CADTH Reimbursement Review
Lumasiran (Oxlumo)
Sponsor: Alnylam Netherlands B.V.
Therapeutic area: Primary hyperoxaluria type 1
This multi-part report includes:
Clinical Review
Pharmacoeconomic Review
Ethics Review
Stakeholder Input
Clinical Review
Abbreviations
ADA
antidrug antibody
AE
adverse event
AGT
alanine-glyoxylate aminotransferase
ALT
alanine aminotransferase
ANCOVA
analysis of covariance
AST
aspartate aminotransferase
AUC
area under the curve
BSA
body surface area
CI
confidence interval
CKD
chronic kidney disease
DB
double-blind
eGFR
estimated glomerular filtration rate
ESKD
end-stage kidney disease
ESRD
end-stage renal disease
EQ-5D-5L
EuroQol-5 Dimensions-5 Levels
EQ-5D-Y
EuroQol-5 Dimensions-Youth
FAS
full analysis set
GFR
glomerular filtration rate
GO
glycolate oxidase
GRHPR
glyoxylate reductase/hydroxypyruvate reductase
HAO1
hydroxyacid oxidase 1
HRQoL
health-related quality of life
HOGA1
4-hydroxy-2-oxoglutarate aldolase
ICC
intraclass correlation
KDQOL
Kidney Disease Quality of Life Questionnaire
LLOQ
lower limit of quantitation
LSM
least squares mean
MCS
mental component summary
MID
minimal important difference
MMRM
Mixed-Effect Model Repeated Measures
OLE
open-label extension
PCS
physical component summary
PD
pharmacodynamic
PedsQL
Pediatric Quality of Life Inventory
PH
primary hyperoxaluria
PH1
primary hyperoxaluria type 1
PK
pharmacokinetic
RCT
randomized controlled trial
REML
restricted maximum likelihood
SAE
serious adverse event
SD
standard deviation
SEM
standard error of the mean
SF-12
Short Form-12
siRNA
small interfering ribonucleic acid
ULN
upper limit of normal
VAS
visual analogue scale
WDAE
withdrawal due to adverse event
Executive Summary
An overview of the submission details for the drug under review is provided in Table 1.
Item | Description |
|---|---|
Drug product | Lumasiran (Oxlumo), 94.5 mg/0.5 mL lumasiran (as lumasiran sodium), subcutaneous injection |
Indication | For the treatment of primary hyperoxaluria type 1 to lower urinary oxalate levels in pediatric and adult patients |
Reimbursement request | As per indication |
Health Canada approval status | NOC |
Health Canada review pathway | Priority review |
NOC date | March 7, 2022 |
Sponsor | Alnylam Netherlands B.V. |
NOC = Notice of Compliance.
Source: Sponsor’s submission package for review of lumasiran;1 Oxlumo product monograph.2
Introduction
Primary hyperoxaluria type 1 (PH1) is an ultrarare, autosomal recessive metabolic condition caused by a pathogenic variant of the alanine:glyoxylate aminotransferase (AGT) gene.3 There is considerable heterogeneity with PH1 in the age of onset, severity of disease, residual enzyme activity, and genotype.4 The AGT enzyme catalyzes the conversion of glyoxylate to glycine in peroxisomes and without it (i.e., in patients with PH1), glyoxylate is converted to oxalate in the cytosol.3 Oxalate binds to calcium, producing insoluble calcium oxalate salts that are difficult for the body to eliminate. The clinical experts consulted by CADTH added that patients with PH1 are prone to kidney stone formation and recurrent episodes of renal colic. Once kidney function declines to an estimated glomerular filtration rate (eGFR) of less than 30 to 45 mL/min/1.73 m2, the kidneys become unable to excrete excess oxalate.5 Plasma oxalate levels increase, leading to systemic oxalosis, in which oxalate builds up in tissues throughout the body (e.g., bone, skin, retina, and cardiovascular and nervous systems).3,5 Patients often progress to end-stage kidney disease (ESKD), which, combined with complications of systemic oxalosis, results in early death.3 Laboratory tests showing urine oxalate levels consistently higher than 0.7 mmol/1.73 m2/day3 or 40 to 45 mg/day (500 µmol/day),5 elevated urine glycolate concentration, or plasma oxalate levels greater than 50 µmol/L when glomerular filtration rate (GFR) is less than 30 mL/min/1.73 m23 also indicate PH1. To confirm the diagnosis, genetic testing is used to identify a pathogenic variant in the AGT gene.3 Due to the variable clinical presentation and age of onset as well as a limited awareness of PH1, it has been suggested that the disease is underdiagnosed.3,6 The incidence of PH1 has been estimated to be between 0.4 and 1 per 100,000 live births in different populations.4 The prevalence has been estimated to be between 1 and 3 per million in European countries, with higher rates among countries with consanguinity.4 No Canadian data for prevalence or incidence have been identified from the literature.
Because hepatic overproduction of oxalate is the main cause of PH1, it is suggested that the best form of management is to reduce oxalate production, which can be further supported by increasing oxalate clearance by the kidneys, though the latter has limited effect.3 An estimated 30% of patients have a form of PH1 that is sensitive to high-dose vitamin B6 (a cofactor for AGT), which helps to ensure proper localization of the enzyme to the liver peroxisomes and may delay the onset of ESKD.3,7 According to the literature and the clinical experts consulted by CADTH, vitamin B6 therapy may be able to lower oxalate levels in some patients; however, not all patients achieve normalization of oxalate levels.7,8 Citrate supplementation to inhibit crystal formation and hyperhydration (2 to 3 L/m2/day) are also used to treat PH1 and preserve kidney function. Both citrate supplementation and hyperhydration can be burdensome for patients and are associated with compliance issues. Moreover, pediatric patients may require a gastrostomy tube to ensure adequate hydration throughout the day. It has been suggested that reducing dietary oxalate will have little effect because the main problem is endogenous overproduction.9 New therapeutics consisting of small interfering ribonucleic acid (siRNA) such as lumasiran and nedosiran have been developed to treat primary hyperoxaluria (PH).3 Patients may also undergo shockwave lithotripsy, ureteroscopy, or percutaneous nephrolithotomy to treat kidney stones. When kidney function declines to less than 30 mL/min/1.73 m2, patients may require hemodialysis to remove oxalate that cannot be excreted through urine. The major limitation with dialysis is that oxalate production often exceeds clearance, and while hemodialysis can dramatically lower plasma oxalate levels, this effect is transient, with a return to supersaturated levels (i.e., greater than 30 to 45 µmol/L) within a few hours of completing each dialysis treatment.3,9 The clinical experts consulted by CADTH stated that current standard-of-care treatments require lifelong adherence, are noncurative, and only partially alleviate the oxalate burden in patients. Liver-kidney transplant is considered the only cure for PH1 because it corrects AGT function (endogenous oxalate production is returned to normal levels) and restores kidney function, but is associated with high morbidity, mortality, and lifelong immunosuppression.3,5,9
Lumasiran (Oxlumo) is indicated for the treatment of PH1 to lower urinary oxalate levels in pediatric and adult patients.1 The drug is available as a solution of 94.5 mg/0.5 mL lumasiran for subcutaneous injection with weight-based loading and maintenance dosing.2 According to the product monograph, patients weighing less than 10 kg receive a loading dose of 6 mg/kg once monthly for 3 doses and a maintenance dose of 3 mg/kg once monthly, patients weighing 10 kg to less than 20 kg receive a loading dose of 6 mg/kg once monthly for 3 doses and a maintenance dose of 6 mg/kg once every 3 months (quarterly), and patients weighing 20 kg or more receive a loading dose of 3 mg/kg once monthly for 3 doses and a maintenance dose of 3 mg/kg once every 3 months (quarterly).2
The objective of the CADTH review is to perform a systematic review of the beneficial and harmful effects of lumasiran 94.5 mg/0.5 mL, subcutaneous, for the treatment of PH1 to lower urinary oxalate levels in pediatric and adult patients.
Stakeholder Perspectives
The information in this section is a summary of input provided by patient groups that responded to CADTH’s call for patient input and from clinical experts consulted by CADTH for the purpose of this review.
Patient Input
Two patient groups (the Oxalosis and Hyperoxaluria Foundation and the Canadian Organization for Rare Disorders) provided input as a joint submission to the CADTH review of lumasiran for the treatment of PH1. The responses were collected through an online survey and a virtual focus group with caregivers and patients. In total, 43 respondents completed the entire survey (18.6% Canadian and 41.9% American). Of the 43 responders, one-third indicated they were patients with PH and two-thirds identified as caregivers. In addition, 3 Canadians, 7 Americans, 6 non–North Americans from the online survey, and 2 Canadian children from the focus group reported having experience with lumasiran.
Patients reported that the greatest burden of PH1 was the physical toll (e.g., frequent dialysis, multiple hospitalizations, fractures) and emotional stress (e.g., anxiety and/or depression over concerns about kidney failure, liver-kidney transplant, not having an approved treatment). Respondents also highlighted issues with receiving appropriate and timely care as well as misdiagnoses. Patients and caregivers described the challenges associated with treatment such as gastrostomy tube insertion for infants and children, ureteroscopy and/or surgery to remove stones, vitamin B6 losing efficacy over time, noncompliance, and intensive dialysis. Patients who have received lumasiran described experiencing an improvement in PH1 management and quality of life.
The survey participants responded that current treatments and dialysis are insufficient and that therapies that decrease the likelihood of kidney stones, need for kidney and/or liver transplant, kidney failure, oxalosis, and the amount of medication are critical. Patients and families said that they need access to treatments that improve physical well-being, thereby mitigating stress and anxiety for the entire family. The respondents described how the physical, emotional, and financial challenges associated with PH1 have profound effects on quality of life, which is further compounded by a lack of knowledge among clinicians as well as access to treatments and affordability issues.
Clinician Input
Input From Clinical Experts Consulted by CADTH
The clinical experts consulted by CADTH emphasized the need for a therapy to treat PH1 that effectively lowers hepatic oxalate production, reduces kidney stone formation, and prevents the development of ESKD. The experts stated that current treatments are noncurative and do not lower hepatic oxalate production or total oxalate burden in patients. The clinical experts also noted that there is a small subset of patients whose PH1 is partially or completely vitamin B6 sensitive, but that vitamin B6 therapy only partially alleviates oxalate accumulation in these patients.
Two therapies, lumasiran and nedosiran, were identified by the clinicians as being possible pharmacotherapies for PH1. The experts expected lumasiran to cause a shift in the current treatment paradigm, becoming the first-line treatment for patients with PH1 and specifically for patients who are insensitive or only partially sensitive to vitamin B6 therapy. The clinicians noted that treatment with lumasiran is expected to be lifelong or until the patient receives a liver transplant. Further, the clinical experts stated the importance of continuing current standard-of-care treatments along with lumasiran.
As per the clinical experts, patients with PH1 would typically be identified based on clinical symptoms, laboratory testing of oxalate levels, and a diagnosis confirmed by genetic testing. Because there are hundreds of genetic variants currently identified10 as being related to PH1, 1 clinical expert noted that it may take time for new mutations to be accepted as pathogenic.
The clinical experts stated that patients would be candidates for lumasiran if they have genetically confirmed PH1 and are unable to normalize urine oxalate excretion. The clinicians were uncertain if or when lumasiran would be used for patients who are sensitive to vitamin B6 therapy and are able to normalize urine oxalate excretion but suggested it may be reasonable to begin treatment if these patients showed signs of disease progression. The experts felt that early intervention and treatment with lumasiran would be reasonable for all patients who still have kidney function and would not wait until GFR falls to 60 mL/min/1.73 m2, given that starting treatment early would help reduce kidney stone formation and slow down the progression of kidney function impairment. The clinical experts indicated that patients with little or no urine oxalate excretion who are relying solely on dialysis to remove oxalate from the body are at a very high risk of systemic oxalosis and would benefit from lumasiran. They stated that hemodialysis only temporarily lowers plasma oxalate levels, which rise to predialysis levels within a few hours. The clinical experts noted that lumasiran may be effective in avoiding the need for liver transplant in patients with ESKD and that it would be reasonable to treat patients with lumasiran before and after a kidney transplant to lower both plasma and urine oxalate levels.
The clinical experts noted that urine oxalate excretion and plasma oxalate are surrogate markers for oxalate production in patients with PH1 and that there is no widely accepted method for measuring total body oxalate, making it difficult to assess how effective a treatment is. Per the clinical experts, patients in earlier stages of PH1 may be monitored for urine oxalate excretion, plasma oxalate levels, kidney function (eGFR), and nephrocalcinosis via radiological imaging. Because patients in later stages of PH1 and on dialysis would not have reliable urine oxalate measures, clinicians would instead measure predialysis plasma oxalate every 1 to 3 months. The clinical experts stated that patients who have received a kidney or combined liver-kidney transplant may have plasma oxalate levels measured initially on a daily basis, transitioning to weekly and then monthly frequency as levels stabilize. The clinicians expected that there would be a noticeable improvement after an initial 6-month treatment duration, but that this is unlikely to be long enough to see normalization of urine or plasma oxalate levels. The experts suggested that it is important to consider treatment success in light of how severe the patient’s disease is before treatment and that it might be reasonable to treat a patient for at least 12 months (total) before deciding to continue lumasiran or not. According to the clinical experts, renewal of lumasiran would depend on adequate response to treatment as well as an assessment of potential treatment issues (e.g., adverse events [AEs], antidrug antibodies [ADAs], or compliance).
The clinical experts stated that patients who have received a liver transplant would not be treated with lumasiran because the new liver has functional enzyme, and there would be no need for the drug. Other possible reasons for stopping treatment suggested by the clinicians were no response to treatment, or severe untreatable or intolerable AEs.
The clinical experts agreed that a specialist (e.g., nephrologist or metabolic physician) should monitor patients with PH1 and that lumasiran can be administered by a health care professional in a community setting. One clinical expert suggested the potential for the patient or caregiver to self-administer lumasiran at home because subcutaneous injections can be routinely performed for other medications; however, other clinicians did not expect lumasiran to be self-administered.
According to the experts, it is unlikely that treatment would exceed the Health Canada recommended dose for most patients, although a higher dose may be warranted in infants due to their larger liver surface area to body surface area (BSA) ratio or to overcome potential neutralizing ADAs. The latter was based on experience with other drugs and has been suggested in the literature,11 though there is a lack of clinical evidence supporting higher doses of lumasiran at this time. The clinical experts identified the need for additional consideration of patients who have limited access to health care resources (e.g., living in remote areas, no primary care physician or access to specialists, and lack of health insurance). The clinical experts also indicated that other ethical issues were the burden of knowing there is a treatment for PH1 but not being able to access it, especially given the severity of the disease; the inadequacy of current treatments; and the overall burden of care on patients and families.
Drug Program Input
The drug programs described the lack of approved pharmacological treatments for PH1, different dosing for loading and maintenance, and dosing based on body mass. The drug programs also asked questions about the potential for newborn screening, the use of lumasiran in small infants, the relationship between trial outcomes and complications related to PH1, the likelihood of routine urine testing, identifying a loss of treatment response, prescribing and administration of lumasiran, and product wastage.
The clinical experts consulted by CADTH did not expect newborn screening to take place at this time and felt it would be reasonable to treat infants with PH1 who are aged less than 2 years and weigh less than 10 kg. The experts noted that the end points used in the ILLUMINATE trials are not perfect surrogates for PH1 complications but are satisfactory markers depending on how far a patient’s disease has progressed. The clinicians stated that 24-hour urine oxalate excretion is routinely measured for continent patients and spot oxalate:creatinine ratios for noncontinent children, which is considered an imperfect substitute and must be compared to normal ranges based on age. The clinical experts suggested that a loss of response would appear as a failure to show a progressive reduction in urine oxalate excretion over time in patients with preserved kidney function or failure to lower predialysis plasma oxalate in dialysis patients. A lack of response could also be due to patients not receiving treatment (e.g., missed dose), developing neutralizing ADAs; taking vitamin C, which increases oxalate production; or if GFR has declined, which would likely result in a rise in plasma oxalate. The clinical experts stated that it may be reasonable to stop lumasiran if there was documented failure to respond, serious untreatable or intolerable side effects, or the patient received a liver transplant. According to the experts, nephrologists or genetic/metabolic specialists would prescribe lumasiran while a health care professional, rather than the patient, would administer the drug, though the clinical experts had differing opinions on self-administration. The clinicians stated that a patient’s weight would be assessed at the time of the injection and the dose calculated based on the current weight (measured within 1 week for an infant, 2 weeks for a child, and 1 month for an adult). The clinical experts stated that product wastage would be inevitable given the current available formulation and weight-based dosing.
Clinical Evidence
Pivotal Studies and Protocol-Selected Studies
Description of Studies
The 3 included studies (ILLUMINATE-A, ILLUMINATE-B, and ILLUMINATE-C) are ongoing, phase III trials investigating the efficacy and safety of lumasiran in patients with PH1. All patients received study drug based on weight-based loading and maintenance-dosing schedules consistent with the Health Canada product monograph. The 3 trials were structured similarly with a 6-month primary analysis period followed by a 54-month extension period (3-month blinded extension and 51-month open-label extension [OLE] in the ILLUMINATE-A trial).
The ILLUMINATE-A trial (N = 39) is a placebo-controlled, double-blind (DB), randomized controlled trial (RCT) that included patients who were aged 6 years and older. Patients were randomized 2:1 to receive lumasiran or placebo. During the 6-month DB period, patients received study drug (lumasiran 3 mg/kg or matching placebo) administered as a subcutaneous injection once per month for the first 3 months (loading doses), followed by a single administration of study drug 1 month later (maintenance dose for the next 3 months). At month 6, patients entered the 3-month blinded treatment-extension period, in which all patients received active treatment (i.e., patients switched from placebo to lumasiran). At month 9, the 51-month OLE began, and all patients were on the maintenance-dosing schedule. The primary end point was percent change in 24-hour urinary oxalate excretion from baseline to month 6, corrected for BSA. The secondary end points were absolute change in urinary oxalate at month 6, percent change in urinary oxalate:creatinine ratio at month 6, percent and absolute changes in plasma oxalate at month 6, proportion of patients with urinary oxalate level near normal (at or below 1.5 times the upper limit of normal [ULN]) and normal (at or below the ULN) at month 6, and change in eGFR at month 6. At baseline, patients had a mean age of 18.1 years (standard deviation [SD] = █████ years; median = 14.0 years; range, 6 years to 60 years); 66.7% were male and 33.3% were female; and 76.9% were white, 15.4% were Asian, 5.1% were another race, and 2.6% identified as being of more than 1 race. Baseline mean 24-hour urine oxalate excretion corrected for BSA was 1.82 mmol/24 hour/1.73 m2 (SD = 0.62 mmol/24 hour/1.73 m2).
The ILLUMINATE-B trial (N = 18) is a single-arm trial that included patients who were aged less than 6 years. The primary end point was percent change in urinary oxalate excretion from baseline to month 6. The secondary end points were proportion of patients with urinary oxalate near normal and normal, plasma oxalate, and eGFR levels. At baseline, patients had a mean age of ████ months (SD = █████ months; median = 50.1 months; range, 3 to 72 months); 55.6% were female and 44.4% were male; and 88.9% were white while 11.1% identified as another race. Baseline mean spot urine oxalate:creatinine ratio was 0.63 mmol/mmol (SD = 0.43 mmol/mmol).
The ILLUMINATE-C trial (N = 21) is a single-arm trial that included patients who had an eGFR of 45 mL/min/1.73 m2 or lower and were either not receiving hemodialysis (Cohort A) or had begun stable hemodialysis (Cohort B). The primary end point was percent change in plasma oxalate from baseline to month 6 (predialysis for Cohort B). The secondary end points were plasma oxalate area under the curve (AUC) between dialysis sessions (Cohort B), urinary oxalate, urinary oxalate:creatinine ratio, Pediatric Quality of Life Inventory (PedsQL) and Kidney Disease Quality of Life Questionnaire (KDQOL) scores, and eGFR. At baseline, patients had a mean age of ████ years (SD = ████ years; median = 8.0 years; range, 0 to 59 years); 57.1% were male and 42.9% were female; and 76.2% were white, 19.0% were Asian, and 4.8% identified as another race. Mean baseline plasma oxalate was █████ μmol/L (SD = █████ μmol/L) for Cohort A and ██████ μmol/L (SD = █████ μmol/L) for Cohort B.
Efficacy Results
Statistical testing was conducted based on a gatekeeping procedure in the ILLUMINATE-A trial and the primary and secondary outcomes (except for eGFR) were controlled for multiplicity. Efficacy results are summarized in Table 2 for the ILLUMINATE-A trial and Table 3 for the ILLUMINATE-B and ILLUMINATE-C trials.
Kidney Function
During the 6-month DB period of the ILLUMINATE-A trial, eGFR declined from study baseline by a mean of 2.57 mL/min/1.73 m2 (SD = 10.65 mL/min/1.73 m2) in the lumasiran group and 0.11 mL/min/1.73 m2 (SD = 6.49 mL/min/1.73 m2) in the placebo group. Data at month 18 of extended lumasiran treatment showed that eGFR increased by a mean of ████ mL/min/1.73 m2 (SD = ████ mL/min/1.73 m2) in the lumasiran followed by lumasiran treatment group and decreased by a mean of ████ mL/min/1.73 m2 (SD = █████ mL/min/1.73 m2) in the placebo followed by lumasiran treatment group.
In the ILLUMINATE-B trial, eGFR declined from study baseline by a mean of 0.26 mL/min/1.73 m2 (SD = 15.38 mL/min/1.73 m2) for all patients during the first 6 months of treatment. By month 12 of treatment on lumasiran, eGFR increased by a mean of █████ mL/min/1.73 m2 (no SD) for 1 patient weighing less than 10 kg and decreased by a mean of ████ mL/min/1.73 m2 (SD = █████ mL/min/1.73 m2) and mean of ████ mL/min/1.73 m2 (SD = █████ mL/min/1.73 m2) in the groups of patients weighing between 10 and 20 kg and patients weighing more than 20 kg, respectively. In the ILLUMINATE-C trial, eGFR declined from study baseline by a mean of ████ mL/min/1.73 m2 (SD = ████ mL/min/1.73 m2) for patients in Cohort A during the first 6 months of treatment.
Loss of kidney function over time and prevention of dialysis and/or liver-kidney transplant were not assessed in the trials.
Kidney Stone Events
During the DB period of the ILLUMINATE-A trial, 5 patients (19.2%) in the lumasiran group experienced 13 kidney stone events and 2 patients (15.2%) in the placebo group experienced 4 kidney stone events. Some events (████% for the lumasiran group and ████% for the placebo group) were graded as ████████ severity and the rest were ████. The rate of events was 0.30 and 0.18 events per 100 person-days for the lumasiran and placebo groups, respectively. The rate of events generally appeared to decrease in the lumasiran followed by lumasiran treatment group from 1.09 events per person-year (95% confidence interval [CI], 0.63 events to 1.88 events per person-year) between day 1 and month 6 to ████ events per person-year (95% CI, ████ to ████ events per person-year) between months 18 and 24 of lumasiran treatment. In the placebo followed by lumasiran treatment group, rates appeared to fluctuate over the same period and remained less than 1 event per person-year.
In the ILLUMINATE-B trial, █████████ had █ kidney stone █████ each (████████ from each weight group) and all events were graded as mild severity. The rate of events was 0.11 renal stone events per person-year for the whole group. In the ILLUMINATE-C trial, █████████ in Cohort A had a total of █ kidney stone events and all events were graded as ████████████. The rate of events was 1.52 renal stone events per person-year for Cohort A.
Health-Related Quality of Life
In the ILLUMINATE-A trial, results from the KDQOL, PedsQL, EuroQol-5 Dimensions-5 Levels (EQ-5D-5L), EuroQol-5 Dimensions-Youth (EQ-5D-Y), and visual analogue scale (VAS) generally showed ████████████ ███████ ████████ from baseline to month 6 and during extended lumasiran treatment. Data at month 18 showed mean scores ██████ ███████ ████ and were ██████ ███████ ██████ with the results from the DB period.
Health-related quality of life (HRQoL) was not assessed in the ILLUMINATE-B trial and results were very limited due to small patient numbers and short treatment duration in the ILLUMINATE-C trial.
Urine Oxalate Excretion Corrected for BSA
In the ILLUMINATE-A trial, the least squares mean (LSM) percent change from baseline to the average of months 3 to 6 for urine oxalate excretion was –65.39% (95% CI, –71.32% to –59.45%) for the lumasiran group and –11.84% (95% CI, –19.53% to –4.15%) for the placebo group. The treatment difference between groups was –53.55% (95% CI, –62.31% to –44.78%; P < 0.001). For absolute change, the LSM treatment difference between groups was –0.98 mmol/24 hour/1.73 m2 (95% CI, –1.18 to –0.77 mmol/24 hour/1.73 m2; P < 0.001). For patients who achieved near normalization (at or below 1.5 times ULN), the difference in proportions was 0.84 (95% CI, 0.55 to 0.94; P < 0.001). For patients who achieved normalization (at or below ULN), the difference in proportions was 0.52 (95% CI, 0.23 to 0.70; P = 0.0010). Data from extended treatment on lumasiran indicated decreases in 24-hour urine oxalate at month 6 that appeared to be maintained for both lumasiran followed by lumasiran and placebo followed by lumasiran treatment groups to month 18.
Urine oxalate assessments were based on urine oxalate:creatinine ratios and are described later for the ILLUMINATE-B trial. In the ILLUMINATE-C trial, the LSM absolute change from baseline to the average of months 3 to 6 was –0.53 mmol/24 hour/1.73 m2 (95% CI, –0.89 to –0.18 mmol/24 hour/1.73 m2). The LSM percent change from baseline to the average of months 3 to 6 was –10.56% (95% CI, –31.99% to 10.87%).
Plasma Oxalate
In the ILLUMINATE-A trial, for absolute change, the treatment difference between groups for plasma oxalate was –8.71 µmol/L (95% CI, –11.45 to –5.98 µmol/L; P < 0.001). For percent change, the treatment difference between groups was –39.48% (95% CI, –50.10% to –28.87%; P < 0.001).
In the ILLUMINATE-B trial, the mean absolute change from baseline was –5.03 µmol/L (SD = ████ µmol/L), while the mean percent change from baseline was –32.06% (SD = █████%) at month 6. Data from the extension period indicated that decreases in plasma oxalate at month 6 appeared to be ██████████ for patients ██████ ████████████ ████████████. In the ILLUMINATE-C trial, the LSM percent change from baseline to the average of months 3 to 6 was –33.33% (95% CI, –81.82% to 15.16%) for Cohort A and –42.43% (95% CI, –50.71% to –34.15%) for Cohort B. The LSM absolute change from baseline to the average of months 3 to 6 was –35.28 µmol/L (95% CI, –56.32 to –14.24 µmol/L) for Cohort A and –48.33 µmol/L (95% CI, –55.85 to –40.80 µmol/L) for Cohort B.
Urine Oxalate:Creatinine Ratio
In the ILLUMINATE-A trial, for percent change, the treatment difference between groups for urine oxalate:creatinine ratio was –51.77% (95% CI, –64.27% to –39.28%; P < 0.001). Data from extended treatment on lumasiran indicated that decreases at month 6 appeared to be maintained for both lumasiran followed by lumasiran and placebo followed by lumasiran treatment groups.
In the ILLUMINATE-B trial, the LSM percent change from baseline to the average of months 3 to 6 for all patients was –71.97% (95% CI, –77.52% to –66.42%). At month 6, 9 (50.0%) patients had achieved near normalization, while 1 (5.6%) patient had achieved normalization. Data from the extension period indicated decreases in spot urine oxalate:creatinine ratio by month 6 that appeared to be ██████████ for patients ██████████████████████████████. Additionally, ██ of the ██ patients who had data at that time point achieved near normalization and █ patients achieved normalization.
In the ILLUMINATE-C trial, the LSM absolute change from baseline to the average of months 3 to 6 was –0.19 mmol/mmol (95% CI, –0.23 to –0.15 mmol/mmol). The LSM percent change from baseline to the average of months 3 to 6 was –39.51% (95% CI, –64.13% to –14.90%).
Harms Results
Harms results are summarized in Table 2 for the ILLUMINATE-A trial and Table 3 for the ILLUMINATE-B and ILLUMINATE-C trials.
Table 2: Summary of Key Results From the ILLUMINATE-A Trial
Outcome | ILLUMINATE-A | |
|---|---|---|
Placebo (N = 13) | Lumasiran (N = 26) | |
Kidney function — eGFR (mL/min/1.73 m2)a: FAS | ||
Baseline, n (%) | 13 (100) | 26 (100) |
Mean (SD) | 78.95 (26.83) | 82.97 (25.55) |
Month 6, n (%) | 13 (100) | 25 (96.2) |
Mean (SD) | 78.83 (█████) | 78.53 (█████) |
Mean change from baseline (SD) | –0.11 (6.49) | –2.57 (10.65) |
Kidney stone events: FAS | ||
Patients with at least 1 kidney stone event, n (%) | 2 (15.4) | 5 (19.2) |
Total number of kidney stone events, n | 4 | 13 |
Severity of event | ||
Mild | █ (████) | ██ (████) |
Moderate | █ (████) | █ (████) |
Rate of renal stone events per 100 person-days during DB period (95% CI)b | 0.18 (████, ████) | 0.30 (████, ████) |
24-hour urinary oxalate excretion corrected for BSA (mmol/24 hour/1.73 m2): FAS | ||
Baseline, n (%) | 13 (100) | 26 (100) |
Mean (SEM) | 1.79 (0.19) | 1.84 (0.12) |
Mean of months 3 to 6 | ||
Change from baseline to average of months 3 to 6, LSM (SEM) (95% CI)c | –0.27 (0.08) (–0.44, –0.10) | –1.24 (0.06) (–1.37, –1.12) |
LSM (SEM) treatment group difference (lumasiran – placebo) (95% CI)c | Reference | –0.98 (0.10) (–1.18, –0.77) |
P valuec,d | Reference | < 0.001 |
Percent change from baseline to average of months 3 to 6, LSM (SEM) (95% CI)c | –11.84 (3.81) (–19.53, –4.15) | –65.39 (2.94) (–71.32, –59.45) |
LSM (SEM) treatment group difference (lumasiran – placebo) (95% CI)c | Reference | –53.55 (4.32) (–62.31, –44.78) |
P valuec,d | Reference | < 0.001 |
24-hour urinary oxalate excretion corrected for BSA ≤ 1.5 × ULN or ≤ ULN: FAS | ||
Number of patients contributing to the analysis, n (%) | 13 (100) | 25 (96.2) |
Number of patients with ≤ 1.5 × ULN | 0 | 21 |
Proportion of patients with ≤ 1.5 × ULN (95% CI)e | 0.00 (0.00, 0.25) | 0.84 (0.64, 0.95) |
Difference in proportions (95% CI)f | Reference | 0.84 (0.55, 0.94) |
P valued,g | Reference | < 0.001 |
Number of patients with ≤ ULN | 0 | 13 |
Proportion of patients with ≤ ULN (95% CI)e | 0.00 (0.00, 0.25) | 0.52 (0.31, 0.72) |
Difference in proportions (95% CI)f | Reference | 0.52 (0.23, 0.70) |
P valued,g | Reference | 0.0010 |
Plasma oxalate (µmol/L): plasma oxalate analysis set | ||
Baseline, n (%) | 10 (100) | 23 (100) |
Mean (SEM) | 17.76 (2.17) | 15.73 (1.59) |
Mean of months 3 to 6 | ||
Change from baseline to average of months 3 to 6, LSM (SEM) (95% CI)c | 1.25 (1.12) (–1.04, 3.54) | –7.46 (0.77) (–9.03, –5.90) |
LSM (SEM) treatment group difference (lumasiran – placebo) (95% CI)c | Reference | –8.71 (1.34) (–11.45, –5.98) |
P valuec,d | Reference | < 0.001 |
Percent change from baseline to average of months 3 to 6, LSM (SEM) (95% CI)c | –0.32 (████) (–9.12, 8.48) | –39.80 (████) (–45.81, –33.80) |
LSM (SEM) treatment group difference (lumasiran – placebo) (95% CI)c | Reference | –39.48 (████) (–50.10, –28.87) |
P valuec,d | Reference | < 0.001 |
Urinary oxalate:creatinine ratio (mmol/mmol): FAS | ||
Baseline, n (%) | 13 (100) | 26 (100) |
Mean (SEM) | 0.24 (████) | 0.21 (████) |
Mean of months 3 to 6 | ||
Percent change from baseline to average of months 3 to 6, LSM (SEM) (95% CI)c | –10.78 (████) (–21.58, 0.03) | –62.55 (████) (–70.71, –54.39) |
LSM (SEM) treatment group difference (lumasiran – placebo) (95% CI)c | Reference | –51.77 (█████) (–64.27, –39.28) |
P valuec,d | Reference | < 0.001 |
Harms, n (%): Safety analysis set | ||
AEs | 9 (69.2) | 22 (84.6) |
SAEs | 0 | 0 |
WDAE (from study treatment) | 0 | 1 (3.8) |
Deaths | 0 | 0 |
Notable harms | ||
Injection site reaction, n (%) | 0 | 6 (23.1) |
Renal events, n (%) | 0 | █ (███) |
Complications from systemic oxalosis | NR | NR |
Headache | 3 (23.1) | 3 (11.5) |
Rhinitis | 2 (15.4) | 2 (7.7) |
Upper respiratory infection | 2 (15.4) | 2 (7.7) |
Hypersensitivity reactions | 0 | 1 (3.8) |
ADA positive at any time | 0 | 1 (3.8) |
ADA = antidrug antibody; AE = adverse event; BSA = body surface area; CI = confidence interval; DB = double-blind; eGFR = estimated glomerular filtration rate; FAS = full analysis set; LSM = least squares mean; SAE = serious adverse events; SD = standard deviation; SEM = standard error of the mean; ULN = upper limit of normal; WDAE = withdrawal due to adverse events.
aThe eGFR is calculated from serum creatinine based on the Modification of Diet in Renal Disease formula for patients at least 18 years of age and the Schwartz Bedside Formula for patients aged younger than 18 years at screening.
bRate is calculated as total number of renal stone events divided by total person-days at risk, defined as time from first dose to end of the DB period.
cBased on Mixed-Effect Model Repeated Measures model with the corresponding value at baseline as a continuous fixed covariate, visit, and treatment as fixed effects, and patient as a random effect. Visit is fitted as a categorical variable, and the variance-covariance matrix is assumed to be unstructured. Satterthwaite approximation is used to estimate denominator degrees of freedom. A difference less than 0 represents a favourable outcome for lumasiran.
dP value has been adjusted for multiple testing (i.e., the type I error rate has been controlled).
eClopper Pearson exact confidence interval.
fCalculated using the Newcombe method based on the Wilson score.
gP value is based on Cochran-Mantel-Haenszel test stratified by baseline 24-hour urine oxalate corrected for BSA (less than or equal to 1.70 vs. greater than 1.70 mmol/24 hour/1.73 m2).
Source: ILLUMINATE-A Clinical Study Report.12
Table 3: Summary of Key Results From the ILLUMINATE-B and ILLUMINATE-C Trials
Characteristic | ILLUMINATE-Ba | ILLUMINATE-Cb | |||
|---|---|---|---|---|---|
All patients (N = 18) | Cohort A: no dialysis (N = 6) | Cohort B: dialysis (N = 15) | |||
Kidney function: eGFR (mL/min/1.73 m2)c | |||||
Baseline, n (%) | 16 (88.9) | 5 (83.3) | NR | ||
Mean (SD) | 112.80 (27.63) | 19.85 (9.64) | NR | ||
Month 6, n (%) | 16 (88.9) | 5 (83.3) | NR | ||
Mean (SD) | ██████ (█████) | 16.43 (9.82) | NR | ||
Mean change from baseline (SD) | –0.26 (15.38) | █████ (████) | NR | ||
Kidney stone events | |||||
Patients with at least 1 kidney stone event, n (%) | 3 (16.7) | █ (████) | █ | ||
Total number of kidney stone events, n | █ | █ | █ | ||
Severity of event: | |||||
Mild | █ (████) | █ (███) | █ | ||
Rate of renal stone events per person-year during lumasiran treatment (95% CI)d | 0.11 (████, ████) | 1.52 (████, ████) | 0.00 (0.00, ████) | ||
24-hour urinary oxalate excretion corrected for BSA (mmol/24 hour/1.73 m2) | |||||
Baseline, n (%) | NR | 5 (83.3) | NR | ||
Mean (SD) | NR | ████ (████) | NR | ||
Mean of months 3 to 6 | |||||
Change from baseline, LSM (SEM) (95% CI)e | NR | –0.53 (0.11) (–0.89, –0.18) | NR | ||
Change from baseline, P valuee,f | NR | ██████ | NR | ||
Percent change from baseline, LSM (SEM) (95% CI)e | NR | –10.56 (6.81) (–31.99, 10.87) | NR | ||
Percent change from baseline, P valuee,f | NR | ██████ | NR | ||
Plasma oxalate (µmol/L) | |||||
Baseline, n (%) | 18 (100) | 6 (100) | 15 (100) | ||
Mean (SD) | 13.24 (6.50) | █████ (█████) | ██████ (█████) | ||
Month 6, n (%) | 18 (100) | NA | NA | ||
Mean (SD) (µmol/L) | 8.21 (████) | NA | NA | ||
Change from baseline, mean (SD) (µmol/L) | –5.03 (████) | NA | NA | ||
Percent change from baseline, mean (SD) | –32.06 (█████) | NA | NA | ||
Mean of months 3 to 6 | NA | NA | NA | ||
Change from baseline, LSM (SEM) (95% CI)g | NA | –35.28 (7.40) (–56.32, –14.24) | –48.33 (3.63) (–55.85, –40.80) | ||
Change from baseline, P valuef,g | NA | ██████ | ██████ | ||
Percent change from baseline, LSM (SEM) (95% CI)g | NA | –33.33 (17.63) (–81.82, 15.16) | –42.43 (3.95) (–50.71, –34.15) | ||
Percent change from baseline, P valuef,g | NA | 0.1299 | < 0.001 | ||
Urinary oxalate:creatinine ratio (mmol/mmol) | |||||
Baseline, n (%) | 18 (100) | 6 (100) | NR | ||
Mean (SD) | 0.63 (0.43) | ████ (████) | NR | ||
Month 6 | |||||
Percent change from baseline to average of months 3 to 6, LSM (SEM) (95% CI)h | –71.97 (2.71) (–77.52, –66.42) | NA | NA | ||
P valuef,h | < 0.001 | NA | NA | ||
Mean of months 3 to 6 | |||||
Change from baseline, LSM (SEM) (95% CI)i | NA | –0.19 (0.02) (–0.23, –0.15) | NR | ||
Change from baseline, P valuef,i | NA | ██████ | NR | ||
Percent change from baseline, LSM (SEM) (95% CI)i | NA | –39.51 (9.43) (–64.13, –14.90) | NR | ||
Percent change from baseline, P valuef,i | NA | ██████ | NR | ||
24-hour urinary oxalate excretion corrected for BSA ≤ 1.5 × ULN or ≤ ULN: FAS | |||||
Baseline,a n (%) | 18 (100) | NA | NA | ||
Proportion of patients with ≤ 1.5 × ULN | 0 | NA | NA | ||
Proportion of patients with ≤ ULN | 0 | NA | NA | ||
Month 6, n (%) | 18 (100) | NA | NA | ||
Proportion of patients with ≤ 1.5 × ULN | 9 (50.0) | NA | NA | ||
Proportion of patients with ≤ ULN | 1 (5.6) | NA | NA | ||
Harms, n (%): safety analysis set | < 10 kg (N = 3) | 10 to < 20 kg (N = 12) | ≥ 20 kg (N = 3) | Cohort A: no dialysis (N = 6) | Cohort B: dialysis (N = 15) |
AEs | 3 (100) | 12 (100) | 3 (100) | 5 (83.3) | 13 (86.7) |
SAEs | 0 | 0 | 1 (33.3) | 1 (16.7) | 8 (53.3) |
WDAE (from study treatment) | 0 | 0 | 0 | 0 | 2 (13.3) |
Deaths | 0 | 0 | 0 | 0 | 0 |
Notable harms n (%) | |||||
Injection site reaction | 0 | 2 (16.7) | 1 (33.3) | 1 (16.7) | 4 (26.7) |
Renal events | █ | █ (███) | █ | █ (████) | █ |
Complications from systemic oxalosis | NR | NR | NR | NR | NR |
Headache | 0 | 0 | 2 (66.7) | NR | NR |
Rhinitis | 1 (33.3) | 3 (25.0) | 0 | NR | NR |
Upper respiratory infection | 1 (33.3) | 2 (16.7) | 1 (33.3) | █ (████) | █ (███) |
Hypersensitivity reactions | NR | NR | NR | NR | NR |
ADA positive at any time | 1 (33.3) | 2 (16.7) | 0 | 0 | 0 |
ADA = antidrug antibody; AE = adverse event; BSA = body surface area; CI = confidence interval; eGFR = estimated glomerular filtration rate; FAS = full analysis set; LSM = least squares mean; MMRM = Mixed-Effect Model Repeated Measures; NA = not applicable; NR = not reported; REML = restricted maximum likelihood; SAE = serious adverse events; SD = standard deviation; SEM = standard error of the mean; ULN = upper limit of normal; WDAE = withdrawal due to adverse events.
aILLUMINATE-B analysis population was the efficacy analysis set.
bILLUMINATE-C analysis population was the FAS.
cThe eGFR is calculated based on the Schwartz Bedside Formula in patients aged at least 12 months at the time of the assessment.
dRate is calculated as total number of renal stone events divided by total person-years during lumasiran treatment. The 95% CI for the event rate was obtained using a generalized linear model for a Poisson distribution unless the rate was 0, in which case the upper bound of the 95% CI was calculated using the exact Poisson method.
eBased on REML-based MMRM model to test against the null hypothesis of mean change from baseline outcome being equal to 0. The model includes scheduled visits and baseline 24-hour urine oxalate corrected for BSA (mmol/24 hour/1.73 m2) as fixed effects and patient as a random factor. Autoregressive (1) was used to model the within-patient variability.
fP value has not been adjusted for multiple testing (i.e., the type I error rate has not been controlled).
gBased on REML-based MMRM model to test against the null hypothesis of mean change from baseline outcome being equal to 0. The model includes scheduled visits and baseline plasma oxalate (μmol/L) as fixed effects and patient as a random factor. Autoregressive (1) was used to model the within-patient variability.
hBased on REML-based MMRM model to test against the null hypothesis of mean percent change from baseline output being equal to 0. The model includes fixed effects of scheduled visits and baseline spot urine oxalate:creatinine ratio value (mmol/mmol), including patient as a random factor. Autoregressive (1) was used to model the within-patient error.
iBased on REML-based MMRM model to test against the null hypothesis of mean change from baseline outcome being equal to 0. The model includes scheduled visits and baseline spot urine oxalate:creatinine ratio as fixed effects and patient as a random factor. Autoregressive (1) was used to model the within-patient variability.
Source: ILLUMINATE-B Clinical Study Report,13 ILLUMINATE-C Clinical Study Report.14
During the primary analysis period, in the ILLUMINATE-A trial, a larger proportion of patients in the lumasiran group reported an AE compared to the placebo group (84.6% versus 69.2%). All patients in the ILLUMINATE-B trial reported at least 1 AE. In the ILLUMINATE-C trial, the percentage of patients reporting an AE was similar between the groups (83.3% for no dialysis and 86.7% for dialysis). The most frequently reported AEs were injection site reaction (the ILLUMINATE-A and ILLUMINATE-C trials), headache (the ILLUMINATE-A trial), and pyrexia (the ILLUMINATE-B and ILLUMINATE-C trials) with injection site reaction occurring only among patients treated with lumasiran. During the overall period of receiving lumasiran treatment, injection site reaction (██████████), abdominal pain (█████████), and headache (█████████) were the most frequently reported AEs in the ILLUMINATE-A trial. In the ILLUMINATE-B trial, pyrexia (8 patients) and vomiting (5 patients) were the most frequently reported AEs.
During the primary analysis period, there were no serious adverse events (SAEs) in the ILLUMINATE-A trial. One patient weighing more than 20 kg (33.3%) in the ILLUMINATE-B trial reported a viral infection SAE. In the ILLUMINATE-C trial, 9 patients reported an SAE: 1 (16.7%) patient not on dialysis and 8 (53.3%) patients on dialysis. ███████████████████████ and device-related infection were reported in 2 patients for each SAE (all patients were on dialysis). All other SAEs were single-patient events. During the overall period of receiving lumasiran treatment, █████████ reported SAEs of █████████████, urosepsis, and ██████████████████████████ in the ILLUMINATE-A trial, while 1 patient reported viral infection in the ILLUMINATE-B trial.
During the primary analysis period, 1 patient receiving lumasiran in the ILLUMINATE-A trial stopped treatment due to an AE (fatigue and disturbance in attention) while ████████████ ███████ in the ILLUMINATE-C trial ████████ ███ ██████████████ ██████ █████████████████. There were no new reports of patients stopping treatment due to AEs during the extended treatment for either the ILLUMINATE-A or ILLUMINATE-B trials. No deaths were reported for any patients during the 6-month primary analysis period for any of the 3 studies or during the extension periods up to the data cut-off dates.
Notable Harms
Complications from systemic oxalosis were not reported in the clinical study reports at the given cut-off dates.
Injection site reactions were reported among 6 patients receiving lumasiran in the ILLUMINATE-A trial, 3 patients (2 patients weighing between 10 kg and 20 kg, 1 patient weighing more than 20 kg) in the ILLUMINATE-B trial, and 5 patients (4 patients on dialysis, 1 patient not on dialysis) in the ILLUMINATE-C trial. During the overall period of receiving lumasiran treatment, █████████ in the ILLUMINATE-A trial and 3 patients in the ILLUMINATE-B trial reported an injection site reaction, with the most common symptom being erythema.
Kidney stone events were captured as an efficacy outcome and were not reported as harms. All renal events were single-patient events and were generally infrequent: █████████ in the ILLUMINATE-A trial, ████████ in the ILLUMINATE-B trial, and █████████ in the ILLUMINATE-C trial. During the overall period of receiving lumasiran treatment, █████████ in the ILLUMINATE-A trial reported renal events, with the most frequent events being ███████ (█████████) and █████████ (█████████). In the ILLUMINATE-B trial, ████████ reported █████████.
Six patients reported headache in the ILLUMINATE-A trial (3 patients each on placebo and lumasiran) and 2 patients in the ILLUMINATE-B trial (███████████████████). No patients reported headache in the ILLUMINATE-C trial. During the overall period of receiving lumasiran treatment, █████████ in the ILLUMINATE-A trial and █████████ in the ILLUMINATE-B trial reported headache.
Four patients reported rhinitis in the ILLUMINATE-A trial (2 patients each on placebo and lumasiran) and 4 patients in the ILLUMINATE-B trial (1 patient weighing less than 10 kg and 3 patients weighing between 10 kg and 20 kg). No patients reported rhinitis in the ILLUMINATE-C trial. During the overall period of receiving lumasiran treatment, █████████ in the ILLUMINATE-A trial and █████████ in the ILLUMINATE-B trial reported rhinitis.
Four patients reported upper respiratory infection in the ILLUMINATE-A trial (2 patients each on placebo and lumasiran), 4 patients in the ILLUMINATE-B trial (1 patient less than 10 kg, 2 patients weighing between 10 kg and 20 kg, and 1 patient weighing more than 20 kg), and █████████ in the ILLUMINATE-C trial (████████ each not receiving dialysis and on dialysis). During the overall period of receiving lumasiran treatment, 4 patients reported upper respiratory infection each in the ILLUMINATE-A and ILLUMINATE-B trials.
One patient receiving lumasiran in the ILLUMINATE-A trial reported a hypersensitivity reaction. Hypersensitivity reactions were not reported in the ILLUMINATE-B or ILLUMINATE-C trials. There were no additional reports in the ILLUMINATE-A trial during extended lumasiran treatment.
One patient tested positive for ADAs in the ILLUMINATE-A trial, while 3 patients tested positive for ADAs in the ILLUMINATE-B trial. The sponsor concluded that the ADAs did not appear to affect efficacy or safety results for these patients. No patients tested positive for ADAs in the ILLUMINATE-C trial. During the overall period of receiving lumasiran treatment, in the ILLUMINATE-A trial, 1 patient originally randomized to placebo tested positive for ADAs. There were no additional reports of patients testing positive for ADAs in the ILLUMINATE-B trial during extended lumasiran treatment.
Critical Appraisal
The ILLUMINATE-A trial appeared to have appropriate methods for blinding of treatment assignment, randomization, and adequate power, and the primary and secondary outcomes (except eGFR) were controlled for multiplicity. The primary and key secondary outcomes were objective in nature, centrally assessed, relevant to PH1, and supported by regulatory agencies, which reduce bias in the results.12,15 The ILLUMINATE-B and ILLUMINATE-C sample sizes were based on feasibility considerations rather than power calculations, were single-arm trials, and end points were not controlled for multiplicity. The sponsor noted that patient heterogeneity, disease heterogeneity, rarity of PH1, lack of available approved therapies, objectively measured end points, and the sponsor’s feasibility results justified the use of a single-arm trial design.13,14 Baseline characteristics were mostly balanced in the ILLUMINATE-A trial, suggesting that randomization was generally successful, and it is possible that the imbalances were due to the small patient numbers. There were imbalances in sex; race; patients’ medical history, specifically for PH1-related symptoms; and vitamin B6 use, which may have introduced bias, though the magnitude or direction of the bias is uncertain. More specifically, the proportion of patients using vitamin B6 varied among treatment groups in the trials and, because it may also lower oxalate levels, it is unclear how much of the treatment effect could be attributed to vitamin B6 compared to lumasiran. Subgroup analyses of baseline vitamin B6 use (yes versus no) did not indicate a clear difference between the groups, though limitations of the subgroup analyses prevent firm conclusions from being made. Because patients in the ILLUMINATE-B and ILLUMINATE-C trials were not randomized to their treatment group, but rather were categorized based on body mass and use of dialysis, respectively, imbalances between groups are likely to occur. During the 6-month primary analysis periods, few patients discontinued lumasiran during the trials and few withdrew from the trials, suggesting there was little risk of attrition bias. Due to the small amount of missing data among the 3 trials and sensitivity analyses supporting the primary outcomes, the risk of bias due to missing data appears to be low.
One of the main limitations is the small number of patients in each trial (N = 39, 18, and 21 in the ILLUMINATE-A, ILLUMINATE-B, and ILLUMINATE-C trials, respectively), though consideration must be given for the rarity of PH1. The small number of patients in each treatment group makes it challenging to interpret the results and to estimate how meaningful they are. Although there are data for up to 24 months of lumasiran treatment in the ILLUMINATE-A trial, a second major limitation is the relatively short duration of evidence available, given that the clinical experts expect lumasiran to be a lifelong treatment or until liver transplant occurs. The short duration makes it difficult to be certain if the efficacy and safety results will persist long-term. A third limitation is the lack of minimal important differences (MIDs) for patients with PH1 identified from the literature for all outcomes in the trials. Without published MIDs, there is uncertainty around how meaningful the absolute and percent changes from baseline were. The sponsor performed analyses for the proportion of patients who achieved near normalization or normalization for 24-hour urine oxalate in the ILLUMINATE-A trial and spot urine oxalate:creatinine ratio in the ILLUMINATE-B trial, but not for plasma oxalate in the ILLUMINATE-C trial. According to the clinical experts, normalization of elevated oxalate levels may result in clinical benefits, but it is unclear if achieving near normalization prevents long-term kidney outcomes, and long-term evidence will be needed to support this.
Given the lack of details for screening failures for all 3 trials, it is unknown if this biased results or how this limits the generalizability to the entire population of patients who could receive lumasiran. Patients enrolled in the 3 ILLUMINATE trials included both adult and pediatric patients (age range, 0 to 60 years) with a range of kidney function (eGFR range, 8.61 to 174.06 mL/min/1.73 m2 and included patients on dialysis) and presenting symptoms related to PH1. Patients with possible hepatic impairment (alanine aminotransferase [ALT] or aspartate aminotransferase [AST] reading greater than 2 times ULN for age or total bilirubin greater than 1.5 times ULN), history of kidney transplant, evidence of systemic oxalosis (in the ILLUMINATE-A or ILLUMINATE-B trials), or receiving peritoneal dialysis (in the ILLUMINATE-C trial) were excluded. Thus, treatment with lumasiran is uncertain in patients with these characteristics. Aside from these limitations, the clinical experts generally felt that the trial results could be generalized to the Canadian population with PH1. The clinical experts confirmed that the trial outcomes, all of which are surrogate measures, were typical measures used when assessing and managing patients with PH1. However, it is unclear how the main outcomes of the trials lead to treatment goals such as prevention of kidney stones and progression to ESKD, and the clinical experts emphasized the need for long-term data to better understand how the surrogate outcomes are related to clinical benefit.
Other Relevant Evidence
Description of Studies
The ALN-GO1 to 001 trial was a phase I/II study conducted in 2 parts: single ascending dose (Part A) in 32 healthy adult volunteers aged between 18 and 64 years and multiple ascending dose (Part B) in 20 patients with PH1 who were aged at least 6 years and had relatively preserved kidney function (eGFR at least 45 mL/min/1.73m2). The ALN-GO1 to 002 trial is a phase II, multicentre, open-label, extension study to evaluate the long-term safety and efficacy of lumasiran in patients with PH1 who have completed Part B of the ALN-GO1 to 001 trial. Patients received lumasiran according to their initiation-dosing regimen in Part B of the ALN-GO1 to 001 trial for up to 54 months.
Efficacy Results
Results are presented for the baseline for Part B of the ALN-GO1 to 001 trial and postbaseline for the ALN-GO1 to 002 trial. Mean eGFR was 77.34 mL/min/1.73 m2 (SD = 22.11 mL/min/1.73 m2) at baseline and █████ mL/min/1.73 m2 (SD = █████ mL/min/1.73 m2) at month 30, and appeared to be stable throughout the study. Three (15%) patients had at least 1 kidney stone event during the study period and the rate of kidney stone events per person-year during treatment was 0.06 (95% CI, ████ to ████). No data on HRQoL were reported in the clinical study reports. Mean 24-hour urinary oxalate corrected for BSA was 2.24 mmol/24 hour/1.73 m2 (SD = ████ mmol/24 hour/1.73 m2) at baseline, ████ mmol/24 hour/1.73 m2 (SD = ████ mmol/24 hour/1.73 m2) at month 30, and appeared to be stable after the first 6 months. At any postbaseline visit, 100% and ██% of patients achieved near-normal and normal 24-hour urinary oxalate corrected for BSA levels, respectively. Mean plasma oxalate level was 15.28 µmol/L (SD = ████ µmol/L) at baseline, ████ µmol/L (SD = ████ µmol/L) at month 30, and appeared to be stable after the first 6 months. Mean 24-hour urinary oxalate:creatinine ratio was 0.28 mmol/mmol (SD = ████ mmol/mmol) at baseline and ████ mmol/mmol (SD = ████ mmol/mmol) at month 30, and appeared to be stable after the first 6 months.
Harms Results
All patients in the ALN-GO1 to 002 trial experienced at least 1 AE. The most commonly reported AEs were injection site reaction (40%), vomiting (20%), headache (15%), limb injury (15%), and oropharyngeal pain (15%). Four (20%) patients reported SAEs of blood creatinine increase, pyelonephritis, renal colic, and ureterolithiasis. One patient experienced 2 SAEs, a craniocerebral injury and bone (rib) contusion, from road traffic accidents. There were no withdrawals due to AEs (WDAEs), no patients discontinued treatment due to AEs, and no deaths reported during the study.
Of the notable harms identified in the CADTH systematic review protocol, 40% of patients reported injection site reaction. Three (15%) patients experienced kidney and urinary disorders, such as nephrolithiasis, renal colic, and ureterolithiasis. Headache, ██████ ██████████████ ██████████, and ████████ were reported by 3, █, and █ patients, respectively. Complications caused by systemic oxalosis and hypersensitivity were not reported during the study period. ██ ████████ █████ █████████ █████████████████ ███████████████████████ ███████████ █████ █████ ██████ ██ █ █ █████ █████████ ███████.
Critical Appraisal
The limitations for the ALN-GO1 to 002 trial are similar to those for the ILLUMINATE trials. The ALN-GO1 to 002 trial was a phase II, OLE study, and statistical analyses, adjustments for multiplicity, and imputations for missing data points were not performed. Because vitamin B6 may help to reduce oxalate levels, it is unclear how much of the effect seen in this trial could be attributed to the concomitant treatment. The sample size was not determined using a power calculation and was likely too small to make definitive conclusions about safety and efficacy. Considering the wide range of clinical manifestations with PH1, it is uncertain if the sample population adequately represents patients with PH1 living in Canada, which limits generalizability of the results. Additionally, none of the trial sites were in Canada. The follow-up time may be sufficient for observing an immediate treatment effect (mean duration of exposure was 28.8 months) because the clinical experts stated that 2 to 3 years are deemed appropriate in a kidney disease–related clinical trial setting. However, it is unlikely that the duration of exposure is long enough to draw long-term conclusions for lumasiran treatment given that it is expected to be a lifelong treatment. Although the safety data suggest that lumasiran is safe for the first 30 months of treatment, the clinical experts emphasized that longer-term data for efficacy and safety are warranted.
Conclusions
The ILLUMINATE-A, ILLUMINATE-B, and ILLUMINATE-C trials are ongoing trials that have provided evidence of the efficacy and safety of lumasiran in patients with PH1 who were aged 6 years and older, younger than 6 years, and any age with an eGFR at or below 45 mL/min/1.73 m2 (receiving dialysis or not), respectively. Lumasiran demonstrated improvements in urine oxalate corrected for BSA, plasma oxalate, and urine oxalate:creatinine ratio in the 3 trials. In the DB, placebo-controlled ILLUMINATE-A trial, all primary and key secondary outcomes were for objective measures, controlled for multiplicity (except eGFR), and most were deemed clinically meaningful (except eGFR) based on clinical expert opinion because there were no MIDs identified from the literature. Results for single-arm ILLUMINATE-B and ILLUMINATE-C trials were generally consistent with those observed in the ILLUMINATE-A trial, which the clinical experts agreed were also meaningful for those populations. Changes in eGFR and HRQoL were numerically small, the latter outcome was not controlled for multiplicity, and conclusions could not be drawn about whether lumasiran had an impact on these outcomes due to the small number of patients and short treatment duration of the trials so far.
Efficacy results for up to 30 months on lumasiran in the ALN-GO1 to 002 study indicated similar findings as the ILLUMINATE trials, although the same limitations apply to these longer-term data. The clinical experts had no major concerns with the harms profile and there were few SAEs, WDAEs, and no deaths reported. Lumasiran treatment for up to 30 months in the ALN-GO1 to 002 trial showed a similar harms profile as the ILLUMINATE trials, with no new safety signals identified. In the ILLUMINATE trials, there were no patients aged 60 years or older patients were excluded if they had a history of kidney transplant or had hepatic impairment (ALT or AST greater than 2 times ULN for age or total bilirubin greater than 1.5 times ULN).
Therefore, further research showing adequate efficacy and safety is needed to inform broader treatment with lumasiran. According to the clinical experts, given the meaningful reductions in urine and plasma oxalate levels compared to placebo for up to 24 months of treatment, acceptable safety profile so far, lack of other effective treatments, and easy administration, lumasiran appears to be an important treatment option for patients with PH1. The experts and CADTH review team agreed that long-term efficacy and safety data will be necessary to confirm the findings in the ILLUMINATE trials and to better understand how the main trial outcomes translate to improved long-term outcomes of maintained lowering of hepatic oxalate production, prevention of kidney stones, and prevention of progression to ESKD.
Introduction
Disease Background
PH1 is an ultrarare, autosomal recessive metabolic condition caused by a pathogenic variant of the AGT gene.3 There is considerable heterogeneity with PH1 in the age of onset, severity of disease, residual enzyme activity, and genotype.4 It has been estimated that there are about 200 genetic variants of the AGT gene10 and that the genotype does not reliably predict the phenotype.3 Further, the level of enzyme function may not be indicative of disease severity because some patients may have functional enzyme that is incorrectly localized to mitochondria rather than peroxisomes in the liver.3,4 The enzyme catalyzes the conversion of glyoxylate to glycine in peroxisomes and without it (i.e., in patients with PH1), glyoxylate is converted to oxalate in the cytosol.3 Oxalate binds to calcium, producing insoluble calcium oxalate salts that are difficult for the body to eliminate. The clinical experts stated that PH1 usually manifests with the formation of kidney stones. Once kidney function declines to an eGFR of less than 30 to 45 mL/min/1.73 m2, the kidneys become unable to excrete excess oxalate.5 Plasma oxalate levels increase, leading to systemic oxalosis in which oxalate builds up in tissues throughout the body (e.g., bone, skin, retina, and cardiovascular and nervous systems).3,5 Patients often progress to ESKD, which, combined with complications of systemic oxalosis, results in early death.3
Due to the variable clinical presentation and age of onset as well as a limited awareness of PH1, it has been suggested that the disease is underdiagnosed.3,6 The incidence of PH1 has been estimated to be between 0.4 and 1 per 100,000 live births in different populations.4 The prevalence has been estimated to be between 1 and 3 per million in European countries, with higher rates among countries with consanguinity.4 Patient survival has been estimated in a study16 of 155 patients of families from Western Europe, North Africa, and the Middle East to be 95%, 86%, and 74% at 10, 30, and 50 years of age, respectively, and based on a European study17 of 526 patients to be 95%, 93%, 85%, and 74% at 5, 10, 30, and 50 years of age, respectively. No Canadian data for prevalence, incidence, or survival have been identified from the literature.
There is notable heterogeneity in the presentation of PH1 and Milliner et al. described 5 groups of patients who are differentiated by kidney manifestations.3 Approximately 10% of patients show early nephrocalcinosis and kidney failure in infancy or early childhood. Most patients present with recurrent nephrolithiasis and progressive kidney failure in childhood to mid-adulthood. About 10% of patients are diagnosed after ESKD based on oxalate deposits from kidney biopsy, recurrent oxalate nephropathy after kidney transplant, or systemic oxalosis with chronic dialysis. Less than 10% of patients are considered late-onset and have occasional kidney stones in adulthood. Finally, less than 10% of patients are diagnosed presymptomatically based on family screening and having a close relative with PH1. The median age for symptom onset has been reported to be about 4 to 6 years (ranging from infancy to 60 years of age) and can be higher (i.e., 25 years) for patients who are diagnosed after ESKD.3
Symptoms suggestive of PH1 in pediatric patients consist of recurrent kidney stones, nephrocalcinosis, oxalate deposits in tissues, or impaired kidney function leading to failure to thrive.3 Laboratory tests showing urine oxalate levels consistently higher than 0.7 mmol/1.73 m2/day3 or 40 to 45 mg/day (500 µmol/day),5 elevated urine glycolate concentration, or plasma oxalate levels greater than 50 µmol/L when GFR is less than 30 mL/min/1.73 m23 also indicate PH1. It is recommended, both in the literature and by the clinical experts consulted by CADTH, that 24-hour urine collection corrected for BSA be used over spot urine analyses, where possible, and assessments such as that for oxalate:creatinine ratio be interpreted with an age-related reference.18 The clinical experts CADTH consulted stated that patients suspected of having PH1 (who do not yet have ESKD) will have urine biochemistry testing with a hyperoxaluria panel. Then, to confirm a diagnosis, genetic testing is used to identify a pathogenic variant in the AGT gene.3 Of the 3 types of PH, PH1 makes up approximately 80%.10 The types can be differentiated from each other based on genetic testing: AGT gene for PH1, glyoxylate reductase/hydroxypyruvate reductase (GRHPR) gene for PH2, and 4-hydroxy-2-oxoglutarate aldolase (HOGA1) gene for PH3.3 Additionally, PH2 and PH3 have a less severe phenotype than PH1.3 It has also been recommended that siblings of a proband be screened even if they are asymptomatic because their clinical course can be similar and they may benefit from early treatment.19
Standards of Therapy
Because hepatic overproduction of oxalate is the main cause of PH1, it is suggested that the best form of management is to reduce oxalate production, which can be further supported by increasing oxalate clearance, though the latter has limited effect.3 An estimated 30% of patients have a form of PH1 that is sensitive to high-dose vitamin B6 (a cofactor for AGT), which helps to ensure proper localization of the enzyme to the liver peroxisomes and may delay the onset of ESKD.3,7 According to the literature and the clinical experts consulted by CADTH, vitamin B6 therapy may be able to lower oxalate levels in some patients; however, not all patients achieve normalization of oxalate levels.7,8 Citrate supplementation to inhibit crystal formation and hyperhydration (2 to 3 L/m2/day) are also used to treat PH1 and preserve kidney function. Both citrate supplementation and hyperhydration can be burdensome for patients and are associated with compliance issues. Moreover, pediatric patients may require a gastrostomy tube to ensure adequate hydration throughout the day. It has been suggested that reducing dietary oxalate will have little effect because the main problem is endogenous overproduction.9 New therapeutics consisting of siRNA, such as lumasiran and nedosiran, have been developed to treat PH.3 Patients may also undergo shockwave lithotripsy, ureteroscopy, or percutaneous nephrolithotomy to treat kidney stones. When kidney function declines to less than 30 mL/min/1.73 m2, patients may require hemodialysis to remove oxalate that cannot be excreted through urine. The major limitation with dialysis is that oxalate production often exceeds clearance and intensive hemodialysis (consisting of many hours per day and multiple days per week) only reduces plasma oxalate levels transiently for a few hours before returning to supersaturated levels (i.e., greater than 30 to 45 µmol/L).3,9 The clinical experts consulted by CADTH noted that current standard-of-care treatments require lifelong adherence, are noncurative, and only partially alleviate the oxalate burden in patients. Liver-kidney transplant and complete removal of the non-functional liver is considered the only cure for PH1 because it corrects AGT function (endogenous oxalate production is returned to normal levels) and restores kidney function, but is associated with high morbidity, mortality, and lifelong immunosuppression.3,5,9 It has been estimated that 5-year survival is higher with dual-organ transplant compared to isolated kidney transplant at 67% versus 45%, respectively, in adults20 and 76% versus 14%, respectively, in children.21 After liver-kidney transplant, systemic oxalosis may be reversible, but the resolubilization of oxalate from tissues can put the new kidneys at risk of nephrocalcinosis and can take years to completely clear oxalate stores.3,9,18 Hemodialysis may also be used as a bridge to organ transplant and can be continued posttransplant in some patients to clear systemic stores of calcium oxalate and limit damage to the transplanted kidney.9,18
Milliner et al. suggested monitoring patients with PH1 based on kidney function.3 For example, patients with preserved function (GFR at least 60 mL/min/1.73 m2) may have regular kidney ultrasounds, fundoscopic eye exams for oxalate deposition, and urinalysis for oxalate and creatinine measures. In patients with reduced renal function (GFR less than 60 mL/min/1.73 m2) plasma oxalate may be included with the previously listed assessments. Those with greatly reduced renal function (GFR less than 30 mL/min/1.73 m2) or rapid deterioration of function may have bone X-rays, anemia testing, electrocardiogram for conduction abnormalities, echocardiogram for oxalate cardiomyopathy, and imaging for tissue calcification, along with the previously listed assessments.
The clinical experts consulted by CADTH stated that the current goals of therapy are to lower hepatic oxalate production, reduce kidney stone formation, and prevent the development of ESKD.
Drug
Lumasiran (Oxlumo) is indicated for the treatment of PH1 to lower urinary oxalate levels in pediatric and adult patients.1 The drug is available as a solution of 94.5 mg/0.5 mL lumasiran for subcutaneous injection with weight-based loading and maintenance dosing.2 According to the product monograph, patients weighing less than 10 kg receive a loading dose of 6 mg/kg once monthly for 3 doses and a maintenance dose of 3 mg/kg once monthly, patients weighing 10 kg to less than 20 kg receive a loading dose of 6 mg/kg once monthly for 3 doses and a maintenance dose of 6 mg/kg once every 3 months (quarterly), and patients weighing 20 kg or more receive a loading dose of 3 mg/kg once monthly for 3 doses and a maintenance dose of 3 mg/kg once every 3 months (quarterly).2
Lumasiran is a double-stranded siRNA that targets hydroxyacid oxidase 1 (HAO1) messenger RNA (mRNA) in hepatocytes and reduces glycolate oxidase (GO) levels through RNA interference.2 Lower GO levels reduce the amount of glyoxylate available for oxalate production, which results in a reduction of urine and plasma oxalate levels, the underlying cause of disease manifestations in patients with PH1. Since GO is upstream of AGT, the deficiency of which causes PH1, the mechanism of action of lumasiran is independent of the underlying gene mutation encoding AGT. Lumasiran is not expected to be effective in PH2 or PH3 because its mechanism of action does not affect the metabolic pathways causing PH2 and PH3.
Lumasiran underwent a priority review at Health Canada and was issued a Notice of Compliance on March 7, 2022. The sponsor has requested reimbursement as per the approved Health Canada indication.1 Lumasiran has not been previously reviewed by CADTH.
Stakeholder Perspectives
Patient Group Input
This section was prepared by CADTH staff based on the input provided by 1 patient group. The full original patient input received by CADTH has been included in the stakeholder section at the end of this report.
About the Patient Groups and Information Gathered
Two patient groups provided input as a joint submission to the CADTH review of lumasiran for the treatment of PH1. The Oxalosis and Hyperoxaluria Foundation is the first patient advocacy organization in the world dedicated to finding treatments, and ultimately a cure, for hyperoxaluria and is the largest private funder of hyperoxaluria research in the world. The Canadian Organization for Rare Disorders is Canada’s national network for organizations representing those with rare disorders. The network advocates for health policy and a health care system that is supportive of rare disorders and works with stakeholders to promote research, diagnosis, treatment, and services for all rare disorders in Canada.
The responses have been collected through an online survey (Survey Monkey, available from May 19, 2022, to May 31, 2022) and a virtual focus group (3 Canadian caregivers for children less than 12 years old diagnosed with PH1 and 1 Canadian patient diagnosed with PH1). In total, 43 respondents completed the entire survey (18.6% Canadian from Alberta, British Columbia, Ontario, and Yukon; 41.9% American). Of the 43 responders, one-third indicated that they were patients with PH and two-thirds identified as caregivers. In addition, 3 Canadians, 7 Americans, 6 non–North Americans from the online survey, and 2 Canadian children from the focus group reported having experience with lumasiran.
Disease Experience
Patients reported that the greatest burden of PH1 was the physical toll and emotional stress. Physical burdens included frequent dialysis, multiple hospitalizations, or emergency visits to remove stones and manage pain, fractures, repeated urinary or kidney infections, delayed development, infertility, and many systemic symptoms including nausea, stomach pain, and headaches. Emotional stress included anxiety and/or depression, concerns about kidney failure, liver-kidney transplant, disease prognosis, pregnancy, dying at a younger age, not having an approved treatment, and not being able to live as 1 wishes. Younger patients felt additional emotional stress because they wondered why they have the disease or why they are different. Also, responders highlighted the complexity of diagnosis for PH — for example, the time it took to get appropriate care and the preceding years of misdiagnoses. Responders cited challenges associated with treatment that included gastrostomy tube insertion for some infants and children, ureteroscopy and/or surgery to remove stones, loss of efficacy over time with vitamin B6, noncompliance, and intensive dialysis. Patients who have received lumasiran described experiencing an improvement in PH1 management and quality of life.
Improved Outcomes
The participants responded that current treatments and dialysis are insufficient and that therapies that decrease the likelihood of kidney stones, need for kidney and/or liver transplant, kidney failure, oxalosis, and the amount of medication are critical. Patients and families said they need access to treatments that improve physical well-being, thereby mitigating stress and anxiety for the entire family.
The respondents described the many physical, emotional, and financial challenges associated with PH1 having profound impacts on the quality of life of patients, caregivers, and families. These are compounded by a lack of knowledge among clinicians as well as access and affordability issues to treatments. One respondent stated, “There is a lack of clinical expertise within Canada that creates additional barriers to diagnosis and treatment. Just getting to a diagnosis has been a painful and exhausting marathon.”
Clinician Input
Input From Clinical Experts Consulted by CADTH
All CADTH review teams include at least 1 clinical specialist with expertise regarding the diagnosis and management of the condition for which the drug is indicated. Clinical experts are a critical part of the review team and are involved in all phases of the review process (e.g., providing guidance on the development of the review protocol, assisting in the critical appraisal of clinical evidence, interpreting the clinical relevance of the results, and providing guidance on the potential place in therapy). In addition, as part of the lumasiran review, a panel of 4 clinical experts from across Canada was convened to characterize unmet therapeutic needs, assist in identifying and communicating situations in which there are gaps in the evidence that could be addressed through the collection of additional data, promote the early identification of potential implementation challenges, gain further insight into the clinical management of patients living with a condition, and explore the potential place in therapy of the drug (e.g., potential reimbursement conditions). The following is a summary of this panel discussion.
Unmet Needs
The clinical experts consulted by CADTH emphasized the need for a therapy to treat PH1 that effectively lowers hepatic oxalate production, reduces kidney stone formation, and prevents the development of ESKD. The experts stated that current treatments, such as hyperhydration, oxalate crystal inhibitors, and dialysis, are noncurative and do not lower hepatic oxalate production or the total oxalate burden in patients. The clinical experts also noted that there is a small subset of patients whose PH1 is partially or completely vitamin B6 sensitive, but who may still progress to ESKD. One expert stated that administration of vitamin B6 in patients with pyridoxine-sensitive mutations only sometimes partially alleviates oxalate accumulation in these patients.
Place in Therapy
According to the clinical experts, a liver transplant is currently considered the only cure for PH1, but this is associated with high morbidity and lifelong immunosuppression. Two therapies, lumasiran and nedosiran, were identified by the clinicians as being possible pharmacotherapies for PH1. The experts expected lumasiran to cause a shift in the current treatment paradigm, becoming the first-line treatment for patients with PH1 and specifically for patients who are insensitive or only partially sensitive to vitamin B6 therapy. The clinicians noted that treatment with lumasiran is expected to be lifelong or until the patient receives a liver transplant. Long-term safety and efficacy data are limited, and it is uncertain what long-term outcomes or potential side effects there could be with lumasiran. Further, the clinical experts stated the importance of continuing current standard-of-care treatments along with lumasiran, particularly post–kidney transplant or when on dialysis, at least until there is normalization of urine oxalate excretion and plasma oxalate levels.
Patient Population
As per the clinical experts, patients with PH1 would typically be identified based on clinical symptoms, laboratory testing of oxalate levels, and a diagnosis confirmed by genetic testing. The clinicians suggested that a diagnosis could be missed if clinical signs were not further investigated, such as kidney stones in adults, which are more common than in children and do not immediately indicate PH1. Otherwise, the experts indicated that a diagnosis of PH1 is unlikely to be missed with genetic testing, which is generally not difficult to access, and which drug companies may subsidize. One clinical expert noted that it may take time for mutations that have not been previously documented to be accepted as being pathogenic, which may occur more frequently in underrepresented ethnic groups.
As noted earlier, the clinical experts stated that patients would be candidates for lumasiran if they have genetically confirmed PH1 and are unable to normalize urine oxalate excretion. The clinicians were uncertain if or when lumasiran would be used for patients who are sensitive to vitamin B6 therapy and are able to normalize urine oxalate excretion. The experts suggested that it may be reasonable to treat these latter patients with lumasiran if, despite adequate standard of care, they experience any of the following: inability to maintain normalized urine oxalate excretion, elevated plasma oxalate levels, progressive nephrocalcinosis, ongoing kidney stone formation, or decline in GFR (to less than 60 mL/min/1.73 m2). The clinicians explained that patients with normal renal function but who have evidence of nephrocalcinosis or elevated plasma oxalate levels may benefit from lumasiran because it is very unlikely these patients will maintain normal kidney function long-term. The experts felt that early intervention and treatment with lumasiran would be reasonable for patients who still have kidney function, rather than waiting until GFR falls to 60 mL/min/1.73 m2. As PH1 progresses and GFR declines, the clinical experts stated that lumasiran could reduce urine oxalate excretion and plasma oxalate levels and prevent systemic oxalosis.
One expert explained that patients with limited kidney function may have low urine oxalate excretion, though this is not indicative of the extent of disease and the urine oxalate level is inaccurate in patients who have ESKD. The clinical experts indicated that patients with little or no urine oxalate excretion and who rely solely on dialysis to remove oxalate from the body are at very high risk of systemic oxalosis with clinical deterioration and would benefit from lumasiran. The experts stated that hemodialysis only temporarily lowers plasma oxalate levels, with a typical drop of 50% in a 2.5-hour dialysis, after which plasma oxalate rises to predialysis levels within minutes to hours. Moreover, an expert emphasized that daily dialysis is insufficient to remove the daily production of oxalate, resulting in persistent tissue deposition of oxalate. Currently, there is a lack of long-term data in patients on dialysis who have been treated with lumasiran.
The clinical experts noted that lumasiran may be effective in avoiding the need for liver transplant in patients with ESKD and identified some evidence22 for treating pediatric patients with ESKD or with markedly reduced GFR (e.g., less than 30 mL/min/1.73 m2) with lumasiran and kidney-only transplants. The experts explained that it would be reasonable to treat patients with lumasiran before and after a kidney transplant to lower plasma and urine oxalate levels and prevent damage to the transplanted kidney from oxalate deposition as well as reduce stored oxalate that is excreted post–kidney transplant. One expert noted that patients who receive a kidney-only transplant would be required to continue lumasiran treatment indefinitely because the allograft would be otherwise damaged by endogenous oxalate overproduction.
Assessing Response to Treatment
The clinical experts noted that urine oxalate excretion and plasma oxalate are surrogate markers for oxalate production in patients with PH1 and that there is no widely accepted method for measuring total body oxalate, making it difficult to assess how effective a treatment is. The expert also stated that in patients with ESKD who receive dialysis, predialysis oxalate levels would be measured to assess adequate suppression of oxalate production, which should slowly decline, indicating effective treatment, but may take time because dialysis is continually removing stored oxalate from the body.
The clinicians expected that there would be a noticeable improvement after an initial treatment duration of lumasiran for 6 months, but that this is unlikely to be long enough to see a lowering of urine or plasma oxalate to normal levels, especially in patients on dialysis or with advanced chronic kidney disease (CKD). The experts suggested that successful treatment must consider how progressed a patient is before treatment; for example, a patient with established kidney failure and on dialysis will not see normalization of oxalate levels very quickly. A clinician indicated that if no observable changes occurred during the first 6 months of treatment, it might be reasonable to treat a patient for 12 months (total) before deciding to continue lumasiran or not.
Per the clinical experts, patients in earlier stages of PH1 may be monitored for urine oxalate excretion (24-hour urine preferred over spot urine sampling depending on the patient’s age), plasma oxalate levels, kidney function (eGFR), and nephrocalcinosis via radiological imaging. Because patients in later stages of PH1 and on dialysis would not have reliable urine oxalate measures, clinicians would instead measure predialysis plasma oxalate every 1 to 3 months to assess response to therapy. The clinical experts stated that patients who have received a kidney or combined liver-kidney transplant may have plasma oxalate levels measured initially on a daily basis, transitioning to weekly and then monthly frequency as levels stabilize.
The clinicians noted that a 30% reduction in urine oxalate excretion may not be sufficient to declare successful treatment and would rather see normalization of urine and plasma oxalate for a full response. Clinicians of patients with systemic oxalosis would want to see an improvement in symptoms such as clearance of skin deposits, normal cardiac ejection fraction, and improvement in musculoskeletal and vascular issues. The experts described how patients (post–liver transplant or on lumasiran) with substantial systemic oxalate burden may require years to normalize urinary excretion because the body is slowly clearing stored oxalate.
According to the clinical experts, renewal of lumasiran would depend on adequate response to treatment as well as an assessment of potential treatment issues (e.g., AEs, ADAs, compliance). The clinicians indicated that it would be important to have urine and plasma measurements at least 2 times per year and to see patients in the clinic at least annually.
Discontinuing Treatment
The clinical experts stated that patients who have received a liver transplant would not be treated with lumasiran because the new liver has functional enzyme and there would be no need for the drug. Other possible reasons for stopping treatment suggested by the clinicians were no response to treatment, or severe untreatable or intolerable adverse effects.
Prescribing Conditions
The clinical experts agreed that a specialist (e.g., nephrologist or metabolic physician) should monitor patients with PH1, depending on who is available to the patient in their area. The experts also stated that lumasiran can be administered by a health care professional, such as by a nurse, in a community setting. One clinical expert suggested the potential for the patient or caregiver to self-administer lumasiran at home because subcutaneous injections can be routinely performed for other medications, but other clinicians did not expect lumasiran to be self-administered.
According to the experts, it is unlikely that treatment would exceed the Health Canada recommended dose for most patients. The clinicians suggested that a higher dose may be used in infants due to their larger liver surface area to BSA ratio and that a higher dose might overcome neutralization occurring in patients who have measurable neutralizing ADAs. This was based on experience with other drugs and has been suggested in the literature,11 although there is a lack of clinical evidence supporting higher doses of lumasiran at this time.
Additional Considerations
The clinical experts identified the need for additional consideration of patients who have limited access to health care resources (e.g., individuals living in remote areas, who do not have a primary care physician or access to specialists, and who lack health insurance or a means to afford treatments). The clinicians also noted that access to pediatric hemodialysis is limited to major cities across Canada (e.g., Vancouver, Calgary, Edmonton, Winnipeg, London, Hamilton, Toronto, Ottawa, Montreal, and Halifax), requiring patients and families to relocate to access treatment. The experts stated that lowering hepatic oxalate production with medications such as lumasiran would potentially allow treatment of ESKD with peritoneal dialysis, preventing the need for relocation to access pediatric hemodialysis. The clinical experts also indicated that other ethical issues were the burden of knowing there is a treatment for PH1, but not being able to access it, especially given the severity of the disease, inadequacy of current treatments, and overall burden of care on patients and families.
Drug Program Input
The drug programs provide input on each drug being reviewed through CADTH’s reimbursement review processes by identifying issues that may affect their ability to implement a recommendation. The implementation questions and corresponding responses from the clinical experts consulted by CADTH are summarized in Table 4.
Table 4: Summary of Drug Plan Input and Clinical Expert Response
Drug program implementation questions | Clinical expert response |
|---|---|
Relevant comparators | |
There are no approved pharmacological treatments for PH1. Other treatments for management of PH1 include dietary or over-the-counter measures that may not be covered by drug plans:
| For CDEC consideration. |
Initiation criteria | |
PH1 is a rare disease with an estimated prevalence of 1 to 3 per million. PH1 is a genetic disorder of oxalate metabolism that leads to manifestations such as recurrent kidney stones; nephrocalcinosis; progressive renal failure, which can lead to end-stage kidney disease; and multiorgan damage systemic deposition of toxic oxalate crystals. Diagnosis of PH is determined by genetic testing. Is there potential for newborn screening? | The clinical experts do not expect there will be newborn screening for PH1 at this time and there are limitations with newborn screening that will have to be addressed before this can be implemented. |
Health Canada has authorized use for pediatric patients aged younger than 18 years; however, there is limited data for patients aged younger than 2 years and weighing less than 10 kg. Would patients with PH1 who are aged less than 2 years or weighing less than 10 kg be treated with lumasiran? | The clinical experts agreed that infants with PH1 who are aged younger than 2 years and weigh less than 10 kg could be treated with lumasiran. |
Renewal criteria | |
The primary end points in the clinical trials are reduction in urine oxalate excretion corrected for BSA averaged over months 3 to 6 (ILLUMINATE-A) and percent reduction from baseline in spot urine oxalate:creatinine ratio (averaged over months 3 to 6). How do these outcomes relate to complications associated with PH1 such as recurrent kidney stones, nephrocalcinosis, progressive renal failure, end-stage kidney disease, and multiorgan damage? | According to the experts, the end points used in the ILLUMINATE trials are not perfect surrogates for PH1 complications and it is important to consider the population being assessed and PH1 disease severity. The clinical experts described the clinical progression many patients experience and how, early in PH1, patients will have normal kidney function and plasma oxalate but increased urine oxalate excretion. As the disease progresses, eGFR declines, plasma oxalate increases, and urine oxalate remains high. Once a patient reaches ESKD and starts hemodialysis, urine oxalate excretion will decline to normal or even below normal. The experts stated that there is no single biomarker that will be useful in all stages of this disease. The experts agreed that early in the disease course, when patients have preserved kidney function, urine oxalate is a satisfactory marker, but measuring plasma oxalate levels should be added as kidney function falls. The experts noted that urine oxalate is not helpful for patients with ESKD or on dialysis and instead should have predialysis plasma oxalate levels measured. The experts suggested that plasma oxalate may be a better assessment for systemic outcomes, especially in patients with ESKD, because it is readily measurable and likely predicts clinical outcomes, but noted that there is currently a lack of data supporting this. |
The provincial laboratory (in 1 jurisdiction) confirmed that it can perform urine (24 hour) oxalate tests, although it was suggested that this is not very practical for patients. Studies used an average over 3 to 6 months. How would this be done in a real-world setting and how would it translate to demonstration of efficacy of drug treatment? | The clinical experts agreed that 24-hour urine oxalate excretion is routinely performed for continent patients though noncontinent children can be assessed using spot oxalate:creatinine ratios, which is considered an imperfect substitute. The clinicians would look for a progressive lowering of urine oxalate on timed or spot urine accounting for age-specific changes and suggested that measurements be taken at least twice per year to monitor therapeutic response. |
Random urine oxalate testing is also an option for measuring the oxalate:creatinine ratio; however, it would be difficult to determine an average over 3 to 6 months unless testing was performed frequently. Can CDEC and the clinical experts comment on how response should be monitored or reported for patients receiving this therapy? | One clinical expert stated that urine oxalate:creatinine ratio, while simpler to collect, is less accurate and 24-hour urine oxalate excretion is preferred. Other clinical experts who treat pediatric patients stated that spot urine oxalate:creatinine is monitored approximately every 1 to 3 months (more frequently at the beginning of therapy) and at least every 6 months. The experts also noted that the measurements must be compared to normal ranges for oxalate:creatinine ratio based on age. |
Discontinuation criteria | |
The disease appears to be progressive over time, which may make stopping treatment difficult. Can CDEC and the clinical experts define what loss of response or absence of clinical benefit would look like? | The clinical experts suggested that a loss of response would appear as a failure to lower predialysis plasma oxalate in a patient on dialysis or a failure to show a progressive reduction in urine oxalate excretion over time in patients with preserved kidney function. One expert explained that the latter response could take an extended amount of time if there was a high tissue oxalate burden that was being slowly released. Furthermore, the expert would expect normalization of elevated plasma oxalate in patients with normal kidney function. Lastly, the experts stated that an increase of plasma oxalate or increase in urine oxalate after an initial improvement would also be a loss of response. If a patient appeared to show a lack of response, the clinical experts stated that it would be important to check if the patient was receiving treatment (or if they had missed any doses); had developed neutralizing ADAs; was taking vitamin C, which increases oxalate production; or if GFR has declined, which would likely result in a rise in plasma oxalate. Because there are many factors that can influence plasma oxalate levels, the experts emphasized that a rise in plasma oxalate alone would not be sufficient to indicate a lack of treatment response and other reasons would need to be investigated. The clinical experts stated that it may be reasonable to stop treatment with lumasiran if there was documented failure to respond, serious untreatable or intolerable side effects, or the patient received a liver transplant. |
Prescribing criteria | |
For all patients, the first 3 doses are administered monthly. The maintenance regimen should start 1 month after the last loading dose. After the first 3 doses, the dosing regimen is different for patients weighing less than 10 kg and those weighing more than 10 kg:
| For CDEC consideration. |
Lumasiran is administered via subcutaneous injection. The product monograph notes that the product will be administered by a health care professional. Who would be the main prescribers of this drug (e.g., nephrologists)? Would they also be administering the drug? | The clinical experts agreed that nephrologists or genetic/metabolic specialists would both prescribe and supervise the administration of lumasiran. One clinician suggested that it is possible, but less likely, that a urologist would prescribe or supervise administration of lumasiran. One clinical expert stated that given the limited information regarding adverse effects of lumasiran, the drug should be administered by a health care professional and not self-administered by the patient. Another clinical expert suggested that lumasiran could be administered in a hospital outpatient clinic, an injection facility, or at home by a visiting nurse or by the patient or caregiver. This clinician further noted that it would be unlikely that the prescriber would do the administration because subcutaneous injections are typically done by registered nurses or by the patient at home. |
Special implementation issues and generalizability | |
Certain relevant populations were not included or only minimally included in the trial. | For CDEC consideration. |
Care provisions issues | |
Weight should be measured and dose should be calculated before each dose being administered. Dispensing of product may be delayed until a weight and dose are determined for each patient; otherwise, wastage or insufficient dosing may result. Could the clinical expert explain more about the prescribing and administration process; other care requirements for providers or informal caregivers; and challenges or limitations on access to testing necessary to use drug? | One clinical expert stated that if lumasiran were administered at an injection facility (e.g., Innomar) or hospital, the patient’s weight would be assessed at the time of the injection and the dose calculated based on the current weight. Alternatively, if administered at home, the patient’s weight could be taken on a reliable scale in the home, and dosing based on the current weight. A clinical expert who treats pediatric patients noted that a weight checked within 1 week for an infant, 2 weeks for a child, and 1 month for an adult would likely be acceptable if done in a doctor’s office. One clinician stated that, for adults, weight can be checked every 3 to 6 months to adjust drug dosage. According to the product monograph, dosing is determined based on mg/kg body weight, which the clinical expert noted is a simple calculation once the weight is obtained. |
Pricing conditions | |
The price of lumasiran is $96,855.33 per single-use vial (94.5 mg/0.5 mL as a single-use vial). National budget impact is anticipated to be $61 million over 3 years. The sponsor states that a significant portion of this budget impact will be offset by cost savings from a reduction in dialysis costs of $5.8 million over 3 years. Savings realized through a reduction in need for dialysis are not direct savings to drug programs. | For CDEC consideration. |
Wastage might be a consideration for patients of certain weights. Dosage is weight based and the product is formulated as a single-use vial (94.5 mg of lumasiran per 0.5 mL). Given that dosage is weight based and the product is formulated as a single-use vial (94.5 mg of lumasiran per 0.5 mL), do you expect there will be wastage for patients of certain weights? | The clinical experts agreed that wastage would be inevitable given the current available formulation. One clinician suggested that multiple vial sizes would allow for use of the closest combination of vials to minimize wastage. |
ADA = antidrug antibody; BSA = body surface area; CDEC = CADTH Canadian Drug Expert Committee; eGFR = estimated glomerular filtration rate; ESKD = end-stage kidney disease; GFR = glomerular filtration rate; PH1 = primary hyperoxaluria type 1.
Clinical Evidence
The clinical evidence included in the review of lumasiran (Oxlumo) is presented in 3 sections. The first section, the Systematic Review, includes pivotal studies provided in the sponsor’s submission to CADTH and Health Canada, as well as those studies that were selected according to an a priori protocol. The second section includes sponsor-submitted long-term extension studies and additional relevant studies that were considered to address important gaps in the evidence included in the systematic review.
Systematic Review (Pivotal and Protocol-Selected Studies)
Objectives
To perform a systematic review of the beneficial and harmful effects of lumasiran 94.5 mg/0.5 mL, subcutaneous, for the treatment of PH1 to lower urinary oxalate levels in pediatric and adult patients.
Methods
Studies selected for inclusion in the systematic review included pivotal studies provided in the sponsor’s submission to CADTH and Health Canada, as well as those meeting the selection criteria presented in Table 5. Outcomes included in the CADTH review protocol reflect outcomes considered to be important to patients, clinicians, and drug plans.
Table 5: Inclusion Criteria for the Systematic Review
Criteria | Description |
|---|---|
Population | Pediatric and adult patients with primary hyperoxaluria type 1 Subgroups:
|
Intervention | Lumasiran administered via subcutaneous injection with weight-based loading and maintenance dosing:
|
Comparator | Standard of care (e.g., dietary changes, hyperhydration, citrate supplementation, vitamin B6, dialysis, liver-kidney transplant) |
Outcomes | Efficacy outcomes:
Harms outcomes:
|
Study Designs | Published and unpublished phase III and IV RCTs |
ADA = antidrug antibody; AE = adverse event; eGFR = estimated glomerular filtration rate; HRQoL = health-related quality of life; RCT = randomized controlled trial; SAE = serious adverse event; WDAE = withdrawal due to adverse events.
The literature search for clinical studies was performed by an information specialist using a peer-reviewed search strategy according to the PRESS Peer Review of Electronic Search Strategies checklist.23
Two CADTH clinical reviewers independently selected studies for inclusion in the review based on titles and abstracts, according to the predetermined protocol. Full-text articles of all citations considered potentially relevant by at least 1 reviewer were acquired. Reviewers independently made the final selection of studies to be included in the review, and differences were resolved through discussion.
Published literature was identified by searching the following bibliographic databases: MEDLINE All (1946–) via Ovid and Embase (1974–) via Ovid. All Ovid searches were run simultaneously as a multifile search. Duplicates were removed using Ovid deduplication for multifile searches, followed by manual deduplication in EndNote. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s Medical Subject Headings, and keywords. The main search concepts were Oxlumo (lumasiran). Clinical trials registries were searched: the US National Institutes of Health’s clinicaltrials.gov, the WHO’s International Clinical Trials Registry Platform search portal, Health Canada’s Clinical Trials Database, and the European Union Clinical Trials Register.
No filters were applied to limit the retrieval by study type. Retrieval was not limited by publication date or language. Conference abstracts were excluded from the search results. Refer to Appendix 1 for the detailed search strategies.
The initial search was completed on June 9, 2022. Regular alerts updated the search until the meeting of the CADTH Canadian Drug Expert Committee on September 28, 2022.
Grey literature (i.e., literature that is not commercially published) was identified by searching relevant websites from the Grey Matters: A Practical Tool For Searching Health-Related Grey Literature checklist.24 Included in this search were the websites of regulatory agencies (US FDA and the European Medicines Agency). Google was used to search for additional internet-based materials. Refer to Appendix 1 for more information on the grey literature search strategy.
These searches were supplemented by reviewing bibliographies of key papers and through contacts with appropriate experts. In addition, the sponsor of the drug was contacted for information regarding unpublished studies.
Findings From the Literature
A total of 3 reports from 2 studies were identified from the literature for inclusion in the systematic review (Figure 1). The included studies are summarized in Table 6. A list of excluded studies is presented in Appendix 2.
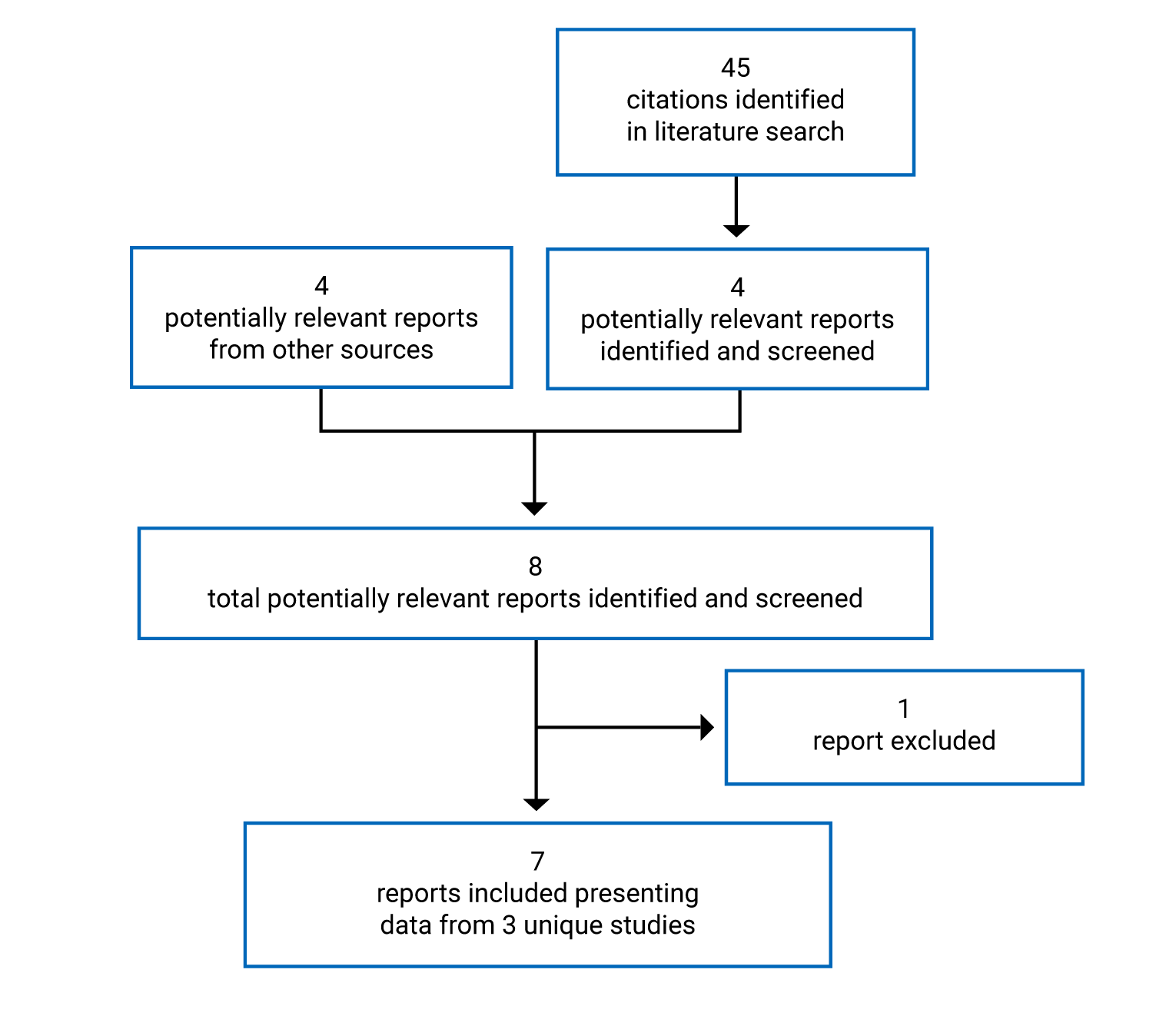
Table 6: Details of Included Studies
Characteristic | ILLUMINATE-A | ILLUMINATE-B | ILLUMINATE-C |
|---|---|---|---|
Designs and populations | |||
Study design | Phase III, DB, RCT with placebo control and parallel groups | Phase III, single-arm | Phase III, single-arm |
Locations | 16 study centres in 8 countries in North America, Europe, and Middle East | 9 study centres in 5 countries in North America, Europe, and Middle East | 13 study centres in 10 countries in North America, Europe, Middle East, and Australia |
Study initiation date | December 13, 2018 | April 22, 2019 | January 22, 2020 |
Randomized | N = 39
| N = 18 | N = 21 |
Inclusion criteria |
| ||
|
|
| |
Exclusion criteria |
| ||
|
|
| |
Drugs | |||
Intervention | Lumasiran administered with weight-based loading and maintenance-dosing schedule with dose adjustments for interval weight gain:
| ||
Comparator(s) | Placebo administered on a matching schedule | NA | NA |
Duration | |||
Phase | |||
Screening | Maximum 60 days | Maximum 60 days | Maximum 120 days |
Primary analysis | 6 months DB | 6 months | 6 months |
Extension | 3 months blinded treatment extension 51 months OLE | 54 months | 54 months |
Follow-up | Maximum 12 months | Maximum 84 days | Maximum 12 months |
Outcomes | |||
Primary end point | Percent change in 24-hour urinary oxalate excretion from baseline to month 6 corrected for BSA | Percent change in urinary oxalate excretion from baseline to month 6 |
|
Secondary and exploratory end points | Secondary:
Extension period: Change from baseline (percent and absolute) in 24-hour urinary oxalate excretion, 24-hour urinary oxalate:creatinine ratios, and eGFR; and percentage of time that 24-hour urinary oxalate is ≤ 1.5 x ULN Exploratory:
Safety: Frequency of AEs | Secondary for the extension phase:
Secondary for duration of trial:
Exploratory:
Safety: Frequency of AEs | Secondary for the primary analysis period:
Secondary for the extension phase:
Exploratory:
Safety: Frequency of AEs |
Notes | |||
Publications | Sas et al. (2022)27 | None | |
ADA = antidrug antibody; AE = adverse event; ALT = alanine aminotransferase; AST = aspartate aminotransferase; AUC = area under the curve; BSA = body surface area; DB = double-blind; eGFR = estimated glomerular filtration rate; ESRD = end-stage renal disease; INR = international normalized ratio; KDQOL = Kidney Disease Quality of Life Questionnaire; MCS = mental component summary; NA = not applicable; OLE = open-label extension; PCS = physical component summary; PedsQL = Pediatric Quality of Life Inventory; PH1 = primary hyperoxaluria type 1; PK = pharmacokinetic; RCT = randomized controlled trial; SF-12 = Short Form-12; ULN = upper limit of normal; VAS = visual analogue scale.
aeGFR calculated by the Modification of Diet in Renal Disease formula if aged at least 18 years, or Schwartz Bedside Formula if aged at least 12 months to less than 18 years, or patients aged less than 12 months with serum creatinine that was considered elevated for age at consent.
Source: ILLUMINATE-A Clinical Study Report,12 ILLUMINATE-B Clinical Study Report,13 ILLUMINATE-C Clinical Study Report.14
Description of Studies
All 3 trials were ongoing at the time of the CADTH review of lumasiran.
ILLUMINATE-A Trial
The ILLUMINATE-A trial is a phase III, DB, RCT investigating the efficacy and safety of lumasiran in patients with PH1 who were aged 6 years and older. The trial took place at 16 study centres in 8 countries and screening for eligibility occurred within 60 days of the first administration of the study drug. Overall, 39 patients were randomized 2:1 to receive lumasiran or placebo. Randomization was conducted using an interactive response system and treatment patients were stratified by mean urine oxalate excretion (greater than versus less than or equal to 1.70 mmol/24 hour/1.73 m2). Patients received study drug based on weight-based loading and maintenance-dosing schedules. During the 6-month primary analysis period (DB period), patients received study drug (lumasiran 3 mg/kg or matching placebo) administered as a subcutaneous injection once per month for the first 3 months (loading dose at day 1, month 1, and month 2) followed by a single administration of study drug 1 month later (maintenance dose for the next 3 months at month 3). At month 6, patients entered the 3-month blinded treatment-extension period in which all patients received active treatment. Patients randomized to lumasiran continued the maintenance-dosing schedule, consisting of a single administration of lumasiran and matching placebo for the next 2 injections to maintain treatment blinding (referred to as lumasiran followed by lumasiran). Patients randomized to placebo started receiving active treatment and began the loading dose schedule (lumasiran 3 mg/kg each month; referred to as placebo followed by lumasiran). At month 9, the 51-month OLE began, and all patients were on the maintenance-dosing schedule. Efficacy and safety assessments were conducted every month through month 9, then every 3 months through month 24 and every 6 months until month 60 at the end of the trial. Data are available from primary analysis safety and efficacy results with an interim data cut-off date of November 6, 2019.
Urine and plasma oxalate testing was performed by a central laboratory and the investigator was blinded to the results from the first dose to unblinding (when the last patient completed month 9 assessments). If laboratory measurements were taken locally as part of routine clinical care, steps were taken to avoid informing the patient and site personnel of the result until unblinding occurred.
The baseline for the DB period was based on the last valid measurements before the first dose of study drug. For the all lumasiran–treated set, baseline for patients randomized to lumasiran was the same as described for the DB period. For patients randomized to placebo and crossed over to lumasiran, baseline was defined as the last valid measurement before the first dose of lumasiran (i.e., month 6).
Protocol amendment 2 contained changes that lowered the exclusion threshold for GFR from at or below 45 mL/min/1.73 m2 to less than 30 mL/min/1.73 m2, moved the evaluation of long-term plasma oxalate measures from exploratory to secondary end points, and clarified that specific study assessments may be performed outside of the trial centre by a home health care professional. As a result of the first amendment, the subgroup analysis by baseline eGFR changed from at or below versus greater than 60 mL/min/1.73 m2 to less than versus at least 60 mL/min/1.73 m2.
ILLUMINATE-B Trial
The ILLUMINATE-B trial is a phase III, single-arm trial investigating the efficacy and safety of lumasiran in patients with PH1 who were aged younger than 6 years. The trial took place at 9 study centres in 5 countries and screening for eligibility was similar to ILLUMINATE-A. At screening, for those who were able to comply, patients had a 24-hour urine collection to establish baseline urine oxalate excretion. Otherwise, where allowed and at the discretion of the investigator and patient’s guardian, baseline and month 6 measures may have been taken using a single catheterized 24-hour collection. Due to the challenges of pediatric patients providing 24-hour urine samples, single-void urine samples were collected throughout the trial. Overall, 18 patients were included in the trial. Patients received the study drug based on weight-based loading and maintenance-dosing schedules. Efficacy and safety assessments were conducted every 2 weeks for the first month and every month for the rest of the 6-month primary analysis period. During the 54-month long-term extension period, assessments occurred at least once every 3 months until the end of the trial. Data are available from primary analysis safety and efficacy results with an interim data cut-off date of June 30, 2020.
As a single-arm trial, there was no blinding of treatment assignments. All efficacy and pharmacodynamic (PD) analyses were performed centrally, and data were distributed to study sites only after the last patient had completed the month 6 visit.
Protocol amendment 1 contained changes that increased the sample size to 20 patients, due to a lower-than-expected screening failure rate; moved the evaluation of plasma oxalate from exploratory to secondary end points; included the percentage of time that the spot urine oxalate:creatinine ratio was at or below 1.5 times ULN, as a secondary end point in the extension period; and clarified that specific study assessments might be performed outside of the trial centre by a home health care professional and that specific laboratory tests could be performed locally, with abnormalities being confirmed by a central laboratory.
An interim analysis was conducted based on data available up to October 25, 2019, with an updated report dated March 9, 2020, for regulatory submission purposes. Analyses were descriptive and did not contain formal hypothesis testing.
ILLUMINATE-C Trial
The ILLUMINATE-C trial is a phase III, single-arm trial investigating the efficacy and safety of lumasiran in patients with PH1 who had an eGFR of 45 mL/min/1.73 m2 or lower and were either not receiving hemodialysis (Cohort A) or had begun hemodialysis (Cohort B). The trial took place at 13 study centres in 10 countries and screening for eligibility occurred within 120 days of the first administration of the study drug. Overall, 21 patients were included in the trial. Patients received the study drug based on weight-based loading and maintenance-dosing schedules. Dose administration and efficacy and safety assessment scheduling were similar to the ILLUMINATE-B trial. Data are available from primary analysis safety and efficacy results with an interim data cut-off date of May 20, 2021.
Similar to the ILLUMINATE-B trial, there was no blinding of treatment assignments and data were not distributed until after the last patient’s month 6 visit.
Cohort A included patients who did not require hemodialysis, while Cohort B included those who did. Patients in Cohort A who began requiring hemodialysis due to progressive renal impairment could cross over to Cohort B. At the time of the data cut-off for the primary analysis, no patients had crossed over to Cohort B. According to the study protocol and at the sponsor’s discretion, patients may have been replaced if they discontinued the study drug or stopped participating before month 6, or if patients crossed over from Cohort A to Cohort B. Patients who discontinued study drug or participation after month 6 were not replaced.
Protocol amendment 1 increased the sample size from 16 to 20 patients.
An interim analysis was conducted based on plasma oxalate data available up to May 14, 2021, from 4 patients in Cohort B to support responses directed to questions from a health agency. Analyses were descriptive.
Populations
Inclusion Criteria
All patients included in the 3 trials must have had documented or confirmed diagnosis of PH1 by genetic testing and, if taking therapeutic vitamin B6, were on a stable regimen for at least 90 days before screening and maintained the regimen for at least 6 months during the trial. The ILLUMINATE-A trial included patients who were aged 6 years or older with a mean 24-hour urine oxalate excretion of at least 0.70 mmol/24 hour/1.73 m2 based on 24-hour urine collections. The ILLUMINATE-B trial included patients who were aged younger than 6 years with a urine oxalate:creatinine ratio greater than the ULN based on age. The ILLUMINATE-C trial included patients of any age who had an eGFR at or below 45 mL/min/1.73 m2 and plasma oxalate of at least 20 μmol/L. Patients on hemodialysis (Cohort B) must have had a stable regimen for at least 4 weeks before screening and maintained this regimen through the month 6 visit.
Exclusion Criteria
Patients in the 3 trials were not eligible if they had an ALT or AST reading greater than 2 times ULN for age or total bilirubin greater than 1.5 times ULN. Of note, individuals were excluded from the ILLUMINATE-A or ILLUMINATE-B trials if they had an eGFR less than 30 mL/min/1.73 m2 or 45 mL/min/1.73 m2 and lower, respectively; had clinical evidence of extrarenal systemic oxalosis, past liver or kidney transplant, or anticipated a liver transplant within 6 months. Individuals were excluded from the ILLUMINATE-C trial if they had a condition other than PH1 that resulted in renal insufficiency, were receiving peritoneal dialysis, had a history of liver transplant or kidney transplant and were receiving immunosuppression for it, or anticipated a liver transplant within 6 months.
Baseline Characteristics
Baseline characteristics are summarized in Table 7. Due to the different eligibility criteria and data reported for each trial, meaningful comparisons between trials could not be made.
ILLUMINATE-A Trial
The mean age of patients was 18.1 years (SD = █████ years; median = 14.0 years; range, 6 years to 60 years); 66.7% were male and 33.3% were female; and 76.9% were white, 15.4% were Asian, 5.1% were another race, and 2.6% identified as being of more than 1 race. The mean age at diagnosis was ███ years (SD = █████ years). Patients had a mean 24-hour urine oxalate excretion corrected for BSA of 1.82 mmol/24 hour/1.73 m2 (SD = 0.62 mmol/24 hour/1.73 m2) and mean plasma oxalate of 15.01 μmol/L (SD = 7.44 μmol/L). Most patients had an eGFR of at least 60 mL/min/1.73 m2 (82.0%), while fewer had an eGFR between 45 and 60 mL/min/1.73 m2 (███%) or between 30 and 45 mL/min/1.73 m2 (████%). In general, baseline characteristics appeared to be balanced between lumasiran and placebo groups.
A higher percentage of patients in the lumasiran group had history of kidney stones (88.5% versus 76.9% in placebo), whereas a higher percentage of patients in the placebo group had history of vitamin B6 use (69.2% versus 50.0% in lumasiran), pyelonephritis (38.5% versus 19.2% in lumasiran), and nephrocalcinosis (69.2% versus 46.2% in lumasiran). At diagnosis, a higher percentage of patients in the lumasiran group reported presenting symptoms of kidney stones (80.8% versus 53.8% in placebo), whereas a higher percentage of patients in the placebo group reported presenting with nephrocalcinosis (53.8% versus 38.5% in lumasiran) or were asymptomatic (23.1% versus 7.7% in lumasiran).
ILLUMINATE-B Trial
The mean age of patients was ████ months (SD = █████ months; median = 50.1 months; range, 3 months to 72 months); 55.6% were female and 44.4% were male; and 88.9% were white while 11.1% identified as another race. The mean age at diagnosis was ████ months (SD = █████ months). Patients had a mean spot urine oxalate:creatinine ratio of 0.63 mmol/mmol (SD = 0.43 mmol/mmol) and mean plasma oxalate of 13.24 μmol/L (SD = 6.50 μmol/L). The mean eGFR was 112.80 mL/min/1.73 m2 (SD = 27.63 mL/min/1.73 m2). Due to the small number of patients in each group and because treatment groups were differentiated by body mass, which is related to age, some baseline characteristics did not appear balanced. There were more females than males in the 10 kg to 20 kg group and all patients in the 20 kg or more group were male. One-third of patients in the 10 kg or less group and all patients in the 10 kg or more group were white. Mean spot urine oxalate:creatinine ratio, plasma oxalate measures, and eGFR were highest in the 10 kg or less group.
Mean plasma oxalate was higher in the less than 10 kg group compared to the other treatment groups. More than half of patients in each weight category reported using vitamin B6 (66.7%, 58.3%, and 66.7% by increasing weight category, respectively). A larger percentage of patients in the 20 kg or more group reported a history of kidney stone events (33.3% versus 16.7%) and nephrocalcinosis (███% versus ████%) compared to the group of patients weighing between 10 kg and 20 kg. At diagnosis, a larger proportion of patients weighing less than 10 kg were identified through familial screening (66.7%) compared to the other groups. A higher percentage of patients in the 20 kg or more group presented with nephrocalcinosis (66.7%) compared to the other groups.
ILLUMINATE-C Trial
The mean age of patients was ████ years (SD = ████ years; median = 8.0 years; range, 0 years to 59 years); 57.1% were male and 42.9% were female; and 76.2% were white, 19.0% were Asian, and 4.8% identified as another race. The mean age at diagnosis was ████ years (SD = ████ years). Patients had a mean plasma oxalate of █████ μmol/L (SD = █████ μmol/L). The mean eGFR was 19.85 mL/min/1.73 m2 (SD = 9.64 mL/min/1.73 m2) for Cohort A and eGFR was not available for Cohort B. In general, baseline characteristics appeared to be balanced between cohorts A and B. Urinary measures were not available for most patients in Cohort B.
Mean plasma oxalate was higher in Cohort B compared to Cohort A. A larger proportion of patients in Cohort A had a history of kidney stone events (█████ versus ████ in Cohort B) and vitamin B6 use (66.7% versus 46.7% in Cohort B), while a larger proportion of patients in Cohort B had a history of pyelonephritis (████% versus ████% in Cohort A). At diagnosis, a higher percentage of patients presented with nephrocalcinosis (████% versus ████%), ESKD (███% versus ████%), and other symptoms (████% versus ████%) in Cohort B versus Cohort A. A larger proportion of patients in Cohort A presented with kidney stones (████% versus ████% in Cohort B) or were asymptomatic at diagnosis (████% versus █% in Cohort B).
Table 7: Summary of Baseline Characteristics, Safety Analysis Set
Characteristic | ILLUMINATE-A | ILLUMINATE-B | ILLUMINATE-C | ||||
|---|---|---|---|---|---|---|---|
Placebo (N = 13) | Lumasiran (N = 26) | < 10 kg (N = 3) | 10 to < 20 kg (N = 12) | ≥ 20 kg (N = 3) | Cohort A: no dialysis (N = 6) | Cohort B: dialysis (N = 15) | |
Demographics | |||||||
Age | |||||||
Mean (SD)a | 17.0 (15.19) | 18.7 (11.52) | ███ (████) | ████ (█████) | ████ (████) | ████ (████) | ████ (████) |
Median (min, max)a | 11.0 (6, 60) | 16.5 (6, 47) | 10.1 (3, 14) | 50.1 (23, 72) | 62.2 (54, 72) | 9.0 (0, 40) | 6.0 (1, 59) |
0 to < 1 year, n (%) | NA | NA | 2 (66.7) | 0 | 0 | NA | NA |
1 to < 2 years, n (%) | NA | NA | 1 (33.3) | 1 (8.3) | 0 | NA | NA |
2 to < 6 years, n (%) | NA | NA | 0 | 11 (91.7) | 3 (100) | NA | NA |
< 18 years, n (%) | 8 (61.5) | 14 (53.8) | NA | NA | NA | █ (████) | ██ (████) |
≥ 18 years, n (%) | 5 (38.5) | 12 (46.2) | NA | NA | NA | █ (████) | █ (████) |
Sex, n (%) | |||||||
Male | 8 (61.5) | 18 (69.2) | 2 (66.7) | 3 (25.0) | 3 (100) | 3 (50.0) | 9 (60.0) |
Female | 5 (38.5) | 8 (30.8) | 1 (33.3) | 9 (75.0) | 0 | 3 (50.0) | 6 (40.0) |
Race, n (%) | |||||||
White | 9 (69.2) | 21 (80.8) | 1 (33.3) | 12 (100) | 3 (100) | 4 (66.7) | 12 (80.0) |
Asian | 3 (23.1) | 3 (11.5) | 0 | 0 | 0 | 1 (16.7) | 3 (20.0) |
Other | 0 | 2 (7.7) | 2 (66.7) | 0 | 0 | 1 (16.7) | 0 |
More than 1 race | 1 (7.7) | 0 | 0 | 0 | 0 | 0 | 0 |
Baseline disease characteristics and medical historyb | |||||||
Age at diagnosisa | |||||||
Mean (SD) | ███ (█████) | ███ (████) | ███ (████) | ████ (█████) | ████ (█████) | ███ (████) | ████ (████) |
Median (min, max) | NR (–1b, 59) | NR (0, 36) | 0.8 (█, █) | 22.7 (█, ██) | 27.0 (█, ███ | █████, ███ | █████, ███ |
24-hour urine oxalate excretion corrected for BSA (mmol/24 hour/1.73 m2) | |||||||
n (%) | 13 (100) | 26 (100) | 0 | 3 (25.0) | 2 (66.7) | 5 (83.3) | 1 (6.7) |
Mean (SD) | 1.79 (0.68) | 1.84 (0.60) | NR | ████ (████) | ████ (████) | ████ (████) | ████ (NA) |
Median (min, max) | 1.68 (0.68, 2.84) | 1.77 (0.76, 3.05) | NR | 1.94 (1.03, 2.02) | 2.72 (2.54, 2.89) | 2.01 (0.56, 2.47) | 1.28 (1.28, 1.28) |
24-hour urine oxalate:creatinine ratio (mmol/mmol) | |||||||
n (%) | 13 (100) | 26 (100) | 0 | 3 (25.0) | 3 (100) | 5 (83.3) | 1 (6.7) |
Mean (SD) | 0.24 (0.11) | 0.21 (0.10) | NR | ████ (████) | ████ (████) | ████ (████) | ████ (NA) |
Median (min, max) | ████ (████, ████) | ████ (████, ████) | NR | 0.31 (0.17, 0.48) | 0.37 (0.28, 0.43) | ████ (████, ████) | ████ (████, ████) |
Spot urine oxalate:creatinine ratio (mmol/mmol) | |||||||
n (%) | 13 (100) | 26 (100) | 3 (100) | 12 (100) | 3 (100) | 6 (100) | 2 (13.3) |
Mean (SD) | 0.24 (0.14) | 0.23 (0.11) | ████ (████) | ████ (████) | ████ (████) | ████ (████) | ████ (████) |
Median (min, max) | ████ (█████ ████) | ████ (█████ ████) | 1.25 (1.13, 1.71) | 0.45 (0.17, 1.21) | 0.35 (0.26, 0.69) | 0.33 (0.08, 1.38) | 0.53 (0.45, 0.62) |
Plasma oxalate (μmol/L) | |||||||
n (%) | 13 (100) | 26 (100) | 3 (100) | 12 (100) | 3 (100) | 6 (100) | 15 (100) |
Mean (SD) | 15.49 (7.34) | 14.77 (7.63) | █████ (████) | █████ (████) | █████ (████) | █████ (█████) | ██████ (█████) |
Median (min, max) | 13.10 (7.8, 28.4) | 13.05 (7.0, 43.5) | 22.25 (17.2, 30.6) | 9.58 (6.6, 19.9) | 11.70 (7.2, 18.7) | 57.94 (22.7, 134.0) | 103.65 (56.3, 167.0) |
eGFR (mL/min/1.73 m2) | |||||||
n (%) | 13 (100) | 26 (100) | 1 (33.3) | 12 (100) | 3 (100) | 5 (83.3) | NA |
Mean (SD) | 78.95 (26.83) | 82.97 (25.55) | ██████ (NR) | ██████ (█████) | █████ (█████) | 19.85 (9.64) | NA |
Median (min, max) | █████ (█████, ██████) | 84.67 (31.70, 131.35) | 134.52 (134.52, 134.52) | 110.65 (75.82, 174.06) | 90.12 (64.67, 134.87) | 16.54 (8.61, 34.09) | NA |
eGFR CKD stage (mL/min/1.73 m2) | |||||||
≥ 90 | 4 (30.8) | 9 (34.6) | NR | NR | NR | NR | NR |
60 to < 90 | 6 (46.2) | 13 (50.0) | NR | NR | NR | NR | NR |
45 to < 60 | 1 (7.7) | 2 (7.7) | NR | NR | NR | NR | NR |
30 to < 45 | 2 (15.4) | 2 (7.7) | NR | NR | NR | NR | NR |
History of the following, n (%) | |||||||
Symptomatic kidney stone events | 10 (76.9) | 23 (88.5) | 0 | 2 (16.7) | 1 (33.3) | █ (████) | █ (███) |
Lithotripsy or stone removal procedure in past 12 months | 3 (23.1) | 4 (15.4) | █ | █ (████) | █ | █ | █ |
Vitamin B6 use | 9 (69.2) | 13 (50.0) | 2 (66.7) | 7 (58.3) | 2 (66.7) | 4 (66.7) | 7 (46.7) |
Pyelonephritis | 5 (38.5) | 5 (19.2) | 0 | 2 (16.7) | 0 | █ (████) | █ (████) |
Urinary tract infections | 5 (38.5) | 11 (42.3) | 0 | 3 (25.0) | 1 (33.3) | █ (████) | █ (████) |
Nephrocalcinosis | 9 (69.2) | 12 (46.2) | 3 (100) | 6 (50.0) | 3 (100) | █ (████) | ██ (████) |
Presenting symptoms,d n (%) | |||||||
Asymptomatic (familial screening) | 3 (23.1) | 2 (7.7) | 2 (66.7) | 2 (16.7) | 1 (33.3) | █ (████) | █ |
Kidney stone | 7 (53.8) | 21 (80.8) | 0 | 4 (33.3) | 1 (33.3) | █ (████) | █ (████) |
Nephrocalcinosis | 7 (53.8) | 10 (38.5) | 1 (33.3) | 5 (41.7) | 2 (66.7) | █ (████) | ██ (████) |
ESKD | 0 | 0 | 0 | 0 | 0 | █ (████) | ██ (█████) |
Othere | 3 (23.1) | 4 (15.4) | 0 | 5 (41.7) | 0 | █ (████) | █ (████) |
History of other comorbidities,f n (%) | |||||||
Dysuria | █ | █ (███) | NR | NR | NR | NR | NR |
Urinoma | █ | █ (███) | NR | NR | NR | NR | NR |
Kidney fibrosis | █ | █ (███) | NR | NR | NR | NR | NR |
Acute kidney injury | █ (████) | █ | █ | █ (███) | █ | █ (████) | █ |
Anuria | NR | NR | NR | NR | NR | █ | ██ (████) |
CKD | █ (███) | █ (███) | █ (████) | █ | █ | █ (████) | █ (███) |
ESKD | NR | NR | NR | NR | NR | █ (████) | █ |
Renal impairment | █ | █ (███) | NR | NR | NR | NR | NR |
Renal hypertension | █ | █ | NR | NR | NR | █ | █ (███) |
Nephrolithiasis | █ | █ (███) | █ | █ (████) | █ | █ (████) | █ (███) |
Small kidney | █ | █ (███) | NR | NR | NR | NR | NR |
Hypercalciuria | █ | █ (███) | NR | NR | NR | NR | NR |
Proteinuria | █ | █ (███) | NR | NR | NR | NR | NR |
Urethral stenosis | NR | NR | NR | NR | NR | █ | █ (███) |
Renal colic | █ | █ (███) | NR | NR | NR | █ | █ (███) |
Renal pain | █ | █ (███) | NR | NR | NR | NR | NR |
Microalbuminuria | NR | NR | █ | █ (███) | █ | NR | NR |
Hypertension | █ (████) | █ (███) | NR | NR | NR | █ (████) | █ (████) |
Diabetes | NR | NR | NR | NR | NR | NR | NR |
Systemic oxalosis | NR | NR | NR | NR | NR | █ | █ (████) |
BSA = body surface area; CKD = chronic kidney disease; DB = double-blind; eGFR = estimated glomerular filtration rate; ESKD = end-stage kidney disease; NA = not applicable; NR = not reported; SD = standard deviation.
aAge is in years for ILLUMINATE-A, months for ILLUMINATE-B, and years for ILLUMINATE-C.
bData presented are from patients who could complete testing (e.g., 24-hour urine oxalate was evaluated in a limited subset of patients who were able to complete a 24-hour urine collection). Percentages are based on the number of patients in each treatment group for whom data are available.
cMinimum reflects 1 patient with a prebirth diagnosis.
dIncludes all symptoms that a patient experienced before diagnosis. A patient may check more than 1 category; therefore, percentages may exceed 100%.
eIncluded metabolic acidosis, weight loss, whewellite crystals in urine, acute renal injury, and urinary tract infection.
fIdentified by CADTH and clinical experts consulted by CADTH as being potentially important.
Note: Percentages are based on the number of patients in each treatment group for whom data are available.
Source: ILLUMINATE-A Clinical Study Report,12 ILLUMINATE-B Clinical Study Report,13 ILLUMINATE-C Clinical Study Report.14
Interventions
For all 3 trials, lumasiran for subcutaneous injection (189 mg/mL concentration of lumasiran in sterile solution) was the active treatment. In the ILLUMINATE-A trial, placebo was sterile saline solution for subcutaneous injection, and site pharmacists covered syringes in yellow transparent film to mask the identity of the treatment being administered. Preferred injection site was the abdomen, with optional injection in the upper arms or thighs.
Doses and scheduling were based on results from the phase I/II study ALN-GO1 to 001, with consideration for the younger age, lower body weight, and physiologic differences between children and adults for pediatric patients in the ILLUMINATE-B and ILLUMINATE-C trials. Dose administration was based on total body weight, which was measured within 3 months of dosing or collected on the day of dosing (ILLUMINATE-A trial), or within 7 days for patients weighing less than 20 kg (ILLUMINATE-B trial) or aged younger than 6 years (ILLUMINATE-C trial). For the ILLUMINATE-C trial, the sponsor noted that preclinical and clinical data indicated that renal impairment did not affect the systemic exposure, PD, or safety of siRNA compounds; thus, weight-based dosing was used.
For patients weighing less than 10 kg, the loading dose was lumasiran 6.0 mg/kg for 3 months followed by the maintenance dose of lumasiran 3.0 mg/kg monthly. For patients weighing 10 kg to less than 20 kg, the loading dose was lumasiran 6.0 mg/kg for 3 months followed by the maintenance dose of lumasiran 6.0 mg/kg every 3 months. For patients weighing 20 kg or more, the loading dose was lumasiran 3.0 mg/kg for 3 months followed by the maintenance dose of lumasiran 3.0 mg/kg every 3 months. In the ILLUMINATE-B and ILLUMINATE-C trials, patients whose weight increased past the next weight-based dose threshold continued with the increased dose during the study (i.e., patients did not return to a lower weight-based dose if their weight decreased). Monthly doses were required to be administered at least 21 days apart. In the ILLUMINATE-C trial, lumasiran was required to be administered within 120 minutes after dialysis.
Due to the COVID-19 pandemic restricting patient and health care professional travel, the study drug may have been administered at home by the patient’s caregiver after adequate training, under the oversight of the investigator, in consultation with the medical monitor, and where local regulations and infrastructure allowed. In the ILLUMINATE-A trial, patients who demonstrated tolerability could begin receiving at-home administration starting at month 15, while those in the ILLUMINATE-B and ILLUMINATE-C trials must have tolerated at least 1 dose of lumasiran in the clinic.
Standard-of-care therapies for PH1 (e.g., hyperhydration, vitamin B6, crystallization inhibitors) were continued throughout month 6 (ILLUMINATE-B and ILLUMINATE-C) or month 12 (ILLUMINATE-A) of the trial. Patients using vitamin B6 for the treatment of PH1 must have been on a stable regimen for at least 9 months before the trial and continue for at least 6 months (ILLUMINATE-B and ILLUMINATE-C) or 12 months (ILLUMINATE-A) from the start of the trial. Other restrictions on concomitant treatments included not applying topical steroids near the injection site, avoiding high doses of vitamin C 4 days before oxalate measures, and not injecting concomitant subcutaneous medications in the same site within 7 days of the study drug.
Outcomes
A list of efficacy end points identified in the CADTH review protocol that were assessed in the clinical trials included in this review is provided in Table 8. These end points are further summarized subsequently. A detailed discussion and critical appraisal of the outcome measures is provided in Appendix 4.
Most biochemical assessments and collections were made before the study drug was administered. Sponsor-developed assays for urine and plasma oxalate assessments had characteristics that met FDA and European Medicines Agency guidance and were validated early on during the trial at QPS Holdings LLC, a sponsor contract research organization partner. Randomization was stratified in the ILLUMINATE-A trial based on 24-hour urine oxalate measures. Initially, the measures were based on a clinical assay (Mayo Clinical Laboratories), and included the first 5 patients, before assessments were transitioned to the validated PD assay (QPS). Once the QPS assay was validated and available, patient screening and stratification were performed based on both assays. During the trial, 24-hour urine oxalate samples were analyzed using the QPS assay and plasma oxalate samples were analyzed using both assays.
Table 8: Summary of Outcomes of Interest Identified in the CADTH Review Protocol
Outcome measure | ILLUMINATE-A | ILLUMINATE-B | ILLUMINATE-C |
|---|---|---|---|
Kidney function (e.g., eGFR or creatinine levels) | Secondary | Secondary | Secondary |
Loss of kidney function over time | NR | NR | NR |
Prevention of dialysis and/or liver-kidney transplant | NR | NR | NR |
Kidney stone events (e.g., severity) | Exploratory | Exploratory | Secondary |
HRQoL | Exploratory | NR | Secondary/exploratory |
Urinary oxalate levels | Primary/secondary | Primary/secondary | Secondary |
Plasma oxalate levels | Secondary | Secondary | Primary/secondary |
Urinary oxalate:creatinine measures | Secondary/exploratory | Primary/secondary | Secondary |
eGFR = estimated glomerular filtration rate; HRQoL = health-related quality of life; NR = not reported.
The sponsor noted that all urine oxalate and creatinine samples were analyzed within established long-term stability limits (i.e., for storage). Seven and 5 plasma oxalate samples in the ILLUMINATE-A and ILLUMINATE-B trials, respectively, were analyzed outside of the established stability limit. In the ILLUMINATE-C trial, all plasma oxalate samples were analyzed within the established stability limit. The Clinical Study Report presented efficacy and PD data using the QPS assays.
Kidney Function
Serum creatinine from blood samples was measured and eGFR (mL/min/1.73 m2) was calculated to assess kidney function. The Modification of Diet in Renal Disease method was used for patients aged 18 years and older while the Schwartz Bedside Formula was used for patients aged 12 months to 18 years. In the ILLUMINATE-B trial, eGFR was calculated for patients aged at least 12 months. In the ILLUMINATE-C trial, eGFR was calculated for patients in Cohort A.
According to the Kidney Disease Improving Global Outcomes guideline, CKD is defined as abnormalities in kidney function or structure that have been present for at least 3 months.28 For patients with kidney damage, GFR (mL/min/1.73 m2) maps to levels of kidney function as follows: GFR of at least 90 is normal or high, 60 to 89 is mildly decreased relative to young adult level, 45 to 59 is mildly to moderately decreased, 30 to 44 is moderately to severely decreased, 15 to 29 is severely decreased, and less than 15 is kidney failure.28
Loss of kidney function over time and prevention of dialysis and/or liver-kidney transplant were identified as important outcomes in the CADTH review of lumasiran but were not assessed in the trials.
Kidney Stone Events
A kidney stone event was defined as having at least 1 of the following occur:
visit to health care provider (e.g., outpatient clinic, urgent care, emergency department, or procedure) due to a kidney stone
medication taken for renal colic
stone passage
macroscopic hematuria due to a kidney stone.
All events were assessed by the investigator.
Health-Related Quality of Life
In the ILLUMINATE-A and ILLUMINATE-C trials, adult patients (aged 18 years or older) completed the KDQOL-36 while pediatric patients (aged 2 to 18 years) completed the PedsQL, including the generic and end-stage renal disease (ESRD) modules. Both parent- and self-report versions were available for pediatric patients in the trials. Adult patients also completed the EQ-5D-5L and VAS, while pediatric patients completed the EQ-5D-Y and VAS. HRQoL was not assessed in the ILLUMINATE-B trial.
The KDQOL-36 is a self-reported questionnaire made up of 36 items in 5 scales: Physical component summary (PCS), mental component summary (MCS), burden of kidney disease, symptoms and problems with kidney disease, and effects of kidney disease.29,30 Although the instrument was intended to assess HRQoL in patients on dialysis, patients who have had a transplant and/or are at the predialysis stage can also complete it by excluding 2 items asking about access and catheter sites.31 Scores are transformed into a scale from 0 to 100,32 with higher scores representing better HRQoL. The instrument has been shown to have adequate construct validity supported by moderate to strong correlations33 (r = 0.40 to 0.52) between the SF-12 (PCS and MCS) scores and the kidney-specific subscale scores as well as statistically significant differences (P < 0.001 to 0.05) between distinct patient groups.29 Internal consistency (alpha = 0.83 to 0.85) and dialysis facility-level reliability (alpha = 0.72 to 0.83) were acceptable (alpha > 0.7).29,34 Most items within each scale demonstrated acceptable internal consistency (alpha = 0.31 to 0.73).29 No MID was identified from the literature.
The PedsQL survey consists of 23 items from the 4.0 Generic Core Scales and 34 items from the 3.0 ESRD Module for measuring HRQoL in healthy and/or pediatric patient populations using a Likert scale for each item.35 Raw scores are transformed to a scale of 0 to 100, with higher scores indicative of better HRQoL.35 The Psychosocial Health Summary Score consists of the emotional, social, and school functioning scores. For the Generic Core Scales, construct validity has been demonstrated using the known-groups approach: healthy versus acutely ill versus chronically ill children,36 no chronic illness versus complex or noncomplex chronic illness,37 and healthy children versus children with ESRD.38 Internal consistency for total scale scores was acceptable: self-report (alpha = 0.88) and proxy-report (alpha = 0.90) in pediatric population (healthy, acutely or chronically ill pediatric population),36 alpha was about 0.9 in pediatric patients who are healthy and/or have ESRD.38 Also, a strong correlation (Pearson r = 0.6) was found between patient self-report and parent-proxy report of patients on dialysis.39 Evidence for responsiveness to change was identified from pediatric patients admitted to hospital: total score changed from upon admission to during follow-up (mean difference = 22.1; SD = 22.7).37 No MID was identified from the literature.
For the PedsQL 3.0 ESRD Module, content validity was assessed using focus groups, cognitive interviews, pretesting, and field-testing protocols in population of children with ESRD.38 Internal consistency was acceptable in most of the self-report and parent-proxy report scales, though child self-reports tended to show lower reliability.38 Moderate agreements (intraclass correlation [ICC] = 0.41 to 0.60) between child self-reports and parent-proxy reports were found in 7 of 10 scales and fair agreements (ICC = 0.21 to 0.40) were found in 3 of 10 scales of PedsQL 4.0 Generic Core Scales and 3.0 ESRD Module. No MID was identified from the literature.
The EQ-5D-5L is a generic, preference-based HRQoL measure consisting of descriptive questions and a VAS.40 The descriptive questions cover 5 dimensions (mobility, self-care, usual activities, pain/discomfort, and anxiety/depression) in which each dimension is divided into 5 levels (no, slight, moderate, severe, and extreme) of perceived problems.41,42 Higher scores indicate worse quality of life in individual scores and better quality of life in population index scores. The VAS records the patient’s self-rated health on a 10 cm scale with end points 0 to 100 labelled “the worst health you can imagine” and “the best health you can imagine,” respectively.40,42 Validity, reliability, and responsiveness to change have not been studied in patients with kidney disease or PH1. No MID was identified from the literature.
The EQ-5D-Y is a generic, preference-based HRQoL measure with child-friendly wording intended for younger populations.43 Self-completion (ages 8 to 15 years) and proxy (ages 4 to 7 years) versions are available. Like the EQ-5D questionnaire, the descriptive system comprises the same 5 dimensions, with each dimension having 3 levels (no problems, some problems, and a lot of problems) with wording that is more child-appropriate.43,44 The VAS is the same as that for the EQ-5D. Scoring is consistent with the EQ-5D and VAS. Validity, reliability, and responsiveness to change have not been studied in pediatric patients with kidney disease or PH1. No MID was identified from the literature.
Urine Oxalate Levels
In the ILLUMINATE-A trial, 24-hour urine samples were collected to assess urine oxalate excretion corrected for BSA (mmol/24 hour/1.73 m2). To be a valid collection, the sample must have been between 22 and 26 hours in duration, no voids were missed between start and end times (based on patient collection diary), and the 24-hour creatinine content was at least 10 mg/kg, as determined by the central laboratory. A sample was not collected if it was within 14 days after a dialysis session.
In the ILLUMINATE-B trial, 24-hour urine collections could not be collected by all patients and single-void urine samples were collected instead. A noncatheterized 24-hour urine collection was valid if the samples were between 18 and 26 hours in duration, no voids were missed between start and end times, and the 24-hour creatinine content was at least 5 mg/kg, as determined by the central laboratory.
In the ILLUMINATE-C trial, some patients were anuric (unable to produce more than 100 mL/day) and did not require collection assessments. Otherwise, 24-hour samples were collected from patients who were not anuric, or single-void urine samples were collected from those who could not comply with 24-hour collections. Urine oxalate excretion was assessed for patients who provided 24-hour collections. A urine sample was valid if collected between 18 and 26 hours in duration, no missed voids, and, for Cohort A, 24-hour creatinine was at least 5 mg/kg for patients aged younger than 6 years or weighing at least 10 mg/kg for patients aged 6 years and older as determined by the central laboratory. Patients in Cohort B did not have a minimum creatinine threshold to be considered valid.
Urine oxalate excretion is thought to be in the causal pathway to stone formation and kidney damage in CKD (especially stages 1 to 3a) and is a surrogate outcome to measure total body oxalate in patients with PH1.45 Analysis of data from the Rare Kidney Stone Consortium PH registry of 297 patients with all types of PH (65% of whom had PH1) demonstrated that kidney outcomes were correlated with baseline urine oxalate excretion stratified by quartile, with a kidney failure hazard ratio for quartile 4 (Q4) versus Q1 to Q3 of 3.4 (95% CI, 1.4 to 7.9).46 Based on the literature, normal values for urine oxalate from 24-hour urine samples are less than 0.50 mmol or less than 45 mg/1.73 m2/day, although readings may vary based on laboratory or methods of analysis used.3 Further, oxalate excretion results should be corrected to a BSA of 1.73 m2 in children to be properly interpreted.45 It has been suggested that PH1 should be suspected in an individual with elevated urine oxalate excretion persistently greater than 0.7 mmol/1.73 m2/day.47 The magnitude of reduction needed for clinical benefit is uncertain.3
Plasma Oxalate Levels
In the ILLUMINATE-A and ILLUMINATE-B trials, blood samples were collected post–drug administration for plasma oxalate measures (µmol/L).
In the ILLUMINATE-C trial, blood samples were collected pre–drug administration and predialysis for patients in Cohort B. Up to 8 samples were collected over a 24-hour period to produce plasma oxalate profiles and calculate AUC between dialysis sessions and may have been taken before, during, or after dialysis.
Similar to urine oxalate excretion, plasma oxalate is a surrogate measure for total body oxalate in patients with PH1.45 It has been suggested that plasma oxalate may not correlate well with the loss of kidney function at higher eGFR levels (greater than 45 mL/min/1.73 m2) because of the kidney’s ability to excrete excess oxalate, and therefore measures in patients with advanced CKD may be more accurate.45 A study noted that plasma oxalate increased as eGFR fell and plasma oxalate exceeded 35 to 40 μmol/L (threshold for supersaturation) in samples from patients with PH almost universally when eGFR fell to less than 10 mL/min/1.73m2.48 These results are supported in a recent study that found a moderate to strong inverse correlation between eGFR and plasma oxalate levels for patients with CKD stages 1 to 3b, though the relationship is nonlinear across eGFR values.49 Normal plasma oxalate levels are about 1 to 3 µmol/L,45 while normative plasma oxalate values range from less than 50.0 µmol/L50-55 to 89.9 µmol/L.56
Urine Oxalate:Creatinine Measures
In the trials, 24-hour and spot urine samples were collected for oxalate:creatinine measures (mmol/mmol). When available, 24-hour urine samples were collected for oxalate excretion corrected by BSA and oxalate:creatinine ratios.
Similar to urine oxalate excretion, urine oxalate:creatinine ratio is a surrogate measure for total body oxalate in patients with PH1.45 As noted by the sponsor, although 24-hour urine collections are the preferred method for assessing urine oxalate excretion, many pediatric patients were not able to comply with 24-hour urine collection procedures. Therefore, in the ILLUMINATE-B and ILLUMINATE-C trials, multiple spot urine samples were collected to calculate the oxalate:creatinine ratio (mmol/mmol). The sponsor identified literature that indicated spot urine oxalate:creatinine measures were an appropriate alternative for 24-hour urine oxalate measures. Data from individuals (N = 5,580) with and without PH showed a moderate correlation between spot urine oxalate:creatinine ratios and 24-hour urine oxalate (R2 = 0.63),57 though there were notable limitations (described in Appendix 4). These results were consistent with a small population (N = 94) of groups of children aged 5 to 14 years without PH (R2 = 0.75).58 A cross-sectional study found a weak correlation between 24-hour urine oxalate excretion and spot urine oxalate:creatinine (Spearman correlation r = 0.289, P < 0.005) in 62 patients with a history of kidney stones and it was concluded that a random spot urine test could not replace the 24-hour urine oxalate estimation in patients with urolithiasis.59 Based on the literature, normal values for urine oxalate:creatinine ratio in spot urine samples are less than 325 to 360 mmol/mol for individuals aged 0 to 6 months, 132 to 174 mmol/mol for individuals aged 7 to 24 months, less than 98 to 101 mmol/mol for individuals aged 2 to 5 years, 70 to 82 mmol/mol for individuals aged 5 to 14 years, and less than 40 mmol/mol for individuals aged greater than 16 years.3 Again, measurements are expected to vary based on laboratory, methods of analysis used, or literature reference, which was confirmed by the clinical experts consulted by CADTH. It was also noted that values are inconsistent before 5 years of age and differ based on sex,45,57 and the clinical experts stated that there is a gradual decline in the oxalate:creatinine ratio with age.
Harms
Incidence and seriousness of AEs, WDAEs, and deaths were reported for the safety population during the primary analysis and extension period of the 3 trials. AEs, SAEs, and protocol-defined notable harms were described based on preferred term and associated system organ class. Notable harms from the CADTH systematic review protocol included injection site reactions, renal events, complications from systemic oxalosis, headache, rhinitis, upper respiratory infection, hypersensitivity reactions, and ADAs. Kidney stone events were considered an efficacy outcome and were not captured as an AE or SAE. Blood samples were collected before study drug administration to assess ADAs using a validated enzyme-linked immunosorbent assay.
Statistical Analysis
The statistical analysis of efficacy end points conducted in the trials is summarized in Table 9.
Primary Outcome
In the ILLUMINATE-A trial, the percent change from baseline to month 6 for 24-hour urine oxalate corrected for BSA (mmol/24 hour/1.73 m2) was the primary end point and was estimated based on the mean percent change from baseline across months 3 to 6 (when treatment was expected to have reached a steady state). The primary analysis used a restricted maximum likelihood (REML)–based Mixed-Effect Model Repeated Measures (MMRM) method. The LSM treatment differences (lumasiran – placebo), standard errors of the mean (SEMs), 95% CIs, and P values have been reported.
In the ILLUMINATE-B trial, the percent change from baseline to month 6 for spot urine oxalate:creatinine ratios (mmol/mmol) was the primary end point and was based on the mean percent change from baseline across months 3 to 6. The primary analysis used a REML-based MMRM method. Because the sample size was small for this trial, an autoregressive (1) covariance structure was used to model the within-patient error. If the autoregressive (1) covariance structure matrix failed to converge, an analysis of covariance (ANCOVA) model with covariate of baseline spot urine oxalate:creatinine ratio value was used. The LSM treatment averaged from months 3 to 6, SEMs, 95% CIs, and P values has been reported.
In the ILLUMINATE-C trial, the percent change from baseline to month 6 for plasma oxalate (μmol/L; Cohort A) or predialysis plasma oxalate (Cohort B) was the primary end point and was based on the mean percent change from baseline across months 3 to 6. The primary analysis used a REML-based MMRM method. Similar to the ILLUMINATE-B trial, an autoregressive (1) covariance structure and ANCOVA model with covariate of baseline plasma oxalate (predialysis for Cohort B) was used. The LSM treatment averaged from months 3 to 66, SEMs, 95% CIs, and P values have been reported.
Sample Size and Power Calculation
In the ILLUMINATE-A trial, patients were randomized 2:1 to lumasiran or placebo. The power calculation was based on an assumption that the placebo group would have a mean reduction from baseline to month 6 in 24-hour urine oxalate corrected for BSA of 17% and both treatment groups would have an SD of 25%. The sponsor determined that 24 patients would be required to provide 90% power to detect a treatment difference of 37% at a 2-sided 5% significance level, or a 54% reduction in the lumasiran group. Enrolment of up to 30 patients was planned to account for potential dropouts.
In the ILLUMINATE-B trial, the sample size was based on feasibility considerations rather than power calculations. The sponsor planned to enrol 8 patients based on the original trial protocol and, as outlined in protocol amendment 1, the number was increased to 20 patients (with at least 1 patient aged younger than 12 months and weighing less than 10 kg) due to a lower-than-expected screening failure rate.
In the ILLUMINATE-C trial, the sample size was based on feasibility considerations, as in the ILLUMINATE-B trial. The sponsor planned to enrol at least 20 patients with at least 6 patients in each cohort, 4 patients aged younger than 6 years, and 2 patients aged between 6 and 18 years.
Statistical Testing
In the ILLUMINATE-A trial, a gatekeeping testing strategy was used to control for overall type I error rate for primary and secondary end points. The primary end point (percent change in 24-hour urine oxalate from baseline to month 6) was compared between treatment groups at a 2-sided significance level of 0.05. Subsequent testing proceeded only if the previous test was statistically significant at the 0.05 level. Change in eGFR was a secondary end point, but not included in the hierarchy because it was not expected that a significant difference would occur within 6 months.25 Tests for secondary outcomes were conducted in the following order:
absolute change in 24-hour urinary oxalate from baseline to month 6 (full analysis set [FAS])
percent change in 24-hour urinary oxalate:creatinine ratio from baseline to month 6 (FAS)
percent change in plasma oxalate from baseline to month 6 (plasma oxalate analysis set)
proportion of patients with 24-hour urinary oxalate at or below 1.5 times ULN at month 6 (FAS)
proportion of patients with 24-hour urinary oxalate at or below ULN at month 6 (FAS)
absolute change in plasma oxalate from baseline to month 6 (plasma oxalate analysis set)
In the ILLUMINATE-B and ILLUMINATE-C trials, there was no formal hypothesis testing and no control for multiplicity.
Data Imputation
In the ILLUMINATE-A trial, data missing for the primary end point were imputed by treatment group using the Markov Chain Monte Carlo method, assuming data were missing at random, with adjustments for baseline 24-hour urine oxalate level and visit. After imputation, data were analyzed using an ANCOVA model.
In the ILLUMINATE-B trial, data missing for 24-hour urine oxalate and 24-hour urine oxalate:creatinine ratio values were imputed using spot urine oxalate:creatinine ratio measures. Imputation was applied for patients who had valid baseline values only; patients with missing baseline values were not included in the analysis. This method for imputing values was deemed to be valid by the sponsor based on 156 paired samples and 16 patients from a phase I study of lumasiran (ALN-GO1 to 001) demonstrating correlation between time-matched oxalate:creatinine ratios from spot urine samples and oxalate excretion from 24-hour urine collections (Pearson correlation coefficient = ████; 95% CI, ████ to ████). Like the ILLUMINATE-A trial, data were analyzed using an ANCOVA model.
In the ILLUMINATE-C trial, linear interpolation or extrapolation may have been used for missing plasma oxalate AUC values, if appropriate. Imputation of missing data was not further described.
Sensitivity Analyses
In the ILLUMINATE-A trial, 2 sensitivity analyses were performed to estimate the treatment effect of the primary end point without assuming an equal treatment effect across months 3 to 6. The first sensitivity analysis includes the interaction of visit and treatment to the primary MMRM model. The second sensitivity analysis includes all postbaseline data, such as that from months 1 and 2.
In the ILLUMINATE-B trial, 3 sensitivity analyses were performed to estimate the treatment effect of the primary end point by visits for the efficacy analysis set, from months 3 to 6 for the safety analysis set, and for the percent change from baseline in ULN ratio (ratio of measured spot urine oxalate:creatinine to ULN) from months 3 to 6 for the efficacy analysis set.
In the ILLUMINATE-C trial, 1 sensitivity analysis was performed to estimate the treatment effect of the primary end point by cohorts in the safety analysis set, which included patients who lacked plasma oxalate assessments at month 3 or after.
Subgroup Analyses
In the ILLUMINATE-A trial, prespecified subgroups included age (6 to younger than 12 years, versus 12 to younger than 18 years, versus 18 years and older), sex (male versus female), race (white versus any other race), baseline 24-hour urine oxalate corrected for BSA (at or below versus greater than 1.70 mmol/24 hour/1.73 m2), baseline eGFR (less than versus at least 60 mL/min/1.73 m2), history of renal stones (yes versus no), baseline vitamin B6 use (yes versus no), region 1: North America (Canada and US) versus other (outside of North America), and region 2: Europe versus other (outside of Europe). When there were fewer than 5 patients in a subgroup treatment group, only descriptive statistics were presented. These analyses were not controlled for multiplicity.
In the ILLUMINATE-B trial, prespecified subgroups included age (0 to younger than 1 year versus 1 to younger than 6 years) and weight-based dosing categories (less than 10 kg, versus 10 to less than 20 kg, versus 20 kg or more).
In the ILLUMINATE-C trial, prespecified subgroups included age (younger than 2 years, versus 2 to younger than 6 years, versus 6 to 18 years, versus 18 years or older) and weight-based dosing categories (same as the ILLUMINATE-B trial).
The CADTH review team and clinical experts identified subgroups based on age, kidney function, baseline urine and/or plasma oxalate levels, and genetic status as being relevant.
Secondary Outcomes
In the ILLUMINATE-A trial, secondary outcomes of absolute change in 24-hour urine oxalate, percent change in 24-hour urine oxalate:creatinine ratio, percent change in plasma oxalate, and absolute change in plasma oxalate from baseline to month 6 were analyzed using a similar MMRM model as the primary end point. The proportion of patients with 24-hour urine oxalate at or below 1.5 times ULN and at or below ULN at month 6 were analyzed using a Cochran-Mantel-Haenszel test stratified by baseline urine oxalate (at or below versus greater than 1.70 mmol/24 hour/1.73 m2). The number and percentage of patients, odds ratio, 95% CI, and P values were reported. The differences in proportion of responders and their 95% CIs, which were calculated using the Newcombe method based on the Wilson score, were reported. Continuous data were presented using descriptive statistics, LSMs, and SEs. Reporting for the extension period end points was limited by the data available at the cut-off date for the Clinical Study Report.
In the ILLUMINATE-B trial, the secondary outcome for the extension period (month 6 to end of study) was the percent change in spot urine oxalate:creatinine ratio from baseline for all post–month 6 visits using the efficacy analysis set. For the entire duration of study (baseline to end of study), the secondary outcomes included absolute change in spot urine oxalate:creatinine ratio and percent and absolute change in plasma oxalate from baseline for the efficacy analysis set. Descriptive statistics were presented for eGFR and the percentage of time a patient met the 1.5 times ULN threshold during the study. Counts and percentages were presented for the number of patients with urine oxalate excretion at or below 1.5 times ULN and at or below ULN.
In the ILLUMINATE-C trial, the secondary outcome for percent change from baseline in plasma oxalate AUC0 to 24 hours was calculated using the linear-trapezoidal method and the LSM and 95% CI were estimated using an MMRM model. Absolute change from baseline to month 6 for plasma oxalate, percent and absolute change from baseline to month 6 for 24-hour urine oxalate, and percent and absolute change for spot urine oxalate:creatinine ratio were analyzed using a REML-based MMRM method. Results for HRQoL instruments were summarized. The number of patients with kidney stone events, total events, and rate were calculated and reported. Continuous data were presented using descriptive statistics and categorical data were presented using counts and percentages.
Table 9: Statistical Analysis of Efficacy End Points
End point | Statistical model | Adjustment factors | Sensitivity analyses |
|---|---|---|---|
ILLUMINATE-A | |||
Percent change from baseline to month 6 for 24-hour urinary oxalate corrected for BSA | REML-based MMRM | Treatment arm (lumasiran vs. placebo), scheduled visits (months 3, 4, 5, and 6), baseline 24-hour urinary oxalate corrected for BSA level (mmol/24 hour/1.73 m2), and patient (random factor) |
|
Absolute change in 24-hour urinary oxalate from baseline to month 6 | MMRM | Treatment arm (lumasiran vs. placebo), scheduled visits (months 3, 4, 5, and 6), baseline 24-hour urinary oxalate corrected for BSA level (mmol/24 hour/1.73 m2), and patient (random factor) | None |
Percent change in 24-hour urinary oxalate:creatinine ratio from baseline to month 6 | MMRM | Treatment arm (lumasiran vs. placebo), scheduled visits (months 3, 4, 5, and 6), baseline 24-hour urine oxalate:creatinine ratio, and patient (random factor) | None |
Percent change in plasma oxalate from baseline to month 6 | MMRM | Treatment arm (lumasiran vs. placebo), scheduled visits (months 3, 4, 5, and 6), baseline plasma oxalate, and patient (random factor) | None |
Proportion of patients with 24-hour urinary oxalate ≤ 1.5 x ULN at month 6 | CMH | Baseline urinary oxalate (≤ 1.70 vs. > 1.70 mmol/24 hour/1.73 m2) | None |
Proportion of patients with 24-hour urinary oxalate ≤ ULN at month 6 | CMH | Baseline urinary oxalate (≤ 1.70 vs. > 1.70 mmol/24 hour/1.73 m2) | None |
Absolute change in plasma oxalate from baseline to month 6 | MMRM | Treatment arm (lumasiran vs. placebo), scheduled visits (months 3, 4, 5, and 6), baseline plasma oxalate, and patient (random factor) | None |
ILLUMINATE-B | |||
Percent change in spot urinary oxalate:creatinine ratios from baseline to the mean across month 3 to month 6 | REML-based MMRM | Scheduled visits and baseline spot urine oxalate:creatinine ratio value (mmol/mmol), and patient (random factor) |
|
ILLUMINATE-C | |||
Percent change in plasma oxalate (Cohort A) or predialysis plasma oxalate (Cohort B) from baseline to month 6 | REML-based MMRM | Scheduled visits and baseline plasma oxalate value (μmol/L), patient (random factor) | Same as primary analysis but by cohorts in safety analysis set |
Percent change from baseline in plasma oxalate AUC (0 to 24 hours) | MMRM | Scheduled visits and baseline plasma oxalate value (μmol/L), patient (random factor) | None |
Absolute change from baseline to month 6 for plasma oxalate | REML-based MMRM | Scheduled visits and baseline plasma oxalate value (μmol/L), patient (random factor) | None |
Percent and absolute change from baseline to month 6 for 24-hour urinary oxalate | REML-based MMRM | Scheduled visits and baseline plasma oxalate value (μmol/L), patient (random factor) | None |
Percent and absolute change for spot urinary oxalate:creatinine ratio | REML-based MMRM | Scheduled visits and baseline plasma oxalate value (μmol/L), patient (random factor) | None |
AUC = area under the curve; BSA = body surface area; CMH = Cochran-Mantel-Haenszel; MMRM = Mixed-Effect Model Repeated Measures; REML = restricted maximum likelihood; ULN = upper limit of normal.
Source: ILLUMINATE-A Clinical Study Report,12 ILLUMINATE-B Clinical Study Report,13 ILLUMINATE-C Clinical Study Report.14
Analysis Populations
ILLUMINATE-A Trial
The FAS included all randomized patients who received any study drug and was used to assess efficacy end points during the DB period. Patients were analyzed according to the treatment to which they were randomized.
The safety analysis set included all patients who received any study drug and was used to assess safety end points. Patients were analyzed according to the treatment they received.
The PK analysis set included all patients who received any study drug and have at least 1 PK concentration measurement and was used to assess PK end points.
The all lumasiran–treated set included all patients who received any lumasiran (both patients randomized to lumasiran and patients who crossed over from placebo to lumasiran). Long-term efficacy and safety were assessed using the all lumasiran–treated set.
The plasma oxalate analysis set included all patients who received any study drug and had a baseline plasma oxalate level of at least 1.5 times the lower limit of quantitation (LLOQ; 5.55 μmol/L) and was used to assess plasma oxalate end points.
ILLUMINATE-B Trial
The efficacy analysis set included all patients who received any lumasiran and have at least 1 valid spot urine oxalate:creatinine value at baseline and from assessments at months 3 to 6.
The PK analysis set included all patients who received a full dose of lumasiran and have at least 1 postdose blood sample for PK parameters and have evaluable PK data.
The safety analysis set included all patients who received any lumasiran and was used to assess safety end points.
ILLUMINATE-C Trial
The FAS included all randomized patients who received any lumasiran, have at least 1 evaluable plasma oxalate value (predialysis in Cohort B) at baseline, and have at least 1 evaluable plasma oxalate value from assessments at months 3 through 6. The FAS was used to assess efficacy end points.
The safety analysis set included all patients who received any lumasiran. The safety analysis set was used to assess safety end points and the sensitivity analysis of efficacy.
The PK analysis set included all patients who received any lumasiran, have at least 1 postdose blood sample for PK parameters, and have evaluable PK data. The PK analysis set was used to assess PK end points.
Results
Patient Disposition
Patient disposition is summarized in Table 10.
In the ILLUMINATE-A trial, 52 individuals were screened, of whom 13 were screened out based on eligibility criteria and withdrawal by the individual. The resulting 39 patients were randomized to lumasiran (N = 29) or placebo (N = 13). All but 1 patient in the lumasiran group (96.2%) and all patients in the placebo group completed the month 6 visit. Two (7.7%) patients in the lumasiran group discontinued the study drug due to fatigue and disturbance in attention and parent/caregiver choice. One (3.8%) patient withdrew from the study due to parent/caregiver choice. All but 2 patients (92.3%) in the lumasiran group and all patients in the placebo group entered the OLE.
In the ILLUMINATE-B trial, the number of individuals screened was not reported, although 18 patients participated: 3 weighing less than 10 kg, 12 weighing between 10 and 20 kg, and 3 weighing more than 20 kg. All patients completed the month 6 visit and entered the OLE. There were no discontinuations or withdrawals from the 6-month primary analysis period.
Similarly, in the ILLUMINATE-C trial, the screening numbers were not reported but 21 patients participated: 6 in Cohort A (no dialysis) and 15 in Cohort B (on dialysis). All patients completed the month 6 visit and entered the OLE. ███ (████%) patients discontinued treatment and █ (███%) withdrew from the study, all due to █████████ ██████████ █████, which was considered an AE.
Patient disposition | ILLUMINATE-A | ILLUMINATE-B | ILLUMINATE-C | ||||
|---|---|---|---|---|---|---|---|
Placebo | Lumasiran | < 10 kg | 10 to < 20 kg | ≥ 20 kg | Cohort A: no dialysis | Cohort B: dialysis | |
Screened, N | 52 | NR | NR | ||||
Primary analysis period | |||||||
Participants,a N (%) | 13 (100) | 26 (100) | 3 (100) | 12 (100) | 3 (100) | 6 (100) | 15 (100) |
Completed month 6 visit, n (%) | 13 (100) | 25 (96.2) | 3 (100) | 12 (100) | 3 (100) | 6 (100) | 15 (100) |
Discontinued study drug, n (%) | 0 | 2 (7.7) | 0 | 0 | 0 | 0 | █ (████) |
Adverse event | 0 | 1 (3.8) | 0 | 0 | 0 | 0 | █ (████) |
Other | 0 | 1 (3.8) | 0 | 0 | 0 | 0 | █ |
Withdrew from study, n (%) | 0 | 1 (3.8) | 0 | 0 | 0 | 0 | █ (███) |
Parent/guardian stopped patient’s participation | 0 | 1 (3.8) | 0 | 0 | 0 | 0 | █ |
Adverse event | 0 | 0 | 0 | 0 | 0 | 0 | █ (███) |
Extension periodb | |||||||
Entered OLE, n (%) | 13 (100.0) | 24 (92.3) | 3 (100) | 12 (100) | 3 (100) | 6 (100) | 15 (100) |
Discontinued study drug, n (%) | 0 | 0 | 0 | 0 | 0 | 0 | █ (█████ |
Withdrew from study, n (%) | 0 | 0 | 0 | 0 | 0 | 0 | █ (███) |
Analysis sets | |||||||
FAS, N (%) | 13 (100) | 26 (100) | 3 (100) | 12 (100) | 3 (100) | 6 (100.0) | 15 (100.0) |
Safety analysis set, N (%) | 13 (100) | 26 (100) | 3 (100) | 12 (100) | 3 (100) | 6 (100.0) | 15 (100.0) |
PK analysis set, N (%) | 13 (100) | 26 (100) | 3 (100) | 12 (100) | 3 (100) | 6 (100.0) | 15 (100.0) |
All lumasiran–treated set, N (%) | 13 (100) | 26 (100) | NA | NA | NA | NA | NA |
Plasma oxalate analysis set, N (%) | 10 (76.9) | 23 (88.5) | NA | NA | NA | NA | NA |
FAS = full analysis set; NA = not applicable; NR = not reported; OLE = open-label extension; PK = pharmacokinetic.
aIn ILLUMINATE-A, patients were randomized 2:1 to receive either lumasiran or placebo.
bIn ILLUMINATE-A, patients randomized to placebo began lumasiran treatment after the 6-month DB primary analysis period.
Source: ILLUMINATE-A Clinical Study Report,12 ILLUMINATE-B Clinical Study Report,13 ILLUMINATE-C Clinical Study Report.14
Exposure to Study Treatments
Exposure to study treatments is summarized in Table 11.
In the ILLUMINATE-A trial, the mean duration of treatment was ████ months (range, ███ to ████ months) in the lumasiran group and ████ months (range, ████ to ████ months) in the placebo group. Most patients (████%) had at least 18 months of treatment on lumasiran and █ patients (████%) had at least 24 months of exposure.
In the ILLUMINATE-B trial, the mean duration of treatment was about ████ months for all weight groups (range, ████ to ████ months). ████ of the patients had at least 18 months of treatment on lumasiran.
In the ILLUMINATE-C trial, the mean durations of treatment were ███ months (range, ███ to ███ months) for Cohort A and █████ months (range ███ to ████ months) for Cohort B. Most patients (████%) had at least 6 months of treatment on lumasiran and █ (████%) patients had at least 12 months of exposure.
Table 11: Overall Treatment Exposure — ILLUMINATE-A, ILLUMINATE-B, and ILLUMINATE-C Trials
Treatment exposure | ILLUMINATE-A All lumasiran–treated set | ILLUMINATE-B Safety analysis set | ILLUMINATE-C Safety analysis set | ||||
|---|---|---|---|---|---|---|---|
Placebo (N = 13) | Lumasiran (N = 26) | < 10 kg (N = 3) | 10 to < 20 kg (N = 12) | ≥ 20 kg (N = 3) | Cohort A: no dialysis (N = 6) | Cohort B: dialysis (N = 15) | |
Duration of lumasiran exposure (months)a | |||||||
Mean (SD) | █████ (████) | █████ (████) | █████ (████) | █████ (████) | █████ (████) | ████ (████) | █████ (████) |
Median (min, max) | █████ (████, ████) | █████ (███, ████) | █████ (████, ████) | █████ (███, ████) | ████ (███, ████) | ████ (███, ███) | ████ (███, ████) |
Number of patients (%) on lumasiran for at least | |||||||
1 day | ██ (█████) | ██ (█████) | █ (███) | ██ (███) | █ (███) | █ (█████) | ██ (█████) |
3 months | ██ (█████) | ██ (████) | █ (███) | ██ (███) | █ (███) | █ (█████) | ██ (█████) |
6 months | ██ (█████) | ██ (████) | █ (███) | ██ (███) | █ (███) | █ (████) | ██ (█████) |
9 months | ██ (█████) | ██ (████) | █ (███) | ██ (███) | █ (███) | █ (████) | █ (████) |
12 months | ██ (█████) | ██ (████) | █ (███) | ██ (███) | █ (███) | █ | █ (████) |
18 months | █ (████) | ██ (████) | █ (████) | █ (████) | █ (████) | █ | █ |
24 months | █ | █ (████) | █ | █ | █ | █ | █ |
SD = standard deviation.
aIndividual duration of exposure (months) = individual duration of treatment (days) / 30.44. Study visits and drug administration were scheduled based on 28-day intervals (e.g., month 3 visit corresponds to 85 days or 2.8 months).
Source: ILLUMINATE-A Clinical Study Report,12 ILLUMINATE-B Clinical Study Report,13 ILLUMINATE-C Clinical Study Report.14
Protocol Deviations
In the ILLUMINATE-A trial, 5 major protocol deviations were reported for 4 patients: █████████ in the lumasiran group and ████████ in the placebo group. These were related to study procedures or assessments (24-hour urine sample not valid or not collected and signed consent not properly collected) and concomitant medication (pause in stable vitamin B6 regimen [2 events for 1 patient]).
In the ILLUMINATE-B trial, █ major protocol deviations were reported for █ patients related to study procedures or assessments (signed consent not properly collected) and concomitant medication (pause in stable vitamin B6 regimen).
In the ILLUMINATE-C trial, █ major protocol deviations were reported for █ patients in Cohort B (failure to collect blood samples for plasma oxalate assessment).
Efficacy
Only those efficacy outcomes and analyses of subgroups identified in the review protocol are reported in the sections that follow. Refer to Appendix 3 for detailed efficacy data.
Kidney Function
ILLUMINATE-A Trial
Change from baseline in eGFR during the DB and extension periods were secondary outcomes and are summarized in Table 12 and Table 37, respectively. During the 6-month DB period, eGFR declined from study baseline by a mean of 2.57 mL/min/1.73 m2 (SD = 10.65 mL/min/1.73 m2) in the lumasiran group and 0.11 mL/min/1.73 m2 (SD = 6.49 mL/min/1.73 m2) in the placebo group. Data at month 18 of lumasiran treatment showed that eGFR increased by a mean of ████ mL/min/1.73 m2 (SD = ████ mL/min/1.73 m2) in the lumasiran group and decreased by a mean of ████ mL/min/1.73 m2 (SD = █████ mL/min/1.73 m2) in the placebo group.
The shift from baseline eGFR to worst postbaseline eGFR during the DB period is summarized in Table 38 and during the overall period of receiving lumasiran treatment in Table 39. During the DB period, █████████ in the placebo group decreased 1 step in eGFR category (e.g., from at least 90 mL/min/1.73 m2 at baseline to between 60 and less than 90 mL/min/1.73 m2) whereas ████████ increased 1 step during that time. In the lumasiran group, ██ patients decreased 1 step in eGFR category. During the overall period of receiving lumasiran treatment, █ patients in the placebo followed by lumasiran treatment group decreased 1 step in eGFR category while ██ decreased 1 step and █ patients decreased 2 steps in the lumasiran followed by lumasiran treatment group.
ILLUMINATE-B Trial
Change from baseline in eGFR during the study was a secondary outcome and is summarized in Table 13. By month 12 of treatment on lumasiran, eGFR increased by a mean of █████ mL/min/1.73 m2 (no SD) for 1 patient weighing less than 10 kg and decreased by a mean of ████ mL/min/1.73 m2 (SD = █████ mL/min/1.73 m2) and mean of ████ mL/min/1.73 m2 (SD = █████ mL/min/1.73 m2) in the groups of patients weighing between 10 and 20 kg and patients weighing greater than 20 kg, respectively.
The shift from baseline eGFR to worst postbaseline eGFR during the overall period of receiving lumasiran treatment is summarized in Table 40. Overall, █████████ in the 10 to less than 20 kg group decreased 1 step in eGFR category, while ████████ decreased 1 step and ████████ decreased 2 steps in the 20 kg or more group.
ILLUMINATE-C Trial
Change from baseline in eGFR during the study was a secondary outcome and is summarized in Table 14. By month 6 of treatment on lumasiran, eGFR decreased by a mean of ████ mL/min/1.73 m2 (SD = ████ mL/min/1.73 m2) in Cohort A.
The shift from baseline eGFR to worst postbaseline eGFR during the overall period of receiving lumasiran treatment is summarized in Table 41. Overall, █ patients in Cohort A decreased 1 step in eGFR category.
Table 12: Change From Baseline to Month 6 in eGFR During DB Period (Secondary Outcome): ILLUMINATE-A Trial, FAS
Outcome | ILLUMINATE-A | |
|---|---|---|
Placebo (N = 13) | Lumasiran (N = 26) | |
Baseline,a n (%) | 13 (100) | 26 (100) |
Mean eGFR (SD) (mL/min/1.73 m2) | 78.95 (26.83) | 82.97 (25.55) |
Month 6, n (%) | 13 (100) | 25 (83.3) |
Mean eGFR (SD) (mL/min/1.73 m2) | 78.83 (█████) | 78.53 (█████) |
Mean change from baseline (SD) (mL/min/1.73 m2) | –0.11 (6.49) | –2.57 (10.65) |
DB = double-blind; eGFR = estimated glomerular filtration rate; FAS = full analysis set; SD = standard deviation.
aBaseline is the last assessment before the first dose of study drug (placebo or lumasiran) in the 6-month double-blind period.
Note: The eGFR is calculated from serum creatinine based on the Modification of Diet in Renal Disease formula for patients aged at least 18 years and the Schwartz Bedside Formula for patients aged less than 18 years at screening.
Source: ILLUMINATE-A Clinical Study Report.12
Table 13: Change From Baseline in eGFR (Secondary Outcome): ILLUMINATE-B Trial, Efficacy Analysis Set
Outcome | ILLUMINATE-B | |||
|---|---|---|---|---|
< 10 kg (N = 3) | 10 to < 20 kg (N = 12) | ≥ 20 kg (N = 3) | All patients (N = 18) | |
Baseline,a n (%) | 1 (33.3) | 12 (100) | 3 (100) | 16 (88.9) |
Mean eGFR (SD) (mL/min/1.73 m2) | ██████ (NA) | ██████ (█████) | █████ (█████) | 112.80 (27.63) |
Month 6, n (%) | 1 (33.3) | 12 (100) | 3 (100) | 16 (88.9) |
Mean eGFR (SD) (mL/min/1.73 m2) | ██████ (█████) | ██████ (█████) | █████ (█████) | ██████ (█████) |
Mean change from baseline (SD) (mL/min/1.73 m2) | ██████ (NA) | ████ (█████) | ████ (████) | █████ (█████) |
Month 12, n (%) | 1 (33.3) | 12 (100) | 3 (100) | 16 (88.9) |
Mean eGFR (SD) (mL/min/1.73 m2) | ██████ (█████) | ██████ (█████) | █████ (█████) | ██████ (█████) |
Mean change from baseline (SD) (mL/min/1.73 m2) | █████ (NA) | █████ (█████) | █████ (█████) | █████ (█████) |
eGFR = estimated glomerular filtration rate; NA = not applicable; SD = standard deviation.
aBaseline is the last nonmissing value collected before the first dose of lumasiran.
Note: The eGFR is calculated based on the Schwartz Bedside Formula in patients aged at least 12 months at the time of the assessment.
Source: ILLUMINATE-B Clinical Study Report.13
Table 14: Change From Baseline in eGFR (Secondary Outcome): ILLUMINATE-C Trial, FAS
Outcome | ILLUMINATE-C |
|---|---|
Cohort A: no dialysis (N = 6) | |
Baseline,a n (%) | 5 (83.3) |
Mean eGFR (SD) (mL/min/1.73 m2) | 19.85 (9.64) |
Month 3, n (%) | 5 (83.3) |
Mean eGFR (SD) (mL/min/1.73 m2) | █████ (████) |
Mean change from baseline (SD) (mL/min/1.73 m2) | █████ (████) |
Month 6, n (%) | 5 (83.3) |
Mean eGFR (SD) (mL/min/1.73 m2) | 16.43 (9.82) |
Mean change from baseline (SD) (mL/min/1.73 m2) | █████ (████) |
eGFR = estimated glomerular filtration rate; FAS = full analysis set; SD = standard deviation.
aBaseline is defined as last nonmissing value collected before the first dose of lumasiran.
Note: The eGFR is calculated in patients aged at least 12 months at the time of the assessment.
Loss of kidney function over time and prevention of dialysis and/or liver-kidney transplant were not assessed in the trials.
Source: ILLUMINATE-C Clinical Study Report.14
Kidney Stone Events
ILLUMINATE-A Trial
Kidney stone events was an exploratory outcome and is summarized in Table 15 for the DB period. Five (19.2%) patients in the lumasiran group experienced 13 kidney stone events and 2 (15.2%) patients in the placebo group experienced 4 kidney stone events. Some events were graded as moderate severity (████% for the lumasiran group and ████% for the placebo group) and the rest were mild. The rate of events was 0.30 and 0.18 events per 100 person-days for the lumasiran and placebo groups, respectively.
Rates of kidney stone events per person-year by time period are summarized in Table 42. During the 12 months before informed consent, the rate was 3.19 events per person-year (95% CI, 2.57 to 3.96 events per person-year) for the lumasiran followed by lumasiran treatment group and 0.54 events per person-year (95% CI, 0.26 to 1.13 events per person-year) for the placebo followed by lumasiran treatment group. The rate of events generally appeared to decrease in the lumasiran followed by lumasiran treatment group from 1.09 events per person-year (95% CI, 0.63 to 1.88 events per person-year) between day 1 and month 6 to 0.63 events per person-year (95% CI, 0.30 to 1.33 events per person-year) between months 18 and 24 of lumasiran treatment. In the placebo followed by lumasiran treatment group, rates appeared to fluctuate over the same period and remained less than 1 event per person-year.
ILLUMINATE-B Trial
Kidney stone events was an exploratory outcome and is summarized in Table 16. In total, █ patients had 1 kidney stone event each (████ ████████████████████ ███) and ███ events were graded as mild severity. The rate of events was 0.11 renal stone events per person-year for the whole group.
ILLUMINATE-C Trial
Kidney stone events was a secondary outcome and is summarized in Table 17. ███ patients in Cohort A had a total of █ kidney stone events and ███ events were graded as mild severity. The rate of events was 1.52 renal stone events per person-year for Cohort A.
Table 15: Kidney Stone Events During DB Period (Exploratory Outcome): ILLUMINATE-A Trial, FAS
Outcome | ILLUMINATE-A | |
|---|---|---|
Placebo (N = 13) | Lumasiran (N = 26) | |
Patients with at least 1 kidney stone event, n (%) | 2 (15.4) | 5 (19.2) |
Patients with the following number of kidney stone events (%): | NA | NA |
0 | ██ (████) | ██ (████) |
1 | █ (███) | █ (███) |
2 to 5 | █ (███) | █ (████) |
Total number of kidney stone events, n | 4 | 13 |
Severity of event: | NA | NA |
Mild | █ (████) | ██ (████) |
Moderate | █ (████) | █ (████) |
Number of kidney stone events meeting at least 1 of the criteria: | NA | NA |
Visit to health care provider | █ | █ |
Medication for renal colic | █ | █ |
Stone passage | █ | ██ |
Macroscopic hematuria | █ | █ |
Rate of renal stone events per 100 person-days for patients reporting any events: (95% CI)a | 0.18 (0.07 to 0.48) | 0.30 (0.17 to 0.51) |
DB = double-blind; CI = confidence interval; FAS = full analysis set; NA = not applicable.
aRate is calculated as total number of renal stone events divided by total person-days at risk, defined as time from first dose to end of the DB period.
Source: ILLUMINATE-A Clinical Study Report.12
Table 16: Kidney Stone Events During the Overall Period of Receiving Lumasiran Treatment (Exploratory Outcome): ILLUMINATE-B Trial, Efficacy Analysis Set
Outcome | ILLUMINATE-B | |||
|---|---|---|---|---|
< 10 kg (N = 3) | 10 to < 20 kg (N = 12) | ≥ 20 kg (N = 3) | All patients (N = 18) | |
Patients with at least 1 kidney stone event, n (%) | █ (████) | █ (███) | █ (████) | 3 (16.7) |
Patients with the following number of kidney stone events (%) | NA | NA | NA | NA |
0 | █ (████) | ██ (████) | █ (████) | ██ (████) |
1 | █ (████) | █ (███) | █ (███) | █ (████) |
Total number of kidney stone events, n | █ | █ | █ | 3 |
Severity of event: | NA | NA | NA | NA |
Mild | █ (████) | █ (███) | █ (████) | █ (████) |
Number of kidney stone events meeting at least 1 of the criteria: | NA | NA | NA | NA |
Visit to health care provider | █ | █ | █ | █ |
Medication for renal colic | █ | █ | █ | █ |
Stone passage | █ | █ | █ | █ |
Macroscopic hematuria | █ | █ | █ | █ |
Rate of renal stone events per person-year during lumasiran treatment (95% CI)a | ████ (████, ████) | ████ (████, ████) | ████ (████, ████) | 0.11 (████, ████) |
CI = confidence interval; NA = not applicable.
aRate is calculated as total number of renal stone events divided by total person-years during the respective period. The 95% CI for the event rate was obtained using a generalized linear model for a Poisson distribution unless the rate was 0, in which case the upper bound of the 95% CI was calculated using the exact Poisson method.
Source: ILLUMINATE-B Clinical Study Report.13
Table 17: Kidney Stone Events During the Overall Period of Receiving Lumasiran Treatment (Secondary Outcome): ILLUMINATE-C Trial, FAS
Outcome | ILLUMINATE-C | |
|---|---|---|
Cohort A: no dialysis (N = 6) | Cohort B: dialysis (N = 15) | |
Patients with at least 1 kidney stone event, n (%) | █ (████) | █ |
Patients with the following number of kidney stone events (%) | NA | NA |
0 | █ (████) | ██ (█████) |
1 | █ | █ |
2 to 5 | █ (████) | █ |
Total number of kidney stone events, n | █ | █ |
Severity of event: | NA | NA |
Mild | █ (███) | █ |
Number of kidney stone events meeting at least 1 of the criteria: | NA | NA |
Visit to health care provider | █ | █ |
Medication for renal colic | █ | █ |
Stone passage | █ | █ |
Macroscopic hematuria | █ | █ |
Rate of renal stone events per person-year during lumasiran treatmenta (95% CI) | 1.52 (████, ████) | ████ (████, ████) |
CI = confidence interval; FAS = full analysis set; NA = not applicable.
aRate is calculated as total number of renal stone events divided by total patient-years during the respective period. The 95% CI for the event rate was obtained using a generalized linear model for a Poisson distribution unless the rate was 0, in which case the upper bound of the 95% CI was calculated using the exact Poisson method.
Source: ILLUMINATE-C Clinical Study Report.14
Health-Related Quality of Life
ILLUMINATE-A Trial
The KDQOL and PedsQL results were captured for patients aged at least 18 years and younger than 18 years, respectively, and are summarized in Table 18 and Table 43 for the DB and extension periods, respectively. The EQ-5D-5L and EQ-5D-Y results (data not presented) were captured for the same age cut-offs, respectively, and the VAS results are summarized in Table 19 and Table 44 for the DB and extension periods, respectively. Results for HRQoL were exploratory outcomes.
Kidney Disease Quality of Life Questionnaire
During the DB period, mean scores on the SF-12 PCS █████████ from baseline by ████ points (SD = ████ points) by month 6 and █████████ by ████ points (SD = ████ points) for the lumasiran and placebo groups, respectively. Mean scores on the SF-12 MCS █████████ from baseline by ████ points (SD = █████ points) and █████████ by ████ points (SD = ████ points) for the lumasiran and placebo groups, respectively. Mean scores on the symptoms/problems subscale █████████ from baseline by █████ points (SD = █████ points) and █████████ by ████ points (SD = █████ points) for the lumasiran and placebo groups, respectively. Mean scores on the effects of kidney disease subscale █████████ from baseline by ████ points (SD = ████ points) and █████████ by ████ points (SD = █████ points) for the lumasiran and placebo groups, respectively. Mean scores on the burden of kidney disease (BKD) subscale █████████ from baseline by ████ points (SD = █████ points) and █████████ by ████ points (SD = █████ points) for the lumasiran and placebo groups, respectively.
Data at month 18 for the KDQOL showed mean scores for SF-12 PCS and MCS generally appeared to ████████ and kidney-specific subscales appeared to █████ ████████████████████ ██████ ███ ████. Mean scores at month 18 did not differ by more than ██ points between placebo followed by lumasiran and lumasiran followed by lumasiran treatment groups.
Pediatric Quality of Life Inventory
During the DB period, mean physical functioning scores █████████ from baseline by ████ points (SD = ████ points) and █████████ by ████ points (SD = █████ points) for the lumasiran and placebo groups, respectively. Mean psychosocial health summary scores █████████ from baseline by ████ points (SD = █████ points) and █████████ by ████ points (SD = ████ points) for the lumasiran and placebo groups, respectively. Mean total scores █████████ from baseline by ████ points (SD = █████ points) and █████████ by ████ points (SD = ████ points) for the lumasiran and placebo groups, respectively. Mean ESRD total score – patient █████████ from baseline by ███ points (SD = █████ points) and █████████ by ███ points (SD = ████ points) for the lumasiran and placebo groups, respectively. Mean ESRD total score – caregiver █████████ from baseline by ███ points (SD = █████ points) and █████████ by ████ points (SD = █████ points) for the lumasiran and placebo groups, respectively.
Data at month 18 for the PedsQL showed the mean physical functioning score generally seemed to █████ ███, Psychosocial Health Summary Score appeared to █████████ ██████████, and total score appeared to ██ ██████ ███████████ for the lumasiran followed by lumasiran treatment group and ████ ████████ for the placebo followed by lumasiran treatment group. The ESRD total score – patient seemed to ███ ████████████████ for the lumasiran followed by lumasiran treatment group and ███ █████ ████ for the placebo followed by lumasiran treatment group, while the ESRD total score – caregiver score generally appeared to ███████ for both groups. Only the mean ESRD total score – patient at month 18 differed by more than ██ points between placebo followed by lumasiran and lumasiran followed by lumasiran treatment groups.
EQ-5D-5L, EQ-5D-Y, and VAS
During the DB period, adults who completed the EQ-5D-5L ████ █████ ██████████████ ████████████████ ███ ████ █████████ ██████████████ ████ █████████ ████ ███ █ ███████ ████████████ ████████████ ██████ █████████ ██████████ ██████ ██ ██████████ ████████████ ████████████████ █████ █████████████████ ██████████ ████████ ███ ███████████ ██████ █████████ ██████████████████. Long-term results were consistent with those observed during the DB period.
During the DB period, most pediatric patients who completed the EQ-5D-Y █████ █████ ███████ ██████████ ███ █████ ██ ████ ███ ██████████ ██████ ██████████████ ██ ██████ █ █ ██████ █████ ████ ███ ███ ████████████ █ ███████████████ ███ ██ ████ █████████ █████████ ████ ██████ ██ ██ █████ ███ ███ ███████ █ ███████████ ██████ ████████████████ ███ █████ ████████████ ██ █████ ██████ █████ ██ █████████ ██████ ██ ██████████ ██████ ██████ ███ ████ █████ ████. Long-term results were generally consistent with those observed during the DB period.
During the DB period, VAS scores appeared to ████████ from baseline by ███ (SD = █████) in the lumasiran group and ████████ by ███ (SD = ████) in the placebo group. Data at month 18 showed that mean scores seemed to █████████ and were generally consistent with the results from the DB period. Results at month 18 appeared to be similar between groups.
ILLUMINATE-B Trial
HRQoL was not captured in the trial.
ILLUMINATE-C Trial
No information for HRQoL has been presented in the CADTH report due to the small number of patients who completed each questionnaire based on age and therefore meaningful conclusions could not be drawn from the results.
Table 18: Change in KDQOL and PedsQL During DB Period (Exploratory Outcome): ILLUMINATE-A Trial, FAS
Outcome | ILLUMINATE-A | |
|---|---|---|
Time point | Placebo (N = 13) | Lumasiran (N = 26) |
KDQOL-36 (≥ 18 years) | ||
SF-12 PCS | N = █ | N = ██ |
Baseline, n (%) | ██████ | ████████ |
Mean (SD) | ███████████ | ███████████ |
Month 6, n (%) | ██████ | ████████ |
Change from baseline, mean (SD) | ██████████ | ███████████ |
SF-12 MCS | N = █ | N = ██ |
Baseline, n (%) | ██████ | ████████ |
Mean (SD) | ███████████ | ████████████ |
Month 6, n (%) | ██████ | ███████ |
Change from baseline, mean (SD) | █████ ██████ | ███████████ |
Symptoms/problems | N = █ | N = ██ |
Baseline, n (%) | ██████ | ████████ |
Mean (SD) | ████████████ | ████████████ |
Month 6, n (%) | ██████ | ████████ |
Change from baseline, mean (SD) | ███████████ | ████████████ |
Effects of kidney disease | N = █ | N = ██ |
Baseline, n (%) | ██████ | ████████ |
Mean (SD) | ███████████ | ████████████ |
Month 6, n (%) | █████ | ████████ |
Change from baseline, mean (SD) | ████████████ | ██████████ |
Burden of kidney disease | N = █ | N = ██ |
Baseline, n (%) | ██████ | ███████ |
Mean (SD) | ███████████ | ████████████ |
Month 6, n (%) | ██████ | ███████ |
Change from baseline, mean (SD) | ███████████ | ███████████ |
PedsQL (< 18 years) | ||
Physical functioning | N = █ | N = ██ |
Baseline, n (%) | ███████ | ███████ |
Mean (SD) | ████████████ | ████████████ |
Month 6, n (%) | ███████ | ████████ |
Change from baseline, mean (SD) | ███████████ | ███████████ |
Psychosocial health summary score | N = █ | N = ██ |
Baseline, n (%) | ███████ | ████████ |
Mean (SD) | ████████████ | ████████████ |
Month 6, n (%) | ███████ | ████████ |
Change from baseline, mean (SD) | ██████████ | ███████████ |
Total score | N = █ | N = ██ |
Baseline, n (%) | ███████ | ████████ |
Mean (SD) | ████████████ | ████████████ |
Month 6, n (%) | ███████ | ████████ |
Change from baseline, mean (SD) | ██████████ | ███████████ |
ESRD total score: patient | N = █ | N = ██ |
Baseline, n (%) | ███████ | ████████ |
Mean (SD) | ██████████ | ███████████ |
Month 6, n (%) | ███████ | ███████ |
Change from baseline, mean (SD) | ██████████ | ██████████ |
ESRD total score: caregiver | N = █ | N = ██ |
Baseline, n (%) | ██████ | ████████ |
Mean (SD) | ███████████ | ███████████ |
Month 6, n (%) | ███████ | ███████ |
Change from baseline, mean (SD) | ███████████ | ███████████ |
DB = double-blind; ESRD = end-stage renal disease; FAS = full analysis set; KDQOL-36 = Kidney Disease Quality of Life Questionnaire-36; MCS = mental component summary; PCS = physical component summary; PedsQL = Pediatric Quality of Life Inventory; SD = standard deviation; SF-12 = Short Form-12.
Source: ILLUMINATE-A Clinical Study Report.12
Table 19: Change in EQ VAS During DB Period (Exploratory Outcome): ILLUMINATE-A Trial, FAS
Outcome | ILLUMINATE-A | |
|---|---|---|
Time point | Placebo (N = 13) | Lumasiran (N = 26) |
Baseline, n (%) | ████████ | ████████ |
Mean (SD) | ███████████ | ███████████ |
Month 6, n (%) | ████████ | ███████ |
Mean (SD) | ███████████ | ███████████ |
Change from baseline, mean (SD) | ██████████ | █████████ |
DB = double-blind; EQ = EuroQol; FAS = full analysis set; SD = standard deviation; VAS = visual analogue scale.
Source: ILLUMINATE-A Clinical Study Report.12
Urine Oxalate Levels
ILLUMINATE-A Trial
Percent change from baseline to month 6 in 24-hour urine oxalate corrected for BSA was the primary outcome in the trial and is summarized in Table 20. The LSM percent change from baseline to the average of months 3 to 6 was –65.39% (95% CI, –71.32% to –59.45%) for the lumasiran group and –11.84% (95% CI, –19.53% to –4.15%) for the placebo group. The treatment difference between groups was –53.55% (95% CI, –62.31% to –44.78%; P < 0.001). The results of the 2 sensitivity analyses supported the primary outcome. Subgroup analyses for the primary outcome are summarized in Figure 2. Treatment estimates for subgroups of age, kidney function (baseline eGFR), and baseline urine oxalate level, which were identified as subgroups of interest in the CADTH systematic review protocol, indicated a benefit with lumasiran over placebo and were consistent with the overall analysis.
Absolute change from baseline to month 6 in 24-hour urine oxalate corrected for BSA was a secondary outcome in the trial and is summarized in Table 20. The LSM absolute change from baseline to the average of months 3 to 6 was –1.24 mmol/24 hour/1.73 m2 (95% CI, –1.37 to –1.12 mmol/24 hour/1.73 m2) for the lumasiran group and –0.27 mmol/24 hour/1.73 m2 (95% CI, –0.44 to –0.10 mmol/24 hour/1.73 m2). The treatment difference between groups was –0.98 mmol/24 hour/1.73 m2 (95% CI, –1.18 to –0.77 mmol/24 hour/1.73 m2; P < 0.001).
The proportion of patients with 24-hour urine oxalate corrected for BSA at or less than 1.5 times ULN and at or less than the ULN at month 6 were secondary outcomes and are summarized in Table 21. In the lumasiran group, 84% (95% CI, 64% to 95%) of patients had a 24-hour urine oxalate measure at month 6 that was at or less than 1.5 times ULN, while no patients in the placebo group achieved this. The difference in proportions was 0.84 (95% CI, 0.55 to 0.94; P < 0.001). In the lumasiran group, 52% (95% CI, 31% to 72%) of patients had a 24-hour urine oxalate measure at month 6 that was at or less than the ULN, while no patients in the placebo group achieved this. The difference in proportions was 0.52 (95% CI, 0.23 to 0.70; P = 0.0010).
Absolute and percent change from baseline in 24-hour urine oxalate corrected for BSA were secondary outcomes for the extension period and are summarized in Table 45. Data from treatment on lumasiran indicated decreases in 24-hour urine oxalate at month 6 that appeared to be maintained for both lumasiran followed by lumasiran and placebo followed by lumasiran treatment groups to month 18.
ILLUMINATE-B Trial
Urine oxalate assessments were based on urine oxalate:creatinine ratios and are described later in the report.
ILLUMINATE-C Trial
Absolute and percent change from baseline in 24-hour urine oxalate corrected for BSA was a secondary outcome and is summarized in Table 22 for Cohort A. Patients who were anuric were not assessed. The LSM absolute change from baseline to the average of months 3 to 6 was –0.53 mmol/24 hour/1.73 m2 (95% CI, –0.89 to –0.18 mmol/24 hour/1.73 m2). The LSM percent change from baseline to the average of months 3 to 6 was –10.56% (95% CI, –31.99% to 10.87%).
Table 20: Change From Baseline to Month 6 in 24-Hour Urine Oxalate Corrected for BSA (Primary and Secondary Outcomes): ILLUMINATE-A Trial, FAS
Outcome | ILLUMINATE-A | |
|---|---|---|
Placebo (N = 13) | Lumasiran (N = 26) | |
Baseline,a n (%) | 13 (100) | 26 (100) |
Mean (SEM) (mmol/24 hour/1.73 m2) | 1.79 (0.19) | 1.84 (0.12) |
Mean of months 3 to 6 | NA | NA |
Change from baseline to average of months 3 to 6, LSM (SEM) (mmol/24 hour/1.73 m2) (95% CI)b | –0.27 (0.08) (–0.44 to –0.10) | –1.24 (0.06) (–1.37 to –1.12) |
LSM (SEM) treatment group difference (lumasiran – placebo) (mmol/24 hour/1.73 m2)b (95% CI)b | Reference | –0.98 (0.10) (–1.18, –0.77) |
P valueb,c | Reference | < 0.001 |
Percent change from baseline to average of months 3 to 6, LSM (SEM) (95% CI)b | –11.84 (3.81) (–19.53 to –4.15) | –65.39 (2.94) (–71.32 to –59.45) |
LSM (SEM) treatment group difference (lumasiran – placebo) (mmol/24 hour/1.73 m2)b (95% CI)b | Reference | –53.55 (4.32) (–62.31 to –44.78) |
P valueb,c | Reference | < 0.001 |
BSA = body surface area; CI = confidence interval; FAS = full analysis set; LSM = least squares mean; NA = not applicable; SEM = standard error of the mean.
aBaseline is the median of all valid 24-hour urine assessments collected before the first dose date/time of study drug (lumasiran or placebo) without any nonprotocol-related sample issues.
bBased on Mixed-Effect Model Repeated Measures model with the corresponding value at baseline as a continuous fixed covariate, visit, and treatment as fixed effects, and patient as a random effect. Visit is fitted as a categorical variable, and the variance-covariance matrix is assumed to be unstructured. Satterthwaite approximation is used to estimate denominator degrees of freedom. A difference less than 0 represents a favourable outcome for lumasiran.
cP value has been adjusted for multiple testing (i.e., the type I error rate has been controlled).
Source: ILLUMINATE-A Clinical Study Report.12
Table 21: 24-Hour Urine Oxalate Corrected for BSA at Month 6 ≤ 1.5 × ULN or ≤ ULN (Secondary Outcome): ILLUMINATE-A Trial, FAS
Outcome | ILLUMINATE-A | |
|---|---|---|
Placebo (N = 13) | Lumasiran (N = 26) | |
Number of patients contributing to the analysis, n (%) | 13 (100) | 25 (96.2) |
Number of patients with ≤ 1.5 x ULN | 0 | 21 |
Proportion of patients with ≤ 1.5 x ULN (95% CI)a | 0.00 (0.00, 0.25) | 0.84 (0.64, 0.95) |
Difference in proportions (95% CI)b | Reference | 0.84 (0.55, 0.94) |
P valuec,d | Reference | < 0.001 |
Number of patients with ≤ ULN | 0 | 13 |
Proportion of patients with ≤ ULN (95% CI)a | 0.00 (0.00, 0.25) | 0.52 (0.31, 0.72) |
Difference in proportions (95% CI)b | Reference | 0.52 (0.23, 0.70) |
P valuec,d | Reference | 0.0010 |
BSA = body surface area; CI = confidence interval; FAS = full analysis set; ULN = upper limit of normal.
aClopper Pearson exact confidence interval.
bCalculated using the Newcombe method based on the Wilson score.
cP value is based on the Cochran-Mantel-Haenszel test stratified by baseline 24-hour urine oxalate corrected for BSA (less than or equal to 1.70 vs. greater than 1.70 mmol/24 hour/1.73 m2).
dP value has been adjusted for multiple testing (i.e., the type I error rate has been controlled).
Source: ILLUMINATE-A Clinical Study Report.12
Table 22: Change From Baseline in 24-Hour Urine Oxalate Corrected for BSA (Secondary Outcome): ILLUMINATE-C Trial, FAS
Outcome | ILLUMINATE-C |
|---|---|
Cohort A – no dialysis (N = 6) | |
Baseline,a n (%) | 5 (83.3) |
Mean (SD) (mmol/24 hour/1.73 m2) | ████ (████) |
Month 3 | NA |
Change from baseline, LSM (SEM) (mmol/24 hour/1.73 m2)b (95% CI) | █████ (████) ██████, █████) |
Percent change from baseline, LSM (SEM)b (95% CI) | █████ (████) (██████, █████) |
Month 6 | NA |
Change from baseline, LSM (SEM) (mmol/24 hour/1.73 m2)b (95% CI) | █████ (████) (█████, █████) |
Percent change from baseline, LSM (SEM)b (95% CI) | ██████ (████) (██████, ████) |
Mean of months 3 to 6 | NA |
Change from baseline, LSM (SEM) (mmol/24 hour/1.73 m2)b (95% CI) | –0.53 (0.11) (–0.89 to –0.18) |
Change from baseline, P valueb,c | ██████ |
Percent change from baseline, LSM (SEM)b (95% CI) | –10.56 (6.81) (–31.99 to 10.87) |
Percent change from baseline, P valueb,c | ██████ |
BSA = body surface area; CI = confidence interval; FAS = full analysis set; LSM = least squares mean; NA = not applicable; SD = standard deviation; SEM = standard error of the mean.
aBaseline is defined as the median of all valid 24-hour urine assessments collected before the first dose date or time of lumasiran without any nonprotocol-related sample issues.
bBased on the restricted maximum likelihood–based Mixed-Effect Model Repeated Measures model to test against the null hypothesis of mean change from baseline outcome being equal to 0. The model includes scheduled visits and baseline 24-hour urine oxalate corrected for BSA (mmol/24 hour/1.73 m2) as fixed effects and patient as a random factor. Autoregressive (1) was used to model the within-patient variability.
cP value has not been adjusted for multiple testing (i.e., the type I error rate has not been controlled).
Source: ILLUMINATE-C Clinical Study Report.14
Plasma Oxalate Levels
ILLUMINATE-A Trial
The plasma oxalate analysis set was used and included only patients who had a baseline plasma oxalate measurement of at least 1.5 times LLOQ. Patients who had a postbaseline measurement less than the LLOQ were assigned a value of 5.55 µmol/L (the LLOQ). Percent and absolute changes from baseline to month 6 in plasma oxalate were secondary outcomes in the trial and are summarized in Table 23. The LSM absolute change from baseline to the average of months 3 to 6 was –7.46 µmol/L (95% CI, –9.03 to –5.90 µmol/L) for the lumasiran group and 1.25 µmol/L (95% CI, –1.04 to 3.54 µmol/L) for the placebo group. The treatment difference between groups was –8.71 µmol/L (95% CI, –11.45 to –5.98 µmol/L; P < 0.001). The LSM percent change from baseline to the average of months 3 to 6 was –39.80% (95% CI, –45.81% to –33.80%) for the lumasiran group and –0.32% (95% CI, –9.12% to 8.48%) for the placebo group. The treatment difference between groups was –39.48% (95% CI, –50.10% to –28.87%; P < 0.001).
ILLUMINATE-B Trial
Absolute and percent changes from baseline in plasma oxalate were secondary outcomes and are summarized in Table 24. The mean absolute change from baseline at month 6 was ██████ µmol/L (SD = ████ µmol/L), █████ µmol/L (SD = ████ µmol/L), and █████ µmol/L (SD = ████ µmol/L) for the 3 weight groups by increasing weight, respectively. The mean percent change from baseline at month 6 was ██████% (SD = █████%), ██████% (SD = █████%), and ██████% (SD = █████%) for the 3 weight groups by increasing weight, respectively. Data from the extension period indicated that decreases in plasma oxalate at month 6 appeared to be maintained for patients across all weight groups to month 18.
ILLUMINATE-C Trial
Percent change from baseline to month 6 in plasma oxalate was the primary outcome and is summarized in Table 25. The LSM percent change from baseline to the average of months 3 to 6 was –33.33% (95% CI, –81.82% to 15.16%) for Cohort A and –42.43% (95% CI, –50.71% to –34.15%) for Cohort B. The results of the sensitivity analysis supported the primary outcome. Due to the small sample size in Cohort A, subgroup analyses by age groups were performed for Cohort B only. Subgroup treatment estimates by age group indicated a benefit with lumasiran over placebo, though patient numbers were small.
Absolute change from baseline to month 6 in plasma oxalate was the secondary outcome and is summarized in Table 25. The LSM absolute change from baseline to the average of months 3 to 6 was –35.28 µmol/L (95% CI, –56.32 to –14.24 µmol/L) for Cohort A and –48.33 µmol/L (95% CI, –55.85 to –40.80 µmol/L) for Cohort B.
Percent change in plasma oxalate AUC0 to 24 hours between dialysis sessions was a secondary outcome and is summarized in Table 26 for Cohort B. The LSM percent change from baseline to the average of months 3 to 6 was –41.4% (95% CI, –51.0% to –31.8%).
Table 23: Change From Baseline to Month 6 in Plasma Oxalate (Secondary Outcome): ILLUMINATE-A Trial, Plasma Oxalate Analysis Set
Outcome | ILLUMINATE-A | |
|---|---|---|
Placebo (N = 10) | Lumasiran (N = 23) | |
Baseline,a n (%) | 10 (100) | 23 (100) |
Mean (SEM) (µmol/L) | 17.76 (2.17) | 15.73 (1.59) |
Mean of months 3 to 6 | NA | NA |
Change from baseline to average of months 3 to 6, LSM (SEM) (µmol/L)b (95% CI) | 1.25 (1.12) (–1.04 to 3.54) | –7.46 (0.77) (–9.03 to –5.90) |
LSM (SEM) treatment group difference (lumasiran – placebo) (µmol/L)b (95% CI) | Reference | –8.71 (1.34) (–11.45 to –5.98) |
P valueb,c | Reference | < 0.001 |
Percent change from baseline to average of months 3 to 6, LSM (SEM)b (95% CI) | –0.32 (████) (–9.12 to 8.48) | –39.80 (████) (–45.81 to –33.80) |
LSM (SEM) treatment group difference (lumasiran – placebo)b (95% CI) | Reference | –39.48 (████) (–50.10 to –28.87) |
P valueb,c | Reference | < 0.001 |
CI = confidence interval; LSM = least squares mean; SEM = standard error of the mean.
aBaseline is defined as the mean of all assessments before the first dose date/time of study drug in the study (placebo or lumasiran).
bBased on the Mixed-Effect Model Repeated Measures model with the corresponding value at baseline as a continuous fixed covariate, visit, and treatment as fixed effects, and patient as a random effect. Visit is fitted as a categorical variable, and the variance-covariance matrix is assumed to be unstructured. Satterthwaite approximation is used to estimate denominator degrees of freedom. A difference less than 0 represents a favourable outcome for lumasiran.
cP value has been adjusted for multiple testing (i.e., the type I error rate has been controlled).
Source: ILLUMINATE-A Clinical Study Report.12
Table 24: Change From Baseline in Plasma Oxalate (Secondary Outcome): ILLUMINATE-B Trial, Efficacy Analysis Set
Outcome | ILLUMINATE-B | |||
|---|---|---|---|---|
< 10 kg (N = 3) | 10 to < 20 kg (N = 12) | ≥ 20 kg (N = 3) | All patients (N = 18) | |
Baseline,a n (%) | █ (███) | ██ (███) | █ (███) | 18 (100) |
Mean (SD) (µmol/L) | █████ (████) | █████ (████) | █████ (████) | 13.24 (6.50) |
Month 6, n (%) | 3 (100) | 12 (100) | 3 (100) | 18 (100) |
Mean (SD) (µmol/L) | █████ (████) | ████ (████) | ████ (████) | 8.21 (████) |
Change from baseline, mean (SD) (µmol/L) | ██████ (████) | █████ (████) | █████ (████) | –5.03 (████) |
Percent change from baseline, mean (SD) | ██████ (█████) | ██████ (█████) | ██████ (█████) | –32.06 (█████) |
Month 12, n (%) | 3 (100) | 12 (100) | 3 (100) | 18 (100) |
Mean (SD) (µmol/L) | 5.55 (0.00) | 5.82 (0.49) | 6.62 (1.85) | 5.91 (████) |
Change from baseline, mean (SD) (µmol/L) | –17.77 (6.76) | –5.08 (3.82) | –5.92 (4.14) | –7.33 (████) |
Percent change from baseline, mean (SD) | –74.84 (7.10) | –41.27 (16.45) | –42.95 (17.17) | –47.14 (█████) |
Month 18, n (%) | █ (███) | ██ (████) | █ (████) | ██ (████) |
Mean (SD) (µmol/L) | ████ (████) | ████ (████) | ████ (████) | ████ (████) |
Change from baseline, mean (SD) (µmol/L) | ██████ (████) | █████ (████) | █████ (████) | █████ (████) |
Percent change from baseline, mean (SD) | ██████ (████) | ██████ (█████) | ██████ (█████) | ██████ (█████) |
SD = standard deviation.
aBaseline is the mean of all assessments collected before the first dose of lumasiran.
Source: ILLUMINATE-B Clinical Study Report.13
Table 25: Change From Baseline in Plasma Oxalate to Month 6 (Primary and Secondary Outcomes): ILLUMINATE-C Trial, Safety Analysis Set
Outcome | ILLUMINATE-C | |
|---|---|---|
Cohort A: no dialysis (N = 6) | Cohort B: dialysis (N = 15) | |
Baseline,a n (%) | 6 (100) | 15 (100) |
Mean (SD) (µmol/L) | █████ (█████) | ██████ (█████) |
Month 3 | NA | NA |
Change from baseline, LSM (SEM) (µmol/L)b (95% CI) | ██████████████████ | ██████████████████ |
Percent change from baseline, LSM (SEM)b (95% CI) | ████████████████ | █████████████████ |
Month 6 | NA | NA |
Change from baseline, LSM (SEM) (µmol/L)b (95% CI) | ████████████████████ | █████████████████ |
Percent change from baseline, LSM (SEM)b (95% CI) | ███████████████ | ███████████████ |
Mean of months 3 to 6 | NA | NA |
Change from baseline, LSM (SEM) (µmol/L)b (95% CI) | –35.28 (7.40) (–56.32 to –14.24) | –48.33 (3.63) (–55.85 to –40.80) |
P valueb,c | ██████ | ██████ |
Percent change from baseline, LSM (SEM)b (95% CI) | –33.33 (17.63) (–81.82 to 15.16) | –42.43 (3.95) (–50.71 to –34.15) |
P valueb,c | 0.1299 | < 0.001 |
CI = confidence interval; LSM = least squares mean; NA = not applicable; SD = standard deviation; SEM = standard error of the mean.
aFor Cohort A, the baseline is defined as the mean of all plasma oxalate samples collected before the first dose of lumasiran. For Cohort B, the baseline is defined as the mean of the last 4 predialysis plasma oxalate samples collected before the first dose of lumasiran. In Cohort B, only predialysis samples are utilized.
bBased on the restricted maximum likelihood–based Mixed-Effect Model Repeated Measures model to test against the null hypothesis of mean change from baseline outcome being equal to 0. The model includes scheduled visits and baseline plasma oxalate (μmol/L) as fixed effects and patient as a random factor. Autoregressive (1) was used to model the within-patient variability.
cP value has not been adjusted for multiple testing (i.e., the type I error rate has not been controlled).
Source: ILLUMINATE-C Clinical Study Report.14
Table 26: Percent Change in Plasma Oxalate AUC0 to 24 Hours Between Dialysis Sessions (Secondary Outcome): ILLUMINATE-C Trial, FAS
Outcome | ILLUMINATE-C |
|---|---|
Cohort B: dialysis (N = 15) | |
Baseline,a n (%) | 15 (100) |
Mean (SD) | ██████ (█████) |
Month 3 | NA |
LSM (SEM)b (95% CI) | ███████████████████████ |
Month 6 | NA |
LSM (SEM)b (95% CI) | ████████████████████████ |
Mean of months 3 to 6 | NA |
LSM (SEM)b (95% CI) | –41.4 (4.4) (–51.0 to –31.8) |
P valueb,c | ██████ |
AUC = area under the curve; CI = confidence interval; FAS = full analysis set; LSM = least squares mean; NA = not applicable; SD = standard deviation; SEM = standard error of the mean.
aBaseline is defined as mean value of all valid AUC profiles being computed before the first dose of lumasiran.
bBased on the restricted maximum likelihood–based Mixed-Effect Model Repeated Measures used to test against the null hypothesis of mean change from baseline outcome being equal to 0. The model includes scheduled visits and baseline plasma oxalate AUC0 to 24 hours as fixed effects and patient as a random factor. Autoregressive (1) was used to model the within-patient variability.
cP value has not been adjusted for multiple testing (i.e., the type I error rate has not been controlled).
Source: ILLUMINATE-C Clinical Study Report.14
Urine Oxalate:Creatinine Levels
ILLUMINATE-A Trial
Percent change from baseline to month 6 in 24-hour urine oxalate:creatinine was a secondary outcome in the trial and is summarized in Table 27. The LSM percent change from baseline to the average of months 3 to 6 was –62.55% (95% CI, –70.71% to –54.39%) for the lumasiran group and –10.78% (95% CI, –21.58% to 0.03%) for the placebo group. The treatment difference between groups was –51.77% (95% CI, –64.27% to –39.28%; P < 0.001).
Percent and absolute change from baseline in 24-hour urine oxalate:creatinine were secondary outcomes for the extension period and are summarized in Table 46. Data from treatment on lumasiran indicated decreases in 24-hour urine oxalate:creatinine at month 6 that appeared to be maintained for both lumasiran followed by lumasiran and placebo followed by lumasiran treatment groups.
ILLUMINATE-B Trial
Percent change from baseline to month 6 in spot urine oxalate:creatinine ratio was the primary outcome in the trial and is summarized in Table 28. The LSM percent change from baseline to the average of months 3 to 6 for all patients was –71.97% (95% CI, –77.52% to –66.42%). The results of the 3 sensitivity analyses supported the primary outcome. Subgroup analysis results for age had very few patients and meaningful conclusions could not made.
The proportion of patients with a spot urine oxalate:creatinine ratio at or below 1.5 times ULN and at or below the ULN during the study were secondary outcomes and are summarized in Table 29. By month 6, 9 patients in the trial were at or below 1.5 times ULN and 1 patient was at or below the ULN. By month 18, ██ of the ██ patients who had data at that time point were at or below 1.5 times ULN and █ patients were at or below the ULN.
Absolute and percent change from baseline in spot urine oxalate:creatinine ratio were secondary outcomes and are summarized in Table 47. Data from the extension period indicated decreases in spot urine oxalate:creatinine ratio by month 6 that appeared to be maintained for patients across all weight groups to month 18.
ILLUMINATE-C Trial
Absolute and percent changes from baseline in spot urine oxalate:creatinine ratio were secondary outcomes and are summarized in Table 30 for Cohort A. The LSM absolute change from baseline to the average of months 3 to 6 was –0.19 mmol/mmol (95% CI, –0.23 to –0.15 mmol/mmol). The LSM percent change from baseline to the average of months 3 to 6 was –39.51% (95% CI, –64.13% to –14.90%).
Table 27: Percent Change From Baseline to Month 6 in 24-Hour Urine Oxalate:Creatinine Ratio (Secondary Outcome): ILLUMINATE-A Trial, FAS
Outcome | ILLUMINATE-A | |
|---|---|---|
Placebo (N = 13) | Lumasiran (N = 26) | |
Baseline,a n (%) | 13 (100) | 26 (100) |
Mean (SEM) | 0.24 (████) | 0.21 (████) |
Month 6 | NA | NA |
Percent change from baseline to average of months 3 to 6, LSM (SEM) (95% CI)b | –10.78 (████) (–21.58 to 0.03) | –62.55 (████) (–70.71 to –54.39) |
LSM (SEM) treatment group difference (lumasiran – placebo) (95% CI)b | Reference | –51.77 (████) (–64.27 to –39.28) |
P valueb,c | Reference | < 0.001 |
CI = confidence interval; FAS = full analysis set; LSM = least squares mean; NA = not applicable; SEM = standard error of the mean.
aBaseline is the median of all valid 24-hour urine assessments collected before the first dose date/time of study drug (lumasiran or placebo) without any nonprotocol-related sample issues.
bBased on the Mixed-Effect Model Repeated Measures model with the corresponding value at baseline as a continuous fixed covariate, visit, and treatment as fixed effects, and patient as a random effect. Visit is fitted as a categorical variable, and the variance-covariance matrix is assumed to be unstructured. Satterthwaite approximation is used to estimate denominator degrees of freedom. A difference less than 0 represents a favourable outcome for lumasiran.
bP value has been adjusted for multiple testing (i.e., the type I error rate has been controlled).
Source: ILLUMINATE-A Clinical Study Report.12
Table 28: Percent Change From Baseline to Month 6 in Spot Urine Oxalate:Creatinine Ratio (Primary Outcome): ILLUMINATE-B Trial, Efficacy Analysis Set
Outcome | ILLUMINATE-B |
|---|---|
All patients (N = 18) | |
Baseline,a n (%) | 18 (100) |
Mean (SD) (mmol/mmol) | 0.63 (0.43) |
Month 6 | NA |
Percent change from baseline to months 3 to 6, LSM (SEM)b (95% CI) | –71.97 (2.71) (–77.52 to –66.42) |
P valueb,c | < 0.001 |
CI = confidence interval; LSM = least squares mean; NA = not applicable; SD = standard deviation; SEM = standard error of the mean.
aBaseline is the mean of all assessments collected before the first dose of lumasiran. The mean of data within a visit was used as the postdose value at each visit.
bBased on the restricted maximum likelihood–based Mixed-Effect Model Repeated Measures model used to test against the null hypothesis of mean percent change from baseline output being equal to 0. The model includes fixed effects of scheduled visits and baseline spot urine oxalate:creatinine ratio value (mmol/mmol), including patient as a random factor. Autoregressive (1) was used to model the within-patient error.
cP value has not been adjusted for multiple testing (i.e., the type I error rate has not been controlled).
Source: ILLUMINATE-B Clinical Study Report.13
Table 29: Spot Urine Oxalate:Creatinine Ratio ≤ 1.5 × ULN or ≤ ULN (Secondary Outcomes): ILLUMINATE-B Trial, Efficacy Analysis Set
Outcome | ILLUMINATE-B | |||
|---|---|---|---|---|
< 10 kg (N = 3) | 10 to < 20 kg (N = 12) | ≥ 20 kg (N = 3) | All patients (N = 18) | |
Baseline,a n (%) | 3 (100) | 12 (100) | 3 (100) | 18 (100) |
Proportion of patients with ≤ 1.5 × ULN | 0 | 0 | 0 | 0 |
Proportion of patients with ≤ ULN | 0 | 0 | 0 | 0 |
Month 6, n (%) | 3 (100) | 12 (100) | 3 (100) | 18 (100) |
Proportion of patients with ≤ 1.5 × ULN | ███████ | ███████ | ███████ | 9 (50.0) |
Proportion of patients with ≤ ULN | █ | ██████ | █ | 1 (5.6) |
Month 12, n (%) | 3 (100) | 12 (100) | 3 (100) | 12 (100) |
Proportion of patients with ≤ 1.5 × ULN | ███████ | ███████ | ███████ | 10 (55.6) |
Proportion of patients with ≤ ULN | ███████ | ██████ | █ | 2 (11.1) |
Month 18, n (%) | ██████ | ████████ | ███████ | ████████ |
Proportion of patients with ≤ 1.5 × ULN | ███████ | ███████ | ███████ | ████████ |
Proportion of patients with ≤ ULN | █ | ███████ | █ | ███████ |
ULN = upper limit of normal.
aBaseline is the mean of all assessments collected before the first dose of lumasiran. The mean of data within a visit was used as the postdose value at each visit.
Note: Age-dependent ULN based on Matos et al.60
Source: ILLUMINATE-B Clinical Study Report.13
Table 30: Change From Baseline in Spot Urine Oxalate:Creatinine Ratio (Secondary Outcome): ILLUMINATE-C Trial, FAS
Outcome | ILLUMINATE-C |
|---|---|
Cohort A: no dialysis (N = 6) | |
Baseline,a n (%) | 6 (100) |
Mean (SD) (mmol/mmol) | ████ (████) |
Month 3 | NA |
Change from baseline, LSM (SEM) (mmol/mmol)b (95% CI) | █████████████████████████ |
Percent change from baseline, LSM (SEM)b (95% CI) | █████████████████████████████ |
Month 6 | NA |
Change from baseline, LSM (SEM) (mmol/mmol)b (95% CI) | █████████████████████████ |
Percent change from baseline, LSM (SEM)b (95% CI) | █████████████████████████████ |
Mean of months 3 to 6 | NA |
Change from baseline, LSM (SEM) (mmol/mmol)b (95% CI) | –0.19 (0.02) (–0.23 to –0.15) |
Change from baseline, P valueb,c | ██████ |
Percent change from baseline, LSM (SEM)b (95% CI) | –39.51 (9.43) (–64.13 to –14.90) |
Percent change from baseline, P valueb,c | ██████ |
CI = confidence interval; FAS = full analysis set; LSM = least squares mean; NA = not applicable; SD = standard deviation; SEM = standard error of the mean.
aBaseline is defined as the mean of all assessments before the first dose date/time of lumasiran.
bBased on the restricted maximum likelihood–based Mixed-Effect Model Repeated Measures model used to test against the null hypothesis of mean change from baseline outcome being equal to 0. The model includes scheduled visits and baseline spot urine oxalate:creatinine ratio as fixed effects and patient as a random factor. Autoregressive (1) was used to model the within-patient variability.
cP value has not been adjusted for multiple testing (i.e., the type I error rate has not been controlled).
Source: ILLUMINATE-C Clinical Study Report.14
Harms
Only those harms identified in the review protocol are reported below. Harms outcomes for the 6-month primary analysis periods of the 3 studies are summarized in Table 31 and long-term harms while receiving lumasiran for up to 24 months for the ILLUMINATE-A trial and 12 months of treatment for the ILLUMINATE-B trial are summarized in Table 48.
Adverse Events
Most patients in the ILLUMINATE-A and ILLUMINATE-C trials and all patients in the ILLUMINATE-B trial reported at least 1 AE during the 6-month primary analysis period. In the ILLUMINATE-A trial, a larger proportion of patients in the lumasiran group reported an AE compared to the placebo group (84.6% versus 69.2%). In the ILLUMINATE-C trial, the percentage of patients reporting an AE was similar between the groups (83.3% for no dialysis and 86.7% for dialysis).
In the ILLUMINATE-A trial, injection site reaction and headache were the most frequently reported AEs. All 6 patients (23.1%) who experienced an injection site reaction were in the lumasiran group, while 3 patients reported headache in either of the lumasiran and placebo groups (11.5% and 23.1%, respectively). In the ILLUMINATE-B trial, pyrexia was the most frequently reported AE for 2 (66.7%) patients weighing less than 10 kg, 4 (33.3%) patients weighing between 10 kg and 20 kg, and 1 (33.3%) patient weighing more than 20 kg. In the ILLUMINATE-C trial, pyrexia and injection site reaction were the most frequently reported AEs. One (16.7%) patient not on dialysis and 7 (46.7%) patients on dialysis reported pyrexia, while 1 (16.7%) patient not on dialysis and 4 (26.7%) patients on dialysis reported injection site reaction.
During the overall period of receiving lumasiran treatment, injection site reaction (██████████), abdominal pain (█████████), and headache (█████████) were the most frequently reported AEs in the ILLUMINATE-A trial. In the ILLUMINATE-B trial, pyrexia (8 patients) and vomiting (5 patients) were the most frequently reported AEs.
Serious Adverse Events
Overall, SAEs were not reported in the ILLUMINATE-A trial (0 patients) and were infrequent in the ILLUMINATE-B trial (1 patient weighing at least 20 kg). In the ILLUMINATE-C trial, 9 patients reported a SAE: 1 (16.7%) patient not on dialysis and 8 (53.3%) patients on dialysis. ████ ████████████████ ███ and device-related infection were reported in 2 patients for each SAE (all patients were on dialysis). All other SAEs were single-patient events.
During the overall period of receiving lumasiran treatment, ████████ reported SAEs of █████████████, urosepsis, and ███ ████████ ████████ ██████ in the ILLUMINATE-A trial, while 1 patient reported viral infection in the ILLUMINATE-B trial.
Withdrawals Due to AEs
One patient receiving lumasiran in the ILLUMINATE-A trial stopped treatment due to an AE (fatigue and disturbance in attention), while █ patients on dialysis in the ILLUMINATE-C trial stopped treatment due to an AE (both due to █████ ██████████ █████).
No additional withdrawals due to AEs were reported during the overall period of receiving lumasiran treatment.
Mortality
No deaths were reported during the 6-month primary analysis period for any of the 3 studies.
No deaths due to AEs were reported during the overall period of receiving lumasiran treatment.
Notable Harms
Complications from systemic oxalosis were not reported in the clinical study reports at the given cut-off dates.
Injection Site Reactions
Injection site reactions were reported among 6 patients receiving lumasiran in the ILLUMINATE-A trial, 3 patients (2 patients weighing between 10 kg and 20 kg, 1 patient weighing more than 20 kg) in the ILLUMINATE-B trial, and 5 patients (4 patients on dialysis, 1 patient not on dialysis) in the ILLUMINATE-C trial. Symptoms included injection site erythema, pain, pruritus, discomfort, swelling, discoloration, and hematoma.
During the overall period of receiving lumasiran treatment, ██ patients in the ILLUMINATE-A trial and █ patients in the ILLUMINATE-B trial reported an injection site reaction, with the most common symptom being erythema.
Renal Events
Kidney stone events were captured as an efficacy outcome and were not reported as harms. All renal events were single-patient events. ████████ and █████████ were reported by patients receiving lumasiran in the ILLUMINATE-A trial. ████ █████ was reported in a patient weighing between 10 kg and 20 kg in the ILLUMINATE-B trial. ███████████ and ██ ████ ████████ █ were reported by patients not on dialysis in the ILLUMINATE-C trial.
During the overall period of receiving lumasiran treatment, █████████ in the ILLUMINATE-A trial reported renal events, with the most frequent events being ███████ (█████████) and █████████ (█████████). In the ILLUMINATE-B trial, ████████ reported █████████.
Headache
Six patients reported headache in the ILLUMINATE-A trial (3 patients each on placebo and lumasiran), and 2 patients in the ILLUMINATE-B trial (████ ██████ ██████████). No patients reported headache in the ILLUMINATE-C trial.
During the overall period of receiving lumasiran treatment, █████████ in the ILLUMINATE-A trial and █████████ in the ILLUMINATE-B trial reported headache.
Rhinitis
Four patients reported rhinitis in the ILLUMINATE-A trial (2 patients each on placebo and lumasiran) and 4 patients in the ILLUMINATE-B trial (1 patient weighing less than 10 kg and 3 patients weighing between 10 kg and 20 kg). No patients reported rhinitis in the ILLUMINATE-C trial.
During the overall period of receiving lumasiran treatment, ████████ in the ILLUMINATE-A trial and █████████ in the ILLUMINATE-B trial reported rhinitis.
Upper Respiratory Infection
Four patients reported upper respiratory infection in the ILLUMINATE-A trial (2 patients each on placebo and lumasiran), 4 patients in the ILLUMINATE-B trial (1 patient weighing less than 10 kg, 2 patients weighing between 10 kg and 20 kg, and 1 patient weighing more than 20 kg), and █████████ in the ILLUMINATE-C trial (████████████ not receiving dialysis and on dialysis).
During the overall period of receiving lumasiran treatment, 4 patients reported upper respiratory infection each in the ILLUMINATE-A and ILLUMINATE-B trials.
Hypersensitivity Reactions
One patient receiving lumasiran in the ILLUMINATE-A trial reported a hypersensitivity reaction. Hypersensitivity reactions were not reported in the ILLUMINATE-B or ILLUMINATE-C trials.
No additional reports of hypersensitivity were captured during lumasiran treatment.
Antidrug Antibodies
In the ILLUMINATE-A trial, 1 patient tested positive for ADAs during the trial. The patient tested negative before first receiving lumasiran and at months 1 and 3, but tested positive at month 6. The sponsor concluded that the ADAs did not appear to affect the 24-hour urine oxalate corrected for BSA outcome.
In the ILLUMINATE-B trial, 3 patients tested positive for ADAs during the trial, with 1 patient weighing less than 10 kg and 2 patients weighing between 10 kg and 20 kg. The patient weighing less than 10 kg tested positive at month 6, but tested negative at month 9. One of the patients weighing between 10 kg and 20 kg tested positive at month 1, while the other patient tested positive at month 3. Both patients tested negative for ADAs at later time points (e.g., months 3, 6, 9 and months 6, 9, 12, respectively). Similarly, the sponsor concluded that there did not appear to be an impact on efficacy (assessed based on spot urine oxalate:creatinine ratio) or safety results for these patients.
No patients tested positive for ADAs in the ILLUMINATE-C trial.
During the overall period of receiving lumasiran treatment in the ILLUMINATE-A trial, 1 patient originally randomized to placebo tested positive for ADAs. There were no additional reports of patients testing positive for ADAs in the ILLUMINATE-B trial during extended lumasiran treatment.
Table 31: Summary of Harms During 6-Month Primary Analysis Period: ILLUMINATE-A, ILLUMINATE-B, ILLUMINATE-C Trials, Safety Analysis Set
Harms | ILLUMINATE-A | ILLUMINATE-B | ILLUMINATE-C | ||||
|---|---|---|---|---|---|---|---|
Placebo (N = 13) | Lumasiran (N = 26) | < 10 kg (N = 3) | 10 to < 20 kg (N = 12) | ≥ 20 kg (N = 3) | Cohort A: no dialysis (N = 6) | Cohort B: dialysis (N = 15) | |
Patients with ≥ 1 adverse event | |||||||
n (%) | 9 (69.2) | 22 (84.6) | 3 (100) | 12 (100) | 3 (100) | 5 (83.3) | ██ (████) |
Most common events,a n (%) | |||||||
Injection site reaction | 0 | 6 (23.1) | 0 | 2 (16.7) | 1 (33.3) | 1 (16.7) | 4 (26.7) |
Headache | 3 (23.1) | 3 (11.5) | █ | █ | █ ██████ | NR | NR |
Injection site erythema | 0 | 3 (11.5) | █ | ███████ | █ | █ | ██████ |
Injection site pain | 0 | 3 (11.5) | █ | █ | ██████ | NR | NR |
Rhinitis | 2 (15.4) | 2 (7.7) | 1 (33.3) | 3 (25.0) | 0 | NR | NR |
Upper respiratory infection | 2 (15.4) | 2 (7.7) | 1 (33.3) | 2 (16.7) | 1 (33.3) | ██████ | ██████ |
Oropharyngeal pain | 1 (7.7) | 1 (3.8) | █ | ███████ | █ | NR | NR |
Constipation | 0 | 1 (3.8) | NR | NR | NR | ███████ | █████ |
Cough | 0 | 1 (3.8) | ██████ | █████ | █ | █ | ██████ |
Nasopharyngitis | 0 | 1 (3.8) | ██████ | █ | ██████ | NR | NR |
Nausea | 0 | 1 (3.8) | █ | ██████ | ██████ | NR | NR |
Pyrexia | NR | NR | 2 (66.7) | 4 (33.3) | 1 (33.3) | 1 (16.7) | █ (████) |
Vomiting | NR | NR | 1 (33.3) | 2 (16.7) | 1 (33.3) | 1 (16.7) | 1 (6.7) |
Bronchitis | NR | NR | █ | ██████ | ██████ | NR | NR |
Diarrhea | NR | NR | █ | ███████ | █ | ██████ | ██████ |
Gastroenteritis | NR | NR | █ | ███████ | █ | NR | NR |
Teething | NR | NR | ██████ | █ | █ | NR | NR |
Device-related infection | NR | NR | NR | NR | NR | 0 | 2 (13.3) |
Hypokalemia | NR | NR | NR | NR | NR | ███████ | ███████ |
Renal and liver transplant | NR | NR | NR | NR | NR | █ | ███████ |
Patients with ≥ 1 SAE | |||||||
n (%) | 0 | 0 | 0 | 0 | 1 (33.3) | 1 (16.7) | ███████ |
Viral infection | NR | NR | 0 | 0 | 1 (33.3) | NR | NR |
Device-related infection | NR | NR | NR | NR | NR | 0 | 2 (13.3) |
Renal and liver transplant | NR | NR | NR | NR | NR | █ | ███████ |
Abdominal pain | NR | NR | NR | NR | NR | 0 | 1 (6.7) |
Anemia | NR | NR | NR | NR | NR | █ | ██████ |
Arteriovenous fistula operation | NR | NR | NR | NR | NR | 0 | 1 (6.7) |
Arteriovenous fistula thrombosis | NR | NR | NR | NR | NR | 0 | 1 (6.7) |
Catheter site swelling | NR | NR | NR | NR | NR | 0 | 1 (6.7) |
Cholecystitis acute | NR | NR | NR | NR | NR | █ | █████ |
Device-related thrombosis | NR | NR | NR | NR | NR | 0 | 1 (6.7) |
Dialysis device insertion | NR | NR | NR | NR | NR | 0 | 1 (6.7) |
General physical condition abnormal | NR | NR | NR | NR | NR | █ | █████ |
Hemorrhage | NR | NR | NR | NR | NR | 0 | 1 (6.7) |
Pancreatitis | NR | NR | NR | NR | NR | █ | ██████ |
Pyrexia | NR | NR | NR | NR | NR | 0 | 1 (6.7) |
Renal transplant | NR | NR | NR | NR | NR | █ | ██████ |
Seizure | NR | NR | NR | NR | NR | 0 | 1 (6.7) |
Skin scar contracture | NR | NR | NR | NR | NR | 0 | 1 (6.7) |
Spontaneous hematoma | NR | NR | NR | NR | NR | 0 | 1 (6.7) |
Hypokalemia | NR | NR | NR | NR | NR | 1 (16.7) | 0 |
Vomiting | NR | NR | NR | NR | NR | 1 (16.7) | 0 |
Patients who stopped treatment due to adverse events | |||||||
n (%) | 0 | 1 (3.8) | 0 | 0 | 0 | █ | ██████ |
Fatigue and disturbance in attention, n (%) | 0 | 1 (3.8) | NR | NR | NR | NR | NR |
Renal and liver transplant | NR | NR | NR | NR | NR | █ | ███████ |
Deaths | |||||||
n (%) | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
Notable harms, n (%) | |||||||
Injection site reaction | 0 | 6 (23.1) | 0 | 2 (16.7) | 1 (33.3) | 1 (16.7) | 4 (26.7) |
Injection site erythema | 0 | ███████ | █ | ███████ | █ | █ | ███████ |
Injection site pain | 0 | 3 (11.5) | █ | █ | ██████ | NR | NR |
Injection site pruritus | 0 | ███████ | NR | NR | NR | NR | NR |
Injection site discomfort | 0 | ███████ | NR | NR | NR | NR | NR |
Injection site reaction | 0 | ███████ | NR | NR | NR | NR | NR |
Injection site swelling | 0 | ███████ | NR | NR | NR | NR | NR |
Injection site discoloration | NR | NR | █ | ███████ | █ | ███████ | █ |
Injection site hematoma | NR | NR | NR | NR | NR | █ | ███████ |
Renal eventsb | █ | ███████ | █ | ███████ | █ | ███████ | █ |
Polyuria | █ | ███████ | NR | NR | NR | NR | NR |
Renal pain | █ | ███████ | NR | NR | NR | NR | NR |
Hematuria | NR | NR | █ | ███████ | █ | NR | NR |
Proteinuria | NR | NR | NR | NR | NR | ███████ | █ |
Renal impairment | NR | NR | NR | NR | NR | ███████ | █ |
Complications from systemic oxalosis | NR | NR | NR | NR | NR | NR | NR |
Headache | 3 (23.1) | 3 (11.5) | █ | █ | ██████ | NR | NR |
Rhinitis | 2 (15.4) | 2 (7.7) | 1 (33.3) | 3 (25.0) | 0 | NR | NR |
Upper respiratory infection | 2 (15.4) | 2 (7.7) | 1 (33.3) | 2 (16.7) | 1 (33.3) | ███████ | ███████ |
Hypersensitivity reactions | 0 | 1 (3.8) | NR | NR | NR | NR | NR |
ADA positive at any time | 0 | 1 (3.8) | 1 (33.3) | 2 (16.7) | 0 | 0 | 0 |
ADA = antidrug antibody; NR = not reported; SAE = serious adverse event.
aFrequency of at least 10% in any treatment group in ILLUMINATE-A and at least 2 patients in ILLUMINATE-B or -C.
bKidney stone events were captured as an efficacy outcome in the 3 studies and not reported as harms.
Source: ILLUMINATE-A Clinical Study Report,12 ILLUMINATE-B Clinical Study Report,13 ILLUMINATE-C Clinical Study Report.14
Critical Appraisal
Internal Validity
The ILLUMINATE-A, ILLUMINATE-B, and ILLUMINATE-C trials all generally had acceptable trial designs. All 3 are multicentre, international trials investigating the efficacy and safety of lumasiran in patients with PH1 and have ongoing extension periods for a total treatment time of up to 60 months. The ILLUMINATE-A trial was sufficiently powered to detect a treatment difference between lumasiran and placebo. An interactive response system was used to ensure that treatment allocation was concealed and randomization between treatment groups was stratified by urinary oxalate excretion with a cut point of 1.70 mmol/24 hour/1.73 m2 based on the median baseline excretion of patients in the ALN-GO1 to 001 study. At the time of protocol finalization, there were no approved therapies for PH1 preventing the inclusion of an active comparator.12 The trial had a 6-month, DB, placebo-controlled period and patients remained blinded for an additional 3 months, while those randomized to placebo crossed over to receive lumasiran. Further measures were taken to maintain blinding (e.g., if patients had laboratory tests performed locally for routine care, patients and trial site personnel were to remain blinded to the results). There did not appear to be clear differences in HRQoL results between placebo and lumasiran groups and the risk of unblinding was likely low. AEs during the DB period were slightly higher in the lumasiran group in the ILLUMINATE-A trial. Injection site reaction was the most frequently reported AE in the trial and occurred only in the lumasiran group (23.1%) during the 6-month DB period and in both groups (34.6% and 38.5% in the lumasiran followed by lumasiran and placebo followed by lumasiran groups, respectively) during all lumasiran treatment (placebo patients crossed over to lumasiran). Due to the imbalance, it is possible there was some risk of unblinding during the DB period, though there were no reports of study withdrawals due to injection site reaction. The ILLUMINATE-A trial also had a prespecified testing procedure of trial end points to control for multiplicity. All primary and key secondary outcomes were objective in nature, centrally assessed, relevant to PH1, and supported by regulatory agencies, which reduce bias in the results.12,15 The ILLUMINATE-B and ILLUMINATE-C trials were based on feasibility considerations rather than power calculations, were single-arm trials, and end points were not controlled for multiplicity. Although these trials did not have a comparator or control arm, the clinical experts felt that the results were consistent with those in the ILLUMINATE-A trial and were meaningful. The sponsor noted that patient heterogeneity, disease heterogeneity, rarity of PH1, lack of available approved therapies, objectively measured end points, and the sponsor’s feasibility results justified the use of a single-arm trial design.13,14
Baseline characteristics were mostly balanced in the ILLUMINATE-A trial, suggesting that randomization was generally successful, and it is possible that the imbalances were due to the small patient numbers. There was a larger proportion of males than females and patients who were white compared to other races. The clinical experts indicated that there is no reason to expect a difference in PH1 prevalence based on sex and that the limited number of races represented in the trial may not reflect the general patient population in Canada. There were also imbalances in patients’ medical history, specifically for PH1-related symptoms and vitamin B6 use, which may have introduced bias, although the magnitude or direction of the bias is uncertain. Because patients in the ILLUMINATE-B and ILLUMINATE-C trials were not randomized to their treatment group, they were categorized based on body mass and use of dialysis, respectively, and imbalances between groups are likely to occur, making it challenging to compare results between groups.
During the 6-month primary analysis periods, few patients discontinued lumasiran during the trials (████ █████ ███████ █ █ ██████████ ████) and few withdrew from the trials (█ ███████████ ████████ █████████ ██), suggesting there was little risk of attrition bias. In the ILLUMINATE-A trial, all patients were included in the MMRM analysis for the primary end point, which used the average of months 3 to 6, thus allowing more flexibility because any measurements from those months could be used in the analysis, rather than specifying month 6 only. The sponsor noted that 4 of 39 patients had some missing data from months 3 to 6 but did not expect that this would greatly affect the results. Two sensitivity analyses were performed to estimate the treatment effect of the primary end point without assuming an equal treatment effect across months 3 to 6 and both supported the main findings. For plasma oxalate outcomes, patients were included in the plasma oxalate analysis set (N = 33) if they had a baseline measurement of at least 1.5 times LLOQ. In total, 32 patients contributed to the MMRM analysis (1 patient withdrew from the study). The sponsor noted that, in the ILLUMINATE-B trial, all patients had data for urine oxalate levels at all time points at the data cut-off date, and it appears as though nearly all patients had data for plasma oxalate. In the ILLUMINATE-C trial, all patients contributed to the MMRM analysis for the primary end point, which used the average of months 3 to 6. The sponsor noted that 3 patients in Cohort B had some missing data from months 3 to 6 but did not expect that this would greatly affect the results. A sensitivity analysis was performed to estimate the treatment effect of the primary end point by cohorts in the safety analysis set, which included patients who lacked plasma oxalate assessments at month 3 or after, and the results supported the main findings. Both the MMRM and imputation for missing data assumed that the data were missing at random, which is difficult to verify and could have biased the results. However, due to the overall small amount of missing data among the 3 trials and sensitivity analyses supporting the primary outcomes, the risk of bias due to missing data appears to be low.
One of the main limitations is the small number of patients in each trial (N = 39, 18, and 21 in the ILLUMINATE-A, ILLUMINATE-B, and ILLUMINATE-C trials, respectively), though consideration must be given for the rarity of PH1. The small number of patients in each treatment group makes it challenging to interpret the results, particularly for outcomes such as kidney stone events. Likewise, although subgroup analyses were prespecified, they were not powered to detect a treatment difference, none were controlled for type I error, and they all had few patients in each group, limiting interpretation of the results. The results were consistent with the overall study findings; however, they should be interpreted as supportive evidence only for the overall effect of lumasiran.
Although there are data for up to 24 months of lumasiran treatment in the ILLUMINATE-A trial, a second major limitation is the relatively short duration of evidence available given that the clinical experts expect lumasiran to be a lifelong treatment or until liver transplant occurs. The short duration makes it difficult to be certain if the efficacy and safety results will persist long-term, particularly for clinically important outcomes such as kidney function (eGFR) and kidney stone events. Furthermore, it is unclear if or how lumasiran affects HRQoL over time, which is important to patients.
A third limitation is the lack of MIDs for patients with PH1 identified from the literature for all outcomes in the trials. Without published MIDs, there is uncertainty about how meaningful the absolute and percent changes from baseline were. Normal ranges for the biochemical outcomes were identified, but it is not immediately clear from population-level data of changes from baseline if normalization was achieved. The sponsor performed analyses for the proportion of patients who achieved near normalization (at or below 1.5 times ULN) or normalization (at or below the ULN) for 24-hour urine oxalate in the ILLUMINATE-A trial and spot urine oxalate:creatinine ratio in the ILLUMINATE-B trial, but not for plasma oxalate in the ILLUMINATE-C trial. Based on the laboratory assay used to measure plasma oxalate, the LLOQ was 5.55 μmol/L which is greater than the normal values of 1 to 3 μmol/L identified from the literature,45 indicating that determining the proportion of patients who achieved normalization was not possible due to the assay’s sensitivity. According to the clinical experts, normalization of elevated oxalate levels may result in clinical benefits, but it is unclear if achieving near normalization prevents long-term kidney outcomes, and long-term evidence will be needed to support this.
There were other issues in the trials that limit the interpretation of the results. Specifically, the proportion of patients using vitamin B6 in the trials varied among treatment groups and because it may also lower oxalate levels, it is unclear how much of the treatment effect could be attributed to vitamin B6 versus lumasiran. Subgroup analyses of baseline vitamin B6 use (yes versus no) did not indicate a clear difference between the groups, though limitations of the subgroup analyses prevent firm conclusions from being made. Based on the data available up to the cut-off date, the rate of kidney stone events appeared to be lower for the lumasiran followed by lumasiran treatment group compared to before enrolling in the ILLUMINATE-A trial. However, patients randomized to lumasiran in the trial appeared to have a higher instance of history of kidney stone events compared to the placebo group, which may confound the interpretation of this outcome. For HRQoL outcomes, baseline scores for some instrument scales appeared to be imbalanced between treatment groups in the ILLUMINATE-A trial and there were no MIDs identified from the literature for patients with PH1, making it challenging to draw conclusions from these results.
External Validity
In the ILLUMINATE-A trial, 13 individuals were screened out: ██ due to eligibility criteria and █ from withdrawal by patient. Screening failures were not discussed in either the ILLUMINATE-B or ILLUMINATE-C trial. Given the lack of details for all 3 trials, it is unknown if this biased results or how this limits the generalizability to the entire population of patients who could receive lumasiran.
Patients enrolled in the 3 ILLUMINATE trials included both adult and pediatric patients (age range 0 to 60 years) with a range of kidney function (eGFR ranged from 8.61 to 174.06 mL/min/1.73 m2 and included patients on dialysis) and PH1-presenting symptoms. The oldest patient among the studies was aged 60 years and the clinical experts expect most patients to be younger than 60 years and that those older than that would likely have mild disease. Although it has been noted2 that there is limited evidence in patients younger than 2 years and weighing less than 10 kg, the clinical experts felt it would be appropriate to treat these patients with lumasiran. Based on the wide range of patients included in the 3 trials and the baseline characteristics, the clinical experts consulted by CADTH indicated that the trials were mostly applicable to patients living in Canada with PH1 who may receive lumasiran.
Administration of lumasiran in the trial appeared to align with the product monograph. Currently there are no approved treatments for PH1 beyond standard of care and placebo was the only comparator used (ILLUMINATE-A). In all 3 trials, patients were to continue their current standard-of-care treatments, which the clinical experts stated was expected practice with lumasiran. The clinical experts also stated the importance of having more data on the use of lumasiran in patients who have a vitamin B6–sensitive mutation to determine how the drug is used in these patients.
The 3 trials included patients with PH1 who would be the most likely candidates for lumasiran: the ILLUMINATE-A trial consisted of patients aged at least 6 years with a mean 24-hour urine oxalate excretion of at least 0.70 mmol/24 hour/1.73 m2; the ILLUMINATE-B trial included patients aged less than 6 years with a urine oxalate:creatinine ratio greater than the ULN; and the ILLUMINATE-C trial included patients with an eGFR of 45 mL/min/1.73 m2 or lower, with plasma oxalate of at least 20 μmol/L (with or without dialysis). Patients with possible hepatic impairment (ALT or AST reading greater than 2 times ULN for age or total bilirubin greater than 1.5 times ULN), history of kidney transplant, evidence of systemic oxalosis (ILLUMINATE-A or ILLUMINATE-B), or receiving peritoneal dialysis (ILLUMINATE-C) were excluded. Thus, treatment with lumasiran is uncertain in patients with these characteristics. Aside from these limitations, the clinical experts generally felt that the trial results could be generalized to the Canadian population with PH1. Specifically for dialysis, the clinical experts stated that the type of dialysis (peritoneal or hemodialysis) should not prevent a patient from receiving lumasiran. Further, patients who have received a kidney-only transplant would be required to continue lumasiran treatment posttransplant to reduce endogenous oxalate overproduction and protect the allografts. Therefore, the exclusion of these patients is a limitation and more evidence is needed to be certain of the efficacy and safety in patients with these characteristics.
The clinical experts confirmed that the trial outcomes were typical measures used when assessing and managing patients with PH1. Although improvements in urine and plasma oxalate levels are clinically important, they may be less relevant to patients compared to outcomes such as preventing kidney stone formation, dialysis, transplant, and progression to ESKD. As mentioned earlier, a major limitation is the relatively short duration of treatment on lumasiran so far and the clinical experts emphasized the need for long-term data to better understand how the surrogate measures relate to clinical outcomes.
The clinical experts stated that there is no way to measure total body oxalate, making it challenging to accurately assess treatment efficacy. Moreover, there are uncertainties about what the most appropriate or relevant trial outcomes are, which limits the interpretation and generalizability of the results. Kidney stone burden is clinically meaningful, but there are issues with assessing stones and using it as a trial end point.61 Additionally, kidney function is not expected to rapidly decline in patients with PH1, with studies reporting a decrease of 1 to 2 mL/min/1.73 m2 per year, though this is generally higher in patients with advanced CKD.61 Thus, it is unclear if eGFR can be used as a trial end point.
The clinical experts confirmed that the trial outcomes, all of which are surrogate measures, were typical measures used when assessing and managing patients with PH1. However, it is unclear how the main outcomes of the trials lead to treatment goals such as prevention of kidney stones and progression to ESKD. The clinical experts explained how, as kidney function declines with progression of PH1, the kidneys lose their ability to excrete oxalate, making urinary oxalate levels unreliable and/or not used in favour of plasma oxalate measures. Therefore, in patients who have preserved kidney function (and are removing excess oxalate through urine), it is unclear how meaningful changes in plasma oxalate are, while in patients with very low kidney function, it is unclear how meaningful changes in urine oxalate are. One study suggested that urine oxalate and plasma oxalate measures be used as surrogate outcomes for patients with CKD stages 1 to 3a and CKD stages 3 to 5b, respectively.9 Another study noted the challenges with accurately measuring plasma oxalate, how it does not correlate well with eGFR, and that there can be variation among patients with PH1.5,61 The experts also noted that while 24-hour urine is the standard method for measuring urine oxalate, this is not feasible for all patients (e.g., incontinent patients) and spot urine is an acceptable, but imperfect, substitute. Results from the literature are variable, with some studies finding no or weak correlation62,63 between 24-hour and spot urine tests for oxalate and others finding some correlation64,65 between the measures. Evidence from the literature is also mixed for how related urine oxalate and urine oxalate:creatinine ratio measures are, with a study finding no correlation (r = 0.02),63 while others have found a moderate (r = 0.63)57 to strong correlation (r = 0.75)58 between the measures. Despite the correlation, it was noted that there was some variability in results, and that age-specific references are needed when interpreting oxalate:creatinine values.58
Other Relevant Evidence
This section includes a long-term extension study included in the sponsor’s submission to CADTH that was considered to address important gaps in the evidence included in the systematic review.
Long-Term Extension Studies
The sponsor submitted the ALN-GO1 to 001 and ALN-GO1 to 002 trials to CADTH as supportive evidence of lumasiran for the treatment of PH1.
ALN-GO1 to 001 Trial (Parts A and B)
The ALN-GO1 to 001 trial was a first-in-human, phase I/II study conducted in 2 parts: single ascending dose (Part A) in 32 healthy adult volunteers who were aged between 18 and 64 years; and multiple ascending dose (Part B) in 20 patients with PH1 who were aged at least 6 years and had relatively preserved kidney function (eGFR at least 45 mL/min/1.73m2).
Part A was conducted at 1 clinical study centre in the UK. The total duration of Part A of the study, including screening, for each healthy volunteer was up to 405 days. Data from Part A demonstrated the safety profile of lumasiran and a dose-dependent response in plasma and urinary glycolate concentration across 1.0 mg/kg, 3.0 mg/kg, and 6.0 mg/kg lumasiran dosing regimens. (Note: In healthy individuals, because their oxalate level is within reference range, glycolate was chosen as a biomarker instead of oxalate. Plasma glycolate levels were measured as an indicator of the reduction of GO messenger RNA by lumasiran.)
Part 2 was a randomized, placebo-controlled, single-blind study in which lumasiran was administered as 3 monthly doses of 1 mg/kg (Cohort 1, n = 7) or 3 mg/kg (Cohort 2, n = 7) or, alternatively, 2 quarterly doses of 3 mg/kg (Cohort 3, n = 3). One patient in each cohort received placebo (n = 3 for placebo) and subsequently crossed over to receive lumasiran at day 85, according to their respective cohort. The duration of treatment and estimated total time for Part B, including screening, for each patient on once-monthly dosing group was 57 days (from first to last dose) and up to 462 days, respectively, for active treatment arm; and 141 days and up to 546 days, respectively, for the placebo arm. For those in the once-every-3-month dosing group, duration of treatment (from first to last dose) was 85 days and the total time on study was up to 490 days in both lumasiran and placebo groups. Data from Part B demonstrated acceptable safety and tolerability of lumasiran. The majority of AEs reported in 58.8% of lumasiran-treated patients and 66.7% of placebo-treated patients were mild in severity. SAEs were reported in 2 (11.8%) lumasiran-treated patients and 1 (33.3%) placebo-controlled patient, with nephrolithiasis as the most commonly reported SAE. No deaths or WDAEs were reported during Part B. All lumasiran–treated patients in Part B showed a mean maximal reduction of ████% (range = ████% to ████%) in BSA-corrected 24-hour urinary oxalate excretion from baseline (a mean baseline urinary oxalate excretion of 1.71 mmol/24h/1.73m2) and achieved urinary oxalate level at or below 1.5 times ULN (at or below 0.69 mmol/24h/1.73m2) by day 197. Reductions in urine oxalate:creatinine ratios from both 24-hour urine samples and spot urine samples were consistent with the results seen in BSA-corrected, 24-hour urine oxalate assessments. The 3.0 mg/kg monthly dosing showed more rapid and higher magnitude of reduction in 24-hour urinary oxalate with lower interpatient variability compared to the 1.0 mg/kg monthly and 3.0 mg/kg quarterly dosing regimens. Also, the 3.0 mg/kg quarterly dosing showed sustained urinary oxalate reduction throughout the 3-month dosing interval.
ALN-GO1 to 001 Part B became the parent trial of the ALN-GO1 to 002 trial, which is discussed in more detail in the following section.
ALN-GO1 to 002 Trial (OLE Study)
The ALN-GO1 to 002 trial was a phase II, multicentre, open-label, extension study to evaluate the long-term safety and efficacy of lumasiran in patients with PH1 who have completed Part B of the ALN-GO1 to 001 trial within 12 months. Patients were enrolled from a total of 9 clinical sites (7 sites in the European Union and 2 sites in Israel). Patients enrolled in the ALN-GO1 to 002 trial received lumasiran according to their respective initiation-dosing regimen in Part B of the ALN-GO1 to 001 trial for up to 54 months.
In addition to the completion of Part B of the ALN-GO1 to 001 trial, to be eligible for the ALN-GO-002 study, patients must have had 24-hour urine oxalate excretion of at least 0.7 mmol/1.73 m2/day and eGFR of at least 45 mL/min/1.73 m2 at baseline. If patients were on vitamin B6, they must have been on stable dosage for at least 90 days before study entry and were to remain on a stable regimen for the study duration. Patients were excluded if they required chronic dialysis, had electrocardiogram abnormalities, left ventricular ejection fraction less than 55%, or AST or ALT level abnormalities at baseline. If patients progressed to require dialysis while on the trial, they continued with lumasiran, which would be dosed as soon as possible at the end of dialysis (e.g., within 2 hours of completing the dialysis session). During the trial, patients would continue standard-of-care treatments. Patients received lumasiran in the same dose and regimen as they had received in Part B of the ALN-GO1 to 001 study.
The primary end point was the incidence of AEs. Secondary end points were the change in 24-hour urinary oxalate corrected for BSA over time, change in 24-hour urinary oxalate:creatinine ratio over time, and change in eGFR over time. Exploratory end points included change in plasma oxalate concentration and spot urine oxalate:creatinine ratio from baseline over the course of the study, incidence of ADAs, and HRQoL as assessed by KDQOL (for adults at least 18 years old), PedsQL Generic and ESRD modules (for pediatric patients aged under 18 years). Of note, the protocol was amended to extend the study duration from up to 2 years to up to 54 months.
No formal statistical analyses were performed, including statistical analyses that adjust for possible covariate effects and imputations for missing data points. The sample size was not determined through a power calculation. All results were descriptive in nature and did not involve any formal hypothesis testing. Safety and clinical activity data (e.g., eGFR) were analyzed for the safety analysis set (N = 20), which included all patients who received any amount of lumasiran. For main efficacy parameters (e.g., 24-hour urinary oxalate), the PD analysis set (N = 20) was used, which included all patients who received any amount of study drug and who had at least 1 postdose urine sample for PD. Additional analyses on exploratory end points (e.g., plasma oxalate, spot urine oxalate:creatinine ratio) were also performed on the PD analysis set. Patients’ eGFR was calculated based on the Modification of Diet in Renal Disease formula for patients at least 18 years of age at enrolment and the Schwartz Bedside Formula for patients younger than 18 years of age at enrolment.
The duration of follow-up in the ALN-GO1 to 002 study varied between patients (range, 112 to 401 days). At screening, the mean age of all lumasiran–treated patients (N = 20) was 14.9 years (SD, 10.18 years): 80% were aged less than 18 years and none was aged older than 65 years. Thirteen patients (65%) were female and 7 patients (35%) were male; 15 patients (75%) were white, while 4 patients (20%) were Asian and 1 patient (5%) was another race. Two patients (10%) were identified as having any type of genotype that is responsive to vitamin B6 and 13 (65%) patients were being treated with vitamin B6 at baseline. The mean age at diagnosis was 4.4 years (SD = 3.65 years) and mean time since diagnosis to first dose of lumasiran was ████ years (SD = ████ years).
Baseline is defined as the derived baseline value in Part B of the ALN-GO1 to 001 study: all measurements before the first dose date of lumasiran for patients in active study drug arm and the last 3 measurements collected before the first dose date of lumasiran for patients in placebo arm. For data not collected in Part B of the ALN-GO1 to 001 study, such as KDQOL-36 and PedsQL, baseline is defined as the last measurement before the first of lumasiran in the ALN-GO1 to 002 study.
The median age among all patients was ████ years (range 6 to 43 years; mean age = 14.9 years [SD = █████ years]; min, max = 6, 43 years) and most patients (80%) were younger than aged 18 years with ████████ being aged less than 12 years at the time of enrolment in Part B of the ALN-GO1 to 001 study. More than half (65%) of the patients were female and 7 patients (35%) were male; 15 patients (75%) were white, 4 patients (20%) were Asian, and 1 patient (5%) was another race. The mean age at diagnosis among all patients was 4.4 years (SD = 3.65 years) and the mean time since diagnosis before the first dose of lumasiran was ████ years (SD = ████ years). A majority of patients (65.0%) were taking vitamin B6 at baseline. Most patients (██%) had at least 1 PH1 symptom before entry into Part B of the ALN-GO1 to 001 study: ██████ █████ █████████████████ █ █ ██ ████████ ██████████ █████ █ ██████ ████. Finally, 2 (10%) patients had a genotype that was vitamin B6 responsive and were on vitamin B6. These 2 patients were in the 1.0 mg/kg once monthly or 3.0 mg/kg once-quarterly dosing arm (n = 13) and none in the 3.0 mg/kg once-monthly dosing arm (n = 7) had a vitamin B6–responsive genotype.
At baseline, among all patients treated with lumasiran (N = 20), mean 24-hour urinary oxalate excretion corrected for BSA and urinary oxalate:creatinine ratio were 2.24 mmol/24 hour/1.73m2 (SD = ████ mmol/24 hour/1.73m2) and 0.28 mmol/mmol (SD = ████ mmol/mmol), respectively, based on the validated PD assay performed at QPS. The ULNs for both parameters are 0.514 mmol/24 hour/1.73 m2 and 0.0799 mmol/mmol for patients aged 6 years or older, respectively. Mean baseline plasma oxalate based on validated PD assay performed at QPS was 15.28 µmol/L (SD = ████ µmol/L) among all lumasiran–treated patients. The ULN is less than 2 µmol/L according to the Mayo Clinic reference as noted by the clinical expert consulted by CADTH. Of note, the mean 24-hour urinary oxalate corrected for BSA at baseline was higher among patients in the 3.0 mg/kg monthly dosing cohort (n = 7; ████ mmol/24 hour/1.73 m2, SD = ████ mmol/24 hour/1.73 m2) compared to those in 1.0 mg/kg monthly or 3.0 mg/kg quarterly dosing cohorts (n = 13; ████ mmol/24 hour/1.73 m2, SD = ████ mmol/24 hour/1.73 m2). Similarly, the mean plasma oxalate level at baseline was higher among patients in the 3.0 mg/kg monthly dosing cohort (n = 7; █████ µmol/L, SD = ████ µmol/L) compared to those in the 1.0 mg/kg monthly or 3.0 mg/kg quarterly dosing cohorts (n = 13; █████ µmol/L, SD = ████ µmol/L). There was no difference in baseline mean spot urinary oxalate:creatinine ratio, which was ████ mmol/mmol (SD = ████ mmol/mmol) for all lumasiran–treated patients. Of all the patients, ██% had an eGFR equal to or greater than 45 mL/min/1.73 m2 and ████████████ had an eGFR between 30 and 44 mL/min/1.73 m2 at baseline. No explanation was provided by the sponsor regarding inclusion of ██████████ whose eGFR was less than 45 mL/min/1.73 m2 at baseline.
At the data cut-off date of March 1, 2021, the mean duration of drug exposure among all lumasiran–treated patients was ████ months (SD = ████ months), with a median of 28.0 months (Q1, Q3 = ██, ██ months; min, max = 24, 35 months). Because patients were enrolled sequentially by dose cohort, patients in the earlier dose cohort (i.e., 1.0 mg/kg monthly or 3.0 mg/kg quarterly), had a longer duration of exposure than those in the 3.0 mg/kg monthly cohort by a few months.
Efficacy
To assess the efficacy of lumasiran in the long-term treatment of patients with PH1, intragroup comparisons are made based on baseline values. One patient did not have a valid baseline collection from Part B of the ALN-GO1 to 001 trial (creatinine excretion less than 10 mg/kg); therefore, this patient was not included in the analyses for 24-hour urinary oxalate and plasma oxalate changes.
The mean eGFR for all patients was 77.34 mL/min/1.73 m2 (SD = 22.11 mL/min/1.73 m2) at baseline in Part B of the ALN-GO1 to 001 trial, and remained stable before dosing (day 1) in the ALN-GO1 to 002 trial with █████ mL/min/1.73 m2 (SD = █████ mL/min/1.73 m2). Throughout the study period, mean eGFR levels appeared to remain stable. For all lumasiran–treated patients, mean eGFR was █████ mL/min/1.73 m2 (SD = █████ mL/min/1.73 m2), █████ mL/min/1.73 m2 (SD = █████ mL/min/1.73 m2), █████ mL/min/1.73 m2 (SD = 24.70 mL/min/1.73 m2), and █████ mL/min/1.73 m2 (SD = █████ mL/min/1.73 m2) at months 6, 12, 24, and 30, respectively (Table 32). The results for loss of kidney function over time estimated by measures other than eGFR and results for prevention of dialysis and/or liver-kidney transplant were not reported in the study.
Prior to Part B of the ALN-GO1 to 001 trial, ██████████████ had at least 1 symptomatic kidney stone episode. During the treatment in Part B of the ALN-GO1 to 001 trial, 4 (20%) patients had an episode. After resuming treatment in the ALN-GO1 to 002 trial, an additional 3 (15%) patients had at least 1 kidney stone event during a total 30 (or 36) months period. The rate of kidney stone events per person-year during the ALN-GO1 to 002 trial was 0.06 (95% CI, ████ to ████) for the total population (Table 32).
Assessments of HRQoL (KDQOL and PedsQL) were not performed before the first lumasiran dose in Part B of the ALN-GO1 to 001 trial and changes from baseline were not assessed. The data were not reported by the sponsor and were not summarized in this report.
The mean 24-hour urinary oxalate corrected for BSA was 2.24 mmol/24 hour/1.73 m2 (SD = ████ mmol/24 hour/1.73 m2, ULN = 0.514 mmol/24 hour/1.73 m2) at baseline in Part B of the ALN-GO1 to 001 trial and was lower (████ mmol/24 hour/1.73 m2, SD = ████ mmol/24 hour/1.73 m2) at the start of the ALN-GO1 to 002 trial, indicating persistence of treatment effect of lumasiran. Levels of 24-hour urinary oxalate corrected for BSA decreased upon resuming treatment in the ALN-GO1 to 002 trial and then stabilized afterward. For all lumasiran–treated patients (n = 19), 24-hour urinary oxalate corrected for BSA was ████ mmol/24 hour/1.73 m2 (SD = ████ mmol/24 hour/1.73 m2), ████ mmol/24 hour/1.73 m2 (SD = ████ mmol/24 hour/1.73 m2), ████ mmol/24 hour/1.73 m2 (SD = ████ mmol/24 hour/1.73 m2), and ████ mmol/24 hour/1.73 m2 (SD = ████ mmol/24 hour/1.73 m2) at months 6, 12, 24, and 30, respectively. Between the groups, patients who received 3.0 mg/kg once monthly had a █████% (SD = ████%) to █████% (SD = ████%) reduction in urinary oxalate, whereas those who received either 1.0 mg/kg once monthly or 3.0 mg/kg every 3 months achieved a █████% (SD = █████%) to █████% (SD = █████%) decrease in urinary oxalate during the study period. Of note, the 3.0 mg/kg once-monthly group had a higher baseline urinary oxalate level (████ mmol/24 hour/1.73 m2, SD = ████ mmol/24 hour/1.73 m2) compared to the other groups that received either 1.0 mg/kg once monthly or 3.0 mg/kg quarterly (████ mmol/24 hour/1.73 m2, SD = ████ mmol/24 hour/1.73 m2). Similarly, the proportion of patients achieving 24-hour urinary oxalate corrected for BSA of near-normal (1.5 times ULN) and normal (ULN) levels appeared to stabilize after 6 months. At any postbaseline visit, 100% and 65% of all lumasiran–treated patients showed near-normal and normal values, respectively, for 24-hour urinary oxalate corrected for BSA (Table 32).
Results from changes in plasma oxalate level were consistent with the observations in 24-hour urinary oxalate. Patients showed a reduction in plasma oxalate level in the first 6 months and maintained the reduction throughout the study period. For all lumasiran–treated patients (n = 19), plasma oxalate level was ████ µmol/L (SD = ████ µmol/L), ████ µmol/L (SD = ████ µmol/L), ████ µmol/L (SD = ████ µmol/L), ████ µmol/L (SD = ███ µmol/L), and ████ µmol/L (SD = ████ µmol/L) at day 1 and months 6, 12, 24, and 30, respectively. Similar to 24-hour urinary oxalate results, patients in the 3.0 mg/kg once-monthly group had a higher baseline plasma oxalate level (█████ µmol/L, SD = ████ µmol/L) and showed a greater reduction with lumasiran (ranges from █████% [SD = █████%] to █████% [SD was not reported]) compared to those in the 1.0 mg/kg once monthly or 3.0 mg/kg quarterly groups (█████ µmol/L [SD = ████ µmol/L] at baseline; decrease ranges from █████% [SD = █████%] to █████% [SD = █████%]) (Table 32).
Similarly, mean 24-hour and spot urinary oxalate:creatinine ratios declined after resuming treatment in ALN-GO1 to 002 for the first 6 months and stabilized thereafter. For all lumasiran–treated patients (N = 20), 24-hour urinary oxalate:creatinine ratio was ████ mmol/mmol (SD = ████ mmol/mmol), ████ mmol/mmol (SD = ████ mmol/mmol), ████ mmol/mmol (SD = ████ mmol/mmol), ████ mmol/mmol (SD = ████ mmol/mmol), and ████ mmol/mmol (SD = ████ mmol/mmol) at day –1 and months 6, 12, 24, and 30, respectively. Patients in the 3.0 mg/kg once-monthly group had a higher baseline value (████ mmol/mmol [SD = ████ mmol/mmol]) and greater reduction in 24-hour oxalate:creatinine ratio (ranges from █████% [█████%] to █████% [SD = ████%]) than those in the 1.0 mg/kg once monthly or 3.0 mg/kg quarterly groups (████ mmol/mmol [SD = ████ mmol/mmol] at baseline, reduction ranges from █████% [SD = █████%] to █████% [SD = █████%]). For all lumasiran–treated patients (N = 20), spot urinary oxalate:creatinine ratio was ████ mmol/mmol (SD = ████ mmol/mmol), ████ mmol/mmol (SD = ████ mmol/mmol), ████ mmol/mmol (SD = ████ mmol/mmol), ████ mmol/mmol (SD = ████ mmol/mmol), and ████ mmol/mmol (SD = ████ mmol/mmol) at day 1 and months 6, 12, 24, and 30, respectively. In terms of between-group comparison, baseline values were similar (0.26 mmol/mmol [SD = ████ mmol/mmol] in the 1.0 mg/kg once-monthly or 3.0 mg/kg quarterly groups versus ████ mmol/mmol [SD = ████ mmol/mmol] in the 3.0 mg/kg once monthly group). The magnitude of reduction with lumasiran ranged from █████% (SD = █████%) to █████% (SD = █████%) in the 1.0 mg/kg once monthly or 3.0 mg/kg quarterly groups compared to ranges from █████% (SD = █████%) to █████% (SD not reported) in the 3.0 mg/kg once-monthly group) for spot urinary oxalate:creatinine ratio (Table 32).
Table 32: Secondary and Exploratory Efficacy End Points: ALN-GO1 to 002 Trial
Outcome | 1.0 mg/kg QM or 3.0 mg/kg Q3M (N = 13) | 3.0 mg/kg QM (N = 7) | All lumasiran–treated (N = 20) | |
|---|---|---|---|---|
eGFRa (mL/min/1.73 m2): safety analysis set | ||||
Number of patients contributing to the analysis, n (%) | ███████ | ███████ | ███████ | |
Baseline, mean (SD) | ███████ | ███████ | 77.34 (22.11) | |
Number of patients contributing to the analysis, n (%) | ███████ | ███████ | ███████ | |
Day 1, mean (SD) | ███████ | ███████ | ███████ | |
Change from baseline, mean (SD) | ███████ | ███████ | ███████ | |
% change from baseline, mean (SD) | ███████ | ███████ | ███████ | |
Number of patients contributing to the analysis, n (%) | ███████ | ███████ | ███████ | |
Month 6, mean (SD) | ███████ | ███████ | ███████ | |
Change from baseline, mean (SD) | ███████ | ███████ | ███████ | |
% change from baseline, mean (SD) | ███████ | ███████ | ███████ | |
Number of patients contributing to the analysis, n (%) | ███████ | ███████ | ███████ | |
Month 12, mean (SD) | ███████ | ███████ | ███████ | |
Change from baseline, mean (SD) | ███████ | ███████ | ███████ | |
% change from baseline, mean (SD) | ███████ | ███████ | ███████ | |
Number of patients contributing to the analysis, n (%) | ███████ | ███████ | ███████ | |
Month 24, mean (SD) | ███████ | ███████ | ███████ | |
Change from baseline, mean (SD) | ███████ | ███████ | ███████ | |
% change from baseline, mean (SD) | ███████ | ███████ | ███████ | |
Number of patients contributing to the analysis, n (%) | ███████ | ███████ | ███████ | |
Month 30, mean (SD) | ███████ | ███████ | ███████ | |
Change from baseline, mean (SD) | ███████ | ███████ | ███████ | |
% change from baseline, mean (SD) | ███████ | ███████ | ███████ | |
Kidney stone eventsb: safety analysis set | ||||
Number of patients contributing to the analysis | 1.0 mg/kg QM (N = 8) | 3.0 mg/kg Q3M (N = 4) | 3.0 mg/kg QM (N = 8) | All lumasiran (N = 20) |
Number of patients with at least 1 symptomatic kidney stone episode, n (%) | ||||
12-month period before informed consent | ███████ | ███████ | ███████ | ███████ |
Lumasiran treatment in ALN-GO1 to 001 Part B | ███████ | ███████ | ███████ | ███████ |
Number of patients with at least 1 kidney stone adverse event during lumasiran treatment in ALN-GO1 to 002, n (%) | ||||
Day 1 to month 6 | ███████ | ███████ | ███████ | █ |
Month 6 to month 12 | ███████ | ███████ | ███████ | ███████ |
Month 12 to month 24 | ███████ | ███████ | ███████ | ███████ |
Month 24 to month 30 | ███████ | ███████ | ███████ | ███████ |
Overall | ███████ | ███████ | ███████ | ███████ |
Ratec of kidney stone AEs per person-year (95% CI) during lumasiran treatment in ALN-GO1 to 002d | ███████ | ███████ | ███████ | 0.06 (█████ ████) |
24-hour urinary oxalate corrected for BSA (mmol/24 hour/1.73 m2): PD analysis set | ||||
Number of patients contributing to the analysis, n (%) | ███████ | ███████ | ███████ | |
Baseline, mean (SD) | ███████ | ███████ | 2.24 (████) | |
Number of patients contributing to the analysis, n (%) | ███████ | ███████ | ███████ | |
Day –1, mean (SD) | ███████ | ███████ | ███████ | |
Change from baseline, mean (SD) | ███████ | ███████ | ███████ | |
% change from baseline, mean (SD) | ███████ | ███████ | ███████ | |
Number of patients contributing to the analysis, n (%) | ███████ | ███████ | ███████ | |
Month 6, mean (SD) | ███████ | ███████ | ███████ | |
Change from baseline, mean (SD) | ███████ | ███████ | ███████ | |
% change from baseline, mean (SD) | ███████ | ███████ | ███████ | |
Number of patients contributing to the analysis, n (%) | ███████ | ███████ | ███████ | |
Month 12, mean (SD) | ███████ | ███████ | ███████ | |
Change from baseline, mean (SD) | ███████ | ███████ | ███████ | |
% change from baseline, mean (SD) | ███████ | ███████ | ███████ | |
Number of patients contributing to the analysis, n (%) | ███████ | ███████ | ███████ | |
Month 24, mean (SD) | ███████ | ███████ | ███████ | |
Change from baseline, mean (SD) | ███████ | ███████ | ███████ | |
% change from baseline, mean (SD) | ███████ | ███████ | ███████ | |
Number of patients contributing to the analysis, n (%) | ███████ | ███████ | ███████ | |
Month 30, mean (SD) | ███████ | ███████ | ███████ | |
Change from baseline, mean (SD) | ███████ | ███████ | ███████ | |
% change from baseline, mean (SD) | ███████ | ███████ | ███████ | |
Percentage of patients with 24-hour urinary oxalate corrected for BSA ≤ 1.5 × ULN,e n/N (%) | ||||
Baseline | ███████ | ███████ | ███████ | |
Day –1 | ███████ | ███████ | ███████ | |
Month 6 | ███████ | ███████ | ███████ | |
Month 12 | ███████ | ███████ | ███████ | |
Month 24 | ███████ | ███████ | ███████ | |
Month 30 | ███████ | ███████ | ███████ | |
At any postbaseline visit | ███████ | ███████ | ███████ | |
Percentage of patients with 24-hour urinary oxalate corrected for BSA ≤ ULNe, n/N (%) | ||||
Baseline | ███████ | ███████ | ███████ | |
Day –1 | ███████ | ███████ | ███████ | |
Month 6 | ███████ | ███████ | ███████ | |
Month 12 | ███████ | ███████ | ███████ | |
Month 24 | ███████ | ███████ | ███████ | |
Month 30 | ███████ | ███████ | ███████ | |
At any postbaseline visit | ███████ | ███████ | ███████ | |
Plasma oxalate (µmol/L): PD analysis set | ||||
Number of patients contributing to the analysis, n (%) | ███████ | ███████ | ███████ | |
Baseline, mean (SD) | ███████ | ███████ | 15.28 (████) | |
Number of patients contributing to the analysis, n (%) | ███████ | ███████ | ███████ | |
Day 1, mean (SD) | ███████ | ███████ | ███████ | |
Change from baseline, mean (SD) | ███████ | ███████ | ███████ | |
% change from baseline, mean (SD) | ███████ | ███████ | ███████ | |
Number of patients contributing to the analysis, n (%) | ███████ | ███████ | ███████ | |
Month 6, mean (SD) | ███████ | ███████ | ███████ | |
Change from baseline, mean (SD) | ███████ | ███████ | ███████ | |
% change from baseline, mean (SD) | ███████ | ███████ | ███████ | |
Number of patients contributing to the analysis, n (%) | ███████ | ███████ | ███████ | |
Month 12, mean (SD) | ███████ | ███████ | ███████ | |
Change from baseline, mean (SD) | ███████ | ███████ | ███████ | |
% change from baseline, mean (SD) | ███████ | ███████ | ███████ | |
Number of patients contributing to the analysis, n (%) | ███████ | ███████ | ███████ | |
Month 24, mean (SD) | ███████ | ███████ | ███████ | |
Change from baseline, mean (SD) | ███████ | ███████ | ███████ | |
% change from baseline, mean (SD) | ███████ | ███████ | ███████ | |
Number of patients contributing to the analysis, n (%) | ███████ | ███████ | ███████ | |
Month 30, mean (SD) | ███████ | ███████ | ███████ | |
Change from baseline, mean (SD) | ███████ | ███████ | ███████ | |
% change from baseline, mean (SD) | ███████ | ███████ | ███████ | |
24-hour urinary oxalate:creatinine ratiof (mmol/mmol): PD analysis set | ||||
Number of patients contributing to the analysis, n (%) | ███████ | ███████ | ███████ | |
Baseline, mean (SD) | ███████ | ███████ | 0.28 (████) | |
Number of patients contributing to the analysis, n (%) | ███████ | ███████ | ███████ | |
Day –1, mean (SD) | ███████ | ███████ | ███████ | |
Change from baseline, mean (SD) | ███████ | ███████ | ███████ | |
% change from baseline, mean (SD) | ███████ | ███████ | ███████ | |
Number of patients contributing to the analysis, n (%) | ███████ | ███████ | ███████ | |
Month 6, mean (SD) | ███████ | ███████ | ███████ | |
Change from baseline, mean (SD) | ███████ | ███████ | ███████ | |
% change from baseline, mean (SD) | ███████ | ███████ | ███████ | |
Number of patients contributing to the analysis, n (%) | ███████ | ███████ | ███████ | |
Month 12, mean (SD) | ███████ | ███████ | ███████ | |
Change from baseline, mean (SD) | ███████ | ███████ | ███████ | |
% change from baseline, mean (SD) | ███████ | ███████ | ███████ | |
Number of patients contributing to the analysis, n (%) | ███████ | ███████ | ███████ | |
Month 24, mean (SD) | ███████ | ███████ | ███████ | |
Change from baseline, mean (SD) | ███████ | ███████ | ███████ | |
% change from baseline, mean (SD) | ███████ | ███████ | ███████ | |
Number of patients contributing to the analysis, n (%) | ███████ | ███████ | ███████ | |
Month 30, mean (SD) | ███████ | ███████ | ███████ | |
Change from baseline, mean (SD) | ███████ | ███████ | ███████ | |
% change from baseline, mean (SD) | ███████ | ███████ | ███████ | |
Spot urinary oxalate:creatinine ratiof (mmol/mmol): PD analysis set | ||||
Number of patients contributing to the analysis, n (%) | ███████ | ███████ | ███████ | |
Baseline, mean (SD) | ███████ | ███████ | ███████ | |
Number of patients contributing to the analysis, n (%) | ███████ | ███████ | ███████ | |
Day 1, mean (SD) | ███████ | ███████ | ███████ | |
Change from baseline, mean (SD) | ███████ | ███████ | ███████ | |
% change from baseline, mean (SD) | ███████ | ███████ | ███████ | |
Number of patients contributing to the analysis, n (%) | ███████ | ███████ | ███████ | |
Month 6, mean (SD) | ███████ | ███████ | ███████ | |
Change from baseline, mean (SD) | ███████ | ███████ | ███████ | |
% change from baseline, mean (SD) | ███████ | ███████ | ███████ | |
Number of patients contributing to the analysis, n (%) | ███████ | ███████ | ███████ | |
Month 12, mean (SD) | ███████ | ███████ | ███████ | |
Change from baseline, mean (SD) | ███████ | ███████ | ███████ | |
% change from baseline, mean (SD) | ███████ | ███████ | ███████ | |
Number of patients contributing to the analysis, n (%) | ███████ | ███████ | ███████ | |
Month 24, mean (SD) | ███████ | ███████ | ███████ | |
Change from baseline, mean (SD) | ███████ | ███████ | ███████ | |
% change from baseline, mean (SD) | ███████ | ███████ | ███████ | |
Number of patients contributing to the analysis, n (%) | ███████ | ███████ | ███████ | |
Month 30, mean (SD) | ███████ | ███████ | ███████ | |
Change from baseline, mean (SD) | ███████ | ███████ | ███████ | |
% change from baseline, mean (SD) | ███████ | ███████ | ███████ | |
BSA = body surface area; CI = confidence interval; eGFR = estimated glomerular filtration rate; NA = not applicable; NR = not reported; PD = pharmacodynamic; Q3M = once every 3 months or quarterly; QM = once monthly; SD = standard deviation; ULN = upper limit of normal.
Baseline is defined as the last measurement before the first dose of lumasiran in the ALN-GO1 to 001 study.
Day –1 is defined as the median of all measurements within 30 days of the first dose of lumasiran in the ALN-GO1 to 002 study.
Day 1 is the latest measurement before the first dose of lumasiran in the ALN-GO1 to 002 study.
aeGFR is calculated based on the Modification of Diet in Renal Disease formula for patients aged at least 18 years at enrolment and the Schwartz Bedside Formula for patients aged less than 18 years at enrolment.
bRate of symptomatic kidney stone episodes and kidney stone adverse events.
cRate is calculated as the total number of kidney stone adverse events divided by total person-years at risk, with years at risk defined as (time from first lumasiran dose until 84 days after the last dose of lumasiran) / 365.25. The 95% CI for the event rate was obtained using a generalized linear model for a Poisson distribution unless the rate was 0, in which case the upper bound of the 95% CI was calculated using the exact Poisson method.
dPatients who received the specified initial dose of lumasiran in ALN-GO1 to 001 Part B either received the same dose or changed dose when they transitioned into ALN-GO1 to 002.
eThe ULN for QPS equals 0.514 mmol/24 hour/1.73 m2.
fBased on validated PD assay (QPS).
Source: CSR (ALN-GO1 to 002 month 24 data; data cut-off: March 01, 2021).66
The sponsor provided data for shift from baseline to worst postbaseline eGFR values. For all lumasiran–treated patients (N = 20), █ (██%), ██ (██%), █ (██%), and █ (█%) patients had an eGFR of at least 90, 60 to less than 90, 45 to less than 60, and 30 to less than 45 mL/min/1.73 m2 at baseline, respectively. At any postbaseline visit, █ (██%), ██ (██%), █ (██%), and █ (██%) patients had a worst eGFR of at least 90, 60 to less than 90, 45 to less than 60, and 30 to less than 45 mL/min/1.73 m2, respectively. For eGFR categories of 45 to less than 60 and 15 to less than 30 mL/min/1.73 m2, the number of patients █████████ from █ (██%) to █ (██%) and █ (█%) to █ (██%), respectively, from baseline to postbaseline. For eGFR category 60 to less than 90 mL/min/1.73 m2, the number of patients who fell in that category ██████ ███ ████ from baseline to postbaseline. For the eGFR category at least 90 mL/min/1.73 m2, the number of patients ████ from █ (██%) to █ (██%) from baseline to postbaseline (Table 33).
Table 33: Shift From Baseline to Worst Postbaseline eGFR (mL/min/1.73 m2): ALN-GO1 to 002 Trial, Safety Analysis Set
Outcome | 1.0 mg/kg QM or 3.0 mg/kg Q3M (N = 13) | 3.0 mg/kg QM (N = 7) | All lumasiran–treated (N = 20) | |||
|---|---|---|---|---|---|---|
eGFR (mL/min/1.73 m2) | Baseline eGFR categorization, n (%) | Worst value postbaseline, n (%) | Baseline eGFR categorization, n (%) | Worst value postbaseline, n (%) | Baseline eGFR categorization, n (%) | Worst value postbaseline, n (%) |
≥ 90 | ███████ | ███████ | ███████ | ███████ | ███████ | ███████ |
60 to < 90 | ███████ | ███████ | ███████ | ███████ | ███████ | ███████ |
45 to < 60 | ███████ | ███████ | ███████ | ███████ | ███████ | ███████ |
30 to < 45 | ███████ | ███████ | ███████ | ███████ | ███████ | ███████ |
15 to < 30 | ███████ | ███████ | ███████ | ███████ | ███████ | ███████ |
< 15 | ███████ | ███████ | ███████ | ███████ | ███████ | ███████ |
Total | ███████ | ███████ | ███████ | ███████ | ███████ | ███████ |
eGFR = estimated glomerular filtration rate; Q3M = once every 3 months or quarterly; QM = once monthly.
Baseline data are the derived baseline in the ALN-GO1 to 001 study.
Source: CSR (ALN-GO1 to 002 Month 24 data; data cut-off: March 1, 2021).66
Harms
All patients (N = 20) who had received at least 1 dose of lumasiran experienced at least 1 AE. The most commonly reported AEs (that are experienced by at least 2 patients) were injection site reaction (40%), vomiting (20%), headache (15%), limb injury (15%), and oropharyngeal pain (15%) (Table 34).
A total of 4 (20%) patients reported SAEs that included ██ ████████ ████████ ████████████████ ████████ ██ ██ ████ ████████ ██ ██████████ █████████ ████████ ███. One patient experienced 2 SAEs, a craniocerebral injury and bone (rib) contusion, from road traffic accidents (Table 34).
No patients discontinued treatment or withdrew from the study due to AEs.
There were no deaths reported during the study.
Of the notable harms, the most frequently reported (40%) was injection site reaction: ██████ ██████████ █ █ ███ ██████ ███ ██████████ ████ ██ ███████ ████████████████ █████████████ ███████ █████ ████████ ███████ █████ █████ ████████ ████ █████ ████████ ████████████████████ ███. Three (15%) patients experienced kidney and urinary disorders, such as nephrolithiasis (██), renal colic (██), and ureterolithiasis (██). Headache, ███ ███████ █████ ████████ ████████ ███████████ were reported by 3 (███), ███ ██████████ ██████████████████████ ███. Complications caused by systemic oxalosis or hypersensitivity were not reported during the study period. ██████ ██████████████████ ██████████ ███████ ████████ ██ ████ ██ ██████████████████████ ███ (Table 34).
A total of 20 patients contributed to the analysis of ADAs, which were assessed every 6 months during the study. ███ ███████ █████████ ████ █████████ █████████ ███████████████████████ ██████████████████ █████ █████████████ ████████████████ █████████████ ████████████████ ███████████████████ █████ ██ █████████████████ ██████ ██████████ ████████ ██████████████ ██ ██ ████ ███ ████████████████ █████████ ████████████████████████████████████████ ███ ███ ███ ███ █████ █████████ ██████ ██████ ████████ ███████ █ █████████ █████████. Of note, ADA assessment was an exploratory outcome in the ALN-GO1 to 002 trial.
Table 34: Summary of Harms (Primary End Point): ALN-GO1 to 002 Trial, Safety Analysis Set
Harms | 1.0 mg/kg QM or 3.0 mg/kg Q3M (N = 13) | 3.0 mg/kg QM (N = 7) | All lumasiran–treated (N = 20) |
|---|---|---|---|
Patients with ≥ 1 adverse event | |||
n (%) | █████████ | ████████ | 20 (100.0) |
Most common eventsa, n (%) | NA | NA | NA |
Injection site reaction | ███████ | ███████ | 8 (40.0) |
Vomiting | ███████ | ███████ | 4 (20.0) |
Headache | ███████ | ███████ | 3 (15.0) |
Limb injury | ███████ | ███████ | 3 (15.0) |
Oropharyngeal pain | ██████ | ███████ | 3 (15.0) |
Abdominal pain upper | █ | ███████ | ███████ |
Back pain | ██████ | ███████ | ███████ |
Cough | ██████ | ███████ | ███████ |
Gastroenteritis | ██████ | ███████ | ███████ |
Gastroenteritis viral | ██████ | █ | ███████ |
Influenza | ███████ | █ | ███████ |
Nasopharyngitis | ███████ | █ | ███████ |
Nausea | █ | ███████ | ███████ |
Pharyngitis | ██████ | █ | ███████ |
Pyrexia | ██████ | ███████ | ███████ |
Upper respiratory infection | █ | ███████ | ███████ |
Vitamin D deficiency | █ | ███████ | ███████ |
Patients with ≥ 1 SAEb | |||
n (%) | ███████ | ██████ | 4 (20.0) |
Blood creatinine increased | █ | ███████ | 1 (5.0) |
Bone contusion | ██████ | █ | 1 (5.0) |
Craniocerebral injury | ██████ | █ | 1 (5.0) |
Pyelonephritis | █ | ██████ | 1 (5.0) |
Renal colic | ██████ | █ | 1 (5.0) |
Ureterolithiasis | █ | ██████ | 1 (5.0) |
Patients who stopped treatment or withdrew due to adverse events | |||
n (%) | 0 | 0 | 0 |
Deaths | |||
n (%) | 0 | 0 | 0 |
Notable harms, n (%) | |||
Injection site reaction | ███████ | ███████ | 8 (40.0) |
Injection site erythema | ███████ | ███████ | ███████ |
Injection site swelling | ██████ | ███████ | ███████ |
Injection site discoloration | █ | ███████ | ███████ |
Injection site hematoma | ██████ | █ | ██████ |
Injection site induration | ██████ | █ | ██████ |
Injection site pain | █ | ███████ | ██████ |
Injection site pruritus | ██████ | █ | ██████ |
At least 1 kidney stone adverse event | ██████ | ███████ | 3 (15.0) |
Renal and urinary disorders | ███████ | ███████ | 3 (15.0) |
Nephrolithiasis | ██████ | █ | ██████ |
Renal colic | ██████ | █ | ██████ |
Ureterolithiasis | █ | ███████ | ██████ |
Complications from systemic oxalosis | NR | NR | NR |
Headache | ███████ | ███████ | 3 (15.0) |
Rhinitis | ██████ | █ | ██████ |
Upper respiratory infection | █ | ███████ | ███████ |
Hypersensitivity reaction | NR | NR | NR |
ADAs | ██████ | █ | ██████ |
Hypertension | █ | ███████ | ██████ |
Blood creatinine increased | █ | ███████ | ██████ |
ADA = antidrug antibody; NA = not applicable; NR = not reported; Q3M = once every 3 months or quarterly; QM = once monthly; SAE = serious adverse event.
aAt least 2 patients experienced an adverse event.
bIf a patient experienced more than 1 SAE in a given category, the patient was counted only once for that category.
Source: CSR (ALN-GO1 to 002 Month 24 data; data cut-off: March 1, 2021).66
Critical Appraisal
Internal Validity
The ALN-GO1 to 002 trial was a phase II, open-label, extension study to evaluate the long-term safety and efficacy of lumasiran in patients with PH1. As such, the study was not designed to test a hypothesis. Also, hierarchical statistical analyses, adjustments for multiplicity and type I error, and imputations for missing data points were not performed. Subgroup analyses or statistical adjustments to account for important factors such as vitamin B6–sensitive mutations were not conducted either. For example, there were 2 patients in the 1.0 mg/kg once monthly or 3.0 mg/kg once-quarterly dosing group (n = 13) who had a vitamin B6–sensitive mutation and were on vitamin B6, whereas none in the 3.0 mg/kg once-monthly dosing group (n = 7) had a vitamin B6–responsive genotype. Because vitamin B6 may also reduce oxalate levels, it is unclear how much of the effect seen in this trial could be attributed to this effect. In addition, results for HRQoL were not reported. The sample size was not determined using a power calculation and was likely too small to make a definitive conclusion about safety and efficacy. Finally, without a comparator, it is not possible to interpret comparative efficacy of lumasiran to other treatments. Therefore, all results are descriptive in nature, including efficacy outcomes that are secondary or exploratory end points in the ALN-GO1 to 002 trial.
External Validity
Based on clinical expert opinion, patients enrolled in the ALN-GO1 to 002 trial are considered similar to those seen in a Canadian clinical setting. However, considering the wide range of clinical manifestations with PH1, it is uncertain if the sample population adequately represents patients living in Canada with PH1. For example, the mean age of patients was 14.9 years (SD = █████ years) and the maximum age was 43 years. According to the clinical experts, younger patients may be considered to have more severe disease compared to older patients who had manifestation of PH1 later in life. Furthermore, most patients (██%) had at least 1 PH1 symptom before entry into Part B of the ALN-GO1 to 001 trial, with ███████ ███ ██████%) and ███ █████ ████ ████ (████%) being the most frequent symptoms, indicating these patients may have more severe disease. In addition, none of the trial sites selected were in Canada. Taken together, there may be some generalizability issues.
The follow-up time may be sufficient for observing an immediate treatment effect with a mean duration of exposure of ████ months (SD = ████ months) because the clinical experts stated that 2 to 3 years are deemed appropriate in a kidney disease–related clinical trial setting. It is unlikely that the duration of exposure is long enough to draw long-term conclusions for lumasiran treatment given that it is expected to be a lifelong treatment, according to the experts. During the ALN-GO1 to 002 treatment period, no patients withdrew from study or died due to AEs. Most AEs were related to injection site reactions that were local. Also, most of the reported SAEs were kidney related. These data suggest that lumasiran is safe for the first 30 months of treatment. However, as the clinical expert emphasized, longer-term data for ADAs, efficacy, and safety are warranted because ADAs can affect treatment efficacy.
In conclusion, based on the phase I/II study, efficacy cannot be determined for the reasons previously noted. Considering the available data, lumasiran appears to be safe for the first few years of treatment for patients with PH1.
Discussion
Summary of Available Evidence
One DB, phase III, placebo-controlled RCT (ILLUMINATE-A) and 2 phase III, single-arm trials (ILLUMINATE-B and ILLUMINATE-C) were included in the systematic review. All 3 trials are currently ongoing and were designed to assess the safety and efficacy of lumasiran in patients with a confirmed diagnosis of PH1. The ILLUMINATE-A trial (N = 36) compared lumasiran to placebo in patients who were aged 6 years or older and had a mean 24-hour urinary oxalate excretion of at least 0.70 mmol/24 hour/1.73 m2. After the 6-month DB period, patients randomized to the placebo group received lumasiran for the rest of the trial. The mean age of patients was 18.1 years (SD = █████ years; median = 14.0 years; range, 6 to 60 years); 66.7% were male and 33.3% were female; 76.9% were white, 15.4% were Asian, 5.1% were another race, and 2.6% identified as more than 1 race. The primary outcome was the percent change in 24-hour urinary oxalate excretion from baseline to month 6 corrected for BSA, and key secondary outcomes were absolute change in 24-hour urinary oxalate, 24-hour urinary oxalate:creatinine ratio, plasma oxalate, proportion of patients with 24-hour urinary oxalate level near-normal (at or less than 1.5 times ULN) or normal (at or less than ULN), and eGFR. The ILLUMINATE-B trial (N = 18) included patients who were aged younger than 6 years and had a urinary oxalate:creatinine ratio greater than the ULN. The mean age of patients was ████ months (SD = █████ months; median = 50.1 months; range, 3 to 72 months); 55.6% were female and 44.4% were male; and 88.9% were white while 11.1% identified as being another race. The primary outcome was percent change in urinary oxalate excretion from baseline to month 6, and key secondary outcomes were time and proportion of patients with urinary oxalate excretion near normal or normal, plasma oxalate, and eGFR. The ILLUMINATE-C trial (N = 21) included patients who had an eGFR of 45 mL/min/1.73 m2 or lower and who were either not on hemodialysis (Cohort A) or receiving stable hemodialysis (Cohort B). The mean age of patients was ████ years (SD = ████ years; median = 8.0 years; range, 0 to 59 years); 57.1% were male and 42.9% were female; and 76.2% were white, 19.0% were Asian, and 4.8% identified as another race. The primary outcome was percent change in plasma oxalate from baseline to month 6 (using a predialysis reading for Cohort B), and key secondary outcomes were plasma oxalate AUC between dialysis sessions, urinary oxalate, urinary oxalate:creatinine ratio, and PedsQL and KDQOL instruments. Other outcomes in the trials that were important to the CADTH review included kidney function (e.g., eGFR), kidney stone events, and HRQoL. Harms and notable harms (identified in the CADTH systematic review protocol) were assessed.
Two other relevant studies were summarized for this review that provided long-term safety and efficacy data on lumasiran treatment for up to 30 months in patients with PH1. The ALN-GO1 to 001 trial (32 healthy volunteers and 20 patients with PH1) and ALN-GO1 to 002 trial (N = 20) were phase I/II and phase II trials, respectively. The ALN-GO1 to 002 trial was the long-term, OLE that included patients with PH1 who had completed the ALN-GO1 to 001 trial, were aged at least 6 years, and had an eGFR of at least 45 mL/min/1.73 m2. The mean age of patients was 14.9 years (SD = 10.2 years; median = ████ years; range, 6 years to 43 years); 13 patients (65%) were female and 7 patients (35%) were male; and 15 patients (75%) were white, 4 patients (20%) were Asian, and 1 patient (5%) was of another race. The primary outcome was safety, and secondary end points were 24-hour urinary oxalate, 24-hour urinary oxalate:creatinine ratio, and eGFR.
Interpretation of Results
Efficacy
Current standard-of-care treatments for PH1 leave patients with many unmet needs such as challenges with compliance, treatments being burdensome, not addressing the underlying issue of hepatic oxalate overproduction, and having limited or no impact on the long-term complications of PH1.67 Liver (or combined liver-kidney) transplant has been identified as the only cure for these patients and is associated with high morbidity and mortality, lifelong immunosuppression, and limited survival of the allograft.67
The clinical experts consulted by CADTH noted the importance of preserving kidney function and preventing progression to ESKD in patients with PH1. Evidence from the literature suggests that there is a relationship between urine oxalate46 and kidney function, though the relationship is less clear for plasma oxalate.68-72 Changes in eGFR during the primary analysis period were numerically small during the 6-month primary analysis period across all 3 trials. The clinical experts noted that a duration of 6 months is not long enough to have a large change in eGFR, which is consistent with the published literature (expected decline of 1 to 2 mL/min/1.73 m2 per year for patients with PH1 and a larger decline for patients with advanced CKD).61 Results were also available for the shift from baseline to worst postbaseline eGFR category. Although the CADTH reviewers and clinical experts felt that this may provide useful information, interpretation of the data are challenging due to the lack of MID from the literature, small number of patients in the trials, short duration of treatment, and possible processes that were active when the patient was enrolled, causing a continual decline in eGFR during the study. Based on the available evidence, it is unclear how lumasiran affects kidney function and the experts stated the need for long-term data, ideally from more patients, to better understand what effect lumasiran has on eGFR and delaying dialysis or kidney failure. From the patient input submission, survey respondents felt it was very important (rated at least 9 out of a maximum 10) to have a treatment that prolonged or maintained kidney function. Data up to month 30 of lumasiran treatment from the ALN-GO1 to 002 trial indicated that mean eGFR appeared to be mostly maintained over the course of lumasiran treatment, though the same limitations to interpretation of results apply as in the main trials. Loss of kidney function over time and prevention of dialysis and/or liver-kidney transplant were identified as important outcomes in the CADTH systematic review protocol and by the patient groups who submitted input for the review but were not assessed in the trials.
According to the clinical experts, preventing kidney stones is 1 of the main treatment goals for PH1. In the ILLUMINATE-A trial, the rate of kidney stone events appeared to be lower for the lumasiran followed by lumasiran treatment group compared to before enrolling in the trial. However, patients randomized to lumasiran in the ILLUMINATE-A trial appeared to have higher instances of kidney stone events based on baseline characteristics compared to the placebo group, which may confound the interpretation of this outcome. Comparison with the placebo followed by lumasiran treatment group is challenging due to the low number of events, few patients, and apparent fluctuations in rate of events during lumasiran treatment. The clinical experts stated that there are many factors influencing the rate of stone growth and kidney stones may be present for years without symptoms. As a result, it is unclear if lumasiran conveys a benefit over placebo in reducing kidney stone events over time. Information from the patient input submission noted that it is critical to have treatments that can decrease the likelihood of kidney stones, organ transplant, kidney failure, and oxalosis. Firm conclusions from the ALN-GO1 to 002 trial regarding if or how lumasiran affects kidney stone events cannot be made due to the same limitations as those listed for the main trials.
Results presented in the CADTH report were limited to those from the ILLUMINATE-A trial, which captured HRQoL data using both disease-specific and generic instruments (i.e., KDQOL, PedsQL, EQ-5D-5L, EQ-5D-Y, and VAS). First, decreases in urine and plasma oxalate levels (discussed in the following paragraphs) were not clearly reflected as benefits in HRQoL. There were no MIDs identified from the literature for patients with PH1, baseline scores for some instruments appeared imbalanced, and there was a lack of notable difference in scores between lumasiran and placebo groups that would indicate that 1 treatment was favourable over the other. Additionally, the small number of patients was further split by age-specific instruments, making it challenging to interpret the results for the relatively short duration of treatment. Therefore, it is not clear if or how lumasiran affects HRQoL for patients with PH1, and particularly for those aged younger than 6 years and those with decreased kidney function due to the lack of data and meaningful results from the ILLUMINATE-B and ILLUMINATE-C trials, respectively. Long-term data from the extension periods of the trials (up to 60 months of treatment) will be necessary. The patient input submission also noted that improving clinical outcomes and physical well-being would help to mitigate stress and anxiety for patients and families when managing PH1.
Ability to thrive during childhood was a patient-important outcome identified from the patient group input. However, growth parameters and developmental milestones for pediatric patients were exploratory outcomes in the ILLUMINATE-B and ILLUMINATE-C trials, and there were no meaningful changes observed as of the cut-off date for the clinical study reports. Therefore, no firm conclusions could be drawn from the data.
Compared to placebo, patients treated with lumasiran demonstrated a decrease in urine oxalate excretion compared to patients treated with placebo in the ILLUMINATE-A trial. The LSM treatment difference between lumasiran and placebo was approximately 54% from baseline to the average of months 3 to 6 in the ILLUMINATE-A trial. When compared to vitamin B6 therapy, in which a 30% reduction in urine oxalate excretion is considered successful treatment,3 the clinical experts agreed that the trial results were meaningful. Although the change from baseline appeared to be numerically lower in ILLUMINATE-C Cohort A patients compared to those treated with lumasiran in the ILLUMINATE-A trial, the clinical experts did not expect the same magnitude of response because the former patients already had CKD whereas the latter group had some kidney function. The proportions of patients reaching normal and near-normal levels were captured in the ILLUMINATE-A trial but not the ILLUMINATE-C trial. The experts noted that although this is a meaningful outcome, achieving normalization or near normalization does not clearly indicate whether this will lead to clinical improvements (e.g., preventing kidney stones and progression to ESKD). There is evidence that higher levels of urine oxalate are related to increased risk of ESKD, suggesting that this is an acceptable surrogate outcome for PH1.73 However, there were no published MIDs for percent or absolute changes identified and the magnitude of reduction in urine oxalate needed for clinical benefit is unclear at this time.3 Long-term data will be necessary to determine if the decline in urine oxalate observed in the first 6 months of treatment will be sustained because patients are expected to continue receiving treatment for the rest of their lives or until liver transplant.
Data for up to 30 months of lumasiran treatment in the ALN-GO1 to 002 trial indicated a similar magnitude and decrease in mean urine oxalate excretion as that observed in the ILLUMINATE-A trial, which appeared to be sustained over the course of the study. The same limitations apply to interpreting the results as those outlined for the main trials.
Compared to placebo, patients treated with lumasiran demonstrated a decrease in plasma oxalate excretion compared to patients treated with placebo in the ILLUMINATE-A trial. Based on the available data, it is unclear if patients in any of the studies achieved normal levels (not a trial end point), but the clinical experts stated that the observed decreases appeared to be consistent across the studies and were clinically meaningful for these patients. The experts explained that plasma levels may not change during early treatment because the oxalate stored in tissues is remobilizing and replacing that which is lost through urine or dialysis. This makes it challenging to interpret changes in plasma oxalate and, therefore, the potential magnitude of benefit of lumasiran may not be immediately apparent based on this outcome and the short time on treatment. The clinical experts also stated that there is currently no accurate method for measuring total oxalate burden in the body and that plasma levels may only partially reflect changes in total body oxalate. Given the lack of MID from the literature and limited data available (small number of patients and short duration of treatment), it is uncertain what the long-term benefit is for lowering plasma oxalate and whether this will directly translate to important outcomes such as preventing nephrocalcinosis or systemic oxalosis. There is a clear need for follow-up data to better understand how lumasiran affects total body oxalate. The clinical experts suggested that after years of effective treatment, if plasma oxalate levels declined to the point of normal levels, it may indicate that total body oxalate stores are being depleted.
The literature suggests that plasma oxalate may be an acceptable predictor of ESKD risk given its association with CKD stages 3a and 3b.73 The clinical experts explained that the goal of treatment in patients with advanced CKD and on dialysis (i.e., patients in the ILLUMINATE-C trial) is to use lumasiran treatment as a bridge to organ transplant. Lumasiran is expected to lower endogenous oxalate overproduction and alleviate the body of the existing oxalate burden as dialysis removes oxalate from the blood. In doing so, it is expected that treatment will improve the patient’s health before transplant, though this is yet to be confirmed with evidence. The clinical experts noted that the ILLUMINATE-C Cohort B results are of interest because they show the effect of the drug when essentially no oxalate is excreted through urine and oxalate removal is limited to hemodialysis. For example, the experts suggested that the lower predialysis readings indicate that lumasiran is working to reduce hepatic production, but any conclusions are limited by the small number of patients and short treatment duration so far. Additionally, the AUC results appear to be meaningful because they indicate that levels are low between dialysis sessions, though firm conclusions cannot be drawn due to the mentioned limitations.
Data for up to 30 months of lumasiran treatment in the ALN-GO1 to 002 trial indicated a similar magnitude and decrease in mean plasma oxalate levels as that observed in the ILLUMINATE-A trial, which appeared to be sustained over the course of the study. The same limitations apply to interpreting the results as those outlined for the main trials.
Compared to placebo, patients treated with lumasiran demonstrated a decrease in urine oxalate:creatinine ratio compared to patients treated with placebo in the ILLUMINATE-A trial. Interpretation of the results is challenging because there is no published MID for a treatment difference, normal values from the literature are based on patient age rather than body mass (i.e., how patients were categorized in the ILLUMINATE-B trial), and there is some variability among reference values. The clinical experts felt that the observed decreases were consistent across the studies and were clinically meaningful for these patients. Similar to urine oxalate in the ILLUMINATE-A trial, the proportions of patients who achieved normal values and near-normal values were captured in the ILLUMINATE-B trial and, as with the former study, it is unclear if achieving near-normal values will translate to overall improvements in complications due to PH1. As with all the efficacy outcomes discussed, there is a need for long-term data from more patients to be more certain of lumasiran’s effect on lowering urine oxalate:creatinine ratio.
Data for up to 30 months of lumasiran treatment in the ALN-GO1 to 002 trial indicated a similar magnitude and decrease in mean urine oxalate:creatinine ratio as that observed in the ILLUMINATE-A trial, which appeared to be sustained over the course of the study. It may be worth noting that the ILLUMINATE-A trial used 24-hour urine oxalate:creatinine ratios, whereas Part B of the ALN-GO1 to 001 trial used spot urine oxalate:creatinine ratios, and the same limitations apply to interpreting the results as those outlined for the main trials.
Harms
The clinical experts felt that the overall safety profile was generally acceptable based on the types and frequencies of reported AEs, SAEs, few WDAEs, and no deaths for the data available so far from the 3 studies. In the ILLUMINATE-A trial, injection site reactions occurred only with lumasiran treatment (no events were reported for patients who received placebo and events occurred once placebo patients began receiving lumasiran in the extension period). The experts stated that injection site reactions are expected with this medication but did not raise major safety concerns because none resulted in patients withdrawing from the trial, administration is infrequent (once every 3 months), and administration can be alternated among different injection sites. Most SAEs were single-patient events and most occurred in ILLUMINATE-C Cohort B, which included patients with poor kidney function (eGFR at or below 45 mL/min/1.73 m2) and on hemodialysis. Across all 3 trials, individuals with hepatic impairment were excluded from the trial (ALT or AST greater than 2 times ULN for age and total bilirubin greater than 1.5 times ULN) and all patients were aged younger than 60 years when enrolled. As a result, there are no safety data for lumasiran treatment in these patients. ADAs were generally infrequent across the studies for the first 6 months of treatment and the sponsor concluded that they had no impact on treatment efficacy. However, the clinical experts stated that it will be necessary to follow patients in the coming years to better understand if there is any impact on long-term efficacy or safety. The experts emphasized the need for long-term safety results beyond the available 2 years of data because patients continue treatment on lumasiran during the extension studies.
Safety data for up to 30 months of lumasiran treatment in the ALN-GO1 to 002 trial were mostly consistent in type and frequency as those in the main trials, with injection site reaction being the most frequently reported AE. In the ALN-GO1 to 002 trial, SAEs were infrequent (20%) and single-patient events. There were no patients who stopped treatment or withdrew due to an AE and no deaths were reported. Likewise, ADAs were infrequent (████████), and the sponsor concluded that the positive result did not appear to affect the efficacy of lumasiran. Safety follow-ups will be necessary because patients are expected to continue receiving treatment for years.
Based on the patient input submission for CADTH’s review of lumasiran, patients experienced side effects with standard-of-care treatments (e.g., vitamin B6 therapy, citrate). Currently, there is no information from patients to know if the AEs from 1 treatment are more acceptable to patients over the other. There is also a lack of evidence showing that lumasiran treatment prevents or delays the time to organ transplant, but this would be an important clinical outcome to patients due to the anxiety they have expressed over the eventual need for a transplant, high morbidity and mortality associated with transplant, and subsequent need for lifelong immunosuppression.
The Health Canada product monograph notes that lumasiran causes a chronic, stable increase in plasma glycolate in the body and further states that patients with severe kidney disease or ESKD are at an increased risk of metabolic acidosis.2 It is unknown what risks there are in patients with metabolic acidosis who are exposed to high levels of plasma glycolate; therefore, the product monograph warns that caution should be taken to monitor signs and symptoms of metabolic acidosis in patients being treated with lumasiran.2
Conclusions
The ILLUMINATE-A, ILLUMINATE-B, and ILLUMINATE-C studies are ongoing trials that have provided evidence of the efficacy and safety of lumasiran in patients with PH1 who were aged 6 years and older, younger than 6 years, and any age with an eGFR at or below 45 mL/min/1.73 m2 (receiving dialysis or not), respectively. Lumasiran demonstrated improvements in urine oxalate corrected for BSA, plasma oxalate, and urine oxalate:creatinine ratio in the 3 trials. In the DB, placebo-controlled ILLUMINATE-A trial, all primary and key secondary outcomes were for objective measures, controlled for multiplicity (except eGFR), and most were deemed clinically meaningful (except eGFR) based on clinical expert opinion because there were no MIDs identified from the literature. Results for the single-arm ILLUMINATE-B and ILLUMINATE-C trials were generally consistent with those observed in the ILLUMINATE-A trial, which the clinical experts agreed were also meaningful for those populations. Changes in eGFR and HRQoL were numerically small, the latter outcome was not controlled for multiplicity, and conclusions could not be drawn about whether lumasiran had an impact on these outcomes due to the small number of patients and short treatment duration of the trials so far. Efficacy results for up to 30 months on lumasiran in the ALN-GO1 to 002 trial indicated similar findings as the ILLUMINATE trials, though the same limitations apply to these longer-term data. The clinical experts had no major concerns with the harms profile and there were few SAEs or WDAEs, and no deaths reported. Lumasiran treatment for up to 30 months in the ALN-GO1 to 002 trial showed a similar harms profile as the ILLUMINATE trials with no new safety signals identified. In the ILLUMINATE trials, there were no patients aged older than 60 years and patients were excluded if they had a history of kidney transplant or had hepatic impairment (ALT or AST greater than 2 times ULN for age or total bilirubin greater than 1.5 times ULN). Therefore, further research showing adequate efficacy and safety is needed to inform broader treatment with lumasiran. According to the clinical experts, given the meaningful reductions in urine and plasma oxalate levels compared to placebo for up to 24 months of treatment, acceptable safety profile so far, lack of other effective treatments, and easy administration, lumasiran appears to be an important treatment option for patients with PH1. The experts and CADTH review team agreed that long-term efficacy and safety data will be necessary to confirm the findings in the ILLUMINATE trials and to better understand how the main trial outcomes translate to improved long-term outcomes of maintained lowering of hepatic oxalate production, prevention of kidney stones, and prevention of progression to ESKD.
References
1.Drug Reimbursement Review sponsor submission: Oxlumo (lumasiran), 94.5 mg/0.5 mL for subcutaneous injection [internal sponsor's package]. Mississauga (ON): Alnylam Pharmaceuticals Canada ULC; 2022 May 10.
2.Oxlumo (lumasiran): solution, 94.5 mg/0.5 mL lumasiran (as lumasiran sodium), subcutaneous injection [product monograph]. Amsterdam (NL): Alnylam Netherlands B.V.; 2022 Mar 3.
3.Milliner DS, Harris PC, Sas DJ, Cogal AG, JC L. Primary hyperoxaluria type 1. GeneReviews®. Seattle (WA): University of Washington; 2002 Jun 19 [Updated 2022 Feb 10]: https://www.ncbi.nlm.nih.gov/sites/books/NBK1283/. Accessed 2022 Sep 9.
4.Coulter-Mackie MB, Rumsby G. Genetic heterogeneity in primary hyperoxaluria type 1: impact on diagnosis. Mol Genet Metab. 2004;83(1-2):38-46. PubMed
5.Demoulin N, Aydin S, Gillion V, Morelle J, Jadoul M. Pathophysiology and management of hyperoxaluria and oxalate nephropathy: a review. Am J Kidney Dis. 2022;79(5):717-727. PubMed
6.Cochat P, Groothoff J. Primary hyperoxaluria type 1: practical and ethical issues. Pediatr Nephrol. 2013;28(12):2273-2281. PubMed
7.Bobrowski AE, Langman CB. Hyperoxaluria and systemic oxalosis: current therapy and future directions. Expert Opin Pharmacother. 2006;7(14):1887-1896. PubMed
8.Mandrile G, Beck B, Acquaviva C, et al. Genetic assessment in primary hyperoxaluria: why it matters. Pediatr Nephrol. 2022. PubMed
9.Gupta A, Somers MJG, Baum MA. Treatment of primary hyperoxaluria type 1. Clin Kidney J. 2022;15(Suppl 1):i9-i13. PubMed
10.Fargue S, Acquaviva Bourdain C. Primary hyperoxaluria type 1: pathophysiology and genetics. Clin Kidney J. 2022;15(Suppl 1):i4-i8. PubMed
11.Meaux MN, Sellier-Leclerc AL, Acquaviva-Bourdain C, Harambat J, Allard L, Bacchetta J. The effect of lumasiran therapy for primary hyperoxaluria type 1 in small infants. Pediatr Nephrol. 2022;37(4):907-911. PubMed
12.Clinical Study Report: ILLUMINATE-A. A phase 3 randomized, double-blind, placebo-controlled study with an extended dosing period to evaluate the efficacy and safety of lumasiran in children and adults with primary hyperoxaluria type 1 [internal sponsor's report]. Cambridge (MA): Alnylam Pharmaceuticals, Inc.; 2020.
13.Clinical Study Report: ILLUMINATE-B. An open-label study to evaluate the efficacy, safety, pharmacokinetics, and pharmacodynamics of lumasiran in infants and young children with primary hyperoxaluria type 1 (lumasiran) [internal sponsor's report]. Cambridge (MA): Alnylam Pharmaceuticals, Inc.; 2020.
14.Clinical Study Report: ILLUMINATE-C. A single arm study to evaluate efficacy, safety, pharmacokinetics, and pharmacodynamics of lumasiran in patients with advanced primary hyperoxaluria type 1 (PH1) [internal sponsor's report]. Cambridge (MA): Alnylam Pharmaceuticals, Inc.; 2021.
15.Highly Specialised Technology Evaluation: Lumasiran for treating primary hyperoxaluria type 1 [ID3765]. Evaluation Report. London (GB): National Institute for Health and Care Excellence; 2022: https://www.nice.org.uk/guidance/gid-ta10660/documents/committee-papers. Accessed 2022 Jul 26.
16.Harambat J, Fargue S, Acquaviva C, et al. Genotype-phenotype correlation in primary hyperoxaluria type 1: the p.Gly170Arg AGXT mutation is associated with a better outcome. Kidney Int. 2010;77(5):443-449. PubMed
17.Mandrile G, van Woerden CS, Berchialla P, et al. Data from a large European study indicate that the outcome of primary hyperoxaluria type 1 correlates with the AGXT mutation type. Kidney Int. 2014;86(6):1197-1204. PubMed
18.Cochat P, Hulton SA, Acquaviva C, et al. Primary hyperoxaluria Type 1: indications for screening and guidance for diagnosis and treatment. Nephrol Dial Transplant. 2012;27(5):1729-1736. PubMed
19.Sas DJ, Enders FT, Mehta RA, et al. Clinical features of genetically confirmed patients with primary hyperoxaluria identified by clinical indication versus familial screening. Kidney Int. 2020;97(4):786-792. PubMed
20.Bergstralh EJ, Monico CG, Lieske JC, et al. Transplantation outcomes in primary hyperoxaluria. Am J Transplant. 2010;10(11):2493-2501. PubMed
21.Harambat J, van Stralen KJ, Espinosa L, et al. Characteristics and outcomes of children with primary oxalosis requiring renal replacement therapy. Clin J Am Soc Nephrol. 2012;7(3):458-465. PubMed
22.Abstracts of the 54th ESPN Annual Meeting, Ljubljana, Slovenia. Pediatr Nephrol. 2022.
23.McGowan J, Sampson M, Salzwedel DM, Cogo E, Foerster V, Lefebvre C. PRESS Peer Review of Electronic Search Strategies: 2015 guideline statement. J Clin Epidemiol. 2016;75:40-46. PubMed
24.Grey matters: a practical tool for searching health-related grey literature. Ottawa (ON): CADTH; 2019: https://www.cadth.ca/grey-matters. Accessed 2022 May 27.
25.Garrelfs SF, Frishberg Y, Hulton SA, et al. Lumasiran, an RNAi therapeutic for primary hyperoxaluria type 1. N Engl J Med. 2021;384(13):1216-1226. PubMed
26.Hulton SA, Groothoff JW, Frishberg Y, et al. Randomized clinical trial on the long-term efficacy and safety of lumasiran in patients with primary hyperoxaluria type 1. Kidney Int Rep. 2022;7(3):494-506. PubMed
27.Sas DJ, Magen D, Hayes W, et al. Phase 3 trial of lumasiran for primary hyperoxaluria type 1: A new RNAi therapeutic in infants and young children. Genet Med. 2022;24(3):654-662. PubMed
28.Kidney Disease Improving Global Outcomes (KDIGO) CKD Work Group. KDIGO 2012 clinical practice guideline for the evaluation and management of chronic kidney disease. Kidney International Supplements. 2013;3(1):1–150. https://kdigo.org/wp-content/uploads/2017/02/KDIGO_2012_CKD_GL.pdf. Accessed 2022 Jul 26.
29.Peipert JD, Bentler PM, Klicko K, Hays RD. Psychometric properties of the Kidney Disease Quality of Life 36-Item Short-Form Survey (KDQOL-36) in the United States. Am J Kidney Dis. 2018;71(4):461-468. PubMed
30.Schatell D, Witten B. Measuring dialysis patients’ health-related quality of life with the KDQOL-36™. Madison (WI): Medical Education Institute, Inc.; 2012: https://www.kdqol-complete.org/pdfs/kdqol-36.pdf. Accessed 2022 Sep 9.
31.RAND Corporation. Kidney Disease Quality of Life Instrument (KDQOL). 2022; https://www.rand.org/health-care/surveys_tools/kdqol.html. Accessed 2022 Jun 24.
32.Hays RD, Kallich JD, Mapes DL, Coons SJ, Carter WB. Development of the kidney disease quality of life (KDQOL) instrument. Qual Life Res. 1994;3(5):329-338. PubMed
33.Cohen J. A power primer. Psychol Bull. 1992;112(1):155-159. PubMed
34.Reeve BB, Wyrwich KW, Wu AW, et al. ISOQOL recommends minimum standards for patient-reported outcome measures used in patient-centered outcomes and comparative effectiveness research. Qual Life Res. 2013;22(8):1889-1905. PubMed
35.Varni JW, Seid M, Rode CA. The PedsQL: measurement model for the pediatric quality of life inventory. Med Care. 1999;37(2):126-139. PubMed
36.Varni JW, Seid M, Kurtin PS. PedsQL 4.0: reliability and validity of the Pediatric Quality of Life Inventory version 4.0 generic core scales in healthy and patient populations. Med Care. 2001;39(8):800-812. PubMed
37.Desai AD, Zhou C, Stanford S, Haaland W, Varni JW, Mangione-Smith RM. Validity and responsiveness of the pediatric quality of life inventory (PedsQL) 4.0 generic core scales in the pediatric inpatient setting. JAMA Pediatr. 2014;168(12):1114-1121. PubMed
38.Goldstein SL, Graham N, Warady BA, et al. Measuring health-related quality of life in children with ESRD: performance of the generic and ESRD-specific instrument of the Pediatric Quality of Life Inventory (PedsQL). Am J Kidney Dis. 2008;51(2):285-297. PubMed
39.Stockard KL, Seidel KD, Flynn JT. Routine use of the PedsQL for assessment of quality of life in pediatric dialysis patients. National Kidney Foundation Journal of Nephrology Social Work. 2014;38(1-2):24-32.
40.van Reenen M. EQ-5D-5L User Guide. Basic information on how to use the EQ-5D-5L instrument. Rotterdam (NL): EuroQol Research Foundation; 2015.
41.McClure NS, Sayah FA, Xie F, Luo N, Johnson JA. Instrument-defined estimates of the minimally important difference for EQ-5D-5L index scores. Value Health. 2017;20(4):644-650. PubMed
42.2014 Alberta population norms for EQ-5D-5L. Calgary (AB): Health Quality Council of Alberta; 2014 https://hqca.ca/wp-content/uploads/2018/05/2014_EQ_5D_5L_report_FINALFINAL-1.pdf. Accessed 2022 Sep 8.
43.EuroQol. EQ-5D-Y (Youth): about. 2021; https://euroqol.org/eq-5d-instruments/eq-5d-y-about/. Accessed 2022 Jun 27.
44.Hsu CN, Lin HW, Pickard AS, Tain YL. EQ-5D-Y for the assessment of health-related quality of life among Taiwanese youth with mild-to-moderate chronic kidney disease. Int J Qual Health Care. 2018;30(4):298-305. PubMed
45.Milliner DS. The primary hyperoxalurias: an algorithm for diagnosis. Am J Nephrol. 2005;25(2):154-160. PubMed
46.Zhao F, Bergstralh EJ, Mehta RA, et al. Predictors of incident ESRD among patients with primary hyperoxaluria presenting prior to kidney failure. Clin J Am Soc Nephrol. 2016;11(1):119-126. PubMed
47.Dutta C, Avitahl-Curtis N, Pursell N, et al. Inhibition of glycolate oxidase with Dicer-substrate siRNA reduces calcium oxalate deposition in a mouse model of primary hyperoxaluria type 1. Mol Ther. 2016;24(4):770-778. PubMed
48.Perinpam M, Enders FT, Mara KC, et al. Plasma oxalate in relation to eGFR in patients with primary hyperoxaluria, enteric hyperoxaluria and urinary stone disease. Clin Biochem. 2017;50(18):1014-1019. PubMed
49.Milliner DS, Cochat P, Hulton SA, et al. Plasma oxalate and eGFR are correlated in primary hyperoxaluria patients with maintained kidney function-data from three placebo-controlled studies. Pediatr Nephrol. 2021;36(7):1785-1793. PubMed
50.Ladwig PM, Liedtke RR, Larson TS, Lieske JC. Sensitive spectrophotometric assay for plasma oxalate. Clin Chem. 2005;51(12):2377-2380. PubMed
51.Thakur M, Goyal L, Pundir CS. Discrete analysis of plasma oxalate with alkylamine glass bound sorghum oxalate oxidase and horseradish peroxidase. J Biochem Biophys Methods. 2000;44(1-2):77-88. PubMed
52.Ogura H. [Determinations of oxalate in urine and plasma by capillary electrophoresis]. Nihon Hinyokika Gakkai Zasshi. 2000;91(6):547-555. PubMed
53.Honow R, Hesse A. Comparison of extraction methods for the determination of soluble and total oxalate in foods by HPLC-enzyme-reactor. Food Chem. 2002;78(4):511-521.
54.Porowski T, Gałasiński W. A semi-micromethod for determination of oxalate in human plasma. Acta Pol Pharm. 2003;60(4):239-245. PubMed
55.Harris AH, Freel RW, Hatch M. Serum oxalate in human beings and rats as determined with the use of ion chromatography. J Lab Clin Med. 2004;144(1):45-52. PubMed
56.Zarembski PM, Hodgkinson A. The fluorimetric determination of oxalic acid in blood and other biological materials. Biochem J. 1965;96(3):717-721. PubMed
57.Clifford-Mobley O, Tims C, Rumsby G. The comparability of oxalate excretion and oxalate:creatinine ratio in the investigation of primary hyperoxaluria: review of data from a referral centre. Ann Clin Biochem. 2015;52(Pt 1):113-121. PubMed
58.Reusz GS, Dobos M, Byrd D, Sallay P, Miltényi M, Tulassay T. Urinary calcium and oxalate excretion in children. Pediatr Nephrol. 1995;9(1):39-44. PubMed
59.Hashmi SB, Jafri L, Majid H, Talati J, Aziz W, Khan AH. Relationship of spot urine oxalate to creatinine ratio and 24 hours urinary oxalate excretion in patients with urolithiasis. Ann Med Surg (Lond). 2020;60:330-333. PubMed
60.Matos V, Van Melle G, Werner D, Bardy D, Guignard JP. Urinary oxalate and urate to creatinine ratios in a healthy pediatric population. Am J Kidney Dis. 1999;34(2):e1. PubMed
61.Milliner DS, McGregor TL, Thompson A, et al. End points for clinical trials in primary hyperoxaluria. Clin J Am Soc Nephrol. 2020;15(7):1056-1065. PubMed
62.Hong YH, Dublin N, Razack AH, Mohd MA, Husain R. Twenty-four hour and spot urine metabolic evaluations: correlations versus agreements. Urology. 2010;75(6):1294-1298. PubMed
63.Ogawa Y, Yonou H, Hokama S, Oda M, Morozumi M, Sugaya K. Urinary saturation and risk factors for calcium oxalate stone disease based on spot and 24-hour urine specimens. Front Biosci. 2003;8:a167-176. PubMed
64.Habtemariam B, Shahraz A, Lu J, McGregor T. 110 24hr and random spot urine collections were comparable in assessing oxalate excretion and response to treatment in primary hyperoxaluria type 1. Am J Kidney Dis. 2021;77(4):601.
65.von Schnakenburg C, Byrd DJ, Latta K, Reusz GS, Graf D, Brodehl J. Determination of oxalate excretion in spot urines of healthy children by ion chromatography. Eur J Clin Chem Clin Biochem. 1994;32(1):27-29. PubMed
66.Clinical Study Report: ALN-GO1-002 A phase 2, multicenter, open-label, extension study to evaluate the long-term administration of ALN-GO1 in patients with primary hyperoxaluria type 1 [internal sponsor's report]. Cambridge (MA): Alnylam Pharmaceuticals, Inc.; 2020.
67.Pharmaceutical Safety and Efficacy Assessment: (supplemental) new drug submission for Oxlumo (lumasiran) [internal sponsor's report]. Ottawa (ON): Health Canada; 2022.
68.Hoppe B, Kemper MJ, Hvizd MG, Sailer DE, Langman CB. Simultaneous determination of oxalate, citrate and sulfate in children's plasma with ion chromatography. Kidney Int. 1998;53(5):1348-1352. PubMed
69.Marangella M, Petrarulo M, Vitale C, et al. Serum calcium oxalate saturation in patients on maintenance haemodialysis for primary hyperoxaluria or oxalosis-unrelated renal diseases. Clin Sci (Lond). 1991;81(4):483-490. PubMed
70.Cochat P, Rumsby G. Primary hyperoxaluria. N Engl J Med. 2013;369(7):649-658. PubMed
71.Hoppe B, Beck BB, Milliner DS. The primary hyperoxalurias. Kidney Int. 2009;75(12):1264-1271. PubMed
72.Hillebrand P, Hoppe B. Plasma oxalate levels in primary hyperoxaluria type I show significant intra-individual variation and do not correlate with kidney function. Pediatr Nephrol. 2020;35(7):1227-1233. PubMed
73.Shah RJ, Vaughan LE, Enders FT, Milliner DS, Lieske JC. Plasma oxalate as a predictor of kidney function decline in a primary hyperoxaluria cohort. Int J Mol Sci. 2020;21(10):3608. PubMed
74.Monico CG, Rossetti S, Olson JB, Milliner DS. Pyridoxine effect in type I primary hyperoxaluria is associated with the most common mutant allele. Kidney Int. 2005;67(5):1704-1709. PubMed
75.Hopp K, Cogal AG, Bergstralh EJ, et al. Phenotype-genotype correlations and estimated carrier frequencies of primary hyperoxaluria. J Am Soc Nephrol. 2015;26(10):2559-2570. PubMed
76.Lorenz EC, Lieske JC, Seide BM, et al. Sustained pyridoxine response in primary hyperoxaluria type 1 recipients of kidney alone transplant. Am J Transplant. 2014;14(6):1433-1438. PubMed
77.Kemper MJ, Nolkemper D, Rogiers X, et al. Preemptive liver transplantation in primary hyperoxaluria type 1: timing and preliminary results. J Nephrol. 1998;11 Suppl 1:46-48. PubMed
78.Galanti M, Contreras A. Excellent renal function and reversal of nephrocalcinosis 8 years after isolated liver transplantation in an infant with primary hyperoxaluria type 1. Pediatr Nephrol. 2010;25(11):2359-2362. PubMed
79.Perera MT, Sharif K, Lloyd C, et al. Pre-emptive liver transplantation for primary hyperoxaluria (PH-I) arrests long-term renal function deterioration. Nephrol Dial Transplant. 2011;26(1):354-359. PubMed
80.Broyer M, Jouvet P, Niaudet P, Daudon M, Revillon Y. Management of oxalosis. Kidney Int Suppl. 1996;53:S93-98. PubMed
81.Varni JW, Burwinkle TM, Seid M, Skarr D. The PedsQL 4.0 as a pediatric population health measure: feasibility, reliability, and validity. Ambul Pediatr. 2003;3(6):329-341. PubMed
82.Jin X, McClure NS, Le CY, et al. Minimally Important Differences for EQ-5D instruments: a systematic review of estimates in published literature. Poster presented at: 2019 Canadian Agency for Drugs and Technologies in Health Symposium. Edmonton (AB): CADTH; 2019 Apr 14 - 16.
83.Hoppe B. An update on primary hyperoxaluria. Nat Rev Nephrol. 2012;8(8):467-475. PubMed
84.Vahlensieck EW, Bach D, Hesse A. Circadian rhythm of lithogenic substances in the urine. Urol Res. 1982;10(4):195-203. PubMed
85.Remer T, Neubert A, Maser-Gluth C. Anthropometry-based reference values for 24-h urinary creatinine excretion during growth and their use in endocrine and nutritional research. Am J Clin Nutr. 2002;75(3):561-569. PubMed
86.Marangella M, Vitale C, Petrarulo M, et al. Bony content of oxalate in patients with primary hyperoxaluria or oxalosis-unrelated renal failure. Kidney Int. 1995;48(1):182-187. PubMed
87.Morgenstern BZ, Milliner DS, Murphy ME, et al. Urinary oxalate and glycolate excretion patterns in the first year of life: a longitudinal study. J Pediatr. 1993;123(2):248-251. PubMed
88.Barratt TM, Kasidas GP, Murdoch I, Rose GA. Urinary oxalate and glycolate excretion and plasma oxalate concentration. Arch Dis Child. 1991;66(4):501-503. PubMed
89.Leumann EP, Dietl A, Matasovic A. Urinary oxalate and glycolate excretion in healthy infants and children. Pediatr Nephrol. 1990;4(5):493-497. PubMed
90.Scheinman JI. Primary hyperoxaluria: therapeutic strategies for the 90's. Kidney Int. 1991;40(3):389-399. PubMed
91.Elgstoen KB, Johnsen LF, Woldseth B, Morkrid L, Hartmann A. Plasma oxalate following kidney transplantation in patients without primary hyperoxaluria. Nephrol Dial Transplant. 2010;25(7):2341-2345. PubMed
92.Marangella M, Cosseddu D, Petrarulo M, Vitale C, Linari F. Thresholds of serum calcium oxalate supersaturation in relation to renal function in patients with or without primary hyperoxaluria. Nephrol Dial Transplant. 1993;8(12):1333-1337. PubMed
93.Hoppe B, Kemper MJ, Bökenkamp A, Portale AA, Cohn RA, Langman CB. Plasma calcium oxalate supersaturation in children with primary hyperoxaluria and end-stage renal failure. Kidney Int. 1999;56(1):268-274. PubMed
94.Elgstoen KB. Liquid chromatography-tandem mass spectrometry method for routine measurement of oxalic acid in human plasma. J Chromatogr B Analyt Technol Biomed Life Sci. 2008;873(1):31-36. PubMed
95.Stokes F, Acquaviva-Bourdain C, Hoppe B, et al. Plasma oxalate: comparison of methodologies. Urolithiasis. 2020;48(6):473-480. PubMed
96.Mayo Clinic Laboratories. Oxalate, plasma - Test ID: POXA1. 2022; https://www.mayocliniclabs.com/test-catalog/Overview/606472. Accessed 2022 Jun 28.
97.Raju DL, Cantarovich M, Brisson ML, Tchervenkov J, Lipman ML. Primary hyperoxaluria: clinical course, diagnosis, and treatment after kidney failure. Am J Kidney Dis. 2008;51(1):e1-5. PubMed
98.Porowski T, Konstantynowicz J, Zoch-Zwierz W. A need to establish normative data for plasma oxalates. Am J Kidney Dis. 2008;51(6):1071-1072. PubMed
99.Cohen DE, Lee A, Sibbel S, Benner D, Brunelli SM, Tentori F. Use of the KDQOL-36™ for assessment of health-related quality of life among dialysis patients in the United States. BMC Nephrol. 2019;20(1):112. PubMed
100.KDQOL-36 TM scoring program (v1.0). Santa Monica (CA): RAND Corporation; 2000: https://www.rand.org/health-care/surveys_tools/kdqol.html. Accessed 2022 Sep 9.
101.Ware J, Kosinski MA, Keller SD. SF-12: How to score the SF-12 Physical and Mental Health Summary Scales. 2nd ed. Boston (MA): The Health Institute, New England Medical Center; 1995.
102.Mapes DL, Bragg-Gresham JL, Bommer J, et al. Health-related quality of life in the Dialysis Outcomes and Practice Patterns Study (DOPPS). Am J Kidney Dis. 2004;44(5 Suppl 2):54-60. PubMed
103.Herdman M, Gudex C, Lloyd A, et al. Development and preliminary testing of the new five-level version of EQ-5D (EQ-5D-5L). Qual Life Res. 2011;20(10):1727-1736. PubMed
104.van Reenen M, Janssen B, Stolk E, et al. EQ-5D-5L User Guide: Basic information on how to use the EQ-5D-5L instrument. Rotterdam (NL): EuroQol Research Foundation 2019: https://euroqol.org/publications/user-guides/. Accessed 2022 Sep 9.
105.EuroQol. EQ-5D-Y: available modes of administration. 2022; https://euroqol.org/eq-5d-instruments/eq-5d-y-available-modes-of-administration/. Accessed 2022 Jun 27.
106.van Reenen M, Janssen B, Oppe M, et al. EQ-5D-Y User Guide. Rotterdam (NL): EuroQol Research Foundation; 2020: https://euroqol.org/publications/user-guides/. Accessed 2022 Sep 9.
Appendix 1: Literature Search Strategy
Note that this appendix has not been copy-edited.
Clinical Literature Search
Overview
Interface: Ovid
Databases:
MEDLINE All (1946 to present)
Embase (1974 to present)
Note: Subject headings and search fields have been customized for each database. Duplicates between databases were removed in Ovid.
Date of search: June 9, 2022
Alerts: Bi-monthly search updates until project completion
Search filters applied: No filters were applied to limit the retrieval by study type.
Limits:
No date or language limits were used
Conference abstracts: excluded
Syntax | Description |
|---|---|
/ | At the end of a phrase, searches the phrase as a subject heading |
MeSH | Medical Subject Heading |
exp | Explode a subject heading |
* | Before a word, indicates that the marked subject heading is a primary topic; or, after a word, a truncation symbol (wildcard) to retrieve plurals or varying endings |
.ti | Title |
.ot | Original title |
.ab | Abstract |
.hw | Heading word; usually includes subject headings and controlled vocabulary |
.kf | Author keyword heading word (MEDLINE) |
.dq | Candidate term word (Embase) |
.rn | Registry number |
.nm | Name of substance word (MEDLINE) |
medall | Ovid database code: MEDLINE All, 1946 to present, updated daily |
oemezd | Ovid database code; Embase, 1974 to present, updated daily |
Multidatabase Strategy
(lumasiran* or Oxlumo* or ad 65585 or ad65585 or aln 65585 or aln65585 or aln g01 or alng01 or aln go1 or alngo1 or RZT8C352O1 or 67P6XH37HD).ti,ab,kf,ot,hw,rn,nm.
1 use medal.
*lumasiran/ or (lumasiran* or Oxlumo* or ad 65585 or ad65585 or aln 65585 or aln65585 or aln g01 or alng01 or aln go1 or alngo1).ti,ab,kf,dq.
3 use oemezd.
4 not (conference review or conference abstract).pt.
2 or 5.
remove duplicates from 6.
Clinical Trials Registries
ClinicalTrials.gov
Produced by the US National Library of Medicine. Targeted search used to capture registered clinical trials.
[Search -- Studies with results ██ Oxlumo or lumasiran]
WHO ICTRP
International Clinical Trials Registry Platform, produced by WHO. Targeted search used to capture registered clinical trials.
[Search terms -- Oxlumo or lumasiran]
Health Canada’s Clinical Trials Database
Produced by Health Canada. Targeted search used to capture registered clinical trials.
[Search terms -- Oxlumo or lumasiran]
EU Clinical Trials Register
European Union Clinical Trials Register, produced by the European Union. Targeted search used to capture registered clinical trials.
[Search terms -- Oxlumo or lumasiran]
Grey Literature
Search dates: May 27, 2022, to June 3, 2022
Keywords: Oxlumo, lumasiran, primary hyperoxaluria
Limits: None
Updated: Search updated before the completion of stakeholder feedback period
Relevant websites from the following sections of the CADTH grey literature checklist Grey Matters: A Practical Tool for Searching Health-Related Grey Literature were searched:
Health Technology Assessment Agencies
Health Economics
Clinical Practice Guidelines
Drug and Device Regulatory Approvals
Advisories and Warnings
Drug Class Reviews
Clinical Trials Registries
Databases (free)
Health Statistics
Internet Search
Appendix 2: Excluded Studies
Note that this appendix has not been copy-edited.
Reference | Reason for exclusion |
|---|---|
Saland, J., et al. (2021). “243 Lumasiran Lowered Urinary Oxalate in Patients with Primary Hyperoxaluria Type 1 Irrespective of Pyridoxine Use, Hydration Status, and Genotype in the Phase 3 Clinical Trial Illuminate-A.” American Journal of Kidney Diseases 77(4): 644 | Abstract |
Appendix 3: Detailed Outcome Data
Note that this appendix has not been copy-edited.
Table 37: Change From Baseline in eGFR During Extension Period (Secondary Outcome) – ILLUMINATE-A Trial, All Lumasiran-Treated Set
Outcome | ILLUMINATE-A | |
|---|---|---|
Time pointa | Placebo / lumasiran (N = 13) | Lumasiran / lumasiran (N = 26) |
Baseline, n (%) | 13 (100) | 26 (100) |
Mean eGFR (SD) (mL/min/1.73 m2) | █████████ | █████████ |
Month 6, n (%) | 13 (100) | 25 (96.2) |
Mean eGFR (SD) (mL/min/1.73 m2) | █████████ | █████████ |
Mean change from baseline (SD) (mL/min/1.73 m2) | █████████ | █████████ |
Month 12, n (%) | 13 (100) | 24 (92.3) |
Mean eGFR (SD) (mL/min/1.73 m2) | █████████ | █████████ |
Mean change from baseline (SD) (mL/min/1.73 m2) | █████████ | █████████ |
Month 18, n (%) | 13 (100) | 24 (92.3) |
Mean eGFR (SD) (mL/min/1.73 m2) | █████████ | █████████ |
Mean change from baseline (SD) (mL/min/1.73 m2) | █████████ | █████████ |
Month 24, n (%) | 0 | █████████ |
Mean eGFR (SD) (mL/min/1.73 m2) | 0 | █████████ |
Mean change from baseline (SD) (mL/min/1.73 m2) | NA | █████████ |
eGFR = estimated glomerular filtration rate; NA = not applicable; SD = standard deviation.
aTime points are relative to first dose of lumasiran. Baseline is the last assessment collected before the first dose date or time of lumasiran.
Note: Placebo / lumasiran includes patients who received placebo during the 6-month DB period and switched to lumasiran during the Extension period. Lumasiran / lumasiran includes patients who received lumasiran during the 6-month DB period. The eGFR is calculated from serum creatinine based on the Modification of Diet in Renal Disease formula for patients at least 18 years of age and the Schwartz Bedside Formula for patients less than 18 years of age at screening.
Source: ILLUMINATE-A Clinical Study Report.12
Table 38: Shift From Baseline to Worst Postbaseline in eGFR During DB Period – ILLUMINATE-A Trial, FAS
Outcome | Baseline category | Worst postbaseline category (mL/min/1.73 m2) | |||||||
|---|---|---|---|---|---|---|---|---|---|
≥ 90 n (%) | 60 to < 90 n (%) | 45 to < 60 n (%) | 30 to < 45 n (%) | 15 to < 30 n (%) | < 15 n (%) | Missing n (%) | Total n (%) | ||
Placebo (N = 13) | ≥ 90 | ████ | ████ | ████ | ████ | ████ | ████ | ████ | ████ |
60 to < 90 | ████ | ████ | ████ | ████ | ████ | ████ | ████ | ████ | |
45 to < 60 | ████ | ████ | ████ | ████ | ████ | ████ | ████ | ████ | |
30 to < 45 | ████ | ████ | ████ | ████ | ████ | ████ | ████ | ████ | |
Missing | ████ | ████ | ████ | ████ | ████ | ████ | ████ | ████ | |
Total | ████ | ████ | ████ | ████ | ████ | ████ | ████ | ████ | |
Lumasiran (N = 26) | ≥ 90 | ████ | ████ | ████ | ████ | ████ | ████ | ████ | ████ |
60 to < 90 | ████ | ████ | ████ | ████ | ████ | ████ | ████ | ████ | |
45 to < 60 | ████ | ████ | ████ | ████ | ████ | ████ | ████ | ████ | |
30 to < 45 | ████ | ████ | ████ | ████ | ████ | ████ | ████ | ████ | |
Missing | ████ | ████ | ████ | ████ | ████ | ████ | ████ | ████ | |
Total | ████ | ████ | ████ | ████ | ████ | ████ | ████ | ████ | |
DB = double-blind; eGFR = estimated glomerular filtration rate; FAS = full analysis set.
Source: ILLUMINATE-A Clinical Study Report.12
Table 39: Shift From Baseline to Worst Postbaseline in eGFR During the Overall Period of Receiving Lumasiran Treatment – ILLUMINATE-A Trial, All Lumasiran-Treated Set
Outcome | Baseline categorya | Worst postbaseline category (mL/min/1.73 m2) | |||||||
|---|---|---|---|---|---|---|---|---|---|
≥ 90 n (%) | 60 to < 90 n (%) | 45 to < 60 n (%) | 30 to < 45 n (%) | 15 to < 30 n (%) | < 15 n (%) | Missing n (%) | Total n (%) | ||
Placebo / lumasiran (N = 13) | ≥ 90 | ████ | ████ | ████ | ████ | ████ | ████ | ████ | ████ |
60 to < 90 | ████ | ████ | ████ | ████ | ████ | ████ | ████ | ████ | |
45 to < 60 | ████ | ████ | ████ | ████ | ████ | ████ | ████ | ████ | |
30 to < 45 | ████ | ████ | ████ | ████ | ████ | ████ | ████ | ████ | |
Missing | ████ | ████ | ████ | ████ | ████ | ████ | ████ | ████ | |
Total | ████ | ████ | ████ | ████ | ████ | ████ | ████ | ████ | |
Lumasiran / lumasiran (N = 26) | ≥ 90 | ████ | ████ | ████ | ████ | ████ | ████ | ████ | ████ |
60 to < 90 | ████ | ████ | ████ | ████ | ████ | ████ | ████ | ████ | |
45 to < 60 | ████ | ████ | ████ | ████ | ████ | ████ | ████ | ████ | |
30 to < 45 | ████ | ████ | ████ | ████ | ████ | ████ | ████ | ████ | |
Missing | ████ | ████ | ████ | ████ | ████ | ████ | ████ | ████ | |
Total | ████ | ████ | ████ | ████ | ████ | ████ | ████ | ████ | |
All lumasiran-treated (N = 39) | ≥ 90 | ████ | ████ | ████ | ████ | ████ | ████ | ████ | ████ |
60 to < 90 | ████ | ████ | ████ | ████ | ████ | ████ | ████ | ████ | |
45 to < 60 | ████ | ████ | ████ | ████ | ████ | ████ | ████ | ████ | |
30 to < 45 | ████ | ████ | ████ | ████ | ████ | ████ | ████ | ████ | |
Missing | ████ | ████ | ████ | ████ | ████ | ████ | ████ | ████ | |
Total | ████ | ████ | ████ | ████ | ████ | ████ | ████ | ████ | |
eGFR = estimated glomerular filtration rate.
aBaseline is defined as the last nonmissing value available up to the first dose of lumasiran. Postbaseline assessments include tests taken after the first dose of lumasiran and through 84 days after the last dose of lumasiran.
Note: Placebo / lumasiran includes patients who receive placebo during the 6-month DB period and switch to lumasiran during the Extension period. Lumasiran / lumasiran includes patients who receive lumasiran during the 6-month DB period. All lumasiran includes all patients who receive any lumasiran during the study.
Source: ILLUMINATE-A Clinical Study Report.12
Table 40: Shift From Baseline to Worst Postbaseline in eGFR During the Overall Period of Receiving Lumasiran Treatment – ILLUMINATE-B Trial, Efficacy Analysis Set
Outcome | Baseline categorya | Worst postbaseline category (mL/min/1.73 m2) | |||||||
|---|---|---|---|---|---|---|---|---|---|
≥ 90 n (%) | 60 to < 90 n (%) | 45 to < 60 n (%) | 30 to < 45 n (%) | 15 to < 30 n (%) | < 15 n (%) | Missing n (%) | Total n (%) | ||
< 10 kg (N = 3) | ≥ 90 | ████ | ████ | ████ | ████ | ████ | ████ | ████ | ████ |
60 to < 90 | ████ | ████ | ████ | ████ | ████ | ████ | ████ | ████ | |
45 to < 60 | ████ | ████ | ████ | ████ | ████ | ████ | ████ | ████ | |
30 to < 45 | ████ | ████ | ████ | ████ | ████ | ████ | ████ | ████ | |
Missing | ████ | ████ | ████ | ████ | ████ | ████ | ████ | ████ | |
Total | ████ | ████ | ████ | ████ | ████ | ████ | ████ | ████ | |
10 to < 20 kg (N = 12) | ≥ 90 | ████ | ████ | ████ | ████ | ████ | ████ | ████ | ████ |
60 to < 90 | ████ | ████ | ████ | ████ | ████ | ████ | ████ | ████ | |
45 to < 60 | ████ | ████ | ████ | ████ | ████ | ████ | ████ | ████ | |
30 to < 45 | ████ | ████ | ████ | ████ | ████ | ████ | ████ | ████ | |
Missing | ████ | ████ | ████ | ████ | ████ | ████ | ████ | ████ | |
Total | ████ | ████ | ████ | ████ | ████ | ████ | ████ | ████ | |
≥ 20 kg (N = 3) | ≥ 90 | ████ | ████ | ████ | ████ | ████ | ████ | ████ | ████ |
60 to < 90 | ████ | ████ | ████ | ████ | ████ | ████ | ████ | ████ | |
45 to < 60 | ████ | ████ | ████ | ████ | ████ | ████ | ████ | ████ | |
30 to < 45 | ████ | ████ | ████ | ████ | ████ | ████ | ████ | ████ | |
Missing | ████ | ████ | ████ | ████ | ████ | ████ | ████ | ████ | |
Total | ████ | ████ | ████ | ████ | ████ | ████ | ████ | ████ | |
All lumasiran-treated (N = 18) | ≥ 90 | ████ | ████ | ████ | ████ | ████ | ████ | ████ | ████ |
60 to < 90 | ████ | ████ | ████ | ████ | ████ | ████ | ████ | ████ | |
45 to < 60 | ████ | ████ | ████ | ████ | ████ | ████ | ████ | ████ | |
30 to < 45 | ████ | ████ | ████ | ████ | ████ | ████ | ████ | ████ | |
Missing | ████ | ████ | ████ | ████ | ████ | ████ | ████ | ████ | |
Total | ████ | ████ | ████ | ████ | ████ | ████ | ████ | ████ | |
eGFR = estimated glomerular filtration rate.
Note: eGFR is calculated based on the Schwartz Bedside Formula in patients ≥ 12 months of age at the time of the assessment.
Source: ILLUMINATE-B Clinical Study Report.13
Table 41: Shift From Baseline to Worst Postbaseline in eGFR During the Overall Period of Receiving Lumasiran Treatment – ILLUMINATE-C Trial, Safety Analysis Set
Outcome | Baseline categorya | Worst postbaseline category (mL/min/1.73 m2) | |||||||
|---|---|---|---|---|---|---|---|---|---|
≥ 90 n (%) | 60 to < 90 n (%) | 45 to < 60 n (%) | 30 to < 45 n (%) | 15 to < 30 n (%) | < 15 n (%) | Missing n (%) | Total n (%) | ||
Cohort A (N = 6) | ≥ 90 | ████ | ████ | ████ | ████ | ████ | ████ | ████ | ████ |
60 to < 90 | ████ | ████ | ████ | ████ | ████ | ████ | ████ | ████ | |
45 to < 60 | ████ | ████ | ████ | ████ | ████ | ████ | ████ | ████ | |
30 to < 45 | ████ | ████ | ████ | ████ | ████ | ████ | ████ | ████ | |
15 to < 30 | ████ | ████ | ████ | ████ | ████ | ████ | ████ | ████ | |
< 15 | ████ | ████ | ████ | ████ | ████ | ████ | ████ | ████ | |
Missing | ████ | ████ | ████ | ████ | ████ | ████ | ████ | ████ | |
Total | ████ | ████ | ████ | ████ | ████ | ████ | ████ | ████ | |
eGFR = estimated glomerular filtration rate.
Note: eGFR is calculated based on the Schwartz Bedside Formula in patients ≥ 12 months of age at the time of the assessment.
Source: ILLUMINATE-C Clinical Study Report.14
Table 42: Rate of Kidney Stone Events by Time Period – ILLUMINATE-A Trial, All Lumasiran-Treated Set
Outcome | ILLUMINATE-A | |
|---|---|---|
Placebo / lumasiran (N = 13) | Lumasiran / lumasiran (N = 26) | |
Rate of renal stone events per person-year (95% CI)a | ||
12-month period before informed consent | 0.54 (0.26, 1.13) | 3.19 (2.57, 3.96) |
Screening | ████ | ████ |
DB periodb | NR | 1.09 (0.63, 1.88) |
Screening and placebo DB period | ████ | NR |
Lumasiran treatment day 1 to month 6 | ████ | 1.09 (0.63, 1.88) |
Lumasiran treatment month 6 to month 12 | ████ | ████ |
Lumasiran treatment month 12 to month 18 | ████ | ████ |
Lumasiran treatment month 18 to month 24 | ████ | ████ |
Lumasiran treatment month 24 to month 30 | NR | ████ |
DB = double-blind; CI = confidence interval; NR = not reported.
aRate is calculated as total number of renal stone events divided by total person-years. The 95% CI for the event rate was obtained using a generalized linear model for a Poisson distribution unless the rate was 0, in which case the upper bound of the 95% CI was calculated using the exact Poisson method.
bIncludes data for only the patients treated with lumasiran during the 6-month DB period.
Note: Placebo / lumasiran includes patients who received placebo during the 6-month DB period and switched to lumasiran during the Extension period. Lumasiran / lumasiran includes patients who received lumasiran during the 6-month DB period.
Source: ILLUMINATE-A Clinical Study Report.12
Table 43: Change in KDQOL and PedsQL During the Overall Period of Receiving Lumasiran Treatment (Exploratory Outcome) – ILLUMINATE-A Trial, All Lumasiran-Treated Set
Outcome | ILLUMINATE-A | |
|---|---|---|
Time pointa | Placebo / lumasiran | Lumasiran / lumasiran |
KDQOL-36 (≥ 18 years) | ||
SF-12 PCS | N = 5 | N = 12 |
Baseline, n (%) | ████ | ████ |
Mean (SD) | ████ | ████ |
Month 6, n (%) | ████ | ████ |
Change from baseline, mean (SD) | ████ | ████ |
Month 12, n (%) | ████ | ████ |
Change from baseline, mean (SD) | ████ | ████ |
Month 18, n (%) | ████ | ████ |
Change from baseline, mean (SD) | ████ | ████ |
Month 24, n (%) | ████ | ████ |
Change from baseline, mean (SD) | ████ | ████ |
SF-12 MCS | N = 5 | N = 12 |
Baseline, n (%) | ████ | ████ |
Mean (SD) | ████ | ████ |
Month 6, n (%) | ████ | ████ |
Change from baseline, mean (SD) | ████ | ████ |
Month 12, n (%) | ████ | ████ |
Change from baseline, mean (SD) | ████ | ████ |
Month 18, n (%) | ████ | ████ |
Change from baseline, mean (SD) | ████ | ████ |
Month 24, n (%) | ████ | ████ |
Change from baseline, mean (SD) | ████ | ████ |
Symptoms/problems | N = 5 | N = 12 |
Baseline, n (%) | ████ | ████ |
Mean (SD) | ████ | ████ |
Month 6, n (%) | ████ | ████ |
Change from baseline, mean (SD) | ████ | ████ |
Month 12, n (%) | ████ | ████ |
Change from baseline, mean (SD) | ████ | ████ |
Month 18, n (%) | ████ | ████ |
Change from baseline, mean (SD) | ████ | ████ |
Month 24, n (%) | ████ | ████ |
Change from baseline, mean (SD) | ████ | ████ |
Effects of kidney disease | N = 5 | N = 12 |
Baseline, n (%) | ████ | ████ |
Mean (SD) | ████ | ████ |
Month 6, n (%) | ████ | ████ |
Change from baseline, mean (SD) | ████ | ████ |
Month 12, n (%) | ████ | ████ |
Change from baseline, mean (SD) | ████ | ████ |
Month 18, n (%) | ████ | ████ |
Change from baseline, mean (SD) | ████ | ████ |
Month 24, n (%) | ████ | ████ |
Change from baseline, mean (SD) | ████ | ████ |
Burden of kidney disease | N = 5 | N = 12 |
Baseline, n (%) | ████ | ████ |
Mean (SD) | ████ | ████ |
Month 6, n (%) | ████ | ████ |
Change from baseline, mean (SD) | ████ | ████ |
Month 12, n (%) | ████ | ████ |
Change from baseline, mean (SD) | ████ | ████ |
Month 18, n (%) | ████ | ████ |
Change from baseline, mean (SD) | ████ | ████ |
Month 24, n (%) | ████ | ████ |
Change from baseline, mean (SD) | ████ | ████ |
PedsQL (< 18 years) | ||
Physical functioning | N = 8 | N = 14 |
Baseline, n (%) | ████ | ████ |
Mean (SD) | ████ | ████ |
Month 6, n (%) | ████ | ████ |
Change from baseline, mean (SD) | ████ | ████ |
Month 12, n (%) | ████ | ████ |
Change from baseline, mean (SD) | ████ | ████ |
Month 18, n (%) | ████ | ████ |
Change from baseline, mean (SD) | ████ | ████ |
Month 24, n (%) | ████ | ████ |
Change from baseline, mean (SD) | ████ | ████ |
Psychosocial health summary score | N = 8 | N = 14 |
Baseline, n (%) | ████ | ████ |
Mean (SD) | ████ | ████ |
Month 6, n (%) | ████ | ████ |
Change from baseline, mean (SD) | ████ | ████ |
Month 12, n (%) | ████ | ████ |
Change from baseline, mean (SD) | ████ | ████ |
Month 18, n (%) | ████ | ████ |
Change from baseline, mean (SD) | ████ | ████ |
Month 24, n (%) | ████ | ████ |
Change from baseline, mean (SD) | ████ | ████ |
Total score | N = 8 | N = 14 |
Baseline, n (%) | ████ | ████ |
Mean (SD) | ████ | ████ |
Month 6, n (%) | ████ | ████ |
Change from baseline, mean (SD) | ████ | ████ |
Month 12, n (%) | ████ | ████ |
Change from baseline, mean (SD) | ████ | ████ |
Month 18, n (%) | ████ | ████ |
Change from baseline, mean (SD) | ████ | ████ |
Month 24, n (%) | 0 | ████ |
Change from baseline, mean (SD) | NA | ████ |
ESRD total score – patient | N = 8 | N = 14 |
Baseline, n (%) | ████ | ████ |
Mean (SD) | ████ | ████ |
Month 6, n (%) | ████ | ████ |
Change from baseline, mean (SD) | ████ | ████ |
Month 12, n (%) | ████ | ████ |
Change from baseline, mean (SD) | ████ | ████ |
Month 18, n (%) | ████ | ████ |
Change from baseline, mean (SD) | ████ | ████ |
Month 24, n (%) | 0 | ████ |
Change from baseline, mean (SD) | NA | ████ |
ESRD total score – caregiver | N = 8 | N = 14 |
Baseline, n (%) | ████ | ████ |
Mean (SD) | ████ | ████ |
Month 6, n (%) | ████ | ████ |
Change from baseline, mean (SD) | ████ | ████ |
Month 12, n (%) | ████ | ████ |
Change from baseline, mean (SD) | ████ | ████ |
Month 18, n (%) | ████ | ████ |
Change from baseline, mean (SD) | ████ | ████ |
Month 24, n (%) | 0 | ████ |
Change from baseline, mean (SD) | NA | ████ |
ESRD = end-stage renal disease; KDQOL-36 = Kidney disease Quality of Life Questionnaire-36; MCS = Mental Component Summary; NA = not applicable; PCS = Physical Component Summary; PedsQL = Pediatric Quality of Life Inventory; SD = standard deviation; SF-12 = Short Form-12.
aTime points are relative to first dose of lumasiran. Baseline is the last assessment before the first dose of lumasiran.
Note: Placebo / lumasiran includes patients who received placebo during the 6-month DB period and switched to lumasiran during the Extension period. Lumasiran / lumasiran includes patients who received lumasiran during the 6-month DB period.
Source: ILLUMINATE-A Clinical Study Report.12
Table 44: Change in EQ VAS During the Overall Period of Receiving Lumasiran Treatment (Exploratory Outcome) – ILLUMINATE-A Trial, All Lumasiran-Treated Set
Outcome | ILLUMINATE-A | |
|---|---|---|
Time pointa | Placebo / lumasiran (N = 13) | Lumasiran / lumasiran (N = 26) |
Baseline, n (%) | ████ | ████ |
Mean (SD) | ████ | ████ |
Month 6, n (%) | ████ | ████ |
Change from baseline, mean (SD) | ████ | ████ |
Month 12, n (%) | ████ | ████ |
Change from baseline, mean (SD) | ████ | ████ |
Month 18, n (%) | ████ | ████ |
Change from baseline, mean (SD) | ████ | ████ |
Month 24, n (%) | 0 | ████ |
Change from baseline, mean (SD) | NA | ████ |
SD = standard deviation; VAS = visual analogue scale.
aTime points are relative to first dose of lumasiran. Baseline is the last assessment before the first dose of lumasiran.
Note: Placebo / lumasiran includes patients who received placebo during the 6-month DB period and switched to lumasiran during the Extension period. Lumasiran / lumasiran includes patients who received lumasiran during the 6-month DB period.
Source: ILLUMINATE-A Clinical Study Report.12
Figure 2: Subgroup Analyses for Treatment Difference in Percent Change From Baseline to Month 6 in 24-Hour Urine Oxalate Corrected for BSA – ILLUMINATE-A Trial, FAS
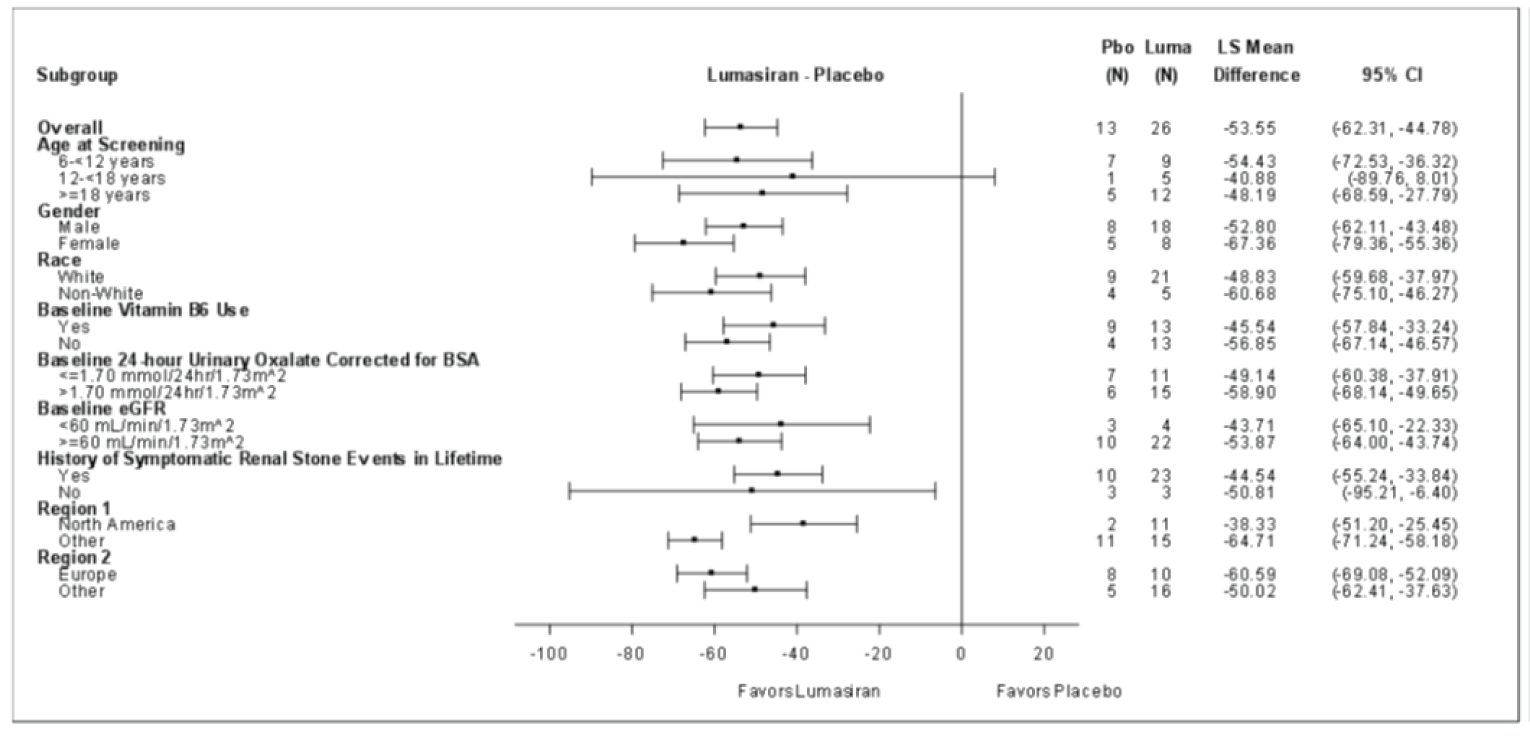
BSA = body surface area; CI = confidence interval; eGFR = estimated glomerular filtration rate; FAS = full analysis set; Luma = lumasiran; LS Mean = least squares mean; Pbo = placebo.
Note: The LSM, treatment difference in LSM, 95% CIs, and P values for comparing lumasiran versus placebo are derived using a REML-based MMRM model with the corresponding value at baseline as a continuous fixed covariate, and visit as fixed effects, and patient as a random effect. Visit is fitted as a categorical variable, and the variance-covariance matrix is assumed to be unstructured. Satterthwaite approximation is used to estimate denominator degrees of freedom.
Source: ILLUMINATE-A Clinical Study Report.12
Table 45: Change From Baseline in 24-Hour Urine Oxalate Corrected for BSA During Extension Period (Secondary Outcome) – ILLUMINATE-A Trial, All Lumasiran-Treated Set
Outcome | ILLUMINATE-A | |
|---|---|---|
Time pointa | Placebo / lumasiran (N = 13) | Lumasiran / lumasiran (N = 26) |
Baseline, n (%) | 13 (100) | 26 (100) |
Mean (SD) (mmol/24 hour/1.73 m2) | 1.63 (0.67) | 1.84 (0.60) |
Month 6, n (%) | 13 (100) | 25 (96.2) |
Mean (SD) (mmol/24 hour/1.73 m2) | ████ | ████ |
Change from baseline, mean (SD) (mmol/24 hour/1.73 m2) | ████ | ████ |
Percent change from baseline, mean (SD) | –57.25 (████) | –66.89 (████) |
Month 12, n (%) | 12 (92.3) | 24 (92.3) |
Mean (SD) (mmol/24 hour/1.73 m2) | ████ | ████ |
Change from baseline, mean (SD) (mmol/24 hour/1.73 m2) | ████ | ████ |
Percent change from baseline, mean (SD) | ████ | –64.12 (████) |
Month 18, n (%) | ████ | ████ |
Mean (SD) (mmol/24 hour/1.73 m2) | ████ | ████ |
Change from baseline, mean (SD) (mmol/24 hour/1.73 m2) | ████ | ████ |
Percent change from baseline, mean (SD) | ████ | ████ |
Month 24, n (%) | 0 | ████ |
Mean (SD) (mmol/24 hour/1.73 m2) | 0 | ████ |
Change from baseline, mean (SD) (mmol/24 hour/1.73 m2) | NA | ████ |
Percent change from baseline, mean (SD) | NA | ████ |
BSA = body surface area; NA = not applicable; SD = standard deviation.
aTime points are relative first dose of lumasiran. For the lumasiran / lumasiran treatment sequence, baseline is the median of all valid 24-hour urine assessments collected before the first dose date or time of lumasiran without any nonprotocol-related sample issues. For the placebo / lumasiran treatment sequence, baseline is the median of all valid 24-hour urine assessments at month 6 without any nonprotocol-related sample issues (or, if the patient did not have 2 valid 24-hour urine PD assessments at month 6, then the baseline was calculated using the latest 3 valid 24-hour urine PD collections before the first dose date or time of lumasiran).
Source: ILLUMINATE-A Clinical Study Report.12
Table 46: Change From Baseline in 24-Hour Urine Oxalate:Creatinine Ratio (Secondary Outcome) – ILLUMINATE-A Trial, All Lumasiran-Treated Set
Outcome | ILLUMINATE-A | |
|---|---|---|
Time pointa | Placebo / lumasiran (N = 13) | Lumasiran / lumasiran (N = 26) |
Baseline, n (%) | 13 (100) | 26 (100) |
Mean (SD) (mmol/mmol) | ████ | ████ |
Month 6, n (%) | 13 (100) | 25 (96.2) |
Mean (SD) (mmol/mmol) | ████ | ████ |
Change from baseline, mean (SD) (mmol/mmol) | ████ | ████ |
Percent change from baseline, mean (SD) | –54.31 (████) | –66.21 (████) |
Month 12, n (%) | 12 (92.3) | 24 (92.3) |
Mean (SD) (mmol/mmol) | ████ | ████ |
Change from baseline, mean (SD) (mmol/mmol) | ████ | ████ |
Percent change from baseline, mean (SD) | ████ | –62.94 (████) |
Month 18, n (%) | 13 (100) | 24 (92.3) |
Mean (SD) (mmol/mmol) | ████ | ████ |
Change from baseline, mean (SD) (mmol/mmol) | ████ | ████ |
Percent change from baseline, mean (SD) | ████ | ████ |
Month 24, n (%) | 0 | ████ |
Mean (SD) (mmol/mmol) | 0 | ████ |
Change from baseline, mean (SD) (mmol/mmol) | NA | ████ |
Percent change from baseline, mean (SD) | NA | ████ |
NA = not applicable; SD = standard deviation.
aTime points are relative to first dose of lumasiran. For lumasiran / lumasiran treatment sequence, baseline is the median of all 24-hour urine assessments collected before the first dose date or time of lumasiran without any nonprotocol-related sample issues. For placebo / lumasiran treatment sequence, baseline is the median of all 24-hour urine assessments without any nonprotocol-related sample issues at Month 6 of the DB treatment period.
Note: Placebo / lumasiran includes patients who received placebo during the 6-month DB period and switched to lumasiran during the Extension period. Lumasiran / lumasiran includes patients who received lumasiran during the 6-month DB period.
Source: ILLUMINATE-A Clinical Study Report.12
Table 47: Change From Baseline in Spot Urine Oxalate:Creatinine Ratio (Secondary Outcome) – ILLUMINATE-B Trial, Efficacy Analysis Set
Outcome | ILLUMINATE-B | |||
|---|---|---|---|---|
< 10 kg (N = 3) | 10 to < 20 kg (N = 12) | ≥ 20 kg (N = 3) | All patients (N = 18) | |
Baseline,a n (%) | 3 (100) | 12 (100) | 3 (100) | 18 (100) |
Mean (SD) (mmol/mmol) | ████ | ████ | 0.43 (0.23) | 0.63 (0.43) |
Month 6, n (%) | 3 (100) | 12 (100) | 3 (100) | 18 (100) |
Mean (SD) (mmol/mmol) | ████ | ████ | ████ | ████ |
Change from baseline, mean (SD) (mmol/mmol) | ████ | ████ | ████ | ████ |
Percent change from baseline, mean (SD) | ████ | ████ | ████ | –71.69 (████) |
Month 12, n (%) | 3 (100) | 12 (100) | 3 (100) | 18 (100) |
Mean (SD) (mmol/mmol) | ████ | ████ | ████ | ████ |
Change from baseline, mean (SD) (mmol/mmol) | ████ | ████ | ████ | ████ |
Percent change from baseline, mean (SD) | ████ | ████ | ████ | ████ |
Month 18, n (%) | 3 (100) | 11 (91.7) | 2 (66.7) | 16 (88.9) |
Mean (SD) (mmol/mmol) | ████ | ████ | ████ | ████ |
Change from baseline, mean (SD) (mmol/mmol) | ████ | ████ | ████ | ████ |
Percent change from baseline, mean (SD) | ████ | ████ | ████ | ████ |
NA = not applicable; SD = standard deviation.
aBaseline is the mean of all assessments collected before the first dose of lumasiran. The mean of data within a visit was used as the postdose value at each visit.
Source: ILLUMINATE-B Clinical Study Report.13
Table 48: Summary of Long-Term Harms – ILLUMINATE-A, ILLUMINATE-B Trials
Harms | ILLUMINATE-Aa | ILLUMINATE-Bb | |||
|---|---|---|---|---|---|
Placebo / lumasiran (N = 13) | Lumasiran / lumasiran (N = 26) | < 10 kg (N = 3) | 10 to < 20 kg (N = 12) | ≥ 20 kg (N = 3) | |
Patients with ≥ 1 adverse event | |||||
n (%) | 11 (84.6) | 24 (92.3) | 3 (100.0) | 12 (100.0) | 3 (100.0) |
Most common events,b n (%) | |||||
Injection site reaction | ████ | ████ | ████ | ████ | ████ |
Abdominal pain | ████ | ████ | ████ | ████ | ████ |
Headache | ████ | ████ | ████ | ████ | ████ |
Dysuria | ████ | ████ | NR | NR | NR |
Injection site erythema | ████ | ████ | NR | NR | NR |
Injection site pain | ████ | ████ | NR | NR | NR |
Nasopharyngitis | ████ | ████ | ████ | ████ | ████ |
Upper respiratory tract infection | ████ | ████ | ████ | ████ | ████ |
Flank pain | ████ | ████ | NR | NR | NR |
Abdominal pain upper | ████ | ████ | NR | NR | NR |
Nausea | ████ | ████ | ████ | ████ | ████ |
Pyrexia | ████ | ████ | ████ | ████ | ████ |
Rhinitis | ████ | ████ | ████ | ████ | ████ |
Vomiting | ████ | ████ | ████ | ████ | ████ |
Cough | ████ | ████ | ████ | ████ | ████ |
Oropharyngeal pain | ████ | ████ | ████ | ████ | ████ |
Influenza-like illness | ████ | ████ | ████ | ████ | ████ |
Gastroenteritis | ████ | ████ | ████ | ████ | ████ |
Bronchitis | ████ | ████ | ████ | ████ | ████ |
Diarrhea | ████ | ████ | ████ | ████ | ████ |
Teething | NR | NR | ████ | ████ | ████ |
Patients with ≥ 1 SAE | |||||
n (%) | ████ | ████ | ████ | ████ | ████ |
Abdominal pain | ████ | ████ | NR | NR | NR |
Urosepsis | ████ | ████ | NR | NR | NR |
Postprocedural complication | ████ | ████ | NR | NR | NR |
Viral infection | NR | NR | ████ | ████ | ████ |
Patients who stopped treatment due to adverse events | |||||
n (%) | ████ | ████ | ████ | ████ | ████ |
Fatigue | ████ | ████ | NR | NR | NR |
Disturbance in attention | ████ | ████ | NR | NR | NR |
Deaths | |||||
n (%) | ████ | ████ | ████ | ████ | ████ |
Notable harms, n (%) | |||||
n (%) | |||||
Injection site reaction | ████ | ████ | ████ | ████ | ████ |
Injection site discoloration | ████ | ████ | ████ | ████ | ████ |
Injection site discomfort | ████ | ████ | NR | NR | NR |
Injection site erythema | ████ | ████ | ████ | ████ | ████ |
Injection site exfoliation | ████ | ████ | NR | NR | NR |
Injection site hematoma | ████ | ████ | NR | NR | NR |
Injection site mass | ████ | ████ | NR | NR | NR |
Injection site pain | ████ | ████ | ████ | ████ | ████ |
Injection site pruritus | ████ | ████ | NR | NR | NR |
Injection site rash | ████ | ████ | NR | NR | NR |
Injection site reaction | ████ | ████ | NR | NR | NR |
Injection site swelling | ████ | ████ | NR | NR | NR |
Renal eventsb | ████ | ████ | ████ | ████ | ████ |
Dysuria | ████ | ████ | NR | NR | NR |
Hematuria | NR | NR | ████ | ████ | ████ |
Hypertonic bladder | ████ | ████ | NR | NR | NR |
Microalbuminuria | ████ | ████ | NR | NR | NR |
Polyuria | ████ | ████ | NR | NR | NR |
Renal impairment | ████ | ████ | NR | NR | NR |
Renal pain | ████ | ████ | NR | NR | NR |
Urinary incontinence | ████ | ████ | NR | NR | NR |
Complications from systemic oxalosis | NR | NR | NR | NR | NR |
Headache | ████ | ████ | ████ | ████ | ████ |
Rhinitis | ████ | ████ | ████ | ████ | ████ |
Upper respiratory infection | ████ | ████ | ████ | ████ | ████ |
Hypersensitivity reactions | ████ | ████ | NR | NR | NR |
ADA positive at any time | ████ | ████ | ████ | ████ | ████ |
ADA = antidrug antibody; NR = not reported; SAE = serious adverse event.
aAll lumasiran-treated set. From a Clinical Study Report with data up to 24 months.
bSafety analysis set. From a Clinical Study Report with data up to 12 months.
cFrequency of at least 10% in any treatment group in ILLUMINATE-A and at least 2 patients in ILLUMINATE-B.
dKidney stone events were captured as an efficacy outcome in the studies and not reported as harms.
Note: Placebo / lumasiran includes patients who receive placebo during the 6-month DB period and switch to lumasiran during the Extension period. Lumasiran / lumasiran includes patients who receive lumasiran during the 6-month DB period.
Source: ILLUMINATE-A Clinical Study Report,12 ILLUMINATE-B Clinical Study Report.13
Appendix 4: Description and Appraisal of Outcome Measures
Note that this appendix has not been copy-edited.
Aim
To describe the following outcome measures and review their measurement properties (validity, reliability, responsiveness to change, and MID):
Table 49: Outcome Measures and Trial End Points
Outcome measure | ILLUMINATE-A | ILLUMINATE-B | ILLUMINATE-C |
|---|---|---|---|
Urine oxalate excretion (24-hour collection corrected for BSA) | Primary end point: percent change from baseline to month 6 Secondary end point: absolute change from baseline to month 6, proportion of patients ≤ ULN and ≤ 1.5 × ULN at Month 6 | Primary end point: percent change from baseline to month 6 Secondary end point: absolute change from baseline to month 6, percent change from month 6 to End of Study (Extension Period), proportion of patients ≤ the ULN and ≤ 1.5 × ULN at Month 6 | Secondary end point: percent and absolute change from baseline to month 6 and for the Long-term Extension Period |
Urine oxalate:creatinine ratio (24-hour and spot collection) | Secondary end point: percent changes for 24-hour and spot collection from baseline to month 6 | Secondary end point: percentage of time that spot collection ≤ 1.5 × ULN during the Extension Period | Secondary end point: percent and absolute change in spot collection from baseline to month 6 and for the Long-term Extension Period |
Plasma oxalate | Secondary end point: absolute change from baseline to month 6 | Secondary end point: percent and absolute changes from baseline to month 6 | Primary end point for Cohort A: percent change in level from baseline to month 6 Primary end point for Cohort B: percent change in predialysis level from baseline to month 6 Secondary end point for Cohort B: percent change in AUC between dialysis session from baseline to month 6 and from month 6 to End of Study (Long-term Extension Period) Secondary point: absolute change from baseline to month 6, percent and absolute change for the Long-term Extension Period |
KDQOL-36, PedsQL, EQ-5D-5L, EQ-5D-Y | Exploratory end points:
| NR | Secondary end point:
Exploratory end point:
|
AUC = area under the curve; BSA = body surface area; EQ-5D-5L = EuroQol-5 Dimensions-5 Levels; EQ-5D-Y = EuroQol-5 Dimensions-Youth; ESRD = end-stage renal disease; KDQOL-36 = Kidney Disease and Quality of Life-36; NR = not reported; PedsQL = Pediatric Quality of Life; ULN = upper limit of normal.
Sources: ILLUMINATE-A Clinical Study Report,12 ILLUMINATE-B Clinical Study Report,13 ILLUMINATE-C Clinical Study Report.14
Findings
Table 50: Summary of Outcome Measures and Their Measurement Properties
Outcome measure | Type | Conclusions about measurement properties | MID |
|---|---|---|---|
Urine oxalate excretion | A surrogate outcome to measure total body oxalate burden in patients with PH1. Can be measured either by 24-hour or spot collection. Must be corrected to a BSA of 1.73 m2 in children (< 18 years) for comparison. Higher urine oxalate excretion indicates higher level of total body oxalate level in patients with normal kidney function and mild/moderate kidney damage (CKD 1 to 3a). Appears within reference range in advanced CKD. | Located in the causal pathway to stone formation and kidney damage.45 Several epidemiological data support relationship between urine oxalate and kidney function loss over time46 as well as treatment effects of reducing urine oxalate (with pyridoxine and liver transplant) on clinical benefit of preserving kidney function for a long time.16,74-79 | Unknown |
Urine oxalate:creatinine ratio | A surrogate outcome to measure total body oxalate burden in patients with PH-1. A composite ratio parameter that can be calculated from both 24-hour and spot urine collection. Does not require correction for BSA. Higher value represents higher total body oxalate burden. | Evidence exists to support a moderate correlation with urine oxalate from 24-hour collection in stone formers62 and spot collection from patients with PH80 as well as a strong correlation (r = 0.63) in the same 24-hour collection.57 Contrary evidence also exists, i.e., weak correlation with urine oxalate in spot urine collection (r = 0.29)59 in patients with history of kidney stone. Limitations include inconsistent correlation with urine oxalate, high variability in patients who are < 5 years old, and sex differences requiring sex-related URLs in adults.57 | Unknown |
Plasma oxalate | A surrogate outcome to measure total body oxalate burden in patients with PH1. Methods of sample preparation and procedures for measurement are not standardized across different laboratories making interpretation challenging. Higher level represents higher total body oxalate level, especially in advanced CKD (eGFR < 45 mL/min per 1.73 m2). | Retrospective evidence exists to support moderate-strong relationship with urine oxalate excretion,48 GFR at all levels68-71 (r = –0.44 to –0.55),49 loss of kidney function over time73 and mild/moderate kidney damage (CKD 1 to 3b),49 in addition to severity of oxalosis.68,70,71 Contrary evidence also exists, i.e., no relationship with eGFR.72 Treatment effects of lowering plasma oxalate through intensive dialysis to reduce severity of systemic oxalosis or liver transplant on resolution of oxalosis symptoms have been observed in case reports.20,78 | Unknown |
KDQOL-36 | Self-completed HRQoL measure composed for 36 items in 5 scales: PCS, MCS, BKD, SPKD and EKD. PCS and MCS (both are part of SF-12, a short version of SF-36) are generic scales, whereas BKD, SPKD, and EKD assess issues specific to CKD. Intended to assess HRQoL in patients on dialysis, however, patients who had transplant and/or are at predialysis stage can also use it by excluding 2 items asking about access and catheter sites. Scores are transformed into a scale from 0 to 100 according to the Likert-method32 with higher scores representing better HRQoL. | Validity Construct validity was supported by moderate to strong correlations33 (r = 0.40 to 0.52) between the SF-12 (PCS and MCS) scores and the BKD, SPKD, and EKD scores; statistically significant differences (P < 0.001 to 0.05) between distinct patient groups, e.g., hemodialysis vs. peritoneal dialysis, with diabetes vs. without diabetes, full-time employment vs. other types of employment.29 Reliability Internal consistency (alpha = 0.83 to 0.85) and dialysis facility-level reliability (alpha = 0.72 to 0.83) were acceptable (alpha > 0.7).29,34 Most of items within each scale demonstrated acceptable (alpha > 0.7)34 internal consistency (alpha = 0.31 to 0.73).29 Each kidney-specific subscale mostly measures unique features, however, overlapped with each other to a moderate degree (r = 0.48 to 0.62).29 | Not identified |
PedsQL 4.0 Generic Core Scales and 3.0 ESRD Module | Surveys consisting of 23 items (4.0 Generic Core Scales) and 34 items (3.0 ESRD Module) for measuring HRQoL in healthy and/or pediatric patient populations, with a Likert scale for each item.
Raw scores are transformed to a scale of 0 to 100, with higher scores indicative of better HRQoL. | PedsQL 4.0 Generic Core Scales: Validity: Construct validity has been demonstrated using known-groups approach: healthy vs. acutely ill vs. chronically ill children,36 no chronic illness vs. complex or noncomplex chronic illness,37 healthy children vs. children with ESRD.38 Also, correlation with illness burden and morbidity measures was found.36 Reliability: Internal consistency for total scale scores exceeded the acceptable alpha coefficient of 0.7: self-report (alpha = 0.88) and proxy-report (alpha = 0.90) in pediatric population (healthy, acutely or chronically ill pediatric population),36 alpha approached or exceeded 0.9 in pediatric patients who are healthy and/or with ESRD.38 Also, a strong correlation (Pearson r = 0.6) was found between patient self-report and parent-proxy report of patients on dialysis.39 Responsiveness to change: Evidence exists in pediatric patients admitted to hospital: total score changed from upon admission to during follow-up (mean difference = 22.1, SD = 22.7).37 PedsQL 3.0 ESRD Module: Validity: Content validity has been ensured through focus groups, cognitive interviews, pretesting and field-testing protocols in population of children with ESRD.38 Reliability: Internal consistency was acceptable (alpha > 0.7) in most of self-report and parent-proxy report scales: in general, child self-reports showed lower reliability.38 Moderate agreements (ICC = 0.41 to 0.60) between child self-reports and parent-proxy reports were found in 7 of 10 scales and fair agreements (ICC = 0.21 to 0.40) were found in 3 of 10 scales of PedsQL 4.0 Generic Core Scales and 3.0 ESRD Module. | PedsQL 4.0 Generic Core Scales: Unknown in pediatric patients with kidney disease. 4.4 for self-reported and 4.5 for proxy-reported total scale score when estimated using distribution-based method in healthy and patient pediatric population.81 PedsQL 3.0 ESRD Module: Unknown |
EQ-5D-5L | A generic, preference-based, HRQoL measure consisting of descriptive questions and a VAS. The descriptive questions cover 5 dimensions (mobility, self-care, usual activities, pain/discomfort, and anxiety/depression), while each dimension is divided into 5 levels of (no, slight, moderate, severe, and extreme) perceived problems. Higher scores indicate worse quality of life in individual scores and better quality of life in population index (HUI) scores. The VAS records the patient’s self-rated health on a 10 cm scale with end points 0 to 100 labelled “the worst health you can imagine” and “the best health you can imagine,” respectively. | Validity, reliability, and responsiveness to change: have not been studied in pediatric patients with kidney disease and/or PH1. | Unknown in kidney disease and/or PH1. HUI is estimated to be 0.056 in general Canadian population.41 VAS is estimated to be 10.2 by systematic review.82 |
EQ-5D-Y | A generic, preference-based HRQoL measure with child-friendly wording intended for younger population. Self-completion (ages 8 to 15 years) and proxy (ages 4 to 7 years) versions are available. Based on EQ-5D-3L, descriptive system comprises 5 dimensions (mobility, self-care, usual activities, pain/discomfort, and anxiety/depression) with each dimension having 3 levels (no problems, some problems, and a lot of problems). VAS description is the same as above. Lower scores on 5-digit health status, higher scores on index and VAS represent better HRQoL. | Validity, reliability, and responsiveness to change have not been studied in pediatric patients with kidney disease and/or PH1. | Unknown |
BKD = burden of kidney disease; BSA = body surface area; CKD = chronic kidney disease; eGFR = estimated glomerular filtration rate; EKD = effects of kidney disease; EQ-5D-3L = EuroQol – 5 Dimensions – 3 Levels; EQ-5D-5L = EuroQol – 5 Dimensions – 5 Levels; EQ-5D-Y = EuroQol – 5 Dimensions – Youth; ESRD = end-stage renal disease; GFR = glomerular filtration rate; HRQoL = health-related quality of life; HUI = health utility index; ICC = intraclass correlation; KDQOL = Kidney Disease Quality of Life Questionnaire; MCS = mental component summary; MID = minimal important difference; PCS = physical component summary; PedsQL = Pediatric Quality of Life; PH1 = primary hyperoxaluria type 1; SD = standard deviation; SF-12 = 12-item Short Form survey; SF-16 = 16-item Short Form survey; SPKD = symptoms and problems with kidney disease; URL = upper reference limit; VAS = visual analogue scale.
Urine Oxalate Excretion
In humans, there is no enzyme to degrade oxalate, therefore, it must be eliminated primarily by the kidneys, with a small amount by the gastrointestinal tract. When oxalate is overproduced by the liver, as in the case of PH1, hyperoxaluria results in kidney stones, oxalate nephropathy, and ultimately kidney failure over time.45 Thus, urine oxalate is thought to be in the causal pathway to stone formation and kidney damage in CKD (especially stages 1 to 3a).45
Epidemiologic data show a strong relationship between urine oxalate and long-term kidney function loss. Analysis of data from the Rare Kidney Stone Consortium PH registry of 297 patients with all types of PH (65% PH1) demonstrated that kidney outcomes were correlated with baseline urine oxalate excretion stratified by quartile, with a kidney failure hazard ratio for quartile 4 (Q4) versus Q1 to Q3 of 3.4 (95% CI, 1.4 to 7.9). The 20-year kidney survival was 96% for patients whose oxalate excretion rate at PH diagnosis was less than 1.11 mmol/1.73 m2/24 hours, in contrast to 42% for those with excretions or at least 2.45 mmol/1.73 m2/24 hours.46 When urine oxalate excretion rates over time were analyzed as a continuous time-dependent covariate, the risk of kidney failure was greater with increasing urine oxalate levels, yielding a hazard ratio of 1.8 (95% CI, 1.2 to 2.5) per 1 mmol/1.73 m2/24-hour increase.46 Although it is difficult to draw definitive conclusions from the cross-sectional analysis, the data support that patients with the highest levels of urine oxalate are at greatest risk for PH disease progression.46 However, it is unclear if correction of high oxalate levels leads to long-term kidney preservation.
A retrospective review by Monico et al. (2005)74 showed that pyridoxine therapy reduced mean urine oxalate by 73% from a baseline of 1.5 mmol/1.73 m2/day among 6 patients with PH1 who were homozygous for the most common pyridoxine-responsive AGT mutation (G170R) with 4 patients having achieved normal urine oxalate excretion. In the same study, 8 patients who were heterozygous showed a 45% reduction from a baseline of 2.2 mmol/1.73 m2/day. The pyridoxine effect was sustained during 6.5 and 8.4 years of follow-up, respectively.74 Other PH registry studies showed that patients with PH1 who had the G170R mutation had better preservation of kidney function than those patients without this mutation.16,75 Similarly, in 4 of 5 patients with late diagnosis of PH but with urine oxalate excretions normal or near normal level (less than 0.5 mmol/1.73 m2/day) after initiation of pyridoxine, kidney function was maintained during a median of 8.5 years after a kidney-alone transplant where the only graft loss occurred at 13.9 years posttransplant.76 Normalization of oxalate excretion and stabilization of kidney function has also been observed after preemptive liver transplant, and nephrocalcinosis had resolved after liver-alone transplant in a few reported cases.77-79
Normal value (values are laboratory and method dependent; adapted from Hoppe (2012).83) for urine oxalate in 24-hour urine sample3:
< 0.50 mmol (< 45 mg)/1.73 m2/day
Oxalate excretion (not corrected for BSA) levels out from approximately age 18 years. Therefore, oxalate excretion results should be corrected to a BSA of 1.73 m2 in children to allow interpretation,45 as unadjusted results may appear misleadingly normal. Magnitude of reduction needed for clinical benefit is unclear at this time.3 PH1 should be suspected in a proband with elevated urine oxalate excretion persistently greater than 0.7 mmol/1.73 m2/day.47
To measure urine oxalate excretion rate most accurately, timed 24-hour urine collections are needed, but are challenging, especially in children. In pediatric patients, urine oxalate measurements must account for changes in reference ranges due to maturation of kidney function and growth throughout infancy and childhood.45 The use of 24-hour collection is often preferred over a spot urine sample because it indicates the overall level of oxaluria and should be less subject to variation in oxalate and creatinine excretion, for example from dietary sources in the postprandial phase; however, it has limitations. For example, 24-hour collection smooths out peaks and troughs, thereby, hiding episodic PH. Since the absolute oxalate concentration in the urine affects lithogenesis, it is possible to have a 24-hour output within the reference range but still be at high risk of stone formation.84 Another drawback to 24-hour collection is that accurate timing is problematic and duration can often be either less than or more than 24 hours. In addition, there are other factors affecting the reliability of a 24-hour collection, such as patients missing a urine pass, the quantity of acid added to the container or the possibility of another liquid being added.57
Urine Oxalate:Creatinine Ratio
Oxalate:creatinine ratio is not subject to error from an inaccurately-timed collection and can be calculated from a spot urine sample as well as from a 24-hour collection, which is an advantage especially for children. However, as a ratio, it is a composite parameter that includes 2 variables with associated imprecision.57
Oxalate excretion from a 24-hour collection and oxalate:creatinine ratio calculated from a separate sample have been shown to be moderately correlated using an early morning urine in stone formers62 and using a random sample in a patient with PH.80 Even though the majority of samples from PH cases had both elevated oxalate:creatinine ratio and oxalate excretion, 5 patients with PH had an urine oxalate result within the reference range with 1 patient with PH having both parameters in the reference range (excretion 0.257 mmol/24 hour, ratio 24 mmol/mol). The 1 patient had renal failure and the other 4 patients (oxalate excretions 0.476, 0.415, 0.481, 0.387 mmol/24 hour and oxalate:creatinine ratios 32, 54, 44, 43 mmol/mol, respectively) were on pyridoxine treatment.62
Another comparability study showed that oxalate:creatinine ratio and oxalate excretion were strongly (greater than 0.5)33 correlated (Pearson’s correlation coefficient r = 0.63) in the same 24-hour collections and ratio alone for spot urine samples from patients 18 years and older.57 However, there were several limitations: (1) a large scatter of results was found even after exclusion of obvious under- and over-collections; (2) an overlap was observed in the distribution of results for oxalate:creatinine ratio and oxalate excretion between the PH and non-PH groups, for example, patients with PH having oxalate excretion within reference range whereas ‘normal’ individuals having oxalate excretion above reference range (suggesting undiagnosed PH); (3) oxalate:creatinine ratio and oxalate excretion were discordant in many patients (likely to due to interindividual variation in creatinine output and imprecision in the collection itself), for example, there are a large number (n = 391) of samples with normal oxalate:creatinine ratio but elevated oxalate excretion; (4) sex-related differences were found, for example, both mean oxalate excretion and mean creatinine excretion were significantly higher in males than females (340 versus 281 mmol/24-hour, P < 0.001 and 14.7 versus 9.8 mmol/24-hour, P < 0.001), whereas mean oxalate:creatinine ratio was significantly higher in females than males (32 versus 26 mmol/mmol, P < 0.001 [95th percentile: 39 mmol/mol for all patients, 33 mmol/mol for males and 45 mmol/mol for females]).57
A recent cross-sectional study by Hashmi et al. (2020)59 found correlation between 24-hour urine oxalate excretion and spot urine oxalate:creatinine to be weak (Spearman correlation r = 0.289, P < 0.005) in 62 patients with history of kidney stones. They concluded that random spot urine test cannot replace the 24-hour urine oxalate estimation in patients with urolithiasis.59
Overall, patients with PH can have widely variable urine oxalate concentrations by both measures.57 The variability in results may be a reflection of both preanalytical errors (such as under- and over-collection) and physiologic variation within and/or between individuals. Combination of oxalate excretion and oxalate:creatinine ratio, i.e., elevated levels of both measures, can help diagnose PH.
Normal values (values are laboratory and method dependent; adapted from Hoppe (2012).83) for urine oxalate:creatinine (urinary excretion of creatinine on a per-kg basis differs between males and females and does not stabilize until ages 14 to 18 years;85 to prevent alkaline conversion of ascorbate to oxalate in urine, the sample must be strongly acidified to stabilize ascorbate and minimize formation of calcium crystals.86) molar ratio in spot urine samples3:
0 to 6 months: < 325 to 360 mmol/mol (< 253 to 282 mg/g)
Seven to 24 months: < 132 to 174 mmol/mol (< 103 to 136 mg/g)
Two to 5 years: < 98 to 101 mmol/mol (< 76 to 79 mg/g)
Five to 14 years: < 70 to 82 mmol/mol (< 55 to 64 mg/g)
Greater than 16 years: < 40 mmol/mol (< 32 mg/g)
Oxalate excretion should be corrected to a BSA of 1.73 m2 in children (younger than 18 years) to allow interpretation,45 as unadjusted results may appear misleadingly normal; therefore, the oxalate:creatinine ratio, which does not require BSA correction, can be helpful. Also, oxalate:creatinine ratio falls rapidly over the first years of life and stabilizes from approximately 5 years of age. The inconsistent value before 5 years of age is another limitation for comparability. Lastly, because of differences in production of oxalate and creatinine by body size, sex-related upper reference limits (URLs) for oxalate:creatinine ratio are needed.57
The sponsor cited a study by Matos et al. (1999)60 that provided reference ranges for urine oxalate:creatinine ratios by age range for pediatric patients. Matos et al.60 collected spontaneously voided second morning urine samples from healthy infants, children, and adolescents (N = 384) recruited from 7 nurseries and kindergartens, and 4 schools in Switzerland. The urine collection was repeated after 1 week (total urine samples N = 627) to confirm that there was no order effect between repeated measurements. Oxalate was measured by the oxalate-oxidase method (SIGMA kit procedure 591, Buchs, Switzerland). Matos et al. found that there were no statistically significant sex-related differences in samples collected from patients aged between 1 month and 17 years. They showed that the 95th percentiles decreased markedly over the first years of life, which could be explained by a weight-dependent increase in the creatinine production and excretion as well as a net decrease in the oxalate excretion associated with BSA.65 Also, a decrease in intra- and inter-individual variations were observed with increasing age in the pediatric population. Regarding relatively low URL values observed in their study compared to those previously reported, Matos et al. explained that factors such as differences in diets, sample size, recruitment places (community versus hospitalized infants), and timing of urine collection (first versus second morning urine) in different studies could play a role.58,65,87-89
Suggested URLs (95th percentiles) for urinary oxalate:creatinine ratio in a healthy pediatric population by age60:
One month to 6 months: 0.22 mol/mol (0.175 mg/mg)
Six months to 1 year: 0.17 mol/mol (0.139 mg/mg)
One to 2 years: 0.13 mol/mol (0.103 mg/mg)
Two to 3 years: 0.10 mol/mol (0.080 mg/mg)
Three to 5 years: 0.08 mol/mol (0.064 mg/mg)
Five to 7 years: 0.07 mol/mol (0.056 mg/mg)
Seven to 17 years: 0.06 mol/mol (0.048 mg/mg)
Both Matos et al.60 and Scheinman et al.90 suggested values of 0.1 mol/mol (0.08 mg/mg) and 0.06 mol/mol (0.048 mg/mg) be set for high risk at hyperoxaluria in children aged 1 to 5 years and those older than 5 years, respectively.
Plasma Oxalate
Although oxalate overproduction is a key causal factor in the loss of kidney function, plasma oxalate in isolation may not correlate well with the loss of kidney function at higher eGFR levels (greater than 45 mL/min/1.73 m2) because of the ability of the kidney to excrete the excess load.45 Urine oxalate excretion is expected to decrease as GFR falls to very low levels (less than 15 mL/min/1.73 m2) and ultimately will cease with oligoanuria.45 In patients with advanced CKD, urine oxalate may no longer reflect systemic oxalate burden and plasma oxalate may represent a more accurate biomarker. Besides, collecting 24-hour urine samples can be difficult, especially on a repeated basis or in younger children; therefore, a blood biomarker that predicts urine oxalate and other clinical features of PH is considered clinically valuable.91
In patients with PH, plasma oxalate normal-modestly increased (2 to 10 µmol/L; normal is 1 to 3 µmol/L with most assays) when GFR is well preserved (greater than 60 mL/min/1.73 m2) and markedly increased (greater than 90 to 100 µmol/L) in patients with CKD stage 5.68,70,71 Plasma oxalate concentrations that exceed the supersaturation threshold (35 to 50 µmol/L) for calcium oxalate are typically observed in patients with PH with GFR at or less than 30 to 40 mL/min/1.73 m2 (CKD 3b to 5).68,69 Only patients with PH who have advanced CKD and markedly increased plasma oxalate experience clinically overt systemic deposition of calcium oxalate in multiple body tissues, resulting in severe disease and ultimately death.68,70,71 Dialysis cannot remove enough oxalate to prevent progressive systemic oxalosis, and kidney transplant alone often fails due to recurrent oxalate injury in the allograft.70
To establish relationships between plasma oxalate, GFR, and urine oxalate excretion among patients with PH, Perinpam et al. (2017)48 electronically pulled the most recent plasma oxalate measurement from laboratory information systems on all Mayo Clinic patients between 2005 and 2015 with the closest serum creatinine within 14 days and 24-hour urine measures within 60 days. They found that plasma oxalate increased as eGFR fell (P < 0.0001) or at higher levels of urine oxalate. For a given urine oxalate level, the plasma oxalate level increased as GFR fell. On average, plasma oxalate exceeded 35 to 40 μmol/L (threshold for supersaturation) in PH samples almost universally when eGFR dipped to less than 10 mL/min/1.73m2.48
In a retrospective study on PH registry data, Shah et al. (2020)73 demonstrated that higher plasma oxalate levels both at baseline and during follow-up were significantly associated with loss of kidney function over time. When stratified by quartile, those in plasma oxalate Q4 were at increased risk of ESKD compared to Q1 across CKD stages 2 to 3b. The greatest ESKD rate was found in the CKD 3b in plasma oxalate Q4. After adjusting for follow-up time, eGFR was significantly lower among those with higher plasma oxalate (eGFR reduced by 1.27 mL/min/1.73 m2 per 1 µmol/L increase in plasma; P < 0.001). Furthermore, their results suggest that plasma oxalate is a useful predictor of ESKD risk across CKD stages 2 to 3b, with the effect most pronounced in CKD 3b.
In an analysis of patients with PH1 and stable kidney function from a European registry, no significant correlation between plasma oxalate and eGFR was detected.72 However, a recent study suggested otherwise. Milliner et al. (2021)49 investigated the relationship between plasma oxalate and eGFR in patients with PH (type 1, 2, or 3; PH1 making up more than 83%) and preserved kidney function (eGFR greater than 40 mL/min/1.73 m2, most patients in CKD stage I or II) from 3 randomized, placebo-controlled trials (studies OC3-DB-01, OC3-DB-02, and OC5-DB-01). They found a moderate and statistically significant inverse correlation between eGFR and plasma oxalate across all analyses; Spearman’s correlation coefficients were −0.44 (P = 0.004) in study OC3-DB-01, −0.55 (P = 0.0005) in study OC3-DB-02, −0.51 (P = 0.006) in study OC5-DB-01, and −0.49 (P = 0.0001) in the pooled studies with the same assay types. This study demonstrated that a correlation between plasma oxalate and eGFR is present before substantial loss in kidney function occurs, i.e., at early stages of CKD (stages 1 to 3b) and suggest that the relationship is nonlinear across the range of eGFR values assessed because the observed curve steepens when eGFR approaches and falls below 100 mL/min/1.73 m2.
Evidence that reduction in plasma oxalate reduces the risk or severity of subsequent systemic oxalosis is limited to anecdotal experience with intensive dialysis regimens and the resolution of disease manifestations after transplant. Rapid reduction of plasma oxalate often occurs after liver transplant,20,78 with gradual resolution of oxalosis reported.78 In this regard, plasma oxalate is a likely surrogate for a treatment’s effect on systemic manifestations of the disease. However, the exchange of oxalate between tissue stores and plasma is poorly understood in advanced systemic oxalosis.86,92,93
Measurement of blood oxalate is challenging due to its micromolar concentration and issues related to nonenzymatic generation (ascorbate conversion to oxalate) in vitro. It is complicated by both sample instability and by differences in sample preparation, potentially leading to the impaired recovery of oxalate and differences in results. Currently, methods for measuring oxalate, including sample type, preparation, and analysis, are not interchangeable between laboratories giving rise to different results depending on methods used.50,68,94 Therefore, it is suggested that longitudinal studies on patients be carried out using the same laboratory and methodology. Moreover, it is important that published data acknowledge the methodology used since clinical target setting and evaluation of patient registry data differ by assays used. In an article by Stokes et al.,95 it was mentioned that identifying a definitive method for plasma oxalate, along with a matrix-matched standard reference material would improve the situation as well as quality assurance scheme, co-operation of laboratories to standardize future alterations in calibrators and preanalytic procedures.95
Normal values for plasma oxalate:
Suggested normative plasma oxalate values from literature:
≤ 0.5 mg/L (55.5 µmol/L)97 by unknown method
Mean 0.81 mg/L (89.9 µmol/L) or median 0.29 mg/L (32.19 µmol/L)56 from approximately 30 papers published between 1965 and 2005 using a variety of methods
≤ 0.45 mg/L (50.0 µmol/L): based on mean 0.24 mg/L (26.64 µmol/L) or median 0.22 mg/L (24.42 µmol/L), 5th to 95th percentiles 0.13 to 0.41 mg/L (14.4 µmol/L to 45.51 µmol/L)50-55 from 6 studies published between 2000 and 2005 with participants ranged from 6 to 133
< 0.54 mg/L (59.94 µmol/L)54,55 based on enzymatic method with oxalate oxidase
Taken together, difficulty in sample collection (especially children), variability between labs, and potential for nonlinear kinetics of oxalate in the body make interpretation of changes in oxalate levels on important clinical outcomes highly uncertain. As such, a MID has not been identified for changes in oxalate levels over time.45 Also, there is no distinct upper cut-off point for normal levels of plasma oxalates determined, requiring age- and sex-related normative data based on a large population.98 Some guidelines suggest that the intent of dialysis is to reduce and maintain the plasma oxalate level to less than 30 to 45 µmol/L (the calcium/oxalate supersaturation threshold at which tissue deposition occurs) as much of the time between dialysis sessions as possible. Another source reported supersaturation level to be 25 to 30 µmol/L.96 In addition, continuous dialytic therapies such as continuous veno-venous hemodialysis can maintain plasma oxalate at less than 20 μmol/L for prolonged periods and may be useful in acute situations such as following transplant in an individual with extensive oxalosis whose kidney allograft is functioning poorly.3
Kidney Disease and Quality of Life – 36
Available since 2000,31 the KDQOL-36 is derived from the original 134-item KDQOL instrument (a kidney disease-specific measure of HRQoL developed in 1994) and the later version, 79-item Kidney Disease Quality of Life Short Form Survey (KDQOL-SF).32 The KDQOL-36 comprises the SF-12 (a shorter version of the SF-36) as the generic core portion plus 24 kidney disease-specific questions from the KDQOL-SF v1.3.31 The KDQOL-36 reduced the number of kidney disease-targeted scales from 11 to 3 and includes BKD, symptoms and problems with kidney disease (SPKD), and effects of kidney disease (EKD) scales. Each of the 3 scales contains subsets of items from the KDQOL-SF scales.29,30
The SF-12 PCS subscale and MCS subscale (12 questions): include items about general health, activity limits, ability to accomplish desired tasks, depression and anxiety, energy level, and social activities.
The BKD subscale (4 questions; 5 response options ranging from “definitely true” to “definitely false”): includes items about how much kidney disease interferes with daily life, takes up time, causes frustration, or makes the respondent feel like a burden.
The SPKD subscale (12 questions; 5 response options ranging from “not at all bothered” to “extremely bothered”): includes items about how bothered a respondent feels by sore muscles, chest pain, cramps, itchy or dry skin, shortness of breath, faintness or dizziness, lack of appetite, feeling washed out or drained, numbness in the hands or feet, nausea, or problems with dialysis access.
The EKD subscale (8 questions; 5 response options ranging from “not at all bothered” to “extremely bothered”): includes items about how bothered the respondent feels by fluid limits, diet restrictions, ability to work around the house or travel, feeling dependent on doctors and other medical staff, stress or worries, sex life, and personal appearance.
The PCS and MCS are a generic measure of HRQoL (and are identical to the SF-12), whereas the latter 3 subscales, (i.e., BKD, SPKD, EKD) assess issues specific to patients with ESKD or earlier stages of CKD.99 Scores are reported separately for each of the 5 KDQOL-36 subscales. All items in each scale are transformed to a scale of 0 to 100 with higher scores indicating better HRQoL.100 The PCS and MCS scores are scored on a T-score metric (mean = 50; SD = 10; based on the US general population)101 and are associated with aggregate hospitalization and mortality for groups, not individuals.30 Scores within 1 SD indicate “average” risk when adjusted by age and gender and 1 SD below the mean indicate higher risk. Scores 1 SD above the mean indicate lower than average risk.102 Floor and ceiling effects have been observed with a higher proportion of patients demonstrating ceiling effects than floor effects29 and high frequency of ceiling effect in SPKD compared to other subscales.99 Items that are left blank (missing data) are not taken into account when calculating the scale scores. Hence, scale scores represent the average for all items in the scale that the respondent answered.31 The survey is to be self-completed in about 10 to 15 minutes. Recall period is the past 4 weeks. The KDQOL-36 has been translated into more than 25 different languages.31
Even though KDQOL-36 is intended for patients on dialysis, predialysis patients can also complete the questionnaire by excluding dialysis-specific questions, such as problems with access site (question 28a) and catheter site (question 28b). Users may do the same in using the KDQOL-36 with patients who have received a kidney transplant.31
Validity
Using clinical registry data collected from 70,786 patients in 1,381 US dialysis facilities between June 1, 2015, and May 31, 2016, Peipert et al.29 assessed construct validity by estimating Pearson correlations between BKD, SPKD, and EKD scores with PCS and MCS scores, in addition to known-group analyses with subgroups (dialysis type, diabetes, and employment status). Construct validity was supported by moderate correlations33 (r = 0.40 to 0.52) between the SF-12 (PCS and MCS) scores and the BKD, SPKD, and EKD scores. Also, statistically significant differences (P < 0.001 to 0.05) on the scale scores were observed between patients receiving different types of dialysis (hemodialysis versus peritoneal dialysis), patients with or without diabetes, and patients who were employed full-time versus not.29
Reliability
Peipert et al.29 assessed internal consistency (Cronbach alpha) and dialysis facility-level reliability using 1-way ANOVA. Each of the KDQOL-36’s kidney disease-targeted subscales had acceptable (alpha > 0.7)34 internal consistency reliability (alpha = 0.83 to 0.85) and facility-level reliability (r = 0.75 to 0.83). All items were mostly correlated with the subscales that they were hypothesized to represent (BKD items alpha = 0.56 to 0.73, SPKD items alpha = 0.31 to 0.61, EKD items alpha = 0.47 to 0.68). Lastly, it was shown that each of BKD, SPKD, and EKD subscales mostly measures unique features of kidney disease; however, overlaps of moderate degrees exist among them (Pearson r = 0.48 to 0.62).
MID
An estimated MID that is associated with KDQOL-36 in patients with kidney disease and/or PH1 has not been identified through literature search.
Pediatric Quality of Life Inventory 4.0 Generic Core Scales and 3.0 ESRD Module
The original PedsQL was developed as a HRQoL measure that addressed the paucity of appropriately validated and reliable instruments incorporating both the child and parental experience with chronic health conditions. The PedsQL uses a modular approach and incorporates both generic and disease/symptom-specific items that are appropriate for the assessment of pediatric chronic conditions.35 The generic HRQoL measure was developed using pediatric cancer as the model since the consequences of pediatric cancer (rather than specific cancer symptoms) are applicable to many other pediatric chronic health conditions.35
Pediatric Quality of Life Generic Core Scales
The PedsQL 4.0 Generic Core Scales comprise 23 items under the following modules: (1) Physical Functioning (8 items), (2) Emotional Functioning (5 items), (3) Social Functioning (5 items), and (4) School Functioning (5 items).36 The Generic Core Scales are comprised of both the parent-proxy report and the child self-report formats that assess health perceptions. The child self-report format is specific for ages 5 to 7 years, 8 to 12 years, and 13 to 18 years, while the corresponding parent-proxy reports are specific for toddlers (ages 2 to 4 years, for which there is no child self-assessment report), young children (ages 5 to 7 years), children (ages 8 to 12 years), and adolescents (ages 13 to 18 years). The questions ask how much of a problem each item has been in the past month. A 5-point Likert response scale is used across the child reports (from ages 8 to 18 years) and corresponding parent reports, which include the following responses and scores: 0 = never a problem; 1 = almost never a problem; 2 = sometimes a problem; 3 = often a problem; and 4 = almost always a problem. In addition, a 3-point scale is used for simplification and ease of use for children who are aged 5 to 7 years and include 0 = not at all a problem; 2 = sometimes a problem; and 4 = a lot of a problem, with each of the response choices anchored to a happy face to sad face scale.36 The scores, which are reversed scored, are transformed linearly to a 0 to 100 scale, where 0 = 100, 1 = 75, 2 = 50, 3 = 25, and 4 = 0, with higher scores indicative of a higher HRQoL. To account for missing data, the sum of the items divided by the number of items that are answered is computed to ascertain the scale score. If greater than 50% of the items within the scale are missing, then the scale score cannot be obtained. To create the Psychosocial Health Summary Score (comprised of 15 items), the sum of the items is divided by the items answered in the School Functioning, Emotional, and Social Subscales.36 There are currently more than 60 translations of the PedsQL 4.0 that have been validated.
Validity
Validity of the PedsQL 4.0 was tested in a sample of chronically ill (as reported by their parents in a specialty clinic [n = 683]), acutely ill (parents reported no presence of chronic illness and attended a specialty clinic [n = 207]), and healthy children (identified at their physician’s office during regular visits or using telephone calls [n = 730]) between the ages of 2 to 18 years.36 Construct validity was ascertained using the known-groups method, whereby scale scores were compared across groups that are known to differ in the specific health constructs being examined (healthy versus acute or healthy versus chronic conditions). In addition, potentially confounding factors such as age, sex, and ethnicity were also examined across health states. Hypothesizing that healthy children would have a higher HRQoL, Varni et al. noted that the PedsQL 4.0 differentiated between the different health states (healthy, acute, and chronically ill) and it also correlated with illness burden and morbidity measures.36 Construct validity was further demonstrated by another study: patients with no chronic illness (and their parents) scored higher on the total score, physical domain, and psychosocial domain than patients with either complex or noncomplex chronic illness.37 Construct validity for the Generic Core Scales was also determined by Goldstein et al. by using the known-groups method, which compared scale scores across groups known to differ in the health construct (healthy children and children with ESKD) with independent sample t-tests.38 Large effect size (ES > 0.80) was observed between ESKD and healthy samples (P < 0.001) across all subscales of parent-proxy reported and child self-reported Generic Core Scales except for child self-reported Emotional (ES = 0.50) and Social (ES = 0.70) Functioning subscale in healthy sample.38
Reliability
Internal consistency reliabilities generally exceeded the standard alpha coefficients of 0.70.36 The total scale scores across the ages for the self-report and proxy-report were 0.88 and 0.90, respectively, indicating this as an appropriate primary analysis summary score. The Physical Health and Psychosocial Health Summary Scores were greater than 0.8 for the self-report and the proxy-report; hence, Varni et al. determined they were best for secondary analyses. The Emotional, Social, and School Functioning Subscales generally obtained alpha coefficients around 0.70; therefore, Varnet et al. suggested these be used for descriptive or exploratory analyses.36 Similarly, in study by Goldstein et al. all child self-report and parent-proxy report scales on the Generic Core Scales exceeded the minimum reliability standard of 0.70 required for group comparisons, whereas total scale scores for both child self-report and parent-proxy report approached or exceeded the reliability criterion of 0.90 recommended for analyzing individual patient scores.38 In a study by Stockard et al. with patients (n = 29, ages 2 to 18 years) and parents (n = 41) of patients (ages 2 to 18 years) on dialysis, it was shown that Generic Core Scale was correlated between patient and their parent proxy (Pearson correlation coefficient r = 0.60).39
Responsiveness to Change
In a study by Desai et al.,37 patients admitted to medical or surgical units were administered the PedsQL 4.0 upon admission (64.5%; n = 4,637 out of 7,184) and during follow-up (58.1%; n = 2,694 out of 4,637). The responsiveness of the PedsQL 4.0 was demonstrated upon examination of the mean differences between admission and follow-up; 22.1 (SD = 22.7) for the total score, 29.3 (SD = 32.4) for the physical domain, and 17.1 (SD = 21.0) for the psychosocial domain. Moderate variability in responsiveness was observed by age and minimal variability in responsiveness was observed for patients having been admitted for medical or surgical reasons.37
MID
In a study by Varni et al.,81 the authors mailed a survey to residents in California (of which 10,241 [51%] completed and returned the survey) and estimated the MID by calculating the SEM in the survey responses. They estimated the MID for the Total Scale Score of the child self-report to be a change of 4.4, while the MID for the Total Scale Score for parent-proxy report was a change of 4.5.81 However, an anchor-based approach using a valid patient-reported scale would be a preferable approach to distribution-based method in estimating an MID.
No MID has been identified through literature search for any specific chronic or acute condition, including kidney disease and/or PH1.
Pediatric Quality of Life 3.0 ESRD Module
The 34-item PedsQL 3.0 ESRD Module encompasses 7 scales: (1) General Fatigue (4 items), (2) About My Kidney Disease (5 items), (3) Treatment Problems (4 items), (4) Family and Peer Interaction (3 items), (5) Worry (10 items), (6) Perceived Physical Appearance (3 items), and (7) Communication (5 items). The scales are composed of parallel child self-report and parent-proxy report formats for children aged 5 to 18 years and a parent-proxy report format for children aged 2 to 4 years. For the parent report for toddlers (aged 2 to 4 years) form, there are no Family and Peer Interaction, Perceived Physical Appearance, and Communication Scales. Furthermore, for toddlers, the General Fatigue, About My Kidney Disease, Treatment Problems, and Worry Scales were modified to include fewer items (not all items were applicable for toddlers). The format, instructions, Likert response scale, and scoring method are identical to the PedsQL 4.0 Generic Core Scales, i.e., ESRD Module is scored on a scale of 0 to 100, with higher numbers correlating with better quality of life. The ESRD Module generates a total score and 7 subcategory scores.38
Validity
The ESRD Module scales were developed through focus groups, cognitive interviews, and pretesting and field-testing protocols, ensuring content validity in pediatric patients with ESRD.38
Reliability
Goldstein et al.38 conducted a cross-sectional study comparing child self-reported and parent- or proxy-reported HRQoL of children with ESKD (n = 193 patients between the ages of 5 and 18 years; n = 190 parents of patients aged between 2 and 18 years) with a matched sample (randomly matched by age, sex, and race/ethnicity) of healthy controls across the US. The sample included children receiving hemodialysis (n = 30; 14.4%) and peritoneal dialysis (n = 45; 21.6%) and those with a functioning renal transplant (n = 127; 61.1%). Internal consistency reliability for the PedsQL 3.0 ESRD Module was acceptable (Cronbach coefficient alpha > 0.7) for both parent-proxy report and child self-report, except for 1 parent-proxy report scale (Treatment Problems alpha = 0.61) and 3 child self-report scales (Treatment Problems alpha = 0.39, Perceived Physical Appearance alpha = 0.57, About My Kidney Disease alpha = 0.64) on the ESRD Module. Generally, child self-report showed lower reliability than parent-proxy reports. Scales that met the minimum coefficient standard of 0.70 may be used to examine specific domains of HRQoL, as well as subgroup differences, whereas scales that did not achieve or approach the 0.70 standard should be used only for descriptive analyses. Furthermore, according to the authors, Treatment Problem Scale is not conceptually an HRQoL scale, but a treatment barrier scale, and is not necessarily expected to be highly correlated.38
Agreement between child self-report and parent-proxy report was determined by ICCs by Goldstein et al.38 The ICCs are in the moderate agreement range (between 0.41 and 0.60) for 7 of 10 PedsQL Scales and in the fair agreement range (between 0.21 and 0.40) for 3 of 10 PedsQL Scales (Emotional Functioning = 0.39, Perceived Physical Appearance = 0.36, and Communication = 0.35). The greatest overall agreement is found on the General Fatigue Scale (0.57) and Physical Health Summary Score (0.56). The finding demonstrated that children with ESKD and their parents showed fair to moderate agreement on PedsQL 4.0 Generic Core Scales and PedsQL 3.0 ESRD Module.38
MID
No MID has been identified through literature search for any specific chronic or acute condition, including kidney disease and/or PH1.
EuroQol – 5 Dimensions – 5 Levels
The EQ-5D-5L questionnaire is a generic, preference-based, HRQoL measure consisting of descriptive questions and a VAS.40 The EQ-5D-5L has been validated in terms of feasibility, convergent validity, discriminatory power, and ceiling effects in a diverse patient population from 6 countries with chronic conditions.40 Questions were answered based on how the patient felt that day.
The EQ-5D-5L was developed by the EuroQol Group as an improvement to the EQ-5D 3 level (EQ-5D-3L), to improve sensitivity (measuring small and medium health changes) and reduce ceiling effects.41,42 The instrument comprises 5 dimensions: mobility, self-care, usual activities, pain/discomfort, and anxiety/depression. Each dimension is rated on 5 levels: 1 = “no problems,” 2 = “slight problems,” 3 = “moderate problems,” 4 = “severe problems,” and 5 = “extreme problems” or “unable to perform.” Respondents are asked to choose the level that reflects their health state for each of the 5 dimensions. The numerical values assigned to levels 1 to 5 for each dimension reflect rank order categories of function. Data are not used to produce an individual dimension score. A total of 3,125 unique health states are possible, with 55555 representing the worst health state and 11111 representing the best state.
Results from the EQ-5D-5L descriptive system can be converted into a single, country-specific index score using a scoring algorithm taking the local patient and population preferences into account.103 Therefore, the index score is a country-specific value and the lowest EQ-5D index (utility) score varies depending on the scoring algorithm used.40 In all scoring algorithms of the EQ-5D-5L, a score of 0 represents the health state “dead” and 1.0 reflects “perfect health.” Also, negative values are possible to represent health states that a society, not the patient, considers worse than death. Different utility functions are available that reflect the preferences of specific populations, e.g., US, UK. As an example, a Canadian scoring algorithm results in a score of –0.148 for health state 55555 (worst health state).42
Another component of the EQ-5D-5L is a VAS, which is a 10 cm, continuous scale anchored by 2 verbal descriptors: 0 (worst health imaginable) to 100 (best health imaginable). The respondents are asked to mark an X on the scale that best represents their health on that day.40,42
In summary, the EQ-5D produces 3 types of data for each respondent40,42:
A profile indicating the extent of problems on each of the 5 dimensions represented by a 5-digit descriptor, such as 11121 or 21143.
A population preference-weighted health utility index (HUI) score based on the descriptive system.
A self-reported assessment of health status based on the VAS.
Even though the EQ-5D-5L has been validated in a diverse patient population in 6 countries,104 no literature was identified that assessed the EQ-5D-5L for validity, reliability, or responsiveness in populations with kidney disease and/or PH1.
MID
No MID was estimated either for index or VAS in populations with kidney disease and/or PH1.
An estimated MID for the general population was based off scoring algorithms for 6 countries (Canada, China, Spain, Japan, England, and Uruguay) to be between 0.037 and 0.069.41 The MID estimates for the index score in the Canadian population have a summarized mean of 0.056 (SD = 0.011), and a summarized median of 0.056 (interquartile range [IQR], 0.049 to 0.063).41 Systematic review of 16 anchor-method based studies in mixed population showed that estimated MID for VAS was 10.2 (range, 0.4 to 35.0; IQR = 8.3).82
EuroQol – 5 Dimensions – Youth
In 2009, the EuroQol Group introduced the EQ-5D-Y that is a child-friendly version of EQ-5D and a more comprehensible instrument suitable for children and adolescents. EQ-5D-Y is available in more than 100 languages and in various modes of administration. The EQ-5D-Y is based on the EQ-5D-3L and essentially consists of 2 pages: the EQ-5D descriptive system and the VAS.43 The EQ-5D-Y is designed for self-completion by children and adolescents aged 8 to 15 years. Between the ages of 4 and 7 years, a proxy-completed version should be used. Proxy versions, for completion by a caregiver or someone who knows the person well, are used when children or adolescents are mentally or physically incapable of reporting on their HRQoL, for instance, because of severe intellectual disability or mental health problems. Four proxy versions are currently available.105 For adolescents between the ages of 12 and 15 years, either the EQ-5D-Y or adult version of EQ-5D can be used depending on the study design. All the questions in descriptive questionnaire and VAS ask to describe a health status on the day of administration.106
The EQ-5D-Y descriptive system comprises 5 dimensions: (1) mobility, (2) self-care, (3) usual activities, (4) pain or discomfort, and (5) anxiety/depression.44 Each dimension has 3 levels: no problems, some problems, and a lot of problems. Patients are asked to indicate their health state by ticking the box next to the most appropriate statement in each of the 5 dimensions. Even though the EQ-5D-Y descriptive system comprises the same 5 dimensions as the EQ-5D-3L, it uses more appropriate, child-friendly wording. The most relevant differences with the adult EQ-5D-3L are43:
The “Mobility” dimension header includes “walking about” to facilitate understanding.
The title of the second dimension was changed from “Self-Care” to “Looking After Myself.”
The “Usual Activities” dimension became more child relevant: the new title, “Doing Usual Activities,” is followed by “for example, going to school, hobbies, sports, playing, doing things with family or friends.”
For the fifth dimension, “Anxiety/Depression” was replaced with “Feeling Worried, Sad or Unhappy.”
The wording of the items representing the highest level of severity were changed in all dimensions, from “confined to bed” to “a lot of problems walking about,” in the first dimension, and from “being unable to” to “having a lot of problems” (with washing or dressing myself, or doing usual activities) in the second and third dimensions. In the Pain/Discomfort dimension, the upper (worst) level was changed from “I have extreme pain or discomfort” in the adult 3L version to “I have a lot of pain or discomfort” in the Y version. In the final dimension, the upper level was changed from “I am extremely anxious or depressed” to “I am very worried, sad or unhappy.”
The wording of the first response level in the Looking after Myself dimension was also changed from “I have no problems with self-care” to “I have no problems washing or dressing myself.”
Each dimension results in a 1-digit number and the digits for the 5 dimensions can be combined to form a 5-digit score that describes the patient’s health state. Lower numbers in the 5-digit score indicate better HRQoL. A summary index value can be obtained based on societal preference weights for the health state. The weights or “utilities” are often used to compute quality-adjusted life-years for health economic analyses. Health state index scores generally range from less than 0 (negative values represent a health state worse than dead; 0 = dead) to 1 (the value of full health), with higher scores indicating higher health utility. Health state preferences often represent national or regional values and can therefore differ between countries or regions. The second part of the questionnaire consists of a VAS on which the respondent rates their perceived health from 0 (the worst imaginable health) to 100 (the best imaginable health).106 The VAS records the patient’s self-rated health and can be used as a quantitative measure of health outcome that reflects the younger patient’s own judgment.43 Higher scores on index and VAS represent better HRQoL.
Psychometric properties of EQ-5D-Y have not been assessed in pediatric population with kidney disease and/or PH1. No MID estimate for EQ-5D-Y has been identified from the literature.
Pharmacoeconomic Review
Abbreviations
BIA
budget impact analysis
CKD
chronic kidney disease
cLKT
combined liver-kidney transplant
ECM
established clinical management
eGFR
estimated glomerular filtration rate
ESKD
end-stage kidney disease
FHNHD
frequent home nocturnal dialysis
ICER
incremental cost-effectiveness ratio
PH1
primary hyperoxaluria type 1
QALY
quality-adjusted life-year
SOB
Schedule of Benefits
Executive Summary
The executive summary comprises 2 tables (Table 1 and Table 2) and a conclusion.
Item | Description |
|---|---|
Drug product | Lumasiran (Oxlumo), 94.5 mg per 0.5 mL vial of solution for subcutaneous injection |
Submitted price | Lumasiran: $96,855.33 per vial |
Indication | Treatment of primary hyperoxaluria type 1 (PH1) to lower urinary oxalate levels in pediatric and adult patients |
Health Canada approval status | NOC |
Health Canada review pathway | Priority review |
NOC date | March 7, 2022 |
Reimbursement request | As per indication |
Sponsor | Alnylam Netherlands B.V. |
Submission history | Previously reviewed: No |
NOC = Notice of Compliance.
Table 2: Summary of Economic Evaluation
Component | Description |
|---|---|
Type of economic evaluation | Cost-utility analysis Markov model |
Target populations | Pediatric and adult patients with PH1 |
Treatment | Lumasiran plus ECM |
Comparator | ECM (consisting of oxalate-controlled diet, hyperhydration, and vitamin B6 and oral citrate supplements) |
Perspective | Canadian publicly funded health care payer |
Outcomes | LYs QALYs |
Time horizon | Lifetime |
Key data sources | ILLUMINATE-A, ILLUMINATE-B, and ILLUMINATE-C trials |
Submitted results | Compared to ECM alone, the ICER of lumasiran + ECM was $948,635 per QALY (incremental costs = $20,155,677; incremental QALYs = 21.25) |
Key limitations |
|
CADTH reanalysis results |
|
CKD = chronic kidney disease; ECM = established clinical management; ESKD = end-stage kidney disease; ICER = incremental cost-effectiveness ratio; LY = life-year; QALY = quality-adjusted life-year; PH1 = primary hyperoxaluria type 1.
Conclusions
In the 3 ILLUMINATE trials, lumasiran demonstrated improvements in urine oxalate and plasma oxalate. Changes in estimated glomerular filtration rate (eGFR) and health-related quality of life from baseline were numerically small, and conclusions could not be drawn about whether lumasiran had an impact on these outcomes due to the small number of patients and short treatment duration of the trials so far. The clinical experts and CADTH clinical review team agreed that long-term efficacy and safety data will be necessary to confirm the findings in the ILLUMINATE trials and to better understand how the main trial outcomes translate to improved long-term outcomes of maintained lowering of hepatic oxalate production, prevention of kidney stones, and prevention of progression to end-stage kidney disease (ESKD).
The sponsor’s base case included several assumptions that were not substantiated by quality evidence, were based on unvalidated surrogate outcomes measured in the ILLUMINATE trials, and did not reflect current practice in Canada. First, the sponsor assumed that lumasiran was 100% effective in preventing chronic kidney disease (CKD) progression based on the association of plasma oxalate levels and the rate of eGFR loss per year. The nature of this relationship is speculative: The fixed rate used is uncertain (and likely heterogeneous), and this has not been confirmed in the clinical trials. Second, the assumption regarding high-intensity dialysis for all patients with stage 4 CKD (CKD 4) and those with ESKD on established clinical management (ECM) overestimated costs and favoured lumasiran. Third, the rate of combined liver-kidney transplants (cLKTs) used to inform the model is not appropriate. Clinical experts consulted by CADTH indicate that patients with primary hyperoxaluria type 1 (PH1) approaching ESKD are prioritized for transplants, given that earlier liver transplants will significantly improve health outcomes. This priority setting is even more relevant in the pediatric population. Fourth, a parental caregiver disutility decrement was applied to CKD 4 and ESKD health states for all patients (including adults), despite methodological limitations and uncertainty due to a lack of provided source data. In addition, the inclusion of disutilities from multiple events resulted in negative utility values (worse than death) for the high-intensity dialysis ESKD health states, which was deemed unrealistic by clinical experts consulted by CADTH. Finally, the sponsor’s base case assumed a greater proportion of patients in the late CKD stage at the start of the model, which was in contrast to the distribution of CKD stages seen in the trials.
The CADTH reanalysis addressed the previously mentioned limitations to be more reflective of current care in Canada. The CADTH results were similar to those of the sponsor, in that lumasiran is not considered cost-effective based on conventionally accepted willingness-to-pay thresholds. The CADTH base case incremental cost-effectiveness ratio (ICER) for lumasiran + ECM compared to ECM alone is $2,165,926 per quality-adjusted life-year (QALY) gained; lumasiran has a 0% probability of being cost-effective at a willingness-to-pay threshold of $50,000 per QALY gained. A price reduction of 95% is required for lumasiran to achieve a mean cost-effective estimate of $50,000 per QALY. A key driver of the ICER was the high annual cost and long-term use of lumasiran.
Although the CADTH reanalysis attempted to address limitations in the 4 areas previously described, significant uncertainty still exists in the CADTH base case due to remaining uncertain but optimistic assumptions. Specifically, if lumasiran is not 100% effective in preventing CKD progression, or if more pediatric patients at early stages of disease are treated with lumasiran because of early detection, or if lumasiran treatment continues after kidney transplant, an even greater price reduction is likely required.
Stakeholder Input Relevant to the Economic Review
This section is a summary of the feedback received from the patient groups, registered clinicians, and drug plans that participated in the CADTH review process.
CADTH received a joint patient submission from the Oxalosis and Hyperoxaluria Foundation and the Canadian Organization for Rare Disorders. In total, 43 responders’ inputs were collected through an online survey and virtual focus groups, with 18.6% stating they were Canadian. Of the respondents, 17 identified as patients with PH, with the remaining being caregivers. In addition, 74.4% of respondents indicated that they or the individual(s) they cared for had been diagnosed with PH1. In total, 5 Canadian respondents (2 children), 7 American respondents, and 6 non–North American respondents reported having experience with lumasiran. Patients indicated that the greatest burden of PH-1 was the physical toll and emotional stress associated with the disease. Responders further stressed the complexity of diagnosing PH-1. Patients responded that current treatments and dialysis are insufficient for managing their disease and that therapies that decrease the likelihood of kidney stones, need for kidney and/or liver transplant, kidney failure, oxalosis, and the amount of medication are critical. Patients who have received lumasiran stated they have experienced improvement in PH-1 management and quality of life.
No registered clinician input was received for this review.
Drug plan input was received for this review. The plans had questions about how outcomes from the trials relate to complications associated with PH1 such as recurrent kidney stones, nephrocalcinosis, progressive renal failure, ESKD, and multirenal damage. The drug plans further inquired into how response to lumasiran should be monitored or reported, and what loss of response or absence of clinical benefit would be defined as. Finally, the drug plans sought further clarification on who the prescribers of the drug would be, and noted that savings realized through a reduction in the need for dialysis are not direct savings to drug programs.
Several of these concerns were addressed in the sponsor’s model:
ESKD and cLKT were included as part of the model health states.
Patients on lumasiran were assumed to have better quality of life by halting kidney disease progression and lower intensity of dialysis if needed.
Renal stone events and systemic oxalosis were also included as potential complications in the model.
Economic Review
The current review is for lumasiran (Oxlumo) for patients with PH1.
Economic Evaluation
Summary of Sponsor’s Economic Evaluation
Overview
The sponsor submitted a cost-utility analysis comparing lumasiran plus ECM (lumasiran hereafter) to ECM (oxalate-controlled diet, hyperhydration, and vitamin B6 and oral citrate supplements) for pediatric and adult patients with PH1. This population aligns with the approved Health Canada indication and reimbursement request.
Lumasiran is available in a single-use, ready-to-use vial of solution for subcutaneous injection. The recommended dose consists of loading (first 3 months) and maintenance doses, based on body weight measurements. The number of administrations per quarter is 3 for the loading dose phase and 1 for the maintenance dose phase, regardless of the population. This equates to an average number of vials for the loading phase of 3 (pediatric) and 9 (adult); in the maintenance phase, the average number of vials per quarter is 1 (pediatric) and 3 (adult); or per year 4 (pediatric) and 12 (adult) vials. The list price for lumasiran is $96,855.33 per 94.5-mg vial, equating to an average annual cost of $387,421 for pediatric patients and $1,162,263 for adult patients in the maintenance phase.
The clinical outcomes were QALYs and life-years. The analyses were conducted from the Canadian public payer perspective. The time horizon in the base case was a lifetime (up to 100 years old, approximately 66 to 93 years), with a 1.5% annual discount rate for costs and effects.
Model Structure
A Markov model structure (Figure 1, Appendix 3) was used to assess the costs and health outcomes of lumasiran and ECM in a weighted cohort of pediatric and adult patients with PH1. The Markov cycle length was 6 months. The cohort could transition through 9 health states defined by kidney function including several CKD stages, ESKD, and cLKT status. The CKD4, ESKD, and cLKT health states could also be subcategorized by controlled (Oxc) or uncontrolled (Oxu) plasma oxalate levels (defined as plasma oxalate greater than or equal to or less than 50 μmol/L, respectively). The 10 health states were CKD 1 to 2, CKD 3a, CKD 3b, CKD 4-Oxu, CKD 4-Oxc, end-stage kidney disease (ESKD-Oxu, ESKD-Oxc), and posttransplantation (cLKT-Oxu, cLKT-Oxc) and death.
In each Markov cycle, the cohort starts the simulation in 1 of the 3 early disease stages (i.e., CKD 1 to 2, 3a, or 3b) or 1 of 2 later-stage health states with uncontrolled oxalate (CKD 4-Oxu or ESKD-Oxu). A patient who had not yet undergone transplant could progress to the next CKD stage or remain in the same CKD stage; transition to a less severe CKD stage was not permitted. For the late-stage health states (CKD 4 and ESKD), a transition between the uncontrolled oxalate (Oxu) and controlled oxalate (Oxc) states was permitted for the lumasiran arm only. Treatment with lumasiran or ECM was continued across all health states until transplant.
Model Inputs
The simulated patient cohort in the model was informed by the ILLUMINATE trials and published literature. The initial age for the pediatric and adult population was 6.9 and 34.2 years old, respectively, with a weighted average age of 14.9 years for the entire cohort. The mean weight was 26.2 kg for the pediatric population and 82.0 kg for the adult population. Fifty-nine percent were male and 70.6% were pediatric patients. The proportion of the cohort entering the model in each health state was informed by the pooled distribution of patients on entry in the Singh et al. study: 38% with CKD 1 to 2, 12% with CKD 3a, 12% with CKD 3b, 10% with CKD 4-Oxu, and 28% with ESKD-Oxu (no patients starting in Oxc).1
Patients in the ECM arm of the model may progress to more severe CKD stages over time. The transition probabilities from CKD 1 to CKD 4 were estimated by mapping observed changes in plasma oxalate levels in the placebo arm of the ILLUMINATE-A trial, and the relationship between plasma oxalate and eGFR reported by Shah et al.2 Shah et al. reported a mean absolute eGFR decrease of 1.27 mL/min/1.73 m2 (assumed per year) per 1 μmol/L increase in plasma oxalate.2 The plasma oxalate increased by 2.23 μmol/L in the trial for the placebo group, which was assumed to result in eGFR decrease of 2.83 mL/min/1.73 m2 per year. The model then estimated the time to progress to the next CKD stage by dividing the difference of the mean eGFR from each CKD stage by 2.83 mL/min/1.73 m2, and the annual probability of transitioning to the next more severe health state was the inverse of the mean number of years required to transition. Patients in the ECM cohort progressing beyond CKD 3b or entering the model with late-stage disease were assumed to have uncontrolled oxalate levels. It was assumed that patients in the ECM arm could not transition from uncontrolled oxalate health states to controlled; 100% of the CKD 4 and ESKD health states received high-intensity dialysis in addition to ECM. According to UK experts’ opinion, high-intensity dialysis consists of hemodialysis 6 times a week for pediatric patients and, in adults, 87% received hemodialysis 6 times week and 13% received hemodialysis 6 times a week plus peritoneal dialysis 7 times a week. Time to ESKD was modelled on the ESKD-free survival curves reported by the Harambat et al. study in European patients with PH1.3 Patients in the CKD 4-Oxc health state were assumed to be stable with no progression to ESKD.
For patients in the lumasiran arm, the transition probabilities from CKD 1 to CKD 4 were estimated using 12 months of observed effects of lumasiran on plasma oxalate in the ILLUMINATE-A and ILLUMINATE-B trials. Patients treated with lumasiran were assumed to have no further reduction in eGFR (stayed in same CKD health state) according to the relationship suggested by Shah et al. because the ILLUMINATE-A and ILLUMINATE-B trials indicated reduction of plasma oxalate of 46.32% over 12 months. The transition probability from CKD 4-Oxu or ESKD-Oxu to CKD 4-Oxc or ESKD-Oxc was extrapolated using 6 months of observed effects of lumasiran on plasma oxalate in the ILLUMINATE-C trial. Only the lumasiran cohort was expected to transition from uncontrolled oxalate states to controlled oxalate states. Based on the ILLUMINATE-C trial, the percent reduction in plasma oxalate was 44.15% per cycle, with a baseline plasma oxalate level of 98.93 μmol/L in the trial, it would take 1.1 cycle to reduce to the oxalate level to 50 μmol/L; thus, the transition probability was 0.89 for the first cycle and 1 for the second cycle — that is, after 12 months, all patients in the lumasiran-treated arm had a controlled oxalate level and no progression from CKD 4-Oxc to ESKD-Oxc was assumed. Normal-intensity dialysis (hemodialysis 3 times a week for pediatric patients; 87% hemodialysis 3 times week or 13% peritoneal dialysis 7 times a week for adults, according to UK expert opinions) was assumed only for patients with ESKD on lumasiran.
The model allowed patients reaching CKD4 and ESKD to undergo cLKT. The probability of undergoing cLKT for late-stage CKD with controlled oxalate was assumed to be similar to the cLKT probability observed for patients who do not have PH1; the transplant rate (0.21 per 6 months) obtained from the 2020 Canadian Institute for Health Information e-Statistics Report on Transplant, Waiting List and Donor Statistics (cLKT)4 was applied to CKD 4 and ESKD health states with controlled oxalate for both adult and pediatric cohorts, given the absence of pediatric-specific data. For late-stage CKD cohorts with uncontrolled oxalate (i.e., ECM arm), transplant rates (0.007 per cycle) were estimated using data from the Compagnon et al. study based on 33 French patients with PH1 who underwent combined transplants.5 Both ECM and lumasiran were assumed to cease after liver-kidney transplant.
Upon transplant, patients would remain in the posttransplant health state (cLKT) or death. The cohort receiving a transplant from CKD 4-Oxu or ESKD-Oxu transitioned to cLKT-Oxu and has a worse posttransplant prognosis than the cohort receiving a transplant from the CKD 4-Oxc or ESKD-Oxc who transitioned to cLKT-Oxc, according to the long-term follow-up study of patients with PH1 by Jamieson et al.6 This is because patients in late-stage health states with uncontrolled oxalate levels (i.e., unstable disease) would have greater systemic oxalosis; therefore, they were modelled to have poorer outcomes following transplant. The average of the 2 Kaplan-Meier curves from the Jamieson et al. study that referred to patients in “very good” and “good” preoperative condition was used to estimate posttransplant mortality among patients with controlled oxalate levels. The average of the 2 Kaplan-Meier curves referring to patients in “fair” and “poor” preoperative condition was used to model patients with uncontrolled oxalate levels. The model assumed that a portion of posttransplant patients would undergo retransplant, and retransplant rates were also based on data published by Compagnon et al.
The annualized rate of kidney stone events for CKD 1 to 3b health states was obtained from pooled baseline data in the ILLUMINATE-A and ILLUMINATE-B trials. For the CKD 4 and ESKD health states, the annualized rate was obtained from baseline data in the ILLUMINATE-C study. The probability of experiencing systemic oxalosis complications is assumed to be 0 in the CKD 1 to 3b health states. The prevalence of complications associated with systemic oxalosis in patients with late-stage CKD and uncontrolled oxalate was obtained from a survey of UK clinical experts who treat PH1. The prevalence of systemic oxalosis in patients with CKD 4 and ESKD ranged from 15% to 30% and 35% to 80%, respectively. A 20% reduction in systemic oxalosis complications was assumed among patients in CKD 4 or ESKD with controlled oxalate levels.
A time-on-treatment curve derived from ILLUMINATE-A and ILLUMINATE-B patient-level data was used to simulate the proportion of the CKD 1 to 3b cohorts discontinuing treatment with lumasiran at each cycle of the model. Based on the log-normal extrapolated curve in the model, 8% of patients would discontinue lumasiran by year 10. Following treatment discontinuation, the cohort was assumed to experience the clinical effect observed in the ECM arm. A discontinuation rate of zero was applied to CKD 4 and ESKD cohorts because no discontinuations were observed in the ILLUMINATE-C trial within the first 6 months.
The cohorts in the model could transition to death from any live health state, with probabilities based on national statistics for the age-specific mortality rate in the general population and adjusted by CKD stage-specific mortality multipliers based on a US study.7,8 The same mortality rates were used for each of the late-stage health states (CKD 4 or ESKD) regardless of oxalate levels. The incidences of adverse events associated with lumasiran and ECM in the model were based on 6-month data from ILLUMINATE-A.
Utility values for patients in early-stage disease (CKD 1 to 3b) were obtained from pooled patient-level EQ-5D data collected at baseline, month 6, and month 12 in the ILLUMINATE-A study. For late-stage disease (CKD 4/ESKD) with uncontrolled oxalate and on high-intensity dialysis (ECM arm), EQ-5D data were derived from a sponsor-conducted unpublished health-state vignette study capturing the burden of PH1 in a sample of the general public. Canadian EQ-5D-5L value sets reported by Xie et al. were applied to EQ-5D-5L vignette data to derive utility values.9 For other late-stage disease patients (i.e., controlled oxalate and high-intensity dialysis [ECM arm]), and normal-intensity dialysis with uncontrolled or controlled oxalate (lumasiran arm), utilities obtained from the ILLUMINATE-A study for populations with CKD 1 to 3b were used as a starting point from which to apply utility decrements from the literature due to systemic oxalosis complications and dialysis.10-12 The health-state vignette study was also used to obtain utilities for patients following cLKT. A one-off disutility of transplant,13 graft failure,14 treatment-related adverse events,10 systemic oxalosis complications10,11 and acute kidney stone events15 were obtained from literature. The Canadian utility norms reported by Guertin et al. were used to adjust base utilities by age and sex.16 A caregiver disutility decrement of –0.08 was also applied to all patients in CKD 4 and ESKD health states.17,18
The list price for lumasiran is $96,855.3299 per 94.5 mg vial. The average number of vials per cycle in the model was 4 for cycle 1 (loading dose) and 2 for subsequent cycles for the pediatric population. In the adult population, the average was 12 for cycle 1 (loading dose) and 6 for subsequent cycles. No vial sharing was included, and they assumed 98% compliance. The average cost of lumasiran for a pediatric patient was $378,724 for the first 6-month cycle and $189,362 for subsequent 6-month cycles. The average cost of lumasiran for an adult patient was $1,136,172 for the first 6-month cycle and $568,086 for subsequent cycles. Lumasiran was administered subcutaneously, at a cost of $88.34 per administration. The cost of vitamin B6 ($0.05 per 50 mg tablet) was included as a component of ECM based on the Newfoundland and Labrador Drug Product Database. The average per-cycle cost of vitamin B6 treatment is $23.97 for pediatric patients and $67.12 for adults in the lumasiran arm, and $33.18 for pediatric patients and $92.89 for adults in the ECM arm.
Per-cycle costs of high-intensity ($95,691 to $97,724) and normal-intensity dialysis ($39,407 to $41,010) were based on the unit costs from Interprovincial Health Insurance Agreements Coordinating Committee Outpatient Billing Rates19 for hemodialysis, the average cost of hospital and home peritoneal dialysis (no reference provided), and the frequency of resource use per cycle. Unit costs were assumed to be the same for pediatric and adult patients. Renal stone event costs were obtained from the Ontario Health Insurance Plan Schedule of Benefits (SOB),20 in which systemic oxalosis complications costs and treatment-related adverse event costs were obtained from published Canadian literature.21-27 The one-off liver-kidney transplant cost ($28,430) for the adult population was calculated from the sum of liver and kidney transplant costs according to SOB. The one-off transplant cost for adults was also adjusted based on the proportional difference in costs for adults versus pediatric patients undergoing liver and kidney transplants in the UK, to give a one-off cost for pediatric patients ($46,360). Posttransplant monitoring cost, immunosuppression cost, and retransplant costs were also obtained from SOB, while graft-failure cost was converted from UK National Health Service Costs.28 Disease management costs such as laboratory tests, procedures, and visits by each CKD stage were also derived from SOB. Lastly, an end-of-life cost of $4,107.57 was included in the model as a one-off cost in the last 6 months of life.29
Summary of Sponsor’s Economic Evaluation Results
The sponsor’s cost-effectiveness analysis was based on 5,000 probabilistic iterations, for which findings are presented in Table 3. The results of the deterministic analysis were similar to the results of the probabilistic analysis.
Base-Case Results
In the sponsor’s base-case analysis, the ICER of lumasiran was $948,635 per QALY compared to ECM. Specifically, lumasiran was associated with 21.25 additional QALYs and $20,155,677 additional costs compared to ECM over a lifetime horizon (disaggregated results are presented in Table 10 and Table 11, Appendix 3). The cost-effectiveness acceptability curves found that 0% of the results were cost-effective at the willingness-to-pay threshold of $100,000 per QALY. The results of the deterministic analysis were similar to the results of the probabilistic analysis.
Most of the incremental cost was attributable to the higher drug costs with lumasiran, with cost savings associated with dialysis, systemic oxalosis complications, and post-cLKT (Table 10). The major driver contributing to QALY gains for lumasiran was from the early CKD stages and post-cLKT (Table 11).
Table 3: Summary of the Sponsor’s Economic Evaluation Results
Treatment | Total costs ($) | Incremental costs ($) | Total QALYs | Incremental QALYs | ICER ($ per QALY) |
|---|---|---|---|---|---|
Lumasiran + ECM | 24,927,031 | 20,155,677 | 28.53 | 21.25 | 948,635 |
ECM | 4,771,354 | — | 7.28 | — | — |
ECM = established clinical management; ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year.
Source: Sponsor’s pharmacoeconomic submission.30
Sensitivity and Scenario Analysis Results
Uncertainty was addressed by deterministic 1-way sensitivity analysis, and probabilistic scenario analyses with 1,000 simulations. For the scenario analyses, the largest increase from the base-case ICER was seen when different baseline CKD distributions were used for adult and pediatric populations, which resulted in a 2.7% increase in ICER relative to the base case. The largest decrease from the base-case ICER was seen when the societal perspective was assessed, which resulted in a 4.1% reduction in the ICER ($818,857) relative to the base case.
CADTH Appraisal of the Sponsor’s Economic Evaluation
CADTH identified several key limitations to the sponsor’s analysis that have notable implications on the economic analysis:
Unproven assumptions on the relationship between biochemical end points (serum oxalate) and clinical end points (CKD progression). Numerous assumptions are made by the sponsor to estimate progression of CKD in both the lumasiran and ECM arms, including the association between oxalate levels and the rate of eGFR loss per year. The assumption of a mean absolute eGFR decrease of 1.27 mL/min/1.73 m2 (assumed per year) per 1 μmol/L increase in plasma oxalate based on literature and 6 months of trial data are not validated and highly speculative (refer to the Plasma Oxalate section in the Clinical Review Report for details); while oxalate damages the kidney, at lower levels of kidney function there is less excretion of oxalate, resulting in greater total body oxalate. Thus, the mapping of a biochemical parameter to loss of kidney function is likely not as straightforward as modelled. As such, the progression of kidney disease (slope of eGFR) in the ECM arm is speculative; the rate of progression of CKD in the ECM arm dictates incremental benefit. However, this rate is uncertain (and likely heterogeneous given a heterogeneous phenotype).
CADTH could not address this limitation in its reanalysis due to uncertainty.
Unproven assumption that lumasiran is 100% effective in halting CKD progression. The model assumes that in earlier stages of CKD (stages 1 to 3), lumasiran-treated patients have no progression of kidney disease, under the assumption that normalization or near normalization of plasma oxalate observed in the ILLUMINATE trials is lifelong and completely effective in preventing kidney function loss. As noted previously, the association of oxalate levels with lumasiran treatment and outcomes is assumed; while this relationship may be potentially plausible, it is the most optimistic outcome and has not yet been confirmed in clinical trials. To support this assumption, long-term efficacy data are needed.
CADTH did not address this limitation in its reanalysis and thus the true effect is uncertain.
Assumptions regarding late-stage CKD were not supported by clinical experts consulted by CADTH. The model assumed no progression from CKD 4 to ESKD once oxalate levels were controlled, defined as plasma oxalate level less than 50 μmol/L. However, this was deemed an arbitrary binary threshold by clinical experts consulted by CADTH and may not reflect a valid surrogate (refer to the Plasma Oxalate section in the Clinical Review Report for details). As in the late stages of kidney disease, oxalate levels are determined by production and excretion, the latter of which are impaired, given impaired kidney function. The clinical expert consulted by CADTH indicated that due to the small number of patients in the single-arm ILLUMINATE-C trial, the effectiveness of lumasiran in late-stage patients is uncertain, and no evidence has been provided to support this assumption. Further, it is also possible that severe kidney disease may progress even after the causal factors (e.g., hyperfiltration injury) are removed.
CADTH did not address this limitation in its reanalysis and thus the true relationship and effect in late-stage disease is uncertain.
Uncertain dialysis assumptions, intensity, and costs. The sponsor assumed dialysis started in patients with CKD 4, and high-intensity dialysis was assumed for the ECM arm. While there may be heterogeneity in the approach to treatment, clinical experts consulted by CADTH indicated that adult patients with CKD 4 in Canada would likely not start dialysis; however, this is the standard of care in pediatric patients. There is also heterogeneity in the provision of intensive dialysis. Intensive dialysis that uses both peritoneal dialysis and hemodialysis is not typically used in Canada. Further, frequent home nocturnal dialysis (FHNHD) is emerging as the preferred dialysis modality to deliver high-intensity dialysis, and is associated with similar or lower costs and similar quality of life compared to conventional dialysis.31 Although FHNHD may not be feasible for a significant proportion of patients, the clinical experts consulted by CADTH suggested that 20% of adult patients may be treated by FHNHD, while the remainder would require in-centre intensive dialysis. Finally, the costs of hemodialysis were obtained from Interprovincial Health Insurance Agreements Coordinating Committee Outpatient Billing Rates, which are not concordant (overestimate) with previously reported costs of dialysis in Canada (reported in a previous CADTH Optimal Use Report).31
In the CADTH reanalysis, revisions informed by clinical experts to more closely simulate Canadian practice included sourcing costs from the CADTH Optimal Use Report on dialysis modality costs, only using dialysis in pediatric patients with CKD4, assuming 20% of patients on hemodialysis would be on FHNHD, and assuming no peritoneal dialysis and hemodialysis combination for high-intensity dialysis.
Transplant rate assumptions were dramatically underestimated. The model assumed that a low probability of transplant (0.20759 for lumasiran and 0.00696 for ECM) would apply to all CKD 4/ESKD adult and pediatric patients. However, the evidence source to inform the probability of receiving a cLKT was not appropriate, because sourced rates from the Canadian Institute for Health Information reflected patients with liver failure who also had kidney failure, which is a different patient population. Thus, the transplant rate used for ECM was not plausible, and clinical experts consulted by CADTH indicated that patients with PH1 approaching ESKD are very frequently prioritized for transplant given that an earlier liver transplant may significantly modify health outcome (compared to being waitlisted while on dialysis). This is even more relevant to pediatric populations because they have an even higher priority than the adult population.
Based on clinical experts consulted by CADTH, the CADTH reanalysis assumed an annual transplant rate of 50% for ESKD adults and a 90% transplant rate for pediatric patients (i.e., 6-month cycle of 0.2929 for ESKD adults and 0.6838 for pediatric patients). In addition, to reflect Canadian practice, only ESKD adult patients (not CKD 4) were assumed to be eligible for transplant.
Improper utility estimates overestimated lumasiran incremental QALY gain. A parental caregiver disutility decrement of █████ was applied to CKD 4 and ESKD health states regardless of patient age, potentially underestimating total QALY gain in the ECM arm. The source data to derive caregiver disutility were not provided to CADTH for review, aside from mention in a report from an external group funded by the sponsor, which stated that only demographics were reported as the code to score the EQ-5D-5L results were provided to the sponsor along with a scored dataset. Because this survey to derive EQ-5D-5L recruited caregivers of children and adolescents diagnosed with PH1, the caregiver disutility may not be applicable to adults (because caregiver disutility was applied to both adults and children in the model).
In addition, the additive effects of disutilities from multiple events resulted in negative utility values (worse than death) for some health states (i.e., –0.033 for ESKD-Oxu and high-intensity dialysis [children]; and –0.013 for CKD ESKD-Oxu and high-intensity dialysis [adults]). The clinical experts consulted by CADTH indicated that these states considered worse than death were not plausible and that quality of life is likely slightly worse than other patient on dialysis. This resulted in an assumption that favoured lumasiran because a lower quality of life was assumed for the ECM health states.
In the CADTH reanalysis, CADTH removed caregiver disutility given the uncertainty surrounding its derivation and magnitude, and tested its inclusion in a scenario analysis. Because a reported average utility value for dialysis patients is 0.5,32 CADTH set the baseline utility values in the CADTH base case for CKD 4 and ESKD to 0.4, as recommended by the clinical experts consulted by CADTH.
The proportion of patients in each CKD stage was not reflective of trial data. The initial distribution used in the model of patients in each CKD stage was obtained from published literature (38% of patients started at later stage [CKD 4 and ESKD]). This was not reflective of the ILLUMINATE trials because the relative efficacy from the trials was derived from overall less severe cohorts (only 21 patients from the ILLUMINATE-C trial compared to 57 in the ILLUMINATE-A and ILLUMINATE-B trials). Further, it is possible that if a treatment is available, increased identification of patients through case finding or screening may identify affected patients at a young age. This may also identify genetic PH1 in those with a less severe phenotype, because if this occurs the incremental benefit in these patients is likely lessened.
In the CADTH reanalysis, CADTH used the distribution of baseline CKD stage from the ILLUMINATE trials to inform the initial CKD distribution. CADTH also evaluated an alternative assumption of early identification of CKD as a scenario analysis.
Additionally, the following key assumptions were made by the sponsor and have been appraised by CADTH (refer to Table 4).
Table 4: Key Assumptions of the Submitted Economic Evaluation (Not Noted as Limitations to the Submission)
Sponsor’s key assumption | CADTH comment |
|---|---|
Patients in the CKD 4 or Oxc health state were assumed not to experience disease progression. | Unknown. This assumption was not validated or supported by clinical evidence and was deemed highly optimistic. Further, it was not supported by available clinical evidence with short-term evidence on changes in eGFR, and only inferred by dichotomous biochemical outcomes (plasma oxalate < 50) that have not been validated. |
Patients in CKD 1 to 3 health states treated with lumasiran are expected to have no further reduction in eGFR. Progression to more severe health states (i.e., CKD 4 or ESKD) only applied to the proportion of the CKD 1 to 3b cohort having discontinued lumasiran treatment, at which point ECM transitions are applied. | Unknown. This assumes that lumasiran is 100% effective in preventing progression of CKD. True effectiveness is unknown; this assumption is the most optimistic and does not account for uncertainty, which was not supported by results from clinical trials. |
The treatment efficacy of lumasiran observed over 12 months in the ILLUMINATE-A and ILLUMINATE-B trials, including the benefits of kidney stone, is expected to be maintained over time. Systematic oxalosis complications were also assumed to be less frequent based on UK clinical experts. | Not appropriate. Data on long-term efficacy were not provided and are therefore not clearly established. |
ECM-treated patients with CKD 4 or ESKD cannot transition from uncontrolled to controlled oxalate health states. | Appropriate. |
The probability of undergoing transplant for late-stage CKD cohorts with controlled oxalate is expected to be similar to the transplant probability observed across patients with CKD who do not have PH1. | Not appropriate; according to the clinical experts, this patient group is commonly prioritized for transplant. |
Mortality RRs by health state for PH1 are based on a model of non–PH1-related CKD. | Uncertain. Patients with PH1 are often younger and much healthier than most patients with CKD or ESKD; therefore, the mortality multiplier may overestimate mortality. |
The transplant rate for the pediatric population was assumed to be the same as for the adult population. | Not appropriate. Pediatric populations are highly prioritized, thus resulting in a higher transplant rate. |
CKD = chronic kidney disease; ECM = established clinical management; eGFR = estimated glomerular filtration rate; ESKD = end-stage kidney disease; Oxc = controlled oxalate levels; PH1 = primary hyperoxaluria type 1; RR = relative risk.
CADTH Reanalyses of the Economic Evaluation
Base-Case Results
The CADTH base case was derived by making changes in model parameter values and assumptions in consultation with clinical experts. Although uncertainty exists in multiple parameters, the CADTH base-case modified parameters from the sponsor that were deemed nonreflective of current care and practice in Canada.
Table 5: CADTH Revisions to the Submitted Economic Evaluation
Stepped analysis | Sponsor’s value or assumption | CADTH value or assumption |
|---|---|---|
Corrections to sponsor’s base case | ||
None | — | — |
Changes to derive the CADTH base case | ||
1. Dialysis assumptions, intensity, and costs | The unit HD cost was $524. All patients with CKD 4who were on ECM were assumed to be on high-intensity dialysis, with 13% of adults (0% of pediatric patients) on PD and HD combination dialysis. | The unit HD cost based on the CADTH Optimal Use Report was $368.95 (assumed 20% on FHNHD detailed calculations can be found in Appendix 4). Only pediatric patients with CKD 4 on ECM would start dialysis, and no PD and HD combination for high-intensity dialysis in adults. This reflects current Canadian practice. |
2. Transplant rate assumptions | 6-month probability of 0.20759 for lumasiran and 0.00696 for ECM, applied to all CKD 4 or ESKD adult and pediatric patients. | Six-month probability of 0.2929 for adult patients with ESKD patients and 0.6838 for pediatric patients with CKD 4 and ESKD to more closely reflect Canadian practice. |
3. Utility assumptions | Pediatric patients: 0.11 for CKD 4, 0.10 for ESKD; adults: 0.43 for CKD 4, 0.13 for ESKD; caregiver disutility –0.08. | Children: 0.40 for CKD 4 and ESKD; Adults: 0.43 for CKD 4, 0.40 for ESKD. Remove caregiver disutility. |
4. Baseline distribution of patients by CKD status | CKD 1 to 2, 38%; CKD 3a, 12%; CKD 3b, 12%; CKD 4, 10%; and ESKD 28% from published literature. | CKD 1 to 2, 64%; CKD 3a, 4%; CKD 3b, 7%; CKD, 4 4%; and ESKD 21% from pooled ILLUMINATE trials. |
CADTH base case | 1 + 2 + 3 + 4 | |
CKD = chronic kidney disease; ECM = established clinical management; ESKD = end-stage kidney disease; FHNHD = frequent home nocturnal dialysis; HD = hemodialysis; PD = peritoneal dialysis.
Table 6: Summary of the Stepped Analysis of the CADTH Reanalysis Results
Stepped analysis | Drug | Total costs ($) | Total QALYs | ICER ($ per QALY) |
|---|---|---|---|---|
Sponsor’s base case (probabilistic) | ECM | 4,771,354 | 7.28 | Reference |
Lumasiran + ECM | 24,927,031 | 28.53 | 948,635 | |
Sponsor’s base case | ECM | 4,729,620 | 6.83 | Reference |
Lumasiran + ECM | 24,459,447 | 28.33 | 917,656 | |
CADTH reanalysis 1 | ECM | 3,071,146 | 6.83 | Reference |
Lumasiran + ECM | 24,347,626 | 28.33 | 989,593 | |
CADTH reanalysis 2 | ECM | 955,304 | 15.43 | Reference |
Lumasiran + ECM | 24,722,368 | 27.03 | 2,049,639 | |
CADTH reanalysis 3 | ECM | 4,729,620 | 12.92 | Reference |
Lumasiran + ECM | 24,459,447 | 28.67 | 1,253,313 | |
CADTH reanalysis 4 | ECM | 4,476,988 | 8.77 | Reference |
Lumasiran + ECM | 29,405,467 | 30.14 | 1,166,334 | |
CADTH base case (deterministic) | ECM | 651,397 | 17.09 | Reference |
Lumasiran + ECM | 29,255,241 | 29.55 | 2,295,100 | |
CADTH base case | ECM | 1,035,104 | 16.96 | Reference |
Lumasiran + ECM | 30,853,528 | 30.72 | 2,165,926 |
ECM = established clinical management; ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year.
The CADTH base case demonstrated that, relative to ECM, lumasiran was more expensive by $29,818,424 and more effective by 13.77 QALYs, resulting in an ICER of $2,165,926 per QALY. Deterministic 1-way analyses were also provided to show how the parameters affect the results while holding everything else constant. When more patients started in the less severe CKD stages (reanalysis 4), higher lumasiran drug costs occurred due to the use of lumasiran for a longer period of time. Notably, changing transplant rates (greater) and dialysis costs (lower) to reflect practice in Canada (reanalyses 1 and 2) reduced the total cost of ECM, and thus increased the incremental costs of lumasiran compared to ECM. On the effectiveness side, increasing the baseline utility values for patients with CKD 4 and ESKD (reanalysis 3) increased the total QALYs of ECM when higher proportions of ECM patients transitioned to these health states, resulting in a smaller incremental effectiveness of lumasiran compared to ECM. The largest change in the ICER was observed when more realistic rates of transplant were used, because this reduced the total cost of ECM-treated patients and also led to greater QALYs than the sponsor’s base case because patients did not spend protracted periods of time in more advanced CKD or ESKD before undergoing transplant.
Note that the CADTH reanalysis focuses on assumptions and parameters that are amenable to estimation to reflect patient management and treatment in Canada; however, multiple model assumptions that are likely to be optimistic to lumasiran are still included, including the optimistic assumptions on the incremental benefit of lumasiran on CKD progression. Given the model restrictions and that there remains uncertainty about actual rates and effectiveness, this was not tested. It should be noted that the ICER in the CADTH base case is likely to be greater if lumasiran is not 100% effective in preventing CKD progression.
Scenario Analysis Results
CADTH performed scenario analyses to determine the impact of including the caregiver disutility, having all patients start in the CKD 1 to 2 health state, and allowing ESKD progression in the CKD 4/Oxc health state. The results of these analyses are presented in Table 15, Appendix 4. All scenarios had minimal impact on the CADTH base-case ICER.
CADTH also performed a price reduction analysis to determine the price reduction of lumasiran required to achieve an ICER under $50,000/QALY. It determined that a price reduction of approximately 95% for lumasiran would be required.
Table 7: CADTH Price Reduction Analyses
Analysis | ICERs for lumasiran + ECM vs. ECM ($/QALY) | |
|---|---|---|
Price reduction | Sponsor base case | CADTH reanalysis |
No price reduction | 948,635 | 2,165,926 |
50% | 403,228 | 1,051,322 |
60% | 283,765 | 828,896 |
70% | 166,245 | 606,307 |
80% | 45,512 | 382,958 |
90% | Dominant | 158,619 |
95% | Dominant | 46,767 |
ECM = established clinical management; ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year; vs. = versus.
Issues for Consideration
Potential increase in early detection. The clinical experts consulted by CADTH mentioned that in the near future, there may be neonate screening practices to identify PH1 earlier. In this scenario, more young patients in early CKD stages could be put on lumasiran treatment; analyses that examine pediatric patients with normal kidney function (as might be found through screening) result in an increased ICER. If assuming this scenario in the base case, the ICER increased to $2,277,045/QALY.
Potential identification of genetic PH1 with less severe phenotype. There is significant phenotypic heterogeneity in patients with PH1 mutations. Case finding or screening may result in the identification of patients with a less severe phenotype; as a group, these less severe patients are likely to have a reduced benefit from treatment and thus a greater ICER.
Kidney-only transplant and treatment after transplant. If lumasiran becomes available and is effective, pediatric patients may only undergo kidney transplants (to avoid the higher risk associated with liver transplant). These patients will require lifelong lumasiran after transplant to control their oxalate levels, thus resulting in a greater ICER.
Vial size. A smaller vial size, especially among the pediatric population, was suggested by the clinical experts consulted by CADTH to reduce wastage and potentially reduce drug costs.
Overall Conclusions
In the 3 ILLUMINATE trials, lumasiran demonstrated improvements in urine oxalate and plasma oxalate. Changes in eGFR and health-related quality of life from baseline were numerically small, and conclusions could not be drawn about whether lumasiran had an impact on these outcomes due to the small number of patients and short treatment duration of the trials so far. The clinical experts and CADTH clinical review team agreed that long-term efficacy and safety data will be necessary to confirm the findings in the ILLUMINATE trials and to better understand how the main trial outcomes translate to improved long-term outcomes of maintained lowering of hepatic oxalate production, prevention of kidney stones, and prevention of progression to ESKD.
The sponsor’s base case included several assumptions that were not substantiated by quality evidence, were based on unvalidated surrogate outcomes measured in the ILLUMINATE trials and did not reflect current practice in Canada. First, the sponsor assumed that lumasiran was 100% effective in preventing CKD progression based on the association of plasma oxalate levels and the rate of eGFR loss per year. The nature of this relationship is speculative: The fixed rate used is uncertain (and likely heterogeneous), and this has not been confirmed in the clinical trials. Second, the assumption regarding high-intensity dialysis for all patients with CKD 4 and ESKD on ECM overestimated costs and favoured lumasiran. Third, the rate of cLKTs used to inform the model is not appropriate. Clinical experts consulted by CADTH indicated that patients with PH1 approaching ESKD are prioritized for transplants, given that earlier liver transplants will significantly improve health outcomes. This priority setting is even more relevant in the pediatric population. Fourth, a parental caregiver disutility decrement was applied to CKD 4 and ESKD health states for all patients (including adults) despite methodological limitations and uncertainty due to a lack of provided source data. In addition, the inclusion of disutilities from multiple events resulted in negative utility values (worse than death) for the high-intensity dialysis ESKD health states, which was deemed unrealistic by clinical experts consulted by CADTH. Finally, the sponsor’s base case assumed a greater proportion of patients in the late CKD stage at the start of the model, which was in contrast to the distribution of CKD stages seen in the trials.
The CADTH reanalysis addressed the previously mentioned limitations to be more reflective of current care in Canada. The CADTH results were similar to the sponsors’ in that lumasiran is not considered cost-effective based on conventionally accepted willingness-to-pay thresholds. The CADTH base case ICER for lumasiran plus ECM compared to ECM alone is $2,165,926 per QALY gained; lumasiran has a 0% probability of being cost-effective at a willingness-to-pay threshold of $50,000 per QALY gained. A price reduction of 95% is required for lumasiran to achieve a mean cost-effective estimate of $50,000 per QALY. A key driver of the ICER was the high annual cost and long-term use of lumasiran.
Although the CADTH reanalysis attempted to address limitations in the 4 areas previously described, significant uncertainty still exists in the CADTH base case due to remaining uncertain but optimistic assumptions. Specifically, if lumasiran is not 100% effective in preventing CKD progression, or if more pediatric patients at early stages of disease are treated with lumasiran because of early detection, or if lumasiran treatment continues after kidney transplant, an even greater price reduction is likely required.
References
1.Singh P, Viehman JK, Mehta RA, et al. Clinical characterization of primary hyperoxaluria type 3 in comparison with types 1 and 2. Nephrol Dial Transplant. 2022;37(5):869-875. PubMed
2.Shah RJ, Vaughan LE, Enders FT, Milliner DS, Lieske JC. Plasma oxalate as a predictor of kidney function decline in a primary hyperoxaluria cohort. Int J Mol Sci. 2020;21(10). PubMed
3.Harambat J, Fargue S, Acquaviva C, et al. Genotype-phenotype correlation in primary hyperoxaluria type 1: the p.Gly170Arg AGXT mutation is associated with a better outcome. Kidney Int. 2010;77(5):443-449. PubMed
4.Canadian Institute for Health Information. e-Statistics report on transplant, waiting list and donor statistics, 2020. 2021: https://www.cihi.ca/en/summary-statistics-on-organ-transplants-wait-lists-and-donors. Accessed 2022 Jul 29.
5.Compagnon P, Metzler P, Samuel D, et al. Long-term results of combined liver-kidney transplantation for primary hyperoxaluria type 1: the French experience. Liver Transpl. 2014;20(12):1475-1485. PubMed
6.Jamieson NV. A 20-year experience of combined liver/kidney transplantation for primary hyperoxaluria (PH1): the European PH1 transplant registry experience 1984-2004. Am J Nephrol. 2005;25(3):282-289. PubMed
7.Table: 13-10-0114-01. Life expectancy and other elements of the life table, Canada, all provinces except Prince Edward Island. Ottawa (ON): Statistics Canada; 2022: https://www150.statcan.gc.ca/t1/tbl1/en/tv.action?pid=1310011401. Accessed 2022 May 19.
8.Go AS, Chertow GM, Fan D, McCulloch CE, Hsu CY. Chronic kidney disease and the risks of death, cardiovascular events, and hospitalization. N Engl J Med. 2004;351(13):1296-1305. PubMed
9.Xie F, Pullenayegum E, Gaebel K, et al. A time trade-off-derived value set of the EQ-5D-5L for Canada. Med Care. 2016;54(1):98-105. PubMed
10.Sullivan PW, Slejko JF, Sculpher MJ, Ghushchyan V. Catalogue of EQ-5D scores for the United Kingdom. Med Decis Making. 2011;31(6):800-804. PubMed
11.Torrance N, Lawson KD, Afolabi E, et al. Estimating the burden of disease in chronic pain with and without neuropathic characteristics: does the choice between the EQ-5D and SF-6D matter? Pain. 2014;155(10):1996-2004. PubMed
12.Lee AJ, Morgan CL, Conway P, Currie CJ. Characterisation and comparison of health-related quality of life for patients with renal failure. Curr Med Res Opin. 2005;21(11):1777-1783. PubMed
13.Perl J, Zhang J, Gillespie B, et al. Reduced survival and quality of life following return to dialysis after transplant failure: the Dialysis Outcomes and Practice Patterns Study. Nephrol Dial Transplant. 2012;27(12):4464-4472. PubMed
14.Ratcliffe J, Young T, Longworth L, Buxton M. An assessment of the impact of informative dropout and nonresponse in measuring health-related quality of life using the EuroQol (EQ-5D) descriptive system. Value Health. 2005;8(1):53-58. PubMed
15.Modersitzki F, Milliner DS, Enders FT, Lieske JC, Goldfarb DS, Rare Kidney Stone Consortium. SA-PO271: Stone event proximity determines health-related quality of life (HRQoL) in primary hyperoxaluria (PH). J Am Soc Nephrol. 2019;30:833.
16.Guertin JR, Feeny D, Tarride JE. Age- and sex-specific Canadian utility norms, based on the 2013-2014 Canadian Community Health Survey. CMAJ. 2018;190(6):E155-E161. PubMed
17.Health status assessment of adult caregivers of children with primary hyperoxaluria: Draft summary [internal sponsor's report]. Research Triangle Park (NC): RTI Health Solutions; 2021.
18.A valuation survey to explore public preferences (utilities) for treatment in primary hyperoxaluria type 1 (PH1) [internal sponsor's report]. London (GB): Acaster Lloyd Consulting Ltd.; 2021.
19.Interprovincial/territorial outpatient billing rates for services provided in ON for QC residents. 2021: effective for visits on or after April 1, 2021. Toronto (ON): Ontario Ministry of Health, Ontario Ministry of Long-Term Care; 2021: https://www.health.gov.on.ca/en/pro/programs/ohip/bulletins/redux/docs/2021-22_outpatients_services_billing_rate_sheet.pdf.
20.Schedule of benefits for physician services under the Health Insurance Act: effective October 1, 2021. Toronto (ON): Ontario Ministry of Health; 2022: https://www.health.gov.on.ca/en/pro/programs/ohip/sob/physserv/sob_master.pdf. Accessed 2022 Mar 28.
21.Kobelt G, Andlin-Sobocki P, Maksymowych WP. The cost-effectiveness of infliximab (Remicade) in the treatment of ankylosing spondylitis in Canada. J Rheumatol. 2006;33(4):732-740. PubMed
22.Smolderen KG, Bell A, Lei Y, et al. One-year costs associated with cardiovascular disease in Canada: Insights from the REduction of Atherothrombosis for Continued Health (REACH) registry. Can J Cardiol. 2010;26(8):297-305. PubMed
23.Clarke AE, Urowitz MB, Monga N, Hanly JG. Costs associated with severe and nonsevere systemic lupus erythematosus in Canada. Arthritis Care Res (Hoboken). 2015;67(3):431-436. PubMed
24.Gonder JR, Walker VM, Barbeau M, et al. Costs and quality of life in diabetic macular edema: Canadian burden of diabetic macular edema observational study (C-REALITY). J Ophthalmol. 2014;2014:939315. PubMed
25.Goeree R, Blackhouse G, Petrovic R, Salama S. Cost of stroke in Canada: a 1-year prospective study. J Med Econ. 2005;8(1-4):147-167.
26.Church DL, Davies HD, Mitton C, et al. Clinical and economic evaluation of rapid influenza A virus testing in nursing homes in Calgary, Canada. Clin Infect Dis. 2002;34(6):790-795. PubMed
27.Stokes M, Becker WJ, Lipton RB, et al. Cost of health care among patients with chronic and episodic migraine in Canada and the USA: results from the International Burden of Migraine Study (IBMS). Headache. 2011;51(7):1058-1077. PubMed
28.National schedule of NHS costs. Year 2019/20. Leeds (GB): National Health Service (NHS) England: https://www.england.nhs.uk/wp-content/uploads/2021/06/National_Schedule_of_NHS_Costs_FY1920.xlsx. Accessed 2021 Dec 6.
29.Hollander MJ. Costs of end-of-life care: findings from the province of Saskatchewan. Healthc Q. 2009;12(3):50-58. PubMed
30.Pharmacoeconomic evaluation [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Oxlumo (lumasiran), 94.5 mg/0.5 mL for subcutaneous injection Mississauga (ON): Alnylam Pharmaceuticals Canada ULC; 2022 May 10.
31.Dialysis modalities for the treatment of end-stage kidney disease: a health technology assessment. (CADTH optimal use report vol. 6, no. 2b). Ottawa (ON): CADTH; 2017: https://www.cadth.ca/sites/default/files/pdf/OP0526_Dialysis_Modalities_Science_Report.pdf. Accessed 2022 Jul 29.
32.Cooper JT, Lloyd A, Sanchez JJG, Sorstadius E, Briggs A, McFarlane P. Health related quality of life utility weights for economic evaluation through different stages of chronic kidney disease: a systematic literature review. Health Qual Life Outcomes. 2020;18(1):310. PubMed
33.Oxlumo (lumasiran): solution, 94.5 mg/0.5 mL lumasiran (as lumasiran sodium), subcutaneous injection [product monograph]. Amsterdam (NL): Alnylam Netherlands B.V.; 2022 Mar 3.
34.Budget Impact Analysis [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission:Oxlumo (lumasiran), 94.5 mg/0.5 mL for subcutaneous injection Mississauga (ON): Alnylam Pharmaceuticals Canada ULC; 2022 May 10.
35.Harambat J, Fargue S, Bacchetta J, Acquaviva C, Cochat P. Primary hyperoxaluria. Int J Nephrol. 2011;2011:864580. PubMed
Appendix 1: Cost Comparison Table
Note that this appendix has not been copy-edited.
The comparators presented in the following table have been deemed to be appropriate based on feedback from clinical experts. Comparators may be recommended (appropriate) practice or actual practice. Existing Product Listing Agreements are not reflected in the table and, as such, the table may not represent the actual costs to public drug plans.
Table 8: CADTH Cost Comparison Table for the Treatment of Primary Hyperoxaluria Type 1
Treatment | Strength / concentration | Form | Price | Recommended dosagea | Average daily costb | Annual costb |
|---|---|---|---|---|---|---|
Lumasiran (Oxlumo) | 94.5 mg/0.5 mL | 0.5 mL Solution for subcutaneous injection | $96,855.3299c | ≤ 10 kg: loading dose of 6 mg/kg monthly for 3 doses and maintenance dose of 3 mg/kg monthly 10 to 20 kg: loading dose of 6 mg/kg monthly for 3 doses and maintenance dose of 6 mg/kg once every 3 months ≥ 20 kg: loading dose of 3 mg/kg monthly for 3 doses and maintenance dose of 3 mg/kg once every 3 months | Pediatric Year 1: $1,591.05 Subsequent: $1,060.70 Adult Year 1: $4,773.16 Subsequent: $3,182.11 | Pediatric Year 1: $581,131.98 Subsequent: $387,421.32 Adult Year 1: $1,743,395.94 Subsequent: $1,162,263.96 |
aRecommended doses informed from the product monograph.33
bAverage daily and annual costs were calculated assuming an average pediatric and adult weight of 26.15 kg and 82.02 kg, respectively (aligned with the pooled ILLUMINATE-A, ILLUMINATE-B and ILLUMINATE-C mean weights at baseline).30 Annual costs assumed 365.25 days per year. Calculated costs include wastage where applicable.
cSponsor submitted price.30
Appendix 2: Submission Quality
Note that this appendix has not been copy-edited.
Description | Yes/no | Comments |
|---|---|---|
Population is relevant, with no critical intervention missing, and no relevant outcome missing | Yes | No comment. |
Model has been adequately programmed and has sufficient face validity | Yes | No comment. |
Model structure is adequate for decision problem | Yes | No comment. |
Data incorporation into the model has been done adequately (e.g., parameters for probabilistic analysis) | Yes | No comment. |
Parameter and structural uncertainty were adequately assessed; analyses were adequate to inform the decision problem | No | CKD progression (absolute and incremental) cannot be easily modified in the model. The assumption of treatment continuation after single transplant was not feasible to test in the model. |
The submission was well organized and complete; the information was easy to locate (clear and transparent reporting; technical documentation available in enough details) | Yes | No comment. |
CKD = chronic kidney disease.
Appendix 3: Additional Information on the Submitted Economic Evaluation
Note that this appendix has not been copy-edited.
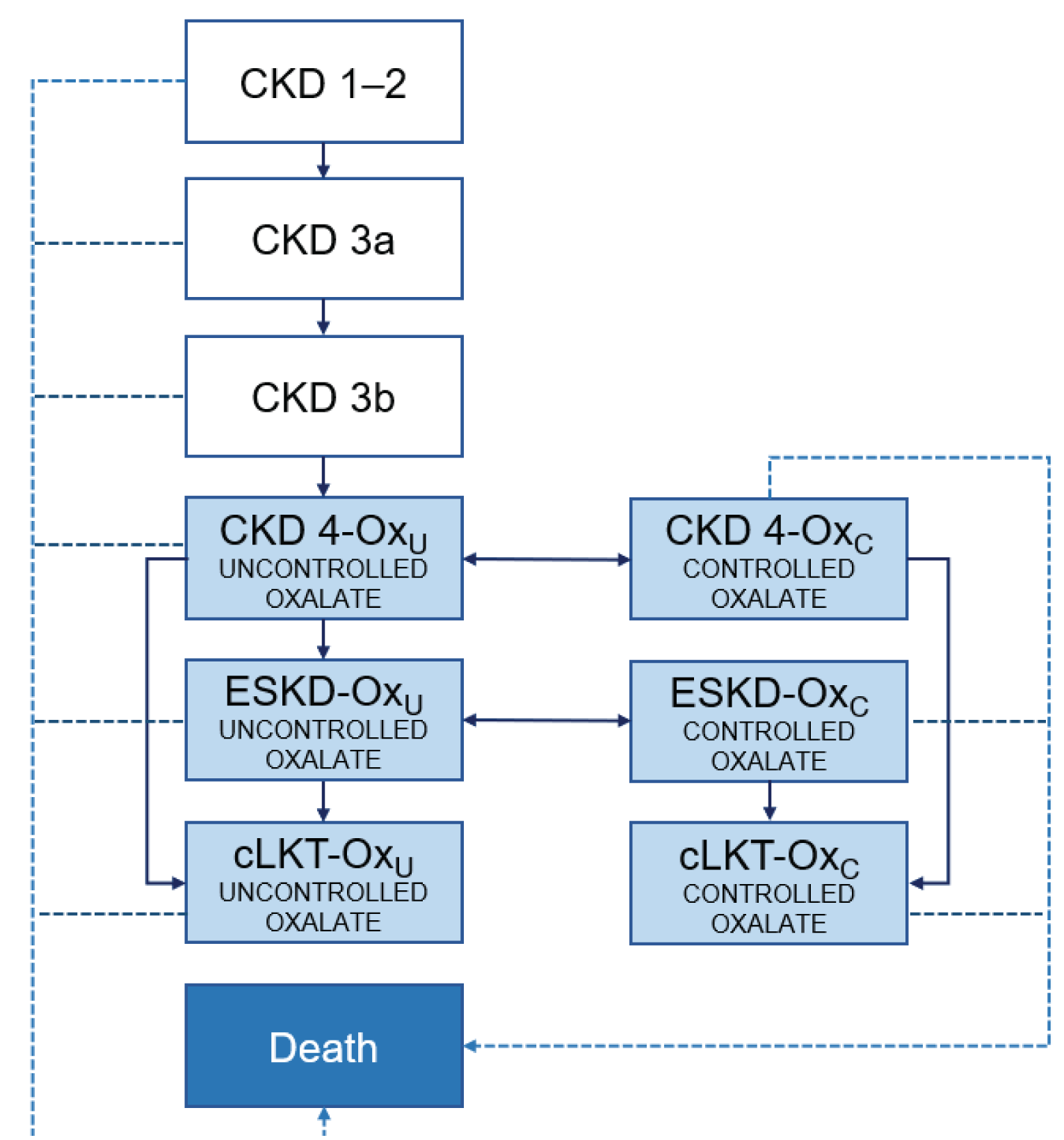
CKD = chronic kidney disease; cLKT = combined liver-kidney transplant; ESKD = end-stage kidney disease; Oxc = controlled oxalate levels; Oxu = uncontrolled oxalate levels; PH1 = primary hyperoxaluria type 1.30
Source: Sponsor’s pharmacoeconomic submission
Detailed Results of the Sponsor’s Base Case
Table 10: Discounted Disaggregated Mean Costs for the Probabilistic Sponsor’s Reference Case Analysis
Cost | Lumasiran ($) | ECM ($) | Incremental ($) |
|---|---|---|---|
Drug | 24,567,698 | 4,198 | 24,563,500 |
Administration | 22,387 | 0 | 22,387 |
Monitoring | 14,179 | 39,273 | −25,094 |
Dialysis | 243,396 | 4,346,285 | −4,102,889 |
Renal stone events | 3,931 | 11,253 | −7,322 |
Systemic oxalosis | 25,914 | 336,007 | −310,093 |
Post-cLKT | 38,338 | 21,405 | 16,932 |
AEs | 9,346 | 10,794 | −1,448 |
End-of-life | 1,842 | 2,138 | −296 |
Total costs | 24,927,031 | 4,771,354 | 20,155,677 |
cLKT = combined liver-kidney transplant; ECM = established clinical management; AEs = adverse events.
Source: Table 49 in sponsor’s submission.
Table 11: Discounted Disaggregated Mean QALYs for the Probabilistic Sponsor’s Reference Case Analysis
Health State | Lumasiran | ECM | Incremental |
|---|---|---|---|
CKD 1 to 2 | 12.56 | 1.81 | 10.75 |
CKD 3a | 3.96 | 0.96 | 2.99 |
CKD 3b | 3.83 | 1.16 | 2.66 |
CKD 4-Oxc | 0.14 | 0.00 | 0.14 |
CKD 4-Oxu | 0.12 | 1.50 | –1.37 |
ESKD-Oxc | 0.19 | 0.00 | 0.19 |
ESKD-Oxu | –0.03 | –1.71 | 1.68 |
cLKT-Oxc | 7.58 | 0.00 | 7.58 |
cLKT-Oxu | 0.18 | 3.56 | –3.39 |
Total QALYs | 28.53 | 7.28 | 21.25 |
CKD = chronic kidney disease; cLKT = combined liver-kidney transplant; ECM = established clinical management; ESKD = end-stage kidney disease; Oxc = controlled oxalate levels; Oxu = uncontrolled oxalate levels; PH1 = primary hyperoxaluria type 1.
Source: Table 48 in sponsor’s submission.
Table 12: Discounted Disaggregated Mean LYs for the Probabilistic Sponsor’s Reference Case Analysis
Health State | Lumasiran | ECM | Incremental |
|---|---|---|---|
CKD 1 to 2 | 14.95 | 2.24 | 12.71 |
CKD 3a | 4.70 | 1.19 | 3.51 |
CKD 3b | 4.53 | 1.44 | 3.09 |
CKD 4-Oxc | 0.23 | 0.00 | 0.23 |
CKD 4-Oxu | 0.61 | 9.45 | –8.84 |
ESKD-Oxc | 0.65 | 0.00 | 0.65 |
ESKD-Oxu | 0.45 | 12.90 | –12.45 |
cLKT-Oxc | 10.77 | 0.00 | 10.77 |
cLKT-Oxu | 0.27 | 5.39 | –5.11 |
Total QALYs | 37.16 | 32.61 | 4.55 |
CKD = chronic kidney disease; cLKT = combined liver-kidney transplant; ECM = established clinical management; ESKD = end-stage kidney disease; Oxc = controlled oxalate levels; Oxu = uncontrolled oxalate levels; PH1 = primary hyperoxaluria type 1.
Source: Table 48 in sponsor’s submission.
Appendix 4: Additional Details on the CADTH Reanalyses and Sensitivity Analyses of the Economic Evaluation
Note that this appendix has not been copy-edited.
Detailed Calculation of Hemodialysis Unit Costs
Annual cost (2015 prices) of in-centre hemodialysis: CA$50,07631
Annual cost (2015 prices) of frequent home nocturnal hemodialysis: CA$36,661
Monthly frequency of normal-intensity hemodialysis in sponsor’s model: 13.04 (3.26 per week)
Unit cost (2022 prices) of in-centre hemodialysis session: 54,551 / 12 / 13.04 = CA$348.61
Unit cost (2022 prices) of frequent home nocturnal hemodialysis session: 39,937 / 12 / 13.04 = CA$255.22
Chronic dialysis weekly team fee = CA$127.2020
Hemodialysis unit cost (assuming 20% FHNHD): (0.8 × 348.61 + 0.2 × 255.22) + 127.20 / 3.26 = $368.95
Detailed Results of CADTH Base Case
Table 13: Disaggregated Summary of CADTH’s Economic Evaluation Results
Cost | Lumasiran ($) | ECM ($) | Incremental ($) |
|---|---|---|---|
Drug | 30,715,228 | 2,559 | 30,712,670 |
Administration | 28,087 | 0 | 28,087 |
Monitoring | 12,512 | 10,930 | 1,582 |
Dialysis | 46,838 | 869,337 | –822,499 |
Renal stone events | 4,557 | 8,259 | –3,701 |
Systemic oxalosis | 8,964 | 87,882 | –78,918 |
Post-cLKT | 24,453 | 46,871 | –22,418 |
AEs | 11,120 | 6,947 | 4,173 |
End-of-life | 1,768 | 2,320 | –552 |
Total costs | 30,853,528 | 1,035,104 | 29,818,424 |
cLKT = combined liver-kidney transplant; ECM = established clinical management; AEs = adverse events.
Table 14: Disaggregated Summary of CADTH’s Economic Evaluation Results
Health State | Lumasiran | ECM | Incremental |
|---|---|---|---|
CKD 1 to 2 | 21.74 | 3.04 | 18.71 |
CKD 3a | 1.39 | 1.31 | 0.08 |
CKD 3b | 2.30 | 1.37 | 0.93 |
CKD 4-Oxc | 0.25 | 0.00 | 0.25 |
CKD 4-Oxu | 0.14 | 2.99 | –2.85 |
ESKD-Oxc | 0.04 | 0.00 | 0.04 |
ESKD-Oxu | 0.02 | 0.04 | –0.02 |
cLKT-Oxc | 2.34 | 0.00 | 2.34 |
cLKT-Oxu | 2.51 | 8.21 | –5.71 |
Total QALYs | 30.72 | 16.96 | 13.77 |
CKD = chronic kidney disease; cLKT = combined liver-kidney transplant; ECM = established clinical management; ESKD = end-stage kidney disease; Oxc = controlled oxalate levels; Oxu = uncontrolled oxalate levels; PH1 = primary hyperoxaluria type 1.
Table 15: Additional Scenario Analysis Results
Analysis | Drug | Total costs ($) | Total QALYs | ICER ($/QALYs) |
|---|---|---|---|---|
CADTH base case | ECM | 1,035,104 | 16.96 | Reference |
Lumasiran + ECM | 30,853,528 | 30.72 | 2,165,926 | |
Inclusion of caregiver disutility to all patients (CKD4 and ESKD) | ECM | 1,034,160 | 16.12 | — |
Lumasiran + ECM | 30,887,587 | 30.64 | 2,056,910 | |
All pediatric population starting in CKD 1 to 2 | ECM | 1,165,507 | 19.44 | — |
Lumasiran + ECM | 41,482,952 | 37.15 | 2,277,045 | |
Allowing ESKD progression for CKD 4-Oxc | ECM | 1,027,082 | 16.98 | — |
Lumasiran + ECM | 30,859,620 | 30.73 | 2,168,343 |
CKD = chronic kidney disease; ECM = established clinical management; ESKD = end-stage kidney disease; Oxc = controlled oxalate levels.
Appendix 5: Submitted Budget Impact Analysis and CADTH Appraisal
Note that this appendix has not been copy-edited.
Table 16: Summary of Key Take-Aways
Key Take-aways of the BIA |
|---|
|
BIA = budget impact analysis; PH1 = primary hyperoxaluria type 1.
Summary of Sponsor’s Budget Impact Analysis
The submitted budget impact analysis (BIA) evaluated the incremental budget impact of introducing lumasiran for the treatment of PH1. The analysis was conducted from the perspective of the Canadian public drug plans (excluding Quebec) with a 3-year time horizon (2022 to 2024; base year = 2021). The patient population size was derived with an epidemiological approach, estimating both a prevalent and incident population to determine the total number of patients with PH1 who would be eligible for treatment each year. The sponsor assumed that all patients would be eligible for treatment. A summary of the epidemiological inputs can be found in Figure 2.
The BIA compared 2 scenarios to determine the incremental budget impact of reimbursing lumasiran. The reference case scenario assumed that 100% of eligible patients would receive ECM, while the new scenario included lumasiran. In the sponsor’s base case, costs related to drug acquisition and lumasiran subcutaneous administration were considered.34 Vial sharing was not included.34 Key inputs to the BIA are documented in Table 17.
Key assumptions included:
Non-Insured Health Benefit program beneficiaries were assumed to be captured by the provincial estimates.
PH1 prevalence and incidence remain constant over the time horizon.
Symptomatic management of PH1 is done with inexpensive therapies and therefore ECM had a treatment cost of $0.
Adherence rate to lumasiran is 97.8%.
Table 17: Summary of Key Model Parameters
Parameter | Sponsor’s estimate (reported as year 1 / year 2 / year 3 if appropriate) |
|---|---|
Target population | |
Prevalent patients | 2 per million individuals35 |
Incident patients | |
Number of patients eligible for drug under review | 70 / 71 / 72 |
Market uptake (3 years) | |
Uptake (reference scenario) ECM | 100% / 100% / 100% |
Uptake (new drug scenario) Lumasiran ECM | 65% / 60% / 55% 35% / 40% / 45% |
Cost of treatment (per patient) | |
Cost of treatment in Year 1 / Year 2+ annually Lumasirana ECM | $███████ / $███████ $0 / $0 |
ECM = established clinical management.
aCost of lumasiran was calculated by weight, where adult patients were assumed to have a weight of 82.02 kg and pediatric patients a weight of 26.15 kg. A weighted population was used to calculate the average annual cost of lumasiran treatment, with 70.6% of patients assumed to be pediatric. Includes administration costs.
Summary of the Sponsor’s BIA Results
The estimated incremental budget impact of funding lumasiran for the treatment of patients with PH1 was $23,462,841 in Year 1, $17,446,728 in Year 2, and $20,454,784 in Year 3, for a 3-year incremental budget impact of $61,364,353. The sponsor also conducted a scenario analysis with a health care payer perspective that included the cost of dialysis, where the 3-year incremental budget impact of lumasiran was $55,548,206.
CADTH Appraisal of the Sponsor’s BIA
CADTH identified several key limitations to the sponsor’s analysis that have notable implications on the results of the BIA:
The estimated number of patients with PH1 who are eligible for treatment is uncertain. The sponsor estimated the total number of patients eligible for PH1 treatment using European data.35 Clinical experts consulted by CADTH stated that although the source used is appropriate to estimate the population of patients with PH1 in Canada, PH1 is likely underdiagnosed. The sponsor further used a conservative approach by rounding up patient numbers to calculate the total budget impact as a result of the rareness of the disease; however, rounding may not accurately represent the total number of patients with PH1, thus overestimating the budget impact.
In the CADTH base case, the budget impact of lumasiran was calculated using unrounded patient numbers.
Lumasiran market shares were underestimated. In the sponsor’s base-case analysis, the pan-Canadian market share values were derived from aggregated provincial patient numbers. Given that the sponsor used rounding to estimate the patient numbers, this therefore skewed the resultant market share values of lumasiran; however, as the sponsor used the conservative approach in rounding up the patient numbers, the overall impact of this implication would overestimate the budget impact of lumasiran.
The market share values of lumasiran in the new therapy scenario were informed by the sponsor’s internal market research. Clinical experts consulted by CADTH noted that the market share values for lumasiran were underestimated, as it is expected to capture the market rapidly due to it being the first therapy available for the indicated population. If available, disease specialists are expected to prescribe this drug to most patients, except those who have access to alternative investigative therapies or who are reluctant to receive further treatment.
To address this limitation, CADTH set the market share values for lumasiran to 80% in year 1, 85% in year 2, and 88% in year 3.
The proportion of pediatric patients is likely overestimated. In the sponsor’s base case, it was assumed that 70.6% of patients were pediatric, aligned with the proportion of patients from the clinical trials. Clinical experts consulted by CADTH stated that the 70.6% of the population may be pediatric at the time of diagnosis; however, the proportion of pediatric patients in the prevalent population is likely lower, as PH1 is underdiagnosed in the adult population.
Due to limitations in available data informing the proportion of pediatric patients with PH1, CADTH was unable to address this limitation. However, because the drug cost of lumasiran was calculated as a weighted average between pediatric and adult patients, a high proportion of pediatric patients would underestimate the 3-year budget impact of reimbursing lumasiran.
Use of treatment adherence to estimate drug costs is not appropriate. In the sponsor’s base case, they assumed that the adherence rate to lumasiran is ████% based on the rate from the pooled data from the ILLUMINATE trials. Usage of the trial’s adherence rate to determine drug costs is not appropriate, as patient adherence rate to a treatment may be influenced by several factors, each of which have different impacts on the drug costs.
In the CADTH reanalysis, treatment adherence of lumasiran was set to 100%.
CADTH Reanalyses of the BIA
Table 18: CADTH Revisions to the Submitted Budget Impact Analysis
Stepped analysis | Sponsor’s value or assumption | CADTH value or assumption |
|---|---|---|
Corrections to sponsor’s base case | ||
1. Administration fees | Included | Excluded |
Changes to derive the CADTH base case | ||
1. Rounded patient numbers | Yes | No |
2. Lumasiran market shares | Year 1: 35% Year 2: 40% Year 3: 45% | Year 1: 80% Year 2: 85% Year 3: 88% |
3. Adherence rate | ████% | 100% |
CADTH base case | 1 + 2 + 3 | |
The results of the CADTH stepwise reanalysis are presented in summary format in Table 18, and a more detailed breakdown is presented in Table 19. Based on the CADTH base case, the estimated incremental budget impact of reimbursing lumasiran is $46,922,574 in year 1, $36,344,252 in year 2, and $38,660,077 in year 3. The 3-year total budget impact was $121,926,903.
Scenario analyses were conducted exploring the inclusion of dialysis costs, including patient rounding and a price reduction of lumasiran, as recommended in the Pharmacoeconomic Report. The 3-year incremental budget impact results of these scenarios are presented in Table 20.
Table 19: Summary of the CADTH Reanalyses of the Budget Impact Analysis
Stepped analysis | Three-year total |
|---|---|
Submitted base case | $61,364,353 |
Submitted base case (corrected) | $61,308,435 |
CADTH reanalysis 1 | $58,625,261 |
CADTH reanalysis 2 | $130,430,690 |
CADTH reanalysis 3 | $62,716,353 |
CADTH base case (1 + 2 + 3) | $121,926,903 |
Table 20: Detailed Breakdown of the CADTH Reanalyses of the Budget Impact Analysis
Stepped analysis | Scenario | Year 0 (current situation) | Year 1 | Year 2 | Year 3 | Three-year total |
|---|---|---|---|---|---|---|
Submitted base case | Reference | $0 | $0 | $0 | $0 | $0 |
New drug | $0 | $23,462,841 | $17,446,728 | $20,454,784 | $61,364,353 | |
Budget impact | $0 | $23,462,841 | $17,446,728 | $20,454,784 | $61,364,353 | |
Submitted base case (corrected) | Reference | $0 | $0 | $0 | $0 | $0 |
New drug | $0 | $23,441,460 | $17,430,829 | $20,436,145 | $61,308,435 | |
Budget impact | $0 | $23,441,460 | $17,430,829 | $20,436,145 | $61,308,435 | |
CADTH base case | Reference | $0 | $0 | $0 | $0 | $0 |
New drug | $0 | $46,922,574 | $36,344,252 | $38,660,077 | $121,926,903 | |
Budget impact | $0 | $46,922,574 | $36,344,252 | $38,660,077 | $121,926,903 | |
CADTH scenario analysis: include patient rounding | Reference | $0 | $0 | $0 | $0 | $0 |
New drug | $0 | $51,648,761 | $39,966,303 | $41,810,902 | $133,425,966 | |
Budget impact | $0 | $51,648,761 | $39,966,303 | $41,810,902 | $133,425,966 | |
CADTH scenario analysis: include dialysis costs | Reference | $4,502,963 | $5,280,348 | $6,075,591 | $6,911,179 | $18,267,119 |
New drug | $4,502,963 | $49,155,043 | $38,562,564 | $40,901,975 | $128,619,582 | |
Budget impact | $0 | $43,874,695 | $32,486,973 | $33,990,795 | $110,352,463 | |
CADTH scenario analysis: 95% price reduction | Reference | $0 | $0 | $0 | $0 | $0 |
New drug | $0 | $2,346,129 | $1,817,213 | $1,933,004 | $6,096,345 | |
Budget impact | $0 | $2,346,129 | $1,817,213 | $1,933,004 | $6,096,345 |
Ethics Review
Abbreviations
AGT
alanine-glyoxylate aminotransferase
PH1
primary hyperoxaluria type 1
Summary
Patient, clinical expert, and drug program input gathered in the course of this CADTH review, in addition to relevant literature, was reviewed to identify ethical considerations relevant to the use of lumasiran for the treatment of primary hyperoxaluria type 1 (PH1) in pediatric and adult patients.
Ethical considerations arising in the context of PH1 highlighted challenges of diagnosis for this rare disease, as well as equity and access challenges related to diagnosis and treatment. The severity of PH1 was noted, as was the burdensome nature of current treatment options. Given the ongoing need for liver and kidney transplants for the treatment of PH1, considerations arise related to the allocation of scarce organs.
Ethical considerations arising in the evidence used to support lumasiran indicated that several evidentiary uncertainties exist, particularly related to the long-term safety and efficacy of this drug, and the use of surrogate end points in clinical trials, as well as their representativeness.
Patients and clinical experts reported improvements in PH1 with the use of lumasiran, but uncertainties remain about efficacy and challenges in prescribing and dispensing.
Ethical considerations for health systems related to the implementation of lumasiran highlight the challenges of funding decisions, population screening, and issues related to high-cost drugs for rare diseases.
Objective
The aim of this report is to identify and describe ethical considerations associated with the use of lumasiran for the treatment of primary hyperoxaluria type 1 (PH1) to lower urinary oxalate levels in pediatric and adult patients, including those related to the context of PH1, the evidentiary basis and use of lumasiran, and considerations relevant to health systems.
Research Questions
This report addresses the following research questions:
What ethical considerations arise in the context of PH1 in pediatric and adult patients?
What ethical considerations arise related to the evidence (e.g., clinical and economic data) related to the validation and approval of lumasiran?
What ethical considerations arise in the use of lumasiran for clinicians, patients, and their caregivers?
What ethical considerations for health systems are involved in the context of lumasiran?
Methods
To identify ethical considerations relevant to the use of lumasiran for the treatment of PH1, this Ethics Review was driven by relevant questions identified in the EUnetHTA Core Model 3.0 Ethics Analysis Domain1 and supplemented by relevant questions from the Equity Checklist for HTA (ECHTA).2 These guiding questions were organized to respond to the research questions posed, and investigated ethical considerations related to:
patients living with PH1 and their caregivers (i.e., disparities in incidence, treatment, or outcomes; challenges related to diagnosis or clinical care; factors that might prevent patients from gaining access to therapies)
the evidence used to demonstrate the benefits, harms, and value of lumasiran (i.e., ethical considerations in relevant clinical trials, including their representativeness, choice of outcome measures, appropriateness of analytical methods and models to all population groups; ethical considerations related to the data or assumptions in the economic evaluation)
the use of lumasiran, including considerations related to benefits and harms to patients, relatives, caregivers, clinicians, or society, and considerations related to access to this therapy
the uptake of the therapy in health systems, including considerations related to the distribution of health care resources.
Data Collection: Review of Project Inputs and Literature
Data to inform this Ethics Review drew from an identification of ethical considerations (e.g., values, norms, or implications related to the harms, benefits, and implications for equity, justice, resource allocation, and ethical considerations in the evidentiary basis) in the patient, clinical expert, and drug program input gathered in the course of this review, as well as a complementary search of the published literature. Ongoing collaboration and communication with the CADTH review team also assisted in the clarification and identification of ethical considerations raised.
As described in the Clinical Review Report, input was collected from clinical experts with experience treating adult and pediatric patients with PH1 in Canada, from drug programs across Canada, and from patients who represent this affected group. In addition to drawing ethical content from these sources, a literature review was conducted to complement and augment these inputs.
Review of Project Inputs
Five main sources of input collected in the course of this CADTH review were reviewed by 1 reviewer to inform the Ethics Report:
The sponsor submission was reviewed for ethical considerations, noting relevant information and external references or sources relevant to each of the research questions driving this report.
Patient input collected by CADTH was reviewed for ethical considerations, relevant to each of the research questions driving this report.
Drug program input was reviewed for ethical considerations relevant to each of the research questions driving this report. Respondents from the drug programs were explicitly asked to identify any ethical issues or questions that arose in their consideration of this therapy.
Clinical experts were engaged by CADTH over the course of this reimbursement review for 2 teleconference discussions (2 clinical experts) and 1 panel discussion (4 clinical experts). These clinical experts were active in relevant clinical roles in Canada, and all had experience treating patients with PH1. During each of the 3 interactions with clinical experts, notes were taken on ethical considerations as they arose. In addition, targeted questions related to ethical considerations were asked of the experts at each of these input calls, corresponding to the research questions driving this report.
Collaboration with the CADTH clinical and economic reviewers identified domains of ethical interest arising in their reviews and identified relevant questions and sources pursued in this report.
Literature Search and Selection Methods
A literature search was conducted by an information specialist on key resources including MEDLINE All (1946‒) via Ovid and Philosopher’s Index via Ovid. Duplicates were removed by manual deduplication in Endnote. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. The main search concepts were Oxlumo (lumasiran) or primary hyperoxaluria type 1.
CADTH-developed search filters were applied to limit retrieval to citations related to empirical and normative ethical considerations. The initial search was completed on May 18, 2022. Retrieval was not limited by publication date or language limits. Due to the iterative nature of the literature review, additional searching was required to capture literature on RNAi therapies. The additional search was completed on June 23, 2022. Retrieval was not limited by publication date or language limits.
Grey literature was identified by searching sources listed in relevant sections of the Grey Matters: A Practical Tool For Searching Health-Related Grey Literature checklist.3 The grey literature search for ethical considerations was conducted on May 26, 2022. The main search concepts were Oxlumo (lumasiran) or primary hyperoxaluria type 1. Retrieval was not limited by publication date or language limits. Google was used to search for additional internet-based materials. These searches were supplemented by reviewing bibliographies of key papers and through contacts with experts, as appropriate.
Literature Screening and Selection
The selection of relevant literature proceeded in 2 stages. In the first stage, the titles and abstracts of citations were screened for relevance by a single reviewer. Articles were retrieved for full-text review if they identified, or provided normative analysis (i.e., focusing on “what ought to be” through argumentation) of, or presented empirical research (i.e., focusing on “what is” through observation) on ethical considerations related to the incidence, diagnosis, treatment, or outcomes of PH1, or arising in the evidence used to support, use, or implications of lumasiran.
As a parallel process, grey literature and other sources drawn from relevant bibliographies or in consultation with experts or other CADTH reviewers were retrieved and reviewed following the selection criteria listed previously.
Data Analysis
Data analysis for this Ethics Report included the collection, coding, and thematic analysis of data drawn from the literature and project inputs, driven by the 4 research questions guiding this report. The reviewer conducted 2 cycles of coding to abstract, identify, and synthesize relevant ethical considerations in the literature and from relevant project inputs.
In the initial coding phase, publications and input sources were reviewed for ethical content (e.g., claims related to potential harms, benefits, equity, justice, resource allocation, and ethical issues in the evidentiary base). Once identified, claims related to ethical content were coded using methods of qualitative description.4 Initial descriptive coding of the reports focused broadly on categories concerning what ethical considerations were described. In the second coding phase, major themes and subcodes were identified through repeated readings of the data,4 and summarized into the thematic categories within each domain or research question. When ethical content emerged that did not fit into the categories or domains outlined in the research questions, this was noted.
Results
Description of Included Sources
Data to inform this Ethics Report drew from a review of the patient input, drug program input, and consultation with clinical experts engaged for this review. A description and summary of these sources are included in the Clinical Report of this review.
A total of 36 citations were identified in the search of the published literature. Following screening of titles and abstracts, 28 citations were excluded and 8 potentially relevant publications from the electronic search were retrieved for full-text review. Of the potentially relevant publications, 2 publications were excluded, as they did not discuss ethical considerations arising in the context of lumasiran for the treatment of PH1. Six publications met the inclusion criteria and were included in this report. In addition, 6 relevant publications were retrieved from other sources, including the grey literature search.
A total of 12 publications were used to inform this report. Four publications examined ethical considerations related to diagnosis, treatment, and outcomes of patients with PH1; 2 publications examined ethical considerations related to lumasiran as a treatment for PH1; and 4 publications examined both ethical considerations in the context of PH1 and the context of treatment with lumasiran. In addition, 2 publications were selected to provide a broader understanding of the context of ethical considerations for rare diseases. Details regarding the characteristics of included publications are reported in Table 1.
Key Ethical Considerations
Diagnosis and Experiences of PH1
PH1 has been categorized as a rare or ultra-rare disease, with estimates of disease prevalence of PH1 ranging from 1 to 3 cases per 1 million people to 1 in 58,000, implying significant underdiagnosis.5 The rarity of this condition also means that cases are geographically widespread,5 leading to challenges in building clinical expertise and health system capacity. Patients with PH1 thus face challenges related to diagnosis, equity of access to treatment, and challenges in the management of a complex and severe genetic disease, particularly for infants and caregivers.
This lack of general clinical expertise in the diagnosis of PH1 can lead to a potential for missed diagnosis among clinicians who may be unfamiliar with the disease, or who may misinterpret clinical signs.6 A 2013 review found the median time between initial symptoms and diagnosis to be more than 5 years, and that this condition is unknown to most medical students and young practitioners.6 The clinical experts engaged for this review characterized diagnosis as relying on a constellation of factors, and indicated that there are currently no known guidelines for the treatment of PH1 and very limited clinical expertise. Clinical experts engaged for this review and the literature consulted described the heterogeneous nature of PH1 presentation and progression, with which even siblings may present differently,7 leading to further challenges in diagnosis. In adults, the presentation of PH1 can be less obvious and more varied than in children, often leading to delayed or missed diagnosis.8
Clinical experts consulted and patient input received by CADTH indicated that when physicians do not recognize or categorize symptoms as part of PH1, they may not advocate for or follow through on the appropriate care and testing of these patients, or refer them for specialist care or genetic diagnosis. These delays in diagnosis can lead to uncertainty and distress for patients, as well as progression to advanced stage or chronic kidney disease for some patients with this disease.6,7
Clinical experts also discussed how the challenges with diagnosis of PH1 include equity and access considerations, as an accurate and timely diagnosis of PH1 can be dependent on where patients live and which health care professionals they have access to. Geographic access challenges that arise in communities where there is no primary care access, or where there is limited access to the health care system, or that are located far from medical centres and specialists, were also discussed. Further, clinical experts identified financial access barriers that can arise for those who cannot afford to travel to treatment centres, as well as the issue of how those in many equity-deserving groups may lack resources for the high caregiver support requirements involved with PH1 care, may have fewer resources for care, and may lack health literacy that would assist in understanding their health conditions.
Once diagnosed, the management of patients with advanced PH1 can be extremely difficult and often requires an individualized approach.6 Both patients and clinicians indicated that the disease burden for patients and their caregivers is significant, both physically and mentally. The patient input indicated significant psychological and emotional stress as it related to anxiety about the uncertainty of PH1 and how it will progress; stress for parents and caregivers of children with PH1, including those related to family planning; anxieties about managing or maintaining kidney function levels; guilt associated with noncompliance to strict management regimes; and uncertainties related to the fluctuating nature of the disease and side effects of medications. Alongside these psychological challenges, patients identified how physical treatments or management regimens for PH1, such as sustained hemodialysis for those with advanced stage disease, can also be difficult to sustain for patients and caregivers. Other forms of supportive care — such as hyperhydration — are also difficult to sustain, especially for children, as this can require the insertion of a gastrostomy tube (G-tube).6,9 However, a lack of adherence to even conservative treatment can enhance the adverse outcomes of the disease.6
PH1 is particularly severe in infants, as patients aged younger than 2 years have a 3.4 times higher risk of early death compared to patients aged older than 2 years at the onset of renal replacement therapy,9 representing a particularly vulnerable population. A 1999 study found that infants had a particularly poor prognosis, with half reaching end-stage renal disease before 5 years of age and requiring combined kidney and liver transplant.10 For these infants, therapeutic withdrawal due to parental, ethical, or financial reasons was seen to be justifiable,10 and in more recent reports, many physicians have accepted palliative care for pediatric patients with PH1 with end-stage kidney disease due to the burden of therapy and the extent of comorbidity.9
A PH1 diagnosis is confirmed by genetic testing for the alanine-glyoxylate aminotransferase (AGT) gene; however, the clinical experts indicated that uncertainties remain about when this genetic testing occurs in practice. Genetic testing also raises considerations for disclosure to family members and the implications for relatives who are not directly tested, and considerations related to learning information that they did not primarily consent to receive.11 In the context of this review, clinical experts described their experiences of screening siblings and parents, and other familial testing for PH1. Prenatal diagnosis of the presence of the AGT gene is available, but holds implications of pregnancy termination, which all may not agree on for personal or religious reasons.6,10
Considerations Related to Treatment and Transplantation
A significant treatment option for PH1 has been combined liver-kidney transplant. However, this raises resource allocation considerations as they relate to the prioritization of patients with PH1 in organ allocation networks.6 The need for 2 donor organs, especially when these are in short supply, presents special challenges in the treatment of this disease.12 Although the liver itself may not appear to be damaged or diseased, a liver transplant is often required with a kidney transplant in the treatment of PH1, raising ethical considerations around the removal of an otherwise healthy liver for transplantation.7 The genetic nature of this disease also poses challenges within organ transplantation networks, where potential related donors may also carry PH1,12 even at low levels that may not be fully detected on genetic assays.6 Transplantation also poses unique risks in an infant population, especially when they reach end-stage renal disease before 1 year of age, due to the risks of immunosuppression and difficulty in placing organs.10 For both adults and children, transplantation comes with risks of severe perioperative complications and the long-term consequences of immunosuppression.13 While it has been suggested that the use of lumasiran might displace the need for kidney and liver transplants,13 clinical experts noted that, depending on the stage of the disease, treatment with lumasiran may still require a kidney and/or liver transplant, posing ongoing challenges related to organ allocation and transplantation.
The clinical experts consulted by CADTH noted that the treatment of PH1 also often requires access to hemodialysis. This poses significant access challenges for most people in Canada, where there are limited sites that can administer this. These challenges are heightened for those in rural or remote communities, or who live far from hemodialysis centres, and for those under the age of 15 years. Clinical experts noted that there are very few centres in Canada that can perform pediatric hemodialysis for this population group (for example, only 4 in Ontario; 4 in Western Canada; and very limited capacity in Eastern Canada), and that accessing pediatric hemodialysis may mean that families need to relocate for children to receive treatment. The clinical experts indicated that if oxalate levels can be lowered, peritoneal dialysis becomes an option, and access can increase as more treatment sites and options are available.
Ethics of Supporting Evidence
Several uncertainties arose in the evidence used to support lumasiran, including those related to the lack of long-term data, the use of surrogate end points, and the representativeness of supporting clinical trials. One of the primary noted uncertainties related to lumasiran, by both clinical experts and in the published literature, is the absence of long-term safety and efficacy data, especially as this drug is expected to be administered for a patient’s entire life,5,14 raising questions about unknown risks to patients.
Another challenge identified was the use of surrogate end points in these clinical trials. Clinical experts indicated that measures of urine or plasma oxalate do not necessarily reflect total body oxalate levels, and acknowledged that there are currently no accepted methods for accurately measuring total body oxalate. The clinical experts identified that the surrogate end points used may not be relevant to patients who do not experience these clinically. Patients may experience symptoms of oxalosis and renal failure, but these were not specifically measured in the trials. In addition, the surrogate outcome of urine oxalate may not always translate to changes in renal function, although it is expected that lowering urinary oxalate levels could prevent further complications associated with PH1 in patients who have retained kidney function. Further, while there is some association between urinary oxalate levels and a decreased risk of kidney failure in the short-term, long-term data on this association is not available.14 Clinical experts also noted that urinary oxalate levels can only be measured for those patients who are still producing urine, and may be a less meaningful indicator for patients with end-stage kidney disease or who lack kidney function. The drug programs also posed the question of how these surrogate outcomes correlate to complications associated with PH1 and other outcomes important to patients and clinicians.
At a practical level, the drug program input indicated that measuring urine oxalate through repeated urine tests would cause challenges for labs conducting these test and burdens for patients to complete. The studies used to support this drug measured urine oxalate levels each month, but it is unclear how this would be collected in a real-world setting or how this would demonstrate drug efficacy over time.
Regarding the representativeness of the clinical trials used to support lumasiran, the ILLUMINATE-A, ILLUMINATE-B, and ILLUMINATE-C trials did not include participants aged older than 60 years; participants were mostly white (76.9% in the ILLUMINATE-A trial, 88.9% in the ILLUMINATE-B trial, and 76.2% in the ILLUMINATE-C trial); and there was a predominance of male participants in the ILLUMINATE-A (66.7%) and ILLUMINATE-C (57.1%) trials. This predominance of white participants may not fully reflect the population of people living in Canada, especially those in equity-deserving groups. However, since this is a rare disease, recruiting a representative sample into clinical trials may pose challenges, and the clinical experts indicated that these limitations did not affect the generalizability of these trials. Despite this, questions remain about their representativeness and applicability to the diverse population of people living in Canada.
Ethical Considerations in the Use of Lumasiran
Alongside uncertainties related to the long-term safety and efficacy of this drug, the clinical experts raised uncertainties related to its shorter-term efficacy, especially in its potential to prevent, delay, or reverse oxalosis.14 The clinical experts also indicated that lumasiran has not been shown to reverse kidney damage in practice, although it may lead to some improvement in kidney function, depending on a patient’s initial oxalate levels.
Despite long-term uncertainties, patient input received for this CADTH review reported lumasiran as providing noticeable improvements in patients’ PH1 symptoms and providing hope, as well as improving their ability to live a “normal life.” Patients were hopeful that the use of lumasiran might decrease the amounts of other medications or aspects of supportive care needed to maintain functioning. The clinical experts also acknowledged the moral dilemma of knowing that a treatment might be available for PH1, without being able to provide patients with access. Given the heterogeneous nature of PH1, clinical experts indicated that lumasiran may be more effective for patients with mild disease rather than more advanced disease, highlighting the need for earlier and accurate diagnosis.
The provincial drug programs identified uncertainties around who would prescribe and administer the drug, and whether these would be the same health care provider. Because lumasiran in its current form must be administered in a clinical setting, this may raise some accessibility challenges for those who may not have access to health care providers who can administer the medication.14 Patients and clinicians raised concerns about costs to patients that might be incurred. If this drug is fully reimbursed, patients may still face costs related to time and travel to receive this therapy, especially if lifelong therapy is required.
The drug programs also raised questions around challenges with dispensing the drug, as it is administered based on weight and must be determined for each patient, leading to concerns about wastage. Some authors have questioned whether oral administration of this therapy might be considered and developed, which would reduce physical, geographical, and financial burdens for patients.5,14
Health System Considerations
The use of lumasiran for patients with PH1 raises several health system and resource considerations related to resource allocation and trade-offs, screening programs, and the high costs of drugs for rare diseases. Provincial drug programs indicated that funding decisions for lumasiran may be complicated by the fact that many therapies for PH1 (e.g., transplantation, dialysis, hyperhydration, and supportive care) are not funded by the drug programs, and so direct comparisons of cost savings across sectors can be difficult to make and justify. As noted previously in this report, the use of lumasiran does not preclude patients with PH1 from requiring kidney and/or liver transplants. Given the overall shortage of donor organs relative to those on the waitlist, resource allocation and prioritization decisions remain, especially those related to how to prioritize patients with PH1 for the receipt of donor organs.
Due to the noted challenges and delays in the diagnosis of PH1, both the provincial drug programs and clinical experts considered whether a population screening program might be implemented, such as genetic screening as part of newborn screening panels. However, the clinical experts noted that this type of population screening should only be undertaken when there are widely available treatments for the condition. In addition, clinical experts consulted by CADTH expressed some concerns that this might be an expensive or complex undertaking to find a very small number of PH1-positive infants, given the rarity of the disease. In international settings, a screening program for potentially affected individuals has also been suggested, requiring high throughput, high sensitivity, a clear definition of the selected population, and a mechanism to manage false positives and provide confirmatory testing to those who screen positive.8
A final significant consideration is related to the high cost of lumasiran, raising questions about access and sustainability.14 As with many drugs targeting rare diseases, the trend toward high costs raises a conundrum between a utilitarian calculation, indicating that it may not be in the broader interest of the population to divert resources to benefit only a few patients with a rare disease at the cost of society at large, and obligations to protect and assist the most vulnerable, drawing on principles of beneficence, nonabandonment, and the rule of rescue.15 When drugs for rare diseases do not meet cost-effectiveness thresholds, nonfinancial justifications for producing and distributing these drugs may be used.15
Limitations
The noted rarity and underdiagnosis of PH1, in combination with the novelty of lumasiran and lack of other PH1-specific therapies available on the market, meant that the published literature that raised ethical considerations in this domain was limited. However, augmenting this limited literature with inputs from patient groups, drug programs, and clinical experts collected in the course of this reimbursement review provided a more comprehensive picture of ethical considerations in the context of lumasiran for the treatment of PH1.
Although this Ethics Report drew and extracted from patient group, clinical expert, and drug program inputs, it is possible that more directed engagement (such as direct interviews with patients, caregivers, or family members) on their specific experiences with lumasiran would have yielded more relevant domains of analysis.
Conclusion
Input from patients, clinical experts, drug programs, and relevant published literature was reviewed for ethical considerations relevant to the use of lumasiran for the treatment of PH1 in pediatric and adult patients. Ethical considerations in the context of PH1 highlighted the challenges of diagnosis and underdiagnosis for this rare disease, especially those that relate to equity and access to diagnosis and treatment. PH1 is a severe disease, posing both physical and mental strains for patients and their caregivers, especially for infants. Treatments for PH1 tend to be burdensome, and access challenges arise for certain groups, as do resource allocation challenges when donor livers and kidneys are required.
Regarding the evidence used to support lumasiran, uncertainties remain about the long-term safety and efficacy of this drug, as do challenges with the use of surrogate end points in clinical trials, and considerations related to the representativeness of these trials. Although patients and clinicians noted noticeable improvements in their condition with the use of lumasiran, uncertainties remain about the efficacy of this drug in preventing end-stage kidney disease, and challenges remain around the prescribing and dispensing of this drug.
Finally, the implementation of lumasiran raises ethical considerations for health systems related to the challenges of making funding decisions when funds must be reallocated from different funding pockets, considerations related to widespread population screening for PH1, and considerations in the context of high-cost drugs for rare diseases.
Lumasiran offers the potential for addressing an underserved, underdiagnosed population who face severe and burdensome disease, and for whom equity and access challenges are present. However, uncertainties remain about the long-term safety and efficacy of this drug, as do implementation challenges related to its prescribing, dispensing, and funding.
References
1.EUnetHTA HTA core model version 3.0. Diemen (NL): European Network for Health Technology Assessment: https://www.eunethta.eu/wp-content/uploads/2018/03/HTACoreModel3.0-1.pdf?x69613. Accessed 2021 Dec 17.
2.Benkhalti M, Espinoza M, Cookson R, Welch V, Tugwell P, Dagenais P. Development of a checklist to guide equity considerations in health technology assessment. Int J Technol Assess Health Care. 2021;37:e17. PubMed
3.Grey matters: a practical tool for searching health-related grey literature. Ottawa (ON): CADTH; 2019: https://www.cadth.ca/grey-matters. Accessed 2022 May 26.
4.Sandelowski M. Whatever happened to qualitative description? Res Nurs Health. 2000;23(4):334-340. PubMed
5.Moya-Garzon MD, Gomez-Vidal JA, Alejo-Armijo A, et al. Small molecule-based enzyme inhibitors in the treatment of primary hyperoxalurias. J Pers Med. 2021;11(2):27. PubMed
6.Cochat P, Groothoff J. Primary hyperoxaluria type 1: practical and ethical issues. Pediatr Nephrol. 2013;28(12):2273-2281. PubMed
7.Hoppe B, Langman CB. A United States survey on diagnosis, treatment, and outcome of primary hyperoxaluria. Pediatr Nephrol. 2003;18(10):986-991. PubMed
8.Moochhala SH, Worcester EM. Primary hyperoxaluria: the adult nephrologist's point of view. Clin Kidney J. 2022;15(Suppl 1):i29-i32. PubMed
9.Ben-Shalom E, Garrelfs SF, Groothoff JW. Primary hyperoxaluria: the pediatric nephrologist's point of view. Clin Kidney J. 2022;15(Suppl 1):i23-i28. PubMed
10.Cochat P, Koch Nogueira PC, Mahmoud MA, Jamieson NV, Scheinman JI, Rolland MO. Primary hyperoxaluria in infants: medical, ethical, and economic issues. J Pediatr. 1999;135(6):746-750. PubMed
11.Kruse J, Mueller R, Aghdassi AA, Lerch MM, Salloch S. Genetic testing for rare diseases: a systematic review of ethical aspects. Front. 2021;12:701988. PubMed
12.Narasimhan G, Govil S, Rajalingam R, Venkataraman C, Shanmugam NP, Rela M. Preserving double equipoise in living donor liver-kidney transplantation for primary hyperoxaluria type 1. Liver Transpl. 2015;21(10):1324-1326. PubMed
13.Bacchetta J, Wood KD. Primary hyperoxaluria type 1: time for prime time? Clin Kidney J. 2022;15(Suppl 1):i1-i3. PubMed
14.Bacchetta J, Lieske JC. Primary hyperoxaluria type 1: novel therapies at a glance. Clin Kidney J. 2022;15(Suppl 1):i17-i22. PubMed
15.Kacetl J, Maresova P, Maskuriy R, Selamat A. Ethical questions linked to rare diseases and orphan drugs - a systematic review. Risk Manag Healthc Policy. 2020;13:2125-2148. PubMed
Appendix 1: Details of Included Publications
Note that this appendix has not been copy-edited.
Table 1: Details of Included Publications
First author, year | Publication type | Objective | Key ethical considerations | Funding source |
|---|---|---|---|---|
Bacchetta 2022a14 | Review | To summarize the current knowledge on RNAi therapies and to discuss other therapeutic possibilities |
| Alnylam Pharmaceuticals, Inc. |
Bacchetta 2022b13 | Commentary | To introduce a journal supplement on PH1 and its treatment options | Potential of lumasiran to manage PH1 and improve quality of life and reduce the need for transplantation is significant | Alnylam Pharmaceuticals, Inc. |
Ben-Shalom, 20229 | Review | To review the manifestations of pediatric hyperoxaluria, treatment options, and medical and ethical dilemmas |
| Alnylam Pharmaceuticals, Inc. |
Cochat, 199910 | Original Research (Survey) | To survey the current (1999) medical approach to and economic issues affecting infants with PH1 |
| None identified |
Cochat, 20136 | Review | To discuss practical barriers and ethical dilemmas that directly affect the outcome of PH patients |
| None identified |
Hoppe, 20037 | Original Research (Survey) | To determine the spectrum of diagnostics, treatment practices and patient outcomes of PHs |
| Oxalosis and Hyperoxaluria Foundation |
Kacetl, 202015 | Systematic Review | To identify ethical questions linked to rare diseases and orphan drugs and ethical principles or approaches applied to solve them |
| University of Hradec Kralove Long Term Development Plan |
Kruse, 202211 | Systematic Review | To present a detailed overview of ethical aspects relevant to genetic testing for rare diseases as discussed in the literature | Ethical aspects arise in the process of testing, consequence of test outcome and contextual challenges for rare diseases | European Union grants |
Moochhala, 20228 | Review | To review considerations relevant to adults with PH |
| Alnylam Pharmaceuticals, Inc. |
Moya-Garzon, 20215 | Review | To describe the most recent advances in the treatment of PHs |
| None identified |
Narasimhan, 201512 | Commentary | To identify considerations related to liver-kidney transplantation in patients with PH1 |
| None identified |
Stakeholder Input
Patient Input
The Oxalosis and Hyperoxaluria Foundation and the Canadian Organization for Rare Disorders
About the Oxalosis and Hyperoxaluria Foundation and the Canadian Organization for Rare Disorders
The Oxalosis and Hyperoxaluria Foundation
Founded in 1989 by families in the hyperoxaluria community, the Oxalosis & Hyperoxaluria Foundation (OHF) is the first patient advocacy organization in the world dedicated to finding treatments, and ultimately a cure, for hyperoxaluria. Today, the OHF is a global leader, a partner, an alliance and a movement. We strive to amplify the patient voice every step of the way, bringing together thousands around the globe to join forces to improve lives and advance towards a cure.
The Oxalosis & Hyperoxaluria Foundation (OHF) is the largest private funder of hyperoxaluria research in the world, investing more than $30 million in the scientific search for causes, preventative measures, and potential treatments. The OHF’s efforts support numerous programs that include patient support, patient and professional education, advocacy and awareness, multiple patient and professional advisory boards, while providing expert perspective on innovations, treatments and care, including discussions with multiple stakeholders: industry, insurance payers, policy makers and regulatory agencies, fundraising and outreach. The OHF is a registered 501(c)(3) nonprofit based in the US, with international outreach. Website: www.ohf.org
Canadian Organization for Rare Disorders
The Canadian Organization for Rare Disorders (CORD) is Canada’s national network for organizations representing all those with rare disorders. CORD provides a strong common voice to advocate for health policy and a healthcare system that works for those with rare disorders. The Canadian Organization for Rare Disorders works with governments, researchers, clinicians and industry to promote research, diagnosis, treatment and services for all rare disorders in Canada. Website: www.raredisorders.ca
Information Gathering
Recruitment: The primary hyperoxaluria patient community provided direct input through an online survey and a virtual focus group. Recruitment for the survey targeted patients and caregivers affected by primary hyperoxaluria type 1, 2, and 3. Recruitment was primarily conducted by the Oxalosis & Hyperoxaluria Foundation, and the Canadian Organization for Rare Disorders, through patient databases and social media. The Oxalosis & Hyperoxaluria Foundation recruited and facilitated the virtual focus group of three Canadian caregivers for children under the age of 12 diagnosed with primary hyperoxaluria type 1, and one Canadian patient diagnosed with primary hyperoxaluria type 1.
Responses: Patients provided input through a survey available on Survey Monkey from May 19 to May 31, 2022. The survey introduction specified that the purpose of the survey was to provide anonymous patient input to the Canadian Agency for Drugs and Technologies in Health; however, both Canadians and non-Canadians were invited to take part. There were 47 respondents, with 43 who completed the entire survey, and the feedback reported here reflects those 43 complete responses. Among these, 8 (18.6%) participants identified as Canadian, 18 (41.9%) as American, 6 (13.95%) as British, 2 (4.65%) as Spanish, 2 (4.65%) as German, 2 (4.65%) as Australian, 1 (2.33%) as Ecuadorian, 1 (2.33%) as Hungarian, 1 (2.33%) as Dutch, 1 (2.33%) as Pakistani, and 1 (2.33%) as Swiss. Canadian respondents reported home provinces of Alberta, British Columbia, Ontario, and Yukon.
Of the 43 respondents who completed the survey, 17 (39.5%) identified as “diagnosed with primary hyperoxaluria”, and 30 (69.8%) as caregivers for an individual or individuals diagnosed with primary hyperoxaluria, indicating some overlap between these groups. Additionally, 32 (74.4%) participants reported that they or the individual(s) they care for had been diagnosed with primary hyperoxaluria type 1; 5 (11.6%) with primary hyperoxaluria type 2; and 6 (14.0%) with primary hyperoxaluria type 3.
The ages of individuals diagnosed primary hyperoxaluria were distributed across 6 groupings, with 18 (41.9%) under the age of 12, 10 (23.3%) between 12 and 17, 8 (18.6%) between 18 and 29, 5 (11.7%) between 30 and 39, 4 (9.3%) between 40 and 49, and 2 (4.65%) between 50 and 59. Survey takers who care for multiple individuals with a primary hyperoxaluria diagnosis were encouraged to select all age ranges that applied.
The demographics and patient experience of Canadian, USA, and non-North American respondents were compared (see Table 1). The demographic breakdown of these groups was found to be similar. A comparable proportion of Canadian, USA, and non-North American respondents were diagnosed with primary hyperoxaluria type 1, and respondents were similarly distributed across age ranges. The experience of Canadian, USA, and non-North American patients was also very comparable. This is illustrated in Table 1, which highlights how patients in the USA, Canada and outside of North America most commonly use the same two currently available therapies to manage their primary hyperoxaluria. In addition, 3 Canadians, 7 Americans and 6 non-North American participants as well as the children of two focus group participants (Canadian) reported receiving Oxlumo (Lumasiran).
Table 1: Characteristics of Respondents in Canada, USA, and Outside North America
Respondents’ Place of Residence | Age (years) | Type of Primary Hyperoxaluri a | Current Treatment Options | ||||||
|---|---|---|---|---|---|---|---|---|---|
<12 | 12-17 | 18-29 | 30-59 | PH1 | PH2 | PH3 | Prescriptions Medications (B-6, Diuretics, Baclofen) | Increased Fluid Intake | |
Canada (n=8, number of patients=8) | 62.5% 5 | 0 | 37.5% 3 | 0 | 75.0% 6 | 0 | 25.0% 2 | 50.0% 4 | 75.0% 6 |
USA (n=18, number of patients=25) | 25.0% 5 | 30.0% 7 | 15.0% 3 | 25.0% 5 | 72.2% 13 | 16.7% 3 | 11.1% 2 | 77.8% 14 | 100.0% 18 |
Outside of North America (n=17, number of patients=19) | 42.1% 8 | 15.8% 3 | 10.5% 2 | 31.6% 6 | 76.5% 13 | 11.8% 2 | 11.8% 2 | 64.7% 11 | 58.8% 10 |
Disease Experience
Primary hyperoxaluria (PH) disease experience was elicited in the survey through (1) open-ended questions asking respondents to describe the experience of patients and caregivers with primary hyperoxaluria, and (2) rating a predefined matrix of symptoms out of 10 for how significantly they “affect the quality of life of the individual living with PH”. Focus group members were also asked to describe their experience with primary hyperoxaluria type 1. While the survey sample size is too small to conduct meaningful statistical analyses, the demographic breakdown and patient experience of respondents from Canada, the USA and outside of North America was found to be similar, as shown in Table 1. The combined results are therefore reported here.
Overall, the physiological impact and emotional stress resulting from primary hyperoxaluria diagnosis and disease management are common themes expressed by patients. Participants reported painful and devastating outcomes, highlighting kidney stones, decreased kidney function, pain in the body, and fatigue as the most impactful in the matrix of physical symptoms. Moreover, they reported equally debilitating anxiety and depression associated with a primary hyperoxaluria diagnosis. Participants shared the fear and stress of not knowing when a painful kidney stone might occur or if kidney failure is imminent. Several children from the same family may have varying degrees of the condition, which can affect the dynamics between family members.
Survey participants were asked what worried them most about the future impact of primary hyperoxaluria. The most commonly reported concerns were “Kidney failure or needing dialysis”, “Kidney and/or liver transplant” and “The stress of not knowing how the disease will progress”, which were highlighted by between 70.8% and 80.4% of respondents. Other frequently reported concerns included “Dying at a younger age”, “Not having an approved treatment”, and “Not being able to live as I want to”, which were raised by over half of survey takers.
Qualitative responses from the focus group and survey participants provide invaluable insights on the physical toll of this rare disease diagnosis on patients and families. Patients and caregivers related the devastating impact of primary hyperoxaluria symptoms, dialysis, surgeries, and organ transplantation on themselves and their children.
“My little boy can’t have a bath; he can’t swim due to his hemodialysis line. He can’t play with his brother as a normal sibling can as he might fracture so easily. His development is delayed due to lack of normal stimulus like playing with other children. He hasn’t been to any baby groups playgroups and has only just started preschool but is hardly there due to his health. I had to give up work to bring him to dialysis 6 times a week so financially it’s a struggle as my husband who also has PH1 is our main income. I have been through liver donation and will be donating a kidney when his oxalate levels are low enough, which has impacted my health. We can’t have a holiday due to the dialysis.”
“My oldest child suffered a great deal in their life with kidney stones, but when the stones became too big, too frequent, we had to have multiple hospital stays to remove the stone and manage pain. The stones were over an inch in size requiring subcutaneous surgery and kidneys could not bounce back from this surgery. My child had to drop out of high school and begin hemodialysis. Dialysis continued for over 2 years until they could get a transplant (last month). This disease has robbed my children of many opportunities and created many complications in their lives.”
“Our major symptom for [our daughter] was failure to thrive and I would rank that out of 10 on the survey as a 10. It was [...] a very broad diagnosis or symptom, but definitely failure to thrive was number one, and she was tiny, tiny, tiny, tiny she was like .1 percentile for height and .1 percentile for weight and very took a long time to figure out exactly why that's the case.”
“Because of recently declining kidney function, I can no longer have a baby that we've been trying for more than a year to have.”
“[Our daughter] was having repeat urinary infections, and then she did end up in the hospital when she was nine or ten with a kidney infection. I guess our big concern would be her kidney function and keeping it where it is right now, because you know it's probably about 56% and kind of goes up and down a little bit.”
“Stones, probably the most continuously bother me, some kind of good years and bad years. It's tough from like the family side as well with my younger brother, he has not had nearly as many stones, as I have but he's had a lot of sorts of systemic symptoms, he’s had a lot of issues with like hypercalciuria and other organ damage so that's hard to deal with as well, certainly wasn't easy for parents.”
“Lots of times, where I missed important school events or whatever, because I was getting another lithotripsy surgery.”
“When I was younger my disease was more severe and affected my ability to participate in school and extracurricular activities. I faced frequent nausea and stomach pain, and headaches. This affected education and ability to form social relationships with peers.”
“I was diagnosed at one year of age with renal failure due to both ureters occluded with stones. I was critically ill.”
“I had to come home early on my college graduation trip to Disney world to have emergency surgery because my favorite roller coaster, space mountain, threw my body around and I ended up having a blockage in my kidney. Had multiple surgeries to remove the stone and blockage. My symptoms experienced were the worst they have ever been due to the size of the stone. I was continuously vomiting and in SEVERE pain as I flew home alone to meet my mom at the airport and rush me to the hospital for immediate help.”
“My daughter would not have survived without her liver/kidney transplant to treat her infant onset PH1.”
Individuals highlighted the complexity of the diagnostic odyssey for primary hyperoxaluria, reflecting on the time it took to get appropriate care, and the preceding years of misdiagnoses. Patients and caregivers also shared how the psychological toll of uncertainty about the future affects them and their families.
“The kidney stones were the biggest symptom for us when [our daughter] was about two and a half. We had had about four or five months prior to that of the nausea and vomiting as well as the pain. And no one could quite figure out what it was, they thought urinary tract infections, they thought constipation. We went through the whole gamut multiple times before they had discovered her kidney stones, and she was actually filled with so many kidney stones in her kidney as well as in her bladder, so she has gone through a few surgeries at that point just to remove everything.”
“It was a constant worry [...] we had no idea what was going on, a lot of stress on me as a breastfeeding mom being like ‘Am I not giving enough, isn't my supply issue, what's happening?’ [...] related to anxiety or depression, I guess that would fall into a symptom of our family, and other significant symptoms there and then in terms of chills, fever or other infections.”
“So yeah, again same thing, anxiety was huge when we first were diagnosed, we're now quite a few years in so definitely settled out, but it is something that affects us daily is the water intake, which has always been a struggle and continues to be. And then, just the appointments I work only part time [...] I don't know how I would be able to work full time just in terms of managing the appointments and getting her.”
“We are planning for the future which is difficult when you don't know what it looks like. I'm in a rural place, right now, and that was really hard to do because I'm away from most medical care, there's a lot of anxiety around that. I'm 26 now, my partner and I are trying to decide whether kids are in our future, and there's just been so so few healthy pregnancies with PH1 patients, and that's something that even like my doctors have no idea about or how to manage it would be like very, very high risk, so those sort of like bigger kind of family planning life decisions.”
“How stressful it is to worry about your child’s health and if they are drinking enough to help minimize stone formation. I especially worry about the future when they go to college and will somewhat be on their own. It also mentally affects younger PH sufferers when they do not understand why they have disease and why they are different.”
Experiences With Currently Available Treatments
Until very recently, there were few specific therapies for treatment of primary hyperoxaluria. Among the 43 survey respondents, the majority utilize prescription medications such as Vitamin B-6, diuretics, or baclofen (29 individuals, 67.4% of respondents), as well as increased fluid intake also known as hyperhydration (34 individuals, 79.1% of respondents), to manage primary hyperoxaluria. In infants and children, hyperhydration often requires placement of a gastrostomy tube (G-tube) to enable sufficient fluid intake and adherence to the otherwise unattainable recommended level of therapeutic hydration.
16 individuals (37.2%) also reported undergoing ureteroscopy to remove stones, and 14 (32.6%) individuals reported undergoing percutaneous nephrolithotomy/surgical removal of stones. 3 Canadians, 7 Americans and 6 non-North American participants reported receiving Oxlumo (Lumasiran). In addition, the children of two focus group participants (Canadian) were also receiving Oxlumo (Lumasiran) through compassionate use from the manufacturer.
In discussion of their experiences in open ended questions, participants reported the challenges of living with the inconsistent efficacy of currently available therapies.
“[B-6] has gotten less effective over time even with higher and higher doses so just knowing that there's another option out there and might end up being the only option other than a transplant is pretty big.”
“[Our daughter] takes about 200 grams of [high dose vitamin B-6] twice a day, and then she also takes a potassium citrate tablet daily, and that has been able to lower her oxalate levels quite substantially. The only thing with her is she really fluctuates so from the time she was young; we were doing monthly urine and blood now about three times every three months we do it. And she has always just kind of been like these last few months, in December, it was like her numbers were the highest they've ever been and then in March, they were the lowest they've ever been so they really kind of fluctuate with her and that's where I think eventually she may end up needing access to something like Lumasiran because, again, the kidney function is where our concern comes in.”
“And just so you know, being in pain, being tired, the kind of ebb and flow of things when sometimes you'll have a couple months where you feel like you're perfectly normal and then all of a sudden you're at the sick person again.”
Individuals also reflected on the challenges of hyperhydration (extreme high fluid intake), dialysis, and the side effects of the treatment options that are available.
“Even, just like the meds that you can be on can cause a lot of side effects, like I know somebody mentioned that one of their kids was on potassium citrate. I could not tolerate that at all I lost so much weight, I was so nauseous all the time, those are like the worst two years of my life was when I was on that so it's things like that, where it's like ‘Oh, even if you find something that starts working and then that causes its own problems.’”
“My hope is to ultimately need to be less dependent on increased fluid intake, which can be very burdensome. TID [3x day] dosing of potassium citrate can also be difficult. The guilt of not maintaining a perfect regimen can be debilitating.”
“Throughout the rest of my life, my activities are often impeded by hyperhydration and for frequent bathroom needs. This impacts my activities every day.”
“It is a silent disease. But powerful if not treated. Drinking a lot of water is very difficult for children. Getting enough fluids every day is nearly impossible.”
“When my son is attached to a machine dialysing his blood for six hours a day six days a week he can do nothing, nothing nothing.our life have changed white PH1, from kidney stones to kidney failure was a hard way, then the hardest way started after with dialysis for three years then the transplant and the end.”
Improved Outcomes
When asked on a scale of 1-10 how important an approved treatment that prolonged or maintained kidney function would be to patients and families living with primary hyperoxaluria, survey participants rated the importance of this possibility as >9 on average.
Patient and caregiver feedback demonstrates that current treatments and dialysis are insufficient and showed that therapies that decrease the likelihood of kidney stones, the need for kidney and liver transplantation, kidney failure, and oxalosis are critical. Responses revealed that patients and families need access to treatments that improve these measures of physical well-being, and thereby mitigate the stress and anxiety surrounding primary hyperoxaluria for the entire family.
“[A treatment that] eventually prevents the need for a transplant, if that's where this road leads, that would be huge, because that is always kind of a hovering fear in the background.”
“I'd even go further than that to say it's not just about the endgame of a transplant, but to be able to lead a more normal, stress free, life [...] remove that kind of high level of stress and planning for [our daughter] and then also for our whole entire family.”
“My biggest goal is to avoid a transplant, but yeah just improving quality of life, not being like just living to see a bunch of numbers on lab reports going up or down and how that affects my day.”
“I hope that, at least for me, it will radically decrease the amount of medication that is needed to help functionality. I hope that it introduces a sense of normality for patients, whilst also greatly reducing the risk of transplant or dialysis.”
Experience With Drug Under Review
A brief summary of RNAi therapies in primary hyperoxaluria was provided. Overall, about 25 (58.1%) survey respondents were familiar with RNAi therapies, and 26 (60.5%) knew of Oxlumo (Lumasiran) prior to completing the survey. A higher proportion of Americans were familiar with RNAi therapies, like Oxlumo (Lumasiran), than Canadians. 100% of American respondents reported prior knowledge of these medications, while 75% of Canadian respondents reported previous familiarity.
Survey participants were asked whether they would expect the life of a patient with primary hyperoxaluria type 1 (PH1) to be improved by Oxlumo (Lumasiran). 100% of respondents stated that they would expect this therapy to improve the lives of patients.
16 of the survey respondents (3 Canadian, 7 American, and 6 non-North American), and two focus group participants (both Canadian) reported direct experience with Oxlumo (Lumasiran). The focus group participants had accessed Oxlumo (Lumasiran) through compassionate access from the company. The two focus group participants whose children have experience with Oxlumo (Lumasiran) were asked how well this drug manages their child’s primary hyperoxaluria type 1. Both participants reported that Oxlumo (Lumasiran) was “Excellent” at managing their primary hyperoxaluria. Survey participants who reported experience with Oxlumo (Lumasiran) were asked on a scale of 1-10 how effective Oxlumo (Lumasiran) was in managing primary hyperoxaluria type 1. Survey participants rated the efficacy of this drug as >9 on average.
When asked to share their experience with Oxlumo (Lumasiran), participants reported dramatic improvements in primary hyperoxaluria type 1 management, and quality of life. Participants particularly noted large improvements in growth and energy, need for organ transplantation, risk of kidney failure and oxalosis, and the anxiety surrounding primary hyperoxaluria type 1 (PH1).
“Worked wonders. I have two children that get it. My oldest got diagnosed with PH1 after a kidney transplant. His plasma oxalate levels started in the 50’s- now it’s in the high teens. It’s kept him from needing another transplant so quickly and staying off dialysis. My youngest was diagnosed after his brother was. His oxalates started at 6 and have been undetected since starting Oxlumo.”
“[Oxlumo] brought her oxalate expression down, it was four times the normal and is now normalized There’s so much hope now with just having access to this drug and at least it's working for my daughter so and then I'm hoping, you know with my son catching it early enough, you know, he may never need a transplant ever in this life. So I yeah I feel you know we're the kids are definitely doing well, but I couldn't imagine not having access to a drug, to help them. I’d just to add to that, like my children just being newly diagnosed was one of the hardest times in my life, it was unbelievable. You know I found so much hope, from the hope that there was a drug available to help them that could possibly help them. I couldn't imagine how I would have felt if I was just told okay just increase the water and take and take potassium citrate and try basics like right now, I probably still would have my head in the hole, I think this drug is working, it brings so much hope you know, imagine like a kidney transplant, you know for a child, or even a teenager even being in your 20s 30s. It’s a life changing event and it is terrifying, and you know it just makes sense that this drug should be available to us.”
“So, she is on Lumasiran right now and it has made a huge difference in her growth trajectory, and we think it's related mostly to that. She's like 75th for weight now 50 percentile for height so huge change and so how that affected our life. I don't know how to emphasize this, but it has made a huge difference in our life. Like now my husband can look at going back to work. She can look at going into daycare and we don't worry with every like sniffle and cold that her kidney function is going to drop or something's going to change. It’s just relieved a huge amount of stress and burden from us. I don't know, I mean she's a lot happier that she doesn't go, so she is so much happier that she doesn't go to the hospital as much and she's so much happier to have like kind of like more of a normal life, like a two-year-old would have that she's in daycare.”
“There is a lack of clinical expertise within Canada that creates additional barriers to diagnosis and treatment. Just getting to a diagnosis has been a painful and exhausting marathon. Then the combination of high level of uncertainty with high stakes of kidney failure and stones result in exceptional stress on a daily basis. Prior to lumasiran, all that existed was fear, now there is hope.”
“It’s a GREAT treatment. Doing wonders for both my children that are in different stages of PH1.”
“This is a game changer for us as parents. He gives us some hope for his life and has helped our child avoid kidney stones and has protected kidney function.”
“It has reduced my urine oxalate and provided me with hope for the future.”
Participants were asked to discuss their expectations for Oxlumo (Lumasiran), and what they believed or hoped it would do for them or those they care for. Based on the overwhelmingly positive results with Oxlumo (Lumasiran), individuals voiced their belief that it would reduce kidney stones, the need for organ transplantation, kidney failure, and oxalosis. Moreover, patients and families shared that this therapy gives them new hope for the future, both for themselves and for other families living with primary hyperoxaluria.
“My hope with this treatment is it's going to prevent one if not both of my children from needing a transplant one day, that's the end game. I want to keep their kidney function, where it is I don't want there to be damage or further damage from stones.”
“This drug has been successful in lowering the urinary oxalate levels in patients with PH1. This job can hopefully protect kidneys and delay requirements for a kidney transplant and effectively obviate the need for liver transplantation. This drug will help children avoid painful kidney stones and may help children avoid other medications and hyperhydration and enable them to live a more normal life.”
“I am a double kidney transplant patient. The failure of my original kidneys was misdiagnosed I only found out I had PH1 when my new kidneys function deteriorated we hope Lumasiran will halt the deterioration”
“There's not really a lot of other options out there, so just having anything new in and of itself is exciting and gets people hope and that could kind of change somebody's trajectory.”
“I feel I’ve been relatively fortunate, having been diagnosed early in life. Being asymptomatic may make it appear that the disease hasn’t affected me, but it is such a part of my daily life that I cannot necessarily articulate how much the worry pervades my existence. Worry about disease progression, being conscious of what I eat, drink, where I go. Planning for the future knowing I will need to continue my current regiment - I knew I probably couldn’t be a surgeon due to my need for water and bathrooms. I am terrified of the dialysis unit knowing that is likely to be me someday. Now I am so hopeful it hurts, that this drug could provide a more hopeful future.”
“I hope that, at least for me, it will radically decrease the amount of medication that is needed to help functionality. I hope that it introduces a sense of normality for patients, whilst also greatly reducing the risk of transplant or dialysis.”
“Unfortunately, it’s too late for my little boy but if he had been given it from diagnosis then it probably would have stopped him requiring a liver transplant and he would have had his kidney transplant by now and he’d be living some kind of life. Instead of constantly being unwell, having fractures, and living on dialysis 6 days a week.”
“The RNAi regime is so incomparably simple. This advance in a real treatment has meant more to me and my family than I can express. I hope for access for all people with PH.”
“I feel like because I will start on this therapy, I'll avoid kidney failure, and live at least an extra 10 years for my husband and daughter... and those donated organs that may have had to go to me (when my kidneys failed) can go to someone else.”
Companion Diagnostic Test
Access to targeted therapies requires genetic testing for primary hyperoxaluria, to ensure the appropriate patients have access to appropriate therapies.
Anything Else?
These patient and caregiver responses are typical of the primary hyperoxaluria community, where diagnosis is delayed, symptoms are debilitating, treatment options are insufficient, and the future is uncertain with the possibility of dialysis and a liver-kidney transplant looming as kidney function declines. Their voices express the profound effect of this disease on quality of life. In summary, living with primary hyperoxaluria presents innumerable physical, emotional and financial challenges to patients, caregivers, and their families.
These challenges are compounded by the lack of knowledge among clinicians, and little hope is offered. Families desperately seek new treatment options to reduce the frequency of kidney stones, the need for organ transplantation, kidney failure, and oxalosis. The option of RNAi therapies like Oxlumo (Lumasiran) for primary hyperoxaluria type 1 (PH1) represents hope for a brighter future to the families who participated in our survey and focus group. These individuals were given the opportunity to provide any additional recommendations or comments to the Canadian Agency for Drugs and Technologies in Health.
“Lumasiran has changed my daughter’s life, my life and our whole family’s life. Without funded access to this medication, we would be living our life 3/10 whereas now we are 8/10! Lumasiran needs to be supported by a federal funding program to allow all affected individuals, patients and caregivers, the opportunity to live their full life.”
“Every rare disease has its challenges. But any rare disease has a risk of lack of access to drug- my greatest concern is the risk of not having access to valuable medication such as Lumasiran which could not just improve but also protect or ‘save’ my child’s life. Due to the disease being rare, the medication could be cost prohibitive. This is a great fear.”
“Allowing access to Oxlumo and other treatments for PH1 is extremely important. Even though it’s a rare disease, those who suffer from it need access to all the advances that may be available.”
“Please help all children and adults have access to this medication.”
“There are people in countries having a hard time getting this medication who can surely use it. Hoping it becomes available and affordable to all.”
“I feel we are extremely fortunate to have a drug available which is working for my children. This disease affects children early in life and it would be heartbreaking if they were unable to access a lifesaving drug. This drug can prevent a transplant from ever being needed. It brings so much hope for their future.”
“A plea to make this drug accessible. We are a small population, and it can be easy to feel forgotten, however understandable it may be. I will need to pay for this, whether coverage happens or not. I’m fortunate I’ll be able to. I cannot imagine finally being on the cusp of a major hope (RNAi treatment), and not being able to afford it.”
“It is difficult to have a rare disease that few people are informed on. It’s more difficult to get treated by knowledgeable individuals who advocate and follow through on proper care and testing for each individual patient. When there are added delays and challenges in getting critical medication to a PH patient, there is the added risk of too little too late. We tried for years to get our oldest child into a clinical trial or access to RNAi treatment, but we just couldn't get it in time due to "red tape" and our child ended up declining to where they suffered for years of dialysis and recently a transplant. Had we gotten this medication when it was first available, we could have avoided all of the struggles. Yes, it is expensive, but so is dialysis, transplant, lifetime transplant related health care. This medication works, it's available, patients need it. fast. There should be no more delays and no more suffering or even death just because someone deems it too expensive to provide it to someone who needs it.”
Finally, participants were asked how important they thought it was for individuals diagnosed with primary hyperoxaluria type 1 to have access to Oxlumo (Lumasiran). An overwhelming majority (97.6%) of respondents rated it “Very important” for individuals to have access to this therapy. As illustrated by one participant's response, the importance of this drug to patients cannot be overstated.
“[These therapies] give patients hope and options. When a patient has the opportunity to get this medication before their health declines, they can potentially eliminate the need for dialysis and transplant and considerably reduce kidney stone formation. If a patient is already in kidney failure, this medication treatment can reduce the oxalate burden in the body to allow for more successful transplant and may only need kidney transplant and not liver and kidney transplant. The longer a patient has to wait for this medication, the sicker they might become and more expensive and invasive the treatment will be.”
This sentiment can be summarized by one focus group particpant’s closing statement:
“I couldn't imagine not having access to this drug.”
Conflict of Interest Declaration — The Oxalosis & Hyperoxaluria Foundation and Canadian Organization for Rare Disorders
To maintain the objectivity and credibility of the CADTH reimbursement review process, all participants in the drug review processes must disclose any real, potential, or perceived conflicts of interest. This Patient Group Conflict of Interest Declaration is required for participation. Declarations made do not negate or preclude the use of the patient group input. CADTH may contact your group with further questions, as needed.
Did you receive help from outside your patient group to complete this submission? If yes, please detail the help and who provided it.
This submission was completed by the staff and volunteers of the Oxalosis & Hyperoxaluria Foundation (OHF) and Canadian Organization for Rare Disorders (CORD). Outside input for this submission came from the patients and caregivers who participated in interviews and those who responded to the online survey.
Did you receive help from outside your patient group to collect or analyze data used in this submission? If yes, please detail the help and who provided it.
Data collection and analysis was completed by the staff of the Oxalosis & Hyperoxaluria Foundation (OHF) and Canadian Organization for Rare Disorders (CORD).
List any companies or organizations that have provided your group with financial payment over the past 2 years AND who may have direct or indirect interest in the drug under review.
The Oxalosis & Hyperoxaluria Foundation (OHF) is committed to being a global leader in patient advocacy. Our priority is to amplify the patient voice and to share the patient experience. The OHF receives funding from a variety of sources with the majority coming from donations from individuals in the US and outside the US. We use these funds to support hyperoxaluria awareness, education, patient support, advocacy and research grant programs to improve patient outcomes.
The Oxalosis & Hyperoxaluria Foundation (OHF) receives some program funding in the form of unrestricted grants from several biotech companies. Grant agreements are established in support of activities initiated by the OHF and prohibit the funder from having any input or influence in program objectives or deliverables.
Table 2: Financial Disclosures for the OHF
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
Alnylam Pharmaceuticals | — | — | — | X |
Table 3: Financial Disclosures for CORD
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
Alnylam Pharmaceuticals | — | — | X | — |
Clinician Input
No clinician group input was received for this review.
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up-to-date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
Redactions: Confidential information in this document may be redacted at the request of the sponsor in accordance with the CADTH Drug Reimbursement Review Confidentiality Guidelines
Stakeholder Input: The views expressed in each submission are those of the submitting organization or individual; not necessarily the views of CADTH or of other organizations. As such, they are independent of CADTH and do not necessarily represent or reflect the view of CADTH. No endorsement by CADTH is intended or should be inferred. By filing with CADTH, the submitting organization or individual agrees to the full disclosure of the information. CADTH does not edit the content of the submissions.
CADTH does use reasonable care to prevent disclosure of personal information in posted material; however, it is ultimately the submitter’s responsibility to ensure no identifying personal information or personal health information is included in the submission. The name of the submitting organization or individual and all conflict of interest information are included in the submission; however, the name of the author, including the name of an individual patient or caregiver submitting the patient input, are not posted.
Accessibility: CADTH is committed to treating people with disabilities in a way that respects their dignity and independence, supports them in accessing material in a timely manner, and provides a robust feedback process to support continuous improvement. All materials prepared by CADTH are available in an accessible format. Where materials provided to CADTH by a submitting organization or individual are not available in an accessible format, CADTH will provide a summary document upon request. More details on CADTH’s accessibility policies can be found here.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.