CADTH Reimbursement Review
Caplacizumab (Cablivi)
Resubmission
Sponsor: Sanofi-Aventis Canada Inc.
Therapeutic area: Acquired thrombotic thrombocytopenic purpura
This multi-part report includes:
Clinical Review
Pharmacoeconomic Review
Stakeholder Input
Clinical Review
Abbreviations
ADAMTS13
a disintegrin and metalloproteinase with thrombospondin type 1 motif, member 13
AE
adverse event
aTTP
acquired thrombotic thrombocytopenic purpura
CAG
Canadian Apheresis Group
CDEC
CADTH Canadian Drug Expert Committee
CI
confidence interval
CNR-MAT
Centre National de Référence sur les Microangiopathies Thrombotiques
HIT-6
Headache Impact Test 6
HR
hazard ratio
HRQoL
health-related quality of life
HTA
health technology assessment
ICU
intensive care unit
IQR
interquartile range
ITO
intent to observe
ITT
intention to treat
iTTP
immune-mediated thrombotic thrombocytopenic purpura
LDH
lactate dehydrogenase
MedDRA
Medical Dictionary for Regulatory Affairs
MID
minimal important difference
OL
open label
PE
plasma exchange
RBANS
Repeatable Battery for the Assessment of Neuropsychological Status
RWE
real-world evidence
SAE
serious adverse event
SC
subcutaneous
SD
standard deviation
SE
standard error
SF-36
Short Form (36) Health Survey
SOC
standard of care
TPE
therapeutic plasma exchange
TTP
thrombotic thrombocytopenic purpura
ULN
upper limit of normal
vWF
von Willebrand factor
Executive Summary
An overview of the resubmission details for the drug under review is provided in Table 1.
Table 1: Resubmitted for Review
Item | Description |
|---|---|
Drug product | Caplacizumab (Cablivi) for injection, powder for solution (11 mg), IV or subcutaneous |
Indication | For the treatment of adults with acquired thrombotic thrombocytopenic purpura in combination with plasma exchange and immunosuppressive therapy |
Reimbursement request | As per indication |
Health Canada approval status | NOC |
Health Canada review pathway | Priority review |
NOC date | February 28, 2020 |
Sponsor | Sanofi-Aventis Canada Inc. |
NOC = Notice of Compliance.
Source: Sponsor’s drug reimbursement review resubmission for caplacizumab.1
Introduction
Thrombotic thrombocytopenic purpura (TTP) is an ultra-rare blood disorder caused by reduced enzymatic activity of the von Willebrand factor (vWF)-cleaving protease, a disintegrin and metalloproteinase with thrombospondin type 1 motif, member 13 (ADAMTS13), resulting in an inability to cleave high molecular weight vWF multimers, and as a consequence, formation of platelet-rich blood clots in small vessels (thrombotic microangiopathy).2 TTP is a medical emergency and acquired TTP (aTTP) (driven by autoantibodies against ADAMTS13) is the dominant form.2-4 Mortality is estimated at approximately 10% to 20%;5 in addition, thrombotic complications and their sequelae contribute to persistent cognitive and physical difficulties that can be life-altering in some patients, compromising health-related quality of life (HRQoL).6 After the presenting episode, recurrence of aTTP (exacerbation: recurrence within 30 days of cessation of plasma exchange [PE]; relapse: recurrence after 30 days of cessation of PE) will occur in up to half of patients, while refractory aTTP (absence of platelet count increase following treatment) will occur in approximately 10% of patients.7
According to the clinical experts consulted by CADTH for this review, diagnosis of aTTP is based on clinical and laboratory findings and is made by a hematologist. The incidence of aTTP is estimated at approximately 2 to 4 cases per million population per year (approximately ||| cases per million adults);8-10 approximately ||| |||||||| with TTP were treated in Canada in 2018.1 According to the clinical experts consulted by CADTH for this review, current management of aTTP in Canada involves PE and immunosuppression with corticosteroids. The sponsor emphasized that the treatment burden associated with PE is significant as PE often requires a transfer to a PE centre, there is a need for surgery (vascular catheter insertion with a risk of infections), and there is potential for exposure to multiple donors (risk of PE reactions).1 In Canada, rituximab is typically not used upfront and is administered to patients with aTTP exacerbations, relapsed aTTP, or refractory aTTP. The clinical experts stated the main goals of treatment are to prolong life and avoid mortality while preventing thrombotic complications and associated disabilities. Treatment goals are accomplished by replenishing ADAMTS13 and removing autoantibodies against ADAMTS13, allowing normalization of ADAMTS13 activity and consequently halting thrombotic microangiopathy.
Caplacizumab is a bivalent humanized nanobody that binds to the A1 domain of vWF, inhibiting the interaction between vWF and platelets, reducing vWF-mediated platelet activation and adhesion, and preventing the formation of ultra-large vWF-rich platelet microthrombi.11 The drug is dosed at 11 mg (IV and subcutaneous [SC] injections on day 1 of PE followed by daily SC injections during PE and for a minimum of 30 days after cessation of PE).11 The Health Canada indication for caplacizumab is “for the treatment of adults with aTTP in combination with PE and immunosuppressive therapy.”11
Caplacizumab was initially reviewed by CADTH for the treatment of adults with aTTP in combination with PE and immunosuppressive therapy and received a negative funding recommendation from the CADTH Canadian Drug Expert Committee (CDEC) on September 1, 2020.12 Key reasons for the recommendation included insufficient evidence of clinically important outcomes (e.g., survival, organ damage, health care use, or long-term aTTP recurrence), lack of long-term clinical outcome data, lack of an identifiable subpopulation most likely to benefit from treatment, generalizability to Canadian clinical practice, and absence of HRQoL data. The recommendation was based on evidence assessed in the CADTH Clinical Review Report for the initial submission of caplacizumab,13 the executive summary of which is reproduced as Appendix 2. The drug was resubmitted for review by the sponsor on the basis of the availability of new evidence on June 7, 2022.1 The new evidence included a prospective long-term follow-up study of patients who completed the HERCULES trial (the post-HERCULES trial),14,15 a variety of post hoc analyses including an integrated analysis of data from the HERCULES and TITAN studies,16 and several real-world evidence (RWE) studies including comparisons of patients treated with caplacizumab with historical controls who received standard of care (SOC) alone in France17-19 and the UK.20
The objective of this report was to perform a systematic review of the beneficial and harmful effects of caplacizumab (11 mg IV bolus plus 11 mg SC injection on day 1 of PE, followed by 11 mg SC injection daily) for the treatment of adults with aTTP in combination with PE and immunosuppressive therapy. This report is an update of the Clinical Review Report for the original submission of caplacizumab;13 new evidence provided by the sponsor or identified through a systematic literature search was included in the report if it addressed an evidence gap identified by CDEC in its final recommendation for the initial submission.
Stakeholder Perspectives
The information in this section is a summary of input provided by the patient groups who responded to CADTH’s call for patient input and from clinical experts consulted by CADTH for the purpose of this review.
Patient Input
One patient group, the Answering TTP Foundation, provided input for this review. The group conducted an online survey in May and June of 2022 (N = 49 respondents including 31 patients with aTTP, 16 family members, caregivers, or friends of patients with aTTP, 1 health care professional, and 1 researcher). Most (80%) survey respondents were women and most (90%) were people living in Canada. Approximately half of respondents (48%) had experienced at least 1 relapse. Patients highlighted delays in diagnosis and treatment as well as the negative impacts of serious and/or frequent symptoms of aTTP (e.g., bruising, fever, fatigue, migraine, confusion, abdominal pain, bleeding, shortness of breath, vision loss, and jaundice) which impose heavy burdens on mental health (e.g., anxiety, depression, and panic attacks). A subset of patients experienced incapacitating or life-threatening complications of aTTP including stroke, myocardial infarction, and kidney problems. Nearly all patients had experience with PE and corticosteroids while approximately two-thirds (65%) had experience with rituximab. Respondents described the challenges of current treatments including lengthy hospital stays, side effects of corticosteroids, and the inconvenience of daily PE; in addition, available treatments are costly, require time off from work, and may require travel to a major centre for access. Respondents identified an unmet need for treatments that can reduce the risk of death or disability from aTTP and ease the mental and emotional burdens of disease (e.g., continuous fear of relapse and impacts on social life and career goals). Specifically, respondents valued new treatments that enable patients to survive an aTTP crisis and thereby reduce the patient’s emotional uncertainty in the early stages of a TTP episode and improve peace of mind during remission. As well, respondents noted that a reduction in the number of PE treatments and ability to plan for the future were important when considering treatment options. Approximately one-third (34%) of respondents had experience with caplacizumab and felt that the drug had contributed to shorter hospitalization, faster remission, and prevention of further disease.
Clinician Input
Input From Clinical Experts Consulted by CADTH
Two clinical specialists with expertise in the diagnosis and management of aTTP provided input for this review. The clinical experts stated that while currently available treatments (PE plus immunosuppression with corticosteroids with or without rituximab) are effective in many patients, not all patients manifest durable responses and thus experience persistent or recurrent thrombotic microangiopathy, which can lead to thrombotic complications and, potentially, mortality. According to the clinical experts, there is an unmet need for additional treatment options especially for patients with aTTP recurrence or refractory aTTP. The clinical experts relayed that caplacizumab would be administered in combination with PE and immunosuppressive therapy. The clinical experts felt that because some patients respond well to PE and immunosuppressive therapy, caplacizumab may be a reasonable option to be reserved for patients with aTTP recurrence or refractory aTTP as these patients currently have limited treatment options. The clinical experts acknowledged that it is currently unclear if delaying access to caplacizumab may impact its efficacy. The HERCULES trial was designed to evaluate the upfront use of caplacizumab in combination with PE and immunosuppressive therapy. The clinical experts also felt that upfront treatment with caplacizumab would be considered in high-risk patients who have neurologic or cardiac abnormalities (including elevated troponin) or are otherwise critically ill. The clinical experts acknowledged that currently there is insufficient evidence to identify patients who are more likely to respond to caplacizumab in combination with PE plus immunosuppression.
The clinical experts stated that clinically meaningful responses to caplacizumab plus PE and immunosuppression would be defined by normalization of platelet count (complete blood count) and lactate dehydrogenase (LDH) level. Reticulocyte count, unconjugated bilirubin, hemoglobin, haptoglobin, creatinine, ADAMTS13 activity, and ADAMTS13 autoantibody levels should also normalize. The clinical experts relayed that although the ultimate mechanistic goal of therapy is to normalize ADAMTS13 activity, results of ADAMTS13 testing are generally not readily available in a timely manner, as compared to platelet count. According to the clinical experts, PE is typically discontinued after 5 days if platelet count, LDH, and other markers are normalized. Patients are then typically monitored for 1 to 2 days while in hospital to determine if their platelet counts decrease again or if the hemolytic markers show signs of aTTP recurrence. If there is no evidence of aTTP recurrence, patients are typically discharged from hospital with a corticosteroid taper plan and close outpatient follow-up. The clinical experts stated that in patients receiving caplacizumab who develop aTTP recurrence or refractory aTTP would be discontinued from therapy, as would patients with serious toxicities such as clinically significant bleeding. The clinical experts relayed that 1 of the challenges of using caplacizumab is that it directly increases platelets through its mechanism, potentially masking an indicator of aTTP disease activity, which would make it difficult to determine when it is time to taper PE.
Clinician Group Input
Clinician group input was received from the Canadian Apheresis Group (CAG), with 5 clinicians contributing to the submission. No major contrary views from those provided by the clinical experts consulted by CADTH for this review were presented. The clinician group echoed the inability of current treatments to accomplish the goals of therapy (avoid mortality and prevent thrombotic complications) in all patients and the unmet need for additional treatment options for patients with aTTP exacerbations, relapsed aTTP, and refractory aTTP as well as patients at high risk of mortality and/or organ damage. The clinician group also highlighted the unmet need for drugs that can rapidly inhibit platelet aggregation while waiting for PE and immunosuppression to take effect.
Drug Program Input
The Formulary Working Group identified the following jurisdictional implementation issues: considerations for initiation of therapy, considerations for continuation or renewal of therapy, considerations for discontinuation of therapy, considerations for prescribing of therapy, generalizability, care provision issues, and system and economic issues. The clinical experts consulted by CADTH for this review weighed evidence from the included study and other clinical considerations to provide responses to drug program implementation questions.
Clinical Evidence
Pivotal Studies and Protocol-Selected Studies
Description of Studies
One phase III, prospective, long-term follow-up study of adult patients with aTTP who completed the HERCULES study (post-HERCULES, N = 104)14,15 contributed evidence to this review. The objectives of the post-HERCULES trial were to evaluate long-term safety and efficacy of caplacizumab, to evaluate the safety and efficacy of repeated use of caplacizumab in participants who experienced a recurrence of aTTP, and to characterize the long-term clinical impact of aTTP. Following the final 4-week follow-up visit in the HERCULES trial, adult patients with aTTP were invited to enrol in the post-HERCULES trial within 1 month. Patients who were not able or willing to comply with study protocol procedures or who enrolled in a clinical study with another investigational drug or device were excluded. Following enrolment at 43 centres in Europe, the US, Canada (3 centres), and Israel, patients were followed for a period of 3 years. Patients attended twice-yearly visits, starting with a baseline visit coinciding with or occurring within 1 month of the final 28-day follow-up visit in the HERCULES study. During the 3-year follow-up period, patients could receive open-label (OL) caplacizumab in combination with PE and immunosuppression (administered as in the HERCULES study, except that 1 PE could be given before initiation of caplacizumab) for aTTP recurrence (defined as recurrence of thrombocytopenia requiring initiation of daily PE).
The overall intent-to-observe (ITO) population was used for analysis of safety. The efficacy ITO population (patients within the overall ITO population who had not experienced aTTP recurrence in the HERCULES study or before the beginning of the post-HERCULES study) was used for analysis of efficacy based on twice-yearly follow-up visits. The recurrence population (patients within the overall ITO population who experienced at least 1 aTTP recurrence during the post-HERCULES study) was used for analysis of data collected during recurrence periods.
All patients who completed the HERCULES study (n = 108) were eligible for the post-HERCULES study, of whom 104 (96.3%) participated. ||||||||||||| ||| |||||| || |||||||||||| || ||||||||||||| |||| ||||| |||||||| ||||||||||||| ||| |||||| ||||||| |||| |||||| ||| ||| ||||||| ||| ||| |||| |||||| |||| |||| |||||||| |||| |||||||||||| || ||| ||||||||||||| |||||||| ||| |||| ||| ||||||| |||||||| |||||||| ||| ||||||
Efficacy Results
Key efficacy results of the post-HERCULES study are summarized in Table 2 In the efficacy ITO population, consisting of patients who completed the HERCULES study, enrolled in the post-HERCULES study, and had not experienced an aTTP recurrence in either the HERCULES study or before the beginning of the post-HERCULES study, aTTP-related events (aTTP-related death, recurrence of aTTP, or major thromboembolic events) occurred in 4 patients (8.2%) randomized to receive caplacizumab in the HERCULES study and in 11 patients (37.9%) randomized to receive SOC alone in the HERCULES study. No patients randomized to receive caplacizumab in the HERCULES study and 1 patient (3.4%) randomized to receive SOC in the HERCULES study died during the post-HERCULES study. Four patients (8.2%) randomized to receive caplacizumab in the HERCULES study and 8 patients (27.6%) randomized to receive SOC in the HERCULES study experienced recurrence of aTTP during the post-HERCULES study. Four patients (8.2%) randomized to receive caplacizumab in the HERCULES study and 11 patients (37.9%) randomized to receive SOC in the HERCULES study experienced major thromboembolic events during the post-HERCULES study; major thromboembolic events other than aTTP occurred in no patients randomized to receive caplacizumab in the HERCULES study and in 3 patients (10.2%) randomized to receive SOC in the HERCULES study.
Table 2: Summary of Key Results From the Post-HERCULES Study (Efficacy ITO Population)
Outcome | Randomized to caplacizumab in HERCULES n = 49 | Randomized to SOC in HERCULES n = 29 |
|---|---|---|
aTTP-related events, n (%) | 4 (8.2) | 11 (37.9) |
aTTP-related death | 0 | 1 (3.4) |
Recurrence of aTTP | 4 (8.2) | 8 (27.6) |
At least 1 major thromboembolic event | 4 (8.2) | 11 (37.9) |
aTTP | 4 (8.2) | 8 (27.6) |
Acute myocardial infarction | 0 | 1 (3.4) |
Embolism venous | 0 | 1 (3.4) |
Renal infarct | 0 | 1 (3.4) |
aTTP = acquired thrombotic thrombocytopenic purpura; ITO = intent to observe; SOC = standard of care.
Source: Post-HERCULES Clinical Study Report (2021).14
Harms Results
Key harms results of the post-HERCULES study are summarized in Table 3. In the overall ITO population, 68 patients (90.7%) treated with caplacizumab in the HERCULES study and 26 patients (89.7%) treated with SOC only in the HERCULES study experienced adverse events (AEs) during the post-HERCULES study. Twenty-eight patients (37.3%) treated with caplacizumab in the HERCULES study and 16 patients (55.2%) treated with SOC only in the HERCULES study experienced serious AEs (SAEs) during the post-HERCULES study. No patients treated with caplacizumab, and 1 patient (3.4%) treated with SOC only in the HERCULES study died during the post-HERCULES study. Sixteen patients (21.3%) treated with caplacizumab in the HERCULES study and 9 patients (31.0%) treated with SOC only in the HERCULES study experienced at least 1 bleeding event during the post-HERCULES study (based on the Standardized Medical Dictionary for Regulatory Affairs [MedDRA] query “Haemorrhage” excluding the preferred term “aTTP”).
Table 3: Summary of Harms in Post-HERCULES (Overall ITO Population)
Outcome | Patients treated with caplacizumab in HERCULES n = 75 | Patients treated with placebo in HERCULES n = 29 |
|---|---|---|
Harms, n (%) | ||
AEs | 68 (90.7) | 26 (89.7) |
aTTP | 11 (14.7) | 8 (27.6) |
SAEs | 28 (37.3) | 16 (55.2) |
AEs leading to death | 0 | 1 (3.4) |
Notable harms, n (%) | ||
≥ 1 bleeding eventa | 16 (21.3) | 9 (31.0) |
≥ 1 bleeding eventb | || |||||| | | |||||| |
Hypersensitivity reactionsc | | ||||| | | ||||| |
Drug-induced ADAs | | |||||| | ||| |
ADA = antidrug antibody; AE = adverse event; aTTP = acquired thrombotic thrombocytopenic purpura; ITO = intent to observe; MedDRA = Medical Dictionary for Regulatory Affairs; SAE = serious adverse event; TTP = thrombotic thrombocytopenic purpura.
aBased on Standardized MedDRA query excluding TTP.
bBased on investigator documentation of event indicating an increased bleeding tendency.
cBased on specific preferred terms “drug hypersensitivity” and “hypersensitivity.”
Source: Post-HERCULES Clinical Study Report (2021).14
Critical Appraisal
Many of the internal validity issues of the HERCULES study affect the post-HERCULES study as well (refer to the Clinical Review Report for the initial submission of caplacizumab for details,13 the executive summary of which is reproduced as Appendix 2). Only patients who completed the HERCULES study (108 of 145, 74.5%) were eligible for the post-HERCULES study, and the study provides no information on patients who discontinued the HERCULES study. Higher proportions of caplacizumab-naive patients (n = 6, 20.7%) than patients who received caplacizumab in the HERCULES study (n = 5, 6.7%) discontinued the post-HERCULES study. The clinical experts consulted by CADTH for this review did not expect that any resulting biases would be directional in favour of caplacizumab. Due to variable rates of missing data, lack of formal statistical testing, potential for bias in patient-reported outcomes in an OL study, and uncertainty in the measurement properties of these instruments in patients for aTTP, changes in HRQoL over time and between the arms of the post-HERCULES efficacy ITO population could not be interpreted.
Many of the external validity issues of the HERCULES study affect the post-HERCULES study as well (refer to Appendix 2). The clinical experts consulted by CADTH felt that the post-HERCULES study population was generally reflective of adult patients with aTTP in Canada. Mortality rates in the HERCULES and post-HERCULES studies were lower than expected in routine clinical practice and patients may have been observed and followed by health care teams for aTTP recurrence and/or thromboembolic events more vigilantly compared to real-world practice. The clinical experts consulted by CADTH stated that the duration of follow-up in the post-HERCULES study was adequate to assess both early recurrence of aTTP (within the first month of presentation) and later recurrences (which often occur within the 2 years following cessation of PE). In the post-HERCULES study, caplacizumab could be administered following up to 1 administration of PE, but this was not a requirement as it was in the HERCULES study. Approximately half (6 of 13, 46.2%) of patients treated for their first recurrence in the post-HERCULES study with caplacizumab received rituximab. The clinical experts consulted by CADTH for this review noted that the proportion of patients living in Canada with aTTP who receive upfront rituximab in addition to PE and corticosteroids is not known with certainty but is likely lower than in the post-HERCULES trial. However, the proportion in clinical practice has increased in recent years due to improved access to rituximab.
Indirect Comparisons
No indirect evidence was identified for this review.
Other Relevant Evidence
Other Clinical Trials
The phase III HERCULES trial21-23 and phase II TITAN trial24-26 were reviewed in the CADTH Clinical Review Report for the initial caplacizumab submission13 (the executive summary of which is reproduced as Appendix 2). Both studies documented statistically significant differences in time to platelet count response that were viewed by the clinical experts consulted by CADTH for the initial review as too small to be clinically relevant. In the HERCULES study, the proportion of patients randomized to receive caplacizumab who experienced recurrence during the HERCULES overall study period was statistically significantly lower compared with patients randomized to receive SOC. The duration and volume of daily PE was shorter in the caplacizumab arm, which the clinical experts consulted by CADTH felt was encouraging and potentially clinically relevant. However, neither the HERCULES nor TITAN studies provided conclusive evidence showing that caplacizumab decreases mortality, minimizes organ damage, reduces health care utilization, or prevents long-term aTTP recurrence beyond the duration of the trials.
Post Hoc Analyses
Description of Studies
Peyvandi et al. (2021)16 conducted an integrated analysis of data from the HERCULES and TITAN trials as suggested by the FDA to increase statistical power for assessing treatment differences in efficacy and safety outcomes. The integrated analysis included all randomly assigned patients from the HERCULES and TITAN studies, which were described in detail in the Clinical Review Report for the initial review of caplacizumab13 (Appendix 2). This study provided an additional evaluation of the clinically important outcomes of mortality, organ damage, health care utilization, and refractory aTTP, but did not address long-term aTTP recurrence.
For the primary analysis of time to platelet count response, treatment groups were compared using a 2-sided log-rank test stratified by trial based on Kaplan-Meier analysis. Hazard ratios (HRs) and 95% confidence intervals (CIs) were calculated using a Cox proportional hazards model with time to platelet count response as a dependent variable, treatment group as an independent variable, and study as a random effect. To compare secondary outcomes (time to normalization of organ damage markers, duration of PE, proportion of patients with aTTP-related death, aTTP recurrence, or major thromboembolic events, and aTTP recurrence) between treatment groups, a stratified Cochran-Mantel-Haenszel test was used as a stratification factor in the trials. Analysis of time to first normalization of organ damage markers was performed as for the primary analysis of time to platelet count response.
Efficacy Results
During blinded study drug treatment, no patients randomized to receive caplacizumab and 4 patients (3.6%) randomized to receive placebo died; during the overall study periods, 1 patient (0.9%) randomized to receive caplacizumab and 5 patients (4.5%) randomized to receive placebo died. The proportion of patients who experienced aTTP-related events (aTTP-related death, major thromboembolic events, or aTTP exacerbation) while receiving blinded study drug treatment was 13.0% in patients randomized to receive caplacizumab versus 47.3% among patients randomized to receive placebo. During blinded study drug treatment, no patients randomized to receive caplacizumab and 8 patients (7.1%) randomized to receive placebo had refractory aTTP. Consistent with the individual studies, treatment with caplacizumab resulted in a numerically faster time to normalization of LDH (HR = 1.43; 95% CI, 1.04 to 1.96), numerically faster time to normalization of troponin (HR = 1.32; 95% CI, 0.86 to 2.04), and numerically faster time to normalization of serum creatinine (HR = 1.68; 95% CI, 0.89 to 3.15). During the overall treatment periods, median duration of PE was numerically shorter in patients randomized to receive caplacizumab (5.0 days; range, 1 to 35 days) compared with patients randomized to receive placebo (7.5 days; range, 2 to 46 days). During the treatment-free follow-up periods, 14 patients (13.0%) randomized to receive caplacizumab and no patients randomized to receive placebo experienced aTTP relapses.
Harms Results
The safety data for the integrated safety population were consistent with the results of the individual studies and no new safety signals were identified. Bleeding excluding aTTP occurred in 58.5% of patients treated with caplacizumab and 42.7% of patients treated with placebo. Serious bleeding excluding aTTP occurred in 11.3% of patients treated with caplacizumab and 1.8% of patients treated with placebo.
Critical Appraisal
Overall, the results of the integrated analysis supported and reinforced the consistent numeric improvements in the clinically important outcomes of survival, refractory aTTP, and duration of PE observed in the clinical development program (phase II TITAN and phase III HERCULES studies). However, internal and external validity issues of the individual HERCULES and TITAN trials affect the integrated analysis as well (refer to the Clinical Review Report for the initial submission of caplacizumab13 for details, the executive summary of which is reproduced as Appendix 2). In particular, the clinical experts consulted by CADTH for this review were concerned that the higher proportion of patients in the placebo arm of the integrated population with recurrent rather than initial aTTP may have contributed to poorer outcomes, including higher mortality. In addition, there were several notable differences between the TITAN and HERCULES studies, including the time they were conducted (2010 to 2014 versus 2015 to 2017) and the administration of caplacizumab (requirement for 1 prior PE session in the HERCULES study and the possibility to extend treatment beyond the first 30 days post-PE in the HERCULES study). Thus, the clinical experts consulted by CADTH for this review relayed their uncertainty that the data from the 2 studies could be naively pooled. Statistical analyses of integrated data in the study by Peyvandi et al. (2021) were post hoc, not adjusted for multiple comparisons, and should be interpreted in descriptive and exploratory fashion.
Real-World Evidence
Description of Studies
Three studies of 2 RWE cohorts of patients treated with caplacizumab from France17-19 and the UK20 are summarized in this report. The RWE studies provided additional supportive evidence regarding the clinically important outcomes of mortality, health care use, and refractory aTTP, but did not address organ damage or long-term aTTP recurrence.
Coppo et al. (2021)18 prospectively analyzed outcome data for 90 patients with aTTP from France treated from September 2018 to December 2019 with a frontline triplet regimen consisting of PE, immunosuppression with corticosteroids and rituximab, and caplacizumab. Outcomes were compared with 180 historical control patients from the Centre National de Référence sur les Microangiopathies Thrombotiques (CNR-MAT) registry treated from June 2015 to September 2018 with standard frontline therapy (PE plus corticosteroids, with rituximab as salvage therapy). CEMKA and Sanofi17,19 conducted an updated reanalysis of the data from this RWE cohort to include all historical controls available in the same registry, and to calculate a propensity score based on disease severity and mortality risk as an adjustment factor in multivariate modelling.
Dutt et al.20 conducted a retrospective analysis of data from 85 patients with aTTP (including 4 children) who received caplacizumab in 22 UK hospitals from May 2018 and January 2020. Outcomes for these patients were compared with data from the HERCULES study and to a group of historical control patients consisting of 39 consecutive cases from the UK TTP registry who received standard treatment (PE plus immunosuppression with corticosteroids and rituximab) from 2014 to 2018.
Efficacy Results
In the RWE cohort of Coppo et al. (2021),18 the percentage of patients receiving the triplet regimen including caplacizumab with the composite primary outcome including death and refractoriness was 2.2% versus 12.2% in historical controls (HR = 6.2; 95% CI, 1.4 to 26.3). One patient (1.1%) treated with the triplet regimen died compared with 12 (6.7%) historical controls. One patient (1.1%) treated with the triplet regimen experienced refractory aTTP compared with 16 (18%) historical controls. Compared with historical controls, patients receiving the triplet regimen had numerically fewer PE sessions (median 5 sessions versus 10 sessions), required numerically lower overall PE volume until remission (median 24.2 L versus 44.2 L), and had numerically shorter duration of hospitalization (median 13 days versus 22 days).
|| ||| ||||||| |||||||||| || ||||| ||| |||||| |||||||||||| ||| ||||||| |||||| ||||||||| ||| ||||||| ||||||| ||||||||| |||||||||||| ||||||||||| ||| ||||||| ||||||| || ||||| |||||| || ||||| ||||| || |||||||| |||||| || |||||||| || ||| |||||||||| |||||| |||| |||||| || ||||| ||| ||||||| |||||| ||||||| |||| ||| ||||||| ||||||| ||||||||||| |||||||||| |||| |||||||| |||| || ||||||| |||||||||| ||||||||| ||| |||||||| |||||| ||||||| |||| ||| ||||||| ||||||| ||||||||||| ||| ||||||||| |||||||| |||||||||||| |||||| |||||||||||||| || ||||| |||||||||||||| |||||| |||||| || |||| |||||| |||||||||| |||| |||||||| |||| || |||||||||| ||||||| |||||||| |||||||| |||||||| |||| |||||||||| ||||||||| |||||||| ||||||||| ||| ||||||| ||||||| ||| ||||||||||| ||||||| |||||||| || || ||||||| ||| |||| || |||| |||||| |||||||| ||||||||||| ||||| ||||||| || |||||| ||||| ||||||||| ||||||| |||| | ||| |||| ||| ||| ||| ||||||||||| ||||||| |||||||| || ||||||||||||||| ||||||| || |||| || || ||||||
In the RWE cohort of Dutt et al. (2021),20 5 patients (6%) in the caplacizumab cohort died and no deaths were reported among historical control patients. aTTP recurrence and refractoriness were not compared between the 2 groups. In 4 of the patients who died, caplacizumab was introduced more than 48 hours after PE initiation (range, 3 to 21 days). Compared with historical controls, patients who received caplacizumab had numerically shorter duration of PE (median 7 days versus 9 days) and numerically shorter time from PE initiation to platelet count normalization (median 4 days versus 6 days). Duration of hospitalization was similar in the caplacizumab cohort (median = 12 days) and the historical control cohort (median = 14 days).
Harms Results
The safety data for the RWE cohorts were generally consistent with the clinical trial data from the HERCULES study. Bleeding events occurred in 12% to 18% of patients. In the RWE cohort of Dutt et al. (2021), 5 patients (5.9%) experienced venous thromboembolism.
Critical Appraisal
Comparisons between the RWE cohorts and historical controls or the HERCULES trial populations were limited by risk of bias in selection of participants and potential for confounding by measured and unmeasured variables including nonoverlapping time frames and differences in treatment, primarily use of rituximab, which was higher in the RWE cohorts. The impact of bias in selection of patients into RWE cohorts as well as selection of historical control groups could not be evaluated and contributed to a high level of uncertainty. Except for the reanalysis of Sanofi and CEMKA (2021),17,19 all comparisons were naive and did not take into account baseline differences between populations, such as cardiac and organ involvement. The rationale for statistical hypothesis testing was not provided and it was unclear whether statistical tests were prespecified or conducted post hoc for some outcomes. Statistical tests were not adjusted for multiple comparisons and should be interpreted in descriptive and exploratory fashion.
Generalizability of the RWE to Canadian clinical practice was limited by high rates of rituximab use, including as upfront therapy. In addition, in the RWE cohort of Coppo et al. (2021),18 caplacizumab was administered upfront only, which may not be consistent with the anticipated use of the drug in Canadian clinical practice, according to the clinical experts consulted for this review. In the RWE cohort of Dutt et al. (2021),20 the baseline characteristics suggested that some had severe disease and/or multiorgan involvement and may have been candidates for upfront therapy with caplacizumab in Canadian practice; however, in approximately half of patients caplacizumab was started 2 days or longer after PE initiation. In the RWE cohort of Dutt et al. (2021)20 administration of caplacizumab was not aligned with the HERCULES study or the product monograph due to high rates of discontinuation before 30 days after PE.
Conclusions
Evidence from the HERCULES study suggested that administration of caplacizumab resulted in a statistically significant decrease in the frequency of aTTP recurrence during the HERCULES study period. In the long term follow-up study of the HERCULES study (the post-HERCULES study), there were no signs that treatment with caplacizumab during the HERCULES study resulted in increased frequency of aTTP relapse post PE discontinuation beyond the follow-up period of the HERCULES trial. A post hoc integrated analysis of data from the HERCULES and TITAN trials provided an additional evaluation of survival, health care use, organ damage, and refractory aTTP; however, due to naive pooling of the data and lack of formal statistical testing of prespecified hypotheses, including adjustment for multiple comparisons, its results supported but were unable to extend the conclusions regarding these outcomes drawn from the individual trials. Two RWE cohorts from France and the UK provided additional supportive evidence regarding the frequency of aTTP-related events, including mortality in patients receiving caplacizumab; however, due to potential for biased patient selection in observational studies, intergroup differences in measured and/or unmeasured confounders including treatments received that could not be accounted for, and absence of formal statistical testing, no conclusions could be drawn that go beyond the HERCULES, post-HERCULES, and TITAN trial data. The combined data from the HERCULES and post-HERCULES studies suggested that caplacizumab may decrease overall aTTP recurrence during treatment and immediately following treatment cessation (HERCULES) without producing an increased frequency of long-term aTTP relapse in the subsequent months and years (post-HERCULES).
Introduction
Disease Background
TTP is an ultra-rare blood disorder cause by reduced enzymatic activity of the vWF-cleaving protease, ADAMTS13, resulting in inability to cleave high molecular weight vWF multimers and as a consequence formation of platelet-rich blood clots in small vessels (thrombotic microangiopathy).2 TTP is an acute, fulminant disorder that is a medical emergency occurring mainly among adults aged 30 to 50 years.2,3 Congenital TTP (involving familial inheritance of ADAMTS13 gene mutations) makes up less than 5% of cases while aTTP, driven by autoantibodies against ADAMTS13), is the dominant form.4 Because there is no specific known cause of aTTP, it is sometimes known as immune TTP.
The incidence of aTTP is estimated at approximately 2 to 4 cases per million population (approximately ||| cases per million adults) per year.8-10 In agreement with incidence estimates, data from the CAG registry indicated that approximately ||| patients with TTP were treated in Canada in 2018;1 data for more recent years were not provided by the sponsor. When diagnosis is made immediately and current SOC treatments are administered rapidly, mortality has been estimated at approximately 10% to 20%.5 After the presenting episode, recurrence of aTTP (exacerbation: recurrence within 30 days of cessation of PE; relapse: recurrence after 30 days of cessation of PE) will occur in up to half of patients, while refractory aTTP (absence of platelet count increase following treatment) will occur in approximately 10% of patients.7 In addition, thrombotic complications and their sequelae (e.g., stroke, myocardial infarction, neurocognitive deficits, kidney injury) contribute to persistent cognitive and physical difficulties that can be life-altering in some patients, compromising HRQoL.6
According to the clinical experts consulted by CADTH for this review, diagnosis of aTTP is based on clinical and laboratory findings and is made by a hematologist, although treatment may also be managed by nephrologists and pathologists or transfusion medicine specialists. The clinical manifestations of aTTP are often nonspecific and may include skin discoloration (e.g., bruising), fatigue, dyspnea, fever, myalgia, arthralgia, and neurological symptoms.2,4 aTTP is a microangiopathic hemolytic anemia and laboratory markers including findings of red blood cell fragments called schistocytes on peripheral blood smear, thrombocytopenia (typically platelets less than 30 × 109/L), low ADAMTS13 activity (typically < 10% of normal), evidence of hemolytic anemia (low hemoglobin, elevated serum LDH, elevated unconjugated bilirubin, elevated reticulocyte count, and low to absent haptoglobin), and elevated creatinine.2,4 Cardiac troponin may also be elevated. Due to the diverse clinical manifestations of aTTP, overlap in clinical presentation with other thrombotic microangiopathies, and limited availability of ADAMTS13 testing, diagnosis at immediate presentation to medication attention can be challenging. Therefore, patients who have a presentation concerning for aTTP (e.g., those who are identified as intermediate or high risk of having aTTP using the PLASMIC [platelets, lysis, active cancer, stem cell, or solid organ transplant, mean corpuscular volume, international normalized ratio, and creatinine] score27) will be treated empirically for aTTP while awaiting the results of ADAMTS13 activity testing and inhibitor titres, which can take days. Empirical treatment for aTTP is initiated in these patients due to the potential consequences of a missed aTTP diagnosis.2
Standards of Therapy
According to the clinical experts consulted by CADTH for this review, current management of aTTP in Canada involves PE and immunosuppression. The sponsor emphasized that the treatment burden associated with PE is significant as PE often requires a transfer to a PE centre, there is a need for surgery (vascular catheter insertion with a risk of infections), and there is potential for exposure to multiple donors (risk of PE reactions).1 PE is administered daily until platelet count and LDH normalize, with the goal of removing ADAMTS13 autoantibodies and ultra-large vWF multimers; if PE is not immediately available, plasma infusion can be used as a bridge while the patient is transferred to a centre that can perform PE. The goal of immunosuppression is to suppress production of ADAMTS13 autoantibodies via administration of corticosteroids (prednisone 1 mg/kg or methylprednisolone 1 g daily for 3 days, followed by prednisone 1 mg/kg; dosing is tapered once a patient is in remission) and, in some patients, rituximab (375 mg/m2 weekly for 4 weeks). In Canada, rituximab is typically not used upfront and is administered to patients with aTTP exacerbations, relapsed aTTP, or refractory aTTP. Use of rituximab may decrease the risk of aTTP relapse.
The clinical experts consulted by CADTH for this review relayed that from a clinical standpoint, the main goals of treatment are to prolong life and avoid mortality while preventing thrombotic complications as well as their sequelae and associated disabilities (e.g., stroke, myocardial infarction, neurocognitive deficits, kidney injury). Treatment goals are accomplished by replenishing ADAMTS13 and removing autoantibodies against ADAMTS13, allowing normalization of ADAMTS13 activity and consequently halting thrombotic microangiopathy.
Drug
Key characteristics of caplacizumab are shown in Table 4. Caplacizumab is a bivalent humanized nanobody that is administered at a dose of 11 mg (IV and SC injections on day 1 of PE followed by daily SC injections during PE and for a minimum of 30 days after cessation of PE).11 Its mechanism of action involves binding to the A1 domain of vWF, inhibition of the interaction between vWF and platelets, reduction of vWF-mediated platelet activation and adhesion, and prevention of the formation of ultra-large vWF-rich platelet microthrombi.11 The Health Canada indication for caplacizumab is “for the treatment of adults with acquired thrombotic thrombocytopenic purpura (aTTP) in combination with plasma exchange (PE) and immunosuppressive therapy.”11 The sponsor’s reimbursement request is the same as the approved Health Canada indication. Caplacizumab underwent priority review at Health Canada and received a Notice of Compliance on February 28, 2020.
Submission History
Caplacizumab was initially reviewed by CADTH for the treatment of adults with aTTP in combination with PE and immunosuppressive therapy and received a negative funding recommendation from CDEC on September 1, 2020.12 The recommendation was based on evidence assessed in the CADTH Clinical Review Report for the initial submission of caplacizumab,13 the executive summary of which is reproduced as Appendix 2. Key reasons for the recommendation included:
insufficient evidence of clinically important outcomes (e.g., survival, organ damage, health care use, or long-term aTTP recurrence), and given caplacizumab’s mechanism of action, uncertainty in the correlation between time to normalization of platelet count and these outcomes
lack of long-term clinical outcome data, including on aTTP recurrence, beyond the relatively short durations of the trials
lack of an identifiable subpopulation most likely to benefit from treatment with caplacizumab, given the variability in the natural history of aTTP
unclear generalizability of the trial results, primarily due to higher rates of rituximab use compared with Canadian clinical practice
absence of HRQoL data.
In response to the draft CDEC recommendation, the sponsor submitted a request for reconsideration in which the potential role caplacizumab might play in reducing aTTP mortality and microvascular thrombosis was emphasized, as was the potential clinical importance of consistent numerical improvements achieved with caplacizumab across many outcomes. In addition, to better align with the views of clinical experts consulted by CADTH, the sponsor’s reimbursement request was narrowed to patients with multiorgan involvement indicating more severe disease as well as patients with refractory aTTP who do not respond well to SOC treatment for a given time period. However, CDEC maintained its initial position that direct evidence showing an advantage for caplacizumab in clinically relevant outcomes was not currently available and that subgroup analyses justifying use of caplacizumab in patients with severe or refractory aTTP were unavailable.
The drug was resubmitted for review by the sponsor on the basis of the availability of new evidence on June 7, 2022.1 The new evidence included a prospective long-term follow-up study of patients who completed the HERCULES study (post-HERCULES),14,15 a variety of post hoc analyses of clinical trial data including an integrated analysis of data from the HERCULES and TITAN studies,16 and several RWE studies including comparisons of patients treated with caplacizumab from France17-19 and the UK20 with historical controls who received SOC alone. The sponsor suggested that the post-HERCULES study addressed CDEC concerns 2 and 5 (lack of long-term clinical outcome data and absence of HRQoL data), while the post hoc analyses addressed CDEC concerns 1 to 4 (insufficient evidence of clinically important outcomes, lack of long-term clinical outcome data, lack of an identifiable subpopulation most likely to benefit, and generalizability to Canadian practice) and the RWE studies addressed CDEC concerns 1 to 3 (insufficient evidence of clinically important outcomes, lack of long-term clinical outcome data, and lack of an identifiable subpopulation most likely to benefit).
The objective of this report was to perform a systematic review of the beneficial and harmful effects of caplacizumab (11 mg IV bolus plus 11 mg SC injection on day 1 of PE, followed by 11 mg SC injection daily) for the treatment of adults with aTTP in combination with PE and immunosuppressive therapy. This report is an update of the Clinical Review Report for the original submission of caplacizumab;13 any new evidence provided by the sponsor or identified through a systematic literature search was included in the report if it addressed an evidence gap identified by CDEC in its final recommendation for the initial submission.
Table 4: Key Characteristics of Caplacizumab, PE, and Immunosuppressive Therapy for Treatment of aTTP
Characteristic | Caplacizumab | PE | IST |
|---|---|---|---|
Mechanism of action | Binding to the A1 domain of vWF, inhibition of the interaction between vWF and platelets, reduction of vWF-mediated platelet activation and adhesion, and prevention of the formation of ultra-large vWF-rich platelet microthrombi | Removal of ADAMTS13 autoantibodies and ultra-large vWF multimers, replenishment of ADAMTS13 activity | Suppression of production of ADAMTS13 autoantibodies |
Indicationa | For the treatment of adults with aTTP in combination with PE and immunosuppressive therapy | NA | Various |
Route of administrationb | IV, SC | IV | Oral (corticosteroids) IV (rituximab) |
Recommended doseb | 11 mg | 1 to 1.5 plasma volumes | 1 mg/kg daily (corticosteroids) 375 mg/m2 once per week (rituximab) |
Serious adverse effects or safety issues | Bleeding | Infection, bleeding, thrombosis, transfusion reactions | Infections, infusion reactions |
ADAMTS13 = a disintegrin and metalloproteinase with thrombospondin type 1 motif, member 13; aTTP = acquired thrombotic thrombocytopenic purpura; IST = immunosuppressive therapy; NA = not applicable; PE = plasma exchange; SC = subcutaneous; vWF = von Willebrand factor.
aHealth Canada–approved indication. Note that rituximab is used off label to treat aTTP.
bThere is some variation in clinical practice related to administration and dosing of corticosteroids and rituximab for treatment of aTTP.
Source: Sponsor’s drug reimbursement review resubmission1 and product monograph for caplacizumab.11
Stakeholder Perspectives
Patient Group Input
This section was prepared by CADTH staff based on the input provided by a patient group. The original patient group submission can be found at the end of this report.
One patient group, the Answering TTP Foundation, provided input for this review. The group conducted an online survey in May and June of 2022 (N = 49 respondents including 31 patients with aTTP, 16 family members, caregivers, or friends of patients with aTTP, 1 health care professional, and 1 researcher). Most (80%) survey respondents were women and most (90%) were living in Canada. Approximately half of respondents (48%) had experienced at least 1 relapse. Patients highlighted delays in diagnosis and treatment as well as the negative impacts of serious and/or frequent symptoms of aTTP (e.g., bruising, fever, fatigue, migraine, confusion, abdominal pain, bleeding, shortness of breath, vision loss, and jaundice) which impose heavy burdens on mental health (e.g., anxiety, depression, and panic attacks). A subset of patients experienced incapacitating or life-threatening complications of aTTP including stroke, myocardial infarction, and kidney problems. Nearly all patients had experience with PE and corticosteroids while approximately two-thirds (65%) had experience with rituximab. Respondents described the challenges of current treatments including lengthy hospital stays, side effects of corticosteroids, and the inconvenience of daily PE; in addition, available treatments are costly, require time off from work, and may require travel to a major centre for access. Respondents identified an unmet need for treatments that can reduce the risk of death or disability from aTTP and ease the mental and emotional burdens of disease (e.g., continuous fear of relapse and impacts on social life and career goals). Specifically, respondents valued new treatments that enable patients to survive an aTTP crisis and thereby reduce the patient’s emotional uncertainty in the early stages of an aTTP episode and improve peace of mind during remission. As well, respondents noted that a reduction in the number of PE treatments and ability to plan for the future were important when considering treatment options. Approximately one-third (34%) of respondents had experience with caplacizumab and felt that the drug had contributed to shorter hospitalization, faster remission, and prevention of further disease.
Clinician Input
Input From Clinical Experts Consulted by CADTH
All CADTH review teams include at least 1 clinical specialist with expertise regarding the diagnosis and management of the condition for which the drug is indicated. Clinical experts are a critical part of the review team and are involved in all phases of the review process (e.g., providing guidance on the development of the review protocol, assisting in the critical appraisal of clinical evidence, interpreting the clinical relevance of the results, and providing guidance on the potential place in therapy). The following input was provided by 2 clinical specialists with expertise in the diagnosis and management of aTTP.
Unmet Needs
The clinical experts consulted by CADTH for this review stated that while currently available treatments are effective in many patients, not all patients manifest durable responses to the current SOC (PE plus immunosuppression with corticosteroids with or without rituximab) and thus experience persistent or recurrent thrombotic microangiopathy, which can lead to thrombotic complications and, potentially, mortality (in 10% to 20% of patients). The clinical experts emphasized that both currently available therapies (PE and immunosuppression) as well as caplacizumab aim to correct the dysfunctions of aTTP (PE removes ADAMTS13 autoantibodies and replaces ADAMTS13, immunosuppression aims to suppress production of ADAMTS13 autoantibodies, and caplacizumab blocks platelet aggregation), but these treatments do not modify the underlying disease mechanism involving loss of self-tolerance and generation of autoantibodies to ADAMTS13. However, the clinical experts relayed that immunosuppression can limit or stop autoantibody production for sustained periods.
According to the clinical experts, there is an unmet need for additional treatment options that improve survival and prevent thrombotic complications and their sequelae (e.g., stroke, myocardial infarction, neurocognitive deficits), especially for patients with aTTP recurrence or refractory aTTP. It is not currently possible to identify which patients will experience these outcomes at the time of presentation. Patients with refractory aTTP are continued on PE (sometimes with increased frequency) and typically receive rituximab if it was not administered upfront. For patients with aTTP recurrence, PE is restarted, doses of corticosteroids are increased (if on a taper) and rituximab is typically administered. Less commonly, other immunosuppressive agents may be used in patients with aTTP recurrence or refractory aTTP such as cyclophosphamide, vincristine, and cyclosporine as well as IV immunoglobulin and splenectomy.
Place in Therapy
The clinical experts relayed that the mechanism of action of caplacizumab (disruption of the interaction between vWF and platelets) differs from that of PE and immunosuppressive therapy. Therefore, caplacizumab would be administered in combination with PE and immunosuppressive therapy. The clinical experts felt that because some patients respond well to PE and immunosuppressive therapy, caplacizumab may be a reasonable option to be reserved for patients with aTTP recurrence or refractory aTTP as these patients currently have limited treatment options. The clinical experts acknowledged that it is currently unclear if delaying access to caplacizumab may impact its efficacy. The HERCULES trial was designed to evaluate the upfront use of caplacizumab in combination with PE and immunosuppressive therapy. According to the clinical experts, upfront treatment with caplacizumab could also be considered in high-risk patients who have neurologic or cardiac abnormalities (including elevated troponin) or are otherwise critically ill. The clinical experts acknowledged that currently there is insufficient evidence to identify patients who are more likely to respond to caplacizumab in combination with PE plus immunosuppression. The clinical experts did not expect that use of caplacizumab would cause a shift in the treatment paradigm for aTTP; PE plus immunosuppression would still be initiated immediately and response to treatment monitored using the same markers.
Patient Population
According to the clinical experts consulted by CADTH, high-risk patients (those with neurologic or cardiac abnormalities or who are otherwise critically ill) would be best suited for caplacizumab. Patients with aTTP recurrence or refractory aTTP (regardless of the presence of high-risk features) would also benefit from the addition of caplacizumab to standard therapy (PE plus immunosuppression). These patients would be identified by the treating hematologist. Low-risk patients (defined by the absence of high-risk features described previously), patients who have responded to PE plus immunosuppression, and patients in clinical remission (clinical response of 1 month or longer) would be least suitable for treatment with caplacizumab. The clinical experts noted that currently it is not possible to identify patients who are more likely to respond to caplacizumab in combination with PE plus immunosuppression.
The clinical experts relayed that misdiagnosis of aTTP is relatively common (overdiagnosis) due to the potential consequences of a missed diagnosis, and that at present there is some uncertainty in diagnostic testing of ADAMTS13 due to lack of standardized testing methods. However, these diagnostic challenges would not affect selection of patients to receive caplacizumab.
Assessing Response to Treatment
The clinical experts consulted by CADTH for this review stated that response to caplacizumab plus PE and immunosuppression would be based on normalization of platelet count (complete blood count) and LDH. Reticulocyte count, unconjugated bilirubin, hemoglobin, haptoglobin, ADAMTS13 activity, and ADAMTS13 autoantibody levels should also normalize. Some clinicians also monitor creatinine, although acute kidney injury in patients with aTTP is typically mild. A clinically meaningful response to treatment would be defined by normalization of platelet count and LDH. During acute aTTP episodes, complete blood count (platelets, hemoglobin), unconjugated bilirubin, LDH, reticulocyte count, and creatinine are monitored daily. Haptoglobin, ADAMTS13 activity, and ADAMTS13 autoantibody levels are typically monitored after completion of 5 days of PE as well as following cessation of PE.
The clinical experts relayed that the ultimate mechanistic goal of therapy is to normalize ADAMTS13 activity. It is possible to use ADAMTS13 levels to monitor response, but these results will not be as available in a timely manner, as compared to platelet count. More typically, if a patient is not demonstrating a clinical response to standard therapy, ADAMTS13 activity may be measured.
Discontinuing Treatment
According to the clinical experts, PE is typically discontinued after 5 days if platelet count, LDH, reticulocyte count, unconjugated bilirubin, and hemoglobin are normalized. Patients are then typically monitored for 1 to 2 days to determine if their platelet counts drop again or if hemolytic or other markers (e.g., LDH, reticulocytes, unconjugated bilirubin) show signs of aTTP recurrence. If there is no evidence of recurrence, patients are typically discharged from hospital and doses of corticosteroids are tapered with close outpatient follow-up. If there is evidence of recurrence, PE is reinitiated and additional treatments such as rituximab are ordered.
The clinical experts stated that in patients receiving caplacizumab who develop aTTP recurrence or refractory aTTP would be discontinued from therapy, as would patients with serious toxicities such as clinically significant bleeding. The clinical experts relayed that 1 of the challenges of using caplacizumab is that it directly increases platelets through its mechanism, potentially masking an indicator of aTTP disease activity, which would make it difficult to determine when it is time to taper PE.
Prescribing Conditions
The clinical experts emphasized that PE is only offered in certain hospitals and therefore patients with aTTP are typically transferred urgently to major centres. Patients are typically managed by a hematologist (either as the admitting or consulting service). Caplacizumab would be administered in centres that have both PE capacity and a hematology service.
Clinician Group Input
This section was prepared by CADTH staff based on the input provided by a clinician group. The original clinician group submission can be found at the end of this report.
Clinician group input was received from the CAG, with 5 clinicians contributing to the submission. No major contrary views from those provided by the clinical experts consulted by CADTH for this review were presented. The clinician group echoed the inability of current treatments to accomplish the goals of therapy (avoid mortality and prevent thrombotic complications) in all patients and the unmet need for additional treatment options for patients with aTTP exacerbations, relapsed aTTP, and refractory aTTP as well as patients at high risk of mortality and/or organ damage. The clinician group also highlighted the unmet need for drugs that can rapidly inhibit platelet aggregation while waiting for PE and immunosuppression to take effect.
Drug Program Input
The drug programs provide input on each drug being reviewed through CADTH’s reimbursement review processes by identifying issues that may impact their ability to implement a recommendation. The implementation questions and corresponding responses from the clinical experts consulted by CADTH are summarized in Table 5.
Table 5: Summary of Drug Plan Input and Clinical Expert Response
Implementation issues | Clinical experts’ response |
|---|---|
Considerations for initiation of therapy | |
FWG noted that there may be patient characteristics other than disease diagnosis for eligibility to receive caplacizumab.
| The clinical experts felt that both the HERCULES and post-HERCULES trial data were generally applicable to the population of patients in Canada living with aTTP. In the HERCULES study, patients received the current standard of care in Canada (PE plus immunosuppression with corticosteroids with or without rituximab). Although most patients in the HERCULES study were women, this is consistent with established trends in the occurrence of aTTP and therefore the results are applicable to Canada. |
FWG noted that eligibility criteria for re-treatment were unclear.
| The clinical experts responded that the post-HERCULES study provided additional relevant evidence regarding the efficacy of caplacizumab beyond the short follow-up period of the original HERCULES trial. The clinical experts relayed that there is currently no clear evidence or guidance to inform the frequency of reuse of caplacizumab. However, in the post-HERCULES study, 9 patients were retreated with caplacizumab and thus it would be reasonable to re-treat patients with caplacizumab if they previously responded to the drug (and did not lose response while receiving the drug) and did not experience major adverse events. |
FWG noted that there may be patient subgroups to consider separately for eligibility.
| The clinical experts responded that high-risk patients (those with neurologic or cardiac abnormalities, including elevated troponin, or who are otherwise critically ill) would likely benefit most from treatment with caplacizumab. However, there is currently insufficient evidence to identify patients who are more likely to respond to caplacizumab in combination with PE plus immunosuppression. |
Considerations for continuation or renewal of therapy | |
FWG noted that there are challenges related to assessment and monitoring of therapeutic response to caplacizumab.
| The clinical experts responded that in addition to clinical deterioration or improvement, including neurological status, all of the following parameters must be monitored to assess response to caplacizumab:
|
Considerations for discontinuation of therapy | |
FWG noted definitions of loss of response or absence of clinical benefit that would justify discontinuation of caplacizumab are unclear.
| The clinical experts relayed that loss of response to caplacizumab would be reflected by refractory aTTP (drop in platelet count or evidence of ongoing or worsening hemolysis) while receiving caplacizumab. As noted previously, the clinical experts relayed that there is currently no clear evidence or guidance to inform the frequency of reuse of caplacizumab. In the absence of such evidence, it would be reasonable to re-treat patients with caplacizumab if they previously responded to the drug (and did not lose their response) and did not experience major adverse events. |
Considerations for prescribing of therapy | |
FWG noted that caplacizumab requires initial IV administration upon initiation of PE with subsequent SC injections during PE and for 30 days following the last daily PE. In certain circumstances (e.g., signs of persistent, underlying disease) treatment may be extended for a maximum of 28 days. | For CDEC consideration. |
FWG noted that because aTTP is an ultra-rare disease, access to clinical specialists and/or care settings may be limited. | For CDEC consideration. |
Generalizability | |
FWG noted that the previous CDEC recommendation indicated that the percentages of patients receiving rituximab in the HERCULES trial (between 40% and 50%) was higher than that expected in Canada.
| The clinical experts responded that the proportion of patients in Canada living with aTTP who receive upfront rituximab in addition to PE and corticosteroids is not known with certainty but is likely lower than in the HERCULES trial (40% in the caplacizumab arm and 49% in the placebo arm). However, this proportion has increased in recent years due to improved access to rituximab. |
Care provision issues | |
FWG noted that caplacizumab is dosed as an initial IV therapy followed by SC injections, including over a 30-day period following completion of PE. | For CDEC consideration. |
FWG noted that additional supportive medication or other health interventions are required for caplacizumab administration because the drug is indicated in combination with PE with or without immunosuppressive therapy. | For CDEC consideration. |
System and economic issues | |
FWG noted that provision of caplacizumab as a first-line treatment in combination with standard of care may have substantial budget impact.
|
|
FWG noted that there could be involvement of additional payers because the initial dose of caplacizumab would be administered by IV bolus in a health care setting followed by SC dosing on an outpatient basis. | For CDEC consideration. |
ADAMTS13 = a disintegrin and metalloproteinase with thrombospondin type 1 motif, member 13; aTTP = acquired thrombotic thrombocytopenic purpura; CDEC = CADTH Canadian Drug Expert Committee; FWG = Formulary Working Group; LDH = lactate dehydrogenase; PE = plasma exchange; SC = subcutaneous.
Clinical Evidence
The clinical evidence included in the review of caplacizumab is presented in 2 sections. The first section, the Systematic Review, includes pivotal studies provided in the sponsor’s submission to CADTH and Health Canada, as well as those studies that were selected according to an a priori protocol. No indirect evidence was submitted by the sponsor and no indirect evidence was selected from the literature that met the selection criteria specified in the review. The second section includes additional relevant studies that were considered to address important gaps in the evidence included in the systematic review.
Systematic Review (Pivotal and Protocol-Selected Studies)
Objectives
To perform a systematic review of the beneficial and harmful effects of caplacizumab (11 mg IV bolus plus 11 mg SC injection on day 1 of PE, followed by 11 mg SC injection daily) for the treatment of adults with aTTP in combination with PE and immunosuppressive therapy.
Methods
Studies selected for inclusion in the systematic review included pivotal studies provided in the sponsor’s resubmission to CADTH and Health Canada, as well as those meeting the selection criteria presented in Table 6. Outcomes included in the CADTH review protocol reflect outcomes considered to be important to patients, clinicians, and drug plans.
Table 6: Inclusion Criteria for the Systematic Review
Criteria | Description |
|---|---|
Patient population | Adults (aged ≥ 18 years) with aTTP Subgroups:
|
Intervention | Caplacizumab plus PE with or without immunosuppressive therapy (e.g., glucocorticoids, rituximab) Caplacizumab dosing:
|
Comparators | PE with or without immunosuppressive therapy (e.g., glucocorticoids, rituximab) |
Outcomes | Efficacy outcomes:
Harms outcomes:
|
Study design | Published and unpublished Phase III and IV RCTs |
ADAMTS13 = a disintegrin and metalloproteinase with thrombospondin type 1 motif, member 13; AE = adverse event; aTTP = acquired thrombotic thrombocytopenic purpura; DVT = deep vein thrombosis; HRQoL = health-related quality of life; LDH = lactate dehydrogenase; MI = myocardial infarction; PE = plasma exchange; RCT = randomized controlled trial; SAE = serious adverse event; SC = subcutaneous; WDAE = withdrawal due to adverse event.
The literature search for clinical studies was performed by an information specialist using a peer-reviewed search strategy according to the PRESS Peer Review of Electronic Search Strategies checklist.28 Published literature was identified by searching the following bibliographic databases: MEDLINE All (1946—) via Ovid and Embase (1974—) via Ovid. All Ovid searches were run simultaneously as a multifile search. Duplicates were removed using Ovid deduplication for multifile searches, followed by manual deduplication in EndNote. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. The main search concept was Cablivi (caplacizumab). Clinical trials registries were searched: the US National Institutes of Health’s clinicaltrials.gov, WHO’s International Clinical Trials Registry Platform (ICTRP) search portal, Health Canada’s Clinical Trials Database, and the European Union Clinical Trials Register.
No filters were applied to limit the retrieval by study type. Retrieval was not limited by publication date or by language. Conference abstracts were excluded from the search results. Refer to Appendix 1 for the detailed search strategies. The initial search was completed on July 6, 2022. Regular alerts updated the search until the meeting of CDEC on October 26, 2022.
Grey literature (literature that is not commercially published) was identified by searching relevant websites from the Grey Matters: A Practical Tool For Searching Health-Related Grey Literature checklist.29 Included in this search were the websites of regulatory agencies (FDA and European Medicines Agency). Google was used to search for additional internet-based materials. Refer to Appendix 1 for more information on the grey literature search strategy.
These searches were supplemented by reviewing bibliographies of key papers and through contacts with appropriate experts. In addition, the manufacturer of the drug was contacted for information regarding unpublished studies.
Two CADTH clinical reviewers independently selected studies for inclusion in the review based on titles and abstracts, according to the predetermined protocol. Full-text articles of all citations considered potentially relevant by at least 1 reviewer were acquired. Reviewers independently made the final selection of studies to be included in the review, and differences were resolved through discussion.
Findings From the Literature
Two reports of a single study14,15 were identified for inclusion in the systematic review (Figure 1). In the previous CADTH Clinical Review Report for the initial submission of caplacizumab,13 the pivotal HERCULES trial was identified and evaluated; therefore, this study was excluded from the systematic review section for the resubmission, as was the CADTH Clinical Review Report for the initial submission of caplacizumab13 itself (the executive summary of which is reproduced as Appendix 2). A table of included and excluded studies is presented in Appendix 3.
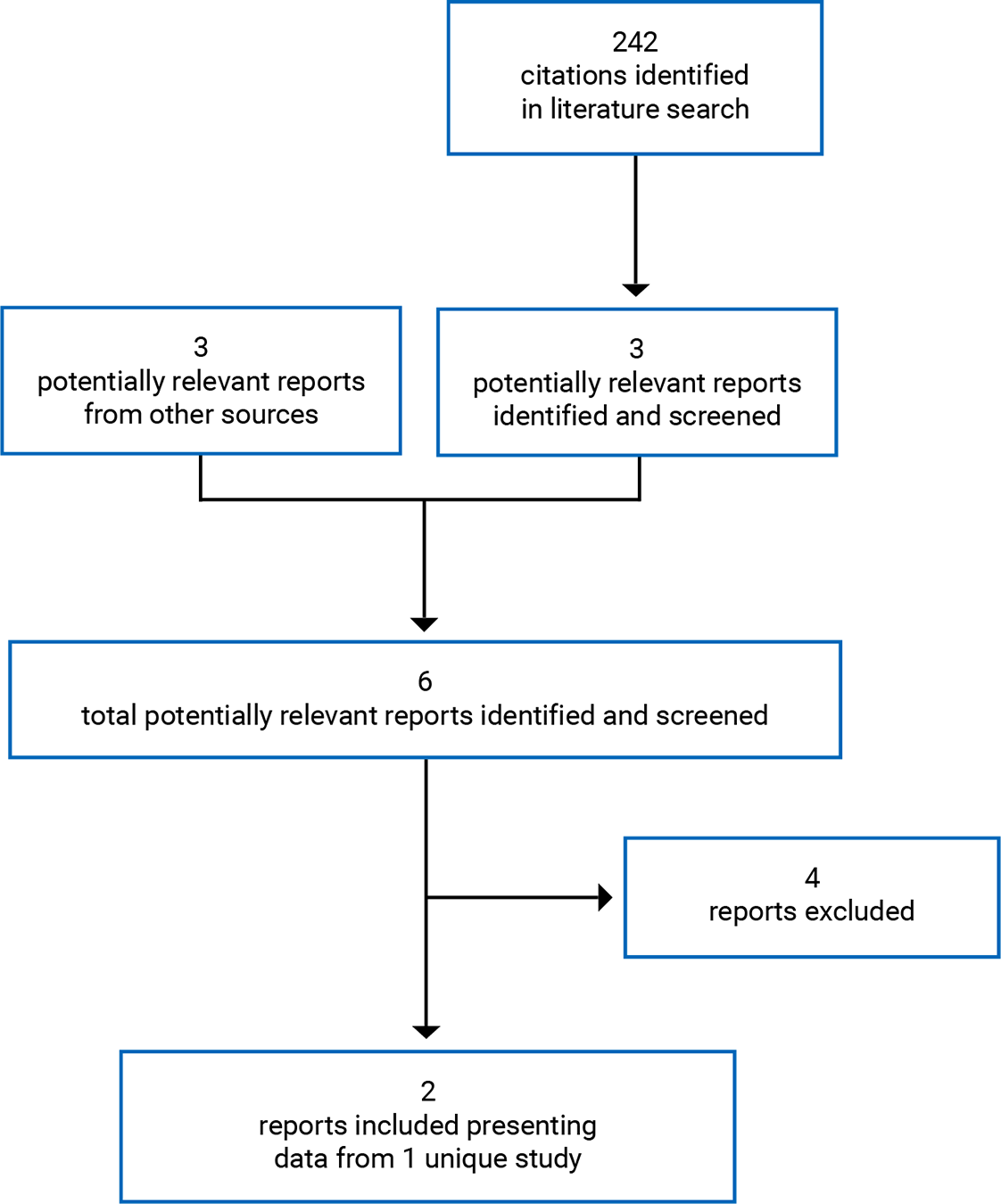
The included study (post-HERCULES) is summarized in Table 7. For ease of reference, the HERCULES study21-23 is summarized alongside the post-HERCULES study, although the evidence from the HERCULES study was previously evaluated by CADTH and is not presented further in the systematic review section of this report.
Table 7: Details of the Included Study
Detail | HERCULESa | Post-HERCULES |
|---|---|---|
Designs and populations | ||
Study design | Phase III, DB, placebo-controlled RCT | Phase III, prospective, long-term follow-up study |
Locations | 55 centres in Europe, the US, Canada, Israel, and Australia | 43 centres in Europe, the US, Canada, and Israel |
Patient enrolment dates | November 2015 to April 2017 | October 2016 to October 2017 |
Data cut-off | June 2018 | October 2020 |
Randomized or enrolled (N) | 145 | 104 |
Inclusion criteria |
|
|
Exclusion criteria |
|
|
Drugs | ||
Intervention | Caplacizumab plus PE with or without immunosuppressive therapy (e.g., glucocorticoids, rituximab) Caplacizumab dosing:
| OL treatment for recurrence: Caplacizumab plus PE with or without immunosuppressive therapy (e.g., glucocorticoids, rituximab) Caplacizumab dosing:
Optional extension period: Daily 11 mg SC injection for a maximum of 28 days if there are signs of persistent underlying disease |
Comparator | PE with or without immunosuppressive therapy (e.g., glucocorticoids, rituximab) | NA |
Duration | ||
Phase | ||
Screening | No minimum or maximum durationa | Within 1 month of the final 4-week follow-up visit in the HERCULES study |
DB or SB treatment |
|
|
Treatment extension period | 7-day to 28-day extension with initial treatment allocated for patients at risk of aTTP relapse | 7-day to 28-day extension with initial treatment allocated for patients at risk of aTTP relapse |
Follow-up | 4 weeks | 3 years |
Outcomes | ||
Primary end point | Time to platelet count response (defined as initial platelet count of 150 × 109/L or greater with discontinuation of PE within 5 days) | None |
Secondary and exploratory end points | Key secondary (hierarchically tested):
Other secondary:
| Exploratory:
Other exploratory:
|
Notes | ||
Publications | Scully et al. (2019)23 Knoebl et al. (2020)22 | Scully et al. (2022)15 |
ASA = acetylsalicylic acid; aTTP = acquired thrombotic thrombocytopenic purpura; AUC = area under the curve; cTnI = cardiac troponin I; CVA = cerebrovascular accident; DB = double blind; DIC = diffuse intravascular coagulation; DVT = deep vein thrombosis; HIT-6 = Headache Impact Test 6; HRQoL = health-related quality of life; HUS = hemolytic uremic syndrome; ICU = intensive care unit; LDH = lactate dehydrogenase; LMWH = low molecular weight heparin; MI = myocardial infarction; MTE = major thromboembolic event; NA = not applicable; OL = open label; PD = pharmacodynamics; PE = plasma exchange; PK = pharmacokinetics; RBANS = Repeatable Battery for the Assessment of Neuropsychological Status; RCT = randomized controlled trial; SB = single blind; SC = subcutaneous; SF-36 = Short Form (36) Health Survey; SMMSE = Standardised Mini-Mental State Examination; TTP = thrombotic thrombocytopenic purpura; ULN = upper limit of normal.
aFor ease of reference, the HERCULES study is summarized alongside the post-HERCULES study, although the evidence from the HERCULES study was previously evaluated by CADTH and is not presented further in the systematic review section of this report.
Note: One additional report was included (post-HERCULES Clinical Study Report).
Source: HERCULES Clinical Study Report (2018)21 and post-HERCULES Clinical Study Report (2021).14
Description of Studies
Key characteristics of the post-HERCULES study14,15 are summarized in Table 7. The post-HERCULES study was a phase III, prospective, long-term follow-up study (N = 104) of patients who completed the HERCULES study (N = 145, n = 108 completed). The objectives of the post-HERCULES study were to evaluate long-term safety and efficacy of caplacizumab, to evaluate the safety and efficacy of repeated use of caplacizumab in participants who experienced a recurrence of aTTP, and to characterize the long-term clinical impact of aTTP. Following the final 4-week follow-up visit in the HERCULES study, adult patients with aTTP were invited to enrol in the post-HERCULES study within 1 month. Patients who were not able or willing to comply with study protocol procedures or who enrolled in a clinical study with another investigational drug or device were excluded.
The design of the post-HERCULES study is illustrated in Figure 2. Following enrolment at 43 centres in Europe, the US, Canada (3 centres), and Israel, patients were followed for a period of 3 years. Patients attended twice-yearly visits, starting with a baseline visit coinciding with or occurring within 1 month of the final 28-day follow-up visit in the HERCULES study. At each twice-yearly visit, patients completed patient-reported outcome measures and underwent clinical and safety assessments. During the 3-year follow-up period, patients could receive OL caplacizumab in combination with PE and immunosuppression (administered as in the HERCULES study, except that 1 administration of PE was optional before initiation of caplacizumab) for aTTP recurrence (defined as recurrence of thrombocytopenia requiring initiation of daily PE). Patients receiving caplacizumab followed a scheduled of visits including at presentation, day 3 of treatment with caplacizumab, weekly visits during treatment with caplacizumab, and a follow-up visit 1 week after the end of treatment of caplacizumab. At each of these visits, information on the aTTP recurrence and treatment was collected and patients underwent clinical and safety assessments. The study is complete (data cut-off October 2020) and was funded by Ablynx (acquired by the sponsor in 2018) and the sponsor.
Figure 2: Design of the Post-HERCULES Trial
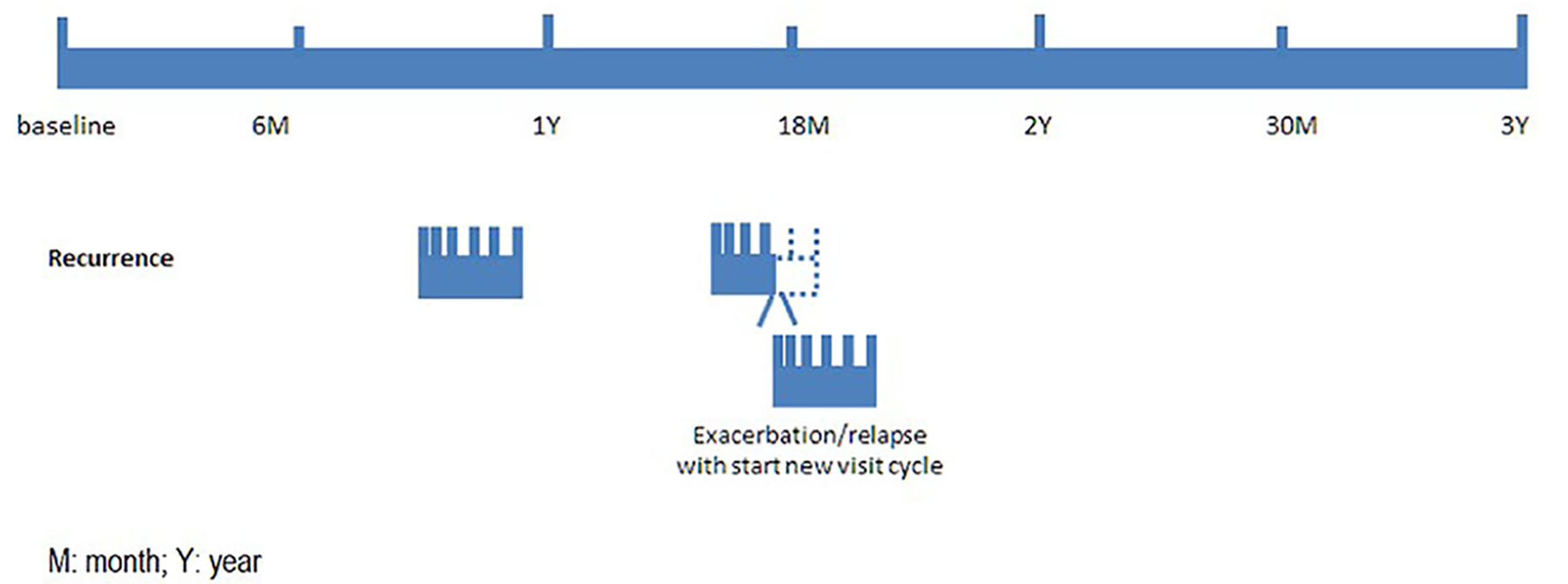
Note: In case of recurrent thrombocytopenia requiring reinitiation of daily plasma exchange during an ongoing recurrence period, a new visit cycle was started, with a recurrence visit on the day of the new recurrence followed by all subsequent visits. All remaining visits of the original schedule were no longer applicable and were not to be performed. Twice-yearly visits that were scheduled within a recurrence period were not held, as assessments at such visits would be confounded by the concurrent recurrence.
Source: Post-HERCULES Clinical Study Report (2021).14
Populations
Inclusion and Exclusion Criteria
All patients who completed the HERCULES study were eligible for the post-HERCULES study. Patients who participated in the HERCULES study but did not complete the study were not eligible. Patients who completed the HERCULES study but were not able or willing to comply with post-HERCULES study protocol procedures or who enrolled in a clinical study with another investigational drug or device were excluded.
Baseline Characteristics
The baseline characteristics of patients in the overall ITO population (refer to the Statistical Analysis section for descriptions of analysis sets) in the post-HERCULES study are shown in Table 8. ||||||||||||| ||| |||||| || |||||||| ||| |||||||||||| || ||||||||||||| |||| |||||| |||||||| ||||||||||||| ||| |||||| ||||||| |||| |||||| ||| ||| ||||||| ||| ||| |||| |||||| No significant imbalances were observed between study groups in the overall ITO population. In general demographic baseline characteristics corresponded with those described for the intention-to-treat (ITT) population of the HERCULES trial. Note that patients were disease-free at the baseline of the post-HERCULES study and thus the average ADAMTS13 activity was |||||.
Separate demographic and TTP disease characteristics for the efficacy ITO population were not provided. The efficacy ITO population included the same patients in the group of “SOC-treated in HERCULES” as the overall ITO population (n = 29) and 60% (n = 49) of patients in the group of “Caplacizumab-Treated in HERCULES” of the overall ITO population.
Table 8: Summary of Baseline Characteristics in Post-HERCULES (Overall ITO Population)
Characteristic | Patients treated with caplacizumab in HERCULES n = 75 | Patients treated with SOC in HERCULES n = 29 | All n = 104 |
|---|---|---|---|
Age (years) | |||
Mean (SD) | 46.0 (11.9) | 51.5 (14.8) | |||| |||||| |
Median (IQR) | 45.0 (37.0 to 55.0) | 48.0 (41.0 to 62.0) | |||| ||||| || ||||| |
Sex, n (%) | |||
Female | 51 (68.0) | 23 (79.3) | || |||||| |
Male | 24 (32.0) | 6 (20.7) | || |||||| |
Race, n (%) | |||
White | 52 (69.3) | 21 (72.4) | || |||||| |
Black or African American | 13 (17.3) | 6 (20.7) | || |||||| |
Asian | 3 (4.0) | 0 | | ||||| |
Other | 2 (2.7) | 0 | | ||||| |
Missing | 5 (6.7) | 2 (6.9) | | ||||| |
Ethnicity, n (%) | |||
Hispanic or Latino | 1 (1.3) | 0 | | ||||| |
Not Hispanic or Latino | 69 (92.0) | 27 (93.1) | || |||||| |
Missing | 5 (6.7) | 2 (6.9) | | ||||| |
Weight (kg) | |||
Mean (SD) | 86.4 (20.9) | 85.6 (30.1) | |||| |||||| |
Median (IQR) | 85.0 (70.0 to 97.5) | 75.6 (61.8 to 108.5) | |||| ||||| || ||||| |
Height (cm) | |||
Mean (SD) | 167.7 (8.8) | 166.0 (10.7) | ||||| ||||| |
Median (IQR) | 167.0 (162.0 to 176.0) | 165.0 (160.0 to 170.0) | ||||| ||||||| |||||| |
ADAMTS13 activity (%), mean (SD) | 60.5 (35.7) | 66.5 (41.0)a | |||| |||||| |
ADAMTS13 = a disintegrin and metalloproteinase with thrombospondin type 1 motif, member 13; IQR = interquartile range; ITO = intent to observe; SD = standard deviation; SOC = standard of care.
aADAMTS13 activity was measured in 28 of 29 patients treated with SOC in the HERCULES study.
Source: Post-HERCULES Clinical Study Report (2021).14
Interventions
There were no scheduled interventions in the post-HERCULES study. In the event of aTTP recurrence (defined as recurrence of thrombocytopenia requiring initiation of daily PE), patients received daily PE and immunosuppression. Immunosuppression with corticosteroids and other immunosuppressive agents (e.g., rituximab) was as per standard practice at each study site. In addition, an IV loading dose of OL caplacizumab (11 mg bolus) could be administered before initiation of daily PE followed by daily SC administration of caplacizumab (11 mg) for the duration of daily PE and for 30 days thereafter. Of note, up to 1 PE could be given before initiation of treatment with caplacizumab as long as it was considered part of the treatment of the presenting aTTP episode. Treatment with caplacizumab could be extended for a maximum of 4 weeks in case of persistent signs and symptoms of underlying disease activity (e.g., ADAMTS13 activity less than 10% based on weekly measurements). The decision to extend caplacizumab treatment with additional 1-week periods was made by the investigator based on ADAMTS13 activity, as well as other signs and symptoms of continued underlying disease activity, such as presence of inhibitors if measured as routine practice by the site. Caplacizumab was stopped when ADAMTS13 activity showed a sustained upward trend above 10% or was stable and there were no other signs and symptoms of disease activity. For recurrences during an existing recurrence period, an IV loading dose of caplacizumab needed to be administered before reinitiation of PE.
Treatment with caplacizumab was not permitted for patients who were pregnant or intended to get pregnant in the near future or for patients with a history of severe or serious hypersensitivity reactions to caplacizumab observed in either the HERCULES or post-HERCULES studies. These patients would receive SOC (PE plus immunosuppression) only.
Outcomes
A list of efficacy end points identified in the CADTH review protocol that were assessed in the clinical trial included in this review is provided in Table 9. These end points are further summarized subsequently. A detailed discussion and critical appraisal of the outcome measures is provided in Appendix 5.
Table 9: Summary of Outcomes of Interest Identified in the CADTH Review Protocol
Outcome measure | Definition | Assessment schedule |
|---|---|---|
aTTP-related death | Investigator judgment | Continuous |
Recurrence of aTTP | Recurrent thrombocytopenia requiring initiation of daily PE | Continuous |
At least 1 major thromboembolic event | Major thromboembolic events (e.g., MI, CVA, pulmonary embolism, DVT) were defined based on the SMQ “Embolic and thrombotic (arterial, venous, and vessel type unspecified and mixed arterial and venous)” | Continuous |
Cognitive assessment (RBANS total score) | NA | Screening/baseline and at study completion (36 months follow-up visit or early termination visit) |
HRQoL (SF-36 subscale scores and HIT-6 total scores) | NA | Screening/baseline, biannual follow-up visits, and at study completion (36 months follow-up visit or early termination visit) In case of aTTP recurrence: SF-36 was administered 1 week after end of caplacizumab treatment. |
aTTP = acquired thrombotic thrombocytopenic purpura; CVA = cerebrovascular accident; DVT = deep vein thrombosis; HIT-6 = Headache Impact Test 6; HRQoL = health-related quality of life; MI = myocardial infarction; NA = not applicable; RBANS = Repeatable Battery for the Assessment of Neuropsychological Status; SMQ = Standardized MedDRA query; SF-36 = Short Form (36) Health Survey.
Source: Post-HERCULES Clinical Study Report (2021).14
Outcomes related to aTTP recurrence were assessed both as a composite outcome (aTTP-related events) and the individual components of this outcome (aTTP-related death, recurrence of aTTP, and major thromboembolic events). For Kaplan-Meier analyses of aTTP-related events, time to event was calculated with reference to the post-HERCULES study baseline visit.
Cognitive status was assessed using the Repeatable Battery for the Assessment of Neuropsychological Status (RBANS)30 at baseline and at study completion. Higher RBANS total scores reflect improvement in cognitive symptoms. HRQoL was assessed using the Headache Impact Test (HIT-6, a 6-item questionnaire used to assess the impact of headache on HRQoL)31 and the Short Form (36) Health Survey (SF-36)32 at baseline, at twice-yearly visits, at study completion, and after the end of caplacizumab treatment for patients who experienced aTTP recurrence. For the SF-36, higher subscale scores reflect better HRQoL. For the HIT-6, higher scores reflect worse HRQoL due to a greater impact of headache. The RBANS, SF-36, and HIT-6 are all patient-reported outcome measures. Note that the measurement properties of these instruments in patients with aTTP have not been studied and no minimal important difference (MID) has been identified. Refer to Appendix 5 for more details.
In the subset of patients who experienced aTTP recurrence, duration of aTTP (defined as time to initial platelet count initial platelet count of ≥ 150 × 109/L with subsequent stop of daily PE within 5 days), time to platelet count of 150 × 109/L or greater, duration of daily PE, and durations of hospitalization and intensive care unit (ICU) stay were also calculated.
Harms outcomes included treatment-emergent AEs, SAEs, AEs requiring dose interruption, withdrawal due to AEs, and deaths. AEs were considered for the overall ITO population during the overall study period. For patients with aTTP recurrence who were treated with caplacizumab during the post-HERCULES study, AEs that began or worsened on or after the start of protocol therapy until 30 days after the last dose of study drug were captured. AEs were defined as any untoward medical occurrence and were coded according to MedDRA version 22.033 and graded according to the National Cancer Institute Common Terminology Criteria for Adverse Events, version 4.0.34
Statistical Analysis
||||||||||| |||||||| || |||||||| |||||||| || ||||||||||||| || |||||||||| || ||||||||| ||| |||||| |||| ||| ||| ||||| || ||||||||||| |||||||||||||| ||| || ||||| |||||||||||| |||| |||||||||| ||||| |||| || ||||||| ||||||||| ||||||||||| |||||||| ||| ||| |||||||| |||||||| ||||||||||| ||| ||||||| ||||||||||| || ||||||||| ||| |||||||| || |||||||||||| |||||| ||| | ||||||||| ||||||| || |||| || ||| |||||||||| ||||||||||| |||||||||||| |||||| |||||||||| || ||||| ||| ||||| |||||||||||||| |||||||| |||||||| ||||||||| |||| ||||||||| ||||| ||| |||||||||||| ||||||| ||||| |||||| ||| ||||||||| ||||||||||| ||||| ||||| |||| |||||||||||| ||||||||| ||||| ||||||||| |||||||| || ||| |||| || |||| ||||||| || ||| ||||| ||| ||| ||||||||| |||| |||| ||| ||||||| ||| ||| |||||||| |||| |||| |||||||| || ||||||||| || |||||||| || || |||||| ||||||||||| |||||||| ||||| |||||||||| || ||||||||||| ||||||||| ||| || ||||||| |||||||| |||||||| |||| |||||||||
Table 10: Statistical Analysis of Efficacy End Points
End point | Statistical model | Adjustment factors | Sensitivity analyses | Missing data |
|---|---|---|---|---|
||||||||||||||||||||||||||||||||| | |||||||||||| ||||||||||||||||||| | ||| | |||| | ||||||||| || |||| || |||| ||||||| |
||||||||| |||||| |||||| ||||| ||| | |||||||||| ||| ||||||| |||||||||| | ||| | ||| | ||| |
||||| ||||||| ||||| ||||| ||||||| | |||||||||| ||| ||||||| |||||||||| | ||| | ||| | ||| |
aTTP = acquired thrombotic thrombocytopenic purpura; CCA = complete case analysis; HIT-6 = Headache Impact Test 6; HRQoL = health-related quality of life; MTE = major thromboembolic event; RBANS = Repeatable Battery for the Assessment of Neuropsychological Status; SF-36 = Short Form (36) Health Survey.
Source: Post-HERCULES Clinical Study Report (2021).14
Analysis Populations
Analysis sets in the post-HERCULES study are described in Table 11. The overall ITO population was used for analysis of safety. The efficacy ITO population (patients within the overall ITO population who had not experienced aTTP recurrence in the HERCULES study or before the beginning of the post-HERCULES study) was used for analysis of efficacy based on twice-yearly follow-up visits. The recurrence population (patients within the overall ITO population who experienced at least 1 aTTP recurrence during the post-HERCULES study) was used for analysis of data collected during recurrence periods. A diagram of patient flow is shown in Figure 3 (refer to Patient Disposition section).
Table 11: Analysis Populations in Post-HERCULES
Population | Definition |
|---|---|
Overall ITO population | All patients enrolled in the post-HERCULES study |
Efficacy ITO population | Patients within the overall ITO population who did not experience a recurrence of aTTP in the HERCULES study or before the beginning of the post-HERCULES study |
Recurrence population | Patients within the overall ITO population who experienced at least 1 recurrence of aTTP during the post-HERCULES study only |
Repeated caplacizumab use population | Patients within the recurrence population treated at least twice with caplacizumab either because they received caplacizumab in the HERCULES study and were treated again with caplacizumab at least once in post-HERCULES, or they were treated for at least 2 recurrence episodes with caplacizumab in the post-HERCULES study |
aTTP = acquired thrombotic thrombocytopenic purpura; ITO = intent to observe.
Source: Post-HERCULES Clinical Study Report (2021).14
Results
Patient Disposition
Patient disposition in the post-HERCULES study is summarized in Table 12. A diagram of patient flow is shown in Figure 3. Of 108 patients who completed the HERCULES study, 104 (96.3%) enrolled in the post-HERCULES study. Among post-HERCULES study participants, 29 patients (27.9%) had received only PE plus immunosuppression in the HERCULES study while 75 patients (72.1%) had received caplacizumab in addition to SOC in the HERCULES study (including 55 patients randomized to receive caplacizumab and 20 patients randomized to received placebo who received OL caplacizumab). Twenty-three patients who received only SOC in the HERCULES study (79.3%) and 70 patients who received caplacizumab in addition to SOC in the HERCULES study (93.3%) completed the post-HERCULES study. Among patients who received only SOC in the HERCULES study (n = 29), the most common reason for discontinuation was loss to follow-up (13.8%). Among patients who received SOC plus caplacizumab in the HERCULES study (n = 75), the most common reason for discontinuation was physician decision (4.0%).
Table 12: Patient Disposition in the Post-HERCULES Study (Overall ITO Population)
Parameter | Patients treated with caplacizumab in HERCULES n = 75 | Patients treated with SOC in HERCULES n = 29 |
|---|---|---|
Enrolled in post-HERCULES, N | 75 | 29 |
Patients with at least 1 recurrence and treated with caplacizumab, n (%) | 8 (10.7) | 5 (17.2) |
Patients with at least 1 recurrence and not treated with caplacizumab, n (%)a | 3 (4.0) | 3 (10.3) |
Completed study period, n (%) | 70 (93.3) | 23 (79.3) |
Did not complete study period, n (%) | 5 (6.7) | 6 (20.7) |
Lost to follow-up | 1 (1.3) | 4 (13.8) |
Withdrawal by patient | 1 (1.3) | 1 (3.4) |
Death | 0 | 1 (3.4) |
Physician decision | 3 (4.0) | 0 |
Overall ITO population, N | 75 | 29 |
Efficacy ITO population, N | 49 | 29 |
Recurrence population, N | 11 | 8 |
Repeated caplacizumab use population, N | 8 | 1 |
ICF = informed consent form; IRB = institutional review board; ITO = intent to observe; ITT = intention to treat; SOC = standard of care.
Note: Definitive treatment discontinuation is defined as the discontinuation of all study drugs. When all study drugs are not discontinued at the same time, the reason for definitive discontinuation is the reason for discontinuation of the last study drug stopped.
aOf the 6 patients who did not receive caplacizumab for recurrence during the post-HERCULES study, 2 discontinued the study upon the recurrence event. Reasons for not receiving caplacizumab included pregnancy, investigator’s decision due to pending IRB approval for latest ICF, patient withdrawal due to neurological deterioration on commencing plasma exchange and transferred to palliative care, receiving more than 1 plasma exchange before initiation of caplacizumab at recurrence.
Source: Post-HERCULES Clinical Study Report (2021).14
Figure 3: Patient Flow in the Post-HERCULES Trial
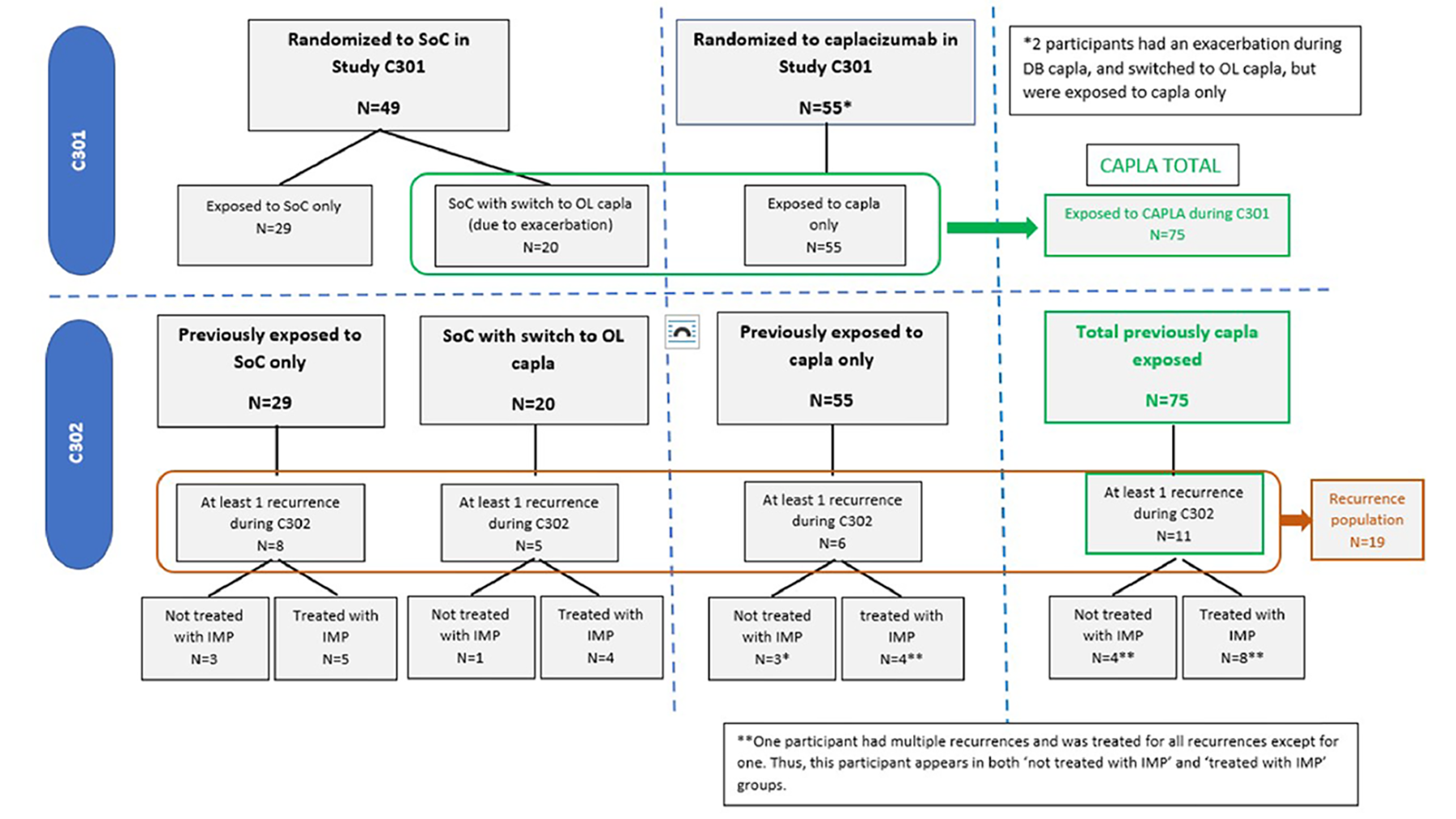
DB = double blind; capla = caplacizumab; C301 = Study ALX0681-C301/HERCULES; C302 = Study ALX0681-C302/Post-HERCULES/LTS16371; IMP = investigational medicinal product; OL = open label; SoC = standard of care.
Source: Post-HERCULES Clinical Study Report (2021).14
|||||||| || ||||| |||||||| |||||||||| || ||| ||||||||||||| ||||| |||||| |||| ||||||||||| |||||||| |||||||| ||||||||| ||||||||||||||| ||||||||||||||| ||| ||||| ||||| || |||||||| |||||||||| || ||| ||||||||| || |||||||||||||| ||| |||||||||| || ||||||||| ||||| ||||||||||||| ||||||||||||| || |||||||| ||||||| ||| |||||||| |||| || |||| ||||||||||||||||| || |||||||| ||||||||||| ||||| || |||||||| |||||||| |||||||||| ||||| || |||||||| ||||||| ||| |||||||| |||||||||||| || |||||||| || ||| || |||||||| ||||||||||| ||||| || |||||||| |||||||| ||||||||||| ||| |||| |||||||| |||||||| |||||||| || |||||||| || ||||| |||||||| |||||||||| ||| |||||||| ||| ||||| |||| ||||||||| ||| || |||||||||| |||||||||||||||| ||||||| |||||||| ||||||| |||||| |||||| ||||||| |||| ||||||||| || |||| ||| |||||||| |||| |||||||| ||||||| ||||||||||
Table 13: Critical or Major Protocol Deviations in the Post-HERCULES Trial (Overall ITO Population)
Deviation category | Patients treated with caplacizumab in HERCULES n = 75 | Patients treated with SOC in HERCULES n = 29 |
|---|---|---|
||| |||||||| || ||||| |||||||| |||||||||| | ||| | || |||||| | || |||||| |
||||||| ||| ||||||||| || ||| |||||||| | | ||||| | ||| |
||||||||| |||||||||||||| | | ||||| | | ||||| |
|||||||| |||||||||| ||||||||| | | ||||| | | ||||| |
||||| | || |||||| | || |||||| |
ITO = intent to observe; SOC = standard of care.
Note: A patient can be counted in multiple deviation categories.
Source: Post-HERCULES Clinical Study Report (2021).14
Exposure to Study Treatments
Among participants in the post-HERCULES study, 5 patients (17.2%) who received only PE plus immunosuppression in the HERCULES study experienced at least 1 recurrence during the post-HERCULES study and were treated with caplacizumab plus SOC while 8 patients (10.7%) who received caplacizumab in addition to SOC in the HERCULES study experienced at least 1 recurrence during the post-HERCULES study and were treated with caplacizumab plus SOC. Three patients (10.3%) who received only PE plus immunosuppression in the HERCULES study experienced at least 1 recurrence during the post-HERCULES study and were not treated with caplacizumab while 3 patients (4.0%) who received caplacizumab in addition to SOC in HERCULES experienced at least 1 recurrence during the post-HERCULES study and were not treated with caplacizumab.
Treatments administered for aTTP recurrence during the post-HERCULES study are summarized in Figure 4. Overall, 13 patients had a first recurrence during the post-HERCULES study that was treated with caplacizumab and 6 patients had a second recurrence of aTTP that was treated with caplacizumab. Only 1 participant had more than 2 recurrences; this patient experienced 8 recurrences, of which 7 were treated with caplacizumab and 1 (recurrence 6) was treated with PE plus immunosuppression alone. For the first recurrence in the post-HERCULES study, the median duration of caplacizumab treatment was 56 days and mean compliance with caplacizumab was ||| during daily PE and ||||| after daily PE. Six patients had a recurrence during the post-HERCULES study and were not treated with caplacizumab. Reasons for not receiving caplacizumab included pregnancy, patient withdrawal due to neurological deterioration on commencing PE and transfer to palliative care, investigator decision due to absence of informed consent, and administration of more than 1 PE before initiation of caplacizumab; 2 patients discontinued the study upon recurrence.
For treatment of the first aTTP recurrence in the post-HERCULES study, 3 of 4 patients (75%) who were treated without caplacizumab received rituximab while 6 of 13 patients (46.2%) who were treated with caplacizumab received rituximab.
Figure 4: Treatment of Patients With Recurrence During the Post-HERCULES Study
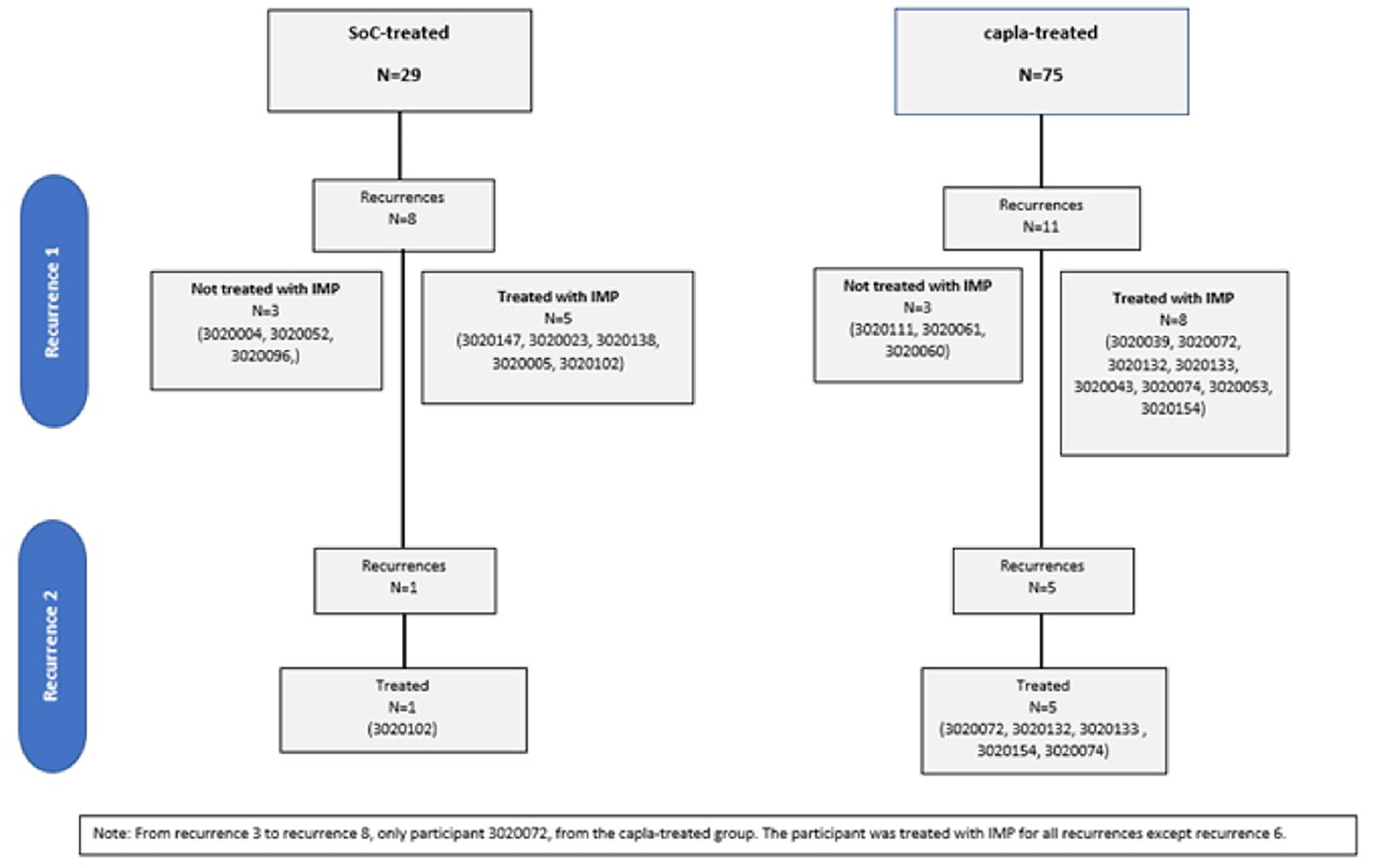
Capla = caplacizumab; IMP = investigational medicinal product; N = number of participants; SoC = standard of care.
Source: Post-HERCULES Clinical Study Report (2021).14
Efficacy
Only those efficacy outcomes and analyses of subgroups identified in the review protocol are reported subsequently. Refer to Appendix 4 for detailed efficacy data.
aTTP-Related Death, Recurrence of aTTP, and Major Thromboembolic Events
aTTP-related death, recurrence of aTTP, and major thromboembolic events were analyzed both as a composite end point and its individual components in the efficacy ITO population. aTTP-related events during the post-HERCULES study are summarized in Table 14. aTTP-related events (TTP-related death, recurrence of aTTP, or major thromboembolic events) occurred in 11 patients (37.9%) randomized to receive SOC in the HERCULES study and in 4 patients (8.2%) randomized to receive caplacizumab in the HERCULES study. One patient (3.4%), who was randomized to receive SOC in the HERCULES study, died during the post-HERCULES study. Eight patients (27.6%) who were randomized to receive SOC in the HERCULES study and 4 patients (8.2%) who were randomized to receive caplacizumab in the HERCULES study experienced recurrence of aTTP during the post-HERCULES study. Eleven patients (37.9%) who were randomized to receive SOC in the HERCULES study and 4 patients (8.2%) who were randomized to receive caplacizumab in the HERCULES study experienced major thromboembolic events during the post-HERCULES study. Major thromboembolic events other than aTTP occurred in 3 patients who were randomized to receive SOC in the HERCULES study.
Table 14: aTTP-Related Events in the Post-HERCULES Trial (Efficacy ITO Population)
Outcome | Randomized to caplacizumab in HERCULES n = 49 | Randomized to SOC in HERCULES n = 29 |
|---|---|---|
aTTP-related events, n (%) | 4 (8.2) | 11 (37.9) |
aTTP-related death | 0 | 1 (3.4) |
Recurrence of aTTP | 4 (8.2) | 8 (27.6) |
At least 1 major thromboembolic event | 4 (8.2) | 11 (37.9) |
aTTP | 4 (8.2) | 8 (27.6) |
Acute myocardial infarction | 0 | 1 (3.4) |
Embolism venous | 0 | 1 (3.4) |
Renal infarct | 0 | 1 (3.4) |
aTTP = acquired thrombotic thrombocytopenic purpura; ITO = intent to observe; SOC = standard of care.
Source: Post-HERCULES Clinical Study Report (2021).14
Kaplan-Meier analyses of time to first aTTP-related event and time to first aTTP relapse during the post-HERCULES study are shown in Figure 5 and Figure 6. Median time to first aTTP-related event and time to first aTTP relapse was not reached in either patients randomized to receive caplacizumab in the HERCULES study or in patients randomized to receive SOC alone in HERCULES study. No formal statistical analysis was performed.
Figure 5: Kaplan-Meier Analysis of Time to First aTTP-Related Event in the Post-HERCULES Trial (Efficacy ITO Population) — Redacted

aTTP = acquired thrombotic thrombocytopenic purpura; C301 = HERCULES study; C302 = post-HERCULES study; Capla = caplacizumab; ITO = intent to observe; SOC = standard of care.
Notes: Figure redacted based on the sponsor request.
Time to event calculated from screening/baseline.
Participants with a recurrence of aTTP in the post-HERCULES study were analyzed up to their first recurrence in the post-HERCULES study. Participants without a recurrence of aTTP in the post-HERCULES study were analyzed up to the end of the study.
Source: Post-HERCULES Clinical Study Report (2021).14
Figure 6: Kaplan-Meier Analysis of Time to First aTTP Relapse in the Post-HERCULES Trial (Efficacy ITO Population) — Redacted

aTTP = acquired thrombotic thrombocytopenic purpura; C301 = HERCULES study; C302 = post-HERCULES study; Capla = caplacizumab; SOC = standard of care.
Notes: Figure redacted based on the sponsor request.
Time to event calculated from screening/baseline.
Participants with a recurrence of aTTP in the post-HERCULES study were analyzed up to their first recurrence in the post-HERCULES study. Participants without a recurrence of aTTP in the post-HERCULES study were analyzed up to the end of the study.
Source: Post-HERCULES Clinical Study Report (2021).14
Reduction in Use of PE
The duration of PE in the recurrence population in the post-HERCULES study (n = 19) is shown in Table 15. Among patients experiencing a first recurrence in the post-HERCULES study who were treated with PE plus immunosuppression only (n = 4), the mean duration of PE was ||| |||| ||| ||| |||||| Among patients experiencing a first recurrence in the post-HERCULES study who were treated with caplacizumab (n = 13), the mean duration of PE was ||| |||| ||| ||| |||||| Among patients experiencing a second recurrence in the post-HERCULES study who were treated with caplacizumab (n = 6), the mean duration of PE was ||| |||| ||| ||| ||||||
Table 15: Duration of PE in the Post-HERCULES Trial (Recurrence Population)
Recurrence | Treated with caplacizumab in post-HERCULES n = 13 | Not treated with caplacizumab in post-HERCULES n = 7 |
|---|---|---|
Recurrence episode 1 | ||
N | 13 | 4 |
Duration of PE, days, mean (SD) | ||| ||||| | ||| ||||| |
Duration of PE, days, median (range) | 5.0 (2 to 19) | 5.5 (4 to 7) |
Recurrence episode 2 | ||
N | 6 | 0 |
Duration of PE, days, mean (SD) | ||| ||||| | |||| |
Duration of PE, days, median (range) | 5.0 (3 to 6) | NA |
Recurrence episode 3 | ||
N | 1 | 0 |
Duration of PE, days, mean (SD) | ||| |||| | |||| |
Duration of PE, days, median (range) | 5 (NC) | NA |
NA = not applicable; NC = not calculable; PE = plasma exchange; SD = standard deviation.
Source: Post-HERCULES Clinical Study Report (2021).14
Health-Related Quality of Life
Total HIT-6 scores in a post-HERCULES study efficacy ITO population are summarized in Table 16. At the post-HERCULES study baseline, all patients completed the HIT-6. The mean total HIT-6 score was 45.0 (standard deviation [SD] = 10.0) in patients randomized to receive SOC alone in the HERCULES study and 48.2 (SD = 9.9) in patients randomized to receive caplacizumab in the HERCULES study. At the 36-month follow-up visit, 14 of 29 patients randomized to receive SOC only in the HERCULES study and 43 of 49 randomized to receive caplacizumab in the HERCULES study completed the HIT-6. The mean total HIT-6 score was 44.1 (SD = 10.1) in patients randomized to receive SOC alone in the HERCULES study and 49.4 (SD = 10.2) in patients randomized to receive caplacizumab in the HERCULES study.
Table 16: Total HIT-6 Score in the Post-HERCULES Trial (Efficacy ITO Population)
Outcome | Randomized to caplacizumab in HERCULES n = 49 | Randomized to SOC in HERCULES n = 29 | All n = 78 |
|---|---|---|---|
Baseline | |||
N | 49 | 29 | 78 |
Mean (SD) | 48.2 (9.9) | 45.0 (10.0) | |||| |||||| |
Median (range) | |||| ||| || ||| | |||| ||| || ||| | |||| ||| || ||| |
6-month follow-up visit | |||
N | 48 | 22 | 70 |
Mean (SD) | 46.9 (9.4) | 44.2 (8.7) | |||| ||||| |
Median (range) | |||| ||| || ||| | |||| ||| || ||| | |||| ||| || ||| |
12-month follow-up visit | |||
N | 43 | 20 | 63 |
Mean (SD) | 48.6 (9.1) | 44.0 (8.5) | |||| ||||| |
Median (range) | |||| ||| || ||| | |||| ||| || ||| | |||| ||| || ||| |
18-month follow-up visit | |||
N | 44 | 18 | 62 |
Mean (SD) | 48.5 (9.8) | 45.6 (8.9) | |||| ||||| |
Median (range) | |||| ||| || ||| | |||| ||| || ||| | |||| ||| || ||| |
24-month follow-up visit | |||
N | 45 | 19 | 64 |
Mean (SD) | 47.3 (10.6) | 43.9 (9.1) | |||| |||||| |
Median (range) | |||| ||| || ||| | |||| ||| || ||| | |||| ||| || ||| |
30-month follow-up visit | |||
N | 42 | 18 | 60 |
Mean (SD) | 48.1 (9.4) | 45.8 (9.5) | |||| ||||| |
Median (range) | |||| ||| || ||| | |||| ||| || ||| | |||| ||| || ||| |
36-month follow-up visit | |||
N | 43 | 14 | 57 |
Mean (SD) | 49.4 (10.2) | 44.4 (10.1) | |||| |||||| |
Median (range) | |||| ||| || ||| | |||| ||| || ||| | |||| ||| || ||| |
HIT-6 = Headache Impact Test 6; ITO = intent to observe; SD = standard deviation; SOC = standard of care.
Source: Post-HERCULES Clinical Study Report (2021).14
SF-36 physical functioning scores in the post-HERCULES study efficacy ITO population are summarized in Table 17. At the post-HERCULES study baseline, all patients completed the SF-36. The mean SF-36 physical functioning score was 68.3 (SD = 28.9) in patients randomized to receive SOC alone in the HERCULES study and 74.1 (SD = 23.6) in patients randomized to receive caplacizumab in the HERCULES study. At the 36-month follow-up visit, 15 of 29 patients randomized to receive SOC only in the HERCULES study and 43 of 49 randomized to receive caplacizumab in the HERCULES study completed the SF-36. The mean SF-36 physical functioning score was 82.0 (SD = 22.9) in patients randomized to receive SOC alone in the HERCULES study and 80.7 (SD = 22.3) in patients randomized to receive caplacizumab in the HERCULES study.
Table 17: Total SF-36 Physical Functioning Score in the Post-HERCULES Trial (Efficacy ITO Population)
Outcome | Randomized to caplacizumab in HERCULES n = 49 | Randomized to SOC in HERCULES n = 29 | All n = 78 |
|---|---|---|---|
Baseline | |||
N | 49 | 29 | 78 |
Mean (SD) | 74.1 (23.6) | 68.3 (28.9) | |||| |||||| |
Median (range) | |||| ||| || |||| | |||| ||| || |||| | |||| ||| || |||| |
6-month follow-up visit | |||
N | 48 | 22 | 70 |
Mean (SD) | 76.9 (23.3) | 75.9 (21.1) | |||| |||||| |
Median (range) | |||| ||| || |||| | |||| || || |||| | |||| || || |||| |
12-month follow-up visit | |||
N | 46 | 20 | 66 |
Mean (SD) | 75.8 (26.3) | 78.8 (19.7) | |||| |||||| |
Median (range) | |||| ||| || |||| | |||| ||| || |||| | |||| ||| || |||| |
18-month follow-up visit | |||
N | 45 | 19 | 64 |
Mean (SD) | 78.3 (24.0) | 80.8 (19.2) | |||| |||||| |
Median (range) | |||| || || |||| | |||| ||| || |||| | |||| || || |||| |
24-month follow-up visit | |||
N | 45 | 20 | 65 |
Mean (SD) | 80.3 (22.4) | 80.5 (22.2) | |||| |||||| |
Median (range) | |||| || || |||| | |||| ||| || |||| | |||| || || |||| |
30-month follow-up visit | |||
N | 43 | 18 | 61 |
Mean (SD) | 80.7 (23.4) | 80.3 (17.5) | |||| |||||| |
Median (range) | |||| || || |||| | |||| ||| || |||| | |||| || || |||| |
36-month follow-up visit | |||
N | 43 | 15 | 58 |
Mean (SD) | 80.7 (22.3) | 82.0 (22.9) | |||| |||||| |
Median (range) | |||| || || |||| | |||| ||| || |||| | |||| || || |||| |
ITO = intent to observe; SD = standard deviation; SF-36 = Short Form (36) Health Survey; SOC = standard of care.
Source: Post-HERCULES Clinical Study Report (2021).14
Productivity
Productivity was not evaluated as an efficacy outcome in the post-HERCULES study.
Organ Damage Markers
Levels of organ damage markers were not evaluated as an efficacy outcome in the post-HERCULES study.
Refractory aTTP
Refractory aTTP was not evaluated as an efficacy outcome in the post-HERCULES study.
Response to Treatment and Change in Platelet Count
Time to platelet count response (defined as initial platelet count of ≥ 150 × 109/L with subsequent stop of daily PE within 5 days) in the post-HERCULES study recurrence population is shown in Table 18. Among patients experiencing a first recurrence in the post-HERCULES study who were treated with PE plus immunosuppression only (n = 5), the mean time to platelet count response was 9.8 days (SD = 4.0 days). Among patients experiencing a first recurrence in the post-HERCULES study who were treated with caplacizumab (n = 13), the mean time to platelet count response was ||| |||| ||| ||| |||||| Among patients experiencing a second recurrence in the post-HERCULES study who were treated with caplacizumab (n = 6), the mean time to platelet count response was ||| |||| ||| ||| ||||||
Table 18: Time to Platelet Count Response in the Post-HERCULES Trial (Recurrence Population)
Recurrence | Treated with caplacizumab in post-HERCULES n = 13 | Not treated with caplacizumab in post-HERCULES n = 7 |
|---|---|---|
Recurrence episode 1 | ||
N | 13 | 5 |
Time to response, days, mean (SD) | ||| ||||| | ||| ||||| |
Time to response, days, median (range) | 7.0 (3 to 24) | 10.0 (5 to 15) |
Recurrence episode 2 | ||
N | 6 | 0 |
Time to response, days, mean (SD) | ||| ||||| | |||| |
Time to response, days, median (range) | 5.5 (3 to 6) | NA |
Recurrence episode 3 | ||
N | 1 | 0 |
Time to response, days, mean (SD) | ||| |||| | |||| |
Time to response, days, median (range) | 5 (NC) | NA |
NA = not applicable; NC = not calculable; SD = standard deviation.
Note: Platelet count response was defined as defined as initial platelet count ≥ 150 × 109/L with subsequent stop of daily plasma exchange within 5 days.
Source: Post-HERCULES Clinical Study Report (2021).14
aTTP Exacerbation
Exacerbation of aTTP was not evaluated as an efficacy outcome in the post-HERCULES study.
Cognitive and Neurological Assessment (RBANS)
Total RBANS scores in the post-HERCULES study efficacy ITO population are summarized in Table 19. At the post-HERCULES study baseline, 26 of 29 patients randomized to receive SOC only in the HERCULES study and 38 of 49 randomized to receive caplacizumab in the HERCULES study completed the RBANS. The mean total RBANS score was 89.7 (SD = 20.3) in patients randomized to receive SOC alone in the HERCULES study and 92.7 (SD = 14.9) in patients randomized to receive caplacizumab in the HERCULES study. At the 36-month follow-up visit, 12 of 29 patients randomized to receive SOC only in the HERCULES study and 32 of 49 randomized to receive caplacizumab in the HERCULES study completed the RBANS. The mean total RBANS score was 98.0 (SD = 16.6) in patients randomized to receive SOC alone in the HERCULES study and 96.5 (SD = 17.0) in patients randomized to receive caplacizumab in the HERCULES study.
Table 19: Total RBANS Score in the Post-HERCULES Trial (Efficacy ITO Population)
Outcome | Randomized to caplacizumab in HERCULES n = 49 | Randomized to SOC in HERCULES n = 29 | All n = 78 |
|---|---|---|---|
Baseline | |||
N | 38 | 26 | 64 |
Mean (SD) | 92.7 (14.9) | 89.7 (20.3) | 91.5 (17.2) |
Median (range) | |||| ||| || |||| | |||| ||| || |||| | |||| ||| || |||| |
36-month follow-up visit | |||
N | 32 | 12 | 44 |
Mean (SD) | 96.5 (17.0) | 98.0 (16.6) | 96.9 (16.7) |
Median (range) | |||| ||| || |||| | ||||| ||| || |||| | |||| ||| || |||| |
Change from baseline | |||
N | 32 | 12 | 44 |
Mean (SD) | 4.2 (8.9) | 2.1 (8.7) | 3.6 (8.8) |
Median (range) | ||| |||| || ||| | |||| ||| || ||| | ||| |||| || ||| |
ITO = intent to observe; RBANS = Repeatable Battery for the Assessment of Neurologic Status; SD = standard deviation; SOC = standard of care.
Source: Post-HERCULES Clinical Study Report (2021).14
Hospitalization
Duration of hospitalization in the post-HERCULES study recurrence population is summarized in Table 20. Among patients experiencing a first recurrence in the post-HERCULES study who were treated with PE plus immunosuppression only (n = 3), the mean duration of hospitalization was |||| |||| ||| ||| |||||. Among patients experiencing a first recurrence in the post-HERCULES study who were treated with caplacizumab (n = 11), the mean duration of hospitalization was ||| |||| ||| ||| |||||| Only 1 patient treated with PE plus immunosuppression in the post-HERCULES study and 3 patients treated with caplacizumab in the post-HERCULES study required intensive care.
Table 20: Duration of Hospitalization in the Post-HERCULES Trial (Recurrence Population)
Recurrence | Treated with caplacizumab in post-HERCULES n = 13 | Not treated with caplacizumab in post-HERCULES n = 7 |
|---|---|---|
Recurrence episode 1 | ||
N | 11 | 3 |
Duration of hospitalization, days, mean (SD) | ||| ||||| | |||| ||||| |
Duration of hospitalization, days, median (range) | 7.0 (4 to 23) | 10.0 (9 to 11) |
Recurrence episode 2 | ||
N | 2 | 0 |
Duration of hospitalization, days, mean (SD) | ||| ||||| | |||| |
Duration of hospitalization, days, median (range) | 7.0 (7 to 7) | NA |
NA = not applicable; SD = standard deviation.
Source: Post-HERCULES Clinical Study Report (2021).14
Harms
Only those harms identified in the review protocol are reported subsequently. Refer to Table 21 and Table 22 for detailed harms data in the overall ITO population and the recurrence population, respectively.
Adverse Events
In the overall ITO population, 90.7% of patients treated with caplacizumab in the HERCULES study and 89.7% of patients treated with SOC only in the HERCULES study experienced AEs. Common AEs in both groups of patients included headache (caplacizumab-treated in HERCULES: 21.3%; SOC-treated in HERCULES: 31.0%) and aTTP (caplacizumab-treated in HERCULES: 14.7%; SOC-treated in HERCULES: 27.6%). Decreased ADAMTS13 activity was observed in 17.3% of patients treated with caplacizumab in the HERCULES study but in no patients treated with SOC only in the HERCULES study.
Among patients who received caplacizumab in the post-HERCULES study in the recurrence population (n = 13) and in the repeat caplacizumab use population (n = 9), 92% and 89%, respectively, experienced AEs.
Serious Adverse Events
In the overall ITO population, 37.3% of patients treated with caplacizumab in the HERCULES study and 55.2% of patients treated with SOC only in the HERCULES study experienced SAEs. The most common SAE was aTTP (caplacizumab-treated in HERCULES: 14.7%; SOC-treated in HERCULES: 27.6%).
Among patients who received caplacizumab in the post-HERCULES study in the recurrence population (n = 13) and in the repeat caplacizumab use population (n = 9), 38% and 44%, respectively, experienced SAEs.
Withdrawals Due to Adverse Events
In the overall ITO population, most patients were not treated in the post-HERCULES study and thus withdrawals due to AEs were not applicable.
Among patients who received caplacizumab in the post-HERCULES study in the recurrence population (n = 13) and in the repeat caplacizumab use population (n = 9), 15% and 22%, respectively, experienced AEs leading to study drug interruption, and 8% and 11%, respectively, experienced SAEs.
Mortality
In the overall ITO population, 1 patient (3.4%) treated with SOC only in the HERCULES study died. The death was aTTP-related.
Among patients who received caplacizumab in the post-HERCULES study in the recurrence population (n = 13) and in the repeat caplacizumab use population (n = 9), no patients died.
Notable Harms
In the overall ITO population, 21.3% of patients treated with caplacizumab in the HERCULES study and 31.0% of patients treated with SOC only in the HERCULES study experienced at least 1 bleeding event (based on Standardized MedDRA query “Haemorrhage” excluding the preferred term “aTTP”). Information on hypersensitivity reactions was not provided. |||||||||||| |||| ||||||||| |||||| ||||||||| || ||||||||| |||| |||||||| || ||||| || |||||||| ||||||| |||| |||||||||||| || |||||||| ||| || || |||||||| ||||||| |||| ||| |||| || |||||||||
Among patients who received caplacizumab in the post-HERCULES study in the recurrence population (n = 13) and in the repeat caplacizumab use population (n = 9), 54% and 56%, respectively, experienced at least 1 bleeding event (based on Standardized MedDRA query “Haemorrhage” excluding the preferred term “aTTP”); 23% and 22%, respectively, experienced hypersensitivity reactions; and ||| ||| |||| ||||||||||||| ||| |||||||||||| |||||
Table 21: Summary of Harms in the Post-HERCULES Trial (Overall ITO Population)
Outcome | Patients treated with caplacizumab in HERCULES n = 75 | Patients treated with placebo in HERCULES n = 29 |
|---|---|---|
Patients with ≥ 1 AE | ||
n (%) | 68 (90.7) | 26 (89.7) |
Common AEs, n (%)a | ||
Headache | 16 (21.3) | 9 (31.0) |
aTTP | 11 (14.7) | 8 (27.6) |
Nasopharyngitis | 6 (8.0) | 6 (20.7) |
Diarrhea | 5 (6.7) | 5 (17.2) |
Paresthesia | 4 (5.3) | 5 (17.2) |
ADAMTS13 activity decreasedb | 13 (17.3) | 0 |
Patients with ≥ 1 SAE | ||
n (%) | 28 (37.3) | 16 (55.2) |
Common SAEs, n (%)c | ||
aTTP | 11 (14.7) | 8 (27.6) |
Patients with AEs leading to death | ||
n (%) | 0 | 1 (3.4) |
Notable harms, n (%) | ||
≥ 1 bleeding eventd | 16 (21.3) | 9 (31.0) |
≥ 1 bleeding evente | || |||||| | | |||||| |
Drug hypersensitivityf | | ||||| | | ||||| |
Hypersensitivityf | | ||||| | | ||||| |
Drug-induced ADAs | | |||||| | ||| |
ADA = antidrug antibody; ADAMTS13 = a disintegrin and metalloproteinase with thrombospondin type 1 motif, member 13; AE = adverse event; aTTP = acquired thrombotic thrombocytopenic purpura; ITO = intent to observe; MedDRA = Medical Dictionary for Regulatory Affairs; NR = not reported; SAE = serious adverse event; TTP = thrombotic thrombocytopenic purpura; WDAE = withdrawal to adverse event.
aFrequency > 15%.
bBased on investigator reporting.
cSAEs occurring in more than 2 patients in either group are reported.
dBased on Standardized MedDRA query excluding TTP.
eBased on investigator documentation of event indicating an increased bleeding tendency.
fBased on specific preferred terms “drug hypersensitivity” and “hypersensitivity.”
Source: Post-HERCULES Clinical Study Report (2021).14
Table 22: Summary of Harms During First Recurrence Period in the Post-HERCULES Trial (Recurrence and Repeat Caplacizumab Use Populations)
Outcome | Treated with caplacizumab in post-HERCULES n = 13 | Repeat caplacizumab use n = 9 |
|---|---|---|
Patients with ≥ 1 AE | ||
n (%) | 12 (92) | 8 (89) |
Common AEs, n (%)a | ||
aTTP | 3 (23) | 2 (22) |
Headache | 3 (23) | 1 (11) |
Constipation | 3 (23) | 3 (33) |
Nausea | 2 (15) | 1 (11) |
Vomiting | 2 (15) | 2 (22) |
Epistaxis | 2 (15) | 2 (22) |
Catheter site hemorrhage | 2 (15) | 1 (11) |
Injection site pain | 2 (15) | 2 (22) |
Pruritis | 2 (15) | 2 (22) |
Hypokalemia | 2 (15) | 2 (22) |
Patients with ≥ 1 SAE | ||
n (%) | 5 (38) | 4 (44) |
Common SAEs, n (%)b | ||
aTTP | 3 (23) | 2 (22) |
Hematuria | 1 (8) | 1 (11) |
Urinary tract hemorrhage | 1 (8) | 1 (11) |
Allergic transfusion reaction | 1 (8) | 1 (11) |
Patients with ≥ 1 AE leading to study drug interruption | ||
n (%) | 2 (15) | 2 (22) |
Patients with WDAEs | ||
n (%) | 1 (8) | 1 (11) |
Patients with AEs leading to death | ||
n (%) | 0 | 0 |
Notable harms, n (%) | ||
≥ 1 bleeding eventc | 7 (54) | 5 (56) |
Hypersensitivity reactionsd | 3 (23) | 2 (22) |
ADAs | | |||| | | |||| |
ADA = antidrug antibody; AE = adverse event; aTTP = acquired thrombotic thrombocytopenic purpura; MedDRA = Medical Dictionary for Regulatory Affairs; NR = not reported; SAE = serious adverse event; TTP = thrombotic thrombocytopenic purpura; WDAE = withdrawal to adverse event.
Note: Recurrence period was defined as the period from recurrence to 1 week post caplacizumab discontinuation.
aFrequency > 15%.
bAll SAEs are reported.
cBased on Standardized MedDRA query excluding TTP.
dBased on Standardized MedDRA queries “Hypersensitivity” (narrow), “Anaphylactic reaction” (narrow), and “Angioedema” (narrow).
Source: Post-HERCULES Clinical Study Report (2021).14
Critical Appraisal
Internal Validity
As a long-term follow-up study, many of the internal validity issues of the HERCULES study affect the post-HERCULES study as well. Refer to the Clinical Review Report for the initial submission of caplacizumab13 for details, the executive summary of which is reproduced as Appendix 2.
The data from the post-HERCULES study should be interpreted within the context of potential for bias inherent to its design. Only patients who completed the HERCULES study (108 of 145, 74.5%) were eligible for the post-HERCULES study, and thus the study provides no information on patients who discontinued the HERCULES study. The most common reasons for discontinuation from the HERCULES study were AEs (11 patients, 7.6%) and withdrawal of consent (10 patients, 6.9%); reasons for discontinuation were broadly similar for both arms of the study. Because of potential for crossover to OL caplacizumab in the HERCULES study, only a small number of participants (n = 29) in the post-HERCULES study overall ITO population were caplacizumab-naive. Higher proportions of caplacizumab-naive patients (n = 6, 20.7%) than patients who received caplacizumab in the HERCULES study (n = 5, 6.7%) discontinued the post-HERCULES study. The clinical experts consulted by CADTH for this review did not expect that any resulting biases would be directional in favour of caplacizumab or limit interpretation of the study findings.
Baseline demographic characteristics were provided for the post-HERCULES study overall ITO population (arranged by prior caplacizumab experience in HERCULES). Although demographic characteristics appeared well balanced between these groups, it should be noted that the protections of randomization against bias and confounding do not apply.
No formal statistical analyses were conducted in the post-HERCULES study and all results were presented in descriptive and exploratory fashion. The study involved no testing of a priori hypotheses, no adjustment for multiple comparisons, no sensitivity analyses, and no subgroup analyses. There were high rates of missing data for some outcomes at later time periods in the study and these were not imputed. Data on aTTP-related events (aTTP-related death, recurrence of aTTP, and major thromboembolic events) were assumed to be complete for patients who did not discontinue the post-HERCULES study.
Because the double blind in the HERCULES study was lifted before the post-HERCULES study, patients and investigators were aware of treatment assignment in the HERCULES as well as in post-HERCULES studies (for patients who experienced aTTP recurrence). The OL nature of the study may have affected evaluation of patient-reported outcomes (HIT-6, SF-36, and RBANS) and safety outcomes. The measurement properties of the patient-reported outcomes used in the post-HERCULES study have not been studied in patients with aTTP and MIDs have not been determined.
External Validity
As a long-term follow-up study, many of the external validity issues of the HERCULES study affect the post-HERCULES study as well. Refer to the Clinical Review Report for the initial submission of caplacizumab13 for details, the executive summary of which is reproduced as Appendix 2.
As for the HERCULES study, the clinical experts consulted by CADTH felt that the post-HERCULES study population was generally reflective of adult patients with aTTP in Canada. Mortality rates in the HERCULES and post-HERCULES studies were lower than expected in routine clinical practice and patients may have been observed and followed by health care teams for aTTP recurrence and/or thromboembolic events more vigilantly compared to real-world practice.
In the post-HERCULES study, caplacizumab could be administered following up to 1 PE, but this was not a requirement as it was in the HERCULES study. Approximately half (6 of 13, 46.2%) of patients treated for their first recurrence in the post-HERCULES study with caplacizumab received rituximab, higher than what would be expected in Canadian practice according to the clinical experts consulted by CADTH for this review. The clinical experts consulted by CADTH for this review noted that the proportion of patients with aTTP in Canada who receive upfront rituximab in addition to PE and corticosteroids is not known with certainty but is likely lower than in the post-HERCULES trial. However, the proportion in clinical practice has increased in recent years due to improved access to rituximab.
The clinical experts consulted by CADTH did not feel that the post-HERCULES study population was likely to be significantly enriched for patients more likely to respond to caplacizumab. This could occur, if for example, patients who experienced AEs in the HERCULES study (n = 11, 7.6%) or withdrew consent (n = 10, 6.9%) were less likely to tolerate or respond to caplacizumab. The clinical experts also emphasized that evaluating the efficacy of caplacizumab for treating aTTP recurrences was not the major purpose of the post-HERCULES study.
The clinical experts consulted by CADTH stated that the duration of follow-up in the post-HERCULES study was adequate to assess both early recurrence of aTTP (within the first month of presentation) and later recurrences (which often occur within the 2 years following cessation of PE). The clinical experts felt that the aTTP-related events (aTTP-related death, recurrence of aTTP, and major thromboembolic events) evaluated in the post-HERCULES study would appropriately capture the burden of disease associated with long-term aTTP recurrence. However, the patient-reported outcomes (HIT-6, SF-36, AND RBANS) administered in the study are not used in clinical practice and their clinical relevance was uncertain. Nevertheless, HRQoL and neurocognitive symptoms were identified by patient groups, clinical experts, and clinician groups as important outcomes for patients with aTTP.
Indirect Evidence
No indirect evidence was submitted by the sponsor. A focused literature search for network meta-analyses dealing with aTTP was run in MEDLINE All (1946–) on July 5, 2022. No limits were applied to the search. No published indirect evidence was identified from the literature search comparing caplacizumab to comparators of interest for this review.
Other Relevant Evidence
This section includes additional relevant studies included in the sponsor’s submission to CADTH that were considered to address important gaps in the evidence included in the systematic review. Studies that were deemed not to address important gaps in the evidence included in the systematic review, or that were not described in sufficient detail to permit critical appraisal as outlined in Appendix 3, are described in Appendix 4 for reference only. In addition, the sponsor’s submission provided an interview with Canadian clinical experts and an Environmental Scan of Health Technology Assessment (HTA) reviews, which have been summarized in Appendix 4.
Other Clinical Trial Evidence
Three clinical trials were included in the sponsor’s resubmission: HERCULES, TITAN, and a phase II/III, OL, single-arm, multicentre trial of caplacizumab conducted among adult patients with aTTP in Japan (NCT04074187, N = 21).35 Because of the noncomparative design of the phase II/III trial and description only in a conference abstract, the results of this study are described in Appendix 4 for reference only.
HERCULES and TITAN
The phase III HERCULES trial21-23 and phase II TITAN trial24-26 were reviewed in the CADTH Clinical Review Report for the initial caplacizumab submission13 (refer to Appendix 2 for details) and were considered relevant evidence for this review. For reference, the designs of the HERCULES and TITAN trials are summarized in Figure 7 and a summary of the main results from the TITAN and HERCULES trials is provided in Table 23.
The primary outcome in both studies was time to platelet response. Statistically tested secondary outcomes in the HERCULES study included the composite end point of aTTP-related events (aTTP-related death, recurrence of aTTP, or at least 1 major thromboembolic event), proportion of patients with aTTP recurrence, proportion of patients with refractory aTTP, and time to normalization of all 3 of the organ damage markers LDH, cardiac troponin, and serum creatinine. There were no statistically tested secondary outcomes in the TITAN trial. Both studies documented statistically significant differences in time to platelet count response that were viewed by the clinical experts consulted by CADTH for the previous review as too small to be clinically relevant. In the HERCULES study, the proportion of patients randomized to receive caplacizumab who experienced recurrence during the HERCULES overall study period was statistically significantly lower compared with patients randomized to receive SOC. Differences between study randomization arms in the proportion of patients with refractory aTTP were not statistically significant, precluding further statistical testing. The duration and volume of daily PE was shorter in the caplacizumab arm, which the clinical experts consulted by CADTH felt was encouraging and potentially clinically relevant. In addition, duration of hospitalization and ICU stay was shorter in the caplacizumab arm, but missing data and absence of statistical testing prevented interpretation of these results. Analysis of mortality and time to normalization of organ damage markers numerically favoured caplacizumab but without formal, prespecified statistical testing, these differences could not be interpreted.
Post Hoc Analyses of Clinical Trial Data
Six post hoc analyses were included in the sponsor’s resubmission: a publication of an integrated analysis of the HERCULES and TITAN16 studies as well as 4 posters and 1 abstract describing subgroup analyses of the HERCULES36 and post-HERCULES37 study data by rituximab use in the HERCULES study, subgroup analyses of the HERCULES study data by baseline disease severity38 and time to platelet count response,39 and a subgroup analysis of patients in the HERCULES study who had suboptimal responses to PE.40 As outlined in Appendix 3, because of their post hoc design and incomplete description, the results of the posters/abstracts are described in Appendix 4 for reference only.
Integrated Analysis of the HERCULES and TITAN Study Data
One post hoc analysis of data from the HERCULES and TITAN trials was summarized to provide additional evidence regarding the clinically important outcomes of survival, health care use, organ damage, and refractory aTTP. The study did not address long-term aTTP recurrence beyond the duration of the trials. Peyvandi et al. (2021) conducted an integrated analysis of data from the HERCULES and TITAN trials as suggested by the FDA.16 The goal was to increase statistical power for assessing treatment differences in efficacy and safety outcomes. The study was funded by the sponsor.
Methods
The integrated analysis included all randomly assigned patients (ITT populations) from the HERCULES and TITAN studies, which were described in detail in the Clinical Review Report for the initial review of caplacizumab (the executive summary of which is reproduced as Appendix 2).
Populations
Baseline demographic and disease characteristics of the integrated ITT population are shown in Table 24. The characteristics of the integrated ITT population reflected the ITT populations of the individual trials. Approximately 3-quarters (74.1%) of patients were white, approximately two-thirds (65.5%) were women, and the average age was 44.6 years. Higher proportions of patients randomized to receive caplacizumab presented with an initial aTTP episode (66.7%) compared with patients randomized to receive placebo (54.5%). Other characteristics were broadly similar in both groups.
Figure 7: Designs of the TITAN (A) and HERCULES (B) Trials
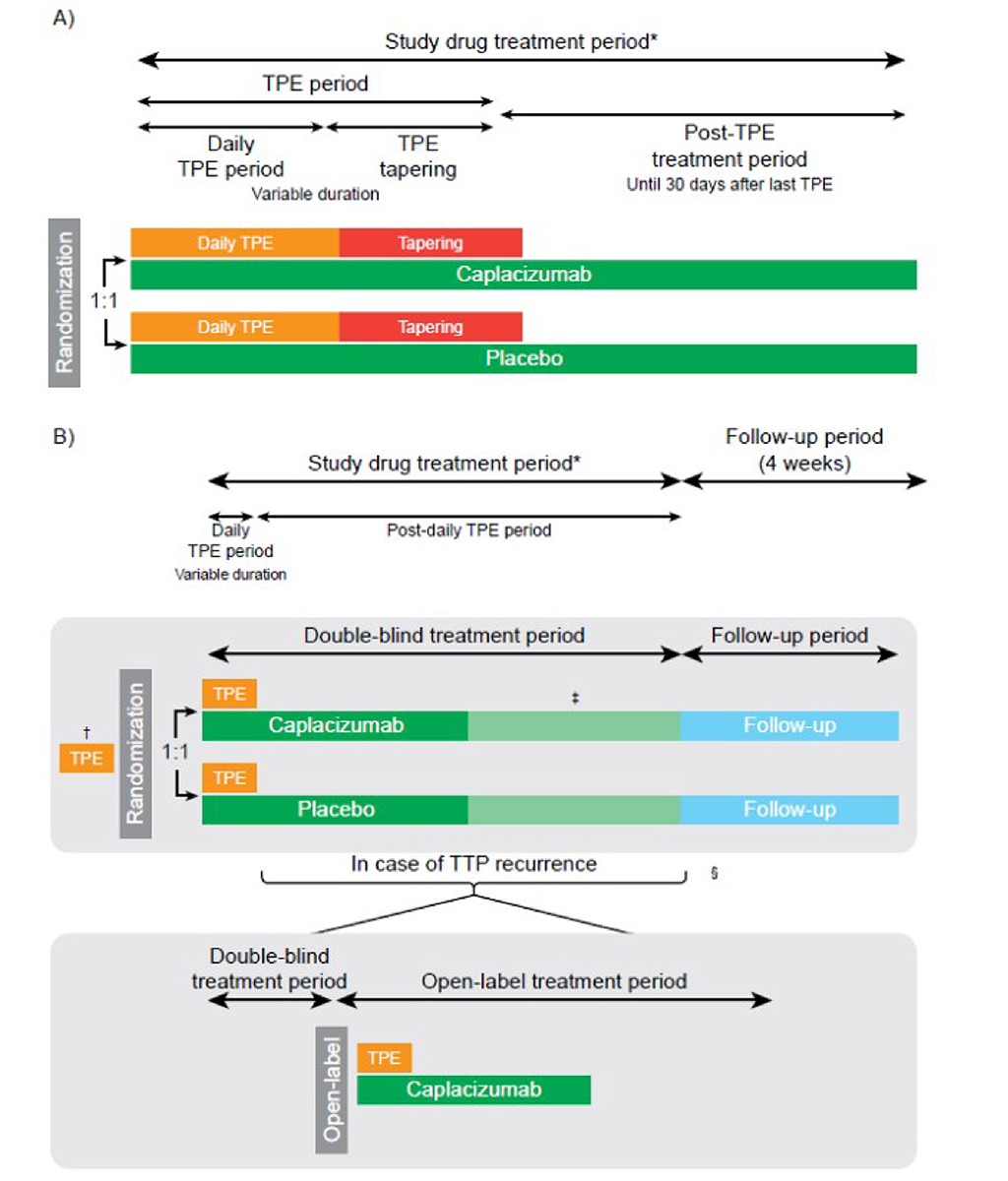
TPE = therapeutic plasma exchange; TTP = thrombotic thrombocytopenic purpura.
Note: Notable differences between the TITAN and HERCULES study designs were the requirement for 1 prior PE session in HERCULES, the possibility to extend treatment beyond the first 30 days after PE in the HERCULES study, and the option to switch to open-label caplacizumab in case of exacerbation or relapse during the HERCULES study.
* Study drug treatment period: covered the period from the date of the first study drug administration until the date of the last study drug administration. The treatment period incorporated a period of variable duration, during which PE was administered and a 30-day post-PE period starting after the date of the last daily PE.
† Participants were randomized prior to the start of PE treatment. After the approval and implementation of Clinical Study Protocol version 12.0, a participant could be randomized after an initial PE session, in which case the next PE session was designated as the first PE on study.
‡ Daily PE: required.
§ PE tapering: optional, per local standard site practice.
Source: Peyvandi et al. (2021).16 Reprinted from Blood Advances, Vol 5/No 8, Peyvandi F, Cataland S, Scully M, et al., Caplacizumab prevents refractoriness and mortality in acquired thrombotic thrombocytopenic purpura: integrated analysis, Pages 2137-2141, Copyright 2021, with permission from The American Society of Hematology.
Table 23: Summary of Key Results From the HERCULES and TITAN Trials
Result | HERCULES | TITAN | ||
|---|---|---|---|---|
Caplacizumab n = 72 (ITT) n = 71 (safety) | Placebo n = 73 (ITT) n = 73 (safety) | Caplacizumab n = 36 (ITT) n = 35 (safety) | Placebo n = 39 (ITT) n = 37 (safety) | |
Mortality, overall study period (ITT population) | ||||
n (%) | 1 (1.4) | 3 (4.1) | 0 | 2 (5.1) |
PE, treatment period (ITT population) | ||||
PE duration, days, mean (SD or SE)a | 5.8 (0.5) | 9.4 (0.8) | 6.7 (3.69) | 8.4 (6.74) |
Total PE volume, L, mean (SD or SE)a | 21.3 (1.6) | 35.9 (4.2) | 22.5 (15.9) | 28.4 (21.3) |
aTTP recurrence, overall study period (ITT population) | ||||
Exacerbations, n (%) | 3 (4.2) | 28 (38.4) | 3 (8.3) | 11 (28.2) |
Relapse, n (%) | 6 (9.1) | 0 | 11 (30.6) | 3 (7.7) |
Patients with ≥ 1 major thromboembolic event, overall study period (ITT population)b | ||||
n (%) | 6 (8.3) | 6 (8.2) | 4 (11.4) | 20 (4.3) |
Normalization of organ damage markers: LDH, cTnI, and serum creatinine, overall study period (ITT population) | ||||
Median time to normalization (95% CI)c | 2.86 (1.93 to 3.86) | 3.36 (1.88 to 7.71) | NR | NR |
Refractory aTTP, DB or SB treatment period (ITT population)b | ||||
n (%) | 0 | 3 (4.2) | 0 | 5 (12.8) |
P valued | 0.0572 | NT | ||
Platelet count response, DB or SB treatment period (ITT population) | ||||
Time to response, days, mean (95% CI)a | 2.69 (1.89 to 2.83) | 2.88 (2.68 to 3.56) | 3.0 (2.7 to 3.9)e 2.4 (1.9 to 3.0)f | 4.9 (3.2 to 6.6)e 4.3 (2.9 to 5.7)r |
P valueg | 0.0099 | 0.005 | ||
Duration of hospitalization, treatment period (ITT population) | ||||
Duration of ICU stay, days, mean (SE) | 3.4 (0.40) | 9.7 (2.12) | NR | NR |
Duration of hospitalization, days, mean (SE) | 9.9 (0.70) | 14.4 (1.22) | NR | NR |
Harms (safety population) | ||||
Patients with ≥ 1 AE, n (%) | 69 (97.2) | 71 (97.3) | 34 (97.1) | 37 (100) |
Patients ≥ 1 SAE, n (%) | 28 (39.4) | 39 (53.4) | 20 (57.1) | 19 (51.4) |
Patients with WDAEs, n (%) | 5 (7.0) | 9 (12.3) | 4 (11.4) | 2 (5.4) |
Deaths, n (%) | 1 (1.4) | 3 (4.1) | 0 | 2 (4.5) |
Patients with > 1 bleeding event, n (%) | 49 (69.0) | 49 (67.1) | 19 (54.3) | 14 (37.8) |
Patients with ≥ 1 hypersensitivity reaction, n (%) | 24 (33.8) | 22 (30.1) | 1 (2.9) | 2 (5.4) |
Patients with drug-induced ADAs, n (%) | 2 (2.8) | 1 (1.4) | 3 (8.6) | 0 |
ADA = antidrug antibody; AE = adverse event; aTTP = acquired thrombotic thrombocytopenic purpura; CI = confidence interval; CMH = Cochran-Mantel-Haenszel; cTnI = cardiac troponin I; DB = double blind; GCS = Glasgow Coma Scale; ICU = intensive care unit; ITT = intention to treat; LDH = lactate dehydrogenase; NR = not reported; NT = not tested; PE = plasma exchange; SAE = serious adverse event; SB = single blind; SD = standard deviation; SE = standard error; ULN = upper limit of normal; WDAE = withdrawal due to adverse event.
Notes: Recurrence was defined as recurrent thrombocytopenia after initial recovery of platelet count requiring reinitiation of daily PE and after discontinuation of caplacizumab. An exacerbation was defined as a recurrence that occurred within 30 days after the last PE. A relapse was defined as a recurrence that occurred more than 30 days after cessation of PE. Refractory was defined as the absence of platelet count doubling after 4 days of treatment and LDH greater than the ULN. Platelet count response was defined as initial platelet count ≥ 150 × 109/L with subsequent stopping of daily PE within 5 days of treatment.
Data on major thromboembolic events during the overall study period and refractory aTTP were not reported in the TITAN Clinical Study Report and are instead inferred from the integrated analysis of Peyvandi et al. (2021).16
aHERCULES trial: SE and TITAN trial: SD.
bFrequencies of major thromboembolic events and refractory aTTP were not presented in the TITAN Clinical Study Report and thus these values are inferred from Peyvandi et al. (2021) by subtracting frequencies from the HERCULES trial from the total for the integrated population.
cFrom Kaplan-Meier analysis.
dFrom stratified CMH test adjusted for GCS category at randomization.
ePatients who had not undergone PE before enrolment (n = 69).
fPatients who had undergone a PE before enrolment (n = 6).
gFrom stratified log-rank test adjusted for GCS category at randomization (HERCULES) or PE before enrolment (TITAN).
Sources: HERCULES Clinical Study Report (2018),21 TITAN Clinical Study Report (2015),24 and Peyvandi et al. (2021).16
Table 24: Study Participant Demographics and Baseline Disease Characteristics (ITT Analysis Set)
Characteristic | Caplacizumab (n = 108) | Placebo (n = 112) | Total (n = 220) |
|---|---|---|---|
Mean (range) age, years | 43.5 (18-77) | 45.6 (21-79) | 44.6 (18-79) |
Female sex, n (%) | 73 (67.6) | 71 (63.4) | 144 (65.5) |
Mean (range) body mass index, kg/m2 | 29.4 (16.2-53.5) | 29.9 (18.9-59.3) | 29.7 (16.2-59.3) |
Race or ethnic group, n (%) | |||
White | 79 (73.1) | 84 (75.0) | 163 (74.1) |
Black or African American | 19 (17.6) | 18 (16.1) | 37 (16.8) |
Asian | 4 (3.7) | 0 (0.0) | 4 (1.8) |
Native Hawaiian or Other Pacific Islander | 1 (0.9) | 0 (0.0) | 1 (0.5) |
Other | 2 (1.9) | 1 (0.9) | 3 (1.4) |
Missing | 3 (2.8) | 9 (8.0) | 12 (5.5) |
Presenting episode of TTP, n (%) | |||
Initial | 72 (66.7) | 61 (54.5) | 133 (60.5) |
Recurrent | 36 (33.3) | 51 (45.5) | 87 (39.5) |
Mean (range) platelet count,a × 109/L | 28 (3-119) | 35 (5-133) | 31 (3-133) |
LDH > ULN, n (%) | 91 (84.3) | 88 (78.6) | 179 (81.4) |
Troponin > ULN, n (%) | 53 (49.1) | 52 (46.4) | 105 (47.7) |
Serum creatinine > ULN, n (%) | 24 (22.2) | 32 (28.6) | 56 (25.5) |
ADAMTS13 activity at admission or baseline,b n (%) | |||
< 10% | 86 (79.6) | 96 (85.7) | 182 (82.7) |
≥ 10% | 15 (13.9) | 13 (11.6) | 28 (12.7) |
Missing | 7 (6.5) | 3 (2.7) | 10 (4.5) |
TPE prior to randomization, n (%) | |||
Yes | 71 (65.7) | 77 (68.8) | 148 (67.3) |
No | 37 (34.3) | 35 (31.3) | 72 (32.7) |
ADAMTS13 = a disintegrin and metalloproteinase with thrombospondin type 1 motif, member 13; ITT = intention to treat; LDH = lactate dehydrogenase; TPE = therapeutic plasma exchange; ULN = upper limit of normal; TTP = thrombotic thrombocytopenic purpura.
Note: This table is reproduced from original source and may not follow CADTH style.
aAlthough inclusion criteria in HERCULES required platelet counts to be < 100 × 109/L at screening, some participants had higher platelet counts by randomization, most likely owing to the prior PE session.
bThe smallest value of ADAMTS13 activity at admission or baseline was summarized as ADAMTS13 activity levels could be substantially affected by prior PE in HERCULES (as well as platelet counts and LDH, troponin, and creatinine levels).
Source: Peyvandi et al. (2021).16 Reprinted from Blood Advances, Vol 5/No 8, Peyvandi F, Cataland S, Scully M, et al., Caplacizumab prevents refractoriness and mortality in acquired thrombotic thrombocytopenic purpura: integrated analysis, Pages 2137-2141, Copyright 2021, with permission from The American Society of Hematology.
Interventions
Patients received either caplacizumab plus PE and immunosuppression or a matching-administration placebo (double blind in the HERCULES study, single blind in the TITAN study) plus PE and immunosuppression. Treatments were administered as described in HERCULES and TITAN studies, which were described in detail in the Clinical Review Report for the initial review of caplacizumab. There were several notable differences in treatment between the TITAN and HERCULES studies, including the requirement for 1 prior PE session in the HERCULES study, the possibility to extend treatment beyond the first 30 days post-PE in the HERCULES study, and the option to switch to OL caplacizumab in case of exacerbation or relapse during the HERCULES study.
Outcomes
Time to platelet count response was assessed during the blinded study periods. Secondary efficacy end points (assessed during blinded study periods unless otherwise specified) included time to normalization of organ damage markers, duration of PE, proportion of participants with aTTP-related death, aTTP recurrence, or major thromboembolic events (assessed both as a composite end point and as individual events), aTTP recurrence (occurring ≤ 30 days after the end of daily PE [exacerbation] or > 30 days after end of daily PE [relapse]) during the blinded treatment period and the overall study period, and refractory aTTP.
Statistical Analysis
For analysis of time to platelet count response, treatment groups were compared using a 2-sided log-rank test stratified by trial based on Kaplan-Meier analysis. HRs and 95% CIs were calculated using a Cox proportional hazards model with time to platelet count response as a dependent variable, treatment group as an independent variable, and study as a random effect. To compare secondary outcomes between treatment groups, a stratified Cochran-Mantel-Haenszel test was used as a stratification factor in the trials. Time to first normalization of organ damage markers was performed as for the primary analysis of time to platelet count response.
Patient Disposition
Patient disposition in the integrated safety populations is presented in Table 25. Higher proportions of patients receiving placebo (35.5%) discontinued from the studies prematurely compared with patients receiving caplacizumab (26.4%). Discontinuations due to AEs occurred with similar frequencies in patients receiving caplacizumab (8.5%) and placebo (9.1%).
Table 25: Study Participant Disposition and Discontinuations (Safety Population)
Caplacizumab | Placebo | Total | |
|---|---|---|---|
Safety population during blinded study periods, n | 106 | 110 | 216 |
Completed study, n (%) | 78 (73.6) | 71 (64.5) | 149 (69.0) |
Discontinued prematurely, n (%) | 28 (26.4) | 39 (35.5) | 67 (31.0) |
Study terminated by sponsora | 9 (8.5) | 10 (9.1) | 19 (8.8) |
Adverse event/drug reaction | 9 (8.5) | 10 (9.1) | 19 (8.8) |
Subject withdrew consent | 4 (3.8) | 8 (7.3) | 12 (5.6) |
Physician decision | 3 (2.8) | 5 (4.5) | 8 (3.7) |
Death | 1 (0.9) | 4 (3.6) | 5 (2.3) |
Other | 1 (0.9) | 1 (0.9) | 2 (0.9) |
Lost to follow-up | 1 (0.9) | 1 (0.9) | 2 (0.9) |
Withdrawal by legal representative | 0 (0.0) | 1 (0.9) | 1 (0.5) |
Noncompliance with study drug | 0 (0.0) | 1 (0.9) | 1 (0.5) |
aThis reason was only relevant for TITAN.
Note: This table is reproduced from original source and may not follow CADTH style.
Source: Peyvandi et al. (2021).16 Reprinted from Blood Advances, Vol 5/No 8, Peyvandi F, Cataland S, Scully M, et al., Caplacizumab prevents refractoriness and mortality in acquired thrombotic thrombocytopenic purpura: integrated analysis, Pages 2137-2141, Copyright 2021, with permission from The American Society of Hematology.
Exposure to Study Treatments
Exposure to caplacizumab and placebo in the HERCULES and TITAN studies is described in detail in the Clinical Review Report for the initial review of caplacizumab (the executive summary of which is reproduced as Appendix 2). Exposure and adherence were high in both studies.
Efficacy
A summary of efficacy outcomes in the integrated ITT population is shown in Table 26. During blinded study drug treatment, no patients randomized to receive caplacizumab and 4 patients (3.6%) randomized to receive placebo died; during the overall study periods, 1 patient (0.9%) randomized to receive caplacizumab and 5 patients (4.5%) randomized to receive placebo died. The proportion of patients who experienced aTTP-related events (aTTP-related death, major thromboembolic events, or aTTP exacerbation) while receiving blinded study drug treatment was 13.0% in patients randomized to receive caplacizumab versus 47.3% among patients randomized to receive placebo. During the treatment-free follow-up periods, 14 patients (13.0%) randomized to receive caplacizumab and no patients randomized to receive placebo experienced aTTP relapses. During blinded study drug treatment, no patients randomized to receive caplacizumab and 8 patients (7.1%) randomized to receive placebo had refractory aTTP.
Table 26: Integrated Efficacy End Points for the Overall ITT Population
Efficacy end points | Caplacizumab n = 108 | Placebo n = 112 | P |
|---|---|---|---|
Proportion of participants with ≥1 of the events below while receiving blinded study drug treatment | 14 (13.0) | 53 (47.3) | <.001 |
TTP-related death | 0 | 4 (3.6) | |
Major thromboembolic eventa | 8 (7.4) | 14 (12.5) | |
TTP exacerbation | 6 (5.6) | 39 (34.8) | |
TTP recurrencesb | |||
TTP exacerbation during blinded treatment period | 6 (5.6) | 39 (34.8) | <.001 |
TTP relapses during treatment-free follow-up period | 14 (13.0) | 0 (0.0) | n/s |
TTP exacerbation or relapse during overall study | 19 (17.6) | 39 (34.8) | 0.0040 |
Refractory to treatmentc | |||
n (%) | 0 (0.0) | 8 (7.1) | <.01 |
Mortality rate | |||
During the blinded treatment periods | 0 (0.0) | 4 (3.6) | .0477 |
During the overall study period | 1 (0.9)d | 5 (4.5)d | n/s |
ADAMTS13 = a disintegrin and metalloproteinase with thrombospondin type 1 motif, member 13; ITT = intention to treat; MedDRA = Medical Dictionary for Regulatory Activities; n/s = not statistically significant (P ≥ 0.05); nt = not tested; TPE = therapeutic plasma exchange; TTP = thrombotic thrombocytopenic purpura.
Note: This table is reproduced from original source and may not follow CADTH style.
aBased on Standardized MedDRA (Medical Dictionary for Regulatory Activities) queries (Standardized MedDRA Query) in the TITAN trial (post hoc); confirmed after adjudication in the HERCULES trial.
bRecurrence was defined as a new drop in platelet count after initial platelet count normalization, necessitating reinitiation of TPE. Exacerbation is a recurrence within 30 days after the end of daily TPE. Relapse is a recurrence occurring more than 30 days after the end of daily TPE.
cDefined as a lack of sustained platelet count increment or platelet counts < 50 × 109/L throughout the assessment period and persistently increased lactate dehydrogenase (> 1.5 × upper limit of normal) despite 5 TPEs and steroid treatment.
dIn the TITAN trial, 1 participant in the placebo group died 2 days after study treatment was permanently discontinued by physician decision and therefore counted as a death during the follow-up period, despite dying from severe refractory disease in the acute setting. In the HERCULES trial, 1 participant in the caplacizumab group died in the follow-up period after completing treatment and reaching complete remission. Both participants had a confirmed TTP diagnosis (ADAMTS13 < 10%).
Source: Peyvandi et al. (2021).16 Reprinted from Blood Advances, Vol 5/No 8, Peyvandi F, Cataland S, Scully M, et al., Caplacizumab prevents refractoriness and mortality in acquired thrombotic thrombocytopenic purpura: integrated analysis, Pages 2137-2141, Copyright 2021, with permission from The American Society of Hematology.
Consistent with the individual studies, treatment with caplacizumab resulted in a numerically faster time to platelet count response (HR = 1.65; 95% CI, 1.24 to 2.20), numerically faster time to normalization of LDH (HR = 1.43; 95% CI, 1.04 to 1.96), numerically faster time to normalization of troponin (HR = 1.32; 95% CI, 0.86 to 2.04), and numerically faster time to normalization of serum creatinine (HR = 1.68; 95% CI, 0.89 to 3.15). Also consistent with the individual studies, median duration of PE was numerically shorter in patients randomized to receive caplacizumab (5.0 days; range, 1 to 35 days) compared with patients randomized to receive placebo (7.5 days; range, 2 to 46 days).
Harms
A summary of safety outcomes in the integrated safety population is shown in Table 27. The safety data were consistent with the results of the individual studies and no new safety signals were identified. Seven patients (6.6%) treated with caplacizumab and 8 patients (7.3%) treated with placebo experienced AEs leading to treatment interruption. Seven patients (6.6%) treated with caplacizumab and 11 patients (10.0%) treated with placebo experienced WDAEs. No patients treated with caplacizumab and 4 patients (3.6%) treated with placebo died. Bleeding excluding aTTP occurred in 58.5% of patients treated with caplacizumab and 42.7% of patients treated with placebo. Serious bleeding excluding aTTP occurred in 11.3% of patients treated with caplacizumab and 1.8% of patients treated with placebo.
Table 27: Summary of TEAEs Occurring in the Blinded Study Periods (Safety Analysis Set)
Preferred term | Overall | |||
|---|---|---|---|---|
Caplacizumab (n = 106) | Placebo (n = 110) | |||
n (%) | No. of events | n (%) | No. of events | |
At least 1 TEAE | 102 (96.2) | 790 | 105 (95.5) | 897 |
At least 1 serious TEAE | 31 (29.2) | 44 | 54 (49.1) | 72 |
Any bleeding TEAE excluding TTPa | 62 (58.5) | 157 | 47 (42.7) | 94 |
Any serious bleeding excluding TTP | 12 (11.3) | 15 | 2 (1.8) | 2 |
Epistaxis | 4 (3.8) | 4 | 0 | 0 |
Subarachnoid hemorrhage | 2 (1.9) | 2 | 0 | 0 |
Gingival bleeding | 1 (0.9) | 1 | 0 | 0 |
Gastric ulcer hemorrhage | 1 (0.9) | 1 | 0 | 0 |
Hematemesis | 1 (0.9) | 1 | 0 | 0 |
Upper gastrointestinal hemorrhage | 1 (0.9) | 1 | 0 | 0 |
Retinal hemorrhage | 1 (0.9) | 1 | 0 | 0 |
Metrorrhagia | 1 (0.9) | 2 | 0 | 0 |
Menorrhagia | 1 (0.9) | 1 | 0 | 0 |
Hemorrhagic ovarian cyst | 1 (0.9) | 1 | 0 | 0 |
Cerebral hemorrhage | 0 | 0 | 1 (0.9) | 1 |
Hemorrhagic transformation stroke | 0 | 0 | 1 (0.9) | 1 |
AE = adverse event; MedDRA = Medical Dictionary for Regulatory Affairs; TEAE = treatment-emergent adverse event; TTP = thrombotic thrombocytopenic purpura.
Notes: This table is reproduced from original source and may not follow CADTH style.
Participants may have had more than 1 adverse event (AE) per preferred term. An individual was counted only once if he or she experienced 1 or more AE.
aA bleeding AE was defined as a Standardized MedDRA Query bleeding TEAE (excluding TTP events), with an onset date on or after the first dose of study medication.
Source: Peyvandi et al. (2021).16 Reprinted from Blood Advances, Vol 5/No 8, Peyvandi F, Cataland S, Scully M, et al., Caplacizumab prevents refractoriness and mortality in acquired thrombotic thrombocytopenic purpura: integrated analysis, Pages 2137-2141, Copyright 2021, with permission from The American Society of Hematology.
Critical Appraisal: Internal Validity
Overall, the results of the integrated analysis supported and reinforced the consistent numeric improvements in the clinically important outcomes of survival, refractory aTTP, and duration of PE observed in the clinical development program (phase II TITAN and phase III HERCULES studies). However, the internal validity issues of the individual HERCULES and TITAN trials affect the integrated analysis as well. Refer to the Clinical Review Report for the initial submission of caplacizumab13 for details, the executive summary of which is reproduced as Appendix 2. In particular, the clinical experts consulted by CADTH for this review were concerned that the higher proportion of patients receiving placebo with recurrent rather than initial aTTP may have contributed to poorer outcomes, including higher mortality.
In addition, there were several notable differences between the TITAN and HERCULES studies, including the time they were conducted (2010 to 2014 versus 2015 to 2017) and the administration of caplacizumab (requirement for 1 prior PE session in HERCULES and the possibility to extend treatment beyond the first 30 days post-PE in HERCULES). Thus, the clinical experts consulted by CADTH for the present review relayed their uncertainty that the data from the 2 studies could be pooled. No poolability assessments or evaluation of heterogeneity of treatment effects of caplacizumab between the 2 studies were conducted. Statistical analyses of integrated data in the study by Peyvandi et al. (2021) were post hoc, not adjusted for multiple comparisons, and should be interpreted in descriptive and exploratory fashion. The results of post hoc analyses are considered hypothesis-generating only.
Critical Appraisal: External Validity
The external validity issues of the individual HERCULES and TITAN trials affect the integrated analysis as well. Refer to the Clinical Review Report for the initial submission of caplacizumab13 for details, the executive summary of which is reproduced as Appendix 2.
Real-World Evidence
Three studies of 2 RWE cohorts in France17-19 and the UK20 describing the efficacy and safety of caplacizumab were summarized to provide additional evidence regarding the clinically important outcomes of survival, refractory aTTP, and health care utilization. The studies did not address organ damage or long-term aTTP recurrence.
In addition, a RWE study of a German cohort41-43 that was included in the sponsor’s submission was not considered by the CADTH review team to address an important gap in the evidence due to the lack of a comparison between patients who received caplacizumab and patients who did not receive caplacizumab, as outlined in Appendix 3. Similarly, 4 abstracts describing other RWE cohorts44-47 were not described in sufficient detail to enable the CADTH review team to rigorously evaluate their conduct and reporting. Finally, 2 additional studies of RWE cohorts48,49 were identified from the literature search results for the Systematic Review section, but also made no comparison between patients who did and did not receive caplacizumab. For reference only, these data have been described in Appendix 4.
French RWE Cohort
Coppo et al. (2021)18 prospectively analyzed outcome data for 90 patients with aTTP from France treated from September 2018 to December 2019 with a compassionate frontline triplet regimen consisting of PE, immunosuppression with corticosteroids and rituximab, and caplacizumab. Outcomes were compared with 180 historical control patients treated from June 2015 to September 2018 with standard frontline therapy (PE plus corticosteroids, with rituximab as salvage therapy).
Methods
All data from French patients with a clinical diagnosis of aTTP and treated with PE, immunosuppression with corticosteroids and rituximab, and caplacizumab from September 2018 to December 2019 were analyzed. The French Mortality in TTP Score (French severity score or French score)50 was calculated in patients with features of thrombotic microangiopathy and no associated condition (cancer, chemotherapy, pregnancy, transplant, severe disseminated intravascular coagulopathy). Diagnosis of aTTP was considered in patients with features of thrombotic microangiopathy and a French score of 1 or 2. Patients with a French severity score of 0 (platelet count ≥ 30 × 103/mm3 and serum creatinine ≥ 200 mmol/L) were considered having an alternative diagnosis, mostly hemolytic and uremic syndrome, and were not part of the cohort. A French severity score of 2 (platelet count < 30 × 103/mm3 and serum creatinine < 200 mmol/L) was highly suggestive of aTTP; patients meeting only 1 of these criteria were considered having probable aTTP, and daily PE with corticosteroids and caplacizumab was immediately started; in this scenario; however, rituximab was started only after aTTP diagnosis was confirmed (ADAMTS13 activity < 10%). The final diagnosis of aTTP was confirmed in patients with ADAMTS13 activity less than 10% and anti-ADAMTS13 antibodies of 15 U/mL or greater. After PE cessation, ADAMTS13 activity was assessed weekly until normalization (activity ≥ 50%).
Severity of aTTP at baseline was assessed using cerebral involvement (including confusion, stupor, coma, or focal deficiency), age, and LDH level. Patients were classified into 2 groups: low-intermediate and high risk of early death, according to age, cerebral involvement, and LDH levels. Cardiac involvement was defined as an increase of troponin and/or electrocardiographic abnormalities. However, troponin assessment was not performed homogeneously through all centres; consequently, troponin was used for initial prognostic evaluation, but detailed prognostic analyses were not performed.
The outcomes of patients treated with the triplet regimen (PE plus immunosuppression with corticosteroids and rituximab plus caplacizumab) was compared with a historical cohort of patients with aTTP (historical cohort) managed with the standard regimen (daily PE and corticosteroids in association with salvage rituximab in patients experiencing refractoriness or an exacerbation of the disease). Patients from the triplet regimen were compared on a 1:2 ratio with the more recent patients of the historical cohort from the CNR-MAT registry. The choice of a 1:2 ratio with the historical cohort was driven by the rarity of aTTP and the desire to include patients with standardized management. The study was conducted according to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) methodology.
Populations
The characteristics of patients treated with the triplet regimen including caplacizumab and historical controls receiving standard therapy are shown in Table 28. Patients receiving the triplet regimen including caplacizumab were treated from September 2018 to December 2019, while the historical controls were treated from June 2015 to September 2018. In both groups, similar proportions of patients had relapsed aTTP (12% to 13%), cerebral involvement (61% to 62%), and cardiac involvement (47% to 56%). Median LDH levels were 5.1 times the upper limit of normal (ULN) in patients receiving the triplet regimen including caplacizumab compared with 3.7 times the ULN in historical controls. All patients receiving the triplet regimen including caplacizumab received frontline rituximab (median time between first infusion and first PE = 2 days), while approximately two-thirds of historical controls received rituximab (68%) as salvage therapy (median time between first infusion and first PE = 7 days).
Table 28: Clinical Features and Concomitant Treatment of Patients on Diagnosis According to the Treatment Regimen
Characteristic | Triplet regimen (N = 90) | Historical cohort (N = 180) | P |
|---|---|---|---|
Age (y) | 45 (34-57) | 43 (30-57) | 1.00 |
Female sex | 63 (70%) | 127 (70%) | .30 |
Weight (kg) | 71 (60-91) | 71 (60-86) | .83 |
Body mass index | 27.2 (22.7-32.2) | 26.6 (23.0-31.7) | .68 |
Ethnicity | |||
White | 74 | 149 | .39 |
African-West Indies | 10 | 25 | |
Asian | 6 | 6 | |
Ongoing antiplatelet agent/anticoagulation | 9 (10%) | 16 (8.9%) | .77 |
Antiplatelet agent | 7 | 11 | |
Anticoagulant | 2 | 5 | |
Relapse | 12 (13.3%) | 21 (11.7%) | .70 |
Cerebral involvement | 55 (61%) | 111 (62%) | .91 |
Headache | 19 | 58 | |
Confusion | 22 | 36 | |
Seizure | 10 | 15 | |
Coma | 2 | 5 | |
Focal deficiency | 20 | 26 | |
Cardiac involvement | 51 (56%) | 86 (47%) | .15 |
Hemoglobin (g/dL) | 8.9 (7.5-10.2) | 8.6 (7.3-10.1) | .54 |
Platelet count (×103/mm3) | 12 (10-20) | 12 (8-23) | .88 |
LDH level ×N (U/L) | 5.1 (4.0-6.5) | 3.7 (2.4-5.6) | .01 |
Serum creatinine level (µmol/L) | 92 (71-120) | 86 (68-133) | .17 |
GFR (mL/min per 1.73 m2) (MDRD) | 74 (51-108) | 80 (46-120) | .85 |
ADAMTS13 activity (%) | <10% | <10% | nt |
Anti-ADAMTS13 antibodies (U/mL) | 78 (39-91) | 80 (36-100) | .44 |
French Severity score | |||
0-2 | 72 (81%)a | 145 (87%)b | .37 |
3-4 | 17 (19%) | 21 (13%) | |
Immunosuppressive therapy | |||
Corticosteroids | 88 (98%) | 166 (92%) | .10 |
Rituximab | 90 (100%) | 123 (68%) | <.01 |
Time between first infusion and first TPE | 2 (1-3) | 7 (4-10) | <.01 |
Other therapies | 0 | 25 (13.9%) | <.01 |
Twice-daily TPE | 20 | ||
Cyclophosphamide | 4 | ||
Splenectomy | 2 | ||
Vincristine | 3 | ||
Bortezomib | 1 | ||
>1 salvage therapy | 4 |
ADAMTS13 = a disintegrin and metalloproteinase with thrombospondin type 1 motif, member 13; GFR = glomerular filtration rate; iTTP = immune-mediated thrombotic thrombocytopenic purpura; LDH = lactate dehydrogenase; MDRD = modification of diet in renal disease; N = normal; nt = not tested; TPE = therapeutic plasma exchange; ULN = upper limit of normal; y = year.
Notes: Table reproduced from original source and may not follow CADTH style.
Data are given as median (25th-75th percentile) for quantitative variables and as n (%) for qualitative variables. Severe ADAMTS13 activity was defined as an activity < 10% (normal range for ADAMTS13 activity: 50% to 100%). The positivity threshold for anti-ADAMTS13 immunoglobulin G (IgG) was 15 U/mL, according to the manufacturer’s instructions (Technoclone). Cardiac involvement was defined as an increase of troponin and/or electrocardiographic abnormalities. Patients at high risk of early death of iTTP were defined by a French severity score ≥ 3 (cerebral involvement: yes = 1/no = 0, LDH: > 10 × ULN = 1/ ≤ 10 × ULN = 0, age: > 60 year = 2/ > 40 and ≤ 60 year = 1/ ≤ 40 year = 0).
aData from 89 patients.
bData from 166 patients.
Source: Coppo et al. (2021).18 Reprinted from Blood, Vol 137/No 6, Coppo P, Bubenheim M, Azoulay E, et al., A regimen with caplacizumab, immunosuppression, and plasma exchange prevents unfavorable outcomes in immune-mediated TTP, Pages 733-742, Copyright 2021, with permission from The American Society of Hematology.
Interventions
The triplet regimen including caplacizumab administered is summarized in Figure 8. Daily PE, corticosteroids (prednisone 1.0 mg/kg per day, maximum dose: 100 mg/day), and caplacizumab (10 mg IV loading dose followed by daily 10 mg SC doses) were started as soon as the clinical diagnosis of aTTP was suspected based on the French score. Rituximab (375 mg/m2) was administered IV on days 1, 4, 8, and 15 of PE; rituximab could be started from day 1 if the French score was highly suggestive for the diagnosis of aTTP (French score = 2) or alternatively by day 4 once severe ADAMTS13 deficiency was ascertained (French score = 1). Caplacizumab was continued for 30 days after PE cessation and could be extended until ADAMTS13 improvement (activity of 20% or greater). PE was performed daily until 2 days of a normal platelet count (150 × 103/mm3) and interrupted with no maintenance. Corticosteroids were administered for 3 weeks.
Outcomes
The primary outcome was a composite of refractoriness and death within 30 days since diagnosis. Key secondary outcomes were refractoriness, death, exacerbations, the time to durable platelet count recovery, the number of PEs, the volume of plasma required to achieve durable platelet count recovery, the length of hospitalization, and caplacizumab-related AEs.
Complete response was defined as full resolution of the neurologic manifestations (or stabilization of neurologic abnormalities in patients considered as having permanent sequelae) and renal failure and recovery of normal platelet count (greater than 150 × 103/mm3) for at least 2 days. Durable remission was defined as complete response with no further thrombocytopenia, renal failure, or clinical worsening for more than 30 consecutive days from the first day of platelet count recovery; at this step, the episode is considered as ended. Exacerbation was defined as initial treatment response but reappearance of clinical manifestations and/or thrombocytopenia (platelets less than 100 × 103 for at least 2 days) before durable remission. Relapse was defined as reappearance of clinical features of aTTP (platelet counts less than 100 × 103/mm3 for at least 2 days, with or without organ involvement; i.e., a new aTTP episode) after durable remission had been achieved. Refractoriness was defined as platelet count less than double the initial count after 4 days of standard intensive treatment, together with persistently elevated LDH levels. The definition of major bleeding and clinically relevant nonmajor bleeding events was adapted from the International Society on Thrombosis and Hemostasis.
Statistical Analysis
Data were presented as descriptive and summary statistics. The sample size was grounded in the hypothesis that the triplet regimen including caplacizumab would result in frequencies of the primary outcome at least 3 times lower than historically observed (10%). It was estimated that at least 65 patients were needed. To assess differences between baseline characteristics and treatment outcomes of the 2 cohorts, the Mann–Whitney-Wilcoxon test was used for ordinal variables, and Freeman-Halton test was used otherwise. Because follow-up time varied between patients, Poisson regression was used for statistical testing of efficacy end points.
Patient Disposition
A summary of patient flow in Coppo et al. (2021)18 is shown in Figure 9. Among 139 patients with a clinical suspicion of aTTP, 3 died before any treatment and 22 were treated without caplacizumab. Of the 114 patients receiving caplacizumab, 6 subsequently received an alternative diagnosis and 18 received caplacizumab as salvage therapy. Thus, a total of 90 patients received the triplet regimen including caplacizumab as frontline therapy. The median follow-up for these patients was 4.2 months.
Figure 8: The CAPLAVIE Regimen
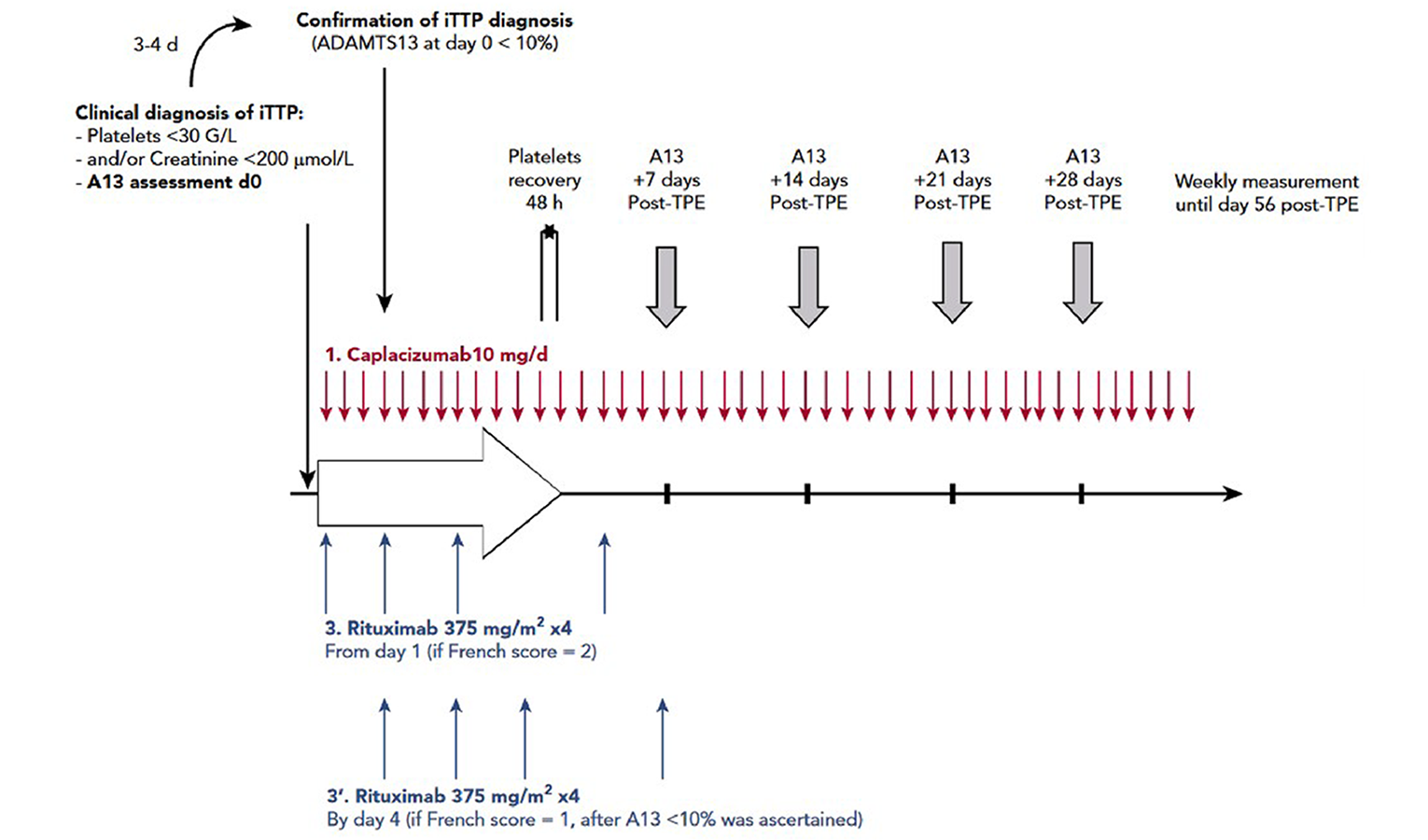
A13 = ADAMTS13; ADAMTS13 = (a disintegrin and metalloproteinase with thrombospondin type 1 motif, member 13); iTTP = immune-mediated thrombotic thrombocytopenic purpura; TPE = therapeutic plasma exchange.
Note: ADAMTS13 activity was assessed weekly until normalization or day 56.
Source: Coppo et al. (2021).18 Reprinted from Blood, Vol 137/No 6, Coppo P, Bubenheim M, Azoulay E, et al., A regimen with caplacizumab, immunosuppression, and plasma exchange prevents unfavorable outcomes in immune-mediated TTP, Pages 733-742, Copyright 2021, with permission from The American Society of Hematology.
Figure 9: Flow Chart of the Study
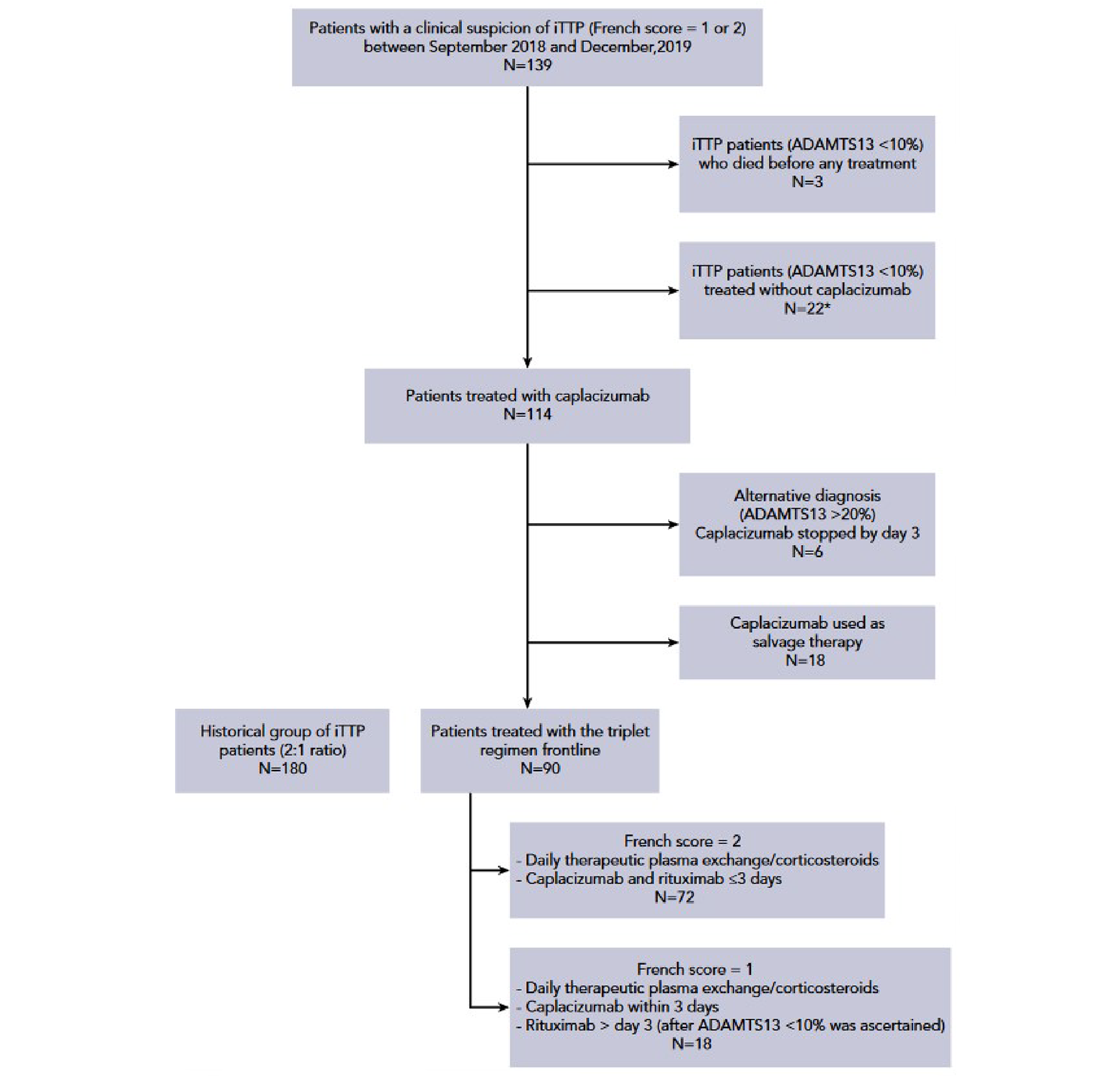
iTTP = immune-mediated thrombotic thrombocytopenic purpura.
* Mostly because of unawareness of practitioners about the availability of the compound (18 cases) or because patients were considered at risk of bleeding (1 case of recent surgery and 3 cases of active bleeding).
Source: Coppo et al. (2021).18 Reprinted from Blood, Vol 137/No 6, Coppo P, Bubenheim M, Azoulay E, et al., A regimen with caplacizumab, immunosuppression, and plasma exchange prevents unfavorable outcomes in immune-mediated TTP, Pages 733-742, Copyright 2021, with permission from The American Society of Hematology.
Exposure to Study Treatments
Information on exposure and compliance was not provided.
Efficacy
Efficacy outcomes for the RWE cohort of Coppo et al. (2021)18 are summarized in Table 29.The percentage of patients receiving the triplet regimen including caplacizumab with the composite primary outcome including death and refractoriness was 2.2% versus 12.2% in historical controls (RR = 6.2; 95% CI, 1.4 to 26.3). One patient (1.1%) treated with the triplet regimen died of pulmonary embolism compared with 12 (6.7%) historical controls. One patient (1.1%) treated with the triplet regimen experienced refractory aTTP compared with 16 (18%) historical controls.
Consistent with data from the HERCULES trial, patients receiving the triplet regimen including caplacizumab experienced fewer exacerbations compared with historical controls (3.4% versus 44% ; RR 16.4, 95% CI 5.2 to 52.1), recovered durable platelet count faster (median time to recovery of 5 days versus 12 days; RR 1.8, 95% CI 1.41 to 2.36), had fewer PE sessions (median 5 versus 10 sessions), required lower overall PE volume until remission (median 24.2 versus 44.2 L), and had shorter duration of hospitalization (median 13 versus 22 days). Patients receiving the triplet regimen including caplacizumab had faster time to ADAMTS13 activity over 20% compared with historical controls (median 28 versus 48 days; RR 4.0, 95% CI 3.03 to 5.26). The frequency of major thromboembolic events was similar in patients receiving the triplet regimen including caplacizumab and in historical controls.
Table 29: Primary and Secondary Outcomes According to the Treatment Regimen
Outcome | Triplet regimen (N = 90) | Historical cohort (N = 180) | P |
|---|---|---|---|
Primary outcome | |||
Composite of death and refractoriness | |||
All patients | 2 (2.2%) | 22 (12.2%)a | .01 |
According to French Severity score | |||
0-2 | 2 (2.8%) | 15 (8.3%) | <.01 |
3-4 | 0 | 7 (33%) | |
Secondary outcomes | |||
Death | 1 (1.1%) | 12 (6.7%) | .06 |
Refractoriness | 1 (1.1%) | 16 (18%)b | .01 |
Exacerbations | 3 (3.4%) | 70 (44%) | <.01 |
Time to durable platelet count recovery | 5 (4-6) | 12 (6-17) | <.01 |
Number of daily TPE until remission | 5 (4-7) | 10 (6-16) | <.01 |
Volume of plasma (L) until remission | 24.2 (18.3-30.2) | 44.4 (26.3-74.3) | <.01 |
Time to ADAMTS13 activity >20% (days) | 28 (14-42) | 48 (24-83) | <.01 |
Length of hospitalization (days) | 13 (9-19) | 22 (15-30) | .01 |
Thromboembolic events | 11 (12%) | 20 (11.1%) | .79 |
ADAMTS13 = a disintegrin and metalloproteinase with thrombospondin type 1 motif, member 13; TPE = therapeutic plasma exchange.
aIncludes 10 refractory patients who survived (only 1 event per patient was considered).
bIncludes 6 deaths.
Notes: This table is reproduced from original source and may not follow CADTH style.
Data are given as median (25th-75th percentile) for quantitative variables and as n (%) for qualitative variables. Patients at high risk of early death from aTTP were defined by a French severity score ≥ 3 (cerebral involvement: yes = 1/no = 0, LDH: > 0 × ULN = 1/ ≤ 10 × ULN = 0, age: > 60 year = 2/ > 40 y and ≤ 60 year = 1/ ≤ 40 y = 0).
Source: Coppo et al. (2021).18 Reprinted from Blood, Vol 137/No 6, Coppo P, Bubenheim M, Azoulay E, et al., A regimen with caplacizumab, immunosuppression, and plasma exchange prevents unfavorable outcomes in immune-mediated TTP, Pages 733-742, Copyright 2021, with permission from The American Society of Hematology.
Harms
Safety outcomes for the RWE cohort of Coppo et al. (2021)18 are summarized in Table 30. Overall, 46 patients (51%) experienced at least 1 caplacizumab-related AE. Two patients (2%) experienced major bleeding and 11 patients (12%) experienced clinically relevant nonmajor bleeding.
Table 30: Caplacizumab-Related Adverse Events
Adverse event | Number of adverse events | Description |
|---|---|---|
Major bleeding | 2 | One with hemorrhagic shock with lower digestive bleeding One with abundant menorrhagia with a decrease in hemoglobin level of 2.5 g/dL |
Clinically relevant nonmajor bleeding | 11 | Three with macroscopic gastrointestinal hemorrhage Seven with epistaxis One with subcutaneous hematoma larger than 25 cm2 |
Non-clinically relevant nonmajor bleeding | 17 | Nine with ecchymosis or small hematoma Six with gingival bleedings Two with catheter site hemorrhage |
Inflammatory reaction | 6 | Inflammatory swelling at the injection site, especially at the end of the treatment course |
Thrombocytosis | 19 | Platelet count (×103/mm3) >450-600: 11 cases >600-900: 7 cases >900: 1 case |
Note: This table is reproduced from original source and may not follow CADTH style.
Source: Coppo et al. (2021).18 Reprinted from Blood, Vol 137/No 6, Coppo P, Bubenheim M, Azoulay E, et al., A regimen with caplacizumab, immunosuppression, and plasma exchange prevents unfavorable outcomes in immune-mediated TTP, Pages 733-742, Copyright 2021, with permission from The American Society of Hematology.
Critical Appraisal: Internal Validity
Comparisons between patients receiving the triplet regimen including caplacizumab and historical controls receiving SOC were limited by risk of bias in selection of participants and potential for confounding. Approximately 16% of patients who were eligible for the triplet regimen were not treated with caplacizumab due to lack of awareness of the drug, and approximately 16% of patients treated with the triplet regimen received caplacizumab as salvage therapy and were excluded from the analysis. As an observational cohort study, comparisons could be biased due to both measured and unmeasured confounders, neither of which were accounted for. In particular, the 2 cohorts analyzed had nonoverlapping time frames, and changes in treatment practice could potentially influence the results. In addition, all patients receiving the triplet regimen including caplacizumab received frontline rituximab, while only approximately two-thirds of historical controls received rituximab as salvage therapy only. Thus, differences in outcomes between the 2 groups of patients are difficult to attribute specifically to caplacizumab and may be partially explained by differences in rituximab use.
The rationale for statistical hypothesis testing was not provided and it was unclear whether statistical tests were prespecified or conducted post hoc for some outcomes. Statistical tests were not adjusted for multiple comparisons and should be interpreted in descriptive and exploratory fashion.
Critical Appraisal: External Validity
According to the clinical experts consulted by CADTH for this review, upfront use of rituximab and upfront-only treatment with caplacizumab (i.e., no salvage therapy) is not consistent with the current or expected use of either drug in Canadian clinical practice.
French RWE Cohort: Reanalysis
||||| ||| |||||| ||||||||||| ||||||||| || ||||||| |||||||||| || ||| |||| |||| ||| ||| |||||| || ||||| || ||| ||||||||| ||| ||||| ||||||||||| || ||| ||||||| |||||||| ||||| ||| ||||||||| || ||| |||||||||| |||||||| || ||| ||||||| |||||||| ||||||| ||||||| ||||||| |||| ||| |||||| ||||| ||| |||| ||||||||||| || | |||||||||| ||||| ||||| || ||||||| |||||||| ||| ||||||||| |||| || || |||| || || |||||||||| |||||| || |||||||||||| ||||||||| ||||||||||| ||| ||| ||||||| |||||||||| || ||||| ||| |||||| ||||||||||| || ||||||||| || |||| |||||| |||| ||||| || ||||||| |||| |||| ||||||||| ||| ||| |||||||| |||||||| || ||||| || ||| |||||||||||||||||||||| |||| ||||||||| ||||||||||||||| ||| |||||||| || ||| ||||||| |||||||| ||| |||||||| ||| ||||||| ||||||| ||||||||| |||||||||||| ||||||||| || ||||| || ||| |||||||| |||| ||||||||| |||| || |||||||| |||| |||||| ||| ||| |||||||| ||||||||| |||||||| || |||| ||| |||| ||||||||||||||||| |||| |||||||||||||||| |||| || ||||||| ||||||||| || ||||||| |||||||| ||||||| ||||||| |||| ||| |||||| |||| |||||||||||||||||||||||| ||||||||||||||| || ||| ||| |||||| || |||||||| || ||| ||||||| ||||||||||| ||| ||||| ||
||||| ||| || |||| ||||||| ||||||| ||||||||||| || |||||||| ||| |||||||| |||| |||| || ||||| |||||||| ||||||||||| |||| || ||||| ||| ||||||| ||||||||||| |||| || ||||| ||| |||||||| ||||||||| ||| ||||||| ||||||| ||||||||| |||||||||||| |||||||| ||||||||| ||||||||| ||||||| |||| ||||||| ||||| |||||||| ||| ||||| ||| ||| |||||| ||||| ||||||||||||| ||| |||||| || |||||||||| |||||||| |||||||| ||||||||| ||||| || ||||||| ||||||| ||||||| |||| ||||||| ||||| |||||||| ||| ||||| ||| ||| |||||| |||| || |||| || ||||| ||||||||| |||||||| |||| ||||||| || ||||||||||||| ||| ||||| || |||||||||| ||||||||||
|||||||||||||| | ||||||| ||||||||||||||||| |||| || |||||||| ||||||||| | |||||||||| ||||||||||| |||| || |||||| |||||||||| |
|---|---|---|
||| ||||||| | ||
|||| |||||| |||||| ||||| | |||| ||||| || ||||| | |||| ||||| || ||| |
||||||| | ||| | ||
|||||| | || |||||| | ||| |||||| |
|||| | || |||||| | || |||||| |
|||| ||||| | ||
|||| |||| | |||| ||||| | |||| ||||| |
|||||||| | ||| | || |||||| | || |||||| |
|||||||||| | ||| | ||
||||||||| | || |||||| | ||| |||||| |
|||||||||||| |||||| | || |||||| | || |||||| |
||||| | | ||||| | | ||||| |
||||||| | ||| | || |||||| |
||||||| |||||||||||| ||||| ||||||||||||||| | ||
| ||| | | |||||| | || ||||| |
|||||||| | ||| | ||| | || |||||| |
|||||||| |||| | ||
| ||| | || |||||| | || ||||| |
|||||||| ||||||||||| | ||
| ||| | || |||||| | ||| |||||| |
|||||||| | ||| | ||| | | ||||| |
||||||| |||||||||||| | ||
| ||| | || |||||| | ||| |||||| |
|||||||| | ||| | | ||||| | | ||||| |
|||||||||| |||||| | ||
|||| |||| | ||| ||||| | ||| ||||| |
|||||||| | ||| | | ||||| | | ||||| |
|||||||| ||||| ||||||||| | ||
|||| |||| | |||| |||||| | |||| |||||| |
||| ||||| || |||| | ||
|||| |||| | ||| ||||| | ||| ||||| |
|||||||| | ||| | | ||||| | || ||||| |
||||| |||||||||| |||||||| | ||
|||| |||| | ||||| |||||| | ||||| ||||||| |
|||||||| | ||| | | ||||| | | ||||| |
||| ||||||| ||| |||| ||| ||||| | ||
|||||| ||||| | ||| | ||| |
|||||||| | ||
||||||||| | | ||| | ||| |
||||||||||||| |||||||||| |||||| | ||
|||| |||| | |||| |||||| | |||| |||||| |
|||||||| | ||| | ||| | | ||||| |
||| ||||||||||| | ||| | | |||||| | ||| |
|||||| |||||||| |||||| | |||| | ||
| || | | || |||||| | ||| |||||| |
| || | | || |||||| | || |||||| |
|||||||| | ||| | | ||||| | || ||||| |
||||||||||||||||| |||||||| | ||| | ||
||||||||||||||| | || |||||| | ||| |||||| |
||||||||| | || ||||| | ||| |||||| |
|||| ||||||| ||||| ||||||||| |||||||| ||| ||||| ||| |||| | ||
|||| |||| | ||| ||||| | ||| ||||| |
|||||||| | ||| | | ||||| | || |||||| |
||||| ||||||||| | ||
| ||| | ||| | || |||||| |
|||||||| | ||| | ||| | || |||||| |
|||| || ||||| |||||||| | ||| | ||
||||||||||| || | ||| | || ||||| |
|||||||||||||||| | ||| | | ||||| |
||||||||||| | ||| | | ||||| |
||||||||||| | ||| | | ||||| |
|||||||||| | ||| | | ||||| |
||| || |||| ||||||| ||||||| | ||| | | ||||| |
Note: Table redacted as per sponsor’s request.
|||||||| | | ||||||||||| |||| | |||||||| |||||||||| |||||||||||||||| |||||||| ||| | |||| |||| |||||| ||| | |||||||||| |||||||||| ||||| ||| | ||||||||||||| |||||| ||| | ||||||| |||||||||||||| |||| | |||||||||||| || |||| || ||||| |||||||| || | ||| ||||||||| || | |||||| ||||||||| || | |||||||| |||||||||| ||| | ||||| ||||| || |||||||||||||||| ||||||||||| ||| ||||||| || || |||||||| || |||||||| |||||| |||||||||||||||||||| |||||||||||||||||||||| |||||||| |||||| |||| ||||||||| ||| || || || |||||||| ||||||||| ||| ||||||| ||||||| ||| ||| || ||| |||||||| || ||| |||||||||| ||||||||||||||| ||||| ||| |||||| ||||||||||||||||||||||||||||||| ||||||||||||| |||||||||||| |||||||| ||||||| ||||||||| |||||||||||| || |||||||| ||||||| |||||||||| || || |||| |||||||||||||||||| |||| || ||||||||| || ||||| || ||| |||||||| ||||||| ||||||||||| || |||||||||| |||||||| || ||| ||||||| ||||||||||| ||||||| |||||||| ||||||||| || ||||||| ||||||| |||||||| |||| ||| |||||||| |||||||| ||||||||||||||||||||| ||||||| |||||||| ||| ||||| |||||| || |||| ||||||||| ||||||||| || ||||| ||||||||| |||||||| |||||||| ||||| || |||||||||| |||||||| | ||||||||| |||||||| || ||||| |||||| || |||| ||| |||||||||| |||||||| ||||| |||||| || |||| || |||||||||| |||||||||||| || ||||| |||||||||| || || ||||| ||| |||||||||||||| |||||| |||| |||| ||||||||| |||||||||| || |||||||| |||||||||||||| |||| |||| ||||||||| |||||||||| || |||||||| |||||||| || ||| || |||||||| |||||| || ||||| || |||||||| ||||| |||||||||| ||||| || |||||| ||||| |||||||||| ||| |||||| || |||||||| ||||||||||||||||| || ||||||||| |||||||||| ||||||||||||| |||||||| ||| |||||||||||||| |||| || ||| ||| || ||||| || ||| |||||| ||| |||| |||||| |||| ||||||||||||||||||| |||||||||| |||||||||| ||||| ||| |||||||||| ||| |||||||| || |||| ||||||| ||||| || |||| ||| |||||||| |||||| |||||||||||| ||| ||||||| |||||||||||||| ||| |||||| ||| |||||||||| |||||||||| ||||| ||||| ||||||||| |||| |||||||||| || |||| ||||||| ||| ||||| || |||||||| ||||||| ||||||||| || |||| |||| ||| ||||||| ||||||||| |||||||||||| ||||||||| |||| ||||||||| ||||||||||||||||| |||||||| || ||| ||||||| |||||||| ||||||||||| || ||||| |||||| || |||| ||||||||| ||||||||||| | |||||| |||||||| ||| ||||||| ||| ||| |||||||||| || ||||| || || |||| ||| ||||||| || |||||||| ||||||||||| ||| |||||||| |||||||| ||| ||| |||||||||| || ||||| |||||| || |||| ||||||||| |||||||||| ||| ||| ||||||||||| |||||||| ||| ||| |||||| || ||||| |||||||| |||| |||||||| ||||||||||||| |||||| |||||| |||||||||| |||||||| | |||||||||||| ||||| ||| ||||||||||| || ||||||||| ||| |||||||||| ||||| || | ||||||||| || || |||||||| ||||| ||| |||| || |||||||||| || |||||||||| |||||| || ||||| || |||||||| ||| |||||||||| || ||| ||||||||| ||| ||||||| |||||||| ||| |||||||| |||| ||| |||||||||| |||||||| ||| |||||||||| || ||| ||||||||| |||| || ||||||||| ||| |||||||||| |||||| ||| |||| ||||||| ||||||||| || ||| |||||||||| ||||| |||| ||| ||| || ||||||||| || ||||||| ||||||||||| ||||||||| ||||| |||| || |||||| | ||||||||| |||||||| |||||||||| ||||| ||||||| |||||||||||| ||| |||| ||||||| |||||||| ||||||||| |||||||||
|||||| ||| ||| |||||||||||| |||||| |||||| ||| ||| |||| || || ||| |||||||| |||||||| || ||||| || ||| |||||||| ||||| ||| |||||||| |||| || |||| ||||||||| ||||||| ||||||| |||| ||| |||||| ||||| |||| |||| |||||||| |||||| |||| |||||||| ||||||| |||| ||| ||| ||||||| ||||

||||| | |||||||| |||||||||| |||||||||||||||| |||||||| ||||||| | |||||| |||||||| || ||||||||| ||| ||| ||||||||||||||||| |||||||||||||| || | |||||| ||||||||||||||||| ||||| ||| |||||| ||||||||||||||||||||| || ||||| |||||||||||||||||||||| || |||||||| ||| |||||||||| ||| ||| ||||||||||||||||||||||||||| |||||||| ||| ||| ||||||| ||||||||||| || ||| |||||| ||| |||||| || ||||| ||| |||||| ||||||||||| ||| |||||||||| ||
||||| ||| |||| |||| ||||| |||||||| ||| |||||||||| ||| || ||| |||| |||| ||||||| |||||||||| ||||||| |||| ||| ||||||| |||||| ||||||||| ||| ||||||| ||||||| ||||||||| |||||||||||| ||||||||||| ||| ||||||| ||||||| || ||||| |||||| || ||||| ||||| || |||||||| |||||| || |||||||| || ||| |||||||||| |||||| |||| |||||| || ||||| |||| ||||||| |||||| ||||||| |||| ||| ||||||| ||||||| ||||||||||| |||||||||| |||| |||||||| |||| || ||||||| |||||||||| ||||||||| ||| |||||||| |||||| ||||||| |||| ||| ||||||| ||||||| ||||||||||| ||| ||||||||| |||||||| || ||||| |||||| || |||| |||||| |||||||||| |||| |||||||| |||| || |||||||||| ||||||| |||||||| ||||||||||||||||||| |||| |||| |||| ||| |||||||| |||||| |||||||| ||||||||| ||| ||||||| ||||||| ||||||||| |||||||||||| ||||||||||| ||||| ||||||||||||| |||||||| |||| |||||||||| |||||||| ||||| || ||||||| ||| ||||||| |||||||| || || ||||||| ||| || |||| |||||| |||||||| ||||| ||||||| || |||||| ||||| ||||||||| ||||||| |||| ||| |||| ||| ||| ||| ||||||| |||||||| || ||||||||||||||| ||||||| || || || |||||| ||| ||||||||| || ||||| |||||||||||||| |||||| ||| ||||||| || |||||||| ||||||||| ||| ||||||| ||||||| ||||||||| |||||||||||| ||| ||
||||||| | ||||||| |||||||||||||||||||| |||||||| |||||||||| |||| | |||||||||| ||||||||||| |||| |||||| ||||||||||||| ||| | |||||||| |
|---|---|---|---|
||||||| ||||||| |||||| |||||| || ||||| | |||
||| ||||||||| | ||| | | ||||| | || ||||| | ||||| |
|||||||| |||| |||||||||| |||||||||| | | ||||| | || ||||| | ||||| |
|||||||||| |||| | |||
||| ||||||||| | ||| | | ||||| | || |||||| | ||||| |
|||||||| |||| |||||||||| |||||| ||| | | ||||| | || |||||| | ||||| |
|||||||| | ||| | ||| | | ||||| | ||| |
||||||||| |||||||||| ||||| || || |||| |||||| |||||||||| |||| | |||
||||||||| |||||||| ||| ||||| || | | ||||| | || |||||| | |||||| |
||||||||| |||||||| ||| ||||||||||| | | ||||| | || |||||| | |||||| |
|||||||| | ||| | ||| | | ||||| | ||| |
|||| |||| ||||||||| || ||||| ||| |||||||| ||| |||| |||||| || |||| | |||
||| | ||| | ||| | ||| |
||||| ||||| |||| |||| | | |||| | ||| ||||| | ||||| |
|||| ||||||||||||| | |||
||| ||||||||| | ||| | | ||||| | || |||||| | |||||| |
|||||||| |||| |||||||||| ||||||| || | | ||||| | || |||||| | |||||| |
|||||||| | ||| | ||| | | ||||| | ||| |
|||||||||||||| |||||| | |||
||| ||||||||| | ||| | || |||||| | || |||||| | ||||| |
|||||||| |||| |||||||||| ||||||| || | || |||||| | || |||||| | ||||| |
|||||||| | ||| | | ||||| | || |||||| | ||| |
|||| || |||||||| ||||| ||||||||||||| | |||
|||||||| |||||||| | ||| | ||| | |||||| |
|||| |||| ||||||||| |||||||||| || |||||||| |||| | |||
|||||||| |||||||| | ||| | ||| | |||||| |
|||||| || ||||| || ||||| ||||||||| | |||
|||| |||| | ||| ||||| | |||| |||||| | |||||| |
|||||||| | ||| | | ||||| | || ||||| | ||| |
|||||| |||||| ||||| ||||||||| ||| | |||
|||| |||| | |||| |||||| | |||| |||||| | |||||| |
|||||||| | ||| | | ||||| | || ||||| | ||| |
|||||| || |||||||| |||| | |||
|||||||| ||||||||| |||||| |||||| | ||| | ||| | ||||||| |
|||||||| | | ||||||||||| ||| ||||||||||||||||| |||| |||||||||||||| |||| | |||||| |||||| ||| |||| | |||||||| |||||||||| |||||||||||||||| |||||||| || | ||| ||||||||||| || | ||| ||||||||| || | |||||| ||||||||| || | |||||||||| |||||| || | |||||||| |||||||||||||||||| |||| | ||||||| |||| || ||| |||| || |||||||| |||||||||||| ||||| | |||||||||||| |||| || ||| |||| || |||||||||||| |||||||||||| ||||| | |||||| ||||| |||| ||| ||||||||||| ||||||||| |||| ||| |||||| ||||| |||| ||| ||| | ||||||||||| |||| ||| ||| ||||| ||||||||||| |||||||||||||||||| ||||| ||| |||||| |||||||||||||||||||||||||| |||||||| || ||| ||||||| ||||||| ||||| | ||||||| || |||||||| |||||||||| ||||||||||| ||||||||| |||||||||| ||| ||||||||||
|||||| ||| ||| |||| ||||| |||| ||| ||||| |||||| || |||| ||||||||| |||||||| ||||||| |||| ||| ||||||| ||||||| ||| |||||||||| |||||||| |||||| |||| |||| || |||||| ||| ||| ||| ||| || |||| ||| |||||||| ||| || ||||||| |||||||||| ||| ||| |||

||||| | ||||||| ||||||||||| |||||||||||||||||| ||||| ||| |||||| |||||||||||||||||||||||||| |||||||| || ||||||||| |||||||| |||| |||||||||| |||| ||| |||||||||| ||||||||||||||||||||| |||||||| |||| ||| |||||||| || ||| ||||||| ||||||||||| || ||| |||||| ||| |||||| || ||||| ||| |||||| ||||||||||||
Critical Appraisal: Internal Validity
The internal validity issues described for the original analysis by Coppo et al. (2021)18 apply to the updated reanalysis as well, including potential for bias and impact of unmeasured confounders. While the clinical experts consulted by CADTH for the present review felt that the variables used for calculation of propensity scores appropriately captured disease severity and mortality risk, they did not account for the major treatment differences between the 2 groups (frontline rituximab in all patients receiving the triplet regimen, and salvage rituximab in approximately two-thirds of historical controls). In addition, the 2 cohorts analyzed had nonoverlapping time frames, and changes in treatment practice could potentially influence the results. An additional source of bias in the updated reanalysis was that some patients ||||| || |||||||||||||||||||| |||||||| ||| ||||| || |||||||||| ||||||||| had missing data for propensity scores and were thus excluded from the multivariate analysis. The impact of this bias was unclear.
Statistical tests were not adjusted for multiple comparisons and should be interpreted in descriptive and exploratory fashion. There was substantial variation evident in the 95% CIs for the odds ratio from logistic regression, and associated P values, depending on the analytical technique used. Use of propensity scores as covariates in adjusted multivariate models can result in biased estimation of HRs,51 although sensitivity analyses using alternative methodological approaches were performed.
Critical Appraisal: External Validity
The external validity issues described for the original analysis by Coppo et al. (2021)18 apply to the updated reanalysis as well.
UK RWE Cohort
Dutt et al. (2021)20 conducted a retrospective analysis of data from 85 patients with aTTP (including 4 children) who received caplacizumab in 22 UK hospitals from May 2018 and January 2020. Outcomes for these patients were compared with data from the HERCULES study and to a group of historical control patients consisting of 39 consecutive cases from the UK TTP registry who received standard treatment (PE plus immunosuppression with corticosteroids and rituximab) from 2014 to 2018.
Methods
An invitation to participate in RWE data collection for patients receiving caplacizumab was sent to all UK TTP registry collaborators. Data were retrospectively collected from consecutive eligible patients’ medical records from UK hospitals between May of 2018 and January of 2020. Inclusion criteria were patients of any age, who had received at least 1 dose of caplacizumab through the patient drug access scheme, following a confirmed diagnosis of acute aTTP. There were no exclusion criteria. Characteristics and outcomes for patients receiving caplacizumab compared with outcome data from the HERCULES study and a historical control group consisting of 39 consecutive cases from the UK TTP registry from 2014 to 2018.
Anonymized data were submitted by participating centres on specific patient characteristics and outcome data. Relevant outcome parameters were identified ahead of data collection, comparable with the HERCULES study end points. These included patient demographics, ADAMTS13 serology, serological markers of organ injury, platelet count recovery, PE, aTTP recurrences, bleeding and thromboembolic complications, and mortality.
Populations
The baseline characteristics of patients treated with caplacizumab in the RWE cohort of Dutt et al. (2021) are shown in Table 33. Approximately two-thirds (66%) of patients were women, approximately two-thirds (67%) were white, and the average age was 46 years. The median cardiac troponin level was 98 ng/mL, the median serum creatinine level was 90 µmol/L, and approximately two-thirds (66%) of patients had neurologic symptoms at presentation. Approximately one-quarter of patients (26%) required intubation during hospitalization for aTTP.
Table 33: Characteristics at Presentation of Patients Receiving Caplacizumab
Baseline characteristics | Caplacizumab cohort (n = 85) |
|---|---|
Age, mean (range), y | 46 (3-82) |
Females | 56 (66) |
Ethnicitya | |
White | 57 (67) |
Black | 16 (19) |
Asian | 6 (7) |
Other | 4 (5) |
Platelet count, median (IQR), ×109/L | 13 (9-21) |
Cardiac troponin, median (IQR), ng/mLb | 98 (31-317) |
Serum creatinine, median (IQR), µmol/L | 90 (71-135) |
Neurological symptoms at presentation | 56 (66) |
ADAMTS13 activity | |
<10 IU/dL | 84 (99) |
≥10 IU/dL | 1 (1) |
Detectable ADAMTS13 inhibitor, U/mLc | 68 (80) |
Immunosuppressive/adjuvant therapy started during admission | |
Glucocorticoids | 84 (99) |
Rituximab | 84 (99) |
Mycophenolate mofetil | 25 (29) |
Bortezomib | 5 (6) |
Ofatumumab | 2 (2) |
Cyclophosphamide | 1 (1) |
N-acetyl cysteine | 1 (1) |
Intensive care intervention | |
Patients requiring intubation | 22 (26) |
Duration of intubation, median (IQR), d | 4 (2-7) |
ADAMTS13 = a disintegrin and metalloproteinase with thrombospondin type 1 motif, member 13; d = day; IQR = interquartile range; IU = international units; NHS = National Health Service; y = year.
Note: This table is reproduced from original source and may not follow CADTH style.
aEthnicity was determined by the hematologist submitting the data for each center. Data on race were missing for 2 patients.
bMedian cardiac troponin on admission is based on n = 81 patients for whom data were available. Data are based on troponin T, the more commonly used cardiac enzyme in the NHS Trusts submitting the data.
cADAMTS13 inhibitor value on admission is based on n = 78 patients for whom data were available. The NHS Trusts included in this study used different assays for ADAMTS13 inhibitor; therefore, the normal values for each laboratory were used to determine whether the ADAMTS13 inhibitor was present/absent.
Source: Dutt et al. (2021).20 Reprinted from Blood, Vol 137/No 13, Dutt T, Shaw RJ, Stubbs M, et al., Real-world experience with caplacizumab in the management of acute TTP, Pages 1731-1740, Copyright 2021, with permission from The American Society of Hematology.
Interventions
Patients in the caplacizumab cohort of Dutt et al. (2021)20 received caplacizumab in addition to standard treatment, while historical controls received standard treatment alone. The standard treatment was as per UK national guidance and included PE plus corticosteroids and rituximab as a component of acute management. In the caplacizumab cohort, 84 patients (99%) received rituximab while in the historical control group 34 patients (87%) received rituximab.
Of note, caplacizumab was administered within 2 days of initiation of PE in approximately half of patients, while in 13% of patients, caplacizumab was initiated 1 week or more from beginning PE. The duration of caplacizumab treatment continuation post-PE ranged from 0 to 92 days (median, 28 days), with 55% of patients (47 of 85) discontinuing caplacizumab ahead of the 30-day period due to increased platelets and/or ADAMTS13 activity. The proportion of patients who continued caplacizumab for more than 30 days post-PE plus a 28-day extension as per the product monograph was not stated.
Outcomes
Time to platelet count normalization was defined in line with the HERCULES study as the time from the first IV administration of caplacizumab to the normalization of platelet count (platelet count of 150 × 109/L or greater with discontinuation of PE within 5 days thereafter). Recurrence of aTTP was defined as a new decrease in platelet count after initial normalization, requiring PE therapy to be reinitiated. A recurrence within 30 days after completion of PE was defined as an “exacerbation,” and a recurrence occurring more than 30 days after completion of PE was defined as a “relapse.” Refractory aTTP was defined as progression of clinical symptoms or persistent thrombocytopenia despite PE.
Statistical Analysis
Statistical analyses included descriptive and summary statistics. In addition, between-group comparisons were performed using a Mann-Whitney U test for continuous data and Fisher exact test for binary variables. The Kaplan-Meier estimator was used to calculate median times to events.
Patient Disposition
Between May 2018 and January 2020, 115 patients (110 adult and 5 pediatric) from 25 UK hospitals received caplacizumab through the free drug patient access scheme. Data were provided from 22 hospitals for 85 of 115 patients. Participation in data submission was voluntary, and no data were received for the remaining 30 patients.
No information was provided on the selection of the historical control group of 39 consecutive cases from the UK TTP registry from 2014 to 2018. The criteria for entry of these patients (approximately 10 patients per year) in the registry were not stated.
The median follow-up time for the caplacizumab cohort was 2.6 months (interquartile range [IQR], 1.9 to 5.5 months).
Exposure to Study Treatments
The median duration of caplacizumab treatment was 32 days (IQR, 22 to 47 days).
Efficacy
Treatment outcomes in the caplacizumab cohort of Dutt et al. (2021)20 are summarized in Table 34. Consistent with the results of the HERCULES trial, median time to platelet count normalization in the caplacizumab cohort was 3 days, median duration of PE was 7 days, and median duration of hospitalization was 12 days. Slightly more than half of patients had normalization of neurological symptoms (61%) and creatinine levels (56%) posttreatment. Five patients (6%) experienced aTTP recurrence (2 exacerbations and 3 relapses). Five patients in the caplacizumab cohort (6%) died.
Table 34: Summary of Outcomes for Patients Receiving Caplacizumab for iTTP
Patient outcomes | Caplacizumab cohort (n = 85) |
|---|---|
Time to normalization of platelet count, median (IQR), da | 3 (2-4) |
Total days of PEX, median (IQR) | 7 (5-14) |
Length of caplacizumab treatment, median (IQR), d | 32 (22-47) |
Caplacizumab discontinued prior to 30 d | 47 (55) |
Caplacizumab continued beyond 30 d | 27 (32) |
Number of days of hospitalization, median (IQR)b | 12 (8-24) |
Normalization of neurological symptomsc | 33 (61) |
Normalization of creatinined | 18 (56) |
Recurrence of TTPe | 5 (6) |
Exacerbation of TTP | 2 (2) |
Relapse of TTP | 3 (4) |
TTP-related deathf | 5 (6) |
Caplacizumab-related death | 0 (0) |
d = day; IQR = interquartile range; iTTP = immune-mediated thrombotic thrombocytopenic purpura; PEX = plasma exchange; TTP = thrombotic thrombocytopenic purpura.
Notes: This table is reproduced from original source and may not follow CADTH style.
Unless otherwise noted, data are n (%).
aTime to normalization of platelet count was defined in line with the HERCULES study as the time from the first IV administration of caplacizumab to normalization of platelet count (i.e., ≥ 150 × 109/L with discontinuation of PEX within 5 days thereafter). Time to normalization of platelet count is based on 81 of 85 patients; the remaining 4 patients did not achieve normalization of their platelet count by 30 days post-PEX discontinuation (1 case because of concomitant diagnosis of immune thrombocytopenia with a history of chronic low-grade thrombocytopenia, 1 case who achieved a normal platelet count by day 43, and 2 patients with multiple organ failure leading to death).
bBased on n = 81 patients, excluding 4 who died prior to discharge from the hospital.
cBased on available data for 54 of 55 patients who presented with neurological symptoms. The most common neurological symptoms on discharge were depressed mood and anxiety.
dBased on available data for 32 of 35 patients who presented with acute kidney injury.
eRecurrence of TTP was defined as a new decrease in platelet count after initial normalization of the platelet count, requiring PEX therapy to be reinitiated. A recurrence within 30 days after completion of PEX therapy was defined as an exacerbation, and a recurrence occurring > 30 days after completion of PEX therapy was defined as a relapse.
fThe cause of death was determined by the hematology clinician submitting the data; in all cases the cause was believed to be secondary to severe and/or refractory TTP.
Source: Dutt et al. (2021).20 Reprinted from Blood, Vol 137/No 13, Dutt T, Shaw RJ, Stubbs M, et al., Real-world experience with caplacizumab in the management of acute TTP, Pages 1731-1740, Copyright 2021, with permission from The American Society of Hematology
A comparison of baseline characteristics and treatment outcomes between the caplacizumab cohort of Dutt et al.20 and historical controls is shown in Table 35. Compared with historical controls, higher proportions of the caplacizumab cohort had elevated cardiac troponin (79% versus 64%) and elevated creatinine (41% versus 26%).
Consistent with the HERCULES study, median duration of PE (median 7 days versus 9 days) and time from PE initiation to platelet count normalization (median 4 days versus 6 days) were shorter in the caplacizumab cohort compared with historical controls. Duration of hospitalization was similar in the caplacizumab cohort (median = 12 days) and the historical control cohort (median = 14 days). aTTP recurrence and refractoriness were not compared between the 2 groups. In the caplacizumab cohort, 5 patients (6%) died but there were no deaths among historical control patients.
Table 35: Comparison of Presentation Characteristics and Outcomes in Caplacizumab Cohort Versus a Precaplacizumab Historical Control
Presentation characteristics and outcomes | Standard-treatment cohorta (n = 39) | Caplacizumab cohort (n = 85) | Pb |
|---|---|---|---|
Age, mean (range), y | 45 (15-93) | 46 (3-82) | .76 |
Females | 31 (80) | 56 (66) | 0.18 |
Platelet count on admission, median (IQR), ×109/L | 10 (6-20) | 13 (9-21) | .51 |
Elevated cardiac troponin | 25 (64) | 67 (79) | .12 |
Elevated serum creatinine | 10 (26) | 35 (41) | .08 |
Neurological symptoms at presentation | 29 (74) | 56 (66) | .74 |
ADAMTS13 activity <10 IU/dL | 39 (100) | 84 (99) | >.99 |
Patients achieving platelet count normalization | 39 (100) | 81 (95) | .31 |
Time from first PEX to normalization of platelet count, median (IQR), d | 6 (4-10) | 4 (3-8)c | .011 |
Days of PEX, median (IQR) | 9 (8-16) | 7 (5-14) | .007 |
Adjuvant therapy with rituximab | 34 (87) | 84 (99) | >.99 |
Patients requiring intubation | 4 (10) | 22 (26) | .06 |
Length of hospitalization, median (IQR), d | 14 (9-17) | 12 (8-24) | .62 |
Patients with bleeding post-admission | 0 (0) | 15 (18) | .003 |
Patients with VTE during admission | 2 (5) | 4 (5) | >.99 |
TTP-related death | 0 (0) | 5 (6) | .32 |
ADAMTS13 = a disintegrin and metalloproteinase with thrombospondin type 1 motif, member 13; d = days; IQR = interquartile range; IU = international units; PEX = plasma exchange; TTP = thrombotic thrombocytopenic purpura; VTE = venous thromboembolism; y = years.
Notes: This table is reproduced from original source and may not follow CADTH style.
Unless otherwise noted, data are n (%).
aStandard treatment cohort is from 39 consecutive cases from unpublished TTP Registry data from 2014 to 2018.
bP values were calculated using the Student t-test/Χ2 test for parametric data and the Mann–Whitney U test for nonparametric data.
cBased on 81 of 85 patients. Four of 85 patients did not achieve a normal platelet count (by 30 days, post-PEX discontinuation); 1 case due to a concomitant diagnosis of immune thrombocytopenia with a history of chronic low-grade thrombocytopenia, 1 case whose platelets returned to normal levels by day 43, and 2 cases with multiple organ failure leading to death.
Source: Dutt et al. (2021).20 Reprinted from Blood, Vol 137/No 13, Dutt T, Shaw RJ, Stubbs M, et al., Real-world experience with caplacizumab in the management of acute TTP, Pages 1731-1740, Copyright 2021, with permission from The American Society of Hematology.
The relationships between ADAMTS13, aTTP recurrence, and mortality in the caplacizumab cohort are shown in Figure 12. In 4 patients who died, caplacizumab was introduced more than 48 hours after PE initiation (range, 3 to 21 days), and in 3 patients who died, caplacizumab was introduced more than 1 week after PE initiation (range, 8 to 21 days). All deaths were believed by the treating hematologist to be secondary to severe and/or refractory TTP.
Figure 12: Drug Initiation, Mortality, and Disease Recurrence in Relation to ADAMTS13 Activity
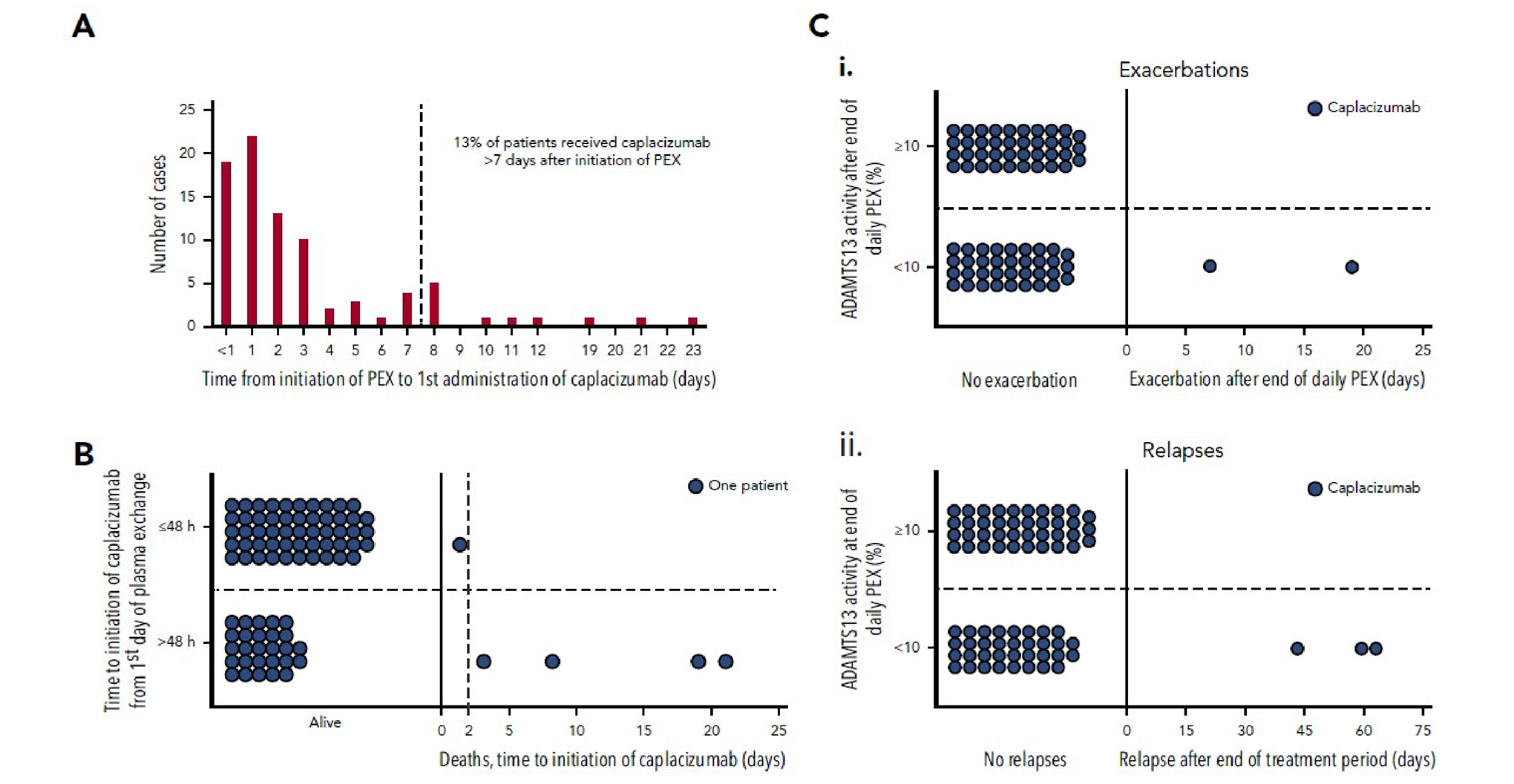
ADAMTS13 = a disintegrin and metalloproteinase with thrombospondin type 1 motif, member 13; PEX = plasma exchange.
Note: (A) Time taken from initiation of PEX therapy to the first dose of caplacizumab (days). < 1 day refers to the first administration of caplacizumab < 24 hours following initiation of PEX. (B) Mortality according to caplacizumab initiation (≤ 48 hours vs > 48 hours). Eighty percent of those who died had caplacizumab initiated > 48 hours after the first PEX. (C) Recurrence status according to ADAMTS13 activity at completion of PEX. (i) Individual patient data with regard to exacerbation status. ADAMTS13 activity after the end of PEX was available for 76 patients. Of these, 37 (48.7%) had ADAMTS13 activity < 10.0% (range, < 1.0 to 5.2); 3 patients experienced exacerbations. The other 39 patients (51.3%) had ADAMTS13 ≥ 10.0% (range, 10.2 to 107.2), without any exacerbations. (ii) Individual patient data with regard to relapse status. No patient with ADAMTS13 activity ≥ 10.0% relapsed, whereas 3 of the 37 patients with ADAMTS13 activity < 10.0% did. Recurrences are termed exacerbations if they occur within 30 days of last PEX and are classified as relapses if they occur > 30 days after last PEX.
Source: Dutt et al. (2021).20 Reprinted from Blood, Vol 137/No 13, Dutt T, Shaw RJ, Stubbs M, et al., Real-world experience with caplacizumab in the management of acute TTP, Pages 1731-1740, Copyright 2021, with permission from The American Society of Hematology.
Harms
Safety outcomes in the caplacizumab cohort of Dutt et al. (2021)20 are summarized in Table 36. Twenty-six patients (30.6%) experienced at least 1 AE, while the numbers of patients who experienced SAEs, AEs leading to treatment interruption, or WDAEs were not reported. Five patients (5.9%) died. Fifteen patients (17.6%) had bleeding AEs, including 17 episodes of which 5 were episodes of major bleeding. Eleven patients (12.9%) had non-bleeding AEs, including 5 patients (5.9%) who experienced venous thromboembolism.
Table 36: Summary of Adverse Events for Patients Receiving Caplacizumab
Episodes | No. episodesa | Episodes with caplacizumab interruption | Major bleedingb |
|---|---|---|---|
Bleeding | |||
Gum bleeding | 6 | 1c | 1 |
Epistaxis | 1 | 0 | 0 |
Bruising | 1 | 0 | 0 |
Hemarthrosis | 1 | 1 | 1 |
Lower gastrointestinal bleeding | 3 | 0 | 0 |
Upper gastrointestinal bleeding | 2d | 2 | 2 |
Intracranial bleeding | 2e | 2 | 2 |
Traumatic | 1 | 1f | 1 |
Total | 17 | 6 | 5 |
Nonbleeding | |||
Venous thromboembolism | 5g | 4h | NA |
Injection site reaction/allergy | 4 | 1 | NA |
Skin rash | 3 | 3i | NA |
LFT derangements | 1 | 1 | NA |
Neutropenic feverj | 1 | 1 | NA |
Total | 14 | 10 | |
LFT = liver function test; NA = not applicable.
Note: This table is reproduced from original source and may not follow CADTH style.
aSome patients were reported to have > 1 adverse event. There were 17 bleeding episodes in 15 patients and 14 nonbleeding episodes in 11 patients.
bMajor bleeding was defined as per the International Society on Thrombosis Haemostasis bleeding scale guideline. Major bleeding in nonsurgical patients includes fatal bleeding and/or symptomatic bleeding in a critical area or organ (e.g., intracranial, intraspinal, intraocular, retroperitoneal, intra-articular, or pericardial, or intramuscular with compartment syndrome) and/or bleeding causing a decrease in hemoglobin levels ≥ 2 g/dL or leading to transfusion of ≥ 2 units of whole blood or red cells.
cThis case was associated with a significant reduction in hemoglobin leading to drug interruption.
dOne case of severe upper gastrointestinal bleeding with subsequent decrease in hemoglobin on background of Barrett’s esophagus, gastroscopy showing small ulcer and esophagitis. One case of minor upper gastrointestinal bleeding.
eOne case of secondary hemorrhage of cerebral infarct and 1 case of intracranial hemorrhage following initial ischemic insult. There were no cases of primary intracerebral hemorrhage while on caplacizumab.
fPostmechanical fall resulting in fractured femoral neck.
gThrombotic episodes included left brachial and right internal jugular thrombosis (n = 1) and pulmonary embolism (n = 4). These 5 episodes occurred in 4 patients. Two of these episodes occurred outside of the time during which the patient was being administered caplacizumab.
hCaplacizumab was interrupted because of concerns managing bleeding risk on concurrent therapeutic anticoagulation in all cases.
iOne case had concurrent thrombosis.
jNot listed on drug summary of product characteristics as a side effect.
Source: Dutt et al. (2021).20 Reprinted from Blood, Vol 137/No 13, Dutt T, Shaw RJ, Stubbs M, et al., Real-world experience with caplacizumab in the management of acute TTP, Pages 1731-1740, Copyright 2021, with permission from The American Society of Hematology.
Critical Appraisal: Internal Validity
Comparisons between patients receiving the triplet regimen including caplacizumab and historical controls receiving SOC were limited by risk of bias in selection of participants. Data for 26% of eligible patients treated with caplacizumab were not submitted for analysis and no data were available for these patients which prevents the evaluation of selection bias for this analysis. Furthermore, data for 115 patients from 2018 and 2019 were in the registry compared with data for 39 consecutive cases for the 4-year period from 2014 to 2018; the lower sample for the comparator group collected over a longer time period suggests that the historical controls represented a small subgroup of the overall population of patients with aTTP treated during this period. Comparisons between the caplacizumab cohort of Dutt et al. (2021)20 and the HERCULES trial data were direct without adjustment, and the baseline characteristics and treatments administered differed substantially; thus, the risk of bias due to measured and unmeasured confounders is high for this comparison. There were baseline differences between the caplacizumab and historical control cohorts in cardiac involvement and serum creatinine level, which could have affected the outcomes including mortality. In addition, the 2 cohorts analyzed had nonoverlapping time frames, and changes in treatment practice could potentially influence the results.
The rationale for statistical hypothesis testing was not provided and it was unclear whether statistical tests were prespecified or conducted post hoc for some outcomes. Statistical tests were not adjusted for multiple comparisons and should be interpreted in descriptive and exploratory fashion.
Critical Appraisal: External Validity
In more than half of patients (55%), caplacizumab was discontinued before 30 days post PE, which is not consistent with the product monograph. The clinical experts consulted by CADTH felt that early discontinuation of treatment could have contributed to worse outcomes in the caplacizumab cohort. In addition, the clinical experts noted that the baseline characteristics of the patients in the caplacizumab cohort reflected severe disease (e.g., cardiac and neurological involvement), which was also supported by intubation of approximately one-quarter of patients; the clinical experts felt it was possible that some patients in the cohort may have been candidates for upfront therapy with caplacizumab but instead received it 2 days or longer after PE initiation. According to the clinical experts consulted by CADTH for this review, upfront use of rituximab is not consistent with the current or expected use of either drug in Canadian clinical practice.
Discussion
Summary of Available Evidence
One phase III, prospective, long-term follow-up study (post-HERCULES, N = 104)14,15 of patients who completed the HERCULES study (N = 145, n = 108 completed) contributed evidence to the systematic review section of this report. The objectives of post-HERCULES were to evaluate long-term safety and efficacy of caplacizumab, to evaluate the safety and efficacy of repeated use of caplacizumab in participants who experienced a recurrence of aTTP, and to characterize the long-term clinical impact of aTTP. Following the final 4-week follow-up visit in the HERCULES study, adult patients with aTTP were invited to enrol in the post-HERCULES study within 1 month and were then followed for a period of 3 years through twice-yearly visits. During the 3-year follow-up period, patients could receive OL caplacizumab in combination with PE and immunosuppression. Outcomes related to aTTP recurrence were assessed both as a composite outcome (aTTP-related events) and the individual components of this outcome (aTTP-related death, recurrence of aTTP, and major thromboembolic events).
Additionally, the phase III HERCULES21-23 and phase II TITAN24-26 trials, which were evaluated in the Clinical Review Report for the initial submission of caplacizumab, were also considered relevant for this review. Refer to the Clinical Review Report for the initial submission of caplacizumab13 for details, the executive summary of which is reproduced as Appendix 2.
One post hoc analysis, an integrated analysis of data from the HERCULES and TITAN trials, provided an additional evaluation of the previously assessed evidence regarding the clinically important outcomes of survival, health care use, organ damage, and refractory aTTP. Peyvandi et al. (2021)16 conducted an integrated analysis of data from the HERCULES and TITAN trials as suggested by the FDA. The goal was to increase statistical power for assessing treatment differences in efficacy and safety outcomes.
Finally, data for 2 RWE cohorts from France17-19 and the UK20 were summarized to provide additional evidence regarding the clinically important outcomes of survival, aTTP recurrence, refractory aTTP, and health care utilization and to provide additional evidence regarding the impacts of caplacizumab beyond the duration of clinical trials. The French RWE cohort of Coppo et al. (2021)18 prospectively analyzed outcome data for 90 patients with aTTP from France treated with a compassionate frontline triplet regimen consisting of PE, immunosuppression with corticosteroids and rituximab, and caplacizumab and compared them with 180 historical control patients treated with standard frontline therapy (PE plus corticosteroids, with rituximab as salvage therapy). ||||| ||| |||||| ||||||||||| ||||||||| || ||||||| |||||||||| || ||| |||| |||| |||| ||| ||||||| || ||||||| ||| |||||||||| ||||||| |||||||| |||||| ||| |||||||| |||||| ||| || ||||||||||| | |||||||||| ||||| ||| ||||||| |||||||| || || |||||||||| |||||| || |||||||||||| ||||||||| The UK RWE cohort of Dutt et al. (2021)20 conducted a retrospective analysis of data from 85 patients with aTTP (including 4 children) who received caplacizumab in 22 UK hospitals from May 2018 to January 2020 and compared them with data from the HERCULES study and to a group of historical control patients consisting of 39 consecutive cases from the UK TTP registry who received standard treatment (PE plus immunosuppression with corticosteroids and rituximab).
Interpretation of Results
Efficacy
The final CDEC recommendation for the initial submission of caplacizumab12 identified the following areas as having insufficient evidence regarding the efficacy and safety of caplacizumab: insufficient evidence of clinically important outcomes, lack of long-term clinical outcome data, lack of an identifiable subpopulation most likely to benefit from treatment, generalizability to Canadian clinical practice, and absence of HRQoL data. Interpretation of efficacy results in the following is organized for each of these points separately.
Insufficient Evidence of Clinically Important Outcomes
In its final recommendation for the initial submission of caplacizumab, CDEC noted that the HERCULES study was not designed to assess the effects of caplacizumab on the clinically important outcomes of survival, reduction in organ damage, health care use, or long-term recurrence of aTTP. Given caplacizumab’s mechanism of action, CDEC could not determine the clinical magnitude of the correlation between time to normalization of platelet count with the aforementioned clinical outcomes. While observational studies have documented correlations between longer times to platelet count response (using various thresholds) and poor outcomes such as mortality52,53 at the time this report was prepared, there remained uncertainty that small differences in time to platelet normalization impacted risk of major thromboembolic events, organ damage, or mortality.
Of the clinically important outcomes identified by CDEC, the post-HERCULES study14,15 was designed to assess long-term aTTP recurrence, and it did not directly address any of the other outcomes. More specifically, since the efficacy ITO population excluded patients who were randomized to receive SOC in the HERCULES study who switched to OL caplacizumab, the study assessed long-term aTTP recurrence among patients who received upfront caplacizumab; importantly, the study was not designed to inform the efficacy of caplacizumab in patients receiving the drug as salvage therapy for aTTP recurrence or refractory aTTP (refer to Interpretation of Harms section), which was suggested by the clinical experts consulted by CADTH for this review as a potential place in therapy for the drug. According to the clinical experts consulted by CADTH for the present resubmission, aTTP recurrence tends to occur within the first month of treatment as well as up to 2 years later. The clinical experts relayed that 1 of the challenges of using caplacizumab is that it directly increases platelets through its mechanism, potentially masking an indicator of aTTP disease activity, which would make it difficult to determine when it is time to taper PE. Thus, the clinical experts relayed that a valid concern regarding the HERCULES study was that with a relatively short 4-week follow-up period, additional recurrences in patients treated with caplacizumab occurring in the subsequent weeks and months might be missed. According to the clinical experts, the post-HERCULES study provided additional supportive evidence to address this concern: during its 3-year follow-up period among patients who completed the HERCULES study and had not experienced aTTP recurrence in the HERCULES study or before the beginning of post-HERCULES (efficacy ITO population), a descriptive comparison showed that the frequency of aTTP recurrence was numerically lower in patients randomized to receive caplacizumab in the HERCULES study (8.2%) compared to those randomized to receive SOC alone and who did not receive caplacizumab during the HERCULES trial (37.9%). Though interpretation of these results was limited by the descriptive nature of the comparison and potential for bias due to limitations in the study design, this evidence is not supportive of the concern that treatment with caplacizumab may result in increased relapses after 30 days post PE discontinuation and beyond the HERCULES trial duration. The clinical experts consulted by CADTH for the present resubmission stated that the mechanisms through which caplacizumab could potentially influence long-term aTTP relapse were unknown.
The post hoc integrated analysis of the HERCULES and TITAN study data by Peyvandi et al.16 provided an additional lens with which to view the results of the HERCULES and TITAN trials, including the clinically important outcomes of survival, health care use, organ damage, and refractory aTTP. This analysis provided no additional information on long-term aTTP recurrence. Consistent with both of the individual trials, the integrated analysis indicated that among patients randomized to receive caplacizumab compared to those randomized to receive placebo, mortality was numerically lower (blinded treatment periods: 0% versus 3.6%, respectively; overall study periods: 0.9% versus 4.5%, respectively), duration of PE was numerically shorter (median 5.0 days versus 7.5 days, respectively), the frequency of aTTP relapse was numerically higher (13.0% versus 0%, respectively), the frequency of aTTP-related events (TTP-related death, major thromboembolic events, or aTTP exacerbation) was numerically lower (13.0% versus 47.3%, respectively), and the frequency of refractory aTTP was numerically lower (0% versus 7.1%, respectively). In addition, caplacizumab was associated with numerically faster normalization of LDH, troponin, and serum creatinine. However, because of the lack of evaluation or justification for naive pooling of the data from 2 distinct trials as well as lack of formal statistical testing of prespecified hypotheses with adjustment for multiple comparisons, the results of the integrated analysis were unable to extend the conclusions regarding these outcomes drawn from the individual trials.
Two additional post hoc analyses were described in a poster and a conference abstract. Coppo et al. (2020)39 conducted a post hoc subgroup analysis of the HERCULES study data by time to platelet count response and reported that caplacizumab was associated with numerically faster time to durable response, numerically longer time to complete remission and numerically longer recurrence-free survival. Scully et al. (2020)40 described outcomes among 8 patients randomized to receive SOC in the HERCULES study who had suboptimal responses to PE; suboptimal response to PE occurred in no patients in the caplacizumab arm. However, these studies did not address an important gap in the evidence for the initial review of caplacizumab due to their limitations (hypothesis-generating only, unclear relevance of surrogate outcomes, described in limited detail in poster or abstract form) and thus data are described for reference only in Appendix 4.
Two RWE cohorts provided additional supportive evidence on survival, health care use, and refractory aTTP. These included a French RWE cohort of 90 patients receiving frontline caplacizumab therapy, PE, corticosteroids, and rituximab versus 180 or 216 historical controls, by Coppo et al. (2021)18 and CEMKA and Sanofi (2021),17,19 respectively; and a UK RWE cohort of 85 patients receiving caplacizumab, PE, corticosteroids and rituximab versus 39 historical controls by Dutt et al. (2021).20 These studies did not address organ damage or long-term recurrence of aTTP. In the French RWE cohort, mortality was numerically lower in patients who received caplacizumab compared with historical controls (1.1% versus 6.7%, Coppo et al. [2021]18 | |||| || ||||| CEMKA and Sanofi [2021]17,19), while in the UK RWE cohort,20 mortality was numerically higher in patients who received caplacizumab compared with historical controls (6% versus 0%). In both RWE cohorts, duration and volume of PE and duration of hospitalization were numerically shorter for patients receiving caplacizumab, although the magnitudes of the differences were smaller for the UK RWE cohort.20 In the French RWE cohort, 1.1% of patients receiving caplacizumab experienced refractory aTTP compared with 10%17,19 to 18%18 of historical controls; refractory aTTP was not compared between patients treated with caplacizumab and SOC in the UK RWE cohort. Except for the reanalysis of Sanofi and CEMKA (2021),17,19 all comparisons were naive and did not take into account baseline differences between populations. None of the analyses accounted for measured and unmeasured confounders including nonoverlapping treatment time frames and differences in treatment, primarily use of rituximab, which was higher in the RWE cohorts. Due to limitations of this evidence related to risk of potential for bias and confounding and lack of formal statistical testing, no conclusions could be drawn that go beyond the HERCULES, post-HERCULES, and TITAN trial data.
Data for an additional German RWE cohort were published by Volker et al. (2020);41-43 however, because there was no comparison of outcomes between patients treated with caplacizumab and SOC, the study did not address an important gap in the evidence for the initial review of caplacizumab. Similarly, 3 additional RWE studies described as conference abstracts were either noncomparative (Maanaoui et al.45) and/or were not described in sufficient detail to enable rigorous evaluation of their conduct and reporting (Vataire et al. [2022]46 and Volker et al. [2021]47). Data for these studies are described for reference only in Appendix 4
Lack of Long-Term Clinical Outcome Data
In its final recommendation for the initial submission of caplacizumab, CDEC noted that the HERCULES and TITAN studies provided data on the effects of caplacizumab versus placebo for up to 2 aTTP episodes only. As such, CDEC could not determine caplacizumab’s benefit, if any, beyond the duration of the trials.
As explained previously, the 3-year follow-up period of the post-HERCULES study14,15 provided additional relevant evidence beyond the duration of the HERCULES trial on long-term aTTP recurrence; the results were not supportive of the concern that treatment with caplacizumab may result in increased relapses after 30 days post PE discontinuation and beyond the HERCULES trial duration. The study was not designed to provide information on the effects of caplacizumab versus placebo for more than 2 aTTP episodes, as patients who had experienced aTTP recurrence in the HERCULES study or before the beginning of the post-HERCULES study were excluded from the post-HERCULES study efficacy ITO population. Only 6 patients in the efficacy ITO population in the post-HERCULES study experienced 2 or more recurrences during the study. The post-HERCULES study was not designed to provide conclusive long-term data on other outcomes of interest to CDEC (e.g., survival, health care utilization, organ damage, refractory aTTP, or prevention of further aTTP relapses beyond the second episode).
The 2 RWE cohorts described in this report were potentially able to provide additional supportive evidence on long-term recurrence of aTTP beyond the duration of the HERCULES trial. Median follow-up in the French17-19 and UK20 RWE cohorts was 4.2 months and 2.6 months, respectively. However, in the French RWE cohort only exacerbation (not long-term relapse) was compared between patients treated with caplacizumab and SOC, and the UK RWE cohort did not compare recurrence rates between patients treated with caplacizumab and SOC. Due to these reasons as well as the limitations noted previously, no conclusions regarding long-term outcomes could be drawn from the RWE that go beyond the HERCULES, post-HERCULES, and TITAN trial data.
Data for an additional German RWE cohort were published by Volker et al. (2020)41-43 were considered not to address an important gap in the evidence for the reasons noted previously. Similarly, 1 additional RWE study described as a conference abstract (Jimenez et al. [2020]44) was not described in sufficient detail to enable rigorous evaluation of its conduct and reporting. Data for these studies are described for reference only in Appendix 4.
Lack of an Identifiable Subpopulation Most Likely to Benefit
In its final recommendation for the initial submission of caplacizumab, CDEC noted that variability in the natural history of aTTP and the limitations in the design and analysis of the HERCULES study prevented CDEC from identifying a subpopulation of patients with aTTP most likely to benefit from treatment with caplacizumab. Post hoc analyses of data from the HERCULES study stratified by disease severity38 and time to platelet count response39 revealed no signals that the impacts of caplacizumab on the occurrence of aTTP-related events in patients varied by subgroup within the HERCULES study (refer to Appendix 4). This result was consistent with the hypothesis, which remains to be tested, that the impact of caplacizumab on the occurrence of aTTP-related events in patients is similar regardless of baseline disease severity or time to platelet count response.
In addition, in the French RWE cohort of Coppo et al. (2021)18 patients were stratified by baseline French severity score (≤ 2 versus ≥ 3) and the results of the primary analysis were similar in both subgroups. The CADTH review team noted that results from post hoc analyses are considered exploratory and hypotheses generating only. Due to the lack of formal inferential statistical testing, the ability to interpret results of such analyses is significantly limited.
Generalizability to Canadian Clinical Practice
In its final recommendation for the initial submission of caplacizumab, CDEC noted that the percentage of patients who received rituximab in the HERCULES study (40%) was higher than what is expected in Canada and that it is thus unclear if the observed effects of caplacizumab in the trial would be observed in Canadian practice. Post hoc analyses of data from the HERCULES36 and post-HERCULES37 studies stratified by rituximab use (Appendix 4) revealed no signals that the impacts of caplacizumab on occurrence of aTTP-related events in patients varied by subgroup, both within the HERCULES study, and for patients who participated in the post-HERCULES study, for up to 3 years thereafter. The clinical experts consulted by CADTH for this review noted that the proportion of patients living in Canada with aTTP who receive upfront rituximab therapy in addition to PE and corticosteroids is not known with certainty but is likely lower than in the post-HERCULES trial. However, the proportion in clinical practice has increased in recent years due to improved access to rituximab.
The CADTH review team noted that results from post hoc analyses are considered exploratory and hypotheses generating only. Due to the lack of formal inferential statistical testing, the ability to interpret results of such analyses is significantly limited.
Absence of HRQoL Data
In the rationale for its final recommendation on the initial submission of caplacizumab, CDEC made no comments on HRQoL data in the rationale or discussion sections; however, the absence of HRQoL data was noted in the “Summary of evidence considered by CDEC” section of the final recommendation.12 HRQoL data were collected using 2 instruments (HIT-6 and SF-36) in the post-HERCULES study.14,15 However, due to variable rates of missing data, lack of formal statistical testing, potential for bias in patient-reported outcomes in an OL study, and uncertainty in the measurement properties of these instruments in patients for aTTP, changes in HRQoL over time and between the arms of the post-HERCULES study efficacy ITO population could not be interpreted.
Harms
Analysis of safety data from the post-HERCULES study,14,15 a post hoc integrated analysis of the HERCULES and TITAN study data,16 and data from RWE cohorts17-20 suggested that the harms profile of caplacizumab is consistent with that observed in the HERCULES and TITAN trials. The post-HERCULES study provided long-term safety data for up to 3 years in 104 patients who participated in the HERCULES trial. No new safety signals were identified. Bleeding AEs were the most common manifestations of caplacizumab treatment. Although 5 patients (5.9%) in the RWE cohort of Dutt et al.20 experienced venous thromboembolism, the clinical experts consulted by CADTH for this review relayed that this was due to the severe disease and poor outcomes of this cohort.
In the post-HERCULES study, harms were evaluated in the overall ITO population (N = 104) while efficacy outcomes were evaluated in the efficacy ITO population (n = 78). All patients who were part of the overall ITO population but excluded from the efficacy ITO population (n = 26) had prior caplacizumab experience in the HERCULES study; the majority (20 of 26; 77%) were randomized to receive double-blind placebo therapy in the HERCULES study and then switched to OL caplacizumab. Comparing the data in Table 14 (in the efficacy ITO population, 4 of 49 patients randomized to receive caplacizumab in the HERCULES study experienced aTTP recurrence in post-HERCULES) and Table 21 (in the overall ITO population, 11 of 75 patients treated with caplacizumab in the HERCULES study experienced aTTP recurrence in the post-HERCULES study) indicated that 7 of 26 patients (27%) who were part of the overall ITO population but excluded from the efficacy ITO population experienced aTTP recurrence during the post-HERCULES study.
Conclusions
Evidence from the HERCULES study suggested that administration of caplacizumab resulted in a statistically significant decrease in the frequency of aTTP recurrence during the HERCULES study period. In the long term follow-up study of the HERCULES study (the post-HERCULES study), there were no signs that treatment with caplacizumab during the HERCULES study resulted in increased frequency of aTTP relapse post PE discontinuation beyond the follow-up period of the HERCULES trial. A post hoc integrated analysis of data from the HERCULES and TITAN trials provided an additional evaluation of survival, health care use, organ damage, and refractory aTTP; however, due to naive pooling of the data and lack of formal statistical testing of prespecified hypotheses, including adjustment for multiple comparisons, its results supported but were unable to extend the conclusions regarding these outcomes drawn from the individual trials. Two RWE cohorts from France and the UK provided additional supportive evidence regarding the frequency of aTTP-related events, including mortality in patients receiving caplacizumab; however, due to potential for biased patient selection in observational studies, intergroup differences in measured and/or unmeasured confounders including treatments received that could not be accounted for, and absence of formal statistical testing, no conclusions could be drawn that go beyond the HERCULES, post-HERCULES, and TITAN trial data. The combined data from the HERCULES and post-HERCULES studies suggested that caplacizumab may decrease overall aTTP recurrence during treatment and immediately following treatment cessation (HERCULES) without producing an increased frequency of long-term aTTP relapse in the subsequent months and years (post-HERCULES).
References
1.Drug Reimbursement Review sponsor submission: Cablivi (caplacizumab), 11 mg powder for solution, for intravenous (IV) or subcutaneous injection [internal sponsor's package]. Laval (QC): sanofi-aventis Canada Inc.; 2022 Jun 22.
2.Joly BS, Coppo P, Veyradier A. Thrombotic thrombocytopenic purpura. Blood. 2017;129(21):2836-2846. PubMed
3.Agosti P, Mancini I, Artoni A, et al. The features of acquired thrombotic thrombocytopenic purpura occurring at advanced age. Thromb Res. 2020;187:197-201. PubMed
4.Scully M, Hunt BJ, Benjamin S, et al. Guidelines on the diagnosis and management of thrombotic thrombocytopenic purpura and other thrombotic microangiopathies. Br J Haematol. 2012;158(3):323-335. PubMed
5.Goel R, King KE, Takemoto CM, Ness PM, Tobian AA. Prognostic risk-stratified score for predicting mortality in hospitalized patients with thrombotic thrombocytopenic purpura: nationally representative data from 2007 to 2012. Transfusion. 2016;56(6):1451-1458. PubMed
6.Lewis QF, Lanneau MS, Mathias SD, Terrell DR, Vesely SK, George JN. Long-term deficits in health-related quality of life after recovery from thrombotic thrombocytopenic purpura. Transfusion. 2009;49(1):118-124. PubMed
7.le Besnerais M, Veyradier A, Benhamou Y, Coppo P. Caplacizumab: a change in the paradigm of thrombotic thrombocytopenic purpura treatment. Expert Opin Biol Ther. 2019;19(11):1127-1134. PubMed
8.Miesbach W, Menne J, Bommer M, et al. Incidence of acquired thrombotic thrombocytopenic purpura in Germany: a hospital level study. Orphanet J Rare Dis. 2019;14(1):260. PubMed
9.Pascual-Izquierdo C, Del Rio-Garma J, de la Rubia J, et al. Incidence, diagnosis, and outcome of immune-mediated thrombotic thrombocytopenic purpura: a nationwide survey by the Spanish registry of thrombotic thrombocytopenic purpura. J Clin Apher. 2021;36(4):563-573. PubMed
10.Merlen C, Pepin E, Barry O, et al. Incidence of thrombotic microangiopathies in Quebec: insight from a laboratory centralizing ADAMTS-13 testing. Orphanet J Rare Dis. 2022;17(1):308. PubMed
11.Cablivi (caplacizumab): 11 mg powder for solution for intravenous (IV) or subcutaneous injection [product monograph]. Laval (QC): sanofi-aventis Canada Inc.; 2022 May 03.
12.CADTH Canadian Drug Expert Committee (CDEC) final recommendation: caplacizumab (Cablivi — Sanofi-Aventis Canada Inc.). Ottawa (ON): CADTH; 2020 Sep 1: https://www.cadth.ca/sites/default/files/cdr/complete/SR0633%20Cablivi%20-%20CDEC%20Final%20Recommendation%20September%201%2C%202020%20for%20posting.pdf. Accessed 2022 Aug 15.
13.Drug Reimbursement Review clinical guidance report: caplacizumab (Cablivi) for the treatment of adults with acquired thrombotic thrombocytopenic purpura (aTTP) in combination with plasma exchange (PE) and immunosuppressive therapy. Ottawa (ON): CADTH; 2020 Oct: https://www.cadth.ca/sites/default/files/cdr/clinical/sr0633-cablivi-clinical-review-report.pdf. Accessed 2022 Aug 15.
14.Clinical Study Report: ALX0681-C302/LTS16371 (Post-HERCULES). Prospective follow-up study for patients who completed study ALX0681-C301 (HERCULES) to evaluate long-term safety and efficacy of caplacizumab (Post-HERCULES) [internal sponsor's report]. Paris (FR): Sanofi Group; 2021 Jun 15.
15.Scully M, de la Rubia J, Pavenski K, et al. Long-term safety and efficacy of caplacizumab for immune-mediated thrombotic thrombocytopenic purpura: the post-HERCULES study. J Thromb Haemost. 2022.
16.Peyvandi F, Cataland S, Scully M, et al. Caplacizumab prevents refractoriness and mortality in acquired thrombotic thrombocytopenic purpura: integrated analysis. Blood Adv. 2021;5(8):2137-2141. PubMed
17.Study report: study of the CNR-MAT registry in autoimmune thrombotic thrombocytopenic purpura [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Cablivi (caplacizumab), 11 mg powder for solution, for intravenous (IV) or subcutaneous injection. Laval (QC): sanofi-aventis Canada Inc; 2022 Jun 22.
18.Coppo P, Bubenheim M, Azoulay E, et al. A regimen with caplacizumab, immunosuppression, and plasma exchange prevents unfavorable outcomes in immune-mediated TTP. Blood. 2021;137(6):733-742. PubMed
19.Vataire AL, Nevoret C, Bouee S, Duvivier A, Coppo P. POSB4 effectiveness of caplacizumab on reducing acute mortality in acquired thrombotic thrombocytopenic purpura: results from a French National Registry (CNR-MAT). Value Health. 2022;25(1):S25.
20.Dutt T, Shaw RJ, Stubbs M, et al. Real-world experience with caplacizumab in the management of acute TTP. Blood. 2021;137(13):1731-1740. PubMed
21.Clinical Study Report: ALX0681-C301 (HERCULES). A phase III double-blind, randomized, parallel group, multicenter placebo-controlled trial to study the efficacy and safety of caplacizumab in patients with acquired thrombotic thrombocytopenic purpura, version 2.0 [internal sponsor's report]. Zwijnaarde (BE): Ablynx NV; 2018 Jun 18.
22.Knoebl P, Cataland S, Peyvandi F, et al. Efficacy and safety of open-label caplacizumab in patients with exacerbations of acquired thrombotic thrombocytopenic purpura in the HERCULES study. J Thromb Haemost. 2020;18(2):479-484. PubMed
23.Scully M, Cataland SR, Peyvandi F, et al. Caplacizumab treatment for acquired thrombotic thrombocytopenic purpura. N Engl J Med. 2019;380(4):335-346. PubMed
24.Clinical Study Report: ALX-0681-2.1/10 (TITAN). A phase II, single-blind, randomized, placebo-controlled trial to study the efficacy and safety of anti-von Willebrand factor nanobody administered as adjunctive treatment to patients with acquired thrombotic thrombocytopenic purpura [internal sponsor's report]. Zwijnaarde (BE): Ablynx NV; 2015 May 29.
25.Peyvandi F, Scully M, Kremer Hovinga JA, et al. Caplacizumab for acquired thrombotic thrombocytopenic purpura. N Engl J Med. 2016;374(6):511-522. PubMed
26.Peyvandi F, Scully M, Kremer Hovinga JA, et al. Caplacizumab reduces the frequency of major thromboembolic events, exacerbations and death in patients with acquired thrombotic thrombocytopenic purpura. J Thromb Haemost. 2017;15(7):1448-1452. PubMed
27.Wynick C, Britto J, Sawler D, et al. Validation of the PLASMIC score for predicting ADAMTS13 activity <10% in patients with suspected thrombotic thrombocytopenic purpura in Alberta, Canada. Thromb Res. 2020;196:335-339. PubMed
28.McGowan J, Sampson M, Salzwedel DM, Cogo E, Foerster V, Lefebvre C. PRESS Peer Review of Electronic Search Strategies: 2015 guideline statement. J Clin Epidemiol. 2016;75:40-46. PubMed
29.Grey matters: a practical tool for searching health-related grey literature. Ottawa (ON): CADTH; 2019: https://www.cadth.ca/grey-matters. Accessed 2022 Jun 22.
30.Randolph C, Tierney MC, Mohr E, Chase TN. The Repeatable Battery for the Assessment of Neuropsychological Status (RBANS): preliminary clinical validity. J Clin Exp Neuropsychol. 1998;20(3):310-319. PubMed
31.Shin HE, Park JW, Kim YI, Lee KS. Headache Impact Test-6 (HIT-6) scores for migraine patients: their relation to disability as measured from a headache diary. J Clin Neurol. 2008;4(4):158-163. PubMed
32.Ware JE, Jr., Sherbourne CD. The MOS 36-item short-form health survey (SF-36). I. Conceptual framework and item selection. Med Care. 1992;30(6):473-483. PubMed
33.Medical Dictionary for Regulatory Activities (MedDRA) version 21.1. Geneva (CH): International Council for Harmonisation of Technical Requirements for Pharmaceuticals for Human Use; 2018: https://www.meddra.org. Accessed 2022 Aug 15.
34.National Cancer Institute. Common Terminology Criteria for Adverse Events (CTCAE v4.0: CTCAE v4.03). 2010: https://ctep.cancer.gov/protocoldevelopment/electronic_applications/ctc.htm. Accessed 2022 Aug 15.
35.Miyakawa Y, Imada K, Ichikawa S, et al. The efficacy and safety of caplacizumab in Japanese patients with immune-mediated thrombotic thrombocytopenic purpura (iTTP): an open-label, phase 2/3 study. Blood Adv. 2021;138(Suppl 1):1009.
36.Pavenski K, Knobl P, Scully M, et al. Efficacy of caplacizumab in patients with aTTP in the HERCULES study according to initial immunosuppression regimen [poster] [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Cablivi (caplacizumab), 11 mg powder for solution, for intravenous (IV) or subcutaneous injection. Laval (QC): sanofi-aventis Canada Inc; 2022 Jun 22.
37.Scully M, De la Rubia J, Pavenski K, et al. Long-term safety and efficacy of capacizumab for acquired thrombotic thrombocytoepnic purpura (ATTP): the post-HERCULES study [poster] [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Cablivi (caplacizumab), 11 mg powder for solution, for intravenous (IV) or subcutaneous injection. Laval (QC): sanofi-aventis Canada Inc; 2022 Jun 22.
38.Coppo P, Cataland S, Peyvandi F, et al. Efficacy of caplacizumab in patients with aTTP in the HERCULES study according to baseline disease severity [poster] [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Cablivi (caplacizumab), 11 mg powder for solution, for intravenous (IV) or subcutaneous injection. Laval (QC): sanofi-aventis Canada Inc; 2022 Jun 22.
39.Coppo P, Scully M, De la Rubia J, et al. Caplacizumab induces fast and durable platelet count responses with improved time to complete remission and recurrence-free survival in patients with acquired thrombotic thrombocytopenic purpura [poster] [internal sponsor's report] In: Drug Reimbursement Review sponsor submission: Cablivi (caplacizumab), 11 mg powder for solution, for intravenous (IV) or subcutaneous injection. Laval (QC): sanofi-aventis Canada Inc; 2022 Jun 22.
40.Scully M, Rubia JL, Peyvandi F, et al. Outcomes of patients with worsening acquired thrombotic thrombocytopenic purpura (TTP) despite daily therapeutic plasma exchange in the phase 3 HERCULES trial. Hematol Transfus Cell Ther. 2020;42(S2):95.
41.Volker LA, Kaufeld J, Miesbach W, et al. Real-world data confirm the effectiveness of caplacizumab in acquired thrombotic thrombocytopenic purpura. Blood Adv. 2020;4(13):3085-3092. PubMed
42.Kaufeld J, Brinkkoetter PT, Schreiber A, et al. Caplacizumab: frequent local skin reactions. Ann Hematol. 2021;100(12):3051-3052. PubMed
43.Volker LA, Kaufeld J, Miesbach W, et al. ADAMTS13 and VWF activities guide individualized caplacizumab treatment in patients with aTTP. Blood Adv. 2020;4(13):3093-3101. PubMed
44.Jimenez MM, Bobillo S, Perez A, et al. Real-world data with the use of caplacizumab in the treatment of acquired thrombotic thrombocytopenic purpura (aTTP). Blood. 2020;136(Suppl 1):3.
45.Maanaoui M, Maury E, Francois A, et al. P0202: First real-life data of patients treated for thrombotic thrombocytopenic purpura from the French Thrombotic Microangiopathies Network. Nephrol Dial Transplant. 2020;35(Suppl 3):iii505.
46.Vataire AL, Duvivier A, Karam P, Coppo P. Comparison of healthcare resource utilization among hospitalized patients with acquired thrombotic thrombocytopenic purpura treated with or without caplacizumab: a French hospital database (PMSI) analysis. Value Health. 2022;25(Suppl 1):S18.
47.Volker LA, Balduin G, Kuhne L, et al. Caplacizumab is effective in treating immune-mediated thrombotic thrombocytopenic purpura in real-world scenarios and may lower mortality: an aggregative analysis. Blood. 2021;138(Suppl 1):1019.
48.Logothetis CN, Patel A, Eatrides J, et al. Post approval experience with caplacizumab for acquired thrombotic thrombocytopenic purpura at a single institution. J Clin Med. 2021;10(15):31. PubMed
49.Kuhne L, Kaufeld J, Volker LA, et al. Alternate-day dosing of caplacizumab for immune-mediated thrombotic thrombocytopenic purpura. J Thromb Haemost. 2022;20(4):951-960. PubMed
50.Benhamou Y, Assie C, Boelle PY, et al. Development and validation of a predictive model for death in acquired severe ADAMTS13 deficiency-associated idiopathic thrombotic thrombocytopenic purpura: the French TMA Reference Center experience. Haematologica. 2012;97(8):1181-1186. PubMed
51.Austin PC. The performance of different propensity score methods for estimating marginal odds ratios. Stat Med. 2007;26(16):3078-3094. PubMed
52.Liu C, Kallogjeri D, Dynis M, Grossman BJ. Platelet recovery rate during plasma exchange predicts early and late responses in patients with thrombotic thrombocytopenic purpura. Transfusion. 2013;53(5):1096-1107. PubMed
53.Staley EM, Cao W, Pham HP, et al. Clinical factors and biomarkers predict outcome in patients with immune-mediated thrombotic thrombocytopenic purpura. Haematologica. 2019;104(1):166-175. PubMed
54.George J, Cuker A. Acquired TTP: clinical manifestations and diagnosis. In: Post TW, ed. UpToDate. Waltham (MA): UpToDate; 2019: www.uptodate.com. Accessed 2020 Jan 30.
55.CDR submission: Cablivi (caplacizumab), 10 mg powder and solvent for injection [CONFIDENTIAL sponsor's submission]. Mississauga (ON): Sanofi Genzyme, a division of sanofi-aventis Canada Inc.; 2019 Sep 23.
56.Sargentini-Maier ML, De Decker P, Tersteeg C, Canvin J, Callewaert F, De Winter H. Clinical pharmacology of caplacizumab for the treatment of patients with acquired thrombotic thrombocytopenic purpura. Expert Rev Clin Pharmacol. 2019;12(6):537-545. PubMed
57.George J, Cuker A. Acquired TTP: management following recovery from an acute episode and during remission. In: Post TW, ed. UpToDate. Waltham (MA): UpToDate; 2019: www.uptodate.com. Accessed 2020 Jan 30.
58.Azoulay E, Bauer PR, Mariotte E, et al. Expert statement on the ICU management of patients with thrombotic thrombocytopenic purpura. Intensive Care Med. 2019;45(11):1518-1539. PubMed
59.Cablivi (caplacizumab): 11 mg, powder for solution, intravenous or subcutaneous injection [product monograph]. Laval (QC): sanofi-aventis Canada Inc.; 2020 Feb 28: https://pdf.hres.ca/dpd_pm/00055326.PDF. Accessed 2022 Aug 15.
60.Clinical Study Report: ALX0681-C301 (HERCULES). A phase III double-blind, randomized, parallel group, multicenter placebo-controlled trial to study the efficacy and safety of caplacizumab in patients with acquired thrombotic thrombocytopenic purpura, version 1.0 [internal sponsor's report]. Zwijnaarde (BE): Ablynx NV; 2018 Mar 5.
61.de la Rubia J, Peyvandi F, Scully M, et al. Safety of caplacizumab in patients without documented severe ADAMTS13 deficiency during the HERCULES study. Blood. 2019;134(Suppl 1):1093. https://ashpublications.org/blood/article/134/Supplement_1/1093/426834/Safety-of-Caplacizumab-in-Patients-Without. Accessed 2022 Aug 15.
62.Scully M, Cataland S, Coppo P, et al. Consensus on the standardization of terminology in thrombotic thrombocytopenic purpura and related thrombotic microangiopathies. J Thromb Haemost. 2017;15(2):312-322. PubMed
63.Cohen J. A power primer. Psychol Bull. 1992;112(1):155-159. PubMed
64.Signorovitch J, Brainsky A, Grotzinger KM. Validation of the FACIT-fatigue subscale, selected items from FACT-thrombocytopenia, and the SF-36v2 in patients with chronic immune thrombocytopenia. Qual Life Res. 2011;20(10):1737-1744. PubMed
65.Reeve BB, Wyrwich KW, Wu AW, et al. ISOQOL recommends minimum standards for patient-reported outcome measures used in patient-centered outcomes and comparative effectiveness research. Qual Life Res. 2013;22(8):1889-1905. PubMed
Appendix 1: Literature Search Strategy
Note that this appendix has not been copy-edited.
Clinical Literature Search
Overview
Interface: Ovid
Databases:
MEDLINE All (1946 to present)
Embase (1974 to present)
Note: Subject headings and search fields have been customized for each database. Duplicates between databases were removed in Ovid.
Date of search: July 6, 2022
Alerts: Biweekly search updates until project completion
Search filters applied: No filters were applied to limit the retrieval by study type.
Limits:
Publication date limit: none
Language limit: none
Conference abstracts: excluded
Syntax | Description |
|---|---|
/ | At the end of a phrase, searches the phrase as a subject heading |
MeSH | Medical Subject Heading |
* | Before a word, indicates that the marked subject heading is a primary topic; or, after a word, a truncation symbol (wildcard) to retrieve plurals or varying endings |
.ti | Title |
.ot | Original title |
.ab | Abstract |
.hw | Heading word; usually includes subject headings and controlled vocabulary |
.kf | Author keyword heading word (MEDLINE) |
.dq | Candidate term word (Embase) |
.pt | Publication type |
.rn | Registry number |
.nm | Name of substance word (MEDLINE) |
medall | Ovid database code: MEDLINE All, 1946 to present, updated daily |
oemezd | Ovid database code; Embase, 1974 to present, updated daily |
Multidatabase Strategy
(cablivi* or caplacizumab* or alx-81 or alx81 or alx-0081 or alx0081 or alx-0681 or alx0681 or 2R27AB6766).ti,ab,kf,ot,hw,nm,rn.
1 use medall
*caplacizumab/
(cablivi* or caplacizumab* or alx-81 or alx81 or alx-0081 or alx0081 or alx-0681 or alx0681).ti,ab,kf,dq.
or/3-4
5 use oemezd
6 not (conference abstract or conference review).pt.
2 or 7
remove duplicates from 8
Clinical Trials Registries
ClinicalTrials.gov
Produced by the US National Library of Medicine. Targeted search used to capture registered clinical trials.
[Search -- Studies with results cablivi OR caplacizumab OR alx-81 OR alx81 OR alx-0081 OR alx0081 OR alx-0681 OR alx0681]
WHO ICTRP
International Clinical Trials Registry Platform, produced by the WHO. Targeted search used to capture registered clinical trials.
[Search terms -- cablivi OR caplacizumab OR alx-81 OR alx81 OR alx-0081 OR alx0081 OR alx-0681 OR alx0681]
Health Canada’s Clinical Trials Database
Produced by Health Canada. Targeted search used to capture registered clinical trials.
[Search terms -- cablivi OR caplacizumab OR alx-81 OR alx81 OR alx-0081 OR alx0081 OR alx-0681 OR alx0681]
EU Clinical Trials Register
European Union Clinical Trials Register, produced by the European Union. Targeted search used to capture registered clinical trials.
[Search terms -- cablivi OR caplacizumab OR alx-81 OR alx81 OR alx-0081 OR alx0081 OR alx-0681 OR alx0681]
Grey Literature
Search dates: June 22, 2022 to June 29, 2022
Keywords: [cablivi OR caplacizumab OR alx-81 OR alx81 OR alx-0081 OR alx0081 OR alx-0681 OR alx0681 acquired thrombotic thrombocytopenic purpura OR aTTP OR acquired TTP OR immune thrombotic thrombocytopenic purpura OR iTTP OR immune TTP]
Limits: Publication years: none
Updated: Search updated before the meeting of CADTH Canadian Drug Expert Committee (CDEC)
Relevant websites from the following sections of the CADTH grey literature checklist Grey Matters: A Practical Tool for Searching Health-Related Grey Literature were searched:
HTA Agencies
Health Economics
Clinical Practice Guidelines
Drug and Device Regulatory Approvals
Advisories and Warnings
Drug Class Reviews
Clinical Trials Registries
Databases (free)
Internet Search
Appendix 2: Executive Summary of CADTH Clinical Review Report for the Initial Submission of Caplacizumab
Note this appendix has not been copy-edited.
Introduction
Thrombotic thrombocytopenic purpura (TTP) is a rare but serious thrombotic microangiopathy.54 It is characterized by small-vessel platelet-rich thrombi that cause thrombocytopenia, microangiopathic hemolytic anemia (MAHA) and, sometimes, organ ischemia.4,54 Acquired TTP (aTTP), which is due to autoantibodies against a disintegrin and metalloproteinase with a thrombospondin type 1 motif, member 13 (ADAMTS13) and is usually associated with an ADAMTS13 activity level of less than 10%, is the most common form of TTP (95%). The incidence of aTTP was reported in the literature to be 1.2 to 13 cases per million. In Canada, the number of patients with aTTP was estimated to be ||| in 2018.55 Since the development of therapeutic plasma exchange (PEX) or plasma infusion in the 1980s, mortality due to aTTP has decreased from 90% to a range of 10% to 20%.5,54 Early diagnosis and treatment of aTTP is essential to the patient’s survival. Despite advances in understanding the disease and evolving treatment regimens, surviving patients with aTTP are still at risk for TTP exacerbation or relapse, refractory disease, or long-term consequences such as cognitive deficits, depression, hypertension, renal impairment, development of systemic lupus erythematosus, and reduced life expectancy.7,56,57
Daily PEX plus immunosuppressive therapies (primarily corticosteroids) are the mainstay of treatment. It allows removal of anti-ADAMTS13 antibodies and replenishment of functional ADAMTS13 and von Willebrand factor (vWF). PEX has substantially reduced mortality rates and enables faster remission in patients with aTTP4,58 although its use is associated with a number of adverse events (AEs). When there is a delay in delivering PEX, large-volume plasma infusions can be provided.4 Rituximab is another immunosuppressive that is also recommended for patients with aTTP, especially for those with refractory or relapsing aTTP, in conjunction with PEX and steroids; however, rituximab does not have an indication for aTTP. Refractory patients can also be treated with cytotoxic drugs such as cyclophosphamide, and splenectomy.
Caplacizumab is a humanized, bivalent nanobody targeting the A1 domain of vWF to inhibit the interaction between vWF and platelets. On February 28, 2020, caplacizumab was approved by Health Canada for the treatment of adults with aTTP in combination with PE and immunosuppressive therapy.59 The recommended dose of caplacizumab is as follows:
First day of treatment: 11 mg IV injection before PEX followed by an 11 mg subcutaneous injection after completion of PEX on that day.
Subsequent days of treatment during PEX: daily 11 mg subcutaneous injection following PEX.
Treatment after PEX period: 11 mg subcutaneous injections once daily for 30 days following the last daily PEX. If, after the initial treatment course, sign(s) of persistent underlying disease such as suppressed ADAMTS13 activity levels remain present, treatment may be extended for a maximum of 28 days.59
The CADTH Canadian Drug Expert Committee (CDEC) recommended that caplacizumab not be reimbursed for the treatment of adults with aTTP in combination with PEX and immunosuppressive therapy (March 6, 2020). A request for reconsideration was received by CADTH for this embargoed CDEC recommendation. The revised reimbursement criteria are for a narrower population: patients with multiorgan involvement indicating a more severe disease or refractory patients who do not respond well to previous treatment for a given time period, as determined by a specialist physician with expertise in treating aTTP.
Stakeholder Engagement
Patient Input
One patient group, the Answering TTP Foundation, submitted patient input for the review of caplacizumab for aTTP. Answering TTP is a volunteer-based organization that aims to provide patients with information about living with TTP by fostering research, providing support, and furthering education initiatives to improve the prognosis for patients living with TTP.
Answering TTP’s submission was completed with assistance from the Canadian Organization for Rare Disorders. The 2 patient groups collaborated to develop the survey and interview questions to collect information from patients about aTTP and caplacizumab. The 2 groups also collaborated to conduct the interviews and summarize the feedback received. In total, 289 individuals provided feedback by completing the online survey or participating in interviews. Most of the respondents (83%) were patients with TTP.
The patient group describes the experience of living with this life-threatening disorder, saying that an aTTP episode has a significant impact on patients’ and family members’ quality of life. Patients also reported stress, altered mood, and the financial burden related to the disorder.
The outcomes patients expect from a new treatment are faster normalization of platelet counts, shorter hospital stays, quicker return to normal life, improved survival, and reduced aTTP episodes. Faster access to rapid care is also desired.
Clinician Input
Although PE and immunosuppressants are effective, not all patients respond to these currently available treatments and, for some patients, the disease becomes refractory. In addition, the available treatment options are limited, especially for the patients with refractory disease. PE is a temporary solution that removes the anti-ADAMTS13 antibodies; however, it is impossible to predict when these patients will have another aTTP episode. Gaining access to the treatments that may be effective is another challenge; some patients may have to go through a special access program to receive access to a specific treatment (e.g., rituximab) or obtain medications for off-label use.
There is a lack of standardization around the treatment protocols for aTTP across the specialized centres; for example, variabilities exist regarding access to PE, when to start immunosuppression therapy such as rituximab and how aggressive the treatment should be, and how to taper PE or steroids. This is associated with variable compliance among patients. There is also a gap in defining what qualifies a patient for more intensive treatment.
Although PE is generally well tolerated, it can be time-intensive to set up (operationally) and requires specially trained personnel. PE is typically available during the day. If patients arrive during off-hours, they will likely be treated with plasma infusion and/or IV immunoglobulin until the appropriate personnel are available. PE also exposes patients to the risks associated with the transfusion of blood products.
The mechanism of caplacizumab is different from the current treatment paradigm. It targets the A1 domain of vWF and can be considered an anti-vWF drug that prevents the binding of vWF to the platelets. The panel indicated that from a resource and cost standpoint, caplacizumab probably wouldn’t be used as first-line management or to replace the standard of care. Other standard-of-care drugs should be used continuously. Caplacizumab might be used for patients with multiorgan involvement indicating a more severe disease, or for refractory patients who do not respond well to previous treatment for a given time period. However, the panel noted that specifying criteria to identify these patients is difficult because of the current limited understanding of the disease and the variation in its natural history, caplacizumab’s effect on natural history, and the lack of clinical data validating such an approach.
Adult patients best suited for treatment with caplacizumab might be those with very low platelet counts or multiorgan involvement in addition to the presentation of thrombocytopenia. They are considered to have more severe disease. However, there is a lack of agreed-upon criteria to quantify the severity of disease. Also, it is unknown if caplacizumab would provide more or less benefit for those with more severe forms of the disease. Patients should at least have a documented low ADAMTS13 level; however, this test is available only in specialized laboratories. Caplacizumab is contraindicated in patients who are hypersensitive to this drug. Caplacizumab should be used with caution in patients with impaired hepatic or renal functions, hemophilia, or coagulopathies. Patients with antidrug antibody formation may not be suitable for this treatment.
In clinical practice, platelet counts are measured to determine whether a patient is responding to treatment for aTTP, with steadily increasing platelet counts and a count of higher than 150 × 109/L as 1 of the first metrics in terms of goals of care. Biochemistry laboratory results, such as lactate dehydrogenase (LDH), renal function (e.g., creatinine), hemoglobin, red blood cell fragments, and reticulocyte count are also measured. Clinically, if the patient is presenting with neurological abnormalities, improvements in the neurological symptoms are evaluated. ADAMTS13 activity and decreasing titres of ADAMTS13 inhibitors are useful measures of response to treatment. This specialized assay is now used in practice as well as in clinical studies. Patients are usually in hospital for at least 5 to 7 days. During their hospitalization, their clinical response alongside the laboratory response are monitored daily. After the cessation of PE, monitoring is still required to assess for relapse, although monitoring is not standardized in its frequency. In the clinical trials, patients were typically monitored for up to 30 days following the last treatment.
Discontinuation of caplacizumab should be considered in cases of worsening symptoms, or in cases where unacceptable AEs are present, such as increased bleeding (particularly in the central nervous system and gastrointestinal tract), injection site issues, autoantibody formation, or thrombosis, or any other AE that would be worth considering for discontinuation of treatment with caplacizumab.
It would be appropriate to have specialists or health care professionals with experience treating patients with TTP to diagnose, treat, and monitor patients who may receive caplacizumab. The clinical experts agreed that the drug would be initiated in the hospital and continued in an outpatient setting, which is appropriate once the patient’s condition has clinically improved and there is no need to stay in the hospital after PE is finished and when PE can be done during an outpatient visit.
Clinical Evidence
Pivotal Studies and Protocol-Selected Studies
Description of Studies
One phase III, double-blind, randomized controlled trial (RCT) (HERCULES, N = 145) submitted by the sponsor is included in this systematic review. The objective of HERCULES was to evaluate the efficacy and safety of caplacizumab in patients with aTTP. The trial included adult patients (≥ 18 years of age) with a clinical diagnosis of aTTP that presented with both thrombocytopenia and microscopic evidence of red blood cell fragmentation. Patients were excluded if they had platelet counts greater than 100 × 109/L at screening, had suspected thrombotic microangiopathies that were not associated with aTTP (such as hemolytic uremic syndrome), or if they had congenital TTP. Patients who had clinically significant active bleeding or a high risk of bleeding or were receiving chronic treatment with anticoagulant therapy that could not be stopped safely were also excluded. Eligible patients were randomized to receive caplacizumab 10 mg or placebo, in addition to standard of care, which consisted of PEX and corticosteroid treatment and other immunosuppressives. Note that even though the clinical trial protocol specified the caplacizumab dose as 10 mg, to be delivered by withdrawing all of the reconstituted solution from the vial and administering the full amount, a dose-recovery study showed that the mean dose that can be withdrawn from a vial is 11 mg, which is indicated in the product monograph for caplacizumab.59 The double-blind treatment periods consisted of a daily PEX period and a 30-day post–daily PEX period. A treatment extension of 7 to 28 days with caplacizumab or placebo was allowed for patients with risk factors for relapse of the presenting TTP episode. During the double-blind treatment period of HERCULES, in the case of first exacerbation or relapse of the presenting TTP episode, patients would receive open-label caplacizumab together with daily PEX irrespective of what the initial treatment allocation was. The primary efficacy outcome of this study was time to platelet count response, which was defined as an initial platelet count of 10 × 109/L or higher with the subsequent stopping of daily PEX within 5 days. Other efficacy outcomes include prevention of recurrence of aTTP, prevention of refractory aTTP, prevention of major thromboembolic events, normalization of organ damage markers, and length of intensive care unit (ICU) or hospital stays related to TTP episodes. Harm outcomes associated with the use of caplacizumab were also examined.
The major limitations of HERCULES include potential biases on the study results due to an imbalance in patients’ baseline characteristics, uncertainty around the validity of using platelet count for treatment effect evaluation, substantial and disproportional missing data for some efficacy outcomes, and a lack of statistical testing for some of the secondary efficacy end points. Subgroup and sensitivity analyses were performed; however, the results should be interpreted with caution, given the small sample size. Long-term clinical benefits and harms could not be explored in HERCULES due to the trial’s short duration.
Efficacy Results
In HERCULES, the treatment effect of caplacizumab on survival, duration, and volume of PE, disease recurrence, refractory disease, organ damage, platelet response, neurological symptoms, cognitive change, and length of ICU and hospital stays related to aTTP episodes was examined.
Four TTP-related deaths were recorded during the overall study period; 1 patient from the caplacizumab group died during the drug-free follow-up period, and 3 patients from the placebo group died during the daily PE period. One death from the placebo group was considered possibly related to the study drug, and all other deaths were considered not related to any of the treatments.
During the overall treatment period, treatment with caplacizumab was related to a shorter duration of PE therapy compared with placebo (mean days on PE: 5.8, standard error [SE] = 0.5 for caplacizumab versus 9.4 days, SE = 0.8 for placebo). Treatment with caplacizumab was also associated with reduced total PE volume compared with placebo (21.3, SE = 1.6 litres versus 35.9, SE = 4.2 litres, respectively). According to the clinical experts consulted for this review, the between-group differences in the number of days on PE and the PE volume were considered clinically relevant.
During the overall study period, a statistically significantly lower percentage of patients in the caplacizumab group (9 patients, 12.7%) compared with the placebo group (28 patients, 38.4%) experienced recurrence of aTTP — either an exacerbation or a relapse. Exacerbations occurred in 3 patients (4.2%) treated with caplacizumab and 28 patients (38.4%) treated with placebo during the double-blind treatment period. During the follow-up period, relapses occurred in 6 patients (9.1%) treated with caplacizumab but in zero patients in the placebo group. The low recurrence of aTTP was attributed to the lower incidence of aTTP exacerbation in the caplacizumab group.
The median time to normalization of organ damage markers (e.g., LDH, cardiac troponin, serum creatinine) was 2.86 days (95% CI, 1.93 to 3.86) in the caplacizumab group and 3.36 days (95% CI, 1.88 to 7.71) in the placebo group, respectively. However, the between-group differences could not be considered statistically significant because the hierarchical statistical analysis plan failed to demonstrate statistical significance at a higher-order comparison.
During the overall treatment period, the number of patients experiencing major thromboembolic events was similar between the caplacizumab group (6 patients, 8.5%) and the placebo group (6 patients, 8.2%). The small number of events in the treatment groups makes it difficult to make conclusions.
During the double-blind treatment period, no patients in the caplacizumab group and 3 patients (4.2%) in the placebo group were considered to have refractory aTTP. The between-group difference in refractory aTTP was not statistically significant (P = 0.0572).
Time to platelet response was the primary efficacy end point in HERCULES. A statistically significantly shorter time to normalization of the platelet count was observed in the caplacizumab group (median = 2.69 days; 95% CI, 1.89 to 2.83) compared with the placebo group (median of 2.88 days; 95% CI, 2.68 to 3.56; P = 0.0099). An HR of 1.55 (95% CI, 1.10 to 2.20) also suggested that at any given time point, patients in the caplacizumab group were 1.55 times more likely to achieve a platelet count response compared with those in the placebo group. However, the difference was not considered clinically relevant, according to the clinical experts consulted for this review.
There were numerical improvements in neurological symptoms and cognitive function from baseline, as well as shorter ICU days and hospitalizations during the overall study period with caplacizumab compared with placebo. However, HERCULES was not designed to assess the effects of caplacizumab on these outcomes, and limitations in the statistical analyses and missing data preclude drawing conclusions on these.
A phase II, single-blind RCT (TITAN) provided supportive evidence on treatment with caplacizumab. The efficacy of caplacizumab compared with placebo was demonstrated based on confirmed platelet response, which was the primary outcome in this study. Patients treated with caplacizumab were more likely to reach a confirmed platelet response compared with placebo based on hazard ratio of 2.20 (95% CI, 1.28 to 3.78), which was statistically significant (P = 0.005).
Harms Results
During the overall study period, almost all patients reported AEs in HERCULES: 97.2% in the caplacizumab group and 97.3% in the placebo group. The majority of the AEs were of mild or moderate severity. The most common AEs reported in the caplacizumab group were epistaxis, headache, gingival bleeding, urticaria, pyrexia, fatigue, nausea, and TTP episodes. In the placebo group, TTP episodes, rash, and contusion were commonly reported. In the open-label caplacizumab therapy period, AEs were reported in 89.3% of patients. Catheter site hemorrhage, epistaxis, gingival bleeding, and gastrointestinal symptoms were commonly reported.
SAEs were reported in 28 patients (39.4%) in the caplacizumab group and 39 patients (53.4%) in the placebo group during the overall study period. TTP episodes were the most commonly reported SAEs, and the incidence of TTP episodes was higher in the placebo group (39.7%) than in the caplacizumab group (12.7%). During the open-label caplacizumab therapy, 7 patients (25%) reported SAEs.
|||||| ||| ||||||| ||||| ||||||| |||| |||||||| |||||| ||||||| |||| |||||||||||| ||| |||| |||||||| ||||||| ||||||| |||| ||||||| |||||||| ||| ||||| || ||||||||| ||| || |||| |||||| ||| |||||||||| |||||||||||| ||||||| ||||||| ||| |||||||
Three patients in the placebo group died during the daily PE treatment period. One patient in the caplacizumab group died in the follow-up period.
In terms of AEs of particular interest during the overall study period, the incidence of bleeding events was similar between treatment groups: 49 patients (69%) in the caplacizumab group and 49 patients (67.1%) in the placebo group. Hypersensitivity was experienced by 24 patients (33.8%) in the caplacizumab group and 22 patients (30.1%) in the placebo group. Antidrug antibodies were found in 2 patients (2.8%) in the caplacizumab group and 1 patient (1.4%) in the placebo group.
|||||| ||| |||||||||| ||||||||| |||| ||||||||||||| || |||||||| |||||||| |||||||| ||||||| || |||||||| ||||||| |||||||| |||||||||||||||| |||| ||||||||| |||||||||| |||| |||| |||||||| || ||| ||||||| |||||||
Results from the TITAN study indicated that almost every patient experienced at least 1 AE, and more than half of them experienced at least 1 serious adverse event (SAE). The most common AEs and SAEs were TTP episodes. The most common AEs following TTP in the caplacizumab group were headache, epistaxis, and nausea, which was consistent with the results from HERCULES.
Table 38: Summary of Key Results From Pivotal and Protocol-Selected Studies
Key results | HERCULES | |
|---|---|---|
Caplacizumab n = 72 | Placebo n = 73 | |
Efficacy outcomes | ||
Death, n (%), overall study period | 1 (1.9) occurred during follow-up period | 3 (4.1) occurred during daily PE period |
Reduction in use of PE, overall treatment period | ||
Duration of PE, days, mean (SE) | 5.8 (0.5) | 9.4 (0.8) |
Total volume of PE, L, mean (SE) | 21.3 (1.6) | 35.9 (4.2) |
Recurrence of aTTP, overall study period | 9 (12.7) | 28 (38.4) |
Exacerbations, n (%) | 3 (4.2) | 28 (38.4) |
Relapses, n (%) | 6 (9.1) | 0 |
Number of patients with ≥ 1 treatment-emergent major thromboembolic event, n (%), overall study period | 6 (8.5) | 6 (8.2) |
Time to normalization of all 3 organ damage markers, days, median (95% CI), P value vs. placeboa | 2.86 (1.93 to 3.86) | 3.36 (1.88 to 7.71) |
Time to normalization of LDH, days, median (95% CI) | |||| ||||| || ||||| | |||| ||||| || ||||| |
Time to normalization of cTnI, days, median (95% CI) | |||| ||||| || ||||| | |||| ||||| || ||||| |
Time to normalization of creatinine, days, median (95% CI) | |||| ||||| || |||||| | |||| ||||| || |||||| |
Number of patients with refractory aTTP, n (%), P value vs. placebo,b DB study treatment period | 0 P = 0.0572 | 3 (4.2) |
Time to platelet count response, days, median (95% CI), P value vs. placeboa | 2.69 (1.89 to 2.83) P = 0.0099 | 2.88 (2.68 to 3.56) |
Days in ICU related to aTTP, mean (SE) | ||
Daily PE period | ||| |||||| | ||| |||||| |
Overall treatment period, including open-label period | 3.4 (0.40) | 9.7 (2.12) |
Overall treatment period, including follow-up period | ||| |||||| | |||| |||||| |
Days in hospital related to aTTP, mean (SE) | ||
Daily PE period | ||| |||||| | ||| |||||| |
Overall treatment period, including open-label period | 9.9 (0.70) | 14.4 (1.22) |
Overall treatment period, including follow-up period | |||| |||||| | |||| |||||| |
Harm outcomes | ||
Patients with ≥ 1 AE, n (%) | 69 (97.2) | 71 (97.3) |
Patients with ≥ 1 SAE, n (%) | 28 (39.4) | 39 (53.4) |
Patients with ≥ 1 WDAE, n (%) | 5 (7.0) | 9 (12.3) |
Notable harms, n (%) | ||
Bleeding event | 49 (69.0) | 49 (67.1) |
Hypersensitivity | || |||||| | || |||||| |
ADA positive | 2 (2.8) | 1 (1.4) |
ADA = antidrug antibody; AE = adverse event; aTTP = acquired thrombotic thrombocytopenic purpura; CI = confidence interval; cTnI = cardiac troponin I; DB = double blind; LDH = lactate dehydrogenase; PE = plasma exchange; SAE = serious adverse event; SE = standard error; TTP = thrombotic thrombocytopenic purpura; WDAE = withdrawal due to adverse event.
Note:
Exacerbation: Defined as a recurrent thrombocytopenia after initial recovery of platelet count.
Relapse: Defined as recurrent thrombocytopenia after initial recovery of platelet count requiring reinitiation of daily PE and after discontinuation of caplacizumab.
Refractory: Defined as the absence of platelet count doubling after 4 days of standard treatment and LDH > upper limit of normal.
Platelet count response: Defined as initial platelet count ≥ 150 × 109/L with the subsequent stopping of daily PE within 5 days of treatment.
aCalculated using stratified log-rank test.
bCochran-Mantel-Haenszel test comparing caplacizumab group with placebo, adjusted for Glasgow Coma Scale at randomization.
Source: Clinical Study Report for HERCULES.60
Critical Appraisal
In HERCULES, appropriate methods were used to randomize patients to treatments and conceal treatment allocation. In general, patient characteristics appear to be balanced at baseline between groups, although some imbalance of these characteristics was also observed. Compared with the placebo group, patients in the caplacizumab group had fewer previous TTP episodes, more severe conditions, higher cardiac troponin I levels, and higher LDH levels at baseline. This imbalance in baseline characteristics may have an impact on data interpretation and could bias the results.
The treatment effects of the study drug were assessed at various periods, such as the double-blind daily PE therapy period, the 30-day post–daily PE period, the extension treatment period, and the open-label caplacizumab therapy period. Some patients who were initially assigned to the placebo group had to switch to caplacizumab therapy due to disease recurrence. This would complicate the data analysis and interpretation of the results for some of the efficacy outcomes, especially longer-term outcomes, for example, the risk of recurrence of aTTP in the future or days on PE. In the analysis of the composite end point comprising TTP-related death, recurrence of aTTP, and occurrence of major thromboembolic events, switching to open-label caplacizumab therapy was not an issue for data analysis, as only events that had occurred before a switch to open-label caplacizumab were evaluated. For time to platelet count response, the primary efficacy outcome in HERCULES, the switch to open-label caplacizumab for those patients who experienced a recurrence of aTTP during the study did not affect the primary efficacy analysis, as a recurrence can occur only after platelet count response, according to the definition for this outcome (i.e., initial platelet count ≥ 150 × 109/L with the subsequent stopping of daily PE within 5 days).
A hierarchical testing procedure was used to account for multiple comparisons among the primary end point and key secondary end points. The hierarchical sequence in the included studies was prespecified and included clinically outcomes that were commonly accepted in thrombocytopenic disorders. Outcomes outside of the testing hierarchy, such as neurological assessment, cognitive assessments, and length of ICU or hospital stays need to be interpreted with caution due to the possible inflated type I error. In HERCULES, efficacy outcomes, except for the primary and key secondary outcomes, were descriptively summarized using the number of observations, means, and SEs. Formal statistical tests were not performed for these outcomes.
The study indicated that efficacy analyses were performed on an intention-to-treat (ITT) population. However, a violation of ITT principles was observed in the analyses of several efficacy outcomes. ||| |||||||| ||| ||| ||||||| || |||||||||| ||||| |||||||| |||||||||||| ||| || |||| || ||||||||| || ||||||| |||||||||| |||||| ||| | |||| |||||||| |||| ||| |||||||. In addition, the proportion of missing data was substantial (> 20%), as was the differential between caplacizumab and placebo for some of the efficacy outcomes, such as time to normalization of organ damage markers and cognitive assessments. Therefore, bias may have been introduced into the results. For the outcomes of platelet count response or days on PE therapy, the impact of missing data would be minimal on the study results because all patients tended to complete the treatment with PE. Missing data were not imputed for most of the outcome measures and no documented procedure was used to account for missing data, except for refractory aTTP, where a multiple imputation approach was adopted. The Clinical Study Report for HERCULES stated that all efficacy analyses were conducted on the ITT population; however, according to the data provided, many of the results were assessed using a subset of the randomized sample, so it seems that a modified ITT (mITT) population was used. Note that the ITT population included 145 patients, while the mITT population included 144 patients.
According to the clinical experts involved in the review, the inclusion and exclusion criteria for the study were reasonable and the included patient population was generally consistent with clinical practice. Misdiagnosis is common for aTTP, as other conditions may mimic aTTP. Although severe ADAMTS13 deficiency (activity < 10%) typically confirms a diagnosis of aTTP, activity less than 10% is not 100% sensitive or specific for aTTP, and patients with aTTP who have received multiple PE containing functional ADAMTS13 may have ADAMTS13 activity of 10% to 20%. In HERCULES, 10% to 18% of study participants had ADAMTS13 activity levels of 10% or higher. All patients received 1 PE before randomization; this may have increased their ADAMTS13 levels at baseline. Four patients (5.6%) in the caplacizumab group and 3 patients (4.1%) in the placebo group who were initially diagnosed with aTTP had an alternative diagnosis later in the trial.61 The misdiagnosis rate was low and is less likely to have had a significant impact on the generalizability of the study results. Due to the relatively short duration (2 to 6 months) of the included study, some important clinical outcomes could not be sufficiently examined, such as survival, TTP relapses, and safety in the long run.
Other Relevant Evidence
Description of Studies
The TITAN study was included to supplement the review of caplacizumab in terms of providing additional safety and efficacy data. The TITAN study was a phase II, multicentre, single-blind, parallel design, placebo-controlled RCT conducted in adult patients who were symptomatic and experiencing acute episodes of aTTP that required treatment with PE. A total of 75 patients were included in the TITAN study: 36 received caplacizumab and 39 received placebo.
Efficacy Results
The efficacy of caplacizumab compared with placebo was demonstrated based on confirmed platelet response, which was the primary outcome in the TITAN study. Patients treated with caplacizumab were more likely to reach a confirmed platelet response compared with placebo, based on a hazard ratio of 2.20 (95% CI, 1.28 to 3.78), which was statistically significant (P = 0.005).
Harms Results
In terms of safety, almost every patient experienced at least 1 AE, and more than half of all patients experienced at least 1 SAE. The most common AE and SAE was TTP. The most common AEs following TTP (37% to 38% in both groups) in the caplacizumab and placebo groups, respectively, were headache (34.3% and 27.0%), epistaxis (31.3% and 10.8%), and nausea (28.6% and 29.7%). Of note, reports of serious TTP and bleeding events were more common among patients treated with caplacizumab compared with placebo, with TTP reported by ||||| ||| ||||| of patients treated with caplacizumab and placebo, respectively, and bleeding events reported by 54.3% and 37.8% of patients.
Critical Appraisal
Overall, the TITAN study demonstrated efficacy and highlighted safety signals that should be considered with the use of caplacizumab; however, the interpretation of the outcome data are limited due to concerns with the study’s internal validity (more specifically, in terms of the single-blind study design, the potentially misleading choice of primary efficacy outcome, and the lack of adjustment for multiplicity and statistical testing), as well as its external validity in terms of generalizability to the Canadian context.
Conclusions
One phase III, double-blind, placebo-controlled, randomized trial provided evidence on the efficacy and safety of caplacizumab in adult patients with aTTP. Patients who received caplacizumab in addition to standard therapy (PE and immunosuppressants) showed benefits in reducing the duration and volume for PE and reducing the frequency of aTTP exacerbations when comparing to placebo. There were no data on the impact of caplacizumab on subsequent aTTP recurrence beyond the trial observation period. Although only 1 of the 4 deaths in the trial occurred in the caplacizumab group and was considered by the blinded assessors as unrelated to treatment, the study was not designed to specifically assess survival. Therefore, it remains uncertain what the impact of caplacizumab is on survival and requires additional research. Caplacizumab improved platelet counts but it is unclear what the clinical relevance of this finding is. Almost all study participants reported treatment-emergent adverse events (TEAEs). A higher frequency of bleeding events occurred in the caplacizumab group, while patients who received placebo reported more TTP episodes. Most of the reported AEs were mild to moderate in intensity. A phase II single-blind RCT provided evidence to support the effect of caplacizumab on platelet response. The safety results in this trial were consistent with those in the phase III trial.
Conclusions regarding the long-term efficacy and safety of caplacizumab in patients with aTTP are lacking due to the short duration of treatment; in addition, the long-term results could be complicated by the use of open-label caplacizumab in some patients.
Appendix 3: Study Flow
Note this appendix has not been copy-edited.
Table 39: Included and Excluded Studies
Study name | Reference(s) | Evidence type | Report type | Location | Reason for exclusion |
|---|---|---|---|---|---|
Post-HERCULES | Post-HERCULES Clinical Study Report (2021)14 Scully et al. (2022)15 | Clinical trial | Clinical study report, publication | Main report, Systematic Review section | NA |
HERCULES | HERCULES Clinical Study Report (2018)21 Scully et al. (2019)23 Knoebl et al. (2020)22 | Clinical trial | Clinical study report, publications | Main report, Other Relevant Evidence section; Appendix 2 | Evaluated in the initial review of caplacizumab |
TITAN | TITAN Clinical Study Report (2015) Peyvandi et al. (2016)25 Peyvandi et al. (2017)26 | Clinical trial | Clinical study report, publications | Main report, Other Relevant Evidence section; Appendix 2 | Evaluated in the initial review of caplacizumab |
NA | Miyakawa et al. (2021)35 | Clinical trial | Abstract | Excluded from main report due to noncomparative nature | |
NA | CADTH Clinical Review Report for initial submission of caplacizumab13 | HTA assessment | Publication | Initial CADTH review of caplacizumab | |
NA | Peyvandi et al. (2021)16 | Post hoc analysis | Publication | Main report, Other Relevant Evidence section | NA |
NA | Pavenski et al. (2019)36 | Post hoc analysis | Poster | No full text available | |
NA | Scully et al. (2021)37 | Post hoc analysis | Poster | No full text available | |
NA | Coppo et al. (2019)38 | Post hoc analysis | Poster | No full text available | |
NA | Coppo et al. (2020)39 | Post hoc analysis | Poster | No full text available | |
NA | Scully et al. (2020)40 | Post hoc analysis | Abstract | No full text available | |
NA | Coppo et al. (2021)18 | RWE | Publication | Main report, Other Relevant Evidence section | NA |
NA | Cemka and Sanofi (2021)17 Vataire et al. (2022)19 | RWE | Study Report, abstract | Main report, Other Relevant Evidence section | NA |
NA | Dutt et al. (2021)20 | RWE | Publication | Main report, Other Relevant Evidence section | NA |
NA | Volker et al. (2020)41 Volker et al. (2020)43 Kaufeld et al. (2021)42 | RWE | Publications | Study design (no comparator) | |
NA | Volker et al. (2021)47 | RWE | Abstract | No full text available | |
NA | Maanaoui et al. (2020)45 | RWE | Abstract | Study design (no comparator); no full text available | |
NA | Jimenez et al. (2020)44 | RWE | Abstract | No full text available | |
NA | Vataire et al. (2022)46 | RWE | Abstract | No full text available | |
NA | Kuhne et al. (2022)49 | RWE | Publication | Study design (no comparator) | |
NA | Logothetis et al. (2021)48 | RWE | Publication | Study design (no comparator) | |
NA | Sponsor’s resubmission1 | Sponsor’s interview with Canadian clinicians | Unpublished document | Study design (no intervention) | |
NA | Sponsor’s resubmission1 | Sponsor’s environmental scan of HTA reviews | Unpublished document | Study design (no intervention) |
HTA = health technology assessment; NA = not applicable; RWE = real-world evidence
Appendix 4: Detailed Outcome Data
Note this appendix has not been copy-edited.
Summary of Outcome Data From All Studies
For reference only, a summary of efficacy outcome data from all studies described in this report, including those in Appendix 4, is provided in Table 40.
Table 40: Summary of Key Outcome Data From All Studies
Trial | aTTP-related death, % | aTTP exacerbation, (%) | aTTP relapse, (%) | aTTP recurrence (%) | Refractory aTTP, (%) | MTEs, (%) | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
Capla | SOC | Capla | SOC | Capla | SOC | Capla | SOC | Capla | SOC | Capla | SOC | |
Clinical trials | ||||||||||||
1.4 | 4.1 | 4.2 | 38.4 | 9.1 | 0 | 11.0 | 38.4 | 0 | 4.2 | 8.3 | 8.2 | |
0 | 3.4 | NA | NA | 8.2 | 27.6 | 8.2 | 27.6 | NR | NR | 0 | 10.3 | |
0 | 5.1 | 8.3 | 28.2 | 30.6 | 7.7 | 38.9 | 35.9 | 0 | 12.8 | 5.6 | 20.5 | |
Miyakawa et al. (2021)35 | 6.7 | NA | NR | NA | NR | NA | 6.7 | NA | 0 | NA | 0 | NA |
Post hoc analyses | ||||||||||||
Peyvandi et al. (2021)16 | 0.9 | 4.5 | 5.6 | 34.8 | 13.0 | 0 | 17.6 | 34.8 | 0 | 7.1 | 7.4 | 12.5 |
RWE | ||||||||||||
Coppo et al. (2021)18 | 1.1 | 6.7 | 3.4 | 44 | NR | NR | NR | NR | 1.1 | 18 | 12 | 11.1 |
||| | ||| | ||| | |||| | |||| | |||| | |||| | |||| | ||| | |||| | |||| | |||| | |
Dutt et al. (2021)20 | 6 | 0 | 2 | NR | 4 | NR | 6 | NR | 3.5 | NR | 5 | 5 |
1.7 | NA | 3.3 | NA | 3.3 | NA | 6.7 | NA | 31.7 | NA | NR | NA | |
Volker et al. (2021)47 | 2.0 | 4.9 | 14 | 39 | NR | NR | NR | NR | NR | NR | NR | NR |
Maanaoui et al. (2020)45 | 0 | NA | 14.6 | NA | NR | NA | NR | NA | 0 | NA | NR | NA |
Jimenez et al. (2020)44 | 0 | 11.1 | 0 | 33.3 | 11.1 | 11.1 | 11.1 | 44.4 | 0 | 44.4 | NR | NR |
Vataire et al. (2022)46 | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR |
Kuhne et al. (2022)49 | 0 | NA | 12 | NA | 8 | NA | 20 | NA | NR | NA | NR | NA |
Logothetis et al. (2021)48 | 0 | NA | 30 | NA | 10 | NA | 40 | NA | 30 | NA | 0 | NA |
ADA = antidrug antibody; AE = adverse event; CI = confidence interval; CMH = Cochran-Mantel-Haenszel; cTnI = cardiac troponin I; DB = double blind; GCS = Glasgow Coma Scale; ICU = intensive care unit; ITT = intention to treat; LDH = lactate dehydrogenase; NA = not applicable; NR = not reported; PE = plasma exchange; SAE = serious adverse event; SB = single blind; SD = standard deviation; SE = standard error; SOC = standard of care; ULN = upper limit of normal; WDAE = withdrawal due to adverse event.
Source: All studies cited in table.
Table 41: Summary of Key Outcome Data From All Studies (Continued)
Trial | Plt Resp, median (95% CI or SD) | Organ damage, median (95% CI) | PE days, mean (SD or SE or range) | PE L, mean (SD or SE) | Hosp days, mean (SE) | |||||
|---|---|---|---|---|---|---|---|---|---|---|
Capla | SOC | Capla | SOC | Capla | SOC | Capla | SOC | Capla | SOC | |
Clinical trials | ||||||||||
2.69 (1.89 to 2.83) | 2.88 (2.68 to3.56) | 2.86 (1.93 to 3.86) | 3.36 (1.88 to 7.71) | 5.8 (0.5) | 9.4 (0.8) | 21.3 (1.6) | 35.9 (4.2) | 9.9 (0.7) | 14.4 (1.22) | |
7.0 (3 to 24) | 10.0 (5 to 15) | NR | NR | 6.6 (4.7) | 5.5 (1.3) | NR | NR | 9.1 (5.8) | 10.0 (1.0) | |
3.0 (2.7 to 3.9)d 2.4 (1.9 to 3.0)e | 4.9 (3.2 to 6.6)d 4.3 (2.9 to 5.7)e | NR | NR | 6.7 (3.69) | 8.4 (6.74) | 22.5 (15.9) | 28.4 (21.3) | NR | NR | |
Miyakawa et al. (2021)35 | 2.79 (1.76 to 3.59) | NA | 2.65 (0.98 to 4.98) | NA | 5.0 (3 to 11) | NA | 24.6 (13.4 to 50.0) | NA | NR | NA |
Post hoc analyses | ||||||||||
Peyvandi et al. (2021)16 | 2.75 (2.65 to 2.87) | 3.51 (2.88 to 3.86) | NR | NR | 5.0 (1 to 35) | 7.5 (2 to 46) | NR | NR | NR | NR |
RWE | ||||||||||
Coppo et al. (2021)18 | 5 (4 to 6) | 12 (6 to 17) | NR | NR | 5 (4 to 7) | 10 (6 to 16) | 24.2 (18.3 to 30.2) | 44.4 (26.3 to 74.3) | 13 (9 to 19) | 22 (15 to 30) |
|||| | |||| | |||| | |||| | ||| ||||| | |||| |||||| | |||| |||||| | |||| |||||| | |||| | |||| | |
Dutt et al. (2021)20 | 4 (3 to 8) | 6 (4 to 10) | NR | NR | 7 (5 to 14) | 9 (8 to 16) | NR | NR | 12 (8 to 24) | 14 (9 to 17) |
3 (1 to 3) | NA | NR | NA | 4 (0 to 22) | NA | NR | NA | 18 (5 to 29) | NA | |
Volker et al. (2021)47 | NR | NR | NR | NR | 7.2 | 10.2 | NR | NR | 14.0 | 18.1 |
Maanaoui et al. (2020)45 | 5 (4 to 6) | NA | NR | NA | 6 (3 to 16) | NA | NR | NR | NR | NA |
Jimenez et al. (2020)44 | 4 (3 to 4) | 6 (5 to 14) | NR | NR | 10 (9 to 11) | 19 (16 to 23) | NR | NR | 12 | 26 |
Vataire et al. (2022)46 | NR | NR | NR | NR | 8.1 (7.9) | 11.5 (9.9) | NR | NR | 18.8 (13.2) | 26.2 (16.9) |
Kuhne et al. (2022)49 | 3 (2 to 7) | NA | NR | NA | NR | NA | NR | NA | NR | NA |
Logothetis et al. (2021)48 | 5 (3 to 10) | NA | 3 (0 to 146) | NA | 12 (1 to 33) | NA | NR | NA | 10 (4 to 37) | NA |
ADA = antidrug antibody; AE = adverse event; CI = confidence interval; CMH = Cochran-Mantel-Haenszel; cTnI = cardiac troponin I; DB = double blind; GCS = Glasgow Coma Scale; ICU = intensive care unit; ITT = intention to treat; LDH = lactate dehydrogenase; NA = not applicable; NR = not reported; PE = plasma exchange; SAE = serious adverse event; SB = single blind; SD = standard deviation; SE = standard error; SOC = standard of care; ULN = upper limit of normal; WDAE = withdrawal due to adverse event.
Source: All studies cited in table.
Other Clinical Trial Evidence
Miyakawa et al. (2021): The Efficacy and Safety of Caplacizumab in Japanese Patients with Immune-Mediated Thrombotic Thrombocytopenic Purpura (iTTP): An Open-Label, Phase II/III Study (Abstract)
One additional phase II/III, OL, single-arm, multicentre trial conducted in Japanese patients with aTTP (NCT04074187)35 was summarized to provide additional supportive evidence regarding the efficacy and safety of caplacizumab among patients in a different region and to provide additional supportive evidence for the TITAN and HERCULES trials.
Methods
A phase II/III, OL, single-arm, multicentre trial was conducted in Japan to evaluate the efficacy and safety of caplacizumab in adult patients with aTTP (N = 21). Patients received OL caplacizumab plus PE and corticosteroids with or without rituximab. The primary outcome was the proportion of patients with recurrence of aTTP. The study started in October 2019 and completed in May 2021 and was funded by the sponsor.
Populations
Japanese adults aged 18 years or older with a clinical diagnosis of aTTP (initial or recurrent) were eligible if they required PE but had received no more than 1 prior PE treatment. Diagnostic criteria for aTTP included thrombocytopenia (platelet count less than 105/µL), microangiopathic hemolytic anemia as evidenced by red blood cell fragmentation, and elevated LDH. Exclusion criteria included platelet counts of 105/µL or above, serum creatinine > 2.3 mg/dL in case platelet counts were above 3 × 104/µL, known other causes of thrombocytopenia, congenital TTP, clinically significant active bleeding or high risk of bleeding, malignant arterial hypertension, known chronic treatment with anticoagulant treatment that could not be safely stopped, previous participation in a caplacizumab study, and clinical condition other than that associated with aTTP with life expectancy less than 6 months.
In the modified ITT population, the median age was 59 years (range, 22 to 86 years), 16 patients (76%) presented with an initial aTTP episode, the median platelet count at baseline was 21.5 × 109/L (range, 8 × 109/L to 78 × 109/L), and 10 patients (48%) received rituximab. All patients in the PP population had ADAMTS13 activity less than 10%.
Interventions
Patients received caplacizumab plus PE and corticosteroids (mandatory) with or without rituximab during daily PE (IV bolus first dose, followed by SC injection) and for a minimum of 30 days after discontinuation of PE (SC injection). Treatment extension was permitted for a maximum of 8 weeks in patients with persistent ADAMTS13 deficiency.
Outcomes
The primary outcome was the proportion of patients with recurrence of aTTP during the overall study period. Secondary outcomes (assessed in the PP population and for key secondary outcomes, the mITT population) included number of aTTP recurrences, proportion of patients with aTTP-related events (e.g., aTTP-related mortality, aTTP recurrence, or at least 1 major thromboembolic event), time to platelet count response (defined as platelet count of 150 × 109 or greater with subsequent stop of daily PE within 5 days), proportion of patients with platelet counts of 1.5 × 105/µL or greater, refractory aTTP, time to normalization of organ damage markers (LDH, cardiac troponin I, and serum creatinine), time to PE cessation, duration and volume of PE, duration of ICU stay and hospitalization, and change from baseline in Standardised Mini-Mental State Examination total score. The follow-up period was 4 weeks after discontinuation of caplacizumab.
Statistical Analysis
All analyses were descriptive only. The PP population consisted of patients who completed treatment and follow-up per-protocol or had a recurrence of aTTP. The mITT and safety populations consisted of patients who received at least 1 dose of caplacizumab.
Patient Disposition
A total of 21 patients were enrolled and treated with caplacizumab. Six patients (29%) discontinued caplacizumab (AEs, n = 2, 10%; physician decision, n = 4, 19%) and 15 patients with included in the PP population.
Exposure to Study Treatments
The median duration of caplacizumab exposure during the overall treatment period was 35 days (range, 7 to 69 days).
Efficacy
Refer to Table 42 for detailed efficacy data. During the overall study period, 1 patient (7%) in the PP population experienced aTTP recurrence. No patients in the PP population experienced aTTP-related death, thromboembolic events, or refractory aTTP. The median time to platelet count response was 2.79 days (95% CI, 1.76 to 3.59 days) and the median time to normalization of all 3 organ damage markers was 2.65 days (95% CI, 0.98 to 4.98 days). The median duration of PE was 5.0 days (range, 3 to 11 days) and median total volume of PE was 24.6 L (range, 13.4 to 50.0 L). Information on duration of hospitalization and ICU stay and change in Standardised Mini-Mental State Examination total scores from baseline was not provided.
Efficacy outcomes | PP population (n=15) |
|---|---|
Primary endpoint: Recurrence of iTTPa, n (%) | 1 (7) |
Composite endpointb: Proportion of patients with ≥1 of the below events, n (%) | 1 (7) |
TTP-related death | 0 |
Recurrence of iTTP, n (%) | 1 (7) |
≥1 treatment-emergent TE | 0 |
Refractory diseasec, n (%) | 0 |
Time to platelet count responsed | |
Median (95% CI), days | 2.79 (1.76-3.59) |
Time to normalization of all 3 organ damage markers (LDH, cTnI, serum creatinine) | |
Median (95% CI), days | 2.65 (0.98-4.98) |
Number of days of TPEb | |
Median (range), days | 5.0 (3-11) |
Total volume of TPEb | |
Median (range), L | 24.6 (13.4-50.0) |
CI = confidence interval; cTnI = cardiac troponin I; iTTP = immune-mediated thrombotic thrombocytopenic purpura; LDH = lactate dehydrogenase; PP = per protocol; TE = thrombolic event; TPE = therapeutic plasma exchange.
Note: This table is reproduced from original source and may not follow CADTH style.
aDuring overall study period.
bDuring overall treatment period.
cDuring the 5 days from the first TPE.
dPlatelet count ≥ 150 × 109 with subsequent stop of daily TPE within 5 days.
Source: Miyakawa et al. (2021).35 Vol 138/Suppl 13, Miyakawa Y, Imada K, Ichikawa S, et al., The efficacy and safety of caplacizumab in Japanese patients with immune-mediated thrombotic thrombocytopenic purpura (iTTP): An open-label, phase 2/3 study, Page 1009, Copyright 2021, with permission from The American Society of Hematology
Harms
Refer to Table 43 for detailed harms data. All patients in the study (n = 21, 100%) experienced at least 1 AE; common AEs were constipation (n = 9, 43%) and insomnia (n = 6, 29%). 5 patients (24%) experienced at least 1 SAE. 5 patients (24%) experienced AEs leading to caplacizumab interruption and 2 patients (10%) experienced withdrawal due to adverse events. No deaths occurred during the study period. Among notable harms identified in this review protocol, bleeding events occurred in 7 patients (33%), thromboembolic events occurred in 2 patients (10%), and hypersensitivity reactions occurred in 12 patients (57%). No information on ADAs was provided.
Safety outcomes | Safety population (n=21) |
|---|---|
≥1 TEAE | 21 (100) |
≥1 TEAE reported in >15% of patients | |
Constipation | 9 (43) |
Insomnia | 6 (29) |
Allergic transfusion reaction | 4 (19) |
Hypokalemia | 4 (19) |
≥1 TEAE considered treatment related | 12 (57) |
≥1 serious TEAE | 5 (24) |
≥1 serious TEAE considered treatment related | 1 (5) |
≥1 TEAE leading to death | 0 |
≥1 TEAE leading to caplacizumab interruption | 5 (24) |
≥1 TEAE leading to caplacizumab withdrawal | 2 (10) |
1 or more bleeding eventa | 7 (33) |
Epistaxis | 2 (10) |
GI hemorrhage | 2 (10) |
Pulmonary alveolar hemorrhage | 1 (5) |
Contusion | 1 (5) |
Wound hemorrhage | 1 (5) |
Hemorrhage subcutaneous | 1 (5) |
Purpura | 1 (5) |
Injection site hemorrhage | 1 (5) |
≥1 thromboembolic eventb | 2 (10) |
≥1 hypersensitivity reactionb | 12 (57) |
≥1 hypersensitivity reaction considered treatment relatedb | 1 (5) |
GI = gastrointestinal; SMQ = standard MedDRA queries; TEAE = treatment-emergent adverse event; TTP = thrombotic thrombocytopenic purpura.
Note: This table is reproduced from original source and may not follow CADTH style.
aBased on SMQ excluding TTP.
bBased on SMQ.
Source: Miyakawa et al. (2021).35 Vol 138/Suppl 13, Miyakawa Y, Imada K, Ichikawa S, et al., The efficacy and safety of caplacizumab in Japanese patients with immune-mediated thrombotic thrombocytopenic purpura (iTTP): An open-label, phase 2/3 study, Page 1009, Copyright 2021, with permission from The American Society of Hematology.
Critical Appraisal
This study could not be critically appraised because it was described in limited detail only in a conference abstract. Notable design limitations of the study were its small sample size, noncomparative design, and short follow-up period (4 weeks post caplacizumab discontinuation).
Post Hoc Analyses of Clinical Trial Data
Pavenski et al. (2019): Post-Hoc Subgroup Analysis of HERCULES Data by Initial Immunosuppressive Regimen (Poster)
Pavenski et al. (2019)36 conducted a subgroup analysis of outcomes in the HERCULES study by initial immunosuppressive regimen (corticosteroids only versus corticosteroids plus rituximab). The analysis was reported in a poster.
Among the 145 randomized patients in the HERCULES study, 112 (77.2%) patients received only corticosteroids as initial immunosuppressive therapy, while 24 (16.6%) patients received corticosteroids and rituximab (initiated within the first 3 days of the study). The remaining patients received another form of immunosuppressive therapy.
The baseline characteristics of patients in HERCULES according to baseline immunosuppressive regimen are shown in Table 44.
Table 44: Baseline Characteristics for Patients in the HERCULES Study (Placebo and Caplacizumab Arms) According to Initial Immunosuppressive Regimen
Characteristic | Cortcosteroids only (n=112) | Corticosteroids + rituximab (n=24) |
|---|---|---|
Age, mean (SD) | 46.6 (13.8) | 43.8 (14.0) |
Female, n (%) | 74 (66.1) | 18 (75.0) |
Previous TTP episodes, n (%) | ||
Initial | 67 (59.8) | 13 (54.2) |
Recurrent | 45 (40.2) | 11 (45.8) |
ADAMTS13a | ||
<10% | 97 (86.6) | 23 (95.8) |
≥10% | 15 (13.4) | 1 (4.2) |
Platelet counts (×109/L), mean (SD) | 35.6 (28.0) | 31.6 (28.4) |
LDH (U/L), mean (SD) | 566 (395) | 604 (689) |
>ULN, n (%) | 92 (89.3) | 19 (82.6) |
Cardiac Troponin I (µg/L), range | 0.077 (0.01; 76.0) | 0.096 (0.01; 4.44) |
>ULN, n (%) | 56 (54.4) | 13 (56.5) |
Serum creatinine (µmol/L), mean (SD) | 100 (87) | 93.8 (45.3) |
>ULN, n (%) | 24 (23.3) | 5 (21.7) |
ADAMTS13 = a disintigren and metalloproteinase with a thrombospondin type 1 motif, member 13; LDH = lactate dehydrogenase; SD = standard deviation; TPE = therapeutic plasma exchange; TTP = thrombotic thrombocytopenic purpura; ULN = upper limit of normal.
Note: This table is reproduced from original source and may not follow CADTH style.
aOne TPE was required for inclusion in the HERCULES trial.
Source: Pavenski et al. (2019).36
Additional interventions used for immunosuppressive therapy intensification in patients in HERCULES according to baseline immunosuppressive regimen are shown in Table 45.
Table 45: Additional Therapies Used for Immunosuppressive Therapy Intensification in Participants Receiving Corticosteroids ± Rituximab in the HERCULES Study
Therapy | Corticosteroids only (n = 112) | Corticosteroids + rituximab (n = 24) | ||
|---|---|---|---|---|
Caplacizumab (n = 58) | Placebo (n = 54) | Caplacizumab (n = 8) | Placebo (n = 16) | |
Any intensification, n (%) | 19 (26.4) | 19 (26.0) | 3 (4.2) | 0 |
Splenectomy | 1 (1.4) | 1 (1.4) | 0 | 0 |
Bortezomib | 1 (1.4) | 0 | 1 (1.4) | 0 |
Hydroxychloroquine | 1 (1.4) | 0 | 0 | 0 |
Mycophenolate Mofetil | 1 (1.4) | 0 | 3 (4.2) | 0 |
Plasma | 0 | 1 (1.4) | 0 | 0 |
Rituximab | 18 (25.0) | 19 (26.0) | 0 | 0 |
Source: Pavenski et al. (2019).36
Efficacy outcomes in the HERCULES study according to baseline immunosuppressive regimen are summarized in Table 46. Analysis of the composite end point of aTTP-related death, exacerbation of aTTP, or major thromboembolic events numerically favoured caplacizumab in both subgroups. Analysis of aTTP recurrence in the overall study period also numerically favoured caplacizumab in both subgroups.
Table 46: Efficacy Outcomes for Patients Treated With Initial Corticosteroids ± Rituximab in the HERCULES Study (Placebo and Caplacizumab Arms)
Outcome | Cortcosteroids only (n=112) | Corticosteroids + rituximab (n=24) | ||
|---|---|---|---|---|
Caplacizumab (n=58) | Placebo (n=54) | Caplacizumab (n=8) | Placebo (n=16) | |
Composite endpointa, n (%) | 7 (12.1) | 26 (48.1) | 1 (12.5) | 9 (56.3) |
TTP-related death, n (%) | 0 | 2 (3.7) | 0 | 0 |
Exacerbation, n (%) | 3 (5.2) | 20 (37.0) | 0 | 8 (50.0) |
Major thromboembolic event, n (%) | 4 (6.9) | 5 (9.3) | 1 (12.5) | 1 (6.3) |
Overall recurrence during the study (exacerbation or relapse), n (%) | 7 (12.1) | 20 (37.0) | 1 (12.5) | 8 (50.0) |
Refractory TTP, n (%) | 0 | 1 (1.9) | 0 | 1 (6.3) |
MTE = major thromboembolic event.
Note: This table is reproduced from original source and may not follow CADTH style.
aComposite end point consists of ≥ 1 of TTP-related death, recurrence (exacerbation), or major thromboembolic event during the blinded treatment period.
Source: Pavenski et al. (2019).36
Safety outcomes in the HERCULES study according to baseline immunosuppressive regimen are summarized in Table 47. The frequencies of AEs and SAEs were similar or higher in patients receiving placebo compared to those receiving caplacizumab in both subgroups.
Table 47: Safety Outcomes for Patients Treated With Initial Corticosteroids ± Rituximab in the HERCULES Study (Placebo and Caplacizumab Arms)
Corticosteroids only (n = 112) | Corticosteroids + rituximab (n = 24) | |||
|---|---|---|---|---|
Caplacizumab (n = 58) | Placebo (n = 54) | Caplacizumab (n = 8) | Placebo (n = 16) | |
At least 1 TEAE, n (%) | 56 (96.6) | 52 (96.3) | 8 (100.0) | 16 (100.0) |
At least 1 treatment-emergent SAE, n (%) | 21 (36.2) | 28 (51.9) | 2 (25.0) | 10 (62.5) |
SAE = serious adverse event; TEAE = treatment-emergent adverse event.
Note: This table is reproduced from original source and may not follow CADTH style.
Source: Pavenski et al. (2019).36
Scully et al. (2021): Post-Hoc Subgroup Analysis of Post-HERCULES Data by Initial Immunosuppressive Regimen (Poster)
Scully et al. (2021)37 conducted a subgroup analysis of outcomes in the Post-HERCULES study by immunosuppressive regimen in HERCULES (corticosteroids only versus corticosteroids plus rituximab). The analysis was reported in a poster.
Among the 78 patients in the Post-HERCULES efficacy ITO population, 33 (42.3%) patients received rituximab. aTTP-related events (aTTP-related death, recurrence of aTTP, and major thromboembolic events) are summarized in Table 48, stratified by use of rituximab in HERCULES. The analysis numerically favoured caplacizumab for both subgroups.
Table 48: TTP-Related Events During the Post-HERCULES Study Period According to Randomization in the HERCULES Study and Subgroups by Rituximab Use (Post Hoc Analysis)
Efficacy ITO population,a n (%) | Randomized to caplacizumab + TPE + IST n = 49 | Randomized to placebo + TPE + IST (n = 29) | ||||
|---|---|---|---|---|---|---|
No rituximab use during HERCULES n = 28 | Used rituximab during HERCULES n = 21 | All patients n = 49 | No rituximab use during HERCULES n = 17 | Used rituximab during HERCULES n = 12 | All patients n = 29 | |
TTP-related events | 2 (7) | 2 (10) | 4 (8) | 8 (47) | 3 (25) | 11 (38) |
TTP-related deathb | 0 | 0 | 0 | 1 (6) | 0 | 1 (3) |
Recurrence of TTP | 2 (7) | 2 (10) | 4 (8) | 6 (35) | 2 (17) | 8 (28) |
≥ 1 major TE event (excluding TTP) | 0 | 0 | 0 | 2 (12) | 1 (8) | 3 (10) |
aTTP = acquired thrombotic thrombocytopenic purpura; IST = immunosuppressive therapy; ITO = intention-to-observe; TE = thromboembolic event; TPE = therapeutic plasma exchange; TTP = thrombotic thrombocytopenic purpura.
aPatients in the ITO population who did not experience an aTTP exacerbation in HERCULES or before the beginning of post-HERCULES; patients were analyzed up to the moment they had an aTTP recurrence.
bA patient who never received caplacizumab died after having a TTP recurrence.
Source: Scully et al. (2021).37
Coppo et al. (2019): Post-Hoc Subgroup Analysis of HERCULES Data by Disease Severity (Poster)
Coppo et al. (2019)38 conducted a subgroup analysis of outcomes in the HERCULES study by baseline aTTP disease severity. Two subgroups of disease severity were analyzed: (i) very severe aTTP, defined as French severity score of 3 or higher, presence of severe neurological involvement (coma, seizures, focal deficit), or cardiac involvement (cardiac troponin I more than 2.5 × ULN) and (ii) less severe aTTP not meeting these criteria. The analysis was reported in a poster.
Baseline characteristics of patients in the HERCULES trial according to baseline disease severity are shown in Table 49.
Table 49: Baseline Characteristics for Patients in the HERCULES Study (Placebo and Caplacizumab Arms) According to Baseline Disease Severity Subgroup
Characteristic | Less severe (n=90) | Very severe (n=55) |
|---|---|---|
Age, mean (SD) | 43 (13.5) | 51.3 (12.8) |
Female, n (%) | 63 (70) | 37 (67.3) |
Previous TTP episodes, n (%) | ||
Initial | 47 (52.2) | 35 (63.6) |
Recurrent | 43 (47.8) | 20 (36.4) |
ADAMTS13 | ||
<10% | 74 (84.1) | 49 (89.1) |
≥10% | 14 (15.9) | 6 (10.9) |
Platelet counts (× 109/L), mean (SD) | 37.2 (27.7) | 32.9 (29.46) |
LDH (U/L), mean (SD) | 434 (255.6) | 748.8 (587.7) |
>ULN, n (%) | 64 (83.1) | 51 (92.7) |
Cardiac Troponin I (µg/L), mean (SD) | 0.036 (0.0391) | 4.86 (14.72) |
>ULN, n (%) | 17 (22.1) | 54 (98.2) |
Serum creatinine (µmol/L), mean (SD) | 87.8 (65.24) | 119.5 (107.01) |
>ULN, n (%) | 10 (13) | 20 (36.4) |
ADAMTS13 = a disintegrin and metalloproteinase with a thrombospondin type 1 motif, member 13; LDH = lactate dehydrogenase; SD = standard deviation; TTP = thrombotic thrombocytopenic purpura; ULN = upper limit of normal.
Notes: This table is reproduced from original source and may not follow CADTH style.
One PE was required for inclusion in the HERCULES trial.
Source: Coppo et al. (2019).38
Efficacy outcomes for patients in the HERCULES trial according to baseline disease severity are shown in Table 50. Time to platelet count numerically favoured caplacizumab in both patients with less severe disease (HR = 1.69; 95% CI, 0.94 to 3.04) and in patients with more severe disease (HR = 1.59; 95% CI, 1.02 to 2.47). The proportion of patients experiencing the composited end point of aTTP-related death, exacerbation of aTTP, or major thromboembolic was lower in patients randomized to receive caplacizumab who had had less severe disease (caplacizumab: 4.9%; placebo: 50.0%) and those who had more severe disease (caplacizumab: 23.3%; placebo: 48.0%).
Table 50: Efficacy Outcomes According to Baseline Disease Severity in the HERCULES Study During the Double-Blind Treatment Period
Outcome | Less severe (n=90) | Very severe (n=55) | ||
|---|---|---|---|---|
Caplacizumab (n=42) | Placebo (n=48) | Caplacizumab (n=30) | Placebo (n=25) | |
Time to platelet count response, HR (95% CI) | 1.69 (0.94; 3.04) | 1.59 (1.02; 2.47) | ||
Composite endpointa, n (%) | 2 (4.9)b | 24 (50.0) | 7 (23.3) | 12 (48.0) |
TTP-related death, n (%) | 0 | 1 (2.1) | 0 | 2 (8.0) |
Exacerbation of TTP, n (%) | 0 | 20 (41.7) | 3 (10.0) | 8 (32.0) |
Treatment-emergent major thromboembolic event, n (%) | 2 (4.9)b | 3 (6.3) | 4 (13.3) | 3 (12.0) |
Refractory TTP, n (%) | 0 | 1 (2.1) | 0 | 2 (8.0) |
CI = confidence interval; HR = hazard ratio; TTP = thrombotic thrombocytopenic purpura.
Note: This table is reproduced from original source and may not follow CADTH style.
aComposite end point consists of ≥ 1 of TTP-related death, recurrence (exacerbation), or major thromboembolic event during the blinded treatment period.
b41 patients were assessable for this event.
Source: Coppo et al. (2019).38
Safety outcomes for patients in the HERCULES trial according to baseline disease severity are shown in Table 51. The frequencies of AEs and SAEs were similar or higher in patients receiving placebo compared to those receiving caplacizumab.
Table 51: Safety Outcomes for Participants With Less Severe or Very Severe Disease Severity at Baseline in the HERCULES Study
Less Severe (n = 90) | More Severe (n = 55) | |||
|---|---|---|---|---|
Caplacizumab (n = 42) | Placebo (n = 48) | Caplacizumab (n = 30) | Placebo (n = 25) | |
At least 1 TEAE, n (%) | 39 (95.1) | 46 (95.8) | 30 (100.0) | 25 (100.0) |
At least 1 treatment-emergent SAE, n (%) | 15 (36.6) | 25 (52.1) | 13 (43.3) | 14 (56.0) |
SAE = serious adverse event; TEAE = treatment-emergent adverse event.
Note: This table is reproduced from original source and may not follow CADTH style.
Source: Coppo et al. (2019).38
Coppo et al. (2020): Post-Hoc Subgroup Analysis of HERCULES Data by Time to Platelet Count Response (Poster)
Coppo et al. (2020)39 conducted a subgroup analysis of outcomes in the HERCULES study by time to platelet count response. The analysis was reported as a poster.
Patients were stratified into 2 groups of fast or slow platelet count response (≤ 3 days or > 3 days); platelet count response was defined as achieving platelet count of ≥ 150 × 109/L followed by cessation of daily PE within 5 days. Frequencies of aTTP exacerbation were compared between these 2 patient subgroups. Exacerbation rates in patients with fast and slow platelet count responses are shown in Table 52. The results numerically favoured caplacizumab for both subgroups.
Table 52: Time to Platelet Count Response and Exacerbation Rate
Time to platelet count responsea | Placebo (n=73) | Caplacizumab (n=72) |
|---|---|---|
Fast response (≤3 days), n (%) | 43 (58.9) | 56 (78.8) |
Patients with exacerbation,b n (%) | 19/43 (44.2) | 2/56 (3.6) |
Slow response (<3 days), n (%) | 30 (41.1) | 15 (20.8) |
Patients with exacerbation, n (%) | 9/30 (30.0) | 1/15 (6.7) |
aTTP = acquired thrombotic thrombocytopenic purpura; TPE = therapeutic plasma exchange.
Note: This table is reproduced from original source and may not follow CADTH style.
aPlatelet count response was defined as restored platelet count ≥ 150 × 109/L.
bExacerbation was defined as having a recurrent aTTP episode ≤ 30 days after daily TPE cessation.
Source: Coppo et al. (2020).39
In addition, the durability of platelet count responses was assessed using Kaplan-Meier analysis of time to durable platelet response (defined as time from first treatment to last daily PE during the overall treatment period), time to complete remission (defined as time to sustained platelet count ≥ 150 × 109/L and LDH < 1.5 × ULN for > 30 days after cessation of daily PE), and recurrence-free survival (defined as absence of exacerbation or relapse during the overall study period).The results of these analyses are shown in Table 53 and Figure 13. Analysis of time to durable platelet count response and time to complete remission, and recurrence-free survival numerically favoured caplacizumab.
Table 53: Time to Durable Platelet Count Response, Complete Remission, and Recurrence-Free Survival (Coppo et al. [2020])
Outcome | Caplacizumab n = 72 | Placebo n = 73 |
|---|---|---|
Time to durable platelet count response, days, median (95% CI)a | 4.5 (4.4 to 4.6) | 10.5 (6.5 to 14.5) |
Time to complete remission, days, median (95% CI)b | 40.0 (37.7 to 41.1) | 44.2 (42.0 to 48.2) |
Recurrence-free survival, days, median (95% CI)b | Not reached | Not reached |
CI = confidence interval; ITT = intention to treat; PE = plasma exchange.
aDefined as time from first treatment to last daily PE during the overall treatment period.
bDefined as time to sustained platelet count ≥ 150 × 109/L and LDH < 1.5 × ULN for > 30 days after cessation of daily PE.
cDefined as absence of exacerbation or relapse during the overall study period among patients who achieved the primary end point.
Source: Coppo et al. (2020).39
Figure 13: Kaplan-Meier Analysis of Time to Durable Platelet Response, Time to Complete Remission, and Recurrence-Free Survival in Coppo et al. (2020)
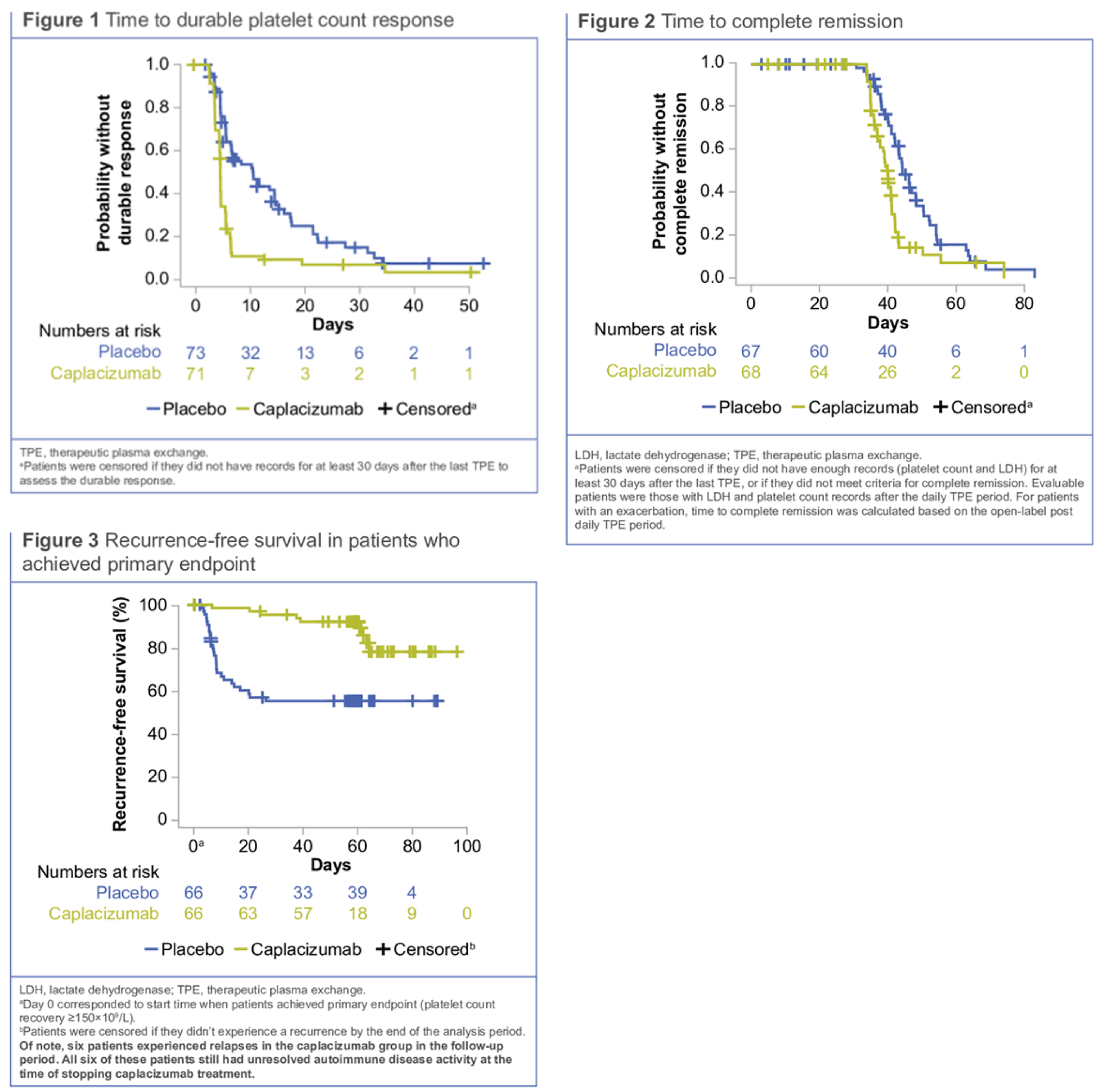
Source: Coppo et al. (2020).39
Scully et al. (2020): Post-Hoc Subgroup Analysis of HERCULES Data for Patients with Worsening aTTP Despite PE (Abstract)
Scully et al. (2020)40 described the outcomes of patients in the HERCULES study with suboptimal response to PE (defined by decreasing platelet counts and increasing LDH after initial but nonsustained improvement of platelet counts and LDH during daily PE). The analysis was reported in an abstract only.
Suboptimal responses to PE occurred in no patients in the caplacizumab arm and in 8 patients in the placebo arm of HERCULES. Suboptimal response to TPE was defined as worsening platelet counts and LDH levels (after initial improvement) despite ongoing TPE.
Disease severity at baseline was defined as follows: (i) a French severity score ≥ 3, or (ii) severe neurological involvement (i.e., coma, seizures, or focal deficit), or (iii) cardiac involvement (cTnI > 2.5 × ULN). The French severity score is a discrete risk score that ranges from 0 to 4 (with severity scores ≥ 3 indicating very severe disease) and involves evaluation of 3 parameters: Cerebral involvement: yes = 1, no = 0; lactate dehydrogenase: > 10 × ULN = 1, ≤ 10 × ULN = 0; age: > 60 years = 2, > 40 and ≤ 60 years = 1, ≤ 40 years = 0.
The baseline disease characteristics of these 8 patients were as follows. Patient A had recurrent aTTP, baseline platelet count of 9 × 109/L, baseline cTnI of 7.025 mcg/mL, baseline LDH of 1,113 U/L, baseline serum creatinine of 82 µmol/L, and baseline disease severity of very severe. Patient B had initial aTTP, baseline platelet count of 15 × 109/L, baseline cTnI of 0.022 mcg/mL, baseline LDH of 520 U/L, baseline serum creatinine of 106 µmol/L, and baseline disease severity of less severe. Patient C had recurrent aTTP, baseline platelet count of 23 × 109/L, baseline cTnI of 4.435 mcg/mL, baseline LDH of 3,343 U/L, baseline serum creatinine of 211 µmol/L, and baseline disease severity of very severe. Patient D had initial aTTP, baseline platelet count of 14 × 109/L, baseline cTnI of 0.213 mcg/mL, baseline LDH of 338 U/L, baseline serum creatinine of 145 µmol/L, and baseline disease severity of very severe. Patient E had recurrent aTTP, baseline platelet count of 82 × 109/L, baseline cTnI of less than 0.010 mcg/mL, baseline LDH of 253 U/L, baseline serum creatinine of 145 µmol/L, and baseline disease severity of less severe. Patient F had recurrent aTTP, baseline platelet count of 12 × 109/L, baseline cTnI of 0.018 mcg/mL, baseline LDH of 346 U/L, baseline serum creatinine of 92 µmol/L, and baseline disease severity of less severe. Patient G had initial aTTP, baseline platelet count of 21 × 109/L, baseline cTnI of 1.020 mcg/mL, baseline LDH of 359 U/L, baseline serum creatinine of 137 µmol/L, and baseline disease severity of very severe. Patient H had recurrent aTTP, baseline platelet count of 30 × 109/L, baseline cTnI was not available, baseline LDH was not available, baseline serum creatinine was not available, and baseline disease severity of less severe.
The treatment outcomes of these 8 patients were as follows. Patient A had a time to platelet count response of 22.37 days, a time to stop of daily TPE of 23 days, no TTP-related death, and no exacerbation. Patient B had a time to platelet count response of 11.97 days, a time to stop of daily TPE of 13 days, no TTP-related death, and exacerbation. Patient C had a time to platelet count response of 5.71 days, a time to stop of daily TPE of 8 days, no TTP-related death, and exacerbation. Patient D had a time to platelet count response of 16.58 days, a time to stop of daily TPE of 20 days, no TTP-related death, and exacerbation. Patient E had a time to platelet count response of 6.75 days, a time to stop of daily TPE of 9 days, no TTP-related death, and no exacerbation. Patient F had a time to platelet count response of 18.79 days, a time to stop of daily TPE of 21 days, no TTP-related death, and exacerbation. Patient G had a time to platelet count response of 6.07 days (censored observation), a time to stop of daily TPE of 7 days, experienced TTP-related death, and no exacerbation. Patient H had a time to platelet count response of 9.79 days, a time to stop of daily TPE of 14 days, no TTP-related death, and exacerbation.
Real-World Evidence
Volker et al. (2020): German RWE Cohort
Volker et al. (2020)41-43 conducted a retrospective observational study of 60 patients treated with caplacizumab in addition to standard treatment (PE plus immunosuppression) at 29 centres in Germany. The characteristics and outcomes of this cohort were naively compared with the HERCULES study population.
Methods
The PLASMIC (platelets, lysis, active cancer, stem cell, or solid organ transplant, mean corpuscular volume, international normalized ratio, and creatinine) score, which was developed as a clinical predictive tool of severe ADAMTS13 deficiency, was determined retrospectively. Day 0 was defined as the day of diagnosis as indicated by the treating physician, beginning of aTTP-specific therapy, or a reported ADAMTS13 activity measurement of less than 10%. It is important to note that the reported date of ADAMTS13 activity measurements may not reflect the time point when the results became available to the treating physician. Testing was not available on site at most centres and results may have been reported with a delay of several days. Retrospectively, aTTP had likely begun before the day of diagnosis in some patients but was not recognized or treated under the presumption of a different diagnosis.
Populations
The baseline characteristics of patients in the caplacizumab cohort of Volker et al. (2020) and of patients in the HERCULES trial ITT population are shown in Table 55. Higher proportions of the German RWE cohort were white (98.3% versus 71.0%) and had initial aTTP occurrence (76.7% versus 57%) compared with the HERCULES ITT population.
Table 55: Baseline Patient Characteristics and Disease Parameters of the Cohort Reported in the Manuscript and the HERCULES Trial
Germanya (n = 60) | HERCULES cohort (N= 145) | Comparison of Germany vs HERCULES (Fisher’s exact test), P | |
|---|---|---|---|
Age, mean (range), y | 45.7 (22-83) | 46 (18-79) | |
Female sex, % (n/total) | 70 (42/60) | 69 (100/145) | >.9999 |
White, % (n/total) | 98.3 (59/60) | 71.0 (97/137) | <0.0001 |
BMI, median (range), kg/m2 (n = 59) | 27 (16.0-42.6) | 30 (18-59) | |
First occurrence of TTP, % (n/total) | 76.7 (46/60) | 57 (82/145) | .0072 |
Hemoglobin, initial, median (range), g/dL | 8.2 (5.0-13.6) | Placebo arm (n = 63), 8.7 (6.4-15.1); verum arm (n = 62), 8.6 (5.9-15.9)b | |
Hemoglobin, minimum, median (range), g/dL | 6.3 (4.5-10.9) | Not reported | |
Platelets, initial, median (range), ×109/L | 13.0 (3-85) | 24 (3-133) | |
Platelets, minimum, median (range), ×109/L | 10 (2 to 62) | Not reported | |
LDH, initial, median (range), U/L | 985 (316-2588) | 422 (120-3343) | |
LDH, maximum, median (range), U/L | 1088 (316-2918) | Not reported | |
Troponin above ULN at any point, % (n/total) (n = 32) | 84.4 (27/32) | cTnI above ULN at baseline, 49.0 (71/145)c | |
Creatinine, initial, median (range), U/L | 96.5 (52.2-470) | 80 (35-717) | |
Creatinine, maximum, median (range), U/L | 120.4 (55.8-470) | Not reported | |
ADAMTS13 activity below 10%, % (n/total) | 100 (60/60) | 85 (123/145) | .0004 |
ADAMTS13 activity above 12 IU/mL (ULN) at any point, % (n/total) | 91.7 (55/60) | Not reported | nt |
Maximum ADAMTS13 antibody concentration, IU/mL | |||
ADAMTS13 antibody concentration, maximum, median (range), IU/ml | 75.5 (0.0-131.6) | Not reported | nt |
Glasgow Coma Scale, % (n/total) | |||
<13 | 13.3 (8/60) | 8 (11/145) | nt |
13-15 | 83.3 (50/60) | 91 (132/145) | |
Missing | 3.3 (2/60) | 1 (2/145) | |
PLASMIC score, % (n/total) | |||
0-4 | 1.7 (1/60) | Not reported | nt |
5-6 | 36.7 (22/60) | Not reported | |
7 | 60.0 (36/60) | Not reported | |
Data missing | 1.7 (1/60) | Not reported | |
ADAMTS13 = a disintegrin and metalloproteinase with thrombospondin type 1 motif, member 13; BMI = body mass index; cTnI = cardiac troponin I; IU = international units; LDH = lactate dehydrogenase; nt = not tested; PLASMIC = platelets, lysis, active cancer, stem cell or solid organ transplant, MCV, INR, and creatinine; TTP = thrombotic thrombocytopenic purpura; ULN = upper limit of normal; y = years.
Note: This table is reproduced from original source and may not follow CADTH style.
an = 60 unless indicated otherwise due to missing data. Differences in the HERCULES cohort were tested using the Fisher’s exact test if sufficient data were available.
bSource data from Sanofi are on file shared by the company.
cData source is the Orphan Maintenance Assessment Report (EMA/541816/2018). Please note the difference in the time point of troponin assessment (at any time point in the German cohort and at baseline in HERCULES).
Note: Bold P values indicate statistical significance (P < 0.05).
Source: Volker et al. (2020).41-43 Reprinted from Blood Advances, Vol 4/No 13, Volker LA, Kaufeld J, Miesbach W, et al., Real-world data confirm the effectiveness of caplacizumab in acquired thrombotic thrombocytopenic purpura, Pages 3085-3092, Copyright 2020, with permission from The American Society of Hematology.
Interventions
The interventions administered to patients in the caplacizumab cohort of Volker et al. (2020) and to patients in the HERCULES trial ITT population are shown in Table 56. Caplacizumab was administered as a frontline drug in 35 patients (60%) in the German RWE cohort. In 2 patients, caplacizumab was administered without PE. Note that only 8 patients (13.3%) were treated according to the HERCULES protocol, defined as caplacizumab started before or after the first PE and continued for a minimum of 30 days and a maximum of 58 days after the last PE. In 5 patients (8.3%), caplacizumab was continued beyond 58 days post-PE, and in 34 patients (56.7%), it was discontinued before 30 days post-PE.
In the German RWE cohort, rituximab was administered in 48 patients (80%), higher than in HERCULES (43%); rituximab was administered frontline in only 11 patients (18.3%). The median duration of PE was 9 days (range, 2 to 41 days) and the median duration of PE during caplacizumab treatment was 4 days (range, 0 to 22 days)
Table 56: Treatment Modalities
Modality | Germany (n=60) | HERCULES cohort (N=145) | Comparison of Germany vs HERCULES (Fisher’s exact test), P |
|---|---|---|---|
Rituximab treatment, % (n/total) | 80 (48/60) | 43 (63/145) | <.0001 |
Rituximab, % (n/total) | |||
Frontline (within 72 h) | 18.3 (11/60) | 17 (25/145) | .8398 |
Delayed | 60.0 (36/60) | ||
Data missing | 1.7 (1/60) | ||
Day of first rituximab after disease onset, median (range),d | 7 (0-35) | Not reported | |
Cumulative rituximab dose, median (range), mg | 2000 (562.5-5000) | Not reported | |
PEX treatment, % (n/total) | 96.7 (58/60) | 100 (145/145) | .0846 |
Days of PEX treatment (n = 58) | |||
Median, no. (range) | 9 (2-41) | Not reported | |
Mean, no. (95% CI) | 11.8 (9.5-14.2) | Not reported | |
Days of PEX under caplacizumab treatment | |||
Median, no. (range) | 4 (0-22) | Verum arm (n = 72), 5 (1-35) | |
Mean, no. (95% CI) | 5.3 (4.2-6.4) | Verum arm (n = 72), 5.8 (4.8-6.8) | |
Caplacizumab doses, median (range), no. | 34.0 (2-89) | Not reported | |
Caplacizumab treatment duration, median (range),d | 34 (2-211) | 35 (1-65)a | |
Caplacizumab as frontline (within 72 h), % (n/total) | 58.3 (35/60) | Not applicable | |
Caplacizumab start after disease onset, median (range),d | 3 (0-27; 27) | Not applicable | |
Treatment according to HERCULES protocolb | |||
Treatment according to HERCULES protocol, % (n/total)b | 13.3 (8.60) | Not applicable | |
Steroid treatment, % (n/total) | |||
Any dose | 98.3 (59/60) | 97 (140/145) | 0.6734 |
High dosec | 76.6 (46/60) | Not reported | |
Non-high dose | 8.3 (5/60) | Not reported | |
Data missing | 13.3 (8/60) | Not reported | |
Steroid initial dose (n = 51), median (range), mg/kg BWd | 1.40 (0.64-15.11) | Not reported | |
Other treatments, % (n/total) | |||
Mycophenolate | 5.9 (3/60) | 4 (6/145) | |
Hydroxychloroquine | 1.7 (1/60) | 2 (3/145) | |
Vincristine | 1.7 (1/60) | Not reported | |
Ciclosporin | 3.3 (2/60) | 1 (2/145) | |
Azathioprine | 5.0 (2/60) | 1 (2/145) | |
Splenectomy | 0.0 (0/60) | 2 (3/145) | |
IVIG | 0.0 (0/60) | 3 (4/145) | |
Bortezomib | 0.0 (0/60) | 1 (2/145) | |
Immunoadsorption | 0.0 (0/60) | 0.7 (1/145) | |
BW = body weight; CI = confidence interval; d = day; IVIG = intravenous immunoglobulin; PEX = plasma exchange.
Notes: This table is reproduced from original source and may not follow CADTH style.
N = 60 unless indicated otherwise.
aData source is the Orphan Maintenance Assessment Report (EMA/541816/2018). Differences from the HERCULES cohort were tested using the Fisher’s exact test if sufficient data were available.
bDefined as caplacizumab start before or after first PEX and caplacizumab continued for a minimum of 30 d after last PEX treatment.
cHigh doses are defined as ≥ 1 mg/kg body weight of prednisone equivalent.
dMilligram of prednisone or prednisone equivalence dose if another glucocorticoid has been used.
Source: Volker et al. (2020).41-43 Reprinted from Blood Advances, Vol 4/No 13, Volker LA, Kaufeld J, Miesbach W, et al., Real-world data confirm the effectiveness of caplacizumab in acquired thrombotic thrombocytopenic purpura, Pages 3085-3092, Copyright 2020, with permission from The American Society of Hematology.
Outcomes
Time to normalization of platelet count after the start of caplacizumab treatment was defined as the first day with a count of 150 × 109/L or greater. Clinical remission, exacerbation, refractory disease, and relapse were defined as per published international guidelines (Scully et al., 2017) with the exception that reinitiation of PE was not a prerequisite of exacerbation and relapse because some of these instances were managed with conservative treatment only. Treatment according to the HERCULES protocol was defined as caplacizumab started before or after the first PE and continued for a minimum of 30 days and a maximum of 58 days after the last PE treatment. Frontline use was defined as a treatment started within 72 hours after diagnosis. Presence of acute kidney injury according to Kidney Disease: Improving Global Outcome (KDIGO) was determined by comparing the highest with the lowest serum creatinine measurement during the follow-up. Lowest serum creatinine was assumed to be the baseline. Urinary output was not taken into consideration because this information was not available.
Statistical Analysis
Only descriptive and summary statistics were provided.
Patient Disposition
The study enrolled patients at 29 German medical centres. In total, 60 patients (approximately 90% of all patients treated in Germany) with aTTP were identified who received caplacizumab between June 2018 and December 2019. The rationale for believing this cohort captured 90% of patients treated in Germany during this period was not stated. The median duration of follow-up was 3.6 months (range: 0.2 to 10.8 months).
Exposure to Study Treatments
The median duration of caplacizumab dosing was 34 days (range: 2 to 211 days).
Efficacy
Efficacy outcomes in the German RWE cohort of Volker et al. (2020) are summarized in Table 57. The median time to platelet normalization was 3 days (range: 1 to 13 days). The median duration of hospitalization was 18 days (range: 5 to 79 days) and the median ICU stay was 4 days (range: 0 to 46 days). One patient (1.7%) died due to aTTP-associated complications. 2 patients (2.2%) experienced exacerbations while on caplacizumab and 2 patients (2.2%) experienced relapse. Data on refractory aTTP during caplacizumab treatment were not provided.
Germany (n = 60) | |
|---|---|
Mortality, % (n/total) | 1.7 (1/60) |
Follow-up, median (range),d | 108.5 (5-330) |
Clinical response, % (n/total)a | |
Achieved | 93.3 (56/60) |
Not achieved | 3.3 (2/60) |
Insufficient follow-up | 3.3 (2/60) |
Exacerbation, % (n/total) | 38.3 (23/60) |
While on caplacizumab | 3.3 (2/60) |
Refractory disease, % (n/total) | 31.7 (19/60) |
Refractoriness, grade, % (n/total)b | |
Severe | 68.4 (13/19) |
Mild | 31.6 (6/19) |
Relapse, % (n/total) | |
Relapsing disease | 3.3 (2/60) |
Insufficient follow-up | 13.3 (8/60) |
Time to final platelet normalization after diagnosis, median (range),d | 12 (3-152) |
Reached at end of follow-up, % (n/total) | 95.0 (57/60) |
Not reached at end of follow-up, % (n/total) | 5.0 (3/60) |
Time to final platelet normalization after caplacizumab start, days (n=64)c, d | |
Median (range) | 3.0 (1-13) |
Mean (95% CI) | 3.78 (3.19-4.38) |
Duration of hospital stay (n = 54),d | |
Median (range) | 18 (5-79) |
Mean (95% CI) | 21.6 (18.0-25.2) |
Duration of ICU stay (n = 54),d | |
Median (range) | 4 (0-46) |
Mean (95% CI) | 5.8 (3.8-7.7) |
CI = confidence interval; ICU = intensive care unit; LDH = lactate dehydrogenase; PEX = plasma exchange.
Note: This table is reproduced from original source and may not follow CADTH style.
aClinical response as defined in Scully et al62: a sustained normalization of platelet counts > 150 × 109/L and of LDH < 1.5 upper limit of normal after cessation of PEX.
bRefractoriness grade as defined in Scully et al.62 Refractory TTP is defined as persistent thrombocytopenia < 50 × 109/L and persistently raised LDH levels despite 5 PEX and steroid treatments. It is defined as severe if thrombocytopenia remains < 30 × 109/L.
cPlatelets > 150 × 109/L. In 3 patients, platelet count did not normalize due to ongoing sepsis or concomitant liver cirrhosis. These cases were excluded from the calculation (patients 10, 49, and 53). One patient (patient 18) was not computed because of aTTP-related death.
dInstances (n = 64) rather than patient numbers are reported here reflecting the fact that, in some patients, caplacizumab treatment was stopped and restarted. Every time caplacizumab was restarted, the time to platelet normalization was measured again.
Source: Volker et al. (2020).41-43 Reprinted from Blood Advances, Vol 4/No 13, Volker LA, Kaufeld J, Miesbach W, et al., Real-world data confirm the effectiveness of caplacizumab in acquired thrombotic thrombocytopenic purpura, Pages 3085-3092, Copyright 2020, with permission from The American Society of Hematology.
Harms
One major bleeding complication in the form of recurrent vaginal hemorrhages 2 weeks after delivery was reported in 1 patient (patient 8); as a result, caplacizumab was initially paused and then stopped. Other minor bleeding complications comprised epistaxis and gingival bleeding without the need to stop caplacizumab. No patient suffered debilitating hemorrhage.
Critical Appraisal: Internal Validity
Comparisons between the German RWE cohort receiving caplacizumab and the HERCULES ITT population, or any other groups of patients, were limited by serious risk of bias in selection of participants as well as confounding of efficacy outcomes. In particular, nearly all patients in the German were white and a high proportion had initial aTTP episodes (76.7%), which the clinical experts consulted by CADTH for this review stated generally has better outcomes than recurrent aTTP. Major treatment differences between the use of caplacizumab (e.g., 56.7% discontinued the drug before 30 days post-PE) and rituximab (used in 80% of the German RWE cohort but only 46% of the HERCULES population) may have affected treatment outcomes.
Critical Appraisal: External Validity
The majority of patients in the German RWE cohort were not treated according to the HERCULES trial or to the product monograph for caplacizumab: 56.7% discontinued caplacizumab before 30 days post-PE, and smaller numbers continued the drug for long periods and/or received it without PE. Thus, the data from this study may not be generalizable to expected clinical practice in Canada. According to the clinical experts consulted by CADTH for this review, rates of rituximab use in the German RWE cohort (80%, upfront use 18.3%) were not consistent with the current use of this drug in Canadian clinical practice.
Volker et al. (2021): Caplacizumab is Effective in Treating Immune-Mediated Thrombotic Thrombocytopenic Purpura in Real-World Scenarios and May Lower Mortality: An Aggregative Analysis (Abstract)47
“Introduction: The treatment of acquired thrombotic thrombocytopenic purpura has been a subject to change lately due to the introduction of caplacizumab as a novel, and potentially life-saving agent. Here, we compare patient-centered outcomes of a historic cohort of 119 aTTP patients and an extended real-world caplacizumab-treated cohort of 113 aTTP patients from Germany and Austria in the context of multiple recently published international cohorts of aTTP patients.
Methods: From October 2018 until May 2021, data from German and Austrian patients presenting with an acute episode of aTTP as defined by an ADAMTS13 activity below 10% treated with caplacizumab were gathered retrospectively. We aggregated data from two published randomized controlled trials (TITAN, HERCULES), 1 single-arm prospective trial and two retrospective cohorts with a historical control cohort. In total, we report 846 aTTP cases, 396 of those treated with caplacizumab and 450 without. For data analysis, placebo groups from randomized trials and historical controls from retrospective analyses were combined.
Results: All cohorts combined reported 30 aTTP-related deaths, predominantly in the non-caplacizumab cohort. Mortality in the caplacizumab cohort (8 cases total) was mainly driven by 5 reported deaths in the UK-cohort, which have been ascribed to a delayed use of caplacizumab by the authors. The number of daily PE was significantly less in the caplacizumab-treated cohort (7.2 vs 10.2 days). In line, the number of hospital (14.0 vs 18.1) and ICU (4.7 vs 8.9) days differed significantly. Exacerbations (14% vs 39%) were significantly reduced in the caplacizumab group. In view of all treatment-related outcomes, the data presented herein argues strongly in favor of an early and consistent use of caplacizumab in all instances of aTTP.”
Maanaoui et al. (2020): First Real-Life Data of Patients Treated for Thrombotic Thrombocytopenic Purpura from the French Thrombotic Microangiopathies Network (Abstract)45
“Background and Aims: Caplacizumab, a bivalent Nanobody, targets the A1 domain of von Willebrand Factor, inhibiting the interaction between ultra-large vWF and platelets in the treatment of Acquired Thrombotic Thrombocytopenic Purpura (aTTP). Results of the Phase 3 HERCULES study confirm that treatment with caplacizumab reduces the time to platelet count response, resulting in faster resolution of aTTP. Treatment with caplacizumab also resulted in a highly clinically meaningful reduction in aTTP-related death, recurrence of aTTP, or a major thromboembolic event during study drug treatment. Data from clinical practice confirming the clinical trial data is still scarce. We report here the first real-world evidence collected in the French thrombotic microangiopathies network.
Method: Patients with an acute episode of aTTP were included in an observational prospective multicentric study. The diagnosis of aTTP was done according to the French score (platelet count < 30 g/l and serum creatinine<200mmol/l) or ADAMTS13 activity if available. Adult patients were proposed to be treated with daily plasma exchange (PE) in addition to corticosteroid and frontline rituximab plus early initiation of caplacizumab. PE was stopped after 2 days of platelet count normalization.
Results: Fifty patients (36 females, median age of 46 years old) were treated for aTTP. 30 patients (60%) had cerebral involvement and 13 (26%) had cardiac involvement. Cardiac troponin I was above upper normal value for 61% of patients. Before treatment, median platelet count was 16 g/l and median serum creatinine was 86 mmol/L. Three initial clinical suspicions of aTTP were finally diagnosed as HUS (2 patients) or vitamin deficiency (1 patient) resulting in the stop of treatment. A median number of 6 plasma exchanges was administered (min:3 - max:16). 375mg/m˙ rituximab injections (3 to 4 for 35/43 patients with reported data) were mostly initiated within 3 days after the first plasma exchange. Caplacizumab treatment was initiated early (37/42 patients with reported data within 2 days after 1st plasma exchange) with a total median duration of treatment of 33 days (min:18 - max:35). The median platelet count normalization was 5 days (min:4 - max:6). 6/41 (14.6%) experienced exacerbations. No deaths and no patients refractory to therapy were reported. Eight adverse events related to caplacizumab therapy were reported, all with good outcomes.
Conclusion: Concomitant start of additional treatments allow to target severe ADAMTS13 deficiency and platelet aggregation which causes early mortality. The clinical French score seems useful in clinical practices.”
Jimenez et al. (2020): Real-World Data With the Use of Caplacizumab in the Treatment of Acquired Thrombotic Thrombocytopenic Purpura (aTTP) (Abstract)44
“Introduction: For more than 2 decades, the treatment of aTTP consisted of therapeutic plasma exchange (TPE) and immunosuppressive agents. The addition of caplacizumab, a nano-antibody that binds to the A1 domain of the von Willebrand factor, inhibiting platelet aggregation, has been shown to reduce the time to resolution of thrombocytopenia, the rate of recurrence, and the aTTP-related death. Real-world evidence of the effectiveness of caplacizumab is limited yet. The objective of our study was to assess the results of the introduction of caplacizumab in our internal protocol and to compare those results with the patients treated before the drug was available.
Methods: A single-center retrospective observational study that evaluates the clinical characteristics and response to treatment of 18 consecutively diagnosed aTTP patients between May/14 to May/20. All patients received initial treatment with TPE and prednisone (PDN) 1 mg/Kg; the control group did not receive any other initial therapy, whereas nine patients received caplacizumab in addition to PE and PDN once ADAMTS-13 deficiency was confirmed. Complete response (CR) was defined as the second of two consecutive days with platelets ≥150x109/L, refractoriness as the lack of platelet increase despite optimal therapy after seven days, exacerbation as the decrease in platelet count during the first 30 days of discontinuation of TPE, and relapse as a new episode of aTTP beyond 30 days after the last TPE. All results are given as median (interquartile range). Statistical analysis was conducted using STATA/IC software.
Results: The clinical characteristics at diagnosis of patients treated with or without caplacizumab were similar, except for a lower percentage of males and lower neurological involvement in the caplacizumab group (Table 58).”
Table 58: Baseline Clinical Characteristics at Diagnosis of Patients Suffering aTTP
Characteristic | Caplacizumab group (n=9) | Control goup (n=9) |
|---|---|---|
Age, median (IQR) | 43 (39-55) | 41 (33-52) |
Female sex, n (%) | 8 (89%) | 6 (67%) |
Hemoglobin g/dL, median (IQR) | 8,6 (8-9,2) | 8,3 (6,6-9,2) |
Platelets ×109/L, median (IQR) | 16 (8-21) | 12 (7-18) |
Creatinine mg/dL median (IQR) | 0.95 (0,73-1,12) | 0,85 (0,81-1,37) |
Severe neurological involvement: Focalization, convulsion | 3 (33%) | 5 (55%) |
Mild neurological involvement: Headache, dizziness | 0 | 1 (11%) |
Fever | 1 (11%) | 0 |
Anemic syndrome | 1 (11%) | 1 (11%) |
Mucocutaneous diathesis, bleeding | 4 (44%) | 2 (22%) |
aTTP = acquired thrombotic thrombocytopenic purpura; IQR = interquartile range.
Note: This table is reproduced from original source and may not follow CADTH style.
Source: Jimenez et al. (2020).44 Reprinted from Blood, Vol 136/Suppl 1, Jimenez et al., Real-World Data With the Use of Caplacizumab in the Treatment of Acquired Thrombotic Thrombocytopenic Purpura (aTTP), Pages 14-16, Copyright 2020, with permission from The American Society of Hematology.
“Caplacizumab was started at a median of 3 days after diagnosis following ADAMTS-13 deficiency determination and was administered during a median of 39 days (IQR 33-39). Adverse events related to caplacizumab were mild: 1 patient presented mild metrorrhagia, 1 developed pain and erythema at the puncture area and 1 suffered an urticarial dermatitis, the last case leading to the suspension of the drug since levels of ADAMTS-13 were recovered.
The caplacizumab group achieved CR after a median of 4 days (IQR 3-4) vs. 6 days (IQR 5-4) in the control group (p = 0.016). Likewise, the number of TPE was lower with caplacizumab (Figure 1), with a median of 10 TPE (IQR 9-11) vs. 19 (IQR 16-23) (p = 0.001). Hospitalization time was also shorter in the caplacizumab group with a median of 12 days (IQR 12-14) vs. 26 (IQR 20-27) (p = 0.002). Finally the time of hospitalization into the intensive care unit was shorter in the caplacizumab group with a median of 3 days (IQR 2-4) versus 4 (IQR 3-13) (p = 0.1).
In the caplacizumab group (median follow-up of 6.8 months), there were no refractory cases. There was 1 exacerbation before initiation of caplacizumab and 1 relapse. Both cases were treated with rituximab. In contrast, in the control group (median follow-up of 51.8 months), we observed 4 refractory cases (1 aTTP-related death), 3 exacerbations and 1 relapse; rituximab was necessary in 8 patients and a 3rd line with vincristine was administered in 4 cases.
Conclusions: The observed benefits of caplacizumab in our series are in line with the ones identified in randomized clinical trials. Caplacizumab can be used in combination with other therapies to attain a faster response and reduce aTTP-related complications.”
Vataire et al. (2022): Comparison of Healthcare Resource Utilization Among Hospitalized Patients with Acquired Thrombotic Thrombocytopenic Purpura Treated With or Without Caplacizumab: A French Hospital Database (PMSI) Analysis (Abstract)46
“Objectives: Caplacizumab is a humanized anti-von Willebrand factor monoclonal antibody fragment indicated for the treatment of acquired thrombotic thrombocytopenic purpura (aTTP). Clinical trials have demonstrated its efficacy and safety along with shorter hospital length of stay (LOS) and intensive care unit duration. However, there is limited real-world data on effectiveness of caplacizumab. This study compares healthcare resource utilization (HCRU) in aTTP patients treated with or without caplacizumab in clinical practice in France. Methods: A retrospective study was conducted using data from a French national hospital discharge database (Programme de Médicalisation des Systèmes d’Information, PMSI). All hospitalized patients receiving caplacizumab between August 2018 and December 2019 and diagnosed with aTTP using a previously published algorithm were evaluated. A cohort of control patients (i.e., not treated with caplacizumab) was selected from a population of patients hospitalized between January 2015 and August 2018 and matched 2:1 with caplacizumab-treated patients by sex, age group, and hospitalization at reference centres. HCRU outcomes including hospital LOS, ICU duration and the number of plasma exchanges (PEX), were compared between cohorts using the Wilcoxon signed-rank test. Results: A total of 89 aTTP patients who were on caplacizumab treatment were identified (67.4% females; mean [SD] age, 46.5 [16.1] years). The control cohort included 178 patients (67.4% females; mean [SD] age, 46.3 [16.1] years). Caplacizumab-treated patients had significantly shorter hospital LOS (mean [SD], 18.8 [13.2] vs. 26.2 [16.9] days, p,0.0001), ICU duration (mean [SD], 9.7 [7.2] vs. 12.9 [12.5] days, p=0.027) and fewer number of PEX (mean [SD], 8.1 [7.9] vs. 11.5 [9.9], p,0.0001) than control cohort. Conclusions: In a real-world setting, caplacizumab treatment is associated with a significantly lower HCRU, and may reduce the hospitalization costs and burden in aTTP patients in France. These findings also corroborate data from the pivotal trial (HERCULES).”
Kuhne et al. (2022): Alternate-Day Dosing of Caplacizumab for Immune-Mediated Thrombotic Thrombocytopenic Purpura49
Refer to the abstract on PubMed.49
Logothetis et al. (2021): Post Approval Experience with Caplacizumab for Acquired Thrombotic Thrombocytopenic Purpura at a Single Institution48
Refer to the abstract on PubMed.48
Other Outcome Data
Interview With Canadian Clinical Experts
The sponsor interviewed 5 Canadian physicians who diagnose and treat patients with aTTP in February 2022. All 5 physicians indicated that while currently available treatments (PE with or without immunosuppressive therapy) can reverse ADAMTS13 inhibition and decrease levels of ADAMTS13 autoantibodies, there is an unmet need for treatments that can address platelet aggregation and microthrombus formation. The interviewed clinicians emphasized the importance of immediate treatment for preventing long-term complications and noted that even if SOC treatment is administered rapidly, patients are at risk of aTTP exacerbation or death during the acute treatment phase. According to the interviewed clinicians, adoption of formal clinical practice guidelines in Canada has been constrained by limited access to rituximab, caplacizumab, and rapid ADAMTS13 testing. Most of the interviewed clinicians identified the inconvenience (e.g., cost, availability of equipment and specialized personnel) and risks (e.g., infection, bleeding, thrombosis, transfusion reactions) of PE as limitations of current treatment approaches, as well as the time required for immunosuppressive therapies (especially rituximab) to produce an effect. Most of the interviewed clinicians had direct experience with caplacizumab and noted that patients who received the drug under their care had good treatment outcomes, were compliant with therapy, and experienced few adverse reactions (e.g., minor bleeding).
Environmental Scan of HTA Reviews
The sponsor summarized the global reimbursement status of caplacizumab as of March 2022. Caplacizumab received positive recommendations for reimbursement following HTA review in the UK, Germany, Spain, Sweden, Denmark, France, Scotland, and Italy; negative recommendations in Canada, Quebec, and Australia; and was not filed for review in New Zealand. The sponsor noted that many of the same issues identified by CDEC in the final recommendation for caplacizumab were highlighted in other HTA reviews, including those that recommended reimbursement. All HTA reviews discussed the relevance of the primary outcome in the HERCULES trial (time to platelet count normalization) as a surrogate measure of long-term aTTP complications and mortality. Some reviews (e.g., NICE) concluded that time to platelet normalization plausibly approximated patient exposure to microthrombi and thus would likely be associated with long-term complications given the correlations between time to platelet normalization and mortality documented in earlier observational studies. Other reviews (e.g., PBAC) concluded that small differences in time to platelet normalization provided little or no evidence regarding risk of major thromboembolic events, organ damage, or mortality. Many HTA reviews mentioned the design limitations of the HERCULES trial and their associated limitations, including crossover from double-blind placebo to OL caplacizumab and its potential impact on results during the overall study period as well as generalizability concerns relating to initiation of caplacizumab after PE which is not aligned with the intended use of the drug in clinical practice. Despite these limitations, many HTA reviews concluded that despite absence of formal statistical testing, reduction of health care resource utilization (e.g., duration and volume of PE, duration of hospitalization and ICU stay) among patients receiving caplacizumab was clinically relevant, as was reduction of aTTP recurrence (exacerbation or relapse) during the double-blind treatment period and the overall study period. However, many HTA reviews noted the absence of long-term efficacy and safety data, including rates of aTTP recurrence beyond the 4-week follow-up period after discontinuing caplacizumab in the HERCULES trial. Sweden was the only country to consider RWE in their HTA review, which noted that caplacizumab use was associated with low mortality rates (between 1% and 6%) in the real world; however, variation in clinical management and patient status at the group level may have contributed to patient outcomes, rendering the effect size uncertain.
Appendix 5: Description and Appraisal of Outcome Measures
Note this appendix has not been copy-edited.
Aim
To describe the following outcome measures and review their measurement properties (validity, reliability, responsiveness to change, and MID):
Repeatable Battery for the Assessment of Neurological Status (RBANS)
HIT-6
SF-36, version 2.0
Findings
Table 59: Summary of Outcome Measures in the Post-HERCULES Trial and Their Measurement Properties
Outcome measure | Description and type of scale | Conclusions about measurement properties | MID |
|---|---|---|---|
RBANS | RBANS is a 30-minute screening test used to assess the cognitive mental status of patients in 5 domains (immediate memory, delayed memory, attention, language, and visuospatial ability).14 The overall score (performance across all 5 domains) and domain scores were based on the normal population values adjusted for age. Scores were standardized to a mean score of 100 with a standard deviation of 15. An increase in the total score indicated improvement.14 | The psychometric properties of the RBANS in the setting of aTTP were not identified in the literature. | An estimated MID in the RBANS in the setting of aTTP was not identified in the literature. |
HIT-6 | HIT-6 is a 6-item questionnaire used to assess the impact of headaches on a patient’s HRQoL. The items were 6 areas of functioning that are most impacted in patients with headaches including pain, role functioning (ability to carry out usual activities), social functioning, vitality (energy/fatigue), cognitive functioning, and psychological/emotional distress.14 Scores ranged from 36 to 78, with higher scores indicating worse condition.14 | The psychometric properties of the HIT-6 in the setting of aTTP were not identified in the literature. | An estimated MID in the HIT-6 in the setting of aTTP was not identified in the literature. |
SF-36 v2.0 | SF-36 v2.0 is a 36-item questionnaire used to assess HRQoL in various disease states. The survey comprised 8 multi-item scales (domains): physical functioning (10 items), social functioning (2 items), role functioning/physical (4 items), role functioning/emotional (3 items), emotional well-being (5 items), vitality (energy/fatigue) (4 items), pain (2 items), and general health (5 items). An additional single item covered change in health status over the past year.14 Two summary measures (PCS and MCS) can be derived using the domain scores. For each domain, item scores were coded, summed, and transformed on to a scale from 0 (worse possible health state) to 100 (best possible health state). A higher score indicated a more favourable health state.14 | The psychometric properties of the SF-36 v2.0 in the setting of aTTP were not identified in the literature. The psychometric properties of the SF-36 v2.0 were assessed in adult patients previously treated for chronic ITP and had participated in 2 clinical studies of eltrombopag.a Validity: For construct validity, moderate to strong63 Pearson correlations (> 0.30) were observed between the baseline and change scores of the SF-36 PF, SF-36 VT, PCS, MEI-SF, FACIT-F, and FACT-Th6.64 Reliability: For internal consistency, all item-to-domain score correlations were sufficientb (> 0.20) and the Cronbach alpha values for the domains were acceptable65 (≥ 0.75). For test-retest reliability in clinically stable patients (mean of 39 to 43 days), the ICC was acceptable65 (> 0.70) in the physical function, general health, and vitality domains in 1 study, and in all domains except for bodily pain and emotional role in the other study. The results of the subgroup analysisc were generally consistent with the primary analysis; ICC was acceptable65 (> 0.70) for all domains and summary measures except for social function and emotional role domains.64 Responsiveness: For responsiveness to change, the PCS was able to discriminate between responders and nonrespondersd (effect size = NR), but the MCS was not able to discriminate. Signorovitch et al.64 concluded the SF-36 v2.0 was less responsive to change in comparison to disease-specific measures. | An estimated MID in the SF-36 v2.0 in the setting of aTTP was not identified in the literature. |
aTTP = acquired thrombotic thrombocytopenic purpura; FACIT-F = fatigue subscale of the functional assessment of chronic illness therapy; FACT-Th6 = 6-item subset from the thrombocytopenia subscale of the functional assessment of cancer therapy; HIT-6 = Headache Impact Test-6; HRQoL = health-related quality of life; ICC = intraclass correlation coefficient; ITP = immune thrombocytopenia; MEI-SF = motivation and energy inventory-short form; MCS = mental component summary; MID = minimal important difference; NR = not reported; PCS = physical component summary; PF = physical function; RBANS = repeatable battery for the assessment of neurological status; SF-36 v2.0 = Short Form health survey version 2.0; VT = vitality.
aGeneralizability of the results in the Signorovitch et al. study64 to patients with aTTP and in patients who receive treatment with a drug other than eltrombopag is uncertain.
bThe Signorovitch et al. study64 prespecified that a correlation coefficient threshold of ≥ 0.20 indicated sufficient internal consistency.
cSubgroup analysis included patients with ≤ 15% change in platelet counts between consecutive visits; time frame for test-retest reliability was 45 to 52 days. Note that the primary analysis used clinically stable patients with 2 consecutive scores for time points when platelet counts were most similar.64
dThe Signorovitch et al. study64 defined responders as patients with either (1) doubling of platelet count relative to baseline or (2) increased platelet counts > 50,000/µL in patients with baseline platelet count < 50,000/µL.
Pharmacoeconomic Review
Abbreviations
ADAMTS13
a disintegrin and metalloproteinase with a thrombospondin type 1 motif, member 13
aTTP
acquired thrombotic thrombocytopenic purpura
BIA
budget impact analysis
CAG
Canadian Apheresis Group
ICER
incremental cost-effectiveness ratio
ICU
intensive care unit
ITO
intent to observe
PE
plasma exchange
QALY
quality-adjusted life-year
SOC
standard of care
TTP
thrombotic thrombocytopenic purpura
Executive Summary
The executive summary comprises 2 tables (Table 1 and Table 2) and a conclusion.
Item | Description |
|---|---|
Drug product | Caplacizumab (Cablivi), IV or subcutaneous injection |
Submitted price | Caplacizumab, 11 mg, powder for solution: $6,200.0000 per single-use vial |
Indication | For the treatment of adults with aTTP in combination with PE and immunosuppressive therapy |
Health Canada approval status | NOC |
Health Canada review pathway | Priority review |
NOC date | February 28, 2020 |
Reimbursement request | As per indication |
Sponsor | Sanofi-Aventis Canada Inc. |
Submission history | Previously reviewed: Yes Indication: For the treatment of adults with aTTP in combination with PE and immunosuppressive therapy Recommendation date: August 26, 2020 Recommendation: Do not reimburse |
aTTP = acquired thrombotic thrombocytopenia purpura; NOC = Notice of Compliance; PE = plasma exchange.
Table 2: Summary of Economic Evaluation
Component | Description |
|---|---|
Type of economic evaluation | Cost-utility analysis Decision tree followed by Markov model |
Target population | Adults experiencing an acute aTTP episode |
Treatment | Caplacizumab, 11 mg IV injection before PE, followed by 11 mg SC afterwards on day 1, then 11 mg SC daily following PE, then 11 mg SC daily for 30 days following the last daily PE in addition to SOC. If, after the initial treatment course, signs of persistent underlying disease such as suppressed ADAMTS13 activity levels remain present, treatment may be extended for a maximum of 28 days. |
Comparator | SOC, defined as PE therapy continuing for at least 2 days after platelet count reaches ≥ 150 × 109/L, corticosteroid treatment of at least 1 mg/kg/day continuing for 1 week after the end of PE therapy, and rituximab as permitted by standard practice at each study centre. |
Perspective | Canadian publicly funded health care payer |
Outcome | QALYs |
Time horizon | Lifetime (53 years) |
Key data source | HERCULES trial and post-HERCULES study |
Submitted results | ICER = $210,903 per QALY (incremental costs: $283,010; incremental QALYs: 1.34) |
Key limitations |
|
CADTH reanalysis results |
|
ADAMTS13 = a disintegrin and metalloproteinase with a thrombospondin type 1 motif, member 13; aTTP = acquired thrombotic thrombocytopenic purpura; ICER = incremental cost-effectiveness ratio; PE = plasma exchange; QALY = quality-adjusted life-year; SC = subcutaneous; SOC = standard of care.
Conclusions
In adult patients with acquired thrombotic thrombocytopenic purpura (aTTP), the use of caplacizumab in addition to standard of care (SOC) reduced the frequency of aTTP recurrence within the active treatment and follow-up period of the HERCULES trial and was associated with 1 patient death (n = 72) within the same time period, compared to 3 deaths in patients treated with SOC alone (n = 73). Fewer patients randomized to receive caplacizumab experienced recurrences (early or late exacerbations) than patients randomized to receive SOC alone during the HERCULES trial. Among patients who completed the HERCULES trial and did not yet experience recurrence of aTTP, the post-HERCULES long-term follow-up study reported that patients who were initially randomized to caplacizumab did not have an increased frequency of long-term aTTP relapse compared to patients who were initially randomized to SOC and remained caplacizumab-naive over the 3-year follow-up period, although these data were associated with limitations due to study design, a lack of statistical testing and a priori hypotheses, and small patient numbers.
CADTH undertook reanalyses limiting the long-term reduction in risk of relapse associated with caplacizumab to 3 years and lowering the duration of neuropsychological impairment associated with an aTTP event to 1 year. With these changes, the addition of caplacizumab to SOC was associated with an incremental cost-effectiveness ratio (ICER) of $269,158 per quality-adjusted life-year (QALY) compared to SOC alone. CADTH results were consistent with those of the sponsor in that caplacizumab would require a substantial (75%) price reduction to be considered cost-effective at a willingness-to-pay threshold of $50,000 per QALY.
The key drivers of the model were the extrapolation of relapse rates reported in the 3-year post-HERCULES study over patients’ entire remaining lifespan, as well as the reduction in relative risk of long-term sequelae assumed for patients who received caplacizumab. In the sponsor’s base case, 73% of the incremental QALYs were gained in the extrapolated period for which there are no clinical data. Cost-effectiveness results were especially sensitive to assumptions in the relative risk of long-term sequelae associated with caplacizumab, which were highly uncertain and which CADTH was unable to address given the lack of data. Furthermore, given the inflexibility in the model structure, CADTH was unable to model the associated costs and outcomes (including long-term sequelae) associated with multiple true relapses given the model only explicitly modelled 1 relapse event. Finally, the use of prevalence rather than incidence data for long-term sequelae following individual aTTP events would overestimate the impact of treatment. Together, these limitations increase the uncertainty in the model’s extrapolated predictions, the time period in which the majority of incremental QALYs were gained.
Stakeholder Input Relevant to the Economic Review
This section is a summary of the feedback received from the patient groups, registered clinicians, and drug plans that participated in the CADTH review process.
Patient input was received from the Answering TTP Foundation, who conducted an online survey receiving 49 responses, of whom 44 lived in Canada. Of the respondents, 31 were patients with thrombotic thrombocytopenic purpura (TTP), with the rest being caregivers, family, or friends of patients. Survey respondents had a variety of symptoms during their TTP episode or as a result of treatment, including “serious and frequent” bruises, fever, fatigue, migraine, confusion, abdominal pain, anxiety, depression, and panic attacks. Eight respondents reported a life-threatening or incapacitating stroke or acute myocardial infarction, and 4 had incapacitating or life-threatening kidney problems. In terms of number of relapses, 47%, 12%, 22%, and 10% of respondents reported experiencing 0, 1 to 2, 3 to 4, and 5 to 6 relapses respectively; 2 respondents had experienced 7 to 10 relapses. Of the 49 respondents, 45 were treated with prednisone, 32 with rituximab, 12 with cyclosporin, 9 had had their spleen removed, and 16 respondents had been treated with caplacizumab. Survey responders emphasized the hardship of long hospital stays, the side effects of steroids, and the negative impact and frightening nature of plasma exchanges (PEs), with at least 1 patient reporting post-traumatic stress disorder. In addition, 68% reported experiencing hives from PE therapy, 37% experienced anaphylaxis, and 2 respondents reported developing transfusion-related acute lung injury. Patients and caregivers reported difficulty and expenses associated with treatment such as travel costs and time off work, with several noting difficulties in treatment affordability due to a lack of coverage for rituximab and/or caplacizumab and an inability to access insurance while off work. Patients with caplacizumab experience noted shorter hospital stays, faster healing, the prevention of further disease, and a reduction in anxiety regarding relapses. The patient group noted that the effects of COVID-19 created a shortage of blood donations, raising concerns about the future plasma capacity in Canada, a burden which the use of caplacizumab could improve by reducing plasma resources.
Clinician group input was received from the Canadian Apheresis Group (CAG). CAG noted that standard treatment is not sufficient in patients who develop refractory disease, which is associated with a high probability of catastrophic organ damage (e.g., stroke) and death. Caplacizumab was noted as a good treatment option for all patients with aTTP, but especially those presenting with significant organ damage to protect from further deterioration while immunosuppression takes effect. CAG proposes that patients who present with a high pretest probability of aTTP have access to caplacizumab without waiting on their a disintegrin and metalloproteinase with a thrombospondin type 1 motif, member 13 (ADAMTS13) assay results, with continuing administration depending on ADAMTS13 levels when received, while patients with an intermediate-to-low pretest probability of aTTP should access caplacizumab only once the ADAMTS13 results are back and show low (< 10%) levels. Patients with ADAMTS13 of greater than 10% without evidence of anti-ADAMTS13 antibodies should not receive caplacizumab. As caplacizumab addresses the thrombotic mechanism of aTTP but not the underlying autoimmune disease, CAG noted there is a risk of recurrence when treatment is discontinued and that clinicians should consider ordering ADAMTS13 activity and antibody levels before discontinuing caplacizumab.
Input from the drug plans noted that provision of caplacizumab in the first line would be associated with substantial budgetary impact. The plans also noted that access to specialists may be limited as aTTP is an ultra-rare disease.
Several of these concerns were addressed in the sponsor’s model:
The comparator, SOC, was defined as PE therapy plus steroids with or without rituximab. This was considered reflective of practice in Canada.
The impact of aTTP on patient quality of life, including the potential for long-term sequelae (i.e., cognitive and neuropsychological impairment) were modelled.
A higher mortality rate was associated with patients who were refractory to standard PE and immunosuppressive treatment compared to those who were not refractory.
CADTH was unable to address the following concerns raised from stakeholder input:
The recurrent nature of aTTP, beyond a single relapse, was not explicitly modelled within the submitted model structure.
The use and the cost of ADAMSTS13 activity testing to guide discontinuation of caplacizumab therapy was not incorporated due to a lack of data.
Economic Review
The current review is for caplacizumab (Cablivi) for the treatment of adults with aTTP.
Economic Evaluation
Summary of Sponsor’s Economic Evaluation
Overview
Caplacizumab is indicated for the treatment of adults with aTTP in combination with PE and immunosuppressive therapy,1 which is aligned with the sponsor’s reimbursement request.2 The sponsor submitted a cost-utility analysis comparing caplacizumab plus SOC to SOC alone in adult patients experiencing an acute aTTP episode. SOC consisted of daily PE until at least 2 days after patient platelet count had normalized at or above 150 × 109/L, corticosteroid treatment (prednisone or methylprednisolone) for the duration of daily PE and then 7 days thereafter, and the option of rituximab.
Caplacizumab is available in single or multivial (7) pack kits containing an 11 mg vial of caplacizumab powder, a prefilled syringe of sterile water for injection, a vial adaptor, a needle, and alcohol swabs.1 The recommended loading dose of caplacizumab is 11 mg by IV injection at least 15 minutes before the PE, followed by an 11 mg subcutaneous injection after completion of the PE on that day. Subsequently, 11 mg of caplacizumab should be administered as a daily maintenance dose by subcutaneous injection following PE administration for the duration of daily PE therapy, then once daily for 30 days following the last daily PE treatment. If, after the initial treatment course, signs of persistent underlying disease such as suppressed ADAMTS13 activity levels remain present, treatment may be extended for a maximum of 28 days.1 At the submitted price of $6,200 per 11 mg dose and the sponsor’s assumed mean duration of treatment of 37.2 days, the average cost of caplacizumab therapy in the model was $236,840 per patient per aTTP episode. SOC in the caplacizumab group consisted of a mean of 5.5 days of PE therapy with a total volume of 21.3 L ($2,602), 1 dose of 100 mg IV methylprednisolone ($6), and 1.6 doses of 375 mg/m2 IV rituximab ($3,707, including wastage), while SOC in the SOC alone group consisted of 6.5 days of PE therapy with a total volume of 35.9 L ($4,384), 1 dose of methylprednisolone ($6), and 1.9 doses of rituximab ($4,562, including wastage).
The clinical outcome of interest was QALYs. The sponsor adopted a lifetime time horizon (53 years), with the analysis conducted from the perspective of a publicly funded health care payer. Future costs and benefits were discounted at a rate of 1.5% per cycle, and the model’s Markov cycle length was 3 months.
Model Structure
The sponsor submitted a hybrid model structure that consisted of a decision tree to model an acute aTTP episode (Figure 1), followed by a 3-state Markov model representing patients’ long-term outcomes in terms of remission, true relapse (i.e., not a late exacerbation),3 or death (Figure 2).
Patients entered the decision tree while experiencing an acute aTTP event and assumed to be admitted to hospital to be treated with either caplacizumab plus SOC or SOC alone. During the 3-month duration of the decision tree, patients could either be responders or initially refractory and then responders to treatment; they could then have an exacerbation or no exacerbation; and they were then either alive or dead at the end of the decision tree. Refractoriness was defined in the sponsor’s model as per the International TTP Working Group consensus definition: lack of a sustained platelet count increment or platelet counts less than 50 × 109/L and persistently raised lactate dehydrogenase (LDH) (> 1.5 × upper limit of normal) despite 5 PEs and steroid treatment.4 The decision tree incorporated both early and late exacerbations, with the former based on the HERCULES trial’s definition for an exacerbation (i.e., recurrence after initial recovery of platelet count requiring re-initiation of daily PE occurring during the first 30 days post daily PE therapy) while the latter was based on the HERCULES trial definition for a relapse (i.e., recurrence within the trial period but after the first 30 days post daily PE therapy).5
After this 3-month initial period, patients then entered the Markov model in either the remission or dead state, as applicable. Patients in remission had a per-cycle chance of experiencing a relapse, defined as a recurrence of disease after initial resolution of disease and after full normalization of ADAMTS13 activity and occurring after the follow-up period of the HERCULES trial.5 Patients who did not die during this relapse did not revert to the remission state in the following cycle, but instead were assigned a “payoff,” in which all costs and outcomes (i.e., life-years and QALYs) from time of relapse until death were applied in the model as a one-off lump sum upon entry into the true relapse state (Figure 3). Such patients were no longer tracked in the Markov model and thus did not have the possibility of relapsing again.
Model Inputs
The sponsor’s modelled population is based on patients enrolled in the HERCULES trial,3,6,7 with 69% of patients being female and having a mean starting age of 46.1 years. SOC was represented by the PE plus placebo group of the HERCULES trial.3 All modelled patients were assumed to receive PE and methylprednisolone with 48% of patients in the SOC arm and 39% in the caplacizumab arm assumed to receive rituximab.3
The primary measures of efficacy in the model were the proportion of patients who were initially refractory to treatment, the proportion experiencing an exacerbation during the initial 3-month period, both derived from the HERCULES trial, as well as the probability of experiencing a relapse each Markov cycle thereafter, derived from the post-HERCULES study. No patients randomized to receive caplacizumab in the HERCULES trial were refractory to treatment, while 6.85% of patients randomized to receive SOC were. In terms of exacerbations in the first 3 months, 12.68% of patients randomized to receive caplacizumab in the HERCULES trial experienced an early or late exacerbation, while 38.36% of patients randomized to receive SOC did. For long-term relapse after remission, among patients who completed the HERCULES trial and did not yet experience recurrence of aTTP, 8.2% of those randomized to receive caplacizumab and 27.6% of those randomized to receive SOC experienced at least 1 relapse during the 3-year observation period of the post-HERCULES study, which the sponsor used to estimate a 0.68% and 2.30% probability of relapse per 3-month model cycle. Patients randomized to SOC who had received open-label caplacizumab after experiencing a recurrence during the HERCULES trial were excluded from this analysis, as were patients randomized to caplacizumab who experienced a recurrence during the HERCULES trial.
During the initial 3-month period, mortality was based on post hoc internal analyses of the HERCULES trial data, where 1 of 70 (1.43%) caplacizumab responders, 2 of 66 (3.03%) SOC responders, and 1 of 5 (20%) refractory patients receiving SOC died during the trial period. For patients in the remission health state, mortality rates from Upreti et al. (2019)8 were used to generate a standardized mortality ratio of 9.03, which was applied to gender- and age-specific general population life tables as reported by Statistics Canada.9 Mortality during a relapse after remission was assumed to be the same as that experienced by responders during the initial aTTP event.
During their initial aTTP event, patients could experience long-term sequelae in the form of cognitive and/or neuropsychological impairments. The proportion of patients in the SOC group experiencing a mild (54%) or moderate to severe (21%) cognitive impairment was based on 24 patients from the Oklahoma TTP-HUS registry who were followed for a median of 4 years after an aTTP episode,10 while the proportion of patients experiencing a neuropsychological impairment (37%) was based on a study on the prevalence of post-traumatic stress disorder and depression in TTP11 (Table 11). Patients in the caplacizumab group were assumed to have a relative risk of each individual sequelae of 0.66, based on the ratio of days spent in hospital or the intensive care unit (ICU) between treatment groups and the sponsor’s clinical expert opinion.5 To determine the probability of patients having 1 of, both, or neither impairment, the Markov model assumed that cognitive and neuropsychological impairments occur independently of each other, while the postrelapse payoff section assumed that all patients with a cognitive impairment only had a cognitive impairment.5
Payoff values for costs, life-years, and QALYs were calculated separately for caplacizumab and SOC. The calculation was based on the remaining life-years at each cycle for patients experiencing a true relapse. Under this payoff approach, relapsing patients were assumed to spend 0.25 years (3 months) in the payoff-relapse state (termed “process”) in which costs and utilities were informed by the expected costs and QALYs calculated from the decision tree and these patients then transitioned to the payoff-remission state for the remainder of their lifespans (termed “output”) in which costs and disutilities were calculated based on the inputs from the remission state.5
Patients in either group could also experience treatment-emergent adverse events, based on those observed in the HERCULES trial and post-HERCULES study. These would have impacts on both utilities and costs.3,7,12
In terms of quality of life, patients were assigned a utility multiplier of 0.644 while hospitalized during the initial acute aTTP episode, derived from differences in average utility between hospital admission and discharge reported in an American influenza vaccine study,13 and 0.736 after discharge, based on a mapping exercise of patients’ health-related quality of life data from Short Form (36) Health Survey (SF-36) observations in the Oklahoma TTP registry to the EQ-5D 3-Level.14 This mapping exercise further informed the utility in the remission health state, which was adjusted to account for age- and gender-matched population norms from the UK14,15 and further modified depending on the presence of cognitive and/or neuropsychological impairment.16,17 It was assumed that cognitive and/or neuropsychological impairment would last a patient’s entire lifetime.
Drug acquisition costs for caplacizumab were based on the sponsor’s submitted price,5 while the Ontario Drug Benefit Formulary informed other drug costs,18 The unit cost of PE therapy was derived from the previous CADTH review on caplacizumab, which had been informed by the sponsor,19 Additional costs during the acute phase included hospitalization in the ICU (3.6 days for patients receiving caplacizumab and 10.1 days for patients receiving SOC) and the general ward (8.4 days for patients receiving caplacizumab and 6.1 days for patients receiving SOC);12 administration of PE; management of adverse events, laboratory testing, and hematology specialist visits. Long-term remission costs included ongoing laboratory testing, hematology specialist visits, occasional rituximab usage (1% of patients in remission), and management of cognitive and/or neuropsychological impairments. Unit costs were sourced from the Canadian Institute of Health Information for ICU and ward stays as well as for the costs associated with adverse events.20 The Ontario Ministry of Health Schedule of Physician Services informed the costs of administration, physician visits, and procedure costs.21
Summary of Sponsor’s Economic Evaluation Results
The sponsor presented a probabilistic base-case analysis based on 5,000 iterations, the results of which are presented in Table 3. Deterministic results were similar to the probabilistic. The submitted analysis is based on publicly available prices for SOC. More detailed results of the sponsor’s economic evaluation are presented in Appendix 3.
Base-Case Results
For the treatment of adult patients with aTTP, the use of caplacizumab in combination with PE and immunosuppressive therapy (SOC) was associated with an incremental cost of $283,010 compared to SOC alone, and 1.34 incremental QALYs, resulting in an incremental cost-effectiveness ratio (ICER) of $210,903 per QALY (Table 3).
Approximately 73% of incremental QALYs were gained after the first 3 years, in the portion of the model which was fully extrapolated (i.e., which occurred later than the mean follow-up of the post-HERCULES study).
Table 3: Summary of the Sponsor’s Economic Evaluation Results
Drug | Total costs ($) | Incremental costs ($) | Total QALYs | Incremental QALYs | ICER vs. SOC ($/QALY) |
|---|---|---|---|---|---|
SOC alone | 74,689 | Reference | 8.95 | Reference | Reference |
Caplacizumab + SOC | 357,700 | 283,010 | 10.29 | 1.34 | 210,903 |
ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year; SOC = standard of care; vs. = versus.
Source: Sponsor’s pharmacoeconomic submission.5
Sensitivity and Scenario Analysis Results
The sponsor considered scenario analyses; none of these analyses had notable impacts on the model’s findings.
CADTH Appraisal of the Sponsor’s Economic Evaluation
CADTH identified several key limitations to the sponsor’s analysis that have notable implications on the economic analysis.
Long-term probability of relapse is highly uncertain: In the efficacy intent-to-observe (efficacy ITO) population of the post-HERCULES study, the cumulative 3-year probability of a patient having a true relapse was reported as 4 of 49 (8%) patients who were randomized to receive caplacizumab during their acute aTTP event in the HERCULES trial, and 8 of 29 (28%) patients who were randomized to SOC.7 As the efficacy ITO population of the post-HERCULES study only included patients who had completed the HERCULES trial and excluded patients initially randomized to SOC but who later received open-label caplacizumab due to exacerbation, as well as patients initially randomized to caplacizumab who had experienced an exacerbation in the HERCULES trial, it should be noted that protections provided by randomization against bias and confounding do not apply to this extension study. As those with a recurrence during the HERCULES trial were eliminated in the efficacy ITO population, bias may be attributed to the effects of the drug. Additionally, no formal statistical analyses were conducted in the post-HERCULES study and all results were presented in descriptive and exploratory fashion, without testing for a priori hypotheses, subgroup or sensitivity analyses, or adjustment for multiple comparisons. While evidence from the post-HERCULES study is not indicative of an increased rate of recurrences among patients receiving caplacizumab after discontinuation, due to these stated limitations, as well as to the small number of caplacizumab-naive patients analyzed, the relapse rates in the post-HERCULES study are associated with uncertainty even within the time period studied (3 years after an aTTP event). Based on the 3-year probabilities of relapse reported in the post-HERCULES study, the sponsor’s model assumed a 0.68% and 2.30% per cycle (3-month) probability of true relapse for patients receiving caplacizumab and SOC,5 respectively, using simple division, and applied these probabilities for the remaining 53-year time horizon, effectively assuming a lifelong benefit in relapse reduction for patients who received caplacizumab during an acute aTTP event relative to SOC. This assumption was not considered plausible based on CADTH-obtained clinical expert feedback, nor according to the sponsor’s own statement in the key assumptions table of the pharmacoeconomic submission: “The probability of true relapse is not dependent on treatment given for the acute episode. Caplacizumab is used to treat the acute episode only. Clinicians did not anticipate differential effects between treatments for true relapse rates.”2 The timing of relapses in the post-HERCULES study is unclear, as the number of patients who had a first relapse when reported at each measured time point (12 months, 24 months, and 36 months) and by ADAMSTS13 activity subgroup (< 10% and ≥ 10%) were inconsistent with the cumulative 3-year data reported.7 As such, CADTH was unable to calculate rates of relapse over shorter intervals of time based on the post-HERCULES study.
In its base case, CADTH made a correction to the sponsor’s per-cycle relapse probabilities by converting the 3-year probabilities to instantaneous rates and then to a 3-month probabilities.22,23 CADTH then assumed these differential relapse probabilities for patients receiving caplacizumab and SOC would apply for the first 3 years after the resolution of the initial aTTP event, after which a per-cycle probability of relapse of 0.5% was applied for both groups. These changes resulted in 43% of patients receiving SOC having a true relapse within their lifetime, a figure that aligns more closely to the 40% estimate of the proportion of patients who will experience relapse that has previously been noted in the literature24-26 and to CADTH-obtained clinical expert feedback, than to the 71% of patients receiving SOC who relapsed within their lifetime under the sponsor’s assumptions. Due to limitations associated with the relapse data from the post-HERCULES study, CADTH explored a scenario analysis where these differential relapse rates were limited to a single year after recovery from the initial aTTP episode (i.e., 1 year after the initial 3-month decision tree ended).
Inflexible model structure leads to uncertainty in the long term model estimates: The sponsor’s model used several simplifying assumptions which made the model inflexible and increased uncertainty in the results. The sponsor’s Markov model included health states for remission, true relapse, and death. For the remission state, the sponsor adopted a typical Markov cohort approach, in which patients accrue costs, life-years, and QALYs based on the duration of time spent in this health state. In contrast, for the true relapse health state, the sponsor employed a payoff approach. Using this approach, the model allowed for the explicit modelling of only a single true relapse. Upon entering the true relapse state, remaining costs and QALYs associated with the relapsing patient’s life were assigned single fixed payoff values and removed the patient from the Markov model. In doing so, the sponsor implicitly assumed that patients who relapsed only did so once, which is not consistent with patient input received in this or the prior review of caplacizumab.27
Second, the sponsor used prevalence data10,11 to estimate the proportion of patients with aTTP who had long-term sequelae in the form of cognitive and/or neuropsychological impairments after their initial aTTP episode, rather than incidence data of these impairments after each aTTP event. In doing so, the sponsor overestimated the rates at which a single aTTP event was likely to lead to long-term sequelae, and thus overestimated the absolute risk reduction impact of caplacizumab on the initial aTTP event in terms of these outcomes. This issue interacted with the payoff approach in that the risk reduction in long-term sequelae that might be associated with caplacizumab use over multiple events was accrued during the first aTTP event, while the costs of treating multiple aTTP events, either with caplacizumab and/or SOC, beyond the first relapse were not considered.
Third, to calculate the payoff values, the approach taken simplified long-term sequelae such that patients who had a true relapse were considered to have a cognitive impairment, a neuropsychological impairment, or neither, without the possibility of having both as was possible within the Markov model. The sponsor stated this simplification was anticipated to have minimal impact on results due to few patients experiencing relapse and fewer still experiencing both impairments. However, CADTH notes that under the sponsor’s base case, 71% of patients receiving SOC and 37% of patients receiving caplacizumab relapsed before the end of their lives; of these, 28% and 12%, respectively, were assumed within the Markov section of the model to have both impairments. Due to this simplifying assumption, altering the duration for which a neuropsychological impairment is assumed to last leads to counterintuitive results on the ICER when applied to the sponsor’s base case (Figure 4). This is discussed further in the following section on the neuropsychological impairment limitation.
Due to the submitted model structure, CADTH was unable to address these limitations.
Neuropsychological impairment is unlikely to be lifelong: The sponsor’s model assumed that neuropsychological impairments arising from aTTP events such as depression and anxiety will be lifelong (i.e., up to 53 years). However, according to clinical expert feedback elicited by CADTH, unlike cognitive impairment, neuropsychological impairment would be expected to resolve for most patients over time and with treatment, if required. Furthermore, as noted previously, the submitted model was not flexible enough to allow for increasing patient proportions or increasing duration of neuropsychological impairments after an increasing number of relapses, as might be expected in clinical practice.
In reanalyses, CADTH limited the duration of neuropsychological impairment to 1 year after an aTTP event. Although this changed the duration of neuropsychological impairments in the remission health state of the Markov model, this change does not get fully implemented in the same fashion within the payoff calculations given the sponsor’s simplifying assumption that all patients with a cognitive impairment only have a cognitive impairment (i.e., there are no patients who have both cognitive and neuropsychological impairments) (Table 11). CADTH was unable to address the inappropriate modelling of neuropsychological impairment in the payoff section of the model. Thus, the full impact on the ICER of reducing the duration of neuropsychological impairment could not be fully explored.
Relative risk of long-term sequelae is uncertain: The sponsor’s model assumes that the relative risk of a patient who received caplacizumab experiencing a cognitive or neuropsychological impairment after an aTTP event is 0.66 compared to that of a patient using SOC, based on clinical expert feedback obtained by the sponsor5 and the ratio of time spent in the hospital or in the ICU among treatment groups in the HERCULES trial. Clinical expert feedback elicited by CADTH did not consider this estimate to be unreasonable; however, in the absence of data to inform this estimate, the magnitude of this assumption was noted to be highly uncertain. CADTH notes that varying the relative risk of long-term sequelae associated with the use of caplacizumab has a large impact on the expected ICER value.
CADTH explored the impact of varying the assumed relative risk of long-term sequelae in scenario analyses.
Poor modelling practices were employed. The sponsor’s submitted model included numerous IFERROR statements, which lead to situations in which the parameter value was over-written with an alternative value without alerting the user to the automatized overwriting. IFERROR statements are problematic in that they should generally be unnecessary within a model. The systematic use of IFERROR statements makes thorough auditing of the sponsor’s model impractical as it remains unclear whether the model is running inappropriately by overriding errors.
CADTH was unable to address these limitations and notes that a thorough validation of the sponsor’s model was not possible.
Additionally, the following key assumptions were made by the sponsor and have been appraised by CADTH (Table 4).
Table 4: Key Assumptions of the Submitted Economic Evaluation (Not Noted as Limitations to the Submission)
Sponsor’s key assumption | CADTH comment |
|---|---|
53-year time horizon represents “lifetime.” | Acceptable. |
Mortality during an acute aTTP event can be represented by that reported in HERCULES | Uncertain. According to CADTH-obtained clinical expert feedback, mortality rates in the HERCULES and post-HERCULES studies were lower than expected in routine clinical practice and patients may have been observed and followed by health care teams for TTP recurrence and/or thromboembolic events more vigilantly compared to real-world practice. Mortality rates in the submitted decision tree model are based on those observed in the HERCULES trial, and as such, the absolute risk of mortality for either treatment group may be higher during an acute aTTP event in the real world than modelled. The magnitude of this issue as well as its potential impact on the observed risk reduction for patients receiving caplacizumab in the real world compared to during the HERCULES trial is uncertain. |
The risks of cognitive and neuropsychological impairments are independent in the Markov model. | Uncertain. Some observational studies have reported a correlation between depression and cognitive impairment following TTP events,28 while others did not support such a correlation.29 While the direction of impact should such a correlation exist is uncertain, it is not expected to have a large impact on the current model. |
Rituximab will be used in clinical practice at a similar rate as in the HERCULES trial. | Uncertain. The previous CADTH review of caplacizumab noted that rituximab was used less often for aTTP in Canada than in the sponsor’s model due to access limitations.19 If true, this may impact modelled morbidity, mortality, PE treatment, and hospital stay for both groups. Clinical expert feedback obtained by CADTH for this review could not validate the proportion of patients with aTTP in Canada currently receiving rituximab due to variation in jurisdiction’s access criteria, but it was noted that rituximab usage has been significantly increasing over the past several years. Therefore, the difference between rituximab usage in the HERCULES trial vs. in Canadian clinical practice is likely smaller than previously noted and is thus likely to have a smaller impact on the uncertainty in the modelled results than in the previous review.19 |
Rituximab administration costs were not included. | Inappropriate. The use of rituximab is associated with IV administration costs. However, given the small differences in the rates of rituximab use between treatment groups and the relatively small cost of administration relative to other costs in the model, this omission was expected to have a minimal impact on model results. |
Caplacizumab administration costs were not included. | Potentially appropriate and unlikely to impact the model results. The first dose is administered by IV while all other injections are administered subcutaneously and may be administered by patients or caregivers after proper training.1 |
The costs of managing treatment-related AEs were separately considered in addition to the cost of hospitalization. | Inappropriate. The sponsor’s model considers the cost of ICU and general ward hospitalization by length of stay in each treatment group, based on the HERCULES trial3,12 and cost data from CIHI.20 The submitted model also considers AEs as reported in the HERCULES trial and post-HERCULES study,7 with costs also based on the average cost associated with the AE as reported by CIHI, including treatment and hospitalization. Given that some modelled AEs would occur while a patient was already hospitalized for their aTTP event, it is likely that hospitalization-related costs are double counted for a proportion of these AEs. However, altering the costs associated with each AE has only minimal impact on the modelled results. |
Costs for oral corticosteroids were not included. | Acceptable. Relative to the costs of caplacizumab, PE, and rituximab, the acquisition cost of oral prednisone is negligible and not expected to differ substantially between treatment groups. |
AE = adverse event; aTTP = acquired thrombotic thrombocytopenic purpura; CIHI = Canadian Institute for Health Information; ICU = intensive care unit; PE = plasma exchange; TTP = thrombotic thrombocytopenic purpura.
CADTH Reanalyses of the Economic Evaluation
Base-Case Results
CADTH reanalyses addressed some of the key limitations of the submitted model (Table 5), by reducing the length of time for which caplacizumab was associated with a lower aTTP relapse rate than SOC from lifetime to 3 years, and by assuming that neuropsychological impairments associated with aTTP events have a duration of 1 year rather than lifetime. Additionally, CADTH corrected the calculations estimating the 3-month-cycle probabilities of relapse from the 3-year probabilities in the post-HERCULES study by using a more established conversion methodology.22 CADTH was unable to address the other aforementioned limitations with the submitted model.
Table 5: CADTH Revisions to the Submitted Economic Evaluation
Stepped analysis | Sponsor’s value or assumption | CADTH value or assumption |
|---|---|---|
Correctionsa to sponsor’s base case | ||
1. Per-cycle probability of relapse | Caplacizumab: 0.68% SOC: 2.30% | Caplacizumab: 0.71% SOC: 2.65% |
Changes to derive the CADTH base case | ||
1. Long-term relapse probability | Extrapolated from post-HERCULES study, lifelong effect. | Based on post-HERCULES study for 3 years, after which both groups have a 0.5% probability of relapse per 3-month cycle |
2. Duration of neuropsychological impairment | Lifelong | 1 Year |
CADTH base case | 1 + 2 | |
SOC = standard of care.
aCorrections are minor errors (e.g., transcription errors between report and model, misapplication of distributions or standard errors in probabilistic analyses, and so on) that are not identified as limitations.
CADTH base-case results are presented in Table 6. Additional reanalyses and disaggregated results are presented in Appendix 4.
In the CADTH base-case reanalysis, the addition of caplacizumab to SOC was associated with 1.03 incremental QALYs and $278,078 incremental costs, for an ICER of $269,158 compared to SOC alone. At a willingness-to-pay threshold of $50,000 per QALY, caplacizumab was the most cost-effective option in 1% of iterations. Approximately 65% of the incremental QALYs were gained after the first 3.25 years, in the portion of the model which was fully extrapolated (i.e., which occurred later than the mean follow-up of the post-HERCULES study).
In CADTH reanalysis 2, the change in the duration of neuropsychological impairment produced a counterintuitive lowering of the predicted ICER compared to the sponsor’s corrected base-case ICER value. Due to the sponsor’s simplifying assumption when calculating the payoff values that relapsed patients could not have both a cognitive and neuropsychological impairment, 36% and 24% of patients receiving SOC and caplacizumab, respectively, in the ”remission” health state (i.e., Markov model) were assumed to have a neuropsychological impairment (with or without a cognitive one), while only 9% and 12% of patients receiving SOC and caplacizumab, respectively, in the “true relapse” payoff section of the model would have a neuropsychological impairment. Due to this oversimplification and the reversal in relative proportions of affected patients in each treatment group, altering the duration of neuropsychological impairment has a differential impact on relative costs and QALYs associated with SOC and caplacizumab depending on the proportions of patients who relapse for each comparator and at what time point they relapse. In the sponsor’s base case, with its continuing high relapse rate for patients receiving SOC, this interaction leads to a decreasing ICER as the duration of neuropsychological impairment is increased from 1 to 7 years, followed by an increasing ICER from 8 to 30 years, and a decreasing ICER thereafter (i.e., up to 53 years) (Figure 4). However, when combined with the CADTH reanalysis that limited differential relapse probabilities between comparators to the first 3 years following an aTTP event, altering the duration of neuropsychological impairment produced the expected effect (i.e., the shorter the assumed duration of impairment associated with an aTTP event, the less neuropsychological health loss difference between caplacizumab and SOC, and the higher the ICER associated with caplacizumab).
Table 6: Summary of the Stepped Analysis of the CADTH Probabilistic Reanalysis Results
Stepped analysis | Drug | Total costs ($) | Total QALYs | ICER ($/QALYs) |
|---|---|---|---|---|
Sponsor’s base case | SOC alone | 74,689 | 8.95 | Reference |
Caplacizumab + SOC | 357,700 | 10.29 | 210,903 | |
Sponsor’s corrected base case | SOC alone | 75,976 | 8.96 | Reference |
Caplacizumab + SOC | 362,084 | 10.28 | 215,724 | |
CADTH reanalysis 1 – long-term relapse probability | SOC alone | 65,664 | 9.24 | Reference |
Caplacizumab + SOC | 345,337 | 10.38 | 245,045 | |
CADTH reanalysis 2 – 1-year neuropsychological impairment | SOC alone | 75,141 | 9.48 | Reference |
Caplacizumab + SOC | 355,585 | 10.85 | 205,180 | |
CADTH base case (1 + 2) | SOC alone | 64,545 | 9.88 | Reference |
Caplacizumab + SOC | 342,623 | 10.91 | 269,158 |
ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year; SOC = standard of care.
Scenario Analysis Results
Scenario analyses were conducted using the CADTH base-case reanalysis to investigate the impact of assuming a lower (0.5) and higher (0.80) relative risk of long-term sequelae with caplacizumab, assuming that caplacizumab only lowers relapse risk for 1 year after the initial aTTP event, and assuming neuropsychological impairment lasts 3 years. These scenarios resulted in ICERs associated with the use of caplacizumab ranging from $207,826 to $340,311, with the model being most sensitive to the scenarios in which the relative risk of long-term sequelae was adjusted. Details and results of these scenario analyses can be found in Table 14 and Table 15, respectively.
CADTH also undertook price reduction analyses based on the sponsor-submitted analysis and CADTH’s base-case reanalysis. Under the CADTH base case, a 75% price reduction would be required for caplacizumab to be considered cost-effective at a willingness-to-pay of $50,000 per QALY (Table 7).
Table 7: CADTH Price Reduction Analyses
Analysis | ICERs for caplacizumab plus SOC vs. SOC alone | |
|---|---|---|
Price reduction | Sponsor base case | CADTH reanalysis |
No price reduction | $210,903 | $269,158 |
10% | $186,926 | $239,948 |
20% | $162,949 | $210,738 |
30% | $138,972 | $181,527 |
40% | $114,995 | $152,317 |
50% | $91,018 | $123,107 |
60% | $67,041 | $93,896 |
67.1% | $50,000 | NA |
70% | $43,064 | $64,686 |
75% | NA | $50,000 |
ICER = incremental cost-effectiveness ratio; NA = not applicable; SOC = standard of care; vs. = versus.
Issues for Consideration
PE therapy: Based on the available clinical evidence, caplacizumab was associated with decreased volume of PE therapy, which was further captured in the cost-effectiveness model. CADTH was unable to independently confirm the unit cost of blood products for infusion and thus the cost of PE therapy. CADTH therefore assumed the same price as used by the sponsor in their original CADTH submission for PE therapy (Table 9). Should the daily cost of blood products be substantially different than assumed, the incremental cost of caplacizumab therapy may change. As noted in the patient input submitted for this review and reported by news agencies,30 there is a current shortage of blood donations in Canada which may lead to reduced plasma capacity and/or increased costs. Should this shortage continue, caplacizumab may be more attractive if it reduces plasma usage during acute aTTP treatment in clinical practice as suggested by the HERCULES trial.
Model assumes no delay in treatment: The sponsor’s model assumes that patients receive treatment for aTTP without delay, or at least without more delay than was experienced by patients entering the HERCULES trial. However, given the rarity of aTTP, the high cost of caplacizumab, and the possibility that reimbursement of caplacizumab may be limited to clinical specialists or based on ADAMTS13 testing as suggested by clinician and drug plan input, it is possible that delays in access to caplacizumab may occur in a real-world clinical setting. This may impact the clinical effectiveness of caplacizumab and, therefore, its cost-effectiveness; however, without more data, it is uncertain how delays in treatment initiation may impact patients’ clinical outcomes.
Outpatient transition: Caplacizumab is initiated in hospital and, upon discharge, continued in an outpatient setting. The transition from hospital budgets to drug plan budgets, as well as the potential offset of costs due to reduced ICU and overall hospital length of stays may be seen by hospital budget holders while drug plan payers would not benefit from these potential offsets, complicating the implementation of caplacizumab therapy.
Therapy decisions: Clinical expert feedback obtained by CADTH indicated that tapering and stopping PE therapy, as well as reinitiating it in the case of recurrence, is often guided in part by normalization or worsening of platelet count, a response measure which may be masked by caplacizumab. Caplacizumab raises platelet count without necessarily resolving the underlying condition, and this artificial rise in platelets may complicate treatment decisions and patient monitoring, as well as potentially delay some exacerbations rather than prevent them. The HERCULES trial administered caplacizumab for the length of daily PE therapy and for an additional 30 days, with the option of up to 4 weeks of additional caplacizumab guided by risk factors for recurrence such as persistent, severe ADAMTS13 deficiency.3 The product monograph states: “Patients, especially those with ADAMTS13 activity < 10% at or near the time of discontinuation of Cablivi, should be closely monitored for platelet counts and signs of aTTP for early diagnosis of relapse after stopping or interrupting use of Cablivi.”1 Input from the clinical group, CAG, further supports this practice as ADAMTS13 activity and antibody levels should be monitored when considering treatment discontinuation given concerns of recurrence. While the clinical trial had a clear maximum duration of treatment (58 days after daily PE cessation) and the product monograph specifies treatment may be extended by a maximum of 28 days and should be discontinued if the patient experiences more than 2 recurrences of aTTP while on caplacizumab, it is not clear how long treatment will continue for patients with persistent recurrence risk factors in real-world clinical practice. As only 1 true relapse of aTTP was possible within the model, the economic impact of either multiple recurrences or discontinuing caplacizumab therapy following 2 recurrences could not be considered.
Development of antidrug antibodies: Antidrug antibodies were detected in 3 patients receiving caplacizumab (9%) in the TITAN trial31 and 2 caplacizumab patients (2.8%) and 1 placebo patient (1.4%, presumably during open-label caplacizumab treatment) in the HERCULES trial.12 No serious adverse events were reported for these patients, and no impact on drug efficacy was observed. The potential impact of developing antidrug antibodies was not considered in the economic analysis.
Resubmission: The sponsor has submitted a resubmission that contains new clinical information and a new pharmacoeconomic model that incorporated some of the new clinical information and adjusted model structure, assumptions, and inputs in response to the limitations identified with the previously submitted model.5,19 A budget impact analysis (BIA) was also developed by the sponsor for this resubmission.32 As such, the pharmacoeconomic findings of the current review are different from those of the previous report.
Overall Conclusions
In adult patients with aTTP, the use of caplacizumab in addition to SOC reduced the frequency of aTTP recurrence within the active treatment and follow-up period of the HERCULES trial and was associated with 1 patient death (n = 72) within the same time period compared to 3 deaths in patients treated with SOC alone (n = 73). Fewer patients randomized to receive caplacizumab experienced recurrences (early or late exacerbations) than patients randomized to receive SOC alone during the HERCULES trial. Among patients who completed the HERCULES trial and did not yet experience recurrence of aTTP, the post-HERCULES extension study reported that patients who were initially randomized to caplacizumab did not have an increased frequency of long-term aTTP relapse compared to patients who were initially randomized to SOC and remained caplacizumab-naive over the 3-year follow-up period, although these data were associated with limitations due to study design, a lack of statistical testing and a priori hypotheses, and small patient numbers. Relative risks of cognitive and neuropsychological impairments were not studied in either the HERCULES trial or post-HERCULES study but were assumed to be lower for patients using caplacizumab than SOC due to reductions in length of ICU and hospital stay observed in the HERCULES trial.
CADTH undertook reanalyses limiting the long-term reduction in risk of relapse associated with caplacizumab to 3 years and lowering the duration of neuropsychological impairment associated with an aTTP event to 1 year. With these changes, the addition of caplacizumab to SOC was associated with an ICER of $269,158 per QALY compared to SOC alone. CADTH results were consistent with those of the sponsor in that caplacizumab would require a substantial (75%) price reduction to be considered cost-effective at a willingness-to-pay threshold of $50,000 per QALY.
The key drivers of the model were the extrapolation of relapse rates reported in the 3-year post-HERCULES study over patients’ entire remaining lifespan, as well as the reduction in relative risk of long-term sequelae assumed for patients who received caplacizumab. In the sponsor’s base case, 73% of the incremental QALYs were gained in the extrapolated period for which there are no clinical data. Cost-effectiveness results were especially sensitive to assumptions in the relative risk of long-term sequelae (cognitive and neuropsychological impairments), which were highly uncertain. Altering the relative risk of long-term sequelae from 0.66 as assumed by the sponsor to 0.50 and 0.80 led to ICERs of $207,826 per QALY and $340,311 per QALY, respectively, when applied to the CADTH base case. Beyond these exploratory analyses, CADTH was unable to address the lack of data regarding the potential reduction in risk of long-term sequelae associated with caplacizumab.
Furthermore, given the inflexibility in the model structure, CADTH was unable to model the associated costs and outcomes (including long-term sequelae) associated with multiple true relapses given the model only explicitly modelled 1 relapse event. Finally, the use of prevalence rather than incidence data for long-term sequelae following individual aTTP events would overestimate the impact of treatment. Together, these limitations increase uncertainty in the model’s extrapolated predictions, the time period in which the majority of incremental QALY were gained.
References
1.Cablivi (caplacizumab): 11 mg powder for solution for intravenous (IV) or subcutaneous injection [product monograph]. Laval (QC): sanofi-aventis Canada Inc.; 2022 May 03.
2.Drug Reimbursement Review sponsor submission: Cablivi (caplacizumab), 11 mg powder for solution, for intravenous (IV) or subcutaneous injection [internal sponsor's package]. Laval (QC): sanofi-aventis Canada Inc.; 2022 Jun 22.
3.Scully M, Cataland SR, Peyvandi F, et al. Caplacizumab treatment for acquired thrombotic thrombocytopenic purpura. N Engl J Med. 2019;380(4):335-346. PubMed
4.Scully M, Cataland S, Coppo P, et al. Consensus on the standardization of terminology in thrombotic thrombocytopenic purpura and related thrombotic microangiopathies. J Thromb Haemost. 2017;15(2):312-322. PubMed
5.Pharmacoeconomic evaluation [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Cablivi (caplacizumab), 11 mg powder for solution, for intravenous (IV) or subcutaneous injection. Laval (QC): sanofi-aventis Canada Inc.; 2022 Jun 22.
6.Clinical Study Report: ALX0681-C301 (HERCULES). A phase III double-blind, randomized, parallel group, multicenter placebo-controlled trial to study the efficacy and safety of caplacizumab in patients with acquired thrombotic thrombocytopenic purpura, version 2.0 [internal sponsor's report]. Zwijnaarde (BE): Ablynx NV; 2018 Jun 18.
7.Clinical Study Report: ALX0681-C302/LTS16371 (Post-HERCULES). Prospective follow-up study for patients who completed study ALX0681-C301 (HERCULES) to evaluate long-term safety and efficacy of caplacizumab (Post-HERCULES) [internal sponsor's report]. Paris (FR): Sanofi Group; 2021 Jun 15.
8.Upreti H, Kasmani J, Dane K, et al. Reduced ADAMTS13 activity during TTP remission is associated with stroke in TTP survivors. Blood. 2019;134(13):1037-1045. PubMed
9.Table 13-10-0114-01: Life expectancy and other elements of the life table, Canada, all provinces except Prince Edward Island. Ottawa (ON): Statistics Canada; 2022: https://www150.statcan.gc.ca/t1/tbl1/en/tv.action?pid=1310011401. Accessed 2022 Jul 05.
10.Kennedy AS, Lewis QF, Scott JG, et al. Cognitive deficits after recovery from thrombotic thrombocytopenic purpura. Transfusion. 2009;49(6):1092-1101. PubMed
11.Chaturvedi S, Oluwole O, Cataland S, McCrae KR. Post-traumatic stress disorder and depression in survivors of thrombotic thrombocytopenic purpura. Thromb Res. 2017;151:51-56. PubMed
12.Clinical Study Report: ALX0681-C301 (HERCULES). A phase III double-blind, randomized, parallel group, multicenter placebo-controlled trial to study the efficacy and safety of caplacizumab in patients with acquired thrombotic thrombocytopenic purpura, version 1.0 [internal sponsor's report]. Zwijnaarde (BE): Ablynx NV; 2018 Mar 5.
13.Chit A, Becker DL, DiazGranados CA, Maschio M, Yau E, Drummond M. Cost-effectiveness of high-dose versus standard-dose inactivated influenza vaccine in adults aged 65 years and older: an economic evaluation of data from a randomised controlled trial. Lancet Infect Dis. 2015;15(12):1459-1466. PubMed
14.Burns D, Lee D, Vesely S, et al. Patient health-related quality of life associated with remission of aTTP, a regression analysis using non-randomised observational data from the Oklahoma TTP registry. Value Health. 2018;21(Suppl 3):S469.
15.Ara R, Brazier JE. Populating an economic model with health state utility values: moving toward better practice. Value Health. 2010;13(5):509-518. PubMed
16.Guertin JR, Humphries B, Feeny D, Tarride J. Health Utilities Index Mark 3 scores for major chronic conditions: population norms for Canada based on the 2013 and 2014 Canadian Community Health Survey. Ottawa (ON): Statistics Canada; 2018 Nov 21: https://www150.statcan.gc.ca/n1/pub/82-003-x/2018011/article/00001-eng.htm. Accessed 2022 Jul 17.
17.Sullivan PW, Slejko JF, Sculpher MJ, Ghushchyan V. Catalogue of EQ-5D scores for the United Kingdom. Med Decis Making. 2011;31(6):800-804. PubMed
18.Ontario Ministry of Health, Ontario Ministry of Long-Term Care. Ontario drug benefit formulary/comparative drug index. 2022; https://www.formulary.health.gov.on.ca/formulary/. Accessed 2022 Aug 22.
19.Drug Reimbursement Review pharmacoeconomic report: caplacizumab (Cablivi) for the treatment of adults with acquired thrombotic thrombocytopenic purpura (aTTP) in combination with plasma exchange (PE) and immunosuppressive therapy. Ottawa (ON): CADTH; 2020 Oct: https://www.cadth.ca/sites/default/files/cdr/pharmacoeconomic/sr0633-cablivi-pharmacoeconomic-review-report.pdf. Accessed 2022 Jun 28.
20.Canadian Institute for Health Information. Patient cost estimator. 2022; https://www.cihi.ca/en/patient-cost-estimator. Accessed 2022 Aug 22.
21.Schedule of benefits for physician services under the Health Insurance Act: effective October 1, 2021. Toronto (ON): Ontario Ministry of Health; 2022: https://www.health.gov.on.ca/en/pro/programs/ohip/sob/physserv/sob_master.pdf. Accessed 2022 Aug 22.
22.Briggs A, Claxton K, Sculpher M. Decision modelling for health economic evaluation. Oxford (UK): Oxford University Press; 2006.
23.Fleurence RL, Hollenbeak CS. Rates and probabilities in economic modelling: transformation, translation and appropriate application. Pharmacoeconomics. 2007;25(1):3-6. PubMed
24.Joly BS, Coppo P, Veyradier A. Thrombotic thrombocytopenic purpura. Blood. 2017;129(21):2836-2846. PubMed
25.Coppo P, Veyradier A. Current management and therapeutical perspectives in thrombotic thrombocytopenic purpura. Presse Med. 2012;41(3 Pt 2):e163-176. PubMed
26.Deford CC, Reese JA, Schwartz LH, et al. Multiple major morbidities and increased mortality during long-term follow-up after recovery from thrombotic thrombocytopenic purpura. Blood. 2013;122(12):2023-2029; quiz 2142. PubMed
27.CADTH Canadian Drug Expert Committee (CDEC) final recommendation: caplacizumab (Cablivi — Sanofi-Aventis Canada Inc.). Ottawa (ON): CADTH; 2020 Sep 1: https://www.cadth.ca/sites/default/files/cdr/complete/SR0633%20Cablivi%20-%20CDEC%20Final%20Recommendation%20September%201%2C%202020%20for%20posting.pdf. Accessed 2022 Jun 28.
28.Falter T, Schmitt V, Herold S, et al. Depression and cognitive deficits as long-term consequences of thrombotic thrombocytopenic purpura. Transfusion. 2017;57(5):1152-1162. PubMed
29.Han B, Page EE, Stewart LM, et al. Depression and cognitive impairment following recovery from thrombotic thrombocytopenic purpura. Am J Hematol. 2015;90(8):709-714. PubMed
30.Sachdeva R. Canada facing critical shortage of O+ and O- blood supply: Canadian Blood Services. CTVNews. 2022; https://www.ctvnews.ca/health/canada-facing-critical-shortage-of-o-and-o-blood-supply-canadian-blood-services-1.6016037. Accessed 2022 Aug 30.
31.Clinical Study Report: ALX-0681-2.1/10 (TITAN). A phase II, single-blind, randomized, placebo-controlled trial to study the efficacy and safety of anti-von Willebrand factor nanobody administered as adjunctive treatment to patients with acquired thrombotic thrombocytopenic purpura [internal sponsor's report]. Zwijnaarde (BE): Ablynx NV; 2015 May 29.
32.Budget Impact Analysis [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Cablivi (caplacizumab), 11 mg powder for solution, for intravenous (IV) or subcutaneous injection. Laval (QC): sanofi-aventis Canada Inc.; 2022 Jun 22.
33.Table 17-10-0057-01: Projected population, by projection scenario, age and sex, as of July 1 (x 1,000). Ottawa (ON: Statistics Canada; 2022: https://www150.statcan.gc.ca/t1/tbl1/en/tv.action?pid=1710005701. Accessed 2022 Jul 15.
34.Indigenous Services Canada. Non-Insured Health Benefits program: First Nations and Inuit Health Branch: annual report 2019 to 2020. 2020: https://www.sac-isc.gc.ca/eng/1624462613080/1624462663098. Accessed 2022 Aug 22.
35.sanofi-aventis Canada Inc response to July 28, 2022 DRR request for additional information regarding Cablivi (caplacizumab) resubmission DRR review: clarification of public funding proportion inputs [internal additional sponsor's information]. Laval (QC): sanofi-aventis Canada Inc; 2022 Aug 9.
36.Government of Saskatchewan. Saskatchewan Drug Plan: search formulary. 2022; https://formulary.drugplan.ehealthsask.ca/SearchFormulary. Accessed 2022 Aug 22.
37.Ontario Ministry of Health, Ontario Ministry of Long-Term Care. Exceptional Access Program (EAP). 2022: https://www.health.gov.on.ca/en/pro/programs/drugs/odbf/odbf_except_access.aspx. Accessed 2022 Aug 22.
38.CADTH reimbursement review pharmacoeconomic report: fostamatinib (Tavalisse) for chronic immune thrombocytopenia. Can J Health Technol. 2022;2(7). https://www.cadth.ca/sites/default/files/DRR/2022/SR0701-Tavalisse-combined.pdf. Accessed 2022 Aug 22.
39.Exceptional access program reimbursement criteria for frequently requested drugs. Toronto (ON): Ontario Ministry of Health; Ontario Ministry of Long-Term Care; 2022: https://www.health.gov.on.ca/en/pro/programs/drugs/docs/frequently_requested_drugs.pdf. Accessed 2022 Aug 22.
40.Ontario Ministry of Health. Get help with high prescription drug costs. 2022; https://www.ontario.ca/page/get-help-high-prescription-drug-costs#:~:text=prescription%2Ddrug%20costs-,What%20is%20covered,through%20the%20Exceptional%20Access%20Program. Accessed 2022 Aug 9.
41.Health PEI. Catastrophic Drug Program. 2022; https://www.princeedwardisland.ca/en/information/health-pei/catastrophic-drug-program. Accessed 22 Aug 2022.
42.Indigenous Services Canada. Non-Insured Health Benefits program: First Nations and Inuit Health Branch: annual report 2020 to 2021. 2021: https://www.sac-isc.gc.ca/eng/1645718409378/1645718500555. Accessed 2022 Aug 22.
Appendix 1: Cost Comparison Table
Note this appendix has not been copy-edited.
The comparators presented in the following table have been deemed to be appropriate based on feedback from clinical experts. Comparators may be recommended (appropriate) practice or actual practice. Existing Product Listing Agreements are not reflected in the table and as such, the table may not represent the actual costs to public drug plans.
Table 8: CADTH Cost Comparison Table of Medications Indicated for the Treatment of Adults With aTTP
Treatment | Strength / concentration | Form | Price ($) | Recommended dosage | Daily cost | Cost per course |
|---|---|---|---|---|---|---|
Caplacizumab (Cablivi) | 11 mg | 11 mg powder for solution | 6,200.0000a | 11 mg | Day 1 of treatment: 12,400 Subsequent days of treatment: 6,200 | Median duration of therapy:b 223,200 Max duration of therapy:b 409,200 |
aTTP = acquired thrombotic thrombocytopenic purpura.
aSponsor’s submitted price.5
bBased on the median duration of caplacizumab therapy of 35 days in the HERCULES trial (i.e., the median 5 days of PE therapy plus an additional 30 days). Maximum duration of therapy is 65 days as reported in the HERCULES trial.6
Table 9: CADTH Cost Comparison Table of Standard-of-Care Therapies for the Treatment of Adults With aTTP
Treatment | Strength / concentration | Form | Price ($) | Recommended dosage | Daily cost ($) | Cost per course |
|---|---|---|---|---|---|---|
Plasma exchange | 250 mL unit | Blood product for infusion | 122.01a | 1.5 Plasma volume (60 mL/kg) | 2,342.59 | 11,713b |
Adjunctive therapies | ||||||
Prednisone (generic, Winpred) | 1 mg 5 mg 50 mg | Tablet | 0.1214 0.0220 0.1900 | 1 mg/kg during daily PE and for the first week thereafter, then tapered at clinician’s discretionc | 0.32 initially | 4b plus taper |
Methylprednisolone (Medrol) | 100mg | 20 mg/mL injectable solution | 14.2400 | 1,000 mg | 142.40 | 427 |
Rituximab (subsequent entry biologics) | 100 mg 500 mg | 10 mg/mL injectable solution | 297.0000 1,485.0000 | 375 mg/m2 weekly for 1 to 4 dosesc | 297.00 | 2,079 to 8,316 |
aTTP = acquired thrombotic thrombocytopenic purpura.
All prices are Ontario Drug Benefit Formulary list prices (June 2022) unless otherwise indicated. For the purposes of dose calculation, the average patient was assumed to weigh 80 kg and have a body surface area of 1.8 m2. Costs include wastage of excess medication in vial.
aCited by the sponsor as from the 2020 CADTH review of Cablivi,19 however the price within that review was originally provided by the sponsor and could not be independently verified by CADTH.
bAssumes 5 days of therapy, the median number of days of plasma exchange reported in the HERCULES trial during the daily plasma exchange stage for both the caplacizumab and standard of care groups.6
cHERCULES trial as reported in Scully, 2019.3 Rituximab does not have a Health Canada indication for the treatment of acute aTTP episodes and is not reimbursed for such in all jurisdictions.
Appendix 2: Submission Quality
Note this appendix has not been copy-edited.
Description | Yes/No | Comments |
|---|---|---|
Population is relevant, with no critical intervention missing, and no relevant outcome missing | Yes | No comment |
Model has been adequately programmed and has sufficient face validity | No | The submitted model does not allow for the possibility of multiple true relapses due to its use of a payoff approach following a true relapse, and also does not allow for differential risk of relapse based on the number of relapses previously experienced. Modelled patients who have experienced a relapse cannot have both a cognitive and a neuropsychological impairment (i.e., as part of the payoff calculation), which is not consistent with clinical feedback or the Markov model. The model further included numerous IFERROR statements, making validation difficult (see key limitation section). |
Model structure is adequate for decision problem | No | The structure of the submitted model was inflexible (see key limitation section). |
Data incorporation into the model has been done adequately (e.g., parameters for probabilistic analysis) | Yes | No comment |
Parameter and structural uncertainty were adequately assessed; analyses were adequate to inform the decision problem | Yes | No comment. |
The submission was well organized and complete; the information was easy to locate (clear and transparent reporting; technical documentation available in enough details) | No | The sponsor’s written report is misleading in parts, particularly in the key assumption table. For example, the table states that the probability of true relapse is not dependent on treatment given for the acute episode, while the modelled rate of true relapse is entirely based on whether a patient received caplacizumab or SOC. Additionally, the table states that neuropsychological impairment is assumed to last one year, however the model applies related utility and cost consequences over the remainder of a patient’s life. |
Appendix 3: Additional Information on the Submitted Economic Evaluation
Note this appendix has not been copy-edited.
Figure 1: Model Structure — Decision Tree, Acute aTTP Episode
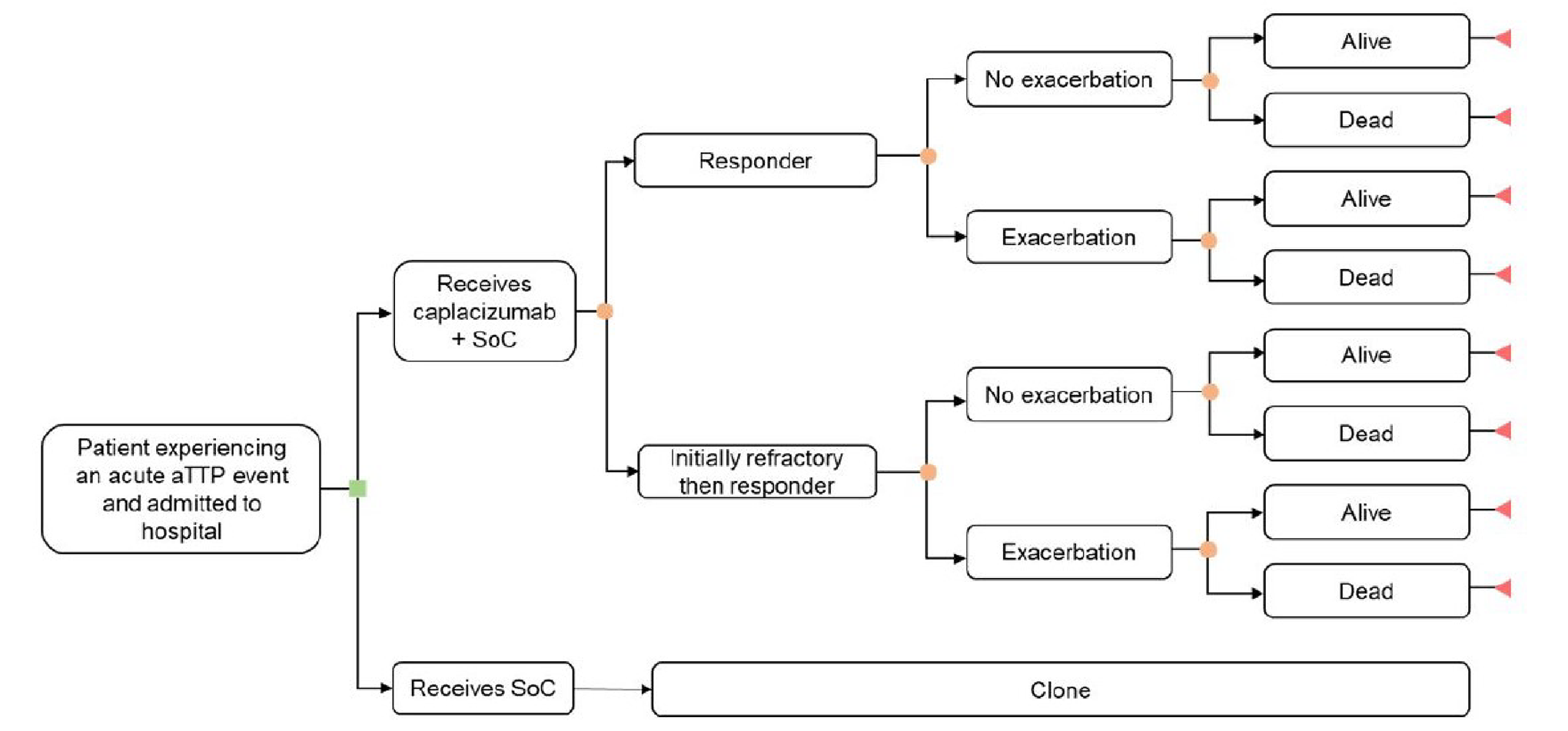
Source: Sponsor’s pharmacoeconomic submission.5
Figure 2: Model Structure — Markov Model, aTTP in Remission
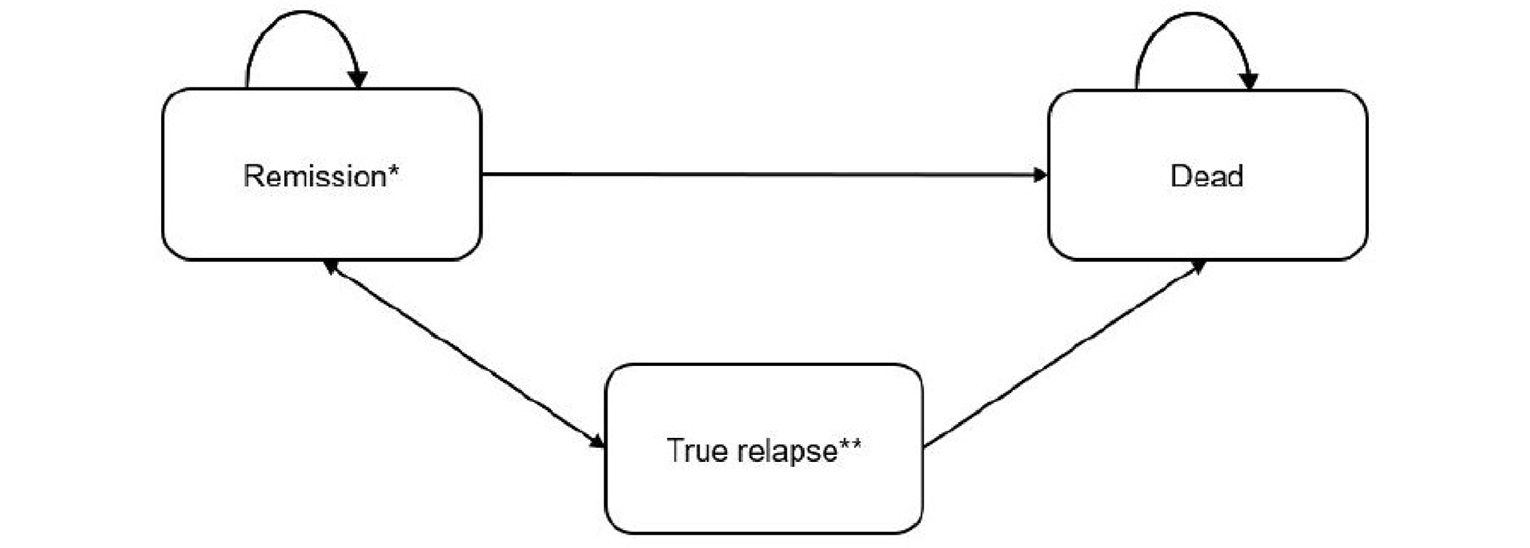
Sponsor’s notes: *The remission state includes patients with no chronic conditions, patients with cognitive impairment, patients with neuro-psychological impairment, and patients with both cognitive and neuro-psychological impairment; **Treatment costs for the acute episode also apply to the true relapse state.
Source: Sponsor’s pharmacoeconomic submission5
Figure 3: Model Structure — Payoff Approach to Relapse
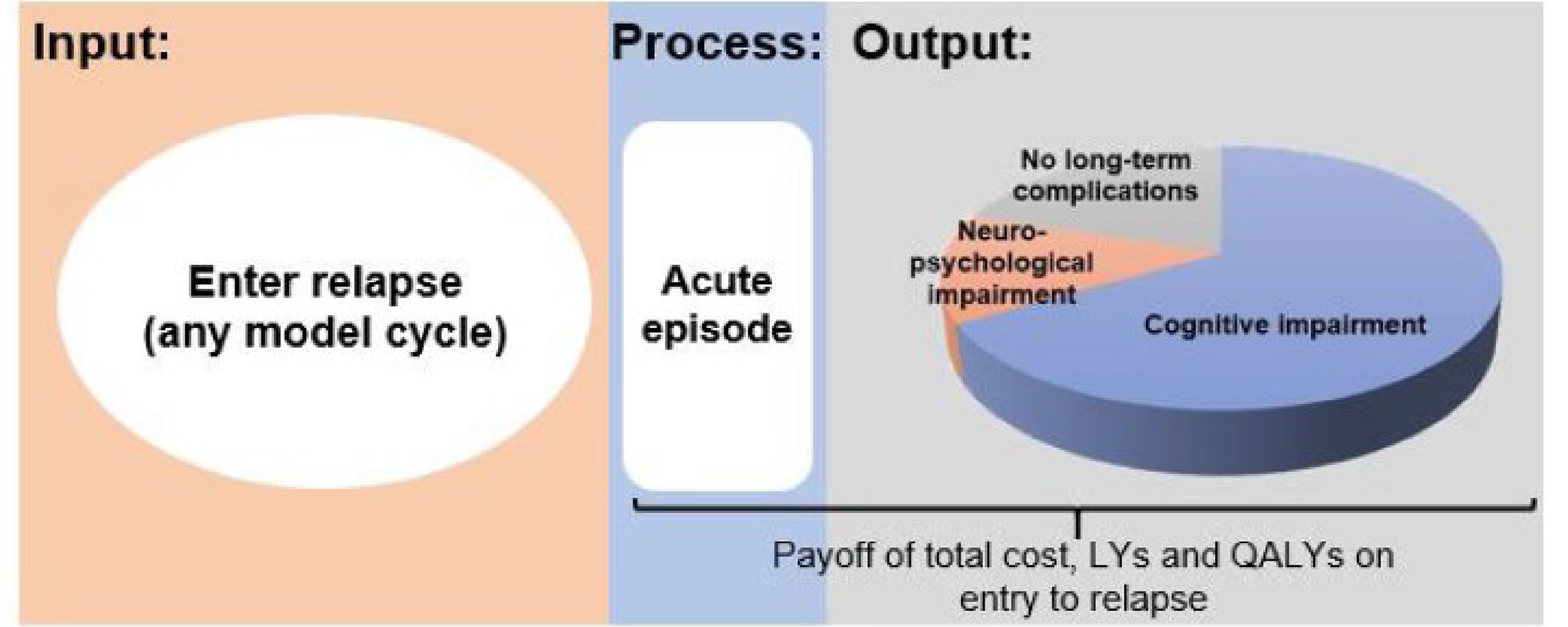
LY = life-year; QALY = quality-adjusted life-year.
Source: Sponsor’s pharmacoeconomic submission5
Table 11: Sponsor’s Health State Proportions for Patients in Remission
Impairment | SOC prevalence | Caplacizumaba prevalence |
|---|---|---|
Mild cognitive | 54%10 | 36% |
Moderate/severe cognitive | 21%10 | 14% |
Neuropsychological | 37%11 | 24% |
Proportion of modelled remission patients in each impairment state (Markov model)b | ||
Cognitive and neuropsychological | 28% | 12% |
Cognitive only | 47% | 37% |
Neuropsychological only | 9% | 12% |
Neither (no impairment) | 16% | 38% |
Proportion of modelled relapsed patients in each impairment state (relapse payoff)c | ||
Cognitive and neuropsychological | 0% | 0% |
Cognitive only | 75% | 50% |
Neuropsychological only | 9% | 12% |
Neither (no impairment) | 16% | 38% |
SOC = standard of care.
aBased on a relative risk of 0.66 vs. standard of care for each individual impairment, informed by clinical experts consulted by the sponsor.
bCognitive and neuropsychological events are assumed to be independent.5
cAll patients with a cognitive impairment were assumed to only have a cognitive impairment in the sponsor’s payoff approach.
Detailed Results of the Sponsor’s Base Case
Table 12: Disaggregated Summary of Sponsor’s Economic Evaluation Results
Parametera | Caplacizumab + SOC | SOC alone | Incremental |
|---|---|---|---|
Discounted LYs | |||
Total | 18.025 | 16.865 | 1.159 |
Initial aTTP episode (decision tree) | 0.247 | 0.241 | 0.006 |
Alive – no chronic conditions | 5.244 | 1.223 | 4.021 |
Alive – cognitive impairment | 5.098 | 3.609 | 1.490 |
Alive – neuropsychological impairment | 1.697 | 0.715 | 0.981 |
Alive – cognitive and neuropsychological impairment | 1.649 | 2.111 | −0.462 |
True relapse – aTTP episode | 0.092 | 0.171 | −0.079 |
Relapsed – no chronic conditions | 1.532 | 1.405 | 0.127 |
Relapsed – cognitive impairment | 1.970 | 6.569 | −4.599 |
Relapsed – neuropsychological impairment | 0.496 | 0.822 | −0.327 |
Discounted QALYs | |||
Total | 10.291 | 8.833 | 1.294 |
Initial aTTP episode (decision tree) | 0.167 | 0.123 | 0.045 |
AE decrement in initial aTTP episode (decision tree) | −0.003 | −0.006 | 0.003 |
Alive – no chronic conditions | 3.537 | 0.873 | 2.664 |
Alive – cognitive impairment | 2.853 | 2.137 | 0.716 |
Alive – neuropsychological impairment | 0.879 | 0.393 | 0.486 |
Alive – cognitive and neuropsychological impairment | 0.709 | 0.960 | −0.251 |
True relapse – aTTP episode | 0.054 | 0.078 | −0.024 |
True relapse – AE decrement | −0.001 | −0.004 | 0.003 |
Relapsed – no chronic conditions | 0.960 | 0.899 | 0.062 |
Relapsed – cognitive impairment | 0.920 | 3.132 | −2.212 |
Relapsed – neuropsychological impairment | 0.215 | 0.364 | −0.149 |
Discounted costs ($) | |||
Total | 357,700 | 74,689 | 283,010 |
Drug costs (decision tree) | $237,551 | $0 | $237,551 |
Administration costs (decision tree) | $0 | $0 | $0 |
Resource use costs (decision tree) | $19,589 | $29,798 | -$10,209 |
AE costs (decision tree) | $4,196 | $8,337 | -$4,141 |
Alive – no chronic conditions | $3,095 | $754 | $2,341 |
Alive – cognitive impairment | $3,635 | $2,690 | $945 |
Alive – neuropsychological impairment | $1,443 | $636 | $807 |
Alive – cognitive and neuropsychological impairment | $1,606 | $2,149 | -$543 |
True relapse – aTTP episode: drug costs | $76,358 | $0 | $76,358 |
True relapse – aTTP episode: Administration costs | $0 | $0 | $0 |
True relapse – aTTP episode: Resource use costs | $6,300 | $19,043 | -$12,743 |
True relapse – aTTP episode AE costs | $1,350 | $5,329 | -$3,979 |
Relapsed – no chronic conditions | $853 | $794 | $58 |
Relapsed – cognitive impairment | $1,325 | $4,488 | -$3,163 |
Relapsed – neuropsychological impairment | $398 | $671 | -$273 |
ICER ($/QALY) | $210,903 | ||
AE = adverse event; aTTP = acquired thrombotic thrombocytopenic purpura; ICER = incremental cost-effectiveness ratio; LY = life-year; QALY = quality-adjusted life-year; SOC = standard of care.
aAll health states refer to those within the Markov section of the sponsor’s model unless otherwise indicated.
Appendix 4: Additional Details on the CADTH Reanalyses and Sensitivity Analyses of the Economic Evaluation
Note this appendix has not been copy-edited.
Detailed Results of CADTH Base Case
Table 13: Disaggregated Summary of CADTH Economic Evaluation Reanalysis Results
Parametera | Caplacizumab plus SOC | SOC alone | Incremental |
|---|---|---|---|
Discounted LYs | |||
Total | 18.172 | 17.527 | 0.645 |
Initial aTTP episode (decision tree) | 0.247 | 0.241 | 0.006 |
Alive – no chronic conditions | 7.248 | 2.850 | 4.397 |
Alive – cognitive impairment | 7.072 | 8.438 | −1.366 |
Alive – neuropsychological impairment | 0.089 | 0.063 | 0.026 |
Alive – cognitive and neuropsychological impairment | 0.087 | 0.189 | −0.102 |
True relapse – aTTP episode | 0.076 | 0.102 | −0.026 |
Relapsed – no chronic conditions | 1.662 | 1.389 | 0.273 |
Relapsed – cognitive impairment | 1.655 | 4.217 | −2.562 |
Relapsed – neuropsychological impairment | 0.036 | 0.037 | −0.001 |
Discounted QALYs | |||
Total | 10.912 | 9.879 | 1.033 |
Initial aTTP episode (decision tree) | 0.167 | 0.123 | 0.045 |
AE decrement in initial aTTP episode (decision tree) | −0.003 | −0.006 | 0.003 |
Alive – no chronic conditions | 4.835 | 1.906 | 2.929 |
Alive – cognitive impairment | 3.927 | 4.698 | −0.772 |
Alive – neuropsychological impairment | 0.055 | 0.039 | 0.016 |
Alive – cognitive and neuropsychological impairment | 0.045 | 0.097 | −0.052 |
True relapse – aTTP episode | 0.045 | 0.048 | −0.003 |
True relapse – AE decrement | −0.001 | −0.002 | 0.001 |
Relapsed – no chronic conditions | 1.044 | 0.896 | 0.148 |
Relapsed – cognitive impairment | 0.780 | 2.059 | −1.279 |
Relapsed – neuropsychological impairment | 0.019 | 0.021 | −0.002 |
Discounted costs ($) | |||
Total | 342,623 | 64,545 | 278,078 |
Drug costs (decision tree) | 237,698 | 0 | 237,698 |
Administration costs (decision tree) | 0 | 0 | 0 |
Resource use costs (decision tree) | 19,565 | 29,744 | −10,179 |
AE costs (decision tree) | 4,196 | 8,362 | −4,166 |
Alive – no chronic conditions | 4,238 | 1,670 | 2,568 |
Alive – cognitive impairment | 4,999 | 5,976 | −977 |
Alive – neuropsychological impairment | 87 | 62 | 25 |
Alive – cognitive and neuropsychological impairment | 97 | 211 | −114 |
True relapse – aTTP episode: drug costs | 63,343 | 0 | 63,343 |
True relapse – aTTP episode: Administration costs | 0 | 0 | 0 |
True relapse – aTTP episode: Resource use costs | 5,210 | 11,535 | −6,325 |
True relapse – aTTP episode AE costs | 1,117 | 3,243 | −2,126 |
Relapsed – no chronic conditions | 926 | 793 | 133 |
Relapsed – cognitive impairment | 1,116 | 2,916 | −1,800 |
Relapsed – neuropsychological impairment | 31 | 33 | −2 |
ICER ($/QALY) | 269,158 | ||
AE = adverse event; aTTP = acquired thrombotic thrombocytopenic purpura; ICER = incremental cost-effectiveness ratio; LY = life-year; QALY = quality-adjusted life-year; SOC = standard of care.
aAll health states refer to those within the Markov section of the sponsor’s model unless otherwise indicated.
Scenario Analyses
Table 14: CADTH Scenario Analyses
Scenario | CADTH base case | CADTH scenario |
|---|---|---|
A. Lower relative risk of long-term sequelae | 0.66 | 0.50 |
B. Higher relative risk of long-term sequelae | 0.66 | 0.80 |
C. Shorter duration of reduced relapse risk | 3 years | 1 year |
D. Longer duration of neuropsychological impairment | 1 year | 3 years |
Table 15: Summary of the Scenario Analysis Results
Stepped analysis | Drug | Total costs ($) | Total QALYs | ICER ($/QALYs) |
|---|---|---|---|---|
CADTH base case | SOC alone | 64,545 | 9.88 | Ref. |
Caplacizumab + SOC | 342,623 | 10.91 | 269,158 | |
Scenario A: long-term sequelae RR = 0.50 | SOC alone | 64,588 | 9.87 | Ref. |
Caplacizumab + SOC | 338,261 | 11.18 | 207,826 | |
Scenario B: long-term sequelae RR = 0.80 | SOC alone | 64,613 | 9.91 | Ref |
Caplacizumab + SOC | 344,153 | 10.73 | 340,311 | |
Scenario C: Caplacizumab reduces relapse risk for 1 year | SOC alone | 60,861 | 9.96 | Ref |
Caplacizumab + SOC | 338,260 | 10.94 | 280,887 | |
Scenario D: neuropsychological impairment lasts 3 years | SOC alone | 64,858 | 9.79 | Ref |
Caplacizumab + SOC | 344,666 | 10.85 | 264,631 |
ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year; Ref. = reference; RR = relative risk; SOC = standard of care.
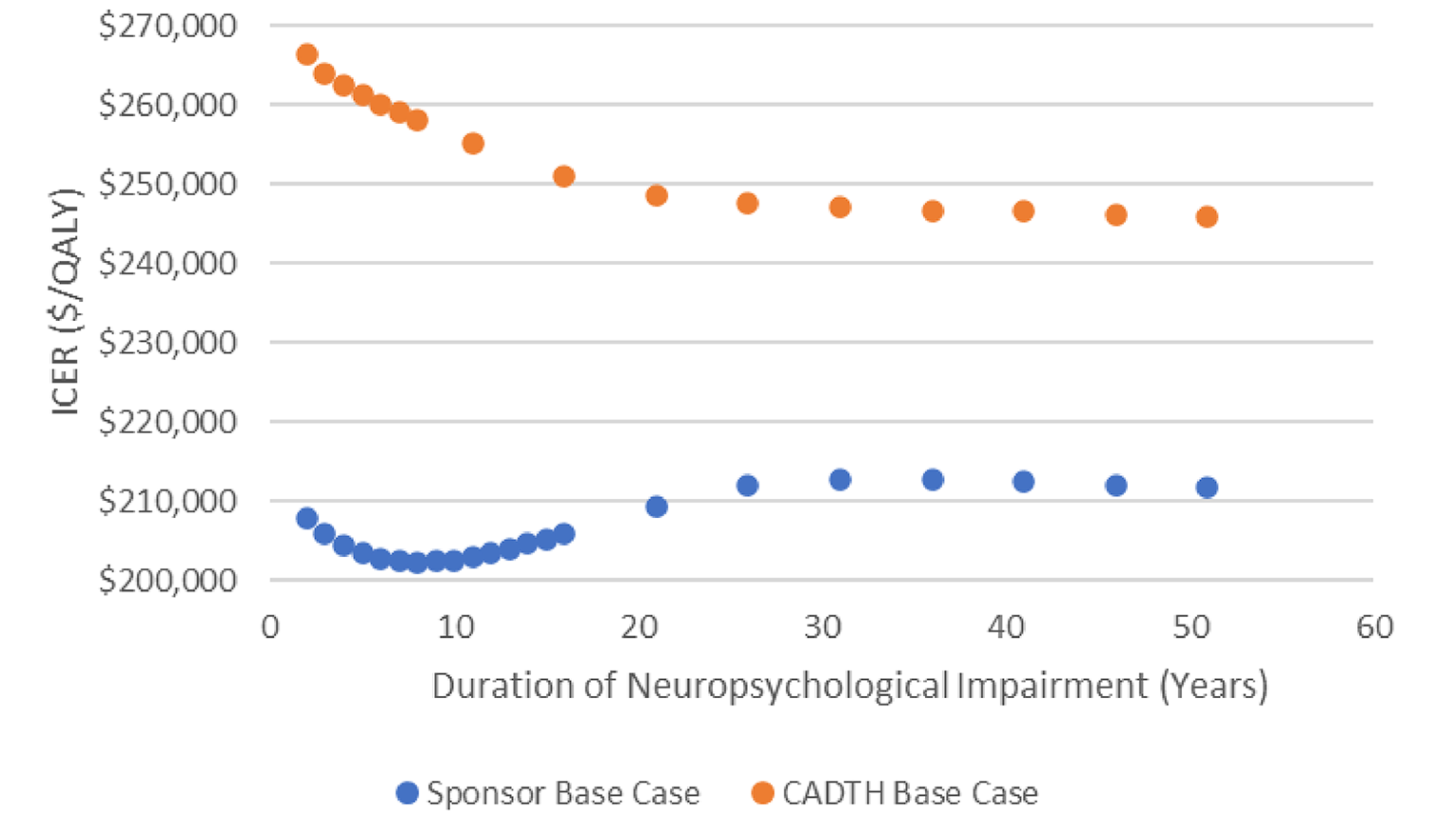
Appendix 5: Submitted BIA and CADTH Appraisal
Note this appendix has not been copy-edited.
Table 16: Summary of Key Take-Aways
Key take-aways of the BIA |
|---|
|
Summary of Sponsor’s BIA
In the submitted BIA, the sponsor assessed the introduction of caplacizumab for the treatment of adults with aTTP in combination with PE and immunosuppressive therapy. The BIA was undertaken from the perspective of a Canadian public drug plan payer over a 3-year time horizon (2023 to 2025) using an epidemiological approach. The sponsor’s analysis included drug acquisition costs for caplacizumab once patients were in the community (outpatients), as well as dispensing fees and markups in the base case. Data from the model were obtained from various sources including Statistics Canada,33 the Non-Insured Health Benefits (NIHB) program,34 confidential CAG registry data,32 the published literature,24 the sponsor’s internal data, and expert opinion.32 Key inputs to the BIA are documented in Table 17.
Key assumptions include:
TTP registry data from 2019 through 2021 was artificially low due to COVID-19 and were excluded when making growth projections for 2023 through 2025.
The growth rate of the aTTP population is the same as the TTP population.
In-hospital caplacizumab costs were not considered as part of drug plan payer perspective.
Caplacizumab will not displace the use of SOC.
Table 17: Summary of Key Model Parameters
Parameter | Sponsor’s estimate (reported as year 1 / year 2 / year 3 if appropriate) |
|---|---|
Target population | |
Total population age 18+ years (year 0, 2022) | 24,026,70833 |
Rate of TTP events per adult in Canada | 0.00056%a |
Proportion of TTP that is aTTP | 95%24 |
Public coverage rate | 60%b |
Annual growth rate of TTP population | 1.56%c |
Number of aTTP events eligible for drug under reviewd | 77 / 79 / 80 |
Market uptake (3 years, reference scenario) | |
Standard of care | 100% / 100% / 100% |
Market uptake (3 years, new drug scenario)e | |
Standard of care | 50% / 40% / 30% |
Caplacizumab | 50% / 60% / 70% |
Cost of treatment (per patient, outpatient setting only)f | |
Standard of care | $0 |
Caplacizumab (assumes 26.8 days of therapy) | $166,160 |
aTTP = acquired thrombotic thrombocytopenic purpura; TTP = thrombotic thrombocytopenic purpura; Y = year
aDerived by projecting Canadian Apheresis Group registry data from 2013 through 2018 to 2022 and dividing by the adult population of Canada in 2021.32
bReported as using Revolade as an analogue to determine the proportion of coverage for a medication used in both a hospital and community setting for a rare condition.
cThe annual growth rate of TTP cases as reported by CAG registry data from 2013 through 2018.32
dAs a final step, the number of patients in the baseline year was rounded up, such that no jurisdiction would have less than 1 patient per year.32
eReported as based on internal market research and external clinician consultation.
fIncludes outpatient costs only and assumes no difference in use of standard of care between groups, thus standard of care was assumed to have no incremental cost.
Summary of the Sponsor’s BIA Results
Results of the sponsor’s analysis suggest that the reimbursement of caplacizumab, when considering only drug plan perspective (i.e., coverage of drug costs, markups and dispensing fees incurred in the outpatient setting), will be associated with an incremental cost of $6,972,127 in year 1, $8,418,279 in year 2, and $9,908,076 in year 3, for a total budget impact of $25,298,482 over the first 3 years.
CADTH Appraisal of the Sponsor’s BIA
CADTH identified several key limitations to the sponsor’s analysis that have notable implications on the results of the BIA:
Annual number of aTTP events is uncertain: The sponsor’s analysis calculated the “prevalence,” or annual rate of TTP events by dividing the total number of TTP patients projected from confidential CAG data by the total adult population of Canada, resulting in a rate of 0.00056% or 5.6 per million adults in Canada.32 These data did not differentiate patients having their first TTP event from those experiencing a recurrent TTP event. However, it is unclear whether all patients reported in these data were adults or whether patients who had multiple events within the same year were counted once or per event. As such, the actual number of aTTP events that may be eligible for treatment with caplacizumab is uncertain.
CADTH corrected a minor inconsistency ensuring both inputs informing this event rate calculation were from the year 2021, resulting in a rate of 5.5 per million adults in Canada. CADTH was otherwise unable to account for this limitation. Rates of 4.5 and 6.5 events per million adults in Canada were explored in scenario analyses.
SOC and downstream cost offsets were not considered: The sponsor’s model does not consider any offsetting of SOC-related costs (e.g., reduced use of PE, rituximab) or downstream avoidance of either drug plan costs or health system costs (e.g., avoidance of stroke, myocardial infarction, cognitive impairment, neuropsychological outcomes, and so on).
CADTH was unable to address this limitation. However, the sponsor’s approach may be conservative as it does not capture the potential savings in downstream costs should caplacizumab improve health outcomes and reduce consumption of health care resources for patients. The magnitude of costs potentially offset by the use of caplacizumab for either the drug plan perspective or the broader health care system perspective is unknown.
Proportion of caplacizumab that will be publicly funded is uncertain: The sponsor’s BIA estimated that 60% of patients who receive caplacizumab will do so through public plans based on the use of eltrombopag (Revolade) claims data as a proxy due to similarities in its use both within the hospital and community setting, the rarity of the indicated patient populations, the expected age of patients, and the overlap in clinicians expected to prescribe both products.32,35 However, CADTH notes that eltrombopag is not funded in all jurisdictions, which the sponsor’s methodology did not account for.35 Additionally, in jurisdictions that do fund it, eltrombopag is subject to strict reimbursement criteria36,37 which may limit the proportion of patients who would be eligible for public funding. The expected use of caplacizumab is not similar to that of eltrombopag as eltrombopag may be used chronically while caplacizumab would be used for a limited duration after an acute aTTP event. This acute usage of caplacizumab may affect implementation of public reimbursement in the form of specialty programs or plans. Finally, the median cost of a course of caplacizumab for an aTTP event ($223,200) is substantially more than the annual cost of eltrombopag for chronic immune thrombocytopenia (range: $23,725 to $71,175 depending on dose and duration, based on public list price),38,39 which may impact the proportion of patients who would either exceed their maximum private plan benefits and/or the proportion of patients who would qualify for public reimbursement through income-based drug programs.40,41
CADTH was unable to fully address this limitation in reanalyses. The impact of assuming 100% of caplacizumab patients would be publicly reimbursed was explored in scenario analysis.
The uptake of caplacizumab is uncertain: The sponsor estimated that caplacizumab would be used for 50%, 60%, and 70% of adult aTTP patients in Years 1, 2, and 3 of its reimbursement, respectively, based on internal forecasts and expert opinion.32 Clinical expert feedback solicited by CADTH did not find these proportions unreasonable, but noted that the estimates were uncertain.
CADTH explored this limitation by assuming 25% more and less uptake of caplacizumab in scenario analyses.
CADTH Reanalyses of the BIA
CADTH made 2 corrections to the sponsor’s base-case analysis, first by estimating the prevalence of aTTP using inputs consistently from 2021. Second, since the sponsor’s analysis was conducted, the 2020–2021 NIHB Annual Report has been published.42 CADTH therefore updated the analysis to reflect this more recent population data.
Due to a lack of data which might reduce uncertainty in the sponsor’s analysis, CADTH did not conduct a base-case reanalysis beyond the corrections previously discussed, but did conduct scenario analyses to explore the areas of uncertainties.
Table 18: CADTH Revisions to the Submitted Budget Impact Analysis
Stepped analysis | Sponsor’s value or assumption | CADTH value or assumption |
|---|---|---|
Corrections to sponsor’s base case | ||
1. Prevalence calculation | 2022 estimate of TTP cases divided by 2021 population = 0.00056% | 2021 estimate of TTP cases divided by 2021 population = 0.00055% |
2. NIHB population updated with 2021 data | 2021 adult NIHB population estimated from 2020 data: 659,09332,34 | 2021 adult NIHB population: 660,74042 |
NIHB = Non-Insured Health Benefits program; TTP = thrombotic thrombocytopenic purpura.
The results of the CADTH corrections to the sponsor’s base case are presented in Table 19. When considering only drug plan perspective (i.e., coverage of drug costs, markups and dispensing fees incurred in the outpatient setting), the reimbursement of caplacizumab may be associated with an incremental cost of $6,870,366 in year 1, $8,294,254 in year 2, and $9,761,116 in year 3, for a 3-year total budget impact of $24,925,736.
Due to the extent of remaining uncertainty in the sponsor’s analysis, CADTH conducted a series of scenario analyses on the sponsor’s corrected base case (Table 19) varying the rate of TTP events per million adults in Canada (Scenarios A and B), varying the uptake of caplacizumab by ± 25% (Scenarios C and D), and assuming 100% of aTTP events would be publicly reimbursed (Scenario E). Scenarios were also conducted which excluded markups and dispensing fees (Scenario F), as well as assuming a 75% price reduction for caplacizumab based on the results of the CADTH pharmacoeconomic reanalysis (Scenario G).
Finally, while appropriate from a drug plan payer perspective, the exclusion of caplacizumab given in the hospital setting fails to account for the total cost of caplacizumab to the public health care system should it be reimbursed. CADTH therefore conducted a scenario where 100% of aTTP events treated with caplacizumab were assumed to be publicly reimbursed for the portion of the event for which the patient was hospitalized, while 60% were assumed to be reimbursed after discharge (Scenario H). It is important to note that this scenario only includes the costs associated with caplacizumab and does not include other hospital costs for treating aTTP events such as SOC, ICU and ward stays, or adverse events, nor does it consider potential immediate or downstream resource use avoided due to the use of caplacizumab.
Table 19: Summary of Sponsor’s BIA and CADTH Scenario Analyses
Stepped analysis | Year 1 | Year 2 | Year 3 | 3-year total |
|---|---|---|---|---|
Sponsor’s base case | 6,972,127 | 8,418,279 | 9,908,076 | 25,298,482 |
Sponsor’s corrected base case | 6,870,366 | 8,294,254 | 9,761,116 | 24,925,736 |
CADTH Scenario A: Annual TTP event rate 4.5 per million | 5,738,080 | 6,845,208 | 8,044,105 | 20,627,393 |
CADTH Scenario B: Annual TTP event rate 6.5 per million | 8,059,298 | 9,743,300 | 11,505,701 | 29,308,299 |
CADTH Scenario C: 25% lower caplacizumab uptake | 5,342,065 | 6,332,437 | 7,411,350 | 19,085,852 |
CADTH Scenario D: 25% higher caplacizumab uptake | 8,497,445 | 10,282,405 | 12,150,299 | 30,930,148 |
CADTH Scenario E: 100% caplacizumab publicly funded | 11,231,784 | 13,649,347 | 16,139,873 | 41,021,005 |
CADTH Scenario F: markups and dispensing fees excluded | 6,511,567 | 7,863,462 | 9,256,157 | 23,631,185 |
CADTH Scenario G: 75% caplacizumab price reduction | 1,720,590 | 2,077,179 | 2,444,530 | 6,242,298 |
CADTH Scenario H: caplacizumab use in hospital included | 11,502,054 | 13,977,825 | 16,528,314 | 42,008,193 |
BIA = budget impact analysis; TTP = thrombotic thrombocytopenic purpura.
Note: As the BIA only considers the cost of caplacizumab, all reference scenarios and year 0 costs are $0, while new drug scenario costs are identical to incremental costs. Thus, only incremental costs (i.e., the budget impact) are presented.
Stakeholder Input
Patient Input
Answering Thrombotic Thrombocytopenic Purpura Foundation
About the Answering Thrombotic Thrombocytopenic Purpura Foundation
Answering TTP Foundation (www.AnsweringTTP.org) is a grassroots patient organization headquartered in Ontario and solely made up of volunteers across Canada who have been directly or indirectly affected by TTP. The organization was founded in 2009 by seven-time TTP survivor Sydney Kodatsky who recognized the need for a patient organization to support the TTP community, act as a unified voice for the patient community, fundraise for TTP research, and drive education and awareness about this rare disease. The foundation’s Board is made of seven Directors with diverse skillsets and three of the seven Directors are also TTP patients.
The operations team is made up of two members of the Board: The Executive Director chairs the annual fundraiser and oversees the accounting with the help from a paid bookkeeper. The Chair runs the annual research competition, maintains the website, manages communications and educational materials, and runs the day-to-day operations of the Foundation. One of the organization’s Board members is also the volunteer Director of Patient Relations. They hold a virtual peer support group meeting for the TTP community four times a year.
Over the years, the Foundation has also supported a research grant program, having understood the crucial need for biomedical, clinical, and population health for a rare disease. Since its inception, Answering TTP has committed over $2 million to research grants through 2023.
In 2021, Answering TTP strengthened the level of support and education to Canadian TTP patients and helped drive greater awareness of TTP to the medical community by creating the Foundation's first national Canadian TTP Medical Advisory Panel comprised of six physicians from different areas of the country. This was also supplemented by the creation of an informal Patient Advisory Panel, comprised of five TTP patients and caregivers who volunteer their time to provide the patient perspective on Answering TTP’s initiatives.
Answering TTP’s work could not be accomplished without its passionate volunteers, who fundraise for the Foundation each year. While the TTP community is small, the experience of having TTP or taking care of someone with TTP propels patients, caregivers, friends, and loved ones to want to draw awareness of this disease and support Answering TTP’s goals to act as a voice for this community.
Information Gathering
During the period of May 18, 2022, to June 8, 2022, Answering TTP Foundation conducted a patient survey through Google Forms. While based on our 2019 patient survey during the first review of caplacizumab, this survey was updated to reflect our group’s growth, as well as changes to the environment since our first survey in 2019. We also conducted two informal Patient Advisory Group meetings where participants were able to review and add survey questions to ensure that it reflected the experience of TTP patients and caregivers.
Survey Recruitment: All interview and survey questions were developed by Answering TTP Foundation with the help of a Patient Advisory Group made up of five Answering TTP volunteers, with outreach to all Answering TTP members through the organization’s website, social media pages (Facebook and Twitter), and direct email. We are also appreciative of the Canadian Apheresis Group and the Canadian Association of Apheresis Nurses, who generously agreed to share the opportunity to participate in the survey with their TTP patients. The summary of feedback was collated by Answering TTP.
Survey Responses: We received completed 49 survey responses. Demographic information:
The survey was mainly completed by TTP patients (31 respondents). However, family members, caregivers, or friends of persons diagnosed with TTP were also invited to participate in the survey, of which made up 16 of the received responses. One healthcare professional that worked with TTP patients also responded, and one researcher provided their input.
29% of respondents were ages 50-59
20% of respondents were ages 30-39
18% of respondents were ages 60-69
14% of respondents were ages 40-49
The age groups of 18-29 and 70 + made up of 8% of respondents respectively
There was one respondent under the age of 18
80% of survey respondents identified as female and 20% identified as male
A significant majority of respondents lived in Canada. Half of the survey’s respondents lived in Ontario, 5 respondents lived in Alberta, 3 respondents lived in each British Columbia and Manitoba respectively and 2 respondents lived in each Quebec and Nova Scotia respectively. There was 1 respondent from the provinces of Saskatchewan, New Brunswick, PEI, and Newfoundland and Labrador each.
Outside of Canada, 3 respondents lived in the United States, and 2 lived in Europe (Germany and Switzerland, respectively).
Disease Experience
TTP is a rare episodic disorder that affects 2-6 people per million and the road to a TTP diagnosis can be fatal as TTP is characterized by the medical community as a true medical emergency requiring immediate treatment. The small blood clots that characterize this disease can have sudden and severe consequences, but because standard therapies are not targeted and take time to “kick-in”, patients are left in a life-threatening state for days and sometimes weeks. During this time up to 20% of patients die and others are left with life altering complications from stroke, heart attack etc.
In our survey, most patients (or the person they cared for) were first diagnosed with TTP between the ages of 20-30 (49% of respondents) and between the ages of 40 and 59 (31% of respondents). 16% were diagnosed when they were over the age of 60 and two (2) patients were under 20 years old at the age of diagnosis.
Between the time of initial symptom onset and treatment, many patients (35%) said it took within a week from their first symptoms to receive treatment, but for many patients, this took longer with 27% of respondents stating that it took more than a week, 9 respondents said it took more than a month.
During an Answering TTP Patient Advisory Group meeting, one patient said:
“A lot of people who are diagnosed late have to deal with collapsed veins and there is no way to insert a central line for treatment… they had given up on me after 5 hours and 40 minutes of trying and I was told I was going. It was an apheresis nurse that begged someone on the floor to keep trying, saying to a resident doctor -this girl is dying, please give it another try- and that resident ended up being successful.”
Persons diagnosed (or cared for) with TTP experience a variety of symptoms during their TTP episode or as a result of the treatment they have received. Survey respondents rated their symptoms on a scale of “no problem, minor, moderate, serious/frequent, and incapacitating/life-threatening” and these were some of the findings:
Bruises, fever, fatigue, migraine, confusion, abdominal pain, and anxiety/depression or panic attacks were noted as “serious and frequent symptoms”. Half of the respondents noted bruising and fever/fatigue/migraine/confusion as “serious, frequent symptoms”.
One-third of respondents listed anxiety/depression/panic attacks as a “serious, frequent” result.
18 respondents cited having abdominal pain and/or kidney problems as a serious frequent symptom.
More alarmingly, 8 respondents had a stroke or acute myocardial infarction in an incapacitating/life- threatening manner, 9 respondents had fever/fatigue/migraine/confusion in a similar incapacitating manner, and 4 respondents noted kidney problems in an incapacitating/life-threatening manner.
Survey respondents added that bleeding from gums/nose, shortness of breath, vision loss from retinal detachment and jaundice were common symptoms/results during a TTP episode.
For TTP patients, a relapse can cause lengthy hospitalizations, disable, or even be fatal. TTP patients live in a state of uncertainty, not knowing if a relapse will occur. Our survey asked how many relapses the person diagnosed with TTP (or the person they care for) has had since the initial episode and diagnosis.
48% at least one relapse, with 22.4% having 3-4 relapses, 12% having 1-2 relapses, 10% having 5-6 relapses, and scarily, 2 respondents said they suffered 7-10 relapses.
47% of respondents said they did not have a relapse.
Due to the unpredictability of this disease, many TTP patients stay an average of 9.7 days in the intensive care unit and an average of 14.4 days in hospital. Our survey respondents echoed this in their responses. In a question asking about the longest amount of time that a TTP patient stayed in hospital during a TTP crisis:
83% of respondents noted that their hospital stay was more than 7 days, with 37% having stayed in hospital for 28 days and more, 31%n hospital for 14-28 days, and 16% for 7-14 days.
One respondent said their hospital stay was for 120 days.
Only 3 respondents said their hospital stay was less than one week.
Experiences With Currently Available Treatments
A TTP episode is always a matter of life or death, especially with the current standard of care. As new treatments like caplacizumab have been released, there is an increasing recognition that TTP patients do not have to face the life-threatening consequences that come with each TTP episode.
Our survey asked which treatments the person diagnosed with TTP has received in the past or present and almost all respondents (44 of 49) noted that they or their loved one had received plasma exchange (plasmapheresis). Other treatments were also used:
45 of 49 respondents were treated with steroids (prednisone), and 32 were treated with Rituximab (Rituxin).
Cyclosporin was used for 12 patients and 9 patients had their spleens removed.
34% (or 16 respondents) to the survey had been treated with Cablivi (caplacizumab).
Other patients were also treated with Cyclophosphamide, Vincristine, CellCept, and Velcade.
When asked what the worst part(s) of treatment was for a TTP patient, many described the hardship of a long hospital stay, the side effects of receiving steroids, and the impact during and after plasma exchange. Many stated that the effects of the steroids resulted in weight gain, hair loss, sore bones, being unable to sleep, retina issues, depression, and Cushing's disease.
“The plasma exchange treatment for 3 months was very draining, and I was scared that I was going to get an infection in my line that was inserted in my neck. Also, getting blood products scared me. After my treatment, I did not feel like talking to anyone. I went into depression for a long time. Mental fog was another symptom.”
“I cannot overemphasize the impact of daily plasmaphereisis treatments… After so many relapses and scarring each line insertion gets more delicate. The risk is real with critically low platelets it takes more time for your bruised neck and chest to heal with low platelets. I'll never forget my best friend pressing bandages against my chest at the direction of my plasmapheresis nurse as they attempted to stop the bleeding from the line early on in my second relapse during a treatment.”
Current standard of care: The current standard of care for TTP is plasma exchange (plasmapheresis), combined with immunosuppressant drugs. Both are administered to deal with the urgent drop in platelets and small blood clots that form throughout the body that characterizes an episode. Some patients may require additional use of immunosuppressants during remission, but until recently, there has been no targeted or indicated treatment for TTP.
Our survey asked respondents that received plasma exchange to note the longest period they received this treatment for.
35% of respondents received plasma exchange for less than 5 days to 3 weeks, with 7 of those respondents receiving plasma for 1-2 weeks and 5 respondents for 2-3 weeks.
56% of respondents received plasma exchange from 3 weeks to more than 12 weeks. 20% of those respondents undergone plasma exchange for 3-4 weeks, and 16% undergone plasma exchange for more than 12 weeks.
Of all patients that received plasma exchange, 68% said they had hives from the treatment, 37% were anaphylaxis (as diagnosed by their doctor), and two respondents developed TRALI (Transfusion- related acute lung injury), a serious complication during transfusion causing rapid lung injury.
Beyond the physical symptoms of plasma exchange, the emotional effects loom larger and are more long- lasting. Plasma exchange is a frightening, risky, and an unpredictable treatment to patients. During a TTP episode, this untargeted treatment can be repeated sometimes multiple times per day, and then tapered-off as tolerated. Sudden life-threatening flares during tapering, or soon after, are not uncommon and requires the process to be started again with daily apheresis treatments. Plasma exchange can only be administered to hospital in-patients and may require weeks and sometimes months of hospital stays. For the duration of this time, the patient remains at risk of severe complications and death.
“It is very difficult with plasma exchange through your arms or through a line in your neck. You may have to stay in the Apheresis clinic for 3-6 hours. You receive other peoples’ plasma which may cause other reactions and so more drugs are required to treat the patient.”
“I cannot underscore enough that plasma exchange is a huge deal to me. Being hospitalized for weeks away from your young family, and having your entire blood volume passed through a machine and fed back to you combined with strangers’ blood is mind boggling. To date I've required over 700 units of blood plasma for plasmapheresis - an extraordinary amount of blood from strangers. I still can't believe that with all the advances in medical care there isn't a safer, more targeted treatment available to me. Instead with every relapse I need to cross my fingers that plasma exchange can "rebalance" my body with blood from strangers.”
“It is a HUGE deal! Even with solvent-detergent plasma, the chance of reaction is still high, and one worries what might happen with each treatment. In our case, there were many side effects and rarely was there a 'straight-forward' session.”
“I had an allergic reaction each time. Hives all over my body and was given steroids and another medication to resolve. It caused confusion, retina issues and swelling. Gained weight and had to use a wheelchair to get around. With my last relapse, I was given plasma exchange for 3 months. Risk of infection was high for my line insertion (neck area) and because I received high number of blood products.”
Our survey wanted to know more about any difficulties with accessing the treatment they or their loved one received (i.e., cost, travel, time off work) during their TTP episode. Many respondents said that the cost of medication was unaffordable, and they had been unable to work during their TTP episode(s). Caregivers of TTP patients also have to take time off work to care for their loved one.
From a caregiver’s perspective: “The cost of Cablivi was not covered. He had to stay in the hospital for over a month, was discharged for a weekend then re-admitted due to nothing else working. The stress around the cost and nothing working was crazy.”
“The insurance I had at the time wouldn't pay for the two treatments - the Rituximab and the caplacizumab. Since I've not been able to return to work, I'm presently trying to get ODSP, I'm having a hard time paying for transportation and parking for my bi-weekly appointments. I was laid off work because of Covid one month before I was diagnosed.”
“I missed 6 months of work and my husband had to miss work as well. He had to be there to communicate with the doctor and nurses. I was not alert on my treatment days and needed him for emotional support.”
Improved Outcomes
The reality is that for TTP patients, there has been no alternative to the current treatment regimen until Health Canada approved caplacizumab on March 2, 2020. Caplacizumab was given a priority review by Health Canada, which signified the need for a therapy of this kind. Which is why when CADTH declined it for reimbursement, the TTP community was extremely disappointed despite the significant unmet need here in Canada.
On a day-to-day basis, during a TTP episode, survey respondents have general anxiety over their treatments not working, having to put their life on hold, and the general depression that ensues with not being able to move forward when life is put on hold due to TTP.
“When having an episode, the biggest fear is that perhaps the treatment won't work and that I am facing a life-threatening disease if not treated and there are no guarantees that it will always work - the risk of heart attack, stroke or death is very real.”
“Rest of life is put on hold; patients need to face risk of serious or fatal outcomes each time, which left me with PTSD.”
“It’s like my entire life is put on pause … in addition to all the physical symptoms, the level of anxiety knowing I have 2 young kids is sometimes unbearable.”
“My daughter was to graduate from her policing course that year she fell ill and had to drop out of school, take medical leave from work for a year. She felt socially isolated from her family and friends.”
As a result, TTP patients and their families have their lives uprooted and the impacts are beyond physical - extending socially, financially, and psychologically. If advancement in treatments reduce the risk of death/irreversible consequences from each TTP crisis, patient’s mental health during remission will improve. It is the uncertainty of the life-threatening timing of the next relapse that brings about real mental stress. A high prevalence of PTSD and depression in TTP survivors has been reported and a study found that 80.8% of individuals with TTP have mild depressive symptoms, compared to 10.5% found in the general population.
Survey respondents have noted financial difficulties, an impact on their mental health, continuous fears of relapses, and impacts to their social life and career goals due to TTP. Simply put, TTP patients deserve a treatment that can ease the burden and significantly reduce their risk of death or disability.
“I’ve lost friends who don’t understand and can’t cope with the illness. I’m unable to return to work, my savings is gone, I’ve maxed out credit cards and I’m having huge issues keeping up with bills.
“Psychologically, I’ve been super depressed. This is the first time in my life that I’ve had serious thoughts about suicide (I got help), that my future doesn’t have an outcome.”
“You never feel safe from this disease as you never know what or when something will trigger a relapse.”
“The threat and anxiety of it returning and whether or not we can access the lifesaving medication Cablivi which was generously funded through an organization.”
“TTP has left me in fear and worrying about having a relapse. It caused me to worry about anything I ate, drank or activities that I did. Most importantly, my husband and I were going to be starting fertility treatments in January however I was diagnosed with TTP in October which put those plans on hold. TTP has potentially caused us not to be able to have another child and if we decide to take the risk, my pregnancy will be high risk.”
“Ultimately, I had to adjust my career goals and how I was going to build my family... Instead of working my way up the corporate ladder, I had to sidestep.”
“We were a dual-income, one-child family before, with plans to have a second. TTP meant that we would not risk having another child. TTP meant that one working parent became a completely disabled dependant for roughly a year, and after that was somewhat disabled, only able to work a small number of hours for pay and not contribute to household chores. The other parent had to pick up the slack and do all the wage-earning, all the child-rearing, all the cooking and cleaning. It is an understatement to say it has been hard. That has social implications: we don't have the energy to socialize.”
The anxiety over treatments and having to delay planning for the future also extends to caregivers. 32% of respondents to the survey were caregivers, family members, or friends of those with TTP and in response to a question about the caregivers’ quality of life during their loved one’s TTP episode, this is what some caregivers had to say:
“Quality of life changed completely. I would say the fear of never know what may happen next.” “The worry and anxiety. Huge impact on work”
“As a caregiver, I had to be with my spouse every day to make sure he got to each department within the hospital and listened to the different doctors. Regular life activities go on hold and I did miss time from my own job. My mental health was fragile but had to be strong for my spouse.”
“I was with her minimum 15hrs daily and away from my other children then when strokes began slept at the hospital with her. She was in hospital for 5 weeks therefore had to quit my job.”
TTP patients and caregivers expect that access to caplacizumab will provide:
The ability to survive the next TTP crisis which carries a 20% mortality rate;
A treatment that provides them with less uncertainty in the early stages of their TTP episode and peace of mind during remission;
A reduction in the number of plasmapheresis treatments, of which respondents have said is an arduous process with risks; and
The ability to plan for the future – something that current TTP patients cannot do.
Experience With Drug Under Review
Of patients and caregivers, 16 respondents (34%) had received access to caplacizumab. This access was varied – 7 patients had participated in a Canadian clinical trial, 6 had received it via the manufacturer’s compassionate access program, and one respondent had received it repeatedly via their private insurance coverage.
Patients and caregivers with experience with caplacizumab were clear about the benefits provided by this therapy, with one respondent saying it is a “total game-changer” for TTP treatment. Respondents with experience on caplacizumab noted shorter hospital stays, faster healing, and prevention of further disease as key benefits, while two respondents emphasized the reduced mental health burden – specifically, the anxiety surrounding relapses.
“My anxiety about relapse during remission has been drastically reduced. I now stress about not only when the next relapse will happen, but if I will survive it. Access to caplacizumab reduces the 20% risk of death with every relapse. Access to caplacizumab has changed everything about my outlook for the future with this disease.”
“My expectations would be that the drug would allow my body to heal quicker and my platelet count would increase and remain at a stable level.”
“Cablivi probably would have prevented stroke, DVT and retinal detachment as these items all happened after diagnosis and treatment for TTP had started.”
“Caplacizumab will keep me safe and reduce the number of risky and unpredictable plasmapheresis treatments I need. It will get me home to my young children and will get me there faster.”
“Cablivi would save my life if I were to get another relapse. In my last relapse, standard therapy did not work. My stay was 3 months in the hospital. I could have lost my life. The drug would shorten my stay in the hospital.”
“We fully believe that being part of that (Capla) clinical trial saved her life. Yes, TTP has been hard, and she has had life-long disability as a result. But it could have been so much worse without Cablivi. We fully expect that if her TTP recurs, that she will be at risk of further organ damage, which might lead to more cognitive impairments, or further affect her kidneys, or add to the muscle weakness.”
On the disadvantages for caplacizumab, patients noted the cost of treatment (for those without private coverage) and overall availability for patients. However, more respondents stated the advantages being:
Shorter treatment time
Less stress on the hospital system, due to duration of hospital stays and plasma resources.
Reduced risk of TTP side effects
“In crisis I would recover from TTP episodes quicker (less immune suppression and cancer risk) to get back to my life so much faster. And with a lower risk of damage to organs and other long-term disabilities associated with TTP from the clots that could potentially change my life tomorrow.”
“A shorter treatment duration will also reduce the amount of immunosuppressant medication that I will need going forward. As a metastatic cancer survivor, this is amazing news as the use of immunosuppressant medications invite the deadly cancer back.”
Our survey respondents truly believe that their quality of life could change if Cablivi was accessible. Respondents said that the simple fact of knowing it is available would be lifechanging as it would take away the stress of TTP episodes, lower anxiety knowing they can resume life again earlier, and create less mental stress about the disease and cost of medication.
“Knowing it is available and its another tool to treat TTP takes a lot of stress away when you know you could potentially relapse at any time and maybe the next time conventional treatments won't work.”
“Less worry about if we would have access to this treatment in future, or if we would have to pay high prices to save the family members life.”
“My anxiety over the next relapse would be greatly reduced because the fear of death would be significantly diminished. The relief would be freeing.”
“PTSD and anxiety related to relapses is one part of the reduced quality-of-life that TTP has caused our family. Having ready access to Cablivi would mean that recurrences would be less terrifying, with a greater hope that she could make it through one without picking up more disabilities and cognitive impairments.”
We believe that this should be available immediately for all TTP patients upon the order of their physician – there is a real and specific value for patients of which the standard of care is ineffective. They die otherwise.
Companion Diagnostic Test
Not applicable.
Anything Else?
Commentary
The Canadian TTP community was devastated to learn of CADTH’s 2020 recommendation – even as the rest of the world (including the United Kingdom’s NICE, the United States, Denmark, Belgium, Netherlands, Finland, Italy) saw the clinical value and recommended its use for patients. This has been incredibly frustrating for Canadian TTP patients, as we watch members of our international community receive access to treatment that, for some reason, our system does not deem beneficial.
The effects of COVID-19 have created surgical backlogs, a need for health human resources, and we understand there is a current blood donation shortage with major concerns about future plasma capacity in Canada.
Caplacizumab not only saves TTP patients’ lives but has the capability to ease the burden on the health system by freeing up hospital beds due to shorter stays and reducing plasma resources needed to save a patient during a TTP episode.
CADTH Review Framework: Significant Unmet Need
As discussed above, TTP is a rare disease with significant unmet need with respect to treatments. We are encouraged by CADTH’s inclusion of Considerations for Significant Unmet Need within the Procedures for CADTH Reimbursement Reviews, and hope that CADTH applies those considerations during the review of caplacizumab.
Survey Responses: “Anything Else?”
The vast majority of our survey respondents provided responses to the open-ended question of “Is there anything else you’d like decision-makers to know as they consider recommending caplacizumab for reimbursement?”.
Selected responses include:
“Please please fund this as if you can minimize hospital stays and reduce the need for life saving plasma, I believe it is a win win situation, hopefully costing the health care system less in the long run.”
“One of my friends lost her battle with TTP days after delivering (early) her second baby girl. She was a kind, thoughtful and lovely person who was taken too young. Her daughters will grow up without their mom because she did not have access to caplacizumab. She'd relapsed more than once, she'd survived before. In the end, she lost the race to tame the TTP with untargeted treatment. Don't let this happen again. It doesn't need to be a race anymore. Caplacizumab can give us the time we need to survive and emerge without life altering disability.”
“Peer countries to Canada support the use of Cablivi. I assume that Canada can benefit from their knowledge and make the right decision to support Canadian TTP patients.”
“Cablivi kept my daughter 19 years old safe from further damage that TTP had already caused her during her 5-week stay in hospital. She fought for 11 days without caplacizumab, sustained 3 strokes, and was moved to ICU hearing all the negative information from doctors that she wasn't responding to the typical treatment plan for TTP. 2 weeks into fighting for her life she was given caplacizumab and within only 13 hours of receiving the drug and not changing any other treatment she was receiving she started seeing improvements with her blood labs. 3 days later she says, "I am feeling better" and her labs are out of the critical range. Caplacizumab is the drug that kept her safe from further damage TTP had planned for her. Caplacizumab bought her the time she needed for her typical treatment plan to work. Caplacizumab was a key factor that saved my daughters life please keep her and other ttp patients safe and grant access to this life saving drug. My daughter is here today to continue her life's journey because of it.”
As noted via the experiences above, our patient community is passionate about access to a proven treatment that can protect their lives during a TTP episode. TTP is a true medical emergency and having immediate access to a life-saving treatment such as caplacizumab could mean the difference between life and death to patients. We firmly urge CADTH to recommend caplacizumab (Cablivi) for TTP in Canada.
Conflict of Interest Declaration — Answering Thrombotic Thrombocytopenic Purpura Foundation
To maintain the objectivity and credibility of the CADTH reimbursement review process, all participants in the drug review processes must disclose any real, potential, or perceived conflicts of interest. This Patient Group Conflict of Interest Declaration is required for participation. Declarations made do not negate or preclude the use of the patient group input. CADTH may contact your group with further questions, as needed.
Did you receive help from outside your patient group to complete this submission? If yes, please detail the help and who provided it.
No.
Did you receive help from outside your patient group to collect or analyze data used in this submission? If yes, please detail the help and who provided it.
No.
List any companies or organizations that have provided your group with financial payment over the past 2 years AND who may have direct or indirect interest in the drug under review.
Answering TTP Foundation has not received any support from any pharmaceutical company in the last two years. We are extremely careful to ensure our reputation remains one of independent regard for the patients we represent.
Table 1: Financial Disclosures for the Answering Thrombotic Thrombocytopenic Purpura Foundation
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
No COI | — | — | — | — |
Clinician Input
Canadian Apheresis Group
About the Canadian Apheresis Group
The Canadian Apheresis Group (CAG) is a national organization representing all practitioners involved in therapeutic apheresis procedures in Canada with members from 42 major medical centres. Apheresis procedures include plasma exchange, therapeutic cytapheresis, photopheresis, and peripheral blood stem cell and lymphocyte collections for the production of CART cells for cancer therapy. Currently, there are 107 physicians involved in the CAG and these include, for the most part, hematologists, nephrologists, pathologists and hematopathologists.
Since it was established in 1980 with funding from the Federal Ministry of Health, the CAG has collected data on all of the apheresis procedures performed in the country. This national database, which is now computerized, has allowed members to evaluate and optimize practice and has resulted in the development and execution of a considerable number of clinical trials some of which have been pivotal in establishing apheresis practice throughout the world. Our activities and data are reviewed by all at our annual general meeting where plans are made regarding future practice.
In fact, it was our CAG 1991 publication in the New England Journal of Medicine (1), indicating that plasma exchange was an effective treatment of thrombotic thrombocytopenic purpura (TTP) resulting in more than 85% survival of patients treated early in the course of disease, that established plasma exchange as the first-line therapy for this disorder.
Subsequently, we have published 13 other papers dealing with the treatment ofTTP (2-14) of which a report published in the British Journal of Hematology in 2015 clearly showed that Rituximab, an anti-B cell agent, would decrease antibody production. However, Rituximab was not immediately effective and took two weeks to reduce the CD 20 levels as shown in Figure 1 (14). At the same time, it was noted that the ADAMTS-13 levels did not return to near normal levels for several weeks thereafter (Figure 2). So, there is a significant delay before immunotherapy has an effect on the course of the disease and during this time the microthrombi continue to be formed, causing morbidity and mortality.
This finding is supported by the data from Pavenski et al (15) which showed that corticosteroids, with or without rituximab, are not immediately effective. They further reported that Caplacizumab reduced the rate of the composite endpoint of TIP-related death, exacerbation, and major thromboembolic events during the double-blind treatment period irrespective of baseline immunosuppression regimen.
The CAG has played a major role in the treatment and understanding of TTP over the years and, since the 1980s, has had a functional working group of experts in the field of TTP who constantly consider our data and information and look for ways to improve practice and therapeutic outcome. Most recently, our chair, Dr. Gail Rock, was invited to participate in the International Society on Thrombosis and Haemostasis (ISTH) panel that made recommendations on the treatment ofTTP (16).
As physicians directly involved in the care of these patients across the country, we offer our advice and are prepared to consult at any time with the committees deciding on the importance of this drug and its relative role in the treatment of TTP.
The Canadian Apheresis Group website can be located by following this link: https:/cagcanada.ca.
Information Gathering
Upon receiving the information that CADTH had recommended against the reimbursement of Caplacizumab to treat patients with TTP, the information was shared with the TTP working group and then circulated to all members of our organization. Comments were requested from our members with the consensus result being that the group disagreed with this recommendation. The TTP working group then prepared documentation which was shared both with CADTH and INESSS in which we requested that their recommendations be reconsidered to allow at least selective use in certain patients with TTP. The document was submitted to both organizations on December 14, 2021, and we requested that Caplacizumab would, at least, be made available for use in patients who have:
Severe presentation requiring ICU care.
Patients presenting with significant organ involvement - neurological (ex. focal deficit seizures or altered LOC), cardiac (arrhythmia, ischemic EKG changes, ventricular dysfunction) or renal involvement requiring dialysis.
Patients with early relapse on standard of care therapy or those who are refractory to standard of care therapy.
Patients who are intolerant of plasma exchange or object to plasma exchange on religious grounds.
Following the publication of several real-life evaluations of the role of Caplacizumab and the continued difficulties in providing the drug to Canadian patients despite the fact that information obtained from international sources indicated that the drug was being reimbursed in 21 other countries, the members of the TTP working group resolved to further pursue the issue. We were then notified that Sanofi would be making a resubmission for reconsideration of reimbursement and we decided, as a group, to support this resubmission by submitting a Clinician Group Input Survey in support of the application.
To do this we have taken the different sections of the six headings and had various members of our TTP working group respond to each. Our central office then correlated the results and circulated the entire report to all working group members for further input. Subsequently, it was sent to every apheresis centre in the country for comments and further input prior to submission (see example, Appendix A).
Current Treatments
Acquired, immune-mediated TTP is caused by severe ADAMTS13 deficiency caused by autoantibodies. It is treated with urgent initiation of daily therapeutic plasma exchange (TPE) with plasma as replacement (to replace ADAMTS13), plus immune suppression with corticosteroids (to suppress production of auto antibodies responsible for ADAMTS13 deficiency). Anti-platelet agents to prevent organ damage by aTTP are also sometimes used (usually ASA, once the platelet count is above 50; efficacy unproven).
Caplacizumab is not routinely available in Canada but is used for this purpose by other countries. Laboratory targets to guide treatment include platelet count and lactate dehydrogenase (LDH), and TPE is typically continued until platelets have normalized (i.e., >150 x 109/L) for at least 48 hours, LDH is improved/normalized, and symptoms and organ damage markers (creatinine, troponin, etc.) have resolved/stabilized. Additional immune suppression with rituximab (or biosimilar) is standard of care for patients who have refractory disease (i.e., persistent thrombocytopenia and persistently elevated LDH level despite five TPE) or who exacerbate (disease recurs shortly after TPE is stopped) or for those who presented with an aTTP relapse (patients who have had at least one relapse have a significantly higher likelihood of having another relapse). Rituximab suppresses production of immune cells which produce antibodies including autoantibodies against ADAMTS13 and is therefore disease-modifying. Efficacy of rituximab has been demonstrated in multiple trials and observational cohorts (and in many cases, it is used first line) (reduces mortality, reduces relapses), and is endorsed by multiple guidelines (most recently, those from the International Society for Thrombosis & Hemostasis, ISTH) and has been shown to be cost-effective (Goshuat et al Blood Advances). This drug is neither licensed by Health Canada nor reimbursed by any province for this indication. Access is usually through compassionate access or private insurance plans. In patients with insufficient response or intolerance to rituximab, additional/alternative immune suppression may be required (e.g., cyclosporine, azathioprine, bortezomib). Immune suppression modifies the underlying disease by suppressing production of anti-ADAMTS13 antibodies, but this process, regardless of therapeutic chosen, takes time and it is essential to normalize platelet count, prevent ongoing microangiopathy and target organ damage (kidneys, heart, brain) as soon as possible.
Treatment Goals
Treatment aims for immune-mediated TTP are broadly two-fold: 1) to rapidly normalize platelet count, which is associated with reduced platelet activation/aggregation and thrombotic obstruction of the microvasculature; and 2) to abolish production of anti-ADAMTS13 autoantibodies. These two, together, are required to successfully achieve the main goal, which is to significantly reduce mortality (90% if untreated). Mortality of treated aTTP (TPE plus immunosuppression) is about 10%, based on real world studies.
Mortality of patients who are refractory to standard treatments is more than 30%. In aTTP, a low platelet count signifies ongoing microthrombosis and organ damage, as platelets are low due to consumption in microthrombi. In this regard, low platelet count is the most significant and direct marker of organ damage. As discussed above, we have several options available to reduce antibody/inhibitor production, but we only have TPE with its inherent risks and side effects to help try to normalize platelet count.
Of note, patients with aTTP require admission to a hospital and, frequently, to the critical care unit. Once the disease starts to respond, the patients are transferred from the ICU to the ward. The patients do not leave the hospital until weaned off TPE (normal platelets, stable/normal LOH and organ damage markers). The patients spend about 10 days in a hospital and another few weeks recovering at home. Those who suffered complications or have refractory disease have longer hospital stays and longer days of disability. A significant proportion of patients suffer from mental health issues, neurocognitive deficits, hypertension, headaches, and have reduced quality of life following recovery. The existing therapies do not adequately address these long-term complications.
Treatment Gaps (Unmet Needs)
Considering the treatment goals, please describe goals (needs) that are not being met by currently available treatments.
As mentioned above, there are several options available to deal with Aim 2 (i.e., immune control of antibody production), even though not all patients respond or may have limited response due to toxicity. Aim 1 above is where more significant treatment gaps remain. To protect patients from ongoing end-organ damage, rapid inhibition of microvascular thrombosis is required, and this is associated with platelet count normalization.
TPE with plasma replacement provides deficienUinhibited ADAMTS and helps rebalance physiologic hemostasis but does not directly inhibit platelet aggregation/thrombosis. Reduction of circulating anti ADAMTS13 antibodies is associated with this but is not immediate; the median onset of the effect of rituximab is 10-12 days (as shown in Figure 1) (14) days, whereas other steroid-sparing agents can take weeks before appreciable benefit is seen. As such, an ability to rapidly inhibit platelet aggregation while waiting for TPE and immune suppression to take proper effect is needed. Moreover, standard treatment will not be sufficient in about 30% of patients who will develop refractorlNESSS; a refractory state is associated with a high probability of suffering catastrophic organ damage (ex. stroke) and/or dying from the disease.
Which patients have the greatest unmet need for an intervention such as the drug under review?
All patients with immune-mediated aTTP are at significant risk of mortality and long-term morbidity if the disease is not controlled fully and rapidly. This holds for any acute presentation, including relapses which can occur in approximately 30% of patients. Patients presenting with already-apparent end-organ damage, including neurologic (e.g., confusion, headache, stroke seizures), renal (e.g., kidney failure, proteinuria), and cardiac (e.g., arrhythmia, myocardial ischemia), among other manifestations are likely at highest risk of severe outcomes if not treated urgently. Moreover, patients with refractory disease are at a high risk of mortality. The microthrombotic damage to the viscera is driven by continued platelet aggregation and thrombosis in the context of severely deficient ADAMTS13 and pathologically elevated levels of ultra large von Willebrand Factor multimers. The drug under review therefore would be expected to (and has been shown to) directly target this unmet issue. (2)
Moreover, patients who object to receiving plasma and hence TPE treatment (for e.g., due to religious objections) do not have good/effective therapeutic options in Canada. Untreated, aTTP leads to mortality in 90% of patients.
Caplacizumab will provide a good treatment option to those presenting with significant organ damage (as it will protect from further deterioration while immunosuppression takes effect), refractory patients (Caplacizumab rapidly normalizes PLT count and eliminates refractorlNESSS, while waiting for immunosuppression to work), and patients objecting to plasma (case reports of patients successfully treated with Caplacizumab and immunosuppression without TPE have been published). Whereas all patients are at risk of organ damage and death from aTTP and all should be considered for Caplacizumab treatment, the subpopulations who stand to benefit the most from this therapy are as above.
Place in Therapy
How would the drug under review fit into the current treatment paradigm?
Caplacizumab directly inhibits binding of von Willebrand Factor to platelets, which is the trigger to microthrombi formation, microvascular thrombosis and organ damage or failure. It is the first and only licensed drug that can directly and quickly inhibit microvascular thrombosis in aTTP. Plasma exchange is effective by restoring ADAMTS13 levels while removing the inhibitor but is not a direct treatment of platelet activation and microthrombi formation. It is through the enzymatic activity of ADAMTS13 that the more active fraction of von Willebrand Factor, the ultra large multimers, will be cleaved into smaller multimers which are less likely to activate platelets spontaneously, which, in turn, will reduce platelet activation, microthrombi formation and platelet consumption. As mentioned previously, plasma exchange is a lifesaving procedure for patients with aTTP but it takes a few days, at a minimum, to show therapeutic activity. The mechanism of action of Rituximab, corticosteroids and immunosuppresslve drugs has been described above and none of these drugs directly target the mechanism responsible for end-organ damage. Caplacizumab has the potential to stop further end-organ damage in a short period of time.
For the subgroup of patients detailed in section 2, access to Caplacizumab will not shift the current treatment paradigm in the sense that all currently recommended treatments will remain. For patients requiring ICU or presenting with significant end-organ damage, they will still require and benefit from plasma exchange and corticosteroids. Because Caplacizumab aims at stopping the consequences of platelet activation rather than targeting the cause of ADAMTS13 deficiency, restoring ADAMTS13 levels with plasma exchange and stopping antibody production against this enzyme will remain the stepping-stones of aTTP treatment. Although the studies supporting the Caplacizumab initial application to CADTH and INESSS were not designed to show specific outcomes related to the total burden of disseminated microthrombi, there is strong indirect evidence to support the hypothesis that the shortest time to platelet count recovery will result in less mid- and long-term morbidity in aTTP patients. The same hypothesis supports its use in relapsing and refractory patients since these patients tend to have a higher microthrombi burden. Caplacizumab may not treat the underlying cause of refractorlNESSS to standard therapy but will allow more time for immunosuppressive treatment to work while protecting patients from further end-organ damage.
Please indicate whether or not it would be appropriate to recommend that patients try other treatments before initiating treatment with the drug under review. Please provide a rationale from your perspective.
Patients with aTTP will be started on currently used therapies. Caplacizumab will be added to these treatments as per the treatment schedule studied in the Hercules trial. There is no other treatment that could be considered specifically interchangeable with this drug.
How would this drug affect the sequencing of therapies for the target condition?
Since Caplacizumab does not act directly on ADAMTS13 deficiency and the subsequent generation of ultra large multimers ofvWfactor, only on its downstream consequences, patients with relapsing or refractory disease would be able to receive further treatments with Caplacizumab while more effective therapies to decrease and stop anti-ADAMTS13 antibody production are worked out. For patients who fail caplacizumab, meaning patients who would not show platelet count recovery or who would show new or progressive end-organ damage while on therapy with Caplacizumab, there are no alternatives available. Caplacizuzmab therapy would be stopped, and treatments would fall back on current strategies for refractory TTP such as high- volume PE, Rituximab if not already used, bortezomib, etc.
Which patients would be best suited for treatment with the drug under review?
Patients who are not early and good responders to plasma exchange would be best suited to receive Caplacizumab. As detailed in section 2, patients with more severe end-organ damage, such as those requiring ICU care for major organ failure or mechanical ventilation for airway protection, are at higher risk of mortality and morbidity. Fortunately, with education and increasing awareness of this disease by physicians, an increasing number of aTTP patients are diagnosed prior to development of major organ failure. But for those who are not, timely access to plasma transfusion, plasma exchange and adequate supportive care is critical to their survival and to reducing the risk of long-term morbidity from this disease. Caplacizumab has the advantage of reducing the time to platelet count recovery, which increases the likelihood of rapid recovery and prevents additional organ damage.
Patients with relapsing or refractory disease have a much less favorable prognosis, in good part due to the recurring and ongoing microthrombi production which increases the risk of end organ damage.
Finally, currently there is no alternative as effective as plasma exchange for the treatment of aTTP. There are reports, however, of patients successfully treated with Caplacizumab alone with potentially comparable outcomes. Therefore, for patients in whom plasma exchange is contra-indicated due to prior serious adverse events, or because of religious objection, there is currently no other effective treatment.
Caplacizumab would address an unmet need in this very rare population of patients.
How would patients best suited for treatment with the drug under review be identified?
Diagnosis of aTTP requires a combination of clinical examination and laboratory test results along with urgent consultation. The basic requirements for diagnosis of TTP are the presence of thrombotic microangiopathy (TMA) associated with low levels of ADAMTS13. TMA refers to anemia with red cell fragments on the blood smear, and thrombocytopenia. After urgent consultation with hematology, nephrology, or internal medicine to confirm the presence of TMA, it is usually recommended to start plasma exchange while the cause of the TMA is being investigated. Because of a long turnaround time to obtain ADAMTS13 levels in many institutions, the management of suspected aTTP cases requires the clinician to estimate the clinical probability of ADAMTS13 deficiency using a clinical scoring system such as the PLASMIC score (Li et al. J Thromb Haemost. 2018).
We propose that patients who present with suspected aTTP and a high pretest probability of aTTP have access to Caplacizumab which should be administered early in the treatment schedule without waiting for the results of the ADAMTS13 assay. The decision to continue will depend on the ADAMTS13 levels. If the pretest probability is intermediate or low, Caplacizumab should only be made available once the ADAMTS13 assay results are back and show low (< 10%) levels.
For patients with suspected aTTP who are started on plasma exchange and become intolerant to a point that plasma exchange can no longer be performed, Caplacizumab should be started as soon as possible considering plasma exchange would normally be done on a daily basis.
For patients who object to plasma exchange on religious grounds, Caplacizumab should replace plasma exchange and be started when TMA is observed while we wait for the ADAMTS13 levels to come back and confirm or not the diagnosis of aTTP.
For patients with early relapse on standard of care therapy or those who are refractory to standard of care therapy but had not received Caplacizumab initially, Caplacizumab should be started as soon as relapse or refractorlNESSS is diagnosed. Relapse is easily diagnosed when there is recurrent thrombocytopenia and elevated LDH level after initial normalization with therapy, whereas refractorlNESSS is defined as persistent thrombocytopenia and persistently elevated LDH level despite five TPE.
Which patients would be least suitable for treatment with the drug under review?
Patients with TMA not caused by ADAMTS13 deficiency should not receive Caplacizumab based on the current evidence. Therefore, patients who have ADAMTS13 levels above 10% without evidence of anti ADAMTS13 antibodies should not receive it. For those whose ADAMTS13 levels are pending but have a low or intermediate pretest probability using a clinical scoring system, Caplacizumab should be withheld and only administered if ADAMTS13 activity is <10%. Patients with confirmed pregnancy should not receive Caplacizumab while there is an absence of evidence to support safely.
For patients who would otherwise be eligible to receive Caplacizumab but have ongoing bleeding, Caplacizumab should be withheld until bleeding is resolved.
Is it possible to identify those patients who are most likely to exhibit a response to treatment with the drug under review?
In studies reported with Caplacizumab, all patients with confirmed TTP who received the drug in addition to standard therapy or in replacement of PE responded with elevation and normalization of platelet counts.
This suggests that all patients with the appropriate diagnosis (TMA with low levels of ADAMTS13) will respond.
What outcomes are used to determine whether a patient is responding to treatment in clinical practice?
There are many outcome measures that need to be monitored for these patients. The time to platelet recovery, normalization of LOH, resolution of neurological signs or symptoms such as seizures, resolution of cardiac ischemia, if present, are all important outcomes. Obviously, we also monitor survival, number of days in ICU, number of days on a ventilator if applicable, length of hospital stay and long term survival.
These are all outcomes also reported in clinical trials and observational studies.
What would be considered a clinically meaningful response to treatment?
The most meaningful responses would be those related to major end-organ damage. In patients experiencing neurological deficits, seizures, cardiac ischemia or hypoxemia, rapid recovery is critical to their survival and long-term morbidity. Time to platelet count recovery correlates with the decrease in microthrombi generation and resolution of clinical signs or symptoms, making it an objective and easily obtainable outcome measure.
How often should treatment response be assessed?
Treatment response should initially be monitored daily while the patients are admitted to hospital. Once the patient has entered remission, the monitoring can be decreased over time until it is being conducted weekly. The time to aTTP remission is different for all patients. Caplacizumab is typically used for 30 days. Patients do require close follow-up after discontinuation of Caplacizumab with ongoing weekly blood work to ensure that disease relapse does not occur.
What factors should be considered when deciding to discontinue treatment?
When discontinuing therapy, the provider should ensure that the patient is in remission. The main risk when discontinuing therapy is the risk of disease relapse. While Caplacizumab directly addresses the thrombotic mechanism of aTTP, it does not address the underlying auto-immune disease. If this has not been successfully treated, there is a risk of recurrence. With this in consideration, the provider should consider ordering ADAMTS-13 activity levels and antibody levels prior to discontinuing Caplacizumab.
What settings are appropriate for treatment with the drug under review?
Typically, Caplacizumab would be initiated in a hospital setting. aTTP is a severe illness and the first dose is administered intravenously. Subsequent doses are administered subcutaneously in the abdomen. Once the patient has entered remission and has been discharged, the remainder of the doses (to complete 30 days) can be given at home by the patient or a care provider, after proper education. These doses could also be given in the community or by a specialty clinic, but this approach would likely be less common.
For non-oncology drugs, is a specialist required to diagnose, treat, and monitor patients who might receive the drug under review?
In general, the diagnosis of aTTP should be made by a Hematologist, Nephrologist or an Apheresis physician. In communities where these specialties are not available, the patient should be transferred to a center capable of providing apheresis with expertise in aTTP.
Rationale for Significant Unmet Need Classification
aTTP is a very rare disease affecting primarily younger women and, despite many efforts and even with the best available treatment, results in 10 to 15% mortality and a very high morbidity rate with serious long-term effects and impairment. Therefore, the CAG requests that CADTH/p/ERC apply the recommendations framework that includes Considerations for Significant Unmet Need as described in the Procedures for CADTH Reimbursement Reviews (March 2022), section 9.3.1.
Appendix: Email Example of a Response the CAG Received
The Clinician Group Input was sent to all 42 Canadian centres for review and final comments. This is an email example of a response the CAG received from St. Joes in Hamilton, Ontario.
From: Gangji, Azim █gangji@mcmaster.ca█ June 8, 2022, 1:52 PM
Sent to: CAG
Subject: Re: CADTH
I reviewed this with the physician group at St Joes Hamilton and no changes were suggested.
Thank you.
Azim
Azim S. Gangji MD MSc FRCPC BSc
Pharm Professor of Medicine, Dept of Medicine
Vice President, Education, St. Joseph's Healthcare Hamilton Chair, Canadian Society of Transplantation Education Committee Co-Chair, RCPSC AFC Accreditation Committee
Co-Chair, RCPSC Solid Organ Transplantation Ctte AFC/AST Director, Solid Organ Transplantation
Fellowship Director, Glomerulonephritis, Home Dialysis, Geriatric Nephrology Chair, Medical Specialties Fellowship Directors
Chair, Medical Specialties UGME Electives Coordinators McMaster University
St. Joseph's Healthcare Hamilton
From: ████████████████████████
Date: Wednesday, June 8, 2022, at 12:56 PM
To: ██████████████████████
Subject: CADTH Dear All,
I hope this email finds everyone well. The CAG will be submitting the Clinician Group Input (see attached) to CADTH next week. If you have any final comments, please send them to ██████████████████ no later than Monday June 13. Thank you in advance.
CAG Office
References
Rock GA, Shumak KH, Buskard NA, Blanchette VS, Kelton JG, Nair RC, Spasoff RA, and the Members of the CASG. Comparison of Plasma Exchange with Plasma Infusion in the Treatment of Thrombotic Thrombocytopenic Purpura. New England Journal of Medicine 1991; 325: 393-397
Rock G, Shumak K, Kelton J, Blanchette V, Buskard N, Spasoff R, and the Members of the CASG. Thrombotic thrombocytopenic purpura: outcome in 24 patients with renal impairment treated with plasma exchange. Transfusion 1992; 32: 710-714
Tandon nn, Rock G, Jamieson GA. Anti-CD36 antibodies in thrombotic thrombocytopenic purpura. British Journal of Haematology 1994; 88: 816-825.
Shumak KH, Rock GA, Nair RC and the Canadian Apheresis Group. Late Relapses in Patients Successfully Treated for Thrombotic Thrombocytopenic Purpura. Annals of Internal Medicine 1995;122: 569-572.
Rock G, Kelton JG, Shumak KH, Buskard NA, Sutton DMC and members of the GAG. Laboratory abnormalities in thrombotic thrombocytopenic purpura. British Journal of Haematology 1998; 103: 1031-1036.
Rock, G. and members of the GAG. Influence of Replacement Fluid on TTP: The Experience of the Canadian Apheresis Group. Transfusion Science 1998; 19(3): 199-200.
Wright J, Wang H, Hornstein A, Hogarth M, Mody M, Garvey M, Blanchette V, Rock G, Freedman J. Characterization of platelet glycoproteins and platelet/endothelial cell antibodies in patients with thrombotic thrombocytopenic purpura. British Journal of Haematology 1999; 107: 546-555.
Tsai H-M, Anping L, Rock G. Inhibitors of von Willebrand Factor-Cleaving Protease in Thrombotic Thrombocytopenic Purpura. Clinical Laboratory 2001; 47: 387-392.
Rock, G., Anderson, D., Clark, W., Leblond, P., Palmer, D., Sternbach, M., Sutton, D., Wells, G., Members of the GAG and members of the Canadian Association of Apheresis Nurses. Does cryosupernatant plasma improve outcome in thrombotic thrombocytopenic purpura? No answer yet. British Journal of Haematology 2005; 129: 79-86.
Foley S, Webert K, Arnold D, Rock G, Clark W, Barth D, Sutton D and members of the Canadian Apheresis Group. A Canadian phase II study evaluating the efficacy of rituximab in the management of patients with relapsed/refractory thrombotic thrombocytopenic purpura. Kidney International, February 2009, 75 (112) S55-S58
Cataland SR., Peyvandi F., Mannucci PM., Lammie B., Kremer Hovinga JA., Machin SJ., Scully M., Rock G., Gilbert JC.Yang S. Wu H., Jilma B., Knoebl P. Initial experience from a double-blind, placebo-controlled, clinical outcome study of ARC1779 in patients with thrombotic thrombocytopenic purpura. American Journal of Hematology, Volume 87, Issue 4, April 2012, pages 430-432
Rock GA., Clark WF., Anderson D., Barrett B., Sutton D., Leblond P., Sternbach M., Sontrop
J. and Members of the CAG. ADAMTS-13 May Not Predict Disease or Outcome in Patients with Thrombotic Thrombocytopenic Purpura. Thromb Res. 2013, 131(4).
Clark, WF., Rock, G., Foley, R., Barth, David; Weber!, K., Yenson, P., Kelton, J., Li, L. A Phase-II sequential case-series study of all patients presenting to four plasma exchange centres with presumed relapsed/refractory TTP treated with Rituximab. Br J Haematol., 2015 Jul;170(2):208-17.
Rock G., Andronov A., Weger S., Abouhadjar H., Barth D., Clark W., Yenson P., Foley R.; Absence of Viral Complications When Using Rituximab to Treat TTP with Plasma Exchange; December 3, 2015; Blood: 126 (23)
Katerina Pavenski, Paul Knoebl, Marie Scully,Johanna A. Kremer Hovinga,
Paul Coppo, Flora Peyvandi, Spero Cataland, Ara Metjian, Javier De La Rubia,Hilde De Winter, Rui de Passos Sousa,Filip Callewaert; Efficacy of Caplacizumab in Patients with aTTP in the HERCULES, Study According to Initial lmmunosuppression Regimen. American Society of Hematology, November 13, 2019; Blood
X.Long Zheng, S. Vesely, S. Cataland, P. Coppo, B. Geldziler, A. Iorio, M. Matsumoto, R. Mustafa, M. Pai, G. Rock, L. Russell, R. Tarawneh, J. Valdes, Good Practice Statements (GPS) for the Clinical Care of Patients with Thrombotic Thrombocytopenic Purpura, Journal of Thrombosis and Haemostasis, July 10, 2020.
Conflict of Interest Declarations — Canadian Apheresis Group
Declaration for Clinician 1
Name: Gail Rock
Position: Chair Canadian Apheresis Group
Date: May 20, 2022
Table 2: COI Declaration for Canadian Apheresis Group — Clinician 1
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
Sanofi | X | — | — | — |
Declaration for Clinician 2
Name: Christopher Patriquin
Position: Hematologist, Clinician Investigator
Date: 22-April-22
Table 3: COI Declaration for Canadian Apheresis Group — Clinician 2
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
Alexion | — | X | — | — |
Apellis | X | — | — | — |
BioCryst | X | — | — | — |
Octapharma | X | — | — | — |
Sanofi | X | — | — | — |
Sobi | — | X | — | — |
Takeda | X | — | — | — |
Declaration for Clinician 3
Name: Katerina Pavenski
Position: Hematologist, St. Michael's Hospital - Unity Health Toronto
Date: June 2, 2022
Table 4: COI Declaration for Canadian Apheresis Group — Clinician 3
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
No COI | — | — | — | — |
I served as site Pl on HERCULES (Caplacizumab in iTTP) and post HERCULES studies (Ablynx/Sanofi), site Pl on SOAR-HI (rADAMTS13 in iTTP) (Shire!Takeda)
I have provided consultative services related to the above trials as well as real world utilization of caplacizumab and rADAMTS13 as well as spoke as invited speaker (my own slides/materials) about iTTP at the industry-sponsored events.
I declined all honoraria from the above sponsors since April 1, 2020.
Prior to 2020, I accepted honoraria to be paid to my institution for conduct of iTTP and related diseases studies.
Declaration for Clinician 4
Name: Vincent Laroche
Position: Hematologist, Blood bank, transfusion service and apheresis medical co-director
Date: 21-04-2022
Table 5: COI Declaration for Canadian Apheresis Group — Clinician 4
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
No COI | — | — | — | — |
Declaration for Clinician 5
Name: Gayatri Sreenivasan
Position: Hematologist, Medical Director Apheresis Program of British Columbia
Date: June 2, 2022
Table 6: COI Declaration for Canadian Apheresis Group — Clinician 5
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
No COI | — | — | — | — |
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up-to-date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
Redactions: Confidential information in this document may be redacted at the request of the sponsor in accordance with the CADTH Drug Reimbursement Review Confidentiality Guidelines.
Stakeholder Input: The views expressed in each submission are those of the submitting organization or individual; not necessarily the views of CADTH or of other organizations. As such, they are independent of CADTH and do not necessarily represent or reflect the view of CADTH. No endorsement by CADTH is intended or should be inferred. By filing with CADTH, the submitting organization or individual agrees to the full disclosure of the information. CADTH does not edit the content of the submissions.
CADTH does use reasonable care to prevent disclosure of personal information in posted material; however, it is ultimately the submitter’s responsibility to ensure no identifying personal information or personal health information is included in the submission. The name of the submitting organization or individual and all conflict of interest information are included in the submission; however, the name of the author, including the name of an individual patient or caregiver submitting the patient input, are not posted.
Accessibility: CADTH is committed to treating people with disabilities in a way that respects their dignity and independence, supports them in accessing material in a timely manner, and provides a robust feedback process to support continuous improvement. All materials prepared by CADTH are available in an accessible format. Where materials provided to CADTH by a submitting organization or individual are not available in an accessible format, CADTH will provide a summary document upon request. More details on CADTH’s accessibility policies can be found here.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.