CADTH Reimbursement Review
Finerenone (Kerendia)
Sponsor: Bayer Inc.
Therapeutic area: Chronic kidney disease
This multi-part report includes:
Clinical Review
Pharmacoeconomic Review
Stakeholder Input
Clinical Review
Abbreviations
ACE
angiotensin-converting enzyme
AE
adverse event
ARB
angiotensin receptor blocker
CI
confidence interval
CKD
chronic kidney disease
eGFR
estimated glomerular filtration rate
EQ-5D-5L
5-level EQ-5D
ESRD
end-stage renal disease
FAS
full analysis set
GCP
good clinical practice
GLP-1
glucagon-like peptide-1
HR
hazard ratio
HRQoL
health-related quality of life
ITC
indirect treatment comparison
KDQOL-36
Kidney Disease Quality of Life survey
LS
least squares
MI
myocardial infarction
MID
minimal important difference
MRA
mineralocorticoid receptor antagonist
NMA
network meta-analysis
NOC
Notice of Compliance
RAAS
renin-angiotensin-aldosterone system
RCT
randomized controlled trial
SAE
serious adverse event
SD
standard deviation
SGLT2
sodium-glucose cotransporter-2
SOC
standard of care
T2D
type 2 diabetes
UACR
urinary albumin-creatinine ratio
Executive Summary
An overview of the submission details for the drug under review is provided in Table 1.
Item | Description |
|---|---|
Drug product | Finerenone (Kerendia) tablets, 10 mg and 20 mg, oral administration |
Indication | As an adjunct to standard of care therapy in adults with chronic kidney disease and type 2 diabetes to reduce the risk of:
|
Reimbursement request | As an adjunct to standard of care therapya in adults with chronic kidney disease and type 2 diabetes to reduce the risk of:
|
Health Canada approval status | NOC |
Health Canada review pathway | Standard |
NOC date | October 14, 2022 |
Sponsor | Bayer Inc. |
NOC = Notice of Compliance.
aStandard of care includes an angiotensin-converting enzyme inhibitor or angiotensin receptor blocker, and a sodium-glucose cotransporter-2 inhibitor, unless contraindicated or not tolerated.
Introduction
Diabetes is the most common cause of kidney disease in Canada, and it is estimated by the sponsor that there are more than 1 million people in Canada living with chronic kidney disease (CKD) and type 2 diabetes (T2D) in 2022.1-3 Older age, low socioeconomic status, obesity, smoking, poor glycemic and blood pressure control, and genetic factors are known risk factors for diabetic kidney disease.4 CKD is the leading cause of kidney failure (previously termed end-stage renal disease [ESRD]), necessitating dialysis or renal transplant; CKD is also associated with cardiovascular complications, leading to decreased quality of life and premature death.1,4,5 In a US survey that evaluated 15,000 patients with diabetes and kidney disease, 10-year mortality was 4-fold and 2.7-fold higher and cardiovascular mortality was 3-fold and 6-fold higher in patients with both CKD and T2D than in patients with, respectively, CKD alone or T2D alone.6 Patients with both CKD and T2D also reported lower health-related quality of life (HRQoL) scores than those with CKD alone or T2D alone.7,8 CKD is clinically diagnosed in patients who are diabetic based on the presence of albuminuria (> 30 mg/g) and/or a decreased estimated glomerular filtration rate (eGFR < 60 mL/min/1.73 m2) in at least 2 out of 3 samples in a 3-month period.4,5 These are also 2 important indicators of disease progression: High urinary albumin-creatinine ratio (UACR) and low eGFR values indicate more severe disease.5,9
According to the clinical experts consulted by CADTH, the primary goal of treatment is to reduce the risk of progression of CKD to ESRD by the application of pharmacologic and lifestyle strategies. The general approach to management of patients with CKD and T2D includes optimization of blood pressure, proteinuria, and glycemic control; dietary changes; and lowering of lipid levels with statins.10 In addition, for several decades, patients with CKD have been treated with either an angiotensin-converting enzyme (ACE) inhibitor or an angiotensin receptor blocker (ARB) that inhibits the renin-angiotensin-aldosterone system (RAAS).10 Recently, guidelines have been revised to encourage the use of sodium-glucose cotransporter-2 (SGLT2) inhibitors in patients with CKD and T2D, particularly for patients with severely increased albuminuria (> 300 mg/g).10-12 Some patients may be intolerant of SGLT2 inhibitors, including patients with poor glycemic control, patients at high risk of genital infections or lower limb amputation, and patients with acute kidney injury.10 According to the clinical experts consulted by CADTH, there is limited access to SGLT2 inhibitors in Canada and access varies by jurisdictions, although access and subsequent use are expected to increase with time. In this review, the sponsor identifies SGLT2 inhibitors, in addition to ACE inhibitors or ARBs, as standard of care (SOC). Despite the application of pharmacologic and lifestyle strategies, the clinical experts indicated that a number of patients with both CKD and T2D continue to progress to kidney failure or develop cardiovascular events and that patients with CKD and T2D could benefit from additional pharmacologic therapies.
The reimbursement request submitted by the sponsor for review by CADTH for finerenone is as an adjunct to SOC therapy to reduce the risk of end-stage kidney disease and a sustained decrease in eGFR, as well as of cardiovascular death, nonfatal myocardial infarction (MI), and hospitalization for heart failure, where SOC includes an ACE inhibitor or ARB, and an SGLT2 inhibitor, unless contraindicated or not tolerated. Finerenone underwent review by Health Canada through the standard review pathway and received a Notice of Compliance (NOC) on October 14, 2022. Finerenone is a nonsteroidal, selective mineralocorticoid receptor antagonist (MRA) that reduces inflammation and fibrosis caused by mineralocorticoid receptor overactivation by selectively binding to these receptors.13 Finerenone has not been previously reviewed by CADTH. Finerenone is available as oral tablets (10 mg and 20 mg). The recommended starting dosage of finerenone is 20 mg once daily for patients with an eGFR greater than or equal to 60 mL/min/1.73 m2 or 10 mg once daily for patients with an eGFR greater than or equal to 25 mL/min/1.73 m2 to less than 60 mL/min/1.73 m2. Four weeks after initiation, restart, or up-titration of finerenone treatment, serum potassium and eGFR should be remeasured to determine continuation of finerenone treatment and dose adjustment. Thereafter, serum potassium should be remeasured periodically and as needed based on patient characteristics and serum potassium levels. Initiation of finerenone treatment is not recommended in patients with an eGFR less than 25 mL/min/1.73 m2 or in patients with serum potassium greater than 5.0 mmol/L. Treatment should be discontinued in patients with ESRD (eGFR < 15 mL/min/1.73 m2).
The objective of this review is to perform a systematic review of the beneficial and harmful effects of finerenone 10 mg and 20 mg tablets to delay the progression of kidney disease and to reduce the risk of major adverse cardiovascular events (cardiovascular death, nonfatal MI, nonfatal stroke) and hospitalization for heart failure in adult patients with CKD and T2D.
Stakeholder Perspectives
The information in this section is a summary of input provided by the patient and clinician groups who responded to CADTH’s call for input and from clinical experts consulted by CADTH for the purpose of this review.
Patient Input
Patient input for the review of finerenone was provided as a joint submission from the Kidney Foundation of Canada and Diabetes Canada. They conducted an online survey of patients with CKD and T2D, and their caregivers, residing across Canada in May 2022 (n = 24; 9 completed and 15 partially completed the survey). Eight respondents identified as patients with CKD, 1 respondent identified as a caregiver of a patient with CKD, and 6 respondents identified as patients with T2D.
Survey respondents who identified themselves as living with both CKD and diabetes reported challenges with fatigue and anemia as well as adhering to dietary restrictions due to the high costs associated with those restrictions and inconvenience when dining with others. Patients with CKD may often present with comorbidities; 7 respondents reported high blood pressure, 3 reported high cholesterol, 1 reported high potassium levels, 1 reported heart disease, and 1 reported having had a heart attack. One survey respondent stated feeling tired and unable to focus on certain tasks due to living with multiple medical conditions. Five respondents reported worsening of their CKD, and 6 respondents indicated they had taken a medication to reduce the risk of worsening kidney disease, of which 3 reported experience with ACE inhibitors and 2 reported experience with ARBs. Respondents also indicated experience with diuretics, tacrolimus, erythropoietin, and dapagliflozin (SGLT2 inhibitor). Of the 6 survey respondents who indicated their level of satisfaction with their current medication(s), 3 were satisfied, 1 was very satisfied, and 2 were neutral.
Survey respondents identified the following factors as the most important considerations for new treatment options in CKD: “Does it make me feel tired?” “Does it interfere with my other medications?” and “How much does it cost?” Survey respondents identified the following outcomes as important for new treatment options for CKD both with or without diabetes: “limiting or arresting the progression of both diseases,” “make kidneys better,” “a longer life span,” and “maintain and improve quality of life overall.”
Finally, the Kidney Foundation of Canada and Diabetes Canada indicated that patients living with CKD may experience significant financial challenges due to reduced income (e.g., missed time from work as a result of their symptoms) and increased expenses (e.g., high costs associated with treatment, frequent visits to the health care team, and hospitalization). According to the organizations, equitable access to medications that slow the progression of kidney disease and reduce the risk of cardiovascular events, such as finerenone, may help relieve the financial burden of CKD and T2D on patients and the health care system.
Clinician Input
Input From the Clinical Experts Consulted by CADTH
The clinical experts mentioned that, despite available therapies for patients with CKD and T2D, there is a need for additional treatment options that reduce the risk of progression to kidney failure or cardiovascular events. There are still patients who progress to these outcomes and who could benefit from additional therapies such as finerenone. The clinical experts noted that the current paradigm aims to reduce progression of CKD to ESRD (kidney failure requiring dialysis or renal transplant). Treatment measures include blood pressure control, RAAS inhibition (ACE inhibitors and/or ARBs), and the use of SGLT2 inhibitors, in addition to lifestyle changes, the use of statins, and glycemic control. The clinical expert noted that finerenone may be combined with SGLT2 inhibitors to reduce cardiorenal risk as they protect kidney function through distinct and complementary pathways.14
According to the clinical experts, finerenone should be considered for patients who retain significant residual proteinuria despite being on a maximum tolerated dose of ACE inhibitor or ARB and SGLT2 inhibitor and noted, based on clinical experience, that finerenone can be added to these therapies 3 months after initiating SGLT2 inhibitor. They also mentioned that patients who are unable to tolerate SGLT2 inhibitor (e.g., due to hypotension or acute kidney injury) should be considered for finerenone. In the opinion of the clinical experts, treatment response can be assessed using surrogate measures such as changes in proteinuria over time and stability of renal function (eGFR). Intervals for monitoring should follow the current guidelines (twice annually according to the American Diabetes Association).15
According to the clinical experts, finerenone is better initiated as an add-on therapy in a specialist setting or in a community setting with specialist guidance and support. The clinical experts noted that finerenone should be discontinued if the patient is unable to tolerate the drug because of adverse events (AEs) such as hyperkalemia that are not amenable to management (e.g., dietary changes and/or diuretic use) or such as hypotension.
Clinician Group Input
The views of the clinician groups were consistent with the views of the clinical experts consulted by CADTH. Clinician group input for the review of finerenone was prepared and submitted by clinicians representing LMC Diabetes and Endocrinology, a single-specialty group endocrinology practice with 13 clinics across 3 provinces (Ontario, Quebec, and Alberta).
The clinician group recognized that there is an unmet need for a medication that will address significant decline in kidney function and cardiovascular disease in patients with T2D despite the availability of RAAS blockers and SGLT2 inhibitors and in patients who experience intolerance to and side effects with the currently available treatment options. The clinician group indicated finerenone would be used as an add-on therapy to RAAS blockers with or without SGLT2 inhibitors in patients with T2D and an ongoing risk of kidney disease progression and cardiovascular disease. Alternatively, finerenone would be used as the first add-on therapy for patients who were unable to tolerate or who developed side effects with RAAS blockers or SGLT2 inhibitors.
With respect to the patient population that will most likely benefit from finerenone, the clinician group identified patients with an eGFR greater than or equal to 25 mL/min/1.73 m2 and a UACR greater than or equal to 34 mg/mmol or patients with an eGFR of 25 mL/min/1.73 m2 to 90 mL/min/1.73 m2 and a UACR of 3.4 mg/mmol to 33.9 mg/mmol. The patient population identified to be the least suitable for treatment with finerenone was patients with a history of clinically significant hyperkalemia. Outcomes used in clinical practice would be preservation of eGFR over time, reduction in UACR, improved symptoms of heart failure or prevention of heart failure, and reduced emergency department visits or hospitalizations.
Drug Program Input
The drug programs identified the following jurisdictional implementation issues: relevant comparators in the randomized controlled trials (RCTs); considerations for initiation of therapy, for prescribing of therapy, and for discontinuation of therapy; and system and economic issues. The clinical experts consulted by CADTH weighed evidence from the FIDELIO and FIGARO studies and other clinical considerations to provide responses to the drug program implementation questions. Refer to Table 5 for more details.
Clinical Evidence
Pivotal Studies and Protocol-Selected Studies
Description of Studies
FIDELIO (N = 5,734) and FIGARO (N = 7,437) are phase III, randomized, double-blind, placebo-controlled, parallel-group, multicentre, event-driven studies of finerenone compared with placebo in patients with CKD and T2D. The 2 studies differed in their primary objective: The primary objective in FIDELIO was time to first occurrence of a renal composite end point in both the finerenone and placebo groups, while the primary objective of FIGARO was time to first occurrence of a cardiovascular composite end point in both the finerenone and placebo groups. Secondary objectives in each study included the primary objective of the other study, as well as time to first occurrence of a more severe renal composite end point, time to all-cause mortality, time to all-cause hospitalization, and change in UACR from baseline to month 4. The studies were sponsored by Bayer and included 30 (FIDELIO) and 31 (FIGARO) study centres in Canada.
After a run-in period of up to 16 weeks and a screening period of up to 2 weeks, eligible patients were randomized in a 1:1 ratio to the finerenone (10 mg or 20 mg) or placebo treatment arm, and stratified by region, eGFR category at screening, and albuminuria interval at screening. Randomization occurred at visit 1, and then there were 3 more planned monthly visits, followed by a visit every 4 months until the end of the study. The finerenone dose could be up-titrated or down-titrated at any point following the start of treatment at visit 1. If patients stopped the study drug prematurely, they remained in the trial and were followed up with until the end of the study.
Patient demographic characteristics and key disease characteristics were balanced between the finerenone and placebo groups in both trials. The mean age in both groups in both studies was approximately 65 years old. Most patients in both trials were male (69.8%) and white (68.1%). The mean baseline body mass index across all groups was 31.3 (standard deviation [SD] = 6.0), 47.5% of patients had never smoked, and 59.8% were alcohol abstinent. In the FIDELIO trial, the mean baseline eGFR was approximately 44 mL/min/1.73 m2 (SD = 12.5) in both groups, and the mean baseline UACR was 798.8 mg/g (SD = 2.7) and 814.7 mg/g (SD = 2.7) in the finerenone and placebo groups, respectively. In FIGARO, the mean baseline eGFR was approximately 68 mL/min/1.73 m2 (SD = 21.7) in both groups, and the mean baseline UACR was 284.3 mg/g (SD = 3.6) and 288.9 mg/g (SD = 3.5) in the finerenone and placebo groups, respectively. Regarding medication use at baseline, 66% of patients in FIDELIO and 57% of patients in FIGARO were on ARBs, and 34% of patients in FIDELIO and 43% of patients in FIGARO were on ACE inhibitors. Across the 2 trials, 97.7% of patients were also on antidiabetic treatment, including 6.7% of patients who were on SGLT2 inhibitors.
Efficacy Results
Key efficacy results of the FIDELIO and FIGARO trials for all randomized patients are summarized in Table 2. In FIDELIO, the primary and key secondary end points met the preplanned criteria for significance, and all-cause mortality (the next secondary end point) was tested hierarchically. It did not reach statistical significance, and so the remaining secondary end points were tested in an exploratory manner. In FIGARO, the primary end point met the preplanned criteria for significance, and the key secondary end point did not; therefore, the remaining secondary end points were tested in an exploratory manner.
The primary outcome in the FIDELIO study was time to first occurrence of the 40% renal composite end point, which comprises onset of kidney failure, a sustained decrease of eGFR greater than or equal to 40% from baseline over at least 4 weeks, or renal death. The 40% renal composite end point was a key secondary end point in FIGARO. In FIDELIO, this composite outcome occurred in 504 patients (17.8%) and 600 patients (21.1%) in the finerenone and placebo groups, respectively, and the hazard ratio (HR) was 0.825 (95% confidence interval [CI], 0.73 to 0.93; P = 0.0014) in favour of finerenone. In FIGARO, this end point occurred in 350 patients (9.5%) and 395 patients (10.8%) in the finerenone and placebo groups, respectively, and the HR was 0.87 (95% CI, 0.76 to 1.01; P = 0.0689), which was not statistically significant. In the pooled analysis of FIDELIO and FIGARO, the HR was 0.85 (95% CI, 0.77 to 0.93) and 0.77 (95% CI, 0.67 to 0.88) for the 40% and 57% renal composite end points, respectively, in favour of finerenone.
The 57% renal composite end point was a secondary end point in both studies. In FIDELIO, it occurred in 252 patients (8.9%) and 326 patients (11.5%) in the finerenone and placebo groups, respectively, and the HR was 0.76 (95% CI, 0.65 to 0.90) in favour of finerenone. In FIGARO, it occurred in 108 patients (2.9%) and 139 patients (3.8%) in the finerenone and placebo groups, respectively, and the HR was 0.77 (95% CI, 0.60 to 0.99) in favour of finerenone. In FIDELIO, the individual components of sustained decrease in eGFR greater than or equal to 40% or of greater than or equal to 57% (relative to baseline) had HRs of 0.815 (95% CI, 0.722 to 0.920) and 0.68 (95% CI, 0.55 to 0.82), respectively, and were the main drivers of the composite outcome results. The treatment effect of finerenone was assessed across the following subgroups of patients: history of cardiovascular disease, eGFR category at baseline, type of albuminuria at baseline, and SGLT2 inhibitor treatment at baseline. In general, the treatment effect of finerenone on the primary end point (time to first occurrence of the 40% renal composite end point) was consistent with the primary analysis across patient subgroups, with the following exception: In FIDELIO, the HR was greater than 1 in patients who were treated with SGLT2 inhibitors at baseline, favouring placebo over finerenone, yet the small sample size and wide CIs in this subgroup reflect uncertainty in the effect estimates. In FIGARO, the HR was also greater than 1 in patients with an eGFR of 45 mL/min/1.73 m2 to less than 60 mL/min/1.73 m2 at baseline and in patients with high albuminuria (30 mg/g to < 300 mg/g) at baseline.
Baseline values of UACR were comparable between the treatment groups but differed between trials according to the inclusion criteria, with higher values in the FIDELIO trial population. Nevertheless, in both trials, the change in UACR from baseline to month 4 was larger in the finerenone group than in the placebo group, with a ratio of least squares (LS) mean change from baseline (95% CI) of 0.69 (0.66 to 0.72) and 0.68 (0.65 to 0.70) in FIDELIO and FIGARO, respectively, with a P value less than 0.0001.
Baseline values of eGFR were comparable between the treatment groups but differed between trials according to the inclusion criteria, with lower values in the FIDELIO trial population. There was a larger acute reduction in eGFR in the finerenone group than in the placebo group, with an LS mean difference between groups at month 4 of –2.38 (95% CI, –2.77 to –1.98) and –2.24 (95% CI, –2.67 to –1.80) in FIDELIO and FIGARO, respectively, with a P value of less than 0.0001. The decrease in eGFR in the finerenone group then slows down, until the difference between both groups becomes positive, indicating a slower rate in eGFR decline in the finerenone group than in the placebo group at month 28 in the FIDELIO trial and month 36 in the FIGARO trial.
The primary outcome in the FIGARO study was time to first occurrence of the cardiovascular composite end point, which comprises cardiovascular death, nonfatal MI, nonfatal stroke, or hospitalization for heart failure. The cardiovascular composite end point was a key secondary end point in FIDELIO. In FIDELIO, this composite outcome occurred in 367 patients (13%) and 420 patients (14.8%) in the finerenone and placebo groups, respectively, and the HR was 0.86 (95% CI, 0.75 to 0.99; P = 0.0339) in favour of finerenone. In FIGARO, this end point occurred in 458 patients (12.4%) and 519 patients (14.2%) in the finerenone and placebo groups, respectively, and the HR was 0.87 (95% CI, 0.76 to 0.98; P = 0.0264) in favour of finerenone. In the pooled analysis of both trials, the HR was 0.86 (95% CI, 0.78 to 0.95) with a P value of 0.0018 in favour of finerenone. In FIGARO, the only individual component of statistical significance was hospitalization for heart failure, which had an HR of 0.71 (95% CI, 0.56 to 0.90) in favour of finerenone. In both trials, there was almost no difference in the risk of nonfatal stroke, with an HR of 0.97 (95% CI, 0.74 to 1.26) in FIDELIO and of 1.03 (95% CI, 0.77 to 1.38) in FIGARO. The treatment effect of finerenone on time to first occurrence of the cardiovascular composite end point was assessed across the following subgroups of patients: history of cardiovascular disease, eGFR category at baseline, type of albuminuria at baseline, and SGLT2 inhibitor treatment at baseline. In general, the treatment effect of finerenone was consistent with the primary analysis across patient subgroups, with the following exception: The HR was approximately 1 in patients who were treated with SGLT2 inhibitors at baseline in FIDELIO, while the HR was 0.49 (95% CI, 0.28 to 0.86) in FIGARO. However, the small sample size of this patient group in both trials reflects uncertainty in the effect estimates.
Incidence of all-cause mortality was similar between both groups in both trials, with 552 deaths (8.5% of patients) and 614 deaths (9.4% of patients) from any cause in the finerenone and placebo groups, respectively. Comparing the finerenone group with the placebo group, the HR was 0.90 (95% CI, 0.75 to 1.07) in FIDELIO and 0.89 (95% CI, 0.77 to 1.04) in FIGARO.
Incidence of all-cause hospitalization was similar between both groups in both trials, with 2,836 patients (43.5%) and 2,926 patients (45.0%) hospitalized for any cause in the finerenone and placebo groups, respectively. More hospitalizations were non–cardiovascular related (35%) than cardiovascular related (19%). Comparing the finerenone group with the placebo group, the HR was 0.95 (95% CI, 0.88 to 1.02) in FIDELIO and 0.97 (95% CI, 0.90 to 1.04) in FIGARO.
At baseline, the mean Kidney Disease Quality of Life survey (KDQOL-36) summary scores in all domains were comparable between treatment groups in each trial, and between both trials, except for the “burden of kidney disease” domain, where patients in the FIGARO group scored higher than those in the FIDELIO group. The quality of life decreased over time for all patients, consistently in all domains, assessed until month 36 in FIDELIO and month 48 in FIGARO. The physical component summary showed a sustained difference in favour of finerenone in FIDELIO at month 12 (LS mean difference = ███ ████ ███ ███ ██ ████ ███████ █ █████) and month 24 (LS mean difference = ███ ████ ███ ███ ██ ████ █████████████), and in FIGARO at month 36 (██ ████ ██████████ ████ ████ ███ ███ ██ ████ ███████ ██████).
Table 2: Summary of Key Results From Pivotal and Protocol-Selected Studies (FAS)
Efficacy outcome | FIDELIO | FIGARO | |||
|---|---|---|---|---|---|
Finerenone N = 2,833 | Placebo N = 2,841 | Finerenone N = 2,833 | Placebo N = 2,841 | ||
40% renal composite end pointa | |||||
n (%) | 504 (17.8) | 600 (21.1) | 350 (9.5) | 395 (10.8) | |
n/100 person-years (95% CI) | 7.6 (6.9 to 8.3) | 9.1 (8.4 to 9.8) | 3.2 (2.8 to 3.5) | 3.6 (3.2 to 3.9) | |
HR (95% CI) | 0.82 (0.73 to 0.93) | 0.87 (0.76 to 1.01) | |||
P valueb | 0.0014 | 0.0689 | |||
57% renal composite end pointa | |||||
n (%) | 252 (8.9) | 326 (11.5) | 108 (2.9) | 139 (3.8) | |
n/100 person-years (95% CI) | 3.64 (3.21 to 4.11) | 4.74 (4.24 to 5.26) | 0.95 (0.78 to 1.13) | 1.23 (1.03 to 1.44) | |
HR (95% CI) | 0.76 (0.65 to 0.90) | 0.77 (0.60 to 0.99) | |||
P valueb | 0.0012 | 0.0406 | |||
Cardiovascular composite end pointc | |||||
n (%) | 367 (13.0) | 420 (14.8) | 458 (12.4) | 519 (14.2) | |
n/100 person-years (95% CI) | 5.11 (4.60 to 5.64) | 5.92 (5.37 to 6.50) | 3.87 (3.52 to 4.23) | 4.45 (4.08 to 4.84) | |
HR (95% CI) | 0.86 (0.75 to 0.99) | 0.87 (0.76 to 0.98) | |||
P valueb | 0.0339 | 0.0264 | |||
Change in UACRd from baseline to month 4 | |||||
Baseline mean value (SD) | 798.79 (2.65) | 814.7 (2.7) | 284.33 (3.58) | 288.87 (3.53) | |
Month 4 mean value (SD)e | 520.39 (3.21) | 769.9 (3.0) | 177.86 (4.24) | 268.01 (3.99) | |
Patients in analysis, n | 2,711 | 2,705 | 3,521 | 3,476 | |
LS mean change (95% CI)e,f | 0.66 (0.64 to 0.67) | 0.95 (0.92 to 0.98) | 0.62 (0.60 to 0.64) | 0.92 (0.90 to 0.95) | |
Ratio of LS means (95% CI)e | 0.69 (0.66 to 0.72) | 0.68 (0.65 to 0.70) | |||
P value of F testg | < 0.0001 | < 0.0001 | |||
Change in eGFR from baselineh | |||||
Baseline mean value (SD) | 44.4 (12.5) | 44.3 (12.6) | 67.6 (21.6) | 68.0 (21.7) | |
LS mean difference, finerenone minus placebo, (95% CI; P value) | |||||
Month 4 | –2.38 (–2.77 to –1.98; < 0.0001) | –2.24 (–2.67 to –1.80; < 0.0001) | |||
Month 12 | –1.49 (–1.95 to –1.04; < 0.0001) | –2.01 (–2.51 to –1.52; < 0.0001) | |||
Month 24 | –0.03 (–0.60 to 0.55; 0.9244) | –1.09 (–1.68 to –0.49; 0.0003) | |||
Month 36 | 0.98 (0.17 to 1.78; 0.0172) | 0.11 (–0.62 to 0.83; 0.7717) | |||
Month 44 | 1.98 (0.83 to 3.13; 0.0008) | 0.37 (–0.47 to 1.21; 0.3899) | |||
CI = confidence interval; eGFR = estimated glomerular filtration rate; FAS = full analysis set; HR = hazard ratio; LS = least squares; SD = standard deviation; UACR = urinary albumin-creatinine ratio.
aRenal composite end point comprises onset of kidney failure, sustained decrease of eGFR greater than or equal to 40% or of greater than or equal to 57% from baseline over at least 4 weeks, or renal death. For composite outcomes and each component, the first event after randomization is considered. Subsequent events of the same type are not shown. The incidence rate is estimated as the number of patients with events divided by the cumulative at-risk time in the reference population, where a patient was no longer at risk once an event occurred. Incidence rates, HRs, and P values were only calculated for predefined efficacy end points.
bTwo-sided P value from log-rank test, stratified. Adjusted for multiplicity for the primary 40% renal composite outcome and the key secondary cardiovascular composite outcome in FIDELIO, and only for the primary cardiovascular composite outcome in FIGARO.
cCardiovascular composite end point comprises cardiovascular death, nonfatal myocardial infarction, nonfatal stroke, or hospitalization for heart failure. Events were adjudicated by an independent adjudication committee and considered from randomization until the end-of-study visit. For composite outcomes and each component, the first event after randomization is considered. Subsequent events of the same type are not shown. The incidence rate is estimated as the number of patients with events divided by the cumulative at-risk time in the reference population, where a patient was no longer at risk once an incident event occurred.
dUACR was determined 3 times at each visit from first morning void urine samples collected on 3 consecutive days and summarized according to the statistical analysis plan. For baseline, only samples with two-thirds of measurements taken on or before the day of randomization were used.
eMonth 4 is the visit closest to day 120 within a time window of 120 ± 30 days after randomization. If no measurements are available in this time window, the patient is excluded from this analysis.
fAnalysis of covariance with factors treatment group, region, eGFR category at screening, type of albuminuria at screening, and log-transformed baseline value as covariate nested within type of albuminuria.
gF test of equal means between the following additional factor levels: region, eGFR category at screening, and type of albuminuria at screening.
hFor the statistical evaluation, a mixed model was applied with factors treatment group, region, eGFR category at screening, type of albuminuria at screening, time, treatment × time, baseline value nested within type of albuminuria, and baseline value × time as covariate.
Source: FIDELIO Clinical Study Report;16 FIGARO Clinical Study Report.17
Harms Results
A summary of harms in the pooled analysis of FIDELIO and FIGARO is presented in Table 3. A total of 5,602 patients (86.1%) in the finerenone group and 5,607 patients (86.4%) in the placebo group experienced at least 1 AE. The most common AE in the finerenone group was hyperkalemia (14% versus 6.9% in the placebo group), and the most common AEs in the placebo group were hypertension (9% versus 6.4% in the finerenone group) and peripheral edema (5.9% versus 9% in the finerenone group). A total of 2,060 patients (31.6%) in the finerenone group and 2,186 patients (33.7%) in the placebo group experienced at least 1 serious AE (SAE). The most commonly reported SAE was pneumonia (2.2% in the finerenone group versus 3.3% in the placebo group).
A total of 414 patients (6.4%) in the finerenone group and 351 patients (5.4%) in the placebo group stopped treatment due to AEs. There were 110 deaths (1.7% of patients) and 151 deaths (2.3% of patients) due to treatment-emergent AEs in the finerenone and placebo groups, respectively.
In terms of notable harms, more patients reported hypotension in the finerenone group than in the placebo group (4.3% versus 2.7%). The number of patients who experienced atrial flutter and atrial fibrillation was less than 1% in each treatment group and comparable between groups. The number of patients who experienced hospitalization due to hyperkalemia was higher in the finerenone group than in the placebo group (0.9% versus 0.2%).
Table 3: Summary of Key Harms Results From the Pooled Analysis (Safety Analysis Set)
Harms outcome | Pooled analysis | |
|---|---|---|
Finerenone N = 6,510 | Placebo N = 6,510 | |
Harms | ||
Patients with ≥ 1 TEAE, n (%) | 5,602 (86.1) | 5,607 (86.4) |
Patients with ≥ 1 SAE, n (%) | 2,060 (31.6) | 2,186 (33.7) |
Patients who stopped treatment due to adverse events, n (%) | 414 (6.4) | 351 (5.4) |
Deaths, n (%) | 110 (1.7) | 151 (2.3) |
Notable harms | ||
Hyperkalemia, n (%) | 912 (14.0) | 448 (6.9) |
Hypotension, n (%) | 282 (4.3) | 177 (2.7) |
Hyperkalemia leading to hospitalization, n (%) | 61 (0.9) | 10 (0.2) |
Atrial fibrillation, n (%) | 49 (0.8) | 47 (0.7) |
Atrial flutter, n (%) | 13 (0.2) | 8 (0.1) |
SAE = serious adverse event; TEAE = treatment-emergent adverse event.
Source: FIDELITY pooled analysis.18
Critical Appraisal
Key baseline demographic and disease characteristics and past history of medication used appear to be balanced between the finerenone and placebo groups in both trials. There were important protocol deviations, balanced between treatment groups, reported in 53% and 58.5% of patients in FIDELIO and FIGARO, respectively. Due to study timelines, more protocol deviations associated with the COVID-19 pandemic were reported in FIGARO than in FIDELIO; however, deviations were balanced between treatment groups, and supportive analyses did not uncover any notable effect of the COVID-19 pandemic on the treatment effect of finerenone. The interpretation of results for the HRQoL instruments (i.e., the ability to assess trends over time and to make comparisons across treatment groups) is limited by the significant decline in patients available to provide assessment over time as well as lack of evidence of validity or minimal important difference (MID) of the HRQoL questionnaires used in the trials in patients with CKD and T2D. In the prespecified FIDELITY pooled analysis combining both trials, patients in FIDELIO had a lower eGFR at baseline than those in FIGARO, and the mean treatment duration was longer in FIGARO (approximately 35 months) than in FIDELIO (approximately 27 months). The statistical analysis in FIDELITY was exploratory and descriptive in nature with no adjustment for multiplicity; however, pooling is considered appropriate.
According to the clinical experts consulted by CADTH for this review, the demographic and disease characteristics of both study populations were generally reflective of the patients with CKD and T2D living in Canada. They agreed that there was an overrepresentation of male patients (70% male to 30% female) and noted there should be a more proportionate representation of patients, given potential differences in treatment efficacy and safety. The product monograph indicates that patients with an eGFR less than or equal to 25 mL/min/1.73 m2 should not start finerenone; however, 2.4% of patients in FIDELIO reported a baseline eGFR less than or equal to 25 mL/min/1.73 m2 (potentially due to decline in eGFR between screening and randomization). While the trials were under way, the SOC for patients with CKD and T2D evolved to include SGLT2 inhibitor. Therefore, only 6.7% of patients in both trials (n = 877) were on an SGLT2 inhibitor at baseline, and patients were not stratified by SGLT2 inhibitor use; however, use at baseline was balanced between the 2 treatment groups in both trials. In addition, the proportion of patients using glucagon-like peptide-1 (GLP-1) agonists with and without SGLT2 inhibitor at baseline was not balanced (18.5% versus 6.4%). This may have confounded the subgroup findings as GLP-1 agonists may also improve cardiorenal outcomes in patients with CKD and T2D.19,20 The clinical experts consulted by CADTH agreed that placebo plus SOC was an appropriate comparator in Canadian clinical practice for patients with CKD and T2D. The clinical experts agreed with the sponsor’s definition of SOC as including an ACE inhibitor or ARB, and ideally an SGLT2 inhibitor, which is still not widely accessible to patients with CKD and T2D living in Canada. The clinical experts pointed out that a combination therapy with the 2 drugs together makes physiologic sense as SGLT2 inhibitors are linked to reductions in the risk of hyperkalemic episodes (serum potassium ≥ 6.0 mmol/L), and finerenone has hyperkalemia as a side effect. There is, however, limited evidence on the positioning of finerenone in relation to SGLT2 inhibitors, and the evidence available for the addition of finerenone to ACE inhibitor or ARB, and an SGLT2 inhibitor, is limited. A non-sponsor-submitted reimbursement review assessing the use of SGLT2 inhibitor in patients with CKD and T2D is currently ongoing. A phase II RCT that will compare finerenone plus placebo, SGLT2 inhibitors plus placebo, and finerenone plus SGLT2 inhibitors (CONFIDENCE trial)21 will begin in 2022, and results may provide more insight into this comparison and the place of finerenone in therapy. Finally, the trials included composite renal and cardiovascular outcomes and were only powered for their respective primary composite outcomes and not for the components of the primary outcome, which include a sustained decrease in eGFR and initiation of ESRD in FIDELIO, and hospitalization for heart failure in FIGARO; hence, the impact of finerenone on each of the components of the composite outcomes is uncertain.
Indirect Comparisons
Indirect evidence from 1 published network meta-analysis (NMA) by Zhao et al. (2022)22 evaluated the effectiveness of finerenone compared to SGLT2 inhibitors in the treatment of CKD and T2D. SGLT2 inhibitors are currently part of the SOC for patients with diabetic kidney disease; however, only 6.7% of patients (877 out of 13,026) in the pivotal trials were concurrently taking SGLT2 inhibitors in the FIDELIO and FIGARO trials. This NMA, therefore, provides an indirect comparison of efficacy outcomes between finerenone and SGLT2 inhibitors.
Description of Studies
The authors include 14 articles reporting 8 placebo-controlled RCTs comprising 30,661 patients. Seven studies involved an assessment of SGLT2 inhibitor (13,246 patients receiving gliflozin versus 11,741 receiving placebo): EMPA-REG OUTCOME,23,24 CANVAS Program,25,26 CREDENCE,27,28 DECLARE–TIMI 58,29 DAPA-CKD,30 VERTIS CV,31,32 and SCORED.33 One study (the pivotal FIDELIO trial)34,35 assessed finerenone (2,833 patients receiving finerenone versus 2,841 receiving placebo). According to risk of bias assessment, there was low risk of bias in all 8 studies.
Major adverse cardiovascular events were defined consistently across the included studies. Kidney function progression, however, was defined differently across the included studies, with composite end points that included ESRD, renal death, and a sustained decrease in eGFR that ranged from 40% to 50%. One trial (EMPA-REG OUTCOME) included patients who had initiated renal replacement therapy, and 2 trials (DAPA-CKD and SCORED) included patients with kidney transplants. One trial (VERTIS CV) did not report a renal composite end point. The authors considered these definitions similar enough to be used in the meta-analysis.
Efficacy Results
NMA results showed that, compared to finerenone, SGLT2 inhibitors significantly reduced the risks of kidney function progression (HR = 0.78; 95% CI, 0.67 to 0.90) and hospitalization for heart failure (HR = 0.71; 95% CI, 0.55 to 0.92). No treatment was favoured when finerenone was compared to SGLT2 inhibitors for the outcomes of major adverse cardiovascular events (HR = 0.95; 95% CI, 0.71 to 1.27), nonfatal MI (HR = 0.91; 95% CI, 0.64 to 1.30), nonfatal stroke (HR = 0.70; 95% CI, 0.35 to 1.39), cardiovascular death (HR = 1.00; 95% CI, 0.78 to 1.29), and all-cause death (HR = 0.96; 95% CI, 0.75 to 1.23). No network plot for any outcome had a closed loop, suggesting a lack of direct evidence between finerenone and SGLT inhibitors, so an inconsistency test was not performed.
Harms Results
The safety outcomes of the treatments were not assessed in this NMA.
Critical Appraisal
This NMA included a limited number of studies, with some heterogeneity in the definition of a key renal outcome across the studies. Only 1 study assessed finerenone, while the other 7 assessed an SGLT2 inhibitor, which limited the statistical power of this NMA. The second pivotal RCT on finerenone from this review (FIGARO) was not included in this NMA; its inclusion may have strengthened this analysis. The authors did not explore the baseline demographic characteristics of the patient populations across the trials and reported that “the cardiorenal risk of participants was possibly different among included trials.”22 The durations of the trials were not reported and may have differed between studies. Moreover, the safety outcomes of the treatments were not assessed in this NMA. The CADTH review team was unable to rigorously assess the methods in this article because insufficient details on the methods were provided (e.g., no details on the retrieved number of records in the systematic review), and there was no discussion on possible adjustments for potential effect modifiers or feasibility assessment. A small proportion of patients in the included FIDELIO trial were using SGLT2 inhibitor at baseline, but no additional analysis including and excluding this subgroup was conducted.
Conclusions
Two RCTs informed the systematic review of finerenone as an adjunct therapy for the treatment of patients with CKD and T2D. The trials demonstrated that treatment with finerenone was associated with a clinically meaningful reduction in the renal composite outcome and the cardiovascular composite outcome, driven by the outcome components of a sustained decrease in eGFR greater than or equal to 40% or greater than or equal to 57% and incidence of hospitalization for heart failure. The trials also demonstrated that finerenone was associated with a significant reduction in UACR from baseline, which the clinical experts referred to as an important marker for reduced risk of progression of CKD to ESRD. The impact of finerenone on HRQoL is uncertain due to difficulty interpreting results from the HRQoL instruments. All patients in both trials were on a maximum tolerated dose of ACE inhibitor or ARB as SOC, but only a small proportion in both trials were on SGLT2 inhibitor at baseline; hence, available evidence on the efficacy and safety of the addition of finerenone to ACE inhibitor or ARB, and an SGLT2 inhibitor, is limited. No significant difference was reported when comparing patients who were on an SGLT2 inhibitor at baseline with patients who were not. Furthermore, although the included NMA favoured SGLT2 inhibitor over finerenone in improving cardiorenal outcomes, this NMA had several limitations that preclude any definitive conclusion.
The safety profile of finerenone in these trials was consistent with the known safety profile of other nonsteroidal MRAs in terms of hyperkalemia and hypotension. No additional safety signals were identified with finerenone in this study.
Introduction
Disease Background
Diabetes is the most common cause of kidney disease in Canada, and it is estimated by the sponsor (applying prevalence estimates) that there are more than 1 million people in Canada living with CKD and T2D in 2022.1-3 Diabetic kidney disease has “numerous overlapping etiologic pathways” where changes in glomerular hemodynamics, inflammation, and fibrosis mediate kidney tissue damage.4 However, the only way to differentiate between CKD caused directly by diabetes (diabetic nephropathy) and CKD from other causes in patients who are diabetic is a kidney biopsy, which is rarely performed, and so the term “diabetic kidney disease” with no pathological phenotype is most commonly used.4 Older age, low socioeconomic status, obesity, smoking, poor glycemic and blood pressure control, and genetic factors are known risk factors for diabetic kidney disease.4 T2D linked to obesity is now common in younger populations, resulting in an earlier and more rapid rate of progression of CKD complications.4
CKD is the leading cause of ESRD, requiring dialysis or renal transplant. CKD is also associated with cardiovascular complications leading to decreased quality of life and premature death.1,4,5 In a US survey that evaluated 15,000 patients with diabetes and kidney disease, 10-year mortality was 4-fold and 2.7-fold higher and cardiovascular mortality was 3-fold and 6-fold higher in patients with both CKD and T2D than in patients with, respectively, CKD alone or T2D alone.6 Patients with both CKD and T2D also reported lower HRQoL scores than those with CKD alone or T2D alone.7,8
CKD is clinically diagnosed in patients who are diabetic based on the presence of albuminuria (> 30 mg/g) and/or decreased eGFR (eGFR < 60 mL/min/1.73 m2) in at least 2 out of 3 samples in a 3-month period.4,5 These are also 2 important indicators of disease progression: High UACR and low eGFR values indicate more severe disease.5,9 In some cases, patients with T2D and CKD may present with only reduced eGFR and normal urine albumin levels (UACR ≤ 30 mg/mmol), referred to as nonproteinuric diabetic CKD.4
Standards of Therapy
According to the clinical experts consulted by CADTH, the primary goal of treatment is to reduce the risk of progression of CKD to ESRD by the application of pharmacologic and lifestyle strategies. The general approach to management of patients with CKD and T2D includes optimization of blood pressure, proteinuria, and glycemic control; dietary changes; and lowering of lipid levels with statins.10 In addition, for several decades, patients with CKD have been treated with either an ACE inhibitor or an ARB that inhibits the RAAS.10 RAAS inhibiters are antihypertensive drugs and have also been linked to decreasing the risk of progression of albuminuria from normal to mildly increased (30 mg/g to 300 mg/g) and from mildly increased to severely increased (> 300 mg/g).10 Assessment of serum creatinine and potassium soon after starting or intensifying RAAS inhibitors is recommended due to their serum creatinine and potassium–elevating effects.10,12
Recently, guidelines have been revised to encourage the use of SGLT2 inhibitors in patients with CKD and T2D, particularly for patients with severely increased albuminuria (> 300 mg/g).10-12 SGLT2 inhibitors can prevent renal disease progression, including the development of ESRD, as well as the incidence of cardiovascular disease in patients with diabetic kidney disease, as demonstrated in 2 large RCTs: CREDENCE and DAPA-CKD.27,32,36 Some patients may be intolerant of SGLT2 inhibitors, including patients with poor glycemic control, patients at high risk of genital infections or lower limb amputation, and patients with acute kidney injury.10 According to the clinical experts consulted by CADTH, there is limited access to SGLT2 inhibitors in Canada, and access varies by jurisdictions, although access and subsequent use are expected to increase with time. In this review, the sponsor identifies SGLT2 inhibitors, in addition to ACE inhibitors or ARBs, as SOC.
In spite of the application of the pharmacologic and lifestyle strategies, the clinical experts indicated that there are patients with CKD and T2D who continue to progress to renal failure or develop cardiovascular events and who could benefit from additional pharmacologic therapies.
According to the clinical experts consulted by CADTH and clinical management guidelines, patients with CKD and T2D should ideally be monitored every 3 months to 6 months to assess blood pressure, glycated hemoglobin, volume status, eGFR based on serum creatinine, serum potassium, and albuminuria.10
Drug
The initial reimbursement request submitted by the sponsor for review by CADTH for finerenone is as an adjunct to SOC therapy to delay progression of kidney disease and to reduce the risk of major adverse cardiovascular events (cardiovascular death, nonfatal MI, nonfatal stroke) and hospitalization for heart failure in adults with CKD and T2D, where SOC includes an ACE inhibitor or ARB, and an SGLT2 inhibitor, unless contraindicated or not tolerated.37 Finerenone underwent review by Health Canada through the standard review pathway and received an NOC on October 14, 2022. The approved indication is as adjunct to SOC therapy in adults with CKD and T2D to reduce the risk of end-stage kidney disease and a sustained decrease in eGFR, as well as of cardiovascular death, nonfatal MI, and hospitalization for heart failure.13 The CADTH review team agreed with the sponsor’s assessment that this revision to the indication does not meaningfully impact the CADTH clinical review, and the reimbursement request was subsequently revised to this approved indication. Finerenone was approved by the FDA on July 9, 2021, to be used to reduce the risk of sustained eGFR decline, end-stage kidney disease, cardiovascular death, nonfatal MI, and hospitalization for heart failure in adult patients with CKD associated with T2D.11 It was approved by the Australian Therapeutic Goods Administration on November 18, 2021, to delay progressive decline of kidney function in adults with CKD associated with T2D (with albuminuria), in addition to SOC.38 Finally, finerenone was approved by the European Medicines Agency on December 16, 2021, for the treatment of CKD (stage 3 and 4 with albuminuria) associated with T2D in adults.39 The sponsor noted that the European Medicines Agency review was based only on the FIDELIO clinical trial and that a European Medicines Agency review based on the FIGARO trial is ongoing. In its draft guidance issued in May 2022, the National Institute for Health and Care Excellence (NICE) was minded not to recommend finerenone as an option for treating stage 3 and 4 CKD with albuminuria associated with T2D in adults.40 The sponsor noted that the institute’s process is ongoing, with a second appraisal committee meeting to be held after requested clarification and analyses are provided. Finerenone is currently under review at the Scottish Medicines Consortium.
Mineralocorticoid receptors are expressed in the kidneys, heart, and blood vessels. Finerenone is a nonsteroidal, selective MRA that reduces inflammation and fibrosis caused by mineralocorticoid receptor overactivation by selectively binding to mineralocorticoid receptors.13 This binding leads to a “specific receptor ligand complex that blocks recruitment of transcriptional coactivators implicated in the expression of proinflammatory and profibrotic mediators.”13 Due to its nonsteroidal structure, finerenone has no relevant affinity for androgen, progesterone, estrogen, or glucocorticoid receptors and therefore does not cause sex hormone–related AEs such as gynecomastia (as is common with other MRAs, such as spironolactone). Finerenone has not been previously reviewed by CADTH.
Key characteristics of finerenone are shown in Table 4. Finerenone is available as oral tablets (10 mg and 20 mg). The recommended starting dosage of finerenone is 20 mg once daily for patients with eGFR greater than or equal to 60 mL/min/1.73 m2 or 10 mg once daily for patients with eGFR greater than or equal to 25 mL/min/1.73 m2 to less than 60 mL/min/1.73 m2. Four weeks after initiation, restart, or up-titration of finerenone treatment, serum potassium and eGFR should be remeasured to determine continuation of finerenone treatment and dose adjustment. Thereafter, serum potassium should be remeasured periodically and as needed based on patient characteristics and serum potassium levels. Initiation of finerenone treatment is not recommended in patients with eGFR less than 25 mL/min/1.73 m2 and for patients with serum potassium greater than 5.0 mmol/L. Treatment with finerenone should be discontinued in patients with ESRD (eGFR < 15 mL/min/1.73 m2).13
Table 4: Key Characteristics of Finerenone and SGLT2 Inhibitors for CKD and T2D
Characteristic | Finerenone | SGLT2 inhibitors |
|---|---|---|
Mechanism of action | Nonsteroidal, selective mineralocorticoid receptor antagonist | Blocking reabsorption of glucose in the proximal tubule through SGLT2, which lowers the renal glucose threshold and leads to substantial glycosuria |
Indicationa | As an adjunct to standard of care therapy in adults with chronic kidney disease and T2D to reduce the risk of:
| To reduce the risk of sustained eGFR decline, end-stage kidney disease, cardiovascular death, and hospitalization for heart failure in adults with CKD at risk of progression (a broader population of patients that includes patients with CKD associated with T2D) |
Route of administration | Oral | Oral |
Recommended dosage |
| Canagliflozin 100 mg once daily Dapagliflozin 10 mg once daily |
Serious adverse effects or safety issues | Hyperkalemia | Increased genital infections Fournier gangrene Higher risk of lower limb amputations |
Other |
| — |
CKD = chronic kidney disease; eGFR = estimated glomerular filtration rate; SGLT2 = sodium-glucose cotransporter-2; T2D = type 2 diabetes.
aHealth Canada–approved indication.
Source: Finerenone product monograph;13 Perkovic et al. (2022).10
Stakeholder Perspectives
Patient Group Input
This section was prepared by CADTH staff based on the input provided by patient groups. The full original patient input received by CADTH has been included in the stakeholder section at the end of this report.
Patient input for the review of finerenone was provided as a joint submission from the Kidney Foundation of Canada and Diabetes Canada. The Kidney Foundation of Canada and Diabetes Canada are charities committed to eliminating the burden of kidney disease and leading the fight against diabetes, respectively, through research, education, and advocacy.
The Kidney Foundation of Canada and Diabetes Canada conducted an online survey of patients with CKD and T2D, and their caregivers, residing across Canada in May 2022 (n = 24; 9 completed and 15 partially completed the survey). Eight respondents identified as patients with CKD, 1 respondent identified as a caregiver of a patient with CKD, and 6 respondents identified as patients with T2D. Of the 8 respondents who reported their current age, or the age of the patient they cared for, 2 patients were aged between 40 years and 54 years, 2 patients were aged between 55 years and 69 years, and 4 patients were 70 years old or older.
Survey respondents who identified themselves as living with both CKD and diabetes reported challenges with fatigue and anemia as well as adhering to dietary restrictions due to the high costs associated with those restrictions and inconvenience when dining with others. Patients with CKD may often present with comorbidities; 7 respondents reported high blood pressure, 3 reported high cholesterol, 1 reported high potassium levels, 1 reported heart disease, and 1 reported having had a heart attack. One survey respondent stated feeling tired and unable to focus on certain tasks due to living with multiple medical conditions.
Five respondents reported worsening of their CKD, and 6 respondents indicated they had taken a medication to reduce the risk of worsening kidney disease, of which 3 reported experience with ACE inhibitors and 2 reported experience with ARBs. Respondents also indicated experience with diuretics, tacrolimus, erythropoietin, and dapagliflozin (SGLT2 inhibitor). Of the 6 survey respondents who indicated their level of satisfaction with their current medication(s), 3 were satisfied, 1 was very satisfied, and 2 were neutral. One respondent reported side effects with tacrolimus (nausea, heartburn, and flushing), while other respondents reported the benefits of their current medication (e.g., controlled the itch and burning sensation in the feet and legs with excess fluid and achieved lab values within acceptable ranges).
Survey respondents identified the following factors as the most important considerations for new treatment options in CKD: “Does it make me feel tired?” “Does it interfere with my other medications?” and “How much does it cost?” Survey respondents identified the following outcomes as important for new treatment options for CKD with or without diabetes: “limiting or arresting the progression of both diseases,” “make kidneys better,” “a longer life span,” and “maintain and improve quality of life overall.”
Finally, the Kidney Foundation of Canada and Diabetes Canada indicated that patients living with CKD may experience significant financial challenges due to reduced income (e.g., missed time from work as a result of their symptoms) and increased expenses (e.g., high costs associated with treatment, frequent visits to the health care team, and hospitalization). According to the organizations, equitable access to medications that slow the progression of kidney disease and reduce the risk of cardiovascular events, such as finerenone, may help relieve the financial burden of CKD and T2D on patients and the health care system.
Clinician Input
Input From Clinical Experts Consulted by CADTH
All CADTH review teams include at least 1 clinical specialist with expertise in the diagnosis and management of the condition for which the drug is indicated. Clinical experts are a critical part of the review team and are involved in all phases of the review process (e.g., providing guidance on the development of the review protocol; assisting in the critical appraisal of clinical evidence; interpreting the clinical relevance of the results; and providing guidance on the potential place in therapy). The following input was provided by 2 clinical specialists with expertise in the diagnosis and management of CKD with T2D and in cardiovascular conditions subsequent to CKD.
Unmet Needs
The clinical experts mentioned that in spite of available therapies for patients with CKD and T2D, there is a need for additional treatment options that reduce the risk of progression to kidney failure or cardiovascular events. There are patients who continue to progress to these outcomes and who could benefit from additional therapies such as finerenone.
Place in Therapy
The clinical experts noted that the current paradigm aims to reduce progression of CKD to ESRD (kidney failure requiring dialysis or renal transplant). Treatment measures include blood pressure control, RAAS inhibition (ACE inhibitors and/or ARBs), and the use of SGLT2 inhibitors, in addition to lifestyle changes, the use of statins, and glycemic control. The clinical experts noted that finerenone may be combined with SGLT2 inhibitors to reduce cardiorenal risk as they protect kidney function through distinct and complementary pathways.14
The clinical experts also mentioned that steroidal MRAs, such as spironolactone and pelerine, are currently used in conjunction with ACE inhibitors (or ARBs) and beta-blockers in the treatment of heart failure with reduced ejection fraction. Replacing steroidal MRAs with nonsteroidal MRAs such as finerenone may have a better safety profile and produce better outcomes for patients (citing a phase II tolerability and safety trial comparing both drugs).41
Patient Population
According to the clinical experts, finerenone should be considered for patients who retain significant residual proteinuria despite being on ACE inhibitor or ARB and SGLT2 inhibitor and noted that finerenone can be added to these therapies 3 months after initiating the SGLT2 inhibitor. They also mentioned that patients who are unable to tolerate SGLT2 inhibitor (e.g., due to hypotension or acute kidney injury) should be considered for finerenone.
Assessing Response to Treatment
In the opinion of the clinical experts, treatment response can be assessed using surrogate measures such as changes in proteinuria over time and stability of renal function (eGFR). Intervals for monitoring should follow the current guidelines (twice annually according to the American Diabetes Association).15
Discontinuing Treatment
The clinical experts noted that finerenone should be discontinued if the patient is unable to tolerate the drug because of AEs such as hyperkalemia that are not amenable to management (e.g., dietary changes and/or diuretic use) or such as hypotension.
Prescribing Conditions
According to the clinical experts, finerenone is better initiated as an add-on therapy in a specialist setting or in a community setting with specialist guidance and support.
Additional Considerations
One clinical expert (a cardiologist) noted that the use of finerenone may be more cost-effective than a combination of steroidal MRAs and potassium binders.
Clinician Group Input
This section was prepared by CADTH staff based on the input provided by clinician groups. The full original clinician group input(s) received by CADTH have been included in the stakeholder section at the end of this report.
Clinician group input for the review of finerenone was prepared and submitted by 2 clinicians representing LMC Diabetes and Endocrinology, a single-specialty group endocrinology practice with 13 clinics across 3 provinces (Ontario, Quebec, and Alberta).
The clinician group recognized that there is an unmet need for a medication that will address significant decline in kidney function and cardiovascular disease in patients with T2D despite the availability of RAAS blockers and SGLT2 inhibitors and in patients who experience intolerance to and side effects with the currently available treatment options.
The clinician group indicated finerenone would be used as an add-on therapy to RAAS blockers with or without SGLT2 inhibitors in patients with T2D and an ongoing risk of kidney disease progression and cardiovascular disease. Alternatively, finerenone would be used as the first add-on therapy for patients who were unable to tolerate or who developed side effects with RAAS blockers or SGLT2 inhibitors.
With respect to the patient population that will most likely benefit from finerenone, the clinician group identified patients with an eGFR greater than or equal to 25 mL/min/1.73 m2 and a UACR greater than or equal to 34 mg/mmol or patients with an eGFR of 25 mL/min/1.73 m2 to 90 mL/min/1.73 m2 and a UACR of 3.4 mg/mmol to 33.9 mg/mmol. The patient population identified to be the least suitable for treatment with finerenone was patients with a history of clinically significant hyperkalemia. Outcomes used in clinical practice would be preservation of eGFR over time, reduction in UACR, improved symptoms of heart failure or prevention of heart failure, and reduced emergency department visits or hospitalizations.
Drug Program Input
The drug programs provide input on each drug being reviewed through CADTH’s reimbursement review processes by identifying issues that may impact their ability to implement a recommendation. The implementation questions and corresponding responses from the clinical experts consulted by CADTH are summarized in Table 5.
Table 5: Summary of Drug Plan Input and Clinical Expert Response
Drug program implementation questions | Clinical expert response |
|---|---|
Relevant comparators | |
Was placebo plus SOC a reasonable comparator to use in these studies? Could there have been an alternative? | The clinical experts consulted by CADTH indicated that placebo plus SOC is a reasonable comparator. |
The sponsor is asking for reimbursement of the drug as adjunctive SOC for patients with CKD and T2D. Does CDEC agree with the SOC defined by the sponsor for the current landscape of therapy for CKD and T2D? The sponsor indicated that SOC therapies include:
| The clinical experts consulted by CADTH indicated that SOC as defined by the sponsor is appropriate and that statins could potentially be added to the SOC (at least 70% of patients in both trials were on statins). |
The benefit status of SGLT2 inhibitor varies across the country and in some jurisdictions is based on indication, such as T2D and HF. Patients in jurisdictions that have SGLT2 inhibitor as restricted would have to meet specific criteria before adding on finerenone. Would the need for this drug in patients with CKD and T2D have an effect on the current benefit status of SGLT2 inhibitor? | The clinical experts consulted by CADTH indicated that the need for finerenone should not directly impact access to SGLT2 inhibitor. |
The sponsor is asking for reimbursement of finerenone to use as adjunctive therapy to reduce hospitalizations for HF. Could there be an indication creep and need to use this medication just in patients with HF? | The clinical experts noted that in cardiology, MRA drugs are a fundamental part of guideline-based therapy, and a newer-generation drug with relative advantages over spironolactone and eplerenone would be welcomed, irrespective of whether the patient had CKD, T2D, or both. This would not be viewed as an “indication creep” so much as an indication. |
Would there be a need for finerenone in patients with either CKD or T2D alone? If so, how would jurisdictions be expected to handle these requests? | The clinical experts noted that there would be a need for finerenone for patients with CKD or T2D alone only in situations where ACE inhibitor or ARBs and/or SGLT2 inhibitor are not tolerated or, in rare instances, are contraindicated. The prescribers can state these reasons to justify access to the medication as needed. This will rarely happen based on current clinical practice experience as there are no data to inform this question. The sponsor also noted that there are no data to inform whether finerenone can be used in patients with either CKD or T2D alone (meaning that treatment in this manner is expected to be rare in current clinical practice) and that the anticipated Health Canada indication is for patients with both CKD and T2D; therefore, use in CKD alone would be off label. A clinical trial planned specifically to evaluate finerenone in patients with nondiabetic CKD is expected to be completed in 2025. |
The sponsor acknowledges that since the conclusion of both trials, Canadian treatment practices have evolved for CKD with T2D; SGLT2 inhibitors have received regulatory approvals, and contemporary guidelines recommend their use to reduce cardiorenal risk in CKD with T2D.
| The clinical experts noted that the beneficial effects of SGLT2 inhibitor on renal outcomes in people with T2D are largely seen as a “class effect” at this point. Data are too limited to be conclusive in people without diabetes. |
Can the committee define intolerance or contraindication to an SGLT2 inhibitor? | The clinical experts indicated that intolerance or contraindication to an SGLT2 inhibitor is defined as patients with persistent hypoglycemia or hypotension, acute kidney injury, and high risk of amputation. |
Considerations for initiation of therapy | |
What would CDEC’s definition of CKD be for patients to meet initiation criteria? Are there specific lab markers or other parameters that would be required from patients? | The clinical experts indicated that the definition of CKD for patients to meet initiation criteria is if they have CKD and persistent residual risk (albuminuria) despite an optimal use of ACE inhibitor or ARB and SGLT2 inhibitor. The use of finerenone will be an add-on therapy to modify risk of CKD in patients already optimized on the SOC (ACE inhibitor or ARB plus SGLT2 inhibitor) who have serum potassium in the normal range (< 5 mmol/L). |
Considerations for discontinuation of therapy | |
What would CDEC define as disease progression for CKD, and when would the medication be discontinued? | The clinical experts indicated that the key factor that may drive discontinuation would be hyperkalemia. This will usually be on a temporary basis to control the hyperkalemia with dietary measures and to reassess and reinitiate therapy. A permanent discontinuation is only warranted in cases of hyperkalemia that are persistent and not amenable to dietary and/or therapeutic measures with ACE inhibitors or ARBs. |
If the patient had a clinically significant CV event or hospitalization for HF while on finerenone, would treatment be discontinued? | The clinical experts indicated that if the patient had a clinically significant CV event or hospitalization for HF while on finerenone, treatment with finerenone should not be discontinued as finerenone would be used in lieu of 1 of the older MRAs. Patients with HF have readmissions for HF or admissions for other cardiac conditions (e.g., arrhythmia) while on an MRA, and these drugs are not stopped just on account of that. In the specific example of arrhythmia, if this was ventricular tachycardia or ventricular fibrillation felt due to hyperkalemia that was due in turn to the MRA, then dosing might be adjusted, but it would not mean that the drug would automatically be stopped. |
Considerations for prescribing of therapy | |
Would this medication only be prescribed by a specialist, or would a GP be able to initiate therapy? If only a specialist, which would be the most appropriate: cardiologist, nephrologist, or endocrinologist? | The clinical experts indicated that GPs will be prescribing the medication, as with the SGLT2 inhibitor, since they see the most patients meeting the eligibility criteria for the drug (i.e., early CKD, stages 1 to 3). |
System and economic issues | |
With generic SGLT2 inhibitor coming out soon, would this have any impact on the substantial estimated incremental costs to the drug programs provided by the sponsor? | For CDEC consideration. |
ACE = angiotensin-converting enzyme; ARB = angiotensin receptor blocker; CDEC = CADTH Canadian Drug Expert Committee; CKD = chronic kidney disease; CV = cardiovascular; GP = general practitioner; HF = heart failure; MRA = mineralocorticoid receptor antagonist; SGLT2 = sodium-glucose cotransporter-2; SOC = standard of care; T2D = type 2 diabetes.
Clinical Evidence
The clinical evidence included in the review of Kerendia (finerenone) is presented in 2 sections. The first section, the systematic review, includes pivotal studies provided in the sponsor’s submission to CADTH and Health Canada, as well as those studies that were selected according to an a priori protocol. The second section includes indirect evidence selected from the literature that met the selection criteria specified in the review (no indirect evidence was submitted by the sponsor).
Systematic Review (Pivotal and Protocol-Selected Studies)
Objectives
To perform a systematic review of the beneficial and harmful effects of finerenone 10 mg and 20 mg tablets, used to delay progression of kidney disease and to reduce the risk of major adverse cardiovascular events (cardiovascular death, nonfatal MI, nonfatal stroke) and hospitalization for heart failure in adult patients with CKD and T2D.
Methods
Studies selected for inclusion in the systematic review will include pivotal studies provided in the sponsor’s submission to CADTH and Health Canada, as well as those meeting the selection criteria presented in Table 6. Outcomes included in the CADTH review protocol reflect outcomes considered to be important to patients, clinicians, and drug plans. Of note, the systematic review protocol presented in the following was established before the granting of an NOC from Health Canada.
Table 6: Inclusion Criteria for the Systematic Review
Criteria | Description |
|---|---|
Patient population | Adults with chronic kidney disease and type 2 diabetes Subgroups:
|
Intervention | Finerenone 10 mg and 20 mg, oral administration |
Comparators | Placebo plus SOCa SGLT2 inhibitor plus SOC |
Outcomes | Efficacy outcomes:
Harms outcomes: AEs, SAEs, WDAEs, mortality, and notable harms or harms of special interest (e.g., hyperkalemia, new onset of atrial fibrillation and atrial flutter, hypotension) |
Study design | Published and unpublished phase III and IV RCTs |
ACE = angiotensin-converting enzyme; AE = adverse event; ARB = angiotensin receptor blocker; eGFR = estimated glomerular filtration rate; HRQoL = health-related quality of life; RCT = randomized controlled trial; SAE = serious adverse event; SGLT2 = sodium-glucose cotransporter-2; SOC = standard of care; WDAE = withdrawal due to adverse event.
aSOC includes an ACE inhibitor or ARB.
The literature search for clinical studies was performed by an information specialist using a peer-reviewed search strategy according to the PRESS Peer Review of Electronic Search Strategies checklist.42
Published literature was identified by searching the following bibliographic databases: MEDLINE All (1946—) via Ovid and Embase (1974—) via Ovid. All Ovid searches were run simultaneously as a multifile search. Duplicates were removed using Ovid deduplication for multifile searches, followed by manual deduplication in Endnote. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. The main search concepts were finerenone and CKD. Clinical trials registries were searched: the US National Institutes of Health’s clinicaltrials.gov, WHO’s International Clinical Trials Registry Platform search portal, Health Canada’s Clinical Trials Database, and the European Union Clinical Trials Register.
No filters were applied to limit the retrieval by study type. Retrieval was not limited by publication date or by language. Conference abstracts were excluded from the search results. Refer to Appendix 1 for the detailed search strategies.
The initial search was completed on June 15, 2022. Regular alerts updated the search until the meeting of the CADTH Canadian Drug Expert Committee on October 26, 2022.
Grey literature (literature that is not commercially published) was identified by searching relevant websites from the Grey Matters: A Practical Tool for Searching Health-Related Grey Literature checklist.43 Included in this search were the websites of regulatory agencies (FDA and the European Medicines Agency). Google was used to search for additional internet-based materials. Refer to Appendix 1 for more information on the grey literature search strategy.
Two CADTH clinical reviewers independently selected studies for inclusion in the review based on titles and abstracts, according to the predetermined protocol. Full-text articles of all citations considered potentially relevant by at least 1 reviewer were acquired. Reviewers independently made the final selection of studies to be included in the review, and differences were resolved through discussion.
A focused literature search for indirect treatment comparisons (ITCs) dealing with diabetes and CKD was run in MEDLINE All (1946–) on June 15, 2022. No search limits were applied.
Findings From the Literature
Fifteen studies were identified from the literature for inclusion in the systematic review (Figure 1). The included studies are summarized in Table 7. A list of excluded studies is presented in Appendix 2.
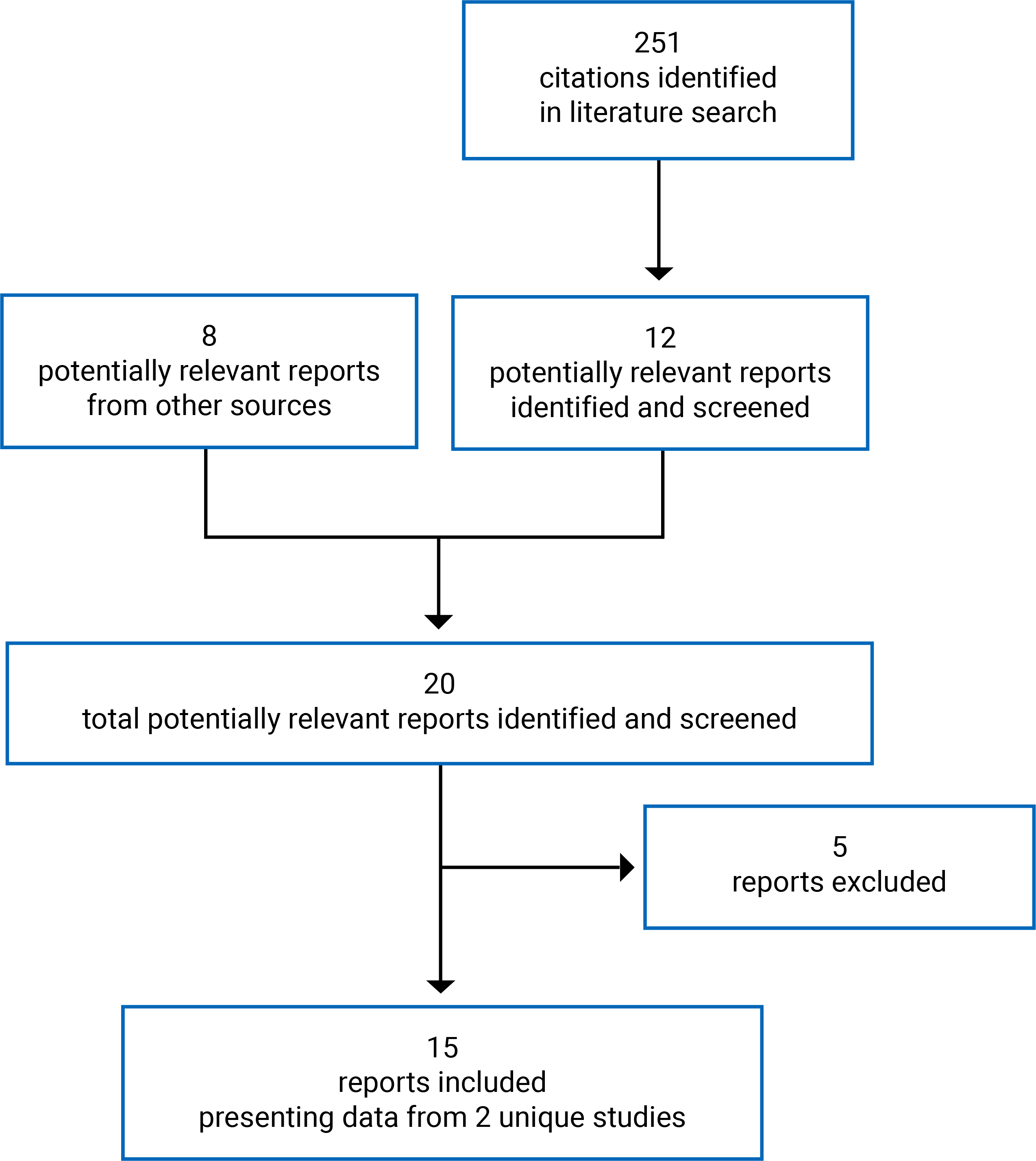
Table 7: Details of Included Studies
Study detail | FIDELIO (more severe CKD) | FIGARO |
|---|---|---|
Designs and populations | ||
Study design | Randomized, double-blind, placebo-controlled, parallel-group, multicentre, event-driven phase III studies | |
Locations | 1,024 study centres in 48 countries including Canada (30) and US (185) | 1,019 study centres in 48 countries including Canada (31) and US (184) |
Patient enrolment dates | First patient visit: September 17, 2015 Last patient visit: April 14, 2020 | First patient visit: September 17, 2015 Last patient visit: February 2, 2021 |
Randomized (N) | 5,734 | 7,437 |
Inclusion criteria |
| |
|
| |
| ||
Exclusion criteria |
| |
Drugs | ||
Intervention | Finerenone:
| |
Comparator(s) | Placebo oral tablet once daily in the morning | |
Background treatment | Standard of care therapy | |
Duration | ||
Phase | ||
Run-in | 4 to 16 weeks | |
Screening | Up to 2 weeks | |
Double-blind | 4 planned visits in the first 4 months, then a visit every 4 months until end of study (up to 4 years) | |
Follow-up | 4 weeks + 5 days after last dose of study drug | |
Outcomes | ||
Primary end point | Time to first occurrence of the 40% renal composite end point: onset of kidney failure, a sustained decrease of eGFR ≥ 40% from baseline over at least 4 weeks, or renal death | Time to first occurrence of the CV composite end point: CV death, nonfatal MI, nonfatal stroke, or hospitalization for heart failure |
Secondary and exploratory end points | Secondary:
| Secondary:
|
| ||
Exploratory:
| ||
Notes | ||
Publications | Agarwal et al. (2022);44 Bakris et al. (2019);45 Bakris et al. (2020);34 Filippatos et al. (2022);46 Rossing et al. (2022)19 | Filippatos et al. (2021);35 Filippatos et al. (2022);47 Filippatos et al. (2021);48 Pitt et al. (2021);49 Ruilope et al. (2019);50 Ruilope et al. (2022)51 |
Pooled analysis | Agarwal et al. (2021)52 | |
ACE = angiotensin-converting enzyme; ARB = angiotensin receptor blocker; CKD = chronic kidney disease; CKD-EPI = Chronic Kidney Disease Epidemiology Collaboration; CV = cardiovascular; DBP = diastolic blood pressure; eGFR = estimated glomerular filtration rate; EQ-5D-5L = 5-level EQ-5D; ESRD = end-stage renal disease; HRQoL = health-related quality of life; KDQOL-36 = Kidney Disease Quality of Life survey; MI = myocardial infarction; MRA = mineralocorticoid receptor antagonist; NYHA = New York Heart Association; SBP = systolic blood pressure; UACR = urinary albumin-creatinine ratio.
Note: Three additional reports were included: sponsor-submitted Clinical Study Reports for FIDELIO and FIGARO and the FIDELITY pooled analysis.16-18
Source: FIDELIO Clinical Study Report;16 FIGARO Clinical Study Report.17
Description of Studies
FIDELIO (N = 5,734) and FIGARO (N = 7,437) are phase III, randomized, double-blind, add-on, parallel-group, multicentre, event-driven studies on the efficacy and safety of finerenone 10 mg or 20 mg once daily compared with placebo in patients with CKD and T2D. The 2 trials were conducted in 48 countries in Europe, Asia, North America, and South America during 2015 to 2021. The study design was completely identical despite some differences in patient inclusion criteria, through which FIDELIO likely included more severe CKD in terms of eGFR than FIGARO.
The primary end point for FIDELIO was time to first occurrence of the 40% renal composite end point: onset of kidney failure, a sustained decrease of eGFR greater than or equal to 40% from baseline over at least 4 weeks, or renal death. The primary end point for FIGARO was time to first occurrence of the cardiovascular composite end point: cardiovascular death, nonfatal MI, nonfatal stroke, or hospitalization for heart failure. Secondary end points in each study included the primary objective of the other study, as well as time to first occurrence of a more severe renal composite end point, time to all-cause mortality, time to all-cause hospitalization, and change in UACR from baseline to month 4. The studies were sponsored by Bayer and included 30 (FIDELIO) and 31 (FIGARO) study centres in Canada.
After a run-in period of up to 16 weeks and a screening period of up to 2 weeks, eligible patients were randomized 1:1 to the finerenone (10 mg or 20 mg) or placebo treatment arm, and stratified by region, eGFR category at screening, and albuminuria interval at screening. Randomization occurred at visit 1, and then there were 3 more planned monthly visits, followed by a visit every 4 months until the end of the study. The finerenone dose could be up-titrated or down-titrated at any point following the start of treatment at visit 1. If patients stopped the study drug prematurely, they remained in the trial and were followed up with until the end of the study.
A summary of the study designs for FIDELIO and FIGARO is shown in Figure 2.
Figure 2: FIDELIO and FIGARO Study Design

eGFR = estimated glomerular filtration rate; EOS = end of study; OD = once daily; PD = permanent discontinuation; Post Trt = posttreatment; V = visit.
* Scheduled visits continued even if treatment with study drug was discontinued.
† PD visit conducted only after permanent withdrawal from treatment.
†† EOS visit conducted after notification of end of study by the sponsor.
‡ Posttreatment visit for all patients on study drug treatment at end of study.
Source: FIDELIO Clinical Study Report;16 FIGARO Clinical Study Report.17
Populations
Inclusion and Exclusion Criteria
Key inclusion and exclusion criteria for FIDELIO and FIGARO are shown in Table 7. Adult patients with T2D mellitus, a diagnosis of CKD, prior treatment with ACE inhibitors or ARBs, and serum potassium levels less than or equal to 4.8 mmol/L were included in both trials. The criteria for CKD severity differed between trials: In FIDELIO, patients had persistent high albuminuria (UACR ≥ 30 mg/g to < 300 mg/g) and eGFR greater than or equal to 25 mL/min/1.73 m2 but less than 60 mL/min/1.73 m2 with the presence of diabetic retinopathy or persistent very high albuminuria (UACR ≥ 300 mg/g) and eGFR greater than or equal to 25 mL/min/1.73 m2 to less than 75 mL/min/1.73 m2, while in FIGARO patients had less severe CKD with persistent high albuminuria and eGFR greater than or equal to 25 mL/min/1.73 m2 but less than or equal to 90 mL/min/1.73 m2 or persistent very high albuminuria and eGFR greater than or equal to 60 mL/min/1.73 m2. Patients were excluded from the studies if they had a known significant nondiabetic renal disease, uncontrolled hypertension or hypotension, cardiovascular events (e.g., stroke) in the 30 days before the screening visit, chronic heart failure, dialysis for acute renal failure within 12 weeks of run-in visit, or renal allograft or planned renal transplant within 12 months.
Baseline Characteristics
The baseline demographic and disease characteristics of all patients in the full analysis set (FAS) are presented in Table 8. The mean age in both groups in both studies was approximately 65 years old, with 58.1% and 52.5% of patients aged 65 years and older in the FIDELIO and FIGARO trials, respectively. Most patients in both trials were male (69.8%) and white (68.1%), and 287 patients (2.2%) were in Canada. The mean baseline body mass index across all groups was 31.3 (SD = 6.0), 47.5% of patients had never smoked, and 59.8% were alcohol abstinent.
In the FIDELIO trial, the mean baseline eGFR was approximately 44 mL/min/1.73 m2 (SD = 12.5) in both groups, and the mean baseline UACR was 798.8 mg/g (SD = 2.7) and 814.7 mg/g (SD = 2.7) in the finerenone and placebo groups, respectively. In FIGARO, the mean baseline eGFR was approximately 68 mL/min/1.73 m2 (SD = 21.7) in both groups, and the mean baseline UACR was 284.3 mg/g (SD = 3.6) and 288.9 mg/g (SD = 3.5) in the finerenone and placebo groups, respectively. Approximately 88% of patients in FIDELIO and 51% of patients in FIGARO had very high albuminuria. Across both trials, the mean baseline serum potassium was 4.35 mmol/L (SD = 0.44), the mean baseline systolic blood pressure was 136.7 mm Hg (SD = 14.2), and the baseline hemoglobin A1C was 7.7% (SD = 1.4). Regarding medication use at baseline, 65.7% of patients (n = 3,725) in FIDELIO and 57% of patients (n = 4,212) in FIGARO were on ARBs, and 34% of patients (n = 1,942) in FIDELIO and 43% of patients (n = 3,137) in FIGARO were on ACE inhibitors. Across the 2 trials, patients were also on statins (72%), diuretics (51.5%), beta-blockers (50%), and antidiabetic treatment (97.7%), including 6.7% (n = 877) of patients who were on SGLT2 inhibitors. Across both trials, 45.6% of patients (n = 5,935) had a history of cardiovascular disease and 96.5% of patients (n = 12,566) had a history of hypertension.
Table 8: Summary of Baseline Characteristics (FAS)
Characteristic | FIDELIO | FIGARO | ||
|---|---|---|---|---|
Finerenone N = 2,833 | Placebo N = 2,841 | Finerenone N = 3,686 | Placebo N = 3,666 | |
Patient demographic characteristics | ||||
Age (years) | ||||
Mean (SD) | 65.4 (8.9) | 65.7 (9.2) | 64.1 (9.7) | 64.1 (10.0) |
Median (Q1, Q3) | 66 (60, 72) | 66 (60, 72) | 65 (58, 71) | 65 (58, 71) |
Age (years), n (%) | ||||
18 to 44 | 49 (1.7) | 65 (2.3) | 127 (3.4) | 123 (3.4) |
45 to 64 | 1,156 (40.8) | 1,109 (39.0) | 1,626 (44.1) | 1,634 (44.6) |
65 to 74 | 1,197 (42.3) | 1,203 (42.3) | 1,438 (39.0) | 1,383 (37.7) |
≥ 75 | 431 (15.2) | 464 (16.3) | 495 (13.4) | 526 (14.3) |
Sex, n (%) | ||||
Male | 1,953 (68.9) | 2,030 (71.5) | 2,528 (68.6) | 2,577 (70.3) |
Female | 880 (31.1) | 811 (28.5) | 1,158 (31.4) | 1,089 (29.7) |
Race, n (%) | ||||
White | 1,777 (62.7) | 1,815 (63.9) | 2,672 (72.5) | 2,605 (71.1) |
Asian | 717 (25.3) | 723 (25.4) | 715 (19.4) | 739 (20.2) |
Black or African American | 140 (4.9) | 124 (4.4) | 113 (3.1) | 145 (4.0) |
American Indian or Alaska Native | 78 (2.8) | 76 (2.7) | 73 (2.0) | 70 (1.9) |
Multiple | 101 (3.6) | 86 (3.0) | 87 (2.4) | 86 (2.3) |
Native Hawaiian or other Pacific Islander | 11 (0.4) | 7 (0.2) | 17 (0.5) | 14 (0.4) |
Not reported | 9 (0.3) | 10 (0.4) | 9 (0.2) | 7 (0.2) |
Region, n (%) | ||||
North America | 467 (16.5) | 477 (16.8) | 559 (15.2) | 548 (14.9) |
Canada | 49 (1.7) | 58 (2.0) | 82 (2.2) | 98 (2.7) |
Europe | 1,182 (41.7) | 1,176 (41.4) | 1,754 (47.6) | 1,750 (47.7) |
Asia | 790 (27.9) | 789 (27.8) | 810 (22.0) | 815 (22.2) |
Latin America | 295 (10.4) | 298 (10.5) | 424 (11.5) | 417 (11.4) |
Rest of the world | 99 (3.5) | 101 (3.6) | 139 (3.8) | 136 (3.7) |
Baseline BMI (kg/m2) | ||||
Mean (SD) | 31.1 (6.0) | 31.1 (6.0) | 31.5 (6.0) | 31.4 (5.9) |
Baseline categories, n (%) | ||||
Missing | 12 (0.4) | 5 (0.2) | 11 (0.3) | 7 (0.2) |
< 20 kg/m2 | 22 (0.8) | 28 (1.0) | 26 (0.7) | 26 (0.7) |
≥ 20 to < 25 kg/m2 | 348 (12.3) | 348 (12.2) | 400 (10.9) | 406 (11.1) |
≥ 25 to < 30 kg/m2 | 950 (33.5) | 966 (34.0) | 1,202 (32.6) | 1,217 (33.2) |
≥ 30 to < 35 kg/m2 | 866 (30.6) | 846 (29.8) | 1,160 (31.5) | 1,130 (30.8) |
≥ 35 kg/m2 | 635 (22.4) | 648 (22.8) | 887 (24.1) | 880 (24.0) |
Smoking history, n (%) | ||||
Never | 1,375 (48.5) | 1,371 (48.3) | 1,760 (47.7) | 1,684 (45.9) |
Former | 1,044 (36.9) | 1,078 (37.9) | 1,275 (34.6) | 1,346 (36.7) |
Current | 414 (14.6) | 392 (13.8) | 651 (17.7) | 636 (17.3) |
Alcohol use, n (%) | ||||
Abstinent | 1,733 (61.2) | 1,722 (60.6) | 2,197 (59.6) | 2,134 (58.2) |
Light | 946 (33.4) | 947 (33.3) | 1,253 (34.0) | 1,278 (34.9) |
Moderate | 143 (5.0) | 155 (5.5) | 216 (5.9) | 239 (6.5) |
Heavy | 11 (0.4) | 16 (0.6) | 17 (0.5) | 15 (0.4) |
Key disease characteristics | ||||
Baseline serum potassium (mmol/L) | ||||
Mean (SD)a | 4.37 (0.46) | 4.38 (0.46) | 4.33 (0.43) | 4.33 (0.43) |
Baseline category, n (%) | ||||
≤ 4.5 mmol/L | 1,881 (66.4) | 1,861 (65.5) | 2,643 (71.7) | 2,612 (71.2) |
> 4.5 mmol/L | 951 (33.6) | 979 (34.5) | 1,043 (28.3) | 1,052 (28.7) |
Baseline systolic blood pressure (mm Hg) | ||||
Mean (SD)a | 138.05 (14.32) | 138.01 (14.42) | 135.81 (13.96) | 135.70 (14.06) |
Baseline category, n (%) | ||||
< 130 mm Hg | 788 (27.8) | 778 (27.4) | 1,187 (32.2) | 1,197 (32.7) |
≥ 130 to < 160 mm Hg | 1,900 (67.1) | 1,922 (67.7) | 2,392 (64.9) | 2,355 (64.2) |
≥ 160 mm Hg | 142 (5.0) | 139 (4.9) | 107 (2.9) | 114 (3.1) |
Baseline eGFR (mL/min/1.73 m2) | ||||
Mean (SD)a | 44.36 (12.54) | 44.32 (12.57) | 67.62 (21.65) | 67.99 (21.74) |
Baseline category, n (%) | ||||
< 25 mL/min/1.73 m2 | 66 (2.3) | 69 (2.4) | 15 (0.4) | 12 (0.3) |
25 to < 45 mL/min/1.73 m2 | 1,476 (52.1) | 1,505 (53.0) | 641 (17.4) | 610 (16.6) |
45 to < 60 mL/min/1.73 m2 | 972 (34.3) | 928 (32.7) | 745 (20.2) | 789 (21.5) |
≥ 60 mL/min/1.73 m2 | 318 (11.2) | 338 (11.9) | 2,285 (62.0) | 2,254 (61.5) |
Baseline albuminuria category (mg/g), n (%) | ||||
Normoalbuminuria (UACR < 30 mg/g) | 11 (0.4) | 12 (0.4) | 109 (3.0) | 98 (2.7) |
High albuminuria (≥ 30 mg/g to < 300 mg/g) | 350 (12.4) | 335 (11.8) | 1,726 (46.8) | 1,688 (46.0) |
Very high albuminuria (≥ 300 mg/g) | 2,470 (87.2) | 2,493 (87.8) | 1,851 (50.2) | 1,878 (51.2) |
Baseline UACR (mg/g) | ||||
Mean (SD)b | 798.79 (2.65) | 814.73 (2.67) | 284.33 (3.58) | 288.87 (3.53) |
Median in FAS (mg/g) | 851.9 | 308.2 | ||
UACR at baseline,c n (%) | ||||
≤ FAS median | 1,442 (50.9) | 1,394 (49.1) | 1,861 (50.5) | 1,814 (49.5) |
> FAS median | 1,389 (49.0) | 1,446 (50.9) | 1,825 (49.5) | 1,850 (50.5) |
Baseline hemoglobin A1C (%) | ||||
Mean (SD)a | 7.66 (1.33) | 7.69 (1.36) | 7.74 (1.39) | 7.69 (1.35) |
Medication use at baseline, n (%) | ||||
ARB | 1,879 (66.3) | 1,846 (65.0) | 2,108 (57.2) | 2,104 (57.4) |
ACE inhibitor | 950 (33.5) | 992 (34.9) | 1,576 (42.8) | 1,561 (42.6) |
Statin | 2,105 (74.3) | 2,110 (74.3) | 2,552 (69.2) | 2,632 (71.8) |
Beta-blocker | 1,462 (51.6) | 1,506 (53.0) | 1,774 (48.1) | 1,762 (48.1) |
Diuretic | 1,577 (55.7) | 1,637 (57.6) | 1,748 (47.4) | 1,748 (47.7) |
Antidiabetic treatment | 2,747 (97.0) | 2,777 (97.7) | 3,607 (97.9) | 3,589 (97.9) |
Insulins and analogues | 1,843 (65.1) | 1,794 (63.1) | 2,023 (54.9) | 1,970 (53.7) |
Biguanides | 1,251 (44.2) | 1,239 (43.6) | 2,561 (69.5) | 2,506 (68.4) |
Dipeptidyl peptidase 4 inhibitors | 764 (27.0) | 758 (26.7) | 896 (24.3) | 860 (23.5) |
Sulfonamides | 654 (23.1) | 673 (23.7) | 1,037 (28.1) | 1,025 (28.0) |
GLP-1 agonists | 189 (6.7) | 205 (7.2) | 308 (8.4) | 242 (6.6) |
SGLT2 inhibitors | 124 (4.4) | 135 (4.8) | 314 (8.5) | 304 (8.3) |
History of CV disease present, n (%) | 1,303 (46.0) | 1,302 (45.8) | 1,676 (45.5) | 1,654 (45.1) |
Duration of diabetes (years) | ||||
Mean (SD)a | 16.58 (8.77) | 16.55 (8.77) | 14.53 (8.60) | 14.44 (8.44) |
Medical history, n (%) | ||||
Hypertension | 2,737 (96.6) | 2,768 (97.4) | 3,544 (96.1) | 3,517 (95.9) |
Diabetic retinopathy | 1,312 (46.3) | 1,351 (47.6) | 1,193 (32.4) | 1,098 (30.0) |
Hyperlipidemia | 1,281 (45.2) | 1,280 (45.1) | 1,515 (41.1) | 1,550 (42.3) |
Diabetic neuropathy | 742 (26.2) | 722 (25.4) | 1,046 (28.4) | 990 (27.0) |
Peripheral arterial occlusive disease | 470 (16.6) | 453 (15.9) | 587 (15.9) | 575 (15.7) |
Ischemic stroke/transient ischemic attack | 425 (15.0) | 423 (14.9) | NR | NR |
Coronary artery disease | 842 (29.7) | 860 (30.3) | 1,148 (31.1) | 1,147 (31.3) |
Myocardial infarction | 378 (13.3) | 388 (13.7) | 640 (17.4) | 616 (16.8) |
Ischemic stroke | 329 (11.6) | 360 (12.7) | 442 (12.0) | 425 (11.6) |
Atrial fibrillation and atrial flutter | 240 (8.5) | 221 (7.8) | 328 (8.9) | 317 (8.6) |
Cardiac failure | 195 (6.9) | 241 (8.5) | 290 (7.9) | 281 (7.7) |
Percutaneous coronary intervention | 151 (5.3) | 135 (4.8) | 217 (5.9) | 198 (5.4) |
ACE = angiotensin-converting enzyme; ARB = angiotensin receptor blocker; BMI = body mass index; CV = cardiovascular; eGFR = estimated glomerular filtration rate; FAS = full analysis set; GLP-1 = glucagon-like peptide-1; NR = not reported; Q = quartile; SD = standard deviation; SGLT2 = sodium-glucose cotransporter-2; UACR = urinary albumin-creatinine ratio.
aArithmetic mean and arithmetic SD.
bGeometric mean and geometric SD.
cBelow median and above median (851.9 mg/g in FIDELIO and 308.2 mg/g in FIDELIO) in the FAS.
Source: FIDELIO Clinical Study Report;16 FIGARO Clinical Study Report.17
Interventions
The patients received 1 of the following: finerenone 10 mg tablet once daily (starting dose for patients with an eGFR between 25 mL/min/1.73 m2 and < 60 mL/min/1.73 m2 at the screening visit) or 20 mg tablet once daily (starting dose for patients with an eGFR ≥ 60 mL/min/1.73 m2 at the screening visit), or a matching placebo tablet once daily. Patients were instructed to take 1 tablet once daily, preferably in the morning.
Dose Modifications
Patients starting at 10 mg would be up-titrated to 20 mg at any visit if they had been on a stable dose for over 4 weeks, provided the potassium concentration was less than or equal to 4.8 mmol/L and eGFR decrease was less than 30% below the value at the previous visit. Patients at 20 mg could be down-titrated to 10 mg at any point during the study if required for safety reasons.
Concomitant Medications
The conditions of prior therapy with ACE inhibitors and ARBs during the time leading up to the screening visit are depicted in Figure 3. For at least 4 weeks before run-in, patients are treated with ACE inhibitors and/or ARBs but then only treated with the maximum tolerated labelled dose of an ACE inhibitor or an ARB starting from the run-in visit for at least 4 weeks before the screening visit. Concomitant therapies not permitted during either study included eplerenone, spironolactone, any renin inhibitor or potassium-sparing diuretic, a combination of ACE inhibitor and an ARB, and potent cytochrome P450 isoenzyme 3A4 (CYP3A4) inhibitors or inducers.
Figure 3: Background Therapy With RAS Blockade
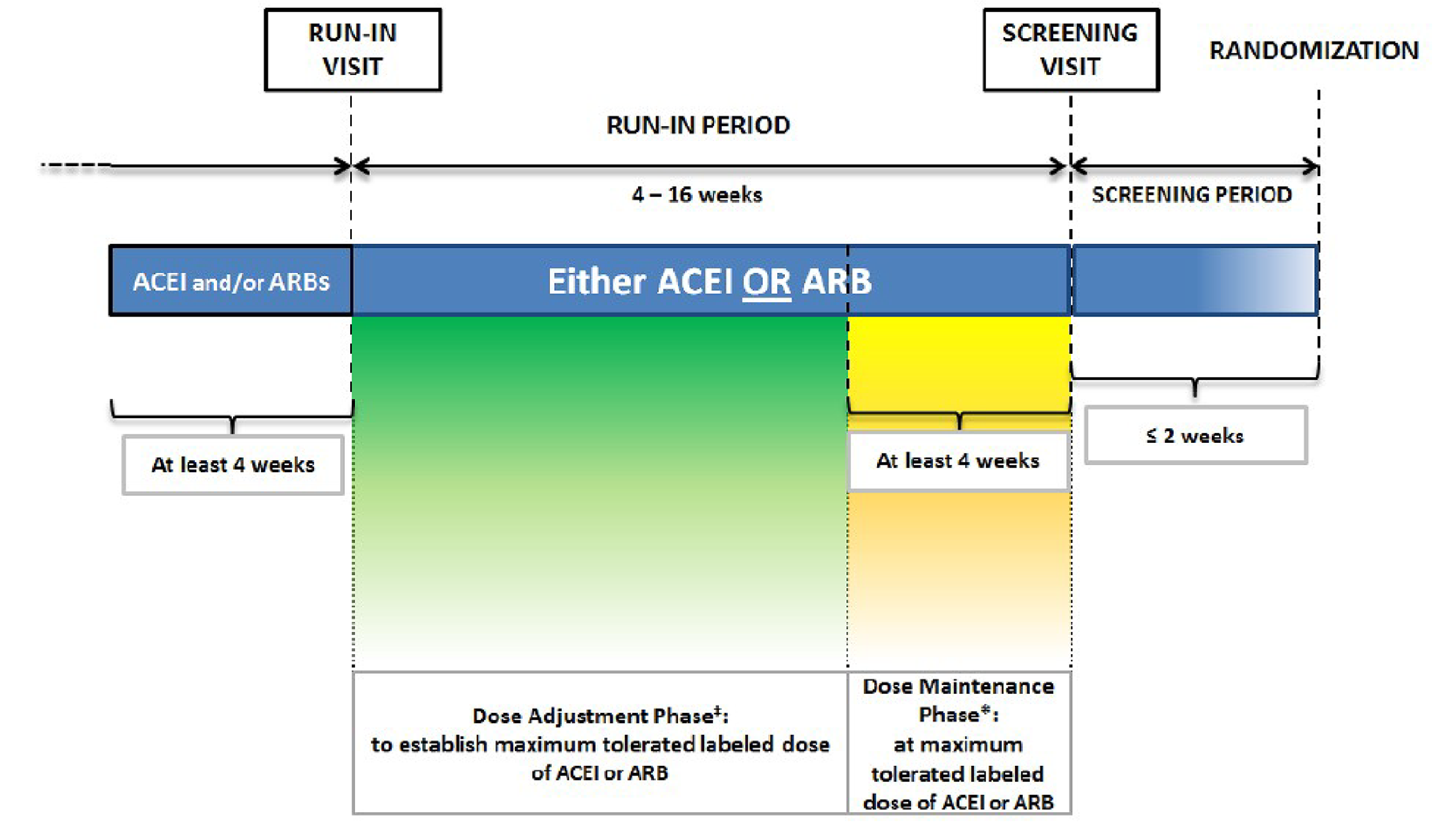
ACEI = angiotensin-converting enzyme inhibitor; ARB = angiotensin receptor blocker; RAS = renin-angiotensin system.
‡ If applicable.
* During the maintenance phase, there should preferably be no adjustments to dose of ACEI or ARB or to any other antihypertensive or antiglycemic treatment.
Source: FIDELIO Clinical Study Report protocol.16
Outcomes
A list of efficacy end points identified in the CADTH review protocol that were assessed in the clinical trials is provided in Table 9. These end points are summarized in the following text. A detailed discussion and critical appraisal of the outcome measures is provided in Appendix 4.
The primary outcome in the FIDELIO study was time to first occurrence of the 40% renal composite end point, which comprises onset of kidney failure, a sustained decrease of eGFR greater than or equal to 40% from baseline over at least 4 weeks, or renal death. Kidney failure was defined as either ESRD (initiation of chronic dialysis for at least 90 days or renal transplant) or 2 measurements of eGFR of less than 15 mL/min/1.73 m2 (KDIGO 2013)53 that were 4 weeks apart. Renal death included deaths where renal replacement therapy was indicated but not started and there were no other likely causes of death. Events were included from visit 1 (randomization day) until the end-of-study visit, or the last visit in cases where there was premature discontinuation. Randomized patients without an event of the renal composite end point at the time of analysis were censored at the date of their last visit when complete information on all components of the composite renal end point was available, up to and including the end of study visit, or date of nonrenal death. Patients without any information about the primary composite end point after baseline were censored at day 1.
The primary outcome in the FIGARO study was time to first occurrence of the cardiovascular composite end point, which comprises cardiovascular death, nonfatal MI, nonfatal stroke, or hospitalization for heart failure. Cardiovascular death included any death resulting from an acute MI, sudden cardiac death, sudden death, death due to heart failure, death due to stroke, and death due to cardiovascular procedures and other cardiovascular causes such as pulmonary embolism. Randomized patients without an event of the primary composite end point at the time of analysis were censored at the date of their last contact up to and including the end of study visit or date of non-CV death. Patients without any information about the primary composite end point after baseline were censored at day 1. All events qualifying for the primary outcome were adjudicated by an independent adjudication committee.
The primary outcome in each trial was a key secondary outcome in the other trial. Additional secondary outcomes in both trials included time to all-cause mortality, time to all-cause hospitalization, change in UACR from baseline to month 4, and time to first occurrence of the second renal composite end point (comprising onset of kidney failure, a sustained decrease in eGFR of ≥ 57% from baseline over at least 4 weeks, or renal death), hereafter referred to as the 57% renal composite end point. Patients were censored on day 1 if there was no subsequent information about the secondary composite end point, or if patients were without an event at the date of noncardiovascular death (in FIDELIO) or nonrenal death (in FIGARO) or at the date of their last visit if they did not experience an event of the secondary composite end point at the time of analysis. Hospitalization events were counted as withdrawal or death, and all-cause mortality was counted as the last visit. Randomized patients without such an event at the time of analysis were censored at the last date vital status could be obtained.
Exploratory outcomes of interest included the components of the renal and cardiovascular composite end points, new diagnosis of atrial fibrillation or atrial flutter, time to noncardiovascular or nonrenal death, change in eGFR and UACR from baseline, and change in HRQoL summary scores.
HRQoL was assessed using the KDQOL-36 and the 5-level EQ-5D (EQ-5D-5L) questionnaires. KDQOL-36 assesses the HRQoL of patients with CKD and consists of generic and disease-specific sections, with higher scores indicating a more favourable HRQoL. EQ-5D-5L comprises a descriptive system and the visual analogue scale, and a higher score indicates better HRQoL. The questionnaires were completed by the patient at visit 1 (baseline) and then completed before other visit procedures every 12 months (visits 5, 8, 11, and so on) and at the last visit (end of study or after permanent discontinuation). The MID in both questionnaires was not identified in the literature in the setting of diabetic CKD. A detailed discussion and critical appraisal of the HRQoL measures is provided in Appendix 4.
Safety and tolerability were assessed using the incidence of AEs and SAEs coded using the Medical Dictionary for Regulatory Activities. Serum potassium concentration was assessed at all visits, and change from baseline and incidence of hyperkalemia and hyperkalemia-related events were reported. In this report, the term hyperkalemia refers to the combined Medical Dictionary for Regulatory Activities preferred terms “blood potassium increased” and “hyperkalemia.”
Table 9: Summary of Outcomes of Interest Identified in the CADTH Review Protocol
Outcome measure | FIDELIO | FIGARO |
|---|---|---|
Time to first occurrence of the 40% renal composite end point: onset of kidney failure, a sustained decrease of eGFR ≥ 40% from baseline over at least 4 weeks, or renal death | Primary | Secondary |
Time to first occurrence of the CV composite end point: CV death, nonfatal MI, nonfatal stroke, or hospitalization for heart failure | Secondary | Primary |
Time to all-cause mortality | Secondary | |
Time to all-cause hospitalization | Secondary | |
Change in UACR from baseline to month 4 | Secondary | |
Time to first occurrence of the following composite end point: onset of kidney failure, a sustained decrease in eGFR of ≥ 57% from baseline over at least 4 weeks, or renal death | Secondary | |
Components of the renal composite end points:
| Exploratory | |
Components of the CV composite end point:
| Exploratory | |
Number of patients with new diagnosis of atrial fibrillation or atrial flutter | Exploratory | |
Time to non-CV, nonrenal death | Exploratory | |
Number of patients with new diagnosis of heart failure | Exploratory | |
Change in UACR from baseline | Exploratory | |
Change in eGFR from baseline | Exploratory | |
Change in quality-of-life summary scores measured by the following HRQoL questionnaires:
| Exploratory | |
Serious adverse events and adverse events leading to discontinuation of treatment with study drug, and adverse events related to hyperkalemia | Exploratory | |
CV = cardiovascular; eGFR = estimated glomerular filtration rate; EQ-5D-5L = 5-Level EQ-5D; ESRD = end-stage renal disease; HRQoL = health-related quality of life; KDQOL-36 = Kidney Disease Quality of Life survey; MI = myocardial infarction; UACR = urinary albumin-creatinine ratio.
Source: FIDELIO Clinical Study Report;16 FIGARO Clinical Study Report.17
Statistical Analysis
Statistical analysis of all efficacy outcomes (specified in the protocol for the systematic literature review) is summarized in Table 10.
Power Calculation
Both event-driven trials were designed to achieve 90% power using a log-rank test (at a 2-sided significance level of 3.33% in FIDELIO and 5% in FIGARO) to detect 20% relative risk reduction in the events of the primary end point with finerenone compared with placebo. In FIDELIO, the total number of primary end point events needed was 1,068 across both treatment groups, and in FIGARO it was 976.
The following assumptions were made: study duration of approximately 44 months, annual placebo event rate of 12% in FIDELIO and 8% in FIGARO, annual loss to follow-up rate of 0.7%, and annual finerenone treatment discontinuation rate of 5%. A slower-than-assumed event rate was observed during the study, so the required number of randomized patients was 5,800 and 7,400 in FIDELIO and FIGARO, respectively.
Statistical Model
Neither study was stopped early in the interim analysis; therefore, the final primary analysis was performed as specified in the studies’ protocols. The statistical analyses followed the intention-to-treat principle and were based primarily on the FAS. Events for inclusion in the primary analysis were counted from randomization at visit 1 until the end-of-study visit or until end-of-study notification ( + 4 weeks).
A group sequential design was used in each study with a single interim analysis when two-thirds of the information was available, with a stopping rule of 2-sided P of less than 0.00270, which required a small adjustment to the significance level of the final analysis to maintain the overall significance level at 5%. To account for multiplicity, a weighted Bonferroni-Holm procedure was used for the primary and key secondary end points, followed by hierarchical testing of the remaining efficacy end points at the adjusted 2-sided significance level of 0.04967388, as shown in Figure 4 and Figure 5. If the testing strategy stopped at 1 point due to a nonsignificant result, the remaining secondary efficacy variables were tested in an exploratory manner.
In FIDELIO, the primary and key secondary end points met the preplanned criteria for significance, and all-cause mortality (the next secondary end point) was tested hierarchically. It did not reach statistical significance, and so the remaining secondary end points were tested in an exploratory manner. In FIGARO, the primary end point met the preplanned criteria for significance, and the key secondary end point did not; therefore, the remaining secondary end points were tested in an exploratory manner.
The primary and secondary time-to-event end points were analyzed using stratified log-rank testing, and a stratified Cox proportional hazard regression model was used to provide a point estimate of the HR and a corresponding 2-sided 95% CI. Kaplan-Meier curves were provided for the cumulative incidence risk of outcome events by treatment group. Stratification factors included region (North America, Latin America, Europe, Asia, other), eGFR category at screening (25 mL/min/1.73 m2 to < 45 mL/min/1.73 m2, 45 mL/min/1.73 m2 to < 60 mL/min/1.73 m2, ≥ 60 mL/min/1.73 m2) type of albuminuria at screening (high albuminuria, very high albuminuria), and — only in FIGARO — history of cardiovascular disease.
An analysis of covariance model was fitted to the logarithmized ratios of UACR at month 4 to UACR at baseline, including the factor treatment group; the stratification factors region, type of albuminuria, and eGFR category; and the logarithmized baseline UACR as covariates. All other exploratory variables were analyzed in the FAS and the per-protocol set (in the per-protocol set only data points and events up to 30 days after stopping of study drug were considered). The eGFR was summarized descriptively by treatment group and visit, including absolute and relative changes from baseline. The absolute change of eGFR from baseline at each visit was analyzed by a mixed model with the factors treatment group, visit, treatment-by-visit interaction, factors for the stratification levels, baseline value as covariate (nested within eGFR category), and baseline by visit interaction. HRQoL analyzed based on KDQOL-36 and EQ-5D, with absolute change of the patient-related outcome from baseline at each visit up to the last visit analyzed by a mixed model.
Subgroup Analyses
Descriptive statistics, graphical display of estimated treatment effects with 95% CIs in a forest plot, and a statistical test for interaction were completed for exploratory subgroup analysis for the primary and secondary efficacy end points. The following subgroups, planned a priori in the statistical analyses plan, aligned with the subgroups prespecified in the protocol for this CADTH review: history of cardiovascular disease, eGFR category at baseline, type of albuminuria at baseline, and SGLT2 inhibitor use at baseline.
Sensitivity Analyses
For the primary end point, the analysis was repeated in the per-protocol set, and patients with a censoring or event date more than 30 days after last study drug intake were censored at the date of last study drug intake ( + 30 days). Additional analyses included an on-treatment analysis (FAS only) — repeating the inferential statistics, the log-rank test, and the Cox regression model without including stratification factors — and a tipping point analysis based on the intention-to-treat approach (FAS only). For the secondary time-to-event end points, the same additional analyses were conducted except for the on-treatment and tipping point analyses, which were only performed for the key secondary end points.
Figure 4: Hierarchical Testing Strategy in FIDELIO Study

CV = cardiovascular; UACR = urinary albumin-creatinine ratio.
Note: Hx refers to the null hypothesis of no treatment effect for each end point, and wx denotes the weight allocated to the test of Hx, which in case of rejection is passed on to the next test as indicated by the arrows.
Figure 5: Hierarchical Testing Strategy in FIGARO Study
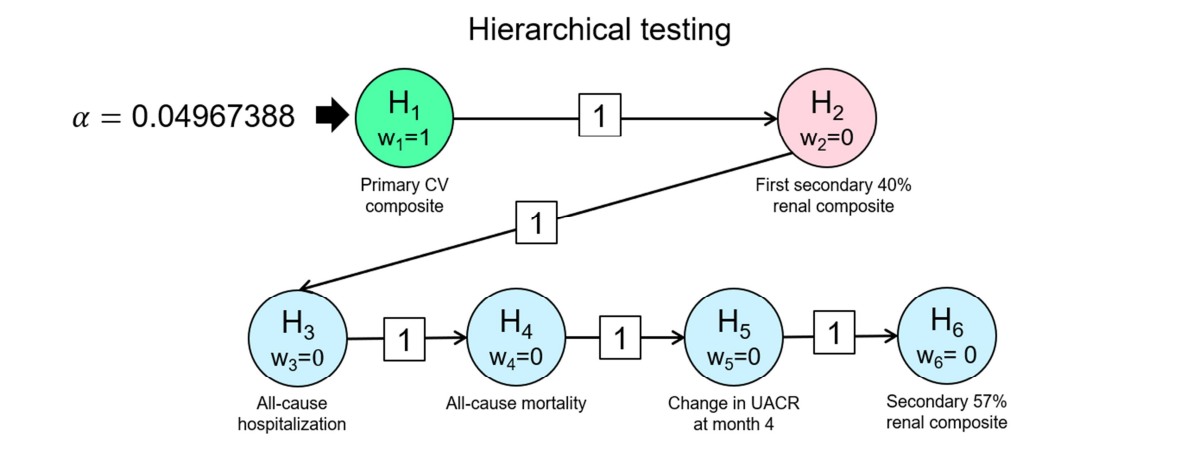
CV = cardiovascular; UACR = urinary albumin-creatinine ratio.
Note: Hx refers to the null hypothesis of no treatment effect for each end point, and wx denotes the weight allocated to the test of Hx, which in case of rejection is passed on to the next test as indicated by the arrows.
Protocol Changes
The major changes to the study protocol are:
In Amendment 3, study duration and site numbers were increased, rescreening rules were amended, an exclusion criterion was modified to allow randomization of patients with a recent cardiovascular disease episode, and the definition of the end point “kidney failure” was added.
In Amendment 4, the posttreatment visit could be performed as a telephone contact, baseline values for patients who did not immediately start with study drug treatment were specified, the time window after last study drug administration was increased from 3 days to 30 days for on-treatment analyses, and the definition of treatment-emergent AEs and interruptions of study treatment were specified.
Table 10: Statistical Analysis of Primary and Secondary Efficacy End Points
End point | Statistical model | Adjustment factors | Sensitivity analyses |
|---|---|---|---|
Primary end point | |||
40% renal composite end point in FIDELIO and CV composite end point in FIGARO |
| Stratification factors:
|
|
Key secondary end point | |||
CV composite end point | Similar to primary end point | Similar to primary end point | Similar to primary end point |
Other secondary end points | |||
Time to all-cause mortality | Similar to primary end point | Similar to primary end point |
|
Time to all-cause hospitalization | |||
57% renal composite end point | |||
Change in UACR from baseline to month 4 |
|
|
|
ANCOVA = analysis of covariance; BOCF = baseline observation carried forward; CI = confidence interval; CV = cardiovascular; eGFR = estimated glomerular filtration rate; FAS = full analysis set; ITT = intention to treat; LOCF = last observation carried forward; PPS = per-protocol set; UACR = urinary albumin-creatinine ratio.
Source: FIDELIO Clinical Study Report;16 FIGARO Clinical Study Report.17
Analysis Populations
The analysis populations are presented in detail in Table 11. The FAS population was used in all efficacy analyses and included all randomized patients without good clinical practice (GCP) violations. The safety analysis set included only patients who took at least 1 dose of the study drug. Per-protocol patients comprised FAS patients without validity findings, such as being younger than 18 years old or not having T2D.
FIDELITY Pooled Analysis
FIDELITY is a prespecified pooled efficacy and safety analysis combining data from FIDELIO and FIGARO, with a prespecified formal statistical analysis plan. Statistical analyses were exploratory and descriptive in nature with no adjustment for multiplicity. Only the primary or secondary outcomes from the complementary studies were included in this pooled analysis.
End points were analyzed using stratified Cox proportional hazards models (stratification factors described earlier) as HRs with corresponding 95% CIs. P values for the comparison of treatment groups were presented based on a stratified log-rank test. For the cardiovascular composite outcome and the key renal composite outcome, cumulative incidences were calculated based on Aalen-Johansen accounting for mortality as competing risk, and corresponding numbers needed to treat were calculated in 6-month intervals. For all-cause mortality, cumulative incidences were calculated based on Kaplan-Meier methods. An on-treatment sensitivity analysis was performed for outcomes, considering only events occurring up to 30 days after study drug discontinuation in the FAS.
Results
Patient Disposition
Patient disposition for the FIDELIO and FIGARO studies is presented in Table 11.
Of the 13,911 patients screened in the FIDELIO study, 5,734 (41%) were randomized and, after excluding 60 patients due to GCP violations, the FAS included 5,674 patients randomized to receive finerenone (n = 2,833) or placebo (n = 2,841). By the end of the study, 1,623 patients (28.6%) had discontinued treatment, most commonly due to an adverse or outcome event (10.9% in the finerenone group and 10.3% in the placebo group). The safety population included 2,827 patients in the finerenone group and 2,831 patients in the placebo group.
Of the 19,381 patients screened in the FIGARO study, 7,437 (38%) were randomized and, after excluding 85 patients due to GCP violations, the FAS included 7,352 patients randomized to receive finerenone (n = 3,686) or placebo (n = 3,666). By the end of the study, a total of 2,023 patients (27.5%) had discontinued treatment, most commonly due to an adverse or outcome event (7.5% in the finerenone group and 7.4% in the placebo group). The safety population included 3,682 patients in the finerenone group and 3,659 patients in the placebo group.
Patient disposition | FIDELIO | FIGARO | ||
|---|---|---|---|---|
Finerenone | Placebo | Finerenone | Placebo | |
Enrolled, N | 13,911 | 19,381 | ||
Screening failures, n | 8,177 | 11,944 | ||
Switched to FIGARO/FIDELIO study,a n | 1,555 | 1,376 | ||
Randomized, N | 2,866 | 2,868 | 3,723 | 3,714 |
GCP violations, n | 33 | 27 | 37 | 48 |
FAS, N (%) | 2,833 (100) | 2,841 (100) | 3,686 (100) | 3,666 (100) |
Discontinued from study, n (%) | 9 (0.3) | 9 (0.3) | 5 (0.1) | 13 (0.4) |
Reason for discontinuation, n (%) | ||||
Consent withdrawn | 4 (0.1) | 6 (0.2) | 1 (< 0.1) | 7 (0.2) |
Loss to follow-up | 5 (0.2) | 3 (0.1) | 4 (0.1) | 6 (0.2) |
Completed study,b n (%) | 2,824 (99.7) | 2,832 (99.7) | 3,681 (99.9) | 3,653 (99.6) |
Discontinued study treatment, n (%) | 822 (29) | 801 (28.2) | 1,009 (27.4) | 1,014 (27.7) |
Most common reason for discontinuation of treatment, n (%) | ||||
Adverse or outcome event | 309 (10.9) | 294 (10.3) | 275 (7.5) | 272 (7.4) |
Withdrawal by patient | 157 (5.5) | 169 (5.9) | 244 (6.6) | 214 (5.8) |
Death | 130 (4.6) | 157 (5.5) | 214 (5.8) | 251 (6.8) |
Physician decision | 148 (5.2) | 109 (3.8) | 143 (3.9) | 123 (3.4) |
Safety, n (%) | 2,827 (98.6) | 2,831 (98.7) | 3,682 (98.9) | 3,659 (98.5) |
PP, n (%) | 2,391 (83.4) | 2,451 (85.5) | 3,157 (84.8) | 3,199 (86.1) |
GCP = good clinical practice; FAS = full analysis set; PP = per protocol.
aPatients who were found to be ineligible for a study during the run-in and screening periods (due to variations in estimated glomerular filtration rate and urinary albumin-creatinine ratio) were permitted to switch from either study to the other only once.
bA patient is considered as having completed the study if there was contact with the patient after the end-of study notification or if the patient died.
Source: FIDELIO Clinical Study Report;16 FIGARO Clinical Study Report.17
Protocol Violations
In FIDELIO, important protocol deviations in the FAS were reported in ████ ███████ patients and ████ ███████ ████████ in the finerenone and placebo groups, respectively. The most frequently reported deviations in the finerenone and placebo groups were up-titration visit not done ██████ ███ ███████; SAE not submitted within 24 hours after initial flagging of event as serious in the electronic case report form ██████ ███ ███████; and up-titration visit not performed in time ██████ ███ ███████. Deviations associated with the COVID-19 pandemic included end-of-study visit not conducted as per protocol ███ ███ █████ and end point not assessable (████ ███ █████).
In FIGARO, important protocol deviations in the FAS were reported in ████ ███████ patients and ████ ███████ patients in the finerenone and placebo groups, respectively. The most frequently reported deviations in the finerenone and placebo groups were COVID-19 — visit not conducted as outlined in the CSP due to logistical reasons; ██████ ███ ███████ up-titration visit not done ██████ ███ ███████; and SAE not submitted within 24 hours after initial flagging of event as serious in the electronic case report form ██████ ███ ███████. Approximately ███ of patients were assigned to the incorrect stratification group. Deviations associated with the COVID-19 pandemic were reported in █████ ███ █████ of patients, specifically a visit was not conducted as outlined in the clinical study protocol due to logistical reasons (█████ ███ ███████ due to patient decision ███ ███ ██████ or physician decision █████ ███ ████).
Table 12: Important Protocol Deviations
Protocol deviation | FIDELIO | FIGARO | ||
|---|---|---|---|---|
Finerenone N = 2,833 | Placebo N = 2,841 | Finerenone N = 3,686 | Placebo N = 3,666 | |
Any important deviation finding, n (%) | ████ ██████ | ████ ██████ | ████ ██████ | ████ ██████ |
Procedure deviations | ███ ██████ | ███ ██████ | ███ ██████ | ███ ██████ |
Other protocol deviationsa | ███ ██████ | ███ ██████ | ████ ██████ | ████ ██████ |
Time schedule deviations | ███ ██████ | ███ ██████ | ███ ██████ | ███ ██████ |
Inclusion or exclusion criteria not met | ███ █████ | ███ ████ | ███ █████ | ███ █████ |
Treatment deviations | ███ █████ | ███ █████ | ███ █████ | ███ █████ |
Randomization errors | ██ █████ | ███ █████ | ███ ██████ | ███ ██████ |
Excluded concomitant medication treatment | ██ █████ | ██ █████ | ██ █████ | ███ █████ |
aCOVID-19-related important protocol deviations were categorized under “other protocol deviations.”
Source: FIDELIO Clinical Study Report;16 FIGARO Clinical Study Report.17
Exposure to Study Treatments
A summary of exposure to study treatments is provided in Table 13. Overall, the mean duration of treatment was similar between treatment groups but differed between both studies. In FIDELIO, the mean duration of treatment in the FAS was 26.9 months (range = 0 months to 51.5 months) in the finerenone group and 27.2 months (range = 0 months to 51.5 months) in the placebo group. In FIGARO, the mean duration of treatment in the FAS was longer, at 35.2 months (range = 0 months to 61 months) in the finerenone group and 35.3 months (range = 0 months to 61.4 months) in the placebo group. In FIDELIO, 58% and 1.8% of patients took the study treatment for at least 24 months and 48 months, respectively, while in FIGARO this corresponded to 81% and 22.6% of patients, respectively.
At the start of the trials, ███ of the patients in FIDELIO (█ ██████) and ███ of patients in FIGARO (█ ██████) were on the 10 mg dose of finerenone; by month 48, the percentage of patients on 10 mg of finerenone was ███ ██ ████ and ███ ██ ██ ███, respectively. Details on the finerenone doses are presented in Table 14.
Table 13: Exposure in FIGARO and FIDELIO (FAS)
Study exposure | FIDELIO | FIGARO | ||
|---|---|---|---|---|
Finerenone N = 2,833 | Placebo N = 2,841 | Finerenone N = 3,686 | Placebo N = 3,666 | |
Treatment (months),a mean (SD) | 26.9 (12.4) | 27.2 (12.2) | 35.2 (14.9) | 35.3 (14.7) |
Cumulative treatment duration, n (%) | ||||
At least 12 months | 2,446 (86.3) | 2,472 (87.0) | 3,321 (90.1) | 3,340 (91.1) |
At least 24 months | 1,631 (57.6) | 1,661 (58.5) | 2,990 (81.1) | 2,959 (80.7) |
At least 48 months | 51 (1.8) | 52 (1.8) | 824 (22.4) | 836 (22.8) |
At least 60 months | NA | NA | 8 (0.2) | 7 (0.2) |
Study duration (months),b mean (SD) | 31.9 (9.9) | 31.8 (10.0) | 40.2 (11.7) | 40.1 (11.9) |
Cumulative study duration, n (%) | ||||
At least 12 months | 2,773 (97.9) | 2,765 (97.3) | 3,611 (98.0) | 3,586 (97.8) |
At least 24 months | 2,100 (74.1) | 2,097 (73.8) | 3,469 (94.1) | 3,439 (93.8) |
At least 48 months | 81 (2.9) | 84 (3.0) | 1,099 (29.8) | 1,100 (30.0) |
At least 60 months | NA | NA | 10 (0.3) | 9 (0.2) |
FAS = full analysis set; NA = not applicable; SD = standard deviation.
aTreatment duration was from first to last intake of study drug.
bStudy duration refers to total observation time from randomization until end-of-study visit or until last contact date if no end-of-study visit took place.
Source: FIDELIO Clinical Study Report;16 FIGARO Clinical Study Report.17
Table 14: Number of Patients on Doses of Finerenone Over Time (FAS)
Time point | FIDELIO | FIGARO | ||||
|---|---|---|---|---|---|---|
N | Finerenone 10 mg | Finerenone 20 mg | N | Finerenone 10 mg | Finerenone 20 mg | |
Day 1 (randomization day), n (%) | ████ | ██ ████ | ███ ████ | ████ | ██ ████ | ███ █████ |
Month 1 | ████ | ██ ███ | ███ █████ | ████ | ███ ████ | ███ █████ |
Month 4 | ████ | ██ ████ | ███ █████ | ████ | ██ █████ | ███ █████ |
Month 12 | ████ | ██ ████ | ███ █████ | ████ | ██ █████ | ███ █████ |
Month 24 | ████ | ██ ████ | ███ █████ | ████ | ██ █████ | ███ █████ |
Month 36 | ███ | ██ ████ | ██ █████ | ████ | ██ █████ | ███ █████ |
Month 48 | ██ | ██ ████ | ██ █████ | ███ | ██ █████ | ██ █████ |
Month 60 | NA | NA | NA | ██ | █ ██████ | ██ █████ |
FAS = full analysis set; N = number of patients who have not yet permanently discontinued study drug up until the respective time point; NA = not applicable.
Source: FIDELIO Clinical Study Report;16 FIGARO Clinical Study Report.17
Efficacy
Only those efficacy outcomes and analyses of subgroups identified in the review protocol are reported as follows.
In FIDELIO, the primary and key secondary end points met the preplanned criteria for statistical significance, and all-cause mortality (the next secondary end point) was tested hierarchically. It did not reach statistical significance, and so the remaining secondary end points were tested in an exploratory manner. In FIGARO, the primary end point met the preplanned criteria for statistical significance, and the key secondary end point did not; therefore, the secondary end points were tested in an exploratory manner.
Renal Outcomes
Renal end points were assessed at every visit up to and including the last visit after premature discontinuation and the end-of-study visit. Results are presented in detail in Table 15. The 40% renal composite end point was the primary end point in FIDELIO and a key secondary end point in FIGARO. In FIDELIO, the composite events occurred in 504 patients (17.8%) and 600 patients (21.1%) in the finerenone and placebo groups, respectively, and the HR was 0.83 (95% CI, 0.73 to 0.93; P = 0.0014), representing a 17% reduction in risk in favour of finerenone. In FIGARO, this event occurred in 350 patients (9.5%) and 395 patients (10.8%) in the finerenone and placebo groups, respectively, and the HR was 0.87 (95% CI, 0.76 to 1.01; P = 0.0689); this end point was not statistically significant.
The 57% renal composite end point was a secondary end point in both studies. In FIDELIO, it occurred in 252 patients (8.9%) and 326 patients (11.5%) in the finerenone and placebo groups, respectively, and the HR was 0.76 (95% CI, 0.65 to 0.90) in favour of finerenone. In FIGARO, it occurred in 108 patients (2.9%) and 139 patients (3.8%) in the finerenone and placebo groups, respectively, and the HR was 0.77 (95% CI, 0.60 to 0.99).
In FIDELIO, the individual components of a sustained decrease in eGFR greater than or equal to 40% and eGFR greater than or equal to 57% (relative to baseline) had HRs of 0.815 (95% CI, 0.722 to 0.920) and 0.68 (95% CI, 0.55 to 0.82), respectively, in favour of finerenone. The HRs of the other individual components of kidney failure, ESRD, and sustained decrease in eGFR to less than 15 mL/min/1.73 m2 were 0.87 (95% CI, 0.72 to 1.05), 0.86 (95% CI, 0.67 to 1.10), and 0.82 (95% CI, 0.67 to 1.01), respectively.
In FIGARO, the individual components of sustained decrease in eGFR greater than or equal to 40% and eGFR greater than or equal to 57% (relative to baseline) had HRs of 0.87 (95% CI, 0.75 to 1.00) and 0.76 (95% CI, 0.58 to 1.00), respectively. The HRs of the other individual components of kidney failure, ESRD, and a sustained decrease in eGFR to less than 15 mL/min/1.73 m2 were 0.72 (95% CI, 0.49 to 1.05), 0.64 (95% CI, 0.41 to 1.00), and 0.71 (95% CI, 0.43 to 1.16), respectively.
In the pooled analysis of FIDELIO and FIGARO, the HR was 0.85 (95% CI, 0.77 to 0.93) and 0.77 (95% CI, 0.67 to 0.88) for the 40% and 57% renal composite end points, respectively, in favour of finerenone. The cumulative incidences based on Aalen-Johansen estimates are presented in Figure 6.
Table 15: Renal Composite End Point (FAS)
Outcome | FIDELIO | FIGARO | Pooled analysis | |||
|---|---|---|---|---|---|---|
Finerenone N = 2,833 | Placebo N = 2,841 | Finerenone N = 3,686 | Placebo N = 3,666 | Finerenone N = 6,519 | Placebo N = 6,507 | |
Patients with the 40% renal composite end point,a n (%) | 504 (17.8) | 600 (21.1) | 350 (9.5) | 395 (10.8) | 854 (13.1) | 995 (15.3) |
Incidence rate (person-years) (95% CI) | 7.6 (6.9 to 8.3) | 9.1 (8.4 to 9.8) | 3.2 (2.8 to 3.5) | 3.6 (3.2 to 3.9) | 4.8 (4.5 to 5.1) | 5.6 (5.3 to 6.0) |
HR (95% CI) | 0.83 (0.73 to 0.93) | 0.87 (0.76 to 1.01) | 0.85 (0.77 to 0.93) | |||
P valueb | 0.0014 | 0.0689 | 0.0004 | |||
Patients with the 57% renal composite end point,c n (%) | 252 (8.9) | 326 (11.5) | 108 (2.9) | 139 (3.8) | 360 (5.5) | 465 (7.1) |
Incidence rate (person-years) (95% CI) | 3.64 (3.2 to 4.1) | 4.74 (4.2 to 5.3) | 0.95 (0.8 to 1.1) | 1.23 (1.0 to 1.4) | 1.96 (1.8 to 2.2) | 2.55 (2.3 to 2.8) |
HR (95% CI) | 0.76 (0.65 to 0.90) | 0.77 (0.60 to 0.99) | 0.77 (0.67 to 0.88) | |||
P valueb | 0.0012 | 0.0406 | 0.0002d | |||
Components of the renal composite end point | ||||||
Patients with kidney failure, n (%) | 208 (7.3) | 235 (8.3) | 46 (1.2) | 62 (1.7) | 254 (3.9) | 297 (4.6) |
Incidence rate (person-years) (95% CI) | 2.99 (2.6 to 3.4) | 3.39 (3.0 to 3.8) | 0.40 (0.3 to 0.5) | 0.54 (0.4 to 0.7) | 1.38 (1.2 to 1.6) | 1.62 (1.4 to 1.8) |
HR (95% CI) | 0.87 (0.72 to 1.05) | 0.72 (0.49 to 1.05) | 0.84 (0.71 to 0.99) | |||
P valueb | 0.1409 | 0.0889 | 0.0392 | |||
Patients with ESRD, n (%) | 119 (4.2) | 139 (4.9) | 32 (0.9) | 49 (1.3) | 151 (2.3) | 188 (2.9) |
Incidence rate (person-years) (95% CI) | 1.6 (1.3 to 1.9) | 1.9 (1.6 to 2.2) | 0.26 (0.2 to 0.4) | 0.40 (0.3 to 0.5) | 0.76 (0.7 to 0.9) | 0.96 (0.8 to 1.1) |
HR (95% CI) | 0.86 (0.67 to 1.10) | 0.64 (0.41 to 1.00) | 0.80 (0.64 to 0.99) | |||
P valueb | 0.2191 | 0.0458 | NR | |||
Patients with sustained decrease in eGFR to < 15 mL/min/1.73 m2, n (%) | 167 (5.9) | 199 (7.0) | 28 (0.8) | 38 (1.0) | 195 (3.0) | 237 (3.6) |
Incidence rate (person-years) (95% CI) | 2.4 (2.1 to 2.8) | 2.9 (2.5 to 3.3) | 0.24 (0.2 to 0.3) | 0.33 (0.2 to 0.5) | 1.06 (0.9 to 1.2) | 1.29 (1.1 to 1.5) |
HR (95% CI) | 0.82 (0.67 to 1.01) | 0.71 (0.43 to 1.16) | 0.81 (0.67 to 0.98) | |||
P valueb | 0.0646 | 0.1711 | NR | |||
Patients with sustained decrease in eGFR ≥ 40% (relative to baseline), n (%) | 479 (16.9) | 577 (20.3) | 338 (9.2) | 385 (10.5) | 817 (12.5) | 962 (14.8) |
Incidence rate (person-years) (95% CI) | 7.2 (6.6 to 7.9) | 8.7 (8.0 to 9.5) | 3.04 (2.7 to 3.4) | 3.49 (3.2 to 3.8) | 4.60 (4.3 to 4.9) | 5.45 (5.1 to 5.8) |
HR (95% CI) | 0.815 (0.72 to 0.92) | 0.87 (0.75 to 1.00) | 0.84 (0.76 to 0.92) | |||
P valueb | 0.0009 | 0.0526 | 0.0002 | |||
Patients experiencing renal death, n (%) | 2 (< 0.1) | 2 (< 0.1) | 0 | 2 (< 0.1) | 2 (< 0.1) | 4 (< 0.1) |
Sustained decrease in eGFR ≥ 57% (relative to baseline) | 167 (5.9) | 245 (8.6) | 90 (2.4) | 116 (3.2) | 257 (3.9) | 361 (5.5) |
Incidence rate (person-years) (95% CI) | 2.41 (2.1 to 2.8) | 3.54 (3.1 to 4.0) | 0.79 (0.6 to 1.0) | 1.02 (0.9 to 1.2) | 1.40 (1.2 to 1.6) | 1.98 (1.8 to 2.2) |
HR (95% CI) | 0.68 (0.55 to 0.82) | 0.76 (0.58 to 1.00) | 0.70 (0.60 to 0.83) | |||
P valueb | < 0.0001 | 0.0533 | < 0.0001 | |||
CI = confidence interval; eGFR = estimated glomerular filtration rate; ESRD = end-stage renal disease; FAS = full analysis set; HR = hazard ratio; NR = not reported.
aRenal composite end point comprises the onset of kidney failure, sustained decrease of eGFR greater than or equal to 40% from baseline over at least 4 weeks, or renal death. For composite outcomes and each component, the first event after randomization is considered. Subsequent events of the same type are not shown. The incidence rate is estimated as the number of patients with events divided by the cumulative at-risk time in the reference population, where a patient was no longer at risk once an event occurred. Incidence rates, HRs, and P values were only calculated for predefined efficacy end points.
bP value: 2-sided P value from log-rank test, stratified. Only adjusted for multiple testing in the FIDELIO 40% renal composite end point.
cRenal composite end point comprises the onset of kidney failure, sustained decrease of eGFR greater than or equal to 57% from baseline over at least 4 weeks, or renal death.
dIn the pooled analysis, statistical analyses were prespecified exploratory evaluations, and no adjustment for multiplicity was performed.
Source: FIDELIO Clinical Study Report;16 FIGARO Clinical Study Report;17 FIDELITY pooled analysis.18
Figure 6: Time to Renal Outcomes From Pooled Analysis
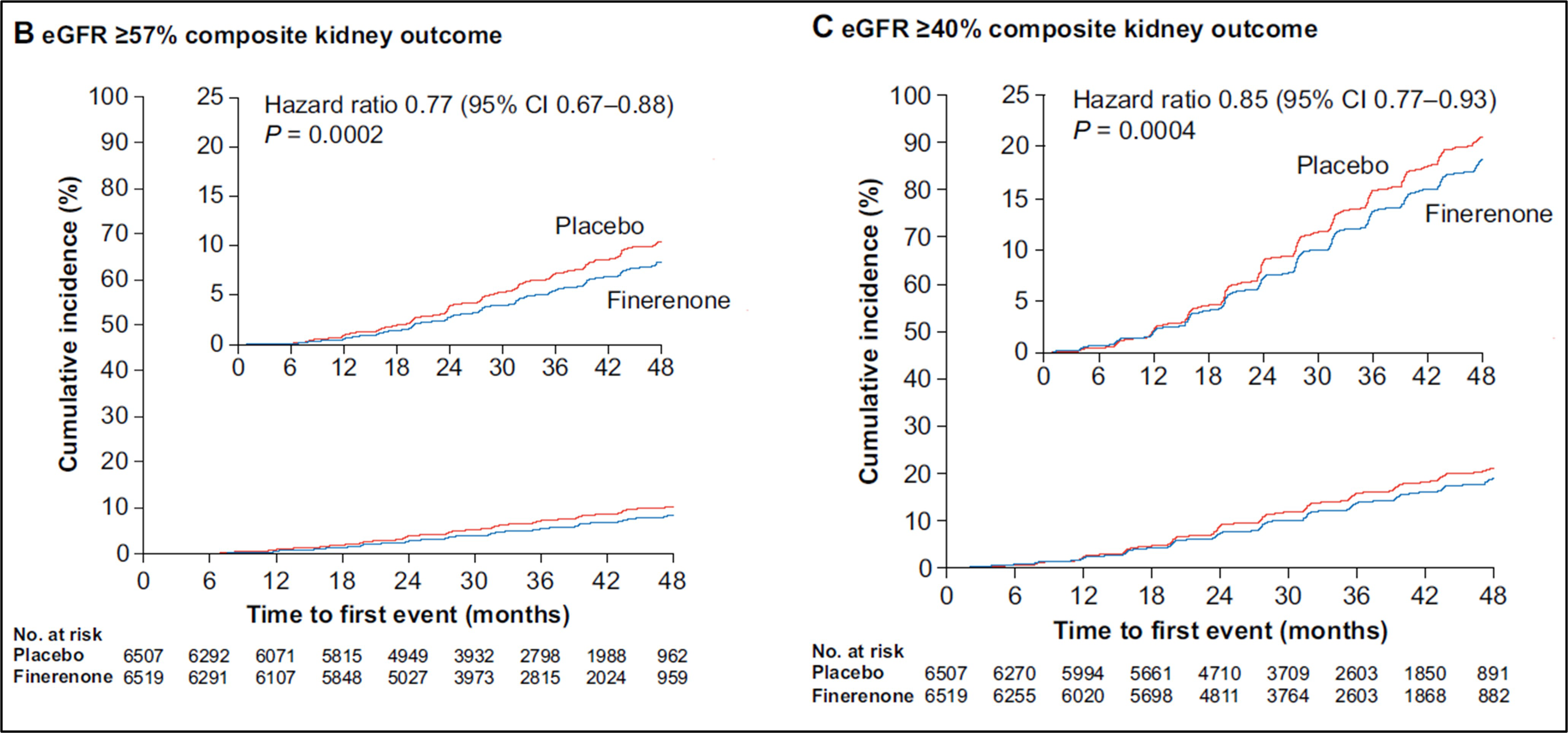
CI = confidence interval; eGFR = estimated glomerular filtration rate.
Source: Agarwal et al. (2021). Copyright © 2021 Oxford University Press. Reprinted in accordance with Creative Commons Attribution License CC BY-NC 4.0.52
Subgroup Analysis
The renal composite results by subgroups of interest, as specified a priori in the protocol for this CADTH review, are summarized in Table 16. In FIDELIO, the HR was greater than 1 in patients who were treated with SGLT2 inhibitors at baseline, favouring placebo over finerenone, yet the small sample size and wide CIs in this subgroup reflect uncertainty in the effect estimates. In FIGARO, the HR was also greater than 1 in patients with an eGFR of 45 mL/min/1.73 m2 to < 60 mL/min/1.73 m2 at baseline and in patients with high albuminuria (30 mg/g to < 300 mg/g) at baseline.
Table 16: Forty Percent Renal Composite Outcomes by Subgroups (FAS)
Outcome | FIDELIO | FIGARO | ||||||
|---|---|---|---|---|---|---|---|---|
Finerenone n/N | Placebo n/N | HR (95% CI)a | P valuea | Finerenone n/N | Placebo n/N | HR (95% CI)a | P valuea | |
History of CV disease | ||||||||
Present | 200/1,303 | 267/1,302 | 0.70 (0.58 to 0.84) | 0.0160 | 159/1,676 | 170/654 | 0.92 (0.74 to 1.15) | 0.4777 |
Absent | 304/1,530 | 333/1,539 | 0.94 (0.80 to 1.09) | 191/2,010 | 225/2,012 | 0.84 (0.69 to 1.02) | ||
eGFR category at baseline | ||||||||
< 25 mL/min/1.73 m2 | 18/66 | 23/69 | 0.88 (0.48 to 1.64) | 0.8451 | 2/15 | 0/12 | NC | 0.2073 |
25 to < 45 mL/min/1.73 m2 | 295/1,476 | 339/1,505 | 0.86 (0.73 to 1.00) | 50/641 | 51/610 | 0.92 (0.62 to 1.37) | ||
45 to < 60 mL/min/1.73 m2 | 138/972 | 168/928 | 0.77 (0.61 to 0.96) | 73/745 | 67/789 | 1.25 (0.88 to 1.77) | ||
≥ 60 mL/min/1.73 m2 | 53/318 | 70/338 | 0.78 (0.55 to 1.12) | 225/2,285 | 277/2,254 | 0.79 (0.66 to 0.94) | ||
Type of albuminuria at baseline | ||||||||
Normoalbuminuria (UACR < 30 mg/g) | 0/11 | 2/12 | NC | NC | 4/109 | 3/98 | 0.58 (0.09 to 3.57) | 0.0188 |
High albuminuria (UACR 30 mg/g to < 300 mg/g) | 19/350 | 20/335 | 0.92 (0.40 to 1.72) | 145/1,726 | 124/1,688 | 1.16 (0.91 to 1.47) | ||
Very high albuminuria (UACR ≥ 300 mg/g) | 485/2,470 | 578/2,493 | 0.83 (0.73 to 0.93) | 201/1,851 | 268/1,878 | 0.74 (0.62 to 0.90) | ||
SGLT2 inhibitor treatment at baseline | ||||||||
No | 490/2,709 | 590/2,706 | 0.82 (0.72 to 0.92) | 0.2114 | 328/3,372 | 371/3,362 | 0.88 (0.76 to 1.03) | 0.6875 |
Yes | 14/124 | 10/135 | 1.38 (0.61 to 3.10) | 22/314 | 24/304 | 0.70 (0.37 to 1.30) | ||
CI = confidence interval; CV = cardiovascular; eGFR = estimated glomerular filtration rate; FAS = full analysis set; HR = hazard ratio; NC = not calculated; SGLT2 = sodium-glucose cotransporter-2; UACR = urinary albumin-creatinine ratio.
aHRs, 95% CIs, and interaction P values (2-sided) are based on stratified Cox proportional models including treatment, subgroup, and a subgroup by treatment interaction term as fixed effects.
Change in UACR From Baseline to Month 48
Baseline values of UACR were comparable between the treatment groups but differed between trials according to the inclusion criteria, with higher values in the FIDELIO trial population. Nevertheless, in both trials, the change in UACR from baseline to month 4 was larger in the finerenone group than in the placebo group, with an LS mean ratio to baseline of 0.69 (95% CI, 0.66 to 0.72) and 0.68 (95% CI, 0.65 to 0.70) in FIDELIO and FIGARO, respectively. This effect was sustained for the duration of the study up to month 36 in FIDELIO and month 48 in FIGARO, as shown in Figure 7 and Figure 8. Further details are provided in Table 17.
Table 17: Change in UACR From Baseline to Month 48 (FAS)
Outcome | FIDELIO | FIGARO | Pooled analysis | ||||||
|---|---|---|---|---|---|---|---|---|---|
Finerenone N = 2,833 | Placebo N = 2,841 | Finerenone N = 3,686 | Placebo N = 3,666 | Finerenone N = 6,519 | Placebo N = 6,507 | ||||
Change in UACRa from baseline to month 4 | |||||||||
Baseline mean value (SD) | 798.79 (2.65) | 814.73 (2.67) | 284.33 (3.58) | 288.87 (3.53) | 445.35 (3.54) | 454.29 (3.52) | |||
Month 4 mean value (SD)b | 520.39 (3.22) | 769.90 (3.04) | 177.86 (4.24) | 268.01 (3.99) | 283.76 (4.20) | 425.28 (3.96) | |||
Patients in analysis, n | 2,711 | 2,705 | 3,521 | 3,476 | 6,232 | 6,181 | |||
LS mean ratio to baseline (95% CI)b,c | 0.66 (0.64 to 0.67) | 0.95 (0.93 to 0.98) | 0.62 (0.61 to 0.64) | 0.92 (0.90 to 0.95) | 0.64 (0.63 to 0.65) | 0.94 (0.92 to 0.95) | |||
LS mean ratio finerenone to placebo (95% CI)b | 0.69 (0.66 to 0.72) | 0.68 (0.65 to 0.70) | 0.68 (0.66 to 0.70) | ||||||
P value of F testd | < 0.0001 | < 0.0001 | < 0.0001 | ||||||
Change in UACRe from baseline to month 12 | |||||||||
Patients in analysis, n | 2,582 | 2,598 | 3,406 | 3,375 | NA | ||||
LS mean ratio to baseline (95% CI) | 0.59 (0.57 to 0.61) | 0.97 (0.94 to 1.00) | 0.556 (0.54 to 0.58) | 0.93 (0.89 to 0.96) | NA | ||||
LS mean ratio finerenone to placebo (95% CI) | 0.60 (0.57 to 0.64) | 0.60 (0.57 to 0.63) | NA | ||||||
Change in UACRe from baseline to month 24 | |||||||||
Patients in analysis, n | 1,841 | 1,825 | 3,026 | 3,004 | NA | ||||
LS mean ratio to baseline (95% CI) | 0.60 (0.57 to 0.63) | 0.98 (0.94 to 1.03) | 0.58 (0.56 to 0.61) | 0.93 (0.89 to 0.98) | NA | ||||
LS mean ratio finerenone to placebo (95% CI) | 0.61 (0.57 to 0.66) | 0.62 (0.59 to 0.66) | NA | ||||||
Change in UACRe from baseline to month 36 | |||||||||
Patients in analysis, n | 856 | 834 | 1,889 | 1,872 | NA | ||||
LS mean ratio to baseline (95% CI) | 0.71 (0.66 to 0.76) | 1.04 (0.97 to 1.12) | 0.62 (0.58 to 0.65) | 0.96 (0.91 to 1.02) | NA | ||||
LS mean ratio finerenone to placebo (95% CI) | 0.68 (0.61 to 0.76) | 0.64 (0.59 to 0.70) | NA | ||||||
Change in UACRe from baseline to month 48 | |||||||||
Patients in analysis, n | NA | 831 | 811 | NA | |||||
LS mean ratio to baseline (95% CI) | NA | 0.71 (0.66 to 0.77) | 0.99 (0.92 to 1.07) | NA | |||||
LS mean ratio finerenone to placebo (95% CI) | NA | 0.72 (0.64 to 0.80) | NA | ||||||
CI = confidence interval; eGFR = estimated glomerular filtration rate; FAS = full analysis set; LS = least squares; NA = not available; SD = standard deviation; UACR = urinary albumin-creatinine ratio.
aUACR was determined 3 times at each visit from first morning void urine samples collected on 3 consecutive days and summarized according to the statistical analysis plan. For baseline, only samples with two-thirds of measurements taken on or before the day of randomization were used.
bMonth 4 is the visit closest to day 120 within a time window of 120 ± 30 days after randomization. If no measurements are available in this time window, the patient is excluded from this analysis.
cAnalysis of covariance with factors treatment group, region, eGFR category at screening, type of albuminuria at screening, and log-transformed baseline value as covariate nested within type of albuminuria.
dF test of equal means between the following additional factor levels: region, eGFR category at screening, and type of albuminuria at screening. Not adjusted for multiplicity.
eFor the statistical evaluation, a mixed model was applied with factors treatment group, region, eGFR category at screening, type of albuminuria at screening, time, treatment × time, log-transformed baseline value nested within type of albuminuria at screening, and log-transformed baseline value × time as covariate. Separate unstructured covariance patterns were estimated for each treatment group. Values after the onset date of end-stage renal disease were excluded from this analysis.
Source: FIDELIO Clinical Study Report;16 FIGARO Clinical Study Report;17 FIDELITY pooled analysis.18
Figure 7: FIDELIO — Least Squares Means of Ratio to Baseline for UACR Values by Visit (FAS)
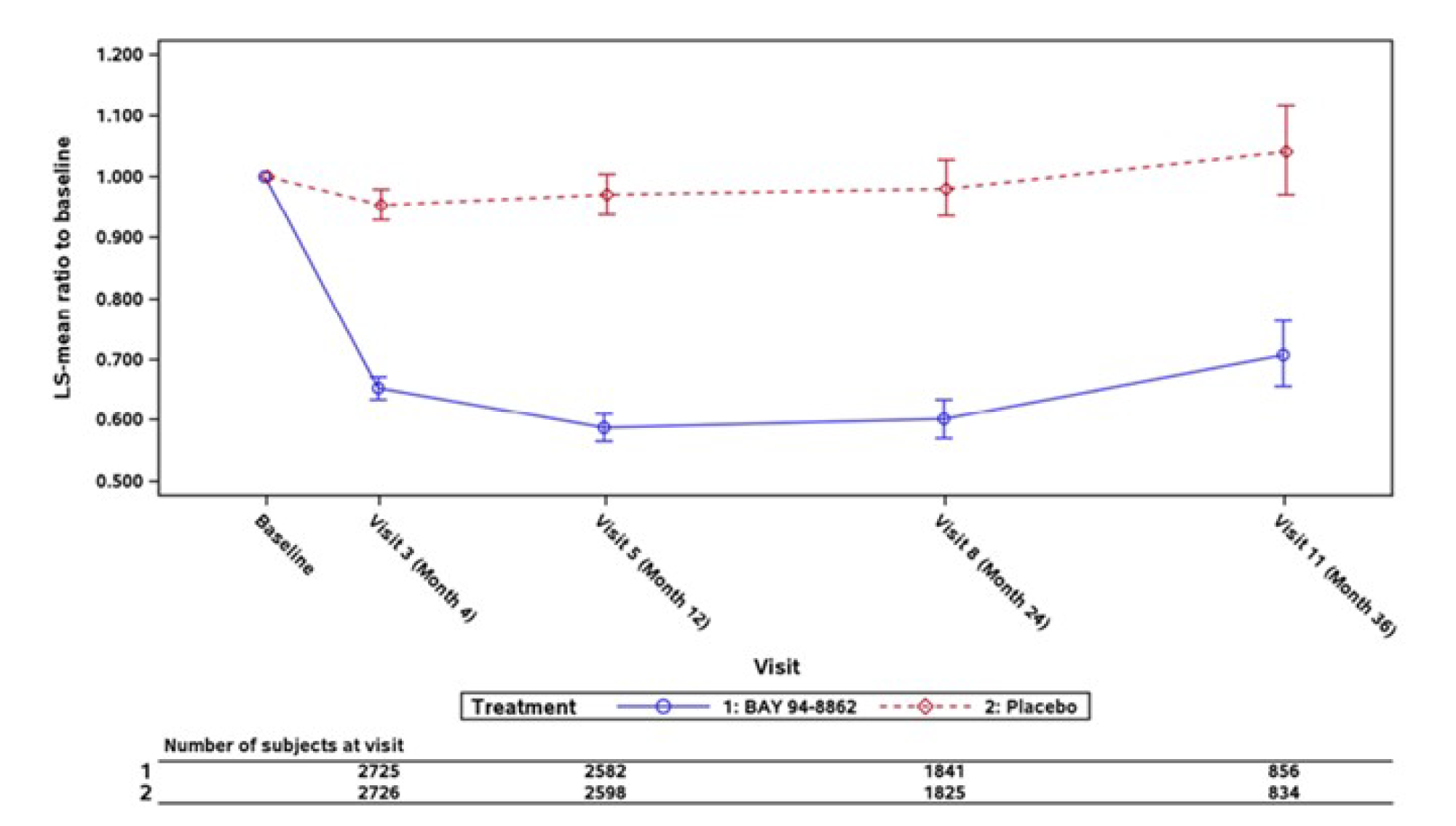
FAS = full analysis set; LS = least squares; UACR = urinary albumin-creatinine ratio.
Note: LS means result from a mixed model with factors treatment group, region, estimated glomerular filtration rate category at screening, type of albuminuria at screening, cardiovascular disease history, time, treatment × time, log-transformed baseline value nested within type of albuminuria at screening, and log-transformed baseline value × time as covariate. Separate unstructured covariance patterns were estimated for each treatment group. Values after the onset date of end-stage renal disease are excluded from this analysis.
Source: FIDELIO Clinical Study Report.16
Figure 8: FIGARO — Least Squares Means of Ratio to Baseline for UACR Values by Visit (FAS)
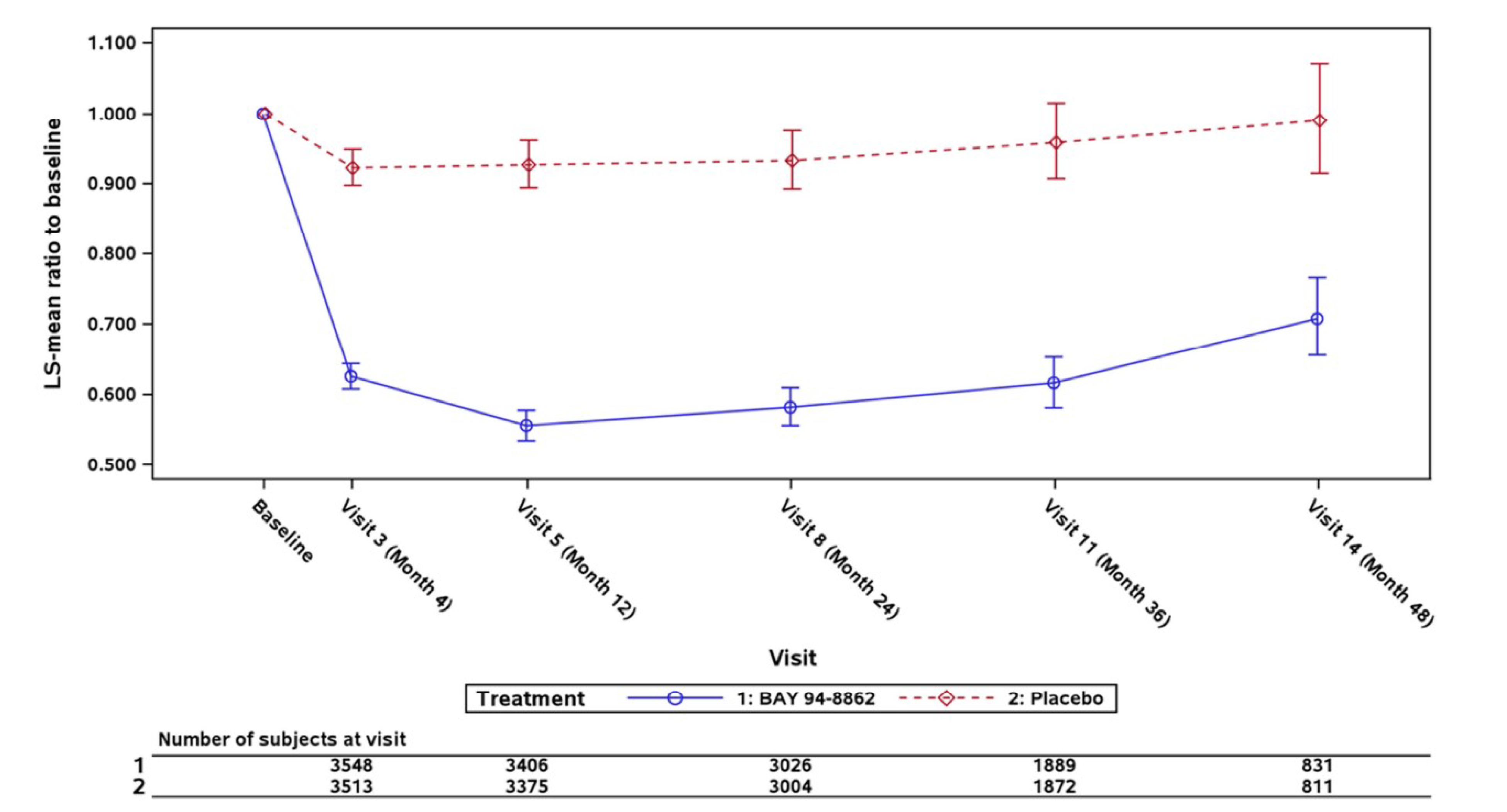
FAS = full analysis set; LS = least squares; UACR = urinary albumin-creatinine ratio.
Note: LS means result from a mixed model with factors treatment group, region, estimated glomerular filtration rate category at screening, type of albuminuria at screening, cardiovascular disease history, time, treatment × time, log-transformed baseline value nested within type of albuminuria at screening, and log-transformed baseline value × time as covariate. Separate unstructured covariance patterns were estimated for each treatment group. Values after the onset date of end-stage renal disease are excluded from this analysis.
Source: FIGARO Clinical Study Report.17
Change in eGFR From Baseline to 48 Months
Baseline values of eGFR were comparable between the treatment groups but differed between trials according to the inclusion criteria, with lower values in the FIDELIO trial population (44.4 mL/min/1.73 m2 and 44.3 mL/min/1.73 m2 in the finerenone and placebo groups, respectively) compared to the FIGARO trial population (67.6 mL/min/1.73 m2 and 68.0 mL/min/1.73 m2 in the finerenone and placebo groups, respectively). Results from the mixed model analysis are presented in Table 18. After baseline, there was a larger acute reduction in eGFR in the finerenone group than in the placebo group, with an LS mean difference at month 4 of –2.38 (95% CI, –2.77 to –1.98) and –2.24 (95% CI, –2.67 to –1.80) in FIDELIO and FIGARO, respectively. The decrease in eGFR in the finerenone group then slows down, as shown in Figure 9 and Figure 10, until the difference becomes positive at month 28 in the FIDELIO trial and month 36 in the FIGARO trial.
Table 18: Mixed Model Analysis of eGFR (FAS)
Time point | FIDELIO | FIGARO | ||||
|---|---|---|---|---|---|---|
Finerenone, N | Placebo, N | LS mean difference (95% CI)a | Finerenone, N | Placebo, N | LS mean difference (95% CI)a | |
Baseline | 2,833 | 2,841 | NA | 3,686 | 3,666 | NA |
Month 1 | 2,799 | 2,800 | –2.13 (–2.48 to –1.78) | 3,629 | 3,606 | –2.17 (–2.57 to –1.77) |
Month 4 | 2,722 | 2,720 | –2.38 (–2.77 to –1.98) | 3,540 | 3,524 | –2.24 (–2.67 to –1.80) |
Month 8 | 2,646 | 2,672 | –1.75 (–2.18 to –1.33) | 3,454 | 3,454 | –2.05 (–2.52 to –1.58) |
Month 12 | 2,613 | 2,611 | –1.49 (–1.95 to –1.04) | 3,402 | 3,380 | –2.01 (–2.51 to –1.52) |
Month 16 | 2,524 | 2,524 | –0.87 (–1.35 to –0.38) | 3,312 | 3,301 | –1.79 (–2.32 to –1.26) |
Month 20 | 2,268 | 2,290 | –0.57 (–1.10 to –0.03) | 3,189 | 3,144 | –1.40 (–1.96 to –0.84) |
Month 24 | 1,870 | 1,846 | –0.03 (–0.60 to 0.55) | 3,053 | 3,026 | –1.09 (–1.68 to –0.49) |
Month 28 | 1,520 | 1,527 | 0.22 (–0.41 to 0.85) | 2,697 | 2,677 | –0.90 (–1.53 to –0.28) |
Month 32 | 1,180 | 1,184 | 0.70 (0.00 to 1.39) | 2,270 | 2,223 | –0.62 (–1.29 to 0.05) |
Month 36 | 867 | 844 | 0.98 (0.17 to 1.78) | 1,900 | 1,883 | 0.11 (–0.62 to 0.83) |
Month 40 | 598 | 602 | 1.65 (0.76 to 2.55) | 1,576 | 1,561 | 0.15 (–0.65 to 0.95) |
Month 44 | 336 | 339 | 1.98 (0.83 to 3.13) | 1,253 | 1,233 | 0.37 (–0.47 to 1.21) |
Month 48 | NA | NA | NA | 841 | 817 | 0.67 (–0.26 to 1.60) |
CI = confidence interval; eGFR = estimated glomerular filtration rate; FAS = full analysis set; LS = least squares; NA = not applicable.
aLS mean difference of finerenone minus placebo. For the statistical evaluation, a mixed model was applied, with factors treatment group, region, eGFR category at screening, type of albuminuria at screening, time, treatment × time, baseline value nested within type of albuminuria, and baseline value × time as covariate.
Source: FIDELIO Clinical Study Report;16 FIGARO Clinical Study Report.17
Figure 9: FIDELIO — Least Squares Means of eGFR Absolute Changes From Baseline by Visit (FAS)
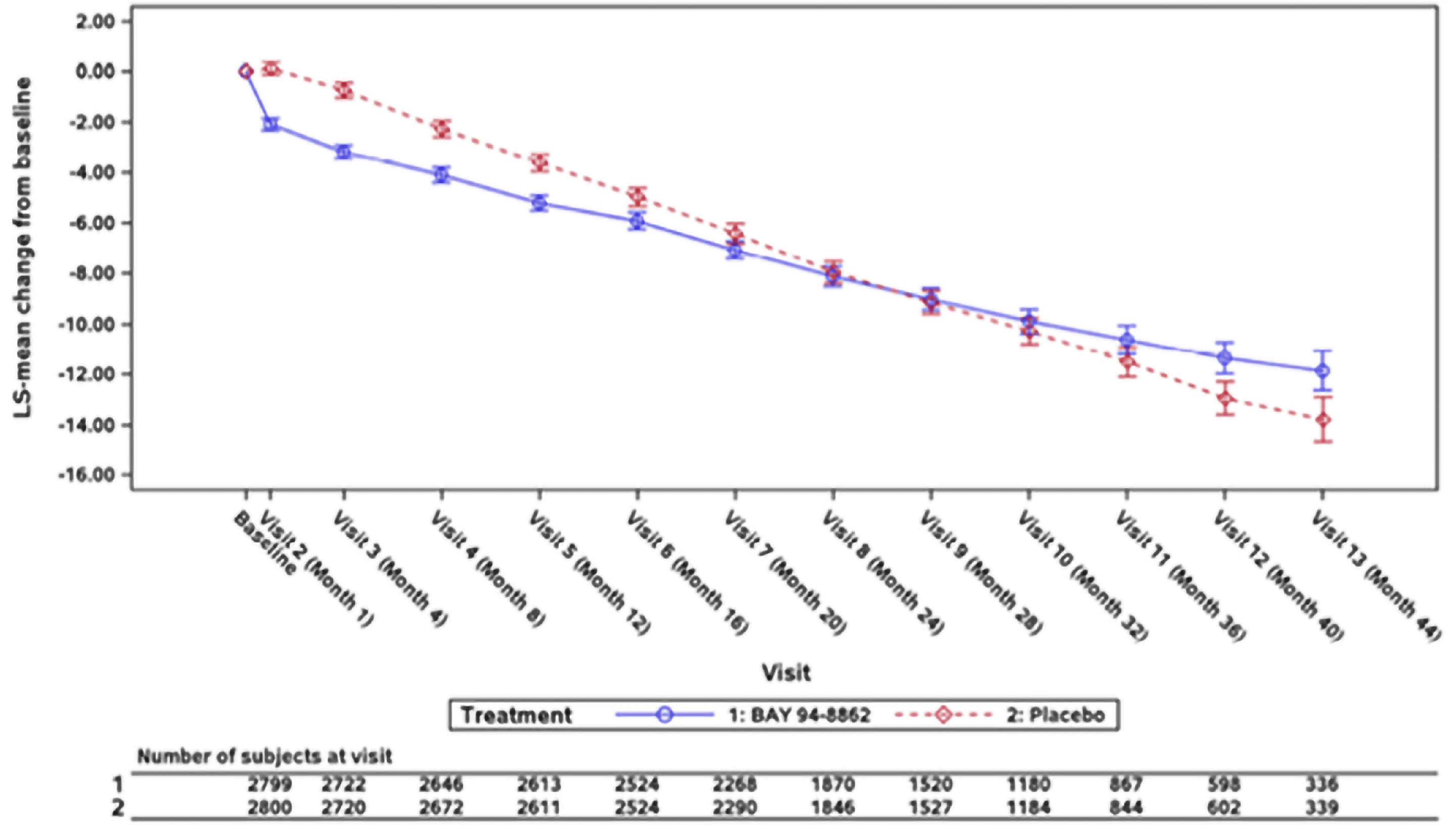
eGFR = estimated glomerular filtration rate; FAS = full analysis set; LS = least squares.
Note: LS means result from a mixed model with factors treatment group, region, eGFR category at screening, type of albuminuria at screening, time, treatment × time, baseline value nested within eGFR category at screening, and baseline value × time as covariate. Separate unstructured covariance patterns were estimated for each treatment group. Values after the onset date of end-stage renal disease are excluded from this analysis.
Source: FIDELIO Clinical Study Report.16
Figure 10: FIGARO — Least Squares Means of eGFR Absolute Changes From Baseline by Visit (FAS)
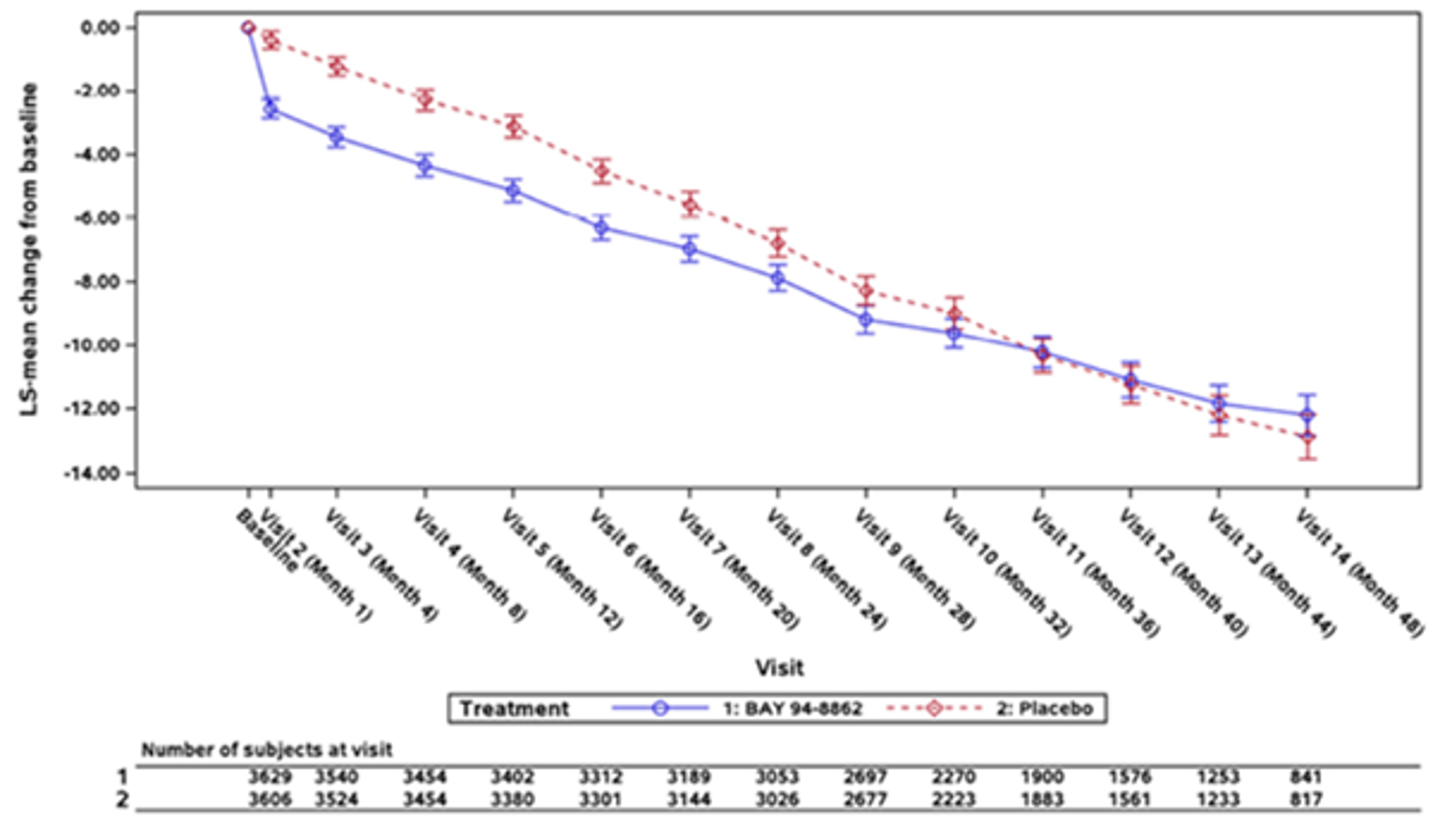
eGFR = estimated glomerular filtration rate; FAS = full analysis set; LS = least squares.
Note: LS means result from a mixed model with factors treatment group, region, eGFR category at screening, type of albuminuria at screening, cardiovascular disease history, time, treatment × time, baseline value nested within eGFR category at screening, and baseline value × time as covariate. Separate unstructured covariance patterns were estimated for each treatment group. Values after the onset date of end-stage renal disease are excluded from this analysis.
Source: FIGARO Clinical Study Report.17
Cardiovascular Outcomes
Cardiovascular end points were assessed at every visit up to and including the last visit after premature discontinuation and the end-of-study visit. Results are presented in detail in Table 19. The cardiovascular composite end point was the primary end point in FIGARO and a key secondary end point in FIDELIO. In FIDELIO, the composite events occurred in 367 patients (13%) and 420 patients (14.8%) in the finerenone and placebo groups, respectively, and the HR was 0.86 (95% CI, 0.75 to 0.99; P = 0.0339), representing a 14% reduction in risk in favour of finerenone. In FIGARO, this end point occurred in 458 patients (12.4%) and 519 patients (14.2%) in the finerenone and placebo groups, respectively, and the HR was 0.87 (95% CI, 0.76 to 0.98; P = 0.0264), representing a 13% reduction in risk in favour of finerenone.
In FIGARO, the only individual component of statistical significance was hospitalization for heart failure, which had an HR of 0.71 (95% CI, 0.56 to 0.90) in favour of finerenone. The individual components of cardiovascular death and nonfatal MI had HRs of 0.90 (95% CI, 0.74 to 1.09) and 0.99 (95% CI, 0.76 to 1.31), respectively. In FIDELIO, the individual components of cardiovascular death, nonfatal MI, and hospitalization for heart failure had HRs of 0.86 (95% CI, 0.68 to 1.08), 0.80 (95% CI, 0.58 to 1.09), and 0.86 (95% CI, 0.68 to 1.08), respectively. In both trials, there was almost no difference in risk of nonfatal stroke, with an HR of 0.97 (95% CI, 0.74 to 1.26) in FIDELIO and of 1.03 (95% CI, 0.77 to 1.38) in FIGARO.
In the pooled analysis of FIDELIO and FIGARO, the HR was 0.86 (95% CI, 0.78 to 0.95) in favour of finerenone. The cumulative incidences based on Aalen-Johansen estimates are presented in Figure 11.
Table 19: Cardiovascular Composite End Point (FAS)
Outcome | FIDELIO | FIGARO | Pooled analysis | |||
|---|---|---|---|---|---|---|
Finerenone N = 2,833 | Placebo N = 2,841 | Finerenone N = 3,686 | Placebo N = 3,666 | Finerenone N = 6,519 | Placebo N = 6,507 | |
Number of patients with a CV composite end point,a n (%) | 367 (13.0) | 420 (14.8) | 458 (12.4) | 519 (14.2) | 825 (12.7) | 939 (14.4) |
Incidence rate (person-years) (95% CI) | 5.11 (4.60 to 5.64) | 5.92 (5.37 to 6.50) | 3.87 (3.52 to 4.23) | 4.45 (4.08 to 4.84) | 4.34 (4.05 to 4.64) | 5.01 (4.69 to 5.33) |
HR (95% CI) | 0.86 (0.75 to 0.99) | 0.87 (0.76 to 0.98) | 0.86 (0.78 to 0.95) | |||
P valueb | 0.0339 | 0.0264 | 0.0018 | |||
Components of the CV composite end point | ||||||
CV death, n (%) | 128 (4.5) | 150 (5.3) | 194 (5.3) | 214 (5.8) | 322 (4.9) | 364 (5.6) |
Incidence rate (person-years) (95% CI) | 1.69 (1.41 to 2.00) | 1.99 (1.68 to 2.32) | 1.56 (1.35 to 1.79) | 1.74 (1.52 to 1.98) | 1.61 (1.44 to 1.79) | 1.84 (1.65 to 2.03) |
HR (95% CI) | 0.86 (0.68 to 1.08) | 0.90 (0.74 to 1.09) | 0.88 (0.76 to 1.02) | |||
P valueb | 0.1927 | 0.2742 | 0.0922 | |||
Nonfatal MI, n (%) | 70 (2.5) | 87 (3.1) | 103 (2.8) | 102 (2.8) | 173 (2.7) | 189 (2.9) |
Incidence rate (person-years) (95% CI) | 0.94 (0.73 to 1.17) | 1.17 (0.94 to 1.43) | 0.85 (0.69 to 1.02) | 0.85 (0.69 to 1.02) | 0.88 (0.75 to 1.02) | 0.97 (0.84 to 1.11) |
HR (95% CI) | 0.80 (0.58 to 1.09) | 0.99 (0.76 to 1.31) | 0.91 (0.74 to 1.12) | |||
P valueb | 0.1540 | 0.9628 | 0.3601 | |||
Nonfatal stroke, n (%) | 90 (3.2) | 87 (3.1) | 108 (2.9) | 111 (3.0) | 198 (3.0) | 198 (3.0) |
Incidence rate (person-years) (95% CI) | 1.21 (0.97 to 1.47) | 1.18 (0.94 to 1.44) | 0.89 (0.73 to 1.06) | 0.92 (0.76 to 1.10) | 1.01 (0.87 to 1.16) | 1.02 (0.88 to 1.17) |
HR (95% CI) | 1.03 (0.77 to 1.38) | 0.97 (0.74 to 1.26) | 0.99 (0.82 to 1.21) | |||
P valueb | 0.8579 | 0.7932 | 0.9460 | |||
Hospitalization for heart failure, n (%) | 139 (4.9) | 162 (5.7) | 117 (3.2) | 163 (4.4) | 256 (3.9) | 325 (5.0) |
Incidence rate (person-years) (95% CI) | 1.89 (1.59 to 2.21) | 2.21 (1.89 to 2.57) | 0.96 (0.80 to 1.14) | 1.36 (1.16 to 1.57) | 1.31 (1.15 to 1.48) | 1.68 (1.50 to 1.87) |
HR (95% CI) | 0.86 (0.68 to 1.08) | 0.71 (0.56 to 0.90) | 0.78 (0.66 to 0.92) | |||
P valueb | 0.1821 | 0.0043 | 0.0030 | |||
CI = confidence interval; CV = cardiovascular; FAS = full analysis set; HR = hazard ratio; MI = myocardial infarction.
aCV composite end point comprises CV death, nonfatal MI, nonfatal stroke, or hospitalization for heart failure. Events were adjudicated by an independent adjudication committee and considered from randomization until the end-of-study visit. For composite outcomes and each component, the first event after randomization is considered. Subsequent events of the same type are not shown. The incidence rate is estimated as the number of patients with events divided by the cumulative at-risk time in the reference population, where a patient was no longer at risk once an incident event occurred.
bTwo-sided P value from log-rank test, stratified. Adjusted for multiplicity in composite outcome in both trials. Not powered for individual components of the composite outcome.
Source: FIDELIO Clinical Study Report;16 FIGARO Clinical Study Report;17 and FIDELITY pooled analysis.18
Figure 11: Time to Cardiovascular Outcome From Pooled FIDELITY Analysis
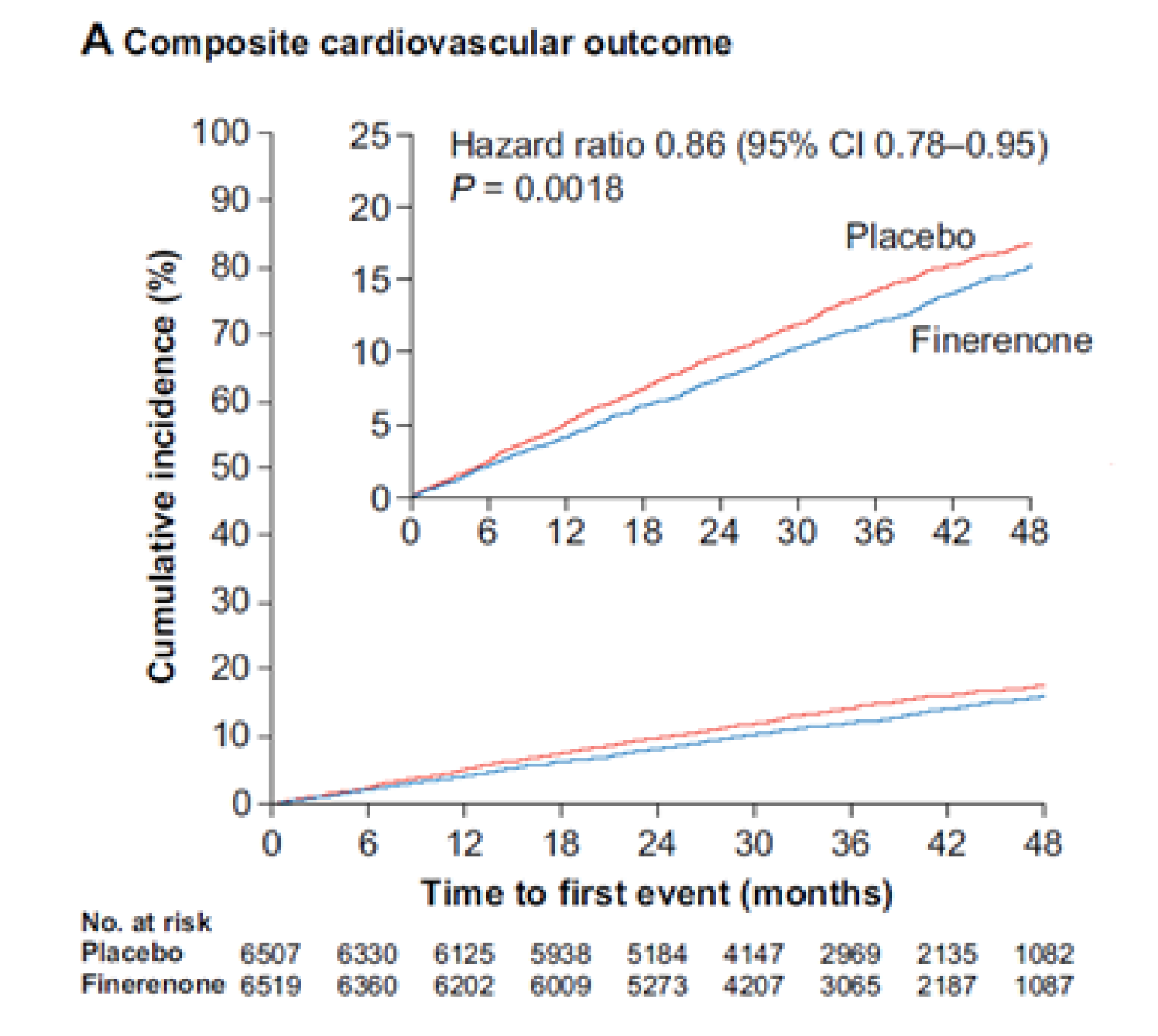
Source: Agarwal et al. (2021). Copyright © 2021 Oxford University Press. Reprinted in accordance with Creative Commons Attribution License CC BY-NC 4.0.52
Subgroup Analysis
The cardiovascular composite results by subgroups of interest, as specified a priori in the protocol for this CADTH review, are summarized in Table 20. The HR was approximately 1 in patients who were treated with SGLT2 inhibitors at baseline in FIDELIO, while the HR was 0.49 (95% CI, 0.28 to 0.86) in FIGARO. However, the small sample size of this patient group in both trials reflects uncertainty in the effect estimates.
Table 20: Cardiovascular Composite Outcome by Subgroups (FAS)
Outcome | FIDELIO | FIGARO | ||||||
|---|---|---|---|---|---|---|---|---|
Finerenone n/N | Placebo n/N | HR (95% CI)a | P valuea | Finerenone n/N | Placebo n/N | HR (95% CI)a | P valuea | |
History of CV disease | ||||||||
Present | 200/1,303 | 267/1,302 | 0.85 (0.71 to 1.01) | 0.8535 | 280/1,676 | 332/1,654 | 0.82 (0.70 to 0.96) | 0.2719 |
Absent | 304/1,530 | 333/1,539 | 0.87 (0.69 to 1.09) | 178/2,010 | 187/2,012 | 0.95 (0.77 to 1.17) | ||
eGFR category at baseline | ||||||||
< 25 mL/min/1.73 m2 | 8/66 | 19/69 | 0.40 (0.18 to 0.92) | 0.1806 | 3/15 | 4/12 | 0.62 (0.10 to 3.83) | 0.6655 |
25 to < 45 mL/min/1.73 m2 | 212/1,476 | 224/1,505 | 0.95 (0.78 to 1.14) | 109/641 | 107/610 | 0.95 (0.73 to 1.25) | ||
45 to < 60 mL/min/1.73 m2 | 106/972 | 126/928 | 0.78 (0.60 to 1.01) | 91/745 | 121/789 | 0.81 (0.61 to 1.06) | ||
≥ 60 mL/min/1.73 m2 | 40/318 | 51/338 | 0.85 (0.56 to 1.28) | 255/2,285 | 286/2,254 | 0.87 (0.73 to 1.03) | ||
Type of albuminuria at baseline | ||||||||
Normoalbuminuria (UACR < 30 mg/g) | 0/11 | 2/12 | NC | NC | 10/109 | 13/98 | 0.67 (0.27 to 1.66) | 0.6023 |
High albuminuria (UACR 30 mg/g to < 300 mg/g) | 34/350 | 41/335 | 0.76 (0.48 to 1.20) | 226/1,726 | 251/1,688 | 0.87 (0.73 to 1.04) | ||
Very high albuminuria (UACR ≥ 300 mg/g) | 332/2,470 | 377/2,493 | 0.87 (0.75 to 1.01) | 222/1,851 | 254/1,878 | 0.90 (0.75 to 1.08) | ||
SGLT2 inhibitor treatment at baseline | ||||||||
No | 352/2,709 | 405/2,706 | 0.85 (0.74 to 0.98) | 0.4553 | 434/3,372 | 482/3,362 | 0.89 (0.78 to 1.01) | 0.1141 |
Yes | 15/124 | 15/135 | 1.12 (0.55 to 2.30) | 24/314 | 37/304 | 0.49 (0.28 to 0.86) | ||
CI = confidence interval; CV = cardiovascular; eGFR = estimated glomerular filtration rate; FAS = full analysis set; HR = hazard ratio; NC = not calculated; SGLT2 = sodium-glucose cotransporter-2; UACR = urinary albumin-creatinine ratio.
aHRs, 95% CIs, and interaction P values (2-sided) are based on stratified Cox proportional hazards models, including treatment, subgroup, and a subgroup by treatment interaction term as fixed effects.
Source: FIDELIO Clinical Study Report;16 FIGARO Clinical Study Report.17
All-Cause Mortality
All-cause mortality was assessed throughout the study and counted up to the last date a vital status could be obtained. Incidence of all-cause mortality was similar between both groups in both trials, with 552 deaths (8.5% of patients) and 614 deaths (9.4% of patients) from any cause in the finerenone and placebo groups, respectively. Comparing the finerenone group with the placebo group, the HR was 0.90 (95% CI, 0.75 to 1.07) in FIDELIO and 0.89 (95% CI, 0.77 to 1.04) in FIGARO. All-cause mortality results are presented in Table 21.
Table 21: All-Cause Mortality (FAS)
Outcome | FIDELIO | FIGARO | FIDELITY pooled analysis | |||
|---|---|---|---|---|---|---|
Finerenone N = 2,833 | Placebo N = 2,841 | Finerenone N = 3,686 | Placebo N = 3,666 | Finerenone N = 6,519 | Placebo N = 6,507 | |
All-cause mortalitya | ||||||
All-cause mortality,a n (%) | 219 (7.7) | 244 (8.6) | 333 (9.0) | 370 (10.1) | 552 (8.5) | 614 (9.4) |
n/100 person-years (95% CI) | 2.90 (2.53 to 3.29) | 3.23 (2.84 to 3.65) | 2.68 (2.40 to 2.98) | 3.01 (2.71 to 3.33) | 2.76 (2.54 to 3.00) | 3.10 (2.86 to 3.35) |
HR (95% CI) | 0.90 (0.75 to 1.07) | 0.89 (0.77 to 1.04) | 0.89 (0.79 to > 1.00) | |||
P valueb | 0.2348 | 0.1337 | 0.9468c | |||
Components of all-cause mortality | ||||||
CV death, n (%) | 128 (4.5) | 150 (5.3) | 194 (5.3) | 214 (5.8) | 322 (4.9) | 364 (5.6) |
Incidence rate (person-years) (95% CI) | 1.69 (1.41 to 2.00) | 1.99 (1.68 to 2.32) | 1.56 (1.35 to 1.79) | 1.74 (1.52 to 1.98) | 1.61 (1.44 to 1.79) | 1.84 (1.65 to 2.03) |
HR (95% CI) | 0.86 (0.68 to 1.08) | 0.90 (0.74 to 1.09) | 0.88 (0.76 to 1.02) | |||
P valueb | 0.1927 | 0.2742 | 0.0922 | |||
Renal death, n (%) | 2 (< 0.1) | 2 (< 0.1) | 0 | 2 (< 0.1) | 2 (< 0.1) | 4 (< 0.1) |
Fatal, non-CV or nonrenal, n (%) | 89 (3.1) | 92 (3.2) | 139 (3.8) | 154 (4.2) | 228 (3.5) | 246 (3.8) |
Incidence rate (person-years) (95% CI) | 1.18 (0.95 to 1.43) | 1.22 (0.98 to 1.48) | 1.12 (0.94 to 1.31) | 1.25 (1.06 to 1.46) | 1.14 (1.00 to 1.29) | 1.24 (1.09 to 1.40) |
HR (95% CI) | 0.96 (0.72 to 1.28) | 0.90 (0.71 to 1.13) | 0.92 (0.77 to 1.10) | |||
P valueb | 0.7751 | 0.3592 | 0.7926c | |||
CI = confidence interval; CV = cardiovascular; FAS = full analysis set; HR = hazard ratio.
aEvents were adjudicated by an independent adjudication committee and considered from randomization until the end-of-study visit. For composite outcomes and each component, the first event after randomization is considered. Subsequent events of the same type are not shown. The incidence rate is estimated as the number of patients with events divided by the cumulative at-risk time in the reference population, where a patient was no longer at risk once an incident event occurred.
bTwo-sided P value from log-rank test, stratified. Not adjusted for multiplicity.
cInteraction P value displays the study treatment interaction based on a stratified model including study, treatment, and study treatment as covariates and removing study as a stratification factor.
Source: FIDELIO Clinical Study Report;16 FIGARO Clinical Study Report;17 and FIDELITY pooled analysis.18
All-Cause Hospitalization
All-cause hospitalization was assessed throughout the studies up to the day of withdrawal from the study, death, or the end-of-study visit. Incidence of all-cause hospitalization was similar between both groups in both trials, with 2,836 patients (43.5%) and 2,926 patients (45.0%) hospitalized for any cause in the finerenone and placebo groups, respectively. More hospitalizations were noncardiovascular related (35%) than cardiovascular related (19%). Comparing the finerenone group with the placebo group, the HR was 0.95 (95% CI, 0.88 to 1.02) in FIDELIO and 0.97 (95% CI, 0.90 to 1.04) in FIGARO. While cardiovascular hospitalizations overall were comparable between both groups in both trials, the risk of hospitalization for heart failure was lower in the finerenone group than in the placebo group in the FIGARO trial, with an HR of 0.71 (95% CI, 0.56 to 0.90). The incidence of other hospitalizations and all-cause hospitalization results are presented in Table 22.
Table 22: All-Cause Hospitalization (FAS)
Outcome | FIDELIO | FIGARO | FIDELITY pooled analysis | |||||
|---|---|---|---|---|---|---|---|---|
Finerenone N = 2,833 | Placebo N = 2,841 | Finerenone N = 3,686 | Placebo N = 3,666 | Finerenone N = 6,519 | Placebo N = 6,507 | |||
All-cause hospitalization,a n (%) | 1,263 (44.6) | 1,321 (46.5) | 1,573 (42.7) | 1,605 (43.8) | 2,836 (43.5) | 2,926 (45.0) | ||
n/100 person-years (95% CI) | 22.56 (21.3 to 23.8) | 23.87 (22.6 to 25.2) | 16.91 (16.09 to 17.76) | 17.52 (16.68 to 18.39) | 19.04 (18.34 to 19.74) | 19.91 (19.20 to 20.64) | ||
HR (95% CI) | 0.95 (0.88 to 1.02) | 0.97 (0.90 to 1.04) | 0.96 (0.91 to 1.01) | |||||
P value | 0.1623b | 0.3558b | 0.5848c | |||||
Components of all-cause hospitalization | ||||||||
CV hospitalization, n (%) | 519 (18.3) | 561 (19.7) | 689 (18.7) | 718 (19.6) | 1,208 (18.5) | 1,279 (19.7) | ||
n/100 person-years (95% CI) | 7.63 (6.99 to 8.30) | 8.33 (7.66 to 9.03) | 6.15 (5.70 to 6.62) | 6.52 (6.05 to 7.01) | 6.71 (6.34 to 7.09) | 7.21 (6.82 to 7.61) | ||
HR (95% CI) | 0.92 (0.81 to 1.03) | 0.94 (0.84 to 1.04) | 0.93 (0.86 to > 1.00) | |||||
P value | 0.1617b | 0.2290b | 0.7036c | |||||
Hospitalization for heart failure, n (%) | 139 (4.9) | 162 (5.7) | 117 (3.2) | 163 (4.4) | 256 (3.9) | 325 (5.0) | ||
n/100 person-years (95% CI) | 1.89 (1.59 to 2.21) | 2.21 (1.89 to 2.57) | 0.96 (0.80 to 1.14) | 1.36 (1.16 to 1.57) | 1.31 (1.15 to 1.48) | 1.68 (1.50 to 1.87) | ||
HR (95% CI) | 0.86 (0.68 to 1.08) | 0.71 (0.56 to 0.90) | 0.78 (0.66 to 0.92) | |||||
P value | 0.1821b | 0.0043b | 0.2629c | |||||
Other hospitalization, n (%) | 1,026 (36.2) | 1,059 (37.3) | 1,246 (33.8) | 1,242 (33.9) | 2,272 (34.9) | 2,301 (35.4) | ||
CI = confidence interval; CV = cardiovascular; FAS = full analysis set; HR = hazard ratio.
aEvents were adjudicated by an independent adjudication committee and considered from randomization until the end-of-study visit. For composite outcomes and each component, the first event after randomization is considered. Subsequent events of the same type are not shown. The incidence rate is estimated as the number of patients with events divided by the cumulative at-risk time in the reference population, where a patient was no longer at risk once an incident event occurred.
bTwo-sided P value from log-rank test, stratified. Not adjusted for multiplicity.
cInteraction P value displays the study treatment interaction based on a stratified model including study, treatment, and study treatment as covariates and removing study as a stratification factor.
Source: FIDELIO Clinical Study Report;16 FIGARO Clinical Study Report;17 FIDELITY pooled analysis.18
Health-Related Quality of Life
Kidney Disease Quality of Life Survey
At baseline, mean KDQOL-36 summary scores in all domains were comparable between treatment groups in each trial, and between both trials, except for the “burden of kidney disease” domain, where patients in the FIGARO group scored higher than those in the FIDELIO group. The quality of life decreased over time in all patients, consistently in all domains, assessed until month 36 in FIDELIO and month 48 in FIGARO. The physical component summary showed a sustained difference in favour of finerenone in FIDELIO at month 12 (LS mean difference = ███ ████ ███ ███ ██ ███) and month 24 (LS mean difference = ███ ████ ███ ███ ██ ███, and in FIGARO at month 36 (LS mean difference = ███ ████ ███ ███ ██ ███. Detailed results are presented in Table 27 in Appendix 3.
EQ-5D-5L Visual Analogue Scale
At baseline, mean EQ-5D-5L visual analogue scale summary scores were comparable between treatment groups in each trial, and between both trials. Quality of life decreased over time in all patients; however, the decrease appears to be more rapid in FIDELIO than in FIGARO. Detailed results are presented in Table 28 in Appendix 3.
Harms
Only those harms identified in the review protocol are reported in the following. Refer to Table 23 for detailed harms data. Results from the FIDELITY pooled analysis are reported.
Adverse Events
A total of 5,602 patients (86.1%) in the finerenone group and 5,607 patients (86.4%) in the placebo group experienced at least 1 AE. The most common AE in the finerenone group was hyperkalemia (14% versus 6.9% in the placebo group) and the most common AEs in the placebo group were hypertension (9% versus 6.4% in the finerenone group) and peripheral edema (9% versus 5.9% in the finerenone group).
Serious AEs
A total of 2,060 patients (31.6%) in the finerenone group and 2,186 patients (33.7%) in the placebo group experienced at least 1 SAE. The most commonly reported SAE was pneumonia (2.2% in the finerenone group versus 3.3% in the placebo group).
Withdrawals due to AEs
A total of 414 patients (6.4%) in the finerenone group and 351 patients (5.4%) in the placebo group stopped treatment due to AEs.
Mortality
There was a total of 110 deaths (1.7% of patients) and 151 deaths (2.3% of patients) due to treatment-emergent AEs in the finerenone and placebo groups, respectively.
Notable Harms
More patients reported hypotension in the finerenone group than in the placebo group (4.3% versus 2.7%). The number of patients who experienced atrial flutter and atrial fibrillation was less than 1% in each treatment group and comparable between groups. The number of patients who experienced hospitalization due to hyperkalemia was higher in the finerenone group than in the placebo group (0.9% versus 0.2%).
Table 23: Summary of Harms (Safety Analysis Set)
Harms | FIDELITY pooled analysis | |
|---|---|---|
Finerenone N = 6,510 | Placebo N = 6,489 | |
Patients with ≥ 1 TEAE | ||
n (%) | 5,602 (86.1) | 5,607 (86.4) |
Most common events,a n (%) | ||
Hyperkalemia | 912 (14.0) | 448 (6.9) |
Nasopharyngitis | 559 (8.6) | 577 (8.9) |
Arthralgia | 496 (7.6) | 459 (7.1) |
Back pain | 436 (6.7) | 428 (6.6) |
Urinary tract infection | 431 (6.6) | 432 (6.7) |
Diarrhea | 423 (6.5) | 411 (6.3) |
Anemia | 425 (6.5) | 397 (6.1) |
Hypertension | 419 (6.4) | 581 (9.0) |
Upper respiratory tract infection | 407 (6.3) | 394 (6.1) |
Peripheral edema | 384 (5.9) | 584 (9.0) |
GFR decreased | 348 (5.3) | 274 (4.2) |
Hypoglycemia | 340 (5.2) | 375 (5.8) |
Dizziness | 341 (5.2) | 322 (5.0) |
Bronchitis | 328 (5.0) | 332 (5.1) |
Constipation | 317 (4.9) | 334 (5.1) |
Pneumonia | 271 (4.2) | 387 (6.0) |
Patients with ≥ 1 SAE | ||
n (%) | 2,060 (31.6) | 2,186 (33.7) |
Most common events,b n (%) | ||
Pneumonia | 143 (2.2) | 216 (3.3) |
Patients who stopped treatment due to adverse events | ||
n (%) | 414 (6.4) | 351 (5.4) |
Deathsc | ||
n (%) | 110 (1.7) | 151 (2.3) |
Notable harms | ||
Hypotension, n (%) | 282 (4.3) | 177 (2.7) |
Hyperkalemia leading to hospitalization, n (%) | 61 (0.9) | 10 (0.2) |
Atrial fibrillation, n (%) | 49 (0.8) | 47 (0.7) |
Atrial flutter, n (%) | 13 (0.2) | 8 (0.1) |
GFR = glomerular filtration rate; SAE = serious adverse event; TEAE = treatment-emergent adverse event.
aFrequency greater than 5% in either group.
bFrequency greater than 2% in either group.
cThe number of patients who died as a result of a treatment-emergent event.
Source: FIDELITY pooled analysis.18
Critical Appraisal
Internal Validity
The included pivotal studies FIDELIO and FIGARO were phase III, randomized, double-blind, placebo-controlled studies of finerenone in adult patients with CKD and T2D. Identical finerenone and placebo tablets were designed to maintain blinding with packaging and labelling; however, it is unclear if unblinding could have occurred due to a difference in the taste of the tablets or due to additional investigations following SAEs (such as hyperkalemia). Randomization codes were broken for ██ patients by the sponsor’s pharmacovigilance department ██████ or by the investigator due to a safety concern ██████ but all patients were included in the FAS and safety analysis set. Randomization was stratified by region, eGFR category at screening, type of albuminuria at screening, and — only in FIGARO — history of cardiovascular disease. Key baseline demographic and disease characteristics, and past history of medication used, appear to be balanced between the finerenone and placebo groups in both trials. Dietary changes, such as reduced sodium intake, are important in the management of patients with CKD and T2D;10 however, there is no mention of diet management in the trials, how closely dietary changes were followed by patients in both trials, and whether there were any differences in diet between patients in the 2 treatment groups.
There were important protocol deviations, balanced between treatment groups, reported in ███ ███ ████% of patients in FIDELIO and FIGARO, respectively. In FIDELIO, more procedure deviations were reported in the finerenone group than in the placebo group. In FIGARO, approximately 10% of patients were assigned to the incorrect stratification group. Due to study timelines, more protocol deviations associated with the COVID-19 pandemic were reported in FIGARO than in FIDELIO; however, deviations were balanced between treatment groups. In FIGARO, supportive analyses were conducted to account for pandemic-related disruptions, and deviations associated with the COVID-19 pandemic had no notable effect on the treatment effect of finerenone. For ███ ██████ ███ ███ ██████ patients in FIDELIO and FIGARO, respectively, the first drug intake was not on the day of randomization; however, for the majority, the difference was 1 day, and no significant impact on the comparative clinical efficacy of finerenone versus placebo would be expected.
Almost all the patients completed the studies; however, a high proportion of patients discontinued treatment in both studies (approximately 28%). This may have biased the studies, although the direction of bias is unknown as the timing of discontinuation is not reported in the clinical study reports.
Maintaining and improving quality of life overall was rated as an important outcome by patients, yet interpretation of the results for the HRQoL instruments (i.e., the ability to assess trends over time and to make comparisons across treatment groups) is limited by the significant decline in patients available to provide assessment over time. The CADTH review team conducted an assessment on the validity of outcome measures and did not find evidence of validity or the MID of the KDQOL-36 or EQ-5D-5L in patients with CKD and T2D. The clinical experts consulted by CADTH pointed out that HRQoL instruments were not used routinely in clinical practice and that more weight is placed on clinical outcomes, which, if improved, would likely improve HRQoL.
In the prespecified FIDELITY pooled analysis, data from both trials were combined. Based on the individual study’s inclusion criteria, patients in FIDELIO had a worse diagnosis of CKD at baseline than those in FIGARO. However, the clinical experts agreed that the pooling of patient data from both trials was appropriate as they represent the wide range of patients with CKD and T2D seen in clinical practice. In addition, the mean treatment duration was longer in FIGARO (approximately 35 months) than in FIDELIO (approximately 27 months). Other than those differences, the study design of both trials was completely identical, and pooling is considered appropriate.
External Validity
According to the clinical experts CADTH consulted for this review, the FIDELIO and FIGARO study population is considered reflective of the requested reimbursement population. The following considerations are of importance regarding the external validity of the study.
Population: According to the clinical experts consulted by CADTH for this review, the demographic and disease characteristics of both study populations were generally reflective of patients with CKD and T2D living in Canada. They agreed that there was an overrepresentation of male patients (70% male to 30% female), and they noted there should be a more proportionate representation of patients, given potential differences in treatment efficacy and safety. The mean age of patients was 65 years old, which they agreed was consistent with the population of patients who develop CKD due to T2D in clinical practice. Most participants were white; however, the clinical experts did not think this would limit generalizability to patients in Canadian clinical practice. The product monograph indicates that patients with an eGFR less than or equal to 25 mL/min/1.73 m2 should not start finerenone; however, 2.4% of patients in FIDELIO reported a baseline eGFR less than or equal to 25 mL/min/1.73 m2 (potentially due to deterioration between screening and randomization). Only patients with persistent high or very high albuminuria were included in the trials; however, approximately 3% of the patients in the FIGARO trial had normal albuminuria levels at baseline. While the trials were under way, the SOC for patients with CKD and T2D evolved to include SGLT2 inhibitor. Therefore, only 6.7% of patients in both trials (n = 877) were on an SGLT2 inhibitor at baseline, and patients were not stratified by SGLT2 inhibitor use; however, use at baseline was balanced between the 2 treatment groups in both trials. The clinical experts agreed that future trials would ideally include a larger population of patients treated with SGLT2 inhibitor. In addition, the proportion of patients using GLP-1 agonists with and without SGLT2 inhibitor at baseline was not balanced (18.5% versus 6.4%). This may have confounded the subgroup findings as GLP-1 agonists may also improve cardiorenal outcomes in patients with CKD and T2D.19,20
Appropriateness of comparator: The clinical experts consulted by CADTH agreed that placebo plus SOC was an appropriate comparator in Canadian clinical practice for patients with CKD and T2D. The clinical experts agreed with the sponsor’s definition of SOC as including an ACE inhibitor or ARB, and ideally an SGLT2 inhibitor, which is still not widely accessible to patients with CKD and T2D living in Canada. The clinical experts pointed out that a combination therapy with the 2 drugs together makes physiologic sense as SGLT2 inhibitors are linked to reductions in the risk of hyperkalemic episodes (serum potassium ≥ 6.0 mmol/L), and finerenone has hyperkalemia as a side effect. There is, however, limited evidence on the positioning of finerenone in relation to SGLT2 inhibitors, and the evidence available for the addition of finerenone to ACE inhibitor or ARB, and an SGLT2 inhibitor, is limited. It is uncertain if results from the pivotal studies would be generalizable for patients who would receive finerenone as an add on to ACE inhibitor or ARB, and an SGLT2 inhibitor. A non-sponsor-submitted reimbursement review assessing the use of SGLT2 inhibitor in patients with CKD and T2D is currently ongoing. A phase II RCT that will compare finerenone plus placebo, SGLT2 inhibitors plus placebo, and finerenone plus SGLT2 inhibitors (CONFIDENCE trial)21 will begin in 2022, and results may provide more insight into this comparison and the place of finerenone in therapy.
Relevance of end points: The clinical experts consulted by CADTH and clinician groups providing input agreed that reducing progression of CKD to ESRD is the most meaningful end point in the treatment of patients with CKD and T2D, since ESRD signifies kidney failure and the need for dialysis or renal transplant. The clinical experts agreed that the most important surrogate marker is reduction in albuminuria and stability of eGFR. The clinician groups also added improved symptoms of or prevention of heart failure and reduced emergency department visits or hospitalizations as important outcomes in clinical practice. The trials included 2 composite renal outcomes that differed in 1 component: sustained decrease in eGFR of 40% or 57% from baseline. The clinical experts mentioned that both end points were clinically meaningful, as any significant decline in eGFR indicates the patient is likely to develop kidney failure. Both studies were only powered for their respective primary composite outcomes and not for the components of the primary outcome; thus, there is some uncertainty about the impact of finerenone on each of the components of the composite outcomes. In the FIDELIO trial, the statistically significant improvement in the composite primary renal outcome was only reproduced for a sustained decrease greater than or equal to 40% in eGFR from baseline. In the FIGARO trial, the statistically significant improvement in the composite primary cardiovascular outcome was only reproduced for hospitalization for heart failure. It is, therefore, not possible to conclude that the treatment has a clinically relevant effect on the composite end points as a whole. Moreover, the sponsor defined ESRD as the initiation of chronic dialysis for at least 90 days or renal transplant but only provided the number of patients who experienced each individual event; therefore, it is not possible to conclude the potential risk of dialysis and renal transplant separately.
Setting: This study was a multinational, multicentre trial. The study population was drawn from a wide variety of sites across the globe, with 13.3% of patients in the US and 2.2% in Canada. The clinical experts indicated that there is no concern in generalizing the findings from the pivotal study to the Canadian clinical setting due to the use of homogenized global management guidelines for CKD with T2D.
Indirect Evidence
Objectives and Methods for the Summary of Indirect Evidence
The objective of this section is to critically appraise available indirect evidence comparing finerenone to relevant comparators for the treatment of diabetic kidney disease. SGLT2 inhibitors are currently part of SOC for patients with diabetic kidney disease; however, only 6.7% of patients (877 out of 13,026) in the FIDELIO and FIGARO trials were concurrently taking SGLT2 inhibitors. Therefore, the focus of this section is on ITCs comparing finerenone and SGLT2 inhibitors.
A focused literature search for ITCs dealing with diabetes and CKD was run in MEDLINE All (1946–) on June 15, 2022. No search limits were applied. In total, 186 articles were retrieved, 10 were potentially relevant, and only 1 published NMA by Zhao et al. (2022)22 was included. This published NMA is summarized in the following.
Methods
Objectives
The objective of this ITC was to assess the relative efficacy of SGLT2 inhibitors versus finerenone on cardiorenal end points in patients with T2D and CKD.
Study Selection Methods
The searches were conducted in March 2021 to capture cardiovascular or renal outcomes in RCTs that compared any SGLT2 inhibitor or finerenone with placebo in patients with CKD and T2D. Two reviewers screened abstracts and full-text articles, conducted data extraction, and assessed the risk of bias of each study. Full details on the study selection methods are presented in Table 24.
Table 24: Study Selection Criteria and Methods
Parameter | Zhao et al. (2022) |
|---|---|
Population | Patients with T2D and CKD (defined as eGFR < 60 mL/min/1.73 m2 and/or urinary albumin-creatinine ratio > 300 mg/g) |
Intervention | Any SGLT2 inhibitor or finerenone |
Comparator | Placebo |
Outcome | Kidney function progression,a hospitalization for heart failure, major adverse cardiovascular events,b nonfatal MI, nonfatal stroke, cardiovascular death, and all-cause death |
Study design | Randomized controlled trials |
Databases searched | Embase, PubMed, and Cochrane Central Register of Controlled Trials (CENTRAL) to identify related articles published before March 26, 2021 |
Selection and data extraction process | Two authors independently performed study selection and data extraction |
Quality assessment | Two authors independently performed risk-of-bias assessment according to the Cochrane risk-of-bias assessment tool (Higgins et al. [2011]). When they encountered inconsistencies, they asked for the arbitration of a third author. |
CKD = chronic kidney disease; eGFR = estimated glomerular filtration rate; MI = myocardial infarction; SGLT2 = sodium-glucose cotransporter-2; T2D = type 2 diabetes.
aKidney function progression was defined as a composite of a sustained decrease of at least 40% in the eGFR from the baseline or a doubling of the serum creatinine level, kidney failure (a composite of end-stage kidney disease or sustained decrease in eGFR to < 15 mL/min/1.73 m2), or renal death. If this composite outcome was not available, another composite renal outcome was used instead.
bA major adverse cardiovascular event was defined as a composite of cardiovascular disease, nonfatal MI, or nonfatal stroke. If data on nonfatal MI and nonfatal stroke were not available, data on total MI and stroke were used instead.
Source: Zhao et al. (2022).22
ITC Analysis Methods
The authors extracted 2 variables from the included study: the number of patients developing events of interest and the total number of patients in the intervention and placebo groups. Treatment effects were presented as risk ratio and 95% CI. The authors first conducted a conventional meta-analysis using the fixed-effects inverse variance method and the random-effects DerSimonian and Laird method (I2 was used to measure statistical heterogeneity, and random effects were reported if I2 was more than 50%). The authors then conducted an NMA using the restricted maximum likelihood method within the frequentist framework using Stata/MP (version 16.0).
Results
Summary of Included Studies
The authors included 14 articles reporting 8 placebo-controlled RCTs comprising 30,661 patients. Seven studies involved an assessment of SGLT2 inhibitor (13,246 patients receiving gliflozin versus 11,741 receiving placebo): EMPA-REG OUTCOME,23,24 CANVAS Program,25,26 CREDENCE,27,28 DECLARE–TIMI 58,29 DAPA-CKD,30 VERTIS CV,31,32 and SCORED.33 One study (the pivotal FIDELIO trial)34,35 assessed finerenone (2,833 patients receiving finerenone versus 2,841 receiving placebo). According to risk-of-bias assessment, there was low risk of bias in all 8 studies.
Major adverse cardiovascular events were defined consistently across the included studies. Kidney function progression, however, was defined differently across the included studies, with composite end points that included ESRD, renal death, and sustained decrease in eGFR that ranged from 40% to 50%. One trial included patients who had initiated renal replacement therapy (EMPA-REG OUTCOME), and 2 trials included patients with kidney transplants (DAPA-CKD and SCORED). One trial (VERTIS CV) did not report a renal composite end point. The authors considered these definitions similar enough to be used in the meta-analysis.
Results
NMA results showed that, compared to finerenone, SGLT2 inhibitors significantly reduced the risk of kidney function progression (HR = 0.78; 95% CI, 0.67 to 0.90) and hospitalization for heart failure (HR = 0.71; 95% CI, 0.55 to 0.92) as shown in Figure 12. No treatment was favoured when finerenone was compared to SGLT2 inhibitors for the outcomes of major adverse cardiovascular events (HR = 0.95; 95% CI, 0.71 to 1.27), nonfatal MI (HR = 0.91; 95% CI, 0.64 to 1.30), nonfatal stroke (HR = 0.70; 95% CI, 0.35 to 1.39), cardiovascular death (HR = 1.00; 95% CI, 0.78 to 1.29), and all-cause death (HR = 0.96; 95% CI, 0.75 to 1.23). No network plot for any outcome had a closed loop, suggesting a lack of direct evidence between finerenone and SGLT inhibitors, so an inconsistency test was not performed.
Figure 12: NMA Treatment Effects for Kidney Function Progression and Hospitalization for Heart Failure
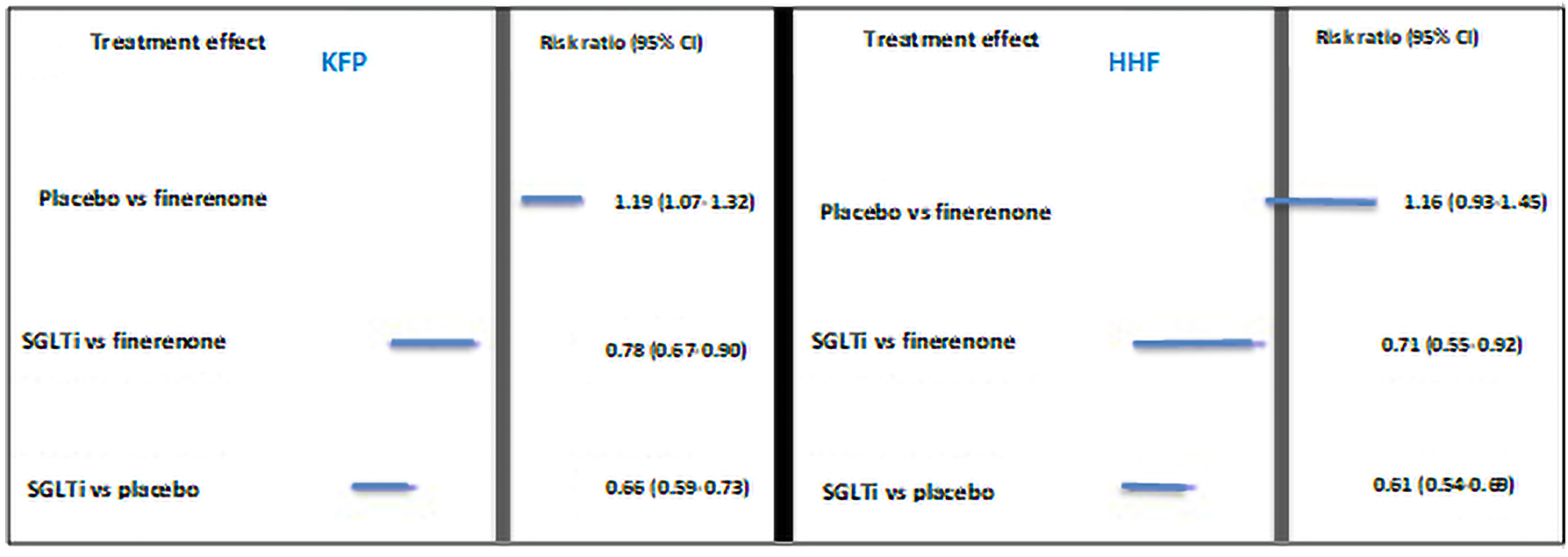
CI = confidence interval; HHF = hospitalization for heart failure; KFP = kidney function progression; NMA = network meta-analysis; SGLTi = sodium-glucose cotransporter inhibitor; vs = versus.
Source: Zhao et al. (2022). Copyright © 2022 Frontiers. Reprinted in accordance with Creative Commons Attribution License CC BY-NC 4.0.22
Critical Appraisal of ITC
This NMA included a limited number of studies with some heterogeneity in the definition of a key renal outcome across the studies. Only 1 study assessed finerenone, while the other 7 assessed an SGLT2 inhibitor, which limited the statistical power of this NMA. The second pivotal RCT on finerenone from this review (FIGARO) was not included in this NMA; its inclusion may have strengthened this analysis. The authors did not explore the baseline demographic characteristics of the patient populations across the trials and reported that “the cardiorenal risk of participants was possibly different among included trials.”22 The durations of the trials were not reported and may have differed between studies. Moreover, the safety outcomes of the treatments were not assessed in this NMA.
The CADTH review team was unable to rigorously assess the methods in this article because insufficient details on the methods were provided (e.g., no details on the retrieved number of records in the systematic review), and there was no discussion on possible adjustments for potential effect modifiers or feasibility assessment. A small proportion of patients in the included FIDELIO trial were using SGLT2 inhibitor at baseline, but no additional analysis including and excluding this subgroup was conducted.
Summary
Indirect evidence from the published NMA evaluated the effectiveness of finerenone compared to SGLT2 inhibitor in the management of patients with CKD and T2D. This analysis suggests that SGLT2 inhibitors are more effective than finerenone at reducing kidney function progression and hospitalization for heart failure events in this population. However, only 1 trial out of the included 8 trials assessed finerenone, which limited the statistical power of this NMA and precluded definitive conclusions being drawn about the comparative effectiveness of finerenone versus SGLT2 inhibitor.
Other Relevant Evidence
No long-term extension studies or additional relevant studies were included in the sponsor’s submission to CADTH.
Discussion
Summary of Available Evidence
The CADTH systematic review included 2 pivotal phase III RCTs (FIDELIO and FIGARO). Both trials are completed double-blind, placebo-controlled, multicentre, superiority studies comparing finerenone to placebo in patients with CKD and T2D. Combined, both trials included a total of 13,026 patients randomized in a 1:1 ratio to receive finerenone (n = 6,519) or placebo (n = 6,489), stratified by region, eGFR at baseline, albuminuria at baseline, and — only in FIGARO — history of cardiovascular disease.
The primary outcome in FIDELIO was a renal composite outcome composed of time to onset of kidney failure, a sustained decrease of eGFR greater than or equal to 40% from baseline over at least 4 weeks, or renal death. The primary outcome in FIGARO was a cardiovascular composite outcome composed of time to first occurrence of the cardiovascular composite end point: cardiovascular death, nonfatal MI, nonfatal stroke, or hospitalization for heart failure. The primary outcome in each trial was a key secondary outcome in the other trial. Other secondary outcomes included time to all-cause mortality, time to all-cause hospitalization, change in UACR from baseline to month 4, and time to first occurrence of a second renal composite end point. Exploratory outcomes of interest included the components of the renal and cardiovascular composite end points, new diagnosis of atrial fibrillation or atrial flutter, time to noncardiovascular and nonrenal death, change in eGFR and UACR from baseline, and change in HRQoL summary scores. Both trials enrolled adult patients with T2D and a diagnosis of CKD with persistent high or very high albuminuria and an eGFR greater than or equal to 25 mL/min/1.73 m2 (the upper eGFR limit was lower in the FIDELIO inclusion criteria than in those of FIGARO). Patients had to be treated with the maximum tolerated dose of an ACE inhibitor or an ARB for at least 4 weeks before the screening visit. The mean age of the patients in both trials was approximately 65 years old, most patients where white (68%) and male (70%), and approximately 6.7% of patients from both trials were treated with SGLT2 inhibitors.
Indirect evidence from 1 published NMA evaluated the effectiveness of finerenone compared to SGLT2 inhibitors in the treatment of CKD and T2D. This analysis suggests that SGLT2 inhibitors are more effective than finerenone at reducing renal failure and hospitalization for heart failure events in this population. However, only 1 trial out of the included 8 trials assessed finerenone, which limited the statistical power of this NMA and precluded definitive conclusions being drawn about the comparative effectiveness of finerenone versus SGLT2 inhibitor.
Interpretation of Results
Efficacy
Input received from both patient groups and clinicians for the review of finerenone indicated that the most important end point in CKD with T2D is reducing progression of CKD to ESRD. Important surrogate markers included reduction of albuminuria and stability of eGFR. In FIDELIO,16 where patients had worse characteristics of CKD at baseline (lower eGFR and higher UACR) and the 40% renal composite outcome was the primary outcome, finerenone reduced the risk of 40% renal composite outcome by 17%. In FIGARO,17 where the cardiovascular composite outcome was the primary outcome, finerenone reduced the risk of the cardiovascular composite outcome by 13%. These effects appeared to be sustained for the duration of the trial. However, the size of the effect on the composite end points is not transferable to the size of the effect on the components, as the trials were not powered for these components. In addition, the statistically significant improvement in the composite primary outcomes was only reproduced for 1 of the disaggregated outcomes in each trial — specifically, a sustained decrease greater than or equal to 40% in eGFR from baseline in the FIDELIO trial and incidence of hospitalization for heart failure in the FIGARO trial.
The clinical experts noted that change in albuminuria has been linked to reduction in incident risk for adverse clinical outcomes of kidney failure,54 cardiovascular events,55 and mortality.56 In both trials, the reduction in UACR from baseline to the end of trial (month 36 in FIDELIO and month 48 in FIGARO) was significantly larger in the finerenone group than in the placebo group, and this between-group difference was considered to be clinically meaningful by the clinical experts.
It is unclear if the benefits of finerenone apply to patients with nonproteinuric diabetic CKD as only 1.8% of the patients in both trials had normal albuminuria levels at baseline and subgroup analysis of baseline albuminuria levels was nonconclusive due to low sample size. However, according to the clinical experts, the management approach and therapeutic targets for this subgroup of patients are similar to those for patients with proteinuric CKD with diabetes.
There was no significant between-group difference in the risk of all-cause mortality and all-cause hospitalization, which the trials were not powered to assess. This lack of difference could be due to the duration of the trials (less than 48 months) or rarity of events (mortality events were less than 10% across all treatment groups in both trials).
The clinical experts consulted by CADTH agreed that finerenone would be an adjunct to SOC therapy that includes ACE inhibitor or ARB, and SGLT2 inhibitor, particularly for patients who cannot tolerate these medications. SGLT2 inhibitor was only added to the management guidelines recently; the trials only included 6.7% of patients who were treated with SGLT2 inhibitor at baseline. Analyses by SGLT2 inhibitor subgroup were not defined before randomization, but use at baseline was balanced between treatment groups in both trials, and there was no significant difference in SGLT2 inhibitor use at baseline across both trials in all primary and secondary outcomes. It is, therefore, uncertain if results from the pivotal studies would be generalizable for patients who would receive finerenone as an add on to ACE inhibitor or ARB, and an SGLT2 inhibitor. A non-sponsor-submitted reimbursement review assessing the use of SGLT2 inhibitor in patients with CKD and T2D is currently ongoing.
The direct comparison of finerenone and SGLT2 inhibitor is limited by the small subpopulation included in the trial. A published NMA was included in this review, comparing finerenone and SGLT2 inhibitor in patients with CKD and T2D, and it concluded that SGLT2 inhibitors are more effective than finerenone at reducing kidney function progression and hospitalization for heart failure events in this population. However, only 1 trial out of the included 8 trials assessed finerenone, which limited the statistical power of this NMA and precluded definitive conclusions being drawn about the comparative effectiveness of finerenone versus SGLT2 inhibitor. A phase II RCT that will compare finerenone plus placebo, SGLT2 inhibitors plus placebo, and finerenone plus SGLT2 inhibitors (CONFIDENCE trial)21 will begin in 2022, and results may provide more insight into this comparison and the place of finerenone in therapy.
Maintaining and improving quality of life overall was rated as an important outcome by patients, yet the interpretation of results for the HRQoL instruments is limited by the decline in patients over time and lack evidence of validity or MID of the instruments in patients with CKD and T2D; hence, the impact of finerenone on HRQoL is uncertain. The clinical experts consulted by CADTH pointed out that HRQoL instruments were not used routinely in clinical practice and that more weight is placed on clinical outcomes, which, if improved, would likely improve HRQoL.
Harms
Approximately 86% of patients in both treatment groups in both trials experienced at least 1 treatment-emergent AE, and the proportion of patients discontinuing study treatment due to AEs is only slightly higher in the finerenone group (6.4%) than in the placebo group (5.4%). SAEs were similar in both groups (31.6% in finerenone and 33.7% in placebo). The incidence of hyperkalemia was 2-fold higher in the finerenone group (14%) than in the placebo group (7%), although hyperkalemia leading to hospitalization was less than 1% in both groups. The clinical experts noted that this hyperkalemia would be clinically manageable with routine monitoring of potassium and temporary or permanent discontinuation of finerenone as needed. Hypotension was more common in the finerenone group (4.3%) than in the placebo group (2.7%), and the clinical experts noted that the effect on blood pressure was minimal in the FIDELITY pooled analysis.52 Atrial flutter and atrial fibrillation were similar in both groups and less than 1%. Peripheral edema was more common in the placebo group (9%) than in the finerenone group (6%); the clinical experts pointed out that its reduction would be especially valued from the cardiology perspective for patients who had also developed heart failure. In the published NMA, the indirect comparison of safety outcomes of finerenone and SGLT2 inhibitor were not assessed.
Conclusions
Two RCTs informed the systematic review of finerenone as an adjunct therapy for the treatment of patients with CKD and T2D. The trials demonstrated that treatment with finerenone was associated with a clinically meaningful reduction in the renal composite outcome and the cardiovascular composite outcome, driven by the outcome components of a sustained decrease in eGFR greater than or equal to 40% or greater than or equal to 57% and incidence of hospitalization for heart failure. The trials also demonstrated that finerenone was associated with a significant reduction in UACR from baseline, which the clinical experts referred to as an important marker for reduced risk of progression of CKD to ESRD. The impact of finerenone on HRQoL is uncertain due to difficulty interpreting results from the HRQoL instruments. All patients in both trials were on a maximum tolerated dose of ACE inhibitor or ARB as SOC, but only a small proportion in both trials were on SGLT2 inhibitor at baseline; hence, available evidence on the efficacy and safety of the addition of finerenone to ACE inhibitor or ARB, and an SGLT2 inhibitor, is limited. No significant difference was reported when comparing patients who were on an SGLT2 inhibitor at baseline with patients who were not. Furthermore, although the included NMA favoured SGLT2 inhibitor over finerenone in improving cardiorenal outcomes, this NMA had several limitations that preclude any definitive conclusion.
The safety profile of finerenone in these trials was consistent with the known safety profile of other nonsteroidal MRAs in terms of hyperkalemia and hypotension. No additional safety signals were identified with finerenone in this study.
References
1.Tonelli M, Wiebe N, Richard J-F, Klarenbach SW, Hemmelgarn BR. Characteristics of adults with type 2 diabetes mellitus by category of chronic kidney disease and presence of cardiovascular disease in Alberta Canada: a cross-sectional study. Can J Kidney Health Dis. 2019;6:2054358119854113. PubMed
2.LeBlanc AG, Gao YJ, McRae L, Pelletier C. At-a-glance-twenty years of diabetes surveillance using the Canadian Chronic Disease Surveillance System. Health Promot Chronic Dis Prev Can. 2019;39(11):306. PubMed
3.Diabetes Mellitus (types combined), excluding gestational diabetes, crude prevalence, percent, age 1 year and older, Canada. Canadian Chronic Disease Surveillance System (CCDSS). Ottawa (ON): Public Health Agency of Canada (PHAC); 2019: https://health-infobase.canada.ca/CCDSS/data-tool/. Accessed 2022 Aug 3.
4.Mottl AK. Diabetic kidney disease: pathogenesis and epidemiology. In: Post TW, ed. UpToDate. Waltham (MA): UpToDate; 2022: https://www.uptodate.com. Accessed 2022 Aug 3.
5.McFarlane P, Cherney D, Gilbert RE, Senior P. Chronic kidney disease in diabetes. Can J Diabetes. 2018;42:S201-S209. PubMed
6.Afkarian M, Sachs MC, Kestenbaum B, et al. Kidney disease and increased mortality risk in type 2 diabetes. J Am Soc Nephrol. 2013;24(2):302-308. PubMed
7.Grandy S, Fox KM, Shield Study Group. Change in health status (EQ-5D) over 5 years among individuals with and without type 2 diabetes mellitus in the SHIELD longitudinal study. Health Qual Life Outcomes. 2012;10(1):99. PubMed
8.Pagels AA, Söderkvist BK, Medin C, Hylander B, Heiwe S. Health-related quality of life in different stages of chronic kidney disease and at initiation of dialysis treatment. Health Qual Life Outcomes. 2012;10(1):1-11. PubMed
9.KDIGO 2020 Clinical practice guideline for diabetes management in chronic kidney disease. Kidney Int. 2020;98(4S):S1-S115. PubMed
10.Perkovic V, Badve SV, Bakris G. Treatment of diabetic kidney disease. In: Post TW, ed. UpToDate. Waltham (MA): UpToDate; 2022: https://www.uptodate.com. Accessed 2022 Aug 3.
11.Center for Drug Evaluation Research. Integrated review(s). Kerendia (Finerenone) administration. Company: Bayer Healthcare Pharmaceuticals. Application No.: 215341. Approval date: 07/09/2021 (FDA approval package). Silver Spring (MD): U.S. Food and Drug Administration (FDA); 2021 Jul 9: https://www.accessdata.fda.gov/drugsatfda_docs/nda/2021/215341Orig1s000IntegratedR.pdf. Accessed 2022 Jul 12.
12.American Diabetes Association Professional Practice Committee, Draznin B, Aroda VR, et al. 11. Chronic kidney disease and risk management: standards of medical care in diabetes-2022. Diabetes Care. 2022;45(Suppl 1):S175-S184. PubMed
13.Kerendia: 10 mg and 20 mg finerenone, oral tablets [product monograph]. Mississauga (ON): Bayer Inc.; 2022.
14.Neuen BL, Jardine MJ. SGLT2 inhibitors and finerenone: one or the other or both? Nephrol Dial Transplant. 2022;37(7):1209-1211. PubMed
15.American Diabetes Association. Standards of medical care in diabetes-2020 abridged for primary care providers. Clin Diabetes. 2020;38(1):10-38. PubMed
16.Clinical Study Report: PH-39746. A randomized, double-blind, placebo-controlled, parallel-group, multicenter, event-driven phase III study to investigate the efficacy and safety of finerenone, in addition to standard of care, on the progression of kidney disease in subjects with type 2 diabetes mellitus and the clinical diagnosis of diabetic kidney disease. [internal sponsor's report]. Whippany (NJ): Bayer Healthcare Pharmaceuticals Inc.; 2020 Sep 22.
17.Clinical Study Report: PH-39747.A randomized, double-blind, placebo-controlled, parallel-group, multicenter, eventdriven phase III study to investigate the efficacy and safety of finerenone on the reduction of cardiovascular morbidity and mortality in subjects with type 2 diabetes mellitus and the clinical diagnosis of diabetic kidney disease in addition to standard of care. [internal sponsor's report]. Whippany (NJ): Bayer Healthcare Pharmaceuticals Inc.; 2021 Aug 20.
18.Integrated analysis statistical report: PH-42134. Integrated analysis of FIDELIO-DKD and FIGARO-DKD [internal sponsor's report]. Wuppertal (DE): Bayer AG; 2021 Jul 30.
19.Rossing P, Filippatos G, Agarwal R, et al. Finerenone in predominantly advanced CKD and type 2 diabetes with or without sodium-glucose cotransporter-2 inhibitor therapy. Kidney Int Rep. 2022;7(1):36-45. PubMed
20.Górriz JL, Romera I, Cobo A, O'Brien PD, Merino-Torres JF. Glucagon-like peptide-1 receptor agonist use in people living with type 2 diabetes mellitus and chronic kidney disease: a narrative review of the key evidence with practical considerations. Diabetes Ther. 2022;13(3):389-421. PubMed
21.Green JB, Mottl AK, Bakris G, et al. Design of the COmbinatioN effect of FInerenone anD EmpaglifloziN in participants with chronic kidney disease and type 2 diabetes using an UACR Endpoint study (CONFIDENCE). Nephrol Dial Transplant. 2022. PubMed
22.Zhao LM, Zhan ZL, Ning J, Qiu M. Network meta-analysis on the effects of SGLT2 inhibitors versus finerenone on cardiorenal outcomes in patients with type 2 diabetes and chronic kidney disease. Front Pharmacol. 2022;12:751496. PubMed
23.Zinman B, Lachin JM, Inzucchi SE. Empagliflozin, cardiovascular outcomes, and mortality in type 2 diabetes. N Engl J Med. 2016;374(11):1094. PubMed
24.Wanner C, Lachin JM, Inzucchi SE, et al. Empagliflozin and clinical outcomes in patients with type 2 diabetes mellitus, established cardiovascular disease, and chronic kidney disease. Circulation. 2018;137(2):119-129. PubMed
25.Neal B, Perkovic V, Mahaffey KW, et al. Canagliflozin and cardiovascular and renal events in type 2 diabetes. N Engl J Med. 2017;377(7):644-657. PubMed
26.Neuen BL, Ohkuma T, Neal B, et al. Cardiovascular and renal outcomes with canagliflozin according to baseline kidney function: data from the CANVAS program. Circulation. 2018;138(15):1537-1550. PubMed
27.Mahaffey KW, Jardine MJ, Bompoint S, et al. Canagliflozin and cardiovascular and renal outcomes in type 2 diabetes mellitus and chronic kidney disease in primary and secondary cardiovascular prevention groups. Circulation. 2019;140(9):739-750. PubMed
28.Perkovic V, Jardine MJ, Neal B, et al. Canagliflozin and renal outcomes in type 2 diabetes and nephropathy. N Engl J Med. 2019;380(24):2295-2306. PubMed
29.Wiviott SD, Raz I, Bonaca MP, et al. Dapagliflozin and cardiovascular outcomes in type 2 diabetes. N Engl J Med. 2019;380(4):347-357. PubMed
30.Cannon CP, Pratley R, Dagogo-Jack S, et al. Cardiovascular outcomes with ertugliflozin in type 2 diabetes. N Engl J Med. 2020;383(15):1425-1435. PubMed
31.Cherney DZI, McGuire DK, Charbonnel B, et al. Gradient of risk and associations with cardiovascular efficacy of ertugliflozin by measures of kidney function observations from VERTIS CV. Circulation. 2021;143(6):602-605. PubMed
32.Wheeler DC, Stefansson BV, Jongs N, et al. Effects of dapagliflozin on major adverse kidney and cardiovascular events in patients with diabetic and non-diabetic chronic kidney disease: a prespecified analysis from the DAPA-CKD trial. Lancet Diabetes Endocrinol. 2021;9(1):22-31. PubMed
33.Bhatt DL, Szarek M, Pitt B, et al. Sotagliflozin in patients with diabetes and chronic kidney disease. N Engl J Med. 2021;384(2):129-139. PubMed
34.Bakris GL, Agarwal R, Anker SD, et al. Effect of finerenone on chronic kidney disease outcomes in type 2 diabetes. N Engl J Med. 2020;383(23):2219-2229. PubMed
35.Filippatos G, Anker SD, Agarwal R, et al. Finerenone and Cardiovascular Outcomes in Patients With Chronic Kidney Disease and Type 2 Diabetes. Circulation. 2021;143(6):540-552. PubMed
36.Palmer SC, Tendal B, Mustafa RA, et al. Sodium-glucose cotransporter protein-2 (SGLT-2) inhibitors and glucagon-like peptide-1 (GLP-1) receptor agonists for type 2 diabetes: systematic review and network meta-analysis of randomised controlled trials. BMJ. 2021;372:m4573. PubMed
37.Drug Reimbursement Review sponsor submission: Kerendia® (finerenone) 10 mg, and 20 mg tablets [internal sponsor's package]. Mississauga (ON): Bayer Inc.; 2022 Jun 3.
38.Australian public assessment report for finerenone. Canberra (AU): Australian Department of Health; 2022: https://www.tga.gov.au/sites/default/files/2022-07/auspar-finerenone-220519.pdf. Accessed 2022 Aug 16.
39.Kerendia: EPAR - Public Assessment Report. Amsterdam (NL): European Medicines Agency; 2021 Dec 16: https://www.ema.europa.eu/en/documents/assessment-report/kerendia-epar-public-assessment-report_en.pdf. Accessed 2022 Aug 16.
40.Finerenone for treating chronic kidney disease in type 2 diabetes. NICE appraisal consultation document. London (UK): National Institute For Health And Care Excellence (NICE); 2022: https://www.nice.org.uk/guidance/gid-ta10820/documents/129. Accessed 2022 Aug 16.
41.Filippatos G, Anker SD, Böhm M, et al. A randomized controlled study of finerenone vs. eplerenone in patients with worsening chronic heart failure and diabetes mellitus and/or chronic kidney disease. Eur Heart J. 2016;37(27):2105-2114. PubMed
42.McGowan J, Sampson M, Salzwedel DM, Cogo E, Foerster V, Lefebvre C. PRESS Peer Review of Electronic Search Strategies: 2015 guideline statement. J Clin Epidemiol. 2016;75:40-46. PubMed
43.Grey matters: a practical tool for searching health-related grey literature. Ottawa (ON): CADTH; 2019: https://www.cadth.ca/grey-matters. Accessed 2022 Jun 30.
44.Agarwal R, Joseph A, Anker SD, et al. Hyperkalemia risk with finerenone: results from the FIDELIO-DKD trial. J Am Soc Nephrol. 2022;33(1):225-237. PubMed
45.Bakris GL, Agarwal R, Anker SD, et al. Design and baseline characteristics of the finerenone in reducing kidney failure and disease progression in diabetic kidney disease trial. Am J Nephrol. 2019;50(5):333-344. PubMed
46.Filippatos G, Pitt B, Agarwal R, et al. Finerenone in patients with chronic kidney disease and type 2 diabetes with and without heart failure: a prespecified subgroup analysis of the FIDELIO-DKD trial. Eur J Heart Fail. 2022;03:03.
47.Filippatos G, Anker SD, Agarwal R, et al. Finerenone reduces risk of incident heart failure in patients with chronic kidney disease and type 2 diabetes: analyses from the FIGARO-DKD trial. Circulation. 2022;145(6):437-447. PubMed
48.Filippatos G, Bakris GL, Pitt B, et al. Finerenone reduces new-onset atrial fibrillation in patients with chronic kidney disease and type 2 diabetes. J Am Coll Cardiol. 2021;78(2):142-152. PubMed
49.Pitt B, Filippatos G, Agarwal R, et al. Cardiovascular events with finerenone in kidney disease and type 2 diabetes. N Engl J Med. 2021;385(24):2252-2263. PubMed
50.Ruilope LM, Agarwal R, Anker SD, et al. Design and baseline characteristics of the finerenone in reducing cardiovascular mortality and morbidity in diabetic kidney disease trial. Am J Nephrol. 2019;50(5):345-356. PubMed
51.Ruilope LM, Pitt B, Anker SD, et al. Kidney outcomes with finerenone: an analysis from the FIGARO-DKD study. Nephrol Dial Transplant. 2022;22:22. PubMed
52.Agarwal R, Filippatos G, Pitt B, et al. Cardiovascular and kidney outcomes with finerenone in patients with type 2 diabetes and chronic kidney disease: the FIDELITY pooled analysis. Eur Heart J. 2021;43(6):474-484. PubMed
53.KDIGO Working Group. Kidney disease: improving global outcomes (KDIGO). KDIGO 2012 clinical practice guideline for the evaluation and management of chronic kidney disease. Kidney Int Suppl. 2013;3(1):1-150.
54.Coresh J, Heerspink HJ, Sang Y, et al. Change in albuminuria and subsequent risk of end-stage kidney disease: an individual participant-level consortium meta-analysis of observational studies. Lancet Diabetes Endocrinol. 2019;7(2):115-127. PubMed
55.Brantsma AH, Bakker SJ, de Zeeuw D, de Jong PE, Gansevoort RT. Extended prognostic value of urinary albumin excretion for cardiovascular events. J Am Soc Nephrol. 2008;19(9):1785-1791. PubMed
56.Schmieder RE, Mann JF, Schumacher H, et al. Changes in albuminuria predict mortality and morbidity in patients with vascular disease. J Am Soc Nephrol. 2011;22(7):1353-1364. PubMed
57.Cohen S, Sternlicht H, Bakris GL. Mineralocorticoid receptor antagonists in the treatment of diabetic kidney disease: their application in the era of SGLT2 inhibitors and GLP-1 receptor agonists. Curr Diab Rep. 2022;22(5):213-218. PubMed
58.Goulooze SC, Heerspink HJL, van Noort M, et al. Dose-exposure-response analysis of the nonsteroidal mineralocorticoid receptor antagonist finerenone on UACR and eGFR: an analysis from FIDELIO-DKD. Clin Pharmacokinet. 2022;61(7):1013-1025. PubMed
59.Goulooze SC, Snelder N, Seelmann A, et al. Finerenone dose-exposure-serum potassium response analysis of FIDELIO-DKD phase III: the role of dosing, titration, and inclusion criteria. Clin Pharmacokinet. 2022;61(3):451-462. PubMed
60.Zhang MZ, Bao W, Zheng QY, Wang YH, Sun LY. Efficacy and Safety of Finerenone in Chronic Kidney Disease: A Systematic Review and Meta-Analysis of Randomized Clinical Trials. Front Pharmacol. 2022;13:819327. PubMed
61.Zuo C, Xu G. Efficacy and safety of mineralocorticoid receptor antagonists with ACEI/ARB treatment for diabetic nephropathy: A meta-analysis. Int J Clin Pract. 2019:e13413. PubMed
Appendix 1: Literature Search Strategy
Note that this appendix has not been copy-edited.
Clinical Literature Search
Overview
Interface: Ovid
Databases:
MEDLINE All (1946–present)
Embase (1974–present)
Note: Subject headings and search fields have been customized for each database. Duplicates between databases were removed in Ovid.
Date of search: June 15, 2022
Alerts: Bi-weekly search updates until project completion
Search filters applied: No filters were applied to limit the retrieval by study type.
Limits: Conference abstracts: excluded
Syntax | Description |
|---|---|
/ | At the end of a phrase, searches the phrase as a subject heading |
MeSH | Medical Subject Heading |
.fs | Floating subheading |
exp | Explode a subject heading |
* | Before a word, indicates that the marked subject heading is a primary topic; or, after a word, a truncation symbol (wildcard) to retrieve plurals or varying endings |
# | Truncation symbol for one character |
? | Truncation symbol for one or no characters only |
adj# | Requires terms to be adjacent to each other within # number of words (in any order) |
.ti | Title |
.ot | Original title |
.ab | Abstract |
.hw | Heading word; usually includes subject headings and controlled vocabulary |
.kf | Keyword heading word |
.dq | Candidate term word (Embase) |
.pt | Publication type |
.mp | Mapped term |
.rn | Registry number |
.nm | Name of substance word (MEDLINE) |
.yr | Publication year |
.jw | Journal title word (MEDLINE) |
.jx | Journal title word (Embase) |
freq = # | Requires terms to occur # number of times in the specified fields |
medall | Ovid database code: MEDLINE All, 1946 to present, updated daily |
oemezd | Ovid database code; Embase, 1974 to present, updated daily |
cctr | Ovid database code; Cochrane Central Register of Controlled Trials |
Multidatabase Strategy
(finerenone* or kerendia* or BAY94-8862 or BAY-94-8862 or BAY948862 or BAY-948862 or DE2O63YV8R).ti,ab,kf,ot,hw,rn,nm.
1 use medall
*finerenone/
(finerenone* or kerendia* or BAY94-8862 or BAY-94-8862 or BAY948862 or BAY-948862).ti,ab,kf,dq.
3 or 4
5 use oemezd
(conference abstract or conference review).pt.
6 not 7
2 or 8
remove duplicates from 9
Clinical Trials Registries
ClinicalTrials.gov
Produced by the US National Library of Medicine. Targeted search used to capture registered clinical trials.
[Search terms: finerenone (Kerendia) AND chronic kidney disease (CKD)]
WHO ICTRP
International Clinical Trials Registry Platform, produced by the WHO. Targeted search used to capture registered clinical trials.
[Search terms: finerenone (Kerendia) AND chronic kidney disease (CKD)]
Health Canada’s Clinical Trials Database
Produced by Health Canada. Targeted search used to capture registered clinical trials.
[Search terms: finerenone (Kerendia) AND chronic kidney disease (CKD)]
EU Clinical Trials Register
European Union Clinical Trials Register, produced by the European Union. Targeted search used to capture registered clinical trials.
[Search terms: finerenone (Kerendia) AND chronic kidney disease (CKD)]
Grey Literature
Search dates: June 10 to 14, 2022
Keywords: (finerenone OR Kerendia) AND (chronic kidney disease AND diabetes)
Limits: None
Updated: Search updated before the completion of stakeholder feedback period
Relevant websites from the following sections of the CADTH grey literature checklist Grey Matters: A Practical Tool for Searching Health-Related Grey Literature were searched:
Health Technology Assessment Agencies
Health Economics
Clinical Practice Guidelines
Drug and Device Regulatory Approvals
Advisories and Warnings
Drug Class Reviews
Clinical Trials Registries
Databases (free)
Health Statistics
Internet Search
Open Access Journals
Appendix 2: Excluded Studies
Note that this appendix has not been copy-edited.
Reference | Reason for exclusion |
|---|---|
Cohen S, Sternlicht H, Bakris GL. Mineralocorticoid receptor antagonists in the treatment of diabetic kidney disease: their application in the era of SGLT2 inhibitors and GLP-1 receptor agonists. Curr Diab Rep. 2022 05;22(5):213-218.57 | Review article |
Goulooze SC, Heerspink HJL, van Noort M, et al. Dose-exposure-response analysis of the nonsteroidal mineralocorticoid receptor antagonist finerenone on UACR and eGFR: an analysis from FIDELIO-DKD. Clin Pharmacokinet. 2022 Jul;61(7):1013-1025.58 | Pharmacokinetic pharmacodynamic analysis |
Goulooze SC, Snelder N, Seelmann A, et al. Finerenone dose-exposure-serum potassium response analysis of FIDELIO-DKD phase III: the role of dosing, titration, and inclusion criteria. Clin Pharmacokinet. 2022 03;61(3):451-462.59 | Pharmacokinetic pharmacodynamic analysis |
Zhang MZ, Bao W, Zheng QY, Wang YH, Sun LY. Efficacy and safety of finerenone in chronic kidney disease: a systematic review and meta-analysis of randomized clinical trials. Front Pharmacol. 2022;13:819327.60 | Systematic Review |
Zuo C, Xu G. Efficacy and safety of mineralocorticoid receptor antagonists with ACEI/ARB treatment for diabetic nephropathy: a meta-analysis. Int J Clin Pract. 2019 Aug 29:e13413.61 | Meta-analysis |
ACE = angiotensin-converting enzyme; ARB = angiotensin receptor blocker; eGFR = estimated glomerular filtration rate; GLP-1 = glucagon-like peptide-1; SGLT2 = sodium-glucose cotransporter-2; UACR = urinary albumin-creatinine ratio.
Appendix 3: Detailed Outcome Data
Note that this appendix has not been copy-edited.
Table 27: Mixed Model Repeated Measures for Changes From Baseline in KDQOL-36 Domain Scores (FAS)
Score | FIDELIO | FIGARO | ||
|---|---|---|---|---|
Finerenone N = 2,833 | Placebo N = 2,841 | Finerenone N = 3,686 | Placebo N = 3,666 | |
Physical component summary | ||||
Baseline score, mean (SD) | ████ ██████ | █████ ██████ | █████ | █████ |
Month 12, n | ████ | ████ | ████ | ████ |
LS mean change from baseline (95% CI) | ███ ████ █ | ███ ████ █ | ███ ████ ████ | ███ ████ █ |
LS mean difference (95% CI) | ████ █████ ██ █████ | ████ ██████ ██ █████ | ||
P value of treatment group comparison | ██████ | ██████ | ||
Month 24, n | ████ | ████ | ████ | ████ |
LS mean change from baseline (95% CI) | ███ ████ █ | ███ ████ ██ | ███ ████ █ | ███ ████ █ |
LS mean difference (95% CI) | ████ █████ ██ █████ | █████ ██████ ██ █████ | ||
P value of treatment group comparison | ██████ | ██████ | ||
Month 36, n | ███ | ███ | ████ | ████ |
LS mean change from baseline (95% CI) | ███ ████ █ | ███ ████ █ | ███ ████ █ | ███ ████ █ |
LS mean difference (95% CI) | ████ ██████ ██ █████ | ████ █████ ██ █████ | ||
P value of treatment group comparison | ██████ | ██████ | ||
Month 48, n | ██ | ███ | ███ | |
LS mean change from baseline (95% CI) | ██ | ███ ███ ██ | ███ ███ █ | |
LS mean difference (95% CI) | ██ | ████ ██████ ██ █████ | ||
P value of treatment group comparison | ██ | ██████ | ||
Mental component summary | ||||
Baseline score, mean (SD) | █████ ██████ | █████ | █████ ██████ | █████ |
Month 12, n | ████ | ████ | ████ | ████ |
LS mean change from baseline (95% CI) | ███ ████ ██ | ███ ████ ██ | ███ ████ ██ | ███ ████ ██ |
LS mean difference (95% CI) | █████ ██████ ██ █████ | ████ ██████ ██ █████ | ||
P value of treatment group comparison | ██████ | ██████ | ||
Month 24, n | ████ | ████ | ████ | ████ |
LS mean change from baseline (95% CI) | ███ ████ ██ | ███ ████ ██ | ███ ████ ██ | ███ ████ ██ |
LS mean difference (95% CI) | █████ ██████ ██ █████ | ████ ██████ ██ █████ | ||
P value of treatment group comparison | ██████ | ██████ | ||
Month 36, n | ███ | ███ | ████ | ████ |
LS mean change from baseline (95% CI) | ███ ████ ██ | ███ ████ ██ | ███ ████ ██ | ███ ████ ██ |
LS mean difference (95% CI) | ████ ██████ ██ █████ | █████ ██████ ██ █████ | ||
P value of treatment group comparison | ██████ | ██████ | ||
Month 48, n | ██ | ███ | ███ | |
LS mean change from baseline (95% CI) | ██ | |||
LS mean difference (95% CI) | ██ | ████ ██████ ██ █████ | ||
P value of treatment group comparison | ██ | ██████ | ||
Burden of kidney disease | ||||
Baseline score, mean (SD) | █████ | █████ | █████ | █████ |
Month 12, n | ████ | ████ | ████ | ████ |
LS mean change from baseline (95% CI) | ██ ████ █ ███ | ██ ████ █ | ██ ████ █ ███ | ██ ████ █ |
LS mean difference (95% CI) | ████ ██████ ██ █████ | ████ ██████ ██ █████ | ||
P value of treatment group comparison | ██████ | ██████ | ||
Month 24, n | ████ | ████ | ████ | ████ |
LS mean change from baseline (95% CI) | ███ ████ █ | ███ ████ █ | ███ ████ █ | ███ ████ █ |
LS mean difference (95% CI) | ████ ██████ ██ █████ | ████ ██████ ██ █████ | ||
P value of treatment group comparison | ██████ | ██████ | ||
Month 36, n | ███ | ███ | ████ | ████ |
LS mean change from baseline (95% CI) | ███ ████ █ | ███ ████ █ | ███ ████ █ | ███ ████ █ |
LS mean difference (95% CI) | ████ ██████ ██ █████ | ████ ██████ ██ █████ | ||
P value of treatment group comparison | ██████ | ██████ | ||
Month 48, n | ██ | ███ | ███ | |
LS mean change from baseline (95% CI) | ██ | ███ ████ █ | ███ ████ █ | |
LS mean difference (95% CI) | ██ | ████ ██████ ██ █████ | ||
P value of treatment group comparison | ██ | ██████ | ||
Symptoms/problems | ||||
Baseline score, mean (SD) | █████ | █████ | █████ | █████ |
Month 12, n | ████ | ████ | ████ | ████ |
LS mean change from baseline (95% CI) | ███ ████ █ | ███ ████ █ | ███ ████ █ | ███ ████ █ |
LS mean difference (95% CI) | ████ ██████ ██ █████ | ████ ██████ ██ █████ | ||
P value of treatment group comparison | ██████ | ██████ | ||
Month 24, n | ████ | ████ | ████ | ████ |
LS mean change from baseline (95% CI) | ███ ████ █ | ███ ████ █ | ███ ████ █ | ███ ████ █ |
LS mean difference (95% CI) | ████ ██████ ██ █████ | ████ ██████ ██ █████ | ||
P value of treatment group comparison | ██████ | ██████ | ||
Month 36, n | ███ | ███ | ████ | ████ |
LS mean change from baseline (95% CI) | ███ ████ █ | ███ ████ █ | ███ ████ █ | ███ ████ █ |
LS mean difference (95% CI) | █████ ██████ ██ █████ | ████ ██████ ██ █████ | ||
P value of treatment group comparison | ██████ | ██████ | ||
Month 48, n | ██ | ███ | ███ | |
LS mean change from baseline (95% CI) | ██ | ████ ████ ██ | ████ ████ ██ | |
LS mean difference (95% CI) | ██ | ████ ██████ ██ █████ | ||
P value of treatment group comparison | ██ | ██████ | ||
Effects of kidney disease | ||||
Baseline score, mean (SD) | █████ | █████ | █████ | █████ |
Month 12, n | ████ | ████ | ████ | ████ |
LS mean change from baseline (95% CI) | ███ ████ █ | ███ ████ █ | ██ ████ ████ | ██ ████ █ |
LS mean difference (95% CI) | ████ ██████ ██ █████ | █████ ██████ ██ █████ | ||
P value of treatment group comparison | ██████ | ██████ | ||
Month 24, n | ████ | ████ | ████ | ████ |
LS mean change from baseline (95% CI) | ███ ████ █ | ███ ████ █ | ███ ████ █ | ███ ████ █ |
LS mean difference (95% CI) | ████ █████ ██ █████ | ████ ██████ ██ █████ | ||
P value of treatment group comparison | ██████ | ██████ | ||
Month 36, n | ███ | ███ | ████ | ████ |
LS mean change from baseline (95% CI) | ███ ████ █ | ███ ████ █ | ███ ████ █ | ███ ████ █ |
LS mean difference (95% CI) | ████ █████ ██ █████ | ████ ██████ ██ █████ | ||
P value of treatment group comparison | ██████ | ██████ | ||
Month 48, n | ██ | ███ | ███ | |
LS mean change from baseline (95% CI) | ██ | ███ ████ █ | ███ ████ █ | |
LS mean difference (95% CI) | ██ | ████ ██████ ██ █████ | ||
P value of treatment group comparison | ██ | ██████ | ||
CI = confidence intervals, eGFR = estimated glomerular filtration rate, FAS = full analysis set, KDQOL = Kidney Disease Quality of Life, LS = Least squares, MMRM = mixed model repeated measures, NA = not applicable.
For the statistical evaluation, a MMRM model was applied with factors treatment group, region, eGFR category at screening, type of albuminuria at screening, time, treatment*time, baseline value and baseline value*time as covariate. Separate unstructured covariance patterns are estimated for each treatment group.
Source: FIDELIO Clinical Study Report16 and FIGARO Clinical Study Report17
Table 28: Mixed Model Repeated Measures for Change From Baseline in EQ-5D Visual Analogue Scale Summary Scores (FAS)
Score | FIDELIO | FIGARO | ||
|---|---|---|---|---|
Finerenone N = 2,833 | Placebo N = 2,841 | Finerenone N = 3,686 | Placebo N = 3,666 | |
Baseline score, mean (SD) | █████ | █████ | █████ | █████ |
Month 12, n | ████ | ████ | ████ | ████ |
LS mean change from baseline (95% CI) | ████ █████ ██ | ████ █████ | ███ █████ ██ | ███ █████ █ |
LS mean difference (95% CI) | ████ █████ ██ █████ | ████ ██████ ██ █████ | ||
P value of treatment group comparison | ██████ | ██████ | ||
Month 24, n | ████ | ████ | ████ | ████ |
LS mean change from baseline (95% CI) | ████ █████ ██ | ████ █████ | ████ █████ ██ | ████ █████ █ |
LS mean difference (95% CI) | ████ ██████ ██ █████ | ████ ██████ ██ █████ | ||
P value of treatment group comparison | ██████ | ██████ | ||
Month 36, n | ███ | ███ | ████ | ████ |
LS mean change from baseline (95% CI) | ████ █████ ██ | ████ █████ | ████ █████ ██ | ████ █████ █ |
LS mean difference (95% CI) | ████ ██████ ██ █████ | ████ ██████ ██ █████ | ||
P value of treatment group comparison | ██████ | ██████ | ||
Month 48, n | ██ | ██ | ███ | ███ |
LS mean change from baseline (95% CI) | ██ | ██ | ████ █████ █ | ████ █████ █ |
LS mean difference (95% CI) | ██ | ████ ██████ ██ █████ | ||
P value of treatment group comparison | ██ | ██████ | ||
CI = confidence interval; FAS = full analysis set; NA = not applicable; LS = least squares; SD = standard deviation.
For the statistical evaluation, a mixed model repeated measures model was applied with factors treatment group, region, eGFR category at screening, type of albuminuria at screening, time, treatment*time, baseline value and baseline value*time as covariate. Separate unstructured covariance patterns are estimated for each treatment group.
Source: FIDELIO Clinical Study Report16 and FIGARO Clinical Study Report.17
Appendix 4: Description and Appraisal of Outcome Measures
Note that this appendix has not been copy-edited.
Aim
To describe the following outcome measures and review their measurement properties (validity, reliability, responsiveness to change, and MID):
KDQOL-36
EQ-5D-5L.
Findings
Table 29: Summary of Outcome Measures and Their Measurement Properties
Outcome measure | Type | Conclusions about measurement properties | MID |
|---|---|---|---|
KDQOL-36 | KDQOL-36 was a 36-item questionnaire used to assess the HRQoL of patients with CKD. The measure consisted of 2 parts: generic and disease-specific. The generic part assessed general health using 12 items which can be further described as the physical and mental component summary. The disease-specific part comprised 3 subscales: (1) burden of kidney disease (4 items), (2) symptoms and problems (12 items), and (3) effects of kidney disease on daily life (8 items). Domain scores were calculated as the sum of the individual, relevant item scores and transformed into a range from 0 to 100, with higher scores indicating a more favourable HRQoL.16,17 | Studies determining the psychometric properties of KDQOL-36 were not identified in the literature in the setting of diabetic CKD. | The MID in the KDQOL-36 was not identified in the literature in the setting of diabetic CKD. |
EQ-5D-5L | EQ-5D-5L comprised (1) a descriptive system and (2) the VAS. The descriptive system had 5 dimensions (mobility, self-care, usual activities, pain/discomfort, and anxiety/depression). Each dimension had 5 levels (no problems, slight problems, moderate problems, severe problems, and extreme problems). Based on the 5 dimensions, summary scores were determined using the scoring instructions from the UK, which represented Europe, and the US and to the EQ-5D-5L Value Sets.16,17 | Studies determining the psychometric properties of EQ-5D-5L were not identified in the literature in the setting of diabetic CKD. | The MID in the EQ-5D-5L was not identified in the literature in the setting of diabetic CKD. |
CKD = chronic kidney disease; EQ-5D-5L = 5-level EQ-5D; HRQoL = health-related quality of life; KDQOL-36 = Kidney Disease Quality of Life; MID = minimal important difference; VAS = visual analogue scale.
Pharmacoeconomic Review
Abbreviations
ACE
angiotensin-converting enzyme
ARB
angiotensin receptor blocker
CKD
chronic kidney disease
CV
cardiovascular
eGFR
estimated glomerular filtration rate
ESRD
end-stage renal disease
HR
hazard ratio
HRQoL
health-related quality of life
ICER
incremental cost-effectiveness ratio
KDIGO
Kidney Disease: Improving Global Outcomes
MI
myocardial infarction
QALY
quality-adjusted life-year
SGLT2
sodium-glucose cotransporter-2
SOC
standard of care
T2D
type 2 diabetes
Executive Summary
The executive summary comprises 2 tables (Table 1 and Table 2) and a conclusion.
Item | Description |
|---|---|
Drug product | Finerenone (Kerendia) |
Submitted price | Finerenone, 10 mg, tablet: $3.340 Finerenone, 20 mg, tablet: $3.340 |
Indication | As an adjunct to standard of care therapy in adults with chronic kidney disease and type 2 diabetes to reduce the risk of:
|
Health Canada approval status | NOC |
Health Canada review pathway | Standard |
NOC date | October 14, 2022 |
Reimbursement request | As an adjunct to standard of care therapy in adults with chronic kidney disease and type 2 diabetes to reduce the risk of:
Standard of care includes an ACE inhibitor or ARB, and an SGLT2 inhibitor, unless contraindicated or not tolerated |
Sponsor | Bayer Inc. |
Submission history | Previously reviewed: No |
ACE = angiotensin converting enzyme; ARB = angiotensin receptor blocker; CKD = chronic kidney disease; NOC = Notice of Compliance; SGLT2 = sodium-glucose cotransporter-2; T2D = type 2 diabetes.
Table 2: Summary of Economic Evaluation
Component | Description |
|---|---|
Type of economic evaluation | Cost-utility analysis Markov model |
Target population | Health Canada indication: adults with CKD and T2D Reimbursement request: adults with CKD and T2D as an adjunct to SOC that consists of an ACE inhibitor or ARB, and an SGLT2 inhibitor, unless contraindicated or not tolerated |
Treatment | Finerenone plus SOC |
Comparator | SOC (consisting of an ACE inhibitor or ARB, and an SGLT2 inhibitor, unless contraindicated or not tolerated) along with other concomitant medications for glucose management and/or CV complications (e.g., beta-blockers, diuretics, calcium antagonists, statins, platelet aggregation inhibitors, insulin, metformin, acarbose, sulfonylurea, DPP-4 inhibitors, GLP-1 agonists) |
Perspective | Canadian publicly funded health care payer |
Outcomes | QALYs, LYs |
Time horizon | Lifetime (35.2 years) |
Key data source | FIDELITY, a prespecified pooled efficacy and safety analysis, combining data from FIDELIO-DKD and FIGARO-DKD: 2 phase III, randomized, double-blind, placebo-controlled, multicentre clinical trials designed to investigate the effect of finerenone on reducing kidney failure and disease progression and on reducing CV mortality and morbidity, respectively |
Submitted results | Health Canada indication: ICER = $18,225 per QALY (incremental costs = $2,559; incremental QALYs = 0.14) Reimbursement request: ICER = $30,822 per QALY (incremental costs = $3,736; incremental QALYs = 0.12) |
Key limitations |
|
CADTH reanalysis results |
|
ACE = angiotensin converting enzyme; ARB = angiotensin receptor blocker; CKD = chronic kidney disease; CV = cardiovascular; DPP-4 = dipeptidyl peptidase 4; eGFR = estimated glomerular filtration rate; GLP-1 = glucagon-like peptide-1; HR = hazard ratio; ICER = incremental cost-effectiveness ratio; LY = life-year; MI = myocardial infarction; QALY = quality-adjusted life-year; SGLT2 = sodium-glucose cotransporter-2; SOC = standard of care; T2D = type 2 diabetes.
Conclusions
Two randomized controlled trials demonstrated that treatment with finerenone was associated with a clinically meaningful reduction in the renal composite outcome and the cardiovascular (CV) composite outcome driven by the outcome components of a sustained decrease in estimated glomerular filtration rate (eGFR) of greater than or equal to 40% and greater than or equal to 57% and incidence of hospitalization for heart failure. The trials also demonstrated that finerenone was associated with a significant reduction in urinary albumin-creatinine ratio from baseline, which the clinical experts referred to as an important marker for the reduced risk of progression of chronic kidney disease (CKD) to end-stage renal disease (ESRD). The impact of finerenone on health-related quality of life (HRQoL) is uncertain due to difficulty interpreting results from the HRQoL instruments. The trials did not demonstrate statistically significant differences in all-cause mortality or CV mortality. All patients in both trials were on angiotensin-converting enzyme (ACE) inhibitors or angiotensin receptor blockers (ARBs) as standard of care (SOC), but only a small proportion in both trials were on sodium-glucose cotransporter-2 (SGLT2) inhibitors at baseline. Hence, the available evidence on the efficacy and safety of the addition of finerenone to ACE inhibitor or ARB, and an SGLT2 inhibitor, is limited.
CADTH noted uncertainty with the sponsor’s modelling approach, which considered a clinical pathway that allowed for substantial improvements in kidney function considered highly unlikely by the clinical experts consulted by CADTH. In addition, CV events were not modelled separately, meaning finerenone reduced strokes and myocardial infarctions (MIs) within the model to an extent not seen in the trial. These aspects of the model could not be fully addressed by CADTH. For these reasons, CADTH could not derive a reliable base-case analysis and instead conducted a series of exploratory analyses to explore different areas of uncertainty. As part of CADTH’s exploratory reanalysis, more appropriate utility values for CKD states were used, more appropriate costs were applied to CKD states, and the risk of dialysis was changed to match the trial outputs. In addition, CADTH conducted additional analyses by removing stroke and MI from the analysis, removing CV mortality reduction associated with finerenone, and further decreasing the reduction in dialysis associated with finerenone.
If results from the trial are fully realized in the Canadian context (i.e., concurrent use of SGLT2 inhibitors has no impact on the benefits seen from finerenone), mortality benefits are realized, and the benefits of finerenone are permanent and enduring (i.e., there is no treatment waning), then the incremental cost-effectiveness ratio (ICER) for finerenone relative to SOC was estimated to be $70,052 per quality-adjusted life-year (QALY). A price reduction of at least 23% would be required for finerenone to be considered cost-effective at a willingness-to-pay threshold of $50,000 per QALY. If CV mortality benefits are not realized, then the ICER increases to $175,549 per QALY. A price reduction of at least 31% may be required to achieve cost-effectiveness. Given the current clinical evidence, whether finerenone will result in a life expectancy gain is unclear. On top of this, if reduction in dialysis use does not continue indefinitely beyond the trial time horizon, then the ICER may exceed $2 million per QALY, with price reductions of more than 55% required to bring the ICER below $50,000 per QALY. CADTH notes that the analysis allows for clinically unsupported improvements in eGFR and reductions in strokes and MIs not seen in the trial and that it may overestimate cost savings from preventing CV events. Therefore, the results may be biased in favour of finerenone across all these analyses, and further price reductions than those cited may be required.
Overall, the sponsor’s analysis shows that improvements in life expectancy have the largest impact on incremental QALYs generated by finerenone relative to SOC. Outside of potential mortality reduction, the main value of finerenone, as estimated by the sponsor’s analysis, is derived from dialysis reduction and reduction in hospitalizations for heart failure, both of which lead to cost savings to the health system. The extent to which these benefits will occur is uncertain given the range of estimates derived from the exploratory reanalyses. As the place in therapy of finerenone relative to SGLT2 inhibitors is uncertain, and because there is a paucity of clinical evidence regarding the efficacy of finerenone when used alongside SGLT2 inhibitors, CADTH was unable to conduct a reliable reanalysis in the sponsor’s reimbursement request population. CADTH notes the analyses only look at finerenone as an add-on therapy that would not displace any component of current SOC, meaning that the cost-effectiveness of finerenone versus SGLT2 inhibitors is unknown.
Stakeholder Input Relevant to the Economic Review
This section is a summary of the feedback received from the patient groups, registered clinicians, and drug plans that participated in the CADTH review process.
CADTH received 1 joint patient group submission from the Kidney Foundation of Canada and Diabetes Canada. Information was collected via surveys directed at people living with CKD and type 2 diabetes (T2D) and their caregivers. Respondents noted that CKD had a negative impact on their daily life, specifically noting fatigue to be a significant problem. In addition, patients noted swelling, itching and dry skin, and dietary restrictions arising from the disease as being concerning. Currently available treatment options being used by patients included ACE inhibitors, ARBs, and other medications (diuretics, tacrolimus, erythropoietin, and dapagliflozin). Of the 6 people who responded to how satisfied they were with their current medication regimens, 4 reported being satisfied or very satisfied and 2 reported being neither satisfied nor unsatisfied. Expectations for a new medication were that it would not make patients feel tired, would not interfere with current medications, and would have an acceptable cost. Other expectations were for preservation of kidney function, delay of dialysis, reduced mortality, and an overall improvement in quality of life. No respondents had experience with finerenone.
Clinician input was received from LMC Diabetes and Endocrinology, a single-specialty group endocrinology practice with clinics in Ontario, Quebec, and Alberta. Current treatment includes renin angiotensin aldosterone system blockers (e.g., ACE inhibitors or ARBs) and, more recently, SGLT2 inhibitors. Clinicians noted that expectations for new treatments included a reduction in the risk of sustained decline in glomerular filtration rate, reduction in the risk of ESRD, and improvement in CV outcomes, which would improve morbidity and quality of life and reduce the burden of disease (e.g., in terms of need for dialysis or hospitalization). Clinicians noted finerenone would be used as an add on to renin angiotensin aldosterone system blockers with or without SGLT2 inhibitors among people with ongoing risk of kidney disease progression and CV disease.
Drug plan input noted that the benefit status of SGLT2 inhibitors varies by jurisdiction, with some jurisdictions reimbursing SGLT2 inhibitors based on indication, such as T2D or heart failure, and questioned how the introduction of finerenone would influence the current benefit status of SGLT2 inhibitors. Drug plan input also queried whether finerenone would be discontinued in patients who experience a CV event or hospitalization for heart failure while taking finerenone. Drug plan input also noted concerns regarding indication creep for heart failure.
Several of these concerns were addressed in the sponsor’s model:
Mortality due to T2D and CKD, CKD progression, CV events (including hospitalization for heart failure) and progression to dialysis were included in the sponsor’s model.
HRQoL was included in the model via health state utility values assigned to CKD stage based on health states.
In addition, CADTH addressed some of these concerns as follows:
CADTH included patients with heart failure, CKD, and T2D mellitus in the budget impact analysis.
CADTH was unable to address the following concerns raised from stakeholder input:
Specific symptoms such as fatigue and swelling, itching and dry skin, and dietary restrictions were not explicitly considered in the model since health states were based on CKD stages defined by eGFR cut-offs.
Discontinuation of finerenone due to experiencing a CV event or hospitalization for heart failure was not included.
The exploration of indication creep for heart failure was not addressed.
Economic Review
The current review is for finerenone (Kerendia) for adults with CKD and T2D.
Economic Evaluation
Summary of Sponsor’s Economic Evaluation
Overview
The sponsor submitted a cost-utility analysis of finerenone compared with SOC (including ACE inhibitors and ARBs) in adult patients with CKD and T2D, aligned with the Health Canada indication.1 The sponsor also submitted a reimbursement request for finerenone as an adjunct to SOC, where SOC included SGLT2 inhibitors.
Finerenone is available as 10 mg and 20 mg tablets.2 The starting dosage for finerenone is based on eGFR (20 mg once daily if eGFR ≥ 60 mL/min/1.73 m2; 10 mg once daily if eGFR ≥ 25 mL/min/1.73 m2 to < 60 mL/min/1.73 m2).2 The recommended target dosage for finerenone is 20 mg once daily.2 At the sponsor’s submitted price of $3.34 per 10 mg or 20 mg tablet, the annual cost of finerenone would be $1,219 if patients remained on treatment for a year. SOC in the model consisted of the medications used as background therapies in the FIDELIO-DKD and FIGARO-DKD studies, which included ACE inhibitors, ARBs, SGLT2 inhibitors, and other medications used to manage T2D and CKD.1,3,4 In the sponsor’s model, SOC was associated with an annual cost of $1,276 per patient. In the sponsor’s model, patients receiving finerenone also received SOC at the same cost as patients receiving SOC alone.
The clinical outcomes of interest were QALYs and life-years. The economic analysis was undertaken over a lifetime (35.2-year) time horizon from the perspective of a Canadian public health care payer. Discounting (1.5% per year) was applied to both costs and outcomes.
Model Structure
A Markov model with 17 health states, defined by CKD stages and history of CV events, was submitted by the sponsor with 4-month cycle lengths (Figure 1).1 CKD stages were defined based on eGFR level (refer to Table 11 for cut-offs).5 Progression through the model is primarily based on CKD stages. Patients enter the model distributed across CKD stages (refer to Table 11 for baseline patient distribution) without any modelled CV events. In each model cycle, patients can remain in their current CKD stage, transition to an improved or worsened CKD stage, or experience a first CV event. The model assumes that the probability of moving between CKD states (i.e., kidney function improving or worsening) is only based on the patient’s current CKD state. For example, a patient can move from CKD stage 5 up to CKD stage 1. This is not represented diagrammatically in the sponsor’s model shown in Figure 1.
Once patients experience a first CV event, they are differentiated from those who have not experienced an event as they transition to a CKD stage health state for those who have experienced a first CV event (e.g., CKD stage 1/2, with a CV event). In the model, patients can move to the dialysis state in CKD stages 3, 4, and 5, and patients can receive a kidney transplant in CKD stage 4 or in CKD stage 5 without dialysis or from dialysis. Patients can transition to death from all health states.
Model Inputs
The model’s baseline population characteristics were characterized by the FIDELITY pooled analysis, a prespecified pooled analysis of the FIDELIO-DKD and FIGARO-DKD clinical trials.3,4,6 FIDELIO-DKD and FIGARO-DKD were both phase III, randomized, double-blind trials designed to evaluate the efficacy and safety of finerenone compared with placebo in reducing kidney disease progression3 and reducing CV mortality and morbidity4 in patients with CKD and T2D. The sponsor assumed that the FIDELITY population (baseline characteristics: mean age 64.8 years; 69.8% male) reflected the population living in Canada.6
Transition probabilities for patients receiving SOC in the model were based on the placebo plus SOC arm of the FIDELITY analysis.6 Patient movement between health states was based on data from FIDELITY. At each 4-month interval, the sponsor estimated the probabilities of moving from 1 state to another. These probabilities were then averaged across the 4-year trial to develop a single transition matrix for the entire model time horizon.6 This approach assumes that the probability of CKD progression does not change over time. The probability of needing a kidney transplant was assumed to be independent of treatment and was based on the placebo arm of the FIDELITY analysis.6 Transition probabilities for finerenone patients were also based on the clinical trials for the CKD stage 1/2, 3, and 4 health states. The probability of transitioning to CKD stage 5, given the patient was on finerenone, was calculated by applying a hazard ratio (HR) of 0.81 to the SOC probability of transitioning to CKD stage 5.6 This HR was taken from the FIDELITY analysis for the onset of an eGFR decrease to less than 15 mL/min/1.73 m2 over at least 4 weeks between finerenone and placebo. Similarly, transitions to dialysis for finerenone were based on SOC transitions to dialysis with an HR for progression to dialysis applied (0.82).6 None of the HRs used in the analysis were time dependent, and therefore the proportional hazard assumption is assumed, meaning the treatment effect is maintained indefinitely while the patient remains on treatment.
The proportion of patients experiencing a first CV event was based on the sponsor’s CV composite end point in the clinical trials, which included nonfatal MI, nonfatal stroke, and hospitalization for heart failure.3,4 To estimate the proportion of SOC patients who experience a first CV event, the sponsor estimated the risk of having a first CV event for each given health state, at 4-month intervals, in the FIDELITY analysis. The average probability of a first CV event in each health state was then taken over 4 years from the placebo arm of the analysis. For finerenone patients, an HR of 0.88 (derived from FIDELITY) was applied to the risks derived for SOC patients.6 To extrapolate the risk of experiencing a first CV event over a longer time horizon, after the first 4 years in the model (i.e., after the trial period ended), the sponsor applied an HR for an increased risk of experiencing a CV event with each year of age (1.03), sourced from the literature.7
Three risks of death were possible in the model: renal death, CV death, and other background mortality. Renal death was only possible in CKD stage 5 without renal replacement therapy. The probability of renal death was derived from a component of the renal composite end point (renal death) from the placebo arm of the FIDELITY analysis for patients receiving SOC. CV death by health state was derived from the placebo arm of the FIDELITY analysis. Renal and CV death for finerenone were estimated by applying HRs from the FIDELITY analysis (0.53 and 0.88, respectively) to SOC mortality estimates.6 Background mortality was based on Canadian life tables, with CV and renal deaths removed to avoid double counting. Background mortality increased in the model with CKD progression by applying literature-derived HRs (refer to Table 12) to background mortality estimates.8,9 Background mortality among those who had a first CV event was increased by applying HRs for a long-term increased mortality risk due to CV events sourced from the literature.10
In addition to events influencing patient transitions through the model, the sponsor incorporated 5 “other health events,” which could be experienced in any living health state and would not impact subsequent renal events, CV events, or death.1 These included subsequent CV event, hyperkalemia leading to hospitalization, hyperkalemia not leading to hospitalization, a sustained decrease in eGFR of greater than or equal to 40% from baseline (over at least 4 weeks), and new onset of atrial fibrillation or atrial flutter.1 The probability of experiencing an “other health event” for those on SOC alone was based on the placebo arm of the FIDELITY analysis, with HRs applied to derive finerenone probabilities. “Other health events” were incorporated in the model by including a cost and utility consequence; they were assumed to last for 4 months, apart from a sustained decrease in eGFR of greater than or equal to 40% from baseline, which was assumed to be permanent and last the remainder of the model time horizon.1
Costs in the model included treatment acquisition, event treatment, follow-up costs, and death costs. The proportion of finerenone patients receiving a 10 mg or 20 mg dose was based on the percentage of their use in the FIDELITY analysis (██% and ██% receiving 10 mg and 20 mg once daily, respectively).6 A discontinuation rate for finerenone was incorporated in the model based on the rate of discontinuation at 4 years observed in FIDELITY; this was assumed to be constant over time.6 Additionally, finerenone was discontinued when patients initiated dialysis, whereas patients remain on SOC during dialysis. SOC costs were estimated based on the proportion using each class of drug from the FIDELITY analysis. A representative drug from each class was selected based on the most common drug used from Ontario claims data. Drug unit costs were based on the Ontario Drug Benefit Formulary.11
Disease management costs for CKD stages 1/2, 3, and 4 were based on an Alberta population-based study on care costs (including hospitalization, physician, and ambulatory care costs) for people with CKD.12 CKD stage 5 costs without dialysis were based on a previous CADTH submission for hyperkalemia.13 Dialysis costs were based on a weighted average cost for hemodialysis and peritoneal dialysis, with the proportion of patients receiving each based on a Canadian Institute for Health Information report.14 Dialysis costs were based on a 2016 dialysis study from Manitoba, inflated to 2021 Canadian dollars, and included human resource, supply, drug, equipment, overhead, and capital costs.15 Transplant costs were sourced from a 2013 Canadian published economic evaluation and inflated to 2021 Canadian dollars.16 First CV event costs were sourced from the literature for each component CV event, inflated to 2021 Canadian values, and weighted by the proportion of patients in FIDELITY experiencing each event.6,17-22 One-time death costs for CV and renal death were incorporated. CV death costs were weighted based on the reasons behind CV death in the FIDELITY analysis, using literature-based sources for the various CV death types.21,23,24 Renal death costs were assumed to be equal to the cost of renal failure.25 Non-CV and nonrenal death were assumed to not incur any costs in the model.1,6
Health state utility values were derived based on 5-level EQ-5D data from FIDELITY, using Canadian-specific tariffs.6,26 Baseline FIDELITY data informed the CKD stage 1/2 health state utility value (0.827). The sponsor then conducted a multivariate regression to estimate utility changes associated with progressive CKD stages to derive CKD stage health state utilities, including dialysis, transplant, and posttransplant states (Table 13).1 Disutilities for CV events and other health events were also derived from a multivariate regression.1
The sponsor conducted a reimbursement request scenario that assumed that SGLT2 inhibitors were part of SOC. In this scenario, 81.5% of patients were receiving SGLT2 inhibitors as part of SOC, based on the sponsor’s market research.1 The sponsor then applied HRs from a randomized controlled trial to adjust baseline CKD and CV risks for the proportion of people in the model receiving an SGLT2 inhibitor.27
Summary of Sponsor’s Economic Evaluation Results
All analyses were run probabilistically (1,000 iterations for the base-case and scenario analyses). The deterministic and probabilistic results were similar. The probabilistic findings are presented in the following.
Base-Case Results
Finerenone was associated with a QALY gain of 0.14 at an additional cost of $2,559, resulting in an ICER of $18,255 compared with SOC (Table 3). At a willingness-to-pay threshold of $50,000 per QALY gained, there was an 85.1% probability of finerenone being cost-effective. Of the 0.14 incremental QALYs gained for finerenone, 0.01 (9%) were accrued during the trial period.
The majority of the QALY gain for finerenone was accrued in the CKD stage 3 health state, followed by CKD stage 4. Total QALYs were higher for SOC across all other health states, meaning patients receiving SOC spent more time in CKD stage 1/2, dialysis, and transplant health states than patients finerenone. Medication costs accounted for all the incremental costs for finerenone compared with SOC. The largest source of cost savings for finerenone was dialysis-related costs, followed by first CV event and other health event costs.
Table 3: Summary of the Sponsor’s Economic Evaluation Results
Drug | Total costs ($) | Incremental costs ($) | Total QALYs | Incremental QALYs | ICER vs. SOC ($/QALY) |
|---|---|---|---|---|---|
SOC | 86,729 | Ref. | 9.40 | Reference | Reference |
Finerenone + SOC | 89,289 | 2,559 | 9.54 | 0.14 | 18,255 |
ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year; SOC = standard of care; vs. = versus.
Source: Sponsor’s pharmacoeconomic submission.1
Sensitivity and Scenario Analysis Results
The sponsor conducted a reimbursement request scenario, whereby the proportion of patients receiving SGLT2 inhibitors as part of SOC was increased to 81.5%, as SGLT2 inhibitors were assumed to be part of SOC for T2D with CKD in the reimbursement request scenario. In the reimbursement request, finerenone was associated with a QALY gain of 0.12 at an additional cost of $3,701, resulting in an ICER of $30,822 compared with SOC.
The sponsor conducted several scenario analyses to examine uncertainty. The results of the model were sensitive to discount rates, with the ICER for finerenone plus SOC compared to SOC decreasing to $15,891 per QALY and increasing to $21,942 per QALY when 0% and 3% discount rates were used, respectively. When a 20-year time horizon was used, the ICER for finerenone plus SOC versus SOC increased to $20,685 per QALY. Finally, adjusting utilities by age resulted in an increase of the ICER to $20,867 per QALY.
CADTH Appraisal of the Sponsor’s Economic Evaluation
CADTH identified several key limitations to the sponsor’s analysis that have notable implications for the economic analysis:
The sponsor’s model structure may not adequately reflect the progressive nature of CKD. The sponsor’s submitted model structure was based on CKD stages defined by eGFR cut-off scores (refer to Table 11) based on Kidney Disease: Improving Global Outcomes (KDIGO) guidelines.1,5 In each cycle in the sponsor’s model, patients could remain in their current CKD stage or transition to an improved CKD stage (regress) or a worsened CKD stage (progress).1 To derive transition probabilities in the model, the sponsor noted movement that occurred between states at each 4-month visit. This meant an individual who has an eGFR of 14 mL/min/1.73 m2 and then at a subsequent visit has an eGFR of 16 mL/min/1.73 m2 would be considered to move from CKD stage 5 to CKD stage 4. The result of moving from CKD stage 5 to CKD stage 4 in the model means that mortality and morbidity dramatically improve and the likelihood of needing dialysis decreases. Consequently, the analysis assumes small changes in eGFR correspond to drastic shifts in management and prognosis. Likewise, large shifts in eGFR (e.g., moving from 29 mL/min/1.73 m2 to 17 mL/min/1.73 m2 in a small time frame) have no impact on health outcomes unless they pass a discrete threshold. As the model also does not track patient movement through the health states, an individual whose eGFR improves by a small amount could experience substantial subsequent improvements in eGFR, implying that eventually their CKD could be effectively cured.
It is uncertain that regression, in terms of substantial decreases in mortality risk related to kidney function, is possible in CKD or a goal of treatment with finerenone. CKD is a progressive, generally irreversible disease.28 According to the KDIGO guidelines, patients should be treated comprehensively to reduce the risk of kidney disease progression.5 Clinician input for this review also indicated that goals for a new treatment would be to delay the progression of kidney disease. This was aligned with the objective of the FIDELIO trial, which was to evaluate the efficacy of finerenone in delaying the progression of kidney disease.3 This is also reflected in the proposed Health Canada indication for finerenone, which is to delay progression of kidney disease.2 Estimated glomerular filtration rate is a surrogate marker for kidney disease, and therefore equating small unsustained changes in this score to substantial improvements in mortality and quality of life is highly uncertain.
Despite the progressive nature of kidney disease, the transition probabilities applied to the sponsor’s model allow for drastic improvements in CKD stages for both finerenone and SOC patients. To illustrate, if all patients receiving SOC alone enter the model in CKD stage 5, after 4 years 4%, 13%, and 7% will have improved to CKD stage 1/2, CKD stage 3, and CKD stage 4, respectively. Therefore after 4 years, the model predicts 4% of patients with an eGFR of less than 15 mL/min/1.73 m2 will return to near normal kidney function. According to the clinical experts consulted by CADTH for this review, CKD stage 5 is considered ESRD, is irreversible, and will require treatment with dialysis or renal transplant. Likewise, the sponsor uses an HR, derived from the FIDELITY analysis, which looks at “Sustained decrease in eGFR to <15 ml/min per 1.73 m2.”6 If patients can move from CKD stage 5 to a less severe CKD state, this would imply the decrease in eGFR is not sustained. CADTH notes that the likelihood of improved kidney function is higher in the finerenone arm; no clinical evidence from the trial is given to support this, and no uncertainty is analyzed around this finding. Given that finerenone is indicated to slow kidney disease progression, not reverse it, there is no clinical evidence that finerenone will improve kidney function.
If patients do improve their eGFR scores such that they shift to an improved CKD stage, it is uncertain whether they would have the same costs and consequences as a patient who had remained in that stage and not yet progressed. It is unclear, for example, if someone who entered the analysis and remained in CKD stage 4 would have the same outcomes as someone who was CKD stage 5 and regressed back to CKD stage 4. If these 2 patients had different expected clinical outcomes and costs, then the CKD state would not represent a homogenous group. Likewise, the state may include individuals with rapidly deteriorating eGFR and individuals with stable eGFR. From a methodological perspective, a health state in an economic model should represent a homogenous group of patients who have similar expected costs and quality-of-life considerations. The implications of heterogeneity in health states have been documented in the literature.29
Finally, CADTH notes that transition probabilities that pertain to regression are deterministic in the sponsor’s analysis. They are assumed to occur with certainty across all probabilistic iterations. The confidence in which these estimates have been generated is unclear; some transitions may be informed by very small patient numbers and be an artifact of chance, for example. Baseline transition matrices were also hard coded, making validation by CADTH difficult.
As all transition probabilities for SOC (and the majority for finerenone) are taken directly from the trial, CADTH could not alter 1 transition probability without considering the implication for other transition probabilities within the model. Given that regression through states is higher in the finerenone arm, this model structure is likely biased in favour of finerenone. As CADTH could not correct this limitation, any result from the analysis is highly uncertain.
The expected place for finerenone in therapy relative to SGLT2 inhibitors is uncertain. The FIDELIO and FIGARO clinical trials investigated the efficacy of finerenone as an add on to SOC in the reduction of CV disease and kidney disease progression. In the clinical trials, SOC consisted of an ACE inhibitor or ARB.6 At the time that the finerenone clinical trials were conducted, 6.7% of patients in the trials were receiving SGLT2 inhibitors as part of SOC.30 More recently, SGLT2 inhibitors have been approved for use in CKD.31 According to KDIGO guidelines, SGLT2 inhibitors are recommended for patients with T2D and CKD.5 Despite this, as the approval of SGLT2 inhibitors for CKD is relatively recent, and because no SGLT2 inhibitors have undergone the CADTH reimbursement review process,32 it is unclear to what extent SGLT2 inhibitors will become part of SOC for CKD in Canada. If finerenone, as an add on to SOC, is listed for T2D and CKD, it is uncertain what SOC will consist of.
The impact of how finerenone and SGLT2 inhibitors would work when used together is also unclear. If SGLT2 inhibitors reduce the rate of underlying events as part of SOC, since finerenone is modelled as a relative benefit over SOC, the benefit of finerenone could be lower than that predicted by the sponsor’s analysis. The sponsor conducted a scenario analysis to explore this, whereby the underlying event frequencies for SOC patients in the model were adjusted using HRs observed from an SGLT2 inhibitor clinical trial.27 In this scenario, finerenone was associated with fewer QALYs compared with the base case. Likewise, there is uncertainty as to whether the treatment effect of finerenone would be impacted by SGLT2 inhibitor use. A subgroup analysis of the patients who were using SGLT2 inhibitors in the clinical trials showed finerenone continued to have improved outcomes relative to placebo. However, given the small patient numbers, this analysis is highly uncertain, and we cannot conclude how efficacious finerenone would be when given in combination with an SGLT2 inhibitor.
CADTH was unable to address this limitation. Exploratory reanalyses were conducted that altered the finerenone efficacy profile. This may represent scenarios in which finerenone efficacy is impacted by concurrent use with an SGLT2 inhibitor.
Application of the proportional hazards assumption. The sponsor uses the proportional hazards assumption for finerenone treatment effects, implying a consistent treatment effect that does not wane over time. The long-term treatment efficacy for finerenone beyond 5 years is uncertain as no long-term data beyond the clinical trials exist. The sponsor provides statistical tests to explore the proportional hazards assumption for time to first CV event and time to eGFR decrease to less than 15 mL/min/1.73 m2. Time to eGFR decrease was noted as potentially violating the proportional hazards assumption but was dismissed for not producing statistically significant P values. CADTH notes that the sponsor assumes benefit with regard to finerenone’s impact on CV mortality and reduction in dialysis, for example, despite not achieving statistical significance. More importantly, within economic evaluations we need to consider the relevance of constant proportional hazards over the lifetime horizon of the model and not just the duration of the clinical trial. Caution has been expressed with assuming proportional hazards within economic evaluations.33 It is therefore uncertain whether the treatment effect observed with finerenone during the trial period would be sustained indefinitely, as assumed by the sponsor. No option was provided to explore uncertainty related to this.
CADTH was unable to address the proportional hazards assumption.
The impact of finerenone on reducing dialysis is uncertain. In the sponsor’s model, the main way a patient enters the dialysis state is through transitioning to CKD stage 5 where their eGFR is less than 15 mL/min/1.73 m2. A small number of patients can transition to the dialysis state from CKD stage 1/2, 3, and 4. According to the clinical expert, only those in stage CKD stage 5 would be considered for chronic dialysis. Therefore, CADTH can only assume those who transition to dialysis from non-CKD stage 5 states do so by rapidly deteriorating within a 4-month period (cycle length of the model). This implies a 4-month cycle length may be too long for the analysis. For finerenone, the rate of dialysis is reduced in 2 ways. First, the likelihood of a patient progressing to CKD stage 5 (likelihood of their eGFR falling below 15 mL/min/1.73 m2) is reduced. Second, the likelihood of receiving dialysis, even for those who are already CKD stage 5, is lowered by applying an HR of 0.82 to the SOC dialysis rate. The sponsor therefore assumes that the likelihood of receiving dialysis is lower for those on finerenone, even if a patient’s eGFR falls below 15 mL/min/1.73 m2.
CADTH notes the Cox proportional hazard model for the dialysis HR estimate was only adjusted for eGFR at baseline, which did not include those who had an eGFR of less than 15 mL/min/1.73 m2. From the trial, the sponsor calculates that the likelihood of receiving dialysis every 4 months for patients in CKD stage 5 is 18.72% for those on SOC alone versus 16.67% for those on finerenone. This implies a reduced likelihood of receiving dialysis for those with CKD stage 5 on finerenone, but the risk reduction in the trial is lower than what is programmed in the model (HR = 0.88 versus 0.82 used in the model). No assessment of uncertainty is provided around these transition probabilities.
Furthermore, the sponsor’s incorporation of dialysis into the model may not accurately estimate the proportion of dialysis occurring in the clinical trials. Figure 2 demonstrates that for SOC, by approximately 36 months, the model is overestimating the proportion of patients receiving dialysis compared to what was observed in FIDELITY.3 Therefore, it appears that the model may be overestimating dialysis rates for SOC, which would result in an overestimate of the dialysis benefit associated with finerenone. As the predictions between the model and FIDELITY begin to diverge during the first 4 years, it is possible that this is amplified over the model time horizon and that the difference in dialysis between finerenone and SOC over a lifetime may be overestimated. Likewise, as shown in Figure 2, the model predictions fall outside the 95% confidence interval (CI) as predicted by data from the trial.
As there is uncertainty regarding the benefit of finerenone in reducing the need for dialysis, as well as the potential that this benefit could be overestimated over a longer time horizon, CADTH changed the dialysis benefit based on the sponsor’s trial-derived transition probabilities as an exploratory analysis. As an additional analysis, the dialysis benefit for finerenone upon progression to CKD stage 5 was removed. In this analysis, dialysis reduction due to finerenone use still occurs through patients progressing to CKD stage 5 at a slower rate.
The sponsor assumes a reduction in MIs and stroke not seen in the trial. The risk of having a first CV event was based on a modification of the composite CV outcome used in the clinical trials (time to first CV event excluding CV death).1 The risk of having a first CV event in the model was based on the average rate over 4 years for placebo patients from the FIDELITY analysis and was CKD stage dependent.6 Finerenone CV event risks were based on placebo risk, with an HR applied. This approach assumes the risk of having a CV event is time independent, which is uncertain.
In terms of the components of the CV composite outcome, the CADTH clinical review report only concluded that finerenone was superior to SOC in reducing hospitalization for heart failure. The HRs from the CADTH clinical review report for nonfatal MI, nonfatal stroke, and hospitalization for heart failure are 0.91, 0.99, and 0.78. In the sponsor’s analysis these events are not modelled separately; instead, at any given point the individual could have a first CV event. A probability is then applied as to what event this could be (MI, stroke, or hospitalization for heart failure) to derive an average cost and health impact for the event.1 The same probabilities are applied to finerenone and SOC. If finerenone mainly reduces hospitalizations for heart failure, with minimal impact on stroke and MI, then the likelihood of a CV event in the finerenone arm being a hospitalization for heart failure must be lower than in the SOC arm. As this adjustment is not made, the model predicts finerenone having an equal impact at reducing strokes and MIs as it does at reducing hospitalizations for heart failure; this runs counter to the trial evidence.
The same issue of composite outcomes applies when considering subsequent CV events as well. As part of an additional information request from CADTH, the sponsor provided HRs for preventing subsequent CV events for each component of the composite outcome. The HRs for MI, stroke, and hospitalizations vary from 0.54 to 1.45, with no individual component achieving statistical significance.34 Again, it appears that a reduction in hospitalization for heart failure is the main reason for the composite outcome being in favour of finerenone. Assuming that finerenone has an equal likelihood of reducing subsequent strokes and MIs runs counter to the evidence. In the data provided by the sponsor, hospitalization for heart failure also made up most subsequent CV events, and stroke events were more common in the finerenone arm, albeit not at a statistically significant level.
CADTH was unable to address these limitations given the structure of the model. CADTH notes that the cost savings derived from CV events in the model are overestimated as they assume finerenone reduces strokes and MIs at the same rate it does hospitalizations for heart failure, counter to what the evidence shows. As part of an exploratory reanalysis, the risk of MIs and strokes was removed from the model, leaving the focus solely on hospitalizations for heart failure.
Health state utility values are uncertain and lack face validity. The sponsor’s utility value for a 65-year-old patient with CKD stage 1/2 and T2D mellitus was estimated to be 0.827, which may be an overestimate.1 A Canadian utility study estimated the mean utility value for people 65 years old in the general population living in Canada to be 0.848.35 Further, a Canadian population utility study for chronic conditions estimated a utility score of 0.766 for people with diabetes.36 According to the clinical experts consulted by CADTH for this review, people with CKD and T2D are expected to have worse quality of life than someone with T2D alone. The sponsor also estimates that patients post–kidney transplant would have better utility than the general population living in Canada (0.879). A recent systematic review of EQ-5D utility values in patients with CKD, summarized by state, found much lower utility estimates for those on dialysis than those predicted by the sponsor (sponsor value: 0.78 versus 0.63).1,37 Likewise, in the 2 studies provided as scenario analyses by the sponsor, the utility in the dialysis state is also shown to be much lower (sponsor value: 0.78 versus scenario analysis values: 0.47 and 0.66).1 In the sponsor’s analysis, dialysis leads to a utility decrement of roughly 0.01 (0.802 for CKD stage 5 without dialysis versus 0.788 for CKD stage 5 with dialysis after 6 months). This decrement is much smaller than what is found in the literature and indicates that dialysis has minimal impact on a patient’s quality of life.
Utility estimates from FIDELITY appear to be consistently higher than those from studies in the literature. This may be due to differences in methodology, such as utilization of the 5-level EQ-5D, or trial populations representing healthier patients. CADTH notes the sponsor’s utility values are for patients with no CV event, though this alone would not explain the large difference between the trial estimates and literature estimates, as CV events are not common in lower CKD stages. Likewise, 46% of patients in the pooled FIDELITY analysis had a history of CV disease, so this will have been captured to an extent.
Finally, in the sponsor’s base case, utilities were not age adjusted, meaning that health state utility values were assumed to not decrease with age, which is not supported by the literature.35
In the exploratory analyses, CADTH used disutility estimates from Cooper et al. to derive utility values, maintaining the utility value for CKD stage 1/2 used by the sponsor and applying disutility to derive estimates for other states.37 Table 13 in Appendix 4 outlines these changes. Although the Cooper et al. values are not without limitations, it was felt that the sponsor’s utility estimates diverged substantially from what has been presented in the literature — indicating, for example, that dialysis has minimal impact on quality of life. Likewise, relative to general population estimates of people living in Canada, utilities from FIDELITY indicate that, relative to many diseases, having CKD and T2D mellitus has minimal to no impact on utility. The values from Cooper et al. were chosen as opposed to the sponsor’s chosen values in the scenario analyses as they aggregated across relevant utility studies rather than relying on a single estimate from 1 study.
Estimation of cost savings is uncertain. The sponsor’s base-case analysis uses costs from Manns et al. to derive health state costs for each CKD stage.12 From this study, the sponsor only uses costs related to kidney care.1 As per the CADTH guidelines, all costs incurred by the health system should be included if they are deemed to be influenced by the intervention being considered.38 As shown by Manns et al., costs increase as patients progresses through CKD stages, and these costs are not all attributable to kidney and cardiac care.12 Likewise, additional costs will be incurred through life extension not pertaining to just kidney care. CADTH notes that the sponsor does not appear to take a consistent approach of only including kidney and CV costs, as in the transplant state all health system costs are included. As per the CADTH guidelines, the distinction between what constitutes a relevant and an irrelevant cost requires careful consideration. In this analysis, only including costs pertaining to kidney care may be misleading given the high health care costs incurred by patients with this condition. By doing so, it appears the sponsor miscalculates the cost savings associated with finerenone.
CADTH further notes that the sponsor assumes increased health care costs after a CV event. However, in the pooled FIDELITY analysis, 46% of patients start the trial with a history of CV disease and would therefore be classed as “post–CV event.” In these patients, it is uncertain what the incremental costs would be after the acute phase of an additional CV event. The sponsor may therefore overestimate CV event costs in the postacute phase.
Finally, the sponsor only includes the cost related to the dialysis itself when considering dialysis costs. Canadian studies have shown dialysis is a high-cost burden outside of just costs related to the dialysis itself. The sponsor also assumes no costs related to kidney care in this state.12,39 This underestimates the potential health care savings from preventing dialysis.
In exploratory analyses, the full cost of CKD was applied to each CKD stage using the Manns et al. study.12 To prevent double counting, costs associated with CV events were excluded from the total estimates provided by Manns et al. Drug costs, as estimated by the sponsor, were also removed from these estimates. For those in CKD stage 5 without renal replacement therapy, dialysis costs were removed from the Manns et al. estimates. For those with CKD stage 5 on renal replacement therapy, the sponsor’s estimated dialysis costs were added. Table 14 in Appendix 4 outlines which costs CADTH used for all CKD states. CADTH notes that this will attribute additional cost savings from slowing CKD progression, outside of hospitalizations, that have not been evidenced in the trial.
In all analyses, CADTH outlines what percentage of cost savings occur in the post-acute phase, thus determining what impact this has on the conclusions.
The mortality benefit associated with finerenone treatment and CKD progression is uncertain. In the sponsor’s model, mortality for SOC was incorporated based on CKD stage using specific CV death and renal death rates, derived from the FIDELITY analysis.3 HRs, also derived from FIDELITY, were applied to these SOC rates to derive finerenone CV and renal death.6 The CADTH clinical review concluded that there was no difference in all-cause, CV, or renal death between finerenone and placebo, based on the HRs for these outcomes being nonsignificant with wide CIs that crossed 1. As such, whether there is a mortality benefit from finerenone remains uncertain, despite the sponsor’s base case predicting 0.16 greater life-years for finerenone compared with SOC.
In addition, the sponsor applied HRs from the literature to account for the increased risk of mortality associated with being in each CKD stage. As CV and renal death had already been incorporated based on the trial, these additional HRs were accounting for deaths that were not due to renal or CV causes. According to clinical experts consulted by CADTH for this review, CV death is the largest driver of mortality for patients with CKD, followed by renal complications. Therefore, the application of additional HRs for death is uncertain and may represent double counting of death if the risk of increased death by CKD stage has already been captured.
Due to the uncertainty in the mortality benefit for finerenone, as a scenario analysis CADTH removed the CV death benefit for finerenone. All-cause mortality is still lower for finerenone in this scenario analysis due to the structure of the model that grants improved mortality for those in lower CKD states.
The assumption that other health events will not impact future events is likely inappropriate. In the model, patients were also at risk of experiencing other health events, including subsequent CV events, hyperkalemia leading to and not leading to hospitalization, new onset of atrial fibrillation or atrial flutter, and a sustained decrease in eGFR of greater than or equal to 40% from baseline (over at least 4 weeks). It was assumed that these events were independent of CKD stage and that they would not influence CKD transitions or mortality, which was deemed inappropriate. Recurrent hospitalizations for heart failure increase the risk of CV mortality.40 There is a mortality risk associated with hyperkalemia, and having hyperkalemia can influence the occurrence of CV events.41 Patients with atrial fibrillation have an increased risk of all-cause death compared to the age- and sex-matched general population,42 and atrial fibrillation is the leading cause of ischemic stroke.43 Finally, having a sustained decrease in eGFR of greater than or equal to 40% from baseline would influence 1’s CKD stage, given that the stages are defined by eGFR.
Additionally, the CADTH clinical review was unable to validate the HRs used to incorporate subsequent health events as these were not included in the FIDELITY analysis; rather, they were reported in a supplemental file that lacked details on how the HRs were calculated.34
CADTH was unable to address this limitation.
Additional limitations were identified but were not considered to be key limitations. These limitations are outlined subsequently (or in Appendix 4).
Background medication use was assumed to be independent of CKD stage. In the sponsor’s model, the proportion of patients using each class of SOC medication was based on FIDELITY and assumed to be generalizable to the general population living in Canada.6 According to the clinical experts consulted for this review, the proportions are largely aligned with Canadian clinical practice, but the experts noted that the proportion of people receiving each of the SOC medications is CKD stage dependent, whereas the sponsor’s approach assumed the same proportion of people would take these medications regardless of CKD stage. For example, the clinical experts noted that when in CKD stage 4 and 5, patients should no longer be taking metformin. Therefore, assuming independence between CKD stage and background medications was deemed to be inappropriate. Additionally, the proportion receiving SGLT2 inhibitors in the sponsor’s base case (10.2%) is not aligned with the FIDELITY analysis (6.7%). Given the low proportion of patients receiving of SGLT2 inhibitor in the sponsor’s base case, this discrepancy is unlikely to influence model results.
CADTH was unable to address this limitation.
Additionally, the following key assumptions were made by the sponsor and have been appraised by CADTH (Table 4).
Table 4: Key Assumptions of the Submitted Economic Evaluation (Not Noted as Limitations to the Submission)
Sponsor’s key assumption | CADTH comment |
|---|---|
Patients in FIDELITY were assumed to be representative of patients in Canada who would be eligible for finerenone. | Likely appropriate according to the clinical experts consulted by CADTH for this review. The clinical experts noted that there was an overrepresentation of male patients compared to Canadian clinical practice. |
It was assumed that finerenone would be discontinued when people initiate RRT but that SOC medications would not be. | Appropriate according to the clinical experts consulted by CADTH for this review. |
The risk of having a first cardiovascular event among those with acute dialysis and post-acute dialysis was equal to that of those with CKD stage 5 without RRT. | Appropriate according to the clinical experts consulted by CADTH for this review. |
CKD = chronic kidney disease; RRT = renal replacement therapy; SOC = standard of care.
CADTH Reanalyses of the Economic Evaluation
Base-Case Results
Due to uncertainties with the sponsor’s model structure and derivation of benefit associated with finerenone, CADTH was unable to conduct a base-case analysis. Instead, CADTH conducted a series of exploratory analyses to explore the impact of various assumptions regarding finerenone benefit and the impact this has on cost-effectiveness.
Table 5: CADTH Revisions to the Submitted Economic Evaluation
Stepped analysis | Sponsor’s value or assumption | CADTH value or assumption |
|---|---|---|
Correctionsa to sponsor’s base case | ||
1. None | — | — |
Changes to derive the CADTH exploratory reanalyses | ||
1. Changes to utility values | Not adjusted for age; small reductions in health state utilities for more severe states. | Adjusted for age; increased disutility. Refer to Table 13 for details. |
2. CKD state costs | Exclude everything but kidney care costs. | Only exclude CV-related, dialysis, and drug costs from Manns et al. estimates to prevent double counting. Add CKD stage 5 costs to dialysis. Refer to Table 14 for details. |
3. Dialysis reduction in line with trial transition probabilities | HR of 0.82 applied. | HR of 0.88 applied. |
4. No difference in CV death | HR of 0.88 applied. | HR of 1 applied, meaning no reduction in CV deaths through finerenone use. |
5. Dialysis reduction only through eGFR delay | HR of 0.82 applied. | HR of 1 applied, meaning probability of dialysis in patients with an eGFR < 15 mL/min/1.73 m2 is the same for those on and off finerenone. |
6. Reduction in hospitalizations for HF only | Finerenone assumed to have an equal impact at reducing stroke, MIs, and hospitalization for heart failure. | Finerenone only reduces hospitalizations for HF. The following was assumed based on data provided by the sponsor:
CV event cost, disutility, and impact on mortality all assumed to come from hospitalization for HF only |
CADTH exploratory reanalysis 1 | 1 + 2 + 3 | |
CADTH exploratory reanalysis 2 | 1 + 2 + 3 + 6 | |
CADTH exploratory reanalysis 3 | 1 + 2 + 3 + 4 | |
CADTH exploratory reanalysis 4 | 1 + 2 + 3 + 5 | |
CADTH exploratory reanalysis 5 | 1 + 2 + 3 + 4 + 5 | |
CKD = chronic kidney disease; CV = cardiovascular; eGFR = estimated glomerular filtration rate; HF = heart failure; HR = hazard ratio; MI = myocardial infarction; SOC = standard of care; vs. = versus.
aCorrections are minor errors (e.g., transcription errors between report and model or misapplication of distributions or standard errors in probabilistic analyses) that are not identified as limitations.
In the first CADTH exploratory reanalysis, finerenone was associated with a total cost of $318,236 and 7.96 QALYs compared to $311,874 and 7.87 for patients receiving SOC alone. The ICER for finerenone compared to SOC was $70,052 per QALY gained with a probability of being cost-effective at a willingness-to-pay threshold of $50,000 of 27%. Of the 0.09 incremental QALYs associated with finerenone, 0.005 (5%) were accrued during the trial period. This analysis potentially overestimates the benefit of finerenone as it assumes a reduction in strokes and MIs not seen from the trial. In an analysis that removes MIs and strokes, the ICER increases to $73,484 per QALY. Three further reanalyses were conducted to explore uncertainties pertaining to CV mortality benefit and dialysis reduction. Removing benefits related to CV deaths, the ICER increases to $175,549 per QALY as mortality reductions make up the majority of incremental QALYs associated with finerenone. By assuming the likelihood of receiving dialysis once eGFR falls below 15 mL/min/1.73 m2 is the same regardless of finerenone use, the ICER increases to $93,752 per QALY. Assuming both no CV mortality reduction and a lower rate of dialysis reduction, the ICER increases to $2,994,490 per QALY. This high ICER is driven largely by very small QALY gains that are close to zero. CADTH notes that uncertainty related to the model structure could not be assessed. Therefore, these analyses still allow for substantial improvements in eGFR scores (e.g., moving from an eGFR < 15 mL/min/1.73 m2 to > 60 mL/min/1.73 m2 without transplant), which are likely not clinically plausible. Detailed information and disaggregated results are presented in Appendix 4.
Table 6: Summary of the Stepped Analysis of the CADTH Reanalysis Results
Stepped analysis | Drug | Total costs ($) | Total LYs | Total QALYs | ICER ($/QALYs) |
|---|---|---|---|---|---|
Sponsor’s base case (probabilistic) | SOC | 86,729 | 11.54 | 9.40 | Reference |
Finerenone + SOC | 89,289 | 11.70 | 9.54 | 18,255 | |
Sponsor’s base case (deterministic) | SOC | 84,671 | 11.50 | 9.35 | Reference |
Finerenone + SOC | 87,188 | 11.67 | 9.50 | 17,398 | |
1 – Changes to health state utilities (deterministic) | SOC | 84,671 | 11.50 | 7.89 | Reference |
Finerenone + SOC | 87,188 | 11.67 | 7.99 | 23,903 | |
2 – CKD state costs (deterministic) | SOC | 310,207 | 11.50 | 9.35 | Reference |
Finerenone + SOC | 316,095 | 11.67 | 9.50 | 40,701 | |
3 – Using transition probability for finerenone for dialysis from trial (deterministic) | SOC | 84,671 | 11.50 | 9.35 | Reference |
Finerenone + SOC | 87,824 | 11.65 | 9.49 | 23,431 | |
4 – No difference in CV death (deterministic) | SOC | 84,671 | 11.50 | 9.35 | Reference |
Finerenone + SOC | 86,364 | 11.55 | 9.41 | 32,172 | |
5 – Dialysis prevention only through slowing progression to CKD stage 5 (deterministic) | SOC | 84,671 | 11.50 | 9.35 | Reference |
Finerenone + SOC | 89,018 | 11.63 | 9.47 | 37,647 | |
6 – Reduction in hospitalizations for heart failure only (deterministic) | SOC | 65,209 | 11.70 | 9.56 | Reference |
Finerenone + SOC | 68,164 | 11.88 | 9.71 | 19,622 | |
CADTH exploratory reanalysis 1 (1 + 2 + 3) (probabilistic) | SOC | 311,874 | 11.50 | 7.87 | Reference |
Finerenone + SOC | 318,236 | 11.64 | 7.96 | 70,052 | |
CADTH exploratory reanalysis 2 (1 + 2 + 3 + 6) (probabilistic) | SOC | 294,176 | 11.63 | 7.96 | Reference |
Finerenone + SOC | 301,111 | 11.79 | 8.05 | 73,484 | |
CADTH exploratory reanalysis 3 (1 + 2 + 3 + 4) (probabilistic) | SOC | 312,179 | 11.51 | 7.83 | Reference |
Finerenone + SOC | 315,472 | 11.55 | 7.85 | 175,549 | |
CADTH exploratory reanalysis 4 (1 + 2 + 3 + 5) (probabilistic) | SOC | 310,716 | 11.48 | 7.86 | Reference |
Finerenone + SOC | 318,049 | 11.61 | 7.94 | 93,752 | |
CADTH exploratory reanalysis 5 (1 + 2 + 3 + 4 + 5) (probabilistic) | SOC | 311,993 | 11.51 | 7.85 | Reference |
Finerenone + SOC | 316,249 | 11.52 | 7.85 | 2,994,490 |
CKD = chronic kidney disease; CV = cardiovascular; ICER = incremental cost-effectiveness ratio; LY = life-year; QALY = quality-adjusted life-year; SOC = standard of care.
Scenario Analysis Results
CADTH performed price reduction analyses based on the sponsor’s base case and CADTH exploratory reanalyses. If results from the trial are fully realized in the Canadian context (i.e., concurrent use of SGLT2 inhibitors has no impact on the benefits seen from finerenone), mortality benefits are realized, and the benefits of finerenone are permanent and enduring (i.e., there is no treatment waning), then the price reduction to achieve an ICER less than $50,000 per QALY will be closer to 23% (exploratory analysis 1). CADTH notes that assessment of mortality is uncertain given the wide CIs around the mortality benefit estimates, as well as SGLT2 inhibitors not appearing in SOC. If finerenone is not expected to influence CV mortality (exploratory reanalysis 3), then a price reduction of closer to 31% is required. If mortality benefits are realized but the reduction in dialysis use over the patient lifetime is smaller than what is seen from the trial, then a price reduction of 44% is required (exploratory reanalysis 4). If mortality benefits are not realized and reductions in dialysis are smaller, then a price reduction of greater than 55% may be required (exploratory analysis 5). If hospitalizations for heart failure are the only nonfatal CV event prevented with finerenone, then the price reduction required to achieve cost-effectiveness increases across all analyses; for example, in exploratory reanalysis 1 the price reduction would increase from 23% to 29% (exploratory reanalysis 2).
CADTH notes that up to 73% of the –$857 to –$1,092 cost savings associated with preventing a first CV event are attributed to savings that occur in the post-acute phase. The degree of cost savings in the post-acute phase is uncertain, as 46% of patients start the analysis with a history of CV disease. These patients may therefore not experience the same increase in health care costs after the acute phase of a CV event (first 4 months) as someone who has never experienced a CV event. A decrease in cost savings would require further price reductions to achieve cost-effectiveness at a $50,000 per QALY threshold.
Finally, CADTH could not address uncertainty in the model structure, which may result in bias in favour of finerenone. It is unclear to what degree this influences the results.
Table 7: CADTH Price Reduction Analyses
Price reduction analysis | Sponsor base case | ICERs for finerenone vs. SOC ($/QALY) | ||||
|---|---|---|---|---|---|---|
CADTH exploratory reanalysis 1 | CADTH exploratory reanalysis 2 | CADTH exploratory reanalysis 3 | CADTH exploratory reanalysis 4 | CADTH exploratory reanalysis 5 | ||
No price reduction | 18,255 | 70,052 | 73,484 | 175,549 | 93,752 | 2,994,490 |
10% | NA | 61,251 | 65,261 | 134,828 | 83,932 | 2,459,563 |
20% | NA | 52,450 | 57,038 | 94,106 | 74,111 | 1,924,635 |
30% | NA | 43,649 | 48,815 | 53,385 | 64,291 | 1,389,708 |
40% | NA | NA | NA | 12,663 | 54,470 | 854,781 |
50% | NA | NA | NA | NA | 44,649 | 319,853 |
60% | NA | NA | NA | NA | NA | Dominant |
70% | NA | NA | NA | NA | NA | NA |
ICER = incremental cost-effectiveness ratio; NA = not applicable; QALY = quality-adjusted life-year; SOC = standard of care; vs. = versus.
Issues for Consideration
Patients were excluded from FIDELIO and FIGARO if they had known chronic heart failure.3,4 Clinical experts consulted for this review indicated that finerenone may be used in patients with heart failure and noted that they would consider heart failure to be an indication to use finerenone. As the clinical studies excluded patients with heart failure, the cost-effectiveness of finerenone in patients with T2D and CKD with concomitant heart failure is not known. As experts indicated that finerenone may be used for heart failure, there is potential for indication creep beyond the T2D-CKD indication.
Only patients with persistently high or very high albuminuria were included in the FIDELIO and FIGARO trials; therefore, the cost-effectiveness of finerenone in patients with normal albuminuria is unknown.3,4 The proposed Health Canada indication for finerenone does not exclude use in patients with normal albuminuria.2
According to clinical experts consulted by CADTH for this review, finerenone may be considered for use in patients with CKD alone in circumstances where ACE inhibitors or ARBs and/or SGLT2 inhibitors are not tolerated or are contraindicated, which is expected to be rare. The finerenone clinical trials were only conducted in patients with T2D and CKD; therefore, the cost-effectiveness of finerenone in patients with CKD alone is unknown.3,4
The patent for dapagliflozin, the only SGLT2 inhibitor with a Health Canada indication for CKD, will expire in May 2023.31,44 If dapagliflozin is considered SOC and if finerenone is reimbursed as an add on to SOC, the genericization of dapagliflozin will not influence cost-effectiveness results. However, if dapagliflozin is a comparator to finerenone, generic dapagliflozin will influence the cost-effectiveness of finerenone. The sponsor did not submit a model including dapagliflozin as a comparator; therefore, the cost-effectiveness of finerenone versus dapagliflozin (generic or patented) is unknown.
Overall Conclusions
Two randomized controlled trials demonstrated that treatment with finerenone was associated with a clinically meaningful reduction in the renal composite outcome and the CV composite outcome driven by the outcome components of a sustained decrease in eGFR of greater than or equal to 40% and greater than or equal to 57% and incidence of hospitalization for heart failure. The trials also demonstrated that finerenone was associated with a significant reduction in urinary albumin-creatinine ratio from baseline, which the clinical experts referred to as an important marker for the reduced risk of progression of CKD to ESRD. The impact of finerenone on HRQoL is uncertain due to difficulty interpreting results from the HRQoL instruments. The trials did not demonstrate statistically significant differences in all-cause mortality or CV mortality. All patients in both trials were on ACE inhibitors or ARBs as SOC, but only a small proportion in both trials were on SGLT2 inhibitors at baseline. Hence, the available evidence on the efficacy and safety of the addition of finerenone to ACE inhibitor or ARB, and an SGLT2 inhibitor, is limited.
CADTH noted uncertainty with the sponsor’s modelling approach, which considered a clinical pathway that allowed for substantial improvements in kidney function. For example, patients with an eGFR of less than 15 mL/min/1.73 m2 could achieve an eGFR of greater than 60 mL/min/1.73 m2 within an 8-month time span, resulting in lower mortality risk, better quality of life, and lower health care costs. This type of improvement was considered highly unlikely by the clinical experts consulted by CADTH for the review, who noted that once eGFR is sustained below 15 mL/min/1.73 m2, kidney damage is irreversible. In addition, CV events were not modelled separately; as such, finerenone had an equal chance of reducing MIs, strokes, and hospitalizations for heart failure. When MIs, strokes, and hospitalizations for heart failure are analyzed separately in the FIDELITY pooled analysis, finerenone has a statistically significant reduction in hospitalizations for heart failure but not for stroke or MIs.6 For example, the HR for finerenone versus placebo when looking at incidence of nonfatal strokes is 0.99 (95% CI, 0.82 to 1.21) in the FIDELITY pooled analysis. However, in the model, the sponsor assumes the HR for nonfatal strokes is 0.88 (the HR for first CV events), resulting in finerenone having a substantial impact on reducing the incidence of strokes. These aspects of the model could not be fully addressed by CADTH. For these reasons, CADTH could not derive a reliable base-case analysis and instead conducted a series of exploratory analyses to explore different areas of uncertainty. As part of CADTH’s exploratory reanalysis, more appropriate utility values for CKD states were used, more appropriate costs were applied to CKD states, and the risk of dialysis was changed to match the trial outputs. In addition, CADTH conducted additional analyses by removing stroke and MI from the analysis, removing CV mortality reduction associated with finerenone, and further decreasing the reduction in dialysis associated with finerenone.
If results from the trial are fully realized in the Canadian context (i.e., concurrent use of SGLT2 inhibitors has no impact on the benefits seen from finerenone), mortality benefits are realized, and the benefits of finerenone are permanent and enduring (i.e., there is no treatment waning), then the ICER for finerenone relative to SOC was estimated to be $70,052 per QALY. A price reduction of 23% would be required to be considered cost-effective at a willingness-to-pay threshold of $50,000 per QALY. If CV mortality benefits are not realized, then the ICER increases to $175,549 per QALY. A price reduction of at least 31% may be required to achieve cost-effectiveness. Given the current clinical evidence, whether finerenone will result in a life expectancy gain is unclear. On top of this, if reduction in dialysis use does not continue indefinitely beyond the trial time horizon, then the ICER may exceed $2 million per QALY, with price reductions of more than 55% required to bring the ICER below $50,000 per QALY. CADTH notes that the analysis allows for clinically unsupported improvements in eGFR and reductions in strokes and MIs that are not seen in the trial and that it may overestimate cost savings from preventing CV events. Therefore, the results may be biased in favour of finerenone across all these analyses, and further price reductions than those cited may be required.
Overall, the sponsor’s analysis shows that improvements in life expectancy have the largest impact on incremental QALYs generated by finerenone relative to SOC. Outside of potential mortality reduction, the main value of finerenone, as estimated by the sponsor’s analysis, is derived from dialysis reduction and reduction in hospitalizations for heart failure, both of which lead to cost savings to the health system. However, the extent of cost savings that could be realized is uncertain. The CREDENCE trial shows that SGLT2 inhibitors also reduce CV events and ESRD.27 If SGLT2 inhibitors become SOC in Canada, then it is unclear what the concurrent benefit of giving patients both SGLT2 inhibitors and finerenone will be. The analysis also assumes that the treatment effect of finerenone does not wane over the patient’s lifetime, with the majority of benefit occurring 5 years after treatment initiation, a period for which there are no data. As the place of finerenone in therapy, relative to SGLT2 inhibitors, is uncertain, and because there is a paucity of clinical evidence regarding the efficacy of finerenone when used alongside SGLT2 inhibitors, CADTH was unable to conduct a reliable reanalysis in the sponsor’s reimbursement request population. CADTH notes that the analyses only looks at finerenone as an add-on therapy that would not displace any component of current SOC, meaning that the cost-effectiveness of finerenone versus SGLT2 inhibitors is unknown.
References
1.Pharmacoeconomic evaluation [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Kerendia (finerenone), 10 mg, and 20 mg tablets. Mississauga (ON): Bayer Inc.; 2022 Jun 3.
2.PrKerendia® (finerenone): 10 mg and 20 mg, oral tablets [draft product monograph]. Mississauga (ON): Bayer Inc.; 2021 Oct 29.
3.Clinical Study Report: PH-39746. A randomized, double-blind, placebo-controlled, parallel-group, multicenter, event-driven phase III study to investigate the efficacy and safety of finerenone, in addition to standard of care, on the progression of kidney disease in subjects with type 2 diabetes mellitus and the clinical diagnosis of diabetic kidney disease [internal sponsor's report]. Mississauga (ON): Bayer Inc.; 2020 Sep 22.
4.Clinical Study Report: PH-39747. A randomized, double-blind, placebo-controlled, parallel-group, multicenter, eventdriven phase III study to investigate the efficacy and safety of finerenone on the reduction of cardiovascular morbidity and mortality in subjects with type 2 diabetes mellitus and the clinical diagnosis of diabetic kidney disease in addition to standard of care [internal sponsor's report]. Mississauga (ON): Bayer Inc.; 2021 Aug 20.
5.de Boer IH, Caramori ML, Chan JC, et al. KDIGO 2020 clinical practice guideline for diabetes management in chronic kidney disease. Kidney Int. 2020;98(4 Suppl):S1-S115. PubMed
6.Integrated analysis statistical report: PH-42134. Integrated analysis of FIDELIO-DKD and FIGARO-DKD [internal sponsor's report]. Mississauga (ON): Bayer Inc.; 2021 Jul 30.
7.Wilson PW, D'Agostino Sr R, Bhatt DL, et al. An international model to predict recurrent cardiovascular disease. Am J Med. 2012;125(7):695-703. e691.
8.Darlington O, Dickerson C, Evans M, et al. Costs and healthcare resource use associated with risk of cardiovascular morbidity in patients with chronic kidney disease: evidence from a systematic literature review. Adv Ther. 2021;38(2):994-1010. PubMed
9.UK renal registry 22nd annual report: data to 31/12/2018. Bristol (UK): The Renal Association; 2020: https://ukkidney.org/sites/renal.org/files/publication/file-attachments/22nd_UKRR_ANNUAL_REPORT_FULL.pdf. Accessed 2022 Jul 18.
10.Erickson KF, Japa S, Owens DK, Chertow GM, Garber AM, Goldhaber-Fiebert JD. Cost-effectiveness of statins for primary cardiovascular prevention in chronic kidney disease. J Am Coll Cardiol. 2013;61(12):1250-1258. PubMed
11.Ontario Ministry of Health, Ontario Ministry of Long-Term Care. Ontario drug benefit formulary/comparative drug index. 2022; https://www.formulary.health.gov.on.ca/formulary/. Accessed 2022 Jul 1.
12.Manns B, Hemmelgarn B, Tonelli M, et al. The cost of care for people with chronic kidney disease. Can J Kidney Health Dis. 2019;6:2054358119835521. PubMed
13.Pharmacoeconomic review report: sodium zirconium cyclosilicate (Lokelma) CADTH common drug review. Ottawa (ON): CADTH; 2020: https://www.cadth.ca/sites/default/files/cdr/pharmacoeconomic/sr0612-lokelma-pharmacoeconomic-review-report.pdf. Accessed 2022 Jul 18.
14.Treatment of end-stage organ failure in Canada, Canadian organ replacement register, 2011 to 2020: end-stage kidney disease and kidney transplants — data tables. Ottawa (ON): Canadian Institute for Health Information (CIHI); 2021.
15.Beaudry A, Ferguson TW, Rigatto C, Tangri N, Dumanski S, Komenda P. Cost of dialysis therapy by modality in Manitoba. Clin J Am Soc Nephrol. 2018;13(8):1197-1203. PubMed
16.Barnieh L, Gill JS, Klarenbach S, Manns BJ. The cost-effectiveness of using payment to increase living donor kidneys for transplantation. Clin J Am Soc Nephrol. 2013;8(12):2165-2173. PubMed
17.Cohen D, Manuel DG, Tugwell P, Sanmartin C, Ramsay T. Direct healthcare costs of acute myocardial infarction in Canada’s elderly across the continuum of care. J Econ Ageing. 2014;3:44-49.
18.Endovascular therapy for acute ischemic stroke. Edmonton (AB): Institute of Health Economics (IHE); 2017.
19.Tawfik A, Wodchis WP, Pechlivanoglou P, Hoch J, Husereau D, Krahn M. Using phase-based costing of real-world data to inform decision–analytic models for atrial fibrillation. Appl Health Econ Health Policy. 2016;14(3):313-322. PubMed
20.Wells G, Coyle D, Cameron C, et al. Safety, effectiveness, and cost-effectiveness of new oral anticoagulants compared with warfarin in preventing stroke and other cardiovascular events in patients with atrial fibrillation. CADTH therapeutic review. Ottawa (ON): CADTH; 2012.
21.Zaour N, Barbeau M, Liu N, Borrelli R, Fischer A. The cost of hospitalization and length of stay for chronic heart failure cases in Canada. Can J Cardiol. 2015;31(10):S273.
22.New drugs for type 2 diabetes: second-line therapy – science report. CADTH therapeutic review. Vol. 4 No.1b. Ottawa (ON): CADTH; 2017: https://www.cadth.ca/sites/default/files/pdf/TR0012_T2D_Science_Report.pdf. Accessed 2022 Jul 12.
23.Health Quality Ontario. Left atrial appendage closure device with delivery system: a health technology assessment. Ont Health Technol Assess Ser. 2017;17(9):1-106. PubMed
24.Smolderen KG, Bell A, Lei Y, et al. One-year costs associated with cardiovascular disease in Canada: insights from the REduction of Atherothrombosis for Continued Health (REACH) registry. Can J Cardiol. 2010;26(8):e297-e305. PubMed
25.Patient cost estimator. 2022; https://www.cihi.ca/en/patient-cost-estimator. Accessed 2022 May 20.
26.Xie F, Pullenayegum E, Gaebel K, et al. A time trade-off-derived value set of the EQ-5D-5L for Canada. Med Care. 2016;54(1):98. PubMed
27.Perkovic V, Jardine MJ, Neal B, et al. Canagliflozin and renal outcomes in type 2 diabetes and nephropathy. N Engl J Med. 2019;380(24):2295-2306. PubMed
28.Slow progression & reduce complications. Bethesda (MD): National Institutes of Health (NIH); 2022: https://www.niddk.nih.gov/health-information/professionals/clinical-tools-patient-management/kidney-disease/identify-manage-patients/manage-ckd/slow-progression-reduce-complications#:~:text=Although%20CKD%20is%20generally%20progressive,need%20for%20renal%20replacement%20therapy. Accessed 2022 Jul 27.
29.Zaric GS. The impact of ignoring population heterogeneity when Markov models are used in cost-effectiveness analysis. Med Decis Making. 2003;23(5):379-386. PubMed
30.Integrated analysis statistical report: PH-42131. Additional integrated exposure and safety analysis of the phase III FIDELIO-DKD and FIGARO-DKD studies and the five finerenone phase II studies [internal sponsor's report]. Mississauga (ON): Bayer Inc.; 2021 Aug 9.
31.PrForxiga® (dapagliflozin propanediol monohydrate): 5 mg and 10 mg tablets [product monograph ]. Mississauga (ON): AstraZeneca Canada; 2021 Aug 6: https://pdf.hres.ca/dpd_pm/00062416.PDF. Accessed 2022 Jul 25.
32.Foxiga (dapagliflozin). CADTH drug reimbursement review - not filed by the manufacturer 2021; https://www.cadth.ca/dapagliflozin-2. Accessed July 27 2022.
33.Davies C, Briggs A, Lorgelly P, Garellick G, Malchau H. The “hazards” of extrapolating survival curves. Med Decis Making. 2013;33(3):369-380. PubMed
34.Bayer Inc. response to 2022 Jul 16 DRR request for additional information regarding Kerendia (finerenone) for the treatment of patients with chronic kidney disease (CKD) and type 2 diabetes (T2D) [internal additional sponsor's information]. Mississauga (ON): Bayer Inc.; 2022 Jul 22.
35.Guertin JR, Feeny D, Tarride J-E. Age-and sex-specific Canadian utility norms, based on the 2013–2014 Canadian Community Health Survey. CMAJ. 2018;190(6):E155-E161. PubMed
36.Guertin JR, Humphries B, Feeny D, Tarride J-E. Health utilities index mark 3 scores for major chronic conditions: population norms for Canada based on the 2013-2014 Canadian Community Health Survey. Health Rep. 2018;29(11):12-19. PubMed
37.Cooper JT, Lloyd A, Sanchez JJG, Sörstadius E, Briggs A, McFarlane P. Health related quality of life utility weights for economic evaluation through different stages of chronic kidney disease: a systematic literature review. Health Qual Life Outcomes. 2020;18(1):1-11. PubMed
38.Guidelines for the economic evaluation of health technologies: Canada. 4th ed. Ottawa (ON): CADTH; 2017: https://www.cadth.ca/guidelines-economic-evaluation-health-technologies-canada-4th-edition. Accessed 2022 Jun 21.
39.Krahn MD, Bremner KE, de Oliveira C, et al. Home dialysis is associated with lower costs and better survival than other modalities: a population-based study in Ontario, Canada. Perit Dial Int. 2019;39(6):553-561. PubMed
40.Lahoz R, Fagan A, McSharry M, Proudfoot C, Corda S, Studer R. Recurrent heart failure hospitalizations are associated with increased cardiovascular mortality in patients with heart failure in Clinical Practice Research Datalink. ESC Heart Fail. 2020;7(4):1688-1699. PubMed
41.Hougen I, Leon SJ, Whitlock R, et al. Hyperkalemia and its association with mortality, cardiovascular events, hospitalizations, and intensive care unit admissions in a population-based retrospective cohort. Kidney Int Rep. 2021;6(5):1309-1316. PubMed
42.Lee E, Choi EK, Han KD, et al. Mortality and causes of death in patients with atrial fibrillation: a nationwide population-based study. PLoS One. 2018;13(12):e0209687. PubMed
43.Alshehri AM. Stroke in atrial fibrillation: review of risk stratification and preventive therapy. J Family Community Med. 2019;26(2):92-97. PubMed
44.Patent register - form IV summaries. Ottawa (ON): Health Canada; 2022.
45.Consumer Price Index, annual average, not seasonally adjusted. 2022; https://www150.statcan.gc.ca/t1/tbl1/en/tv.action?pid=1810000501&pickMembers%5B0%5D=1.2&cubeTimeFrame.startYear=2015&cubeTimeFrame.endYear=2021&referencePeriods=20150101%2C20210101. Accessed 2022 Aug 12.
46.Budget Impact Analysis [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Kerendia (finerenone), 10 mg, and 20 mg tablets. Mississauga (ON): Bayer Inc.; 2022 Jun 3.
47.Table 17-10-0009-01. Population estimates, quarterly. Ottawa (ON): Statistics Canada; 2022: https://www150.statcan.gc.ca/t1/tbl1/en/tv.action?pid=1710000901 Accessed 2022 Mar 17.
48.Chu L, Fuller M, Jervis K, Ciaccia A, Abitbol A. Prevalence of chronic kidney disease in type 2 diabetes: The Canadian Registry of Chronic Kidney Disease in Diabetes Outcomes (CREDO) study. Clin Ther. 2021;43(9):1558-1573. PubMed
49.Tonelli M, Wiebe N, Richard J-F, Klarenbach SW, Hemmelgarn BR. Characteristics of adults with type 2 diabetes mellitus by category of chronic kidney disease and presence of cardiovascular disease in Alberta Canada: a cross-sectional study. Can J Kidney Health Dis. 2019;6:2054358119854113. PubMed
50.Canadian Chronic Disease Surveillance System. 2019; https://health-infobase.canada.ca/CCDSS/data-tool/ Accessed 2022 Apr 26.
51.LeBlanc AG, Jun Gao Y, McRae L, Pelletier C. At-a-glance - Twenty years of diabetes surveillance using the Canadian Chronic Disease Surveillance System. Health Promot Chronic Dis Prev Can. 2019;39(11):306-309. PubMed
52.Armstrong M, Weaver R, Pannu N. Prevalence and quality of care in chronic kidney disease. Alberta kidney care report. Edmonton (AB): Alberta Health Services; 2019: https://www.albertahealthservices.ca/assets/about/scn/ahs-scn-kh-ckd-report-2019.pdf. Accessed 2022 Jul 13.
53.Dinh T, Sutherland G. Understanding the gap: a pan-Canadian analysis of prescription drug insurance coverage. Ottawa (ON): The Conference Board of Canada; 2017: https://www.conferenceboard.ca/e-library/abstract.aspx?did=9326. Accessed 2022 Jun 21.
54.Liu P, Quinn RR, Lam NN, et al. Progression and regression of chronic kidney disease by age among adults in a population-based cohort in Alberta, Canada. JAMA Netw Open. 2021;4(6):e2112828-e2112828. PubMed
Appendix 1: Cost Comparison Table
Note that this appendix has not been copy-edited.
The comparators presented in the following table have been deemed to be appropriate based on feedback from clinical experts. Comparators may be recommended (appropriate) practice or actual practice. Existing Product Listing Agreements are not reflected in the table and as such, the table may not represent the actual costs to public drug plans.
Table 8: CADTH Cost Comparison Table for Patients With T2D and CKD
Treatment | Strength / concentration | Form | Price | Recommended dosage | Daily cost | Annual cost |
|---|---|---|---|---|---|---|
Kerendia (finerenone) | 10 mg 20 mg | Tablet | 3.3400a | Starting:
Target: 20 mg once daily | 3.34 | 1,219 |
CKD = chronic kidney disease; T2D = type 2 diabetes
aSponsor submitted price1
Table 9: CADTH Cost Comparison Table for Other Treatments With a Health Canada Indication for CKD
Treatment | Strength / concentration | Form | Price | Recommended dosage | Daily cost | Annual cost |
|---|---|---|---|---|---|---|
SGLT2 inhibitors | ||||||
Forxiga (Dapagliflozin) | 5 mg 10 mg | Tablet | 2.7300 2.7300 | 10 mg once daily | 2.73 | 996 |
CKD = chronic kidney disease
Note: All prices are from the Ontario Drug Benefit Formulary (accessed July 2022), unless otherwise indicated, and do not include dispensing fees.11
Note: Other SGLT2 inhibitors are also available in Canada (e.g., empagliflozin and canagliflozin), however, these medications do not currently have a Health Canada indication for CKD.
Appendix 2: Submission Quality
Note that this appendix has not been copy-edited.
Description | Yes/No | Comments |
|---|---|---|
Population is relevant, with no critical intervention missing, and no relevant outcome missing | Yes | No comment |
Model has been adequately programmed and has sufficient face validity | Yes | CADTH notes the trace is transparent and outcomes from the model can be compared against trial outcomes. |
Model structure is adequate for decision problem | No | The model allows for substantial regression through CKD stages which was deemed clinically unlikely. The model also applies equal treatment efficacy to the prevention of MI, strokes and HF hospitalizations despite showing no evidence of a reduction in strokes. |
Data incorporation into the model has been done adequately (e.g., parameters for probabilistic analysis) | Yes | No comment |
Parameter and structural uncertainty were adequately assessed; analyses were adequate to inform the decision problem | No | Uncertainty around transition probabilities between health states was not captured in the probabilistic analysis. |
The submission was well organized and complete; the information was easy to locate (clear and transparent reporting; technical documentation available in enough details) | Yes | CADTH notes the sponsor was accommodating in all additional information requests providing all data requested. |
Appendix 3: Additional Information on the Submitted Economic Evaluation
Note that this appendix has not been copy-edited.
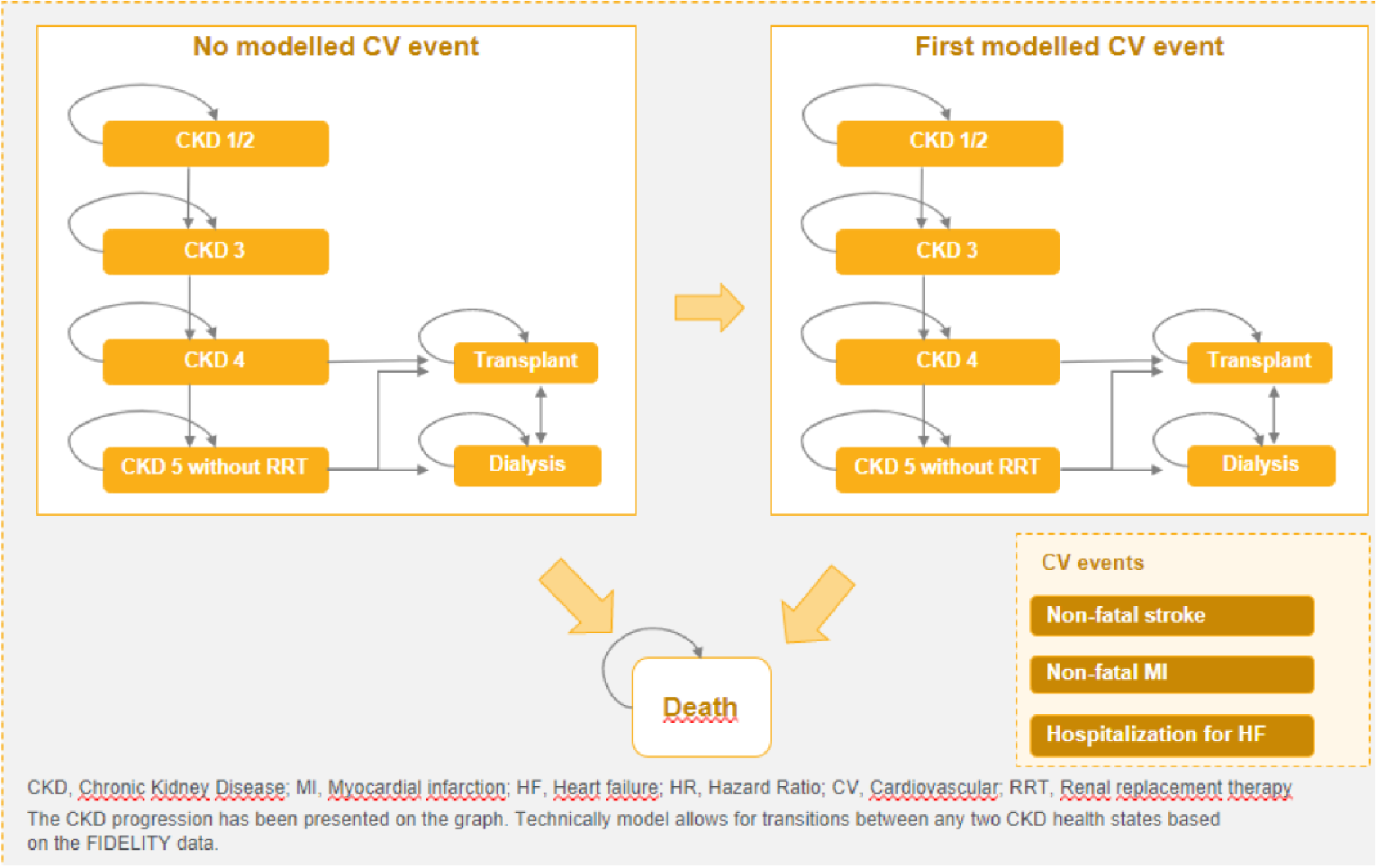
Detailed Results of the Sponsor’s Base Case
Table 11: CKD Stage eGFR Cut-Offs and Baseline Patient Distribution Across CKD-Health States
Health state | eGFR cut-off for state (mL/min/1.73 m2) | Baseline patient distribution |
|---|---|---|
CKD1/2 | ≥ 60 | 39.9% |
CKD3 | 30 to 59 | 53.3% |
CKD4 | 15 to 29 | 6.8% |
CKD5 w/o RRT | < 15 | 0.0% |
Dialysis | NA | 0.0% |
Kidney Transplant | NA | 0.0% |
CKD = chronic kidney disease; NA = not applicable; RRT = renal replacement therapy
Source: Sponsor’s pharmacoeconomic analysis1
Table 12: Hazard Ratios Used to Derive Increased Mortality Risk due to CKD Progression
CKD stage | Hazard ratio | Source |
|---|---|---|
CKD1/2 | 1.14 | Darlington 2028 |
CKD3 | 1.32 | |
CKD4 | 6.42 | |
CKD 5 w/o RRT | 9.49 | |
Dialysis (acute) | 10.04 | UKKR Annual Report9 |
Dialysis (post-acute) | 10.04 | |
Kidney Transplant (acute) | 1.59 | |
Kidney Transplant (post-acute) | 1.59 |
CKD = chronic kidney disease; RRT = renal replacement therapy
Figure 2: Time to Dialysis for SOC From the Model Versus FIDELITY Analysis
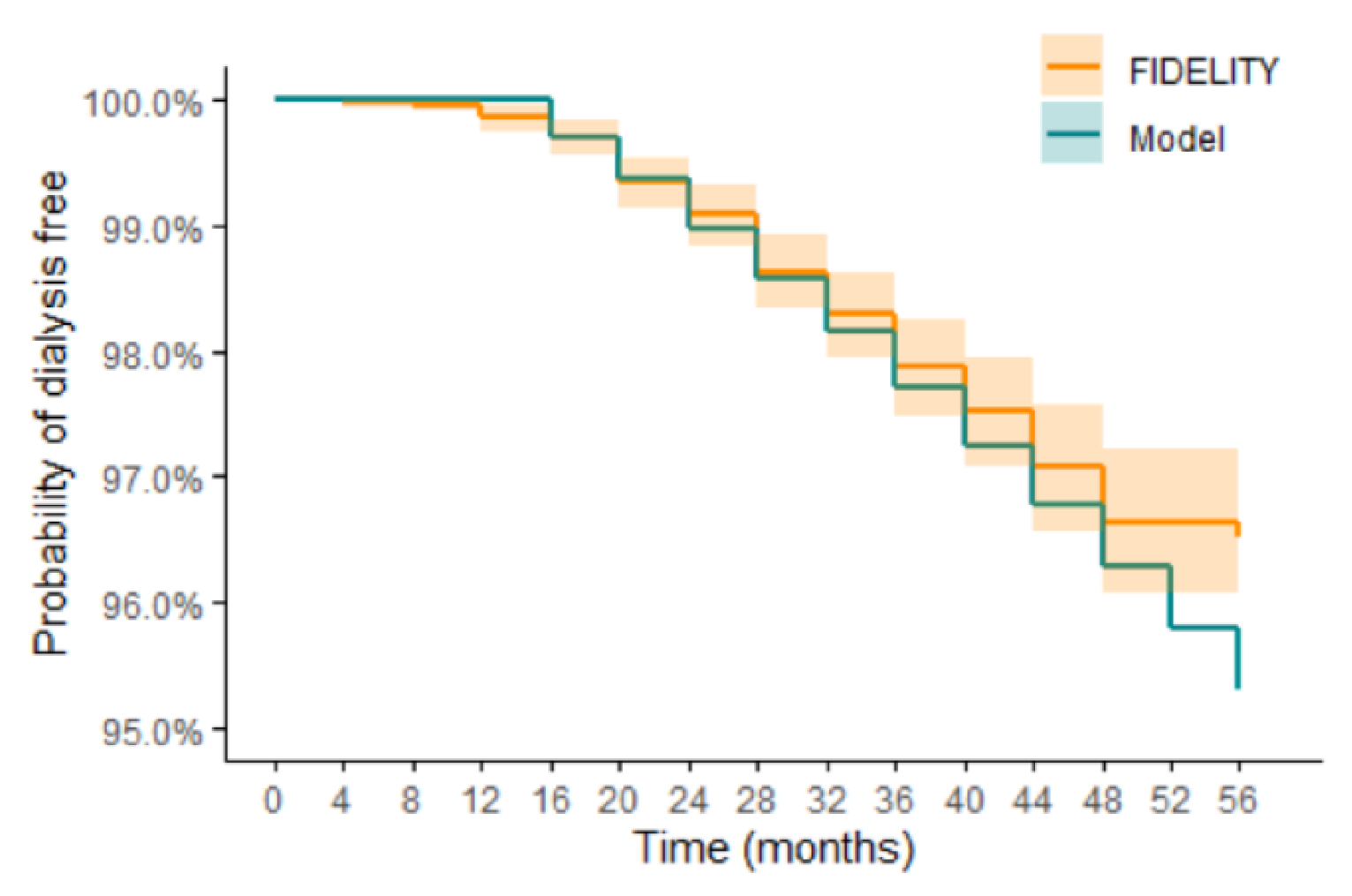
Source: Sponsor’s pharmacoeconomic analysis.1
Figure 3: Time to Dialysis for Finerenone From the Model Versus FIDELITY Analysis
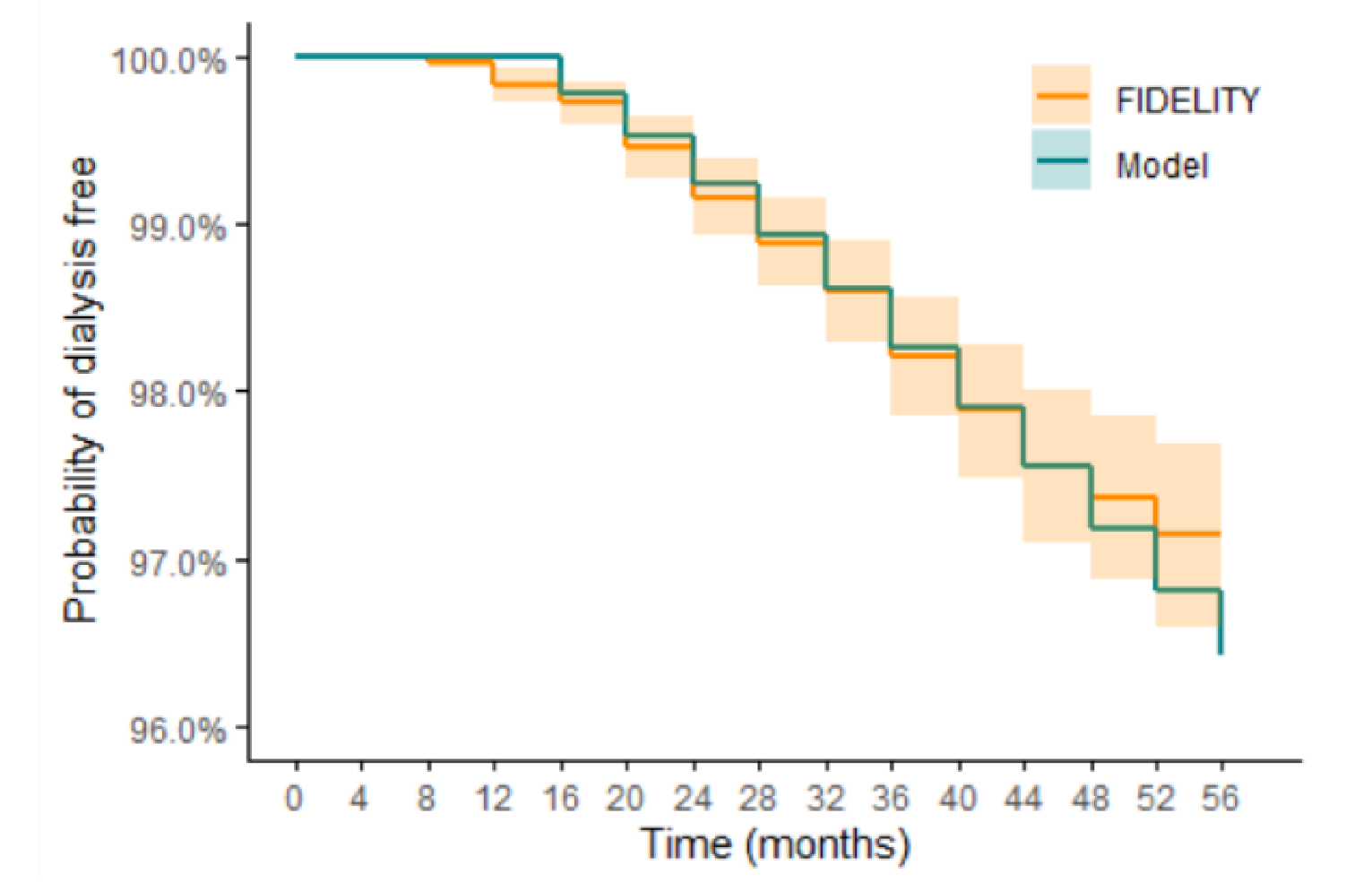
Source: Sponsor’s pharmacoeconomic analysis1
Appendix 4: Additional Details on the CADTH Reanalyses and Sensitivity Analyses of the Economic Evaluation
Note that this appendix has not been copy-edited.
Table 13: Utilities by CKD Stage
Health state | Sponsor base case | Cooper et al.37 | Utility in CADTH exploratory reanalysis |
|---|---|---|---|
CKD1/2 | 0.827 | 0.85 | 0.827a |
CKD3 | 0.825 | 0.73 | 0.707b |
CKD4 | 0.813 | 0.74d | 0.717b |
CKD5 | 0.802 | 0.73 | 0.707b |
Dialysis | 0.761 (acute) 0.788 (post-acute) | 0.67 (hemodialysis) 0.57 (peritoneal dialysis) | 0.627 (acute)b,c 0.627 (post-acute)b,c |
Kidney Transplant | 0.824 (acute) 0.879 (post-acute) | 0.74 (pretransplant) 0.83 (posttransplant) | 0.717 (acute)b 0.807 (post-acute)b |
CKD = chronic kidney disease; NA = not applicable; RRT = renal replacement therapy
aDerived from FIDELITY6
bApplied utility reductions relative to CKD 2 as per Cooper et al.37
cAssumed 79.4% of patients are on hemodialysis and 20.6% are on peritoneal dialysis as per sponsor’s assumptions.
dIt was noted that utility would not likely increase upon progression to CKD4, however this has minimal impact on the results given the small differences.
Table 14: Costs by CKD Stage per Cycle (4 Months)
Health state | Sponsor base case (annual) | Manns et al.12 adjusted for albuminuria and CKD 3 (annual)a, b | Costs related to dialysis, drug costs included in model and cardiac care (annual)c | Costs used in CADTH exploratory reanalysis adjusted to 2021 CAD (annual)d |
|---|---|---|---|---|
CKD1/2 | $27 | $16,468 | Dialysis costs: $0 Cardiac care: $270 (moderate albuminuria); $552 (severe albuminuria) Drug costs: $1,277 | $15,976 |
CKD3 | $123 | $20,368 | Dialysis costs: $0 Cardiac care: $646 (CKD 3a); $1,414 (CKD 3b) Drug costs: $1,277 | $19,875 |
CKD4 | $1,419 | $26,349 | Dialysis costs: $1,000 (moderate/severe albuminuria only) Cardiac care: $2,157 Drug costs: $1,277 | $24,269 |
CKD5 without RRT | $5,739 | $46,105 (includes CKD5 with RRT) | Dialysis costs: $8,000 (no significant albuminuria); $12,000 (moderate/severe albuminuria) Cardiac care: $2,395 Drug costs: $1,277 | $33,235 |
Dialysis | $62,799 (acute) $62,799 (post-acute) | NR | NR | $96,034.08 (acute)e $96,034.08 (post-acute)e |
Kidney Transplant | $122,814 (acute) $25,671 (post-acute) | NR | NR | $122,814 (acute) $25,671 (post-acute) |
CKD = chronic kidney disease; NR = not reported; RRT = renal replacement therapy
aSource: Manns et al. 201912
bIt was assumed that 1.8% of patients had no significant albuminuria, 31.5% had moderate, and 66.7% had severe as per FIDELITY trial.6 Further, it was assumed 68% of CKD 3 are 3a and 32% are 3b based on patients numbers reported in Manns et al. 2019.12
cDialysis costs were sourced from Figure 1 in Manns et al. 2019.12 Drug costs are taken from the sponsor’s analysis and cardiac care costs are taken from Figure 3 in Manns et al.201912
dAdjusted for inflation using consumer price index from Statistics Canada.45
eHealth state costs for dialysis are CADTH’s CKD 5 without RRT costs plus the sponsor’s dialysis costs ($62,799 + $33,235 = $96,034)
Detailed Results of CADTH Base Case
Table 15: Disaggregated Summary of CADTH’s Reanalysis 1 Results
Parameter | Finerenone + SOC | SOC | Incremental |
|---|---|---|---|
Discounted LYs | |||
Total | 11.64 | 11.50 | 0.15 |
Discounted QALYs | |||
Total | 7.96 | 7.87 | 0.09 |
CKD 1/2 | 2.50 | 2.58 | −0.09 |
CKD 3 | 3.93 | 3.79 | 0.15 |
CKD 4 | 1.14 | 1.07 | 0.07 |
CKD 5 without dialysis | 0.11 | 0.11 | −0.01 |
Dialysis (acute) | 0.02 | 0.03 | 0.00 |
Dialysis (post-acute) | 0.21 | 0.23 | −0.02 |
Kidney transplant (acute) | 0.00 | 0.00 | 0.00 |
Kidney transplant (post-acute) | 0.05 | 0.06 | −0.01 |
Discounted costs ($) | |||
Total | 318,236 | 311,874 | 6,362 |
Acquisition | 22,565 | 1,470 | 7,863 |
CKD-related costs | 261,182 | 260,943 | 239 |
First CV event costs | 22,117 | 22,974 | −857 |
Other health events costs | 11,682 | 12,534 | −853 |
Death costs | 690 | 721 | −31 |
ICER ($/QALY) | 70,052 | ||
CKD = chronic kidney disease; CV = cardiovascular; ICER = incremental cost-effectiveness ratio; LY = life-year; QALY = quality-adjusted life-year; SOC = standard of care.
Table 16: Disaggregated Summary of CADTH’s Reanalysis 2 Results
Parameter | Finerenone + SOC | SOC | Incremental |
|---|---|---|---|
Discounted LYs | |||
Total | 11.79 | 11.63 | 0.15 |
Discounted QALYs | |||
Total | 8.05 | 7.96 | 0.09 |
CKD 1/2 | 2.54 | 2.62 | −0.09 |
CKD 3 | 3.97 | 3.82 | 0.15 |
CKD 4 | 1.13 | 1.07 | 0.07 |
CKD 5 without dialysis | 0.11 | 0.11 | −0.01 |
Dialysis (acute) | 0.02 | 0.03 | 0.00 |
Dialysis (post-acute) | 0.23 | 0.25 | −0.02 |
Kidney transplant (acute) | 0.00 | 0.00 | 0.00 |
Kidney transplant (post-acute) | 0.05 | 0.06 | −0.01 |
Discounted costs ($) | |||
Total | 301,111 | 294,176 | 6,935 |
Acquisition | 22,781 | 14,868 | 7,913 |
CKD-related costs | 265,511 | 265,323 | 188 |
First CV event costs | 9,644 | 10,662 | −1,018 |
Other health events costs | 2,373 | 2,488 | −115 |
Death costs | 802 | 835 | −33 |
ICER ($/QALY) | 73,484 | ||
CKD = chronic kidney disease; CV = cardiovascular; ICER = incremental cost-effectiveness ratio; LY = life-year; QALY = quality-adjusted life-year; SOC = standard of care.
Table 17: Disaggregated Summary of CADTH’s Reanalysis 3 Results
Parameter | Finerenone + SOC | SOC | Incremental |
|---|---|---|---|
Discounted LYs | |||
Total | 11.55 | 11.51 | 0.04 |
Discounted QALYs | |||
Total | 7.85 | 7.83 | 0.02 |
CKD 1/2 | 2.46 | 2.57 | −0.11 |
CKD 3 | 3.87 | 3.76 | 0.11 |
CKD 4 | 1.13 | 1.08 | 0.06 |
CKD 5 without dialysis | 0.10 | 0.11 | −0.01 |
Dialysis (acute) | 0.02 | 0.03 | 0.00 |
Dialysis (post-acute) | 0.21 | 0.24 | −0.03 |
Kidney transplant (acute) | 0.00 | 0.00 | 0.00 |
Kidney transplant (post-acute) | 0.05 | 0.06 | −0.01 |
Discounted costs ($) | |||
Total | 315,472 | 312,179 | 3,293 |
Acquisition | 22,275 | 14,623 | 7,653 |
CKD-related costs | 258,868 | 261,220 | −2,351 |
First CV event costs | 21,969 | 23,033 | −1,064 |
Other health events costs | 11,626 | 12,583 | −956 |
Death costs | 733 | 721 | 11 |
ICER ($/QALY) | 175,549 | ||
CKD = chronic kidney disease; CV = cardiovascular; ICER = incremental cost-effectiveness ratio; LY = life-year; QALY = quality-adjusted life-year; SOC = standard of care.
Table 18: Disaggregated Summary of CADTH’s Reanalysis 4 Results
Parameter | Finerenone + SOC | SOC | Incremental |
|---|---|---|---|
Discounted LYs | |||
Total | 11.61 | 11.48 | 0.13 |
Discounted QALYs | |||
Total | 7.94 | 7.86 | 0.08 |
CKD 1/2 | 2.49 | 2.58 | −0.09 |
CKD 3 | 3.93 | 3.79 | 0.14 |
CKD 4 | 1.12 | 1.06 | 0.06 |
CKD 5 without dialysis | 0.10 | 0.11 | −0.01 |
Dialysis (acute) | 0.02 | 0.03 | 0.00 |
Dialysis (post-acute) | 0.22 | 0.23 | −0.01 |
Kidney transplant (acute) | 0.00 | 0.00 | 0.00 |
Kidney transplant (post-acute) | 0.05 | 0.06 | 0.00 |
Discounted costs ($) | |||
Total | 318,049 | 310,716 | 7,333 |
Acquisition | 22,355 | 14,550 | 7,806 |
CKD-related costs | 261,527 | 260,214 | 1,313 |
First CV event costs | 21,967 | 22,836 | −869 |
Other health events costs | 11,512 | 12,399 | −886 |
Death costs | 687 | 718 | −31 |
ICER ($/QALY) | 93,752 | ||
CKD = chronic kidney disease; CV = cardiovascular; ICER = incremental cost-effectiveness ratio; LY = life-year; QALY = quality-adjusted life-year; SOC = standard of care.
Table 19: Disaggregated Summary of CADTH’s Reanalysis 5 Results
Parameter | Finerenone + SOC | SOC | Incremental |
|---|---|---|---|
Discounted LYs | |||
Total | 11.52 | 11.51 | 0.02 |
Discounted QALYs | |||
Total | 7.85 | 7.85 | > 0.01 |
CKD 1/2 | 2.48 | 2.59 | −0.11 |
CKD 3 | 3.85 | 3.75 | 0.10 |
CKD 4 | 1.11 | 1.07 | 0.05 |
CKD 5 without dialysis | 0.10 | 0.12 | −0.01 |
Dialysis (acute) | 0.02 | 0.03 | 0.00 |
Dialysis (post-acute) | 0.22 | 0.24 | −0.01 |
Kidney transplant (acute) | 0.00 | 0.00 | 0.00 |
Kidney transplant (post-acute) | 0.05 | 0.06 | 0.00 |
Discounted costs ($) | |||
Total | 316,249 | 311,993 | 4,256 |
Acquisition | 22,258 | 14,663 | 7,596 |
CKD-related costs | 259,867 | 261,144 | −1,277 |
First CV event costs | 21,854 | 22,946 | −1,092 |
Other health events costs | 11,538 | 12,520 | −982 |
Death costs | 732 | 720 | 12 |
ICER ($/QALY) | 2,994,490 | ||
CKD = chronic kidney disease; CV = cardiovascular; ICER = incremental cost-effectiveness ratio; LY = life-year; QALY = quality-adjusted life-year; SOC = standard of care.
Appendix 5: Submitted Budget Impact Analysis and CADTH Appraisal
Note that this appendix has not been copy-edited.
Table 20: Summary of Key Take-Aways
Key take-aways of the budget impact analysis |
|---|
|
Summary of Sponsor’s Budget Impact Analysis
The sponsor submitted a budget impact analysis (BIA) estimating the incremental budget impact of reimbursing finerenone for patients with T2D and CKD from a publicly funded drug plan payer perspective over a 3-year time horizon, considering only drug costs in the base-case analysis.46 The analytic framework, which used an epidemiology-based approach, leveraged data from multiple sources in the literature and assumptions based on clinical expert input to determine the estimated population size (Figure 4). New patients were added to the BIA by projecting jurisdictional population sizes by an adult population growth rate based on the past 6 years.47
The sponsor compared a reference scenario in which finerenone is not reimbursed for T2D CKD with a new drug scenario, where finerenone is funded according to the Health Canada indication.46 In the reference scenario, patients were assumed to receive SOC alone, while patients in the whereas in the new drug scenario patients were stratified across available treatment options which included SOC alone and finerenone + SOC, with uptake rates for finerenone informed by the sponsor’s internal market research.46 SOC costs included 100% of patients receiving an ACE inhibitor or ARB, with the distribution based on a real world utilization study.48 Additionally, a proportion of patients were assumed to receive SGLT2 inhibitors as part of SOC, with the proportion based on an Alberta administrative data study from 2018, and applying a yearly growth rate of SGLT2 inhibitor use based on SGLT2 inhibitor public and private claims data from IQVIA.49 This resulted in an estimate that 35.2%, 39.0%, and 42.8% of patients with CKD and T2D would be using an SGLT2 inhibitor as part of SOC. As finerenone costs is used in addition to SOC, SOC therapy costs do not influence incremental finerenone costs. Key inputs to the BIA are documented in Table 22.
Figure 4: Sponsor’s Estimation of the Size of the Eligible Population
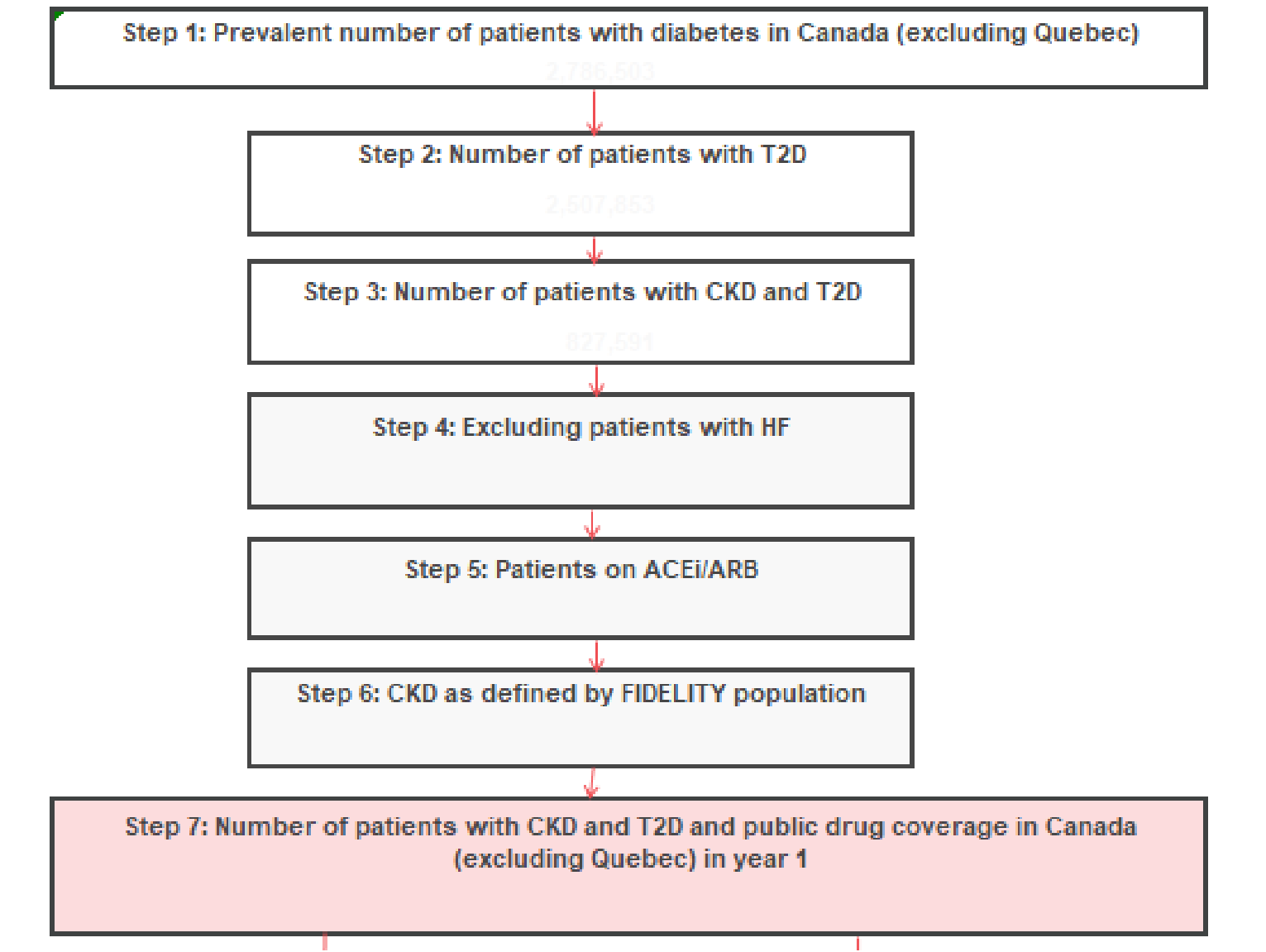
ACEi = angiotensin converting enzyme inhibitor; ARB = angiotensin receptor blocker; CKD = chronic kidney disease; HF = heart failure; T2D = type 2 diabetes;
Table 21: Summary of Key Model Parameters
Parameter | Sponsor’s estimate (reported as Year 1 / Year 2 / Year 3 if appropriate) |
|---|---|
Target Population | |
Prevalence of diabetes | 9.16%50 |
Prevalence of diabetes that is T2D | 90%51 |
CKD prevalence in adult T2D patients | 33%49 |
Proportion of CKD-T2D patients with heart failure (excluded from BIA) | 20%49 |
Proportion of CKD-T2D patients receiving an ACE inhibitor/ARB | 77.7%52 |
Proportion of CKD-T2D patients receiving an ACE inhibitor/ARB with persistent high or very high albuminuria | 47.5%49 |
Proportion eligible for public drug plan coverage | 71.71%53 |
Number of patients eligible for drug under review | 177,401 / 179,606 / 181,839 |
Market Uptake (3 years) | |
Uptake (reference scenario) Standard of care | 100% / 100% / 100% |
Uptake (new drug scenario) Finerenone Standard of care | 5.78% / 16.62% / 26.88% 94.22% / 83.38% / 73.12% |
Cost of treatment (per patient) | |
Cost of treatment over one year’ Finerenone alone Standard of care-Year 1a Standard of care-Year 2 Standard of care-Year 3 | $1,219.10 $401.67 $439.53 $477.40 |
ACE = angiotensin converting enzyme; ARB = angiotensin receptor blocker; CKD = chronic kidney disease; HF = heart failure; T2D = type 2 diabetes;
aDifferent costs for standard of care were calculated for each year as the proportion of people using SGLT2 inhibitors as standard of care increased over time (35.2% / 39.0% / 42.8% in Year 1, 2, and 3, respectively). The proportion of patients using ACE inhibitor and ARB remained consistent across all years (51.6% and 48.4%, respectively)
Summary of the Sponsor’s BIA Results
The sponsor estimated the net budget impact of introducing finerenone for the treatment of adult patients with T2D and CKD who have persistent high or very high albuminuria be $12,491,153 in Year 1, $36,394,767 in Year 2 and $59,588,681 in Year 3 for a total budget impact $108,474,600 over 3 years.
CADTH Appraisal of the Sponsor’s BIA
CADTH identified several key limitations to the sponsor’s analysis that have notable implications on the results of the BIA:
The sponsor underestimated the size of the eligible population. The sponsor’s approach to calculating the size of the eligible population excluded T2D-CKD patients with concomitant chronic heart failure.46 According to clinical experts consulted by CADTH for this review, finerenone would be prescribed to patients T2D-CKD patients with heart failure. The clinical experts also noted that finerenone is undergoing clinical trials for a heart failure indication, and that there could be indication creep for use of finerenone in patients with heart failure. Therefore, it is highly likely that CKD-T2D patients with heart failure would receive finerenone.
In the CADTH base case, patients with concomitant heart failure were included in the eligible population size.
The prevalence of CKD in T2D is uncertain. The sponsor’s base-case estimate for the prevalence of CKD in patients with T2D was 33%, estimated from a cohort of patients with T2D from the Alberta Kidney Network database.49 The sponsor provided a second estimate of 47.9% of T2D patients having CKD, estimated using data from the LMC Diabetes Registry, which holds records for patients with diabetes from a group of 13 endocrinology clinics in Ontario, Quebec, and Alberta.48 Clinical experts consulted by CADTH for this review noted that the proportion of T2D patients with CKD was uncertain.
As a scenario analysis, CADTH explored the budget impact if 47.9% of T2D patients had CKD.
The proportion of people using SGLT2 inhibitor as SOC is uncertain. In the sponsor’s base case, the sponsor assumed that 35.2%, 39.0% and 42.8% of all patients would be using SGLT2 inhibitors as part of SOC in Year 1, 2, and 3, respectively. According to drug plan input received for this review, reimbursement of SGLT2 inhibitors is restricted in some jurisdictions to indications such as T2D and heart failure. This is reflected in the sponsor’s comparator reimbursement status table, which shows that dapagliflozin, the only SGLT2 inhibitor with a Health Canada indication for CKD, is a restricted benefit in nearly all jurisdictions. Therefore, the status of SGLT2 inhibitors as SOC for T2D CKD is uncertain.
No changes were made in the CADTH base case. As the sponsor assumed finerenone would be added on to SOC, and that SGLT2 inhibitors were part of SOC, changing the proportion of people receiving SOC does not influence the incremental budget impact.
The sponsor’s estimated eligible population does not reflect the proposed Health Indication. In calculating the size of the population eligible for finerenone, the sponsor excluded T2D-CKD patients who did not have persistent high or very high albuminuria to align with the inclusion criteria of the FIDELIO-DKD and FIGARO-DKD trials.3,4 However, the proposed Health Canada indication does not restrict eligibility of finerenone by albuminuria. According to clinical experts consulted by CADTH for this review, they would be unlikely to prescribe finerenone to a patient who did not did not have persistent high or very high albuminuria. Nonetheless, it is uncertain whether all physicians prescribing finerenone would only initiate use in those with persistent high or very high albuminuria.
In a scenario analysis, CADTH explored the budget impact if finerenone was reimbursed for T2D-CKD patients regardless of their albuminuria.
The uptake of finerenone is not aligned with clinical expert expectations. In the sponsor’s base case the sponsor assumed that 6%, 17% and 27% of patients eligible for finerenone would uptake it in its first, second, and third year of reimbursement, respectively. Clinical experts noted that the proportion of people who will uptake finerenone is uncertain. This uncertainty is compounded by the uncertainty regarding the place in therapy of finerenone relative to SGLT2 inhibitors.
To explore the influence uncertainty in finerenone uptake, as a scenario analysis, CADTH explored increasing uptake of finerenone by 50% in all years relative to the sponsor’s base-case estimates.
No incidence incident CKD cases were added to the analysis. In the sponsor’s base case, new patients were only added to the analysis via a population growth rate. This was deemed to be inappropriate as the annual incidence of CKD increases with advancing age.54
As estimates for incidence of CKD among patients with T2D were not available, CADTH was unable to address this limitation. If the incidence of CKD among T2D is expected to be greater than mortality in this population, the CADTH and sponsor base case will underestimate the population size, and therefore will also underestimate the expected budget impact of reimbursing finerenone.
Additional limitations were identified, but were not considered to be key limitations. These limitations include: uncertainty regarding the inclusion of dispensing fees and mark-ups in a drug program perspective.
CADTH Reanalyses of the BIA
CADTH revised the sponsor’s base case by: assuming patients with concomitant chronic heart failure will be eligible for finerenone and including drug mark-ups and dispensing fees. Table 22 notes the assumptions used by the sponsor in comparison to those used by CADTH in its reanalysis.
Table 22: CADTH Revisions to the Submitted BIA
Stepped analysis | Sponsor’s value or assumption | CADTH value or assumption |
|---|---|---|
Correctionsa to sponsor’s base case | ||
1. None | — | — |
Changes to derive the CADTH base case | ||
1. Exclude patients with concomitant CHF from eligible population | Yes | No |
2. Drug mark-ups and dispensing fees included in base-case analysis | No | Yes |
CADTH base case | 1 + 2 | |
BIA = budget impact analysis; CHF = chronic heart failure.
aCorrections are minor errors (e.g., transcription errors between report and model, misapplication of distributions or SEs in probabilistic analyses) that are not identified as limitations.
The results of the CADTH step-wise reanalysis are presented in summary format in Table 23 and a more detailed breakdown is presented in Table 24. In the CADTH reanalysis, the 3-year budget impact of reimbursing finerenone adult patients with CKD and T2D, was $148,282,507 (Year 1: $17,075,144; Year 2: $49,750,884; Year 3: $81,456,478).
Table 23: Summary of the CADTH Reanalyses of the BIA
Stepped analysis | Three-year total |
|---|---|
Submitted base case | $108,474,600 |
CADTH reanalysis 1 - Not excluding CHF patients | $135,593,250 |
CADTH reanalysis 2 - Drug mark-ups and dispensing fees | $118,626,005 |
CADTH base case | $148,282,507 |
BIA = budget impact analysis; CHF = chronic heart failure
CADTH also conducted additional scenario analyses to address remaining uncertainty, using the CADTH base case. Results are provided in Table 24:
Excluding dispensing fees and mark-up (i.e., only drug costs included).
Assuming that 47.9% of patients with T2D have CKD .
Aligning the eligible population with the Health Canada indication (i.e., removing the need to have persistent high or very high albuminuria to be eligible for finerenone).
Increasing the sponsor’s base-case uptake estimates for finerenone by 50%.
Table 24: Detailed Breakdown of the CADTH Reanalyses of the BIA
Stepped analysis | Scenario | Year 0 (current situation) | Year 1 | Year 2 | Year 3 | Three-year total |
|---|---|---|---|---|---|---|
Submitted base case | Reference | $70,381,724 | $71,256,570 | $72,142,291 | $73,039,021 | $286,819,606 |
New drug | $70,381,724 | $83,747,723 | $108,537,058 | $132,627,701 | $395,294,206 | |
Budget impact | $0 | $12,491,153 | $36,394,767 | $59,588,681 | $108,474,600 | |
CADTH base case | Reference | $119,941,258 | $121,432,130 | $122,941,534 | $124,469,699 | $488,784,621 |
New drug | $119,941,258 | $138,507,274 | $172,692,418 | $205,926,177 | $637,067,128 | |
Budget impact | $0 | $17,075,144 | $49,750,884 | $81,456,478 | $148,282,507 | |
CADTH base case: drug costs only | Reference | $87,977,155 | $89,070,713 | $90,177,863 | $91,298,776 | $358,524,507 |
New drug | $87,977,155 | $104,684,654 | $135,671,322 | $165,784,627 | $494,117,758 | |
Budget impact | $0 | $15,613,941 | $45,493,459 | $74,485,851 | $135,593,250 | |
CADTH sensitivity analysis: 47.9% prevalence | Reference | $174,096,554 | $176,260,577 | $178,451,499 | $180,669,654 | $709,478,283 |
New drug | $174,096,554 | $201,045,407 | $250,665,661 | $298,904,967 | $924,712,589 | |
Budget impact | $0 | $24,784,830 | $72,214,162 | $118,235,313 | $215,234,305 | |
CADTH sensitivity analysis: all patients receive finerenone, regardless of albuminuria | Reference | $252,507,912 | $255,646,590 | $258,824,281 | $262,041,472 | $1,029,020,255 |
New drug | $252,507,912 | $291,594,261 | $363,562,985 | $433,528,795 | $1,341,193,953 | |
Budget impact | $0 | $35,947,671 | $104,738,704 | $171,487,323 | $312,173,698 | |
CADTH sensitivity analysis: increasing uptake rate of finerenone | Reference | $119,941,258 | $121,432,130 | $122,941,534 | $124,469,699 | $488,784,621 |
New drug | $119,941,258 | $147,044,846 | $197,567,860 | $246,654,417 | $711,208,381 | |
Budget impact | $0 | $25,612,716 | $74,626,326 | $122,184,718 | $222,423,760 |
BIA = budget impact analysis.
Stakeholder Input
Patient Input
The Kidney Foundation of Canada and Diabetes Canada
About the Kidney Foundation of Canada and Diabetes Canada
Kidney Foundation of Canada
Over nearly six decades, the Kidney Foundation of Canada has been guided by the fundamental principles of innovation, leadership, and collaboration, and has been committed to excellent kidney health, optimal quality of life for those affected by kidney disease, and a cure.
The Kidney Foundation of Canada is the leading charity committed to eliminating the burden of kidney disease through:
Funding and stimulating innovative research for better prevention, treatments and a cure;
Providing education and support to prevent kidney disease in those at risk and empower those with kidney disease to optimize their health status;
Advocating for improved access to high quality health care;
Increasing public awareness and commitment to advancing kidney health and organ donation.
For more information, please visit kidney.cahttps://www.kidney.ca/
Diabetes Canada
Diabetes Canada is a national health charity representing millions of Canadians affected by diabetes. Diabetes Canada leads the fight against diabetes by helping people live healthy lives, preventing the onset and consequences of diabetes, and discovering a cure. It has a heritage of excellence and leadership, and its co-founder, Dr. Charles Best, along with Dr. Frederick Banting, is credited with the co-discovery of insulin. Diabetes Canada is supported in its efforts by a community-based network of volunteers, employees, health care professionals, researchers, and partners. By providing education and services, advocating on behalf of people living with diabetes, supporting research and translating it into practical applications, Diabetes Canada is delivering on its mission. Diabetes Canada will continue to change the world for those affected by diabetes through healthier communities, exceptional care, and high-impact research.
A world free of the effects of diabetes is our vision. That’s why we’re working together to improve the quality of life of people living with diabetes. We’re sharing knowledge and creating connections for individuals and the health professionals who care for them; advocating through public policy; and funding research to improve treatments and find a cure to end diabetes.
For more information, please visit: diabetes.ca
Information Gathering
Patient input was collected in May 2022 by the Kidney Foundation of Canada in both official languages via a self-administered questionnaire to people across Canada. The survey was directed at people living with chronic kidney disease and type 2 diabetes and their caregivers and inquired about respondents’ lived experience with chronic kidney disease and medications and expectations for new drug therapies in Canada. The survey posed a number of questions specifically about the drug under review, finerenone. Awareness about the surveys was generated through the Kidney Foundation’s social media channels (Twitter and Facebook), as well as the website and e-newsletter.
A link to the survey was also shared via Diabetes Canada’s social media channels (Twitter and Facebook), as well as via an online portal for health-care providers in Diabetes Canada’s Professional Section.
A total of 24 people responded to the survey with 9 completed and 15 partially completed surveys. Of the 8 people who responded to the questions about their current age or the current age of the person they care for, 2 were between the ages of 40 and 54, 2 were 55 to 69 years old, and 4 were over 70 years old.
8 respondents identified as being a person living with chronic kidney disease and 1 identified as being a caregiver for a person with chronic kidney disease. 8 respondents answered the questions about how long they had lived with kidney disease. 2 respondents reported living with chronic kidney disease for 1 to 2 years, 2 for 3 to 5 years, 1 for 6 to 10 years, 2 for 11 to 20 years and 1 respondent reported more than 20 years living with the disease.
10 respondents answered the question about whether they live with diabetes. Of those, 6 identified as people living with type 2 diabetes, and 4 reported that they do not have diabetes. 6 respondents answered the questions about how long they had lived with type 2 diabetes. 1 respondent reported living with type 2 diabetes for 1 to 2 years, 1 for 11 to 20 years and 4 respondents reported more than 20 years living with the disease.
Disease Experience
Kidney disease describes a variety of disease and disorders that affect the kidneys. Most diseases of the kidney attack the nephrons and damage their ability to eliminate wastes and excess fluids. Diseases of the kidney are a common finding in people with diabetes, with up to one-half demonstrating signs of renal damage in their lifetime. Diabetes is the leading cause of kidney failure, and people living with kidney disease often experience additional medical conditions such as high blood pressure and heart disease.
Chronic kidney disease (CKD) is the presence of kidney damage, or a decreased level of kidney function, for a period of three months or more. Kidney disease can range from mild to severe and in some cases, lead to kidney failure (sometimes referred to as end-stage kidney disease, or ESKD). There are usually no specific symptoms of kidney disease until the damage is severe. When the kidneys fail, wastes accumulate in the body and dialysis treatments, or a kidney transplant are needed to survive.
Dialysis is the most common treatment for kidney failure, with kidney transplant being another option. There are two types of dialysis: peritoneal dialysis and hemodialysis. Canadians with kidney failure and their families face significant out-of-pocket costs. This burden is further compounded by the loss of income that is often associated with starting dialysis. It is important to note that poverty is a determinant of health. This means that patients and their families that live in poverty may not be able to achieve optimal management of their medical issues.
In the early stages of chronic kidney disease, self-management strategies such as lifestyle changes; engaging in regular physical activity, maintaining a healthy body weight, stopping smoking and reducing sodium, managing other medical conditions and medications may slow or stop damage to the kidneys.
Normally, healthy kidneys balance the body’s minerals, however if the kidneys are not working well, potassium, sodium, calcium, and phosphate levels can be too high or too low. Depending on the stage of chronic kidney disease, a restricted diet and/or medications may be necessary. For example, some people in the early stages of CKD do not need to limit their potassium intake, while others may need to restrict it via dietary restrictions. People on dialysis usually need to limit potassium intake to avoid hyperkalemia between treatments. This diet is highly restrictive and negatively impacts quality of life for patients with CKD.
Most survey respondents reported that chronic kidney disease has had a negative effect on their daily life, especially with regard to fatigue. One respondent said, “I’m constantly fatigued, find it extremely hard to balance work and family life”, while another said “I’ve had to leave my job at 55, fatigued, hard on myself for not having energy to do stuff, think I’m just being lazy.” Two respondents reported trouble sleeping, with one saying that they “have to take meds to sleep, don’t get to sleep through the night.” Swelling, itching and dry skin were also mentioned, as were the limitations of the dietary restrictions associated with the disease. Two respondents talked about the difficulty of eating at restaurants or friends’ houses, with one stating: “Very rarely eat out as difficult to choose foods that follow the diet.”
Most survey respondents who participated in the survey spoke negatively of their experience living with both CKD and diabetes. Respondents talked about the challenges of fatigue and anemia. They said, “sometimes if my blood sugars are high this brings fatigue along with fatigue from CKD”. Many also said that their diet is a constant challenge, and two mentioned the high cost of healthy foods.
“It is a constant challenge trying to keep my glucose levels at a reasonable level due to a lack of funds needed to buy fresh meats, veggies and fruit.” One person said that a “low carb, low Na [sodium] and low fat [diet] can be difficult when you’re cooking for others as well as yourself”.
“It appears as if one chronic disease diet does not corelate (sic) with the other very well. Especially in the foods I enjoy”.
Many people dealing with CKD have a number of other conditions. 7 respondents reported having or having had high blood pressure, 3 reported high cholesterol, and 1 said their potassium levels have been high. 5 reported that their chronic kidney disease is worsening, one person reported heart disease, and 1 reported having had a heart attack. One respondent said, “I have been very tired and unable to focus on certain tasks as a result of my multiple conditions”.
Experiences With Currently Available Treatments
Of the 10 respondents to a question about whether they’ve ever taken medication to reduce the risk of worsening kidney disease, 6 said that they had, and 4 said that they had not. 3 take or have taken angiotensin-converting enzyme (ACE) inhibitors, 2 reported taking angiotensin-receptor blockers (ARBs), and other medications mentioned including diuretics, tacrolimus, erythropoietin, and dapagliflozin.
6 people responded to a question about how satisfied they are with their current medication/blend of medications, and of those 3 reported being satisfied, 1 very satisfied, and 2 neither satisfied nor unsatisfied. One respondent said that “Tacrolimus causes nausea, heartburn and flushing for me,” and others said, “My kidneys have got better” and “It keeps my numbers within range.” One person reported that their medication “helps maintain the itch and burning feeling in the feet and legs with the excess fluid.”
Improved Outcomes
When asked about their expectations for CKD therapies, respondents rated these questions as most important: “Does it make me tired? Does it interfere with my other medications? How much does it cost?” Respondents mentioned that side effects were important and said that it was important that kidney disease medication “preserves my one remaining kidney,” and that it delays dialysis.
Respondents’ hopes for new therapies for CKD or for CKD and diabetes together are “limiting or arresting the progression of both diseases”, “make kidneys better,” “a longer life span,” and “maintain and improve quality of life overall.”
Experience With Drug Under Review
This drug is not available in Canada and therefore patients and caregivers have no experience with the medication.
Companion Diagnostic Test
Not applicable to this submission.
Anything Else?
Living with chronic kidney disease can involve not only health and quality of life challenges, but significant financial challenges as well. People may experience a decrease in income if they limit their working hours due to their symptoms, and out-of-pocket costs increase as they change their diet and follow up more often with their health care team. Those living with kidney disease also tend to be part of a low income and high-cost population, and government coverage and financial support varies across jurisdictions, which can lead to inequities. For more on the financial burden of kidney disease, visit https://kidney.ca/Get-Involved/Be-Their-Voice/Financial-Burden-of-Kidney-Disease.
Should chronic kidney disease progress to kidney failure, hemodialysis is the most common treatment. The cost of hemodialysis to the health care system per person per year ranges from $56,000 to $107,000, so the savings to the system associated with slowing the progression of kidney disease are significant. Hospitalization and treatment of cardiac events in patients with chronic kidney disease also represent a significant cost to the health care system.
Canadians living with both chronic kidney disease and type 2 diabetes often experience additional health and financial challenges. Medication, equipment, devices, and supplies required to treat diabetes can cost people thousands of dollars annually. A 2011 Statistics Canada survey showed that 32 percent of people with diabetes take three to four medications, 40 percent take five to nine medications and 12 percent take 10 medications or more, as part of their treatment. In a Diabetes Canada survey from 2015, 25 percent of all people with diabetes indicated treatment adherence was affected by cost. Every day, diabetes costs the Canadian health-care system almost $50 million to treat.
The combined financial burden of these illnesses means that many would benefit from effective, affordable treatments that they can access equitably and in a timely manner. As finerenone may slow the progression of kidney disease and reduce the risk of cardiac events, it should be available as an option for people living with CKD and type 2 diabetes.
Conflict of Interest Declarations — The Kidney Foundation of Canada
To maintain the objectivity and credibility of the CADTH reimbursement review process, all participants in the drug review processes must disclose any real, potential, or perceived conflicts of interest. This Patient Group Conflict of Interest Declaration is required for participation. Declarations made do not negate or preclude the use of the patient group input. CADTH may contact your group with further questions, as needed.
Did you receive help from outside your patient group to complete this submission?
Yes, there was collaboration with Diabetes Canada on the survey questions and with increasing awareness of the survey via social media.
Did you receive help from outside your patient group to collect or analyze data used in this submission?
There was no external assistance with data collection or analysis for this submission.
List any companies or organizations that have provided your group with financial payment over the past 2 years AND who may have direct or indirect interest in the drug under review.
Table 1: Financial Disclosures for The Kidney Foundation of Canada
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
Alexion Pharma Canada Corp | — | X | — | — |
Amgen Canada | — | — | — | X |
Astra Zeneca Canada | — | — | — | X |
Bayer | — | X | — | — |
Horizon Pharma Inc. | — | — | — | X |
Janssen Pharmaceutical Companies | — | — | — | X |
Otsuka Canada Pharmaceutical Inc. | — | — | — | X |
Paladin | — | — | X | — |
Takeda | X | — | — | — |
Conflict of Interest Declarations — Diabetes Canada
To maintain the objectivity and credibility of the CADTH reimbursement review process, all participants in the drug review processes must disclose any real, potential, or perceived conflicts of interest. This Patient Group Conflict of Interest Declaration is required for participation. Declarations made do not negate or preclude the use of the patient group input. CADTH may contact your group with further questions, as needed.
Did you receive help from outside your patient group to complete this submission?
Yes, there was collaboration with the Kidney Foundation of Canada on the survey questions and with increasing awareness of the survey via social media.
Did you receive help from outside your patient group to collect or analyze data used in this submission?
The Kidney Foundation of Canada completed the data collection and analysis for this submission.
List any companies or organizations that have provided your group with financial payment over the past 2 years AND who may have direct or indirect interest in the drug under review.
Table 2: Financial Disclosures for Diabetes Canada
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
AstraZeneca | — | — | — | X |
Bayer | — | — | X | — |
Janssen | — | — | — | X |
Lilly | — | — | X | — |
Novo Nordisk | — | — | — | X |
Paladin | — | — | X | — |
Sanofi | — | — | — | X |
Takeda | — | — | X | — |
Clinician Group Input
LMC Diabetes & Endocrinology
About LMC Diabetes & Endocrinology
LMC Diabetes & Endocrinology is the largest single-specialty group endocrinology practice with 13 clinics in 3 provinces (Ontario, Quebec, Alberta) evaluating a wide range of patients with diabetes and endocrine disorders. Our offices are also comprised of the largest team of certified diabetes educators (dieticians, nurses and pharmacists), clinical research coordinators, optometrists, and chiropodists.
Information Gathering
Author and Dr. Ronald Goldenberg prepared the submission, which was presented and shared with LMC endocrinologists, who were invited to contribute and participate.
Current Treatments and Treatment Goals
Presently, patients with type 2 diabetes at risk of progression of kidney disease are presecribed agents with proven benefit to reduce the risk of kidney disease progression and cardiovascular disease. The mainstay of these therapies in Canada are renin angiotensinaldosterone system (RAAS) blockers, and more recently SGLT2 inhibitors. Despite the use of these agents, there is still a significant residual risk of cardiorenal disease amongst patients affected with diabetic kidney disease. Finerenone has demonstrated a clinically significant reduction in the risk of sustained decline in glomerular filtration rate, end stage kidney disease, cardiovascular death, heart attacks, and hospitalization due to heart failure in adults with chronic kidney disease and type 2 diabetes. These beneficial outcomes would directly diminish morbidity, improve quality of life, and reduce the burden of disease (dialysis, hospitalization) on the healthcare system.
Treatment Gaps (Unmet Needs)
Considering the treatment goals, please describe goals (needs) that are not being met by currently available treatments.
There are many patients affected with type 2 diabetes who have significant decline in kidney function and who are affected by cardiovascular disease despite the availability of RAAS blockers and SGLT2 inhibitors. Others who might benefit but who are unable to tolerate these agents or who develop adverse effects while taking them.
Place in Therapy
How would the drug under review fit into the current treatment paradigm?
In type 2 diabetes as an add-on to RAAS blockers with or without SGLT2i for patients demonstrating an ongoing risk for kidney disease progression and cardiovascular disease. Alternatively, as a first add-on therapy for patients’ intolerant or unable to take RAAS blockers or SGLT2i. Finerenone as a nonsteroidal mineralocorticoid receptor antagonist has a different and complementary mechanism of action for kidney protection.
Which patients would be best suited for treatment with the drug under review? Which patients would be least suitable for treatment with the drug under review?
Criteria are based on routine lab assessments, including serum creatinine, eGFR and urine albumin to creatinine ratio (uACR). Patients likely to benefit include those with eGFR ≥25 ml/min/1.73m2 with ACR ≥34 mg/mmol or with eGFR 25-90 ml/min/1.73 ml/min/173m2 with ACR 3.4 to 33.9 mg/mmol. Those least suitable would be those with a history of clinically significant hyperkalemia.
What outcomes are used to determine whether a patient is responding to treatment in clinical practice? How often should treatment response be assessed?
Outcomes used in clinical practice would preservation of eGFR over time, reduction in uACR, improved symptoms of or prevention of heart failure and reduced ER visits/hospitalizations.
What factors should be considered when deciding to discontinue treatment with the drug under review?
Clinically significant hyperkalemia, especially if not corrected by dietary changes of potassium binders, or hypotension.
What settings are appropriate for treatment with [drug under review]? Is a specialist required to diagnose, treat, and monitor patients who might receive [drug under review]?
Community, hospital, and specialty care settings are all appropriate. Both specialists and primary care physicians are well-suited to initiate and monitor therapy.
Additional Information
Progressive kidney disease and heart failure represent two of the most significant complications of diabetes. Finerenone has demonstrated clinically significant benefits in cardiovascular and renal outcomes amongst patients with type 2 diabetes and chronic kidney disease. Finerenone was approved in the USA in 2021. American Diabetes Association 2022 Guidelines state: “For patients with type 2 diabetes and chronic kidney disease treated with maximum tolerated doses of ACE inhibitors or angiotensin receptor blockers, addition of finerenone should be considered to improve cardiovascular outcomes and reduce the risk of chronic kidney disease progression.” The ADA Guidelines also state: “In patients with chronic kidney disease who are at increased risk for cardiovascular events or chronic kidney disease progression or are unable to use a sodium–glucose cotransporter 2 inhibitor, a nonsteroidal mineralocorticoid receptor antagonist (finerenone) is recommended to reduce chronic kidney disease progression and cardiovascular events.”
Conflict of Interest Declarations — LMC Diabetes & Endocrinology
To maintain the objectivity and credibility of the CADTH drug review programs, all participants in the drug review processes must disclose any real, potential, or perceived conflicts of interest.
Did you receive help from outside your clinician group to complete this submission?
No.
Did you receive help from outside your clinician group to collect or analyze any information used in this submission?
No.
List any companies or organizations that have provided your group with financial payment over the past two years AND who may have direct or indirect interest in the drug under review.
Declaration for Clinician 1
Name: Dr. Alex Abitbol
Position: Endocrinologist
Date: June 2, 2022
Table 3: COI Declaration for LMC Diabetes & Endocrinology — Clinician 1
Company | $0 to $5,000 | $5,001 to $10,000 | $10,001 to 50,000 | In excess of $50,000 |
|---|---|---|---|---|
Novo Nordisk | — | — | X | — |
Janssen | — | X | — | — |
Eli Lilly | — | X | — | — |
Boehringer-Ingelheim | — | X | — | — |
Astra Zeneca | X | — | — | — |
Abbott | X | — | — | — |
Amgen | X | — | — | — |
Bayer | X | — | — | — |
Dexcom | X | — | — | — |
Declaration for Clinician 2
Name: Dr. Ronald Goldenberg
Position: Endocrinologist
Date: June 2, 2022
Table 4: COI Declaration for LMC Diabetes & Endocrinology — Clinician 2
Company | $0 to $5,000 | $5,001 to $10,000 | $10,001 to 50,000 | In excess of $50,000 |
|---|---|---|---|---|
Bayer | — | X | — | — |
BI-Lilly | — | — | X | — |
Astra Zeneca | — | — | X | — |
Janssen | — | — | X | — |
Declaration for Clinician 3
Name: Dr. Robert Schlosser
Position: Endocrinologist
Date: June 8, 2022
Table 5: COI Declaration for LMC Diabetes & Endocrinology — Clinician 3
Company | $0 to $5,000 | $5,001 to $10,000 | $10,001 to 50,000 | In excess of $50,000 |
|---|---|---|---|---|
Novo Nordisk | — | — | X | — |
Astra Zeneca | — | X | — | — |
Janssen | — | X | — | — |
BI-Eli Lilly | — | X | — | — |
Sanofi | — | X | — | — |
Dexcom | X | — | — | — |
Bayer | X | — | — | — |
Declaration for Clinician 4
Name: Dr Jean-François Yale
Position: Endocrinologist
Date: June 8, 2022
Table 6: COI Declaration for LMC Diabetes & Endocrinology — Clinician 4
Company | $0 to $5,000 | $5,001 to $10,000 | $10,001 to 50,000 | In excess of $50,000 |
|---|---|---|---|---|
Eli Lilly | — | — | X | — |
Novo Nordisk | — | — | — | X |
Sanofi | — | — | X | — |
Bayer | — | — | X | — |
Abbott | — | — | X | — |
Dexcom | — | X | — | — |
Astra Zeneca | — | X | — | — |
Merck | — | X | — | — |
Pfizer | X | — | — | — |
Declaration for Clinician 5
Name: Dr. Ronnie Aronson
Position: Endocrinologist
Date: June 10, 2022
Table 7: COI Declaration for LMC Diabetes & Endocrinology — Clinician 5
Company | $0 to $5,000 | $5,001 to $10,000 | $10,001 to 50,000 | In excess of $50,000 |
|---|---|---|---|---|
Eli Lilly | — | X | — | — |
Novo Nordisk | — | — | X | — |
Abbott | — | X | — | — |
Takeda | — | X | — | — |
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up-to-date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
Redactions: Confidential information in this document may be redacted at the request of the sponsor in accordance with the CADTH Drug Reimbursement Review Confidentiality Guidelines.
Stakeholder Input: The views expressed in each submission are those of the submitting organization or individual; not necessarily the views of CADTH or of other organizations. As such, they are independent of CADTH and do not necessarily represent or reflect the view of CADTH. No endorsement by CADTH is intended or should be inferred. By filing with CADTH, the submitting organization or individual agrees to the full disclosure of the information. CADTH does not edit the content of the submissions.
CADTH does use reasonable care to prevent disclosure of personal information in posted material; however, it is ultimately the submitter’s responsibility to ensure no identifying personal information or personal health information is included in the submission. The name of the submitting organization or individual and all conflict of interest information are included in the submission; however, the name of the author, including the name of an individual patient or caregiver submitting the patient input, are not posted.
Accessibility: CADTH is committed to treating people with disabilities in a way that respects their dignity and independence, supports them in accessing material in a timely manner, and provides a robust feedback process to support continuous improvement. All materials prepared by CADTH are available in an accessible format. Where materials provided to CADTH by a submitting organization or individual are not available in an accessible format, CADTH will provide a summary document upon request. More details on CADTH’s accessibility policies can be found here.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.