CADTH Reimbursement Review
Setmelanotide (Imcivree)
Sponsor: Rhythm Pharmaceuticals, Inc.
Therapeutic area: Bardet-Biedl syndrome
This multi-part report includes:
Clinical Review
Pharmacoeconomic Review
Ethics Review
Stakeholder Input
Clinical Review
Abbreviations
AE
adverse event
AS
Alström syndrome
BBS
Bardet-Biedl syndrome
BMI
body mass index
CI
confidence interval
CRIBBS
Clinical Registry Investigating Bardet-Biedl Syndrome
FAS
full analysis set
GLP1
glucagon-like peptide 1
HRQoL
health-related quality of life
IWQoL-Lite
Impact of Weight on Quality of Life – Lite
LEPR
leptin receptor
LTE
long-term extension
MC4R
melanocortin-4 receptor
MID
minimally important difference
PCSK1
proprotein convertase subtilisin/kexin type 1
PedsQL
Pediatric Quality of Life Inventory
POMC
pro-opiomelanocortin
PRO
patient-reported outcome
QoL
quality of life
RCT
randomized controlled trial
SAE
serious adverse event
SAS
safety analysis set
SC
subcutaneous
SD
standard deviation
TEAE
treatment-emergent adverse event
Executive Summary
An overview of the submission details for the drug under review is provided in Table 1.
Table 1: Background Information on the Application Submitted for Review
Item | Description |
|---|---|
Information on drug submitted for review | |
Drug product | Setmelanotide (Imcivree), 10 mg/mL solution in a 1 mL multiple-dose vial, administered through once-daily SC injection |
Sponsor | Rhythm Pharmaceuticals, Inc. |
Indication | For weight management in adult and pediatric patients aged 6 years and older with obesity due to:
|
Reimbursement request | For weight management in adult and pediatric patients aged 6 years and older with obesity due to BBS |
Health Canada approval status | NOC |
Health Canada review pathway | Priority review |
NOC date | May 5, 2023 |
Recommended dose | Patients aged 18 years and older
Patients aged 6 years to 17 years of age
|
BBS = Bardet-Biedl syndrome; LEPR = leptin receptor; NOC = Notice of Compliance; PCSK1 = proprotein convertase subtilisin/kexin type 1; POMC = pro-opiomelanocortin; SC = subcutaneously.
Introduction
Bardet-Biedl syndrome (BBS) is a rare genetic disease with highly heterogeneous ciliopathy that affects multiple body systems and causes many variable symptoms, such as retinal degeneration, obesity, renal anomalies, polydactyly, hypogonadism, and intellectual impairments.
Despite a normal weight at birth, a quick weight gain that leads to obesity is considered a major clinical feature of BBS. This rapid weight gain is a common component of BBS that occurs during the first year of life in 72% to 92% of patients. Hyperphagia associated with obesity is also considered a hallmark of BBS. It is thought to be caused by the impairment of the melanocortin-4 receptor (MC4R) pathway, and can affect satiety, appetite regulation, food intake, and energy expenditure. Excessive food-seeking behaviour negatively affects the lives of patients and caregivers. It can create difficulties with productivity and concentration at work and school, affect patients’ emotional and psychosocial status, and impair their relationships and quality of life (QoL). Additionally, uncontrolled hyperphagia can increase the risk of obesity-related morbidities, such as cardiometabolic diseases, liver disease, and diabetes.
The prevalence of BBS is estimated to range from 1 in 100,000 to 1 in 160,000 in the populations of North America and Europe. Approximately 300 to 400 individuals in Canada have BBS; the disorder occurs with greater frequency in certain populations of Newfoundland and Labrador (from 1 in 16,000 to 1 in 18,000).
BBS can be diagnosed based on clinical features (e.g., retinal dystrophy, obesity, postaxial polydactyly) using the Beales diagnostic criteria. The diagnosis may be supported by out-of-country genetic testing. Given that there are no targeted therapies for BBS, management of obesity follows the same approaches as those used for the general population, such as diet and lifestyle modifications. However, adherence to these practices and sustainability of weight loss are especially low in this population.
There are no Health Canada–approved treatments for obesity or control of hunger in patients with BBS. Some pharmacotherapies may be used off-label,1 such as glucagon-like peptide 1 (GLP1) receptor agonists (e.g., semaglutide injection or liraglutide injection) or gastrointestinal lipase inhibitors (e.g., orlistat). Both types of treatments are reimbursed in some Canadian jurisdictions for adults with type 2 diabetes (semaglutide) or in patients with obesity and 1 weight-related comorbid condition (liraglutide, orlistat).2,3 The clinical experts consulted by CADTH indicated that only semaglutide was likely to be prescribed off-label for patients with BBS due to its potential to reduce hunger; however, they noted that it does not target the underlying mechanism of BBS-induced hyperphagia and that there are no clinical studies available specifically in populations with BBS. Other pharmacotherapies for obesity management that were not indicated as potentially used off-label in BBS include lixisenatide, naltrexone and bupropion, lisdexamfetamine, and topiramate.1
Bariatric surgery with gastric banding or sleeve surgery may be used as a last resort in patients with a body mass index (BMI) greater than 40 kg/m2 or greater than 35 kg/m2 with comorbidities.4,5 However, there are significant limitations associated with bariatric surgery. For example, it may be dangerous and lack durability for patients with hyperphagia if the patient’s food environment is not tightly controlled. Additionally, cognitive impairment is common in patients with BBS (affecting approximately 62% of patients).6
The objective of this review is to review the beneficial and harmful effects of setmelanotide 10 mg/mL injectable solution for weight management in adult and pediatric patients aged 6 years and older with obesity due to BBS.
Stakeholder Perspectives
The information in this section is a summary of the input provided by the patient and clinician groups that responded to CADTH’s call for input and from the clinical expert(s) consulted by CADTH for the purpose of this review.
Patient Input
CADTH received 1 input from the Bardet Biedl Syndrome Foundation, which conducted an online survey and 1-on-1 telephone or video conference interviews with people who have BBS. The majority of survey respondents (61%) were from the US.
According to the input, 71% of patient and caregiver respondents indicated that they or their loved ones currently live with obesity. Patients with BBS think about food constantly and take a long time to feel full after eating. According to the input, BBS-related obesity and hyperphagia affected the emotional and psychological well-being of patients along with their social lives and work or school lives.
The patient input stated that there is no approved treatment for BBS or BBS-related hunger and obesity in Canada. Patients reported that they used environmental tools, such as exercise, supervision from others, calorie-restricted diets, and meal schedules for weight management and found these measures to be somewhat to very effective. However, caregiver respondents noted that these strategies are challenging to implement.
Two patient and 2 caregiver respondents indicated that they or their loved ones had experience with some off-label weight management medications, such as semaglutide and phentermine. They reported that these treatments were somewhat to very effective. One respondent stated that they were using semaglutide at the same time as setmelanotide.
Four patient respondents and 13 caregiver respondents reported having experience with setmelanotide and said the treatment had helped control appetite and hunger, manage weight, and improve QoL.
Patient and caregiver respondents identified not thinking about food constantly, not feeling hungry right after eating, and reducing stigma and/or judgment and stress as key outcomes for the treatment of BBS-related hunger.
Interviews with 1 patient and 4 caregivers who had experience with setmelanotide were provided in the patient input. The results were consistent with the survey input in terms of disease symptoms, improved outcomes, and the recommendation that the drug be available and accessible for all patients living with BBS.
Clinician Input
Input From Clinical Experts Consulted by CADTH
The information in this section is based on input received from a panel of 4 clinical specialists consulted by CADTH for the purpose of this review.
The clinical experts indicated that the primary unmet need is for targeted treatment options for patients with BBS. BBS is a very rare genetic ciliopathy with multisystem manifestations, commonly including early-onset obesity and hyperphagia. The clinical experts indicated that lifestyle interventions for obesity management are particularly inefficient and unsustainable in this population because of biologically driven hyperphagia and other potential manifestations of BBS, such as vision loss, behavioural issues, food-seeking behaviours, cognitive impairment, and others. The experts also highlighted that patients with early-onset obesity due to BBS and hyperphagia may be exposed to their obesity for a substantially longer period of time than people with late-onset common obesity, which places them at greater risk for obesity-related comorbidities.
The clinical expert panel agreed that setmelanotide would be considered a first-line therapy for patients with BBS who have hyperphagia and obesity, and would be used in combination with obesity management recommendations, such as intensive diet and lifestyle changes. It was noted that setmelanotide would be the first available therapy to target the underlying mechanism of BBS-associated hyperphagia, and that setmelanotide would not be expected to have an impact on manifestations in other body systems (e.g., ocular manifestations). The experts reported that, despite a lack of data, combination therapy consisting of setmelanotide and GLP1 receptor agonists was likely to occur in some circumstances, including comorbidity involving BBS with type 2 diabetes. The experts noted that there is some evidence that the response to bariatric surgery may be less durable in populations with hyperphagic obesity, and that there are no data for any other pharmacotherapies in the treatment of patients with BBS.
The experts indicated that genetic testing for the suite of known BBS mutations is currently not available in Canada. It is requested through the provincial ministries of health as an out-of-country test, but does not cause out-of-pocket expenses for patients. The experts stated that clinical diagnosis using the Beales criteria was considered common and sufficient, and that misdiagnosis was unlikely, but that the majority of patients do seek genetic confirmation as well. There was a diversity of opinion among the clinical experts on whether genetic testing should be a requirement for receiving BBS-targeted therapies because there may yet be unknown mutations that cause BBS.
The clinical experts indicated that it is currently unknown which patients are the most or least likely to demonstrate a clinically meaningful response to treatment with setmelanotide. However, it is clinically plausible that differences in the underlying mutation(s) may be relevant for prognosis and treatment effect and that more data are needed in this area. In terms of assessing response, the experts indicated that a 1-year trial period was reasonable and that a meaningful response would consist of a qualitative improvement in hunger and/or health-related quality of life (HRQoL) and a reduction of greater than or equal to 5% of body weight in adults or greater than or equal to 5% BMI in pediatric patients. There were variable opinions on approaches to treatment for patients who do not achieve greater than or equal to 5% weight loss. In 1 approach, setmelanotide would be discontinued, but in another, continuing on setmelanotide would be considered if there were other positive changes; or combination therapy might be considered. Other discontinuation criteria may include severe adverse events (AEs) that cannot be managed by dose reductions or pausing the medication, a lack of impact on hyperphagia after 12 months of treatment, or significant issues with nonadherence. The clinical experts also noted that patient registries for BBS would be of great value because there are still evidence gaps, especially regarding long-term efficacy and safety, given that obesity is a chronic, long-term, relapsing condition.
Clinician Group Input
Input from 1 clinician group, the Canadian endocrinologists treating BBS, was received. Overall, the input aligned with that of the clinical experts consulted by CADTH.
The clinician group reported that BBS is characterized by multisystem manifestations, such as early-onset obesity with hyperphagia and related complications, intellectual and cognitive impairment, delayed development, renal anomalies, polydactyly, retinal dystrophy, hypogonadism, and hypogenitalism. The input stated that 72% to 92% of patients with BBS have obesity and hyperphagia caused by hypothalamic dysfunction leading to reduced MC4R activation. The clinician group commented that obesity should be recognized as a complex, chronic, progressive, and relapsing condition.
The clinician group stated that no targeted therapy exists for the treatment of BBS; the disease is managed symptomatically. The clinicians indicated that hyperphagia is considered the most distressing symptom associated with BBS and is associated with many negative effects on the QoL and physical and mental health of patients with BBS and obesity. They stated that some environmental and lifestyle interventions that are used to manage obesity, such as food supervision, energy intake reduction, and meal schedules, are challenging to implement and not sustainable because these do not address persistent hyperphagia. In addition to that, other symptoms associated with BBS, such as vision impairment, lack of balance or coordination, and intellectual disabilities, could make the implementation of these interventions more complicated.
The clinicians’ input noted that some procedures — such as bariatric surgery and off-label therapies, like liraglutide, semaglutide, and naltrexone hydrochloride plus bupropion hydrochloride — have no evidence of safety or effectiveness in patients living with BBS because these options do not address biologically driven hyperphagia.
The clinician group also indicated that obesity management goals should consider the prevention of morbidities associated with obesity, including but not limited to cardiometabolic disease, diabetes, liver disease, and sleep apnea.
The input suggested that setmelanotide could serve as an additional treatment option in therapy plans along with lifestyle and environmental interventions to address obesity in patients with genetically confirmed BBS aged 6 years or older. The clinician group input indicated that treatment response would be assessed after 12 weeks to 16 weeks of therapy. The input agreed that discontinuation should be considered if a decrease of 5% or greater in weight or baseline BMI has not been achieved, during pregnancy and/or breastfeeding, or if the patient experiences a lack of response, side effects, or renal impairment, or has a contraindication to setmelanotide. The clinician group reported that a holistic multidisciplinary approach is required to care for patients with BBS.
Drug Program Input
The drug programs identified the following jurisdictional implementation issues or questions: relevant comparators, considerations for initiation of therapy, considerations for discontinuation of therapy, and considerations for prescribing of therapy. Refer to Table 3 for details.
Clinical Evidence
Pivotal Studies and Randomized Controlled Trial Evidence
Description of Studies
Study 023 was a phase III, open-label trial with a 14-week, randomized, double-blind, placebo-controlled period followed by a 52-week, open-label period that aimed to evaluate the efficacy and safety of setmelanotide (1 mg to 3 mg daily by subcutaneous [SC] injection) in patients aged greater than or equal to 6 years with BBS or Alström syndrome (AS) and obesity. For the purposes of this review, only the patients with BBS were of interest; results from this subgroup of patients were provided in a posthoc analysis.
Patients were also divided into “pivotal” and “supplemental” cohorts. Pivotal patients were defined as all those enrolled up to the sixth patient with AS; this group included 32 patients with BBS and 6 patients with AS. The supplementary patients (12 patients with BBS and 2 with AS) were included in some secondary and all safety outcomes. Outcomes assessed at 52 weeks of setmelanotide treatment, such as the primary and key secondary outcomes, were measured from the “active treatment baseline” as opposed to the true baseline of the study, which would have been after week 14 for patients who were initially randomized to placebo; this was done so that patients would have approximately 52 weeks of active treatment experience for single-arm outcomes. In contrast, outcomes assessed during the first 14 weeks as placebo-controlled outcomes were measured from “placebo-controlled baseline” (i.e., the true baseline of the study).
The primary outcome of Study 023 was the proportion of pivotal patients aged greater than or equal to 12 years at baseline who were treated with setmelanotide for approximately 52 weeks and achieved a greater than or equal to 10% reduction in body weight, as measured from the active treatment baseline. This single-arm outcome was compared against an external control, sourced from the Clinical Registry Investigating Bardet-Biedl Syndrome (CRIBBS), in which 6.4% of adult patients with BBS were shown to achieve greater than or equal to 10% weight loss over a 1-year period, on average. The CRIBBS data did not include any information regarding significant efforts to lose weight; the data reflect a heterogeneous, real-world approach to BBS management. In Study 023, the prespecified threshold was rounded up to 10% from 6.4% of patients expected to achieve a greater than or equal to 10% reduction in body weight without setmelanotide treatment.
Hunger score was assessed as a key secondary outcome in patients aged greater than or equal to 12 years without cognitive impairment using daily questionnaires developed by the sponsor. Patients rated hunger in terms of average daily hunger, morning hunger, and worst or most hunger over 24 hours, each on a scale of 0 to 10 wherein 10 represented the hungriest possible. Other secondary outcomes included placebo-controlled metrics of weight loss and hunger scores at 14 weeks, measured from a placebo-controlled baseline. Exploratory outcomes included change in waist circumference, change in fasting lipids, and change in HRQoL (| || || || || || || |, Impact of Weight on Quality of Life – Lite [IWQoL-Lite], the Pediatric Quality of Life Inventory [PedsQL], and | || || || || || || || || || || || || || |) as well as safety.
At baseline, patients with BBS included 32 pivotal patients and 12 supplemental patients. Patients were mostly white (68.2% and 86.4% in the setmelanotide and placebo arms, respectively), with mean ages of 18.5 years (standard deviation [SD] = 9.7 years) and 21.5 years (SD = 12.6 years), respectively. There was a high prevalence of cognitive impairment (54.5% and 36.4%, respectively). The mean BMIs were 41.4 kg/m2 (SD = 10.0 kg/m2) and 41.6 kg/m2 (SD = 10.1 kg/m2) kg/m2, respectively. Although genetic confirmation was not required, more than 90% of patients had genetic confirmation of BBS, which was defined as homozygous or compound heterozygous loss-of-function mutation in BBS genes. Of the 22 pivotal and supplemental patients with BBS who were assigned to setmelanotide, 4 were aged less than 12 years and 12 were aged less than 17 years; among the 22 assigned to placebo, 4 were aged less than 12 years and 10 were aged less than 17 years.
Efficacy Results
Key efficacy results of Study 023 are summarized in Table 2.
Body Weight Change After 52 Weeks of Setmelanotide Treatment
Among pivotal patients aged greater than or equal to 12 years with BBS (N = 28), 35.7% (95% confidence interval [CI], 18.6% to 55.9%) had a greater than or equal to 10% reduction in body weight from the active treatment baseline after 52 weeks of treatment with setmelanotide, which was greater than the prespecified assumption of 10% of patients with BBS achieving a greater than or equal to 10% reduction in body weight without setmelanotide treatment. The mean and percent changes in weight among pivotal patients with BBS (N = 28) were −7.24 kg (SD = 8.208 kg) and −6.47 kg (SD = 6.970 kg), respectively. Results were similar when supplemental patients with BBS were also included.
As an ad hoc analysis in response to a request by CADTH to reflect the Health Canada recommendations, the sponsor also provided the estimated proportion of pivotal patients with BBS aged greater than or equal to 12 years who achieved a greater than or equal to 5% reduction in total body weight | || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || |7
Change in Hunger Scores After 52 Weeks of Setmelanotide Treatment
Among pivotal patients with BBS aged greater than or equal to 12 years and without cognitive impairment (N = 14), the mean percent change in hunger score after 52 weeks of setmelanotide treatment was −31.80% (95% CI, −48.81% to −14.79%). Of these patients, 71.4% experienced at least a 1-point (≥ 10%) reduction, and 42.9% experienced at least a 2-point (≥ 20%) reduction in the most or worst hunger score. Additionally, 57.1% experienced at least a 25% improvement in the weekly average of the 3 evaluated hunger scores (most or worst score over 24 hours, average score over 24 hours, or morning hunger score). Results were similar when supplemental patients with BBS were also included. There is no known minimally important difference (MID) for these hunger scores.
Body Weight Change After 14 Weeks of Setmelanotide Treatment Compared to Placebo
In the placebo-controlled analysis of pivotal patients aged greater than or equal to 12 years with BBS, patients receiving setmelanotide (N = 14) had a greater mean percentage body weight change (−3.31%; SD = 4.474%) than patients receiving placebo (N = 15) (−0.25%; SD = 2.353%). The difference in mean percent change was −2.96% (95% CI, −5.65% to −0.26%). Similar results were observed when considering both pivotal and supplemental patients with BBS.
Change in Hunger Scores After 14 Weeks of Setmelanotide Treatment Compared to Placebo
Among pivotal patients with BBS aged greater than or equal to 12 years without cognitive impairment, patients treated with setmelanotide (N = 5) had a greater reduction in hunger score than patients treated with placebo (N = 9) in the mean change in average daily hunger score and most or worst hunger score from placebo-controlled baseline to week 14. However, sample sizes were small, and the 95% CI of the difference was very wide and included the null value in the case of the percent change in hunger over 24 hours, mean change in morning hunger, and percent change in morning hunger. Results were similar when considering both pivotal and supplemental patients with BBS.
Subgroup Analyses of Change in Body Weight and Hunger Scores
There were 8 patients with BBS who were aged less than 12 years in Study 023. All had decreases of | || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || |. Including all patients aged greater than or equal to 6 years to less than 12 years with either AS or BBS (n = 11), during the 14-week placebo-controlled period, patients treated with setmelanotide (n = 6) had | || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || | (n = 5) in the same age group.
Subgroup results were directionally consistent among other age-specific subgroups of patients with BBS, including patients aged less than 18 years and greater than or equal to 18 years.
Hunger was also assessed in patients with cognitive impairments by caregiver assessment using the | || || || || || || || || || || || || || || || || || || || || || || || | because there is no validated hunger assessment for this population, and patients with | || || || || || || | share the symptoms of early obesity, intense hunger, and cognitive impairment. The scale ranges from 0 to 30, with higher scores indicating more severe hyperphagia-related behaviours. The mean change from active treatment baseline in the 11 assessed patients was | || || || || || || || || || || || || || |
Health-Related Quality of Life
Exploratory HRQoL outcomes based on the IWQoL-Lite (patients aged ≥ 18 years without cognitive impairment; n = 11) and PedsQL (pivotal patients aged < 18 years without cognitive impairment; n = 9) generally showed improvement from the active treatment baseline to week 52 of setmelanotide treatment; the mean change in IWQoL-Lite was + 11.75 (SD = 10.297), and the mean change in PedsQL was + 11.2 (SD = 14.4). Although no MIDs have been identified in BBS populations specifically for either scale, a general population survey of children identified MIDs for PedsQL as 4.4 (self-report) or 4.5 (parent proxy-report);8 MIDs using IWQoL-Lite in patients with general obesity range from 7.7 points to 12 points.1,2
Some assessed patients had impaired HRQoL at baseline, according to the IWQoL-Lite (n = 8 of 11) and PedsQL (n = 4 of 9); the majority of these patients experienced improved scores after 52 weeks of setmelanotide treatment.
The results of the | || || || || in pivotal patients aged greater than or equal to 16 years without cognitive impairment (n = 13) differed by health state score: | || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || | were identified specific to BBS, obesity, or hyperphagia.
Harms Results
Results for key harms in Study 023 are summarized in Table 2. The harms results discussed here are based on the safety analysis set (SAS; N = 57), which includes patients with BBS or AS to maximize sample size. The results were similar in the BBS subgroup. The sponsor and clinical experts identified a number of AEs of special interest: injection-site reactions, anaphylaxis, bradycardia, hyperpigmentation, melanoma, sexual events, sexually inappropriate behaviours, and select psychiatric events, including anxiety, depression or depressed mood, suicidal ideation, suicide attempts, and aggression.
Common Treatment-Emergent AEs and Serious AEs
The most common treatment-emergent adverse events (TEAEs) experienced by patients were injection-site reactions (erythema, pruritus, bruising, and induration and pain), skin hyperpigmentation, nausea, vomiting, and diarrhea.
Incidences of injection-site reactions, diarrhea, and nausea were similar between treatment arms during the placebo-controlled period, but vomiting was experienced only by setmelanotide-treated patients (n = 7; 25.9%). Incidents of vomiting also occurred in patients initially randomized to placebo when they later received setmelanotide (n = 7; 28.0%) during the open-label period; these tended to occur in the first month of setmelanotide treatment. No events of severe nausea or vomiting occurred.
Over the entire study, 100% of patients with BBS or AS experienced at least 1 AE, and 3 patients (5.8%) experienced at least 1 serious adverse event (SAE). The SAEs experienced over the entire study period included anemia, blindness, suicidal ideation, and anaphylactic reaction (as previously described in a placebo-treated patient), none of which were considered by study investigators to be caused by the study drug.
Discontinuation Due to AEs
During the placebo-controlled period, 2 setmelanotide-treated patients and 3 placebo-treated patients discontinued treatment due to AEs. Of these, 1 placebo-treated patient and 1 setmelanotide-treated patient discontinued due to nausea, and 1 setmelanotide-treated patient but 0 placebo-treated patients discontinued due to vomiting. In the setmelanotide treatment group, other AEs leading to discontinuation included 1 instance each of ocular hyperemia and face edema. In the placebo group, other AEs leading to discontinuation included 1 instance each of anaphylactic reaction, headache, acne, hidradenitis, and hot flush.
Over the entire study, | || || || || || || | discontinued due to any TEAE. The reasons for discontinuation over the entire 66-week study period (N = 57 with BBS or AS) included nausea (n = 3) and vomiting (n = 3), and 1 instance each of discontinuation due to ocular hyperemia, anaphylactic reaction, headache, acne, hidradenitis, hot flush, skin hyperpigmentation, and abdominal pain.
AEs of Special Interest
Hyperpigmentation was experienced frequently and exclusively in setmelanotide-treated patients (63.0% during the placebo-controlled period and 63.5% over the full study period). These events were expected due to the effect of melanocortin receptor agonism during setmelanotide treatment.
Sexual events occurred in some patients: | || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || | during the study period.
The other AEs of special interest were either | || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || |
Deaths
No deaths occurred during the study.
Table 2: Summary of Key Results From Study 023
Outcome | Result | |
|---|---|---|
Single-arm outcomes after 52 weeks of setmelanotide treatment | ||
Proportion achieving ≥ 10% body weight reduction from ATB a,b | ||
N | 28 | |
Estimated % (95% CI)c | 35.7 (18.6 to 55.9) | |
P valuec | 0.0002 | |
Percent change in body weight from ATBa,b | ||
N | 28 | |
Mean % (SD) | −6.47 (6.970) | |
P valued | < 0.0001 | |
Proportion achieving a ≥ 25% improvement in average daily hunger score from ATBa,b | ||
Estimated % (95% CI)d | 57.1 (28.9 to 82.3) | |
P valued | < 0.0001 | |
Harms, n (%)e | ||
AEs | 52 (100.0) | |
SAEs | 3 (5.8) | |
WDAEs (from study treatment) | 6 (11.5) | |
Deaths | 0 | |
Placebo-controlled outcomes after 14 weeks | ||
Percentage body weight change from PCPBa | Setmelanotide | Placebo |
N | 14 | 15 |
Mean % (SD) | −3.21 (4.474) | −0.25 (2.353) |
Median % (95% CI) | −2.77 (−5.79 to −0.62) | 0.32 (−1.55 to 1.05) |
Difference (95% CI)d | −2.96 (−5.65 to −0.26) | |
P valued | 0.0164 | |
Percent change in the weekly average of daily hunger scores from PCPBa | Setmelanotide | Placebo |
N | | || || || || | | | || || || || | |
Mean % (SD) | | || || || || | | | || || || || | |
Difference (95% CI)d | | || || || || | | |
P valued | | || || || || | | |
Harms, n (%)e | Setmelanotide | Placebo |
AEs | 26 (96.3) | 24 (96.0) |
SAEs | 1 (3.7) | 2 (8.0) |
WDAEs (from study treatment) | 2 (7.4) | 3 (12.0) |
Deaths | 0 | 0 |
AS = Alström syndrome; ATB = active treatment baseline; BBS = Bardet-Biedl syndrome; CI = confidence interval; FAS = full analysis set; PCPB = placebo-controlled period baseline; PRO = patient-reported outcome; SD = standard deviation.
aPatients with BBS (pivotal) aged greater than or equal to 12 years. Hunger and PRO outcomes do not include patients with cognitive impairment. Active treatment baseline refers to when the patient began treatment with setmelanotide (which would have been after week 14 for patients initially randomized to placebo), while placebo-controlled baseline refers to the baseline of the study overall.
bSix patients (19.35% of the full pivotal population; 21.42% of the pivotal BBS population) had missing measurements at 52 weeks due to study discontinuation and were conservatively considered to have treatment failure. Active treatment baseline refers to when the patient began treatment with setmelanotide (which would have been after week 14 for patients initially randomized to placebo), while placebo-controlled baseline refers to the baseline of the study overall.
cThe estimated percentage, 95% CI, and P value are based on Rubin’s rule testing the prespecified assumption of 10% of patients with BBS achieving a greater than or equal to 10% reduction in body weight without treatment. Multiplicity adjustment was not conducted. Values are from the posthoc analysis of patients with BBS and should be used for descriptive purposes only.
dThe P value is 1-sided, based on Rubin’s rule testing the assumption of no change from baseline; the key secondary end point (percent change after 52 weeks) was analyzed first in the prespecified hierarchy at alpha = 0.025. Multiplicity adjustment was not conducted. Values are from the posthoc analysis of patients with BBS and should be used for descriptive purposes only.
eSafety analysis population (BBS and AS). Difference, 95% CI of difference, and P value are based on Rubin’s rule, and difference is calculated as setmelanotide minus placebo. Multiplicity adjustment was not conducted. Values are from the posthoc analysis of patients with BBS and should be used for descriptive purposes only.
Sources: Study 023 Clinical Study Report9 and the report of patients with BBS from Study 023.10 Details in the table have been taken from the sponsor’s Summary of Clinical Evidence.
Critical Appraisal
Study 023 was a phase III, multicentre study that consisted of a 14-week, randomized, placebo-controlled, double-blind period followed by a 52-week, open-label, single-arm period. To reflect the requested reimbursement criteria, all efficacy outcomes considered in this report were posthoc reanalyses based on the subgroup of patients with BBS; these patients comprised the majority of the overall population. The results of the posthoc analysis were consistent with the results of the prespecified analyses in the full analysis set (FAS). Although the population size was small, BBS is a rare disease with a small patient population, and the sample size exceeded the minimum power calculation conducted by the sponsor. However, the already-small sample size was further restricted for hunger-related outcomes (because cognitively impaired patients were excluded), for exploratory outcomes related to HRQoL (because of the different age requirements associated with the validated scales and the exclusion of cognitively impaired patients), and across many other outcomes (because of missing data). There are inherent risks of bias, confounding, and uncertainty in the estimation of treatment effects from single-arm data due to unidentified, uncontrolled prognostic factors. Moreover, the open-label design of the single-arm period increases the risk of detection bias and performance bias and may lead to overestimation of the treatment effect for subjective outcomes. The duration of treatment for this period was considered appropriate by CADTH clinical experts for evaluating weight loss and hunger; however, longer-term data are also needed, given that obesity in patients with BBS is a long-term, chronic, relapsing condition.
The primary outcome of the proportion of patients achieving a greater than or equal to 10% reduction in body weight at 52 weeks was considered to be conservative, given that a greater than or equal to 5% reduction in body weight is widely accepted by clinical experts as clinically meaningful in patients with BBS and obesity. The trial result was compared to a prespecified threshold of 10% responders based on historical control data. The key secondary hunger-related outcomes were based on a hunger scale that has not been externally validated, confounding the interpretation of a MID; moreover, the results were compared against an assumption of no effect without treatment, which does not control for the possibility of the placebo effect and may be biased in favour of setmelanotide, given that this is a subjective patient-reported outcome (PRO). Primary and key secondary results from the 52-week analyses are supported by the exploratory placebo-controlled outcomes in which, at week 14, a higher percentage of patients in the setmelanotide treatment group had improvement in parameters related to weight loss and hunger compared to patients who received placebo.
The eligibility criteria and population characteristics at baseline were considered to be appropriate and generalizable to the population of interest (i.e., adult and pediatric patients with BBS, obesity, and hyperphagia who may or may not have cognitive impairment or genetic confirmation of diagnosis). Although patients aged greater than or equal to 6 years were included, most outcomes were analyzed in patients aged 12 years and older, and very few patients aged less than 12 years were enrolled in the trial (n = 8). Additionally, although patients with cognitive impairment were enrolled, they were not included in the key secondary and exploratory outcomes related to hunger and HRQoL due to the practical limitations of assessing these outcomes in cognitively impaired populations. Subgroup analyses of younger and cognitively impaired populations generally aligned with the primary and secondary outcomes described, but the interpretation of results was limited due to the small sample sizes. There are also concerns about generalizability of the results to pediatric patients, given that the average maintenance dose in pediatric patients in Study 023 (| || || || || |) exceeded the maximum recommended dose of 2 mg daily. The clinical experts consulted by CADTH indicated that dosing in real-world practice would mostly follow the product monograph, with occasional exceptions for patients aged older than 16 years, who may begin to receive adult dosages based on clinical judgment.
Long-Term Extension Studies
Description of Studies
Study 022 is an ongoing, long-term extension (LTE) study that is nonrandomized, open-label, and single-arm, and includes patients aged greater than or equal to 6 years with BBS and obesity. Enrolled patients are “responders” who have completed 1 of the phase II or phase III studies (i.e., Study 014 or Study 023, respectively), demonstrated tolerability, and achieved a body weight reduction of greater than or equal to 10% (patients aged ≥ 18 years) or a greater than or equal to 0.3 reduction in BMI z score (patients aged < 18 years) after 52 weeks of setmelanotide treatment. Patients received personalized setmelanotide doses titrated to a target of 3 mg once daily. The primary objective was to evaluate safety and tolerability; secondary objectives were to evaluate changes in weight and hunger.
Efficacy Results
At the time of this review, Study 022 was still ongoing, and not all patients had completed the 36-month assessment. However, early findings from 12-month, 18-month, and 24-month assessments indicate that weight-related parameters have tended to stabilize in | || || || || | patients with BBS and obesity. | || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || ||.
Harm Results
During Study 022, 100% of patients experienced at least 1 TEAE. The most common TEAEs were injection-site reactions, skin hyperpigmentation, nausea, and vomiting. Three patients (10%) experienced SAEs. No death related to AEs was reported. It was not reported whether deaths were observed in general.
Critical Appraisal
The open-label design of Study 022 is considered a limitation that could increase the risk of detection bias and performance bias and lead to the overestimation of treatment effect for subjective outcomes. The small sample size, immature data, lack of a control arm, and lack of adjustment for covariates are considered key constraints that limit the interpretation of study outcomes. Additionally, only a brief summary of the trial was available for this review, with limited reporting. Hunger and HRQoL outcomes were not reported.
Indirect Comparisons
The sponsor conducted a feasibility assessment to determine if an indirect treatment comparison of setmelanotide versus 8 general obesity treatments — including semaglutide, lixisenatide, lisdexamfetamine, topiramate, liraglutide, naltrexone-bupropion, orlistat, and bariatric surgery — can be undertaken. Systematic literature reviews were conducted to identify prospective or retrospective clinical studies, published or unpublished, pertaining to the treatment of patients with BBS and obesity. No relevant articles were identified in this patient population; therefore, indirect comparisons were not feasible.
Conclusions
There is an unmet need for targeted treatments that address the underlying biological cause of hyperphagia and obesity caused by BBS, which is a rare, incurable, genetic ciliopathy with multisystem manifestations. Patients and clinicians highlighted that early-onset obesity and hyperphagia are 2 of the most distressing symptoms of BBS, causing significant HRQoL impairment and caregiver burden, and that typical obesity management strategies (such as restricted diet) are less feasible and less sustainable in this population than in general obesity. One completed phase III trial (Study 023) and an ongoing LTE (Study 022) were included in this review. There were notable concerns with the internal validity of the studies. These were driven primarily by the single-arm, open-label design, which introduces significant risk of bias to all subjective clinical outcomes and limits the interpretation of the magnitude of effect attributable to the intervention. However, it is worth noting that BBS is a rare disease with a small patient population for which there are no other targeted pharmacotherapies.
The data submitted to CADTH were considered clinically relevant to the target patient population. Setmelanotide results were consistent with a clinically meaningful reduction in all weight-related parameters — such as change in body weight and BMI across all reported analysis populations and subgroup analyses at 52 weeks — and the results were supported by the exploratory, comparative, 14-week, placebo-controlled outcomes. The results also suggested a consistent reduction in hunger score in both the placebo-controlled and open-label periods. However, the scale used to measure hunger has not been externally validated; therefore, it is inconclusive whether these results are clinically meaningful. Similarly, results for HRQoL outcomes at 52 weeks appeared to support a beneficial effect, but small sample sizes and the single-arm study design made interpreting events attributable to setmelanotide challenging. The long-term efficacy of setmelanotide is unknown because efficacy data from the LTE (Study 022) were immature at the time of this review. There is no evidence of effect regarding other BBS-related manifestations or prognoses aside from obesity. There are concerns about the generalizability of the clinical data to pediatric patients, given that the average maintenance dose in pediatric patients in Study 023 (| || || || || |) exceeded the maximum Health-Canada–recommended dose of 2 mg daily. There are also inherent risks of bias, confounding, and uncertainty in the estimation of treatment effects from single-arm data due to unidentified, uncontrolled prognostic factors. Moreover, the open-label design of the single-arm period increases the risk of detection bias and performance bias, and may lead to an overestimation of the treatment effect for subjective outcomes.
There are potentially notable harms from setmelanotide, including hyperpigmentation and sexual events or inappropriate behaviours. However, these events were generally uncommon, and no treatment-related melanoma has been observed in any setmelanotide trial to date. Behavioural or psychiatric disturbances, such as depression or aggression, were observed in the setmelanotide trials, but are unlikely to be related to study medication. All patients in Study 023 experienced at least 1 AE, but very few were serious; setmelanotide was generally well-tolerated. The most common AEs in patients treated with setmelanotide were injection-site reactions, skin hyperpigmentation, nausea, vomiting, and diarrhea. Vomiting was commonly and exclusively observed in patients treated with setmelanotide, and tended to occur during the first month of treatment; however, no events were severe. No new safety signals have been identified in the ongoing LTE (Study 022).
Overall, the results of Study 023 and Study 022 were consistent with setmelanotide improving important weight-related outcomes for patients with BBS, but the ability to draw firm conclusions on the magnitude of clinical benefit in hunger, HRQoL, and other outcomes was limited. There are uncertainties regarding the long-term efficacy and safety of setmelanotide, given that it is potentially a lifelong treatment.
Introduction
The objective of this report is to review and critically appraise the evidence submitted by the sponsor on the beneficial and harmful effects of setmelanotide 10 mg/mL solution administered as a once-daily SC injection for weight management in adult and pediatric patients aged 6 years and older with obesity due to BBS.
Disease Background
Contents within this section have been informed by materials submitted by the sponsor and clinical expert input. The following information has been summarized and validated by the CADTH review team.
Disease Overview
BBS is a rare and highly heterogeneous ciliopathy caused by genetic variants that lead to dysfunction in the MC4R pathway. It is characterized by various clinical manifestations, including hyperphagia, obesity, postaxial polydactyly, renal anomalies, retinal cone-red dystrophy, learning disabilities, developmental delays, and diabetes.12 Additionally, cognitive impairment is common in patients with BBS (approximately 62%6).
Despite the clinical heterogeneity of BBS, hyperphagia is common, and approximately 72% to 92% of patients with BBS have obesity as a major clinical finding.6,12 Childhood obesity is considered a dominant feature of BBS that develops early in life.13 An analysis of the largest international BBS registry revealed that the proportion of patients with BBS who were overweight or obese exceeded 90% after the age of 6 years, despite most birth weights being in the normal range.13 This very early onset of obesity in BBS cases is atypical of general obesity and should raise the possibility of diagnostic screening for BBS and other rare obesity syndromes;13 it is thought to be driven by hyperphagia.14-16 Obesity and hyperphagia in BBS are thought to be associated with genetic defects resulting in impairment of the MC4R pathway, leading to insatiable hunger, decreased metabolism, and severe obesity.12 Hyperphagia is associated with a severe preoccupation with food, persistent and potentially extreme food-seeking behaviours, and distress or inappropriate behaviours if denied food.17,18
According to patients and caregivers, hyperphagia and obesity are 2 of the most distressing features of BBS13 that significantly decrease their QoL.18 Weight management is an ongoing struggle for most patients. In particular, patients or caregivers of patients with BBS can experience guilt, stigmatization by family or peers, and judgment regarding their perceived incompetency in managing their or their child’s behaviours and weight.19 Hyperphagia also has broad negative effects on patients’ emotional state and relationships as well as negative effects on productivity at work and school.20
The prognostic implications of hyperphagia and obesity in BBS are uncertain, although general obesity is acknowledged as a chronic disease that impairs health, increases the risk of long-term medical complications, and reduces lifespan.21-23 Obesity, especially in children, is a complex disease associated with numerous comorbid conditions, including type 2 diabetes, gallbladder disease, nonalcoholic fatty liver disease, gout, and various cancers.21 Moreover, obesity is linked to depression and social isolation24,25 as well as stigma and discrimination,26 which can be sources of suffering, morbidity, and even mortality.21 Obesity accelerates long-term, coexisting health problems in patients with BBS, such as cardiovascular disease, obstructive sleep apnea, liver disease, and diabetes, and impairs QoL.13,27-31
Prevalence
The overall prevalence of BBS is estimated at approximately 1 case per 100,000 to 1 case per 160,000 population in North America and Europe.12,32,33 However, it is significantly more prevalent in isolated communities or where consanguinity is common.6 For example, the prevalence reaches approximately 1 case per 16,000 to 1 case per 18,000 population in Newfoundland and Labrador.32,34 It is estimated that approximately 300 to 400 individuals in Canada have BBS, 215 to 370 of whom may have obesity, based on a prevalence estimate of 72% to 92%.6,12
Diagnosis
Diagnostic Testing Requirements
A diagnosis of BBS is established based on clinical features, which may include rod-cone dystrophy (93% of patients), obesity (72% to 92%), polydactyly (63% to 81%), genital malformations (59% to 98%), learning difficulties (61%), and renal abnormalities (53%).12 Symptoms may vary significantly across patients; as a result, a clinical diagnosis requires the presence of at least 4 major features or 3 major features plus at least 2 minor features from the diagnostic criteria published by Beales et al.35
Primary features include:
rod-cone dystrophy
polydactyly
obesity
learning disabilities
hypogonadism in males
renal abnormalities.
Secondary features include:
speech disorder and/or delay
strabismus and/or cataracts and/or astigmatism
brachydactyly and/or syndactyly
developmental delay
polyuria and/or polydipsia (nephrogenic diabetes insipidus)
mild spasticity (especially of the lower limbs)
diabetes mellitus
dental crowding and/or hypodontia and/or small roots and/or high, arched palate
hepatic fibrosis.
However, many of the manifestations of BBS are progressive and may evolve as children grow, complicating physicians’ ability to make a clinical diagnosis based on the diagnostic criteria.6 At birth, many individuals with BBS may appear healthy unless they have polydactyly, and some symptoms may emerge gradually during or after the first decade of life.28 Therefore, symptoms may be missed in early childhood, and an ongoing assessment framework is needed to support the diagnosis of suspected BBS.
Availability of Diagnostic Testing
Genetic testing may be conducted to confirm a diagnosis of BBS, but it is not required.36 A genetic testing panel that can identify 12 of the 22 known BBS genes is currently available through some Canadian treatment centres. However, a genetic test that can identify all 22 BBS genes is not currently available in Canada and must be ordered as an out-of-country test. | || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || ||
Standards of Therapy
Contents within this section have been informed by materials submitted by the sponsor and by clinical expert input. The following information has been summarized and validated by the CADTH review team.
Currently, there is no cure for BBS; nor are there any targeted therapies available for the treatment of BBS and its related hyperphagia or obesity. Interdisciplinary symptomatic treatment for patients with BBS aims to aggressively manage diabetes, hypertension, and metabolic syndrome.12,37 Management of obesity in patients with BBS is similar to management of obesity in the general population, and includes lifestyle modifications, restricted calorie diets, exercise, and psychological interventions, in most cases; it does not address the underlying hyperphagia.10 The clinical experts consulted by CADTH noted that, although some patients with BBS with obesity and hyperphagia may achieve a greater than or equal to 5% weight loss through lifestyle changes, this is uncommon; the ability to sustain weight loss is especially low in this population.
There are no Health Canada–approved treatments for obesity or control of hunger in patients with BBS. Some pharmacotherapies may be used off-label,1 such as GLP1 receptor agonists (e.g., semaglutide injection or liraglutide injection) or gastrointestinal lipase inhibitors (e.g., orlistat), which are reimbursed in some Canadian jurisdictions for adults with type 2 diabetes (semaglutide) or in patients with obesity and 1 weight-related comorbid condition (liraglutide, orlistat).2,3 The clinical experts consulted by CADTH indicated that only semaglutide was likely to be prescribed off-label for patients with BBS (because of its potential to reduce hunger); however, they noted that it does not target the underlying mechanism of BBS-induced hyperphagia and that there are no clinical trials currently available in populations with BBS. Other pharmacotherapies for obesity management that were not indicated as potentially used off-label in BBS include lixisenatide, naltrexone-bupropion, lisdexamfetamine, and topiramate.1
Bariatric surgery with gastric banding or sleeve surgery may be used as a last resort in a few patients with a BMI of greater than 40 kg/m2 or those with a BMI of greater than 35 kg/m2 and comorbidities.4,5 However, there are significant limitations associated with bariatric surgery. For example, it may be dangerous and lack durability for patients with hyperphagia if the patient’s food environment is not tightly controlled.
Drug Under Review
Setmelanotide is an MC4R agonist.38 MC4Rs in the brain are involved in regulating hunger, satiety, and energy expenditure. In genetic forms of obesity related to the leptin-melanocortin pathway associated with insufficient activation of the MC4R, setmelanotide is believed to reestablish the MC4R pathway activity to reduce hunger and promote weight loss through decreased caloric intake and increased energy expenditure.38 Setmelanotide is indicated for weight management in adult and pediatric patients aged 6 years and older with obesity due to BBS.38 It is also indicated for weight management in adult and pediatric patients aged 6 years and older with obesity due to genetically confirmed biallelic pro-opiomelanocortin (POMC), proprotein convertase subtilisin/kexin type 1 (PCSK1), or leptin receptor (LEPR) deficiency due to variants interpreted as pathogenic, likely pathogenic, or of uncertain significance. Setmelanotide is not indicated for the treatment of patients with obesity due to suspected POMC, PCSK1, or LEPR deficiency with POMC, PCSK1, or LEPR variants classified as benign or likely benign, or other types of obesity not related to POMC, PCSK1, or LEPR deficiency or BBS, including obesity associated with other genetic syndromes and general (polygenic) obesity.38
The product monograph notes the following:
Setmelanotide should be prescribed and supervised by a physician with expertise in obesity with underlying genetic etiology.
Setmelanotide should be administered once daily, at the beginning of the day, without regard to meals.
Patients selected for treatment with setmelanotide should have a genetically determined deficiency of POMC, PCSK1, or LEPR or a clinical diagnosis of BBS.
Response to setmelanotide therapy should be assessed regularly.
In patients with BBS, weight loss should be evaluated after 22 weeks of treatment. If a patient has not lost at least 5% of baseline body weight (or 5% of baseline BMI for patients with continued growth potential), setmelanotide should be discontinued, because it is unlikely that the patient will achieve and sustain clinically meaningful weight loss with continued treatment.
In pediatric patients, the impact of weight loss on growth and maturation should be evaluated.38
Setmelanotide is available as a 10 mg/mL solution in a 1 mL multiple-dose vial. The recommended dosage for the treatment of patients with BBS aged 18 years and older is as follows:38
The starting dose of setmelanotide is 1 mg (0.1 mL) injected SC once daily for 2 weeks.
Monitor patients for gastrointestinal adverse reactions to adjust dosage.
The dose may be increased by 0.5 mg daily every 2 weeks, if tolerated, to a maximum dose of 3.0 mg daily.
If the starting dose is not tolerated, setmelanotide should be discontinued.
For patients with mild to moderate renal impairment, no dosing adjustments are required.
For patients with severe renal impairment, the starting dose is 0.5 mg (0.05 mL) and may be increased by 0.5 mg daily every 2 weeks, if tolerated, to a maximum of 1.5 mg daily.
Setmelanotide is not recommended in patients with any degree of hepatic impairment.
For patients with BBS aged 6 years to 17 years, the recommended dosage is as follows:38
The starting dose of setmelanotide is 0.5 mg (0.05 mL) injected SC once daily for 2 weeks.
Monitor patients for gastrointestinal adverse reactions to adjust dosage.
The dose may be increased by 0.5 mg daily every 2 weeks, if tolerated, to a maximum dose of 2.0 mg daily.
If the starting dose is not tolerated, setmelanotide should be discontinued.
It is not recommended to treat pediatric patients who have severe renal impairment with setmelanotide.
Setmelanotide is not recommended in patients with any degree of hepatic impairment.
It is worth noting that the dosage in the pivotal study (Study 023) differed from the currently recommended dosing:
During the 14-week, double-blind treatment period, patients aged greater than or equal to16 years were started on setmelanotide once daily through SC injection at 2 mg or matching placebo for 2 weeks, after which they were increased to the target dose of 3 mg SC once daily (or matching placebo) at the beginning of week 3 for the duration of the double-blind period.
Patients aged less than 16 years were started on setmelanotide 1 mg SC once daily or matching placebo during week 1. This dosage was increased to 2 mg SC once daily or matching placebo at the beginning of week 2, and increased to 3 mg SC once daily or matching placebo at the beginning of week 3 for the duration of the double-blind period.
After the initial 14-week, double-blind treatment period, all patients immediately transitioned to open-label setmelanotide once daily, administered through SC injection. To preserve the blind, all patients were restarted at their initial age-based dose and re-escalated to the 3 mg target dose. Thus, beginning at week 15, patients aged greater than or equal to 16 years of age received open-label setmelanotide 2 mg SC once daily for 2 weeks, followed by a dose increase to 3 mg SC once daily beginning at week 17 for the duration of the trial; patients aged less than 16 years received open-label setmelanotide 1 mg SC once daily during week 15, 2 mg SC once daily during week 16, and 3 mg SC once daily beginning at week 17 for the duration of the trial.
Setmelanotide was approved by Health Canada through the priority review process. The sponsor has requested reimbursement according to the indication for patients with BBS (i.e., for weight management in adult and pediatric patients aged 6 years and older with obesity due to BBS). This drug has not been previously reviewed by CADTH. No other therapies are currently approved by Health Canada for the treatment of obesity due to BBS.39
Stakeholder Perspectives
Patient Group Input
This section was prepared by the CADTH review team based on the input provided by patient groups. The full original patient input received by CADTH is included in the stakeholder section at the end of this report.
One patient group, the Bardet Biedl Syndrome Foundation, submitted patient input for this review. The foundation connects families and shares information on research, treatment, and therapies for BBS. The input was based on a 30-minute online survey and 1-on-1 telephone or video conference interviews. Of the 41 survey participants, 61% were from the US and 29% were from Canada; 34 respondents were caregivers of patients aged 3 years to 18 years, and 7 were adult patients living with BBS. Additional information was also gathered through interviews with 1 patient and 4 caregivers, all of whom had direct experience with setmelanotide.
Among the patient respondents, 57% indicated that their childhood weight was of concern, and 71% said they are currently living with obesity, with a BMI of greater than or equal to 30.0 kg/m2. Among the caregiver respondents, 71% indicated that their loved ones currently live with obesity related to their BBS. Regarding hunger-related symptoms and behaviours, 86% of the patient respondents stated that they take a longer time to feel full after eating and indicated that managing hunger is crucial. In addition, 71% of patient respondents indicated that they think about food constantly. Similarly, most caregiver respondents (85%) stated that their loved ones take a longer time to feel full after eating, and 91% indicated that their loved ones constantly think about food. Nearly half (43%) of patient respondents noted that BBS-related hunger negatively affects their emotional and psychological well-being, their social life, and their ability to travel. Half of caregiver respondents indicated that BBS-related hunger affects their loved one’s social life; similar proportions indicated that it affects their loved one’s emotional and psychological well-being (47%) and work or school life (44%).
The patient input stated that there is no approved treatment for BBS or BBS-related hunger and obesity in Canada. Patient and caregiver respondents discussed their own and their loved ones’ experiences with weight management strategies, such as environmental factors and pharmacologic therapies. Patient respondents found regular exercise plans to be somewhat effective (43%) or very effective (43%), and supervision from others to be somewhat effective (29%) or very effective (29%), in managing their weight. The strategies identified by most caregivers as somewhat to very effective included regular exercise (74%), supervision from others (85%), calorie-restricted diets (56%), and adherence to meal schedules (73%).
However, caregivers noted that despite these strategies, challenges remained in aiding patients with constant hunger, and that the strategies are challenging to implement. When asked to identify the most important outcome of treatment for BBS-related hunger, caregivers identified not thinking about food so much (80%), not feeling hungry right after eating (68%), and reducing stigma and/or judgment (63%). They also identified that effective treatment of BBS-related hunger would reduce stress from the perspective of caregivers and their families.
Two patient respondents had experience with other weight management medications: 1 reported that semaglutide was very effective, and another reported that phentermine was somewhat effective. Two caregiver respondents reported that their loved ones had tried semaglutide. They indicated that it was effective in managing their weight; however, 1 of these respondents stated that semaglutide was being used at the same time as setmelanotide.
Four patient respondents and 13 caregiver respondents from the patient input stated that they or their caregivers had experience with setmelanotide; they indicated that setmelanotide improved appetite and hunger control and management, weight loss, travel, and QoL.
In addition to the survey responses, the patient input summarized the results of interviews with 1 patient and 4 caregivers who had experience with setmelanotide. Their input aligned with the survey answers in terms of symptoms and improved outcomes of weight, hunger control, QoL, and the recommendation that the drug be available and accessible for all patients living with BBS.
Clinician Input
Input From Clinical Experts Consulted by CADTH
All CADTH review teams include at least 1 clinical specialist with expertise regarding the diagnosis and management of the condition for which the drug is indicated. Clinical experts are a critical part of the review team and are involved in all phases of the review process (e.g., assisting in the critical appraisal of clinical evidence; interpreting the clinical relevance of the results; and providing guidance on the potential place in therapy). In addition, as part of the setmelanotide review, a panel of 4 clinical experts from across Canada was convened to characterize unmet therapeutic needs, assist in identifying and communicating situations where there are gaps in the evidence that could be addressed through the collection of additional data, promote the early identification of potential implementation challenges, gain further insight into the clinical management of patients living with the condition, and explore the potential place in therapy of the drug under review (e.g., potential reimbursement conditions). A summary of this panel discussion is presented in this section.
Unmet Needs
The clinical experts indicated that the primary unmet need is for targeted treatment options for patients with BBS, a genetic ciliopathy that results in multisystem manifestations. The experts highlighted that key features of BBS can include hyperphagia, early-onset obesity, polydactyly, renal disease, genitourinary malformations, ophthalmic manifestations, anosmia or hyposmia, dental abnormalities, developmental delay, cognitive impairment, and gastrointestinal manifestations; moreover, potential consequences of obesity can include hyperglycemia, type 2 diabetes, metabolic syndrome, dyslipidemia, fatty liver disease, hypertension, cardiovascular diseases, obstructive sleep apnea, and hypogonadism, among others, as well as premature death.
The clinical experts indicated that lifestyle interventions for obesity management are particularly inefficient and unsustainable in this population because of biologically driven hyperphagia, the potential for hyperphagia-related behavioural challenges related to food-seeking (particularly in children), and the potential for cognitive impairment as a consequence of BBS. The experts also highlighted that patients with early-onset obesity due to BBS and hyperphagia may be exposed to their obesity for a substantially longer time period than people with late-onset common obesity, placing them at greater risk for downstream obesity-related comorbidities.
Place in Therapy
The clinical expert panel agreed that setmelanotide would be considered first-line therapy for patients with BBS who have hyperphagia and obesity, in combination with obesity management recommendations, such as intensive diet and lifestyle changes. Setmelanotide was noted as the first therapy that would target the mechanism of hyperphagia in BBS, which is a major obstacle in the maintenance of obesity management activities in this population.
The experts noted that, although some patients with BBS with obesity and hyperphagia may achieve weight loss of greater than or equal to 5% through lifestyle changes, the sustainability of weight loss is especially low in this patient population, and it would be clinically and ethically inappropriate to withhold or delay access to pharmacologic treatment for those patients, due to their underlying, biologically driven hyperphagia.
The experts indicated that off-label treatments, such as GLP1 receptor agonists (e.g., semaglutide), have been reported in case studies of adult patients with BBS for the control of hunger obesity, but there is a lack of robust clinical data in this patient population; and, unlike setmelanotide, GLP1 receptor agonists do not address the underlying disease mechanisms of hyperphagia caused by BBS. Moreover, semaglutide is not approved by Health Canada in pediatric patients. For these reasons, the experts agreed that it would be inappropriate to begin treatment with a trial of semaglutide before allowing access to setmelanotide in patients with BBS for the control of obesity and hyperphagia.
Despite a lack of data, the experts believed that combination therapy of setmelanotide and GLP1 receptor agonists was likely to occur in some circumstances, including in patients with BBS who also have type 2 diabetes (i.e., comorbidity). The preferred approach to combination therapy varied among panel members in the case of insufficient response to setmelanotide. One approach would be to initiate combination therapy with setmelanotide and pharmacological therapies, such as GLP1 receptor agonists; another would be to discontinue setmelanotide and not pursue combination therapies. However, it was agreed that a combination of setmelanotide and GLP1 receptor agonists may have a synergistic treatment effect in reducing hunger and helping patients with BBS to improve or maintain weight loss, but there is a lack of clinical data.
The experts noted that there is some evidence that the response to bariatric surgery may be less durable in populations with hyperphagic obesity.
Patient Population
The clinical experts noted that BBS is a very rare disease with elevated prevalence in some locations (e.g., Newfoundland and Labrador), and that approximately 90% of patients with BBS have comorbid obesity by adulthood. The clinical experts agreed that the target population for treatment with setmelanotide would be adult and pediatric patients with BBS, obesity, and hyperphagia, and that reasonable thresholds for obesity were a BMI of greater than or equal to 30 kg/m2 for patients aged greater than or equal to 16, or weight greater than the 97th percentile for age and sex in patients aged less than 16 years.
Expert opinion on clinical versus genetic diagnosis of BBS was variable among panel members. In 1 approach, clinical diagnosis of BBS based on the Beales criteria was considered by the experts to be sufficient for treatment with targeted therapies, such as setmelanotide; the experts believed it would be inappropriate to strictly require genetic confirmation because additional BBS-causing mutations are still being discovered. In another approach, the diagnosis of BBS should be based on the clinical diagnosis of BBS using the Beales criteria as well as genetic confirmation. The experts noted that the majority of patients, especially pediatric patients, generally seek genetic confirmation of diagnosis. It is worth noting that the Health Canada–approved product monograph indicates that patients selected for treatment with setmelanotide should have a genetically determined deficiency of POMC, PCSK1, or LEPR, or a clinical diagnosis of BBS; they did not indicate that genetic diagnosis of BBS was needed.38
The experts indicated that genetic testing for the suite of known BBS mutations is currently not available in Canada but can be requested through the provincial ministries of health as an out-of-country test. This does not cause out-of-pocket expense for the patients. The specialists most commonly diagnosing BBS were identified to be pediatricians, pediatric endocrinologists, and pediatric geneticists; however, owing to the multisystem effects and heterogeneous presentation of other symptoms in BBS, some patients may be first identified by specialists working in nephrology or ophthalmology, or by developmental pediatricians. It was also noted by the clinical experts that the average age of diagnosis with BBS is approximately 9 years, and that limited access to pediatric weight management clinics may contribute to delayed obesity management. Although there are no studies of the sensitivity and specificity of the Beales criteria, misdiagnosis was considered by the experts to be unlikely.
The pivotal study (Study 023) of setmelanotide for the treatment of obesity and hunger in patients with BBS excluded patients under 6 years of age; the majority of outcomes were assessed in the population aged greater than or equal to 12 years without cognitive impairment. Although this limits generalizability to patients aged greater than or equal to 6 years to less than 12 years, and those with cognitive impairment, the experts indicated that these are still populations of interest with substantial unmet needs. Moreover, there are practical limitations to the assessment of hunger and PROs in these subpopulations, and to the assessment of weight loss in growing children aged less than 12 years.
Patients who had recently undergone intensive weight control strategies were excluded from the pivotal study of setmelanotide. The clinical experts agreed that this would not reflect clinical practice, given that patients would be expected to combine obesity management strategies with setmelanotide and would not be excluded from treatment for recency of weight-loss activities. However, for the purpose of interpreting the trial results, the clinical experts agreed that this was a conservative trial design element and was not a cause for concern in the implementation of setmelanotide in clinical practice.
The clinical experts indicated that it is currently unknown which patients are the most or least likely to demonstrate a clinically meaningful response to treatment with setmelanotide. However, it is clinically plausible that differences in the underlying mutation may be relevant for prognosis and treatment effect. More data are needed in this area.
Assessing the Response to Treatment
The experts indicated that the most important assessments are changes in hunger, weight, and BMI in adults (or BMI percentile in pediatric patients), and that patients may also be monitored for changes in related biomarkers, such as lipid and glycemic profiles. For the measurement of hunger, formal scales or questionnaires are not currently used in clinical practice, but could feasibly be adopted in the circumstances of a treatment that directly addresses hyperphagia; different approaches would be required for pediatric and cognitively impaired patients. In current clinical practice, hunger is assessed during discussions between physicians and patients or caregivers, with a focus on the frequency and intensity of perceived experiences with hunger, food-seeking behaviours, and behavioural issues that may arise as a result of hunger. Similarly, HRQoL is not formally quantified. Rather, it is elucidated through discussions with patients. When initiating a targeted therapy for BBS, the experts indicated that they would monitor patients approximately once every 3 months in adults and from every month to every 3 months in pediatric patients for the first year of treatment. For stable patients, the frequency of monitoring would be approximately once every 4 months to 6 months.
The approach to assessing response varied slightly between clinical experts. Overall, the experts agreed that a 1-year trial period was reasonable for determining whether a patient was responding to setmelanotide. Generally, a meaningful response during the 1-year trial period would assess as a qualitative improvement in hunger and/or HRQoL and a reduction of greater than or equal to 5% in total body weight in adults or greater than or equal to 5% BMI in pediatric patients. With regards to the threshold of meaningful weight loss, some experts considered this metric of meaningful response to be a potential requirement for treatment renewal after a trial of 1 year. However, it was noted that weight loss takes longer in adults who have long-standing obesity and comorbidities, that BBS is a complex multisystem disease that includes neurologic and behavioural symptoms that add to the complexity of the response criteria, and that many patients with BBS with hyperphagia would continue to gain weight over time when untreated; for these reasons, and because of the potential to prevent or delay downstream comorbidities, some experts expressed that setmelanotide renewal may be more circumstantial and could include patients whose weight has stabilized, but not meaningfully reduced, if they have demonstrated improvement in other key areas, such as hunger, HRQoL, and/or biomarkers of metabolic health, like lipid/glycemic profiles. With regards to qualitative improvements in hunger and/or HRQoL, it was noted that these assessments become more challenging and must be approached differently, such as by relying on assessment by caregivers, if possible, in young pediatric patients and patients with cognitive impairment. It is worth noting that the Health Canada–approved product monograph recommended that in patients with BBS, evaluation of weight loss should occur after 22 weeks of treatment with setmelanotide.38 If a patient has not lost at least 5% of baseline body weight (or 5% of baseline BMI for patients with continued growth potential), then setmelanotide should be discontinued because it is unlikely that the patient will achieve and sustain clinically meaningful weight loss with continued treatment.38 | || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || |40
Although there is a lack of long-term data for setmelanotide, the clinical experts agreed that weight loss would be expected to eventually plateau, and that subsequent maintenance of weight would be considered as treatment response in the long-term, after the first year of treatment. Therefore, patients who initially respond and then maintain their weight would be expected to continue with setmelanotide treatment in the absence of any major discontinuation criteria. Patients with an initial response who thereafter regain significant weight would also be expected to continue treatment, with additional assessment to identify and address what factors have changed and caused the weight gain, such as poorly controlled lifestyle modification, nonadherence, or complicating comorbidities. In the opinion of some experts, combining other pharmacotherapies with setmelanotide may also be considered in the circumstances of initial response followed by weight regain, and/or in the circumstances of initial weight maintenance without clinically significant weight loss but with notable improvements in HRQoL, hunger, or lipid and/or glycemic profiles. In general, it was agreed that clinical decision-making would be highly case-by-case for patients with initial response (weight loss) but subsequent weight gain, and that it is not plausible that patients will become resistant to treatment with setmelanotide, based on current data.
Discontinuing Treatment
The clinical experts agreed that treatment would be discontinued in the case of severe AEs that cannot be managed, including but not limited to moderate to severe allergic reactions, significant gastrointestinal symptoms, serious sexual events, suicidal ideation, or depression. In circumstances such as suicidal ideation or depression, a pause in treatment may be considered, rather than permanent discontinuation, to determine whether the AE re-emerges. Treatment may also be discontinued if there is no impact on hyperphagia after 12 months of treatment, or when there are significant issues with nonadherence.
Some clinical experts indicated that discontinuation would be considered in the absence of a clinically meaningful (i.e., ≥ 5%) reduction in total body weight. However, other experts indicated that patients may still be better off with treatment than without, despite a lack of weight loss. Their clinical approach would be to continue treatment on a case-by-case basis, as previously described.
Prescribing Considerations
The experts indicated that BBS is a rare disease with multisystem involvement. Patients may initially be identified through a variety of avenues dictated by their symptoms, and should ideally be followed by a multidisciplinary team, including specialist medical doctors as well as mental health professionals and registered dietitians. The most common prescribing physicians for setmelanotide would likely be endocrinologists or pediatric endocrinologists, but specialists in weight management or genetics may also prescribe. Access to some specialists or supports may be challenging, depending on patients’ geographic locations and other circumstances.
The prescribed dose of setmelanotide would not be expected to exceed 3 mg per day and would include titration of the dose from 1 mg or 2 mg per day according to age and tolerance.
Prescription in combination with other pharmacotherapies was not described to be of interest in the first-line setting, specifically for the treatment of weight loss and hyperphagia in BBS. However, as previously described, the clinical experts considered combination therapy to be a viable approach in some circumstances (with specific approaches differing among experts). Combination therapy with setmelanotide is expected to occur due to necessary treatment for comorbidities, such as the use of semaglutide for treating type 2 diabetes. In some approaches, combination therapy, such as with GLP1 receptor agonists or other appetite-limiting therapies, may be considered, depending on the patient’s experience with and response to setmelanotide (e.g., inadequate response after 1 year or clinically meaningful initial response followed by subsequent weight regain).
Additional Considerations
The clinical experts described that stigma related to obesity may cause patients to be reluctant to access care and is an important consideration when evaluating the impacts of weight loss on HRQoL. The transition from pediatric to adult care may also result in loss of patient follow-up. Also of particular importance is the impact of highly prevalent cognitive impairment in patients with BBS, which can affect the continuity of care, the ability to self-inject (or to measure the injection from a vial), compliance with a treatment regimen, concurrent lifestyle and dietary modifications, and the ability of physicians and caregivers to estimate subjective outcomes, such as HRQoL and hunger. The clinical experts also noted that patient registries for BBS would be of great value because there are still evidence gaps, especially regarding long-term efficacy and safety.
Clinician Group Input
This section was prepared by the CADTH review team based on the input provided by clinician groups. The full original clinician group input(s) received by CADTH have been included in the stakeholder section at the end of this report.
One clinician group provided input for this review: the Canadian endocrinologists treating BBS. Overall, the views of this clinician group were consistent with those of the clinical experts consulted by CADTH.
The clinician group reported that BBS is characterized by early-onset obesity with hyperphagia, intellectual impairment, renal anomalies, polydactyly, retinal degeneration, hypogonadism, and hypogenitalism, and that people with BBS may also have musculoskeletal complications, such as scoliosis, hip dysplasia, and difficulties with balance and coordination. The clinician group indicated that there is an unmet need for treating patients with BBS because there is currently no available targeted therapy. Complications associated with BBS are treated symptomatically, similarly to how they are treated or managed in the general population. Obesity was noted as highly prevalent in patients with BBS (72% to 92% of patients); it is thought to be driven by hyperphagia (insatiable appetite) caused by hypothalamic dysfunction leading to reduced MC4R activation. The clinician group commented that obesity is recognized as a complex, chronic, progressive, and relapsing condition.
The clinician group input stated that most available interventions for weight loss are complicated by hyperphagia, which is considered among the most distressing symptoms of BBS and associated with negative impacts on physical health, mental health, QoL, mobility, finances, activities of daily life, and judgment or discrimination. While environmental control interventions — such as food supervision, energy intake reduction, and meal schedules — are essential to managing and regulating weight for those with BBS, these interventions can be ineffective, unsustainable, and challenging to implement because these do not address persistent hyperphagia. The clinician group also noted that patient engagement in lifestyle interventions can be complicated by other coexisting issues related to BBS, such as low vision, difficulties in balance or coordination, intellectual disabilities, and mental health concerns.
According to the clinician group input, some pharmacologic therapies, such as liraglutide, are now approved for use in those with obesity aged 12 years and older. Semaglutide and naltrexone hydrochloride plus bupropion hydrochloride are approved for those aged 18 years and older. However, there is no evidence of the effectiveness or safety of these drugs in patients living with BBS. Also, these drugs do not address biologically driven hyperphagia. In addition, the safety, efficacy, and durability of the effects of bariatric surgery in this population remain largely unknown.
The clinician group indicated that the most essential obesity management goals include the prevention of weight-related health complications, including cardiometabolic risk, type 2 diabetes, abnormalities in lipid metabolism, nonalcoholic fatty liver disease, obstructive sleep apnea, musculoskeletal pain/discomfort, and difficulties with activities of daily living.
The clinician group input suggested that setmelanotide could serve as a part of the therapy plan, combined with lifestyle interventions for weight management, and could benefit patients with genetically confirmed BBS and obesity who are aged 6 years or older by addressing the underlying cause of hyperphagia. In the opinion of the clinician group, the treatment should be reassessed after 12 weeks to 16 weeks of therapy; if a decrease of 5% or greater in weight or baseline BMI has not been achieved, then the individual is unlikely to experience benefit from setmelanotide. It is unknown which individuals with BBS and obesity are most likely to respond to setmelanotide. The clinician group noted that setmelanotide should be discontinued during pregnancy and/or breastfeeding because the drug’s safety is unknown. Other reasons for discontinuation may include lack of response, presence of side effects, co-existent moderate to severe renal impairment, and contraindication. The clinician group reported that care of patients with BBS requires a multidisciplinary team approach, involving a physician who has expertise in weight management in consultation with other health care providers, such as ophthalmologists, nephrologists, endocrinologists, internal medicine specialists, gastroenterologists, primary care physicians, dietitians, and mental health care providers.
Drug Program Input
The drug programs provide input on each drug being reviewed through CADTH’s reimbursement review processes by identifying issues that may affect their ability to implement a recommendation. The implementation questions and corresponding responses from the clinical experts consulted by CADTH are summarized in Table 3.
Table 3: Summary of Drug Plan Input and Clinical Expert Response
Drug program implementation questions | Clinical experts’ responses |
|---|---|
Relevant comparators | |
The comparator in the submitted trial was a placebo, so there is no evidence comparing setmelanotide with other medications for weight loss. Is it possible that other medications for weight loss (e.g., liraglutide, semaglutide, naltrexone with bupropion, orlistat) would have been more appropriate comparators than placebo? (Public drug plans do not generally fund the previously noted drugs for weight loss. An exception is that orlistat is funded for obesity by the Canadian Armed Forces.) | Placebo is the most relevant comparator for weight loss in patients with BBS because there are no other pharmacotherapies currently studied for the treatment of this specific population, and setmelanotide is the first therapy that directly addresses the underlying cause of hyperphagia and obesity in BBS. There is no evidence available outside of case reports for the efficacy of other appetite-reducing drugs, such as semaglutide 2.4 mg in patients with BBS; additionally, semaglutide 2.4 mg is approved only in adult patients (i.e., those aged ≥ 18 years) in Canada. (Approval for an indication for adolescents aged 12 years and older is pending.) |
Considerations for the initiation of therapy | |
Patients included in the pivotal trial had a clinical diagnosis of BBS. Should patients require genetic (or other) testing to confirm BBS? If so, is such testing routinely available? | Although the majority of patients do pursue genetic confirmation of diagnosis, more BBS mutations may yet be discovered. As a result, there is a diversity of expert opinion on whether genetic testing should be required before treatment. In 1 approach, it is considered inappropriate to require patients to undergo genetic testing to access targeted therapies for BBS because of the possibility of currently unknown mutations. In another approach, genetic testing is always sought and is considered appropriate to confirm diagnosis of BBS. There is no genetic test available in Canada that includes all currently known BBS-causing mutations. While this test is commonly covered by the provincial MOH (through special application as an out-of-country test), the cost to the public system is nontrivial. | || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || | Given that BBS is a genetic ciliopathy that causes multisystem manifestations, clinical misdiagnosis is unlikely, although diagnosis may be delayed by the rarity of the disease and resulting lack of familiarity among physicians, by the progressive development of symptoms in childhood, and by stigma around obesity and hyperphagia. |
The exclusion criteria for the pivotal trial included:
Given the cost of setmelanotide, should patients be required to have insufficient clinical response to other interventions before access to therapy is provided? | Setmelanotide is considered the most clinically appropriate first-line therapy for patients with BBS who have hyperphagia and obesity because it is the only available therapy that targets the underlying disease mechanism of BBS. There is also a lack of data for other pharmacological therapies in the treatment of BBS outside of very few case studies. Behaviour modification, intensive dietary regimens, and exercise should be considered in combination with setmelanotide as first-line treatments. Notably, these nonpharmacological interventions are particularly challenging in this population due to the biologically driven hyperphagia, high prevalence of cognitive impairment and other comorbidities, and early-age onset of disease. As such, it is considered inappropriate to withhold or delay pharmacological treatment to trial behaviour and lifestyle modification alone. |
Considerations for discontinuation of therapy | |
The sponsor noted that a 10% reduction in body weight from baseline is clinically meaningful. The sponsor also noted that: “If an adult patient has not lost ≥ 5% of baseline body weight, or ≥ 5% of baseline BMI for patients aged less than 18 years, setmelanotide treatment should be discontinued as it is unlikely that the patient will achieve and sustain clinically meaningful weight loss with continued treatment.” How should clinically meaningful weight loss be defined? What duration of treatment is appropriate for assessing response to therapy? | The clinical experts noted that a 1-year trial period is reasonable for determining whether a patient is responding to setmelanotide. Meaningful response in the 1-year trial period would be a qualitative improvement in hunger and/or HRQoL, and a reduction of ≥ 5% in body weight in adults (aged ≥ 16 years) or ≥ 5% in BMI in pediatric patients (aged < 16 years). However, the measure of hunger and HRQoL are subjective, and the approaches must differ by age of patient and by the presence or absence of cognitive impairment. Lack of improvement in hyperphagia after 1 year of treatment would trigger consideration of discontinuing therapy. Additionally, there is diversity in clinical expert opinion on whether setmelanotide should be discontinued if the threshold of ≥ 5% reduction in weight or BMI has not been achieved after 1 year of treatment. In the opinion of some clinical experts, maintenance of weight instead of persistent weight gain is still an indicator of treatment response in circumstances where the patient would have otherwise been gaining weight if untreated, and if there are other benefits observed after 1 year, such as reduction in hyperphagia, improvement in HRQoL, and improvement in markers of metabolic health. Additionally, some experts expressed that continuation of setmelanotide and additional lifestyle changes and/or combination pharmacotherapy could be considered on a case-by-case basis. It is worth noting that the Health Canada–approved product monograph recommended that in patients with BBS, evaluation of weight loss should occur after 22 weeks of treatment with setmelanotide. If a patient has not lost at least 5% of baseline body weight (or 5% of baseline BMI for patients with continued growth potential), then discontinuation is recommended because it is unlikely that the patient will achieve and sustain clinically meaningful weight loss with continued treatment. |
Considerations for prescribing therapy | |
Which specialists should be responsible for overseeing therapy with setmelanotide? Are such specialists widely accessible? | The most common prescribing physicians for setmelanotide would likely be endocrinologists or pediatric endocrinologists. However, specialists in weight management may also prescribe. Ideally, an interdisciplinary team of specialist medical doctors, mental health professionals, and registered dieticians should oversee the care of patients with BBS. Access to some specialists or supports may be challenging because of geographic location or other circumstances. |
BBS = Bardet-Biedl syndrome; BMI = body mass index; HRQoL = health-related quality of life; MOH = Ministry of Health.
Clinical Evidence
The objective of CADTH’s Clinical Review Report is to review and critically appraise the clinical evidence submitted by the sponsor on the beneficial and harmful effects of setmelanotide 10 mg/mL solution in 1 mL, multiple-dose vials administered by SC injection for weight management in adult and pediatric patients aged 6 years and older with obesity due to BBS. The focus will be on comparing setmelanotide to relevant comparators and identifying gaps in the current evidence.
A summary of the clinical evidence included by the sponsor in the review of setmelanotide is presented in 2 sections, and CADTH’s critical appraisal of the evidence is included after each section. The first section, the systematic review, includes pivotal studies and randomized controlled trials (RCTs) that were selected according to the sponsor’s systematic review protocol. The second section includes a sponsor-submitted LTE study. There was no available indirect evidence, and no additional studies were included.
Included Studies
Clinical evidence from the following studies is included in the CADTH review and appraised in this document:
One pivotal study
One LTE study
Pivotal Studies and RCT Evidence
Contents within this section have been informed by materials submitted by the sponsor. The following information has been summarized and validated by the CADTH review team.
Description of Studies
Characteristics of the included studies are summarized in Table 4.
Table 4: Details of the Pivotal Study 023 Identified by the Sponsor
Study 023 (RM-493 to 023) | |
|---|---|
Designs and populations | |
Study design | A 52-week, phase III, open-label trial with a 14-week, randomized, double-blind, placebo-controlled period |
Locations | 12 sites in the US, Canada, the UK, France, and Spain |
Patient enrolment dates | Start: November 23, 2018 End: March 8, 2021 |
Randomized (N) | 52 patients in total: 44 patients with BBS and 8 patients with AS. 19 pivotal patients and 8 supplemental patients were randomized to setmelanotide; 17 pivotal and 6 supplemental patients were randomized to placebo. Among the patients with BBS (n = 44, including 32 pivotal and 12 supplemental), 22 patients were randomized to setmelanotide and 22 patients were randomized to placebo. Among pivotal patients with BBS, 16 patients were randomized to setmelanotide and 16 patients were randomized to placebo. |
Inclusion criteria | |
Exclusion criteria |
|
Drugs | |
Intervention | Setmelanotide 1 mg to 3 mg through once-daily subcutaneous injection with dose escalation |
Comparators | Matched placebo during the randomized controlled period, none during the open-label phases |
Study duration | |
Screening phase | 2 weeks to 3 weeks |
Dose escalation phase | Conducted during the 14-week randomized, placebo-controlled phase. The dose for all patients was retitrated after the randomized, placebo-controlled phase to maintain the blinding from that phase into the open-label phase. |
Treatment phase | Treatment up to 66 weeks, including the 14-week, double-blind, placebo-controlled phase |
Follow-up phase | Patients were eligible to enrol in a long-term extension study (RM493 to 022, NCT03651765). |
Outcomes | |
Primary end point | Proportion of pivotal patients aged ≥ 12 years at baseline treated with setmelanotide for ~52 weeks who achieved a clinically meaningful reduction in body weight from active treatment baseline (≥ 10%) |
Secondary and exploratory end points | Key secondary:
Other secondary:
Exploratory:
|
Publication status | |
Publications | Haqq et al. (2022)37 and Forsythe et al. (2023)20 NCT03746522 |
AS = Alström syndrome; BBS = Bardet-Biedl syndrome; BMI = body mass index; | || || || || || || | || || | || || |; IWQoL-Lite = Impact of Weight on Quality of Life – Lite; PedsQL = Pediatric Quality of Life Inventory; QoL = quality of life; | || || || || || || || || || || || || || || || || || || || || || || || || || || || .vs. = versus.
Source: Clinical Study Report for Study 023.9 Details in the table have been taken from the sponsor’s Summary of Clinical Evidence.
Study 023 included patients who were aged greater than or equal to 6 years, obese, and had a clinical diagnosis of BBS or a diagnosis of AS. These patients were randomized 1:1 through an interactive website response system to receive setmelanotide or matched-administration placebo for 14 weeks (period 1), followed by a 38-week period wherein all patients received open-label setmelanotide treatment (period 2) and then a 14-week period of open-label setmelanotide treatment (period 3) (Figure 1). Stratification was performed according to age group (≥ 12 years versus < 12 years) and disease (BBS versus AS).
Study 023 included 12 sites in Canada (1 site, 6 patients), the US (6 sites), France (2 sites), Puerto Rico (1 site), Spain (1 site), and the UK (1 site).
During the 14-week, double-blind treatment period, patients aged greater than or equal to 16 years were started on setmelanotide once daily through SC injection at 2 mg or matching placebo for 2 weeks. The target dose was increased to 3 mg SC once daily (or matching placebo) at the beginning of week 3 for the duration of the double-blind period.
Patients aged less than 16 years were started on setmelanotide 1 mg SC once daily or matching placebo during week 1. This dose was increased to 2 mg SC once daily or matching placebo at the beginning of week 2, and to 3 mg SC once daily or matching placebo at the beginning of week 3 for the duration of the double-blind period.
After the initial 14-week, double-blind treatment period, all patients immediately transitioned to open-label setmelanotide once daily through SC injection. To preserve the blind, all patients were restarted at their initial age-based dose and re-escalated to the 3 mg target dose. Thus, beginning at week 15, patients aged greater than or equal to 16 years received open-label setmelanotide 2 mg SC once daily for 2 weeks, followed by 3 mg SC once daily beginning at week 17 for the duration of the trial; and patients aged less than 16 years received open-label setmelanotide 1 mg SC once daily during week 15, 2 mg SC once daily during week 16, and 3 mg SC once daily beginning at week 17 for the duration of the trial.
Dose adjustment was not required for patients with mild to moderate renal impairment, although lower starting and target doses were used for patients with severe impairment. The exact values were not reported.
The primary analysis was performed after approximately 52 weeks of setmelanotide treatment; it is important to note that, as a result, patients initially randomized to placebo would require an evaluation at week 66 to reach approximately 52 weeks of setmelanotide treatment, as presented in Figure 1. Dose escalation was repeated for patients in both arms at the start of the 38-week, open-label period to maintain the blinding from during the placebo-controlled period. For the analysis of the primary end point and key secondary end points, baseline was defined as active treatment baseline (i.e., rather than as inclusion in the trial).
Populations
Inclusion and Exclusion Criteria
Study 023 included patients who were aged greater than or equal to 6 years, obese, and had a clinical diagnosis of BBS or a diagnosis of AS. Only the patients with BBS are relevant for the purposes of this review.
Patients with BBS were eligible for Study 023 if they had a clinical diagnosis of BBS based on Beales criteria. Patients were not required to have genetically confirmed diagnoses. Genetically confirmed BBS was defined as homozygous or compound heterozygous loss-of-function mutation in BBS genes. Patients were also required to be obese; obesity was measured using absolute BMI (≥ 30 kg/m2 for patients aged ≥ 16 years) or BMI percentile (≥ 97th on growth chart for patients aged 6 years to 15 years). Different measures of obesity and changes in weight were used for different age groups due to the confounding effects of normal weight gains during childhood growth and development.
Patients were considered ineligible if they had recent intensive diet or exercise therapy, recent or current medication related to obesity treatment, or gastric bypass surgery resulting in greater than 10% weight loss with no evidence of weight regain. These exclusion criteria were applied to avoid confounding of weight loss findings and to ensure that weight loss effects could be attributed to setmelanotide treatment. In addition, no specific guidance regarding diet or exercise was given during the trial, although it is possible that patients may have been familiar with, or may have previously attempted, lifestyle modifications to control body weight.
Figure 1: Schema for Study 023

Escal = escalation; SET = setmelanotide.
aDuring dose escalation, participants aged greater than or equal to 16 years receive setmelanotide 2 mg once daily for 2 weeks, increasing to 3 mg at the beginning of week 3; participants aged less than 16 years receive setmelanotide 1 mg once daily for the first week, 2 mg for the second week, and 3 mg at the beginning of week 3.
Source: Study 023 Clinical Study Report.9
Interventions
Patients enrolled in Study 023 received double-blind treatment using setmelanotide (in a mPEG-DSPE formulation) or a matched-administration vehicle placebo during the 14-week, randomized, double-blind, placebo-controlled period (period 1). The placebo formulation had similar excipients to the active formulation. The 2 treatments were indistinguishable: both were clear, colourless to slightly opalescent solutions essentially free of visible particles and were contained in identical vials. A placebo control arm was used because there are no approved treatments to control hunger and obesity in patients with BBS.
Both treatments were administered once daily through SC injection, with the setmelanotide dose started at a lower dose and then escalated toward a target of 3.0 mg/day to improve tolerability. Based on historical data that patients aged greater than or equal to 16 years have minimal (if any) height increase, a daily starting setmelanotide dose of 2.0 mg was selected for patients who were at least 16 years of age at the time of enrolment, with planned dose escalation to 3.0 mg after 2 weeks. As a measure of added caution for patients who were less than 16 years of age, the starting dose was lowered to 1.0 mg, with planned escalation to 2.0 mg at the end of week 1 and then to 3.0 mg at the end of week 2. Similarly, to maintain blinding, setmelanotide dose escalation was performed at the start of the 38-week, open-label period for all patients, regardless of whether they had originally been assigned to receive placebo or setmelanotide. Doses were not to be adjusted after the dose escalation phase unless discussed with and approved by the sponsor.
Patients and/or their caregivers were trained in SC injection (including through practice sessions and education materials) and were responsible for drawing up and administering setmelanotide (or matched placebo) at home in each morning. If patients or their caregivers were unable to successfully administer the drug, assistance was provided by a home health care practitioner. Patients and/or caregivers were given a drug diary to monitor compliance.
Outcomes
A list of efficacy end points assessed in this clinical review report are provided in Table 5. These end points are further summarized in this section. Summarized end points are based on those included in the sponsor’s Summary of Clinical Evidence along with any identified as important to this review, according to stakeholders (such as the clinical expert, clinician groups, or patient groups).
Body Weight
All body weight measurements were done in triplicate at regular time points. Whenever possible, the same scale was used throughout the trial, including at the screening visit, and calibrated on a regular basis. Weight was measured at approximately the same time at each visit and after fasting for at least 8 hours. Patients were to be in light clothing or underwear, with no shoes, and to have emptied their bladder.
Table 5: Outcomes Summarized From Study 023
Outcome measure | Time point | Study 023 |
|---|---|---|
Proportion of pivotal patients (aged ≥ 12 years) in the FAS population who achieve a ≥ 10% reduction from ATB in body weighta | After ~52 weeks of setmelanotide treatment (multiple imputation was used for patients who had not completed the 52-week assessment) | Primary |
Mean percent change in body weight for pivotal patientsa | After ~52 weeks of setmelanotide treatment | Key secondary |
Mean percent change in daily hunger score in pivotal patientsa | After ~52 weeks of setmelanotide treatment | Key secondary |
Proportion of pivotal patients who achieved a ≥ 25% reduction in weekly average of daily hunger scorea | After ~52 weeks of setmelanotide treatment | Key secondary |
Mean percent change in body weight for pivotal patients | After 14 weeks of treatment (placebo or setmelanotide) | Secondary |
Mean percent change in the weekly average of daily hunger score for pivotal patients | After 14 weeks of treatment (placebo or setmelanotide) | Secondary |
Change from baseline in waist circumference | After ~52 weeks of setmelanotide treatment | Exploratory |
Change from baseline in fasting lipids | After ~52 weeks of setmelanotide treatment | Exploratory |
Change and percent change | || || || || || || | scoresb | After ~52 weeks of setmelanotide treatment | Exploratory |
Change in IWQoL-Lite, PedsQL, and | || || || | After ~52 weeks of setmelanotide treatment | Exploratory |
Safety | After 14 weeks and ~52 weeks of setmelanotide treatment | Exploratory |
ATB = active treatment baseline; BMI = body mass index | || || || || || || || || || |; FAS = full analysis set; IWQoL-Lite = Impact of Weight on Quality of Life – Lite; PedsQL = Pediatric Quality of Life Inventory; | || || || || || || || || || || || || || || || || || || || || || || || || || || || .
aOutcomes were also assessed for patients who were aged 6 years to less than 12 years and for all patients regardless of age.
bResults for only the patients with BBS were not provided.
Source: Study 023 Clinical Study Report.9 Details in the table have been taken from the sponsor’s Summary of Clinical Evidence.
Height for Determination of BMI
Height was measured in centimetres, without shoes, using a wall-mounted stadiometer. All measurements were done in triplicate at regular time points. Height was used along with body weight to determine BMI at different time points in the trial.
Body Mass Index
BMI was calculated for all patients using the following formula: weight (kg) ÷ [height (m)].2 BMI accounts for linear growth, assessed by changes in height, observed in the pediatric population.
BMI z Score
The BMI z score was calculated for patients aged less than 18 years. The BMI z score indicates how many standard deviations a given patient’s BMI is from the normal mean of age-matched and sex-matched peers based on normative data from WHO.
BMI 95th Percentile Score
The percentage of the BMI 95th percentile score was calculated for patients aged less than 18 years. The percentage of the BMI 95th percentile score expresses the patient’s BMI as a percentage of the Centers for Disease Control and Prevention 95th percentile in age and sex-matched peers.
Daily Hunger Questionnaire
The daily hunger questionnaire (Figure 2) was administered to patients with no cognitive impairment (per the investigator’s judgment). Due to the unsuitability of using the hunger score tool in younger patients, this was administered only in patients greater than or equal to 12 years of age at baseline. The questionnaire assessed 3 aspects of hunger daily: average hunger in the last 24 hours, most or worst hunger in the last 24 hours, and morning hunger. Responses to the daily hunger questionnaire were recorded in an electronic diary. Each of the 3 items was scored separately (rather than combined) and averaged on a weekly basis.
In addition, hunger was assessed in patients aged 6 years to less than 12 years who were able to assess their own hunger using a pictorial (smiley face) version of the Likert rating scale, with scores from 0 to 4, where 0 = not hungry at all and 4 = hungriest possible. Data for this assessment were not reported because only a small number of patients completed this questionnaire.
In patients who were assessed as cognitively impaired, hunger was evaluated using | || || || || || || || || || || || || || |, a caregiver-completed questionnaire designed to assess behaviours associated with hunger in patients with | || || || || || || || || || | The | || || || was used in patients with BBS because there is no validated hunger assessment specifically for patients who have BBS with cognitive impairment, and patients with | || || | share many of the same obesity-related symptoms as those with BBS, including intense hunger.42 The | || || || was administered to caregivers of patients who were assessed as having cognitive impairment. The | || || || is a 10-item, observer-reported outcome measure designed by the sponsor to capture food-related behaviours commonly exhibited by people with | || || ||. As previously noted, the | || || || was used in patients with BBS because there is no validated hunger assessment tool specifically for patients with BBS who have cognitive impairment, and patients with | || | share many of the same obesity-related symptoms as those with BBS, including intense hunger.42
Items 1 to 5 of the | || || || address behaviours that are commonly exhibited more than once in a 24-hour period. These items are answered using a 4-point ordinal response scale ranging from “never” to “more than 4 times.” Items 6 to 10 address behaviours that are less common and potentially indicative of more severe hyperphagia and/or food-seeking behaviour; these items are answered using a dichotomous response scale (i.e., yes or no).
Responses to Items 1 to 5 were assigned scores of 0 (never), 1 (1 to 2 times), 2 (3 to 4 times), or 3 (more than 4 times) over the past 24 hours. Responses to items 6 to 10 were assigned scores of 0 (no) or 3 (yes). A total score was created as the average of the nonmissing items multiplied by 10, yielding a range from 0 to 30, with higher scores suggestive of more severe hyperphagia and/or food-related behaviours. To create weekly scores, the nonmissing daily | || || || total scores were averaged across predesignated 7-day periods. If more than 3 daily total scores were missing, the weekly score was set to missing for that individual. A copy of the | || || || is shown here (Figure 3).
Impact of Weight on IWQoL-Lite
The IWQoL-Lite was administered to patients aged greater than or equal to 18 years without cognitive impairment. The IWQoL-Lite is a validated, 31-item, self-reported, obesity-specific, QoL questionnaire that provides a total score inclusive of 5 domains: physical function, self-esteem, sex life, public distress, and work. The questionnaire is responsive to weight loss and gain and sensitive to both treatment-seeking status and the degree of obesity.43
Pediatric Quality of Life Inventory
The PedsQL was administered to children aged less than 18 years without cognitive impairment and their parent(s). The PedsQL Measurement Model is a validated modular approach to measuring HRQoL in healthy children and adolescents as well as those with acute and chronic health conditions. It is a 23-item reported measure with 4 domains: physical functioning, emotional functioning, social functioning, and school functioning. The total score is the mean score of the transformed items across the 4 domains. The PedsQL Measurement Model integrates both generic core scales and disease-specific modules into 1 measurement system, with instruments developed for children of specific age groups to self-report as well as parent proxies.8,44 The age-appropriate instrument was administered for children aged less than18 years and their parent(s).
| || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || | || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || | || || || || || || || || || || || || || || || || || || || || || || || || || | | || || || || || || || || || | || || || || || || || || || || || || || || || || || || || || || || || || || || || || | || || || || || || || || || || || || || || || || || || || || || || || ||
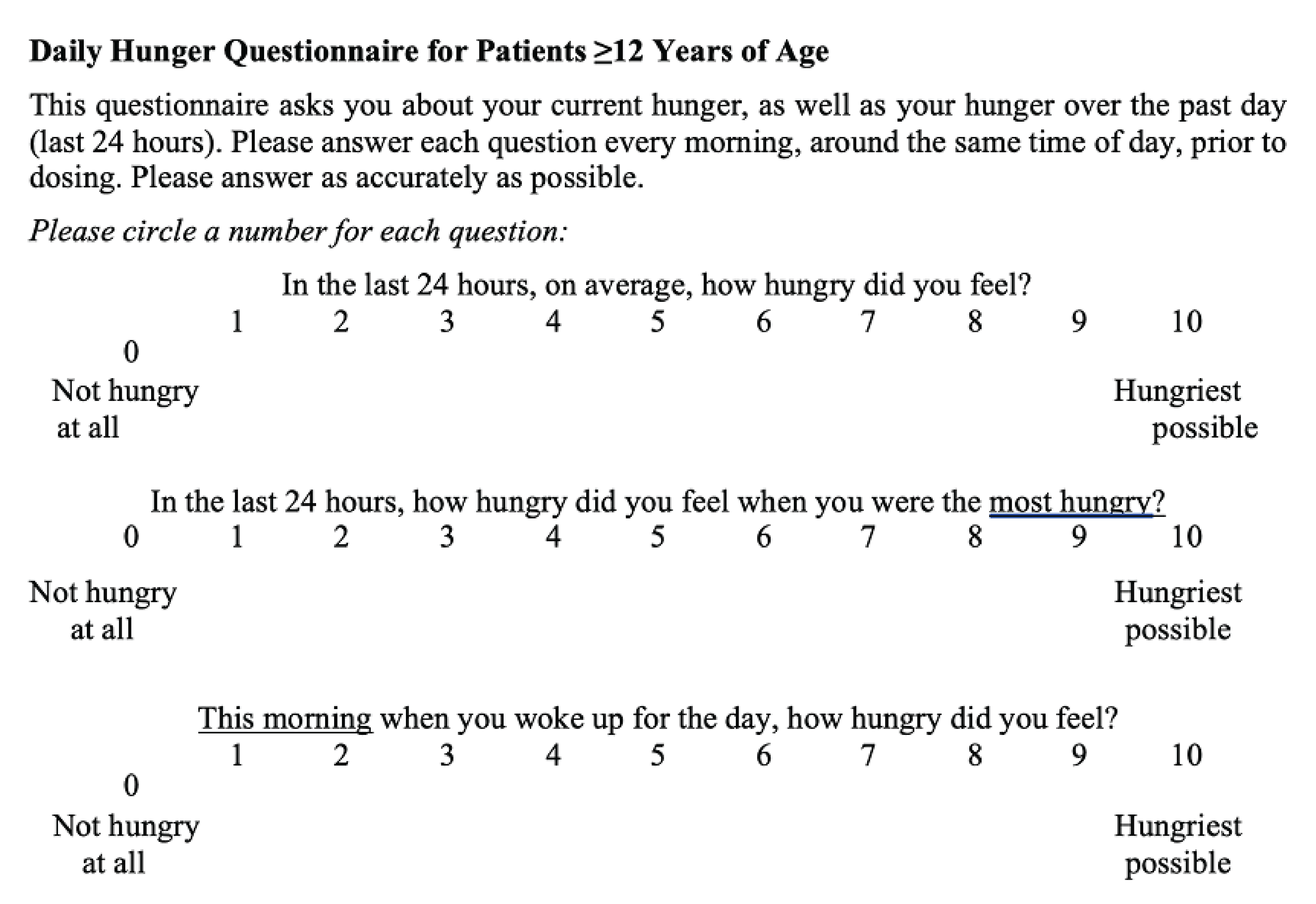
| || || || || | || || || || || || || || || || || || || || ||

Waist Circumference
Waist circumference (cm) was measured according to the National Heart, Lung, and Blood Institute criteria46 at regular time points. It was measured at approximately the same time at each visit when patients were fasting, wearing light clothing, and had emptied their bladder.
Lipid Profile
Blood samples for lipid profiles were collected at regular time points when patients were in the fasted state. The lipid profile included total cholesterol, high-density lipoprotein cholesterol, low-density lipoprotein cholesterol, and triglycerides.
Safety Assessments
Safety in patients with BBS was assessed by evaluating TEAEs, SAEs, and treatment discontinuations. Safety in the combined population of patients with BBS and AS was also assessed through physical, skin, and vital signs examinations, electrocardiograms, and clinical laboratory testing.
Table 6: Summary of Outcome Measures and Their Measurement Properties
Outcome measure | Type | Conclusions about measurement properties | MID |
|---|---|---|---|
Weight loss | Body weight:
BMI:
Proportion (of pediatric patients) in the 95th percentile of BMI according to age and sex BMI z score (for pediatric patients) | Not applicable; objective measurements | Clinically meaningful body weight loss is often defined as a decrease of > 5% in body weight in general obesity.47,48 The 95th percentile of BMI is commonly used as a threshold for obesity in children.49 For BMI z score in pediatric patients, reported MIDs range from −0.20 to −0.3 in general pediatric obesity.50-52 Although no specific MIDs have been developed regarding weight loss in patients with BBS, it is clinically plausible that the MIDs for weight loss in BBS would be the same as for the general population. This assumption was supported by the clinical experts consulted by CADTH. |
Daily hunger questionnaire | Mean change and mean percent change in weekly average of daily hunger score. The self-reported daily hunger questionnaire evaluated 3 aspects of hunger on an 11-point Likert scale, where 0 = not hungry at all and 10 = hungriest possible for each aspect:
Patients aged < 12 years could respond using a pictorial (smiley face) version, scoring from 0 (not hungry at all) to 4 (hungriest possible). Parents and caregivers could complete the questionnaire for patients who were unable to respond accurately due to age or cognitive dysfunction. | No literature validating the measurement properties of this questionnaire was identified. | Based on a psychometric analysis conducted by the sponsor (as recommended by the FDA patient-reported outcome guidance documents), a 1- to 2-point reduction (i.e., a 10% to 20% reduction) for the most or worst hunger score was considered a meaningful within-patient reduction. The sponsor selected a threshold of a 25% reduction in the weekly average of the daily hunger score as a key secondary outcome of interest. This was conservative relative to the sponsor-conducted analysis described here. There are no externally published estimations of MID for this outcome. |
| || || || || | | | || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || | | | || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || | | || || || || || || || || || || || || || || || || || || || || || || || || || || || || |
IWQoL-Lite | The IWQoL-Lite is a self-reported, 31-item measure of obesity-specific HRQoL with 5 domains:
Scores range from 0 to 100, with 100 representing the best HRQoL. | Validity, reliability, and responsiveness have been evaluated in populations with obesity, but not specifically in populations with BBS. Validity: strong convergent validity,54 discriminant validity,54 construct validity,43 and content validity55 in populations with general obesity. Reliability: strong internal consistency and test-retest results in a population with general obesity.43 Responsiveness: Demonstrated good responsiveness to change in weight in patients with general obesity.43 | There were no MIDs identified specific to patients with BBS. Published MIDs in patients with general obesity range from 7.7 points to 12 points.1,2 |
PedsQL Measurement Model | Self- or parent-reported HRQoL for children and adolescents and those with acute or chronic conditions. 4 components:
Summary scores:
Each item is scored on a 5-point Likert scale (0 to 4) where 0 = never a problem and 4 = almost always a problem. Components are transformed into 3 summary scores that range from to 0 to 100 in scale, with higher numbers correlating to better HRQoL. | Validity, reliability, and responsiveness to change have been documented as strong in several populations of both healthy children and children with acute or chronic health conditions (including type 1 and 2 diabetes) as well as in a general pediatric population aged 2 years to 16 years from 20,031 families enrolled in the California Children’s Health Insurance program.8 No literature specific to populations with BBS was identified. | No BBS-specific or obesity-specific MID has been identified. However, approximately 4.4 points (self-report) or 4.5 points (parent proxy report) were reported as the MIDs in a survey of children aged 2 years to 16 years from 20,031 families enrolled in the California Children’s Health Insurance program.8 |
BBS = Bardet-Biedl syndrome; BMI = body mass index; HRQoL = health-related quality of life; IWQoL-Lite = Impact of Weight on Quality of Life – Lite; MID = minimal important difference; PedsQL = Pediatric Quality of Life Inventory.
Statistical Analysis
Sample Size and Power Calculation
The sample size for Study 023 was driven by the primary hypothesis and rarity of the patient population. The primary hypothesis was that the proportion of pivotal patients experiencing a weight reduction of greater than or equal to 10% at 52 weeks would be greater than a historical control rate of 10% (refer to the Historical Control Response Rate section).
Early clinical data (from a phase II trial, RM-493 to 014, Study 014) regarding setmelanotide revealed that the anticipated response rate was 66% in patients with BBS or AS.39 Based on that response rate and a 1-sided alpha of 0.025, a sample of 7 patients would provide 91% power to detect a statistically significant difference versus the historical control rate. Nevertheless, to better understand the effect of setmelanotide in this rare patient population, the sponsor planned to enrol approximately 30 patients (including 6 patients with AS) for the pivotal cohort (i.e., all patients enrolled up to the sixth patient with AS), which ultimately included 38 patients (32 patients with BBS and 6 patients with AS).
A cohort of supplemental patients was added to the study protocol midcourse to gain additional treatment experience. The supplemental patients were not included in the primary analysis. Thus, a total of 52 patients were enrolled (44 with BBS and 8 with AS), including 14 supplemental patients. Note that the sample of patients with BBS included all 44 patients with BBS for the 14-week, double-blind, placebo-controlled period, but only 31 patients with BBS from the pivotal cohort had data to 52 weeks; thus, data from the 13 patients with BBS in the supplemental cohort were not included for the 52-week analyses. Pivotal patients were considered to have completed the study if they attended their week 66 visit, while supplemental patients were considered to have completed the study once they completed at least the week 24 visit, after which they were eligible to enrol in a separate LTE study (Study 022).
Historical Control Response Rate
CRIBBS (https://www.bbs-registry.org) is a global registry of patients with BBS that is housed at the Marshfield Research Center in Madison, Wisconsin and led by Dr. Robert Haws, principal investigator of the BBS cohort in Study 023. The registry aims to improve the understanding of BBS clinical features, progression, and management. Patients are assessed approximately once per year (during 1 to 4 annual visits), and data are collected through patient interviews, health provider assessments, and medical records. Approximately 500 patients with BBS from around the world have contributed data to the CRIBBS registry.
Rhythm Pharmaceuticals, Inc. received deidentified, individual patient data from the CRIBBS registry, including longitudinal body weight records, from 371 patients with BBS (aged 0 years to 68 years old, with approximately equal numbers of male and female patients). An analysis of baseline weight (i.e., at entry to the registry) showed that most adult patients with BBS were obese or extremely obese (43.1% and 32.1%, respectively), while only a small proportion were underweight or at normal weight (8.1%) (Table 7).
Table 7: Historical Obesity Data From Adult Patients (≥ 18 Years) With BBS in CRIBBS
Time point | Underweight (BMI < 18.5 kg/m2) | Normal weight (BMI 18.5 kg/m2 to 24.9 kg/m2) | Overweight (BMI 25 kg/m2 to 29.9 kg/m2) | Obese (BMI 30 kg/m2 to 39.9 kg/m2) | Extremely obese (BMI ≥ 40 kg/m2) |
|---|---|---|---|---|---|
Baseline | 1.5% (2 of 137) | 6.6% (9 of 137) | 16.8% (23 of 137) | 43.1% (59 of 137) | 32.1% (44 of 137) |
Year 1 | 1.8% (2 of 110) | 6.4% (7 of 110) | 21.8% (24 of 110) | 37.3% (41 of 110) | 32.7% (36 of 110) |
Year 2 | 0.0% (0 of 85) | 3.5% (3 of 85) | 20.0% (17 of 85) | 49.4% (42 of 85) | 27.1% (23 of 85) |
Year 3 | 0.0% (0 of 36) | 8.3% (3 of 36) | 19.4% (7 of 36) | 38.9% (14 of 36) | 33.3% (12 of 36) |
BBS = Bardet-Biedl syndrome; BMI = body mass index; CRIBBS = Clinical Registry Investigating Bardet-Biedl Syndrome.
Source: Study 023 Clinical Study Report.9 Details in the table have been taken from the sponsor’s Summary of Clinical Evidence.
To estimate the historical control response rate within the pivotal population age group (≥ 12 years), data for 1-year changes in weight were collected for patients with BBS who were greater than or equal to 12 years old (i.e., 153 patients contributing 313 one-year periods for the analysis). After applying a response criterion of greater than or equal to 10% weight lost over a 1-year period, the historical control response rate was calculated to be 6.4% of patients (Table 8). Lower 1-year historical control response rates were observed when the analyses were broadened to patients with BBS who were greater than 6 years of age (i.e., ≥ 5% decrease = 11.5% of patients; ≥ 7.5% decrease = 6.9% of patients; ≥ 10% decrease = 5.2% of patients), which likely reflects the natural growth and weight gain of pediatric patients. Therefore, the historical control response rate was set conservatively (i.e., numerically higher than the CRIBBS estimate) at 10% of patients with BBS who were greater than or equal to 12 years of age achieving a greater than or equal to 10% decrease in body weight.
The CRIBBS data received by the sponsor did not include any information regarding significant efforts to lose weight, although patients with BBS and obesity are encouraged to control and lose weight through diet and exercise; pharmacological and surgical approaches are occasionally used. The protocol for Study 023 also prohibited active diet or weight-loss interventions.
Table 8: Historical Control Response Rates for Categorical Weight Loss Thresholds Over a 1-Year Period
Time point | ≥ 5% decrease | ≥ 7.5% decrease | ≥ 10% decrease |
|---|---|---|---|
Baseline to year 1 | 17.0% (26 of 153) | 11.1% (17 of 153) | 7.2% (11 of 153) |
Year 1 to year 2 | 12.0% (13 of 108) | 5.6% (6 of 108) | 5.6% (6 of 108) |
Year 2 to year 3 | 13.5% (7 of 52) | 7.7% (4 of 52) | 5.8% (3 of 52) |
Across all years and all observations | 14.7% (46 of 313) | 8.6% (27 of 313) | 6.4% (20 of 313) |
Source: Study 023 Clinical Study Report.9 Details in the table have been taken from the sponsor’s Summary of Clinical Evidence.
Statistical Testing
The primary end point was the proportion of pivotal patients (i.e., all patients enrolled up to the sixth patient with AS; 32 patients with BBS and 6 patients with AS) aged greater than or equal to 12 years in the FAS who achieved a greater than or equal to 10% reduction in body weight after approximately 52 weeks of setmelanotide treatment.56 The primary and secondary analyses considered all pivotal patients regardless of disease (i.e., including pivotal patients with BBS and pivotal patients with AS);56 however, the sponsor conducted analyses of the BBS subpopulation in the same manner described herein, which is the primary focus of the review.57
The primary analysis was conducted with an exact binomial test with a 1-sided, 0.025 significance level and a 2-sided, 95% CI calculated using the exact Clopper-Pearson method. No formal test of the difference between BBS and AS was planned, although separate efficacy estimates were planned. Due to the small target sample size, no formal statistical analyses were planned to adjust for possible covariate effects.
The study had several key secondary end points planned for which a prespecified step-down procedure was used to control type I error for the each of the following key secondary analyses:
body weight percent change from baseline in patients greater than or equal to 12 years of age (mean percent change from baseline in body weight after approximately 52 weeks of treatment for patients in the FAS population)
daily hunger score percent change from baseline in patients greater than or equal to 12 years of age (mean percent change from baseline in the weekly average of daily hunger scores after approximately 52 weeks of treatment for patients in the FAS population)
daily hunger score reduction (threshold of 25%) in patients greater than or equal to 12 years of age (the proportion of patients in the FAS population who achieve a greater than or equal to 25% improvement from baseline in the weekly average of the daily hunger score after approximately 52 weeks of treatment).
However, this hierarchical testing procedure was specified for the primary analysis of the original study; thus, it cannot be applied to the posthoc analysis of patients with BBS, who are the focus of this review.
Additional secondary end points (body weight percent change from baseline at 14 weeks and daily hunger score percent change from baseline at 14 weeks) were analyzed in a similar manner. Exploratory end points, including PROs, were summarized using descriptive statistics and analyzed similarly to the primary, key secondary, and secondary end points as appropriate.
Because of the placebo-controlled period, analyses based on approximately 52 weeks of setmelanotide treatment used the active treatment baseline, which was defined as the last available measurement before the first dose of setmelanotide. It is important to note that as a result, pivotal patients randomized to receive placebo during the first 14-week period would not reach 52 weeks of active treatment until approximately week 66; some of these patients had not completed their week 66 visit at the time of the primary analysis. Therefore, the primary analysis included multiple imputation (linear mixed-effect model) to impute the weight measurements to a time point of approximately 52 weeks for patients with less than 52 weeks of active setmelanotide treatment. The final multiple imputed datasets were analyzed using Rubin’s rule.
The same multiple imputation approach was also performed for patients with missing values for reasons not related to study design (e.g., loss to follow-up, early dropout or discontinuation, missed visits). However, these imputed values were then set to the baseline value (i.e., no treatment effect) for the primary analysis, key secondary analyses, and exploratory analyses that were similar to the primary and key secondary analyses. A sensitivity analysis was planned, using the imputed values (i.e., no baseline replacement). For secondary and exploratory end points that were not similar to the primary or key secondary analyses, the imputed values were included in the analyzed dataset and were not replaced with the baseline values.
Subgroup Analyses
Formal subgroup analyses of the pivotal patient group (i.e., patients ≥ 12 years of age in the FAS) were not planned, given the small sample size of the study. However, separate descriptive statistics were provided according to the stratification factors (i.e., ≥ 12 years of age or less, BBS or AS). A separate report was also generated to describe the findings in patients with BBS as a posthoc analysis.
Analysis Populations
Analysis sets are summarized in Table 9.
Table 9: Data Sets Used for the Analyses in Study 023
Study | Population | Definition | Application |
|---|---|---|---|
Study 023 | SAS | All patients who received at least 1 dose of study drug (placebo or setmelanotide) | Safety summary |
FAS | All patients, regardless of age and initial randomization, who received ≥ 1 setmelanotide dose at any point during the study and had baseline data | Primary, secondary, and exploratory efficacy analyses | |
Pivotal population | All patients enrolled up to the sixth patient with AS (i.e., 32 patients with BBS and 6 patients with AS) who were ≥ 12 years of age in the FAS | Primary, secondary, and exploratory efficacy analyses | |
DUS | All patients in the FAS with ≥ 5 kg weight loss (or ≥ 5% if baseline weight < 100 kg) over the first 14 weeks of setmelanotide treatment, regardless of later disposition | Select secondary and exploratory efficacy analyses | |
PCS | All randomized patients during the 14-week, placebo-controlled period who had baseline data and received ≥ 1 dose of placebo or setmelanotide | Select secondary and exploratory efficacy analyses | |
Per-protocol set at end of period 1 | All patients in PCS without any major protocol violations | Select secondary and exploratory efficacy analyses | |
Per-protocol set at end of period 1 | All patients in FAS without any major protocol violations | Select secondary and exploratory efficacy analyses | |
Completers set | All patients in the per-protocol set at the end of period 1 who completed their assigned treatment during the 14-week, placebo-controlled period | Select secondary and exploratory efficacy analyses |
AS = Alström syndrome; BBS = Bardet-Biedl syndrome; DUS = designated use set; FAS = full analysis set; PCS = placebo-controlled set; SAS = safety analysis set.
Source: Study 023 Clinical Study Report.9 Details in the table have been taken from the sponsor’s Summary of Clinical Evidence.
Table 10: Statistical Analysis of Efficacy End Points in Study 023
End point | Age group | Statistical model | Adjustment factors | Missing data | Analysis set | Sensitivity sets | Baseline |
|---|---|---|---|---|---|---|---|
Primary analysis (~52 weeks of setmelanotide treatment) | |||||||
Proportion of patients who achieved a ≥ 10% reduction in body weight at ~52 weeks | ≥ 12 yearsa | Exact binomial test | None | Multiple imputation with linear mixed-effect model | FAS |
| ATB |
Key secondary analysis (~52 weeks of setmelanotide treatment) | |||||||
Mean percent change in body weight at ~52 weeks | ≥ 12 years of agea | 1-sample t test (i.e., setmelanotide vs. assumption of no treatment effect) | None | Multiple imputation with linear mixed-effect model | DUS | None | ATB |
Mean percent change in weekly average of daily hunger score | ≥ 12 years and without cognitive impairmenta | 1-sample t test (i.e., setmelanotide vs. assumption of no treatment effect) | None | Multiple imputation with linear mixed-effect model | DUS | None | ATB |
Proportion of patients who achieved a ≥ 25% reduction in weekly average of daily hunger score | ≥ 12 years of age and without cognitive impairmenta | 1-sample t test (i.e., setmelanotide vs. assumption of no treatment effect) | None | Multiple imputation with linear mixed-effect model | FAS | None | ATB |
Secondary analysis (after 14-week placebo-controlled period) | |||||||
Secondary end points after the 14-week placebo-controlled period | ≥ 12 years of agea | 2-sample t test (i.e., setmelanotide vs. placebo) | None | Multiple imputation with linear mixed-effect model | PCS |
| PCPB |
Exploratory analysis (after 14 weeks or 52 weeks, as appropriate) | |||||||
Various end points, including patient-reported outcomes | Specified in results | Descriptive statistics | None | None | FAS, PCS, or DUS | None | ATB or PCPB |
AG = active growth analysis set; ATB = active treatment baseline; CS = completers’ set; DUS = designated use set; FAS = full analysis set; PCPB = placebo-controlled period baseline; PCS = placebo-controlled analysis set; PPS at EOP1 = per-protocol set at end of period 1; PPS at EOP2 = per-protocol set at end of period 2; SH = stable height; vs. = versus.
Note: Multiplicity adjustment was not required for the primary analysis (a single primary end point) and was not used for secondary end points because of the rarity of the diseases and the small, expected sample size. Nominal P values were used to interpret each end point separately, although a step-down procedure (hierarchical order of testing) was prespecified to control type I error if needed.
aSubgroup analyses were also performed for patients less than 12 years of age as well as patients with BBS and patients with AS.
Source: Study 023 Clinical Study Report.9 Details in the table have been taken from the sponsor’s Summary of Clinical Evidence.
Results
Patient Disposition
A total of 60 patients with BBS or AS were screened, and 8 patients failed screening; among patients with BBS, 51 patients were screened and 44 were randomized to setmelanotide (N = 22) or placebo (N = 22). Reasons for screening failure were not identified in the Clinical Study Report.
Among patients with BBS, trial discontinuation was observed for 2 patients (9.1%) who were randomized to receive setmelanotide and for 6 patients (27.3%) who were randomized to receive placebo. One patient with BBS who was randomized to receive placebo discontinued the trial during the placebo-controlled, double-blind period and before completing active treatment baseline assessments. Therefore, this patient was included in the analyses of the placebo-controlled period, but not in the FAS for the approximately 52-week efficacy analyses.
Pivotal patients were considered to have completed the study if they attended their week 66 visit, while supplemental patients were considered to have completed the study once they had completed at least the week 24 visit, after which they were eligible to enrol in a separate LTE study (Study 022). Among patients with BBS, 90.9% of patients randomized to setmelanotide and 72.7% of those randomized to placebo completed the study.
Table 11: Summary of Patient Disposition for Patients With BBS From Study 023
Parameter | Overall | Pivotal | Supplemental | |||
|---|---|---|---|---|---|---|
Setmelanotide | Placebo | Setmelanotide | Placebo | Setmelanotide | Placebo | |
Screened | 51 | |||||
Randomized | 22 | 22 | 16 | 16 | 6 | 6 |
Completed trial, n (%) | 20 (90.9) | 16 (72.7) | 14 (87.5) | 12 (75.0) | 6 (100) | 4 (66.7) |
Discontinued trial, n (%) | 2 (9.1) | 6 (27.3) | 2 (12.5) | 4 (25.0) | 0 | 2 (3.33) |
Primary reason for early trial discontinuation | ||||||
AE, n (%) | 0 | 3 (13.6) | 0 | 3 (18.8) | 0 | 0 |
Death, n (%) | 0 | 0 | 0 | 0 | 0 | 0 |
Lack of efficacy, n (%) | 0 | 0 | 0 | 0 | 0 | 0 |
Lost to follow-up, n (%) | 1 (4.5) | 1 (4.5) | 1 (6.3) | 1 (6.3) | 0 | 0 |
Noncompliance with trial drug, n (%) | 0 | 0 | 0 | 0 | 0 | 0 |
Withdrawal by parent or guardian, n (%) | 0 | 0 | 0 | 0 | 0 | 0 |
Withdrawal by patient, n (%) | 1 (4.5) | 0 | 1 (6.3) | 0 | 0 | 0 |
Transfer to extension trial, n (%) | 0 | 2 (9.1)a | 0 | 0 | 0 | 2 (33.3)a |
AE = adverse event; BBS = Bardet-Biedl syndrome.
aSupplemental patients were considered completed if they enrolled in the extension trial; however, these 2 patients enrolled in the extension trial and were counted as discontinued.
Source: Clinical Study Report of patients with BBS from Study 023.10 Details in the table have been taken from the sponsor’s Summary of Clinical Evidence.
Baseline Characteristics
The baseline characteristics outlined in the following table are limited to those that are most relevant to this review or were felt to affect the outcomes or interpretation of the study results. Population sets included are the SAS (which includes both patients with BBS and patients with AS) and the cohort of patients with BBS (pivotal alone as well as pivotal plus supplemental) to reflect the various populations considered in the efficacy and safety results.
Among patients with BBS, a greater proportion were female in the placebo group (15 patients of 22 patients [68.2%]) than the setmelanotide group (9 patients of 44 patients [40.9%]). At the placebo-controlled baseline, the placebo group was slightly older than the setmelanotide group in terms of mean age. Weight, height, race, and BMI were similar at the placebo-controlled baseline between the 2 arms. There were more cognitively impaired patients in the placebo arm (14 patients of 22 patients [63.5%]) compared to the setmelanotide arm (10 patients of 22 patients [45.5%]).
Table 12: Summary of Baseline Characteristics in Study 023
Characteristic | Safety analysis set (BBS or AS) (N = 52) | Only patients with BBS (pivotal) (N = 32) | Only patients with BBS (pivotal + supplemental) (N = 44) | |||
|---|---|---|---|---|---|---|
Pivotal (n = 38) | Supplemental (n = 14) | Setmelanotide (n = 16) | Placebo (n = 16) | Setmelanotide (n = 22) | Placebo (n = 22) | |
Age at PCPB (years), mean (SD) | 19.8 (10.20) | 18.6 (13.21) | 19.1 (9.8) | 21.2 (10.7) | 18.5 (9.7) | 21.5 (12.6) |
< 12 years of age, n (%) | 5 (13.2) | 6 (42.9) | 2 (12.5) | 1 (6.3) | 4 (18.2) | 4 (18.2) |
< 17 years of age, n (%) | 19 (50.0) | 7 (50.0) | 9 (56.3) | 7 (43.8) | 12 (54.5) | 10 (45.5) |
Sex, n (%) | ||||||
Female | 23 (60.5) | 8 (57.1) | 7 (43.8) | 10 (62.5) | 9 (40.9) | 15 (68.2) |
Male | 15 (39.5) | 6 (42.9) | 9 (56.3) | 6 (37.5) | 13 (59.1) | 7 (31.8) |
Race, n (%) | ||||||
Asian | 1 (2.6) | 1 (7.1) | 0 | 0 | 0 | 1 (4.5) |
Black or African American | 3 (7.9) | 1 (7.1) | 0 | 1 (6.3) | 1 (4.5) | 1 (4.5) |
Other | 3 (7.9) | 5 (35.7) | 3 (18.8) | 0 | 6 (27.3) | 1 (4.5) |
White | 31 (81.6) | 7 (50.0) | 13 (81.3) | 15 (93.8) | 15 (68.2) | 19 (86.4) |
Clinically defined disease subgroup, n (%) | ||||||
BBS | 32 (84.2) | 12 (85.7) | 16 (100.0) | 16 (100.0) | 22 (100) | 22 (100) |
AS | 6 (15.8) | 2 (14.3) | NA | NA | NA | NA |
Cognitively impaired, n (%) | ||||||
No | 19 (50.0) | 11 (78.6) | 6 (37.5) | 9 (56.3) | 10 (45.5) | 14 (63.6) |
Yes | 19 (50.0) | 3 (21.4) | 10 (62.5) | 7 (43.8) | 12 (54.5) | 8 (36.4) |
Height in cm, mean (SD) | ||||||
PCPB | 162.31 (10.79) | 151.40 (19.05) | 164.34 (12.32) | 163.30 (9.89) | 161.70 (14.64) | 158.92 (14.38) |
ATB | 162.63 (10.89)a | 151.90 (18.61) | 164.34 (12.32) | 163.57 (9.96) | 161.70 (14.64) | 159.25 (14.07) |
Weight in kg, mean (SD) | ||||||
PCPB | 111.67 (30.41) | 97.25 (43.54) | 113.43 (30.06) | 111.22 (26.43) | 110.45 (35.8) | 106.5 (31.8) |
ATB | 112.00 (31.00)a | 97.86 (42.90) | 113.43 (30.06) | 112.37 (27.12) | 110.45 (35.81) | 107.54 (31.86) |
BMI in kg/m2, mean (SD) | ||||||
PCPB | 42.25 (11.03) | 40.51 (11.67) | 41.72 (9.71) | 41.55 (8.54) | 41.4 (10.0) | 41.6 (10.1) |
ATB | 42.18 (11.14)a | 40.61 (11.58) | 41.72 (9.71) | 41.78 (8.53) | 41.35 (10.02) | 41.87 (10.05) |
AS = Alström syndrome; ATB = active treatment baseline; BBS = Bardet-Biedl syndrome; BMI = body mass index; PCPB = placebo-controlled period baseline; NA = not applicable; SD = standard deviation.
aCalculated for 36 patients in the pivotal group with ATB data.
Sources: Study 023 Clinical Study Report;9 the report of patients with BBS from Study 023;10 the sponsor’s response to the CADTH request for additional information.57 Details in the table have been taken from the sponsor’s Summary of Clinical Evidence.
Exposure to Study Treatments
Treatment exposure is summarized for the double-blind, placebo-controlled treatment period in Table 13 and for the full study period in Table 14. The median total setmelanotide exposure was 258 mg over the 14-week, double-blind, placebo-controlled period. Similar numbers of doses were administered during that period in the setmelanotide and placebo groups. The median total setmelanotide exposure during the full study was | || || || || || || | for all patients and for patients with BBS. During the study period, 5 patients had dose reductions (setmelanotide = 2 patients; placebo = 3 patients) after discussion with and approval by the sponsor. However, 4 of these patients resumed the full 3.0 mg dosage following a brief reduction. All patients with BBS were titrated to a therapeutic dose of 3 mg daily.
Medications for treating general obesity (e.g., orlistat, lorcaserin, phentermine-topiramate, naltrexone-bupropion) were not allowed within 3 months of randomization and were prohibited during the study. Use of a GLP1 receptor agonist was permitted up to the dose approved for the treatment of diabetes mellitus as long as 4 conditions were met: it was not prescribed for the treatment of obesity; the dose had been stable for at least 3 months before randomization; the patient had not experienced weight loss during the previous 3 months; and the patient intended to keep the dose stable throughout the course of the study. One patient (1.9% of the SAS population) who was initially randomized to the setmelanotide group in the supplemental cohort had received semaglutide (a GLP1 receptor agonist) as a prior or concomitant medication (not specified in the Clinical Study Report).
| || || || || || || | | | || || || || || || | | | || || || || || || | | | || || || || || || | |
|---|---|---|---|
| || || || || || || | | |||
| || || || || || || | | | || || || || || || | | | || || || || || || | | | || || || || || || | |
| || || || || || || | | | || || || || || || | | | || || || || || || | | | || || || || || || | |
| || || || || || || | | | || || || || || || | | | || || || || || || | | | || || || || || || | |
| || || || || || || | | |||
| || || || || || || | | | || || || || || || | | | || || || || || || | | | || || || || || || | |
| || || || || || || | | | || || || || || || | | | || || || || || || | | | || || || || || || | |
| || || || || || || | | | || || || || || || | | | || || || || || || | | | || || || || || || | |
| || || || || || || | | |||
| || || || || || || | | | || || || || || || | | | || || || || || || | | | || || || || || || | |
| || || || || || || | | | || || || || || || | | | || || || || || || | | | || || || || || || | |
| || || || || || || | | | || || || || || || | | | || || || || || || | | | || || || || || || | |
| || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || |
| || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || |
Source: Study 023 Clinical Study Report.9 Details in the table have been taken from the sponsor’s Summary of Clinical Evidence.
| || || || || || || | | | || || || || || || | | | || || || || || || | |
|---|---|---|
| || || || || || || | | ||
| || || || || || || | | | || || || || || || | | | || || || || || || | |
| || || || || || || | | | || || || || || || | | | || || || || || || | |
| || || || || || || | | | || || || || || || | | | || || || || || || | |
| || || || || || || | | | || || || || || || | | | || || || || || || | |
| || || || || || || | | | || || || || || || | | | || || || || || || | |
| || || || || || || | | ||
| || || || || || || | | | || || || || || || | | | || || || || || || | |
| || || || || || || | | | || || || || || || | | | || || || || || || | |
| || || || || || || | | | || || || || || || | | | || || || || || || | |
| || || || || || || | | | || || || || || || | | | || || || || || || | |
| || || || || || || | | | || || || || || || | | | || || || || || || | |
| || || || || || || | | ||
| || || || || || || | | | || || || || || || | | | || || || || || || | |
| || || || || || || | | | || || || || || || | | | || || || || || || | |
| || || || || || || | | | || || || || || || | | | || || || || || || | |
| || || || || || || | | | || || || || || || | | | || || || || || || | |
| || || || || || || | | | || || || || || || | | | || || || || || || | |
| || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || |
| || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || | || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || | || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || |
Source: Study 023 Clinical Study Report.9 Details in the table have been taken from the sponsor’s Summary of Clinical Evidence.
Table 15: Prior and Concomitant Medications Used Throughout Study 023 by Patients With BBS or AS (> 10% of Total Patients)
Parameter, n (%) | Setmelanotide (N = 27) | Placebo (N = 25) | Total (N = 52) |
|---|---|---|---|
Patients with ≥ 1 concomitant medication | 27 (100.0) | 25 (100.0) | 52 (100.0) |
Vitamin D and analogues | 14 (51.9) | 15 (60.0) | 29 (55.8) |
Angiotensin-converting enzyme inhibitors | 4 (14.8) | 10 (40.0) | 14 (26.9) |
Anilides | 7 (25.9) | 7 (28.0) | 14 (26.9) |
Osmotically acting laxatives | 5 (22.2) | 7 (20.0) | 11 (21.2) |
Biguanides | 3 (11.1) | 6 (28.0) | 10 (19.2) |
Combinations of vitamins | 4 (14.8) | 5 (20.0) | 9 (17.3) |
Corticosteroids | 5 (14.8) | 5 (20.0) | 9 (17.3) |
Selective beta2-adrenoreceptor agonists | 3 (11.1) | 6 (24.0) | 9 (17.3) |
Progestogens and estrogens, fixed combinations | 3 (11.1) | 5 (20.0) | 8 (15.4) |
Thyroid hormones | 4 (14.8) | 4 (16.0) | 8 (15.4) |
Glucocorticoids | 2 (7.4) | 5 (20.0) | 7 (13.5) |
Other antihistamines for systemic use | 4 (14.8) | 3 (12.0) | 7 (13.5) |
Aminoalkyl ethers | 4 (14.8) | 2 (8.0) | 6 (11.5) |
Corticosteroids, weak (group I) | 3 (11.1) | 3 (12.0) | 6 (11.5) |
AS = Alström syndrome; BBS = Bardet-Biedl syndrome.
Source: Study 023 Clinical Study Report.9 Details in the table have been taken from the sponsor’s Summary of Clinical Evidence.
At least 1 concomitant procedure was performed for 44% of patients (n = 23 patients of 52 patients) in the SAS population (setmelanotide = 37% [n = 10 patients of 27 patients]; placebo = 52% [n = 13 patients of 25 patients]). The only concomitant procedures performed for greater than 10% of patients were limb operations (11.5%; n = 6 patients of 52 patients). No patients underwent any form of bariatric surgery before or during the study.
No subsequent treatment was mandated after patients completed their setmelanotide treatments.
Efficacy
Primary End Point: Proportion of Patients Achieving a Reduction in Body Weight Greater Than or Equal to 10% After 52 Weeks of Setmelanotide
Among pivotal patients with BBS (N = 28), 35.7% (95% CI, 18.6% to 55.9%) had a greater than or equal to 10% reduction in body weight after 52 weeks of setmelanotide treatment, as measured from the active treatment baseline. Results were similar when considering both pivotal and supplemental patients with BBS. The numbers achieving this in both groups exceeded the prespecified assumption that 10% of patients with BBS would achieve a body weight reduction of greater than or equal to 10% without treatment.
Table 16: Proportion of Patients (Aged ≥ 12 Years) With Greater Than or Equal to 10% Reduction in Body Weight After 52 Weeks of Setmelanotide Treatment
Statistica | Patients with BBS (pivotal, aged ≥ 12 years) | Patients with BBS (pivotal + supplemental, aged ≥ 12 years) |
|---|---|---|
N | 28b | 35c |
Estimated % | 35.7 | 33.7 |
95% CIa | (18.6 to 55.9) | (16.9 to 50.6) |
P valuea | 0.0002 | 0.0029 |
BBS = Bardet-Biedl syndrome; CI = confidence interval.
aThe estimated percentage, 95% CI, and P value are based on Rubin's Rule. The P value is 1-sided, based on testing the prespecified assumption of 10% of patients with BBS achieving a greater than or equal to 10% reduction in body weight without treatment. Multiplicity adjustment was not conducted. Values are from the posthoc analysis of BBS patients and should be used for descriptive purposes only.
bSix patients (19.35% of the full pivotal population, 21.42% of pivotal BBS population) had missing measurements at 52 weeks due to study discontinuation and were conservatively considered to have treatment failure.
cN value provided by sponsor in response to CADTH request for additional information.58
Sources: Study 023 Clinical Study Report9 and the report of patients with BBS from Study 023.10
Key Secondary End Point: Mean Percent Change in Body Weight After 52 Weeks of Setmelanotide
At 52 weeks, the mean and percent changes in weight among pivotal patients with BBS (N = 28) were −7.24 kg (SD = 8.208 kg; 95% CI, −10.60 kg to −4.24 kg) and −6.47% (SD = 6.970%; 95% CI, −9.17% to −3.77%), respectively. Results considering both pivotal and supplemental patients were similar. Both were greater than the background assumption of no treatment effect in untreated patients with BBS.
Key Secondary End Point: Mean Percent Change in Weekly Average of the Daily Hunger Score After 52 Weeks of Setmelanotide
Among pivotal patients aged greater than or equal to 12 years with BBS and no cognitive impairment (N = 14), the mean percent change in hunger score after 52 weeks of setmelanotide treatment was −31.80% (95% CI, −48.81% to −14.79%). Similar results were observed among the group of pivotal plus supplemental patients with BBS for most or worst hunger over 24 hours and for morning hunger scores (Table 18).
Based on a psychometric analysis of the Study 023 data, which was conducted as recommended in US FDA PRO guidance documents, a 1-point to 2-point reduction (i.e., a 10% to 20% reduction) for the most or worst hunger score was considered a meaningful within-patient reduction by the sponsor. Among pivotal patients with BBS in Study 023 (aged ≥ 12 years old without cognitive impairment), 71.4% of patients experienced a greater than or equal to 1-point reduction, and 42.9% of patients experienced a greater than or equal to 2-point reduction.
Table 17: Body Weight Change and Percent Change From ATB in Patients (Aged ≥ 12 Years) After 52 Weeks of Setmelanotide Treatment
Statistic | Patients with BBS (pivotal, aged ≥ 12 years) | Patients with BBS (pivotal + supplemental, aged ≥ 12 years) |
|---|---|---|
Change after 52 weeks (kg) | ||
Na | 28 | 35 |
Mean (SD) | −7.42 (8.208) | −7.51 (8.067) |
95% CI | −10.60 to −4.24 | −10.36 to −4.66 |
P valueb | < 0.0001 | < 0.0001 |
Percent change after 52 weeks (%) | ||
Na | 28 | 35 |
Mean (SD) | −6.47 (6.970) | −6.44 (6.795) |
95% CI | −9.17 to −3.77 | −8.83 to −4.05 |
P valueb | < 0.0001 | < 0.0001 |
ATB = active treatment baseline; BBS = Bardet-Biedl syndrome; CI = confidence interval; SD = standard deviation.
aSix patients (19.35%) had missing measurements at 52 weeks due to study discontinuation. Their percent change was considered as 0.
bThe P value is 1-sided, based on Rubin’s rule testing the assumption of no change from baseline. Multiplicity adjustment was not conducted. Values are from the posthoc analysis of BBS patients and should be used for descriptive purposes only.
Sources: Study 023 Clinical Study Report9 and the report of patients with BBS from Study 023.10
Key Secondary End Point: Proportion of Patients Achieving a Greater Than or Equal to 25% Improvement in the Weekly Average of Daily Hunger Scores After 52 Weeks of Setmelanotide
An estimated 57.1% (95% CI, 28.9 to 82.3) of pivotal patients with BBS (aged ≥ 12 years old without cognitive impairment; N = 14) achieved a greater than or equal to 25% improvement in the weekly average | || || || || || || || || || || || (most or worst score over 24 hours, | || || || || || || || || || || || || || || || || || || || | after 52 weeks of setmelanotide treatment (Table 18).
Secondary End Point: Mean Percent Change From Baseline in Body Weight After 14 Weeks of Setmelanotide Compared With Placebo
In the placebo-controlled analysis of pivotal patients with BBS aged greater than or equal to 12 years, those receiving setmelanotide (N = 14) had an estimated reduction in mean body weight compared to patients receiving placebo (N = 15) (difference = −3.81 kg; 95% CI, −7.03 kg to −0.58 kg). Patients receiving setmelanotide also had a greater mean body weight percent change than those receiving placebo (difference = −2.96%; 95% CI, −5.65% to −0.26%). | || || || || || || || || || || || || || || || || || || || || || || || || || || || |
Notably, patients receiving placebo had very little change in body weight over the 14-week RCT period (mean = −0.21 kg or −0.25% in the pivotal cohort of patients with BBS, | || || || || || || || || || || || || || || || || || || || || |).
Table 18: Change in the Weekly Average of Daily Hunger Score From ATB After 52 Weeks of Setmelanotide Treatment Among Patients (Aged ≥ 12 Years) Without Cognitive Impairment
Statistica | Patients with BBS (pivotal, aged ≥ 12 years) | | || || || || || || || || || || || || || || || || || || || || | | ||||
|---|---|---|---|---|---|---|
| || || || || || || || || || || || || || | | Most or worst hunger over 24 hours | | || || || || || || | | | || || || || || || || || || || || || || | | | || || || || || || || || || || || || || | | | || || || || || || | | |
Weekly average changeb,c,d | ||||||
N | | || || || || || || | | 14 | | || || || || || || | | | || || || || || || | | | || || || || || || | | | || || || || || || | |
Mean (SD) | | || || || || || || | | −2.12 (2.051) | | || || || || || || | | | || || || || || || | | | || || || || || || | | | || || || || || || | |
Median | | || || || || || || | | −1.69 | | || || || || || || | | | || || || || || || | | | || || || || || || | | | || || || || || || | |
95% CIa | | || || || || || || | | −3.31 to −0.94 | | || || || || || || | | | || || || || || || | | | || || || || || || | | | || || || || || || | |
P valuea | | || || || || || || | | 0.0010 | | || || || || || || | | | || || || || || || | | | || || || || || || | | | || || || || || || | |
Weekly average percent changeb,c,d | ||||||
N | | || || || || || || | | 14 | | || || || || || || | | | || || || || || || | | | || || || || || || | | | || || || || || || | |
Mean (SD) | | || || || || || || | | −30.45 (26.485) | | || || || || || || | | | || || || || || || | | | || || || || || || | | | || || || || || || | |
Median | | || || || || || || | | −25.00 | | || || || || || || | | | || || || || || || | | | || || || || || || | | | || || || || || || | |
95% CIa | | || || || || || || | | −45.74 to −15.16 | | || || || || || || | | | || || || || || || | | | || || || || || || | | | || || || || || || | |
P valuea | | || || || || || || | | 0.0004 | | || || || || || || | | | || || || || || || | | | || || || || || || | | | || || || || || || | |
Proportion of patients achieving ≥ 25% improvement in weekly average of daily hunger scoresb,c,d | ||||||
Estimated %a | | || || || || || || | | 57.1 | | || || || || || || | | | || || || || || || | | | || || || || || || | | | || || || || || || | |
95% CIa | | || || || || || || | | (28.9 to 82.3) | | || || || || || || | | | || || || || || || | | | || || || || || || | | | || || || || || || | |
P valuea | | || || || || || || | | < 0.0001 | | || || || || || || | | | || || || || || || | | | || || || || || || | | | || || || || || || | |
ATB = active treatment baseline; BBS = Bardet-Biedl syndrome; CI = confidence interval; SD = standard deviation.
aThe estimated percentage, 95% CI, and P values are based on Rubin’s rule. The P values for change and percent change were testing the assumption of no change from baseline; the key secondary end point (percent change after 52 weeks) was analyzed first in the prespecified hierarchy at alpha = 0.025. The P values for the proportion of patients achieving a greater than or equal to 25% improvement were calculated against a reference value of 10%. Multiplicity adjustment was not conducted. Values are from the posthoc analysis of BBS patients and should be used for descriptive purposes only.
bIf there were missing measurements after 52 weeks, a multiple imputation model was used to impute the measurements for patients with fewer than 52 weeks of setmelanotide treatment to a time point that approximated 52 weeks of setmelanotide treatment.
cIf there were missing measurements after 52 weeks due to a reason other than study design, the patient was considered to have failed treatment.
dThree patients (18.75%) had missing measurements at 52 weeks due to study discontinuation and were considered to have a percent change of 0.
Sources: Study 023 Clinical Study Report9 and the report of patients with BBS from Study 023.10
Table 19: Body Weight Change and Percent Change From Placebo-Controlled Period Baseline After 14 Weeks of Treatment
Statistica | Patients with BBS (pivotal, aged ≥ 12 years)b | | || || || || || || || || || || || || || | | ||
|---|---|---|---|---|
Setmelanotide | Placebo | | || || || || || || | | | || || || || || || | | |
Mean body weight at PCPB | ||||
N | 14 | 15 | | || || || || || || | | | || || || || || || | |
Mean (SD) | 119.27 (25.796) | 111.63 (27.308) | | || || || || || || | | | || || || || || || | |
Median | 120.48 | 113.77 | | || || || || || || | | | || || || || || || | |
Min, max | 68.1, 173.8 | 70.7, 166.0 | | || || || || || || | | | || || || || || || | |
Mean body weight change from PCPB after 14 weeks of treatment | ||||
N | 14 | 15 | | || || || || || || | | | || || || || || || | |
Mean (SD) | −4.02 (5.312) | −0.21 (2.890) | | || || || || || || | | | || || || || || || | |
Median | −3.20 | 0.40 | | || || || || || || | | | || || || || || || | |
95% CI | −7.08 to −0.95 | −1.81 to 1.39 | | || || || || || || | | | || || || || || || | |
Differencea | −3.81 | | || || || || || || | | ||
95% CI of differencea | −7.03 to −0.58 | | || || || || || || | | ||
P valuea | 0.0113 | | || || || || || || | | ||
Mean body weight percent change from PCPB after 14 weeks of treatment | ||||
N | 14 | 15 | | || || || || || || | | | || || || || || || | |
Mean (SD) | −3.21 (4.474) | −0.25 (2.353) | | || || || || || || | | | || || || || || || | |
Median | −2.77 | 0.32 | | || || || || || || | | | || || || || || || | |
95% CI | −5.79 to −0.62 | −1.55 to 1.05 | | || || || || || || | | | || || || || || || | |
Differencea | −2.96 | | || || || || || || | | ||
95% CI of differencea | −5.65 to −0.26 | | || || || || || || | | ||
P valuea | 0.0164 | | || || || || || || | | ||
BBS = Bardet-Biedl syndrome; CI = confidence interval; PCPB = placebo-controlled period baseline; SD = standard deviation.
Note: P values were calculated for each end point without adjustment for multiplicity.
aDifference, 95% CI of difference, and P value are based on Rubin’s rule, and difference is calculated as setmelanotide minus placebo. Multiplicity adjustment was not conducted. Values are from the posthoc analysis of BBS patients and should be used for descriptive purposes only.
bIf there were missing measurements after approximately 14 weeks, a multiple imputation model was used to impute the measurements for patients with fewer than approximately 14 weeks of setmelanotide or placebo treatment to a time point that approximated 14 weeks of setmelanotide or placebo treatment.
Sources: Study 023 Clinical Study Report9 and the report of patients with BBS from Study 023.10
Secondary End Point: Mean Percent Change in the Weekly Average of the Daily Hunger Score After 14 Weeks of Setmelanotide Treatment in Comparison to Placebo
Pivotal patients with BBS treated with setmelanotide (N = 5) had an estimated reduction in hunger score compared with patients treated with placebo (N = 9) in | || || || || || || || || || || || || || | and in most or worst hunger over 24 hours (percent change) (Table 20). However, results were inconclusive for some metrics of hunger due to wide 95% CIs that included the null value: | || || || || || || || || || || || || || || || || most or worst hunger over 24 hours (mean change) and | || || || || || || || || || || || || || |
Table 20: Change in the Weekly Average of Daily Hunger Score From Placebo-Controlled Period Baseline After 14 Weeks Among Patients (Aged ≥ 12 Years) With No Cognitive Impairment in Placebo-Controlled Analysis
Statistica | | || || || || || || || || || || || || || |b | Patients with BBS (pivotal + supplemental, aged ≥ 12 years)b,c | ||
|---|---|---|---|---|
| || || || || || || | | | || || || || || || | | Setmelanotide | Placebo | |
| || || || || || || || || || || || || || | | ||||
N | | || || || || || || | | | || || || || || || | | | || || || || || || | | | || || || || || || | |
Mean change (SD) | | || || || || || || | | | || || || || || || | | | || || || || || || | | | || || || || || || | |
95% CIa | | || || || || || || | | | || || || || || || | | | || || || || || || | | | || || || || || || | |
Differenceb | | || || || || || || | | | || || || || || || | | ||
95% CI of differenceb | | || || || || || || | | | || || || || || || | | ||
P valueb | | || || || || || || | | | || || || || || || | | ||
| || || || || || || || || || || || || | || || || || || || | | | ||||
N | | || || || || || || | | | || || || || || || | | | || || || || || || | | | || || || || || || | |
Mean change (SD) | | || || || || || || | | | || || || || || || | | | || || || || || || | | | || || || || || || | |
95% CIa | | || || || || || || | | | || || || || || || | | | || || || || || || | | | || || || || || || | |
Differenceb | | || || || || || || | | | || || || || || || | | ||
95% CI of differenceb | | || || || || || || | | | || || || || || || | | ||
P valueb | | || || || || || || | | | || || || || || || | | ||
| || || || || || || || || || || || || || || || || || || || || | | ||||
N | | || || || || || || | | | || || || || || || | | | || || || || || || | | | || || || || || || | |
Mean change (SD) | | || || || || || || | | | || || || || || || | | | || || || || || || | | | || || || || || || | |
95% CIa | | || || || || || || | | | || || || || || || | | | || || || || || || | | | || || || || || || | |
Differenceb | | || || || || || || | | | || || || || || || | | ||
95% CI of differenceb | | || || || || || || | | | || || || || || || | | ||
P valueb | | || || || || || || | | | || || || || || || | | ||
Most or worst hunger over 24 hours (percent change) | ||||
N | | || || || || || || | | | || || || || || || | | 6 | 12 |
Mean change (SD) | | || || || || || || | | | || || || || || || | | −30.09 (20.264) | −15.71 (14.513) |
95% CIa | | || || || || || || | | | || || || || || || | | −51.35 to −8.82 | −24.93 to −6.48 |
Differenceb | | || || || || || || | | −14.38 | ||
95% CI of differenceb | | || || || || || || | | −31.90 to 3.14 | ||
P valueb | | || || || || || || | | 0.0505 | ||
| || || || || || || || || || || || || || | | ||||
N | | || || || || || || | | | || || || || || || | | | || || || || || || | | | || || || || || || | |
Mean change (SD) | | || || || || || || | | | || || || || || || | | | || || || || || || | | | || || || || || || | |
95% CIa | | || || || || || || | | | || || || || || || | | | || || || || || || | | | || || || || || || | |
Differenceb | | || || || || || || | | | || || || || || || | | ||
95% CI of differenceb | | || || || || || || | | | || || || || || || | | ||
P valueb | | || || || || || || | | | || || || || || || | | ||
Morning Hunger (Percent Change) | ||||
N | | || || || || || || | | | || || || || || || | | | || || || || || || | | | || || || || || || | |
Mean change (SD) | | || || || || || || | | | || || || || || || | | | || || || || || || | | | || || || || || || | |
95% CIa | | || || || || || || | | | || || || || || || | | | || || || || || || | | | || || || || || || | |
Differenceb | | || || || || || || | | | || || || || || || | | ||
95% CI of differenceb | | || || || || || || | | | || || || || || || | | ||
P valueb | | || || || || || || | | | || || || || || || | | ||
AS = Alström syndrome; BBS = Bardet-Biedl syndrome; CI = confidence interval; pcgh = percent change; PCPB = placebo-controlled period baseline; SD = standard deviation.
Notes: PCPB is the placebo-controlled period baseline, defined as the last available measurement before the first dose of setmelanotide or placebo.
If there were missing measurements after approximately 14 weeks, a multiple imputation model was used to impute the measurements for patients with fewer than approximately 14 weeks of setmelanotide or placebo treatment to a time point that approximated 14 weeks of setmelanotide or placebo treatment. One patient (5.88%) had missing measurements at 52 weeks due to study discontinuation. Their values were imputed.
aThe 95% CI of the mean is based on Rubin’s rule. If no imputation is needed for a given treatment, then the 95% CI of the mean reflects an observed CI.
bThe difference, 95% CI of difference, and P value are based on Rubin’s rule, and the difference is calculated as setmelanotide minus placebo. The null hypothesis (H0) to be tested is that the mean difference in daily hunger scores (calculated as setmelanotide minus placebo) is greater than or equal to 0. The alternative hypothesis (H1) is that the percent change is less than 0 (i.e., H0 pchg ≥ 0 vs. H1 pchg < 0). The P value is 1-sided. Values are from the posthoc analysis of patients with BBS and should be used for descriptive purposes only.
Sources: Study 023 Clinical Study Report9 and the report of patients with BBS from Study 023.10
Exploratory End Points: QoL
QoL assessments were conducted in patients with BBS without cognitive impairment. Assessment tools varied by age: IWQoL-Lite scores were reported for patients greater than or equal to 18 years old, PedsQL scores for patients less than 18 years old, and | || || for patients greater than or equal to 16 years old.
Adult patients assessed using the IWQoL-Lite (N = 11) had a 12.0-point mean total score improvement from the active treatment baseline to 52 weeks of setmelanotide treatment (Table 21). At the active treatment baseline, the mean total score was 74.9 (SD = 12.6), which falls within the range of moderate impairment (i.e., 71.9 to 79.4) and is much lower than seen in comparative populations without obesity (94.7; SD = 7.6).2 Of the assessed patients, 8 of 11 (72.7%) had impaired HRQoL at baseline according to the IWQoL-Lite, and 5 of these patients (62.5%) experienced improvement in their IWQoL-Lite scores over 52 weeks; the remaining 3 had stable IWQoL scores over 52 weeks.
Pediatric patients assessed using the PedsQL (N = 9) had a 11.2-point mean total score improvement from the active treatment baseline to 52 weeks of setmelanotide treatment (Table 21). At the active treatment baseline, the mean total score was 67.2 (SD = 20.1), which is beneath the threshold of 68.2 points that is indicative of impairment.31 Of the assessed patients, 4 patients of 9 patients (44.4%) had impaired HRQoL at baseline, according to the PedsQL, and each of the 4 patients experienced improved scores after 52 weeks of setmelanotide.
Patients aged greater than or equal to 16 years assessed using | || || || (N = 13; Table 21) reported some improvements (decreases) in | || || || health state scores from the active treatment baseline to 52 weeks of treatment, with the greatest improvements seen in the scores for mobility and usual activities. No improvement or worsening was seen in self-care scores. Scores for pain and/or discomfort worsened (i.e., increased).
Table 21: Change in QoL Assessment Scores From the Active Treatment Baseline to Week 52 in Pivotal Patients With BBS Without Cognitive Impairment
Parameter | Baseline (ATB) | Change from ATB at week 52 |
|---|---|---|
IWQoL-Lite in pivotal patients with BBS aged ≥ 18 years without cognitive impairmenta | ||
N | 11 | 11 |
Total score, mean (SD) | 74.9 (12.6) | + 12.0 (10.8) |
Physical function score, mean (SD) | 63.0 (13.9) | + 15.3 (12.1) |
Sexual life score, mean (SD) | 90.1 (14.9) | + 9.3 (14.1) |
Work score, mean (SD) | 83.7 (17.0) | + 9.5 (14.7) |
Public distress score, mean (SD) | 75.0 (20.0) | + 12.7 (15.7) |
Self-esteem score, mean (SD) | 79.1 (20.0) | + 11.1 (16.7) |
PedsQL in pivotal patients with BBS aged < 18 years without cognitive impairmentb | ||
N | 9 | 9 |
Total score, mean (SD) | 67.2 (20.1) | + 11.2 (14.4) |
Physical function score, mean (SD) | 60.4 (29.8) | + 14.0 (29.3) |
Psychosocial score, mean (SD) | 70.7 (17.3) | + 9.3 (10.5) |
| || || || || || || | in pivotal patients with BBS aged ≥ 16 years without cognitive impairmentc | ||
N | | || || || || || || | | | || || || || || || | |
Mobility score, mean (SD) | | || || || || || || | | | || || || || || || | |
Self-care score, mean (SD) | | || || || || || || | | | || || || || || || | |
Usual activities score, mean (SD) | | || || || || || || | | | || || || || || || | |
Pain and/or discomfort score, mean (SD) | | || || || || || || | | | || || || || || || | |
Anxiety and/or depression score, mean (SD) | | || || || || || || | | | || || || || || || | |
VAS score, mean (SD) | | || || || || || || | | | || || || || || || | |
ATB = active treatment baseline; BBS = Bardet-Biedl syndrome; | || || || || || || || || || || || || || |; IWQoL-Lite = Impact of Weight on Quality of Life – Lite; PedsQL = Pediatric Quality of Life Inventory; QoL = quality of life; SD = standard deviation, VAS = visual analogue scale.
aHigher scores represent higher QoL (range = 0 to 100, where 100 = best QoL).
bHigher scores represent higher QoL (range = 0 to 100, where 100 = best QoL).
c| || || || || || || |, lower scores represent higher QoL (range = 1 to 5, where 5 = extreme problems). However, in VAS, higher scores represent higher QoL (range = 0 to 100, where 100 = best QoL).
Sources: Study 023 Clinical Study Report9 and the report of patients with BBS from Study 023.10
Subgroup and Sensitivity Analyses
Pivotal Patients With BBS, All Ages
Among | || || || || || || || || || || || || || || || || || || || || |, after 52 weeks of setmelanotide treatment, the mean BMI change from the active treatment baseline was | || || || || || || || || || || || || || || || || || || and the mean percent change in BMI was | || || || || || || || || || || || || || | After the 14-week, double-blind, placebo-controlled period, patients treated with setmelanotide had a decrease in BMI relative to patients assigned to placebo | || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || |
Pediatric Patients With BBS Aged Less Than 12 Years
There were 8 patients aged less than 12 years with BBS in Study 023. | || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || |
Including all patients aged from greater than or equal to 6 years to less than 12 years with either AS or BBS, during the 14-week placebo-controlled period, those treated with setmelanotide (N = 6) | || || || || || || || || || || || || || || || || || || || || | compared to placebo-treated patients (N = 5) in the same age group.
Patients With BBS Aged Less Than 18 Years
Among pivotal patients with BBS who were less than 18 years of age (N = 14 to 16), the mean BMI z score dropped by 0.75 points ± 0.46 points (95% CI, −1.02 to −0.49) after 52 weeks of setmelanotide treatment. Of these patients, after 52 weeks of setmelanotide treatment, 85.7% achieved a 0.2-point reduction, and 71.4% achieved a 0.3-point reduction in BMI z score. Mean BMI fell by 3.36 kg/m2 ± 2.07 kg/m2 (95% CI, −4.55 kg/m2 to −2.16 kg/m2), and percent BMI dropped by 9.50 ± 6.44% (95% CI, −13.22 to −5.78). Additionally, there was a reduction in the percentage of patients with BMI 95th percentile scores (−17.30 ± 7.67%; 95% CI, −21.73 to −12.87). This change reflects a shift from class 3 (high-risk) obesity (≥ 140% of the 95th percentile) to class 2 (moderate-risk) obesity (120% to < 140% of the 95th percentile).59
During the 14-week, placebo-controlled period, among pivotal patients with BBS aged less than 18 years (N = 22), treatment with setmelanotide was associated with | || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || |
Pivotal Patients With BBS Greater Than or Equal to 18 years of Age
Among pivotal patients with BBS who were greater than or equal to 18 years of age (N = 15), an estimated 60% (95% CI, 32.3% to 83.7%) achieved a greater than or equal to 5% reduction in body weight, and an estimated 46.7% (95% CI, 21.3% to 73.4%) achieved a greater than or equal to 10% reduction in body weight after 52 weeks of setmelanotide treatment. The mean weight change was −9.42 kg ± 9.39 kg (95% CI, −14.63 kg to −4.22 kg) and mean percent weight change was −7.57% ± 7.13% (95% CI, 11.52% to −3.62%). The mean change in BMI was −4.22 kg/m2 ± 3.34 kg/m2 (95% CI, −6.34 kg/m2 to −2.10 kg/m2), and the mean percent BMI change was −9.09% ± 6.76% (95% CI, −13.39% to −4.80%).
During the 14-week placebo-controlled period, patients assigned to setmelanotide had | || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || placebo-treated patients achieved greater than or equal to 5% weight loss.
Hunger Assessments in Cognitively Impaired Patients With BBS
Hunger was also assessed in cognitively impaired patients (aged ≥ 12 years). These assessments were done by caregivers using the | || || || || because there is no validated hunger assessment for this population, and | || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || |.There is no known MID for patients with BBS.
Harms
Refer to Table 22 for the summary of harms in Study 023 among patients with BBS and AS, and Table 23 for data pertaining to the most common harms (≥ 5%) in patients with BBS.
In Study 023, the safety analysis population (SAS) consisted of all patients who received at least 1 dose of the study drug (i.e., placebo or setmelanotide), with results reported for the 14-week, placebo-controlled, double-blind period and full study period. All AEs were coded using the Medical Dictionary for Regulatory Activities system organ class and graded by the investigators using the National Cancer Institute Common Terminology Criteria for Adverse Events.
The definition of a TEAE was any AE with onset after the first administration of study medication through the end of the study (i.e., 28 days after the last dose administered); any event that was present at baseline, but worsened in intensity or was considered drug-related by the investigator by the end of the study; or any event that was deemed related to study drug exposure. In the AE calculations, each patient contributed only once (i.e., the most related occurrence or the most intense occurrence) to each of the incidence rates in the descriptive analysis, regardless of the number of episodes.
No AEs of special interest were prespecified in the protocol. However, the sponsor recognized events that were appropriate for special monitoring, including injection-site reactions, skin hyperpigmentation, and sexual events (male or female). Additional AEs identified by clinical experts as AEs of special interest are also discussed in the Notable Harms section.
Adverse Events
During the 14-week, placebo-controlled period in patients with either BBS (n = 44) or AS (n = 8), 26 of 27 (96.3%) setmelanotide-treated patients and 24 of 25 (96.0%) placebo-treated patients experienced at least 1 TEAE. In the overall study period, 100% of patients experienced at least 1 TEAE (Table 22). Results were similar in the BBS subpopulation (Table 23). The most common TEAEs were injection-site reactions (erythema, pruritus, bruising, induration, pain), skin hyperpigmentation, nausea, vomiting, and diarrhea.
Rates of injection-site reactions were similar between the treatment groups during the 14-week, placebo-controlled period.
There were also similar rates of nausea between the setmelanotide-treated patients (25.9%) and placebo-treated patients (24.0%), although vomiting was observed only in patients treated with setmelanotide (25.9%). Among all patients, nausea and vomiting tended to occur soon after starting setmelanotide treatment, and most events were mild or moderate in severity. These events were infrequent after the first month of setmelanotide treatment. No events of severe nausea or severe vomiting occurred among all patients.
| || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || |

Serious Adverse Events
SAEs were uncommon. During the 14-week, placebo-controlled period in patients with BBS or AS, 1 patient randomized to setmelanotide (3.7%) and 2 patients randomized to placebo (5.8%) experienced at least 1 SAE. In the setmelanotide-treated patient, the SAE was anemia caused by gynecological bleeding, which was judged by the investigator to be related to the initiation of oral contraceptives. In the patients treated with placebo, the SAEs were blindness and anaphylactic reaction.
Over the full study period in patients with BBS or AS, a total of 3 patients (5.8%) experienced at least 1 SAE, which included the previously described events in addition to 2 events of suicidal ideation. Of the 3 patients with SAEs, 1 patient experienced both blindness and 2 events of suicidal ideation that resolved without a change in study medication. These were considered by the investigator to be attributable to concomitant disease.
Withdrawals Due to Adverse Events
During the 14-week, placebo-controlled period in patients with BBS or AS, 2 patients randomized to setmelanotide (7.4%) and 3 patients assigned to placebo (12.0%) withdrew due to any TEAE. The TEAEs leading to withdrawal in setmelanotide-treated patients were nausea, vomiting, ocular hyperemia, and face edema. In placebo-treated patients, the TEAEs were nausea, anaphylactic reaction, headache, acne, hidradenitis, and hot flush. Similar rates of treatment discontinuation due to nausea were observed in the setmelanotide group (3.7%) and placebo group (4.0%) during the placebo-controlled phase, while 1 patient (3.7%) in the setmelanotide group and 0 in the placebo group discontinued treatment due to vomiting.
Over the full study period in patients with BBS or AS, a total of 6 patients withdrew due to any TEAE. These included the previously listed TEAEs with the addition of skin hyperpigmentation and abdominal pain.
Mortality
No deaths were observed.
Notable Harms
Although no AEs of special interest were prespecified in the trial protocol, the sponsor conducted in-depth evaluation of injection-site reactions, hyperpigmentation, and sexual events.
Similar rates of injection-site reactions were observed between the setmelanotide and placebo groups during the double-blind period, which suggests that these reactions were related to the injection and/or excipients (i.e., not to the setmelanotide, but to the mPEG-DSPE vehicle). Results were consistent between the full population (i.e., BBS and AS) and the BBS subpopulation.
Hyperpigmentation events (e.g., changes in skin tone, new mole development, and changes in an existing mole) occurred with setmelanotide treatment during the double-blind period (63.0% versus 0% with placebo) and in the full study period (63.5%) in patients with BBS or AS. Consistent results were observed between the full study population and among the patients with BBS. Just 1 patient (1.9%) discontinued treatment because of hyperpigmentation during the full study period. There were no reports of melanoma related to the observed hyperpigmentation in clinical trials of setmelanotide, including Study 023.
| || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || |. None of the male patients experienced priapism (prolonged or painful erection) that required intervention.
Additional notable harms to consider, as recommended by experts consulted by CADTH, were suicide attempts, depression or depressed mood, anxiety, anaphylaxis, bradycardia, cold abscess at the injection site, aggression, and sexually inappropriate behaviours. There were no suicide attempts recorded during the study. Depression and depressed mood each occurred in 1 patient over the full study period (1 patient who was initially randomized to placebo and another who was initially randomized to setmelanotide). Anxiety was not reported. Anaphylaxis occurred in 1 placebo-treated patient during the double-blind period, as previously described. Bradycardia was not reported. Abscesses occurred in 2 patients over the study period, but these were not specified as cold abscesses, and the location of the occurrences was not specified. Aggression occurred in 3 patients. Finally, sexually inappropriate behaviour occurred in 1 patient over the full study period.
Table 22: Summary of Harms in Study 023 (SAS, BBS and AS)
Adverse events | Double-blind, placebo-controlled period (14 weeks) | Full study period (66 weeks) | ||
|---|---|---|---|---|
Setmelanotide (N = 27) | Placebo (N = 25) | Setmelanotide to setmelanotide (N = 27) | Placebo to setmelanotide (N = 25) | |
Most common TEAEs with incidence ≥ 5%, n (%) | ||||
≥ 1 TEAE | 26 (96.3) | 24 (96.0) | 27 (100.0) | 25 (100.0) |
General disorders and administration-site conditions | 17 (63.0) | 20 (80.0) | 19 (70.4) | 20 (80.0) |
Injection-site erythema | 12 (44.4) | 11 (44.0) | 13 (48.1) | 13 (52.0) |
Injection-site pruritus | 8 (29.6) | 9 (36.0) | 10 (37.0) | 10 (40.0) |
Injection-site bruising | 6 (22.2) | 9 (36.0) | 7 (25.9) | 11 (44.0) |
Injection-site pain | 3 (11.1) | 8 (32.0) | 4 (14.8) | 10 (40.0) |
Injection-site induration | 6 (22.2) | 4 (16.0) | 6 (22.2) | 8 (32.0) |
Injection-site hemorrhage | 3 (11.1) | 2 (8.0) | 4 (14.8) | 2 (8.0) |
Fatigue | 1 (3.7) | 2 (8.0) | 1 (3.7) | 5 (20.0) |
Injection-site edema | 2 (7.4) | 1 (4.0) | 4 (14.8) | 2 (8.0) |
Injection-site reaction | 1 (3.7) | 2 (8.0) | 1 (3.7) | 2 (8.0) |
Skin and subcutaneous tissue disorders | 20 (74.1) | 4 (16.0) | 24 (88.9) | 15 (60.0) |
Skin hyperpigmentation | 17 (63.0) | 0 | 21 (77.8) | 12 (48.0) |
Acne | 1 (3.7) | 1 (4.0) | 2 (7.4) | 1 (4.0) |
Dermatitis atopic | 2 (7.4) | 1 (4.0) | 3 (11.1) | 0 |
Dry skin | 0 | 2 (8.0) | 0 | 3 (12.0) |
Skin striae | 1 (3.7) | 0 | 3 (11.1) | 0 |
Gastrointestinal disorders | 12 (44.4) | 8 (32.0) | 17 (63.0) | 19 (76.0) |
Nausea | 7 (25.9) | 6 (24.0) | 9 (33.3) | 10 (40.0) |
Vomiting | 7 (25.9) | 0 | 7 (25.9) | 7 (28.0) |
Diarrhea | 2 (7.4) | 1 (4.0) | 5 (18.5) | 5 (20.0) |
Abdominal pain | 0 | 1 (4.0) | 1 (3.7) | 3 (12.0) |
Abdominal pain upper | 0 | 1 (4.0) | 2 (7.4) | 2 (8.0) |
Infections and infestations | 7 (25.9) | 10 (40.0) | 10 (37.0) | 16 (64.0) |
Nasopharyngitis | 2 (7.4) | 1 (4.0) | 2 (7.4) | 2 (8.0) |
Urinary tract infection | 1 (3.7) | 1 (4.0) | 2 (7.4) | 2 (8.0) |
Ear infection | 0 | 1 (4.0) | 2 (7.4) | 1 (4.0) |
Pharyngitis streptococcal | 0 | 2 (8.0) | 1 (3.7) | 2 (8.0) |
Upper respiratory tract infection | 1 (3.7) | 1 (4.0) | 1 (3.7) | 2 (8.0) |
Abscess | 0 | 1 (4.0) | 1 (3.7) | 1 (4.0) |
Nervous system disorders | 6 (22.2) | 7 (28.0) | 7 (25.9) | 9 (36.0) |
Headache | 1 (3.7) | 6 (24.0) | 4 (14.8) | 8 (32.0) |
Dizziness | 1 (3.7) | 2 (8.0) | 2 (7.4) | 2 (8.0) |
Musculoskeletal and connective tissue disorders | 3 (11.1) | 1 (4.0) | 7 (25.9) | 8 (32.0) |
Back pain | 0 | 1 (4.0) | 1 (3.7) | 4 (16.0) |
Arthralgia | NR | NR | 2 (7.4) | 1 (4.0) |
Metabolism and nutrition disorders | 4 (14.8) | 3 (12.0) | 7 (25.9) | 6 (24.0) |
Dyslipidemia | 1 (3.7) | 0 | 2 (7.4) | 1 (4.0) |
Impaired glucose tolerance | 0 | 2 (8.0) | 1 (3.7) | 2 (8.0) |
Respiratory, thoracic, and mediastinal disorders | 4 (14.8) | 4 (16.0) | 7 (25.9) | 6 (24.0) |
Nasal congestion | 3 (11.1) | 0 | 3 (11.1) | 0 |
Cough | 0 | 2 (8.0) | 2 (7.4) | 3 (12.0) |
Rhinorrhea | 0 | 2 (8.0) | 1 (3.7) | 2 (8.0) |
Reproductive system and breast disorders | 2 (10.5) | 0 | 6 (22.2) | 6 (24.0) |
Spontaneous penile erection | 1 (5.3) | 0 | 3 (11.1) | 2 (8.0) |
Menorrhagia | 1 (5.3) | 0 | 1 (3.7) | 2 (8.0) |
Investigations | 6 (22.2) | 0 | 7 (25.9) | 3 (12.0) |
Decreased high-density lipoprotein | 4 (14.8) | 0 | 4 (14.8) | 0 |
Neoplasms (benign, malignant, and unspecified, (including cysts and polyps) | 1 (3.7) | 0 | 4 (14.8) | 4 (16.0) |
Melanocytic nevus | 1 (3.7) | 0 | 3 (11.1) | 3 (12.0) |
Serious TEAEs, n (%) | ||||
Patients with ≥ 1 SAE | 1 (3.7) | 2 (8.0) | 1 (3.7) | 2 (8.0) |
Anemia | 1 (3.7) | 0 | 1 (3.7) | 0 |
Blindness | 0 | 1 (4.0) | 0 | 1 (4.0) |
Anaphylactic reaction | 0 | 1 (4.0) | 0 | 1 (4.0) |
Suicidal ideation | NR | NR | 0 | 1 (4.0) |
Patients who stopped treatment due to adverse events, n (%) | ||||
Due to treatment-related AE | 0 | 0 | 2 (7.4) | 3 (12.0) |
Due to any TEAEa | 2 (7.4) | 3 (12.0) | 2 (7.4) | 4 (16.0) |
Nausea | 1 (3.7) | 1 (4.0) | 1 (3.7) | 2 (8.0) |
Vomiting | 1 (3.7) | 0 | 1 (3.7) | 2 (8.0) |
Ocular hyperemia | 1 (3.7) | 0 | 1 (3.7) | 0 |
Face edema | 1 (3.7) | 0 | 1 (3.7) | 0 |
Anaphylactic reaction | 0 | 1 (4.0) | 0 | 1 (4.0) |
Headache | 0 | 1 (4.0) | 0 | 1 (4.0) |
Acne | 0 | 1 (4.0) | 0 | 1 (4.0) |
Hidradenitis | 0 | 1 (4.0) | 0 | 1 (4.0) |
Hot flush | 0 | 1 (4.0) | 0 | 1 (4.0) |
Skin hyperpigmentation | NR | NR | 1 (3.7) | 0 |
Abdominal pain | NR | NR | 0 | 1 (4.0) |
Deaths, n (%) | ||||
Patients who died | 0 | 0 | 0 | 0 |
Additional TEAEs of special interest, n (%) | ||||
Psychiatric disorders | 1 (5.3) | 2 (10.5) | 5 (18.5) | 3 (12.0) |
Anxiety | NR | NR | NR | NR |
Aggression | 1 (5.3) | 0 | 2 (7.4) | 1 (4.0) |
Depression | 0 | 1 (5.3) | 0 | 1 (4.0) |
Depressed mood | 1 (3.7) | 0 | 1 (3.7) | 0 |
Mood altered | 0 | 1 (5.3) | 0 | 1 (4.0) |
Suicidal ideation | 0 | 1 (5.3) | 0 | 1 (4.0) |
Disturbance in sexual arousal | NR | NR | 1 (3.7) | 0 |
Insomnia | 1 (3.7) | 0 | 1 (3.7) | 0 |
Increased libido | NR | NR | 1 (3.7) | 0 |
Sexually inappropriate behaviour | NR | NR | 1 (3.7) | 0 |
Cardiac disorders | 0 | 1 (5.3) | 1 (3.7) | 1 (4.0) |
Bradycardia | NR | NR | 1 (3.7) | 0 |
Immune system disorders | 0 | 1 (5.3) | 0 | 1 (4.0) |
Anaphylactic reaction | 0 | 1 (5.3) | 0 | 1 (4.0) |
AE = adverse event; AS = Alström syndrome; BBS = Bardet-Biedl syndrome; NR = not reported; SAE = serious adverse event; SAS = safety analysis set; TEAE = treatment-emergent adverse event.
aStudy drug permanently withdrawn.
Sources: Study 023 Clinical Study Report9 and the report of patients with BBS from Study 023.10 Details in the table have been taken from the sponsor’s Summary of Clinical Evidence.
Table 23: Summary of Harms Occurring in Greater Than or Equal to 5% of All BBS Patients (Double-Blind, Placebo-Controlled Period and Full Study)
Adverse events | Double-blind, placebo-controlled period (14 weeks) | Full study period (66 weeks) | ||
|---|---|---|---|---|
Setmelanotide (N = 22) | Placebo (N = 22) | Setmelanotide to Setmelanotide (N = 22) | Placebo to Setmelanotide (N = 22) | |
Most common TEAEs with incidence ≥ 5%, n (%) | ||||
≥ 1 TEAE | 21 (95.5) | 21 (95.5) | 22 (100.0) | 22 (100.0) |
General disorders and administration-site conditions | 14 (63.6) | 18 (81.8) | 15 (68.2) | 18 (81.8) |
Injection-site erythema | 10 (45.5) | 11 (50.0) | 11 (50.0) | 12 (54.5) |
Injection-site pruritus | 7 (31.8) | 9 (40.9) | 8 (36.4) | 10 (45.5) |
Injection-site bruising | 6 (27.3) | 9 (40.9) | 7 (31.8) | 11 (50.0) |
Injection-site pain | 3 (13.6) | 7 (31.8) | 4 (18.2) | 9 (40.9) |
Injection-site induration | 5 (22.7) | 4 (18.2) | 5 (22.7) | 8 (36.4) |
Injection-site hemorrhage | 3 (13.6) | 2 (9.1) | 4 (18.2) | 2 (9.1) |
Injection-site edema | 2 (9.1) | 1 (4.5) | 4 (18.2) | 2 (9.1) |
Fatigue | 0 | 2 (9.1) | 0 | 5 (22.7) |
Skin and subcutaneous tissue disorders | 16 (72.7) | 3 (13.6) | 19 (86.4) | 13 (59.1) |
Skin hyperpigmentation | 13 (59.1) | 0 | 16 (72.7) | 10 (45.5) |
Dry skin | 0 | 2 (9.1) | 0 | 3 (13.6) |
Skin striae | 1 (4.5) | 0 | 3 (13.6) | 0 |
Gastrointestinal disorders | 10 (45.5) | 8 (36.4) | 13 (59.1) | 18 (81.8) |
Nausea | 5 (22.7) | 6 (27.3) | 6 (27.3) | 10 (45.5) |
Vomiting | 6 (27.3) | 0 | 6 (27.3) | 7 (31.8) |
Diarrhea | 2 (9.1) | 1 (4.5) | 5 (22.7) | 5 (22.7) |
Abdominal pain, upper | 0 | 1 (4.5) | 1 (4.5) | 2 (9.1) |
Infections and infestations | 6 (27.3) | 8 (36.4) | 9 (40.9) | 14 (63.6) |
Urinary tract infection | 1 (4.5) | 1 (4.5) | 2 (9.1) | 2 (9.1) |
Nasopharyngitis | 1 (4.5) | 1 (4.5) | 1 (4.5) | 2 (9.1) |
Nervous system disorders | 5 (22.7) | 7 (31.8) | 6 (27.3) | 9 (40.9) |
Headache | 0 | 6 (27.3) | 3 (13.6) | 8 (36.4) |
Dizziness | 1 (4.5) | 2 (9.1) | 2 (9.1) | 2 (9.1) |
Musculoskeletal and connective tissue disorders | 2 (9.1) | 1 (4.5) | 5 (22.7) | 7 (31.8) |
Back pain | 0 | 1 (4.5) | 0 | 3 (13.6) |
Respiratory, thoracic, and mediastinal disorders | 3 (13.6) | 3 (13.6) | 6 (27.3) | 5 (22.7) |
Cough | 0 | 1 (4.5) | 1 (4.5) | 2 (9.1) |
Nasal congestion | 3 (13.6) | 0 | 3 (13.6) | 0 |
Rhinorrhea | 0 | 2 (9.1) | 1 (4.5) | 2 (9.1) |
Metabolism and nutrition disorders | 3 (13.6) | 1 (4.5) | 6 (27.3) | 4 (18.2) |
Dyslipidemia | 1 (4.5) | 0 | 2 (9.1) | 1 (4.5) |
Reproductive system and breast disorders | 3 (13.6) | 1 (4.5) | 5 (22.7) | 5 (22.7) |
Spontaneous penile erection | 1 (4.5) | 0 | 3 (13.6) | 2 (9.1) |
Neoplasms (benign, malignant, and unspecified, including cysts and polyps) | 1 (4.5) | 0 | 4 (18.2) | 4 (18.2) |
Melanocytic nevus | 1 (4.5) | 0 | 3 (13.6) | 3 (13.6) |
Psychiatric disorders | 3 (13.6) | 3 (13.6) | 5 (22.7) | 3 (13.6) |
Aggression | 1 (4.5) | 1 (4.5) | 2 (9.1) | 1 (4.5) |
Eye disorders | 0 | 4 (18.2) | 2 (9.1) | 5 (22.7) |
Investigations | 4 (18.2) | 0 | 5 (22.7) | 2 (9.1) |
Decreased high-density lipoprotein | 3 (13.6) | 0 | 3 (13.6) | 0 |
Injury, poisoning, and procedural complications | 2 (9.1) | 1 (4.5) | 3 (13.6) | 2 (9.1) |
Vascular disorders | 1 (4.5) | 1 (4.5) | 1 (4.5) | 2 (9.1) |
BBS = Bardet-Biedl syndrome; TEAE = treatment-emergent adverse event.
Sources: Study 023 Clinical Study Report9 and the report of patients with BBS from Study 023.10 Details in the table have been taken from the sponsor’s Summary of Clinical Evidence.
Critical Appraisal
Internal Validity
Study 023, the only study included in this review, was a phase III, multicentre study that consisted of a 14-week, randomized, placebo-controlled, double-blind period followed by a 52-week, open-label, single-arm period. The original study protocol and all key primary and secondary outcomes were designed to include patients with either AS or BBS. To reflect the requested reimbursement criteria, all efficacy outcomes considered in this report were posthoc reanalyses based solely on the subgroup of patients with BBS, who comprised the majority of the overall population. The results of the posthoc analysis were consistent with the results of the prespecified analyses in the FAS. Although the population size was small, BBS is a rare disease with a small patient population, and the sample size exceeded the minimum power calculation conducted by the sponsor.
The primary and secondary outcomes pertained to the 52-week, single-arm period, while some exploratory outcomes were evaluated in the context of the 14-week, placebo-controlled period. It is important to note that for 52-week outcomes, the baseline values were selected at the active treatment baseline as opposed to the baseline of enrolment in the trial; as such, for patients initially randomized to placebo, the active treatment baseline would have been at the end of the initial 14-week, placebo-controlled period. Therefore, patients randomized to placebo would also require an evaluation at approximately week 66 of the trial to reach approximately 52 weeks of setmelanotide treatment; multiple imputation was used for patients who had not reached this time point. The approaches taken to handling missing data were considered to be appropriate and potentially conservative. While a step-down procedure (i.e., a hierarchical order of testing) was prespecified to control for type I error in the original study, this procedure would not apply to the posthoc analysis of patients with BBS. As a result, all results from these analyses must be interpreted with consideration for the potential risk of increased type I error. Due to the small target sample size, no formal statistical analyses were planned to adjust for possible covariate effects.
There are inherent risks of bias, confounding, and uncertainty due to the open-label and single-arm design of the study. However, BBS is a rare disease with a small patient population for which there are no other targeted pharmacotherapies. Single-arm data are limited in the estimation of treatment effects due to unidentified, uncontrolled prognostic factors (e.g., age, weight, severity of hyperphagia, and BBS genotype). The open-label design of the single-arm period increases the risk of detection bias and performance bias, and may lead to an overestimation of the treatment effect in subjective outcomes, such as the hunger surveys. The duration of treatment for this period was considered by CADTH clinical experts to be appropriate for evaluating weight loss and hyperphagia. However, longer-term data are also needed, given that obesity is a long-term, chronic, relapsing condition.
The key outcomes assessed during the 52-week, single-arm period included metrics of weight loss and hunger, with additional exploratory outcomes pertaining to HRQoL and metrics of metabolic health. The primary outcome of Study 023 was the percentage of patients aged at least 12 years who achieved a greater than or equal to 10% reduction in body weight after 52 weeks of active treatment, which was compared against an assumption of 10% response without treatment. The threshold of greater than or equal to 10% reduction in body weight exceeds the MID identified by the clinical experts (5% to 7%) in obesity management. The threshold of 10% for the response rate was also agreed to be conservative. It was based on historical control data illustrating that fewer than approximately 7% of patients with BBS lost greater than or equal to 10% of their body weight over a 3-year period in a heterogenous, real-world population. These real-world patients may also have been engaged in intensive weight loss activities or receiving interventions that would have been disallowed in Study 023, which further supports the view that the threshold was conservative.
The measurement of hunger was based on daily hunger questionnaires designed by the sponsor, and the estimation of MIDs was conducted using data from the same trial. As such, the questionnaire and its MIDs are not externally validated for validity, reliability, and responsiveness, which limits the interpretability of these results. Statistical analyses were performed against an assumption of no response without treatment; while it is clinically plausible that hunger does not spontaneously resolve in patients with BBS, the measurement of subjective outcomes in single-arm trials is nonetheless confounded by the placebo effect, which may introduce bias leading to overestimation of the treatment effect; as such, the lack of control arm limits interpretability. The clinical experts consulted by CADTH considered the relatively high proportion of patients achieving a 25% improvement in hunger on setmelanotide treatment at 52 weeks to be an encouraging result, but they did not have specific experience with this or other hunger-related questionnaires in clinical practice.
During the 14-week, placebo-controlled period, randomization and concealment were carried out appropriately, and maintenance of blinding was preserved during the transition to the open-label phase by re-escalating patients to setmelanotide after week 14 regardless of their initial randomization. Treatment with placebo or setmelanotide during the RCT was administered in the same manner, with indistinguishable, clear, colourless to opalescent solutions in identical vials; the placebo formulation had similar excipients to the active formulation. However, hyperpigmentation occurred in more than half of setmelanotide-treated patients and in no placebo-treated patients, which may have allowed patients or clinicians to guess treatment assignments. Similarly, vomiting occurred in more than a quarter of setmelanotide-treated patients, but in no placebo-treated patients during the placebo-controlled period, and again in more than a third of patients who had been initially randomized to placebo when they transitioned to setmelanotide during the single-arm period; this also may have unblinded patients or clinicians to their initial randomization.
The baseline and disease characteristics between treatment groups were considered by clinical experts consulted by CADTH to be reasonably similar to 1 another; the observed differences in the proportion of females between the active and placebo groups were not considered to confound the treatment effect. While differences in the proportion of patients with cognitive impairment were also not expected to confound the treatment effect, these did further reduce the available sample size for outcomes — such as the key secondary hunger-related metrics that excluded patients with cognitive impairment — due to the practical limitations of assessing PROs in cognitively impaired populations. The duration of the 14-week, placebo-controlled period has inherent limitations for the assessment of weight loss; however, it was considered appropriate for the assessment of reductions in hyperphagia, according to clinical experts consulted by CADTH.
In both patients with BBS and patients with AS, drop-outs occurred during the placebo-controlled phase in 2 patients assigned to placebo, but in 0 patients assigned to setmelanotide. Over the full study period, among patients with BBS, a total of 8 patients discontinued prematurely; however, 2 of these patients were counted as discontinued due to transferring to the extension trial when they were meant to be counted as completed. As such, there were no concerns about imbalanced or excessive dropout. However, there was substantial missingness in all exploratory outcomes. Low sample sizes in the exploratory QoL and hunger outcomes were due to many patients being ineligible for inclusion in the analyses due to cognitive impairment or age.
External Validity
In discussions with clinical experts consulted by CADTH, the inclusion and exclusion criteria of Study 023 were appropriate and generalizable to the population of interest (i.e., adult and pediatric patients with BBS, obesity, and hyperphagia who may or may not have cognitive impairment and may or may not have genetic confirmation of diagnosis). Although patients aged greater than or equal to 6 years were included, most outcomes analyzed only patients aged greater than or equal to 12 years; very few patients aged less than 12 years were enrolled in the trial (n = 8). Additionally, although patients with cognitive impairment were enrolled, they were not considered in the key secondary and exploratory outcomes related to hunger and QoL due to the practical limitations of assessing these outcomes in cognitively impaired populations. The subgroup analyses of younger and cognitively impaired populations had small sample sizes and used different metrics for measurement by necessity. Although reasonable from the perspective of trial design, the generalizability of the trial results for these subpopulations is nonetheless more uncertain. Overall, the primary, secondary, and exploratory outcomes were considered to be appropriately selected.
The clinical experts noted that the eligibility criterion disallowing recent intensive weight-loss activities would not reflect clinical practice, but that this was not a cause for concern in the implementation of setmelanotide in real-world clinical practice. In clinical practice, patients would be expected to be engaged in other obesity management strategies, such as calorie-reduced diets, and would not be excluded from pharmacotherapy for recency of weight-loss activities. This limitation in the generalizability of results is beneficial from an internal validity standpoint because it removes the potentially confounding factor of lifestyle intervention.
The baseline characteristics of the trial population were also considered by the experts to be appropriately generalizable to the Canadian context of patients with BBS and obesity. Although there were some differences identified between the setmelanotide and placebo arms of the placebo-controlled period, these differences were not considered to be concerning by the consulted experts. Moreover, the differences do not complicate the interpretation of the 52-week outcomes, which include patients regardless of initial randomization.
The dosing in Study 023 differed from that recommended in the product monograph. According to the product monograph, patients 18 years of age and older should be started on 1 mg daily, increasing by 0.5 mg daily every 2 weeks to a maximum of 3.0 mg daily, if tolerated; during the trial, patients 16 years of age or older started on 2 mg daily for 2 weeks, then increased to 3 mg daily, if tolerated. For pediatric patients, the recommended starting dose is 0.5 mg, increased by 0.5 mg daily every 2 weeks to a maximum of 2.0 mg daily. In Study 023, patients age less than 16 started at 1 mg daily for 1 week, increased to 2 mg daily for 1 week, and increased to a maximum of 3 mg daily, if tolerated. In summary, the trial had higher starting doses and shorter periods of intermediate dosing during the titration phase for all ages, and higher target doses for patients aged 16 years or older. The clinical experts consulted by CADTH indicated that dosing in real-world practice would mostly follow the product monograph, with occasional exceptions for patients older than 16, who may begin to receive adult dosing, based on clinical judgment.
Given that there are no other Health Canada–approved treatments that target the underlying mechanism of BBS-related hyperphagia and obesity, there were no appropriate comparators aside from placebo. There is a lack of data on the efficacy and safety of the potential off-label use of semaglutide and other pharmacotherapies; by extension, there is an evidence gap regarding the comparative efficacy between setmelanotide and these therapies.
Of the locations participating in the clinical trial, 1 was in Canada and included 6 enrolled patients. Given the rarity of the disease and the locations of other participating sites (i.e., in the US and western Europe), this was considered acceptable for generalization to the Canadian context.
One potential difference from clinical practice in Study 023 may be the level of background care provided in the study, such as training and, if needed, at-home assistance with self-injection. In real-world practice, adherence is often lower than in clinical trials. Given the high prevalence of cognitive impairment in patients with BBS and the lifelong, incurable nature of the disease, equitable access to training and support should be considered.
LTE Studies
Contents within this section have been informed by materials submitted by the sponsor. The following information has been summarized and validated by the CADTH review team.
Description of Studies
One LTE study was submitted for review. Study 02260 is an ongoing, open-label extension study of the index trial Study 0239 to examine the long-term safety and tolerability of setmelanotide in patients greater than or equal to 6 years old with BBS and obesity for up to 36 months of treatment. The primary objective is to evaluate safety and tolerability. The secondary objectives are to evaluate changes in weight and hunger.
Populations
Patients were eligible to enrol in Study 022 if they had completed 1 of the index trials (i.e., Study 01461 or Study 0239) and had been were considered “responders” and demonstrated acceptable tolerability in the index trial. A responder was defined as a patient who achieved a greater than or equal to 10% body weight reduction (for patients aged ≥ 18 years) or a greater than or equal to 0.3 reduction in BMI z score (for patients aged < 18 years) after 52 weeks of setmelanotide treatment in the index trial. Responder patients began the LTE trial after index trial completion without a gap between visits. Visits occurred every 3 months throughout the study. The study started on March 18, 2021, and is still ongoing.
Interventions
Patients enrolled in Study 022 continued their personalized setmelanotide dose (titrated for each patient with a target of 3 mg once daily) without any specific guidance regarding diet or exercise.
Outcomes
Efficacy variables included measurements of change in BMI up to 36 months from the Study 023 baseline, including absolute and percentage change in BMI and body weight for adult patients (i.e., ≥ 18 years of age) and BMI z score in the 95th percentile for patients aged less than 18 years.
Hunger was assessed once every 3 months. However, hunger scores were not reported. The justification provided was that hunger scores are relative and are most informative when comparing pretreatment with posttreatment scores.
The frequency and severity of TEAEs, SAEs, AEs leading to discontinuation, and AEs leading to death were assessed and summarized as of June 2022.
Statistical Analysis
No statistical analysis for hypothesis testing was planned.
Results
Patient Disposition
Patient disposition is summarized in Table 24. Out of the 44 patients with BBS who were randomized in Study 023, 23 participants enrolled in the LTE study. Patients could also enrol after completing Study RM-493 to 014, a phase II basket trial in patients with rare genetic diseases of the MC4R pathway, including BBS (ClinicalTrails.gov identification number: NCT03013543); in total, 7 patients from RM-493 to 014 enrolled in Study 022.
Three patients discontinued the LTE trial: 1 due to an AE (auditory hallucination) that was considered unlikely to be related to treatment; 1 based on their own decision; and 1 because they transitioned to another setmelanotide clinical trial. The remainder (90%) are ongoing.
Parameter | Study 022 |
|---|---|
Enrolled in Study 023, N | 44 |
Completed Study 023, N | 30 |
Enrolled in LTE, N | 30 (23 from Study 022) |
Ongoing, N (%) | 27 (90) |
Completed study | 10 |
Discontinued study, N (%) | 3 (10) |
Reasons for discontinuation, N (%) | |
Adverse eventa | 1 (3.3) |
Withdrawal by patient | 1 (3.3) |
Transitioned to another setmelanotide trial | 1 (3.3) |
LTE = long-term extension.
aAuditory hallucination that was determined to be unlikely to be related to treatment.
Source: Study 022 Clinical Study Report.60 Details in the table have been taken from the sponsor’s Summary of Clinical Evidence.
Baseline Characteristics
Patient characteristics at baseline are summarized in Table 25.
Table 25: Summary of Baseline Characteristics of the LTE Submitted by the Sponsor
Characteristic | Study 022 (N = 30) |
|---|---|
Female, n (%) | | || || || || | |
Age, years, mean (SD) at index trial baseline | |
Mean (SD) | | || || || || | |
Median | | || || || || | |
Min, max | | || || || || | |
Age categories at index trial baseline, n (%) | |
< 18 years of age | | || || || || | |
≥ 18 years of age | | || || || || | |
Race, n (%) | |
White | | || || || || | |
Black or African American | | || || || || | |
Asian | | || || || || | |
Other | | || || || || | |
Weight at index trial baseline (kg) | |
Mean (SD) | | || || || || | |
Median | | || || || || | |
Min, max | | || || || || | |
Height at index trial baseline (cm) | |
Mean (SD) | | || || || || | |
Median | | || || || || | |
Min, max | | || || || || | |
BMI at LTE baseline (kg/m2) | |
Mean (SD) | | || || || || | |
Median | | || || || || | |
Min, max | | || || || || | |
BMI z score at LTE baseline in patients aged < 18 years, n = 19 | |
Mean (SD) | | || || || || | |
Median | | || || || || | |
Min, max | | || || || || | |
BMI body mass index; LTE = long-term extension; SD = standard deviation.
Source: Study 022 Clinical Study Report.60 Details in the table have been taken from the sponsor’s Summary of Clinical Evidence.
Exposure to Study Treatments
Not reported.
Efficacy
At the time of this review, Study 022 was still ongoing, and not all patients had completed the 36-month assessment. Early findings from the 12-month, 18-month, and 24-month assessments were available.
Change in BMI up to 36 Months Among All Patients With BBS
Changes from baseline in BMI for all patients (11 adult patients and 19 pediatric patients) were −13.78% ± 4.58% (n = 30) at month 12; −11.97% ± 9.33% (n = 29) at month 18; −10.74% ± 12.24% (n = 24) at month 24; and | || || || || || || || || || || || || || || |. The proportions of all patients who achieved a greater than or equal to 10% reduction in BMI from the index trial baseline were 76.7% (23 of 30 patients) at month 12; 62.1% (18 of 29 patients) at month 18; 54.2% (13 of 24 patients) at month 24; and | || || || || || || || || || || || || || || | adult patients experienced BMI increases above baseline at months 18, 24, and/or 36.
Table 26: Changes in BMI After up to 36 Months of Setmelanotide Treatment
Time point | Statistic | Patients with BBS (N = 30) | |
|---|---|---|---|
BMI at index trial baseline | Actual (kg/m2) | N | 30 |
Mean (SD) | 39.65 (8.97) | ||
90% CI | 36.87 to 42.44 | ||
Median | 42.37 | ||
Min, max | 24.4, 59.0 | ||
BMI at month 12 | Change from baseline (kg/m2) | N | 30 |
Mean (SD) | −5.53 (2.26) | ||
90% CI | −6.23 to −4.82 | ||
Median | −4.94 | ||
Min, max | −10.2, −1.3 | ||
Percentage change from baseline | N | 30 | |
Mean (SD) | −13.78 (4.58) | ||
90% CI | −15.20 to −12.36 | ||
Median | −13.61 | ||
Min, max | −25.4, −4.8 | ||
BMI at month 18 | Change from baseline (kg/m2) | N | 29 |
Mean (SD) | −4.76 (4.11) | ||
90% CI | −6.06 to −3.46 | ||
Median | −4.31 | ||
Min, max | −13.5, 3.3 | ||
Percentage change from baseline | N | 29 | |
Mean (SD) | −11.97 (9.33) | ||
90% CI | −14.91 to −9.02 | ||
Median | −10.56 | ||
Min, max | −30.7, 7.0 | ||
BMI at month 24 | Change from baseline (kg/m2) | N | 24 |
Mean (SD) | −4.35 (5.26) | ||
90% CI | −6.19 to −2.51 | ||
Median | −4.64 | ||
Min, max | −15.4, 6.6 | ||
Percentage change from baseline | N | 24 | |
Mean (SD) | −10.74 (12.24) | ||
90% CI | −15.02 to −6.45 | ||
Median | −11.10 | ||
Min, max | −35.0, 13.8 | ||
| || || || || | | | || || || || || || || || || | | | || || || || | | | || || || || | |
| || || || || | | | || || || || | | ||
| || || || || | | | || || || || | | ||
| || || || || | | | || || || || | | ||
| || || || || | | | || || || || | | ||
| || || || || || || || || || | | | || || || || | | | || || || || | | |
| || || || || | | | || || || || | | ||
| || || || || | | | || || || || | | ||
| || || || || | | | || || || || | | ||
| || || || || | | | || || || || | | ||
BBS = Bardet-Biedl syndrome; BMI = body mass index; CI = confidence interval; SD = standard deviation.
Source: Study 022 Clinical Study Report.60 Details in the table have been taken from the sponsor’s Summary of Clinical Evidence.
Change in Body Weight up to 36 Months Among Adult Patients With BBS
Changes from baseline in BMI for all patients (i.e., 11 adult patients, 19 pediatric patients) were −14.34% ± 3.14% (n = 11); −12.42% ± 9.83% (n = 11); −11.73% ± 11.11% (n = 10), and | || || || || || || || || || | for months 12, 18, 24, and 36, respectively. The proportions of adult patients who achieved a greater than or equal to 10% weight reduction from baseline were 63.6% at month 18 (7 patients of 11 patients); 60.0% at month 24 (6 patients of 10 patients), and | || || || || || || || || || |
Table 27: Changes in Body Weight in Adults After up to 36 Months of Setmelanotide Treatment
Time point | Statistic | Patients with BBS (N = 30) | |
|---|---|---|---|
Weight at index trial baseline | Actual (kg) | N | 11 |
Mean (SD) | 131.60 (21.07) | ||
90% CI | 120.08 to 143.12 | ||
Median | 127.50 | ||
Min, max | 99.3, 168.4 | ||
Weight at month 12 | Change from baseline (kg) | N | 11 |
Mean (SD) | −18.94 (5.65) | ||
90% CI | −22.03 to −15.85 | ||
Median | −16.70 | ||
Min, max | −27.3, −12.7 | ||
Percentage change from baseline | N | 11 | |
Mean (SD) | −14.34 (3.14) | ||
90% CI | −16.05 to −12.62 | ||
Median | −14.45 | ||
Min, max | −18.6, −10.0 | ||
Weight at month 18 | Change from baseline (kg) | N | 11 |
Mean (SD) | −16.70 (14.06) | ||
90% CI | −24.39 to −9.01 | ||
Median | −14.20 | ||
Min, max | −44.9, 2.0 | ||
Percentage change from baseline | N | 11 | |
Mean (SD) | −12.42 (9.83) | ||
90% CI | −17.79 to −7.05 | ||
Median | −12.03 | ||
Min, max | −30.5, 1.6 | ||
Weight at month 24 | Change from baseline (kg) | N | 10 |
Mean (SD) | −15.05 (15.48) | ||
90% CI | −24.03 to −6.07 | ||
Median | −13.77 | ||
Min, max | −51.2, 1.7 | ||
Percentage change from baseline | N | 10 | |
Mean (SD) | −11.73, (11.11) | ||
90% CI | −18.17 to −5.29 | ||
Median | −11.63 | ||
Min, max | −34.8, 1.5 | ||
| || || || || | | | || || || || || || || || || | | | || || || || | | | || || || || | |
| || || || || | | | || || || || | | ||
| || || || || | | | || || || || | | ||
| || || || || | | | || || || || | | ||
| || || || || | | | || || || || | | ||
| || || || || || || || || || | | | || || || || | | | || || || || | | |
| || || || || | | | || || || || | | ||
| || || || || | | | || || || || | | ||
| || || || || | | | || || || || | | ||
| || || || || | | | || || || || | | ||
BBS = Bardet-Biedl syndrome; CI = confidence interval; SD = standard deviation.
Source: Study 022 Clinical Study Report.60 Details in the table have been taken from the sponsor’s Summary of Clinical Evidence.
Change in BMI z Score up to 36 Months Among Pediatric Patients With BBS
Changes from baseline in BMI z score were −0.82 ± 0.35 (n = 19), −0.92 ± 0.41 (n = 17), −0.85 ± 0.45 (n = 19), and | || || || || || || | at months 12, 18, 24, and 36, respectively. The proportions of pediatric patients who achieved a greater than or equal to 0.3 change in BMI z score from baseline were 100.0% at month 18 (17 of 17 patients), 92.3% at month 24 (12 of 13 patients), and | || || || | | || || | at month 36 (| || || | patients).
Change in Weight-Related Parameters Beyond 36 Months
The results of | || || patients who received setmelanotide treatment for greater than 36 months were available. The longest time on treatment was 5 years (| || || || || || || || || || || || || || || || || || || || |). Findings are consistent with previous months’ measures, with BMI reduction tending to decrease or stabilize. However, | || pediatric patients experienced an increase in their BMI at months 24 and 36.
Table 28: Changes in BMI z Score Among Pediatric Patients After up to 36 Months of Setmelanotide Treatment
Time point | Statistic | Index trial baseline value | Month 12 and latest time point |
|---|---|---|---|
BMI z score at index trial baseline | Actual | N | 19 |
Mean (SD) | 3.57 (0.89) | ||
90% CI | 3.21 to 3.92 | ||
Median | 3.60 | ||
Min, max | 1.8, 5.7 | ||
BMI z score at month 12 | Change from baseline | N | 19 |
Mean (SD) | −0.82 (0.35) | ||
90% CI | −0.96 to −0.68 | ||
Median | −0.75 | ||
Min, max | −1.9, −0.4 | ||
BMI z score at month 18 | Change from baseline | N | 17 |
Mean (SD) | −0.92 (0.41) | ||
90% CI | −1.09 to −0.74 | ||
Median | −0.82 | ||
Min, max | −2.2, −0.4 | ||
BMI z score at month 24 | Change from baseline | N | 13 |
Mean (SD) | −0.85 (0.45) | ||
90% CI | −1.07 to −0.63 | ||
Median | −0.85 | ||
Min, max | −1.6, 0.1 | ||
| || || || || || || || || | | || || || || | | | || || || || | | | || || || || | |
| || || || || | | | || || || || | | ||
| || || || || | | | || || || || | | ||
| || || || || | | | || || || || | | ||
| || || || || | | | || || || || | | | || || || || | |
BMI = body mass index; CI = confidence interval; SD = standard deviation.
Source: Study 022 Clinical Study Report.60 Details in the table have been taken from the sponsor’s Summary of Clinical Evidence.
Harms
All AEs presented in the following table were treatment-emergent and analyzed in the SAS.
In Study 022, AEs were reported for all enrolled patients at the time of the data cut-off; however, setmelanotide was well-tolerated, and no patients experienced SAEs related to the treatment except for 1 patient who discontinued due to auditory hallucination, which was believed to be unrelated to the study medication. The most frequently reported TEAEs included injection-site pruritis (73.3%) and erythema (70.0%), skin hyperpigmentation (66.7%), injection-site bruising (53.3%), and induration and pain (46.7%). Injection-site edema, nausea, and vomiting occurred in greater than or equal to 33.3% of patients. SAEs were reported by 3 participants (10.0%). No death related to AEs was reported.
The sponsor concluded that the systemic safety profile of Study 022 was generally consistent with the safety findings from Study 023 and suggested that this medication is effective and safe for the long-term treatment of obesity and control of hunger in adult and pediatric patients greater than or equal to 6 years of age with BBS and obesity.
Table 29: Summary of Harms in Study 022
TEAEs, n (%) | Study 022 (N = 30) |
|---|---|
Any TEAE | 30 (100) |
Any SAE | 3 (10.0) |
Any TEAE leading to discontinuation | 1 (3.3) |
Any TEAE leading to death | 0 |
Any TEAE related to study drug | 30 (100) |
TEAEs occurring in ≥ 10% of patients | |
Injection-site pruritis | 22 (73.3) |
Injection-site erythema | 21 (70.0) |
Skin hyperpigmentation | 20 (66.7) |
Injection-site bruising | 16 (53.3) |
Injection-site induration | 14 (46.7) |
Injection-site pain | 14 (46.7) |
Injection-site edema | 10 (33.3) |
Nausea | 10 (33.3) |
Vomiting | 10 (33.3) |
SAE = serious adverse event; TEAE = treatment-emergent adverse event.
Note: The data cut-off date was June 2022. The study is still ongoing.
Source: Study 022 Clinical Study Report.60 Details in the table have been taken from the sponsor’s Summary of Clinical Evidence.
Critical Appraisal
Internal Validity
Study 022 was designed as an open-label extension study to assess the long-term efficacy and safety of setmelanotide dosing regimens in the treatment of adult and pediatric patients with BBS. The open-label and single-arm design could bias the magnitude of the efficacy of outcomes and subjective safety parameters due to unblinded exposure to the study medication during the treatment period.
The lack of hunger and HRQoL measures, the lack of adjustment for covariates, and the absence of statistical testing are considered limitations.
External Validity
The external validity of the LTE is similar to that reported for the parent trial. It is reasonable to expect that the same strengths and limitations related to generalizability apply to the extension study, with the addition that this is an inherently enriched population, given that patients needed to complete the parent study before enrolling; this introduces some selection bias for responders.
Indirect Evidence
Contents within this section have been informed by materials submitted by the sponsor. The following information has been summarized and validated by the CADTH review team.
A feasibility assessment was conducted for indirect treatment comparisons of setmelanotide versus 8 general obesity treatments, including semaglutide, lixisenatide, lisdexamfetamine, topiramate, liraglutide, naltrexone-bupropion, orlistat, and bariatric surgery. Systematic literature reviews were conducted to identify prospective or retrospective clinical studies, published or unpublished, pertaining to the treatment of patients with BBS and obesity. No relevant articles were identified in this patient population; therefore, indirect comparisons were not feasible.
Discussion
Summary of Available Evidence
One phase III, 52-week, open-label trial with a 14-week, randomized, double-blind, placebo-controlled period was included in this review (Study 023), as well as an associated LTE (Study 022). Study 023 enrolled 52 patients, 44 of whom had BBS and 8 of whom had AS; only the patients with BBS are of interest for this review. The patients with BBS had a clinical diagnosis per the Beales criteria, were greater than or equal to 6 years of age, were obese (BMI ≥ 30 kg/m2 for patients ≥ 16 years of age, or weight > 97th percentile for age and sex on growth chart assessment for patients 6 years to 15 years of age), and had not participated in recent or current intensive diet and/or exercise regimens or recently received pharmacotherapies that could affect the efficacy results related to obesity. Patients were randomized to either setmelanotide at an age-specific starting dose of 1 mg or 2 mg (escalating toward a target dose of 3 mg once daily through SC injection) or a matching-administration placebo for the first 14 weeks of the study. Thereafter, all patients received setmelanotide with the same starting and target dose, with dosing re-escalated to preserve the initial blinding, for 52 weeks. The primary outcome of Study 023 was the proportion of pivotal patients age greater than or equal to 12 years at baseline treated with setmelanotide for approximately 52 weeks who achieved a greater than or equal to 10% reduction in body weight from the active treatment baseline. Secondary outcomes included change in body weight and hunger scores after 52 weeks on setmelanotide and at 14 weeks compared to placebo. Additional exploratory outcomes included safety and tolerability, PROs related to hunger and HRQoL (e.g., based on hunger questionnaires, the IWQoL-Lite, the PedsQL, and | || || ||) and pharmacokinetics. For this review, the focus was on the BBS subgroup, including both pivotal and supplemental patients for all outcomes where possible.
At baseline, the patients with BBS included in Study 023 had a mean age of 18.5 years in the group randomized to setmelanotide and 21.5 years in the group randomized to placebo; in each group, 12 patients and 10 patients were under 17 years of age, and there were 9 female patients (40.9%) and 15 female patients (68.2%), respectively. Cognitive impairment was present in 12 patients (54.5%) and 8 patients (36.4%). The mean weights at placebo-controlled baseline were 110.45 kg and 106.5 kg, respectively, and the mean BMIs were 41.4 and 41.6, respectively.
The associated LTE, Study 022, is an ongoing, 36-month, open-label extension study that recruited a total of 30 responders with BBS and obesity, aged greater than or equal to 6 years, who completed either Study 023 (n = 23) or the phase II trial, Study 014 (n = 7). Of the 30 recruited patients, 27 are still ongoing in the trial. Early findings from months 12, 18, and 24 are available.
It was not feasible to conduct indirect treatment comparisons of setmelanotide to other active therapies due to a lack of data in patients with BBS.
Efficacy
There are limitations to the interpretability of the efficacy results from Study 023 due to the single-arm, open-label design. These design elements increase the risk of bias for subjective clinical outcome assessments and may lead to the overestimation of treatment effects for both benefits and harms. However, BBS is a rare disease with a small patient population for which there are no other targeted pharmacotherapies, and the 14-week, exploratory, placebo-controlled outcomes provide some supportive comparative effectiveness evidence. Additionally, the trial incorporated conservative design elements that could partially mitigate the increased risk of bias introduced from the study design. However, ultimately, the final direction and magnitude of bias are unknown.
Additionally, dosing in Study 023 differed from the recommended dosing described in the product monograph. The product monograph indicates that patients aged 18 years and older should start on 1 mg daily, increasing by 0.5 mg daily every 2 weeks to a maximum of 3.0 mg daily, if tolerated; however, during the trial, patients aged 16 years or older started on 2 mg daily for 2 weeks and then increased to 3 mg daily, if tolerated. For pediatric patients, the recommended starting dose in the product monograph is 0.5 mg, increasing by 0.5 mg daily every 2 weeks to a maximum of 2.0 mg daily; however, in Study 023, patients aged less than 16 years started at 1 mg daily for 1 week, increasing to 2 mg daily for 1 week, and then to a maximum of 3 mg daily, if tolerated. In summary, the trial had higher starting doses and shorter periods of intermediate dosing during the titration phase for all ages, and higher target doses for patients aged 16 years or older. Given that the average maintenance dose for pediatric patients with BBS was | || || || per day after titration,11 which exceeds the maximum recommended dose, this presents some uncertainty in generalizability. The average dose in adults after titration was | || || | per day, which aligns with the recommended dosing.11 The clinical experts consulted by CADTH indicated that dosing in real-world practice would mostly follow the product monograph, with occasional exceptions for patients who are older than 16 years and may begin to receive adult dosing, based on clinical judgment.
For the primary outcome of the proportion of patients who achieved a weight-loss response, both the target of weight loss (≥ 10% reduction in total body weight, compared to the well-accepted MID of ≥ 5%) and the prespecified target for the proportion of responders (≥ 10% responders, rounded up from the observed 6.4% in historical control data) were considered to be quite conservative. These conservative design elements could partially mitigate the increased risk of bias introduced from the study design. However, ultimately, the final direction and magnitude of bias are unknown. The estimated response rate of 33.7% (95% CI, 16.9% to 50.6%) exceeded the target of 10% responders after 52 weeks of setmelanotide treatment in pivotal patients aged greater than or equal to 12 years.
In the exploratory, placebo-controlled analyses assessed at 14 weeks, setmelanotide was associated with a greater difference in mean percentage change in body weight (i.e., −3.43%; 95% CI, −5.67% to −1.19), and placebo-treated patients had a mean change of 0 kg or −0.23% body weight (SD = 2.137%). These results are supportive of the treatment effect of setmelanotide.
Input from clinician and patient groups indicated that hyperphagia is among the most distressing symptoms of BBS and represents an important unmet need. In Study 023, although there appears to be an improvement in hunger at 52 weeks (and in comparison to placebo at 14 weeks), the hunger questionnaires developed by the sponsor and the associated MIDs have not been externally validated. Therefore, it is not possible to conclude on whether the observed benefits in hunger scores are clinically meaningful or can be interpreted as attributable to setmelanotide.
Exploratory HRQoL outcomes based on the IWQoL-Lite and PedsQL in patients without cognitive impairment generally showed a trend toward improvement greater than the reported MIDs (in general populations or general obesity) after 52 weeks of setmelanotide treatment. No MIDs were provided for the | || || ||, and results were inconsistent between the health state scales. No outcomes comparing setmelanotide to placebo were available for HRQoL-related outcomes. However, very small sample sizes, the lack of MIDs specific to BBS, and the single-arm, open-label nature of these assessments reduce the certainty associated with these results. As a result, the effect of setmelanotide on HRQoL is inconclusive.
The exploratory outcomes of waist circumference and lipid profile changes also suggest some improvement after 52 weeks of setmelanotide treatment. The clinical experts consulted by CADTH indicated that there are no firm MIDs established, but that improvement in these parameters is encouraging in clinical practice. Ultimately, it is not possible to conclude on whether these changes are clinically meaningful.
Subgroup analyses were conducted with different analysis sets based on age among pivotal patients with BBS for weight-related outcomes, and the results were consistent with the primary and secondary outcomes previously described. Age groups considered include all ages (≥ 6 years), less than 12 years, less than 18 years, and greater than or equal to 18 years. The results for patients aged less than 12 years and greater than or equal to 18 years will be highlighted here. Among pivotal patients with BBS who were less than 12 years of age (n = 8), | || || || || || || || || || || || || || || || || || || || || |; this magnitude of change in BMI z score is greater than reported clinically meaningful reductions in pediatric BMI z scores (−0.15 to −0.20).59 Among pivotal patients with BBS who were greater than or equal to 18 years of age, | || || || || | of patients achieved a clinically meaningful (≥ 5%) reduction in body weight and | || || || achieved a greater than or equal to 10% reduction in body weight after 52 weeks of setmelanotide treatment. As previously described, the interpretability of the magnitude of effect at 52 weeks is limited due to the open-label, single-arm nature of the trial. However, the exploratory 14-week outcomes for weight-related parameters in the age-specific subgroups support the possibility of a treatment effect associated with setmelanotide versus placebo in terms of weight loss measured according to body weight change, BMI, or BMI z score.
The clinical experts consulted by CADTH indicated that weight loss is expected to plateau over time, and that maintenance of weight loss would be considered a continued treatment response after the first year of setmelanotide. At the time of this review, the LTE (Study 022) was still ongoing, and not all patients had completed the 36-month assessment. Early findings from 12-month, 18-month, and 24-month assessments indicate that weight-related parameters tended to stabilize in 26 patients of the 30 patients with BBS and obesity, while the remaining 4 patients experienced BMI increases above baseline. However, due to the immaturity of the data and the potentially lifelong treatment period for patients with BBS, the long-term efficacy of setmelanotide is highly uncertain. There is also a data gap regarding the efficacy of off-label treatments for general obesity in BBS populations, and by extension, the comparative efficacy of setmelanotide versus off-label therapies in BBS. The efficacy and safety of combination therapies are also unknown but may be used in clinical practice for this population, such as for patients with BBS who are also receiving semaglutide for comorbid diabetes. The clinical experts consulted by CADTH suggested that it is clinically plausible that combination therapies have a synergistic effect on control of hunger and weight loss.
Notably, Health Canada recommends discontinuation of setmelanotide for patients who have not lost at least 5% of baseline total body weight (or 5% of baseline BMI for patients with continued growth potential) after 22 weeks of treatment, inclusive of the approximately 8 weeks required for initial dose titration and the minimum of 14 weeks on a therapeutic dose (for patients requiring the maximum dose).38 It was concluded that patients who are not responders at 22 weeks are unlikely to achieve and sustain clinically meaningful weight loss with continued treatment. The 5% threshold for weight loss is consistent with both widely accepted MIDs and the clinical expert opinion provided to CADTH. However, the timing of the 22-week assessment differs from Study 023 in which, based on the study design, key outcomes were assessed at 52 weeks of active therapy, and exploratory, placebo-controlled outcomes were assessed at 14 weeks from baseline; additionally, it differs from the recommendations given by the clinical experts consulted by CADTH, who proposed a 1-year trial period of setmelanotide. As an ad hoc analysis in response to a request by CADTH to reflect the Health Canada recommendations, the sponsor also provided the estimated proportion of pivotal patients with BBS aged greater than or equal to 12 years who achieved a greater than or equal to 5% reduction in total body weight after | | || || || || || || || || || || || || || || | || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || |.7
Harms
To maximize the available sample size, the analysis of harms is based on the SAS of Study 023, which included all 52 enrolled patients with either AS or BBS. Results were consistent between this cohort and the subgroup of patients with BBS. Overall, nonserious AEs were very common during the 14-week, placebo-controlled period and were similar between setmelanotide-treated patients and placebo-treated patients (96.3% and 96.0% of whom experienced at least 1 AE, respectively). Over the 52-week, open-label period, 100% of patients experienced at least 1 AE. The most common TEAEs were injection-site reactions (erythema, pruritus, bruising, and induration and pain), skin hyperpigmentation, nausea, vomiting, and diarrhea. Injection-site reactions were similar between treatment arms during the placebo-controlled period. It is important to note that the placebo formulation contained excipients that were similar to those used in the active formulation. Given this fact, it would not be unexpected to observe a similar rate of injection-site reactions in the placebo-treated group, and it is unlikely that these reactions were due to setmelanotide. Local injection-site tolerance has been assessed in all setmelanotide toxicity studies, and the most common findings were that inflammatory injection-site reactions related mainly to the primary excipient, mPEG-DSPE, with the possible involvement of setmelanotide at high doses. Although rates of nausea and diarrhea were very similar between treatment arms, vomiting occurred in setmelanotide-treated patients only (25.9%); 1 setmelanotide-treated patient withdrew due to vomiting. | || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || ||. No events of severe vomiting or nausea occurred. SAEs were uncommon and occurred in only 3 patients over the study period; none were considered related to the study drug by study investigators. TEAEs that led to study drug withdrawal were otherwise similar between treatment arms during the placebo-controlled period. No deaths occurred.
AEs of special interest identified by the sponsor and/or by clinical experts included injection-site reactions (as previously described), anaphylaxis, bradycardia, hyperpigmentation, melanoma, sexual events, and select psychiatric events, including anxiety, depression, suicidal ideation, suicide attempts, and aggression. Anxiety was not reported in the study. No patients experienced melanoma or suicide attempts. Anaphylaxis was experienced by only 1 placebo-treated patient, who withdrew during the placebo-controlled period as a result. Hyperpigmentation was experienced frequently and exclusively in setmelanotide-treated patients (in 63.0% during the RCT period and 63.5% over the full study period); these events were expected due to the effect of melanocortin receptor agonism during setmelanotide treatment. One patient discontinued due to hyperpigmentation. Sexual events occurred in some patients: | || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || || during the study period. Depression and depressed mood each occurred in 1 patient over the full study period. One patient experienced 2 events of suicidal ideation that resolved without study drug discontinuation and were concurrent with an SAE (blindness); none of these were considered related to the study drug. Aggression occurred in 3 patients.
Preliminary results of the LTE study, Study 022, supported the safety-related conclusions of Study 023. No new safety signals were identified. However, the study is ongoing, and more data are needed to support the long-term safety of setmelanotide. Overall, the clinical experts consulted by CADTH considered the safety profile of setmelanotide to be acceptable.
Conclusion
There is an unmet need for targeted treatments that address the underlying biological causes of hyperphagia and obesity in BBS, a very rare, incurable, genetic ciliopathy with multisystem manifestations. Patients and clinicians highlighted that early-onset obesity and hyperphagia are 2 of the most distressing symptoms, causing significant caregiver burden and impairment to HRQoL, and that typical obesity management strategies — such as restricted diet — are less feasible and less sustainable in this population than in general obesity. One completed phase III trial (Study 023) and an ongoing LTE (Study 022) were included in this review. There were notable concerns about the internal validity of these studies. These concerns were driven primarily by the single-arm, open-label trial designs, which introduce significant risk of bias to all subjective clinical outcomes and limit the interpretation of the magnitude of effect attributable to the intervention. However, BBS is a rare disease with a small patient population for which there are no other targeted pharmacotherapies.
The data submitted to CADTH were considered clinically relevant to the target patient population. Setmelanotide results were consistent with a clinically meaningful reduction in all weight-related parameters, such as change in body weight and BMI, across all reported analysis populations and subgroup analyses at 52 weeks, and the results were supported by the exploratory, comparative, 14-week, placebo-controlled outcomes. The results also suggested a consistent reduction in hunger scores in both the placebo-controlled and open-label periods; however, the scale used to measure hunger has not been externally validated. Therefore, whether these results are clinically meaningful is inconclusive. Similarly, results of the HRQoL outcomes at 52 weeks appeared to support a beneficial effect of setmelanotide, but small sample sizes and the single-arm study design made interpreting these events challenging. The long-term efficacy of setmelanotide is unknown because efficacy data from the LTE (Study 022) were immature at the time of this review. There is no evidence of effect regarding other BBS-related manifestations or prognosis aside from obesity. There are concerns about the generalizability of the clinical data to pediatric patients, given that the average maintenance dose in pediatric patients in Study 023 (| || || || || || || || || ||11) exceeded the maximum recommended dose of 2 mg daily. There are also inherent risks of bias, confounding, and uncertainty in the estimation of treatment effects from single-arm data due to unidentified, uncontrolled prognostic factors. Moreover, the open-label design of the single-arm period increases the risk of detection bias and performance bias, and may lead to an overestimation of the treatment effect for subjective outcomes.
There are potentially notable harms of setmelanotide — including hyperpigmentation, sexual events, or inappropriate behaviours — but these events were generally uncommon, and no treatment-related melanoma has been observed in any setmelanotide trial to date. Behavioural or psychiatric disturbances, such as depression or aggression, were observed in the setmelanotide trials, but were unlikely to be related to study medication. All patients in Study 023 experienced at least 1 AE, but very few were serious; setmelanotide was generally well-tolerated. The most common AEs in setmelanotide-treated patients were injection-site reactions, skin hyperpigmentation, nausea, vomiting, and diarrhea. Vomiting was commonly and exclusively observed in patients treated with setmelanotide, and tended to occur during the first month of treatment; however, no events were severe. No new safety signals have been identified in the ongoing LTE (Study 022).
Overall, the results of Study 023 and Study 022 were consistent with setmelanotide improving important weight-related outcomes for patients with BBS. However, the ability to draw firm conclusions about the magnitude of clinical benefit in hunger, HRQoL, and other outcomes was limited. There are uncertainties regarding the long-term efficacy and safety of setmelanotide, given that it is potentially a lifelong treatment.
References
1.Kroes M, Osei-Assibey G, Baker-Searle R, Huang J. Impact of weight change on quality of life in adults with overweight/obesity in the United States: a systematic review. Curr Med Res Opin. 2016;32(3):485-508. PubMed
2.Crosby RD, Kolotkin RL, Williams GR. An integrated method to determine meaningful changes in health-related quality of life. J Clin Epidemiol. 2004;57(11):1153-1160. PubMed
3.Warkentin LM, Das D, Majumdar SR, Johnson JA, Padwal RS. The effect of weight loss on health-related quality of life: systematic review and meta-analysis of randomized trials. Obes Rev. 2014;15(3):169-182. PubMed
4.Wolfe BM, Kvach E, Eckel RH. Treatment of Obesity: Weight Loss and Bariatric Surgery. Circ Res. 2016;118(11):1844-1855. PubMed
5.Frühbeck G. Bariatric and metabolic surgery: a shift in eligibility and success criteria. Nat Rev Endocrinol. 2015;11(8):465-477. PubMed
6.Forsythe E, Beales PL. Bardet–Biedl syndrome. Eur J Hum Genet. 2013;21(1):8-13. PubMed
7.Rhythm Pharmaceuticals response to May 24, 2023 CADTH request for additional information regarding setmelanotide review. Boston (MA): Rhythm Pharmaceuticals Inc; 2023 May 26.
8.Varni JW, Burwinkle TM, Seid M, Skarr D. The PedsQL 4.0 as a pediatric population health measure: feasibility, reliability, and validity. Ambul Pediatr. 2003;3(6):329-341. PubMed
9.Clinical Study Report: RM-493-023. A phase 3 trial of setmelanotide (RM-493), a melanocortin-4 receptor (MC4R) agonist, in Bardet-Biedl Syndrome (BBS) and Alstrom Syndrome (AS) patients with moderate to severe obesity. [internal sponsor's report]. Boston (MA): Rhythm Pharmaceuticals Inc; 2022 Jun 16.
10.Report on the effects of setmelanotide in patients with Bardet-Biedl syndrome (BBS) from trial RM-493-023 [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Imcivree (setmelanotide) 10 mg/mL subcutaneous. Boston (MA): Rhythm Pharmaceuticals Inc; 2022 Jun 16.
11.Ad-hoc table: Average Setmelanotide Dosing Query for BBS patients [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Imcivree (setmelanotide) 10 mg/mL subcutaneous. Boston (MA): Rhythm Pharmaceuticals Inc 2022 Apr 25.
12.Forsythe E, Kenny J, Bacchelli C, Beales PL. Managing Bardet–Biedl Syndrome—Now and in the Future. Front Pediatr. 2018;6. PubMed
13.Pomeroy J, Krentz AD, Richardson JG, Berg RL, VanWormer JJ, Haws RM. Bardet‐Biedl syndrome: Weight patterns and genetics in a rare obesity syndrome. Pediatr Obes. 2020;16(2). PubMed
14.Feuillan PP, Ng D, Han JC, et al. Patients with Bardet-Biedl Syndrome Have Hyperleptinemia Suggestive of Leptin Resistance. J Clin Endocr. 2011;96(3):E528-E535. PubMed
15.Sherafat-Kazemzadeh R, Ivey L, Kahn SR, et al. Hyperphagia among patients with Bardet-Biedl syndrome. Pediatr Obes. 2013;8(5):e64-e67. PubMed
16.Han JC, Reyes-Capo DP, Liu C-Y, et al. Comprehensive Endocrine-Metabolic Evaluation of Patients With Alström Syndrome Compared With BMI-Matched Controls. J Clin Endocr. 2018;103(7):2707-2719. PubMed
17.Kleinendorst L, van Haelst MM, van den Akker ELT. Genetics of Obesity. Exp Suppl. 2019;111:419-441. PubMed
18.Heymsfield SB, Avena NM, Baier L, et al. Hyperphagia: Current concepts and future directions proceedings of the 2nd international conference on hyperphagia. Obesity. 2014;22(S1):S1-S17. PubMed
19.Hamlington B, Ivey LE, Brenna E, Biesecker LG, Biesecker BB, Sapp JC. Characterization of Courtesy Stigma Perceived by Parents of Overweight Children with Bardet-Biedl Syndrome. PLoS One. 2015;10(10):e0140705. PubMed
20.Forsythe E, Haws RM, Argente J, et al. Quality of life improvements following one year of setmelanotide in children and adult patients with Bardet–Biedl syndrome: phase 3 trial results. Orphanet J Rare Dis. 2023;18(1). PubMed
21.Wharton S, Lau DCW, Vallis M, et al. Obesity in adults: a clinical practice guideline. Can Med Assoc J. 2020;192(31):E875-E891. PubMed
22.Di Angelantonio E, Bhupathiraju SN, Wormser D, et al. Body-mass index and all-cause mortality: individual-participant-data meta-analysis of 239 prospective studies in four continents. Lancet. 2016;388(10046):776-786. PubMed
23.Prospective Studies Collaboration, Whitlock G, Lewington S, et al. Body-mass index and cause-specific mortality in 900 000 adults: collaborative analyses of 57 prospective studies. Lancet. 2009;373(9669):1083-1096. PubMed
24.Aykut A, Özen S, Gökşen D, et al. Melanocortin 4 receptor (MC4R) gene variants in children and adolescents having familial early-onset obesity: genetic and clinical characteristics. Eur J Pediatr. 2020;179(9):1445-1452. PubMed
25.Hilbert A, Rief W, Braehler E. Stigmatizing Attitudes Toward Obesity in a Representative Population-based Sample. Obesity. 2008;16(7):1529-1534. PubMed
26.Puhl RM, Heuer CA. The Stigma of Obesity: A Review and Update. Obesity. 2009;17(5):941-964. PubMed
27.Yeung JC, Katwa UA, Lee GS. Sleep disordered breathing in Bardet-Biedl Syndrome. Int J Pediatr Otorhinolaryngol. 2017;102:127-132. PubMed
28.Suspitsin EN, Imyanitov EN. Bardet-Biedl Syndrome. Mol Syndromol. 2016;7(2):62-71. PubMed
29.Polyzos SA, Kountouras J, Mantzoros CS. Obesity and nonalcoholic fatty liver disease: From pathophysiology to therapeutics. Metabolism. 2019;92:82-97. PubMed
30.Kuhl ES, Rausch JR, Varni JW, Stark LJ. Impaired Health-Related Quality of Life in Preschoolers With Obesity. J Pediatr Psychol. 2012;37(10):1148-1156. PubMed
31.Schwimmer JB. Health-Related Quality of Life of Severely Obese Children and Adolescents. JAMA. 2003;289(14). PubMed
32.Moore SJ, Green JS, Fan Y, et al. Clinical and genetic epidemiology of Bardet-Biedl syndrome in Newfoundland: A 22-year prospective, population-based, cohort study. Am J Med Genet A. 2005;132A(4):352-360. PubMed
33.National Organization for Rare Disorders. Bardet-Biedl Syndrome. 2022; https://rarediseases.org/rare-diseases/bardet-biedl-syndrome/?filter=ovr-ds-resources. Accessed 2023 Apr 21.
34.Woods MO, Young T-L, Parfrey PS, Hefferton D, Green JS, Davidson WS. Genetic Heterogeneity of Bardet–Biedl Syndrome in a Distinct Canadian Population: Evidence for a Fifth Locus. Genomics. 1999;55(1):2-9. PubMed
35.Beales PL, Elcioglu N, Woolf AS, Parker D, Flinter FA. New criteria for improved diagnosis of Bardet-Biedl syndrome: results of a population survey. J Med Genet. 1999;36(6):437-446. PubMed
36.Haws R, Brady S, Davis E, et al. Effect of setmelanotide, a melanocortin‐4 receptor agonist, on obesity in Bardet‐Biedl syndrome. Diabetes Obes Metab. 2020;22(11):2133-2140. PubMed
37.Haqq AM, Chung WK, Dollfus H, et al. Efficacy and safety of setmelanotide, a melanocortin-4 receptor agonist, in patients with Bardet-Biedl syndrome and Alström syndrome: a multicentre, randomised, double-blind, placebo-controlled, phase 3 trial with an open-label period. Lancet Diabetes Endocrinol. 2022;10(12):P859-868. PubMed
38.Imcivree (setmelanotide): 10 mg/mL solution for subcutaneous injection [product monograph]. Boston (MA): Rhythm Pharmaceuticals Inc; 2023 Apr 24.
39.Setmelanotide (IMCIVREE™) in adult and pediatric patients 6 years of age and older with impairments in the MC4R pathway due to genetic diseases, for the treatment of obesity and control of hunger in Bardet-Biedl syndrome (BBS) [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Imcivree (setmelanotide), 10 mg/mL subcutaneous injection. Boston (MA): Rhythm Pharmaceuticals Inc; 2022 Nov.
40.Health Canada clarimail: Imcivree (setmelanotide) [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Imcivree (setmelanotide) 10 mg/mL subcutaneous. Boston (MA): Rhythm Pharmaceuticals Inc; 2023 Mar 7.
41.Marshall JD, Beck S, Maffei P, Naggert JK. Alström Syndrome. Eur J Hum Genet. 2007;15(12):1193-1202. PubMed
42.Driscoll DJ, Miller JL, Schwartz S, Cassidy SB. Prader-Willi Syndrome. In: Adam MP, Ardinger HH, Pagon RA, et al., editors. GeneReviews® [Internet]. 1998 [updated 2017 Dec 14]; https://www.ncbi.nlm.nih.gov/books/NBK1330/. Accessed 2023 Apr 26.
43.Kolotkin RL, Crosby RD, Kosloski KD, Williams GR. Development of a Brief Measure to Assess Quality of Life in Obesity. Obes Res. 2001;9(2):102-111. PubMed
44.Varni JW, Seid M, Kurtin PS. PedsQL 4.0: reliability and validity of the Pediatric Quality of Life Inventory version 4.0 generic core scales in healthy and patient populations. Med Care. 2001;39(8):800-812. PubMed
45.Herdman M, Gudex C, Lloyd A, et al. Development and preliminary testing of the new five-level version of EQ-5D (EQ-5D-5L). Qual Life Res. 2011;20(10):1727-1736. PubMed
46.The practical guide: identification, evaluation, and treatment of overweight and obesity in adults. (NIH Publication No. 00-4084). Bethesda (MD): National Heart Lung and Blood Institute; 2000: https://www.nhlbi.nih.gov/files/docs/guidelines/prctgd_c.pdf. Accessed 2023 Apr 21.
47.Colman E. Food and Drug Administration's Obesity Drug Guidance Document. Circulation. 2012;125(17):2156-2164. PubMed
48.Guideline on clinical evaluation of medicinal products used in weight management. London (GB): European Medicines Agency; 2017: https://www.ema.europa.eu/en/documents/scientific-guideline/guideline-clinical-evaluation-medicinal-products-used-weight-management-revision-1_en.pdf. Accessed 2023 Mar 23.
49.Centers for Disease Control and Prevention. Defining child BMI categories. 2022; https://www.cdc.gov/obesity/basics/childhood-defining.html. Accessed 2023 May 4.
50.Ells LJ, Rees K, Brown T, et al. Interventions for treating children and adolescents with overweight and obesity: an overview of Cochrane reviews. Int J Obes. 2018;42(11):1823-1833. PubMed
51.Wiegand S, Keller K-M, Lob-Corzilius T, et al. Predicting Weight Loss and Maintenance in Overweight/Obese Pediatric Patients. Horm Res Paediatr. 2014;82(6):380-387. PubMed
52.Grossman DC, Bibbins-Domingo K, Curry SJ, et al. Screening for Obesity in Children and Adolescents. JAMA. 2017;317(23):2417-2426. PubMed
53.Feng YS, Kohlmann T, Janssen MF, Buchholz I. Psychometric properties of the EQ-5D-5L: a systematic review of the literature. Qual Life Res. 2021;30(3):647-673. PubMed
54.Kolotkin RL, Crosby RD. Psychometric evaluation of the impact of weight on quality of life-lite questionnaire (IWQOL-lite) in a community sample. Qual Life Res. 2002;11(2):157-171. PubMed
55.Tessier A, Mayo NE, Cieza A. Content identification of the IWQOL-Lite with the International Classification of Functioning, Disability and Health. Qual Life Res. 2011;20(4):467-477. PubMed
56.Clinical Study Report: RM-493-023. A phase 3 trial of setmelanotide (RM-493), a melanocortin-4 receptor (MC4R) agonist, in Bardet-Biedl Syndrome (BBS) and Alstrom Syndrome (AS) patients with moderate to severe obesity [internal sponsor's report]. Boston (MA): Rhythm Pharmaceuticals; 2022 Jun 16.
57.Rhythm Pharmaceuticals response to April 14, 2023 CADTH request for additional information regarding setmelanotide review. Boston (MA): Rhythm Pharmaceuticals Inc; 2023 Apr 20.
58.Rhythm Pharmaceuticals response to May 5, 2023 CADTH request for additional information regarding setmelanotide review. Boston (MA): Rhythm Pharmaceuticals Inc; 2023 May 9.
59.Kumar S, King EC, Christison AL, et al. Health Outcomes of Youth in Clinical Pediatric Weight Management Programs in POWER. J Pediatr. 2019;208:57-65.e54. PubMed
60.Clinical Study Report: RM-493-022. Long-term extension trial of setmelanotide (RM-493) for patients who have completed a trial of setmelanotide for the treatment of obesity associated with genetic defects upstream of the MC4 receptor in the leptin-melanocortin pathway. [internal sponsor's report]. Boston (MA): Rhythm Pharmaceuticals Inc; 2022 Sep 19.
61.Rhythm Pharmaceuticals Inc. NCT03013543: Setmelanotide (RM-493) phase 2 treatment trial in patients with rare genetic disorders of obesity. Bethesda (MD): U.S. National Library of Medicine; 2022: https://clinicaltrials.gov/ct2/show/NCT03013543. Accessed 2023 May 10.
Appendix 1: Detailed Outcome Data
Note that this appendix has not been copy-edited.
| || || || || || || || || || || | | || || || || || || || || || || || || || || || |
|---|---|
| || || || || || | | || || || || || |
| || || || || || | | || || || || || |
| || || || || || | | || || || || || |
| || || || || || | | || || || || || |
| || || || || || | | || || || || || |
| || || || || || | | || || || || || |
| || || || || || | | || || || || || |
| || || || || || | | || || || || || |
| || || || || || | | || || || || || |
| || || || || || || || || || || || || || || || || || || || || | || || || || || | || || || || || | || || || || || | || || || || || | || || || || || | || || || || || |
Exploratory End Point: Change in Waist Circumference After 52 Weeks of Setmelanotide
Consistent with its effects on hunger and weight reduction, all 36 patients in the FAS (all ages) had measurable reductions in waist circumference after 52 weeks of setmelanotide treatment. Among 31 patients with BBS in the FAS (all ages), the mean waist circumference at active treatment baseline was 117.89 ± 18.02 cm. After 52 weeks of setmelanotide treatment, the mean absolute change was −7.18 ± 7.40 cm and the mean percent change was −6.33 ± 7.41%.
Exploratory End Point: Changes in Lipid Profile After 52 Weeks of Setmelanotide
Among all patients in the FAS (all ages) and patients with BBS in the FAS (all ages), 52 weeks of setmelanotide treatment resulted in reduced concentrations of total cholesterol, low-density lipoprotein cholesterol, and triglycerides, as well as increased concentrations of high-density lipoprotein cholesterol (Table 31).
Table 31: Lipid Profiles and Changes From Active Treatment Baseline After 52 Weeks of Setmelanotide Among All Patients and Among BBS Patients in the FAS
Parameter | Statistic | Patients with BBS in FAS (N = 31) |
|---|---|---|
Total cholesterol (mmol/L) | ||
Actual at ATB | N | 31 |
Mean (SD) | 4.39 (1.027) | |
Change from ATB | N | 23 |
Mean (SD) | 0.27 (0.437) | |
% change from ATB | N | 23 |
Mean (SD) | 6.09 (10.566) | |
High-density lipoprotein cholesterol (mmol/L) | ||
Actual at ATB | N | 31 |
Mean (SD) | 1.08 (0.193) | |
Change from ATB | N | 23 |
Mean (SD) | 0.06 (0.137) | |
% change from ATB | N | 23 |
Mean (SD) | 5.30 (11.561) | |
Low-density lipoprotein cholesterol (mmol/L) | ||
Actual at ATB | N | 31 |
Mean (SD) | 2.99 (1.014) | |
Change from ATB | N | 23 |
Mean (SD) | −0.21 (0.436) | |
% change from ATB | N | 23 |
Mean (SD) | −7.82 (16.775) | |
Triglycerides (mmol/L) | ||
Actual at ATB | N | 31 |
Mean (SD) | 1.86 (0.920) | |
Change from ATB | N | 23 |
Mean (SD) | −0.22 (0.620) | |
% change from ATB | N | 23 |
Mean (SD) | −9.62 (32.543) | |
ATB = active treatment baseline; BBS = Bardet-Biedl syndrome; FAS = full analysis set; HDL = high-density lipoprotein; LDL = low-density lipoprotein; SD = standard deviation
Sources: Study 023 Clinical Study Report9 and the report of patients with BBS from Study 023.10
Pharmacoeconomic Review
Abbreviations
BBS
Bardet-Biedl syndrome
BMI
body mass index
BSC
best supportive care
CV
cardiovascular
DAH
daily average hunger
HRQoL
health-related quality of life
ICER
incremental cost-effectiveness ratio
NAFLD
nonalcoholic fatty liver disease
NASH
nonalcoholic steatohepatitis
QALY
quality-adjusted life-year
SMR
standardized mortality ratio
Executive Summary
The executive summary comprises 2 tables (Table 1 and Table 2) and a conclusion.
Item | Description |
|---|---|
Drug product | Setmelanotide (IMCIVREE), 10 mg/mL solution in a 1 mL, multiple-dose vial for self-administered subcutaneous injection |
Submitted price | Setmelanotide, $402.70 per mg |
Indication | For weight management in adult and pediatric patients aged 6 years and older with obesity due to:
|
Health Canada approval status | NOC |
Health Canada review pathway | Priority review |
NOC date | May 5, 2023 |
Reimbursement request | Weight management in adult and pediatric patients aged 6 years and older with obesity due to Bardet-Biedl syndrome |
Sponsor | Rhythm Pharmaceuticals, Inc. |
Submission history | Not previously reviewed |
NOC = Notice of Compliance.
Table 2: Summary of Economic Evaluation
Component | Description |
|---|---|
Type of economic evaluation | Cost-utility analysis Markov model |
Target populations | Weight management in adult and pediatric patients aged 6 years and older with obesity due to Bardet-Biedl syndrome |
Treatment | Setmelanotide |
Comparators | BSC alone (nutrition, exercise, and non-pharmacological interventions) |
Perspective | Canadian publicly funded health care payer |
Outcomes | QALYs and LYs |
Time horizon | Lifetime (85 years for pediatric-initiated patients; 71 years for adult-initiated patients) |
Key data source | Pivotal trial RM-493 to 023 |
Submitted results | Pediatric-initiated: $1,185,599 per QALY gained (incremental costs = $11,457,751; incremental QALYs = 9.66) Adult-initiated: $1,288,761 per QALY gained (incremental costs = $5,353,700; incremental QALYs = 4.15) |
Key limitations |
|
CADTH reanalysis results |
|
BMI = body mass index; BSC = best supportive care; ICER = incremental cost-effectiveness ratio; LY = life-year; QALY = quality-adjusted life-year; QoL = quality of life.
Conclusions
The results of Study 022 (a long-term extension study) and Study 023 (a completed phase III trial) were consistent with setmelanotide improving important weight-related outcomes for patients with Bardet-Biedl syndrome (BBS). However, the ability to draw firm conclusions about the magnitude of clinical benefit in hunger, health-related quality of life (HRQoL), and other outcomes was limited. There are uncertainties regarding the long-term efficacy and safety of setmelanotide, given that it may be a potentially lifelong treatment.
The sponsor’s base case was derived using various assumptions and data sources that were uncertain. First, including additional hospitalization and specialty care visits as body mass index (BMI) increases in addition to obesity-related comorbidity resource use likely double-counts the resource use associated with obesity. Second, applying a disutility associated with weight class as well as weight-related comorbidities likely double-counts the quality of life impact associated with obesity. Third, assuming that the same comorbidity prevalence rate applies across different age groups likely overestimates the proportions of patients with comorbidities in younger age groups. Fourth, the utility value used for severe hyperphagia from the sponsored vignette study was relatively low compared to the value in another hyperphagia study. Finally, the model assumed that all patients with moderate and severe hyperphagia transitioned to a state of mild hyperphagia, which was not shown in the pivotal trial. The CADTH reanalysis addressed these limitations.
The CADTH base-case results were similar to the sponsor’s assessment in that both incremental cost-effectiveness ratios (ICERs) exceeded $1 million per quality-adjusted life-year (QALY) gained and were driven primarily by the cost of setmelanotide. In the CADTH base case, for the pediatric-initiated population, setmelanotide resulted in an additional 4.46 QALYs gained at an additional cost of $10,425,770 to the health system, resulting in an ICER of $2,336,431 per QALY gained, relative to best supportive care (BSC) alone. In the adult-initiated population, setmelanotide resulted in an additional 1.94 QALYs gained at an additional cost of $5,293,917 to the health system, resulting in an ICER of $2,702,877 per QALY gained, relative to BSC alone. At the recommended dose, the annual cost of setmelanotide per patient is $441,258 for adults and $294,172 for pediatric patients, assuming no wastage. In the model, this translated into lifetime setmelanotide drug costs of $10,438,536 for patients who initiate under the age of 18 and $5,298,918 for patients who initiate over the age of 18.
CADTH notes that the QALY gains in the base case were driven by large improvements in quality of life due to a reduction in hyperphagia and to mortality improvements. The CADTH reanalysis predicts life-year gains of 1.74 years for patients who initiate setmelanotide under the age of 18 years. CADTH notes that the model structure and assumptions were inappropriate for assessing the impact on weight-related comorbidities and that there is limited evidence to support improvements in mortality. Assuming that there is no impact on comorbidities increases the ICER to $2,948,725 per QALY gained in the pediatric-initiated population.
At a 90% price reduction, the annual per-patient cost of setmelanotide decreases to $44,126 in adult patients and to $29,417 in pediatric patients, resulting in ICERs of $268,963 and $229,545 per QALY gained, respectively. Therefore, price reductions of more than 90% would be required to achieve ICER thresholds below $200,000 per QALY. At a $50,000 per QALY threshold, a price reduction of approximately 98% would be required.
Stakeholder Input Relevant to the Economic Review
This section is a summary of the feedback received from the patient groups, registered clinicians, and drug plans that participated in the CADTH review process.
CADTH received patient input from the Bardet Biedl Syndrome Foundation. Forty-one individuals submitted responses to a survey about their experiences with BBS. Thirty-four respondents were caregivers to patients living with BBS, and the remaining 7 respondents were BBS patients. Many respondents were from the US (61%) or Canada (29%), with the remainder from Germany, Ireland, Spain, and the UK. Respondents noted concerns about lack of access to treatment, given that there is currently no cure for BBS and no available, targeted, publicly funded treatments in Canada, whether overall or for BBS-related hunger and obesity. From a quality of life perspective, respondents indicated that BBS-related hunger has the greatest impact on their social lives and emotional and psychological well-being. Among all survey respondents, 17 had experience with setmelanotide: 4 patients reported that they were currently taking it, and 13 caregivers indicated that their loved ones were taking it. When asked about any negative impacts experienced with setmelanotide, the most commonly mentioned ones were darkening of the skin and bruises and scars being more noticeable. Nausea and gastrointestinal upset were mentioned to a lesser extent, as well itchiness and/or pain at the injection site. Several respondents noted that the method of administration (daily injections) was challenging for patients who have vision impairments, which can be a symptom of BBS, and for younger patients, for whom it could limit activities of daily living, such as field trips and sleepovers.
CADTH received clinical input from a group of endocrinologists in Canada who treat BBS in adult and pediatric populations. The group stated that 72% to 92% of patients with BBS have obesity, with most having onset before 6 years of age. The prevalence of hyperphagia and obesity in BBS patient populations are thought to be related to hypothalamic dysfunction. There are no targeted therapies; therefore, current weight management approaches for individuals with BBS are similar to those for the general population. The cornerstone of obesity management is lifestyle intervention, which includes counselling and interventions to ensure optimized nutrition, appropriate physical activity, improved sleep patterns, and psychosocial and/or mental health supports. Pharmacotherapeutic options and bariatric surgery are now available for a subset of people living with obesity. For those living with BBS, engagement in lifestyle interventions is complicated by coexisting, biologically driven hyperphagia (i.e., deregulation of appetite), as well as by low vision, balance and coordination difficulties, intellectual disabilities, and mental health concerns. The effectiveness and safety of existing pharmacotherapeutic options for patients living with BBS have not been studied. Furthermore, these drugs do not directly address the hypothalamic dysfunction in patients living with BBS. The safety, efficacy, and durability of bariatric surgery in this population remain largely unknown. Setmelanotide would become part of the therapy plan (in combination with existing lifestyle interventions) for those aged 6 years or older with obesity. The addition of setmelanotide would allow for more successful weight management, given that it addresses the underlying hyperphagia directly. The responsiveness to lifestyle interventions would be expected to improve significantly. Therefore, 1 could also expect a decrease in the prevalence of weight-related health complications, such as cardiometabolic risk, type 2 diabetes, hypertension, nonalcoholic fatty liver disease (NAFLD), obstructive sleep apnea, and musculoskeletal pain and/or discomfort.
The input received from participating drug plans noted concerns with the fact that the comparator in the submitted trial was a placebo and that, as a result, there is no evidence comparing setmelanotide with other medications for weight loss. Moreover, drug plans were concerned with whether the weight loss reported in the submitted trial was clinically meaningful. Drug plans were also concerned with the availability of the genetic testing required to diagnose patients with BBS and whether patients would have access to the specialists who might be required to oversee the usage of setmelanotide and determine its place in therapy.
Several of these concerns were addressed in the sponsor’s model:
Utility estimates associated with hyperphagia were included.
Reduction in weight-related health complications, such as cardiometabolic risk, type 2 diabetes, hypertension, NAFLD, and obstructive sleep apnea, were assessed.
Economic Review
The current review is for setmelanotide (Imcivree) for weight management in adult and pediatric patients aged 6 years and older with obesity due to BBS.
Economic Evaluation
Summary of Sponsor’s Economic Evaluation
Overview
The sponsor submitted a cost-utility analysis comparing setmelanotide with BSC (i.e., nutrition, exercise, and non-pharmacological, psychological interventions) for patients with BBS. This population is narrower than the Health Canada indication, but aligns with the reimbursement request.
The drug acquisition cost for setmelanotide is $402.70 per mg (10 mg/mL solution in a 1 mL multiple-dose vial). It is self-administered once daily by subcutaneous injection (in the abdomen). The annual costs of setmelanotide based on actual dosing from the pivotal clinical trial, RM-493 to 023, were $419,195.60 (||||||| |||| |||| ||) in the first year and $428,020.77 from year 2 onward (|||| ||) for pediatric patients, and $423,608.18 in the first year (|||| ||) and $429,491.63 from year 2 onward (|||| ||) for adult patients, assuming no wastage. CADTH notes that the product monograph recommends a maximum dose of 3 mg for adults and 2 mg for pediatric patients.
The clinical outcomes reported were QALYs and life-years. The analyses were conducted from the Canadian public payer perspective. The time horizon in the base case was lifetime (i.e., 85 years for pediatric-initiated patients and 71 years for adult-initiated patients), and a 1.5% annual discount rate was applied for costs and effects.
Model Structure
A Markov model structure (refer to Appendix 3), with treatment effect on both obesity and hyperphagia (each modelled separately), was used to assess the cost-effectiveness of setmelanotide versus BSC. The Markov cycle length was 1 year. Patients entered the model with a distribution by BMI and hyperphagia severity aligned with participants at baseline in the pivotal trial, RM-493 to 023. Setmelanotide initiated in pediatric patients (aged 6 years to < 18 years) was modelled separately from adults (aged ≥ 18 years). When the pediatric cohort reached age 18 years, their pediatric BMI z scores were mapped to BMI using the WHO algorithm, assuming that a z score greater than or equal to 4.0 would equally be distributed into BMI classes of 40 to 45, 45 to 50, and greater than or equal to 50. Health states included 7 BMI or BMI z score states (< 25 or 0 to 1.0; 25 to < 30 or 1.0 to < 2.0; 30 to < 35 or 2.0 to < 2.5; 35 to < 40 or 2.5 to < 3.0; 40 to < 45 or 3.0 to < 3.5; 45 to < 50 or 3.5 to < 4.0; and ≥ 50 or ≥ 4.0) as well as 3 hyperphagia severity states (a mild daily average hunger [DAH] score [< 3.5], a moderate DAH score [3.5 to 6.4], or a severe DAH score [≥ 6.5]) and death.
Model Inputs
The patient baseline characteristics and the safety and efficacy of setmelanotide in adult and pediatric patients aged 6 years and older were obtained from a 66-week clinical study, which included a 14-week, randomized, double-blind, placebo-controlled period and a 52-week, open-label period during which all patients received setmelanotide (Study RM-493 to 023). The primary end point was the proportion of patients aged 12 years or older who achieved a greater than or equal to 10% reduction in body weight from baseline after 52 weeks of treatment. Analyses of outcomes among BBS patients were also performed after stratification by age (i.e., ≥ 18 years and < 18 years). Response rates were defined by greater than or equal to 10% weight loss and a BMI z score decrease of greater than or equal to 0.2 by 52 weeks for patients aged greater than or equal to 18 years and patients aged less than 18 years at baseline, respectively. Setmelanotide responders (defined as experiencing a ≥ 0.2 reduction in BMI z score or a ≥ 10% weight loss at week 52) had treatment effects related to BMI or BMI z score reduction and hyperphagia improvement modelled as a 1-time health state transition in the first cycle. Nonresponders remained at their baseline BMI or BMI z scores. In the base case, it was assumed that all setmelanotide responders transitioned from their baseline hyperphagia severity to mild hyperphagia, while DAH scores obtained from the trial were used in the scenario analysis. A discontinuation rate of 1% per year was assumed for setmelanotide responders; people who discontinued treatment were assumed to revert to their baseline BMI or BMI z scores and hyperphagia categories immediately upon discontinuation, with no tapering in treatment effects. All nonresponders were assumed to stop setmelanotide indefinitely.
Mortality was modelled using Canadian general population life tables, and treatment effect on mortality was modelled indirectly through impacts on BMI or BMI z score. Standardized mortality ratios (SMRs) by BMI were informed by a population-based cohort study of 3.6 million UK adults in which a hazard ratio of all-cause mortality of 1.21 was associated with every 5-point increase in BMI above 25.1 The pediatric SMRs were assumed to be equivalent to the adult SMRs after mapping from BMI to BMI z score category. The model also includes an additional increase in mortality risk associated with early-onset obesity. Given that less than 5% of patients in either treatment arm experienced serious treatment-emergent adverse events, these were not incorporated into the base case.
Utility values (EQ-5D) were determined by BMI level and age based on published Medical Expenditure Panel Survey data and a UK clinical study for the pediatric population2,3 using a mapping algorithm from the Pediatric Quality of Life Inventory to the EQ-5D in Khan et al. HRQoL values were measured in the RM-493 to 023 trial, but the sponsor’s clinical experts found that those values (i.e., a visual analogue scale of 69.38 at baseline) did not reflect the experience of BBS patients, given that these were only slightly below population norms. Additional utility multipliers for mild, moderate, and severe hyperphagia were obtained from a vignette study.4 Further utility decrements for obesity-related comorbidities (sleep apnea, osteoarthritis, type II diabetes, myocardial infarction, angina, stroke, and transient ischemic attack) were also obtained from UK literature.5,6 A composite cardiovascular (CV) event disutility was calculated by weighting the individual event disutilities by how common each event is when it occurs.
The proposed unit cost for setmelanotide is $402.70 per mg. Annual costs for setmelanotide were calculated using the average daily patient dosage from the trial for day 1, during titration, and after titration, instead of according to the planned dosing schedule. Administration costs were not included in the model, given that patients are expected to be able to self-administer setmelanotide with the help of a caregiver.
Disease management costs associated with routine patient monitoring (laboratory tests and primary and specialty physician visits) were informed by a combination of available published literature and feedback from the sponsor’s clinician experts in Canada; the sponsor’s clinician experts indicated that health care resource usage for disease management increases with age and BMI or BMI z score. An annual hospitalization visit was also assumed for pediatric patients with BMI z scores greater than or equal to 2.0. The unit costs for physician visits were obtained from the Ontario Ministry of Health Schedule of Benefits for Physician Services, while the unit costs for laboratory tests were obtained from the Ontario Schedule of Benefits for Laboratory Services. Unit costs for family physician and specialist visits were sourced from the Ontario Schedule of Benefits for Physicians. No costs were associated with hyperphagia severity. Additional costs for obesity-related comorbidities (i.e., osteoarthritis, nonalcoholic steatohepatitis [NASH], type 2 diabetes, and CV events) were applied as annual costs for the time horizon of the model using Canadian literature sources,7-14 except for the annual cost of NASH, for which a UK source was used.14 The model also assumed increasing costs by BMI or BMI z score category using a loglinear distribution. Productivity losses were considered in scenario analyses.
Summary of Sponsor’s Economic Evaluation Results
The sponsor’s cost-effectiveness analysis was based on 1,500 probabilistic iterations due to model convergence for both treatment arms; findings are presented here. The results of the deterministic analysis were similar to the results of the probabilistic analysis.
Base-Case Results
In the sponsor’s base-case analysis for the pediatric-initiated population, the ICER of setmelanotide was $1,185,599 per QALY when compared to BSC. Specifically, setmelanotide was associated with 9.66 additional QALYs and $11,457,751 additional costs compared to BSC over a lifetime horizon. (Disaggregated results are presented in Appendix 3.) The cost-effectiveness acceptability curves indicated that 0% of the results were cost-effective at the willingness-to-pay threshold of $50,000 per QALY.
For the adult-initiated population, the ICER of setmelanotide was $1,288,761 per QALY when compared to BSC. Setmelanotide was associated with 4.15 additional QALYs and $5,353,700 additional costs compared to BSC over a lifetime horizon. (Disaggregated results are presented in tables 12 to 17 in Appendix 3.) The cost-effectiveness acceptability curves indicated that 0% of the results were cost-effective at willingness-to-pay thresholds of up to $900,000 per QALY.
For both populations, most of the incremental costs (pediatric-initiated population = $11,522,640; adult-initiated population = $5,362,211) were attributable to the drug acquisition costs of setmelanotide, with cost savings (pediatric-initiated population = $64,645; adult-initiated population = $8,466) in health care monitoring costs, health care visit costs, and comorbidity costs in the setmelanotide arm. The key driver contributing to QALY gains (pediatric-initiated population = 62%; adult-initiated population = 65%) for setmelanotide was a reduction in hyperphagia severity (refer to Table 13 and Table 16 in Appendix 3). Ninety-six percent to 97% of the QALYs gained were accrued after the 52-week trial period. The life-years gained from the mortality benefit were 1.74 and 0.81 for the pediatric-initiated and adult-initiated populations, respectively.
Table 3: Summary of the Sponsor’s Economic Evaluation Results (Pediatric-Initiated Population)
Treatment | Total costs ($) | Incremental costs ($) | Total QALYs | Incremental QALYs | ICER vs. BSC ($/QALY) |
|---|---|---|---|---|---|
BSC | $541,833 | Reference | 15.02 | Reference | Reference |
Setmelanotide | $11,999,584 | $11,457,751 | 24.69 | 9.66 | $1,185,599 |
BSC = best supportive care; ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year; vs. = versus.
Source: Sponsor’s pharmacoeconomic submission.
Table 4: Summary of the Sponsor’s Economic Evaluation Results (Adult-Initiated Population)
Treatment | Total costs ($) | Incremental costs ($) | Total QALYs | Incremental QALYs | ICER vs. BSC ($/QALY) |
|---|---|---|---|---|---|
BSC | $527,125 | Reference | 10.58 | Reference | Reference |
Setmelanotide | $5,880,825 | $5,353,700 | 14.73 | 4.15 | $1,288,761 |
BSC = best supportive care; ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year; vs. = versus.
Source: Sponsor’s pharmacoeconomic submission.
Sensitivity and Scenario Analysis Results
The sponsor conducted several scenario analyses to test the impact of alternative parameters and assumptions on the modelled results. The largest change to the ICER from the base-case results was seen when excluding comorbidity disutilities (pediatric-initiated = $1,402,744 per QALY gained; adult-initiated = $1,471,270 per QALY gained), using DAH score improvements from the trial as an effect of hyperphagia treatment (pediatric-initiated = $1,402,283 per QALY gained; adult-initiated = 1,535,370 per QALY gained), or setting severe hyperphagia to be 100% at baseline (pediatric-initiated = $794,437 per QALY gained; adult-initiated = $848,717 per QALY gained). When using the societal perspective, with caregiver disutility and indirect costs, the ICERs were $705,620 and $897,071 per QALY for the pediatric-initiated and adult-initiated populations, respectively.
CADTH Appraisal of the Sponsor’s Economic Evaluation
CADTH identified several key limitations to the sponsor’s analysis that have notable implications on the economic analysis:
Hyperphagia response and quality of life. Based on the views of the sponsor’s experts, the sponsor assumed that 100% of setmelanotide responders would transition to mild hyperphagia severity. However, this is not supported by the pivotal trial data, which indicate that only 50% and 75% of severe and moderate hyperphagia cases, respectively, transitioned to mild hyperphagia. In addition, the hyperphagia-related quality of life was obtained from a vignette study in which the use of the lead-time trade-off method (a variant of the traditional time trade-off method) resulted in very low utility scores. For example, severe hyperphagia (0.218) was comparable to other severe health states, such as acute stroke or progressive and metastatic cancers. In addition, the definition of hyperphagia severity in this study does not align with the DAH scores used in the trial. These assumptions likely overestimated the quality of life gains associated with setmelanotide.
The CADTH reanalysis used hyperphagia response based on reported pivotal trial data. An alternate quality of life value (0.677) from Lavelle et al.15 on hyperphagia in Prader-Willi syndrome was also applied to moderate and severe hyperphagia. Clinical experts consulted by CADTH agreed that this value held more face validity.
Resource use associated with BMI in addition to obesity-related comorbidity resource use. The model assumed increasing hospitalization and specialty care visits with increasing BMI, based on the sponsor’s clinician expert opinion; this is in addition to the resource use associated with obesity-related conditions. The clinical experts consulted by CADTH indicated that BBS alone is not a reason for hospitalization, and that any hospitalizations would likely result from obesity-related comorbidities. Given that the model includes the costs of managing obesity-related comorbidities, the assumption of increased hospitalization and specialty care visits with greater BMI alone likely double-counts the costs of BBS. This assumption overestimated the cost savings from disease management associated with setmelanotide.
In the CADTH reanalysis, only the costs associated with obesity-related comorbid conditions were retained.
Obesity-related comorbidity prevalence rates: Obesity-related comorbidity prevalence rates by BMI and age were obtained from the literature. However, most estimates were not age-specific (i.e., for osteoarthritis, type 2 diabetes, and CV events), with most rates coming from a largely older, adult population. However, these were applied to pediatric and young adult populations, which likely overestimates the prevalence of comorbidities in younger age groups. In addition, the assumption that the rate of NAFLD is equivalent to the rate of NASH was neither justified nor supported by the clinical experts consulted by CADTH. These prevalence assumptions overestimated the proportions of BBS patients with comorbidities, especially among the younger age groups.
CADTH notes that the model structure for assessing comorbidities lacks clinical plausibility. For example, it is assumed that as cohort weight decreases, the prevalence of all comorbidities decreases. While this may be true for some comorbidities, such as sleep apnea, other comorbidities are chronic once they have developed. For example, the prevalence of type 2 diabetes will never decrease because once type 2 diabetes has developed, it is incurable (although it can go into remission). A more appropriate decision model would have looked at the prevalence and incidence of comorbidities based on BMI to account for this using the sponsor-submitted model structure.
In the CADTH reanalysis, population prevalence rates from the Canadian Chronic Disease Surveillance System were used for the younger age groups at baseline (i.e., BMI 20 to 25). Multipliers were then applied to the sponsor’s estimates for the different BMI classes. Detailed calculations are provided in Appendix 4.
CADTH notes that issues related to the incorporation of comorbidities within the model structure could not be addressed and that the model structure likely overestimates the impact of weight loss on comorbidities. As a scenario analysis, the impact of comorbidities was removed to explore the impact these had on the model’s output.
Assumption using both obesity-related quality of life and disutility due to comorbidity. The model used the baseline health state utility values by BMI and age from the literature using US Medical Expenditure Panel Survey data;16 this estimate does not adjust for obesity-related comorbidities (likely to be more common at greater BMIs) and therefore captures both BMI alone and obesity-related comorbidity disutility. Including additional disutility for obesity-related comorbidities likely double-counts the quality of life impact of obesity in BBS patients. This assumption overestimates the quality of life improvement associated with weight loss caused by setmelanotide.
In the CADTH reanalysis, the disutilities associated with comorbidities were excluded because these were captured by utility reductions associated with higher BMI scores.
Assumption of mortality benefit and comorbidity benefit with setmelanotide: The model assumed mortality benefits linked to BMI and not comorbidities. The impact of weight loss alone on mortality is not well understood. A Canadian study by Doumouras et al. (2020), which looked at mortality outcomes in patients in Ontario undergoing bariatric surgery, found that postsurgery mortality differences were seen after approximately 1.5 years.17 However, a mortality benefit may be derived from mechanisms related to the surgery, such as its impact on type 2 diabetes remission, as opposed to being derived from weight loss. Likewise, the study found no difference in mortality for those with a BMI under 40 kg/m2 (hazard ratio = 1; 95% confidence interval, 0.67 to 1.53) or any statistical difference in those under the age of 55.
In addition, a reduction in comorbidity prevalence associated with weight loss was based on literature estimates because there were no trial data to support this. This may overestimate the benefits associated with setmelanotide.
In the CADTH scenario analysis, mortality and comorbidity rates were assumed to be equal among all BMI classes.
The pediatric dose exceeded the maximum recommended dose in the product monograph. The product monograph states that the maximum recommended dose for individuals under the age of 18 years is 2 mg per day. However, the model assumed that, on average, pediatric patients would receive a dose of |||| || according to the pivotal trial. These assumptions might overestimate the drug costs of setmelanotide.
In the CADTH reanalysis, a maximum dose of 2 mg was used for the pediatric population. This assumes that the same clinical efficacy is achieved in pediatric patients at a lower dose, which may overestimate the benefits associated with setmelanotide.
Assumption about response rates and long-term discontinuation. The model used the trial response rates of 85.7% and 46.7% among the pediatric and adult populations, respectively. This assumes that after 1 year of treatment, 14% of pediatric patients would discontinue and 54% of adult patients would discontinue setmelanotide. The model also assumed an annual discontinuation rate of 1%. According to the clinical experts consulted by CADTH, clinicians may keep patients on setmelanotide even if the trial-specified treatment effect was not achieved (i.e., in the case of a ≥ 0.2 BMI z score decrease or a ≥ 10% decrease in weight, as defined in the pivotal trial). There is also no evidence from the extension trial on drug discontinuation among responders. These assumptions might underestimate the true costs associated with setmelanotide. CADTH also notes that the product monograph suggests assessing response at 22 weeks, albeit at a lower weight threshold (with response defined as a 5% reduction in baseline body weight or a 5% reduction in baseline BMI for patients with continued growth).
The sponsor’s model was not programmed to adequately assess different response thresholds. Therefore, this could not be explored.
Additionally, the key assumptions shown in Table 5 were made by the sponsor and have been appraised by CADTH.
Table 5: Key Assumptions of the Submitted Economic Evaluation (Not Noted as Limitations to the Submission)
Sponsor’s key assumption | CADTH comment |
|---|---|
The BMI z score was mapped onto the appropriate BMI group at age 18, and adult response rates were applied to the pediatric cohort when they reached age 18. | Uncertain. With the WHO mapping algorithm, a z score ≥ 4.0 would be distributed equally into BMI categories of 40 to 45, 45 to 50, and ≥ 50, resulting in smaller proportions of morbidly obese patients. However, this should not affect the cost-effectiveness of setmelanotide, given that this algorithm was applied to both the setmelanotide and BSC arms. |
The treatment effect of setmelanotide on hyperphagia that occurs during the 1-year clinical trial period is sustained throughout patients’ lifetimes if they continue to use setmelanotide. Nonresponders revert to their original BMIs or BMI z score levels upon discontinuation. Patients on BSC retain their original BMIs or BMI z score levels throughout the model time horizon. | Uncertain. The pivotal trial RM-493 to 023 was only 1 year long, and the results from the ongoing long-term extension trial are not yet available. However, 3 out of 30 responders from the extension trial did gain weight by the 2-year mark. |
Patients with BBS with obesity maintain the same BMIs or BMI z scores as they age. | Uncertain. However, this assumption was applied to both the setmelanotide and BSC arms. |
BBS = Bardet-Biedl Syndrome; BMI = body mass index; BSC = best supportive care.
CADTH Reanalyses of the Economic Evaluation
Base-Case Results
The CADTH base case was derived by making changes in model parameter values and assumptions in consultation with clinical experts. These changes, summarized in Table 6, involved the removal of obesity-related hospitalization and specialty care costs, the removal of comorbidity disutilities, the editing of comorbidity prevalence rates, and the use of alternate hyperphagia utility and hyperphagia response rates based on the pivotal trial.
Table 6: CADTH Revisions to the Submitted Economic Evaluation
Stepped analysis | Sponsor’s value or assumption | CADTH value or assumption |
|---|---|---|
Corrections to sponsor’s base case | ||
None | — | — |
Changes to derive the CADTH base case | ||
1. Hospitalization and specialty care costs attributed to BMI alone | The costs of hospitalization and specialty care visits were included as obesity-related comorbidity management costs. | The costs of hospitalization and specialty care visits attributed to BMI alone were excluded. |
2. Comorbidity disutilities | Comorbidity disutilities (ranging from 0.03 for sleep apnea to 0.19 for osteoarthritis) were included in the model in addition to BMI-specific disutility. | Comorbidity disutilities were set to 0 to prevent double-counting because the study population informing the BMI-associated disutility also had obesity-related comorbidity. |
3. Comorbidity prevalence rates | Comorbidity prevalence rates (except for sleep apnea) obtained from a largely adult population were used across different age groups. | New estimated rates based on Canadian prevalence rates were used for younger age groups (refer to Appendix 4 for details). |
4. Hyperphagia utility | 0.702 for moderate hyperphagia and 0.218 for severe hyperphagia | 0.677 for both moderate and severe hyperphagia |
5. Hyperphagia response rate | Assumed that 100% of setmelanotide responders would transition to a mild hyperphagia severity. | 50% and 75% of cases of severe and moderate hyperphagia transitioned to mild hyperphagia, based on the pivotal trial. |
6. 2 mg per day for patients aged < 18 years (applies only to pediatric-initiated population) | Average pediatric patients would receive a dose of |||| || from the pivotal study. | A maximum dose of 2 mg was used for pediatric patients, according to the product monograph. |
CADTH base case | 1 + 2 + 3 + 4 + 5 + (6 for the pediatric-initiated population only) | — |
The CADTH base case for pediatric-initiated patients demonstrated that, compared to BSC, setmelanotide was more costly by $10,425,770 and more effective by 4.46 QALYs, resulting in an ICER of $2,336,431 per QALY. For the adult-initiated population, the base case demonstrated that, compared to BSC, setmelanotide was more expensive by $5,293,917 and more effective by 1.94 QALYs, resulting in an ICER of $2,726,591 per QALY.
The change to the CADTH base case that had the greatest impact on the results was the use of an alternate hyperphagia utility value (reanalysis 4); this change reduced the sponsor’s base-case QALYs gained to 7.6 from 9.66 in pediatric patients and to 3.2 from 4.15 in adult patients. Excluding the obesity-related hospitalization and specialty care costs (reanalysis 1) also significantly reduced the total costs of BSC.
Table 7: Summary of the Stepped Analysis of the CADTH Reanalysis Results (Pediatric-Initiated Population)
Stepped analysis | Drug | Total costs ($) | Total QALYs | ICER ($/QALYs) |
|---|---|---|---|---|
Sponsor’s base case | BSC | $541,833 | 15.02 | Reference |
Setmelanotide | $11,999,584 | 24.69 | $1,185,599 | |
CADTH reanalysis 1 | BSC | $90,355 | 15.00 | Reference |
Setmelanotide | $11,620,388 | 24.71 | $1,187,458 | |
CADTH reanalysis 2 | BSC | $540,978 | 18.33 | Reference |
Setmelanotide | $12,011,245 | 26.51 | $1,402,744 | |
CADTH reanalysis 3 | BSC | $506,472 | 16.88 | Reference |
Setmelanotide | $12,101,654 | 25.63 | $1,325,184 | |
CADTH reanalysis 4 | BSC | $540,450 | 18.08 | Reference |
Setmelanotide | $12,098,739 | 25.68 | $1,521,175 | |
CADTH reanalysis 5 | BSC | $541,544 | 15.04 | Reference |
Setmelanotide | $12,096,525 | 23.28 | $1,402,283 | |
CADTH reanalysis 6 | BSC | $542,962 | 15.00 | Reference |
Setmelanotide | $10,884,030 | 24.71 | $1,065,378 | |
CADTH base case | BSC | $54,919 | 21.48 | Reference |
Setmelanotide | $10,480,689 | 25.94 | $2,336,431 |
BSC = best supportive care; ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year.
Note: Reanalyses 2 and 5 are taken directly from the sponsor’s sensitivity analysis.
Table 8: Summary of the Stepped Analysis of the CADTH Reanalysis Results (Adult-Initiated Population)
Stepped analysis | Drug | Total costs ($) | Total QALYs | ICER ($/QALYs) |
|---|---|---|---|---|
Sponsor’s base case | BSC | $527,125 | 10.58 | Reference |
Setmelanotide | $5,880,825 | 14.73 | $1,288,761 | |
CADTH reanalysis 1 | BSC | $100,845 | 10.56 | Reference |
Setmelanotide | $5,357,236 | 14.65 | $1,286,166 | |
CADTH reanalysis 2 | BSC | $524,110 | 13.90 | Reference |
Setmelanotide | $5,790,584 | 17.48 | $1,471,270 | |
CADTH reanalysis 3 | BSC | $491,704 | 12.03 | Reference |
Setmelanotide | $5,753,256 | 15.82 | $1,387,440 | |
CADTH reanalysis 4 | BSC | $524,776 | 12.91 | Reference |
Setmelanotide | $5,879,387 | 16.11 | $1,672,098 | |
CADTH reanalysis 5 | BSC | $526,454 | 10.57 | Reference |
Setmelanotide | $5,784,329 | 14.00 | $1,535,370 | |
CADTH base case | BSC | $65,526 | 16.26 | Reference |
Setmelanotide | $5,359,443 | 18.20 | $2,726,591 |
BSC = best supportive care; ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year.
Note: Reanalyses 2 and 5 are directly taken from the sponsor’s sensitivity analysis.
CADTH notes that the reanalysis focused on modifying the sponsor model assumptions and parameters to reflect the clinical course, patient management, and treatment more accurately in Canada, where possible. However, it should be noted that significant uncertainty exists in this reanalysis due to limitations that could not be addressed or were only addressed as part of scenario analyses. This includes multiple optimistic model assumptions in favour of setmelanotide that remained as part of the CADTH base case. The assumption that patients’ BMIs would stabilize after 52 weeks regardless of treatment arm could not be tested due to model restrictions.
Scenario Analysis Results
To address additional uncertainty, CADTH performed scenario analyses to determine the impact of assuming no mortality and comorbidity benefits with changes in BMI. The results of these analyses are presented in Table 9 and Table 10. The ICER is also sensitive to the range of hyperphagia utility values used in the model (refer to Appendix 4 for details).
Table 9: Scenario Analysis Results (Pediatric-Initiated Population)
Analysis | Drug | Total costs ($) | Total QALYs | ICER ($/QALYs) |
|---|---|---|---|---|
CADTH base case | BSC | 54,919 | 21.48 | Reference |
Setmelanotide | 10,480,689 | 25.94 | $2,336,431 | |
1. Remove mortality benefit | BSC | 29,330 | 25.31 | Reference |
Setmelanotide | 11,268,830 | 29.12 | $2,948,725 |
BSC = best supportive care; ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year.
Table 10: Scenario Analysis Results (Adult-Initiated Population)
Analysis | Drug | Total costs ($) | Total QALYs | ICER ($/QALYs) |
|---|---|---|---|---|
CADTH base case | BSC | 65,526 | 16.26 | Reference |
Setmelanotide | 5,359,443 | 18.20 | $2,726,591 | |
1. Remove mortality benefit | BSC | 35,545 | 21.51 | Reference |
Setmelanotide | 6,365,645 | 23.32 | $3,487,669 |
BSC = best supportive care; ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year.
CADTH undertook a price reduction analysis based on the sponsor’s base case and the CADTH base case to determine the price reduction of setmelanotide required to achieve an ICER of less than $50,000 per QALY (Table 11 and Table 12). These analyses demonstrated that a price reduction of 98% for setmelanotide would be required to reach this willingness-to-pay threshold in the CADTH base case. In the pooled population, covering both adult and pediatric patients, a 98% price reduction reduces the ICER to $46,241 per QALY gained.
Table 11: CADTH Price Reduction Analyses (Pediatric-Initiated Population)
Analysis | ICERs for setmelanotide vs. BSC ($/QALY) | |
|---|---|---|
Price reduction | Sponsor base case | CADTH reanalysis |
No price reduction | $1,185,599 | $2,336,431 |
10% | $1,066,367 | $2,102,502 |
20% | $947,135 | $1,868,573 |
30% | $827,903 | $1,634,644 |
40% | $708,671 | $1,400,715 |
50% | $589,439 | $1,166,786 |
60% | $470,207 | $932,857 |
70% | $350,975 | $698,928 |
80% | $231,743 | $464,999 |
90% | $112,511 | $231,070 |
98% | $17,125 | $43,927 |
BSC = best supportive care; ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year; vs. = versus.
Table 12: CADTH Price Reduction Analyses (Adult-Initiated Population)
Analysis | ICERs for setmelanotide vs. BSC ($/QALY) | |
|---|---|---|
Price reduction | Sponsor base case | CADTH reanalysis |
No price reduction | $1,288,761 | $2,726,591 |
10% | $1,159,680 | $2,453,675 |
20% | $1,030,599 | $2,180,759 |
30% | $901,518 | $1,907,843 |
40% | $772,437 | $1,634,927 |
50% | $643,356 | $1,362,011 |
60% | $514,275 | $1,089,095 |
70% | $385,194 | $816,179 |
80% | $256,113 | $543,263 |
90% | $127,032 | $270,347 |
99% | $23,767 | $52,014 |
BSC = best supportive care; ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year; vs. = versus.
Issues for Consideration
According to the clinical expert feedback obtained by CADTH, 1 criteria for setmelanotide prescription may be confirmation of BBS from genetic testing, which is performed out of the country. The cost of this testing has not been included.
According to the clinical experts consulted by CADTH, setmelanotide might also be used in combination with other obesity treatments that target different mechanisms to treat BBS patients.
Overall Conclusions
The results of Study 022 (a long-term extension study) and Study 023 (a completed phase III trial) were consistent with setmelanotide improving important weight-related outcomes for patients with Bardet-Biedl syndrome (BBS). However, the ability to draw firm conclusions about the magnitude of clinical benefit in hunger, HRQoL, and other outcomes was limited. There are uncertainties regarding the long-term efficacy and safety of setmelanotide, given that it may be a potentially lifelong treatment.
The sponsor’s base case was derived using various assumptions and data sources that were uncertain. First, including additional hospitalization and specialty care visits as BMI increases — in addition to obesity-related comorbidity resource use — likely double-counts the resource use associated with obesity. Second, applying a disutility associated with weight class as well as weight-related comorbidities likely double-counts the quality of life impact associated with obesity. Third, assuming that the same comorbidity prevalence rate applies across different age groups likely overestimates the proportions of patients with comorbidities in younger age groups. Fourth, the utility value used for severe hyperphagia (from the sponsored vignette study) was relatively low compared to the value in another hyperphagia study. Finally, the model assumed that all moderate and severe hyperphagia cases transitioned to mild hyperphagia, which was not shown in the pivotal trial. The CADTH reanalysis addressed these limitations.
The CADTH base-case results were similar to the sponsor’s assessment in that both ICERs exceeded $1 million per QALY gained and were driven primarily by the cost of setmelanotide. In the CADTH base case, for the pediatric-initiated population, setmelanotide resulted in an additional 4.46 QALYs gained at an additional cost of $10,425,770 to the health system, resulting in an ICER of $2,336,431 per QALY gained, relative to BSC alone. In the adult-initiated population, setmelanotide resulted in an additional 1.94 QALYs gained at an additional cost of $5,293,917 to the health system, resulting in an ICER of $2,702,877 per QALY gained, relative to BSC alone.
At the recommended dose, the annual cost of setmelanotide per patient is $441,258 for adults and $294,172 for pediatric patients, assuming no wastage. In the model, this translated into lifetime setmelanotide drug costs of $10,438,536 for a patient who initiates treatment when under the age of 18 years and $5,298,918 for a patient who initiates treatment when over the age of 18 years. Although the model predicts cost savings attributed to preventing obesity-related comorbidities ($12,407 in the pediatric-initiated population and $4,967 in the adult-initiated population), these are small relative to the drug cost of setmelanotide.
CADTH notes that QALY gains in the base case were driven by mortality improvements and large improvements in quality of life due to reduced hyperphagia. The CADTH reanalysis predicts life-year gains of 1.74 years for patients who initiate setmelanotide under the age of 18 years. CADTH notes that the model structure and assumptions were inappropriate for assessing the impact on weight-related comorbidities and that there is limited evidence to support improvements in mortality. Assuming no impact on mortality increases the ICER to $2,948,725 per QALY gained in the pediatric-initiated population.
At a 90% price reduction, the annual per-patient cost of setmelanotide decreases to $44,126 in adults and to $29,417 in pediatric patients, resulting in ICERs of $268,963 per QALY gained in adults and $229,545 per QALY gained in pediatric patients. Therefore, a price reduction of more than 90% would be required to achieve ICER thresholds below $200,000 per QALY. At a threshold of $50,000 per QALY, a price reduction of approximately 98% would be required.
References
1.Bhaskaran K, Dos-Santos-Silva I, Leon DA, Douglas IJ, Smeeth L. Association of BMI with overall and cause-specific mortality: a population-based cohort study of 3.6 million adults in the UK. Lancet Diabetes Endocrinol. 2018;6(12):944-953. PubMed
2.Riazi A, Shakoor S, Dundas I, Eiser C, McKenzie SA. Health-related quality of life in a clinical sample of obese children and adolescents. Health Qual Life Outcomes. 2010;8:134. PubMed
3.Khan KA, Petrou S, Rivero-Arias O, Walters SJ, Boyle SE. Mapping EQ-5D utility scores from the PedsQL generic core scales. PharmacoEcon. 2014;32(7):693-706. PubMed
4.Howell TA, Matza LS, Mallya UG, Goldstone AP, Butsch WS, Lazarus E. Health state utilities associated with hyperphagia: Data for use in cost‐utility models. Obes Sci Pract. 2023. PubMed
5.Soltoft F, Hammer M, Kragh N. The association of body mass index and health-related quality of life in the general population: data from the 2003 Health Survey of England. Qual Life Res. 2009;18(10):1293-1299. PubMed
6.Sullivan PW, Slejko JF, Sculpher MJ, Ghushchyan V. Catalogue of EQ-5D scores for the United Kingdom. Med Decis Making. 2011;31(6):800-804. PubMed
7.Guidelines for the economic evaluation of health technologies: Canada. 4th ed. Ottawa (ON): CADTH; 2017: https://www.cadth.ca/guidelines-economic-evaluation-health-technologies-canada-4th-edition. Accessed 2023 Jul 26.
8.Ontario Ministry of Health. Schedule of benefits for physician services under the Health Insurance Act: (January 25, 2022 (effective July 1, 2022)). Toronto (ON): Ontario Ministry of Health; 2022: https://www.health.gov.on.ca/en/pro/programs/ohip/sob/physserv/sob_master.pdf. Accessed 2023 Jul 26.
9.Sharif B, Kopec JA, Wong H, Anis AH. Distribution and Drivers of Average Direct Cost of Osteoarthritis in Canada From 2003 to 2010. Arthritis Care Res (Hoboken). 2017;69(2):243-251. PubMed
10.Rosella LC, Lebenbaum M, Fitzpatrick T, et al. Impact of diabetes on healthcare costs in a population-based cohort: a cost analysis. Diabet Med. 2016;33(3):395-403. PubMed
11.Cohen D, Manuel DG, Tugwell P, Sanmartin C, Ramsay T. Direct healthcare costs of acute myocardial infarction in Canada’s elderly across the continuum of care. J Econ Ageing. 2014;3:44-49.
12.McGillion MH, Croxford R, Watt-Watson J, Lefort S, Stevens B, Coyte P. Cost of illness for chronic stable angina patients enrolled in a self-management education trial. Can J Cardiol. 2008;24(10):759-764. PubMed
13.Assasi N, Blackhouse G, Xie F, et al. Ablation procedures for rhythm control in patients with atrial fibrillation: clinical and cost-effectiveness analyses. CADTH Technol Overv. 2012;2(1):e2101. PubMed
14.Morgan A, Hartmanis S, Tsochatzis E, et al. Disease burden and economic impact of diagnosed non-alcoholic steatohepatitis (NASH) in the United Kingdom (UK) in 2018. Eur J Health Econ. 2021;22(4):505-518. PubMed
15.Lavelle TA, Crossnohere NL, Bridges JFP. Quantifying the Burden of Hyperphagia in Prader-Willi Syndrome Using Quality-Adjusted Life-years. Clin Ther. 2021;43(7):1164-1178 e1164. PubMed
16.Alsumali A, Eguale T, Bairdain S, Samnaliev M. Cost-Effectiveness Analysis of Bariatric Surgery for Morbid Obesity. Obes Surg. 2018;28(8):2203-2214. PubMed
17.Doumouras AG, Hong D, Lee Y, Tarride JE, Paterson JM, Anvari M. Association Between Bariatric Surgery and All-Cause Mortality: A Population-Based Matched Cohort Study in a Universal Health Care System. Ann Intern Med. 2020;173(9):694-703. PubMed
18.Pharmacoeconomic evaluation [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Imcivree (setmelanotide), solution, 10 mg/mL, subcutaneous. Boston (MA): Rhythym Pharmaceuticals; 2023 Oct 4.
19.Government of Canada. Canadian Chronic Disease Surveillance System (CCDSS). 2023; https://health-infobase.canada.ca/ccdss/data-tool/. Accessed 2023 Jun 26.
20.Hamid O, Eltelbany A, Mohammed A, Alsabbagh Alchirazi K, Trakroo S, Asaad I. The epidemiology of non-alcoholic steatohepatitis (NASH) in the United States between 2010-2020: a population-based study. Ann Hepatol. 2022;27(5):100727. PubMed
21.Webb MP, Dicks EL, Green JS, et al. Autosomal recessive Bardet-Biedl syndrome: first-degree relatives have no predisposition to metabolic and renal disorders. Kidney Int. 2009;76(2):215-223. PubMed
22.Understanding the gap 2.0: a pan-Canadian analysis of prescription drug insurance coverage. Ottawa (ON): The Conference Board of Canada; 2022: https://www.conferenceboard.ca/product/understanding-the-gap-2-0-a-pan-canadian-analysis-of-prescription-drug-insurance-coverage-2/. Accessed 2023 Jun 21.
Appendix 1: Cost Comparison Table
Note this appendix has not been copy-edited.
The comparators presented in the following table have been deemed to be appropriate based on feedback from clinical expert(s) drug plans. Comparators may be recommended (appropriate) practice or actual practice. Existing Product Listing Agreements are not reflected in the table and as such, the table may not represent the actual costs to public drug plans.
Table 13: CADTH Cost Comparison Table for BBS
Treatment | Strength / concentration | Form | Price | Recommended dosage | Daily cost | Annual cost |
|---|---|---|---|---|---|---|
Setmelanotide (IMCIVREE) | 10 mg/mL solution for subcutaneous injection | 1-mL multiple-dose vial | $4,027.0000 | Adult Patients 18 years of Age and Older: Initiate at 1mg and titrate up by 0.5mg per day every 2 weeks up to 3mg once daily. Pediatric Patients 17 Years of Age and younger: Initiate at 0.5mg and titrate up by 0.5mg per day every 2 weeks up to 2mg once daily. | Adult Patients 18 years of Age and Older: $402 - $1,208 Pediatric Patients 6 to Less than 12 Years of Age: $201 - $805 | Adult Patients 18 years of Age and Older First year: $411,559 Subsequent years: $441,258 Pediatric Patients 6 to Less than 12 Years of Age First year: $276,252 Subsequent years: $294,172 |
Notes: The drug price is based on the sponsor-submitted price. No drug wastage is assumed.
Annual drug prices were calculated under the assumption that there are 365.25 days in a year.
Appendix 2: Submission Quality
Note this appendix has not been copy-edited.
Description | Yes/No | Comments |
|---|---|---|
Population is relevant, with no critical intervention missing, and no relevant outcome missing | Yes | No comment |
Model has been adequately programmed and has sufficient face validity | No | Certain parameters (e.g., quality of life) needed to be edited multiple times in the model to make changes to the model |
Model structure is adequate for decision problem | No | The impact of weight loss on comorbidities was not accurately modelled |
Data incorporation into the model has been done adequately (e.g., parameters for probabilistic analysis) | Yes | No comment |
Parameter and structural uncertainty were adequately assessed; analyses were adequate to inform the decision problem | Yes | No comment |
The submission was well organized and complete; the information was easy to locate (clear and transparent reporting; technical documentation available in enough details) | Yes | No comment |
Appendix 3: Additional Information on the Submitted Economic Evaluation
Note this appendix has not been copy-edited.

Detailed Results of the Sponsor’s Base Case
Table 15: Discounted Disaggregated Mean Costs for the Sponsor’s Reference Case Analysis (Probabilistic, Pediatric-Initiated Population)
Cost ($) | Setmelanotide | BSC | Incremental |
|---|---|---|---|
Treatment acquisition costs | $11,522,640 | $0 | $11,522,640 |
Health care monitoring cost unrelated to weight-related comorbidities | $3,049 | $3,171 | -$122 |
Health care visit costs unrelated to weight-related comorbidities | $415,893 | $457,757 | -$41,864 |
Health care costs associated with weight-related comorbidities | $58,003 | $80,905 | -$22,903 |
Total costs | $11,999,584 | $541,833 | $11,457,751 |
BSC = best supportive care.
Source: Sponsor’s pharmacoeconomic submission.
Table 16: Discounted Disaggregated Mean QALYs for the Sponsor’s Reference Case Analysis (Probabilistic, Pediatric-Initiated Population)
BMI/BMI Z score | Setmelanotide | BSC | Incremental |
|---|---|---|---|
20 to 25/0.0 to 1.0 | 3.12 | 0.00 | 3.12 |
25 to 30/1.0 to 2.0 | 3.32 | 2.30 | 1.02 |
30 to 35/2.0 to 2.5 | 8.98 | 5.13 | 3.85 |
35 to 40/2.5 to 3.0 | 8.36 | 5.45 | 2.91 |
40 to 45/3.0 to 3.5 | 5.49 | 7.91 | −2.42 |
45 to 50/3.5 to 4.0 | 1.90 | 4.00 | −2.10 |
≥ 50/ ≥ 4.0 | 1.19 | 5.40 | −4.21 |
Comorbidities decrement | −1.85 | −3.33 | 1.47 |
Hyperphagia | −5.82 | −11.84 | 6.02 |
Total QALYs | 24.69 | 15.02 | 9.66 |
Total LYs | 38.77 | 37.03 | 1.74 |
BSC = best supportive care; QALY = quality-adjusted life-year.
Source: Sponsor’s pharmacoeconomic submission.
Table 17: Discounted Disaggregated Mean Costs for the Sponsor’s Reference Case Analysis (Probabilistic, Adult-Initiated Population)
Cost ($) | Setmelanotide | BSC | Incremental |
|---|---|---|---|
Treatment acquisition costs | $5,362,211 | $0 | $5,362,211 |
Health care monitoring cost unrelated to weight-related comorbidities | $2,603 | $2,573 | $30 |
Health care visit costs unrelated to weight-related comorbiditiesa | $432,513 | $432,438 | $75 |
Health care costs associated with weight-related comorbidities | $83,498 | $92,114 | -$8,616 |
Total costs | $5,880,825 | $527,125 | $5,353,700 |
BSC = best supportive care.
aThe sponsor assumed that as BMI increases, a patient would have more primary care, specialty, and hospital visits unrelated to any weight-related comorbidity.
Source: Sponsor’s pharmacoeconomic submission.
Table 18: Discounted Disaggregated Mean QALYs for the Sponsor’s Reference Case Analysis (Probabilistic, Adult-Initiated Population)
BMI/BMI Z score | Setmelanotide | BSC | Incremental |
|---|---|---|---|
20 to 25/0.0 to 1.0 | 0.00 | 0.00 | 0.00 |
25 to 30/1.0 to 2.0 | 0.73 | 0.00 | 0.73 |
30 to 35/2.0 to 2.5 | 2.48 | 1.79 | 0.69 |
35 to 40/2.5 to 3.0 | 5.88 | 3.32 | 2.56 |
40 to 45/3.0 to 3.5 | 7.22 | 8.94 | −1.72 |
45 to 50/3.5 to 4.0 | 4.68 | 4.15 | 0.53 |
≥ 50/ ≥ 4.0 | 2.85 | 4.71 | −1.86 |
Comorbidities decrement | −2.84 | −3.35 | 0.51 |
Hyperphagia | −6.27 | −8.99 | 2.71 |
Total QALYs | 14.73 | 10.58 | 4.15 |
Total LYs | 29.83 | 29.01 | 0.81 |
BSC = best supportive care; QALY = quality-adjusted life-year.
Source: Sponsor’s pharmacoeconomic submission.
Appendix 4: Additional Details on the CADTH Reanalyses and Sensitivity Analyses of the Economic Evaluation
Note this appendix has not been copy-edited.
The prevalence of osteoarthritis, diabetes, and CV events are relatively high in the younger age groups as the sponsor assumes the same rates across all age groups. Given that age is a significant risk factor, this assumption appears questionable. An alternative approach is to use the Canadian population prevalence by age as our baseline rates (BMI 20 to 25),19 then apply multiplier from the sponsor suggested literature to estimate increased risk due to obesity) for the younger age groups. If calculated rates were higher than the sponsor’s rates, sponsor’s rates were used in the CADTH base case.
For NASH, the sponsor used the NAFLD rates for NASH, which was considered inappropriate according to clinical experts consulted by CADTH. Baseline NASH rates in the CADTH base case were obtained from a US population prevalence study,20 and the multiplier was obtained from the sponsor suggested literature. Clinical experts consulted by CADTH also advised to set the osteoarthritis and NASH rates to 0% for individuals under 18 years old.
The final prevalence rates used in the CADTH base case are listed in Table 19.
Table 19: Alternative Prevalence Rates of Obesity-Related Comorbidities Stratified by BMI or BMI z Score and Age
Cormorbidities | BMI Z score | BMI | Pediatric (< 18 years old)a | Adult (≥ 18 years old) | ||||
|---|---|---|---|---|---|---|---|---|
18 to 29 | 30 to 39 | 40 to 49 | 50 to 59 | 60+ | ||||
Sleep Apnea | 0.0 to 1.0 | 20 to 25 | 4.50% | 4.50% | 4.50% | 4.50% | 14.59% | 14.59% |
1.0 to 2.0 | 25 to 30 | 14.27% | 11.97% | 11.97% | 11.97% | 29.24% | 29.24% | |
2.0 to 2.5 | 30 to 35 | 24.04% | 30.64% | 30.64% | 30.64% | 52.29% | 52.29% | |
2.5 to 3.0 | 35 to 40 | 33.81% | 30.64% | 30.64% | 30.64% | 52.29% | 52.29% | |
3.0 to 3.5 | 40 to 45 | 43.58% | 63.11% | 63.11% | 63.11% | 76.11% | 76.11% | |
3.5 to 4.0 | 45 to 50 | 53.34% | 63.11% | 63.11% | 63.11% | 76.11% | 76.11% | |
≥ 4.0 | ≥ 50 | 63.11% | 63.11% | 63.11% | 63.11% | 76.11% | 76.11% | |
Osteoarthritis | 0.0 to 1.0 | 20 to 25 | 0.00%b | 0.50% | 0.50% | 3.62% | 6.10% | 6.10% |
1.0 to 2.0 | 25 to 30 | 0.00%b | 0.54% | 0.54% | 3.92% | 6.60% | 6.60% | |
2.0 to 2.5 | 30 to 35 | 0.00%b | 0.85% | 0.85% | 6.17% | 10.40% | 10.40% | |
2.5 to 3.0 | 35 to 40 | 0.00%b | 1.33% | 1.33% | 9.61% | 16.20% | 16.20% | |
3.0 to 3.5 | 40 to 45 | 0.00%b | 1.39% | 1.39% | 10.09% | 17.00% | 17.00% | |
3.5 to 4.0 | 45 to 50 | 0.00%b | 1.73% | 1.73% | 12.52% | 21.10% | 21.10% | |
≥ 4.0 | ≥ 50 | 0.00%b | 2.20% | 2.20% | 15.96% | 26.90% | 26.90% | |
NASH | 0.0 to 1.0 | 20 to 25 | 0.00%b | 3.20% | 8.60% | 14.10% | 24.50% | 21.65% |
1.0 to 2.0 | 25 to 30 | 0.00%b | 3.20% | 8.60% | 14.10% | 24.50% | 21.65% | |
2.0 to 2.5 | 30 to 35 | 0.00%b | 14.44% | 18.5% | 18.5% | 24.50% | 21.65% | |
2.5 to 3.0 | 35 to 40 | 0.00%b | 14.44% | 18.5% | 18.5% | 24.50% | 21.65% | |
3.0 to 3.5 | 40 to 45 | 0.00%b | 25.76% | 33% | 33% | 33% | 33% | |
3.5 to 4.0 | 45 to 50 | 0.00%b | 25.76% | 33% | 33% | 33% | 33% | |
≥ 4.0 | ≥ 50 | 0.00%b | 25.76% | 33% | 33% | 33% | 33% | |
Type 2 diabetes | 0.0 to 1.0 | 20 to 25 | 0.00% | 1.24% | 2.80% | 2.80% | 2.80% | 2.80% |
1.0 to 2.0 | 25 to 30 | 0.00% | 1.42% | 3.20% | 3.20% | 3.20% | 3.20% | |
2.0 to 2.5 | 30 to 35 | 0.00% | 2.30% | 5.20% | 5.20% | 5.20% | 5.20% | |
2.5 to 3.0 | 35 to 40 | 0.00% | 3.90% | 8.80% | 8.80% | 8.80% | 8.80% | |
3.0 to 3.5 | 40 to 45 | 0.00% | 4.81% | 10.85% | 10.85% | 10.85% | 10.85% | |
3.5 to 4.0 | 45 to 50 | 0.00% | 7.40% | 16.70% | 16.70% | 16.70% | 16.70% | |
≥ 4.0 | ≥ 50 | 0.00% | 9.96% | 22.50% | 22.50% | 22.50% | 22.50% | |
CV Events | 0.0 to 1.0 | 20 to 25 | 0.00% | 0.36% | 2.18% | 2.18% | 3.80% | 3.80% |
1.0 to 2.0 | 25 to 30 | 0.00% | 0.42% | 2.52% | 2.52% | 4.40% | 4.40% | |
2.0 to 2.5 | 30 to 35 | 0.00% | 0.50% | 3.01% | 3.01% | 5.25% | 5.25% | |
2.5 to 3.0 | 35 to 40 | 0.00% | 0.79% | 4.76% | 4.76% | 8.30% | 8.30% | |
3.0 to 3.5 | 40 to 45 | 0.00% | 0.72% | 4.39% | 4.39% | 7.65% | 7.65% | |
3.5 to 4.0 | 45 to 50 | 0.00% | 0.99% | 6.02% | 6.02% | 10.50% | 10.50% | |
≥ 4.0 | ≥ 50 | 0.00% | 1.59% | 9.64% | 9.64% | 16.80% | 16.80% | |
BMI = body mass index; CI = confidence interval; CV = cardiovascular; NASH = nonalcoholic steatohepatitis; OSA = osteoarthritis.
aPediatric prevalence was linearly extrapolated between BMI z score 0.0 to 1.0 and BMI z score ≥ 4.0, assuming pediatric prevalence for BM z score ≥ 4.0 group the same as adult BMI ≥ 50 group. It was assumed that no type 2 diabetes or CV comorbidities were prevalent for patients < 18 years old.
b0% was assumed based on feedback from clinical experts consulted by CADTH.
Note: rates in bold indicate different values used in the CADTH base case relative to the sponsor’s.
Detailed Results of CADTH Base Case
Table 20: Discounted Disaggregated Mean Costs for the CADTH Reference Case Analysis (Probabilistic, Pediatric-Initiated Population)
Cost ($) | Setmelanotide | BSC | Incremental |
|---|---|---|---|
Treatment acquisition costs | $10,438,536 | $0 | $10,438,536 |
Health care monitoring cost unrelated to weight-related comorbidities | $3,058 | $3,182 | -$124 |
Health care visit costs unrelated to weight-related comorbidities | $5,853 | $6,088 | -$235 |
Health care costs associated with weight-related comorbidities | $33,242 | $45,649 | -$12,407 |
Total costs | $10,480,689 | $54,919 | $10,425,770 |
BSC = best supportive care.
Table 21: Discounted Disaggregated Mean QALYs for the CADTH Reference Case Analysis (Probabilistic, Pediatric-Initiated Population)
BMI/BMI Z score | Setmelanotide | BSC | Incremental |
|---|---|---|---|
20 to 25/0.0 to 1.0 | 3.15 | 0.00 | 3.17 |
25 to 30/1.0 to 2.0 | 3.38 | 2.25 | 1.07 |
30 to 35/2.0 to 2.5 | 8.98 | 5.21 | 3.73 |
35 to 40/2.5 to 3.0 | 8.36 | 5.35 | 3.02 |
40 to 45/3.0 to 3.5 | 5.50 | 7.92 | −2.44 |
45 to 50/3.5 to 4.0 | 1.89 | 4.02 | −2.13 |
≥ 50/ ≥ 4.0 | 1.17 | 5.40 | −4.24 |
Hyperphagia | −6.49 | −8.79 | 2.30 |
Total QALYs | 25.94 | 21.48 | 4.46 |
Total LYs | 38.81 | 37.07 | 1.74 |
BSC = best supportive care; QALY = quality-adjusted life-year.
Table 22: Discounted Disaggregated Mean Costs for the CADTH Reference Case Analysis (Probabilistic, Adult-Initiated Population)
Cost ($) | Setmelanotide | BSC | Incremental |
|---|---|---|---|
Treatment acquisition costs | $5,298,918 | $0 | $5,298,918 |
Health care monitoring cost unrelated to weight-related comorbidities | $2,612 | $2,584 | $29 |
Health care visit costs unrelated to weight-related comorbidities | $6,168 | $6,231 | -$62 |
Health care costs associated with weight-related comorbidities | $51,745 | $56,712 | -$4,967 |
Total costs | $5,359,443 | $65,526 | $5,293,917 |
BSC = best supportive care.
Table 23: Discounted Disaggregated Mean QALYs for the CADTH Reference Case Analysis (Probabilistic, Adult-Initiated Population)
BMI/BMI Z score | Setmelanotide | BSC | Incremental |
|---|---|---|---|
20 to 25/0.0 to 1.0 | 0.00 | 0.00 | 0.00 |
25 to 30/1.0 to 2.0 | 0.74 | 0.00 | 0.74 |
30 to 35/2.0 to 2.5 | 2.49 | 1.83 | 0.66 |
35 to 40/2.5 to 3.0 | 5.78 | 3.30 | 2.48 |
40 to 45/3.0 to 3.5 | 7.22 | 8.85 | −1.63 |
45 to 50/3.5 to 4.0 | 4.71 | 4.17 | 0.54 |
≥ 50/ ≥ 4.0 | 2.90 | 4.77 | −1.86 |
Hyperphagia | −5.63 | −6.66 | 1.02 |
Total QALYs | 18.20 | 16.26 | 1.94 |
Total LYs | 29.84 | 29.04 | 0.8 |
BSC = best supportive care; LY = life-year; QALY = quality-adjusted life-year.
Table 24: Pooled Results Across Both Adult and Pediatric-Initiated Populations
Drug | Total costs ($) | Total QALYs | ICER ($/QALYs) |
|---|---|---|---|
BSC | $60,010 | 18.97 | Reference |
Setmelanotide | $8,022,491 | 22.22 | $2,448,232 |
BSC = best supportive care; ICER = incremental cost-effectiveness ratio; QoL = quality of life.
Additional Scenario Analyses
Table 25: Additional Scenario Analysis Results (Pediatric-Initiated Population)
Analysis | Drug | Total costs ($) | Total QALYs | ICER ($/QALYs) |
|---|---|---|---|---|
CADTH base case | BSC | $54,919 | 21.48 | Reference |
Setmelanotide | $10,480,689 | 25.94 | $2,336,431 | |
1. Increase hyperphagia QoL by 25% | BSC | $54,628 | 25.78 | Reference |
Setmelanotide | $10,477,446 | 28.43 | $3,934,096 | |
2. Decrease hyperphagia QoL by 25% | BSC | $54,947 | 17.00 | Reference |
Setmelanotide | $10,525,920 | 23.31 | $1,659,894 |
BSC = best s supportive care; ICER = incremental cost-effectiveness ratio; QoL = quality of life.
Table 26: Additional Scenario Analysis Results (Adult-Initiated Population)
Analysis | Drug | Total costs ($) | Total QALYs | ICER ($/QALYs) |
|---|---|---|---|---|
CADTH base case | BSC | $65,526 | 16.26 | Reference |
Setmelanotide | $5,359,443 | 18.20 | $2,726,591 | |
1. Increase hyperphagia QoL by 25% | BSC | $65,173 | 19.52 | Reference |
Setmelanotide | $5,426,202 | 20.67 | $4,666,624 | |
2. Decrease hyperphagia QoL by 25% | BSC | $65,334 | 12.88 | Reference |
Setmelanotide | $5,412,450 | 15.65 | $1,930,961 |
BSC = best supportive care; ICER = incremental cost-effectiveness ratio; QoL = quality of life.
Appendix 5: Submitted Budget Impact Analysis and CADTH Appraisal
Note this appendix has not been copy-edited.
Table 27: Summary of Key Takeaways
Key takeaways of the budget impact analysis |
|---|
|
Summary of Sponsor’s Budget Impact Analysis
The submitted budget impact analysis (BIA) assessed the introduction of setmelanotide for weight management in adult and pediatric patients 6 years of age and older with obesity due to BBS. The analysis took the perspective of Canadian public drug plans. A time horizon of 3 years was taken. The model used epidemiological data to estimate the number of adults and pediatric patients with obesity associated with BBS in each jurisdiction. The analysis compared the cost of a reference drug scenario without setmelanotide to a new drug scenario with setmelanotide to determine the expected financial implications related to reimbursing setmelanotide for the treatment of obesity and control of hunger in patients with BBS. Key inputs to the BIA are documented in Table 28.
Key assumptions to the sponsor’s BIA included:
Only ||% of BBS patients are diagnosed.
Individuals would only receive ||% of the maximum dose, an assumed ||% compliance.
33.15% of BBS patients eligible for setmelanotide would receive public coverage.
Market uptake for setmelanotide would be 24% in year 1, 32% in year 2, 40% in Year 3.
Table 28: Summary of Key Model Parameters
Parameter | Sponsor’s estimate (reported as year 1 / year 2 / year 3 if appropriate) |
|---|---|
Target population | |
Prevalence of BBS in the general population in Canada Alberta British Columbia Manitoba New Brunswick Newfoundland and Labrador Nova Scotia Ontario Prince Edward Island Saskatchewan NIHB | (1/160,000) (1/160,000) (1/160,000) (1/160,000) (1/17,000) (1/160,000) (1/160,000) (1/160,000) (1/160,000) (1/160,000) |
Proportion of patients diagnosed with BBS | ||| |
Proportion of patients with BBS who experience obesity | 82% |
Proportion of BBS patients by age group: Proportion of patients aged less than 6 years and therefore ineligible for setmelanotide Pediatric (6 ≥ to < 18 years) Adult (≥ 18 years) | 8% 44% 48% |
Proportion of patients eligible for treatment with setmelanotide with no contraindications | 95% |
Response Rate: Pediatric (6 ≥ to < 18 years) Adult (≥ 18 years) | 55% 55% |
Proportion of people in Canada covered by public drug plans: CADTH-participating drug plans Alberta British Columbia Manitoba New Brunswick Newfoundland and Labrador Nova Scotia Ontario Prince Edward Island Saskatchewan NIHB | 35.13% 36.83% 37.38% 39.29% 44.31% 35.92% 36.24% 31.08% 23.25% 34.41% 100.00% |
Number of patients eligible for public coverage for setmelanotide | 19 / 19 / 20 |
Market Uptake (3 years) – All Participating Drug Programs Except Ontario | |
Uptake (reference scenario) Setmelanotide + BSC Semaglutide + BSC Orlistat + BSC BSC | 0% / 0% / 0% 10% / 10% / 10% 0% / 0% / 0% 90% / 90% / 90% |
Uptake (new drug scenario) Setmelanotide + BSC Semaglutide + BSC Orlistat + BSC BSC | 24% / 32% / 40% 8% / 7% / 6% 0% / 0% / 0% 68% / 61% / 54% |
Market Uptake (3 years) – Ontario Drug Programs | |
Uptake (reference scenario) Setmelanotide + BSC Semaglutide + BSC Orlistat + BSC BSC only | 0% / 0% / 0% 10% / 10% / 10% 9% / 9% / 9% 81% / 81% / 81% |
Uptake (new drug scenario) Setmelanotide + BSC Semaglutide + BSC Orlistat + BSC BSC only | 24% / 32% / 40% 8% / 7% / 6% 7% / 6% / 5% 62% / 55% / 49% |
Cost of treatment (per patient per year) | |
Setmelanotide compliance rate Setmelanotide + BSC (pediatric dose) Setmelanotide + BSC (adult dose) Semaglutide + BSC Orlistat + BSC BSC | ||| $225,190 (first year) - $235,338 (subsequent years) $338,349 (first year) - $353,007 (subsequent years) $5,294 $1,816 $0 |
BSC = best supportive care.
Note: Sponsor separated Ontario market shares and market uptake approximates from other jurisdictions due to the fact that orlistat is only reimbursed in this jurisdiction under the Exceptional Access Program.
Summary of the Sponsor’s BIA Results
The sponsor’s estimated budget impact of funding setmelanotide as a treatment for obesity and control of hunger in adult and pediatric patients 6 years of age and older living with BBS was $952,269 in Year 1, $1,511,333 in Year 2, $2,031,542 in Year 3, for a 3-year total of $4,495,145.
The sponsor conducted several sensitive and scenario analyses testing alternative assumptions. The changes with the greatest impact on the results included a change in prevalence of BBS, a change in the proportion of patients diagnosed with BBS and a change in the proportion of patients with no contraindications.
CADTH Appraisal of the Sponsor’s BIA
CADTH identified several key limitations to the sponsor’s analysis that have notable implications on the results of the BIA:
The anticipated market uptake of setmelanotide is underestimated: The sponsor assumed that setmelanotide would achieve a 40% market share over a 3-year time horizon. The sponsor noted in the US market setmelanotide achieved a market uptake of ||| across all reimbursement markets in the first 12 months postlaunch. A |||||||| adjustment factor was applied to Canada || || ||| ||||| ||||| |||||| |||||||||| || |||||| |||||||| || ||| || |||||| ||| |||| |||||| ||||||||||| || |||||| |||| || ||| || || ||| |||| || ||||||| |||||||
Clinical experts consulted by CADTH indicated that physicians would be likely to prescribe setmelanotide to a far greater proportion of eligible patients due to the lack of therapies indicated for BBS. Given the rarity of BBS, experts confirmed that awareness of this new treatment was high. It is unlikely that any specialist who is managing a patient with BBS would be unaware of setmelanotide given the absence of any dedicated treatment options. It was noted that the only patients who would likely not receive setmelanotide would be those who fall outside the indication or have contraindications. These considerations have already been explicitly accounted for in the BIA therefore including them in the market uptake assessment would double-count their impact. The BIA is looking at market uptake of setmelanotide in individuals who have a confirmed diagnosis of BBS, meet the eligibility criteria, have no contraindications, and are eligible for public reimbursement. In this patient cohort it is unclear why some would not receive setmelanotide given the absence of any dedicated treatment options in the space.
Clinical expert input obtained by CADTH indicated that setmelanotide could achieve a market share of 90% in 3 years for those eligible for public reimbursement of setmelanotide. This translates into a 50% uptake in year 1 which is still ||| less than market penetration in the US after 1 year. 70% in year 2 ||||| ||||||| |||| ||| |||| || ||| || and then 90% in year 3.
CADTH addressed this limitation by revising the market uptake of setmelanotide to 50% in Year 1, 70% in Year 2 and 90% in Year 3 in the CADTH base case.
The comparators included in the BIA were inappropriate for this patient population: in the sponsor’s BIA it was assumed that setmelanotide would take market share from weight loss medications such as orlistat and semaglutide. CADTH notes that semaglutide is reimbursed for the treatment of type 2 diabetes in Canada and received a negative recommendation by CADTH for weight loss in 2022. Given this, setmelanotide would not displace semaglutide as this would be used for type 2 diabetes. Secondly, experts consulted by CADTH noted that due to the unique mechanism of action, setmelanotide would likely be used alongside any current weight loss pharmacotherapy to improve chances of weight loss. Therefore, even if semaglutide was publicly reimbursed for weight loss it would still be used in combination with setmelanotide.
CADTH addressed this limitation by reducing the market shares of semaglutide and orlistat to 0% in all jurisdictions.
There is uncertainty associated with the anticipated diagnosis rate for BBS patients: The sponsor assumed that ||| of BBS patients would receive a diagnosis. This estimate was derived by the sponsor using internal research on the number of patients diagnosed with BBS in Canada. Physicians in the research reported managing || patients with BBS |||||| |||| ||||||| ||| |||||||||| |||||||| || |||||||||| |||||||||| || |||||||| |||| |||||||||| |||||||| || |||||||| ||| |||||||| |||||||||| || |||||||||||||| 46 patients were identified in Eastern Canada from work by Webb et al.21 Therefore, the sponsor assumed, in total, ||| diagnosed BBS patients across Canada. It was noted this may be an overestimate as there will likely be some double-counting of patients from the internal research and the patients identified by Webb. Assuming an estimated prevalence rate of 1/17,000 in Newfoundland and Labrador and 1/100,000 in the rest of Canada yields approximately 400 patients across the country with BBS. Therefore ||| ||| ||||||| || |||||||| ||| || ||||. Clinical experts consulted by CADTH confirmed this diagnosis rate to be accurate. However, if setmelanotide was reimbursed then having a targeted treatment option for BBS may elevate diagnosis rates.
CADTH performed a scenario analysis with a hypothetical 50% diagnosis rate for BBS patients.
CADTH performed a scenario analysis where the number of identified BBS patients was reduced by 20% to account for the possibility of overlap between the patients identified in the sponsor’s internal research and the Webb study.
There is uncertainty associated with the maintenance dose compliance rate: the maximum recommended dose is 3mg per day for adults and 2mg for individuals under the age of 18. Individuals start on a lower dose and then the dose is titrated upwards to the maximum if the higher dose is tolerated. The sponsor assumed that compliance would reach 80% of the maximum dose, therefore in adults it was assumed a dose of 2.6 mg would be administered in adults and 1.6 mg would be administered in children. The sponsor estimated a compliance rate of ||| by reviewing the proportion of active patients in Rhythm’s patient support program in the US who received a shipment of setmelanotide monthly ||| was the average between June 2022 – February 2023. CADTH notes that the sponsor assumes many patients discontinue setmelanotide in the first year as they do not achieve a response. It is unclear how this was accounted for in the data the sponsor quotes. As response is already accounted for in the BIA it is important the compliance rate only applies for those who continue therapy lifelong. In the RM-493-023 trial patients achieved an average daily maintenance dose of |||| || and |||| || for adults and pediatric patients respectively after 1 year. In the trial compliance was therefore estimated to be 97% based on the maximum allowed dose in the trial noting that in the trial a maximum dose of 3mg was allowed for children.
CADTH changed the maintenance dose compliance rate to 97% and performed a scenario analysis with an 80% maintenance dose compliance rate.
There is uncertainty associated with the proportion of BBS patients eligible for public coverage: The sponsor estimated the proportion of BBS patients in Canada eligible for public coverage based on the ‘2022 Understanding the Gap 2.0: A Pan-Canadian Analysis of Prescription Drug Insurance Coverage’ Report.22 Based on this source, the sponsor assumed 35.13% of BBS patients eligible for setmelanotide would be eligible for public coverage. CADTH notes the report looks at average public coverage rates across provinces for all disease areas and age groups. However, public coverage will be highly dependent on the disease and age demographics of the cohort, given that public plans have coverage programs contingent on age and income relative to drug cost. Given that BBS is a rare disease with a large pediatric population and that the annual cost of setmelanotide exceeds median family incomes, it is likely that there will be a higher rate of public coverage of setmelanotide for patients living with BBS relative to the average public coverage rates across all diseases.
In the base case CADTH assumed 75% public coverage, however given the uncertainty surrounding this parameter, CADTH performed a sensitivity analysis where 100% of patients were eligible for public coverage.
Patients discontinuing due to lack of response is uncertain: in the sponsor’s BIA it was assumed that response would be assessed at 22 weeks and would be assessed according to whether weight loss of greater or equal to 5% was achieved. In consultation with clinical experts, it was noted that some patients may continue setmelanotide beyond 22 weeks even if 5% weight loss was not achieved if the treatment had a noticeable impact on hyperphagia. In data submitted by the sponsor 12/22 (54.5%) of patients over the age of 12 had achieved a response after 22 weeks. CADTH notes that data from the trial shows that 47% of adults achieved 10% weight loss at 52 weeks and 86% of pediatrics achieved a 0.2 reduction in BMI Z score at 52 weeks. This suggests that response rates in pediatrics may be underestimated by the sponsor, given that the data used are an average of patients over the age of 12 years.
As a scenario analysis, CADTH assumed that 86% of pediatrics would remain on setmelanotide after 22 weeks.
CADTH Reanalyses of the BIA
CADTH revised the sponsor’s base case by updating market shares to align with the expected market uptake of setmelanotide in clinical practice, Table 16.
Table 29: CADTH Revisions to the Submitted BIA
Stepped analysis | Sponsor’s value or assumption | CADTH value or assumption |
|---|---|---|
Corrections to sponsor’s base case | ||
None | — | — |
Changes to derive the CADTH base case | ||
1. Market uptake of setmelanotide over a 3-year period | 24% in Year 1, 32% in Year 2, 40% in Year 3 | 50% in Year 1, 70% in Year 2, 90% in Year 3 |
2. 0% market shares for semaglutide and orlistat in all jurisdictions | Semaglutide 10% market share in all CADTH-participating drug plans, orlistat 9% market share in Ontario | Semaglutide and orlistat given 0% market share in all CADTH-participating drug plans under the assumption market uptake for these medications will be unaffected by reimbursement of setmelanotide |
3. Maintenance dose compliance rate | ||% Maintenance Dose Compliance Rate | 97% Maintenance Dose Compliance Rate |
4. 75% public coverage for BBS patients in all CADTH-participating drug plans | 35.13% of patients in CADTH-participating drug programs will receive public coverage for this medication (100% assumed for NIHB) | 75% of patients in CADTH-participating drug programs will receive public coverage for this medication (100% assumed for NIHB) |
CADTH base case | Reanalysis 1 + 2 + 3 + 4 | |
The results of the CADTH stepwise reanalysis are presented in summary format in Table 30 and a more detailed breakdown is presented in Table 31. Based on the CADTH base case, the expected budget impact of setmelanotide for the treatment of patients with BBS was $4,679,772 in year 1, $7,830,216 in year 2, $10,859,642 in year 3, for a 3-year total of $23,369,630.
Scenario analyses were conducted to assess alternative assumptions, and these included changes related to the proportion of BBS patients that would be diagnosed (50% instead of the 26% assumed in the sponsor-submitted base case) and the proportion of patients who would be eligible for public coverage (100% instead of the 35.13% assumed in the sponsor-submitted base case). The results of these scenario analyses ranged from $19,533,077 to $44,941,596 over a 3-year period.
Table 30: Summary of the CADTH Reanalyses of the BIA
Stepped analysis | 3-year total |
|---|---|
Submitted base case | $4,495,145 |
CADTH reanalysis 1 | $9,800,480 |
CADTH reanalysis 2 | $4,506,321 |
CADTH reanalysis 3 | $5,381,575 |
CADTH reanalysis 4 | $8,936,752 |
CADTH base case | $23,369,630 |
BIA = budget impact analysis.
Table 31: Detailed Breakdown of the CADTH Reanalyses of the BIA
Stepped analysis | Scenario | Year 0 (current situation) | Year 1 | Year 2 | Year 3 | 3-year total |
|---|---|---|---|---|---|---|
Submitted base case | Reference | $11,382 | $11,502 | $11,622 | $11,742 | $34,865 |
New drug | $11,382 | $963,771 | $1,522,955 | $2,043,284 | $4,530,010 | |
Budget impact | $0 | $952,269 | $1,511,333 | $2,031,542 | $4,495,145 | |
CADTH base case | Reference | $0 | $0 | $0 | $0 | $0 |
New drug | $0 | $4,679,772 | $7,830,216 | $10,859,642 | $23,369,630 | |
Budget impact | $0 | $4,679,772 | $7,830,216 | $10,859,642 | $23,369,630 | |
CADTH scenario analysis: 50% diagnosis rate for BBS patients | Reference | $0 | $0 | $0 | $0 | $0 |
New drug | $0 | $8,999,561 | $15,058,107 | $20,883,928 | $44,941,596 | |
Budget impact | $0 | $8,999,561 | $15,058,107 | $20,883,928 | $44,941,596 | |
CADTH scenario analysis: 100% public coverage for BBS patients across CADTH-participating drug plans | Reference | $0 | $0 | $0 | $0 | $0 |
New drug | $0 | $6,184,770 | $10,348,252 | $14,351,687 | $30,884,709 | |
Budget impact | $0 | $6,184,770 | $10,348,252 | $14,351,687 | $30,884,709 | |
CADTH scenario analysis: 80% Maintenance Dose Compliance Rate | Reference | $0 | $0 | $0 | $0 | $0 |
New drug | $0 | $3,956,065 | $6,541,742 | $9,035,271 | $19,533,077 | |
Budget impact | $0 | $3,956,065 | $6,541,742 | $9,035,271 | $19,533,077 | |
CADTH scenario analysis: 86% response rate in pediatrics | Reference | $0 | $0 | $0 | $0 | $0 |
New drug | $0 | $5,156,919 | $8,292,988 | $11,188,889 | $24,638,797 | |
Budget impact | $0 | $5,156,919 | $8,292,988 | $11,188,889 | $24,638,797 | |
CADTH scenario analysis: 20% reduction in the number of identified BBS patients | Reference | $0 | $0 | $0 | $0 | $0 |
New drug | $0 | $3,743,818 | $6,264,173 | $8,687,714 | $18,695,704 | |
Budget impact | $0 | $3,743,818 | $6,264,173 | $8,687,714 | $18,695,704 |
BIA = budget impact analysis.
Ethics Review
Objectives
To identify and describe the ethical considerations associated with the use of setmelanotide for weight management in adult and pediatric patients 6 years of age and older with obesity due to BBS. These considerations will include those related to the broader context of BBS, the evidentiary basis of setmelanotide, the use of setmelanotide, and health systems more broadly.
Research Questions
This report addresses the following research questions:
What ethical considerations arise in the context of BBS, including those related to diagnosis, treatment, and outcomes?
What ethical considerations arise related to the evidence (e.g., clinical and economic data) used to evaluate setmelanotide?
What ethical considerations arise in the use of setmelanotide for patients, their caregivers, and clinicians?
What ethical considerations for health systems are involved in the context of setmelanotide?
Methods
To identify ethical considerations relevant to the use of setmelanotide for weight management in adult and pediatric patients 6 years of age and older with obesity due to BBS, this ethics report was driven by relevant questions identified in the European Network for Health Technology Assessment Core Model 3.0, Ethics Analysis Domain,1 and supplemented by relevant questions from the Equity Checklist for Health Technology Assessment (ECHTA).2 These guiding questions were organized to respond to the research questions posed, and investigated ethical considerations related to:
patients living with BBS and their caregivers (i.e., disparities in incidence, treatment, or outcomes; challenges related to diagnosis or clinical care; factors that might prevent patients from gaining access to therapies)
the evidence used to demonstrate the benefits, harms, and value of setmelanotide (i.e., ethical considerations in relevant clinical trials, including their representativeness, choice of outcome measures, and appropriateness of analytical methods and models to all population groups; ethical considerations related to the data or assumptions in the economic evaluation)
the use of setmelanotide, including considerations related to benefits and harms to patients, relatives, caregivers, or clinicians, and considerations related to access to these therapies
the uptake of setmelanotide in health systems, including considerations related to the distribution of health care resources.
These were explored through a review and synthesis of project inputs and relevant literature to highlight ethical considerations across each of the domains.
Data Collection: Review of Project Inputs and Literature
Data to inform this ethics report were drawn from an identification of ethical considerations (e.g., values, norms, or implications related to the harms, benefits, and implications for equity, justice, resource allocation, and ethical considerations in the evidentiary basis) in the patient and clinician group, clinical expert, and drug program input collected by CADTH to inform this review, as well as from a complementary search of the published literature. Ongoing collaboration and communication with CADTH reviewers working on the clinical and economic reviews for this submission also assisted in the clarification and identification of ethical considerations raised.
Review of Project Inputs
During this CADTH review, a single reviewer collected and considered input from 6 main sources for content related to ethical considerations relevant to addressing the research questions guiding this ethics report. In addition to published literature, this report considered the following sources:
the sponsor submission, including noting information and external references or sources relevant to each of the research questions driving this report
the clinician group input received by CADTH from a group of endocrinologists in Canada with expertise in treating BBS (referred to as “clinician input”)
the patient input received by CADTH from the Bardet-Biedl Syndrome Foundation
the drug program input received by CADTH from drug programs participating in the CADTH reimbursement review process
discussions with 4 clinical experts directly engaged by CADTH during this reimbursement review (referred to in the text as “clinical experts”), including through a clinical consultation meeting involving 3 experts, 1 panel discussion involving 4 experts, and an economic consultation meeting involving 2 experts. During each of the 3 discussions, clinical experts were asked targeted questions related to ethical considerations corresponding to the research questions driving this report. All clinical experts were endocrinologists, with 3 specializing in adult populations and 1 in pediatrics.
engagement with CADTH clinical and economic reviewers to identify domains of ethical interest arising from their respective reviews as well as relevant questions and sources to further pursue in this report.
Literature Search Methods
An information specialist conducted a literature search using key resources, including MEDLINE through Ovid, Philosopher’s Index through Ovid, the Cumulative Index to Nursing and Allied Health Literature through EBSCO, and Scopus. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. The main search concepts were setmelanotide and BBS.
CADTH-developed search filters were applied, where applicable, to limit retrieval to citations related to ethical, equity, and natural history concepts or considerations. Duplicates were removed by manual deduplication in EndNote. Retrieval was limited to the English language. The search was completed on April 10, 2023.
Literature Screening and Selection
Literature retrieved according to the search and selection methods previously detailed was screened in 2 stages. First, titles and abstracts of citations retrieved were screened for relevance by a single reviewer. Articles were identified and retrieved for full-text review by a single reviewer if their titles or abstracts identified ethical considerations, provided normative analysis (i.e., focusing on “what ought to be” through argumentation), or presented empirical research (i.e., focusing on “what is” through observation) of ethical considerations related to the experiences, incidence, diagnosis, treatment, or outcomes of obesity or uncontrolled hunger associated with BBS or the evidence on, use of, or implications of setmelanotide for patients with BBS. In the second stage, full-text publications categorized as “retrieve” were reviewed by the same reviewer. Texts that included substantive information meeting the criteria were included in the review, and reports that did not meet these criteria were excluded. As a parallel process, other sources drawn from relevant bibliographies, relevant key concepts, or in consultation with experts or other CADTH reviewers were retrieved and reviewed using the previously described selection criteria.
Data Analysis
The data analysis was driven by the 4 research questions guiding this report and included the collection, coding, and thematic analysis of data drawn from the literature and project inputs. The reviewer conducted 2 iterative cycles of coding and analysis to abstract, identify, and synthesize relevant ethical considerations in the literature and from relevant project inputs.
In the initial coding phase, publications and input sources were reviewed for ethical content (e.g., claims related to potential harms, benefits, equity, justice, resource allocation, and ethical issues in the evidentiary basis). Once identified, claims related to ethical content were coded using methods of qualitative description.3 In the second coding phase, major themes and subcodes were identified through repeated readings of the data3 and summarized into thematic categories within each guiding domain or research question. Where ethical content did not fit into the categories or domains outlined in the research questions, this was noted, as were discrepancies or conflicts between ethical considerations or values identified between project sources or within thematic categories. Data analysis was iterative, and the themes identified in the literature, in project inputs, and during consultations with the clinical experts were used to further refine and reinterpret the ethical considerations identified.
Data collected and analyzed from these sources were thematically organized and described according to the 4 research questions and domains driving this report. The results of this analysis and its limitations and conclusions are described in the next section.
Results
Description of Included Sources
Data to inform this ethics report drew from a review of patient group input, clinician group input, drug program input, and consultations with clinical experts engaged by CADTH for this review. All clinical experts were active in relevant clinical roles as practising endocrinologists in Canada, and at least 3 had experience treating patients with BBS. A description and summary of these sources are included in the Clinical Review Report.
The literature search identified 349 results and the grey literature search identified 13 additional results, for a total of 362 results. Following title and abstract screening, 343 citations were excluded, and 20 potentially relevant publications from the electronic searches were retrieved for full-text review. Of the potentially relevant publications, 11 publications were excluded because they did not discuss ethical considerations of setmelanotide or BBS (n = 10) or were not published in English (n = 1). Nine publications met the inclusion criteria and were included in this report. Five additional publications were retrieved from backward searching of the included publications’ reference lists or manual searching.
A total of 14 publications were used to inform this report. Of these, 8 publications discussed ethical considerations in the context of BBS, including related to diagnosis and treatment; 4 publications discussed patient and/or family and caregiver experiences in the context of BBS; and 2 publications were selected to provide a broader understanding of the context of ethical considerations for drugs for rare diseases. Details regarding the characteristics of the included publications are reported in Table 1.
Key Ethical Considerations
Diagnosis, Treatment, and Experiences of BBS
Diagnosis
BBS is a rare, multisystem, autosomal recessive ciliopathy with a high degree of phenotypic and genetic variability.4-6 While clinical manifestations are heterogeneous, BBS is clinically characterized by 6 primary features, including retinal degeneration, truncal obesity, polydactyly, genital abnormalities, learning difficulties, and renal anomalies.4-7 In addition to these 6 primary features, some secondary features include neurodevelopmental abnormalities (e.g., developmental and/or speech delay, ataxia), metabolic abnormalities (e.g., metabolic syndrome), cardiovascular abnormalities, liver or gastrointestinal diseases, brachydactyly or syndactyly, olfactory dysfunction, and dental anomalies.4,5
The prevalence of BBS is estimated to range from 1 in 100,000 to 1 in 160,000 in North America and Europe.4,7,8 However, its prevalence can be much higher in certain isolated communities, such as Newfoundland and Labrador, where incidence is estimated to range from 1 in 16,000 to 1 in 18,000.4 Based on these prevalence data, the Clinical Review Report has indicated that there are an estimated 300 to 400 people living with BBS in Canada. However, both the sponsor and clinical experts indicated that there is some uncertainty around the accuracy of the diagnostic rate for BBS (estimated by the sponsor to be as low as 26%, as discussed in the CADTH Pharmacoeconomic Review), which could mean there is a significant underestimation of people living with BBS and may imply a severe unmet need for this population.
BBS is clinically diagnosed based on the Beales criteria, which require the presence of at least 4 primary features or 3 primary and at least 2 secondary features.4 While clinical experts indicated that the Beales criteria are sufficient as a diagnostic tool and do not often result in misdiagnosis, the progressive onset of many of these features can delay the ability of physicians to correctly identify patients as living with BBS.4,7,9 Although BBS can be misdiagnosed, which does present challenges for families,9 delays in diagnosis are more common. Children with BBS are typically diagnosed between the ages of 5 years and 10 years.4
The clinical experts indicated that the rarity of BBS means most primary care providers would be too unfamiliar with it to make a diagnosis. As such, BBS is typically diagnosed by specialists in pediatric endocrinology or genetics, although other specialists may also diagnose it, depending on where the patient is first referred. For patients living in rural or remote locations, this referral process (and the ultimate diagnosis) may be further delayed due to the more limited availability of appropriate specialists. These delays can be distressing for parents or caregivers struggling to find support for their child’s symptoms and support for themselves as they navigate what it means to be a good parent or caregiver.9,10
It is also possible to confirm a clinical diagnosis of BBS with a genetic test. While a genetic confirmation of BBS is not a requirement to access current treatment options in Canada, the clinical experts indicated that genetic confirmation is common practice in pediatric endocrinology, which is where most cases will be identified. The clinical experts noted that, as far as they were aware, all genetic testing for BBS required sending genetic material outside of Canada; they did not know of any jurisdiction that had in-house capacity to conduct genetic testing for BBS. However, they agreed that the provincial ministries of health typically granted appeal-based funding for out-of-country testing. While there are currently 26 genes that have been associated with BBS,5 genetic mutations have not been identified for 20% to 30% of individuals who have a clinical diagnosis of BBS.7 Some clinical experts consulted during this review worried that, if genetic confirmation were to become a requirement for accessing BBS-related treatment or care services, this gap in knowledge could result in undue harm for people whose genetic variants are not yet identified or understood, given that this may delay their access to treatment or care.
Treatment of BBS and Related Obesity and Hyperphagia
BBS-related obesity has an early onset and is 1 of the more common primary features of the disease, with a prevalence of 72% to 92% among people with BBS.4 Children with BBS typically have a normal birth weight. However, 90% of children with BBS gain excess weight within their first year of life, and by 3 years old, many can be classified as obese.5 The exact mechanism driving obesity in people with BBS remains poorly understood. However, a prominent hypothesis is that hypothalamic dysfunction associated with the melanocortin-4 receptor pathway leads to hyperphagia (i.e., severe and insatiable hunger), which ultimately results in overeating and obesity.11 The excessive food-seeking behaviours associated with hyperphagia can negatively affect the lives of people with BBS and their families. As will be discussed, hyperphagia can affect the emotional and social well-being of people with BBS and their families, make concentrating at school or work challenging, and interfere with relationship-building.8,12 Accordingly, the patient and clinician input, clinical experts’ views, and published literature8,12 all stressed the importance of attending to the severe impact that obesity and hyperphagia have on quality of life and overall health for people with BBS and their families.
The clinician group input and clinical experts indicated that there are currently no targeted treatment options for any clinical features of BBS aside from the drug under review. In the absence of any targeted treatment options, these sources described how the current standard approach in BBS care is symptom management, consistent with approaches used in the general population. For BBS-related obesity specifically, they indicated that the current treatment options are lifestyle interventions, off-label use of some pharmacotherapies (e.g., orlistat, semaglutide, liraglutide), and — though not recommended — bariatric surgery. None of these options was considered ideal, and all were described as having insufficient effect on weight loss and limited to no effect on hunger, given that they do not directly address the leptin signalling and melanocortin-4 receptor activation that are presumed to be at the root of hyperphagia in BBS. Dieting can be particularly distressing in this population because hyperphagia causes feelings of extreme hunger and can prevent or delay the feeling of satiety after eating. Similarly, exercise regimens may be difficult to follow for people with BBS because other clinical features (e.g., cognitive impairment or vision loss) may complicate their ability to participate.
The clinician group input, clinical experts, and published literature all pointed to the importance of accessing early, ongoing care for BBS-related obesity, given that these patients may be at elevated risk for developing common obesity-related comorbidities (e.g., type 2 diabetes, metabolic syndrome, dyslipidemia, hypertension, and obstructive sleep apnea).11 However, accessing early and supportive weight-related care was described as challenging, given the limitations to current treatment options highlighted previously in this report and the small number of pediatric weight-management programs across Canada. As with diagnosis, limited availability of weight-management programs in some geographic areas may lead to inequitable delays in accessing care, particularly for those who live outside of urban settings. Further published literature highlighted that, for people with rare forms of genetic obesity (e.g., BBS), transitioning from pediatric to adult care often involves disruptions to both social and medical components of care.11 Not only could this disrupt patients’ integration into broader medico-social support systems for adults, but it could also hamper their ability to access comprehensive and coordinated health care services.11
Patient, Family, and Caregiver Experiences of BBS
The published literature and patient group input received by CADTH reported significant psychosocial and emotional burdens for people living with BBS and their families.9,10,12 Prior to diagnosis, parents found the uncertainty around their children’s symptoms distressing and reported that this fostered feelings of depression or guilt.9 These may be reinforced by stigmatizing experiences with care providers or relatives who blame the parents for their children’s behaviours and suggest they are not doing enough to help.9,12 While these pressures may be alleviated for some as the child ages and is diagnosed,9 they do not disappear altogether, and people with BBS, or their parents, commonly report ongoing stigmatizing experiences with relatives, care providers, and the general public.9,10,12 The clinical experts suggested that these stigmatizing experiences, along with general societal stigma around obesity, may cause delays to both diagnosis and care for children living with BBS-related obesity.
The psychosocial and emotional burdens of living with BBS were described as particularly onerous for people living with hyperphagia related to their BBS. The patient group input and 1 mixed-methods study of patients with hyperphagia due BBS, but no cognitive impairments repeatedly described how challenging it can be to focus on something other than food.12 Not only could this limit concentration at school or work, but it may also lead to feelings of irritability or anxiety around eating and guilt or frustration with one’s self at not being able to control hunger.12 Similarly, building relationships and engaging in social environments were described by adults living with BBS-related hyperphagia as challenging activities that fostered feelings of isolation and loneliness.12
Caring for a child with BBS was also described as affecting both internal family dynamics and family members’ ability to fully engage with their peers and local communities or even to find time for themselves.9,12 As noted in the patient group input, this can be particularly challenging for parents of children with hyperphagia because their child’s persistent hunger may lead to confrontations with siblings over food or public experiences like eating off of the floor, out of waste-bins, or off other children’s plates.12 Having supportive family members, care providers, colleagues, and school staff may help to alleviate some of the burdens of caring for a child with BBS.9 Similarly, parents of children with BBS may benefit from targeted counselling on how to navigate both their child’s BBS symptoms and others’ responses to these.10
Because BBS is a genetic condition that affects several systems throughout the body, patients require a broad, multidisciplinary care team. Depending on which clinical features are present, these care providers may be specialists in fields as diverse as endocrinology, cardiology, nutrition, clinical psychology, ophthalmology, speech pathology, nephrology, neurology, occupational therapy, and medical genetics. Coordinating care across all these disciplines can be challenging for parents of children with BBS and may present major obstacles to accessing the right care at the right time.9 The clinical experts suggested that this situation may be exacerbated during the transition from pediatric to adult care as the responsibility to coordinate a patients’ care shifts onto patients and away from their families.
Ethics of Evidence and Evaluation of Setmelanotide
As is explained in more detail in the CADTH Clinical Review Report for this reimbursement review, the primary clinical evidence used to evaluate setmelanotide in the treatment of obesity associated with BBS is derived from a completed pivotal study (Study 023) and a long-term extension (LTE) study (Study 022).
Study 023 was a phase III, open-label trial that evaluated the efficacy and safety of setmelanotide in patients aged greater than or equal to 6 years with obesity related to BBS or Alström syndrome over 52 weeks, with an initial 14-week, randomized, double-blind, placebo-controlled period. The primary outcome was the proportion of participants achieving a reduction of greater than or equal to 10% of their overall body weight after 52 weeks. Key secondary outcomes of interest included the mean percent change in overall body weight from baseline and, given the proposed relationship between hyperphagia and obesity, the impact of setmelanotide on daily hunger. These secondary outcomes were evaluated following both the 14-week, placebo-controlled period and at 52 weeks. In addition, Study 023 had exploratory outcomes of safety, patient-reported outcomes, and health-related quality of life (HRQoL). By and large, the clinical experts and clinician group input indicated that the results for both the primary and secondary end points were promising. In particular, the clinical experts suggested that a greater than or equal to 10% reduction in body weight was a conservative goal (given the clinically meaningful impact that a ≥ 5% reduction could have on comorbidities associated with obesity), and they felt that 33.7% of participants achieving this greater than or equal to 10% reduction after 52 weeks was a strong indicator of the value of setmelanotide. Nonetheless, the CADTH Clinical Review Report’s critical appraisal and discussion highlight several limitations to the overall interpretability (and generalizability) of the safety and magnitude of effect of setmelanotide in a BBS population. Briefly, these limitations stem from the small sample size and the trial’s single-arm, open-label design, which made it challenging to control for bias, confounding, and magnitude of effect. As will be discussed, while the results may be considered promising, the uncertainty of the clinical evidence has implications for the use of setmelanotide, including those related to determining eligibility and assessing treatment response.
The clinical experts considered the trial population to be generalizable to the Canadian context. However, given that assessment of hunger was a key secondary end point in Study 023, it is important to note that the trial evaluated hunger scores only for trial participants without cognitive impairments. While the clinical experts agreed with the sponsor’s reasoning that it can be challenging to collect subjective data from people with cognitive impairments, the fact that this information is missing makes the generalizability of hunger score results to people with cognitive impairments more uncertain. Similarly, while patients aged greater than or equal to 6 years were included in Study 023, most trial outcomes were measured only for patients greater than or equal to 12 years of age, and few trial participants were less than 12 years of age (n = 8). As with cognitive impairment, this smaller sample size does make the generalizability of the trial results more uncertain for this population.
Study 022 is a 36-month LTE study that includes 30 patients with BBS and is meant as an exploratory evaluation of the durability of weight-related outcomes. While weight-related outcomes stabilized in the majority of participants over 24 months of assessment, the Clinical Review Report indicates that the long-term efficacy of setmelanotide is highly uncertain, adding to the challenge of interpreting its long-term clinical benefit. As will be discussed further, given the high costs of setmelanotide and the uncertainty around the durability of effect, this can complicate decisions about discontinuation.
However, while the clinical experts and clinician group input noted that it would be helpful to have stronger evidence on the safety and magnitude of benefit of setmelanotide in people with BBS — as well as on which BBS subtypes are more likely to benefit — these limitations are not uncommon in studies involving rare diseases like BBS. Nonetheless, given the limitations to the current evidence base on setmelanotide, the clinical experts also indicated the importance of collecting long-term data on the durability of effect, safety, and subtypes likely to create a greater benefit and adding these data to a patient registry. Not only could this help inform clinical decision-making regarding the balance of harm and benefit for individual patients, but it may also be particularly important for the use of setmelanotide in future, given that it is expected to be used as a lifelong medication.
The CADTH Pharmacoeconomic Review Report indicates that, without clear evidence leading to definitive conclusions about the clinical benefit and comparative effectiveness of setmelanotide, it is challenging to accurately model and assess its cost-effectiveness. This limitation — which may affect cost-effectiveness analyses for oncology drugs and drugs for rare diseases more generally — presents challenges for assessing the opportunity costs (or forgone benefits) associated with reimbursing and resourcing a particular intervention over others. However, these opportunity costs are important for informing resource allocation decisions at a health systems level.13
Ethical Considerations in the Use of Setmelanotide
There are several ethical considerations pertaining to the use of setmelanotide for BBS-related obesity, including those related to the harms and benefits associated with the use of setmelanotide, how eligibility and assessment of treatment response are determined, and access.
Balancing Benefits and Harms
According to the sponsor’s submission for this review, the value of setmelanotide rests in its ability to target the specific molecular pathway believed to be responsible for hyperphagia and the subsequent development of obesity in people living with BBS. This value is unique relative to other, nonspecific pharmacotherapies used to help regulate weight in BBS populations (e.g., orlistat, liraglutide, and semaglutide); setmelanotide is the first targeted therapy available for people with BBS. As such, the patient and clinician group input, clinical experts, and published literature expressed a general sense of excitement surrounding setmelanotide and what it represented as a potentially life-changing pharmacotherapy for this population.14
Indeed, setmelanotide has demonstrated results consistent with improving weight-related outcomes for patients with BBS in both the pivotal trial, Study 023, and in early data from the LTE study, Study 022. In addition to the positive impacts being seen on body weight and hunger, the clinical experts and clinician input indicated that setmelanotide could potentially help prevent or delay the onset of cardiometabolic disease that is common to people living with obesity. Generally positive evidence on the exploratory end point, HRQoL, from Study 0238,12 was complemented by the patient input received by CADTH, which described setmelanotide as improving mental health and well-being for patients and their families. For those providing feedback through patient input, there was near-unanimous support for recommending setmelanotide for public reimbursement. Similarly, the clinical experts suggested that setmelanotide would likely be used as a first-line therapy for people with BBS-related obesity, and that there would be a high level of uptake in clinical practice if reimbursed. However, as described previously (and more thoroughly in the Clinical Review Report), there are limitations to the ability to interpret the magnitude, generalizability, and durability of the clinical benefit and safety of setmelanotide, and no definitive conclusions can be drawn at this time on its clinical effectiveness or, as a result, its cost-effectiveness. This complicates deliberations on the value of its potential use in clinical practice.
Further, there are some potential harms associated with the use of setmelanotide. As detailed in the Clinical Review Report, a frequent adverse event noted in Study 023 was hyperpigmentation of the area surrounding the injection site due to melanocortin-1 receptor activation.11,14 While this was well-tolerated during the trial, and no cases of melanoma were reported, the authors noted that ongoing attention should be paid to the chronic stimulation of the melanocytes,11,14 given that some melanocortin-1 receptor variants may predispose persons to melanoma.15 Other potential harms of particular interest to the clinical experts were injection-site reactions, anaphylaxis, bradycardia, sexual events, sexually inappropriate behaviours, and psychiatric events (e.g., depression, anxiety, and suicidal ideation). The clinical experts highlighted the importance of monitoring for potential psychiatric events (sexually aggressive behaviour, in particular), but did note that cases of these events were either unreported (i.e., anxiety), uncommon (i.e., sexually aggressive behaviour and depression), or not associated with the use of setmelanotide (i.e.,1 case of suicidal ideation).14
Nonetheless, the clinical experts described being satisfied with the safety profile of setmelanotide. They noted that evidentiary limitations are common to novel rare-disease pharmacotherapies. As such, both the clinical experts and clinician group input indicated that they would be sufficiently comfortable with the currently available evidence to prescribe setmelanotide for patients who meet the eligibility criteria. Given the high level of unmet need for targeted therapy for BBS-related obesity, the clinical experts and patient input suggested that the uncertainty around the long-term safety and effectiveness of setmelanotide would be accepted by patients and their families, were it to be reimbursed. With this in mind, there are several ethical considerations around eligibility, assessment of treatment response, and access that are relevant to the potential implementation and use of setmelanotide in this population. These considerations are discussed in the next sections.
Eligibility
The clinical experts discussed whether eligibility for setmelanotide ought to be determined based on a clinical diagnosis using the Beales criteria or whether confirmatory genetic testing should also be required. Either way, the clinician group input and clinical experts alike indicated that they would prescribe setmelanotide to their patients living with obesity, hyperphagia, and a diagnosis of BBS.
While the clinician group input suggested that genetic confirmation of clinical diagnosis should be required to access setmelanotide, the clinical experts were more equivocal. On the 1 hand, some experts felt that requiring a genetic diagnosis carried the risk of denying access for people who have a clinical diagnosis of BBS but do not test positive for a known genetic variant. Given that only 70% to 80% of clinical diagnoses have a clear relationship to known BBS-related genetic variants,7 this concern is not without cause. However, given the significant financial burden that setmelanotide may represent to the health care system — and the importance of ensuring that people with BBS are the ones accessing setmelanotide (because there is currently no evidence indicating whether setmelanotide would be beneficial or harmful for those without BBS) — the clinical experts suggested that genetic testing could be a valuable tool. Given the progressive onset of some of the primary clinical features of BBS (e.g., vision loss and renal complications), genetic testing may be particularly helpful in cases in which only non–BBS-specific primary clinical features (e.g., learning difficulties and obesity) are presently identifiable and the clinical diagnostic criteria are only partially met. Further, pediatric endocrinologists indicated that genetic testing was already common practice and would not present an additional practice burden.
Assessment of Response
Given that obesity is a chronic condition, and setmelanotide is expected to be a lifelong intervention, the participating drug programs sought clarity around what qualified as an appropriate and sufficiently durable treatment response for a patient to remain on setmelanotide.
Health Canada has suggested that the assessment of treatment response should be conducted at 22 weeks. The reasoning is that if a patient does not notice a reduction of at least 5% in total body weight (or a ≥ 5% reduction in baseline body mass index [BMI], for patients aged < 18 years) by this time, then they are unlikely to experience a benefit from setmelanotide. This represents a significant departure from the sponsor’s original proposal and from the clinical experts’ agreement that 52 weeks was a reasonable time point for this assessment. As such, there is considerable uncertainty around whether a 22-week assessment of response would be followed in practice without any hard-stopping rules. This could inadvertently introduce inequities related to patients’ access to and long-term use of setmelanotide in practice.
Similarly, what was considered an appropriate treatment response by clinical experts is somewhat divergent from the Health Canada–approved product monograph. While the clinical experts agreed that a reduction in total body weight of greater than or equal to 5% (or a ≥ 5% reduction in baseline BMI for patients < 18 years) was a valuable metric for assessing the benefit of setmelanotide, they argued that emphasizing ever-increasing weight reduction over the long-term would be inappropriate because it does not account for the biological nature of obesity and enforces an unrealistic expectation for this population. Instead, they suggested that the effect of setmelanotide on hyperphagia could be a driving metric in considerations of discontinuation. While reductions in overall body weight and BMI were seen as positive, the experts indicated that they would continue treatment even if weight stabilized (or, for some, even if it fluctuated), as long as patients were seeing improvements to hyperphagia and overall quality of life. Given the concerns around the interpretability and generalizability of the hunger scores and HRQoL measures that were collected as part of Study 023, and their absence from the LTE study, the clinical experts’ approach to considering discontinuation may complicate deliberations on the appropriate implementation of setmelanotide.
Access
In addition to the challenges associated with determining eligibility and assessing treatment response, the clinical experts highlighted 2 overarching access challenges that would need to be navigated: administration and ongoing access to a multidisciplinary care team.
Setmelanotide is a subcutaneous injection administered once daily by the patient or their caregiver(s). Depending on their age and tolerance of the drug, the patient (or their caregiver) will need draw their dose of 1 mg to 3 mg (0.1 mL to 0.3 mL) from a 10 mg/mL multiple-dose vial. Although the patient input and clinical experts indicated that this is a generally accessible mode of delivery, they also indicated that some people with BBS may find it challenging to self-administer setmelanotide. Given that vision impairment and cognitive challenges are common features of BBS, patients with these characteristics may find self-administration challenging. However, the clinical experts noted that extra nursing support may be available through weight-management programs for those struggling with self-administration. That said, as described earlier, access to such programs may be limited for those living outside of major metropolitan areas and could result in inequitable access (to extra nursing supports) for those living in rural or remote locations. Because dose compliance may still ultimately be less than 100% using this approach (e.g., because the patient may not be home or the nurse may be unable to visit), the clinical experts did suggest that in the future, it could be helpful to provide setmelanotide in a pen-like format, similar to insulin.
While setmelanotide is most likely to be prescribed by a pediatric (or adult) endocrinologist, given the potential psychological and behavioural adverse events associated with its use (e.g., suicidal ideation or aggressive sexual behaviour), the clinical experts indicated that having access to a clinical psychologist would be particularly important for people on setmelanotide. Similarly, given that setmelanotide is posited to work on weight by suppressing appetite, the clinical experts indicated that ongoing access to dieticians or nutritionists would be important. While these specialists are already indicated for people with BBS-related hyperphagia and obesity, the limited availability of pediatric weight clinics across Canada may impede equitable access to these specialists and necessary care. The clinical experts indicated that this challenge may be exacerbated for those living in more rural or remote geographic locations.
Health System Considerations
The reimbursement and use of setmelanotide for BBS raises several ethical considerations related to health systems and resource allocation. Expensive drugs for rare diseases, such as setmelanotide, raise various ethical considerations related to distributive justice and equitable access, the sustainability of health care budgets, and the fair pricing of pharmaceuticals.13,16 Although there is a significant unmet need for an effective, targeted therapy for BBS, assessing the opportunity costs of reimbursing setmelanotide is complicated by uncertainty regarding the magnitude and generalizability of its clinical benefit and safety, given the limitations discussed in this report and the heterogeneity of disease presentation in this population.
The clinical experts acknowledged the high cost of setmelanotide and felt that justifying its use in the Canadian health care system would require careful consideration of the eligibility criteria as well as the creation of a patient registry to track whether some BBS subtypes respond better than others. This may be particularly valuable for Newfoundland and Labrador, given the higher prevalence rate of BBS and the potentially increased budget impact of setmelanotide for this jurisdiction. However, as described earlier, defining eligibility criteria is complicated, given the heterogeneity and progressive onset of BBS clinical features and the concern that genetic causes are unclear in 20% to 30% of people with a clinical diagnosis.7 This, paired with the lack of clinical evidence clearly indicating whether some BBS subtypes would be more likely than others to benefit from setmelanotide, presents a challenge for providers and funders when considering whether setmelanotide has a role for their patients or in their jurisdictions. Therefore, while there was some disagreement among clinical experts as to whether confirmatory genetic testing should be a required for access to setmelanotide, the clinician input and some clinical experts indicated that genetic testing could be used as a means of attending to patients’ needs for targeted therapy and addressing both the opportunity costs of reimbursing setmelanotide and health system budgetary constraints. However, as some clinical experts noted, genetic testing could also run the risk of denying access to patients with a clinical diagnosis of BBS, but no known genetic cause.
As described earlier, the clinical experts and clinician input indicated the importance of ensuring that people using setmelanotide have access to a multidisciplinary team of specialists. However, the clinical experts noted that the need for specialist care could diminish over time for patients who respond positively to setmelanotide. The clinician group input and clinical experts also noted that they would expect health care resource utilization associated with weight-related comorbidities (e.g., diabetes mellitus, cardiovascular disease, and liver disease) to decrease or be delayed, were setmelanotide used.
The clinical experts also recommended that the sponsor build a BBS-specific patient registry to track whether certain subtypes of BBS were more likely to benefit from setmelanotide. Such a registry could be used to limit future expenditures for persons unlikely to benefit. While this is not an immediate solution (given that building an evidentiary base would take time) — and bearing in mind that delisting the BBS subtypes unlikely to benefit would be difficult in practice — with the CADTH budget impact analysis estimating (based on conversations with clinical experts) a clinical uptake of setmelanotide at 50%, 70%, and 90% over the first 3 years respectively, it is possible that future budgets would experience a great benefit from such a registry. According to the clinical experts, the sponsor has already developed a patient registry in Europe for conditions that have not received Health Canada approval. However, it is unclear whether the sponsor intends to develop a BBS-specific registry. If not, the cost of developing and managing 1 could have further resource implications for Canadian jurisdictions.
Limitations
This review is limited by the paucity of published literature examining the ethical issues directly related to the use of setmelanotide for the treatment of adult and pediatric patients (aged ≥ 6 years) living with obesity due to BBS. Given the rarity of the condition and the novelty of the drug under review, this is not unexpected; nor does it suggest that there are no ethical issues related to the use of setmelanotide. As such, the review has been augmented by drawing from patient group, clinician group, and drug program input, as well as from discussions with clinical experts and engagement with CADTH clinical and pharmacoeconomic review teams, to provide a more comprehensive understanding of the ethical considerations related to the use of setmelanotide for BBS-related obesity and hyperphagia.
While these discussions have certainly been supportive of identifying some of the high-level ethical challenges associated with the use of setmelanotide, it is possible that more directed engagement with key stakeholders beyond clinical experts (e.g., patients, their caregivers, and health care decision-makers) may have offered additional insights into the ethical considerations highlighted throughout this report or may have raised considerations that it does not identify.
Conclusion
Inputs from patient and clinician groups, drug programs, and relevant published literature were reviewed alongside direct engagement with clinical experts to identify and describe ethical considerations relevant to the use of setmelanotide for the treatment of adult and pediatric patients (aged ≥ 6 years) living with obesity due to BBS. Ethical considerations in the context of BBS highlighted the significant unmet treatment needs for this population, given the lack of any existing BBS-targeted pharmacotherapy and the general reliance on lifestyle interventions (e.g., exercise and diet) that have limited effectiveness for BBS-related hyperphagia and obesity. As a multisystem condition with a highly heterogenous phenotypic expression, BBS presents significant physical and psychosocial burdens for patients and their caregivers. For those living with hyperphagia and obesity, these burdens may be even further exacerbated. While clinical trial evidence regarding the effect of setmelanotide on weight, hyperphagia, and quality of life is promising, considerable uncertainty around the safety and magnitude of its effect limits the ability to make definitive statements about its benefits and harms based on currently available evidence. Limited long-term data and the absence of any comparative data (beyond placebo) also limit the assessment of the durability of clinical benefit and cost-effectiveness.
Although the clinical experts, patients, and published literature all indicated a level of comfort with the safety profile of setmelanotide, it is not without risk; patients on setmelanotide will need to be monitored for sexual dysfunction, depression, suicidal ideation, and melanoma. Nonetheless, if reimbursed, setmelanotide is expected to experience a high uptake in clinical practice. Challenges around the definition of appropriate eligibility and discontinuation criteria will need to be navigated. Equitable access to setmelanotide will require attending to common geographic barriers that can limit patients’ access to specialist care and monitoring. In addition, there is the possibility that some patients with cognitive or vision impairment related to BBS may require additional supports to fully access and achieve dose compliance on setmelanotide. For health systems, the ethical considerations connected to setmelanotide highlight the challenges inherent in the funding decisions and opportunity cost assessments for expensive drugs to treat rare diseases. Given the uncertainty around the long-term safety and efficacy of setmelanotide — and around whether some BBS subtypes may respond better than others — the development of a BBS-specific patient registry could ensure better clinical decision-making and resource stewardship in the future. However, building such a database is a project that carries potential cost and infrastructural implications for budgets.
References
1.EUnetHTA Joint Action 2 Work Package 8. HTA Core Model ® version 3.0. Diemen (NL): European Network for Health Technology Assessment (EUnetHTA); 2016: https://www.htacoremodel.info/BrowseModel.aspx. Accessed 2022 Nov 18.
2.Benkhalti M, Espinoza M, Cookson R, Welch V, Tugwell P, Dagenais P. Development of a checklist to guide equity considerations in health technology assessment. Int J Technol Assess Health Care. 2021;37(1):e17. PubMed
3.Sandelowski M. Whatever happened to qualitative description? Res Nurs Health. 2000;23(4):334-340. PubMed
4.Forsythe E, Kenny J, Bacchelli C, Beales PL. Managing Bardet–Biedl Syndrome—Now and in the Future. Front Pediatr. 2018;6. PubMed
5.Melluso A, Secondulfo F, Capolongo G, Capasso G, Zacchia M. Bardet-Biedl Syndrome: Current Perspectives and Clinical Outlook. Ther Clin Risk Manag. 2023;19:115-132. PubMed
6.Kenny J, Forsythe E, Beales P, Bacchelli C. Toward personalized medicine in Bardet–Biedl syndrome. Per Med. 2017;14(5):447-456. PubMed
7.National Organization for Rare Disorders. Bardet-Biedl Syndrome. 2022; https://rarediseases.org/rare-diseases/bardet-biedl-syndrome/?filter=ovr-ds-resources. Accessed 2023 May 18.
8.Forsythe E, Haws RM, Argente J, et al. Quality of life improvements following one year of setmelanotide in children and adult patients with Bardet-Biedl syndrome: phase 3 trial results. Orphanet J Rare Dis. 2023;18(1):12. PubMed
9.Zelihic D, Hjardemaal FR, Lippe CV. Caring for a child with Bardet-Biedl syndrome: A qualitative study of the parental experiences of daily coping and support. Eur J Med Genet. 2020;63(4):103856. PubMed
10.Hamlington B, Ivey LE, Brenna E, Biesecker LG, Biesecker BB, Sapp JC. Characterization of Courtesy Stigma Perceived by Parents of Overweight Children with Bardet-Biedl Syndrome. PLoS One. 2015;10(10):e0140705. PubMed
11.Poitou C, Mosbah H, Clement K. MECHANISMS IN ENDOCRINOLOGY: Update on treatments for patients with genetic obesity. Eur J Endocrinol. 2020;183(5):R149-R166. PubMed
12.Ervin C, Norcross L, Mallya UG, et al. Interview-Based Patient- and Caregiver-Reported Experiences of Hunger and Improved Quality of Life with Setmelanotide Treatment in Bardet-Biedl Syndrome. Adv Ther. 2023;24:24. PubMed
13.Kacetl J, Marešová P, Maskuriy R, Selamat A. Ethical Questions Linked to Rare Diseases and Orphan Drugs – A Systematic Review. Risk Manag Healthc Policy. 2020;13:2125-2148. PubMed
14.Lazareva J, Brady SM, Yanovski JA. An evaluation of setmelanotide injection for chronic weight management in adult and pediatric patients with obesity due to Bardet-Biedl syndrome. Expert Opin Pharmacother. 2023:1-8. PubMed
15.Hinney A, Korner A, Fischer-Posovszky P. The promise of new anti-obesity therapies arising from knowledge of genetic obesity traits. Nat Rev Endocrinol. 2022;18(10):623-637. PubMed
16.Wagner M, Goetghebeur MM, Ganache I, et al. HTA challenges for appraising rare disease interventions viewed through the lens of an institutional multidimensional value framework. Expert Rev Pharmacoecon Outcomes Res. 2023;23(2):143-152. PubMed
17.Ryan DH. Drugs for Treating Obesity. In: Michel MC, ed. Handbook of Experimental Pharmacology. Vol 274. Basel (CH): Springer Nature Switzerland AG; 2022:387-414.
Appendix 1: Details of Included Publications
Note this appendix has not been copy-edited.
Table 1: Details of Included Publications
First author, year | Publication type | Objective | Key ethical considerations | Funding source |
|---|---|---|---|---|
Ervin 202312 | Qualitative interview study | To characterize the nature, severity, and effect of hyperphagia on patient and caregiver HRQoL before and during clinical trials for setmelanotide | Significant caregiver burden associated with BBS Significant courtesy stigma experienced by parents of children with BBS Hyperphagia presents significant challenges for HRQoL for people living with BBS (hard to focus on anything aside from food) and their families | Rhythm Pharmaceuticals, Inc. |
Forsythe 20238 | Multicenter phase III trial | To evaluate changes in HRQoL in adults and children with BBS following 1 year of treatment with setmelanotide | Substantial physical and psychosocial burden for patients and caregivers No targeted treatment for BBS Hyperphagia associated with BBS has been reported as severely impacting HRQoL of patients and caregivers Obesity and hyperphagia are early onset and often lifelong for those with BBS Lack of evidence of HRQoL for patients with hyperphagia related to BBS and how pharmacological management may impact HRQoL Interpretation of self-reported outcomes in patients with cognitive impairment can be challenging | Rhythm Pharmaceuticals, Inc. |
Lazareva 202314 | Review and expert opinion | To review and provide clinical expert assessment of data from clinical trials for setmelanotide for adult and pediatric patients with obesity due to BBS | Depression and suicidal ideation should be monitored for people on setmelanotide Given how long it took to note the effect of setmelanotide on trial, it should be offered for a full year before assessing impact There is still a significant unmet need for pharmacological interventions for obesity in BBS given that 40% of patients with BBS did not experience a reduction in weight justifying continued use of setmelanotide at a cost of $30,000 / month Genetic heterogeneity of BBS may mean that several factors contribute to obesity in people with BBS, each of which may require different interventions. Currently unable to distinguish which subtypes of BBS are most likely to experience a reduction of hyperphagia and weight when using setmelanotide | Intramural Research Program of the Eunice Kennedy Shriver National Institute of Child Health and Human Development, of the US National Institutes of Health, grant ZIAHD00641 |
Hinney 202215 | Review | To consider the heritability of body weight and genetic classifications of obesity; to discuss the clinical features of monogenic obesity; and to highlight novel pharmacological treatment options for monogenic obesity targeting the central melanocortin pathway | A known adverse event of setmelanotide is that it can activate MC1R pathway and can cause skin darkening Certain variants in MC1R may predispose people to developing melanoma | No funding reported, but one author indicated providing unpaid advice to Rhythm Pharmaceuticals |
Ryan 202217 | Review | To review medications (current or anticipated) indicated for chronic weight management as well as those approved for genetic and syndromic conditions | Use of setmelanotide for BBS, or other conditions with proven genetic defects in the leptin-melanocortin pathway, may lead to increases in genetic testing for patients with history of early onset obesity Pediatric clinicians receiving referrals for children with severe obesity likely to be primary prescribers of setmelanotide Need for guidance on when to offer genetic testing to adults living with severe obesity but no current diagnosis | Author reported personal fees and nonfinancial support from Boeringer Ingelheim, Calibrate (ReDesign Health) Epitomee, Gila Therapeutics, IFA Celtic, Janssen, Novo Nordisk, Phenomix, Real Appeal (United Health), Ro, Sanofi, Scientific Intake and Wondr Health |
Wagner 202316 | Review and expert opinion | To identify ethical challenges for appraising interventions for rare diseases, including key ethical tensions as well as approaches and principles for addressing these challenges | Health technology assessment challenges in the appraisal of interventions for rare diseases span assessments of clinical, population, economic, organization, and sociocultural value | Institut national d'excellence en santé et en services sociaux (INESSS) |
Kacetl, 202013 | Systematic Review | To identify ethical questions related to rare diseases and orphan drugs and ethical principles or approaches applied to address them | Noneconomic values and nonutilitarian reasoning, including a variety distributive justice considerations, are significant in decision-making about orphan drugs and rare diseases | University of Hradec Kralove Long-term Development Plan |
Poitou 202011 | Review | To describe care management approaches and new therapeutic opportunities in genetic obesity | The mechanisms driving obesity in BBS are poorly understood, but hyperphagia associated with hypothalamic dysfunction represents one current hypothesis Setmelanotide activates off-target MC1R pathway, which leads to skin darkening. The long-term consequences of chronic stimulation of melanocytes should be monitored Early diagnosis and multidisciplinary management of rare genetic obesity can lead to better long-term prognosis Transition from pediatric to adult care is often associated with disruptions in medical and social care for people with rare genetic obesity | None reported |
Zelihic 20209 | Qualitative interview study | To explore Norwegian parents’ experiences of having a child with BBS | BBS diagnosis is often delayed due to progressive onset of some clinical features and overlap with clinical features of other rare genetic conditions Parents reported:
| None Reported |
Hamlington 201510 | Qualitative interview study | To understand the experiences of courtesy stigma for parents of children with obesity due to BBS | Parents reported that:
The authors suggest that parents may benefit from targeted counselling focused on stigma and their child’s BBS. | Intramural Research Program of the National Human Genome Research Institute |
Stakeholder Input
Patient Input
Bardet Biedl Syndrome Foundation
About Bardet Biedl Syndrome Foundation
The Bardet Biedl Syndrome Foundation (https://www.bardetbiedl.org/) is a registered 501(c)3 non-profit agency that connects families and shares information on research, treatment and therapies for Bardet Biedl Syndrome (BBS). It is registered in Delaware.
Information Gathering
The information contained in this submission was gathered by the BBS Foundation through a 30-minute online survey and one-on-one interviews conducted by telephone/videoconference. All data were contributed anonymously.
The online survey was disseminated in English and responses were collected between January 30 and February 10, 2023. Survey respondents were recruited by the BBS Foundation through promotion via email and social media, and through the BBS registry maintained by Fighting Blindness Canada. The following populations were invited to take part: people living with BBS (“patients”) and caregivers and/or family members of people living with BBS (“caregivers”).
There was a total of 41 respondents to the online survey. Most (n=34) were caregivers, and the remainder (n=7) were patients. The majority of respondents were from the U.S. (61%) and Canada (29%), with the remainder from Germany, Ireland, Spain and the U.K.
Of the caregivers who completed the survey, 79% reported that their loved one with BBS is 18 years of age or younger, with 41% of all caregiver respondents reporting that their loved one is 3 to 10 years of age. All of the patients who responded to the survey are adults.
In February 2023, the information gathered through the survey was supplemented through telephone/videoconference interviews with one patient and four caregivers, all of whom have experience with setmelanotide.
Given the indication of the drug under review, information gathering focused on understanding patient and caregiver experiences with BBS-related obesity and hunger, and no other symptoms of the disease.
Disease Experience
Bardet Biedl Syndrome is a rare genetic disorder. It is associated with the following primary symptoms: visual impairment caused by retinal abnormalities; obesity, typically apparent by age one; polydactyly (extra fingers or toes); hypogonadism; renal anomalies (kidney malformations and/or malfunctions); fewer common symptoms include ASD, learning disabilities, anosmia, Legg-Perthes disease.
While there are more than 20 genes associated with BBS, the underlying cause regardless of gene is malfunction of primary cilia, a key component of cellular communication. BBS is therefore categorized as a ciliopathy, or a disease of the cilia.
BBS is a rare disease affecting approximately 1 in 250,000 people around the world. Based on general population trends, there are likely about 3,000 people in the United States and Canada living with BBS. It is more common in some areas of the world including Newfoundland, where prevalence is estimated to be 1 in 17,500, and in the Middle East (among Bedouin populations).
There is currently no cure for BBS and no available, targeted treatments for BBS either overall, or for BBS-related hunger and obesity, other than setmelanotide which has been approved by the FDA in the United States.
Obesity
Of patients who responded to the survey, 57% said that as a toddler or young child, doctors or medical professionals had identified that their weight was a concern and 71% said they are currently obese (having a body mass index of 30.0 or higher). Of caregivers who responded to the survey, 71% stated that their loved one is currently obese because of their BBS.
Hunger-Related Symptoms and Behaviours
Survey respondents were asked to indicate the degree to which they (or their loved ones, in the case of caregivers) were affected by symptoms related to their hunger.
As shown in Table 1, a large majority of patients (86%) responded that they sometimes, often or always take a longer time to feel full after eating. Thinking about food constantly was reported by 71% of patients to occur sometimes, often or always.
Table 1: Patient Responses About Hunger-Related Symptoms and Behaviours
Response option | Never | Sometimes | Often | Always |
|---|---|---|---|---|
Taking a longer time to feel full after eating | 14.29% | 28.57% | 42.86% | 14.29% |
Feeling hungry again right after a meal | 0 | 100% | 0 | 0 |
Thinking about food constantly | 28.57% | 28.57% | 28.57% | 14.29% |
Feeling stressed out due to hunger, or worrying about food | 42.86% | 42.86% | 14.29% | 0 |
Many people with BBS experience intense, hard-to-control hunger.
When asked to rank the importance of being able to manage these symptoms of hunger, all but one of the seven patients who responded (86%) ranked “taking a longer time to feel full after eating” as 4/5 or 5/5 on a five-point scale, with 5 ranking as extremely important.
When asked to describe in their own words how hunger affected their behaviour, patients said:
“I was diagnosed with a binge eating disorder at the age of 22. I had done therapy for it, and nothing seemed to help. I often find my hunger to be the worst at night, typically I can ignore it by keeping busy during the day. I was diagnosed about 8 weeks ago with BBS at age 31 and now I am questioning the past 9 years of living with the eating disorder. I don't think anything worked because it's not really a mental health/eating disorder problem.”
“I would get upset with anyone who was withholding food from me.”
“Having negative self-esteem and body image, never feeling like a normal person, and being susceptible to bullying by others, not feeling comfortable in regular chairs, or other public venues.”
“I used to sneak food when no one was watching.”
Similarly, an equally large majority of caregivers (85%) responded that their loved ones sometimes, often or always take a longer time to feel full after eating. As shown in Table 2, 91% of caregivers responded that their loved ones sometimes, often or always seem preoccupied with food or talk about it a lot.
Table 2: Caregiver Responses About Hunger-Related Symptoms and Behaviours
Response option | Never | Sometimes | Often | Always |
|---|---|---|---|---|
Compared to others, taking a longer time to seem full while eating | 14.71% | 26.47% | 26.47% | 32.35% |
Seeming constantly hungry regardless of how much they’ve already eaten | 11.76% | 35.29% | 29.41% | 23.53% |
Seeming preoccupied by food or talking about it a lot | 8.82% | 20.59% | 47.06% | 23.53% |
Seeming stressed out or worried about hunger or food | 14.71% | 38.24% | 26.47% | 20.59% |
Many people with BBS experience intense, hard-to-control hunger.
When asked to describe in their own words how they observed hunger affecting their loved one’s behaviour, caregivers said:
“He wakes up in the middle of the night to eat or he will not sleep because he says he is hungry. We have started to limit his food as he will eat everything and will beg his siblings for their food, or he brings them so he can have their food.”
“Celebrations are impossible for him.”
“At birthday parties or celebrations, she will take other kids’ food if they leave it on their plate.”
“My son was always focused on food. It took a lot to distract him, and other parents didn’t want to deal with that, so he never was invited to other kids’ parties or for sleepovers.”
“Used to sneak food constantly but not so much anymore. We lock cabinets and fridge so they cannot get to food, so they don’t try.”
“She will get up at night and sneak food.”
“Things were so bad, that I needed to put locks in the pantry and fridge doors. As he got older and cognitively able to understand why we have a feeding schedule, he no longer roots for food, but still asks constantly and watches the clock and is hyper focused on when he can eat again.”
“Does not know when he is full, frequently saying he’s hungry, crying at the end of every meal, and steals brother’s food.”
“Had to lock fridge. Child would be angry if I forgot because she knew she had no self-control.”
Quality of Life
From a quality of live perspective, BBS-related hunger has the greatest impact on social life and emotional/psychological well-being. This was reported both by patients and by caregivers when responding about the observed impact on loved ones, as well as impact on their own quality of life, as shown in Table 3. A significant number of patients and caregivers also noted that BBS-related hunger has an impact on work or school life, as well as their relationships with family.
Table 3: Patient and Caregiver Responses About Quality of Life Impacts
Response option | Patient self-reported impacta | Caregiver observed impact on loved oneb | Caregiver self-reported impactc |
|---|---|---|---|
Relationship with family members in general/family life | 14.29% | 38.24% | 44.12% |
Relationship specifically with spouse/partner | 28.57% | 0 | 35.29% |
Relationship specifically with children | 14.29% | 14.71% | 17.65% |
Emotional/psychological well-being | 42.86% | 47.06% | 52.94% |
Social life | 42.86% | 50% | 41.18% |
Work or school life | 28.57% | 44.12% | 29.41% |
Ability to travel | 42.86% | 11.76% | 20.59% |
Ability to pursue hobbies | 28.57% | 20.59% | 23.53% |
Financial situation | 28.57% | 11.76% | 17.65% |
None of these | 57.14% | 26.47% | 26.47% |
aHas intense, hard-to-control hunger had a negative impact on any aspects of your life? Choose all that apply.
bBased on your observations, how has your loved one’s intense, hard to control hunger had a negative impact on their quality of life? Choose all that apply.
cBased on your observations, how has your loved one’s intense, hard to control hunger had a negative impact on your quality of life? Choose all that apply.
Patients elaborated on how BBS-related obesity and hunger have affected them:
“When I was in middle school other kids would try to see how much they could feed me and tease me.”
“Not feeling worthy enough of a dating relationship, having to buy expensive clothes to fit my size and feeling different and judged by others.”
Caregivers commented about on how BBS-related obesity and hunger has affected their loved ones:
“The school has called to ask if we have enough food for him as he seems to not get enough at school. He has lied to the district saying we don't feed him so he can get more food. He has no friends because he hounds them for their meals while at school.”
“Food seems to be on his mind very often. He wants to know what and when we'll be eating next. He often takes food when he thinks no one is watching and definitely eats more than he should. Because he is overweight it affects his mobility and self-esteem.”
“She couldn't focus on school, friends, siblings anything all she thought about was eating.”
“Her focus on food would cause worse mood swings which impacted her socially and the preoccupation impacted her attention at school.”
“My son was not usually invited over friends’ houses because other parents didn’t like telling him no.”
“It was very difficult as a child to bring her to birthday parties. I would turn around for 5 min and she had eaten 5 pieces of pizza. Just no control over food. I would also find wrappers hidden everywhere in her room, she would steal food and hide to eat it.”
“My daughter was low energy and was depressed about her body weight and image and dissatisfied with herself. She could not keep up with her friends and was often left out of activities or social outings they planned because of it.”
“Her desire to eat more causes her anxiety.”
Caregivers also shared how their loved one’s BBS-related hunger has affected their own quality of life:
“He bullies his younger siblings until they give him their food, or he will just take it…it has caused major fights and resulted in my younger kids and myself going hungry cause he will steal the food.”
“The whole condition of BBS has been trying. The hunger has been difficult along with weight gain and concerns about the social impacts and health impacts. The worry has for sure caused us increased anxiety and stress.”
“It’s always on my mind - how’s she doing physically, how much she’s eating, how much exercise she’s getting…I think about whether it’s ‘okay’ to give her unhealthy foods because I worry, she won’t eat the healthy food that her body needs. We as a family worry about how this will impact her throughout her life as she gets older. How much freedom will we be able to provide to her when it comes to food choices as she grows and matures?”
“Lack of sleep due to 3 to 6 nightly feedings; trouble weaning from breastfeeding, especially during nighttime; time-consuming food-prepping/cooking; own orthopaedic issues due to heavy weight of BBS-impacted child which has to be carried a lot (cannot walk, yet); social isolation due to child's behaviour (screaming).”
“At parties I would be the one trying to keep control on my son's eating and that was stressful. People would tease me and tempt my son because they thought it was funny.”
“People do not understand. He has a typical brother who eats all day and tons of junk food and stays thin. People see him and immediately think I am over feeding him, or he just eats all day, but he doesn’t. I’ve even had social services called on me to investigate if I am over feeding him. It is so tiring and such a struggle.”
Experiences With Currently Available Treatments
In Canada, there is no approved treatment for BBS either overall, or for BBS-related hunger and obesity. Patients and caregivers were asked about weight management strategies they have employed, and their degree of effectiveness.
Environmental Controls
As shown in Table 4, when patients were asked what environmental controls, they have tried to help manage their weight, they identified a regular exercise plan as somewhat (43%) or very (43%) effective. Only one other strategy – supervision from others – was identified by more than half of respondents to be somewhat or very effective.
Table 4: Patient Responses About Environmental Controls
Response option | Ineffective | Somewhat effective | Very effective | N/A or haven’t tried |
|---|---|---|---|---|
Supervision from others | 14.29% | 28.57% | 28.57% | 28.57% |
Securing food sources | 0 | 0 | 0 | 100% |
Reducing energy intake | 14.29% | 28.57% | 0 | 57.14% |
Adhering to meal schedules | 28.57% | 28.57% | 0 | 42.86% |
Regular exercise plan | 14.29% | 42.86% | 42.86% | 0 |
Caregivers identified that a regular exercise plan was a somewhat (56%) or very (18%) effective way for their loved one to manage their weight. Because all caregivers identified that their loved one with BBS is 18 years of age or younger, other strategies were identified to be effective to varying degrees, including:
Supervision from others, reported as somewhat (59%) or very (26%) effective.
Reducing energy intake (calorie-restricted diet), reported as somewhat (47%) or very (9%) effective.
Adhering to meal schedules, reported as somewhat (29%) or very (44%) effective.
Table 5 shows all the response options and the data provided by caregivers.
Table 5: Caregiver Responses About Environmental Controls
Response option | Ineffective | Somewhat effective | Very effective | N/A or haven’t tried |
|---|---|---|---|---|
Supervision from others | 5.88% | 58.82% | 26.47% | 8.82% |
Securing food sources | 2.94% | 20.59% | 26.47% | 50.00% |
Reducing energy intake | 17.65% | 47.06% | 8.82% | 26.47% |
Adhering to meal schedules | 14.71% | 29.41% | 44.12% | 11.76% |
Regular exercise plan | 17.65% | 55.88% | 17.65% | 8.82% |
Even taking these environmental controls into consideration, many caregivers anecdotally shared the challenge of helping their loved one to manage their weight:
“No matter what we did she was always hungry.”
“Food restrictions never worked for us and looking back I think it’s because she was sneaking food. Exercise is still hard because she’s uncoordinated and tires so easily. Keeping food away and schedules helped the most.”
"No diet seems to work. Exercise is hard as he is rapidly out of breath due to excess weight."
“No matter how much exercise and diet restriction my son still gained weight.”
“Did numerous weight loss attempts but my son would always find ways to sneak food.”
“We have tried everything except locking up food, nothing was very effective. I find offering healthier food, and eating regularly, routine has helped with the hunger...but no matter what we did, she still gained weight and fast.”
Medications
Patients and caregivers were asked if they or their loved ones had used any of the following weight management medication for weight regulation related to their BBS: orlistat (Xenical, Alli); phentermine-topiramate (Osymia), naltrexone-bupropion (Contrave), liraglutide (Saxenda), semaglutide (Wegovy, Ozempic, Rybelsus), phentermine, benzphetamine, diethylpropion, and/or phendimetrazine.
Of patients who responded to the survey, only two reported that they had tried any of these medications: one reported that semaglutide was very effective while another reported that phentermine was somewhat effective.
Similarly, of the 34 caregivers who responded to the survey, only semaglutide had been tried, and only in two instances. One respondent indicated it was somewhat effective for their loved one, while the other said it was very effective. Of note, in one of these instances, semaglutide was being used at the same time as setmelanotide. Additionally, vyvanase and metrofmin were mentioned by one respondent.
Improved Outcomes
When asked what would be meaningful for them in a treatment that manages the hunger associated with their BBS, all seven patient respondents said being able to effectively manage their weight. Feeling full faster was named by six of the seven patients, and not thinking about food so much, not feeling hungry right after they’ve eaten, and reduced stigma and/or judgment were each identified by five of the respondents. In the words of one patient:
“So much would be easier if my weight was managed. Travel, interactions with my kids, self-esteem, medical care for problems not associated with weight - the bias of medical professionals because of weight is awful - social life and work environment would be better.”
When thinking about what they believed would be meaningful to their loved one in a treatment that manages BBS-related hunger, caregivers’ top answer was not thinking about food so much (80%), followed by not feeling hungry right after they’ve eaten (68%) and reduced stigma and/or judgment (63%). Given that their loved ones with BBS are all 18 years of age or younger, caregivers’ comments overwhelmingly reflected the hope for their loved ones to have an easier life journey especially in their youth:
“She could be happy and so much less stressed. The ability to not worry about food provides the freedom every child deserves.”
“Improved self-esteem and reduced health concerns.”
“Food won’t be the focus most of the time.”
“Better access to healthcare without judgement when he is older.”
“Less screaming and lower stress level, improved motor skills (ability to walk) due to weight loss.”
“Happier individuals. As parents, that's all we want for them.”
“They could start to focus on other things more and stop letting hunger steal their joy and pleasure in other activities. They could have better control over their weight and not feel shame each time they are weighed.”
“He would have more of a social life and be able to travel easier.”
“We would be able to go longer in doing things without stopping constantly fighting him on wanting food. He would be able to stay healthier.”
“He can move more and be more active. He could focus more on just being a teenager and living life and going on vacations and not being so tired all the time or feeling bad about himself because people can be so mean. His family wouldn’t constantly make comments about his weight and what I’m doing about it.”
“She would not be struggling as much to get around. Her sight is already quite affected by BBS, her balance is not the greatest either.... to add obesity to that, is hard. It's for sure affecting her self-confidence. She would be able to move more freely, and to focus on things that matter, instead of thinking about food and eating all the time.”
Caregivers also acknowledged that a treatment to manage their loved one’s BBS-related hunger would have broader benefits for them personally and their family overall:
“Less emphasis on food would limit the stress built around family meals. Family members need to focus on supporting each other and not on food.”
“We would also be less stressed about food. It would feel like a huge weight had been lifted off our family.”
“We would be able to go out and to parties without someone ‘standing guard’ near the food table.”
“The worry and battle of weight management would not be a priority in our relationship.”
“All of my time and energy would not be focused on keeping him healthy and redirected from his obsession with food and eating. We could have cable TV again without worry of what food commercial may come on. We could go to a fair or carnival or out to eat without his having a meltdown because he needs all the food.”
Experience With Drug Under Review – Setmelanotide
Among all survey respondents, 17 had experience with setmelanotide: four patients reported they are taking it, and 13 caregivers indicated their loved ones are taking it. Clinical trials and private insurance were the most common ways that survey respondents were able to access the drug.
Many patients and caregivers reported positive outcomes as a result of their experience with setmelanotide:
“The benefits were many... after about a month or two of being on setmelanotide... my 12-year-old at the time told me she was not hungry anymore.... for the first time in her life. She herself said, ‘Mom, I am not hungry anymore... and I have never felt this feeling before.’ She said I did not know before what it was to not feel hunger. That broke my heart, but that's when I realized that it was working. She is now cutting down her portion size herself, makes better food choices, not hungry all the time.... she has lost some weight; she feels good about herself.”
“Life changing. He gets full and satisfied. He has lost almost 50 lbs and moves better. He seems excited about not being so obsessed with food and making better food choices, without my constant guidance.”
“It was a game changer in every aspect of our lives, no question about it, and our daughter is healthier and happier overall, and we are happier and feel relieved that there is a medicine out there that can help our child afflicted by something that is not her fault and can make so many wonderful impacts on her life.”
“It is very difficult to reason with someone you know is sick and is also young. If your child has BBS they probably have sight issues or no sight and balance/coordination issues so it is very difficult to get them to try to be active in the usual sense-you have to become creative and when you have so many other extenuating circumstances to a caring for a loved one with BBS it is difficult to only focus on the nutrition aspect of their lives also because you see they derive so much pleasure out of eating. We know that our daughter snuck food, almost always the worst of snacks but we never locked our cabinets or fridge as we didn't want to make her feel bad because of it. We would definitely speak with her about it after the fact and tried to explain to her why it isn't good to do it because of her health, etc. But the brain is definitely wired differently for her and at the end of the day it wasn't her fault - that is why Imcivree is so special because it regulates that for them, and they are not interested in food as irrationally as before - like making sure there are seconds before she even finished the plate in front of her.
“Did well. Lost 50lbs but had to travel to Washington to get the medication and injection was hard for him to manage without help as his vision is very poor.”
“Setmelanotide helped my son lose over 130 pounds and keep it off. He is much happier that he moves around so easily. The first time he didn’t have to use a seatbelt extender on the airplane he was so excited.”
“Slow, steady weight loss, better mental and physical health. Social relationships greatly increased and/or improved.”
“Weight loss, decreased stress, and worry over hunger. Increased focus and attention at school and at home.”
“I lost over 130 pounds during the 5 years that I was in the study for setmelanotide and taking Imcivree now and with regular exercise I am keeping the weight off.”
“For the first time I was able to sustain weight loss due to reduced hunger and cravings.”
“My daughter is currently in the trial for setmelanotide so these answers were our experience prior to that medication. She used to be hyper focused on food. As a 6.5-year-old she does still focus on food in play a lot, but not nearly as much as before the study. She leaves food on her plate now and never did before the study.”
“We are currently in the Setmelanotide study, and it has been life changing! My daughter lost 14 lbs so far from March 2022 to now (as a six-year-old!) and is healthier than she has ever been in her life. We have much less stress and worry and we are so hopeful for more treatments to come with BBS after such a positive experience in this study…. I would recommend [setmelanotide] because the side effects are so minimal, and it is a very easy medicine to take once you are in a routine. The benefits seem to really outweigh the risks in terms of changing the life of the person with BBS as well as their family. The long-term effects of the weight loss cannot be understated. This would decrease risks of weight related health issues in the long run.”
“Setmelanotide has been a life saver; literally.”
When asked about any negative impacts experienced with setmelanotide, the most commonly mentioned ones were the darkening of the skin, and bruises and scars being more noticeable.
Nausea and gastrointestinal upset were mentioned to a lesser extent, as well itchiness and/or pain at the injection site. Several respondents noted the method of administration via daily injection was challenging for patients who were vision-impaired, which is a symptom of BBS, or for younger patients for whom it could limit activities of daily living such as field trips and sleepovers. One respondent reported feeling jittery and limited their caffeine as a result; they have since been able to add it back in. One patient has an allergy to setmelanotide and is unable to take it.
Of the 41 people who responded to the survey, all but one patient and one caregiver would recommend that setmelanotide be made available to people with BBS. Comments about this included:
“Everyone should have the ability to make informed decisions regarding their healthcare. If a medication has shown that it effectively treats a disease, the patient should be able to advocate for themselves and decide if they would like to try a treatment.”
“I think it would provide an option for those with BBS who are struggling with their obesity and the secondary effects of that (diabetes, hypertension, etc.) to be able to manage it more successfully.”
“People with BBS are not lazy and do not overeat [on] purpose. The co-morbidities are so much worse and more expensive than the cost of this life changing treatment. Setmelanotide truly gives a person back their life and health, both physically and mentally. All people with BBS should have access to this medication.”
“Every person with BBS who has a hunger/obesity issue should be able to take this medicine. It is caused by a medical condition, not because they are lazy or at fault - it is the wiring in the brain that causes this - setmelanotide is effective and life altering for anyone afflicted by BBS - it has so many synergies in one's life with health, mental health, school life is easier to focus at school, social aspects are enhanced as one's mood is enhanced - the possibilities exponentially increased once the hunger is addressed.”
“I strongly recommend that this medication be accessible. Prior to starting the trial my husband and I were not sure if we would even notice an impact on our son and were blown away by his immediate progress in not only hunger management but overall development and mood. I have tears in my eyes as I type this. Every person living with BBS should have access to this medication. Observing the changes to all areas of his development are so encouraging and suggest even BBS individuals with controlled weight or hunger may benefit as well. While he is not able to communicate how he feels, I really do think the feeling of being hungry was always there, we just didn't know it. Because of his food aversions he never seemed preoccupied with food until 3 years old (we noticed him asking for crackers more around that age) and he also never seemed to eat more than his older brothers when they were his age. He has always been significantly obese, seemingly regardless of what he ate. Setmelanotide seems to allow him to more fully participate in everything, I'm guessing because his brain doesn't think he is starving. His teachers and therapists have been so impressed with the changes as well. Please make this medication available to every individual with BBS.”
In addition to the survey responses summarized above, one (1) patient and four (4) caregivers were interviewed regarding their experiences with setmelanotide and its impact on their lives. All those who participated in the interviews were from the U.S., and have accessed setmelanotide through clinical trials and private insurance.
Caregiver A says that “Imcivree saved his life” when sharing her experience with her son, Patient A, who was diagnosed with BBS in 2011 when he was a high school senior. The diagnosis was a relief to the family since Patient A’s weight issues were previously attributed to his personal inability to control his hunger and not a medical condition. Caregiver A said, “We just didn't know until he was diagnosed. And then I read everything about it, and I'm like, oh, my God, this totally explains this kid!” Patient A shared how BBS has had a significant impact on his life. As a child, his compulsion to eat “was often made fun of in school” and his mother said that “other parents had misgivings about inviting him over because of his hunger issues.” Because of his weight, Patient A had trouble playing sports and he wasn’t able “to do basic things like learning to ride a bike with training wheels” because the training wheels bent when he sat on the bike, due to his weight. Despite exercise and significant lifestyle changes over many years, Patient A was unable to lose weight until he was able to access setmelanotide through a clinical trial in 2017. At the time he enrolled in the clinical trial, Patient A weighed 325 pounds. Today, he weighs 195 pounds and goes on daily walks with his family and cycles with his father every morning. Caregiver A says that “People can barely recognize my son now”. Patient A says that “I felt I had nothing to lose by trying setmelanotide and my life is so much better for it.”
Caregiver B, a mother of two daughters living with BBS shared the challenges she faced. From birth, this mother noticed that her first-born daughter wanted to nurse constantly, to the point where she wasn’t able to produce enough breast milk. As a first-time mom, she initially thought that this need for constant breast-feeding was a normal part of her baby’s growth cycle. When her daughter became a toddler, she used to “raid the grocery bags” if they were put in the back seat for the drive home. After her second daughter was born, she noticed that both children were “rapidly gaining weight” despite only serving them healthy meals and not allowing her daughters to have dessert “unless it was a special occasion like a birthday or company visiting.” After returning to work full-time, her two daughters would “sneak food” after school, before their mom got home from work, so she began to “hide food in the garage.” Eventually, one of her daughters was diagnosed with diabetes and the other one with kidney disease, as a result of their BBS. Today, Caregiver B credits setmelanotide for helping one of her daughters to “no longer need a kidney transplant” and for dramatically reducing the amount of insulin her diabetic daughter now needs due to improved A1C levels – both thanks to the drug’s effectiveness in addressing their BBS-driven hunger. This caregiver felt it was important to make setmelanotide accessible to all BBS patients who could benefit from it, as it could help “reduce costs to the healthcare system later on” as a result of preventing kidney transplants and the need for diabetes medications.
Caregiver C shared how her daughter was diagnosed with BBS at 2.5 years of age, after one day her eye “turned in and stuck” and she was rushed to the emergency room. Before the diagnosis, her daughter used to have lots of “fits and meltdowns” to the point where she would “beat her head to bleeding” on the wall or the floor during her tantrums. Looking back, this caregiver now believes that her daughter’s tantrums were her way of “just managing feelings and frustrations” of not being able to communicate her insatiable hunger, which “hurts to think about.” The hardest part of her daughter’s BBS diagnosis has been “worrying about what will be in the future and what that [future] looks like for her” considering issues like vision loss, diabetes and kidney failure pose tangible risks to people with BBS. Her daughter was able to receive setmelanotide through a clinical trial and today is doing well at school and is able to be more engaged with friends and family “now that her focus is off food.” She feels that her daughter’s treatment has been “life changing in several areas, we [now] feel like there’s hope.” When it comes to access to setmelanotide, this mother says that “parents need something…with BBS we have so many obstacles and we have so many areas of concern, and not a lot of hope. And [setmelanotide] is what we have right now, and parents need that option.”
Caregiver D’s daughter was born with an extra digit on her hands and was not meeting her development milestones. Her daughter was diagnosed with BBS at one year of age. At the time, Caregiver D had never heard of BBS, but it explained the hunger she observed in her daughter. “It was like a switch was flipped on all the time, she couldn’t focus, she didn’t want to play…everything was about food. It took over our life [as a family]”. When her daughter was nine years old, she started treatment with setmelanotide through a clinical trial and it has been like the “[hunger] switch has been switched off.” Her daughter is losing weight, her Body Mass Index (BMI) is coming down, her energy levels have improved and she’s more focused on school and friends. This mother says that setmelanotide has been “a blessing” and that it “gives her hope” for her daughter’s health in the long-term. Even though her daughter has been on setmelanotide for less than one year, Caregiver D says it’s like a “huge weight has been lifted”. They can finally go out as a family without her daughter having “meltdowns” due to her insatiable hunger. Caregiver D believes that publicly funded access to setmelanotide “should be mandatory. It’s a life-saving medication. Everyone has the right to good health and quality of life.”
Companion Diagnostic Test
Not applicable.
Anything Else?
When asked if there was anything else they wanted to share about their experience with BBS or with setmelanotide, this is what patients and caregivers said:
“Apart from curing BBS overall, which is not yet possible, setmelanotide is the game-changing component to someone affected by BBS, specifically if they are enduring the hunger component of the syndrome. For our family it has been a godsend.”
“It has changed our lives completely ... I can't even begin [to describe the impact setmelanotide has had on my life]. I never thought a medicine could change our lives. I cannot say enough wonderful things. Our daughter does not have constant hunger.”
“…Out-of-control hunger and food seeking is the cause of much of the obesity in BBS… that has been successfully treated with setmelanotide. The excess hunger and food seeking not only result in obesity, but they can also cause, or contribute to mental health challenges and relationship issues. Quality of life suffers.”
“Although BBS is rare, those people who are affected by it need to know that Health Canada is willing to approve a drug specifically for them. If it is helping other people in other countries, it needs to be an option for Canadians as well.... The overall results have shown that it is beneficial for people in helping them with their weight. This directly correlates with their risk for other life-threatening diseases.”
Conflict of Interest Declaration — Bardet Biedl Syndrome Foundation
To maintain the objectivity and credibility of the CADTH reimbursement review process, all participants in the drug review processes must disclose any real, potential, or perceived conflicts of interest. This Patient Group Conflict of Interest Declaration is required for participation. Declarations made do not negate or preclude the use of the patient group input. CADTH may contact your group with further questions, as needed.
Did you receive help from outside your patient group to complete this submission? If yes, please detail the help and who provided it.
The BBS Foundation completed the submission independently with external support from EVERSANA.
Did you receive help from outside your patient group to collect or analyze data used in this submission? If yes, please detail the help and who provided it.
The BBS Foundation completed the submission independently with external support from EVERSANA.
List any companies or organizations that have provided your group with financial payment over the past two years AND who may have direct or indirect interest in the drug under review.
Table 6: Financial Disclosures for Bardet Biedl Syndrome Foundation
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
Rhythm Pharmaceuticals | — | — | — | X |
Clinician Input
Canadian Endocrinologists Treating Bardet-Biedl Syndrome
About Canadian Endocrinologists Treating Bardet-Biedl Syndrome
We are a group of Canadian endocrinologists who treat Bardet-Biedl syndrome (BBS) in pediatric and adult populations. We represent the specialty from across Canada in both academic and community settings and share the goal to improve the health and quality of life of those living with BBS.
Information Gathering
An initial draft was written by Dr. Stasia Hadjiyannakis. The resulting final submission was distributed to a group of Canadian physicians who treat BBS. Physicians who wished to support this Clinician Group Input submission signed the submission.
In addition, the following were referenced for background information and supporting evidence.
Clément K, et al. Efficacy and safety of setmelanotide, an MC4R agonist, in individuals with severe obesity due to LEPR or POMC deficiency: single-arm, open-label, multicentre, phase 3 trials. Lancet Diabetes Endocrinol. 2020;8(12):960-70.
Clinical Trials.gov. Setmelanotide in Pediatric Rare Genetic Diseases of Obesity. Available at: https://clinicaltrials.gov/ct2/show/NCT04966741 (accessed January 3, 2023).
Government of Canada. Meds Entry Watch – New Medicines Approved in 2020. Available at: https://www.canada.ca/en/patented-medicine-prices-review/services/npduis/analytical-studies/meds-entry-watch-6th-edition/new-medicines-approved-2020.html(accessed January 3, 2023).
Haqq AM, et al. Efficacy and safety of setmelanotide, a melanocortin-4 receptor agonist, in patients with Bardet-Biedl syndrome and Alström syndrome: a multicentre, randomised, double-blind, placebo-controlled, phase 3 trial with an open-label period. Lancet Diabetes Endocrinol. 2022;10(12):859-68.
Haws RM, et al. The efficacy and safety of setmelanotide in individuals with Bardet-Biedl syndrome or Alström syndrome: Phase 3 trial design. Contemp Clin Trials Comm. 2021;22:100780. https://doi.org/10.1016/j.conctc.2021.100780.
Imcivree. Beginning Treatment: An Overview. https://www.imcivree.com/hcp/bbs/ (accessed January 3, 2023).
Pomeroy J, et al. Bardet-Biedl syndrome: Weight patterns and genetics in a rare obesity syndrome Pediatr Obes. 2021;16(2):e12703.
Rare Disease Database. Bardet-Biedl Syndrome. https://rarediseases.org/rare-diseases/bardet-biedl-syndrome/.
U.S. Food & Drug Administration. FDA approves treatment for weight management in patients with Bardet-Biedl Syndrome aged 6 or older. https://www.fda.gov/drugs/news-events-human-drugs/fda-approves-treatment-weight-management-patients-bardet-biedl-syndrome-aged-6-or-older (accessed January 3, 2023).
Current Treatments and Treatment Goals
BBS is a rare multi-system genetic condition that falls under the spectrum of ciliopathy disorder. The estimated incidence of BBS is 1:160,000 in Northern European populations, but as high as 1:13,500 and 1:17,000 in isolated communities in Kuwait and Newfoundland and Labrador, respectively. It is characterized classically by early-onset obesity with hyperphagia, intellectual impairment, renal anomalies, polydactyly, retinal degeneration, hypogonadism and hypogenitalism. People with BBS can also have co-existent musculoskeletal complications, such as scoliosis and hip dysplasia, and often have balance and coordination difficulties. Surveillance includes regular ophthalmologic evaluation, monitoring of renal and liver function, glucose and lipid metabolism, endocrine function, blood pressure, weight/growth, and musculoskeletal function. A multidisciplinary team approach is required to effectively manage and support individuals with BBS. There is currently no targeted therapy for BBS. Complications associated with BBS are treated symptomatically in a similar manner to which they are treated or managed in the general population.
The hyperphagia and obesity in BBS are thought to be related to hypothalamic dysfunction. The consequences of BBS include difficulties trafficking leptin-receptor signaling to proopiomelanocortin (POMC), thereby reducing the activation of the melanocortin 4 receptor (MC4R), which is our main signal of satiety. Lack of MC4R activation leads to insatiable hunger (hyperphagia), decreased metabolism and severe obesity. There is currently no available therapy that directly addresses this consequence of BBS. As a result, 72% to 92% of individuals with BBS have obesity, with most having onset prior to 6 years of age.
Current approaches to weight management in individuals with BBS are similar to those for the general population. Obesity is widely recognized as a complex, chronic, progressive and relapsing condition. The cornerstone of obesity management is lifestyle intervention, which includes counselling and interventions to ensure optimized nutrition, appropriate physical activity, improved sleep patterns, as well as psychosocial/mental health supports. There are also now available pharmacotherapeutic options and bariatric surgery for a subset of people living with obesity. For those living with BBS, engagement in lifestyle interventions is complicated by co-existing biologically driven hyperphagia (deregulation of appetite), as well as low vision, balance and coordination difficulties, intellectual disabilities, and mental health concerns.
While liraglutide is now approved for use in those with obesity aged 12 years and older, and semaglutide and naltrexone HCI/buproprion HCI are approved for those aged 18 years and older, the effectiveness and safety of these agents in those living with BBS has not been studied. Furthermore, these agents do not directly address leptin signaling and MC4R activation at the level at which it is impacted in those living with BBS. The safety, efficacy and durability of bariatric surgery in this population remains largely unknown.
Obesity management goals include prevention of weight-related health complications, including cardiometabolic risk, type 2 diabetes, abnormalities in lipid metabolism, non-alcoholic fatty liver disease (NAFLD), obstructive sleep apnea, musculoskeletal pain/discomfort, and difficulties with activities of daily living. For those living with obesity, a sustained decrease in body mass index (BMI) or body weight of 5% or more can lead to a clinically meaningful decrease in risk for complications related to obesity.
Treatment Gaps (Unmet Needs)
Considering the treatment goals, please describe goals (needs) that are not being met by currently available treatments.
There is currently no available targeted therapy for BBS. In those living with BBS, obesity is highly prevalent, impacting 72% to 92% of patients, with onset prior to 6 years of age in most. The driver of obesity is hypothalamic dysfunction (interference of leptin signalling and MC4R activation). Weight management is, therefore, complicated by hyperphagia (insatiable appetite). This sustained hyperphagia is distressing and a significant burden to both the individual living with BBS as well as their family or caregivers. Hyperphagia leads to severe obesity that negatively impacts health, quality of life, mobility, mental health (mood, body image, self-confidence), and finances. Patients are also confronted with weight bias and discrimination in school, work, and healthcare environments. Severe obesity can make activities of daily living more difficult and is often exacerbated by co-existent low vision and balance and coordination difficulties. Environmental controls, such as adult/caregiver supervision around food, securing food sources, reducing energy intake and adhering to meal schedules, are essential management strategies for weight regulation for those with BBS. However, these controls are often ineffective, difficult to implement and sustain, and do not address the persistent hyperphagia that can negatively affect quality of life and social dynamics. Things that most people take for granted, such as social gatherings that include food, restaurants, trips to the grocery store or mall, and even school/work cafeterias, can be challenging to manage and navigate. Even for those without BBS, clinically meaningful weight loss is exceptionally difficult to achieve and sustain. In the context of co-existing hypothalamic dysfunction and hyperphagia, it is near impossible.
Place in Therapy
How would the drug under review fit into the current treatment paradigm?
Hyperphagia is one of the most distressing symptoms associated with BBS and contributes to life-shortening comorbidities, including severe obesity and its consequent increased cardiometabolic risk, type 2 diabetes, obstructive sleep apnea, NAFLD, musculoskeletal difficulties, and impact on activities of daily living. Setmelanotide is a melanocortin 4 (MC4) receptor agonist and a peptide analogue of endogenous melanocortin peptide alpha-melanocyte stimulating hormone (MSH). It binds to the MC4R to transmit a signal of satiety (sense of fullness). Given that MC4R activation is muted in BBS, treatment with setmelanotide effectively addresses this defect, thereby allowing for better recognition of fullness/satiety, decreased hunger and increased metabolism in those living with BBS. Treatment with setmelanotide will, through this mechanism, decrease risk for severe obesity and lead to weight loss for those already living with severe obesity.
In November of 2020, setmelanotide was approved by the U.S. Food & Drug Administration (FDA) for treatment of genetic conditions of obesity including POMC, PCSK1 and leptin receptor deficiency, all of which led to decreased activation of the MC4R. Given the role of the BBS protein in the MC4R signaling pathway, in June of 2022, setmelanotide was also approved by the FDA for treatment of those with BBS and obesity.
A recent clinical trial evaluating the use of setmelanotide in those with BBS and obesity demonstrated a mean decrease in BMI of 7.9% (with 5% weight loss or decrease in BMI considered clinically significant). Sixty-one percent of participants lost 5% or more of their initial BMI and 39% lost 10% or more. Participants reported a decrease in hunger score and experienced improvements in their lipid profile, contributing to decreased overall cardiovascular disease risk.Haws 2021; Haqq 2022
Setmelanotide is the first approved treatment that would address the underlying hypothalamic dysfunction that contributes to hyperphagia for those with obesity and BBS. No other treatment options have been proven to be safe and effective at managing or treating obesity in this population. Lifestyle interventions have limited benefit and are difficult to sustain in the context of ongoing hyperphagia (appetite deregulation). Further complicating things for those with BBS are co-existing low vision, balance and coordination difficulties, hip dysplasia, and scoliosis that make engagement in weight-management strategies such as physical activity more challenging. Obesity can also make management of existing musculoskeletal issues and balance and coordination difficulties more challenging.
Setmelanotide would become part of the therapy plan (in combination with already existing lifestyle interventions) for those aged 6 years or older with obesity. The addition of setmelanotide would allow for more successful weight management, given that it addresses the underlying hyperphagia directly. The responsiveness to lifestyle interventions would be expected to improve significantly. One could therefore also expect a decrease in prevalence of weight-related health complications such as cardiometabolic risk, type 2 diabetes, hypertension, NAFLD, obstructive sleep apnea, and musculoskeletal pain/discomfort.
Which patients would be best suited for treatment with the drug under review? Which patients would be least suitable for treatment with the drug under review?
All individuals with genetically confirmed BBS and obesity who are 6 years of age or older are likely to respond to treatment and benefit from setmelanotide.
At this time, setmelanotide should not be considered for patients under 6 years of age or for those without obesity, as it has not been adequately studied in these populations. It should not be used during pregnancy and/or breast feeding, as the safety of setmelanotide in pregnancy and/or on the fetus and breastfeeding infant is unknown. It is also not recommended in those with moderate to severe renal impairment.
We have no way of identifying which individuals with BBS and obesity are most likely to respond to setmelanotide at this time.
What outcomes are used to determine whether a patient is responding to treatment in clinical practice? How often should treatment response be assessed?
Response to treatment should be reassessed after 12 to 16 weeks of therapy. If a decrease of 5% or greater in weight or baseline BMI has not been achieved by that time, then the individual is unlikely to experience benefit from setmelanotide.
What factors should be considered when deciding to discontinue treatment with the drug under review?
Response to treatment, presence of side effects and/or contraindications to treatment with setmelanotide should be considered when deciding to discontinue treatment. Response to treatment should be seen within 12 to 16 weeks of initiation of therapy. Therapy should be discontinued if the individual becomes pregnant. It should also be discontinued if there is co-existent moderate to severe renal impairment.
What settings are appropriate for treatment with setmelanotide? Is a specialist required to diagnose, treat, and monitor patients who might receive setmelanotide?
Care of patients with BBS requires a multidisciplinary team approach. The diagnosis of BBS should be confirmed through genetic testing. A physician with expertise in weight management should treat and monitor patients with BBS on setmelanotide, in consultation with other healthcare providers involved in their care (e.g., ophthalmologist, nephrologist, endocrinologist, internal medicine specialist, gastroenterologist, primary care physician, dietitian, and mental health care provider).
Additional Information
Parents of children with BBS find obesity and hyperphagia to be two of the most distressing features of BBS. Oftentimes, parents utilize measures such as locking cabinets or refrigerators to limit the child's access to food. Parental guilt and an awareness of stigmatization by extended family or peers, as well as a perception of being negatively judged by healthcare providers, is also frequently reported. Obesity accelerates long-term, co-existing health concerns in BBS, including cardiovascular disease, obstructive sleep apnea, NAFLD, type 2 diabetes, and other negative effects on quality of life. Vision loss resulting from retinal degeneration, poor balance or ataxia, and musculoskeletal disorders including hip dysplasia, talipes equinovarus, and scoliosis all hamper activity in children with BBS, thus aggravating the effects of underlying hyperphagia and obesity.Pomeroy J, 2021
The paucity of reported successful treatments for obesity suggests that current interventions have limited efficacy in the BBS population. Likewise, available pharmacotherapy has been unsuccessful. Targeted therapy with setmelanotide offers significant hope for this population, as it directly addresses the hypothalamic dysfunction that leads to hyperphagia in this condition.
Conflict of Interest Declarations — Canadian Endocrinologists Treating Bardet-Biedl Syndrome
To maintain the objectivity and credibility of the CADTH drug review programs, all participants in the drug review processes must disclose any real, potential, or perceived conflicts of interest. This conflict of interest declaration is required for participation. Declarations made do not negate or preclude the use of the clinician group input. CADTH may contact your group with further questions, as needed. Please refer to the Procedures for CADTH Drug Reimbursement Reviews (section 6.3) for further details.
Did you receive help from outside your clinician group to complete this submission? If yes, please detail the help and who provided it.
Medical writer, Cynthia Lank (Cynthia N. Lank Editorial Services, Halifax, NS), provided logistical support in the form of participating in initial interviews with Dr. Hadjiyannakis, reviewing and proofreading, and incorporating feedback as directed by Dr. Hadjiyannakis.
Did you receive help from outside your clinician group to collect or analyze any information used in this submission? If yes, please detail the help and who provided it.
Medical writer, Cynthia Lank (Cynthia N. Lank Editorial Services, Halifax, NS), provided logistical support in the form of participating in initial interviews with Dr. Hadjiyannakis, reviewing and proofreading, and incorporating feedback as directed by Dr. Hadjiyannakis.
List any companies or organizations that have provided your group with financial payment over the past two years AND who may have direct or indirect interest in the drug under review.
Declaration for Clinician 1
Name: Dr. Stasia Hadjiyannakis
Position: Assistant Professor, University of Ottawa and Medical Director of Centre for Healthy Active Living at the Children’s Hospital of Eastern Ontario (CHEO), Ottawa, Ontario
Date: 03-03-2023
Table 7: COI Declaration for Canadian Endocrinologists Treating Bardet-Biedl Syndrome — Clinician 1
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
NovoNordisk | X | — | — | — |
Declaration for Clinician 2
Name: Dr. Sue D. Pedersen
Position: Endocrinologist and Obesity Specialist (Diplomate of the American Board of Obesity Medicine), C-ENDO Diabetes & Endocrinology, Calgary, Alberta
Date: 28-02-2023
Table 8: COI Declaration for Canadian Endocrinologists Treating Bardet-Biedl Syndrome — Clinician 2
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
No COI | — | — | — | — |
Declaration for Clinician 3
Name: Dr. Laurent Legault
Position: Head of Pediatric Endocrine Division, McGill University, Montreal, Quebec
Date: 28-02-2023
Table 9: COI Declaration for Canadian Endocrinologists Treating Bardet-Biedl Syndrome — Clinician 3
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
No COI | — | — | — | — |
Declaration for Clinician 4
Name: Dr. Jill Hamilton
Position: Professor of Paediatrics, University of Toronto, Head, Division of Endocrinology, Hospital for Sick Children, Toronto, Ontario
Date: 28-02-2023
Table 10: COI Declaration for Canadian Endocrinologists Treating Bardet-Biedl Syndrome — Clinician 4
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
Rhythm Pharmaceuticals | X | — | — | — |
Declaration for Clinician 5
Name: Dr. Munier Nour
Position: Associate Professor, University of Saskatchewan, Saskatoon, Saskatchewan
Date: 28-02-2023
Table 11: COI Declaration for Canadian Endocrinologists Treating Bardet-Biedl Syndrome — Clinician 5
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
Rhythm Pharmaceuticals | X | — | — | — |
Declaration for Clinician 6
Name: Dr. Marie-Phillipe Morin
Position: General Internal Medicine and Bariatric Medicine Specialist, Quebec Heart and Lung Institute; Associate Professor of Department of Medicine, Laval University, Quebec City, Quebec
Date: 28-02-2023
Table 12: COI Declaration for Canadian Endocrinologists Treating Bardet-Biedl Syndrome — Clinician 6
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
No COI | — | — | — | — |
Declaration for Clinician 7
Name: Dr. Andrea Marie Haaq
Position: Professor of Pediatrics, University of Alberta, Edmonton, Alberta
Date: 01-03-2023
Table 13: COI Declaration for Canadian Endocrinologists Treating Bardet-Biedl Syndrome — Clinician 7
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
Rhythm Pharmaceuticals | X | — | — | — |
Declaration for Clinician 8
Name: Dr. Celine Huot
Position: Professor of Pediatrics, University of Montreal, Montreal, Quebec
Date: 02-03-2023
Table 14: COI Declaration for Canadian Endocrinologists Treating Bardet-Biedl Syndrome — Clinician 8
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
No COI | — | — | — | — |
Declaration for Clinician 9
Name: Dr. Shahebina Walji
Position: Clinical Assistant Professor, Department of Family Medicine, University of Calgary, Calgary, Alberta
Date: 03-03-2023
Table 15: COI Declaration for Canadian Endocrinologists Treating Bardet-Biedl Syndrome — Clinician 9
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
Rhythm Pharmaceuticals | X | — | — | — |
Declaration for Clinician 10
Name: Dr. Vasudhevan Chetty
Position: Associate Professor, Pathology and Molecular Medicine, McMaster University, Hamilton, Ontario
Date: 03-03-2023
Table 16: COI Declaration for Canadian Endocrinologists Treating Bardet-Biedl Syndrome — Clinician 10
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
Rhythm Pharmaceuticals | X | — | — | — |
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up-to-date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
Redactions: Confidential information in this document may be redacted at the request of the sponsor in accordance with the CADTH Drug Reimbursement Review Confidentiality Guidelines
Stakeholder Input: The views expressed in each submission are those of the submitting organization or individual; not necessarily the views of CADTH or of other organizations. As such, they are independent of CADTH and do not necessarily represent or reflect the view of CADTH. No endorsement by CADTH is intended or should be inferred. By filing with CADTH, the submitting organization or individual agrees to the full disclosure of the information. CADTH does not edit the content of the submissions.
CADTH does use reasonable care to prevent disclosure of personal information in posted material; however, it is ultimately the submitter’s responsibility to ensure no identifying personal information or personal health information is included in the submission. The name of the submitting organization or individual and all conflict of interest information are included in the submission; however, the name of the author, including the name of an individual patient or caregiver submitting the patient input, are not posted.
Accessibility: CADTH is committed to treating people with disabilities in a way that respects their dignity and independence, supports them in accessing material in a timely manner, and provides a robust feedback process to support continuous improvement. All materials prepared by CADTH are available in an accessible format. Where materials provided to CADTH by a submitting organization or individual are not available in an accessible format, CADTH will provide a summary document upon request. More details on CADTH’s accessibility policies can be found here.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.