CADTH Reimbursement Review
Dexamethasone Intravitreal Implant (Ozurdex)
Sponsor: Allergan, an AbbVie Company
Therapeutic area: Diabetic macular edema
This multi-part report includes:
Clinical Review
Pharmacoeconomic Review
Stakeholder Input
Clinical Review
Abbreviations
AE
adverse event
AUC
area under the curve
BCVA
best corrected visual acuity
CCB
Canadian Council of the Blind
CDEC
CADTH Canadian Drug Expert Committee
CI
confidence interval
CMT
central macular thickness
CNIB
Canadian National Institute for the Blind
CRS
Canadian Retina Society
CRT
central retinal thickness
CST
central subfield thickness
DC
Diabetes Canada
DME
diabetic macular edema
DR
diabetic retinopathy
ECRS
Eastern Canada Retina Specialists
ETDRS
Early Treatment Diabetic Retinopathy Study
FBC
Fighting Blindness Canada
HRQoL
health-related quality of life
IDC
indirect comparison
INESSS
Institut national d’excellence en santé et en services sociaux
IOP
intraocular pressure
ITT
intention-to-treat
LOCF
last observation carried forward
logMAR
logarithm of the minimum angle of resolution
MI
myocardial infarction
MID
minimal important difference
NEI-VFQ-25
National Eye Institute Visual Functioning Questionnaire–25
OCT
optical coherence tomography
RCT
randomized controlled trial
SAE
serious adverse event
SD
standard deviation
SD-OCT
spectral domain optical coherence tomography
TD-OCT
time domain optical coherence tomography
VA
visual acuity
VEGF
vascular endothelial growth factor
VLRC
Vision Loss Rehabilitation Canada
WDAE
withdrawal due to adverse event
Executive Summary
An overview of the submission details for the drug under review is provided in Table 1.
Item | Description |
|---|---|
Drug product | Dexamethasone (Ozurdex) 0.7 mg intravitreal implant |
Indication | For the treatment of adult patients with DME who are pseudophakic |
Reimbursement request | For the treatment of adult patients with DME who are pseudophakic and have had an inadequate response to prior anti-VEGF therapy |
Health Canada approval status | NOC |
Health Canada review pathway | Standard |
NOC date | April 16, 2015 |
Sponsor | Allergan, an Abbvie Inc. company |
DME = diabetic macular edema; NOC = Notice of Compliance; VEGF = vascular endothelial growth factor.
Source: Dexamethasone (Ozurdex) product monograph.1
Introduction
Diabetic macular edema (DME) is a vision-related, microvascular complication of diabetes mellitus (type 1 and type 2) commonly reported in adults of working age.2 It is characterized by multifactorial pathophysiology,2 which is reportedly mediated by angiogenic vascular endothelial growth factor (VEGF) and inflammatory pathways.3-6 Estimates in Canada in 2022 show that more than 4 million patients were diagnosed with type 1 and type 2 diabetes.7 A retrospective study conducted in Canada in 2012 assessing patient records from the southwestern Ontario database estimated the prevalence of DME in adults with diabetes to be 15.7% and the prevalence of vision loss due to DME to be 2.56%.8 DME manifests slowly as progressive vision loss of varying degrees, primarily dependent on the severity, duration, and location of intraretinal fluid, among other factors.3,9 Common signs and symptoms of DME include blurred vision, retinal hemorrhages, retinal detachment, colours appearing “washed out” or faded, changes in contrast sensitivity, impaired colour vision, gaps in vision, and potentially permanent vision loss.10-12
In Canadian practice, pharmacologic and nonpharmacologic therapeutic options are available for patients with DME. Anti-VEGFs are first-line options available for patients, administered intravitreally every month for up to 3 loading doses, and thereafter every 1 month to 3 months. Health Canada–approved anti-VEGFs include ranibizumab and aflibercept, and recent additions such as brolucizumab and faricimab. Bevacizumab, an anti-VEGF drug, is also used in the first-line setting in clinical practice but does not have Health Canada–approved indications for the treatment of DME and is reimbursed only in certain jurisdictions. Intravitreal corticosteroids, such as dexamethasone and triamcinolone, may be considered in patients who do not respond well to anti-VEGF treatment, especially patients who have artificial lens implants (i.e., pseudophakic) because of the increased risk of cataract formation with corticosteroid treatment. In Canada, intravitreal dexamethasone implants are indicated for use in patients with DME who are pseudophakic. Focal laser, vitrectomy, or grid therapy are nonpharmacologic treatment options available in later line settings, according to the clinician group input and the clinical expert consulted by CADTH.
Dexamethasone 0.7 mg biodegradable intravitreal implant (Ozurdex) is a sustained-release, glucocorticoid receptor agonist. Dexamethasone is administered using the Dexamethasone Posterior Segment Drug Delivery System. This is a sterile, single-use system intended to deliver 1 implant into the vitreous cavity and was designed to prolong the duration of the dexamethasone effect in the eye. The product monograph notes that there is “very limited information on repeat dosing intervals less than 6 months”1 and highlights evidence from a 2-year observational study that “the use of more than two consecutive administrations is associated with increases in some adverse reactions; therefore, no more than two consecutive dexamethasone injections should be used, and an interval of approximately 6 months should be allowed between the two injections.”1 However, clinical expert input to CADTH noted that in practice, ophthalmologists readminister the dexamethasone implant approximately every 3 months to 4 months and that treatment discontinuation is based on clinical considerations other than the maximum of 2 consecutive dexamethasone implants recommended in the product monograph. The dexamethasone implant received approval from Health Canada, with a Notice of Compliance granted on April 16, 2015, for the treatment of adult patients with DME who are pseudophakic.
The dexamethasone implant (Ozurdex) was reviewed previously by CADTH, but received a negative recommendation from the CADTH Canadian Drug Expert Committee (CDEC) on October 24, 2018,13 for the treatment of adult patients with DME who are pseudophakic. CDEC identified several gaps in the evidence presented by the sponsor during the submission. Key evidence gaps noted in the CDEC recommendation were the lack of high-quality direct evidence comparing a dexamethasone implant with other active treatments used in Canada for the requested population, uncertainty regarding the magnitude of benefit with a dexamethasone implant in the pseudophakic population, and insufficient data to assess the safety and efficacy of dexamethasone in patients who would use dexamethasone implants as second-line therapy. Appendix 3 presents a summary of the initial CADTH clinical review of Ozurdex,14 which examined the evidence reported in 2 trials — the MEAD-010 and MEAD-011 trials — in the sponsor’s submission. The sponsor provided a resubmission to CADTH for dexamethasone implants for the treatment of patients with DME who are pseudophakic and have inadequate response to prior anti-VEGF therapies. The sponsor’s reimbursement population differs from that of the Health Canada–approved indication in that it focuses on patients who have had an inadequate response to prior anti-VEGF therapies. New evidence (1 randomized controlled trial [RCT] and 10 observational studies) evaluating the use of a dexamethasone intravitreal implant in patients with DME, which was not available during the initial submission to CADTH in 2017, was identified and submitted by the sponsor for this resubmission.
The objective of this report was to perform a systematic review of the beneficial and harmful effects of a 0.7 mg dexamethasone intravitreal implant for the treatment of adult patients with DME who are pseudophakic and have had an inadequate response to prior anti-VEGF therapy.
Stakeholder Perspectives
The information in this section is a summary of input provided by the patient groups that responded to CADTH’s call for patient input and from clinical experts consulted by CADTH for the purpose of this review.
Patient Input
CADTH received a joint patient group submission from 5 organizations: Fighting Blindness Canada (FBC), the Canadian Council of the Blind (CCB), the Canadian National Institute for the Blind (CNIB), Vision Loss Rehabilitation Canada (VLRC), and Diabetes Canada (DC). FBC’s goal is to understand why vision loss occurs, how it can be slowed, and how sight can be restored. CCB is a membership-based not-for-profit organization that brings together Canadians who are living with vision loss — those who are blind, deafblind, and partially sighted — to promote a sense of purpose and self-esteem along with enabling the efforts of each member to achieve an enhanced quality of life. CNIB is a nonprofit organization that delivers programs and advocates to empower people impacted by blindness and remove barriers to inclusion. VLRC is a health services organization that provides training to enable people who are blind or partially sighted to develop or restore key daily living skills, helping enhance their independence, safety, and mobility. DC is a national health charity representing millions of Canadians affected by diabetes. DC’s mission is to provide education and services, advocate on behalf of people living with diabetes, and support research and translate it into practical applications. Data were collected through an online survey made available to Canadians living with diabetic retinopathy (DR) or DME in January 2020 and shared across networks associated with the submitting organizations. A total of 67 patients in Canada responded to the survey. In April 2020, CCB conducted a separate survey of 572 respondents on the impact of the COVID-19 pandemic on Canadians who are blind, deafblind, or partially sighted.
Overall, respondents indicated that both DR and DME had substantial and life-altering impacts, including a negative impact on the ability to perform daily activities such as reading, using a phone, and driving, anxiety over potential worsening of the condition, and reliance on others. In addition, the CCB COVID-19 study showed that fear, anxiety, loneliness, and other psychosocial impacts were intensified for patients with age-related macular edema and DR during the pandemic. Respondents of the joint survey indicated that they had experience with a variety of DR or DME treatments, including anti-VEGF therapies and Ozurdex, and most indicated that intravitreal treatment prevented further loss of vision. When asked about the most difficult part of eye injection appointments, travel and waiting time were central concerns. The submission highlighted that the low number of respondents (4.5%) who received injections less than 3 months ago is disconcerting, potentially indicating low adherence to injections. Respondents indicated the following reasons for cancelling or delaying appointments: being too busy to attend the appointment, not feeling well, being unable to find someone to take them to the appointment, and being “scared to receive the injection.”
Though the survey did not ask patients for their views on improving their experiences and outcomes, the submission highlighted that any treatment that reduces the physical, psychological, and logistical strain on patients would be preferred. A treatment that is less invasive or one that is similarly invasive but that is administered less frequently would be helpful in reducing this strain.
Clinician Input
Input From Clinical Expert Consulted by CADTH
According to the clinical expert consulted by CADTH for this review, the goal in treating patients with DME is to resolve macular edema and to improve vision while minimizing treatment-related complications. The expert highlighted that anti-VEGF therapies are available in the mainstay therapies in the first-line setting for patients with centre-involved DME, while steroids (dexamethasone implant or triamcinolone acetonide) are reserved for pseudophakic patients who have shown inadequate response while on anti-VEGF therapy, those with a contraindication to anti-VEGF therapy (recent stroke, myocardial infarction [MI], or pregnancy), or those who cannot afford the cost of anti-VEGF therapies. The clinical expert consulted cited that although anti-VEGFs have shown effectiveness in patients with DME, up to 40% of patients respond inadequately to repeated injections with anti-VEGFs; thus, there is a need for other treatment options for these patients. In addition, the expert highlighted that treatment with anti-VEGFs requires monthly administration of up to 5 doses, which may be inconvenient for some patients. The expert also noted that anti-VEGFs are associated with high costs, concerns with potential complications, and the possibility of no improvement in vision despite treatment. The expert indicated that patients often remark upon the inconvenience of taking time off work to receive monthly treatments and the discomfort associated with the injection.
The clinical expert consulted highlighted that patients most likely respond to treatment with a dexamethasone implant are patients with chronic DME because they are likely to have inflammation as part of the mechanism of DME. The clinical expert considered central retinal thickness (CRT) measured by optical coherence tomography (OCT) and visual acuity (VA) to be important outcomes used in clinical practice. In the opinion of the clinical expert, a clinically meaningful response to treatment with dexamethasone will include a gain of 5 letters of Snellen acuity, or a reduction of CRT of 50 µm or more as measured by OCT. According to the expert, adverse events (AEs) such as glaucoma, infection, migration of the implant to the anterior chamber, and lack of improvement in treatment will be considered when deciding to discontinue the dexamethasone implant.
The expert noted that the dexamethasone implant can be administered in a community setting, hospital (outpatient clinic), or specialty clinic. An ophthalmologist familiar with the diagnosis and treatment of patients with DME will be required to diagnose, treat, and monitor patients who receive a dexamethasone implant.
Clinician Group Input
This section was prepared by CADTH staff based on the input provided by clinician groups.
CADTH received 4 clinician group submissions for this review from the following organizations: Eastern Canada Retina Specialists (ECRS) (12 clinicians), the Retina Society of Alberta (8 clinicians), the Canadian Retina Society (CRS) (4 clinicians), and retina specialists from Western Canada (7 clinicians). ECRS is a group of independent retina specialists practising in various locations throughout Eastern Canada. The Retina Society of Alberta is a retina medical and surgical retina subspecialty practice of 8 physicians based in Edmonton who provide retina-related care to the northern half of Alberta. The CRS represents those ophthalmologists in Canada whose primary area of patient care is surgical and/or medical vitreoretinal disease. Retina specialists from Western Canada is a group of retina specialists practising in Western Canada (Manitoba, Saskatchewan, Alberta, and British Columbia). The group clinician input was largely in agreement with the input received from the clinical expert consulted by CADTH.
The clinician groups and the clinical expert consulted generally agreed on the main goals of treatment, the unmet needs of patients, and prescribing conditions. The goals in treating patients with DME are to resolve macular edema and improve vision while minimizing treatment-related complications. In addition to these treatment goals, the clinician groups noted longer duration of action as an important treatment goal. The clinician groups indicated that patients who do not respond to anti-VEGF therapy can be identified after receiving 5 doses to 6 doses or at least 3 months of therapy. According to the ECRS, the retina specialists from Western Canada, and CRS, patients may be switched to another anti-VEGF therapy after inadequate response with initial anti-VEGF therapy. Following anti-VEGF therapy failure (or if the duration of response is shorter than 4 weeks, according to the Retina Society of Alberta), dexamethasone implants and triamcinolone are among the treatment options. In addition, the clinician groups mentioned that dexamethasone was considered particularly well-suited for pseudophakic patients and those with vitrectomized eyes due to the predictable and lower risk of elevated intraocular pressure (IOP) and a longer duration of action (most often about 4 months) compared with triamcinolone.
Clinician groups specified that patients with centre-involving DME who are resistant to first-line anti-VEGF therapy after at least 3 monthly injections would be considered as best suited for the dexamethasone treatment, and also indicated that patients with DME least suited for dexamethasone treatment would include those who have a tractional component (epiretinal membrane or vitreomacular traction), severe glaucoma, a known steroid response with IOP elevation, signs of chronic DME, aphakic eyes, or a compromised posterior capsule.
Clinician groups indicated that clinically meaningful response to dexamethasone treatment would include the resolution of DME (a 30% to 50% reduction in excess central foveal thickness) measured by OCT, VA improvement (20/50 Snellen equivalent or better), decreased frequency of treatment, and/or regression of a diabetic severity score. The ECRS submission also mentioned that patients should be assessed monthly when treatment is initiated and then every 3 months to monitor therapy outcomes and response as well as individual durability of the dexamethasone implant. The clinician groups indicated that chronic DME, potential side effects (e.g., elevated IOP, infection or inflammatory response, migration of the implant to the anterior chamber), and a lack of clinical improvement (retina thickness and fluid that does not improve) would be considered as discontinuation factors.
The clinician groups and the clinical expert consulted agreed that the duration of action for the dexamethasone injections is approximately 3 months to 4 months.
Drug Program Input
The drug programs provide input on each drug being reviewed through CADTH’s reimbursement review processes by identifying issues that may impact their ability to implement a recommendation. The implementation questions and corresponding responses from the clinical experts consulted by CADTH are summarized in Table 3.
Clinical Evidence
Protocol Selected Studies
For this resubmission, the sponsor provided 11 published studies to support the current reimbursement request for the use of dexamethasone implant in pseudophakic patients who have had an inadequate response to anti-VEGF therapy. One of these 11 studies was an RCT that was included in the CADTH systematic review. No additional studies, other than the pivotal MEAD trials reviewed as part of the original Ozurdex submission, were identified in the literature.
Description of Studies
The study authored by Shah et al. (2016)15 was a prospective, randomized, patient-masked, phase III trial conducted at a single site in the US. The study was supported by an investigator-initiated trial grant provided by Allergan Inc. Patients with DME and inadequate response to prior anti-VEGF therapy who met the eligibility criteria were randomized to 1 of 2 treatment groups: bevacizumab or dexamethasone implant. Patients whose right eye and left eye both met the eligibility criteria had 1 eye randomized to 1 treatment, with the other eye assigned to the other treatment. The study lasted 7 months, and patients received monthly follow-up.
Eligible patients were adults 18 years and older with type 1 or type 2 diabetes mellitus with best corrected visual acuity (BCVA) scores of between 24 and 78 Early Treatment Diabetic Retinopathy Study (ETDRS) letters (20/32 to 20/320 Snellen equivalent). Patients were required to have persistent DME, which was defined as a central subfield thickness (CST) of greater than 340 mm measured by spectral domain optical coherence tomography (SD-OCT) despite at least 3 anti-VEGF injections within the previous 5 months. The mean changes from baseline to month 7 in VA and CST were assessed as the primary outcomes. Other outcomes included safety outcomes and the proportion of 10-letter and 15-letter gainers from baseline to month 7.
Between January 29, 2014, and October 15, 2014, 50 eyes in 45 patients (mean age of 61 [standard deviation or SD = 10] years) were enrolled in the study, of which 23 eyes were assigned to the bevacizumab group and 27 eyes to the dexamethasone implant group. Most eyes were in patients with type 2 diabetes (20 [87%] eyes in the bevacizumab group and 27 [100%] eyes in the dexamethasone implant group). Nine (39%) eyes were pseudophakic in the bevacizumab group versus 14 (52%) eyes in the dexamethasone implant group; the rest of the eyes were phakic. The mean BCVA was 59 (SD = 13) ETDRS letters in the bevacizumab group and 59 (SD = 12) ETDRS letters in the dexamethasone group.
The bevacizumab group received a 1.25 mg (in 0.05 mL) intravitreal injection of bevacizumab at baseline and every month thereafter, if re-treatment criteria were met. The dexamethasone implant group received a 0.7 mg dexamethasone implant at baseline, month 3, and month 6. In the event that the eye did not meet the re-treatment criteria at month 3, the dexamethasone implant was administered at month 4. In the case where the patient eye did not meet re-treatment criteria at month 6, a sham injection was administered. Re-treatment was administered only if VA was less than 83 letters or if CST was 300 µm or more.
The mean number of previous intravitreal anti-VEGF injections in the bevacizumab group was 15 (SD = 11) and 18 (SD = 12) in the dexamethasone implant group. Eleven eyes in the bevacizumab group and 29 eyes in the dexamethasone implant group had previously received intravitreal triamcinolone injections. The mean number of prior intravitreal triamcinolone injections in the bevacizumab group was 8 (SD = 6) and 9 (SD = 6) in the dexamethasone implant group. Three eyes in each group had previously received a dexamethasone implant.
Most eyes were in patients with type 2 diabetes (20 [87%] eyes in the bevacizumab group and 27 [100%] eyes in the dexamethasone implant group). Nine (39%) eyes were pseudophakic in the bevacizumab group versus 14 (52%) eyes in the dexamethasone implant group; the rest of the eyes were phakic. The mean BCVA was 59 (SD = 13) ETDRS letters in the bevacizumab group and 59 (SD = 12) ETDRS letters in the dexamethasone group.15
Efficacy Results
Visual Acuity
The mean BCVA at month 7 was 64 (SD = 11) ETDRS letters in eyes receiving the dexamethasone implant and 65 (SD = 16) ETDRS letters in eyes receiving bevacizumab. The mean change in BCVA from baseline to month 7 in eyes receiving the dexamethasone implant was 5.8 (SD = 7.6) ETDRS letters and 5.6 (SD = 6.1) ETDRS letters in eyes receiving bevacizumab, with a P value of 0.785 for the between-group comparison. The mean number of eyes considered as 10-letter gainers from baseline to month 7 was 9 (33%) in the dexamethasone implant group and 6 (26%) in the bevacizumab group. The mean number of eyes considered as 15-letter gainers from baseline to month 7 was 4 (15%) in the dexamethasone implant group and 3 (13%) in the bevacizumab group. In both treatment groups, no eyes were considered 10-letter or 15-letter losers. The mean time to a 10-letter gain was 3.5 (SD = 1.9) months in the dexamethasone implant group versus 3.6 (SD = 1.9) months in the bevacizumab group.15
Central Subfield Thickness
CST measurements were missing at 1 visit for 1 eye and at 3 visits for another eye in the bevacizumab group as well as at 1 visit each for 2 eyes in the dexamethasone implant group.
The mean CST at month 7 in eyes receiving dexamethasone implants was 336 (SD = 89) μm compared to 471 (SD = 157) μm in eyes receiving bevacizumab. The mean change in CST decreased by 122 (SD = 120) μm in the dexamethasone implant group compared to a decrease of 13 (SD = 105) μm in eyes receiving bevacizumab (P = 0.001).15
Harms Results
AEs were not systematically reported aside from specific harms, ocular serious adverse events (SAEs), and systemic SAEs. No withdrawals from study treatment due to AEs and no deaths were reported. Two (7%) eyes in the dexamethasone implant group and 3 (13%) eyes in the bevacizumab group had ocular SAEs. One (4%) eye in the dexamethasone group and 4 (17%) eyes in the bevacizumab group were in patients who had serious systemic AEs.
An IOP of greater than 21 mm Hg was reported for at least 1 visit in 14 (52%) eyes of the dexamethasone implant group and in no eyes in the bevacizumab group. A greater proportion of eyes receiving the dexamethasone implant presented with elevated IOP requiring glaucoma drugs to control it (13 [50%] eyes) compared to eyes in the bevacizumab group (1 [5%] eye). No eyes required laser or incisional surgery for glaucoma in either group.15 Cataract progression was reported in 7 (26%) eyes in the dexamethasone implant group and 4 (17%) eyes in the bevacizumab group.15 There were no reports of endophthalmitis in either study group.
Critical Appraisal
Despite randomization, there appeared to be differences between groups in some baseline characteristics; for instance, pseudophakia was more common in the dexamethasone group and type 1 diabetes was more common in the bevacizumab group. Given the relatively small sample sizes in each group, these numerical differences may not be clinically important. Nevertheless, the differences undermine the RCT design of the study and suggest that characteristics of patients that may influence outcomes were not evenly distributed between treatment groups. Additionally, other potential confounders (e.g., baseline diabetes control measured by glycated hemoglobin; hyperlipidemia, which can worsen the retinal exudate) were not reported.
There was no clearly stated hypothesis or adjustment for multiple outcomes and it was likely that the trial was not powered to detect statistically significant differences between the 2 groups. There were no subgroup analyses in pseudophakic eyes. Patient history of cataract at baseline and cataract progression and cataract surgery during the study may have impacted the VA and CST findings because the study enrolled phakic eyes; however, this information was not clearly reported and the potential impact is unknown.
There is a potential for selection bias in favour of the dexamethasone implant given the possibility that patients were poor responders to anti-VEGF therapy based on their treatment history (the mean number of prior anti-VEGF injections was 15 in the bevacizumab group and 18 in the dexamethasone implant group). According to the clinical expert consulted by CADTH, inflammation may have played a greater role in the etiology of DME in the study population compared with patients who have received fewer anti-VEGF injections. However, the influence of treatment history on treatment response in this study (which also included triamcinolone acetonide injections and dexamethasone implants for some patients) remains unclear.
Bevacizumab may not have been the most appropriate anti-VEGF comparator in the RCT given that patients who were enrolled had already received a mean of 15 anti-VEGF injections to 18 anti-VEGF injections before being enrolled in the study. It was unclear whether patients were previously treated with bevacizumab only or switched to other anti-VEGFs. According to the clinical expert consulted by CADTH, patients who show inadequate response after receiving their first anti-VEGF will likely be switched to another anti-VEGF therapy before a corticosteroid such as a dexamethasone implant is considered.
The frequency of administration of dexamethasone differed from the recommended dosage in the Health Canada–approved product monograph. However, it was consistent with the treatment interval of 3 months to 4 months identified as appropriate and aligned with how dexamethasone is used in practice, according to clinical expert input.
Indirect Comparisons
No relevant indirect evidence was included in the sponsor’s submission to CADTH or identified in the literature search conducted by CADTH.
Other Relevant Evidence
Of the remaining 10 studies in the sponsor’s resubmission, 2 were retrospective observational studies with relevant comparisons (Busch et al. [2018]16 and Thomas et al. [2016]17) and were summarized and appraised. The rest of the submitted studies were published observational studies; however, none included a relevant comparison and all had significant limitations. Therefore, they do not adequately address the evidence gaps identified by CDEC. These other studies are briefly summarized in Table 14, along with their main limitations in regard to informing this review.
Description of Studies
Busch et al. (2018)16 was a multicentre, retrospective, case-control study designed to compare the effectiveness of the continued use of anti-VEGF therapy versus switching to a dexamethasone implant on functional and anatomic outcomes in eyes of patients with DME, with inadequate response following 3 initial anti-VEGF injections. Eligible eyes were treatment-naive at presentation and were initially treated with 3 monthly anti-VEGF injections at the loading phase (aflibercept, ranibizumab, or bevacizumab), leading to an inadequate response. Inadequate response was defined as “5 or less letter gain in VA (including vision loss), or reduction of less than 20% of CST on SD-OCT 1 month after the third anti-VEGF injection.”16
Eligible eyes either continued with an anti-VEGF therapy or switched to a dexamethasone implant after a maximum of 1 additional anti-VEGF injection. Patients were also required to have VA and CST measurements at baseline, month 3 (after 3 loading anti-VEGF injections), at either month 6 or month 9, and at month 12. Follow-up lasted 9 months (from month 3 to month 12). The mean changes in VA and CST from month 3 to month 12 were the primary end points examined; the mean changes in standardized area under the curve (AUC) of VA and CST from month 3 to month 12 — the proportion of eyes gaining 10 or more letters and 5 or more letters — were secondary end points. There were 110 eyes in total in 105 patients, of which 72 eyes (n = 67 patients) were treated with anti-VEGF therapy only, and 38 eyes (n = 38 patients) were switched to the dexamethasone implant.
Each eye receiving anti-VEGF therapy only was propensity score–matched to the eyes in the dexamethasone implant group. In total, 38 eyes (in 38 patients) were included in the matched anti-VEGF group, which was compared with the dexamethasone implant group. The mean age of patients in the matched anti-VEGF group versus the dexamethasone implant group at baseline was 61.2 years and 63.1 years, respectively. There were 15 (39.5%) eyes in the matched anti-VEGF group that were pseudophakic compared to 18 (47.7%) eyes in the dexamethasone implant group. The mean VA at month 3 was 0.52 logarithm of the minimum angle of resolution (logMAR) (approximately 55 ETDRS letters to 61 ETDRS letters) in the matched anti-VEGF group and 0.53 logMAR (approximately 55 ETDRS letters to 61 ETDRS letters) in the dexamethasone implant group. The mean CST at month 3 was 444.0 (SD = 118.3) µm in the matched anti-VEGF group and 472.1 (SD = 124.1) µm in the dexamethasone implant group.
Thomas et al. (2016)17 was a retrospective, comparative case series study designed to assess the effectiveness of therapeutic responses of matched contralateral eyes of patients with “recalcitrant” DME to continued anti-VEGF therapy versus dexamethasone implant. Eligible patients had bilateral DME and had previously undergone consistent monthly bilateral intravitreal injections with an anti-VEGF drug (ranibizumab). Patients were considered to have recalcitrant DME “if regular (monthly) anti-VEGF therapy were maintained for at least 3 months, and there was persistent central macular edema (greater than 300 μm) and/or a minimal response to therapy (less than 25% reduction in central macular thickness [CMT]) in both eyes.” Patients received a dexamethasone implant in 1 eye while being maintained on anti-VEGF therapy at regular intervals in the collateral eye. Patients were followed up every 4 weeks to 6 weeks, and the study lasted 3 months. VA, CMT, and IOP were evaluated during every visit.17 The cohort included 11 eyes treated with dexamethasone implants and 11 paired contralateral eyes that continued treatment with ranibizumab in the 3-month study period.
Of the 11 patients enrolled, the mean age was 62 (range = 51 to 84) years. All patients had type 2 diabetes with a mean glycated hemoglobin A1C of 6.51% (range = 5.9% to 7.0%) (most recent measurement). Eyes receiving dexamethasone implants had received a median of 8.0 prior anti-VEGF injections at treatment baseline versus a median of 8.5 anti-VEGF injections in contralateral eyes receiving ranibizumab. Eight eyes receiving the dexamethasone implant and 7 eyes receiving ranibizumab were pseudophakic.
Effectiveness Results
Visual Acuity
In the Busch et al. (2018) study, eyes that switched to dexamethasone implants had a mean VA of 0.41 logMAR (approximately 61 ETDRS letters to 65 ETDRS letters) at month 12 compared to 0.53 logMAR (approximately 55 ETDRS letters to 61 ETDRS letters) in the matched anti-VEGF group. The mean change in VA from month 3 (after 3 or 4 initial doses of anti-VEGF) to month 12 was an increase of 6.1 ETDRS letters in eyes in the dexamethasone implant group compared to a decrease of 0.4 letters in the anti-VEGF matched eyes (P value = 0.004; multivariate analysis).
The mean change in VA from month 3 to month 12 based on the AUC approach was an increase of 15.2 ETDRS letters in eyes in the dexamethasone implant group compared to an increase of 2.4 ETDRS letters in the matched anti-VEGF group (P = 0.008; multivariate analysis).
In the Thomas et al. study (2016), the mean logMAR VA at baseline in eyes receiving dexamethasone implants was 0.415 (approximately 61 ETDRS letters to 65 ETDRS letters) versus 0.394 (approximately 65 ETDRS letters to 70 ETDRS letters) in eyes continuing with ranibizumab. The mean logMAR VA improved in both groups at month 3 and was 0.261 (approximately 70 ETDRS letters to 76 ETDRS letters) in the dexamethasone implant group and 0.269 (approximately 70 ETDRS letters to 76 ETDRS letters) in eyes continuing with ranibizumab. The difference between the groups was not statistically significant.
Central Subfield Thickness
In the Busch et al. (2018) study, the mean CST at month 12 was 380.3 µm in the dexamethasone implant group compared to 462.5 µm in the matched anti-VEGF group. The mean change in CST from month 3 to month 12 was a decrease of 92.8 µm in eyes receiving dexamethasone implants and an increase of 18.3 µm in the matched group of anti-VEGF eyes.
Central Macular Thickness
The mean CMT from baseline to month 3 also improved in both treatment groups, with a larger decrease in the dexamethasone group (net decrease of 105.8 µm) than in the ranibizumab group (net decrease of 47.9 µm). The mean CMT at month 3 in eyes receiving dexamethasone implants was 355.6 (SD = 110.2) µm compared to 373.2 (SD = 142.6) µm in eyes receiving ranibizumab, but the difference at month 3 was not statistically different.
Harms Results
The Busch et al. (2018)16 study did not present any safety outcomes. No infectious endophthalmitis, vitreous hemorrhage, retinal detachment, or lens disruption or subluxation were reported for either treatment group during the period of the Thomas et al. (2016)17 study. Two eyes receiving dexamethasone reportedly had an IOP of greater than 30 mm Hg during the study, which did not require IOP-lowering medications, and they returned to normal levels at the end of the study.
Critical Appraisal
Several limitations were identified in both studies, which impacts the interpretation of the findings and their generalizability to patients with DME who are pseudophakic and have had an inadequate response to prior anti-VEGF therapy.
It was unclear whether each study site in the Busch et al. (2018) study used standardized methods and procedures to collect data, which may introduce variability in measurements across centres. It was not reported in either study whether outcome measurements were validated for quality before study initiation (completeness, correctness); hence, there is a potential risk of information bias and the direction of bias is uncertain.
In the Busch et al. (2018) study, propensity matching procedures were used to ensure that the 2 groups investigated were comparable for various baseline prognostic factors and potential confounders. Differences in the matched characteristics were assessed using univariate logistic regression (an approach that is not recommended because P values comparing the baseline factors between the treatment groups are influenced by sample size). However, the rationale behind the matching factors used was not provided; it was not clear whether the groups were adequately matched, as few details were provided regarding the balance diagnostics to determine the quality of the matching, and the distribution of these factors was not reported. The Thomas et al. (2016) study included contralateral eyes, which may have reduced variability in some confounders and other measurements. Although key potential confounders important for patients with DME were assessed at baseline and included in the study, there remains a potential risk of confounding bias for other confounders (e.g., background care, concomitant medications), which may have impacted the findings. According to the clinical expert consulted by CADTH, key factors such as type of diabetes, diabetes control, and baseline cataract status (especially because the population was a mix of phakic and pseudophakic eyes) should have been considered.
Treatment exposure (number of injections) was reported in the Busch et al. (2018) study, but it was unclear whether patients who completed the initial anti-VEGF dosing period continued with the same drug afterward or had been allowed to switch to another anti-VEGF. If patients continued receiving the same anti-VEGF that they had an inadequate response to in the initial phase, then this may bias results in favour of the dexamethasone implant. Additional treatments administered to patients (including ocular hypertensives) were reported in the Busch et al. (2018) study. Within the reported data, there appeared to be imbalances in panretinal photocoagulation and cataract surgery during the study period, which is concerning as these treatments are potential confounders in terms of efficacy. It is also unknown whether these imbalances point to underlying differences between the 2 groups. The Thomas et al. (2016) study did not present information on concomitant treatments.
Health-related quality of life (HRQoL) and other important outcomes identified in the CADTH protocol were not reported in either study. The effectiveness of the dexamethasone implant on HRQoL and other outcomes on patients in both study populations is uncertain.
It was unclear what treatment strategies (i.e., doses and treatment intervals) were used in the studies and whether they varied across centres in the Busch et al. (2018) study. This made it challenging to assess the generalizability of the interventions, particularly in the anti-VEGF groups.
Both studies enrolled a mix of phakic and pseudophakic patients, whereas the Health Canada indication only includes pseudophakic patients. The sample sizes were limited and there were no analyses by lens status; thus, the generalizability of the findings to patients with DME who are pseudophakic is uncertain. The studies did not report some important patient characteristics (e.g., type of diabetes, baseline hemoglobin A1C, medications to control glucose levels) and, therefore, it could not be fully determined how generalizable the study population was to populations seen in clinical practice.
The duration of the Thomas et al. study (2016) was considered relatively short by the clinical expert consulted and may not have been appropriate to evaluate the long-term effectiveness and safety of the dexamethasone implant on patient eyes with DME.
Conclusions
The results of 1 RCT and 2 retrospective studies in patients with DME who had experienced inadequate treatment response with 3 or more injections of anti-VEGF therapy suggested that dexamethasone implants administered every 3 months to 4 months was associated with a modest clinical benefit in VA and CST, with the observed changes in VA close to the minimum change considered clinically meaningful by the clinical expert consulted by CADTH. However, there is uncertainty in the magnitude of the clinical benefit due to several limitations of the studies, which included relatively small sample sizes leading to imprecision in the estimates as well as issues with generalizability related to lens status and treatment history in the studied patients and choice of anti-VEGF therapy. Although all 3 studies provided a comparison with an active treatment (anti-VEGF therapy), the comparative efficacy of dexamethasone implants versus anti-VEGF therapies is uncertain due to the aforementioned issues, in addition to observed imbalances in baseline characteristics and sparse reporting of important confounders and effect modifiers. Therefore, it is not possible to conclude based on the studies that a dexamethasone implant is superior in efficacy or effectiveness to any anti-VEGF therapy in patients with DME who are pseudophakic and have had an inadequate response to prior anti-VEGF therapy. The comparative efficacy of dexamethasone implants versus triamcinolone acetonide, a particularly relevant comparator due its use in the post–anti-VEGF setting, remains unknown as no relevant evidence was identified comparing the 2 interventions. Harms outcomes were not comprehensively assessed in any of the studies, but the reported results were consistent with the known safety profile of dexamethasone implants, which includes the risk of IOP elevation and the need for medications to control IOP.
Introduction
Disease Background
DME is a vision-related, microvascular complication of diabetes mellitus (type 1 and type 2) commonly reported in adults of working age.2 It is characterized by multifactorial pathophysiology,2 which is reportedly mediated by angiogenic VEGF and inflammatory pathways.3-6 DME manifests slowly as progressive vision loss of varying degrees, primarily dependent on the severity, duration, and location of intraretinal fluid, among other factors.3,9 Initially, patients experience damage to retinal blood vessels from chronic hyperglycemia, leading to DR.2 Continuous damage to blood vessels due to elevated blood glucose levels causes extracellular fluid accumulation in the retina (macular edema) and swelling, which leads to DME, vision loss, visual disability, or blindness (legal) when left untreated.10-12 Common signs and symptoms of DME include blurred vision, retinal hemorrhages, retinal detachment, colours appearing washed out or faded, changes in contrast sensitivity, impaired colour vision, gaps in vision (scotomas), and potential permanent vision loss.10-12 Vision loss is associated with significant morbidity, including increased falls, hip fracture, and mortality.18 Progressive visual impairment in patients typically results in significant decrements in daily functioning and quality of life, and indirect costs due to lost productivity are high if left untreated.19-21
Estimates in Canada in 2022 show that more than 4 million patients were diagnosed with type 1 and type 2 diabetes.7 In the US, findings reported by the Eye Diseases Prevalence Research Group revealed that 40.3% of adults with diabetes have DR, of which 8.2% was considered sight-threatening retinopathy.22 The Eye Diseases Prevalence Research Group also reported that approximately 11% of patients with type 1 diabetes developed macular edema, while 15% of patients with type 2 diabetes receiving insulin therapy and 4% of patients being treated with antihyperglycemic therapies developed macular edema.23 A retrospective study conducted in Canada in 2012 assessing patient records from the southwestern Ontario database estimated the prevalence of DME in adults with diabetes to be 15.7% and the prevalence of vision loss due to DME to be 2.56%.8 This study revealed that more than 50% of patients with DME experiencing vision loss were older than 60 years and more than 22% of patients with DME experiencing vision loss were Indigenous Peoples.8 Another study showed that Indigenous populations in Canada are disproportionally affected by diabetes,24 with higher prevalence rates of DR compared to the general population.25,26 However, there is limited accurate data reporting the proportion of patients with vision loss in this population.24
Standards of Therapy
Current therapies for DME in Canada include nonpharmacologic interventions (laser therapy and vitrectomy) and pharmacologic interventions (intravitreal anti-VEGF drugs and intravitreal steroids). Health Canada–approved anti-VEGF drugs for DME treatment include ranibizumab and aflibercept, while approved intravitreal corticosteroids include dexamethasone. Bevacizumab, an anti-VEGF drug, and triamcinolone, a corticosteroid, do not have Health Canada–approved indications for the treatment of DME, but these are used in clinical practice and reimbursed (in only certain jurisdictions for bevacizumab). At the time of writing this review report, 2 new anti-VEGFs were being reviewed in parallel by Health Canada and CADTH for the treatment of DME: faricimab and brolucizumab.
Macular laser photocoagulation (including focal, grid, or panretinal) therapy for DME was the standard of care for more than 25 years before the introduction of anti-VEGF drugs and is still widely used either alone or in combination with anti-VEGF treatment.27 Laser therapy has been shown to slow and/or stabilize vision loss, but has been minimally effective in restoring vision.28 Laser therapy also has the disadvantage of causing permanent destruction of retinal tissue during treatment.29-31
VEGF has been implicated in the pathobiology of DME, given it is a promoter of vascular permeability.4-6 Clinical studies have demonstrated the efficacy and safety for monthly or bimonthly anti-VEGF injections for the treatment of patients with DME.32-35 The results from these trials demonstrated that treatment with anti-VEGF drugs improved visual and anatomic outcomes compared with laser photocoagulation, and avoided the ocular side effects associated with laser treatment. Canadian evidence-based guidelines and clinical treatment algorithms recommend anti-VEGF injections as therapy (alone or in conjunction with focal laser therapy) for most patients with clinically significant DME involving central macular thickening. Cases without central macular thickening are recommended to receive focal laser, while eyes with vitreomacular traction and macular edema are recommended as candidates for vitrectomy.24
The goals in treating patients with DME are to resolve macular edema and to improve vision, while minimizing treatment-related complications. According to the clinical expert consulted by CADTH for this review, the successful treatment of DME will reduce the severity of symptoms, improve HRQoL, increase ability to maintain employment for the working population, increase ability to maintain independence, and reduce burden on caregivers and society. Although anti-VEGF therapies are widely accepted as the standard of care for DME, they are also associated with an increased risk of cerebrovascular and cardiovascular events such as thromboembolic events;36 therefore, they may not be appropriate in all patients with DME, especially in patients with prior stroke or other cardiovascular comorbidities. Some patients have an inadequate response to anti-VEGF treatment, although the frequency of suboptimal response is unclear. There is limited evidence of the benefit and risk of continuous anti-VEGF injections among patients who did not respond well to prior anti-VEGF therapy.37
Intravitreal corticosteroids, such as dexamethasone and triamcinolone, may be considered in patients who do not respond well to anti-VEGF treatment, especially for patients who have artificial lens implants (i.e., pseudophakic) because of the increased risk of cataract formation with corticosteroid treatment. In Canada, intravitreal dexamethasone implants are indicated for use in patients with DME who are pseudophakic. Focal laser, vitrectomy, or grid therapy are nonpharmacologic treatment options available in later line settings, according to the clinician group input and the clinical expert consulted.
Drug
Dexamethasone (Ozurdex) 0.7 mg biodegradable intravitreal implant is a sustained-release, glucocorticoid receptor agonist. The mechanism of action in ocular inflammatory disease is suggested to be due to dexamethasone’s potent antiinflammatory activity; however, the mechanism of action in the treatment of posterior segment diseases of the eye, such as DME, is not completely understood. Dexamethasone, in addition to its antiinflammatory effects, is reported to inhibit the expression of VEGF.1
Dexamethasone is administered using the Dexamethasone Posterior Segment Drug Delivery System. This is a sterile, single-use system intended to deliver 1 implant into the vitreous cavity and was designed to prolong the duration of the dexamethasone effect in the eye. Additional key characteristics of a dexamethasone implant are presented in Table 2.1 Reinjection of the dexamethasone 0.7 mg implant for DME is recommended when macular edema persists after the first dose. The product monograph notes that there is “very limited information on repeat dosing intervals less than 6 months.”1 The product monograph highlights evidence from a 2-year observational study that “the use of more than two consecutive administrations is associated with increases in some adverse reactions; therefore, no more than two consecutive dexamethasone injections should be used, and an interval of approximately 6 months should be allowed between the two injections.”1 However, clinical expert input given to CADTH noted that in practice, ophthalmologists readminister the dexamethasone implant approximately every 3 months to 4 months and that treatment discontinuation is based on clinical considerations other than the maximum of 2 consecutive dexamethasone implants recommended in the product monograph. According to the expert input, dexamethasone is used primarily in patients who have not responded to 1 or more treatment courses with anti-VEGFs, and that — in their opinion — the reduced interval for repeat dosing leads to improved vision and anatomic outcomes over waiting until 6 months.
The dexamethasone implant received approval from Health Canada, with a Notice of Compliance granted on April 16 2015, for the treatment of adult patients with DME who are pseudophakic. The sponsor’s reimbursement population differs from the Health Canada–approved indication and specifies patients with DME who are pseudophakic and have had an inadequate response to prior anti-VEGF therapies.
Table 2: Key Characteristics of Dexamethasone, Triamcinolone Acetonide, Aflibercept, Ranibizumab, and Bevacizumab
Characteristic | Dexamethasone1 | Triamcinolone acetonide38 | Aflibercept39 | Ranibizumab40 | Bevacizumab41,a |
|---|---|---|---|---|---|
Mechanism of action | Corticosteroid with antiinflammatory activity; possible inhibition of VEGF The exact mechanism of action in DME is unclear | Corticosteroid with antiinflammatory action The exact mechanism of action in DME is unclear. | VEGF inhibitor (soluble decoy receptor, targets VEGFA and PIGF) | VEGF inhibitor (mAb, targets VEGFA isoforms) | VEGF inhibitor (mAb, targets VEGF) |
Indicationb | For the treatment of patients with DME who are pseudophakic | No approved indication for DME (off-label) | For the treatment of DME | For the treatment of DME | No approved indication for DME (off-label) |
Route of administration | IVT implant injection | IVT injection | IVT injection | IVT injection | IVT injection |
Recommended dosage | 0.7 mg implant (single use) per eye as needed Reinjection is recommended when there is persisting macular edema after the initial injection. A maximum of 2 consecutive injections with an interval of approximately 6 months between the 2 injections is recommended. | 4 mg (in 0.1 mL)42 | 2 mg once every 4 weeks for 5 doses, then 1 dose every 8 weeks After first year, may extend the interval by up to 2-week increments (maximum of 4 months between injections) based upon disease activity | 0.5 mg once every 4 weeks until maximum VA is achieved and stable for 3 months Thereafter, monitor monthly, resume monthly injections if VA lost | 1.25 mg once every 4 weeks for approximately 6 loading doses, after which interval may be extended based on disease activity |
Serious adverse effects or safety issues | Endophthalmitis, eye inflammation, eye infections, retinal detachment, increased IOP, ATE,c dislocated implants, glaucoma, damage to optic nerve, defects in VA and visual field, necrotizing retinitis, conjunctival hemorrhage, vitreous hemorrhage Cataract in phakic eyes Dislocated implant | Subcapsular cataracts or glaucoma with possible damage to the optic nerve Cataract in phakic eyes | IVT injection-related reactions Transient increase in IOP ATEc | IVT injection-related reactions Transient increase in IOP ATEc | IVT injection-related reactions Transient increase in IOP ATEc |
ATE = arterial thromboembolic event; DME = diabetic macular edema; IVT = intravitreal; IOP = intraocular pressure; mAb = monoclonal antibody; PIGF = placental growth factor; VA = visual acuity; VEGF = vascular endothelial growth factor.
aBevacizumab is used off-label in the treatment of DME.
bHealth Canada–approved indication.
cATE includes nonfatal stroke, nonfatal myocardial infarction, and vascular death.
Submission History
The dexamethasone implant was previously reviewed by CADTH for the treatment of adult patients with DME who are pseudophakic, but received a recommendation not to reimburse from CDEC on October 24, 2018.13 CDEC identified several gaps in the evidence submitted by the sponsor, which included the pivotal MEAD-010 and MEAD-011 trials. Key gaps in evidence highlighted in the final recommendation of October 2018 include the following.
There was no high-quality direct evidence identified comparing the dexamethasone implant with other active treatments used in Canada for the treatment of adult patients with DME who are pseudophakic (e.g., laser therapy, intravitreal steroid, anti-VEGF therapies). The 2 phase III, sham-controlled RCTs identified in the systematic review (the MEAD-010 trial and MEAD-011 trial) were designed to compare dexamethasone implants with the sham treatment.
Compared with sham, the mean change from baseline in BCVA in the prespecified subgroup of patients with DME who were pseudophakic did not exceed a 10-letter improvement (5.9 letters and 3.6 letters in the MEAD-010 and MEAD-011 trials, respectively). As well, between-treatment differences in the proportion of patients achieving an improvement of 15 or more letters favouring dexamethasone were modest: 18.1% (95% confidence interval [CI], 0.8 to 35.4) and 6.0% (95% CI, –5.7 to 17.8) in the MEAD-010 and MEAD-011 trials, respectively. Further, the lack of stratification by lens status and failure to control for multiplicity resulted in uncertainty regarding the magnitude of benefit.
Between 9.1% and 16.0% of patients in the subgroup of pseudophakic patients included in the MEAD-010 and MEAD-011 trials, respectively, had prior experience with anti-VEGF therapy. However, the responses of these patients to anti-VEGF treatment (i.e., whether they had suboptimal responses or simply had been treated previously) is unknown. Therefore, there are insufficient data to assess the safety and efficacy of dexamethasone in patients who would use dexamethasone implants as second-line therapy (e.g., those who had had an inadequate response to or did not tolerate prior anti-VEGF therapy).
The sponsor has provided a resubmission to CADTH for a dexamethasone implant for the treatment of patients with DME who are pseudophakic and have inadequate response to prior anti-VEGF therapies. The sponsor’s resubmission indicated there is a lack of publicly funded treatments to address the inflammatory component of DME for patients experiencing inadequate response to first-line anti-VEGFs and that a dexamethasone implant may fill an unmet need for patients. New evidence (1 RCT and 10 observational studies) evaluating the use of a dexamethasone intravitreal implant in patients with DME, which was not available during the initial submission to CADTH in 2017, was identified and submitted by the sponsor for this resubmission.
The dexamethasone implant received a recommendation in 2016 from Institut national d’excellence en santé et en services sociaux (INESSS) to reimburse for the treatment of DME in pseudophakic patients when treatment with an anti-VEGF is not appropriate, and was added to the list of drugs under Régie de l'assurance maladie du Québec.43 The clinical rationale for the recommendation was based on the drug’s therapeutic value demonstrated in the subgroup of patients who were pseudophakic in the MEAD-010 and MEAD-011 studies, although INESSS noted the treatment effect was modest. INESSS also noted that the magnitude of the treatment effect was smaller compared with anti-VEGFs, which remain the treatment of choice in those with DME. However, INESSS concluded that the benefits observed with a dexamethasone implant may fill unmet needs in patients for whom anti-VEGF therapy is not appropriate. INESSS’s recommendation stipulated a condition for a reduction in the price of the dexamethasone implant to achieve cost-effectiveness in the subpopulation identified.43
Stakeholder Perspectives
Patient Group Input
This section was prepared by CADTH staff based on the input provided by patient groups. The full original patient input received by CADTH has been included in the stakeholder section at the end of this report.
CADTH received a joint patient group submission from 5 organizations: FBC, CCB, CNIB, VLRC, and DC. FBC’s goal is to understand why vision loss occurs, how it can be slowed, and how sight can be restored. CCB is a membership-based not-for-profit organization that brings together Canadians who are living with vision loss — those who are blind, deafblind, and partially sighted — to promote a sense of purpose and self-esteem along with enabling the efforts of each member to achieve an enhanced quality of life. CNIB is a nonprofit organization that delivers programs and advocates to empower people impacted by blindness and remove barriers to inclusion. VLRC is a health services organization that provides training to enable people who are blind or partially sighted to develop or restore key daily living skills, helping enhance their independence, safety, and mobility. DC is a national health charity representing millions of Canadians affected by diabetes. DC’s mission is to provide education and services, advocate on behalf of people living with diabetes, and support research and translate it into practical applications. Data were collected through an online survey made available to Canadians living with DR or DME in January 2020 and shared across networks associated with the submitting organizations. A total of 67 patients in Canada responded to the survey. In April 2020, CCB conducted a separate survey of 572 respondents on the impact of the COVID-19 pandemic on Canadians who are blind, deafblind, or partially sighted.
Overall, respondents indicated that both DR and DME had substantial and life-altering impacts, including a negative impact on the ability to perform daily activities such as reading, using a phone, and driving, anxiety over potential worsening of the condition, and reliance on others. In addition, the CCB COVID-19 study showed that fear, anxiety, loneliness, and other psychosocial impacts were intensified for patients with age-related macular edema and DR during the pandemic. Respondents of the joint survey indicated that they had experience with a variety of DR or DME treatments, including anti-VEGF therapies and Ozurdex, and most indicated that intravitreal treatment prevented further loss of vision. When asked about the most difficult part of eye injection appointments, travel and waiting time were central concerns. The submission highlighted that the low number of respondents (4.5%) who received injections less than 3 months ago is disconcerting, potentially indicating low adherence to injections. Respondents indicated the following reasons for cancelling or delaying appointments: being too busy to attend the appointment, not feeling well, being unable to find someone to take them to the appointment, and being “scared to receive the injection.”
Though the survey did not ask patients for their views on improving their experiences and outcomes, the submission highlighted that any treatment that reduces the physical, psychological, and logistical strain on patients would be preferred. A treatment that is less invasive, or 1 that is similarly invasive but that is administered less frequently, would be helpful in reducing this strain.
Clinician Input
Input From Clinical Experts Consulted by CADTH
All CADTH review teams include at least 1 clinical specialist with expertise regarding the diagnosis and management of the condition for which the drug is indicated. Clinical experts are a critical part of the review team and are involved in all phases of the review process (e.g., providing guidance on the development of the review protocol, assisting in the critical appraisal of clinical evidence, interpreting the clinical relevance of the results, providing guidance on the potential place in therapy). The following input was provided by 1 clinical specialist with expertise in the diagnosis and management of DME.
Unmet Needs
According to the clinical expert, the goal in treating patients with DME is to resolve macular edema and to improve vision while minimizing treatment-related complications. The expert highlighted that anti-VEGFs are the mainstay therapies in the first-line setting for patients with centre-involved DME. Steroids (dexamethasone implants or triamcinolone acetonide) are preferably administered to pseudophakic patients who have shown inadequate response (or not improved) after treatment with anti-VEGFs, to patients with a contraindication to an anti-VEGF (recent stroke, MI, or pregnancy), or to patients who cannot afford anti-VEGFs due to the treatment costs.
The clinical expert consulted noted that although anti-VEGFs have shown effectiveness in patients with DME, up to 40% of patients respond inadequately to repeated injections with anti-VEGFs; thus, there is a need for other treatment options for these patients in current practice. In addition, the expert highlighted that treatment with anti-VEGFs requires monthly administration of up to 5 doses, which may be inconvenient for some patients. The expert also noted that anti-VEGFs are associated with high costs, concerns with potential complications, and the possibility of no improvement in vision despite treatment. The expert indicated that patients often remark upon the inconvenience of taking time off work to receive monthly treatments and the discomfort associated with the injection. The expert pointed out that although there are newer anti-VEGF therapies (brolucizumab and faricimab) with longer durability of up to 3 months, there are some risk concerns associated with their use (e.g., increased incidence of intraocular inflammation, retinal vasculitis associated with the use of brolucizumab). Although both triamcinolone acetonide and dexamethasone intravitreal implants can cause glaucoma and cataract formation, these side effects are more frequently reported with the use of triamcinolone acetonide.
Place in Therapy
The clinical expert highlighted that a dexamethasone implant is typically administered after anti-VEGF therapies have already been used, owing to the potential for cataract formation in phakic eyes, but a dexamethasone implant can be used as a first-line treatment in the event that anti-VEGF use in the patient is inappropriate (such as with recent stroke, MI, or pregnancy), or in patients who demonstrate intolerance to anti-VEGF therapies. The expert noted that the dexamethasone implant mechanism of action is different from that of anti-VEGFs as it acts on the inflammatory pathway to reduce inflammation, which is associated with DME. The expert noted that there is a potential for the use of dexamethasone in combination with anti-VEGFs for treating some nonresponders in practice.
Patient Population
The clinical expert consulted highlighted that patients most likely to respond to treatment with a dexamethasone implant are patients with chronic DME because they are likely to have inflammation as part of the mechanism of DME. The expert noted that patients with centre-involved DME and decreased VA have the greatest need for treatment with a dexamethasone implant (Ozurdex).
According to the expert, patients with DME are identified following clinical assessment. The expert highlighted that this patient group is possibly underdiagnosed in clinical practice.
Assessing Response to Treatment
The clinical expert considered CRT measured by OCT and VA to be important outcomes used in clinical practice; this also aligns with the outcomes identified in the sponsor-submitted studies. In the opinion of the clinical expert, a clinically meaningful response to treatment with dexamethasone will include a gain of 5 letters of Snellen acuity, or a reduction of CRT of 50 µm or more as measured by OCT. As noted by the expert, this assessment is less vigorous compared to some outcomes used in clinical trials (e.g., at least a 15-letter gain or 100 µm change of CRT on OCT). The expert noted that this assessment varies across different physicians as clinicians do not generally use clinical trial outcome definitions for real-life patient management.
Discontinuing Treatment
The expert highlighted that AEs such as glaucoma, infection, migration of the implant to the anterior chamber, and lack of improvement in treatment are factors that will be considered when deciding to discontinue treatment with dexamethasone implants.
Prescribing Conditions
The expert consulted noted that a dexamethasone implant can be administered in a community setting, hospital (outpatient clinic), or specialty clinic. An ophthalmologist familiar with the diagnosis and treatment of patients with DME will be required to diagnose, treat, and monitor patients who receive dexamethasone implants.
Clinician Group Input
This section was prepared by CADTH staff based on the input provided by clinician groups. The full clinician group inputs received by CADTH have been included in the stakeholder section at the end of this report.
CADTH received 4 clinician group submissions for this review from the following organizations: ECRS (12 clinicians), the Retina Society of Alberta (8 clinicians), CRS (4 clinicians), and retina specialists from Western Canada (7 clinicians). ECRS is a group of independent retina specialists practising in various locations throughout Eastern Canada. The Retina Society of Alberta is a retina medical and surgical retina subspecialty practice of 8 physicians based in Edmonton who provide retina-related care to the northern half of Alberta. The CRS represents those ophthalmologists in Canada whose primary area of patient care is surgical and/or medical vitreoretinal disease. Retina specialists from Western Canada is a group of retina specialists practising in Western Canada (Manitoba, Saskatchewan, Alberta, and British Columbia). The group clinician input was largely in agreement with the input received from the clinical expert consulted by CADTH.
The clinician groups and the clinical expert consulted generally agreed on the main goals of treatment, the unmet needs of patients, and prescribing conditions. The goals in treating patients with DME are to resolve macular edema and improve vision while minimizing treatment-related complications. In addition to these treatment goals, the clinician groups noted longer duration of action as an important treatment goal. The clinician groups indicated that patients who do not respond to anti-VEGF therapy can be identified after receiving 5 doses to 6 doses or at least 3 months of therapy. According to the ECRS, retina specialists from Western Canada, and CRS, patients may be switched to another anti-VEGF therapy after inadequate response with initial anti-VEGF therapy. Following anti-VEGF therapy failure (or if the duration of response is shorter than 4 weeks, according to the Retina Society of Alberta), dexamethasone implants and triamcinolone are among the treatment options. In addition, the clinician groups mentioned that dexamethasone was considered particularly well-suited for pseudophakic patients and those with vitrectomized eyes due to the predictable and lower risk of elevated IOP and a longer duration of action (most often about 4 months) compared with triamcinolone.
Clinician groups specified that patients with centre-involving DME who are resistant to first-line anti-VEGF therapy after at least 3 monthly injections would be considered as best suited for the dexamethasone treatment, and also indicated that patients with DME least suited for dexamethasone treatment would include those who have a tractional component (epiretinal membrane or vitreomacular traction), severe glaucoma, a known steroid response with IOP elevation, signs of chronic DME, aphakic eyes, or a compromised posterior capsule.
Clinician groups indicated that a clinically meaningful response to dexamethasone treatment would include the resolution of DME (a 30% to 50% reduction in excess central foveal thickness) measured by OCT, VA improvement (20/50 Snellen equivalent or better), decreased frequency of treatment, and/or regression of a diabetic severity score. The ECRS submission also mentioned that patients should be assessed monthly when treatment is initiated and then every 3 months to monitor therapy outcomes and response as well as individual durability of the dexamethasone implant. The clinician groups indicated that chronic DME, potential side effects (elevated IOP, infection or inflammatory response, migration of the implant to the anterior chamber), and a lack of clinical improvement (retina thickness and fluid that does not improve) would be considered as discontinuation factors.
The clinician groups and the clinical expert consulted agreed that the duration of action for the dexamethasone injections is approximately 3 months to 4 months.
Drug Program Input
The drug programs provide input on each drug being reviewed through CADTH’s reimbursement review processes by identifying issues that may impact their ability to implement a recommendation. The implementation questions and corresponding responses from the clinical experts consulted by CADTH are summarized in Table 3.
Table 3: Summary of Drug Plan Input and Clinical Expert Response
Drug program implementation questions | Clinical expert response |
|---|---|
Considerations for initiation of therapy | |
The reimbursement request specifies that inadequate response to prior anti-VEGF therapy is needed.
| According to the clinical expert, inadequate response to prior anti-VEGF therapy is usually defined as lack of treatment response:
The requested population should not include the inability to access anti-VEGF therapy or nonadherence to therapy; these can be the reasons why patients may consider another treatment. |
Eligibility for re-treatment:
| According to the clinical expert, the implant can be readministered every 3 months to 4 months in practice. The expert stated that the treatment effect starts to wear off after 3 months to 4 months, with the macular edema returning. |
Considerations for discontinuation of therapy | |
There is a need for a clear definition of refractory disease. What parameters would be used? | The clinical expert stated that if after repeated treatment, there is no reduction in CST and no change in VA, the disease may be considered refractory. As long as there are continuing changes in CST or VA, even if they are small amounts, the disease is not considered as refractory and treatment should continue. |
Should therapy end after a certain number of implants or after 1 year, or is there a limit to how long it can be continued if needed? | According to the clinical expert, the maximum number of implants per year should be 4, assuming treatment is repeated every 3 months. Realistically, this will likely mean 3 treatments per year. As long as the patient is responding, treatment should not stop. |
Considerations for prescribing of therapy | |
How many implants per eye should be funded? Should there be a duration of the treatment? | According to the clinical expert, 3 implants per eye per year should be funded as the duration of treatment is 3 months to 4 months. The treatment duration depends on the patient’s needs. |
Could dexamethasone implants be used in conjunction with other treatments such as anti-VEGF? | The clinical expert indicated that combined dexamethasone implant and anti-VEGF treatment is usually not necessary. |
There is limited access to specialists in some regions. | For consideration by CDEC. |
The drug needs to be administered by a qualified ophthalmologist experienced in intravitreal injections. | For consideration by CDEC. |
Care provision issues | |
The drug must be administered by a qualified ophthalmologist experienced in intravitreal injections. This may not be readily available for all patients. | For consideration by CDEC. |
Regular monitoring for IOP changes is needed. | For consideration by CDEC. |
System and economic issues | |
Eligible patients may need to travel to specialists. | For consideration by CDEC. |
Anti-VEGF drugs all have varying pricing between jurisdictions based on negotiations. | For consideration by CDEC. |
This drug is covered by RAMQ, which may be a possible issue for federal plans. | For consideration by CDEC. |
CDEC = CADTH Canadian Drug Expert Committee; CST = central subfield thickness; IOP = intraocular pressure; OCT = optical coherence tomography; RAMQ = Régie de l'assurance maladie du Québec; VA = visual acuity; VEGF = vascular endothelial growth factor.
Clinical Evidence Selection
The clinical evidence included in the review of dexamethasone (Ozurdex) is presented in 3 sections. The first section, the systematic review, includes pivotal studies provided in the sponsor’s submission to CADTH as well as those studies that were selected according to an a priori protocol. The second section may include indirect evidence selected from the literature that met the selection criteria specified in the review. The third section may include sponsor-submitted, long-term extension studies and additional relevant studies that were considered to address important gaps in the evidence included in the systematic review.
Systematic Review (Pivotal and Protocol Selected Studies)
Objectives
To perform a systematic review of the beneficial and harmful effects of a 0.7 mg dexamethasone intravitreal implant for the treatment of adult patients with DME who are pseudophakic and have had an inadequate response to prior anti-VEGF therapy.
Studies selected for inclusion in the systematic review included pivotal studies provided in the sponsor’s submission to CADTH, as well as those meeting the selection criteria presented in Table 4. Outcomes included in the CADTH review protocol reflect outcomes considered to be important to patients, clinicians, and drug plans.
Table 4: Inclusion Criteria for the Systematic Review
Criteria | Description |
|---|---|
Patient population | For the treatment of adult patients with DME who are pseudophakic and have had an inadequate response to prior anti-VEGF therapy Subgroups:
|
Intervention | 0.7 mg dexamethasone intravitreal implant |
Comparators |
|
Outcomes | Efficacy outcomes:
Harms outcomes: AEs, SAEs, WDAEs, mortality Notable harms: Endophthalmitis, eye inflammation, eye infections, retinal detachment, increased IOP, ATE, dislocated implants, glaucoma, damage to optic nerve, defects in visual acuity and visual field, necrotizing retinitis, conjunctival hemorrhage, vitreous hemorrhage |
Study design | Published and unpublished phase III and phase IV RCTs |
AE = adverse event; ATE = arterial thromboembolic event; CST = central subfield thickness; CRT = central retina thickness; DME = diabetic macular edema; HRQoL = health-related quality of life; IOP = intraocular pressure; NEI-VFQ-25 = National Eye Institute Visual Functioning Questionnaire–25; RCT = randomized controlled trial; SAE = serious adverse event; VEGF = vascular endothelial growth factor; WDAE = withdrawal due to adverse event.
The literature search for clinical studies was performed by an information specialist using a peer-reviewed search strategy according to the PRESS Peer Review of Electronic Search Strategies checklist.44
Published literature was identified by searching the following bibliographic databases: MEDLINE All (1946–) via Ovid and Embase (1974–) via Ovid. All Ovid searches were run simultaneously as a multifile search. Duplicates were removed using Ovid deduplication for multifile searches, followed by manual deduplication in Endnote. The search strategy consisted of both controlled vocabulary, such as the US National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. The main search concepts were Ozurdex or dexamethasone implants, and DME. Clinical trials registries were searched: the US National Institutes of Health’s ClinicalTrials.gov, WHO’s International Clinical Trials Registry Platform search portal, Health Canada’s Clinical Trials Database, and the European Union Clinical Trials Register.
No filters were applied to limit the retrieval by study type. Retrieval was not limited by publication date or by language. Conference abstracts were excluded from the search results. Refer to Appendix 1 for the detailed search strategies.
The initial search was completed on July 7, 2022. Regular alerts updated the search until the meeting of CDEC on October 24, 2022.
Grey literature (literature that is not commercially published) was identified by searching relevant websites from the Grey Matters: A Practical Tool For Searching Health-Related Grey Literature reference.45 Included in this search were the websites of regulatory agencies (US FDA and European Medicines Agency). Google was used to search for additional internet-based materials. Refer to Appendix 1 for more information on the grey literature search strategy.
Two CADTH clinical reviewers independently selected studies for inclusion in the review based on titles and abstracts, according to the predetermined protocol. Full-text articles of all citations considered potentially relevant by at least 1 reviewer were acquired. Reviewers independently made the final selection of studies to be included in the review, and differences were resolved through discussion.
Findings From the Literature
Three studies were identified for inclusion in the systematic review section (Figure 1). The included studies are summarized in the next section. A list of excluded studies is presented in Appendix 2.
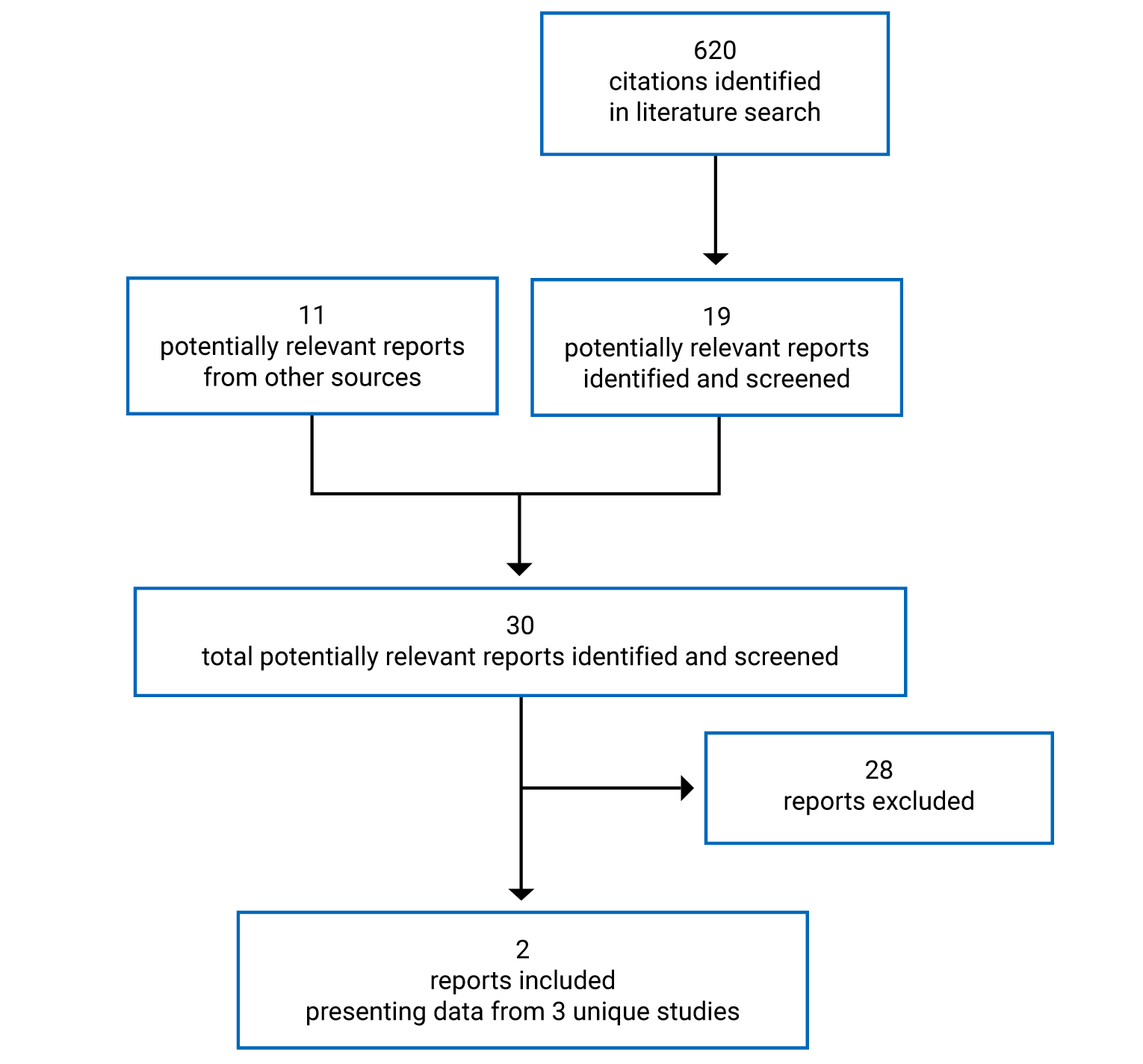
Table 5: Details of the Included Study
Description | Shah et al. (2016)15 |
|---|---|
Designs and populations | |
Study design | Phase III prospective, patient-masked RCT |
Locations | 1 site, US |
Patient enrolment dates | January 29, 2014, through October 15, 2014 |
Randomized (N) | 50 eyes (45 patients):
|
Inclusion criteria |
|
Exclusion criteria |
|
Drugs | |
Intervention | Intravitreal injection of the dexamethasone implant 0.7 mg |
Comparator | Intravitreal injection of bevacizumab 1.25 mg in 0.05 mL |
Duration | |
Treatment period | 7 months |
Outcomes | |
Primary end point |
|
Secondary and exploratory end points | Secondary outcomes:
Safety:
|
Publications | Shah et al. (2016)15 |
BCVA = best corrected visual acuity; CST = central subfield thickness; DME = diabetic macular edema; ETDRS = Early Treatment Diabetic Retinopathy Study; IOP = intraocular pressure; OCT = optical coherence tomography; RCT = randomized controlled trial; VA = visual acuity; VEGF = vascular endothelial growth factor.
Source: Shah et al. (2016).15
Description of Studies
The MEAD-010 and MEAD-011 trials were the pivotal studies for the dexamethasone (0.7 mg) implant for the indication for the treatment of DME. A summary of the evidence reviewed in the original submission to CADTH, which included analyses of the pseudophakic subgroup in the trials, is presented in Appendix 3. For the full details of the clinical review for the original submission, please refer to the CADTH Clinical Review Report for Dexamethasone Implant (Ozurdex).14 As noted in the CADTH recommendation,46 between 9.1% and 16.0% of patients in the subgroup of pseudophakic patients included in the MEAD-010 and MEAD-011 trials had prior experience with anti-VEGF therapy but the responses of these patients to anti-VEGF treatment were unknown. Given the uncertainty regarding response to prior anti-VEGF therapy and the fact that the MEAD trials were not designed or analyzed in a way to determine the efficacy of dexamethasone implants in pseudophakic patients with DME who had had an inadequate response to anti-VEGF treatment, the data from these trials could not be used to inform the present resubmission for a dexamethasone implant.
The study authored by Shah et al. (2016)15 was a prospective, randomized, patient-masked, phase III trial conducted at a single site in the US. This study was the only RCT submitted by the sponsor for the resubmission, and it provides a comparison of dexamethasone implants with an active treatment in patients with prior anti-VEGF treatment. The study was supported by an investigator-initiated trial grant provided by Allergan Inc.
Patients who met the eligibility criteria were randomized to 1 of 2 treatment groups: intravitreal bevacizumab monotherapy or dexamethasone implant monotherapy. Patients whose right eye and left eye both met the eligibility criteria had 1 eye randomized to 1 treatment, with the other eye assigned to the other treatment. The study lasted 7 months, and patients received monthly follow-up.
Between January 29, 2014, and October 15, 2014, 50 eyes in 45 patients were enrolled in the study, of which 23 eyes were assigned to the intravitreal bevacizumab group and 27 eyes to the dexamethasone implant group. There were no OCT data available for 2 eyes in the intravitreal bevacizumab group (at 1 visit for 1 eye and at 3 visits for the other eye) and for 2 eyes in the dexamethasone implant group (at 1 visit for both eyes).
Population
Inclusion and Exclusion Criteria
Eligible patients were adults 18 years and older with type 1 or type 2 diabetes mellitus with BCVA scores between 24 ETDRS letters and 78 ETDRS letters (20/32 to 20/320 Snellen equivalent). Patients were required to have persistent DME, which was defined as a CST of greater than 340 mm measured by SD-OCT despite at least 3 anti-VEGF injections within the previous 5 months.
Patients were excluded if they had had any of the following: an intravitreal anti-VEGF injection 4 weeks before the study, an intravitreal triamcinolone injection 8 weeks before the study, intravitreal dexamethasone 16 weeks before the study, or laser photocoagulation of the retina 16 weeks before the study.
Baseline Characteristics
The mean ages of patients were 61 (SD = 9) years in the bevacizumab group and 65 (SD = 11) years in the dexamethasone implant group. Thirteen (57%) eyes and 12 (44%) eyes were in male patients in the bevacizumab and dexamethasone implant groups, respectively; 10 (44%) eyes and 15 (56%) eyes were in female patients in the bevacizumab and dexamethasone implant groups, respectively. Patients were white (22 [96%] eyes in the bevacizumab group and 24 [89%] eyes in the dexamethasone implant group) or African American (1 [4%] eye in the bevacizumab group and 3 [11%] eyes in the dexamethasone implant group). Most eyes were in patients with type 2 diabetes (20 [87%] eyes in the bevacizumab group and 27 [100%] eyes in the dexamethasone implant group). Nine (39%) eyes were pseudophakic in the bevacizumab group versus 14 (52%) eyes in the dexamethasone implant group; the rest of the eyes were phakic. The mean BCVA was 59 (SD = 13) ETDRS letters in the bevacizumab group and 59 (SD = 12) ETDRS letters in the dexamethasone group. The mean baseline IOP in eyes assigned to the bevacizumab group was 16 (SD = 2) mm Hg and 15 (SD = 2) mm Hg in the dexamethasone implant group. The mean CST was 485 (SD = 122) µm in the bevacizumab group versus 458 (SD = 100) µm in the dexamethasone implant group. The mean total macular volume was 12.0 (SD = 1.9) mm3 in the bevacizumab group versus 11.7 (SD = 1.9) mm3 in the dexamethasone implant group.
Treatment History
Patients had received intravitreal treatments before baseline as follows.
The mean number of previous intravitreal anti-VEGF injections in the bevacizumab group was 15 (SD = 11) and 18 (SD = 12) in the dexamethasone implant group. The mean duration from the last intravitreal anti-VEGF injection was 6 (SD = 6) weeks in the bevacizumab group and 6 (SD = 4) weeks in the dexamethasone implant group.
Eleven eyes in the bevacizumab group and 29 eyes in the dexamethasone implant group had previously received intravitreal triamcinolone injections. The mean number of prior intravitreal triamcinolone injections in the bevacizumab group was 8 (SD = 6) and 9 (SD = 6) in the dexamethasone implant group. The mean duration from the last intravitreal triamcinolone injection was 41 (SD = 19) weeks in the bevacizumab group and 89 (SD = 111) weeks in the dexamethasone implant group.
Three eyes in each group had previously received dexamethasone implants. The mean number of prior dexamethasone implant injections was 2 (SD = 1) in both the bevacizumab group and the dexamethasone implant group. The mean duration from the last intravitreal dexamethasone implant was 85 (SD = 46) weeks in the bevacizumab group and 81 (SD = 8) weeks in the dexamethasone implant group.
Intervention
Eyes assigned to the bevacizumab group received a 1.25 mg (in 0.05 mL) intravitreal injection of bevacizumab (Avastin) at baseline and every month thereafter, if re-treatment criteria were met (described as follows). In the event that a patient did not meet the re-treatment criteria at any of the monthly visits, a sham injection was administered.15
Eyes assigned to the dexamethasone implant group received a 0.7 mg dexamethasone implant at baseline, month 3, and month 6. These eyes received sham injections at month 1, month 2, month 4, and month 5. In the event that the patient did not meet the re-treatment criteria at month 3, a sham injection was administered, and the dexamethasone implant was administered at month 4. In the case where a patient eye did not meet re-treatment criteria at month 6, a sham injection was administered.
Re-treatment was administered only if VA was less than 83 letters or if CST was 300 µm or more. Re-treatment was withheld if VA was 83 letters or more and CST was less than 300 µm. Patients in either group could be withdrawn from the study at the investigator’s discretion if the escape criterion of an increase of CST by 200 µm or more from baseline at any of month 2 through month 6 was met. Permitted and prohibited concomitant medications were not described.
Outcomes
A detailed discussion and critical appraisal of the outcome measures is provided in Appendix 4.
VA Assessed by the ETDRS Letter Score
One of the primary end points was mean change in BCVA from baseline to month 7. VA was also assessed by the following secondary end points: the proportions of eyes with at least a 10-letter gain and at least a 15-letter gain, and the mean time to a 10-letter gain (all assessed using the ETDRS charts).
The ETDRS charts, a modified version of the Snellen chart, are commonly used in clinical research.47 The ETDRS charts present a series of 5 letters of equal difficulty of reading in each row, with standardized spacing between letters and rows — a total of 14 lines (70 letters). Letters range from 58.18 mm to 2.92 mm in height, corresponding to Snellen VA fractions of 20/200 to 20/10, respectively. Letter size increases geometrically and equivalently in every line by a factor of 1.2589 (or 0.1 log unit) moving up the chart. Scores are based on the number of letters correctly read by a patient. The patient reads each letter on each row down the chart and is allowed 1 attempt for each letter. The ETDRS letter score could result in a maximum score of 100.48
Scoring for ETDRS charts is designed to produce a logMAR score suitable for statistical analysis in which individual letters score 0.02 log units.
Central Subfield Thickness
The mean change in CST from baseline to month 7 was a primary end point. Both were measured using OCT, though further details were not provided.
OCT is a noninvasive instrument used to create cross-sectional maps of the retinal structures and to quantify retinal thickness in patients with macular edema.30 OCT machines can differentiate 3 reflecting layers thought to be the interfaces between the vitreous and retina, the inner and outer photoreceptor segments, and the retinal pigment epithelium and choriocapillaris. Ultra high-resolution machines can differentiate a fourth layer. In a previous meta-analysis of the diagnostic test accuracy of OCT-measured foveal thickness for the diagnosis of DME, the pooled estimates of sensitivity and specificity were 0.79 and 0.85, respectively, for a thickness threshold of 250 µm for time domain optical coherence tomography (TD-OCT) and 300 µm for newer SD-OCT.49
Safety Outcomes
Safety measures including cataracts, endophthalmitis, other ocular SAEs, and systemic SAEs were collected during monthly visits throughout the study period.
Statistical Analysis
All efficacy and safety measures were analyzed using the Mann–Whitney U test and Fisher exact t-test.15 There was no information reported regarding control for multiplicity and the statistical significance level was not stated. The end points were analyzed using eyes with available data only, with no imputation for missing data.
The study protocol was not included as part of the publication and there was no mention of a published protocol for the study.
Results
Patient Disposition
No eyes (and hence, no patients) were withdrawn from the study and there was no mention of treatment discontinuations.
Exposure to Study Treatments
In total, 19 (70%) eyes in the dexamethasone implant group met the re-treatment criteria at each scheduled visit and received 3 dexamethasone injections in total. Eight eyes received 2 dexamethasone injections because they did not meet the re-treatment criteria at 1 visit.
In the bevacizumab group, 22 (96%) eyes met the re-treatment criteria at all visits and so received 7 injections of bevacizumab. One eye did not meet the re-treatment criteria at 1 visit and, thus, was treated with 6 injections of bevacizumab.
Efficacy
Only those efficacy outcomes and subgroups identified in the review protocol are reported as follows.
Visual Acuity
The mean BCVA at month 7 was 64 (SD = 11) ETDRS letters in eyes receiving the dexamethasone implant and 65 (SD = 16) ETDRS letters in eyes receiving bevacizumab. The mean change in BCVA from baseline to month 7 in eyes receiving the dexamethasone implant was 5.8 (SD = 7.6) ETDRS letters and 5.6 (SD = 6.1) ETDRS letters in eyes receiving bevacizumab, with a P value of 0.785 for the between-group comparison. The mean number of eyes considered as 10-letter gainers from baseline to month 7 was 9 (33%) in the dexamethasone implant group and 6 (26%) in the bevacizumab group. The mean number of eyes considered as 15-letter gainers from baseline to month 7 was 4 (15%) in the dexamethasone implant group and 3 (13%) in the bevacizumab group. In both treatment groups, no eyes were considered 10-letter or 15-letter losers. The mean time to 10-letter gain was 3.5 (SD = 1.9) months in the dexamethasone implant group versus 3.6 (SD = 1.9) months in the bevacizumab group.15
Central Subfield Thickness
CST measurements were missing at 1 visit for 1 eye and 3 visits for another eye in the bevacizumab group as well as at 1 visit each for 2 eyes in the dexamethasone implant group.
The mean CST at month 7 in eyes receiving dexamethasone implants was 336 (SD = 89) μm compared to 471 (SD = 157) μm in eyes receiving bevacizumab. The mean change in CST decreased by 122 (SD = 120) μm in the dexamethasone implant group compared to a decrease of 13 (SD = 105) μm in eyes receiving bevacizumab (P = 0.001).15
Vision-Related Function
Vision-related function was not reported.
Change in Diabetic Retinopathy Severity
Change in DR severity was not reported.
Health-Related Quality of Life
HRQoL was not reported.
Blindness (Legal)
Blindness (legal) was not reported.
Harms
Only those harms identified in the CADTH review protocol are reported in this section.
Adverse Events
AEs were not systematically reported aside from specific harms, ocular SAEs, and systemic SAEs.
Serious Adverse Events
Two (7%) eyes in the dexamethasone implant group and 3 (13%) eyes in the bevacizumab group had ocular SAEs. One (4%) eye in the dexamethasone group and 4 (17%) eyes in the bevacizumab group were in patients who had systemic SAEs.
Withdrawals Due to Adverse Events
No withdrawals from study treatment due to AEs were reported.
Mortality
No deaths were reported.
Notable Harms
An IOP of greater than 21 mm Hg was reported for at least 1 visit in 14 (52%) eyes of the dexamethasone implant group and none in the bevacizumab group. A greater proportion of eyes receiving dexamethasone implants presented with elevated IOP requiring glaucoma drugs to control it (13 [50%] eyes) compared to eyes in the bevacizumab group (1 [5%] eye). No eyes required laser or incisional surgery for glaucoma in either group.15
Cataract progression was reported in 7 (26%) eyes in the dexamethasone implant group and 4 (17%) eyes in the bevacizumab group.15 There were no reports of endophthalmitis in either study group.
Table 6 presents the summary of safety outcomes in the 2 study groups.
Table 6: Safety Outcomes at Month 7 in the Bevacizumab Versus Dexamethasone Group — Shah et al. (2016)15
— | — |
|---|---|
Note: For complete table contents, please refer to Table 5 in the following article: Shah SU, Harless A, Bleau L, Maturi RK. Prospective randomized subject-masked study of intravitreal bevacizumab monotherapy versus dexamethasone implant monotherapy in the treatment of persistent diabetic macular edema. Retina. 2016;36(10):1986-1996.15 | — |
Critical Appraisal
Internal Validity
Shah et al. (2016)15 is a randomized, patient-masked, phase III trial. Randomization was conducted in a 1:1 ratio using a computer-generated sequence and allocation concealment was achieved by nonstudy personnel. Despite randomization, there appeared to be differences in some baseline characteristics. For instance, the proportion of eyes with pseudophakic lens status was imbalanced between the 2 groups (52% in the dexamethasone group and 39% in the bevacizumab group). Also, the proportion of eyes in patients with type 2 diabetes was 100% in the dexamethasone implant group compared to 87% in the bevacizumab group. Given the relatively small sample sizes in each group, these numerical differences may not be clinically important. Nevertheless, the differences undermine the RCT design of the study and suggest that characteristics of patients that may influence outcomes (e.g., patents with type 1 diabetes experience more severe DME symptoms and are most likely to respond poorly to treatment compared to patients with type 2 diabetes) were not evenly distributed between treatment groups. Additionally, other potential confounders were not reported (e.g., baseline diabetes control measured by hemoglobin A1C, hyperlipidemia, which can worsen the retinal exudate). The analyses of the primary outcomes were not adjusted for baseline CST or other factors. The impacts of these limitations on the outcomes could not be determined.
Patient history of cataracts at baseline and cataract progression and cataract surgery during the study may have also impacted the VA and CST findings because the study enrolled phakic eyes. However, this information (other than the incidence of cataract formation) was not clearly stated in the study and, therefore, the impact of the potential bias is unknown.
There is a potential for selection bias in favour of the dexamethasone implant, given the possibility that patients were poor responders to anti-VEGF therapy based on their treatment history (the mean number of prior anti-VEGF injections was 18 in the dexamethasone implant group and 15 in the bevacizumab group). According to the clinical expert consulted by CADTH, inflammation may have played a greater role in the etiology of DME in the study population compared with patients who have received fewer anti-VEGF injections. However, the influence of treatment history in this study (which also included triamcinolone acetonide injections and dexamethasone implants for some patients) on treatment response remains unclear.
Hypotheses for tests to determine statistical significance were not clearly stated in the study. Although the authors expressed an expectation that the efficacy of dexamethasone could be equivalent to that of bevacizumab, the study appeared to be designed to test for superiority as between-group differences were commonly described as being statistically significant or not. The authors did not describe a 2-sided equivalence margin, which would imply a test for equivalence, or a noninferiority margin for testing noninferiority between the treatments. Therefore, the lack of a clearly stated hypothesis to be tested (not the general-purpose statement of “to compare intravitreal bevacizumab monotherapy with intravitreal dexamethasone delayed delivery system monotherapy for persistent diabetic macular edema”15) makes it difficult to interpret the results of the study. The mean changes in BCVA and CST from baseline to month 7 were primary end points investigated in the trial. The authors did not report a prespecified alpha to determine whether the null hypothesis was rejected or not. It was also unclear whether multiplicity adjustments were implemented to adjust for type I error.
The sample size was relatively small and there were no sample size considerations described to suggest that the study was powered to detect a statistically significant difference between the 2 groups.
It was unclear whether the initial statistical analysis plan was prespecified to follow the intention-to-treat (ITT) population approach, given that the authors did not describe any methods to handle data and they mentioned that data were analyzed as observed. No discontinuations or eyes (patients) withdrawn from the trial were reported in either treatment group. It is unclear from the study if there were any protocol deviations that may have impacted the findings.
External Validity
The sponsor’s reimbursement request is for adult patients with DME who are pseudophakic and have had an inadequate response to prior anti-VEGF therapy. The study population in the Shah et al. (2016)15 trial does not exactly match the reimbursement request as its population included a mix of pseudophakic and phakic eyes. The benefit of dexamethasone implants on pseudophakic patients who have had inadequate response to prior anti-VEGF therapy is uncertain in the absence of a well-controlled subgroup analysis in pseudophakic patients. Thus, the noted issues with the enrolled population and the aforementioned internal validity issues in the Shah et al. (2016) trial mean the findings cannot be generalized to patients with DME who are pseudophakic and have had an inadequate response to prior anti-VEGF therapy.
The study lasted 7 months and patients underwent monthly follow-ups. The clinical expert noted that a minimum study duration of 6 months is needed to evaluate the efficacy of dexamethasone implants in patient eyes with DME. However, the study duration was short for determining the longer-term comparative effects and safety of the dexamethasone implant versus bevacizumab, and the authors of the article themselves note this in several instances, especially regarding the comparative harms. The monthly follow-up schedules and procedures implemented in the Shah et al. (2016) study may not reflect real-world practice. According to the clinical expert and clinician groups consulted, patients with DME are assessed monthly at treatment initiation for IOP changes and once the patient is stabilized, patients are followed up every 3 months to monitor DME.
The dose of dexamethasone administered in the Shah et. al 2016 trial aligns with the one recommended by Health Canada. However, the frequency of administration or re-treatment criteria differs from the recommended dosage in the Health Canada–approved product monograph. The product monograph recommends re-treatment with the dexamethasone implant after a 6-month interval (based on the MEAD protocols). In the Shah et al. (2016) study, eyes were retreated 3 months after initial dexamethasone implant administration if patients met the re-treatment criteria; otherwise, they were retreated 4 months after the first administration. The clinical expert highlighted that it has been observed in practice that the efficacy of the dexamethasone implant declines after 3 months, requiring that patients receive additional implants, as needed, before the recommended 6-month interval is up to stabilize DME and improve VA and anatomic outcomes if symptoms persist. The expert considered a treatment interval of 3 months to 4 months to be appropriate and in alignment with how dexamethasone is used in practice settings.
Bevacizumab was identified as a comparator of interest for the CADTH review. The expert consulted by CADTH stated that bevacizumab is used to treat patients with DME in Canada and, in some jurisdictions, it is the first-line medication. However, patients had received 15 to 18 previous anti-VEGF injections on average up to approximately 6 weeks before entering the Shah et al. (2016) trial; therefore, the choice of using bevacizumab in this trial may not have been appropriate. According to the clinical expert, patients who show inadequate response after receiving an anti-VEGF (e.g., bevacizumab) in the first-line setting will likely be switched to another anti-VEGF therapy (such as aflibercept) before a corticosteroid such as a dexamethasone implant is considered. There was no information on the specific anti-VEGF therapies patients had received and whether patients had already been treated with more than 1 anti-VEGF therapy before being enrolled in the study. The clinical expert noted that in current practice, patients are considered to have inadequate response to anti-VEGF therapy after up to 6 anti-VEGF injections have been administered. The use of bevacizumab as a comparator in this circumstance may not have been optimal. Triamcinolone may have been a more informative comparator, given that the eyes of the population enrolled in the study appeared to no longer be achieving an expected magnitude of benefit from anti-VEGF treatment. Some patient eyes received prior triamcinolone injections at some point before the trial and given the much longer mean treatment intervals from the last triamcinolone injection versus those for anti-VEGF therapy, it is most likely that they received triamcinolone before anti-VEGF treatment. However, as with anti-VEGF treatment history, treatment outcomes with previous triamcinolone treatment were not reported in the study.
The clinical expert consulted noted that the long durations of prior therapy and the number of prior anti-VEGF and triamcinolone injections may not reflect clinical practice; however, the expert indicated that the population selected (i.e., poor responders to anti-VEGF therapy) is consistent with the population that corticosteroids, including dexamethasone implants, are considered for in practice.
HRQoL and other outcomes highlighted in the CADTH protocol (vision-related function, change in DR severity, and blindness) were not reported in the study. The efficacy of a dexamethasone implant on these outcomes is unknown.
Indirect Evidence
No relevant indirect evidence was included in the sponsor’s submission to CADTH or identified in the literature search conducted by CADTH. A focused literature search for indirect treatment comparisons dealing with Ozurdex, dexamethasone implants, or DME was run in MEDLINE All (1946–) on July 6, 2022. No limits were applied to the search.
Other Relevant Evidence
This section includes additional relevant studies included in the sponsor’s submission to CADTH that were considered to address important gaps in the evidence included in the systematic review section. Both comparative and noncomparative published observational studies were included in the sponsor’s submission, evaluating the use of a dexamethasone implant in patients with DME. Given that the CDEC recommendation for the original Ozurdex submission highlighted the lack of comparative evidence between a dexamethasone implant and other active treatments, the focus of this section is on the studies comparing a dexamethasone implant with 1 of the relevant comparators identified in the CADTH systematic review protocol. Two studies — by Busch et al. (2018)16 and Thomas et al. (2016)17 — met this criterion as they included a comparison of a dexamethasone implant with anti-VEGF therapy in patients who had an inadequate response to prior anti-VEGF therapy. Table 7 presents details of these studies. The other 8 studies were either noncomparative or did not have a relevant comparison. These other studies are briefly summarized in Table 14, along with their main limitations in regard to informing this review.
BCVA measurements derived using the Snellen scale approach were converted to their nearest approximations in ETDRS letters using VA conversion charts presented in Heeren (2021),50 adapted from Gregori et al. (2010).51
Table 7: Details of the Busch et al. (2018) and Thomas et al. (2016) Studies
Detail | Busch et al. (2018)16 | Thomas et al. (2016)17 |
|---|---|---|
Designs and populations | ||
Study design | International, multicentre, retrospective, case-control study | Single-centre, retrospective, consecutive case series study |
Locations | 14 sites (Argentina, Israel, Australia, Türkiye, Thailand, India, Germany, France, Mexico, Portugal, and Italy) | 1 site (US) |
Patient enrolment dates | Patient records reviewed from January 1, 2010, to December 31, 2016 | NR |
Enrolled (N) |
| 11 patients, each with 1 eye treated with dexamethasone implants and 1 eye treated with anti-VEGF therapy |
Inclusion criteria |
|
|
Exclusion criteria |
|
|
Drugs | ||
Intervention | Dexamethasone implant | Dexamethasone implant |
Comparator(s) | Anti-VEGF therapy (aflibercept, ranibizumab, or bevacizumab) | Anti-VEGF therapy (ranibizumab) |
Duration | ||
Follow-up | 9 months | 3 months |
Outcomes | ||
Primary end points |
|
|
Secondary and exploratory end points |
| IOP (eyes with IOP greater than 30 mm Hg and eyes requiring IOP-lowering therapy) |
Publications | Busch et al. (2018)16 | Thomas et al. (2016)17 |
AUC = area under the curve; BCVA = best corrected visual acuity; CMT = central macular thickness; CST = central subfield thickness; DME = diabetic macular edema; IOP = intraocular pressure; logMAR = logarithm of the minimum angle of resolution; NR = not reported; SD-OCT = spectral domain optical coherence tomography; VA = visual acuity; VEGF = vascular endothelial growth factor.
Sources: Busch et al. (2018)16 and Thomas et al. (2016).17
Description of Studies
Busch et al. (2018)
Busch et al. (2018)16 was a multicentre, retrospective, case-control study designed to compare the effectiveness of the continued use of anti-VEGF therapy versus switching to a dexamethasone implant with regard to functional and anatomic outcomes in eyes of patients with DME, with inadequate response following 3 initial anti-VEGF injections. Eligible eyes were required to be treatment-naive at presentation and were initially treated with 3 monthly anti-VEGF injections at the loading phase (aflibercept, ranibizumab, or bevacizumab), leading to a suboptimal response to the treatment. Inadequate response was defined as “5 or less letter gain in VA (including vision loss), or reduction of less than 20% of CST on SD-OCT 1 month after the third anti-VEGF injection.”16
Eligible eyes either continued with an anti-VEGF therapy or switched to a dexamethasone implant after a maximum of 1 additional anti-VEGF injection. Patients were also required to have VA and CST measurements at baseline, month 3 (after 3 loading anti-VEGF injections), at either month 6 or month 9, and at month 12. Follow-up lasted 9 months (from month 3 to month 12). The mean changes in VA and CST from month 3 to month 12 were the primary end points examined; the mean changes in standardized AUC of VA and CST from month 3 to month 12, the proportion of eyes gaining 10 or more letters and 5 or more letters, were secondary end points.16 There were 110 eyes in total in 105 patients, of which 72 eyes (n = 67 patients) were treated with anti-VEGF therapy only, and 38 eyes (n = 38 patients) were switched to dexamethasone implants (after 3 anti-VEGF injections to 4 anti-VEGF injections).
Thomas et al. (2016)
Thomas et al. (2016)17 was a retrospective, comparative case series study designed to assess the effectiveness of therapeutic responses of matched contralateral eyes of patients with recalcitrant DME to continued anti-VEGF therapy versus a dexamethasone implant. Eligible patients had bilateral DME and had previously undergone consistent monthly bilateral intravitreal injections with an anti-VEGF drug (ranibizumab). Patients were considered to have recalcitrant DME “if regular (monthly) anti-VEGF therapy were maintained for at least 3 months, and there was persistent central macular edema (greater than 300 μm) and/or a minimal response to therapy (less than 25% reduction in CMT) in both eyes.” Patients received a dexamethasone implant in 1 eye while being maintained on anti-VEGF therapy at regular intervals in the collateral eye. Patients were followed up every 4 weeks to 6 weeks, and the study lasted 3 months. VA, CMT, and IOP were evaluated on every visit.17 The cohort included 11 eyes treated with the dexamethasone implant and 11 paired contralateral eyes that continued treatment with ranibizumab in the 3-month study period.
The inclusion and exclusion criteria for Busch et al. (2018) and Thomas et al. (2016) are presented in Table 7.
Baseline Characteristics
Busch et al. (2018)
Each eye receiving anti-VEGF therapy only was propensity score–matched to the eyes in the dexamethasone implant group. In total, 38 eyes (in 38 patients) were included in the matched anti-VEGF group, which was compared with the dexamethasone implant group.16
The mean age of patients in the matched anti-VEGF group versus the dexamethasone implant group at baseline was 61.2 years and 63.1 years, respectively. Seventeen eyes in the anti-VEGF group and 22 eyes in the dexamethasone implant group were in male patients. Proliferative DR was identified in 12 (31.6%) eyes in the matched anti-VEGF group and 15 (39.5%) eyes in the dexamethasone implant group. In total, 15 (39.5%) eyes in the matched anti-VEGF group were pseudophakic compared to 18 (47.7%) eyes in the dexamethasone implant group. Prior panretinal photocoagulation was observed in 13 (34.2%) eyes in the matched anti-VEGF group and 17 (44.7%) eyes in the dexamethasone implant.16 Table 8 presents the baseline and demographics of patients enrolled in the Busch et al. (2018) study. The mean VA at month 3 was 0.52 logMAR (approximately 55 ETDRS letters to 61 ETDRS letters) in the matched anti-VEGF group and 0.53 logMAR (approximately 55 ETDRS letters to 61 ETDRS letters) in the dexamethasone implant group. The mean CST at month 3 was 444.0 (SD = 118.3) µm in the matched anti-VEGF group and 472.1 (SD = 124.1) µm in the dexamethasone implant group.16
Table 8: Characterization of the Included Eyes in the Busch et al. (2018) Study16
— | — |
|---|---|
Note: For complete table contents, please refer to Table 1 in the following article: Busch C, Zur D, Fraser-Bell S, et al. Shall we stay, or shall we switch? Continued anti-VEGF therapy versus early switch to dexamethasone implant in refractory diabetic macular edema. Acta Diabetol. 2018;55(8):789-796.16 | — |
Thomas et al. (2016)
Of the 11 patients enrolled, the mean age was 62 (range = 51 to 84) years; 7 patients were female and 4 were male. All patients had type 2 diabetes with a mean glycated hemoglobin A1C of 6.51% (range = 5.9% to 7.0%) (most recent measurement). Eyes receiving dexamethasone implants had received a median of 8.0 prior anti-VEGF injections at treatment baseline versus a median of 8.5 anti-VEGF injections in contralateral eyes receiving ranibizumab. Eight eyes receiving the dexamethasone implant and 7 eyes receiving ranibizumab were pseudophakic. Table 9 presents baseline ophthalmic features of paired contralateral eyes at treatment onset.17
Outcomes
A list of effectiveness end points identified in the CADTH review protocol that were assessed in the studies included in this review is provided in Table 10.
Table 9: Features of Matched Contralateral Eyes at Treatment Outset
Feature | Eye receiving intravitreal dexamethasone implant (N = 11) | Eye receiving intravitreal ranibizumab (N = 11) | P value |
|---|---|---|---|
Duration of prior treatment, months, mean (range) | 19.4 (5 to 50) | — | — |
Laterality, n (%) | |||
Right eye (OD) | 5 (45.5) | 6 (54.5) | — |
Left eye (OS) | 6 (54.5) | 5 (45.5) | — |
Lens status, n (%) | |||
Phakic | 3 (27.3) | 4 (36.4) | — |
Pseudophakic | 8 (72.7) | 7 (63.6) | — |
Prior anti-VEGF injections, mean (median) | 8.91 (8.0) | 9.10 (8.5) | 0.944 |
Visual acuity, logMAR, mean (SD) | 0.415 (0.165) | 0.394 (0.313) | 0.294 |
CMT, µm, mean (SD) | 461.3 (156.8) | 421.1 (146.8) | 0.795 |
IOP, mm Hg, mean (SD) | 17.1 (4.18) | 16.0 (3.87) | 0.535 |
CMT = central macular thickness; IOP = intraocular pressure; logMAR = logarithm of the minimum angle of resolution; SD = standard deviation; VEGF = vascular endothelial growth factor.
Source: Thomas et al. Clinical Ophthalmology. 2016;10:1679 to 1684.17 Originally published by and used with permission from Dove Medical Press Ltd.
Table 10: Outcomes Evaluated in the Included Studies
Outcome | Busch et al. (2018)16 | Thomas et al. (2016)17 |
|---|---|---|
Change from baseline of visual acuity | Yes | Yes |
Change in CRT or CST | Yes | Yes |
Vision-related function | No | No |
Change in diabetic retinopathy severity | No | No |
HRQoL | No | No |
Blindness (legal) | No | No |
Safety | No | Yes |
CRT = central retinal thickness; CST = central subfield thickness; HRQoL = health-related quality of life.
Statistical Analysis
Busch et al. (2018)
The AUC of VA and CST changes from month 3 to month 12 were calculated using the trapezoidal rule.
Propensity matching methods were applied to account for imbalances between groups. Variables in the matching process included age, gender, duration of diabetes, type of DR, lens status, prior panretinal photocoagulation, ellipsoid zone disruption, VA, and CST at month 0 and month 3.16 A regression model was used to assess the differences between the matched anti-VEGF group and the dexamethasone implant group.
A multivariable regression model was used to assess differences in outcome measures between the matched anti-VEGF and dexamethasone implant group.16 The model’s variables included age, gender, stage of DR, ellipsoid zone disruption at baseline, lens status at baseline and after 12 months, postpanretinal photocoagulation status at baseline and after 12 months, and baseline (VA outcomes) and baseline CST (for CST outcomes).
Missing data were imputed using the last observation carried forward (LOCF) method.16
The study protocol was not included as part of the publication and there was no mention of a published protocol for the study.
Thomas et al. (2016)
Snellen BCVA measurements were converted to logMAR units in the statistical analyses.17
A Mann–Whitney U-test and the Wilcoxon signed rank test were used to evaluate differences in each group. Alpha for statistical significance was set at 0.05.17
The study protocol was not included as part of the publication and there was no mention of a published protocol for the study.
Results
Treatment Exposure
Busch et al. (2018)
In the matched anti-VEGF group, the mean number of injections received was 4.2 (SD = 2.4) compared to 1.4 (SD = 0.5) for eyes in the dexamethasone implant group after switching from the anti-VEGF group. In total, 25 (65.8%) eyes switched to the dexamethasone implant after 3 anti-VEGF injections and 13 (34.2%) eyes switched to the dexamethasone implant after 4 injections.16 In the dexamethasone implant group, 17 (44.7%) eyes received 2 implants and the mean interval between the first and second implant injections was 136.5 (SD = 23.9) days.
In terms of concomitant ocular treatments during the 12-month period in the matched anti-VEGF group and the dexamethasone implant group, respectively, 1 of 38 (2.6%) eyes and 1 of 35 (2.9%) eyes had macular laser, 10 of 38 (26.3%) eyes and 1 of 37 (2.7%) eyes had panretinal photocoagulation, 2 of 23 (8.7%) eyes and 5 of 19 (26.3%) eyes had cataract surgery, and no eyes had pars plana vitrectomy. Table 11 presents treatment exposure information in the Busch et al. (2018) study.
Thomas et al. (2016)
No treatment exposure data were reported.
Table 11: Treatment Characteristics in the Busch et al. (2018) Study16
— | — |
|---|---|
Note: For complete table contents, please refer to Table 2 in the following article: Busch C, Zur D, Fraser-Bell S, et al. Shall we stay, or shall we switch? Continued anti-VEGF therapy versus early switch to dexamethasone implant in refractory diabetic macular edema. Acta Diabetol. 2018;55(8):789-796.16 | — |
Effectiveness
Only those outcomes and subgroups identified in the CADTH review protocol are reported as follows.
Busch et al. (2018)
Visual Acuity
VA was measured at baseline, month 3, and at month 12. At the 6-month evaluation, 2 eyes in each of the entire anti-VEGF group and the dexamethasone implant group had missing data (2.8% of the entire anti-VEGF group and 5.2% of the dexamethasone implant group; data for the matched group were not reported). At 9 months, data on VA were missing for 17 eyes in the entire anti-VEGF group (26.3%; data for the matched group were not reported) and 1 eye in the dexamethasone implant group (2.6%). Mean change in VA was calculated between month 3 and month 12.16
Eyes that switched to a dexamethasone implant had a mean VA of 0.41 logMAR (approximately 61 ETDRS letters to 65 ETDRS letters) at month 12 compared to 0.53 logMAR (approximately 55 ETDRS letters to 61 ETDRS letters) in the matched anti-VEGF group. The mean change in VA from month 3 to month 12 was an increase of 6.1 ETDRS letters in eyes in the dexamethasone implant group compared to a decrease of 0.4 letters in the anti-VEGF matched eyes (P value = 0.004; multivariate analysis).16
The mean change in VA from month 3 to month 12 based on the AUC approach was an increase of 15.2 ETDRS letters in eyes in the dexamethasone implant group compared to an increase of 2.4 ETDRS letters in the matched anti-VEGF group (P = 0.008; multivariate analysis).16
Central Subfield Thickness: CST was measured at baseline, at month 3, and at month 12. The mean CST at month 12 was 380.3 µm in the dexamethasone implant group compared to 462.5 µm in the matched anti-VEGF group. The mean change in CST from month 3 to month 12 was a decrease of 92.8 µm in eyes receiving dexamethasone implants and an increase of 18.3 µm in the matched group of anti-VEGF eyes.16 Table 12 presents the VA and CST after 12 months of treatment.
Table 12: Twelve-Month Outcomes in the Busch et al. (2018) Study16
— | — |
|---|---|
Note: For complete table contents, please refer to Table 3 in the following article: Busch C, Zur D, Fraser-Bell S, et al. Shall we stay, or shall we switch? Continued anti-VEGF therapy versus early switch to dexamethasone implant in refractory diabetic macular edema. Acta Diabetol. 2018;55(8):789-796.16 | — |
Thomas et al. (2016)
The mean logMAR VA at baseline in eyes receiving dexamethasone implants was 0.415 (approximately 61 ETDRS letters to 65 ETDRS letters) versus 0.394 (approximately 65 ETDRS letters to 70 ETDRS letters) in eyes continuing with ranibizumab. The mean logMAR VA improved in both groups at month 3 and was 0.261 (approximately 70 ETDRS letters to 76 ETDRS letters) in the dexamethasone implant group and 0.269 (approximately 70 ETDRS letters to 76 ETDRS letters) in eyes continuing with ranibizumab.17 The difference between the groups was not statistically different.
The mean CMT from baseline to month 3 also improved in both treatment groups, with a larger decrease in the dexamethasone group (net decrease of 105.8 µm) than in the ranibizumab group (net decrease of 47.9 µm). The mean CMT at month 3 in eyes receiving dexamethasone implants was 355.6 (SD = 110.2) µm compared to 373.2 (SD = 142.6) µm in eyes receiving ranibizumab, but the difference at month 3 was not statistically different.17 VA and anatomic changes in the 2 study groups are presented in Table 13.
Table 13: Treatment Outcomes at Baseline, Month 1 to Month 3, in the Thomas et al. (2016) Study
Feature | Eye receiving intravitreal dexamethasone implant (N = 11) | Eye receiving intravitreal ranibizumab (N = 11) | P value (dexamethasone vs. ranibizumab) |
|---|---|---|---|
Mean VA, logMAR (SD) | |||
Baseline | 0.415 (0.165) | 0.394 (0.313) | 0.294 |
Month 1 | 0.334 (0.172) | 0.378 (0.282) | 0.873 |
Month 2 | 0.366 (0.171) | 0.338 (0.183) | 0.818 |
Month 3 | 0.261 (0.182) | 0.269 (0.186) | 0.976 |
Net gain | 0.153 | 0.125 | 0.624 |
P value (baseline to month 3) | 0.004 | 0.058 | |
Mean CMT, µm (SD) | |||
Baseline | 461.3 (156.8) | 421.1 (146.8) | 0.795 |
Month 1 | 353.3 (99.8) | 413.1 (117.1) | 0.490 |
Month 2 | 314.6 (86.4) | 406.9 (128.9) | 0.509 |
Month 3 | 355.6 (110.2) | 373.2 (142.6) | 1.0 |
Net decrease | 105.8 | 47.9 | 0.332 |
P value (baseline to month 3) | 0.01 | 0.26 | |
CMT = central macular thickness; logMAR = logarithm of the minimum angle of resolution; SD = standard deviation; VA = visual acuity; vs. = versus.
Source: Thomas et al. Clinical Ophthalmology. 2016;10:1679 to 1684.17 Originally published by and used with permission from Dove Medical Press Ltd.
Harms
Only those harms identified in the CADTH review protocol are reported in this section.
Adverse Events
Busch et al. (2018)
No safety data were reported.
Thomas et al. (2016)
No infectious endophthalmitis, vitreous hemorrhage, retinal detachment, or lens disruption or subluxation were reported for either treatment group during the study period of the Thomas et al. (2016) study. Two eyes receiving dexamethasone reportedly had an IOP of greater than 30 mm Hg during the study, which did not require IOP-lowering medications, and they returned to normal levels at the end of the study. The mean IOP observed was 17.1 mm Hg and 16.0 mm Hg in eyes receiving dexamethasone implant and ranibizumab, respectively.17
Critical Appraisal
Internal Validity
Data in the Busch et al. (2018) study were collected from medical records at each of the participating study sites. It was unclear whether study sites in the Busch et al. (2018) study used similar and standardized methods and procedures to collect data at baseline. The Busch et al. (2018) study did not report whether each participating site used the same instrument calibration approach, treatment procedures, and testing conditions. The Thomas et al. (2016) study collected baseline data at patient presentation. The risk of variability in treatment procedures, testing conditions, and diabetic control of patients was likely lower in the Thomas et al. (2016) study because the study was conducted in a single centre. As well, contralateral eyes with bilateral, symmetric DME (in terms of VA and CMT) were included in the study; this provided control for some potential confounders (patient adherence, testing conditions, treatment procedures, diabetic control) that may impact findings.
Data used to assess outcomes in both studies were not specifically collected for the studies given the retrospective design and were collected from multiple sites in the Busch et al. (2018) study. It was not reported in either study whether outcome measurements were validated for quality (completeness, correctness) before study initiation; hence, there is a potential risk of information bias and the direction of bias is uncertain. In the Busch et al. (2018) study, it was unclear whether a similar protocol was used across participating centres for diagnosing DME and for identifying nonresponders to anti-VEGF therapy. Investigators in the Busch et al. (2018) study were blinded to treatment when assessing the patient charts, which would have helped reduce assessment bias. Performance bias was considered low in the Busch et al. (2018) study because OCT scans were graded by independent masked graders. It was unclear in the Thomas et al. (2016) study whether OCT scans were evaluated by independent graders, which would have reduced performance bias.
The Busch et al. (2018) study used propensity score matching procedures to match baseline characteristics in the dexamethasone group and a subset of the continuing anti-VEGF group. While there were limited details, it appeared that the investigators followed recommended approaches to matching, using propensity scores and checking differences between the matched characteristics. However, the rationale behind the matching factors used was not provided. The clinical expert consulted by CADTH stated that the factors used were relevant but that key factors such as type of diabetes, diabetes control (e.g., baseline levels of hemoglobin A1C) and baseline cataract status (especially because the population was a mix of phakic and pseudophakic eyes) should have been considered. The distribution of these factors was not reported and their impact on the results could not be determined. The authors did report variability in definitions of cataract progression across sites and inconsistencies in the availability of hemoglobin A1C levels. As mentioned, few details were provided regarding the balance diagnostics to determine the quality of the matching. The study only states that similarity between the matched groups was assessed using P vales from univariate logistic regression. This approach is not recommended because P values comparing the baseline factors between treatment groups are influenced by sample size.52 There appeared to be differences between the matched groups based on the percentages — for example, 39.5% versus 47.7% of patient eyes were pseudophakic at baseline in the anti-VEGF and dexamethasone groups, respectively — yet the P value for the difference between these was 0.49. Therefore, it is not clear whether the groups were adequately matched, and this may reflect the small sample sizes per group. The Thomas et al. (2016) study included contralateral eyes, which may have reduced variability in some confounders and other measurements. Although key potential confounders important for patients with DME were assessed at baseline, there remains a potential risk of confounding bias for other confounders (e.g., background care, concomitant medications), which may have impacted the findings.
Outcomes investigated in both studies were considered appropriate and validated. OCT measurements for anatomic outcomes may have varied across centres and across scanners if calibrating techniques were inconsistent across centres in the Busch et al. (2018) study, resulting in imprecise findings (variability between readers of about 10 µm, according to the clinical expert consulted for this review). The Thomas et al. (2016) study was conducted in 1 site, and 1 OCT scanner was used to obtain measurements. Assessment bias and the impact on findings were considered low in both studies.
Treatment exposure (number of injections) was reported in the Busch et al. (2018) study, but it was unclear whether patients who completed the initial anti-VEGF dosing period continued with the same drug afterward or had been allowed to switch to another anti-VEGF. If patients continued receiving the same anti-VEGF that they had an inadequate response to in the initial phase, then this may have biased results in favour of the dexamethasone implant.
Additional treatments administered to patients (including ocular hypertensives) were reported in the Busch et al. (2018) study. A greater proportion of eyes in the dexamethasone group received prior panretinal photocoagulation (34.2% in the matched anti-VEGF group and 44.7% in the dexamethasone implant group) and more eyes in the matched anti-VEGF group (10 [26.3%] eyes) received additional panretinal photocoagulation between month 0 and month 12 compared to the dexamethasone implant group (1 [2.7%] eye). Further, a greater proportion of eyes underwent cataract surgery in the dexamethasone implant group (26.3%) compared to the matched anti-VEGF group (8.7%), which may impact VA as patients with cataracts may have worsened VA and may have improved VA upon surgery. Baseline data on cataracts and data on cataract progression during treatment were not reported. The imbalances in the reported concomitant ocular treatments are concerning as these treatments are potential confounders in terms of efficacy; it is also unknown whether these imbalances point to underlying differences between the 2 groups. The Thomas et al. (2016) study did not present information on concomitant medications.
No published protocols were identified, and no sample size or power calculations were provided in either study. The Busch et al. study (2018) matched 38 eyes per group and 11 eyes per group were matched in the Thomas et al. (2016) study; this appears to represent relatively small sample sizes upon which to draw concrete conclusions. No patient was lost to follow-up in either study; thus, the risk of attrition bias was low. However, the LOCF method was used to impute missing data in the Busch et al. (2018) study; this is based on numerous assumptions, including data missing at random and that the natural history of DME would not impact the validity of this approach. The authors did not report sensitivity analyses or use other methods of imputation that are used to assess the appropriateness of LOCF as the method for imputation. The Thomas et al. (2016) study did not report any methods for handling missing data.
External Validity
The patient population in both studies included a mix of phakic and pseudophakic eyes with DME. The Busch et al. (2018) study used lens status in the propensity score matching procedure, and lens status at baseline and after 12 months was a covariate included in the regression model used to evaluate the outcomes. However, results were not reported by lens status and in the absence of subgroup analyses, it is unclear how generalizable the results are to patients who are pseudophakic and have had an inadequate response to prior anti-VEGF therapy.
The clinical expert noted that baseline characteristics of patients recruited in the Busch et al. (2018) study may not be representative of patients with DME in current practice. For instance, the expert noted that patients with proliferative DR usually present with severe DME in practice and these patients represent only 20% to 25% of the population. The Busch et al. study (2018) had 31.6% and 39.5% of patients with proliferative disease in the matched anti-VEGF and dexamethasone groups, respectively. The clinical expert highlighted that the study did not present data on other important patient characteristics (i.e., type of diabetes, baseline hemoglobin A1C, and medications to control glucose levels) and, therefore, it could not be fully determined how generalizable the study population was to that of clinical practice. The clinical expert considered the baseline characteristics presented in the Thomas et al. (2016) study similar to those in patients with DME in current practice. However, several key baseline characteristics were not reported and generalizability to practice could also not be fully determined for this study.
The outcomes investigated (VA using ETDRS letters and Snellen scales) in both studies were considered appropriate by the clinical expert consulted and reflective of clinical practice. The clinical expert highlighted that CMT, CRT, and CST are similar measures assessing anatomic outcomes in eyes with DME, which are valid measures in current practice. HRQoL and other important outcomes identified in the CADTH protocol were not reported in either study. The effectiveness of the dexamethasone implant on HRQoL and other patient outcomes in both study populations is uncertain.
The Busch et al. (2018) study did not present any safety outcomes while the Thomas et al. (2016) study did not present comprehensive data on the differences in safety outcomes reported in patients receiving treatments in both eyes.
It was unclear what treatment strategies (i.e., doses and treatment intervals) were used in the studies and whether they varied across centres in the Busch et al. (2018) study. This made it challenging to assess the generalizability of the interventions, particularly in the anti-VEGF groups.
The duration of the Thomas study was considered relatively short by the clinical expert consulted and may not be reflective of clinical practice. The short duration may not have been appropriate to observe the true effect of a dexamethasone implant on patient eyes with DME. The study duration in Bush et al. (2018) was considered appropriate to assess the true effect of the dexamethasone implant on DME and the dosing frequency aligned with clinical practice.
Other Sponsor-Submitted Studies
Table 14 presents a summary of study characteristics and main findings from 8 other published observational studies submitted by the sponsor.
Wang et al. (2021)
Wang et al. (2021)53 was a single-centre, retrospective observational study that investigated the effectiveness and safety of dexamethasone implants in eyes that were inadequately responding to anti-VEGF therapy (group 1) and treatment-naive eyes (no treatment within the 3 months before the study) (group 2) over a 6-month follow-up time point. Medical charts of patients with consecutive pseudophakic eyes with centre-involved DME were reviewed retrospectively from May 2015 to May 2017 to identify cases.53
Both groups received dexamethasone implants. Patients in group 1 had received an intravitreal dexamethasone implant at least 1 month after the last anti-VEGF administration. The administration of 1 dexamethasone implant plus as-needed dosing to eyes was performed by 2 surgeons. Eyes were allowed to receive repeated injections at least within a 4-month interval, with CFT greater than 300 μm or a BCVA of less than Snellen 20/25 (approximately 80 ETDRS letters). Patients were followed up every 6 months and measurements of changes in VA and CFT after 6 months were the primary outcomes. Changes in IOP, injection number, and complications were also evaluated. The Fisher exact test was used to assess categorical comparison between groups, the Wilcoxon signed rank test was used within the group and the Wilcoxon rank sum test was used between groups. A P value of less than 0.05 was considered statistically significant.53
At baseline, 34 eyes (in 31 patients) were included in group 1 and 41 eyes (from 38 patients) were included in group 2. The mean change in BCVA from baseline to month 6 in ETDRS was 7.29 (SD = 16.22) letters in group 1 versus 16.42 (SD = 14.38) letters (P value for ETDRS letters = 0.0008) in group 2. The mean number of dexamethasone implants at 6 months was 1.82 in group 1 and 1.54 in group 2. The mean change in CFT in group 1 at 6 months was –155.44 (SD = 112.67) µm and –172.42 (SD = 133.79) µm (P value = 0.27) in group 2. The final IOP mean at 6 months in group 1 was 17.87 (SD = 4.94) mm Hg and 18.52 (SD = 3.43) mm Hg in group 2.53
Table 14: Summary of Other Sponsor-Submitted Studies
Study citation | Study design | Population and characteristics | Treatment | Main study findings |
|---|---|---|---|---|
Wang et al. (2021)53 | Retrospective observational study | Population: Adult patients, pseudophakic eyes with centre-involved DME (including treatment-naive or inadequate response to anti-VEGF treatment) Characteristics Of 75 eyes (69 patients):
|
|
|
Iglicki et al. (2019)54 | Retrospective observational study (chart review) | Population: Adult patients with DME (including treatment-naive or inadequate response to anti-VEGF therapy) Characteristics Of 130 eyes (125 patients):
|
|
|
Pareja-Ríos et al. (2018)55 | Retrospective observational study (case series) | Population: Adult patients with DME who had shown no improvement after prior standard treatments or anti-VEGF therapy Characteristics Of 116 eyes (85 patients):
| Intravitreal dexamethasone implant | Findings specific to pseudophakic eyes were as follows:
|
Wallsh et al. (2020)56,a | Retrospective observational study (chart review) | Population: Patients with branch retinal vein occlusion, central retinal vein occlusion, uveitis, and/or DME who were receiving dexamethasone implant treatment Characteristics In 62 eyes (43 patients) with DME:
|
| Over a mean period of 63.9 (SD = 4.6) weeks (approximately 14.7 months):
|
Cicinelli et al. (2017)57 | Retrospective observational study | Population: Adult patients with DME Characteristics Of 45 eyes (45 patients) with DME:
| Patients received monthly ranibizumab injections and then switched to dexamethasone implant injections at 4-month intervals until stable BCVA was reached. | Here are findings 12 months after the start of dexamethasone implant treatment:
|
Chatziralli et al. (2017)58 | Prospective observational study | Population: Adult patients with DME refractory to previous treatment with anti-VEGF therapy Characteristics Of 54 eyes (54 patients) with DME:
| Intravitreal dexamethasone implant injection |
|
Pacella et al. (2016)59 | Retrospective observational study | Population: Adult patients with DME resistant to previous treatment with anti-VEGF therapy Characteristics Of 32 eyes (32 patients) with DME:
| Patients received 1 injection of 0.7 mg dexamethasone intravitreal implant at baseline and reinjection was performed at 4 months based on the patient’s condition. |
|
Degoumois et al. (2015)60,a | Retrospective cohort study | Population: Patients with DME refractory to previous treatment with anti-VEGF therapy, patients who had undergone retinal detachment surgery, patients with macular edema due to Irvine-Gass Syndrome, and patients with endophthalmitis infection or type 1 macular telangiectasia who received at least 1 injection of intravitreal dexamethasone implant Characteristics: The study did not report specific demographic information for the DME cohort. For the total enrolled population, the majority of patients was pseudophakic (88%). | The study did not report the treatment information for the DME cohort. All patients having diffuse macular edema had received at least 1 injection of dexamethasone implant. |
|
BCVA = best corrected visual acuity; CFT = central foveal thickness; CI = confidence interval; CMT = central macular thickness; CST = central subfield thickness; DME = diabetic macular edema; ETDRS = Early Treatment Diabetic Retinopathy Study; IOP = intraocular pressure; logMAR = logarithm of the minimum angle of resolution; SD = standard deviation; SEM = standard error of the mean; VA = visual acuity; VEGF = vascular endothelial growth factor; vs. = versus.
Iglicki et al. (2019)
Iglicki et al. (2019)54 was a multicentre, retrospective chart review using data from 10 sites. The study investigated the effectiveness and safety of the repeated administration of dexamethasone implants in treatment-naive eyes with DME compared to eyes with an inadequate response to the repeated administration of anti-VEGF injections, within a 24-month follow-up period. Eyes not responding to anti-VEGF treatment were defined as the worsening of BCVA by 2 ETDRS lines or a reduction of less than 10% of retinal thickness on SD-OCT measured 1 month after at least 3 anti-VEGF injections had been administered to the patient at monthly intervals. Patient records available between January 1, 2011, to August 1, 2017, in participating centres were reviewed to identify cases. The study assessed visual and anatomic changes 24 months after the first dexamethasone implant was administered as the primary outcome. BCVA and CST measured after 6 months and 12 months, IOP, and the proportion of cataract extractions were other secondary outcomes assessed. Multivariate logistic regression models were used to assess changes in primary outcomes at baseline, 6, months 12 months, and 24 months. The LOCF method was used to impute missing data. A generalized estimating equation was used to adjust correlations between data.54
There were 130 eyes in 125 patients, of which 71 (54.6%) eyes were treatment-naive and 59 (45.6%) eyes were not responding to anti-VEGF injections. In the inadequate response group, 63% of eyes were pseudophakic at baseline and the mean number of prior anti-VEGF injections was 7.4 (SD = 3.6). The mean number of dexamethasone implants administered in inadequate response eyes within the 24-month period was 3.1 (range = 1 to 4; 37 eyes received 4 implants). The mean (range) duration between the first and second treatment (with the dexamethasone implant) in the inadequate response eyes was 214 (11 to 686) days. Thirteen (22.8%) eyes required IOP-lowering topical treatments.54
The mean BCVA at baseline in eyes in the anti-VEGF inadequate response group was 0.61 logMAR (approximately 55 ETDRS letters) and 0.59 logMAR (approximately 55 ETDRS letters to 58 ETDRS letters) in the treatment-naive group. At month 24, patient eyes in the anti-VEGF inadequate response group reportedly gained a mean of 7.3 (SD = 12.7) letters (P = 0.01) compared to the treatment-naive group (mean of 11.3 [SD = 10.0] letters). The mean CMT at baseline was 583 µm in the treatment-naive group and 565 µm in the anti-VEGF inadequate response group. The mean CST at 24 months was 279 µm (SD = 61) in the treatment-naive group versus 313 (SD = 125) µm in the anti-VEGF inadequate response group (P value = 0.1).54
Pareja-Ríos et al. (2018)
Pareja-Ríos et al. (2018)55 was a single-centre, retrospective, case series study that assessed the safety and effectiveness of dexamethasone implants in adult patients with DME who had shown no improvement (in retinal thickness and VA) after prior standard treatments (macular focal laser or modified grid laser, or anti-VEGF therapy) had been administered for at least 3 months. The medical records of patients who had been diagnosed and consecutively treated with the dexamethasone implant between January 2013 and February 2014 were reviewed. The interval from the last laser treatment to the dexamethasone implant treatment was at least 6 months while the last anti-VEGF injection was performed 3 months before the administration of the dexamethasone implant. Patients could receive up to 2 additional treatments with dexamethasone after the initial 1, as needed. The re-treatment of eyes was based on whether a significant loss of BCVA (greater than 10 ETDRS letters) with respect to the best reached value was observed after the use of the dexamethasone implant or a CMT value that returned to baseline values. The study period was 1 year. The study assessed outcomes in the entire cohort and in 3 subgroup analyses (treatment-naive, pseudophakic, and phakic eyes). A Student’s t-test was used to compare outcomes between visits, and a 1-way analysis of variance was used to assess between-group differences.55
In total, 116 eyes in 85 patients were included in the study, of which 113 had complete 1-year follow-up data. Three eyes were lost to follow-up. Of the 113 eyes with complete data, 72 (63.7%) were pseudophakic eyes, 11 (9.7%) were treatment-naive eyes, and 30 (26.6%) were phakic eyes. Eleven (9.8%) eyes had received an anti-VEGF treatment, 34 (30%) eyes had received laser treatment, and 57 (50.4%) eyes had received a combined laser and anti-VEGF treatment before receiving the dexamethasone implant treatment.55
VA findings specific to pseudophakic eyes were as follows. The mean baseline VA was 42.2 (range = 4 to 80). At month 12, the mean VA in ETDRS letters was 45.6 (range = 8 to 80) letters. The maximum mean increase in BCVA from baseline occurred at 3 months. There was an increase in 6.9 ETDRS letters for eyes in the pseudophakic subgroup. The CMT at month 12 in the pseudophakic subgroup was 425 µm (between 400 µm and 450 µm). Safety outcomes reported included mild vitritis (1 eye), which did not require treatment. Increases in IOP of 5 mm Hg or greater were observed in 16 (14%) eyes, of which 5 (4%) eyes showed an increase of IOP of 10 mm Hg or greater when compared to baseline values. No other major ocular events or major systemic complications were observed.55
Wallsh et al. (2020)
Wallsh et al. (2020)56 was a noncomparative, retrospective chart review. The study investigated the effectiveness and safety of repeated intravitreal dexamethasone implants over a mean follow-up period of 63.9 (SD = 4.6) weeks (approximately 14.7 months). The study had 4 cohorts of patients who were treatment-naive or had been previously treated (with laser, intravitreal or periocular corticosteroid injections, or intravitreal anti-VEGF injections); 1 of the study cohorts was for patients with DME. In the previously treated patients, dexamethasone implant treatment was initiated for failure to respond to previous treatment, inadequate response to previous treatment, or a patient’s desire to decrease injections and/or drop treatment burden. Failure to respond to and inadequate response to previous treatment were determined based on multiple modalities, including persistent macular edema on OCT. Final visit measurements were assessed at the visit closest to 6 weeks after the last dexamethasone implant treatment, but no less than 28 days after that treatment.56
Only the results from the DME cohort are in scope for the CADTH review. There were 62 eyes in 43 patients with DME, of which 44 (71.0%) eyes were pseudophakic, 57 (91.0%) eyes had previous anti-VEGF treatments, and 32 (51.6%) eyes had concurrent anti-VEGF treatments. The number of previous anti-VEGF treatments was not reported for the DME cohort. Patients with DME received a total of 153 dexamethasone implant injections for all eyes in the DME cohort, with a mean length of treatment of 247.4 (SEM = 35.3) days (approximately 8 months). There were no data reported for the mean dexamethasone implant treatment interval for the DME cohort; the study only reported that the mean interval between dexamethasone implant treatments for all eyes was 126.0 (SEM = 5.1) days (approximately 4 months).
The VA for the DME cohort improved from 0.73 (SEM = 0.06) logMAR (approximately 50 ETDRS letters) at baseline to 0.61 (SEM = 0.06) logMAR (approximately 55 ETDRS letters) at final visit (P < 0.05) and CMT improved from 428.4 (SEM = 23.3) μm to 320.1 (SEM = 10.7) μm (P < 0.05). The study did not provide detailed subgroup analysis results of eyes with DME from baseline to final visit based on lens status (neither for those pseudophakic throughout, phakic throughout, or who underwent cataract surgery during study) but stated that the results demonstrated similar improvements in BCVA and CMT for all subgroups. IOP increased from 15.1 (SEM = 0.7) mm Hg at baseline to 16.3 (SEM = 0.6) mm Hg at final visit. The study did not provide specific anti-glaucoma medication results for the DME cohort; for the pooled population, the amount of anti-glaucoma medications being used significantly increased from 0.71 (SD = 0.06) drops to 1.50 (SD = 0.07) drops with 105 (33.0%) eyes using anti-glaucoma medications at baseline and 213 (67.6%) eyes using anti-glaucoma medications at the final visit. Overall, 133 (42.2%) eyes required an additional or initial anti-glaucoma medication following intravitreal dexamethasone implant treatment.56
Cicinelli et al. (2017)
Cicinelli et al. (2017)57 was a noncomparative, retrospective, observational study. The study aimed at analyzing the effects of intravitreal dexamethasone implants in patients with DME, based on their visual and functional response to initial anti-VEGF (ranibizumab) treatment. The study enrolled consecutive patients with DME who were treated at a single ophthalmology clinic in Italy. All patients included in the study underwent intravitreal injections of ranibizumab performed at fixed 4-week intervals for the first 12 weeks. Then, all patients, regardless of functional and anatomic characteristics, were switched to 0.7 mg dexamethasone implant injections that continued at 4-month intervals until stable BCVA was reached. The study assessed BCVA and CMT at week 12 (end of ranibizumab treatment, baseline for dexamethasone implant treatment), and at 1 month, 4 months, and 12 months after the initiation of dexamethasone implant injections.57
In the ranibizumab loading phase (to week 12), patients received 3.5 (SD = 1.1) ranibizumab injections. Patients who had a poor response to ranibizumab were defined as eyes gaining less than 5 letters measured by ETDRS after 3 intravitreal ranibizumab injections administered monthly. Based on the visual and anatomic changes at week 12, patients were stratified as poor visual response to ranibizumab (n = 30; BCVA mean change = −4.3 [SD = 10.7] letters) versus good visual response to ranibizumab (n = 15; BCVA mean change = 13.9 [SD = 9.2] letters); edema lowering worsening (n = 18) versus improving (n = 27) was also noted. After 12 months from the start of dexamethasone implant treatment, patients with poor response to anti-VEGF treatment showed improvements in BCVA. Stratified by BCVA, the results went from 58.5 (SD = 17.8) letters to 64.1 (SD = 23) letters (P = 0.02). Stratified by CMT, the results went from 58.2 (SD = 25.8) letters to 59.2 (SD = 24) letters (P = 0.03).
Patients with poor response to anti-VEGF treatment also showed a reduction in CMT. Stratified by BCVA, the results went from 529 (SD = 180.9) µm to 363.6 (SD = 32.5) µm (P = 0.9). Stratified by CMT, the results went from 571 (SD = 186.3) µm to 368 (SD = 131.3) µm (P = 0.8). The study did not report IOP at 12 months but observed increased IOP at month 1 (16.76 [SD = 3.04] mm Hg; P = 0.001) and month 4 (16.74 [SD = 3.22] mm Hg; P = 0.004) compared with baseline IOP (14.89 [SD = 1.66] mm Hg).57
Chatziralli et al. (2017)
Chatziralli et al. (2017)58 was a prospective observational study conducted at 3 retina departments in Greece between March 2015 and June 2016. The study aimed to evaluate the effectiveness and safety of 0.7 mg dexamethasone intravitreal implants in patients with DME seen in clinical practice with a follow-up of 12 months. The study enrolled patients with DME who were not responding to previous anti-VEGF treatment (defined as no increase in VA and no reduction in CST after at least 3 anti-VEGF injections). The study assessed BCVA and CST at baseline, 1 month, 3 months, 6 months, 9 months, and 12 months. The study used the Bonferroni correction to adjust for multiplicity in statistical analysis; the level of statistical significance was set at 0.05/5 = 0.01.58
The study included 54 eyes of 54 patients with DME. The study reported improvement in BCVA at all time points. At the end of the 12-month follow-up period, patients received 2.1 (SD = 0.6) dexamethasone implant injections and gained 5.2 letters; 53.7% of patients gained 5 or more letters. With respect to CST, the study reported a reduction at all time points. At month 12, the CST was decreased by 181 µm and 31 (57.4%) patients presented a total resolution of macular edema (defined as no intraretinal or subretinal fluid). There was no statistically significant increase in IOP at month 12 compared to baseline.58
Pacella et al. (2016)
Pacella et al. (2016)59 was a retrospective observational study conducted in Italy. The reported objective of the study was to evaluate the long-term efficacy and safety of dexamethasone implants in patients affected by DME resistant to anti-VEGF therapy. Patients resistant to anti-VEGF therapy were defined as having no improvements in CMT and BCVA values after the loading phase of 3 monthly anti-VEGF intravitreal injections. The study included 32 eyes in 32 patients with DME. In terms of previous anti-VEGF treatments, 16 (50%) patients had bevacizumab, 13 (41%) patients had ranibizumab and 3 (9%) patients had pegaptanib (not available in Canada).59
At baseline, the mean BCVA was 16.54 (SD = 10.85) letters and CMT was 521.8 (SD = 174.5) µm. The study reported that ETDRS values improved at all follow-up visits as compared to baseline. Similar changes were observed for CMT. The changes in BCVA and CMT tended to be smaller toward the end of the 18-month follow-up period as compared to the beginning of the dexamethasone implant treatment. There was no statistically significant increase in IOP at 18 months compared to baseline.59
Degoumois et al. (2015)
Degoumois et al. (2015)60 was a retrospective cohort study conducted from January 2012 to December 2013 in France. The study assessed the effectiveness and safety of dexamethasone implants in treating patients with macular edema in the context of DR or following a retinal detachment surgery. The study included 6 cohorts of patients, including 1 with those patients with diabetes and DME who did not respond to 3 consecutive injections of anti-VEGF (53%). The study compared preinjection and postinjection VA, ocular pressure, and CMT.60
For the DME cohort, the mean VA was 55 ETDRS letters preinjection; this increased to 61.4 letters after dexamethasone implant injections. The average VA gain was 6.7 letters (95% CI, 4.53 to 8.84; P < 0.001). In total, 38% of patients experienced VA improvement greater than 5 letters, another 15% of patients improved more than 10 letters, and 8% of patients improved more than 15 letters. The mean CMT was 510 μm preinjection; this was reduced to 335 μm after dexamethasone implant treatments with a median reduction of 175 μm (95% CI, 142 to 208). The study did not report specific IOP results for the DME cohort.60
Critical Appraisal
The key limitation of the additional sponsor-provided studies was that they lacked a comparator treatment group and, thus, the results observed cannot be attributed to the treatment with a dexamethasone implant. No published protocol was specified or identified for any of the studies, limited details were reported with regard to how patients were chosen, and no sample size or power calculations were provided. As well, potential confounding factors, such as types of diabetes, DR severity, duration of DME before therapy, the treatment interval for dexamethasone implant injections and the duration of the treatment, and methods for adjusting for these were underreported, which means the extent to which these factors may have influenced the results is unknown. Relatedly, it was unclear to what extent patients received concomitant therapies, except in the study by Wallsh et al. In that study, the population was predominantly a mix of patients who received concomitant therapy with anti-VEGF medications, focal or panretinal photocoagulation, or surgical intervention; thus, it is difficult to determine whether the observed treatment effects were due to dexamethasone implants or the combination of these treatments. Most studies did not report methods of controlling for multiplicity, and given the number of statistical analyses conducted within each study, including at multiple time points, there is the potential for type I error. Generally, patients received a smaller number of dexamethasone implant injections (the mean ranged from 1.64 to 2.1) during the study follow-up periods (ranging from 12 months to 18 months) compared to what would be expected in Canadian practice (i.e., repeated injections every 3 months to 4 months), based on input from the clinical expert consulted by CADTH. It is, therefore, unclear how reflective the treatment and results are of Canadian practice.
Discussion
Summary of Available Evidence
Dexamethasone implant (Ozurdex) was previously reviewed by CADTH in 2018 for the treatment of adult patients with DME who are pseudophakic; for this review, it received a recommendation from CDEC not to reimburse in the indicated population. CDEC highlighted the following gaps in evidence: the lack of high-quality direct evidence comparing dexamethasone implants with an active treatment, the fact that pseudophakic patients only formed a subgroup of the study populations in the MEAD trials, uncertainty regarding the magnitude of benefit with dexamethasone implants in the pseudophakic subgroup, and limited data (few patients and limited information for treatment history) to assess the safety and efficacy of dexamethasone implants in patients with prior anti-VEGF therapy.
For this resubmission, the sponsor provided 11 studies to support the current reimbursement request for the use of dexamethasone implants in pseudophakic patients who have had an inadequate response to anti-VEGF therapy. The studies were not available at the time of the initial submission. Of these 11 studies, 1 RCT (Shah et al. [2016]15) that met the CADTH systematic review protocol criteria and 2 retrospective observational studies (Busch et al. [2018]16 and Thomas et al. [2016]17) were summarized and appraised. Eight other published observational studies were also reviewed; however, due to the limitations identified in these studies (including the lack of a relevant comparison), they do not adequately address the evidence gaps identified by CDEC. These other studies are briefly summarized in Table 14, along with their main limitations in regard to informing this review.
Interpretation of Results
Efficacy and Effectiveness
The studies provided for the resubmission only partly address the limitations identified by CDEC with the original submission, which was based primarily on the MEAD trials. An overarching issue with the MEAD trials was that they were not designed to evaluate the efficacy and safety of dexamethasone implants in patients with DME who were pseudophakic, nor were they adequately designed to evaluate the effects of dexamethasone in patients who had had an inadequate response to anti-VEGF treatment. Clinician input for the original submission and resubmission stated that anti-VEGF treatment is the preferred initial therapy for DME. Intravitreal corticosteroids, such as the dexamethasone implant, are usually considered in patients who have not shown improvement in VA and/or edema with 1 or more anti-VEGF treatments and who are pseudophakic (due to the elevated risk of cataract formation in native lenses with intravitreal corticosteroid treatment). Thus, the sponsor’s reimbursement request aligns with the current use of dexamethasone implants by clinicians and the reimbursement criteria set in other jurisdictions (e.g., Quebec [INESSS],62 England [National Institute for Health and Care Excellence]63).
The Shah et al. (2016) RCT appears to have enrolled patients who were not responding as expected to anti-VEGF treatment despite an average of 15 prior anti-VEGF injections to 18 prior anti-VEGF injections. As well, the bevacizumab group only had a mean of 5.6 (SD = 6.1) in improvement in VA from baseline, suggesting patients were indeed not responding well to anti-VEGF treatment. However, only 39% and 52% of patients, respectively, in the bevacizumab and dexamethasone groups had pseudophakic eyes. The imbalance between the groups regarding lens status, the lack of details reported about baseline cataract status, and the lack of a prespecified subgroup analysis makes it difficult to determine what impact these factors had on the study results and how well the results can be extrapolated to the reimbursement population. Likewise, the Busch et al. (2018) and Thomas et al. (2016) studies only enrolled subgroups of patients with a pseudophakic lens (48% and 73% in the dexamethasone groups of the respective studies). As well, in the Busch et al. (2018) study, it was unclear whether patients were truly inadequate responders after 3 doses to 4 doses of a single anti-VEGF drug. The 2 retrospective studies were also variable in terms of how well the enrolled populations matched the target population for treatment in practice and the reimbursement request. Of note, these 2 studies had many design and analysis limitations, in addition to limitations associated with the enrolled populations, that preclude drawing conclusions on their results. Therefore, the new studies do not clearly address the population gaps identified by CDEC.
Another key limitation with the original submission was the comparative data. The MEAD trials compared dexamethasone to sham injection, which is important for establishing efficacy and safety, especially for regulatory approval, but is less informative for reimbursement assessments for which direct comparisons between the treatment and other available active treatments are preferred. The original submission included a network meta-analysis to indirectly compare dexamethasone implants with other treatments for DME; however, limitations with the methods and unaccounted-for between-trial heterogeneity precluded drawing conclusions on the results of the analysis. Phase II RCT comparisons between dexamethasone implants and ranibizumab and bevacizumab were reviewed in the original submission, but again, design and analysis limitations prevented determination of the comparative efficacy or the effectiveness and safety of dexamethasone implants. The Shah et al. (2016), Busch et al. (2018), and Thomas et al. (2016) studies in the resubmission provide direct comparative data; however, as was described in the critical appraisals of these studies, there are serious limitations with the designs and analyses that make it difficult to determine how the effects compare between dexamethasone implants and the comparators — primarily, anti-VEGF therapies. For example, imbalances in patient characteristics and lack of reporting on all important confounders and/or effect modifiers mean that the treatment effects observed in the studies may not be due to dexamethasone implants. As well, while anti-VEGF therapies were identified as relevant comparators for this review, it could not be determined to what extent prior anti-VEGF treatment and inadequate response influenced the effects observed between the studied anti-VEGF and dexamethasone implant groups. As discussed with the clinical expert consulted for the review, the use of bevacizumab as the comparator in the Shah et al. (2016) study may not have been appropriate because of what the expert described as an extensive anti-VEGF treatment history before enrolling in the study. The clinical expert also noted the lack of improvement in CST to accompany the improvement in VA in the bevacizumab group, which was not consistent with clinical experience. None of the submitted studies compared dexamethasone implants with triamcinolone, and no such studies were identified in the search of the literature. Given that triamcinolone is the other available corticosteroid used to treat DME in Canada and was not evaluated in the studies, the data for the resubmission does not completely address this evidence gap.
The magnitude of the treatment effect with dexamethasone implant remains uncertain. Across the reviewed studies, dexamethasone appeared to provide improvement in VA by approximately 5 ETDRS letters to 8 ETDRS letters from baseline. This change from baseline may be clinically important for certain patients, primarily those with worse VA at baseline. The clinical expert consulted by CADTH noted that a 5-letter improvement in ETDRS letters is the minimum change that would be perceptible by patients and, as in the original review of dexamethasone, the benefit with treatment appears to be modest. The observed reductions in CST across the studies from baseline were greater than the 50 µm that the clinical expert considered to be the minimum for a clinically meaningful change. Importantly, the between-group differences in the Shah et al. (2016), Busch et al. (2018), and Thomas et al. (2016) studies are difficult to interpret because of the aforementioned study design and analysis limitations, as well as the limited precision in the between-group estimates based on the generally wide CIs and measures of variance for between-group mean differences. The clinical expert consulted by CADTH noted that there is variability in the response to intravitreal corticosteroids, including dexamethasone, in practice. The expert suggested that patients who are more likely to achieve a meaningful response with intravitreal corticosteroids are those who have persistent inflammation after treatment with anti-VEGF therapies because of the different pathways on which each drug class acts. Nonetheless, the provided evidence, while suggestive of benefit and seemingly aligned with clinical practice, does not conclusively establish the comparative efficacy or effectiveness between dexamethasone and other relevant treatments.
The studies in the resubmission indicated that patients in the population of interest required fewer injections with dexamethasone implants than with anti-VEGF therapies, even with the 3-month to 4-month interval for administration instead of the 6-month interval recommended in the product monograph. This finding is not surprising given the administration schedule differences between dexamethasone and the anti-VEGFs. Patient and clinician input to CADTH highlighted the monthly frequency of administration with the anti-VEGF therapies as burdensome and a key factor in adherence to treatment, and noted the desire for a treatment that allows for a longer interval between administrations. While dexamethasone implants may offer this, there were no data regarding the impact on patient HRQoL, preferences, or ability to engage in daily activities, nor were there sufficient data on longer-term adherence to treatment. The clinical expert consulted by CADTH noted that patients who switch to dexamethasone from other injected treatments appreciate the longer interval between dose administrations. However, the expert acknowledged that it is not always clear whether frequency alone improves HRQoL, given there is a trade-off for increased monitoring of AEs and additional treatments to manage the effects (e.g., increased IOP), not to mention whether patients have responded sufficiently to dexamethasone. Therefore, the proposed benefits with the administration schedule for dexamethasone implants have not been conclusively determined yet.
Harms
The AEs of interest with dexamethasone implants are those related to all intravitreal injections (e.g., injection-related infections) and corticosteroids (e.g., increased IOP), and specific to dexamethasone is migration of the implant. The studies provided in the resubmission were not adequately designed to investigate AEs (particularly the design of relatively short follow-up times) and AE reporting in the studies was considered to be poor by CADTH reviewers and the expert consulted for the review.
In Shah et al. (2016), a greater proportion of eyes receiving dexamethasone implants versus bevacizumab reported AEs related to elevated IOP and requiring glaucoma drugs to control. In total, 14 (52%) eyes had an IOP of greater than 21 mm Hg at 1 or more visits versus none in the bevacizumab group. Cataract progression was reported in 7 (26%) eyes receiving dexamethasone implants and 4 (17%) eyes in the bevacizumab group. Ocular SAEs were reported for 2 (7%) eyes on dexamethasone implants versus 3 (13%) eyes in the bevacizumab group; systemic SAEs were reported for 1 (4%) patient in the dexamethasone implant group and 4 (17%) patients in the bevacizumab group. AEs other than the aforementioned outcomes were not assessed in the trial.
There was selective reporting of safety outcomes identified in both studies. The Busch et al. (2018) study did not present any safety outcomes and the Thomas et al. (2016) study did not present comprehensive data on safety outcomes. The Thomas et al. (2016) study reported no significant complications in eyes receiving dexamethasone implants or ranibizumab. The study reported increases in IOP in 2 eyes in the dexamethasone implant group and none in the ranibizumab group, though the increases did not require IOP-lowering medications and these eyes returned to normal IOP at the end of the study. No deaths were reported in any of the studies reviewed.
The clinical expert consulted highlighted that raised IOP is a known risk following the use of dexamethasone implants and IOP is expected to be higher in the first few months of treatment. According to the expert, patients are followed closely in practice for changes in IOP in the first few weeks after the implant has been administered, given that the concentration of the drug peaks within a month of administration. The expert noted that patients presenting with increased IOP are managed in practice with the use of concomitant ocular hypertensives. The expert also mentioned that if patients do not present with increased IOP in the first month of therapy, treating clinicians have fewer concerns that they may experience these symptoms in subsequent months, given that the concentration of dexamethasone in the implant slowly declines, and the effectiveness reduces over time. The expert noted that the proportion of eyes that required ocular hypertensives in the Shah et al. (2016) study was greater than the findings in the MEAD-010 and MEAD-011 trials. The expert indicated that in real-world practice, patients who receive the implant are followed closely initially after the treatment is administered to ensure they do not develop increased IOP. However, if the patients do not present with raised IOP upon receiving the first treatment, the patient will be followed less frequently.
Conclusions
The results of 1 RCT and 2 retrospective studies in patients with DME who had experienced inadequate treatment response with 3 or more injections of anti-VEGF therapy suggested that dexamethasone implants administered every 3 months to 4 months was associated with a modest clinical benefit in VA and CST, with the observed changes in VA close to the minimum change considered clinically meaningful by the clinical expert consulted by CADTH. However, there is uncertainty in the magnitude of the clinical benefit due to several limitations of the studies, which included relatively small sample sizes leading to imprecision in the estimates as well as issues with generalizability related to lens status and treatment history in the studied patients and choice of anti-VEGF therapy. Although all 3 studies provided a comparison with an active treatment (anti-VEGF therapy), the comparative efficacy of dexamethasone implants versus anti-VEGF therapies is uncertain due to the aforementioned issues in addition to observed imbalances in baseline characteristics and sparse reporting of important confounders and effect modifiers. Therefore, it is not possible to conclude based on the studies that the dexamethasone implant is superior in efficacy or effectiveness to any anti-VEGF therapy in patients with DME who are pseudophakic and have had an inadequate response to prior anti-VEGF therapy. The comparative efficacy of dexamethasone implants versus triamcinolone acetonide, a particularly relevant comparator due its use in the post–anti-VEGF setting, remains unknown as no relevant evidence was identified comparing the 2 interventions. Harms outcomes were not comprehensively assessed in any of the studies, but the reported results were consistent with the known safety profile of dexamethasone implants, which includes the risk of IOP elevation and the need for medications to control IOP.
References
1.Ozurdex (dexamethasone): intravitreal implant 0.7 mg [product monograph]. Markham (ON): Allergan Inc.; 2019 Aug 21.
2.Romero-Aroca P. Targeting the pathophysiology of diabetic macular edema. Diabetes Care. 2010;33(11):2484-2485. PubMed
3.Drug Reimbursement Review sponsor submission: Ozurdex (dexamethasone intravitreal implant), 0.7 mg [internal sponsor's package]. Markham (ON): Allergan Inc.; 2022 Jun 7.
4.Bandello F, Lattanzio R, Zucchiatti I, Del Turco C. Pathophysiology and treatment of diabetic retinopathy. Acta Diabetol. 2013;50(1):1-20. PubMed
5.Mrugacz M, Bryl A, Zorena K. Retinal vascular endothelial cell dysfunction and neuroretinal degeneration in diabetic patients. J Clin Med. 2021;10(3). PubMed
6.Romero-Aroca P, Baget-Bernaldiz M, Pareja-Rios A, Lopez-Galvez M, Navarro-Gil R, Verges R. Diabetic macular edema pathophysiology: vasogenic versus inflammatory. J Diabetes Res. 2016;2016:2156273. PubMed
7.Diabetes Canada. Diabetes in Canada: 2022 backgrounder. 2022; https://www.diabetes.ca/DiabetesCanadaWebsite/media/Advocacy-and-Policy/Backgrounder/2022_Backgrounder_Canada_English_1.pdf. Accessed 2022 Aug 14.
8.Petrella RJ, Blouin J, Davies B, Barbeau M. Prevalence, demographics, and treatment characteristics of visual impairment due to diabetic macular edema in a representative Canadian cohort. J Ophthalmol. 2012;2012:159167. PubMed
9.Cade WT. Diabetes-related microvascular and macrovascular diseases in the physical therapy setting. Phys Ther. 2008;88(11):1322-1335. PubMed
10.Ciulla TA, Amador AG, Zinman B. Diabetic retinopathy and diabetic macular edema: pathophysiology, screening, and novel therapies. Diabetes Care. 2003;26(9):2653-2664. PubMed
11.Mohamed Q, Gillies MC, Wong TY. Management of diabetic retinopathy: a systematic review. JAMA. 2007;298(8):902-916. PubMed
12.Williams R, Airey M, Baxter H, Forrester J, Kennedy-Martin T, Girach A. Epidemiology of diabetic retinopathy and macular oedema: a systematic review. Eye (Lond). 2004;18(10):963-983. PubMed
13.CADTH Canadian Drug Expert Committee (CDEC) final recommendation: dexamethasone (Ozurdex - Allergan Canada Inc.) for the treatment of adult patients with diabetic macular edema who are pseudophakic. Ottawa (ON): CADTH; 2018: https://www.cadth.ca/sites/default/files/cdr/complete/SR0535_Ozurdex_Oct-26-18.pdf. Accessed 2022 Oct 4.
14.CADTH Clinical Review Report: dexamethasone (Ozurdex - Allergan Canada Inc.) for the treatment of adult patients with diabetic macular edema who are pseudophakic. Ottawa (ON): CADTH; 2018: https://www.cadth.ca/sites/default/files/cdr/clinical/SR0535_Ozurdex%20_CL_Report.pdf. Accessed 2022 Oct 4.
15.Shah SU, Harless A, Bleau L, Maturi RK. Prospective randomized subject-masked study of intravitreal bevacizumab monotherapy versus dexamethasone implant monotherapy in the treatment of persistent diabetic macular edema. Retina. 2016;36(10):1986-1996. PubMed
16.Busch C, Zur D, Fraser-Bell S, et al. Shall we stay, or shall we switch? Continued anti-VEGF therapy versus early switch to dexamethasone implant in refractory diabetic macular edema. Acta Diabetol. 2018;55(8):789-796. PubMed
17.Thomas BJ, Yonekawa Y, Wolfe JD, Hassan TS. Contralateral eye-to-eye comparison of intravitreal ranibizumab and a sustained-release dexamethasone intravitreal implant in recalcitrant diabetic macular edema. Clin Ophthalmol. 2016;10:1679-1684. PubMed
18.Vu HT, Keeffe JE, McCarty CA, Taylor HR. Impact of unilateral and bilateral vision loss on quality of life. Br J Ophthalmol. 2005;89(3):360-363. PubMed
19.Davidov E, Breitscheidel L, Clouth J, Reips M, Happich M. Diabetic retinopathy and health-related quality of life. Graefes Arch Clin Exp Ophthalmol. 2009;247(2):267-272. PubMed
20.Gonder JR, Walker VM, Barbeau M, et al. Costs and quality of life in diabetic macular edema: Canadian burden of diabetic macular edema observational study (C-REALITY). J Ophthalmol. 2014;2014:939315. PubMed
21.Happich M, Reitberger U, Breitscheidel L, Ulbig M, Watkins J. The economic burden of diabetic retinopathy in Germany in 2002. Graefes Arch Clin Exp Ophthalmol. 2008;246(1):151-159. PubMed
22.Kempen JH, O'Colmain BJ, Leske MC, et al. The prevalence of diabetic retinopathy among adults in the United States. Arch Ophthalmol. 2004;122(4):552-563. PubMed
23.Klein R, Klein BE, Moss SE, Davis MD, DeMets DL. The Wisconsin epidemiologic study of diabetic retinopathy. IV. Diabetic macular edema. Ophthalmology. 1984;91(12):1464-1474. PubMed
24.Hooper P, Boucher MC, Cruess A, et al. Excerpt from the Canadian Ophthalmological Society evidence-based clinical practice guidelines for the management of diabetic retinopathy. Can J Ophthalmol. 2017;52 Suppl 1:S45-s74. PubMed
25.Kaur H, Maberley D, Chang A, Hay D. The current status of diabetes care, diabetic retinopathy screening and eye-care in British Columbia's First Nations communities. Int J Circumpolar Health. 2004;63(3):277-285. PubMed
26.Maberley D, Walker H, Koushik A, Cruess A. Screening for diabetic retinopathy in James Bay, Ontario: a cost-effectiveness analysis. CMAJ. 2003;168(2):160-164. PubMed
27.Tennant MT. Ocular treatment of diabetic macular edema in Canada: where are we going? Can J Ophthalmol. 2011;46(3):221-224. PubMed
28.Photocoagulation for diabetic macular edema. Early Treatment Diabetic Retinopathy Study report number 1. Early Treatment Diabetic Retinopathy Study research group. Arch Ophthalmol. 1985;103(12):1796-1806. PubMed
29.Antithrombotic Trialists C. Collaborative meta-analysis of randomised trials of antiplatelet therapy for prevention of death, myocardial infarction, and stroke in high risk patients. BMJ. 2002;324(7329):71-86. PubMed
30.Goatman KA. A reference standard for the measurement of macular oedema. Br J Ophthalmol. 2006;90(9):1197-1202. PubMed
31.Jain A, Varshney N, Smith C. The evolving treatment options for diabetic macular edema. Int J Inflam. 2013:689276.
32.Diabetic Retinopathy Clinical Research N, Wells JA, Glassman AR, et al. Aflibercept, bevacizumab, or ranibizumab for diabetic macular edema. N Engl J Med. 2015;372(13):1193-1203. PubMed
33.Korobelnik JF, Do DV, Schmidt-Erfurth U, et al. Intravitreal aflibercept for diabetic macular edema. Ophthalmology. 2014;121(11):2247-2254. PubMed
34.Mitchell P. Three-year safety and efficacy of ranibizumab in patients with visual impairment due to diabetic macular edema: the RESTORE Extension Study. Abstract presented at: American Academy of Ophthalmology Annual Meeting; 2012 Nov 12; Chicago IL. 2017: https://secure.aao.org/aao/meeting-archive. Accessed 2022 Oct 4.
35.Mitchell P, Bandello F, Schmidt-Erfurth U, et al. The RESTORE study: ranibizumab monotherapy or combined with laser versus laser monotherapy for diabetic macular edema. Ophthalmology. Vol 1182011. Accessed 4/2011.
36.Porta M, Striglia E. Intravitreal anti-VEGF agents and cardiovascular risk. Intern Emerg Med. 2020;15(2):199-210. PubMed
37.Gonzalez VH, Campbell J, Holekamp NM, et al. Early and long-term responses to anti-vascular endothelial growth factor therapy in diabetic macular edema: analysis of protocol I data. Am J Ophthalmol. 2016;172:72-79. PubMed
38.Kenalog-10 injection (triamcinolone acetonide injectable suspension (U.S.P)); 10 mg/mL [prescribing information]. Montréal (QC): Bristol-Myers Squibb Canada; 2021: https://pdf.hres.ca/dpd_pm/00062329.PDF. Accessed 2022 Aug 14.
39.Eylea (aflibercept injection): single use pre-filled syringes and single use vials for the treatment of a single eye, 2 mg / 0.05 mL solution for intravitreal injection [product monograph]. Mississauga (ON): Bayer Inc.; 2022: https://pdf.hres.ca/dpd_pm/00064757.PDF. Accessed 2022 Oct 4.
40.Lucentis (ranibizumab injection): single use vials, single use pre-filled syringes, 10 mg/mL solution for injection [product monograph]. Dorval (QC): Novartis Pharmaceuticals Canada Inc.; 2021: https://pdf.hres.ca/dpd_pm/00064117.PDF. Accessed August 14, 2022.
41.Abevmy (bevacizumab for injection): 100 mg and 400 mg vials, 25 mg/mL solution for injection [product monograph]. Etobicoke (ON): BGP Pharma ULC; 2022: https://pdf.hres.ca/dpd_pm/00065758.PDF. Accessed 2022 May 2.
42.Elman MJ, Aiello LP, Beck RW, et al. Randomized trial evaluating ranibizumab plus prompt or deferred laser or triamcinolone plus prompt laser for diabetic macular edema. Ophthalmology. 2010;117(6):1064-1077.e1035. PubMed
43.Ozurdex – Œdème maculaire diabétique. Quebec (QC): Institut national d'excellence en santé et en services sociaux (INESSS); 2016: https://www.inesss.qc.ca/fileadmin/doc/INESSS/Inscription_medicaments/Avis_au_ministre/Fevrier_2016/Ozurdex_2016_02_cav.pdf.
44.McGowan J, Sampson M, Salzwedel DM, Cogo E, Foerster V, Lefebvre C. PRESS Peer Review of Electronic Search Strategies: 2015 guideline statement. J Clin Epidemiol. 2016;75:40-46. PubMed
45.Grey matters: a tool for searching health-related grey literature. Ottawa (ON): CADTH; 2019: https://greymatters.cadth.ca/. Accessed 2022 Jul 6.
46.Drug Reimbursement Review: dexamethasone (Ozurdex - Allergan Canada Inc.) for diabetic macular edema. Ottawa (ON): CADTH; 2018: https://www.cadth.ca/dexamethasone. Accessed 2022 Oct 4.
47.Tewari HK, Kori V, Sony P, Venkatesh P, Garg S. Snellen chart may be preferable over early treatment diabetic retinopathy study charts for rapid visual acuity assessment. Indian J Ophthalmol. 2006;54(3):214. PubMed
48.Beck RW, Maguire MG, Bressler NM, Glassman AR, Lindblad AS, Ferris FL. Visual acuity as an outcome measure in clinical trials of retinal diseases. Ophthalmology. 2007;114(10):1804-1809. PubMed
49.Tangelder GJ, Van der Heijde RG, Polak BC, Ringens PJ. Precision and reliability of retinal thickness measurements in foveal and extrafoveal areas of healthy and diabetic eyes. Invest Ophthalmol Vis Sci. 2008;49(6):2627-2634. PubMed
50.Heeren T. See more with eye. 2021; https://cran.r-project.org/web/packages/eye/vignettes/eye.html. Accessed 2022 Aug 23.
51.Gregori NZ, Feuer W, Rosenfeld PJ. Novel method for analyzing Snellen visual acuity measurements. Retina. 2010;30(7). PubMed
52.Austin PC. A critical appraisal of propensity-score matching in the medical literature between 1996 and 2003. Stat Med. 2008;27(12):2037-2049. PubMed
53.Wang JK, Huang TL, Chang PY, et al. Comparison of intravitreal dexamethasone implant and ranibizumab in vitrectomized eyes with diabetic macular edema. J Ophthalmol. 2021;2021:8882539. PubMed
54.Iglicki M, Busch C, Zur D, et al. Dexamethasone implant for diabetic macular edema in naive compared with refractory eyes: the International Retina Group Real-Life 24-Month Multicenter Study. The IRGREL-DEX Study. Retina. 2019;39(1):44-51. PubMed
55.Pareja-Rios A, Ruiz-de la Fuente-Rodriguez P, Bonaque-Gonzalez S, Lopez-Galvez M, Lozano-Lopez V, Romero-Aroca P. Intravitreal dexamethasone implants for diabetic macular edema. Int J Ophthalmol. 2018;11(1):77-82. PubMed
56.Wallsh J, Luths C, Kil H, Gallemore R. Initial ten years of experience with the intravitreal dexamethasone implant: a retrospective chart review. Clin Ophthalmol. 2020;14:3097-3108. PubMed
57.Cicinelli MV, Cavalleri M, Querques L, Rabiolo A, Bandello F, Querques G. Early response to ranibizumab predictive of functional outcome after dexamethasone for unresponsive diabetic macular oedema. Br J Ophthalmol. 2017;101(12):1689-1693. PubMed
58.Chatziralli I, Theodossiadis P, Parikakis E, et al. Dexamethasone intravitreal implant in diabetic macular edema: Real-life data from a prospective study and predictive factors for visual outcome. Diabetes Therapy Research, Treatment and Education of Diabetes and Related Disorders. 2017;8(6):1393-1404. PubMed
59.Pacella F, Romano MR, Turchetti P, et al. An eighteen-month follow-up study on the effects of Intravitreal Dexamethasone Implant in diabetic macular edema refractory to anti-VEGF therapy. Int J Ophthalmol. 2016;9(10):1427-1432. PubMed
60.Degoumois A, Akesbi J, Laurens C, et al. [Efficacy of intravitreal dexamethasone implants in macular edema excluding venous occlusions: results for a cohort of 80 patients]. Journal Francais d Opthalmologie. 2015;38(2):126-133.
61.Gillies MC, Lim LL, Campain A, et al. A randomized clinical trial of intravitreal bevacizumab versus intravitreal dexamethasone for diabetic macular edema: the BEVORDEX study. Ophthalmology. 2014;121(12):2473-2481. PubMed
62.Ozurdex – Œdème maculaire diabétique. Avis d’ajout d’une indication reconnue aux listes de médicaments – Médicament d’exception – Avec conditions. Québec (QC): Institut national d'excellence en santé et en services sociaux (INESSS); 2016: https://www.inesss.qc.ca/fileadmin/doc/INESSS/Inscription_medicaments/Avis_au_ministre/Fevrier_2016/Ozurdex_2016_02_cav.pdf. Accessed 2022 Sep 10.
63.National Institute for Health and Care Excellence. Dexamethasone intravitreal implant for treating diabetic macular oedema. (Technology appraisal guidance TA349) 2015; https://www.nice.org.uk/guidance/ta349/resources/macular-oedema-diabetic-dexamethasone-intravitreal-implant-final-appraisal-determination-document2.
64.Altun A, Hacimustafaoglu AM. Effect of Dexamethasone Implant on Subfoveal Choroidal Thickness in Early Period in Vitrectomized Eyes with Diabetic Macular Edema. J Ophthalmol. 2021;2021:8840689. PubMed
65.Callanan DG, Loewenstein A, Patel SS, et al. A multicenter, 12-month randomized study comparing dexamethasone intravitreal implant with ranibizumab in patients with diabetic macular edema. Graefes Arch Clin Exp Ophthalmol. 2017;255(3):463-473. PubMed
66.Cornish EE, Teo KY, Gillies MC, et al. Five-year outcomes of eyes initially enrolled in the 2-year BEVORDEX trial of bevacizumab or dexamethasone implants for diabetic macular oedema. Br J Ophthalmol. 2021;02:02.
67.Gupta PC, Ram J, Kumar MP, et al. Effect of sustained-release long-acting intravitreal dexamethasone implant in patients of non-proliferative diabetic retinopathy undergoing phacoemulsification: A randomized controlled trial. Indian J Ophthalmol. 2021;69(11):3263-3272. PubMed
68.Haller JA, Kuppermann BD, Blumenkranz MS, et al. Randomized controlled trial of an intravitreous dexamethasone drug delivery system in patients with diabetic macular edema. Arch Ophthalmol. 2010;128(3):289-296. PubMed
69.Heng LZ, Sivaprasad S, Crosby-Nwaobi R, et al. A prospective randomised controlled clinical trial comparing a combination of repeated intravitreal Ozurdex and macular laser therapy versus macular laser only in centre-involving diabetic macular oedema (OZLASE study). Br J Ophthalmol. 2016;100(6):802-807. PubMed
70.Li X, Wang N, Liang X, et al. Safety and efficacy of dexamethasone intravitreal implant for treatment of macular edema secondary to retinal vein occlusion in Chinese patients: randomized, sham-controlled, multicenter study. Graefes Arch Clin Exp Ophthalmol. 2018;256(1):59-69. PubMed
71.Meyer J, Fry C, Turner A, Razavi H. Intravitreal dexamethasone versus bevacizumab in Aboriginal and Torres Strait Islander patients with diabetic macular oedema: The OASIS study (a randomised control trial). Clin Experiment Ophthalmol. 2022;30:30. PubMed
72.Mishra SK, Sinha S, Chauhan R, Kumar A. Intravitreal Dexamethasone Implant versus Intravitreal Ranibizumab Injection for Treatment of Non-Proliferative Diabetic Macular Edema: A Prospective, Randomized and Blinded Trial. Curr Drug Deliv. 2021;18(6):825-832. PubMed
73.Mishra SK, Gupta A, Patyal S, et al. Intravitreal dexamethasone implant versus triamcinolone acetonide for macular oedema of central retinal vein occlusion: quantifying efficacy and safety. Int J Retina Vitreous. 2018;4:13. PubMed
74.Ramu J, Yang Y, Menon G, et al. A randomized clinical trial comparing fixed vs pro-re-nata dosing of Ozurdex in refractory diabetic macular oedema (OZDRY study). Eye. 2015;29(12):1603-1612. PubMed
75.Mehta H, Fraser-Bell S, Yeung A, et al. Efficacy of dexamethasone versus bevacizumab on regression of hard exudates in diabetic maculopathy: data from the BEVORDEX randomised clinical trial. Br J Ophthalmol. 2016;100(7):1000-1004. PubMed
76.Sarao V, Veritti D, Furino C, et al. Dexamethasone implant with fixed or individualized regimen in the treatment of diabetic macular oedema: six-month outcomes of the UDBASA study. Acta Ophthalmol (Oxf). 2017;95(4):e255-e260. PubMed
77.Simsek M, Citirik M, Ozates S, Tekin K, Ozkoyuncu D. The efficacy of single-dose intravitreal dexamethasone implant for diabetic macular edema refractory to anti-VEGF therapy: real-life results. Beyoglu eye j. 2020;5(1):43-48. PubMed
78.Wei W, Chen Y, Hu B, et al. Multicenter, prospective, randomized study of dexamethasone intravitreal implant in patients with center-involved diabetic macular edema in the Asia-Pacific region. Clin Ophthalmol. 2021;15:4097-4108. PubMed
79.Gumus G, Erdogan G, Gunay BO, Karatas Durusoy G. Comparison of intravitreal dexamethasone implant and posterior subtenon triamcinolone injection in the treatment of diabetic macular edema in vitrectomized eyes. Ophthalmologica. 2022. PubMed
80.Sánchez-González MC, García-Oliver R, Sánchez-González JM, Bautista-Llamas MJ, Jiménez-Rejano JJ, De-Hita-Cantalejo C. Minimum detectable change of visual acuity measurements using ETDRS charts (Early Treatment Diabetic Retinopathy Study). Int J Environ Res Public Health. 2021;18(15). PubMed
81.Beck RW, Moke PS, Turpin AH, et al. A computerized method of visual acuity testing: adaptation of the early treatment of diabetic retinopathy study testing protocol. Am J Ophthalmol. 2003;135(2):194-205. PubMed
82.Center for Drug Evaluation and Research. Statistical review(s). Ozurdex (dexamethasone implant). Company: Allergan, Inc. Application no.: 022315. Approval date: 6/17/2009 (FDA drug approval package). Rockville (MD): U.S. Food and Drug Administration (FDA); 2009: https://www.accessdata.fda.gov/drugsatfda_docs/nda/2009/022315_ozurdex_toc.cfm. Accessed 2022 Jun 1.
83.Center for Drug Evaluation and Research. Medical review(s). Lucentis (ranibizumab) injection. Company: Genentech Inc. Application no.: 125156. Approval date: 06/30/2006 (FDA drug approval package). Rockville (MD): U.S. Food and Drug Administration (FDA); 2006: https://www.accessdata.fda.gov/drugsatfda_docs/nda/2006/125156s0000_LucentisTOC.cfm?msclkid=4347785ecfa611ec9d8762763eaf760e. Accessed 2022 Jun 1.
84.Fundus photographic risk factors for progression of diabetic retinopathy. ETDRS report number 12. Early Treatment Diabetic Retinopathy Study Research Group. Ophthalmology. 1991;98(5 Suppl):823-833. PubMed
85.Davis MD, Bressler SB, Aiello LP, et al. Comparison of time-domain OCT and fundus photographic assessments of retinal thickening in eyes with diabetic macular edema. Invest Ophthalmol Vis Sci. 2008;49(5):1745-1752. PubMed
86.Nunes S, Pereira I, Santos A, Bernardes R, Cunha-Vaz J. Central retinal thickness measured with HD-OCT shows a weak correlation with visual acuity in eyes with CSME. Br J Ophthalmol. 2010;94(9):1201-1204. PubMed
87.Lammer J, Scholda C, Prünte C, Benesch T, Schmidt-Erfurth U, Bolz M. Retinal thickness and volume measurements in diabetic macular edema: a comparison of four optical coherence tomography systems. Retina. 2011;31(1):48-55. PubMed
88.Bressler SB, Edwards AR, Chalam KV, et al. Reproducibility of spectral-domain optical coherence tomography retinal thickness measurements and conversion to equivalent time-domain metrics in diabetic macular edema. JAMA Ophthalmol. 2014;132(9):1113-1122. PubMed
89.Kniestedt C, Stamper RL. Visual acuity and its measurement. Ophthalmol Clin North Am. 2003;16(2):155-170, v. PubMed
90.Recommended stardard procedures for the clinical measurement and specification of visual acuity. Report of working group 39. Committee on vision. Assembly of Behavioral and Social Sciences, National Research Council, National Academy of Sciences, Washington, D.C. Adv Ophthalmol. 1980;41:103-148. PubMed
91.Ricci F, Cedrone C, Cerulli L. Standardized measurement of visual acuity. Ophthalmic Epidemiol. 1998;5(1):41-53. PubMed
92.Rosser DA, Cousens SN, Murdoch IE, Fitzke FW, Laidlaw DAH. How sensitive to clinical change are ETDRS logMAR visual acuity measurements? Invest Ophthalmol Vis Sci. 2003;44(8):3278-3281. PubMed
93.Agelis LE, Peh KK, Chen FK. ETDRS letter score equivalents of Snellen fractions in 158 patients. Invest Ophthalmol Vis Sci. 2012;53(14):4787-4787.
94.Matt G, Sacu S, Buehl W, et al. Comparison of retinal thickness values and segmentation performance of different OCT devices in acute branch retinal vein occlusion. Eye (Lond). 2011;25(4):511-518. PubMed
95.Virgili G, Menchini F, Casazza G, et al. Optical coherence tomography (OCT) for detection of macular oedema in patients with diabetic retinopathy. Cochrane Database Syst Rev. 2015;1:Cd008081. PubMed
96.Browning DJ, Glassman AR, Aiello LP, et al. Relationship between optical coherence tomography-measured central retinal thickness and visual acuity in diabetic macular edema. Ophthalmology. 2007;114(3):525-536. PubMed
Appendix 1: Literature Search Strategy
Note that this appendix has not been copy-edited.
Clinical Literature Search
Overview
Interface: Ovid
Databases:
MEDLINE All (1946-present)
Embase (1974-present)
Note: Subject headings and search fields have been customized for each database. Duplicates between databases were removed in Ovid.
Date of search: July 7, 2022
Alerts: Biweekly search updates until project completion (every other week)
Search filters applied: No filters were applied to limit the retrieval by study type.
Limits:
No publication date or language limits
Conference abstracts: excluded
Syntax | Description |
|---|---|
/ | At the end of a phrase, searches the phrase as a subject heading |
MeSH | Medical Subject Heading |
exp | Explode a subject heading |
* | Before a word, indicates that the marked subject heading is a primary topic; or, after a word, a truncation symbol (wildcard) to retrieve plurals or varying endings |
adj# | Requires terms to be adjacent to each other within # number of words (in any order) |
.ti | Title |
.ot | Original title |
.ab | Abstract |
.hw | Heading word; usually includes subject headings and controlled vocabulary |
.kf | Keyword heading word |
.dq | Candidate term word (Embase) |
.pt | Publication type |
.rn | Registry number |
.nm | Name of substance word (MEDLINE) |
medall | Ovid database code: MEDLINE All, 1946 to present, updated daily |
oemezd | Ovid database code; Embase, 1974 to present, updated daily |
Multi-Database Strategy
(Ozurdex* or Posurdex* or DEX implant* or (dexamethasone adj2 implant*)).ti,ab,kf,ot.
exp dexamethasone/
(dexamethason* or dexametason* or S02BA06 or 7S5I7G3JQL).ti,ab,kf,ot,hw,rn,nm.
2 or 3
Drug Implants/
implant*.ti,ab,kf.
5 or 6
4 and 7
1 or 8
exp diabetes mellitus/
diabet*.ti,ab,kf.
10 or 11
Macular Edema/
(macula* adj3 (edema* or oedema*)).ti,ab,kf.
13 or 14
12 and 15
9 and 16
use medall
(Ozurdex* or Posurdex* or DEX implant* or (dexamethasone adj2 implant*)).ti,ab,kf,dq.
*dexamethasone/
(dexamethason* or dexametason*).ti,ab,kf,dq.
20 or 21
intravitreal implant/ or drug implant/
implant*.ti,ab,kf.
23 or 24
22 and 25
19 or 26
diabetic macular edema/
exp diabetes mellitus/
diabet*.ti,ab,kf.
29 or 30
macular edema/ or retina macula cystoid edema/
(macula* adj3 (edema* or oedema*)).ti,ab,kf.
32 or 33
31 and 34
28 or 35
27 and 36
use oemezd
not (conference abstract or conference review).pt.
18 or 39
remove duplicates from 40
Clinical Trials Registries
Date of search: July 7, 2022
ClinicalTrials.gov
Produced by the U.S. National Library of Medicine. Targeted search used to capture registered clinical trials.
Search: Other field: (Ozurdex OR Posurdex OR "DEX Implant" OR (dexamethasone AND (implant OR implants OR implantation))) AND (diabetes OR diabetic) AND macular AND (edema OR oedema)
WHO ICTRP
International Clinical Trials Registry Platform, produced by the World Health Organization. Targeted search used to capture registered clinical trials.
Search: Home search: (Ozurdex OR Posurdex OR "DEX Implant" OR (dexamethason* AND (implant OR implants OR implant*))) AND (diabetes OR diabetic OR diabet*) AND macular AND (edema* OR oedema*) NOT NCT*
Health Canada’s Clinical Trials Database
Produced by Health Canada. Targeted search used to capture registered clinical trials.
Search terms: Ozurdex, dexamethasone implant, dex implant, diabetic macular edema AND dexamethasone, or diabetic macular oedema
EU Clinical Trials Register
European Union Clinical Trials Register, produced by the European Union. Targeted search used to capture registered clinical trials.
Search: (Ozurdex OR Posurdex OR "DEX Implant" OR (dexamethasone AND (implant OR implants OR implant*))) AND (diabetes OR diabetic OR diabet*) AND macular AND (edema OR oedema)
Grey Literature
Search dates: June 29 – July 4, 2022
Keywords: Ozurdex, Posurdex, dexamethasone (implant), diabetic macular edema/oedema, diabetic retinopathy
Limits: No date limits
Updated: Search updated prior to the completion of stakeholder feedback period
Relevant websites from the following sections of the CADTH grey literature checklist Grey Matters: A Practical Tool for Searching Health-Related Grey Literature were searched:
Health Technology Assessment Agencies
Health Economics
Clinical Practice Guidelines
Drug and Device Regulatory Approvals
Advisories and Warnings
Drug Class Reviews
Clinical Trials Registries
Databases (free)
Internet Search
Appendix 2: Excluded Studies
Note that this appendix has not been copy-edited.
Reference | Reason for exclusion |
|---|---|
Altun et al. (2021)64 | Intervention |
Callanan et al. (2017)65 | Population |
Cornish et al. (2021)66 | Population |
Gillies et al. (2014)61 | Population |
Gupta et al. (2021)67 | Population |
Haller et al. (2010)68 | Population |
Heng et al. (2016)69 | Intervention |
Li et al. (2018)70 | Population |
Meyer et al. (2022)71 | Population |
Mishra et al. (2021)72 | Population |
Mishra et al. (2018)73 | Population |
Ramu et al. (2015)74 | Population |
Mehta et al. (2016)75 | Population |
Sarao76 | Population |
SIMSEK et al. (2020)77 | Population |
Wei et al. (2021)78 | Population |
Gumus et al. (2022)79 | Study design |
Appendix 3: Additional Data
Note that this appendix has not been copy-edited.
The following is an excerpt of the executive summary of the CADTH Clinical Review report for the original Ozurdex submission.
Results and Interpretation
Included Studies
No trials were identified that exclusively enrolled the patient population of interest for this review (i.e., adults with DME who are pseudophakic). Rather, the evidence for this review as it pertains to the use of dexamethasone 700 mcg intravitreal injection was derived from subgroups of adult patients with DME who were pseudophakic from 2 similarly designed masked phase III, multicentre, multinational and sham-controlled pivotal RCTs. MEAD-010 (N = 494) and MEAD-011 (N = 554) randomized DME patients to a 1:1:1 ratio of dexamethasone 700 mcg, dexamethasone 350 mcg (not of a Health Canada–approved dose) or sham treatment. Overall, only a subset of the enrolled population (a prespecified subgroup of adult patients with DME who are pseudophakic [MEAD-010, n = 94; MEAD-011, n = 93] derived from the ITT population and the safety population) met the Health Canada–approved indication. The primary efficacy outcome was the average BCVA mean change from baseline evaluated after 3 years of follow-up based on ETDRS charts using an AUC approach. The MEAD trials were not initially designed to assess the average BCVA mean change from baseline as the primary end point. Rather, the original end point was the proportion of patients who achieved at least a 15-letter improvement by end of study. Subsequent to a protocol amendment was the primary end point changed to include the average BCVA mean change from baseline. Secondary outcomes included other BCVA end points, retinal thickness, HRQoL, and vision-related quality of life.
Key limitations associated with the interpretation results of the subgroup of adult patients who are pseudophakic, as drawn from the MEAD trials, include lack of subgroup stratification leading to imbalances in patient characteristics and therefore concerns with randomization potentially leading to confounding; lack of adjustments for multiple statistical testing across end points, subgroups and sensitivity analyses; variability of treatment effect at different time points; imbalances in patient disposition and patient characteristics; and uncertain generalizability to the Canadian setting.
As there were no studies identified that compared dexamethasone against other active treatments for DME, according to the selection criteria outlined in Table 4, the results of the manufacturer’s indirect comparison (IDC) for the treatment of adult patients with DME were reviewed. In addition, 3 nonpivotal phase II trials comparing dexamethasone with other active treatments for DME were reviewed.
Efficacy
The efficacy results presented from the MEAD trials are for the Health Canada–approved dose of dexamethasone, as a 700 mcg intravitreal injection for the subgroup of patients who are pseudophakic.
The adjusted least squares mean differences in average BCVA mean change from baseline between dexamethasone 700 mcg and sham treatment as measured by ETDRS and using the AUC approach (the primary outcome) in the ITT population were 5.9 letters (||||||||||||||||||||); P < 0.001 and 3.6 letters (||||||||||||||||||||); P = 0.018 in MEAD-010 and MEAD-011, respectively. Sensitivity analyses using a per-protocol population in both MEAD-010 and MEAD-011 were consistent with the primary analysis. According to the clinical expert consulted for this review, the degree of improvement reported in the MEAD trials may be considered clinically relevant, especially for patient with poor VA. However, between-group differences did not exceed a 10-letter improvement. The difference in the proportion of patients achieving an improvement of 15 or more letters versus sham was 18.1% (95% CI, 0.8 to 35.4; P = 0.043) and 6.0% (95% CI, –5.7 to 17.8; P = 0.461) in MEAD-010 and MEAD-011, respectively.
The adjusted least squares mean differences in average CRT, as measured by OCT using the AUC approach, were –117.9 µm |||||||||||||||||||| P < 0.001 and –61.5 µm |||||||||||||||||||| P = 0.007 in MEAD-010 and MEAD-011, respectively. The changes from baseline in CRT as measured by OCT were also evaluated at the last study visit and in a sensitivity analysis using the per-protocol population and were consistent with the AUC method.
The MEAD trials evaluated vision-related outcomes using the using the National Eye Institute Visual Functioning Questionnaire–25 (NEI-VFQ-25). Overall, no statistically significant differences were observed between treatment groups with adjusted average least squares mean differences for the overall composite score of 2.4 (95% CI, –2.0 to 6.8) P = 0.288 and –1.5 (95% CI, –6.2 to 3.3) P = 0.542 in MEAD-010 and MEAD-011, respectively. Minimal clinically important differences for the NEI-VFQ-25 (among the general DME population) between 3.3 and 6.13 points in the overall composite score have been reported.20 No postbaseline data associated to HRQoL measures using the Short Form (36) Health Survey or the EQ-5D health questionnaire were provided for the subgroup of patients who are pseudophakic in the MEAD trials.
No trials were identified that directly compared dexamethasone against other active treatments for DME according to the criteria outlined in the CADTH review protocol (Table 4). The manufacturer submitted an unpublished IDC to assess the comparative efficacy and safety of dexamethasone for use in the treatment of DME. The manufacturer-submitted IDC was originally prepared for the National Institute for Health and Care Excellence in 2014. The analysis included 3 types of treatments for adult patients with DME (intravitreal steroids therapies, laser photocoagulation and intravitreal anti-VEGF drugs) and focused on VA improvement (10-letter analysis) as the primary outcome. Ten letter worsening was also reported as a secondary outcome. ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Three phase II studies (the RAN study, BEVORDEX study, and COMB study) that evaluated the effects of dexamethasone compared with anti-VEGF therapies (ranibizumab, bevacizumab) for the treatment of adult patients with DME were also summarized in Appendix 7. The study findings suggested a similar change from baseline in the BCVA letters between treatment with dexamethasone and anti-VEGF therapy. However, these studies were designed to evaluate the effects of dexamethasone in the general DME population, not the pseudophakic subgroup of patients that is of interest for this review. Of the overall number of enrolled patients, 24% to 50% were pseudophakic. Some pseudophakic subgroup results were reported, however the lack of stratification at randomization based on this factor, as well as the absence of reporting on baseline characteristics for the pseudophakic population make it difficult to assess the comparative efficacy and harms between dexamethasone and anti-VEGF drugs (i.e., bevacizumab and ranibizumab). These studies were also likely underpowered to detect differences between treatments in the pseudophakic subgroup, there was no control for multiple statistical testing, study durations were short, and no Canadian sites were included.
Harms
Frequencies of AEs, SAEs, withdrawal due to adverse events (WDAEs), and notable harms were provided for the individual MEAD trials; however, the most common AEs, SAEs, WDAEs, and notable harms were only reported based on a pooled analysis of the 2 MEAD trials.
A greater proportion of patients in the dexamethasone group experienced AEs compared with the sham group. AEs that occurred more frequently in the dexamethasone treatment groups compared with the sham groups were elevated IOP and secondary cataracts, which is consistent with the AE profile of intravitreal steroid therapies.12,19 The frequency of blepharitis in the dexamethasone groups was lower than those observed in the sham groups. Similar frequencies of SAEs were reported in the dexamethasone groups compared with the sham groups. No data were provided for the subgroup of patients who are pseudophakic regarding the most common reasons for ocular SAEs. The overall WDAEs were similar between treatment groups, however; no data regarding the withdrawals due to ocular AEs were provided for the subgroup of adult patients with DME who are pseudophakic in the MEAD trials.
The occurrence of the remaining notable harms — specifically, eye inflammation, retinal detachment, arterial thrombotic event, dislocated implants, glaucoma, damage to optic nerve, conjunctival hemorrhage, and vitreous hemorrhage — was similar in both treatment groups across the MEAD trials. Endophthalmitis, eye infection, defects in VA and visual field, and necrotizing retinitis were not reported in the MEAD trials.
Other Considerations
In consideration of the potential place in therapy for dexamethasone 700 mcg intravitreal injection (first- or second-line), the protocol for CADTH’s Reimbursement Reviews included the examination of a subgroup of patients with DME who are pseudophakic and who are either unsuitable for anti-VEGF therapy or have had an inadequate response to prior anti-VEGF therapy. However, only between 9.1% and 16.0% of patients included in the MEAD trials had prior experience with anti-VEGF therapy; therefore, it is unclear if the results of the MEAD trials can be generalized to patients with prior experience or prior inadequate response to anti-VEGF therapy. Studies by Pacella et al. and Gonzalez et al. as well as a systematic review and meta-analysis conducted by Khan et al. evaluated the effects of dexamethasone in the general DME population who were refractory to anti-VEGF therapy; however, results in patients with DME who are pseudophakic were not reported.9,21,22 Furthermore, the criteria for anti-VEGF therapy being unsuitable mostly remains unclear. The clinical expert consulted for this CADTH review noted that there are different circumstances that may define a lack of suitability, such as history of glaucoma, allergies to anti-VEGF drugs and its components, pregnancy, phakic lens status with or without recent MI, ischemic heart disease, or stroke. Similarly, patients may be considered unsuitable if they are unable to return for their regular monthly or bimonthly intraocular injection of anti-VEGF either due to transportation difficulties or work demands, which are especially common among younger patients who are actively employed.
Potential Place in Therapy
This information is based on information provided in draft form by the clinical expert consulted by CADTH for the purpose of this review.
The current standard of care for patients requiring treatment of centre-involved DME is intraocular injection of anti-VEGF drugs. While the beneficial effects of anti-VEGF drugs typically only last between 4 and 6 weeks at the most, some patients may not adequately respond to treatment. Furthermore, treating DME with anti-VEGF drugs usually requires monthly or bimonthly injections which create barriers to adherence and therefore optimized treatment. In these cases, further improvement in BCVA is still possible; however, a switch to another anti-VEGF may not be effective or appropriate. According to the clinical expert consulted for this CADTH review, all clinical studies associated to the treatment of DME with anti-VEGF therapy or intravitreal steroid therapy compared favourably to laser treatment. Therefore, currently preferred clinical practice for centre-involved DME is either anti-VEGF or intravitreal steroid injections, with laser therapy being reserved for those with non–centre-involved DME.
For some patients, switching to treatment with an intravitreal steroid such as dexamethasone may be a reasonable alternative; however, the use of this medication class for many patients is currently limited due to elevated IOPs as well as the development and progression of cataracts. The clinical expert consulted for this CADTH review highlighted potential issues in the prescribing of dexamethasone given that treatment is typically associated with increased frequency of elevated IOP, likely requiring IOP-lowering drugs, which may add to the treatment burden (number of concomitant treatments) and the overall cost of treatment. However, the expert noted that IOP-lowering treatments would mostly entail the use of topical medications, which should not be too bothersome. Furthermore, the development and progression of secondary cataracts as a result of intravitreal steroid injections would likely require further treatment to address the issue. For patients who have had complete removal of their natural lens, secondary cataracts will not form on the artificial lens. Generally, treatment regimens with intravitreal steroids are less frequent than those associated with anti-VEGF drugs (quarterly or biannual injections).
The clinical expert consulted for this CADTH review noted that there are different circumstances where alternate therapies such as a dexamethasone implant should be considered, such as in patients who are allergic to anti-VEGF drugs and the components or in women during pregnancy given the teratogenicity of anti-VEGF therapies. In clinical practice, patients with DME who are pseudophakic without any history of glaucoma would be the best candidates to receive treatment with dexamethasone. The same clinical expert noted that intravitreal steroid injections should be particularly considered in those who are pseudophakic with or without recent MI, ischemic heart disease, or stroke. Similarly, dexamethasone may also be considered in patient who are unable to return for their regular monthly or bimonthly anti-VEGF intraocular injection either due to transportation difficulties or work demands, which are especially common among younger patients who are actively employed. Patients who do not respond to the anti-VEGF treatment after 3 consecutive monthly intraocular injections or who have inadequate response to anti-VEGF therapy would also be considered for treatment with dexamethasone.
The clinical expert also highlighted that, overall, the effects of dexamethasone on BCVA reported in the MEAD trials (especially in MEAD-011) were found to be modest when compared with the change in BCVA that has been reported for anti-VEGF therapies. The same clinical expert noted that no specialized diagnostic test would be needed to identify patients in whom dexamethasone may be appropriate and that clinicians would likely base their decision on BCVA as well as OCT CRT, which would be routinely requested in this patient population.
Conclusions
The CADTH systematic review included 2 masked, phase III, sham-controlled RCTs designed to assess the benefits and harms of dexamethasone in adult patients with DME. Given the Health Canada–approved indication for dexamethasone, the CADTH review focused on the results of a subgroup of patients from the MEAD trials (i.e., adult patients with DME who are pseudophakic [MEAD-010 n = 94; MEAD-011 n = 93]).
Overall, dexamethasone was associated with a statistically significant improvement when compared with sham for the primary outcome (average BCVA mean change from baseline as measured by ETDRS based on the AUC approach) for patients with DME who are pseudophakic in both MEAD trials, while the proportion of patients achieving an improvement of 15 or more letters was reported to be statistically significantly greater in the dexamethasone group in MEAD-010 only. However, between-group differences did not exceed a 10-letter improvement in either MEAD-010 or MEAD-011 (differences of 5.9 and 3.6 letters, respectively) and were considered modest by the clinical expert consulted for this review. Further, the magnitude of improvement in VA with dexamethasone compared with sham is uncertain, given the results are for a subgroup that was not subject to stratification at randomization and for which there was no adjustment for multiple testing. More patients in the dexamethasone group experienced AEs compared with the sham group in the MEAD trials. The most commonly reported AEs that occurred more frequently in the dexamethasone treatment groups compared with the sham groups were elevated IOP, which is consistent with the AE risk profile of intravitreal steroid therapies.
No data from the MEAD trials were available to assess the efficacy and safety of dexamethasone 700 mcg in adults with DME who are pseudophakic and who are either unsuitable for anti-VEGF therapy or have had an inadequate response to prior anti-VEGF therapy).
Due to the lack of direct evidence of dexamethasone versus other drugs in the MEAD trials, and the limitations with the supportive evidence including the manufacturer-submitted IDC, no definitive conclusions could be made regarding the comparative efficacy and safety of dexamethasone versus other drugs (including anti-VEGFs) for the treatment of patients with DME who are pseudophakic.
Table 17: Summary of the Efficacy Results for the MEAD Trials — Pseudophakic Subgroup
Outcome | MEAD-010 | MEAD-011 | ||||
|---|---|---|---|---|---|---|
DEX 700 N = 44 | Sham N = 50 | DEX 700 N = 42 | Sham N = 51 | |||
Baseline BCVA | ||||||
Baseline, n (%) | 44 (100) | 50 (100) | 42 (100) | 51 (100) | ||
Mean letters (SD) | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||
BCVA average change from baselinea, b | ||||||
Baseline, n (%) | 44 (100) | 50 (100) | 42 (100) | 51 (100) | ||
Adjusted LSM change from baseline, letters (SD) | 8.1 (|||||) | 2.1 (|||||) | 4.9 (|||||) | 1.3 (|||||) | ||
Adjusted LSM difference vs. sham (95% CI) | 5.9 (|||||||||||) P < 0.001 | 3.6 (||||||||||) P = 0.018 | ||||
BCVA ≥ 15 letter improvement from baseline (last visit) | ||||||
Proportion of patients, n/N (%) | 15/44 (34.1) | 8/50 (16.0) | 5/42 (11.9) | 3/51 (5.9) | ||
Difference vs. sham (95% CI) | 18.1% (0.8 to 35.4) P = 0.042 | 6.0% (–5.7 to 17.8) P = 0.461 | ||||
CRT as measured by OCT average change from baselinea, b | ||||||
Baseline, n (%) | 44 (100) | 50 (100) | 42 (100) | 50 (98) | ||
Adjusted LSM change from baseline, µm (SD) | –137.4 (|||||) | –43.3 (|||||) | –125.9 (|||||) | –58.3 (|||||) | ||
Adjusted LSM difference vs. sham (95% CI) | ||||||||||||||||||||||||| P < 0.001 | ||||||||||||||||||||||||| P = 0.007 | ||||
NEI-VFQ-25 | ||||||
Overall composite scorec | ||||||
Baseline, n (%) | ||||||||||||||| | ||||||||||||||| | ||||||||||||||| | ||||||||||||||| | ||
Baseline, mean (SD) | ||||||||||||||| | ||||||||||||||| | ||||||||||||||| | ||||||||||||||| | ||
Adjusted LSM change from baseline at last visit (SD) | ||||||||||||||| | ||||||||||||||| | ||||||||||||||| | ||||||||||||||| | ||
Adjusted LSM average change from baseline (SD)d | ||||||||||||||| | ||||||||||||||| | ||||||||||||||| | ||||||||||||||| | ||
Adjusted average LSM difference vs. comparator (95% CI) | |||||||||||||||||||||||||||||| | |||||||||||||||||||||||||||||| | ||||
ANCOVA = analysis of covariance; ANOVA = analysis of variance; BCVA = best corrected visual acuity; CI = confidence interval; CRT = central retinal thickness; Dex = dexamethasone; ITT = intention-to-treat; LSM = least squares mean; NEI-VFQ-25 = National Eye Institute Visual Functioning Questionnaire–25; OCT = optical coherence tomography; SD = standard deviation; vs. = versus.
Notes: Last visit refers to either month 39 or month 36 which ever was the final visit.
Outcomes were evaluated using an ITT analysis.
No adjustments for multiple statistical tests were made for any outcomes in the subgroup of adult patients with DME who were pseudophakic.
LOCF was used to impute missing data. Patients without postbaseline BCVA were set to value 0 in the analysis.
The overall composite score was calculated by averaging all 11 vision-targeted subscale scores, excluding general health score.
Means and mean differences were analyzed using an ANCOVA model stratified by treatment and study as fixed effects and baseline BCVA as the covariate, with the exception of OCT retinal outcomes which used baseline CRT as measured by OCT as the covariate.
P values from ANOVA with treatment as a factor for baseline and ANCOVA with treatment as a factor and baseline value as a covariate for postbaseline visits.
aBased on AUC approach and observed data.
bMissing data were not imputed.
cLOCF was used to impute missing data.
dBased on AUC approach and observed data and missing data were not imputed.
Sources: MEAD-010 CSR23 and MEAD-011 CSR.24
Table 18: Summary of the Harms for the MEAD Trials — Pseudophakic Subgroup
Outcome | Pooled data (MEAD-010 and MEAD-011) | |
|---|---|---|
DEX 700 N = 85 | Sham N = 100 | |
AEs, n (%) | ||
Subjects with > 0 AEs | 63 (74.1) | 61 (61.0) |
Most common AEsa | ||
Conjunctival hyperaemia | ||||||||||||||| | ||||||||||||||| |
Posterior capsule opacification | 4 (4.7) | 6 (6.0) |
Blepharitis | ||||||||||||||| | ||||||||||||||| |
SAEs, n (%) | ||
Subjects with > 0 SAEs | ||||||||||||||| | ||||||||||||||| |
Treatment-related | ||||||||||||||| | ||||||||||||||| |
WDAEs, n (%) | ||||||||||||||| | ||||||||||||||| |
Most common reasons | ||||||||||||||| | ||||||||||||||| |
Deaths | ||
Number of deaths, n (%) | 1 (1.2) | 2 (2.0) |
Most common reasons | ||
Acute renal failure | ||||||||||||||| | ||||||||||||||| |
Cardiac arrest | ||||||||||||||| | ||||||||||||||| |
Myocardial ischemia | ||||||||||||||| | ||||||||||||||| |
Notable Harms, n (%) | ||
Elevated IOP | 25 (29.4) | 9 (9.0) |
IOP increased | ||||||||||||||| | ||||||||||||||| |
Ocular hypertension | ||||||||||||||| | ||||||||||||||| |
Open angle glaucoma | ||||||||||||||| | ||||||||||||||| |
Glaucoma | ||||||||||||||| | ||||||||||||||| |
Conjunctival hemorrhage | ||||||||||||||| | ||||||||||||||| |
Secondary cataract | 5 (5.9) | 2 (2.0) |
Vitreous detachment | ||||||||||||||| | ||||||||||||||| |
Vitreous hemorrhage | ||||||||||||||| | ||||||||||||||| |
Anterior chamber inflammation | ||||||||||||||| | ||||||||||||||| |
Detachment of retinal pigment epithelium | ||||||||||||||| | ||||||||||||||| |
Retinal detachment | ||||||||||||||| | ||||||||||||||| |
Device dislocation | ||||||||||||||| | ||||||||||||||| |
Optic nerve cupping | ||||||||||||||| | ||||||||||||||| |
Endophthalmitis | ||||||||||||||| | ||||||||||||||| |
Eye infection | ||||||||||||||| | ||||||||||||||| |
Defects in visual acuity and visual field | ||||||||||||||| | ||||||||||||||| |
Necrotizing retinitis | ||||||||||||||| | ||||||||||||||| |
AE = adverse event; Dex = dexamethasone; IOP = intraocular pressure; NR = not reported; SAE = serious adverse event; WDAE = withdrawal due to adverse event.
Note: Ocular harms were evaluated in the Safety Population.
aFrequency of greater than 5%.
Sources: MEAD-010 CSR23 and MEAD-011 CSR.2
Appendix 4: Description and Appraisal of Outcome Measures
Note that this appendix has not been copy-edited.
Aim
To describe the following outcome measures and review their measurement properties (validity, reliability, responsiveness to change, and minimal important difference [MID]):
VA assessed by the ETDRS letter score
CST assessed by SD-OCT
Findings
Table 19: Summary of Outcome Measures and Their Measurement Properties
Outcome measure | Type | Conclusions about measurement properties | MID |
|---|---|---|---|
Visual acuity assessed by the ETDRS letter score | A chart that measures visual acuity. Represents a series of 5 letters of equal difficulty of reading on each row, with standardized spacing between letters and rows: a total of 14 lines (70 letters). A maximum score is 100.48 | Validity: No relevant evidence of validity found in patients with DME. Reliability: Test-retest reliability: 2 studies reported almost perfect agreements (ICC ranged from 0.866 to 0.96) in health participants or patients with various eye diseases including diabetic retinopathy.80,81 Responsiveness: No relevant evidence of responsiveness found in patients with DME. | There has been no derivation of an MID for the ETDRS in patients with DME; the FDA recommends a mean change of 15 letters or more on an ETDRS chart as clinically relevant outcomes in studies of patients with DME.82,83 |
CST assessed by OCT | An instrument to create cross-sectional maps of the retinal structures and quantify retina thickness in patients with macular edema.30 | Validity: Construct validity: A moderate correlation between visual acuity and OCT centre point thickness has been observed (r ranged from – 0.459 to 0.67) in health patients with DME or macular oedema.49,84-86 Reliability: In a study of 30 patients with DME, a comparison of measurements with 4 different OCT devices found good intradevice repeatability(ICC greater than 0.9 ), but statistically significant differences in retinal thickness values across different devices.87 SD-OCT using Heidelberg Spectralis was found to be less variable compared with TD-OCT using Zeiss Stratus and SD-OCT using Zeiss Cirrus scans (Bland-Altman coefficient of repeatability 7%, 12 to 15%, and 14%, respectively) in patients with DME.88 Responsiveness: No relevant evidence of responsiveness found in patients with DME. | The MID for OCT has not been estimated in patient population with DME. |
CST = central subfield thickness; DME = diabetic macular edema; ETDRS = Early Treatment Diabetic Retinopathy Study; ICC = intraclass correlation coefficient; MID = minimal important difference; OCT = optical coherence tomography; SD-OCT = spectral domain optical coherence tomography; TD-OCT = time domain optical coherence tomography.
VA Measured by ETDRS Letter Score
The ETDRS charts, a modified version of the Snellen chart, are based on a design by Bailey and Lovie, and are commonly used in clinical research.47 ETDRS charts present a series of 5 letters of equal difficulty of reading in each row, with standardized spacing between letters and rows; a total of 14 lines (70 letters). Letters range from 58.18 mm to 2.92 mm in height, corresponding to Snellen VA fractions of 20/200 to 20/10, respectively. Letter size increases geometrically and equivalently in every line by a factor of 1.2589 (or 0.1 log unit) moving up the chart. Charts are used in a standard light box, with a background illumination of approximately 150 cd/m.2,89,90 Luminance of the chart can affect VA score and should be reported.47,89
Scores are based on the number of letters correctly read by a patient. The patient reads each letter on each row down the chart and is allowed 1 attempt for each letter. The test continues until the patient reads all of the letters on the chart or cannot read any of the letters on a line. An ETDRS letter score can be calculated when 20 or more letters are read correctly at 4.0 metres (i.e., the VA letter score is equal to the total number of letters read correctly at 4.0 m plus 30. Shorter distances may be used when vision is severely impaired). If fewer than 20 letters are read correctly at 4.0 m, the VA letter score is equal to the total number of letters read correctly at 4.0 m (the number recorded on line 1.0), plus the total number of letters read correctly at 1.0 m in the first 6 lines. The ETDRS letter score could result in a maximum score of 100.48
Scoring for ETDRS charts is designed to produce a logMAR score suitable for statistical analysis in which individual letters score 0.02 log units. ETDRS results can be converted to Snellen fractions, another common measure of VA, in which the numerator indicates the distance at which the chart was read, and the denominator the distance at which a person may discern letters of a particular size. A larger denominator indicates worsening vision. For example, a person with 20/100 vision can read letters at 20 feet that a person with 20/20 vision can read at 100 feet.89,91
A study of 50 participants who were absent of any ocular abnormality reported that a loss of 3 or more lines (≥ 15 letters) on an ETDRS chart corresponds to a doubling of the visual angle and is considered moderate visual loss, while a loss of 6 or more lines (≥ 30 letters) corresponds to a quadrupling of the visual angle and is considered severe.92 The study also indicated that the limitation of ETDRS charts is that it may reliably identify changes in VA of 2 lines (10 letters) or more, but not changes of 1 line (5 letters) or less.92
Assessment of Validity, Reliability, and Responsiveness
Validity: No relevant evidence of validity for ETDRS charts was found in patients with DME.
Reliability: Two studies (study 1, n = 40 health eyes; study 2, n = 265, including 53 healthy eyes and 212 eyes with uncorrected refractive error, age-related macular degeneration, DR, cataract, optic nerve, cornea, uveitis, glaucoma, amblyopia, or other) had accessed the test-retest reliability of the ETDRS charts and reported almost perfect agreements (study 1 intraclass correlation coefficient [ICC]=0.866; study 2 ICC=0.99).80,81
In addition, the reliability of ETDRS charts depends on the baseline VA. For eyes with acuity better than 20/100, a change in VA of 5 or more letters has a greater than 90% probability of being a real change, while for eyes worse than 20/100, a change of 10 or more letters is required for the same reliability.48 Lastly, a floor and ceiling effect of the ETDRS and Snellen charts have been reported when patients are unable to read all letters on the 6/24 lines, or, able to read all the letters on the 6/4 line, respectively.93
Responsiveness
No relevant evidence of responsiveness for ETDRS charts was found in patients with DME.
Minimal Important Difference
To our knowledge, there has been no derivation of an MID for the ETDRS in patients with DME. The US FDA recommends a mean change of 15 letters or more on an ETDRS chart, or a statistically significant difference in the proportion of patients with a change in VA of 15 or more letters, as clinically relevant outcomes in studies of patients with DME.82,83 The 15-letter reference point is still a topic of discussion for the FDA.
Central Subfield Thickness Measured by OCT
OCT is a fast, noninvasive instrument used to create cross-sectional maps of the retinal structures and to quantify retinal thickness in patients with macular edema.30 OCT uses lasers centred on infrared wavelengths to record light reflected from interfaces between materials with different refractive indices, and from materials that scatter light. OCT machines can differentiate 3 reflecting layers thought to be the vitreous/retina, inner/outer photoreceptor segments, and the retinal pigment epithelium/choriocapillaris interfaces. Ultra high-resolution machines can differentiate a fourth layer. During the OCT scan, a series of intersecting, radial cross-sections of the retina are measured. Resolution depends on the software as well as the hardware used and is better around the central axis than lateral areas.30,94 A recent advancement in OCT device technology has been the shift from TD-OCT to SD-OCT, as the latter can acquire data at a higher speed with better image resolution and reduced motion artifact.88
In a previous meta-analysis of the diagnostic test accuracy of OCT-measured foveal thickness for the diagnosis of DME, the pooled estimates of sensitivity and specificity were 0.79 and 0.85, respectively, for a thickness threshold of 250 µm for TD-OCT and 300 µm for newer SD-OCT.95 Additionally, the presence of macular edema can influence OCT measurement precision. In 1 study, the 95% limits of agreement (the scale at which an instrument can detect changes in a patient) for average foveal thickness in healthy eyes was 8 µm, whereas in patients with DME it was 36 µm.95
Assessment of Validity, Reliability, and Responsiveness
Validity: In 2 studies of patients with DME (study 1, n = 251 eyes from 210, study 2 n = 323 eyes), the association between OCT-measured retinal thickness and BCVA has been evaluated to assess the construct validity. A moderate correlation between VA and OCT centre point thickness has been observed (r ranged from 0.52 to 0.67).84,85For every 100 µm decrease in centre point thickness, VA increased by 4.4 letters (95% CI, 3.5 to 5.3).96 A study of 62 eyes (36 patients) with macular oedema have shown similarly weak to modest correlations between VA and CRT determined by OCT(r = –0.459; 95% CI, –0.667 to –0.184).86 A study of 21 eyes with DME of 15 patients treated by laser photocoagulation, changes in centre point thickness were associated with changes in VA, with moderate correlation coefficients of 0.44, 0.30, and 0.43 at 3.5, 8, and 12 months, respectively.49
Reliability: Intradevice repeatability and interdevice reproducibility of measurements depend on a number of factors including retinal pathology, retinal region, region size, OCT model, equipment settings, manual or automated analysis, and operator experience.30 In a study of 30 patients with DME, a comparison of measurements with 4 different OCT devices found good intradevice repeatability(ICC greater than 0.9 ), but statistically significant differences in retinal thickness values across different devices.87 Another study that compared the reproducibility of retinal thickness measurements from OCT images of eyes with DME, 531 eyes measured by TD-OCT using Zeiss Stratus and 717 eyes by SD-OCT using Zeiss Cirrus and Heidelberg Spectralis instruments, and found that SD-OCT devices reported that the Bland-Altman coefficient of repeatability for relative change in CST (the degree of change that could be expected from measurement variability) was lower on SD-OCT using Heidelberg Spectralis compared with TD-OCT using Zeiss Stratus and SD-OCT using Zeiss Cirrus scans (7%, 12 to 15%, and 14%, respectively).88
Responsiveness
No relevant evidence of responsiveness for CST measured by OCT was found in patients with DME.
Minimal Important Difference: MID for CST measured by OCT has not been estimated in patient population with DME.
Pharmacoeconomic Review
Abbreviations
AE
adverse event
BIA
budget impact analysis
DME
diabetic macular edema
DR
diabetic retinopathy
QALY
quality-adjusted life-year
RCT
randomized controlled trial
VEGF
vascular endothelial growth factor
Executive Summary
The executive summary comprises 2 tables (Table 1 and Table 2) and a conclusion.
Item | Description |
|---|---|
Drug product | Dexamethasone (Ozurdex), intravitreal implant |
Submitted price | Dexamethasone intravitreal implant, 0.7 mg, single-use injection: $1,446.03 |
Indication | For the treatment of adult patients with DME who are pseudophakic |
Health Canada approval status | NOC |
Health Canada review pathway | Standard review |
NOC date | April 16, 2015 |
Reimbursement request | For the treatment of adult patients with DME who are pseudophakic and have had an inadequate response to prior anti-VEGF therapy |
Sponsor | Allergan Inc. |
Submission history | Previously reviewed: Yes Indication: DME Recommendation date: October 24, 2018 Recommendation: Do not reimburse Indication: Macular edema, central retinal vein occlusion Recommendation date: April 25, 2012 Recommendation: Do not reimburse |
DME = diabetic macular edema; NOC = Notice of Compliance; VEGF = vascular endothelial growth factor.
Table 2: Summary of Economic Evaluation
Component | Description |
|---|---|
Type of economic evaluation | Cost-utility analysis Markov model |
Target population | Adult patients with DME who are pseudophakic and have had an inadequate response to prior anti-VEGF therapy |
Treatment | Dexamethasone intravitreal implants |
Comparators |
|
Perspective | Canadian publicly funded health care payer |
Outcomes | QALYs, LYs |
Time horizon | 15 years |
Key data sources |
|
Submitted results | Dexamethasone intravitreal implants were dominated by triamcinolone (i.e., dexamethasone intravitreal implants were more costly and equally effective compared to triamcinolone). |
Key limitations |
|
CADTH reanalysis results |
|
DME = diabetic macular edema; LY = life-year; QALY = quality-adjusted life-year; RCT = randomized controlled trial; VEGF = vascular endothelial growth factor.
Conclusions
The CADTH clinical review of the sponsor’s submitted evidence concluded that dexamethasone implants may have a modest clinical benefit in improving visual acuity and reducing central subfield thickness in adult patients with DME who are pseudophakic and have had a prior inadequate response to anti–vascular endothelial growth factor (VEGF) therapy, with uncertainty in the magnitude of the clinical benefit compared to anti-VEGF therapy. Compared to triamcinolone, the comparative efficacy of dexamethasone implants is unknown as no relevant evidence was identified. Thus, the sponsor’s assumption of equivalent efficacy in this patient population between dexamethasone implants and comparators (triamcinolone and a basket of anti-VEGF drugs [aflibercept, ranibizumab]) is uncertain, given methodological and generalizability concerns with the studies used to support these assumptions. These studies, submitted to support the equivalence assumptions, included patients with diabetic macular edema (DME) who had both phakic and pseudophakic eyes, which is not aligned with the reimbursement request). These studies had methodological limitations that affected the interpretation of the results and the generalizability of the findings to the target population. These limitations with the available clinical evidence affected the interpretability of the sponsor’s pharmacoeconomic submission.
Due to limitations with the available comparative evidence, CADTH reanalyses assumed that there would be no difference in treatment effects (i.e., no difference in total quality-adjusted life-years [QALYs] accrued). CADTH therefore conducted a cost comparison assessing the annual drug costs. The annual cost for dexamethasone implants is $2,892 (based on 2 injections per year), which is more costly than bevacizumab and triamcinolone at publicly available list prices. The submitted price of dexamethasone implants would need to be reduced by more than 99% to be equivalent to the lowest-priced comparator (triamcinolone) and by more than 97% to be equivalent to the lowest-priced anti-VEGF drug (bevacizumab). Should re-treatment with dexamethasone implants be more frequent in clinical practice compared with the Health Canada monograph–recommended frequency (2 per year), as indicated by the clinical expert consulted by CADTH for this review, the annual cost of dexamethasone implants would be higher, and a greater price reduction would be required for the annual cost of dexamethasone implants to be equivalent to triamcinolone or bevacizumab.
Based on the CADTH clinical and economic reviews, there is insufficient evidence to support a price premium for dexamethasone implants compared to other available treatments for adult patients with DME who are pseudophakic and have had an inadequate response to prior anti-VEGF therapy. CADTH’s cost comparison analysis assumes that dexamethasone implants will be equally effective compared to other available treatments, which is considered highly uncertain based on the submitted evidence. It remains possible that the incremental benefit with dexamethasone implants may be negative (i.e., lower QALYs gained relative to comparators) and that dexamethasone implants may be more costly and less effective than triamcinolone and/or anti-VEGF drugs. Should dexamethasone be less effective than comparators, even a 100% price reduction may not make dexamethasone implants cost-effective given the reduction in population health. CADTH was unable to explore this uncertainty due to limitations in the available clinical evidence and, therefore, the possibility that dexamethasone implants generate fewer QALYs at a higher cost than comparators should be considered.
Stakeholder Input Relevant to the Economic Review
This section is a summary of the feedback received from the patient groups, registered clinicians, and drug plans that participated in the CADTH review process.
A joint patient input submission was received from 5 groups (Fighting Blindness Canada, the Canadian Council of the Blind, the Canadian National Institute for the Blind, Vision Loss Rehabilitation Canada, and Diabetes Canada). A total of 67 Canadians living with diabetic retinopathy (DR) and DME responded to the survey. Most respondents indicated that they were receiving injections for the treatment of DR or DME, including ranibizumab, aflibercept, and bevacizumab, as well as dexamethasone intravitreal implants. Many respondents had received their last injection 1 year to 5 years ago. Of the respondents, more than half indicated that they were satisfied with their injections and that the injections helped prevent loss of eyesight. Patients noted that an ideal treatment for DR or DME would be one that reduces physical pain from injection, anxiety or fear about the injection, and logistical strain; for example, a treatment that is less invasive or similarly invasive but is administered less frequently requires fewer appointments and/or reduces dependency on caregivers. In addition, patient input noted that those living outside Canada’s urban centres and vulnerable populations experience greater burden. One patient reported experience with dexamethasone implants, which has helped their vision remain stable after progression on other anti-VEGF treatments.
Four clinician groups provided input: the Retina Society of Alberta, the Canadian Retina Society, Eastern Canada Retina Specialists, and retinal specialists from Western Canada. Clinicians indicated that the first-line therapy for DME is an anti-VEGF injection (aflibercept, ranibizumab, bevacizumab, or brolucizumab). However, clinicians noted that not all patients respond to anti-VEGF therapy and such patients would typically be switched to a steroid injection (e.g., triamcinolone acetonide) after receiving approximately 3 months of anti-VEGF therapy without effect. Clinician input indicated that this second-line setting is the expected place in therapy of dexamethasone intravitreal implants. Clinician input noted the potential for dexamethasone intravitreal implants to be used as a complementary drug to further reduce macular edema in patients receiving anti-VEGF injections.
CADTH-participating drug plans sought clarification on what would be considered an inadequate response to anti-VEGF therapy to determine eligibility for dexamethasone implants. The plans also sought clarification on the treatment intervals required for dexamethasone implants, the conditions under which a patient would receive re-treatment, and the maximum duration of treatment. The plans noted that dexamethasone implants need to be administered by a qualified ophthalmologist experienced in intravitreal injections and that there is limited access to specialists in some regions. The plans highlighted the need for regular monitoring of intraocular pressure changes. Finally, the plans noted the presence of confidential negotiated prices for comparators.
Several of these concerns were addressed in the sponsor’s model:
The sponsor’s model compared dexamethasone implants to triamcinolone and a basket of anti-VEGF treatments (ranibizumab and aflibercept). The sponsor assumed that all treatments would have equivalent efficacy.
In addition, CADTH addressed some of these concerns as follows:
CADTH conducted a cost comparison between dexamethasone implants and comparators (including triamcinolone and anti-VEGF drugs [aflibercept, ranibizumab, bevacizumab, brolucizumab]).
CADTH was unable to address the following concerns raised from stakeholder input:
CADTH was unable to assess the cost-effectiveness of dexamethasone implants when used in combination with anti-VEGF treatments.
The CADTH cost comparison is based on publicly available prices and does not consider the presence of confidential negotiated prices.
Economic Review
The current review is for dexamethasone intravitreal implants (Ozurdex) for adult patients with DME who are pseudophakic and have had an inadequate response to prior anti-VEGF therapy.
Economic Evaluation
Summary of Sponsor’s Economic Evaluation
Overview
The sponsor submitted a cost-utility analysis assessing dexamethasone intravitreal implants compared with anti-VEGF treatments (a weighted basket consisting of aflibercept and ranibizumab) and triamcinolone acetonide, an intravitreal steroid.1 The Health Canada indication for dexamethasone implants is for the treatment of adult patients with DME who are pseudophakic,2 which is broader than the sponsor’s reimbursement request (i.e., adult patients with DME who are pseudophakic and have had an inadequate response to prior anti-VEGF therapy).3 The sponsor submitted a request for deviation to restrict its analysis to this reimbursement population. This deviation request was granted by CADTH in September 2021.
Dexamethasone implants are biodegradable intravitreal implants containing 0.7 mg dexamethasone in a single-use device.2 The recommended dose of dexamethasone implants is 0.7 mg per eye (the entire contents of 1 device), with a treatment interval of approximately 6 months between injections and no more than 2 consecutive injections.2 The reinjection of dexamethasone implants is not recommended for patients who experience and retain improved vision or for those who experience a deterioration in vision that is not slowed by dexamethasone implants. Repeat doses should only be considered for patients who experience an initial response to treatment followed by a subsequent loss in visual acuity and for those who, in the physician’s opinion, may benefit from re-treatment without being exposed to “significant risk.”2
The sponsor’s submitted price is $1,446.03 per 0.7 mg dexamethasone implant,3 with an estimated annual cost of $2,892 based on 2 injections per year. Anti-VEGF treatment was assumed by the sponsor to be a weighted basket consisting of 33% ranibizumab (12 injections per year) and 67% aflibercept (6.5 injections per year). This resulted in a per-injection cost of $1,483.52 (8.3 administrations per year) and an annual cost of $12,577 for anti-VEGF treatment. Triamcinolone acetonide was assumed to be administered every 3.5 months (4 mg per injection), resulting in an annual cost of approximately $31.
The clinical outcomes of interest were QALYs and life-years over a 15-year time horizon. Discounting (1.5% per annum) was applied to both costs and outcomes, and a cycle length of 3 months was used. The base-case perspective was that of the Canadian publicly funded health care payer.
Model Structure
The sponsor submitted a Markov model consisting of 12 mutually exclusive health states that categorized patients’ eyes by treatment status (i.e., on treatment, previously treated), better-seeing and worse-seeing eyes, and bilateral or unilateral disease. Patients could enter the model on treatment in their better-seeing eye, worse-seeing eye, or both eyes (i.e., on treatment for bilateral DME). Patients who entered the model with unilateral disease were at risk of developing bilateral DME over time. Patients could remain on treatment for a maximum of 5 years, after which time they received no additional treatment for DME, and their vision was assumed to follow the natural history of vision in eyes with DME. Patients could discontinue treatment before 5 years owing to adverse events (AEs) or a lack or loss of efficacy, after which they were assumed to receive supportive care (a basket consisting of 50% anti-VEGF therapy and 50% watchful waiting with laser treatment). Patients were assumed to be able to either improve or worsen by a maximum of 1 visual acuity state per cycle. A summary of the sponsor’s model structure is available in Appendix 3 (Figure 1).
Model Inputs
The baseline characteristics in the model were based on pooled data from the MEAD trials (MEAD-010 and MEAD-011) for the pseudophakic subgroup. The mean age in this subgroup was 67.5 years and 61.2% of patients were male).4 At baseline, 36.5% of patients had bilateral disease. The sponsor assumed that patients who entered the model with unilateral disease could also develop bilateral disease at the end of year 1 or year 2. The baseline distribution of patients across health states was based on the pseudophakic subgroup of the MEAD trials.4 Transition probabilities for dexamethasone implants were derived from pseudophakic subgroup data observed in the dexamethasone group of the MEAD trials.4
The clinical efficacy and safety inputs for the pharmacoeconomic model were derived from various sources. The sponsor assumed that dexamethasone implants and anti-VEGF treatments are equally effective, based on the findings of a randomized controlled trial (RCT) comparing dexamethasone implants to bevacizumab in patients with diabetes mellitus and persistent DME,5 and that bevacizumab and aflibercept or ranibizumab are equally effective, based on the findings of systematic reviews.6-9 Finally, the sponsor additionally assumed that dexamethasone implants and triamcinolone would be equally effective, based on the findings of a case series involving patients with no DR or mild DR following surgery.10 As a result of these assumptions, the sponsor assumed that there were no differences in the efficacy of dexamethasone implants, triamcinolone, and anti-VEGF treatments. Regarding safety, the following AEs were included in the model: raised intraocular pressure, retinal detachment, endophthalmitis, and vitreous hemorrhage. The rates of AEs for dexamethasone implants were derived from the MEAD trials, while the rates for triamcinolone were assumed to be the same as those of dexamethasone implants.4 The rates of AEs for anti-VEGF treatments were obtained from a published trial of ranibizumab versus laser therapy.11
All-cause mortality data were derived from Canadian life tables, with additional mortality hazards for patients with diabetes relative to the general population (1.93)12 and for those with DME relative to a diabetes population (1.27).13
Utility values for each health state were based on an analysis of Visual Function Questionnaire–Utility Index data obtained from the MEAD clinical trials, which related vision in both the better-seeing eye and the worse-seeing eye simultaneously to derive utility values for DME patients.14,15 A linear regression was performed that included a constant value, along with coefficients modifying the best corrected visual acuity in each eye, which resulted in utility values ranging from ||||||| in the worst state to ||||||| in the best state. Disutilities due to AEs were not included.
The economic model included costs related to drugs (acquisition, administration), AEs, disease management and monitoring, severe vision loss, and subsequent treatment. The dosing for dexamethasone implants and comparators was based on product monographs.2,16-18 Drug acquisition costs for dexamethasone implants were based on the sponsor’s submitted price, and the acquisition costs for comparators were obtained from the Ontario Drug Benefit Formulary.19 Intravitreal administration costs were considered for all treatments.20 Monitoring consisted of the cost of routine monitoring visits, optical coherence tomography, and fluorescein angiography. Patients receiving dexamethasone implants were assumed to require 7 monitoring visits in year 1, while 12 visits were assumed to be required for anti-VEGF treatments and triamcinolone. Costs for severe vision loss attributable to community and residential care for vision loss, along with low vision aids, were included. Costs for the pharmacologic and nonpharmacologic management of AEs were available from the Ontario Drug Benefit Formulary and the Ontario schedules of benefits.19-21
Summary of Sponsor’s Economic Evaluation Results
All analyses were run probabilistically (1,000 iterations for the base-case and scenario analyses). The deterministic and probabilistic results were similar. The probabilistic findings are presented as follows.
Base-Case Results
In the sponsor’s base case, dexamethasone implants were associated with estimated costs of $23,001 and 5.71 QALYs over the 15-year time horizon (Table 3). In sequential analyses, dexamethasone implants were dominated by triamcinolone; that is, dexamethasone implants were more costly and produced the same QALYs compared with triamcinolone (incremental costs = $5,119; incremental QALYs = 0). In the sponsor’s sequential analysis, dexamethasone implants had a 41% probability of being cost-effective at a $50,000 willingness-to-pay threshold. Additional results from the sponsor’s submitted economic evaluation base case are available in Appendix 3.
Table 3: Summary of the Sponsor’s Economic Evaluation Results
Drug | Total costs ($) | Total QALYs | Incremental costs ($) | Incremental QALYs | Sequential ICER ($/QALY) |
|---|---|---|---|---|---|
Triamcinolone | 17,882 | 5.71 | Reference | Reference | Reference |
Dexamethasone implants | 23,001 | 5.71 | 5,119 | 0.00 | Dominated |
Anti-VEGF treatments | 42,460 | 5.71 | 24,578 | 0.00 | Dominated |
ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year; VEGF = vascular endothelial growth factor.
Note: The submitted analyses were based on the publicly available prices of comparators and may not reflect confidential negotiated prices.
Source: Sponsor’s Pharmacoeconomic Submission.3
Sensitivity and Scenario Analysis Results
The sponsor conducted several scenario analyses, including adopting a societal perspective, adopting alternative health state utility values, changing the composition of the anti-VEGF basket, and adopting an alternative discount rate and time horizon. Due to the sponsor’s assumption of equivalent efficacy, none of the scenarios had a meaningful impact on the results. In all scenarios, dexamethasone implants remained dominated by triamcinolone.
CADTH Appraisal of the Sponsor’s Economic Evaluation
CADTH identified several key limitations to the sponsor’s analysis that have notable implications on the economic analysis.
There is uncertainty in the assumption of equivalent efficacy between dexamethasone implants and comparators. The sponsor assumed equivalent efficacy between dexamethasone implants and anti-VEGF treatments (ranibizumab and aflibercept) based on an RCT5 comparing dexamethasone implants to bevacizumab and 2 observational nonrandomized studies involving dexamethasone and ranibizumab22 or anti-VEGF treatments23 (not specified). The assumption of equivalent efficacy between dexamethasone implants and triamcinolone was based on a nonrandomized case series.10 No head-to-head RCTs have been performed comparing dexamethasone implants to ranibizumab, aflibercept, or triamcinolone, and the sponsor determined that an indirect treatment comparison was not feasible. The sponsor justified its assumption of the equivalent effectiveness of dexamethasone implants compared with ranibizumab and aflibercept based on an RCT comparing dexamethasone implants to bevacizumab in patients with diabetes mellitus and persistent DME (Shah et al., [2016]).5 The clinical expert consulted by CADTH for this review indicated that it may be inappropriate to generalize the findings pertaining to bevacizumab to other anti-VEGF drugs (i.e., ranibizumab and aflibercept) in the reimbursement population. Further, as noted in the CADTH Clinical Review report, it is unclear whether the results of the Shah et al. study are generalizable to the reimbursement population, given that 52% of eyes in the dexamethasone implant group were pseudophakic and the included patients had received many prior anti-VEGF injections (15 to 18 injections), which was noted by the clinical expert consulted by CADTH to be in excess of the number of injections typically given to patients with an inadequate response. Additional methodological limitations were noted in the CADTH Clinical Review report pertaining to the Shah et al. trial, as well as limitations with the additional studies provided by the sponsor to support its assumption of equal effectiveness,22,23 which greatly affect the interpretability of the results, as well as their generalizability to the reimbursement population (refer to the CADTH Clinical Review report for details).
CADTH notes that although the sponsor used the findings of the Shah et al. trial to justify its assumption of equivalent efficacy of dexamethasone compared to anti-VEGF treatments, no data from the Shah et al. trial were used in the sponsor’s analysis. Instead, efficacy inputs were based on a pooled analysis of the MEAD trials, which were reviewed as part of an earlier submission to CADTH.24 The MEAD trials compared dexamethasone implants to a watch-and-wait approach and do not provide comparative evidence to support the relationship between dexamethasone implants and relevant comparators (i.e., anti-VEGF drugs and triamcinolone). As noted in the CADTH Clinical Review report, the MEAD trials involved a small proportion of patients who were pseudophakic and had received prior anti-VEGF therapy (9.1% to 16.0%).14,15
The sponsor additionally assumed equivalent efficacy and safety between dexamethasone implants and triamcinolone. The sponsor based this assumption on a prospective, nonrandomized case series of dexamethasone implants or intravitreal triamcinolone in patients with no DR or mild DR following surgery.10 This study included patients with pseudophakic cystoid macular edema with no DR or mild DR, which is a different population than that of the reimbursement request. The clinical expert consulted by CADTH for this review indicated that the results of this study are not generalizable to patients with pseudophakic DME. Thus, the sponsor’s assumption of equivalent effectiveness and safety between dexamethasone implants and triamcinolone in the reimbursement population is not supported by the submitted data.
CADTH was unable to address this fundamental limitation with the sponsor’s analysis. In reanalysis, CADTH assumed that there would be no differences in total QALYs accrued between treatments. This assumption is conservative as there is insufficient evidence to conclude that dexamethasone implants are not less effective than anti-VEGF drugs or triamcinolone in the reimbursement population.
Relevant comparators were omitted. The sponsor compared dexamethasone implants to a weighted basket of anti-VEGF drugs that included aflibercept and ranibizumab. The sponsor assumed that bevacizumab would not be used after an inadequate response to aflibercept or ranibizumab. The clinical expert consulted by CADTH indicated that this is not consistent with Canadian clinical practice, where bevacizumab may be used off-label in this population, although the use of bevacizumab past the first-line setting may be determined, at least in part, by jurisdiction-specific reimbursement policies for anti-VEGF drugs. The clinical expert consulted by CADTH for this review additionally indicated that brolucizumab may be used off-label in this population. Brolucizumab is indicated for the treatment of neovascular (wet) age-related macular degeneration and is currently undergoing review by CADTH for the treatment of DME.25,26
In the CADTH cost comparison, bevacizumab and brolucizumab were included as comparators.
Comparators were not adequately modelled. The sponsor modelled anti-VEGF therapy as a weighted basket instead of modelling each anti-VEGF drug as an individual intervention. The sponsor justified this assumption on the basis of systematic reviews from the literature.6-9 CADTH notes that these reviews are not specific to patients with DME who are pseudophakic and it is unclear whether these drugs would be equally effective and safe in the reimbursement population. According to the clinical expert consulted by CADTH for this review, each anti-VEGF drug has its own efficacy and safety profile in this population, which is not captured by the sponsor’s use of a weighted basket to reflect anti-VEGF therapy. The clinical expert noted that there may be differences in safety between anti-VEGF drugs due to different mechanisms of action. As per CADTH submission requirements, individual comparators should be modelled separately, with relevant AE and discontinuation rates included in the model. Additionally, because treatment sequence was not explored in the model, the use of a basket comparator may lead to patients receiving the same anti-VEGF drug after a prior inadequate response to that drug, which is inappropriate based on clinical expert input.
CADTH was unable to address this limitation in reanalysis. In the CADTH cost comparison, each anti-VEGF drug was considered independently.
The frequency of administration of dexamethasone implants is uncertain. In the pharmacoeconomic model, the sponsor assumed that dexamethasone implants would be received once every 6 months for up to 5 years. While a 6-month injection frequency for dexamethasone implants is consistent with the MEAD trials, the clinical expert consulted by CADTH for this review indicated that, in clinical practice, the injection frequency is tailored to the individual patient and that re-treatment may be more frequent (e.g., up to 4 injections per year), with no maximum number of injections. Further, the Shah et al. trial (used by the sponsor to justify its assumption of equivalent effectiveness between dexamethasone implants and anti-VEGF drugs) used a 3-month injection frequency for dexamethasone implants. Thus, the frequency of administration (and, hence, drug acquisition costs) for dexamethasone implants in the sponsor’s model may be underestimated compared to expected clinical practice and the frequency of administration in the Shah et al. trial. CADTH additionally notes that, as per the Health Canada monograph for dexamethasone implants, a maximum of 2 consecutive injections with an interval of approximately 6 months between injections is recommended.2 The sponsor’s model does not reflect this restriction (i.e., a maximum of 2 consecutive injections); however, clinical expert input indicated that treatment discontinuation is based on clinical considerations rather than the maximum of 2 consecutive dexamethasone implants recommended in the product monograph.
In the CADTH cost comparison, the frequency of dexamethasone implants was considered to be 2 injections per year, in line with the monograph dosing. In scenario analyses, CADTH considered that patients may receive more frequent injections as per clinical expert opinion and the dosing frequency in the Shah et al. trial.
The sponsor’s pharmacoeconomic model lacked transparency. The sponsor’s model relied heavily on visual basic application programming and hard-coded values. In addition, the model contained more than ||||||| IFERROR statements. Both these features make thorough auditing of the sponsor’s model impractical, and it is unclear whether the model is running inappropriately by overriding errors. In addition, the sponsor’s model produced results that lacked face validity given the assumption of equivalent efficacy and safety between treatments. For example, while the sponsor’s model assumed equivalent rates of AEs between dexamethasone implants and triamcinolone, the costs related to AE management differed between treatments (Table 9). Additionally, despite an assumed equivalent discontinuation rate for all treatments, the model predicted different costs related to subsequent treatment for each comparator.
CADTH was unable to address this limitation.
Additionally, the following key assumptions were made by the sponsor and have been appraised by CADTH (refer to Table 4).
Table 4: Key Assumptions of the Submitted Economic Evaluation (Not Noted as Limitations to the Submission)
Sponsor’s key assumption | CADTH comment |
|---|---|
The sponsor submitted a request for deviation to focus its analysis on its reimbursement request (i.e., adult patients who are pseudophakic and have had an inadequate response to prior anti-VEGF therapy) rather than the Health Canada–indicated population, which was granted by CADTH. | Reasonable. The clinical expert consulted by CADTH for this review indicated that dexamethasone implants are typically administered after anti-VEGF therapy. Dexamethasone implants may additionally be used as first-line treatment in the event that anti-VEGF use is inappropriate (e.g., patients with recent stroke, recent myocardial infarction, pregnancy), or in patients who demonstrate intolerance to anti-VEGF therapies. The cost-effectiveness of dexamethasone implants in the first-line setting is unknown. |
Patients who discontinue from treatment are assumed to move to a supportive care strategy that includes a mix of further anti-VEGF therapy (50%) and watchful waiting with laser treatment (50%). | The clinical expert consulted by CADTH for this review noted that this assumption was reasonable. CADTH notes, however, that the sponsor assumed that further anti-VEGF treatment would include only aflibercept or ranibizumab, and additional anti-VEGF treatments such as bevacizumab and brolucizumab were not considered. CADTH notes that bevacizumab and brolucizumab use would be off-label in this population, although brolucizumab is currently under review by CADTH for DME.25 |
Patients switching to another anti-VEGF therapy in the third-line setting would not receive the loading doses but would move directly to the maintenance schedule. | Not appropriate, according to the clinical expert consulted by CADTH, who indicated that patients switching to anti-VEGF treatments would still receive the loading dose before moving to maintenance therapy. The total drug acquisition costs for anti-VEGF treatments may therefore be underestimated. |
Subsequent treatment was assumed to affect costs only, with no effect on outcomes. | Not appropriate, according to the clinical expert consulted by CADTH, who indicated that laser therapy could have some effectiveness in stabilizing vision in the third-line setting. |
Only 1 dose of triamcinolone (4 mg) is assumed to be used per vial, despite it being available in a 40 mg multidose vial.18 | Uncertain. The clinical expert consulted by CADTH noted that vial splitting may not be done for triamcinolone in clinical practice given the risk of infections with compounding. CADTH conducted scenario analyses to explore the impact of vial splitting for triamcinolone. |
Patients receiving anti-VEGF treatments were assumed to require monthly monitoring visits in year 1. | Uncertain. Clinical experts consulted by CADTH indicated that it is unlikely that patients would be monitored outside their injection visits. Given that the sponsor assumed that anti-VEGF treatments would be administered 8.3 times per year (based on a weighted basket of 6.5 injections of aflibercept and 12 injections of ranibizumab), it is likely that costs for monitoring visits are overestimated in the sponsor’s analysis. Dexamethasone implants may be associated with fewer monitoring visits, though this is predicated on the assumption of equal efficacy, which is uncertain. This is unlikely to affect the results due to the relatively small cost of monitoring. |
The sponsor assumed that a watch-and-wait approach and/or best supportive care are not relevant comparators in this population. | Appropriate. The clinical expert consulted by CADTH for this review noted that, while patients with a true nonresponse to anti-VEGF treatments in the first-line setting would be unlikely to receive a subsequent anti-VEGF drug, patients with an inadequate response to initial anti-VEGF therapy typically receive active treatment in the second-line setting. |
Utility values for each health state were based on an analysis of data obtained from MEAD-010 and MEAD-011. | Uncertain whether the patients included in the utility analysis reflect the target population, as 9% to 16% of patients in the MEAD trials were pseudophakic with prior anti-VEGF treatment. |
Disutilities due to adverse events were not included. | Inappropriate but unlikely to affect the conclusion that dexamethasone is dominated by triamcinolone, given the lack of robust comparative data. |
DME = diabetic macular edema; VEGF = vascular endothelial growth factor.
CADTH Reanalyses of the Economic Evaluation
Base-Case Results
Key limitations were identified with the available clinical data informing the treatment benefit of dexamethasone implants in the reimbursement population (i.e., patients with pseudophakic DME and an inadequate response to prior anti-VEGF therapy). Notably, the sponsor assumed that dexamethasone implants would be equally as effective as anti-VEGF drugs and triamcinolone. The CADTH clinical review concluded that, based on the evidence submitted by the sponsor, there is insufficient evidence to conclude that dexamethasone implants are equally as effective as comparators in this population.
In the absence of robust comparative evidence to support a treatment benefit with dexamethasone implants in comparison with relevant comparators, CADTH was unable to derive a base-case estimate of the cost-effectiveness of dexamethasone implants in the reimbursement population. CADTH undertook a cost comparison based on drug acquisition costs (summarized in Table 5), assuming no difference in treatment effects between treatments (i.e., no difference in total QALYs).
In CADTH reanalysis, the annual drug acquisition cost for dexamethasone implants was $2,892 per patient, based on the Health Canada–recommended interval of 6 months between doses (i.e., 2 doses per year). The annual cost of anti-VEGF drugs ranged from $46 (bevacizumab) to $19,399 (ranibizumab), while the annual cost of triamcinolone ranged from $2 to $17 (Table 7). The price reductions required for the annual treatment cost of dexamethasone implants to be equivalent to that of lower cost comparators are shown in Table 5.
Table 5: Summary of the CADTH Cost Comparison Analysis
Price reduction scenario | Annual cost of dexamethasone implant ($)a | Reduction needed (%)b | Reduced annual treatment cost of dexamethasone implant ($) | Savings in treatment cost ($) |
|---|---|---|---|---|
VEGF inhibitors | ||||
Aflibercept | 2,892 | NA | NA | NA |
Bevacizumab (Avastin) | 2,892 | 95.2% to 97.6% | 69 to 138 | 2,754 to 2,823 |
Bevacizumab (Mvasi, generic) | 2,892 | 96.8% to 98.4% | 46 to 93 | 2,800 to 2,846 |
Brolucizumab | 2,892 | NA | NA | NA |
Ranibizumab | 2,892 | NA | NA | NA |
Corticosteroids | ||||
Triamcinolone (Kenalog-40, generic) | 2,892 | 99.9% | 2 | 2,890 |
Triamcinolone (Triesence) | 2,892 | 99.4% to 99.9% | 3 to 17 | 2,875 to 2,889 |
NA = not applicable; VEGF = vascular endothelial growth factor.
Note: CADTH’s reanalysis is based on publicly available prices of the comparator treatments.
aAssumes 2 injections per year as per Health Canada monograph dosing.2
bCalculations based on the following injection frequencies: aflibercept 9 injections in year 1 (7 injections in subsequent years); bevacizumab 6 to 8 injections in year 1 (4 to 7 injections in subsequent years); brolucizumab 7 to 8 injections in year 1 (4 to 7 injections in subsequent years); ranibizumab 12 injections per year; and triamcinolone 3 to 4 injections per year. No price reductions were calculated for dexamethasone implants vs. aflibercept, brolucizumab, or ranibizumab owing to lower annual treatment costs. Full cost details are presented in Appendix 1.
Price Reduction Analysis
In the absence of clinical information to justify a price premium for dexamethasone implants and given that the annual cost of dexamethasone implants is higher than some comparators (i.e., bevacizumab and triamcinolone), a price reduction analysis was performed to understand the percentage price reductions required for dexamethasone implants to be priced similarly to lower-priced comparators (Table 6).
When considering the Health Canada–recommended dosing frequency of 2 dexamethasone implants per year, the sponsor’s submitted price would need to be reduced by 96.8% to 98.4% to be equivalent to those of the lowest-priced anti-VEGF drug (bevacizumab). Compared with triamcinolone, the submitted price of dexamethasone implants would need to be reduced by 99.9% to be equivalent to the lowest-priced drug.
Table 6: Price Reduction Analysis on the CADTH Cost Comparison
Scenario | Sponsor’s submitted price ($) | Reduction needed (%) | Reduced price ($) |
|---|---|---|---|
VEGF inhibitors | |||
Bevacizumab (Mvasi, generic) | 1,446 | 96.8% to 98.4% | 23 to 46 |
Corticosteroids | |||
Triamcinolone (Kenalog-40, generic) | 1,446 | 99.9% | 1 |
VEGF = vascular endothelial growth factor.
Note: CADTH’s reanalysis was based on publicly available prices of the comparator treatments. Drug wastage was included in estimating costs.
Scenario Analyses
CADTH performed scenario analyses to explore uncertainty owing to dosing considerations (Table 10). Clinical expert input received by CADTH for this review indicated that patients may receive up to 4 dexamethasone implants per year in clinical practice. Under this assumption, the submitted price of dexamethasone implants would need to be reduced by more than 98% for the annual cost of treatment to be equivalent between dexamethasone implants and bevacizumab and by more than 99% for the annual cost to be equivalent to triamcinolone.
In a second scenario, CADTH assumed that vial sharing for triamcinolone would not occur (i.e., that unused portions of a vial would be discarded). In this scenario, the submitted price of dexamethasone implants would need to be reduced by more than 99% for the annual treatment costs to be equivalent to triamcinolone.
Issues for Consideration
Brolucizumab is currently undergoing review by CADTH for the treatment of DME.25 Brolucizumab is currently indicated for the treatment of neovascular (wet) age-related macular degeneration; however, clinical expert input noted that brolucizumab is currently used off-label in the reimbursement population. An additional anti-VEGF drug, faricimab, is currently under review by CADTH for the treatment of DME.27 The cost-effectiveness of dexamethasone implants compared to these drugs is unknown.
Clinician group input received for this submission noted the potential for dexamethasone intravitreal implants to be used in combination with anti-VEGF drugs. The clinical effectiveness and, hence, the cost-effectiveness of this treatment approach is unknown.
A biosimilar for ranibizumab (Byooviz) has been recently approved by Health Canada28 and may affect the cost-effectiveness of dexamethasone implants versus ranibizumab depending on the list price.
The sponsor has submitted a resubmission that contains new clinical information and a new pharmacoeconomic model with an adjusted model structure, comparators, assumptions, and inputs in response to the limitations identified with the previously submitted model.29 A budget impact analysis (BIA) was also developed by the sponsor for this resubmission.30 As such, the pharmacoeconomic findings of the current review are different from those in the previous report.
Overall Conclusions
The CADTH clinical review of the sponsor’s submitted evidence concluded that dexamethasone implants may have a modest clinical benefit in improving visual acuity and reducing central subfield thickness in adult patients with DME who are pseudophakic and have had a prior inadequate response to anti-VEGF therapy, with uncertainty in the magnitude of the clinical benefit compared to anti-VEGF therapy. Compared to triamcinolone, the comparative efficacy of dexamethasone implants is unknown as no relevant evidence was identified. Thus, the sponsor’s assumption of equivalent efficacy in this patient population between dexamethasone implants and comparators (triamcinolone, a basket of anti-VEGFs [aflibercept, ranibizumab]) is uncertain given methodological and generalizability concerns with the studies used to support these assumptions. These studies included patients with DME who had both phakic and pseudophakic eyes (i.e., not aligned with the reimbursement request); these studies had methodological limitations that affected the interpretation of the results and the generalizability of the findings to the target population. These limitations with the available clinical evidence affected the interpretability of the sponsor’s pharmacoeconomic submission.
Due to limitations with the available comparative evidence, CADTH reanalyses assumed that there would be no difference in treatment effects (i.e., no difference in total QALYs accrued). CADTH therefore conducted a cost comparison assessing the annual drug costs. The annual cost for dexamethasone implants is $2,892 (based on 2 injections per year), which is more costly than bevacizumab and triamcinolone at publicly available list prices. The submitted price of dexamethasone implants would need to be reduced by more than 99% to be equivalent to the lowest-priced comparator (triamcinolone) and by more than 97% to be equivalent to the lowest-priced anti-VEGF drug (bevacizumab). Should re-treatment with dexamethasone implants be more frequent in clinical practice compared with the Health Canada monograph–recommended frequency (2 per year), the annual cost of dexamethasone implants would be higher, and a greater price reduction would be required for the annual cost of dexamethasone implants to be equivalent to triamcinolone or bevacizumab.
Based on the CADTH clinical and economic reviews, there is insufficient evidence to support a price premium for dexamethasone implants compared to other available treatments for adult patients with DME who are pseudophakic and have had an inadequate response to prior anti-VEGF therapy. CADTH’s cost comparison analysis assumes that dexamethasone implants will be equally effective compared to other available treatments, which is considered highly uncertain based on the submitted evidence. It remains possible that the incremental benefit with dexamethasone implants may be negative (i.e., lower QALYs gained relative to comparators) and that dexamethasone implants may be more costly and less effective than triamcinolone and/or anti-VEGF drugs. Should dexamethasone be less effective than comparators, even a 100% price reduction may not make dexamethasone implants cost-effective given the reduction in population health. CADTH was unable to explore this uncertainty due to limitations in the available clinical evidence, and therefore the possibility that dexamethasone implants generate fewer QALYs at a higher cost than comparators should be considered.
References
1.Pharmacoeconomic evaluation [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Ozurdex (dexamethasone intravitreal implant), 0.7 mg. Markham (ON): Allergan Inc.; 2022 Jun 7.
2.Ozurdex (dexamethasone): intravitreal implant 0.7 mg [product monograph]. Markham (ON): Allergan Inc.; 2019 Aug 21.
3.Saskatchewan drug plan: search formulary. 2022; https://formulary.drugplan.ehealthsask.ca/SearchFormulary. Accessed 2022 Jul.
4.Boyer D, Yoon Y, Belfort R, et al. 3-year randomized sham-controlled trial of dexamethasone intravitreal implant in patients with diabetic macular edema. Ophthalmology. 2014;121:1904-1914. PubMed
5.Shah S, Harless A, Bleau L, Maturi R. Prospective randomized subject-mased study of intravitreal bevacizumab monotherapy versus dexamethasone implant monotherapy in the treatment of persistent diabetic macular edema. Retina. 2016;36(10):1986-1996. PubMed
6.Veritti D, Sarao V, Soppelsa V, Lanzetta P. Managing diabetic macular edema in clinical practice: systematic review and meta-analysis of current strategies and treatment options. Clin Ophthalmol. 2021;15:375-385. PubMed
7.Pham B, Thomas SM, Lillie E, et al. Anti-vascular endothelial growth factor treatment for retinal conditions: a systematic review and meta-analysis. BMJ Open. 2019;9(5):e022031. PubMed
8.Sarohia GS, Nanji K, Khan M, et al. Treat-and-extend versus alternate dosing strategies with anti-vascular endothelial growth factor agents to treat center involving diabetic macular edema: a systematic review and meta-analysis of 2,346 eyes. Surv Ophthalmol. 2022;67(5):1346-1363. PubMed
9.Cai S, Bressler NM. Aflibercept, bevacizumab or ranibizumab for diabetic macular oedema: recent clinically relevant findings from DRCR.net Protocol T. Curr Opin Ophthalmol. 2017;28(6):636-643. PubMed
10.Dang Y, Mu Y, Li L, et al. Comparison of dexamethasone intravitreal implant and intravitreal triamcinolone acetonide for the treatment of pseudophakic cystoid macular edema in diabetic patients. Drug Des Devel Ther. 2014;8:1441-1449. PubMed
11.Mitchell P, Bandello F, Schmidt-Erfurth U. The RESTORE study: ranibizumab monotherapy or combined with laser versus laser monotherapy for diabetic macular edema. Ophthalmology. 2011;120(10):2004-2012. PubMed
12.Mulnier H, Seaman H, Raleigh V, Soedamah-Muthu S, Colhoun H, Lawrenson R. Mortality in people with type 2 diabetes in the UK. Diabet Med. 2006;23(5):516-521. PubMed
13.Hirai F, Knudtson M, Klein B, Klein R. Clinically significant macular edema and survival in type 1 and type 2 diabetes. Am J Ophthalmol. 2008;145(4):700-706. PubMed
14.Clinical Study Report: 206207-010 (MEAD-010). A 3-year, phase 3, multicenter, masked, randomized, sham-controlled trial to assess the safety and efficacy of 700 µg and 350 µg Dexamethasone Posterior Segment Drug Delivery System (DEX PS DDS) applicator system in the treatment of patients with diabetic macular edema [internal sponsor's report]. Irvine (CA): Allergan Inc.; 2013.
15.Clinical Study Report: 206207-011 (MEAD-011). A 3-year, phase 3, multicenter, masked, randomized, sham-controlled trial to assess the safety and efficacy of 700 µg and 350 µg Dexamethasone Posterior Segment Drug Delivery System (DEX PS DDS) applicator system in the treatment of patients with diabetic macular edema [internal sponsor's report]. Irvine (CA): Allergan Inc.; 2013.
16.Eylea (aflibercept injection): single use pre-filled syringes and single use vials for the treatment of a single eye, 2 mg / 0.05 mL solution for intravitreal injection [product monograph]. 2022; https://pdf.hres.ca/dpd_pm/00064757.PDF. Accessed 2022 Jul 15.
17.Lucentis (ranibizumab injection): single use vials, single use pre-filled syringes, 10 mg/mL solution for injection [product monograph]. 2021; https://pdf.hres.ca/dpd_pm/00064117.PDF. Accessed 2022 Jul 15.
18.Triamcinolone acetonide injectable: suspension USP 40 mg/mL [product monograph]. Oakville (ON): SteriMax Inc; 2022: https://pdf.hres.ca/dpd_pm/00066303.PDF.
19.Ontario Ministry of Health, Ontario Ministry of Long-Term Care. Ontario drug benefit formulary/comparative drug index. 2022; https://www.formulary.health.gov.on.ca/formulary/. Accessed 2022 Jul.
20.Schedule of benefits for physician services under the Health Insurance Act: effective October 1, 2021. Toronto (ON): Ontario Ministry of Health; 2022: https://www.health.gov.on.ca/en/pro/programs/ohip/sob/physserv/sob_master.pdf. Accessed 2022 Jul.
21.Schedule of benefits for laboratory services: effective July 1, 2020. Toronto (ON): Ontario Ministry of Health; 2020: https://www.health.gov.on.ca/en/pro/programs/ohip/sob/lab/lab_mn2020.pdf. Accessed 2022 Jul.
22.Thomas B, Yonekawa Y, Wolfe J, Tarek S. Contralateral eye-to-eye comparison of intravitreal ranibizumab and a sustained-release dexamethasone intravitreal implant in recalcitrant diabetic macular edema. Clin Ophthalmol. 2016;10:1679-1684. PubMed
23.Busch C, Zur D, Fraser-Bell S, et al. Shall we stay, or shall we switch? Continued anti-VEGF therapy versus early switch to dexamethasone implant in refractory diabetic macular edema. Acta Diabetol. 2018. PubMed
24.Drug Reimbursement Review: dexamethasone (Ozurdex, Allergan Inc.) for diabetic macular edema. Ottawa (ON): CADTH; 2018: https://www.cadth.ca/dexamethasone.
25.Drug Reimbursement Review: brolucizumab (Beovu, Novartis) for diabetic macular edema. 2022; https://www.cadth.ca/brolucizumab-0. Accessed 2022 Oct 3.
26.Beovu (brolucizumab-dbll) injection, for intravitreal use [highlights of prescribing information]. East Hanover (NJ): Novartis Pharmaceuticals; 2022 May: https://www.novartis.com/us-en/sites/novartis_us/files/beovu.pdf. Accessed 2022 Aug 29.
27.Drug Reimbursement Review: faricimab (Vabysmo, Hoffman-La Roche) for diabetic macular edema. 2022; https://www.cadth.ca/faricimab-0. Accessed 2022 Oct 3.
28.Jeremias S. Health Canada approves first ranibizumab biosimilar. AJMC The Center for Biosimilars. 2022 Mar 10. https://www.centerforbiosimilars.com/view/health-canada-approves-first-ranibizumab-biosimilar. Accessed 2022 Apr 12.
29.Drug Reimbursement Review pharmacoeconomic report: dexamethasone (Ozurdex, Allergan Inc.) for the treatment of adult patients with diabetic macular edema who are pseudophakic. Ottawa (ON): CADTH; 2018: https://www.cadth.ca/sites/default/files/cdr/pharmacoeconomic/SR0535_Ozurdex_PE_Report%20.pdf. Accessed 2022 Oct 3.
30.Budget Impact Analysis [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Ozurdex (dexamethasone intravitreal implant), 0.7 mg. Markham (ON): Allergan Inc.; 2022 Jun 7.
31.Avastin (bevacizumab for injection): 100 mg and 400 mg vials (25 mg/mL solution for injection) [product monograph]. 2022; https://pdf.hres.ca/dpd_pm/00065643.PDF. Accessed 2022 Jul 15.
32.DeltaPA. [Ottawa (ON)]: IQVIA; 2022: https://www.iqvia.com/. Accessed 2022 Jul.
33.Cancer Care Ontario. Funded evidence-informed regimens. 2022; https://www.cancercareontario.ca/en/drugformulary/regimens. Accessed 2022 Jul.
34.Statistics Canada. Population estimates on July 1st, by age and sex. Table: 17-10-0005-01. 2022; https://www150.statcan.gc.ca/t1/tbl1/en/tv.action?pid=1710000501. Accessed 2022 Jul 21.
35.Diabetes Canada. National and provincial backgrounders 2022. 2022; https://www.diabetes.ca/advocacy---policies/advocacy-reports/national-and-provincial-backgrounders. Accessed 2022 Oct 4.
36.Diabetes Canada. Indigenous communities and diabetes. 2022; https://www.diabetes.ca/resources/tools---resources/indigenous-communities-and-diabetes. Accessed 2022 Oct 4.
37.Petrella RJ, Blouin J, Davies B, Barbeau M. Prevalence, demographics, and treatment characteristics of visual impairment due to diabetic macular edema in a representative Canadian cohort. J Ophthalmol. 2012;2012:159167. PubMed
38.Gonzalez VH, Campbell J, Holekamp NM, et al. Early and long-term responses to anti-vascular endothelial growth factor therapy in diabetic macular edema: analysis of Protocol I data. Am J Ophthalmol. 2016;172:72-79. PubMed
39.Dinh T, Sutherland G. Understanding the gap: a pan-Canadian analysis of prescription drug insurance coverage. Ottawa (ON): The Conference Board of Canada; 2017: https://www.conferenceboard.ca/e-library/abstract.aspx?did=9326. Accessed 2022 Oct 3.
Appendix 1: Cost Comparison Table
Note that this appendix has not been copy-edited.
The comparators presented in the following table have been deemed to be appropriate based on feedback from clinical experts. Comparators may be recommended (appropriate) practice or actual practice. Existing Product Listing Agreements are not reflected in the table and as such, the table may not represent the actual costs to public drug plans.
Table 7: CADTH Cost Comparison Table for Diabetic Macular Edema
Treatment | Strength/concentration | Form (vial size if single-use) | Price ($) | Recommended dosagea | Daily cost ($) | Annual cost ($) |
|---|---|---|---|---|---|---|
Dexamethasone intravitreal implants (Ozurdex) | 0.7 mg | Intravitreal implant | 1,446.0300b | 0.7 mg, with 6 months between doses | 7.92 to 15.84 | 2,892 to 5,784 (2 to 4 injections)c |
VEGF inhibitors | ||||||
Aflibercept (Eylea) | 40 mg/mL | 0.05 mL Solution for intravitreal injection | 1,418.0000 | 2 mg every 4 weeks for the first 5 doses followed by 2 mg every 8 weeks. After 12 months the treatment interval may be extended in 2-week increments | Year 1: 34.94 Subsequent: 27.18 | Year 1: 12,762 (9 injections) Subsequent: 9,926 (7 injections) |
Bevacizumab (Avastin) | 25 mg/mL | 4 mL 16 mL Solution for intravitreal injection | 519.1800d 2,076.7104 | 1.25 mg every 4 weeks for the first 3 doses followed by 1.25 mg every 8 to 12 weekse | Year 1: 0.28 to 0.38f Subsequent: 0.19 to 0.33f | Year 1: 104 to 138 (6 to 8 injections)f Subsequent: 69 to 121 (4 to 7 injections)f |
Bevacizumab (Mvasi, generic) | 25 mg/mL | 4 mL 16 mL Solution for intravitreal injection | 347.0000d 1,388.0000 | 1.25 mg every 4 weeks for the first 3 doses followed by 1.25 mg every 8 to 12 weekse | Year 1: 0.19 to 0.25f Subsequent: 0.13 to 0.22f | Year 1: 69 to 93 (6 to 8 injections)f Subsequent: 46 to 81 (4 to 7 injections)f |
Brolucizumab (Beovu) | 120 mg/mL | 0.05 mL Solution for intravitreal injection | 1,390.0000 | 6 mg every 6 weeks for the first 5 doses followed by 6 mg every 8 to 12 weeks | Year 1: 34.25 Subsequent: 26.64 | Year 1: 9,730 to 11,120 (7 to 8 injections) Subsequent: 5,560 to 9,730 (4 to 7 injections) |
Ranibizumab (Lucentis) | 10 mg/mL | 0.23 mL Solution for intravitreal injection | 1,616.5500 | 0.5 mg monthly | Year 1 and subsequent: 53.11 | Year 1 and subsequent: 19,399 (12 injections) |
Corticosteroids | ||||||
Triamcinolone acetonide (Kenalog-40, generic) | 40 mg/mL | Injectable suspension | 5.7750d | 4 mg every 3 to 4 monthsg | 0.01 | 2h |
Triamcinolone acetonide (Triesence) | 40 mg/mL | Suspension for intravitreal injection | 42.5900d | 1 to 4 mg every 3 to 4 monthsg | 0.01 to 0.05 | 3 to 17h |
VEGF = vascular endothelial growth factor.
Note: All prices are from the Ontario Drug Benefit Formulary (accessed July 2022),19 unless otherwise indicated, and do not include dispensing fees. Annual costs are based on 365.25 days per year.
aRecommended doses are from the respective product monographs, unless otherwise indicated.16-18,31 Brolucizumab dosing is based on the FDA product monograph (DME indication).26
bSponsor submitted price.3
cThe product monograph indicates a dosing interval of 6 months between dexamethasone implants. The clinical expert consulted by CADTH for this review indicated that a dosing interval of 3 months may be used in clinical practice.
dPrice from IQVIA DeltaPA (accessed July 2022).32
eBevacizumab is used off-label in this population and, as such, does not have a recommended dosage for DME in the product monograph. Dosing for bevacizumab was based on clinical expert input received by CADTH for this review.
fCosts for bevacizumab were calculated based on the assumption that 30 doses could be obtained per 100 mg (4 mL) vial. This assumption was validated by the clinical expert.
gDose from previous CADTH review of dexamethasone implants.29
hTriamcinolone is available in multidose vials,18 and vial splitting is reflected in the daily and annual cost estimates. Should vial splitting not occur, the annual costs for triamcinolone range from $17 to $23 for Kenalog-40 and from $128 to $170 for Triesence.
Appendix 2: Submission Quality
Note that this appendix has not been copy-edited.
Description | Yes/no | Comments |
|---|---|---|
Population is relevant, with no critical intervention missing, and no relevant outcome missing | No | The sponsor’s analysis did not consider bevacizumab or brolucizumab, which may be relevant comparators according to the clinical expert consulted by CADTH for this review. |
Model has been adequately programmed and has sufficient face validity | No | Numerous IFERROR statements and hard-coding made a thorough validation of the model impractical. The sponsor’s results lack face validity, for example, in that the model predicted different costs related to AEs with dexamethasone implants and triamcinolone, despite the sponsor’s assumption that the rates of AEs would be equal for these treatments. |
Model structure is adequate for decision problem | Yes | No comment. |
Data incorporation into the model has been done adequately (e.g., parameters for probabilistic analysis) | No | Despite the total QALYs being equal in the sponsor’s analysis, the disaggregated QALY breakdown shows slight variation between health states, which lacks face validity given the sponsor’s assumption of equal efficacy. |
Parameter and structural uncertainty were adequately assessed; analyses were adequate to inform the decision problem | No | The sponsor’s base case predicted dexamethasone would be cost-effective at a $50,000 per QALY threshold in 41% of probabilistic iterations, a result that is unreasonable given the assumption of equal efficacy. |
The submission was well organized and complete; the information was easy to locate (clear and transparent reporting; technical documentation available in enough details) | No | Some details were lacking in the technical guidance report pertaining to baseline characteristics, utility values, and discontinuation assumptions. Mean number of injections was not available as a model output. |
AE = adverse event; QALY = quality-adjusted life-year.
Appendix 3: Additional Information on the Submitted Economic Evaluation
Note that this appendix has not been copy-edited.
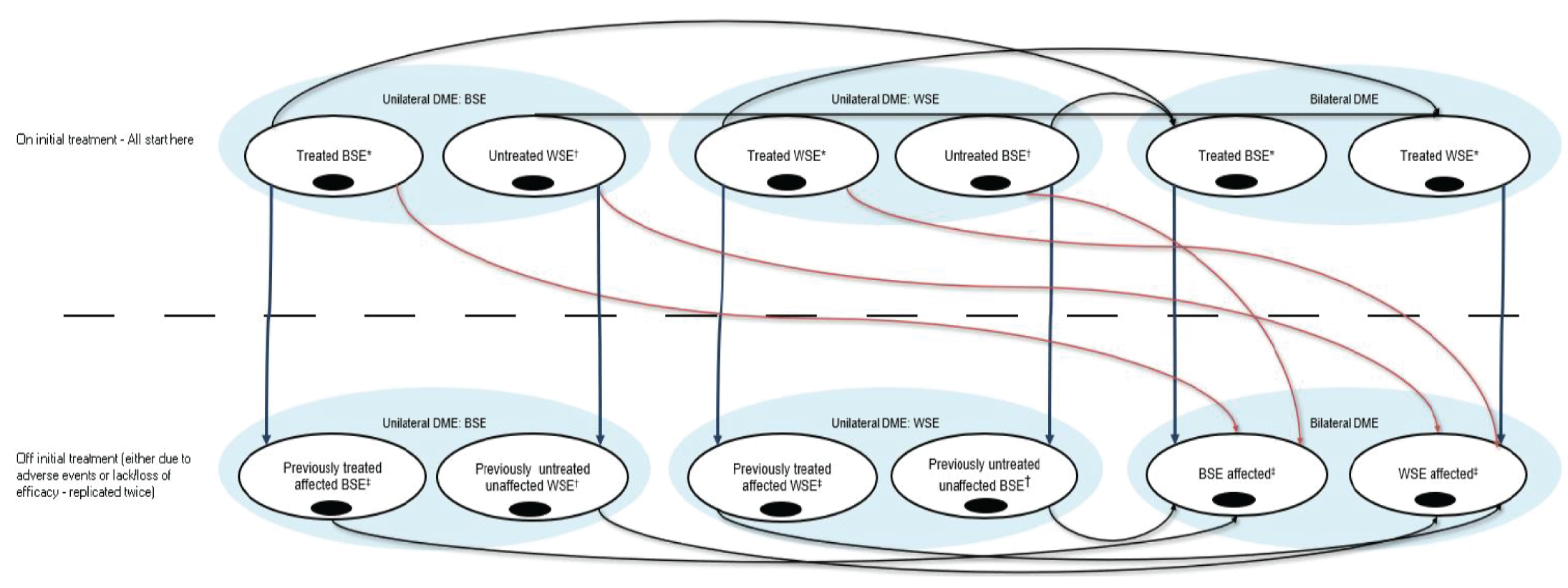
BSE = better-seeing eye; DME = diabetic macular edema; WSE = worse-seeing eye.
Source: Sponsor’s Pharmacoeconomic Submission.3
Detailed Results of the Sponsor’s Base Case
Table 9: Disaggregated Results of the Sponsor’s Base Case
Parameter | Dexamethasone implants | Anti-VEGF treatmentsa | Triamcinolone |
|---|---|---|---|
Discounted LYsb | |||
Total | 9.36 | 9.36 | 9.36 |
Discounted QALYs | |||
Total | 5.71 | 5.71 | 5.71 |
Unilateral BSE | 0.57 | 0.59 | 0.58 |
Unilateral WSE | 1.90 | 2.00 | 1.93 |
Bilateral disease | 3.24 | 3.12 | 3.20 |
Discounted costs ($) | |||
Total | 23,001 | 42,460 | 17,882 |
Drug acquisition | 7,498 | 23,340 | 56 |
Administration | 810 | 2,472 | 984 |
Severe vision loss | 1,881 | 1,777 | 1,804 |
Adverse events | 220 | 0 | 165 |
Medical resource use | 3,419 | 4,949 | 5,012 |
Next line treatment (discontinuation | 5,083 | 6,401 | 6,105 |
Next line treatment (discontinuation | 4,161 | 3,521 | 3,757 |
Pairwise ICER of dexamethasone ($/QALY) | NA | Dexamethasone implants are dominant over anti-VEGFs | Dexamethasone implants are dominated by triamcinolone |
AE = adverse event; BSE = better-seeing eye; LY = life-year; NA = not applicable; QALY = quality-adjusted life-year; VEGF = vascular endothelial growth factor; WSE = worse-seeing eye.
aAnti-VEGF treatments are considered as a basket comparator comprising aflibercept (67%) and ranibizumab (33%).
bDisaggregated LYs are presented deterministically as the sponsor did not report probabilistic LYs gained.
Source: Sponsor’s Pharmacoeconomic Submission.3
Appendix 4: Additional Details on the CADTH Reanalyses and Sensitivity Analyses of the Economic Evaluation
Note that this appendix has not been copy-edited.
Scenario Analyses
Table 10: Summary of Scenario Analyses Conducted on the CADTH Cost Comparison
Price reduction scenario | Annual cost of dexamethasone implant ($) | Reduction needed (%) | Reduced annual treatment cost of dexamethasone implant ($) | Savings in treatment cost ($) |
|---|---|---|---|---|
Scenario 1: Four dexamethasone implants per year | ||||
Bevacizumab (Mvasi, generic) | 5,784 | 98.40% to 99.20% | 46 to 93 | 5,692 to 5,738 |
Triamcinolone (Kenalog-40, generic) | 5,784 | 99.96% to 99.97% | 2 | 5,782 |
Scenario 2: No vial sharing for triamcinolone | ||||
Triamcinolone (Kenalog-40, generic) | 2,892 | 99.20% to 99.40% | 17 to 23 | 2,722 to 2,764 |
VEGF = vascular endothelial growth factor.
Appendix 5: Submitted BIA and CADTH Appraisal
Note that this appendix has not been copy-edited.
Table 11: Summary of Key Take-Aways
Key take-aways of the budget impact analysis |
|---|
|
Summary of Sponsor’s BIA
The submitted BIA assessed the introduction of dexamethasone implants for the treatment of adult patients with DME who are pseudophakic and who have had an inadequate response to prior anti-VEGF therapy.33 The analysis was taken from the perspective of the Canadian public drug plans using an epidemiology-based approach, with only drug acquisition costs included. A 3-year time horizon was used, from fiscal year 2023/24 to fiscal year 2025/26, with fiscal year 2022/23 as a base year. The population size was estimated starting with the prevalence of diabetes followed by a series of attritions. Key inputs to the BIA are documented in Table 12.
The reference case included triamcinolone and a weighted basket of anti-VEGF drugs (i.e., aflibercept and ranibizumab). The market share estimates for these products were based on the opinion of clinical experts consulted by the sponsor. In the new drug scenario, dexamethasone implants were assumed to equally displace triamcinolone and anti-VEGFs.
Key assumptions included:
Patients will receive 2 dexamethasone implants per year.
Dexamethasone implants will displace triamcinolone, aflibercept, and ranibizumab, but not bevacizumab.
Table 12: Summary of Key Model Parameters
Parameter | Sponsor’s estimate (reported as year 1/year 2/year 3 if appropriate) |
|---|---|
Target population | |
Population of CADTH-participating jurisdictions | 30,207,33234 |
Prevalence of diabetesa | |
Proportion of diabetes patients with DME | 15.7%37 |
Proportion of DME patients with vision impairment requiring treatment | 2.56%37 |
Proportion of patients who are pseudophakic | 32%38 |
Proportion of patients with inadequate response to prior anti-VEGF therapy | 40%38 |
Proportion of patients with public drug coverage | Jurisdiction-specific: 32.2% to 100%39 |
Proportion of DME patients with bilateral disease (both eyes) | 12%37 |
Number of patients eligible for drug under review | 1,256/1,271/1,287 |
Number of eyes eligible for drug under review | 1,407/1,424/1,441 |
Market uptake (3 years) | |
Uptake (reference scenario) Anti-VEGF (ranibizumab, aflibercept) Triamcinolone | 80%/80%/80% 20%/20%/20% |
Uptake (new drug scenario) Dexamethasone implants Anti-VEGF (ranibizumab, aflibercept) Triamcinolone | 20%/25%/30% 70%/67.5%/65% 10%/7.5%/5.0% |
Annual cost of treatment (per patient)b | |
Dexamethasone implantsc Anti-VEGF (ranibizumab, aflibercept)d Triamcinolonee | $2,892 $12,577 $31 |
DME = diabetic macular edema; VEGF = vascular endothelial growth factor.
aIncludes Type I and II diabetes.
bThe sponsor used jurisdiction-specific cost data for the individual jurisdictions. The costs for Ontario are presented here.
cAssumed 2 administrations annually.
dAssumed 12 administrations annually for ranibizumab and 6.5 administrations annually for aflibercept. The anti-VEGF comparator is weighted 67% for aflibercept and 33% for ranibizumab.
eAssumed 3.5 administrations annually.
Source: Sponsor’s Budget Impact Submission.33
Summary of the Sponsor’s BIA Results
The estimated cost savings of funding dexamethasone implants for the treatment of adults with DME who are pseudophakic and have had an inadequate response to prior anti-VEGF therapy was $959,445 in year 1, $1,213,983 in year 2, and $1,474,617 in year 3, for a cumulative cost savings of $3,648,045 over the 3-year time horizon.
CADTH Appraisal of the Sponsor’s BIA
CADTH identified several key limitations to the sponsor’s analysis that have notable implications on the results of the BIA:
The proportion of triamcinolone use may be overestimated. The sponsor assumed, in the reference scenario, that 80% of eligible patients would receive anti-VEGF drugs and that 20% would receive triamcinolone. Clinical expert feedback suggested that, in Canadian clinical practice, the proportion of triamcinolone use may be lower than assumed by the sponsor, in the range of 10%. Clinician feedback additionally suggested that, if dexamethasone implants become publicly reimbursed, triamcinolone would be entirely replaced by dexamethasone implants. As such, the expected market share of triamcinolone in the new drug scenario may be closer to 0%.
As part of the base case, CADTH assumed 10% use of triamcinolone in the reference scenario, with the remaining 90% being allocated to anti-VEGFs. In the new drug scenario, triamcinolone use was assumed to be 0%, and the market share of dexamethasone implants was not modified; the remaining treatment share was allocated to anti-VEGFs based on clinical expert input.
Uncertainty regarding the frequency of administration. In the BIA, the annual cost of treatment with dexamethasone implants and anti-VEGF drugs was estimated based on an assumed frequency of administrations. The sponsor assumed that dexamethasone implants would be administered twice annually, which is consistent with the Health Canada–recommended dosing frequency.2 The clinical expert consulted by CADTH for this review indicated that, in clinical practice, the injection frequency is tailored to the individual patient and that re-treatment with dexamethasone implants may be required up to every 3 months. As noted in the CADTH appraisal of the economic evaluation, the sponsor’s assumptions about dexamethasone implant frequency may underestimated usage, and hence drug costs, compared to expected clinical practice.
In the base case, CADTH assumed 2 dexamethasone implants would be received per patient per year. In scenario analyses, CADTH explored the impact of more frequent injections.
Uncertainty regarding the proportion of DME patients with visual impairment. The sponsor assumed that 2.56% of patients with DME would require treatment for their visual impairment, based on a longitudinal study.37 This was felt to be an underestimate by the clinical expert consulted by CADTH for this review, who indicated that, in practice, this proportion may be higher but would likely be influenced by the setting in which patients are diagnosed (i.e., family medicine versus retinal specialist, with higher values expected at retinal specialist clinics).
Due to uncertainty in the proportion of patients treated for visual impairment, CADTH was unable to address this limitation in reanalysis.
Potentially relevant comparators were excluded. In the sponsor’s base case, dexamethasone implants were assumed to displace aflibercept, ranibizumab, and triamcinolone. As noted in the CADTH appraisal of the sponsor’s economic evaluation, bevacizumab and brolucizumab are relevant comparators in this population. The clinical expert consulted by CADTH for this review indicated that bevacizumab is a relevant comparator after an inadequate response to aflibercept or ranibizumab. Although bevacizumab use for this purpose would be off-label in some jurisdictions, the expert noted that it is still used routinely in clinical practice due to its lower price compared to other anti-VEGFs. The clinical expert indicated that the use of bevacizumab for pseudophakic patients with DME after a prior inadequate response to anti-VEGF therapy varies by jurisdiction owing to reimbursement policies.
CADTH was unable to address this limitation in reanalysis.
CADTH Reanalyses of the BIA
Based on the identified limitations, CADTH’s base case included changes to the market shares of triamcinolone and anti-VEGFs.
Table 13: CADTH Revisions to the Submitted Budget Impact Analysis
Stepped analysis | Sponsor’s value or assumption | CADTH value or assumption |
|---|---|---|
Changes to derive the CADTH base case | ||
1. Market shares (year 1/year 2/year 3) | Reference scenario: Anti-VEGFs — 80%/80%/80% Triamcinolone — 20%/20%/20% New scenario: Dexamethasone — 20%/25%/30% Anti-VEGFs — 70%/67.5%/65% Triamcinolone — 10%/7.5%/5.0% | Reference scenario: Anti-VEGFs — 90%/90%/90% Triamcinolone — 10%/10%/10% New scenario: Dexamethasone — 20%/25%/30% Anti-VEGFs — 80%/75%/70% Triamcinolone — 0%/0%/0% |
CADTH base case | Reanalysis 1 | |
VEGF = vascular endothelial growth factor.
The results of the CADTH step-wise reanalysis are presented in summary format in Table 14 and a more detailed breakdown is presented in Table 15. Based on the CADTH base case, the estimated cost savings of the reimbursement of dexamethasone implants for the treatment of adult patients with DME who are pseudophakic and have had an inadequate response to anti-VEGF therapy are expected to be $959,445 in year 1, $1,660,656 in year 2, and $2,378,903 in year 3, for a 3-year total cost savings of $4,999,004. This analysis assumes that patients will receive 2 implants per year.
CADTH performed several scenario analyses to explore uncertainty in these estimates. The scenario in which a higher frequency of dexamethasone implants was assumed (4 per year) resulted in 3-year cost savings of $1,905,534. Assumptions related to triamcinolone wastage had little impact on the estimate owing to low market share.
As noted earlier, CADTH was not able to address the exclusion of additional anti-VEGF drugs owing to the structure of the sponsor’s model and a lack of market share data. Given the lower price of bevacizumab compared to the submitted price for dexamethasone implants, the reimbursement of dexamethasone implants could increase costs to the drug plans should bevacizumab usage be displaced.
Table 14: Summary of the CADTH Reanalyses of the Budget Impact Analysis
Stepped analysis | 3-year total |
|---|---|
Submitted base case | –$3,648,045 |
CADTH reanalysis 1 and base case | –$4,999,004 |
BIA = budget impact analysis.
Table 15: Detailed Breakdown of the CADTH Reanalyses of the Budget Impact Analysis
Stepped analysis | Scenario | Year 0 (current situation) | Year 1 | Year 2 | Year 3 | 3-year total |
|---|---|---|---|---|---|---|
Submitted base case | Reference | $13,989,395 | $14,160,471 | $14,333,749 | $14,509,256 | $43,003,477 |
New drug | $13,989,395 | $13,201,026 | $13,119,766 | $13,034,639 | $39,355,432 | |
Budget impact | $0 | –$959,445 | –$1,213,983 | –$1,474,617 | –$3,648,045 | |
CADTH base case | Reference | $15,733,167 | $15,925,568 | $16,120,444 | $16,317,827 | $48,363,839 |
New drug | $15,733,167 | $14,966,122 | $14,459,787 | $13,938,925 | $43,364,835 | |
Budget impact | $0 | –$959,445 | –$1,660,656 | –$2,378,903 | –$4,999,004 | |
CADTH scenario 1: Four dexamethasone implants annually | Reference | $15,733,167 | $15,925,568 | $16,120,444 | $16,317,827 | $48,363,839 |
New drug | $15,733,167 | $15,779,713 | $15,489,221 | $15,189,371 | $46,458,305 | |
Budget impact | $0 | –$145,854 | –$631,223 | –$1,128,457 | –$1,905,534 | |
CADTH scenario 2: Triamcinolone vial sharing | Reference | $15,729,637 | $15,921,995 | $16,116,827 | $16,314,166 | $48,352,987 |
New drug | $15,729,637 | $14,966,122 | $14,459,787 | $13,938,925 | $43,364,835 | |
Budget impact | $0 | –$955,872 | –$1,657,039 | –$2,375,241 | –$4,988,152 |
BIA = budget impact analysis.
Stakeholder Input
Patient Input
Fighting Blindness Canada, The Canadian Council of the Blind, CNIB, Vision Loss Rehabilitation Canada, Diabetes Canada
About Fighting Blindness Canada, The Canadian Council of the Blind, CNIB, Vision Loss Rehabilitation Canada, and Diabetes Canada
Fighting Blindness Canada (FBC) is the largest charitable funder of vision research in Canada.
Over our 48-year history, FBC has contributed critical funding for the development of sight-saving treatments and cures for blinding eye diseases. By raising and stewarding funds, FBC is helping drive forward research that supports our goal of understanding why vision loss occurs, how it can be slowed and how sight can be restored.
We are an invaluable resource for individuals and families impacted by blindness, providing accurate eye health information through our website and educational events, as well as engaging with government and other stakeholders to advance better vision health policies.
The Canadian Council of the Blind (CCB) was founded in 1944 by schools of the blind and by returning blind Canadian war veterans and is recognized as the Voice of the Blind™ in Canada. The CCB is a membership-based not-for-profit, that brings together Canadians who are living with vision loss, those who are blind, deaf-blind, and the partially sighted. In doing so the Council maintains a vibrant network of active members in 80 chapters across Canada. Each chapter is unique to its geographic area and engages in a variety of social, recreational and community activities based on the interests of their local members.
A tireless advocate of the vision loss community the CCB works to promote a sense of purpose and self-esteem along with enabling the efforts of each member to achieve an enhanced quality of life. The Council through its lived experience constituency is proud of its efforts to break down barriers and remains dedicated to building public awareness and improving the well-being of people with seeing disabilities.
The Canadian Council of the Blind offers numerous programs to assist people living with vision loss, increase accessibility in all areas of vision loss life and bring awareness of vision issues to the public and government. The CCB leads initiatives that call for the provision of the very best in available medical treatments, research, and the fostering of patients’ rights without limitation or discrimination. It does this all while recognizing that vision loss and blindness are preventable.
Founded in 1918, CNIB is a non-profit organization driven to change what it is to be blind today. We deliver innovative programs and powerful advocacy that empower people impacted by blindness to live their dreams and tear down barriers to inclusion. Our work as a blind foundation is powered by a network of volunteers, donors and partners from coast to coast to coast.
Vision Loss Rehabilitation Canada (VLRC) is a health services organization. We provide training that enables people who are blind or partially sighted to develop or restore key daily living skills, helping enhance their independence, safety and mobility. Our certified specialists work closely with ophthalmologists, optometrists and other health care professionals, providing essential care on a referral basis in homes and communities.
The Vision of VLRC is to maximize health and independence for Canadians impacted by vision loss and our mission is to provide high-quality, integrated and accessible rehabilitation and health care services that enable Canadians impacted by vision loss to live the lives they choose.
Diabetes Canada (DC) is a national health charity representing millions of Canadians affected by diabetes. Diabetes Canada leads the fight against diabetes by helping people live healthy lives, preventing the onset and consequences of diabetes, and discovering a cure. It has a heritage of excellence and leadership, and its co-founder, Dr. Charles Best, along with Dr. Frederick Banting, is credited with the co-discovery of insulin. Diabetes Canada is supported in its efforts by a community-based network of volunteers, employees, health care professionals, researchers, and partners. By providing education and services, advocating on behalf of people living with diabetes, supporting research and translating it into practical applications, Diabetes Canada is delivering on its mission. Diabetes Canada will continue to change the world for those affected by diabetes through healthier communities, exceptional care, and high-impact research.
Information Gathering
Data shared in this submission were collected through an online survey made available to Canadians living with diabetic retinopathy (DR) or diabetic macular edema (DME) during the first months of 2020. Shared across networks associated with the submitting organizations, the survey is part of a larger research project titled VIEW DR/DME (Valuation and Interpretation of Experiences with DR/DME) that received ethics approval from Advarra, one of the largest independent providers of institutional review board (IRB) services in Canada.
The intent of the survey was to learn more about the lived experiences of Canadians living with DR and DME. The goal was not to learn more about experiences of Ozurdex or any other specific treatment (though we did gather data and insights related to experiences of treatment general).
Instead, the data and analysis that follows provide insights into the lives of those who live with DR and DME, and who must manage and navigate the often-daily barriers and burdens that accompany these diseases. Our belief is that these perspectives are crucial, and that they can be used to guide decision-making related to treatments that can address the physical, psychological, and socioeconomic burdens associated with DR and DME.
Overview of Respondents
A total of 67 Canadians responded to the survey. Seeing as DR affects approximately 500,000 Canadians, (Ballios BG, Park T, Chaudhary V, Hurley B, et al. Identifying gaps in patient access to diabetic screening eye examinations in Ontario: a provincially representative cross-sectional study. Can J Ophthalmol. 2021;56(4):223-230. https://doi.org/10.1016/j.jcjo.2020.10.018) this number may seem small, but it is difficult locating and engaging with individuals with DR and DME, at least partially as a result of low disease awareness. These challenges have been discussed in various research efforts, including an article published recently by researchers associated with FBC. (Andrews C, Yoganathan P, Pereira JA. Blind Spots: Gaps in Disease Knowledge and the Role of Patient Education for Canadians with Diabetic Macular Edema. Can J Diabetes. 2021;45(4):375-378. https://doi.org/10.1016/j.jcjd.2020.10.001)
Out of these respondents, most were between either 61 and 80 (44.4%) or 41 and 60 (37%), with a mean age of 56.8 (SD = 13.2). Most were either working full time (38.9%) or retired (33.3%), and a majority resided in urban regions within Ontario (41.8%), British Columbia (14.9%), Alberta (13.4%), and Quebec (11.9%), followed by smaller groups within other provinces.
Table 1: Baseline Characteristics of Respondents (n = 67)
Characteristic | n (%) |
|---|---|
Age (n = 54) | |
Mean age (SD) | 56.8 (13.2) |
18 - 40 years | 9 (16.7) |
41 - 60 years | 20 (37.0) |
61 - 80 years | 24 (44.4) |
Over 80 years | 1 (1.9) |
Biological Sex (n = 54) | |
Female | 23 (42.6) |
Male | 31 (57.4) |
Intersex | 0 (0.0) |
Province (n = 67) | |
Ontario | 28 (41.8) |
British Columbia | 10 (14.9) |
Alberta | 9 (13.4) |
Quebec | 8 (11.9) |
Manitoba | 3 (4.5) |
Nova Scotia | 3 (4.5) |
Newfoundland | 2 (3.0) |
Yukon | 2 (3.0) |
New Brunswick | 1 (1.5) |
Saskatchewan | 1 (1.5) |
Location (n = 67) | |
Urban | 62 (92.5) |
Rural | 5 (7.5) |
DME/DR in one eye or both eyes (n = 67) | |
Both eyes | 51 (76.1) |
One eye | 10 (14.9) |
I don’t know | 6 (9.0) |
Other household members (n = 60) | |
Partner/spouse | 43 (71.7) |
My child(ren) | 16 (26.7) |
No one | 9 (15.0) |
Family member(s) other than partner and child | 3 (5.0) |
I live in a retirement home | 2 (3.3) |
Roommate/friend | 2 (3.3) |
I live in a nursing home/long-term care facility | 1 (1.7) |
Employment Status (n = 54) | |
Retired | 18 (33.3) |
Employed, working full-time | 21 (38.9) |
Employed, working part-time | 0 (0.0) |
Not employed, looking for work | 2 (3.7) |
Student | 1 (1.9) |
Unemployed due to illness or disability | 8 (14.8) |
Homemaker | 0 (0.0) |
Parental leave | 0 (0.0) |
Taking care of a family member | 1 (1.9) |
Other: Employed but on disability (2), self-employed (1) | 3 (5.6) |
Disease Experience
Respondents made it clear that both DR and DME have substantial and life-altering impacts on daily life. When asked which activities are most impact by their disease, they emphasized effects on reading, using a phone, and driving, activities that many individuals take for granted.
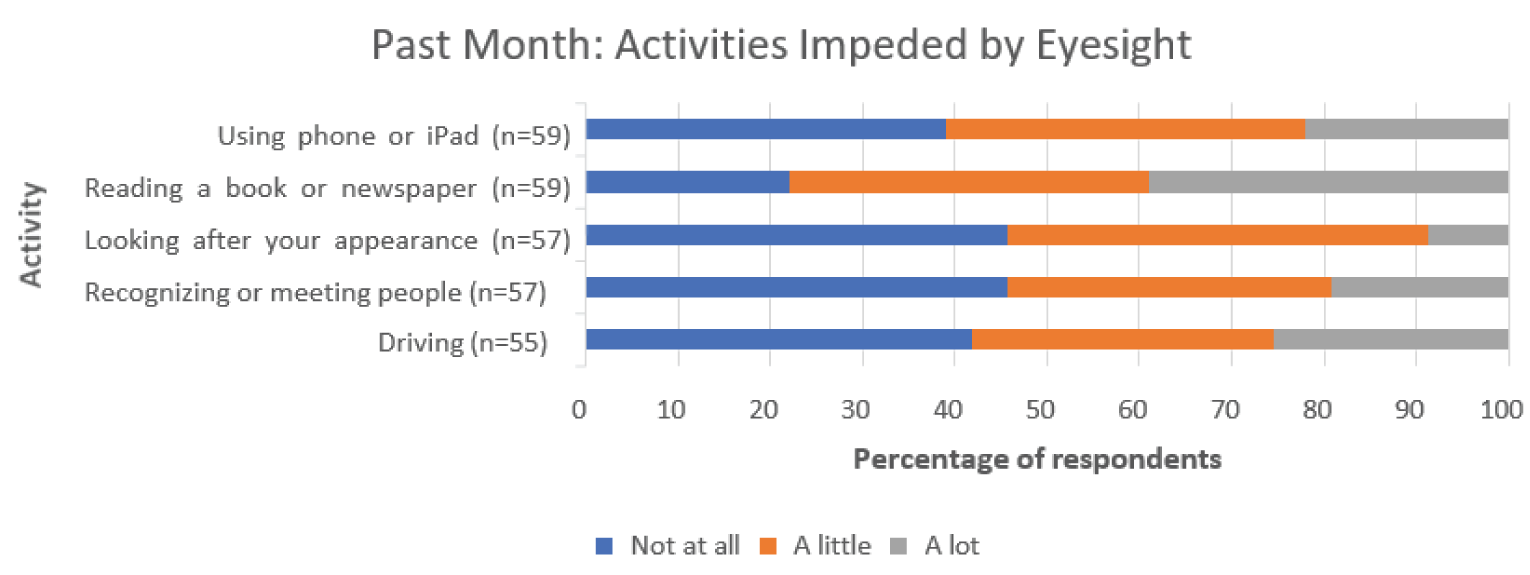
These difficulties were also framed in terms of “challenges.” When asked about the kinds of challenges they face as a result of DR or DME, a significant majority of respondents selected “worry that my condition might worsen in the future” (80.3%), followed by “not being able to do the daily activities I used to” (45.9%) and “explaining my condition to family and friends” (36.1%).
Table 2: Challenges With DMR/DR (n = 61)
Challenges | n (%) |
|---|---|
Worry that my condition might worsen in the future | 49 (80.3) |
Not being able to do the daily activities I used to | 28 (45.9) |
The long wait times for appointments | 18 (29.5) |
Explaining my condition to family and friends | 22 (36.1) |
Lack of social support | 14 (23.0) |
Finding answers to my questions about my condition | 18 (29.5) |
Socializing | 19 (31.1) |
Other* | 5 (8.2) |
*Getting the test I need prior to injections, working/finding work, no funding for technology or training, how long it takes to learn technology, getting appointments with my very busy retinologist
The strong emphasis on worry in relation to the condition worsening implies the existence of emotional and psychological burdens as well; DR and DME may affect daily life as a result of lower visual acuity, but they may also lead to significant psychological strain in the form of a generalized anxiety related to the future. Following up on this notion, respondents were asked to specify their concerns over the last month, with many selecting that they are concerned about their eyesight worsening “all the time” or “a lot of the time.” Respondents also emphasized “coping with everyday life” and “general safety when out of the home” as notable concerns.
Recognizing that both DR and DME are complications of diabetes, it is useful to frame these considerations within the broader experiences of diabetes as a complex and impactful disease. Common symptoms of diabetes include extreme fatigue, unusual thirst, frequent urination and weight change (gain or loss). Diabetes requires considerable selfmanagement, including eating well, engaging in regular physical activity, maintaining a healthy body weight, taking medication as prescribed, monitoring blood glucose, and managing stress. When Diabetes Canada asked Canadian diabetes patients how the disease impacts their lives, several described diabetes as a condition that must be dealt with 24 hours a day, 7 days a week, 365 days a year with no breaks and no holidays or time off. It is physically and mentally exhausting.
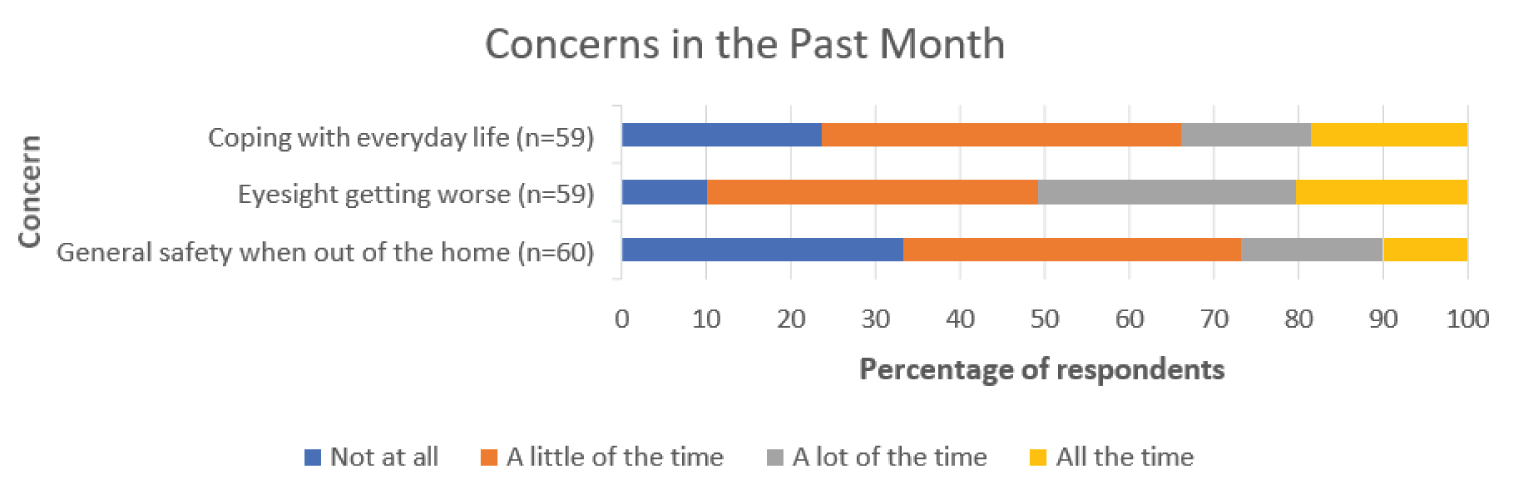
It is clear that DR and DME weigh heavily on the minds of affected individuals, here shown as persistent emotional and psychological factors. This notion was again carried forward in relation to both requiring assistance as well as feelings of loneliness and isolation. In both cases, a majority of respondents replied that they had both experiences (needing assistance and feelings of isolation) at least “a little of the time.”
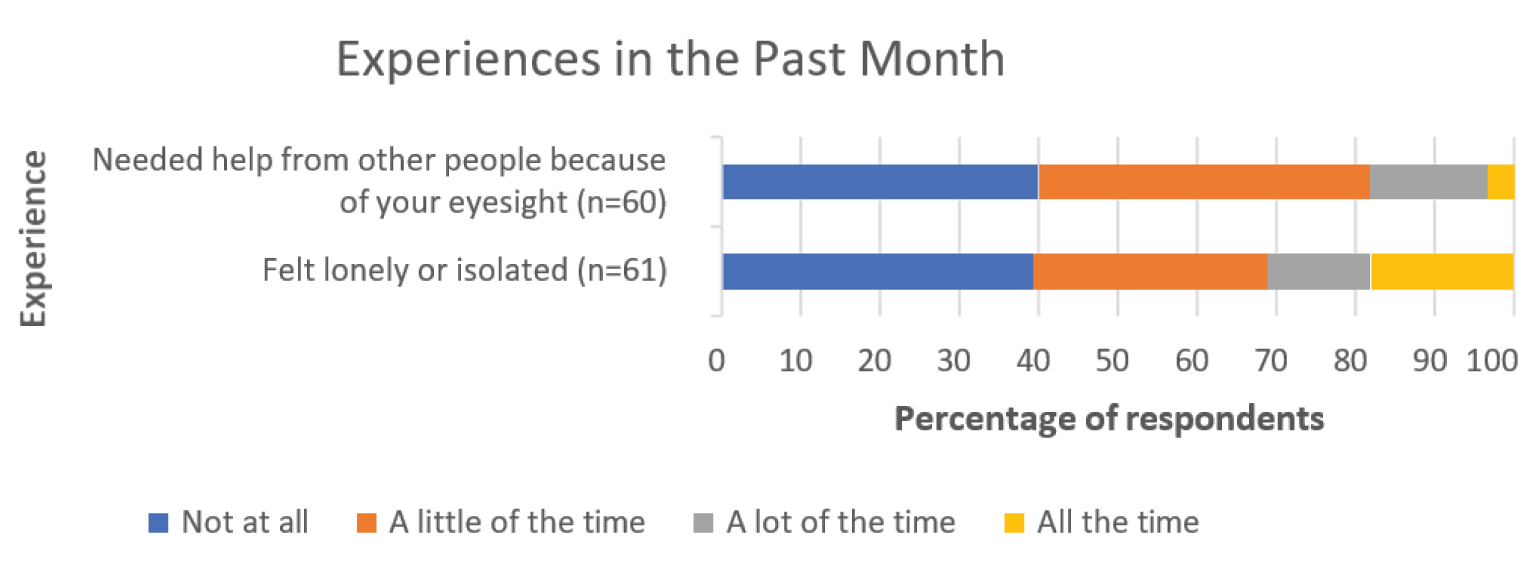
The experience of needing help also highlights the social dimensions of DR and DME, implying that the impacts of the diseases extend beyond one’s personal life to touch on friends and family members. Any analysis of these diseases should take into account the social dimensions of lived experience that are common across eye disease that affect visual acuity and make daily life more challenging.
Overall, it is clear that DR and DME have significant and life-altering impacts on the lives of those who are affected by them. Whether it be in relation to reading or worrying or relying on others, the diseases tend to affect the details and complexities of everyday living in a pervasive manner (as opposed to being a secondary or background consideration). For this reason, it is reasonable to conceptualize DR and DME as considerable burdens on the daily lives of patients. Importantly, it is also reasonable to assume that these impacts have been more intensely felt during the COVID-19 pandemic, especially in relation to loneliness and isolation. This survey collected information before the full scale of the pandemic was known (or even possible to conceptualize)—as a result, the responses do not reflect the full impact of COVID-19 on the lives of patients with DR and DME. That said, the CCB conducted a separate survey in April of 2020 that was exclusively focused on the pandemic and its effects; it showed that fear, anxiety, loneliness, and other psychosocial impacts were intensified for patients with age-related macular edema (AMD) and DR during the pandemic. A follow-up study showed that almost 70,000 fewer eye injections for AMD and DR were performed in 2020 compared to 2019, and that 1,500 fewer patients received injections for AMD and 458 fewer patients received injections for DR in 2020 compared with 2019. A summary of these findings is below.
CCB Summary of the Impacts of COVID-19 for Patients Living with Vision Loss
In April 2020, the CCB conducted a survey on the impact of the COVID-19 pandemic on Canadians who are blind, deafblind or partially-sighted. (Gordon K. “The impact of the COVID-19 pandemic on Canadians who are blind, deaf-blind, and partially-sighted” (2020). Available at: https://ccbnational.net/shaggy/wp-content/uploads/2020/05/COVID-19-Survey-Report-Final-wb.pdf). What we discovered was a community experiencing loneliness and living with considerable stress. Almost half the 572 respondents to the CCB survey (46%) said they hadn’t felt safe going outside the home since the initial lockdown. 47% of respondents said that they needed a sighted guide to assist them when they left home. Respondents said they were concerned about maintaining social distancing and having others maintain social distancing with them. Since most hospitals and doctors’ offices were not permitting anyone to accompany their patient, this meant that a substantial barrier existed for anyone requiring a sighted guide to access their doctor. This undoubtedly resulted in many people missing their regular appointments for anti-VEGF injections. Furthermore, 42% of respondents were worried about their ability to have someone accompany them to a doctor and almost half (49%) were worried about their ability to get transportation to a doctor, hospital, or testing site. About one third of respondents (36%) said that they had had an important medical appointment cancelled as a result of the COVID-19 pandemic.
Many also expressed special concerns about treatment for their eye condition and were afraid that they may lose more vision as a result of missing appointments.
A subsequent study, commissioned by CCB and FBC,(Deloitte Access Economics, Addendum to the cost of vision loss and blindness in Canada. The impact of COVID-19. (report commissioned by the Canadian Council of the Blind), August 2021. Available at: https://ccbnational.net/shaggy/2021/10/12/thehttps://ccbnational.net/shaggy/2021/10/12/the-impact-of-covid-19-an- addendum-to-the-cost-of-vision-loss-in-canada-study/impact-of-covid-19-an-addendum-to-the-cost-of-vision-loss-in-canada- study/) reported the extent of the cancelled appointments for anti-VEGF injections. This report estimated that almost 70,000 fewer eye injections for the treatment of age-related macular degeneration (AMD) and diabetic retinopathy/DME were performed in 2020 compared with 2019.
This study also reported that 458 fewer patients received injections for diabetic retinopathy and 1,500 fewer patients received injections for AMD in 2020 compared with 2019. When combined with other delayed or cancelled eye examinations and treatments it was estimated that an additional 1,437 people experienced vision loss due to the pandemic.
Any treatment that can extend the time between required injections can be expected to be a great advantage to people living with vision loss who are not venturing out of their homes for medical appointments. Such a medication would carry significant potential to minimize unnecessary vision loss.
Experiences With Currently Available Treatments
A majority of survey participants (56.4%) indicated that they currently receive injections as a treatment for DR or DME, with the most common brand being Lucentis (29.4%), followed by Eylea (24.6%), Avastin (20.2%), and Ozurdex (13.5%). The remainder of patients indicated that they did not know the brand of their injection.
Most respondents selected that their last injection was 1-5 years ago (26.9%), followed by more than 5 years ago (16.4%), 3-11 months ago (10.4%), and less than 3 months ago (4.5%).
Table 3: Timing of First Injection (n = 67)
First Injection | n (%) |
|---|---|
Less than 3 months ago | 3 (4.5) |
3-11 months ago | 7 (10.4) |
1-5 years ago | 18 (26.9) |
More than 5 years ago | 11 (16.4) |
I’ve never received injections for DME or DR | 28 (41.8) |
The low number of respondents (4.5%) who received injections more recently is disconcerting, potentially indicating high drop-off and nonadherence in relation to injections. If this is the case, it aligns with existing research showing that nonadherence to intravitreal injections is quite high (Okada M, Mitchell P, Finger RP, Eldem B, et al. Nonadherence and Nonpersistence to Intravitreal Injection Therapy for Neovascular Age-Related Macular Degeneration: A Mixed-Methods Systematic Review. Ophthalmology. 2021;128;2;234-247. https://doi.org/10.1016/j.ophtha.2020.07.060)
Satisfaction, Adherence, and Assistance
The largest number of respondents showed that they are “satisfied” with their injections (54.5%) and that “they helped me avoid losing more eyesight” (63.6%).
Table 4: Level of Satisfaction With Injections (n = 22)
Satisfaction | n (%) |
|---|---|
Very dissatisfied | 1 (4.5) |
Dissatisfied | 1 (4.5) |
Neither satisfied nor dissatisfied | 7 (31.8) |
Satisfied | 12 (54.5) |
Very satisfied | 1 (4.5) |
Table 5: How the Injections Have Helped (n = 22)
Effects | n (%) |
|---|---|
They helped me avoid losing more eyesight | 14 (63.6) |
They dried up fluid/blood in my eye(s) | 10 (45.4) |
They improved my eyesight | 7 (31.8) |
They have had no effect but I receive injections because my doctor recommends them | 3 (13.6) |
I don't know | 1 (4.5) |
Other* | 3 (13.6) |
*Think it’s helping, stopped proliferation of blood vessels, have tunnel vision in one eye but it started to get tightened much more than last year
A majority of respondents who receive injections also indicated that they have not missed an injection in the last year (68.2%). Despite this, the number of patients who have missed injections is sizeable (31.8%) and deserving of attention. Further, in a similar study on AMD conducted by our groups, the percentage of missed appointments was just below 20%. It is worth considering why patients with DR and DME appear to be missing more appointments that those with AMD. Additionally, since this data were collected before COVID, it is safe to assume that more appointments are being missed today then at the beginning of 2020. This notion is supported by findings from the CCB COVID study, which is referenced at the end of section 3 in this submission: “This study also reported that 1,500 fewer patients received injections for AMD and 458 fewer patients received injections for diabetic retinopathy in 2020 compared with 2019. When combined with other delayed or cancelled eye examinations and treatments it was estimated that an additional 1,437 people experienced vision loss due to the pandemic.” Clearly, missed injection appointments— and by extension all forms of nonadherence and non-persistence—require serious attention when developing policies and treatments for DR and DME and support the development and approval of new treatments which can reduce treatment burden.
Following up on this, our survey asked respondents why they have cancelled or delayed appointments in the past. Although the response rate for this question was quite low, most respondents indicated that they were too busy to attend the appointment (50%), followed by not feeling well (33.3%), being “unable to find someone to take me to the appointment” (16.7%), and being “scared to receive the injection” (16.7%).
Table 6: Reason for Cancellation or Delay (n = 6)
Reason | n (%) |
|---|---|
Unable to find someone to take me to the appointment | 1 (16.7) |
Unable to travel to appointment | 0 (0.0) |
Could not afford attending the appointment | 0 (0.0) |
Too busy to attend appointment | 3 (50.0) |
Did not know how important the injection was to my sight | 0 (0.0) |
Scared to receive the injection | 1 (16.7) |
Did not find previous injections helpful | 0 (0.0) |
I forgot about the appointment | 0 (0.0) |
I was not feeling well | 2 (33.3) |
Other | 0 (0.0) |
Regarding the inability to find someone to assist with travel, our questions did uncover a significant reliance on assistance in this area. When asked who helps them attend their injections appointments, over 80% of participants indicating receiving travel from either a spouse, family member, or friend. These individuals helped in a number of ways, including with travel (93.3%), with waiting at the appointment (80%), and with assistance in everyday tasks after the injection (33.3%).
Table 7: Type of Help Provided (n = 15)
Benefit | n (%) |
|---|---|
Help me after the injections with everyday tasks | 5 (33.3) |
Wait with me at the appointment | 12 (80.0) |
Travel with me or drive me to/from the appointment | 14 (93.3) |
Take care of things at home while I am away | 1 (6.7) |
Physical support at my appointment | 4 (26.7) |
Other | 1 (6.7) |
These responses once again underscore the degree to which DR and DME lead to a reliance on family and friends for caregiving and other forms of assistance, most commonly for travel to and from appointments.
Travel and Time Commitment
Almost half of the respondents indicating facing travel time of less than 30 minutes (45.5%) to get to their injection appointment, followed by 31 - 60 minutes (40.9%) and 1 - 2 hours (9.1%).
Table 8: Travel Time (One-Way) to Injection Appointment (n = 22)
Time | n (%) |
|---|---|
Less than 30 minutes | 10 (45.5) |
31-60 minutes | 9 (40.9) |
More than 1 hour, and less than 2 hours | 2 (9.1) |
More than 2 hour, and less than 4 hours | 0 (0.0) |
4 hours or longer | 1 (4.5) |
When asked how long they spend at their injection appointments, the larges group reported less than 1 hour (42.9%), followed by 1 - 2 hours (33.3%) and 2 - 4 hours (14.3%).
Table 9: Total Time Spent per Appointment at Office of Doctor/Clinician for Injection Appointment (n = 21)
Time | n (%) |
|---|---|
Less than 1 hour | 9 (42.9) |
More than 1 hour, and less than 2 hours | 7 (33.3) |
2 hours or more, but less than 4 hours | 3 (14.3) |
4 hours or more, but less than 6 hours | 1 (4.8) |
More than 6 hours | 1 (4.8) |
In terms of the ease or difficulty of travel, responses were varied but skewed towards the easy end of the spectrum, with most respondents selecting that travel is either very easy (27.3%), easy (27.3%), or neither easy nor difficult (27.3%).
Table 10: What Is it Like to Travel to Your Injection Appointments? (n = 22)
Ease of travel | n (%) |
|---|---|
Very difficult | 0 (0.0) |
Difficult | 4 (18.2) |
Neither easy nor difficult | 6 (27.3) |
Easy | 6 (27.3) |
Very easy | 6 (27.3) |
That said, 4 individuals did report difficulty related to their travel, and when asked about the reasons, they selected distance from home (50%), poor condition of vehicle (25%), cost (25%), and difficultly related to taking public transit (25%).
Table 11: What Makes it Difficult for You to Travel to Your Injection Appointments (n = 4)
Reason | n (%) |
|---|---|
It is far from home | 2 (50.0) |
My vehicle is in poor condition | 1 (25.0) |
Poor road conditions | 0 (0.0) |
It is expensive to travel | 1 (25.0) |
Other* | 1 (25.0) |
*Alone it is impossible to take the metro, but with my daughter, difficulty is when I don’t hold her arm.
Interestingly, although in these responses both travel and waiting appear as somewhat minimal concerns, both are flagged as the most difficult aspects of the injection routine in data from a different question. When asked what makes it difficult to travel to injection appointments, half of the respondents selected long wait times, while the remainder selected difficulties such as “finding someone to drive me to/from the appointment” (31.8%) and “taking time off work to attend” (27.3%).
Table 12: Most Difficult Part of Eye Injection Appointments (n = 22)
Reason | n (%) |
|---|---|
Anxiety or fear about the injection | 6 (27.3) |
Long waiting time at the appointment | 11 (50.0) |
Cost of travel to/from the appointment | 0 (0.0) |
Finding someone to drive me to/from the appointment | 7 (31.8) |
Finding someone to help me with my daily tasks after the injection | 0 (0.0) |
I don't find any part difficult | 4 (18.2) |
Scratchiness or pain in my eye after the appointment | 4 (18.2) |
Taking time off work to attend | 6 (27.3) |
Other* | 3 (13.6) |
*Spouse must take time off work to drive me, if I didn’t have my daughter, I’d find difficulties in everything, hotel stay required (travel from Yukon to Vancouver) which is expensive.
When framed or conceptualized in terms of what is most difficult, then, both travel and waiting emerge as central concerns. It is also worth considering whether these issues are exacerbated in rural parts of Canada. Although a regional sub-analysis has not be conducted for this study, it is entirely possible that travel, waiting, and strain on caregivers are even more challenging for Canadians living in rural and remote parts of the country. This is certainly a factor that needs to be considered in the development of new treatments for these diseases.
Emotional and Physical Effects
In response to the question about difficulty, a significant number of patients also selected “anxiety or fear about the injection” (27.3%), highlighting the fact that injections into the eye are emotionally burdensome for some patients. This is interesting, considering that many patients also indicated being “satisfied” with their injections, as well as appreciative of the impact on their sight. It may show that those with DR or DME tend to manage their fear and anxiety in relation to injections as a matter of course. Injections still carry an emotional or psychological impact, but this has become internally managed in such a way as to be common or matter of fact.
The physical burdens of injections are not to ignored either. In response to the same question about the difficult aspects of injections, 18.2% of patients indicated “scratchiness or pain in the back of my eye” as a difficulty worth noting. It is clear that physical impacts are a factor for some patients, then. This is supported to some degree by the number of patients who experience some pain during the injection: when asked to indicate their pain level, a significant majority selected that the injections are “slightly painful” (81.8%). The remainder selected “not painful at all” (9.1%) and “painful” (9.1%).
Table 13: How Painful Is the Injection for You? (n = 22)
Reason | n (%) |
|---|---|
Not painful at all | 2 (9.1) |
Slightly painful | 18 (81.8) |
Painful | 2 (9.1) |
Extremely painful | 0 (0.0) |
Moving into the evening after the injection, our respondents showed an overall transition into a more painful experience. while 45.5% of patients indicated that the evenings are “not painful at all,” 40.9% selected “slightly painful” and 13.6% chose “painful.” as a result, over half of respondents indicated some form of eye pain lingering into the evening.
Table 14: How Painful Is the Injection for You in the Evening After? (n = 22)
Reason | n (%) |
|---|---|
Not painful at all | 10 (45.5) |
Slightly painful | 9 (40.9) |
Painful | 3 (13.6) |
Extremely painful | 0 (0.0) |
Vision was shown to be impacted post-injection as well, with the largest group of respondents selecting that their vision stayed blurry “until I go to sleep that night” (31.6%). This was followed by vision being blurry for 1 - 3 hours (26.3%) and for 4 - 6 hours (21.1%).
Table 15: After an Injection, for How Long Is Your Vision Blurry? (n = 19)
Frequency | n (%) |
|---|---|
Less than 1 hour | 3 (15.8) |
1-3 hours | 5 (26.3) |
4-6 hours | 4 (21.1) |
For at least 24 hours | 1 (5.3) |
Until I go to sleep that night | 6 (31.6) |
Given the prevalence of blurry vision among the cohort, it is unsurprising that they indicated a number of daily activities that become difficult or impossible post-injection. When asked about which activities they can longer do after an injection, the largest groups chose “watch TV” (57.1%) and “read” (57.1%), followed by “drive” (28.6%), “work” (21.4%), and “prepare meals (14.3%). All respondents to this question choose at least one activity that they can no longer do.
Table 16: Which of the Following Are You Unable to Do After an Injection? (n = 14)
Activity | n (%) |
|---|---|
Watch TV | 8 (57.1) |
Read | 8 (57.1) |
Drive | 4 (28.6) |
Prepare meals | 2 (14.3) |
Provide care to family members | 0 (0.0) |
Work | 3 (21.4) |
None of the above activities | 0 (0.0) |
These responses emphasize the emotional and physical impacts of living with and treating DR and DME, making it clear that the diseases exact a physical and psychological toll that exists alongside the logistical and financial challenges associated with travel and time.
Improved Outcomes
Our survey did not ask patients for their views on improving their experiences and outcomes. That said, the responses to our survey make it clear that any treatment that reduces the physical, psychological, and logistical strain on patients would be preferred. In terms of physical and psychological strain, this could take the form of a treatment that is less invasive, or one that is similarly invasive but that is administered less frequently. The frequency of the treatment could play a role in the reduction of logistical demands as well: a treatment that is taken or received less often would require fewer travel appointment, would decrease dependency on caregivers, and potentially more.
Experience With Drug Under Review
We conducted an interview with a patient, living in Alberta who is currently using Ozurdex. These are her words: “I started losing my vision 15 years ago, and went through a three-year period of one eye surgery and treatment after the next. I stopped driving, had to leave the job that I loved, and dealt with mental health challenges as a result. It all started with my diagnosis of type 2 diabetes in 1992 – although I didn’t realize the connection at the time. In fact, I wasn’t made aware that vision loss was a complication of diabetes until the damage had been done.
In 2005, I developed a cataract in one eye. The cataract surgery didn’t go well. When I went to the doctor a couple weeks later for a check-up, he told me that my eye was hemorrhaging (bleeding) and referred me to a retina specialist. My visit to this specialist was a rude awakening. He told me that all the trouble I was having with my eye had begun with my diabetic retinopathy (DR). I had no idea what he was talking about. ‘You’ve known that you had DR for a couple years, right?’ he asked. Not only did I not know, but I’d never even heard the term before. The specialist was stunned, as was I.
My DR – which I’d just learned I had – had progressed to diabetic macular edema. Despite multiple surgeries and 16 rounds of laser surgery, the treatment didn’t work. I started taking anti-VEGFs and they worked for a short time, but I had to go from an eye injection every six weeks to every three and a half weeks eventually, to reduce and manage the bleeding and edema in my eye.
When my anti-VEGF treatments stopped working, I was put on a steroid treatment that has dramatically improved the bleeding in my eye. Unfortunately, it’s not covered by Alberta’s drug benefit program. For years, I was able to take advantage of my partner’s private plan, which covered a portion of the medication, but eventually the relationship ended, and so did my access to treatment.
Despite the cost, fortunately, today I’m miraculously stable due to the longevity of this drug, but I make sacrifices to save the vision I have left.”
Companion Diagnostic Test
Not applicable.
Anything Else?
Researchers, health practitioners, policy experts, and others agree that diabetes is a growing and evolving epidemic, both globally and in Canada. As the incidence of diabetes grow, DR and DME will grow as well. A patient’s life is impacted by these diseases through a range of factors: life changes, loss of productivity, missed work/school hours, and more. As our data shows, DR and DME are diseases that weigh heavily on a patient’s mind, suggesting a strong psychological burden. Caregivers are impacted by the diseases as well, and in complex ways that are not always easy to measure or quantify.
DR and DME have these impacts, surely, but it is safe to assume that those impacts and associated burdens are more pronounced among vulnerable populations and those living outside of Canada’s urban centres. And during the COVID pandemic, it is also safe to assume that the burdens and challenges highlighted in patient responses have only become more pronounced. As the number of people living with diabetes in Canada increases, more patients in rural communities will need options that are effective, that help them comply with treatment programs, and that reduce the psychological toll of the disease.
In the context of diabetes, different people with diabetes require different medications and treatment modalities to help them effectively manage their disease. Their unique clinical profile, preferences and tolerance of therapy should direct prescribers to the most appropriate choice and combination of treatments for disease management. Many individuals with diabetic macular edema are also managing multiple other health conditions, highlighting the need for treatments that reduce the risk of non-compliance.
This submission is a snapshot of the experiences of a small number of DR and DME patients in Canada—not a complete or final one, of course, because no overview can be, but nevertheless one that is grounded in the lived experiences of patients who offered their time, expertise, and insights to participate in this process. The focus of this submission has been on expanding our understanding of how these individuals perceive their diseases and treatments; the burdens that impact their lives; the barriers they face as a result of vision loss and other factors; and the psychological and emotional tolls of the diseases. As organizations that represent patients with DR, DME, and other eye diseases, our overarching goal is to contribute meaningfully to the discussion and potential implementation of new treatments in this space—in particular, to guide that discussion along lines that are patient- centered, that focus on optimal and equitable outcomes, and that recognize the expertise of patients with lived experience of DR/DME and their value in the review process of new treatments.
We look forward to continuing to work with CADTH to support Canadians living with DR and DME, and to advance our collective understanding of how the diseases impact their lives.
Conflict of Interest Declaration — Fighting Blindness Canada, The Canadian Council of the Blind, CNIB, Vision Loss Rehabilitation Canada, Diabetes Canada
Did you receive help from outside your patient group to complete this submission? If yes, please detail the help and who provided it.
FBC contracted Dr. Chad Andrews as an independent consultant with expertise in patient centered research to draft this submission.
Did you receive help from outside your patient group to collect or analyze data used in this submission? If yes, please detail the help and who provided it.
FBC contracted JRL Research & Consulting to program and test the survey, perform qualitative interviews and clean and analyze the data.
List any companies or organizations that have provided your group with financial payment over the past 2 years AND who may have direct or indirect interest in the drug under review.
Table 17: Conflict of Interest Declaration for Fighting Blindness Canada
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
Bayer | — | — | — | X |
Novartis | — | — | — | X |
Roche | — | — | — | X |
Abbvie-Allergan | — | — | — | X |
Table 18: Conflict of Interest Declaration for the Canadian Council of the Blind
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
Bayer | — | — | — | X |
Novartis | — | — | — | X |
Table 19: Conflict of Interest Declaration for CNIB
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
Astra Zeneca (CNIB) | — | — | X | — |
Bausch Foundation (CNIB) | — | — | X | — |
Bayer (CNIB) | — | — | — | X |
Johnson & Johnson (CNIB) | — | — | X | — |
Novartis (CNIB) | — | — | — | X |
Table 20: Conflict of Interest Declaration for Vision Loss Rehabilitation Canada
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
None | — | — | — | — |
Table 21: Conflict of Interest Declaration for Diabetes Canada
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
Novo Nordisk | — | — | — | X |
AstraZeneca | — | — | — | X |
Janssen | — | — | — | X |
Sanofi | — | — | — | X |
Bayer | — | — | X | — |
Clinician Input
Eastern Canada Retina Specialists
About Eastern Canada Retina Specialists
We are a group of independent retina specialists practicing in various locations throughout eastern Canada.
Information Gathering
On March 28th, 2022, a group of retinal and ophthalmology specialists from Eastern Canada met virtually to discuss unmet needs in the current diabetic macular edema (DME) treatment pathway and the role of Ozurdex® in addressing these needs. Physicians were asked to provide their guidance on reconstructing the DME management pathway, identifying patient profiles best suited to Ozurdex® therapy, fulfilling unmet needs and optimizing treatment goals.
Current Treatments and Treatment Goals Current treatments
The current Canadian treatment pathway for DME, as described by fellow physician peers, places Ozurdex® therapy, along with other intravitreal steroids, as the second-line option.
Metabolic control (such as improved glycemic and hypertension control) to drive positive systemic changes should be advocated throughout the treatment pathway as this can impact the underlying disease mechanism.
First-line therapy is anti-VEGF injection (Avastin®, Lucentis®, Eylea®, and Beovu®).
A trial of up to six monthly injections is attempted before switching within this class to another agent.
Should this class fail to provide an adequate response (improved visual acuity and sufficient drying of the retina) then second-line treatments will be the next recourse.
Patients typically receive 5-6 doses of anti-VEGF in order to effectively gauge response prior to being considered a sub- optimal responder.
Second-line options for DME include steroid injections (Triesence®, Kenalog®, and Ozurdex®) and perhaps focal laser therapy, depending on the specific clinical and optical coherence tomography (OCT) appearance.
Triamcinolone (Triesence® and Kenalog®) is currently covered but has a higher risk profile due to elevated intraocular pressure (IOP) and increased need for trabeculectomy compared to dexamethasone (Ozurdex®).
Ozurdex® was also observed to offer greater potency and a longer duration of action in comparison to Triamcinolone.
Ozurdex® appears to be particularly well-suited as a steroid option for pseudophakic patients and those with vitrectomized eyes (where triescence and Kenalog are rapidly cleared from the eye, reducing effectiveness).
In DME with extra-macular focal leakage (which may be clinically exemplified by an extra-macular circinate ring), laser therapy may be the best next option
In DME refractory to anti-VEGF and steroid therapy, surgery (peeling the internal limiting membrane [ILM], vitrectomy) or grid therapy may be appropriate and reasonable third-line therapies.
Treatment Goals:
Patients with DME should be assessed monthly when treatment is initiated and then every three months to monitor once stabilized. The main goals of treatment include:
The prevention of disease progression and improvement of visual acuity
The reduction of treatment burden (frequency of therapy) with a minimally invasive therapy that has a long duration of action with minimal adverse effects
The elimination of retinal fluid, prevention of further vision loss, or improved visual acuity while conserving the retina structurally
The reduction of time off work, restoration/maintenance of patient independence, and lessened burden on caregivers
Treatment Gaps (Unmet Needs)
Considering the treatment goals, please describe goals (needs) that are not being met by currently available treatments.
Many patients with diabetes are still not being referred for eye examinations and remain undiagnosed due to this breakdown in referral pathways.
Limited access for patients in primary care to subspecialty metabolic management and uncoordinated multidisciplinary care is a concern as specialists operate in separate silos.
Patients have a high burden of treatment (frequency of therapy) with first-line therapy (monthly anti-VEGF injections) with up to a third responding sub-optimally (30–40%).
Anti-VEGF therapy targets only the VEGF pathway. In DME, this may pose as a limitation, as there are other pathologic pathways and cytokines at play that may go unchecked (eg. through non-VEGF mediated inflammatory pathways).
Anti-VEGF therapy and vitrectomy are costly. At the same time, there is a lack of access to coverage for better-performing and more cost-effective steroid therapies as second-line options.
There are higher risks of adverse effects (glaucoma, cataract progression, variable IOP) with inexpensive steroid options (eg. triamcinolone) compared to Ozurdex®.
Some patients may react to the preservative used in Kenalog® as it incites inflammation and triamcinolone has been associated with a higher incidence of endophthalmitis than anti-VEGF therapies.
Preservative-free triamcinolone (Triesence®), is sometimes backordered and unavailable due to manufacturing issues.
Access to focal laser therapy is lacking for many patients especially those living in rural areas. Furthermore focal laser therapy may not be efficacious in patients with central macular fluid as the laser cannot be applied in this region directly.
Place in Therapy
How would the drug under review fit into the current treatment paradigm?
Ozurdex® would be considered a second-line steroid option in DME along with triamcinolone (Triesence® and Kenalog®).
If Ozurdex® was reimbursed, it would be the first option chosen after failing first-line anti-VEGF therapy and would require fewer visits to clinic to receive injections and given its enhanced safety protocol.
When considering the MoA of Ozurdex®:
The slow-release nature of this implant is preferable to the bolus required with both anti-VEGF and triamcinolone. The release of medication is consistent over time with Ozurdex®, which helps avoid peaks and troughs in IOP.
Similarly, the medication delivery mode of this implant reduces the risk of complications (steroid migration to the anterior chamber).
The longer duration of action is preferable to lessen treatment burden compared to other agents (anti-VEGF and triamcinolone are both administered more frequently).
Ozurdex® is sometimes used in combination with anti-VEGF therapy to elicit a treatment response but the benefit of this is uncertain.
Following Ozurdex® failure, focal laser, grid therapy, or surgery (peeling of the ILM) may be options.
Which patients would be best suited for treatment with the drug under review? Which patients would be least suitable for treatment with the drug under review?
Patient profiles best suited to Ozurdex:
DME patients best suited to Ozurdex® are:
Those with diffuse focal edema that are sub-optimal responders to anti-VEGF
Patients who had a recent myocardial infarction or stroke that would preclude anti-VEGF therapy
Patients with other concurrent conditions that make travelling to appointments difficult (mobility issues, dialysis, located remotely)
Those that are pseudophakic, have vitrectomized eyes, chronic macular edema, subretinal fluid, chronic cystic macular edema (CME) identified with OCT characteristics, retinal pigment epithelial (RPE) cell migration and atrophy, and the presence of hyperreflective material.
Patients best suited for Ozurdex® can be identified using OCT as well as fluorescein angiography (if necessary).
Patients poorly suited for Ozurdex® treatments include those with advanced or uncontrolled glaucoma. Patients who are phakic would be less ideal, due to the development of cataract, but should still be considered as an inability to control the edema will affect acuity more significantly and long term than cataract if not controlled.
Outcomes to determine response in DME treatment include changes detected on OCT that show central thickness, macular volume, and the disappearance of cysts; improvement of visual acuity; and patient satisfaction with functioning vision and QoL (i.e. fewer missed days of work, less frequent treatments, etc.).
All but the last outcome to capture QoL align with those used in clinical trials. Vision-related QoL may be quantified in trials (VFQ-25) but is noted more qualitatively in practice.
What outcomes are used to determine whether a patient is responding to treatment in clinical practice? How often should treatment response be assessed?
Meaningful response to standard of care:
DME patients should be assessed monthly when treatment is initiated and then every three months to monitor therapy outcomes and response as well as individual durability of the Ozurdex implant.
A meaningful therapeutic outcome would include:
A dry, structurally sound retina
Improved/satisfactory visual acuity (20/50 or better) that allows patients to drive or function well enough to perform important activities; a recurrence of fluid or a small amount remaining should not immediately prompt more treatment if the disease is stable and the patient is satisfied with their vision
A 30–50% reduction in excess central fovea thickness on OCT
In terms of variability of the definition of “meaningful response” among advisors, there are two perspectives:
Those who consider objective clinical end points in studies (retinal thickness < 300 microns and a visual acuity of 20/50 or better)
Those who consider patient-reported outcomes and want to stabilize disease and optimize psycho-social outcomes (quality of life [QoL], patient perception, and patient/caregiver burden)
What factors should be considered when deciding to discontinue treatment with the drug under review?
Discontinuation of standard of care (SoC) therapy would be prompted by:
Control of the disease and stable visual acuity at which point patients would be assessed every 12–16 weeks for recurrence of DME.
Infection or an inflammatory response to the administered medication.
An unsustained rise in IOP or a major steroid response.
Instances where aphakic patients experience anterior chamber migration of the steroid would preclude the use of injections.
What settings are appropriate for treatment with [drug under review]? Is a specialist required to diagnose, treat, and monitor patients who might receive [drug under review]?
Ophthalmologists and Retina Specialists with experience in treating patients with diabetic macular edema would be the most appropriate ones to utilize Ozurdex. These injections may take place in either outpatient offices or clinics (within community or hospital settings).
Additional Information
Not applicable.
Conflict of Interest Declarations — Eastern Canada Retina Specialists
To maintain the objectivity and credibility of the CADTH drug review programs, all participants in the drug review processes must disclose any real, potential, or perceived conflicts of interest. This conflict of interest declaration is required for participation. Declarations made do not negate or preclude the use of the clinician group input. CADTH may contact your group with further questions, as needed. Please refer to the Procedures for CADTH Drug Reimbursement Reviews (section 6.3) for further details.
Did you receive help from outside your clinician group to complete this submission? If yes, please detail the help and who provided it.
No.
Did you receive help from outside your clinician group to collect or analyze any information used in this submission? If yes, please detail the help and who provided it.
An independent third-party medical communications firm, Kataka Medical, assisted in recording the feedback from our group meeting.
List any companies or organizations that have provided your group with financial payment over the past two years AND who may have direct or indirect interest in the drug under review. Please note that this is required for each clinician who contributed to the input — please add more tables as needed (copy and paste). It is preferred for all declarations to be included in a single document.
Declaration for Clinician 1
Name: Dr. Sohel Somani
Position: Physician, Medical Retina Specialist
Date: 25-05-2022
Table 22: Conflict of Interest Declaration for Eastern Canada Retina Specialists — Clinician 1
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
Bayer | X | — | — | — |
Novartis | X | — | — | — |
AbbVie | X | — | — | — |
Bausch & Lomb | X | — | — | — |
Ripple Therapeutics | X | — | — | — |
Declaration for Clinician 2
Name: Dr. Peter Kertes
Position: Vitreoretinal Surgeon
Date: 01-05-2022
Table 23: Conflict of Interest Declaration for Eastern Canada Retina Specialists — Clinician 2
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
Novartis | — | — | X | — |
Bayer | — | — | X | — |
Roche | — | — | X | — |
Novelty Nobility | — | — | X | — |
Arctic Dx | — | — | X | — |
Boehringer Ingelheim | X | — | — | — |
Pfizer | X | — | — | — |
Zeiss | X | — | — | — |
Declaration for Clinician 3
Name: Dr. Netan Choudhry
Position: Vitreoretinal Surgeon
Date: 31-05-2022
Table 24: Conflict of Interest Declaration for Eastern Canada Retina Specialists — Clinician 3
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
Topcon | — | — | — | X |
Allergan | X | — | — | — |
Johnson & Johnson | X | — | — | — |
Zeiss | X | — | — | — |
Bayer | — | — | — | X |
Optos PLC | — | X | — | — |
Novartis | — | X | — | — |
Ellex | X | — | — | — |
Apellis | — | X | — | — |
Hoffman La Roche | — | X | — | — |
Viatris | X | — | — | — |
Declaration for Clinician 4
Name: Dr. Alejandro Oliver
Position: Retina and Vitreous Specialist
Date: 31-05-2022
Table 25: Conflict of Interest Declaration for Eastern Canada Retina Specialists — Clinician 4
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
Allergan | X | — | — | — |
Novartis | X | — | — | — |
Roche | X | — | — | — |
Knight | X | — | — | — |
Declaration for Clinician 5
Name: Dr. Thomas Sheidow
Position: Vitreoretinal Surgeon
Date: 30-05-2022
Table 26: Conflict of Interest Declaration for Eastern Canada Retina Specialists — Clinician 5
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
Roche | X | — | — | — |
Apellis | X | — | — | — |
Novartis | X | — | — | — |
Bayer | X | — | — | — |
Declaration for Clinician 6
Name: Dr. Rajeev Muni
Position: Vitreoretinal Surgeon
Date: 02-06-2022
Table 27: Conflict of Interest Declaration for Eastern Canada Retina Specialists — Clinician 6
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
Novartis | X | — | — | — |
Bayer | X | — | — | — |
Roche | X | — | — | — |
Bausch & Lomb | X | — | — | — |
Alcon | X | — | — | — |
Declaration for Clinician 7
Name: Dr. Bernard Hurley
Position: Vitreoretinal Surgeon
Date: 02-06-2022
Table 28: Conflict of Interest Declaration for Eastern Canada Retina Specialists — Clinician 7
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
Alcon | X | — | — | — |
Novartis | — | X | — | — |
Allergan | X | — | — | — |
Bayer | X | — | — | — |
Declaration for Clinician 8
Name: Dr. Peng Yan
Position: Assistant Professor & Vitreoretinal Surgeon
Date: 02-06-2022
Table 29: Conflict of Interest Declaration for Eastern Canada Retina Specialists — Clinician 8
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
Bayer | X | — | — | — |
Novartis | X | — | — | — |
Alcon | X | — | — | — |
MedPharmacy | X | — | — | — |
Declaration for Clinician 9
Name: Dr. Murari Patodia
Position: Ophthalmologist
Date: 03-06-2022
Table 30: Conflict of Interest Declaration for Eastern Canada Retina Specialists — Clinician 9
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
Allergan | X | — | — | — |
Declaration for Clinician 10
Name: Dr. David Chow
Position: Ophthalmologist
Date: 14-06-2022
Table 31: Conflict of Interest Declaration for Eastern Canada Retina Specialists — Clinician 10
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
AbbVie | X | — | — | — |
Declaration for Clinician 11
Name: Dr. Danny Gauthier
Position: Vitreoretinal ophthalmologist & Assistant Professor of Ophthalmology
Date: 14-06-2022
Table 32: Conflict of Interest Declaration for Eastern Canada Retina Specialists — Clinician 11
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
Novartis | X | — | — | — |
Bayer | X | — | — | — |
AbbVie | X | — | — | — |
Declaration for Clinician 12
Name: Dr. David T. Wong
Position: Ophthalmologist & Associate Professor
Date: 23-06-2022
Table 33: Conflict of Interest Declaration for Eastern Canada Retina Specialists — Clinician 12
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
AbbVie | X | — | — | — |
Alcon | X | — | — | — |
Bayer | — | — | X | — |
Novartis | — | — | X | — |
Roche | — | — | X | — |
Retina Specialists From Western Canada
About Retina Specialists From Western Canada
Group of retinal specialists practicing in western Canada (Manitoba, Saskatchewan, Alberta, British Columbia).
Information Gathering
Phase 3 randomized controlled studies, systematic review, expert opinion
Current Treatments and Treatment Goals
In Canada, the estimated prevalence of diabetic macular edema in 15.7% in patients with diabetes. The prevalence of visual impairment due to DME is 2.6% (R.J.Petrella et al, 2012). Composite scores for vision-related quality of life declined with increase visual acuity loss in a study of 145 Canadian patients with DME (Gonder J et al, 2014).
Current first-line therapy for DME in Canada consists of intravitreal injection of various anti-VEGF agents. These agents have been shown in multiple phase 3 registration trial to be safe and effective in decreasing DME and preserving or improving visual acuity. Despite these excellent treatment options, a significant portion of patients do not respond to these first line agents. Treatment of these refractory patients presents a significant challenge in clinical practice.
All major landmarks phase 3 randomized controlled trial of DME treatments have shown that a decrease in the amount of DME is associated with an improvement in visual acuity. Furthermore, a delay in the resolution of DME is associated with a reduced potential for improvement in visual acuity. There is strong evidence that anti-VEGF agents modify the underlying disease mechanisms of diabetic retinopathy. Multiple studies have shown that anti-VEGF therapy leads to regression of Diabetic Severity Scores (DRSS), slowing of the progression of retinal non-perfusion and decreasing therapeutic need after the first year of treatment.
Ozurdex is a sustained-release biodegradable 0.7mg dexamethasone implant with duration of action between 4-6 months. The MEAD phase 3 trial of Ozurdex for DME has shown a significant decrease in DME and improvement in visual acuity in pseudophakic patients. Furthermore, subgroup analysis of patients with previously treated DME (laser, anti-VEGF or triamcinolone) showed significant improvement in DME and visual acuity. This demonstrates that Ozurdex is an effective option for second line treatment of DME.
Triesence (triamcinolone suspension) is a minimally water-soluble steroid suspension that is injected intravitreally. It has been used as an off-label agent for the treatment of DME, as a second line agent. Triamcinolone has been shown to be more effective than placebo (Gillies et al, 2006). Furthermore, when combined with macular laser, it has shown similar efficacy as ranibizumab in pseudophakic patients.
Macular photocoagulation is no longer a first or second line treatment option in the Canadian context. It is mostly reserved for the treatment of non-central DME, in which anti-VEGF or steroid injections are not indicated.
Important goals of DME treatment are safe and effective pharmaceutical agents while reducing the treatment burden of patients.
Treatment Gaps (Unmet Needs)
Considering the treatment goals, please describe goals (needs) that are not being met by currently available treatments.
Non-responder or sub-responders to anti-vegf agents present a significant therapeutic challenge. There is no clear definition of a DME sub/non-responder. Generally they have been defined as less than 30% improvement in OCT edema. Non-response can be identified as soon as after 3 months of anti-VEGF treatment. The prevalence of persistent DME while on anti-VEGF treatment has been reported to range between 45% and 65% at 24 weeks of treatment, depending on the agent used (Bressler et al, 2018).
In Canadian clinical practice, those patients are switched to another agent and anti-vegf treatment is continued on average for 6 months. At that stage if non-response is persistent, second line therapies are considered. This second line treatment is often a corticosteroid injection. Ozurdex is currently the only injectable corticosteroid that is approved by Health Canada for the treatment of DME. In most Canadian provinces, Ozurdex is not covered by government programs, and hence only accessible with private insurance or out-of-pocket expense. Triamcinolone (Triesence, Kenalog) is also used for the treatment of DME in an off-label manner.
While both Ozurdex and triamcinolone have been shown to be effective in treating DME, their safety profiles are quite different. Intraocular pressure (IOP) elevations beyond 21mmHg following tramcinolone have been shown in studies to vary between 35-52% (Degenring et al, Oum et al).. This experience is comparable with that of the community of Canadian retinal specialists. Furthermore, these elevations of IOP have been been found to be unpredictable in range. This may be related to the suspension nature of Triesence. The initial bolus is variable in amount of steroid injected and the suspension may migrate to the anterior chamber, further increasing the risk of IOP elevation. In contrast, in the MEAD study, the incidence of IOP elevation above 25mmHg was 32%. This IOP elevation was found to be predictable (peaking at 2 months, resolving at 4 months).
The duration of action of triamcinolone is variable and unpredictable, varying between 2 and 4 months. In vitrectomized patients, it is even shorter. The duration of action of Ozurdex is more predicatable, most often about 4 months. In both vitrectomized and nonvitrectomized patients, the duration of action of Ozurdex is the same.
Place in Therapy
How would the drug under review fit into the current treatment paradigm?
Anti-VEGFs target VEGF-A whereas corticosteroids such as Ozurdex target VEGF-A as well as multiple other inflammatory cytokines that are involved in the pathogenesis of DME. The use of Ozurdex as a second line agent could be additive to ongoing anti-VEGF treatment or possibly as monotherapy as per the clinical judgement of the treating physician.
Ozurdex has been shown to slow the progression of the underlying diabetic retinopathy (https://pubmed.ncbi.nlm.nih.gov/26581718/).
Ozurdex is aimed to be used as a second line therapy in pseudophakic DME patients with suboptimal response to initial anti-VEGF therapy. Ozurdex can be used either in monotherapy or in combination with ongoing anti0VEGF treatment, depending on the treating physician’s clinical judgement.
Ozurdex would be used in pseudophakic patients with suboptimal initial response to anti-VEGF.
It is not expected that there would be a shift in treatment paradigm. Ozurdex is already used as a second line agent in patients who can currently have access to the drug.
Ozurdex presents a more favorable therapeutic and safety profile to other injectable corticosteroids (Triesence) currently used as second line therapy agents. Its duration of action is more consistent and predictable, in both non- vitrectimized and vitrectomized eyes. Furthermore, the risk of IOP elevation is lower and more predictable than that of Triesence.
Which patients would be best suited for treatment with the drug under review? Which patients would be least suitable for treatment with the drug under review?
Patients most likely to respond to Ozurdex treatment are patients with centre-involving DME that is resistant to first line antiVEGF therapy.
Patients most in need of intervention are DME patients with persistent DME, progressive vision loss, and those needing a robust therapeutic response. The need for a robust treatment response may be indicated for those patients with treatment anxiety, or difficulty with travel to regular monthly treatment appointments.
Patients least suited for Ozurdex treatment would include:
DME with tractional component (eg. epiretinal membrane, vitreomacular traction)
Signs of chronicity where there is limited prognosis for visual acuity improvement may not be favorable candidates for Ozurdex treatment.
Aphakic patients and patients with compromised posterior capsule
Patients with a known steroid response with IOP elevation
Patients with severe glaucoma
Patients that may be best suited for Ozurdex treatment are identified by their treating physician bases on clinical evaluation in combination with ancillary retinal imaging. There are no issues related to diagnosis. These patients are often managed by ophthalmologists with extensive training and experience in the management of retinal diseases.
Patients with DME and good vision are likely to maintain their vision. In clinical trials, patients with all levels of baseline vision have shown improvement with treatment.
What outcomes are used to determine whether a patient is responding to treatment in clinical practice? How often should treatment response be assessed?
Real world outcomes differ from those in clinical trials for a number of reasons – patient selection, adherence to treatment and monitoring schedules.
A clinically meaningful response would include a reduction in DME, visual acuity improvement, decrease frequency or treatment, regression of diabetic severity score.
What factors should be considered when deciding to discontinue treatment with the drug under review?
Treatment cessation could be considered in scenarios such as:
Chronic DME where the visual prognosis is very guarded regardless of treatment,
Patients who have not shown significant clinical improvement with multiple treatment modalities, including Ozurdex
Patients in which treatment of the DME may not lead to a significant quality of life improvement as a result of a systemic condition (e.g., dementia, cancer, stroke, etc.)
What settings are appropriate for treatment with [drug under review]? Is a specialist required to diagnose, treat, and monitor patients who might receive [drug under review]?
Patients should be managed by an ophthalmologist in all clinical settings (community or hospital setting).
Additional Information
Is there any additional information you feel is pertinent to this review?
None.
Conflict of Interest Declarations — Retina Specialists From Western Canada
To maintain the objectivity and credibility of the CADTH drug review programs, all participants in the drug review processes must disclose any real, potential, or perceived conflicts of interest. This conflict of interest declaration is required for participation. Declarations made do not negate or preclude the use of the clinician group input. CADTH may contact your group with further questions, as needed. Please refer to the Procedures for CADTH Drug Reimbursement Reviews (section 6.3) for further details.
Did you receive help from outside your clinician group to complete this submission? If yes, please detail the help and who provided it.
Not applicable.
Did you receive help from outside your clinician group to collect or analyze any information used in this submission? If yes, please detail the help and who provided it.
Not applicable.
List any companies or organizations that have provided your group with financial payment over the past two years AND who may have direct or indirect interest in the drug under review. Please note that this is required for each clinician who contributed to the input — please add more tables as needed (copy and paste). It is preferred for all declarations to be included in a single document.
Declaration for Clinician 1
Name: Robert Gizicki
Position: Clinical instructor, University of British Columbia
Date: 15-05-2022
Table 34: Conflict of Interest Declaration for Retina Specialists From Western Canada — Clinician 1
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
Novartis | X | — | — | — |
Alcon | X | — | — | — |
AbbVie | — | X | — | — |
Apellis | X | — | — | — |
Declaration for Clinician 2
Name: Ravi Dookeran
Position: Vitreo-Retinal Surgeon and Specialist
Date: 13-06-2022
Table 35: Conflict of Interest Declaration for Retina Specialists From Western Canada — Clinician 2
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
Bayer | X | — | — | — |
Allergan | X | — | — | — |
Bausch and Lomb | X | — | — | — |
Declaration for Clinician 3
Name: Geoff Williams
Position: Physician, Ophthalmologist and Retinal Subspecialist
Date: 13-06-2022
Table 36: Conflict of Interest Declaration for Retina Specialists From Western Canada — Clinician 3
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
Advisory Board or equivalent: AbbVie/Allergan, Alcon, Bayer, Bausch and Lomb, Novartis, Appellis, Roche (ad board, working group, moderator, or host of group learning event | — | X | — | — |
Clinical Trials: Novartis, Ophthotech, Chengdu Kanghong, Regeneron, Regenexbio, Roche/Genentech, Inc, Iveric Bio, Opthea, Alexion, Bayer | — | — | — | X |
MD Collaborate, Arctic Dx | X | — | — | — |
Declaration for Clinician 4
Name: Dr. Amin Kherani
Position: Physician, Ophthalmologist and Retinal Subspecialist
Date: 23-06-2022
Table 37: Conflict of Interest Declaration for Retina Specialists From Western Canada — Clinician 4
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
Advisory Board or equivalent: AbbVie/Allergan, Alcon, Bayer, Bausch and Lomb, Novartis, Apellis, Roche (ad board, working group, moderator, or host of group learning event) | X | — | — | — |
Clinical Trials: Novartis, Ophthotech, Chengdu Kanghong, Regeneron, Regenexbio, Roche/Genentech, Inc, Iveric Bio, Opthea, Alexion, Bayer | — | — | — | X |
MD Collaborate | X | — | — | — |
Declaration for Clinician 5
Name: Michael Butler
Position: Assistant Clinical Professor, UBC Dept of Ophthalmology + Visual Sciences
Date: 02-06-2022
Table 38: Conflict of Interest Declaration for Retina Specialists From Western Canada — Clinician 5
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
Novartis | X | — | — | — |
Sun Pharma | X | — | — | — |
Johnson & Johnson | X | — | — | — |
Allergan | X | — | — | — |
Declaration for Clinician 6
Name: Leah Wittenberg
Position: Ophthalmologist
Date: 29-06-2022
Table 39: Conflict of Interest Declaration for Retina Specialists From Western Canada — Clinician 6
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
Bausch and Lomb | X | — | — | — |
Alcon | X | — | — | — |
Allergan | X | — | — | — |
Declaration for Clinician 7
Name: Patrick Ma
Position: Clinical Professor, UBC Ophthalmologist
Date: 30-06-2022
Table 40: Conflict of Interest Declaration for Retina Specialists From Western Canada — Clinician 7
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
Allergan | — | X | — | — |
Alcon | X | — | — | — |
Bausch and Lomb | X | — | — | — |
AbbVie | — | X | — | — |
Novartis | X | — | — | — |
Retina Society of Alberta
About the Retina Society of Alberta
Alberta Retina Consultants is a group retina medical and surgical retina subspecialty practice of 8 physicians based in Edmonton, Alberta. We provided retina related care to the northern half of Alberta. www.alberta-retina.com
Information Gathering
We surveyed all 8 retina specialists in our practice to see if they were supportive of coverage of Ozurdex for patients with Diabetic macular edema or Central retinal vein occlusion with macular edema.
Current Treatments and Treatment Goals
Current treatment for Diabetic macular edema (DME) and central vein occlusion with cystoid macular edema is most commonly intravitreal anti-vegf injections (Bevacizumab, ranibizumab, aflibercept. Focal laser is occasionally used to treat DME. These treatments are supported by clinical practice guidelines. For those eyes that do not respond to anti-vegf therapy or where the duration of response is less than 4 weeks, alternative therapies may be tried including intravitreal steroid injections (primarily tramcinolone). Intravitreal triamcinolone will often have a longer duration of action when compared to anti-vegf therapy.
Current therapies including anti-vegf and triamcinolone intravitreal injections and laser therapy does modify disease by reducing macular edema and improving visual acuity.
The most important goal of new treatments would be longer duration of action with more powerful effect for those eyes that are nonresponders to anti-vegf therapy.
Treatment Gaps (Unmet Needs)
Considering the treatment goals, please describe goals (needs) that are not being met by currently available treatments.
There are a subset of eyes that do not respond to Anti-vegf therapy or where the duration of action for treatment is less than 4 weeks. These eyes would benefit for an alternative solution that is more powerful and longer acting.
Place in Therapy
How would the drug under review fit into the current treatment paradigm?
It is likely that intravitreal dexamethasone implant would be used in eyes that have failed to respond to anti-vegf injections or where the duration of action of anti-vegf therapy is less than 4 weeks.
There is the potential for it to be used as a complementary agent to further reduce macular edema when patients are receiving intravitreal anti-vegf injections.
It is unlikely that there would be a shift in paradigm with inclusion of intravitreal dexamethasone implant. Instead it would be used in those eyes that have failed conventional anti-vegf therapy.
We would suggest trialing anti-vegf injections for a period of at least 3 months prior to using an intravitreal dexamethasone implant.
Which patients would be best suited for treatment with the drug under review? Which patients would be least suitable for treatment with the drug under review?
A patient with CRVO or DME that has failed anti-vegf therapy after at least 3 monthly injections. Failure would be defined of incomplete resolution of fluid within the retina – ie retinal thickness remains greater than 300 um.
What outcomes are used to determine whether a patient is responding to treatment in clinical practice? How often should treatment response be assessed?
Response to treatment for DME and CRVO is resolution of macular edema as identified clinically and by Optical coherence tomography result.
What factors should be considered when deciding to discontinue treatment with the drug under review?
Potential side effects including elevation of eye pressure or lack of response to treatment (retina thickness and fluid that does not improve)
What settings are appropriate for treatment with [drug under review]? Is a specialist required to diagnose, treat, and monitor patients who might receive [drug under review]?
Ophthalmologist expertise in a community or hospital setting would be required to diagnosis, treat and monitor patients receiving intravitreal dexamethasone implant.
Additional Information
This medication should not be used in patients who have not had previous cataract surgery or are known steroid responders.
Conflict of Interest Declarations — Retina Society of Alberta
To maintain the objectivity and credibility of the CADTH drug review programs, all participants in the drug review processes must disclose any real, potential, or perceived conflicts of interest. This conflict of interest declaration is required for participation. Declarations made do not negate or preclude the use of the clinician group input. CADTH may contact your group with further questions, as needed. Please refer to the Procedures for CADTH Drug Reimbursement Reviews (section 6.3) for further details.
Did you receive help from outside your clinician group to complete this submission? If yes, please detail the help and who provided it.
No, we completed this document without external assistance.
Did you receive help from outside your clinician group to collect or analyze any information used in this submission? If yes, please detail the help and who provided it.
No.
List any companies or organizations that have provided your group with financial payment over the past two years AND who may have direct or indirect interest in the drug under review. Please note that this is required for each clinician who contributed to the input — please add more tables as needed (copy and paste). It is preferred for all declarations to be included in a single document.
Declaration for Clinician 1
Name: Matthew T.S. Tennant, MD
Position: Clinical professor, Department of Ophthalmology, University of Alberta
Date: April 12, 2022
Table 41: Conflict of Interest Declaration for Retina Society of Alberta — Clinician 1
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
No COI | — | — | — | — |
Declaration for Clinician 2
Name: Mark Seamone
Position: Assistant clinical professor, University of Alberta, Department of Ophthalmology
Date: May 16, 2022
Table 42: Conflict of Interest Declaration for Retina Society of Alberta — Clinician 2
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
No COI | — | — | — | — |
Declaration for Clinician 3
Name: Chad Baker
Position: Clinical assistant clinical professor, University of Alberta, Department of Ophthalmology
Date: May 16, 2022
Table 43: Conflict of Interest Declaration for Retina Society of Alberta — Clinician 3
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
No COI | — | — | — | — |
Declaration for Clinician 4
Name: Mark D.J. Greve
Position: Associate Clinical Professor, Department of Ophthalmology, University of Alberta
Date: May 16, 2022
Table 44: Conflict of Interest Declaration for Retina Society of Alberta — Clinician 4
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
No COI | — | — | — | — |
Declaration for Clinician 5
Name: David Ehmann
Position: Assistant Clinical Professor, Department of Ophthalmology, University of Alberta
Date: May 16, 2022
Table 45: Conflict of Interest Declaration for Retina Society of Alberta — Clinician 5
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
No COI | — | — | — | — |
Declaration for Clinician 6
Name: Brad J. Hinz
Position: Assistant Clinical Professor, Department of Ophthalmology, University of Alberta
Date: May 16, 2022
Table 46: Conflict of Interest Declaration for Retina Society of Alberta — Clinician 6
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
No COI | — | — | — | — |
Declaration for Clinician 7
Name: Parampal Grewal
Position: Assistant Clinical Professor, Department of Ophthalmology, University of Alberta
Date: May 16, 2022
Table 47: Conflict of Interest Declaration for Retina Society of Alberta — Clinician 7
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
No COI | — | — | — | — |
Declaration for Clinician 8
Name: Rizwan Somani
Position: Assistant Clinical Professor, Department of Ophthalmology, University of Alberta
Date: May 16, 2022
Table 48: Conflict of Interest Declaration for Retina Society of Alberta — Clinician 8
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
No COI | — | — | — | — |
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up-to-date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
Redactions: Confidential information in this document may be redacted at the request of the sponsor in accordance with the CADTH Drug Reimbursement Review Confidentiality Guidelines
Stakeholder Input: The views expressed in each submission are those of the submitting organization or individual; not necessarily the views of CADTH or of other organizations. As such, they are independent of CADTH and do not necessarily represent or reflect the view of CADTH. No endorsement by CADTH is intended or should be inferred. By filing with CADTH, the submitting organization or individual agrees to the full disclosure of the information. CADTH does not edit the content of the submissions.
CADTH does use reasonable care to prevent disclosure of personal information in posted material; however, it is ultimately the submitter’s responsibility to ensure no identifying personal information or personal health information is included in the submission. The name of the submitting organization or individual and all conflict of interest information are included in the submission; however, the name of the author, including the name of an individual patient or caregiver submitting the patient input, are not posted.
Accessibility: CADTH is committed to treating people with disabilities in a way that respects their dignity and independence, supports them in accessing material in a timely manner, and provides a robust feedback process to support continuous improvement. All materials prepared by CADTH are available in an accessible format. Where materials provided to CADTH by a submitting organization or individual are not available in an accessible format, CADTH will provide a summary document upon request. More details on CADTH’s accessibility policies can be found here.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.