CADTH Reimbursement Review
Deucravacitinib (Sotyktu)
Sponsor: Bristol Myers Squibb
Therapeutic area: Psoriasis, moderate to severe plaque
This multi-part report includes:
Clinical Review
Pharmacoeconomic Review
Stakeholder Input
Clinical Review
Abbreviations
AE
adverse event
BSA
body surface area
CAPP
Canadian Association of Psoriasis Patients
CI
confidence interval
CPN
Canadian Psoriasis Network
CrI
credible interval
DLQI
Dermatology Life Quality Index
HRQoL
health-related quality of life
IL
interleukin
IR
incidence rate
ITC
indirect treatment comparison
LTE
long-term extension
MCS
Mental Component Score
MID
minimal important difference
NMA
network meta-analysis
OR
odds ratio
PASI
Psoriasis Area and Severity Index
PASI 50
50% reduction in Psoriasis Area and Severity Index score
PASI 75
75% reduction in Psoriasis Area Severity Index score
PASI 90
90% reduction in Psoriasis Area Severity Index score
PASI 100
100% reduction in Psoriasis Area Severity Index score
PCS
Physical Component Score
PGA
Physician’s Global Assessment
PSSD
Psoriasis Symptoms and Signs Diary
PY
patient-year
RCT
randomized controlled trial
RD
risk difference
RE
random effects
SAE
serious adverse event
SD
standard deviation
SF-36
Short Form (36) Health Survey
SOC
system organ class
sPGA
static Physician’s Global Assessment
ss-PGA
scalp severity Physician's Global Assessment
TNF
tumour necrosis factor
VAS
visual analogue scale
Executive Summary
An overview of the submission details for the drug under review is provided in Table 1.
Item | Description |
|---|---|
Drug product | Deucravacitinib (Sotyktu), 6 mg tablet, oral |
Indication | For the treatment of adult patients with moderate to severe plaque psoriasis who are candidates for systemic therapy or phototherapy |
Reimbursement request | As per indication |
Health Canada approval status | Approved |
Health Canada review pathway | Standard |
NOC date | November 23, 2022 |
Sponsor | Bristol Myers Squibb |
NOC = Notice of Compliance.
Introduction
Plaque psoriasis is a chronic inflammatory skin disease characterized by erythematous inflammatory plaques that may be itchy or painful and are usually covered by silver, flaking scales.1 In addition to the dermatological symptoms, plaque psoriasis is often associated with psychosocial symptoms and can impact self-esteem, interpersonal relationships, and performance at school or work. Several comorbid conditions have been linked to psoriasis, such as depression, cardiovascular disease, and psoriatic arthritis.1-3 It is estimated that up to 1 million people living in Canada are living with a type of psoriasis, 90% of whom have plaque psoriasis.4
Most patients with moderate to severe plaque psoriasis will require systemic therapies to control their symptoms.1 Traditional systemic drugs include cyclosporine, methotrexate, and acitretin. Advanced therapy, which is usually reserved for patients who fail or are intolerant of traditional systemic therapies, include apremilast and biologic agents (tumour necrosis factor [TNF] alpha inhibitors, interleukin [IL]-23 inhibitors, IL-12 and IL-23 inhibitors, and IL-17 inhibitors).
Deucravacitinib is a tyrosine kinase 2 inhibitor that impedes the release of proinflammatory cytokines and chemokines.5 It was approved by Health Canada for the treatment of adults with moderate to severe plaque psoriasis who are candidates for systemic therapy or phototherapy.6 It is available as a 6 mg oral tablet and the recommended dose is 6 mg daily.5
The objective of this report is to perform a systematic review of the beneficial and harmful effects of deucravacitinib 6 mg oral tablet for the treatment of adults with moderate to severe plaque psoriasis who are candidates for systemic therapy or phototherapy.
Stakeholder Perspectives
The information in this section is a summary of input provided by the patient groups who responded to CADTH’s call for patient input and from the clinical expert consulted by CADTH for the purpose of this review.
Patient Input
Two patient groups submitted a joint input: Canadian Psoriasis Network (CPN) and the Canadian Association of Psoriasis Patients (CAPP). The patient input was based on English and French surveys that received a total 22 responses and another survey entitled, “2022 Survey of People with Psoriatic Disease in Canada and their Caregivers” commissioned by the CPN that collected responses from 502 patients. The symptoms most frequently experienced by patients were flaking, itching, pain and burning, silvery scaly plaques, and dry skin that may crack or bleed. Many patients indicated that psoriasis negatively affected their mental health, self-esteem, social life, ability to exercise, and sleep. Further, some patients were financially impacted and missed work due to psoriasis.
Regarding patients’ expectations for new medications, improved symptoms, better quality of life, and reduced side effects were mentioned. Other responses included “affordable” and “easier to take, e.g., dosing schedule, route of administration.”
Clinician Input
Input From Clinical Expert Consulted by CADTH
According to the clinical expert consulted by CADTH, the goals of treatment are to reduce signs and symptoms of psoriasis and improve quality of life and function. With available treatments, 80% to 90% of patients achieve a 90% reduction in Psoriasis Area and Severity Index score (PASI 90) and approximately 50% to 60% achieve a 100% reduction in Psoriasis Area and Severity Index score (PASI 100). Approximately 10% of patients may not respond to initial induction therapy with a biologic (i.e., primary failure) or may lose response over time (secondary failure). The expert indicated that there is an unmet need for treatments that can be remittive and allow drug discontinuation or intermittent (rather than continuous) therapy, as well as for treatments that can modify the disease pathophysiology and have a beneficial effect on its natural history.
The clinical expert indicated that deucravacitinib does not address any of the unmet needs in plaque psoriasis and the expert did not anticipate that it would cause a shift in the current treatment paradigm. The expert stated that it would be difficult to define a role for deucravacitinib except as an oral alternative to the biologics for patients who prefer oral treatment.
Advanced therapy, such as deucravacitinib, should be reserved for patients who have failed first-line traditional systemics (methotrexate, acitretin, cyclosporine), according to the clinical expert. Treatment response is usually assessed after 12 to 16 weeks and then at 1 year. Deucravacitinib should be discontinued if patients experience a significant adverse effect (e.g., hypersensitivity, serious infection). In addition, the expert stated that deucravacitinib ought to be discontinued if it fails to provide at least a 75% reduction in Psoriasis Area and Severity Index score (PASI 75). Like biologics, the expert stated that deucravacitinib should be prescribed by dermatologists.
Clinician Group Input
No input was received from clinician groups.
Drug Program Input
The drug programs identified the following issues that may impact their ability to implement a recommendation: relevant comparators, consideration for initiation of therapy, consideration for continuation or renewal of therapy, consideration for discontinuation of therapy, and consideration for prescribing of therapy. Refer to Table 5.
Clinical Evidence
Pivotal Studies and Protocol-Selected Studies
Description of Studies
Two 52-week, double-blind, randomized controlled trials (RCTs) met the inclusion criteria for the systematic review. The POETYK PSO-1 (N = 666) and POETYK PSO-2 (N = 1,020) trials (hereafter referred to as POETYK-1 and POETYK-2) used a parallel study design, with POETYK-2 adding a randomized withdrawal design for responders at week 24. The studies enrolled adults (≥ 18 years) who had moderate to severe plaque psoriasis and were candidates for systemic psoriasis therapy and/or phototherapy. Patients were required to have a baseline Psoriasis Area and Severity Index (PASI) score of 12 or higher, with greater than 10% of body surface area (BSA) affected, and with a static Physician’s Global Assessment (sPGA) score of at least 3 on a 5-point scale.
Both studies randomized eligible patients (2:1:1) to deucravacitinib 6 mg daily, apremilast 30 mg twice daily, or placebo. All patients in the placebo groups switched to deucravacitinib at week 16. Both studies included a 24-week crossover to deucravacitinib for patients in the apremilast group that did not show an adequate response to therapy (i.e., did not achieve a 50% reduction in Psoriasis Area and Severity Index score [PASI 50] in the POETYK-1 study or PASI 75 in the POETYK-2 study). At week 24 in the POETYK-2 study, patients in the deucravacitinib group who achieved a PASI 75 response were rerandomized to placebo or to continue deucravacitinib, and patients in the apremilast group who achieved a PASI 75 response were switched to placebo.
The coprimary outcomes in both studies were the proportion of patients who achieved an sPGA score of 0 or 1 (with at least a 2-point change from baseline) and PASI 75 response at week 16, compared with placebo. The sPGA is a composite score of the physician’s assessment of the overall severity of the patient’s psoriatic lesions using a 5-point scale, described as clear (0), almost clear (1), mild (2), moderate (3), or severe (4). PASI grades the extent and severity of psoriatic lesions and combines an assessment of the BSA affected with the severity of desquamation, erythema, and plaque induration or infiltration. It is scored from 0 to 72, with higher scores representing more severe disease. A PASI response is the percentage improvement in PASI score, with PASI 75 considered the minimum clinically relevant change.
Key secondary outcomes included other PASI or sPGA response thresholds, health-related quality of life (HRQoL) and symptoms of psoriasis for deucravacitinib versus placebo or apremilast at week 16, 24, or 52. The POETYK-2 study also evaluated the time to relapse among patients in the deucravacitinib group that achieved a PASI 75 response at week 24.
The mean age of patients enrolled in the pivotal trials ranged from 44.7 years (standard deviation [SD] = 12.1) to 47.9 years (SD = 14.0) per treatment group. The majority of patients were men (62% to 71%) and the minority were women (29% to 38%). Most patients were white (77% to 93%), and fewer patients were Asian (3% to 21%) Black (1% to 4%), or other races (≤ 2%). The patients enrolled had been diagnosed with psoriasis for a median of 13.4 years to 18.2 years, with a mean PASI score at baseline ranging from 20.7 (SD = 8.0) to 21.8 (SD = 8.6). The majority of patients had received prior systemic therapy for psoriasis (54% to 66%), including biologics (31% to 39%).
Efficacy Results
In the POETYK-1 study, 53.6%, 7.2%, and 32.1% of patients in the deucravacitinib, placebo, and apremilast groups, respectively, met the sPGA 0 or 1 response criteria at week 16. The between-group differences favoured deucravacitinib versus placebo (risk difference [RD] = 46.7%; 95% confidence interval [CI], 40.2% to 53.2%; P < 0.0001) and versus apremilast (RD = 21.4%; 95% CI, 12.7% to 30.1%; P < 0.0001). The proportion of responders was 49.5%, 8.6%, and 33.9% in the deucravacitinib, placebo, and apremilast groups, respectively, of the POETYK-2 study. The between-group RD was 40.9% (95% CI, 35.4% to 46.4%) for deucravacitinib versus placebo, and 15.8% (95% CI, 8.8% to 22.9%) versus apremilast. For both comparisons, the difference favoured deucravacitinib with P values less than 0.0001 (Table 2).
The proportion of patients in the POETYK-1 study who achieved a PASI 75 response at week 16 was 58.4%, 12.7%, and 35.1% in the deucravacitinib, placebo, and apremilast groups, respectively, with a RD of 46.1%, (95% CI, 38.9% to 53.2%) for deucravacitinib versus placebo (P < 0.0001), and 23.0% (95% CI, 14.1% to 31.8%) versus apremilast (P < 0.0001). The results were similar in the POETYK-2 study with 53.0%, 9.4%, and 39.8% of patients in the deucravacitinib, placebo, and apremilast groups, respectively, achieving a PASI 75 response at week 16. The RD was 43.7% (95% CI, 38.0% to 49.3%; P < 0.0001) for deucravacitinib versus placebo, and 13.4% (95% CI, 6.2% to 20.7%; P = 0.0004) versus apremilast (Table 2).
The results of the key secondary outcomes, PASI 90 and PASI 100 at week 16, favoured deucravacitinib versus placebo in both studies. In addition, the PASI 90 response also favoured deucravacitinib versus apremilast at week 16. The proportion of patients who achieved a PASI 90 response ranged from 27.0% to 35.5% in the deucravacitinib groups, 2.7% to 4.2% in the placebo groups, and 18.1% to 19.6% in the apremilast groups, in the POETYK-1 and POETYK-2 studies. Few patients in any group achieved a PASI 100 response at week 16 (deucravacitinib: 10.2% to 14.2%, apremilast: 3.0% to 4.3%, placebo: 1%) and although numerically the proportion of PASI 100 responders was higher for deucravacitinib versus apremilast, this comparison was not controlled for type I error rate.
The Dermatology Life Quality Index (DLQI) was used to assess the impact of treatment on HRQoL. It is a patient-reported 10-item questionnaire that covers 6 domains: symptoms and feeling, daily activities, leisure, work and school, personal relationships, and bother with psoriasis treatment, each assessed over the past week. The overall DLQI score ranges from 0 to 30, with lower scores indicating better quality of life. A score of 0 or 1 may be interpreted as the disease has no impact on the patient’s HRQoL. The proportion of patients who achieved a DLQI score of 0 or 1 at week 16 was 41.0%, 10.6%, and 28.6% for the POETYK-1 study and 37.6%, 9.8%, and 23.1% for the POETYK-2 study in the deucravacitinib, placebo, and apremilast groups, respectively. The between-group differences favoured deucravacitinib versus placebo (POETYK-1: RD = 30.5%; 95% CI, 23.4% to 37.6%; POETYK-2: RD = 27.9%; 95% CI, 22.2% to 33.7%), with P values less than 0.0001. Although numerically more patients reported a DLQI response in the deucravacitinib groups than in the apremilast groups (RD = 12.3% and 14.6%), these comparison were not controlled for type I error rate.
The patient-reported Psoriasis Symptoms and Signs Diary (PSSD) was used to evaluate symptom severity in both studies. PSSD symptom score includes 5 symptoms (itch, pain, stinging, burning, and skin tightness) and is scored from 0 to 100 with 0 indicating a complete absence of symptoms. Among patients who have a baseline PSSD symptom score of at least 1, the proportion of patients who had a symptom score of 0 at week 16 was 7.9%, 0.7%, and 4.4% in the POETYK-1 study and 7.5%, 1.3%, and 4.3% in the POETYK-2 study in the deucravacitinib, placebo, and apremilast groups, respectively. In both studies, the differences favoured deucravacitinib versus placebo (P < 0.01), but with no statistically significant difference detected for deucravacitinib versus apremilast.
The trials were 52 weeks in duration and analyzed longer-term outcomes for the randomized population (POETYK-1) and for the subgroup of patients who achieved a PASI 75 response at week 24 (POETYK-2). In the POETYK-1 study, 56.3% of patients achieved a PASI 75 response at week 24 and week 52, in comparison to 30.5% of patients who had received apremilast (RD = 25.5%; 95% CI, 16.9% to 34.0%; P < 0.0001). Data from the POETYK-2 study indicate that patients who achieved a PASI 75 response with deucravacitinib, and who remained on treatment, were less likely to relapse than patients who were switched to placebo (P < 0.0001).
Harms Results
During the first 16 weeks of the POETYK-1 and POETYK-2 studies (before any treatment switching), the frequency of adverse events (AEs) was generally similar across groups with 53% and 58% of patients in the deucravacitinib groups, 42% and 54% of patients who received placebo, and 55% and 59% who received apremilast reporting 1 or more AEs (Table 3). The most commonly reported events in the deucravacitinib group were nasopharyngitis (6% to 11%), upper respiratory tract infection (5% to 6%), diarrhea and headache (each reported in 4% to 5%). The frequency of these events was comparable in the placebo and apremilast groups, except for gastrointestinal AEs, which appeared to be more common among patients who received apremilast.
The frequency of serious AEs (SAEs) was generally low during the trials, with 2% of patients in the deucravacitinib group, 1% to 5% in the placebo group, and 0.4% to 2% in the apremilast group reporting an event during the first 16 weeks. Among patients who received deucravacitinib at any time during the 52-week trials, 3% to 6% of patients experienced a SAE, compared with 1% to 4% of those who received apremilast at any time. A total of 4 patients died during the studies. One patient in the placebo group of the POETYK-1 study died of hypertensive cardiovascular disease, 2 patients in the deucravacitinib group of the POETYK-2 study died of heart failure and sepsis, and hepatocellular carcinoma, and 1 patient in the apremilast group in the POETYK-2 study died of lung cancer and gastrointestinal hemorrhage.
The proportion of patients who stopped treatment due to AEs was 2% and 3% for deucravacitinib, 4% and 4% for placebo, and 6% and 5% for apremilast, in the POETYK-1 and POETYK-2 studies, respectively, during the first 16 weeks of the trials.
During the first 16 weeks of the studies, infections and infestations were reported by 26% to 31% of patients in the deucravacitinib groups, 15% to 26% in the placebo groups, and 18% to 25% in the apremilast groups. Few patients in any groups experienced an infection or infestation that was a SAE, and there were no opportunistic infections or tuberculosis events reported in either study. The proportion of patients with at least a grade 2 increase in creatine kinase levels was 3% for the deucravacitinib groups, 1% to 4% in the placebo groups, and 0% to 4% in the apremilast groups during week 0 to 16. Over the 52-week study period, 6% of patients receiving deucravacitinib and 4% to 5% receiving apremilast reported grade 2 or higher elevated creatinine kinase levels. None of these events were considered SAEs. In both trials, the frequency of other AEs which may be associated with drugs that work through the Janus kinase pathway (major adverse cardiovascular events, thromboembolic events, malignancy, elevated liver enzymes, lymphopenia, or neutropenia) was generally low.
Table 2: Summary of Key Efficacy Results From Pivotal and Protocol-Selected Studies
Outcome | POETYK-1 | POETYK-2 | ||||
|---|---|---|---|---|---|---|
DEUC n = 332 | PBO n = 166 | APREM n = 168 | DEUC n = 511 | PBO n = 255 | APREM n = 254 | |
sPGA 0 or 1 at week 16a,b | ||||||
Responders, n (%) | 178 (53.6) | 12 (7.2) | 54 (32.1) | 253 (49.5) | 22 (8.6) | 86 (33.9) |
DEUC vs. PBO | ||||||
RD (95% CI) | 46.7 (40.2 to 53.2) | Reference | NA | 40.9 (35.4 to 46.4) | Reference | NA |
P value | < 0.0001c | Reference | NA | < 0.0001c | Reference | NA |
DEUC vs. APREM | ||||||
RD (95% CI) | 21.4 (12.7 to 30.1) | NA | Reference | 15.8 (8.8 to 22.9) | NA | Reference |
P value | < 0.0001d | NA | Reference | < 0.0001d | NA | Reference |
PASI 75 response at week 16a | ||||||
Responders, n (%) | 194 (58.4) | 21 (12.7) | 59 (35.1) | 271 (53.0) | 24 (9.4) | 101 (39.8) |
DEUC vs. PBO | ||||||
RD (95% CI) | 46.1 (38.9 to 53.2) | Reference | NA | 43.7 (38.0 to 49.3) | Reference | NA |
P value | < 0.0001c | Reference | NA | < 0.0001c | Reference | NA |
DEUC vs. APREM | ||||||
RD (95% CI) | 23.0 (14.1 to 31.8) | NA | Reference | 13.4 (6.2 to 20.7) | NA | Reference |
P value | < 0.0001d | NA | Reference | 0.0004d | NA | Reference |
PASI 90 response at week 16a | ||||||
Responders, n (%) | 118 (35.5) | 7 (4.2) | 33 (19.6) | 138 (27.0) | 7 (2.7) | 46 (18.1) |
DEUC vs. PBO | ||||||
RD (95% CI) | 31.6 (25.8 to 37.5) | Reference | NA | 24.3 (19.9 to 28.7) | Reference | NA |
P value | < 0.0001d | Reference | NA | < 0.0001d | Reference | NA |
DEUC vs. APREM | ||||||
RD (95% CI) | 15.8 (8.2 to 23.5) | NA | Reference | 9.0 (3.1 to 14.9) | NA | Reference |
P value | 0.0002d | NA | Reference | 0.0046d | NA | Reference |
APREM = apremilast; CI = confidence interval; DEUC = deucravacitinib; FAS = full analysis set; NA = not applicable; PASI 75 = 75% reduction in Psoriasis Area and Severity Index score; PASI 90 = 90% reduction in Psoriasis Area and Severity Index score; PBO = placebo; RD = risk difference; sPGA = static Physician’s Global Assessment; vs. = versus.
aCochran-Mantel-Haenszel test stratified by geographic region, body weight, and prior biologic use. Nonresponder imputation for missing data.
bPatients must also have at least a 2-point improvement in their sPGA score vs. baseline.
cCoprimary end points tested using a 2-sided alpha of 0.05.
dKey secondary end points tested using a 2-sided alpha of 0.025.
Source: Clinical Study Reports for POETYK-17 and POETYK-2.8
Table 3: Summary of Key Safety Results From Pivotal and Protocol-Selected Studies
Adverse event | POETYK-1 | POETYK-2 | ||||
|---|---|---|---|---|---|---|
DEUC | PBO | APREM | DEUC | PBO | APREM | |
Week 0 to 16, n (%) | ||||||
Safety population,a N | 332 | 165 | 168 | 510 | 254 | 254 |
AE | 176 (53) | 70 (42) | 93 (55) | 293 (58) | 138 (54) | 150 (59) |
SAE | 7 (2) | 9 (5) | 4 (2) | 8 (2) | 3 (1) | 1 (0.4) |
Stopped treatment due to AE | 6 (2) | 7 (4) | 10 (6) | 14 (3) | 9 (4) | 12 (5) |
Infections and infestations (system organ class) | 87 (26) | 24 (15) | 30 (18) | 158 (31) | 66 (26) | 63 (25) |
Infections and infestations (system organ class) SAE | 1 (0.3) | 1 (0.6) | 2 (1.2) | 4 (1) | 1 (0.4) | 0 |
Increased creatine kinase, ≥ grade 2 | 11 (3.3) | 2 (1.2) | 0 | 17 (3.4) | 11 (4.4) | 9 (3.6) |
AE = adverse event; APREM = apremilast; DEUC = deucravacitinib; PBO = placebo; SAE = serious adverse event.
aBased on the as-treated population which included all randomized patients who took at least 1 dose of study drug and who were analyzed according to the drug received. Data reported as number of patients with a treatment-emergent AE including events that occurred up to 30 days after the last dose of study drug.
Source: Clinical Study Reports for POETYK-17 and POETYK-2.8
Critical Appraisal
The POETYK-1 and POETYK-2 studies appear to have a low risk of bias with regards to randomization, allocation concealment, and blinding. In general, the baseline characteristics of patients appeared to be balanced between groups within trials. The efficacy outcomes reported were relevant to patients (i.e., skin clearance, psoriasis symptoms, and HRQoL), had evidence to support their validity, and key patient-reported outcomes were part of the statistical testing procedure to control the type I error rate. However, the coprimary outcome, PASI 75, may be considered the minimum clinically relevant response, whereas, in clinical practice a PASI 90 response is generally the expected goal of therapy. Key skin clearance outcomes were analyzed based on the intention-to-treat population and using nonresponder imputation for patients who stopped treatment or with missing data. This composite estimand may be considered a conservative estimate of effects. However, up to 10% of patients were excluded from the DLQI or PSSD response end points (depending on the treatment group). The potential impact of these missing patients on the findings is unclear.
Overall, the clinical expert consulted for this review considered that the patients enrolled would represent patients with moderate to severe psoriasis who may be treated with advanced therapies in Canada, including those who had received with prior systemic or biologic therapy. However, the clinical expert identified some issues with apremilast as an active comparator. While apremilast is another oral advanced therapy, it is infrequently prescribed in Canada for the treatment of moderate to severe plaque psoriasis. The expert stated that efficacy of apremilast is considered to be low for an advanced therapy, and most dermatologists would select a biologic over apremilast. Thus, based on current practice, apremilast may not be as relevant a comparator as biologics for patients with moderate to severe disease.
Indirect Comparisons
Description of Studies
The sponsor-submitted indirect treatment comparison (ITC) conducted a systematic review and used a Bayesian network meta-analysis (NMA) to evaluate the relative efficacy of deucravacitinib to other comparators for the treatment of patients with moderate to severe plaque psoriasis. The NMA was based on a systematic review of the literature and data from up to 84 trials were used to inform the analyses. The main efficacy outcome of interest was PASI response.
Efficacy Results
The sponsor-submitted ITC reported that in the short-term (at 10 weeks to 16 weeks) with 84 RCTs included, deucravacitinib was favoured over placebo, apremilast, and etanercept in achieving PASI response. Also, no differences were detected between deucravacitinib and tildrakizumab for all PASI levels, or versus tildrakizumab, certolizumab, and ustekinumab on the PASI 100 level, as these comparisons showed 95% credible intervals (CrIs) that overlapped the null. All other comparisons versus deucravacitinib were in favour of the biologic comparator, typically an IL-17 or IL-23 inhibitor.
The ITC reported that in the midterm (at 24 weeks to 28 weeks) with 48 trials included, deucravacitinib was favoured to placebo and apremilast in attaining all levels of PASI responses at weeks 24 to 28. Compared to the rest of the treatments, there was variability in the relative effect of deucravacitinib in attaining different levels of PASI responses. No differences were found for deucravacitinib compared to ustekinumab, secukinumab, and tildrakizumab in attaining PASI 50, tildrakizumab 100 mg and 200 mg attaining PASI 75, and tildrakizumab 100 mg in attaining PASI 100. All other biologic comparators were favoured over deucravacitinib across all PASI response levels.
The sponsor-submitted ITC reported that in the long-term (at 44 weeks to 60 weeks) with 32 trials included, deucravacitinib was favoured to placebo and apremilast in attaining all levels of PASI as found at other time points. No difference was found when comparing deucravacitinib with secukinumab, ustekinumab, and the TNF alpha inhibitors included in the long term analyses, as the 95% CrI included the null. All other treatments were favoured versus deucravacitinib in attaining all levels of PASI score.
Critical Appraisal
The sponsor-submitted ITC involved a rich evidence base with a large network of RCTs and sample size, which strengthened the robustness of the NMA analyses. Nonetheless, the sponsor-submitted ITC had several limitations including heterogeneity present for many patient and study characteristics in the NMA analyses, incorporation of studies that included patients with mild disease, discordance between the sponsor’s assumption of patient treatment adherence and true clinical practice, and lack of data for certain subgroup analyses. Given these limitations, the results from the sponsor-submitted ITC are at some risk of bias for the comparison of deucravacitinib with other treatments in patients with moderate to severe plaque psoriasis. Only 1 measure of efficacy was analyzed, and no harms or quality of life end points were available.
Other Relevant Evidence
Description of Studies
Interim data for a single-arm, open-label extension study, IM011075, was submitted by the sponsor. Patients who completed the POETYK-1 and POETYK-2 studies were eligible to enrol. A total of 1,221 patients entered the extension study, which represented 72% of the patients randomized in the parent trials. All patients received deucravacitinib 6 mg daily. At the time of interim analysis, 90% of patients were ongoing in the study and receiving treatment, and 95%, 61%, and 20% of patients provided data at 24, 48, and 60 weeks, respectively.
Efficacy Results
In the total extension population, sPGA 0 or 1 response rates were 50.9% (95% CI, 48.1% to 53.8%; N = 1,221) at the start of the extension phase (week 0), and 56.4% (95% CI, 52.7% to 60.0%; N = 745) at week 48. PASI 75 response rates were 65.1% (95% CI, 62.4% to 67.8%) at week 0 and 75.7% (95% CI, 68.7% to 80.6%) at week 48.
Harms Results
AEs were reported by 707 of 1,211 patients (58%). The most frequently reported events were COVID-19 (9%) and nasopharyngitis (4%). Seven percent of patients experienced a SAE and 2% stopped treatment due to AEs. In total, 6 deaths occurred, including 5 due to COVID-19 and 1 due to a ruptured thoracic aortic aneurysm. Infections and infestations were reported by 29% of patients and 4% experienced SAEs. At the time of the interim analysis, 45 patients (4%) had at least a grade 2 increase in creatinine kinase levels but only 1 patient stopped treatment due to these events. No new safety signals were identified.
Critical Appraisal
Limitations of the extension study include selection bias, lack of a control group, and lack of blinding. Reporting of harms and subjective measures (such as those included in the PASI score) may be biased by knowledge of treatment received. Since only descriptive statistics were published in this interim report, which were based on observed data with no imputation for missing data, and since there were no comparator groups, the interpretation of the results is limited. Moreover, there is potential for selection bias, as patients who discontinued the parent RCTs due to AEs, lack of efficacy, or other reasons were excluded.
Conclusions
In adults with moderate to severe plaque psoriasis who were candidates for systemic therapy or phototherapy, deucravacitinib showed improvement versus placebo in skin and HRQoL in the short-term, with some data showing skin improvements in the intermediate term (up to 52 weeks). For most outcomes, deucravacitinib was also superior to the active comparator apremilast. However, the clinical relevance of these comparator in the Canadian context is limited. AEs were generally similar between deucravacitinib and apremilast, and no new safety signals were identified in longer-term follow-up or an ongoing extension study. Based on ITCs, deucravacitinib is less effective in producing skin improvement than several biologics established in Canada. Collection of data on long-term safety and duration of effect is ongoing. At present, it is unknown whether deucravacitinib could be combined with other treatments or whether it produces immunosuppression or expresses any of the rare AEs associated with medications that affect the Janus kinase pathway. Given that alternative treatments appear generally more effective, deucravacitinib is not expected to alter the overall treatment paradigm for psoriasis. Since response to treatments can be patient specific, patients are concerned about having treatment options and a minority may prefer to avoid injections.
Introduction
Disease Background
Plaque psoriasis is a chronic inflammatory skin disease characterized by erythematous inflammatory plaques that may be itchy or painful and are usually covered by silver, flaking scales.1 It is a complex immune-mediated disorder, in which dysregulation of components of the innate and adaptive immune systems, keratinocyte function, and vascular structure contribute to the manifestations of the disease.9
In addition to the overt dermatological symptoms, plaque psoriasis is often associated with psychosocial symptoms, including poor self-esteem, and may affect various aspects of social functioning, including interpersonal relationships and performance at school or work. Psoriasis is associated with several comorbid conditions, including depressive symptoms, conditions associated with an increased risk of cardiovascular disease (such as type 2 diabetes, metabolic syndrome, and obesity), and psoriatic arthritis.1-3
The severity of psoriasis may be classified as mild, moderate, or severe, based on the extent of BSA affected, with 10% or more of BSA affected generally considered more severe disease.3 However, for patients with involvement of the hands, feet, scalp, face, or genital area, or those experiencing significant physical discomfort or emotional impacts from the disease, psoriasis may also be considered severe, regardless of BSA affected.3 For most patients with moderate to severe plaque psoriasis, the disease cannot be adequately controlled with topical treatments or phototherapy alone.3
There are multiple forms of psoriasis, including plaque, guttate, inverse, pustular, and erythrodermic psoriasis, but plaque psoriasis is the most common form and represents approximately 90% of cases.4 It is estimated that up to 1 million people living in Canada are living with a type of psoriasis.4 In Ontario, the estimated the age- and sex-standardized cumulative prevalence of psoriasis in 2015 was 2.32%.10 Up to one-third of patients with psoriasis have moderate to severe disease.11,12
Standards of Therapy
Plaque psoriasis requires lifelong treatment. Measures of treatment success include clearance (absence of signs of disease), control (satisfactory response to therapy as defined by the patient and/or physician), and remission (suppression of signs and symptoms over time). Clearance and symptom control have been identified as treatment outcomes that are important to patients, and treatment decisions depend largely on the patient’s perception of their disease.
In patients with mild psoriasis, topical treatments (such as corticosteroids, vitamin D3 analogues, retinoids, anthralin, and tars) may be sufficient to control the disease; however, for those with moderate to severe psoriasis, systemic therapies are often required.1 Traditional systemic drugs include cyclosporine, methotrexate, and acitretin. Advanced therapy, which is usually reserved for patients who fail or are intolerant of traditional systemic therapies, includes apremilast and biologic agents. In Canada, there are several biologic drugs approved for the treatment of plaque psoriasis including the TNF alpha inhibitors (infliximab, etanercept, adalimumab, and certolizumab pegol), IL-23 inhibitors (risankizumab, guselkumab, and tildrakizumab), IL-12/23 inhibitor (ustekinumab), and IL-17 inhibitors (bimekizumab, secukinumab, ixekizumab, and brodalumab) (Table 4). According to the clinical expert consulted for this review, IL-17 and IL-23 inhibitors are now chosen more frequently by dermatologists in Canada over TNF alpha inhibitors as the first biologic for the treatment of plaque psoriasis.
Drug
Deucravacitinib is a tyrosine kinase 2 inhibitor that impedes the release of proinflammatory cytokines and chemokines.5 It was approved by Health Canada through the standard review process for the treatment of adults with moderate to severe plaque psoriasis who are candidates for systemic therapy or phototherapy.6 It is available as a 6 mg oral tablet and the recommended dose is 6 mg daily.5
Deucravacitinib has not previously been reviewed by CADTH. The sponsor has requested reimbursement as per the indication.6
Table 4: Key Characteristics of Drugs for Moderate to Severe Plaque Psoriasis
Drug and drug class | Indicationa | Recommended dose | Serious adverse effects or safety issues |
|---|---|---|---|
Tyrosine kinase inhibitor | |||
Deucravacitinib (Sotyktu) | Proposed: Treatment of adult patients with moderate to severe plaque psoriasis who are candidates for systemic therapy or phototherapy | 6 mg oral tablet once daily | Infections |
IL-17 inhibitors | |||
Bimekizumab (Bimzelx) | Treatment of moderate to severe plaque psoriasis in adult patients who are candidates for systemic therapy or phototherapy | 320 mg SC every 4 weeks for the first 16 weeks, then 320 mg SC every 8 weeks thereafter Note: For patients with a body weight ≥ 120 kg who did not achieve a complete skin response, a dose of 320 mg every 4 weeks after week 16 may be considered | Infections, including candidiasis and other fungal infections Use with caution in patients with inflammatory bowel disease |
Brodalumab (Siliq) | Treatment of moderate to severe plaque psoriasis in adult patients who are candidates for systemic therapy or phototherapy | 210 mg SC at weeks 0, 1, and 2, followed by 210 mg SC every 2 weeks | Suicidal ideation and behaviour Crohn disease Infection |
Secukinumab (Cosentyx) | Treatment of moderate to severe plaque psoriasis in adult patients who are candidates for systemic therapy or phototherapy Treatment of severe plaque psoriasis in pediatric patients 12 years to under 18 years of age who are candidates for systemic therapy or phototherapy and have a body weight ≥ 50 kg | Adults: 300 mg SC at weeks 0, 1, 2, 3, and 4, followed by monthly maintenance administration Pediatric patients > 12 years and ≥ 50 kg: 150 mg (may be increased to 300 mg) at weeks 0, 1, 2, 3, and 4, followed by monthly maintenance administration | Infection Inflammatory bowel disease Serious hypersensitivity reactions |
Ixekizumab (Taltz) | Treatment of adult patients with moderate to severe plaque psoriasis who are candidates for systemic therapy or phototherapy Treatment of pediatric patients aged 6 years to < 18 years with moderate to severe plaque psoriasis who are candidates for systemic therapy or phototherapy | Adults: 160 mg SC at week 0, followed by 80 mg SC at weeks 2, 4, 6, 8, 10, and 12, then 80 mg SC every 4 weeks Pediatric patients ≥ 6 years: > 50 kg: 160 mg at week 0, then 80 mg every 4 weeks 25 kg to 50 kg: 80 mg at week 0, then 40 mg every 4 weeks < 25 kg: 40 mg at week 0, then 20 mg every 4 weeks | Infection Serious hypersensitivity reactions Inflammatory bowel disease |
IL-23 inhibitors | |||
Tildrakizumab (Ilumya) | Treatment of adult patients with moderate to severe plaque psoriasis who are candidates for systemic therapy or phototherapy | 100 mg administered by SC injection at weeks 0 and 4, and every 12 weeks thereafter | Infection |
Risankizumab (Skyrizi) | Treatment of adult patients with moderate to severe plaque psoriasis who are candidates for systemic therapy or phototherapy | 150 mg administered by SC injection at weeks 0 and 4, and every 12 weeks thereafter | Infection Hypersensitivity reactions |
Guselkumab (Tremfya) | Treatment of adult patients with moderate to severe plaque psoriasis who are candidates for systemic therapy or phototherapy | 100 mg administered SC at weeks 0 and 4, followed by maintenance administration every 8 weeks thereafter | Infection Hypersensitivity reactions |
IL-12/23 inhibitors | |||
Ustekinumab (Stelara) | Treatment of adult patients with chronic moderate to severe plaque psoriasis who are candidates for phototherapy or systemic therapy Treatment of chronic moderate to severe plaque psoriasis in adolescent patients aged 12 years to 17 years, whose psoriasis is inadequately controlled by, or who are intolerant to, other systemic therapies or phototherapies | 45 mg SC at weeks 0 and 4, then every 12 weeks thereafter. Alternatively, 90 mg SC may be used in patients with a body weight > 100 kg. For patients who respond inadequately to administration every 12 weeks, consideration may be given to treating as often as every 8 weeks Dose of 0.75 mg/kg is recommended in pediatric patients weighing < 60 kg | Infection Malignancy Serious hypersensitivity reactions |
TNF alpha inhibitors | |||
Adalimumab (Humira and biosimilars) | Treatment of adult patients with chronic moderate to severe plaque psoriasis who are candidates for systemic therapy; for patients with chronic moderate plaque psoriasis, adalimumab should be used after phototherapy has been shown to be ineffective or inappropriate | Initial dose of 80 mg SC followed by 40 mg SC every other week starting 1 week after the initial dose Continued therapy beyond 16 weeks should be carefully reconsidered in a patient not responding within this time period | Malignancies Infection Congestive heart failure Hematologic events Hypersensitivity reactions Autoimmunity and immunosuppression Neurologic events |
Certolizumab pegol (Cimzia) | Treatment of adult patients with moderate to severe plaque psoriasis who are candidates for systemic therapy | 400 mg SC every 2 weeks A dose of 400 mg SC initially (week 0) and at weeks 2 and 4 followed by 200 mg every 2 weeks may be considered | Malignancies Infection Heart failure Hematologic events Hypersensitivity reactions Autoimmunity and immunosuppression Neurologic events |
Etanercept (Enbrel and biosimilars) | Treatment of adult patients with chronic moderate to severe plaque psoriasis who are candidates for systemic therapy or phototherapy Treatment of pediatric patients aged 4 years to 17 years with chronic severe psoriasis who are candidates for systemic therapy or phototherapy | Adults: Starting dose of 50 mg SC given twice weekly (administered 3 or 4 days apart) for 3 months, followed by a reduction to a maintenance dosage of 50 mg SC per week. A maintenance dosage of 50 mg SC given twice weekly has also been shown to be efficacious Pediatric patients: 0.8 mg/kg per week (up to a maximum of 50 mg per week) | Infections Malignancies Neurologic events Hematologic events Congestive heart failure Autoimmunity |
Infliximab (Remicade and biosimilars) | Treatment of adult patients with chronic moderate to severe plaque psoriasis who are candidates for systemic therapy; for patients with chronic moderate plaque psoriasis, infliximab should be used after phototherapy has been shown to be ineffective or inappropriate | 5 mg/kg IV followed by additional 5 mg/kg IV doses at 2 and 6 weeks after the first infusion, then every 8 weeks thereafter. If a patient does not show an adequate response at week 14, no additional treatment with infliximab should be given | Infection Malignancies Cardiovascular events Hematologic abnormalities Hepatic abnormalities Hypersensitivity reactions Autoimmunity and immunogenicity Neurologic events |
Phosphodiesterase 4 inhibitor | |||
Apremilast (Otezla) | Treatment of adult patients with moderate to severe plaque psoriasis who are candidates for systemic therapy or phototherapy. Apremilast is not indicated in combination with other systemic (conventional or biologic) therapies or phototherapy. | 30 mg twice daily, oral | Tachyarrhythmia Weight loss Gastrointestinal adverse events |
IL = interleukin; SC = subcutaneous.
aHealth Canada indication.
Source: Product monographs.5,13-25
Stakeholder Perspectives
Patient Group Input
This section was prepared by CADTH staff based on the input provided by patient groups. The full original patient input(s) received by CADTH have been included in the stakeholder section at the end of this report.
Two patient groups submitted a joint input. Both the CPN and CAPP are national, not-for-profit organizations that strive to improve lives of people in Canada who live with psoriasis. The CPN provides information on research and treatment options, builds awareness, and advocates about the complexity of psoriatic diseases. The CAPP’s mission is to be a resource and advocate for patients and their families to improve patient care and quality of life. A survey conducted between August and September 2022 in English and French was hosted by the CPN and distributed by both organizations’ communication channels as well as sent to clinics that conducted deucravacitinib trials in Canada. This survey collected a total 22 responses from across Canada except for 1 response, which was from outside Canada. Another survey entitled, “2022 Survey of People with Psoriatic Disease in Canada and their Caregivers” commissioned by the CPN In June 2022, collected responses (N = 809) from patients (n = 502) and their caregivers (n = 307). The patient groups received assistance from 2 medical student volunteers in developing and circulating the survey used to inform the submission.
Approximately one-third of participants from the English survey (33%; n = 3) and June 2022 survey (33%; n = 267) said that they have psoriatic arthritis. From the June 2022 survey, 445 (55%) people responded that they live with plaque psoriasis. Four (33%) and 2 (40%) patients from the English and French survey, respectively, said their severity was “moderate” (between 3% to 10% of BSA). Three (25%) and 2 (40%) patients from the English and French survey, respectively, said that their disease was “severe” (≥ 10% BSA). According to the English survey, symptoms most frequently experienced by patients were flaking and itch (79% each), skin colour change (71%), flares (64%), and pain or burning (50%). French survey respondents said flaking, itch, pain/burning (100% each) were the most frequent symptoms they experienced. The CPN’s June 2022 survey showed the most common symptoms reported by people with psoriatic disease (n = 502) were itching, burning, or painful skin (70%); silvery, scaly plaques (66%); and dry skin that may crack or bleed (58%). The English survey showed that mental health (50%; n = 6) and self-esteem (42%; n = 5) were extremely negatively impacted and social life (58%; n = 7) and finances (42%; n = 7) were moderately negatively impacted. Of the French participants, social life (80%; n = 4), ability to exercise (80%; n = 4), and sleep (80%; n = 4) were the areas of life that were negatively impacted by psoriatic disease. In the June 2022 survey, 63% of participants said their disease made quality of life worse with the most impact felt when choosing clothes to wear (54%) or having to change day-to-day life due to psoriasis (52%). In addition, the participants said they felt less confident in themselves (48%), lost sleep (47%), missed work (26%), and changed career (14%) due to psoriasis and/or psoriatic arthritis.
Regarding patients’ expectations for new medications, all English survey participants (n = 10) said “improved symptoms” and all French survey participants said “better quality of life” and “reduced side effects” (n = 3). Other responses for desirable outcomes included “affordable” (60%; n = 6, and 67%; n = 2, from the English and French surveys, respectively) and “easier to take, e.g., dosing schedule, route of administration” (40%; n = 4, and 67%; n = 2, from English and French surveys, respectively). In the June 2022 survey, participants (n = 502) identified that reducing pain (69%), reducing anxiety (64%), reducing sleep disturbances (59%), addressing side effects (51%), and improving ability to work (44%) were the outcomes most patients wished to improve. Approximately 10% of respondents to the June 2022 survey had concerns about self-injection, and people with severe psoriatic disease were concerned about the availability of treatments and/or treatment modalities that are feasible and accessible to them.
The patient group input also emphasized that management of psoriasis can be complex, partly due to varied patient response to treatments, differences in social determinants of health, lifestyle considerations, and other factors that affect one’s condition. Also, patients are worried about recurrence and resistance to therapies.
Clinician Input
Input From Clinical Expert Consulted by CADTH
All CADTH review teams include at least 1 clinical specialist with expertise regarding the diagnosis and management of the condition for which the drug is indicated. Clinical experts are a critical part of the review team and are involved in all phases of the review process (e.g., providing guidance on the development of the review protocol, assisting in the critical appraisal of clinical evidence, interpreting the clinical relevance of the results, and providing guidance on the potential place in therapy). The following input was provided by 1 clinical specialist with expertise in the diagnosis and management of plaque psoriasis.
Unmet Needs
The expert stated that goals of treatment are to reduce signs and symptoms of psoriasis and improve quality of life and function. Although the currently available treatments, especially the biologics, are highly effective, there is no evidence that they modify the disease pathophysiology. With available treatments, 80% to 90% of patients achieve a PASI 90 response and approximately 50% to 60% achieve a PASI 100 response. Approximately 10% of patients may not respond to initial induction therapy with a biologic (i.e., primary failure) or may lose response over time (secondary failure). The expert indicated that there is an unmet need for treatments that are remittive and allow drug discontinuation or intermittent (rather than continuous) therapy, as well as for treatments that can modify the disease pathophysiology and have a beneficial effect on its natural history.
Place in Therapy
According to the clinical expert, deucravacitinib does not address any of the unmet needs in plaque psoriasis and the expert did not anticipate that it would cause a shift in the current treatment paradigm. The expert stated that it would be difficult to define a role for deucravacitinib except as an oral alternative to the biologics for patients who prefer oral treatment. In their opinion, many patients with moderate to severe psoriasis, including those who are needle-phobic, would prefer an injectable biologic (due to its efficacy and infrequent subcutaneous administration), over daily oral medication.
The expert noted that deucravacitinib may replace apremilast; however, apremilast has low efficacy and is infrequently used in Canada for moderate to severe psoriasis. Apremilast is not an immunosuppressant and may have a limited role in patients who need to avoid immunosuppressive medication (e.g., patient with hepatitis B), but deucravacitinib does not have this advantage.
Patient Population
Advanced therapy, such as deucravacitinib, should be reserved for patients who have failed first-line traditional systemics (methotrexate, acitretin, cyclosporine), according to the clinical expert. Evidence is needed to determine if deucravacitinib is more effective than traditional systematic therapies, such as methotrexate, and if it is effective in patients who have failed traditional systemic or biologic therapies.
The expert noted that there may be interest in using deucravacitinib in patients with mild plaque psoriasis; however, the drug is not approved for this population.
Assessing Response to Treatment
Treatment response for biologics is usually assessed at 12 weeks to 16 weeks (following the induction phase) and then at 1 year. With deucravacitinib, assessment of response may be the same or more frequent for (e.g., every 3 months) because of its efficacy. Physicians are asked to report PASI 75 response and treatment coverage may be discontinued if the patient fails to achieve a PASI 75 response. However, in practice, most physicians would assess response based on gestalt or the Physician’s Global Assessment (PGA) rather than a PASI assessment. In the expert’s experience, once a patient is approved for coverage, few actually discontinue treatment for failing to achieve PASI 75. The expert noted that PASI assessment is subjective and arbitrary, and there is no objective parameter to determine disease severity.
Both patients and physicians expect a PASI 90 response with newer treatment options and may not be satisfied with a PASI 75 response.
Discontinuing Treatment
Deucravacitinib should be discontinued if patients experience a significant adverse effect (e.g., hypersensitivity, serious infection). In addition, the expert stated that deucravacitinib should be discontinued if it fails to provide at least a PASI 75 response. However, the expert noted that once coverage is provided, the drug is often not discontinued even if the response is suboptimal because having some improvement is better than none. Patients who fail deucravacitinib may be treated with biologics that have shown high response rates, but some patients who do not want biologic therapy may elect to stay with deucravacitinib even though the response is suboptimal.
Prescribing Conditions
Advanced treatment such as deucravacitinib should be prescribed by dermatologists, as in the case with the biologics. This is to ensure that the prescriber can diagnose moderate to severe psoriasis and has good knowledge of the treatment paradigm.
Additional Considerations
Deucravacitinib works through the Janus kinase pathway, and it is unclear if it has the same safety concerns as the Janus kinase inhibitors. It has only been studied in patients with psoriasis in the clinical trial setting and the results may not be extrapolated to a wider population that may include vulnerable patients. It is not known if deucravacitinib would induce immunosuppression.
Clinician Group Input
No input was received from clinician groups.
Drug Program Input
The drug programs provide input on each drug being reviewed through CADTH’s reimbursement review processes by identifying issues that may impact their ability to implement a recommendation. The implementation questions and corresponding responses from the clinical experts consulted by CADTH are summarized in Table 5.
Table 5: Summary of Drug Plan Input and Clinical Expert Response
Drug program implementation questions | Clinical expert response |
|---|---|
Relevant comparators | |
The 2 pivotal phase III trials POETYK-1 and POETYK-2 compared deucravacitinib to placebo and apremilast (Otezla). Apremilast (Otezla) concluded pCPA negotiations in March 2021 without an agreement and is not publicly funded in most jurisdictions (funded only in Canadian Armed Forces as an RB). Other products, including biologics, that are publicly funded for the treatment of moderate to severe plaque psoriasis may have been appropriate comparators. | For CDEC consideration. |
Other drug products indicated for the treatment of moderate to severe psoriasis include topical agents, conventional nonbiologic systemic agents (acitretin, cyclosporine, and methotrexate), biologics, and oral systemic nonbiologic therapies. Availability of relevant biologic comparators among jurisdictions is as follows:
| For CDEC consideration. |
Considerations for initiation of therapy | |
The eligibility criteria for the submitted pivotal clinical trials were a diagnosis of plaque psoriasis for at least 6 months, moderate to severe disease, and being a candidate for phototherapy or systemic therapy. Exclusion criteria were other forms of psoriasis, history of recent infection, and prior exposure to deucravacitinib or apremilast. Question to CADTH: Should prior therapy and/or concurrent therapy with other comparators, such as other nonbiologic systemic or biologic therapies, be considered when determining eligibility for reimbursement of deucravacitinib? | The expert indicated that patients should have documented inadequate response, contraindication, or intolerance to conventional systemic therapies, such as methotrexate and cyclosporine, before initiating deucravacitinib. Evidence is lacking for the use of deucravacitinib in combination with biologics or systemic therapies. The product monograph states deucravacitinib is not recommended for use in combination with other potent immunosuppressants. |
Is alignment with CDEC-recommended initiation criteria for apremilast appropriate? | The clinical expert stated that the initiation criteria for deucravacitinib should limited to patients with documented inadequate response, contraindication, or intolerance to conventional systemic therapies, such as methotrexate and cyclosporine. |
Considerations for continuation or renewal of therapy | |
Is alignment with CDEC-recommended renewal criteria for apremilast appropriate? | The clinical expert agreed that the renewal criteria for deucravacitinib should be consistent with those for apremilast. |
Considerations for discontinuation of therapy | |
Is alignment with CDEC-recommended discontinuation criteria for apremilast appropriate? | The expert agreed that the discontinuation criteria should be similar to apremilast, which states that treatment should be discontinued if a PASI 75 response has not been demonstrated after 16 weeks of treatment. |
Considerations for prescribing of therapy | |
Should prescribing of deucravacitinib be restricted to dermatologists? | The expert stated that deucravacitinib should be prescribed by dermatologists as in the case with biologics. |
PASI 75 = 75% reduction in Psoriasis Area and Severity Index score; pCPA = pan-Canadian Pharmaceutical Alliance; RB = restricted benefit.
Clinical Evidence
The clinical evidence included in the review of deucravacitinib is presented in 3 sections. The first section, the systematic review, includes pivotal studies provided in the sponsor’s submission to CADTH and Health Canada, as well as those studies that were selected according to an a priori protocol. The second section includes indirect evidence from the sponsor and indirect evidence selected from the literature that met the selection criteria specified in the review. The third section includes sponsor-submitted long-term extension (LTE) studies and additional relevant studies that were considered to address important gaps in the evidence included in the systematic review.
Systematic Review (Pivotal and Protocol-Selected Studies)
Objectives
To perform a systematic review of the beneficial and harmful effects of deucravacitinib 6 mg oral tablet for the treatment of adults with moderate to severe plaque psoriasis who are candidate for systemic therapy or phototherapy.
Methods
Studies selected for inclusion in the systematic review included pivotal studies provided in the sponsor’s submission to CADTH and Health Canada, as well as those meeting the selection criteria presented in Table 6. Outcomes included in the CADTH review protocol reflect outcomes considered to be important to patients, clinicians, and drug plans.
Table 6: Inclusion Criteria for the Systematic Review
Criteria | Description |
|---|---|
Population | Adults with moderate to severe plaque psoriasis who are candidate for systemic therapy or phototherapy Subgroups:
|
Intervention | Deucravacitinib 6 mg oral tablet daily |
Comparator | The following drugs when used as monotherapy or in combination with nonbiologic systemic drugs:
|
Outcomes | Efficacy outcomes:
Harms outcomes: AEs, SAEs, WDAEs, mortality, notable harms (infections, MACE, thromboembolic events, malignancy, elevated liver enzymes or creatinine kinase, lymphopenia, or neutropenia) |
Study designs | Published and unpublished phase III and IV RCTs |
AE = adverse event; BSA = body surface area; DLQI = Dermatology Life Quality Index; HRQoL = health-related quality of life; MACE = major adverse cardiovascular events; PASI = Psoriasis Area and Severity Index; RCT = randomized controlled trial; SAE = serious adverse event; SF-36 = Short Form (36) Health Survey; TNF = tumour necrosis factor; WDAE = withdrawal due to adverse event.
The literature search for clinical studies was performed by an information specialist using a peer-reviewed search strategy according to the PRESS Peer Review of Electronic Search Strategies checklist.26
Published literature was identified by searching the following bibliographic databases: MEDLINE All (1946–) via Ovid and Embase (1974–) via Ovid. All Ovid searches were run simultaneously as a multifile search. Duplicates were removed using Ovid deduplication for multifile searches, followed by manual deduplication in Endnote. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. The main search concept was deucravacitinib. Clinical trials registries were searched: the US National Institutes of Health’s clinicaltrials.gov, WHO’s International Clinical Trials Registry Platform search portal, Health Canada’s Clinical Trials Database, and the European Union Clinical Trials Register.
No filters were applied to limit the retrieval by study type. Retrieval was not limited by publication date or by language. Conference abstracts were excluded from the search results. Refer to Appendix 1 for the detailed search strategies.
The initial search was completed on October 26, 2022. Regular alerts updated the search until the meeting of the CADTH Canadian Drug Expert Committee on February 23, 2022.
Grey literature (literature that is not commercially published) was identified by searching relevant websites from the Grey Matters: A Practical Tool For Searching Health-Related Grey Literature checklist.27 Included in this search were the websites of regulatory agencies (FDA and European Medicines Agency). Google was used to search for additional internet-based materials. Refer to Appendix 1 for more information on the grey literature search strategy. In addition, the manufacturer of the drug was contacted for information regarding unpublished studies.
Two CADTH clinical reviewers independently selected studies for inclusion in the review based on titles and abstracts, according to the predetermined protocol. Full-text articles of all citations considered potentially relevant by at least 1 reviewer were acquired. Reviewers independently made the final selection of studies to be included in the review, and differences were resolved through discussion.
Findings From the Literature
A total of 2 studies were identified from the literature for inclusion in the systematic review (Figure 1). The included studies are summarized in Table 7. A list of excluded studies is presented in Appendix 2.
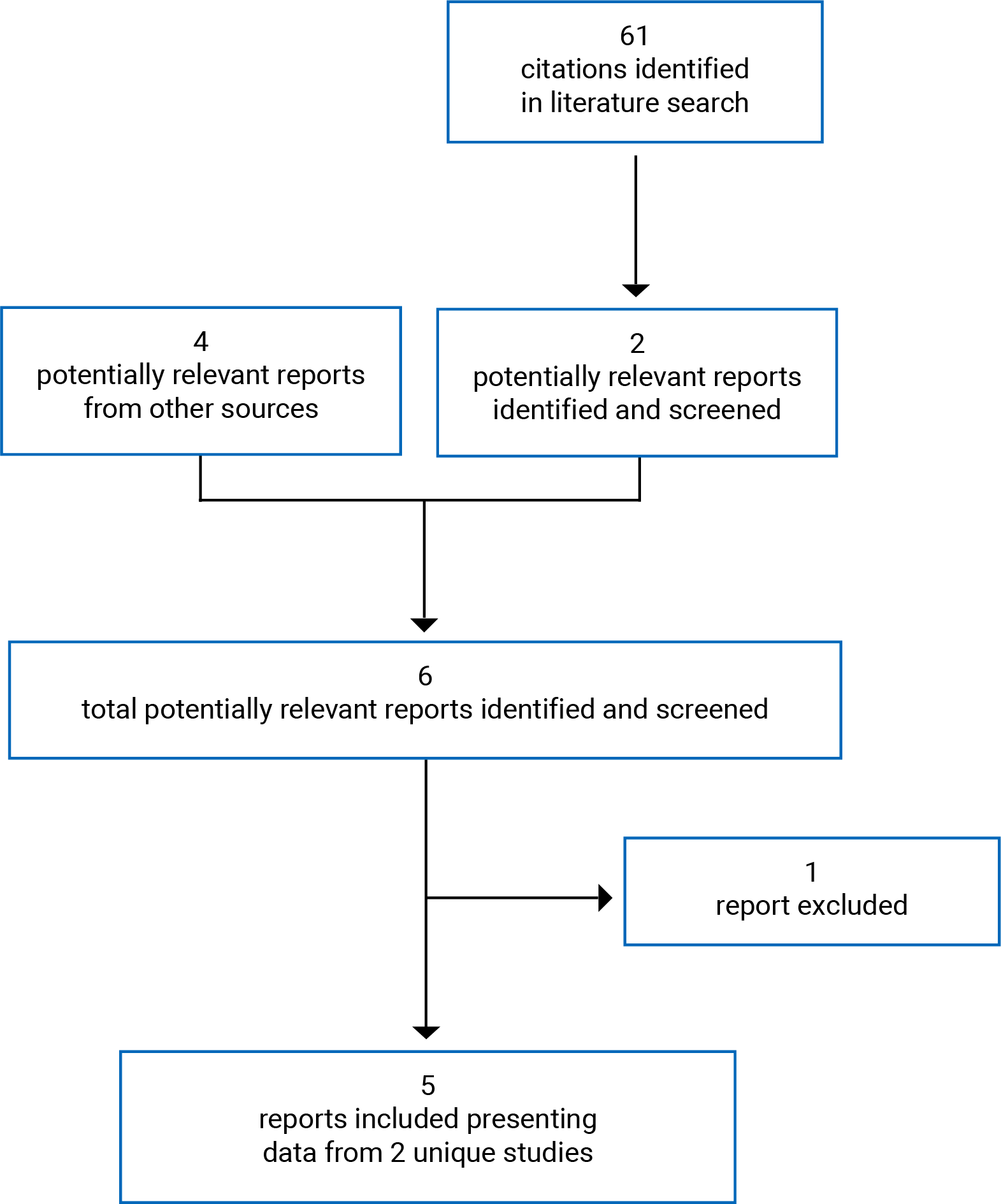
Table 7: Details of Included Studies
Detail | POETYK-1 (IM011046) | POETYK-2 (IM011047) |
|---|---|---|
Designs and populations | ||
Study design | DB RCT | DB RCT, withdrawal design |
Locations | Canada, US, Europe, Asia | Canada, US, Europe, Israel, Australia, New Zealand |
Patient enrolment dates | August 7, 2018, to September 2, 2020 (last patient visit date) | July 26, 2018, to November 30, 2020 (last patient visit date) |
Randomized (N) | 666 | 1,020 |
Inclusion criteria | Adults (≥ 18 years) with moderate to severe plaque psoriasis for at least 6 months, PASI ≥ 12, ≥ 10% of BSA affected, PGA score of ≥ 3 on a 5-point scale, and were candidates for systemic psoriasis therapy and/or phototherapy | Same as POETYK-1 |
Exclusion criteria |
| Same as POETYK-1 |
Drugs | ||
Intervention | Deucravacitinib 6 mg orally once daily (week 0 to 52) | Deucravacitinib 6 mg orally once daily (week 0 to 24). At week 24 patients who achieved PASI 75 response were rerandomized to deucravacitinib 6 mg daily or placebo;a patients who did not achieve PASI 75 response remained on deucravacitinib 6 mg daily until week 52 |
Comparator(s) | Apremilast 30 mg orally twice daily (at week 24, PASI 50 responders continue DB apremilast until week 52; PASI 50 nonresponders switched to DB deucravacitinib 6 mg until week 52) Placebo (at week 16, all patients switched to DB deucravacitinib 6 mg daily until week 52) | Apremilast 30 mg orally twice daily (week 0 to 24). At week 24, PASI 75 responders switched to placeboa Patients who did not achieve PASI 75 response were switched to deucravacitinib 6 mg daily until week 52 Placebo (at week 16, all patients switched to DB deucravacitinib 6 mg daily until week 52) |
Duration | ||
Phase | ||
Screening | 4 weeks | 4 weeks |
Treatment | 52 weeks | 24 weeks |
Withdrawal | NA | 28 |
Follow-up | 4 weeksb | 4 weeksb |
Outcomes | ||
Primary end point | Coprimary:
| Coprimary:
|
Secondary and exploratory end points | Secondary
Other
| Secondary
Other
|
Notes | ||
Publications | Armstrong et al. (2022)28 | Strober et al. (2022)29 |
BSA = body surface area; CV = cardiovascular; DB = double blind; DLQI = Dermatology Life Quality Index; EQ-5D-3L = 3-Level EQ-5D; HADS = Hospital Anxiety and Depression Scale; mNAPSI = modified mail psoriasis severity index; NA = not applicable; PASI = Psoriasis Area and Severity Index score; PASI 50 = 50% reduction in Psoriasis Area and Severity Index score;; PASI 75 = 75% reduction in Psoriasis Area and Severity Index score; PASI 90 = 90% reduction in Psoriasis Area and Severity Index score; PASI 100 = 100% reduction in Psoriasis Area and Severity Index score; PGA = Physician’s Global Assessment; pp-PASI = palmoplantar Psoriasis Area and Severity Index; PGI-C = Patient’s Global Impression of Change; PSSD = Psoriasis Symptoms and Signs Diary; PSSI = Psoriasis Scalp Severity Index; RCT = randomized controlled trial. SF-36 PCS and MCS = Short Form (36) Health Survey Physical Component Score and Mental Component Score; sPGA = static Physician’s Global Assessment; TB = tuberculosis; VAS = visual analogue scale; WLQ = Work Limitations Questionnaire.
Note: Three additional reports were included (FDA Multidisciplinary Review,30 Armstrong et al. [2022],28 and Strober et al. [2022]29).
aIf the patients switched to placebo at week 24 experienced a relapse (defined as at least a 50% loss of week 24 PASI percent improvement from baseline at any visit) they were switched to deucravacitinib 6 mg daily.
bFour-week follow-up period for patients who did not enter the long-term extension study.
Source: Clinical Study Reports for POETYK-17 and POETYK-28.
Description of Studies
Two 52-week double-blind RCTs met the inclusion criteria for the systematic review. The POETYK-1 study (N = 666) used a parallel study design (Figure 2) and the POETYK-2 study (N = 1,020) used a parallel study design followed by a randomized withdrawal design for responders at week 24 (Figure 3).
The objectives of the pivotal studies were to evaluate the safety and efficacy of deucravacitinib versus placebo and apremilast in adults with moderate to severe plaque psoriasis. Both studies randomized eligible patients (2:1:1) to deucravacitinib 6 mg daily, apremilast 30 mg twice daily, or placebo using a central interactive response technology system and stratified computer-generated randomization schedule. The POETYK-1 study was stratified by geographic region (US, Japan, China, and rest of world), previous biologic use for psoriasis, psoriatic arthritis, or other diseases (yes or no), and body weight (≥ 90 kg and < 90 kg for patients enrolled from all countries except China and Japan). The POETYK-2 study was stratified by geographic region (US and rest of world), previous biologic use for psoriasis, psoriatic arthritis, or other diseases (yes or no), and body weight (≥ 90 kg and < 90 kg).
All patients in the placebo groups switched to deucravacitinib at week 16. Both studies included a 24-week crossover to deucravacitinib for patients in the apremilast group that did not show an adequate response to therapy (i.e., did not achieve a PASI 50 response in the POETYK-1 study or PASI 75 in the POETYK-2 study). At week 24 in the POETYK-2 study, patients in the deucravacitinib group who achieved a PASI 75 response were rerandomized to placebo or to continue deucravacitinib, and patients in the apremilast group who achieved a PASI 75 response were switched to placebo.
The coprimary outcomes in both studies were the proportion of patients who met the sPGA response and PASI 75 response criteria at week 16 compared with placebo. Secondary outcomes included other PASI or sPGA response thresholds, HRQoL, and symptoms of psoriasis for deucravacitinib versus placebo or apremilast at week 16, 24, or 52. The POETYK-2 study also evaluated the time to relapse among patients in the deucravacitinib group that achieved a PASI 75 response at week 24.
The trials included sites from Canada (11 sites in POETYK-1; 15 sites in POETYK-2), US, and Europe. The POETYK-1 study also included sites in Asia, and the POETYK-2 study included sites from Israel, New Zealand, and Australia.
At the end of the pivotal studies, patients were eligible to enter the LTE study (IM011075) and receive open-label deucravacitinib.
Populations
Inclusion and Exclusion Criteria
The POETYK-1 and POETYK-2 studies enrolled adults (≥ 18 years) who had moderate to severe plaque psoriasis that was stable (defined as no morphology changes or significant flares) for at least 6 months and who were candidates for systemic psoriasis therapy and/or phototherapy. Patients were required to have a baseline PASI score of 12 or higher, with greater than 10% of BSA affected, and with a sPGA score of at least 3 on a 5-point scale.
Patients with prior exposure to deucravacitinib or apremilast were excluded from the study, but prior exposure to biologic, or nonbiologic systemic or topical therapies for psoriasis were permitted provided the patient had undergone the protocol-specified washout period before enrolment. Other exclusion criteria included patients with nonplaque forms of psoriasis, with active chronic infection, or unstable cardiovascular, neuropsychiatric, or other medical conditions (Table 7).
Figure 2: Study Schematic of POETYK-1
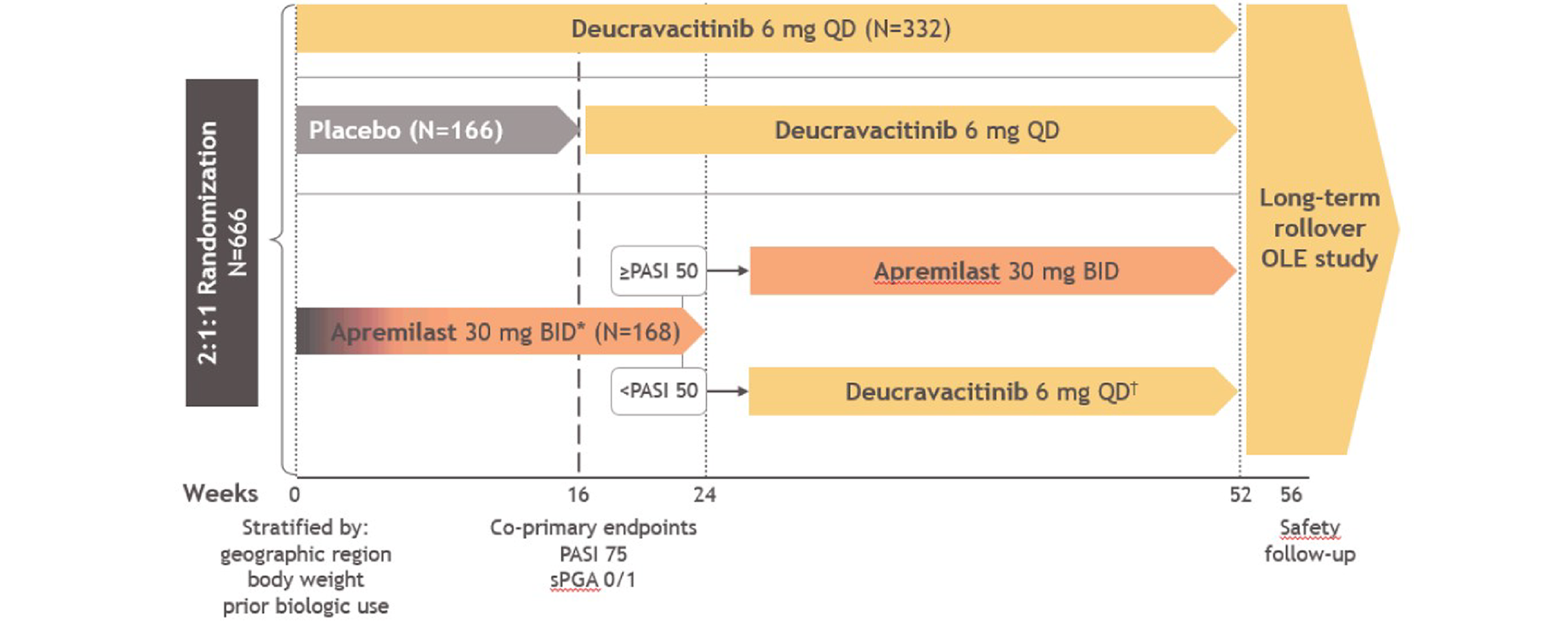
BID = twice daily; OLE = open-label extension; PASI 50 = 50% reduction in Psoriasis Area and Severity Index score; PASI 75 = 75% reduction in Psoriasis Area and Severity Index score; QD = daily; sPGA = static Physician’s Global Assessment.
*Apremilast is titrated from 10 mg QD to 30 mg BID over the first 5 days of dosing.
††Patients in the apremilast group who did not achieve PASI 50 response at week 24 were switched in a blinded fashion to deucravacitinib.
Source: Clinical Study Report for POETYK-1.7
Figure 3: Study Schematic of POETYK-2
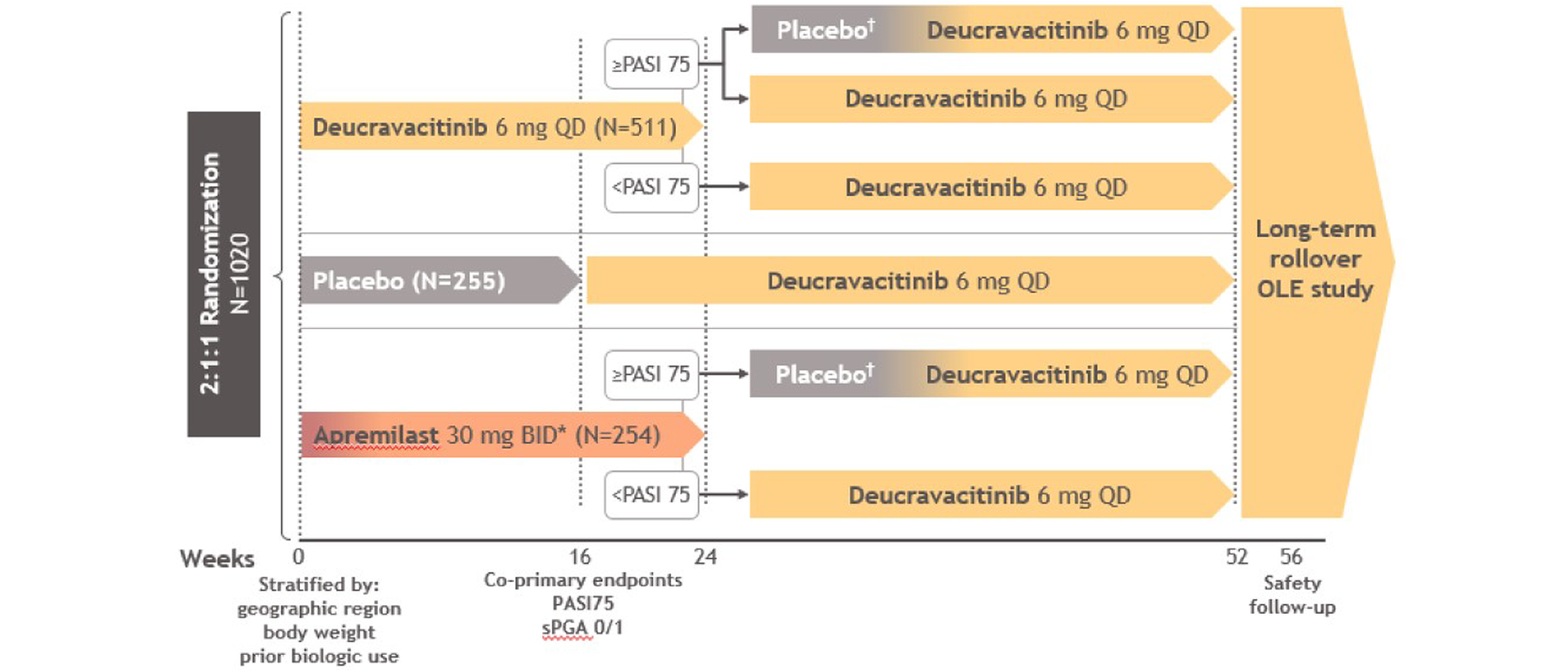
BID = twice daily; OLE = open-label extension; PASI 50 = 50% reduction in Psoriasis Area and Severity Index score; PASI 75 = 75% reduction in Psoriasis Area and Severity Index score; QD = daily; sPGA = static Physician’s Global Assessment.
† Upon relapse (at least a 50% loss of week 24 PASI percent improvement from baseline), subjects were switched to deucravacitinib 6 mg QD.
* Apremilast was titrated from 10 mg QD to 30 mg BID over the first 5 days of dosing.
Source: Clinical Study Report for POETYK-2.8
Baseline Characteristics
In general, the baseline characteristics of patients enrolled in the POETYK-1 and POETYK-2 studies were similar between groups within trials. The mean age of patients enrolled in the pivotal trials ranged from 44.7 years (SD = 12.1) to 47.9 (SD = 14.0) per treatment group. The majority of patients were men (62% to 71%), and the minority were women (29% to 38% per treatment group). Most patients were white (77% to 93%), with fewer patients who were Asian (3% to 21%) or Black (1% to 4%). The patients enrolled had been diagnosed with psoriasis for a median of 13.4 years to 18.2 years, with a mean PASI score at baseline ranging from 20.7 (SD = 8.0) to 21.8 (SD = 8.6). The majority of patients had received prior systemic therapy for psoriasis (54% to 66%) including biologics (31% to 39%). Between 34% and 45% of patients per treatment group had received prior phototherapy (Table 8).
Table 8: Summary of Baseline Characteristics — POETYK-1 and POETYK-2 (FAS)
Characteristic | POETYK-1 | POETYK-2 | ||||
|---|---|---|---|---|---|---|
DEUC n = 332 | Placebo n = 166 | APREM n = 168 | DEUC n = 511 | Placebo n = 255 | APREM n = 254 | |
Age (years), mean (SD) | 45.9 (13.7) | 47.9 (14.0) | 44.7 (12.1) | 46.9 (13.4) | 47.3 (13.6) | 46.4 (13.3) |
Female, n (%) | 102 (31) | 53 (32) | 58 (35) | 175 (34) | 74 (29) | 97 (38) |
Male, n (%) | 230 (69) | 113 (68) | 110 (66) | 336 (66) | 181 (71) | 157 (62) |
Race, n (%) | ||||||
Asian | 59 (18) | 34 (21) | 28 (17) | 24 (5) | 8 (3) | 12 (5) |
Black | 2 (1) | 3 (2) | 1 (1) | 8 (2) | 9 (4) | 9 (4) |
White | 267 (80) | 128 (77) | 139 (83) | 474 (93) | 232 (91) | 229 (90) |
Other | 4 (1) | 1 (1) | 0 | 5 (1) | 6 (2) | 4 (2) |
Ethnicity, n (%) | ||||||
Hispanic or Latino | 50 (15) | 26 (16) | 30 (18) | 58 (11) | 29 (11) | 29 (11) |
Not Hispanic or Latino | 282 (85) | 140 (84) | 138 (82) | 445 (87) | 226 (89) | 223 (88) |
BMI (kg/m2), mean (SD) | 29.8 (7.0) | 30.2 (7.4) | 29.6 (6.7) | 31.0 (6.8) | 30.4 (6.3) | 31.6 (7.2) |
Duration of psoriasis (years), mean (SD) | 17.1 (12.4) | 17.3 (12.8) | 17.7 (11.8) | 19.6 (12.9) | 19.9 (12.8) | 18.9 (12.4) |
Duration of psoriasis (years), median (range) | 13.4 (0.7 to 57.8) | 14.7 (0.9 to 62.3) | 16.3 (0.7 to 56.4) | 17.6 (0.6 to 67.5) | 18.2 (1.1 to 61.5) | 16.0 (0.7 to 60.6) |
Baseline PASI score, mean (SD) | 21.8 (8.6) | 20.7 (8.0) | 21.4 (9.0) | 20.7 (7.5) | 21.1 (9.0) | 21.6 (8.4) |
PASI score > 20, n (%) | 155 (47) | 64 (39) | 70 (42) | 213 (42) | 103 (40) | 111 (44) |
sPGA score, n (%) | ||||||
2 (mild) | 0 | 1 (1) | 0 | 0 | 0 | 0 |
3 (moderate) | 257 (77) | 128 (77) | 139 (83) | 408 (80) | 217 (85) | 196 (77) |
4 (severe) | 75 (23) | 37 (22) | 29 (17) | 103 (20) | 38 (15) | 58 (23) |
% BSA, mean (SD) | 26.6 (15.9) | 25.3 (16.9) | 26.6 (16.1) | 26.3 (15.8) | 25.3 (15.7) | 28.3 (16.5) |
DLQI total score, mean (SD) | 12.0 (6.7) | 11.4 (6.6) | 12.4 (6.8) | 11.8 (6.5) | 11.8 (6.8) | 12.5 (6.7) |
Prior psoriasis therapy, n (%) | ||||||
Any systemic therapy | 200 (60) | 109 (66) | 109 (65) | 274 (54) | 139 (55) | 140 (55) |
Biologic therapy | 130 (39) | 63 (38) | 66 (39) | 165 (32) | 83 (33) | 79 (31) |
Phototherapy | 118 (36) | 57 (34) | 64 (38) | 228 (45) | 105 (41) | 102 (40) |
APREM = apremilast; BMI = body mass index; BSA = body surface area; DEUC = deucravacitinib; DLQI = Dermatology Life Quality Index; FAS = full analysis set; PASI = Psoriasis Area and Severity Index; SD = standard deviation; sPGA = static Physician’s Global Assessment.
Source: Clinical Study Reports for POETYK-17 and POETYK-2.8
Interventions
Patients enrolled in the POETYK-1 and POETYK-2 studies were randomized to deucravacitinib 6 mg daily, apremilast 30 mg twice daily, or placebo. Blinding was maintained using double-dummy methods with placebo tablets that were identical to deucravacitinib and apremilast. Apremilast was titrated up to 30 mg twice daily over 5 days, starting with 10 mg daily on day 1. Patients receiving placebo also received a placebo titration kit to match the apremilast regimen.
In both studies, patients in the placebo groups were switched to blinded deucravacitinib 6 mg daily at week 16.
In the POETYK-1 study, patients in the deucravacitinib group remained on this therapy for the full 52 weeks, regardless of treatment response. Patients in the apremilast group who did not achieve at least a PASI 50 response at week 24 were switched to blinded deucravacitinib 6 mg daily and those who met the PASI 50 response criteria remained on apremilast until week 52.
In the POETYK-2 study, patients randomized to deucravacitinib who met the PASI 75 response criteria at week 24 were rerandomized to either remain on deucravacitinib or switch to blinded placebo. Also, patients in the apremilast group who met the PASI 75 response criteria at week 24 were switched to blinded placebo. Any patients in the deucravacitinib or apremilast groups who did not meet the PASI 75 response criteria at week 24 received blinded deucravacitinib 6 mg daily from week 24 to week 52. Among patients switched from active treatment to placebo, those who experienced a relapse received blinded deucravacitinib for the rest of the 52 week period.
There was no protocol provision for dose adjustments of study treatments. Treatment could be resumed after interruption for an AE with consultation with the sponsor.
In both studies, patients were prohibited from receiving any strong cytochrome P450 inducers as per the US apremilast product monograph (e.g., rifampin, phenobarbital, carbamazepine, phenytoin), live vaccines, any drugs that may worsen psoriasis (e.g., lithium, antimalarial drugs, propranolol, indomethacin), opioid analgesics, phototherapy, biologic medications, oral psoriasis medications, oral corticosteroids, or topical medications or medicated shampoos that may affect the evaluation of psoriasis (e.g., corticosteroids, vitamin D derivatives, or salicylic acid). In both studies, patients with an sPGA score or scalp severity Physician’s Global Assessment (ss-PGA) score of 3 or higher at week 24 were eligible to start restricted topical therapies or shampoos at the investigator’s discretion. These topical treatments included high potency corticosteroids (Classes I to V), greater than 3% salicylic acid, urea, alpha- or beta-hydroxy acids, anthralin, calcipotriene, vitamin D derivatives, retinoids, or tazarotene.
Outcomes
A list of efficacy end points identified in the CADTH review protocol that were assessed in the clinical trials included in this review is provided in Table 9. These end points are further summarized in the following. A detailed discussion and critical appraisal of the outcome measures is provided in Appendix 4.
Table 9: Summary of Outcomes of Interest Identified in the CADTH Review Protocol
Outcome measure | Time point | Comparator | POETYK-1 | POETYK-2 |
|---|---|---|---|---|
sPGA 0 or 1a | Week 16 | Placebo | Coprimary | Coprimary |
PASI 75 | Week 16 | Placebo | Coprimary | Coprimary |
sPGA 0 or 1a | Week 16 | Apremilast | Key secondary | Key secondary |
sPGA 0 or 1a | Week 24 | Apremilast | Key secondary | Key secondary |
sPGA 0 or 1a | Week 52 and week 24 | Apremilast | Key secondary | Additional |
sPGA 0a | Week 16 | Placebo, apremilast | Key secondary | Key secondary |
PASI 100 | Week 16 | Placebo | Key secondary | Key secondary |
PASI 90 | Week 16 | Placebo, apremilast | Key secondary | Key secondary |
PASI 90 | Week 24 | Apremilast | Key secondary | Key secondary |
PASI 90 | Week 52 and week 24 | Apremilast | Key secondary | — |
PASI 75 | Week 16 | Apremilast | Key secondary | Key secondary |
PASI 75 | Week 24 | Apremilast | Key secondary | Key secondary |
PASI 75 | Week 52 and week 24 | Apremilast | Key secondary | Additional |
ss-PGA 0 or 1a,b | Week 16 | Placebo, apremilast | Key secondary | Key secondary |
Fingernail PGA 0 or 1a,b | Week 16 | Placebo | Key secondary | Key secondary |
PSSD symptom score of 0c | Week 16 | Placebo, apremilast | Key secondary | Key secondary |
Change from baseline in PSSD symptom score | Week 16 | Apremilast | Key secondary | Key secondary |
DLQI 0 or 1d | Week 16 | Placebo | Key secondary | Key secondary |
Change from baseline in SF-36 PCS and MCS | Week 16 | Placebo, apremilast | Additional | Additional |
Change from baseline in EQ-5D-3L VAS | Week 16 | Placebo, apremilast | Additional | Additional |
Time to relapse | Week 52 | Placebo | — | Key secondary |
DLQI = Dermatology Life Quality Index; EQ-5D-3L = 3-Level EQ-5D; PASI 75 = 75% reduction in Psoriasis Area and Severity Index score; PASI 90 = 90% reduction in Psoriasis Area and Severity Index score; PASI 100 = 100% reduction in Psoriasis Area and Severity Index score; PGA-F = Physician’s Global Assessment–Fingernail; PSSD = Psoriasis Symptoms and Signs Diary; SF-36 PCS and MCS = Short Form (36) Health Survey Physical Component Score and Mental Component Score; sPGA = static Physician’s Global Assessment; ss-PGA = scalp severity Physician’s Global Assessment; VAS = visual analogue scale.
aWith at least a 2-point improvement from baseline.
bIn the subgroup of patients with a baseline ss-PGA or PGA-F score of at least 3.
cIn the subgroup of patients with a baseline PSSD score of at least 1.
dAnalyzed in patients with a baseline DLQI score of at least 2.
Source: Clinical Study Reports for POETYK-17 and POETYK-2.8
Efficacy assessments were conducted by dermatologists or trained investigators who were experienced in the assessment of patients with psoriasis. Where possible, the same investigator conducted all assessments for a given patient. Outcome assessors underwent training provided by the Group for Research and Assessment of Psoriasis and Psoriatic Arthritis.
Both trials were conducted during the COVID-19 pandemic, which disrupted some study visits and assessments due to site closures and concerns for risk of COVID-19. In the POETYK-1 study, 30 patients had 50 visits impacted, including 25 patients with visits not performed and 5 patients with visits performed virtually. All disruptions occurred after week 24 and only 1 patient had missing data due to COVID-19 at week 52. In the POETYK-2 study, disruptions occurred at the week 20 visit or later and affected 51 patients and 88 visits (45 patients with missed visits and 6 with remote visits). Ten patients missed the week 24 visit (including 2 who had stopped study drug) and 6 patients missed the week 52 visit. The Clinical Study Reports state the disruptions did not affect efficacy outcomes up to week 16 and had a minor impact for outcomes assessed at subsequent time points.
Psoriasis Area and Severity Index
The PASI is widely used in psoriasis trials to grade the extent and severity of psoriatic lesions. It combines an assessment of the BSA affected in 4 anatomic regions (head, trunk, arms, and legs) and the severity of desquamation, erythema, and plaque induration or infiltration (thickness) in each region. Scores range from 0 to 72 points. The percent improvement in PASI score is calculated as the baseline PASI score minus postbaseline PASI score, divided by baseline PASI score, multiplied by 100. Patients with a 50%, 75%, 90%, or 100% improvement are categorized as achieving a PASI 50, PASI 75, PASI 90, or PASI 100 response. PASI scores have shown weak to moderate correlation with DLQI scores and good interrater and moderate intrarater reliability.31,32 Responsiveness may be weak, especially when the BSA affected is less than 10%.33,34
A reduction of PASI score by 75% (PASI 75) is a benchmark in psoriasis clinical trials,35 while more aggressive treatment goals such as reduction of PASI scores by 90% or 100% (total clearance) are also used as end points in psoriasis clinical trials.36,37
Static Physician’s Global Assessment
The sPGA is a composite score of the physician’s assessment of the overall severity of the patient’s psoriatic lesions at a given point of time. The investigator assessed the overall severity of psoriasis based on erythema, scaling, and induration, using a 5-point scale, described as clear (0), almost clear (1), mild (2), moderate (3), or severe (4). The scores are then averaged, with equal weights for each item, to obtain a single score. The sPGA has shown moderate correlation with DLQI, and strong correlation with PASI scores.38,39 The sPGA has shown acceptable test-retest reliability,38 but no information on responsiveness was found.
In both studies, the coprimary outcome of sPGA response was defined as a sPGA score of “clear” or “almost clear” (i.e., 0 or 1), with at least a 2-category improvement from baseline, which is generally accepted as a clinically meaningful score.40,41
The same scale and responder definition was used for separate analyses in the subgroup of patients with fingernail psoriasis who had a baseline Physician’s Global Assessment–Fingernail score of at least 3.7 In patients with scalp psoriasis at baseline, ss-PGA was rated on a 5-point scale; absence of disease (0), very mild (1), mild (2), moderate (3), and severe disease (4). The same responder definition was applied to patients with scalp psoriasis.7
Time to Relapse
In the POETYK-2 study, disease relapse was defined as at least a 50% loss of week 24 PASI percent improvement from baseline among patients who had achieved at least a PASI 75 response at week 24.
Psoriasis Symptoms and Signs Diary
The PSSD is a patient-reported 11-item instrument used to assess the severity of symptoms and signs associated with plaque psoriasis. It includes 5 symptoms (itch, pain stinging, burning, and skin tightness) and 6 signs (skin dryness, cracking, scaling, shedding or flaking, redness, and bleeding) which are assessed on a 0 (absent) to 10 (worst imaginable) scale over the past 24 hours. The symptom score, the signs score, and the total score are the average of the relevant item scores multiplied by 10 and range from 0 (absence of symptoms or signs) to 100 (most severe). In both studies, patients completed the PSSD each day using and eDiary and scores were averaged over at least 4 of the past 7 days. The PSSD has shown acceptable convergent validity, internal consistency, and test-retest reliability.42,43 Estimates for the minimal important difference (MID) of the PSSD total score range from 9 to 12 using anchor-based methods and 5.7 to 13.1 using distribution-based methods.43 No MID was identified for the PSSD symptom score based on the 24-hour recall version, but a 9.1 point MID was reported for the 7-day recall version of the questionnaire.43
Health-Related Quality of Life
The DLQI is a dermatology-specific questionnaire that has been used to assess the impact of the disease on a patient’s HRQoL. It is a patient-reported 10-item questionnaire that covers 6 domains: symptoms and feeling, daily activities, leisure, work and school, personal relationships, and bother with psoriasis treatment, each assessed over the past week. Each item is scored on a 4-point Likert scale: 0 (not at all affected or not relevant), 1 (a little affected), 2 (a lot affected), and 3 (very much affected). The overall DLQI score is a numeric score between 0 to 30, with lower scores indicating better quality of life. The final numeric score translates to the effect of the patient’s disease on their quality of life, where 0 to 1 = no effect, 2 to 5 = small effect, 6 to 10 = moderate effect, 11 to 20 = very large effect, and 21 to 30 = extremely large effect.44 The DLQI has shown strong correlation with the EQ-5D index score and the bodily pain and social functioning domains of the Short Form (36) Health Survey (SF-36).45 It may, however, lack conceptual validity for the psychological impact of psoriasis. There is evidence of responsiveness and test-retest reliability.45,46 Estimates of the MID range from 2.2 to 6.9.45,47,48
The 3-Level EQ-5D questionnaire is a generic, preference-based, HRQoL measure. It includes 5 dimensions: mobility, self-care, usual activities, pain or discomfort, and anxiety or depression. Each dimension is divided into 3 levels representing “no problems,” “some problems,” and “extreme problems” (1, 2, and 3, respectively). The 5 questions are scored and together contribute to the EQ-5D index (utility) score between 0 and 1, where 0 represents death, and 1 represents perfect health. Different utility functions are available that reflect the preferences of specific populations (e.g., US, UK). The EQ-5D also includes a visual analogue scale (VAS) of the patient’s self-rated health status on a vertical 20 cm scale that ranges from 0 (worst imaginable health status) to 100 (best imaginable health status). In patients with psoriasis, MID estimates for the VAS range from 3.82 to 8.43 based on PASI improvement and PGA score and was 10.34 based on distributional methods.45
The SF-36 is a 36-item, general health status instrument that consists of 8 health domains: physical functioning, role physical, bodily pain, general health, vitality, social functioning, role emotional, and mental health. The SF-36 also provides 2 component summaries, the Physical Component Score (PCS) and the Mental Component Score (MCS), derived from aggregating the 8 domains according to a scoring algorithm. All domain and component scores are based on a scale of 0 to 100, with higher scores indicating higher health status. An MID of at least 3 points for the SF-36 PCS or MCS has been reported in the literature.49,50
Harms
Data were collected on treatment-emergent AEs, SAEs, AEs leading to treatment discontinuation, and deaths, including events that occurred up to 30 days after the last dose of study drug. Safety data beyond the 16-week placebo-controlled period were reported using exposure-adjusted incidence rates (IR) per 100 patient-years (PYs) that took into consideration switches between treatments. In addition, the studies’ protocols identified specific AEs of special interest (infection, malignancy, skin-related AEs, and creatine kinase elevation) as well as specific events that were adjudicated by independent external blinded evaluators (cardiovascular events, infections, and suicidal ideation or behaviour). The infections of interest were selected based on the immunomodulatory mechanism of action of deucravacitinib and included herpes zoster, influenza, opportunistic infections, and tuberculosis.
Statistical Analysis
Statistical Models
In both studies, the coprimary outcomes (proportion of patients with sPGA score of 0 or 1, and PASI 75 response at week 16 versus placebo) were tested using a stratified Cochran-Mantel-Haenszel test, which was stratified by the factors used a randomization (geographic region, prior biologic use, and body weight). If expected cell counts were insufficient for each strata, then strata levels were combined. Nonresponder imputation was used for patients who prematurely discontinued the study or the study drug, or those with missing outcome data at that time point (i.e., analyzed as not having met the response criteria). The Clinical Study Report states that this represents an implicit composite estimand analysis strategy. Sensitivity analyses for the coprimary outcomes are listed in Table 10.
Other binary end points were analyzed using the same methods as the primary end points. Continuous end points were analyzed using an analysis of covariance model that included the baseline value and stratification factors. Baseline observation carried forward was used for patients who discontinued the study treatment due to lack of efficacy or AEs, otherwise the last observation was carried forward for other missing data. In the POETYK-1 study, patients in the apremilast group who did not achieve a PASI 50 response at week 24 were considered to be nonresponders for binary end points or had baseline observation carried forward for continuous end points that were analyzed for later time points.
The time to relapse between week 24 and week 52 was reported in the POETYK-2 study for the patients in the deucravacitinib group (who were rerandomized to placebo or deucravacitinib) and patients in the apremilast group (who remained on apremilast) that achieved a PASI 75 response at week 24. The Kaplan-Meier product limit method was used to generate the survival curves, with the difference between deucravacitinib and placebo tested using a stratified log-rank test. Patients who discontinued the study or treatment, had missing data, and did not have relapse by week 52 were censored and the date they experienced these criteria.
Table 10: Statistical Analysis of Efficacy End Points
End point | Statistical model | Adjustment factors | Sensitivity analyses |
|---|---|---|---|
POETYK-1 | |||
Coprimary end points vs. placebo at week 16: sPGA 0 or 1 response PASI 75 response | Cochran-Mantel-Haenszel (FAS) Nonresponder imputation for missing dataa |
|
|
Other binary end points | Same as above | Same as above | Binary GEE model |
Continuous end points | ANCOVA (FAS) Modified BOCF method for missing datab) |
| MMRM |
POETYK-2 | |||
Coprimary end points vs. placebo at week 16: sPGA 0 or 1 response PASI 75 response | Cochran-Mantel-Haenszel (FAS) Nonresponder imputation for missing dataa |
|
|
Other binary end points | Same as above | Same as above | Binary GEE model |
Continuous end points | ANCOVA (FAS) Modified BOCF method for missing datab) |
| MMRM |
Time to relapse among PASI 75 responders at week 24 | Kaplan-Meier product limit method; stratified log-rank test |
| None |
ANCOVA = analysis of covariance; BOCF = baseline observation carried forward; FAS = full analysis set; GEE = general estimating equation; LOCF = last observation carried forward; MMRM = mixed effect model with repeated measures; NRI = nonresponder imputation; PASI 75 = 75% reduction in Psoriasis Area and Severity Index score; sPGA = static Physician’s Global Assessment.
aNonresponder imputation for patients who discontinued the treatment or the study before that time point or had missing data for any reason at that time point.
bThe baseline value was carried forward for patients who discontinued study treatment for all time points after discontinuation due to lack of efficacy or adverse events. Patients who stopped study drug for other reasons or had missing data at the time point of comparison had the last valid observation carried forward. Patients with missing baseline values were excluded from the change from baseline analyses.
Source: Clinical Study Reports for POETYK-17 and POETYK-2.8
Statistical Power
Both studies were estimated to have greater than 99% power to detect superiority (2-sided significance level of 0.05) of deucravacitinib versus placebo for each of the coprimary outcomes, based on a planned enrolment of 600 patients (300 to deucravacitinib and 150 each to placebo and apremilast groups) for the POETYK-1 study and 1,000 patients (500 to deucravacitinib, and 250 each to placebo and apremilast) for the POETYK-2 study. These calculations assumed response rates for PASI 75 and sPGA response at week 16 of 60% for deucravacitinib, 35% for apremilast, and 10% for placebo, based on deucravacitinib data from a phase II study (Bristol Myers Squibb study IM011011), and published response rates for placebo and apremilast. Based on a 2-sided chi-square test with an alpha of 0.025, the trials also had greater than 99% power to detect superiority versus apremilast for both coprimary end points at week 16.
Control of Type I Error Rate
The trials used a similar hierarchical testing procedure to control for the family-wise type I error rate. The coprimary outcomes were tested first at an alpha of 0.05 and if both achieved statistical significance, then the key secondary outcomes were tested in the order listed in Table 11. Two independent fixed-sequence testing branches that compared deucravacitinib to placebo, and to apremilast, proceeded with a 2-sided alpha of 0.025 for each branch. The testing of each branch could proceed only if the prior outcome in the sequence achieved statistical significance. If an outcome failed, then any subsequent outcomes were considered descriptive. Of note, there were 2 testing hierarchies, 1 for the US submission and 1 for submissions to other regulators. For the POETYK-1 study, the DLQI responder outcome was included the global testing procedure but not the US, and in the POETYK-2 study the DLQI responder and time to relapse outcomes were included the global procedure only. For any other outcomes not listed in Table 11, the P values reported are nominal.
Table 11: Statistical Testing Order
Outcome | Time point |
|---|---|
POETYK-1: Comparison to placebo (type I error 0.025) | |
1. PASI 90 | 16 |
2. ss-PGA 0 or 1 with ≥ 2-point improvementa | 16 |
3. sPGA 0 | 16 |
4. PASI 100 | 16 |
5. PSSD symptom score of 0b | 16 |
6. DLQI 0 or 1c,d | 16 |
7. PGA-F 0 or 1 with ≥ 2-point improvementa | 16 |
POETYK-1: Comparison to apremilast (type I error 0.025) | |
1. sPGA 0 or 1 with ≥ 2-point improvement | 16 |
2. PASI 75 | 16 |
3. PASI 90 | 16 |
4. sPGA 0 or 1 with ≥ 2-point improvement | 24 |
5. PASI 75 | 24 |
6. PASI 90 | 24 |
7. Change from baseline in PSSD symptoms score | 16 |
8. ss-PGA 0 or 1 with ≥ 2-point improvementa | 16 |
9. sPGA 0 or 1 with ≥ 2-point improvement | 52 and 24 |
10. PASI 75 | 52 and 24 |
11. PASI 90 | 52 and 24 |
12. sPGA 0 | 16 |
13. PSSD symptom score of 0b | 16 |
POETYK-2: Comparison to placebo (type I error 0.025) | |
1. PASI 90 | 16 |
2. ss-PGA 0 or 1 with ≥ 2-point improvementa | 16 |
3. sPGA 0 | 16 |
4. PASI 100 | 16 |
5. PSSD symptom score of 0b | 16 |
6. DLQI 0 or 1c,d | 16 |
7. Time to relapse until week 52 for week 24 deucravacitinib PASI 75 respondersd,e | 52 |
8. PGA-F 0 or 1 with ≥ 2-point improvementa | 16 |
POETYK-2: Comparison to apremilast (type I error 0.025) | |
1. sPGA 0 or 1 with ≥ 2-point improvement | 16 |
2. PASI 75 | 16 |
3. PASI 90 | 16 |
4. sPGA 0 or 1 with ≥ 2-point improvement | 24 |
5. PASI 75 | 24 |
6. PASI 90 | 24 |
7. Change from baseline in PSSD symptoms score | 16 |
8. ss-PGA 0 or 1 with ≥ 2-point improvementa | 16 |
9. sPGA 0 | 16 |
10. PSSD symptom score of 0b | 16 |
DLQI = Dermatology Life Quality Index; PASI 75 = 75% reduction in Psoriasis Area and Severity Index score; PASI 90 = 90% reduction in Psoriasis Area and Severity Index score; PASI 100 = 100% reduction in Psoriasis Area and Severity Index score; PGA-F = Physician’s Global Assessment–Fingernail; PSSD = Psoriasis Symptoms and Signs Diary; sPGA = static Physician’s Global Assessment; ss-PGA = scalp severity Physician’s Global Assessment.
aAmong patients with baseline score ≥ 3 points.
bAmong patients with baseline PSSD symptom score ≥ 1.
cAmong patients with baseline DLQI score ≥ 2 points.
dThis outcome was controlled for type I error rate in the global testing hierarchy, but not in the US-based testing procedure.
eAmong patients who initially randomized to deucravacitinib who achieved PASI 75 response at week 24.
Source: Clinical Study Reports for POETYK-17 and POETYK-2.8
Adverse Events
AE data were presented as the number and percentage of patients with an event, with events counted only once per patient for recurring AEs within each system organ class (SOC) or preferred term, starting with the first dispensation date within a period in the as-treated population. Due to the treatment switches that occurred after week 16, AEs for the total study period were reporting using the exposure-adjusted IR. The exposure-adjusted IR was calculated by multiplying the total number of patients with an AE divided by the sum of exposure time for that AE under each treatment that patients were exposed to, multiplied by 100 and 365. Individual patient’s exposure time was calculated separately for each treatment a patient received (if the patient switched therapy) based on that treatment’s start date until the first occurrence of that AE (for patients with an event) or until the treatment stop date (for patients with no events and who continued into the extension study), or the treatment stop date plus 30 days (for patients with no events who completed the safety follow-up period).
Subgroup Analyses
Both studies conducted several preplanned subgroup analyses for the coprimary outcomes. Of these, the analyses based on prior biologic use (yes or no) were of interest to this systematic review. Other planned subgroups included gender, age category, race, body weight categories, and geographic region. These subgroup analyses were conducted using the same methods as the primary end point analyses.
Analysis Populations
In the POETYK-1 and POETYK-2 studies, efficacy analyses were based on the full analysis set that included all patients randomized, who were analyzed according to the treatment groups assigned at randomization. The as-treated (i.e., safety) population included all randomized patients who took at least 1 dose of study drug and who were analyzed according to the drug received.
Of note, patients with missing data due to COVID-19 at week 24 or 52 were excluded from the analyses.
Protocol Amendments
||| ||||||||| || |||| ||||||| |||| ||||||| ||||| ||| ||||| || ||| ||||||| ||||| || ||||| ||||||||||| |||||||| |||| ||||||| || |||| || ||||||| ||||| |||| ||||||||| || |||| ||||| |||| ||| ||||| ||||| |||||||| ||||||||||| |||||| |||||| |||||| || |||||||||| || ||| ||||||||||||| |||||||| ||||| ||||||| ||||||||| || |||||||| |||| ||||||||||||||||| || ||||||||||| ||| ||| |||||| |||||| ||| ||||||||| |||||||| |||| |||||||| || ||||||| ||||||||||| |||| |||||||| |||| || ||||| ||||||||| |||||||| || ||||||||| ||||||||| |||| |||| || ||| |||||||| |||||||| ||| ||| ||||| || ||||||| || ||||||||||| |||||||||| ||| |||| ||| ||||||| |||||||| |||| |||||||||| ||| ||||||||||||| || ||| ||||| ||||||| |||| |||| || ||||||| ||| |||||||| |||||||||.
Results
Patient Disposition
A total of 965 patients were screened for inclusion in the POETYK-1 study, of which 666 patients (69%) were randomized (Table 12). During the first 16 weeks of the trial, 8%, 12%, and 14% of patients in the deucravacitinib, placebo, and apremilast groups, respectively, discontinued study treatment. Between week 16 and 24, 2% to 3% of patients per group stopped treatment (Table 13). From week 24 to 52, another 11% of patients randomized to deucravacitinib stopped treatment, as did 8% of the patients switched from placebo to deucravacitinib, 5% of the responders who continued apremilast, and 13% of nonresponders who switched from apremilast to deucravacitinib (Table 14).
In the POETYK-2 study, 1,519 patients were screened, and 1,020 patients were randomized (67%). The proportion of patients who stopped treatment during the first 16 weeks was 11%, 17%, and 15% in the deucravacitinib, placebo, and apremilast groups, respectively (Table 15). Between week 16 and 24, 4% of patients per group stopped treatment (Table 16). Among PASI 75 responders who had received deucravacitinib throughout the study, 7% stopped treatment between week 24 and 52, compared with 11% of responders who switched from deucravacitinib to placebo, and 16% of responders to apremilast who were switched to placebo (Table 17). Among PASI nonresponders at week 24, 12% of those who remained on deucravacitinib and 18% who were switched from apremilast to deucravacitinib, stopped treatment between week 24 and 52, as did 11% of patients who initially received placebo and were switched to deucravacitinib at week 16. The reasons for discontinuation as well as the number of patients switched between treatments at week 16 and 24 are listed in Table 16 and Table 17.
|| ||| |||||||| |||||| | |||||||| |||||||||||| ||||| ||||||||| ||| || |||||||||||||||| ||||||| || |||| |||||||||||||||| | |||| |||||||| ||| | |||| |||||||||| |||||||| ||| || ||||| |||||||| ||||||| |||| || ||| ||| || |||||||| |||||||||||| ||||| ||||||||| ||| || || ||||||| ||||| || ||||||||| || ||||||||| | ||||| ||| || |||||||| |||||||||||| ||| ||||| |||| ||| || |||||||| |||||||||||||||| || ||||||||| ||||||| | ||||||||| ||| |||||||||| | |||||||| ||| |||| |||||| || |||||| ||||| |||||| ||| |||||||||| |||||||||| || ||||||| || |||||||||| || ||||||| ||||| || |||||||| || |||||||||| ||||| || ||| |||||||| |||||||||||| ||||||| |||| || ||| ||| ||| || |||||||| |||||||||||| ||||||| |||| || ||| |||.
Table 12: Patient Disposition — POETYK-1 (Screening to Week 16)
Disposition | POETYK-1 | ||
|---|---|---|---|
DEUC | PBO | APREM | |
Screened, N | 965 | ||
Randomized, N (%) | 666 (69)a | ||
Randomized per group, N | 332 | 166b | 168 |
Treated, N | 332 | 165 | 168 |
Discontinued study treatment week 0 to 16, N (%) | 25 (8) | 20 (12) | 23 (14) |
Reason for discontinuation week 0 to 16, N (%) | |||
Adverse events | 5 (2) | 7 (4) | 10 (6) |
Lost to follow-up | 7 (2) | 2 (1) | 4 (2) |
Lack of efficacy | 0 | 1 (0.6) | 1 (0.6) |
Nonadherence with protocol | 1 (0.3) | 1 (0.6) | 2 (1) |
Withdrawal by patient | 4 (1) | 3 (2) | 3 (2) |
Death | 0 | 1 (0.6) | 0 |
Other | 8 (2) | 5 (3) | 3 (2) |
FAS, N | 332 | 166 | 168 |
Safety (As-treated), N | 332 | 165 | 168 |
APREM = apremilast; DEUC = deucravacitinib; FAS = full analysis set; PBO = placebo.
||||| |||||| ||||||| ||| ||||||||| ||||||| |||| ||| |||||||| ||| ||| |||| ||||||| |||||||| ||||||||| |||||||| |||||| |||| || ||||| || ||| ||||||||| |||||||| || |||||||| |||| |||| || ||||||||||||||||||| ||||||| ||||||| || ||| ||||||||| |||||| |.
bOne patient in the placebo group was not treated. ||| ||||||| |||||||||||| ||| ||||| |||||| ||| ||||| || ||||||||| ||| || ||||||||| ||||||||||||| |||||| ||| ||| |||| ||||||||| |||||||| ||| |||| ||| |||| ||||||||.
Source: Clinical Study Report for POETYK-1.7
Table 13: Patient Disposition — POETYK-1 (Week 16 to Week 24)
Disposition | POETYK-1 | ||
|---|---|---|---|
DEUC | PBO then DEUCa | APREM | |
Continued at week 16, N | 307 | 145 | 145 |
Discontinued study treatment week 16 to 24, N (%) | | ||| | | ||| | 4 (3) |
Reason for discontinuation week 16 to 24, N (%) | |||
Adverse events | | ||||| | ||| | 1 (0.7) |
Lost to follow-up | ||| | ||| | 2 (1) |
Lack of efficacy | | ||||| | | ||| | 0 |
Nonadherence with protocol | | ||||| | ||| | 0 |
Withdrawal by patient | | ||||| | | ||||| | 1 (0.7) |
Other | | ||||| | | ||| | 0 |
APREM = apremilast; DEUC = deucravacitinib; PBO = placebo.
aAt week 16, all patients in the placebo group switched to deucravacitinib 6 mg daily until week 52.
Source: Clinical Study Report for POETYK-1.7
Table 14: Patient Disposition — POETYK-1 (Week 24 to Week 52)
Disposition | POETYK-1 | |||
|---|---|---|---|---|
DEUC | PBO then DEUCa | APREMb PASI 50 responder | APREM then DEUCb PASI 50 nonresponder | |
Continued at week 24, N | ||| | ||| | 87 | 54 |
Discontinued study treatment week 24 to 52, N (%) | || |||| | || ||| | 4 (5) | | |||| |
Reason for discontinuation week 24 to 52, N (%) | ||||
Adverse events | | ||| | ||| | 1 (1) | | ||| |
Lost to follow-up | | ||| | | ||| | 1 (1) | ||| |
Lack of efficacy | | ||| | ||| | 0 | | ||| |
Nonadherence with protocol | | ||||| | | ||||| | 0 | ||| |
Withdrawal by patient | | ||| | | ||| | 0 | | ||| |
Site terminated by sponsor | | ||||| | ||| | 0 | ||| |
Other | || ||| | | ||| | 2 (2) | | ||| |
APREM = apremilast; DEUC = deucravacitinib; PASI 50 = 50% reduction in Psoriasis Area Activity Index score; PBO = placebo.
aAt week 16 all patients randomized to the placebo group switched to deucravacitinib 6 mg daily until week 52.
bAt week 24, patients randomized to the apremilast group who met the PASI 50 response criteria continued to receive apremilast until week 52. Those who did not achieve a PASI 50 response were switched to deucravacitinib 6 mg daily.
Source: Clinical Study Report for POETYK-1.7
Table 15: Patient Disposition — POETYK-2 (Screening to Week 16)
Disposition | POETYK-2 | ||
|---|---|---|---|
DEUC | PBO | APREM | |
Screened, N | 1,519 | ||
Randomized, N (%) | 1,020 (67)a | ||
Randomized per group, N | 510b | 254b | 254 |
Treated, N | 509 | 253 | 254 |
Discontinued study treatment week 0 to 16, N (%) | 54 (11) | 42 (17) | 37 (15) |
Reason for discontinuation week 0 to 16, N (%) | |||
Adverse events | 11 (2) | 7 (3) | 12 (5) |
Lost to follow-up | 5 (1) | 6 (2) | 2 (0.8) |
Lack of efficacy | 6 (1) | 9 (4) | 4 (2) |
Nonadherence with protocol | 5 (1) | 2 (0.8) | 1 (0.4) |
Withdrawal by patient | 14 (3) | 9 (4) | 9 (4) |
Death | 0 | 0 | 1 (0.4) |
Other | 13 (3) | 9 (4) | 7 (3) |
FAS, N | 511 | 255 | 254 |
Safety (as-treated), N | 510 | 254 | 254 |
APREM = apremilast; DEUC = deucravacitinib; FAS = full analysis set; PBO = placebo; PP = per protocol.
||||| |||||| |||||| ||| ||||||||| ||||||| |||| ||| |||||||| ||| ||| |||| ||||||| |||||||| ||||||||| |||||||| |||||| |||| || ||||| || ||| ||||||||| |||||||| || |||||||| |||| |||| || ||||||||| || |||||| |||| |||||||||||| ||| |||||||||| |||||||||| || ||||||||||| |.
bOne patient was not treated.
Source: Clinical Study Report for POETYK-2.8
Table 16: Patient Disposition — POETYK-2 (Week 16 to Week 24)
Disposition | POETYK-2 | ||
|---|---|---|---|
DEUC | PBO then DEUCa | APREM | |
Continued at week 16, N | 455b | 212 | 217 |
Discontinued study treatment week 16 to 24, N (%) | 16 (4) | 9 (4) | 9 (4) |
Reason for discontinuation week 16 to 24, N (%) | |||
Adverse events | 5 (1) | 2 (0.9) | 2 (0.9) |
Lost to follow-up | 2 (0.4) | 0 | 0 |
Lack of efficacy | 4 (0.9) | 4 (2) | 1 (0.5) |
Nonadherence with protocol | 2 (0.4) | 1 (0.5) | 1 (0.5) |
Withdrawal by patient | 1 (0.2) | 1 (0.5) | 1 (0.5) |
Pregnancy | 1 (0.2) | 0 | 1 (0.5) |
Other | 1 (0.2) | 1 (0.5) | 3 (1) |
APREM = apremilast; DEUC = deucravacitinib; PBO = placebo.
aAt week 16, all patients in the placebo group switched to deucravacitinib 6 mg daily until week 52.
Source: Clinical Study Report for POETYK-2.8
Table 17: Patient Disposition — POETYK-2 (Week 24 to Week 52)
Disposition | POETYK-2 | |||||
|---|---|---|---|---|---|---|
DEUCa PASI 75 responder | DEUC then PBOa PASI 75 responder | DEUCa PASI 75 nonresponder | PBO then DEUCb | APREM then PBOc PASI 75 responder | APREM then DEUCc PASI 75 nonresponder | |
Continued at week 24, N | 148 | 150 | 142 | 203 | 97 | 111 |
Discontinued study treatment week 24 to 52, N (%) | 10 (7) | 17 (11) | 17 (12) | 22 (11) | 16 (16) | 20 (18) |
Reason for discontinuation week 24 to 52, N (%) | ||||||
Adverse events | 1 (0.7) | 2 (1) | 3 (2) | 7 (3) | 5 (5) | 3 (3) |
Lost to follow-up | 2 (1) | 3 (2) | 2 (1) | 2 (1) | 1 (1) | 3 (3) |
Lack of efficacy | 0 | 4 (3) | 3 (2) | 0 | 4 (4) | 5 (5) |
Nonadherence with protocol | 1 (0.7) | 0 | 0 | 0 | 0 | 1 (0.9) |
Withdrawal by patient | 1 (0.7) | 4 (3) | 0 | 5 (2) | 2 (2) | 2 (2) |
Pregnancy | 0 | 0 | 0 | 0 | 1 (1) | 0 |
Other | 5 (3) | 4 (3) | 9 (6) | 8 (4) | 3 (3) | 6 (5) |
APREM = apremilast; DEUC = deucravacitinib; PASI 75 = 75% reduction in Psoriasis Area Activity Index score; PBO = placebo.
aAt week 24, patients randomized to the deucravacitinib group who achieved a PASI 75 response were rerandomized to deucravacitinib or placebo. Patients who did not achieve PASI 75 response remained on deucravacitinib 6 mg daily until week 52.
bAt week 16 all patients in the placebo group switched to deucravacitinib 6 mg daily until week 52.
cAt week 24, patients randomized to the apremilast group who met the PASI 75 response criteria were switched to placebo. Patients who did not achieve PASI 75 response were switched to deucravacitinib 6 mg daily until week 52.
Source: Clinical Study Report for POETYK-2.8
Exposure to Study Treatments
|||||| ||| ||||| || ||||| || ||| ||||||| ||||||| ||| |||||| |||||||| || |||||||| ||| ||| |||| ||| ||| ||||||||| ||||||| |||| || ||||||| ||||||||| |||||||| ||||||| |||| | ||| || | ||||||| || ||| |||| | ||. Across the 52-week study period and including treatment switches, the total PYs of exposure was 419.1 and 549.9 PYs for deucravacitinib, 46.9 and 194.0 PYs for placebo, and 115.8 and 105.3 PY for apremilast in the POETYK-1 and POETYK-2 studies, respectively.
|| ||| |||||||| |||||| || |||||||| ||| ||||||||| ||||||||||| ||||||| |||| || ||| || ||| || ||||||||| |||| ||||||||||||| ||||||| ||||||| | ||| || ||||| || ||||||||| || |||||||| ||| ||||||||| ||||||||||| ||| || ||||||||| ||| ||||||||||||| |||||||| ||||| |||| ||| |||| |||| ||||||| |||| || ||| ||| ||| |||||||| || |||||||||||| |||||| |||| | |||| || || |||||.
Table 18: Duration of Exposure to Study Drug — POETYK-1 and POETYK-2 (Safety Population)
Characteristic | POETYK-1 | POETYK-2 | ||||
|---|---|---|---|---|---|---|
DEUC | PBO | APREM | DEUC | PBO | APREM | |
Week 0 to week 16, N | 332 | 165 | 168 | 510 | 254 | 254 |
Duration of exposure, mean days (SD) | 108.2 (19.9) | 103.9 (26.2) | 103.6 (26.0) | 105.5 (24.2) | 102.1 (26.8) | 104.6 (24.2) |
Duration of exposure, median days (range) | 112 (1 to 196) | 112 (2 to 126) | 112 (3 to 127) | 112 (2 to 142) | 112 (4 to 126) | 112 (7 to 133) |
Week 0 to week 52, N | 531a | 165 | 168 | 833a | 501b | 254 |
Duration of exposure, mean days (SD) | 288.3 (92.4) | 103.9 (26.2) | 251.7 (121.9) | 241.1 (101.4) | 141.4 (51.9) | 151.5 (42.1) |
Duration of exposure, median days (range) | 357 (1 to 396) | 112 (2 to 126) | 327 (3 to 392) | 251 (1 to 400) | 114 (1 to 210) | 168 (7 to 196) |
Total patient-years | 419.1 | 46.9 | 115.8 | 549.9 | 194.0 | 105.3 |
APREM = apremilast; DEUC = deucravacitinib; PBO = placebo; SD = standard deviation.
aIncludes all patients who received DEUC at any time during the 52 week study period.
bIncludes patients initially randomized to PBO and those switched from active treatment to PBO at week 24.
Source: Clinical Study Reports for POETYK-17 and POETYK-2.8
Efficacy
Only those efficacy outcomes and analyses of subgroups identified in the review protocol are reported in the following. Refer to Appendix 3 for detailed efficacy data.
Skin Clearance and Psoriasis Scores
Induction Therapy
In the POETYK-1 study, 53.6%, 7.2%, and 32.1% of patients in the deucravacitinib, placebo, and apremilast groups, respectively, met the sPGA 0 or 1 response criteria (with at least a 2-point decrease from baseline) at week 16. The between-group differences favoured deucravacitinib versus placebo (RD = 46.7%; 95% CI, 40.2% to 53.2%; P < 0.0001) and versus apremilast (RD = 21.4%; 95% CI, 12.7% to 30.1%; P < 0.0001) (Table 19).
The proportion of patients who met sPGA 0 or 1 response criteria at week 16 was 49.5%, 8.6%, and 33.9% in the deucravacitinib, placebo, and apremilast groups, respectively, in the POETYK-2 study. The between-group RD was 40.9% (95% CI, 35.4% to 46.4%) for deucravacitinib versus placebo, and 15.8% (95% CI, 8.8% to 22.9%) versus apremilast. For both comparisons, the difference favoured deucravacitinib with P values less than 0.0001.
For both studies, the results for the proportion of patients with an sPGA score of 0 at week 16 also favoured deucravacitinib versus placebo and versus apremilast, with P values below the testing boundary (Table 19).
Data on the PASI response at week 16 are reported in Table 20. In the POETYK-1 study, 58.4%, 12.7%, and 35.1% of patients achieved PASI 75 response at week 16 in the deucravacitinib, placebo, and apremilast groups, respectively, with a RD of 46.1% (95% CI, 38.9% to 53.2%) for deucravacitinib versus placebo (P < 0.0001), and 23.0% (95% CI, 14.1% to 31.8%) versus apremilast (P < 0.0001). The results were similar in the POETYK-2 study with 53.0%, 9.4%, and 39.8% of patients in the deucravacitinib, placebo, and apremilast groups, respectively, achieving a PASI 75 response at week 16. The RD was 43.7% (95% CI, 38.0% to 49.3%; P < 0.0001) for deucravacitinib versus placebo, and 13.4% (95% CI, 6.2% to 20.7%; P = 0.0004) versus apremilast.
The results of the key secondary outcomes, PASI 90 and PASI 100 at week 16, favoured deucravacitinib versus placebo in both studies. In addition, the PASI 90 response also favoured deucravacitinib versus apremilast at week 16. The proportion of patients who achieved a PASI 90 response ranged from 27.0% to 35.5% in the deucravacitinib groups, 2.7% to 4.2% in the placebo groups and 18.1% to 19.6% in the apremilast groups. Few patients in any group achieved a PASI 100 response at week 16 (deucravacitinib: 10.2% to 14.2%, apremilast: 3.0% to 4.3%, placebo: 1%) and although numerically the proportion of responders was higher for deucravacitinib versus apremilast, this comparison was not controlled for type I error rate.
In both studies the results of the sensitivity analyses for the coprimary end points showed results that were supportive of the primary efficacy analyses. The subgroup analyses also reported sPGA 0 or 1 and PASI 75 response results that were consistent for patients based on prior biologic therapy (yes or no), prior systemic therapy (yes or no), baseline sPGA score (moderate or severe), and baseline PASI score (≤ 20 or > 20) (Appendix 3, Table 39, and Table 40).
Both studies reported 16-week response data for the subgroup of patients that had moderate to severe scalp or fingernail psoriasis at baseline. Approximately two-thirds of patients enrolled had scalp psoriasis at baseline (60% to 73% per treatment group), with only 10% to 20% of patients reporting fingernail psoriasis at the start of the trials. Among those with scalp psoriasis, the proportion of responders who achieved an ss-PGA score of 0 or 1 at week 16 favoured deucravacitinib versus placebo in the POETYK-1 study (RD = 52.8%; 95% CI, 43.7% to 62.0%) and the POETYK-2 study (RD = 42.3%; 95% CI, 34.3% to 50.3%), both with P values of less than 0.0001. The 16-week differences also favoured deucravacitinib versus apremilast in both studies with a P value of less than 0.0001 (POETYK-1: RD = 29.6%; 95% CI, 18.7% to 40.6%; POETYK-2: RD = 23.5%; 95% CI, 14.3% to 32.6%) (Appendix 3, Table 41). Neither study detected a difference between deucravacitinib and placebo or apremilast in the proportion of patients who achieved a Physician’s Global Assessment–Fingernail score of 0 or 1 at week 16.
The POETYK-1 and POETYK-2 studies reported the proportion of patients who achieved a sPGA 0 or 1, PASI 75, or PASI 90 response at week 24 in the deucravacitinib versus apremilast groups. All comparisons favoured deucravacitinib versus apremilast with absolute differences of 20.4% to 27.5% for an sPGA 0 or 1 response, 21.1% to 31.0% for PASI 75, and 13.0% to 20.0% for PASI 90 response at week 24, (all comparisons with a P value of less than 0.0001). Full details are shown in Appendix 3, Table 42.
Table 19: sPGA Response at Week 16 — POETYK-1 and POETYK-2 (FAS)
Outcome | POETYK-1 | POETYK-2 | ||||
|---|---|---|---|---|---|---|
DEUC n = 332 | PBO n = 166 | APREM n = 168 | DEUC n = 511 | PBO n = 255 | APREM n = 254 | |
Number of patients contributing to the analysis | 332 | 166 | 168 | 511 | 255 | 254 |
sPGA 0 or 1 at week 16a,b | ||||||
Responders, n (%) | 178 (53.6) | 12 (7.2) | 54 (32.1) | 253 (49.5) | 22 (8.6) | 86 (33.9) |
DEUC vs. PBO | ||||||
RD (95% CI) | 46.7 (40.2 to 53.2) | Reference | NA | 40.9 (35.4 to 46.4) | Reference | NA |
OR (95% CI), P value | 18.71 (9.51 to 36.81), < 0.0001 | Reference | NA | 10.55 (6.54 to 17.00), < 0.0001 | Reference | NA |
DEUC vs. APREM | ||||||
RD (95% CI) | 21.4 (12.7 to 30.1) | Reference | Reference | 15.8 (8.8 to 22.9) | NA | Reference |
OR (95% CI), P value | 2.53 (1.70 to 3.78), < 0.0001c | NA | Reference | 2.01 (1.45 to 2.78), < 0.0001c | NA | Reference |
sPGA 0 at week 16a,b | ||||||
Responders, n (%) | 58 (17.5) | 1 (0.6) | 8 (4.8) | 80 (15.7) | 3 (1.2) | 16 (6.3) |
DEUC vs. PBO | ||||||
RD (95% CI) | 17.1 (12.8 to 21.3) | Reference | NA | 14.5 (11.0 to 17.9) | Reference | NA |
OR (95% CI), P value | Reference | Reference | NA | Reference | Reference | NA |
DEUC vs. APREM | ||||||
RD (95% CI) | 12.9 (7.7 to 18.0) | NA | Reference | 9.4 (5.1 to 13.7) | NA | Reference |
OR (95% CI), P value | 4.52 (2.07 to 9.84), < 0.0001c | NA | Reference | 2.85 (1.61 to 5.03), 0.0002c | NA | Reference |
APREM = apremilast; CI = confidence interval; DEUC = deucravacitinib; FAS = full analysis set; NA = not applicable; OR = odds ratio; PBO = placebo; RD = risk difference; sPGA = static Physician’s Global Assessment; vs. = versus.
Note: For the coprimary end point (sPGA 0 or 1) in the POETYK-1 study, 8%, 13%, and 13% of patients in the DEUC, PBO, and APREM groups, respectively, had stopped treatment or had missing data at week 16 and had data imputed as nonresponders. In POETYK-2 study, 11%, 16%, and 14% of patients in the DEUC, PBO, and APREM groups, respectively, had data imputed.
aCochran-Mantel-Haenszel test stratified by geographic region, body weight, and prior biologic use. Nonresponder imputation for missing data.
bPatients must also have at least a 2-point improvement in their sPGA score vs. baseline.
cTested using a 2-sided alpha of 0.025.
Table 20: PASI Response at Week 16 — POETYK-1 and POETYK-2 (FAS)
Outcome | POETYK-1 | POETYK-2 | ||||
|---|---|---|---|---|---|---|
DEUC n = 332 | PBO n = 166 | APREM n = 168 | DEUC n = 511 | PBO n = 255 | APREM n = 254 | |
Number of patients contributing to the analysis | 332 | 166 | 168 | 511 | 255 | 254 |
PASI 75 response at week 16a | ||||||
Responders, n (%) | 194 (58.4) | 21 (12.7) | 59 (35.1) | 271 (53.0) | 24 (9.4) | 101 (39.8) |
DEUC vs. PBO | ||||||
RD (95% CI) | 46.1 (38.9 to 53.2) | Reference | NA | 43.7 (38.0 to 49.3) | Reference | NA |
OR (95% CI), P value | 11.09 (6.49 to 18.95), < 0.0001 | Reference | NA | 10.49 (6.65 to 16.55), < 0.0001 | Reference | NA |
DEUC vs. APREM | ||||||
RD (95% CI) | 23.0 (14.1 to 31.8) | NA | Reference | 13.4 (6.2 to 20.7) | NA | Reference |
OR (95% CI), P value | 2.64 (1.78 to 3.91), < 0.0001b | NA | Reference | 1.76 (1.29 to 2.41), 0.0004b | NA | Reference |
PASI 90 response at week 16a | ||||||
Responders, n (%) | 118 (35.5) | 7 (4.2) | 33 (19.6) | 138 (27.0) | 7 (2.7) | 46 (18.1) |
DEUC vs. PBO | ||||||
RD (95% CI) | 31.6 (25.8 to 37.5) | Reference | NA | 24.3 (19.9 to 28.7) | Reference | NA |
OR (95% CI), P value | ||||| ||||| || ||||||| ||||||||| | ||| | || | ||||| ||||| || ||||||| |||||||| | | ||| | || |
DEUC vs. APREM | ||||||
RD (95% CI) | 15.8 (8.2 to 23.5) | NA | Reference | 9.0 (3.1 to 14.9) | NA | Reference |
OR (95% CI), P value | |||| ||||| || |||||| |||||||| | | || | ||| | |||| ||||| || |||||| |||||||| | | || | ||| |
PASI 100 response at week 16a | ||||||
Responders, n (%) | 47 (14.2) | 1 (0.6) | 5 (3.0) | 52 (10.2) | 3 (1.2) | 11 (4.3) |
DEUC vs. PBO | ||||||
RD (95% CI) | 13.7 (9.8 to 17.6) | Reference | NA | 9.0 (6.0 to 11.9) | Reference | NA |
OR (95% CI), P value | |||| ||||| || |||||||| ||||||||| | ||| | || | |||| ||||| || ||||||| |||||||| | | ||| | || |
DEUC vs. APREM | ||||||
RD (95% CI) | 11.3 (6.8 to 15.8) | NA | Reference | 5.9 (2.3 to 9.4) | NA | Reference |
OR (95% CI), P value | |||| ||||| || ||||||| ||||||||| | || | ||| | |||| ||||| || |||||| ||||||||| | || | ||| |
APREM = apremilast; CI = confidence interval; DEUC = deucravacitinib; FAS = full analysis set; NA = not applicable; OR = odds ratio; PASI 75 = 75% reduction in Psoriasis Area and Severity Index score; PASI 90 = 90% reduction in Psoriasis Area and Severity Index score; PASI 100 = 100% reduction in Psoriasis Area and Severity Index score; PBO = placebo; RD = risk difference; vs. = versus.
Note: For the coprimary end point (PASI 75) in the POETYK-1 study, 8%, 13%, and 13% of patients in the DEUC, PBO, and APREM groups, respectively, had stopped treatment or had missing data at week 16 and had data imputed as nonresponders. In POETYK-2 study, 11%, 16%, and 14% of patients in the DEUC, PBO, and APREM groups, respectively, had data imputed.
aCochran-Mantel-Haenszel test stratified by geographic region, body weight, and prior biologic use. Nonresponder imputation for missing data.
bTested using a 2-sided alpha of 0.025.
cP value has not been adjusted for multiple testing (i.e., the type I error rate has not been controlled).
Maintenance Therapy
In the POETYK-1 study, patients in the apremilast group who achieved at least a PASI 50 response at week 24 continued to receive apremilast until week 52, whereas patients randomized to deucravacitinib remained on this therapy until week 52, regardless of the 24-week treatment response. Maintenance of treatment response was analyzed based on the proportion of patients who achieved an sPGA 0 or 1 response, PASI 75, or PASI 90 response at week 24 and week 52 in the full analysis set (i.e., intention-to-treat population with nonresponder imputation for patients with missing data or who had stopped the study drug) (Table 21). The proportion of patients who maintained sPGA 0 or 1 response favoured deucravacitinib (45.5%) versus apremilast (22.2%) with an absolute difference of 23.0% (95% CI, 14.9% to 31.1%; P < 0.0001). PASI response rates also favoured deucravacitinib versus apremilast. PASI 75 response at week 24 and week 52 was achieved by 56.3% and 30.5% of patients in the deucravacitinib and apremilast groups, respectively, and the absolute difference was 25.5% (95% CI, 16.9% to 34.0%; P < 0.0001). PASI 90 response was reported in 31.0% and 15.6% of patients in the deucravacitinib and apremilast groups, respectively, and the absolute difference was 15.2% (95% CI, 8.0% to 22.4%; P = 0.0002).
In the POETYK-2 study, maintenance of treatment response (at week 24 and week 52) was reported for patients in the deucravacitinib group who achieved at least a PASI 75 response at week 24 and were rerandomized to receive deucravacitinib or placebo during the maintenance phases of the trial. Among patients who continued on deucravacitinib, 72% achieved an sPGA 0 or 1 response at week 24 and week 52, compared with 23.5% of patients switched to placebo (absolute difference 47.8%; 95% CI, 36.6% to 59.0%) (Table 22). PASI 75 response at week 24 and week 52 was achieved by 82.1% versus 31.3% among patients who received maintenance deucravacitinib versus placebo, with an absolute difference of 50.6% (95% CI, 40.9% to 60.4%). These data were reported descriptively, with no statistical testing performed.
Table 21: Maintenance of sPGA and PASI Response at Week 52 — POETYK-1 (FAS)
Outcome | POETYK-1 | |
|---|---|---|
DEUC n = 332 | APREMa n = 168 | |
Number of patients contributing to the analysis | 332 | 167 |
sPGA 0 or 1 at week 24 and week 52b,c | ||
Responders, n (%) | 151 (45.5) | 37 (22.2) |
RD (95% CI) | 23.0 (14.9 to 31.1) | Reference |
|| |||| |||| | ||||| | |||| ||||| || |||||| ||||||||| | ||| |
PASI 75 response at week 24 and week 52b | ||
Responders, n (%) | 187 (56.3) | 51 (30.5) |
RD (95% CI) | 25.5 (16.9 to 34.0) | Reference |
|| |||| |||| | ||||| | |||| ||||| || |||||| ||||||||| | ||| |
PASI 90 response at week 24 and week 52b | ||
Responders, n (%) | 103 (31.0) | 26 (15.6) |
RD (95% CI) | 15.2 (8.0 to 22.4) | Reference |
|| |||| |||| | ||||| | |||| ||||| || |||||| ||||||||| | ||| |
APREM = apremilast; CI = confidence interval; DEUC = deucravacitinib; FAS = full analysis set; NA = not applicable; OR = odds ratio; PASI = Psoriasis Area and Severity Index; PASI 50 = 50% reduction in Psoriasis Area and Severity Index score; PASI 75 = 75% reduction in Psoriasis Area and Severity Index score; PASI 90 = 90% reduction in Psoriasis Area and Severity Index score; PBO = placebo; RD = risk difference; sPGA = static Physician’s Global Assessment.
aPatients in the APREM group who did not achieve a PASI 50 response at week 24 were switched to DEUC. Patients with at least a PASI 50 response, continued on APREM.
bCochran-Mantel-Haenszel test stratified by geographic region, body weight, and prior biologic use. Nonresponder imputation for missing data.
cPatients must also have at least a 2-point improvement in their sPGA score versus baseline.
dTested using a 2-sided alpha of 0.025.
Source: Clinical Study Report for POETYK-1.7
Table 22: Maintenance of sPGA and PASI Response at Week 52 — POETYK-2 (FAS)
Outcome | POETYK-2 | |
|---|---|---|
DEUC n = 148a | DEUC then PBO n = 150a | |
sPGA 0 or 1 at week 24 and 52 | ||
Number of patients contributing to the analysis | 118 | 119 |
Responders, n (%) | 85 (72.0) | 28 (23.5) |
RD (95% CI) | 47.8 (36.6 to 59.0) | Reference |
PASI 75 response at week 24 and 52 | ||
Number of patients contributing to the analysis | 145 | 150 |
Responders, n (%) | 119 (82.1) | 47 (31.3) |
RD (95% CI) | 50.6 (40.9 to 60.4) | Reference |
CI = confidence interval; DEUC = deucravacitinib; FAS = full analysis set; PASI = Psoriasis Area and Severity Index; PASI 75 = 75% reduction in Psoriasis Area and Severity Index score; PBO = placebo; RD = risk difference; sPGA = static Physician’s Global Assessment.
aAmong patients initially randomized to DEUC who achieved at least a PASI 75 response at week 24 and who were rerandomized to DEUC or PBO.
Source: Clinical Study Reports for POETYK-17 and POETYK-2.8
Relapse
In the POETYK-2 study, time to relapse was tested for patients in the deucravacitinib group who achieved a PASI 75 response at week 24 and were rerandomized to deucravacitinib or placebo. Among responders, |||| of patients who remained on deucravacitinib experienced a relapse, compared with ||||| who were switched to placebo |||||||||| (Table 23). Of note, this outcome was controlled for multiple testing based on the global statistical testing procedure but not the US statistical hierarchy.
Relapse was reported by ||||| of patients who achieved a PASI 75 response with apremilast and were then switched to placebo, with a median time to relapse of ||| |||| |||| || ||| |||| || ||| |||||||||||.
Table 23: Time to Relapse Among Patients With PASI 75 Response at Week 24 — POETYK-2 (FAS)
Outcome | DEUC responders | APREM responders | |
|---|---|---|---|
DEUC then PBO n = 150 | DEUC n = 145 | APREM then PBO n = 95 | |
Relapse after week 24, n (%) | 68 (45.3) | 8 (5.5) | 48 (50.5) |
Censored, n (%) | 82 (54.7) | 137 (94.5) | 47 (49.5) |
Time to relapsea, median days (95% CI) | NE | NE | 197.0 (125.0 to NE) |
P value DEUC vs. PBO | Reference | < 0.0001b | NA |
APREM = apremilast; CI = confidence interval; DEUC = deucravacitinib; FAS = full analysis set; NA = not applicable; NE = not estimable; PASI = Psoriasis Area and Severity Index; PASI 75 = 75% reduction in Psoriasis Area and Severity Index score; PBO = placebo.
aRelapse was defined as at least a 50% loss of week 24 PASI percent improvement from baseline in the 224 day period after the week 24 visit. The analyses included patients who achieved PASI 75 response at week 24. The time to relapse was based on the Kaplan-Meier product limit method, with P value based on a log-rank test that was stratified by geographic region, body weight, and prior biologic use. Patients who had a relapse after the 224 day follow-up period were censored at day 224.
bTested at the alpha 0.025 level in the global testing hierarchy. This end point was not controlled for type I error rate according to the US testing hierarchy.
Source: Clinical Study Report for POETYK-2.8
Health-Related Quality of Life
HRQoL was measured using the disease-specific DLQI questionnaire, as well as the generic instruments, EQ-5D VAS and SF-36. The analyses of the change from baseline in the SF-36 and EQ-5D VAS scores were not controlled for type I error rate. A MID of at least 3 points for the SF-36 PCS or MCS has been reported in the literature.49,50 In patients with psoriasis, MID estimates for the EQ-5D VAS range from 3.82 to 8.43 using anchor-based methods and was 10.34 based on distributional methods.45 Not all randomized patients were included in these analyses. At week 16, the DLQI response analyses were missing 3% to 4%, ||| ||||| ||||| |||||||| |||| ||||||| || || || || |||||||| ||| ||||||||| ||||||.
The proportion of patients who achieved a DLQI score of 0 or 1 at week 16 (classified as no impact of disease on HRQoL) was 41.0%, 10.6%, and 28.6% for the POETYK-1 study and 37.6%, 9.8%, and 23.1% for the POETYK-2 study in the deucravacitinib, placebo, and apremilast groups, respectively. The between-group differences favoured deucravacitinib versus placebo, with P values less than 0.0001. Although numerically more patients reported a DLQI response in the deucravacitinib group than in the apremilast group, this comparison was not controlled for type I error rate (Table 24).
||| ||||||| ||||| |||||||||| || ||| |||||| |||| |||||||| || ||| ||||| ||| ||| ||| || |||| || |||||| |||||| ||| || |||| |||||||| ||| ||||| || ||| |||||| ||| ||||||| ||||| |||||| |||| |||||||| ||| ||| |||||| ||| ||||||| ||| |||||||| || ||| |||||||||| | ||||| ||| ||| |||||| |||| |||||||| || |||| || || ||| ||||| |||| ||| ||||| |||||| |||| |||| |||||| || ||| ||||||||||||||| ||||| ||| ||||||||| ||||||| || ||| ||||||||||||||| |||||| |||||| ||||||| ||||||| ||| |||| ||| |||||||| ||||| |||||| ||||||| ||||| ||||||||||| |||| |||||||| ||| |||||| ||| |||||||| ||||| ||||||| |||||||| || ||| ||||||||||| || |||||||| || ||||||||||||| ||||||||||| |||||||||| ||| |||||||| ||||||| ||||||||||||||| |||||| |||||||||| || ||| |||||| || ||| |||||| ||| ||| ||||||| ||||| |||||||||| || |||||||| ||| ||| |||||| ||| |||||| ||| ||||| | ||.
Table 24: DLQI Score 0 or 1 at Week 16 — POETYK-1 and POETYK-2 (FAS)
Outcome | POETYK-1 | POETYK-2 | ||||
|---|---|---|---|---|---|---|
DEUC n = 332 | PBO n = 166 | APREM n = 168 | DEUC n = 511 | PBO n = 255 | APREM n = 254 | |
DLQI Score 0 or 1 at week 16a,b | ||||||
Number of patients contributing to the analysis | 322 (97) | 160 (96) | 161 (96) | 495 (97) | 246 (96) | 247 (97) |
Responders, n (%) | 132 (41.0) | 17 (10.6) | 46 (28.6) | 186 (37.6) | 24 (9.8) | 57 (23.1) |
DEUC vs. PBO | ||||||
RD (95% CI) | 30.5 (23.4 to 37.6) | Reference | NA | 27.9 (22.2 to 33.7) | Reference | NA |
OR (95% CI), P value | 6.04 (3.46 to 10.53), < 0.0001c | Reference | NA | 5.38 (3.42 to 8.47), < 0.0001c | Reference | NA |
DEUC vs. APREM | ||||||
RD (95% CI) | 12.3 (3.4 to 21.1) | NA | Reference | 14.6 (7.8 to 21.3) | NA | Reference |
OR (95% CI), P value | 1.73 (1.15 to 2.60), 0.0088d | NA | Reference | 2.01 (1.42 to 2.85), < 0.0001d | NA | Reference |
APREM = apremilast; CI = confidence interval; DEUC = deucravacitinib; DLQI = Dermatology Life Quality Index; FAS = full analysis set; NA = not applicable; OR = odds ratio; PBO = placebo; RD = risk difference; vs. = versus.
aCochran-Mantel-Haenszel test stratified by geographic region, body weight, and prior biologic use. Nonresponder imputation for missing data.
bAnalyzed in patients with a baseline DLQI score of at least 2.
cTested at the alpha 0.025 level in the global testing hierarchy. This end point was not controlled for type I error rate according to the US testing hierarchy.
dP value has not been adjusted for multiple testing (i.e., the type I error rate has not been controlled).
Source: Clinical Study Reports for POETYK-17 and POETYK-2.8
Table 25: Change in EQ-5D and SF-36 at Week 16 — POETYK-1 and POETYK-2 (FAS)
Outcome | POETYK-1 | POETYK-2 | ||||
|---|---|---|---|---|---|---|
DEUC n = 332 | PBO n = 166 | APREM n = 168 | DEUC n = 511 | PBO n = 255 | APREM n = 254 | |
SF-36 MCS change from baseline to week 16a | ||||||
Number of patients contributing to the analysis, (%) | ||| |||| | ||| |||| | ||| |||| | ||| |||| | ||| |||| | ||| |||| |
Baseline, mean (SD) | |||| ||||| | |||| ||||| | |||| ||||| | |||| ||||| | |||| ||||| | |||| ||||| |
Week 16, mean (SD) | |||| ||||| | |||| ||||| | |||| ||||| | |||| ||||| | |||| ||||| | |||| ||||| |
Change from baseline to week 16, LS mean (SE) | ||| ||||| | ||| ||||| | ||| ||||| | ||| ||||| | |||| ||||| | ||| ||||| |
DEUC vs. PBO | ||||||
LS mean difference (95% CI) | ||| |||| || |||| ||||||| | ||| | || | ||| |||| |||| |||||| | | ||| | || |
DEUC vs. APREM | ||||||
LS mean difference (95% CI) | ||| |||| || ||||||||||| | | || | ||| | |||| ||||| ||||||||| | | || | ||| |
SF-36 PCS change from baseline to week 16a | ||||||
Number of patients contributing to the analysis | ||| |||| | ||| |||| | ||| |||| | ||| |||| | ||| |||| | ||| |||| |
Baseline, mean (SD) | |||| ||||| | |||| ||||| | |||| ||||| | |||| ||||| | |||| ||||| | |||| ||||| |
Week 16, mean (SD) | |||| ||||| | |||| ||||| | |||| ||||| | |||| ||||| | |||| ||||| | |||| ||||| |
Change from baseline to week 16, LS mean (SE) | ||| ||||| | ||| ||||| | ||| ||||| | ||| ||||| | ||| ||||| | ||| ||||| |
DEUC vs. PBO | ||||||
LS mean difference (95% CI) | ||| ||||| |||| |||||||| | | ||| | || | ||| ||||| ||| |||||| | | ||| | || |
DEUC vs. APREM | ||||||
LS mean difference (95% CI) | ||| |||||| ||||| ||||||| | || | ||| | ||| ||| || | ||||||| | | || | ||| |
EQ-5D VAS change from baseline to week 16a | ||||||
Number of patients contributing to the analysis | ||| |||| | ||| |||| | ||| |||| | ||| |||| | ||| |||| | ||| |||| |
Baseline, mean (SD) | |||| |||||| | |||| |||||| | |||| |||||| | |||| |||||| | |||| |||||| | |||| |||||| |
Week 16, mean (SD) | |||| |||||| | |||| |||||| | |||| |||||| | |||| |||||| | |||| |||||| | |||| |||||| |
Change from baseline to week 16, LS mean (SE) | ||| ||||| | ||| ||||| | ||| ||||| | ||| ||||| | ||| ||||| | ||| ||||| |
DEUC vs. PBO | ||||||
LS mean difference (95% CI) | ||| ||| || ||||| ||||||||| | ||| | || | ||| || || ||||||||||| | ||| | || |
DEUC vs. APREM | ||||||
LS mean difference (95% CI) | ||| ||| || ||||| ||||||| | | || | ||| | ||| ||| ||||| |||| | | || | ||| |
APREM = apremilast; CI = confidence interval; DEUC = deucravacitinib; FAS = full analysis set; LS = least squares; MCS = Mental Component Score; PBO = placebo; PCS = Physical Component Score; RD = risk difference; SD = standard deviation; SE = standard error; SF-36 = Short Form (36) Health Survey; VAS = visual analogue scale; vs. = versus.
aAnalysis of covariance model with factors for geographic region, body weight, and prior biologic use, and baseline value as covariate (modified baseline observation carried forward for missing data).
bP value has not been adjusted for multiple testing (i.e., the type I error rate has not been controlled).
Source: Clinical Study Reports for POETYK-17 and POETYK-2.8
Symptoms
The patient-reported PSSD symptom questionnaire was used to evaluate symptom severity in both studies. PSSD symptom score includes 5 symptoms (itch, pain, stinging, burning, and skin tightness) and is scored from 0 to 100 with 0 indicating a complete absence of symptoms. A 9.1-point MID has been reported for the 7-day version of the PSSD symptoms score.43 Of note, 6% to 10% of patients per treatment group were missing from these analyses.
Among patients who have a baseline PSSD symptom score of at least 1, the proportion of patients who had a symptom score of 0 at week 16 was 7.9%, 0.7%, and 4.4% in the POETYK-1 study and 7.5%, 1.3%, and 4.3% in the POETYK-2 study in the deucravacitinib, placebo, and apremilast groups, respectively (Table 26). The differences favoured deucravacitinib versus placebo, but with no statistically significant difference detected versus apremilast in both studies.
The LS mean difference the change from baseline in the PSSD symptom score was ||||| ||| ||||| for deucravacitinib versus placebo, and −8.8 and −7.2 for deucravacitinib versus apremilast, respectively in the POETYK-1 and POETYK-2 studies. While the comparisons with apremilast were part of the statistical testing hierarchy and were controlled for multiplicity, the between-group difference did not exceed MID estimates. There was no control of the type I error rate for the comparison with placebo.
Table 26: PSSD Symptoms Score 0 at Week 16 — POETYK-1 and POETYK-2 (FAS)
Outcome | POETYK-1 | POETYK-2 | ||||
|---|---|---|---|---|---|---|
DEUC n = 332 | PBO n = 166 | APREM n = 168 | DEUC n = 511 | PBO n = 255 | APREM n = 254 | |
PSSD symptom score 0 at week 16a,b | ||||||
Number of patients contributing to the analysis (%) | 305 (92) | 149 (90) | 158 (94) | 466 (91) | 238 (93) | 232 (91) |
Responders, n (%) | 24 (7.9) | 1 (0.7) | 7 (4.4) | 35 (7.5) | 3 (1.3) | 10 (4.3) |
DEUC vs. PBO | ||||||
RD (95% CI) | 7.4 (4.1 to 10.7) | Reference | NA | 6.2 (3.4 to 8.9) | Reference | NA |
OR (95% CI), P value | 13.67 (1.77 to 105.50), 0.0013c | Reference | NA | 6.40 (1.94 to 21.15), 0.0005c | Reference | NA |
DEUC vs. APREM | ||||||
RD (95% CI) | 3.3 (−1.0 to 7.7) | NA | Reference | 3.3 (−0.3 to 6.9) | NA | Reference |
OR (95% CI), P value | 1.84 (0.76 to 4.42), 0.17c | NA | Reference | 1.82 (0.89 to 3.71), 0.093c | NA | Reference |
PSSD symptom score change from baseline to week 16d | ||||||
Number of patients contributing to the analysis | 306 (92) | 151 (91) | 158 (94) | 466 (91) | 239 (94) | 233 (92) |
Baseline, mean (SD) | 51.7 (25.2) | 51.4 (26.8) | 56.2 (25.2) | 52.3 (26.3) | 50.1 (24.8) | 51.9 (25.4) |
Week 16, mean (SD) | 22.4 (22.1) | 45.3 (28.8) | 33.8 (25.0) | 23.5 (24.0) | 45.6 (26.3) | 31.1 (26.3) |
Change from baseline to week 16, LS mean (SE) | −26.7 (1.8) | −3.6 (−2.1) | −17.8 (2.2) | −28.3 (1.1) | −4.7 (1.4) | −21.1 (1.4) |
DEUC vs. PBO | ||||||
LS mean difference (95% CI), P value | −23.1 (−27.0 to −19.1), < 0.0001e | Reference | NA | −23.6 (−26.9 to −20.3), < 0.0001e | Reference | NA |
DEUC vs. APREM | ||||||
LS mean difference (95% CI), P value | −8.8 (−12.8 to −4.9), < 0.0001c | NA | Reference | −7.2 (−10.5 to −3.9), < 0.0001c | NA | Reference |
APREM = apremilast; CI = confidence interval; DEUC = deucravacitinib; FAS = full analysis set; LS = least squares; NA = not applicable; OR = odds ratio; PBO = placebo; PSSD = Psoriasis Symptoms and Signs Diary; RD = risk difference; SD = standard deviation; SE = standard error; vs. = versus.
aCochran-Mantel-Haenszel test stratified by geographic region, body weight, and prior biologic use. Nonresponder imputation for missing data.
bIn the subgroup of patients with a baseline PSSD score of at least 1.
cTested using a 2-sided alpha of 0.025.
dAnalysis of covariance model with factors for geographic region, body weight, and prior biologic use, and baseline value as covariate (modified best observation carried forward for missing data).
eP value has not been adjusted for multiple testing (i.e., the type I error rate has not been controlled).
Source: Clinical Study Reports for POETYK-17 and POETYK-2.8
Harms
Only those harms identified in the review protocol are reported in the following. Refer to Table 27 and Table 28 for detailed harms data.
Adverse Events
During the first 16 weeks of the POETYK-1 and POETYK-2 studies, 53% and 58% of patients in the deucravacitinib groups reported an AE compared with 42% and 54% of patients who received placebo, and 55% and 59% who received apremilast. The most commonly reported events in the deucravacitinib group were nasopharyngitis (6% to 11%), upper respiratory tract infection (5% to 6%), diarrhea and headache (each reported in 4% to 5%), and in the apremilast groups, nausea and diarrhea (9% to 13%), headache (10% to 11%), and nasopharyngitis (8% to 9%) were most common. In the placebo group, 4% to 11% of patients reported nasopharyngitis, 4% reported upper respiratory tract infection, 4% to 8% reported diarrhea and 3% to 6% reported headache.
For the 52-week study period, the AE IR was similar in the deucravacitinib (212 events per 100 PY) and apremilast groups (234 per 100 PY) in the POETYK-1 study, and for the deucravacitinib (242 per 100 PY) and placebo groups (222 per 100 PY) in the POETYK-2 study, but higher in the apremilast group (330 per 100 PY) in the POETYK-2 study.
Serious Adverse Events
In the first 16 weeks of the POETYK-1 study, 7 patients (2%), 9 patients (5%), and 4 patients (2%) reported a SAE in the deucravacitinib, placebo, and apremilast groups, respectively. In the POETYK-2 study, 8 patients (2%), 3 patients (1%), and 1 patient (0.4%) in the deucravacitinib, placebo, and apremilast groups, respectively, experienced a SAE. No specific events were reported in 2 patients or more up to week 16.
Over the entire POETYK-1 study duration, the exposure-adjusted IR for SAEs was 7.5 and 5.2 events per 100 PYs in the deucravacitinib and apremilast groups, respectively. The exposure-adjusted IR in the POETYK-2 study was 4.3 per 100 PYs in the deucravacitinib group compared with 2.5 and 2.8 per 100 PYs in the placebo and apremilast groups. Events that were reported in 2 or more patients in the deucravacitinib groups included pericarditis (2 patients in the POETYK-1 study), cholecystitis acute (2 patients in the POETYK-1 study), and pneumonia (3 patients the POETYK-2 study). No other SAEs were reported in 2 or more patients per group.
Withdrawals Due to AEs
The proportion of patients who stopped treatment due to AEs was 2% and 3% for deucravacitinib, 4% for placebo, and 5% and 6% for apremilast during the first 16 weeks in the POETYK-1 and POETYK-2 studies. In the POETYK-1 study, no events were reported in more than 1 patient in the deucravacitinib or placebo groups | || ||||||||| |||||||||| |||||||||| |||| |||||||||| ||||||||| |||||||| ||| ||||||| ||| || ||||||||||||||| || ||||||||||||||| || | || |||| ||||||||. In the placebo group of the POETYK-2 study, 3 patients stopped therapy due to psoriasis. In both studies gastrointestinal AEs were the most common reason for stopping therapy in the apremilast groups.
The 52-week IR for withdrawals due to AEs was 3.3 and 10.3 per 100 PYs in the deucravacitinib and apremilast groups, respectively, in the POETYK-1 study, and 5.2, 8.0, 13.1 per 100 PYs in the deucravacitinib, placebo, and apremilast groups in the POETYK-2 study. Two patients in the deucravacitinib group,1 patient in the apremilast group, and no patients in the placebo group stopped treatment due to increased creatinine kinase levels in the POETYK-2 study. No patients in the POETYK-1 study stopped therapy due to increase creatinine kinase levels.
Mortality
In the POETYK-1 study, 1 patient in the placebo group died of hypertensive cardiovascular disease. No deaths were reported in the deucravacitinib and apremilast groups.
There were 3 deaths during the 52 week POETYK-2 study, including 1 patient of heart failure and sepsis, and 1 patient due to hepatocellular carcinoma, both in the deucravacitinib group, and 1 patient in the apremilast group due to lung cancer and gastrointestinal hemorrhage.
Notable Harms
During the first 16 weeks of the studies, infections and infestations SOC were reported || ||| || ||| || |||||||| || ||| ||||||||||||||| ||||||| ||| || ||| || ||| ||||||| |||||| ||| ||| || ||| || ||| |||||||||| |||||||. Overall, the IR of infections and infestations SOC was |||| ||| ||||| |||||| ||| ||| || ||| |||||||| ||||||||| |||||||||||||||| ||| |||| ||| |||| ||| ||| || ||| ||||| ||||||||| ||||||||||| ||| |||||||| || ||| |||||| ||||||||||| || ||||||||| || ||||||||||| |||| ||| | ||||||| ||||||| |||||| ||| ||||| |||| || ||||||||||||| |||||||||| || |||||||||||| |||||| |||||||| || |||||| |||||||. With regards to adjudicated major adverse cardiovascular events, a total of | |||||| ||||||||||| ||||||||||| |||||||| ||||||| ||||||| ||||||| ||| ||||||||||||||| ||||||||| |||| |||||||| ||||| |||||||| ||| |||||||| ||||||||||||||| || |||||| |||||| ||||| |||||||| || ||| ||||||| |||||| |||||||| |||| |||||| || ||||| |||||||||| ||||||||||| |||||||||||| ||||| ||||||| ||| |||||||| ||||||| ||| | |||||||| || ||| |||||||||| |||||| |||||||| |||||||| |||||| || ||||||||| ||| |||||||||| |||||||||||. No adjudicated thromboembolic SAEs occurred in the POETYK-2 study, and 1 patient experienced a pulmonary embolism in the deucravacitinib group in the POETYK-1 study. Other thromboembolic events reported included ischemic clot of right leg, and thrombosis of right radial vein in 2 patients receiving deucravacitinib, and thrombosis of superficial vein of lower limb in a patient receiving apremilast in the POETYK-2 study.
||| | |||||||||||| || |||||||| ||||| |||| |||||||| || ||| ||||||||||||||| |||||| |||||| |||||||| |||||||| |||||| ||||||| ||||||||| |||||||| ||||||||| ||||| ||||| |||||||| ||| ||||| |||| |||||||||| || |||||||| ||||| | ||||| || | |||||||| |||||||| | ||||||||||| | || ||| ||||||||||||||| ||||| ||| | || ||| |||||||||| |||||| ||| ||||||| |||| |||||||||||| |||| ||||||| ||| | |||| ||||| |||||| ||||||||||||||| ||||||||| || ||| ||||||||||||||| ||||| ||| |||| |||||||||||||| || ||| |||||||||| |||||||.
In both studies, the proportion of patients that reported a grade 2 or higher increase in aspartate aminotransferase, alanine aminotransferase, or bilirubin levels ranged from 0% to 2% across all treatment groups during week 0 to 16. In the overall study period of the POETYK-1 study, 1 patient who received deucravacitinib had elevated alanine aminotransferase and aspartate aminotransferase levels greater than 3 times the upper limit of normal and total bilirubin 2 or more times the upper limit of normal; however, this patient also had a history of alcohol dependence and fatty liver, thus did not meet the criteria for drug-induced liver disease. Liver function tests returned to the patient’s normal after the drug was discontinued. The proportion of patients with a grade 2 or higher decrease in the neutrophil or lymphocyte count during week 0 to week 16 was generally similar between groups and did not exceed 3% in the deucravacitinib groups.
The proportion of patients with at least a grade 2 increase in creatinine kinase levels was 3% for the deucravacitinib groups, 1% to 4% in the placebo groups, and 0% to 4% in the apremilast groups during week 0 to 16. Over the 52-week study period, 6% of patients receiving deucravacitinib and 4% to 5% receiving apremilast reported grade 2 or greater elevated creatinine kinase levels. None of these events were considered SAEs.
Table 27: Summary of Harms — POETYK-1 (Safety Population)
Adverse event | Week 0 to 16 | Week 0 to 52 | |||
|---|---|---|---|---|---|
DEUC n = 332 | PBO n = 165 | APREM n = 168 | DEUC n = 531 | APREM n = 168 | |
Total exposure in PY | — | — | — | 419.1 | 115.8 |
Patients with ≥ 1 adverse event | |||||
n (%) | 176 (53) | 70 (42) | 93 (55) | 395 (74) | 127 (76) |
IR per 100 PY | — | — | — | 211.8 | 234.3 |
Most common events,a n (%) | |||||
Nasopharyngitis | 21 (6) | 7 (4) | 14 (8) | 96 (18) | 26 (16) |
URTI | 21 (6) | 6 (4) | 3 (2) | 50 (9) | 6 (4) |
Diarrhea | 13 (4) | 6 (4) | 17 (10) | 30 (6) | 19 (11) |
Nausea | 7 (2) | 4 (2) | 19 (11) | 7 (1) | 21 (13) |
Headache | 16 (5) | 5 (3) | 17 (10) | 35 (7) | 23 (14) |
Hypertension | 6 (2) | 0 | 6 (4) | 14 (3) | 9 (5) |
Patients with ≥ 1 SAE | |||||
n (%) | 7 (2) | 9 (5) | 4 (2) | 31 (6) | 6 (4) |
IR per 100 PY | — | — | — | 7.5 | 5.2 |
Patients who stopped treatment due to adverse events | |||||
n (%) | 6 (2) | 7 (4) | 10 (6) | 14 (3) | 12 (7) |
IR per 100 PY | — | — | — | 3.3 | 10.3 |
Most common events,b n (%) | |||||
|||||||| | ||| | | ||| | | ||| | ||| | | ||| |
|||||| | ||| | ||| | | ||| | ||| | | ||| |
|||||||| | ||| | ||| | | ||| | ||| | | ||| |
|||||||| | ||| | | ||| | | ||| | ||| | | ||| |
Deaths | |||||
n (%) | 0 | 1 (0.6) | 0 | 0 | 0 |
Notable harms | |||||
Infections and infestations SOC, n (%) | || |||| | || |||| | || |||| | ||| |||| | || |||| |
Infections and infestations SOC, IR per 100 PY | ||| | ||| | ||| | |||| | |||| |
Infections and infestations SOC SAE, n (%) | | ||||| | | ||||| | | ||||| | | ||||| | | ||||| |
Infections and infestations SOC SAE, IR per 100 PY | ||| | ||| | ||| | ||| | ||| |
Infections of interest to the sponsor,c n (%) | | ||||| | ||| | ||| | || ||||| | | ||||| |
Infections of interest to the sponsor,c IR per 100 PY | ||| | ||| | ||| | ||| | ||| |
Adjudicated extended MACE,d n (%) | 1 (0.3) | 3 (1.8) | 1 (0.6) | 2 (0.4) | 2 (1.2) |
Adjudicated thromboembolic SAE, n (%) | 0 | 0 | 0 | 1 (0.2) | 0 |
Malignancy, n (%) | 1 (0.3) | 0 | 0 | 4 (0.8) | 0 |
Increased ALT, grade 2 or higher, n (%) | 3 (0.9) | 0 | 0 | NR | NR |
Increased AST, grade 2 or higher, n (%) | 7 (2.1) | 0 | 0 | NR | NR |
Increased blood bilirubin, grade 2 or higher, n (%) | 5 (1.5) | 1 (0.6) | 1 (0.6) | NR | NR |
Increased CK, grade 2 or higher, n (%) | 11 (3.3) | 2 (1.2) | 0 | 35 (6.6) | 8 (4.8) |
Decreased neutrophil count, grade 2 or higher, n (%) | 4 (1.2) | 2 (1.2) | 1 (0.6) | NR | NR |
Decreased lymphocyte count, grade 2 or higher, n (%) | 9 (2.7) | 10 (6.1) | 5 (3.0) | NR | NR |
ALT = alanine aminotransferase; APREM = apremilast; AST = aspartate aminotransferase; CK = creatine kinase; DEUC = deucravacitinib; IR = incidence rate; MACE = major adverse cardiovascular events; NR = not reported; PBO = placebo; PY = patient-years; SAE = serious adverse event; SOC = system organ class; URTI = upper respiratory tract infection.
aFrequency > 5% per group in either pivotal trial.
bReported in 2 or more patients per group.
cIncludes herpes zoster, influenza, opportunistic infections, and tuberculosis. Events were adjudicated by a blinded independent committee.
dIncludes nonfatal stroke, nonfatal myocardial infarction, cardiovascular death, and unstable angina requiring hospitalization.
Source: Clinical Study Report for POETYK-1.7
Table 28: Summary of Harms — POETYK-2 (Safety Population)
Adverse event | Week 0 to 16 | Week 0 to 52 | ||||
|---|---|---|---|---|---|---|
DEUC N = 510 | PBO N = 254 | APREM N = 254 | DEUC N = 833 | Placebo N = 501 | APREM N = 254 | |
Total exposure in PY | — | — | — | 549.9 | 194.0 | 105.3 |
Patients with ≥ 1 adverse event | ||||||
n (%) | 293 (58) | 138 (54) | 150 (59) | 600 (72) | 277 (55) | 172 (68) |
IR per 100 PY | — | — | — | 242.4 | 221.5 | 329.6 |
Most common events,a n (%) | ||||||
Nasopharyngitis | 55 (11) | 29 (11) | 23 (9) | 133 (16) | 47 (9) | 28 (11) |
URTI | 25 (5) | 11 (4) | 14 (6) | 74 (9) | 27 (5) | 21 (8) |
Diarrhea | 24 (5) | 19 (8) | 33 (13) | 39 (5) | 22 (4) | 35 (14) |
Nausea | 7 (1) | 3 (1) | 23 (9) | 13 (2) | 6 (1) | 26 (10) |
Headache | 22 (4) | 14 (6) | 28 (11) | 45 (5) | 16 (3.2) | 30 (12) |
Hypertension | 9 (2) | 1 (0.4) | 5 (2) | 25 (3) | 5 (1) | 7 (3) |
Patients with ≥ 1 SAE | ||||||
n (%) | 8 (2) | 3 (1) | 1 (0.4) | 24 (3) | 5 (1) | 3 (1) |
IR per 100 PY | — | — | — | 4.3 | 2.5 | 2.8 |
Most common events,b n (%) | ||||||
Pneumonia | NR | NR | NR | 3 (0.4) | 0 | 0 |
Patients who stopped treatment due to adverse events | ||||||
n (%) | 14 (3) | 9 (4) | 12 (5) | 29 (4) | 16 (3) | 14 (6) |
IR per 100 PY | — | — | — | 5.2 | 8.0 | 13.1 |
Most common events,b n (%) | ||||||
|||||||||| |||||||||| |||| ||||||||| | | ||||| | | ||||| | | ||||| | | ||||| | | ||||| | | ||||| |
||||| || ||||||||| | | ||||| | | ||||| | | ||||| | | ||||| | | ||||| | | ||||| |
|||||||| | | ||||| | | ||||| | | ||||| | | ||||| | | ||||| | | ||||| |
|||||||| | | ||||| | | ||||| | | ||||| | | ||||| | | ||||| | | ||||| |
|||||||| | | ||||| | | ||||| | | ||||| | | ||||| | | ||||| | | ||||| |
||||||||| |||| | | ||||| | | ||||| | | ||||| | | ||||| | | ||||| | | ||||| |
|||||| | | ||||| | | ||||| | | ||||| | | ||||| | | ||||| | | ||||| |
||||||| | | ||||| | | ||||| | | ||||| | | ||||| | | ||||| | | ||||| |
||||||| | | ||||| | | ||||| | | ||||| | | ||||| | | ||||| | | ||||| |
|||||||| | | ||||| | | ||||| | | ||||| | | ||||| | | ||||| | | ||||| |
||||||| | | ||||| | | ||||| | | ||||| | | ||||| | | ||||| | | ||||| |
|||| | | ||||| | | ||||| | | ||||| | | ||||| | | ||||| | | ||||| |
||||||||| | | ||||| | | ||||| | | ||||| | | ||||| | | ||||| | | ||||| |
Deaths | ||||||
n (%) | 1 (0.2) | 0 | 1 (0.4) | 2 (0.2) | 0 | 1 (0.4) |
Notable harms | ||||||
Infections and infestations SOC, n (%) | 158 (31) | 66 (26) | 63 (25) | 381 (46) | 134 (27) | 83 (33) |
Infections and infestations SOC, IR per 100 PY | — | — | — | 101.8 | 80.0 | 94.5 |
Infections and infestations SOC SAE, n (%) | 4 (1) | 1 (0.4) | 0 | 11 (1) | 1 (0.2) | 1 (0.4) |
Infections and infestations SOC SAE, IR per 100 PY | — | — | — | 2.0 | 0.5 | 0.9 |
Infections of interest to the sponsor,c n (%) | 3 (0.6) | 4 (1.6) | 1 (0.4) | 13 (1.6) | 7 (1.4) | 3 (1.2) |
Infections of interest to the sponsor,c IR per 100 PY | — | — | — | 2.3 | 3.5 | 2.8 |
Adjudicated extended MACE,d n (%) | 1 (0.2) | 0 | 1 (0.4) | 2 (0.2) | 0 | 1 (0.4) |
Adjudicated thromboembolic SAE, n (%) | 0 | 0 | 0 | 0 | 0 | 0 |
Malignancy, n (%) | 0 | 0 | 2 (0.8) | 6 (0.7) | 0 | 2 (0.8) |
Increased ALT, grade 2 or higher, n (%) | 2 (0.4) | 0 | 2 (0.8) | NR | NR | NR |
Increased AST, grade 2 or higher, n (%) | 0 | 1 (0.4) | 2 (0.8) | NR | NR | NR |
Increased blood bilirubin, grade 2 or higher, n (%) | 2 (0.4) | 3 (1.2) | 0 | NR | NR | NR |
Increased CK, grade 2 or higher, n (%) | 17 (3.4) | 11 (4.4) | 9 (3.6) | 47 (5.6) | 21 (4.2) | 11 (4.3) |
Decreased neutrophil count, grade 2 or higher, n (%) | 2 (0.4) | 2 (0.8) | 3 (1.2) | NR | NR | NR |
Decreased lymphocyte count, grade 2 or higher, n (%) | 16 (3.2) | 9 (3.6) | 8 (3.2) | NR | NR | NR |
ALT = alanine aminotransferase; APREM = apremilast; AST = aspartate aminotransferase; CK = creatine kinase; DEUC = deucravacitinib; IR = incidence rate; MACE = major adverse cardiovascular events; NR = not reported; PBO = placebo; PY = patient-years; SAE = serious adverse event; SOC = system organ class; URTI = upper respiratory tract infection.
aFrequency > 5% per group in either pivotal trial.
bReported in 2 or more patients per group.
cIncludes herpes zoster, influenza, opportunistic infections, and tuberculosis. Events were adjudicated by a blinded independent committee.
dIncludes nonfatal stroke, nonfatal myocardial infarction, cardiovascular death, and unstable angina requiring hospitalization.
Source: Clinical Study Report for POETYK-2.8
Critical Appraisal
Internal Validity
The POETYK-1 and POETYK-2 studies appear to have a low risk of bias with regards to randomization and allocation concealment. Randomization was conducted using a central interactive response technology system and stratified computer-generated randomization schedule. In general, the baseline characteristics appear to be balanced between groups within trials, and any variances observed were not thought to have an important impact on the studies’ findings.
Both trials used a double-dummy design to maintain blinding throughout the trial, even for patients who switched therapy at later time points. No substantial differences between groups were observed in the distribution of AEs, thus the occurrence of known AEs was unlikely to be a major source of unblinding. Given the subjective nature of the key efficacy outcomes, maintenance of blinding is important to avoid potential bias in outcome assessment. The dosing of apremilast was consist with Health Canada recommendations and current clinical practice.
Drug discontinuation in first 16 weeks was reported for 8%, 12%, and 14% of patients in the POETYK-1 study and 11%, 17%, and 15% of patients in the POETYK-2 study in the deucravacitinib, placebo, and apremilast groups, respectively. Although there were some differences between groups in the frequency of drug discontinuation, the key efficacy outcomes were based on the intention-to-treat population, with any patients who stopped the study or study drug, or with missing information, imputed as nonresponders. The nonresponder imputation represents an implicit composite estimand analysis strategy, which may be considered a conservative estimate of treatment effects. Continuous outcomes were imputed using a modified baseline observation carried forward method, where patients who discontinued the study treatment due to lack of efficacy or AEs had baseline values carried forward, otherwise the last observation was carried forward for any other missing data. This may also be seen as a conservative approach to impute missing data. Both studies did sensitivity analysis using other methods to impute missing data (such as last observation carried forward, multiple imputation, and a tipping point analysis) and these showed results that were consistent with the primary analyses.
The efficacy outcomes reported were relevant to patients, and included skin clearance, psoriasis symptoms, and HRQoL. Skin clearance assessments were conducted by dermatologists or investigators who were experienced in the assessment of patients with psoriasis and who had undergone standardized training in psoriasis outcome measures, which should improve the consistency of these subjective measures. Due to the COVID-19 pandemic, study visits were disrupted (i.e., visits were delayed, missed, or performed remotely) or study drug treatment was interrupted for some patients. As most COVID-related disruptions occurred between week 24 and week 52 in the trials, the sponsor stated there was no impact on 16-week outcomes and minor impacts on key secondary outcomes at later time points. Patients with missing data due to COVID-19 at week 24 or week 52 were excluded from the analyses, but the number of patients affected was small for key end points, and sensitivity analyses that included these patients as nonresponders showed consistent findings.
The trials looked at shorter-term (16 weeks and 24 weeks) and longer-term outcomes (52 weeks); however, interpretation of the 52-week efficacy and safety end points needs to consider the treatment switching that occurred in most groups. There is the possibility that patients switched to deucravacitinib due inadequate initial treatment response may be more refractory to therapy. Also, there may be carry-over effects which may impact the frequency of AEs reported after a change in therapy; however, the direction of any potential bias is unclear. The POETYK-2 study examined the time to relapse using the Kaplan-Meier product limit method and a stratified log-rank test. Patients who discontinued the study or treatment, had missing data, or who did not have relapse by week 52 were censored. More patients in the placebo group discontinued study drug than in the deucravacitinib group (11% versus 7%), but the potential impact of the differential discontinuations is unclear. Relapse was defined as a loss of at least 50% of the week 24 PASI percent improvement from baseline (among patients who had achieved at least a PASI 75 response at week 24). A similar definition has been used in other psoriasis clinical trials,51 but given that PASI 75 is considered the minimum treatment response for currently available advanced therapies, any loss of response that falls below the PASI 75 threshold may be considered suboptimal. Other clinical trials for biologics have used failure to maintain at least a PASI 75 response as indicative of relapse.52
The trials were powered for the coprimary end points at week 16 to test for superiority versus placebo and apremilast. Multiple secondary outcomes were part of the statistical testing procedure that controlled the type I error rate. Of note, there was a US and global statistical testing procedure. The US procedure included fewer end points and excluded the proportion of patients who achieve DLQI 0 or 1 at 16 weeks (both studies), and the time to relapse (POETYK-2 study only). Thus, if the US testing procedure is preferred, then these outcomes should be interpreted with caution due to the potential inflated risk of type I error.
The outcomes for scalp or fingernail psoriasis were based on the subgroups of patients with psoriasis affecting these areas. Randomization was not stratified by these subgroups so there is the potential for imbalances in confounders or prognostic factors to be present at baseline. The impact of this on the outcomes is unclear. Also of note, relatively few patients had fingernail psoriasis (10% to 20% per group), which could impact the ability to detect a treatment effect. The sample size for the subgroup with moderate to severe scalp psoriasis at baseline was larger (60% to 73% per group). Other subgroup analyses of interest to this review (i.e., based on prior therapy or disease severity) were prespecified, but these data were only reported descriptively, with no planned statistical hypotheses of differences in efficacy or statistical tests (i.e., interaction effects). Except for prior biologic treatment, randomization was not stratified for the subgroups of interest, and thus it is possible the baseline characteristics of patients may not be balanced across treatment subgroups. These factors should be taken into consideration when interpreting the results of the subgroup analyses.
The patient-reported outcomes used in the trials had evidence to support their validity and reliability. However, it was noted that data were missing for up to 10% of patients, depending on the treatment group and outcome. The DLQI responder analyses excluded 3% to 4% of patients randomized. These analyses were restricted to patients who had a baseline DLQI score of at least 2, which may explain why some patients were missing, but the Clinical Study Report did not provide a detailed explanation. For other outcomes, 1% to 4% of patients were excluded from the change in SF-36 component scores, 1% to 7% from the change in EQ-5D VAS, and 6% to 10% from the PSSD symptom score outcomes. The reason for the exclusions and their impact on the findings is unclear. Also, SF-36 and EQ-5D, and some PSSD comparisons were designated as “additional” end points in the trials’ protocols and were not part of the statistical testing hierarchies.
External Validity
Overall, the clinical expert consulted for this review considered that the patients enrolled would represent patients with moderate to severe psoriasis who may be treated with advanced therapies in Canada, including those who had received prior systemic or biologic therapy. The patients enrolled were predominantly middle-aged, with a mean body mass index of approximately 30 kg/m2, and mean PASI score of approximately 21. There was limited information available on the 30% of patients who were screened but were not randomized; thus, it is impossible to assess whether the characteristics of these patients were different from those enrolled. In the trials, there was a higher proportion of men than women, but the expert stated that this would not be expected to affect the generalizability. Although 9% of participants were living in Canada, the overall study population may not reflect the racial distribution of Canada. Most patients were white, and few patients were Black (< 4%), Asian (4% to 18%), or other races (≤ 2%). Approximately 60% of patients had received systemic therapy for their psoriasis, including one-third of patients who had received prior biologic therapy. No information was available on patients’ response to prior treatments; thus, it is unclear if a significant proportion would be classified as having failed previous therapies or if they stopped treatment due to intolerance or for other reasons. More than 40% of the study population had received no prior systemic therapies. In Canada, advanced therapies are typically reserved for patients who have had an inadequate response or are intolerant to or have contraindications to standard systemic therapies.
The clinical expert identified issues with apremilast as an active comparator. While apremilast is another oral advanced therapy, it is infrequently prescribed in Canada for the treatment of moderate to severe plaque psoriasis. The expert stated that efficacy of apremilast is considered to be low for an advanced therapy, and most dermatologists would select a biologic over apremilast. Thus, based on current practice, apremilast may not be as relevant a comparator as biologics. Patients were prohibited from receiving other treatments for psoriasis, with the exception of protocol-specified topical therapies after week 24. Therefore, these trials do not provide evidence on the efficacy and safety of deucravacitinib when used in combination with other systemic therapies.
The outcomes measured were relevant to patients, which included HRQoL as well as symptoms and skin clearance measures. The duration of the trials was 52 weeks (mean deucravacitinib exposure was < 10 months), which may be considered relatively short for a chronic condition. The withdrawal period results of the POETYK-2 study were based on an enriched population who had responded to deucravacitinib. As a result, the 52-week response rate may be inflated relative to an unselected patient population. For the longer-term analyses, treatment response was evaluated at 24 weeks, but according to the expert consulted, most patients and physicians would be unwilling to wait 24 weeks to evaluate response to induction therapy. Thus, the treatment patterns in the trial may not reflect clinical practice.
Indirect Evidence
Objectives and Methods for the Summary of Indirect Evidence
The sponsor submitted an ITC to assess the comparative efficacy of deucravacitinib versus other biologic or nonbiologic treatments for adult patients with moderate to severe plaque psoriasis in the UK. CADTH also conducted a literature search to identify other potentially relevant ITCs in adult patients with moderate to severe plaque psoriasis. The Ovid MEDLINE database was searched using a combination of MeSH (Medical Patient Headings) and keywords. The main search concept was adult patients with moderate to severe plaque psoriasis. A NMA filter was applied to limit study type to NMAs. Retrieval was not limited by publication date or by language. Titles, abstracts, and full-text articles were screened for inclusion by 1 reviewer based on the population, intervention, comparator, and outcome criteria outlined in the CADTH systematic review protocol (Table 6). The systematic review did not identify any relevant ITCs in the literature; therefore, this section will appraise the sponsor-submitted ITC.
One sponsor-submitted ITC was summarized and critically appraised.6,53 The sponsor-submitted ITC was used to inform the pharmacoeconomic model.
Description of Indirect Comparison
The sponsor-submitted ITC, which is an NMA, aimed to evaluate the relative efficacy of deucravacitinib versus other biologic or nonbiologic treatments for moderate to severe plaque psoriasis in adult patients. The sponsor performed a systematic review to identify relevant studies for inclusion in the ITC. Outcomes that were included in the review were efficacy and safety outcomes. The population, interventions, comparators, outcomes, and design of studies included in the sponsor’s ITC are provided in detail in Table 29.
Table 29: Study Selection Criteria and Methods for ITCs
Sponsor-submitted ITC | Inclusion criteria | Exclusion criteria |
|---|---|---|
Population | Adult (≥ 18 years) patients with moderate to severea plaque PsO who are candidates for systemic therapies |
|
Intervention | Systemic biologics:
Systemic nonbiologicsc
| Studies that do not include a treatment arm with any of the selected comparators of interest |
Comparator |
| NA |
Outcome |
|
|
Study design | RCTs (phase II, III, IV) (including follow-up studies of RCTs) |
|
Publication characteristics | English language | Non-English languages |
Subgroups |
| NA |
Other limits |
| Studies published outside the time frame of interest |
Databases searched | MEDLINE, Embase, CENTRAL, Cochrane Database of Systematic Reviews, PsycINFO | NA |
Selection process | Articles screened independently by 2 researchers | NA |
Data extraction process | Data extraction was performed by pairs of reviewers and compared for discrepancies by a third reviewer | NA |
Quality assessment | Cochrane Risk of Bias Assessment Tool 2.0 (RoB 2.0) | NA |
b.i.d. = twice a day; BSA = body surface area; DLQI = Dermatology Life Quality Index; EOW = every other week; IGA = Investigator Global Assessment; IL = interleukin; ITC = indirect treatment comparison; NA = not applicable; NMA = network meta-analysis; PASI = Psoriasis Area and Severity Index; PASI 50 = 50% reduction in Psoriasis Area and Severity Index score; PASI 75 = 75% reduction in Psoriasis Area and Severity Index score; PASI 90 = 90% reduction in Psoriasis Area and Severity Index score; PASI 100 = 100% reduction in Psoriasis Area and Severity Index score; PGA = Physician’s Global Assessment; PRO = patient-reported outcome; PsA = psoriatic arthritis; PsO = plaque psoriasis; PSSD = Psoriasis Symptoms and Signs Diary; q.2.w. = every 2 weeks; q.4.w. = every 4 weeks; q.8.w. = every 8 weeks; q.12.w. = every 12 weeks; RCT = randomized controlled trial; SF-36 = Short Form (36) Health Survey; SLR = systematic literature review.
aIf “moderate to severe” was mentioned, then that was sufficient criteria for inclusion regardless of definition. However, if “moderate to severe” was not mentioned, a decision on inclusion was made with clear documentation based on any of the following criteria: PGA ≥ 3, PASI ≥ 10, BSA ≥ 10 and/or DLQI ≥ 10.
bStudies or treatment arms only evaluating ustekinumab 45 mg were excluded from the SLR and NMA, as the ustekinumab 45 mg body weight requirement results in limited available data, comparability to the population for other treatments and generalizability of the findings.
cAny dose of systemic nonbiologic treatments was included, as doses are often modified or titrated.
dSystematic reviews, meta-analyses, and pooled analyses of RCTs were tagged separately during the screening phase and the list of included studies from each publication were reviewed to identify any additionally relevant RCTs not otherwise captured by the database searches. These publications themselves were be included in the SLR unless unique data were available that are not published elsewhere.
Source: Sponsor-submitted ITC.53
Methods of Sponsor-Submitted ITC
Study Selection Methods
As part of the sponsor’s ITC, a systematic literature review was conducted to identify the current available evidence in terms of clinical efficacy of deucravacitinib versus competing interventions for moderate to severe plaque psoriasis in adults. The systematic literature review was conducted in adherence to the criteria required by the National Institute for Health and Care Excellence and other guidelines including Preferred Reporting Items for Systematic Reviews and Meta-analyses and the Cochrane Handbook for Systematic Reviews of Interventions, according to the sponsor.
Literature searches were conducted from November 2020 to October 11, 2021. Systematic searches were conducted across electronic databases including MEDLINE and MEDLINE In-Process, Embase, Cochrane Central Register of Controlled Trials, Cochrane Database of Systematic Reviews, and PsycINFO. Searches in unpublished literature sources were conducted to supplement the peer-reviewed literature. Searches were conducted to identify abstracts of conference proceedings from 2019 to 2021 that were available to the public. The conference proceedings and websites of relevant conferences that were searched included the American Academy of Dermatology, British Association of Dermatologists, European Society for Dermatological Research, European Association of Dermatology and Venereology, Society for Investigative Dermatology, World Congress of Dermatology, clinical trial directories in the US, European Union, and WHO, and the International Clinical Trial Registry Platform.
Studies were considered for inclusion if the population was adults older than 18 years and had “moderate to severe” plaque psoriasis, and if the disease severity was described using PGA, PASI, BSA, or DLQI criteria (PGA ≥ 3, PASI ≥ 10, BSA ≥ 10, or DLQI ≥ 10). In addition, RCTs reporting on a patient population presenting with mixed disease severity (i.e., mild, moderate, and severe) were considered for inclusion if more than 80% of the population had moderate to severe plaque psoriasis. Trials that did not include a treatment arm with any of the selected comparators of interest were considered as ineligible for inclusion. Interventions of interest were FDA-approved biologics and nonbiologics. Trials reporting on a combination of interventions and trials comparing doses or dosing schedules of the same drug were not included. In addition, a study which did not report any efficacy or safety outcome measured between 10 weeks and 60 weeks of study initiation was not treated as eligible for inclusion. To prevent double counting of primary studies, identified systematic literature reviews of relevance were also not included in this review.
Study selection was conducted via a 2-stage screening procedure. In the first stage (level 1), titles and abstracts of studies identified by the search strategies were reviewed by 2 independent researchers to ascertain eligibility according to the inclusion and exclusion criteria. Discrepancies between the reviewers were resolved by a third reviewer, as required. In the second stage (level 2), all full-text articles determined to be eligible in level 1 were reviewed by 2 independent researchers to determine eligibility according to the inclusion and exclusion criteria. Trials at level 2 that satisfied all inclusion criteria and none of the exclusion criteria were included in the systematic literature review. Discrepancies between the reviewers were resolved by a third reviewer, as required.
Data from the included full-text articles were extracted by 1 researcher. Data extraction was validated by another independent researcher. Data elements of interest included details of study characteristics (e.g., author, publication year, sponsor, study objectives), patient characteristics (e.g., sample size, age, gender, comorbidities), treatment regimen (e.g., name, route of administration, dose), and efficacy and safety outcomes. Furthermore, data for the subgroup analyses (previous use of biologic therapy and severity of psoriasis) were extracted by the treatment arm in each RCT, if available.
A risk of bias assessment was conducted for the RCTs included in the NMA. The risk of bias assessment was conducted using the Cochrane Risk of Bias Assessment Tool 2.0 (RoB 2.0). The risk of bias was assessed for all trials in the NMA that had PASI outcomes at 10 weeks to 16 weeks. As such, the assessment was based on the trial design employed up to 16 weeks postrandomization.
ITC Analysis Methods
The authors of the submitted ITC used a Bayesian NMA approach. Both fixed-effect and random-effect models were considered. Only models of interest and relevance to CADTH for the purpose of this review were summarized and appraised.
To assess the appropriateness of conducting an NMA, a feasibility assessment was conducted. The feasibility assessment was performed to ensure the 2 main NMA assumptions, consistency and similarity, were satisfied across the included trials. In particular, whether the characteristics of the RCTs identified in the systematic literature review and connected in the network (i.e., study design, patient characteristics, interventions and comparators, and outcomes) were sufficiently similar to be quantitatively synthesized was investigated as part of the sponsor’s feasibility assessment. Imbalance in potential effect modifiers was also investigated. Baseline risk was adjusted using the different statistical models described in the following, and prior biologic experience was adjusted with subgroup analyses.
The sponsor conducted several sensitivity analyses using the binomial logit model instead of the multinomial logit model to assess the impact of analyzing PASI response levels separately versus combined as in the multinomial model. The sponsor also conducted sensitivity analyses in which trials that were classified as outliers by the sponsor were removed from analysis. The sensitivity analysis that is of greatest interest from CADTH’s point of view for the purpose of this review is the analysis that compares the PASI response of deucravacitinib 6 mg at 24 weeks versus other comparators at 10 weeks to 16 weeks. All main, subgroup, and sensitivity analyses were performed on PASI response level. The sponsor did not analyze other clinical or safety outcomes without justification. Networks of treatments differ across the 3 time points; details of treatment comparisons are found in the corresponding network diagrams in the results section.
A multinomial analysis was conducted for each time point of interest to compare the clinical efficacy of deucravacitinib to other treatments of moderate to severe plaque psoriasis as the main analysis. The time points of interest were 10 weeks to 16 weeks, 24 weeks to 28 weeks, and 44 weeks to 60 weeks. Multinomial categories of 50%, 75%, 90%, and 100% PASI responses were modelled. Details of all analyses conducted are in Table 30. In addition, 2 types of adjustments were considered for the NMA models.
Adjustment for baseline risk (binomial and multinomial models): a component for baseline risk was added as relative effects as drugs in autoimmune diseases often depend on baseline risk. A baseline risk model was assumed, and the base-case model included a parameter for baseline risk.
“REZ” model; allowing treatments to vary in efficacy across PASI cut-offs (multinomial model): This modification introduced a random effects (RE) component that enabled each treatment’s increase in difficulty to the next-highest PASI cut-off to vary around a common mean, thus allowing “borrowed strength” across PASI cut-offs but also letting treatments have different efficacies for different levels of PASI. This enhanced model is referred to as the “REZ” model because it introduces an RE component to the parameter that reflects the potential change in measured efficacy between 1 PASI cut-off and the next.
The sponsor also conducted a subgroup analysis with binomial NMAs on the 75% PASI response on the biologic-naive and biologic-experienced subpopulations.
Multinomial analyses were conducted with fixed-effects and RE models for relative treatment effects and REZ models, and with and without adjustment for baseline risk, across all time points (Table 31).
In all Bayesian models, noninformative priors were selected for all non-RE parameters. In the RE models, a Uniform(0,1) prior was selected for the treatment effect heterogeneity SD (tau). In the REZ model, a Uniform(0,0.5) prior was used for the SD around the value between probit cut-offs. Other priors for the Bayesian models were investigated via sensitivity analyses. Sensitivity analyses using different prior values (between Uniform[0,0.25] and Uniform[0,1]) were conducted to assess the sensitivity to the choice of priors, but none were discovered due to large sample size in the network.
All Bayesian models were conducted with Markov chain Monte Carlo simulations, with 100,000 burn-in iterations followed by 100,000 iterations for estimation of parameters. Convergence was verified by assessing the 3-chain, Brooks-Gelman-Rubin plots and values of R-hat (potential scale reduction factor, considered converged if R-hat < 1.05 for all parameters being estimated), and the ratios of Monte Carlo error to the SDs of the posteriors. The median of the posterior samples for each effect was used as the parameter estimate (e.g., probit differences between treatments). The 2.5th and 97.5th percentiles of the posterior samples were used as 95% CrI. Moreover, these posterior samples were used to compute the rank probability of a treatment being the best, the probability of a treatment being better than each comparator, and each treatment’s surface under the cumulative ranking curve index.
Goodness of fit of the different models was compared using the posterior mean residual deviance and deviance information criteria. A model with a deviance information criteria smaller by more than 5 points was considered a better-fitting model. Network inconsistency was investigated using residual deviance scores in each arm in each trial in the multinomial model, as a measurement of absolute model fit to the data. Substantial arm-level deviances from different models were investigated. Arm-level outliers were defined as those with residual deviance contribution greater than 4. In addition, statistical heterogeneity was evaluated by investigating the estimates of the between-trial SDs from the multinomial models.
Among the included RCTs, the main potential sources of heterogeneity identified were variation in age and sex, body weight and/or body mass index, race, disease severity, previous biologic use, and comorbid psoriatic arthritis. In the sponsor’s feasibility analysis, literature support was found for body weight, race, severity, and prior treatment with biologics as potential treatment effect modifiers. Sensitivity analyses were proposed for body weight and race and found not to be feasible for severity due to lack of subgroup reporting. Subgroup analyses were conducted for prior exposure to biologics.
Each of the RCTs in the NMA reported the PASI response at 4 percentage levels (PASI 50, 75, 90, and 100), such that if a patient attained PASI 50, for example, this meant their PASI score had improved by 50% or more from baseline. The NMA analyses reported odds ratios (ORs) for achieving a percentage level of PASI score (50, 75, 90, and 100) of deucravacitinib versus other comparators, for each time point of interest. PASI scores from the following time points were analyzed: 10 weeks to 16 weeks (short-term), 24 weeks to 28 weeks (midterm), and 44 weeks to 60 weeks (long-term). The posterior distributions of relative treatment effects were summarized by the median and 95% CrIs. The results of the NMA were presented as forest plots.
Table 30: Summary of Relevant NMA Analyses and Models Conducted
Analysis | Outcome | NMA model | Justification | Adjustment | Treatment effect model |
|---|---|---|---|---|---|
Base case | PASI 50, 75, 90, 100 | Multinomial | A multinomial (probit) model is a hierarchical NMA that allows the analysis to model the relationship between the PASI scores, while keeping the randomization of the original trials. | REZa | Fixed, random |
Subgroup | PASI 75 biologic-naive and biologic-treated subgroups | Binomial | Due to limited data availability, only a binomial (logit) NMA was feasible for the subgroup analysis testing the impact of previous exposure to biologics as a treatment modifier. | Unadjusted, baseline adjustment | Fixed, random |
NMA = network meta-analysis; PASI = Psoriasis Area and Severity Index; PASI 50 = 50% reduction in Psoriasis Area and Severity Index score; PASI 75 = 75% reduction in Psoriasis Area and Severity Index score; PASI 90 = 90% reduction in Psoriasis Area and Severity Index score; PASI 100 = 100% reduction in Psoriasis Area and Severity Index score.
aThe REZ model allowed treatments to vary in efficacy across PASI cut-offs by adding a random effects component that enabled each treatment’s increase in difficulty to the next-highest PASI cut-off to vary around a common mean,
Source: Sponsor-submitted indirect treatment comparison.53
Table 31: ITC Analysis Methods
Analysis | ITC1 |
|---|---|
ITC methods | Fixed and random effects network meta-analysis under a Bayesian framework (multinomial and binomial models) |
Priors | Partially informed priors |
Assessment of model fit | Posterior residual deviance, deviance information criterion |
Assessment of consistency | Residual deviance scores and contribution of each arm in each trial |
Assessment of convergence | Visual inspection of Brook-Gelman-Rubin plots, potential scale reduction factor, ratios of Monte Carlo error to the standard deviations of the posterior samples |
Outcomes | PASI percentage scores (50, 75, 90, 100) |
Follow-up time points | 10 to 16 weeks, 24 to 28 weeks, 44 to 60 weeks |
Construction of nodes | Not reported |
ITC = indirect treatment comparison; PASI = Psoriasis Area and Severity Index.
Source: Sponsor-submitted ITC.53
Results of Sponsor-Submitted ITC
Summary of Included Studies
A systematic literature review was conducted, and 7,487 citations were identified. After removing duplicates, 4,450 citations were screened and resulted in 818 citations eligible for full-text review. Of these, 383 citations pertaining to 84 unique RCTs (of 251 RCTs included in the systematic literature review) met the inclusion criteria for the NMA.
Of the included trials, deucravacitinib intervention has been evaluated in 3 RCTs: a phase II trial (NCT02931838) completed in 2017 and 2 phase III trials (POETYK-1 and POETYK-2) completed in 2020. Patients older than 18 years with a diagnosis of moderate to severe plaque psoriasis for more than 6 months were eligible to participate in these trials. All 3 trials were placebo controlled and both POETYK trials also included an apremilast arm. Outcomes of interest were PASI scores, PGA scores, PSSD symptom scores, and DLQI scores, with time points of evaluation ranging between 16 weeks and 52 weeks.
Of the 84 included RCTs in the NMA, 9 were phase II, 4 were phase II and III, 60 were phase III, and 4 were phase IV. The phase could not be determined for 7 RCTs. Primary outcomes were assessed most commonly at 12 weeks (49 RCTs) or 16 weeks (30 RCTs). Additional primary end point time frames contained 10 weeks (3 RCTs) and 14 weeks (1 RCT).
Study and Patient Characteristics
Trial populations were overall similar with respect to age and sex. In the included RCTs, participants were, on average, aged between 38.7 to 53.3 years, and most participants in the RCTs were men. A minority of men or roughly equal proportions of men and women were observed in 3 RCTs. The sample size varied widely across the RCTs from 20 participants to 2,000 participants, with most of them enrolling more than 100 participants. Psoriatic arthritis and duration of psoriasis before study enrolment were less frequently reported, and some differences were observed across trial populations about these characteristics. RCTs in which all participants had comorbid psoriatic arthritis were removed from the systematic literature review, but most RCTs did not remove patients with psoriatic arthritis. Among 51 RCTs that reported comorbid psoriatic arthritis, between 4.55% to 36.7% of participants reported comorbid psoriatic arthritis, and 33 trials (including the POETYK-1 and POETYK-2 studies) did not report the proportion of participants with comorbid psoriatic arthritis. On average, patients had moderate to severe psoriasis for 10.93 years to 23 years while 13 RCTs did not report disease duration. The average mean body weight of patients across trials varied from 65.8 kg to 108.6 kg; however, the average mean body weight for most trials was between 80 kg and 100 kg, and 19 trials did not report mean body weight. Mean body mass index varied from 23.6 kg/m2 to 38.8 kg/m2, and most trials reported a mean body mass index of 27 kg/m2 to 30 kg/m2; 35 trials did not report body mass index. Most RCTs that reported race included white patients as the largest percentage of their cohort, except for RCTs trials which included Asian patients only; 12 did not report race.
Exposure to prior biologic treatment differed across the RCTs, varying from 0% to 60%, but the majority of RCTs reported exposure to previous biologic treatment from 10% to 40%. The POETYK-1 and POETYK-2 trials reported percentages of patients previously receiving biologic therapies varying from 31.1% to 39.3%, similar to the majority of the trials. Also, 12 trials had fully biologic-naive patient populations; however, these RCTs were mostly published before 2010, before biologic treatments were available. Eight trials did not report the proportion of patients that received prior biologic therapy. The previous biologic therapies that were received by patients were often not reported; however, 5 RCTs reported this information. Previous biologics varied across RCTs and included IL inhibitors such as ustekinumab, T-cell modulating agents including alefacept and efalizumab, and TNF alpha inhibitors including adalimumab and etanercept. Disease severity and exposure to prior biologic treatment was noted by the sponsor as the most important source of between-trial heterogeneity and subgroup analyses were conducted to investigate its impact.
Trial populations were also overall similar with respect to disease severity at baseline. Mean PASI score at baseline varied from 8.0 to 30.3, with most patients having a mean PASI score between 17 and 25. Moreover, 8 RCTs reported PGA score at baseline which varied from 2.8 to 9.8. Mean DLQI score at baseline varied from 7.4 to 16.6, with most patients having a score between 9.8 to 14.6. Patients enrolled in the POETYK trials were similar to most participants enrolled in the plaque psoriasis RCTs, with mean PASI score varying from 20.6 to 21.7 and mean DLQI score varying from 11.4 to 12.4. Differences in PASI scores were noted by clinical experts CADTH consulted for this review as an indication of inclusion of patients with mild psoriasis in the trial populations.
Interventions and Comparators
Interventions and comparators were restricted to only FDA or European Medicines Agency-approved treatment doses. In total, 20 active treatments from 84 RCTs assessing nonbiologic systemic therapies and/or biologic therapies were included (Table 32). Of the included biologics, TNF alpha inhibitors were the most commonly investigated (n = 36), followed by IL-17 family or receptor inhibitors (n = 31), IL-23 inhibitors (n = 16), IL12/IL-23 inhibitors (ustekinumab; n = 13), and lastly tyrosine kinase 2 inhibitors (deucravacitinib; n = 2). Of the TNF alpha and IL inhibitors, etanercept (n = 16) and secukinumab (n = 14) were the most frequently studied interventions. Apremilast was the most frequently studied nonbiologic treatment, evaluated in 8 RCTs. The majority of RCTs were placebo controlled in design (n = 72) rather than only having an active control arm (n = 12).
The midterm and long-term analyses were limited to patients who stayed on the treatment to which they were initially randomized through the time point of assessment, decreasing the number of included RCTs and the number of active treatments in these scenarios. In particular, certolizumab pegol was not eligible for inclusion in either of the analyses beyond the induction phase and tildrakizumab was not included in the long term analyses.
Table 32: Treatments Included in the NMA at Different Time Points
Treatment | 10 week to 16 week analysis (84 trials) | 24 week to 28 week analysis (48 trials) | 44 week to 60 week analysis (32 trials) |
|---|---|---|---|
Adalimumab | Yes | Yes | Yes |
Apremilast | Yes | Yes | Yes |
Bimekizumab | Yes | Yes | Yes |
Brodalumab | Yes | Yes | Yes |
Certolizumab pegol 200 mg | Yes | No | No |
Certolizumab pegol 400 mg | Yes | No | No |
Deucravacitinib | Yes | Yes | Yes |
Dimethyl fumarate | Yes | No | No |
Etanercept 25 mg twice a week or 50 mg once a week | Yes | Yes | No |
Etanercept 50 mg twice a week | Yes | Yes | Yes |
Guselkumab | Yes | Yes | Yes |
Infliximab | Yes | Yes | Yes |
Ixekizumab | Yes | Yes | Yes |
Risankizumab | Yes | Yes | Yes |
Secukinumab 150 mg | Yes | Yes | Yes |
Secukinumab 300 mg | Yes | Yes | Yes |
Tildrakizumab 100 mg | Yes | Yes | No |
Tildrakizumab 200 mg | Yes | Yes | No |
Ustekinumab 45 or 90 mg | Yes | Yes | Yes |
Ustekinumab 90 mg | Yes | Yes | Yes |
Total number of treatments | 20 | 17 | 14 |
Source: Sponsor-submitted indirect treatment comparison.53
Quality Assessment
Of the 84 RCTs included in the NMA, 36 (43%) were rated at overall low risk of bias, 34 (41%) at some concerns, and 13 (16%) at high risk of bias. The main drivers were missing outcome data and departure from intended interventions (7 of 84, 8% of the RCTs judged at high risk of bias; and 6 of 84, 7% of the RCTs judged at high risk of bias, respectively, for each domain).
Most of the included RCTs were of good quality regarding study design (i.e., phase III, double-blinded, controlled trials). The sponsor assumed that any minor differences in study design across the included RCTs would not impact the relative treatment effects. No RCTs were excluded from the analyses because of inadequate study quality.
Results
The results of the multinomial Bayesian NMAs are presented as comparisons of deucravacitinib versus other treatments, for each time point of interest. Interpretation of results was based on evaluation of forest plots and focused on interpretation of the REZ baseline-adjusted multinomial results due to the relative strengths compared to other methods as deemed by the sponsor.
Figure 4: Network of Trials Included in the Network Meta-Analysis (Base Case)
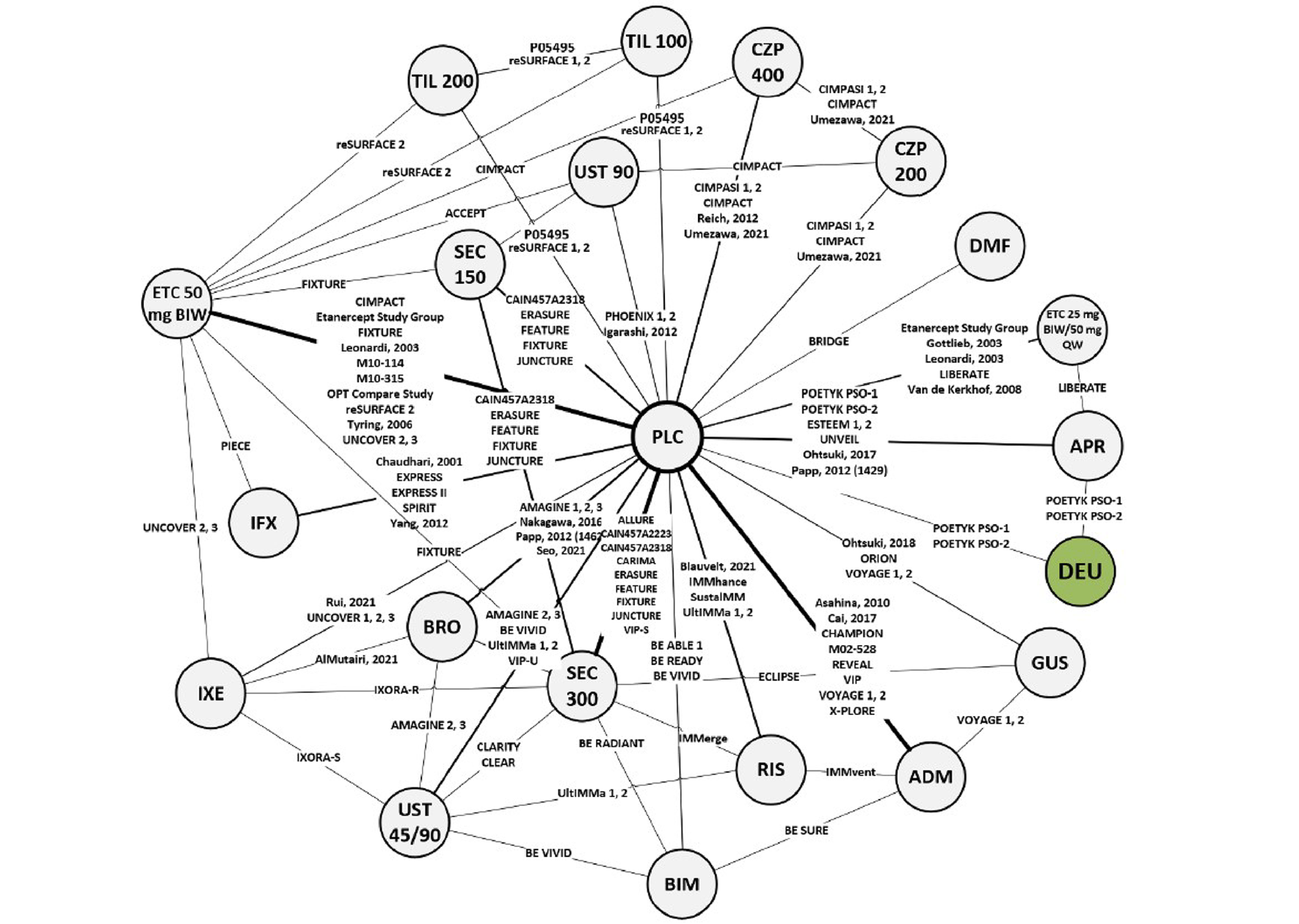
ADM = adalimumab; APR = apremilast; BIM = bimekizumab; BIW = twice per week; BRO = brodalumab; CZP 200 = certolizumab pegol 200 mg; CZP 400 = certolizumab pegol 400 mg; DEU = deucravacitinib; DMF = dimethyl fumarate; ETC 25 = etanercept 25 mg; ETC 50 = etanercept 50 mg; GUS = guselkumab; IFX = infliximab; IXE = ixekizumab; PLC = placebo; QW = weekly; RIS = risankizumab; SEC 150 = secukinumab 150 mg; SEC 300 = secukinumab 300 mg; TIL 100 = tildrakizumab 100 mg; TIL 200 = tildrakizumab 200 mg; UST 45/90 = ustekinumab 45 mg or 90 mg; UST 90 = ustekinumab 90 mg.
Source: Sponsor-submitted indirect treatment comparison.53
Short-Term (10 Weeks to 16 Weeks) PASI NMA Findings
The baseline risk-adjusted random effects REZ multinomial model was chosen. The network diagram is shown in Figure 4.
Overall, little inconsistency is observed in the chosen base-case model, with only 5 study arms of the 197 included in the model being singled out as outliers, therefore showing an overall robust fit of the model to the data.
Deucravacitinib 6 mg is favoured over placebo, apremilast, and etanercept 50 mg weekly (25 mg twice weekly or 50 mg weekly) in attaining PASI response at weeks 10 to 16. For placebo, apremilast, and etanercept 50 mg weekly, the difference was seen across the 4 PASI levels. The comparisons with etanercept 50 mg twice weekly show that deucravacitinib 6 mg gains in relative efficacy with each level of PASI score, from no difference for PASI 50, showing a numerical difference for PASI 75 and PASI 90, and at last reaching statistical significance for PASI 100 (i.e., with 95% CrI that excluded the null).
All other comparisons versus deucravacitinib are in favour of the comparator, with the exception of tildrakizumab, certolizumab, and ustekinumab. No difference was seen between deucravacitinib 6 mg and tildrakizumab 100 mg on any of the PASI response levels, and between deucravacitinib and tildrakizumab 200 mg, certolizumab 200 mg, and ustekinumab 90 mg for PASI 100, as the 95% CrI included the null.
The ORs and associated 95% CrIs for all these comparisons are represented in Figure 5, Figure 6, and Figure 7, arranged by treatment class to facilitate the interpretation.
Figure 5: PASI 75 at 10 Weeks to 16 Weeks — Deucravacitinib 6 mg Versus Other Treatments (RE, Baseline Risk-Adjusted, REZ Multinomial NMA)
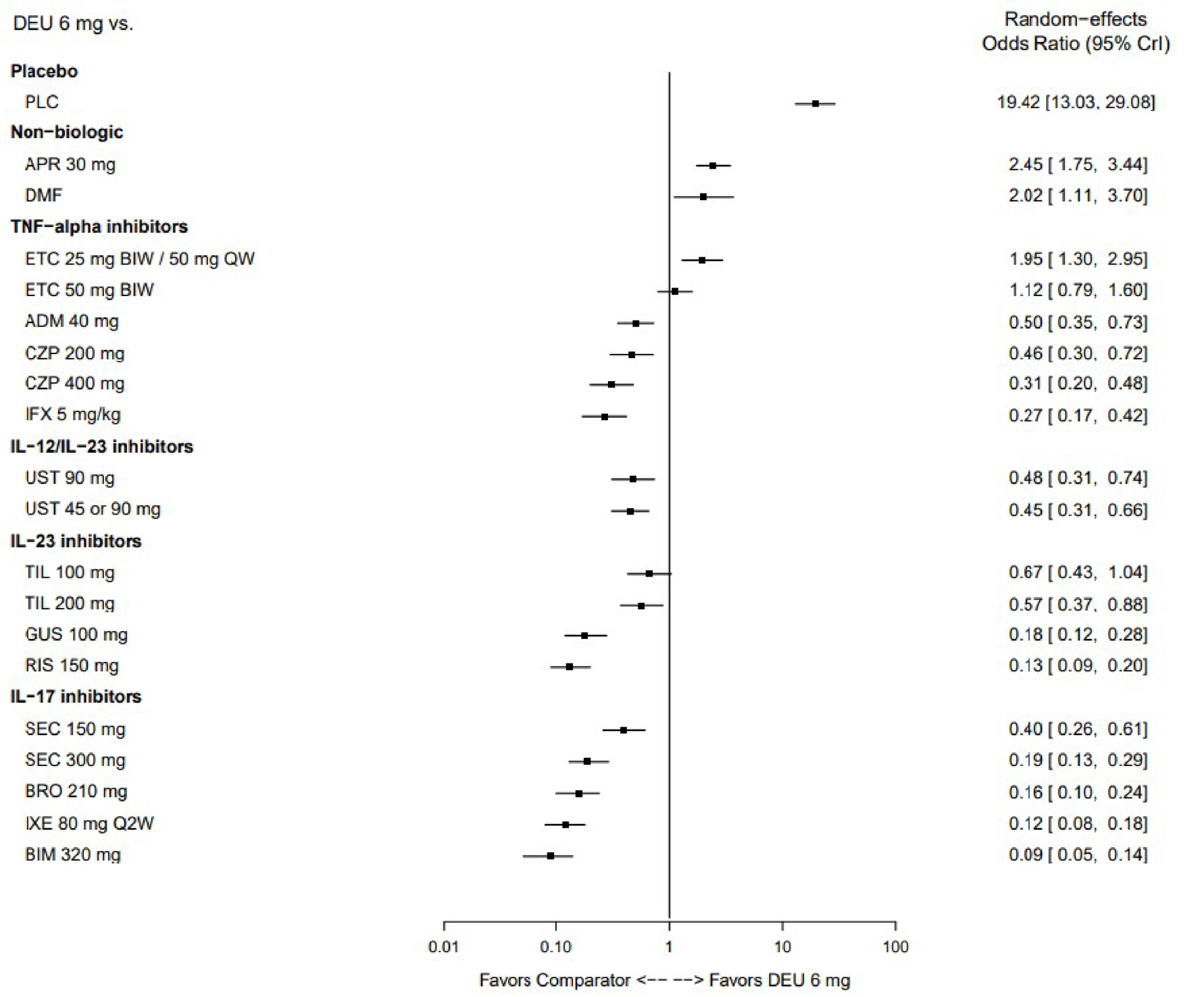
ADM = adalimumab; APR = apremilast; BIM = bimekizumab; BIW = twice per week; BRO = brodalumab; CrI = credible interval; CZP = certolizumab pegol; DEU = deucravacitinib; DMF = dimethyl fumarate; ETC = etanercept; GUS = guselkumab; IFX = infliximab; IL = interleukin; IXE = ixekizumab; NMA = network meta-analysis; PASI 75 = 75% reduction in Psoriasis Area and Severity Index score; PLC = placebo; Q2W = every 2 weeks; QW = weekly; RE = random effects; RIS = risankizumab; SEC = secukinumab; TIL = tildrakizumab; TNF = tumour necrosis factor; UST = ustekinumab; vs. = versus.
Source: Sponsor-submitted indirect treatment comparison.53
Figure 6: PASI 90 at 10 Weeks to 16 Weeks — Deucravacitinib 6 mg Versus Other Treatments (RE, Baseline Risk-Adjusted, REZ Multinomial NMA)
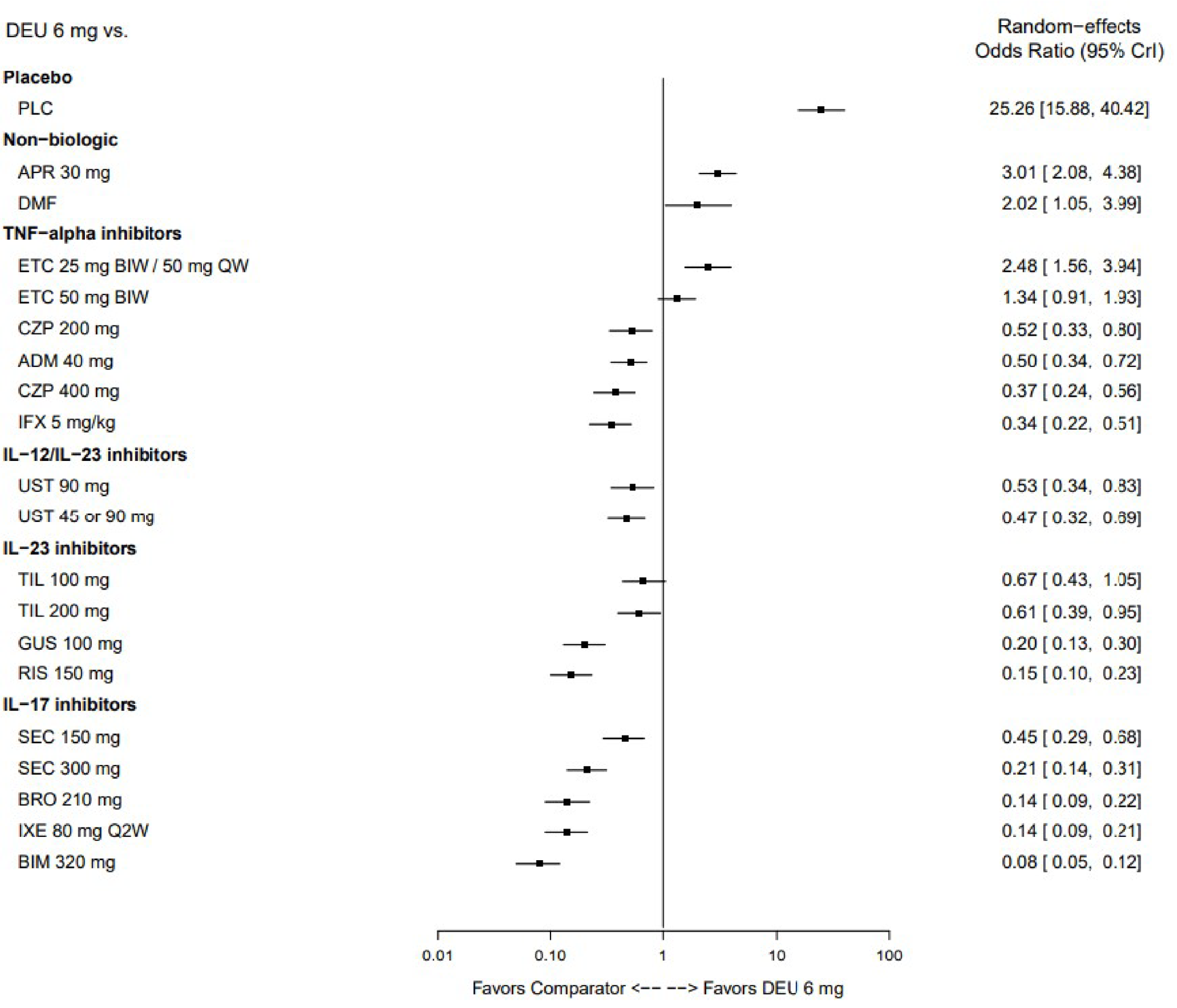
ADM = adalimumab; APR = apremilast; BIM = bimekizumab; BIW = twice per week; BRO = brodalumab; CrI = credible interval; CZP = certolizumab pegol; DEU = deucravacitinib; DMF = dimethyl fumarate; ETC = etanercept; GUS = guselkumab; IFX = infliximab; IL = interleukin; IXE = ixekizumab; NMA = network meta-analysis; PASI 90 = 90% reduction in Psoriasis Area and Severity Index score; PLC = placebo; Q2W = every 2 weeks; QW = weekly; RE = random effects; RIS = risankizumab; SEC = secukinumab; TIL = tildrakizumab; TNF = tumour necrosis factor; UST = ustekinumab; vs. = versus.
Source: Sponsor-submitted indirect treatment comparison.53
Figure 7: PASI 100 at 10 to 16 Weeks — Deucravacitinib 6 mg Versus Other Treatments (RE, Baseline Risk-Adjusted, REZ Multinomial NMA)
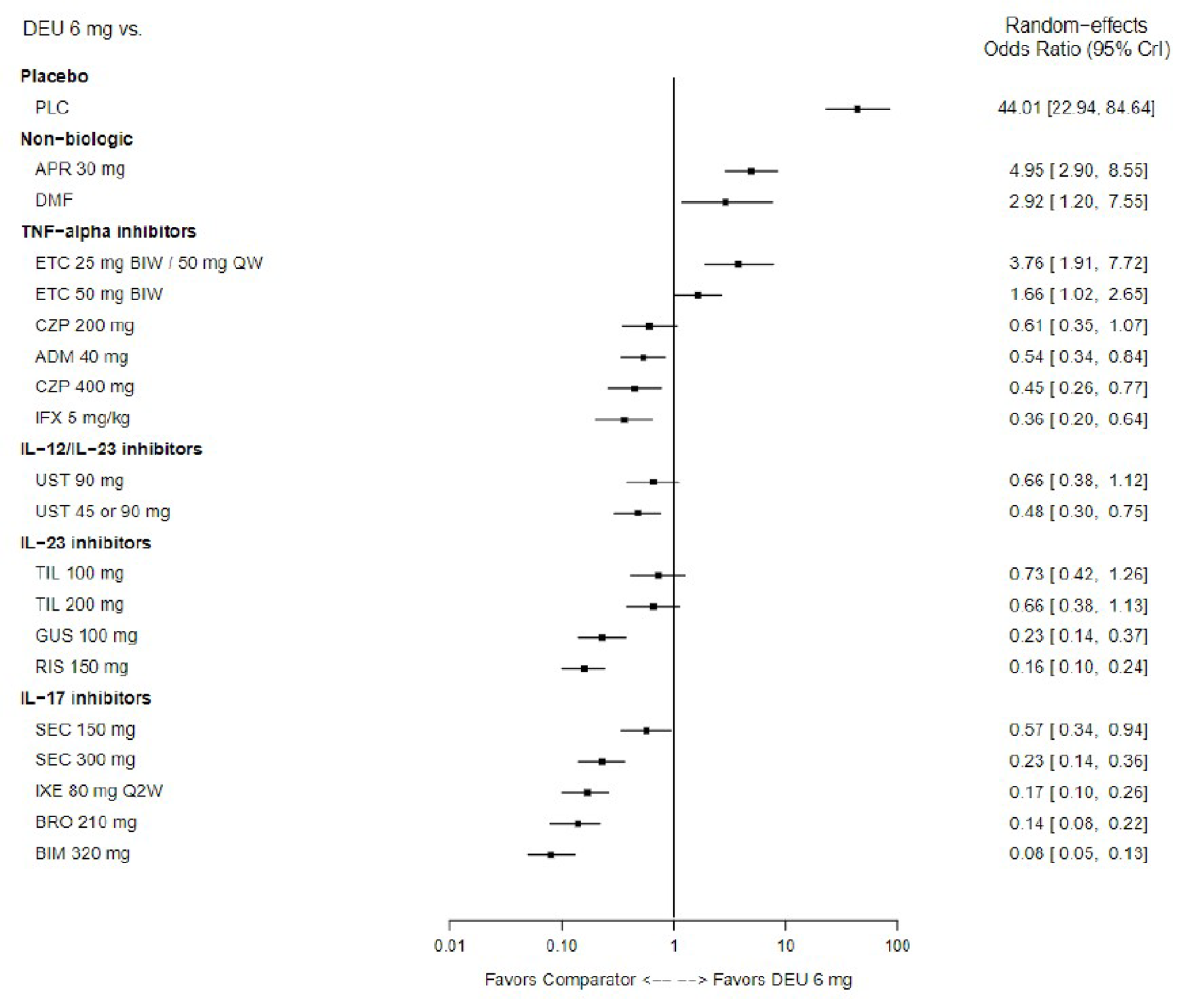
Source: Sponsor-submitted indirect treatment comparison.53
Short-Term (10 Weeks to 16 Weeks) PASI NMA Findings: Subgroup Analysis, Biologic-Naive
Among biologic-naive patients, 27 RCTs contributed data to the subgroup analysis for PASI 75 responses (Figure 8). Due to limited data availability, analyses on the biologic-naive population were limited to PASI 75 percentage level, using a binomial approach (baseline risk-adjusted RE model). The network diagram is shown in Figure 8.
Similar to the overall population, all treatments were more effective than placebo. In the biologic-naive subpopulation, deucravacitinib 6 mg is favoured over placebo and apremilast in attaining PASI 75 response levels at weeks 10 to weeks 16. No differences were detected from either regimen of etanercept 50 mg weekly (difference in favour of deucravacitinib) and etanercept 50 mg twice weekly, certolizumab 200 mg, and ustekinumab 90 mg (differences in favour of the comparators). All other differences are in favour of the other treatments (Figure 9).
Figure 8: Evidence Network — PASI 75, Biologic-Naive Subgroup
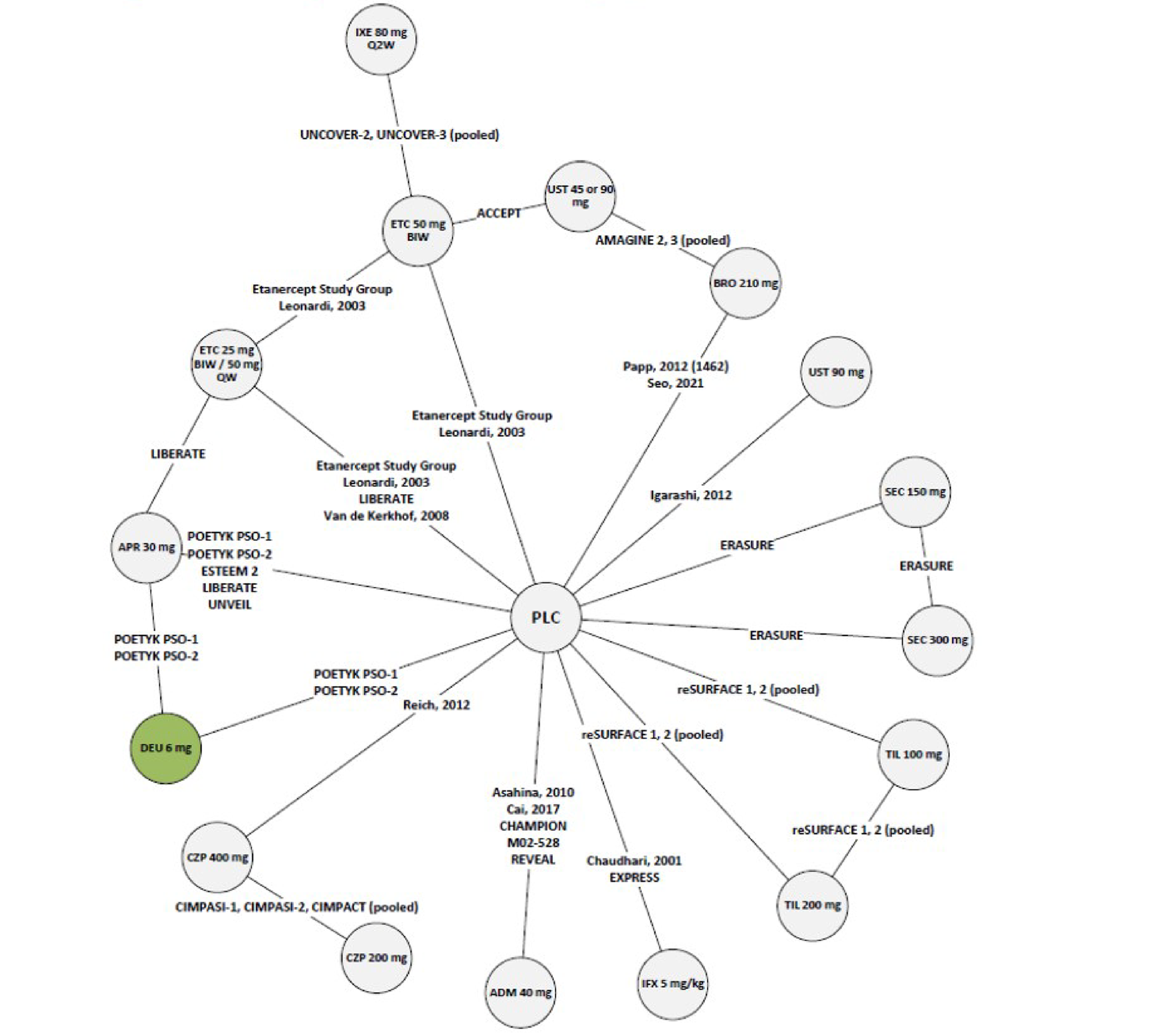
ADM = adalimumab; APR = apremilast; BIW = twice per week; BRO = brodalumab; CZP = certolizumab pegol; DEU = deucravacitinib; ETC = etanercept; IFX = infliximab; IXE = ixekizumab; PASI 75 = 75% reduction in Psoriasis Area and Severity Index score; PLC = placebo; Q2W = every 2 weeks; QW = weekly; SEC = secukinumab; TIL = tildrakizumab; UST = ustekinumab.
Source: Sponsor-submitted indirect treatment comparison.53
Figure 9: PASI 75 at 10 Weeks to 16 Weeks — Deucravacitinib 6 mg Versus Other Treatments (RE, Baseline-adjusted Binomial NMA), Biologic-Naive Subgroup
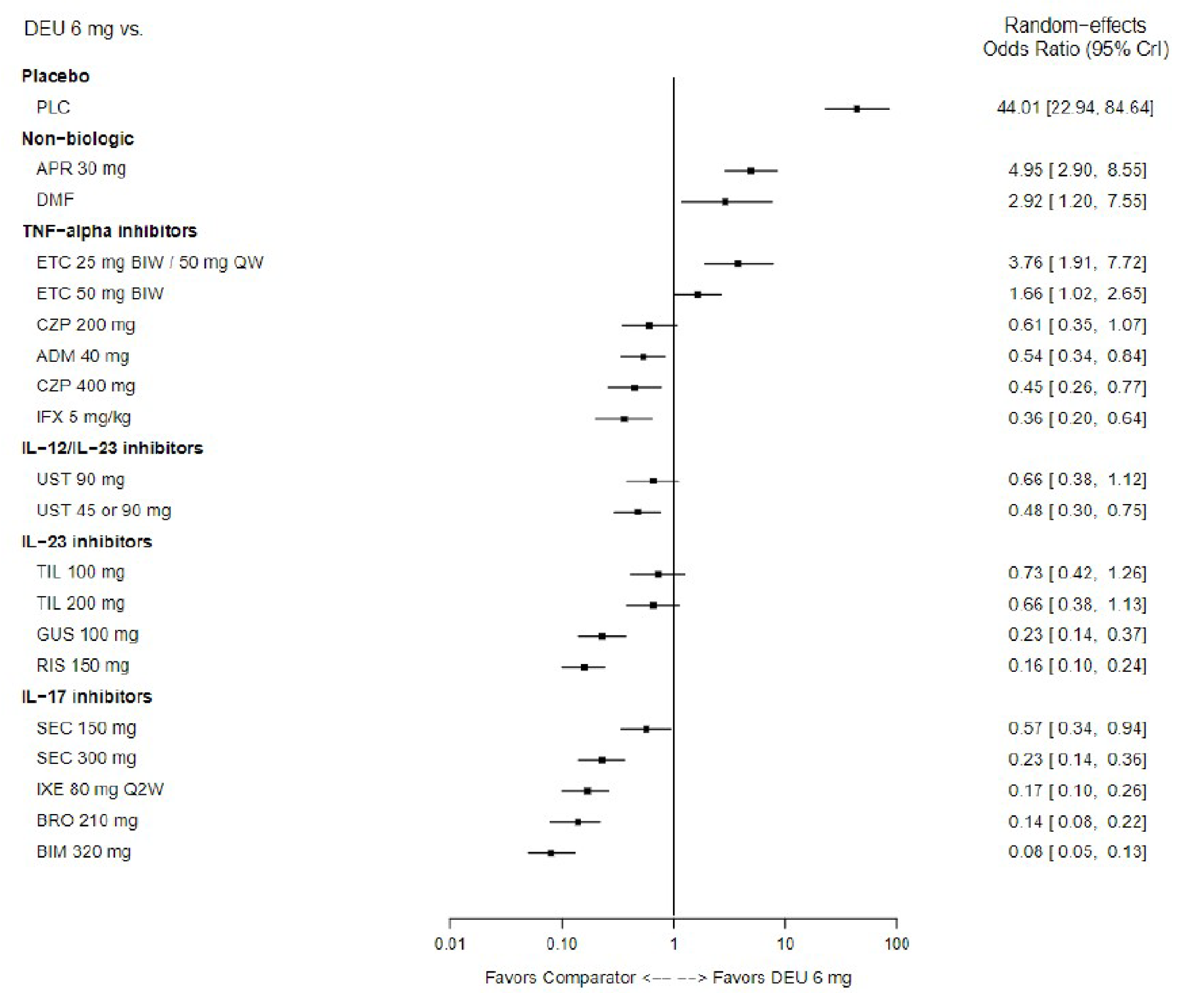
ADM = adalimumab; APR = apremilast; BIM = bimekizumab; BIW = twice per week; BRO = brodalumab; CrI = credible interval; CZP = certolizumab pegol; DEU = deucravacitinib; DMF = dimethyl fumarate; ETC = etanercept; GUS = guselkumab; IFX = infliximab; IL = interleukin; IXE = ixekizumab; NMA = network meta-analysis; PASI 75 = 75% reduction in Psoriasis Area and Severity Index score; PLC = placebo; Q2W = every 2 weeks; QW = weekly; RE = random effects; RIS = risankizumab; SEC = secukinumab; TIL = tildrakizumab; TNF = tumour necrosis factor; UST = ustekinumab; vs. = versus.
Source: Sponsor-submitted indirect treatment comparison.53
Short-Term (10 Weeks to 16 Weeks) PASI NMA Findings: Subgroup Analysis, Biologic-Experienced
Among patients previously treated with biologic agents, 11 RCTs contributed data to the subgroup analysis for PASI 75 responses. Due to limited data availability, analyses on the biologic-naive population were limited to PASI 75 percentage level, using a binomial approach (unadjusted RE model).
All estimates were highly imprecise, as indicated by the width of the CrIs around the ORs (Figure 10). The sponsor did not recommend pursuing this analysis further and deemed potential alternative analyses were not likely to reduce the imprecision and uncertainties.
Midterm (24 Weeks to 28 Weeks) PASI NMA Findings
The baseline risk-adjusted random effects REZ multinomial model was chosen. The network diagram is shown in Figure 11.
Figure 10: PASI 75 at 10 to 16 Weeks — Deucravacitinib 6 mg Versus Other Treatments (RE, Unadjusted Binomial NMA), Biologic-Experienced Subgroup
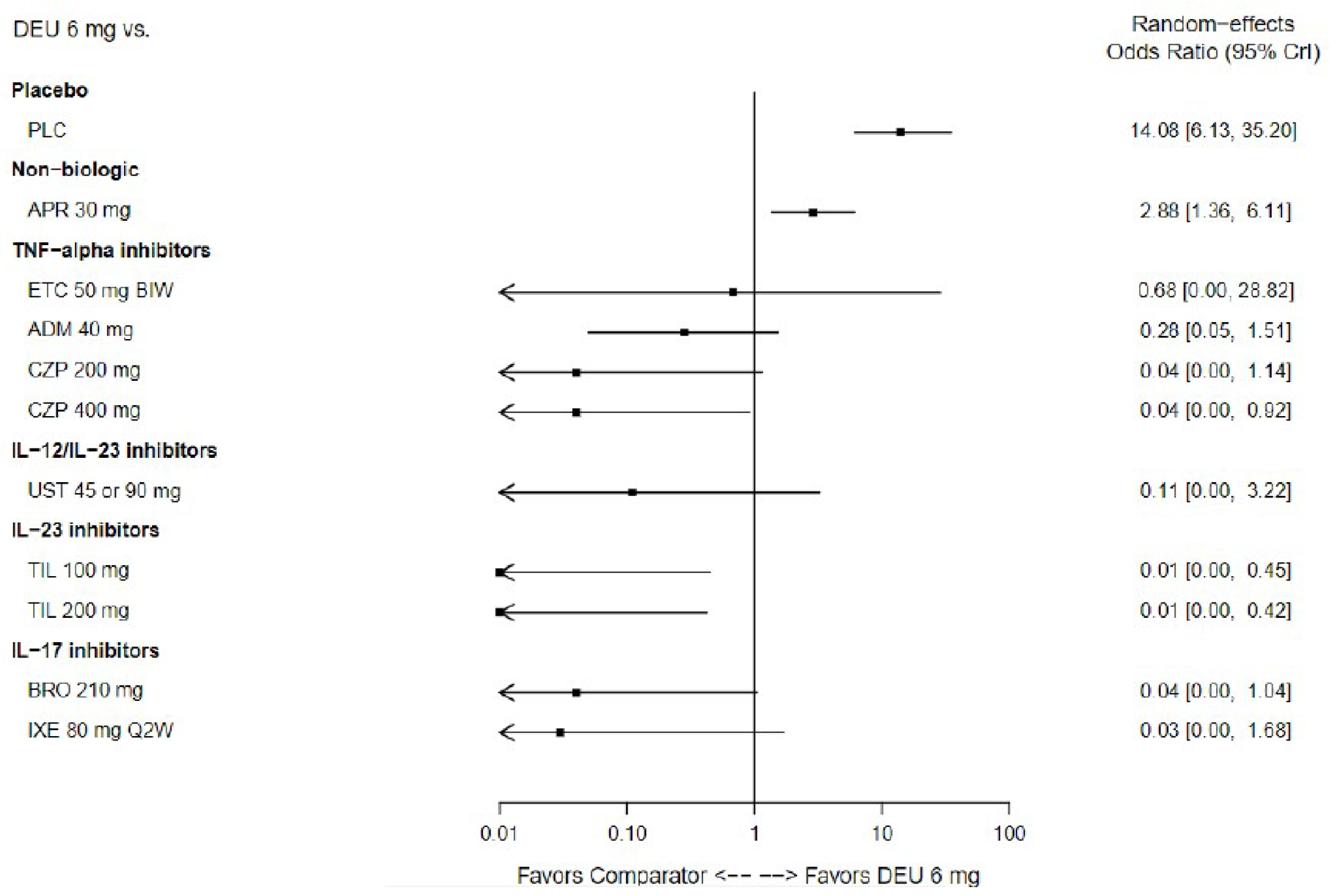
ADM = adalimumab; APR = apremilast; BIW = twice per week; BRO = brodalumab; CrI = credible interval; CZP = certolizumab pegol; DEU = deucravacitinib; ETC = etanercept; IL = interleukin; IXE = ixekizumab; NMA = network meta-analysis; PASI 75 = 75% reduction in Psoriasis Area and Severity Index score; PLC = placebo; Q2W = every 2 weeks; RE = random effects; TIL = tildrakizumab; TNF = tumour necrosis factor; UST = ustekinumab; vs. = versus.
Source: Sponsor-submitted indirect treatment comparison.53
Figure 11: Evidence Network — PASI Response (24 Weeks to 28 Weeks)
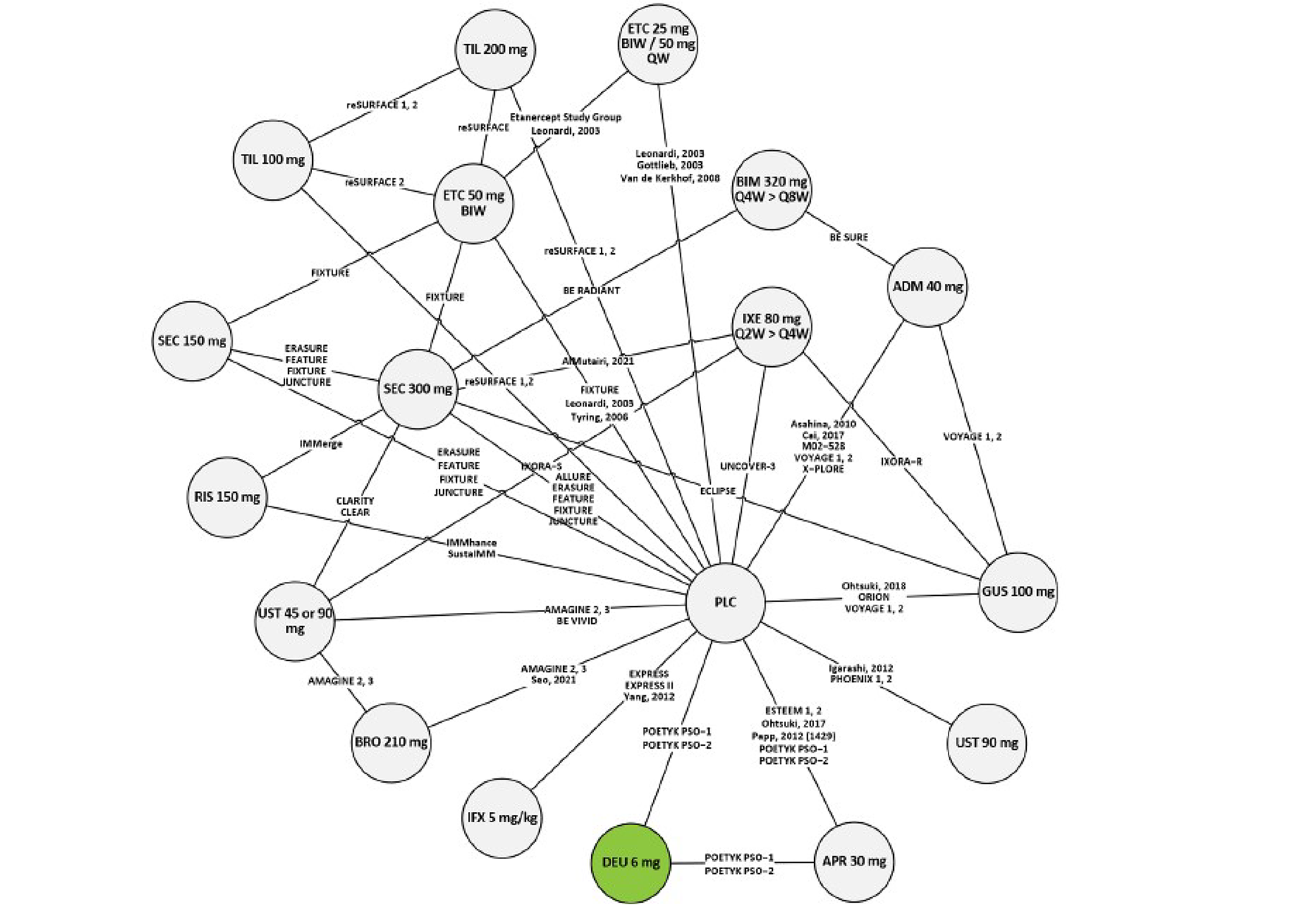
APR = apremilast; BIM = bimekizumab; BIW = twice per week; BRO = brodalumab; DEU = deucravacitinib; ETC = etanercept; GUS = guselkumab; IFX = infliximab; IXE = ixekizumab; PASI = Psoriasis Area and Severity Index; PLC = placebo; Q2W = every 2 weeks; Q4W = every 4 weeks; Q8W = every 8 weeks; QW = weekly; RIS = risankizumab; SEC = secukinumab; TIL = tildrakizumab; UST = ustekinumab.
Source: Sponsor-submitted indirect treatment comparison.53
Overall, little inconsistency is observed in the chosen base-case model, with only 6 study arms out of the 112 included in the model being singled out as outliers, therefore showing an overall robust fit of the model to the data.
Deucravacitinib 6 mg is favoured over placebo and apremilast in attaining all levels of PASI responses at weeks 24 to weeks 28. Compared to the rest of the treatments, there was variability in the relative effect of deucravacitinib 6 mg in attaining different levels of PASI responses at 24 weeks to 28 weeks. Deucravacitinib 6 mg was no different from etanercept 25 mg twice weekly or 50 mg weekly and etanercept 50 mg twice weekly in achieving PASI 50 and 100; whereas it was favoured to etanercept 25 mg twice weekly or 50 mg weekly at achieving PASI 75 and 90. No differences were found for deucravacitinib 6 mg compared to ustekinumab 45 mg or 90 mg, secukinumab 150 mg, and tildrakizumab 100 mg and 200 mg in attaining PASI 50, tildrakizumab 100 mg and 200 mg attaining PASI 75, and tildrakizumab 100 mg in attaining PASI 100. All other biologic comparators were favoured to deucravacitinib 6 mg across all PASI response levels.
The ORs and associated 95% CrIs for all these comparisons are represented on Figure 12, Figure 13, and Figure 14, arranged by treatment class to facilitate the interpretation.
Figure 12: PASI 75 at 24 Weeks to 28 Weeks — Deucravacitinib 6 mg Versus Other Treatments (RE, Baseline Risk-Adjusted, REZ Multinomial NMA)
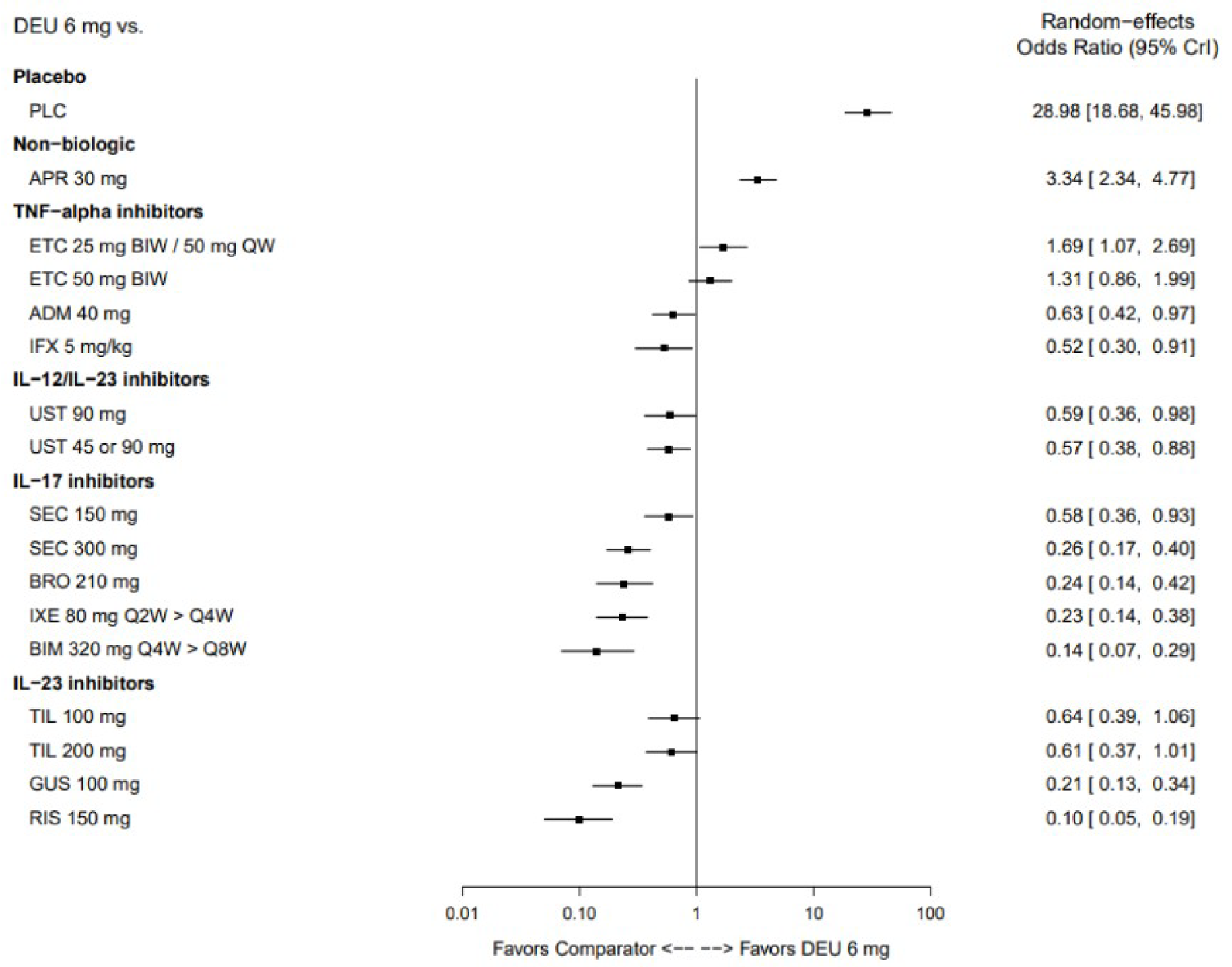
ADM = adalimumab; APR = apremilast; BIM = bimekizumab; BIW = twice per week; BRO = brodalumab; CrI = credible interval; DEU = deucravacitinib; ETC = etanercept; GUS = guselkumab; IFX = infliximab; IL = interleukin; IXE = ixekizumab; NMA = network meta-analysis; PASI 75 = 75% reduction in Psoriasis Area and Severity Index score; PLC = placebo; Q2W = every 2 weeks; Q4W = every 4 weeks; Q8W = every 8 weeks; QW = weekly; RE = random effects; RIS = risankizumab; SEC = secukinumab; TIL = tildrakizumab; TNF = tumour necrosis factor; UST = ustekinumab; vs. = versus.
Source: Sponsor-submitted indirect treatment comparison.53
Figure 13: PASI 90 at 24 Weeks to 28 Weeks — Deucravacitinib 6 mg Versus Other Treatments (RE, Baseline Risk-Adjusted, REZ Multinomial NMA)
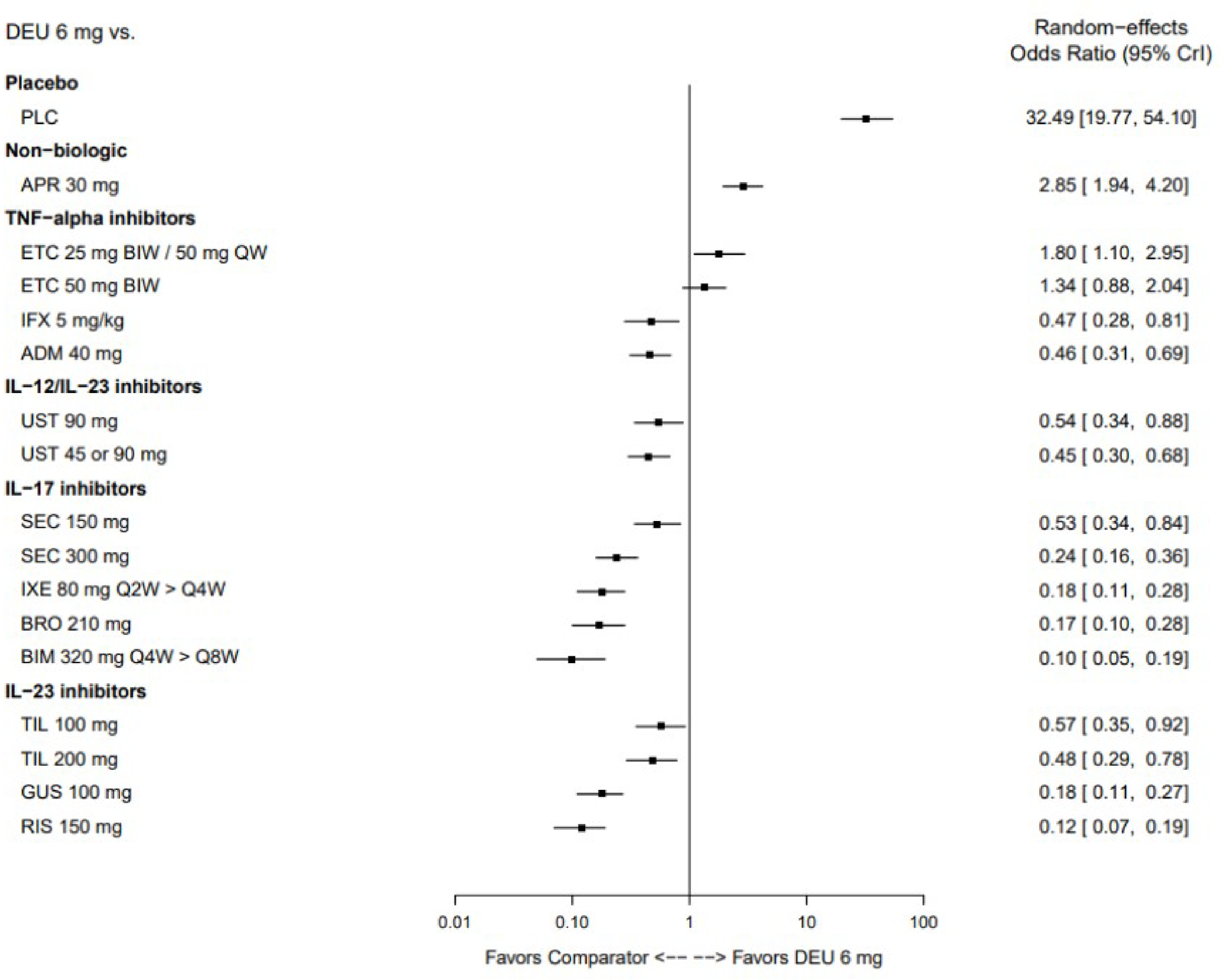
ADM = adalimumab; APR = apremilast; BIM = bimekizumab; BIW = twice per week; BRO = brodalumab; CrI = credible interval; DEU = deucravacitinib; ETC = etanercept; GUS = guselkumab; IFX = infliximab; IL = interleukin; IXE = ixekizumab; NMA = network meta-analysis; PASI 90 = 90% reduction in Psoriasis Area and Severity Index score; PLC = placebo; Q2W = every 2 weeks; Q4W = every 4 weeks; Q8W = every 8 weeks; QW = weekly; RE = random effects; RIS = risankizumab; SEC = secukinumab; TIL = tildrakizumab; TNF = tumour necrosis factor; UST = ustekinumab; vs. = versus.
Source: Sponsor-submitted indirect treatment comparison.53
Figure 14: PASI 100 at 24 Weeks to 28 Weeks —Deucravacitinib 6 mg Versus Other Treatments (RE, Baseline Risk-Adjusted, REZ Multinomial NMA)
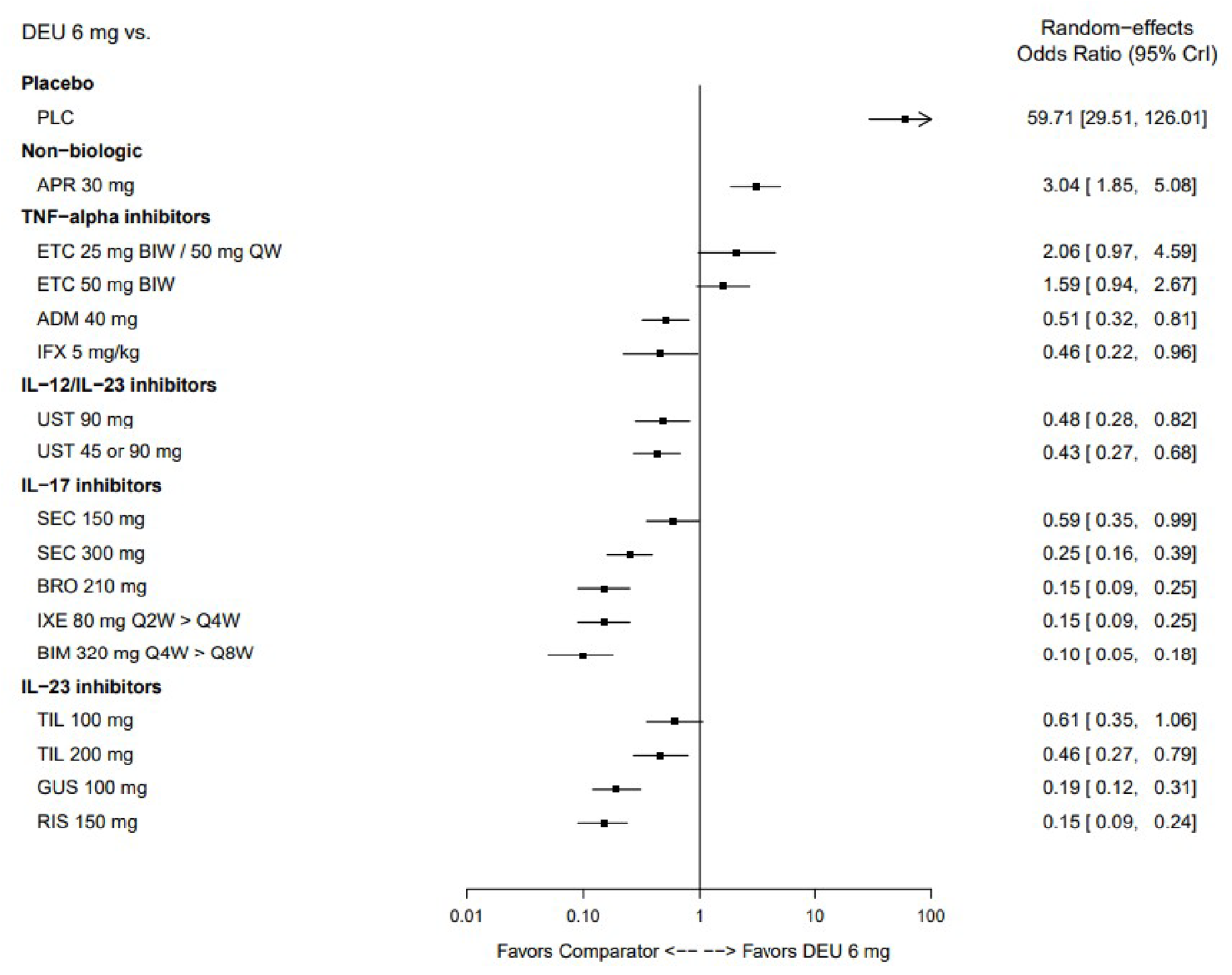
ADM = adalimumab; APR = apremilast; BIM = bimekizumab; BIW = twice per week; BRO = brodalumab; CrI = credible interval; DEU = deucravacitinib; ETC = etanercept; GUS = guselkumab; IFX = infliximab; IL = interleukin; IXE = ixekizumab; NMA = network meta-analysis; PASI 100 = 100% reduction in Psoriasis Area and Severity Index score; PLC = placebo; Q2W = every 2 weeks; Q4W = every 4 weeks; Q8W = every 8 weeks; QW = weekly; RE = random effects; RIS = risankizumab; SEC = secukinumab; TIL = tildrakizumab; TNF = tumour necrosis factor; UST = ustekinumab; vs. = versus.
Source: Sponsor-submitted indirect treatment comparison.53
Long-Term (44 Weeks to 60 Weeks) PASI NMA Findings
The baseline risk-adjusted random effects REZ multinomial model was chosen. The network diagram is shown in Figure 15.
Figure 15: Evidence Network — PASI Response (44 Weeks to 60 Weeks)
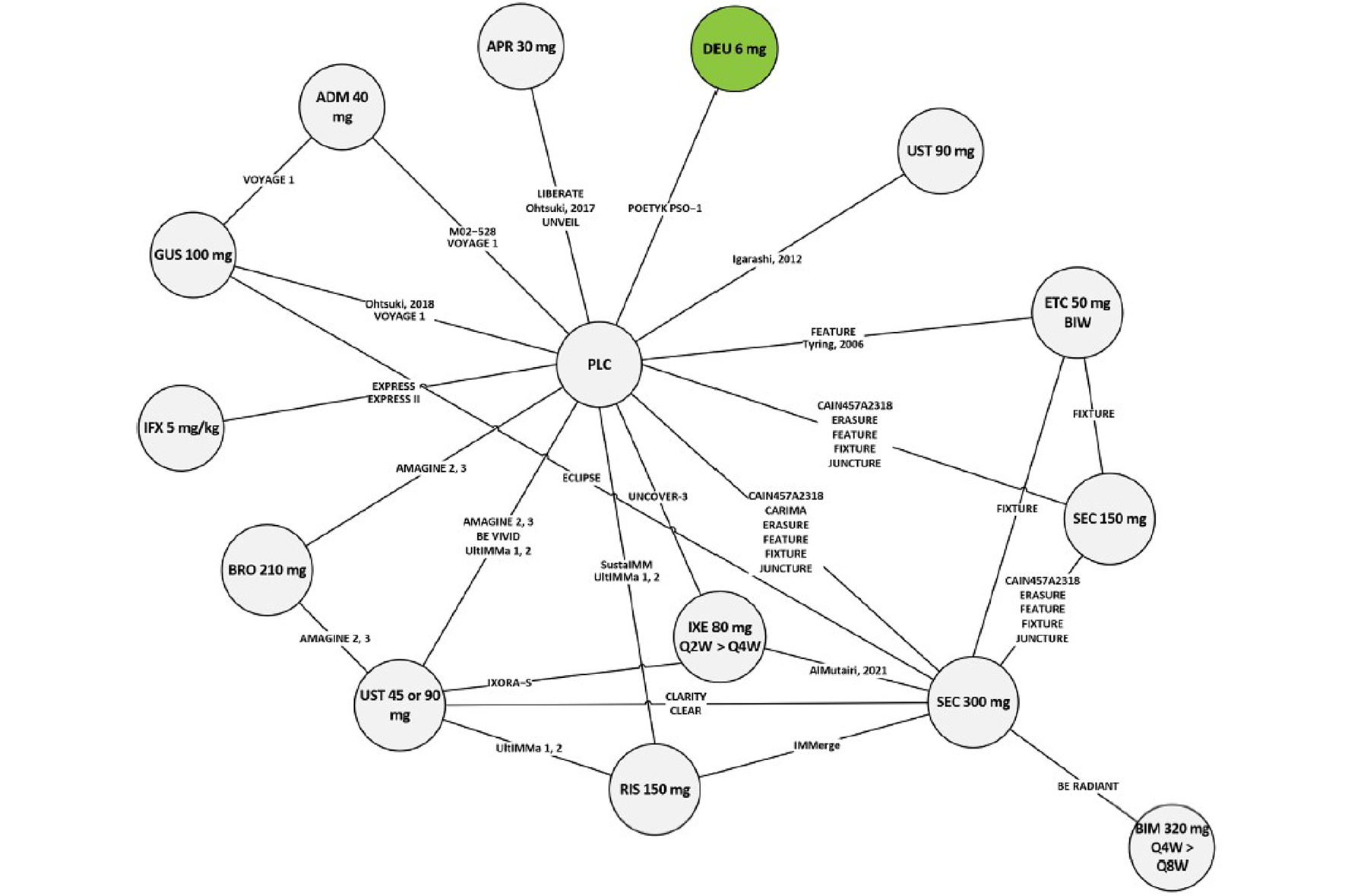
ADM = adalimumab; APR = apremilast; BIM = bimekizumab; BIW = twice per week; BRO = brodalumab; DEU = deucravacitinib; ETC = etanercept; GUS = guselkumab; IFX = infliximab; IXE = ixekizumab; PASI = Psoriasis Area and Severity Index; PLC = placebo; Q2W = every 2 weeks; Q4W = every 4 weeks; Q8W = every 8 weeks; RIS = risankizumab; SEC = secukinumab; UST = ustekinumab.
Source: Sponsor-submitted indirect treatment comparison.53
Overall, little inconsistency is observed in the chosen base-case model, with only 4 study arms out of the 75 included in the model being singled out as outliers, therefore showing an overall robust fit of the model to the data.
Similar to the analysis results at 10 weeks to 16 weeks and 24 weeks to 28 weeks, deucravacitinib 6 mg was favoured to placebo and apremilast in attaining all levels of PASI levels at 44 weeks to 60 week.
No difference was found when comparing deucravacitinib 6 mg to the TNF alpha inhibitors involved in the long term analyses as the 95% CrIs included the null (i.e., included the value of 1). Also, no difference was found when comparing deucravacitinib 6 mg with the IL-15 inhibitor secukinumab 150 mg and the IL-12/23 inhibitor ustekinumab (in doses of 45 mg or 90 mg and 90 mg). All remaining comparisons favour the biologic versus deucravacitinib for all PASI levels.
The ORs and associated 95% CrIs for all these comparisons are represented on Figure 16, Figure 17, and Figure 18, arranged by treatment class to facilitate the interpretation.
Figure 16: PASI 75 at 44 Weeks to 60 Weeks — Deucravacitinib 6 mg Versus Other Treatments (RE, Baseline Risk-Adjusted, REZ Multinomial NMA)
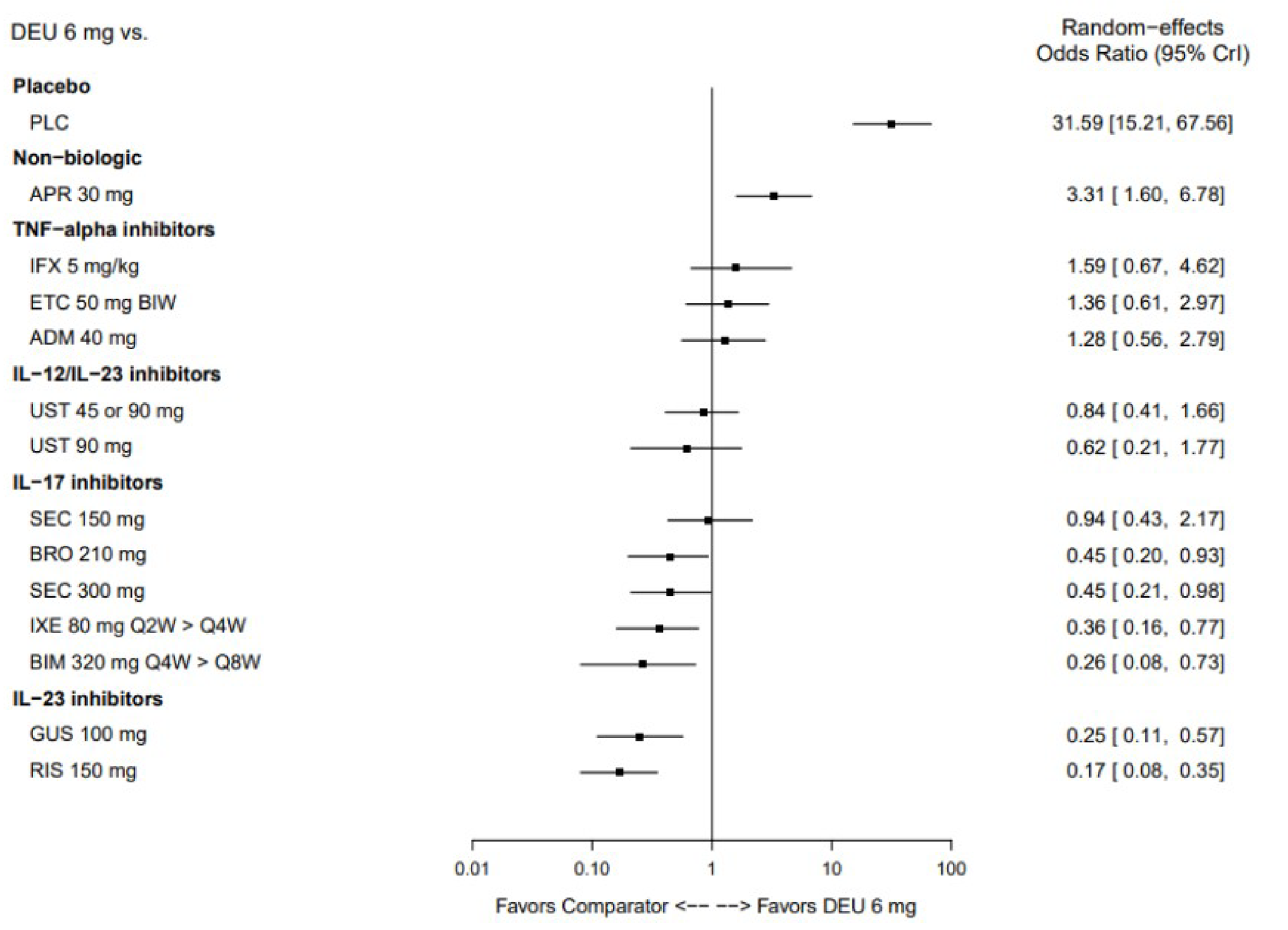
ADM = adalimumab; APR = apremilast; BIM = bimekizumab; BIW = twice per week; BRO = brodalumab; CrI = credible interval; DEU = deucravacitinib; ETC = etanercept; GUS = guselkumab; IFX = infliximab; IL = interleukin; IXE = ixekizumab; NMA = network meta-analysis; PASI 75 = 75% reduction in Psoriasis Area and Severity Index score; PLC = placebo; Q2W = every 2 weeks; Q4W = every 4 weeks; Q8W = every 8 weeks; RE = random effects; RIS = risankizumab; SEC = secukinumab; TNF = tumour necrosis factor; UST = ustekinumab; vs. = versus.
Source: Sponsor-submitted indirect treatment comparison.53
Figure 17: PASI 90 at 44 Weeks to 60 Weeks — Deucravacitinib 6 mg Versus Other Treatments (RE, Baseline Risk-Adjusted, REZ Multinomial NMA)
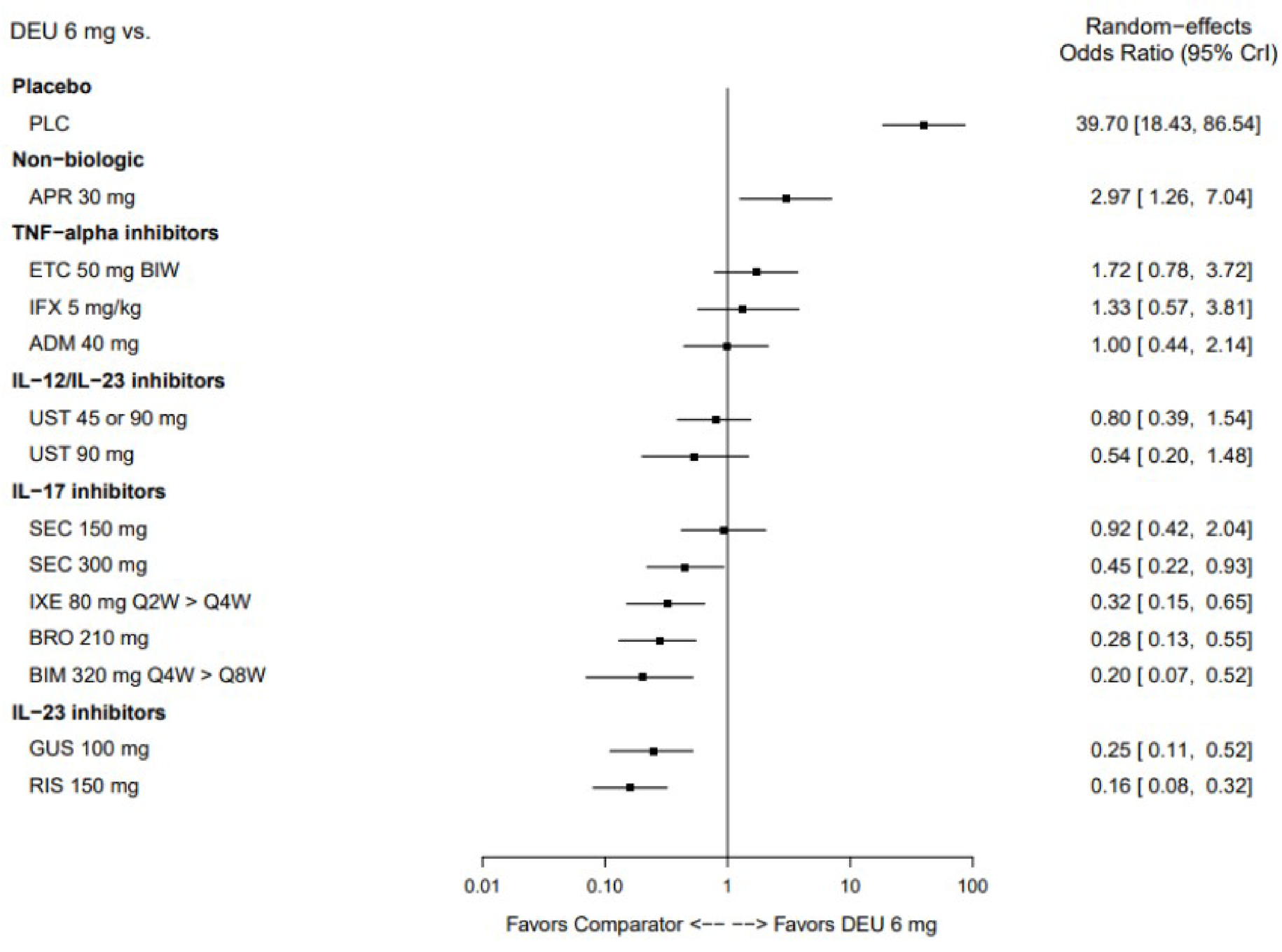
ADM = adalimumab; APR = apremilast; BIM = bimekizumab; BIW = twice per week; BRO = brodalumab; CrI = credible interval; DEU = deucravacitinib; ETC = etanercept; GUS = guselkumab; IFX = infliximab; IL = interleukin; IXE = ixekizumab; NMA = network meta-analysis; PASI 90 = 90% reduction in Psoriasis Area and Severity Index score; PLC = placebo; Q2W = every 2 weeks; Q4W = every 4 weeks; Q8W = every 8 weeks; RE = random effects; RIS = risankizumab; SEC = secukinumab; TNF = tumour necrosis factor; UST = ustekinumab; vs. = versus.
Source: Sponsor-submitted indirect treatment comparison.53
Figure 18: PASI 100 at 44 Weeks to 60 Weeks — Deucravacitinib 6 mg Versus Other Treatments (RE, Baseline Risk-Adjusted, REZ Multinomial NMA)
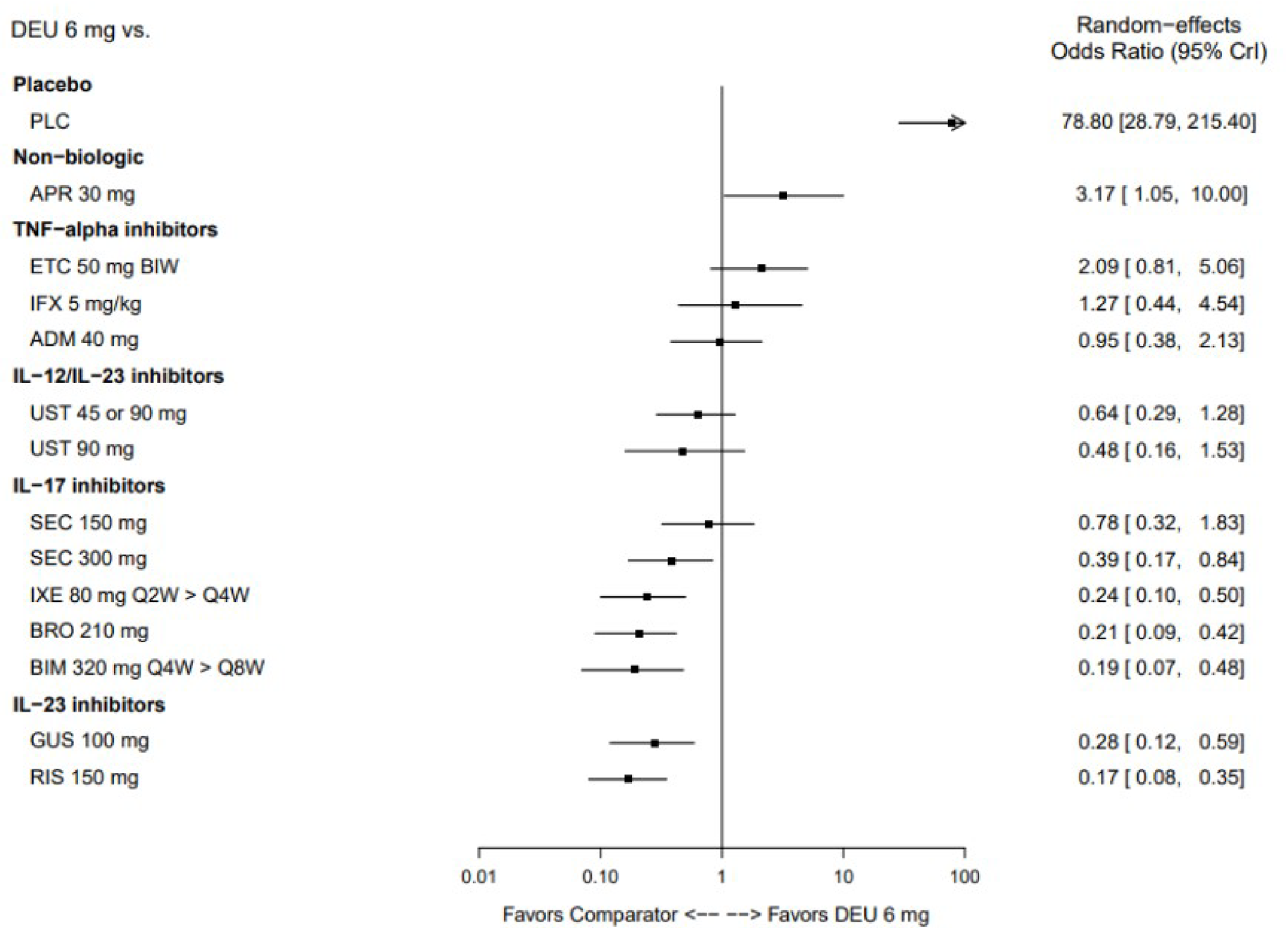
ADM = adalimumab; APR = apremilast; BIM = bimekizumab; BIW = twice per week; BRO = brodalumab; CrI = credible interval; DEU = deucravacitinib; ETC = etanercept; GUS = guselkumab; IFX = infliximab; IL = interleukin; IXE = ixekizumab; NMA = network meta-analysis; PASI 100 = 100% reduction in Psoriasis Area and Severity Index score; PLC = placebo; Q2W = every 2 weeks; Q4W = every 4 weeks; Q8W = every 8 weeks; RE = random effects; RIS = risankizumab; SEC = secukinumab; TNF = tumour necrosis factor; UST = ustekinumab; vs. = versus.
Source: Sponsor-submitted indirect treatment comparison.53
Sensitivity Analysis: Deucravacitinib at 24 Weeks Versus Other Comparators at 10 Weeks to 16 Weeks
This sensitivity analysis replaced the 16-week data for deucravacitinib with 24-week data. The baseline risk-adjusted random effects REZ multinomial model was chosen. The network structure and model settings remained the same as the main analysis (short-term, 10 weeks to 16 weeks) PASI NMA findings.
The sensitivity analysis with 24-week data for deucravacitinib 6 mg resulted in slight shifts in the point estimates of the ORs to be more favourable for deucravacitinib 6 mg across all PASI response levels. Compared to the original scenario used in the main analysis, tildrakizumab 200 mg and adalimumab 40 mg changed from being favoured versus deucravacitinib 6 mg to showing no difference for PASI 50. For PASI 75, deucravacitinib 6 mg changed from no difference to being favoured versus etanercept 50 mg twice weekly, and adalimumab 40 mg, ustekinumab 90 mg, and tildrakizumab 200 mg shifted from being favoured over deucravacitinib 6 mg to no difference. For PASI 90, deucravacitinib 6 mg changed from showing no difference to being favoured versus etanercept 50 mg twice weekly and certolizumab pegol 200 mg, ustekinumab 90 mg, and tildrakizumab 200 mg changed from being favoured versus deucravacitinib 6 mg to no difference. For PASI 100, tildrakizumab 100 mg and 200 mg, ustekinumab 90 mg, secukinumab 150 mg, and adalimumab 40 mg changed from being favoured versus deucravacitinib 6 mg to showing no difference.
Critical Appraisal of Sponsor-Submitted ITC
The sponsor’s rationale for conducting the ITC (i.e., absence of head-to-head trials that have compared deucravacitinib versus other treatments in adult patients with moderate to severe plaque psoriasis) were clearly specified. A comprehensive systematic review was conducted, with multiple efficacy and safety outcomes prespecified. One efficacy outcome, PASI response, was reported. No patient-reported outcomes or AEs were analyzed.
The search and selection of the systematic review were restricted to trials published in English. The latest search update was October 2021. While this is an appropriate level of recency by established standards, it does not include any late-breaking or more recently published information. The impact of potential publication bias was also not explored in the review.
Trials were eligible first if the patients included were described as having moderate to severe psoriasis; if that was not available, thresholds based on scales were applied. Mean PASI score at baseline ranged from 8.0 to 30.3 across trials, and mean DLQI score at baseline ranged from 7.4 to 16.6 across trials, with most patients having a score between 9.8 to 14.6. According to the clinical expert CADTH consulted for this review, a patient who has a PASI score lower than 12.0 or a DLQI score lower than 12.0 would not qualify as having moderate to severe plaque psoriasis. Therefore, the expert believed a proportion of the patients included in the NMA had mild plaque psoriasis instead of moderate to severe plaque psoriasis, although it is thought to be a relatively small proportion.
Clinical heterogeneity was present in the analysis due to varying patient characteristics, including prior exposure to biologic treatment, PASI score at baseline, PGA score, and DLQI score, across trials. As part of the feasibility assessment conducted before pooling of studies, the sponsor selected patient characteristics for sensitivity and subgroup analyses. These included a subgroup analysis that analyzes outcomes for biologic-naive and biologic-experienced patients that was deemed to be important by the clinical expert CADTH consulted for this review. Adjustment for disease severity or presence of psoriatic arthritis was considered but found not feasible due to lack of reporting of subgroups within trials, and its impact on bias is undetermined. Adjustment for baseline risk, as reflected in placebo response rate, was included in the main statistical model. No additional important effect modifiers were identified by the clinical experts, therefore the impact of heterogeneity in unadjusted characteristics on the NMA results is not expected to be substantial. However, exchangeability of patients in the trials included in the NMA was not guaranteed.
The majority of trials included in the NMA were assessed as being at low risk of bias. The most common reasons for bias were missing data and inadequate reporting. The feasibility study assessed missingness and incorporated nonresponder imputation as a conservative approach to missing assessments of response.
Considerations and justification for the choices of pooling of nodes in the NMA network were not provided by the sponsor, that is, whether doses were separated or combined. Thus, it was difficult to assess the appropriateness of the sponsor’s choices for pooling of treatments for different doses. The analyses assumed patients remained on their initial treatment assigned at randomization for 1 year for the analysis of 44-week to 60-week outcomes. This may not align with true clinical practice as patients may cycle on and off different treatments over time, and this assumption limited the evidence network such that RCTs with re-randomization and/or switches to other active treatments were considered ineligible for inclusion in the NMA.
Statistical models were prespecified and appropriate to the data (multinomial model to allow incorporation of multiple PASI levels), and the method for model selection was described. An informative prior distribution was used for the variance parameter that modelled variability in effect differences between PASI cut-offs, and sensitivity analyses conducted to assess its influence.
The sensitivity analysis that compared deucravacitinib 6 mg at 24 weeks against other comparators at 10 weeks to 16 weeks was used for the sponsor’s economic model but is at high risk of bias. Combining treatment outcomes and analysis results from different time points inherently introduces potential issues. The main issue is that the best response for each patient may not have been achieved during the shorter follow-up times, and therefore the full drug effect might not have been measured. This in turn induces substantial bias in treatment efficacy.
While the ITC analyses are largely based on data-rich networks with most treatment comparisons having multiple RCTs per comparison, this feature does not extend to the subgroup analyses, with only 11 trials reporting sufficient information to inform the biologic-experienced network. This is potentially a consequence of that fact that in the past, the precise number of prior biologic treatment or type of biologic received has not been clearly reported in trials of patients with psoriasis. As a result, not only were comparisons of deucravacitinib to several of the newer biologics not available for this subpopulation, but also the subgroups reported within these RCTs were also not sufficiently large to provide precise estimates of comparative treatment effects. Studies did not necessarily stratify randomization by prior biologic exposure, meaning that randomization was not preserved in the subgroups. Given these considerations, the comparative effectiveness in the biologic-experienced subgroup remains unclear.
Given these limitations, the results from the sponsor-submitted ITC are at some risk of bias for the main comparison of deucravacitinib with other treatments in patients with moderate to severe plaque psoriasis, and highly imprecise for the biologic-experienced subgroup. Only 1 measure of efficacy and none of safety or quality of life are available.
Summary
The sponsor-submitted ITC conducted a systematic review and used a Bayesian NMA to evaluate the relative efficacy of deucravacitinib to other comparators for the treatment of patients with moderate to severe plaque psoriasis. The NMA was based on a systematic review of the literature and data from up to 84 trials were used to inform the analyses. The main efficacy outcome of interest was PASI response.
The sponsor-submitted ITC reported that in the short-term (at 10 weeks to 16 weeks), deucravacitinib is favoured versus placebo, apremilast, and etanercept in achieving all levels of PASI responses. Also, no differences were detected between deucravacitinib and tildrakizumab for all PASI levels, or to tildrakizumab, certolizumab, and ustekinumab at the PASI 100 level. All other comparisons versus deucravacitinib are in favour of the biologic comparator, typically an IL-17 or IL-23 inhibitor.
The ITC reported that in the midterm (at 24 weeks to 28 weeks), deucravacitinib was favoured versus placebo and apremilast in attaining all levels of PASI responses at weeks 24 to weeks 28. Compared to the rest of the treatments, there was variability in the relative effect of deucravacitinib in attaining different levels of PASI responses. No differences were found for deucravacitinib compared to ustekinumab, or secukinumab, in attaining PASI 50, and versus tildrakizumab in attaining PASI 50, PASI 75, or PASI 100. All other biologic comparators were favoured over deucravacitinib across all PASI response levels.
In the longer term (at 44 weeks to 60 weeks), deucravacitinib was favoured over placebo and apremilast in attaining all levels of PASI as found at other time points. No difference was found when comparing deucravacitinib with secukinumab, ustekinumab, and the TNF alpha inhibitors included in the long term analyses (adalimumab, etanercept, and infliximab). All other treatments were favoured over deucravacitinib in attaining all levels of PASI score.
The sponsor-submitted ITC involved a rich evidence base with a large network of RCTs and sample size, which strengthened the robustness of the NMA analyses. Nonetheless, the ITC had several limitations including heterogeneity present for many patient and study characteristics in the NMA analyses, incorporation of studies that included patients with mild disease, discordance between the sponsor’s assumption of patient treatment adherence and true clinical practice, and lack of data for certain subgroup analyses. Consequentially, there is uncertainty around the ITC results, and conclusions drawn regarding the efficacy of deucravacitinib versus relevant comparators should not be interpreted with full confidence.
Other Relevant Evidence
This section includes submitted LTE studies and additional relevant studies included in the sponsor’s submission to CADTH that were considered to address important gaps in the evidence included in the systematic review.
LTE Studies
One LTE study, IM011075, submitted by the sponsor has been summarized to provide evidence regarding the long-term safety and efficacy of deucravacitinib in patients with moderate to severe plaque psoriasis.54
Methods
The LTE entitled, “An Open-Label, Multi-Center Extension Study to Characterize the Long-Term Safety and Efficacy of BMS-986165 (Deucravacitinib) in Subjects with Moderate-to-Severe Plaque Psoriasis” was submitted by the sponsor. The submitted evidence is from interim analyses for the ongoing, phase IIIb LTE to the parent studies, POETYK-1 and POETYK-2 (both global studies). Applicable parent trials include POETYK-1, POETYK-2, IM011065 (regional study), and IM011066 (regional study). However, the IM011065 (regional study) and IM011066 (regional study) are ongoing at the time of the data cut-off and patients from these studies were not allowed to participate in the LTE.
A total of 1,221 patients were enrolled and treated at 264 sites in 19 countries including Canada. Data are for all patient visits and events occurring from the first patient visit (or initiation: August 12, 2019) up to and including June 15, 2021 (last patient visit or data cut-off date). The data freeze was on July 15, 2021. The duration of study participation for individual patients is expected to be 240 weeks, with 30 additional days for safety follow-up.
The primary objective is to characterize the safety and tolerability (end points: AE and SAEs) of long-term use of deucravacitinib in patients with moderate to severe plaque psoriasis. The secondary objective is to characterize the maintenance of response to deucravacitinib (end points: sPGA 0 or 1 response, PASI 75 response) in the treatment of patients with moderate to severe plaque psoriasis. Results for additional end points submitted by the sponsor are not included in this report.
All patients were assigned to deucravacitinib at the baseline visit and instructed to take it for the duration of the study. Individual patients, and investigative site and study staff remained blinded to the POETYK-1 and POETYK-2 parent study treatment assignments before patients switching to open-label deucravacitinib in the LTE study.
Populations
All qualified patients who successfully completed the protocol-required treatment period or final treatment visit from parent studies, POETYK-1 and POETYK-2, were eligible to participate. The LTE study included adult patients who had moderate to severe plaque psoriasis (PASI score ≥ 12, sPGA ≥ 3, and BSA involvement ≥ 10% at both screening visit and day 1 of the relevant parent study). Patients were required to have stable plaque psoriasis (no morphology changes or significant flares of plaque psoriasis in the opinion of the investigator) for 6 months or more. To be eligible, patients also had to be deemed a candidate for phototherapy or systemic therapy by the investigator.
Patients with any disease or medical condition that, in the opinion of the investigator, would make the patient unsuitable for the LTE study, would interfere with the interpretation of safety or study results, or was considered unsuitable by the investigator for any other reason were excluded from the study. Prior permanent discontinuation of study treatment in the parent study or evidence of active tuberculosis were additional reasons for exclusion.
For the total population enrolled in the LTE (N = 1,221), the mean age was 46.7 years (SD = 13.17), and the mean weight was 89.44 kg (SD = 21.22 kg) at baseline in the parent studies. Approximately two-thirds (67.9%) were male, and one-third (32.1%) were female. At baseline, the majority of participants were white (86.6%) in the parent studies. At the last visit in the parent studies, disease severity scores for patients last treated with deucravacitinib (sPGA score of 3 or 4, 12.8%; PASI > 20, 1.6%; BSA ≥ 10%, 17.5%) or apremilast (sPGA score 3 or 4, 16.3%; PASI > 20, 1.3%; BSA ≥ 10%, 22.6%) suggested less severe disease than for those last treated with placebo (sPGA score 3 or 4, 39.1%; PASI > 20, 8.6%; BSA ≥ 10%, 42.7%).
Interventions
All patients received an oral tablet of deucravacitinib 6 mg daily in the morning. For the LTE, patients are grouped according to the treatment received previously during the parent study (i.e., deucravacitinib to deucravacitinib, placebo to deucravacitinib, and apremilast to deucravacitinib).
Per-protocol topical treatments or medications, medicated shampoos, and phototherapy could be used as additional treatment for psoriasis per the investigator’s discretion at any time point during the study. None and 3 patients reported use of additional phototherapy and medicated shampoos, respectively. As for very potent (group IV) corticosteroids, 24 (2.0%) patients reported using them. Any lower potency corticosteroid (groups I to III) use occurred in 91 (7.4%) of patients. Use of other antipsoriatic topical treatments occurred in a total of 50 (4.1%) patients, the most common treatment being betamethasone dipropionate and calcipotriol combination.
Outcomes
In this report, primary outcomes, AEs, and SAEs, as well as secondary outcomes, sPGA and PASI, are included. Definitions of these end points are the same as the parent studies. Certain AEs including infections, major adverse cardiovascular events, and venous thromboembolism, were adjudicated by independent, external, blinded, subspecialty expert adjudicators.
Events that were ongoing during the parent studies and worsened once the study drug was initiated in the LTE study were considered treatment-emergent AEs. With regards to efficacy, the baseline measurement from the parent studies was used as the baseline efficacy analyses in this LTE study.
Statistical Analysis
Since this study was a single-arm, LTE for observational purposes only, neither statistical comparisons nor formal calculations of sample size and power determination were conducted. Also, no imputation method was applied. Efficacy and safety summaries were provided for the “as-treated” population for 3 subgroups based on the last treatment received in the parent studies (i.e., deucravacitinib, placebo, and apremilast), as well as the total extension study population.
Patient Disposition
A total of 1,221 patients were enrolled and treated in the LTE, which represented 72% of the 1,686 patients randomized in the parent studies. At the time of the data freeze, the majority of patients were ongoing in the study (90.5%) and were receiving treatment (90.0%). Approximately 10.0% patients discontinued treatment and 9.5% patients discontinued study participation. The most common reasons for not completing treatment were other reasons (3.6%), withdrawal by the patient (2.1%), and AEs (1.3%). The most common study discontinuation reasons were patient withdrawal (4.1%), other (2.5%), and lost to follow-up (1.1%) (Table 33).
Table 33: Patient Disposition — Study IM011075
Status, n (%) | DEUC | |||
|---|---|---|---|---|
DEUC to DEUC | Placebo to DEUCa | Apremilast to DEUCa | Total | |
Screened | 1,221 (100) | |||
Enrolled and treated | 944 (100) | 197 (100) | 80 (100) | 1,221 (100) |
Completed the treatment | 0 | 0 | 0 | 0 |
Ongoing treatment | 841 (89.1) | 186 (94.4) | 72 (90.0) | 1,099 (90.0) |
Discontinued study treatment | 103 (10.9) | 11 (5.6) | 8 (10.0) | 122 (10.0) |
AE | 14 (1.5) | 0 | 2 (2.5) | 16 (1.3) |
Death | 3 (0.3) | 1 (0.5) | 0 | 4 (0.3) |
Lack of efficacy | 12 (1.3) | 1 (0.5) | 0 | 13 (1.1) |
Lost of follow-up | 13 (1.4) | 0 | 0 | 13 (1.1) |
Nonadherence with protocol | 3 (0.3) | 1 (0.5) | 0 | 4 (0.3) |
Pregnancy | 2 (0.2) | 0 | 0 | 2 (0.2) |
Patient withdrawal | 20 (2.1) | 2 (1.0) | 4 (5.0) | 26 (2.1) |
Other | 36 (3.8) | 6 (3.0) | 2 (2.5) | 44 (3.6) |
Completed the study | 0 | 0 | 0 | 0 |
Ongoing study participation | 847 (89.7) | 186 (94.4) | 72 (90.0) | 1,105 (90.5) |
Discontinued study participation | 97 (10.3) | 11 (5.6) | 8 (10.0) | 116 (9.5) |
AE | 11 (1.2) | 0 | 1 (1.3) | 12 (1.0) |
Death | 5 (0.5) | 1 (0.5) | 0 | 6 (0.5) |
Lost of follow-up | 14 (1.5) | 0 | 0 | 14 (1.1) |
Nonadherence with protocol | 3 (0.3) | 0 | 0 | 3 (0.2) |
Patient withdrawal | 40 (4.2) | 5 (2.5) | 5 (6.3) | 50 (4.1) |
Other | 24 (2.5) | 5 (2.5) | 2 (2.5) | 31 (2.5) |
Enrolled populationb | 944 | 197 | 80 | 1,221 |
As-treated populationc | 944 | 197 | 80 | 1,221 |
AE = adverse event; DEUC = deucravacitinib; LTE = long-term extension.
aPatients last received placebo and/or apremilast, respectively, in either the POETYK-1 and POETYK-2 parent studies and were switched to DEUC upon enrolment to the LTE study.
bAll patients who sign informed consent for entry into LTE.
cAll enrolled patients who took at least 1 dose of study treatment in the LTE (patients from parent studies POETYK-1 and POETYK-2 only).
Source: Clinical Study Report for IM01107554 (data cut-off of January 15, 2021; database freeze of July 15, 2021).
Exposure to Study Treatments
A total 1,187 (97.2%) patients had at least 16 weeks of exposure during the LTE. However, less than half of patients (46.9%) had exposure to deucravacitinib for 52 weeks: deucravacitinib to deucravacitinib (47.9%), placebo to deucravacitinib (37.6%), and apremilast to deucravacitinib (58.8%). Median duration of exposure for a total population was 357 days (range, 8 days to 686 days) with no meaningful differences across different categories: deucravacitinib to deucravacitinib (358 days; range, 21 days to 686 days), placebo to deucravacitinib (344 days; range, 41 days to 666 days), and apremilast to deucravacitinib (375 days; range, 8 days to 639 days). The majority of patients (70%) showed adherence rates between 75% and 100%: deucravacitinib to deucravacitinib (69.5%), placebo to deucravacitinib (72.6%), and apremilast to deucravacitinib (70%). Treatment adherence was monitored using standard drug accountability procedures (comparing the number of tablets returned to number dispensed, considering the expected regimen and any reported missed doses). Of patients (78.1%) who reported concomitant medication use, COVID-19 vaccine (21.1%), acetaminophen (10.7%), and ibuprofen (7.9%) were the most commonly used concomitant therapies reported.
Of note, patients in the largest treatment group (deucravacitinib to deucravacitinib) could have received deucravacitinib for 28, 36, or 52 weeks in the parent study before enrolling in the LTE study, depending upon their randomized treatment assignment and response.
Efficacy
Only those efficacy outcomes and analyses of subgroups identified in the review protocol are reported in the following. Efficacy was a secondary end point for this LTE study. As this was an open-label, single-arm study, data analyses are based on observed data and no statistical tests were conducted.
Response as Measured by SPGA 0 or 1
Sponsor-submitted data for the secondary efficacy end points were from week 0 through week 84. The proportion of patients reporting efficacy data was 95%, 61%, and 20% at week 24, week 48, and week 60, respectively. Due to the limited number of patients with data at later time points, the results beyond week 48 are not included in this report. Based on observed data, treatment of deucravacitinib maintained clinical efficacy through week 48.
In the total population, sPGA 0 or 1 response rates were 50.9% (95% CI, 48.1% to 53.8%; N = 1,221) at week 0 and maintained at 56.4% (95% CI, 52.7% to 60.0%; N = 745) through week 48 (Table 34).
Patients who had received active treatment (either deucravacitinib or apremilast) as the last treatment in parent trials maintained efficacy from week 0 through week 48. At week 0, response rate as measured by sPGA 0 or 1 for the deucravacitinib to deucravacitinib group was 56%, which was maintained at 53.8% at week 48. Similarly, at week 0, the apremilast to deucravacitinib group showed a response rate of 53.8% as measured by sPGA 0 or 1, which was maintained at 66.1% at week 48. In contrast, those who had received placebo in the parent study and switched to deucravacitinib in the LTE study showed improved response rate as measured by sPGA 0 or 1, from 25.4% at week 0 to 66.0% at week 48 (Table 34).
Table 34: sPGA 0 or 1 Response by Week — Study IM011075 As-Treated Population (Data as Observed)
Outcome | DEUC to DEUC n = 944 | Placebo to DEUC n = 197 | Apremilast to DEUC n = 80 | Total N = 1,221 |
|---|---|---|---|---|
Week 0 (last visit in parent studies) | ||||
Responders, n of N | 529 of 944 | 50 of 197 | 43 of 80 | 622 of 1,221 |
Response rate, % (95% CI) | 56.0 (52.8 to 59.2) | 25.4 (19.5 to 32.1) | 53.8 (42.2 to 65.0) | 50.9 (48.1 to 53.8) |
Week 24 | ||||
Responders, n of N | 508 of 903 | 140 of 190 | 50 of 73 | 698 of 1,166 |
Response rate, % (95% CI) | 56.3 (53.0 to 59.5) | 73.7 (66.8 to 79.8) | 68.5 (56.6 to 78.9) | 59.9 (57.0 to 62.7) |
Week 48 | ||||
Responders, n of N | 315 of 586 | 66 of 100 | 39 of 59 | 420 of 745 |
Response rate, % (95% CI) | 53.8 (49.6 to 57.8) | 66.0 (55.8 to 75.2) | 66.1 (52.6 to 77.9) | 56.4 (52.7 to 60.0) |
CI = confidence interval; DEUC = deucravacitinib; sPGA = static Physician’s Global Assessment.
Source: Clinical Study Report for IM011075.54
Response as Measured by PASI
The sponsor submitted data for another secondary efficacy end point, PASI 75 response from week 0 through week 84. Based on observed data, treatment of deucravacitinib maintained clinical efficacy through week 48. In the total population, PASI 75 response rates were 65.1% (95% CI, 62.4% to 67.8%; N = 1,221) at week 0 and maintained at 75.7% (95% CI, 68.7% to 80.6%; N = 745) through week 48 (Table 35).
Patients who had received active treatment (either deucravacitinib or apremilast) as the last treatment in the parent trials maintained efficacy from week 0 through week 48. At week 0, response rate as measured by PASI 75 for the deucravacitinib to deucravacitinib group was 70.8%, which was maintained at 72.9% at week 60. Similarly, at week 0, the apremilast to deucravacitinib group showed a response rate of 73.8% as measured by PASI 75, which was maintained at 81.4% at week 48. In contrast, those who had received placebo in the parent study and switched to deucravacitinib in the LTE study, showed an improved response rate as measured by PASI 75, from 34.5% at week 0 to 89.0% at week 48 (Table 35).
Table 35: PASI 75 Response by Week — Study IM011075 As-Treated Population (Data as Observed)
Outcome | DEUC to DEUC n = 944 | Placebo to DEUC n = 197 | Apremilast to DEUC n = 80 | Total N = 1,221 |
|---|---|---|---|---|
Week 0 (last visit in parent studies) | ||||
Responders, n of N | 668 of 944 | 68 of 197 | 59 of 80 | 795 of 1,221 |
Response rate, % (95% CI) | 70.8 (67.7 to 73.6) | 34.5 (27.9 to 41.6) | 73.8 (62.7 to 83.0) | 65.1 (62.4 to 67.8) |
Week 24 | ||||
Responders, n of N | 685 of 903 | 171 of 190 | 65 of 73 | 921 of 1,166 |
Response rate, % (95% CI) | 75.9 (72.9 to 78.6) | 90.0 (84.8 to 93.9) | 89.0 (79.5 to 95.1) | 79.0 (76.5 to 81.3) |
Week 48 | ||||
Responders, n of N | 427 of 586 | 89 of 100 | 48 of 59 | 564 of 745 |
Response rate, % (95% CI) | 72.9 (69.1 to 76.4) | 89.0 (81.2 to 94.4) | 81.4 (69.1 to 90.3) | 75.7 (72.5 to 78.7) |
CI = confidence interval; DEUC = deucravacitinib.
Source: Clinical Study Report for IM011075.54
Harms
Only those harms identified in the review protocol are reported in the following. Refer to Table 36 for detailed harms data.
Adverse Events
Overall, AEs were reported in 707 (57.9%) patients, which were similar across the 3 prior treatment categories. The most frequently reported AEs were COVID-19 (9.2%) and nasopharyngitis (4.4%). For the majority of subjects (90.1%), the AEs were reported as mild (27.8%) or moderate (24.3%) in severity (Table 36).
Serious Adverse Events
For the total population, 83 (6.8%) patients reported having at least 1 SAE. The most frequently reported SAEs were COVID-19 (2.0%) and COVID-19 pneumonia (1.1%) (Table 36).
Withdrawals Due to Adverse Events
The frequency of AEs leading to discontinuation was reported in 23 (1.9%) patients. The most frequently reported AEs leading to study discontinuation were COVID-19 (0.2%), malignant melanoma (0.2%), and psoriasis (0.2%) (Table 36).
Mortality
In total population, 6 patients died during the study period: 5 deaths were due to COVID-19 and 1 death was due to ruptured hemopericardium, thoracic aortic aneurysm (Table 36).
Notable Harms
Infection Events
The most frequently reported AEs were COVID-19 (9.2%), nasopharyngitis (4.4%), and upper respiratory tract infection (2.5%). As for specific infection types, influenza (0.7%), herpes zoster (0.6%), latent tuberculosis that did not convert to active (0.2%), cytomegalovirus infection localized to gut (0.1%), pulmonary tuberculosis (0.11%), and mild varicella (0.1%) were the most reported events. Based on the Clinical Study Report, there were no invasive fungal or disseminated viral infections. None of these specific infections was considered serious; only the event of pulmonary tuberculosis led to treatment discontinuation (Table 36).
Major Adverse Cardiovascular Events and Thromboembolic Events
Based on the adjudicated results, 6 patients experienced extended major adverse cardiovascular events including acute myocardial infarctions (0.2%), unstable angina requiring hospitalization (0.2%), ischemic stroke or cerebrovascular accident (0.1%), and myocardial infarction (0.1%). There was an event of deep vein thrombosis (0.1%) reported in a patient with a history of factor V Leiden mutation and a previous pulmonary embolism (Table 36).
Malignancy Events
There was a total of 16 malignancy events reported in 12 patients (1.0%). The most commonly reported malignancy events were basal cell carcinoma (0.2%), squamous cell carcinoma (0.2%), and malignant melanoma (0.2%). One patient had 2 events of intraductal proliferative breast lesion (0.1%) and invasive ductal breast carcinoma (0.1%). Events reported in 1 patient each were Bowen disease (0.1%), colorectal cancer (0.1%), acute promyelocytic leukemia (0.1%), B-cell lymphoma (0.1%), and nodal marginal zone B-cell lymphoma (0.1%). The number of patients reported to have malignancy (10 of 12) were from a category of patients previously treated with deucravacitinib. However, the frequency of malignancy appears to be similar across the 3 categories of patients: 1.1% in deucravacitinib to deucravacitinib, 0.5% in placebo to deucravacitinib, and 1.3% in apremilast to deucravacitinib (Table 36).
Creatinine Kinase Elevation Events
There were 45 (3.7%) patients who experienced creatinine kinase elevation of grade 2 or greater and 12 (1.0%) patients experienced signs and symptoms associated with the event. One patient (0.1%) discontinued treatment due to the event and none of the patients required treatment for the event. No rhabdomyolysis was reported, and 27 patients were known to have exercised in the previous 7 days before the event (Table 36).
Elevation of Aspartate Aminotransferase or Alanine Aminotransferase Events
There were 19 (1.6%) and 13 (1.1%) patients who experienced elevated alanine aminotransferase and aspartate aminotransferase, respectively. Of those, abnormalities of grade 3 or greater of increased alanine aminotransferase and aspartate aminotransferase were reported in 5 (0.4%) and 11 (0.5%) patients, respectively. Two (0.2%) patients who experienced alanine aminotransferase elevation had drug interruption due to the event (Table 36).
Decreased Neutrophil Count and White Blood Cell Count
As for grade 3 abnormalities in hematologic parameters, there were 2 (0.2%) and 1 (0.1%) patients who had decreased neutrophil and white blood cell count, respectively. There was 1 (0.1%) grade 4 abnormality of decreased neutrophil count and 1 (0.1%) grade 4 event of decreased white blood cell count. All events of grade 3 or greater decreased neutrophil (0.3%) and white blood cell count (0.2%) occurred in the deucravacitinib to deucravacitinib category whereas none of these events were reported in the other 2 categories (Table 36).
Table 36: Summary of Harms — Study IM011075 As-Treated Population
Adverse event | DEUC to DEUC N = 944 | Placebo to DEUC N = 197 | Apremilast to DEUC N = 80 | Total N = 1,221 |
|---|---|---|---|---|
Patients with ≥ 1 adverse event | ||||
n (%) | 559 (59.2) | 104 (52.8) | 44 (55.0) | 707 (57.9) |
Most common events,a n (%) | ||||
COVID-19 | 85 (9.0) | 25 (12.7) | 2 (2.5) | 112 (9.2) |
Nasopharyngitis | 48 (5.1) | 3 (1.5) | 3 (3.8) | 54 (4.4) |
Hypertension | 23 (2.4) | 7 (3.6) | 1 (1.3) | 31 (2.5) |
Upper respiratory tract infection | 28 (3.0) | 2 (1.0) | 1 (1.3) | 31 (2.5) |
Blood creatinine phosphokinase increased | 22 (2.3) | 3 (1.5) | 3 (3.8) | 28 (2.3) |
Psoriasis | 23 (2.4) | 2 (1.0) | 3 (3.8) | 28 (2.3) |
Headache | 21 (2.2) | 3 (1.5) | 2 (2.5) | 26 (2.1) |
Arthralgia | 16 (1.7) | 7 (3.6) | 2 (2.5) | 25 (2.0) |
ALT increased | 16 (1.7) | 2 (1.0) | 1 (1.3) | 19 (1.6) |
Back pain | 14 (1.5) | 5 (2.5) | 0 | 19 (1.6) |
Diarrhea | 15 (1.6) | 1 (0.5) | 0 | 16 (1.3) |
COVID-19 pneumonia | 10 (1.1) | 4 (2.0) | 1 (1.3) | 15 (1.2) |
Pharyngitis | 8 (0.8) | 2 (1.0) | 4 (5.0) | 14 (1.1) |
AST increased | 11 (1.2) | 2 (1.0) | 0 | 13 (1.1) |
Blood glucose increased | 11 (1.2) | 0 | 1 (1.3) | 12 (1.0) |
Dermatitis contact | 10 (1.1) | 1 (0.5) | 1 (1.3) | 12 (1.0) |
Urinary tract infection | 11 (1.2) | 1 (0.5) | 0 | 12 (1.0) |
By severity, n (%) | ||||
Mild | 262 (27.8) | 55 (27.9) | 23 (29.8) | 340 (27.8) |
Moderate | 243 (25.7) | 35 (17.8) | 19 (23.8) | 297 (24.3) |
Severe | 54 (5.7) | 14 (7.1) | 2 (2.5) | 70 (5.7) |
Patients with ≥ 1 SAE | ||||
n (%) | 66 (7.0) | 13 (6.6) | 4 (5.0) | 83 (6.8) |
Most common events,b n (%) | ||||
COVID-19 | 19 (2.0) | 6 (3.0) | 0 | 25 (2.0) |
COVID-19 pneumonia | 8 (0.8) | 4 (2.0) | 1 (1.3) | 13 (1.1) |
Patients who stopped treatment due to adverse events | ||||
n (%) | 19 (2.0) | 1 (0.5) | 3 (3.8) | 23 (1.9) |
Most common events,c n (%) | ||||
COVID-19 | 2 (0.2) | 1 (0.5) | 0 | 3 (0.2) |
Malignant melanoma | 2 (0.2) | 0 | 0 | 2 (0.2) |
Psoriasis | 2 (0.2) | 0 | 0 | 2 (0.2) |
Deaths | ||||
n (%) | 5 (0.5) | 1 (0.5) | 0 | 6 (0.5) |
COVID-19 | 5 (0.5) | 0 | 0 | 5 (0.4) |
Thoracic aortic aneurysm, ruptured, n (%) | 0 | 1 (0.5) | 0 | 1 (0.1) |
Notable harms | ||||
Infections and infestations SOC, n (%) | 280 (29.7) | 50 (25.4) | 21 (26.3) | 351 (28.7) |
Infections and infestations SOC SAE, n (%) | 32 (3.4) | 10 (5.1) | 1 (1.3) | 43 (3.5) |
Infections of interest to sponsor, n (%) | 15 (1.6) | 2 (1.0) | 4 (5.0) | 21 (1.7) |
Influenza | 7 (0.7) | 1 (0.5) | 0 | 8 (0.7) |
Herpes zoster | 4 (0.4) | 1 (0.5) | 2 (2.5) | 7 (0.6) |
Latent tuberculosis | 2 (0.2) | 0 | 1 (1.3) | 3 (0.2) |
Cytomegalovirus infection | 1 (0.1) | 0 | 0 | 1 (0.1) |
Pulmonary tuberculosis | 0 | 0 | 1 (1.3) | 1 (0.1) |
Varicella | 1 (0.1) | 0 | 0 | 1 (0.1) |
Extended MACE,d n (%) | 5 (0.5) | 0 | 1 (1.3) | 6 (0.5) |
Acute myocardial infarction | 2 (0.2) | 0 | 0 | 2 (0.2) |
Angina unstable | 2 (0.2) | 0 | 0 | 2 (0.2) |
Cerebrovascular accident | 1 (0.1) | 0 | 0 | 1 (0.1) |
Myocardial infarction | 0 | 0 | 1 (1.3) | 1 (0.1) |
Adjudicated VTE, n (%) | NR | NR | NR | NR |
Thrombosis, n (%) | 0 | 1 (0.5) | 0 | 1 (0.1) |
Post-thrombotic syndrome, n (%) | 1 (0.1) | 0 | 0 | 1 (0.1) |
Malignancy, n (%) | 10 (1.1) | 1 (0.5) | 1 (1.3) | 12 (1.0) |
Basal cell carcinoma | 2 (0.2) | 1 (0.5) | 0 | 3 (0.2) |
Squamous cell carcinoma of skin | 3 (0.3) | 0 | 0 | 3 (0.2) |
Malignant melanoma | 2 (0.2) | 0 | 0 | 2 (0.2) |
Acute promyelocytic leukemia | 1 (0.1) | 0 | 0 | 1 (0.1) |
B-cell lymphoma | 1 (0.1) | 0 | 0 | 1 (0.1) |
Bowen disease | 1 (0.1) | 0 | 0 | 1 (0.1) |
Colorectal cancer | 0 | 0 | 1 (1.3) | 1 (0.1) |
Intraductal proliferative breast lesion | 1 (0.1) | 0 | 0 | 1 (0.1) |
Invasive ductal breast carcinoma | 1 (0.1) | 0 | 0 | 1 (0.1) |
Nodal marginal zone B-cell lymphoma | 1 (0.1) | 0 | 0 | 1 (0.1) |
Squamous cell carcinoma | 1 (0.1) | 0 | 0 | 1 (0.1) |
CK elevation, n (%) | ||||
CTC grade ≥ 2 | 36 (3.8) | 7 (3.6) | 2 (2.5) | 45 (3.7) |
CTC grade ≥ 3 | 16 (1.7) | 1 (0.5) | 2 (2.5) | 19 (1.6) |
Signs or symptoms present | 11 (1.2) | 1 (0.5) | 0 | 12 (1.0) |
Treatment given | 0 | 0 | 0 | 0 |
Led to discontinuation | 1 (0.1) | 0 | 0 | 1 (0.1) |
ALT increased, n (%) | 16 (1.7) | 2 (1.0) | 1 (1.3) | 19 (1.6) |
CTC grade ≥ 3 | 3 (0.3) | 1 (0.5) | 1 (1.3) | 5 (0.4) |
AST increased, n (%) | 11 (1.2) | 2 (1.0) | 0 | 13 (1.1) |
CTC grade ≥ 3 | 8 (0.8) | 1 (0.5) | 2 (2.5) | 11 (0.9) |
WBC count decreased, CTC grade ≥ 3, n (%) | 2 (0.2) | 0 | 0 | 2 (0.2) |
Neutrophil count decreased, CTC grade ≥ 3, n (%) | 3 (0.3) | 0 | 0 | 3 (0.3) |
ALT = alanine aminotransferase; AST = aspartate aminotransferase; CK = creatinine phosphokinase; CTC = Common Terminology Criteria; DEUC = deucravacitinib; MACE = major cardiovascular adverse events; NR = not reported; SAE = serious adverse event; SOC = system organ class; VTE = venous thromboembolism; WBC = white blood cell.
Note: Adjudicated adverse events included select infection adverse events and certain cardiovascular events (MACE, VTE). These events were adjudicated by independent, external, blinded, subspecialty expert adjudicators.
aFrequency ≥ 1% in total treatment category.
bFrequency > 1% in any treatment category.
cFrequency ≥ 0.2% in any treatment category.
dExtended MACE includes cardiovascular death, nonfatal myocardial infarction, nonfatal stroke, and unstable angina requiring hospitalization.
Source: Clinical Study Report for IM011075.54
Critical Appraisal
Internal Validity
This LTE study is still ongoing with a planned duration of 240 weeks for individual participants. None of the patients have completed the treatment and study with more than 90% of patients still actively being treated. Therefore, it is difficult to make definitive conclusions regarding long-term safety and efficacy at this point with only approximately 20% of patients having completed treatment at week 60 and even fewer at week 84. Also, the open-label, single-arm design of the study does not allow a conclusion about the comparative efficacy or safety of deucravacitinib. Without data on duration of response and with the proportion of patients at certain time points only, it is not possible to ascertain whether the responders from the parent trials were the same responders in the LTE study. Since initiation visits were conducted remotely due to COVID-19, this may introduce performance bias. For example, PASI and sPGA scales have only been validated for in-person use but have not been validated to be used remotely. No detailed information on procedure was provided regarding measuring outcomes remotely. Therefore, the magnitude and direction of this performance bias is uncertain. Of 1,686 patients screened, 1,286 patients (76.3%) completed the POETYK-1 and POETYK-2 studies. Of the patients who completed the 2 parent studies, 1,221 (72.4%) were enrolled in the LTE. This could be a source of selection bias since only those who were able to complete the parent trials were allowed to enrol. Also, the sponsor did not provide reasons for those patients (approximately 5%) who had completed parent trials but did not enrol in the LTE study. Moreover, since patients who completed the 2 parent studies and rolled over to the LTE are a subset of the population, the baseline characteristics for the LTE study population might differ from those who completed the 2 parent studies. However, the sponsor did not provide detailed baseline characteristics of the patients at the beginning of LTE study. Therefore, the effect of this selection bias (i.e., direction and magnitude) are uncertain.
External Validity
Since patients enrolled in the LTE study are rolled over from the 2 parent studies, the same external validity points as the parent trials would apply to the LTE study.
Discussion
Summary of Available Evidence
Two 52-week double-blind, RCTs met the inclusion criteria for the systematic review. Both the POETYK-1 (N = 666) and POETYK-2 (N = 1,020) studies used a parallel design, with the POETYK-2 study adding a randomized withdrawal design for responders at week 24. The studies enrolled adults (≥ 18 years) who had moderate to severe plaque psoriasis and were candidates for systemic psoriasis therapy and/or phototherapy. Both studies randomized eligible patients (2:1:1) to deucravacitinib 6 mg daily, apremilast 30 mg twice daily, or placebo. All patients in the placebo groups switched to deucravacitinib at week 16, and patients in the apremilast groups who did not show an adequate response to therapy at 24 weeks were crossed over to deucravacitinib. The coprimary outcomes in both studies were the proportion of patients who achieved an sPGA score of 0 or 1 and PASI 75 response at week 16, compared with placebo. Secondary outcomes included other PASI or sPGA response thresholds, DLQI response, and PSSD symptom score for deucravacitinib versus placebo or apremilast at week 16, 24, or 52. The POETYK-2 study also evaluated the time to relapse among patients In the deucravacitinib group who achieved a PASI 75 response at week 24. These patients were rerandomized to blinded deucravacitinib or placebo and followed until week 52.
The mean age of patients enrolled in the pivotal trials ranged from 44.7 years (SD = 12.1) to 47.9 years (SD = 14.0) per treatment group. The majority of patients were men (62% to 71%), and the minority were women (29% to 38%). Most patients were white (77% to 93%), with fewer patients who were Asian (3% to 21%), Black (≤ 4%) or other races (≤ 2%). The patients enrolled had been diagnosed with psoriasis for a median of 13.4 years to 18.2 years, with a mean PASI score at baseline ranging from 20.7 (SD = 8.0) to 21.8 (SD = 8.6). The majority of patients had received prior systemic therapy for psoriasis (54% to 66%), including biologics (31% to 39%).
Indirect evidence included a sponsor-submitted Bayesian NMA that evaluated the comparative efficacy of deucravacitinib versus other biologic and nonbiologic systemic therapies in patients with moderate to severe plaque psoriasis. The NMA analyzed PASI response during induction therapy (10 weeks to 16 weeks) as well as maintenance therapy, measured at week 24 to week 28, and week 44 to week 60. A total of 84 RCTs informed the NMA.
Supplementary longer-term safety and efficacy data were available from 1 open-label, uncontrolled, extension study (IM011075), that was submitted by the sponsor. This study enrolled 1,221 patients who had completed 1 of the pivotal trials, and all patients received deucravacitinib 6 mg daily during the extension period.
Interpretation of Results
Efficacy
Both pivotal trials met their primary objectives and demonstrated superiority of deucravacitinib versus placebo in the proportion of patients who achieved an sPGA 0 or 1 response and PASI 75 response at week 16. Superiority was also shown versus apremilast for the coprimary end points. Key secondary outcomes favoured deucravacitinib versus placebo and apremilast for the proportion of patients with PASI 90 or PASI 100 response at week 16, although the PASI 100 comparison with apremilast was not part of the statistical testing procedure and thus should be interpreted considering the potential for inflated type I error rate. While the differences consistently favoured deucravacitinib, the proportion of patients who met the sPGA or PASI response levels was considered low by the clinical expert consulted by CADTH. In the trials, 53% to 58% of patients in the deucravacitinib groups achieved a PASI 75 response, 27% to 36% achieved PASI 90, and 10% to 14% achieved PASI 100 response at week 16. The expert stated that although PASI 75 is the minimal response threshold that may be accepted as clinically relevant, with currently available therapies PASI 90 and PASI 100 are the desired response levels. The expert also noted that apremilast is infrequently used in Canada, in part due to its relatively low efficacy compared to other advanced therapies. Biologics, particularly the IL-17 and IL-23 inhibitors, are the advanced therapies of choice by dermatologists for patients with moderate to severe plaque psoriasis who have shown an inadequate response to standard systemic therapies. Thus, while deucravacitinib may have demonstrated superiority over apremilast, the clinical relevance of difference is unclear due the limited role of apremilast in the management of psoriasis in Canada.
The key secondary patient-reported end points were generally supportive of the superiority of deucravacitinib versus placebo, but not consistently versus apremilast. More patients who received deucravacitinib for 16 weeks achieved a DLQI score of 0 or 1 (which is categorized has the disease having no impact on HRQoL) than patients who received placebo (RD, 28% to 31%) or apremilast (RD, 12% to 15%). However, the comparison with apremilast was not controlled for the type I error rate. The treatment effects observed for the change from baseline in the SF-36 MCS and PCS, and EQ-5D VAS were variable, with some comparisons showing a 95% CI that included the null, and others suggesting a possible difference, but the within- and between-group change scores did not consistently exceed the MID estimates available from the literature. Moreover, the SF-36 and EQ-5D end points were not part of the statistical testing procedure to control the type I error rate. Both trials detected a statistically significant difference in the proportion of patients who achieved a PSSD symptom score of 0 at week 16 for deucravacitinib versus placebo, but the point estimate for the RD was only 6% and 7%. No statistically significant difference was detected for the PSSD responder analysis versus apremilast, and although a statistically significant difference was detected in the change from baseline in the PSSD symptom score versus apremilast, the least squares mean difference did not exceed the MID estimates. All the patient-reported end points were missing some patients, with up to 10% of patients excluded depending on the treatment group and the outcome. As a whole, the interpretation of these end points should take into consideration the limitations of the data (i.e., inflated risk of type I error rate for some end points, missing data) as well as the clinical relevance of the treatment effects observed.
The trials were 52 weeks In duration and analyzed longer-term outcomes for the randomized population (POETYK-1) and for the subgroup of patients who achieved a PASI 75 response at week 24 (POETYK-2). In the POETYK-1 study, 56% of patients achieved a PASI 75 response at week 24 and week 52, in comparison to 31% of patients who had received apremilast. Data from the POETYK-2 study indicate that patients who achieved a PASI 75 response with deucravacitinib, and who remained on treatment, were less likely to relapse than patients who were switched to placebo. Among responders, 82% had maintained a PASI 75 response at week 52 with deucravacitinib, compared with 31% who were switched to placebo. These data suggest that response to treatment may be maintained for some patients up to 1 year. Interim data from the open-label extension study also suggest that treatment response may be maintained longer term, although the results may be limited by selection, attrition, and performance bias.
Overall, the risk of bias was rated as low for the pivotal trials, with no major concerns with bias related to randomization, allocation concealment, or blinding. There were some differences in the frequency of withdrawals across treatment groups, but since the trials use the intention-to-treat population with nonresponder imputation for patients who stopped treatment or withdrew, the potential for attrition bias was generally low for the key binary end points. The subgroup and sensitivity analyses generally showed results that were consistent with the primary analyses. Both trials failed to detect a difference between groups for patients with psoriasis of the fingernails, however this subgroup was small and may have not been adequately powered. With regards to external validity, the clinical expert consulted for this review considered that the patients enrolled would represent patients with moderate to severe psoriasis who may be treated with advanced therapies in Canada. Patients were prohibited from receiving other treatments for psoriasis, with the exception of protocol-specified topical therapies after week 24. Therefore, these trials do not provide evidence on the efficacy and safety of deucravacitinib when used In combination with other systemic therapies. Of note, the clinical expert suggested there may be interest in using deucravacitinib in patients with mild psoriasis; however, the trials excluded patients with mild disease thus the efficacy of deucravacitinib in these patients is unknown.
Indirect evidence of the comparative efficacy of deucravacitinib versus biologic and nonbiologic systemic therapies was available from the sponsor-submitted NMA. The results of the short-term (10 weeks to 16 weeks) analysis favoured deucravacitinib versus placebo, apremilast, and etanercept 50 mg weekly in achieving all levels of PASI responses, and versus etanercept 50 mg biweekly for PASI 100. The OR 95% CrI overlapped the null for deucravacitinib versus tildrakizumab 100 mg for all PASI levels, and tildrakizumab 200 mg, certolizumab 200 mg, and ustekinumab 90 mg for the PASI 100 level. All other comparisons versus deucravacitinib were in favour of the biologic comparator, typically an IL-17 or IL-23 inhibitor. The results of the midterm and long-term analyses were generally similar and favoured many biologics over deucravacitinib. Given the effect size estimates for deucravacitinib versus some comparators, specifically the IL-17 inhibitors and the IL-23 inhibitors risankizumab and guselkumab, the indirect evidence suggests that deucravacitinib is less effective at inducing PASI response than many biologics.
The sponsor-submitted ITC involved a rich evidence base with a large network of RCTs and sample size, which strengthened the robustness of the NMA analyses. Nonetheless, the NMA has limitations including heterogeneity present for many patient and study characteristics in the NMA analyses, incorporation of studies that included patients with mild disease, discordance between the sponsor’s assumption of patient treatment adherence and true clinical practice, and lack of data for certain subgroup analyses. Given these limitations, the results from the sponsor-submitted ITC are at some risk of bias for the main comparison of deucravacitinib with other treatments in patients with moderate to severe plaque psoriasis, and highly imprecise for the biologic-experienced subgroup. Only 1 measure of efficacy was analyzed, and no quality of life end points were available.
Harms
Overall, the frequency of AEs was generally similar across treatment groups in the short-term. SAEs and drug discontinuation due to AEs were infrequent. Infections and infestations were reported by 26% and 31% of patients in the deucravacitinib groups, compared with 15% and 26% in the placebo groups, and 18% and 25% in the apremilast groups over the first 16 weeks, the POETYK-1 and POETYK-2 studies, respectively. However, few events were classified as SAEs and no opportunistic infections or tuberculosis cases were reported in either trial. The overall safety data for the 52 week study periods showed similar trends as the induction phase data, although the later follow-up periods are more difficult to interpret due to the treatment switching that occurred after week 16. No new safety signals were identified in the open-label extension study.
Deucravacitinib is the first tyrosine kinase 2 inhibitor to be approved in Canada for psoriasis. Its mechanism of action is similar to the Janus kinase inhibitors, which carry warnings for major adverse cardiovascular events, thromboembolic events, elevated creatinine kinase levels, as well as low white blood count. Overall, the frequency of these events was generally low in the clinical trials; however, the sample size and duration of follow-up may not have been sufficient to detect rare events. Moreover, the AE rates observed in the clinical trials may not reflect the rates observed in practice once a wider population that may include vulnerable patients is exposed. The safety of deucravacitinib in patients who have an active or chronic infection (e.g., hepatitis C, HIV, tuberculosis), or comorbidities such as cardiovascular, neuropsychiatric, or substance use disorders is unknown, as these patients were excluded from the trials. Direct comparative safety data were limited to relatively short-term events versus apremilast. The sponsor-submitted NMA did not report any safety outcomes, thus the comparative safety versus biologics is unknown.
Conclusions
In adults with moderate to severe plaque psoriasis who were candidates for systemic therapy or phototherapy, deucravacitinib showed improvement versus placebo in skin and HRQoL in the short term, with some data showing skin improvements in the intermediate term (up to 52 weeks). For most outcomes, deucravacitinib was also superior to the active comparator apremilast. However, the clinical relevance of these comparator in the Canadian context is limited. AEs were generally similar between deucravacitinib and apremilast, and no new safety signals were identified in longer-term follow-up or an ongoing extension study. Based on ITCs, deucravacitinib is less effective in producing skin improvement than several biologics established in Canada. Collection of data on long-term safety and duration of effect is ongoing. At present, it is unknown whether deucravacitinib could be combined with other treatments or whether it produces immunosuppression or expresses any of the rare AEs associated with medications that affect the Janus kinase pathway. Given that alternative treatments appear generally more effective, deucravacitinib is not expected to alter the overall treatment paradigm for psoriasis. Since response to treatments can be patient specific, patients are concerned about having treatment options and a minority may prefer to avoid injections.
References
1.Feldman S. Treatment of psoriasis in adults. In: Post TW, ed. UpToDate. Waltham (MA): UpToDate. 2022: www.updodate.com. Accessed 2022 Nov 30.
2.Dowlatshahi EA, Wakkee M, Arends LR, Nijsten T. The prevalence and odds of depressive symptoms and clinical depression in psoriasis patients: a systematic review and meta-analysis. J Invest Dermatol. 2014;134(6):1542-1551. PubMed
3.Menter A, Strober B, Kaplan D, et al. Joint AAD-NPF guidelines of care for the management and treatment of psoriasis with biologics. J Am Acad Dermatol. 2019;80(4):1029-1072. PubMed
4.Canadian Dermatology Association. Psoriasis. 2022; https://dermatology.ca/public-patients/skin/psoriasis/. Accessed 2022 Nov 30.
5.Sotyktu (deucravacitinib): film-coated tablets, 6 mg, oral [product monograph]. Montreal (QC): Bristol-Myers Squibb Canada; 2021 Nov 12.
6.Drug Reimbursement Review sponsor submission: Sotyktu® (deucravacitinib) 6 mg [internal sponsor's package]. Montreal (QC): Bristol-Myers Squibb Canada; 2022 Sep 27.
7.Clinical Study Report: IM011046. A Multi-Center, Randomized, Double-Blind, Placebo- and Active Comparator-Controlled Phase 3 Study to Evaluate the Efficacy and Safety of BMS-986165 in Subjects with Moderate-to Severe Plaque Psoriasis [internal sponsor's report]. Lawrenceville (NJ): Bristol-Myers Squibb; 2021 Aug 13.
8.Clinical Study Report: IM011047. A multi-center, randomized, double-blind, placebo-and active comparator-controlled phase 3 study with randomized withdrawal and retreatment to evaluate the efficacy and safety of BMS-986165 in subjects with moderate-to-severe plaque psoriasis [internal sponsor's report]. Lawrenceville (NJ): Bristol-Myers Squibb; 2021 Aug 19.
9.Baluvelt A, Ehst BD. Pathophysiology of plaque psoriasis. In: Post TW, ed. UpToDate. Waltham (MA): UpToDate. 2021: www.updodate.com. Accessed 2022 Nov 30.
10.Eder L, Widdifield J, Rosen CF, et al. Trends in the Prevalence and Incidence of Psoriasis and Psoriatic Arthritis in Ontario, Canada: A Population-Based Study. Arthritis Care Res (Hoboken). 2019;71(8):1084-1091. PubMed
11.Levy AR, Davie AM, Brazier NC, et al. Economic burden of moderate to severe plaque psoriasis in Canada. Int J Dermatol. 2012;51(12):1432-1440. PubMed
12.Petrella RJ GV, Luciani L, Barbeau M. Characteristics of chronic plaque psoriasis in Canada: a retrospective database study. Value Health. 2014;17(3):PA284.
13.Siliq (brodalumab): 140 mg/mL solution for subcutaneous injection [product monograph]. Laval (QC): Bausch Health, Canada Inc; 2019 Jun 7: https://pdf.hres.ca/dpd_pm/00051682.PDF. Accessed 2022 Nov 30.
14.Cimzia (certolizumab pegol): 200 mg/mL solution for injection [product monograph]. Oakville (ON): UCB Canada Inc; 2019 Nov 13: https://pdf.hres.ca/dpd_pm/00053920.PDF. Accessed 2022 Nov 30.
15.Remicade (infliximab): 100 mg/vial powder for solution, sterile, lyophilized [product monograph]. Toronto (ON): Janssen Inc; 2022 Oct 7: https://pdf.hres.ca/dpd_pm/00067676.PDF. Accessed 2022 Nov 30.
16.Humira (adalimumab): 40 mg in 0.8 mL sterile solution (50 mg/mL), 10 mg in 0.1 mL sterile solution (100 mg/mL), 20 mg in 0.2 mL sterile solution (100 mg/mL), 40 mg in 0.4 mL sterile solution (100 mg/mL), 80 mg in 0.8 mL sterile solution (100 mg/mL), subcutaneous injection [product monograph]. St-Laurent (QC): AbbVie Corporation; 2022 Sep 16: https://pdf.hres.ca/dpd_pm/00067414.PDF. Accessed 2022 Nov 30.
17.Skyrizi (risankizumab): 75 mg in 0.83 mL sterile solution (90 mg/mL), 150 mg in 1 mL sterile solution (150 mg/mL), subcutaneous injection [product monograph]. St-Laurent (QC): AbbVie Corporation; 2022 Oct 19: https://pdf.hres.ca/dpd_pm/00067871.PDF. Accessed 2022 Nov 30.
18.Enbrel (etanercept): 50 mg/mL solution in a prefilled syringe, 25 mg/vial lyophilized powder in a vial for reconstitution, subcutaneous injection [product monograph]. Mississauga (ON): Amgen Canada Inc.; 2021 Mar 19: https://pdf.hres.ca/dpd_pm/00060454.PDF. Accessed 2022 Nov 30.
19.Taltz (ixekizumab): 80 mg/1.0 mL solution for injection [product monograph]. Toronto (ON): Eli Lilly Canada Inc.; 2021 Mar 29: https://pdf.hres.ca/dpd_pm/00060574.PDF. Accessed 2022 Nov 30.
20.Ilumya (tildrakizumab): 100 mg / 1 mL solution (100 mg/mL) for subcutaneous injection [product monograph]. Burlington (ON): C.R.I.; 2022 Jan 24: https://pdf.hres.ca/dpd_pm/00064464.PDF. Accessed 2022 Nov 30.
21.Cosentyx (secukinumab): 150 mg/mL solution for injection, powder for solution for injection [product monograph]. Dorval (QC): Novartis Pharmaceuticals Canada Inc.; 2022 Sep 20: https://pdf.hres.ca/dpd_pm/00067634.PDF. Accessed 2022 Nov 30.
22.Stelera (ustekinumab): 45 mg//0.5 mL, 90 mg/1/0 mL solution for subcutaneous injection; 130 mg/26 mL (5 mg/mL) solution for intravenous infusion [product monograph]. Toronto (ON): Janssen Inc; 2021 Sep 9: https://pdf.hres.ca/dpd_pm/00062938.PDF. Accessed 2022 Nov 30.
23.Tremfya (guselkumab): 100 mg/1 mL solution for injection, pre-filled syringe; Tremfya One-Press (guselkumab): 100 mg/1 mL solution for injection, patient-controlled injector [product monograph]. Toronto (ON): Janssen Inc; 2022 Nov 8: https://pdf.hres.ca/dpd_pm/00068091.PDF. Accessed 2022 Nov 30.
24.Bimzelx (bimekizumab): 160 mg/mL solution subcutaneous injection [product monograph]. Oakville (ON): UCB Canada Inc; 2022 Feb 14: https://pdf.hres.ca/dpd_pm/00064702.PDF. Accessed 2022 Nov 30.
25.Otezla (apremilast); 10 mg, 20 mg and 30 mg oral tablets [product monograph]. Amgen; 2020 Aug 5: https://pdf.hres.ca/dpd_pm/00057499.PDF. Accessed 2022 Nov 30.
26.McGowan J, Sampson M, Salzwedel DM, Cogo E, Foerster V, Lefebvre C. PRESS Peer Review of Electronic Search Strategies: 2015 guideline statement. Journal of clinical epidemiology. 2016;75:40-46. PubMed
27.Grey matters: a practical tool for searching health-related grey literature. Ottawa (ON): CADTH; 2019: https://www.cadth.ca/grey-matters. Accessed 2022 Oct 14.
28.Armstrong AW, Gooderham M, Warren RB, et al. Deucravacitinib versus placebo and apremilast in moderate to severe plaque psoriasis: efficacy and safety results from the 52-week, randomized, double-blinded, placebo-controlled phase 3 POETYK PSO-1 trial. J Am Acad Dermatol. 2022;09:09.
29.Strober B, Thaci D, Sofen H, et al. Deucravacitinib versus placebo and apremilast in moderate to severe plaque psoriasis: efficacy and safety results from the 52-week, randomized, double-blinded, phase 3 POETYK PSO-2 trial. J Am Acad Dermatol. 2022;14:14.
30.Center for Drug Evaluation and Research. Multidiscipline review(s). Sotyktu (deucravacitinib) administration. Company: Bristol-Myers Squibb Company Application Number: 214958 Approval Date: 9/9/2022 (FDA approval package). Silver Spring (MD): U.S. Food and Drug Administration (FDA); 2022: https://www.accessdata.fda.gov/drugsatfda_docs/nda/2022/214958Orig1s000MultidisciplineR.pdf Accessed 31 Oct 2022.
31.Berth-Jones J, Grotzinger K, Rainville C, et al. A study examining inter- and intrarater reliability of three scales for measuring severity of psoriasis: Psoriasis Area and Severity Index, Physician's Global Assessment and Lattice System Physician's Global Assessment. Br J Dermatol. 2006;155(4):707-713. PubMed
32.Bożek A, Reich A. The reliability of three psoriasis assessment tools: Psoriasis area and severity index, body surface area and physician global assessment. Adv Clin Exp Med. 2017;26(5):851-856. PubMed
33.Puzenat E, Bronsard V, Prey S, et al. What are the best outcome measures for assessing plaque psoriasis severity? A systematic review of the literature. J Eur Acad Dermatol Venereol. 2010;24 Suppl 2:10-16. PubMed
34.Spuls PI, Lecluse LL, Poulsen ML, Bos JD, Stern RS, Nijsten T. How good are clinical severity and outcome measures for psoriasis?: quantitative evaluation in a systematic review. J Invest Dermatol. 2010;130(4):933-943. PubMed
35.Weisman S, Pollack CR, Gottschalk RW. Psoriasis disease severity measures: comparing efficacy of treatments for severe psoriasis. J Dermatolog Treat. 2003;14(3):158-165. PubMed
36.Carlin CS, Feldman SR, Krueger JG, Menter A, Krueger GG. A 50% reduction in the Psoriasis Area and Severity Index (PASI 50) is a clinically significant endpoint in the assessment of psoriasis. J Am Acad Dermatol. 2004;50(6):859-866. PubMed
37.Belinchón Romero I, Dauden E, Ferrándiz Foraster C, González-Cantero Á, Carrascosa Carrillo JM. PASI 100 response rates in moderate to severe psoriasis: a systematic literature review and analysis of clinical practice guidelines. J Dermatolog Treat. 2022;33(3):1661-1669. PubMed
38.Callis Duffin K, Bushmakin AG, Cappelleri JC, Mallbris L, Mamolo C. A multi-item Physician Global Assessment scale to assess psoriasis disease severity: validation based on four phase III tofacitinib studies. BMC Dermatol. 2019;19(1):8. PubMed
39.Cappelleri JC, Bushmakin AG, Harness J, Mamolo C. Psychometric validation of the physician global assessment scale for assessing severity of psoriasis disease activity. Qual Life Res. 2013;22(9):2489-2499. PubMed
40.Langley RG, Feldman SR, Nyirady J, van de Kerkhof P, Papavassilis C. The 5-point Investigator's Global Assessment (IGA) Scale: A modified tool for evaluating plaque psoriasis severity in clinical trials. J Dermatolog Treat. 2015;26(1):23-31. PubMed
41.Robinson A, Kardos M, Kimball AB. Physician Global Assessment (PGA) and Psoriasis Area and Severity Index (PASI): why do both? A systematic analysis of randomized controlled trials of biologic agents for moderate to severe plaque psoriasis. J Am Acad Dermatol. 2012;66(3):369-375. PubMed
42.Reeve BB, Wyrwich KW, Wu AW, et al. ISOQOL recommends minimum standards for patient-reported outcome measures used in patient-centered outcomes and comparative effectiveness research. Qual Life Res. 2013;22(8):1889-1905. PubMed
43.Mathias SD, Feldman SR, Crosby RD, Colwell HH, McQuarrie K, Han C. Measurement properties of a patient-reported outcome measure assessing psoriasis severity: The psoriasis symptoms and signs diary. J Dermatolog Treat. 2016;27(4):322-327. PubMed
44.Hongbo Y, Thomas CL, Harrison MA, Salek MS, Finlay AY. Translating the science of quality of life into practice: What do dermatology life quality index scores mean? J Invest Dermatol. 2005;125(4):659-664. PubMed
45.Shikiar R, Willian MK, Okun MM, Thompson CS, Revicki DA. The validity and responsiveness of three quality of life measures in the assessment of psoriasis patients: results of a phase II study. Health Qual Life Outcomes. 2006;4:71. PubMed
46.Finlay AY, Khan GK. Dermatology Life Quality Index (DLQI)--a simple practical measure for routine clinical use. Clin Exp Dermatol. 1994;19(3):210-216. PubMed
47.Melilli L SR, Thompson C. . Minimal clinically important difference in Dermatology Life Quality Index in moderate to severe plaque psoriasis patients treated with adalimumab. J Am Acad Dermatol. 2006;54:AB221.
48.Ali FM, Salek S, Finlay AY, Piguet V. Validation of the electronic Psoriasis Area and Severity Index application: Establishing measurement equivalence. J Am Acad Dermatol. 2019;81(6):1439-1441. PubMed
49.Frendl DM, Ware JE, Jr. Patient-reported functional health and well-being outcomes with drug therapy: a systematic review of randomized trials using the SF-36 health survey. Med Care. 2014;52(5):439-445. PubMed
50.ME M. Determining important differences in scores. User's manual for the SF-36v2 health survey. Lincoln (RI): Quality Metric Incorporated. 2011(3rd ed.):169-177.
51.Reich K, Papp KA, Blauvelt A, et al. Tildrakizumab versus placebo or etanercept for chronic plaque psoriasis (reSURFACE 1 and reSURFACE 2): results from two randomised controlled, phase 3 trials. Lancet (London, England). 2017;390(10091):276-288. PubMed
52.Gordon KB, Foley P, Krueger JG, et al. Bimekizumab efficacy and safety in moderate to severe plaque psoriasis (BE READY): a multicentre, double-blind, placebo-controlled, randomised withdrawal phase 3 trial. Lancet (London, England). 2021;397(10273):475-486. PubMed
53.Systematic literature review and network meta-analysis of systematic biologics and non-biologics in patients with moderate-to-severe plaque psoriasis [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Sotyktu® (deucravacitinib) 6 mg. Montreal (QC): Bristol-Myers Squibb Canada; 2022 Sep 27.
54.Clinical Study Report: IM011075. An open-label, multi-center extension study to characterize the long-term safety and efficacy of BMS-986165 in subjects with moderate-to-severe plaque psoriasis [internal sponsor's report]. Lawrenceville (NJ): Bristol-Myers Squibb; 2021 Aug 23.
55.Simpson MJ, Chow C, Morgenstern H, Luger TA, Ellis CN. Comparison of three methods for measuring psoriasis severity in clinical studies (Part 2 of 2): use of quality of life to assess construct validity of the Lattice System Physician's Global Assessment, Psoriasis Area and Severity Index and Static Physician's Global Assessment. J Eur Acad Dermatol Venereol. 2015;29(7):1415-1420. PubMed
56.Feldman SR, Krueger GG. Psoriasis assessment tools in clinical trials. Ann Rheum Dis. 2005;64 Suppl 2(Suppl 2):ii65-68; discussion ii69-73.
57.Hudgens S, Rich P, Geng Z, Williams D, Fleischer A, Ganguli A. Development and validation of the Physician's Global Assessment of Fingernail Psoriasis. J Eur Acad Dermatol Venereol. 2021;35(11):2324-2330. PubMed
58.Hudgens S, Gugiu C, Guobyte A, et al. Validation of the Physician's Global Assessment of Fingernail Psoriasis by Rheumatologists Treating Psoriatic Arthritis. Value Health. 2022;25(9):1582-1589. PubMed
59.Landis JR, Koch GG. The Measurement of Observer Agreement for Categorical Data. Biometrics. 1977;33(1):159. PubMed
60.Armstrong A, Puig L, Langley R, et al. Validation of psychometric properties and development of response criteria for the psoriasis symptoms and signs diary (PSSD): results from a phase 3 clinical trial. J Dermatolog Treat. 2019;30(1):27-34. PubMed
61.EuroQol--a new facility for the measurement of health-related quality of life. Health Policy. 1990;16(3):199-208. PubMed
62.Ware JE, Jr., Sherbourne CD. The MOS 36-item short-form health survey (SF-36). I. Conceptual framework and item selection. Med Care. 1992;30(6):473-483. PubMed
Appendix 1: Literature Search Strategy
Note this appendix has not been copy-edited.
Clinical Literature Search
Overview
Interface: Ovid
Databases
MEDLINE All (1946 to present)
Embase (1974 to present)
Note: Subject headings and search fields have been customized for each database. Duplicates between databases were removed in Ovid.
Date of search: October 26, 2022
Alerts: Biweekly search updates until project completion
Search filters applied: None
Limits
Conference abstracts: excluded
Syntax | Description |
|---|---|
/ | At the end of a phrase, searches the phrase as a subject heading |
MeSH | Medical Subject Heading |
.fs | Floating subheading |
exp | Explode a subject heading |
* | Before a word, indicates that the marked subject heading is a primary topic; or, after a word, a truncation symbol (wildcard) to retrieve plurals or varying endings |
# | Truncation symbol for 1 character |
? | Truncation symbol for 1 or no characters only |
adj# | Requires terms to be adjacent to each other within # number of words (in any order) |
.ti | Title |
.ot | Original title |
.ab | Abstract |
.hw | Heading word; usually includes subject headings and controlled vocabulary |
.kf | Keyword heading word |
.dq | Candidate term word (Embase) |
.pt | Publication type |
.mp | Mapped term |
.rn | Registry number |
.nm | Name of substance word (MEDLINE) |
.yr | Publication year |
.jw | Journal title word (MEDLINE) |
.jx | Journal title word (Embase) |
freq = # | Requires terms to occur # number of times in the specified fields |
medall | Ovid database code: MEDLINE All, 1946 to present, updated daily |
oemezd | Ovid database code; Embase, 1974 to present, updated daily |
Multidatabase Strategy
(sotyktu* or deucravacitinib* or BMS-986165 or BMS986165 or BMS-98616501 or BMS98616501 or WHO 11342 or WHO11342 or tyk2-in-4 or GTPL10432 or EX-A3154 or BDBM50507816 or MFCD31715455 or NSC825520 or s8879 or AT18623 or NSC-825520 or NCGC00687789-01 or AC-31543 or HY-117287 or CS-0065044 or D11817 or GTPL 10432 or EXA3154 or BDBM 50507816 or MFCD 31715455 or NSC 825520 or s 8879 or AT 18623 or NSC825520 or NCGC 00687789-01 or AC31543 or HY117287 or CS0065044 or D 11817 or N0A21N6RAU or 95C5558CF4).ti,ab,kf,ot,hw,rn,nm.
1 use medall
*Deucravacitinib/
(sotyktu* or deucravacitinib* or BMS-986165 or BMS986165 or BMS-98616501 or BMS98616501 or WHO 11342 or WHO11342 or tyk2-in-4 or GTPL10432 or EX-A3154 or BDBM50507816 or MFCD31715455 or NSC825520 or s8879 or AT18623 or NSC-825520 or NCGC00687789-01 or AC-31543 or HY-117287 or CS-0065044 or D11817 or GTPL 10432 or EXA3154 or BDBM 50507816 or MFCD 31715455 or NSC 825520 or s 8879 or AT 18623 or NSC825520 or NCGC 00687789-01 or AC31543 or HY117287 or CS0065044 or D 11817).ti,ab,kf,dq.
3 or 4
5 not (conference abstract or conference review).pt.
6 use oemezd
2 or 7
remove duplicates from 8
Clinical Trials Registries
ClinicalTrials.gov
Produced by the US National Library of Medicine. Targeted search used to capture registered clinical trials.
[Search – sotyktu OR deucravacitinib OR “BMS-986165” OR BMS986165 OR “BMS-98616501” OR BMS98616501 OR “WHO 11342” OR WHO11342 OR “tyk2-in-4”]
WHO ICTRP
International Clinical Trials Registry Platform, produced by the WHO. Targeted search used to capture registered clinical trials.
[Search – sotyktu OR deucravacitinib OR “BMS-986165” OR BMS986165 OR “BMS-98616501” OR BMS98616501 OR “WHO 11342” OR WHO11342 OR “tyk2-in-4”]
Health Canada’s Clinical Trials Database
Produced by Health Canada. Targeted search used to capture registered clinical trials.
[Search – sotyktu OR deucravacitinib OR “BMS-986165” OR BMS986165 OR “BMS-98616501” OR BMS98616501 OR “WHO 11342” OR WHO11342 OR “tyk2-in-4”]
EU Clinical Trials Register
European Union Clinical Trials Register, produced by the European Union. Targeted search used to capture registered clinical trials.
[Search – sotyktu OR deucravacitinib OR “BMS-986165” OR BMS986165 OR “BMS-98616501” OR BMS98616501 OR “WHO 11342” OR WHO11342 OR “tyk2-in-4”]
Grey Literature
Search dates: October 14, 2022, to October 20, 2022
Keywords: [Search – sotyktu OR deucravacitinib OR “BMS-986165” OR BMS986165 OR “BMS-98616501” OR BMS98616501 OR “WHO 11342” OR WHO11342 OR “tyk2-in-4”]
Limits: None
Updated: Search updated before the completion of stakeholder feedback period
Relevant websites from the following sections of the CADTH grey literature checklist Grey Matters: A Practical Tool for Searching Health-Related Grey Literature were searched:
Health Technology Assessment Agencies
Health Economics
Clinical Practice Guidelines
Drug and Device Regulatory Approvals
Advisories and Warnings
Drug Class Reviews
Clinical Trials Registries
Databases (free)
Health Statistics
Internet Search
Appendix 2: Excluded Studies
Note this appendix has not been copy-edited.
Reference | Reason for exclusion |
|---|---|
Clinical Study Report: IM011075. An open-label, multi-centre extension study to characterize the long-term safety and efficacy of BMS-986165 in subjects with moderate-to-severe plaque psoriasis [internal sponsor’s report]. Lawrenceville (NJ): Bristol Myers Squibb; 2021 August 23.54 | Study design |
Appendix 3: Detailed Outcome Data
Note this appendix has not been copy-edited.
Table 39: sPGA 0 or 1 Response at Week 16 by Subgroup — POETYK-1 and POETYK-2 (FAS)
Outcome, Subgroup | POETYK-1 | POETYK-2 | ||||
|---|---|---|---|---|---|---|
DEUC N = 332 | PBO N = 166 | APREM N = 168 | DEUC N = 511 | PBO N = 255 | APREM N = 254 | |
Prior biologic use: No | ||||||
Number of patients | 202 | 103 | 102 | 346 | 172 | 175 |
Responders, n (%) | 113 (55.9) | 8 (7.8) | 37 (36.3) | 177 (51.2) | 16 (9.3) | 69 (39.4) |
DEUC vs. PBO RD (95%CI) ab | 48.5 (40.2 to 56.9) | ref | NA | 42.0 (35.1 to 48.9) | ref | NA |
DEUC vs. APREM RD (95%CI) ab | 18.6 (7.2 to 30.0) | NA | ref | 11.9 (3.2 to 20.6) | NA | ref |
Prior biologic use: Yes | ||||||
Number of patients | 130 | 63 | 66 | 165 | 83 | 79 |
Responders, n (%) | 65 (50.0) | 4 (6.3) | 17 (25.8) | 76 (46.1) | 6 (7.2) | 17 (21.5) |
DEUC vs. PBO RD (95%CI)ab | 43.6 (33.4 to 53.9) | ref | NA | 38.5 (29.3 to 47.6) | ref | NA |
DEUC vs. APREM RD (95%CI)ab | 25.7 (12.2 to 39.3) | NA | ref | 24.5 (12.9 to 36.0) | NA | ref |
Prior systemic treatment use: No | ||||||
Number of patients | 132 | 57 | 59 | 237 | 116 | 114 |
Responders, n (%) | 70 (53.0) | 3 (5.3) | 22 (37.3) | 119 (50.2) | 11 (9.5) | 44 (38.6) |
DEUC vs. PBO RD (95%CI)ab | 47.6 (37.3 to 57.8) | ref | NA | 42.4 (34.0 to 50.8) | ref | NA |
DEUC vs. APREM RD (95%CI)ab | 15.0 (0.2 to 29.9) | NA | ref | 13.3 (2.7 to 23.8) | NA | ref |
Prior systemic treatment use: Yes | ||||||
Number of patients | 200 | 109 | 109 | 274 | 139 | 140 |
Responders, n (%) | 108 (54.0) | 9 (8.3) | 32 (29.4) | 134 (48.9) | 11 (7.9) | 42 (30) |
DEUC vs. PBO RD (95%CI)ab | 47.1 (38.9 to 55.2) | ref | NA | 40.3 (32.9 to 47.7) | ref | NA |
DEUC vs. APREM RD (95%CI)ab | 24.1 (13.4 to 34.9) | NA | ref | 18.1 (8.7 to 27.5) | NA | ref |
Baseline sPGA score: Moderate | ||||||
Number of patients | 257 | 128 | 139 | 408 | 217 | 196 |
Responders, n (%) | 134 (52.1) | 11 (8.6) | 45 (32.4) | 208 (51.0) | 21 (9.7) | 70 (35.7) |
DEUC vs. PBO RD (95%CI)ab | 43.7 (36.1 to 51.4) | ref | NA | 41.7 (35.4 to 47.9) | ref | NA |
DEUC vs. APREM RD (95%CI)ab | 19.8 (10.0 to 29.6) | NA | ref | 16.0 (8.0 to 24.1) | NA | ref |
Baseline sPGA score: Severe | ||||||
Number of patients | 75 | 37 | 29 | 103 | 38 | 58 |
Responders, n (%) | 44 (58.7) | 1 (2.7) | 9 (31.0) | 45 (43.7) | 1 (2.6) | 16 (27.6) |
DEUC vs. PBO RD (95%CI)ab | 54.5 (42.0 to 67.0) | ref | NA | 40.6 (29.2 to 52.0) | ref | NA |
DEUC vs. APREM RD (95%CI)ab | 15.1 (−5.2 to 35.4) | NA | ref | 14.2 (−1.3 to 29.6) | NA | ref |
Baseline PASI score: ≤ 20 | ||||||
Number of patients | 177 | 102 | 98 | 298 | 152 | 143 |
Responders, n (%) | 89 (50.3) | 10 (9.8) | 33 (33.7) | 154 (51.7) | 16 (10.5) | 47 (32.9) |
DEUC vs. PBO RD (95%CI)ab | 40.9 (31.8 to 50.0) | ref | NA | 41.1 (33.7 to 48.5) | ref | NA |
DEUC vs. APREM RD (95%CI)ab | 19.3 (7.8 to 30.9) | NA | ref | 18.3 (9.0 to 27.6) | NA | ref |
Baseline PASI score: > 20 | ||||||
Number of patients | 155 | 64 | 70 | 213 | 103 | 111 |
Responders, n (%) | 89 (57.4) | 2 (3.1) | 21 (30.0) | 99 (46.5) | 6 (5.8) | 39 (35.1) |
DEUC vs. PBO RD (95%CI)ab | 55.6 (46.8 to 64.4) | ref | NA | 40.8 (32.5 to 49.0) | ref | NA |
DEUC vs. APREM RD (95%CI)ab | 25.2 (12.0 to 38.4) | NA | ref | 12.7 (1.8 to 23.7) | NA | ref |
APREM = apremilast; CI = confidence interval; DEUC = deucravacitinib; FAS = full analysis set; NA = not applicable; PASI = Psoriasis Area and Severity Index; PBO = placebo; RD = risk difference; ref = reference; sPGA = static Physician’s Global Assessment.
aCochran-Mantel-Haenszel test stratified by geographic region and body weight. Nonresponder imputation for missing data.
bPatients must also have at least a 2-point improvement in their sPGA score vs. baseline.
Source: Clinical Study Report for POETYK-1,7 and POETYK-2.8
Table 40: PASI 75 Response at Week 16 by Subgroup — POETYK-1 and POETYK-2 (FAS)
Subgroup, Outcome | POETYK-1 | POETYK-2 | ||||
|---|---|---|---|---|---|---|
DEUC N = 332 | PBO N = 166 | APREM N = 168 | DEUC N = 511 | PBO N = 255 | APREM N = 254 | |
Prior biologic use: No | ||||||
Number of patients | 202 | 103 | 102 | 346 | 172 | 175 |
Responders, n (%) | 121 (59.9) | 16 (15.5) | 42 (41.2) | 195 (56.4) | 18 (10.5) | 80 (45.7) |
DEUC vs. PBO RD (95%CI)a | 44.8 (35.3 to 54.3) | ref | NA | 46.0 (38.9 to 53.1) | ref | NA |
DEUC vs. APREM RD (95%CI)a | 17.6 (6.0 to 29.2) | NA | ref | 10.8 (1.9 to 19.7) | NA | ref |
Prior biologic use: Yes | ||||||
Number of patients | 130 | 63 | 66 | 165 | 83 | 79 |
Responders, n (%) | 73 (56.2) | 5 (7.9) | 17 (25.8) | 76 (46.1) | 6 (7.2) | 21 (26.6) |
DEUC vs. PBO RD (95%CI)a | 48.2 (37.4 to 59.0) | ref | NA | 38.8 (29.6 to 48.1) | ref | NA |
DEUC vs. APREM RD (95%CI)a | 30.6 (16.9 to 44.2) | NA | ref | 19.3 (7.3 to 31.4) | NA | ref |
Prior systemic treatment use: No | ||||||
Number of patients | 132 | 57 | 59 | 237 | 116 | 114 |
Responders, n (%) | 75 (56.8) | 12 (21.1) | 24 (40.7) | 133 (56.1) | 16 (13.8) | 53 (46.5) |
DEUC vs. PBO RD (95%CI)a | 35.6 (22.2 to 49.0) | ref | NA | 43.5 (34.3 to 52.7) | ref | NA |
DEUC vs. APREM RD (95%CI)a | 15.6 (0.4 to 30.8) | NA | ref | 10.7 (−0.3 to 21.6) | NA | ref |
Prior systemic treatment use: Yes | ||||||
Number of patients | 200 | 109 | 109 | 274 | 139 | 140 |
Responders, n (%) | 119 (59.5) | 9 (8.3) | 35 (32.1) | 138 (50.4) | 8 (5.8) | 48 (34.3) |
DEUC vs. PBO RD (95%CI)a | 52.4 (44.3 to 60.6) | ref | NA | 43.6 (36.5 to 50.7) | ref | NA |
DEUC vs. APREM RD (95%CI)a | 26.5 (15.5 to 37.4) | NA | ref | 15.3 (5.6 to 25.0) | NA | ref |
Baseline sPGA score: Moderate | ||||||
Number of patients | 257 | 128 | 139 | 408 | 217 | 196 |
Responders, n (%) | 145 (56.4) | 18 (14.1) | 48 (34.5) | 221 (54.2) | 22 (10.1) | 82 (41.8) |
DEUC vs. PBO RD (95%CI)a | 42.8 (34.4 to 51.2) | ref | NA | 44.4 (38.1 to 50.7) | ref | NA |
DEUC vs. APREM RD (95%CI)a | 21.4 (11.5 to 31.3) | NA | ref | 13.0 (4.8 to 21.3) | NA | ref |
Baseline sPGA score: Severe | ||||||
Number of patients | 75 | 37 | 29 | 103 | 38 | 58 |
Responders, n (%) | 49 (65.3) | 3 (8.1) | 11 (37.9) | 50 (48.5) | 2 (5.3) | 19 (32.8) |
DEUC vs. PBO RD (95%CI)a | 56.4 (41.7 to 71.0) | ref | NA | 43.3 (30.5 to 56.0) | ref | NA |
DEUC vs. APREM RD (95%CI)a | 18.6 (−1.7 to 38.8) | NA | ref | 14.3 (−2.2 to 30.8) | NA | ref |
Baseline PASI score: ≤ 20 | ||||||
Number of patients | 177 | 102 | 98 | 298 | 152 | 143 |
Responders, n (%) | 94 (53.1) | 13 (12.7) | 32 (32.7) | 154 (51.7) | 16 (10.5) | 56 (39.2) |
DEUC vs. PBO RD (95%CI)a | 40.1 (30.5 to 49.8) | ref | NA | 41.3 (33.9 to 48.8) | ref | NA |
DEUC vs. APREM RD (95%CI)a | 22.4 (10.8 to 33.9) | NA | ref | 12.0 (2.4 to 21.6) | NA | ref |
Baseline PASI score: > 20 | ||||||
Number of patients | 155 | 64 | 70 | 213 | 103 | 111 |
Responders, n (%) | 100 (64.5) | 8 (12.5) | 27 (38.6) | 117 (54.9) | 8 (7.8) | 45 (40.5) |
DEUC vs. PBO RD (95%CI)a | 52.4 (41.2 to 63.5) | ref | NA | 47.4 (38.5 to 56.2) | ref | NA |
DEUC vs. APREM RD (95%CI)a | 23.9 (10.0 to 37.8) | NA | ref | 14.7 (3.5 to 26.0) | NA | ref |
APREM = apremilast; CI = confidence interval; DEUC = deucravacitinib; FAS = full analysis set; NA = not applicable; PASI = Psoriasis Area and Severity Index; PASI 75 = At least a 75% improvement in the Psoriasis Area and Severity Index; PBO = placebo; RD = risk difference; ref = reference; sPGA = static Physician’s Global Assessment.
aCMH test stratified by geographic region and body weight. Nonresponder imputation for missing data.
Source: Clinical Study Reports for POETYK-17 and POETYK-2.8
Table 41: Scalp-Specific and Fingernail-Specific PGA Response at Week 16 — POETYK-1 and POETYK-2 (FAS)
Outcome | POETYK-1 | POETYK-2 | ||||
|---|---|---|---|---|---|---|
DEUC N = 332 | PBO N = 166 | APREM N = 168 | DEUC N = 511 | PBO N = 255 | APREM N = 254 | |
ss-PGA 0 or 1 at week 16ab | ||||||
Number of patients contributing to the analysis (%) | 209 (63) | 121 (73) | 110 (65) | 305 (60) | 173 (68) | 166 (65) |
Responders, n (%) | 147 (70.3) | 21 (17.4) | 43 (39.1) | 182 (59.7) | 30 (17.3) | 61 (36.7) |
DEUC vs. PBO | ||||||
RD (95%CI) | 52.8 (43.7 to 62.0) | ref | NA | 42.3 (34.3 to 50.3) | ref | NA |
OR (95% CI), P value | 11.92 (6.69 to 21.25), P < 0.0001c | ref | NA | 6.85 (4.34 to 10.81), P < 0.0001c | ref | NA |
DEUC vs. APREM | ||||||
RD (95%CI) | 29.6 (18.7 to 40.6) | NA | ref | 23.5 (14.3 to 32.6) | NA | ref |
OR (95% CI), P value | 3.65 (2.21 to 6.04), P < 0.0001c | NA | ref | 2.63 (1.77 to 3.91), P < 0.0001c | NA | ref |
PGA-F 0 or 1 at week 16ab | ||||||
Number of patients contributing to the analysis (%) | 43 (13) | 34 (20) | 17 (10) | 69 (14) | 38 (15) | 47 (19) |
Responders, n (%) | 9 (20.9) | 3 (8.8) | 6 (35.3) | 14 (20.3) | 3 (7.9) | 13 (27.7) |
DEUC vs. PBO | ||||||
RD (95%CI) | 14.3 (−2.6 to 31.1) | ref | NA | 15.2 (0.7 to 29.7) | ref | NA |
OR (95% CI), P value | 2.84 (0.73 to 10.96), P = 0.10c | ref | NA | 3.21 (0.88 to 11.79), P = 0.06c | ref | NA |
DEUC vs. APREM | ||||||
RD (95%CI) | −9.3 (−38.5 to 19.9) | NA | ref | −7.1 (−23.4 to 9.1) | NA | ref |
OR (95% CI), P value | 0.64 (0.16 to 2.57), P = 0.55d | NA | ref | 0.68 (0.28 to 1.62), P = 0.39d | NA | ref |
APREM = apremilast; CI = confidence interval; DEUC = deucravacitinib; FAS = full analysis set; LS = least squares; OR = odds ratio; PBO = placebo; PGA-F = Physician’s Global Assessment – fingernail; RD = risk difference; ref = reference; ss-PGA = scalp-specific Physician’s Global Assessment.
aPatients must also have at least a 2-point improvement vs. baseline.
bCMH test stratified by geographic region, body weight, and prior biologic use. Nonresponder imputation for missing data.
cTested using a 2-sided alpha of 0.025.
dP value has not been adjusted for multiple testing (i.e., the type I error rate has not been controlled).
Source: Clinical Study Report for POETYK-1,7 and POETYK-2.8
Table 42: PASI and sPGA Response at Week 24 — POETYK-1 and POETYK-2 (FAS)
Outcome | POETYK-1 | POETYK-2 | ||
|---|---|---|---|---|
DEUC N = 332 | APREM N = 168 | DEUC N = 511 | APREM N = 254 | |
Number of patients contributing to the analysis (%) | 332 (100) | 168 (100) | 504 (99) | 254 (100) |
sPGA 0 or 1 at week 24ab | ||||
Responders, n (%) | 195 (58.7) | 52 (31.0) | 251 (49.8) | 75 (29.5) |
RD (95%CI) | 27.5 (18.8 to 36.2) | ref | 20.4 (13.5 to 27.4) | ref |
OR (95% CI), P value | 3.23 (2.16 to 4.83), P < 0.0001c | ref | 2.47 (1.78 to 3.43), P < 0.0001c | ref |
PASI 75 response at week 24a | ||||
Responders, n (%) | 230 (69.3) | 64 (38.1) | 296 (58.7) | 96 (37.8) |
RD (95%CI) | 31.0 (22.2 to 39.8) | ref | 21.1 (13.9 to 28.3) | ref |
OR (95% CI), P value | 3.76 (2.53 to 5.60), P < 0.0001c | ref | 2.44 (1.78 to 3.36), P < 0.0001c | ref |
PASI 90 response at week 24 a | ||||
Responders, n (%) | 140 (42.2) | 37 (22.0) | 164 (32.5) | 50 (19.7) |
RD (95%CI) | 20.0 (11.9 to 28.2) | ref | 13.0 (6.9 to 19.2) | ref |
OR (95% CI), P value | 2.63 (1.71 to 4.05), P < 0.0001c | ref | 2.07 (1.43 to 3.01), P < 0.0001c | ref |
APREM = apremilast; CI = confidence interval; DEUC = deucravacitinib; FAS = full analysis set; NA = not applicable; OR = odds ratio; PASI 75 or 90 = At least a 75% or 90% improvement in the Psoriasis Area and Severity Index; PBO = placebo; RD = risk difference; ref = reference; sPGA = static Physician’s Global Assessment.
aCMH test stratified by geographic region, body weight, and prior biologic use. Nonresponder imputation for missing data.
bPatients must also have at least a 2-point improvement in their sPGA score vs. baseline.
cTested using a 2-sided alpha of 0.025.
Appendix 4: Description and Appraisal of Outcome Measures
Note this appendix has not been copy-edited.
Aim
To describe the following outcome measures and review their measurement properties (validity, reliability, responsiveness to change, and MID) in population with (plaque) psoriasis.
The PASI and sPGA are coprimary end points in the 2 pivotal trials (POETYK 1 and 2) under review. The patient-reported symptom scale, PSSD score is the key secondary outcome in POETYK 1 and 2 trials. The HRQoL measurements including dermatology-specific tool, i.e., DLQI, and generic tools, i.e., EQ-5D-3L and SF-36, are other outcomes in POETYK-1 and −2 trials.
Findings
Table 43: Summary of Outcome Measures and Their Measurement Properties
Outcome measure | Type | Conclusions about measurement properties | MID |
|---|---|---|---|
PASI 75, 90, or 100 | Disease-specific composite severity index based on an average score of erythema, scaling, and thickness of the lesions in 4 major body areas (head, upper extremities, trunk, and lower extremities) weighted by the area of involvement (BSA). PASI scores range from 0 to 72, with higher scores indicating greater severity. A reduction of PASI score by 75% (PASI 75) is a benchmark in psoriasis clinical trials,35 while more aggressive treatment goals such as reduction of PASI scores 90% or 100% (total clearance) are also used as end points in psoriasis clinical trials.36,37 | Validity: Construct validity was demonstrated through correlation of the PASI and DLQI scores (0.36 ≤ r ≤ 0.54).55 Correlation between the LS-IGA and IGA (Spearman rank correlation 0.92 and 0.73).31 Reliability: PASI was shown to have good interrater reliability (ICC > 0.75). The coefficient of variation for the PASI score was 36.9, indicating moderate inter-rater reliability.32 Responsiveness: Responsiveness was found to be low when the affected BSA is < 10%.33,34 | Unknown |
sPGA | A clinician-reported, 5-point scale to measure the clinical signs of psoriasis at a single point in time not relying on the investigator’s recall of the patient’s disease severity observed at baseline or previous visit.41,56 Individual psoriatic lesions are graded for induration, erythema, and scaling based on scales of 0 (clear) to 4 (severe), then averaged with equal weight for each item to obtain a single estimate of the patient’s overall severity of disease.39 Higher score indicates a more severe condition.40 | Validity: Relatively high correlation with both the PASI and PtGA (Pearson correlation coefficient > 0.5),38,39 moderate correlation with DLQI,55 and a low correlation with the OCI,39 supporting convergent and divergent validity. Reliability: Acceptable test-retest reliability (ICC 0.8).38 High internal consistency reliability in PGA scores, Cronbach coefficient alpha > 0.80 at week 2 and onwards39 and ≥ 0.90 in 4 examined trials.38 | A score of 0 or 1 Is generally accepted that a clinically meaningful.40 Some trials define efficacy as a 2-point reduction in the total score.41 Clinically important difference estimates included point changes of about half of a PGA category; 0.52 and 0.55 points in 2 studies, respectively.38,39 |
PGA-F | A clinician-reported, 5-point ordinal response scale to assess severity of signs of disease in patients’ nail bed and nail matrix. Severity levels are categorized into “clear (0)”, “minimal (1)”, “mild (2)”, “moderate (3)”, and “severe (4)”. Three scores can be derived: nail bed signs, nail matrix signs, and overall global score (worse of the nail bed or matrix score). Higher score indicates more severe disease in fingernail. | Validity: Content validity has been ensured during development, i.e., literature review, clinical expert feedback, cognitive interviews, in accordance with FDA Guidance.57 Concurrent validity was confirmed with mNAPSI at baseline (Pearson r = 0.44; Spearman r = 0.43) and at week 26 (Pearson r = 0.76; Spearman r = 0.77).57 Construct validity was confirmed with significantly increasing mNAPSI scores corresponding to increasing categories of PGA-F (P < 0.0001 for all severity categories, except for “severe” [4] P = 0.03).58 Reliability: ICC between screening (Day −35 to −3) and baseline was 0.78 with a subset of patients showing little change was 0.83.57 Inter-rater agreement was fair (Kappa 0.2 to 0.4)59 for nail bed (0.20 to 0.22), nail matrix (0.28 to 0.29) and global (0.25) scores.58 Responsiveness: In general, PGA-F was able to track changes in fingernail health status as measured by mNAPSI over a 24-week period within and between individuals (P < 0.0001 to 0.7622).58 | Unknown |
ss-PGA | A physician-rated scale to assess scalp psoriasis severity based on erythema and scale characteristics. Score categories are: “Absence of disease (0)”, “very mild disease (1)”, “mild disease (2)”, “moderate disease (3)”, “severe disease (4)”. Higher score presents more severe scalp psoriasis.7 | No evidence was found through literature search to support measurement properties. | Unknown |
DLQI | Ten-item dermatology-specific quality of life questionnaire to assess limitations related to the impact of skin disease. The response options range from 0 (not affected at all) to 3 (very much affected). DLQI scores range from 0 to 30, with lower scores indicating better quality of life. | Validity: Correlated with the bodily pain (r = 0.61) and social functioning domains (r = 0.68) of the SF-36, and the EQ-5D index score (r = 0.71).45 Reliability: The test-retest reliability correlation coefficients were high for both the overall score (Spearman rank correlation 0.99) and for individual questions (0.95 to 0.98).46 Responsiveness: Equal responsiveness to the PASI and IGA scores with correlation coefficients of r = 0.69 and r = 0.71.45 | The MID estimates ranged from 2.2 to 6.9 using 3 anchor-based methods.45 A study in patients with psoriasis treated with adalimumab reported an MID of 3.2.47 In a review of RCTs in psoriasis, the MID was reported to be a score change of 5.48 |
PSSD | A self-administered, disease-specific instrument assessing of 5 symptoms (itch, pain, stinging, burning, skin tightness) and 6 patient-observable signs (skin dryness, cracking, scaling, shedding/flaking, redness, and bleeding) in 2 versions: PSSD-24h (24-hour recall period) and PSSD-7d (7-day recall period). Both versions contain the same 11 items.43 Two summary scores (symptoms and signs [range, 0 to 100 each]) are derived based on individual item scores (0 to 10 [absent-worst imaginable]). In addition, the PSSD-7d asks about frequency of each symptom on a 5-point scale: “None of the days” (0 days), “A small number of days” (1 or 2 days), “Some days” (3 or 4 days), “Most days” (5 or 6 days), “All of the days” (7 days). Higher scores indicate more severe or more frequent signs and symptoms of psoriasis.60 | Validity: Content validity has been ensured in accordance with the FDA’s PRO Guidance, i.e., concept elicitation and cognitive interviews, expert clinical opinion input, extensive literature reviews. Convergent validity was demonstrated between PSSD-24h and DLQI total score (Pearson r = 0.489).43 Another study showed convergent validity between PSSD-7d symptom score and 6 DLQI domain scores (r = 0.782), PASI responses (r = 0.565), and IGA (r = 0.525) at week 16 of treatment.43 Divergent validity between PSSD-24h and SF-36 (PCS r = −0.437, MCS r = −0.203) was found.43 Patients with most severe/lowest HRQoL group based on PASI score, PGI rating, and DLQI score the highest PSSD scores (no P values provided).43 Another study confirmed that PSSD-7d scores at week 16 after treatment can distinguish PASI, IGA, DLGI subgroups (P < 0.001).60 Reliability: Internal consistency was acceptable (alpha > 0.7)42 for PSSD-24h (alpha = 0.96) and −7d (alpha = 0.95) symptom scores.43 Test-retest reliability with 1-week interval for PSSD-24h (ICC = 0.92 to 0.95) and −7d (0.94 to 0.95) was acceptable.43 Responsiveness to change: Significant differences in mean improvement in PSSD-7d symptom scores at week 16 of treatment were detected by subgroups of improvement levels of PASI and IGA (both P < 0.0001), as well as various levels of changes in DLQI. In contrast, patients with no change or worsening in PASI or DLQI had a slight increase (worsening) in PSSD-7d symptoms. Those with no change or worsening in IGA had only marginal improvement in PSSD-7d symptoms.60 | In patients with moderate to severe plaque psoriasis:43 Using anchor-based methods (PGA and PGI-Sx), MID estimates for PSSD 24h total severity scores range from 9 to 12 points and PSSD 7d range from 9.1 to 12.5. Using distribution-based method, MID estimates for PSSD 24h severity scores range from 5.7 to 8.5 (SEM) and from 12.6 to 13.1 (SES), while for PSSD 7d severity scores range from 6.7 to 8.6 (SEM) and from 13.1 to 14.3 (SES). An MID range of 8 to 10 is conservative and from 10 to 12 is reasonable for both 24h and 7d versions.43 |
EQ-5D-3L utility score and VAS | Generic, preference-based, health-related quality of life measure consisting of 6 descriptive questions comprising 5 dimensions.61 | The evidence for the validity of EQ-5D-3L in the psoriasis population is limited. The EQ-5D-3L was found to be highly correlated with the DLQI, though not as responsive to change in patient status.45 EQ-5D-3L showed similar responsiveness as the SF-36 version 1.45 | Based on PASI improvement estimated MID for index score ranges from 0.1 to 0.2. Based on PGA response, MID estimate for index is 0.09. MID estimates based on distribution-based method (0.14 to 0.22) agree with these estimates.45 MID estimated for VAS based on PASI improvement and PGA range from 3.82 to 8.43, as opposed to distributional method based estimate, 10.34.45 |
SF-36 PCS and MCS | 36-item, general health status instrument consisting of 8 domains. A Physical Component Score and a Mental Component Score can be computed.62 | In a systematic review examining both version 1 and 2 of the SF-36, the instrument was observed to be responsive (when compared with primary clinical measures) in patients with psoriasis.45,49 | A review examining both version 1 and 2 of the SF-36 indicated PCS or MCS improvement of at least 3 points in patients with RA, psoriatic arthritis in psoriasis.49,50 |
BSA = body surface area (A patient’s handprint including fingers and thumb representing 1% of the BSA involved); DLQI = Dermatology Life Quality Index; ICC = intraclass coefficient; IGA = Investigator’s Global Assessment; LS-IGA = Lattice System Physician’s Global Assessment; MID = minimal important difference; mNAPSI = modified Nail Psoriasis Severity Index; OCI = Ocular Comfort Index; PASI 75 or 90 or 100 = At least a 75%, 90% or 100% improvement in the Psoriasis Area and Severity Index; PGA = Physician’s Global Assessment; PRO = patient-reported outcome; PSSD = Psoriasis Scalp Severity Index; PtGA = Patient Global Assessment; RCT = randomized clinical trial; SF-36 PCS and MCS = Short Form (36) Health Survey Physical Component Score and Mental Component Score; PGA = Physician’s Global Assessment; PGI-Sx = Patient Global Impression change; RA = rheumatoid arthritis; SEM = standard error of the mean; SES = standard effect size; sPGA = Static Physician's Global Assessment; ss-PGA = Scalp-Specific Physician’s Global Assessment or Scalp Severity Physician’s Global Assessment.
Pharmacoeconomic Review
Abbreviations
AE
adverse event
AQPP
Association québécoise des pharmaciens propriétaires
BIA
budget impact analysis
BoB
basket of biologics
BSC
best supportive care
EAP
Exceptional Access Program
IL
interleukin
NMA
network meta-analysis
NMSC
nonmelanoma skin cancer
PASI
Psoriasis Area and Severity Index
PASI 50
50% reduction in Psoriasis Area and Severity Index score
PASI 75
75% reduction in Psoriasis Area Severity Index score
PASI 90
90% reduction in Psoriasis Area Severity Index score
PASI 100
100% reduction in Psoriasis Area Severity Index score
QALY
quality-adjusted life-year
RAMQ
Régie de l’assurance maladie du Québec
Executive Summary
The executive summary comprises 2 tables (Table 1 and Table 2) and a conclusion.
Item | Description |
|---|---|
Drug product | Deucravacitinib (Sotyktu), tablets |
Submitted price | Deucravacitinib, 6 mg tablets: $39.45 |
Indication | The treatment of adult patients with moderate to severe plaque psoriasis who are candidates for systemic therapy or phototherapy. |
Health Canada approval status | NOC |
Health Canada review pathway | Standard |
NOC date | November 23, 2022 |
Reimbursement request | As per indication |
Sponsor | Bristol Myers Squibb |
Submission history | Previously reviewed: No |
NOC = Notice of Compliance.
Table 2: Summary of Economic Evaluation
Component | Description |
|---|---|
Type of economic evaluation | Cost-utility analysis Markov model |
Target population | Adult patients with moderate to severe PsO who are candidates for systemic therapy or phototherapy, which aligns with the reimbursement request |
Treatmenta | Deucravacitinib |
Comparatorsa | Adalimumab, apremilast, bimekizumab, brodalumab, certolizumab pegol, etanercept, guselkumab, infliximab, ixekizumab, risankizumab, secukinumab, tildrakizumab, ustekinumab |
Perspective | Canadian publicly funded health care payer |
Outcomes | QALYs, LYs |
Time horizon | 10 years |
Key data source | A sponsor-commissioned NMA of 84 clinical trials was used to compare the ability of deucravacitinib to achieve PASI outcomes at 10 weeks to 60 weeks compared to the other biologics. This network included 2 phase III clinical trials for deucravacitinib: POETYK PSO-1 and POETYK PSO-2. |
Submitted results | The 3 treatments on the efficacy frontier were adalimumab, brodalumab, and bimekizumab. Deucravacitinib was dominated by adalimumab (i.e., less effective, more costly) and was less effective and less costly when compared to all other biologic comparators (i.e., not including apremilast). |
Key limitations |
|
CADTH reanalysis results | In CADTH reanalyses, deucravacitinib response was assessed at 16 weeks, tildrakizumab was dosed as per its Health Canada recommendation, and the basket of biologics representing subsequent therapy was assumed to be the same for all initial comparators. CADTH was unable to address the lack of direct evidence against relevant comparators and uncertainty in discontinuation rates and long-term efficacy.
|
LY = life-year; NMA = network meta-analysis; PASI = Psoriasis Area and Severity Index; PsO = plaque psoriasis; QALY = quality-adjusted life-year.
aAll treatments were sequences which began with the noted comparator, followed by a basket of biologic comparators, followed by best supportive care.
Conclusions
The CADTH clinical review concluded that in adults with moderate to severe plaque psoriasis, deucravacitinib is more effective in terms of skin clearance and health-related quality of life than placebo in the short term and is superior to apremilast for most outcomes. However, the relevance of placebo or apremilast as comparators is limited, as apremilast is only reimbursed by the province of Québec and the Canadian Armed Forces in Canada, and there are many active treatment options for adults with moderate to severe plaque psoriasis. The indirect evidence suggests that deucravacitinib is less effective at inducing Psoriasis Area and Severity Index (PASI) response than many biologics, and deucravacitinib is not expected to alter the overall treatment paradigm for moderate to severe psoriasis. The sponsor-submitted network meta-analysis (NMA) did not report any safety outcomes; thus, the comparative safety of deucravacitinib versus biologics is unknown.
In CADTH’s base case, CADTH assumed a 16-week assessment time point for deucravacitinib, assumed tildrakizumab would be dosed according to Health Canada recommendations, and assumed subsequent therapies would be equivalent between comparators. The CADTH base-case results align with the available clinical evidence and were consistent with that of the sponsor. Deucravacitinib was less effective than most other publicly reimbursed biologic comparators at their publicly available list prices. The CADTH base case indicated that deucravacitinib was associated with $5,512 in incremental costs and 0.027 fewer quality-adjusted life-years (QALYs) (i.e., dominated) compared with adalimumab. As deucravacitinib is less effective than several other reimbursed biologics, cost savings are required to compensate for the potential health losses. Therefore, the price of deucravacitinib would need to be reduced by more than 15% to result in enough cost savings relative to the next most optimal treatment (adalimumab) for the cost-effectiveness of adalimumab to be greater than $50,000 per QALY gained compared to deucravacitinib.
Stakeholder Input Relevant to the Economic Review
This section is a summary of the feedback received from the patient groups, registered clinicians, and drug plans that participated in the CADTH review process.
A joint submission from 2 patient groups was received for this review. The Canadian Psoriasis Network and the Canadian Association of Psoriasis Patients conducted a survey hosted on the Canadian Psoriasis Network’s website which received 22 responses, 21 of which were from respondents in Canada, and 20 of whom identified as having psoriasis themselves. One phone interview with a person who had received deucravacitinib as part of a clinical trial was also conducted. Based on survey responses, the main symptoms reported were flaking (n = 16), itching (n = 16), change in skin colour (e.g., redness; n = 13), flares (n = 12), and pain or burning (n = 12). Patients reported experience with topical therapies, apremilast, cyclosporine, methotrexate, oral retinoids, oral steroids, biologic therapies, phototherapies, and medical cannabis. The 3 participants who reported experience with a biologic therapy (unspecified) found it effective or very effective, while the single respondent who reported apremilast experience found it ineffective. Two participants indicated they were taking deucravacitinib as part of a clinical trial, with both reporting that deucravacitinib was easier to use and was better at managing symptoms than their other therapies, and 1 of 2 agreed that deucravacitinib had more tolerable side effects. Neither of these patients reported prior use of apremilast or biologic therapies. The patient who participated in the phone interview stated deucravacitinib has been very effective for them even after 3 years on treatment. They also noted an issue with needles and that they would not be on therapy if the drug was an injection, despite reporting previously severe symptoms. When asked about expectations for new medications, respondents reported symptom improvement (n = 12), better quality of life (n = 10), reduced side effects (n = 9) affordable (n = 8), and easier to take (n = 2). Eight participants noted financial hardships paying for their medications, with 3 reporting taking less than prescribed or stopping taking their medication due to cost. Additionally, information was used from the 2022 Survey of People with Psoriatic Disease in Canada and Their Caregivers, which included 809 survey participants of which 502 were patients themselves, 55% of whom reported having plaque psoriasis. Of respondents to this survey, 30% were using employer benefits to access their therapies, 28% were using public plans, 15% were using a partner’s benefits, and 27% were paying out of pocket.
No clinician group input was received for this review.
Drug plan input for this review noted that apremilast, the comparator in the POETYK PSO-1 and POETYK PSO-2 trials, is not funded in most jurisdictions, and that other products which are publicly funded may have been more appropriate comparators. The public drug plans sought guidance as to whether prior or concurrent therapies, including systemic nonbiologic or biologic therapies, should be considered when determining eligibility for deucravacitinib.
Several of these concerns were addressed in the sponsor’s model.
All biologic and targeted synthetic disease-modifying antirheumatic drugs available in Canada were considered as comparators.
Treatment administration costs were considered.
CADTH was unable to address the following concerns raised from stakeholder input.
An absence of cost-effectiveness results for subgroups of patients who were naive or experienced with biologics.
Economic Review
The current review is for deucravacitinib (Sotyktu) for adult patients with moderate to severe plaque psoriasis who are candidates for systemic therapy or phototherapy.
Economic Evaluation
Summary of Sponsor’s Economic Evaluation
Overview
The sponsor submitted a cost-utility analysis of deucravacitinib compared with other biologic and targeted synthetic comparators in patients with moderate to severe plaque psoriasis who are candidates for systemic therapy or phototherapy. The modelled population was consistent with the POETYK PSO-1 and POETYK PSO-2 trials1-3 and is aligned with the reimbursement request4 and the Health Canada indication.5
Deucravacitinib is available in 6 mg oral tablets, with a recommended dose of 6 mg once daily.5 At the submitted price of $39.45 per tablet, and at the recommended dose, the cost of deucravacitinib is $14,409 per patient per year (365.25 days). The comparators in the sponsor’s analysis were apremilast, adalimumab, bimekizumab, brodalumab, certolizumab pegol, etanercept, guselkumab, infliximab, ixekizumab, risankizumab, secukinumab, tildrakizumab, and ustekinumab. The recommended dosing regimens for each comparator were derived from their respective product monographs and are summarized in Table 8. Wastage was not considered by the sponsor as most comparator treatments use recommended dosing based on prefilled syringes, autoinjectors, or on oral tablets. The exception is infliximab, which has weight-based dosing and a single vial size, and for which wastage was not considered. Annual maintenance costs as considered by the sponsor ranged from $12,295 for adalimumab to $32,615 for tildrakizumab. The sponsor assumed patients would receive up to 3 lines of therapy with the second line composed of a “basket of biologics” (BoB) consisting of the unweighted average cost of all other comparators, excluding apremilast, deucravacitinib, and the product used as first line for that sequence. The third line for all sequences consisted of best supportive care (BSC), where BSC was the weighted average cost of the oral systemics acitretin (15%), cyclosporine (10%), and methotrexate (75%), or $579 per patient per year.
Outcomes of the model included QALYs and life-years which, alongside costs, were assessed over a 10-year time horizon. The base-case analysis was from the perspective of a Canadian publicly funded health care system with discounting of 1.5% per annum applied to both costs and outcomes. The cycle length was 2 weeks, and a half-cycle correction was not applied.
Model Structure
The sponsor submitted a Markov model with health states based on PASI score categories. Patients entered the model and received their initial treatment for 10 weeks (infliximab), 12 weeks (brodalumab, etanercept, ixekizumab, secukinumab, tildrakizumab), 16 weeks (adalimumab, apremilast, bimekizumab, certolizumab, guselkumab, risankizumab, ustekinumab), or 24 weeks (deucravacitinib), after which they were assessed for treatment response according to their PASI score. Those achieving a 75% reduction in PASI score (PASI 75) or greater at their assessment time point continued on maintenance treatment with that therapy until later discontinuation, at which point they moved onto the next line of therapy, which was a BoB as defined above, or death. Those not achieving a treatment response at their assessment time point (< PASI 75) also moved to a BoB. A figure describing the sponsor’s model is available in Appendix 3 (Figure 1).
Model Inputs
The target population for this analysis includes adult patients with moderate to severe plaque psoriasis who are candidates for systemic therapy or phototherapy. Mean baseline demographic characteristics used in the model were based on pooled patient data from the POETYK PSO-1 and POETYK PSO-2 clinical trials.2,3 The mean age and body weight of the population were 46.6 years and 90.7 kg, respectively, and 33.1% of the population were female.
After the initial treatment period of 24 weeks for deucravacitinib and 10 weeks to 16 weeks for the comparators, patients were assigned to health states based on their PASI score: less than a 50% reduction in PASI score (PASI < 50); PASI 50 to a 74% reduction in PASI score (50 ≤ PASI < 75); PASI 75 to an 89% reduction in PASI score (75 ≤ PASI < 90); a 90% reduction in PASI score to a 99% reduction in PASI score (90 ≤ PASI < 100); and a 100% reduction in PASI score (PASI 100). Assignment to these health states was based on the sponsor’s submitted NMA,6 which used a multinomial random effects, baseline risk-adjusted model. The sponsor’s analysis presented the probability of achieving each PASI score for each comparator, converted to proportions of patients achieving each PASI score at the end of the initial treatment period (Table 10). The probability of response to a BoB, and patient assignment to each health state when receiving a BoB, was based on the average probability of response at each PASI level of the comparators included within it and therefore differed when used after each initial therapy.
Beyond the initial induction phase and assessment, the model assumed all patients remain in the same health state, receiving the same treatment for the duration of the model time horizon, unless they discontinued to the next line of treatment in the sequence. An annual discontinuation rate was applied per treatment: 12.4% (deucravacitinib), 31.0% (apremilast), 10.0% (brodalumab, guselkumab, ixekizumab, risankizumab, secukinumab, tildrakizumab), or 15% (certolizumab pegol, etanercept, infliximab, ustekinumab). Patients who discontinued moved onto the next line of treatment, represented by an unweighted average BoB for efficacy (i.e., average PASI response category and thus health state attained after induction of a first-line treatment) and costs. Discontinuation from a BoB was calculated at 0.9% annually using the equation outlined in the Van de Wetering et al. study,7 based on the average discontinuation rate of comparators included in the BoB (12.1% annually), the assumption of 3 lines of therapy within a BoB, and the 10-year time horizon. The sponsor also applied an odds ratio of 1.24 for treatment failure for later lines (second and third lines) of therapy with a BoB.8 Patients who discontinued from a BoB were assumed to receive BSC until death or for the rest of the time horizon. All-cause mortality was based on age- and gender-specific data from Statistics Canada9 and was not affected by a patient’s psoriasis. Adverse events (AEs) considered in the model included severe infections, nonmelanoma skin cancer (NMSC), and malignancies other than NMSC and were sourced from a variety of publications depending on the comparator.1,10-19
Dosing for each comparator was consistent with the relevant product monograph (refer to Table 8), with the dosing of infliximab and ustekinumab, which have different dosing depending on patient weight, based on distributions of patients in each weight category as observed in the POETYK PSO-1 and POETYK PSO-2 trials.20,21 The sponsor also assumed that patients using tildrakizumab who weighed more than 90 kg would receive 200 mg per dose rather than 100 mg as recommended in the product monograph.
Health state utilities were calculated for the various PASI score categories based on the utility values used in the National Institute for Health and Care Excellence appraisal of ixekizumab for plaque psoriasis22 and previously used in the CADTH review of bimekizumab for plaque psoriasis.23 Patients discontinuing from a treatment and moving on to the induction phase of the next treatment would revert to the utility assigned for baseline PASI score. Only severe infections were associated with a utility decrement, which was assumed to be 0.014 per event, on the basis of a 0.986 utility multiplier associated with serious infections in a previous cost-effectiveness model for rheumatoid arthritis.24
The annual maintenance drug acquisition costs for the biologics used in the model ranged from $12,295 for the biosimilar adalimumab to $32,615 for tildrakizumab. Costs for most biologics were derived from the Ontario Drug Benefit Formulary25 and the Ontario Exceptional Access Program (EAP),26 while the costs for bimekizumab and guselkumab were from their respective CADTH reviews23,27,28 and the cost of apremilast was from the Régie de l'assurance maladie du Québec (RAMQ) List of Medications.29 The costs for the BoB was calculated as the unweighted average cost of comparators included after each initial therapy. Monitoring costs included dermatologist visits and laboratory tests (full blood count, urea, electrolytes, and liver function) and were assumed to occur twice during the initiation phase of any new treatment with the exception of infliximab where 3 visits were assumed ($200 to $300), and twice annually during the maintenance phase for all treatments ($200 annually). Infliximab, as the only IV comparator, was assumed to incur a $212 administration cost per infusion, while all subcutaneous comparators were assumed to incur a one-time administration cost of $18 accounting for 21 minutes of self-administration training by a nurse, and an additional $2 per subcutaneous administration was applied under the assumption that 10% of patients would continue having a health care provider administer the injections.30 Severe infections were associated with a cost of $8,819 per event, while NMSC and malignancies other than NMSC were associated with costs of $10,063 and $8,277, respectively.31
Summary of Sponsor’s Economic Evaluation Results
All analyses were run probabilistically (2,000 iterations). The deterministic and probabilistic results were similar. The probabilistic findings are presented subsequently. The submitted analyses are based on publicly available prices for all comparators. Additional results from the sponsor’s submitted base case are available in Appendix 3.
Base-Case Results
The sponsor’s base case demonstrated that 3 drug sequences were on the cost-effectiveness frontier: adalimumab, brodalumab, and bimekizumab. All other products, including deucravacitinib, were dominated or extendedly dominated.
Compared to adalimumab, deucravacitinib was associated with incremental costs of $1,479 and 0.018 fewer QALYs, meaning deucravacitinib was dominated by adalimumab.
Table 3: Summary of the Sponsor’s Economic Evaluation Results
Drug | Total costs ($) | Total QALYs | Sequential ICER ($ per QALY) |
|---|---|---|---|
Adalimumab | 138,687 | 6.968 | Reference |
Brodalumab | 153,558 | 7.047 | 187,202 |
Bimekizumab | 196,124 | 7.063 | 2,639,512 |
Deucravacitinib | 140,270 | 6.949 | Dominated by adalimumab |
ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year.
Note: The submitted analyses are based on publicly available prices of comparators and may not reflect confidential, negotiated prices. Only treatments that are on the efficiency frontier, as well as the drug under review, are reported. All listed comparators are followed in sequence by a basket of biologics and then by best supportive care.
Source: Sponsor’s pharmacoeconomic submission.30
Sensitivity and Scenario Analysis Results
The sponsor conducted a series of scenario and sensitivity analyses involving using a PASI 90 response threshold, using 16-week data for deucravacitinib, using utility values derived from the POETYK PSO-1 and POETYK PSO-2 trials, increasing discontinuation in subsequent lines of therapy, including administration disutilities, excluding AE costs and disutilities, and varying the time horizon, discount rate, and percentage of uncertainty assumed around point estimates. In most scenarios, deucravacitinib remained dominated by adalimumab, although the sponsor reported deucravacitinib as being less costly and less effective than adalimumab in scenarios using a PASI 90 response threshold and when a lifetime time horizon was assumed, and more costly and more effective when disutilities due to format of administration were assumed.
CADTH Appraisal of the Sponsor’s Economic Evaluation
CADTH identified several key limitations to the sponsor’s analysis that have notable implications on the economic analysis.
Uncertainty in relative clinical efficacy, safety, and indirect evidence: The POETYK PSO-1 and POETYK PSO-2 trials compared deucravacitinib to placebo and to apremilast, both of which are of limited clinical relevance in Canada; apremilast due to its lack of public funding in most jurisdictions, and placebo given the likely use of active therapies by patients. In the absence of direct evidence, the sponsor submitted an NMA comparing deucravacitinib to most other therapies available for the treatment of plaque psoriasis in Canada, which was used to calculate the proportion of patients in each PASI state at the time point of assessment for each comparator. The results of the short-term (10 weeks to 16 weeks) analysis favoured deucravacitinib versus placebo, apremilast, and etanercept 50 mg weekly in achieving all levels of PASI responses, and versus etanercept 50 mg biweekly for PASI 100. Most other comparisons of deucravacitinib with relevant comparators were in favour of the biologic comparator, typically an interleukin (IL)-17 or IL-23 inhibitor. The results of the midterm and long-term analyses were generally similar and favoured many biologics over deucravacitinib. Given the effect size estimates for deucravacitinib versus some comparators, specifically the IL-17 inhibitors and the IL-23 inhibitors risankizumab and guselkumab, the indirect evidence suggests that deucravacitinib is less effective at inducing PASI response than many biologics. However, CADTH identified limitations with the sponsor-submitted NMA (heterogeneity present for many patient and study characteristics, incorporation of studies that included patients with mild disease, discordance between patient treatment adherence assumptions and true clinical practice), which suggest the results of the NMA are at some risk of bias.
In terms of safety, the frequency of AEs in the pivotal trials was generally similar between deucravacitinib and comparators; however, the sample size and duration of follow-up may not have been sufficient to detect rare events, thus longer-term safety is uncertain. The submitted NMA did not report safety outcomes, and the submitted pharmacoeconomic analysis naively compared event rates from different trials,1,10-19 yielding a high degree of uncertainty in the comparative safety of deucravacitinib versus biologics.
CADTH conducted a scenario analysis in which the costs and quality of life decrements associated with AEs were not considered, effectively assuming equal safety between comparators.
Inappropriate comparison of time points: In their base-case analysis, the sponsor compared the proportions of patients in each PASI category at 24 weeks for deucravacitinib to the proportions of patients in each PASI category at 10 weeks to 16 weeks for the other comparators based a scenario analysis of the submitted NMA. The sponsor’s rationale for combining these time points was that response to deucravacitinib did not peak until 24 weeks of therapy in the clinical trials,20,21,30 and thus it was expected that patients in clinical practice using deucravacitinib will be assessed at 24 weeks to determine response and thus continuation of therapy. This combination of time points was deemed methodologically inappropriate within the CADTH clinical review, due to the introduction of bias associated with such temporal gaps. Additionally, expert input solicited by CADTH did not agree with the assumption that patients using deucravacitinib in clinical practice will be assessed at 24 weeks to determine whether to continue on maintenance therapy, stating that like other therapies, patients would be assessed at 12 weeks to 16 weeks, with the longer time to peak action for deucravacitinib seen as a reason to choose alternate, faster therapies rather than extend the assessment period, especially given the lower comparative efficacy of deucravacitinib compared to injectable therapies even at 24 weeks.
As part of the revised base-case analysis, CADTH considered PASI 75 response at 16 weeks for deucravacitinib and 10 weeks to 16 weeks for the comparators, using the model’s programmed option to do so.
Uncertainty in the modelling of the BoB: The sponsor assumed that when patients discontinued their first-line therapy, either due to initial lack of response, later loss of response, or other reason, they would then begin their second and later lines of therapy as represented by a BoB, an unweighted average of the efficacy and costs associated with all other comparators with the exception of deucravacitinib, apremilast, and the biologic used in first line, if applicable. As such, the costs and benefits associated with the BoB differed between comparators and thus have varying impacts on the overall cost-effectiveness of the full sequence of therapy. However, this unweighted average is unlikely to represent the actual usage of biologics in later lines in clinical practice, as patients are not equally likely to receive any available biologic at any line of therapy. According to the clinical expert input obtained by CADTH, the choice of the next comparator used may depend on the class of the drug that has failed or lost efficacy, the reason for its discontinuation, the changing market landscape as newer and more effective comparators become available and funded, and patient or clinician preference. Furthermore, the sponsor’s use of efficacy data from first-line treatment with a treatment failure multiplier is associated with uncertainty. Moreover, as the BoB represents 3 lines of therapy rather than 1, and only the initial therapy used was excluded (plus deucravacitinib and apremilast) rather than each therapy used in previous lines, this approach to define BoB biases results against initial comparators with a lower cost-to-QALY ratio and favours those with a higher cost-to-QALY ratio. Due to the complexity of modelling all potential sequences of therapy and the absence of data to inform such sequences, a less biased, simplifying assumption would be to include an identical definition of the BoB across all comparators. In effect, this removes the impact of subsequent lines of therapies from driving the overall cost-effectiveness results.
CADTH reanalyses assumed that the BoB would have the same cost and efficacy for all comparators, using the sponsor-provided option to do so.
Discontinuation rates are uncertain: The sponsor assumed that anti–tumour necrosis factor comparators would have a long-term annual discontinuation rate of 15% for patients who had initially responded, while IL-17 and IL-23 comparators would have a 10% annual discontinuation rate, based on a scenario conducted during the CADTH review of bimekizumab for plaque psoriasis.23 This assumption was based on clinical expert opinion and the expected efficacy increases of newer products, and supported by a retrospective cohort study. Historically, a flat discontinuation rate of 15% has been assumed for all comparators. As apremilast and deucravacitinib were not included in the bimekizumab review, the sponsor assumed a 12.4% annual discontinuation rate after initial response for deucravacitinib based on the proportion of PASI 75 responders who later discontinued deucravacitinib between weeks 24 and weeks 52 of the POETYK PSO-2 clinical trial. The generalizability of the rate at which patients discontinued therapy within a clinical trial and within 6 months of initial response over a longer term and in clinical practice is highly uncertain. The sponsor also assumed an annual discontinuation rate of 31% for patients who had initially responded to apremilast, cited as from a Cochrane NMA on treatments for plaque psoriasis. Although CADTH was unable to identify this data within the source,32 a rough calculation from the sponsor’s POETYK PSO-2 trial indicated a similar discontinuation rate for apremilast (albeit using short-term data). Clinical expert input obtained by CADTH estimated that in clinical practice, the expected discontinuation rate of deucravacitinib would be similar to that of apremilast given their relatively low efficacy rates compared to biologic options, and their shared oral mode of administration.
To explore these uncertainties, CADTH conducted a scenario which assumed that all comparators had a 15% annual discontinuation rate after initial response was established, as well as a scenario where the long-term discontinuation rate of deucravacitinib was assumed to be the same as that of apremilast.
Uncertainty surrounding the appropriate threshold by which to assess treatment response: In the sponsor’s base case, patients were assumed to respond to and maintain their current therapy provided they had achieved a PASI 75 at 10 weeks to 24 weeks, depending on the comparator. CADTH-obtained clinical expert input noted that, especially for newer biologics entering the market, a PASI 90 score would be a more appropriate measure of treatment response, especially in early lines of therapy. This factor was also noted in the CADTH reviews of tildrakizumab, risankizumab, and bimekizumab. In contrast, at later lines of therapy (e.g., third line or later), CADTH-obtained clinical expert input indicated many patients remain on their advanced therapies provided they experience some improvement, even if a PASI response at a set threshold has not been achieved.
As part of a scenario analysis, CADTH considered a PASI 90 threshold for treatment response, using the sponsor-provided option to do so. The sponsor’s model was not sufficiently flexible to explore the impact of changing the PASI response threshold at different lines of therapy. CADTH additionally conducted a scenario assuming patients had an additional round of BoB and did not have long-term discontinuation from it (0% discontinuation) due to an unwillingness to cease using advanced therapies entirely.
Dosing of tildrakizumab was inappropriate: The sponsor assumed that patients who weighed less than 90 kg (48% of patients) would receive 100 mg of tildrakizumab per dose, while those who weighed more than 90 kg would receive 200 mg per dose. This is consistent with the dose outlined in the Summary of Product Characteristics for tildrakizumab as authorized by the European Medicines Agency.33 However, the Health Canada product monograph does not differentiate dosing of tildrakizumab by weight, and instead recommends only the 100 mg dose,34 as does the FDA.35 This difference in dose has a large impact on the average cost of treatment of tildrakizumab, as well as a smaller impact on the cost of the BoB, which includes tildrakizumab for all other comparators.
CADTH reanalyses used a dose of 100 mg per administration of tildrakizumab for all patients.
Treatment waning was not considered: In the sponsor’s base case, it was assumed that patients would achieve different PASI scores based on treatment received according to the proportions derived from the NMA. Patients were assumed to remain in this PASI state until discontinuation for any reason, at which point they would transition to the next line of therapy, where they would acquire a new PASI health state consistent to response rates for that line of therapy (BoB or BSC). This methodology does not allow for consideration of treatment waning, a reality supported by the clinical expert. The expert noted that, while PASI 75 or PASI 90 may be considered a relevant threshold by which to assess response, particularly in early lines of treatment, patients may not actually switch therapy until their score drops below PASI 50. Thus, patients could experience treatment waning in which their condition progresses, and quality of life decreases, while still remaining on the same therapy, a factor not accounted for in the sponsor’s discontinuation assumptions. It is uncertain what effect this has on the cost-effectiveness results.
Due to limitations in the model structure CADTH was unable to address this in reanalysis.
Model was cumbersome and lacked transparency: CADTH notes the sponsor’s submission was overly complex making simple validation checks very difficult. For example, there was duplication of key parameters across multiple sheets making it unclear which parameter needed to be edited to implement a change. Likewise, the sponsor’s submitted model also included numerous IFERROR and IFNA statements, which lead to situations in which the parameter value is overwritten with an alternative value without alerting the user to the automatized overwriting. The systematic use of IFERROR and similar statements makes thorough auditing of the sponsor’s model impractical, as it remains unclear whether the model is running inappropriately by overriding errors.
CADTH was unable to address this limitation and notes that results from the analysis could not be fully validated.
Additionally, the following key assumptions were made by the sponsor and have been appraised by CADTH (refer to Table 4).
Table 4: Key Assumptions of the Submitted Economic Evaluation (Not Noted as Limitations to the Submission)
Sponsor’s key assumption | CADTH comment |
|---|---|
A 10-year time horizon was considered appropriate. | Reasonable. Given the continually evolving field of plaque psoriasis treatments, a shorter time horizon is appropriate as new biologics will likely be added to the treatment paradigm in the future. |
All-cause mortality included in the model, with no additional risk of mortality associated with moderate to severe plaque psoriasis. | Appropriate. Plaque psoriasis is not expected to influence survival. |
Serious infections are associated with a utility decrement of 0.014. | Inappropriate. The source of this assumption is a 2014 cost-effectiveness study for rheumatoid arthritis which applied a utility multiplier of 0.9858 to all bDMARDs on the basis of higher frequencies of serious infections using a utility associated with pneumonia from an earlier study. The assumption that a utility modifier previously applied to all biologic comparators may be used to represent a one-time utility decrement of 0.014 which may be applied to each infection event is inappropriate. However, removing this decrement does not have a substantial impact on results. |
Monitoring occurs 2 to 3 times during induction phase and twice annually thereafter, always including lab tests. | Uncertain. Clinical expert input obtained by CADTH indicated that patients would be seen at the start of any new medication initiation and again to assess response, without laboratory testing being necessary. Thereafter, patients continuing on the medication would be seen once annually. This expert input indicated that the use of deucravacitinib might result in additional lab testing to ensure the side effects associated with JAK inhibitors were not affecting deucravacitinib patients, at least in the early days of its availability. However, the sponsor’s potential overestimation of monitoring costs and additional lab testing for deucravacitinib relative to other comparators for plaque psoriasis did not have a substantial impact on results. |
Later lines of therapy have lower efficacy than earlier lines. | Uncertain. The sponsor assumed that the second and third lines of therapy used within the BoB (the third and fourth lines of therapy overall) would have an odds ratio of treatment failure of 1.24 compared to that of the same drug when used as first-line therapy, based on Gniadecki et al. (2015),8 which compared biologic drug survival between patients who were naive and those who had previously been exposed to a biologic. Clinical expert input elicited by CADTH observed that this ratio would depend on the reason for discontinuation of the previous biologic (e.g., failure to respond, loss of response, loss of reimbursement status) and is not easily generalized to comparators beyond those initially studied (i.e., adalimumab, infliximab, etanercept). However, altering this parameter does not have a substantial impact on results. Of note, the sponsor seemed to consider this parameter to represent treatment waning, but it does not model a potential loss in efficacy and thus quality of life within a single treatment over time. |
bDMARD = biologic disease-modifying antirheumatic drug; BoB = basket of biologics; JAK = Janus kinase.
CADTH Reanalyses of the Economic Evaluation
Base-Case Results
The CADTH base case was derived by altering the assessment time point of deucravacitinib to 16 weeks, incorporating the Health Canada–recommended dosing for tildrakizumab, and assuming the same BoB would be used for all comparators. CADTH also corrected a minor error where the sponsor had reversed the utility weights for 2 PASI-defined health states relative to the original source data.22,23
Table 5: CADTH Revisions to the Submitted Economic Evaluation
Stepped analysis | Sponsor’s value or assumption | CADTH value or assumption |
|---|---|---|
Correctionsa to sponsor’s base case | ||
1. Error in utility values for 2 PASI-defined health states | PASI 75 to 89: 0.791 PASI 90 to 99: 0.778 | PASI 75 to 89: 0.778 PASI 90 to 99: 0.791 |
Changes to derive the CADTH base case | ||
1. Deucravacitinib response assessment time point | 24 weeks | 16 weeks |
2. Tildrakizumab dosing | As per European Medicines Agency Summaries of Product Characteristics, patients with body weights > 90 kg receive 200 mg per dose | As per Health Canada Product Monograph, all patients receive 100 mg per dose |
3. Basket of biologics | Unweighted average cost, safety, and efficacy of all biologics, with the exception of deucravacitinib, apremilast, and the biologic initially used, if applicable. | Unweighted average cost, safety, and efficacy of all biologics, with the exception of deucravacitinib and apremilast. |
CADTH base case | 1 + 2 + 3 | |
PASI = Psoriasis Area Severity Index.
aCorrections are minor errors (e.g., transcription errors between report and model, misapplication of distributions or standard errors in probabilistic analyses, and so forth) that are not identified as limitations.
Results of the CADTH reanalysis are similar to those of the sponsor in that the same 3 drugs remained on the cost-effectiveness frontier, adalimumab, brodalumab, and bimekizumab, with all other products being dominated or subject to extended dominance. Step-wise results of the CADTH reanalysis are presented in Table 6.
In the CADTH base case, deucravacitinib was less effective (fewer QALYs) to most comparators except apremilast and etanercept. This aligns with the available direct and indirect clinical evidence. Deucravacitinib was dominated by adalimumab, being associated with $5,512 in incremental costs, and 0.027 fewer QALYs. The probability of deucravacitinib being the most cost-effective option did not rise above 2% regardless of the willingness-to-pay threshold. The key drivers of the results are the relative efficacy assumptions and drug costs.
Table 6: Summary of the Stepped Analysis of the CADTH Sequential Reanalysis Results
Stepped analysis | Drug | Total costs ($) | Total QALYs | Sequential ICER ($ per QALYs) |
|---|---|---|---|---|
Sponsor’s base case | Adalimumab | 138,687 | 6.968 | Reference |
Brodalumab | 153,558 | 7.047 | 187,202 | |
Bimekizumab | 196,124 | 7.063 | 2,639,512 | |
Deucravacitinib | 140,270 | 6.949 | Dominated by adalimumab | |
Sponsor’s corrected base case | Adalimumab | 138,619 | 6.972 | Reference |
Brodalumab | 153,501 | 7.061 | 167,921 | |
Bimekizumab | 195,486 | 7.079 | 2,316,592 | |
Deucravacitinib | 140,184 | 6.949 | Dominated by adalimumab | |
CADTH reanalysis 1 to 16-week deucravacitinib assessment | Adalimumab | 138,639 | 6.971 | Reference |
Brodalumab | 153,530 | 7.058 | 170,331 | |
Bimekizumab | 195,754 | 7.075 | 2,477,387 | |
Deucravacitinib | 140,330 | 6.937 | Dominated by adalimumab | |
CADTH reanalysis 2 – tildrakizumab 100 mg dosing | Adalimumab | 134,470 | 6.974 | Reference |
Brodalumab | 150,719 | 7.062 | 184,377 | |
Bimekizumab | 193,150 | 7.080 | 2,324,317 | |
Deucravacitinib | 136,459 | 6.859 | Dominated by adalimumab | |
CADTH reanalysis 3 – equal basket of biologics | Adalimumab | 134,452 | 6.968 | Reference |
Brodalumab | 153,252 | 7.068 | 187,929 | |
Bimekizumab | 197,363 | 7.085 | 2,587,908 | |
Deucravacitinib | 140,150 | 6.951 | Dominated by adalimumab | |
CADTH base case (1 + 2 + 3) | Adalimumab | 130,710 | 6.960 | Reference |
Brodalumab | 150,625 | 7.058 | 202,164 | |
Bimekizumab | 194,959 | 7.076 | 2,447,734 | |
Deucravacitinib | 136,222 | 6.933 | Dominated by adalimumab |
ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year.
Note: All analyses are based on the publicly available prices of comparators and may not reflect confidential, negotiated prices. Only treatments that are on the efficiency frontier, as well as the drug under review, are reported. Full results of the CADTH base case are reported in Appendix 3. All listed comparators are followed in sequence by the basket of biologics for an additional 3 lines of therapy and then by best supportive care. All analyses were conducted probabilistically.
Scenario Analysis Results
CADTH undertook price reduction analyses based on the sponsor’s corrected and CADTH’s base case. Based on the CADTH base case, a price reduction of 12.5% would be necessary for deucravacitinib to enter the cost-effectiveness frontier (i.e., to no longer be dominated by adalimumab); however, at this price reduction, adalimumab would remain the most cost-effective treatment at a willingness-to-pay threshold of $50,000 per QALY. A price reduction for deucravacitinib of 15.5% would be necessary to result in enough cost savings relative to the next most optimal treatment (adalimumab) for the cost-effectiveness of adalimumab to be greater than $50,000 per QALY gained compared to deucravacitinib (Table 7).
Table 7: CADTH Price Reduction Analyses
Analysis | ICERs for deucravacitinib vs. comparators ($ per QALY) | |
|---|---|---|
Price reduction | Sponsor’s corrected base case | CADTH reanalysis |
Deucravacitinib at submitted price | WTP threshold < $167,921: adalimumab $167,921 < WTP threshold < $2,316,592: brodalumab $2,316,592 < WTP threshold: bimekizumab | WTP threshold < $202,164: adalimumab $202,164 < WTP threshold < $2,447,734: brodalumab $2,447,734 < WTP threshold: bimekizumab |
3.1% | WTP threshold < $3,469: deucravacitinib $3,469 < WTP threshold < $172,861: adalimumab $172,961 < WTP threshold < $2,452,071: brodalumab $2,452,071 < WTP threshold: bimekizumab | |
5.4% | WTP threshold < $51,128: deucravacitinib $51,128 < WTP threshold < $167,148: adalimumab $167,148 < WTP threshold < $2,306,772: brodalumab $2,306,772 < WTP threshold: bimekizumab | |
10% | WTP threshold < $153,101: deucravacitinib $153,101 < WTP threshold < $167,965: adalimumab $167,965 < WTP threshold < $2,259,012: brodalumab $2,259,012 < WTP threshold: bimekizumab | |
12.5% | WTP threshold < $320: deucravacitinib $320 < WTP threshold < $196,800: adalimumab $196,800 < WTP threshold < $2,332,864: brodalumab $2,332,864 < WTP threshold: bimekizumab | |
15% | WTP threshold < $39,714: deucravacitinib $39,714 < WTP threshold < $198,045: adalimumab $198,045 < WTP threshold < $2,206,479: brodalumab $2,206,479 < WTP threshold: bimekizumab | |
15.6% | WTP threshold < $50,919: deucravacitinib $50,919 < WTP threshold < $200,591: adalimumab $200,591 < WTP threshold < $2,205,315: brodalumab $2,205,315 < WTP threshold: bimekizumab | |
ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year; WTP = willingness to pay; vs. = versus.
Note: All analyses are based on the publicly available prices of comparators and may not reflect confidential, negotiated prices. Only treatments that are on the efficiency frontier, as well as the drug under review, are reported. All listed comparators are followed in sequence by the basket of biologics for an additional 3 lines of therapy and then by best supportive care. All analyses were conducted probabilistically. Reported points were chosen based on the price reduction at which deucravacitinib entered the cost-effectiveness frontier and the price reduction at which the ICER for adalimumab compared to deucravacitinib rose above $50,000 per QALY.
CADTH undertook a series of scenario analyses exploring the impact of alternative assumptions on the cost-effectiveness of deucravacitinib, which are outlined as follows.
Costs and disutilities associated with AEs were removed from the analysis.
A constant long-term discontinuation rate of 15% was used for all comparators.
A discontinuation rate of 31% was used for deucravacitinib to match that of apremilast, the other available oral comparator.
A PASI 90 threshold was considered for treatment response.
Patients were assumed to continue on a BoB for an additional round and had a 0% long-term discontinuation rate.
Newly available generic pricing was used for apremilast.
The results of these analyses are presented in Table 16. In all scenarios, deucravacitinib remained dominated by adalimumab (i.e., deucravacitinib was more costly and less effective).
Issues for Consideration
Generic apremilast is available: For apremilast, the sponsor assumed30 the RAMQ list price for the originator brand, Otezla, of $18.91 per tablet, which is the same as the Association québécoise des pharmaciens propriétaires (AQPP) list price.36 However, several generic versions of apremilast have recently been approved by Health Canada and have begun being marketed. It is likely that the RAMQ list price for apremilast will decrease in the near future. As apremilast is not a benefit in most CADTH-participating public drug plans, and the wholesale list price of generic apremilast outside of Québec was, at the time of this review, similar to the RAMQ list price for Otezla, CADTH did not alter this pricing in its base-case analysis. However, a scenario analysis was conducted which considered the AQPP price for PMS-Apremilast of $14.18 per 30 mg tablet.36 The cost of the Otezla titration pack was not altered in this scenario.
Patents for some comparators have recently expired: The patents for ustekinumab and certolizumab expired in June 2021 and August 2021, respectively.37,38 As such, it is possible that biosimilar versions of 1 or both products could become available within the next few years. Should these biosimilars become available, deucravacitinib may no longer achieve cost savings relative to publicly available prices of ustekinumab and/or certolizumab pegol.
Potential for indication creep: While deucravacitinib is indicated for patients with moderate to severe plaque psoriasis, its oral mode of administration may lead to use in patients with milder forms of psoriasis. If used in this manner, this would increase the overall cost of care for the treatment of plaque psoriasis at an unknown cost-effectiveness.
Place in therapy: As per the sponsor’s NMA, deucravacitinib is less effective in terms of PASI response and takes longer to reach peak response rates than biologics.6,30 Given that the use of more aggressive and effective treatment earlier on may lead to improved patient outcomes,39 it is unclear that the use of deucravacitinib rather than biologics among eligible patients represents a clinically or economically desirable option. As per CADTH-obtained clinical expert feedback, conventional systemic therapies and biologics serve patients’ needs, very few patients are refractory to these therapies, and most patients would opt for a higher efficacy treatment where available. Like apremilast, deucravacitinib may be considered for patients who would prefer oral therapy; however, according to clinical expert feedback, many patients with moderate to severe psoriasis would prefer an injectable biologic, due to its efficacy and infrequent subcutaneous administration, over a daily oral medication. Clinical expert feedback also indicated that even patients who are needle-phobic are usually able to tolerate injections when administered by a caregiver, nurse, or other health care practitioner, especially given the availability of biologics with treatment intervals of up to 12 weeks.
Overall Conclusions
The CADTH clinical review concluded that in adults with moderate to severe plaque psoriasis, deucravacitinib is more effective in terms of skin clearance than placebo or apremilast in the short-term. Patient-reported end points suggest a benefit with deucravacitinib in health-related quality of life versus placebo, but no clinically relevant difference versus apremilast in the short-term. The relevance of placebo or apremilast as comparators is limited, given apremilast is only reimbursed by the province of Québec and the Canadian Armed Forces in Canada, and there are many active treatment options for adults with moderate to severe plaque psoriasis. The sponsor-submitted NMA comparing deucravacitinib with other biologics reimbursed in Canada suggested that in the short-term (10 weeks to 16 weeks), deucravacitinib was superior to apremilast and etanercept in achieving all levels of PASI response, and not significantly different from tildrakizumab for all levels of PASI response, or certolizumab and ustekinumab in terms of PASI 100 response. For all other comparisons, the comparator treatment was statistically superior to deucravacitinib. The sponsor-submitted NMA did not report any safety outcomes; thus, the comparative safety of deucravacitinib versus biologics is unknown. While the sponsor submitted a scenario analysis for the NMA comparing deucravacitinib response at 24 weeks to the comparators at 10 weeks to 16 weeks of therapy and used it as the basis of their pharmacoeconomic analysis, this analysis was deemed methodologically inappropriate in the CADTH clinical review and not representative of what will occur in clinical practice according to CADTH-obtained clinical expert feedback. Given the effect size estimates for deucravacitinib and the comparators, the indirect evidence suggests that deucravacitinib is less effective at inducing PASI response than many biologics, and thus deucravacitinib is not expected to alter the overall treatment paradigm for moderate or severe psoriasis.
CADTH identified several limitations with the sponsor’s pharmacoeconomic model including the clinical evidence used to inform the model, especially the time points of assessment chosen, the modelling of the BoB used to represent subsequent therapies, uncertainty in long-term discontinuation rates, the lack of treatment waning, the PASI threshold used to assess response, tildrakizumab dosing, and poor modelling practices. As part of its base case, CADTH assumed a 16-week assessment time point for deucravacitinib, assumed tildrakizumab would be dosed according to Health Canada recommendations, and assumed subsequent therapies would be equivalent between comparators.
The CADTH base-case analysis was consistent with that of the sponsor, suggesting that deucravacitinib was associated with $5,512 in incremental costs and 0.027 fewer QALYs (i.e., dominated) compared with adalimumab, and was less effective but less expensive than other publicly reimbursed biologic comparators at their publicly available list prices. The probability of deucravacitinib being the most cost-effective option did not rise above 2% regardless of the willingness-to-pay threshold assumed at its submitted price. A price reduction of 15.5% would be required for deucravacitinib to result in a cost savings of at least $50,000 per QALY foregone compared to adalimumab.
References
1.Le AM, Puig L, Torres T. Deucravacitinib for the Treatment of Psoriatic Disease. Am J Clin Dermatol. 2022;23(6):813-822. PubMed
2.Strober B, Thaci D, Sofen H, et al. Deucravacitinib versus placebo and apremilast in moderate to severe plaque psoriasis: efficacy and safety results from the 52-week, randomized, double-blinded, phase 3 POETYK PSO-2 trial. J Am Acad Dermatol. 2022;14:14.
3.Armstrong AW, Gooderham M, Warren RB, et al. Deucravacitinib versus placebo and apremilast in moderate to severe plaque psoriasis: efficacy and safety results from the 52-week, randomized, double-blinded, placebo-controlled phase 3 POETYK PSO-1 trial. J Am Acad Dermatol. 2022;09:09.
4.Drug Reimbursement Review sponsor submission: Sotyktu® (deucravacitinib) 6 mg [internal sponsor's package]. Montreal (QC): Bristol-Myers Squibb Canada; 2022 Sep 27.
5.Sotyktu (deucravacitinib): film-coated tablets, 6 mg, oral [product monograph]. Montreal (QC): Bristol-Myers Squibb Canada; 2022 Nov 23. 2023: https://pdf.hres.ca/dpd_pm/00068437.PDF.
6.Sponsor's NMA report title [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Sotyktu® (deucravacitinib) 6 mg. Montreal (QC): Bristol-Myers Squibb Canada; 2022 Sep 27.
7.van de Wetering G, Ignacio T, Dhanda D, Patel V, Zhang Y, Zhuo J. Modification of treatment-sequence model with a customizable number of treatments to better reflect contemporary and future clinical practice in moderate to severe psoriasis. J Med Econ. 2022;25(1):421-427. PubMed
8.Gniadecki R, Bang B, Bryld LE, Iversen L, Lasthein S, Skov L. Comparison of long-term drug survival and safety of biologic agents in patients with psoriasis vulgaris. Br J Dermatol. 2015;172(1):244-252. PubMed
9.Table: 13-10-0114-01. Life expectancy and other elements of the life table, Canada, all provinces except Prince Edward Island. Ottawa (ON): Statistics Canada; 2022: https://www150.statcan.gc.ca/t1/tbl1/en/tv.action?pid=1310011401. Accessed 2022 Nov 10.
10.Dixon WG, Watson K, Lunt M, et al. Rates of serious infection, including site-specific and bacterial intracellular infection, in rheumatoid arthritis patients receiving anti-tumor necrosis factor therapy: results from the British Society for Rheumatology Biologics Register. Arthritis Rheum. 2006;54(8):2368-2376. PubMed
11.Reich K, Mrowietz U, Radtke MA, et al. Drug safety of systemic treatments for psoriasis: results from The German Psoriasis Registry PsoBest. Arch Dermatol Res. 2015;307(10):875-883. PubMed
12.Reich K, Papp KA, Blauvelt A, et al. Bimekizumab versus ustekinumab for the treatment of moderate to severe plaque psoriasis (BE VIVID): efficacy and safety from a 52-week, multicentre, double-blind, active comparator and placebo controlled phase 3 trial. Lancet. 2021;397(10273):487-498. PubMed
13.Lebwohl M, Strober B, Menter A, et al. Phase 3 Studies Comparing Brodalumab with Ustekinumab in Psoriasis. N Engl J Med. 2015;373(14):1318-1328. PubMed
14.Blauvelt A, Papp KA, Griffiths CE, et al. Efficacy and safety of guselkumab, an anti-interleukin-23 monoclonal antibody, compared with adalimumab for the continuous treatment of patients with moderate to severe psoriasis: Results from the phase III, double-blinded, placebo- and active comparator-controlled VOYAGE 1 trial. J Am Acad Dermatol. 2017;76(3):405-417. PubMed
15.Gordon KB, Blauvelt A, Papp KA, et al. Phase 3 Trials of Ixekizumab in Moderate-to-Severe Plaque Psoriasis. N Engl J Med. 2016;375(4):345-356. PubMed
16.Reich K, Warren RB, Iversen L, et al. Long-term efficacy and safety of tildrakizumab for moderate-to-severe psoriasis: pooled analyses of two randomized phase III clinical trials (reSURFACE 1 and reSURFACE 2) through 148 weeks. Br J Dermatol. 2020;182(3):605-617. PubMed
17.Gordon KB, Strober B, Lebwohl M, et al. Efficacy and safety of risankizumab in moderate-to-severe plaque psoriasis (UltIMMa-1 and UltIMMa-2): results from two double-blind, randomised, placebo-controlled and ustekinumab-controlled phase 3 trials. Lancet. 2018;392(10148):650-661. PubMed
18.Stelara (ustekinumab): 45 mg/0.5 mL, 90 mg/1.0 mL solution for subcutaneous injection; Stelara I.V. (ustekinumab): 130 mg/26 mL (5 mg/mL) solution for intravenous infusion [product monograph]. Toronto (ON): Janssen Inc; 2021: https://pdf.hres.ca/dpd_pm/00062938.PDF. Accessed 2022 Nov 7.
19.Hyrimoz (adalimumab): 20 mg in 0.4 mL sterile solution (50 mg/mL) subcutaneous injection in pre-filled syringe, 40 mg in 0.8 mL sterile solution (50 mg/mL) subcutaneous injection in a pre-filled syringe, 40 mg in 0.8 mL sterile solution (50 mg/mL) subcutaneous injection in a pre-filled autoinjector [product monograph]. Boucherville (QC): Sandoz Canada Inc; 2022 Oct 11: https://pdf.hres.ca/dpd_pm/00067757.PDF. Accessed 2022 Nov 7.
20.Clinical Study Report: IM011046. A Multi-Center, Randomized, Double-Blind, Placebo- and Active Comparator-Controlled Phase 3 Study to Evaluate the Efficacy and Safety of BMS-986165 in Subjects with Moderate-to Severe Plaque Psoriasis [internal sponsor's report]. Lawrenceville (NJ): Bristol-Myers Squibb; 2021 Aug 13.
21.Clinical Study Report: IM011047. A multi-center, randomized, double-blind, placebo-and active comparator-controlled phase 3 study with randomized withdrawal and retreatment to evaluate the efficacy and safety BMS-986165 in subjects with moderate-to-severe plaque psoriasis [internal sponsor's report]. Lawrenceville (NJ): Bristol-Myers Squibb; 2021 Aug 19.
22.Single Technology Appraisal. Ixekizumab for treating moderate to severe plaque psoriasis [ID904]. Committee Papers London (GB): National Institute for Health and Care Excellence; 2016: https://www.nice.org.uk/guidance/ta442/documents/committee-papers-3.
23.CADTH Reimbursement Review: Bimekizumab (Bimzelx) for Moderate to Severe Plaque Psoriasis. Ottawa (ON): CADTH; 2022: https://www.cadth.ca/sites/default/files/DRR/2022/SR0698-Bimzelx.pdf. Accessed 2022 Nov 7.
24.Diamantopoulos A, Finckh A, Huizinga T, et al. Tocilizumab in the treatment of rheumatoid arthritis: a cost-effectiveness analysis in the UK. Pharmacoeconomics. 2014;32(8):775-787. PubMed
25.Ontario Ministry of Health, Ontario Ministry of Long-Term Care. Ontario drug benefit formulary/comparative drug index. 2022; https://www.formulary.health.gov.on.ca/formulary/.
26.Exceptional Access Program (EAP). Toronto (ON): Ontario Ministry of Health; Ontario Ministry of Long-Term Care; 2022: https://www.health.gov.on.ca/en/pro/programs/drugs/odbf/odbf_except_access.aspx. Accessed 2022 Oct 30.
27.CADTH Reimbursement Recommendation (Draft): Guselkumab (Tremfya) for Psoriatic Arthritis. Ottawa (ON): CADTH; 2022: https://www.cadth.ca/sites/default/files/DRR/2022/SR0733%20Tremfya%20PsA%20-%20Draft%20CADTH%20Recommendation%20for%20Posting%20October%2020%2C%202022.pdf. Accessed 2022 Nov 7.
28.CADTH Pharmacoeconomic Review Report: Guselkumab (Tremfya) for Moderate to Severe Plaque Psoriasis. Ottawa (ON): CADTH; 2018: https://www.cadth.ca/sites/default/files/cdr/pharmacoeconomic/SR0530_Tremfya_PE_Report.pdf. Accessed 2022 Nov 7.
29.Gouvernement du Québec. Régie de l’assurance maladie - List of Medications. 2022; 2022 May 6:https://www.ramq.gouv.qc.ca/en/about-us/list-medications. Accessed 2022 Jun 28.
30.Pharmacoeconomic evaluation [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Sotyktu® (deucravacitinib) 6 mg. Montreal (QC): Bristol-Myers Squibb Canada; 2022 Sep 27.
31.Ontario Case Costing Initiative (OCCI). Toronto (ON): Ontario Health and Long-Term Care; 2017: https://data.ontario.ca/dataset/ontario-case-costing-initiative-occi. Accessed 2018 May.
32.Sbidian E, Chaimani A, Afach S, et al. Systemic pharmacological treatments for chronic plaque psoriasis: a network meta-analysis. Cochrane Database Syst Rev. 2020;1(1):CD011535. PubMed
33.European Medicines Agency. Summary of product characteristics - Ilumetri. 2022; https://www.ema.europa.eu/en/documents/product-information/ilumetri-epar-product-information_en.pdf. Accessed 2022 Nov 17.
34.Ilumya (tildrakizumab): 100 mg in 1 mL sterile solution (100 mg/mL) for subcutaneous injection [product monograph]. Brampton ON: Sun Pharma Canada Inc; 2022: https://pdf.hres.ca/dpd_pm/00064464.PDF. Accessed 2022 Nov 7.
35.Full Prescribing Information: Tildrakizumab. Silver Spring (MD): U.S. Food and Drug Administration; 2018: https://www.accessdata.fda.gov/drugsatfda_docs/label/2018/761067s000lbl.pdf. Accessed 08 Dec 2022.
36.DeltaPA. [Ottawa (ON)]: IQVIA; 2022: https://www.iqvia.com/. Accessed 2022 Dec 05.
37.Health Canada. Patent Register - Form IV summaries - Ustekinumab. 2022; https://pr-rdb.hc-sc.gc.ca/pr-rdb/index-eng.jsp. Accessed 2022 Dec 05.
38.Health Canada. Patent Register - Form IV summaries - Certolizumab pegol. 2022; https://pr-rdb.hc-sc.gc.ca/pr-rdb/index-eng.jsp. Accessed 2022 Dec 05.
39.Winterfield LS, Menter A, Gordon K, Gottlieb A. Psoriasis treatment: current and emerging directed therapies. Ann Rheum Dis. 2005;64 Suppl 2(Suppl 2):ii87-90; discussion ii91-82.
40.Siliq (brodalumab): 140 mg/mL solution for subcutaneous injection [product monograph]. Laval (QC): Bausch Health, Canada Inc; 2019: https://pdf.hres.ca/dpd_pm/00051682.PDF. Accessed 2022 Nov 7.
41.Cimzia (certolizumab pegol): 200 mg/mL solution for injection [product monograph]. Oakville (ON): UCB Canada Inc; 2019: https://pdf.hres.ca/dpd_pm/00053920.PDF. Accessed 2022 Nov 7.
42.Erelzi (etanercept): 50 mg/mL solution for injection in a prefilled syringe, 50 mg/mL solution for injection in a prefilled autoinjector [product monograph]. Boucherville (QC): Sandoz Canada Inc; 2021: https://pdf.hres.ca/dpd_pm/00064146.PDF. Accessed 2022 Nov 7.
43.Tremfya (guselkumab): 100 mg/1 mL solution for injection pre-filled syringe, Tremfya One-Press (guselkumab): 100 mg/1 mL solution for injection patient-controlled injector [product monograph]. Toronto (ON): Janssen Inc; 2022: https://pdf.hres.ca/dpd_pm/00065455.PDF. Accessed 2022 Nov 7.
44.Renflexis (infliximab): 100 mg/vial powder for solution, sterile, lyophilized [product monograph]. Kirkland (QC): Merck Canada Inc; 2020: https://pdf.hres.ca/dpd_pm/00055165.PDF. Accessed 2022 Nov 7.
45.Taltz (ixekizumab): 80 mg / 1.0 mL solution for injection [product monograph]. Toronto (ON): Eli Lilly Canada Inc; 2022 https://pdf.hres.ca/dpd_pm/00067635.PDF. Accessed 2022 Nov 7.
46.Skyrizi (risankizumab): 150 mg in 1 mL sterile solution (150 mg/mL), 75 mg in 0.83 mL sterile solution (90 mg/mL), subcutaneous injection [product monograph]. St-Laurent (QC): AbbVie Corporation; 2022: https://pdf.hres.ca/dpd_pm/00067871.PDF. Accessed 2022 Nov 7.
47.Cosentyx (secukinumab): 150 mg/mL powder for solution for injection [product monograph]. Dorval (QC): Novartis Pharmaceuticals Canada Inc; 2022: https://pdf.hres.ca/dpd_pm/00067634.PDF. Accessed 2022 Nov 7.
48.Bimzelx (bimekizumab): 160 mg/mL solution subcutaneous injection [product monograph]. Oakville (ON): UCB Canada Inc; 2022: https://pdf.hres.ca/dpd_pm/00064702.PDF. Accessed 2022 Nov 7.
49.Otezla (apremilast): 10 mg, 20 mg 30 mg tablets [product monograph]. Mississauga ON: Amgen Canada Inc; 2020: https://pdf.hres.ca/dpd_pm/00057499.PDF. Accessed 2022 Nov 7.
50.Statistics Canada. Annual demographic estimates, census metropolitan areas and census agglomerations: Interactive dashboard. 2021; https://www150.statcan.gc.ca/n1/pub/71-607-x/71-607-x2020003-eng.htm.
51.Papp KA, Gniadecki R, Beecker J, et al. Psoriasis Prevalence and Severity by Expert Elicitation. Dermatol Ther (Heidelb). 2021;11(3):1053-1064. PubMed
52.Canadian Dermatology Association. Psoriasis. 2022; https://dermatology.ca/public-patients/skin/psoriasis/. Accessed 2022 Nov 14.
53.pan-Canadian Pharmaceutical Alliance. Bimzelx (bimekizumab). 2022; https://www.pcpacanada.ca/negotiation/21821. Accessed 2022-Dec-15.
54.Indigenous Services Canada. Non-Insured Health Benefits program: First Nations and Inuit Health Branch: annual report 2019 to 2020. 2020: https://www.sac-isc.gc.ca/eng/1624462613080/1624462663098. Accessed 2022 Nov 14.
55.Indigenous Services Canada. Non-Insured Health Benefits program: First Nations and Inuit Health Branch: annual report 2020 to 2021. 2021: https://www.sac-isc.gc.ca/eng/1645718409378/1645718500555. Accessed 2022 Nov 14.
56.Table: 17-10-0057-01 Projected population, by projection scenario, age and sex, as of July 1 (x 1,000). Ottawa (ON: Statistics Canada; 2022: https://www150.statcan.gc.ca/t1/tbl1/en/tv.action?pid=1710005701. Accessed 2022 Dec 09.
57.PharmaStat. [Ottawa (ON)]: IQVIA; 2022: https://www.iqvia.com/. Accessed 2022 Nov 16.
58.Canadian Institute for Health Information. Trends in public drug program spending in Canada. . 2022; https://www.cihi.ca/en/trends-in-public-drug-program-spending-in-canada. Accessed 2022 Dec 9.
59.European Medicines Agency. Annex I Summary of Product Characteristics: Ilumetri, INN-tildrakizumab. https://www.ema.europa.eu/en/documents/product-information/ilumetri-epar-product-information_en.pdf. Accessed 2022 Nov 17.
Appendix 1: Cost Comparison Table
Note this appendix has not been copy-edited.
The comparators presented in Table 8 have been deemed to be appropriate based on feedback from clinical experts. Comparators may be recommended (appropriate) practice or actual practice. Existing Product Listing Agreements are not reflected in the table and as such, the table may not represent the actual costs to public drug plans.
Table 8: CADTH Cost Comparison Table for Moderate to Severe Plaque Psoriasis
Treatment | Strength / concentration | Form | Price | Recommended dosage | Annual cost |
|---|---|---|---|---|---|
Deucravacitinib (Sotyktu) | 6 mg | Tablet | $39.4500a | 6 mg daily | $14,409 |
Adalimumab (Hyrimoz - biosimilar) | 50 mg/mL | 0.4 mL 0.8 mL Prefilled syringe | $235.6350 $471.2700 | 80 mg at week 0 followed by 40 mg every 2 weeks starting 1 week after initial dose | First year: $13,002 Subsequent years: $12,295 |
Apremilast (Otezla) | 10 mg 20 mg 30 mg | Tablet | $18.9041b $18.9041b $18.9041b | 30 mg twice daily after initial titration | $13,809 |
Bimekizumab (Bimzelx) | 160 mg/mL | 1 mL Prefilled syringe or autoinjector | $1,625.0000c | 320 mg at weeks 0, 4, 8, 12, 16 followed by 320 mg every 8 weeks (or every 4 weeks for those ≥ 120 kg) | First year: $27,698 Subsequent years: $21,198 For ≥ 120 kg First year: $42,395 Subsequent years: $42,395 |
Brodalumab (Siliq) | 140 mg/mL | 1.5 mL Prefilled syringe | $645.0000 | 210 mg at weeks 0, 1, 2 followed by 210 mg every 2 weeks | First year: $17,473 Subsequent years: $16,828 |
Certolizumab pegol (Cimzia) | 200 mg/mL | 1 mL Prefilled syringe | $664.5100d | 400 mg at weeks 0, 2, 4 followed by 200 mg or 400 mg every 2 weeks | First year: $19,935 to $35,884 Subsequent years: $17,277 to $34,555 |
Etanercept (Erelzi - biosimilar) | 50 mg/mL | 0.5 mL 1 mL Prefilled syringe or autoinjector | $120.5000 $241.0000 | 50 mg twice per week for 12 weeks followed by 50 mg per week | First year: $15,467 Subsequent years: $12,575 |
Guselkumab (Tremfya) | 100 mg/mL | 1 mL Prefilled syringe or autoinjector | $3,059.7400e | 100 mg at weeks 0 and 4 followed by 100 mg every 8 weeks | First year: $20,722 Subsequent years: $19,957 |
Infliximab (Renflexis - biosimilar) | 0.4 mg/mL | 100 mg Powder for IV injection | $493.0000 | 5 mg/kg at weeks 0, 2, 6 followed by 5 mg/kg every 8 weeks | First year: $19,159 Subsequent years: $16,078 |
Ixekizumab (Taltz) | 80 mg | 1 mL Prefilled syringe | $1,670.4400 | 160 mg at week 0 followed by 80 mg at weeks 2, 4, 6, 8, 10, 12 followed by 80 mg every 4 weeks | First year: $28,472 Subsequent years: $21,790 |
Risankizumab (Skyrizi) | 90 mg/mL | 0.83 mL Prefilled syringe | $2,467.5000 | 150 mg at weeks 0, 4 followed by 150 mg every 12 weeks | First year: $24,748 Subsequent years: $21,458 |
Secukinumab (Cosentyx) | 150 mg/mL | 1 mL Prefilled syringe | $840.0000 | 300 mg at weeks 0, 1, 2, 3, 4 followed by 300 mg monthly | First year: $28,560 Subsequent years: $21,840 |
Tildrakizumab (Ilumya) | 100 mg/mL | 1 mL Prefilled syringe | $4,935.0000 | 100 mg at weeks 0, 4 followed by 100 mg every 12 weeksf | First year: $24,748 Subsequent years: $21,458 |
Ustekinumab (Stelara) | 90 mg/mL | 0.5 mL 1 mL Prefilled syringe | $4,593.1400 | 45 mg to 90 mg at weeks 0, 4, followed by 45 mg to 90 mg every 12 weeksg | First year: $23,034 Subsequent years: $19,972 |
Note: All prices are from the Ontario Drug Benefit Formulary (accessed October 2022), unless otherwise indicated, and do not include dispensing fees. Recommended dosages are from the respective product monographs.5,18,19,34,40-49 Assumes a year length of 365.25 days, and a mean body weight of 90.7 kg for products with weight-based dosing, consistent with pooled POETYK trial data.30
aSponsor’s submitted price.30
bRégie de l'assurance maladie du Québec list price (accessed October 2022).29 The wholesale price of Otezla-brand apremilast was $22.0280 per tablet in jurisdictions outside Québec, which would be $16,091 per patient per year. The least expensive Association québécoise des pharmaciens propriétaires list price per 30 mg tablet of generic apremilast was $14.1780 per tablet, which would be $10,357 per patient per maintenance year of therapy.36
cPrice taken from CADTH review of Bimzelx.23
dODB EAP list price (accessed October 2022).26
ePrice taken from CADTH reviews of Tremfya (accessed October 2022).27,28
fThe sponsor’s base case assumes that patients weighing more than 90 kg will receive 200 mg of tildrakizumab per dose, although this dose is not recommended in the product monograph.34
g90 mg dose is for patients weighing more than 100 kg.18
Appendix 2: Submission Quality
Note this appendix has not been copy-edited.
Description | Yes/No | Comments |
|---|---|---|
Population is relevant, with no critical intervention missing, and no relevant outcome missing | Yes | No comment |
Model has been adequately programmed and has sufficient face validity | No | The models include numerous IFERROR and IFNA statements. The systematic use of IFERROR and IFNA statements makes thorough auditing of the sponsor’s model impractical, as it remains unclear whether the model is running inappropriately by overriding errors. |
Model structure is adequate for decision problem | Yes | No comment |
Data incorporation into the model has been done adequately (e.g., parameters for probabilistic analysis) | Yes | No comment |
Parameter and structural uncertainty were adequately assessed; analyses were adequate to inform the decision problem | Yes | No comment |
The submission was well organized and complete; the information was easy to locate (clear and transparent reporting; technical documentation available in enough details) | No | The submission contradicted itself in several places, complicating validation. For example, Table 5.9 and 5.10 in the sponsor’s submitted PE report states infliximab has an induction phase duration of 14 weeks in the base case, while the model uses a duration of 10 weeks. The submitted PE report also states that BoB was used as second- and third-line therapy with BSC as fourth line in the base case on page 46, however page 50 and the model file include 3 lines of therapy when calculating the discontinuation rate of BoB. |
BSC = best supportive care; BoB = basket of biologics; PE = pharmacoeconomic.
Appendix 3: Additional Information on the Submitted Economic Evaluation
Note this appendix has not been copy-edited.
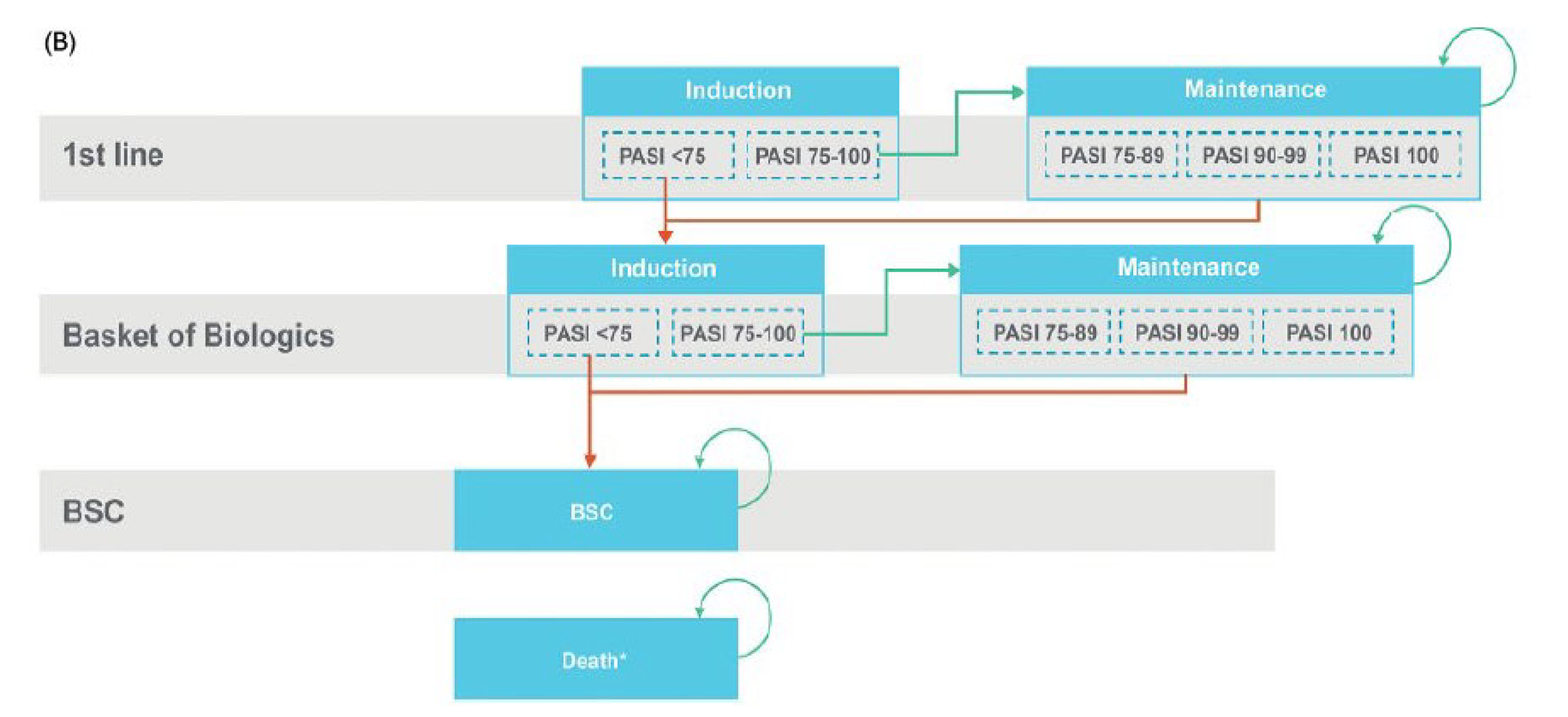
BSC = best supportive care; PASI = Psoriasis Area and Severity Index.
Note: Green arrow: treatment response and continuation of same; orange arrow: treatment failure and transition to the next treatment, remaining in the same health phase. Patients can transition to death from any health state.
Source: Sponsor’s Pharmacoeconomic submission.30
Table 10: Distributions of Patients in Each PASI Response Category After Induction Phase
Treatment (Assessment time point) | PASI < 50 | 50 ≤ PASI < 75 | 75 ≤ PASI < 90 | 90 ≤ PASI < 100 | PASI 100 |
|---|---|---|---|---|---|
Deucravacitinib (24 weeks) | 0.612 | 0.083 | 0.133 | 0.108 | 0.066 |
Adalimumab (16 weeks) | 0.575 | 0.078 | 0.123 | 0.138 | 0.087 |
Apremilast (16 weeks) | 0.721 | 0.120 | 0.101 | 0.048 | 0.011 |
Bimekizumab (16 weeks) | 0.511 | 0.026 | 0.045 | 0.131 | 0.289 |
Brodalumab (12 weeks) | 0.521 | 0.040 | 0.071 | 0.143 | 0.226 |
Certolizumab pegol (16 weeks) | 0.564 | 0.080 | 0.137 | 0.142 | 0.078 |
Etanercept (12 weeks) | 0.625 | 0.123 | 0.137 | 0.084 | 0.032 |
Guselkumab (16 weeks) | 0.523 | 0.046 | 0.099 | 0.170 | 0.163 |
Infliximab (10 weeks) | 0.537 | 0.059 | 0.132 | 0.155 | 0.119 |
Ixekizumab (12 weeks) | 0.515 | 0.033 | 0.084 | 0.169 | 0.201 |
Risankizumab (16 weeks) | 0.517 | 0.036 | 0.086 | 0.153 | 0.209 |
Secukinumab (12 weeks) | 0.529 | 0.044 | 0.098 | 0.165 | 0.165 |
Tildrakizumab (12 weeks) | 0.584 | 0.091 | 0.131 | 0.124 | 0.070 |
Ustekinumab (16 weeks) | 0.562 | 0.079 | 0.129 | 0.135 | 0.096 |
NMA = network meta-analysis; PASI = psoriasis area severity index.
Source: Sponsor’s pharmacoeconomic submission.30
Detailed Results of the Sponsor’s Base Case
Table 11: Full Summary of the Sponsor’s Economic Evaluation Results
Drug | Total costs ($) | Total QALYs | Sequential ICER ($/QALY) |
|---|---|---|---|
Adalimumab | 138,687 | 6.968 | Ref. |
Brodalumab | 153,558 | 7.047 | 187,202 |
Bimekizumab | 196,124 | 7.063 | 2,639,512 |
Dominated therapies | |||
Deucravacitinib | $140,270 | 6.949 | Dominated by adalimumab |
Apremilast | $140,686 | 6.858 | Dominated by adalimumab, deucravacitinib |
Etanercept | $146,412 | 6.951 | Dominated by adalimumab |
Infliximab | $152,750 | 6.989 | Extendedly dominated by mixes of adalimumab plus brodalumab, ixekizumab, or bimekizumab |
Certolizumab | $157,458 | 6.969 | Dominated by brodalumab, infliximab |
Ustekinumab | $168,769 | 6.972 | Dominated by brodalumab, infliximab |
Guselkumab | $170,622 | 7.031 | Dominated by brodalumab |
Secukinumab | $183,071 | 7.035 | Dominated by brodalumab |
Risankizumab | $183,901 | 7.046 | Dominated by brodalumab |
Ixekizumab | $185,759 | 7.047 | Extendedly dominated by mix of brodalumab and bimekizumab |
Tildrakizumab | $216,373 | 6.992 | Dominated by brodalumab, guselkumab, secukinumab, risankizumab, ixekizumab, bimekizumab |
ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year; Ref. = reference.
Note: All comparators are followed in sequence by the basket of biologics and then by best supportive care.
Source: Sponsor’s pharmacoeconomic submission.30
Appendix 4: Additional Details on the CADTH Reanalyses and Sensitivity Analyses of the Economic Evaluation
Note this appendix has not been copy-edited.
Detailed Results of CADTH Base Case
Table 12: Full Summary of CADTH’s Economic Evaluation Results
Drug | Total costs ($) | Total QALYs | Sequential ICER ($/QALY) |
|---|---|---|---|
Adalimumab | 130,710 | 6.960 | Ref. |
Brodalumab | 150,625 | 7.058 | 202,164 |
Bimekizumab | 194,959 | 7.076 | 2,447,734 |
Dominated therapies | |||
Apremilast | 135,185 | 6.853 | Dominated by adalimumab |
Etanercept | 135,219 | 6.917 | Dominated by adalimumab |
Deucravacitinib | 136,222 | 6.933 | Dominated by adalimumab |
Infliximab | 147,424 | 6.989 | Extendedly dominated by mixes of adalimumab and brodalumab, ixekizumab, or bimekizumab |
Certolizumab | 151,734 | 6.961 | Dominated by brodalumab, infliximab |
Ustekinumab | 164,385 | 6.964 | Dominated by brodalumab, infliximab |
Guselkumab | 168,345 | 7.041 | Dominated by brodalumab |
Tildrakizumab | 173,923 | 6.978 | Dominated by brodalumab, infliximab, guselkumab |
Secukinumab | 181,442 | 7.043 | Dominated by brodalumab |
Risankizumab | 182,650 | 7.056 | Dominated by brodalumab |
Ixekizumab | 184,726 | 7.060 | Extendedly dominated by mix of brodalumab and bimekizumab |
ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year; Ref. = reference.
Note: All comparators are followed in sequence by the basket of biologics and then by best supportive care.
Table 13: Disaggregated Costs in the CADTH Base Case
Treatment | Drug acquisition – first line | Drug acquisition – BoB | Drug administration | Monitoring costs | Safety costs | BSC costs | Nonresponder costs | Total costs |
|---|---|---|---|---|---|---|---|---|
Deucravacitinib | $43,813 | $88,373 | $695 | $1,759 | $498 | $941 | $144 | $136,222 |
Adalimumab | $44,133 | $82,081 | $819 | $1,788 | $884 | $862 | $142 | $130,710 |
Apremilast | $15,648 | $115,022 | $903 | $1,674 | $523 | $1,245 | $171 | $135,185 |
Bimekizumab | $138,179 | $53,430 | $507 | $1,871 | $323 | $541 | $108 | $194,959 |
Brodalumab | $89,216 | $57,817 | $716 | $1,874 | $299 | $592 | $112 | $150,625 |
Certolizumab pegol | $64,767 | $81,131 | $815 | $1,788 | $782 | $850 | $142 | $151,734 |
Etanercept | $35,151 | $95,070 | $994 | $1,754 | $1,082 | $1,016 | $152 | $135,219 |
Guselkumab | $106,488 | $58,405 | $532 | $1,846 | $363 | $599 | $112 | $168,345 |
Infliximab | $61,176 | $76,207 | $6,405 | $1,926 | $780 | $793 | $138 | $147,424 |
Ixekizumab | $125,221 | $55,902 | $584 | $1,876 | $465 | $569 | $110 | $184,726 |
Risankizumab | $123,767 | $55,583 | $492 | $1,857 | $275 | $566 | $109 | $182,650 |
Secukinumab | $118,167 | $59,745 | $607 | $1,863 | $332 | $614 | $114 | $181,442 |
Tildrakizumab | $94,500 | $75,782 | $635 | $1,811 | $265 | $801 | $128 | $173,923 |
Ustekinumab | $79,450 | $80,972 | $673 | $1,788 | $512 | $848 | $142 | $164,385 |
BSC = best supportive care; BoB = basket of biologics.
Table 14: Disaggregated QALYs Gained in the CADTH Base Case
Treatment | PASI < 50 | 50 ≤ PASI < 75 | 75 ≤ PASI < 90 | 90 ≤ PASI < 100 | PASI 100 | Total |
|---|---|---|---|---|---|---|
Deucravacitinib | 1.115 | 0.172 | 2.068 | 2.039 | 1.585 | 6.933 |
Adalimumab | 1.028 | 0.155 | 1.891 | 2.204 | 1.725 | 6.960 |
Apremilast | 1.441 | 0.222 | 1.822 | 1.865 | 1.565 | 6.853 |
Bimekizumab | 0.687 | 0.093 | 1.025 | 1.942 | 3.356 | 7.076 |
Brodalumab | 0.714 | 0.102 | 1.316 | 2.123 | 2.832 | 7.058 |
Certolizumab pegol | 1.014 | 0.153 | 1.978 | 2.203 | 1.654 | 6.961 |
Etanercept | 1.160 | 0.181 | 2.150 | 1.993 | 1.485 | 6.917 |
Guselkumab | 0.748 | 0.107 | 1.578 | 2.376 | 2.263 | 7.041 |
Infliximab | 0.911 | 0.135 | 1.874 | 2.219 | 1.890 | 6.989 |
Ixekizumab | 0.691 | 0.097 | 1.407 | 2.318 | 2.575 | 7.060 |
Risankizumab | 0.714 | 0.099 | 1.433 | 2.182 | 2.657 | 7.056 |
Secukinumab | 0.738 | 0.106 | 1.585 | 2.348 | 2.296 | 7.043 |
Tildrakizumab | 0.934 | 0.142 | 2.087 | 2.215 | 1.640 | 6.978 |
Ustekinumab | 1.012 | 0.153 | 1.913 | 2.153 | 1.776 | 6.964 |
QALY = quality-adjusted life-year; PASI = psoriatic area severity index.
Scenario Analyses
Table 15: CADTH Scenario Analyses
Scenario | CADTH Base Case | CADTH Scenario |
|---|---|---|
Scenario Analyses | ||
1. AEs | As programmed by sponsor. | Removed from the analysis. |
2. Annual long-term discontinuation rate | Deucravacitinib: 12.4% Apremilast: 31% Brodalumab, guselkumab, ixekizumab, risankizumab, secukinumab, tildrakizumab: 10% Certolizumab pegol, etanercept, infliximab, ustekinumab: 15% | All comparators: 15% |
3. Deucravacitinib has same long-term discontinuation as apremilast | Deucravacitinib: 12.4% Apremilast: 31% | Deucravacitinib: 31% Apremilast: 31% |
4. Response threshold | Response assessment based on achieving PASI75 improvement | Response assessment based on achieving PASI90 improvement |
5. BoB discontinuation | With 3 lines of BoB and then discontinuation to BSC, the calculated annual long-term discontinuation rate for BoB was 0.9% | BoB discontinuation = 0% |
6. Apremilast pricing | $18.90 per 30 mg tablet, consistent with RAMQ and AQPP list price for Otezla. | $14.18 per 30 mg tablet, consistent with AQPP list price for PMS-Apremilast. |
AQPP = Association québécoise des pharmaciens propriétaires; BoB = basket of biologics; BSC = best supportive care; PASI = psoriasis area and severity index; RAMQ = Régie de l'assurance maladie du Québec.
Table 16: Summary of Sequential CADTH Scenario Results
Stepped analysis | Drug | Total costs ($) | Total QALYs | Sequential ICER ($/QALYs) |
|---|---|---|---|---|
CADTH scenario 1: AEs removed | Adalimumab | 129,841 | 6.961 | Reference |
Brodalumab | 150,313 | 7.062 | 202,469 | |
Bimekizumab | 194,503 | 7.082 | 2,214,731 | |
Deucravacitinib | 135,700 | 6.935 | Dominated by adalimumab | |
CADTH scenario 2: All long-term discontinuation = 15% | Adalimumab | 129,103 | 6.948 | Reference |
Brodalumab | 147,446 | 7.013 | 283,694 | |
Bimekizumab | 185,999 | 7.032 | 2,103,988 | |
Deucravacitinib | 134,381 | 6.908 | Dominated by adalimumab | |
CADTH scenario 3: Deucravacitinib discontinuation same as apremilast | Adalimumab | 130,833 | 6.963 | Reference |
Brodalumab | 150,710 | 7.065 | 194,791 | |
Bimekizumab | 195,192 | 7.085 | 2,316,558 | |
Deucravacitinib | 136,451 | 6.885 | Dominated by adalimumab | |
CADTH scenario 4: PASI90 threshold | Apremilast | 102,579 | 6.615 | Reference |
Adalimumab | 106,846 | 6.752 | 31,222 | |
Brodalumab | 130,563 | 6.922 | 139,456 | |
Bimekizumab | 175,197 | 6.968 | 960,400 | |
Deucravacitinib | 107,782 | 6.706 | Dominated by adalimumab | |
CADTH scenario 5: no discontinuation from BoB | Adalimumab | 153,739 | 7.124 | Reference |
Brodalumab | 166,613 | 7.175 | 251,811 | |
Bimekizumab | 210,005 | 7.186 | 4,240,096 | |
Deucravacitinib | 161,240 | 7.112 | Dominated by adalimumab | |
CADTH scenario 6: generic apremilast | Adalimumab | 130,896 | 6.996 | Reference |
Brodalumab | 150,798 | 7.067 | 196,491 | |
Bimekizumab | 194,961 | 7.085 | 2,378,158 | |
Deucravacitinib | 136,392 | 6.939 | Dominated by adalimumab |
BoB = basket of biologics; ICER = incremental cost-effectiveness ratio; PASI = psoriasis area and severity index; QALY = quality-adjusted life-year.
Note: Only treatments that are on the efficiency frontier, as well as the drug under review, are reported. All listed comparators are followed in sequence by the basket of biologics for an additional 3 lines of therapy and then by best supportive care, with the exception of scenario 4 which assumed the BoB continued for the entire time horizon. All analyses were conducted probabilistically.
Appendix 5: Submitted BIA and CADTH Appraisal
Note this appendix has not been copy-edited.
Table 17: Summary of Key Take-Aways
Key take-aways of the BIA |
|---|
|
Summary of Sponsor’s BIA
The submitted budget impact analysis (BIA) assessed the introduction of deucravacitinib for the treatment of adult patients with moderate to severe plaque psoriasis who are candidates for systemic or phototherapy. The analysis was undertaken from the perspective of the Canadian public health care payer using an epidemiological approach and included drug acquisition costs as well as the costs of administration, routine care and monitoring, extra switching costs, and treatment of AEs. Response rates and long-term discontinuation rates as used in the pharmacoeconomic analysis were considered for all comparators to inform treatment discontinuation within the BIA. A 3-year time horizon was used, from July 2023 to June 2026, with July 2022 to June 2023 as the base year. Data from the model were obtained from various sources including the sponsor’s NMA, Statistics Canada,50 the published literature,51,52 the Summaries of Product Characteristics published by the European Medicines Agency33 for each comparator and an unspecific clinical expert survey (not provided).
Key inputs to the BIA are documented in Table 18. Key assumptions included:
Comparators include those incorporated into the cost-effectiveness model, although apremilast, certolizumab pegol, and guselkumab are assumed to have no market share as they are not funded by public drug plans for plaque psoriasis and thus do not contribute to the analysis. Bimekizumab is not yet reimbursed by public plans, but has successful concluded negotiations with the pan-Canadian Pharmaceutical Alliance53 and was assumed to be entering the market.
Modelled patients may only receive deucravacitinib as first-line therapy within the model, although patients who are assumed to be bio-experienced will have already used a biologic therapy before entering the model.
Displacement by deucravacitinib was proportional to each comparator’s reference scenario market share.
Patients who have discontinued 1 brand of a drug may use another brand of the same drug in subsequent therapy.
All psoriasis patients are reimbursed by public drug plans.
20% of all prevalent patients will switch therapies in a given year, in addition to those who switched in previous years.
Response rates and discontinuation rates are incorporated as in the cost-effectiveness model.
Table 18: Summary of Key Model Parameters
Parameter | Sponsor’s estimate (reported as Year 1 / Year 2 / Year 3 if appropriate) |
|---|---|
Target population | |
Total pan-Canadian population (excluding QC, year 0) | 30,646,304a |
Annual population growth rate | 0.5%b |
Prevalence of psoriasis | 3.37%51 |
Proportion with plaque psoriasis | 90%52 |
Proportion with moderate to severe psoriasis | 41%c |
Treatment rate | 84%c |
Percentage of patients initiating a new treatment in a given year | 20%c |
Number of patients eligible for drug under review who are added to the model each year (including base year) | 64,024 / 64,344 / 64,666 / 64,989 Cumulative: 64,024 / 128,368 / 193,034 / 258,024 |
Proportion of patients who are biologic-experienced/biologic-naive | 75.9% / 24.1%d |
Market uptake (pooled new drug scenario, 3 years) | |
Deucravacitinib | 2.7% / 11.1% / 15.9% |
Adalimumab (Humira) | 3.3% / 2.4% / 1.8% |
Adalimumab (biosimilar) | 6.6% / 6.7% / 7.4% |
Bimekizumab | 3.1% / 12.9% / 18.7% |
Brodalumab | 8.7% / 6.5% / 5.1% |
Certolizumab pegol | 0% / 0% / 0% |
Etanercept (Enbrel) | 0.4% / 0.3% / 0.2% |
Etanercept (biosimilar) | 0.9% / 0.7% / 0.5% |
Infliximab (Remicade) | 2.0% / 1.4% / 1.1% |
Infliximab (biosimilars, combined) | 1.3% / 1.0% / 0.7% |
Ixekizumab | 10.7% / 8.1% / 6.5% |
Risankizumab | 43.8% / 35.2% / 29.7% |
Secukinumab | 9.6% / 7.1% / 5.7% |
Tildrakizumab | 0.6% / 2.3% / 3.1% |
Ustekinumab | 6.4% / 4.4% / 3.3% |
Cost of treatment (maintenance year) | |
Deucravacitinib | $14,409 |
Adalimumab (Humira) | $20,718 |
Adalimumab (biosimilar) | $12,295 |
Bimekizumab | $23,317 |
Brodalumab | $16,828 |
Certolizumab pegol | $17,337 |
Etanercept (Enbrel) | $21,184 |
Etanercept (biosimilar) | $12,575 |
Infliximab (Remicade) | $29,209 |
Infliximab (biosimilars, combined) | $15,528 or $14,581 (2 biosimilar brands) |
Ixekizumab | $21,790 |
Risankizumab | $21,458 |
Secukinumab | $21,915 |
Tildrakizumab | $32,615 |
Ustekinumab | $19,972 |
QC = Québec.
Note: After discontinuation, patients switch to a basket of biologics which consists of the following, with the product they were previously using removed: Adalimumab 3.7%, Adalimumab biosimilar 6.3%, bimekizumab 10%, brodalumab 10%, etanercept 3.6%, etanercept biosimilar 6.4%, infliximab 6.1%, infliximab biosimilars 3.9%, ixekizumab 10%, risankizumab 10%, secukinumab 10%, tildrakizumab 10%, ustekinumab 10%.
aModelled as the sum of the populations of the 9 provinces (i.e., excluding Québec) and the NIHB population, which were cited as Statistics Canada annual demographic estimates from July 1, 2021. CADTH was unable to duplicate this total.50
bBased on the change in the Canadian population from July 1, 2020 to July 1, 2021.50
cCited as an unspecified clinical expert survey.
dCited as forecasting by Bristol Myers Squibb.
Summary of the Sponsor’s BIA Results
The sponsor’s estimated budget impact of funding deucravacitinib for the treatment of adult patients with moderate to severe plaque psoriasis was a savings of $14,753,887 in year 1, $71,085,139 in year 2, and $130,811,175 in year 3, for a 3-year budgetary savings of $216,650,200.
CADTH Appraisal of the Sponsor’s BIA
CADTH identified several key limitations to the sponsor’s analysis that have notable implications on the results of the BIA:
The eligible patient population was inappropriately estimated: The sponsor’s model estimated a pan-Canadian population of 30,646,304 in the base year (July 2022 to June 2023), the total of the 9 CADTH-participating provinces (i.e., excluding Québec) plus the NIHB population, citing annual demographic estimates from Statistics Canada for 2021 as well as the NIHB annual report of the same year.50 CADTH was unable to duplicate the retrieval of the included data from this source or that listed in the BIA report. Additionally, the sponsor used an annual population growth rate of 0.5% based on the population growth between July 2020 and July 2021.50 Due to the excess deaths and border closures associated with the COVID-19 pandemic, population growth between 2020 and 2021 is unlikely to be representative of the future growth of the Canadian population; previous years within the same dataset reported growth rates between 0.7% and 1.4% per year. Finally, the sponsor added the NIHB client population54,55 to that of the provincial populations, despite the NIHB population being included within provincial population data as collected by Statistics Canada, leading to the double counting of much of the NIHB population.
Additionally, the psoriasis prevalence rate used by the sponsor of 3.37% was presented in its original source as the prevalence of plaque psoriasis in adults.51 Therefore, rather than assuming that 3.37% of the overall Canadian population has psoriasis, of which 90% have plaque psoriasis, the estimate should instead be that 3.37% of adult Canadians have plaque psoriasis. Finally, the sponsor’s BIA implicitly assumed that all patients with moderate to severe plaque psoriasis using biologic therapies are reimbursed by public drug programs. However, according to IQVIA Pharmastat data for Q3 2021 to Q2 2022 (excluding Québec), 57.6% of claims for the comparators included within the sponsor’s BIA were funded by public drug plans. While much of the use of these comparators is not for psoriasis, this figure represents a reasonable proxy for the proportion of patients with plaque psoriasis who are publicly reimbursed).
CADTH undertook exploratory analyses using the M1 medium growth 3 projection from Statistics Canada to estimate the adult population (18+ years) within each jurisdiction for each analysis year, e.g., the average of the projected population for 2022 and 2023 was used to represent the population of the base year (July 2022 to June 2023).56 A linear projection was used to estimate the future NIHB population based on 2017 to 2021 data.54,55 The adult population of NIHB clients residing within the borders of each provincial jurisdiction was subtracted from that jurisdiction, with the exception of those in Ontario who were younger than 25 or older than 65 years due to such patients being primarily reimbursed by the Ontario Drug Benefit program. The plaque psoriasis prevalence rate of 3.37% was then applied to this adult population, without further reduction to account for plaque psoriasis, and it was assumed that only 57.6% of otherwise eligible patients were publicly funded.
The model was poorly conceptualized and results did not meet face validity: The sponsor estimated that $3.1 billion, $4.5 billion, and $5.9 billion in Years 1, 2, and 3 of the analysis will be spent on advanced therapies to treat modelled patients with plaque psoriasis. For reference, the total cost paid by IQVIA-participating public and private payers from April 2021 to March 2022 for the included comparators, without limitation by jurisdiction, payer, or indication, was $3.0 billion.57 As the included comparators are used for a range of conditions including psoriasis, rheumatoid arthritis, Crohn disease, ulcerative colitis, ankylosing spondylitis, and so forth, it is unlikely that treatment for plaque psoriasis alone will double the total spending on these drugs within 4 years. Additionally, the cost to public plans for all biologic drugs was estimated to be $4.4 billion in 2021;58 again, substantially less than the sponsor’s model projects the treatment of plaque psoriasis alone will cost by 2026.
A major cause of the overinflated budgetary estimates appears to be the method by which new patients entered the model. The sponsor assumed that 20% of all prevalent patients initiated a new therapy each year, and would therefore be added to the model, starting from the base year. In doing so, the sponsor failed to adjust the number of patients eligible to enter the model each year by the number who had already done so. The sponsor additionally failed to adjust the number of prevalent patients initiating a new therapy per year (i.e., 20%) by the number who were initiating new therapies that year within the model. As such, the sponsor’s model adds more patients than is plausible to the eligible group, and double or triple counts such patients in the overall proportion of prevalent patients who are initiating a new therapy, resulting in total cost estimates that far exceed plausible ranges for the reimbursement of biologic therapies for the treatment of psoriasis.
Without conducting a full de novo budget impact analysis, CADTH was unable to fully address this limitation in the conceptualization and programming of the sponsor’s BIA. In exploratory analyses, CADTH attempted to mitigate the double counting of the prevalent patient population entering the model by removing those already in the model from model entry eligibility as well as including patients switching therapies within the model as part of the 20% of overall patients assumed to initiate a new therapy each year, assuming a weighted average of proportion of patients who did not respond to therapy or who discontinued after response in 1 year would be part of the switching population the next. Due to the lack of flexibility with the sponsor’s model structure, this reanalysis is considered exploratory.
Clinical input assumptions are uncertain: The submitted BIA uses PASI 75 response rates derived from the submitted NMA to estimate the proportion of patients who will discontinue their initial therapy within the model and begin subsequent therapies represented by the BoB. In line with the submitted pharmacoeconomic analysis, the proportions of patients within each PASI category at 24 weeks for deucravacitinib and 10 to 16 weeks for the comparators were used to inform the BIA. The same long-term (postinitial response) discontinuation rates assumed with the submitted pharmacoeconomic analysis were also used within the BIA. As such, the limitations described regarding the appropriateness of combining multiple time points of PASI response, the uncertainty in the use of the PASI 75 threshold, and uncertainties in the long term discontinuation rates described in the CADTH Pharmacoeconomic Review also apply to the submitted BIA.
CADTH adjusted the time point of response assessment for deucravacitinib to 16 weeks for consistency with the CADTH base-case pharmacoeconomic reanalysis within its exploratory reanalyses.
Health care payer perspective inappropriate: CADTH submission guidelines stipulate that the BIA base case should represent the difference in costs that will be seen by a jurisdictional drug plan due to the introduction of the drug under review. As such, the perspective of such an analysis should primarily be that of a public drug plan. Although the sponsor’s base case suggests it is from the public drug plan perspective, the sponsor included the costs of treating AEs as well as administration costs, monitoring costs such as physician visits and lab tests, and “switching costs.” While the model technically allowed for a change in perspective from that of a health care payer to a drug plan payer, toggling this option made a series of unexpected changes to model parameters including changing the number of patients within the model as well as drug acquisition costs throughout, resulting in the 3-year budgetary impact of deucravacitinib implausibly changing from a saving of $217 million to an incremental cost of more than $15 million. Due to the use of IFERROR and IFNA functions embedded within calculations, a reliance on macros, multiple inputs for the same parameter across sheets, and poor labelling, tracing the full impact of altering the provided perspective function was not feasible, which in turn increased uncertain in all aspects of the model.
In exploratory reanalyses, CADTH manually removed costs associated with AEs, administration, monitoring, physician visits by setting all such costs to $0 within the model. The inability to fully validate the impacts of these changes increases uncertainty with the modelled results. A scenario analysis was conducted reintroducing costs related to drug administration.
Market uptake is highly uncertain: The sponsor’s model assumes that deucravacitinib, if funded, will capture 2.7% of the market in year 1, 11.1% in year 2, and 15.9% in year 3, displacing all comparators in proportions equal to their reference case market shares. Within the model, this is presented as a weighted average market share of patients who were biologic-naive (24.1%) and biologic-experienced (75.9%), with the uptake of deucravacitinib assumed to be 6.6% in year 1, 26.0% in Year 2, and 36.8% in year 3 in the biologic-naive population. Clinical expert opinion obtained by CADTH indicated that “very few” patients with moderate to severe psoriasis would prefer the option of a new oral medication of lower efficacy to injectable options with higher efficacies, even if previously biologic-naive. Additionally, clinical expert input also indicated that patients who had already used a biologic therapy would be very unlikely to subsequently try an oral therapy with a lower response rate rather than switching to an alternate injectable biologic therapy. Indeed, the sponsor’s model does not allow deucravacitinib to form a part of the BoB representing subsequent lines of therapy which, while not allowing the full costs associated with reimbursing deucravacitinib in the manner indicated by the sponsor, implies it is not expected to be used in patients with previous exposure to advanced therapies. Finally, it is unlikely that deucravacitinib will displace all comparators similarly, but may instead be more likely to displace older, less expensive comparators than newer therapies.
In exploratory reanalyses, CADTH halved the estimated uptake of deucravacitinib in the bio-naive and bio-experienced populations. CADTH conducted an additional scenario analysis where the estimated uptake of deucravacitinib was halved in the biologic-naive population and zero in the bio-experienced population. CADTH was unable to address the likelihood that deucravacitinib may displace older therapies more frequently than newer ones due to hardcoding within the model and a lack of alternate inputs; if it is the case that deucravacitinib primarily displaces older comparators, the estimated budgetary savings associated with its reimbursement may be further decreased.
Biosimilar use was underestimated: The sponsor’s base case assumed that many patients using adalimumab, etanercept, and infliximab are using the originator products, citing in-house research for market share inputs overall. However, public drug plans have instituted or are planning to institute policies limiting reimbursement of biologic products to less expensive subsequent entry biologics (also known as biosimilars) where available. As such, it is expected that publicly funded biosimilar use will increase and therefore become the most relevant comparator for new entries into affected therapeutic spaces. The cost-utility analysis submitted by the sponsor assumes 100% biosimilar use for adalimumab, etanercept, and infliximab, therefore the BIA should also do so to ensure consistency between the analyses.
CADTH exploratory reanalyses assumed that all adalimumab, etanercept, and infliximab use is of biosimilar products.
Uncertainty in the modelling of the BoB: The sponsor took the same approach to modelling subsequent therapy in the BIA as the economic evaluation; although for the BIA, the BoB excluded deucravacitinib, apremilast, certolizumab pegol, guselkumab, and the biologic used in first line, if applicable; and allowed patients to switch brands but remain on the same treatment, e.g., patients who discontinued Humira-brand adalimumab could receive biosimilar adalimumab as a subsequent treatment, or vice versa. As such, the costs and benefits associated with the BoB differed between comparators and thus have varying impacts on the overall cost of the full sequence of therapy. However, as described in the similar limitation regarding the submitted pharmacoeconomic analysis, this unweighted average is unlikely to represent the actual usage of biologics in later lines in clinical practice and biases results against initial comparators with a lower cost and in favour of those with a higher cost. For consistency with the CADTH base-case pharmacoeconomic reanalysis, the BoB was assumed to be equal between comparators.
CADTH exploratory reanalyses assumed that the BoB would have the same cost for all comparators, set to equal that assumed by the sponsor for deucravacitinib. The sponsor’s error in allowing alternate versions of the same product to be used in subsequent therapy is negated by this assumption. The option to include deucravacitinib within the BoB was not possible due to the structure of the model.
Dosing of tildrakizumab was inappropriate: As in the pharmacoeconomic submission, the sponsor assumed that patients who weighed less than 90 kg (48% of patients) would receive 100 mg of tildrakizumab per dose within the BIA model, while those who weighed above 90kg would receive 200 mg per dose. This is consistent with the dose outlined in the Summary of Product Characteristics for tildrakizumab as authorized by the EMA.33 However, the Health Canada product monograph does not differentiate dosing of tildrakizumab by weight, and instead recommends only the 100 mg dose,34 as does the FDA of the US.35
CADTH exploratory reanalyses assumed the dose of tildrakizumab would be 100 mg per administration for all patients.
Analysis assumed that deucravacitinib will not grow the advanced therapy market: The sponsor’s analysis assumed that patients will only receive deucravacitinib if they would otherwise have received a different biologic therapy, despite noting that deucravacitinib may be used in patients who are needle-phobic or concerned about injection-site reactions (i.e., would not receive a biologic).30 Additionally, while deucravacitinib is indicated for patients with moderate to severe plaque psoriasis, its oral mode of administration may lead to use in patients with milder psoriasis. If used in this manner, this would increase the overall cost of care for the treatment of plaque psoriasis at an unknown cost-effectiveness. Finally, at the submitted price, deucravacitinib is less expensive per treatment year than most available biologics currently reimbursed for plaque psoriasis at their publicly available prices, and thus the use of deucravacitinib may result in cost savings to jurisdictional drug plans over the short-term (i.e., within a 3-year time horizon) as more expensive therapies may be displaced. However, due to its lower efficacy than most biologics, and potential for higher discontinuation due to lack of response, it is likely that the use of deucravacitinib will delay rather than prevent the use of more expensive, more effective therapies, and thus its reimbursement may result in an overall increase in costs over the course of each patients’ life.
The sponsor’s model was insufficiently flexible to explore the possibility that deucravacitinib would be used to treat patients who would not otherwise receive a biologic therapy. Under such an assumption, the budget impact of reimbursing deucravacitinib may be associated with increased budgetary costs rather than savings, especially if used in patients with milder forms of psoriasis.
CADTH Reanalyses of the BIA
Due to the extent of limitations associated with the submitted BIA, CADTH was unable to derive a base-case reanalysis. Instead, CADTH conducted a series of exploratory analyses exploring some of these limitations and incorporated them into a combined analysis, refer to Table 19.
Table 19: CADTH Revisions to the Submitted Budget Impact Analysis
Stepped analysis | Sponsor’s value or assumption | CADTH value or assumption |
|---|---|---|
Corrections to sponsor’s base case | ||
None. | — | — |
Changes to derive the CADTH base case | ||
1. Starting population and growth | Base year: Data of unclear source cited as from July 2021,50 total population Subsequent years: 0.5% growth rate applied50 NIHB population added to provincial jurisdictions Base year: 30,646,304 | Base year: Average of 2022 and 2023 M1 Projection from Statistics Canada for each jurisdiction, adults only Subsequent years: Continuing M1 projection from Statistics Canada, adults only NIHB population removed from each provincial jurisdiction, except those in Ontario aged < 25 and 65+ years. Base year: 24,710,171 |
2. Prevalence data source | Applied 3.37% prevalence to entire pan-Canadian population. Assumed 90% have plaque psoriasis | Applied 3.37% prevalence to the adult pan-Canadian population. Assumed 100% have plaque psoriasis |
3. Proportion of publicly funded patients | 100% | 57.6% |
4. Overcounting switching patients | Each year, 20% of all prevalent patients assumed to switch and are added to the previously modelled patients. Patients entering model in each of Years 0 through 3: 64,024 / 64,344 / 64,666 / 64,989 | Each year, 20% of all prevalent patients not already within the model are assumed to switch and are added, minus the number of patients already within the model who are switching therapies based on a weighted average of those who failed their previous therapy and those who otherwise discontinued. Patients entering model in each of Years 0 through 3: 64,024 / 35,553 / 27,318 / 19,363 (without considering other revisions) |
5. Time point of deucravacitinib response | 24 weeks | 16 weeks |
6. Drug plan perspective | Includes monitoring costs, administration costs, AE treatment costs. | a. All such costs excluded using the sponsor’s programmed options to do so b. All such costs excluded by manually setting them to $0. |
7. Deucravacitinib uptake | Biologic-naive: 6.6% / 26.0% / 36.8% Biologic-experienced: 1.5% / 6.4% / 9.3% | Biologic-naive: 3.3% / 13.0% / 18.4% Biologic-experienced: 0.8% / 3.2% / 4.7% |
8. Assume 100% biosimilar use for available products and remove ability to use same molecule at second line | Market share split between originator brands and biosimilars | All adalimumab, etanercept, and infliximab use assumed to be biosimilar for consistency with CUA model |
9. BoB equal for all comparators | The BoB following each comparator is an unweighted average of all other comparators with the exception of apremilast, deucravacitinib, certolizumab pegol, and guselkumab. | The BoB following each comparator is equal in composition to the BoB following deucravacitinib. |
10. Tildrakizumab dosing | As per European Medicines Agency: 100 mg per dose, or 200 mg per dose for patients above 90 kg body weight.59 | As per Health Canada: 100 mg per dose for all patients.34 |
CADTH combined exploratory reanalysis | 1 through 5, 6b, 7 through 10 | |
AE = adverse event; BoB = basket of biologics; CUA = cost-utility analysis.
The results of the CADTH step-wise exploratory reanalysis are presented in summary format in Table 20 and a more detailed breakdown of the combined reanalysis is presented in Table 21. CADTH’s combined exploratory reanalysis suggested that the reimbursement of deucravacitinib is likely to result in substantially less savings than predicted by the sponsor’s model, with a 3-year incremental budgetary savings of $24,462,738.
Table 20: Summary of the CADTH Exploratory Reanalyses of the BIA
Stepped analysis | Three-year total |
|---|---|
Submitted base case | –$216,650,200 |
CADTH Reanalysis 1 – NIHB corrections and limitation to adult population | –$178,841,797 |
CADTH Reanalysis 2 – Prevalence already excludes nonplaque psoriasis | –$240,722,445 |
CADTH Reanalysis 3 – Publicly reimbursed patients only | –$124,790,515 |
CADTH Reanalysis 4 – Overcounting switching patients | –$82,506,796 |
CADTH Reanalysis 5 – Deucravacitinib 16-week data | –$244,926,648 |
CADTH Reanalysis 6a – drug plan payer, as programmed | $15,505,755 |
CADTH Reanalysis 6b – drug plan perspective, manual removal by CADTH | –$216,950,189 |
CADTH Reanalysis 7 - Deucravacitinib uptake | –$108,325,100 |
CADTH Reanalysis 8 to 100% biosimilar use | –$208,942,194 |
CADTH Reanalysis 9 – equal BoB | –$217,202,543 |
CADTH Reanalysis 10 – tildrakizumab dosing | –$212,129,961 |
CADTH combined exploratory analysis (1 through 5, 6b, 7 through 10) | –$24,462,738 |
BIA = budget impact analysis; BoB = basket of biologics; NIHB = Non-Insured Health Benefits.
These results are exploratory and thus are associated with considerable uncertainty. All analyses assume publicly available prices for the comparators and also assume that deucravacitinib will only be used in patients with moderate to severe plaque psoriasis who would otherwise receive an injectable biologic therapy.
CADTH conducted additional scenario analyses exploring: no uptake of deucravacitinib in the bio-experienced population, reintroducing administration costs to the analysis, and assuming a 15.5% price reduction consistent with that estimated by the CADTH base-case pharmacoeconomic reanalysis.
Table 21: Detailed Breakdown of the CADTH Reanalyses of the BIA
Stepped analysis | Scenario | Base year | Year 1 | Year 2 | Year 3 | Three-year total |
|---|---|---|---|---|---|---|
Submitted base case | Reference | $1,822,308,490 | $3,190,581,095 | $4,603,865,126 | $5,985,923,266 | $15,602,677,978 |
New drug | $1,822,308,490 | $3,175,827,208 | $4,532,779,987 | $5,855,112,091 | $15,386,027,778 | |
Budget impact | $0 | –$14,753,887 | –$71,085,139 | –$130,811,175 | –$216,650,200 | |
CADTH combined exploratory analysis | Reference | $889,469,527 | $1,158,154,236 | $1,426,707,033 | $1,592,835,632 | $4,177,696,901 |
New drug | $889,469,527 | $1,155,685,044 | $1,417,479,938 | $1,580,069,180 | $4,153,234,163 | |
Budget impact | $0 | –$2,469,191 | –$9,227,095 | –$12,766,452 | –$24,462,738 | |
CADTH scenario 1 to 0% bio-experienced deucravacitinib uptake | Reference | $889,469,527 | $1,159,655,342 | $1,431,707,347 | $1,601,060,223 | $4,192,422,912 |
New Drug | $889,469,527 | $1,158,240,057 | $1,426,442,380 | $1,593,716,974 | $4,178,399,411 | |
Budget Impact | $0 | –$1,415,285 | –$5,264,967 | –$7,343,249 | –$14,023,501 | |
CADTH scenario 2 – administration costs included | Reference | $896,113,825 | $1,164,923,862 | $1,434,360,212 | $1,601,245,700 | $4,200,529,774 |
New drug | $896,113,825 | $1,162,428,729 | $1,425,068,693 | $1,588,427,621 | $4,175,925,043 | |
Budget impact | $0 | –$2,495,133 | –$9,291,519 | –$12,818,079 | –$24,604,731 | |
CADTH scenario 3 to 15.5% price reduction | Reference | $889,469,527 | $1,158,154,236 | $1,426,707,033 | $1,592,835,632 | $4,177,696,901 |
New drug | $889,469,527 | $1,155,262,565 | $1,415,856,580 | $1,577,547,324 | $4,148,666,469 | |
Budget impact | $0 | –$2,891,670 | –$10,850,453 | –$15,288,308 | –$29,030,432 |
BIA = budget impact analysis.
Stakeholder Input
Patient Input
Canadian Psoriasis Network and Canadian Association of Psoriasis Patients
About Canadian Psoriasis Network and Canadian Association of Psoriasis Patients
The Canadian Psoriasis Network (CPN) is working in collaboration with the Canadian Association of Psoriasis Patients (CAPP) for the completion of this submission. CPN is a national, not-for-profit organization dedicated to improving the lives of people in Canada who live with psoriasis and psoriatic arthritis (psoriatic disease). We do this in part by providing current information on research and treatment options and by working with others to build awareness and advocacy about the complexity of these conditions. CAPP is a national, not-for-profit organization formed to better serve the needs of psoriasis patients across the country and strives to improve the quality of life for all Canadian psoriasis patients. CAPP’s mission is to be a resource and advocate for psoriatic patients and their families to improve patient care and quality of life.
Information Gathering
Data Gathering
Information for this submission was obtained primarily through a survey hosted on CPN’s website and made available on both organizations’ communications channels from August 1-September 22, 2022, in English and French. Throughout this submission, we report on English survey participants distinctly from French survey participants as this data was collected separately, though the survey content was the same. CPN and CAPP also sent the survey to clinics in Canada that conducted deucravacitinib trials and asked that they share it with patients. We received a total of 22 survey responses (16 in English and 6 in French) from various provinces and territories. There were no responses from participants in the Northwest Territories, Yukon, Saskatchewan, New Brunswick, and Newfoundland and Labrador. One response was received from outside of Canada.
Another information source for questions three to five is the 2022 Survey of People with Psoriatic Disease in Canada and their Caregivers commissioned by CPN, which included 809 survey participants (502 people with psoriatic disease and 307 people who identified as caregivers). The survey was in field between June 1-16, 2022.
We also conducted a phone interview with one person who has experience with deucravacitinib through participation in a clinical trial. We connected with this person through their clinic and are including a summary of their input as an example of one person’s experience with the drug under review.
Regional Data
Of respondents who indicated their location, most English survey responses were from Ontario (50%, n=7). One response (7%, n=1) each was received from Nunavut, British Columbia, Alberta, Manitoba, Nova Scotia, Prince Edward Island, and outside of Canada. The French survey responses (n=6) were from Quebec. The responses of people with psoriatic disease from CPN’s 2022 Survey of People with Psoriatic Disease in Canada and their Caregivers were from:
Quebec (36%, n=502), Ontario (28%, n=502), British Columbia (13%, n=502), Saskatchewan and Manitoba (8%, n=502), Alberta (7%, n=502), and Atlantic provinces (7%, n=502).
Survey Demographics
Fourteen of the English survey participants (88%, n=14) identified as living with psoriasis, while two participants (13%, n=2) identified as a caregiver or family member of a person who has psoriasis. Of the two caregivers, none indicated that the patient in their life takes deucravacitinib. The six French survey participants identified as living with psoriasis.
Three of the English survey participants (27%) indicated that they were between ages 35-44; one participant (9%) was between ages 45-54; six participants (55%) were between ages 55-64; and one participant (9%) was over age 65. Seven participants identified as female (63%), and four identified as male (36%). Of the three French survey participants who answered this question, all identified as female and ranged between the ages of 25 and 64.
Just over a third of the participants of the English survey (33%, n=3) live with psoriatic arthritis and two (22%) live with another type of arthritis. Some participants indicated living with comorbidities, including anxiety (56%, n=5), diabetes (11%, n=1), depression (33%, n=3), another inflammatory condition (11%, n=1), another skin condition (11%, n=1), cancer (11%, n=1), and liver disease (11%, n=1). In the open-ended text option for this question, a participant mentioned living with hypertension, vitiligo (“which complicates UV treatment”), celiac disease, aura with migraines, and osteoporosis. Of the three French survey participants who responded to this question, all indicated that they live with psoriatic arthritis, one reported having anxiety, and two reported having other conditions (not specified).
As indicated above, the 2022 Survey of People with Psoriatic Disease in Canada and their Caregivers included 502 people living with psoriasis / psoriatic arthritis (psoriatic disease) and 307 caregivers for someone living with these diseases. Of participants who live with psoriatic disease, 55% said they live with plaque psoriasis and 33% have psoriatic arthritis.
Disease Severity
Nearly half of English survey participants (42%, n=5) who responded to this question described their psoriasis severity as “mild” (less than 3% of body surface area, or BSA); 33% (n=4) described their severity as “moderate” (between 3- 10% of BSA); and 25% (n=3) described their severity as “severe” (greater than 10% of BSA). Of the French participants who answered this question, 20% (n=1) said their symptoms are “mild”; 40% (n=2) said their symptoms are “moderate”; and 40% (n=2) report their symptoms as “severe”.
Disease Experience
Survey participants were asked to identify the symptoms they experience. Their responses are broken down by English survey responses and French survey responses in Table 1.
Table 1: Symptoms That Patient Survey Participants Experience That Affect Their Ability to Participate in Day-to-Day Life and/or Quality of Life
Symptom | Total (n, %) English survey | Total (n, %) French survey |
|---|---|---|
Flaking | 11 (79%) | 5 (100%) |
Itch | 11 (79%) | 5 (100%) |
Change in skin colour depending on underlying skin tone (e.g. redness) | 10 (71%) | 3 (60%) |
Flares | 9 (64%) | 3 (60%) |
Pain/Burning | 7 (50%) | 5 (100%) |
Additionally, in CPN’s 2022 Survey of People with Psoriatic Disease in Canada and their Caregivers, the most common symptoms reported by people with psoriatic disease (n=502) were “itching, burning, or painful skin” (70%), “silvery, scaly plaques” (66%), and “dry skin that may crack or bleed” (58%).
When asked what areas of life are negatively affected, English survey participants indicated the following.
Table 2: Impact on Areas of Life That (English) Patient Survey Participants Experience Due to Psoriasis
Life Aspect | Extremely Negative Impact (n, %) | Moderately Negative Impact (n, %) | Mildly Negative Impact (n, %) | No Impact (n, %) | N/A (n, %) |
|---|---|---|---|---|---|
Sleep | 0 (0%) | 3 (25%) | 5 (42%) | 4 (33%) | 0 (0%) |
Work | 0 (0%) | 2 (17%) | 4 (33%) | 3 (25%) | 3 (25%) |
School | 0 (0%) | 0 (0%) | 1 (8%) | 0 (0%) | 11 (92%) |
Social life | 1 (8%) | 7 (58%) | 2 (17%) | 2 (17%) | 0 (0%) |
Intimate life | 2 (17%) | 3 (25%) | 1 (8%) | 4 (33%) | 2 (17%) |
Self-esteem | 5 (42%) | 3 (25%) | 3 (25%) | 1 (8%) | 0 (0%) |
Mental health | 6 (50%) | 2 (17%) | 1 (8%) | 3 (25%) | 0 (0%) |
Exercise | 2 (17%) | 3 (25%) | 3 (25%) | 3 (25%) | 1 (8%) |
Finances | 0 (0%) | 5 (42%) | 3 (25%) | 2 (17%) | 2 (17%) |
Family life | 2 (17%) | 3 (25%) | 2 (17%) | 4 (33%) | 1 (8%) |
Of the French participants, who answered this question, many indicated that psoriatic disease has negative impacts on their social life (80%, n=4), ability to exercise (80%, n=4), and sleep (80%, n=4), followed by family life (60%, n=3), self-esteem (40%, n=2), and mental health (40%, n=2).
When asked to share any additional information about the challenges of living with psoriasis that are important to them, one survey participant told us:
“My skin can't be wet for long. Doing dishes is sometimes painful & little splits sometimes occur, then they burn. I wear thin non-latex gloves then heavy duty latex gloves. Same when scrubbing the tub or washing a car” and another reflected, “Difficulté à concilier travail/famille et traitement du psoriasis…”
In addition, in the 2022 Survey of People with Psoriatic Disease in Canada and their Caregivers, the top impacts of psoriatic disease were identified to be: “I pick certain clothes to wear” (54%, n=502), “I change how I go about day-to-day life” (51%, n=502), “I have less confidence in myself” (48%, n=502), and “I have lost sleep” (47%, n=502). Other responses included “I have missed work” (26%, n=502) and “I have changed careers due to my psoriasis and/or psoriatic arthritis (14%, n=502). Overall, 63% participants say that the disease has made their quality of life worse.
Experiences With Currently Available Treatments
Survey participants were asked to identify the treatments that they have used for psoriasis and to rate how effective they were at treating symptoms. Table 3 provides a full breakdown of responses from English survey participants.
Table 3: (English) Patient Survey Participant Rating of Effectiveness of Psoriasis Treatments They Have Used
Treatment | Very effective (n, %) | Effective (n, %) | Ineffective (n, %) | Very ineffective (n, %) | N/A (n, %) |
|---|---|---|---|---|---|
Topical corticosteroid (e.g., betamethasone,mometasone, etc.) | 0 (0%) | 3 (25%) | 6 (50%) | 1 (8%) | 2 (17%) |
Topical vitamin D derivatives (e.g., Dovonex, Silkis, etc.) | 0 (0%) | 1 (8%) | 5 (42%) | 1 (8%) | 5 (42%) |
Topical combination treatment (e.g., Dovobet, Enstilar, etc.) | 0 (0%) | 4 (33%) | 4 (33%) | 1 (8%) | 3 (35%) |
Topical retinoids (e.g., Tazorac) | 0 (0%) | 0 (0%) | 1 (9%) | 1 (8%) | 9 (75%) |
Apremilast | 0 (0%) | 0 (0%) | 1 (9%) | 0 (0%) | 9 (75%) |
Cyclosporine | 0 (0%) | 0 (0%) | 1 (9%) | 0 (0%) | 10 (83%) |
Methotrexate | 1 (8%) | 2 (17%) | 2 (17%) | 6 (50%) | 6 (50%) |
Oral retinoids | 0 (0%) | 0 (0%) | 1 (8%) | 0 (0%) | 10 (83%) |
Oral steroids | 0 (0%) | 0 (0%) | 1 (8%) | 0 (0%) | 10 (83%) |
Biologics (e.g., adalimumab, certolizumab pegol, infliximab, etc.) | 1 (8%) | 2 (17%) | 0 (0%) | 0 (0%) | 7 (58%) |
Phototherapy | 0 (0%) | 2 (17%) | 1 (8%) | 1 (8%) | 7 (58%) |
Medical cannabis | 0 (0%) | 1 (8%) | 1 (8%) | 1 (8%) | 8 (67%) |
Overall, most participants (including those who are on a clinical trial for deucravacitinib) (72%, n=8) indicated that their current treatment allows them to resume daily activities (e.g., work, household tasks, caring for children) but 9% (n=1) disagreed this was the case for them.
Of French survey participants who responded to this question (n=4), none had experience with biologics, topical retinoids, or apremilast. No respondents found any treatment they tried to be “very effective”. Only one (25%) response for “effective” was selected for each of the following: topical corticosteroids, topical combination treatments, methotrexate, oral retinoids, oral steroids, phototherapy, and medicinal marijuana. French participants also reported the following as “ineffective”: topical corticosteroids (75%, n=3), topical combination treatments (25%, n=1), cyclosporine (25%, n=1), and methotrexate (25%, n=1).
When asked if participants experience any side effects of treatments that are difficult to tolerate or manage, the most common responses from English survey participants are depicted in Table 4. There were nine responses to this section.
Table 4: Side Effects of Treatment That Are Difficult to Tolerate or Manage for (English) Patient Survey Participants
Side effect | Respondents who found it difficult to tolerate (n, %) | Side effect | Respondents who found it difficult to tolerate (n, %) |
|---|---|---|---|
Skin itching | 6 (67%) | Development of new rash/acne | 1 (11%) |
Changes in skin pigmentation (i.e., affected skin turns lighter or darker) | 6 (67%) | Hair loss | 1 (11%) |
Skin thinning | 4 (44%) | Nausea or vomiting | 1 (11%) |
Muscle soreness or joint stiffness | 3 (33%) | Weight loss | 0 (0%) |
Unexplained fatigue | 3 (33%) | Diarrhea | 0 (0%) |
Skin irritation or redness | 3 (33%) | Headache | 0 (0%) |
Dry skin, eyes, or lips | 3 (33%) | Confusion | 0 (0%) |
Pain | 1 (11%) | Other | 0 (0%) |
Two participants (17%) said they take medications or over-the-counter products to help manage the side effects noted in Table 4, including a 3-step hair/scalp care program and a cream for rosacea.
The French survey respondents to this question said that they experienced itching (100%, n=4) as a side effect followed by muscle pain or joint stiffness (75%, n=3). Other responses included skin thinning (50%, n=2), fatigue (50%, n=2), development of new rash/acne (50%, n=2), and headache (50%, n=2).
The diversity in responses exemplifies the heterogenous experiences of people when it comes to psoriasis treatments and emphasizes for us the need for a range of accessible treatment options and for approaching treatment planning and drug policy in a way that considers the needs of the individual patient.
Affordability of Treatment
Survey participants were asked to respond to a series of statements regarding their current treatments. In terms of affordability, three English survey participants said they do not think their current treatment is affordable and disagreed with the statement “I can afford my medication.” Six participants indicated they have had financial hardships paying for medications. Of these six participants, three stated they were able to manage, while others shared that they took less than prescribed (n=1), stopped taking their medications (n=1), or didn’t fill their prescription at the pharmacy (n=1).
English survey participants also reported paying for their medications in various ways. Most participants who responded to this question (54%, n=6) have private insurance either through their employer, union, or professional association, or through their partner/spouse. Others (36%, n=4) are covered through a provincial/territorial and/or federal public drug program. Other ways that people accessed their treatments included: participating in a clinical trial (18%, n=2) or paying for medications out of pocket (18%, n=2). One participant (n=1, 9%), stated the following:
“My provincial medical only covers the costs for a few options though I would like to find an alternative medication from what I'm on now.”
Three participants responded to questions about access to treatments in the French patient survey. Each accessed their prescription medication in different ways: private insurance either through their employer, union, or professional association, or through their spouse’s plan, and through public drug programs. Two indicated that they have financial hardships paying for medications, though they manage.
The 2022 Survey of People with Psoriatic Disease in Canada and their Caregivers shows similar results: 30% (n=502) participants use employer benefits to access treatments, 28% (n=502) use public drug plans, 15% (n=502) use partner’s benefits, and the remaining 27% (n=502) of the participants are paying out of pocket.
Accessibility of Treatment
In terms of being prescribed the treatment they need, 72% (n=8) of English survey participants who answered this question agreed that their doctor can prescribe the preferred/appropriate treatment for their circumstances. However, only 45% (n=5) indicated that they are receiving their preferred choice of treatment. The dissonance between these responses was not explored in the current survey, however it is important to recognize that survey participants expressed some level of dissatisfaction with being able to access the treatment that they would prefer. The vast majority (90%, n=10) agreed that instructions for using their current treatment are easy to follow and 27% (n=8) agreed that their current dosing schedule is convenient.
For French survey participants, only one participant (of three) agreed that their prescriber can prescribe the preferred/appropriate treatment for their circumstances and two said that they disagree with the statement that they are receiving their preferred choice of treatment.
Five English survey participants were neutral with regards to the statement “Overall, my needs are met with the treatment I receive”, although no participants (0%, n=0) disagreed with this statement. No participants (0%, n=0) felt that that the travel to and from medical appointments was not manageable.
Improved Outcomes
When asked what survey participants’ expectations for a new medication are, given their experience with existing treatments for psoriasis, all English survey participants who answered this question included “improves my symptoms” (n=10). Other responses included “better quality of life (e.g., return to work, able to socialize more, mental wellbeing, fewer doctor visits)” (70%, n=7); “help with symptom(s) I still have” (70%, n=7); “reduced side effects” (60%, n=6); “affordable” (60%, n=6); and “easier to take (e.g., easier to follow dosing schedule, pills are easier to swallow)” (40%, n=4).
Of the respondents to this question in the French survey, all participants said, “better quality of life” (100%, n=3) and “reduced side effects” (100%, n=3). Other responses in the French survey included, “improves my symptoms” (67%, n=2), “easier to take” (67%, n=2), and “affordable” (67%, n=2).
When asked, “What is the biggest improvement that you would like to see in psoriasis treatment?” participants shared a range of responses including the following:
“Less itching and flaking.”
“Affordable, accessible psoriasis medication that doesn't have crazy side effects.”
“Easy to dose and maintain schedule and access to proper medication that prevents flares or worsening of psoriasis symptoms.”
“Something that actually works.”
“Clearer skin, no more flakes/irritation on my scalp, fewer flare ups and fewer side effects.”
“A reduction in inflammation thereby reducing plaques and a longer remission time would be fantastic.”
“Cure for sure. But clear skin without scarring.”
Most participants who responded to this question provided some form of “clear skin” and/or “fewer flare ups” as responses. Affordability and reduced side effects were also common responses from participants.
In the 2022 Survey of People with Psoriatic Disease in Canada and their Caregivers, top areas participants with psoriasis (n=502) wished to improve included: reducing pain (69%); reducing anxiety (64%); reducing sleep disturbances (59%); addressing treatment side effects (51%); and improving ability to work (44%). This survey also explored concerns that people have with their treatment. The top three concerns identified by participants with psoriatic disease were: “I worry about the risks related to medications”, “I worry about the cost of medications”, and “I have concerns about self-injections”.
Experience With Drug Under Review
Summary of Participants
Of the 14 participants of the English survey, two indicated that they were taking deucravacitinib for their psoriasis. Both respondents accessed deucravacitinib by participating in a clinical trial. No French survey participants had experience with deucravacitinib. We also conducted a phone interview with one male patient on a clinical trial for deucravacitinib who we connected to through their clinic. We are including a summary of their input as an example of one person’s experience with this drug.
Past Medications Trialed by Participants
Of the English survey participants who indicated that they have taken deucravacitinib, the following number also report having tried the other treatments: topical corticosteroids (100%, n=2), topical vitamin D derivatives (50%, n=1), topical combination treatments (100%, n=2), methotrexate (50%, n=1), and phototherapy (50%, n=1). All these treatments were rated from “ineffective” to “very ineffective” by the 2 survey participants and caused them to develop skin thinning (50%, n=1), skin itching (50%, n=1), and develop a new rash/acne (50%, n=1).
Values That Are Important to Patients
With deucravacitinib, the participants were hoping for better quality of life such as return to work, able to socialize more, mental wellbeing, fewer doctor visits (100%, n=2), and improvement in symptoms (100%, n=2).
The Impact of Deucravacitinib of Participants/Patients
When asked to share their experiences with deucravacitinib, one survey participant shared the following:
“Clear skin. No thought of my skin”
Table 5 describes English survey participant responses when asked to rate the following statements related to their experience with using deucravacitinib compared to other treatments.
Table 5: Experience With Deucravacitinib Statement Rating
Statement | Strongly agree / Agree (n, %) | Neutral (n, %) | Statement | Strongly agree / Agree (n, %) | Neutral (n, %) |
|---|---|---|---|---|---|
Deucravacitinib is easier to use than other therapies | 2 (100%) | N/A | Deucravacitinib improved my quality of life (i.e.return to work, able to socialize more, mental well being) | 2 (100%) | N/A |
Deucravacitinib is better at managing my psoriasis symptoms than other therapies | 2 (100%) | N/A | Deucravacitinib helped me return to my day-to-day activities | 1 (50%) | 1 (50%) |
Deucravacitinib's side effects are more tolerable than other therapies | 1 (50%) | 1 (50%) | Deucravacitinib reduced my flares | 2 (100%) | N/A |
Deucravacitinib's instructions are easier to follow than other therapies | 2 (100%) | N/A | Overall, my needs are better met with deucravacitinib | 2 (100%) | N/A |
I expect that deucravacitinib will improve my long-term health and well-being | 1 (50%) | 1 (50%) | — | — | — |
One participant stated that the deucravacitinib caused skin redness and irritation (50%, n=1).
Summary of Interview With Male, Age 55-64, Ontario Who is Taking Deucravacitinib for Plaque Psoriasis
Interviewee reports having first flare about 3 years ago – he was “98% covered”. It was the first time he had a flare. He reports having peeling skin.
“Looks horrible, all red, blotchy. Looks like water blisters, scaly water blisters. It does get painful, itchy, and like a burning [sensation].”
He shares that his symptoms had major impacts on his life. He wore only long sleeves which interfered with the type of work he does. He said his symptoms put a tremendous strain on his marriage. He reports getting to a point where his relationship with his wife was under significant stress because he had psoriasis all over his body and they had difficulty figuring out how to deal with it. He says he was “not happy” living with psoriasis – he shares that he
“I wouldn’t wear shorts, wouldn’t wear anything, would try to keep my face covered.”
Interviewee reports that he went to his doctor who at first gave him some form of topical treatment that was ineffective for him because the psoriasis was all over his body. He reports that his wife would have to help him apply creams all over his body. He shares that:
“She would say: ‘Why are we doing this? This isn’t doing anything. There must be something more that we can do’”. He reports that applying topical treatment to 98% of body was “frustrating” – they wanted to know “what it was and how to get rid of it.”
Interviewee describes that he was eventually referred to a dermatologist who he got an appointment with after three months. He reports that the dermatologist diagnosed him with plaque psoriasis and that when he was told there was no cure, “I was like, are you kidding?” He reports that his dermatologist informed him about the clinical trial and at first, when he learned that they would have to do blood tests throughout the trial, he was hesitant because of his issue with needles – interviewee was adamant that “I hate needles” – but he shared that he had to endure this because of the major impacts that psoriasis was having on his life. Interviewee states that if the clinical trial was for an injectable drug, “I wouldn’t be able to take an injection.”
Interviewee reports that in two months on the drug his psoriasis was down to 10% body surface area. He says that he takes one pill once a day which he reports is convenient for him. He reports having missed a pill early on and that “it came back with a vengeance” but that his skin cleared again once he resumed his medication. He says he recently missed four days of treatment, and that the effect was not as significant. He says that although it was noticeable, “it was not as bad as the first time”; he reports that his skin is “getting back to normal” after he resumed his treatment schedule.
Interviewee does not report any side effects or negative effects.
“Just some itching from the skin healing.”
“I recommend this drug to everyone.”
Three years later, he reports that the treatment is still very effective:
“It’s been a god send for me. Having this is painful, itchy, it bleeds, but once you get passed all that, if you get a dermatologist and he gives you what you need, and if this drug hits the market, it’s going to be fantastic for people. I’m glad I got to participate in being a lab rat. This drug is a miracle drug – for something that they said there’s no cure for this is as close as it gets”.
Interviewee emphasized again that he “hates needles” and that he wouldn’t be on this drug if it was an injection.
For more information about the challenges of living with psoriasis, please refer to the following resources:
CPN and CAPP’s joint report, Journey to Stability
CAPP’s report Pso Serious 2018: A Report on Access to Care and Treatment for Psoriasis Patients in Canada
CPN and CAPP’s joint infographic on Impact of COVID-19 on the Psoriasis and Psoriatic Community in Canada – Highlights from a National Survey
CPN’s fact sheet for health care providers on Women and Psoriasis: Findings from a Survey of Women-identified People with Psoriatic Disease
Patients are looking for a treatment that will control all of their symptoms but ultimately, they want and value a cure for psoriasis.
When interviewee had symptoms, he says he had to wear long sleeved shirts all the time, which was problematic for the type of work he does. This caused distress and disruption. He reports that this is no longer an issue for him now that he’s on effective treatment. Interviewee reiterated that psoriasis put a “big damper” on his relationship with his wife because of “the way it was and the way it looked”– but “that’s been a lot better.” He reports that things were rocky for them even after over 40 years of marriage. He says that successful treatment has helped this area of his life tremendously. Interviewee reports that they gave him a notebook at the clinic that asked about his experiences with psoriasis, including his feelings. He said, “I wasn’t depressed or suicidal, I just wanted this to go away”. However, he reflects that he can “imagine how other people are”. He says that he’s not going to let this disease win over his life.
Companion Diagnostic Test
Not applicable.
Anything Else?
Psoriasis is a chronic and potentially debilitating disease that poses many challenges, including high prevalence, chronicity, disfiguration, disability, and associated comorbidities. Psoriasis is linked to anxiety, depression, and social isolation, and can interfere with relationships, productivity, family life and work life. The physical, psychological, social, and economic impact of psoriasis can significantly burden patients and their families. Access to effective care and appropriate treatment is needed but management of psoriasis can be complex partly due to varied patient response to treatments, differences in social determinants of health, lifestyle considerations, and other factors that affect one’s condition. Moreover, due to the chronicity of this disease, patients are concerned about recurrence and resistance to earlier therapies.
The modality of treatment delivery matters. Almost 10% of CPN’s 2022 survey participants have concerns about self-injections. The patient we interviewed for this submission was adamant against injections. In particular, people with severe forms of psoriatic disease that cause significant disruptions to their health, lives, and well-being need options for treatments and treatment modalities that are feasible and accessible to them.
Psoriasis is more than a skin condition. It is an inflammatory disease that can impact several organ systems. It is estimated that up to 30 percent of people with psoriasis develop psoriatic arthritis. People with psoriatic disease also are at greater risk of developing cardiovascular disease, depression and anxiety, diabetes, and cancer.
Conflict of Interest Declaration — Canadian Psoriasis Network and Canadian Association of Psoriasis Patients
To maintain the objectivity and credibility of the CADTH reimbursement review process, all participants in the drug review processes must disclose any real, potential, or perceived conflicts of interest. This Patient Group Conflict of Interest Declaration is required for participation. Declarations made do not negate or preclude the use of the patient group input. CADTH may contact your group with further questions, as needed.
Did you receive help from outside your patient group to complete this submission? If yes, please detail the help and who provided it.
We received help with developing the survey and outreach to clinical trial sites by two medical student volunteers. We received help from a few clinical trial sites to share the survey with their patients and from one clinical trial site to connect us with patients who were willing to be interviewed.
Did you receive help from outside your patient group to collect or analyze data used in this submission? If yes, please detail the help and who provided it.
CPN and CAPP also sent the survey to clinics in Canada that conducted deucravacitinib trials and asked that they share it with patients. One clinic connected us to the patient who we interviewed for this submission.
List any companies or organizations that have provided your group with financial payment over the past 2 years AND who may have direct or indirect interest in the drug under review.
Table 6: Financial Disclosures for Canadian Psoriasis Network
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
AbbVie Canada | — | — | — | X |
Amgen Canada | — | — | X | — |
Bausch Health | — | — | X | — |
Bristol Myers Squibb | — | — | X | — |
Boehringer Ingelheim International | — | X | — | — |
Boehringer Ingelheim Canada | — | — | X | — |
Janssen Canada | — | — | X | — |
LEO Pharma Canada | — | — | X | — |
Novartis Canada | — | — | X | — |
Pfizer | — | — | X | — |
Sun Pharma | — | — | X | — |
UCB Canada | — | — | X | — |
Table 7: Financial Disclosures for Canadian Association of Psoriasis Patients
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
AbbVie Canada | — | — | X | — |
Amgen Canada | — | — | X | — |
Bausch Health | — | X | — | — |
Bristol Myers Squibb | X | — | — | — |
Boehringer Ingelheim | — | — | X | — |
Janssen Canada | — | X | — | — |
LEO Pharma Canada | — | — | X | — |
Novartis Canada | — | — | X | — |
Pfizer | — | — | X | — |
Sun Pharma | — | — | X | — |
UCB Canada | — | — | X | — |
Clinician Input
There is no clinician input.
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up-to-date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
Redactions: Confidential information in this document may be redacted at the request of the sponsor in accordance with the CADTH Drug Reimbursement Review Confidentiality Guidelines
Stakeholder Input: The views expressed in each submission are those of the submitting organization or individual; not necessarily the views of CADTH or of other organizations. As such, they are independent of CADTH and do not necessarily represent or reflect the view of CADTH. No endorsement by CADTH is intended or should be inferred. By filing with CADTH, the submitting organization or individual agrees to the full disclosure of the information. CADTH does not edit the content of the submissions.
CADTH does use reasonable care to prevent disclosure of personal information in posted material; however, it is ultimately the submitter’s responsibility to ensure no identifying personal information or personal health information is included in the submission. The name of the submitting organization or individual and all conflict of interest information are included in the submission; however, the name of the author, including the name of an individual patient or caregiver submitting the patient input, are not posted.
Accessibility: CADTH is committed to treating people with disabilities in a way that respects their dignity and independence, supports them in accessing material in a timely manner, and provides a robust feedback process to support continuous improvement. All materials prepared by CADTH are available in an accessible format. Where materials provided to CADTH by a submitting organization or individual are not available in an accessible format, CADTH will provide a summary document upon request. More details on CADTH’s accessibility policies can be found here.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.