0 (absent) to 3 (severe). The surface area of atopic dermatitis involvement is assessed as a percentage by BSA of head, trunk, upper limbs, and lower limbs, then converted to a score from 0 to 6. The total EASI score ranges from 0 to 72 points with a higher score indicating more severe disease.34 | Validity: Adequate construct and content validity, estimated between the EASI and SCORAD, reports of moderate to high correlation (r = 0.84 to 0.93) between the 2 tools.72-75 Reliability: Internal consistency of the EASI was also adequate, with Spearman and Cronbach alpha values of 0.86 and 0.94, respectively. Intra- and interrater test-retest reliability kappa values of 0.76.75 Responsiveness: Responsiveness (sensitivity to change) was judged as adequate.73 | MID of 6.6 points using a 1-point improvement on the IGA as an anchor.73,75 |
Itch NRS | A tool for patients with atopic dermatitis to report the intensity of their itch. Patients rate average and maximum intensity in the past 24 hours based on an 11-point scale of 0 (no itch) to 10 (worst itch possible).76 | No information on the validity, reliability, or responsiveness in pediatric patients with atopic dermatitis was identified. | A responder is defined as having an improvement of 3 to 4 points on the NRS when using the EASI and IGA as anchors.76 |
BSA affected by atopic dermatitis | Assessed for each section of the body: head, torso, lower extremities, and upper extremities.37 The proportion assigned to different body regions varies by age in young children: from 14% to 18% for the head, 36% for the torso, from 28% to 32% for the lower extremities, and 18% for the upper extremities.37 | No information on the validity, reliability, or responsiveness in pediatric patients with atopic dermatitis was identified. | None identified. |
POEM | A 7-item (dryness, itching, flaking, cracking, sleep loss, bleeding, and weeping) questionnaire used in clinical trials to assess disease symptoms in children and adults with eczema. Items are assessed using a 5-point scale: 0 indicates no days, 1 indicates 1 to 2 days, 2 indicates 3 to 4 days, 3 indicates 5 to 6 days, and 4 indicates every day. The maximum total score is 28, where a high score indicates more severe disease (0 to 2 for clear or almost clear; 3 to 7 for mild eczema; 8 to 16 for moderate eczema; 17 to 24 for severe eczema; 25 to 28 for very severe eczema).77 | Validity: Moderate concurrent validity (Spearman = 0.56) was detected in adults. Good convergent validity when compared to the Dermatology Life Quality Index questionnaire, but moderate to weak when compared to the EASI and NRS. Poor discriminant validity in predicting self-reported global severity. Poor to moderate content validity as a measurement of clinical signs of atopic dermatitis in children.75,77 Reliability: Good reliability (ICC = 0.90)78 Responsiveness: No information on responsiveness in pediatric patients with atopic dermatitis was identified. | The overall mean MID of the POEM was 3.4 points (SD = 4.8), using a 1-point improvement on the IGA as an anchor.73 A recent study79 suggested the following thresholds to be employed to interpret MID of POEM in children: a score of 3 to 3.9 indicates a probably clinically important change; a score ≥ 4 indicates a very likely clinically important change. |
SCORAD | A tool used in clinical research to assess the extent and severity of atopic dermatitis. Percent BSA is used. The intensity of the disease is measured by assigning values to 5 types of lesions and dryness (erythema, swelling, oozing, excoriation, and lichenification). The maximum possible total score of SCORAD is 103, where a higher score indicates more severe disease. | Validity: Valid and reliable for the objective assessment of eczema clinical signs.80 Two systematic reviews found excellent agreement with global assessments of disease severity.75,81 Content validity was deemed adequate, good construct validity (Spearman rank correlation coefficient ranging from 0.53 to 0.92) and internal consistency. Reliability: Interobserver reliability was adequate with several measurements of ICC from 0.84 to 0.99. Intraobserver reliability (test-retest) was unclear.75 Responsiveness: Sensitivity to change was considered adequate.75 | |
Sleep quality NRS | A sleep diary is completed by the parent or caregiver and includes 2 questions assessing the caregiver’s sleep, and 6 questions assessing the child’s sleep. It is measured using an 11-point NRS in which 0 is the worst possible sleep and 10 is the best possible sleep. | No information on the validity, reliability, or responsiveness in pediatric patients with atopic dermatitis was identified. | None identified. |
Skin pain NRS | An 11-point NRS in which 0 is no pain while 10 is worst pain imaginable to describe the worst level of skin pain in the past 24 hours during a 1-week interval.82,83 | Validity: High content and construct validity.82 Reliability: Considered highly reliable (ICC = 0.753 to 0.845).82 Responsiveness: Considered responsive.82 | Anchor-based estimates of the meaningful change estimation (minimal, moderate, and large) for skin pain NRS were a 4.0-point change, also equivalent to a moderate degree of change in adult patients with moderate-to-severe atopic dermatitis.82 |
DFI | An atopic dermatitis-specific, self-administered, 10-item questionnaire designed to assess the impact of disease on the quality of life of families of children affected by disease based on a 1-week recall. Responses are scored on a 4-point Likert scale (from 0 to 3). The total score ranges from 0 to 30 with higher scores indicating greater impairment in family quality of life.84,85 | Validity: Good construct validity.86 Reliability: Good test-retest reliability (r = 0.95) and good internal consistency with a Cronbach alpha value of (0.85 to 0.90).86 Responsiveness: No information on responsiveness in pediatric patients with atopic dermatitis was identified. | None identified. |
CDLQI | A questionnaire completed by the child (aged 3 years to 16 years) designed to measure the impact of any skin disease on the quality of life with a recall period of 7 days.87,88 It consists of 10 questions asking about the impact of a skin disease on the life of the affected child, including symptoms, embarrassment, friendships, clothes, playing, sports, bullying, sleep, and impact of treatment. Each response is rated on a 4-point Likert scale (from 0 to 3). The total score ranges from 0 to 30 with higher scores indicating a greater degree of impairment in HRQoL.88 | Validity: Adequate concurrent validity vs. Cardiff Acne Disability Index and the Childhood Atopic Dermatitis Impact Scale. Good convergent construct validity and divergent construct validity.87 Reliability: Good internal consistency (examined in 6 studies) with Cronbach alpha values ranging from 0.82 to 0.92. Test-retest reliability is adequate, with Spearman rank order correlation coefficient calculated in 4 studies (range, 0.74 to 0.97). One study calculated an ICC of 0.80.87 Responsiveness: Good responsiveness to change was found in studies using Wilcoxon rank sum test and repeated measures ANOVA.87 | One study89 conducted among 211 children and adolescents, using SD reported for the mean total CDLQI score reported for children with psoriasis, estimated the MID of the CDLQI in these patients to be 2.5. Another study90 in adolescents (aged 12 years to < 18 years) with moderate-to-severe atopic dermatitis indicated a within-person change of 6 to 8 points to be a reasonable responder threshold for clinically meaningful change. |
IDQOL | A questionnaire designed to measure the impact of the skin disease on the quality of life of infants and preschool children aged < 4 years.91 It consists of 10 questions that examine the impact of the disease on the life of the affected child and includes, but is not limited to, the following areas: mood, sleep, and daily activities. Each question is rated on a 4-point Likert scale (from 0 to 3). The total score ranges from 0 to 30 with higher scores indicating worse quality of life. | Validity: High-quality evidence for adequate content validity and construct validity.92 Reliability: Acceptable internal consistency with a Cronbach alpha value of 0.89. Adequate test-retest reliability, with the Spearman rank order correlation coefficient (range, 0.74 to 0.97).92 Responsiveness: No information on responsiveness in pediatric patients with atopic dermatitis was identified. | None identified. |
ANOVA = analysis of variance; BSA = body surface area; CDLQI = Children’s Dermatology Life Quality Index; DFI = Dermatitis Family Impact; EASI = Eczema Area and Severity Index; HRQoL = health-related quality of life; ICC = intraclass correlation coefficient; IDQOL = Infants’ Dermatitis Quality of Life Index; IGA = Investigator’s Global Assessment; MID = minimal important difference; NRS = numeric rating scale; POEM = Patient-Oriented Eczema Measure; SCORAD = Scoring Atopic Dermatitis; SD = standard deviation.
Incidence and seriousness of AEs, withdrawals due to AEs, and deaths were reported for the safety analysis set during the trials. AEs, SAEs, and protocol-defined notable harms were described based on preferred term and associated system organ class. Notable harms included those that were prespecified by the sponsor and confirmed by the clinical experts consulted by CADTH, such as anaphylactic reactions, hypersensitivity, helminthic infections, conjunctivitis, blepharitis, keratitis, eosinophilia, facial erythema, and pain with administration.
Statistical Analysis
Details of the statistical analysis of efficacy end points are summarized in Table 8.
Sample Size and Power Calculation
For the LIBERTY AD PRESCHOOL trial, it was estimated that a sample size of 160 patients (80 patients per treatment group), at the 2-sided 5% significance level using Fisher exact test, would provide an 88% power to detect a treatment difference of 21.4% between the dupilumab and placebo groups in the percentage of patients who experience an IGA score of 0 to 1 at week 16 and a 99% power to detect a treatment difference of 42.9% in the percentage of patients who experience an EASI-75 response at week 16. The assumptions used for the above power calculations were based on results from patients in the LIBERTY AD PEDS study.
Table 8: Statistical Analysis of Efficacy End Points From Pivotal Studies Identified by the Sponsor
End point | Statistical model | Adjustment factors | Handling of missing data | Sensitivity analyses |
|---|---|---|---|---|
LIBERTY AD PRESCHOOL | ||||
Proportion of patients with IGA 0 to 1 at week 16 | CMHa | Randomization stratab | Nonrespondersc MId | Posthoc sensitivity analyses using all observed values regardless of rescue treatment use, and LOCF method after first rescue treatment |
Proportion of patients with EASI-75 at week 16 | CMHa | Randomization stratab | Nonrespondersc MId | Posthoc sensitivity analyses using all observed values regardless of rescue treatment use, and LOCF method after first rescue treatment |
Percent change in EASI score from baseline to week 16 | ANCOVA | Treatment, randomization strata,b and baseline value | WOCFe MId | Posthoc sensitivity analyses using all observed values regardless of rescue treatment use, and LOCF method after first rescue treatment |
Percent change from baseline to week 16 in weekly average of daily worst itch NRS score | ANCOVA | Treatment, randomization strata,b and baseline value | WOCFe MId | Posthoc sensitivity analyses using all observed values regardless of rescue treatment use, and LOCF method after first rescue treatment |
Proportion of patients with improvement (reduction) of weekly average of daily worst itch NRS score ≥ 4 from baseline | CMH | Randomization stratab | Nonrespondersc MId | Posthoc sensitivity analyses using all observed values regardless of rescue treatment use, and LOCF method after first rescue treatment |
Proportion of patients with improvement (reduction) of weekly average of daily worst itch NRS score ≥ 3 from baseline | CMH | Randomization stratab | Nonrespondersc MId | None |
Proportion of patients with EASI-50 at week 16 | CMH | Randomization stratab | Nonrespondersc MId | None |
Proportion of patients with EASI-90 at week 16 | CMH | Randomization stratab | Nonrespondersc MId | None |
Change from baseline in percent BSA affected | ANCOVA | Treatment, randomization stratab, and baseline value | WOCFe MId | None |
Change from baseline to week 16 in POEM | ANCOVA | Treatment, randomization stratab, and baseline value | WOCFe MId | None |
Percent change from baseline to week 16 in SCORAD | ANCOVA | Treatment, randomization stratab, and baseline value | WOCFe MId | None |
Change from baseline in sleep quality NRS | ANCOVA | Treatment, randomization stratab, and baseline value | WOCFe MId | None |
Change from baseline in skin pain NRS | ANCOVA | Treatment, randomization stratab, and baseline value | WOCFe MId | None |
Change from baseline in DFI | ANCOVA | Treatment, randomization stratab, and baseline value | WOCFe MId | None |
Change from baseline to week 16 in CDLQI | ANCOVA | Treatment, randomization stratab, and baseline value | WOCFe MId | None |
Change from baseline to week 16 in IDQOL | ANCOVA | Treatment, randomization stratab, and baseline value | WOCFe MId | None |
LIBERTY AD PEDS | ||||
Proportion of patients with IGA 0 to 1 at week 16 | CMH | Randomization stratab | Nonrespondersc | LOCF after rescue treatment use or study withdrawal, and mFAS and PP analyses |
Proportion of patients with EASI-75 at week 16 | CMH | Randomization stratab | Nonrespondersc | LOCF after rescue treatment use or study withdrawal, and mFAS and PP analyses |
Percent change in EASI score from baseline to week 16 | ANCOVA | Treatment, randomization strata,b and baseline value | MIf | MI using all observed data regardless if rescue treatment used or data collected after treatment withdrawal, and LOCF and WOCF after rescue treatment use |
Proportion of patients with EASI-50 at week 16 | CMH | Randomization stratab | Nonrespondersc | None |
Percent change from baseline to week 16 in weekly average of daily worst itch NRS score | ANCOVA | Treatment, randomization strata,b and baseline value | MIf | MI using all observed data regardless if rescue treatment used or data collected after treatment withdrawal, and LOCF and WOCF after rescue treatment use |
Proportion of patients with improvement (reduction) of weekly average of daily worst itch NRS score ≥ 4 from baseline at week 16 | CMH | Randomization stratab | Nonrespondersc | MI using all observed data regardless if rescue treatment used or data collected after treatment withdrawal, and LOCF and WOCF after rescue treatment use |
Proportion of patients with improvement (reduction) of weekly average of daily worst itch NRS score ≥ 3 from baseline at week 16 | CMH | Randomization stratab | Nonrespondersc | None |
Proportion of patients with EASI-90 at week 16 | CMH | Randomization stratab | Nonrespondersc | None |
Change from baseline to week 16 in POEM | ANCOVA | Treatment, randomization strata,b and baseline value | MIf | None |
Change from baseline to week 16 in CDLQI | ANCOVA | Treatment, randomization strata,b and baseline value | MIf | None |
Percent change from baseline to week 16 in SCORAD | ANCOVA | Treatment, randomization strata,b and baseline value | MIf | None |
ANCOVA = analysis of covariance; BSA = body surface area; CDLQI = Children’s Dermatology Life Quality Index; CMH = Cochran-Mantel-Haenszel; DFI = Dermatitis Family Impact; EASI = Eczema Area and Severity Index; EASI-50 = 50% reduction in Eczema Area and Severity Index score; EASI-75 = 75% reduction in Eczema Area and Severity Index score; EASI-90 = 90% reduction in Eczema Area and Severity Index score; IDQOL = Infants’ Dermatitis Quality of Life Index; IGA = Investigator’s Global Assessment; LOCF = last observation carried forward; mFAS = modified full analysis set; MI = multiple imputation; NRS = numeric rating scale; POEM = Patient-Oriented Eczema Measure; PP = per protocol; SCORAD = Scoring Atopic Dermatitis; WOCF = worst observation carried forward.
aDue to the small number of patients, those in the Europe region, baseline body mass < 15 kg, and IGA 3 stratum were combined with those in the Europe region, baseline body mass ≥ 15 kg, and IGA 3 stratum.
bRandomization strata included baseline body mass group (LIBERTY AD PRESCHOOL: 5 kg to < 15 kg, 15 kg to < 30 kg; LIBERTY AD PEDS: < 30 kg, ≥ 30 kg), disease severity (IGA 3, IGA 4), and region (North America, Europe).
cPatients with missing data due to patient withdrawal (consent, AE, lack of efficacy), use of rescue treatment, or missing data at week 16 were considered nonresponders.
dPatients with missing data due to other reasons were imputed using MI methods. MI methods involved data being imputed 40 times to generate 40 complete datasets. The monotone missing pattern was induced by Markov chain Monte Carlo method. After the first missing visit, subsequent missing data were imputed using the regression method for continuous variables and using the logistic regression method for categorical variables.
ePatients with missing data due to patient withdrawal (consent, AE, lack of efficacy) or use of rescue treatment were imputed using WOCF methods.
fPatients with missing data due to use of rescue medication were imputed using MI methods.
Source: LIBERTY AD PRESCHOOL Clinical Study Report and LIBERTY AD PEDS Clinical Study Report.36,37
At the time the LIBERTY AD PEDS trial was designed, there were no data available on the effects of dupilumab in pediatric patients. The assumptions used for the power calculations were estimated based on results from the R668-AD-1224 study (phase III combination study with TCS for adults with atopic dermatitis) and R668-AD-1021 study (a phase IIb dose ranging study in adults with atopic dermatitis) for patients with an IGA score of 4 at baseline. For the primary outcome (IGA 0 or 1), it was initially estimated that with 80 patients per group, at the 2-sided 5% significance level, would provide 97% power to detect a 23% treatment difference between the dupilumab every 2 weeks and placebo groups and would provide 87% power to detect a 17% treatment difference between the dupilumab every 4 weeks and placebo groups. For the key secondary outcome of EASI-75 at week 16, 80 patients per group would provide 99% power to detect a 51% treatment difference between the dupilumab every 2 weeks and placebo groups and would provide 99% power to detect a 45% treatment difference between the dupilumab every 4 weeks and placebo groups.
Due to an inadvertent operational error, 68 patients were potentially unblinded (30 patients in the every 2 weeks group and 19 patients in each of the every 4 weeks and placebo groups) in the LIBERTY AD PEDS trial. These patients were excluded from the mFAS (supportive analyses). Additional patients were enrolled in the study to maintain study balance and power and to ensure that the original number of blinded patients for all treatment groups was available for sensitivity analyses that excluded the potentially unblinded patients.
Statistical Testing and Data Imputation Methods
In both trials, the proportion of patients with an IGA score of 0 or 1 at week 16 was the primary end point and the proportion of patients with EASI-75 at week 16 was a key secondary end point for the US and its reference markets. For Europe and European reference markets, the IGA and EASI-75 outcomes were co-primary end points.
In the LIBERTY AD PRESCHOOL trial, primary and secondary end points were analyzed using the full analysis set (FAS). The primary outcome of percentage of patients with an IGA score of 0 or 1 at week 16 used the Cochran-Mantel-Haenszel test adjusted by randomization strata (baseline body mass group [5 kg to < 15 kg, 15 kg to < 30 kg], baseline disease severity [IGA 3, IGA 4], and region [North America, Europe]). Similar procedures were used for the key secondary outcome of percentage of patients with EASI-75 at week 16. If a patient withdrew from the study or discontinued due to an AE or lack of efficacy, the patient was considered a nonresponder for the time points after withdrawal. If a patient used a rescue treatment, the patient was considered a nonresponder from when the rescue treatment was used. If the patient had the value missing at week 16 due to any other reasons, the data were imputed using multiple imputation based on all observed values. The underlying continuous (e.g., EASI) or categorical variables (e.g., IGA) were imputed 40 times to generate 40 complete datasets. Multiple imputation using the monotone missing pattern was induced by Markov chain Monte Carlo method in a multiple imputation procedure using seed number 12345. The missing data at subsequent visits were imputed using the regression method for the monotone pattern with seed number 54321 with adjustment for covariates including treatment groups, randomization strata, and relevant baseline variables. For the categorical variable, a logistic regression under monotone option was used. Binary secondary efficacy end points were analyzed using the same approaches used for the analysis of the primary end point. Continuous end points (e.g., EASI, worst itch NRS score) were analyzed using an analysis of covariance (ANCOVA) model with treatment, randomization strata, baseline disease severity, region, and relevant baseline values included in the model as the primary analysis method. Missing data for continuous end points were imputed by the pattern-mixture approach (multiple imputation-worst observation carried forward [WOCF] method). The WOCF approach was used for data after rescue or missing due to withdrawn consent, AE, and lack of efficacy. Missing data were imputed by postbaseline WOCF if there was at least 1 nonmissing postbaseline value or by baseline value if there was no postbaseline value. The multiple imputation approach was used for missing data due to other reasons as described for the primary end point.
In the LIBERTY AD PEDS trial, primary and secondary end points were analyzed using the FAS. The primary outcome of percentage of patients with an IGA score of 0 or 1 at week 16 and key secondary outcome of percentage of patients with EASI-75 at week 16 used the Cochran-Mantel-Haenszel test adjusted by randomization strata. A patient was considered a nonresponder if they withdrew from the study, used a rescue treatment, or had a missing value at week 16. All binary and continuous secondary end points were analyzed using the same approaches as outlined for the LIBERTY AD PRESCHOOL trial. The ANCOVA model used treatment, randomization strata, and relevant baseline variable as covariates.
Multiple Testing Procedure
A hierarchical procedure was used to control the overall type I error rate at 0.05 for the primary and secondary end points of dupilumab versus placebo. Each hypothesis was formally tested only if the preceding test was significant at the 2-sided 0.05 significance level. The hierarchical testing order for the 2 trials is summarized in Table 9.
Table 9: Hierarchical Testing in Pivotal Studies Identified by the Sponsor
Outcome level | End point | Testing order | ||
|---|---|---|---|---|
LIBERTY AD PRESCHOOL | ||||
Outcome level | End point | Testing order: Dupilumab q.2.w. vs. placebo | ||
Primary | Proportion of patients with IGA 0 to 1 at week 16 | 1 | ||
Key secondary | Proportion of patients with EASI-75 at week 16 | 2 | ||
Key secondary | Percent change in EASI score from baseline to week 16 | 3 | ||
Key secondary | Percent change from baseline to week 16 in weekly average of daily worst itch NRS score | 4 | ||
Secondary | Proportion of patients with improvement of weekly average of daily worst itch NRS score ≥ 4 from baseline | 5 | ||
Secondary | Proportion of patients with improvement of weekly average of daily worst itch NRS score ≥ 3 from baseline | 6 | ||
Secondary | Proportion of patients with EASI-50 at week 16 | 7 | ||
Secondary | Proportion of patients with EASI-90 at week 16 | 8 | ||
Secondary | Change from baseline in percent BSA affected by atopic dermatitis | 9 | ||
Secondary | Change from baseline to week 16 in POEM | 10 | ||
Secondary | Percent change from baseline to week 16 in SCORAD | 11 | ||
Secondary | Change from baseline in patient’s sleep quality NRS | 12 | ||
Secondary | Change from baseline in patient’s skin pain NRS | 13 | ||
Secondary | Change from baseline in DFI | 14 | ||
Secondary | Change from baseline to week 16 in CDLQI | 15 | ||
Secondary | Change from baseline to week 16 in IDQOL | 16 | ||
LIBERTY AD PEDS | ||||
Outcome level | End point | Testing order: dupilumab q.2.w. vs. placebo | Testing order: dupilumab q.4.w. vs. placebo | |
Primary | Proportion of patients with IGA 0 to 1 at week 16 | 1 | 7 | |
Key secondary | Proportion of patients with EASI-75 at week 16 | 2 | 8 | |
Key secondary | Percent change in EASI score from baseline to week 16 | 3 | 9 | |
Secondary | Proportion of patients with EASI-50 at week 16 | 4 | 10 | |
Key secondary | Percent change from baseline to week 16 in weekly average of daily worst itch NRS score | 5 | 11 | |
Secondary | Proportion of patients with improvement of weekly average of daily worst itch NRS score ≥ 4 from baseline at week 16 | 6 | 12 | |
Secondary | Proportion of patients with improvement of weekly average of daily worst itch NRS score ≥ 3 from baseline at week 16 | 13 | 15 | |
Secondary | Proportion of patients with EASI-90 at week 16 | 14 | 16 | |
Secondary | Change from baseline to week 16 in POEM | 17 | 20 | |
Secondary | Change from baseline to week 16 in CDLQI | 18 | 21 | |
Secondary | Percent change from baseline to week 16 in SCORAD | 19 | 22 | |
BSA = body surface area; CDLQI = Children’s Dermatology Life Quality Index; DFI = Dermatitis Family Impact; EASI = Eczema Area and Severity Index; EASI-50 = 50% reduction in Eczema Area and Severity Index score; EASI-75 = 75% reduction in Eczema Area and Severity Index score; EASI-90 = 90% reduction in Eczema Area and Severity Index score; IDQOL = Infants’ Dermatitis Quality of Life Index; IGA = Investigator’s Global Assessment; NRS = numeric rating scale; POEM = Patient-Oriented Eczema Measure; q.2.w. = every 2 weeks; q.4.w. = every 4 weeks; SCORAD = Scoring Atopic Dermatitis; vs. = versus.
Source: LIBERTY AD PRESCHOOL Clinical Study Report and LIBERTY AD PEDS Clinical Study Report.36,37
Subgroup Analyses
In the LIBERTY AD PRESCHOOL trial, prespecified subgroups for the primary and key secondary end points were analyzed based on the FAS. These included: age group, sex, ethnicity, race, duration of atopic dermatitis, body mass index, body mass group, age of disease onset, family history of atopic disease, region, baseline EASI, baseline worst itch, percent BSA, baseline SCORAD, previous use of cyclosporine, previous use of systemic immunosuppressants (systemic corticosteroids and systemic nonsteroidal immunosuppressant for atopic dermatitis), history of asthma, history of allergic rhinitis, and history of food allergies. Primary and secondary end points were analyzed in a similar manner as the main analysis for the severe atopic dermatitis subgroup (IGA 4) and nominal P values were provided. The sponsor noted that subgroup analyses for age group, ethnicity, duration of atopic dermatitis, baseline SCORAD score, and previous usage of cyclosporine were not conducted because subgroups were too small for meaningful conclusions to be drawn.
In the LIBERTY AD PEDS trial, prespecified subgroups for the primary and key secondary end points were analyzed based on the FAS. These included: age group, sex, ethnicity, race, duration of atopic dermatitis, age of disease onset, family history of atopic disease, baseline body mass group, body mass index, region, baseline severe or moderate-to-severe EASI, baseline worst itch, percent BSA, baseline SCORAD, previous use of cyclosporine, previous use of methotrexate, previous use of azathioprine, previous use of systemic immunosuppressants for atopic dermatitis, history of asthma, history of nasal polyps, history of allergic rhinitis, and history of food allergies. Subgroup analyses were analyzed in a similar manner as the main analysis. Interactions between the subgroups and treatment groups were tested using the logistic regression model for the categorical end points and using the ANCOVA model for the continuous end points. The model included randomization strata, treatment group, subgroup, treatment by randomization strata interaction, and treatment by subgroup interaction as factors. P values for the interaction term were reported and interaction effects were considered as significant if the P value was greater than 0.1. The sponsor noted that subgroup analyses for Hispanic or Latino patients, duration of atopic dermatitis of less than 5 years, patients aged 5 years or older at onset of atopic dermatitis, baseline EASI score of less than 25, baseline EASI score of less than 20, BSA of 10% to 30%, SCORAD score of less than 50, previous use of methotrexate for atopic dermatitis, previous use of azathioprine, and history of nasal polyps were too small for meaningful conclusions to be drawn.
The sponsor’s systematic review protocol listed 4 subgroups of interest: disease severity (e.g., moderate, severe), number of previous topical prescription therapies, previous immunosuppressant treatment (yes, no), and age (6 months to < 6 years, 6 years to < 12 years).
Sensitivity Analyses
In the LIBERTY AD PRESCHOOL trial, a sensitivity analysis on the co-primary end points was planned using the tipping point analysis method to assess the robustness of primary analysis results, but was not conducted because multiple imputation methods were implemented for only 1 patient.
In the LIBERTY AD PEDS trial, 2 sensitivity analyses were planned and used the FAS. In the first analysis, a postbaseline last observation carried forward approach after censoring for rescue treatment use or study withdrawal to determine a patient’s status at week 16 assessed the robustness of the primary efficacy analysis with regards to handling of missing data. In the second, all observed data were included for analysis, regardless of if rescue treatment was used or data were collected after withdrawal from study treatment. Patients with missing values were counted as nonresponders. Additional sensitivity analyses with the mFAS (due to potential unblinding of 68 patients) and per-protocol populations were used to analyze the primary and key secondary (i.e., IGA and EASI-75) end points.
Analysis Populations
Descriptions of the analysis populations used in the pivotal trials are summarized in Table 10.
Table 10: Analysis Populations of Pivotal Studies Identified by the Sponsor
Study | Population | Definition | Application |
|---|---|---|---|
LIBERTY AD PRESCHOOL | FAS | All randomized patients | All efficacy analyses |
SAS | All randomized patients who receive ≥ 1 dose of study drug and were analyzed as treated | Treatment compliance and administration and all clinical safety variables | |
LIBERTY AD PEDS | FAS | All randomized patients | All efficacy analyses |
mFAS | All randomized patients but excluded potentially unblinded patients | Primary end point and selected secondary end points were evaluated as sensitivity analyses | |
PP | All patients in the FAS except those who were excluded due to major protocol violations | Primary end point and selected secondary end points | |
SAS | All randomized patients who receive ≥ 1 dose of study drug and were analyzed as treated | Treatment compliance and administration and all clinical safety variables |
FAS = full analysis set; mFAS = modified full analysis set; PP = per protocol; SAS = safety analysis set.
Source: Sponsor’s Summary of Clinical Evidence.3 (Note: Details from the table have been taken from the sponsor’s Summary of Clinical Evidence.)
Results
Patient Disposition
Patient disposition is summarized in Table 11.
In the LIBERTY AD PRESCHOOL trial, 197 individuals were screened, of which 162 patients met the eligibility criteria and were randomized to either the dupilumab or placebo group. One patient in the placebo group was randomized in error but did not receive study drug and was not included in the safety analysis set. In total, 83 (100%) patients in the dupilumab group and 76 (96.2%) patients in the placebo group completed the week 16 end-of-treatment visit. Three patients discontinued the study before week 16 and were from the placebo group.
In the LIBERTY AD PEDS trial, 474 individuals were screened, of which 367 patients met the eligibility criteria and were randomized into 1 of 3 treatment groups. Five of the randomized patients were not treated (3 patients in the combined dupilumab group and 2 patients in the placebo group) and were included in the FAS. In total, 237 (97.1%) patients in the combined dupilumab group and 114 (92.7%) patients in the placebo group completed treatment. Thirteen patients discontinued the study (7 patients in the combined dupilumab group and 6 patients in the placebo group) and reasons were balanced across treatment groups.
Table 11: Summary of Patient Disposition From Pivotal Studies
Patient disposition | LIBERTY AD PRESCHOOL | LIBERTY AD PEDS | |||
|---|---|---|---|---|---|
Dupilumab 200 mg or 300 mg q.4.w. + TCS | Placebo + TCS | Dupilumab 300 mg q.4.w. + TCS | Dupilumab 100 mg or 200 mg q.2.w. + TCS | Placebo + TCS | |
Screened, N | 197 | 474 | |||
Reason for screening failure, n (%) | 35 (17.8) | 107 (22.6) | |||
Eligibility criteria not met | 27 (13.7) | 79 (16.7) | |||
Patient withdrew consent | 7 (3.6) | 8 (1.7) | |||
Lost to follow-up | 1 (0.5) | 1 (0.2) | |||
Adverse event | 0 (0.0) | 1 (0.2) | |||
Other | 0 (0.0) | 18 (3.8) | |||
Randomized, N | 83 | 79 | 122 | 122 | 123 |
Discontinued from study, n (%) | 0 (0.0) | 3 (3.8) | 3 (2.5) | 4 (3.3) | 6 (4.9) |
Reason for discontinuation, n (%) | |||||
Patient withdrew consent | 0 (0.0) | 1 (1.3) | 1 (0.8) | 2 (1.6) | 5 (4.1) |
Patient randomized in error | 0 (0.0) | 1 (1.3) | 1 (0.8) | 1 (0.8) | 1 (0.8) |
Lost to follow-up | 0 (0.0) | 1 (1.3) | 0 (0.0) | 0 (0.0) | 0 (0.0) |
Physician or investigator decision | 0 (0.0) | 0 (0.0) | 1 (0.8) | 1 (0.8) | 0 (0.0) |
FAS, n (%) | 83 (100) | 79 (100) | 122 (100) | 122 (100) | 123 (100) |
mFAS, n (%) | NA | NA | 103 (84.4) | 92 (75.4) | 104 (84.6) |
PP, n (%) | NA | NA | || |||||| | || |||||| | || |||||| |
SAS, n (%) | 83 (100) | 78 (98.7) | 120 (98.4) | 122 (100) | 120 (97.6) |
FAS = full analysis set; mFAS = modified full analysis set; NA = not applicable; PP = per protocol; q.2.w. = every 2 weeks; q.4.w. = every 4 weeks; SAS = safety analysis set; TCS = topical corticosteroid.
Source: Sponsor’s Summary of Clinical Evidence, LIBERTY AD PRESCHOOL Clinical Study Report, and LIBERTY AD PEDS Clinical Study Report.3,36,37 (Note: Details from the table have been taken from the sponsor’s Summary of Clinical Evidence.)
Baseline Characteristics
Baseline patient characteristics and medical history are summarized in Table 12. The baseline characteristics outlined in the table are limited to those that are most relevant to this review or were likely to impact the outcomes or interpretation of the study results.
Overall, most characteristics were balanced among treatment groups in either trial. In the LIBERTY AD PRESCHOOL trial, the mean age of patients was 3.8 years, there were fewer females (38.9%) than males (61.1%), and the mean EASI score of patients was 34.1. In the LIBERTY AD PEDS trial, the mean age of patients was 8.5 years, males and females were evenly balanced, and the mean EASI score of patients was ||||. There was an imbalance in race between the dupilumab and placebo groups, and more patients in the placebo group had previously received methotrexate, while more patients in the dupilumab group had previously received systemic corticosteroids for atopic dermatitis.
Table 12: Summary of Baseline Characteristics From Pivotal Studies
Characteristic | LIBERTY AD PRESCHOOL | LIBERTY AD PEDS | |||
|---|---|---|---|---|---|
Dupilumab 200 mg or 300 mg q.4.w. + TCS N = 83 | Placebo + TCS N = 79 | Dupilumab 300 mg q.4.w. + TCS N = 122 | Dupilumab 100 mg or 200 mg q.2.w. + TCS N = 122 | Placebo + TCS N = 123 | |
Demographics and patient characteristics — FAS | |||||
Age (years) | |||||
Mean (SD) | 3.91 (1.23) | 3.78 (1.26) | 8.5 (1.74) | 8.5 (1.68) | 8.3 (1.76) |
Median (min, max) | 4.17 (0.8, 5.8) | 3.83 (0.6, 5.9) | ||| ||||| ||||| | ||| ||||| ||||| | ||| ||||| ||||| |
6 months to < 2 years, n (%) | 6 (7.2) | 5 (6.3) | NA | NA | NA |
≥ 2 years and < 6 years, n (%) | 77 (92.8) | 74 (93.7) | NA | NA | NA |
6 years to < 9 years, n (%) | NA | NA | || |||||| | || |||||| | || |||||| |
9 years to < 12 years, n (%) | NA | NA | || |||||| | || |||||| | || |||||| |
Sex, n (%) | |||||
Male | 44 (53.0) | 55 (69.6) | 57 (46.7) | 65 (53.3) | 61 (49.6) |
Female | 39 (47.0) | 24 (30.4) | 65 (53.3) | 57 (46.7) | 62 (50.4) |
Race, n (%) | |||||
White | 58 (69.9) | 53 (67.1) | 89 (73.0) | 88 (72.1) | 77 (62.6) |
Black | 14 (16.9) | 16 (20.3) | 19 (15.6) | 20 (16.4) | 23 (18.7) |
Asian | 6 (7.2) | 4 (5.1) | 5 (4.1) | 10 (8.2) | 13 (10.6) |
Hawaiian or Other Pacific Islander | 0 (0.0) | 1 (1.3) | 0 (0.0) | 0 (0.0) | 0 (0.0) |
Not reported | 2 (2.4) | 1 (1.3) | 1 (0.8) | 2 (1.6) | 1 (0.8) |
Other | 3 (3.6) | 4 (5.1) | 8 (6.6) | 2 (1.6) | 9 (7.3) |
Weight (kg) | |||||
Mean (SD) | 17.08 (4.41) | 16.66 (3.63) | 31.0 (9.40) | 32.1 (10.79) | 31.5 (10.82) |
5 to < 15, n (%) | 26 (31.3) | 25 (31.6) | NA | NA | NA |
15 to 30, n (%) | 57 (68.7) | 54 (68.4) | 61 (50.0) | 63 (51.6) | 61 (49.6) |
≥ 30, n (%) | NA | NA | 61 (50.0) | 59 (48.4) | 62 (50.4) |
Age at disease onset, n (%) | |||||
< 6 months | 50 (60.2) | 57 (72.2) | NA | NA | NA |
≥ 6 months | 33 (39.8) | 22 (27.8) | NA | NA | NA |
Age at chronic diagnosis, n (%) | |||||
< 5 years | NA | NA | ||| |||||| | ||| |||||| | ||| |||||| |
6 years to 11 years | NA | NA | | ||||| | | ||||| | | ||||| |
Unsure | NA | NA | | ||||| | ||| | | ||||| |
Duration of atopic dermatitis (years) | |||||
Mean (SD) | 3.4 (1.33) | 3.4 (1.30) | 7.4 (2.44) | 7.2 (2.31) | 7.2 (2.15) |
Median (min, max) | 3.6 (0, 6) | 3.4 (0, 6) | ||| ||| ||| | ||| ||| ||| | ||| ||| ||| |
Baseline IGA (range, 0 to 4) | |||||
IGA = 3 | 20 (24.1) | 17 (21.5) | | ||||| | ||| | ||| |
IGA = 4 | 63 (75.9) | 62 (78.5) | ||| |||||| | ||| ||||| | ||| ||||| |
Baseline EASI (range, 0 to 72) | |||||
Mean (SD) | 35.1 (13.88) | 33.1 (12.18) | 37.4 (12.45) | 37.3 (10.86) | 39.0 (12.01) |
Median (min, max) | 33.2 (16, 72) | 32.0 (12, 72) | |||| |||||| ||||| | |||| |||||| ||||| | |||| |||||| ||||| |
Weekly average of daily worse itch NRS score (range, 0 to 10) | |||||
Mean (SD) | 7.5 (1.32) | 7.6 (1.49) | 7.8 (1.58) | 7.8 (1.52) | 7.7 (1.54) |
Median (min, max) | 7.4 (4.0, 10.0) | 7.7 (2.0, 10.0) | ||| ||||| ||||| | ||| ||||| ||||| | ||| ||||| ||||| |
≥ 7, n (%) | 54 (65.1) | 57 (72.2) | || |||||| | || |||||| | || |||||| |
< 7, n (%) | 29 (34.9) | 22 (27.8) | || |||||| | || |||||| | || |||||| |
Percent BSA affected | |||||
Mean (SD) | 59.3 (22.51) | 57.4 (20.91) | 54.8 (21.58) | 57.8 (20.04) | 60.2 (21.46) |
Median (min, max) | 56.0 (19, 100) | 54.5 (14, 100) | |||| |||||| ||||| | |||| |||||| ||||| | |||| |||||| |||||| |
POEM (range, 0 to 28) | |||||
Mean (SD) | 23.1 (4.49) | 23.3 (4.04) | 21.3 (5.51) | 20.5 (5.50) | 20.7 (5.48) |
Median (min, max) | 24.0 (9.0, 28.0) | 24.0 (9.0, 28.0) | |||| ||||| ||||| | |||| ||||| ||||| | |||| ||||| ||||| |
SCORAD (range, 0 to 103) | |||||
Mean (SD) | 72.7 (12.95) | 72.2 (11.44) | 75.6 (11.71) | 72.3 (10.83) | 72.9 (12.01) |
Median (min, max) | 73.6 (47, 98) | 72.1 (41, 98) | |||| |||||| ||||| | |||| |||||| ||||| | |||| |||||| |||||| |
Weekly average of patient’s daily sleep quality NRS score (range, 0 to 10) | |||||
N | 81 | 79 | NA | NA | NA |
Mean (SD) | 4.9 (1.90) | 4.6 (2.09) | NA | NA | NA |
Median (min, max) | 5.0 (0, 9) | 4.7 (0, 9) | NA | NA | NA |
Weekly average of caregiver’s daily sleep quality NRS score (range, 0 to 10) | |||||
N | 81 | 79 | NA | NA | NA |
Mean (SD) | 5.1 (1.91) | 4.7 (2.06) | NA | NA | NA |
Median (min, max) | 5.2 (0, 9) | 5.0 (0, 9) | NA | NA | NA |
Weekly average daily skin pain NRS score (range, 0 to 10) | |||||
N | 81 | 78 | NA | NA | NA |
Mean (SD) | 6.8 (1.76) | 7.2 (1.84) | NA | NA | NA |
Median (min, max) | 6.8 (1, 10) | 7.6 (2, 10) | NA | NA | NA |
DFI (range, 0 to 30) | |||||
N | 83 | 79 | 122 | 122 | 123 |
Mean (SD) | 17.2 (5.99) | 17.6 (7.24) | 16.9 (8.65) | 14.9 (7.05) | 15.0 (7.54) |
Median (min, max) | 17.0 (5, 30) | 19.0 (3, 29) | |||| ||| ||| | |||| ||| ||| | |||| ||| ||| |
CDLQI (range, 0 to 30) | |||||
N | 48 | 38 | 122 | 122 | 123 |
Mean (SD) | 17.5 (5.43) | 17.7 (6.25) | 16.2 (7.85) | 14.5 (6.78) | 14.6 (7.41) |
Median (min, max) | 18.0 (7, 29) | 17.5 (5, 28) | |||| ||| ||| | |||| ||| ||| | |||| ||| ||| |
IDQOL (range, 0 to 30) | |||||
N | 35 | 41 | NA | NA | NA |
Mean (SD) | 17.4 (5.41) | 17.1 (5.37) | NA | NA | NA |
Median (min, max) | 17.0 (7, 29) | 17.0 (5, 28) | NA | NA | NA |
Medical and treatment history — SAS | |||||
Patients with current history of atopic or allergic conditions excluding atopic dermatitis, n (%) | 66 (79.5) | 65 (83.3) | 107 (89.2) | 114 (93.4) | 111 (92.5) |
Patients receiving prior systemic corticosteroids and/or systemic nonsteroidal immunosuppressants for atopic dermatitis, n (%) | 24 (28.9) | 22 (28.2) | 42 (35.0) | 40 (32.8) | 36 (30.0) |
Patients receiving prior systemic corticosteroids | 16 (19.3) | 14 (17.9) | 25 (20.8) | 30 (24.6) | 17 (14.2) |
Patients receiving prior systemic nonsteroidal immunosuppressants | 13 (15.7) | 12 (15.4) | 23 (19.2) | 16 (13.1) | 22 (18.3) |
Azathioprine | 0 (0.0) | 1 (1.3) | 2 (1.7) | 2 (1.6) | 0 (0.0) |
Cyclosporine | 10 (12.0) | 7 (9.0) | 17 (14.2) | 11 (9.0) | 12 (10.0) |
Methotrexate | 4 (4.8) | 7 (9.0) | 7 (5.8) | 3 (2.5) | 11 (9.2) |
Mycophenolate | 1 (1.2) | 1 (1.3) | 2 (1.7) | 1 (0.8) | 2 (1.7) |
BSA = body surface area; CDLQI = Children’s Dermatology Life Quality Index; DFI = Dermatitis Family Impact; EASI = Eczema Area and Severity Index; FAS = full analysis set; IDQOL = Infants’ Dermatitis Quality of Life Index; IGA = Investigator’s Global Assessment; max = maximum; min = minimum; NA = not applicable; NRS = numeric rating scale; POEM = Patient-Oriented Eczema Measure; q.2.w. = every 2 weeks; q.4.w. = every 4 weeks; SAS = safety analysis set; SCORAD = Scoring Atopic Dermatitis; SD = standard deviation; TCS = topical corticosteroid.
Source: Sponsor’s Summary of Clinical Evidence.3 (Note: Details from the table have been taken from the sponsor’s Summary of Clinical Evidence.)
Exposure to Study Treatments
Exposure to study treatments is summarized in Table 13.
The duration of exposure to study drug was similar among treatment groups as was adherence to injections. Adherence to emollient use was lower than injection adherence and was lower in the LIBERTY AD PRESCHOOL trial compared to the LIBERTY AD PEDS trial. Also, in both trials, more patients who received placebo used at least 1 rescue medication compared to patients who received dupilumab with the most common being TCSs and rare use of systemic corticosteroids or noncorticosteroids. Note that the placebo group in the LIBERTY AD PEDS trial consisted of patients who received placebo every 4 weeks and patients who received placebo every 2 weeks in a 1:1 ratio explaining the mean and larger standard deviation (SD) compared to either dupilumab group.
Table 13: Summary of Patient Exposure From Pivotal Studies — SAS
Exposure | LIBERTY AD PRESCHOOL | LIBERTY AD PEDS | |||
|---|---|---|---|---|---|
Dupilumab 200 mg or 300 mg q.4.w. + TCS N = 83 | Placebo + TCS N = 78 | Dupilumab 300 mg q.4.w. + TCS N = 120 | Dupilumab 100 mg or 200 mg q.2.w. + TCS N = 122 | Placebo + TCS N = 120 | |
Number of study drug administrations, mean (SD) | 4.0 (0.27) | 3.9 (0.37) | ||| |||||| | ||| |||||| | ||| |||||| |
Duration (days), mean (SD) | 112.1 (7.84) | 110.7 (9.81) | ||||| |||||| | ||||| ||||||| | ||||| ||||||| |
Duration (days), median (min, max) | 112.0 (57, 126) | 112.0 (56, 126) | ||||| |||||| |||||| | ||||| |||||| |||||| | ||||| |||||| |||||| |
Injection adherence, mean (SD) | 99.70 (2.74) | 99.36 (3.98) | ||| ||| | ||||| |||||| | ||||| |||||| |
Emollient adherence, mean (SD)a | 80.9 (20.36) | 78.3 (24.43) | |||| |||||| | |||| ||||||| | |||| |||||| |
Patients who used ≥ 1 rescue medication, n (%) | 16 (19.3) | 49 (62.8) | 3 (2.5) | 6 (4.9) | 23 (19.2) |
Dermatological preparation of corticosteroids | 16 (19.3) | 49 (62.8) | | ||||| | | ||||| | || |||||| |
Systemic corticosteroids | 1 (1.2) | 2 (2.6) | ||| | | ||||| | | ||||| |
Other noncorticosteroids, including TCIs | | ||||| | | ||||| | ||| | | ||||| | | ||||| |
FAS = full analysis set; max = maximum; min = minimum; q.2.w. = every 2 weeks; q.4.w. = every 4 weeks; SAS = safety analysis set; SD = standard deviation; TCI = topical calcineurin inhibitor; TCS = topical corticosteroid.
aAnalyzed using the FAS.
Source: Sponsor’s Summary of Clinical Evidence, LIBERTY AD PRESCHOOL Clinical Study Report, and LIBERTY AD PEDS Clinical Study Report.3,36,37 (Note: Details from the table have been taken from the sponsor’s Summary of Clinical Evidence.)
Protocol Deviations
Protocol deviations are summarized in Table 14.
Most patients in either trial had at least 1 protocol deviation and less than 15% of patients had a deviation that was considered important or major. In the LIBERTY AD PRESCHOOL trial, the most common deviation was for receiving a prohibited treatment, whereas for the LIBERTY AD PEDS trial, the most common reason was patients entering the study despite entry criteria not being satisfied.
Table 14: Summary of Protocol Deviations From Pivotal Studies — FAS
Deviations | LIBERTY AD PRESCHOOL | LIBERTY AD PEDS | |||
|---|---|---|---|---|---|
Dupilumab 200 mg or 300 mg q.4.w. + TCS N = 83 | Placebo + TCS N = 79 | Dupilumab 300 mg q.4.w. + TCS N = 122 | Dupilumab 100 mg or 200 mg q.2.w. + TCS N = 122 | Placebo + TCS N = 123 | |
Patients with any protocol deviation, n (%) | 78 (94.0) | 77 (97.5) | ||| |||||| | ||| |||||| | ||| |||||| |
Important or major protocol deviations, n | 12 | 8 | || | || | || |
Patients with any important or major protocol deviation, n (%)a | 11 (13.3) | 7 (8.9) | 12 (9.8) | 15 (12.3) | 14 (11.4) |
Received an excluded treatment | 6 (7.2) | 5 (6.3) | || | | ||||| | | ||||| |
Entered study even though entry criteria were not satisfied | 4 (4.8) | 1 (1.3) | | ||||| | | ||||| | | ||||| |
Procedure not performed | 1 (1.2) | 1 (1.3) | | ||||| | || | | ||||| |
Inadequate informed consent administration | 1 (1.2) | 0 (0.0) | || | | ||||| | || |
Visit not performed | NA | NA | | ||||| | | ||||| | | ||||| |
Personnel not qualified and/or designated to perform study-related activities | NA | NA | || | | ||||| | || |
Randomization error – patient randomized to wrong treatment | NA | NA | || | | ||||| | || |
Other (laboratory, randomization, AESI) | NA | NA | | ||||| | | ||||| | | ||||| |
AESI = adverse event of special interest; FAS = full analysis set; NA = not applicable; q.2.w. = every 2 weeks; q.4.w. = every 4 weeks; TCS = topical corticosteroid.
aIn LIBERTY AD PRESCHOOL, 1 patient in had 5 deviations of “procedure not performed” (TCS dispensation not performed at 2 visits, TCS accountability not performed and vital signs not collected at 2 visits), 1 patient had 2 deviations of “procedure not performed” (TCS dispensation not performed, TCS accountability not performed), and 1 deviation of “visit performed out of window.” Another patient had a deviation of “visit performed out of window” and 2 patients had deviations of “visit not performed” (information from datasets). The case of inadequate informed consent was for a patient who became 4 years old at the end-of-treatment visit and therefore should have signed the assent form. However, the assent form was not signed before rolling over to the long-term extension study. Among the patients who received excluded concomitant treatment, 1 received a concomitant live (attenuated) measles, mumps, and rubella vaccine, and 2 received measles, mumps, and rubella and varicella vaccines.
Source: Sponsor’s Summary of Clinical Evidence, LIBERTY AD PRESCHOOL Clinical Study Report, and LIBERTY AD PEDS Clinical Study Report.3,36,37 (Note: Details from the table have been taken from the sponsor’s Summary of Clinical Evidence.)
Efficacy
IGA — Primary Outcome
Results for the IGA are summarized in Table 15.
In the LIBERTY AD PRESCHOOL trial, there was a larger proportion of patients in the dupilumab group who experienced an IGA score of 0 or 1 compared to the placebo group at week 16; the treatment difference was 23.8% (95% CI, 13.27% to 34.37%; P < 0.0001). Results from posthoc sensitivity analyses and prespecified subgroup analyses were consistent with the primary analysis.
In the LIBERTY AD PEDS trial, there was a larger proportion of patients in both the dupilumab every 4 weeks and every 2 weeks groups who experienced an IGA score of 0 or 1 compared to the placebo group at week 16; the treatment differences versus placebo were 21.4% (95% CI, 11.36% to 31.45%; P < 0.0001) and 18.1% (95% CI, 8.28% to 27.97%; P < 0.0001), respectively. Results from sensitivity analyses and prespecified subgroup analyses were consistent with the primary analysis.
Table 15: Summary of IGA Results From Pivotal Studies — FAS
Outcome | LIBERTY AD PRESCHOOL | LIBERTY AD PEDS | |||
|---|---|---|---|---|---|
Dupilumab 200 mg or 300 mg q.4.w. + TCS N = 83 | Placebo + TCS N = 79 | Dupilumab 300 mg q.4.w. + TCS N = 122 | Dupilumab 100 mg or 200 mg q.2.w. + TCS N = 122 | Placebo + TCS N = 123 | |
Primary outcome: proportion of patients with IGA 0 to 1 at week 16 | |||||
Proportion of patients with IGA 0 to 1 at week 16, n (%) | 23 (27.7) | 3 (3.9) | 40 (32.8) | 36 (29.5) | 14 (11.4) |
95% CI | 18.45 to 38.62 | –0.42 to 8.21 | 24.56 to 41.87 | 21.60 to 38.44 | 6.36 to 18.36 |
Difference vs. placebo (95% CI) | 23.8 (13.27 to 34.37) | Reference | 21.4 (11.36 to 31.45) | 18.1 (8.28 to 27.97) | Reference |
P value | < 0.0001a,b | Reference | < 0.0001a,c | 0.0004a,c | Reference |
CI = confidence interval; FAS = full analysis set; IGA = Investigator’s Global Assessment; q.2.w. = every 2 weeks; q.4.w. = every 4 weeks; TCS = topical corticosteroid.
aP value has been adjusted for multiple testing.
bP values were derived by Cochran-Mantel-Haenszel test stratified by region (North America, Europe), baseline disease severity (IGA 3, IGA 4), and baseline body mass (5 kg to < 15 kg, 15 kg to < 30 kg). Two strata were combined (Europe region, baseline body mass < 15 kg, and IGA 3 with Europe region, baseline body mass ≥ 15 kg, and IGA 3) as 1 of the strata had only 2 patients.
cP values were derived by Cochran-Mantel-Haenszel test stratified by region (North America, Europe) and baseline body mass (< 30 kg, ≥ 30 kg).
Source: Sponsor’s Summary of Clinical Evidence, LIBERTY AD PRESCHOOL Clinical Study Report, and LIBERTY AD PEDS Clinical Study Report.3,36,37 (Note: Details from the table have been taken from the sponsor’s Summary of Clinical Evidence.)
EASI — Secondary Outcomes
Results for the EASI are summarized in Table 16.
In the LIBERTY AD PRESCHOOL trial, there was a larger proportion of patients in the dupilumab group who experienced EASI-75 compared to the placebo group at week 16; the treatment difference was 42.3% (95% CI, 29.47% to 55.16%; P < 0.0001). Similarly, there was a larger percent change from baseline to week 16 EASI score observed in the dupilumab group compared to the placebo group; the LSM difference was –50.4% (95% CI, –62.38% to –38.40%; P < 0.0001). Results for the proportion of patients experiencing a 50% reduction in Eczema Area and Severity Index score (EASI-50) and EASI-90 at week 16 also favoured treatment with dupilumab. For EASI-75 and percent change from baseline to week 16 in EASI score outcomes, results from posthoc sensitivity analyses and prespecified subgroup analyses were consistent with the primary analysis.
In the LIBERTY AD PEDS trial, there was a larger proportion of patients in both the dupilumab every 4 weeks and every 2 weeks groups who experienced EASI-75 compared to the placebo group at week 16; the treatment differences versus placebo were 42.8% (95% CI, 31.54% to 54.15%; P < 0.0001) and 40.4% (95% CI, 28.95% to 51.82%; P < 0.0001), respectively. Likewise, there was a larger percent change from baseline to week 16 in EASI score observed in both the dupilumab every 4 weeks and every 2 weeks groups compared to the placebo group; the LSM differences versus placebo were –33.4% (95% CI, –40.06% to –26.82%; P < 0.0001) and –29.8% (95% CI, –36.33% to –23.24%; P < 0.0001), respectively. Results for the proportion of patients experiencing EASI-50 and EASI-90 at week 16 also favoured treatment with dupilumab. For EASI-75 and percent change from baseline to week 16 in EASI score outcomes, results from sensitivity analyses and prespecified subgroup analyses were consistent with the primary analysis.
Itch NRS Score — Secondary Outcomes
Results for the itch NRS are summarized in Table 17.
In the LIBERTY AD PRESCHOOL trial, there was a larger percent change from baseline to week 16 in the itch NRS score observed in the dupilumab group compared to the placebo group; the LSM difference was –47.1% (95% CI, –59.47% to –34.79%; P < 0.0001). Results for the proportion of patients experiencing an improvement of at least 3 points and at least 4 points in itch NRS score from baseline to week 16 also favoured treatment with dupilumab. For the percent change from baseline to week 16 in the itch NRS score outcome, results from post hoc sensitivity analyses and prespecified subgroup analyses were consistent with the primary analysis.
In the LIBERTY AD PEDS trial, there was a larger percent change from baseline to week 16 in the itch NRS score observed in both the dupilumab every 4 weeks and every 2 weeks groups compared to the placebo group; the LSM differences versus placebo were –28.6% (95% CI, –36.47% to –20.82%; P < 0.0001) and –31.0% (95% CI, –38.76% to –23.26%; P < 0.0001), respectively. Results for the proportion of patients experiencing an improvement of at least 3 points and at least 4 points in the itch NRS score from baseline to week 16 also favoured treatment with dupilumab. For the percent change from baseline to week 16 in the itch NRS score outcome, results from sensitivity analyses and prespecified subgroup analyses were consistent with the primary analysis.
Percent BSA Affected by Atopic Dermatitis — Secondary Outcome
Results for the percent BSA affected by atopic dermatitis are summarized in Table 18.
In the LIBERTY AD PRESCHOOL trial, there was a larger change from baseline to week 16 for percent BSA affected by atopic dermatitis observed in the dupilumab group compared to the placebo group; the LSM difference was –24.27% (95% CI, –31.20% to –17.33%; P < 0.0001).
In the LIBERTY AD PEDS trial, there was a larger change from baseline to week 16 for percent BSA affected by atopic dermatitis observed in both the dupilumab every 4 weeks and every 2 weeks groups compared to the placebo group; the LSM differences versus placebo were –18.88% |||| ||| ||||||| || |||||||) and –17.72% |||| ||| ||||||| || |||||||), respectively.
POEM — Secondary Outcome
Results for the POEM are summarized in Table 18.
In the LIBERTY AD PRESCHOOL trial, there was a larger change from baseline to week 16 in POEM score observed in the dupilumab group compared to the placebo group; the LSM difference was –9.1 (95% CI, –11.26 to –6.89; P < 0.0001).
In the LIBERTY AD PEDS trial, there was a larger change from baseline to week 16 in POEM score observed in both the dupilumab every 4 weeks and every 2 weeks groups compared to the placebo group; the LSM differences versus placebo were –8.3 |||| ||| |||||| || |||||| | | ||||||| and –8.1 |||| ||| ||||| || |||||| | | |||||||, respectively.
Table 16: Summary of EASI Results From Pivotal Studies — FAS
Outcome | LIBERTY AD PRESCHOOL | LIBERTY AD PEDS | |||
|---|---|---|---|---|---|
Dupilumab 200 mg or 300 mg q.4.w. + TCS N = 83 | Placebo + TCS N = 79 | Dupilumab 300 mg q.4.w. + TCS N = 122 | Dupilumab 100 mg or 200 mg q.2.w. + TCS N = 122 | Placebo + TCS N = 123 | |
Secondary: proportion of patients with EASI-75 at week 16 | |||||
Proportion of patients with EASI-75 at week 16, n (%) | 44 (53.0) | 8 (10.7) | 85 (69.7) | 82 (67.2) | 33 (26.8) |
95% CI | 41.74 to 64.07 | 3.65 to 17.74 | 60.70 to 77.67 | 58.13 to 75.44 | 19.24 to 35.57 |
Difference vs. placebo (95% CI) | 42.3 (29.47 to 55.16) | Reference | 42.8 (31.54 to 54.15) | 40.4 (28.95 to 51.82) | Reference |
P value | < 0.0001a,b | Reference | < 0.0001a,c | < 0.0001a,c | Reference |
Secondary outcome: percent change in EASI from baseline to week 16 | |||||
Baseline mean (SD) | 35.13 (13.89) | 33.07 (12.18) | 37.35 (12.45) | 37.29 (10.86) | 38.96 (12.01) |
LSM percent change (SE) | –70.0 (4.85) | –19.6 (5.13) | –82.1 (2.37) | –78.4 (2.35) | –48.6 (2.46) |
LSM percent change 95% CI | –79.5 to –60.5 | –29.7 to –9.6 | –86.7 to –77.4 | –83.0 to –73.8 | –53.4 to –43.8 |
LSM difference vs. placebo (95% CI) | –50.4 (–62.38 to –38.40)d | Reference | –33.4 (–40.06 to –26.82)e | –29.8 (–36.33 to –23.24)e | Reference |
P value | < 0.0001a,d | Reference | < 0.0001a,e | < 0.0001a,e | Reference |
Secondary outcome: proportion of patients with EASI-50 at week 16 | |||||
Proportion of patients with EASI-50 at week 16, n (%) | 57 (68.7) | 16 (20.2) | 111 (91.0) | 101 (82.8) | 53 (43.1) |
95% CI | 57.56 to 78.41 | 11.09 to 29.23 | ||||||| |||||| | ||||||| |||||| | ||||||| |||||| |
Difference vs. placebo (95% CI) | 48.5 (35.03 to 62.00) | Reference | 47.9 ||||||| |||||| | 39.7 ||||||| |||||| | Reference |
P value | < 0.0001a,b | Reference | < 0.0001a,c | < 0.0001a,c | Reference |
Secondary outcome: proportion of patients with EASI-90 at week 16 | |||||
Patients with EASI-90 at week 16, n (%) | 21 (25.3) | 2 (2.8) | 51 (41.8) | 37 (30.3) | 9 (7.3) |
95% CI | 16.39 to 36.04 | –1.02 to 6.66 | ||||||| |||||| | ||||||| |||||| | |||||| |||||| |
Difference vs. placebo (95% CI) | 22.5 (12.37 to 32.60) | Reference | 34.5 ||||||| |||||| | 23.0 ||||||| |||||| | Reference |
95% CI | 16.39 to 36.04 | –1.02 to 6.66 | ||||||| |||||| | ||||||| |||||| | |||||| |||||| |
P value | 0.0001a,b | Reference | < 0.0001a,c | < 0.0001a,c | Reference |
CI = confidence interval; EASI = Eczema Area and Severity Index; EASI-50 = 50% reduction in Eczema Area and Severity Index score; EASI-75 = 75% reduction in Eczema Area and Severity Index score; EASI-90 = 90% reduction in Eczema Area and Severity Index score; FAS = full analysis set; LSM = least squares mean; q.2.w. = every 2 weeks; q.4.w. = every 4 weeks; SD = standard deviation; SE = standard error; TCS = topical corticosteroid.
aP value has been adjusted for multiple testing.
bP values were derived by Cochran-Mantel-Haenszel test stratified by region (North America, Europe), baseline disease severity (IGA 3, IGA 4), and baseline body mass (5 kg to < 15 kg, 15 kg to < 30 kg). Two strata were combined (Europe region, baseline body mass < 15 kg, and IGA 3 with Europe region, baseline body mass ≥ 15 kg, and IGA 3) as 1 of the strata had only 2 patients.
cP values were derived by Cochran-Mantel-Haenszel test stratified by region (North America, Europe) and baseline body mass (< 30 kg, ≥ 30 kg).
dThe CI and P value were based on treatment difference (dupilumab, placebo) of the LSM percent change using an analysis of covariance model with baseline measurement as covariate and the treatment, randomization strata (North America, Europe), baseline disease severity (IGA 3, IGA 4), and baseline body mass (5 kg to < 15 kg, 15 kg to < 30 kg) as fixed factors.
eThe CI and P value were based on treatment difference (dupilumab, placebo) of the LSM percent change using an analysis of covariance model with baseline measurement as covariate and the treatment, randomization strata (North America, Europe), and baseline body mass (< 30 kg, ≥ 30 kg) as fixed factors.
Source: Sponsor’s Summary of Clinical Evidence, LIBERTY AD PRESCHOOL Clinical Study Report, and LIBERTY AD PEDS Clinical Study Report.3,36,37 (Note: Details from the table have been taken from the sponsor’s Summary of Clinical Evidence.)
Table 17: Summary of Itch NRS Results From Pivotal Studies — FAS
Outcome | LIBERTY AD PRESCHOOL | LIBERTY AD PEDS | |||
|---|---|---|---|---|---|
Dupilumab 200 mg or 300 mg q.4.w. + TCS N = 83 | Placebo + TCS N = 79 | Dupilumab 300 mg q.4.w. + TCS N = 12 | Dupilumab 100 mg or 200 mg q.2.w. + TCS N = 122 | Placebo + TCS N = 123 | |
Secondary outcome: percent change from baseline to week 16 in weekly average of daily worst itch NRS score at week 16 | |||||
Baseline mean (SD) | 7.51 (1.32) | 7.63 (1.49) | 7.81 (1.58) | 7.78 (1.52) | 7.73 (1.54) |
LSM percent change (SE) | –49.4 (5.03) | –2.2 (5.22) | –54.6 (2.89) | –57.0 (2.77) | –25.9 (2.90) |
LSM percent change 95% CI | –59.2 to –39.5 | –12.5 to 8.0 | –60.3 to –48.9 | –62.4 to –51.5 | –31.6 to –20.3 |
LSM difference vs. placebo (95% CI) | –47.1 (–59.47 to –34.79)a | Reference | –28.6 (–36.47 to –20.82)b | –31.0 (–38.76 to –23.26)b | Reference |
P value | < 0.0001a,c | Reference | < 0.0001b,c | < 0.0001b.c | Reference |
Secondary outcome: proportion of patients with improvement (reduction) of weekly average of daily worst itch NRS score ≥ 4 from baseline at week 16 | |||||
Patients with reduction of NRS from baseline ≥ 4 at week 16, n of N1d (%) | 40 of 83 (48.1) | 7 of 78 (8.9) | 61 of 120 (50.8) | 70 of 120 (58.3) | 15 of 122 (12.3) |
95% CI | 37.05 to 59.15 | 2.25 to 15.51 | 41.55 to 60.07 | 48.98 to 67.26 | 7.05 to 19.47 |
Difference vs. placebo (95% CI) | 39.2 (26.18 to 52.27) | Reference | 38.5 (27.86 to 49.21) | 46.0 (35.47 to 56.61) | Reference |
P value | < 0.0001c,e | Reference | < 0.0001c,f | < 0.0001c,f | Reference |
Secondary outcome: proportion of patients with improvement (reduction) of weekly average of daily worst itch NRS score ≥ 3 from baseline to week 16 | |||||
Patients with reduction of NRS from baseline ≥ 3 at week 16, n of N1g (%) | 44 of 83 (53.3) | 8 of 78 (9.9) | 73 of 121 (60.3) | 81 of 120 (67.5) | 26 of 123 (21.1) |
95% CI | 42.29 to 64.22 | 2.59 to 17.22 | ||||||| |||||| | ||||||| |||||| | ||||||| |||||| |
Difference vs. placebo (95% CI) | 43.3 (30.03 to 56.67) | Reference | 39.2 ||||||| |||||| | 46.4 ||||||| |||||| | Reference |
P value | < 0.0001c,e | Reference | < 0.0001c,f | < 0.0001c,f | Reference |
CI = confidence interval; FAS = full analysis set; LSM = least squares mean; NRS = numeric rating scale; q.2.w. = every 2 weeks; q.4.w. = every 4 weeks; SD = standard deviation; SE = standard error; TCS = topical corticosteroid.
aThe CI and P value were based on treatment difference (dupilumab, placebo) of the LSM percent change using an analysis of covariance model with baseline measurement as covariate and the treatment, randomization strata (North America, Europe), baseline disease severity (IGA 3, IGA 4), and baseline body mass (5 kg to < 15 kg, 15 kg to < 30 kg) as fixed factors.
bThe CI and P value were based on treatment difference (dupilumab, placebo) of the LSM percent change using an analysis of covariance model with baseline measurement as covariate and the treatment, randomization strata (North America, Europe) and baseline body mass (< 30 kg, ≥ 30 kg) as fixed factors.
cP value has been adjusted for multiple testing.
dN1 is the number of patients with baseline NRS score of at least 4.
eP values were derived by Cochran-Mantel-Haenszel test stratified by region (North America, Europe), baseline disease severity (IGA 3, IGA 4), and baseline body mass (5 kg to < 15 kg, 15 kg to < 30 kg). Two strata were combined (Europe region, baseline body mass < 15 kg, and IGA 3 with Europe region, baseline body mass ≥ 15 kg, and IGA 3) as 1 of the strata had only 2 patients.
fP values were derived by Cochran-Mantel-Haenszel test stratified by region (North America, Europe) and baseline body mass (< 30 kg, ≥ 30 kg).
gN1 is the number of patients with baseline NRS score of at least 3.
Source: Sponsor’s Summary of Clinical Evidence, LIBERTY AD PRESCHOOL Clinical Study Report, and LIBERTY AD PEDS Clinical Study Report.3,36,37(Note: Details from the table have been taken from the sponsor’s Summary of Clinical Evidence.)
SCORAD — Secondary Outcome
Results for the SCORAD are summarized in Table 18.
In the LIBERTY AD PRESCHOOL trial, there was a larger percent change from baseline to week 16 in SCORAD score observed in the dupilumab group compared to the placebo group; the LSM difference was –38.4% (95% CI, –46.65% to –30.21%; P < 0.0001).
In the LIBERTY AD PEDS trial, there was a larger percent change from baseline to week 16 in SCORAD score observed in both the dupilumab every 4 weeks and every 2 weeks groups compared to the placebo group; the LSM differences versus placebo were –32.6% |||| ||| ||||||| || |||||||| | | ||||||| and –30.4% |||| ||| ||||||| || |||||||| | | ||||||), respectively.
Patient Sleep Quality NRS — Secondary Outcome
Results for the patient sleep quality NRS are summarized in Table 18.
In the LIBERTY AD PRESCHOOL trial, there was a larger change from baseline to week 16 in patients’ sleep quality NRS score observed in the dupilumab group compared to the placebo group; the LSM difference was 1.70 (95% CI, 1.09 to 2.32; P < 0.0001).
This was not an outcome in the LIBERTY AD PEDS trial.
Patient Skin Pain NRS — Secondary Outcome
Results for the patient skin pain NRS are summarized in Table 18.
In the LIBERTY AD PRESCHOOL trial, there was a larger change from baseline to week 16 in patients’ skin pain NRS score observed in the dupilumab group compared to the placebo group; the LSM difference was –3.31 (95% CI, –4.03 to –2.60; P < 0.0001).
This was not an outcome in the LIBERTY AD PEDS trial.
Table 18: Summary of Other Disease-Related Outcome Results From Pivotal Studies — FAS
Outcome | LIBERTY AD PRESCHOOL | LIBERTY AD PEDS | |||
|---|---|---|---|---|---|
Dupilumab 200 mg or 300 mg q.4.w. + TCS N = 83 | Placebo + TCS N = 79 | Dupilumab 300 mg q.4.w. + TCS N = 122 | Dupilumab 100 mg or 200 mg q.2.w. + TCS N = 122 | Placebo + TCS N = 123 | |
Secondary outcome: change from baseline to week 16 in percent BSA affected | |||||
Baseline mean (SD) | 59.27 (22.51) | 57.39 (20.91) | 54.77 (21.58) | 57.82 (20.04) | 60.20 (21.46) |
LSM change (SE) | –35.00 (2.82) | –10.74 (2.93) | –40.53 (1.65) | –39.37 (1.63) | –21.65 (1.72) |
LSM change 95% CI | –40.52 to –29.49 | –16.47 to –5.00 | |||||||| ||||||| | |||||||| ||||||| | |||||||| ||||||| |
LSM difference vs. placebo (95% CI) | –24.27 (–31.20 to –17.33)a | Reference | –18.88 |||||||| |||||||| | –17.72 |||||||| |||||||| | Reference |
P value | < 0.0001a,c | Reference | < 0.0001b | < 0.0001b | Reference |
Secondary outcome: change from baseline to week 16 in POEM | |||||
Baseline mean (SD) | 23.1 (4.49) | 23.3 (4.04) | 21.3 (5.51) | 20.5 (5.50) | 20.7 (5.48) |
LSM change (SE) | –12.9 (0.89) | –3.8 (0.92) | –13.6 (0.65) | –13.4 (0.65) | –5.3 (0.69) |
LSM change 95% CI | –14.6 to –11.1 | –5.6 to –2.0 | ||||||| |||||| | ||||||| |||||| | |||||| ||||| |
LSM difference vs. placebo (95% CI) | –9.1 (–11.26 to –6.89)a | Reference | –8.3 |||||||| ||||||| | –8.1 ||||||| ||||||| | Reference |
P value | < 0.0001a,c | Reference | < 0.0001b,c | < 0.0001b,c | Reference |
Secondary outcome: percent change from baseline to week 16 in SCORAD | |||||
Baseline mean (SD) | 72.66 (12.95) | 72.19 (11.44) | 75.62 (11.71) | 72.30 (10.83) | 72.92 (12.01) |
LSM percent change (SE) | –54.7 (3.39) | –16.2 (3.54) | –62.4 (2.13) | –60.2 (2.11) | –29.8 (2.26) |
LSM percent change 95% CI | –61.3 to –48.0 | –23.2 to –9.3 | ||||||| |||||| | ||||||| |||||| | ||||||| |||||| |
LSM difference vs. placebo (95% CI) | –38.4 (–46.65 to –30.21)a | Reference | –32.6 |||||||| |||||||| | –30.4 |||||||| |||||||| | Reference |
P value | < 0.0001a,c | Reference | < 0.0001b,c | < 0.0001b,c | Reference |
Secondary outcome: change from baseline to week 16 in patient’s sleep quality NRS | |||||
Baseline mean (SD) | 4.95 (1.90) | 4.62 (2.09) | NA | NA | NA |
LSM change (SE) | 2.04 (0.25) | 0.34 (0.26) | NA | NA | NA |
LSM change 95% CI | 1.55 to 2.53 | –0.17 to 0.84 | NA | NA | NA |
LSM difference vs. placebo (95% CI) | 1.70 (1.09 to 2.32)a | Reference | NA | NA | NA |
P value | < 0.0001a,c | Reference | NA | NA | NA |
Secondary outcome: change from baseline to week 16 in weekly average of skin pain NRS | |||||
Baseline mean (SD) | 6.83 (1.76) | 7.16 (1.84) | NA | NA | NA |
LSM change (SE) | –3.93 (0.30) | –0.62 (0.30) | NA | NA | NA |
LSM change 95% CI | –4.51 to –3.35 | –1.21 to –0.02 | NA | NA | NA |
LSM difference vs. placebo (95% CI) | –3.31 (–4.03 to –2.60)a | Reference | NA | NA | NA |
P value | < 0.0001a,c | Reference | NA | NA | NA |
BSA = body surface area; CI = confidence interval; FAS = full analysis set; LSM = least squares mean; NA = not applicable; NRS = numeric rating scale; POEM = Patient-Oriented Eczema Measure; q.2.w. = every 2 weeks; q.4.w. = every 4 weeks; SCORAD = Scoring Atopic Dermatitis; SD = standard deviation; SE = standard error; TCS = topical corticosteroid.
aThe CI and P value were based on treatment difference (dupilumab, placebo) of the LSM percent change using an analysis of covariance model with baseline measurement as covariate and the treatment, randomization strata (North America, Europe), baseline disease severity (IGA 3, IGA 4), and baseline body mass (5 kg to < 15 kg, 15 kg to < 30 kg) as fixed factors.
bThe CI and P value were based on treatment difference (dupilumab, placebo) of the LSM percent change using an analysis of covariance model with baseline measurement as covariate and the treatment, randomization strata (North America, Europe), and baseline body mass (< 30 kg, ≥ 30 kg) as fixed factors.
cP value has been adjusted for multiple testing.
Source: Sponsor’s Summary of Clinical Evidence, LIBERTY AD PRESCHOOL Clinical Study Report, and LIBERTY AD PEDS Clinical Study Report.3,36,37 (Note: Details from the table have been taken from the sponsor’s Summary of Clinical Evidence.)
DFI — Secondary Outcomes
Results for the DFI are summarized in Table 19.
In the LIBERTY AD PRESCHOOL trial, there was a larger change from baseline to week 16 in DFI score observed in the dupilumab group compared to the placebo group; the LSM difference was –7.80 (95% CI, –9.79 to –5.81; P < 0.0001).
In the LIBERTY AD PEDS trial, there was a larger change from baseline to week 16 in DFI score observed in both the dupilumab every 4 weeks and every 2 weeks groups compared to the placebo group; the LSM differences versus placebo was –3.98 |||| ||| ||||| || |||||| and –4.11 |||| ||| ||||| || ||||||, respectively.
CDLQI — Secondary Outcome
Results for the CDLQI are summarized in Table 19.
In the LIBERTY AD PRESCHOOL trial, there was a larger change from baseline to week 16 in CDLQI score observed in the dupilumab group compared to the placebo group; the LSM difference was –7.5 (95% CI, –10.29 to –4.75; P < 0.0001).
In the LIBERTY AD PEDS trial, there was a larger change from baseline to week 16 in CDLQI score observed in both the dupilumab every 4 weeks and every 2 weeks groups compared to the placebo group; the LSM differences versus placebo were –4.2 |||| ||| ||||| || |||||| | | ||||||| and –4.3 |||| ||| ||||| || |||||| | | ||||||), respectively.
IDQOL — Secondary Outcome
Results for the IDQOL are summarized in Table 19.
In the LIBERTY AD PRESCHOOL trial, there was a larger change from baseline to week 16 in IDQOL score observed in the dupilumab group compared to the placebo group; the LSM difference was –8.96 (95% CI, –11.71 to –6.20; P < 0.0001).
This was not an outcome in the LIBERTY AD PEDS trial.
Table 19: Summary of HRQoL Results From Pivotal Studies — FAS
Outcome | LIBERTY AD PRESCHOOL | LIBERTY AD PEDS | |||
|---|---|---|---|---|---|
Dupilumab 200 mg or 300 mg q.4.w. + TCS N = 83 | Placebo + TCS N = 79 | Dupilumab 300 mg q.4.w. + TCS N = 122 | Dupilumab 100 mg or 200 mg q.2.w. + TCS N = 122 | Placebo + TCS N = 123 | |
Secondary outcome: change from baseline to week 16 in DFI | |||||
Baseline mean (SD) | 17.20 (5.99) | 17.58 (7.24) | 16.92 (8.65) | 14.91 (7.05) | 15.05 (7.54) |
LSM change (SE) | –10.48 (0.81) | –2.68 (0.84) | –10.75 (0.48) | –10.89 (0.47) | –6.77 (0.50) |
LSM change 95% CI | –12.06 to –8.90 | –4.32 to –1.04 | |||||||| |||||| | |||||||| |||||| | ||||||| |||||| |
LSM difference vs. placebo (95% CI) | –7.80 (–9.79 to –5.81)a | Reference | –3.98 ||||||| ||||||| | –4.11 ||||||| ||||||| | Reference |
P value | < 0.0001a,c | Reference | < 0.0001b | < 0.0001b | Reference |
Secondary outcome: change from baseline to week 16 in CDLQI | |||||
Baseline mean (SD) | 17.5 (5.48) | 17.7 (6.25) | 16.2 (7.85) | 14.5 (6.78) | 14.6 (7.41) |
LSM change (SE) | –10.0 (1.56) | –2.5 (1.66) | –10.6 (0.47) | –10.7 (0.46) | –6.4 (0.51) |
LSM change 95% CI | –13.1 to –7.0 | –5.8 to 0.7 | ||||||| ||||| | ||||||| ||||| | |||||| ||||| |
LSM difference vs. placebo (95% CI) | –7.5 (–10.29 to –4.75)a | Reference | –4.2 ||||||| ||||||| | –4.3 ||||||| ||||||| | Reference |
P value | < 0.0001a,c | Reference | < 0.0001b,c | < 0.0001b,c | Reference |
Secondary outcome: change from baseline to week 16 in IDQOL | |||||
Baseline mean (SD) | 17.37 (5.41) | 17.10 (5.37) | NA | NA | NA |
LSM change (SE) | –10.91 (1.16) | –1.95 (1.08) | NA | NA | NA |
LSM change 95% CI | –13.18 to –8.64 | –4.07 to 0.16 | NA | NA | NA |
LSM difference vs. placebo (95% CI) | –8.96 (–11.71 to –6.20)a | Reference | NA | NA | NA |
P value | < 0.0001a,c | Reference | NA | NA | NA |
CDLQI = Children’s Dermatology Life Quality Index; CI = confidence interval; DFI = Dermatitis Family Impact; FAS = full analysis set; HRQoL = health-related quality of life; IDQOL = Infants’ Dermatitis Quality of Life Index; LSM = least squares mean; NA = not applicable; q.2.w. = every 2 weeks; q.4.w. = every 4 weeks; SD = standard deviation; SE = standard error; TCS = topical corticosteroid.
aThe CI and P value were based on treatment difference (dupilumab, placebo) of the LSM percent change using an analysis of covariance model with baseline measurement as covariate and the treatment, randomization strata (North America, Europe), baseline disease severity (IGA 3, IGA 4), and baseline body mass (5 kg to < 15 kg, 15 kg to < 30 kg) as fixed factors.
bThe CI and P value were based on treatment difference (dupilumab, placebo) of the LSM percent change using an analysis of covariance model with baseline measurement as covariate and the treatment, randomization strata (North America, Europe), and baseline body mass (< 30 kg, ≥ 30 kg) as fixed factors.
cP value has been adjusted for multiple testing.
Source: Sponsor’s Summary of Clinical Evidence, LIBERTY AD PRESCHOOL Clinical Study Report, and LIBERTY AD PEDS Clinical Study Report.3,36,37 (Note: Details from the table have been taken from the sponsor’s Summary of Clinical Evidence.)
Harms
Harms are summarized in Table 20.
Adverse Events
More than half of patients in any treatment group for either trial experienced at least 1 TEAE. In both trials, more patients in the placebo group than the dupilumab groups experienced a TEAE and the most frequently reported TEAEs were atopic dermatitis, nasopharyngitis, and upper respiratory tract infection. In the LIBERTY AD PRESCHOOL trial, conjunctivitis occurred more frequently in the dupilumab group than the placebo group (3.6% and 0%, respectively), as did injection site erythema (1.2% and 0%, respectively). Similarly, in the LIBERTY AD PEDS trial, TEAEs that occurred more frequently in 1 or both of the every 4 weeks and every 2 weeks groups compared to the placebo group included conjunctivitis (4.2%, 5.7%, and 2.5%, respectively), injection site erythema (4.2%, 5.7%, and 1.7%, respectively), and nasopharyngitis (12.5%, 6.6%, and 6.7%, respectively).
Serious Adverse Events
There were 4 SAEs reported in the placebo group of the LIBERTY AD PRESCHOOL trial and none in the dupilumab group. In the LIBERTY AD PEDS trial, there were 2 SAEs reported in the dupilumab every 4 weeks group, 0 in the dupilumab every 2 weeks group, and 2 in the placebo group. No SAE was reported by more than 1 patient per trial.
Withdrawals Due to Adverse Events
Two patients stopped treatment due to AEs in the LIBERTY AD PRESCHOOL trial due to atopic dermatitis (dupilumab group) and nightmare (placebo group). Four patients stopped treatment due to AEs in the LIBERTY AD PEDS trial: 2 in the dupilumab every 2 weeks group due to food allergy and bacterial conjunctivitis and 2 in the placebo group due to atopic dermatitis and asthma.
Mortality
There were no patient deaths in either trial.
Notable Harms
There were no reports of anaphylactic reaction in either trial.
There were no reports of hypersensitivity in the LIBERTY AD PRESCHOOL trial. In the LIBERTY AD PEDS trial, no treatment-related events of hypersensitivity or anaphylaxis occurred during the study.
There were no reports of helminthic infection in the LIBERTY AD PRESCHOOL trial. In the LIBERTY AD PEDS trial, | ||||||| in each of the dupilumab every 4 weeks and placebo groups reported a helminthic infection and || |||||||| in the dupilumab every 2 weeks group.
In the LIBERTY AD PRESCHOOL trial, 3 patients in the dupilumab group and 0 patients in the placebo group reported conjunctivitis. In the LIBERTY AD PEDS trial, 5 patients, 7 patients, and 3 patients in the dupilumab every 4 weeks, dupilumab every 2 weeks, and placebo groups, respectively, reported conjunctivitis.
In the LIBERTY AD PRESCHOOL trial, 2 patients in the dupilumab group and 0 patients in the placebo group reported blepharitis. In the LIBERTY AD PEDS trial, | ||||||| and | |||||||| in the dupilumab every 2 weeks and placebo groups, respectively, reported blepharitis and no patients in the dupilumab every 4 weeks group.
In the LIBERTY AD PRESCHOOL trial, 1 patient in the dupilumab group and 0 patients in the placebo group reported keratitis. In the LIBERTY AD PEDS trial, 1 patient in the dupilumab every 2 weeks group reported keratitis and no patients in either the dupilumab every 4 weeks or placebo groups.
In the LIBERTY AD PRESCHOOL trial, 2 patients in the dupilumab group and 0 patients in the placebo group reported eosinophilia. In the LIBERTY AD PEDS trial, 1 patient in the dupilumab every 2 weeks group reported eosinophilia and no patients in either the dupilumab every 4 weeks or placebo groups.
Facial erythema was not captured in either trial.
Injection site pain was not captured in the LIBERTY AD PRESCHOOL trial. In the LIBERTY AD PEDS trial, 3 patients, 2 patients, and 3 patients in the dupilumab every 4 weeks, dupilumab every 2 weeks, and placebo groups, respectively, reported injection site pain.
Table 20: Summary of Harms From Pivotal Studies — SAS
Exposure | LIBERTY AD PRESCHOOL | LIBERTY AD PEDS | |||
|---|---|---|---|---|---|
Dupilumab 200 mg or 300 mg q.4.w. + TCS N = 83 | Placebo + TCS N = 78 | Dupilumab 300 mg q.4.w. + TCS N = 120 | Dupilumab 100 mg or 200 mg q.2.w. + TCS N = 122 | Placebo + TCS N = 120 | |
Most common TEAEs, n (%) | |||||
Patients with ≥ 1 TEAE | 53 (63.9) | 58 (74.4) | 78 (65.0) | 82 (67.2) | 88 (73.3) |
TEAEs reported in ≥ 5% of patients | |||||
Atopic dermatitis | 11 (13.3) | 25 (32.1) | 8 (6.7) | 10 (8.2) | 17 (14.2) |
Nasopharyngitis | 7 (8.4) | 7 (9.0) | 15 (12.5) | 8 (6.6) | 8 (6.7) |
Upper respiratory tract infection | 5 (6.0) | 6 (7.7) | 13 (10.8) | 10 (8.2) | 12 (10.0) |
Impetigo | 3 (3.6) | 6 (7.7) | | ||||| | | ||||| | | ||||| |
Lymphadenopathy | 3 (3.6) | 6 (7.7) | ||| | ||| | ||| |
Asthma | 3 (3.6) | 5 (6.4) | 2 (1.7) | 4 (3.3) | 12 (10.0) |
Conjunctivitis | 3 (3.6) | 0 (0.0) | 5 (4.2) | 7 (5.7) | 3 (2.5) |
Pyrexia | 1 (1.2) | 7 (9.0) | | ||||| | | ||||| | | ||||| |
Urticaria | 1 (1.2) | 4 (5.1) | | ||||| | | ||||| | | ||||| |
Headache | | ||||| | | ||||| | 6 (5.0) | 7 (5.7) | 10 (8.3) |
Injection site erythema | 1 (1.2) | 0 (0.0) | 5 (4.2) | 7 (5.7) | 2 (1.7) |
Cough | 0 (0.0) | 5 (6.4) | 3 (2.5) | 5 (4.1) | 9 (7.5) |
SAEs, n (%) | |||||
Patients with ≥ 1 SAE | 0 (0.0) | 4 (5.1) | 2 (1.7) | 0 (0.0) | 2 (1.7) |
Atopic dermatitis | 0 (0.0) | 1 (1.3) | 0 (0.0) | 0 (0.0) | 1 (0.8) |
Hypersensitivity | 0 (0.0) | 1 (1.3) | 0 (0.0) | 0 (0.0) | 0 (0.0) |
Cellulitis staphylococcal | 0 (0.0) | 1 (1.3) | 0 (0.0) | 0 (0.0) | 0 (0.0) |
Dermatitis infected | 0 (0.0) | 1 (1.3) | 0 (0.0) | 0 (0.0) | 0 (0.0) |
Staphylococcal bacteremia | 0 (0.0) | 1 (1.3) | 0 (0.0) | 0 (0.0) | 0 (0.0) |
Food allergy | 0 (0.0) | 0 (0.0) | 1 (0.8) | 0 (0.0) | 0 (0.0) |
Urinary tract infection | 0 (0.0) | 0 (0.0) | 1 (0.8) | 0 (0.0) | 0 (0.0) |
Asthma | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 1 (0.8) |
Patients who stopped treatment due to adverse events, n (%) | |||||
Patients who stopped | 1 (1.2) | 1 (1.3) | 0 (0.0) | 2 (1.6) | 2 (1.7) |
Atopic dermatitis | 1 (1.2) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 1 (0.8) |
Nightmare | 0 (0.0) | 1 (1.3) | 0 (0.0) | 0 (0.0) | 0 (0.0) |
Food allergy | 0 (0.0) | 0 (0.0) | 0 (0.0) | 1 (0.8) | 0 (0.0) |
Conjunctivitis bacterial | 0 (0.0) | 0 (0.0) | 0 (0.0) | 1 (0.8) | 0 (0.0) |
Asthma | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 1 (0.8) |
Deaths, n (%) | |||||
Patients who died | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) |
Notable harms, n (%) | |||||
Anaphylactic reaction | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) |
Hypersensitivity | 0 (0.0) | 1 (1.3) | 0 (0.0) | 0 (0.0) | 0 (0.0) |
Helminthic infection | 0 (0.0) | 0 (0.0) | | ||||| | || | | ||||| |
Conjunctivitis | 3 (3.6) | 0 (0.0) | 5 (4.2) | 7 (5.7) | 3 (2.5) |
Blepharitis | 2 (2.4) | 0 (0.0) | || | | ||||| | | ||||| |
Keratitis | 1 (1.2) | 0 (0.0) | 0 (0.0) | 1 (0.8) | 0 (0.0) |
Eosinophilia | 2 (2.4) | 0 (0.0) | 0 (0.0) | 1 (0.8) | 0 (0.0) |
Facial erythema | NR | NR | NR | NR | NR |
Injection site pain | NR | NR | 3 (2.5) | 2 (1.6) | 3 (2.5) |
NR = not reported; q.2.w. = every 2 weeks; q.4.w. = every 4 weeks; SAE = serious adverse event; SAS = safety analysis set; TCS = topical corticosteroid; TEAE = treatment-emergent adverse event.
Source: Sponsor’s Summary of Clinical Evidence, LIBERTY AD PRESCHOOL Clinical Study Report, and LIBERTY AD PEDS Clinical Study Report.3,36,37 (Note: Details from the table have been taken from the sponsor’s Summary of Clinical Evidence.)
Critical Appraisal
Internal Validity
In both the LIBERTY AD PRESCHOOL and LIBERTY AD PEDS trials, randomization was stratified and performed centrally. Baseline characteristics were generally balanced between treatment groups with a few notable differences; however, these were mostly small imbalances that could have been due to chance. The clinical experts consulted by CADTH were not aware of any reason that the imbalances would change treatment outcomes. Therefore, the risk of bias arising from the randomization process was likely low.
Both pivotal trials used matching placebos and in the LIBERTY AD PRESCHOOL trial, blinding was adequate. During the LIBERTY AD PEDS trial, product was inadvertently delivered in an open-label manner and, consequently, 68 patients may have been unblinded to their treatment assignment. To mitigate the issue, the sponsor increased patient enrolment to maintain adequate power for the IGA and EASI-75 end points and added the mFAS supportive analyses that excluded data from these patients. The number of patients with major protocol deviations was similar across treatment groups for both trials and reasons were generally balanced, although more patients (6% to 7%) received protocol-excluded treatments in the LIBERTY AD PRESCHOOL trial. The proportion of patients with conjunctivitis, an AE associated with the drug, was higher in dupilumab groups, but the relatively low frequency (< 6% of patients in any group) make it less likely that this would result in unblinding of treatment allocations. Study and treatment discontinuations were also low (< 5% in any group) in both trials.
In both trials, a much smaller proportion of patients in the dupilumab groups used rescue treatment compared to the placebo groups: 19.3% (dupilumab) and 62.8% (placebo) of patients in the LIBERTY AD PRESCHOOL trial and 2.5% (dupilumab every 4 weeks), 4.9% (dupilumab every 2 weeks), and 19.2% (placebo) of patients in the LIBERTY AD PEDS trial. To disentangle the impact of rescue treatment on the assessment of treatment effect, the sponsor defined the following rule: “Values after first rescue treatment used were set to missing. Patients with missing values at week 16 due to rescue treatment, withdrawn consent, adverse event, and lack of efficacy were considered as nonresponders.”37 According to this rule, upon first use of rescue treatment, a patient was counted as a nonresponder, regardless of the subsequent status of this patient. Therefore, there was no impact on responder analysis from the rescue treatment. However, the significant differences in rescue treatment use between dupilumab and placebo groups could impact how other outcomes (e.g., harms, HRQoL) that occurred after the use of rescue treatment were assessed.
Week 16 data for the primary outcome (IGA) and key secondary outcome (EASI-75) were missing for 3 (1.9%) patients in the LIBERTY AD PRESCHOOL trial and 9 (2.5%) patients in the LIBERTY AD PEDS trial. The small amount of missing data are not expected to have a major impact on the results and the risk of bias is low.
There was a lack of validity and reliability evidence in the literature for the itch NRS, percent BSA affected, and sleep quality NRS for patients with atopic dermatitis. Additionally, there were no MIDs identified from the literature for the IGA, percent BSA affected, sleep quality NRS, DFI, or IDQOL scores for patients with atopic dermatitis. However, the estimation of treatment effect based on the IGA and EASI are likely valid and reliable based on the current available literature. Overall, the treatment effects, as observed in the 2 trials and by various different outcome measures, were consistent.
External Validity
According to the clinical experts consulted by CADTH, the patients in both pivotal trials were similar to those seen in practice who could receive dupilumab. The LIBERTY AD PRESCHOOL trial included patients with moderate-to-severe atopic dermatitis, while the LIBERTY AD PEDS trial included only patients with severe atopic dermatitis. The clinical experts were of the opinion that the results from the latter trial would be generalizable to patients with moderate atopic dermatitis based on trial results for age groups both younger and older that included patients with moderate disease but noted that patients with severe disease have a higher ceiling for improvement on continuous efficacy outcomes. The experts suggested that, in practice, some patients with an EASI score less than 16 may be eligible for dupilumab, and this is supported by the literature showing that patients with moderate atopic dermatitis can have an EASI score as low as 6.34,35 For example, a patient with severe lesions but low percent BSA affected or with lesions localized to special areas (e.g., hands, feet, scalp), whose disease is not adequately controlled with prescription topical therapies, could have a low EASI score and be treated with dupilumab. It was unclear if patients in whom topical prescription therapies are not advisable were included in the trials, though according to the clinical experts consulted by CADTH, this would be a very small proportion of patients and would not greatly impact generalizability to the population who could receive dupilumab. Patients with a history of important side effects to TCSs were excluded from the trials, but the clinical experts stated that side effects are rare when TCSs are used properly and that it would be reasonable for patients who cannot tolerate TCSs or other topical therapies to receive dupilumab. This could be a gap in the evidence for dupilumab, but would likely have a minor impact.
The clinical experts confirmed that the types of treatments (both background therapies and rescue therapies) used in the trials were acceptable; however, the way in which nonresponders were defined in the trials was inconsistent with clinical practice. In both pivotal trials, TCS was the only permitted concomitant treatment; other topical therapies such as TCIs and crisaborole had to be discontinued at least 2 weeks before baseline (or were used as rescue treatment) and prescription moisturizers could not be initiated during the trial. This differs from clinical practice and, as per the clinical experts, non-TCS therapies would also be acceptable add-on treatment while receiving dupilumab. The clinical experts thought that the use of rescue treatments, as defined in the trials, would not necessarily mean a patient was a nonresponder and that higher-potency TCSs, other prescription topical treatments, and a short course of systemic therapies (< 8 weeks) would be acceptable to use alongside dupilumab. They also stated that patients may improve while on dupilumab (i.e., be responders), but may still require additional therapy.
The clinical experts stated that although the trials’ assessments are common in clinical trials, they are generally not used in practice. Instead, clinicians often use a gestalt approach, asking how a patient feels and observing clinical changes. The assessments used in the trials may provide an approximation of what clinicians use in practice and are relevant to the most important treatment goals. Based on the input from patient groups and what was highlighted as being the greatest concerns (i.e., symptom management, HRQoL, and safety of systemic treatments), the trial outcomes were relevant to patients. The patient group input also noted that topical regimens are burdensome to administer. It is unclear from the trial if dupilumab injections every 2 weeks or every 4 weeks (with or without topical therapies) address the need for a simpler treatment, particularly if patients or caregivers cannot perform at-home injections (all patients in the LIBERTY AD PRESCHOOL trial and those whose caregivers were uncomfortable with at-home administration in the LIBERTY AD PEDS trial) or if patients are especially afraid of needles. Based on their experience, the experts felt that the trade-off between topical and injectable therapies may be acceptable for some and that many patients who improve on dupilumab are willing to continue. Lastly, it should be noted that the pivotal trials were 16 weeks long and provide short-term results for what is expected to be a long-term treatment.
LTE Studies
Contents within this section have been informed by materials submitted by the sponsor. The following have been summarized and validated by the CADTH review team.
Description of Studies
Study 1434 is an ongoing, global, open-label, single-group, LTE study of patients aged 6 months to younger than 18 years with atopic dermatitis.38,39 The aim of the study is to assess the long-term safety and efficacy of dupilumab following the parent LIBERTY trials for dupilumab for up to 260 weeks of treatment. Presented in this summary are data for patients aged 6 months to younger than 6 years (N = 180) and patients aged 6 years to younger than 12 years (N = 368) who participated in the pivotal trials described in the main report. The primary outcome was the incidence rate (events per patient-year) of TEAEs. The study started on October 15, 2015, and results presented in this document were based on a prespecified second-step analysis conducted on data from patients aged 6 years to younger than 12 years (data cut-off on July 22, 2019) and from a third-step analysis conducted on data from patients aged 6 months to younger than 6 years (data cut-off on July 31, 2021).
Populations
Patients were eligible to enrol in Study 1434 if they were aged 6 months to younger than 18 years and completed at least 50% of the visits during the treatment and follow-up periods in 1 of the parent dupilumab studies. Patients were excluded if they developed a SAE deemed related to the treatment during their participation in a parent study, or an AE related to the study drug that led to discontinuation or withdrawal by the investigator from the study because of noncompliance and/or inability to complete required study assessments. Patients who had sustained disease remission, as defined by maintenance of an IGA score of 0 or 1 continuously for a 12-week period, after week 40, were discontinued from dupilumab. Patients were closely monitored after discontinuing due to disease remission and upon relapse (IGA ≥ 2), dupilumab could be reinitiated.
Interventions
Dupilumab was provided at the following doses and dosing schedules:
body mass 60 kg or greater: 300 mg every 2 weeks
body mass 30 kg to less than 60 kg: 200 mg every 2 weeks
body mass 15 kg to less than 30 kg: 300 mg every 4 weeks
body mass 5 kg to less than 15 kg: 200 mg every 4 weeks.
Outcomes
The primary end points in the study were the incidence and rate of TEAEs from baseline through the last study visit. Incidence was defined as:
TEAE rate per patient-year
number of patients with at least 1 TEAE per patient-year.
The secondary end points included:
incidence of treatment-emergent SAEs from baseline through the last study visit
incidence of TEAEs of special interest from baseline through the last study visit
proportion of patients with an IGA score of 0 or 1 at all in-clinic visits postbaseline
proportion of patients with EASI-75 response (from baseline of parent study) at all in-clinic visits postbaseline
change and percent change from baseline in EASI at all in-clinic visits postbaseline
change from baseline in percent BSA affected by atopic dermatitis at all in-clinic visits postbaseline
percent change from baseline in SCORAD score at all in-clinic visits postbaseline
change from baseline in CDLQI score for patients aged 4 years or older at all in-clinic visits postbaseline in which the assessments were planned
change from baseline in IDQOL score for patients aged younger than 4 years at all in-clinic visits postbaseline in which the assessments were planned
assessment of maintenance of treatment effect:
proportion of responders (defined as patients with IGA 0 or 1) who maintain an IGA score of 0 or 1 during at least 75% of the subsequent visits during the treatment period
for responders (defined as patients with IGA 0 or 1), median percentage of subsequent visits during the treatment period in which an IGA score of 0 or 1 is maintained
assessment of flares:
number and annualized event rate of atopic dermatitis flares during the study
proportion of patients with at least 1 flare during the study
assessment of well-controlled weeks:
proportion of well-controlled weeks during the study.
The sponsor also assessed the following end points; however, the sponsor stated that these end points were not analyzed in the interim Clinical Study Report as the number of patients was too small to conduct meaningful analyses, and they would be available in the final Clinical Study Report:
relapse during off-treatment period by measuring the following variables:
proportion of patients experiencing relapse
annualized event rate of relapse during the off-treatment period
median time to first relapse
assessment of potential rebound (defined as worsening of EASI score [i.e., at least 25% increase from baseline of the parent study] within 12 weeks after the study treatment had been discontinued):
proportion of patients experiencing potential rebound
annualized event rate of potential rebound during the off-treatment period
median time to first potential rebound (from last dose of study drug).
Safety Evaluation Plan
The investigator recorded all AEs that occurred from the time of informed consent to the end of the study. All SAEs, regardless of assessment of causal relationship to the study drug, were reported to the sponsor within 24 hours.
An AE was any untoward medical occurrence in a patient administered a study drug, regardless of relationship to the study drug. Therefore, an AE was any unfavourable and unintended sign (including abnormal laboratory finding), symptom, or disease, which was temporally associated with the use of a study drug. An AE also included any worsening (i.e., any clinically significant change in frequency and/or intensity) of a preexisting condition that was temporally associated with the use of the study drug.
An SAE was any untoward medical occurrence that at any dose:
resulted in death
was life-threatening
required inpatient hospitalization or prolongation of existing hospitalization
resulted in persistent or significant disability or incapacity
was a congenital anomaly or birth defect
was an important medical event.
Notable harms that were prespecified by the sponsor and confirmed by the clinical experts consulted by CADTH are summarized in this review.
Statistical Analysis
No hypothesis-testing statistical analysis was planned. The sponsor did a safety analysis that included all patients who received any study drug.
Baseline Characteristics
Patient characteristics at baseline are summarized in Table 21. For patients aged 6 months to younger than 6 years, 64.4% were male and 35.6% were female and the mean age was 3.86 years (SD = 1.32 years). Approximately, ||||| of patients had an IGA score of 0 to 2, ||||| had an IGA score of 3, and ||||| had an IGA score of 4. The mean baseline EASI, BSA, and SCORAD scores were 17.29 (SD = 14.47), |||| ||| | ||||||, and 46.8 (SD = 22.81), respectively. Overall, ||||| of patients reported prior use of systemic corticosteroid and/or systemic nonsteroidal immunosuppressants, of whom ||||| received systemic corticosteroids and ||||| patients received prior systemic nonsteroidal immunosuppressants. The most commonly used nonsteroidal immunosuppressant was cyclosporine (|||||).
For patients aged 6 years to younger than 12 years, ||||| of patients were male and ||||| were female and the mean age was ||| ||||| ||| | |||| ||||||. Approximately half of patients had an IGA score of 0 to 2, 29.9% had an IGA score of 3, and 19.6% had an IGA score of 4. The mean baseline EASI, BSA, and SCORAD scores were 15.70 (SD = 15.88), 28.6 (SD = 25.52); and |||| ||| | ||||||, respectively. Overall, ||||| of patients reported prior use of systemic corticosteroid and/or systemic nonsteroidal immunosuppressants, of whom ||||| received systemic corticosteroids and ||||| patients received prior systemic nonsteroidal immunosuppressants. The most commonly used nonsteroidal immunosuppressant was cyclosporine (|||||).
Table 21: Summary of Baseline and Disease Characteristics — Study 1434
Characteristic | 6 months to < 6 years N = 180 | 6 years to < 12 years N = 368 |
|---|---|---|
Sex, n (%) | ||
Male | 116 (64.4) | ||| |||||| |
Female | 64 (35.6) | ||| |||||| |
Age (years) | ||
Mean (SD) | 3.86 (1.32) | ||| |||||| |
Median (min, max) | |||| ||||| |||| | ||| ||| ||| |
Age group, n (%) | ||
0.5 years to < 2 years | 19 (10.6) | || |
2 years to < 6 years | 161 (89.4) | || |
6 years to < 9 years | NA | ||| |||||| |
9 years to < 12 years | NA | ||| |||||| |
Race, n (%) | ||
White | 119 (66.1) | ||| |||||| |
Black or African American | 34 (18.9) | || |||||| |
Asian | 13 (7.2) | || ||||| |
Other | 8 (4.4) | || ||||| |
Not reported | 6 (3.3) | | ||||| |
Weight (kg) | ||
Mean (SD) | 16.96 (4.58) | ||||| ||||||| |
Median (min, max) | ||||| ||||| ||||| | ||||| |||||| ||||| |
BMI (kg/m2) | ||
Mean (SD) | 16.46 (2.04) | ||||| |||||| |
Median (min, max) | ||||| |||||| ||||| | ||||| |||||| ||||| |
Country, n (%) | ||
Canada | || | || ||||| |
Czech Republic | || | || ||||| |
Germany | | ||||| | || ||||| |
Hungary | || | | ||||| |
Poland | || |||||| | || |||||| |
UK | || ||||| | || ||||| |
US | ||| |||||| | ||| |||||| |
Duration of atopic dermatitis (years) | ||
Mean (SD) | ||| |||||| | ||| |||||| |
Median (min, max) | ||| ||| || | ||| ||| ||||| |
IGA score | ||
N | ||| | 368 |
Mean (SD) | ||| |||||| | ||| |||||| |
Median (min, max) | ||| ||| || | ||| ||| || |
IGA score, n (%) | ||
0, clear | | ||||| | | ||||| |
1, almost clear | || |||||| | || |||||| |
2, mild disease | || |||||| | ||| |||||| |
3, moderate disease | || |||||| | 110 (29.9) |
4, severe disease | || |||||| | 72 (19.6) |
Missing | | ||||| | || |
EASI score | ||
Mean (SD) | 17.29 (14.47) | 15.70 (15.88) |
Median (min, max) | ||||| ||| ||||| | |||| ||| ||||| |
Percent BSA affected | ||
N | ||| | ||| |
Mean (SD) | |||| ||||||| | 28.6 (25.52) |
Median (min, max) | |||| ||| |||||| | || ||| |||||| |
SCORAD score | ||
N | ||| | ||| |
Mean (SD) | |||| ||||||| | |||| ||||||| |
Median (min, max) | |||| ||| ||||| | |||| ||| |||||| |
CDLQI score | ||
N | || | ||| |
Mean (SD) | ||| |||||| | ||| |||||| |
Median (min, max) | ||| ||| ||||| | ||| ||| ||| |
IDQOL score | ||
N | || | NA |
Mean (SD) | |||| |||||| | NA |
Median (min, max) | |||| ||| ||| | NA |
Patients with current atopic and/or allergic conditions excluding atopic dermatitis, n (%) | ||| |||||| | ||| |||||| |
Prior systemic corticosteroids and/or systemic nonsteroidal immunosuppressants, n (%) | || |||||| | ||| |||||| |
Prior systemic corticosteroids, n (%) | || |||||| | ||| |||||| |
Prior systemic nonsteroidal immunosuppressants, n (%) | || |||||| | ||| |||||| |
Azathioprine | | ||||| | | ||||| |
Methotrexate | || ||||| | || ||||| |
Cyclosporine | || |||||| | || |||||| |
Mycophenolate | | ||||| | | ||||| |
BMI = body mass index; BSA = body surface area; CDLQI = Children’s Dermatology Life Quality Index; EASI = Eczema Area and Severity Index; IDQOL = Infants’ Dermatitis Quality of Life Index; IGA = Investigator’s Global Assessment; max = maximum; min = minimum; NA = not applicable; SCORAD = Scoring Atopic Dermatitis; SD = standard deviation.
Source: Sponsor’s Summary of Clinical Evidence, Study 1434 (6 months to < 6 years) Clinical Study Report, and Study 1434 (6 years to < 12 years) Clinical Study Report.3,38,39 (Note: Details from the table have been taken from the sponsor’s Summary of Clinical Evidence.)
Protocol Deviations
A total of ||| ||||||| patients aged 6 months to younger than 6 years had at least 1 protocol deviation, of whom ||||| of patients had major deviations. The most common reasons for major deviation were inadequate informed consent administration (|||||), due to the COVID-19 pandemic (||||), and personnel not designated to perform study-related activities (||||).
A total of ||| ||||||| patients aged 6 years to 12 years had at least 1 protocol deviation, of whom ||||| of patients had major deviations. The most common reasons for major deviation were dosing noncompliance (|||||), procedure not performed (|||||), and inadequate informed consent administration (||||).
Results
Patient Disposition
Patient disposition is summarized in Table 22. A total of 180 patients aged 6 months to younger than 6 years were screened and enrolled in the study before the data cut-off of July 31, 2021. Of them, 167 patients were ongoing in the study at the time of the cut-off point for the third-step analysis. Reasons for discontinuation included AEs (||||), physician decision (||||), withdrawal by the patient (||||), lack of efficacy (||||), and for other unreported reasons (||||).
A total of ||| patients aged 6 years to younger than 12 years were screened in the study, of whom 368 (|||||) were enrolled. Among the || patients were screened out, || did not meet eligibility criteria and || withdrew consent before the baseline visit. Also, ||| patients had discontinued the study before the data cut-off date. Reasons for discontinuation included AEs (||||), physician decision (||||), withdrawal by the patient (||||), and for lack of efficacy (||||). Accordingly, a total of ||| patients were ongoing in the study at the time of the data cut-off point of July 22, 2019.
Exposure to Study Treatments
Patient exposure to study treatment is summarized in Table 23. Among the 180 patients aged 6 months to younger than 6 years, 122 (67.8%) patients completed 16 weeks, 74 (41.1%) completed 26 weeks, 68 (37.8%) completed 26 weeks, 30 (16.7%) completed 52 weeks, 29 (16.1%) completed 104 weeks, and 15 (8.3%) completed 156 weeks of the treatment period. The mean treatment exposure at the data cut-off date (July 31, 2021) was ||||| ||||| and the median treatment exposure was |||| ||||| ||||||| ||| ||||| || ||||| ||||||.
For patients aged 6 years to younger than 12 years, 282 (76.6%) patients had completed 16 weeks, 217 (59.0%) completed 26 weeks, 39 (10.6%) completed 52 weeks, || |||||| completed 78 weeks, || |||||| completed 104 weeks, and || |||||| completed 156 weeks of the treatment period. The mean treatment exposure at the data cut-off date (July 22, 2019) was ||||| weeks and the median treatment exposure was |||| ||||| (range, ||| ||||| to ||||| |||||).
Table 22: Summary of Patient Disposition — Study 1434
Patient disposition | 6 months to < 6 years N = 180 | 6 years to < 12 years N = 368 |
|---|---|---|
Patients screened, n | 180 | ||| |
From parent study | ||
LIBERTY AD PRESCHOOL part A | 36 (20.0) | NA |
LIBERTY AD PRESCHOOL part B | 144 (80.0) | NA |
R668-AD-1412 | NA | || ||||| |
LIBERTY AD PEDS | NA | ||| |||||| |
Patients enrolled | 180 (100) | ||| |||||| |
Patients screened out | 0 (0.0) | | ||||| |
Patient in SAS | 180 (100) | ||| ||||| |
Patients ongoing | 167 (92.8) | ||| |||||| |
Patients who did not complete study | 13 (7.2) | || ||||| |
Reason for not completing the study | ||
AE | 1 (0.6) | | ||||| |
Physician decision | 0 (0.0) | | ||||| |
Withdrawal by participant | 10 (5.6) | | ||||| |
Lack of efficacy | 1 (0.6) | | ||||| |
Lost to follow-up | 1 (0.6) | | ||||| |
Death | 0 (0.0) | ||| |
Other | 0 (0.0) | | ||||| |
Patient who completed | ||
≥ week 16 | 122 (67.8) | 282 (76.6) |
≥ week 24 | 74 (41.1) | ||| |||||| |
≥ week 26 | 68 (37.8) | 217 (59.0) |
≥ week 52 | 30 (16.7) | 39 (10.6) |
≥ week 78 | 30 (16.7) | || ||||| |
≥ week 104 | 29 (16.1) | || ||||| |
≥ week 156 | 15 (8.3) | || ||||| |
≥ week 208 | 0 (0.0) | ||| |
≥ week 260 | 0 (0.0) | ||| |
AE = adverse event; NA = not applicable; SAS = safety analysis set.
Note: Values are n (%) unless otherwise indicated.
Source: Sponsor’s Summary of Clinical Evidence, Study 1434 (6 months to < 6 years) Clinical Study Report, and Study 1434 (6 years to < 12 years) Clinical Study Report.3,38,39 (Note: Details From the table have been taken from the sponsor’s Summary of Clinical Evidence.)
Table 23: Summary of Patient Exposure — Study 1434, SAS
Exposure | 6 months to < 6 years N = 180 | 6 years to < 12 years N = 368 |
|---|---|---|
Overall exposure (weeks) | ||
Mean (SD) | ||||| ||||||| | ||||| ||||||| |
Median (min, max) | |||| ||||| |||||| | |||| ||||| |||||| |
Number of study drug injections administered | ||
Mean (SD) | |||| ||||||| | |||| ||||||| |
Median (min, max) | ||| ||||| |||||| | ||| ||||| |||||| |
Injection adherence (%) | ||
Mean (SD) | ||||| |||||| | ||||| |||||| |
Median (min, max) | ||||| |||||| |||||| | ||||| |||||| |||||| |
max = maximum; min = minimum; SAS = safety analysis set; SD = standard deviation.
Source: Sponsor’s Summary of Clinical Evidence, Study 1434 (6 months to < 6 years) Clinical Study Report, and Study 1434 (6 years to < 12 years) Clinical Study Report.3,38,39 (Note: Details from the table have been taken from the sponsor’s Summary of Clinical Evidence.)
Concomitant Medications and Co-Interventions
Concomitant medications and co-interventions are summarized in Table 24. Of the patients aged 6 months to younger than 6 years, ||| ||||||| patients used permitted concomitant topical medications during the study, ||| ||||||| used TCSs for atopic dermatitis and || ||||||| used TCIs for atopic dermatitis. A total of | |||||| patients used at least 1 rescue medication (systemic corticosteroids).
Of the patients aged 6 years to younger than 12 years, ||| ||||||| patients used permitted concomitant topical medications during the study, ||| ||||||) used TCSs for atopic dermatitis, and || |||||| used TCIs for atopic dermatitis, mostly tacrolimus (||||). A total of || |||||| patients used at least 1 rescue medication (systemic corticosteroids).
Table 24: Summary of Concomitant Medications and Co-Interventions — Study 1434, SAS
Patient disposition | 6 months to < 6 years N = 180 | 6 years to < 12 years N = 368 |
|---|---|---|
Patients on topical medication for atopic dermatitis, n (%) | ||| |||||| | ||| |||||| |
TCS | ||| |||||| | ||| |||||| |
Mild potency | ||| |||||| | ||| |||||| |
Moderate potency | || |||||| | ||| |||||| |
Potent | || |||||| | ||| |||||| |
Very potent | | ||||| | | ||||| |
TCI | || |||||| | || ||||| |
Tacrolimus | || ||||| | || ||||| |
Pimecrolimus | | ||||| | || ||||| |
Crisaborole | | ||||| | | ||||| |
Used rescue treatment | | ||||| | || ||||| |
Corticosteroids for systemic use | | ||||| | || ||||| |
SAS = safety analysis set; TCI = topical calcineurin inhibitor; TCS = topical corticosteroid.
Source: Sponsor’s Summary of Clinical Evidence, Study 1434 (6 months to < 6 years) Clinical Study Report, and Study 1434 (6 years to < 12 years) Clinical Study Report.3,38,39 (Note: Details from the table have been taken from the sponsor’s Summary of Clinical Evidence.)
Efficacy
At the time of this review, Study 1434 was ongoing and no patients had completed the 260-week assessment. Also, very limited data were available beyond week 16. Early findings for primary and secondary efficacy end points from baseline, 4, 16, 28, 52, and 104 weeks are presented in Table 25.
Proportion of Patients Experiencing an IGA Score of 0 or 1
Of the patients aged 6 months to younger than 6 years, the proportion who experienced an IGA score of 0 or 1 was || || ||| ||||||| patients at baseline of Study 1434, || || ||| ||||||| patients at week 16, || || || ||||||| patients at week 52, and || || || ||||||| patients at week 104. Of the ||| patients who completed 52 weeks of treatment, || ||||| patients experienced sustained remission. |||||||| of the || ||||||| patients experienced disease relapse and subsequently reinitiated dupilumab. Patients may have restarted dupilumab at an unscheduled visit making the mean time between remission and restarting the drug an estimate of |||| ||||| ||| | |||| ||||||.
Of the patients aged 6 years to younger than 12 years, the proportion who experienced an IGA score of 0 or 1 was 65 of 368 (17.7%) patients at baseline of Study 1434, 96 of 281 (34.2%) patients at week 16, 20 of 40 (50.0%) patients at week 52, and 17 of 33 (51.5%) patients at week 104. During the study, patients were transitioned from a weight-based dosing regimen to a fixed dose of 300 mg every 4 weeks and the results for remission were reported for patients who received weight-based dosing under the original protocol. Of the 33 patients who completed 52 weeks of treatment, || ||||||| patients experienced sustained remission. Eleven of the || ||||||| patients experienced disease relapse and subsequently reinitiated dupilumab. Patients may have restarted dupilumab at an unscheduled visit making the mean time between remission and restarting the drug an estimate of |||| ||||| (SD = |||| |||||).
Proportion of Patients Experiencing EASI-75 Relative to Baseline of Parent Study
Of the patients aged 6 months to younger than 6 years, the proportion who experienced EASI-75 was 53 of 180 (29.4%) patients at baseline, 89 of 123 (72.4%) patients at week 16, 26 of 29 (89.7%) patients at week 52, and 25 of 27 (92.6%) patients at week 104.
Of the patients aged 6 years to younger than 12 years, the proportion who experienced EASI-75 was 151 of 368 (41.0%) patients at baseline, 195 of 281 (69.4%) patients at week 16, 33 of 40 (82.5%) patients at week 52, and 23 of 30 (76.7%) patients at week 104.
Proportion of Patients Experiencing EASI-50 Relative to Baseline of Parent Study
Of the patients aged 6 months to younger than 6 years, the proportion who experienced EASI-50 was 103 of 180 (57.2%) patients at baseline, 108 of 123 (87.8%) patients at week 16, 26 of 29 (89.7%) patients at week 52, and 26 of 27 (96.3%) patients at week 104.
Of the patients aged 6 years to younger than 12 years, the proportion who experienced EASI-50 was 251 of 368 (68.2%) patients at baseline, 254 of 281 (90.4%) patients at week 16, 37 of 40 (92.5%) patients at week 52, and 29 of 30 (96.7%) patients at week 104.
Proportion of Patients Experiencing EASI-90 Relative to Baseline of Parent Study
Of the patients aged 6 months to younger than 6 years, the proportion who experienced EASI-90 was 26 of 180 (14.4%) patients at baseline, 54 of 123 (43.9%) patients at week 16, 17 of 29 (58.6%) patients at week 52, and 20 of 27 (74.1%) patients at week 104.
Of the patients aged 6 years to younger than 12 years, the proportion who experienced EASI-90 was 77 of 368 (20.9%) patients at baseline, 108 of 281 (38.4%) patients at week 16, 22 of 40 (55.0%) patients at week 52, and 19 of 30 (63.3%) patients at week 104.
Mean Percent Change in EASI Score From Baseline of Parent Study
Of the patients aged 6 months to younger than 6 years, the mean percent change in EASI score from baseline of the parent study was −50.26% at baseline of the LTE, −79.79% at week 16, −86.44% at week 52, and −90.97 at week 104.
Of the patients aged 6 years to younger than 12 years, the mean percent change in EASI score from baseline of the parent study was −59.05% at baseline of the LTE, −78.56% at week 16, −87.36% at week 52, and −87.25 at week 104.
Mean Percent Change in BSA Involved From Baseline of Parent Study
Of the patients aged 6 months to younger than 6 years, the mean percent change in BSA affected from baseline of the parent study was |||||| at baseline of the LTE, –||||| at week 16, |||||| at week 52, and |||||| at week 104.
Of the patients aged 6 years to younger than 12 years, the mean percent change in BSA affected from baseline of the parent study was |||||| at baseline of the LTE, |||||| at week 16, |||||| at week 52, and |||||| at week 104.
Subgroup Analysis: Previous Usage of Systemic Immunosuppressants
Of the patients aged 6 months to younger than 6 years, consistency of the dupilumab with TCS treatment effect was observed among all the subgroups, including those with prior systemic immunosuppressant usage.
Of the patients aged 6 years to younger than 12 years, a total of ||| out of ||| patients had previous usage of systemic immunosuppressants for atopic dermatitis. At baseline of the LTE, only || || ||| |||||| patients had experienced an IGA score of 0 or 1. The proportion of patients experiencing an IGA score of 0 or 1 generally increased throughout study. By week 28, || || || ||||||| patients experienced an IGA score of 0 or 1.
At baseline of the LTE, || || ||| ||||||| patients had experienced EASI-75. The proportion of patients experiencing EASI-75 generally increased throughout study. By week 25, || || || ||||||| patients EASI-75. The data for this subgroup were consistent with the whole population for the key efficacy end points.
Table 25: Summary of Key Efficacy Outcomes — Study 1434, SAS
Outcome | 6 months to < 6 years N = 180 | 6 years to < 12 years N = 368 |
|---|---|---|
Proportion of patients experiencing IGA 0 or 1, n of N1 (%) | ||
Baseline of Study 1434 | 23 of 179 (12.8) | 65 of 368 (17.7) |
Week 4 | 36 of 172 (20.9) | 80 of 315 (25.4) |
Week 16 | 41 of 123 (33.3) | 96 of 281 (34.2) |
Week 28 | 22 of 55 (40.0) | 75 of 191 (39.3) |
Week 52 | 13 of 30 (43.3) | 20 of 40 (50.0) |
Week 104 | 14 of 27 (51.9) | 17 of 33 (51.5) |
Proportion of patients experiencing EASI-75 relative to baseline of parent study, n of N1 (%) | ||
Baseline of Study 1434 | 53 of 180 (29.4) | 151 of 368 (41.0) |
Week 4 | 98 of 172 (57.0) | 170 of 315 (54.0) |
Week 16 | 89 of 123 (72.4) | 195 of 281 (69.4) |
Week 28 | 43 of 55 (78.2) | 139 of 191 (72.8) |
Week 52 | 26 of 29 (89.7) | 33 of 40 (82.5) |
Week 104 | 25 of 27 (92.6) | 23 of 30 (76.7) |
Proportion of patients experiencing EASI-50 relative to baseline of parent study, n of N1 (%) | ||
Baseline of Study 1434 | 103 of 180 (57.2) | 251 of 368 (68.2) |
Week 4 | 143 of 172 (83.1) | 261 of 315 (82.9) |
Week 16 | 108 of 123 (87.8) | 254 of 281 (90.4) |
Week 28 | 49 of 55 (89.1) | 181 of 191 (94.8) |
Week 52 | 26 of 29 (89.7) | 37 of 40 (92.5) |
Week 104 | 26 of 27 (96.3) | 29 of 30 (96.7) |
Proportion of patients experiencing EASI-90 relative to baseline of parent study, n of N1 (%) | ||
Baseline of Study 1434 | 26 of 180 (14.4) | 77 of 368 (20.9) |
Week 4 | 54 of 172 (31.4) | 93 of 315 (29.5) |
Week 16 | 54 of 123 (43.9) | 108 of 281 (38.4) |
Week 28 | 31 of 55 (56.4) | 86 of 191 (45.0) |
Week 52 | 17 of 29 (58.6) | 22 of 40 (55.0) |
Week 104 | 20 of 27 (74.1) | 19 of 30 (63.3) |
Percent change in EASI score from baseline of parent study, mean (SD) | ||
Baseline of the Study 1434 | –50.3 (35.68) | –59.05 (36.56) |
Week 4 | –71.0 (28.07) | –71.04 (26.06) |
Week 16 | –79.8 (23.95) | –78.56 (23.71) |
Week 28 | –82.1 (25.03) | –82.20 (17.84) |
Week 52 | –86.4 (19.78) | –87.36 (16.71) |
Week 104 | –91.0 (11.18) | –87.25 (18.22) |
Percent change in BSA affected from baseline of parent study, mean (SD) | ||
Baseline of the Study 1434 | –26.3 (23.72) | ||||| ||||||| |
Week 4 | –37.2 (23.72) | ||||| ||||||| |
Week 16 | –42.8 (22.91) | ||||| ||||||| |
Week 28 | –41.8 (23.16) | ||||| ||||||| |
Week 52 | –45.6 (20.03) | ||||| ||||||| |
Week 104 | –51.2 (17.76) | ||||| ||||||| |
BSA = body surface area; EASI = Eczema Area and Severity Index; EASI-50 = 50% reduction in Eczema Area and Severity Index score; EASI-75 = 75% reduction in Eczema Area and Severity Index score; EASI-90 = 90% reduction in Eczema Area and Severity Index score; IGA = Investigator’s Global Assessment; n = number of patients who were responders; N1 = number of patients with observed data at the visit; SAS = safety analysis set; SD = standard deviation.
Source: Sponsor’s Summary of Clinical Evidence, Study 1434 (6 months to < 6 years) Clinical Study Report, and Study 1434 (6 years to < 12 years) Clinical Study Report.3,38,39 (Note: Details from the table have been taken from the sponsor’s Summary of Clinical Evidence.)
Harms
A summary of harms for Study 1434 is presented in Table 26.
Adverse Events
For patients 6 months to younger than 6 years, 109 (60.6%) had at least 1 TEAE. The most common TEAEs were nasopharyngitis (12.8%), upper respiratory tract infection (11.7%), pyrexia (11.7%), cough (8.3%), urticaria (7.2%), dermatitis atopic (6.7%), rhinorrhea (6.1%), and food allergy (5.0%).
For patients aged 6 years to younger than 12 years, ||| ||||||| had at least 1 TEAE. The most common TEAEs were |||||| |||||||||| |||||||| ||||||||||||||| |||||||| ||||| ||||||||||| ||||| ||||||||| ||||||| ||||| ||||||| |||||||||||||| |||||||| ||||||| ||| |||||||| ||||||.
Serious Adverse Events
For patients aged 6 months to younger than 6 years | | |||||| reported SAEs of |||||||||||| |||||||| |||||| and ||||||||| |||||||||| |||||||
For patients aged 6 years to younger than 12 years, | |||||| reported SAEs. |||| of the reported SAEs led to permanent treatment discontinuation.
Withdrawals Due to Adverse Events
For patients aged 6 months to younger than 6 years, | |||||| withdrew from the study due to urticaria.
For patients aged 6 years to younger than 12 years, | |||||| withdrew from the study due to an atopic dermatitis flare and intracranial pressure.
Notable Harms
Patients aged 6 months to younger than 6 years reported the following notable harms: |||||||||||| |||||||| ||||||| |||||||||||||||| ||||||| |||||||||| ||||||||| ||||||| |||||||||||||| ||||||| ||||||||||| ||||||| ||||||||| ||||||| ||| ||||||||| |||| |||| ||||||. |||| led to discontinuation of dupilumab. ||| ||||| was serious (severe anaphylactic reaction) and resolved over time with treatment. The ||||||||| |||||||||| and ||||||||||| |||||||| |||||| resolved over time with treatment and did not lead to discontinuation of study drug.
Patients aged 6 years to younger than 12 years reported the following notable harms: patients experienced |||||||||||| |||||||| ||||||| |||||||||||||||| ||||||| |||||||||| ||||||||| ||||||| |||||||||||||| ||||||| ||||||||||| ||||||| ||||||||| ||||||| |||||||||||| ||||||| ||| ||||||||| |||| |||| ||||||. The |||||||||| |||||||||| resolved after treatment |||| ||||||||||||||| ||||||||||. The ||||||||| || |||| |||| ||| | |||||||| ||||| and |||||||||||||| || |||||| ||||| events resolved over time with treatment and did not lead to discontinuation of study drug.
Table 26: Summary of Harms — Study 1434, SAS
Harms | 6 months to < 6 years N = 180 | 6 years to < 12 years N = 368 |
|---|---|---|
Most common TEAEs, n (%) | ||
Patients with ≥ 1 TEAE | 109 (60.6) | 219 (59.5%) |
TEAE ≥ 5% of patients | ||
Nasopharyngitis | 23 (12.8) | || ||||||| |
Upper respiratory tract infection | 21 (11.7) | || |||||| |
Cough | 15 (8.3) | || |||||| |
Rhinorrhea | 11 (6.1) | || |
Urticaria | 13 (7.2) | | |||||| |
Dermatitis atopic | 12 (6.7) | || ||||||| |
Pyrexia | 21 (11.7) | || |||||| |
Food allergy | 9 (5.0) | || |
Conjunctivitis allergic | ||| | 24 (6.5) |
Headache | ||| | || |||||| |
SAEs, n (%) | ||
Patients with ≥ 1 SAE, n (%) | | ||||| | 9 (2.4) |
Anaphylactic reaction | | ||||| | | ||||| |
Pneumonia mycoplasma | | ||||| | || |
Impetigo | ||| | | ||||| |
Pneumonia | ||| | | ||||| |
Postprocedural hemorrhage | ||| | | ||||| |
Upper limb fracture | ||| | | ||||| |
Lymphadenopathy | ||| | | ||||| |
Cryptorchism | ||| | | ||||| |
Abdominal pain | ||| | | ||||| |
Allergy test | ||| | | ||||| |
Arthralgia | ||| | | ||||| |
Complex regional pain syndrome | ||| | | ||||| |
Dizziness postural | ||| | | ||||| |
Asthma | ||| | | ||||| |
Tonsillar hypertrophy | ||| | | ||||| |
Patients who stopped treatment due to adverse events, n (%) | ||
Patients who stopped | | ||||| | | |||||| |
Urticaria | | ||||| | ||| |
Atopic dermatitis flare | ||| | | |||||| |
Intracranial pressure | ||| | | |||||| |
Deaths, n (%) | ||
Patients who died | 0 (0.0) | 0 (0.0) |
Notable harms, n (%) | ||
Anaphylactic reaction | | ||||| | | ||||| |
Hypersensitivity | | ||||| | | ||||| |
Helminthic infection | | ||||| | | ||||| |
Conjunctivitis | | ||||| | | ||||| |
Blepharitis | | ||||| | | ||||| |
Keratitis | | ||||| | | ||||| |
Eosinophilia | || | | ||||| |
Facial erythema | || | || |
Injection site pain | | ||||| | | ||||| |
NR = not reported; SAE = serious adverse event; SAS = safety analysis set; TEAE = treatment-emergent adverse event.
Source: Sponsor’s Summary of Clinical Evidence, Study 1434 (6 months to < 6 years) Clinical Study Report, and Study 1434 (6 years to < 12 years) Clinical Study Report.3,38,39 (Note: Details from the table have been taken from the sponsor’s Summary of Clinical Evidence.)
Critical Appraisal
Internal Validity
The limited availability of long-term data (i.e., mature data) beyond week 16 makes it challenging to draw firm conclusions about the long-term efficacy and safety of dupilumab. The open-label design could bias the magnitude of treatment effect for subjective efficacy outcomes and reporting of safety parameters. Statistical hypothesis testing was not part of the design and there was no active comparator or placebo arm.
External Validity
Because the extension study consisted of patients who took part in the parent (pivotal) studies, it is reasonable to expect that the same strengths and limitations related to generalizability apply to the LTE, with the added possibility of selection bias due to patients having to complete at least 50% of the visits during the treatment and follow-up periods of the parent study before enrolling in the extension study.
Indirect Evidence
Contents within this section have been informed by materials submitted by the sponsor. The following have been summarized and validated by the CADTH review team.
Objectives and Methods for the Summary of Indirect Evidence
No direct comparative data for the use of dupilumab for the treatment of patients aged 6 months to younger than 12 years with moderate-to-severe atopic dermatitis whose disease is not adequately controlled with topical prescription therapies were identified by the sponsor. As a result, the sponsor conducted a systematic literature review and targeted literature review for evidence of dupilumab versus other treatments (e.g., targeted immunomodulators [biologics, Janus kinase inhibitors], systemic immunosuppressants, and phototherapies) to assess the feasibility of conducting an indirect comparison.3
Due to the lack of a common comparator among trials of adequate size, an evidence network was unable to be established, ruling out a network meta-analysis. Unanchored indirect comparisons via simulated treatment comparison or matching-adjusted indirect comparison were then assessed for feasibility. Based on the assessment, it was determined that due to the assumptions that would be made (e.g., comparability of analysis time points and outcome definitions across the trials) and limitations (e.g., small sample sizes in comparator trials, notable differences in trial durations, and limited variables available for adjustment) of the available data, it was not feasible to conduct any indirect comparisons.
CADTH’s review of the sponsor’s feasibility assessment is provided here.
Appraisal of the Feasibility Assessment
The sponsor conducted a feasibility assessment to determine if the clinical trials identified from the literature search for treatment of pediatric patients aged 6 months to younger than 6 years and 6 years to younger than 12 years with moderate-to-severe atopic dermatitis were sufficiently similar to permit valid comparison in an ITC.3 The study selection criteria were similar to that used for the pivotal trials and appeared to be reasonable.
For the group of participants aged 6 months to younger than 6 years, no relevant results met the inclusion criteria for data extraction from either the systematic literature review or the targeted literature review and an ITC was deemed to be not feasible. Other studies for baricitinib versus TCS or placebo, nemolizumab (single arm), systemic cyclosporine versus dupilumab, and methotrexate versus systemic cyclosporine for pediatric patients with moderate-to-severe atopic dermatitis were identified from the searches. However, these were ongoing trials and did not have published results, and could be of interest for future indirect comparisons.
For the group of participants aged 6 years to younger than 12 years, a total of 4 studies were included in the feasibility assessment: 2 studies identified from the systematic literature review, 1 study identified from the targeted literature review, and data from the LIBERTY AD PEDS trial were provided by the sponsor. Only the SCORAD score, percent BSA affected by atopic dermatitis, and aggregate safety outcomes were reported across all studies; other efficacy and HRQoL outcomes important to the CADTH review were inconsistently reported among studies or data were not available preventing their comparison. Treatment durations varied across studies from 6 weeks to 52 weeks, as did analysis time points with the closest to week 16 (in the LIBERTY AD PEDS trial) being week 12 in 2 studies and week 6 in 1 study.
The sponsor’s literature search went to December 2019 and it is possible that there could have been studies published since then. The authors of the feasibility assessment stated that the lack of common comparator among the studies prevented use of a network meta-analysis. Limited reporting of potential prognostic factors and treatment effect modifiers prevented adjustments that could reduce bias in the analyses, and without the adjustments, it would be necessary to assume that unmeasured effect modifiers were balanced across studies, which was unlikely. The authors also noted that the age range of patients varied considerably, which could not be adjusted for in a matching-adjusted indirect comparison and would require additional assumptions (for a relationship between age and outcomes) that may not be valid. Simulated treatment comparison methods could allow for data extrapolation, but the results would be for a population outside of the age range of interest. Another notable difference was the variable use of concomitant corticosteroids across studies. Without detailed reporting of baseline patient characteristics and differences in study designs, it is difficult to assess the similarity and homogeneity assumptions and with no head-to-head comparisons, no conclusions on consistency can be made. Additionally, the authors indicated that studies for cyclosporine and methotrexate were deemed to have small sample sizes and be of low quality that raised concerns about the validity of comparisons. The CADTH review team agreed that based on the results of the feasibility analysis, namely the between-study heterogeneity, limited available data, and inclusion of small and low-quality studies, conducting an ITC would not be feasible.
Studies Addressing Gaps in the Pivotal and RCT Evidence
Contents within this section have been informed by materials submitted by the sponsor. The following have been summarized and validated by the CADTH review team.
One observational study assessing real-world treatment of patients aged younger than 12 years with moderate-to-severe atopic dermatitis has been summarized for the CADTH report.3 The sponsor indicated that this study may address the gap in evidence comparing dupilumab to other treatments such as methotrexate or cyclosporine for this patient population.
Description of Studies
PEDISTAD is an ongoing, international, 5-year, prospective study that was initiated on September 28, 2018.3 The primary objective of the study was to describe the characteristics of pediatric patients with moderate-to-severe atopic dermatitis whose disease is not adequately controlled with topical therapies or when those therapies are not advisable and to evaluate the time course of atopic dermatitis and selected atopic comorbidities. The secondary objectives were to characterize disease burden and unmet need and to describe real-world treatment patterns, effectiveness, and safety.
Eligibility Criteria
Patients were eligible to enrol if they were aged younger than 12 years at baseline with moderate-to-severe atopic dermatitis and currently receiving systemic treatment for atopic dermatitis (including biologics), UV therapy, and immunosuppressants (e.g., cyclosporine, azathioprine, methotrexate, mycophenolate mofetil, or corticosteroids), or were currently on topical treatment but would be candidates for systemic treatment. Patients were recruited into 3 age cohorts (aged < 2 years, 2 years to < 6 years, and 6 years to < 12 years) and were to be followed for 5 years. A total of 12 visits were planned for each patient.
Choice of treatment was based on the medical judgment of enrolled physicians who assessed patients’ eligibility and disease severity using the assessments of their choice. Patients could start therapies that became commercially available during the course of the study. Treatment effect from the start of therapy through 2 years’ follow-up was assessed using the EASI, percent BSA, and patient- or proxy-reported outcome scores (CDLQI, IDLQI, POEM, peak itch NRS, and DFI). Treatment discontinuations and TEAEs, regardless of seriousness, were also assessed.
Statistical Analysis
Hypothesis-testing statistical analyses were not planned and all statistical analyses were performed descriptively with no formal comparison between study treatments.
Results
A total of 1,329 patients were enrolled across 21 countries with 103 patients from Canada. Globally, approximately 61% of patients had at least 1 atopic or allergic comorbidity. Overall, 32% of patients were receiving any systemic treatment, which included dupilumab (12.0%), corticosteroids (10.2%), cyclosporine (9.3%), methotrexate (8.7%), and mycophenolate (1.0%).
Two-year interim efficacy and safety results from the global subgroup of patients showed that 144 patients received SC dupilumab 300 mg every 2 weeks for a median treatment observation period of 8.1 months, 114 patients received methotrexate for 13.0 months, and 121 patients received cyclosporine for 10.7 months.
Of the patients receiving dupilumab, methotrexate, or cyclosporine, there appeared to be greater numerical improvements in the EASI total score, percent BSA affected by atopic dermatitis, and POEM score among those receiving dupilumab. Also, there was a numerical improvement in the combined CDLQI or IDQOL score among patients receiving dupilumab.
AEs and discontinuation rates were lower in the dupilumab group compared to methotrexate or cyclosporine.
Critical Appraisal
Internal Validity
Several limitations prevent firm conclusions from being drawn for the comparison of dupilumab to methotrexate and cyclosporine. First, the data informing this study were based on the sponsor’s Summary of Clinical Evidence. Published manuscripts or clinical study reports with more detailed information were not available. Second, the results were descriptive and there was no hypothesis testing. Third, there is a possibility of selection bias due to the selection of physicians, especially since the population of eligible physicians and the response rate were not reported. Fourth, it is unclear how many patients were lost to follow-up, how many patients were censored, and how this affects interpretation of the findings. For these reasons, it was challenging to draw any meaningful conclusions about the comparative efficacy of dupilumab versus other systemic treatments.
External Validity
Data on the available treatments were limited; it is unknown what doses were used, if they were pooled, or what background therapies were acceptable. According to the sponsor, treatment selection was at the discretion of the treating physician, rather than patients being randomized to treatment, which is understandable given the real-world setting. However, as per the sponsor, the reason for choice of therapy was not collected, and it is unknown if there was any bias in the choice of selection. Furthermore, reporting was limited to the 3 systemic treatments, and it would be of interest to know the results for other comparators. Data for baseline patient characteristics were available by age cohort, but results were presented based on treatment received; therefore, it was not possible to know how similar or heterogenous the treatment groups were to 1 another and if comparison of groups would be reasonable. The data informing this study included a small number of patients living in Canada and it is unclear how representative the findings are to the population of pediatric patients with atopic dermatitis living in Canada and being managed in clinical practice.
Discussion
Summary of Available Evidence
Two phase III, double-blind RCTs were submitted for the CADTH review of dupilumab for the treatment of patients aged 6 months and older with moderate-to-severe atopic dermatitis whose disease is not adequately controlled with topical prescription therapies or when those therapies are not advisable and can be used with or without TCSs.36,37 Patients in the LIBERTY AD PRESCHOOL trial (N = 162) were randomized to receive either dupilumab every 4 weeks with TCS or placebo with TCS while those in the LIBERTY AD PEDS trial (N = 367) were randomized to receive dupilumab every 2 weeks with TCS, dupilumab every 4 weeks with TCS, or placebo with TCS. Treatment in both trials was for 16 weeks. The primary end point was the proportion of patients with an IGA score of either 0 or 1 at week 16 and key secondary end points included the proportion of patients with EASI-75, percent change from baseline in EASI score, and percent change from baseline in weekly average of daily worst itch NRS score at week 16. Additional secondary end points in the testing hierarchy included other disease-related outcomes (e.g., SCORAD, POEM, skin pain NRS, sleep quality NRS) and HRQoL measures (e.g., DFI, CDLQI, IDQOL). Patients eligible to participate in the LIBERTY AD PRESCHOOL trial must have been aged 6 months to younger than 6 years with moderate-to-severe atopic dermatitis (IGA ≥ 3, EASI ≥ 16, and BSA affected ≥ 10%) while those in the LIBERTY AD PEDS trial must have been aged 6 years to younger than 12 years with severe atopic dermatitis (IGA 4, EASI ≥ 21, and BSA affected ≥ 15%). Patients in the LIBERTY AD PRESCHOOL trial had a mean age of 3.8 years, there were fewer females (38.9%) than males (61.1%), and the mean EASI score was 34.1, while in those in LIBERTY AD PRESCHOOL trial had a mean age of 8.5 years, males and females were evenly balanced, and the mean EASI score was 37.9.
One ongoing, LTE study (Study 1434) was included in the CADTH report that provided longer-term safety and efficacy evidence for patients who had rolled over from the pivotal trials to continue receiving dupilumab.38,39 There was no indirect evidence identified for this patient population and the sponsor performed a feasibility of assessment for an ITC. Sponsor-submitted data addressing gaps in the RCT evidence included 1 ongoing, observational study (PEDISTAD) for pediatric patients with moderate-to-severe atopic dermatitis receiving systemic treatments such as dupilumab, methotrexate, and cyclosporine.3
Interpretation of Results
Efficacy
The LIBERTY AD PRESCHOOL and LIBERTY AD PEDS trials both showed that dupilumab in combination with TCS experienced a clinically significant improvement in IGA score of 0 or 1 at week 16 compared to TCS alone. Patients in the dupilumab group were also more likely to experience EASI-75, greater reduction in EASI score, and greater reduction in itch NRS. The clinical experts consulted by CADTH stated that the results for the primary and key secondary outcomes were clinically meaningful and patients in the dupilumab group consistently showed improvements on other EASI and itch NRS outcomes. The clinical experts also indicated that the dupilumab groups showed a meaningful reduction in percent BSA affected compared to placebo despite no MID being identified. Absolute reductions in the POEM and SCORAD scores, both measures of disease severity, among patients in the dupilumab groups met the MIDs of 3.4 points and 8.7 points, respectively, for the trials. Results from these outcomes indicated that compared to placebo, treatment with dupilumab reduced BSA affected, and improved disease severity and itch. However, there was less certainty of a clinically meaningful treatment effect based on the symptom-specific outcomes of sleep quality NRS and skin pain NRS in the LIBERTY AD PRESCHOOL trial of patients aged 6 months to younger than 6 years due to their subjective nature and the uncertain accuracy of being proxy-reported for a group of patients who may not be able to communicate their condition. There was no evidence of validity nor MID identified from the literature for the sleep quality NRS and the clinical experts noted that it may be difficult to see a change in sleep during a 16-week period. Additionally, for the skin pain NRS, the LSM treatment difference versus placebo did not reach the MID of 4 points identified from the literature. HRQoL was assessed in both trials and showed greater improvements for patients who received dupilumab compared to placebo. There was no MID identified from the literature for the DFI or IDQOL scores making it unclear if the changes observed in the LIBERTY AD PRESCHOOL trial were clinically meaningful. The LIBERTY AD PRESCHOOL trial CDLQI treatment difference met the within-patient MID range of 6 points to 8 points, but the LIBERTY AD PEDS trial did not. Overall, the clinical experts stated that the HRQoL questionnaires are not part of common practice, and it is difficult to contextualize the results in clinical practice.
Risk of bias arising from the randomization process, unblinding of treatment allocation, and missing data were likely low. In the trials, a much smaller proportion of patients in the dupilumab groups used rescue treatment than the respective placebo groups. Once patients used rescue treatment, their values were set to missing and these patients were considered nonresponders, regardless of their subsequent status throughout the rest of the trial. Based on this rule, rescue treatment did not impact the responder analysis, though discrepancies in rescue use could impact how other outcomes, such as harms and HRQoL, were assessed. There was a lack of validity and reliability evidence from the literature and MIDs were not identified for a number of outcomes; however, the overall treatment effects were consistent among the outcomes in both trials.
The trial outcomes, although not typically used in clinical practice, are relevant to the treatment goals of reducing symptom severity and improving HRQoL with minimal harms. The outcomes also addressed some of the most important patient needs for new medications that safely manage the disease and improve the psychosocial aspects of living with atopic dermatitis. Input submitted to CADTH from the patient groups also noted that topical regimens can be burdensome, though it is unclear from the trial if dupilumab injections every 2 weeks or every 4 weeks address the need for a simpler treatment, particularly if patients and caregivers are uncomfortable with at-home administration or if patients are especially afraid of needles. There is a lack of safe and effective treatments for patients younger than 12 years with moderate-to-severe atopic dermatitis and current treatments may be ineffective at controlling the disease (e.g., topical therapies), are used off-label and have a poor safety profile (e.g., systemic immunosuppressants), or may be inappropriate or inaccessible (e.g., phototherapy).
Longer-term efficacy and safety data were available from the LTE, Study 1434, which indicated that the treatment effect was generally maintained for patients who continued treatment on dupilumab. However, there were limited long-term data available beyond week 16 due to the low number of patients who had completed later study time points and the ongoing nature of the study, and these data will be important for drawing firm conclusions on the sustainability of treatment effect for dupilumab. No direct or indirect evidence was identified for the use of dupilumab versus any alternative treatments for atopic dermatitis in patients aged 6 months to younger than 12 years with moderate-to-severe atopic dermatitis. The sponsor conducted a feasibility assessment to identify data that could support an ITC, but due to the between-study heterogeneity, limited available data, and inclusion of small and low-quality studies, it was determined that an ITC would not be able to provide valid evidence. Real-world evidence from an observational study, PEDISTAD, that included patients aged younger than 12 years who were receiving systemic treatment for moderate-to-severe atopic dermatitis had a number of limitations that prevented useful comparisons from being made between dupilumab, methotrexate, cyclosporine, or other interventions of interest.
Although the patient populations differed in severity of atopic dermatitis between the pivotal trials, the clinical experts were of the opinion that the results for patients with severe disease would likely be generalizable to those with moderate disease. They had also suggested that, in practice, a patient with an EASI score less than 16 may be eligible for dupilumab if, for example, the patient had severe lesions, but low percent BSA affected or had lesions localized to special areas (e.g., hands, feet, scalp). This is supported by the literature showing that patients with moderate atopic dermatitis can have an EASI score as low as 6.34,35
Part of the indication for dupilumab notes that the drug would be for patients in whom topical prescription therapies are not advisable. The sponsor has stated that these patients include, but are not limited to, “those with side effects or safety risks, including hypersensitivity reactions, significant skin atrophy, and side effects related to systemic absorption as assessed by the investigator or by the patient’s treating physician.”93 This is consistent with what the clinical experts suggested with the addition of patients who have chronic atopic dermatitis around sensitive areas, such as the eyes. It was not clear if patients with these characteristics were included in the pivotal trials and the sponsor noted that information for the number of patients in whom topical prescription therapies are not advisable was not collected. The experts expected that this would be a very small proportion of patients and would not greatly impact generalizability to those who could receive dupilumab. On a related note, patients were excluded from the pivotal trials if they had a history of important side effects to TCSs, and non-TCS prescription therapies were not permitted as background therapy, which leaves a gap in the evidence for patients who could receive dupilumab while on other topical treatments. The clinical experts stated that, with proper use, it is rare for patients to have side effects with TCSs and that non-TCS treatments would be acceptable background therapy in practice.
The clinical experts also discussed that while it is possible for childhood atopic dermatitis to decrease in severity or resolve in adolescence, this is less likely for patients with more severe disease, a family history of atopy (particularly paternal history), or a higher SCORAD score.94 Of the patients aged 6 months to younger than 6 years in the LTE study, 60% of those who completed 52 weeks of treatment experienced remission and discontinued dupilumab treatment. Subsequently, 78% of those patients experienced disease relapse and reinitiated dupilumab after an estimated mean time of 18 weeks off dupilumab. Among patients aged 6 years to younger than 12 years in the LTE study, 64% of patients who completed 52 weeks of treatment experienced remission. Afterwards, 53% of those patients experienced disease relapse and reinitiated dupilumab after an estimated mean time of 24 weeks off dupilumab. Although the trials were not designed to inform how management and treatment of atopic dermatitis change with age in pediatric patients, the experts stated that it would be reasonable for patients (at any age) and their caregivers to discuss with their physician about increasing the time between injections or holding dupilumab and seeing if the atopic dermatitis has resolved or can be managed with topical therapies alone; however, this is a nuanced decision to be made by patients, caregivers, and clinicians, and should not be forced.
Harms
Greater than half of patients who received dupilumab (63.9% to 67.2%) or placebo (73.3% to 74.4%) in the pivotal trials experienced at least 1 TEAE. More patients in the placebo groups (19.2% to 62.8%) than the dupilumab groups (2.5% to 19.3%) used rescue treatment during the pivotal trials, which may have biased the harms results if patients experienced adverse effects from rescue therapies. There were no new safety concerns during the 16-week trials or the LTE, though data for the latter are limited at this time. Conjunctivitis and injection site erythema were more frequent in the dupilumab group, more so in the LIBERTY AD PEDS trial, and conjunctivitis is known to be associated with dupilumab. The clinical experts indicated that for most patients, these were manageable side effects. SAEs and withdrawals due to AEs were generally low among treatment groups for the pivotal trials and LTE study and there were no deaths. There was no direct or indirect safety evidence available for dupilumab versus other active comparators in this patient population.
Conclusion
Currently dupilumab is available for patients aged 12 years and older with moderate-to-severe atopic dermatitis whose condition is not adequately controlled with prescription topical therapy or when those treatments are not advisable. There are few treatments available for patients who are aged 6 months to younger than 12 years and often these treatments, such as systemic immunosuppressants or phototherapy, are not recommended, used off-label, are inappropriate or inaccessible, and are therefore not preferred in this patient population. Evidence from 2 phase III trials demonstrated that dupilumab in combination with TCS was clinically significantly more effective at improving all disease-related symptoms, including itching, disease severity, and also significantly improving HRQoL compared to TCS alone during 16 weeks of treatment. The treatment effect of dupilumab was likely maintained, though conclusions of long-term efficacy and safety are limited by the number of patients with long-term data at this time and the lack of long-term comparative evidence. No direct or indirect evidence was available on comparative effectiveness of dupilumab versus any alternative therapies including systemic therapies (such as cyclosporine, methotrexate, azathioprine, mycophenolate mofetil), and the ongoing observational study could not fill the evidence gaps of dupilumab treatment efficacy and safety versus other drugs for atopic dermatitis. The indication for dupilumab notes that the drug would be for patients in whom topical prescription therapies are not advisable; however, whether such patients were enrolled and the efficacy of dupilumab in this patient population were unclear. Finally, the Health Canada–approved indication for dupilumab is for the treatment of patients aged 6 months and older with moderate-to-severe atopic dermatitis, though there is no evidence available for patients with moderate atopic dermatitis who are aged 6 years to 12 years, and the magnitude of treatment effect of dupilumab in this patient population is unknown due to lack of data.
References
1.Dupixent (dupilumab): 300 mg single-use syringe (300 mg/2 mL), 300 mg single-use pen (300 mg/2 mL), 200 mg single-use syringe (200 mg/1.14 mL). 200 mg single-use pen (200 mg/1.14 mL), 100 mg single-use syringe (100 mg/0.67 mL) for subcutaneous injection [product monograph]. Laval (QC): Sanofi-aventis Canada Inc; 2023 Apr 14.
2.Drug Reimbursement Review sponsor submission: Dupixent (dupilumab), 300 mg single-use syringe (300 mg/2 mL), 200 mg single-use syringe (200 mg/1.14 mL) for subcutaneous injection [internal sponsor's package]. Toronto (ON): Sanofi-aventis Canada Inc; 2023 Mar 29.
3.Dupixent (Dupilumab Injection) for pediatrics (6 months to <6 years of age) and children (6 to <12 years of age) with moderate to severe atopic dermatitis: clinical summary [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Dupixent, 300 mg single-use syringe (300 mg/2 mL), 200 mg single-use syringe (200 mg/1.14 mL) for subcutaneous injection. Toronto (ON). Sanofi-aventis Canada Inc; 2023 Mar 29.
4.Davari DR, Nieman EL, McShane DB, Morrell DS. Current perspectives on the management of infantile atopic dermatitis. J Asthma Allergy. 2020;13:563-573. PubMed
5.Leung DY, Boguniewicz M, Howell MD, Nomura I, Hamid QA. New insights into atopic dermatitis. J Clin Invest. 2004;113(5):651-657. PubMed
6.Wollenberg A, Christen-Zäch S, Taieb A, et al. ETFAD/EADV Eczema task force 2020 position paper on diagnosis and treatment of atopic dermatitis in adults and children. J Eur Acad Dermatol Venereol. 2020;34(12):2717-2744. PubMed
7.Nutten S. Atopic dermatitis: global epidemiology and risk factors. Ann Nutr Metab. 2015;66 Suppl 1:8-16. PubMed
8.Wollenberg A, Barbarot S, Bieber T, et al. Consensus-based European guidelines for treatment of atopic eczema (atopic dermatitis) in adults and children: part I. J Eur Acad Dermatol Venereol. 2018;32(5):657-682. PubMed
9.Spergel JM. Epidemiology of atopic dermatitis and atopic march in children. Immunol Allergy Clin North Am. 2010;30(3):269-280. PubMed
10.Zhang Z, Li H, Zhang H, et al. Factors associated with persistence of early-onset atopic dermatitis up to the age of 12 years: a prospective cohort study in China. Eur J Dermatol. 2021;31(3):403-408. PubMed
11.Al-Naqeeb J, Danner S, Fagnan LJ, et al. The burden of childhood atopic dermatitis in the primary care setting: a report from the meta-LARC consortium. J Am Board Fam Med. 2019;32(2):191-200. PubMed
12.Galli E, Maiello N, Cipriani F, et al. Atopic dermatitis phenotypes in preschool and school-age children: a latent class analysis. J Investig Allergol Clin Immunol. 2020;30(2):108-116. PubMed
13.Huang CC, Chiang TL, Chen PC, Lin SJ, Wen HJ, Guo YL. Risk factors for asthma occurrence in children with early-onset atopic dermatitis: an 8-year follow-up study. Pediatr Allergy Immunol. 2018;29(2):159-165. PubMed
14.Lee CY, Chen MH, Jeng MJ, et al. Longitudinal association between early atopic dermatitis and subsequent attention-deficit or autistic disorder: a population-based case-control study. Medicine. 2016;95(39):e5005. PubMed
15.Ruge IF, Thorsteinsdottir S, Norgaard S, et al. Symptom burden of atopic dermatitis in early childhood assessed from daily monitoring of symptoms and topical steroid use. J Am Acad Dermatol. 2021;84(3):725-734. PubMed
16.Ramirez FD, Chen S, Langan SM, et al. Assessment of sleep disturbances and exhaustion in mothers of children with atopic dermatitis. JAMA Dermatol. 2019;155(5):556-563. PubMed
17.Balekian DS, Linnemann RW, Castro VM, Perlis R, Thadhani R, Camargo CA, Jr. Pre-birth cohort study of atopic dermatitis and severe bronchiolitis during infancy. Pediatr Allergy Immunol. 2016;27(4):413-418. PubMed
18.Low DW, Jamil A, Md Nor N, Kader Ibrahim SB, Poh BK. Food restriction, nutrition status, and growth in toddlers with atopic dermatitis. Pediatr Dermatol. 2020;37(1):69-77. PubMed
19.Narla S, Silverberg JI. Association between childhood atopic dermatitis and cutaneous, extracutaneous and systemic infections. Br J Dermatol. 2018;178(6):1467-1468. PubMed
20.Paller AS, Mina-Osorio P, Vekeman F, et al. Prevalence of type 2 inflammatory diseases in pediatric patients with atopic dermatitis: real-world evidence. J Am Acad Dermatol. 2021;28:28. PubMed
21.Senna G, Micheletto C, Piacentini G, et al. Multidisciplinary management in type 2 inflammatory disease. Multidiscip Respir Med. 2022;17. PubMed
22.Eczema Society of Canada. Atopic dermatitis quality of life report- moderate to severe disease: 2016/2017 survey results. 2017; https://altogethereczema.org/images/files/ESC_QUALITY_OF_LIFE_REPORT_2017.pdf. Accessed 2023 Feb 1.
23.Manzoni AP, Weber MB, Nagatomi AR, Pereira RL, Townsend RZ, Cestari TF. Assessing depression and anxiety in the caregivers of pediatric patients with chronic skin disorders. An Bras Dermatol. 2013;88(6):894-899. PubMed
24.Andersen YMF, Egeberg A, Skov L, Thyssen JP. Demographics, healthcare utilization and drug use in children and adults with atopic dermatitis in Denmark: a population-based cross-sectional study. J Eur Acad Dermatol Venereol. 2019;33(6):1133-1142. PubMed
25.Drucker AM, Wang AR, Li W-Q, Sevetson E, Block JK, Qureshi AA. The burden of atopic dermatitis: summary of a report for the National Eczema Association. J Invest Dermatol. 2017;137(1):26-30. PubMed
26.Filanovsky MG, Pootongkam S, Tamburro JE, Smith MC, Ganocy SJ, Nedorost ST. The financial and emotional impact of atopic dermatitis on children and their families. J Pediatr. 2016;169:284-290.e285. PubMed
27.Olsson M, Bajpai R, Yew YW, et al. Associations between health-related quality of life and health care costs among children with atopic dermatitis and their caregivers: a cross-sectional study. Pediatr Dermatol. 2020;37(2):284-293. PubMed
28.Ortsater G, Geale K, Dun AR, et al. Clinical and economic burden of pediatric mild-to-moderate atopic dermatitis: a population-based nested case-control study in Sweden. Dermatol Ther (Heidelb). 2021;11(1):161-172. PubMed
29.Ramien M, Gooderham M, Prajapati VH, et al. Suboptimal control of atopic dermatitis in young children in Canada: results from the EPI-CARE survey. International Society of Atopic Dermatitis (ISAD) symposium; 2022 Oct 17-19, 2022; Montreal (QC).
30.Sandhu JK, Salame N, Ehsani-Chimeh N, Armstrong AW. Economic burden of cutaneous infections in children and adults with atopic dermatitis. Pediatr Dermatol. 2019;36(3):303-310. PubMed
31.Lansang P, Lara-Corrales I, Bergman JN, et al. Approach to the assessment and management of pediatric patients with atopic dermatitis: a consensus document. Section IV: consensus statements on the assessment and management of pediatric atopic dermatitis. J Cutan Med Surg. 2019;23(5_suppl):32S-39S. PubMed
32.Spergel JM. Management of severe atopic dermatitis (eczema) in children. In: Post TW, ed. UpToDate. Waltham (MA): UpToDate; 2023: https://www.uptodate.com/. Accessed 2023 Apr 12.
33.CADTH Reimbursement final recommendation: dupilumab (Dupixent) Can J Health Technol. 2023;3(2). https://www.cadth.ca/sites/default/files/DRR/2023/SF0754REC-Dupixent-RfA.pdf. Accessed 2023 Feb 7.
34.Leshem YA, Hajar T, Hanifin JM, Simpson EL. What the Eczema Area and Severity Index Score tells us about the severity of atopic dermatitis: an interpretability study. Br J Dermatol. 2015;172(5):1353-1357. PubMed
35.Chopra R, Vakharia PP, Sacotte R, et al. Severity strata for Eczema Area and Severity Index (EASI), modified EASI, Scoring Atopic Dermatitis (SCORAD), objective SCORAD, Atopic Dermatitis Severity Index and body surface area in adolescents and adults with atopic dermatitis. Br J Dermatol. 2017;177(5):1316-1321. PubMed
36.Clinical Study Report: LIBERTY AD-PEDS (R668-AD-1652). A randomized, double-blind, placebo-controlled study to investigate the efficacy and safety of dupilumab administered concomitantly with topical corticosteroids in patients, ≥6 years to <12 years of age, with severe atopic dermatitis [internal sponsor's report]. Tarrytown (NY): Regeneron Pharmaceuticals, Inc; 2019 Nov 19.
37.Clinical Study Report: LIBERTY AD-PRESCHOOL Part B (R668-AD-1539). A phase 2/3 study investigating the pharmacokinetics, safety, and efficacy of dupilumab in patients aged ≥6 months to <6 years with moderate-to-severe atopic dermatitis [internal sponsor's report]. Tarrytown (NY): Regeneron Pharmaceuticals, Inc; 2021 Sep 16.
38.Clinical Study Report: LIBERTY AD-PEDS (R668-AD-1434). An open-label extension study to assess the long-term safety and efficacy of dupilumab in patients ≥6 months to <18 years of age with atopic dermatitis [internal sponsor's report]. Tarrytown (NY): Regeneron Pharmaceuticals, Inc; 2019 Nov 18.
39.Clinical Study Report: LIBERTY AD-PEDS (R668-AD-1434). An open-label extension study to assess the long-term safety and efficacy of dupilumab in patients ≥6 months to <18 years of age with atopic dermatitis [internal sponsor's report]. Tarrytown (NY): Regeneron Pharmaceuticals, Inc; 2021 Nov 24.
40.Bieber T. Atopic dermatitis 2.0: from the clinical phenotype to the molecular taxonomy and stratified medicine. Allergy. 2012;67(12):1475-1482. PubMed
41.Suárez-Fariñas M, Tintle SJ, Shemer A, et al. Nonlesional atopic dermatitis skin is characterized by broad terminal differentiation defects and variable immune abnormalities. J Allergy Clin Immunol. 2011;127(4):954-964.e951-954.
42.Gandhi NA, Bennett BL, Graham NM, Pirozzi G, Stahl N, Yancopoulos GD. Targeting key proximal drivers of type 2 inflammation in disease. Nat Rev Drug Discov. 2016;15(1):35-50. PubMed
43.Elias PM, Steinhoff M. “Outside-to-inside” (and now back to “outside”) pathogenic mechanisms in atopic dermatitis. J Invest Dermatol. 2008;128(5):1067-1070. PubMed
44.De Benedetto A, Rafaels NM, McGirt LY, et al. Tight junction defects in patients with atopic dermatitis. J Allergy Clin Immunol. 2011;127(3):773-786.e771-777.
45.Leung DY, Guttman-Yassky E. Deciphering the complexities of atopic dermatitis: shifting paradigms in treatment approaches. J Allergy Clin Immunol. 2014;134(4):769-779. PubMed
46.Gallay C, Meylan P, Mermoud S, et al. Genetic predisposition and environmental factors associated with the development of atopic dermatitis in infancy: a prospective birth cohort study. Eur J Pediatr. 2020;179(9):1367-1377. PubMed
47.Roduit C, Frei R, Depner M, et al. Phenotypes of atopic dermatitis depending on the timing of onset and progression in childhood. Jama, Pediatr. 2017;171(7):655-662. PubMed
48.Yonezawa K, Haruna M. Short-term skin problems in infants aged 0-3 months affect food allergies or atopic dermatitis until 2 years of age, among infants of the general population. Allergy Asthma Clin Immunol. 2019;15:74. PubMed
49.Rossberg S, Gerhold K, Geske T, et al. Elevated blood eosinophils in early infancy are predictive of atopic dermatitis in children with risk for atopy. Pediatr Allergy Immunol. 2016;27(7):702-708. PubMed
50.Mohn CH, Blix HS, Halvorsen JA, Nafstad P, Valberg M, Lagerlov P. Incidence trends of atopic dermatitis in infancy and early childhood in a Nationwide Prescription Registry Study in Norway. JAMA netw. 2018;1(7):e184145.
51.Silverberg JI, Simpson EL. Association between severe eczema in children and multiple comorbid conditions and increased healthcare utilization. Pediatr Allergy Immunol. 2013;24(5):476-486. PubMed
52.Djurovic MR, Jankovic J, Cirkovic A, et al. Quality of life in infants with atopic dermatitis and their families. Postepy Dermatol. 2020;37(1):66-72. PubMed
53.Siafaka V, Zioga A, Evrenoglou T, Mavridis D, Tsabouri S. Illness perceptions and quality of life in families with child with atopic dermatitis. Allergol Immunopathol (Madr). 2020;48(6):603-611. PubMed
54.Zhou NY, Nili A, Blackwell CK, et al. Parent report of sleep health and attention regulation in a cross-sectional study of infants and preschool-aged children with atopic dermatitis. Pediatr Dermatol. 2021;21:21. PubMed
55.Torun EG, Ertugrul A, Tekguc DC, Bostanci I. Sleep patterns and development of children with atopic dermatitis. Int Arch Allergy Immunol. 2020;181(11):871-878. PubMed
56.Ramirez FD, Chen S, Langan SM, et al. Association of atopic dermatitis with sleep quality in children. Jama, Pediatr. 2019;173(5):e190025. PubMed
57.Rudzki E, Samochocki Z, Rebandel P, et al. Frequency and significance of the major and minor features of Hanifin and Rajka among patients with atopic dermatitis. Dermatology. 1994;189(1):41-46. PubMed
58.Samochocki Z, Dejewska J. A comparison of criteria for diagnosis of atopic dermatitis in children. World J Pediatr. 2012;8(4):355-358. PubMed
59.Firooz A, Davoudi SM, Farahmand AN, Majdzadeh R, Kashani N, Dowlati Y. Validation of the diagnostic criteria for atopic dermatitis. Arch Dermatol. 1999;135(5):514-516. PubMed
60.Moore K, David TJ, Murray CS, Child F, Arkwright PD. Effect of childhood eczema and asthma on parental sleep and well-being: a prospective comparative study. Br J Dermatol. 2006;154(3):514-518. PubMed
61.Eucrisa (crisaborole): 2% oinment for topical use [product monograph]. Kirkland (QC): Pfizer Canada ULC; 2021 May 18: https://pdf.hres.ca/dpd_pm/00060960.PDF. Accessed 2023 Apr 25.
62.Azathioprine: 50 mg oral tablets [product monograph]. Toronto (ON): Teva Canada Limited; 2022 Nov 23: https://pdf.hres.ca/dpd_pm/00068436.PDF. Accessed 2023 Apr 25.
63.Neopral (cyclosporine): 10, 25, 50 and 100 mg soft gelatin capsules; 100 mg/mL oral use solution [product monograph]. Montreal (QC): Novartis Pharmaceuticals Canada Inc; 2023 Feb 23: https://pdf.hres.ca/dpd_pm/00069722.PDF. Accessed 2023 Apr 25.
64.Mycophenolate (mycophenolate mofetil): 500 mg oral film-coated tablets [product monograph]. Boucherville (QC): JAMP Pharma Corporation; 2023 Jan 19: https://pdf.hres.ca/dpd_pm/00069410.PDF. Accessed 2023 Apr 25.
65.Methotrexate: 2.5 mg oral tablets [product monograph]. Brossard (QC): Mantra Pharma Inc; 2023 Feb 1: https://pdf.hres.ca/dpd_pm/00069449.PDF. Accessed 2023 Apr 25.
66.Paller AS, Simpson EL, Siegfried EC, et al. Dupilumab in children aged 6 months to younger than 6 years with uncontrolled atopic dermatitis: a randomised, double-blind, placebo-controlled, phase 3 trial. Lancet. 2022;400(10356):908-919. PubMed
67.Paller AS, Siegfried EC, Thaçi D, et al. Efficacy and safety of dupilumab with concomitant topical corticosteroids in children 6 to 11 years old with severe atopic dermatitis: a randomized, double-blinded, placebo-controlled phase 3 trial. J Am Acad Dermatol. 2020;83(5):1282-1293. PubMed
68.Futamura M, Leshem YA, Thomas KS, Nankervis H, Williams HC, Simpson EL. A systematic review of Investigator Global Assessment (IGA) in atopic dermatitis (AD) trials: many options, no standards. J Am Acad Dermatol. 2016;74(2):288-294. PubMed
69.Eichenfield LF, Tom WL, Chamlin SL, et al. Guidelines of care for the management of atopic dermatitis: section 1. Diagnosis and assessment of atopic dermatitis. J Am Acad Dermatol. 2014;70(2):338-351. PubMed
70.Bożek A, Reich A. Assessment of intra- and inter-rater reliability of three methods for measuring atopic dermatitis severity: EASI, Objective SCORAD, and IGA. Dermatology. 2017;233(1):16-22. PubMed
71.Zhao CY, Hao EY, Oh DD, et al. A comparison study of clinician-rated atopic dermatitis outcome measures for intermediate- to dark-skinned patients. Br J Dermatol. 2017;176(4):985-992. PubMed
72.Hanifin JM, Thurston M, Omoto M, Cherill R, Tofte SJ, Graeber M. The eczema area and severity index (EASI): assessment of reliability in atopic dermatitis. EASI Evaluator Group. Exp Dermatol. 2001;10(1):11-18. PubMed
73.Schram ME, Spuls PI, Leeflang MM, Lindeboom R, Bos JD, Schmitt J. EASI, (objective) SCORAD and POEM for atopic eczema: responsiveness and minimal clinically important difference. Allergy. 2012;67(1):99-106. PubMed
74.Badia-Tahull MB, Cobo-Sacristán S, Leiva-Badosa E, et al. Use of Subjective Global Assessment, Patient-Generated Subjective Global Assessment and Nutritional Risk Screening 2002 to evaluate the nutritional status of non-critically ill patients on parenteral nutrition. Nutr Hosp. 2014;29(2):411-419. PubMed
75.Schmitt J, Langan S, Deckert S, et al. Assessment of clinical signs of atopic dermatitis: a systematic review and recommendation. J Allergy Clin Immunol. 2013;132(6):1337-1347. PubMed
76.Simpson EL, Bruin-Weller M, Flohr C, et al. When does atopic dermatitis warrant systemic therapy? Recommendations from an expert panel of the International Eczema Council. J Am Acad Dermatol. 2017;77(4):623-633. PubMed
77.Charman CR, Venn AJ, Williams HC. The patient-oriented eczema measure: development and initial validation of a new tool for measuring atopic eczema severity from the patients' perspective. Arch Dermatol. 2004;140(12):1513-1519. PubMed
78.Silverberg JI, Lei D, Yousaf M, et al. Comparison of Patient-Oriented Eczema Measure and Patient-Oriented Scoring Atopic Dermatitis vs Eczema Area and Severity Index and other measures of atopic dermatitis: A validation study. Ann Allergy Asthma Immunol. 2020;125(1):78-83. PubMed
79.Howells L, Ratib S, Chalmers JR, Bradshaw L, Thomas KS. How should minimally important change scores for the Patient-Oriented Eczema Measure be interpreted? A validation using varied methods. Br J Dermatol. 2018;178(5):1135-1142. PubMed
80.Chalmers JR, Schmitt J, Apfelbacher C, et al. Report from the third international consensus meeting to harmonise core outcome measures for atopic eczema/dermatitis clinical trials (HOME). Br J Dermatol. 2014;171(6):1318-1325. PubMed
81.Rehal B, Armstrong AW. Health outcome measures in atopic dermatitis: a systematic review of trends in disease severity and quality-of-life instruments 1985-2010. PLoS One. 2011;6(4):e17520-e17520. PubMed
82.Silverberg JI, DeLozier A, Sun L, et al. Psychometric properties of the itch numeric rating scale, skin pain numeric rating scale, and atopic dermatitis sleep scale in adult patients with moderate-to-severe atopic dermatitis. Health Qual Life Outcomes. 2021;19(1):247. PubMed
83.Newton L, Randall JA, Hunter T, et al. A qualitative study exploring the health-related quality of life and symptomatic experiences of adults and adolescents with ulcerative colitis. J Patient Rep Outcomes. 2019;3(1):66. PubMed
84.Lawson V, Lewis-Jones MS, Finlay AY, Reid P, Owens RG. The family impact of childhood atopic dermatitis: the Dermatitis Family Impact Questionnaire. Br J Dermatol. 1998;138(1):107-113. PubMed
85.Beattie PE, Lewis-Jones MS. An audit of the impact of a consultation with a paediatric dermatology team on quality of life in infants with atopic eczema and their families: further validation of the Infants' Dermatitis Quality of Life Index and Dermatitis Family Impact score. Br J Dermatol. 2006;155(6):1249-1255. PubMed
86.Dodington SR, Basra MK, Finlay AY, Salek MS. The Dermatitis Family Impact questionnaire: a review of its measurement properties and clinical application. Br J Dermatol. 2013;169(1):31-46. PubMed
87.Salek MS, Jung S, Brincat-Ruffini LA, et al. Clinical experience and psychometric properties of the Children's Dermatology Life Quality Index (CDLQI), 1995-2012. Br J Dermatol. 2013;169(4):734-759. PubMed
88.Lewis-Jones MS, Finlay AY. The Children's Dermatology Life Quality Index (CDLQI): initial validation and practical use. Br J Dermatol. 1995;132(6):942-949. PubMed
89.Langley RG, Paller AS, Hebert AA, et al. Patient-reported outcomes in pediatric patients with psoriasis undergoing etanercept treatment: 12-week results from a phase III randomized controlled trial. J Am Acad Dermatol. 2011;64(1):64-70. PubMed
90.Simpson EL, de Bruin-Weller M, Eckert L, et al. Responder Threshold for Patient-Oriented Eczema Measure (POEM) and Children's Dermatology Life Quality Index (CDLQI) in adolescents with atopic dermatitis. Dermatol Ther (Heidelb). 2019;9(4):799-805. PubMed
91.Lewis-Jones MS, Finlay AY, Dykes PJ. The Infants' Dermatitis Quality of Life Index. Br J Dermatol. 2001;144(1):104-110. PubMed
92.Neri E, Agostini F, Gremigni P, et al. Italian validation of the Childhood Atopic Dermatitis Impact Scale: a contribution to its clinical application. J Invest Dermatol. 2012;132(11):2534-2543. PubMed
93.Sanofi-aventis Canada response to April 25, 2023 CADTH request for additional information regarding Dupixent (dupilumab) CADTH review [internal sponsor's report]. Mississauga (ON): Sanofi-aventis Canada Inc.; 2023 May 8.
94.Thorsteinsdottir S, Stokholm J, Thyssen JP, et al. Genetic, clinical, and environmental factors associated with persistent atopic dermatitis in childhood. JAMA Dermatol. 2019;155(1):50-57. PubMed
Pharmacoeconomic Review
Abbreviations
AD
atopic dermatitis
BIA
budget impact analysis
BSC
best supportive care
EASI
Eczema Area and Severity Index
EASI-75
75% reduction in Eczema Area and Severity Index score
HRQoL
health-related quality of life
ICER
incremental cost-effectiveness ratio
LY
life-year
NIHB
Non-Insured Health Benefits
ODB
Ontario Drug Benefit
QALY
quality-adjusted life-year
TCI
topical calcineurin inhibitor
TCS
topical corticosteroid
WTP
willingness to pay
Executive Summary
The executive summary comprises 2 tables (Table 1 and Table 2) and a conclusion.
Item | Description |
|---|---|
Drug product | Dupilumab (Dupixent), solution for subcutaneous injection (200 mg per 1.14 mL prefilled syringe [175 mg/mL]; 300 mg per 2 mL prefilled syringe [150 mg/mL]) |
Submitted price | Dupilumab, 200 mg, 300 mg: $978.70 per prefilled syringe |
Indication | For the treatment of patients aged 6 months and older with moderate-to-severe AD whose disease is not adequately controlled with topical prescription therapies or when those therapies are not advisable. Dupilumab can be used with or without topical corticosteroids. |
Health Canada approval status | NOC |
Health Canada review pathway | Standard review |
NOC date | April 18, 2023 |
Reimbursement request | For the treatment of patients aged 6 months to < 12 years with moderate-to-severe AD whose disease is not adequately controlled with topical prescription therapies or when those therapies are not advisable. |
Sponsor | sanofi-aventis Canada Inc. |
Submission history | Previously reviewed: Yes Indication: For the treatment of patients aged 12 years and older with moderate-to-severe AD whose disease is not adequately controlled with topical prescription therapies or when those therapies are not advisable and/or who are refractory to or ineligible for systemic immunosuppressant therapies (i.e., due to contraindications, intolerance, or need for long-term treatment). Recommendation date: April 22, 2020 Recommendation: Reimburse with clinical criteria and/or conditions Indication: Adult patients with moderate-to-severe AD whose disease is not adequately controlled with topical prescription therapies or when those therapies are not advisable. Recommendation date: June 27, 2018 Recommendation: Do not reimburse Indication: Add-on maintenance treatment in patients aged 12 years and older with severe asthma with a type 2 or eosinophilic phenotype or oral corticosteroid-dependent asthma. Recommendation date: June 8, 2021 Recommendation: Reimburse with clinical criteria and/or conditions Indication: Add-on maintenance treatment in patients aged 6 years and older with severe asthma with a type 2 or eosinophilic phenotype or oral corticosteroid-dependent asthma. Recommendation date: January 20, 2023 Recommendation: Reimburse with clinical criteria and/or conditions |
AD = atopic dermatitis; NOC = Notice of Compliance.
Table 2: Summary of Economic Evaluation
Component | Description |
|---|---|
Type of economic evaluation | Cost-utility analysis Decision tree and Markov model hybrid |
Target population | Patients aged 6 months to < 12 years with moderate-to-severe AD whose disease is not adequately controlled with topical prescription therapies or when those therapies are not advisable |
Treatment | Dupilumab plus BSC (topical corticosteroids and topical calcineurin inhibitors) |
Comparator | BSC |
Perspective | Canadian publicly funded health care payer |
Outcome | QALYs, LYs |
Time horizon | Lifetime (100 years) |
Key data source | LIBERTY AD PRESCHOOL, LIBERTY AD PEDS clinical trials |
Submitted results | ICER = $47,298 per QALY gained (incremental costs: $88,539; incremental QALYs: 1.87) |
Key limitations |
|
CADTH reanalysis results |
|
AD = atopic dermatitis; BSC = best supportive care; ICER = incremental cost-effectiveness ratio; LY = life-year; QALY = quality-adjusted life-year; vs. = versus.
Conclusions
Based on data from the submitted pivotal trials for the reimbursement population, dupilumab plus topical corticosteroids (TCSs) is more effective than TCSs alone at reducing disease-related symptoms and improving health-related quality of life (HRQoL) in patients aged 6 months to younger than 12 years with moderate-to-severe atopic dermatitis (AD) after 16 weeks of treatment. As noted in the CADTH clinical review, evidence from a single-arm extension study suggests that the effect of dupilumab may be maintained beyond 16 weeks; however, the magnitude of any long-term comparative effects relative to best supportive care (BSC) alone is highly uncertain owing to a lack of comparative data beyond 16 weeks. CADTH additionally notes that, for patients aged 6 to younger than 12 years with moderate AD, the magnitude of any treatment benefit between dupilumab plus BSC versus BSC alone is unknown due to a lack of clinical data. As such, the cost-effectiveness of dupilumab in this subgroup, and thus for the full reimbursement population, is highly uncertain.
CADTH undertook a reanalysis to address several limitations in the sponsor’s analysis, which included adopting alternative estimates for the durability of BSC treatment response, health state utility values, and costs related to health care resource use. The CADTH base case suggests that, at a willingness-to-pay (WTP) threshold of $50,000 per quality-adjusted life-year (QALY) gained, dupilumab plus BSC is not a cost-effective treatment option compared with BSC alone, with a 0% probability of dupilumab plus BSC being the optimal treatment strategy at this threshold: dupilumab plus BSC compared with BSC alone is associated with an incremental cost-effectiveness ratio (ICER) of $130,945 per QALY gained. A price reduction of 54% for dupilumab would be required for dupilumab plus BSC to be considered cost-effective at a WTP threshold of $50,000 per QALY gained.
The CADTH reanalysis attempted to address the identified limitations of the sponsor’s economic submission; however, a high degree of uncertainty remains. Notably, the cost-effectiveness of dupilumab plus BSC relative to other systemic treatments is unknown owing to a lack of comparative clinical data. CADTH notes that, although the CADTH base case estimated a gain in QALYs with dupilumab plus BSC compared to BSC alone (incremental: 0.91), most of this benefit (97%) was realized in the extrapolated period (i.e., after 16 weeks) based on data from adult dupilumab trials. In the absence of comparative evidence beyond 16 weeks for the reimbursement population, and for patients aged 6 years to 12 years with moderate AD, the incremental QALYs for dupilumab plus BSC predicted in CADTH’s base case may be overestimated. Similarly, it is highly uncertain whether the predicted savings in health care costs will be realized in clinical practice. Additional price reductions may therefore be required.
Stakeholder Input Relevant to the Economic Review
This section is a summary of the feedback received from the patient groups, registered clinicians, and drug plans that participated in the CADTH review process.
Patient group input was received from Eczema Society of Canada and Canadian Skin Patient Alliance, Eczéma Québec, and Eczema Society of Canada based on written questionnaires, surveys, interviews, statements, and testimonials. Patients and caregivers described how AD severely impacts HRQoL, mental health, social lives, and daily routines. Respondents reported frustration, treatment fatigue, and financial strain from the trial-and-error approach of current treatments and expressed concerns about the safety profile of some treatment options because of potential adverse effects with long-term use. Respondents expressed a desire for a treatment that would be easily accessible, time efficient, and improve or eliminate skin inflammation, flares and rashes, itch, burning sensations, and pain.
Clinician input was received from the Canadian Dermatology Association. Clinician input indicated that if topical therapies are required for treatment, the most commonly prescribed treatments are TCSs, topical calcineurin inhibitors (TCIs), and topical phosphodiesterase type 4 inhibitors, with phototherapy and off-label systemic agents used occasionally. Clinician input indicated that dupilumab would likely be the preferred systemic treatment for AD in patients aged 6 months to 11 years because of the absence of other indicated systemic treatments in this age group. Clinicians noted that dupilumab does not require laboratory testing like other immunosuppressive medications, which reduces the monitoring required by physicians.
CADTH-participating drug plans indicated that an ideal treatment for moderate-to-severe AD would have a proven safety record in this age group and would also be able to reduce symptoms and improve sleep, concentration at school, and the overall quality of life for both patients and caregivers. Plans noted that systemic therapies (e.g., methotrexate, cyclosporine, azathioprine, mycophenolate mofetil) are used off-label for treatment of uncontrolled moderate-to-severe AD in children. It was also emphasized that a trial of systemic immunosuppression should not be a prerequisite for dupilumab coverage in patients aged 6 months to 5 years. Additionally, drug plans expressed concern regarding the uncertainty of how to assess patients when they become 12 years old, as patients may no longer meet the initiation criteria for dupilumab after age 12. Lastly, drug plans expressed concern about the predicted 3-year budget impact of reimbursing dupilumab.
Several of these concerns were addressed in the sponsor’s model:
The sponsor’s model incorporated health states based on treatment response, defined by use of the Eczema Area and Severity Index (EASI) score.
HRQoL was included in the model for patients with AD. Caregiver HRQoL was included in a scenario analysis.
Costs associated with adverse events were included in the model; however, HRQoL impacts of adverse events were not considered.
CADTH was unable to address the following concerns raised from stakeholder input:
CADTH was unable to consider the relative cost-effectiveness of dupilumab versus systemic treatments (i.e., methotrexate, cyclosporine, azathioprine, and mycophenolate mofetil).
Economic Review
The current review is for dupilumab (Dupixent) for patients aged 6 months to younger than 12 years with moderate-to-severe AD whose disease is not adequately controlled with topical prescription therapies or when those therapies are not advisable.
Economic Evaluation
Summary of Sponsor’s Economic Evaluation
Overview
The sponsor submitted a cost-utility analysis of dupilumab plus BSC compared to BSC alone among patients aged 6 months to younger than 12 years with moderate-to-severe AD whose disease is not adequately controlled with topical prescription therapies or when those therapies are not advisable,1 based on the LIBERTY AD PRESCHOOL and LIBERTY AD PEDS trials,2,3 which enrolled patients aged 6 months to younger than 12 years with moderate-to-severe and severe AD, respectively. The modelled population was aligned with the reimbursement request, which is a subset of the Health Canada–indicated population that is restricted to those aged 6 months to younger than 12 years.2,3
Dupilumab is available as 200 mg or 300 mg single-use prefilled syringes at a submitted price of $978.70 per syringe.1,4 The recommended dose of dupilumab varies by age and weight. For those aged 6 months to 5 years, the recommended dosage of dupilumab is 200 mg or 300 mg initially, followed by 200 mg or 300 mg every 4 weeks depending on the patient’s weight.4 For those aged 6 to 17 years, the recommended dosage of dupilumab is 400 mg or 600 mg initially, followed by 200 mg or 300 mg every 2 weeks or every 4 weeks, depending on the patient’s weight.4
In the sponsor’s model, the estimated annual cost of dupilumab was based on the monograph-recommended age and weight dosing,1 with an estimated first-year cost of dupilumab of $12,723 for those aged 6 months to younger than 6 years weighing 30 kg or less, $13,702 for patients aged 6 years to younger than 12 years weighing less than 30 kg, and $26,425 for those aged 6 years to younger than 12 years weighing more than 30 kg.1 Costs of treatment in subsequent years were $12,723 for those weighing less than 30 kg and $25,446 for those weighing 30 kg or more. BSC was assumed by the sponsor to include TCS (0.1% mometasone) and TCI (tacrolimus), with an estimated annual cost of $4,639 for responders and $11,622 for nonresponders in the first year of treatment.1
The analysis was conducted from the perspective of the Canadian public health care payer. Costs and clinical outcomes (life-years [LYs] and QALYs) were estimated over a lifetime time horizon of 100 years (1-year cycle length), discounted at an annual rate of 1.5% per annum.
Model Structure
The model structure included a short-term (1 year) phase encompassing the first year of treatment (with 16-week and 52-week response assessments) and a maintenance phase for the remainder of the lifetime horizon. The short-term phase was based on a decision tree (Figure 1),1 in which all patients start at baseline receiving either dupilumab plus BSC or BSC alone. Response to treatment was first assessed at 16 weeks based on whether EASI scores improved by at least 75% from baseline (EASI-75).1 In the dupilumab arm, patients who responded to treatment at 16 weeks continued to receive dupilumab until week 52, at which time patients were assessed for sustained response. Patients who did not respond to dupilumab at 16 weeks received BSC for the remainder of the model horizon. The long-term maintenance phase (Figure 2) consisted of a Markov model with 3 health states: maintenance treatment, BSC treatment, and death.1 Patients in the dupilumab arm who had sustained response at 52 weeks entered the Markov model in the maintenance treatment health state, while those receiving BSC at 52 weeks entered the BSC treatment health state. In each cycle, patients in the maintenance treatment health state could discontinue dupilumab (based on lack of long-term efficacy, adverse events, and patient or physician preference) and transition to the BSC treatment state or die. Patients in the BSC treatment health state remained on BSC until death.
Model Inputs
The pharmacoeconomic model was informed by inputs from the phase III randomized LIBERTY AD PRESCHOOL and LIBERTY AD PEDS trials (16-week duration),2,3 based on the reimbursement request for the subgroup of patients aged 6 months to younger than 12 years. The model assumed that 50% of patients would be aged 6 months to younger than 6 years and 50% would be aged 6 years to younger than 12 years at baseline. The sponsor assumed that patients aged 6 months to younger than 12 years entered the model at age 4 (61.1% male) based on the LIBERTY AD PRESCHOOL trial and that patients aged 6 years to younger than 12 years entered the model at age 8 (49.9% male) based on the LIBERTY AD PEDS trial.2,3
Response to treatment at 16 weeks was informed by clinical efficacy data from the LIBERTY AD PRESCHOOL and LIBERTY AD PEDS trials,2,3 based on the proportion of patients achieving at least EASI-75 from baseline.2,3 The sponsor assumed that patients who received rescue treatment in the trials were nonresponders and that they would discontinue dupilumab. Treatment response at 52 weeks for those receiving dupilumab was estimated by applying a conditional relative risk (RR) derived from the long-term adult dupilumab CHRONOS trial, based on the proportion of 16-week responders who maintained response at 52 weeks (RR = 0.822 for dupilumab plus BSC).5 For patients receiving BSC alone, an RR was calculated for week 52 regardless of response status at week 16 from the adult CHRONOS trial (RR = 0.595 for BSC alone).5 Sustained treatment response for years 2 to 5 was based on a survey of clinical experts that estimated the probability of sustaining year 1 quality of life benefits for dupilumab plus BSC and BSC alone. The model assumes that the estimate for year 5 carries forward for the remainder of the model time horizon. The proportion of patients who discontinued dupilumab was assumed to be 6.3% per year and is applied to patients in the maintenance phase of treatment, based on data from the adult SOLO trials.6
The sponsor assumed that treatment did not affect mortality risk. All-cause age- and sex-specific mortality from the National Life Tables for Canada was modelled annually and were weighted by the cohort’s proportion of males and females.7
Utilities in the sponsor’s model were assumed to vary by age group (< 18 years, ≥ 18 years), by treatment received (dupilumab plus BSC, BSC alone), and by treatment response (responder, nonresponder). Utility values were derived by the sponsor using a mixed-model regression approach using 3-Level EQ-5D data (with UK tariffs) from the SOLO and CHRONOS dupilumab trials, both of which enrolled patients aged 18 years and older.1,5,6 In the model, the sponsor used utilities derived from the CHRONOS trial to inform utilities for patients aged 6 months to younger than 12 years5 and utilities derived from a subgroup of patients aged 18 years to 25 years from the SOLO trial to inform utilities for patients aged 18 years and older.6
Costs included in the model were dupilumab acquisition costs, medication costs associated with treating AD flares, training costs associated with subcutaneous administration, health care resource costs (including background medication use), adverse events costs, and monitoring costs. Drug acquisition costs for dupilumab were based on the sponsor’s submitted price,1 adjusted by patient age and weight. Patient weight was estimated by the sponsor using a distribution of patient weights derived from the 2017 Health Survey for England.8 Acquisition costs for BSC (i.e., TCSs and TCIs) and for drugs used to treat flare-ups (i.e., TCSs, systemic steroids, or immunosuppressants) were obtained from the Ontario Drug Benefit (OBD) formulary. The cost per flare-up derived by the sponsor (dupilumab plus BSC: $3.65; BSC alone: $21.24) incorporated the proportion of patients from the adult CHRONOS trial who required at least 1 rescue medication from each treatment class for those receiving dupilumab plus BSC or BSC alone.1,9 A one-time cost of training for subcutaneous injection was applied for patients receiving dupilumab, based on the Ontario Nurses’ Association Collective Agreement.10 Health care resource use was assumed by the sponsor to vary by response status (responder versus nonresponder) and by treatment received (dupilumab plus BSC, BSC alone), and included primary care visits, dermatologist visits, emergency room visits, hospitalizations, full blood counts, dermatology nurse visits, and the cost of BSC, with the frequency of use estimated by clinical expert input.1 Costs of adverse events were included for allergic conjunctivitis, infectious conjunctivitis, oral herpes, skin infection, and injection site reaction.1 All health care resource use cost estimates were sourced from the Ontario Schedule of Benefits, Ontario Case Costing Initiative, and the Ontario Schedule of Benefits for Laboratory Services.9,11-13
Summary of Sponsor’s Economic Evaluation Results
All analyses were run probabilistically (5,000 iterations for the base case and 1,000 iterations for scenario analyses). The deterministic and probabilistic results were similar. The probabilistic findings are presented in the following section. Additional results from the sponsor’s submitted economic evaluation base case are presented in Appendix 3.
Base-Case Results
In the sponsor’s base-case analysis, dupilumab plus BSC was associated with an estimated cost of $514,738 and 28.59 QALYs over the 100-year horizon, resulting in an ICER of $47,298 per QALY gained (incremental costs: $88,539; incremental QALYs: 1.87) compared to BSC alone (Table 3). In the sponsor’s analysis, dupilumab plus BSC had a 57% probability of being cost-effective at a WTP threshold of $50,000.
Results were driven by the drug acquisition costs of dupilumab (incremental drug acquisition costs: $141,810), predicted gain in QALYs (incremental: 1.87), and savings in health care resource use (incremental: –$53,420). The sponsor’s model estimated that approximately 1% of the incremental benefits were accrued during the 16-week trial period of assessment.
Table 3: Summary of the Sponsor’s Economic Evaluation Results
Drug | Total costs ($) | Incremental costs ($) | Total QALYs | Incremental QALYs | ICER vs. BSC ($/QALY) |
|---|---|---|---|---|---|
BSC | 426,200 | Reference | 26.71 | Reference | Reference |
Dupilumab plus BSC | 514,738 | 88,539 | 28.59 | 1.87 | 47,298 |
BSC = best supportive care; ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year; vs. = versus.
Note: The submitted analysis is based on the publicly available prices of all treatments including comparator treatments. BSC was assumed by the sponsor to comprise topical corticosteroids (0.1% mometasone) and topical calcineurin inhibitors (tacrolimus).
Source: Sponsor’s pharmacoeconomic submission.1
Sensitivity and Scenario Analysis Results
The sponsor provided several scenario analyses, including adopting weight distributions from the pivotal trials, applying alternate utility values, adopting alternate resource use assumptions, assessing specific age groups (e.g., 6 months to < 6 years; 6 years to < 12 years), including caregiver utilities, and adopting a shorter time horizon (10 years, 20 years). The ICER for dupilumab plus BSC compared to BSC alone was between $31,027 and $63,119 across all scenarios.
CADTH Appraisal of the Sponsor’s Economic Evaluation
CADTH identified several key limitations to the sponsor’s analysis that have notable implications on the economic analysis.
The majority of inputs in the pharmacoeconomic model were derived from adults. Dupilumab is indicated for use in patients aged 6 months and older, with reimbursement requested for patients aged 6 months to 12 years.4 While the sponsor submitted 2 pivotal trials (LIBERTY AD PEDS and LIBERTY AD PRESCHOOL) pertaining to patients in the requested reimbursement population, the majority of inputs in the pharmacoeconomic model were informed by data from adult dupilumab trials, with the exception of initial response to treatment at 16 weeks. That is, treatment response in the economic model at 16 weeks was informed by EASI-75 observations from the LIBERTY AD PEDS and LIBERTY AD PRESCHOOL trials, while all efficacy inputs beyond 16 weeks were informed by data from studies involving adults (52-week response: CHRONOS trial; probability of treatment discontinuation: SOLO trial; flare medication use: CHRONOS trial; background medication costs: CAFÉ trial; health state utility values: SOLO and CHRONOS trials) or expert opinion. CADTH notes that approximately 1% of incremental QALYs predicted by the sponsor’s model to be gained with dupilumab plus BSC compared to BSC alone are accrued during the 16-week trial period; as such, approximately 99% of the predicted QALYs gained with dupilumab are predicated on the assumption that treatment response in adults is equal among children aged 6 months to 12 years. This assumption was not justified by the sponsor, and expert input received by CADTH for this review noted that the natural history of AD differs between children and adults.
The incremental QALYs predicted by the sponsor’s model with the use of dupilumab plus BSC compared to BSC alone are highly uncertain owing to the use of primarily adult data to inform the model. CADTH was unable to address this limitation owing to a lack of comparative efficacy data for the reimbursement population beyond 16 weeks.
Durability of treatment response is highly uncertain. The sponsor’s model included treatment-specific assumptions based on expert opinion to incorporate the durability of treatment response for dupilumab plus BSC and BSC alone. Notably, the sponsor assumed that utility gains for responders to dupilumab plus BSC would remain relatively stable over time (year 2: 98%; year 3: 95%; year 4: 93%; year 5+: 92%), whereas the gains in utility experienced by responders to BSC were assumed to diminish rapidly, such that by year 4 all BSC responders would return to their baseline utility (year 2: 37.0%; year 3: 37%; year 4+: 0%). Owing to the lack of comparative efficacy data beyond 16 weeks for the reimbursement population (as noted previously), the magnitude of any differences over time is highly uncertain. CADTH notes that the sponsor’s single-arm, long-term extension study (Study 1434) may provide additional information about the long-term durability of the treatment effect of dupilumab; however, as noted in the CADTH clinical review, Study 1434 is ongoing and limited data are currently available beyond 16 weeks. CADTH additionally notes that clinical expert input obtained by CADTH for this review suggests that, for patients who experience a treatment response, the effect of treatment on HRQoL is expected to remain stable, regardless of treatment received. Further, expert input indicated that it was unlikely that patients who continue to respond to BSC (i.e., maintain EASI-75) would lose all HRQoL benefit from treatment by year 4. Expert input noted that the number of patients expected to respond to BSC over time would generally remain stable based on expected natural history of AD.14-16
In the CADTH base case, CADTH adopted alternate assumptions about the durability of BSC treatment effect. CADTH maintained the sponsor’s assumptions regarding the durability of dupilumab effect but notes that the relative magnitude of any difference in the waning of treatment effect between dupilumab plus BSC and BSC alone is highly uncertain owing to a lack of clinical data.
The efficacy of dupilumab among some subgroups is uncertain. The requested reimbursement population includes patients with moderate-to-severe AD for whom the disease is not adequately controlled with topical prescription therapies or for whom these therapies are not advisable. In the sponsor’s model, treatment response at 16 weeks for patients aged 6 to younger than 12 years was informed by data from the LIBERTY AD PEDS trial, which enrolled patients with severe AD, and the sponsor assumed that the treatment response would be equivalent among those with moderate AD. As noted in the CADTH clinical review, patients with severe disease may have a higher ceiling for improvement on continuous efficacy outcomes, such as EASI. CADTH additionally notes that patients for whom topical therapies are not advisable may not be reflected in the sponsor’s pharmacoeconomic analysis. As noted in the CADTH clinical review, it is unclear whether such patients were enrolled in the LIBERTY AD PEDS and the LIBERTY AD PRESCHOOL trials and the efficacy of dupilumab in this patient population. However, clinical expert input received by CADTH suggests that this subgroup may comprise a small proportion of the indicated population.
CADTH was unable to address this limitation owing to a lack of clinical data.
Comparative effectiveness of dupilumab to other relevant comparators is unknown. In the sponsor’s model, dupilumab plus BSC was compared to BSC alone. Clinical expert input obtained by CADTH, as well as the results of a survey submitted by the sponsor,1 indicate that additional treatments may be used for pediatric patients with moderate-to-severe AD that has not responded to topical therapies, including cyclosporine, methotrexate, azathioprine, and mycophenolate mofetil. The sponsor justified the omission of these drugs from their analysis because of “known serious side effects.”1 However, the results of the sponsor’s survey of 15 clinicians in Canada suggest that systemic therapies are used in up to 16% of patients aged 6 months to younger than 12 years.1 Similarly, the sponsor’s ongoing PEDISTAD study, which enrolled patients aged younger than 12 years (including 103 patients from Canada), suggests that up to approximately 10% of patients receive systemic treatments including cyclosporine, methotrexate, and mycophenolate.17 As noted in the CADTH clinical review, there is no direct evidence comparing dupilumab to other systemic treatments, and an indirect treatment comparison was deemed to not be feasible by the sponsor. As such, the clinical effectiveness, and hence the cost-effectiveness, of dupilumab relative to other systemic treatments is unknown.
CADTH was unable to address this limitation owing to the lack of comparative clinical efficacy data for dupilumab versus other drugs used in this population.
Inappropriate use of treatment-dependent utilities. The sponsor incorporated treatment-specific utility values for dupilumab plus BSC and BSC alone. As per CADTH Guidelines for Economic Evaluations, utilities should reflect the health states within the model and should not be specific to treatment.18 The sponsor did not provide justification to support the use of treatment-specific utility values. CADTH notes that the utility values adopted by the sponsor for dupilumab responders were higher than those for BSC responders for all age groups, which was deemed to lack face validity according to clinical expert input obtained by CADTH. That is, expert input indicated that all patients who achieved EASI-75 would be expected to have similar HRQoL regardless of treatment received.
In the CADTH base case, all treatments were assumed to have the same utility value for a given health state.
Utility estimates lack face validity. CADTH noted several issues related to the face validity of the health state utility values incorporated in the sponsor’s model. First, the utility values were derived from 3-Level EQ-5D observations from the CHRONOS trial (mean age 41 years) and a subgroup of the SOLO trial (aged 18 years to 25 years). Although the use of the 3-Level EQ-5D aligns with CADTH’s recommendations to use a generic preference-based instrument,18 it is highly uncertain whether the domains included in EQ-5D would be relevant to the reimbursement population (i.e., patients aged 6 months to younger than 12 years). For example, the EQ-5D “self-care” domain is unlikely to be relevant to children at the lower end of the reimbursement age range (i.e., 6 months). It would have been more appropriate for the sponsor to assess HRQoL for the reimbursement population, for example, in the LIBERTY AD PEDS and LIBERTY AD PRESCHOOL trials using an instrument intended for use among pediatric patients.
Second, the sponsor included utility values estimated from different sources for patients aged older or younger than 18 years (< 18 years: CHRONOS trial; ≥ 18 years: SOLO trial subgroup 18 years to 25 years), which resulted in dupilumab responders receiving a utility benefit at age 18 and BSC responders receiving a utility decrement at age 18. No justification was provided by the sponsor for the use of utilities derived from different populations, and there is no methodological or clinical justification to support a treatment-specific change in utility at age 18.
Third, the sponsor’s model was programmed in such a way that nonresponders reverted to the baseline utility value (0.59) instead of being assigned the nonresponder utility value (e.g., 0.71 for BSC responders aged 6 months to < 12 years). Clinical expert input obtained by CADTH suggests that all patients who receive treatment are likely to experience an improvement, regardless of whether EASI-75 is achieved. That is, patients classified as nonresponders in the sponsor’s model may still experience a treatment response (e.g., if they experienced a 50% improvement in EASI score) and a corresponding increase in utility.
CADTH was unable to address the use of adult data to inform utilities for the pediatric reimbursement population. In the CADTH base case, all utilities were adopted from the adult SOLO trial population, and CADTH assumed that nonresponders to would receive the nonresponder utility value instead of reverting to baseline.
Impact of dupilumab on health care resource use is highly uncertain: The sponsor’s model predicts cost savings in terms of medical costs (i.e., health care resource use, background medication use) with dupilumab plus BSC compared to BSC alone (incremental: –$53,420), based on expert opinion about medical care for responders and nonresponders. In the model, the sponsor adopted a micro-level costing approach, using clinical expert opinion to inform the annual number of each resource used by responders and nonresponders. Clinical expert input received by CADTH for this review suggests that several response-specific frequencies do not align with clinical practice in Canada and that the sponsor’s model likely overestimates annual costs for nonresponders. For example, nonresponders were assumed to require 4 additional emergency room visits, 6 additional dermatologist visits, and approximately 5 to 6 additional primary care visits compared to responders in any 1 given year of treatment. Clinical expert input noted that the combination of this frequency of additional resource use did not meet face validity. Further, although clinical experts agreed that it is reasonable to assume that nonresponders will incur more background BSC medication costs, the sponsor’s calculation of background medication cost was based on data from the adult LIBERTY AD CAFÉ trial and likely overestimated the amount of TCS required for a pediatric population based on a small surface area, thus overestimating drug acquisition costs.
In the CADTH base case, CADTH applied alternative estimates of annual health care costs incurred by patients with AD, using the sponsor-provided macro-level costing option to do so. CADTH notes that the derivation of these values was not transparently described by the sponsor but were similarly adopted by CADTH in a previous review of dupilumab.19 Owing to a lack of health care resource utilization data for the reimbursement population, there remains considerable uncertainty in the true annual cost of resource utilization in the reimbursement population.
Poor modelling practices were employed: The sponsor’s model was poorly organized, with parameters repeated across multiple sheets. In many instances, the user-facing cells in the input sheets did not affect calculations in the model. For example, the derivation of health state utility values was spread across 15 individual sheets, and altering values on the user-facing sheets did not affect the values being used in the Markov trace calculations. Finally, the sponsor’s submitted model included numerous IFERROR statements, which led to situations in which the parameter value was over-written with an alternative value without alerting the user to the automatized overwriting. The systematic use of IFERROR statements, as well as inputs repeated across multiple sheets, makes thorough auditing of the sponsor’s model impractical.
CADTH was unable to address these limitations and notes that a thorough validation of the sponsor’s model was not possible.
Additionally, the following key assumptions were made by the sponsor and have been appraised by CADTH (Table 4).
Table 4: Key Assumptions of the Submitted Economic Evaluation (Not Noted as Limitations to the Submission)
Sponsor’s key assumption | CADTH comment |
|---|---|
Patients enrolled in the LIBERTY AD PEDS and LIBERTY AD PRESCHOOL trials were assumed to be representative of patients in Canada who would be eligible for dupilumab. | Uncertain. Clinical expert input obtained by CADTH noted that the pivotal trial participant characteristics were generally representative of patients seen in clinical practice; however, the trials enrolled patients with a higher EASI score than that of patients who may be considered for dupilumab in clinical practice. The score cut-offs for IGA and EASI-75 in the pivotal trials are therefore not reflective of all child and pediatric patients with moderate and severe AD. |
Efficacy (modelled as change in EASI score and utility weights) was assumed to occur at 8 weeks (halfway through the initial clinical assessment period of 16 weeks). | Likely reasonable. Clinical expert input obtained by CADTH noted that response is expected to occur shortly after treatment initiation. |
No utility impacts associated with adverse events. | Uncertain. The sponsor’s model included costs related to the treatment of allergic conjunctivitis, infectious conjunctivitis, oral herpes, skin infection, and injection site reaction; however, no health-related quality of life impacts were included. |
The distributions of patient weight by age were based on a 2017 National Health Service Health Survey for England and assumed to apply to pediatric patients with moderate-to-severe AD in Canada. | Reasonable. Clinical expert input obtained by CADTH noted the weight of pediatric patients with moderate-to-severe AD is expected to be similar to that of the general population and that the weight distribution of pediatric patients in Canada should be comparable to that of the UK. |
Adherence was assumed to be 100% for all scheduled doses of dupilumab. | Uncertain. Clinical expert input obtained by CADTH suggests that adherence to dupilumab may be affected by needle aversion in the reimbursement population. Expert input also suggests that adherence may be less than 100% with topical treatments (i.e., BSC) in clinical practice. |
Patients receiving rescue treatment were assumed to be nonresponders. | Likely reasonable. Efficacy in the model was based on an analysis that classified patients who received rescue treatment as nonresponders. Clinical expert input received by CADTH indicated that patients requiring rescue therapy would not be defined as nonresponders in clinical practice; however, the impact of this assumption on the cost-effectiveness of dupilumab plus BSC vs. BSC alone is likely minimal given that the proportion of patients who achieved EASI-75 was similar across analysis methods. |
AD = atopic dermatitis; BSC = best supportive care; EASI = Eczema Area and Severity Index; EASI-75 = 75% reduction in Eczema Area and Severity Index; IGA = Investigator’s Global Assessment.
CADTH Reanalyses of the Economic Evaluation
Base-Case Results
CADTH undertook reanalyses that addressed key limitations within the submitted economic model, as summarized in Table 5. The CADTH base case was derived by making changes in model parameter values and assumptions, in consultation with clinical experts. CADTH was unable to address the other limitations of the model, including the lack of clinical data for the reimbursement population beyond 16 weeks.
Table 5: CADTH Revisions to the Submitted Economic Evaluation
Stepped analysis | Sponsor’s value or assumption | CADTH value or assumption |
|---|---|---|
Corrections to sponsor’s base | ||
None | — | — |
Changes to derive the CADTH base case | ||
1. Durability of response beyond the trial duration | Proportion of BSC responders who maintained HRQoL benefit:
| Proportion of BSC responders who maintained HRQoL benefit:
|
2. Treatment-specific utility values | Treatment-specific utility values were applied, such that responders and nonresponders to dupilumab received higher utility values than responders and nonresponders to BSC, respectively | Utility values were assigned based on health status (i.e., responder, nonresponder), regardless of treatment received |
3. Utility estimates lacked face validity |
|
|
4. Resource utilization and costs | Expert-elicited estimates of health care resource usea by response status | Annual cost estimates by response status:
|
CADTH base case | — | Reanalysis 1 + 2 + 3 + 4 |
BSC = best supportive care; HRQoL = health-related quality of life.
aIncludes background medication use and health care resources (i.e., primary care visit, dermatologist visit, emergency room visit, hospitalization, full blood count, dermatology nurse visit).
CADTH undertook a stepped analysis, incorporating each change proposed in Table 5 to the sponsor’s base case to highlight the impact of each change (Table 6; disaggregated results are presented in Appendix 4: Table 12). All CADTH probabilistic reanalyses were based on 5,000 iterations.
Results from the CADTH base case suggest that dupilumab plus BSC was associated with higher costs (incremental: $118,787) and higher QALYs (0.91) compared with BSC alone over a lifetime time horizon, resulting in an ICER of $130,945 per QALY gained. In the CADTH base case, dupilumab plus BSC had a 0% probability of being cost-effective at a WTP threshold of $50,000 per QALY.
In the CADTH base case, results were driven by the drug acquisition costs of dupilumab (incremental: $141,775) (Table 12), as well as an incremental gain of 0.91 QALYs with dupilumab plus BSC. Consistent with the sponsor’s submission, the CADTH base case predicts that nearly all of the incremental QALYs (97%) gained with dupilumab are accrued after the trial period. As noted in the CADTH Appraisal of the Sponsor’s Economic Evaluation, all efficacy data used to inform the post-trial period in the model is based on adult populations. The CADTH base case predicts a savings in “other medical costs” (i.e., health care resource and background medication use) which has not been shown in clinical trials. Thus, it is possible that the CADTH base case may not fully reflect the true impact (i.e., benefits and costs) associated with the use of dupilumab in the reimbursement population (i.e., patients aged 6 months to < 12 years).
Table 6: Summary of the Stepped Analysis of the CADTH Reanalysis Results
Stepped analysisa | Drug | Total costs ($) | Total QALYs | ICER ($/QALY) |
|---|---|---|---|---|
Sponsor’s base case | BSC | 426,527 | 26.73 | Reference |
Dupilumab plus BSC | 508,619 | 28.48 | 46,793 | |
CADTH reanalysis 1 — durability of BSC response | BSC | 414,608 | 29.07 | Reference |
Dupilumab plus BSC | 498,264 | 30.55 | 56,244 | |
CADTH reanalysis 2 — utilities based on response status | BSC | 426,527 | 26.76 | Reference |
Dupilumab plus BSC | 508,619 | 28.51 | 46,904 | |
CADTH reanalysis 3 — utilities (face validity) | BSC | 426,527 | 29.04 | Reference |
Dupilumab plus BSC | 508,619 | 30.34 | 63,313 | |
CADTH reanalysis 4 — resource utilization | BSC | 193,257 | 26.73 | Reference |
Dupilumab plus BSC | 304,161 | 28.48 | 63,217 | |
CADTH base case (reanalysis 1 + 2 + 3 + 4) | BSC | 186,162 | 32.89 | Reference |
Dupilumab plus BSC | 297,870 | 33.75 | 130,253 | |
CADTH base case (reanalysis 1 + 2 + 3 + 4) — probabilistic | BSC | 186,139 | 32.88 | Reference |
Dupilumab plus BSC | 304,925 | 33.79 | 130,945 |
BSC = best supportive care; ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year.
Note: CADTH reanalyses are based on publicly available prices of comparator treatments and do not reflect confidential, negotiated prices.
aDeterministic analysis, unless otherwise stated. The probabilistic and deterministic results of the sponsor’s base case were similar.
Scenario Analysis Results
CADTH undertook price reduction analyses based on the sponsor’s results and CADTH’s base case. The CADTH base case suggested that a 54% price reduction for dupilumab would be required to achieve cost-effectiveness of dupilumab plus BSC relative to BSC alone at a $50,000 per QALY threshold (Table 9).
Table 7: CADTH Price Reduction Analyses
Analysis | ICERs for dupilumab plus BSC vs. BSC alone ($/QALY) | |
|---|---|---|
Price reduction | Sponsor base case | CADTH reanalysis |
No price reduction | 47,298 | 130,945 |
10% | 40,086 | 115,891 |
20% | 32,874 | 100,837 |
30% | 25,661 | 85,783 |
40% | 18,449 | 70,729 |
50% | 11,237 | 55,675 |
60% | 4,025 | 40,621 |
BSC = best supportive care; ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year; vs. = versus.
CADTH undertook scenario analyses to explore the impact of alternative assumptions on the cost-effectiveness of dupilumab, which are outlined as follows.
The sponsor’s micro-level costing approach for health care resource utilization and background medication use was adopted.
The sponsor’s micro-level costing estimates of health care resource utilization were adopted, assuming no difference in resource and background medication use between responders and nonresponders, owing to a lack of clinical evidence.
The results of these analyses are presented in Appendix 4 (Table 13). The scenarios involving alternative assumptions about health care resource utilization resulted in ICERs ranging from $99,140 to $156,634, highlighting the impact of uncertainty in estimates for health care resource use.
Issues for Consideration
Dupilumab has been previously reviewed by CADTH for the treatment of patients aged 12 years and older with moderate-to-severe AD whose disease is not adequately controlled with topical prescription therapies or when those therapies are not advisable. The CADTH Canadian Drug Expert Committee recommended that dupilumab be reimbursed with clinical criteria and/or conditions, including a reduction in price.20
Tralokinumab is currently under review by CADTH for the treatment of moderate-to-severe AD in patients aged 12 years and older whose disease is not adequately controlled with topical prescription therapies or when those therapies are not advisable, and clinical studies of tralokinumab in children younger than 12 years are currently ongoing.21 Clinical expert input indicated that the other biologic treatments currently indicated for adult patients are expected to be trialled in pediatric populations. The cost-effectiveness of dupilumab versus other biologic treatments for moderate or severe AD in the reimbursement population is unknown.
Overall Conclusions
Based on data from the submitted pivotal trials for the reimbursement population, dupilumab plus TCS is more effective than TCS alone at reducing disease-related symptoms and improving HRQoL in patients aged 6 months to younger than 12 years with moderate-to-severe AD after 16 weeks of treatment. As noted in the CADTH clinical review, evidence from a single-arm extension study suggests that the effect of dupilumab may be maintained beyond 16 weeks; however, the magnitude of any long-term comparative effects relative to BSC alone is highly uncertain owing to a lack of comparative data beyond 16 weeks. CADTH additionally notes that, for patients aged 6 to younger than 12 years with moderate AD, the magnitude of any treatment benefit between dupilumab plus BSC versus BSC alone is unknown due to a lack of clinical data and as such, the cost-effectiveness of dupilumab in this subgroup, and for the full reimbursement population, is highly uncertain.
The sponsor submitted an economic analysis comparing the cost-effectiveness of dupilumab plus BSC versus BSC alone, based on the proportion of patients achieving EASI-75 at week 16 in the LIBERTY AD PEDS and LIBERTY AD PRESCHOOL trials. To inform efficacy inputs beyond 16 weeks, the sponsor adopted data from adult dupilumab trials, implicitly assuming that treatment response to dupilumab among pediatric patients will be equivalent to that observed among adults. CADTH was unable to explore the validity of this assumption owing to the lack of comparative clinical data for the reimbursement population beyond the 16-week pivotal trials. CADTH identified additional limitations with the sponsor’s economic submission, including those related to the durability of BSC treatment response, omission of relevant comparators, health state utility values, and health care resource use.
CADTH undertook a reanalysis to address several limitations in the sponsor’s analysis, which included adopting alternative estimates for the durability of BSC treatment response, health state utility values, and costs related to health care resource use. The CADTH base case suggests that, at a WTP threshold of $50,000 per QALY gained, dupilumab plus BSC is not a cost-effective treatment option compared with BSC alone, with a 0% probability of dupilumab plus BSC being the optimal treatment strategy at this threshold; dupilumab plus BSC compared with BSC alone is associated with an ICER of $130,945 per QALY gained. A price reduction of 54% for dupilumab would be required for dupilumab plus BSC to be considered cost-effective at a WTP threshold of $50,000 per QALY gained.
The CADTH reanalysis attempted to address the identified limitations of the sponsor’s economic submission; however, a high degree of uncertainty remains. Notably, the cost-effectiveness of dupilumab plus BSC relative to other systemic treatments is unknown owing to a lack of comparative clinical data. CADTH notes that, although the CADTH base case estimated a gain in QALYs with dupilumab plus BSC compared to BSC alone (incremental: 0.91), most of this benefit (97%) was realized in the extrapolated period (i.e., after 16 weeks) based on data from adult dupilumab trials. In the absence of comparative evidence beyond 16 weeks for the reimbursement population, and for patients aged 6 years to 12 years with moderate AD, the incremental QALYs for dupilumab plus BSC predicted in CADTH’s base case may be overestimated. Similarly, it is highly uncertain whether the predicted savings in health care costs will be realized in clinical practice. Additional price reductions may therefore be required.
References
1.Pharmacoeconomic evaluation [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Dupixent (dupilumab), 300 mg single-use syringe (300 mg/2 mL), 200 mg single-use syringe (200 mg/1.14 mL) for subcutaneous injection. Toronto (ON): Sanofi-aventis Canada Inc; 2023 Mar 29.
2.Clinical Study Report: R668-AD-1539 - Part B. [LIBERTY AD-PRESCHOOL]. A phase 2/3 study investigating the pharmacokinetics, safety, and efficacy of dupilumab in patients aged ≥6 months to <6 years with moderate-to-severe atopic dermatitis [internal sponsor's report]. Tarrytown (NY): Regeneron Pharmaceuticals, Inc; 2021 Nov 18.
3.Clinical Study Report: R668-AD-1652. [LIBERTY AD-PEDS]. A randomized, double-blind, placebo-controlled study to investigate the efficacy and safety of dupilumab administered concomitantly with topical corticosteroids in patients, ≥6 years to <12 years of age, with severe atopic dermatitis [internal sponsor's report]. Tarrytown (NY): Regeneron Pharmaceuticals, Inc; 2019 Nov 13.
4.Dupixent (dupilumab): 300 mg single-use syringe (300 mg/2 mL), 300 mg single-use pen (300 mg/2 mL), 200 mg single-use syringe (200 mg/1.14 mL). 200 mg single-use pen (200 mg/1.14 mL), 100 mg single-use syringe (100 mg/0.67 mL) solution for subcutaneous injection [product monograph]. Laval (QC): Sanofi-aventis Canada Inc; 2023 Apr 14.
5.Blauvelt A, de Bruin-Weller M, Gooderham M, et al. Long-term management of moderate-to-severe atopic dermatitis with dupilumab and concomitant topical corticosteroids (LIBERTY AD CHRONOS): a 1-year, randomised, double-blinded, placebo-controlled, phase 3 trial. Lancet. 2017;389(10086):2287-2303. PubMed
6.Thaci D, E LS, Deleuran M, et al. Efficacy and safety of dupilumab monotherapy in adults with moderate-to-severe atopic dermatitis: a pooled analysis of two phase 3 randomized trials (LIBERTY AD SOLO 1 and LIBERTY AD SOLO 2). J Dermatol Sci. 2019;94(2):266-275. PubMed
7.Table: 13-10-0114-01. Life expectancy and other elements of the life table, Canada, all provinces except Prince Edward Island. Ottawa (ON): Statistics Canada; 2022: https://www150.statcan.gc.ca/t1/tbl1/en/tv.action?pid=1310011401. Accessed 2023 Mar 29.
8.NHS Digital. Health survey for England 2017: adult and child overweight and obesity. 2019 Nov 27.
9.Ontario Ministry of Health, Ontario Ministry of Long-Term Care. Ontario drug benefit formulary/comparative drug index. 2022; https://www.formulary.health.gov.on.ca/formulary/. Accessed 2023 Mar 29.
10.Collective agreement. Toronto (ON): Ontario Nurses' Association; 2023 Mar 31: https://www.ona.org/wp-content/uploads/20230331_hospcentralagreement.pdf. Accessed 2023 Jun 5.
11.Schedule of benefits for laboratory services: effective July 1, 2020. Toronto (ON): Ontario Ministry of Health; 2020: http://www.health.gov.on.ca/en/pro/programs/ohip/sob/lab/lab_mn2020.pdf. Accessed 2023 Mar 29.
12.Schedule of benefits for physician services under the Health Insurance Act: (January 25, 2022 (effective July 1, 2022)). Toronto (ON): Ontario Ministry of Health; 2022: https://www.health.gov.on.ca/en/pro/programs/ohip/sob/physserv/sob_master.pdf. Accessed 2023 Mar 29.
13.Ontario Case Costing Initiative (OCCI). Toronto (ON): Ontario Health and Long-Term Care; 2017: https://data.ontario.ca/dataset/ontario-case-costing-initiative-occi. Accessed 2023 Mar 29.
14.Abuabara K, Langan SM. Atopic dermatitis across the life course. Br J Dermatol. 2023;188(6):709-717. PubMed
15.Abuabara K, Magyari A, McCulloch CE, Linos E, Margolis DJ, Langan SM. Prevalence of atopic eczema among patients seen in primary care: data from the health improvement network. Ann Intern Med. 2019;170(5):354-356. PubMed
16.Paternoster L, Savenije OEM, Heron J, et al. Identification of atopic dermatitis subgroups in children from 2 longitudinal birth cohorts. J Allergy Clin Immunol. 2018;141(3):964-971. PubMed
17.Dupixent (dupilumab injection) for pediatrics (6 months to <6 years of age) and Children (6 to <12 years of age) with moderate to severe atopic dermatitis: clinical summary [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Dupixent, 300 mg single-use syringe (300 mg/2 mL), 200 mg single-use syringe (200 mg/1.14 mL) for subcutaneous injection. Toronto (ON): Sanofi-aventis Canada Inc; 2023 Mar 29.
18.Guidelines for the economic evaluation of health technologies: Canada. 4th ed. Ottawa (ON): CADTH; 2017: https://www.cadth.ca/guidelines-economic-evaluation-health-technologies-canada-4th-edition. Accessed 2023 Jun 13.
19.Drug Reimbursement Review pharmacoeconomic report: dupilumab (Dupixent) for the treatment of patients aged 12 years and older with moderate-to-severe atopic dermatitis whose disease is not adequately controlled with topical prescription therapies or when those therapies are not advisable. Ottawa (ON): CADTH; 2020 Jun: https://www.cadth.ca/sites/default/files/cdr/pharmacoeconomic/sr0636-dupixent-pharmacoeconomic-review-report.pdf. Accessed 2023 Jun 22.
20.CADTH reimbursement recommendation: dupilumab (Dupixent — Sanofi Genzyme). Can J Health Technol. 2021;1(6). https://www.cadth.ca/sites/default/files/attachments/2021-06/CADTH_reimbursement_recommendation_dupilumab_%28dupixent%29_1.pdf. Accessed 2023 Jun 13.
21.LEO Pharma. NCT05388760: Tralokinumab monotherapy for children with moderate-to-severe atopic dermatitis - TRAPEDS 1 (TRAlokinumab PEDiatric Trial no. 1). ClinicalTrials.gov. Bethesda (MD): U.S. National Library of Medicine; 2023: https://www.clinicaltrials.gov/study/NCT05388760?term=NCT05388760&rank=1. Accessed 2023 Jun 22.
22.Azathioprine: 50 mg tablets [product monograph]. Toronto (ON): Apotex Inc; 2020 Oct 28: https://pdf.hres.ca/dpd_pm/00059993.PDF. Accessed 2023 May 3.
23.Methotrexate: 2.5 mg tablets [product monograph]. Toronto (ON): Apotex Inc; 2021 Jun 30: https://pdf.hres.ca/dpd_pm/00062029.PDF. Accessed 2023 May 4.
24.Sidbury R, Davis DM, Cohen DE, et al. Guidelines of care for the management of atopic dermatitis: section 3. Management and treatment with phototherapy and systemic agents. J Am Acad Dermatol. 2014;71(2):327-349. PubMed
25.Saskatchewan Drug Plan: search formulary. 2022; http://formulary.drugplan.ehealthsask.ca/SearchFormulary. Accessed 2023 Jun 4.
26.DeltaPA. Ottawa (ON): IQVIA; 2022: https://www.iqvia.com/. Accessed 2023 May 3.
27.Government of Alberta. Interactive drug benefit list. 2022; https://idbl.ab.bluecross.ca/idbl/load.do. Accessed 2023 Jun 5.
28.B.C. Government. BC PharmaCare formulary search. 2022; https://pharmacareformularysearch.gov.bc.ca. Accessed 2023 Jun 5.
29.Eichenfield LF, DiBonaventura M, Xenakis J, et al. Costs and treatment patterns among patients with atopic dermatitis using advanced therapies in the United States: analysis of a retrospective claims database. Dermatol Ther (Heidelb). 2020;10(4):791-806. PubMed
30.CADTH Canadian Drug Expert Committee (CDEC) final recommendation: crisaborole (Eucrisa — Pfizer Canada Inc.). Ottawa (ON): CADTH; 2019 Apr: https://cadth.ca/sites/default/files/cdr/complete/SR0570-Eucrisa-cdec-rec-april-2-2019.pdf. Accessed 2023 May 4.
31.Budget Impact Analysis [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Drug Reimbursement Review sponsor submission: Dupixent (dupilumab), 300 mg single-use syringe (300 mg/2 mL), 200 mg single-use syringe (200 mg/1.14 mL) for subcutaneous injection. Toronto (ON): Sanofi-aventis Canada Inc; 2023 Mar 29.
32.Statistics Canada. Table: 17-10-005-01. Population estimates on July 1st, by age and sex. Ottawa (ON): Statistics Canada; 2022: 10.25318/1710000501-eng. Accessed 2022 Jul.
33.Silverberg JI, Barbarot S, Gadkari A, et al. Atopic dermatitis in the pediatric population: a cross-sectional, international epidemiologic study. Ann Allergy Asthma Immunol. 2021;126(4):417-428.e412. PubMed
34.Paller AS, Siegfried EC, Vekeman F, et al. Treatment patterns of pediatric patients with atopic dermatitis: a claims data analysis. J Am Acad Dermatol. 2020;82(3):651-660. PubMed
35.Sutherland G, Dihn T. Understanding the gap: a pan-Canadian analysis of prescription drug insurance coverage. Ottawa (ON): The Conference Board of Canada; 2017: https://www.conferenceboard.ca/e-library/abstract.aspx?did=9326. Accessed 2023 May 4.
36.Bergman J, Jain V, Lara-Corrales I, Marcoux D, Ramien M. Prescribing preferences and practices of Canadian dermatologists for the treatment of moderate-to-severe atopic dermatitis (AD) in the pediatric population (<12 years old). Presented at: International Society of Atopic Dermatitis; Aug 31-Sep 2, 2023; Gdańsk (PL) [reference provided by the sponsor].
Appendix 1: Cost Comparison Table
Note that this appendix has not been copy-edited.
The comparators presented in the following table have been deemed to be appropriate based on feedback from clinical experts. Comparators may be recommended (appropriate) practice or actual practice. Existing Product Listing Agreements are not reflected in the table and as such, the table may not represent the actual costs to public drug plans.
Table 8: CADTH Cost Comparison Table for Systemic Treatments for Atopic Dermatitis
Treatment | Strength | Form | Price ($) | Recommended dosage | Cost per day ($) | Annual cost ($) |
|---|---|---|---|---|---|---|
Dupilumab (Dupixent) | 300 mg/2 mL 200 mg/1.14 mL | Prefilled syringe | 978.7000a | For patients 6 months to 5 years: 200 mg or 300 mg initially, followed by 200 mg or 300 mg every 4 weeks. For patients 6 to 11 years: 400 to 600 mg initially, followed by 300 mg every 4 weeks or 200 or 300 mg every 2 weeks. | 6 months to 5 years: 34.86b 6 to 11 years: Year 1: 72.40 Subsequent: 69.72 | 6 months to 5 years: 12,723b 6 to 11 years: Year 1: 26,425 Subsequent: 25,446 |
Immunosuppressants | ||||||
Azathioprine (generic) | 50 mg | Tab | 0.2405 | 2.5 mg/kg per day for 24 weeks. Dose adjusted based on patient response | 0.36c | 61c |
Cyclosporine (generic) | 10 mg 25 mg 50 mg 100 mg | Cap | 0.7115 0.7870 1.5350 3.0720 | 3 to 5 mg/kg per day for 24 weeks | 3.07 to 4.61 | 516 to 774 |
Methotrexate (generic) | 2.5 mg | Tab | 0.2513 | 0.2 to 0.7 mg/kg per week (to a maximum of 20 mg per week) for 24 weeks | 0.09 to 0.29c | 15 to 48c |
Mycophenolate mofetil | 250 mg 500 mg | Cap | 0.3712 0.7423 | 30 to 50 mg/kg per day for 24 weeksd | 1.48 to 2.23 | 249 to 374 |
Note: All prices are from the Ontario Drug Benefit Formulary9 (accessed June 2023), unless otherwise indicated, and do not include dispensing fees. Recommended doses based on clinical expert input for patients aged 6 months to 12 years, unless otherwise indicated. For dosing that depends on weight, CADTH assumed a patient weight of 30 kg, unless otherwise indicated.
aSponsor’s submitted price for each dosage.
bAssumes a patient weight of 15 kg.
cAssumes that tablets can be split in half based on the tablet description in the product monograph.22,23
dRecommended dosage based on the American Atopic Dermatology Guidelines.24
Table 9: CADTH Cost Comparison Table for Topical Treatments for Atopic Dermatitis
Treatment | Strength | Package size | Dosage form | Price per gram ($) | Recommended dose |
|---|---|---|---|---|---|
Topical corticosteroids | |||||
Amcinonide (generics) | 0.1% | 60 g tube 60 mL bottle 60 g tube | Cream Lotion Ointment | 0.4522 0.2997a 0.3069a | Thin amount to affected area twice daily, max 5 days on face, axillae, scrotum or scalp, 2 to 3 weeks elsewhere. |
Betamethasone dipropionate (generic) | 0.05% | 50 g tube 75 mL bottle 50 g tube | Cream Lotion Ointment | 0.2048 0.1980 0.2152 | Thin film to affected area twice daily; duration of therapy varies and should be reassessed at least every 4 weeks. |
Betamethasone valerate (generic) | 0.1% | 450 g jar 30 mL, 60 mL bottles 450 g jar | Cream Lotion Ointment | 0.0889 0.3125 0.0889 | No recommended daily dose. Use as directed by clinicians. |
Clobetasol propionate (generic) | 0.05% | 15 g, 50 g tubes, 450 g jar 15 g, 50 g tubes | Cream Ointment | 0.2279 0.2279 | Thin amount to affected area twice daily. Weekly application should not exceed 50 g and treatment should be reviewed weekly. |
Desonide (generic) | 0.05% | 15 g, 60 g tubes, 454 g jar 60 g tube | Cream Ointment | 0.2650 0.2647 | Thin amount to affected area twice daily, may be increased in refractory cases. |
Desoximetasone (Topicort) | 0.25% 0.25% 0.05% | 20 g, 60 g tubes 60 g tube 60 g tube | Cream Ointment Gel | 0.7790a 0.7812a 0.6060a | Thin amount to affected area twice daily. |
Fluocinonide (Lyderm, Lidex) | 0.05% | 15 g, 60 g tubes, 400 g jar 15 g, 60 g tubes 15 g, 60 g tubes | Cream Gel Ointment | 0.2378 0.3076 0.3035 | Thin amount to affected area twice daily. Weekly application should not exceed 45 g. |
Fluocinonide (Tiamol) | 0.05% | 25 g tube 100 g jar | Emollient Cream | 0.1980 | Thin amount 2 to 4 times daily. |
Fusidic acid and betamethasone valerate (Fucibet) | 2% / 0.1% | 15 g, 30 g tubes | Cream | 1.8687b | Twice daily until a satisfactory response is obtained. A single treatment course should not exceed 2 weeks. |
Fusidic acid and Hydrocortisone acetate (Fucidin H) | 2% / 1% | 30 g tube | Cream | 1.6770a | Apply 3 times a day to affected areas for a max of 2 weeks. |
Halobetasol propionate (Ultravate) | 0.05% | 15 g, 50 g tubes 50 g tube | Cream Ointment | 1.0445c 1.2871d | Thin amount to affected area twice daily, limited to 50 g weekly. |
Hydrocortisone (various) | 1% 1% | 45 g tube 60 mL bottle | Cream Lotion | 0.1718 0.1587 | No recommended daily dose. Use as directed by clinicians. |
0.5% 1% | 15 g tube, 454 g jar | Ointment | 0.1400 0.0390 | ||
Hydrocortisone acetate | 0.5% 1% | 15 g, 30 g tubes 28.4 g tube | Cream Ointment | 0.2087a 0.2056 | Twice-daily application is generally recommended initially; intermittent use 1 to 2 times per week on areas that commonly flare for maintenance therapy. |
Hydrocortisone valerate (Hydroval) | 0.2% | 15 g, 45 g, 60 g tubes 15 g, 60 g tubes | Cream Ointment | 0.1667 | Small amount to affected area twice daily. Discontinue as soon as lesions heal or if no response. |
Mometasone furoate (generic) | 0.1% | 15 g, 50 g tubes 15 g, 50 g tubes | Cream Ointment | 0.5542 0.2252 | Thin film to affected areas once daily. |
Prednicarbate (Dermatop) | 0.1% | 20 g, 60 g tubes 60 g tube | Cream Ointment | 1.9772b 1.8831b | Apply a thin film to affected areas of skin twice daily. |
Triamcinolone acetonide (various) | 0.1% | 30 g tube 15 g tube | Cream Ointment | 0.0533 0.1711 | No recommended daily dose. Use as directed by clinicians. |
Topical calcineurin inhibitors | |||||
Pimecrolimus (Elidel) | 1% | 10 g, 30 g tubes | Cream | 2.7935 | Thin layer to affected area twice daily, discontinue when resolved or after 3 weeks if no improvement or exacerbation. |
Tacrolimus (Protopic) | 0.03% 0.10% | 30 g tube | Ointment | 2.8884 3.0899 | Thin layer to affected area twice daily. Discontinue after 6 weeks if no improvement or exacerbation. |
Phosphodiesterase type 4 inhibitor | |||||
Crisaborole (Eucrisa)e | 2% | 60 g tube | Ointment | 2.3000b | Thin layer to affected area twice daily. |
Phototherapy | |||||
UV light therapy | NA | NA | NA | 7.85f per treatment | Administered 2 to 3 times per week.g |
NA = not applicable.
Note: All prices are from the Ontario Drug Benefit Formulary9 (accessed June 2023), unless otherwise indicated, and do not include dispensing fees. Recommended doses are from the product monograph unless otherwise specified.
aSaskatchewan Formulary list price25 (June 2023).
bIQVIA Delta PA list price26 (May 2023).
cAlberta Formulary list price27 (June 2023).
dBritish Columbia Formulary list price,28 as reported by IQVIA Delta PA26 (May 2023).
eCrisaborole received a do not reimburse recommendation from CDEC in March 2019 for treatment of mild to moderate atopic dermatitis in patients 2 years of age and older who have failed or are intolerant to a topical corticosteroid treatment.29,30
fOntario Schedule of Benefits for Physician Services, code G470 “Ultraviolet Light Therapy,” accessed June 2023.12
gBased on clinical expert input.
Appendix 2: Submission Quality
Note that this appendix has not been copy-edited.
Description | Yes or no | Comments |
|---|---|---|
Population is relevant, with no critical intervention missing, and no relevant outcome missing | No | Refer to CADTH appraisal regarding the omission of relevant comparators and modelling of the reimbursement population. The sponsor’s model lacked flexibility to assess the cost-effectiveness of dupilumab plus BSC in relevant subgroups (e.g., moderate AD, severe AD). |
Model has been adequately programmed and has sufficient face validity | No | Refer to CADTH appraisal regarding poor modelling practices and assumptions surrounding treatment response and resource utilization. |
Model structure is adequate for decision problem | Yes | No comment. |
Data incorporation into the model has been done adequately (e.g., parameters for probabilistic analysis) | No | Refer to CADTH appraisal regarding poor modelling practices. |
Parameter and structural uncertainty were adequately assessed; analyses were adequate to inform the decision problem | Yes | No comment. |
The submission was well organized and complete; the information was easy to locate (clear and transparent reporting; technical documentation available in enough details) | No | Refer to CADTH appraisal regarding poor modelling practices. The submission lacked clarity and detail in the technical report (i.e., calculation of resource utilization costs, calculations regarding response). The model was poorly organized and the implementation of utility values in the analysis is misleading and does not fully align with the values presented in the “Utility” sheet. The utility value used for responders on BSC alone in the calculation of QALYs did not match the value under “BSC responder” in the “Utility” sheet, but rather is the “BSC All Patients” utility value derived from the sponsor’s regression model. Values also appeared across various sheets which affected clarity of the submission. |
AD = atopic dermatitis; BSC = best supportive care; QALY = quality-adjusted life-year.
Appendix 3: Additional Information on the Submitted Economic Evaluation
Note that this appendix has not been copy-edited.
Figure 1: Model Structure — Decision Tree
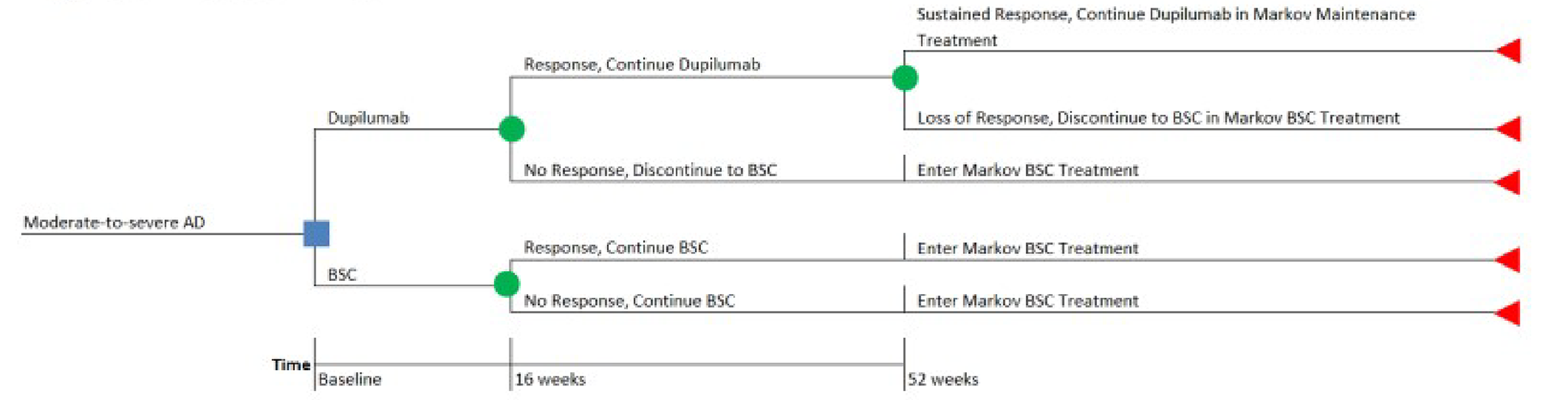
AD = atopic dermatitis; BSC = best supportive care.
Source: Sponsor’s pharmacoeconomic submission.1
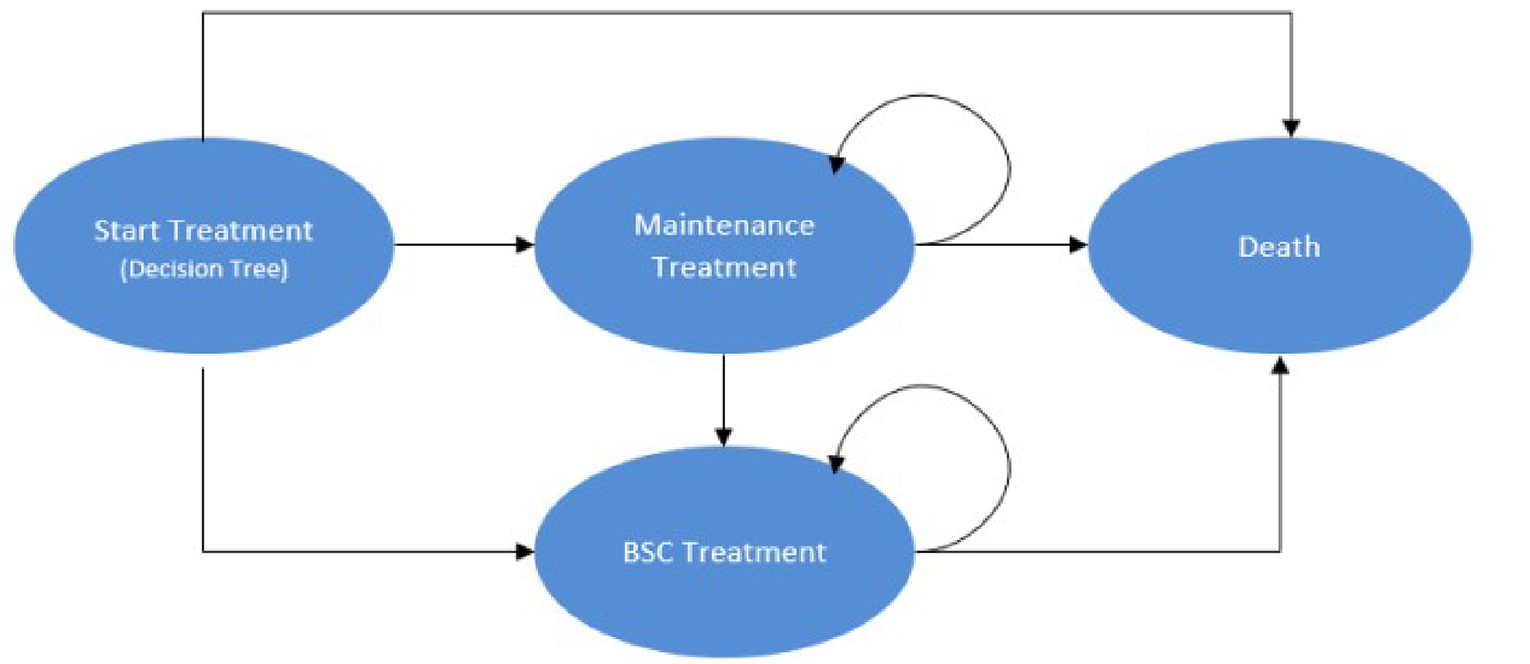
Detailed Results of the Sponsor’s Base Case
Table 11: Disaggregated Summary of the Sponsor’s Economic Evaluation Results
Parameter | Dupilumab + BSC | BSC alone | Incremental |
|---|---|---|---|
Discounted LYs | |||
Total | 45.92 | 45.92 | 0.00 |
Discounted QALYs | |||
Total | 28.48 | 26.73 | 1.75 |
First year of treatment (decision tree) | 0.81 | 0.73 | 0.08 |
Year 2+ (Markov model) | 27.67 | 26.00 | 1.67 |
Discounted costs ($) | |||
Total | 514,738 | 426,200 | 88,539 |
Active treatment | 141,810 | 0 | 141,810 |
Flare medication | 866 | 977 | –111 |
Other medical costsa | 371,389 | 424,809 | –53,420 |
Administration | 57 | 0 | 57 |
Adverse event | 616 | 413 | 203 |
ICER ($/QALY) | 47,298 | ||
BSC = best supportive care; ICER = incremental cost-effectiveness ratio; LY = life-year; QALY = quality-adjusted life-year.
aOther medical costs included background drug costs associated with BSC and health care resource use costs.
Source: Sponsor’s pharmacoeconomic submission.1
Appendix 4: Additional Details on the CADTH Reanalyses and Sensitivity Analyses of the Economic Evaluation
Note that this appendix has not been copy-edited.
Detailed Results of CADTH Base Case
Table 12: Disaggregated Summary of CADTH’s Economic Evaluation Results
Parameter | Dupilumab + BSC | BSC alone | Incremental |
|---|---|---|---|
Discounted LYs | |||
Total | 45.92 | 45.92 | 0.00 |
Discounted QALYs | |||
Total | 33.79 | 32.88 | 0.91 |
First year of treatment (decision tree) | 0.79 | 0.69 | 0.11 |
Year 2+ (Markov model) | 33.00 | 32.20 | 0.80 |
Discounted costs ($) | |||
Total | 304,925 | 186,139 | 118,787 |
Active treatment | 141,775 | 0 | 141,775 |
Flare medication | 865 | 976 | –111 |
Other medical costsa | 161,613 | 184,751 | –23,138 |
Administration | 57 | 0 | 57 |
Adverse event | 616 | 413 | 204 |
ICER ($/QALY) | 130,945 | ||
BSC = best supportive care; ICER = incremental cost-effectiveness ratio; LY = life-year; QALY = quality-adjusted life-year.
aOther medical costs included background drug costs associated with BSC and health care resource use costs.
Scenario Analyses
Table 13: Scenario Analyses Conducted on the CADTH Reanalysis
Stepped analysis | Drug | Total costs ($) | Total QALYs | ICER ($/QALY) |
|---|---|---|---|---|
CADTH base case | BSC | 186,139 | 32.88 | Reference |
Dupilumab + BSC | 304,925 | 33.79 | 130,945 | |
CADTH scenario 1 – micro-level costing | BSC | 414,393 | 32.89 | Reference |
Dupilumab + BSC | 504,695 | 33.80 | 99,140 | |
CADTH scenario 2 – micro-level costing and equal resource use | BSC | 97,418 | 32.89 | Reference |
Dupilumab + BSC | 239,756 | 33.80 | 156,634 |
BSC = best supportive care; ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year.
Appendix 5: Submitted Budget Impact Analysis and CADTH Appraisal
Note that this appendix has not been copy-edited.
Table 14: Summary of Key Take-Aways
Key take-aways of the budget impact analysis |
|---|
|
Summary of Sponsor’s Budget Impact Analysis
In the submitted budget impact analysis (BIA), the sponsor assessed the budget impact of reimbursing dupilumab for use by patients aged 6 months to younger than 12 years with moderate-to-severe AD whose disease is not adequately controlled with topical prescription therapies.31 The BIA was undertaken from the perspective of a Canadian public payer over a 3-year time horizon (January 2025 to December 2027) using an epidemiologic approach. The sponsor’s pan-Canadian estimates reflect the aggregated results from provincial budgets (excluding Quebec), as well as the Non-Insured Health Benefits (NIHB) Program. Data to inform the model were obtained from various sources, including the published literature, the sponsor’s internal data, and input from clinical experts consulted by the sponsor. Key inputs to the BIA are documented in Table 15.
The sponsor compared a reference scenario in which patients received BSC alone to a new drug scenario in which patients received dupilumab as an add-on therapy to BSC, with dupilumab plus BSC assumed to capture 50% of the total market share by year 3 based on the sponsor’s internal data and input from clinical experts in Canada.31 The sponsor’s analysis included drug acquisition costs for dupilumab, with the expected number of annual doses of dupilumab based on patient age and weight. The sponsor assumed that all patients receiving dupilumab would remain on treatment throughout the model’s 3-year time horizon, with an annual estimated cost of dupilumab of $12,758 for patients aged 6 months to < 6 years and $20,063 in the first year of treatment (subsequent years: $19,085) for patients aged 6 years to < 12 years. BSC was assumed by the sponsor to comprise TCIs and TCSs; however, no costs for BSC were included in the model.
Table 15: Summary of Key Model Parameters
Parameter | Sponsor’s estimate (year 1 / year 2 / year 3) | |||
|---|---|---|---|---|
6 months to < 6 years | ≥ 6 to < 12 years | |||
Target population | ||||
Children aged 0 to < 12 years | 3,781,78232 | |||
Proportion of children with AD | 16.3%33 | 13.3%33 | ||
Proportion of children with moderate AD | 29.7%33 | 29.7%33 | ||
Proportion of children with severe AD | 6.5%33 | 6.5%33 | ||
Proportion with uncontrolled ADa post-TCS | 68.5%34 | 71%34 | ||
Proportion who receive advanced therapy | 15%b | 20%b | ||
Proportion covered by public drug plans | Jurisdiction-specific: 3% to 100%31 | |||
Number of patients eligible for drug under review | 5,920 / 5,996 / 6,072 | |||
Market uptake (3 years) | ||||
Uptake (reference scenario) Dupilumab + BSC BSC | 0% / 0% / 0% 100% / 100% / 100% | |||
Uptake (new drug scenario) Dupilumab + BSC BSC | 30% / 40% / 50% 70% / 60% / 50% | |||
Annual cost of treatment (per patient) | ||||
Dupilumab + BSC | $12,758 | First year: $20,064c; subsequent years: $19,085c | ||
BSCd | $0 | $0 | ||
AD = atopic dermatitis; BSC = best supportive care; TCS = topical corticosteroid.
aUncontrolled AD is not defined by the sponsor.
bBased on sponsor’s internal estimates.
cAnnual cost was determined by the sponsor by estimating of the proportion of the population in each weight group (< 30 kg = 50.41%; 30 kg to 60 kg = 46.87%; ≥ 60 kg = 2.72%) based on the participants enrolled in the LIBERTY AD PEDS trial.3
dAssumed by the sponsor to comprise topical corticosteroids and topical calcineurin inhibitors.
Summary of the Sponsor’s BIA Results
The sponsor estimated that the 3-year budget impact of reimbursing dupilumab for the treatment of moderate-to-severe AD in patients aged 6 months to younger than 12 years would be $119,428,852 (year 1: $29,980,625; year 2: $39,508,441; year 3: $49,939,787).
CADTH Appraisal of the Sponsor’s BIA
CADTH identified several key limitations to the sponsor’s analysis that have notable implications on the results of the BIA:
The number of patients eligible to receive dupilumab is underestimated. The sponsor used an epidemiologic approach to estimate the number of patients eligible for dupilumab, starting with the estimated proportion of children with AD.33 Of patients estimated to have uncontrolled AD despite use of TCS treatments, the sponsor assumed that 15% of those aged 6 months to younger than 6 years and 20% of those aged 6 years to younger than 12 years would receive advanced biologic therapy, based on use of the market penetrance of advanced therapy among patients with psoriasis in France, Germany, Italy, Spain the UK, Japan, and the US from 2019 to 2021.31 However, as per the Health Canada–approved indication for dupilumab,4 any patient whose moderate-to-severe AD remains inadequately controlled despite the use of topical prescription therapies would be eligible for dupilumab; thus, the eligible population should not be based on the proportion of patients who have historically received advanced therapy. Clinical expert input received by CADTH indicated that in clinical practice, dupilumab is expected to be used in line with the Health Canada–approved indication and considered after the failure of topical prescription treatments. By imposing this assumption related to advanced therapy in their analysis, the sponsor has severely underestimated the number of patients in the requested reimbursement population eligible to receive dupilumab.
CADTH additionally notes that there is uncertainty regarding the proportion of patients whose moderate-to-severe AD is not adequately controlled with topical prescription therapies. While the sponsor assumed that 68.5% of patients aged 6 months to younger than 6 years and 71.0% of patients aged 6 to younger than 12 years have uncontrolled AD despite receiving treatment with topical therapies,34 CADTH was unable to verify these estimates, and clinical expert input received by CADTH for this review suggests that the values adopted by the sponsor may overestimate the proportion of patients whose AD remains inadequately controlled AD despite topical treatments, although proportion of patients whose disease responds to topical treatments may vary by age and disease severity.
Finally, CADTH notes that the full reimbursement population was not modelled. In addition to patients whose disease is not adequately controlled with topical prescription therapies, the Health Canada–approved indication for dupilumab additionally includes patients for whom topical prescription therapies are not advisable; this subgroup of patients was not included in the sponsor’s BIA estimates. However, clinician input received by CADTH for this review suggests that topical prescription therapies would be considered for the majority of patients and that the proportion for whom such treatments would be inadvisable is low.
In the CADTH base case, it was assumed that all patients whose moderate-to-severe AD is not adequately controlled with topical prescription therapies would be eligible to receive dupilumab, in line with the Health Canada–approved indication and sponsor’s reimbursement request. The impact of restricting dupilumab usage to patients who would be considered eligible for currently available systemic treatments was explored in scenario analyses.
CADTH was unable to address uncertainty in the proportion of patients whose moderate-to-severe AD is not adequately controlled with topical treatments or the exclusion of patients for whom topical prescription therapies is inadvisable owing to a lack of data and the structure of the sponsor’s model.
The proportion of patients eligible for public drug plan coverage is likely underestimated. The sponsor estimated the number of patients eligible for dupilumab by incorporating the proportion of patients covered by public plans for each jurisdiction after accounting for those with private insurance.31 CADTH notes that it is more appropriate to use the proportion of patients eligible for public coverage, rather than enrolled in public plans, as the market size will be determined by all eligible for public coverage. For example, the sponsor estimated that 11% of children in British Columbia aged 6 months to younger than 12 years would be covered by the public plan,31 whereas 100% of patients in this age group are expected to be eligible for public plan coverage.35 Should dupilumab be reimbursed by public plans, it is assumed that all eligible patients for this treatment would enrol for public coverage.
CADTH additionally notes that the NIHB population was inappropriately calculated by the sponsor. NIHB clients residing within Ontario who are under 25 years of age are eligible for reimbursement by the ODB Program and thus should be counted as ODB clients rather than NIHB clients for the purposes of the modelling the budgetary impact of reimbursing dupilumab.
In the CADTH base case, the jurisdiction-specific proportion of patients eligible for public drug plan coverage was used to estimate the market size for dupilumab,35 and the eligible population of NIHB clients was recalculated by considering NIHB clients residing in Ontario to be part of Ontario’s eligible population. CADTH notes that there is uncertainty in the proportion of patients enrolled in public drug plans, and hence the size of the eligible population.
Potentially relevant comparators were excluded. In the sponsor’s base case, the budgetary impact of reimbursing dupilumab was compared to the impact of BSC, which was assumed by the sponsor to be comprised of TCIs and TCSs. As noted in CADTH’s appraisal of the sponsor’s economic evaluation, additional relevant comparators in this population include systemic therapies such as methotrexate, cyclosporine, azathioprine, and mycophenolate mofetil; these were not included in the sponsor’s analysis. Based on a survey of 15 clinicians from Canada undertaken by the sponsor, systemic therapies are used in up to 16% of patients under 12 years of age.36 Clinical expert input received by CADTH for this review indicated that these treatments are currently used off-label for some children with moderate-to-severe AD and may be displaced by dupilumab, given that dupilumab would be the first indicated treatment for this age group and that there may be safety concerns with the use of other systemic therapies in this age group.
CADTH was unable to address this limitation in reanalysis owing to a lack of market share data and the structure of the sponsor’s model.
The market uptake of dupilumab is uncertain: The sponsor’s submitted base case assumed that 30%, 40%, and 50% of eligible patients would receive dupilumab plus BSC in year 1, year 2, and year 3, respectively, based on the sponsor’s internal estimates and expert opinion.31 Clinician input received by CADTH for this review suggests that the uptake of dupilumab may vary depending on jurisdiction, disease severity, patient age, and patient preference.
CADTH explored uncertainty in the uptake of dupilumab in scenario analyses.
Additional limitations were identified, but were not considered to be key limitations. These limitations include:
Misalignment of model inputs between the sponsor-submitted economic analysis and BIA. CADTH noted that several model inputs and assumptions in the BIA were not aligned with the cost-utility analysis submitted by the sponsor. First, the sponsor used different methods between the economic evaluation and BIA to calculate the annual cost of dupilumab, resulting in different annual estimates for dupilumab acquisition. Second, in economic analysis, the sponsor assumed an annual rate of discontinuation from dupilumab (6.3% per year) while assuming in the BIA that all patients remain on treatment for the full 3-year horizon. Neither misalignment is expected to have a notable impact on the estimated budgetary impact of reimbursing dupilumab.
CADTH Reanalyses of the BIA
CADTH revised the sponsor’s base case by aligning the eligibility of dupilumab with the reimbursement request, incorporating the proportion of patients eligible for public drug plan coverage, and correcting the NIHB and ODB population size (Table 16).
Table 16: CADTH Revisions to the Submitted Budget Impact Analysis
Stepped analysis | Sponsor’s value or assumption | CADTH value or assumption |
|---|---|---|
Corrections to sponsor’s base case | ||
None | — | — |
Changes to derive the CADTH base case | ||
1. Eligible population | The number of eligible patients was based on historical market penetrance of advanced therapy (15% for patients 6 months to 5 years old; 20% for patients 6 to 11 years old) among patients with psoriasis from non-Canadian jurisdictions; this assumption is not aligned with the Health Canada–approved indication for dupilumab or the sponsor’s reimbursement request. | The number of eligible patients was aligned with the sponsor’s reimbursement request for patients aged 6 months to < 12 years; that is, all patients whose moderate-to-severe AD is not adequately controlled by topical prescription therapies were assumed to be eligible for dupilumab. |
2a. Public drug plan coverage | Based on the proportion of patients covered by public drug programs (jurisdiction-specific; range 3% to 100%) | Based on the proportion of patients eligible for public drug programs (jurisdiction-specific; range 7% to 100%) |
2b. NIHB and Ontario population | NIHB population (base year) = 123,581 Ontario population (base year) = 1,819,577 | NIHB population (base year) = 96,016 Ontario population (base year) = 1,847,142 |
CADTH base case | Reanalyses 1 + 2a + 2b | |
AD = atopic dermatitis; NIHB = Non-Insured Health Benefits.
The results of the CADTH step-wise reanalysis are presented in summary format in Table 17 and a more detailed breakdown is presented in Table 18. In the CADTH base case, the 3-year budget impact is expected to be $1,523,349,925 (year 1: $381,570,740; year 2: $504,258,676; year 3: $637,520,510) should dupilumab be reimbursed as per the sponsor’s reimbursement request (i.e., for use by patients aged 6 months to younger than 12 years old with moderate-to-severe AD whose disease is not adequately controlled with topical prescription therapies or when those therapies are not advisable).
Table 17: Summary of the CADTH Reanalyses of the BIA
Stepped analysis | Three-year total |
|---|---|
Submitted base case | $119,428,852 |
CADTH reanalysis 1: Number of eligible patients | $663,883,241 |
CADTH reanalysis 2a: Public drug plan coverage | $276,411,516 |
CADTH reanalysis 2b: NIHB and Ontario population | $116,832,026 |
CADTH base case | $1,523,349,925 |
BIA = budget impact analysis; NIHB = Non-Insured Health Benefits.
Note: CADTH reanalyses are based on publicly available prices of comparator treatments and do not reflect confidential, negotiated prices.
CADTH conducted the following scenario analyses to address remaining uncertainty, using the CADTH base case (results are provided in Table 18):
assuming uptake of dupilumab is 10% higher each year
assuming uptake of dupilumab is 10% lower each year
assuming that only patients with severe AD are eligible for dupilumab
assuming that 15% of those aged 6 months to younger than 6 years and 20% of those aged 6 years to younger than 12 years would receive advanced biologic therapy, based on market penetrance of advanced therapy among patients with psoriasis in France, Germany, Italy, Spain the UK, Japan, and the US from 2019 to 202131
assuming that the price of dupilumab is reduced by 54%, the price reduction at which dupilumab would be considered cost-effective at a WTP threshold of $50,000 per QALY in the CADTH reanalysis of the cost-utility analysis (refer to Table 7).
Table 18: Detailed Breakdown of the CADTH Reanalyses of the BIA
Stepped analysis | Scenario | Year 0 (current situation) | Year 1 | Year 2 | Year 3 | Three-year total |
|---|---|---|---|---|---|---|
Submitted base case | Reference | $0 | $0 | $0 | $0 | $0 |
New drug | $0 | $29,980,625 | $39,508,441 | $49,939,787 | $119,428,852 | |
Budget impact | $0 | $29,980,625 | $39,508,441 | $49,939,787 | $119,428,852 | |
CADTH base case | Reference | $0 | $0 | $0 | $0 | $0 |
New drug | $0 | $381,570,740 | $504,258,676 | $637,520,510 | $1,523,349,925 | |
Budget impact | $0 | $381,570,740 | $504,258,676 | $637,520,510 | $1,523,349,925 | |
CADTH scenario 1: 10% increase in uptake of dupilumab | Reference | $0 | $0 | $0 | $0 | $0 |
New drug | $0 | $254,380,493 | $379,116,117 | $510,763,613 | $1,144,260,223 | |
Budget impact | $0 | $254,380,493 | $379,116,117 | $510,763,613 | $1,144,260,223 | |
CADTH scenario 2: 10% decrease in uptake of dupilumab | Reference | $0 | $0 | $0 | $0 | $0 |
New drug | $0 | $508,760,986 | $629,401,234 | $764,277,407 | $1,902,439,627 | |
Budget impact | $0 | $508,760,986 | $629,401,234 | $764,277,407 | $1,902,439,627 | |
CADTH scenario 3: severe AD only | Reference | $0 | $0 | $0 | $0 | $0 |
New drug | $0 | $68,168,371 | $90,086,815 | $113,894,306 | $272,149,492 | |
Budget impact | $0 | $68,168,371 | $90,086,815 | $113,894,306 | $272,149,492 | |
CADTH scenario 4: 15% of patients aged 6 months to 6 years and 20% of patients aged 6 to < 12 years are eligible for dupilumab | Reference | $0 | $0 | $0 | $0 | $0 |
New drug | $0 | $68,577,762 | $90,403,489 | $114,275,316 | $273,256,567 | |
Budget impact | $0 | $68,577,762 | $90,403,489 | $114,275,316 | $273,256,567 | |
CADTH scenario 5: 54% price reduction for dupilumab | Reference | $0 | $0 | $0 | $0 | $0 |
New drug | $0 | $175,522,540 | $231,958,991 | $293,259,435 | $700,740,966 | |
Budget impact | $0 | $175,522,540 | $231,958,991 | $293,259,435 | $700,740,966 |
BIA = budget impact analysis.
Stakeholder Input
Patient Input
Canadian Skin Patient Alliance and Eczéma Québec
About Canadian Skin Patient Alliance and Eczéma Québec
The Canadian Skin Patient Alliance (CSPA) is a national non-profit organization dedicated to advocating, educating, and supporting Canadians impacted by skin, hair, and nail disorders. Our mission is to promote skin health and improve the quality of life of Canadians living with skin disorders through advocacy, education, and awareness, supporting research and working with our Affiliate Member organizations that serve specific patient communities such as eczema, melanoma, and psoriasis.
Eczéma Québec was created as a branch of the McGill University Hospital Network Center of Excellence for Atopic Dermatitis (COE AD), Eczéma Québec is a Patient Advisory Committee (PAC) and registered non-profit organization. It established a network of adult AD patients and healthcare practitioners in the field of AD (encompassing specialist clinician dermatologists, GPs, nurse practitioners, and more), with a goal of building resources based on international best-practice guidelines. Eczéma Québec works with the COE AD to iterate on knowledge translation tools featuring validated information to improve education and experience of care and promote awareness and the health outcomes of this population.
Information Gathering
The CSPA and Eczéma Québec collaborated to hold discussions with atopic dermatitis (AD) patients and caregivers to young AD patients, which inform this submission. To reach these individuals, the CSPA shared a request for participants on its social media channels (Facebook, Instagram), in its newsletter, and via email to dermatologists in its network, and were forwarded by the University of Toronto Division of Dermatology and Toronto Dermatology Society, and to other email contacts of the recipients. Eczéma Québec also shared information about these discussions through its social channels. Eczéma Québec disseminated a community survey and reached out to its patient advisory committee (PAC) members by email.
One of the CSPA’s medical advisors is a clinical trial investigator for pediatric dupilumab and, when asked by the CSPA Executive Director, she connected us with one caregiver of two children, aged 8 and 10, who were part of a pediatric dupilumab clinical trial in Quebec. Eczéma Québec met her for a 1h individual interview. Adult patients who lived with moderate to severe AD as a child and a parent of an adult patient (who experienced AD as a child) were interviewed one-on-one by the Eczéma Québec Co- Director for between 30-60 minutes. The Eczéma Québec Co-Director has also lived experience with the disease and her experience is included in this submission. The interviews were conducted online using the platform Teams and the sessions were recorded. Additionally, the information gathered in this submission also includes material from the current literature on AD in children. Reference material are provided below.
Disease Experience
“Look at him, his skin is bleeding – head to toe his skin is like sandpaper.”1 (Translated)
“When I sit on a black surface or like a black couch, you can see all those skin flakes are all over the place.”2
Atopic dermatitis (AD) is not only the most common chronic inflammatory skin disease, it also ranks highest among all skin disorders as a cause of lost disability-adjusted life-years in patients worldwide. The severity of AD correlates with impact on health-related quality of life (HRQL) as well as lost productivity at school and burden on health systems (Maintz, Bieber, Bissonnette, & Jack, 2021). One in five children have missed school due to their AD (CSPA, 2018).
The disease affects up to 17% of individuals in Canada. The impact of AD varies considerably depending on severity. Impairment in children with chronic skin disease is similar to the experience of children suffering from other chronic diseases of childhood, with AD and psoriasis having the greatest impact on HRQL among chronic skin disorders and only cerebral palsy scoring higher than AD (Beattie & Lewis-Jones, 2006). It is common for people suffering from AD to not view their disease as a chronic condition requiring long-term treatment. Research with parents and children identified the hope these patients expressed of outgrowing their condition. These studies also report that patients often experienced being told they would outgrow their AD. Many patients hope to discover an underlying cause (to “cure”) their AD, which further contributed to a perception of AD as short-term condition. This had implications for the perceived necessity of long-term treatment and was linked with frustration at the perceived ‘simplicity’ of AD management in targeting symptom control rather than underlying causes (Teasdale et al., 2020). We heard from a mom of two children on a clinical trial for dupilumab (ages 6-11) that she was initially told that her son’s symptoms would be temporary, but were not:
“When my children were around two or three years old, [they started showing rashes on their skin], that’s when I realized something was wrong. […] In the first follow-up year, the doctors said, ‘it will go away’. [They said] my child would ‘outgrow’ his eczema.”3 (Translated)
The previous lack of knowledge about how to diagnose, treat and manage moderate to severe AD, as well as the limited treatment options led to many patients experiencing repeated failures with the healthcare system:
“All my life, I have struggled with itch. The constant, debilitating itch that would never leave me alone. As an infant, my parents helped me as best as they could with the limited knowledge they had about eczema.”4
Quality of Life
“Shame, that is a feeling I experienced a lot. I was ashamed of the way I looked, I was ashamed not to be like everyone else, and I was especially ashamed of wanting accommodations for what others considered ‘just a skin problem’.”5
Over the last decade, many studies have been published that highlight the medical and psychosocial burden of moderate to severe AD in Canadian children. Quality of life, access to care, and disease management are all areas of concern for patients and their families and warrant attention from individual clinicians and the health care system (Bridgman, Eshtiaghi, Cresswell-Melville, Ramien, & Drucker, 2018). Patients often report having to change or adapt their behaviours around their condition and modify everyday routines in response to AD symptoms in a desire to avoid potential irritants and adhere to treatment regimens. This can lead to patients having to miss school and restrict their social activities. Patients also reported that they were cautious in choosing a physical activity to practice or would simply give them up (Teasdale et al., 2020):
“It felt like [my kids] were missing out on life. They were not able to go in swimming pool and had to avoid other activities because they felt pain. So, they were left out of many activities.”6 (Translated)
In addition, patients and caregivers often report that they need to purchase special supplies that are often not covered by insurance in order to care for their AD. This can lead to a significant financial burden on families.
Comorbidities
Atopic comorbidities such as food allergies, asthma, allergic rhino-conjunctivitis, and eosinophilic esophagitis, are more common in pediatric AD, especially in those with severe and early-onset disease and can require multidisciplinary management (Lansang et al., 2019). Studies suggest that children who receive a diagnosis of AD were significantly more likely to report a learning disability diagnosis compared to those with clear or almost clear skin. A higher disease severity was associated with greater rates of learning disabilities (Wan, Mitra, Hooper, Hoffstad, & Margolis, 2021). Non-atopic comorbidities such as anxiety, depression, and attention-deficit hyperactivity disorder (ADHD) are also more common in pediatric patients with AD (Lansang et al., 2019). Studies suggest that AD is associated with learning problems and that children with more severe skin disease should undergo screening and treatment for any learning difficulties (Schmidt et al., 2021). Yet many patients report not having been recommended for a screening.
“In elementary school, I remember not [being] able to solve questions or do my homework because I [would get so] itchy that I could not concentrate.”7
Mental Health
With AD being a disease that others can see, many patients experience repeated unwanted comments and stigma from others about their appearance:
“When I first started providing care for my son’s eczema, I did not know where to place my focus, I listened to all the advice and tips everyone gave me like, ‘try this cream/ointment and this other cream’. It ended up being costing me a lot of money and it caused me a lot of stress.”8 (Translated)
Pediatric AD can result in psychosocial impacts, effects on family functioning, disturbance of school performance, sleep loss, and impairment of daily functioning. Seven in 10 children report experiencing sleep loss due to their disease (CSPA, 2018).
“As I grew up, my disease got worse and worse, until it got to the point where I frequently had to miss school and had trouble sleeping at night. On days when I could attend school, I was teased because of the way my skin looked, and people stared or made comments on my appearance. I was not able to skip gym class even though the sensation of burning from sweat on my lesions would make me cry in front of my classmates. I felt as though no one understood what it was like living in my skin.”9
“When [my skin] flares [it feels like my whole] body is burning. I cannot do any sports. I cannot participate in any activities.”10
There is also an increased risk of suicidal ideation in pediatric AD patients. Screening, appropriate management - which may include specialist referral – and treatment of symptoms can reduce the psychosocial impact (Lansang et al., 2019). The increased mental health burden of pediatric AD is the main contributor to the increased risk of death by suicide of these patients (Drucker, Thiruchelvam, & Redelmeier, 2018).
“In elementary school, my AD dictated the way I would dress… I always felt like I needed to hide my disgusting skin.”11
Caregivers’ Experience
Pediatric AD affects many spheres of functioning for patients and families and is associated with significant psychosocial, educational, financial, and occupational burden (Lansang et al., 2019).
“This was stressful because sometimes at night their pajamas were full of blood. I even went to Emergency because I found blood in the diaper [of my son]. Of course, this was due to eczema.”12
“Each night in the bathroom their skin was red, and I applied cream all over [their bodies]; during a trip at the beach in Cuba they felt like their feet were on fire. They were experiencing a great deal of pain.”13
“That was the worst part for me. It was unbearable to see my child suffering and not being able to do anything about it. I spend many nights crying after I put her to bed because I thought I was not doing my job right. I prayed that I could take some of her pain away.”14
“At that point one of my children ended up in the Emergency and was intubated for 1 week with [an] infection all over his body. That was a super stressful and difficult time for me. I lost it. I had to go on a leave from my job; it was too much for me, I needed a break.”15
A common impact among parents was dealing with the extra burden on daily life of caring for a child with eczema. Many parents described carrying out extra tasks to manage their child’s eczema, e.g., applying topical treatments, extra washing, and cleaning, buying specific clothing and products for the house (“Collecting and summarizing research on people’s views of managing eczema,” 2021). Caregivers report being helpless in the face of their child's condition. They frequently feel that they have failed when the disease severity intensifies and feel responsible for the flares of AD affecting their children. Consequently, some caregivers are emotionally exhausted by the burden of the illness, which can affect their overall mental health and well-being. People caring for children suffering from AD often manage the burden themselves: they manage the administration and supply of treatments (renewals, purchasing), the medical appointments, and navigating insurance coverage. This can lead to emotional fatigue and a sense of loneliness:
“Keeping the kids at the hospital was so difficult. I wanted to protect them, and I tried to stay strong for them. I do not think they noticed how I was feeling. I tried to turn the situation around and told them that going to the hospital made us spend time together, but sometimes it is so hard. My oldest son saw me cry.”16
Additionally, where children have separated parents with shared custody, there can be discrepancy between the environments at each home. This underscores how sensitive pediatric AD patients are to changes in their routine and management of their AD:
“My children would come back from their dad’s house and their AD would be worse. Change of environment is a problem, the treatment plan is not performed the same way. [Their dad] knows but maybe the beds are not as clean/aseptic as at my house. The routine is not followed like it is with me. I tell myself the kids are having fun and it is best for them. They must see their dad. It is complicated.”17
Experiences With Currently Available Treatments
Topical therapies such as corticosteroids (TCS), calcineurin inhibitors, and phosphodiesterase 4 (PDE4) inhibitors are the recommended first-line treatments for pediatric AD. TCS failure is associated with nonadherence and/or corticosteroid phobia despite being counselled on treatment adherence (Lansang et al., 2019). However, both patients and caregivers reported that currently available treatments have limited effect. Caregivers often opt for non-prescription options, possibly due to fear of using potentially harsh medications on their children; they may also be instructed by their healthcare providers to be cautious of using such treatment in younger patients. Of prescribed treatments, TCS seem to offer the most improvement, though patients worry of their long-term use and the associated side effects and can face barriers complying with the treatment over a long period of time. Several patients described experiences of steroid withdrawal after years of use.
“Methotrexate and other immune- suppressors are treatment options but have severe complications and require constant monitoring from a doctor. These options do not actually target the disease specifically and cannot control severe AD. Itching still remains and eczema can still be found on the entire body. This is not an adequate treatment option when compared to Dupixent.”18
This corroborates a 2006 survey of Canadian patients which found that 71% were concerned about the safety profile of topical corticosteroids (Barbeau & Bpharm, 2006). While patients and caregivers are clearly willing to try effective medications to treat this condition, safe, effective, and long-term options are limited. Phototherapy may be considered when available, accessible, and deemed appropriate in pediatric patients with AD. Narrowband UVB therapy is the preferred choice of phototherapy but is not widely available throughout Canada. Systemic therapy is warranted for pediatric patients with AD who have inadequate disease control based on clinical signs, symptoms, or QoL impact despite appropriate topical therapy and/or phototherapy.
Other methods of controlling and preventing symptoms used by patients with moderate to severe AD include skin care maintenance such as specific bathing routines (e.g., oatmeal baths, bleach baths), moisturizers, natural and herbal remedies, and acupuncture. Those with AD also report that they avoid certain foods and clothing, refrain from hot baths and wear long sleeves to prevent symptoms or reduce exacerbations.
However, there was strong consensus that several therapeutic strategies commonly tried by patients with AD are not effective in treating disease and may lead to negative outcomes. Food avoidance and elimination diets are not routinely recommended in the absence of specific food allergy nor advised, particularly in younger children. There is no evidence for the use of bath additives in managing signs and symptoms of AD; in fact, some ingredients may aggravate disease or lead to irritant and allergic contact dermatitis. Topical and oral antihistamines have little evidence to support their use. Oral first-generation antihistamines have adverse effects including prolongation of QT interval and sedation. They may interfere with school performance and/or driving in adolescents. Oral second-generation antihistamines used in management of pruritus do not have any added benefit in the treatment of AD (Lansang et al., 2019).
Furthermore, many misconceptions about AD circulate in the public sphere making it challenging for people living with (or caring for someone living with) the disease to find evidence-based information. Many online groups on social media advertise the dangers of TCS usage over long periods of time. A dominant concern is that using topical corticosteroids can lead to skin damage, particularly skin thinning and possibly other long-term negative effects, e.g., weakened bones, weight gain and delayed growth.
Many AD patients are frustrated with the disappointing results of topicals and other treatments for their moderate to severe AD. Consequently, AD patients and caregivers often avoid interactions with the healthcare system and are skeptical about the advice that is provided to them.
Treatment Burden
With complex and time-consuming skin maintenance and treatment routines, the treatment burden, and its impact on people with AD and family life is apparent:
“The doctor prescribed my children with medications that I had to prepare at home and apply to my son’s skin 3 times per day. He trained me on how to mix at home on my own. This mixture took 10-12 minutes to make and could take up 45 minutes to apply [on both of my sons].”19
“I was also given instructions on another treatment to re-hydrate the skin involving applying Vaseline (light type) to the skin, then put on the children’s pajamas that were made wet with water. This treatment had to be done before other medication (pills) were given.”20
Patients and caregivers report feeling that this burden was not acknowledged by others (“Collecting and summarizing research on people’s views of managing eczema,” 2021).
AD patients often experience treatment fatigue, where one treatment that has proven effective for them gradually becomes less effective, leaving them faced with the trial-and-error process of determining which other treatment may provide them with some benefit. A new treatment option can provide relief for some patients whose moderate to severe AD is currently well-controlled but may not be in the near future. The unpredictability of the disease over time is a concern for most patients.
“It was extremely difficult to stick to a treatment routine, it was hard to find the right products, and between my place, her dad’s, school, dance class… Sometimes we could not keep up.”21
“The costs associated with the trial-and-error nature of treatment regimens is very frustrating.”22
Improved Outcomes
Patients living with moderate to severe AD describe the excruciating, “disfiguring” and debilitating nature of their symptoms. As described above, AD causes itching, burning and pain, each of which can decrease patients’ ability to sleep, work, attend school, parent, and complete activities of daily living.
Where the symptoms of AD are adequately controlled, patients will be better able to participate in social occasions without the fear of stigmatization, improving their mental and emotional health. Over the years, patients have reported wanting a therapy that is not only easily accessible to them, they also favour treatments that do not take a long time to use (e.g., applying several topicals to different parts of the body). Patients and caregivers alike express the wish to reduce the frequency of administration of treatment and hope for treatments showing great efficacy and safety. One patient shared that:
“I would almost never go out with my friends or was left out of social activities, like in school, I would never get picked for sports and had to be creative in finding an activity I could practice without experiencing too much pain.”23 (Translation)
Experience With Drug Under Review
We heard from one caregiver, the mother of two children in a clinical trial for dupilumab: one son aged 8 and another son aged 10. She shared that prior to a dupilumab clinical trial, there was a very extensive routine of bathing at specific temperatures (different for each child), five different creams for different parts of each child’s body and specific laundry detergent.
At this time, she had a separate calendar with all this information for each child which was so extensive that it did not fit on a single calendar. If the children’s elaborate routines were not followed by their father (in a separate house), grandparents or babysitters, they would experience a flare and significant discomfort from their AD. As well, wounds were a critical issue for her children despite using five creams and faithfully adhering to their topical treatments.
“[B]efore trying Dupixent injections, my children were at home sick with large wounds all over so bad that my eldest son could not put his shoes on because of large wounds and dressings. He had difficulty at school because he would take his shoes off to scratch. The other children were making fun of him. His feet were bleeding, and the teacher did not know what to do.”24 (Translation)
When asked about her expectations for dupilumab injections, she responded:
“I was expecting their skin would stop itching. That was my expectation. But it was better. They ended up with [b]eautiful skin. [And there] was the fact there were extraordinarily little side effects. I ask[ed] myself “Will it damage their immune systems?” The only negative effect was the dryness of the eyes of my youngest son. I now put eye drops to prevent the dryness. I will notice their eyes becoming red and dry, but it is okay, it is much better like this. You just put eye drops in their eyes. [I mostly used hydrating eye drops during allergy season and did not need a prescription for these.] They now have soft and normal skin. I never could feel the softness of their skin since they were babies! Since the doctor prescribed Dupixent injections, now they are living so well. It is wonderful. Their skin is beautiful – colour is great; their skin is soft. This is so exciting!”25 (Translation)
The change in her sons’ skin was so remarkable that she was afraid she would accidentally do something that would cause their eczema to reappear:
"I did not want to give them a bath in case it affected the skin; I didn’t want to ruin this change in their skin. [I kept feeling like] if I do something [different], it will come back.”26 (Translation)
From her perspective as a caregiver, the successful use of dupilumab for her children was transformative:
“Dupixent changed my life, and I started living. I have nothing to do now [to help manage my kids’ eczema since we started Dupixent injections].”27 (Translation)
The successful use of dupilumab changed many things in terms of the children’s previous treatment routines:
“Since starting Dupixent injections, they do not need [as many] creams. Before, they needed five different creams for different parts of their bodies...no more cortisone I used to use five jars of cream per week and now I just use one.”28 (Translation)
“I looked for AD on their bodies and I could not find any signs of AD They could dress themselves now. I do not have to supervise their baths. What a beautiful summer we had. It was marvelous. In the fall, I kept checking their skin — it was well hydrated. Wow, it was marvelous. I think it is changing now. It is wonderful for the kids. For sure, there are moments where the spots reappear under the ears and on their hands — but less so - probably because there is a bit of stress, and it is allergy time.”29 (Translation)
Despite extra handwashing during the COVID-19 pandemic, her children continue to have positive outcomes:
“Due to COVID-19, they will have plaques on their hands because they wash their hands more often and [a few days before] the injections are due ... their skin becomes itchier [and so] I apply a bit of cream at night.”30 (Translation)
Companion Diagnostic Test
Not applicable.
Anything Else?
Skin disorders are often diminished, disregarded, and dismissed. They are more than “just a rash”. Skin disorders often reflect imbalances in inflammatory and other systems, and can be caused by allergens, viruses, cancer, bacteria, fungi, genetics, wounds, hormones, and other disorders, and can cause devastating impacts. Many of the medicines available to treat skin disorders were initially developed for other diseases or organ systems and have become part of the skin treatment toolbox (e.g., methotrexate developed for cancer, cyclosporine developed for preventing organ rejection, etc.) (Wikipedia, 2021).
The development of more tailored treatment options for skin disorders on the horizon provides new hope that treatments will address the underlying pathology of skin disorders, rather than only treating the symptoms. Skin patients deserve to be treated with respect and dignity by the health system, which includes its embrace of new and tailored treatment options.
1 Participant 1: Caregiver of two children, aged 8 and 10 enrolled in the dupilumab trial for extension 6-11
2 Participant 3: Adult patient living with severe atopic dermatitis who experienced AD as a child, currently on dupilumab.
3 Participant 1: Caregiver of two children, aged 8 and 10 enrolled in the dupilumab trial for extension 6-11
4 Participant 2: Adult patient living with severe atopic dermatitis who experienced AD as a child, currently on dupilumab.
5 Participant 2: Adult patient living with severe atopic dermatitis who experienced AD as a child, currently on dupilumab.
6 Participant 1: Caregiver of two children, aged 8 and 10 enrolled in the dupilumab trial for extension 6-11
7 Participant 3: Adult patient living with severe atopic dermatitis who experienced AD as a child, currently on dupilumab.
8 Participant 1: Caregiver of two children, aged 8 and 10 enrolled in the dupilumab trial for extension 6-11
9 Participant 2: Adult patient living with severe atopic dermatitis who experienced AD as a child, currently on dupilumab.
10 Participant 3: Adult patient living with severe atopic dermatitis who experienced AD as a child, currently on dupilumab
11 Participant 4: Adult patient living with severe atopic dermatitis who experienced AD as a child, currently on dupilumab.
12 Participant 1: Caregiver of two children, aged 8 and 10 enrolled in the dupilumab trial for extension 6-11
13 Participant 1: Caregiver of two children, aged 8 and 10 enrolled in the dupilumab trial for extension 6-11
14 Participant 5: Caregiver of an adult patient who experienced AD as a child.
15 Participant 1: Caregiver of two children, aged 8 and 10 enrolled in the dupilumab trial for extension 6-11
16 Participant 1: Caregiver of two children, aged 8 and 10 enrolled in the dupilumab trial for extension 6-11
17 Participant 1: Caregiver of two children, aged 8 and 10 enrolled in the dupilumab trial for extension 6-11
18 Previously interviewed patient with severe AD who later used dupilumab.
19 Participant 1: Caregiver of two children, aged 8 and 10 enrolled in the dupilumab trial for extension 6-11
20 Participant 1: Caregiver of two children, aged 8 and 10 enrolled in the dupilumab trial for extension 6-11
21 Participant 5: Caregiver of an adult patient who experienced AD as a child.
22 Participant 1: Caregiver of two children, aged 8 and 10 enrolled in the dupilumab trial for extension 6-11
23 Participant 4: Adult patient living with severe atopic dermatitis who experienced AD as a child, currently on dupilumab.
24 Participant 1: Caregiver of two children, aged 8 and 10 enrolled in the dupilumab trial for extension 6-11
25 Participant 1: Caregiver of two children, aged 8 and 10 enrolled in the dupilumab trial for extension 6-11
26 Participant 1: Caregiver of two children, aged 8 and 10 enrolled in the dupilumab trial for extension 6-11
27 Participant 1: Caregiver of two children, aged 8 and 10 enrolled in the dupilumab trial for extension 6-11
28 Participant 1: Caregiver of two children, aged 8 and 10 enrolled in the dupilumab trial for extension 6-11
29 Participant 1: Caregiver of two children, aged 8 and 10 enrolled in the dupilumab trial for extension 6-11
30 Participant 1: Caregiver of two children, aged 8 and 10 enrolled in the dupilumab trial for extension 6-11
Reference Material
1. Beattie, P. E., & Lewis-Jones, M. S. (2006). A comparative study of impairment of quality of life in children with skin disease and children with other chronic childhood diseases. British Journal of Dermatology, 155(1), 145–151. https://doi.org/10.1111/j.1365-2133.2006.07185.x
2. Bridgman, A. C., Eshtiaghi, P., Cresswell-Melville, A., Ramien, M., & Drucker, A. M. (2018). The Burden of Moderate to Severe Atopic Dermatitis in Canadian Children: A Cross-Sectional Survey. Journal of Cutaneous Medicine and Surgery, 22(4), 443–444. https://doi.org/10.1177/1203475418761859
3. Canadian Skin Patient Alliance. (2018). The Skin I’m In: A National Report of the Patient and Caregiver Experience with Atopic Dermatitis. Online: https://www.canadianskin.ca/images/Documents/Atopic_report/CSPA_Atopic_Dermatitis_report_Feb_2_2018_FINAL_.pdf
4. Wan, J., Mitra, N., Hooper, S. R., Hoffstad, O. J., & Margolis, D. J. (2021). Association of Atopic Dermatitis Severity With Learning Disability in Children. JAMA Dermatology. https://doi.org/10.1001/jamadermatol.2021.0008
5. Schmidt, S. A. J., Mailhac, A., Darvalics, B., Mulick, A., Deleuran, M. S., Sørensen, H. T., … Langan, S. M. (2021). Association Between Atopic Dermatitis and Educational Attainment in Denmark. JAMA Dermatology. https://doi.org/10.1001/jamadermatol.2021.0009
6. Collecting and summarizing research on people’s views of managing eczema. (2021). British Journal of Dermatology, 184(4). https://doi.org/10.1111/bjd.19839
7. Lansang, P., Lara-Corrales, I., Bergman, J. N., Hong, C., Joseph, M., Kim, V. H. D., … Spring, S. (2019). Approach to the Assessment and Management of Pediatric Patients With Atopic Dermatitis: A Consensus Document. Section IV: Consensus Statements on the Assessment and Management of Pediatric Atopic Dermatitis. Journal of Cutaneous Medicine and Surgery, 23(5_suppl), 32S39S. https://doi.org/10.1177/1203475419882654
8. Drucker, A. M., Thiruchelvam, D., & Redelmeier, D. A. (2018). Eczema and subsequent suicide: a matched case–control study. BMJ Open, 8(11), e023776. https://doi.org/10.1136/bmjopen-2018- 023776
9. Teasdale, E., Muller, I., Sivyer, K., Ghio, D., Greenwell, K., Wilczynska, S., … Santer, M. (2020). Views and experiences of managing eczema: systematic review and thematic synthesis of qualitative studies*. British Journal of Dermatology, 184(4), 627–637. https://doi.org/10.1111/bjd.19299
10. Maintz, L., Bieber, T., Bissonnette, R., & Jack, C. (2021). Measuring Atopic Dermatitis Disease Severity: The Potential for Electronic Tools to Benefit Clinical Care. The Journal of Allergy and Clinical Immunology: In Practice, 9(4), 1473-1486.e2. https://doi.org/10.1016/j.jaip.2021.02.027
11. Barbeau, M., & Bpharm, H. L. (2006). Burden of Atopic dermatitis in Canada. International Journal of Dermatology, 45(1), 31–36. https://doi.org/10.1111/j.1365-4632.2004.02345.x
12. Wikipedia, Methotrexate - History, online: https://en.wikipedia.org/wiki/Methotrexate#History, last accessed: April 20, 2021.
13. Wikipedia, Ciclosporin – History, online: https://en.wikipedia.org/wiki/Ciclosporin#History; last accessed: April 20, 2021.
Conflict of Interest Declaration — Canadian Skin Patient Alliance (CSPA) and Eczéma Québec
To maintain the objectivity and credibility of the CADTH CDR and pCODR programs, all participants in the drug review processes must disclose any real, potential, or perceived conflicts of interest. This Patient Group Conflict of Interest Declaration is required for participation. Declarations made do not negate or preclude the use of the patient group input. CADTH may contact your group with further questions, as needed.
Did you receive help from outside your patient group to complete this submission? If yes, please detail the help and who provided it.
This submission was prepared by the CSPA and Eczéma Québec without help from outside the organization.
Did you receive help from outside your patient group to collect or analyze data used in this submission? If yes, please detail the help and who provided it.
The data used to support this submission was collected and analyzed by the CSPA and Eczéma Québec.
List any companies or organizations that have provided your group with financial payment over the past two years AND who may have direct or indirect interest in the drug under review.
Table 1: Financial Disclosure for Canadian Skin Patient Alliance
Company | $0 to $5,000 | $5,0001 to $10,000 | $10,001 to $50,000 | In Excess of $50,000 |
|---|---|---|---|---|
Sanofi Canada | — | — | — | X |
Pfizer Canada | — | — | — | X |
Abbvie Canada | — | — | — | X |
LEO Pharma Canada | — | — | X | — |
Table 2: Financial Disclosure for Eczéma Québec
Company | $0 to $5,000 | $5,0001 to $10,000 | $10,001 to $50,000 | In Excess of $50,000 |
|---|---|---|---|---|
Sanofi Genzyme | — | — | X | — |
McGill COE-AD and its pharmaceutical industry sponsors (Pfizer Canada, AbbVie Canada, LEO Pharma Canada, Novartis, Sanofi Genzyme, Eli Lilly) | — | — | — | X |
McGill COE-AD and its dermo-cosmetic industry sponsors (CUTIMed, Beirsdorf, L’Oréal) | — | — | X | — |
Eczema Society of Canada
About Eczema Society of Canada
The Eczema Society of Canada (ESC) is a registered Canadian charity dedicated to improving the lives of Canadians living with eczema, with a mission of support, education, awareness, and research. For more information, please visit http://www.eczemahelp.ca.
Information Gathering
Information for this submission was gathered via written questionnaires, surveys, interviews, statements, and testimonials by patients who live with uncontrolled moderate or severe atopic dermatitis (AD) and/or their caregivers (reporting on patient experience for those aged 17 and younger). Patients and/or caregivers who shared their experiences using dupilumab accessed the drug through clinical trials, compassionate care programs, and/or private or provincial drug coverage. In some cases, patients and/or caregivers paid out of pocket to fund their treatment. All responses and testimonials are anonymous.
Survey data in this submission includes data from: 1057 respondents regarding the AD patient journey; 299 respondents regarding AD systemic treatment experience; and 1035 respondents regarding AD quality of life impact.
Disease Experience
AD is an inflammatory skin condition that causes dry, itchy skin which develops rash/lesions that can crack, ooze, and bleed. It is the most common form of eczema, and severity can range from mild to severe. The symptoms of moderate and severe AD include debilitating itch and pain, and can be life altering for patients, their caregivers, and their family members.
AD is typically characterized by periods of flare (worsening of the condition) and periods of remission (clear skin or improvement of the condition). The condition is chronic, and many patients suffer with it their entire lives. Some patients never experience periods of clear skin, and constantly suffer with some baseline flare activity.
Living with the chronic itch and pain of AD can take a significant toll on quality of life. 70% of paediatric survey respondents with moderate or severe AD suffer from interrupted sleep due to their symptoms, with 18% having poor sleep more than 14 nights per month. Studies show that sleep is important for general health and growth for children, (Zhou Y, Aris IM, Tan SS, et al. Sleep duration and growth outcomes across the first two years of life in the GUSTO study. Sleep Med. 2015 Oct;16(10):1281-6. doi: 10.1016/j.sleep.2015.07.006. Epub 2015 Jul 17. PMID: 26429758.) and sleep is significantly impacted due to the itch and discomfort caused by AD. This is also a distressing aspect of the condition for caregivers, as they frequently report being up throughout the night, or having to sleep with their child in an attempt to stop their child from scratching and damaging the skin, as well as to provide comfort to their child.
“My son would sleep in my bed so I could hold his hands and stop him from biting and scratching until he would bleed, even with all of the oral and topical meds, nothing worked.”
“My child was constantly itchy and would scratch until they bled. We tried everything – topical steroids, prednisone, changing diet, wet wraps, you name it. But nothing helped.
Patients consistently rate itch as the most bothersome symptom of AD. The intense itch can drive patients to scratch uncontrollably and further damage broken skin, especially while asleep when the urge to scratch is uninhibited and can be intense. Patients and caregivers also reported bleeding from skin damage due to scratching and needing to frequently change clothing and bedding as a result. Children can experience feelings of embarrassment and shame when their clothes exhibit visible blood stains, when bandages are required, and when their skin rash has visible crusting, bleeding, and scabbing.
“Some days I was ashamed and embarrassed that I couldn’t help [my child] when people would stare at his skin.”
Paediatric patients can also experience devastating impacts during flares, contributing to missed school, feelings of social isolation, and bullying. Survey data reveals that days of school missed is positively correlated to AD severity. Caregivers reported that their child could not participate in sports or gym class because extending their arms and legs would be too painful and cause their skin to crack. Others reported not being able to participate in activities like swimming and being limited to certain activities or holidays as a family in order to accommodate their child with AD. Paediatric patients have reported to ESC that these circumstances make them feel embarrassed, sad, and like a burden to their family.
“I felt like a bad mother, as if I was not taking proper care of my child, when in reality we were working so hard, applying so many creams and medicines, and nothing was helping our child.”
Caregivers reported that the condition places a significant emotional toll and burden on the whole family. Feelings of guilt, frustration, anger, and sadness is common. Survey results indicated 69% of caregivers reported experiencing anxiety due to managing a child with AD, and 25% reported experiencing depression related to their child’s condition. 41% of caregivers reported they feel like a failure when they cannot control their child’s flares. Watching your child suffer daily is very difficult for caregivers of children with unmanaged AD. Numerous caregivers reported that simple acts like bathing can be excruciating and bring their child to tears.
“I try to stay positive, but I can feel myself melting away as a mother. I get frustrated and angry and have been forced to disconnect from my other children because I simply can’t provide them with the attention they deserve [while caring for my child with AD]. I wouldn’t wish this upon anyone.”
Experiences With Currently Available Treatments
Typical management of AD includes trigger avoidance, skin care, and the use of topical medications to manage inflammation when flares occur. However, for a small group of patients with more severe forms of uncontrolled AD, these strategies often only provide temporary relief, or no relief at all. For this group of patients, their dermatologist may recommend a systemic therapy as the next step.
“Our child has literally suffered with this all his life - since he could control his hands he has scratched. We've tried every topical medication, faithfully, and they never clear his skin or offer relief.”
Before dupilumab was approved, systemic therapies for patients with AD included phototherapy/light therapy, oral corticosteroids, and off-label systemic immunosuppressants. While oral corticosteroids can offer control of symptoms in the short-term, they are not recommended for long-term use, and even short- term use can carry significant risks of side effects. Patients also reported terrible rebound flares after stopping even a short course of these medicines.
Off-label systemic medications like methotrexate and cyclosporine are sometimes used however these immunosuppressive medications are not approved for use in patients with AD. Patients and caregivers report concerns related to serious side effects both in the short-term (e.g., nausea) and long-term (e.g., organ damage). The caregiver community is particularly wary of using systemic therapies that have not been approved for use in children, or that carry significant side effects.
“As parents, we have struggled. [My child and I] have butt heads about their treatment. Every morning, we find dried skin and blood on his sheets. It hurts to see your child hole up in their room and not want to come out. As a parent, how do we support them through this?”
Patient and caregiver concerns related to side effects vary greatly from patient to patient and caregiver to caregiver. Some are very concerned and cautious about risks and side effects related to their child taking any medication(s). Others reported willingness to weigh the risk / benefit ratio in relation to the severity of their child’s condition and the suffering they are enduring.
“As parents, we would get so hopeful when we would see a new doctor or treatment only to feel let down because they didn’t understand our struggle, or the meds didn’t help.”
Improved Outcomes
Patients and caregivers are seeking treatments that reduce or ideally eliminate skin inflammation, skin symptoms, and itch. Many caregivers reported deep frustration in navigating the cycles of recurrent flares when medications fail. For some, it can feel like an endless cycle of topical medications, which result in little or no improvement. Some patients and caregivers reported that despite trying numerous topical treatments and over-the-counter products (often at great personal expense), diligently following the instructions of their health care providers, and modifying their family’s lifestyle to avoid triggers, their child still experienced devastating flares with no relief or improvement of symptoms.
“When his flares were severe, I would be bathing and medicating him constantly and going to see doctors 2-3 times a week and nothing would help. I felt like such a failure as a mom because I couldn’t help him.”
“We would have tried anything, done anything, or paid anything to give our child relief. His eczema was impacting his mental health, his confidence, his desire to go to school. We were desperate.”
Experience with Drug Under Review
Caregivers of patients who were part of the dupilumab clinical trial reported significant improvements in their child’s skin symptoms and quality of life. They all reported that the improvements were life changing, and that dupilumab is the first medication in their child’s life that has worked to improve their child’s skin and reduce itch.
This experience with dupilumab is also reflected in survey data which reported that patients who took dupilumab experienced improved sleep, improved mood, increased concentration at school, improved social relationships, and the renewed ability to exercise.
“We saw drastic results. [Our child] was sleeping better. The difference was night and day.”
“In short, I would characterize my experience taking dupilumab as transformational. I was much less itchy, slept better, and additionally my allergic rhinitis in response to household allergies completely disappeared. My overall quality of life made phenomenal improvement.”
Of the systemic survey respondents who have taken dupilumab, 80% agreed it has contributed to the optimal management of their AD. One family reported that while they knew of the potential side effects, they were willing to accept the risk in exchange for finding something – anything – that could finally provide relief for their child’s suffering. One family interviewed reported noticing redness in their child’s eye, but it did not cause them to stop using the medication.
A caregiver reported that at first, they were in disbelief of the improvement dupilumab made, because their child had been suffering for so long and they didn’t believe relief was even possible. Another caregiver reported that the insatiable itch and fear of flares was eliminated. One family shared that dupilumab changed their child’s life, as their AD is now better than it has ever been.
“We weighed the pros and the cons of the side effects, but nothing else has helped. Our child has never had clear skin until now. People need to know and need to understand that this is not ‘just an itch.’ This affects your whole life.”
“We were originally skeptical of side effects, but those concerns fell away after one week of being on dupilumab. We saw immediate improvement. It was life changing.”
Companion Diagnostic Test
Not applicable.
Anything Else?
Uncontrolled AD can be life altering for a child and can significantly diminish quality of life. These patients and their caregivers are desperate for safe and effective treatments. Based on ESC’s interviews and survey data, dupilumab is reported as a life-altering medication. Patients in need deserve access to this groundbreaking medication. Patients have also reported that the lack of access to dupilumab through provincial drug programs (other than Quebec and NIHB programs) has been devastating, frustrating, and inequitable. Equitable access to novel medications is critically important to patients with AD in Canada.
“After seeing six dermatologists, our son was finally prescribed [dupilumab], and then our private insurance denied him because he hasn't taken Cyclosporine. Ridiculous and infuriating. ODB doesn’t cover it. It’s the carrot dangled in front of an exhausted horse.”
“Why is a biologic drug that has been proven to significantly help patients with eczema been put off by our government? I understand that in some cases there are a lot of people with mild eczema but what about the 10% of people with severe eczema? How much longer do we need to suffer before something is done?”
“We would have loved to keep using it but we couldn’t afford paying out of pocket. We feel awful as parents.”
Conflict of Interest Declaration — Eczema Society of Canada
Did you receive help from outside your patient group to complete this submission?
No.
Did you receive help from outside your patient group to collect or analyze data used in this submission?
No.
List any companies or organizations that have provided your group with financial payment over the past two years AND who may have direct or indirect interest in the drug under review.
ESC receives funding from funding organizations, donations, and corporations, which include pharmaceutical companies.
Table 3: Financial Disclosure for Eczema Society of Canada
Company | $0 to $5,000 | $5,0001 to $10,000 | $10,001 to $50,000 | In Excess of $50,000 |
|---|---|---|---|---|
Sanofi Genzyme Canada | — | — | — | X |
Clinician Input
Canadian Dermatology Association
About Canadian Dermatology Association
The Canadian Dermatology Association, founded in 1925, is the national medical specialty association that represents Canadian certified dermatologists. The association exists to advance the science and art of medicine and surgery related to the care of the skin, hair and nails; provide continuing professional development for its members; support and advance patient care; provide public education on sun protection and other aspects of skin health; and promote a lifetime of healthier skin, hair and nails.
Clinical review and oversight are provided by the Canadian Dermatology Association’s Pharmacy and Therapeutics Advisory Board and the CDA Board of Directors.
Website: https://dermatology.ca/
Information Gathering
Information was gathered from clinical experience, medical literature, and published trial (NCT03346434).
Current Treatments and Treatment Goals
Current treatments for atopic dermatitis in children aged 6 months to 11 years start with education around general measures such as advice on bathing practices and moisturizer use. The most commonly used therapies are topicals: topical corticosteroids, topical calcineurin inhibitors, and topical phosphodiesterase 4 inhibitor. There is occasional use of phototherapy and off-label systemic agents such as short courses of prednisone, and longer courses of methotrexate or cyclosporine. Dupilumab is the only on-label systemic treatment for atopic dermatitis in this age group and is considered the treatment of choice for a child in this age group requiring a systemic agent.
Treatment Gaps (Unmet Needs)
Considering the treatment goals, please describe goals (needs) that are not being met by currently available treatments.
There has been a lack of options for approved systemic medications for atopic dermatitis in this age group. For patients with severe atopic dermatitis not responding to topicals, safe and proven therapies to reduce pruritus, improve sleep, improve concentration at school, and improve overall quality of life for both children with atopic dermatitis and their parents are needed, and dupilumab currently is the only medication that fills this gap.
Atopic dermatitis (AD), especially in its moderate-to-severe form and poorly controlled, is a debilitating disease characterized by well documented significant functional impairment and wide-reaching physical, psychosocial, academic, occupational and economic impact on the growing child. The role of chronic itch can often be analogized to burdens of chronic pain. This can lead to daytime fatigue and irritability, and concentration and behavioural issues at school or work, for example, leading to lost productivity (Barbeau & Lalonde, 2006). The odds of having attention deficit hyperactivity disorder (ADHD) are significantly increased in children with AD with a clear relationship between the prevalence of ADHD and the severity of the skin disease (Yaghmaie, Koudelka, & Simpson, 2013). The severity and impact on the mental health on patients suffering from skin conditions and the increased rates of anxiety and depression in both children who suffer from AD cannot be understated. Estimations show that moderate to severe AD has a greater impact than diabetes on pediatric caregivers (Barbeau & Lalonde, 2006). When under poor control, AD frequently complicated by both short- and long-term problems such as secondary bacterial or viral skin infection (eg. impetigo, MRSA or eczema herpeticum), sleep disturbances and other physical and mental health comorbidities such as anxiety, depression, insomnia and suicidality and due to chronic itching, pain and discomfort (ESC 2017; Weidinger & Novak, 2016).
Unmet Needs
In the Eczema Society of Canada’s 2017 quality of life survey report for moderate-to-severe AD, respondent concerns raised include timely access to specialists, and wait times for those caring for children affected by AD. 85% of survey respondents reported that their child living with moderate to severe AD is not well controlled. For those in more severe categories, many respondents reported failing topical steroids, moisturizers, oral antihistamines, topical calcineurin inhibitors, and even systemic steroids. The majority (78%) used 4 or more different treatments for AD, with over 1/3 of patients using 10 or more different treatments, and 1 in 5 using 15 or more treatments for their AD. This also presents in caregiver/parental impacts due to the multi-regimented nature of AD lifestyle and management, for example, 80% of caregivers in the same survey reported treatment regimens challenging. Over half of caregivers reported sleep loss due to their child’s AD, and 69% experiencing anxiety related to their child’s AD, amongst other impacts such as stress, financial burdens, and feelings of lack of support (ESC, 2017). Clinicians who see with moderate-to-severe AD in pediatric patients see significant impacts on both pediatric patients and caregivers. Furthermore, such extensive regimens can be time-consuming, overwhelming, and place extra burdens on the counseling and prescribing physician who already has limited time.
In the Canadian context, although severe spectrum AD patients represent a minority of children affected, the impact of itch and quality of life impairments are well described. Effects on mood (55%), concentration, (47%) and school (23%) have been reported in Eczema Society of Canada’s ‘Itch in Atopic Dermatitis Survey’ (ESC, 2021). The majority of respondents described their itch as unpredictable and underestimated, often triggered by external and unavoidable factors such as stress, weather changes, fabrics, and exercise. The majority of respondents reported difficulty falling asleep (74%), staying asleep (67%), and woken from sleep (76%) due to their itch. Since both these surveys were published, we are not aware of any FDA approved new options for moderate-to severe AD in this pediatric age group. We need to be able to expand our armamentarium from both a safety and efficacy standpoint, especially when treatment ladders are exhausted. Furthermore, often, pediatric patients have recurrent courses of oral steroids prescribed by multiple physicians, which can lead to both short- and long-term side effects in which the risk far outweighs the benefit of dupilumab’s safety profile.
References
Barbeau, M., & Lalonde, H. (2004). Burden of Atopic dermatitis in Canada. International journal of dermatology, 45(1), 31–36. https://doi.org/10.1111/j.1365-4632.2004.02345.x
Eczema Society of Canada (2017). Atopic Dermatitis Quality of Life Report.
Eczema Society of Canada (2021). Itch in Atopic Dermatitis.
Weidinger, S., & Novak, N. (2016). Atopic dermatitis. Lancet (London, England), 387(10023), 1109–1122. https://doi.org/10.1016/S0140-6736(15)00149-X
Yaghmaie, P., Koudelka, C., & Simpson, E. (2013). Mental health comorbidity in patients with atopic dermatitis. Journal of Allergy and Clinical Immunology, 131(2), 428–433. https://doi.org/10.1016/j.jaci.2012.10.041
Place in Therapy
How would the drug under review fit into the current treatment paradigm?
Dupilumab would be for a child with moderate to severe atopic dermatitis who has failed management with topical therapies [Please refer to the notes above].
Which patients would be best suited for treatment with the drug under review? Which patients would be least suitable for treatment with the drug under review?
Best suited:
Moderate to severe atopic dermatitis
Failed topical management
Poor quality of life
Caregiver impact, complicated regimens with topical therapy
Recurrent courses of oral steroids
Those with severe comorbid asthma
Poorly suited:
Mild atopic dermatitis
Responding to topical management
What outcomes are used to determine whether a patient is responding to treatment in clinical practice? How often should treatment response be assessed?
Clinically meaningful responses include reduced EASI scores; improvement in symptoms - clearer skin, less itch, less body surface area involvement; improvements in daily living – less activity/lifestyle restrictions, more rested and engaged; and improvements in mental health and outlook.
Treatment is assessed initially at monthly intervals and then every 4 to 6 months depending on response to therapy.
What factors should be considered when deciding to discontinue treatment with the drug under review?
Lack of response after 3-4 months or intolerance to Dupilumab
What settings are appropriate for treatment with [drug under review]? Is a specialist required to diagnose, treat, and monitor patients who might receive [drug under review]?
Atopic dermatitis is best diagnosed by a dermatologist. This medication should be prescribed by and monitored by a dermatologist. As dupilumab does not require labwork, this relieves much of the burden of extensive paperwork and safety (eg. laboratory, baseline, imaging) monitoring required by physicians.
Additional Information
Due to inherent skin barrier and cutaneous immune system dysfunction, those with uncontrolled AD are at elevated baseline risk for bacterial skin infections such as impetigo and cellulitis (Bieber, 2010; ESC 2021; Weidinger & Novak 2016; Silverberg 2017). Environmental factors amongst other numerous barriers faced by remote Indigenous communities can play a role in exacerbation of chronic skin disease and secondary infection (eg. crowded housing, poverty, communicable disease burdens, cost/accessibility of basic skin care products such as soap, bleach, moisturizers or other hygiene fundamentals, as well as water supply and healthcare access). Those with low incomes on or from reserve may not be able to afford expenses required to maintain basic skin (bathing/moisturizing/washing) regimes required to control AD, and on top of this, those in remote areas may even face higher costs of over-the-counter products such as cleaning products due to inflated shipping costs. Numerous medical service visits for moderate to severe eczema and its complications (eg. secondary infection), hospitalization, and consequences from absenteeism/loss of productivity are observed in pediatric moderate to severe AD patients by clinicians caring for them, although this needs to be more formally documented (Van Eaton et al., 2022; Asiniwasis et al., 2021). The impacts of AD are often magnified in remote Indigenous communities due to barriers and inherent health disparities and lack of healthcare practitioner access including long waiting lists for dermatologist assessment.
Crowded housing conditions can lead to increased transmission of contagious diseases such as scabies, impetigo, or MRSA. This further complicates care and management of patients with skin disease and compromised skin barrier as seen in AD, and in fact such infections may be worsened with traditional systemic immunosuppressants used in moderate to severe AD. In these situations, we need better options and better access to safer and efficacious treatment, particularly for pediatric patients with moderate to severe disease. As one clinician providing input who has provided outreach services for almost a decade for remote and rural Canadian Indigenous communities in western Canada, severe pediatric atopic dermatitis is a poorly recognized crisis in these communities (Asiniwasis et al., 2021). These same concerns have been shared by physician colleagues in family medicine, dermatology, pediatrics and allergy/immunology – who believe these cases are often too complex and comorbid to deal with at the primary care level. Due to a fundamentally impaired skin barrier in AD, care can become complicated as high rates of secondary skin infection and infestations are reported as concerns in Indigenous children and youth living with AD in both Canadian media (Please refer to reference list ‘Canadian Media References’) and academia (Asiniwasis et al., 2021; Asiniwasis et al., 2022; Schrieber et al., 2023; Van Eaton et al., 2022; others). Clinician R. Asiniwasis has personally observed that addition to improving moderate to severe AD, these rates of skin infections become almost negligible in patients who face recurrent episodes after starting dupilumab which have not been observed in any other AD therapies to date. This is further backed by literature, suggesting that dupilumab may assist with normalizing the cutaneous microbiome and decreasing S. aureus colonizations and bacterial skin infections (Callewaert et al., 2019; Eichenfield et al., 2019) . From an academic and clinical standpoint, dupilumab may represent the first FDA-approved opportunity to help these children grow into healthy adolescents and adults suffering from severe AD and comorbid skin infections, whereas dupilumab may end up being a surprisingly potential straightforward solution to multi-layered burdens and complex barriers already faced by many of these communities - although further observational studies are needed. Additionally, dupliumab is not considered broadly immunosuppressive, and labwork isn’t required like with other immune-suppressing systemic medications. This provides a benefit for those who do not have optimal access to labs and primary care at short notice for safety monitoring.
References
Asiniwasis, R. N., Heck, E., Amir Ali, A., Ogunyemi, B., & Hardin, J. (2021). Atopic dermatitis and skin infections are a poorly documented crisis in Canada's Indigenous pediatric population: It's time to start the conversation. Pediatric dermatology, 38 Suppl 2, 188–189. https://doi.org/10.1111/pde.14759
Asiniwasis R, Campbell T, Odeshi O, Richels L, Eglington T, Phillips Z, Hinther K, Merati N, Pandey M. (2021). Virtual Care for Skin Conditions in Remote and Northern Saskatchewan Indigenous Communities: Addressing Challenges and Exploring Opportunities. Presented at Saskatchewan Healthcare Research Showcase.
Bieber T. (2010). Atopic dermatitis. Annals of dermatology, 22(2)125–137. https://doi.org/10.5021/ad.2010.22.2.125
Callewaert, C., Nakatsuji, T., Knight, R., Kosciolek, T., Vrbanac, A., Kotol, P., Ardeleanu, M., Hultsch, T., Guttman-Yassky, E., Bissonnette, R., Silverberg, J. I., Krueger, J., Menter, A., Graham, N. M. H., Pirozzi, G., Hamilton, J. D., & Gallo, R. L. (2020). IL-4Rα Blockade by Dupilumab Decreases Staphylococcus aureus Colonization and Increases Microbial Diversity in Atopic Dermatitis. The Journal of investigative dermatology, 140(1), 191–202.e7. https://doi.org/10.1016/j.jid.2019.05.024
Eczema Society of Canada (2021). Itch in Atopic Dermatitis.
Eichenfield, L. F., Bieber, T., Beck, L. A., Simpson, E. L., Thaçi, D., de Bruin-Weller, M., Deleuran, M., Silverberg, J. I., Ferrandiz, C., Fölster-Holst, R., Chen, Z., Graham, N. M. H., Pirozzi, G., Akinlade, B., Yancopoulos, G. D., & Ardeleanu, M. (2019). Infections in Dupilumab Clinical Trials in Atopic Dermatitis: A Comprehensive Pooled Analysis. American journal of clinical dermatology, 20(3), 443–456. https://doi.org/10.1007/s40257-019-00445-7
Schreiber, Y., Mallach, G., Barrowman, N., Tsampalieros, A., Kelly, L., Gordon, J., McKay, M., Wong, C. L., & Kovesi, T. (2023). Skin morbidity in Indigenous children in relation to housing conditions in remote communities in Northwestern Ontario, Canada. Clinical and Experimental Dermatology, Volume 48, Issue 3, March 2023, Pages 218–224, https://doi.org/10.1093/ced/llac082
Van Eaton, M, Campbell T, Dixon E, Pandey M, Asiniwasis R. Indigenous Pediatric Atopic Dermatitis in Canada: A Retrospective Chart Review. Presented at USask Dean’s Presentations, Sept 2022
Canadian Media References
Poorly controlled, severe pediatric atopic dermatitis impacts with secondary skin infections seen in remote and northern Canadian Indigenous communities — Can modern therapeutics help address this crisis?
1. Dehaas, J. (2016, Mar 23.) ‘Social emergency’: Kashechewan skin problems blamed on
poverty, overcrowding. CTV News. Retrieved from: https://www.ctvnews.ca/canada/social-emergency-kashechewan-skin-problems-blamed-on-poverty-overcrowding-1.2830199
2. Dehaas, J. (2016, March 24.) Kashechewan skin infections exacerbated by ‘social emergency’. CTV News. Retrieved from: https://www.ctvnews.ca/canada/kashechewan-skin- infections-exacerbated-by-social-emergency-1.2831317
3. Kirkup, K.(2016, March 29). Doctors treating Indigenous children’s rashes cite medical crisis. The Globe and Mail. Retrieved from: https://www.theglobeandmail.com/news/national/doctors-treating-indigenous-childrens-rashes-cite-medical-crisis/article29414627/
4. Martens, K. (2018). Retrieved from: https://www.aptnnews.ca/national-news/kashechewan-mother-says-she-was-told-to-give-daughter-a-bleach-bath-to-cure-her-daughters-skin-sores/
5. Bell, S., and Stewart, D. (2021, Nov 18). Police called on Cree family for trying to access care for baby in distress in northern Quebec. CBC News. Retrieved from: https://www.cbc.ca/news/canada/north/cree-health-board-whapmagoostui-eczema-discrimination-1.6253641
6. CBC News (2016, Mar 18). Kashechewan family wants answers after baby plagued by skin infections. Retrieved from: https://www.cbc.ca/news/canada/sudbury/kashechewan-water-health-skin-rash-1.3498710
7. CBC News (No Author listed). (2016, Mar 21.) Kashechewan children’s skin lesions not caused by water: health minister. CBC News. Retrieved from: https://www.cbc.ca/news/canada/sudbury/kashechewan-water-health-skin-rash-update-1.3500631
8. CBC Radio (2016, Mar 25). Kashechewan rash outbreak highlights woeful First Nations health care, says critics. Retrieved from: https://www.cbc.ca/radio/thecurrent/the-current-for-march-25
Conflict of Interest Declarations — Canadian Dermatology Association
To maintain the objectivity and credibility of the CADTH drug review programs, all participants in the drug review processes must disclose any real, potential, or perceived conflicts of interest. This conflict of interest declaration is required for participation. Declarations made do not negate or preclude the use of the clinician group input. CADTH may contact your group with further questions, as needed. Please refer to the Procedures for CADTH Drug Reimbursement Reviews (section 6.3) for further details.
Did you receive help from outside your clinician group to complete this submission? If yes, please detail the help and who provided it.
No.
Did you receive help from outside your clinician group to collect or analyze any information used in this submission? If yes, please detail the help and who provided it.
No.
List any companies or organizations that have provided your group with financial payment over the past two years AND who may have direct or indirect interest in the drug under review.
Declaration for Clinician 1
Name: Alexandra Kuritzky, MD, FRCPC
Position: Member, CDA Pharmacy and Therapeutics Advisory Board
Date: 24-04-2023
Table 4: COI Declaration for Canadian Dermatology Association — Clinician 1
Company | $0 to $5,000 | $5,0001 to $10,000 | $10,001 to $50,000 | In Excess of $50,000 |
|---|---|---|---|---|
Sanofi | X | — | — | — |
Lilly | X | — | — | — |
AbbVie | X | — | — | — |
Pfizer | X | — | — | — |
Bausch Health | X | — | — | — |
UCB | X | — | — | — |
Janssen | X | — | — | — |
Sun Pharma | X | — | — | — |
Declaration for Clinician 2
Name: Rachel Asiniwasis, MD, MD(HS), FRCPC
Position: Expert Advisor, CDA Pharmacy and Therapeutics Advisory Board
Date: 22-04-2023
Table 5: COI Declaration for Canadian Dermatology Association — Clinician 2
Company | $0 to $5,000 | $5,0001 to $10,000 | $10,001 to $50,000 | In Excess of $50,000 |
|---|---|---|---|---|
Sanofi (AD Advisory Board) | — | X | — | — |
Pfizer (AD Advisory Board) | X | — | — | — |
Leo (AD Advisory Board) | X | — | — | — |
Abbvie (AD Advisory Board) | X | — | — | — |
Declaration for Clinician 3
Name: Susan Poelman, MD, FRCPC
Position: Chair, CDA Pharmacy and Therapeutics Advisory Board
Date: 24-04-2023
Table 6: COI Declaration for Canadian Dermatology Association — Clinician 3
Company | $0 to $5,000 | $5,0001 to $10,000 | $10,001 to $50,000 | In Excess of $50,000 |
|---|---|---|---|---|
Sanofi-Genzyme | X | — | — | — |
Abbvie | — | X | — | — |
Pfizer | X | — | — | — |
Leo Pharma | X | — | — | — |
April 27, 2023
Dear CADTH Committee,
RE: Dupilumab FDA Approval in age 6 months to 5 years, pediatric indication for AD.
As an addendum, further clinician input includes a request to CADTH’s committee to consider not including traditional systemic immunosuppression (Methotrexate, Cyclosporine) as a pre-requisite for dupilumab coverage in this younger age group. The main reasons are as follows:
Traditional systemic immunosuppression such as methotrexate and cyclosporine are associated with significant risk of cytopenias, multiorgan impairment (liver, renal), increased risk of infection, malignancy, and others.
We have attached the monographs of Methotrexate and Cyclosporine to this email for reference.
We believe that the potential risk outweighs the benefit for prescribing these medications in young children and infants. We do not fully understand short- and long-term implications, or impact on the growing child of broad antimetabolite therapy/immunosuppression. Furthermore, parents will raise concerns around this indication, which will leave extra burdens on counseling of risk-benefit, and questions we may not be able to fully answer.
Most dermatologists in Canada are not trained in or comfortable managing pediatric safety labwork in context of systemic immunosuppression. In our residency programs, we have an adult internal-medicine basis to our training. The minority of pediatric dermatologists who carry either fellowships with extra training or residencies in pediatrics are limited and located in large urban centers and may face waiting lists.
In some provinces, such as Saskatchewan, we do not have a pediatric dermatologist. Here, dermatologists manage patients of all ages, including these pediatric patients. As generalists lacking extra training in pediatric dermatology, we may not be fully comfortable in interpreting pediatric safety labwork or confidently managing pediatric patients on this level of immunosuppression.
Should traditional systemic immunosuppression be required, many patients, especially in underserviced areas, will have to be transferred out of province to consult with pediatric dermatology.
Dupilumab does not carry the same profile risks as traditional systemic immunosuppression by data or mechanism. Furthermore, we now have excellent safety data with dupilumab in this age group, where data on traditional systemic immunosuppression is sparse.
Thank you very much for this consideration! We understand rationale for adults requiring certain prerequisites, but we would like to make this special request for the younger children and infants.
Respectfully submitted,
The Canadian Dermatology Association
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up-to-date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
Redactions: Confidential information in this document may be redacted at the request of the sponsor in accordance with the CADTH Drug Reimbursement Review Confidentiality Guidelines.
Stakeholder Input: The views expressed in each submission are those of the submitting organization or individual; not necessarily the views of CADTH or of other organizations. As such, they are independent of CADTH and do not necessarily represent or reflect the view of CADTH. No endorsement by CADTH is intended or should be inferred. By filing with CADTH, the submitting organization or individual agrees to the full disclosure of the information. CADTH does not edit the content of the submissions.
CADTH does use reasonable care to prevent disclosure of personal information in posted material; however, it is ultimately the submitter’s responsibility to ensure no identifying personal information or personal health information is included in the submission. The name of the submitting organization or individual and all conflict of interest information are included in the submission; however, the name of the author, including the name of an individual patient or caregiver submitting the patient input, are not posted.
Accessibility: CADTH is committed to treating people with disabilities in a way that respects their dignity and independence, supports them in accessing material in a timely manner, and provides a robust feedback process to support continuous improvement. All materials prepared by CADTH are available in an accessible format. Where materials provided to CADTH by a submitting organization or individual are not available in an accessible format, CADTH will provide a summary document upon request. More details on CADTH’s accessibility policies can be found here.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.