CADTH Reimbursement Review
Avacopan (Tavneos)
Sponsor: Otsuka Canada Pharmaceutical Inc.
Therapeutic area: Antineutrophil cytoplasmic autoantibody–associated vasculitis
This multi-part report includes:
Clinical Review
Pharmacoeconomic Review
Stakeholder Input
Clinical Review
Abbreviations
AE
adverse event
ALT
alanine aminotransferase
ANCA
antineutrophil cytoplasmic autoantibody
ANCA-AV
antineutrophil cytoplasmic autoantibody–associated vasculitis
AST
aspartate aminotransferase
BVAS
Birmingham Vasculitis Activity Score
CI
confidence interval
eGFR
estimated glomerular filtration rate
ESKD
end-stage kidney disease
EQ-5D-5L
5-Level EQ-5D
GPA
granulomatosis with polyangiitis
GTI
Glucocorticoid Toxicity Index
GTI-AIS
Glucocorticoid Toxicity Index Aggregate Improvement Score
GTI-CWS
Glucocorticoid Toxicity Index Cumulative Worsening Score
HRQoL
health-related quality of life
ITT
intention to treat
KM
Kaplan-Meier
LSM
least squares mean
MID
minimal important difference
MPA
microscopic polyangiitis
PP
per protocol
SAE
serious adverse event
SD
standard deviation
SF-36v2
Short Form (36) Health Survey version 2
TEAE
treatment-emergent adverse event
UACR
urinary albumin–creatinine ratio
VAS
visual analogue scale
VDI
Vasculitis Damage Index
Executive Summary
An overview of the submission details for the drug under review is provided in Table 1.
Item | Description |
|---|---|
Drug product | Avacopan (Tavneos), 30 mg (3 oral capsules of 10 mg each), twice daily |
Indication | For the adjunctive treatment of adult patients with severe ANCA-AV (GPA and MPA) in combination with standard background therapy including glucocorticoids. Avacopan does not eliminate glucocorticoid use. |
Reimbursement request | As per indication |
Health Canada approval status | NOC |
Health Canada review pathway | Standard |
NOC date | April 14, 2022 |
Sponsor | Otsuka Canada Pharmaceutical Inc. |
ANCA-AV = antineutrophil cytoplasmic autoantibody–associated vasculitis; GPA = granulomatosis with polyangiitis; MPA = microscopic polyangiitis; NOC = Notice of Compliance.
Sources: Sponsor’s submission package for review of avacopan;1 Tavneos product monograph.2
Introduction
Antineutrophil cytoplasmic autoantibody (ANCA)–associated vasculitis (ANCA-AV) is a group of inflammatory disorders affecting mostly small- to medium-sized blood vessels that include granulomatosis with polyangiitis (GPA), microscopic polyangiitis (MPA), and other vasculitides.3 Patients often initially present with nonspecific symptoms that progress to involve the ears, nose, and throat; the respiratory system; the kidneys; the skin; or the nervous system.4 ANCA-AV can vary from non-life-threatening to severe disease —major organs are affected in the latter — and from limited disease (i.e., affecting a single organ) to systemic disease.5 As defined by the 2012 Chapel Hill Consensus Conference, GPA causes necrotizing granulomatous inflammation, often involving the lungs and kidneys, and more commonly leads to ear, nose, and throat manifestations than MPA does.3,6,7 MPA also causes necrotizing inflammation, usually without immune deposits, often affecting the kidneys and lungs as well.6,7 Limited information exists about the incidence and prevalence of GPA and MPA in Canada. According to the clinical expert consulted by CADTH, the total incidence of GPA and MPA in Canada is estimated to be 10 to 50 cases per million people per year and their prevalence is estimated to be between 75 and 300 cases per million people, or approximately 1,700 to 2,500 total patients living in Canada. Patients with ANCA-AV are at risk of increased morbidity and mortality, largely due to the disease causing irreversible inflammatory organ damage and the consequences of long-term and often high-dose immunosuppressant drugs and glucocorticoids.5 It is expected that at least 80% of untreated patients will die within 1 year of diagnosis. Even with treatment, patients are at increased risk of developing malignancies, serious infection, and end-stage kidney disease (ESKD), largely due to progressive disease and/or as a consequence of treatment.5,8
GPA and MPA have been treated in the same manner, which consists of 2 main components: induction of remission and maintenance of remission to prevent relapse.5 According to the 2020 CanVasc consensus recommendations for the management of ANCA-AV, IV methylprednisolone pulses are recommended for patients with life-threatening ANCA-AV, followed by oral prednisone for those with severe disease.9 Patients with life-threatening disease are given cyclophosphamide or rituximab for a minimum of 3 to 6 months, with glucocorticoids, to induce remission.7,9 Cyclophosphamide and rituximab have shown similar efficacy for inducing remission;10-13 however, cyclophosphamide has been associated with fertility issues, alopecia, and malignancies, and rituximab may be preferred for specific patients (e.g., children, young adults concerned with infertility, and older adults).5,14 Once patients begin induction therapy with cyclophosphamide or rituximab, tapering of glucocorticoids should begin within 2 weeks to reduce exposure to glucocorticoids and their associated risks.5 Once remission is achieved, patients should be transitioned to maintenance therapy, preferably rituximab (or azathioprine or methotrexate when rituximab cannot be used).7,9 It has been emphasized in the literature and by the clinical expert consulted by CADTH that maintenance treatment should last for at least 2 years and that continued treatment should be considered for patients in high-risk groups (e.g., those with anti-PR3 ANCA, prior relapse, pulmonary involvement, or upper respiratory tract involvement).5,9,15-18 The CanVasc recommendations state that the optimal duration for low-dose glucocorticoid use once remission is achieved is currently unknown.9
Avacopan (Tavneos) is a C5a receptor antagonist indicated for the adjunctive treatment of adult patients with severe active ANCA-AV (GPA and MPA) in combination with standard background therapy, including glucocorticoids.2 Avacopan does not eliminate glucocorticoid use.2 The recommended dosage is 30 mg (3 oral capsules of 10 mg each) taken twice daily.2 The Health Canada product monograph did not specify the duration of treatment with avacopan.
The objective of this report is to perform a systematic review of the beneficial and harmful effects of avacopan 30 mg (3 oral capsules of 10 mg each) twice daily for the adjunctive treatment of adult patients with severe active ANCA-AV (GPA and MPA) in combination with standard background therapy, including glucocorticoids.
Stakeholder Perspectives
The information in this section is a summary of the input provided by 1 patient group that responded to CADTH’s call for patient input, 1 clinical expert consulted by CADTH, 1 clinical group that responded to CADTH’s call for clinician input, and the Canadian public drug programs.
Patient Input
CADTH received 1 patient group submission from Vasculitis Foundation Canada, an organization that aims to increase disease awareness and research support for all forms of vasculitis. Vasculitis Foundation Canada invited its mailing list subscribers to complete an online survey and received input from 46 patients (35 with GPA and 11 with MPA) living in Canada and the US who have experience using prednisone or avacopan. The patient group reported that GPA and MPA impact patients’ daily lives and that patients experience a host of physical manifestations that lead to chronic fatigue, mood swings, poor sleep, chronic infections, and stress due to fear of relapse. Patients treated with prednisone reported side effects that significantly affect quality of life, including body disfiguration, steroid-induced diabetes or hypertension, infections requiring medical care, anxiety, and depression. Vasculitis Foundation Canada reported that patients with GPA or MPA indicated a need for treatment that improves symptoms and quality of life that would also result in a reduction or elimination of the use of prednisone.
Clinician Input
Input From 1 Clinical Expert Consulted by CADTH
The clinical expert consulted by CADTH stated that patients need treatments that result in sustained remission, with limited organ damage (or better recovery from damage); limit the risk of severe infections; require less time on treatment (treatment shorter than 24 months has been associated with unacceptably high rates of relapse to date); and are safe for use in special populations (i.e., pediatric, pregnant, and older adult populations). The expert added that the disease and current ANCA-AV treatments have significant impact on patients’ health-related quality of life (HRQoL) and ability to work.
According to the clinical expert, avacopan would be used as a first-line treatment for adult patients with severe GPA or MPA in line with the patient population for the ADVOCATE trial. Although patients with the most severe forms of disease were excluded from the trial, the expert suggested that these patients may also be candidates for the drug after the disease is controlled with high-dose glucocorticoids. In practice, the expert stated that avacopan would be administered to induce remission alongside IV or oral cyclophosphamide or IV rituximab with glucocorticoids. Once remission is achieved, the clinical expert noted that patients should receive appropriate maintenance therapy, such as rituximab at month 6 and every 6 months thereafter for at least 24 months. There is currently a lack of clinical trial evidence for optimal patient management after 12 months of avacopan.
According to the expert, all adult patients with severe GPA or MPA could be treated with avacopan and it is not clear from the available evidence if any subpopulations would respond better to the drug than other patients.
The clinical expert noted that survival is the most important outcome. Other response measures include improvement of major organ disease (e.g., renal recovery, reduced use of mechanical ventilation), achievement of remission (typically assessed at month 3, then month 6), and sustained remission (at months 12, 18, and 24). The expert stated that it is also important to evaluate and limit the side effects caused by treatments. Although there are instruments to measure disease- and treatment-related changes in studies, the expert indicated that these instruments are not used in routine clinical practice.
The clinical expert stated that avacopan should be administered for 12 months, as was done in the ADVOCATE trial, and suggested that although the drug could be used for longer, there are limited data available for stopping the drug before 1 year or using it beyond that. According to the expert, discontinuing treatment should be considered if there are intolerable side effects, continual disease progression with clinical decline, or repeated relapses. In the expert’s opinion, another reason to discontinue avacopan is if it does not allow for reduced use of glucocorticoids.
Since GPA and MPA are rare diseases and require close monitoring, the clinical expert indicated that patients should be referred to a specialist with expertise in the disease area. In the clinical expert’s opinion, a rheumatologist, nephrologist, general internal medicine specialist, respirologist, or intensive care unit doctor should be able to prescribe avacopan in a hospital setting, and it was noted that restricting the prescription to only rheumatologists or nephrologists with expertise in vasculitis would likely delay treatment initiation by many weeks. However, in community clinics, the expert believed it would be reasonable to restrict access to rheumatologists or nephologists with experience treating vasculitis.
The clinical expert emphasized that treatment with avacopan should be associated with a mandate to stop or significantly decrease glucocorticoids within the first weeks of initiating avacopan; otherwise, the continued use of avacopan should be clinically justified. Given the lack of long-term data, the expert expressed uncertainty about patient management after 12 months of avacopan and about the long-term outcomes after stopping avacopan. Lastly, the clinical expert suggested that alongside the implementation of avacopan in Canada, it would be useful to set up a registry to track the drug’s use and patterns of use and to monitor safety and efficacy.
Clinician Group Input
CanVasc, a Canadian research network for vasculitis, provided input for this review. The clinician group expressed similar views to those of the clinical expert consulted by CADTH.
Drug Program Input
The drug programs described uncertainty around the following: how the ADVOCATE trial showed that avacopan could reduce the use of glucocorticoids, the possibility of aligning initiation and renewal criteria between avacopan and rituximab, and the possibility that avacopan could be used for other autoimmune diseases. The drug programs also asked questions about the patient population that could receive avacopan, the drug’s place in therapy, re-treatment after relapse, assessment of continued need for treatment, definition of refractory disease, duration of therapy, and definition of sustained remission. They also asked whether there are concerns with combining therapies for ANCA-AV.
The clinical expert consulted by CADTH agreed that many patients in the ADVOCATE trial received nonstudy glucocorticoids during the 52-week treatment period, which complicates interpretation of the results and of whether treatment with avacopan can reduce the use of glucocorticoids. According to the clinical expert, patients with active ANCA-AV, whether newly diagnosed or with relapsing disease, could be treated with avacopan as was done in the ADVOCATE trial. Regarding the place in therapy, the clinical expert stated that avacopan would be used as a first-line treatment and that standard of care treatment with immunosuppressants (i.e., IV rituximab or IV or oral cyclophosphamide) would remain the same, with the addition of glucocorticoids and/or avacopan. Based on clinical experience, the expert believed that most physicians and treating teams would be comfortable initially treating patients with standard of care immunosuppressants and glucocorticoids but that once a patient was referred to a specialist for ANCA-AV, avacopan could replace glucocorticoids. The clinical expert indicated that relapse is not common with rituximab maintenance and that if a patient relapsed, they would immediately be started on intensive treatment to reinduce remission. In most situations, the expert emphasized that patients should continue treatment for more than 1 year because — based on clinical experience — any less generally does not result in long-term sustained remission. After 1 year of avacopan treatment, the clinical expert expects that most patients would continue some form of maintenance therapy, such as rituximab or continuing with avacopan, but that it would be unlikely for a patient to receive no additional treatment after 1 year. The clinical expert indicated that it would be reasonable for a patient to continue receiving avacopan after their first relapse but that avacopan should be stopped after the second relapse and the patient should instead be treated with glucocorticoids. The expert stated that a patient may have refractory disease if no treatments work to induce remission and the disease continues to progress or that a patient may have clinical manifestations if most symptoms improve but remission is not achieved and there is still lingering disease activity despite having exhausted all standard of care treatments. The clinical expert expects avacopan to be used for 12 months, similar to the ADVOCATE trial, with the possibility of continuing the drug for longer. However, there is limited evidence for a treatment duration less than 12 months or more than 12 months, and there is uncertainty over how to manage patients after stopping avacopan. It is unclear how avacopan treatment compares to rituximab maintenance therapy, which is currently the standard. The expert typically assesses remission at 6 months and sustained remission at 12 months and every 6 months thereafter, then if the patient remains in remission at those subsequent 6 month time points, assesses if it is safe for the patient to stop maintenance therapy. The clinical expert had no concerns about interactions between the drug combinations typically used to treat ANCA-AV but noted a lack of data on the efficacy and safety of combining rituximab maintenance therapy with avacopan.
Clinical Evidence
Pivotal Studies and Protocol-Selected Studies
Description of Studies
The ADVOCATE trial (N = 331) was a phase III, double-blind, randomized controlled trial designed to investigate the efficacy and safety of avacopan in patients with ANCA-AV with the aim to determine if avacopan could induce and sustain remission without chronic glucocorticoid use at levels currently used in standard of care regimens. The trial compared avacopan (30 mg twice daily, oral) to prednisone (60 mg/day tapered over 20 weeks, oral), with respective matching placebos, in addition to standard of care therapy (IV or oral cyclophosphamide followed by azathioprine, or IV rituximab without maintenance treatment), over 52 weeks with an 8-week follow-up. Patients were permitted to receive nonprotocol-specified, low-dosage oral glucocorticoids (10 mg/day or less) for the treatment of adrenal insufficiency or allergic reaction. Eligible patients included adults who had a clinical diagnosis of GPA or MPA, were ANCA positive for either anti-PR3 or antimyeloperoxidase (anti-MPO) antibodies, and had active disease at screening. Patients with limited disease or with the most severe disease (patients with alveolar hemorrhage requiring mechanical ventilation or with an estimated glomerular filtration rate [eGFR] less than 15 mL/min/1.73 m2 at baseline) were not eligible. The primary outcomes were the proportions of patients who achieved disease remission at week 26 and sustained disease remission at week 52. Key secondary outcomes included glucocorticoid toxicity (Glucocorticoid Toxicity Index [GTI]), HRQoL (Short Form [36] Health Survey version 2 [SF-36v2], 5-Level EQ-5D [EQ-5D-5L], and EQ visual analogue scale [VAS]), kidney function (eGFR and urinary albumin–creatinine ratio [UACR]), systemic damage (Vasculitis Damage Index [VDI]), and the proportion of patients experiencing disease relapse. Harms and notable harms identified in the CADTH systematic review protocol were also assessed.
At baseline, the mean age of patients was 60.9 years (standard deviation [SD] = 14.5 years), more than half were male (56.5%), and most were white (84.3%). Most patients (69.4%) were newly diagnosed with ANCA-AV, and 30.6% had relapsing disease. More than half (54.8%) of patients had GPA, and 45.2% had MPA (45.2%). Less than half (43.0%) were positive for anti-PR3 antibodies, and 57.0% were positive for anti-MPO antibodies.
Efficacy Results
Efficacy results are summarized in Table 2 for the ADVOCATE trial. Survival was not assessed as an efficacy outcome in the trial but was captured as deaths in the assessment of harm outcomes. Hospitalizations were not assessed in the trial. Symptoms (e.g., fatigue) were not assessed as an efficacy outcome, but some symptoms may have been captured as harm outcomes. Only the primary outcomes of disease remission at week 26 and sustained disease remission at week 52 were controlled for multiple testing.
Disease Remission (Induction and Sustained Remission)
Based on the intention-to-treat (ITT) analyses, 72.3% (95% confidence interval [CI], 64.8% to 78.9%) of patients randomized to the avacopan group and 70.1% (95% CI, 62.5% to 77.0%) of patients randomized to the prednisone group achieved remission at week 26. The estimate of common difference in remission rates between groups was 3.4% (95% CI, –6.0% to 12.8%; noninferiority P < 0.0001; superiority P = 0.2387). Findings for the per-protocol (PP) population were similar.
At week 52, 65.7% (95% CI, 57.9% to 72.8%) of patients randomized to the avacopan group and 54.9% (95% CI, 46.9% to 62.6%) of patients randomized to the prednisone group achieved sustained remission. The estimate of common difference in sustained remission rates between groups was 12.5% (95% CI, 2.6% to 22.3%; noninferiority P < 0.0001; superiority P = 0.0066). Findings for the PP population were similar.
Renal Function (e.g., eGFR, Progression to ESKD)
For patients with renal disease at baseline (based on the Birmingham Vasculitis Activity Score [BVAS] renal component), the least squares mean (LSM) difference in change from baseline between treatment groups for eGFR was 2.9 mL/min/1.73 m2 (95% CI, 0.1 mL/min/1.73 m2 to 5.8 mL/min/1.73 m2) at week 26, 3.2 mL/min/1.73 m2 (95% CI, 0.3 mL/min/1.73 m2 to 6.1 mL/min/1.73 m2) at week 52, and ||| ||||||||||| || |||| || |||| || || ||||||||||| at week 60. Seven patients required dialysis during the trial: 3 patients (1.8%) in the avacopan group and 4 patients (2.4%) in the prednisone group.
For patients with renal disease (based on the BVAS renal component) and albuminuria (defined as a UACR of at least 10 mg/g creatinine) at baseline, the LSM difference in change from baseline between groups for UACR was 1.3 mg/g (95% CI, 1.0 mg/g to 1.6 mg/g) at week 26, 1.1 mg/g (95% CI, 0.9 mg/g to 1.5 mg/g) at week 52, and ||| |||| |||| || || || || ||||| at week 60.
Systemic Damage (Measured by VDI)
Based on the data assessed by the adjudication committee, the LSM difference in change from baseline between treatment groups for VDI score was 0.1 (95% CI, –0.1 to 0.3) at week 26, 0.0 (95% CI, –0.2 to 0.3) at week 52, and ||| |||| || |||| || |||| at week 60.
Disease Relapse (e.g., Time to Relapse or Duration of Remission, Minor Versus Major)
For patients who achieved remission at week 26 (n = 120 in the avacopan group; n = 115 in the prednisone group), 7.5% |||| || |||| || |||||| of patients in the avacopan group and 12.2% |||| || |||| || |||||| of patients in the prednisone group experienced disease relapse. The estimate of common difference in rates was –6.0% (95% CI, –14.4% to 2.4%). The hazard ratio was 0.46 (95% CI, 0.25 to 0.84) for avacopan versus prednisone. Due to the small number of patients who relapsed, the median time to relapse was not estimable and Kaplan-Meier (KM) estimates were not calculated. During the 8-week follow-up period, 3.8% of patients in the avacopan group and 4.5% of patients in the prednisone group experienced disease relapse.
Glucocorticoid Use and Related Toxicities and Safety
The LSM difference between treatment groups for the GTI Cumulative Worsening Score (GTI-CWS) was –11.0 (95% CI, –19.7 to –2.2) at week 13 and –16.8 (95% CI, –25.6 to –8.0) at week 26. The LSM difference between treatment groups for the GTI Aggregate Improvement Score (GTI-AIS) was –13.3 (95% CI, –22.2 to –4.4) at week 13 and –12.1 (95% CI, –21.1 to –3.2) at week 26.
Health-Related Quality of Life
The LSM difference in change from baseline between treatment groups for the SF-36v2 mental component summary was 1.6 (95% CI, –0.6 to 3.8) at week 26, 1.7 (95% CI, –0.5 to 3.9) at week 52, and ||| |||| || |||| || |||| at week 60. The LSM difference between treatment groups for the SF-36v2 physical component summary was 3.1 (95% CI, 1.2 to 5.0) at week 26, 2.4 (95% CI, 0.4 to 4.3) at week 52, and ||| |||| || |||| || |||| at week 60.
The LSM difference in change from baseline between treatment groups for the EQ VAS was 3.6 (95% CI, –0.1 to 7.2) at week 26, 5.9 (95% CI, 2.3 to 9.6) at week 52, and ||| |||| || |||| || |||| at week 60. The LSM difference between treatment groups for the EQ-5D-5L index score was 0.0 (95% CI, 0.0 to 0.1) at week 26, 0.1 (95% CI, 0.0 to 0.1) at week 52, and ||| |||| || || || |||| at week 60.
Harms Results
Harms results are summarized in Table 2 for the ADVOCATE trial.
Nearly all patients in the avacopan group (98.8%) and prednisone group (98.2%) experienced at least 1 treatment-emergent adverse event (TEAE). The 3 most common TEAEs in the avacopan group were nausea (23.5% avacopan versus 20.7% prednisone), peripheral edema (21.1% avacopan versus 24.4% prednisone), and headache (20.5% avacopan versus 14.0% prednisone). The 3 most common TEAEs in the prednisone group were peripheral edema, muscle spasms (22.6% prednisone versus 10.8% avacopan), and arthralgia (22.0% prednisone versus 18.7% avacopan).
Overall, 42.2% of patients in the avacopan group and 45.1% of patients in the prednisone group experienced a serious adverse event (SAE). The most common SAEs were ANCA-positive vasculitis (7.2% avacopan versus 12.2% prednisone) and pneumonia (5.4% avacopan versus 5.5% prednisone).
In total, 15.7% of patients in the avacopan group and 17.7% of patients in the prednisone group stopped treatment due to adverse events (AEs). The most common AE that led to withdrawal from treatment was ANCA-positive vasculitis (2.4% avacopan versus 4.9% prednisone); other AEs that led to withdrawal from treatment occurred at a frequency of less than 2% for either group.
Six patients died during the treatment period in the ADVOCATE trial (2 patients receiving avacopan and 4 patients receiving prednisone) and causes of death were reported by a single patient for each cause.
Notable Harms
Treatment-emergent infections were reported in 68.1% and 75.6% of patients in the avacopan and prednisone groups, respectively. Serious treatment-emergent infections were reported in 13.3% and 15.2% of patients in the avacopan and prednisone groups, respectively, of which pneumonia was the most common serious infection-related TEAE (experienced by 5.4% and 5.5% of patients in the avacopan and prednisone groups, respectively). Infections resulted in 9 patients withdrawing from the trial and 3 deaths.
Elevated alanine aminotransferase (ALT) was reported by 4% and 2% of patients in the avacopan and prednisone groups, respectively; elevated aspartate aminotransferase (AST) was reported in 2% of patients and no patients in the avacopan and prednisone groups, respectively; and elevated blood bilirubin was reported in 2% and 1% of patients in the avacopan and prednisone groups, respectively.
Acute myocardial infarction was reported by 0.6% of patients in the avacopan group and 1.2% of patients in the prednisone group; cardiac failure was reported by 1.2% of patients in the avacopan group and no patients in the prednisone group. Cardiac vasculitis was not reported in the trial.
In the avacopan and prednisone groups, respectively, nausea was reported by 23.5% and 20.7% of patients, diarrhea was reported by 15.1% and 14.6% of patients, vomiting was reported by 15.1% and 12.8% of patients, and dyspepsia was reported by 3.0% and 6.1% of patients.
Angioedema was reported by 1.2% of patients in the avacopan group and no patients in the prednisone group.
Table 2: Summary of Key Results From Pivotal Study
Outcome | Prednisone (N = 164) | Avacopan (N = 166) |
|---|---|---|
Disease remission at week 26 (ITT population) | ||
Patients who achieved remission, n (%) 95% CIa | 115 (70.1) (62.5 to 77.0) | 120 (72.3) (64.8 to 78.9) |
Difference (%) | Reference | 2.2 |
Estimate of common difference (%)b 2-sided 95% CI for common difference (%)c | Reference | 3.4 (–6.0 to 12.8) |
Noninferiority P valued,e | Reference | < 0.0001 |
Superiority P valued,e | Reference | 0.2387 |
Sustained remission at week 52 (ITT population) | ||
Patients who achieved remission, n (%) 95% CIa | 90 (54.9) (46.9 to 62.6) | 109 (65.7) (57.9 to 72.8) |
Difference (%) | Reference | 10.8 |
Estimate of common difference (%)b 2-sided 95% CI for common difference (%)c | Reference | 12.5 (2.6 to 22.3) |
Noninferiority P valued,e | Reference | < 0.0001 |
Superiority P valued,e | Reference | 0.0066 |
eGFR (ITT population) | ||
Week 52, n (%) | 125 (76.2) | 119 (71.7) |
LSM change from baseline (SEM) (mL/min/1.73 m2) | 4.1 (1.0) | 7.3 (1.1) |
LSM difference (95% CI) (mL/min/1.73 m2)f | Reference | 3.2 (0.3 to 6.1) |
P valuef,g | Reference | 0.0294 |
UACR (ITT population) | ||
Week 52, n (%) | 114 (69.5) | 109 (65.7) |
LSM change from baseline (SEM) (mg albumin/g creatinine)h | 0.2 (1.1) | 0.3 (1.1) |
LSM ratio (95% CI) (mg albumin/g creatinine)h | Reference | 1.1 (0.9 to 1.5) |
P valuef,h | Reference | 0.3991 |
VDI (ITT population) | ||
Week 52, n (%) | 151 (92.1) | 150 (90.4) |
LSM change from baseline (SEM)i | 1.2 (0.1) | 1.2 (0.1) |
LSM difference (95% CI)i | Reference | 0.0 (–0.2 to 0.3) |
P valuef,i | Reference | 0.8660 |
Disease relapse (ITT population) | ||
Patients who achieved remission at week 26, n (%)j | 115 (70.1) | 120 (72.3) |
Patients who relapsed, n (%) 95% CIa | 14 (12.2) (6.8 to 19.6) | 9 (7.5) (3.5 to 13.8) |
Difference (%) | Reference | –4.7 |
Estimate of common difference (%)b 2-sided 95% CI for difference (%)c | Reference | –6.0 (–14.4 to 2.4) |
Superiority P valuef | Reference | 0.0810 |
GTI-CWS (ITT population) | ||
Week 13, n (%) | 161 (98.1) | 160 (96.4) |
LSM (SEM)k | 36.6 (3.4) | 25.7 (3.4) |
LSM difference (95% CI)k | Reference | –11.0 (–19.7 to –2.2) |
P valuef,k | Reference | 0.0140 |
Week 26, n (%) | 153 (93.3) | 154 (92.7) |
LSM (SEM)k | 56.6 (3.5) | 39.7 (3.4) |
LSM difference (95% CI)k | Reference | –16.8 (–25.6 to –8.0) |
P valuef,k | Reference | 0.0002 |
GTI-AIS (ITT population) | ||
Week 13, n (%) | 161 (98.2) | 160 (96.4) |
LSM (SEM)k | 23.2 (3.5) | 9.9 (3.5) |
LSM difference (95% CI)k | Reference | –13.3 (–22.2 to –4.4) |
P valuef,k | Reference | 0.0034 |
Week 26, n (%) | 153 (93.3) | 154 (92.3) |
LSM (SEM)k | 23.4 (3.5) | 11.2 (3.5) |
LSM difference (95% CI)k | Reference | –12.1 (–21.1 to –3.2) |
P valuef,k | Reference | 0.0082 |
SF-36v2 MCS (ITT population) | ||
Week 52, n (%) | 144 (87.8) | 148 (89.2) |
LSM change from baseline (SEM)l | 4.7 (0.9) | 6.4 (0.8) |
LSM difference (95% CI)l | Reference | 1.7 (–0.5 to 3.9) |
P valuef,l | Reference | 0.1333 |
SF-36v2 PCS (ITT population) | ||
Week 52, n (%) | 144 (87.8) | 147 (88.6) |
LSM change from baseline (SEM)l | 2.6 (0.8) | 5.0 (0.7) |
LSM difference (95% CI)l | Reference | 2.4 (0.4 to 4.3) |
P valuef,l | Reference | 0.0183 |
EQ VAS (ITT population) | ||
Week 52, n (%) | 146 (89.0) | 149 (89.8) |
LSM change from baseline (SEM)l | 7.1 (1.4) | 13.0 (1.4) |
LSM difference (95% CI)l | Reference | 5.9 (2.3 to 9.6) |
P valuef,l | Reference | 0.0015 |
EQ-5D-5L index score (ITT population) | ||
Week 52, n (%) | 145 (88.4) | 149 (89.8) |
LSM change from baseline (SEM)l | 0.0 (0.0) | 0.1 (0.0) |
LSM difference (95% CI)l | Reference | 0.1 (0.0 to 0.1) |
P valuef,l | Reference | 0.0088 |
Harms, n (%) (safety population) | ||
TEAEs | 161 (98.2) | 164 (98.8) |
SAEs | 74 (45.1) | 70 (42.2) |
WDAEs, from study treatment | 29 (17.7) | 26 (15.7) |
Deaths | 4 (2.4) | 2 (1.2) |
Notable harms, n (%) (safety population) | ||
Serious infection | ||
Any treatment-emergent infection | 124 (75.6) | 113 (68.1) |
Any serious treatment-emergent infection | 25 (15.2) | 22 (13.3) |
Any treatment-emergent infection leading to study withdrawal | 5 (3.0) | 4 (2.4) |
Any treatment-emergent infection leading to death | 2 (1.2) | 1 (0.6) |
Most common serious TEAEs of infectionm | ||
Pneumonia | 9 (5.5) | 9 (5.4) |
Urinary tract infection | 2 (1.2) | 3 (1.8) |
Device-related infection | 0 | 2 (1.2) |
Influenza | 1 (0.6) | 2 (1.2) |
Herpes zoster | 2 (1.2) | 0 |
Infectious pleural effusion | 2 (1.2) | 0 |
Pneumonia bacterial | 2 (1.2) | 0 |
Respiratory syncytial virus infection | 2 (1.2) | 0 |
Hepatic injury | ||
Elevated ALT | 4 (2) | 6 (4) |
Elevated AST | 0 | 3 (2) |
Elevated blood bilirubin | 1 (1) | 3 (2) |
Cardiovascular AEs | ||
Acute myocardial infarction | 2 (1.2) | 1 (0.6) |
Cardiac failure | 0 | 2 (1.2) |
Cardiac vasculitis | NR | NR |
Gastrointestinal AEs | ||
Nausea | 34 (20.7) | 39 (23.5) |
Diarrhea | 24 (14.6) | 25 (15.1) |
Vomiting | 21 (12.8) | 25 (15.1) |
Dyspepsia | 10 (6.1) | 5 (3.0) |
Immune-related AEs | ||
Angioedema | 0 | 2 (1.2) |
AE = adverse event; ALT = alanine aminotransferase; ANCA = antineutrophil cytoplasmic autoantibody; ANCA-AV = antineutrophil cytoplasmic autoantibody–associated vasculitis; AST = aspartate aminotransferase; CI = confidence interval; eGFR = estimated glomerular filtration rate; EQ-5D-5L = 5-Level EQ-5D; GTI-AIS = Glucocorticoid Toxicity Index Aggregate Improvement Score; GTI-CWS = Glucocorticoid Toxicity Index Cumulative Worsening Score; ITT = intention to treat; LSM = least squares mean; MCS = mental component summary; MMRM = mixed model for repeated measures; MPO = myeloperoxidase; NR = not reported; PCS = physical component summary; SAE = serious adverse event; SEM = standard error of the mean; SF-36v2 = Short Form (36) Health Survey version 2; TEAE = treatment-emergent adverse event; UACR = urinary albumin–creatinine ratio; VAS = visual analogue scale; VDI = Vasculitis Damage Index; WDAE = withdrawal due to adverse event.
aClopper and Pearson exact CI.
bSummary score estimate of the common difference in remission rates using inverse-variance stratum weights.
cMiettinen-Nurminen (score) confidence limits for the common difference in remission rates.
dP value has been adjusted for multiple testing (i.e., the type I error rate has been controlled).
eResults for the per-protocol analyses were similar to those of the ITT analyses (data included in table).
fP value has not been adjusted for multiple testing (i.e., the type I error rate has not been controlled).
gAnalysis used MMRMs, with treatment group, visit, and treatment-by-visit interaction as factors and baseline as a covariate. MMRM results by visit use the treatment-by-visit interaction term.
hAnalysis used MMRMs, with treatment group, visit, and treatment-by-visit interaction as factors and baseline as a covariate. Logarithmic transformations were applied to the data before fitting the model. The 95% CI was transformed back to the original scale. MMRM results by visit use the treatment-by-visit interaction term.
iAnalysis used MMRMs, with baseline VDI, treatment group, visit, treatment-by-visit interaction, and stratification factors (newly diagnosed or relapsed ANCA-AV, anti-PR3 or anti-MPO ANCA, and IV rituximab or IV or oral cyclophosphamide standard of care treatment) as covariates. MMRM results by visit use the treatment-by-visit interaction term.
jPatients who achieved remission at week 26 is also the denominator for percentage calculations.
kAnalysis used MMRMs, with treatment group, visit, treatment-by-visit interaction, and stratification factors (newly diagnosed or relapsed ANCA-AV, anti-PR3 or anti-MPO ANCA, and IV rituximab or IV or oral cyclophosphamide standard of care treatment) as covariates. MMRM results by visit use the treatment-by-visit interaction term.
lAnalysis used MMRM models, with treatment group, visit, treatment-by-visit interaction, and randomization strata (newly diagnosed or relapsed ANCA-AV, anti-PR3 or anti-MPO ANCA, and IV rituximab or IV or oral cyclophosphamide standard of care treatment) as factors and baseline as a covariate. MMRM results by visit use the treatment-by-visit interaction term.
mFrequency of greater than 2% in either treatment group.
Source: ADVOCATE Clinical Study Report.19
Critical Appraisal
The first notable limitations with the ADVOCATE trial were that rituximab was not used as maintenance therapy in the trial and that patients induced with rituximab did not receive any maintenance therapy, neither of which aligns with the current recommendation for using rituximab as first-line standard of care maintenance therapy for ANCA-AV.9 This was due to rituximab not being approved as a maintenance therapy when the protocol for the ADVOCATE trial was being developed. Further, it is unclear if the addition of avacopan to rituximab maintenance therapy would make a meaningful difference if these treatments were to be used in clinical practice today, and there is currently a lack of clinical data on such usage. The next major limitation was the use of nonstudy immunosuppressants (19.7% of patients) and glucocorticoids (89.1% of patients) during the trial. Nonstudy medication use is problematic for quantifying the effect of avacopan treatment alone on both efficacy and harms outcomes, and data for patients who did not use glucocorticoids were unavailable. The Health Canada indication has specified avacopan as an add-on or adjunctive therapy to standard treatment rather than as a glucocorticoid-sparing drug.2,20 These deviations from current recommended standard of care maintenance therapy9 and from the protocol likely biased the results, although the magnitude and direction of the bias are unknown. Other issues included the relatively large number of discontinuations from treatment (more than 20% in each group), which resulted in missing data for nearly all outcomes, multiple outcome measures not being validated for ANCA-AV, and the absence of published minimal important differences (MIDs) for this population.
Patients with ANCA-AV who have only ever had negative antibody results, as well as those with very severe disease, were excluded from the ADVOCATE trial, and it is uncertain if the results of the trial can be generalized to patients with these characteristics. Also, the apparent difference in glucocorticoid use between treatment groups is more likely attributable to the trial design than to a change in disease activity such as avacopan effectively controlling ANCA-AV.21 The instruments used in the ADVOCATE trial are not used in clinical practice, secondary outcomes were not controlled for multiplicity, and between-group differences for multiple secondary outcomes (week 4 BVAS, UACR, VDI, patients experiencing disease relapse, SF-36v2, and EQ-5D-5L) were relatively small with wide CIs. Lastly, there was no rationale for the trial duration being 52 weeks or the follow-up being 8 weeks, and it is uncertain what long-term (beneficial or harmful) effects there are after discontinuing avacopan treatment. There was no indication from the trial about what posttreatment strategies should be used to manage patients with ANCA-AV, and there is a lack of data to inform such strategies or to indicate whether avacopan can be continued for longer than 12 months.
Conclusions
Avacopan 30 mg (3 capsules of 10 mg each) twice daily with nonprotocol-specified glucocorticoids was compared to oral prednisone tapered over 20 weeks in addition to nonprotocol-specified glucocorticoids over a 12-month treatment period. Treatments were combined with background therapy of IV or oral cyclophosphamide followed by azathioprine, or IV rituximab without maintenance therapy. Avacopan 30 mg twice daily was noninferior to oral prednisone in achieving disease remission at week 26 and was superior for sustained disease remission at week 52. Notably, 89% of patients received nonprotocol-specified glucocorticoids at some point during the ADVOCATE trial. Outcomes related to kidney function, systemic damage, disease relapse, glucocorticoid toxicity, and HRQoL provided limited support for the primary outcomes. Harms were generally balanced between groups in the trial, and no notable safety concerns were identified. The relevance of the findings to current standards of practice is unclear due to the lack of rituximab maintenance in both treatment groups, which is the current gold standard. It is unclear whether the findings would be generalizable to patients who are ANCA negative or who have very severe disease (e.g., patients who have alveolar hemorrhage requiring invasive pulmonary ventilation support or dialysis or patients who have an eGFR less than 15 mL/min/1.73 m2). Although the clinical expert suggested that avacopan could be used beyond 1 year, data to support long-term efficacy and safety beyond 12 months are not available at this time, and how patients should be managed after stopping avacopan is unknown. More evidence is needed to better understand the long-term efficacy and safety of avacopan and whether it can be used to effectively eliminate glucocorticoid use.
Introduction
Disease Background
ANCA-AV is a group of inflammatory disorders affecting mostly small- to medium-sized blood vessels that include GPA, MPA, and other vasculitides.3 With ANCA-AV, white blood cells attack and cause inflammation in the blood vessel walls, leading to loss of vessel integrity, bleeding, tissue ischemia, and necrosis.4 Patients often initially present with nonspecific symptoms such as fever, malaise, weight loss, myalgia, or arthralgia, which may last for weeks or months before there is clear evidence of organ involvement.4 As the disease progresses, there can be involvement of the ears, nose, and throat; respiratory system; kidneys; skin; and nervous system.4 ANCA-AV can vary from non-life-threatening to severe disease — major organs are affected in the latter — and from limited (i.e., affecting a single organ) to systemic disease.5 As defined by the 2012 Chapel Hill Consensus Conference, GPA causes necrotizing granulomatous inflammation, often involving the lungs and kidneys, and more commonly leads to ear, nose, and throat manifestations than MPA does.3,6,7 MPA also causes necrotizing inflammation, usually without immune deposits, often affecting the kidneys and lungs as well.6,7 There is evidence from the National Institutes of Health in the US that although less than one-fifth of patients with GPA or MPA may initially present with disease affecting the kidneys, more than 75% of patients will show evidence of glomerulonephritis within the first 2 years of disease onset.3,8,22 Less common clinical manifestations include involvement of the gastrointestinal tract, heart, and other major organs.3
Limited information exists about the incidence and prevalence of GPA and MPA in Canada. The clinical expert consulted by CADTH estimated that the total incidence of GPA and MPA in Canada is 10 to 50 cases per million people per year and that their prevalence is between 75 and 300 cases per million people, or approximately 1,700 to 2,500 total patients living in Canada. Although cases of GPA and MPA vary with geography, GPA appears to be more common in populations with European ancestry, whereas MPA is more common in populations with East Asian ancestry.3 The 2 forms of ANCA-AV affect males and females equally and tend to occur more frequently in adults (typical age of onset is 45 years to 65 years for GPA and 55 years to 75 years for MPA).23 Patients with ANCA-AV are at risk of increased morbidity and mortality, largely due to the disease causing irreversible inflammatory damage to organs and the consequences of long-term and often high-dose immunosuppressant drugs and glucocorticoids.5 It is expected that at least 80% of untreated patients will die within 1 year of diagnosis. Even with treatment, patients are at increased risk of developing malignancies, serious infections, and ESKD, largely due to progressive disease and/or as a consequence of treatment. Based on pooled data from an international cohort of 535 patients with GPA or MPA who had participated in 4 randomized controlled trials, cumulative survival at 1, 2, and 5 years was estimated to be 88%, 85%, and 78%, respectively,24 which aligns with the clinical expert’s experience of 75% survival at 5 years in Canada. The clinical expert also indicated that, in their experience, around 30% of patients relapse within 5 years and that rates are reported to be higher among those with GPA than among those with MPA.23 Key indicators of poor prognosis at presentation include renal failure, older age, and a high BVAS.23,24
According to the literature and the clinical expert, ANCA-AV may be misdiagnosed, albeit rarely, or there can be delays in getting a proper diagnosis.3 ANCA-AV is suspected in patients who display the initial symptoms discussed in the first paragraph in this section and show evidence of kidney, respiratory, or nervous system involvement.3 Patients can be tested for the presence of anti-PR3 or anti-MPO ANCA, and other assessments of the affected organ(s) can be conducted to confirm a diagnosis.3 Also according to the literature and the clinical expert, approximately 65% to 75% of GPA cases are positive for PR3 ANCA and 55% to 85% of MPA cases are positive for MPO ANCA; however, some patients (20% to 30%) are positive for the other type of ANCA and a small proportion (around 10%) are ANCA negative.23 There is increasing recognition that the type of ANCA positivity (PR3 or MPO) has greater prognostic and clinical meaning than the disease type (GPA or MPA).4 Other assessments can include biopsy of the affected organ, blood or urine tests, and imaging studies.4 Specialists such as rheumatologists, nephrologists, or pulmonologists may be involved in the diagnosis and are often involved in the management of the disease.4
Standards of Therapy
The clinical expert described the main goals of treatment to be achieving sustained remission and preventing relapse, reducing treatment-related side effects, and reducing glucocorticoid use, all of which are challenges with current treatments. Lasting organ damage, reduced HRQoL, the inability to continue working, and insufficient access to expertise and treatments for vasculitis are other issues patients face. The input submitted by patient and clinician groups and by the clinical expert noted the side effects associated with extended and/or high-dose glucocorticoid use and the need for treatments that reduce glucocorticoid use in managing ANCA-AV.
GPA and MPA are treated in the same manner, which consists of 2 main components: induction of disease remission and maintenance of remission to prevent relapse.5 Approaches to treatment and management largely depend on the severity of disease and on which organs are involved.5 According to the 2020 CanVasc consensus recommendations for the management of ANCA-AV, IV methylprednisolone pulses of 500 mg/day to 1,000 mg/day for 1 to 3 days is recommended for patients with life-threatening ANCA-AV.9 This treatment is usually followed by an oral prednisone equivalent dosage of 1 mg/kg/day (not exceeding 80 mg/day) for those with severe disease.9 Patients with life-threatening disease and organ involvement are given cyclophosphamide or rituximab for a minimum of 3 to 6 months, with glucocorticoids to induce remission.7,9 Either oral cyclophosphamide is given at a dosage of 2 mg/kg/day (to a maximum of 200 mg/day) or IV cyclophosphamide is given at a dosage of 15 mg/kg (to a maximum of 1,200 mg) every 2 weeks for the first 3 doses, then every 3 weeks for the next 3 to 6 doses.7 IV rituximab for the induction of remission is given at a dosage of 375 mg/m2 weekly for 4 doses or 1,000 mg at days 1 and 15.7 Cyclophosphamide and rituximab have shown similar efficacy for inducing remission;10-13 however, cyclophosphamide has been associated with fertility issues, alopecia, and malignancies, and rituximab may be preferred for specific patients (e.g., children, young adults concerned with infertility, and older adults).5,14 Once patients begin induction with cyclophosphamide or rituximab, glucocorticoid tapering should begin within 2 weeks to reduce the exposure to glucocorticoids and their associated risks.5 The clinical expert stated that, in their experience, the glucocorticoid dose can gradually be tapered to a final daily dose of 10 mg to 20 mg by month 3 and from 5 mg to 10 mg by month 6. The latest addendum (2022) to the CanVasc recommendations states that with avacopan, clinicians can consider tapering glucocorticoids using a faster protocol, with the aim of discontinuation by the end of week 4, and that this tapering should be done “in conjunction with best clinical judgement” and “close clinical monitoring for disease worsening.”25
Once remission is achieved, patients should be transitioned to maintenance therapy, such as rituximab infusions of 500 mg to 1,000 mg every 4 to 6 months (often 500 mg every 6 months is used) for at least 24 months (4 doses).7,9 Azathioprine (2 mg/kg/day oral to a maximum of 200 mg/day) or methotrexate (0.3 mg/kg/week oral or subcutaneous to a maximum of 25 mg/week) can be used instead of rituximab for maintenance therapy for patients who cannot receive or access the latter.7,9 Mycophenolate mofetil or leflunomide have also been listed as options for maintenance therapy if contraindications, poor tolerance, or poor response occur with other drugs.7,9 It has been stated in the literature and by the clinical expert that maintenance treatment should last for at least 2 years and that continued treatment should be considered for patients in high-risk groups (e.g., those with PR3 ANCA, prior relapse, pulmonary involvement, or upper respiratory tract involvement).5,9,15-18 The CanVasc recommendations state that the optimal duration for low-dose glucocorticoid use once remission is achieved is currently unknown.9
Patients experiencing nonsevere (non-life-threatening or non-organ-threatening) relapse should receive an increased dose of glucocorticoids, and their current immunosuppressive treatment should be optimized.9 For those with severe relapse, reinduction of remission is necessary, and patients who were previously treated with cyclophosphamide should subsequently receive rituximab.9 The 2020 CanVasc recommendations also advise that patients with refractory disease and those with contraindications or poor tolerance to medications should be referred to and managed at a referral centre for vasculitis.9 Patients should also be followed for life, with regularly scheduled full clinical assessments to track disease activity and damage related to the disease or treatments.5,9
Drug
The key characteristics of avacopan, prednisone, rituximab, and cyclophosphamide are summarized in Table 3. Rituximab and cyclophosphamide are included in the standard of care treatment for ANCA-AV and are to be used alongside avacopan.
Avacopan (Tavneos) is indicated for the adjunctive treatment of adult patients with severe active ANCA-AV (GPA and MPA) in combination with standard background therapy, including glucocorticoids.2 Avacopan does not eliminate glucocorticoid use.2 The drug is available in 10 mg capsules to be taken orally at a dosage of 30 mg twice per day.2 The specific and selective blockade of C5aR1 by avacopan reduces the proinflammatory effects of C5a, which include neutrophil activation and migration, and decreases adherence to sites of small blood vessel inflammation, and vascular endothelial cell retraction and increased permeability.2 The Health Canada product monograph did not specify the duration of treatment with avacopan.
Avacopan underwent a standard review at Health Canada and was issued a Notice of Compliance on April 14, 2022.1 The sponsor has requested reimbursement as per the approved Health Canada indication.1 Avacopan has not been previously reviewed by CADTH.
Table 3: Key Characteristics of Avacopan, Prednisone, Rituximab, and Cyclophosphamide
Characteristic | Avacopan | Prednisone | Rituximab | Cyclophosphamide |
|---|---|---|---|---|
Mechanism of action | The specific and selective blockade of C5aR1 by avacopan reduces the proinflammatory effects of C5a, which include neutrophil activation and migration, and decreases adherence to sites of small blood vessel inflammation, and vascular endothelial cell retraction and increased permeability. | Glucocorticoids are associated with the inhibition of inflammatory processes, decreased production of immune response mediators and decreased immunoglobulin binding to cell surfaces, and the inhibition of later stages of wound healing, among other process. | The monoclonal antibody binds B lymphocytes and recruits immune effector functions to mediate B-cell lysis in vitro. Possible mechanisms of cell lysis include complement-dependent cytotoxicity and antibody-dependent, cell-mediated cytotoxicity. | The active metabolite of cyclophosphamide, phosphoramide mustard, exhibits cytotoxic action by crosslinking DNA and RNA strands, as well as inhibiting DNA synthesis. Cyclophosphamide is a potent immunosuppressive drug that also causes marked and persistent inhibition of cholinesterase activity. |
Indicationa | For the adjunctive treatment of adult patients with severe active ANCA-AV (GPA and MPA) in combination with standard background therapy including glucocorticoids. Avacopan does not eliminate glucocorticoid use. | None for ANCA-AV. | In combination with glucocorticoids is indicated for the induction of remission in adult patients with severely active GPA and MPA. Consideration should be given to current treatment guidelines for vasculitis. | None for ANCA-AV. |
Route of administration | Oral | Oral | IV infusion | IV or oral |
Recommended dose | 30 mg (3 capsules of 10 mg each) taken orally twice daily with food. | Adult dosage is 5 mg/day to 60 mg/day, single or divided doses, to a maximum of 250 mg/day. The lowest possible dose of glucocorticoid should be used to control the condition, and when reduction in dose is possible, the reduction should be gradual. | 375 mg/m2 body surface area, administered as an IV infusion once weekly for 4 weeks. Initial infusion rate is 50 mg/hour; subsequently, the rate can be escalated in 50 mg/hour increments every 30 minutes to a maximum of 400 mg/hour. Subsequent infusions can be started at a rate of 100 mg/hour and increased by 100 mg/hour increments every 30 minutes to a maximum of 400 mg/hour. | Initial dosage: For adults with normal hematologic and bone marrow function, 40 mg/kg to 50 mg/kg (1.5 g/m2 to 1.8 g/m2) as 10 mg/kg/day to 20 mg/kg/day for 2 to 5 days, IV. For adults with compromised bone marrow function, 1 mg/kg/day to 5 mg/kg/day, oral, depending on patient tolerance. Maintenance dosage: For adults, 10 mg/kg to 15 mg/kg (350 mg/m2 to 550 mg/m2) every 7 to 10 days or 3 mg/kg to 5 mg/kg (110 mg/m2 to 185 mg/m2) twice weekly, IV, or 1 mg/kg/day to 5 mg/kg/day, oral. |
Serious adverse effects or safety issues |
|
|
|
|
ALT = alanine aminotransferase; ANCA-AV = antineutrophil cytoplasmic autoantibody–associated vasculitis; AST = aspartate aminotransferase; GPA = granulomatosis with polyangiitis; HBV = hepatitis B virus; INR = international normalized ratio; MPA = microscopic polyangiitis; RNA = ribonucleic acid; ULN = upper limit of normal.
aHealth Canada–approved indication.
bThe thresholds are leukopenia (white blood cell count less than 2 × 109/L), neutropenia (neutrophils less than 1 × 109/L), or lymphopenia (lymphocytes less than 0.2 × 109/L).
cA treatment regimen based on the combination with cyclophosphamide followed by azathioprine may carry an increased risk for cardiac disorders compared to a regimen based on the combination with rituximab.
Sources: Product monographs for Tavneos,2 Apo-Prednisone,26 Riximyo,27 cyclophosphamide for injection,28 and Procytox.29
Stakeholder Perspectives
Patient Group Input
This section was prepared by CADTH staff based on the input provided by 1 patient group. The full original patient input received by CADTH has been included in the stakeholder section at the end of this report.
CADTH received 1 patient group submission from Vasculitis Foundation Canada. The organization aims to increase disease awareness and research support for all forms of vasculitis through collaborations with the medical community, patients, and the general public. Vasculitis Foundation Canada invited subscribers on its mailing list to complete an online survey and received input from 46 patients (35 with GPA and 11 with MPA) living in Canada and the US who have experience using prednisone or avacopan.
The patient group reported that GPA and MPA are uncommon but life-threatening diseases that impact patients’ daily lives and quality of life. Patients commonly reported kidney damage leading to chronic kidney disease, kidney failure, dialysis, and transplant. Many patients described experiencing a host of physical manifestations (e.g., breathing difficulties, weight gain, joint or nerve pain, loss of hearing, cataracts, disfigurements) that negatively impacted their well-being and led to chronic fatigue, mood swings, poor sleep, chronic infections, and stress due to fear of relapse. The group reported that patients experienced deteriorations in their quality of life, such as experiencing “anxiety and depression for the past 13 years,” job loss or unplanned early retirement, and/or overall reduced quality of life, highlighted by 1 patient in the following words: “Vasculitis eats away at you, your family, your quality of life and relationships.” For some patients, the devastating toll of the disease takes away their desire to live.
Vasculitis Foundation Canada stated that individuals with GPA or MPA require treatment with powerful immune suppressive medications to induce and maintain disease remission. All the patients surveyed had experience with oral glucocorticoids (i.e., prednisone) and 25 patients (53%) had required IV steroids at some point during the disease course. Patients who require steroids are commonly on high dosages (e.g., 1 g/day IV for 3 days or 60 mg/day for weeks), which may be slowly tapered, ranging from 6 months to 27 years. Patients treated with prednisone reported side effects that significantly affect quality of life, including body disfiguration, steroid-induced diabetes or hypertension, infections requiring medical care, anxiety, and depression. The conflict experienced by patients who rely on prednisone is highlighted in the following quote: “Prednisone saved my life (the benefit), but destroyed my body (the side effect!).” Only 1 patient surveyed had experience with avacopan in a clinical trial. Given the choice, 30 out of 46 respondents (63.8%) stated they would opt for avacopan, despite their limited experience and knowledge of the new drug, given the side effects of prednisone.
Vasculitis Foundation Canada reported that patients with GPA or MPA indicated a need for treatment that improves symptoms and quality of life and that would reduce or eliminate the use of prednisone.
Clinician Input
Input From the Clinical Expert Consulted by CADTH
All CADTH review teams include at least 1 clinical specialist with expertise in the diagnosis and management of the condition under review, in this case, adult patients with severe ANCA-AV. Clinical experts are a critical part of the review team and are involved in all phases of the review process (e.g., providing guidance on the development of the review protocol, assisting in the critical appraisal of clinical evidence, interpreting the clinical relevance of the results, and providing guidance on the potential place in therapy). The following input was provided by 1 clinical specialist with expertise in the diagnosis and management of adult patients with severe ANCA-AV (GPA and MPA).
Unmet Needs
The clinical expert consulted by CADTH noted that the main goals of treatment include achieving sustained remission, preventing relapse, reducing treatment side effects, and reducing glucocorticoid use, all of which are challenges with current treatments. According to the clinical expert, approximately 10% of patients with severe GPA or MPA have very severe, acute disease resulting in death within the first weeks after diagnosis. Even with treatment, approximately 30% of patients experience disease relapse within 5 years. Other challenges include patient access to expert centres and treatments as well as considerable side effects from treatments, particularly glucocorticoids. The clinical expert stated that patients need treatments that result in sustained remission, limit organ damage (or allow for better recovery from damage), limit the risk of severe infections, require less time on treatment (currently, patients are treated for at least 24 months, and treatment shorter than that has been associated with unacceptable rates of relapse), and are safe for use in special populations (i.e., pediatric, pregnant, and older adult populations). It was also noted that both ANCA-AV and current treatments have significant impacts on patients’ HRQoL and ability to work.
Place in Therapy
According to the clinical expert, avacopan would be used as a first-line treatment for adults with severe GPA or MPA, similar to its use in the ADVOCATE trial, but the expert noted that the trial did not enrol patients with very severe disease or who were ANCA negative. The clinical expert suggested that patients with very severe disease may also be candidates for avacopan after the disease is controlled with high-dose glucocorticoids. The expert indicated that avacopan may allow for a reduction in glucocorticoids, which is particularly important for patients who are receiving glucocorticoid in high doses as well as for those who are at elevated risk of the side effects associated with glucocorticoids. The expert stated that, in practice, avacopan would be administered as it was in the ADVOCATE trial: to induce remission alongside IV or oral cyclophosphamide or IV rituximab with glucocorticoids. The clinical expert noted that, in general and following current guidelines, after remission is achieved with standard treatments patients should receive appropriate maintenance therapy, such as rituximab at month 6 and every 6 months thereafter for at least 24 months of total treatment. The clinical expert noted a current lack of clinical trial evidence on optimal patient management after 12 months of avacopan.
Patient Population
While GPA and MPA are rarely misdiagnosed, there are often delays in the diagnosis. The clinical expert indicated that all adult patients with severe active GPA or MPA need new treatment options and would be treated with avacopan. Given the available evidence, the clinical expert indicated that it is unclear if any subpopulations would respond better to avacopan than other patients. The expert described how avoiding glucocorticoids is ideal in all patients and more so in those who have a medical history of significant side effects as well as those who have concurrent infections because the infections can be exacerbated by glucocorticoids. It is in these patients that avacopan may be particularly useful for treating ANCA-AV according to the expert.
Assessing Response to Treatment
The clinical expert stated that survival is the most important outcome, particularly in the first weeks after diagnosis. Other response measures include improvement of major organ disease (e.g., renal recovery, reduced use of mechanical ventilation), achievement of remission (typically assessed at month 3, then at month 6), and sustained remission (assessed at months 12, 18, and 24). The expert also indicated that it would be important to evaluate and limit the side effects from treatments. The expert also noted that disease- and treatment-related instruments are available, such as the BVAS to assess remission and residual disease activity, the VDI to measure cumulative damage burden as of month 3, and the GTI to evaluate glucocorticoid-related toxicities, as well as other symptom and HRQoL scales, although these have been developed for clinical studies and are not used in routine clinical practice.
Discontinuing Treatment
The clinical expert stated that avacopan should be administered for 12 months, as was done in the ADVOCATE trial, with the possibility of continuing the drug for longer, but noted that there are limited data on stopping the drug before 1 year or using it beyond that. According to the expert, discontinuing treatment should be considered if there are intolerable side effects, continual disease progression with clinical decline, or repeated relapses. With disease progression or relapse, the expert would recommend that the patient be treated with glucocorticoids for a few weeks (either starting glucocorticoids or increasing the dose) while maintaining the same avacopan dose. If the patient relapsed a second time, the expert indicated that avacopan would likely be stopped. Further, disease progression and relapse would also indicate a need to reassess the treatment regimen; for example, a patient on cyclophosphamide induction therapy could be switched to rituximab, or rituximab could be added after 6 months of avacopan for maintenance therapy. In the expert’s opinion, another reason to discontinue avacopan would be if its use did not allow for reduced use of glucocorticoids.
Prescribing Conditions
Since GPA and MPA are rare diseases and require close monitoring, the clinical expert indicated that patients should be referred to a specialist with expertise in the disease area. The expert noted that once a patient is diagnosed, most physicians are able to begin treatment with glucocorticoids but suggested that many are not familiar with, or may not be comfortable, initiating and/or prescribing cyclophosphamide or rituximab before a specialist (e.g., rheumatologist) is involved. In the clinical expert’s opinion, a rheumatologist, nephrologist, general internal medicine specialist, respirologist, or intensive care unit doctor should be able to prescribe avacopan in a hospital setting, and the expert noted that restricting the prescription to only rheumatologists or nephrologists with expertise in vasculitis would likely delay treatment initiation by weeks. However, in community clinics, it would be reasonable to restrict access to only rheumatologists or nephologists with experience treating vasculitis. Additionally, the expert indicated that a patient should begin avacopan treatment as soon as possible after receiving the diagnosis to stop or rapidly reduce glucocorticoid use and limit the risk of glucocorticoid-associated side effects.
Additional Considerations
The clinical expert emphasized that treatment with avacopan should be associated with a mandate to stop or significantly decrease glucocorticoid use within the first weeks of initiating avacopan; otherwise, the continued use of avacopan should be clinically justified. Given the lack of long-term data, the expert expressed uncertainty about patient management after 12 months of avacopan use and about the long-term outcomes after stopping the drug. Lastly, the clinical expert suggested that alongside the implementation of avacopan in Canada, it would be useful to set up a registry to track the drug’s use and patterns of use and to monitor safety and efficacy.
Clinician Group Input
This section was prepared by CADTH staff based on the input provided by 1 clinician group. The full original clinician group input received by CADTH has been included in the stakeholder section at the end of this report.
CanVasc, a Canadian research network for vasculitis, provided input for this review. The clinician group expressed similar views to those of the clinical expert consulted by CADTH. The group highlighted the main unmet needs of patients with severe GPA or MPA as better survival, improved renal and neurologic recovery, induced remission (e.g., at 6 months) followed by sustained remission, reduced reliance on high-dose and prolonged glucocorticoid use due to associated toxicities, and access plus coverage for new treatments other than conventional therapies. CanVasc also advocated for a treatment regimen that is convenient and practical for patients and specialists (oral administration preferred over infusion, and without a complex tapering regimen). The clinician group anticipated that avacopan would be used in clinical practice initially as a combined treatment with rituximab, with or without steroids, for 12 months (benefits and harms beyond this time point are unknown). Discontinuation may be considered if relapse is observed at 6 months followed by a subsequent relapse, or earlier if AEs are detected. The respondents for the clinician group did not indicate having direct experience with the drug under review.
Drug Program Input
The drug programs provide input on each drug being reviewed through CADTH’s reimbursement review processes by identifying issues that may impact the programs’ ability to implement a recommendation. The implementation questions and corresponding responses from the clinical experts consulted by CADTH are summarized in Table 4.
Table 4: Summary of Drug Plan Input and Clinical Expert Response
Drug program implementation questions | Clinical expert response |
|---|---|
Relevant comparators | |
Rituximab, cyclophosphamide, and other immunosuppressive medications are relevant comparators in this disease state; however, they were used as standard therapy in the ADVOCATE trial. According to the indication, avacopan is intended to be used as an adjunct to the continued use of these medications. In the ADVOCATE trial, avacopan was compared to prednisone taper in conjunction with standard therapy. The primary objectives were to achieve and sustain remission. A secondary objective was to show a reduction in glucocorticoid usage in remission. Certain limitations or other factors may have played into the study results. Glucocorticoid usage was not well controlled in the study. Avacopan was compared to prednisone use in conjunction with standard therapy, but the avacopan arm was not completely steroid-free because patients could still take steroids for other conditions and for flares. The drug programs are uncertain how the study showed avacopan would reduce glucocorticoid usage, as rituximab and cyclophosphamide were used as well. Avacopan was not found to be superior for induction but possibly for sustained remission. Longer, more extensive studies are likely needed. | As noted in the CanVasc recommendations and by the clinical expert consulted for the CADTH review, standard of care for patients with ANCA-AV includes immunosuppressant therapy of rituximab, IV or oral cyclophosphamide for induction of remission, followed by maintenance therapy once remission is achieved.9 The clinical expert agreed that many patients in the ADVOCATE trial received nonstudy glucocorticoids during the 52-week treatment period, which complicates interpretation of the results and interpretation of whether treatment with avacopan can reduce glucocorticoid use in practice. The expert was of the opinion that avacopan should be used in addition to standard therapy (immunosuppressants and glucocorticoids) only if there is a meaningful reduction in glucocorticoid use once avacopan is started. |
Initiation criteria | |
Is avacopan intended for all newly diagnosed patients as per the study or for all patients to achieve higher remission rates? Do patients need to be newly diagnosed with ANCA-AV? | Approximately 30% of patients in the ADVOCATE trial had relapsing ANCA-AV. According to the clinical expert, patients with active ANCA-AV, whether newly diagnosed or relapsing, could be treated with avacopan, as was done in the ADVOCATE trial. |
What is the place in therapy? Since there are several options for induction of remission, do they need to be tried in a certain order, or is this simply an addition to current therapies? | The clinical expert stated that avacopan would be a first-line treatment and that standard of care ANCA-AV treatment with immunosuppressants (i.e., IV rituximab or IV or oral cyclophosphamide) would remain the same, with the addition of glucocorticoids and/or avacopan. Based on clinical experience, the expert believed that most physicians or treating teams (including specialists) would be comfortable initially treating patients with standard of care immunosuppressants and glucocorticoids. Once a patient is referred to a specialist for ANCA-AV, the expert suggested that avacopan could replace glucocorticoids. Furthermore, if a patient relapsed, the clinical expert believed it would be reasonable to switch therapies (e.g., from rituximab to cyclophosphamide or from glucocorticoids to avacopan). |
Relapse is common with this condition. What would be the appropriate timing of re-treatment and how often would re-treatment occur? | The clinical expert indicated that relapse is not common with rituximab maintenance (5% of patients have a major relapse on 2-year maintenance therapy with rituximab). The expert confirmed that once a patient relapses, there would be no need to wait to re-treat the patient: intensive treatment would be administered to reinduce remission. The expert also stated that it would be reasonable for a patient to continue receiving avacopan after the first relapse but felt that avacopan should be stopped after the second relapse and the patient should be treated with glucocorticoids instead. |
Rituximab is also used for this condition, but the indication is different. Avacopan is intended to be used in conjunction with rituximab, so alignment considerations for initiation may not be possible. | For CDEC consideration. |
Renewal criteria | |
What would be needed to assess continued need? Glucocorticoids and rituximab are used to treat disease relapses. Does this drug continue if a patient relapses? | The clinical expert explained that many factors could influence how avacopan would be used in practice, such as ANCA-AV type (MPA or GPA), ANCA positivity (MPO or PR3 positive), the persistence of ANCA positivity, new diagnosis or relapse, achievement of remission, successfully stopping of glucocorticoid use, and evidence of disease activity. In most situations, the expert felt that patients should continue treatment for more than 1 year because, based on clinical experience, 1 year of treatment generally does not put a patient into long-term sustained remission. After 1 year of avacopan treatment, the clinical expert expected that most patients would continue some form of maintenance therapy, such as rituximab, or would continue with avacopan and that it would be unlikely for a patient to stop all treatment after 1 year. Given the lack of long-term evidence with avacopan, the expert stated that it is very uncertain how the drug would be used, what its effects beyond 1 year would be, and how it would compare to rituximab maintenance therapy, which is currently the standard for maintenance therapy. The clinical expert stated that avacopan should be stopped after the second relapse and the patient should instead be treated with glucocorticoids. |
If possible, consistency in renewal criteria with rituximab would be useful, also due to ANCA-AV being a rare disease, but their indications differ so it may not be possible. | For CDEC consideration. |
Discontinuation criteria | |
What is the definition of refractory disease? What would be the parameters? This is important in determining if and when repeated attempts of this therapy should be halted. | According to the clinical expert, not many patients have refractory disease and there is no standard definition. A patient may have refractory disease if no treatments work to induce remission and the disease continues to progress. Alternatively, a patient may have clinical manifestations where most symptoms improve but remission is not achieved and there is still lingering disease activity despite having exhausted all standard of care treatments |
What is the expected duration of therapy for avacopan? | The clinical expert expects avacopan to be used for 12 months, as it was in the ADVOCATE trial, with the possibility of continuing the drug for longer. There is limited evidence for treatment duration less than or more than 12 months, and it has been noted that there is uncertainty over how to manage patients after stopping avacopan. |
How is sustained remission defined? Is remission for 18 to 24 months considered sustained remission? Can sustained remission only occur once, or can it be repeated? If there were relapses along the way, does sustained remission start after the last relapse? | There is no standard definition for sustained remission, and it can occur more than once. Sustained remission is also different from the initial remission, which is usually assessed at month 3 or month 6. The clinical expert typically makes assessments for sustained remission at 12 months and every 6 months thereafter. The expert also stated that the next step would be to stop maintenance therapy and assess if the patient remained in sustained remission. |
Prescribing criteria | |
This drug is intended to be used as an adjunct therapy. Are there any concerns with the different combinations of standard treatments? (Please consider induction and maintenance therapies.) | The clinical expert had no concerns about interactions between the drug combinations typically used to treat ANCA-AV but noted that there is a lack of data on the efficacy and safety of rituximab maintenance therapy with avacopan. The expert’s main concern was that physicians may give avacopan without reducing glucocorticoids; this reduction was the aim of the ADVOCATE trial. |
Special implementation issues and generalizability | |
Avacopan targets a component of the inflammatory process. There is potential for use in other autoimmune diseases. | For CDEC consideration. |
System and economic issues | |
If avacopan is to be added on and used for all patients to induce remission, it may have a budget impact. | For CDEC consideration. |
Rituximab has been successfully negotiated, although it is for a slightly different indication. Other comparators are older drugs and much less expensive. | For CDEC consideration. |
ANCA-AV = antineutrophil cytoplasmic autoantibody–associated vasculitis; CDEC = CADTH Canadian Drug Expert Committee; GPA = granulomatosis with polyangiitis; MPA = microscopic polyangiitis; MPO = myeloperoxidase.
Clinical Evidence
The clinical evidence included in the review of avacopan is presented in the systematic review, which includes the pivotal studies provided in the sponsor’s submission to CADTH and Health Canada, as well as studies selected according to an a priori protocol. No indirect evidence, long-term extension studies, or additional relevant studies were identified in the literature.
Systematic Review (Pivotal and Protocol-Selected Studies)
Objectives
To perform a systematic review of the beneficial and harmful effects of avacopan 30 mg (3 oral capsules of 10 mg each) twice daily, for the adjunctive treatment of adult patients with severe active ANCA-AV (GPA and MPA) in combination with standard background therapy, including glucocorticoids. Avacopan does not eliminate glucocorticoid use.
Methods
The studies selected for inclusion in the systematic review included the pivotal studies provided in the sponsor’s submission to CADTH and Health Canada, as well as studies meeting the selection criteria presented in Table 5. Outcomes included in the CADTH systematic review protocol reflect outcomes considered to be important to patients, clinicians, and drug plans.
Table 5: Inclusion Criteria for the Systematic Review
Criteria | Description |
|---|---|
Population | Adults with severe active ANCA-AV (GPA and MPA) Subgroups:
|
Intervention | Avacopan 30 mg (3 oral capsules of 10 mg each) twice daily with standard of care (e.g., rituximab or cyclophosphamide) with or without glucocorticoids |
Comparator | Glucocorticoids (e.g., prednisone) with standard of care (e.g., rituximab or cyclophosphamide) |
Outcomes | Efficacy outcomes:
Harms outcomes:
|
Study designs | Published and unpublished phase III and IV RCTs |
AE = adverse event; ALT = alanine aminotransferase; ANCA-AV = antineutrophil cytoplasmic autoantibody–associated vasculitis; AST = aspartate aminotransferase; eGFR = estimated glomerular filtration rate; ESKD = end-stage kidney disease; GPA = granulomatosis with polyangiitis; HRQoL = health-related quality of life; MPA = microscopic polyangiitis; MPO = myeloperoxidase; RCT = randomized controlled trial; SAE = serious adverse event; VDI = Vasculitis Damage Index; WDAE = withdrawal due to adverse event.
The literature search for clinical studies was performed by an information specialist using a peer-reviewed search strategy according to the PRESS Peer Review of Electronic Search Strategies checklist.30
Published literature was identified by searching the following bibliographic databases: MEDLINE All (1946–) via Ovid and Embase (1974–) via Ovid. All Ovid searches were run simultaneously as a multifile search. Duplicates were removed using Ovid deduplication for multifile searches, followed by manual deduplication in Endnote. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. The main search concept was avacopan. The following clinical trial registries were searched: the US National Institutes of Health’s clinicaltrials.gov, WHO’s International Clinical Trials Registry Platform search portal, Health Canada’s Clinical Trials Database, and the European Union Clinical Trials Register.
No filters were applied to limit the retrieval by study type. Retrieval was not limited by publication date or by language. Conference abstracts were excluded from the search results. Refer to Appendix 1 for the detailed search strategies.
The initial search was completed on November 9, 2022. Regular alerts updated the search until the meeting of the CADTH Canadian Drug Expert Committee on March 22, 2023.
Grey literature (literature that is not commercially published) was identified by searching relevant websites from the Grey Matters: A Practical Tool For Searching Health-Related Grey Literature checklist.31 Included in this search were the websites of regulatory agencies (FDA and the European Medicines Agency). Google was used to search for additional internet-based materials. Refer to Appendix 1 for more information on the grey literature search strategy.
These searches were supplemented through contacts with appropriate experts. In addition, the sponsor of the drug was contacted for information regarding unpublished evidence.
Two CADTH clinical reviewers independently selected studies for inclusion in the review based on titles and abstracts, according to the predetermined protocol. Full-text articles of all citations considered potentially relevant by at least 1 reviewer were acquired. Reviewers independently made the final selection of studies to be included in the review, and differences were resolved through discussion.
Findings From the Literature
Two reports19,32 of a single study were identified from the literature for inclusion in the systematic review (Figure 1). The included study is summarized in Table 6. A list of excluded studies is presented in Appendix 2.
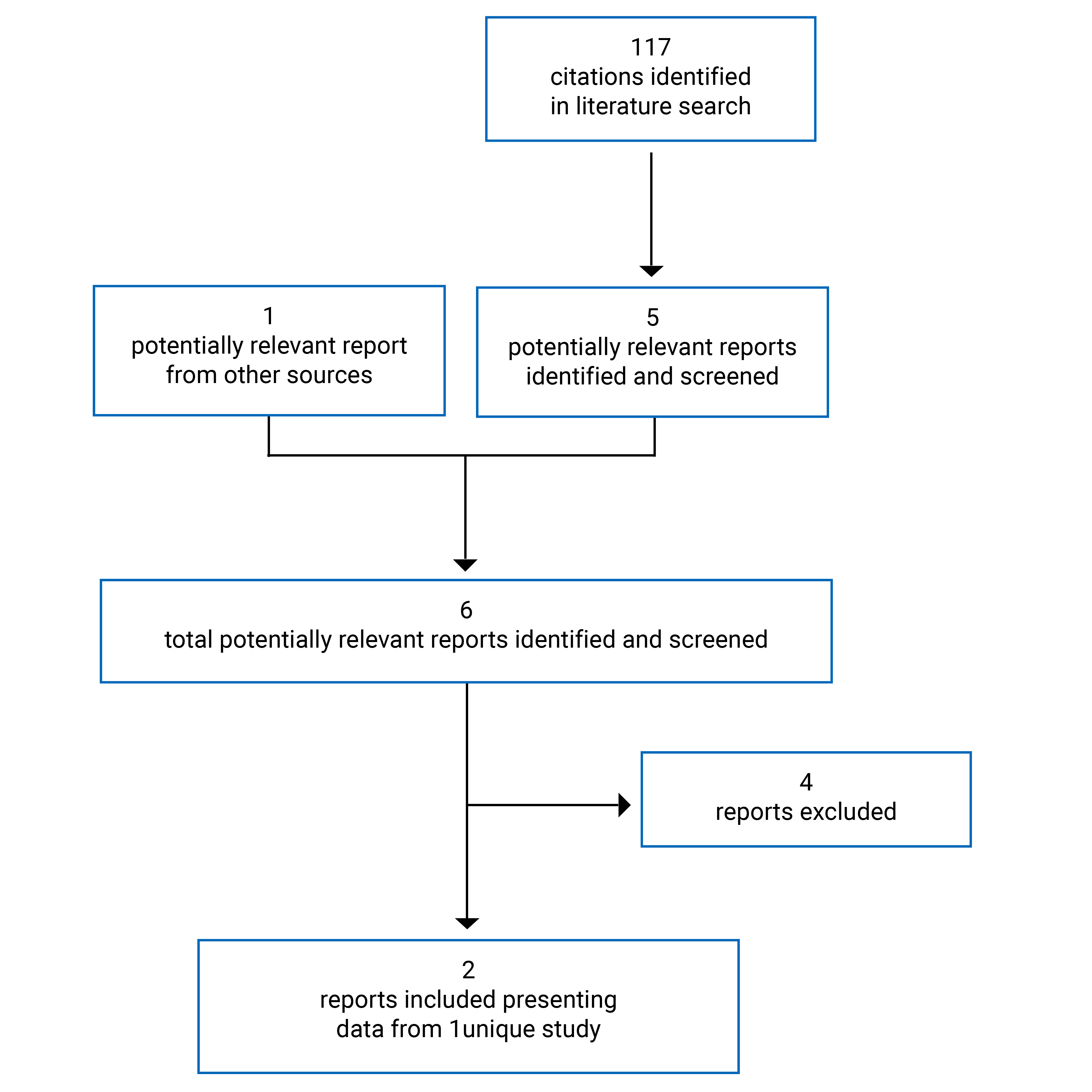
Table 6: Details of Included Study
Study details | ADVOCATE |
|---|---|
Design and population | |
Study design | Phase III, multicentre, DB RCT with placebo and active controls and parallel groups |
Locations | 143 study centres in North America (9 Canadian centres), Europe, Australia, New Zealand, and Japan |
Patient enrolment dates | First patient enrolled March 15, 2017; last patient enrolment date not reported |
Randomized | N = 331
|
Inclusion criteria |
|
Exclusion criteria |
|
Drugs | |
Intervention |
|
Comparator |
|
Phase and duration | |
Screening | Up to 2 weeks |
DB treatment | 52 weeks |
Follow-up | 8 weeks |
Outcomes | |
Primary end points |
|
Secondary end points |
|
Notes | |
Publications | Jayne et al. (2021)32 |
AE = adverse event; ALT = alanine aminotransferase; ANCA-AV = antineutrophil cytoplasmic autoantibody–associated vasculitis; AST = aspartate aminotransferase; BVAS = Birmingham Vasculitis Activity Score; DB = double blind; ECG = electrocardiogram; eGFR = estimated glomerular filtration rate; EGPA = eosinophilic granulomatosis with polyangiitis; EQ-5D-5L = 5-level EQ-5D; GPA = granulomatosis with polyangiitis; GTI = Glucocorticoid Toxicity Index; HRQoL = health-related quality of life; MDRD = modification of diet in renal disease; MPA = microscopic polyangiitis; MPO = myeloperoxidase; RCT = randomized controlled trial; SAE = serious adverse event; SF-36v2 = Short Form (36) Health Survey version 2; TNF = tumour necrosis factor; UACR = urinary albumin–creatinine ratio; ULN = upper limit of normal; VDI = Vasculitis Damage Index; WDAE = withdrawal due to adverse event.
Note: Three additional reports were included (FDA, European Medicines Agency, and Health Canada reports).19,21,33
aPatients received either IV cyclophosphamide (15 mg/kg, up to 1.2 g maximum, at each of the day 1 and week 2, 4, 7, 10, and 13 study visits) or oral cyclophosphamide (2 mg/kg/day, up to 200 mg/day maximum, from day 1 to week 15). The cyclophosphamide dose was adjusted for age, eGFR, and white blood cell count. After week 15, patients received 1 mg/kg/day oral azathioprine up to 2 mg/kg/day at 2 weeks. If azathioprine was not tolerated, 2 g/day mycophenolate mofetil may have been given. If mycophenolate mofetil was not tolerated or not available, 1,440 mg/day enteric coated mycophenolate sodium may have been given.
bPatients received IV rituximab (375 mg/m2 weekly for 4 weeks) where glucocorticoid premedication for rituximab infusions was permitted.
cGlucocorticoid use referred to both the prednisone study medication and other glucocorticoids that were not part of the prednisone study medication given for ANCA-AV for the 4 weeks before the BVAS assessment at weeks 26 and 52. Patients were permitted to receive low-dosage oral glucocorticoids (10 mg/day or less) outside of the trial protocol for treatment of adrenal insufficiency or to receive glucocorticoid treatment for other conditions (e.g., allergic reaction). These patients were to be considered responders if all other requirements for the end points were met.
dRelapse was defined as disease worsening after having previously achieved remission that involved 1 or more major item in the BVAS, or 3 or more minor items in the BVAS, or 1 or 2 minor items in the BVAS recorded at 2 consecutive study visits.
Source: ADVOCATE Clinical Study Report.19
Description of the Study
The ADVOCATE trial (N = 331) was a phase III, double-blind, randomized controlled trial investigating the efficacy and safety of avacopan in patients with ANCA-AV with the intent to determine if avacopan could induce and sustain remission without chronic glucocorticoid use at the levels currently used in standard of care regimens. The trial took place at 143 centres in 20 countries, with 9 sites in Canada enrolling 13 patients.34 The ADVOCATE trial consisted of a 2-week screening period to determine patient eligibility, a 52-week double-blind treatment period, and an 8-week follow-up period. Patients had visits scheduled every week for the first month, then nearly every third week until the end of the trial. Randomization was conducted centrally using an interactive response technology system, and patients were stratified by standard of care immunosuppressant treatment (IV rituximab, IV cyclophosphamide, or oral cyclophosphamide), ANCA positivity (PR3 or MPO) at diagnosis, and disease status (newly diagnosed or relapsed ANCA-AV). Overall, 331 patients were randomized 1:1 to receive either oral avacopan with oral prednisone-matching placebo (N = 166) or oral prednisone with oral avacopan-matching placebo (N = 165) along with, in both groups, background therapy of IV rituximab or oral or IV cyclophosphamide. Patients, investigators, the sponsor, and personnel involved with data monitoring and analysis were blinded to treatment assignment, and a double-dummy design (avacopan- and prednisone-matched placebos) was used.
Patients were withdrawn from the trial if they withdrew their consent or were lost to follow-up. Patients were discontinued from the study drug treatment if they withdrew their consent or if the investigator or sponsor determined that the patient should discontinue the treatment based on clinical judgment or for safety reasons.
Populations
Inclusion Criteria
To be included in the ADVOCATE trial, patients had to be adults (18 years and older, although allowance was made for patients aged 12 years to 17 years at approved trial centres) with newly diagnosed or relapsing ANCA-AV and a clinical diagnosis of GPA or MPA that was consistent with the Chapel Hill Consensus Conference definitions and had to have tested positive (based on historical medical data or at the time of screening) for either anti-PR3 or anti-MPO antibodies.6 At screening, patients had to have at least 1 major item, at least 3 minor items, or at least the 2 renal items of proteinuria and hematuria on the BVAS and an eGFR of at least 15 mL/min/1.73 m2.
Exclusion Criteria
Individuals were excluded if they had severe disease, such as alveolar hemorrhage, requiring invasive pulmonary ventilation support, dialysis, or plasma exchange or if they had another multisystem autoimmune disease (e.g., eosinophilic GPA, systemic lupus erythematosus, immunoglobulin A vasculitis). Other exclusion criteria were administration of cyclophosphamide in the 12 weeks before screening; IV glucocorticoids greater than 3,000 mg methylprednisolone equivalent in the 4 weeks before screening; oral daily glucocorticoids of more than 10 mg prednisone equivalent for more than 6 weeks before screening; or rituximab or other B-cell antibody in the 52 weeks before screening (or 26 weeks, provided B-cell reconstitution had occurred). Evidence of recent cardiovascular symptoms, cancer, tuberculosis, hepatic disease, low white blood cell counts, or hypersensitivity to any of the study drugs were also reasons for exclusion.
Baseline Characteristics
Baseline characteristics are summarized in Table 7.
The mean age of patients in the ADVOCATE trial was 60.9 years (SD = 14.5 years). More than half the patients were male (56.5%), and most were white (84.3%). There was an aim to enrol 10 adolescent patients, but only 3 entered the trial. The mean age at diagnosis was 59.6 years (SD = 15.4 years). Most patients were from Europe (70.1%), and 18.1% were from North America. The proportions of patients by geographic location were imbalanced between treatment groups.
The baseline disease characteristics were generally balanced between treatment groups. Most patients were newly diagnosed with ANCA-AV (69.4%), and 30.6% had relapsing disease. A little more than half the patients had GPA (54.8%), and 45.2% had MPA. Less than half were positive for anti-PR3 antibodies (43.0%), and 57.0% were positive for anti-MPO antibodies. The mean baseline BVAS was 16.2 (SD = 5.8), with the most commonly reported BVAS components being renal (81.2%) and general symptoms (68.2%). Prior immunosuppressant use was generally balanced between treatment groups, with the most common drug being azathioprine (10.3%).
Table 7: Summary of Baseline Characteristics — ADVOCATE
Characteristic | Prednisone | Avacopan |
|---|---|---|
Demographics (all randomized patients) | N = 165 | N = 166 |
Age (years) | ||
Mean (SD) | 60.6 (14.5) | 61.2 (14.6) |
Median (minimum to maximum) | 62.0 (15 to 88) | 65.0 (13 to 83) |
Age category (years), n (%) | ||
12 to 17 | 1 (0.6) | 2 (1.2) |
18 to 50 | 28 (17.0) | 30 (18.1) |
51 to 64 | 61 (37.0) | 48 (28.9) |
65 to 75 | 53 (32.1) | 62 (37.3) |
Older than 75 | 22 (13.3) | 24 (14.5) |
Age at diagnosis of ANCA-AV (years), mean (SD) | 59.4 (15.2) | 59.8 (15.6) |
Sex, n (%) | ||
Male | 89 (53.9) | 98 (59.0) |
Female | 76 (46.1) | 68 (41.0) |
Race, n (%) | ||
White | 141 (85.5) | 138 (83.1) |
Asian | 15 (9.1) | 17 (10.2) |
Black | 2 (1.2) | 3 (1.8) |
Other | 6 (3.6) | 8 (4.8) |
Multiple | 1 (0.6) | 0 |
Geographic region, n (%) | ||
Europe | 123 (74.5) | 109 (65.7) |
North America | 26 (15.8) | 34 (20.5) |
Japan | 10 (6.1) | 11 (6.6) |
Other regions | 6 (3.6) | 12 (7.2) |
Baseline disease characteristics and medical history (ITT population) | N = 164 | N = 166 |
Duration of ANCA-AV (months) | ||
Mean (SD) | 20.1 (40.5) | 22.9 (52.5) |
Median (minimum to maximum) | 0.3 (0 to 212.5) | 0.2 (0 to 362.3) |
ANCA-AV status, n (%) | ||
Newly diagnosed | 114 (69.5) | 115 (69.3) |
Relapsed | 50 (30.5) | 51 (30.7) |
Type of ANCA-AV, n (%) | ||
GPA | 90 (54.9) | 91 (54.8) |
MPA | 74 (45.1) | 75 (45.2) |
ANCA positivity, n (%) | ||
PR3 | 70 (42.7) | 72 (43.4) |
MPO | 94 (57.3) | 94 (56.6) |
BVAS | ||
Mean (SD) | 16.2 (5.7) | 16.3 (5.9) |
Median (minimum to maximum) | |||| || || ||| | |||| || || ||| |
BVAS entry criteria, n (%)a | ||
1 or more major item | 102 (62.2) | 104 (62.7) |
3 or more minor items | 142 (86.6) | 146 (88.0) |
2 renal items of proteinuria and hematuria | 57 (34.8) | 60 (36.1) |
BVAS components, n (%)a | ||
General | 114 (69.5) | 111 (66.9) |
Cutaneous | 23 (14.0) | 24 (14.5) |
Mucous membranes or eyes | 40 (24.4) | 26 (15.7) |
Ear, nose, and throat | 69 (42.1) | 75 (45.2) |
Chest | 71 (43.3) | 71 (42.8) |
Cardiovascular | 3 (1.8) | 6 (3.6) |
Abdominal | 1 (0.6) | 4 (2.4) |
Renal and other (RBC casts and/or glomerulonephritis) | 134 (81.7) | 134 (80.7) |
Nervous system | 31 (18.9) | 38 (22.9) |
VDI score | ||
Mean (SD) | 0.7 (1.39) | 0.7 (1.54) |
Median (minimum to maximum) | | || || | | | || || | |
Prior immunosuppressant useb (safety population) | N = 164 | N = 166 |
||||| ||||||||||||||||||| |||| | | |||||| | | |||||| |
|||||||||||| | | ||||| | | |||||| |
|||||||||||| | | ||||| | | ||||| |
|||||||||||| |||||| | | |||||| | | |||||| |
||||||||| ||||||||||||||||||| |||| | | ||||| | | ||||| |
||||||||||||| ||||||| | | ||||| | | ||||| |
||||||||||||| |||||| | | ||||| | | ||||| |
||||||||||| | | ||||| | | ||||| |
||||||||||||| |||| | | ||||| | | ||||| |
Nitrogen mustard analogues, n (%) | 2 (1.2) | 4 (2.4) |
Cyclophosphamide | 2 (1.2) | 4 (2.4) |
Monoclonal antibodies, n (%) | 4 (2.4) | 1 (0.6) |
Rituximab | 4 (2.4) | 1 (0.5) |
||||||||||| ||||||||||| |||| | | ||||| | | ||||| |
||||||||||| | | ||||| | | ||||| |
|||||||||| | | ||||| | | ||||| |
ANCA-AV = antineutrophil cytoplasmic autoantibody–associated vasculitis; BVAS = Birmingham Vasculitis Activity Score; GPA = granulomatosis with polyangiitis; ITT = intention to treat; MPA = microscopic polyangiitis; MPO = myeloperoxidase; RBC = red blood cell; SD = standard deviation; VDI = Vasculitis Damage Index.
aPatients can appear in more than 1 category.
bPrior medications were defined as those taken in the year before the first dose of the study drug. Medications could be considered both prior and concomitant if started before the first dose of the study drug and continued into the treatment period.
Source: ADVOCATE Clinical Study Report.19
Interventions
Patients in the avacopan group received 30 mg oral avacopan twice daily with prednisone-matched oral placebo; those in the prednisone group received oral prednisone with 30 mg avacopan-matched oral placebo twice daily for 52 weeks. Over the first 20 weeks, prednisone (or matching placebo) was tapered down from a starting dosage of 60 mg/day for patients with a body mass of at least 55 kg or of 45 mg/day for patients with a body mass less than 55 kg. For adolescent patients who received avacopan, the dose was initially dependent on body mass but was further refined based on avacopan plasma exposure; adolescents weighing 37 kg or less received prednisone at 30 mg/day. Patients in both the avacopan and prednisone groups received background immunosuppressant therapy of IV cyclophosphamide for 13 weeks followed by oral azathioprine from week 15 onward, or of oral cyclophosphamide for 14 weeks followed by oral azathioprine from week 15 onwards, or of IV rituximab once weekly for 4 weeks without any subsequent maintenance therapy. Mycophenolate was given if azathioprine was contraindicated. Premedication with glucocorticoids was permitted for rituximab infusions. The choice of background therapy was at the discretion of the trial investigator. Based on previous phase I and II studies of avacopan, a twice daily 30 mg avacopan dose was deemed appropriate.35-37 Dose regimens were consistent with standard clinical practice at the time of protocol development.
Patients who received glucocorticoids during the screening period had to have reduced their dose to 20 mg or less prednisone equivalent by day 1 of the trial, and the dose was to be further tapered to 0 mg within the first 4 weeks of the trial. Glucocorticoid treatments that were outside of the study protocol were to be avoided as much as possible. However, patients who experienced disease relapse or worsening disease involving a major item on the BVAS may have received IV glucocorticoids (0.5 g to 1 g methylprednisolone per day for 3 days) and/or oral glucocorticoids that were tapered according to the patient’s condition. Patients who experienced worsening disease not involving a major item on the BVAS may have received a short burst (2 weeks or less) of oral glucocorticoids to a maximum dose of 20 mg prednisone equivalent. Patients who had at least 1 major item on the BVAS before entering the trial that did not improve or stabilize during the first 4 weeks may have received additional IV or oral glucocorticoids that were tapered according to the patient’s condition. Furthermore, patients who relapsed may have received additional immunosuppressive therapy (e.g., additional rituximab or cyclophosphamide), as discussed with the medical monitor. Despite the use of glucocorticoids outside of the protocol, these patients were to continue in the trial.
Outcomes
A list of efficacy end points identified in the CADTH systematic review protocol and assessed in the clinical trial is provided in Table 8. These end points are further summarized in this section of the report. A detailed discussion and critical appraisal of the outcome measures is provided in Appendix 4.
Survival
Survival was not assessed in the ADVOCATE trial (aside from deaths, which were included in the assessment of harm outcomes).
Table 8: Summary of Efficacy Outcomes of Interest Identified in the CADTH Systematic Review Protocol
Outcome measure | Status within ADVOCATE trial |
|---|---|
Survival | Not reporteda |
Disease remission (induction and sustained remission) | Primary |
Renal function (e.g., eGFR, progression to ESKD) | Secondary |
Systemic damage (e.g., as measured by VDI) | Secondary |
Disease relapse (e.g., time to relapse or duration of remission, minor vs. major) | Secondary |
Glucocorticoid use and related toxicities and safety | Secondary |
HRQoL | Secondary |
Hospitalizations | Not reported |
Symptoms (e.g., fatigue) | Not reported |
eGFR = estimated glomerular filtration rate; ESKD = end-stage kidney disease; HRQoL = health-related quality of life; VDI = Vasculitis Damage Index.
aNot reported as an efficacy outcome; mortality information was reported as deaths in the assessment of harm outcomes.
Disease Remission (Induction and Sustained Remission)
Disease remission was assessed using the BVAS version 3, a comprehensive multisystem clinical assessment of a patient’s current disease activity using a standardized list of 57 clinical items organized into 9 organ systems, with an “other” category.38 Each item is assigned a numerical value based on its perceived clinical relevance according to expert consensus, and only symptoms attributable to active ANCA-AV are reported.19 The BVAS can range from 0 to 63, with 0 indicating no disease activity and any score greater than 0 indicating that active disease is present.39 Face validity and convergent validity were acceptable, and convergent validity was correlated with the physician’s global assessment, treatment decision, and VDI.38 Interobserver and intra-observer reliability were also acceptable, and responsiveness was examined in a cohort of 39 patients with ANCA-AV.38 No MID was identified from the literature for patients with ANCA-AV.
In the ADVOCATE trial, the week 4 BVAS assessment was modified to include disease activity from the past 7 days, rather than 28 days, to exclude the trial’s baseline measurement. Early remission was assessed as a BVAS of 0 at week 4, regardless of glucocorticoid use. All other BVAS assessments considered the previous 28 days. Additionally, the “persistent” disease portion was not evaluated as only the presence or absence of disease was assessed in the trial. BVAS assessments were made at screening and at weeks 4, 10, 16, 26, 39, 52, and 60, and data were confirmed by a blinded adjudication committee.
Disease remission was defined by the adjudication committee as achieving a BVAS of 0, with no glucocorticoids for ANCA-AV in the 4 weeks before week 26 and no BVAS greater than 0 during the 4 weeks before week 26 (if collected for an unscheduled assessment). Sustained disease remission was defined by the adjudication committee as disease remission at week 26 and disease remission at week 52, which was a BVAS of 0 with no glucocorticoids for ANCA-AV in the 4 weeks before week 52 and no disease relapse between week 26 and week 52. Glucocorticoid use referred to both prednisone study medication and other nonstudy glucocorticoids for ANCA-AV during the 4 weeks before the BVAS assessments at week 26 and week 52. Patients were permitted to receive low dosages of oral glucocorticoids (10 mg/day or less) to treat adrenal insufficiency or allergic reaction. Patients were considered responders if all other requirements for the end points were met.
Renal Function (e.g., eGFR, Progression to ESKD)
Renal disease at baseline was defined as having at least 1 renal item on the BVAS at screening (i.e., hypertension, proteinuria greater than 1+ or greater than 0.2 g/g creatinine, hematuria of at least 10 red blood cells per high-power field, elevated serum creatinine [at least 125 μmol/L], or rise in serum creatinine [greater than 30%] or fall in creatinine clearance [greater than 25%] since previous assessment).
The eGFR was calculated for patients with renal disease at baseline from serum creatinine measurements using the modification of diet in renal disease equation for adults and the modified Schwartz equation for adolescents. A different calculation was used for adults identifying as Japanese, although the reason for this was not clear and no reference to literature was available. Serum creatinine measurements for eGFR were taken at screening, at day 1, and at weeks 1, 2, 3, 4, 7, 10, 13, 16, 20, 26, 32, 39, 45, 52, and 60. The number of patients who required dialysis during the trial was reported.
The UACR was calculated for patients with renal disease and albuminuria at baseline through quantitative albumin and creatinine measurements taken from urine samples, which were centrally assessed. Measurements were taken at screening, at day 1, and at weeks 1, 2, 4, 13, 26, 39, 52, and 60.
Systemic Damage (e.g., Measured by VDI)
The VDI is a standardized clinical assessment of damage in systemic vasculitis aimed at distinguishing damage or scarring (which are unlikely to respond to immunosuppression) from disease activity to aid in the selection of therapy.40 The instrument is composed of 64 items, organized into 11 organ-based systems, where damage is defined as disease manifestations that have been present for at least 3 months (to be considered damage as opposed to ongoing activity).40 Comorbidities developed before vasculitis are not scored.40 Each item is scored as being present (1 point) or absent (0 points), and the items are summed.19,40 A VDI score is cumulative and can remain the same or increase over time because previously scored items are carried forward to subsequent assessments (i.e., damage is considered irreversible).40 Content, face, and criterion validity were assessed in patients with a range of systemic vasculitides.40 Convergent and divergent validity were examined for the VDI compared with the Systemic Necrotizing Vasculitis Damage Index and the Systemic Lupus International Cooperating Clinics/American College of Rheumatology Damage Index. Low to moderate correlation was found between the instruments, but the VDI was more sensitive to detecting damage.40 Inter-rater reliability of the VDI was fair to moderate when compared between different assessors, and responsiveness was examined in a group of 100 patients.40 No MID was identified from the literature for patients with ANCA-AV.
VDI assessments were made at screening and at weeks 26, 52, and 60, and data were confirmed by an adjudication committee.
Disease Relapse (e.g., Time to Relapse or Duration of Remission, Minor Versus Major)
Disease relapse was defined as the occurrence of at least 1 major item, 3 or more minor items, or 1 or 2 minor items on the BVAS recorded at 2 consecutive visits, after having achieved remission at week 26 (BVAS of 0 and no glucocorticoids for ANCA-AV within 4 weeks) or after having achieved a BVAS of 0 at any time during the treatment period.
Glucocorticoid Use and Related Toxicities and Safety
The GTI version 2 quantifies and assesses changes in toxicity associated with glucocorticoid use.41,42 It consists of 2 scores: the GTI-CWS and GTI-AIS.41,42 The GTI-CWS measures cumulative toxicity, regardless of whether the toxicity has transient or lasting effects.41,42 New toxicities are added without removing those that have resolved; therefore, the score can remain the same or increase over time.41,42 In contrast, toxicities that improve can be removed from the GTI-AIS, and when overall glucocorticoid toxicity improves, the score can have a negative value.41,42 The GTI-AIS is intended to capture changes in glucocorticoid toxicities over time and whether a treatment is effective at diminishing baseline toxicities.41,42 No evidence of validation of the GTI was identified for patients with ANCA-AV, and Health Canada correspondingly considered it to be unvalidated and too general to be clinically meaningful for ANCA-AV.20 The instrument has been validated in patients with asthma, although it is unclear if it has been validated in other populations.43 A MID of 10 points was identified from the literature, which was based on a mixed population of patients with various inflammatory conditions, including ANCA-AV.43
GTI assessments were made on day 1 and at weeks 13 and 26, the period during which prednisone was given to patients in the prednisone group. The sponsor stated that this was done to focus the assessment on the relevant study period. Data for the GTI did not appear to be confirmed by an adjudication committee.
Health-Related Quality of Life
HRQoL was assessed using the SF-36v2 and the EQ-5D-5L. The SF-36v2 is a generic health survey consisting of 36 questions yielding scores for 8 subscales of functional health and well-being that can be summarized in a physical component summary and a mental component summary.44,45 Scores range from 0 to 100, where a higher score indicates better health status.44 The EQ-5D-5L is a generic health instrument consisting of a descriptive system profile with 5 dimensions measured on a 5-point scale and a VAS measured on a 100-point scale.46 The descriptive system profile can be linked to a “value set” (values or weights for each health state description according to the preferences of the general population or of a country or region) to derive an index score, where 0 represents death and 1.0 represents perfect health.46 The VAS records a respondent’s self-rated health that day on a vertical line, with 0 labelled “worst imaginable health state” and 100 labelled “best imaginable health state.”46 Translations for the instruments were used in the trial, where available. Although some articles indicate that evidence of validity and reliability have been identified for the SF-36v2 for patients with ANCA-AV, CADTH reviewers could not validate such claims. In addition, validity, reliability, and responsiveness were not assessed for the EQ-5D-5L in this population. No MID for either instrument was identified from the literature for patients with ANCA-AV.
The SF-36v2 and the EQ-5D-5L were completed on day 1 and at weeks 4, 10, 16, 26, 39, 52, and 60.
Hospitalizations
Hospitalizations were not assessed in the ADVOCATE trial.
Symptoms (e.g., Fatigue)
Symptoms (aside from those collected under harms) were not assessed in the ADVOCATE trial.
Harms
The incidence and seriousness of AEs, withdrawal due to AEs, and deaths were reported for the safety population during the trial. AEs, SAEs, and protocol-defined notable harms were described based on preferred term and associated system organ class. Notable harms from the CADTH systematic review protocol included serious infection, hepatic injury (e.g., elevated ALT or AST, total bilirubin), cardiovascular AEs (e.g., myocardial infarction, cardiac failure, cardiac vasculitis), gastrointestinal AEs (e.g., dyspepsia, vomiting, nausea, diarrhea), and immune-related AEs (e.g., angioedema).
Statistical Analysis
The statistical analysis of efficacy end points is summarized in Table 9.
Table 9: Statistical Analysis of Efficacy End Points
End point | Statistical model | Adjustment factors | Sensitivity analyses |
|---|---|---|---|
Proportion of patients who achieved disease remission at week 26 | Summary score test for the common difference in remission rates | Stratified by randomization factors: standard of care immunosuppressant treatment (IV rituximab, IV cyclophosphamide, or oral cyclophosphamide); ANCA positivity (PR3 or MPO) at diagnosis; disease status (newly diagnosed or relapsed ANCA-AV) |
|
Proportion of patients who achieved sustained disease remission at week 52 | Summary score test for the common difference in sustained remission rates | Same as above | Same as above |
Proportion of patients who experienced disease relapse and time to relapse | KM, log-rank test | Same as above | None |
BVAS of 0 at week 4 | Summary score test for the common difference in remission rates | Same as above | None |
Change from baseline in eGFR for patients with renal disease at baseline | MMRM | Treatment group, visit, treatment-by-visit interaction, and randomization stratification factors | None |
Change from baseline in UACR for patients with renal disease and albuminuria at baseline | MMRM | Treatment group, visit, treatment-by-visit interaction, and randomization stratification factors | None |
Change from baseline in VDI at week 26 and week 52 | MMRM | Treatment group, visit, treatment-by-visit interaction, baseline VDI score, and randomization stratification factors | Including investigator-assessed VDI data |
Change from baseline in GTI scores at week 13 and week 26 | MMRM | Treatment group, visit, treatment-by-visit interaction, and randomization stratification factors | None |
Change from baseline in HRQoL (SF-36v2 and EQ-5D-5L) | MMRM | Treatment group, visit, treatment-by-visit interaction, baseline values, and randomization stratification factors | None |
ANCA = antineutrophil cytoplasmic autoantibody; ANCA-AV = antineutrophil cytoplasmic autoantibody–associated vasculitis; BVAS = Birmingham Vasculitis Activity Score; eGFR = estimated glomerular filtration rate; EQ-5D-5L = 5-Level EQ-5D; GTI = Glucocorticoid Toxicity Index; HRQoL = health-related quality of life; KM = Kaplan-Meier; MMRM = mixed effects model for repeated measures; MPO = myeloperoxidase; SF-36v2 = Short Form (36) Health Survey version 2; UACR = urinary albumin–creatinine ratio; VDI = Vasculitis Damage Index.
Source: ADVOCATE Clinical Study Report.19
Primary Outcome
The ADVOCATE trial had 2 primary efficacy end points. The first was the proportion of patients who achieved disease remission at week 26, and the second was the proportion of patients who achieved sustained disease remission at week 52. The number of patients adjudicated as having achieved remission at week 26 and week 52 was divided by the total number of patients in the treatment groups for the ITT and PP populations at the respective time points. The primary analysis compared remission rates for the 2 primary efficacy end points using the ITT population based on the stratification variables used for randomization. Data were summarized descriptively by treatment group. Continuous variables were presented as numbers, means, medians, ranges, SDs, and standard errors of the mean, and categorical variables were presented as frequency counts and percentages.
Statistical Testing
The proportion of patients who achieved disease remission at week 26 and sustained disease remission at week 52, and the 2-sided 95% CIs for the difference in proportions (avacopan minus prednisone), were calculated. For both noninferiority and superiority tests, 1-sided P values were presented, and statistical significance was claimed based on the 1-sided type I error of 0.025.
For the stratified analyses of the primary end point of remission, summary score estimates of the common difference in remission rates were calculated using the inverse-variance stratum weights along with their Miettinen-Nurminen (score) confidence limits. The summary score test was used for both noninferiority and superiority tests at week 26 and week 52. For the unstratified sensitivity analyses, Wald confidence limits were calculated for both noninferiority and superiority tests at week 26 and week 52. The Clopper and Pearson exact interval method was used for single proportion data.
A gatekeeping procedure was used to control the overall type I error rate at the 5% level, and the primary outcomes were tested in the following order:
Noninferiority test of the avacopan group compared to the prednisone group for disease remission at week 26. Testing continued if the P value for noninferiority for the 1-sided test was less than 0.025.
Noninferiority test of the avacopan group compared to the prednisone group for sustained disease remission at week 52. Testing continued if the P value for noninferiority for the 1-sided test was less than 0.025.
Superiority test of the avacopan group compared to the prednisone group for sustained disease remission at week 52. Testing continued if the P value for superiority for the 1-sided test was less than 0.025.
Superiority test of the avacopan group compared to the prednisone group for disease remission at week 26.
For noninferiority testing of the first primary end point, avacopan was considered noninferior to prednisone if the lower bound of the 2-sided 95% CI was greater than the noninferiority margin of –0.20 and the prednisone group’s disease remission rate was at least 40% at week 26 (if the observed rate of avacopan was lower than that of the prednisone group). For superiority testing, if the lower bound of the 2-sided 95% CI was greater than 0.0, avacopan was considered superior to prednisone in achieving disease remission at week 26. Similar testing was performed for the second primary end point at week 52.
Noninferiority Margin
A meta-analysis of 20 published studies investigating either rituximab with glucocorticoids or cyclophosphamide with glucocorticoids informed the noninferiority margin used for the first primary end point (–0.20). The lower bound of the 95% CI for remission rate across the studies was approximately 60%. Therefore, the selected noninferiority margin would demonstrate that avacopan retained at least 50% of the effect of the comparator (prednisone).
Sample Size and Power Calculation
Based on remission rates from a previous ANCA-AV study of 64% and 53% for rituximab and for cyclophosphamide with azathioprine, respectively, it was estimated that 60% of patients in the ADVOCATE trial’s prednisone group would experience remission at week 26.13 It was estimated that a sample size of 300 patients (150 per treatment group) would provide more than 90% power for the noninferiority test and 90% power to detect approximately 18% superiority for remission at week 26 if the rate of remission was 60% in the prednisone group. Based on a previous study comparing rituximab to cyclophosphamide with azathioprine, it was estimated that approximately 45% of patients in the prednisone group would achieve sustained remission at 52 weeks.12 A sample size of 300 was expected to provide 85% power to detect approximately 18% superiority if the rate of sustained remission was 45% at week 52 in the prednisone group.
Data Imputation
Missing data for the primary end points were imputed as not achieving remission (week 26) or sustained remission (week 52) for the ITT population and were excluded from the PP population. No imputation was performed for other time points. For the first and second primary end points, patients who withdrew from the trial before week 26 and week 52, respectively, were considered as not achieving remission for the primary end point ITT analyses. Patients who discontinued treatment before the key time points but remained in the trial were adjudicated as achieving remission or not for the primary end point ITT analyses. These patients were imputed as not achieving remission for the PP analyses if they had a less than 75% adherence during the first 26 weeks or 52 weeks of the trial, for the respective primary end points.
Sensitivity Analyses
Sensitivity analyses were performed on the primary end point using unstratified analyses, as well as stratified analyses assessing the impact of nonstudy glucocorticoid use. The analyses assessing the impact of glucocorticoids defined high nonstudy glucocorticoid users as nonremitters or excluded patients with high nonstudy glucocorticoid use. Sensitivity analyses for remission were also performed using investigator-assessed (nonadjudicated) results and excluding results from Japan because patients in this region were only enrolled toward the end of the trial. Finally, analyses using alternative definitions of the primary end points were conducted. In these analyses, remission was defined as a BVAS of 0 at relevant time points, irrespective of glucocorticoid use.
Subgroup Analyses
Prespecified subgroup analyses were performed on the primary end points using 6 stratification factors: IV rituximab, IV or oral cyclophosphamide, PR3 ANCA positive, MPO ANCA positive, newly diagnosed ANCA-AV, and relapsed ANCA-AV.
Subgroups based on ANCA-AV type (GPA versus MPA), ANCA positivity (PR3 versus MPO), disease state (newly diagnosed versus relapsing versus refractory), background therapy (cyclophosphamide versus rituximab), and concomitant use of glucocorticoids (yes versus no) were identified as being relevant to the CADTH systematic review.
Secondary Outcomes
Summary statistics, point estimates for treatment differences and corresponding 95% CIs and P values were provided for secondary efficacy end point measures, although these were tested in parallel and none were controlled for multiplicity. BVAS and VDI data were assessed by a blinded, independent adjudication committee, and analysis of relevant outcomes (e.g., remission, relapse, BVAS at week 4, VDI) used adjudicated data. Glucocorticoid use, an input in remission evaluations, was also adjudicated by the committee.
The proportion of patients who achieved the end point of a BVAS of 0 at week 4 was analyzed similarly to the primary end point.
The change from baseline in eGFR for patients with renal disease at baseline was analyzed for the ITT population using a mixed effects model for repeated measures. Model covariates included treatment group, visit, treatment-by-visit interaction, and randomization stratification factors. Missing data were not imputed, and it was assumed that data were missing at random. The percent change from baseline in UACR for patients with renal disease and albuminuria (defined as UACR of at least 10 mg/g creatinine) at baseline was analyzed similarly to the eGFR outcome. These data were not normally distributed and were loge-transformed before the mixed effects model for repeated measures analysis. LSM differences between treatment groups were back-transformed to calculate the estimate for baseline-adjusted percent reduction from control.
The change from baseline in VDI at week 26 and week 52 was analyzed similarly to the eGFR outcome and included the baseline VDI score in the model. It was found that after the database lock, some VDI scores had decreased (scores can only remain the same or increase). The sponsor concluded that the errors were minor and did not change the conclusions for the outcome.
The proportion of patients who experienced a relapse was determined by the number of patients who relapsed after remission divided by the number of patients who achieved remission at week 26. It was planned that the time to relapse would be analyzed using KM methods and log-rank testing of the treatment group differences; however, due to the small number of patients who relapsed, the median time to relapse was not estimable and KM estimates were not calculated. For patients who did not relapse during the 52 weeks, time to relapse was the time from the week 26 BVAS assessment to the last BVAS assessment during the treatment period, and patients were censored.
The GTI scores at week 13 and week 26 were analyzed for the ITT population similarly to the eGFR and VDI outcomes. The treatment differences at week 13 and week 26 were analyzed using linear contrast from the model. A compound symmetric covariance matrix was used to model the within-patient variance-covariance structure for the model errors.
HRQoL data during the 52-week treatment period were analyzed for the ITT population similarly to the eGFR, VDI, and GTI outcomes, with the same factors and including baseline values as a covariate. A Toeplitz covariance matrix was used to model the within-patient variance-covariance structure for the model errors. If the model did not converge, an autoregressive order 1 covariance matrix was used, and if convergence was not met again, a compound symmetric matrix was used.
Descriptive statistics (proportions) were provided for harms outcomes, and no statistical testing was performed.
Analysis Populations
The randomized population included all patients who provided written informed consent and were randomized in the trial. The ITT population included all patients who were randomized in the trial and who received at least 1 dose of blinded study drug; this was the main population for efficacy analyses. The safety population included all patients who were randomized and had received at least 1 dose of the study drug; this was the main population for safety analyses. The PP population consisted of all patients in the ITT population who were adherent with taking avacopan or placebo and who did not have major protocol deviations that could have significantly affected the interpretation of the results.
Results
Patient Disposition
Patient disposition is summarized in Table 10.
In total, 386 individuals were screened, of whom 55 (14.2%) failed screening, mostly due to not meeting the eligibility criteria. The remaining 331 patients were randomized 1:1 to avacopan (N = 166) or prednisone (N = 165), and all but 1 patient received at least 1 dose of the study drug. The single patient was randomized to the prednisone group but was withdrawn due to their renal biopsy not clearly indicating vasculitis.
Approximately 90% of patients completed all 60 weeks of the trial, and completion rates were balanced between groups. Overall, 22.3% of patients randomized to avacopan and 21.2% of patients randomized to prednisone discontinued early from treatment, with the most common reason being due to AEs (15.7% and 17.6%, respectively). Less than 10% of patients withdrew early from the trial (9.0% and 9.1% in the avacopan and prednisone groups, respectively), with the most common reasons being the patient choosing to withdraw (3.6%) in the avacopan group and AEs (3.6%) in the prednisone group. Reasons for early discontinuation of medication or early discontinuation from the trial were generally balanced between treatment groups.
Patient disposition | Prednisone | Avacopan |
|---|---|---|
Screened, N | 386 | |
Screen failures, n (%) | 55 (14.2) | |
Did not meet eligibility criteria | 41 (10.6) | |
Patient withdrawal | 7 (1.8) | |
Adverse event | 2 (0.5) | |
Other | 5 (1.3) | |
Randomized, N | 165 | 166 |
Completed week 26, n (%) | 154 (93.3) | 155 (93.4) |
Completed week 52, n (%) | 152 (92.1) | 151 (91.0) |
Completed week 60, n (%) | 150 (90.9) | 151 (91.0) |
Early discontinuation from study treatment, n (%) | 35 (21.2) | 37 (22.3) |
Adverse event | 29 (17.6) | 26 (15.7) |
Investigator decision | 4 (2.4) | 4 (2.4) |
Patient withdrawal | 1 (0.6) | 3 (1.8) |
Sponsor decision | 0 | 2 (1.2) |
Lost to follow-up | 0 | 1 (0.6) |
Other | 1 (0.6) | 1 (0.6) |
Early withdrawal from trial, n (%) | 15 (9.1) | 15 (9.0) |
Patient withdrawal | 3 (1.8) | 6 (3.6) |
Adverse event | 6 (3.6) | 3 (1.8) |
Investigator decision | 4 (2.4) | 3 (1.8) |
Lost to follow-up | 2 (1.2) | 1 (0.6) |
Parent or guardian withdrawal | 0 | 1 (0.6) |
Other | 0 | 1 (0.6) |
ITT, n (%) | 164 (99.4) | 166 (100) |
PP, n (%) | 161 (97.6) | 162 (97.6) |
Safety, n (%) | 164 (99.4) | 166 (100) |
ITT = intention to treat; PP = per protocol.
Source: ADVOCATE Clinical Study Report.19
Exposure to Study Treatments
Exposure to study treatments is summarized in Table 11 and Table 12.
The mean adherence to the study drugs was 86.4% for avacopan (91.5% for matching placebo) and 98.4% for prednisone (89.5% for matching placebo). The mean exposure to avacopan was 305.1 days ||| |||||| ||||| in the avacopan group compared to ||||| |||| || ||||| ||||| || |||||||||||||||| ||||||| || || |||||||||| |||||. Likewise, the mean exposure to prednisone-matched placebo was ||||| |||| || ||||| ||||| in the avacopan group compared to the mean exposure to prednisone of 129.2 days ||| ||||| ||||| in the prednisone group. Median exposures were balanced for active and placebo drugs for both groups and were consistent with the expected durations in the trial (364 days for avacopan or matched placebo and 140 days for prednisone or matched placebo). Mean and median daily doses were similar to the expected doses for avacopan (i.e., 60 mg/day), and doses for avacopan and prednisone were similar between treatment arms. Overall adherence to nonbackground medications was lower in the avacopan group (86.4% and 89.5% for avacopan and prednisone-matched placebo, respectively) than in the prednisone group (91.5% and 98.4% for avacopan-matched placebo and prednisone, respectively). The mean overall glucocorticoid use (including both study-supplied and nonstudy-supplied glucocorticoids) was 1,348.9 mg (SD = 2,040.3 mg) and 3,654.5 mg (SD = 1,709.8 mg) in the avacopan and prednisone groups, respectively.
For background immunosuppressant therapy, 102 patients (30.9%) received IV cyclophosphamide, 14 patients (4.2%) received oral cyclophosphamide, and 214 patients (64.8%) received IV rituximab. Mean and median doses tended to be higher in the prednisone group than in the avacopan group for either form of cyclophosphamide, and doses were mostly balanced for IV rituximab.
Prior and concomitant medication use for ANCA-AV is summarized in Table 13.
Most patients were using glucocorticoids during screening: 75.3% and 82.3% for the avacopan and prednisone groups, respectively. Nearly all patients had some exposure to nonstudy glucocorticoids during the treatment period: 87.3% and 90.9% for the avacopan and prednisone groups, respectively, most of whom used them in the first 29 days of the trial (83.1% and 86.0%, respectively). During follow-up, 29.5% and 34.8% of patients in the avacopan and prednisone groups, respectively, received nonstudy glucocorticoids. Doses were reported for the specified period, rather than per day, and for most specified time periods the mean and median doses in the avacopan group were greater than in the prednisone group. Approximately one-fifth of patients had exposure to other nonprotocol-specified immunosuppressants or other treatments for ANCA-AV: 17.5% and 22.0% for the avacopan and prednisone groups, respectively. Overall, 21 patients (12.7%) in the avacopan group and 15 patients (9.1%) in the prednisone group did not receive nonstudy glucocorticoids.
Table 11: Treatment Exposure (ITT Population)
Exposure | Prednisone (N = 164) | Avacopan (N = 166) | ||
|---|---|---|---|---|
Prednisone | Avacopan-matched placebo | Avacopan | Prednisone-matched placebo | |
Duration of exposure (days) | ||||
Mean (SD) | 129.2 |||||| | ||||| |||||| | 305.1 ||||||| | ||||| |||||| |
Median (minimum to maximum) | 140.0 | || |||| | ||||| || || |||| | 364.0 | || |||| | ||||| || || |||| |
||||| |||| |||| | ||||
|||| |||| | |||| ||||| | |||| |||||| | |||| |||||| | |||| ||||| |
|||||| |||| || |||| | |||| || || ||| | |||| || || |||| | |||| || || |||| | |||| || || ||| |
Overall adherencea | ||||
Mean (SD) | 98.4 |||||| | 91.5 |||||| | 86.4 |||||| | 89.5 |||||| |
|||||| |||| || |||| | ||||| || || |||| | |||| || || |||| | |||| || || |||| | |||| || || |||| |
ITT = intention to treat; SD = standard deviation.
aAvacopan and avacopan-matched placebo adherence was calculated as number of capsules taken divided by 6 times the number of days in the randomized treatment period times 100. Number of days in the randomized treatment period was the week 52 visit date (or the early termination visit date) minus the date of the first dose plus 1. For adolescents, the formula was altered, with the number of capsules taken daily based on the placebo starting dose and dose adjustments based on avacopan plasma exposure in adolescents. Prednisone and prednisone-matched placebo adherence was calculated as number of capsules taken divided by the number of expected doses in the randomized treatment period times 100. The number of expected doses during the treatment period was based on the prednisone and matching placebo schedule in the protocol.
Source: ADVOCATE Clinical Study Report.19
Table 12: Background Treatment Exposure (ITT Population)
Exposure | Prednisone (N = 164) | Avacopan (N = 166) |
|---|---|---|
Total study-supplied and nonstudy-supplied glucocorticoid use in prednisone equivalent dose (mg) | ||
Day 1 to end of treatment,a nb (%) | 164 | 145 |
Mean (SD) | 3,654.5 (1,709.8) | 1,348.9 (2,040.3) |
|||||| |||| || |||| | |||||| |||| || |||||| | ||||| || || ||||| |
Study-supplied immunosuppressant use from day 1 to end of treatment | ||
IV cyclophosphamide, n | 51 | 51 |
|||| |||| | |||||| |||||||| | |||||| |||||||| |
|||||| |||| || |||| | |||||| |||||| || |||||||| | |||||| |||| || ||||||| |
Oral cyclophosphamide, n | 6 | 8 |
|||| |||| | ||||||| |||||||| | |||||| |||||||| |
|||||| |||| || |||| | ||||||| ||||||| || |||||||| | |||||| ||||||| || |||||||| |
IV rituximab, n | 107 | 107 |
|||| |||| | |||||| ||||||| | |||||| ||||||| |
|||||| |||| || |||| | |||||| ||||||| || ||||||| | |||||| |||||| || ||||||| |
ITT = intention to treat; SD = standard deviation.
aEnd of treatment is day 365 or early termination visit.
bThe n (the denominator for proportions) is the number of patients who used any glucocorticoids during the period (not all patients in period).
Source: ADVOCATE Clinical Study Report.19
Table 13: Prior and Concomitant Medication Use for ANCA-AV (ITT Population)
Medication use | Prednisone (N = 164) | Avacopan (N = 166) |
|---|---|---|
Concomitant nonstudy glucocorticoid usea in prednisone equivalent dose (mg) | ||
Screening day –14 to –1, nb (%) | 135 (82.3) | 125 (75.3) |
Mean (SD) | 727.8 (787.8) | 654.0 (744.4) |
|||||| |||| || |||| | ||||| || || ||||| | ||||| || || ||||| |
Day 1 to 29, nb (%) | 141 (86.0) | 138 (83.1) |
Mean (SD) | 377 (518.3) | 446.5 (570.2) |
|||||| |||| || |||| | ||||| || || ||||| | ||||| || || ||||| |
Day 30 to 183, nb (%) | 56 (34.1) | 52 (31.3) |
Mean (SD) | 434.3 (962.2) | 645.9 (1,461.9) |
|||||| |||| || |||| | ||||| || || ||||| | |||||| || || ||||| |
Day 1 to 183, nb (%) | 149 (90.9) | 143 (86.1) |
Mean (SD) | 884.2 (1,104.1) | 1,245.5 (1,737.4) |
|||||| |||| || |||| | ||||| || || ||||| | ||||| || || ||||| |
Day 184 to end of treatment,c nb (%) | 64 (39.0) | 45 (27.1) |
Mean (SD) | 489.0 (896.9) | 295.6 (672.0) |
|||||| |||| || |||| | ||||| || || ||||| | ||||| || || ||||| |
Day 1 to end of treatment,c nb (%) | 149 (90.9) | 145 (87.3) |
Mean (SD) | 1,265.3 (1,650.6) | 1,348.9 (2,040.3) |
|||||| |||| || |||| | ||||| || || ||||| | ||||| || || ||||| |
||| || |||||||||| || |||| || || ||| | | |||||| | | |||||| |
|||| |||| | ||||| ||||||| | ||||| ||||||| |
|||||| |||| || |||| | ||||| || || ||||| | ||||| || || ||||| |
Concomitant other nonprotocol-specified immunosuppressant drugs or other treatments for ANCA-AV,d n (%) | ||
Day 1 to 183 | 16 (9.8) | 14 (8.4) |
Day 184 to end of treatmentc | 25 (15.2) | 19 (11.4) |
Day 1 to end of treatmentc | 36 (22.0) | 29 (17.5) |
||| || ||||||||| || |||| || | | |||||| | | |||||| |
Patients who received no glucocorticoids from day 1 to end of treatment,c n (%) | ||
No glucocorticoidse | 0 | 21 (12.7) |
No nonstudy glucocorticoidsf | 15 (9.1) | 21 (12.7) |
ANCA-AV = antineutrophil cytoplasmic autoantibody–associated vasculitis; ITT = intention to treat; SD = standard deviation.
aConcomitant IV or oral glucocorticoids other than the prednisone study medication. Dose is the total dose for the specified period.
bThe n (the denominator for proportions) is the number of patients who used any glucocorticoids during the period (not all patients in the period).
cEnd of treatment is day 365 or early termination visit.
dIncludes nonprotocol-specified rituximab, azathioprine, cyclophosphamide, mycophenolate, methotrexate, methotrexate sodium, cyclosporine, tacrolimus, alemtuzumab, belimumab, abatacept, or other immunosuppressants.
ePatients who did not receive any glucocorticoids during the ADVOCATE trial, including tapered prednisone according to the trial protocol and nonstudy glucocorticoids (e.g., for adrenal insufficiency or allergic reaction).
fPatients who did not receive nonstudy glucocorticoids but may have received tapered prednisone according to the trial protocol.
Source: ADVOCATE Clinical Study Report.19
Protocol Deviations
Protocol deviations are summarized in Table 14.
|||||||||| || ||||| |||||||||| || ||||||||| |||||||| ||||||||||| |||| || |||| |||||| ||||||| || |||||||| ||||||||||| || ||||||| ||||||| ||||| |||||||| |||||||||| || || ||||| |||| ||||||||||| |||||||||| || ||||||| |||||||| ||||| |||| |||||||||| || |||||||||| ||||| || |||||||||| || |||||| || ||||||||| |||| || || ||||||||| ||||| |||||||| |||| |||||||| |||| || || ||||||||||| ||||||||| ||| |||||||| ||||| || ||||||||| || || |||||||||| ||||| || ||||||| ||||| || |||| |||||||||||| ||||| |||||||||| ||||||||||| || || |||||||||||| || ||||| |||| || ||||||| ||||| || |||| ||||||||||| || ||||||| |||||| |||| || ||||| ||||||| || |||||||| |||||||||| |||||| || || |||||||||| ||||||||||||||||| |||||||||| || ||||||||| || ||||| |||||||||| ||||| |||| |||| |||| |||| ||||||||| |||||||||| || |||||||| |||| |||||||||| || |||||| || | ||||| ||||||| |||||||| ||||| ||||||||||| |||||||||| |||||| |||| ||||||||| ||||| |||||||| |||| || || ||||||||||| |||||||||||||| |||||||||||| |||||||| || |||| || ||||| |||||||| |||| ||||||| || ||||||||||||| || ||||| || || || |||||||| ||||| || ||||| || |||||||| || || |||||||| || |||||||||| ||||||| ||||||||||||| || |||||||| |||||||||| |||| |||||||| || ||||| ||||||| ||||| ||||||| || ||||||||||||| || |||| || ||||| ||||| || ||||| || |||||||| || || |||||||||| |||||| |||| ||||||| || ||||||||||||| || |||| |||
|||||||||| | |||||||| | |
|---|---|---|
|||||||||| || ||||| | |||||||| || ||||| | |
||| ||||||||| | | |||||| | | |||||| |
||||| |||||||||| | | |||||| | | |||||| |
|||||||| |||||||||| |||||||| | | |||||| | | |||||| |
||||| |||||||||| | | ||||| | | ||||| |
||| ||||||||| | | ||||| | | ||||| |
||||| |||||||| || ||| | | ||||| | | ||||| |
|||||||| ||||||| | | ||||| | | ||||| |
||| ||||||||| || ||||||||| |||||||||| |||||||| | | ||||| | | ||||| |
||||||||||||||| ||||||| | | ||||| | | ||||| |
||||| |||||||||| | | ||||| | | ||||| |
||||| ||||||||| || ||||||||| |||| |||||||| | | ||||| | | ||||| |
|||||||| |||||||| |||| || ||||||||||| |||| | | ||||| | | ||||| |
||||||| |||| || |||| |||||||||| | | ||||| | | ||||| |
||||| ||||| |||||||||| |||||||||| |||| || || || ||||||||| ||||||||| || ||||||| | | ||||| | | ||||| |
||||||||| |||||||||||| ||||| || ||||||| |||||||| |||| |||||||||| | | ||||| | | ||||| |
|||||||| |||| ||||||| ||||||| || ||||||||||||| || |||| || || |||||||| | | |||||| | | |||||| |
|||||||||||| |||||||||| | | ||||| | | ||||| |
||||||||||||| |||| ||||| |||||||||| | | ||||| | | ||||| |
|||||||||||| |||||||||| || ||||||||||||| |||| ||||| |||||||||| | | ||||| | | ||||| |
|||||||| |||| ||||||| ||||||| || ||||||||||||| || |||| || || ||||||||| | | |||||| | | |||||| |
|||||||||||| |||||||||| | | |||||| | | ||||| |
||||||||||||| |||| ||||| ||||||||| | | ||||| | | |||||| |
|||||||||||| |||||||||| || ||||||||||||| |||| ||||| |||||||||| | | ||||| | | ||||| |
|||| ||||||||||||||| ||||||||||| ||||||||||||| |||| ||||||||||| |||||||||| |||||||| |||||| || |||||||||||||| || |||||||| ||||||| |||||||| |||||||||||| |||||||||| |||||||| |||||||||| ||||||||||||||||| ||||||||||||| |||||||||||||| || |||||||||||| || ||||||||| || ||||||||||| |||| |||| || |||||||| |||| |||||| ||||| |||||||||| ||||| || |||||||| ||||||| ||||||||| |||||||| || |||| |||| |||||||||||| |||||||||| || ||||||||| || |||||||| || || |||| |||| |||| || |||||||| |||| |||||| ||||| ||||||||||||||||||| |||||||| |||||||| ||||| |||||||19
Efficacy
Only those efficacy outcomes and analyses of subgroups identified in the review protocol are reported in this section. Refer to Appendix 3 for detailed efficacy data.
Survival
Survival was not assessed as an efficacy outcome in the ADVOCATE trial but was captured as deaths in the assessment of harm outcomes.
Disease Remission (Induction and Sustained Remission)
Based on the ITT analyses, 72.3% (95% CI, 64.8% to 78.9%) of patients randomized to avacopan and 70.1% (95% CI, 62.5% to 77.0%) of patients randomized to prednisone achieved remission at week 26 (Table 15). The estimate of common difference in remission rates between groups was 3.4% (95% CI, –6.0% to 12.8%; noninferiority P < 0.0001; superiority P = 0.2387). The PP analyses had findings that were consistent with the ITT analyses. The sensitivity analyses results for week 26 were generally consistent with those of the primary outcome. Analyses by randomization stratification factor and subgroup for the primary outcome are summarized in Table 27. Treatment estimates for subgroups were consistent with the primary analysis.
At week 52, 65.7% (95% CI, 57.9% to 72.8%) of patients randomized to avacopan and 54.9% (95% CI, 46.9% to 62.6%) of patients randomized to prednisone achieved sustained remission according to the ITT analyses (Table 15). The estimate of common difference in sustained remission rates between groups was 12.5% (95% CI, 2.6% to 22.3%; noninferiority P < 0.0001; superiority P = 0.0066). The PP analyses had findings that were consistent with the ITT analyses. The week 52 sensitivity analyses and subgroup analyses (Table 28) were generally consistent with those of the week 52 primary outcome.
Table 15: Stratified Analyses of the Proportion of Patients With Disease Remission and Sustained Disease Remission — Primary Outcomes
Outcome | Prednisone | Avacopan |
|---|---|---|
Disease remission at week 26 | ||
ITT population, N | 164 | 166 |
Patients who achieved remission, n (%) 95% CIa | 115 (70.1) (62.5 to 77.0) | 120 (72.3) (64.8 to 78.9) |
Difference (%) | Reference | 2.2 |
Estimate of common difference (%)b 2-sided 95% CI for common difference (%)c | Reference | 3.4 (–6.0 to 12.8) |
Noninferiority P valued | Reference | < 0.0001 |
Superiority P valued | Reference | 0.2387 |
PP population, N | 161 | 162 |
Patients who achieved remission, n (%) 95% CIa | 109 (67.7) ||||| || ||||| | 110 (67.9) ||||| || ||||| |
|||||||||| || ||||||| | ||||||||| | ||||||||| |
Estimate of common difference (%)b 2-sided 95% CI for common difference (%)c | Reference | 2.0 (–7.6 to 11.6) |
Noninferiority P valued | Reference | < 0.0001 |
Superiority P valued | Reference | 0.3419 |
Sustained remission at week 52 | ||
ITT population, N | 164 | 166 |
Patients who achieved remission, n (%) 95% CIa | 90 (54.9) (46.9 to 62.6) | 109 (65.7) (57.9 to 72.8) |
Difference (%) | Reference | 10.8 |
Estimate of common difference (%)b 2-sided 95% CI for common difference (%)c | Reference | 12.5 (2.6 to 22.3) |
Noninferiority P valued | Reference | < 0.0001 |
Superiority P valued | Reference | 0.0066 |
PP population, N | 161 | 162 |
Patients who achieved remission, n (%) 95% CIa | 81 (50.3) ||||| || ||||| | 95 (58.6) ||||| || ||||| |
|||||||||| || ||||||| | ||||||||| | ||||||||| |
Estimate of common difference (%)b 2-sided 95% CI for common difference (%)c | Reference | 11.0 (1.0 to 21.1) |
Noninferiority P valued | Reference | < 0.0001 |
Superiority P valued | Reference | 0.0159 |
CI = confidence interval; ITT = intention to treat; PP = per-protocol; SD = standard deviation.
aClopper and Pearson exact CI.
bSummary score estimate of the common difference in remission rates using inverse-variance stratum weights.
cMiettinen-Nurminen (score) confidence limits for the common difference in remission rates.
dP value has been adjusted for multiple testing (i.e., the type I error rate has been controlled).
Source: ADVOCATE Clinical Study Report.19
At week 4, 62.7% (95% CI, 54.8% to 70.0%) and 68.9% (95% CI, 61.2% to 75.9%) of patients in the avacopan and prednisone groups, respectively, had a BVAS of 0 (use of glucocorticoids during this period was not considered) (Table 16). The estimate of common difference between groups was –5.6% (95% CI, –15.4% to 4.2%).
Renal Function (e.g., eGFR, Progression to ESKD)
For patients with renal disease at baseline (based on the BVAS renal component), the LSM difference in change from baseline between treatment groups for eGFR was 2.9 mL/min/1.73 m2 (95% CI, 0.1 mL/min/1.73 m2 to 5.8 mL/min/1.73 m2) at week 26, 3.2 mL/min/1.73 m2 (95% CI, 0.3 mL/min/1.73 m2 to 6.1 mL/min/1.73 m2) at week 52, and ||| ||||||||||| || |||| || |||| || || ||||||||||| at week 60 (Table 17). Data organized by eGFR category are summarized in Table 29. Seven patients required dialysis during the trial: 3 patients in the avacopan group (1.8%) and 4 patients in the prednisone group (2.4%).
Table 16: Patients Who Achieved BVAS of 0 at Week 4 — Secondary Outcome (ITT Population)
Outcome | Prednisone (N = 164) | Avacopan (N = 166) |
|---|---|---|
Patients with BVAS of 0 at week 4,a n (%) 95% CIb | 113 (68.9) (61.2 to 75.9) | 104 (62.7) (54.8 to 70.0) |
Difference (%) | Reference | –6.2 |
Estimate of common difference (%) 2-sided 95% CI for common difference (%)c | Reference | –5.6 (–15.4 to 4.2) |
Superiority P valued,e | Reference | 0.8695 |
ANCA = antineutrophil cytoplasmic autoantibody; ANCA-AV = antineutrophil cytoplasmic autoantibody–associated vasculitis; BVAS = Birmingham Vasculitis Activity Score; CI = confidence interval; ITT = intention to treat; MPO = myeloperoxidase.
aThis is a modified version of the BVAS in which the week 4 measurement considered the last 7 days (as opposed to the last 28 days, which is the usual range).
bCIs for treatment proportions were calculated using the Clopper and Pearson Method.
cThe 2-sided 95% CI is calculated for the difference in proportions (avacopan minus prednisone), adjusted for randomization strata (newly diagnosed or relapsed ANCA-AV, anti-PR3 or anti-MPO ANCA, and IV rituximab or IV or oral cyclophosphamide standard of care treatment) using the stratified summary score test and the estimate for the common difference in proportions.
dSuperiority P value is 1-sided.
eP value has not been adjusted for multiple testing (i.e., the type I error rate has not been controlled).
Source: ADVOCATE Clinical Study Report.19
Table 17: Change From Baseline in eGFR in Patients With Renal Disease at Baseline — Secondary Outcome (ITT Population)
Outcome | Prednisone (N = 164) | Avacopan (N = 166) |
|---|---|---|
Baseline, n (%) | 134 (81.7) | 131 (78.9) |
Mean (SD) eGFR (mL/min/1.73 m2) | 45.6 (27.3) | 44.6 (27.7) |
Week 26, n (%) | 127 (77.4) | 121 (72.9) |
LSM change from baseline (SEM) eGFR (mL/min/1.73 m2)a | 2.9 (1.0) | 5.8 (1.0) |
LSM difference (95% CI) eGFR (mL/min/1.73 m2)a | Reference | 2.9 (0.1 to 5.8) |
P valuea,b | Reference | 0.0460 |
Week 52, n (%) | 125 (76.2) | 119 (71.7) |
LSM change from baseline (SEM) eGFR (mL/min/1.73 m2)a | 4.1 (1.0) | 7.3 (1.1) |
LSM difference (95% CI) eGFR (mL/min/1.73 m2)a | Reference | 3.2 (0.3 to 6.1) |
P valuea,b | Reference | 0.0294 |
|||| || |||| | ||| |||||| | ||| |||||| |
||| |||||| |||| |||||||| ||||| | ||| ||||| | ||| ||||| |
||| |||||||||| |||| ||| | ||||||||| | ||| ||||| || |||| |
| |||||| | | ||||||||| | |||||| |
CI = confidence interval; eGFR = estimated glomerular filtration rate; ITT = intention to treat; LSM = least squares mean; MMRM = mixed effects model for repeated measures; SD = standard deviation; SEM = standard error of the mean.
aAnalysis used MMRMs, with treatment group, visit, and treatment-by-visit interaction as factors and baseline as a covariate. MMRM results by visit use the treatment-by-visit interaction term.
bP value has not been adjusted for multiple testing (i.e., the type I error rate has not been controlled).
| |||| || || || |||||||| || || ||||||| |||||| |||| || |||| || |||| |||||| |||||| |||| ||||||||| ||||| || ||||||| || |||||||| || ||||||||||
Source: ADVOCATE Clinical Study Report.19
For patients with renal disease (based on the BVAS renal component) and albuminuria (defined as UACR of at least 10 mg/g creatinine) at baseline, the LSM ratio for change from baseline in UACR was 1.3 mg/g (95% CI, 1.0 mg/g to 1.6 mg/g) at week 26, 1.1 mg/g (95% CI, 0.9 mg/g to 1.5 mg/g) at week 52, and ||| |||| |||| || | || || ||||| at week 60 (Table 18).
Table 18: Change From Baseline in UACR in Patients With Renal Disease and Albuminuria at Baseline — Secondary Outcome (ITT Population)
Outcome | Prednisone (N = 164) | Avacopan (N = 166) |
|---|---|---|
Baseline, n (%) | 128 (78.0) | 125 (75.3) |
Geometric mean (mg albumin/g creatinine) | 312.2 | 432.9 |
Week 26, n (%) | 118 (72.0) | 113 (68.1) |
LSM change from baseline (SEM) (mg albumin/g creatinine)a | 0.3 (1.1) | 0.4 (1.1) |
LSM ratio (95% CI) (mg albumin/g creatinine)a | Reference | 1.3 (1.0 to 1.6) |
P valuea,b | Reference | 0.0885 |
Week 52, n (%) | 114 (69.5) | 109 (65.7) |
LSM change from baseline (SEM) (mg albumin/g creatinine)a | 0.2 (1.1) | 0.3 (1.1) |
LSM ratio (95% CI) (mg albumin/g creatinine)a | Reference | 1.1 (0.9 to 1.5) |
P valuea,b | Reference | 0.3991 |
|||| || |||| | ||| |||||| | ||| |||||| |
||| |||||| |||| |||||||| ||||| | ||| ||||| | ||| ||||| |
||| |||||||||| |||| ||| | ||||||||| | ||| |||| || |||| |
| |||||| | | ||||||||| | |||||| |
CI = confidence interval; ITT = intention to treat; LSM = least squares mean; MMRM = mixed effects model for repeated measures; SEM = standard error of the mean; UACR = urinary albumin–creatinine ratio.
aAnalysis for LSM, SEM, CI, and P value used MMRMs, with treatment group, visit, and treatment-by-visit interaction as factors and baseline as a covariate. Logarithmic transformations were applied to the data before fitting the model. The 95% CI was transformed back to the original scale. MMRM results by visit use the treatment-by-visit interaction term.
bP value has not been adjusted for multiple testing (i.e., the type I error rate has not been controlled).
| |||| || || || |||||||| || || ||||||| |||||| |||| || |||| || |||| |||||| |||||| |||| ||||||||| ||||| || |||||| || |||||||| || ||||||||||
Source: ADVOCATE Clinical Study Report.19
Systemic Damage (e.g., Measured by VDI)
Based on the data assessed by the adjudication committee, the LSM difference in change of the VDI from baseline between treatment groups was 0.1 (95% CI, –0.1 to 0.3) at week 26, 0.0 (95% CI, –0.2 to 0.3) at week 52, and ||| |||| || |||| || |||| at week 60 (Table 19).
Table 19: Change From Baseline in VDI Score — Secondary Outcome (ITT Population)
Outcome | Prednisone (N = 164) | Avacopan (N = 166) |
|---|---|---|
Baseline, n (%) | 163 (99.4) | 165 (99.4) |
Mean (SD) | 0.7 (1.5) | 0.7 (1.5) |
Week 26, n (%) | 155 (94.5) | 161 (97.0) |
LSM change from baseline (SEM)a | 1.0 (0.1) | 1.1 (0.1) |
LSM difference (95% CI)a | Reference | 0.1 (–0.1 to 0.3) |
P valuea,b | Reference | 0.4593 |
Week 52, n (%) | 151 (92.1) | 150 (90.4) |
LSM change from baseline (SEM)a | 1.2 (0.1) | 1.2 (0.1) |
LSM difference (95% CI)a | Reference | 0.0 (–0.2 to 0.3) |
P valuea,b | Reference | 0.8660 |
|||| || |||| | ||| |||||| | ||| |||||| |
||| |||||| |||| |||||||| ||||| | ||| ||||| | ||| ||||| |
||| |||||||||| |||| ||| | ||||||||| | ||| ||||| || |||| |
| |||||| | | ||||||||| | |||||| |
ANCA = antineutrophil cytoplasmic autoantibody; ANCA-AV = antineutrophil cytoplasmic autoantibody–associated vasculitis; CI = confidence interval; ITT = intention to treat; LSM = least squares mean; MMRM = mixed effects model for repeated measures; MPO = myeloperoxidase; SD = standard deviation; SEM = standard error of the mean; VDI = Vasculitis Damage Index.
aAnalysis used MMRMs, with baseline VDI, treatment group, visit, treatment-by-visit interaction, and stratification factors (newly diagnosed or relapsed ANCA-AV, anti-PR3 or anti-MPO ANCA, and IV rituximab or IV or oral cyclophosphamide standard of care treatment) as covariates. MMRM results by visit use the treatment-by-visit interaction term.
bP value has not been adjusted for multiple testing (i.e., the type I error rate has not been controlled).
c|||| || || || |||||||| || || ||||||| |||||| |||| || |||| || |||| |||||| |||||| |||| ||||||||| ||||| || ||||||||||||| |||||| |||||| ||||||||| || |||||||| |||||||| |||||||| || |||||||| ||||| | || ||||||||| || |||||||||||||||| || || ||||| |||||||| || |||| |||||||||| || ||||||| || |||||||| || ||||||||||
Source: ADVOCATE Clinical Study Report.19
Disease Relapse (e.g., Time to Relapse or Duration of Remission, Minor Versus Major)
Of the patients who achieved remission at week 26, 7.5% (95% CI, 3.5% to 13.8%) in the avacopan group and 12.2% (95% CI, 6.8% to 19.6%) in the prednisone group experienced disease relapse (Table 20). The estimate of common difference in rates was –6.0% (95% CI, –14.4% to 2.4%).
An exploratory analysis was conducted on the rate of relapse among patients who achieved a BVAS of 0 at any time during the 52-week treatment period (Table 30). Overall, 95.2% of patients in the avacopan group and 95.7% of patients in the prednisone group had a BVAS of 0 at any time point, and 10.1% and 21.0% of these patients in the respective treatment groups experienced disease relapse. The hazard ratio was 0.46 (95% CI, 0.25 to 0.84) for avacopan versus prednisone. Due to the small number of patients who relapsed, the median time to relapse was not estimable and KM estimates were not calculated.
During the follow-up period, from week 52 to week 60, 3.8% of patients in the avacopan group and 4.5% of patients in the prednisone group experienced disease relapse (Table 31). Also, during the 8-week follow-up, 5.7% of patients in the avacopan group and 7.6% of patients in the prednisone group experienced a worsening BVAS.
Table 20: Proportion of Patients With Disease Relapse After Previously Achieving Disease Remission at Week 26 — Secondary Outcome (ITT Population)
Outcome | Prednisone (N = 164) | Avacopan (N = 166) |
|---|---|---|
Patients who achieved remission at week 26, n (%)a | 115 (70.1) | 120 (72.3) |
Patients who relapsed, n (%) 95% CIb | 14 (12.2) (6.8 to 19.6) | 9 (7.5) (3.5 to 13.8) |
Difference (%) | Reference | –4.7 |
Estimate of common difference (%)c 2-sided 95% CI for difference (%)d | Reference | –6.0 (–14.4 to 2.4) |
Superiority P valuee | Reference | 0.0810 |
CI = confidence interval; ITT = intention to treat.
aPatients who achieved remission at week 26, also the denominator for percentage calculations.
bClopper and Pearson exact CI.
cSummary score estimate of the common difference in remission rates using inverse-variance stratum weights.
dMiettinen-Nurminen (score) confidence limits for the common difference in remission rates.
eP value has not been adjusted for multiple testing (i.e., the type I error rate has not been controlled).
Source: ADVOCATE Clinical Study Report.19
Glucocorticoid Use and Related Toxicities and Safety
The LSM difference between treatment groups for the GTI-CWS was –11.0 (95% CI, –19.7 to –2.2) at week 13 and–16.8 (95% CI, –25.6 to –8.0) at week 26 (Table 21). The LSM difference between treatment groups for the GTI-AIS was –13.3 (95% CI, –22.2 to –4.4) at week 13 and –12.1 (95% CI, –21.1 to –3.2) at week 26. This end point was not assessed at later time points.
Table 21: Glucocorticoid-Induced Toxicity by GTI Score — Secondary Outcome (ITT Population)
Outcome | Prednisone (N = 164) | Avacopan (N = 166) |
|---|---|---|
GTI-CWS | ||
Week 13, n (%) | 161 (98.1) | 160 (96.4) |
LSM (SEM)a | 36.6 (3.4) | 25.7 (3.4) |
LSM difference (95% CI)a | Reference | –11.0 (–19.7 to –2.2) |
P valuea,b | Reference | 0.0140 |
Week 26, n (%) | 153 (93.3) | 154 (92.7) |
LSM (SEM)a | 56.6 (3.5) | 39.7 (3.4) |
LSM difference (95% CI)a | Reference | –16.8 (–25.6 to –8.0) |
P valuea,b | Reference | 0.0002 |
GTI-AIS | ||
Week 13, n (%) | 161 (98.2) | 160 (96.4) |
LSM (SEM)a | 23.2 (3.5) | 9.9 (3.5) |
LSM difference (95% CI)a | Reference | –13.3 (–22.2 to –4.4) |
P valuea,b | Reference | 0.0034 |
Week 26, n (%) | 153 (93.3) | 154 (92.3) |
LSM (SEM)a | 23.4 (3.5) | 11.2 (3.5) |
LSM difference (95% CI)a | Reference | –12.1 (–21.1 to –3.2) |
P valuea,b | Reference | 0.0082 |
ANCA = antineutrophil cytoplasmic autoantibody; ANCA-AV = antineutrophil cytoplasmic autoantibody–associated vasculitis; CI = confidence interval; GTI = Glucocorticoid Toxicity Index; GTI-AIS = Glucocorticoid Toxicity Index Aggregate Improvement Score; GTI-CWS = Glucocorticoid Toxicity Index Cumulative Worsening Score; ITT = intention to treat; LSM = least squares mean; MMRM = mixed effects model for repeated measures; MPO = myeloperoxidase; SEM = standard error of the mean.
aAnalysis used MMRMs, with treatment group, visit, treatment-by-visit interaction, and stratification factors (newly diagnosed or relapsed ANCA-AV, anti-PR3 or anti-MPO ANCA, and IV rituximab or IV or oral cyclophosphamide standard of care treatment) as covariates.
bP value has not been adjusted for multiple testing (i.e., the type I error rate has not been controlled).
Source: ADVOCATE Clinical Study Report.19
Health-Related Quality of Life
The LSM difference in change from baseline between treatment groups for the SF-36v2 mental component summary was 1.6 (95% CI, –0.6 to 3.8) at week 26, 1.7 (95% CI, –0.5 to 3.9) at week 52, and ||| |||| || |||| || |||| at week 60 (Table 22). The LSM difference in change from baseline between treatment groups for the SF-36v2 physical component summary was 3.1 (95% CI, 1.2 to 5.0) at week 26, 2.4 (95% CI, 0.4 to 4.3) at week 52, and ||| |||| || |||| || |||| at week 60.
The LSM difference in change from baseline between treatment groups for the EQ VAS was 3.6 (95% CI, –0.1 to 7.2) at week 26, 5.9 (95% CI, 2.3 to 9.6) at week 52, and ||| |||| || |||| || |||| at week 60 (Table 23). The LSM difference in change from baseline between treatment groups for the EQ-5D-5L index score was 0.0 (95% CI, 0.0 to 0.1) at week 26, 0.1 (95% CI, 0.0 to 0.1) at week 52, and ||| |||| || || || |||| at week 60.
Hospitalizations
Hospitalizations were not assessed in the ADVOCATE trial.
Symptoms
Symptoms (e.g., fatigue) were not assessed as an efficacy outcome in the ADVOCATE trial, but some may have been captured as harm outcomes.
Table 22: SF-36v2 Mental Component Summary and Physical Component Summary — Secondary Outcome (ITT Population)
Outcome | Prednisone (N = 164) | Avacopan (N = 166) |
|---|---|---|
Mental component summary | ||
Baseline, n (%) | 160 (97.6) | 166 (100) |
Mean (SD)a | 42.1 (13.3) | 44.2 (12.7) |
Week 26, n (%) | 147 (89.6) | 154 (92.8) |
LSM change from baseline (SEM)a | 3.3 (0.8) | 4.9 (0.8) |
LSM difference (95% CI)a | Reference | 1.6 (–0.6 to 3.8) |
P valuea,b | Reference | 0.1575 |
Week 52, n (%) | 144 (87.8) | 148 (89.2) |
LSM change from baseline (SEM)a | 4.7 (0.9) | 6.4 (0.8) |
LSM difference (95% CI)a | Reference | 1.7 (–0.5 to 3.9) |
P valuea,b | Reference | 0.1333 |
|||| || |||| | ||| |||||| | ||| |||||| |
||| |||||| |||| |||||||| ||||| | ||| ||||| | ||| ||||| |
||| |||||||||| |||| ||| | ||||||||| | ||| ||||| || |||| |
| |||||| | | ||||||||| | |||||| |
Physical component summary | ||
Baseline, n (%) | 160 (97.6) | 165 (99.4) |
Mean (SD) | 40.1 (10.5) | 39.2 (10.3) |
Week 26, n (%) | 147 (89.6) | 153 (92.2) |
LSM change from baseline (SEM)a | 1.3 (0.7) | 4.5 (0.7) |
LSM difference (95% CI)a | Reference | 3.1 (1.2 to 5.0) |
P valuea,b | Reference | 0.0017 |
Week 52, n (%) | 144 (87.8) | 147 (88.6) |
LSM change from baseline (SEM)a | 2.6 (0.8) | 5.0 (0.7) |
LSM difference (95% CI)a | Reference | 2.4 (0.4 to 4.3) |
P valuea,b | Reference | 0.0183 |
|||| || |||| | ||| |||||| | ||| |||||| |
||| |||||| |||| |||||||| ||||| | ||| ||||| | ||| ||||| |
||| |||||||||| |||| ||| | ||||||||| | ||| ||||| || |||| |
| |||||| | | ||||||||| | |||||| |
ANCA = antineutrophil cytoplasmic autoantibody; ANCA-AV = antineutrophil cytoplasmic autoantibody–associated vasculitis; CI = confidence interval; ITT = intention to treat; LSM = least squares mean; MMRM = mixed effects model for repeated measures; MPO = myeloperoxidase; SD = standard deviation; SEM = standard error of the mean; SF-36v2 = Short Form (36) Health Survey version 2.
aAnalysis used MMRMs, with treatment group, visit, treatment-by-visit interaction, and randomization strata (newly diagnosed or relapsed ANCA-AV, anti-PR3 or anti-MPO ANCA, and IV rituximab or IV or oral cyclophosphamide standard of care treatment) as factors and baseline as a covariate. MMRM results by visit use the treatment-by-visit interaction term.
bP value has not been adjusted for multiple testing (i.e., the type I error rate has not been controlled).
| |||| || |||| |||| |||| |||||| |||||| |||| ||||||||| ||||| || ||||||||||||| |||||| |||||| ||||||||| || |||||||| |||||||| |||||||| || |||||||| ||||| | || ||||||||| || |||||||||||||||| || || ||||| |||||||| || |||| |||||||||| || ||||||| || |||||||| || |||||||||.
Source: ADVOCATE Clinical Study Report.19
Table 23: EQ Visual Analogue Scale and EQ-5D-5L Index Scores — Secondary Outcome (ITT Population)
Outcome | Prednisone (N = 164) | Avacopan (N = 166) |
|---|---|---|
EQ visual analogue scale | ||
Baseline, n (%) | 162 (98.8) | 166 (100) |
Mean (SD) | 63.4 (22.7) | 65.8 (19.5) |
Week 26, n (%) | 150 (91.5) | 153 (92.2) |
LSM change from baseline (SEM)a | 5.5 (1.4) | 9.1 (1.4) |
LSM difference (95% CI)a | Reference | 3.6 (–0.1 to 7.2) |
P valuea,b | Reference | 0.0533 |
Week 52, n (%) | 146 (89.0) | 149 (89.8) |
LSM change from baseline (SEM)a | 7.1 (1.4) | 13.0 (1.4) |
LSM difference (95% CI)a | Reference | 5.9 (2.3 to 9.6) |
P valuea,b | Reference | 0.0015 |
|||| || ||| | ||| |||||| | ||| |||||| |
||| |||||| |||| |||||||| ||||| | ||| ||||| | |||| ||||| |
||| |||||||||| |||| ||| | ||||||||| | ||| ||||| || |||| |
| ||||| | | ||||||||| | |||||| |
EQ-5D-5L index score | ||
Baseline, n (%) | 160 (97.6) | 166 (100) |
Mean (SD) | 0.8 (0.2) | 0.8 (0.2) |
Week 26, n (%) | 146 (89.0) | 152 (91.6) |
LSM change from baseline (SEM)a | 0.0 (0.0) | 0.0 (0.0) |
LSM difference (95% CI)a | Reference | 0.0 (0.0 to 0.1) |
P valuea,b | Reference | 0.2168 |
Week 52, n (%) | 145 (88.4) | 149 (89.8) |
LSM change from baseline (SEM)a | 0.0 (0.0) | 0.1 (0.0) |
LSM difference (95% CI)a | Reference | 0.1 (0.0 to 0.1) |
P valuea,b | Reference | 0.0088 |
|||| || |||| | ||| |||||| | ||| |||||| |
||| |||||| |||| |||||||| |||||| | ||| ||||| | ||| ||||| |
||| |||||||||| |||| |||| | ||||||||| | ||| |||| || |||| |
| |||||| | | ||||||||| | |||||| |
ANCA = antineutrophil cytoplasmic autoantibody; ANCA-AV = antineutrophil cytoplasmic autoantibody–associated vasculitis; CI = confidence interval; EQ-5D-5L = 5-Level EQ-5D; ITT = intention to treat; LSM = least squares mean; MMRM = mixed effects model for repeated measures; MPO = myeloperoxidase; SD = standard deviation; SEM = standard error of the mean.
aAnalysis used MMRMs, with treatment group, visit, treatment-by-visit interaction, and randomization strata (newly diagnosed or relapsed ANCA-AV, anti-PR3 or anti-MPO ANCA, and IV rituximab or IV or oral cyclophosphamide standard of care treatment) as factors and baseline as a covariate. MMRM results by visit use the treatment-by-visit interaction term.
bP value has not been adjusted for multiple testing (i.e., the type I error rate has not been controlled).
| |||| || || || |||||||| || || ||||||| |||||| |||| || |||| |||||| |||||| |||| ||||||||| ||||| || ||||||||||||| |||||| |||||| ||||||||| || |||||||| |||| |||||||| || |||||||| ||||| || || ||||||||| || |||||||||||||||| || || ||||| |||||||| || |||| |||||||||| || ||||||| | |||||||| || ||||||||||.
Source: ADVOCATE Clinical Study Report.19
Harms
Only those harms identified in the review protocol are reported in this section; they are also summarized in Table 24.
Adverse Events
Nearly all patients in the avacopan group (98.8%) and prednisone group (98.2%) experienced at least 1 TEAE. The 3 most common AEs in the avacopan group were nausea (23.5% avacopan versus 20.7% prednisone), peripheral edema (21.1% avacopan versus 24.4% prednisone), and headache (20.5% avacopan versus 14.0% prednisone). Other AEs occurred at a frequency of less than 20% in the avacopan group. Headache was the only AE that appeared to be notably more common in the avacopan group than in the prednisone group. The most common AEs in the prednisone group were peripheral edema, muscle spasms (22.6% prednisone versus 10.8% avacopan), arthralgia (22.0% prednisone versus 18.7% avacopan), nausea, and ANCA-positive vasculitis (20.7% prednisone versus 15.7% avacopan), with other AEs occurring at a frequency of less than 20% in the prednisone group. Muscle spasms, ANCA-positive vasculitis, insomnia (15.2% prednisone versus 7.8% avacopan), urinary tract infection (14.0% prednisone versus 7.2% avacopan), hypercholesterolemia (12.2% prednisone versus 7.2% avacopan), lymphopenia (11.0% prednisone versus 3.6% avacopan), and increased weight (10.4% prednisone versus 0.6% avacopan) appeared to be notably more common in the prednisone group than in the avacopan group. Harms categorized by system organ class that had a greater than 10% difference in proportion between treatment groups included eye disorders and endocrine disorders (greater in the prednisone group), as well as gastrointestinal disorders (greater in the avacopan group).
Serious AEs
Overall, 42.2% of patients in the avacopan group and 45.1% of patients in the prednisone group experienced at least 1 SAE. The most common SAEs were ANCA-positive vasculitis (7.2% avacopan versus 12.2% prednisone) and pneumonia (5.4% avacopan versus 5.5% prednisone). ANCA-positive vasculitis had the greatest difference in frequency between treatment groups; other SAEs were generally similar.
Withdrawal Due to AEs
In total, 15.7% of patients in the avacopan group and 17.7% of patients in the prednisone group stopped treatment due to AEs. The most common AE that led to withdrawal from treatment was ANCA-positive vasculitis (2.4% avacopan versus 4.9% prednisone), and other such AEs occurred at a frequency of less than 2% in either group. The frequencies of AEs that led to withdrawal from treatment were generally similar between treatment groups.
Mortality
Six patients died during or after the treatment period in the ADVOCATE trial (2 patients receiving avacopan and 4 patients receiving prednisone), and causes of death were reported by a single patient for each cause.
Notable Harms
Serious Infection
Treatment-emergent infections were reported in 68.1% and 75.6% of patients in the avacopan and prednisone groups, respectively. Serious treatment-emergent infections were reported in 13.3% and 15.2% of patients in the avacopan and prednisone groups, respectively, of which pneumonia was the most common serious infection-related TEAE (5.4% and 5.5%, respectively). Infections resulted in 9 patients (4 in the avacopan group and 5 in the prednisone group) withdrawing from the trial and 3 deaths (1 in the avacopan group and 2 in the prednisone group).
Hepatic Injury (e.g., Increased ALT or AST, Total Bilirubin)
Elevated ALT was reported by 4% and 2% of patients in the avacopan and prednisone groups, respectively; elevated AST was reported in 2% of patients in the avacopan group and no patients in the prednisone group; and elevated blood bilirubin was reported in 2% and 1% of patients in the avacopan and prednisone groups, respectively.
Cardiovascular AEs (e.g., Myocardial Infarction, Cardiac Failure, Cardiac Vasculitis)
Acute myocardial infarction was reported by 1.2% of patients in the prednisone group and 0.6% of patients in the avacopan group, and cardiac failure was reported by 1.2% of patients in the avacopan group and no patients in the prednisone group. Cardiac vasculitis was not reported in the trial.
Gastrointestinal AEs (e.g., Dyspepsia, Vomiting, Nausea, Diarrhea)
Nausea was reported by 23.5% and 20.7% of patients in the avacopan and prednisone groups, respectively; diarrhea was reported by 15.1% and 14.6% of patients, respectively; vomiting was reported by 15.1% and 12.8% of patients, respectively; and dyspepsia was reported by 3.0% and 6.1% of patients, respectively.
Immune-Related AEs (e.g., Angioedema)
Angioedema was reported by 1.2% of patients in the avacopan group and no patients in the prednisone group.
Table 24: Summary of Harms (Safety Population)
Harms | Prednisone (N = 164) | Avacopan (N = 166) |
|---|---|---|
Patients who experienced ≥ 1 TEAE | ||
n (%) | 161 (98.2) | 164 (98.8) |
Most common events, n (%)a | ||
Nausea | 34 (20.7) | 39 (23.5) |
Edema peripheral | 40 (24.4) | 35 (21.1) |
Headache | 23 (14.0) | 34 (20.5) |
Arthralgia | 36 (22.0) | 31 (18.7) |
Hypertension | 29 (17.7) | 30 (18.1) |
ANCA-positive vasculitisb | 34 (20.7) | 26 (15.7) |
Cough | 26 (15.9) | 26 (15.7) |
Nasopharyngitis | 30 (18.3) | 25 (15.1) |
Diarrhea | 24 (14.6) | 25 (15.1) |
Vomiting | 21 (12.8) | 25 (15.1) |
Upper respiratory tract infection | 24 (14.6) | 24 (14.5) |
Rash | 13 (7.9) | 19 (11.4) |
Muscle spasms | 37 (22.6) | 18 (10.8) |
Fatigue | 15 (9.1) | 17 (10.2) |
Back pain | 22 (13.4) | 16 (9.6) |
Myalgia | 22 (13.4) | 16 (9.6) |
Pyrexia | 19 (11.6) | 15 (9.0) |
Epistaxis | 21 (12.8) | 14 (8.4) |
Insomnia | 25 (15.2) | 13 (7.8) |
Anemia | 18 (11.0) | 13 (7.8) |
Urinary tract infection | 23 (14.0) | 12 (7.2) |
Hypercholesterolemia | 20 (12.2) | 12 (7.2) |
Lymphopenia | 18 (11.0) | 6 (3.6) |
Increased weight | 17 (10.4) | 1 (0.6) |
Patients who experienced ≥ 1 SAE | ||
n (%) | 74 (45.1) | 70 (42.2) |
Most common events, n (%)c | ||
ANCA-positive vasculitisb | 20 (12.2) | 12 (7.2) |
Pneumonia | 9 (5.5) | 9 (5.4) |
Granulomatosis with polyangiitis | 1 (0.6) | 5 (3.0) |
Patients who stopped treatment due to AEs | ||
n (%) | 29 (17.7) | 26 (15.7) |
Most common events, n (%)d | ||
ANCA-positive vasculitisb | 8 (4.9) | 4 (2.4) |
Hepatic function abnormal | 0 | 3 (1.8) |
Latent tuberculosis | 0 | 2 (1.2) |
Hepatic enzyme increased | 2 (1.2) | 1 (0.6) |
Lymphopenia | 3 (1.8) | 0 |
Thrombocytopenia | 2 (1.2) | 0 |
Acute myocardial infarction | 2 (1.2) | 0 |
Deaths | ||
n (%) | 4 (2.4) | 2 (1.2) |
GPA | 0 | 1 (0.6) |
Pneumonia | 0 | 1 (0.6) |
Infectious pleural effusion | 1 (0.6) | 0 |
Unknowne | 1 (0.6) | 0 |
Diarrhea, vomiting, and fungal infection | 1 (0.6) | 0 |
Acute myocardial infarction | 1 (0.6) | 0 |
Notable harms, n (%) | ||
Serious infection | ||
Any treatment-emergent infection | 124 (75.6) | 113 (68.1) |
Any serious treatment-emergent infection | 25 (15.2) | 22 (13.3) |
Any treatment-emergent infection leading to study withdrawal | 5 (3.0) | 4 (2.4) |
Any treatment-emergent infection leading to death | 2 (1.2) | 1 (0.6) |
Most common serious TEAEs of infectiond | ||
Pneumonia | 9 (5.5) | 9 (5.4) |
Urinary tract infection | 2 (1.2) | 3 (1.8) |
Device-related infection | 0 | 2 (1.2) |
Influenza | 1 (0.6) | 2 (1.2) |
Herpes zoster | 2 (1.2) | 0 |
Infectious pleural effusion | 2 (1.2) | 0 |
Pneumonia bacterial | 2 (1.2) | 0 |
Respiratory syncytial virus infection | 2 (1.2) | 0 |
Hepatic injury | ||
Elevated ALT | 4 (2) | 6 (4) |
Elevated AST | 0 | 3 (2) |
Elevated blood bilirubin | 1 (1) | 3 (2) |
Cardiovascular AEs | ||
Acute myocardial infarction | 2 (1.2) | 1 (0.6) |
Cardiac failure | 0 | 2 (1.2) |
Cardiac vasculitis | NR | NR |
Gastrointestinal AEs | ||
Nausea | 34 (20.7) | 39 (23.5) |
Diarrhea | 24 (14.6) | 25 (15.1) |
Vomiting | 21 (12.8) | 25 (15.1) |
Dyspepsia | 10 (6.1) | 5 (3.0) |
Immune-related AEs | ||
Angioedema | 0 | 2 (1.2) |
AE = adverse event; ALT = alanine aminotransferase; ANCA = antineutrophil cytoplasmic autoantibody; AST = aspartate aminotransferase; GPA = granulomatosis with polyangiitis; NR = not reported; SAE = serious adverse event; TEAE = treatment-emergent adverse event.
aFrequency of greater than 10% in either treatment group.
bWorsening of vasculitis is reported as the preferred term of “antineutrophil cytoplasmic antibody-positive vasculitis.”
cFrequency of greater than 2% in either treatment group.
dFrequency of greater than 1% in either treatment group.
eNo autopsy was performed.
Source: ADVOCATE Clinical Study Report.19
Critical Appraisal
Internal Validity
In the ADVOCATE trial, the risk of bias arising from the randomization process is low. Stratified randomization was performed centrally, and a few baseline imbalances were noted, which may have been due to chance given the relatively small sample size. The sample size and power calculations were informed by previous studies on the treatment of patients with ANCA-AV and were adequate for noninferiority and superiority testing of the primary outcome.
There are concerns about bias due to deviations from the intended intervention. Patients received active treatment with matching placebos for both prednisone and avacopan, and patients appeared to be adequately blinded to treatments. Discontinuations from treatment were similar between groups, mostly due to AEs; more than 20% of patients in each group discontinued treatment, which is not an insignificant proportion of the total population. Additionally, the use of nonstudy immunosuppressants and glucocorticoids was an issue that likely biased results. The direction and magnitude of the bias are not fully clear. During the 52-week treatment period, 19.7% of patients in the trial used nonstudy immunosuppressants or other ANCA-AV treatments. Nonstudy glucocorticoid use was not considered a protocol violation, and patients could continue in the trial despite receiving glucocorticoids for reasons related to ANCA-AV (e.g., rescue therapy to treat disease relapse or worsening disease involving a major item on the BVAS) or for other reasons (e.g., adrenal insufficiency, allergic reaction). During the 52-week treatment period, 89.1% of patients in the trial used nonstudy glucocorticoids. The intent of the trial was to determine whether avacopan could induce and sustain remission without chronic glucocorticoid use at the levels currently used in standard of care regimens. However, the CADTH review team was unable to determine whether avacopan alone could accomplish this because most patients used nonstudy glucocorticoids and data for those who did not use glucocorticoids were unavailable. Nonstudy medication use is problematic for quantifying the effect of avacopan treatment alone for both efficacy and harm outcomes. Consequently, the Health Canada indication has specified avacopan as an add-on or adjunctive therapy to standard treatment rather than as a glucocorticoid-sparing drug.2,20 Similarly, the FDA stated that the week 26 noninferiority assessment “is not the intended comparison of avacopan versus prednisone, but instead a comparison of avacopan plus lower dose glucocorticoids versus higher dose glucocorticoids.”21
The noninferiority margin was chosen based on a meta-analysis of 20 published studies, but the FDA reported that the noninferiority margin was not informed by a placebo-controlled trial for glucocorticoids as add-on to standard therapy and that, instead, single-arm results from studies were used.21 Further, the FDA noted that it is uncertain how similar or dissimilar the studies used to inform the margin were to the ADVOCATE trial and that there may have been heterogeneity between eligible study populations, patient characteristics, the definition of outcomes, and time points for assessments.21 The results of the ADVOCATE trial’s ITT and PP analyses were generally consistent because the populations were very similar. Patients who used nonstudy immunosuppressants or glucocorticoids could still be included in the PP analyses; the use of nonstudy immunosuppressants was a protocol violation, and patients were imputed as nonremission, whereas the use of glucocorticoids was not considered a protocol violation.
The risk of bias related to missing outcome data are low for the primary outcome. Analyses were based on the ITT population, which is appropriate for assessing the effect of assignment to the intervention. Findings for the PP population were provided for the primary outcomes, which is relevant given that this is likely to provide a more conservative estimate for noninferiority testing. While 9% of patients withdrew early from the study, data imputation methods were conservative for the PP analyses, with a similar amount of imputation between groups for patients who did not achieve remission at week 26 or sustained remission at week 52. For other outcomes, there was no imputation of missing data, which may have introduced bias to varying extents. The potential for bias is most apparent at later time points, due to both early withdrawal from the trial and other reasons, which resulted in data for about 10% of participants being missing (e.g., for HRQoL). Missing data tended to be relatively balanced across groups, resulting in an unclear direction of the potential bias.
Most of the outcome measures are affected by at least some degree of subjectivity, but they were centrally adjudicated, eliminating concerns for bias in the measurement of the outcome. However, there is some potential for bias related to the subjectivity of the patient-reported outcomes, especially if treatment became unblinded (e.g., due to known adverse effects of treatment). According to the literature, only the BVAS and the VDI appear to be adequately validated for ANCA-AV, although this does not apply to the BVAS at week 4, which had a shortened recall period in the ADVOCATE trial; additionally, no published MIDs were identified for a population with ANCA-AV. Additionally, Health Canada found no evidence of validation of the GTI in patients with ANCA-AV, although there is literature supporting validation in patients with asthma;43 Health Canada considered the GTI to be unvalidated and too general to be clinically meaningful for ANCA-AV.20 Additionally, secondary outcomes were not controlled for multiplicity, and between-group differences for several secondary outcomes (e.g., week 4 BVAS, UACR, VDI, patients experiencing disease relapse, SF-36v2, and EQ-5D-5L and EQ VAS) were relatively small with wide CIs.
All analyses were based on a prespecified statistical analysis plan; therefore, there is no concern for bias in the selection of the reported result.
External Validity
The clinical expert confirmed that the baseline demographics and disease characteristics of patients in the trial were similar to those of patients seen in clinical practice. The expert indicated that the proportion of patients with kidney involvement and with MPA in the ADVOCATE trial were higher than global cohorts of patients with ANCA-AV. It was explained that the specialist at a particular clinic will tend to dictate what type of patient attends the site; for instance, nephrologists manage mostly patients with kidney disease and MPA, and rheumatologists manage a mix of patients with GPA or MPA. The clinical expert stated that patients are generally treated in the same manner, regardless of whether they have GPA or MPA, and did not expect the differences to impact generalizability to practice. Overall, 18% of patients enrolled in the trial were from North America, and 13 patients (3.9%) were from Canada. Although this is a relatively small proportion of the total trial population, it helps to support the generalizability to patients with ANCA-AV in Canada. The clinical expert confirmed that the proportions of patients receiving cyclophosphamide or rituximab as induction therapy in the ADVOCATE trial were similar to the estimated proportions in Canada: 35% received cyclophosphamide (oral or IV) and 65% received rituximab in the trial compared to approximately 40% receive cyclophosphamide (oral or IV) and 60% receive rituximab in Canada.
Of the 386 individuals screened in the ADVOCATE trial, 14.2% failed screening, with the most common reason being not meeting eligibility criteria. According to the clinical expert, patients who met the trial’s eligibility criteria were generally similar to those seen in Canadian practice, but there were a few criteria that would prevent generalization to a broader population with ANCA-AV, who might also be treated with avacopan. For instance, the trial included only patients who had tested positive for anti-PR3 or anti-MPO antibodies at screening or historically, essentially ruling out patients who have only had negative antibody results. It has been noted, both in the literature and by the clinical expert, that a small proportion of patients are ANCA negative.23 These patients can have an ANCA-AV status confirmed by other tests, and the clinical expert suggested that they would be treated similarly if the diagnosis was certain (e.g., with renal biopsy). Patients with very severe disease (e.g., patients who have alveolar hemorrhage requiring invasive pulmonary ventilation support or dialysis or patients who have an eGFR less than 15 mL/min/1.73 m2) were also excluded from the ADVOCATE trial. It is possible that these patients could be treated with avacopan, but it is uncertain if they would have comparable outcomes to patients in the trial. Lastly, although the Health Canada indication for avacopan is for adults, there is limited evidence of its use in the pediatric population.
The medications and doses used in the ADVOCATE trial were mostly consistent with those outlined in the CanVasc recommendations and used in clinical practice according to the clinical expert, with an important exception: rituximab was not used as maintenance therapy in the trial.9,47 Understandably, at the time of protocol development, rituximab was not approved as a maintenance therapy for ANCA-AV and therefore was not used. Nevertheless, this is an issue because not only did no patients receive rituximab maintenance therapy (regardless of induction therapy), but patients who received rituximab for induction of remission did not receive any standard of care maintenance therapy in the trial. Furthermore, it was unclear to the CADTH review team and the clinical expert whether the addition of avacopan to rituximab maintenance therapy would make a meaningful difference if these treatments were to be used in clinical practice today, and there is currently a lack of clinical data on this usage. The FDA pointed out that prednisone was tapered at a protocol-defined fixed rate instead of the tapering being determined by disease activity.21 However, the latest addendum (2022) to the CanVasc recommendations states that with avacopan, clinicians can consider tapering glucocorticoids using a faster protocol with the aim of discontinuation by the end of week 4, and this is done “in conjunction with best clinical judgement” and “close clinical monitoring for disease worsening.”25 The FDA also noted that the use of glucocorticoids was similar between treatment groups in the second half of the trial; the notable difference between groups occurred in the first half of the trial, specifically during the first 20 weeks, when prednisone was tapered.21 Therefore, the apparent difference in glucocorticoid use between groups is more likely attributable to the trial design (i.e., the tapering schedule) than to a change in disease activity such as avacopan effectively controlling ANCA-AV.21
The patient group highlighted outcomes relating to quality of life, organ involvement, vasculitis symptoms, and glucocorticoid use as being important, and these mostly aligned with the trial outcomes. The clinical expert also confirmed that the trial outcomes of remission, kidney function, systemic disease, disease relapse, glucocorticoid toxicity, and HRQoL were clinically relevant to ANCA-AV. Nevertheless, some limitations make it challenging to interpret the meaningfulness of the results. For example, the clinical expert confirmed that the instruments used in the ADVOCATE trial are not used in clinical practice (although they may be useful for informing clinicians of treatment effects) and that only the BVAS and the VDI were specific to ANCA-AV (refer to Appendix 4). Hospitalizations and ANCA-AV symptoms were identified as being important to patients but were not specifically assessed in the trial through, for example, hospitalization events or symptom scales.
There was no rationale for the trial duration being 52 weeks or the follow-up being 8 weeks. These are major limitations, and there is a lack of data on the efficacy and safety of avacopan for less than or more than 52 weeks. Also, due to the relatively short follow-up period, it is uncertain what the long-term effects after discontinuing avacopan treatment could be. Moreover, there was no discussion or indication from the trial about what posttreatment strategies should be used to manage patients with ANCA-AV (e.g., continue avacopan beyond 12 months, provide maintenance therapy without avacopan after the 12 months of initial treatment).
Discussion
Summary of Available Evidence
One double-blind, phase III, placebo-controlled randomized controlled trial (ADVOCATE) was included in the CADTH systematic review. The ADVOCATE trial (N = 331) was designed to investigate the efficacy and safety of avacopan in patients with ANCA-AV, with the aim to determine if avacopan could induce and sustain remission without chronic glucocorticoid use at the levels currently used in standard of care regimens. The trial compared avacopan to prednisone tapered over 20 weeks, with respective matching placebos, in addition to standard of care therapy (IV or oral cyclophosphamide followed by azathioprine, or IV rituximab without maintenance therapy) over 52 weeks with an 8-week follow-up. Patients in either group could receive nonstudy-specified glucocorticoids for reasons related to ANCA-AV (e.g., rescue therapy to treat disease relapse or worsening disease involving a major item on the BVAS) or for other reasons (e.g., adrenal insufficiency, allergic reaction). Eligible patients included adults who had a clinical diagnosis of GPA or MPA, were ANCA positive for either anti-PR3 or anti-MPO antibodies, and had active disease at screening. The mean age of patients was 60.9 years (SD = 14.5 years), more than half were male (56.5%), and most were white (84.3%). The primary outcomes were the proportions of patients who achieved disease remission at week 26 and sustained disease remission at week 52. Key secondary outcomes included glucocorticoid toxicity, HRQoL, kidney function, systemic damage, and the proportion of patients experiencing disease relapse. Harms and notable harms identified in the CADTH systematic review protocol were also assessed.
Interpretation of Results
Efficacy
Based on the ADVOCATE trial, avacopan — when provided with nonprotocol glucocorticoids — was noninferior to prednisone for disease remission at week 26 (but not superior at week 26) and was superior to prednisone for sustained disease remission at week 52. Subgroup analyses were aligned with the main analyses. The findings need to be interpreted with consideration of the main limitations of the trial, which include the use of nonstudy immunosuppressants, the use of nonstudy glucocorticoids, and the inclusion of a comparator arm that no longer aligns with present day standards of practice (although was aligned at the time that the protocol was developed). As a result, conclusions about the comparison of avacopan alone to prednisone (as specified in the ADVOCATE protocol) cannot be established because the true comparison described in the study results was avacopan with glucocorticoids versus prednisone, both in the presence of background immunosuppressant treatment. In addition, the relevance of the comparison to clinical practice needs to be interpreted with consideration of changes in practice that have occurred since the development of the study protocol. The clinical expert consulted by CADTH noted that rituximab maintenance (which is the current recommended first-line standard of care maintenance therapy but which was not used in the trial) reduces the rate of relapse to about 5% at 2 years.9 The ADVOCATE trial does not provide information that can be used to determine whether avacopan, with or without glucocorticoids, would be noninferior to the current recommended standard of care maintenance therapy. Finally, there is a lack of long-term data to inform understanding of the efficacy and safety of avacopan beyond 52 weeks.
Overall, only 21 patients (12.7%) in the avacopan group and 15 patients (9.1%) in the prednisone group did not receive nonstudy glucocorticoids in the trial, and data were not available for this subset of patients. The mean doses for any glucocorticoids used in the trial were 1,348.9 mg (SD = 2,040.3 mg) and 3,654.5 mg (SD = 1,709.8 mg) for the avacopan and prednisone groups, respectively, during the treatment period. Removing the protocol-tapered prednisone, the mean doses for just nonstudy glucocorticoids were 1,348.9 mg (SD = 2,040.3 mg) and 1,265.3 mg (SD = 1,650.6 mg) for the avacopan and prednisone groups, respectively, during the treatment period. Although the mean dose for any glucocorticoids is lower in the avacopan group, the difference may be inflated due to the use of protocol-specified prednisone during the first 20 weeks, and the mean dose appears to be greater in the avacopan group when looking at only nonstudy glucocorticoids. It is also unclear if these doses are high enough to effectively treat ANCA-AV or cause additional adverse effects.
The clinical expert indicated that the rates of remission in the trial were lower than what would be expected in practice but explained that it was likely because the trial’s definition of remission specified no glucocorticoids within 4 weeks of assessment, whereas in practice, patients may achieve remission with or without glucocorticoids. Further, the expert clarified that, in practice, remission is determined based on clinical judgment of no disease activity rather than using the BVAS as a formal tool as was done in the trial. According to the expert, the result of the BVAS is dichotomous rather than longitudinal or continuous in nature, such that a patient either has active disease (score greater than 0) or not (score of 0), and as such changes in the score are less meaningful. Although the trial outcomes were related to those considered important to patients according to the stakeholder input CADTH received, there were limitations that make it challenging to be certain of how meaningful the results are. Examples of these limitations are as follows: the clinical expert confirmed that none of the instruments used in the trial (e.g., BVAS, GTI, VDI, SF-36v2, EQ-5D-5L, EQ VAS) are used in routine clinical practice (although they may still inform clinicians of treatment effects), only the BVAS and the VDI were adequately validated for ANCA-AV, none of the trial end points had published MIDs for a population with ANCA-AV, and none of the secondary outcomes were controlled for multiplicity (i.e., there is some risk of a false-positive finding).
The eGFR and UACR results appeared to support avacopan treatment, but changes were small throughout the trial, and without published MIDs from the literature for this population, interpretation relies on clinical expert opinion. The clinical expert suggested that a 5 mL/min/1.73 m2 change in eGFR could be interpreted as meaningful based on the MID for patients with diabetes but confirmed that there is no MID for patients with ANCA-AV and cautioned that the suggested estimate was based on a different patient population. VDI scores showed little to no difference between groups. the clinical expert explained that, as with the BVAS, items on the VDI carry the same weight in score but are not necessarily of equal clinical significance. Therefore, the change in magnitude of the total VDI score is less meaningful than assessing what clinical changes occurred, thus making it challenging to draw meaningful conclusions for this outcome.
The trial did not differentiate between major and minor relapses, which the clinical expert stated was a shortcoming because the reasons for relapse can vary from nasal symptoms to more serious respiratory or kidney failures. The CI was too wide to draw a conclusion about the proportion of relapses in the avacopan group versus in the prednisone group. The GTI scores indicated fewer glucocorticoid-related toxicities for the avacopan group, which the clinical expert felt was reasonable because this group received placebo prednisone instead of active prednisone tapered during the first 20 weeks. Based on evidence from the literature, a MID of 10 was estimated in a mixed population, including patients with ANCA-AV, which the LSM differences between treatment groups met for both GTI-CWS and GTI-AIS at week 26.43 There is evidence of validity of the GTI for patients with asthma, although this validity is unclear for other patient populations.43 Health Canada stated that the GTI was not validated for ANCA-AV and that “the end point was not specific enough to be discriminatory between treatment” groups.20 HRQoL measures showed similarity between treatment groups, with wide CIs. Lastly, the results from the 8-week follow-up for eGFR, VDI, SF-36v2, EQ-5D-5L, and EQ VAS showed that the small differences between groups during the trial may not have been sustained after stopping avacopan and that the treatment differences during follow-up also had wide CIs. Hospitalizations and ANCA-AV symptoms were identified as being important to patients but were not specifically captured in the trial, for example as hospitalization events or through specific symptom scales.
The main limitations were the deviations from both current recommended standard of care treatment (rituximab maintenance) and the trial’s intended comparison (avacopan versus prednisone). The clinical expert indicated that the trial’s tapering regimen (20 weeks, or 5 months) was on the shorter end of what is considered standard (average 6 to 7 months in practice) but confirmed that it was acceptable, which is consistent with the 2022 addendum to the CanVasc recommendations for a faster glucocorticoid taper with clinical judgment and close clinical monitoring.25 The FDA pointed out that the tapering of glucocorticoids was performed at a fixed rate and dictated by the protocol rather than being based on disease activity, the latter of which is used in practice.21 The clinical expert noted that protocolized tapering would be necessary to reduce subjectivity and increase uniformity of treatment for the purposes of a clinical trial. Due to the lack of rituximab maintenance therapy, patients may have been undertreated, putting them at a higher risk of relapse and making them less likely to achieve sustained remission.48 Thus, it is possible that the rates of relapse in the ADVOCATE trial do not accurately reflect expected outcomes with current clinical practice.48 The use of nonstudy glucocorticoids for 89% of the trial’s population and the lack of data for the remaining 11% make it difficult to assess avacopan versus prednisone without additional glucocorticoids. The clinical expert indicated that avacopan along with standard of care immunosuppressant therapy (i.e., rituximab or cyclophosphamide) should be used only if there is a meaningful reduction of glucocorticoids. Although there is no standard definition for what a meaningful reduction would be, the expert stated that it would be ideal if patients were on no glucocorticoids. Another major issue was that treatment duration stopped at 12 months, with only 8 weeks of posttreatment follow-up, and there was no rationale for these time frames. The clinical expert indicated that most patients should receive least 2 years of maintenance therapy to better ensure long-term sustained remission, which could include using avacopan longer than 12 months, although it must be taken into consideration that the limited data for long-term treatment and follow-up with avacopan result in uncertainty about how long avacopan can be used as well as how patients should be managed after discontinuing the drug. More evidence is needed to understand avacopan’s efficacy and safety in addition to rituximab maintenance therapy, long-term patient management with or without avacopan, and whether the drug can eliminate glucocorticoid use.
Harms
Nearly all patients in the trial experienced at least 1 TEAE, with the most common being nausea, peripheral edema, and headache for the avacopan group and peripheral edema, muscle spasms, and arthralgia for the prednisone group. Most events were balanced between treatment groups, and the clinical expert indicated that there was no clear reason for those that appeared imbalanced (e.g., headache, muscle spasms, insomnia). More than 42% of patients in each group experienced at least 1 SAE, and more than 15% of patients in each group stopped treatment due to an AE. There were 6 deaths during the trial (2 patients in the avacopan group and 4 patients in the prednisone group).
Notable harms were generally balanced between treatments, aside from treatment-emergent infections, and there did not appear to be any clear safety signal in the avacopan group. Serious infections were a significant concern raised in the inputs provided by the patient group, the clinician group, and the clinical expert consulted by CADTH. Treatment-emergent infections were higher in the prednisone group than in the avacopan group (75.6% and 68.1%, respectively), although the difference was not as large as would be expected in the ADVOCATE trial, where the aim was to eliminate glucocorticoids and the associated increased risk of infection. The clinical expert noted that rates were lower but still frequent in the avacopan group possibly due to patients in both groups being on immunosuppressants and/or receiving nonstudy glucocorticoids throughout the trial. This was also confirmed by a report from Health Canada.20 Although there did not appear to be a difference in hepatic injury (for events identified as notable harms in the CADTH systematic review), Health Canada noted that hepatic AEs were more frequent in the avacopan group than in the prednisone group, and hepatic AEs have been identified under the warnings and precautions of the product monograph.2,20
Similar to the efficacy results, the major limitations with the safety results re the lack of evidence for avacopan in addition to rituximab maintenance therapy as well as the lack of data for the long-term use of avacopan with or without other treatments for ANCA-AV. Health Canada has noted that the sponsor plans to gather long-term data for up to 36 months through a postauthorization safety study, which will include AEs of special interest such as liver injury, serious infections, malignancies, and cardiovascular events.20 The input provided by the patient group raised concerns over glucocorticoid-related harms as well as symptoms related to kidney damage, fatigue, trouble breathing, infections, and pain. Given the mostly balanced harms results, the use of nonstudy glucocorticoids for the majority of patients, and the challenges with interpreting the GTI scores, it is unclear whether avacopan provides an advantage that would be acceptable to patients. More safety evidence, particularly for avacopan without glucocorticoids, is needed to know if avacopan provides a meaningful benefit over other treatments.
Overall, no clear safety concerns were raised by the clinical expert, and aside from the lower rates of treatment-emergent infections in the avacopan group, harms were generally balanced between the groups. However, this is applicable for only 12 months of treatment of the eligible population under specific trial conditions. More information is needed for patients who may be treated with avacopan but were excluded from the trial as well as for long-term treatment with the drug.
Conclusions
Avacopan 30 mg (3 capsules of 10 mg each) twice daily with nonprotocol-specified glucocorticoids was compared to oral prednisone tapered over 20 weeks in addition to nonprotocol-specified glucocorticoids over a 12-month treatment period. Treatments were combined with background therapy of IV or oral cyclophosphamide followed by azathioprine, or IV rituximab without maintenance therapy. Avacopan 30 mg twice daily was noninferior to oral prednisone in achieving disease remission at week 26 and was superior for sustained disease remission at week 52. Notably, 89% of patients received nonprotocol-specified glucocorticoids at some point during the ADVOCATE trial. Outcomes related to kidney function, systemic damage, disease relapse, glucocorticoid toxicity, and HRQoL provided limited support for the primary outcomes. Harms were generally balanced between groups in the trial, and no notable safety concerns were identified. The relevance of the findings to current standards of practice is unclear due to the lack of rituximab maintenance in both treatment groups, which is the current gold standard. It is unclear whether the findings would be generalizable to patients who are ANCA negative or who have very severe disease (e.g., patients who have alveolar hemorrhage requiring invasive pulmonary ventilation support or dialysis or patients who have an eGFR less than 15 mL/min/1.73 m2). Although the clinical expert suggested that avacopan could be used beyond 1 year, data to support long-term efficacy and safety beyond 12 months are not available at this time, and how patients should be managed after stopping avacopan is unknown. More evidence is needed to better understand the long-term efficacy and safety of avacopan and whether it can be used to effectively eliminate glucocorticoid use.
References
1.Drug Reimbursement Review sponsor submission: Tavneos, 10mg oral capsules [internal sponsor's package]. Saint-Laurent (QC): Otsuka Canada Pharmaceuticals; 2022.
2.Tavneos (avacopan): 10mg oral capsules [product monograph]. Saint-Laurent (QC): Otsuka Canada Pharmaceuticals; 2022: https://www.accessdata.fda.gov/drugsatfda_docs/label/2021/214487s000lbl.pdf. Accessed 2022 Dec 16.
3.Falk RJ, Merkel PA, Talmadge E King J. Granulomatosis with polyangiitis and microscopicpolyangiitis: Clinical manifestations and diagnosis. In: Post TW, ed. Waltham (MA): UpToDate; 2022: www.uptodate.com. Accessed 2022 Oct 31.
4.Merkel PA. Overview of and approach to the vasculitides in adults. In: Post TW, ed. Waltham (MA): UpToDate; 2022: www.uptodate.com. Accessed 2022 Oct 31.
5.Merkel PA, Kaplan AA, Falk RJ. Granulomatosis with polyangiitis and microscopicpolyangiitis: Induction and maintenance therapy. In: Post TW, ed. Waltham (MA): UpToDate; 2022: www.uptodate.com. Accessed 2022 Oct 31.
6.Jennette JC, Falk RJ, Bacon PA, et al. 2012 revised International Chapel Hill Consensus Conference Nomenclature of Vasculitides. Arthritis Rheum. 2013;65(1):1-11. PubMed
7.Ross C, Makhzoum JP, Pagnoux C. Updates in ANCA-associated vasculitis. Eur J Rheumatol. 2022;9(3):153-166. PubMed
8.Fauci AS, Haynes BF, Katz P, Wolff SM. Wegener's granulomatosis: prospective clinical and therapeutic experience with 85 patients for 21 years. Ann Intern Med. 1983;98(1):76-85. PubMed
9.Mendel A, Ennis D, Go E, et al. CanVasc Consensus Recommendations for the Management of Antineutrophil Cytoplasm Antibody-associated Vasculitis: 2020 Update. J Rheumatol. 2021;48(4):555-566. PubMed
10.Jones RB, Tervaert JW, Hauser T, et al. Rituximab versus cyclophosphamide in ANCA-associated renal vasculitis. N Engl J Med. 2010;363(3):211-220. PubMed
11.Jones RB, Furuta S, Tervaert JW, et al. Rituximab versus cyclophosphamide in ANCA-associated renal vasculitis: 2-year results of a randomised trial. Ann Rheum Dis. 2015;74(6):1178-1182. PubMed
12.Specks U, Merkel PA, Seo P, et al. Efficacy of remission-induction regimens for ANCA-associated vasculitis. N Engl J Med. 2013;369(5):417-427. PubMed
13.Stone JH, Merkel PA, Spiera R, et al. Rituximab versus cyclophosphamide for ANCA-associated vasculitis. N Engl J Med. 2010;363(3):221-232. PubMed
14.Rovin BH, Adler SG, Barratt J, et al. Executive summary of the KDIGO 2021 Guideline for the Management of Glomerular Diseases. Kidney Int. 2021;100(4):753-779. PubMed
15.Jayne D, Rasmussen N, Andrassy K, et al. A randomized trial of maintenance therapy for vasculitis associated with antineutrophil cytoplasmic autoantibodies. N Engl J Med. 2003;349(1):36-44. PubMed
16.Pagnoux C, Mahr A, Hamidou MA, et al. Azathioprine or methotrexate maintenance for ANCA-associated vasculitis. N Engl J Med. 2008;359(26):2790-2803. PubMed
17.Wegener's Granulomatosis Etanercept Trial (WGET) Research Group. Etanercept plus standard therapy for Wegener's granulomatosis. N Engl J Med. 2005;352(4):351-361. PubMed
18.Charles P, Perrodeau É, Samson M, et al. Long-Term Rituximab Use to Maintain Remission of Antineutrophil Cytoplasmic Antibody-Associated Vasculitis: A Randomized Trial. Ann Intern Med. 2020;173(3):179-187. PubMed
19.Clinical Study Report: ADVOCATE (CL010_168). A Randomized, Double-blind, Active-controlled, Phase 3 Study to Evaluate the Safety and Efficacy of CCX168 (Avacopan) in Patients with Anti-neutrophil Cytoplasmic Antibody (ANCA)-Associated Vasculitis Treated Concomitantly with Rituximab or Cyclophosphamide/Azathioprine. Mountain View (CA): Otsuka Canada Pharmaceutical Inc.; 2020.
20.Health Canada reviewer's report: Tavneos (avacopan) [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Tavneos, 10mg oral capsules. Saint-Laurent (QC): Otsuka Canada Parmaceuticals; 2022.
21.Center for Drug Evaluation Research. Multidiscipline review(s). Tavneos (avacopan) oral capsules. Company: ChemoCentryx, Inc. Application No.:214487. Approval date: 10/7/2021 (FDA approval package). Silver Spring (MD): U.S. Food and Drug Administration; 2020: https://www.accessdata.fda.gov/drugsatfda_docs/nda/2021/214487Orig1s000MultidisciplineR.pdf. Accessed 2022 Oct 31.
22.Hoffman GS, Kerr GS, Leavitt RY, et al. Wegener granulomatosis: an analysis of 158 patients. Ann Intern Med. 1992;116(6):488-498. PubMed
23.Kitching AR, Anders HJ, Basu N, et al. ANCA-associated vasculitis. Nat Rev Dis Primers. 2020;6(1):71. PubMed
24.Flossmann O, Berden A, de Groot K, et al. Long-term patient survival in ANCA-associated vasculitis. Ann Rheum Dis. 2011;70(3):488-494. PubMed
25.Turgeon D, Bakowsky V, Baldwin C, et al. CanVasc consensus recommendations for the use of avacopan in antineutrophil cytoplasm antibody-associated vasculitis: 2022 addendum. Rheumatology (Oxford). 2023;21:21. PubMed
26.Apo-Prednisone (prednisone): 1 mg, 5 mg, 50 mg oral tablets USP [product monograph]. Toronto (ON): Apotex Inc.; 2015: https://pdf.hres.ca/dpd_pm/00030893.PDF. Accessed 2022 Oct 31.
27.Riximiyo (rituximab): 10 mg/mL intravenous infusion [product monograph]. Boucherville (QC): Sandoz Canada Inc.; 2022: https://pdf.hres.ca/dpd_pm/00064950.PDF. Accessed 2022 Dec 16.
28.Cyclophosphamide for Injection (cyclophosphamide USP): 500 mg, 1000 mg, and 2000 mg per vial [product monograph]. Kirkland (QC): Accord Healthcare Inc.; 2022: https://pdf.hres.ca/dpd_pm/00067461.PDF. Accessed 2022 Dec 10.
29.Procytox (cyclophosphamide): 25 mg, 50 mg oral tablets USP and (cyclophosphamide) 200 mg, 500 mg, 1000 mg, 2000 mg powder for injection per vial [product monograph]. Mississauga (ON): Baxter Corporation; 2012: https://pdf.hres.ca/dpd_pm/00017604.PDF. Accessed 2022 Oct 31.
30.McGowan J, Sampson M, Salzwedel DM, Cogo E, Foerster V, Lefebvre C. PRESS Peer Review of Electronic Search Strategies: 2015 guideline statement. J Clin Epidemiol. 2016;75:40-46. PubMed
31.Grey matters: a practical tool for searching health-related grey literature. Ottawa (ON): CADTH; 2019: https://www.cadth.ca/grey-matters. Accessed 2022 Dec 10.
32.Jayne DRW, Merkel PA, Schall TJ, Bekker P, Group AS. Avacopan for the Treatment of ANCA-Associated Vasculitis. N Engl J Med. 2021;384(7):599-609. PubMed
33.Assessment Report: Tavneos. Amsterdam (NL): European Medicines Agency; 2021: https://www.ema.europa.eu/en/documents/assessment-report/tavneos-epar-public-assessment-report_en.pdf. Accessed 2022 Dec 16.
34.ChemoCentryx. NCT02994927: A Phase 3 Clinical Trial of CCX168 (Avacopan) in Patients With ANCA-Associated Vasculitis (ADVOCATE). ClinicalTrials.gov. Bethesda (MD): U.S. National Library of Medicine; 2022: https://clinicaltrials.gov/ct2/show/NCT02994927. Accessed 2022 Dec 12.
35.Bekker P, Dairaghi D, Seitz L, et al. Characterization of Pharmacologic and Pharmacokinetic Properties of CCX168, a Potent and Selective Orally Administered Complement 5a Receptor Inhibitor, Based on Preclinical Evaluation and Randomized Phase 1 Clinical Study. PLoS One. 2016;11(10):e0164646. PubMed
36.Jayne DRW, Bruchfeld AN, Harper L, et al. Randomized Trial of C5a Receptor Inhibitor Avacopan in ANCA-Associated Vasculitis. J Am Soc Nephrol. 2017;28(9):2756-2767. PubMed
37.Merkel PA, Niles J, Jimenez R, et al. Adjunctive Treatment With Avacopan, an Oral C5a Receptor Inhibitor, in Patients With Antineutrophil Cytoplasmic Antibody-Associated Vasculitis. ACR Open Rheumatol. 2020;2(11):662-671. PubMed
38.Mukhtyar C, Lee R, Brown D, et al. Modification and validation of the Birmingham Vasculitis Activity Score (version 3). Ann Rheum Dis. 2009;68(12):1827-1832. PubMed
39.Suppiah R, Mukhtyar C, Flossmann O, et al. A cross-sectional study of the Birmingham Vasculitis Activity Score version 3 in systemic vasculitis. Rheumatology (Oxford). 2011;50(5):899-905. PubMed
40.Exley AR, Bacon PA, Luqmani RA, et al. Development and initial validation of the vasculitis damage index for the standardized clinical assessment of damage in the systemic vasculitides. Arthritis Rheum. 1997;40(2):371-380. PubMed
41.Miloslavsky EM, Naden RP, Bijlsma JWJ, et al. Development of a Glucocorticoid Toxicity Index (GTI) using multicriteria decision analysis. Ann Rheum Dis. 2017;76(3):543-546. PubMed
42.Ehlers L, Wiebe E, Freier D, et al. AB1310 PROSPECTIVE USE OF THE GLUCOCORTICOID TOXICITY INDEX (GTI) IN A COHORT OF VASCULITIS PATIENTS. Ann Rheum Dis. 2019;78(Suppl 2):2117-2118.
43.Stone JH, McDowell PJ, Jayne DRW, et al. The glucocorticoid toxicity index: Measuring change in glucocorticoid toxicity over time. Semin Arthritis Rheum. 2022;55:152010. PubMed
44.Ware JE, Sherbourne CD. The MOS 36-Item Short-Form Health Survey (SF-36): I. Conceptual Framework and Item Selection. Med Care. 1992;30(6):473-483. PubMed
45.Ware J, Kosinski M, Keller S. SF-36 physical and mental health summary scales: A user's manual. Vol 1994: QualityMetric; 2001.
46.van Reenen M JB, Stolk E, Secnik Boye K, Herdman M, Kennedy-Martin M, et al. EQ-5D-5L user guide: basic information on how to use the EQ-5D-5L instrument. Version 3.0. Rotterdam (Netherlands): EuroQol Group; 2019: https://euroqol.org/publications/user-guides/. Accessed 2022 Nov 16.
47.McGeoch L, Twilt M, Famorca L, et al. CanVasc Recommendations for the Management of Antineutrophil Cytoplasm Antibody-associated Vasculitides. J Rheumatol. 2016;43(1):97-120. PubMed
48.Soulsby WD. Journal Club Review of “Avacopan for the Treatment of ANCA-Associated Vasculitis”. ACR Open Rheumatol. 2022;4(7):558-561. PubMed
49.McDowell PJ, Stone JH, Zhang Y, et al. Quantification of Glucocorticoid-Associated Morbidity in Severe Asthma Using the Glucocorticoid Toxicity Index. J Allergy Clin Immunol Pract. 2021;9(1):365-372.e365. PubMed
50.Merkel PA, Aydin SZ, Boers M, et al. The OMERACT core set of outcome measures for use in clinical trials of ANCA-associated vasculitis. J Rheumatol. 2011;38(7):1480-1486. PubMed
Appendix 1: Literature Search Strategy
Note this appendix has not been copy-edited.
Clinical Literature Search
Overview
Interface: Ovid
Databases:
MEDLINE All (1946-present)
Embase (1974-present)
Note: Subject headings and search fields have been customized for each database. Duplicates between databases were removed in Ovid.
Date of search: November 9, 2022
Alerts: Biweekly search updates until project completion
Search filters applied: None
Limits:
Conference abstracts: excluded
Syntax | Description |
|---|---|
/ | At the end of a phrase, searches the phrase as a subject heading |
MeSH | Medical Subject Heading |
.fs | Floating subheading |
exp | Explode a subject heading |
* | Before a word, indicates that the marked subject heading is a primary topic; or, after a word, a truncation symbol (wildcard) to retrieve plurals or varying endings |
# | Truncation symbol for one character |
? | Truncation symbol for one or no characters only |
adj# | Requires terms to be adjacent to each other within # number of words (in any order) |
.ti | Title |
.ot | Original title |
.ab | Abstract |
.hw | Heading word; usually includes subject headings and controlled vocabulary |
.kf | Keyword heading word |
.dq | Candidate term word (Embase) |
.pt | Publication type |
.mp | Mapped term |
.rn | Registry number |
.nm | Name of substance word (MEDLINE) |
.yr | Publication year |
.jw | Journal title word (MEDLINE) |
.jx | Journal title word (Embase) |
freq = # | Requires terms to occur # number of times in the specified fields |
medall | Ovid database code: MEDLINE All, 1946 to present, updated daily |
oemezd | Ovid database code; Embase, 1974 to present, updated daily |
cctr | Ovid database code; Cochrane Central Register of Controlled Trials |
Multidatabase Strategy
(Tavneos* or avacopan* or CCX168 or CCX 168 or vynpenta*).ti,ab,kf,rn,nm,hw,ot.
O880NM097T.rn,nm.
or/1-2
3 use medall
*Avacopan/
(Tavneos* or avacopan* or CCX168 or CCX 168 or vynpenta*).ti,ab,kf,dq.
or/5-6
7 use oemezd
conference abstract.pt.
8 not 9
or/4,10
remove duplicates from 11
Clinical Trials Registries
ClinicalTrials.gov
Produced by the US National Library of Medicine. Targeted search used to capture registered clinical trials.
[Search -- Studies with results | avacopan]
WHO ICTRP
International Clinical Trials Registry Platform, produced by the WHO. Targeted search used to capture registered clinical trials.
[Search terms -- avacopan]
Health Canada’s Clinical Trials Database
Produced by Health Canada. Targeted search used to capture registered clinical trials.
[Search terms -- avacopan]
EU Clinical Trials Register
European Union Clinical Trials Register, produced by the European Union. Targeted search used to capture registered clinical trials.
[Search terms -- avacopan]
Grey Literature
Search dates: September 23, 2020 – October 4, 2020
Keywords: Tavneos, avacopan, vasculitis, C5aR
Limits: None
Relevant websites from the following sections of the CADTH grey literature checklist Grey Matters: A Practical Tool for Searching Health-Related Grey Literature were searched:
Health Technology Assessment Agencies
Health Economics
Clinical Practice Guidelines
Drug and Device Regulatory Approvals
Advisories and Warnings
Drug Class Reviews
Clinical Trials Registries
Databases (free)
Health Statistics
Internet Search
Open Access Journals.
Appendix 2: Excluded Studies
Note this appendix has not been copy-edited.
Reference | Reason for exclusion |
|---|---|
Gabilan C, Pfirmann P, Ribes D, et al. Avacopan as First-Line Treatment in Antineutrophil Cytoplasmic Antibody-Associated Vasculitis: A Steroid-Sparing Option. KI Rep. 2022;7(5):1115 to 1118. | Study design |
Harigai M, Takada H. Avacopan, a selective C5a receptor antagonist, for anti-neutrophil cytoplasmic antibody-associated vasculitis. Mod Rheumatol. 2022;32(3):475 to 483. | Review article |
Merkel PA, Jayne DR, Wang C, Hillson J, Bekker P. Evaluation of the Safety and Efficacy of Avacopan, a C5a Receptor Inhibitor, in Patients With Antineutrophil Cytoplasmic Antibody-Associated Vasculitis Treated Concomitantly With Rituximab or Cyclophosphamide/Azathioprine: Protocol for a Randomized, Double-Blind, Active-Controlled, Phase 3 Trial. JMIR Res Protoc. 2020;9(4):e16664. | Protocol |
van Leeuwen JR, Bredewold OW, van Dam LS, et al. Compassionate Use of Avacopan in Difficult-to-Treat Antineutrophil Cytoplasmic Antibody-Associated Vasculitis. KI Rep. 2022;7(3):624 to 628. | Study design |
Appendix 3: Detailed Outcome Data
Note this appendix has not been copy-edited.
Table 27: Proportion of Patients With Disease Remission at Week 26 Analyzed by Stratification Factor and by Subgroup (ITT Population)
Outcome | Prednisone | Avacopan |
|---|---|---|
Stratification factors | ||
IV rituximab | 107 | 107 |
Patients who achieved remission, n (%) 95% CIa | 81 (75.7) (66.5 to 83.5) | 83 (77.6) (68.5 to 85.1) |
Difference in percent (95% CI)b | Reference | 1.9 (–9.5 to 13.2) |
IV or oral cyclophosphamide | 57 | 59 |
Patients who achieved remission, n (%) 95% CIa | 34 (59.6) (45.8 to 72.4) | 37 (62.7) (49.1 to 75.0) |
Difference in percent (95% CI)b | Reference | 3.1 (–14.7 to 20.8) |
PR3 ANCA positive | 70 | 72 |
Patients who achieved remission, n (%) 95% CIa | 50 (71.4) (59.4 to 81.6) | 51 (70.8) (58.9 to 81.0) |
Difference in percent (95% CI)b | Reference | –0.6 (–15.5 to 14.3) |
MPO ANCA positive | 94 | 94 |
Patients who achieved remission, n (%) 95% CIa | 65 (69.1) (58.8 to 78.3) | 69 (73.4) (63.3 to 82.0) |
Difference in percent (95% CI)b | Reference | 4.3 (–8.7 to 17.2) |
Newly diagnosed ANCA-AV | 114 | 115 |
Patients who achieved remission, n (%) 95% CIa | 76 (66.7) (7.2 to 75.2) | 76 (66.1) (56.7 to 74.7) |
Difference in percent (95% CI)b | Reference | –0.6 (–12.8 to 11.7) |
Relapsed ANCA-AV | 50 | 51 |
Patients who achieved remission, n (%) 95% CIa | 39 (78.0) (64.0 to 88.5) | 44 (86.3) (73.7 to 94.3) |
Difference in percent (95% CI)b | Reference | 8.3 (–6.6 to 23.1) |
Subgroups | ||
GPA | 90 | 91 |
Patients who achieved remission, n (%) 95% CIa | 65 (72.2) (61.8 to 81.1) | 65 (71.4) (61.0 to 80.4) |
Difference in percent (95% CI)b | Reference | –0.8 (–13.9 to 12.3) |
MPA | 74 | 75 |
Patients who achieved remission, n (%) 95% CIa | 50 (67.6) (55.7 to 78.0) | 55 (73.3) (61.9 to 82.9) |
Difference in percent (95% CI)b | Reference | 5.8 (–8.9 to 20.4) |
ANCA-AV = antineutrophil cytoplasmic autoantibody–associated vasculitis; CI = confidence interval; GPA = granulomatosis with polyangiitis; ITT = intention to treat; MPA = microscopic polyangiitis; MPO = myeloperoxidase.
a95% CIs for treatment proportions are calculated using the Clopper and Pearson Method.
bTwo-sided 95% CIs are calculated for the difference in proportions (avacopan minus prednisone) using the Wald Method.
Source: ADVOCATE Clinical Study Report.19
Table 28: Proportion of Patients With Sustained Disease Remission at Week 52 Analyzed by Stratification Factor and by Subgroup (ITT Population)
Outcome | Prednisone | Avacopan |
|---|---|---|
Stratification factors | ||
IV rituximab | 107 | 107 |
Patients who achieved remission, n (%) 95% CIa | 60 (56.1) (46.1 to 65.7) | 76 (71.0) (61.5 to 79.4) |
Difference in percent (95% CI)b | Reference | 15.0 (2.2 to 27.7) |
IV or oral cyclophosphamide | 57 | 59 |
Patients who achieved remission, n (%) 95% CIa | 30 (52.6) (39.0 to 66.0) | 33 (55.9) (42.4 to 68.8) |
Difference in percent (95% CI)b | Reference | 3.3 (–14.8 to 21.4) |
PR3 ANCA positive | 70 | 72 |
Patients who achieved remission, n (%) 95% CIa | 40 (57.1) (44.7 to 68.9) | 43 (59.7) (47.5 to 71.1) |
Difference in percent (95% CI)b | Reference | 2.6 (–13.6 to 18.8) |
MPO ANCA positive | 94 | 94 |
Patients who achieved remission, n (%) 95% CIa | 50 (53.2) (42.6 to 63.6) | 66 (70.2) (59.9 to 79.2) |
Difference in percent (95% CI)b | Reference | 17.0 (3.3 to 30.7) |
Newly diagnosed ANCA-AV | 114 | 115 |
Patients who achieved remission, n (%) 95% CIa | 66 (57.9) (48.3 to 67.1) | 70 (60.9) (51.3 to 69.8) |
Difference in percent (95% CI)b | Reference | 3.0 (–9.7 to 15.7) |
Relapsed ANCA-AV | 50 | 51 |
Patients who achieved remission, n (%) 95% CIa | 24 (48.0) (33.7 to 62.6) | 39 (76.5) (62.5 to 87.2) |
Difference in percent (95% CI)b | Reference | 28.5 (10.4 to 46.6) |
Subgroups | ||
GPA | 90 | 91 |
Patients who achieved remission, n (%) 95% CIa | 52 (57.8) (46.9 to 68.1) | 56 (61.5) (50.8 to 71.6) |
Difference in percent (95% CI)b | Reference | 3.8 (–10.5 to 18.0) |
MPA | 74 | 75 |
Patients who achieved remission, n (%) 95% CIa | 38 (51.4) (39.4 to 63.1) | 53 (70.7) (59.0 to 80.6) |
Difference in percent (95% CI)b | Reference | 19.3 (4.0 to 34.7) |
ANCA-AV = antineutrophil cytoplasmic autoantibody–associated vasculitis; CI = confidence interval; GPA = granulomatosis with polyangiitis; ITT = intention to treat; MPA = microscopic polyangiitis; MPO = myeloperoxidase.
a95% CIs for treatment proportions are calculated using the Clopper and Pearson Method.
bTwo-sided 95% CIs are calculated for the difference in proportions (avacopan minus prednisone) using the Wald Method.
Source: ADVOCATE Clinical Study Report.19
Table 29: Change From Baseline in eGFR in Patients With Renal Disease at Baseline Based on eGFR Category — Subgroup Analysis (ITT Population)
Outcome | Prednisone (N = 164) | Avacopan (N = 166) |
|---|---|---|
eGFR < 30 mL/min/1.73 m2 | ||
Baseline, n (%) | 48 | 52 |
eGFR (mL/min/1.73 m2), mean (SD) | 21.6 (4.5) | 21.1 (4.2) |
Week 52 | 42 | 45 |
LSM change from baseline (SEM)a | 8.2 (1.4) | 13.7 (1.4) |
LSM difference (95% CI)a | Reference | 5.6 (1.7 to 9.5) |
P valuea, b | Reference | 0.0050 |
eGFR 30 to 59 mL/min/1.73 m2 | ||
Baseline, n (%) | 51 | 46 |
eGFR (mL/min/1.73 m2), mean (SD) | 42.8 (8.5) | 41.2 (8.3) |
Week 52 | 50 | 43 |
LSM change from baseline (SEM)a | 7.8 (1.4) | 10.5 (1.5) |
LSM difference (95% CI)a | Reference | 2.6 (–1.5 to 6.7) |
P valuea, b | Reference | 0.2115 |
eGFR > 59 mL/min/1.73 m2 | ||
Baseline, n (%) | 35 | 33 |
eGFR (mL/min/1.73 m2), mean (SD) | 82.5 | 86.4 |
Week 52 | 33 | 31 |
LSM change from baseline (SEM)a | –7.5 (2.6) | –5.9 (2.7) |
LSM difference (95% CI)a | Reference | 1.6 (–5.8 to 9.0) |
P valuea, b | Reference | 0.6721 |
eGFR = estimated glomerular filtration rate; ITT = intention to treat; LSM = least squares mean; SD = standard deviation; SEM = standard error of the mean.
aAnalysis used MMRM models with treatment group, visit, and treatment-by-visit interaction as factors and baseline as a covariate. MMRM results by visit are provided using the treatment-by-visit interaction term.
bP value has not been adjusted for multiple testing (i.e., the type I error rate has not been controlled).
Source: ADVOCATE Clinical Study Report.19
||||||| | |||||||| | |
|---|---|---|
|||||||||| || ||||| | |||||||| || ||||| | |
|||||||| || |||||||| |||| || || |||| | ||| |||||| | ||| |||||| |
|||||||| || ||||||||||| ||||||| ||||| |||| || || |||| | | |||||| | | |||||| |
|||||||| ||||||||| |||| | ||| |||||| | ||| |||||| |
|||||| ||||| |||| ||| | ||||||||| | |||| ||||| || ||||| |
| |||||| | | ||||||||| | |||||| |
|||| ||||||||||| |||||||||| |||||||| |||||| || ||||||||||| ||||||||| || |||||||||||||||||||||| |||||||| || || ||||| || ||||||| || ||||||| ||||||||| ||||||| ||||| || ||||||||||| || |||||||||| ||||||||||||||| |||||||| || |||||||||||| |||||||||||| ||||| || || |||||||| ||||||| |||||| || || |||| |||||||| || |||||||| ||||||| |||||| || |||| |||||| ||||| || |||| |||||||||||||||||||| |||||||| |||||||| ||||| |||||||19
|||||| | |||||||| | |
|---|---|---|
|||||||||| || ||||| | |||||||| || ||||| | |
|||||||| || |||||||| |||| || || ||| | ||| |||||| | ||| |||||| |
|||||||| || |||||||| ||||||| |||| || || || |||| | | ||||| | | ||||| |
|||||||| |||| ||||||||| |||| ||||||| |||| || || || |||| | | ||||| | | |||| |
|||| ||||||||||| |||||||||| |||||||| |||||| || |||||||||||||||||||||| |||||||| || | ||||| || ||||||| || ||||||| ||||||||| ||||||| ||||| || ||||||||||| || |||||||||| ||||||||||||||||||||| |||||||| |||||||| ||||| |||||||19
Appendix 4: Description and Appraisal of Outcome Measures
Note this appendix has not been copy-edited.
Aim
To describe the following outcome measures and review their measurement properties (validity, reliability, responsiveness to change, and MID):
BVAS version 3
VDI
GTI version 2
SF-36 version 2
EQ-5D-5L
Findings
Table 32: Summary of Outcome Measures and Their Measurement Properties
Outcome measure | Type | Conclusions about measurement properties | MID |
|---|---|---|---|
BVAS version 3 | A comprehensive multisystem clinical assessment of disease activity in systemic vasculitis.38 BVAS v.3 was developed to record persistent disease activity without requiring a separate subscore and comprises 57 clinical features grouped into 9 organ systems plus an “other” category.38 Each feature is given a numerical value based on its perceived clinical relevance (adjudication according to a charter) by an expert consensus blinded to treatment assignment.19 The total score ranges from 0 to 63, with 0 indicating no active disease, and any score higher than 0 indicating that active disease is present.39 | Validity: Face validity was assessed by consensus, reducing the number of items in the previous version, BVAS v.2, from 66 to 56 in BVAS v.3 by omitting or merging items and including a “persistent” option for the entire form.38 In patients with systemic vasculitis, convergent validity was assessed and found that the BVAS v.3 was correlated (Spearman’s correlation coefficient [rs]) with the following:
Reliability: Reliability was assessed using the ICC, and linear weighted kappa statistic for the organ system subscores.38 Interobserver reliability was examined in 99 patients independently assessed by 2 observers on the same day and found an ICC of 0.96 (95% CI, 0.95 to 0.97).38 Intraobserver reliability was examined in the subgroup of 39 patients with a second assessment by the same observer within 9 days of the first assessment and found an ICC of 0.96 (95% CI, 0.92 to 0.97).38 Responsiveness: Sensitivity to change in disease state was assessed in a cohort of 39 patients with newly diagnosed ANCA-AV.38 Analysis was assessed by paired t test and found that BVAS v.3 scores at diagnosis (mean = 18.92 [SD = 6.06]) compared to scores at 3 months (mean = 2.03 [SD = 2.48]) decreased by 16.9 units (95% CI, 14.8 to 18.9; P < 0.001).38 | An MID was not identified for patients with ANCA-AV (GPA or MPA). |
VDI | The VDI is a standardized clinical assessment of damage in systemic vasculitis, aimed at distinguishing damage or scarring (which is unlikely to respond to immunosuppression) from disease activity (as in the BVAS) to aid in the selection of therapy.40 The index comprises 64 items of damage (irreversible scars which have occurred since the onset of vasculitis and present for at least 3 months), grouped into 11 organ systems or categorizations (musculoskeletal, skin/mucous membranes, ocular, ears, nose and throat, pulmonary, cardiovascular, peripheral vascular disease, gastrointestinal, renal, neuropsychiatric, and other).40 The VDI score is a sum of all items of damage, scored as the presence (1 point) or absence (0 points) of an item.19,40 The index is cumulative (all previously score items are counted at each subsequent assessment) and therefore remains stable or increases.40 Newly diagnosed patients with systemic vasculitis usually have a VDI total score of 0.19 | Validity, reliability, and responsiveness of the VDI was assessed in 100 patients with a range of systemic vasculitides.40 Validity: Content and face validity was assessed by applying the VDI to derive scores for each patient.40 Median disease duration from first symptoms to last observation was 6 years (range 3 to 10), with a median VDI score of 3 (range 0 to 8).40 While a wide variety of items were scored among patients, with some items scored in every organ system, 17 items were not used, and no items of damage were scored in 5 (5%) patients.40 Nineteen items recorded once in the “Other features” were considered not representative of damage in systemic vasculitis and not added to the VDI score.40 Using death as the gold standard for damage in systemic vasculitis, criterion validity was assessed by comparing the VDI score for a subgroup of patients with WG comparing nonsurvivors (n = 12) with survivors (n = 47) at last observation; findings demonstrated higher scores for the former group (median = 7 [range 5 to 8] vs. 4 [range 2 to 5]; P = 0.003).40 Convergent validity was assessed by comparing the VDI with the Systemic Necrotizing Vasculitis (SNV) Damage Index and the Systemic Lupus International Cooperating Clinics/American College of Rheumatology (SLICC/ACR) Damage Index.40 There was low correlation between the VDI and weighted scores for the SNV and for the SLICC/ACR (Pearson’s correlation coefficient of 0.594 and 0.570, respectively).40 Somewhat stronger correlations were found between the VDI and unweighted scores for SNV and SLICC/ACR (Pearson’s correlation coefficient of 0.670 and 0.632, respectively).40 The VDI scored more items of damage (median = 3 [range 2 to 5]) than either the unweighted SNV (median = 2 [range 1 to 3]) or the unweighted SLICC/ACR (median = 1 [range 1 to 2]) Damage Indices (P < 0.001).40 The VDI scored more items of damage (median = 3 [range 2 to 5]) than either the weighted SNC (median = 3 [range 1 to 4]) or SLICC/ACR (median = 1 [range 1 to 2]) Damage Indices (P < 0.001).40 Discriminant validity was assessed for the ability of the VDI to detect damage in each vasculitic syndrome and found it demonstrated higher sensitivity to detect more items of damage for numerous syndromes, including WG (median = 2 [IQR 1 to 3]) at last observation.40 Reliability: VDI scores were compared between independent assessors by using paired expert and novice assessments in random order for 6 months postpresentation in 50 patients with systemic vasculitis; paired scores were identical in 64% of patients and within 1 point in 78% of patients.40 In 8 patients, there was complete agreement between all assessors for two-thirds of the VDI where items of damage were scored as absent.40 Restricting analysis to 21 items which any assessor scored damage, the mean kappa per assessor was 0.41, 0.38, 0.36 and 0.34.40 Exley et al. (1997) reported good agreement between all assessors for renal/neurologic systems (mean kappa statistic = 0.61) and ENT system (mean kappa statistic = 0.41).40 Responsiveness: The VDI was assessed for its ability to capture disease change over time and found that among 100 patients with systemic vasculitis, there was a median increased VDI score of 3 (range 1 to 4; P < 0.001) over a median of 5 years (range 2.5 to 8) from disease presentation to last observation.40 | An MID was not identified for patients with ANCA-AV (GPA or MPA). |
Glucocorticoid Toxicity Index (GTI) version 2 | A comprehensive instrument for the assessment of glucocorticoid toxicity, the GTI version 2 uses the Cumulative Worsening Score (GTI-CWS) and the Aggregate Improvement Score (GTI-AIS) to quantify changes in toxicity associated with glucocorticoid use.41,42 The GTI-CWS assesses cumulative glucocorticoid toxicity, regardless of whether the toxicity has lasting effects or is transient; the score can only remain the same or increase over time.41,42 The GTI-AIS includes toxicities (new event or worsening in a specific item compared to baseline) but removes toxicities if improvement occurs. When overall glucocorticoid toxicity improves, the GTI-AIS is negative.41,42 | Validity: The GTI is a tool that appears to be unvalidated in patients with ANCA-AV (though there is evidence of validity in patients with asthma), measures change in glucocorticoid toxicity between 2 points in time, and includes 2 components: a Composite Index, and a Specific List. The GTI assigns systematically determined relative weights to each toxicity item in the Composite Index; these are used to establish a baseline GTI score.49 Notably, Health Canada considered the GTI to be an unvalidated tool for vasculitis, and too general to be clinically meaningful as a measure of glucocorticoid toxicity.20 Reliability: Reliability of the GTI was not assessed for patients with ANCA-AV (GPA or MPA). Responsiveness: Responsiveness of the GTI was not assessed for patients with ANCA-AV (GPA or MPA). | An MID of 10 points was estimated for patients from a mixed population including those with ANCA-AV. |
SF-36 version 2 | The SF-36 is a validated HRQoL instrument developed for use in the MOS that has been used extensively in clinical trials in many disease areas.44 The 36-item scale measures 8 health concepts, each with categorical response options (range 2 to 6 options): 1) physical functioning (PF); 2) role limitations due to physical health problems (RP); 3) bodily pain (BP); 4) general health (GH); 5) vitality (VT); 6) social functioning (SF); 7) role limitations due to emotional problems (RE); and, 8) general mental health (psychological distress and psychological well-being) (MH).44 The first 4 subscales (PF, RP, BP, GH) form the PCS score, and the last 4 subscales form the MCS score.44,45 The SF-36 items and subscales were constructed for scoring using the Likert method of summated ratings.44 Scores for each subscale are converted to norm-based scares based on the 1998 US general population with a mean of 50 (SD = 10).44 Scores for each summary range from 0 to 100 with higher scores indicating better health status.44 | Validity: Evidence of validity could not be verified for patients with ANCA-AV (GPA or MPA).50 Reliability: Evidence of reliability could not be verified for patients with ANCA-AV (GPA or MPA).50 Responsiveness: Responsiveness of the SF-36 was not assessed for patients with ANCA-AV (GPA or MPA). | An MID was not identified for patients with ANCA-AV (GPA or MPA). |
EQ-5D-5L and EQ-5D VAS | The EQ-5D is a standardized measure of health status developed by the EuroQoL Group to provide a simple, generic measure of health across a wide range of disease areas and in the general population. It comprises a short descriptive system and a VAS (EQ-VAS).46 The EQ-5D-5L provides a descriptive profile of a respondent’s health state. It comprises 5 dimensions (mobility, self-care, usual activities, pain/discomfort, and anxiety/depression), each with 5 response levels or levels of severity (no problems = 1, slight problems = 2, moderate problems = 3, severe problems = 4, and unable to/extreme problems = 5). Respondents select the most appropriate response level matching their health state on that day, and these are combined in a 5-digit numerical description or code for each dimension.46 The descriptive system profile can be linked to a ‘value set’ (values or weights for each health state description according to preferences of the general population or a country/region) to derive an index score, where 0 represents the health state “dead” and 1.0 represents “perfect health.”46 The EQ-5D VAS records a respondent’s self-rated health that day on a vertical line with 0 labelled “worst imaginable health state” and 100 as “best imaginable health state.”46 It is intended to complement the EQ-5D index score.46 | Psychometric properties were not identified for patients with ANCA-AV (GPA or MPA). | An MID was not identified for patients with ANCA-AV (GPA or MPA). |
ANCA-AV = antineutrophil cytoplasmic autoantibody–associated vasculitis; ANCOVA = analysis of covariance; BP = bodily pain; BVAS = Birmingham Vasculitis Activity Score; CI = confidence interval; CRP = c-reactive protein; ENT = ear, nose, throat; GH = general health; GPA = granulomatosis with polyangiitis; GTI = Glucocorticoid Toxicity Index; GTI-AIS = Glucocorticoid Toxicity Index Aggregate Improvement Score; GTI-CWS = Glucocorticoid Toxicity Index Cumulative Worsening Score; HRQoL = health-related quality of life; ICC = intraclass correlation coefficient; IQR = interquartile range; MCS = mental component summary; MH = mental health; MID = minimal important difference; MPA = microscopic polyangiitis; PCS = physical component summary; PF = physical functioning; RCT = randomized controlled trial; RE = role emotional; RP = role physical; rs = Spearman’s correlation coefficient; SD = standard deviation; SF = social functioning; SF-36 = Short Form (36) Health Survey; SLICC/ACR = Systemic Lupus International Cooperating Clinics/American College of Rheumatology; SNV = systemic necrotizing vasculitis; VAS = visual analogue scale; VDI = Vasculitis Damage Index; WG = Wegener’s Granulomatosis.
Pharmacoeconomic Review
Abbreviations
ANCA-AV
antineutrophil cytoplasmic autoantibody–associated vasculitis
BIA
budget impact analysis
eGFR
estimated glomerular filtration rate
ESRD
end-stage renal disease
GPA
granulomatosis with polyangiitis
HR
hazard ratio
ICER
incremental cost-effectiveness ratio
MPA
microscopic polyangiitis
QALY
quality-adjusted life-year
SOC
standard of care
WTP
willingness to pay
Executive Summary
The executive summary comprises 2 tables (Table 1 and Table 2) and a conclusion.
Item | Description |
|---|---|
Drug product | Avacopan (Tavneos), oral capsule |
Submitted price | Avacopan, 10 mg: $34.24 per capsule |
Indication | For the adjunctive treatment of adult patients with severe ANCA-AV (GPA and MPA) in combination with standard background therapy including glucocorticoids. Avacopan does not eliminate glucocorticoid use. |
Health Canada approval status | NOC |
Health Canada review pathway | Standard |
NOC date | April 14, 2022 |
Reimbursement request | As per indication |
Sponsor | Otsuka Canada Pharmaceutical Inc. |
Submission history | Previously reviewed: No |
ANCA-AV = anti-neutrophil cytoplasmic autoantibody-associated vasculitis; GPA = granulomatosis with polyangiitis; MPA = microscopic polyangiitis; NOC = Notice of Compliance.
Table 2: Summary of Economic Evaluation
Component | Description |
|---|---|
Type of economic evaluation | Cost-utility analysis Markov model |
Target population | Adults with severe ANCA-AV (GPA and MPA) |
Treatment | Avacopan in combination with SOC (rituximab or cyclophosphamide)a |
Comparators |
|
Perspective | Canadian publicly funded health care payer |
Outcomes | QALYs, LYs |
Time horizon | Lifetime |
Key data source |
|
Submitted results |
|
Key limitations |
|
CADTH reanalysis results |
|
ANCA-AV = antineutrophil cytoplasmic autoantibody–associated vasculitis; eGFR = estimated glomerular filtration rate; ESRD = end-stage renal disease; GPA = granulomatosis with polyangiitis; ICER = incremental cost-effectiveness ratio; LY = life-year; MPA = microscopic polyangiitis; QALY = quality-adjusted life-year; SOC = standard of care.
aThere was uncontrolled use of nonstudy glucocorticoids with a mean dosage of 4 mg per day per patient.
Conclusions
The CADTH clinical review concluded that avacopan was noninferior to cyclophosphamide followed by azathioprine, and to rituximab, for achieving disease remission at week 26 and that is was superior for sustained disease remission at week 52. Outcomes related to disease relapse, systemic damage, kidney function, and health-related quality of life provided limited support for the primary outcomes. The relevance of the findings to current standards of practice are unclear due to the lack of rituximab maintenance in the comparison group, which is the current gold standard. Therefore, the results of the ADVOCATE trial may have limited relevance to current practice, and more evidence is needed to better understand the long-term efficacy and safety of avacopan and whether it can be used to effectively eliminate glucocorticoid use.
CADTH undertook reanalyses to address key limitations in the sponsor’s analysis; these reanalyses included considering a pooled hazard ratio (HR) for end-stage renal disease (ESRD) per change in estimated glomerular filtration rate (eGFR), selecting rituximab as the first-line maintenance therapy, assuming the use of avacopan for reinduction treatment, assuming a treatment duration of 2 years for avacopan, and equating utility values for patients who had a transplant and for patients in remission.
The CADTH results were similar to the sponsor’s in that avacopan plus standard of care (SOC) was not cost-effective at a willingness-to-pay (WTP) threshold of $50,000 per quality-adjusted life-year (QALY) gained. Based on the CADTH base case, in adult patients with severe antineutrophil cytoplasmic autoantibody–associated vasculitis (ANCA-AV), the incremental cost-effectiveness ratio (ICER) of avacopan plus SOC compared to SOC alone is $365,453 per QALY gained. A price reduction of 72.5% is required for avacopan plus SOC to be cost-effective at a WTP threshold of $50,000 per QALY gained.
CADTH was unable to account for the high use of nonstudy glucocorticoids potentially overestimating the efficacy of avacopan, the uncertainty associated with the rate of relapse following remission, and a lack of long-term clinical data on avacopan. These limitations are compounded by the underlying evidence from the trial not being reflective of current clinical practice, where rituximab maintenance therapy is used in place of azathioprine. These factors result in uncertainty in interpreting whether rituximab in combination with avacopan would be equally effective or superior to using rituximab alone, given rituximab’s reported low relapse rate (5% after 2 years). Given these limitations, the cost-effectiveness of avacopan should be interpreted with caution, and even greater price reductions may be required.
Stakeholder Input Relevant to the Economic Review
This section is a summary of the feedback received from the patient groups, registered clinicians, and drug plans that participated in the CADTH review process.
Patient input was received from the Vasculitis Foundation Canada. The foundation gathered patient input through an online survey of 46 patients with ANCA-AV (35 with granulomatosis with polyangiitis [GPA], and 11 with microscopic polyangiitis [MPA]) living in Canada and the US who have experience using prednisone and/or avacopan. One patient had been treated with avacopan through a clinical trial, and all patients had been treated with oral prednisone, with 53% receiving IV steroids. Patients who required glucocorticoids had been treated with higher doses for a prolonged period, ranging from 6 months to 27 years. Patients with ANCA-AV commonly reported renal damage, which could lead to chronic kidney disease, kidney failure, dialysis, and transplant. Moreover, most patients experienced a host of physical manifestations (e.g., breathing difficulties, weight gain, joint or nerve pain, loss of hearing, cataracts, disfigurements) that negatively impacted their quality of life. Patients treated with prednisone reported several adverse events that significantly affected quality of life, including body disfiguration, steroid-induced diabetes or hypertension, infections requiring medical care, bone fractures, and anxiety and depression. The single patient surveyed who had previously used avacopan favoured using avacopan over prednisone. Patients indicated a need for a treatment that would improve symptoms and quality of life while reducing or eliminating prednisone use.
Clinician group input was received from CanVasc, the Canadian network for research on vasculitis. Clinician input noted that the treatment options for patients with ANCA-AV heavily relied on both glucocorticoids and immunosuppressive regimens. The current recommended therapies include cyclophosphamide or rituximab along with glucocorticoids for induction, and then rituximab, azathioprine, or methotrexate for maintenance. Despite these treatments, mortality among patients with ANCA-AV was high, which was mainly attributed to treatment-related complications and sequelae of vasculitis, such as increased cardiovascular disease. The group highlighted the primary unmet needs of patients with severe GPA or MPA as improved survival, improved renal and neurologic recovery, induced remission (e.g., at 6 months) followed by sustained remission, reduced reliance on high-dose and prolonged glucocorticoid use due to the associated toxicities, and access to and coverage of new treatments. There is a need for a treatment regimen that is convenient and practical to patients and specialists (oral administration preferred over infusion, and without a complex tapering regimen). The clinician group anticipates that avacopan will be used in clinical practice initially as a combined treatment with rituximab, with or without steroids, for up to 12 months (benefits and harms beyond this time point are unknown), but the group also raised concerns about stopping avacopan at 12 months in patients who have some lingering minor symptoms or who are ANCA positive. Discontinuation may be considered if relapse is observed at 6 months followed by a subsequent relapse, or earlier if adverse events are detected.
Drug plan input noted that rituximab has been successfully negotiated, although for a slightly different indication. Due to the uncontrolled use of glucocorticoids as well as the use of rituximab and cyclophosphamide in the trial’s avacopan group, there is uncertainty regarding the overall impact of avacopan and whether it will decrease glucocorticoid usage. The drug plans also highlighted that the trial found avacopan not to be superior for induction but to be superior for sustained remission, but this was based on 1 year of data, and therefore the drug plans recommended more extensive studies. Questions were raised regarding the patient population that could receive avacopan, the drug’s place in therapy, the timing of re-treatment after relapse, assessment of continued need for treatment, duration of therapy, and its potential use for reinduction treatment. Further, as avacopan targets a component of the inflammatory process, there is potential for use in other autoimmune diseases.
Several of these concerns were addressed in the sponsor’s model:
The sponsor’s model included relevant comparators (i.e., cyclophosphamide or rituximab along with glucocorticoids).
The model structure captured important aspects of the disease, including induction, remission, relapse, and ESRD.
CADTH was unable to address the following concerns raised from stakeholder input:
The impact the uncontrolled use of nonstudy glucocorticoids in the trial’s avacopan and prednisone groups had on clinical outcomes.
Economic Review
The current review is for avacopan (Tavneos) in combination with rituximab or cyclophosphamide for adult patients with severe ANCA-AV (GPA and MPA).
Economic Evaluation
Summary of Sponsor’s Economic Evaluation
Overview
Avacopan (Tavneos) is indicated for adjunctive treatment for the induction of remission in adult patients with severe ANCA-AV (GPA and MPA) in combination with standard background therapy, including glucocorticoids. Avacopan does not eliminate glucocorticoid use.1 The sponsor submitted a cost-utility analysis of avacopan in combination with SOC (i.e., cyclophosphamide plus glucocorticoids or rituximab plus glucocorticoids followed by azathioprine maintenance therapy) compared to SOC alone in the treatment of adult patients with severe ANCA-AV (GPA and MPA) in Canada.2 This model population aligns with the intention-to-treat population of the ADVOCATE phase III clinical trial,3,4 the Health Canada indication,1 and the reimbursement request.
Avacopan is an add-on treatment and is available in a 10 mg oral capsule. The recommended dosage of avacopan is 30 mg (3 × 10 mg capsules) orally twice daily.1 The cost of avacopan is $34.24 per capsule, equating to an annual cost of $75,051.
The outcomes of the model included QALYs and life-years. The model took a Canadian public health care payer perspective and was run over a lifetime horizon (27 years), with a cycle length of 4 weeks. Both costs and outcomes were discounted at 1.5% per annum.2
Model Structure
The sponsor submitted a Markov cohort model consisting of 9 health states: active disease, 3 disease remission states, 3 disease relapse states, ESRD, and death (Figure 1).2 All patients entered the model with active disease (newly diagnosed or relapsing) and received their first induction therapy. Depending on their response to the treatment, patients could transition to the “remission” or “relapse” state. Patients in remission received maintenance therapy for 2 years, and they could stay in remission or relapse. Patients in relapse were reinducted, and they could progress to the next remission state or stay in relapse state. The model structure allowed for up to 3 induction therapies if remission was not achieved.2 Each induction course in the model was spread over a 6-month period; therefore, patients in remission could only relapse after remaining in the health state for 6 cycles, when induction therapy was completed. Patients who failed their third induction therapy would remain in the relapse (refractory disease) state for the remainder of the time horizon. The model implemented tunnel states for relapse and remission health states to follow patients through the course (Figure 2).2 Patient could develop ESRD or die from any health state at any time.
The treatments chosen for the second and third inductions were the same for avacopan plus SOC and for SOC alone; the sponsor assumed that 64.8% of patients would receive rituximab plus glucocorticoids and 35.2% would receive cyclophosphamide plus glucocorticoids, based on the ADVOCATE trial.3,4 Avacopan was used for the first induction and for a duration of 1 year; it was not used for subsequent inductions or beyond 1 year.
Model Inputs
The baseline characteristics used to inform the model were taken from the ADVOCATE trial. Patients had a mean age of 60 years, an average weight of 77 kg, and a body surface area of 1.92 m2.3,4
The clinical efficacy parameters within the model were primarily informed by the ADVOCATE trial.4,5 The ADVOCATE trial was a multinational, randomized, active-controlled clinical trial that compared avacopan in combination with SOC (i.e., rituximab plus glucocorticoid or cyclophosphamide plus glucocorticoid) against SOC alone in 311 adult patients with severe ANCA-AV (GPA and MPA). Remission rates were estimated based on the proportions of patients in remission at week 26 and week 52 from the ADVOCATE trial; the relapse rate was computed as the difference between the proportion of patients in remission at 26 weeks and at 52 weeks. Based on the trial data, the rate of relapse from patients in remission decreases with time, with an increased risk in the first 2 years of remission.3,6 After 2 years of being in remission, the relapse rate was assumed to be ||| of the trial data from the first 2 years. The rate of relapse between week 52 and week 60 was derived from extension data reported in the ADVOCATE Clinical Study Report. In the absence of data, the rate of relapse after week 60 was assumed to be equal in both the avacopan- and glucocorticoid-based regimens. The rates of remission for rituximab and cyclophosphamide were also assumed to be equal based on the findings of noninferiority of rituximab in the RAVE clinical trial.7 The treatment effect of avacopan was assumed to continue for 2 cycles after week 52 based on the extension data reported in the ADVOCATE trial. Treatment-related adverse events were derived from the ADVOCATE trial.
The baseline probability of ESRD in active disease or relapse was based on the proportion of patients with ESRD in the first 6 months after diagnosis in Robson et al.,7 while long-term data between 6 months and 7 years was used to derive the probability of ESRD in remission. The improvement in eGFR between week 0 and week 26 in the ADVOCATE trial was used to adjust rates of ESRD in the active disease or relapse state; weeks 0 to 52 were used to calculate the risk of ESRD in remission. The corresponding risk for ESRD per eGFR unit decrease was derived from the Gercik et al. study.8 For instance, a 5.8 mL/min (5.8-point) increase in eGFR would lead to a 45.7% decrease in the risk of ESRD. The eGFR was predicted to fall by 10 mL/min with each subsequent relapse, increasing the probability of ESRD.9 The rate of ESRD in refractory disease and relapse was considered to be equal. The sponsor assumed an equal probability of ESRD in sustained remission for patients induced with the avacopan- or glucocorticoid-based regimen.
Background mortality in the model was derived from the Statistics Canada life tables for Canada.10 To account for the increased mortality rate in the population of patients with ANCA-AV and in patients with ESRD, a relative risk of excess mortality was used on the background mortality. This relative risk for ANCA-AV and ESRD was derived from data from the UK and the Republic of Korea, respectively.11,12 Mortality rates in all health states, except ESRD, were assumed to be equal.4
Health state utility values for active disease, remission, and relapse were estimated based on EQ-5D data from the ADVOCATE trial. Utilities corresponding to the 3-Level EQ-5D were derived based on the van Hout crosswalk mapping approach.13,14 The utility of ESRD was computed as the weighted average utility value of patients on peritoneal dialysis and hemodialysis from the literature.15 The utility of transplant recipients (0.82) was estimated from the literature and was higher than that of patients in the remission health state (||||).
Dosing from the ADVOCATE trial was used to inform both avacopan plus SOC and SOC alone.4,5 The drug acquisition costs of avacopan were based on the sponsor’s submitted price, and the costs of comparators were based on data from the Ontario Drug Benefit Formulary.16 The administration cost of rituximab infusion was obtained from the Ontario Schedule of Benefits.17 The dosing and frequency of avacopan and SOC treatments were derived from the ADVOCATE trial. The per-cycle treatment costs were adjusted based on the rate of compliance reported in the ADVOCATE Clinical Study Report, which was 86.4% for avacopan and 98.4% for glucocorticoid. The drug acquisition costs and dosing were consistent with those reported in the Overview section. The treatment cost of ESRD was derived from Ferguson et al.,15 stratified by type of dialysis (19.9% peritoneal dialysis and 75.9% hemodialysis), and the proportion of patients with renal transplant (4.1%) was derived from the Canadian Institute for Health Information Organ Replacement Register annual report.18 In addition to treatment acquisition costs, the following cost inputs were included in the sponsor’s submitted model: cost of monitoring and follow-up visits, cost of hospitalization, and adverse event costs. The cost of monitoring and maintenance for ESRD was assumed to be equal to those costs in the active disease state. Relevant costs were inflated to 2022 Canadian dollars.
Summary of Sponsor’s Economic Evaluation Results
The sponsor presented a probabilistic base-case analysis based on 1,000 iterations. Deterministic results were aligned with the probabilistic results. The probabilistic findings are presented below.
Base-Case Results
The results of the sponsor’s probabilistic base-case analysis demonstrated that avacopan plus SOC was associated with an additional 0.27 QALYs at an incremental cost of $29,626 compared to SOC alone, resulting in an ICER of $110,566 per QALY gained (Table 3).2 At a WTP threshold of $50,000 per QALY, avacopan plus SOC was cost-effective in approximately 2% of the probabilistic iterations. Approximately 91% of the clinical benefit, in terms of QALYs gained, was accumulated outside the 1-year trial period. Further, drug costs accounted for more than 22% and more than 5% of total costs for avacopan plus SOC and SOC alone, respectively. The pairwise and sequential ICER results are presented in Appendix 3, Table 12.
Table 3: Summary of the Sponsor’s Economic Evaluation Results
Drug | Total costs ($) | Incremental costs ($) | Total QALYs | Incremental QALYs | ICER vs. SOC ($ per QALY) |
|---|---|---|---|---|---|
SOC alone | 258,412 | Reference | 7.99 | Reference | Reference |
Avacopan plus SOC | 288,038 | 29,626 | 8.26 | 0.27 | 110,566 |
ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year; SOC = standard of care; vs. = versus.
Source: Sponsor’s pharmacoeconomic submission.2
Sensitivity and Scenario Analysis Results
The sponsor conducted several scenario analyses, including adopting a broader societal perspective that included transportation and productivity costs; using treatment-specific health state utility values; assuming a persistent treatment effect for avacopan; using rituximab as maintenance therapy; and allowing up to 3 reinductions with avacopan plus SOC. In the scenario analyses, avacopan plus SOC was always more costly and more effective than SOC alone. The scenario in which the sponsor assumed a persistent treatment effect for avacopan had the largest impact, with a reduced ICER of $14,294 per QALY gained; it was also the only scenario where avacopan plus SOC was cost-effective at a WTP threshold of $50,000 per QALY. The ICER values were most sensitive to changes in: discount rate, relative risk of death beyond the first year in patients with ANCA-AV, and eGFR recovery at induction and remission.
CADTH Appraisal of the Sponsor’s Economic Evaluation
CADTH identified several key limitations to the sponsor’s analysis that have notable implications for the economic analysis:
The modelled relationship between changes in eGFR and the risk of ESRD is highly uncertain. The sponsor used eGFR improvement in the ADVOCATE trial to calculate the probability of ESRD, which was adjusted based on the HR for ESRD per eGFR unit decrease from Gercik et al. (HR = 0.90; 95% confidence interval, 0.86 to 0.95).8 CADTH was unable to validate the methods behind this single study because it was published as a letter without a detailed methodology. Other studies, such as Brix et al., reported a different HR (HR = 0.96; 95% confidence interval, 0.93 to 0.98).19 As reported in the clinical review, it appears that eGFR results were drawn from a single measure taken during scheduled treatment visits as opposed to an average of replicated measures, the latter of which is more reliable. This, coupled with a lack of published minimal important differences from the literature for patients with AAV and with natural variability in eGFR due to factors such as a patient’s hydration, make it highly uncertain whether an increase in eGFR of 5.8 mL/min would truly result in a 45.7% reduction in the risk of ESRD. The clinical expert consulted for this review noted that the risk of ESRD is dependent on the study population and indicated that the modelled benefits of ESRD risk reduction may be overestimated because the observed eGFR changes in the ADVOCATE trial were insufficient to achieve the sponsor’s claimed impact on the risk of ESRD. Given that the changes in ESRD rates are a key driver of the economic model, alternative estimates using eGFR data and the corresponding risk of ESRD significantly impact the expected incremental QALYs, costs, and cost-effectiveness of avacopan.
CADTH considered the HRs reported by both the Gercik et al. and Brix et al. studies in separate scenario analyses and conducted a base-case reanalysis using a pooled HR (0.947) from the studies. This pooled HR aligns with the expectations of the clinical expert and reflects a similar approach as adopted by the National Institute for Health and Care Excellence (i.e., NICE) in its technology appraisal of avacopan.20
CADTH also performed a scenario analysis in which it was assumed that the eGFR improvements in the avacopan group would be equal to SOC due to the limitations mentioned regarding eGFR measurement in the ADVOCATE trial and insignificant differences in eGFR between trial arms at 60 weeks.
Azathioprine use as a first-line maintenance therapy does not reflect current practice. The sponsor used azathioprine as maintenance therapy for all patients who had cyclophosphamide or rituximab induction therapy. However, the CanVasc guideline21 recommended rituximab every 4 to 6 months as the first-line maintenance therapy. The clinical expert consulted by CADTH for this review confirmed that rituximab administered every 6 months for 2 years as maintenance therapy was considered the current gold standard for treatment of patients with ANCA-AV. The clinical expert stated that rituximab is superior to azathioprine in reducing major relapses and that only 5% of patients on rituximab maintenance therapy relapse after 2 years of treatment (versus 35% for patients on azathioprine), as supported in a Guillevin et al. study that found that at 28 months after remission 5% of patients on rituximab experience a relapse compared to 29% of patients on azathioprine.22 Although azathioprine maintenance therapy has a lower success rate, it can still be used in exceptional circumstances, such as when the patient prefers a less immunosuppressive drug. The clinical expert consulted by CADTH estimated that in Canada, 30% of patients would be induced with cyclophosphamide and receive azathioprine maintenance therapy and the remaining 70% would be induced with rituximab and receive rituximab maintenance therapy. The fact that rituximab was not used as maintenance therapy in the clinical trial could inflate the risk of relapse and the associated costs compared to what would be expected in current clinical practice.
CADTH conducted a base-case reanalysis in which rituximab was considered as first-line maintenance therapy for all patients regardless of their induction treatment. Due to the nature of the model structure, CADTH was unable to perform a base-case reanalysis reflecting the current clinical practice, in which azathioprine maintenance therapy would be used in the 30% of patients who had cyclophosphamide induction therapy.
Avacopan treatment duration and its potential use for reinduction therapy remains unknown. The sponsor used avacopan treatment for 1 year, in line with the ADVOCATE trial, which showed superiority at week 52. Given the lack of long-term data, there is uncertainty in patient management after 12 months of avacopan use and in the long term outcomes after stopping the drug. The clinical expert consulted for this review noted that given avacopan is an add-on treatment, it is unlikely to be discontinued after 1 year and further suggested that it, like other therapies, would be used for up to 2 years while being monitored for safety and efficacy. In the ADVOCATE trial, patients who received rituximab as induction therapy continued to receive avacopan without rituximab from month 6 to month 12, and it remains unknown whether using rituximab in combination with avacopan would be equally effective or superior to using rituximab alone during this period. The clinical expert recommended that avacopan should be used in addition to rituximab for 2 years and advised against stopping treatment after 6 months as it might lead to premature loss of efficacy. Moreover, there is lack of evidence regarding the potential use of avacopan for reinduction therapy. The sponsor’s base-case model allowed induction with avacopan only for the first induction, but the clinical expert indicated that it would be reasonable for a patient to continue receiving avacopan after the first relapse but that avacopan should be stopped after the second relapse and be replaced with glucocorticoids.
CADTH conducted a base-case reanalysis in which it was assumed that avacopan would be used for reinduction treatment. During the reinduction period, avacopan’s potential benefit of reducing the risk of ESRD was assumed to be the same as treatment with SOC.
CADTH conducted a base-case reanalysis in which it was assumed that the treatment duration of avacopan alongside rituximab maintenance therapy was 2 years. For the 2-year treatment duration, avacopan’s HR for the rate of relapse was assumed to wane over time after the ADVOCATE trial’s duration as follows: the benefit seen in the trial continued for week 52 to week 60 and week 60 to week 80 with a HR of 0.39, but after week 80, it was assumed that the rate of relapse waned (HR = 1.0). This is because there is no evidence to warrant that the same benefit in the rate of relapse from week 26 to week 52 would be realized indefinitely while on treatment.
CADTH also performed 2 scenario analyses in which an extended waning period for avacopan was assumed, where relapse benefits seen in the trial continued with same HR of 0.39 up to week 104 in the first scenario and week 130 in the second scenario. In both scenarios, the rate of relapse waned (HR = 1.0) after each respective week.
For patients who achieved remission within 6 months, CADTH was unable to evaluate the effects of using rituximab in combination with avacopan as a maintenance therapy compared to avacopan alone or rituximab alone due to a lack of data.
Higher use of nonstudy glucocorticoids in the avacopan group. In the ADVOCATE trial, nearly all patients had some exposure to non-study-supplied glucocorticoids, which were glucocorticoids administered in addition to those outlined in the protocol. In the first 29 days of the trial, 87.3% and 90.9% of patients in the avacopan group and the prednisone group, respectively, used glucocorticoids.4 Nonstudy medication use is problematic for quantifying the effect of avacopan treatment alone for both efficacy and harms outcomes. The clinical expert consulted by CADTH was in agreement that this nonstudy medication use could have biased the effect estimates from the trial and that it creates added uncertainty around whether treatment with avacopan can reduce glucocorticoid use in practice.
CADTH was unable to address the uncertainties associated with the higher usage of non-study-supplied glucocorticoids among the avacopan group (only 12% of the trial population did not use glucocorticoids outside of protocol).
The transplant utility value lacks face validity. The sponsor’s model estimated that transplant recipients would have a higher quality of life (utility value of 0.82) than those who achieved remission (||||). The clinical expert consulted for this review noted that although the patient’s quality of life would improve following transplant, they would still be on immunosuppressant medication and, therefore, their utility could not be higher than that of patients in the remission health state.
CADTH performed a base-case analysis in which it was assumed that the utility value of patients who had had a transplant would equal the utility value of the remission health state (||||).
The assumption regarding the rate of relapse was optimistic. The sponsor assumed that the rate of relapse for patients in remission would decline after a period of time. Specifically, the rate of relapse would increase over the first 2 years following remission, but after 2 years the relapse rate would be ||| of the first 2 years’ relapse rate.3,6 However, the clinical expert consulted for this review stated that the sponsor’s assumption of 2 years is likely too early, because patients would still be receiving treatment, and major relapses frequently occur after stopping treatment (i.e., between 2 years and 5 years). The clinical expert noted that the risk of relapse from remission is expected to increase over the first 5 years before dropping to a low constant rate.
Due to a lack of data, CADTH was unable to address the uncertainty around the rate of relapse. The direction and the magnitude of the effect on cost-effectiveness are unknown.
The proportion of patients who had a transplant may be inaccurate. The sponsor estimated that 4.1% of patients in the 52-week trial had received a transplant.15 However, data from a 52-week trial is unlikely to be representative of the transplant rate over the lifetime time horizon of the model. The clinical expert consulted by CADTH for this review noted that the sponsor-estimated proportion of patients who had transplants is underestimated and that over a lifetime horizon, the percentage would be closer to 20%.
CADTH performed a scenario analysis that assumed the transplant rate over the lifetime horizon to be 20%.
Treatment adherence on glucocorticoids was overestimated. Based on the ADVOCATE trial, the sponsor estimated a treatment adherence of 86.4% for avacopan and 98.4% for glucocorticoids,3 and the total costs in the model were reduced based on these adherence rates. According to the clinical expert feedback sought by CADTH for this review, the adherence rate of avacopan is reasonable given its oral form; however, the adherence rate for glucocorticoids is anticipated be equivalent to or lower than that for avacopan, primarily due to the severe side effects and toxicity associated with glucocorticoids.
CADTH performed 2 scenario analyses in which it was assumed that adherence to glucocorticoids was equal to adherence to avacopan (86.4%). To rule out cost adjustments based on adherence rate, CADTH performed an additional scenario analysis with the assumption of 100% adherence to avacopan and all comparators.
Additionally, the following key assumptions were made by the sponsor and have been appraised by CADTH (refer to Table 4).
Table 4: Key Assumptions of the Submitted Economic Evaluation
Sponsor’s key assumption | CADTH comment |
|---|---|
Rates of remission for rituximab and cyclophosphamide were considered equal. | Reasonable. The clinical expert consulted by CADTH for this review indicated this was a reasonable assumption. |
For patients with ESRD, each subsequent relapse was assumed to result in a 10 mL/min decrease in eGFR value. | Reasonable. The clinical expert consulted by CADTH for this review noted that it is reasonable to assume a 10 mL/min, and even up to a 20 mL/min, decline in eGFR with each subsequent relapse. |
Cost of HBV serology was not included. | Inappropriate. The sponsor’s base case did not model the costs related to the HBV serology test. This is inappropriate since the avacopan product monograph recommended obtaining an HBV serology test to determine the baseline liver function before initiating the treatment. However, given that the drug acquisition costs and the ESRD-associated costs are the major driver of the results, the impact of omitting the HBV serology test cost is expected to be minimal. |
eGFR = estimated glomerular filtration rate; ESRD = end-stage renal disease; HBV = hepatitis B virus.
CADTH Reanalyses of the Economic Evaluation
Base-Case Results
The CADTH base case was derived by making changes in parameter values, in consultation with clinical experts. CADTH reanalyses addressed several limitations within the economic model, as summarized in Tables 5 and 6, which included considering a pooled HR for ESRD per change in eGFR, selecting rituximab as the first-line maintenance therapy, assuming the use of avacopan for reinduction treatment, assuming avacopan’s treatment duration would be up to 2 years, and equating the utility value for a transplant with the remission health state. CADTH was unable to address limitations regarding non-study-supplied glucocorticoid use or uncertainty associated with relapse rates following remission.
Table 5: CADTH Revisions to the Submitted Economic Evaluation
Stepped analysis | Sponsor’s value or assumption | CADTH value or assumption |
|---|---|---|
Corrections to the sponsor’s base case | ||
None | — | — |
Changes to derive the CADTH base case | ||
1. HR for ESRD per mL/min change in eGFR | HR derived from Gercik et al. (HR = 0.90)8 | A pooled HR from Gercik et al. and Brix et al. (HR = 0.95) |
2. First-line maintenance therapy | Azathioprine | Rituximab |
3. Avacopan treatment duration | 52 weeks | 130 weeks (6 months of induction and 2 years of maintenance therapy) Waning HR for the rate of relapse, with HR = 1 beyond week 80 |
4. Number of reinductions with avacopan | 0 (avacopan not used for reinduction) | 1 reinduction Avacopan’s benefit in reducing the risk of ESRD during this period was assumed to be equal to the benefit of SOC |
5. Utility value of patients who had transplant | Utility of transplant was higher (0.82) than that of the remission health state (||||). | Utility of transplant would be equal to the utility of remission health state (||||) |
CADTH base case | 1 + 2 + 3 + 4 + 5 | |
eGFR = estimated glomerular filtration rate; ESRD = end-stage renal disease; HR = hazard ratio; SOC = standard of care.
Given the changes needed to derive a CADTH base case, a probabilistic reanalysis was not able to be performed on the sponsor’s model without error, primarily due to issues with existing VBA (Visual Basic for Applications) code in the Excel model resetting the CADTH base-case changes. This resulted in probabilistic results that were not reflective of the CADTH base case, which greatly differed from the deterministic results. Therefore, all CADTH reanalyses were run deterministically.
The results of CADTH’s stepped deterministic analysis are presented in Table 6. Compared to SOC alone, avacopan plus SOC had incremental QALY gains of 0.423 and incremental costs of $154,511, resulting in an ICER of $365,453 per QALY gained. The probability that avacopan plus SOC was cost-effective at a WTP threshold of $50,000 per QALY was 0%. In the pairwise comparisons reported in Appendix 3, the addition of avacopan to either cyclophosphamide plus glucocorticoids or rituximab plus glucocorticoids resulted in ICERs of $366,495 and $364,877 per QALY gained, respectively. Similar to the sponsor’s base case, most of the clinical benefit (91% of incremental QALYs) was accumulated outside the trial period; thus, the incurred benefit relied heavily on assumptions and extrapolated data. Also, as in the sponsor’s base case, drug costs accounted for more than 22% and more than 5% of total costs in the avacopan plus SOC and SOC alone treatments, respectively (Table 12).
Table 6: Summary of the Stepped Analysis of the CADTH Reanalysis Results
Stepped analysis | Drug | Total costs ($) | Total QALYs | ICER ($ per QALY) |
|---|---|---|---|---|
Sponsor’s base case (probabilistic) | SOC alone | 258,400 | 7.99 | Reference |
Avacopan plus SOC | 288,509 | 8.26 | 110,566 | |
Sponsor’s base case (deterministic) | SOC alone | 259,602 | 7.95 | Reference |
Avacopan plus SOC | 289,297 | 8.22 | 110,630 | |
CADTH reanalysis 1 (deterministic) | SOC alone | 244,845 | 8.10 | Reference |
Avacopan plus SOC | 278,779 | 8.32 | 154,245 | |
CADTH reanalysis 2 (deterministic) | SOC alone | 251,183 | 8.12 | Reference |
Avacopan plus SOC | 284,519 | 8.35 | 144,939 | |
CADTH reanalysis 3 (deterministic) | SOC alone | 260,021 | 7.95 | Reference |
Avacopan plus SOC | 328,542 | 8.32 | 181,706 | |
CADTH reanalysis 4 (deterministic) | SOC alone | 259,602 | 7.95 | Reference |
Avacopan plus SOC | 320,180 | 8.34 | 153,242 | |
CADTH reanalysis 5 (deterministic) | SOC alone | 259,602 | 7.95 | Reference |
Avacopan plus SOC | 289,297 | 8.21 | 114,212 | |
CADTH base case (1 + 2 + 3 + 4 + 5) (deterministic) | SOC alone | 216,650 | 8.71 | Reference |
Avacopan plus SOC | 371,161 | 9.13 | 365,453 |
ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year; SOC = standard of care.
Scenario Analysis Results
To address remaining uncertainty regarding parameterization of the model, CADTH conducted several scenario analyses. The full results are presented in Table 13. The greatest impacts on the ICER were when it was assumed that avacopan’s relapse benefit seen in the trial continued for up to 130 weeks and when all treatments were assumed to have 100% adherence; these assumptions resulted in ICERs of $194,095 and $433,751 per QALY gained, respectively.
Additionally, CADTH undertook price reduction analyses based on the sponsor’s base case and CADTH’s base case (Table 7). The analyses demonstrated that a price reduction of 32% for the sponsor’s base case and 72.5% for CADTH’s base case would be necessary to achieve cost-effectiveness at a WTP threshold of $50,000 per QALY.
Table 7: CADTH Price Reduction Analyses
Analysis | ICERs ($ per QALY) for avacopan plus SOC vs. SOC alone | |
|---|---|---|
Price reduction | Sponsor base case | CADTH reanalysis |
No price reduction | 110,566 | 365,453 |
10% | 91,148 | 324,019 |
20% | 72,315 | 280,155 |
30% | 53,481 | 236,290 |
40% | 34,648 | 192,426 |
50% | 15,815 | 148,562 |
60% | Dominant | 104,698 |
70% | Dominant | 60,833 |
80% | Dominant | 16,969 |
90% | Dominant | Dominant |
ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year; SOC = standard of care.
Issues for Consideration
Comparator pricing based on publicly available prices. The modelled prices of the comparators are based on publicly accessible list prices and do not reflect any confidential pricing that may have been negotiated by public plans. As cost is 1 of the main drivers of this model, the ICER of avacopan plus SOC is therefore likely to be higher than estimated if confidential discounts have been negotiated for the comparator(s).
Overall Conclusions
The CADTH clinical review concluded that avacopan was noninferior to cyclophosphamide followed by azathioprine, and to rituximab, for achieving disease remission at week 26 and that it was superior for sustained disease remission at week 52. Outcomes related to disease relapse, systemic damage, kidney function, and health-related quality of life provided limited support for the primary outcomes. The relevance of the findings to current standards of practice is unclear, due to the lack of rituximab maintenance in the comparison group, which is the current gold standard. Therefore, the results of the ADVOCATE trial may have limited relevance to current practice, and more evidence is needed to better understand the long-term efficacy and safety of avacopan and whether it can be used to effectively eliminate glucocorticoid use.
CADTH undertook reanalyses to address key limitations in the sponsor’s analysis; these reanalyses included considering a pooled HR for ESRD per change in eGFR, selecting rituximab as the first-line maintenance therapy, assuming the use of avacopan for reinduction treatment, assuming a treatment duration of 2 years for avacopan, and equating utility values for patients who had a transplant and for patients in remission.
The CADTH results were similar to the sponsor’s in that avacopan plus SOC was not cost-effective at a WTP threshold of $50,000 per QALY gained. Based on the CADTH base case, in adult patients with severe ANCA-AV, the ICER of avacopan plus SOC compared to SOC alone is $365,453 per QALY gained. A price reduction of 72.5% is required for avacopan plus SOC to be cost-effective at a WTP threshold of $50,000 per QALY gained.
CADTH was unable to account for the high use of nonstudy glucocorticoids potentially overestimating the efficacy of avacopan, the uncertainty associated with the rate of relapse following remission, and a lack of long-term clinical data on avacopan. These limitations are compounded by the underlying evidence from the trial not being reflective of current clinical practice, where rituximab maintenance therapy is used in place of azathioprine. These factors result in uncertainty in interpreting whether rituximab in combination with avacopan would be equally effective or superior to using rituximab alone, given rituximab’s reported low relapse rate (5% after 2 years). Given these limitations, the cost-effectiveness of avacopan should be interpreted with caution, and even greater price reductions may be required.
References
1.Tavneos (avacopan): 10mg oral capsules [product monograph]. Saint-Laurent (QC): Otsuka Canada Pharmaceuticals; 2022.
2.Pharmacoeconomic evaluation [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Tavneos, 10mg oral capsules. Saint-Laurent (QC): Otsuka Canada Pharmaceuticals; 2022 Oct 14.
3.ChemoCentryx. Clinical study report- A randomized, double-blind, active-controlled, phase 3 study to evaluate the safety and efficacy of CCX168 (avacopan) in patients with anti-neutrophil cytoplasmic antibody (ANCA)-associated vasculitis treated concomitantly with rituximab orcyclophosphamide/azathioprine. ChemoCentryx, Inc; 2020.
4.Jayne DRW, Merkel PA, Schall TJ, Bekker P, Group AS. Avacopan for the Treatment of ANCA-Associated Vasculitis. N Engl J Med. 2021;384(7):599-609. PubMed
5.Merkel PA, Jayne DR, Wang C, Hillson J, Bekker P. Evaluation of the Safety and Efficacy of Avacopan, a C5a Receptor Inhibitor, in Patients With Antineutrophil Cytoplasmic Antibody-Associated Vasculitis Treated Concomitantly With Rituximab or Cyclophosphamide/Azathioprine: Protocol for a Randomized, Double-Blind, Active-Controlled, Phase 3 Trial. JMIR Res Protoc. 2020;9(4):e16664. PubMed
6.Sammon C. An investigation of the adverse outcomes and resource use associated with antineutrophil cytoplasmic antibody (ANCA)-associated vasculitis (AAV) in England and their relationship with glucocorticoid (GC) treatment: A Clinical Practice Research Datalink (CPRD) – Hospital Episode Statistics (HES) study. London (UK): PHMR. 2019. (unpublished).
7.Robson J, Doll H, Suppiah R, et al. Damage in the anca-associated vasculitides: long-term data from the European Vasculitis Study group (EUVAS) therapeutic trials. Ann Rheum Dis 2015;74(1):177. PubMed
8.Gercik O, Bilgin E, Solmaz D, et al. Histopathological subgrouping versus renal risk score for the prediction of end-stage renal disease in ANCA-associated vasculitis. Ann Rheum Dis. 2020;79(5):675-676. PubMed
9.Karras A, Pagnoux C, Haubitz M, et al. Randomised controlled trial of prolonged treatment in the remission phase of ANCA-associated vasculitis. Ann Rheum Dis. 2017;76(10):1662-1668. PubMed
10.Statistics Canada. National Life Tables. https://www150.statcan.gc.ca/n1/en/catalogue/84-537-X. Accessed 2023 Jan 10.
11.Choi H, Kim M, Kim H, et al. Excess mortality among patients on dialysis: Comparison with the general population in Korea. Kidney Res Clin Pract. 2014;33(2):89-94. PubMed
12.Wallace ZS, Lu N, Unizony S, Stone JH, Choi HK. Improved survival in granulomatosis with polyangiitis: A general population-based study. Seminars in Arthritis and Rheumatism 2016;45(4):483-489. PubMed
13.Ara R, Brazier J. Deriving an Algorithm to Convert the Eight Mean SF-36 Dimension Scores into a Mean EQ-5D Preference-Based Score from Published Studies (Where Patient Level Data Are Not Available). Value Heal. 2008;11(7):1131-1143. PubMed
14.Hout B van, Janssen MF, Feng Y-S, et al. Interim Scoring for the EQ-5D-5L: Mapping the EQ-5D-5L to EQ-5D-3L Value Sets. Value Heal. 2012;15(5):708-715. PubMed
15.Ferguson TW, Whitlock RH, Bamforth RJ, et al. Cost-Utility of Dialysis in Canada: Hemodialysis, Peritoneal Dialysis, and Nondialysis Treatment of Kidney Failure. Kidney Med. 2021;3(1):20-30 e21. PubMed
16.Ontario Drug Benefit Formulary/Comparative Drug Index. https://www.formulary.health.gov.on.ca/formulary/. Accessed 2022 Dec 16.
17.Ontario Ministry of Health and Long-Term Schedule of Benefits for Physician Services, Schedule of Benefits and Fees. 2021 https://www.health.gov.on.ca/en/pro/programs/ohip/sob/. Accessed 2022 Dec 20.
18.Canadian Institute for Health Information. Organ replacement in Canada. Canadian Organ Replacement Register (CORR) annual statistics. https://www.cihi.ca/en/organ-replacement-in-canada-corr-annual-statistics. Accessed 2022 Dec 20.
19.Brix SR, Noriega M, Tennstedt P, Vettorazzi E, et al. Development and validation of a renal risk score in ANCA-associated glomerulonephritis. Kidney Int. 2018 Dec;94(6):1177-1188. . PubMed
20.Avacopan for treating severe active granulomatosis with polyangiitis or microscopic polyangiitis technology appraisal guidance [TA825]. London (UK): National Institute for Health and Care Excellence. 2022. https://www.nice.org.uk/guidance/ta825 Accessed 2022 Dec 20.
21.Mendel A, Ennis D, Go E, et al. CanVasc Consensus Recommendations for the Management of Antineutrophil Cytoplasm Antibody-associated Vasculitis: 2020 Update. J Rheumatol. 2021;48(4):555-566. PubMed
22.Guillevin L, Pagnoux C, Karras A, et al. Rituximab versus azathioprine for maintenance in ANCA-associated vasculitis. N Engl J Med. 2014 Nov 6;371(19):1771-80. PubMed
23.Drug Reimbursement Review sponsor submission: Avacopan (TAVNEOS) Oral Capsules,10 mg [internal sponsor's package]. Sait-Laurent (QC): Otsuka Canada Pharmaceutical Inc.; 2022 Sep 22.
24.Fujimoto S, Watts RA, Kobayashi S, et al. Comparison of the epidemiology of anti-neutrophil cytoplasmic antibody-associated vasculitis between Japan and the UK. Rheumatology. 2011;50(10):1916-1920. PubMed
25.Pearce FA, Lanyon PC, Grainge MJ, et al. Incidence of ANCA-associated vasculitis in a UK mixed ethnicity population. Rheumatology (Oxford) 2016;55(9):1656-63. PubMed
26.Watts RA, Mooney J, Skinner J, Scott DGI, Macgregor AJ. The contrasting epidemiology of granulomatosis with polyangiitis (Wegener's) and microscopic polyangiitis. Rheumatology (Oxford). 2012;51(5):926-931. PubMed
27.Anderson K, Klassen J, Stewart SA, Taylor-Gjevre RM. Does geographic location affect incidence of ANCA-associated renal vasculitis in northern Saskatchewan, Canada? Rheumatology (Oxford). Oct 2013;52(10):1840-4. PubMed
28.Mendel A, Pagnoux C. Use of Rituximab for the Treatment of Antineutrophil Cytoplasm Antibody–associated Vasculitis in Canada, 2010–2020. J Rheumatol. 2021;48(11):1755-1756. PubMed
29.Sutherland G and Din T. Understanding the Gap. A Pan-Canadian Analysis of Prescription Drug Insurance Coverage. Ottawa (ON): The Conference Board of Canada. 2017. https://www.conferenceboard.ca/product/understanding-the-gap-a-pan-canadian-analysis-of-prescription-drug-insurance-coverage/ Accessed 2022 Dec 20.
30.Statistics Canada. Population estimates on July 1st, by age and sex. https://www150.statcan.gc.ca/t1/tbl1/en/tv.action?pid=1710000501. 2020. Accessed 2023 Jan 14.
Appendix 1: Cost Comparison Table
Note this appendix has not been copy-edited.
The comparators presented in the following table have been deemed to be appropriate based on feedback from clinical expert and drug plan. Comparators may be recommended (appropriate) practice or actual practice. Existing Product Listing Agreements are not reflected in the table and as such, the table may not represent the actual costs to public drug plans.
Table 8: CADTH Cost Comparison Table for Severe ANCA-AV (GPA and MPA)
Treatment | Strength / concentration | Form | Price ($) | Recommended dosage | Daily cost ($) | Annual cost ($) |
|---|---|---|---|---|---|---|
Avacopan | 10 mg | Oral capsule | 34.2466a | 30 mg twice daily | 205.48 | 75,051 |
Cyclophosphamide | 25 mg 50 mg | Oral tablet | 0.3545 0.4773 | 2mg/kg daily for 14 weeks | 0.48 | 175 |
Rituximab | 10 mg/mL | 10 mg 100 mg 500 mg vial for IV infusion | 29.7000 297.0000 1,485.0000 | 375 mg/m2 weekly for 4 weeks (induction) and 500 mg every 6 months for 2 years (maintenance) | Year 1: 27.50 Year 2+: 8.14 | Year 1 Induction: 8,554 Maintenance: 1,485 Year 2+: 2,970 |
Azathioprine | 50 mg | Oral tablet | 0.2405 | 2mg/kg daily starting at Week 15 for 2 years | Year 1: 0.69 Year 2+: 0.96 | Year 1: 250 Year 2+: 351 |
Prednisone | 1 mg 5 mg 50 mg | Oral tablet | 0.1214 0.0220 0.1735 | Avacopan regimen: 4mg per day for 21 weeks SoC regimen: 12 mg per day for 21 weeks | 0.01 to 0.03 | 3 to 10 |
Avacopan plus SOC (i.e., cyclophosphamide/rituximab) regimen cost | Year 1: 80,453 to 81,681b Year 2+: 74,950 to 77,553b | |||||
Avacopan plus cyclophosphamide regimen cost | Year 1: 75,477 to 76,711b Year 2+: 75,403 to 78,021b | |||||
Avacopan plus rituximab regimen cost | Year 1: 83,855 to 85,090b Year 2+: 75,403 to 78,021b | |||||
SOC alone (i.e., cyclophosphamide/rituximab plus glucocorticoids) regimen cost | Year 1: 5,852 to 7,079b Year 2+: 349 to 2,952b | |||||
Cyclophosphamide plus glucocorticoids regimen cost | Year 1: 425 to 1,660b Year 2+: 351 to 2,970b | |||||
Rituximab plus glucocorticoids regimen cost | Year 1: 8,804 to 10,039b Year 2+: 351 to 2,970b | |||||
Note: All prices are from the Ontario Drug Benefit Formulary (accessed December 2022),17 unless otherwise indicated and do not include dispensing fees. A patient weight of 77 kg and body surface area of 1.92 m2 was assumed.2 When multiple formulations were available, the least expensive type to obtain the recommended dose was used to calculate costs. Calculations assume wastage.
aSponsor’s submitted price23
bDiffering maintenance costs were calculated using azathioprine (lower cost) and rituximab (higher cost).
Appendix 2: Submission Quality
Note this appendix has not been copy-edited.
Description | Yes/No | Comments |
|---|---|---|
Population is relevant, with no critical intervention missing, and no relevant outcome missing | Yes | No comment. |
Model has been adequately programmed and has sufficient face validity | No | The model structure is inflexible to varying the proportion patients receiving azathioprine or rituximab maintenance therapy (refer to key limitation). Further, results were hard coded and required the use of VBA code. |
Model structure is adequate for decision problem | No | No comment. |
Data incorporation into the model has been done adequately (e.g., parameters for probabilistic analysis) | Yes | No comment. |
Parameter and structural uncertainty were adequately assessed; analyses were adequate to inform the decision problem | Yes | No comment. |
The submission was well organized and complete; the information was easy to locate (clear and transparent reporting; technical documentation available in enough details) | No | As per CADTH’s appraisal, the submission lacked details and it was difficult to trace the model parameters used in the analysis. |
Appendix 3: Additional Information on the Submitted Economic Evaluation
Note this appendix has not been copy-edited.
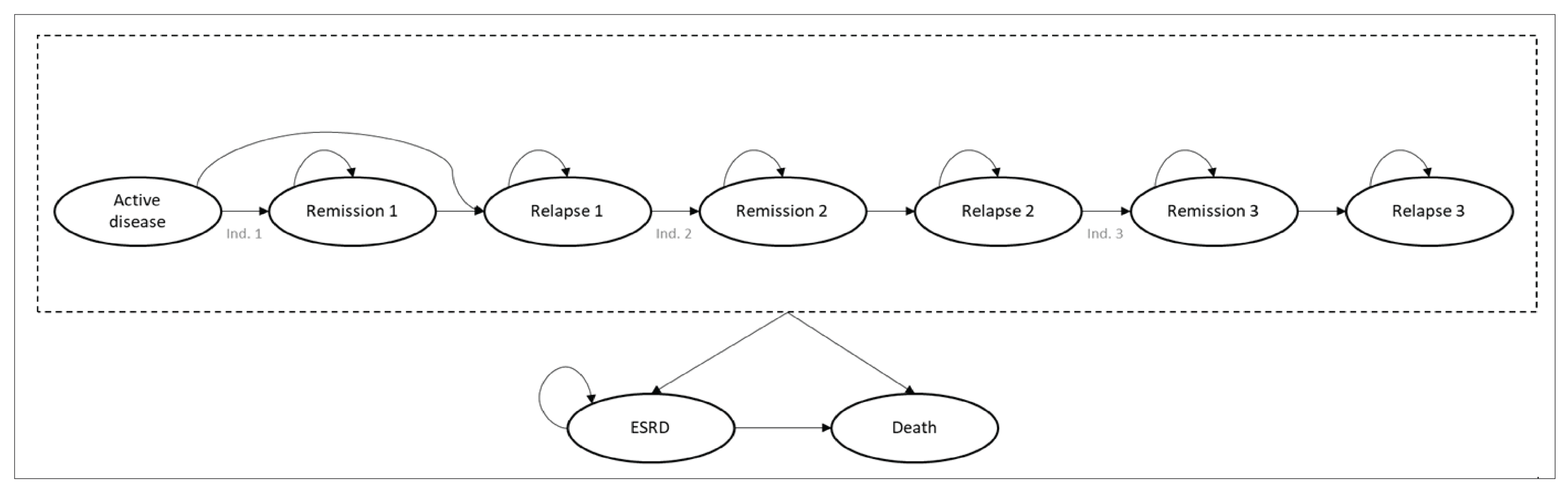
The health states were defined in accordance with the ADVOCATE trial.4
Active disease: patients with a Birmingham vasculitis activity score (BVAS) > 0.
Remission: a BVAS of 0 and no receipt of glucocorticoid for 4 weeks before the end of the 6-month induction period.
Relapse: return of vasculitis activity that involves at least 1 major BVAS item, or at least 3 minor BVAS items, or 1 or 2 minor BVAS items in for at least 2 consecutive study visits.
ESRD: Progression of patient to ESRD was considered when they have GFR/eGFR < 15 mL/min and presented a chronic need for RRT. The source of AE data was grade 3 or 4 AEs reported in the ADVOCATE trial.
Figure 2: Schematic Diagram of Markov States and Tunnel States
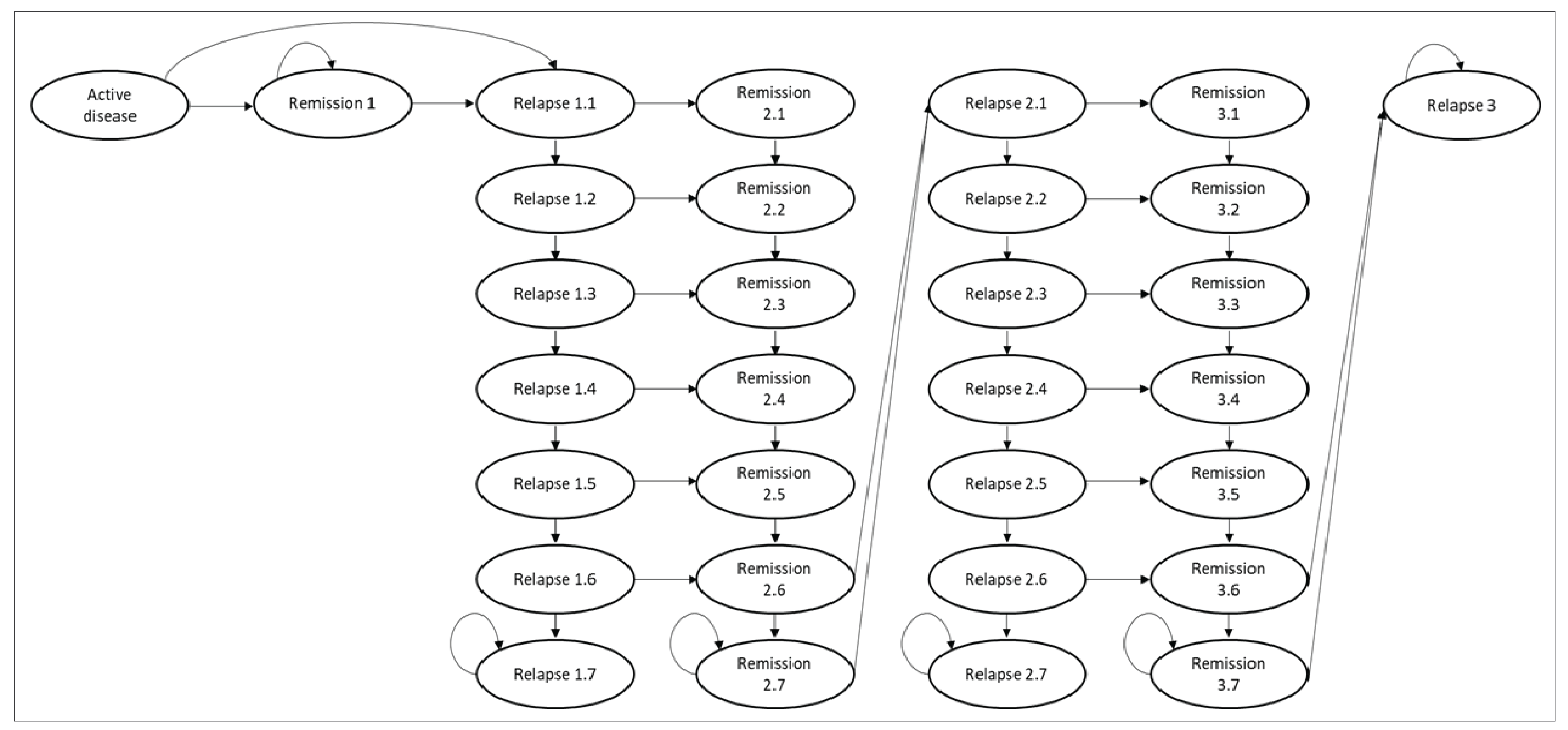
Source: Sponsor’s pharmacoeconomic submission.2
Table 10: Summary of the Sponsor’s Economic Evaluation Pairwise Comparison Results
Drug | Total costs ($) | Total QALYs | Pairwise ICER ($/QALY) |
|---|---|---|---|
Cyclophosphamide-based regimen | |||
Cyclophosphamide plus glucocorticoids | 246,595 | 7.99 | Reference |
Avacopan plus cyclophosphamide | 276,832 | 8.25 | 114,260 |
Rituximab-based regimen | |||
Rituximab plus glucocorticoids | 264,831 | 7.99 | Reference |
Avacopan plus rituximab | 294,126 | 8.26 | 106,015 |
ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year.
Source: Sponsor’s pharmacoeconomic submission.2
Appendix 4: Additional Details on the CADTH Reanalyses and Sensitivity Analyses of the Economic Evaluation
Note this appendix has not been copy-edited.
Table 11: Summary of CADTH Economic Evaluation Pairwise Comparison Results
Drug | Total costs ($) | Total QALYs | Pairwise ICER ($/QALY) |
|---|---|---|---|
Cyclophosphamide-based regimen | |||
Cyclophosphamide plus glucocorticoids | 205,697 | 8.71 | Reference |
Avacopan plus cyclophosphamide | 360,649 | 9.13 | 366,495 |
Rituximab-based regimen | |||
Rituximab plus glucocorticoids | 222,486 | 8.71 | Reference |
Avacopan plus rituximab | 376,754 | 9.13 | 364,877 |
ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year.
Table 12: Disaggregated Summary of CADTH’s Economic Evaluation Results
Parameter | Avacopan plus SOC | SOC alone | Incremental |
|---|---|---|---|
Discounted LYs | |||
Total | 12.32 | 11.96 | 0.36 |
Active disease | 0.27 | 0.28 | −0.01 |
Remission | 7.95 | 6.94 | 1.01 |
Relapse | 1.63 | 1.90 | −0.27 |
ESRD | 2.46 | 2.84 | −0.37 |
Discounted QALYs | |||
Total | 9.13 | 8.71 | 0.42 |
Active disease | 0.21 | 0.21 | −0.01 |
Remission | 6.33 | 5.53 | 0.80 |
Relapse | 1.17 | 1.37 | −0.20 |
ESRD | 1.72 | 1.98 | −0.26 |
Adverse event disutility | −0.31 | −0.40 | 0.09 |
Discounted costs ($) | |||
Total | 371,161 | 216,650 | 154,511 |
Drug costs | 204,309 | 20,729 | 183,579 |
Resources used | 24,113 | 31,565 | −7,452 |
ESRD | 142,740 | 164,356 | −21,616 |
ICER ($/QALY) | 365,453 | ||
CKD = chronic kidney disease; ESRD = end-stage renal disease; ICER = incremental cost-effectiveness ratio; LY = life-year; QALY = quality-adjusted life-year; SOC = standard of care.
Table 13: CADTH Scenario Analyses
Stepped analysis | Drug | Total costs ($) | Total QALYs | ICER ($/QALYs) |
|---|---|---|---|---|
CADTH base case | SOC alone | 216,650 | 8.71 | Reference |
Avacopan plus SOC | 371,161 | 9.13 | 365,453 | |
1. Equal eGFR improvements between comparators during the trial period. | SOC alone | 216,593 | 8.70 | Reference |
Avacopan plus SOC | 371,641 | 9.11 | 380,153 | |
2. HR for ESRD per mL/min change in eGFR derived from Brix et al. (HR = 0.96). | SOC alone | 214,642 | 8.73 | Reference |
Avacopan plus SOC | 369,522 | 9.14 | 375,050 | |
3. HR for ESRD per mL/min change in eGFR derived from Gercik et al. (HR = 0.90). | SOC alone | 227,009 | 8.59 | Reference |
Avacopan plus SOC | 379,817 | 9.05 | 330,263 | |
4. Avacopan relapse benefits seen in the trial continued with same HR of 0.39 for up to week 104 and the rate of relapse waned (HR = 1.0) after week 104. | SOC alone | 216,650 | 8.71 | Reference |
Avacopan plus SOC | 364,504 | 9.24 | 276,677 | |
5. Avacopan relapse benefits seen in the trial continued with same HR of 0.39 for up to week 130 and the rate of relapse waned (HR = 1.0) after week 130. | SOC alone | 216,650 | 8.71 | Reference |
Avacopan plus SOC | 354,559 | 9.42 | 194,095 | |
6. Proportion of patients who had transplant assumed to be 20% | SOC alone | 213,736 | 8.75 | Reference |
Avacopan plus SOC | 368,841 | 9.17 | 372,488 | |
7. Rate of adherence to glucocorticoids assumed to be equal to avacopan (86.4%) | SOC alone | 216,590 | 8.70 | Reference |
Avacopan plus SOC | 371,108 | 9.13 | 365,367 | |
8. Rate of adherence to avacopan and all comparators assumed to be 100% | SOC alone | 216,593 | 8.70 | Reference |
Avacopan plus SOC | 400,032 | 9.13 | 433,751 | |
9. Each relapse associated with a 20 mL/min decline in eGFR | SOC alone | 248,668 | 8.31 | Reference |
Avacopan plus SOC | 397,302 | 8.75 | 335,824 |
ESRD = end-stage renal diseases; GCs = glucocorticoids; HR = hazard ratio; ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year; SOC = standard of care.
Appendix 5: Submitted Budget Impact Analysis and CADTH Appraisal
Note this appendix has not been copy-edited.
Table 14: Summary of Key Takeaways
Key takeaways of the budget impact analysis |
|---|
|
Summary of Sponsor’s Budget Impact Analysis
The sponsor submitted a budget impact analysis (BIA) estimating the budget impact of introducing avacopan for the adjunctive treatment of adult patients with severe ANCA-AV (GPA and MPA) in combination with standard background therapy including glucocorticoids. The base case of the BIA reflects the proposed full Health Canada indication and the reimbursement requested population. The analysis was undertaken from a Canadian public drug plan payer perspective over a 3-year time horizon using an epidemiological approach. The sponsor’s base-case analysis included drug acquisition costs. Data inputs informing the BIA were obtained from the literature and assumptions. Key inputs to the BIA are documented in Table 15.
Key assumptions include:
Azathioprine was considered as the first-line maintenance therapy for all patients, regardless of prior induction treatment.
For drugs that are weight or body surface area dependent, the annual costs were calculated using an average weight of 77 kg and body surface area of 1.92 from patients enrolled in the ADVOCATE trial.4
Cyclophosphamide IV infusion was not included in the analysis and instead it was assumed an oral formulation would be administered in the community setting.
The mean dose of glucocorticoids was estimated to be 4 mg per day per patient in the avacopan plus SOC group and 12 mg per day in the SOC alone based on the ADVOCATE trial, respectively.4
Treatment adherence to avacopan was reported to be 86.4% while adherence to comparators was assumed to be 100%.
Table 15: Summary of Key Model Parameters
Parameter | Sponsor’s estimate (reported as Year 1 / Year 2 / Year 3 if appropriate) |
|---|---|
Target population | |
0.0210% | |
Proportion of prevalent patients not in remissiona | 28.8% |
Incidence of ANCA-AV (GPA plus MPA)27 | 0.0012% |
Proportion of incident patients actively diagnoseda | 95% |
Proportion of prevalent population assessed and treateda | 70% |
Proportion of incident population assessed and treateda | 65% |
53.76% | |
53.76% | |
Annual growth30 | 1.48% |
Number of patients eligible for drug under review | 661 / 671 / 681 |
Market uptake (3 years) | |
Uptake (reference scenario) Rituximab plus glucocorticoids Cyclophosphamide plus glucocorticoids | 65% / 65% / 65% 35% / 35% / 35% |
Uptake (new drug scenario) Avacopan plus SOC (i.e., rituximab or cyclophosphamide) Rituximab plus glucocorticoids Cyclophosphamide plus glucocorticoids | 10% / 20% / 30% 58% / 52% / 45% 32% / 28% / 25% |
Cost of treatment (per patient) | |
Cost of treatment over a year Avacopan plus SOC (i.e., rituximab or cyclophosphamide) Rituximab plus glucocorticoids Cyclophosphamide plus glucocorticoids Azathioprine plus glucocorticoids Glucocorticoids | $65,540 $14,566 $351 $352 $16 |
ANCA-AV = antineutrophil cytoplasmic antibody-associated vasculitis; GPA = granulomatosis with polyangiitis; MPA = microscopic polyangiitis; SOC = standard of care.
Note: Cost calculations do not include markup and dispensing fees.
aClinical expert opinion 2022.
Summary of the Sponsor’s BIA Results
The sponsor estimated that the reimbursement of avacopan for the adjunctive treatment of adult patients with severe ANCA-AV in combination with the SOC will have an estimated budget impact of $3,950,694 in year 1, $8,018,100 in year 2, and $12,204,805 in year 3, for a 3-year total of $24,173,598.
CADTH Appraisal of the Sponsor’s BIA
CADTH identified several key limitations to the sponsor’s analysis that have notable implications on the results of the BIA:
The total population eligible for treatment with avacopan may be inaccurate. The sponsor assumed that 65% of incident patients and 70% of prevalent patients were eligible for treatment with avacopan. Alternatively, the clinical expert consulted by CADTH for this review estimated that 75% of incident patients would be eligible for avacopan treatment. The clinical expert also noted that most prevalent patients would already be in remission, therefore only 20% of patients would be eligible for avacopan treatment based on the ADVOCATE criteria. However, the expert indicated that the sponsor’s estimate may be reasonable if avacopan was intended to entirely substitute glucocorticoids, but this was not demonstrated in the ADVOCATE trial.
In the CADTH reanalysis, the proportion of prevalent and incident patients assessed and treated with avacopan was assumed to be 20% and 75%, respectively.
The anticipated uptake of avacopan is likely underestimated. The sponsor estimated that avacopan plus SOC would have a market share of 10% / 20% / 30% in Year 1, 2, and 3, respectively. However, the clinical expert consulted by CADTH for this review felt that the sponsor’s market share for avacopan plus SOC was underestimated as it is expected to capture the market rapidly due to the hope it can reduce glucocorticoids use for the indicated population; and if publicly funded, avacopan 3-year market share would be closer to 60%.
In the CADTH reanalysis, the uptake of avacopan plus SOC was assumed to be 25% / 50% / 60% in year 1, 2, and 3, respectively.
Treatment adherence on glucocorticoids was overestimated. The sponsor estimated the adherence rate for avacopan and glucocorticoids to be 86.4% and 100%, respectively. However, the clinical expert consulted by CADTH for this review felt that the sponsor's estimate of 100% adherence for glucocorticoids was higher than expected, due to it having a number of severe adverse events which would likely drive it to have lower or equal adherence to avacopan. Additionally, there is inconsistency between the cost-utility analysis and the BIA, as glucocorticoids’ 100% adherence rate does not align with estimates used in the cost-utility analysis (98.6%).
In the CADTH reanalysis, the adherence rate for glucocorticoids was assumed to be equal to avacopan at 86.4%. To rule out drug cost adjustment based on adherence rates, CADTH performed a scenario analysis using a 100% adherence rate to avacopan and all comparators.
The proportion of SOC patients receiving rituximab and cyclophosphamide was inaccurately captured. The sponsor calculated treatment regimen costs based on the assumption that 64.8% of patients would receive rituximab induction therapy and 34.6% would receive cyclophosphamide. When the uptake for SOC changed over time in the new drug scenario (e.g., rituximab changed from 65% in the base year to 45% by Year 3), the proportions remained static for the avacopan regimen. Where avacopan should have been modelled as an add-on treatment to the existing SOC and its fluid ratio, instead of as its own treatment with a fixed SOC ratio.
Due to model structure limitations, CADTH was unable to address this issue. Due to the higher utilization of rituximab in the reference scenario used to calculate the SOC ratio, this limitation likely overestimates the budget impact.
CADTH Reanalyses of the BIA
CADTH revised the sponsor’s base case by changing the proportion of incident and prevalent patients eligible for avacopan treatment, decreasing the adherence rate for glucocorticoids, and changing the market uptake of avacopan. The assumptions used by the sponsor and those used by CADTH in the reanalysis are presented in Table 16.
Table 16: CADTH Revisions to the Submitted Budget Impact Analysis
Stepped analysis | Sponsor’s value or assumption | CADTH value or assumption |
|---|---|---|
1. Proportion of incident patients eligible for treatment with avacopan | 65% | 75% |
2. Proportion of prevalent patients eligible for treatment with avacopan | 70% | 20% |
3. Uptake of avacopan plus SOC Uptake of rituximab plus glucocorticoids Uptake of cyclophosphamide plus glucocorticoids | 10% / 20% / 30% 65% / 65% / 65% 35% / 35% / 35% | 25% / 50% / 60% 49% / 32% / 26% 26% / 18% / 14% |
4. Rate of adherence for glucocorticoids | 100% | 86.4% |
CADTH base case | 1 + 2 + 3 + 4 | |
SOC = standard of care.
The results of the CADTH stepwise reanalysis are presented in summary format in Table 17 and a more detailed breakdown is presented in Table 18. Based on the CADTH base case, the budget impact of reimbursing avacopan is expected to be $4,099,125 in year 1, $8,319,347 in year 2, and $10,130,680 in year 3, for a 3-year total budget impact of $22,549,151
Table 17: Summary of the CADTH Reanalyses of the BIA
Stepped analysis | Three-year total |
|---|---|
Submitted base case | $24,173,598 |
CADTH reanalysis 1 – Incident population eligible for treatment with avacopan | $24,727,570 |
CADTH reanalysis 2 – Prevalent population eligible for treatment with avacopan | $9,478,756 |
CADTH reanalysis 3 – Uptake of avacopan plus SOC, and SOC alone | $54,331,592 |
CADTH reanalysis 4 – Rate of adherence for glucocorticoids | $24,174,180 |
CADTH base case | $22,549,151 |
BIA = budget impact analysis; SOC = standard of care.
To address remaining uncertainty, CADTH conducted 2 scenario analyses which are presented in Table 18. The first assumes 100% adherence to all treatments, which boosts the 3-year budget impact to $26,082,736; while the second uses the 72.5% price reduction derived from the economic model, which drops the 3-year budget impact to $6,263,493.
Table 18: Detailed Breakdown of the CADTH Reanalyses of the BIA
Stepped analysis | Scenario | Year 0 (current situation) | Year 1 | Year 2 | Year 3 | Three-year total |
|---|---|---|---|---|---|---|
Submitted base case | Reference | $6,827,282 | $6,928,129 | $7,030,465 | $7,134,313 | $21,092,908 |
New drug | $6,827,282 | $10,878,822 | $15,048,565 | $19,339,118 | $45,266,505 | |
Budget impact | $0 | $3,950,694 | $8,018,100 | $12,204,805 | $24,173,598 | |
CADTH base case | Reference | $2,833,516 | $2,875,370 | $2,917,842 | $2,960,942 | $8,754,155 |
New drug | $2,833,516 | $6,974,494 | $11,237,189 | $13,091,622 | $31,303,305 | |
Budget impact | $0 | $4,099,125 | $8,319,347 | $10,130,680 | $22,549,151 | |
CADTH scenario 1: 100% adherence to avacopan and all comparators | Reference | $2,833,516 | $2,875,370 | $2,917,842 | $2,960,942 | $8,754,155 |
New drug | $2,833,516 | $7,616,851 | $12,540,880 | $14,679,159 | $34,836,890 | |
Budget impact | $0 | $4,741,481 | $9,623,037 | $11,718,217 | $26,082,736 | |
CADTH scenario 2: 72.5% avacopan price reduction | Reference | $2,833,516 | $2,875,370 | $2,917,842 | $2,960,942 | $8,754,155 |
New drug | $2,833,516 | $4,013,986 | $5,228,713 | $5,774,948 | $15,017,647 | |
Budget impact | $0 | $1,138,617 | $2,310,870 | $2,814,006 | $6,263,493 |
BIA = budget impact analysis.
Stakeholder Input
Patient Input
Vasculitis Foundation Canada
About Vasculitis Foundation Canada
Vasculitis Foundation Canada’s mission is to encourage and support research efforts for the cause and cure for all forms of Vasculitis. To establish rapport with all known Vasculitis patients and try to alleviate the isolation of having an uncommon, life-threatening disease. We want to assist Vasculitis patients and their families with clinical information and coping strategies, to help them develop a strong and positive outlook.
We hope to create greater awareness of Vasculitis within the medical community, as well as the general public. We organize and administer periodic meetings, forums, and conventions for the sharing of information and ideas in the research, treatment and diagnosis of Vasculitis.
Please visit: www.vasculitis.ca
Information Gathering
With input from a group of ~4 vasculitis patients, including 1 PhD (Psychology) vasculitis patient, and Christian Pagnoux M.D. (founder and VP of CanVasc, a Canadian non-profit vasculitis scientific network, (https://canvasc.ca/about-canvasc/), a survey with 38 questions was developed and assembled into an online patient survey (using Google forms). VFC has an email list of ~400 patients and/or caregivers. Several emails requesting patients to complete the survey were made to this list, and survey data was collected from 29.4.22 through 13.5.22. We requested that only patients share their experiences with either prednisone or avacopan. A news post was also placed on the VFC website requesting patients to compete the survey (https://vasculitis.ca/?p=1608). From the survey results a total of 35 GPA patients living in Canada competed the survey, and 9 MPA patients living in Canada and 2 MPA patients living in the United States competed the survey.
Of the 46 completed responses 100% of respondents had taken prednisone (and 25 of 46 had taken IV prednisone in addition to oral), only one had taken avacopan on a trial. The ages ranged from 22 to 80 years old, 36 were female and 11 were male.
The author also has 27 years’ worth of experience taking prednisone.
Prednisone is the sole alternative to the drug under review.
Disease Experience
GPA and MPA are life threatening, and life altering diseases, within the family of ~26 vasculitic diseases.
“For most patients, myself included, GPA/MPA has changed every single aspect of their lives, and not for the better! GPA and MPA are chronic diseases that require powerful immune suppressive medications to induce and maintain remissions. There is a high burden of care with ongoing and repeated lab and diagnostic tests, and often lengthy hospital stays.”
To describe how GPA & MPA impacts patients’ day-to-day life, and quality-of-life, we asked patients to describe what their worst experience with GPA/MPA was, and the responses were eye-opening.
Clearly, the aspects that are more important to control are early diagnosis to prevent organ involvement, organ and tissue damage, and the loss of tissue and organ function. However, on the treatment side, patients can always benefit from modern treatments that are more precisely targeted, but even more importantly it would be treatment that dramatically reduces the impact of prednisone.
Repeatedly, we hear about kidney damage, fatigue, and a broad spectrum of impacts on quality-of-life. Kidney involvement is common and often leads to chronic kidney disease (CKD), kidney failure, dialysis, and transplant. For example, one respondent reported:
“FATIGUE, OSTEOPOROSIS, CATARACTS, FATIGUE, and CKD, I have suffered from anxiety and depression for the past 13 years.”.
Others reported they lost their job, retired early, experienced negative impacts on their family life and relationships, or anxiety and depression. A summation might best be described in this patient quotation:
“Vasculitis eats away at you, your family, your quality of life and relationships.”
Sadly, we are also aware of rare cases of patients who take their lives due to the disease, the treatment and body disfiguration, or they refuse further treatment and simply die rather than continue to fight.
The complete results are reported below.
Patient Responses to Survey — Question 33
In your experience living with vasculitis, briefly describe how vasculitis has impacted your quality-of-life (i.e., your worst experience, or side effect)?
“I lost my old life forever!”
“Inability to breathe due to subglottic stenosis; premature ovarian failure due to cyclophosphamide.”
“Fatigue, and poor sleep.”
“Worst experience was developing tracheal stenosis. That and losing the septum in my nose make breathing difficult sometimes. Very hard to be active. Greatly affects my self-esteem.”
“After initial fear and anxiety and physical manifestations such as loss of hearing and repeated sinus infections were brought under control, worst side remaining is ongoing fatigue.”
“Since 2003, Fatigue, Kidney and Lung Disease, Diabetes, and joint problems made it difficult to continue working on a full-time basis and still do everything at home. In 2016, I took early retirement after my total knee replacement. Since retirement, I’ve had my other knee replaced, and a shoulder arthroscopy, which now needs a full shoulder replacement.”
“Constant pain from the disease and side effects.”
“Moon face, complications of decreased kidney function.”
“Whenever I flare.”
“I needed a kidney transplant.”
“Fear of Relapse.”
“Arthritis like symptoms and inability to breath properly.”
“Mood swings.”
“Chronic malaise and fatigue, but I am managing it.”
“Due to FATIGUE, OSTEOPOROSIS, CATARACTS, FATIGUE, and CKD, I have suffered from anxiety and depression for the past 13 years.”
“The worst experience was the period of relapse with severe joint pain, fatigue, and hemoptomis.”
“With covid isolation and weight gain.”
“Life threatening disease affecting my lungs & kidneys requiring dialysis and plasmapheresis. I was initially misdiagnosed with fibromyalgia and subsequently spent 1 month in hospital because of a delay in accurate diagnosis of Vasculitis. The side effects from medication & mental/emotional impact have been life altering.”
“Fear of a flare up and it effects my kidneys again, but I live life to the fullest while I can.”
“The disease attacked my nerves, paralyzing my left foot/leg and my right hand. While there has been considerable recovery, I still have limited use of both as well as a lot of nerve pain.”
“I find that by the time I am prescribed prednisone, I really, really need it. Vasculitis eats away at you, your family, your quality of life and relationships. As much as I hate taking prednisone, it works.”
“I lost my hearing. For a couple of months, I was completely deaf. Now I can manage with hearing aid. Feeling isolated. Being disfigured (saddle nose deformity, weight gain, moon face, humpback). Being tired all the time physically and mentally, not being able to do things I used to do before, depression, anxiety, afraid of infections, afraid of relapse and complications.”
“Breathing issues with subglottic stenosis, extreme fatigue, sepsis.”
“Currently in stable remission with no flares, prednisone d/c 2017, AZT d/c 2018.”
“I am doing pretty well but I never fully got my energy back. At the worst I just felt like I was falling apart and first no one believed me.”
“I’ve lost my job and friends and rarely see family anymore (some is due to the pandemic also).”
“I have fatigue and can’t do nearly what I used to and severe acute chronic sinusitis.”
“Feeling pain in spurts and feeling tired often.”
“Safety among people because of no immunity.”
“It’s slowed me down a lot.”
“It caused CKD. Fatigue very easily.”
“Symptoms on left side of body, pain in muscles, blocked left nostril, pain in left ear , burning on outside of ear and coughing up phlegm.”
“Vasculitis forced me to be a new person. There isn't too much impact to current quality of life, except fatigue, and extra care to prevent flare ups. However, the journey to this point was several years long and somewhat traumatic. Low points along the way: Refer to answer to Question 32, as well as hair loss, distress over physical appearance changes (while on prednisone) continued eustachian tube dysfunction, and luctuating random symptoms.”
“ICU for 7 days when first diagnosed - separated from 8-month-old baby. Pituitary damage that is not healing itself. Chronic facial pain due to nerve damage.”
“Numbness in feet and fatigue.”
“Kidney failure, swollen leg from nerves effected by vasculitis, multiple, bi-lateral lung blood clots, months on medication with side effects, sore joints, weight gain, and significant, persistent fatigue.”
“1) Heart - Myo-pericarditis, CAD, dilated cardiomyopathy, heart failure with reduced EF 30%, mitral valve regurgitation meaning that I cannot enjoy my pre-existing hobbies; 2) Lungs - repeated collapse on account of bronchial stenosis leading to breathlessness and easily fatigued; 3) Ears - unable to hear due to fluid buildup/thickened mucus; 4) Stress - burden to others, when will it flare, when will I die.”
“Kidney damage and resultant impacts on diet.”
“Extreme fatigue, anxiety, wired, exhausted, very tense, agitated…”
“Without treatment, I was was having chest pain, difficulty breathing, talking, exercising etc., and was extremely tired + had no interest in food due to kidney issues.”
“I am sore all the time and my job require me to be physical. I can no longer do the things I have always done.”
“Kidney failure leading to dialysis.”
“No energy tired all the time no strength change of diet due to kidney failure.”
“Fatigue, get anxious and tired easily if trying to do previously normal workload, anxious in social interactions and can’t volunteer at events like swim meets.”
“Dropped foot so walking any distance is exhausting.”
“Fatigue, weight gain but the worst impact has been major depression after misinformation from doctors to do a horrible life altering procedure (being informed it would be deadly for me to become pregnant and told it was best for my husband to have a vasectomy for my safety). Quality of life if extremely poor!!!”
Experiences With Currently Available Treatments
Generally speaking, GPA and MPA patient care has improved dramatically over the past decade, and this is almost entirely due to the benefit of having Rituximab (and now with biosimilars), approved in 2011 for GPA/MPA treatment in Canada. However, and very regrettably, the actual coverage for Rituximab by private and public insurers/payers dragged on for multiple years after approval which impeded patient access and improved care. This delay in drug approvals and providing coverage and hence access, by both public and private coverage, is one of the single greatest failures in Canada’s healthcare system. It is very simple, access delayed/denied translates into vasculitis lives lost, and reduced quality-of-life for those who manage to survive.
Despite rituximab's huge benefits, the COVID pandemic also introduces significant concerns as high dose prednisone use (>/=15mg’s/day), and B cell depletion, blunts or even prevents COVID-19 antibody production after vaccination, regardless of the number vaccinations. Thus, the pandemic only amplifies the need for newer and improved treatments like avocopan which reduces or eliminates prednisone.
By far, the largest single gap that needs to be improved is to reduce the reliance on glucocorticoids/ steroids/prednisone. Although prednisone is readily available and inexpensive this ~70-year-old medication is the one drug that universally all patients love to hate.
As one patient recently commented:
“Prednisone saved my life (the benefit) but destroyed my body (the side effect)!”
Another patient echoed a common theme, reported numerous times:
“Being extremely tired all the time, Weight gain and disfiguration, insomnia, anxiety, infections.”
To better understand the scope and impact of this gap in treatment our survey asked questions about known areas of specific impact of prednisone, as well as their worst prednisone experience. And, once again the responses were eye-opening.
For GPA/MPA patients there is no escaping the use of oral steroids as 100% of patients have taken, or are taking them, and 25 of 46 have taken IV steroids at some point, and frequently at high doses (1g/day (IV)x3days, or 60mg oral/day for multiple weeks are common, then with slow, or slower, tapering). Although the majority of those who completed our survey were not on prednisone currently (29 off versus 17 on), the range of time they were on prednisone varied from 6 months to 27 years, and respondents reported a dose ranged from 2.5 to 20mg’s/day.
The side effects of prednisone are well known, and most were included as survey questions, these include: negative impacts on quality-of-life, increase in acne, bruising and thinning skin, GI symptoms such as heartburn and GERD, weight gain, insomnia, mood change, anxiety and depression, night sweats, lower self-esteem, body disfiguration such as moon face and torso hump, avascular necrosis, steroid induced diabetes, elevated blood pressure, infections requiring antibiotics, infections requiring hospitalization, bone fractures, osteoporosis, cataracts, loss of tooth mass, and teeth, etc.
When asked on a scale of 1 to 10 (with 1 being low impact and 10 being high impact), patients were asked if prednisone had impacted their quality-life? 39(85%) ticked >/=5, while only 7(15%) ticked </=4 and 29(63%) ticked >/=7.
When asked on a scale of 1 to 10 (with 1 being low impact and 10 being high impact), While on prednisone did you experience an increase in GI (Gastrointestinal) symptoms such as heartburn, or GERD etc? 21(51%) ticked >/=5, while 20(49%) ticked </=4 and 10(24%) ticked >/=7.
When asked on a scale of 1 to 10 (with 1 being low impact and 10 being high impact), patients were asked while on prednisone did you experience insomnia? 34(80%) ticked >/=5, while only 9(20%) ticked </=4 and 31(67%) ticked >/=7.
When asked on a scale of 1 to 10 (with 1 being low impact and 10 being high impact), patients were asked while on prednisone did you experience night sweats? 31(67%) ticked >/=5, while 15(33%) ticked </=4 and 21(46%) ticked >/=7.
Furthermore, avacopan appears to be well tolerated, orally administered, and when asked in our survey respondents indicated a uniform willingness to pay a moderate amount (as an out-of-pocket-cost should public reimbursement be delayed or denied), for avacopan, to avoid using prednisone, if avacopan did not have the side effects of prednisone.
We set out to illustrate eight of the more concerning impacts of prednisone graphically below, and the results are clear to see. We think these results speak for themselves and illustrate the need for a new treatment, without these impacts, to reduce or even replace the use of prednisone.
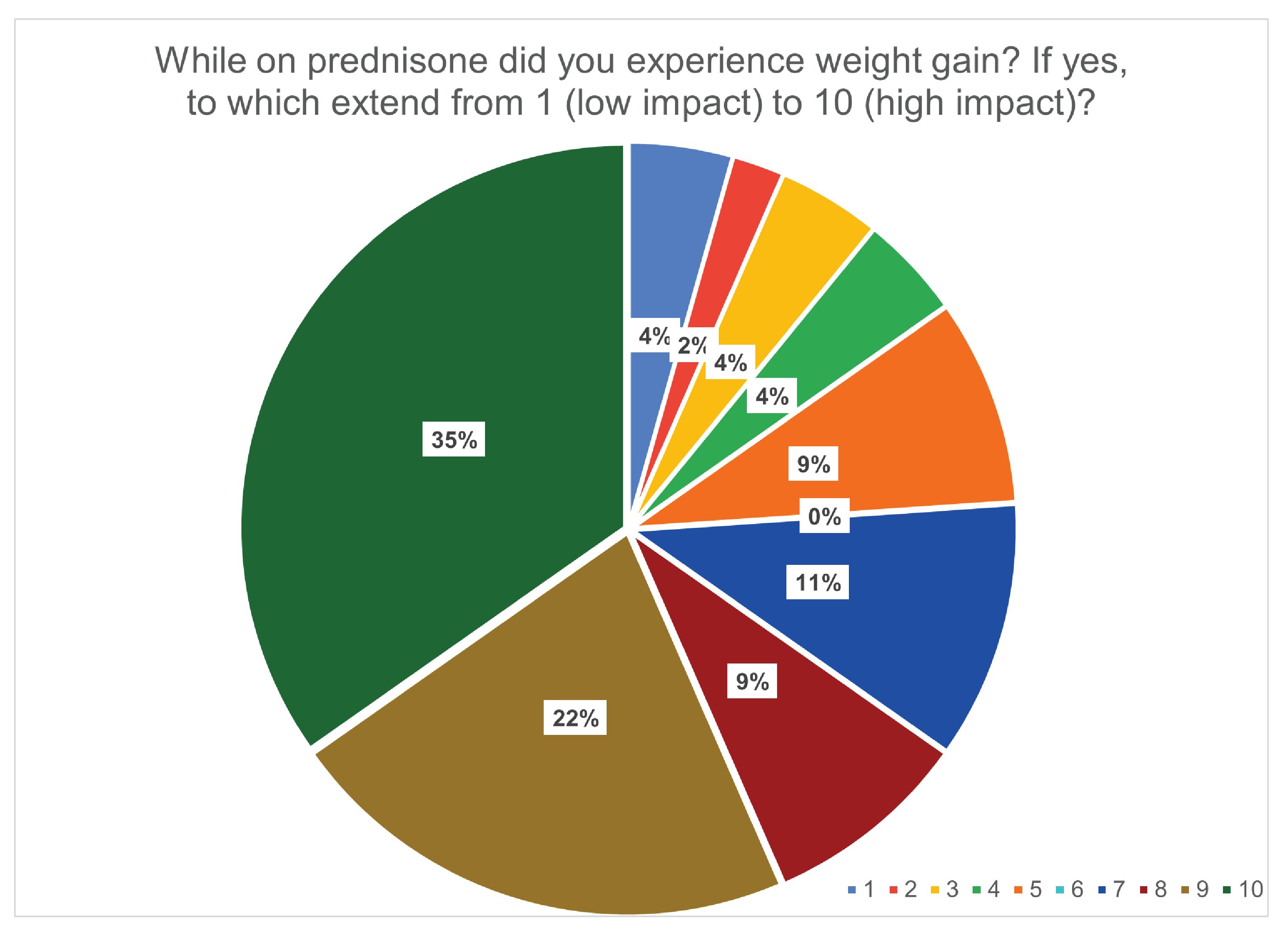
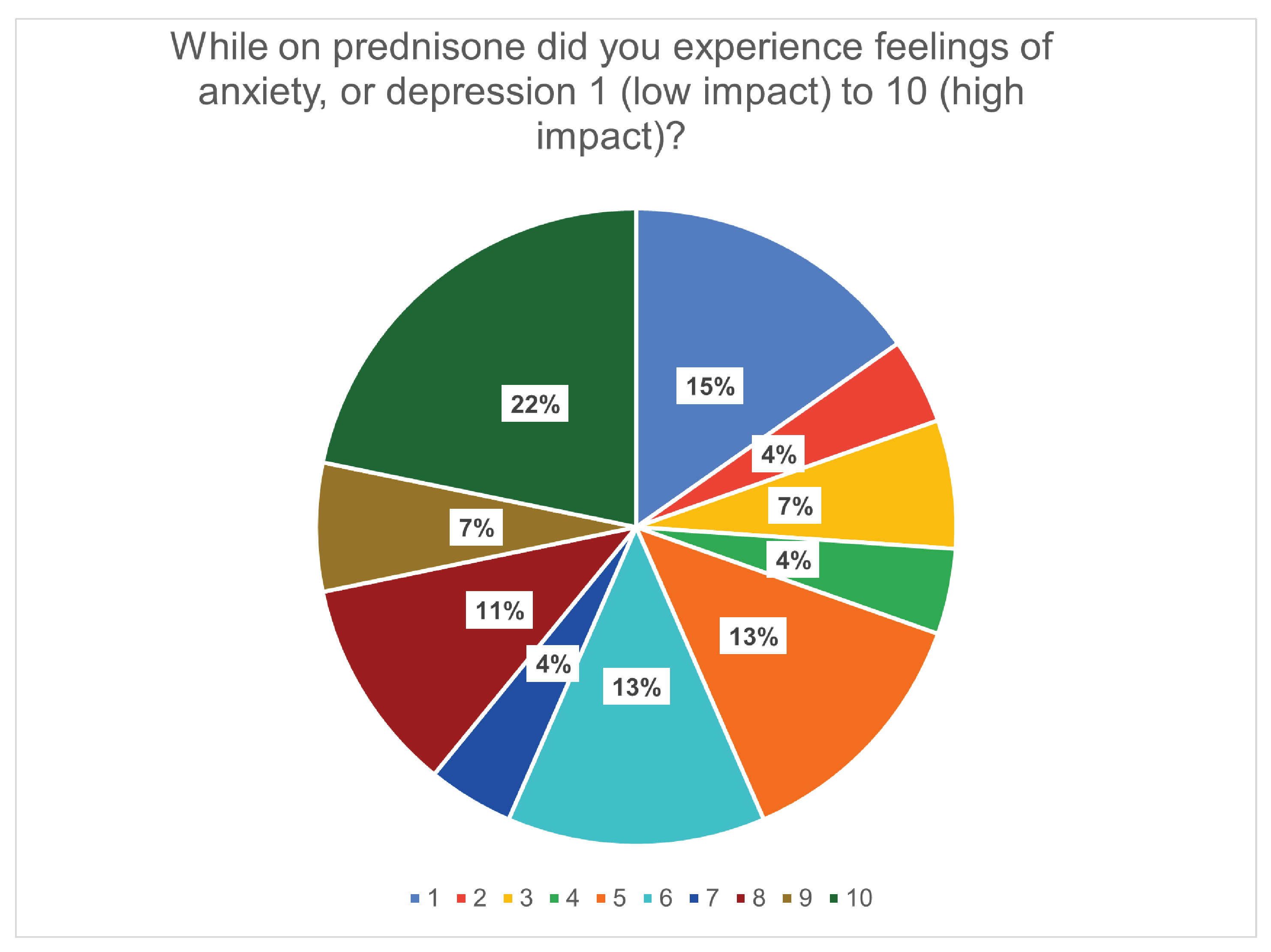
Improved Outcomes
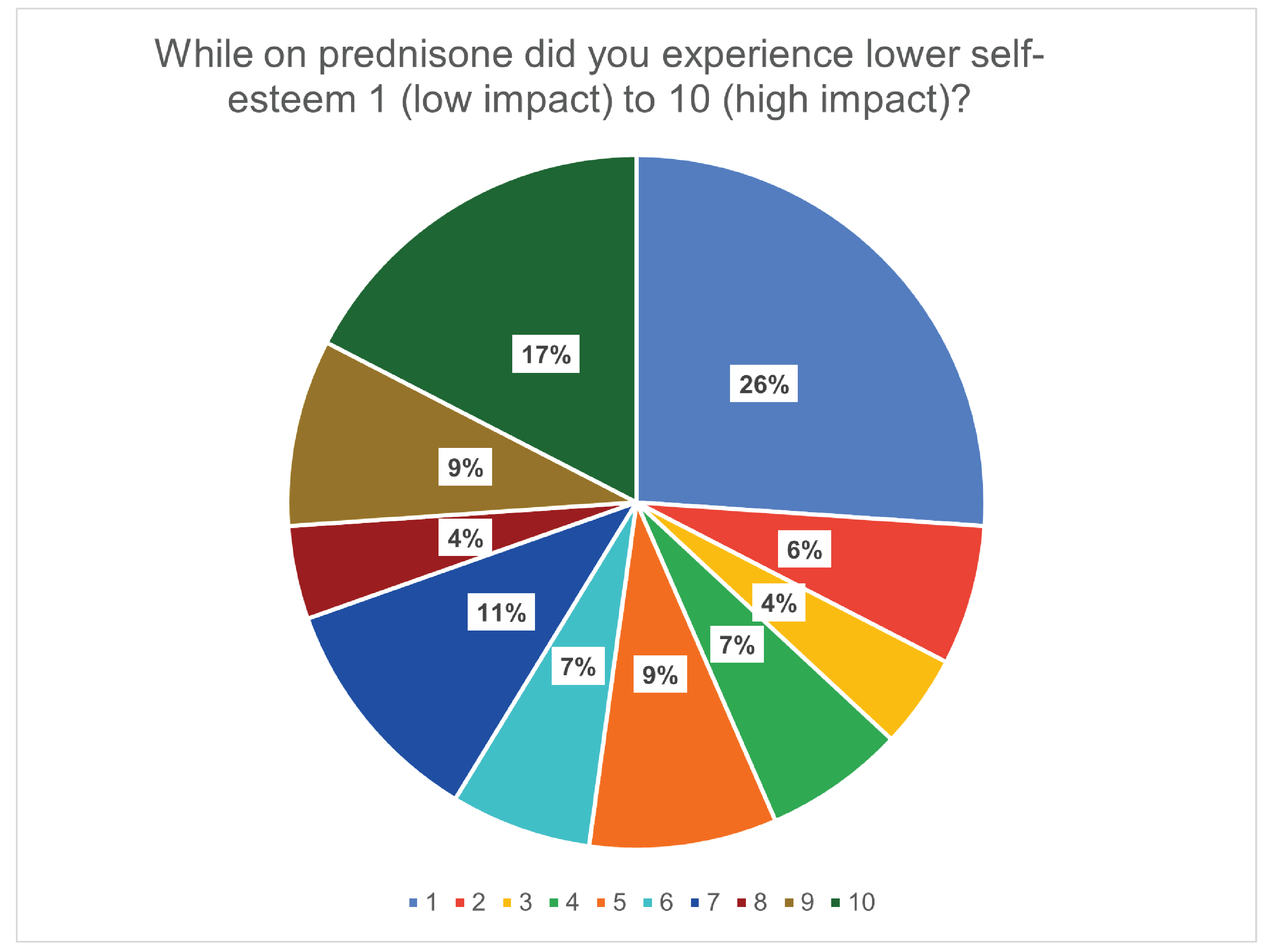
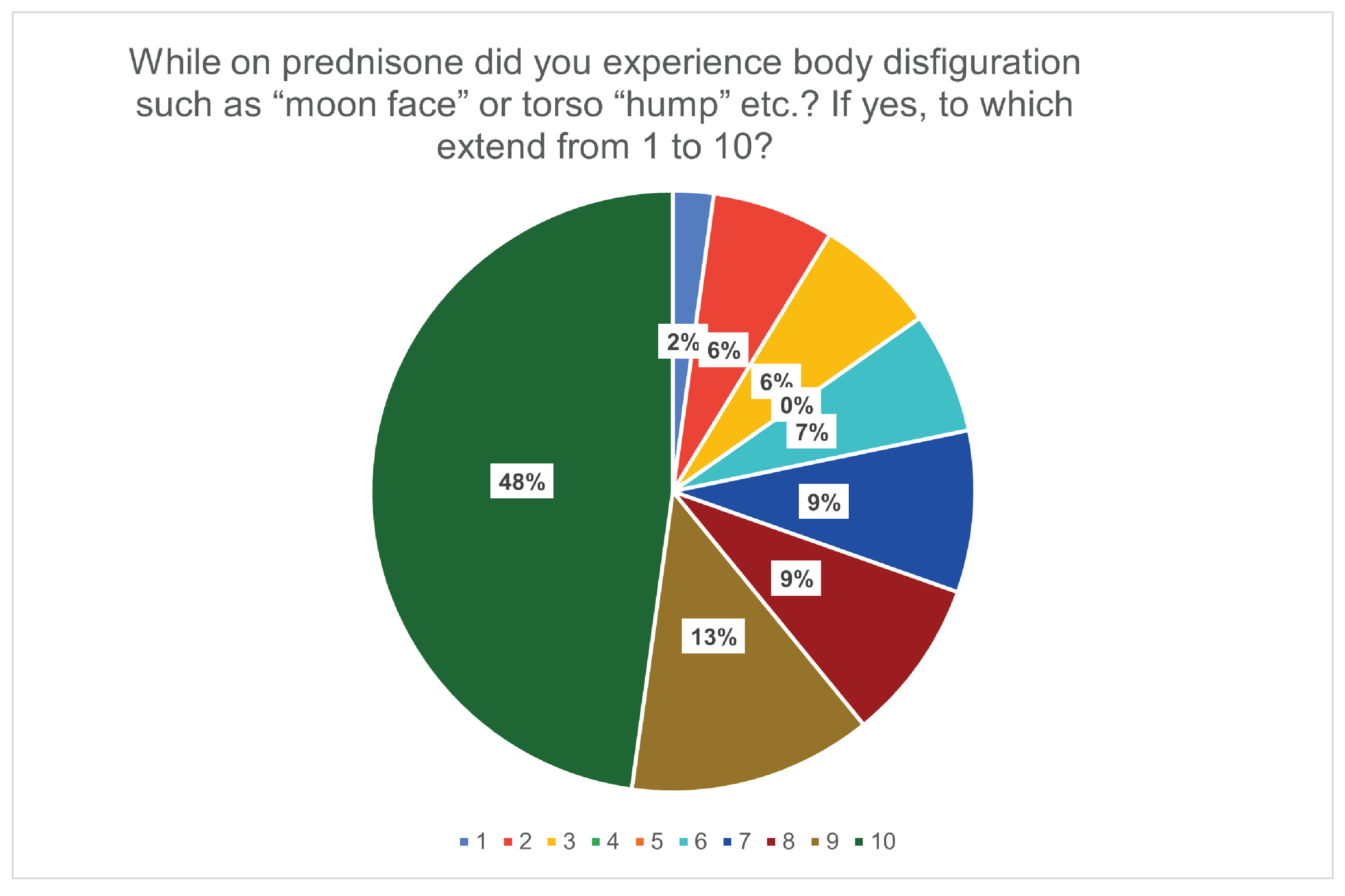
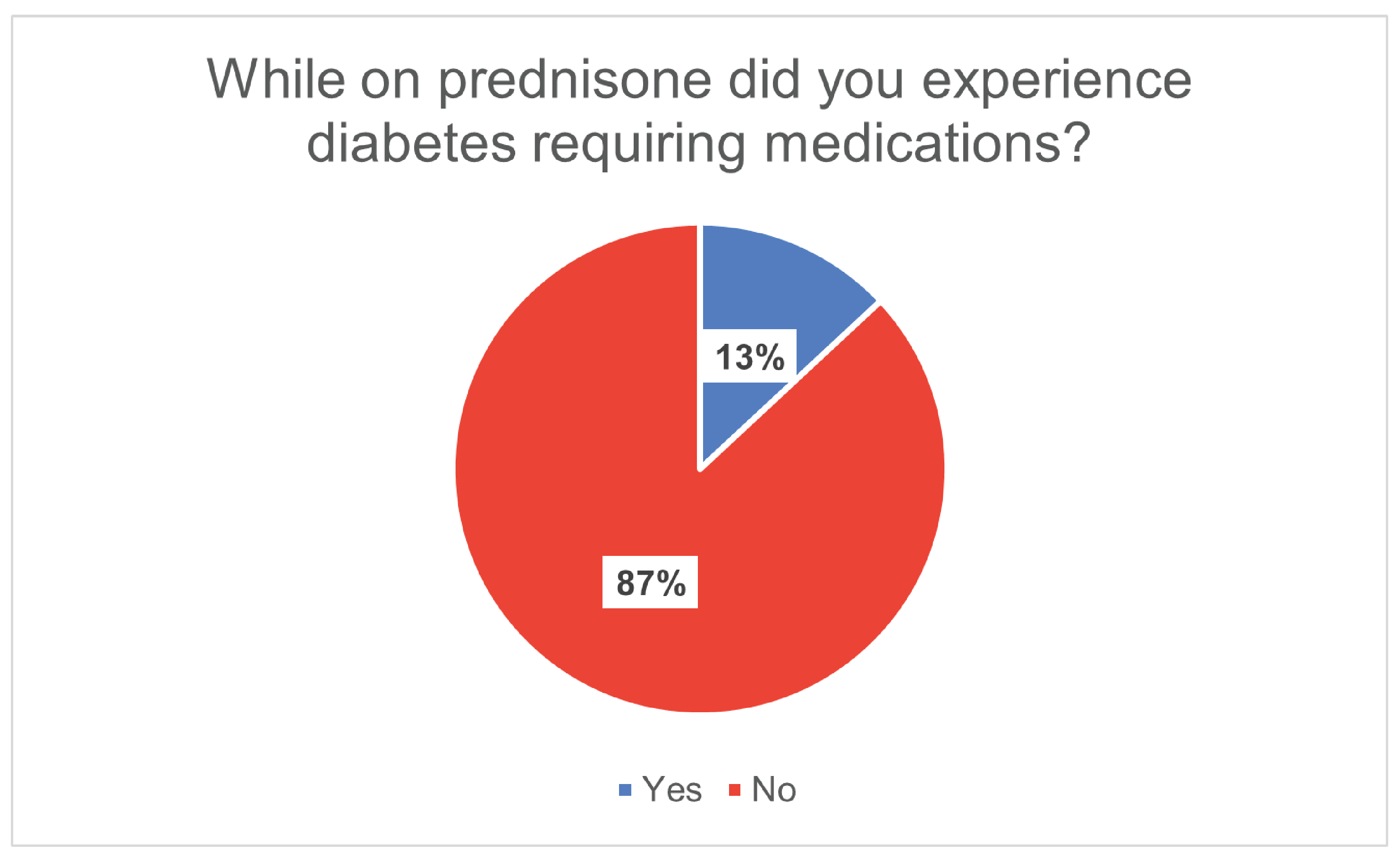
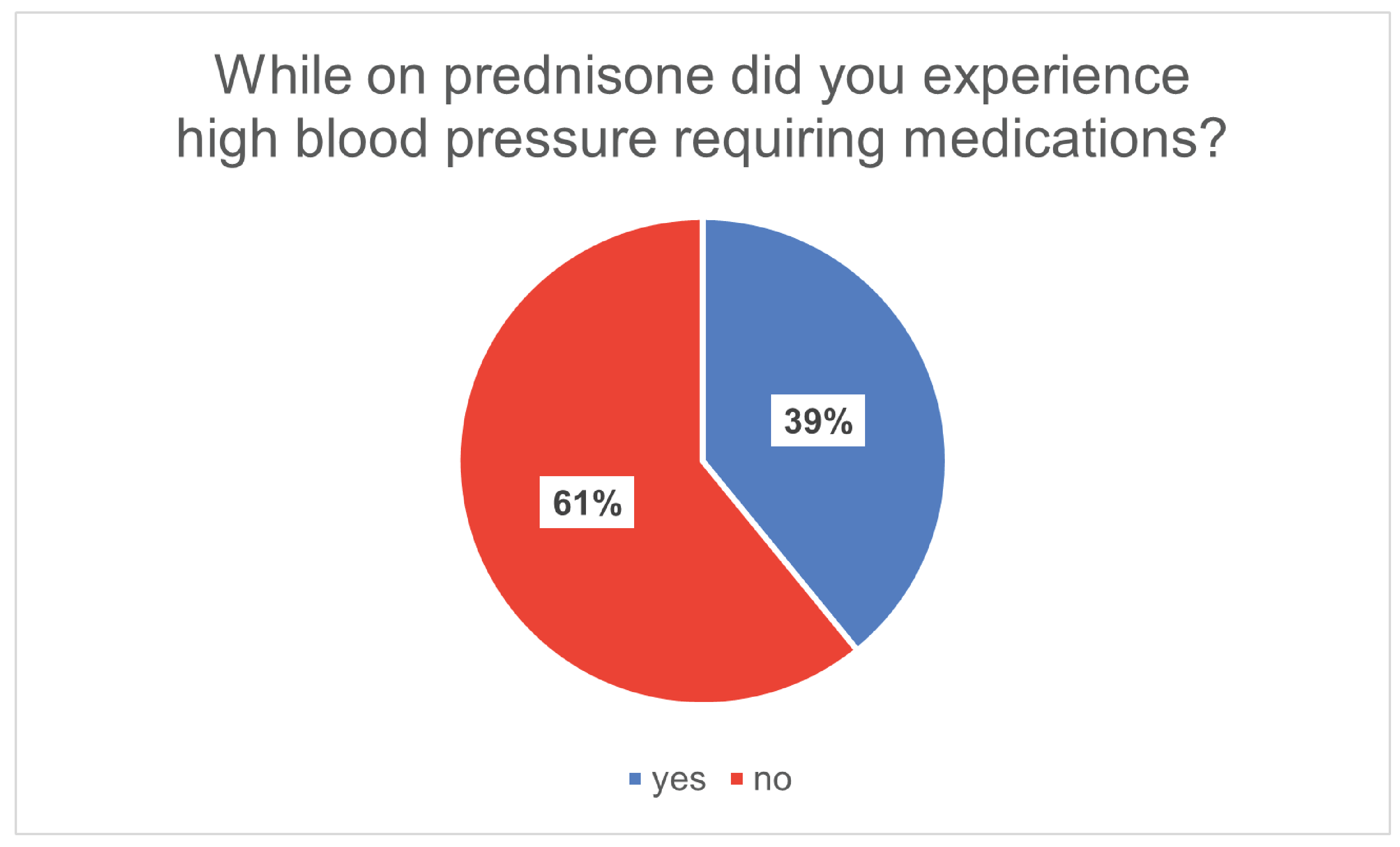
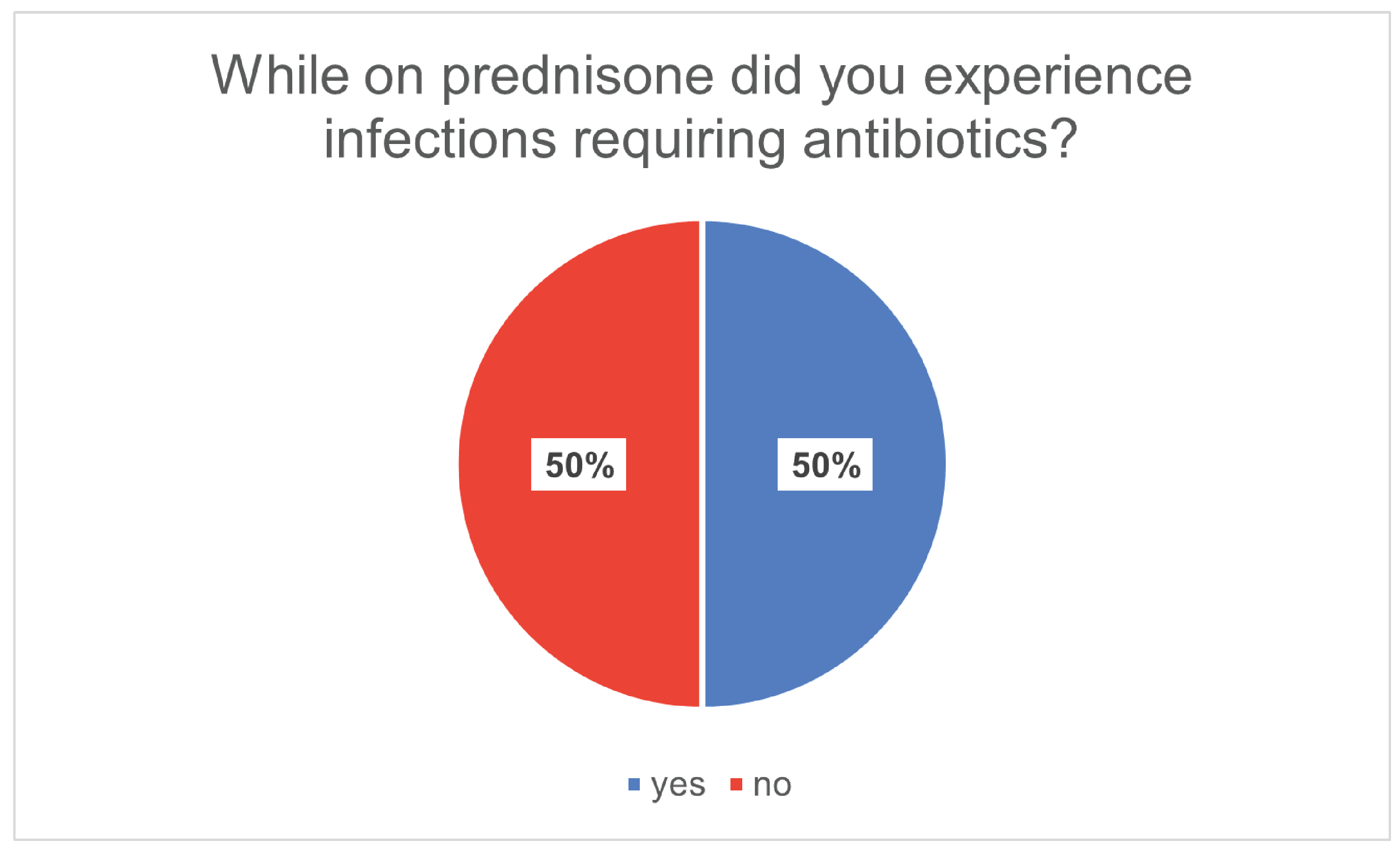
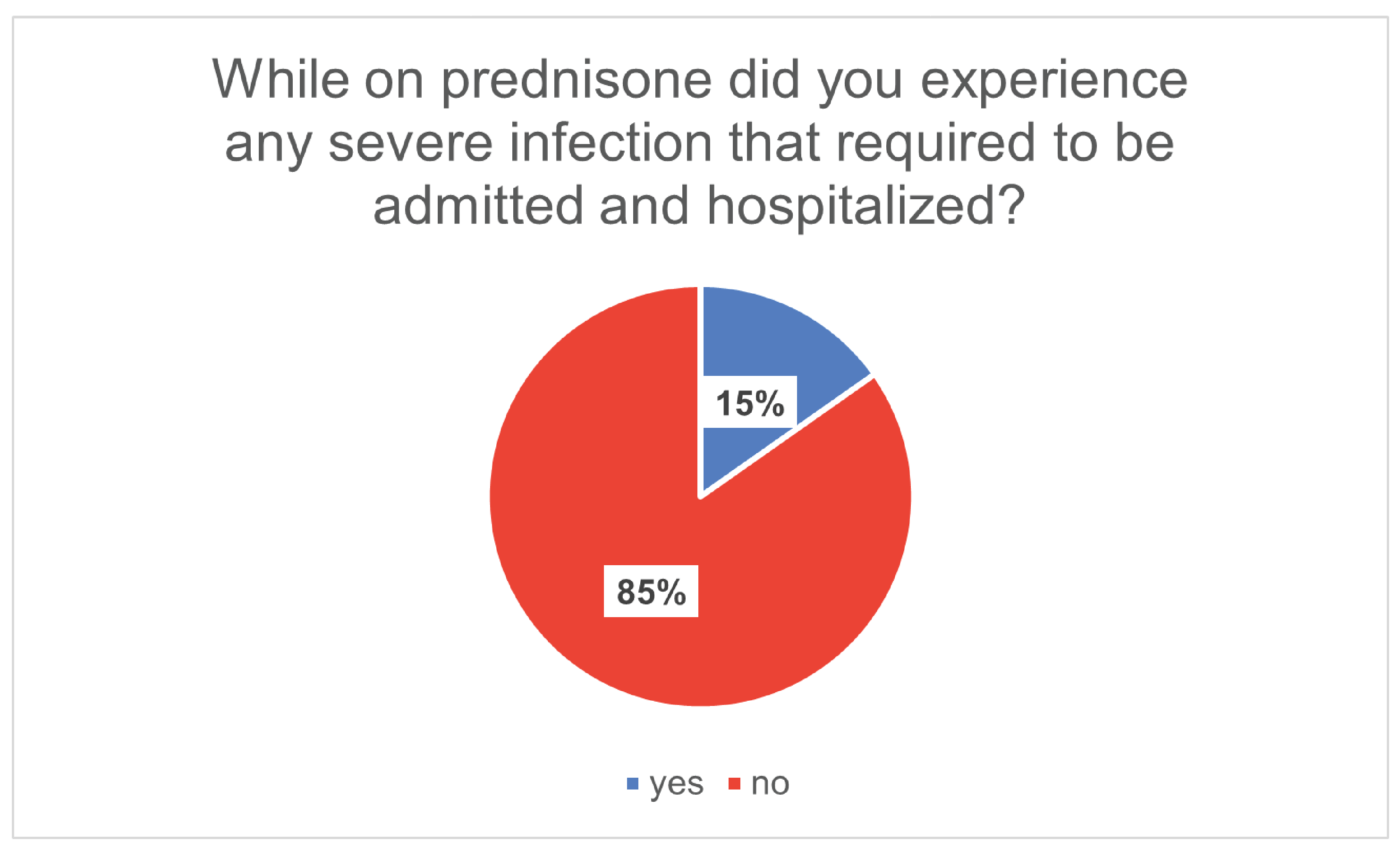
Clearly, patients would like to see improvements in the reduction, or elimination, of the side effects of prednisone, the current and only treatment available. In the absence of even some of prednisone’s side effects, we expect to see a significant improvement in patient quality-of-life and standard of care.
Even when knowing little about a new medication (avacopan), 30 of 46 would out-right choose avacopan over prednisone, 11 would consult their doctor for more info on avacopan, or indicated they needed more info on avacopan, and only 5 of 46 would choose to go back on prednisone if the need arose!
Experience With Drug Under Review
Avocopan is a very new medication to Canada, and to our knowledge only one patient in Canada has taken the drug as part of a clinical trial. Our survey identified one Canadian who actually did take avacopan, but who also had experience taking prednisone at some point as well.
The one person who took the drug reported:
“Any alternative to prednisone would be welcome if I had to use prednisone again.”
In addition to our patient who identified as taking avacopan there are favorable reports in the literature of reduced glucocorticoid adverse events as avacopan is a steroid replacement, or sparing agent.
With avacopan there were impressive reductions in psychological and metabolic AE’s, a similar side effect profile in GI AEs, but overall reductions in the key area of infections especially opportunistic infections. Avacopan use has also been noted for a beneficial effect on kidney function which is a highly impacted organ in GPA/MPA.
Numerous side-effects of prednisone reported in our survey were either not reported in the literature or didn’t occur.
Companion Diagnostic Test
Not applicable.
Anything Else?
On behalf of the Vasculitis Foundation Canada community, I am a strong advocate of faster drug approvals, coverage, and access to new and modern medications that target a specific need within the GPA/MPA treatment sphere. We know that treatment with glucocorticoids save lives, but we also know the damage that is left behind. Canadian patients have clearly revealed the negative side-effects and they want and need solutions, without these negative side-effects, now, not years from now!
Adopting new treatments, as with technology, brings forth new possibilities and can provide for a seismic shift forward in the treatment and care of Canadians with devastating diseases like GPA/MPA. We may not be able to prevent diseases like GPA/MPA, but we can, and should, improve access and availability as expeditiously as possible to modern treatments so as to reduce the negative impacts of such diseases. As was seen with the huge improvements in care with the advance of Rituximab for GPA/MPA a decade ago, we could foresee a similar leap forward with avacopan.
Conflict of Interest Declaration — Vasculitis Foundation Canada
To maintain the objectivity and credibility of the CADTH reimbursement review process, all participants in the drug review processes must disclose any real, potential, or perceived conflicts of interest. This Patient Group Conflict of Interest Declaration is required for participation. Declarations made do not negate or preclude the use of the patient group input. CADTH may contact your group with further questions, as needed.
Did you receive help from outside your patient group to complete this submission?
Not applicable.
Did you receive help from outside your patient group to collect or analyze data used in this submission?
Not applicable.
List any companies or organizations that have provided your group with financial payment over the past 2 years AND who may have direct or indirect interest in the drug under review.
Table 1: Financial Disclosures for Vasculitis Foundation Canada
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
Otsuka Canada Pharmaceutical Inc. | — | — | X | — |
Clinician Input
CanVasc, Canadian Research Network for Vasculitis
About CanVasc, Canadian Research Network for Vasculitis
CanVasc is the Canadian network for research on vasculitides. It was created in November 2010 by Drs. Pagnoux (current president and lead), Carette and Khalidi. The first task was to identify referral medical centers and physicians across Canada with expertise in vasculitis (core members, and referral centers).
Goals of CanVasc are to help conduct studies on vasculitis, provide clinical support and educational material on vasculitis for physicians and health care professionals, optimize the therapeutic management of patients with these rare diseases, and eventually improve their outcomes, wherever they live.
Since its creation, CanVasc core members have worked hard together to develop the first Canadian recommendations for the management of ANCA-associated vasculitides, published in 2015 and updated in 2020, the first Canadian educational case-based textbook on vasculitis (CAVALI, with a 3rd Edition in preparation), and to conduct several cohort studies, a national registry on vasculitis, and participate in many therapeutic trials.
Link to website: https://canvasc.ca/
Information Gathering
CanVasc members are on top of the ongoing research and treatments in vasculitis and have of course followed the development of avacopan from its inception to the recent approval by the FDA. Its president (Dr Pagnoux) participated in 2 trials (CLEAR and ADVOCATE) as site investigator and participated as scientific external expert to the applications made by Otsuka to Health Canada and CADTH. He also co-signed with several lead world-renowned investigators the letter of support for the approval of avacopan by the FDA in early 2021.
As such, CanVasc and Dr Pagnoux are fully aware of the content of this submission.
Current Treatments and Treatment Goals
As written in a recent published review from CanVasc members on avacopan (Avacopan for the treatment of ANCA-associated vasculitis. Osman M, Cohen Tervaert JW, Pagnoux C. Expert Rev Clin Immunol. 2021 Jul;17(7):717-726).: “The current therapeutic options for patients with AAV heavily rely on both GC and immunosuppressive regimens ([7)]. These regimens consist of agents such as cyclophosphamide or rituximab for induction (along with GC), then rituximab ([57)], methotrexate ([58)] or azathioprine ([58)] for maintenance. Cyclophosphamide is a potent but non-selective immunosuppressive, cytotoxic agent. In spite of the availability of these aforementioned agents, the mortality in AAV in the first year of diagnosis has continued to exceed 10%, mostly from complications of the disease, or infections ([2, 12, 626559)]. Indeed, a large component of the mortality in patients with AAV is directly attributed to treatment-related complications, and, later on, sequelae of vasculitis, such as increased cardiovascular disease ([2, 12, 630)]. Prolonged courses of GC are often employed in AAV but can concur in the development, or directly result, in many of these complications, such as infections, cardiovascular disease, diabetes, hypertension, and osteoporosis. Hence, there has been a need for agents’ new approaches that could minimize the use of GC, without any additional risks ([641, 652)].
The ADVOCATE trial ([15)] was a large multicenter, double-blinded, placebo-controlled, randomized controlled trial. Avacopan-based treatment was non-inferior to the conventional glucocorticoid-based treatment at week 26, and superior to it at week 52. Serious adverse events occurred in 37.3% in the patients receiving avacopan, and in 39% in patients receiving prednisone. There were also significant differences in several of the secondary endpoints, with a lower GTI at week 26 in the avacopan group, greater improvement in the GFR in patients with a baseline grade 4 kidney disease (GFR <30 ml/min), and an early change in urinary albumin:creatinine ratio at week 4 in the avacopan recipients.
Avacopan is one the first agents to achieve that key goal for the treatment of AAV to reduce GC exposure and toxicity. Data from the CLEAR, CLASSIC and ADVOCATE studies suggest that blocking the complement pathway may help renal recovery to a greater extent than what can be achieved with other therapeutic options available at present. Avacopan has now to be approved by health authorities but its access and cost, if high, might be limiting factors, at least initially, in its implementation and use.
Treatment Gaps (Unmet Needs)
Considering the treatment goals, please describe goals (needs) that are not being met by currently available treatments.
not all patients respond to conventional treatments.
all patients develop some adverse effects, potentially severe, due to the use of high dose and prolonged use of glucocorticoids, for which no alternative had been available until now.
reducing the use of GC is major and utmost need.
improving further patient recovery is another goal (better renal, neurological recovery especially).
relapses are common with conventional treatments, and sustained remission (not only the remission at month 6) is important to consider.
simple treatment (not with infusions, and not with a complex tapering doing) are more convenient and practical for patients.
Place in Therapy
How would the drug under review fit into the current treatment paradigm?
For the time being, avacopan would be used as it was in the ADVOCATE trial, as a combined treatment for induction of severe GPA and MPA with RTX, and still with some steroids initially at least for the most severely affected patients (GC for a very short time, around 4 weeks). Non-study GC were in fact allowed at the beginning of the ADVOCATE study, in both arms and often given in practice, for a couple to a few weeks in many patients. Patients with severe disease in the ICU were not included in the trial, but could be treated as well, with some steroids initially.
Avacopan can also have an important role in patients with refractory GPA or MPA, despite previous use of other conventional therapies.
Many other questions will have to be answered, and as soon as possible, because I don’t know what should become the strategy after week 52 when you use avacopan.
Which patients would be best suited for treatment with the drug under review? Which patients would be least suitable for treatment with the drug under review?
All patients with active severe GPA or MPA would be candidate for this agent. The diagnosis of GPA and MPA is 99% of the time obvious, as this is not a subtle disease, and there are clear diagnostic tools (ANCA serology, biopsies etc).
In addition, because of the renal improvement observed with avacopan, those patients with active renal disease (up to 80% of the patients with MPA or GPA) would be particularly good candidates for this treatment.
What outcomes are used to determine whether a patient is responding to treatment in clinical practice? How often should treatment response be assessed?
As stated above, AAV are severe condition, and survival is a strong outcome, followed by remission at 6 months, then sustained remission (absence of relapse), and absence of severe damage and severe adverse events. All these outcomes are hard ones and are simple to assess in GPA or MPA. Improvement of quality of life is more complex.
What factors should be considered when deciding to discontinue treatment with the drug under review?
For now, it should be used as done in the ADVOCATE trial. Given for 12 months, unless there is a related side effect. If after 6 months the patient is not in remission, of there is a relapse, avacopan should likely be pursued, but there would be a need to intensify transiently the other co-treatments (increasing the dosing regimen of rituximab or adding steroids for a short course to re-induce remission). In case of a subsequent, other relapse, it might be needed to reconsider the entire treatment strategy with a Canvasc referral center.
What happens after discontinuing avacopan at month 12 remains unknown to date… and of course there will be concern in stopping it then in patients who would still have some lingering minor symptoms, or still ANCA positive… as there are at this time when deciding when to stop rituximab for example (which is systematically given for 2 years at least).
What settings are appropriate for treatment with [drug under review]? Is a specialist required to diagnose, treat, and monitor patients who might receive [drug under review]?
Vasculitis are rare and severe diseases. They should always be managed by specialists in the field, either rheumatologists or nephrologists. CanVasc regroups the main vasculitis expertise centers in Canada.
Additional Information
As stated above, avacopan is being seen as a game changer in GPA and MPA. International experts gathered to support the application to the FDA in 2021, which has been a unique supportive initiative, not seen before for any other agents in GPA or MPA to date. It would apply to almost all patients with GPA and MPA.
My only concerns today include: access to the drug, cost and coverage of the drug, and what to do after month 12… more studies are needed to refine the duration of the treatment, and/or what to do then... it will likely depend on each patient individual characteristics…
Conflict of Interest Declarations — CanVasc, Canadian Research Network for Vasculitis
To maintain the objectivity and credibility of the CADTH drug review programs, all participants in the drug review processes must disclose any real, potential, or perceived conflicts of interest. This conflict of interest declaration is required for participation. Declarations made do not negate or preclude the use of the clinician group input. CADTH may contact your group with further questions, as needed. Please refer to the Procedures for CADTH Drug Reimbursement Reviews (section 6.3) for further details.
Did you receive help from outside your clinician group to complete this submission?
No.
Did you receive help from outside your clinician group to collect or analyze any information used in this submission?
No.
List any companies or organizations that have provided your group with financial payment over the past two years AND who may have direct or indirect interest in the drug under review.
Declaration for Clinician 1
Name: Christian Pagnoux
Position: Founder and President of the CanVasc group
Date: April 1, 2022
Table 2: COI Declaration for CanVasc, Canadian Research Network for Vasculitis — Clinician 1
Company | $0 to $5,000 | $5,001 to $10,000 | $10,001 to $50,000 | In excess of $50,000 |
|---|---|---|---|---|
Otsuka | — | X | — | — |
Pfizer | — | X | — | — |
AstraZeneca | — | X | — | — |
ChemoCentryx | — | X | — | — |
GSK | X | — | — | — |
Roche | X | — | — | — |
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up-to-date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
Redactions: Confidential information in this document may be redacted at the request of the sponsor in accordance with the CADTH Drug Reimbursement Review Confidentiality Guidelines
Stakeholder Input: The views expressed in each submission are those of the submitting organization or individual; not necessarily the views of CADTH or of other organizations. As such, they are independent of CADTH and do not necessarily represent or reflect the view of CADTH. No endorsement by CADTH is intended or should be inferred. By filing with CADTH, the submitting organization or individual agrees to the full disclosure of the information. CADTH does not edit the content of the submissions.
CADTH does use reasonable care to prevent disclosure of personal information in posted material; however, it is ultimately the submitter’s responsibility to ensure no identifying personal information or personal health information is included in the submission. The name of the submitting organization or individual and all conflict of interest information are included in the submission; however, the name of the author, including the name of an individual patient or caregiver submitting the patient input, are not posted.
Accessibility: CADTH is committed to treating people with disabilities in a way that respects their dignity and independence, supports them in accessing material in a timely manner, and provides a robust feedback process to support continuous improvement. All materials prepared by CADTH are available in an accessible format. Where materials provided to CADTH by a submitting organization or individual are not available in an accessible format, CADTH will provide a summary document upon request. More details on CADTH’s accessibility policies can be found here.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.