CADTH Reimbursement Review
Semaglutide (Wegovy)
Sponsor: Novo Nordisk Canada Inc.
Therapeutic area: Weight management
This multi-part report includes:
Clinical Review
Pharmacoeconomic Review
Stakeholder Input
Clinical Review
Abbreviations
AE
adverse event
BMI
body mass index
CI
confidence interval
DB
double-blind
FPG
fasting plasma glucose
GI
gastrointestinal
GI Society
Gastrointestinal Society
GLP-1
glucagon-like peptide 1
HRQoL
health-related quality of life
IBT
intensive behavioural therapy
ITC
indirect treatment comparison
IWQOL
Impact of Weight on Quality of Life
IWQOL-Lite
Impact of Weight on Quality of Life–Lite
IWQOL-Lite-CT
Impact of Weight on Quality of Life–Lite Clinical Trials Version
MCS
mental component summary
MID
minimal important difference
NMA
network meta-analysis
OAD
oral antidiabetic drug
OR
odds ratio
PCS
physical component summary
PHQ-9
Patient Health Questionnaire-9
RCT
randomized controlled trial
SAE
serious adverse event
SC
subcutaneous
SD
standard deviation
SF-36
Short Form (36) Health Survey
Executive Summary
An overview of the submission details for the drug under review is provided in Table 1.
Item | Description |
|---|---|
Drug product | Semaglutide (Wegovy) 2.4 mg subcutaneous injection |
Indication | Indicated as an adjunct to a reduced-calorie diet and increased physical activity for chronic weight management in adult patients with an initial BMI of 30 kg/m2 or greater (obesity), or 27 kg/m2 or greater (overweight) in the presence of at least 1 weight-related comorbidity such as hypertension, type 2 diabetes, dyslipidemia, or obstructive sleep apnea |
Reimbursement request | As an adjunct to a reduced-calorie diet and increased physical activity for chronic weight management in adult patients with an initial BMI of 35 kg/m2 or greater and prediabetes |
Health Canada approval status | NOC |
Health Canada review pathway | Standard |
NOC date | November 23, 2021 |
Sponsor | Novo Nordisk Canada Inc. |
BMI = body mass index; NOC = Notice of Compliance.
Introduction
The WHO defines overweight and obesity as abnormal or excessive fat accumulation that poses a risk to health. A body mass index (BMI) of 25 kg/m2 or greater is considered to be overweight and a BMI of 30 kg/m2 or greater is considered obese.1 In addition to the increasingly recognized role of various biochemical factors in obesity, there are multiple factors that contribute to the condition, including socioeconomic factors, lack of access to healthy foods and easy access to highly palatable processed foods, and living environment. The Canadian Health Measures Survey (2019) found that 35.5% of adults between the ages of 18 and 79 were in the overweight category and 24.3% were living with obesity2 while the Canadian Task Force on Preventive Health Care has reported that 67% of Canadian males and 54% of Canadian females are living with overweight or obesity.3 There is a wide range of comorbidities associated with obesity, including increased risk of type 2 diabetes, certain cancers, hypertension, cardiovascular disease, and gallstones, as well as psychological and psychiatric issues.
The approach to management of overweight and obesity is multi-pronged, and includes modification of physical activity and behaviour in addition to medical nutrition therapy. According to the Canadian Adult Obesity Clinical Practice Guidelines, drug therapy for overweight or obesity is indicated only for those with a BMI of 30 kg/m2 or more, or for those with a BMI of 27 kg/m2 or more with at least 1 weight-related comorbidity. Semaglutide 2.4 mg joins 3 other weight-loss drugs approved in Canada: orlistat, liraglutide, and the combination of naltrexone and bupropion. The clinical expert consulted by CADTH on this review noted that targeting a “normal” BMI of under 25 kg/m2 is neither realistic nor appropriate for many patients living with obesity; rather, the emphasis should be on improving overall health and well-being as well as these weight-related comorbidities.
Semaglutide, a glucagon-like peptide 1 (GLP-1) agonist, is administered by subcutaneous (SC) injection at a dose of 2.4 mg once weekly. It is indicated as an adjunct to a reduced-calorie diet and increased physical activity for chronic weight management in adult patients with an initial BMI of 30 kg/m2 or greater (obesity) or 27 kg/m2 or greater (overweight) in the presence of at least 1 weight-related comorbidity such as hypertension, type 2 diabetes dyslipidemia, or obstructive sleep apnea.4 Semaglutide is also indicated for the management of type 2 diabetes, and was previously reviewed by CADTH for that indication.
The objective was to perform a systematic review of the beneficial and harmful effects of semaglutide 2.4 mg for SC injection as an adjunct to a reduced caloric diet and increased physical activity for chronic weight management in adult patients.
Stakeholder Perspectives
The information in this section is a summary of input provided by the patient groups that responded to CADTH’s call for patient input and from clinical expert(s) consulted by CADTH for the purpose of this review.
Patient Input
A total of 5 patient groups provided 4 submissions (Gastrointestinal Society [GI Society]; Obesity Canada and the Canadian Liver Foundation, which provided a joint input; Diabetes Canada; and Obesity Matters). The GI Society is a national charity that focuses on providing Canadians with trusted, commercial-free, medically sound information on gut and liver diseases and disorders, including obesity. Data for its submission came from a variety of sources, including contact with patients and patient caregivers, the results of published studies, and a survey conducted from October 6, 2020, to January 10, 2021, open to individuals who had experienced obesity. The survey was open internationally, but the majority of the 2,050 (96%) respondents were from Canada. Obesity Canada and the Canadian Liver Foundation provided a joint input. Obesity Canada is Canada’s leading obesity registered charity association for health professionals, researchers, trainees, students, policy-makers, and Canadians living with obesity. The Canadian Liver Foundation is dedicated to supporting education and research into all forms of liver disease. Data for the joint submission of Obesity Canada and the Canadian Liver Foundation was based on a survey, conducted from February to March 2022, that was distributed throughout Obesity Canada and Canadian Liver Foundation networks on social media and newsletter mailing lists as well as within Obesity Canada’s online patient support community. There was a total of 109 responses from Canadians living with obesity. More than half of respondents (66%) indicated past or present experience with prescription medications for obesity management, with 57% reporting experience specifically with semaglutide. Diabetes Canada is a national health charity representing the millions of Canadians who are affected by diabetes and leads the fight against diabetes by helping people live healthy lives, preventing the onset and consequences of diabetes, and discovering a cure. Its submission contains patient input from an online survey conducted in March 2022. A total of 29 people in Canada participated in the survey; 3 identified as living with prediabetes and 26 identified as living with type 2 diabetes. Among those who answered the question (n = 21), 19 (90%) respondents said they identify as living with overweight or obesity. Two people said they have experience with the drug under review. Obesity Matters is a group of people with common experiences and concerns. The goal of Obesity Matters is to provide an opportunity for communities across Canada to share personal feelings, experiences, and coping strategies, and to offer support so they can take action and seek the help they deserve. The input from Obesity Matters was based on a survey conducted from March 2 to 15, 2022, with 104 respondents. A video was also provided in Obesity Matters’ input.
The 4 patient group inputs reported that overweight and obesity affect many areas of life and patients usually present with various comorbid conditions, such as arthritis, hypertension, sleep apnea, gastroesophageal reflux disease, irritable bowel syndrome, high cholesterol, diabetes, fatty liver disease, asthma, osteoarthritis, infertility, cancers, and mental health issues. Overweight and obesity lead to a multitude of negative impacts, including pain and impacts on mobility, regular activities, self image, and patients’ families and relationships. A common theme in the submissions was the stigma associated with the disease, with patients experiencing discrimination from physicians and employers. Regarding current management options, there are very few medication options, and those that are available do not have public or full private coverage. In addition, patients indicated that these drugs have side effects that include nausea, diarrhea, constipation, and headaches. Patients considered it important for them to have a medication for weight management with long-term effectiveness and fewer side effects, and that the medication also be affordable and easy to administer. Key outcomes identified by the patient advocacy groups as important to patients with overweight or obesity were weight loss, reducing weight-related comorbidity, and improving health-related quality of life (HRQoL).
In the input by the GI Society, those who had tried semaglutide found it easier to adhere to lifestyle modifications while taking that medication. In the input by Diabetes Canada, both patients said their ability to maintain or lose weight and meet target blood sugar levels was “much better” on semaglutide injection 2.4 mg than before, though 1 patient indicated improved gastrointestinal (GI) side effects on semaglutide injection while the other patient indicated “much worse” GI side effects. One patient from the Obesity Canada and the Canadian Liver Foundation input stated that semaglutide had been very effective and described increased energy and reduction in medication needed to control blood pressure and cholesterol.
Clinician Input
Input From Clinical Experts Consulted by CADTH
According to the clinical expert consulted by CADTH on this review, current therapies do not fully address the multifaceted nature of obesity, as they only target a few of the known pathways involved in managing weight. The clinical expert believed that the majority of patients who were able to tolerate semaglutide would likely benefit to some extent from treatment; however, patients who have difficulty reducing portion sizes and have significant hunger are likely the ones to benefit most from the drug. Patients who do not report issues with significant hunger and overeating may therefore be least likely to benefit.
Patients most in need of pharmacological intervention are those who are experiencing weight-related comorbidities, according to the clinical expert. To assess response to treatment, markers that are used to monitor improvement in weight-related comorbidities should be measured, such as hemoglobin A1C. With respect to discontinuing treatment, 1 of the key indications for stopping therapy would be the development of gallstones, or treatment failure (gaining weight or failure to lose weight).
The clinical expert also noted that the issue of whether to continue semaglutide immediately after bariatric surgery if a patient happened to be on it before surgery has not been well studied, and there is likely a difference in practice between different surgical centres.
Clinician Group Input
Four groups provided input. These groups were the Calgary Weight Management Centre, Centre de Médecine Métabolique de Lanaudière, Obesity Canada, and the Canadian Association of Bariatric Physicians and Surgeons — the latter 2 of which provided a joint input. The input from the clinician groups was consistent with that provided by the clinical expert consulted by CADTH on this review. The clinician groups believed that semaglutide is likely to replace liraglutide and naltrexone-bupropion for many patients.
Drug Program Input
Input was obtained from the drug programs that participate in the CADTH reimbursement review process. The following were identified as key factors that could potentially impact the implementation of a CADTH recommendation for semaglutide: considerations for initiation, continuation or renewal, and discontinuation of therapy, generalizability, care provision issues, and system and economic issues. The clinical expert consulted by CADTH provided advice on the potential implementation issues raised by the drug programs.
Clinical Evidence
Pivotal Studies and Protocol Selected Studies
Description of Studies
Four placebo-controlled, double-blind (DB) randomized controlled trials (RCTs) — STEP 1 (N = 1,950), STEP 2 (N = 1,210), STEP 3 (N = 611), and STEP 4 (N = 803) — compared semaglutide 2.4 mg to placebo, and 1 open-label RCT compared semaglutide to liraglutide and placebo (STEP 8, N = 338), all over 68 weeks of treatment. All patients in the included studies had overweight (BMI of 27 kg/m2 or greater with at least 1 weight-related comorbidity) or obesity (BMI of 30 kg/m2 or greater), and patients enrolled in STEP 2 also had type 2 diabetes. All studies were funded by the sponsor and all were multi-centre. Two studies (STEP 1 and STEP 2) had Canadian sites. STEP 4 included a 20-week run-in period where all patients were titrated to the target dosage of semaglutide 2.4 mg once weekly before randomization at week 20. All patients in the STEP trials received counselling regarding diet and physical activity. In STEP 3, the first 8 weeks of the study consisted of a 1,000 kcal per day to 1,200 kcal per day liquid calorie diet, after which patients were gradually transitioned to a less strict hypocaloric diet consisting of conventional foods. The primary outcome of all studies was the percentage reduction in body weight from baseline to week 68, and the co-primary outcome of the STEP 1 to STEP 3 studies was patients achieving at least a 5% reduction in body weight by week 68. Other confirmatory secondary outcomes controlled for multiplicity included patients achieving at least a 10% reduction (in 3 studies), a 15% reduction (in 3 studies), and a 20% reduction (in 1 study) in body weight by week 68, and change from baseline to week 68 in the physical function component of the Short Form (36) Health Survey (SF-36) version 2 acute (in 4 studies).
Across studies, the mean age of patients was 46 years to 49 years, with the exception of STEP 2, where the mean age was 55 years. The majority of patients (75% to 80%) was female, with the exception of STEP 2 where there was a roughly equal percentage of females and males in the study. The vast majority of patients across the studies was White (75% to 93%), with the exception of STEP 2, where about 60% of patients were White and 27% were Asian. Baseline body weight in STEP 1, STEP 3, and STEP 8 was approximately 105 kg, and slightly lower (approximately 100 kg) in STEP 2, which focused on patients with type 2 diabetes, and even lower in STEP 4 (approximately 96 kg). Baseline hemoglobin A1C was approximately 5.7% in STEP 1 and STEP 3, 5.5% in STEP 8, and 5.4% in STEP 4, which featured the run-in, and much higher in STEP 2 (8.1%), which enrolled patients with type 2 diabetes.
Efficacy Results
Body Weight
Key efficacy results are presented in Table 2. The percentage change from baseline to week 68 in body weight was a primary outcome in all studies. There was a statistically significant difference in percentage reduction in body weight for semaglutide versus placebo in each of STEP 1 (difference between groups of –12.44% [95% confidence interval, or CI, –13.37% to –11.51%; P < 0.0001]), STEP 2 (difference between groups of –6.21% [95% CI, –7.28% to –5.15%; P < 0.0001]), STEP 3 (difference between groups of –10.27% [95% CI, –11.97% to –8.57%; P < 0.0001]), and STEP 4 (difference between groups of –14.75% [95% CI, – 16.00% to – 13.50%; P < 0.0001]), and a statistically significant difference in percentage reduction in body weight for semaglutide versus liraglutide in STEP 8 (difference between groups of –9.38% [95% CI, –11.97% to –6.80%; P < 0.0001]).
Patients achieving a 5% reduction from baseline in body weight was a co-primary outcome in the STEP 1 to STEP 3 studies, and there were greater percentages of patients in the semaglutide group than in the placebo group who achieved a 5% weight loss by week 68 in each of STEP 1 (odds ratio [OR] = 11.22 [95% CI, 8.88 to 14.19; P < 0.0001]), STEP 2 (OR = 4.88 [95% CI, 3.58 to 6.64; P < 0.0001]), and STEP 3 (OR = 6.11 [95% CI, 4.04 to 9.26; P < 0.0001]). In STEP 4, where it was a supportive secondary outcome, the OR was 8.52 (95% CI, 5.93 to 12.24) for semaglutide versus placebo.
Patients achieving a weight reduction from baseline of at least 10%, 15%, and 20% were confirmatory secondary outcomes in STEP 8, and greater percentages of patients in the semaglutide group than the liraglutide group achieved at least a 10% reduction (OR = ||||| |||| || |||||| | | |||||), at least a 15% reduction (OR = ||||| ||| ||| |||| || |||||| | | ||||||), and at least a 20% reduction (OR = ||||| ||| ||| |||| || |||||| | | ||||||). Similarly, there were statistically significant differences in favour of semaglutide for percentages of patients with at least a 10%, 15%, and 20% reduction in the STEP 1 to STEP 3 studies.
Change from baseline to week 68 in waist circumference was also a confirmatory secondary outcome in the STEP 1 to STEP 4 studies. The mean waist circumference was reduced for semaglutide versus placebo in each of STEP 1 (treatment difference of – 9.42 cm [95% CI, –10.30 to –8.53; P < 0.0001]), STEP 2 (treatment difference of –4.88 cm [95% CI, –5.97 to –3.79; P < 0.0001]), STEP 3 (treatment difference of –8.34 cm [95% CI, –10.08 to –6.59; P < 0.0001]), and STEP 4 (treatment difference of –9.74 cm [95% CI, –10.94 to –8.54; P < 0.0001]). The change from baseline to week 68 was a supportive secondary outcome in STEP 8, and the difference between semaglutide and liraglutide was ||||| || |||| ||| ||||| || |||||||
Body Mass Index
The mean change from baseline to week 68 in BMI was reported as a supportive secondary outcome in the STEP 1 to STEP 4 studies, and thus was not part of the statistical testing hierarchy. The difference between groups with respect to mean change in BMI in STEP 1 was –4.61 kg/m2 (95% CI, –4.96 to –4.27), in STEP 2 was –2.26 kg/m2 (95% CI, –2.63 to –1.88), in STEP 3 was – 3.77 kg/m2 (95% CI, –4.44 to –3.10), and in STEP 4 was –4.74 kg/m2 (95% CI, –5.16 to –4.32).
Health-Related Quality of Life
HRQoL was studied using the SF-36 in the STEP 1 to STEP 4 studies, and the mean change from baseline in physical functioning on the SF-36 was a confirmatory secondary outcome in each of these studies. There was a statistically significant improvement in change in the physical functioning score for semaglutide versus placebo in STEP 1 (1.80 [95% CI, 1.18 to 2.42; P < 0.0001]), STEP 2 (1.52 [95% CI, 0.44 to 2.61; P = 0.0061]), and STEP 4 (2.45 [95% CI, 1.59 to 3.32; P < 0.0001]). In STEP 3, the difference between groups was not statistically significant (0.84 [95% CI, –0.23 to 1.92; P = 0.1249]). The minimal important difference (MID) for the SF-36 physical function score is 3.
Responses on the Impact of Weight on Quality of Life–Lite Clinical Trials Version (IWQOL-Lite-CT) scale physical function score were reported as confirmatory secondary outcomes in the STEP 1 and STEP 2 trials. The difference between semaglutide and placebo in the mean change from baseline to week 68 in scores in STEP 1 was 9.43 (95% CI, 7.50 to 11.35; P < 0.0001) and in STEP 2 was 4.83 (95% CI, 1.79 to 7.86; P = 0.0018). The MID for this instrument is not known.
Normalization of Glucose Parameters
Glycemic status (normoglycemic, prediabetes, diabetes) was assessed in all studies except STEP 2, which enrolled patients who already had type 2 diabetes. In STEP 8, in patients who were normoglycemic at baseline, the percentage of patients transitioning to prediabetes was ||| |||| ||| ||| for semaglutide, liraglutide, and placebo, respectively (Table 31). || |||||||| |||||||||| || ||||||||. In STEP 1, STEP 3, and STEP 4, 3% of semaglutide patients in each study progressed to prediabetes, while 6% to 13% of patients progressed to prediabetes in the placebo group.
In patients who were considered to have prediabetes at baseline, in STEP 8, ||| of semaglutide patients became normoglycemic by the end of the study, compared to ||| of liraglutide patients and ||| of placebo patients, while ||| ||| ||| ||| in the semaglutide, liraglutide, and placebo groups, respectively, progressed to diabetes. In the STEP 1, STEP 3, and STEP 4 trials, 83% to 90% of semaglutide patients became normoglycemic compared to 48% to 68% of placebo patients. In the semaglutide group, no patients in STEP 3 or STEP 4 and 1% of patients in STEP 1 progressed to diabetes while in the placebo group, no patients in STEP 4, 1% of patients in STEP 3, and 3% of patients in STEP 1 progressed to diabetes.
Harms Results
In the STEP 8 study, 95% of patients in each of the semaglutide and placebo groups and 96% of patients in the liraglutide group reported at least 1 adverse event (AE) while on treatment during the study. The most common AEs were GI-related, such as nausea (61% of semaglutide patients versus 59% of liraglutide patients versus 22% of placebo patients) and constipation (39% of semaglutide patients versus 32% of liraglutide patients versus 24% of placebo patients). In the placebo-controlled studies (STEP 1 to STEP 4), AEs occurred in 88% to 96% of semaglutide patients and between 75% and 96% of placebo patients. GI disorders were the most common AE in the semaglutide groups in these studies, including nausea (14% to 58% of semaglutide patients versus 5% to 22% of placebo patients) and diarrhea (14% to 36% of semaglutide patients versus 7% to 22% of placebo patients).
In STEP 8, serious adverse events (SAEs) occurred in 8% of semaglutide-treated patients, in 11% of liraglutide-treated patients, and in 7% of placebo-treated patients. The most common SAEs were in the category of neoplasms — benign, malignant, and unspecified, occurring in 2% of patients in each of the semaglutide and liraglutide groups, and in 1% in the placebo group. In the placebo-controlled studies (STEP 1 to STEP 4), SAEs occurred in 8% to 10% of patients in the semaglutide group and in 3% to 9% of patients in the placebo group.
In STEP 8, permanent discontinuation of trial treatment due to AEs occurred in 3% of semaglutide patients, 13% of liraglutide patients, and 4% of placebo patients. The most common reason for discontinuation of trial treatment was GI disorder, occurring in 1% in each of semaglutide and placebo patients, and 6% of liraglutide patients. Permanent discontinuation of trial treatment due to AEs occurred in 6% to 7% of semaglutide patients and in 3% to 4% of placebo patients in the STEP 1 to STEP 3 studies, and in 2% of semaglutide patients and in 3% of placebo patients in the STEP 4 study, where patients had a 20-week run-in period.
There was no more than 1 death in any group in any of the included trials.
GI disorders were the most common of all the notable harms, as noted previously. In the STEP 8 study, other notable harms included gallbladder-related disorders in 1% in each of semaglutide and placebo patients, and 3% of liraglutide patients. There were no cases of acute pancreatitis or hypoglycemia in the semaglutide or placebo groups, and 1 case of acute pancreatitis and 1 case of hypoglycemia in the liraglutide group. Other notable harms included cardiovascular disorders (13%, 14%, and 11% for semaglutide, liraglutide, and placebo, respectively), injection site reactions (0, 11%, and 6% for semaglutide, liraglutide, and placebo, respectively), and psychiatric disorders (6%, 15%, and 11% for semaglutide, liraglutide, and placebo, respectively).
In the placebo-controlled trials, gallbladder-related disorders occurred in between 0.2% and 5% of semaglutide patients versus between 1% and 3% of placebo patients, with the most common event being cholelithiasis (0.2% to 3% of semaglutide patients versus 1% to 3% of placebo patients). Very few patients had acute pancreatitis — between 0 and 0.2% of patients in each group. Cardiovascular disorders occurred in 5% to 12% of semaglutide patients versus 10% to 12% of placebo patients, adjudicated cardiovascular events occurred in 0.2% to 2% of semaglutide patients versus 0 to 1% of placebo patients, and hypoglycemia occurred in 0.5% to 0.6% of semaglutide patients versus 0 to 1% of placebo patients in the STEP 1, STEP 3, and STEP 4 studies, respectively. In the STEP 2 study, where patients also had type 2 diabetes, cardiovascular events occurred in 6% of semaglutide patients and 3% of placebo patients. Injection site reactions occurred in 3% to 5% of semaglutide patients versus 2% to 7% of placebo patients and psychiatric disorders occurred in 6% to 15% of semaglutide patients versus 4% to 13% of placebo patients.
Table 2: Summary of Key Results From Pivotal and Protocol Selected Studies
Result | STEP 1 | STEP 2 | STEP 3 | STEP 4 | STEP 8 | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
Semaglutide N = 1,306 | Placebo N = 655 | Semaglutide N = 404 | Placebo N = 403 | Semaglutide N = 407 | Placebo N = 204 | Semaglutide N = 535 | Placebo N = 268 | Semaglutide N = 126 | Liraglutide N = 127 | Placebo N = 85 | |
Percentage change from baseline to week 68 in body weight (primary outcome in all studies)a | |||||||||||
Mean (SD) baseline | 105.4 (22.1) N = 1,306 | 105.2 (21.5) N = 655 | 99.9 (22.5) N = 404 | 100.5 (20.9) N = 403 | 106.9 (22.8) N = 407 | 103.7 (22.9) N = 204 | 96.5 (22.5) N = 535 | 95.4 (22.7) N = 268 | 102.5 (25.3) N = 126 | 103.7 (22.5) N = 127 | 108.8 (23.1) N = 85 |
Mean (SD) change | –15.6 (10.1) N = 1,212 | –2.8 (6.5) N = 577 | –9.9 (8.5) N = 388 | –3.4 (6.2) N = 376 | –16.5 (10.1) N = 373 | –5.8 (7.7) N = 189 | –8.3 (8.1) N = 520 | 6.5 (7.7) N = 250 | –16.4 (10.5) N = 117 | –6.4 (7.7) N = 117 | |||| |||||||||| |
Treatment difference (95% CI) | –12.44 (–13.37 to –11.51; P < 0.0001) | –6.21 (–7.28 to –5.15; P < 0.0001) | –10.27 (–11.97 to –8.57; P < 0.0001) | –14.75 P < 0.0001) | Semaglutide vs. liraglutide: –9.38 (–11.97 to –6.80; P < 0.0001) | NA | |||||
Reduction in body weight ≥ 5% by week 68, patients, n (%) (co-primary outcome in STEP 1, STEP 2, and STEP 3)b | |||||||||||
Patients, n (%) | 1,047 (86) | 182 (32) | 267 (69) | 107 (29) | 323 (87) | 90 (48) | 461 (89) | 119 (48) | 102 (87) | 68 (58) | 23 (30) |
OR (95% CI) | 11.22 (8.88 to 14.19; P < 0.0001) | 4.88 (3.58 to 6.64; P < 0.0001) | 6.11 (4.04 to 9.26; P < 0.0001) | 8.52 (5.93 to 12.24; P < 0.0001)c | NA | NA | NA | ||||
Reduction in body weight ≥ 10% by week 68, patients, n (%) | |||||||||||
Patients, n (%) | 838 (69) | 69 (12) | 177 (46) | 31 (8) | 281 (75) | 51 (27) | 411 (79) | 51 (20) | 83 (71) | 30 (26) | 12 (15) |
OR (95% CI) | 14.68 (11.08 to 19.44; P < 0.0001) | 9.63 (6.34 to 14.64; P < 0.0001) | 6.87 (4.68 to 10.09; P < 0.0001) | 14.99 (10.30 to 21.80) | Semaglutide vs. liraglutide: |||| |||||| ||||||| | | |||||| | NA | |||||
Reduction in body weight ≥ 15% by week 68, patients, n (%) | |||||||||||
Patients, n (%) | 612 (51) | 28 (5) | 100 (26) | 12 (3) | 208 (56) | 25 (13) | 331 (64) | 23 (9) | 65 (56) | 14 (12) | 5 (6) |
OR (95% CI) | 19.26 (12.89 to 28.76; P < 0.0001) | 7.65 (4.11 to 14.22; P < 0.0001) | 7.87 (4.90 to 12.63; P < 0.0001) | 19.07 (11.91 to 30.53) | Semaglutide vs. liraglutide: |||| |||||| ||||||| | | |||||| | NA | |||||
Reduction in body weight ≥ 20% by week 68, patients, n (%) | |||||||||||
Patients, n (%) | 388 (32) | 10 (2) | 51 (13) | 6 (2) | 133 (36) | 7 (4) | 206 (40) | 12 (5) | 45 (39) | 7 (6) | 2 (3) |
OR (95% CI) | 26.89 (14.18 to 50.96; P < 0.0001) | 6.84 (2.86 to 16.33; P < 0.0001) | 13.73 (6.23 to 30.29; P < 0.0001) | 14.29 (7.77 to 26.28) | Semaglutide vs. liraglutide: |||| |||||| ||||||| | | |||||| | NA | |||||
Health-related quality of life: SF-36 physical functioning score, mean change from baseline to week 68a | |||||||||||
Mean (SD) baseline | 51.0 (6.9) N = 1,296 | 50.8 (7.9) N = 650 | 49.2 (8.8) N = 397 | 49.6 (8.3) N = 394 | 51.9 (6.7) N = 402 | 52.1 (6.8) N = 203 | 53.8 (5.7) N = 534 | 54.1 (5.0) N = 268 | NR | NR | NR |
Mean (SD) change | 2.3 (6.6) N = 1,195 | 0.4 (7.4) N = 566 | 2.8 (7.7) N = 376 | 0.8 (7.0) N = 365 | 2.5 (5.7) N = 364 | 1.7 (5.7) N = 181 | 1.0 (3.8) N = 515 | –1.2 (4.5) N = 245 | NR | NR | NR |
Treatment difference (95% CI) | 1.80 (1.18 to 2.42; P < 0.0001) | 1.52 (0.44 to 2.61; P = 0.0061) | 0.84 (–0.23 to 1.92; P = 0.1249) | 2.45 (1.59 to 3.32; P < 0.0001) | NA | NA | NA | ||||
Harms | N = 1,306 | N = 655 | N = 403 | N = 402 | N = 407 | N = 204 | N = 535 | N = 268 | N = 126 | N = 127 | N = 85 |
AE, n (%) | 1,171 (90) | 566 (86) | 353 (88) | 309 (77) | 390 (96) | 196 (96) | 434 (81) | 201 (75) | 120 (95) | 122 (96) | 81 (95) |
SAE, n (%) | 128 (10) | 42 (6) | 40 (10) | 37 (9) | 37 (9) | 6 (3) | 41 (8) | 15 (6) | 10 (8) | 14 (11) | 6 (7) |
WDAE, n (%) | 92 (7) | 20 (3) | 25 (6) | 14 (4) | 24 (6) | 6 (3) | 8 (2) | 7 (3) | 4 (3) | 16 (13) | 3 (4) |
AE = adverse event; CI = confidence interval; NA = not applicable; NR = not reported; OR = odds ratio; SAE = serious adverse event; SD = standard deviation; SF-36 = Short Form (36) Health Survey; vs. = versus; WDAE = withdrawal due to adverse event.
Note: Efficacy outcomes were assessed in the full analysis set (all randomized patients) and harms outcomes were assessed in the safety set.
aWeek 68 responses were analyzed using an analysis of covariance model with randomized treatment as factor and baseline value for that outcome as covariate.
bWeek 68 responses were analyzed using a binary logistic regression model with randomized treatment as factor and baseline body weight as covariate.
cThe P value was not adjusted for multiplicity. Critical Appraisal
The included trials were reasonably well conducted with respect to randomization, blinding, and control for multiplicity in statistical testing. Blinding in the STEP 1 to STEP 4 trials may have been compromised somewhat, however, by the fact that the primary outcome is based on a readily measurable, objective measure (weight loss) that patients can self-monitor, and by the large imbalance in GI AEs, a well-known complication of GLP-1 agonists. The only active-controlled trial, STEP 8, lacked blinding between active groups (semaglutide and liraglutide). The relatively long run-in (20 weeks) in STEP 4 may have resulted in a selected population that was already responding to the drug and tolerating semaglutide before being randomized; it may also have resulted in biasing results in favour of semaglutide, as placebo patients experienced rebound weight gain from discontinuing semaglutide.
The structured diet and lifestyle measures that were background therapy in each of the STEP trials may present a generalizability issue, as these measures are unlikely going to be available for the majority of Canadian patients who start semaglutide. The included studies were all 68 weeks in duration, and this is unlikely to be of sufficient duration to assess the long-term efficacy and safety of semaglutide. Most notably, none of the included trials was able to formally assess the impact of semaglutide treatment on the development of comorbidities or the prevention of cardiovascular events.
Indirect Comparisons
Description of Studies
One indirect treatment comparison (ITC), submitted by the sponsor, was reviewed and its objectives were to determine the efficacy and safety of weekly semaglutide 2.4 mg when compared to relevant pharmacological comparators for weight management in patients with overweight or obesity. The study authors conducted a systematic literature review and Bayesian network meta-analysis (NMA).
||||| RCTs of pharmacological interventions for the weight management in overweight or obese patients were included. These trials included comparison of semaglutide, |||||||||||| ||||||||| |||||||||| ||| |||||||||| ||||||||||| ||| ||||||||||| |||||||||||| || ||||||||| |||||||||| || |||| ||| |||||||| |||||||||| |||||||||| |||||||||||| Trials were assessed for risk of bias using the |||||||| ||||||||| ||| |||||| ||| |||| |||||||||| |||||| |||||||||||||| |||||||||. Assessment for network feasibility and heterogeneity were conducted before the ITC. Outcome-specific networks were created, and ||||| ||| |||||||||| |||| |||| || ||||||| |||||| ||| ||||| ||||||| ||||||. The planned efficacy outcomes were |||||||||| || |||||||| |||||| || ||||| ||| |||| ||| ||| || |||||||| ||||||| |||| ||||||| |||||| |||| |||||||| || ||||||| ||||||| |||||| |||| |||||||| || ||||||| |||||| |||| |||||||| || |||||||| ||||| ||||||||| ||||| ||||||||||| |||||||||||| ||| |||||| ||||||||| || |||||||| ||||||||| |||| ||||||||||| || |||||| ||||||| |||||||||| ||||||||| || |||||||| |||||||| |||||||||||||||| ||||||||| ||| ||||||| |||||||| |||||| ||| |||||| |||| |||||||| || ||||| |||||||||||||. The planned safety outcomes were ||||||||| || |||||||||||||| ||||||||| || ||||| ||| |||||||||||||||| ||| || ||||
Sensitivity analyses were conducted ||||||||| ||||||| |||| ||||||||| |||||||||| |||||||| |||||||| |||||||| |||| ||||||||| ||| |||||||||||| |||| |||| | |||||||| ||||||||| |||||||| | |||||||| ||||||||| |||||| ||||||| ||||||||| |||||||| ||| ||||||||||||
Efficacy Results
The models with the best fit (base-case models) are reported as follows:
||||||||||| ||| |||||||||| |||| ||||||| |||| || |||||||| ||||||||| || ||||| || |||||| |||| ||||| || ||||| || ||| |||| ||||||||||| |||||| |||||||| |||| ||||||||||| ||| || ||| |||||||| || || ||||| ||||| ||||| ||||||| ||||||| |||| ||||||| |||||||||||| ||| |||||||||| |||| | ||||||| ||||||| ||||||||| |||| |||||||| || |||||| |||||||| |||| ||||||||||| ||| ||| |||||||||| || || ||| ||||||||| ||| ||| |||||||||| || || ||| ||||||||| ||| ||| |||||||| ||| || ||||| ||||| |||||| ||| |||||||| || || ||||| ||||| ||||| ||| ||||||||||| ||||||||| ||||||| ||| ||||||||||| |||||| |||||||| ||||||||||| |||| ||||||||| ||||||| ||| |||| |||||||| || ||| |||| |||||||| |||||| |||||||||| |||||||| |||| ||| ||||| ||||||||||| || ||| |||||||| || |||||||| |||| ||||| ||||| ||| || |||||||| || | |||||||||| ||||||| ||||||||||| ||| ||||||||||| || |||||||||||||||||||| ||| |||||| ||||||Sensitivity analyses ||||||||| |||||| || ||||||||| ||||||||||| ||||||| ||||| |||| ||||||| |||||||||| |||| ||| |||| ||||||||.
Harms Results
There was no evidence for | |||||||||| || |||| || |||| ||||||| ||||||||||| ||| ||||||||||| ||| ||| |||| ||||||| || |||||||||| ||| ||||||||||| ||| |||||||| ||| || ||||| ||||| ||||| ||| |||||||
Critical Appraisal
The reported ITC was based on a broad systematic literature review, with study inclusion criteria reported transparently. A study protocol was finalized between Novo Nordisk and Mtech Access before conducting the review. Data were extracted in duplicate. The analyses were appropriately conducted and reported. The patients in the included studies match the people who would use this intervention in the real world. Key efficacy and safety outcomes were reported. Follow-up duration was comparable across trials. There was some ||||||||||| |||||||| ||||||||||||| |||| ||||||| || ||| |||||||||||| || |||| ||||||| ||||||| |||| ||| ||| || ||||||| |||||||| ||| ||| |||||||||||||||| || |||| ||||||. Further, it is unclear how the different approaches || |||||||| ||||||| |||| |||||| |||||| might have impacted the results. No ||||||||||| ||||||||||||| was reported. In the event there was ||||||||||||| ||| || ||||||| ||||||| |||||||||||||||| |||||||| |||||||| |||| |||||||||. A sensitivity analysis was also conducted to assess the impact of ||||||||| ||||||| |||| ||| ||||||||||||| which may lead to a ceiling effect. No ||||||||||||||| was presented. |||||||| ||||||||| |||| ||||||||| ||||| |||||| ||| || ||| ||| || |||||| ||||||| ||||||. Reporting of methods was not comprehensive as ||||||| || ||| |||||||| ||||||| was not reported, making it challenging to assess the impact of risk of bias. Sensitivity analyses to explore the impact of outlier studies were not conducted.
Other Relevant Evidence
Description of Studies
STEP 5 was the only 2-year (104-week) RCT in the STEP series of studies. Like the STEP 1 to STEP 4 studies, STEP 5 was a DB placebo-controlled trial, although it was not pivotal and, thus, did not meet the inclusion criteria for the systematic review.
STEP 5 was conducted at 41 sites in Canada, the US and Europe, and randomized 304 patients with overweight or obesity, 1:1, to either semaglutide or placebo. Outcomes were similar to the other STEP trials, with the co-primary outcome being percentage change from baseline in body weight and the percentage of patients achieving a 5% or greater weight reduction. Confirmatory secondary outcomes included the percentage of patients who achieved a 10% or greater reduction in weight by week 104, a 15% or greater reduction in weight by week 104, and change from baseline to week 104 in waist circumference, systolic blood pressure, and SF-36 (physical functioning) score.
Inclusion and exclusion criteria were similar to the STEP 1, STEP 3, STEP 4, and STEP 8 studies. Adults with a BMI of 30.0 kg/m2 or greater or 27.0 kg/m2 or greater with at least 1 weight-related comorbidity and a history of at least 1 unsuccessful attempt at losing weight were included. To be randomized, patients also had to have kept a food diary, have a Patient Health Questionnaire-9 (PHQ-9) score of less than 15 at randomization, and no suicidal behaviour or ideation before randomization.
Patients received a semaglutide SC 2.4 mg injection once weekly as an adjunct to a reduced-calorie diet and increased physical activity, versus matching placebo.
Efficacy Results
Semaglutide evoked a statistically significantly greater percentage reduction in weight from baseline to week 104 versus placebo, with a treatment difference between groups of –12.55% (95% CI, –15.33 to –9.77; P < 0.0001). The other co-primary outcome was patients achieving a 5% or greater reduction in weight from baseline to week 104, and this was achieved by 77% of semaglutide patients and 34% of placebo patients, a statistically significant difference between groups. In patients who were normoglycemic at baseline, || of semaglutide patients and ||| of placebo patients were prediabetic by the end of the trial, and in patients with prediabetes at baseline, ||| in the semaglutide group and ||| in the placebo group became normoglycemic at week 104, and || of patients in the semaglutide group and || of patients in the placebo group went on to develop diabetes by end of trial.
Harms Results
AEs were experienced by ||| of semaglutide patients and ||| of patients in the placebo group, while 8% of semaglutide patients and 12% of placebo patients had an SAE. The most common AEs in terms of semaglutide versus placebo were GI disorders such as nausea (53% of semaglutide patients versus 22% of placebo patients) and diarrhea (35% of semaglutide patients versus 24% of placebo patients). Among other notable harms for semaglutide versus placebo, ||||||||||| ||||||||| |||||||| || || |||||| ||| || ||||||||| || ||| |||||| |||| |||||||||||| || || |||||| ||||| ||||||||| |||| ||||||||| || || |||||| |||| ||| ||||||||||| ||||||||| || ||| |||||| |||| ||||| |||| || ||||| || ||||| |||||||||||||
Critical Appraisal
The limitations of this study are similar to those seen with the other STEP trials, such as the potential for unblinding to occur due to an obvious treatment effect or due to notable harms like GI AEs that occur much more frequently with semaglutide than placebo. The generalizability issues with STEP 5 mirror those of the other STEP trials — notably, the structured weight management regime that patients followed in the trial, which is unlikely to be available to patients in most areas of Canada. Despite the longer follow-up in STEP 5 (104 weeks versus 68 weeks in the other STEP trials), STEP 5 was again not designed or powered to assess the impact of semaglutide on the development of weight-related comorbidities such as cardiovascular disease.
Conclusions
Data from 4 placebo-controlled DB RCTs (the STEP 1, STEP 2, STEP 3, and STEP 4 trials) and 1 open-label RCT comparison to liraglutide (the STEP 8 trial) suggest that treatment with semaglutide injection 2.4 mg for 68 weeks produces a statistically significant weight loss compared to liraglutide and to placebo in patients with overweight or obesity, including patients with comorbid type 2 diabetes. Although the weight loss is considered clinically significant according to the clinical expert consulted by CADTH on this review, there is no clear evidence regarding whether this weight loss reduces the number of patients who may develop various weight-related comorbidities, including type 2 diabetes, cardiovascular disease, and osteoarthritis. There is some evidence of a statistically significant improvement in the physical component of HRQoL versus placebo; however, the clinical significance of this improvement is less clear because it did not meet the MID for 1 instrument (SF36) and the MID is not known for the other (IWQOL-Lite-CT). Longer-term evidence from the STEP 5 trial suggests that the weight loss observed at 104 weeks is consistent with that seen in the other trials at 68 weeks; however, it appears from all the STEP trials that weight loss with semaglutide plateaus before the end of 68 weeks of treatment, and that once patients stop semaglutide treatment, they may regain the majority of the weight lost. The most common tolerability issues with semaglutide are GI-related; these are common with this drug class. Evidence from a sponsor-submitted indirect comparison |||||||| |||| ||||||||||| ||| |||||| | ||||||| |||||| |||| |||| ||||||| ||||| |||||| |||| |||||| ||||||||| |||||||||||| ||||||||| ||| ||||||||||| ||| ||||||||.
Introduction
Disease Background
The WHO defines overweight and obesity as abnormal or excessive fat accumulation that poses a risk to health.1 A BMI of 25 kg/m2 to 30 kg/m2 is considered to be overweight and a BMI of more than 30 kg/m2 is considered obese.1 In addition to the increasingly recognized role of various biochemical factors in obesity, according to the clinical expert consulted by CADTH, multiple factors contribute to the condition, including socioeconomic factors, lack of access to healthy foods and easy access to highly palatable processed foods, and living environment. The gut microbiome may influence 1’s risk of developing obesity, as certain bacteria appear better at extracting calories from food than others, and epigenetics, genetics, and the impact of environmental factors on the endocrine system also play a role. The Canadian Health Measures Survey (2019) found that 35.5% of adults between the ages of 18 and 79 were in the overweight category and 24.3% were living with obesity2 while the Canadian Task Force on Preventive Health Care has reported that 67% of Canadian males and 54% of Canadian females were living with overweight or obesity.3
There is a wide range of comorbidities associated with obesity, including increased risk of type 2 diabetes, certain cancers, hypertension, cardiovascular disease, and gallstones, as well as psychological and psychiatric issues. For example, individuals with obesity are 1.5 times more likely than individuals of normal weight to suffer from anxiety and/or depression,5 and there is an established relationship between obesity and insomnia and obstructive sleep apnea.6 According to the WHO global burden of disease report, more than 4 million people die each year as a result of overweight or obesity, and median survival is reduced by 2 years to 4 years for those with a BMI of 30 kg/m2 to 35 kg/m2, and by 8 years to 10 years for those with a BMI of 40 kg/m2 to 50 kg/m2.1
Standards of Therapy
The approach to management of overweight and obesity is multi-pronged, and includes modification of physical activity and behaviour, in addition to medical nutrition therapy. It is estimated that a diet that provides a deficit of 600 kcal per day may be expected to produce a weight loss of 5 kg over 1 year, whereas exercise and behavioural therapy may induce a weight loss of approximately 2 kg and 8 kg, respectively, when added to a calorie-restricted diet.7 Although it is recognized that these types of interventions are least likely to cause harm, their use alone is difficult to sustain and many individuals regain weight upon discontinuation. This is where drug therapy comes into play.
According to the Canadian Adult Obesity Clinical Practice Guidelines, drug therapy for overweight or obesity is indicated only for those with a BMI of 30 kg/m2 or more, or for those with a BMI of 27 kg/m2 or more with at least 1 comorbidity. Semaglutide joins 3 other weight-loss drugs approved in Canada — orlistat, liraglutide, and the combination of naltrexone and bupropion. Liraglutide is in the same class as semaglutide, a GLP-1 agonist, while orlistat is an older drug that acts locally in the gut, inhibiting GI lipase and preventing fat absorption. Naltrexone is an opioid antagonist that has also been used to treat addiction, and bupropion is an antidepressant, a noradrenaline-dopamine reuptake inhibitor that has been used in addiction disorders, most notably smoking cessation. Although it acts locally, orlistat is known to have a number of unpleasant GI side effects, while bupropion has a number of systemic side effects and is prone to interacting with other drugs. Bariatric surgery is an option for patients with a BMI of 40 kg/m2 or greater or patients with a BMI of 35 kg/m2 or greater and at least 1 weight-related comorbidity. According to the Canadian Adult Obesity Clinical Practice Guidelines, bariatric surgery may also be an option for patients with poorly controlled type 2 diabetes and a BMI of between 30 kg/m2 and 35 kg/m2, or in patients within that BMI range for whom optimal behavioural and medical management have been insufficient to produce significant weight loss.8
Given the significant comorbidities associated with overweight and obesity, the goal of weight management therapy is not simply to reduce weight but to reduce the risk of the patient developing these comorbidities, according to the clinical expert consulted by CADTH on this review. They note that targeting a “normal” BMI of under 25 kg/m2 is neither realistic nor appropriate for many patients living with obesity; rather, the emphasis should be on improving overall health and well-being as well as these weight-related comorbidities. They also note that a 5% to 10% reduction in body weight can result in improvement in clinically relevant parameters such as blood pressure, glycemic control in diabetes, lipids, and symptoms of osteoarthritis.
Drug
Semaglutide is administered by SC injection at a dosage of 2.4 mg once weekly. It is indicated as an adjunct to a reduced-calorie diet and increased physical activity for chronic weight management in adult patients with an initial BMI of 30 kg/m2 or greater (obesity), or 27 kg/m2 or greater (overweight) in the presence of at least 1 weight-related comorbidity such as hypertension, type 2 diabetes, dyslipidemia, or obstructive sleep apnea.4 Semaglutide is also indicated for the management of type 2 diabetes and was previously reviewed by CADTH for that indication, both for a SC formulation (May 2019)9 and an oral formulation (June 2021),10 receiving a positive recommendation for each.
Semaglutide is a GLP-1 agonist. Among other actions, it is believed that this results in enhanced satiety, which reduces hunger and cravings. The sponsor has requested that semaglutide be reimbursed for patients who have a BMI of 35 kg/m2 or greater and prediabetes, which is narrower than the Health Canada indication. The drug was submitted post–Notice of Compliance and did not undergo expedited review at Health Canada.
Table 3: Key Characteristics of GLP-1 Agonists, Naltrexone-Bupropion, and Orlistat
Characteristic | GLP-1 agonists | Naltrexone and bupropion | Orlistat |
|---|---|---|---|
Mechanism of action | GLP-1 agonists are believed to enhance the body’s system for communicating a feeling of fullness from the gut to the brain. Additionally, they delay gastric emptying, which also enhances the feeling of fullness. | Naltrexone is an opioid antagonist and bupropion is a noradrenaline-dopamine reuptake inhibitor. Both drugs have indications in managing addictions and are believed to impact the appetite regulatory centre in the hypothalamus and the dopamine reward pathway; however, their precise mechanism in weight management is unknown. | Reversible GI lipase inhibitor. This inhibits fat absorption. |
Indicationa | Semaglutide: Indicated as an adjunct to a reduced-calorie diet and increased physical activity for chronic weight management in adult patients with an initial BMI of:
Liraglutide Indicated as an adjunct to a reduced-calorie diet and increased physical activity for chronic weight management in adult patients with an initial BMI of:
| Indicated as an adjunct to a reduced-calorie diet and increased physical activity for chronic weight management in adults with an initial BMI of:
| When used in conjunction with a mildly hypocaloric diet, is indicated for:
These indications apply to patients living with obesity (i.e., BMI ≥ 30 kg/m2) or with overweight (i.e., with BMI ≥ 27 kg/m2) in the presence of other risk factors (e.g., hypertension, T2DM, dyslipidemia, excess visceral fat). |
Route of administration | Subcutaneous | Oral | Oral |
Recommended dosage | Semaglutide: The therapeutic and maintenance dosage of 2.4 mg semaglutide once weekly is reached by starting with a dose of 0.25 mg and then following a dose escalation regimen, with dose increases every 4 weeks (to dosages of 0.5 mg per week, 1 mg per week, 1.7 mg per week, and 2.4 mg per week) until the therapeutic/maintenance dosage of 2.4 mg once weekly is reached after 16 weeks. Liraglutide: In adults with an initial BMI of 27 kg/m2 or greater, the recommended daily maintenance dosage is 3 mg per day. Daily doses higher than 3 mg are not recommended. At initiation, doses should be escalated in 0.6 mg increments every week to reduce the likelihood of GI symptoms. Treatment should be discontinued after 12 weeks at the maintenance dosage if the patient has not lost at least 5% of their initial body weight. | Two 8 mg naltrexone hydrochloride and 90 mg bupropion hydrochloride extended-release tablets taken twice daily for a total daily dose of 32 mg and 360 mg. At initiation, dosage should be escalated as follows. Week 1: 1 tablet in the a.m. Week 2: 1 tablet in the a.m. and p.m. each. Week 3: 2 tablets in the a.m. and 1 tablet in the p.m. Week 4 onwards: 2 tablets in the a.m. and p.m. each. The maximum recommended daily dosage is 1 tablet in the a.m. and p.m. each for patients with moderate to severe renal impairment. Treatment should be discontinued after 12 weeks at the maintenance dosage if the patient has not lost at least 5% of their initial body weight. | One 120 mg capsule 3 times daily with each main meal |
Serious adverse effects or safety issues | Semaglutide and liraglutide Contraindicated in patients who:
Serious warning:
Warnings:
Semaglutide
| Contraindicated in:
Warnings based on experience with bupropion hydrochloride:
| Contraindicated in patients with:
Warnings:
|
BMI = body mass index; GI = gastrointestinal; GLP-1 = glucagon-like peptide 1; T2DM = type 2 diabetes mellitus.
aHealth Canada–approved indication.
Source: Product monographs for semaglutide (2020),4 liraglutide (2021),11 naltrexone-bupropion (2018),12 and orlistat (2017).13
Stakeholder Perspectives
Patient Group Input
This section was prepared by CADTH staff based on the input provided by patient groups. The full patient group submissions are included in the Stakeholder Input section at the end of this report.
A total of 5 patient groups provided 4 submissions (GI Society; Obesity Canada and the Canadian Liver Foundation, which provided a joint input; Diabetes Canada; and Obesity Matters). The GI Society is a national charity that focuses on providing Canadians with trusted, commercial-free, medically sound information on gut and liver diseases and disorders, including obesity. Data for its submission came from a variety of sources, including contact with patients and patient caregivers, the results of published studies, and a survey conducted from October 6, 2020, to January 10, 2021, open to individuals who had experienced obesity. The survey was open internationally, but the majority of the 2,050 (96%) respondents were from Canada. Obesity Canada and the Canadian Liver Foundation provided a joint input. Obesity Canada is Canada’s leading obesity registered charity association for health professionals, researchers, trainees, students, policy-makers, and Canadians living with obesity. The Canadian Liver Foundation is dedicated to supporting education and research into all forms of liver disease. Data for the joint submission was based on a survey conducted from February to March 2022, which was distributed throughout Obesity Canada and Canadian Liver Foundation networks, on social media, and via newsletter mailing lists as well as within Obesity Canada’s online patient support community. There was a total of 109 responses from Canadians living with obesity. More than half of respondents (66%) indicated past or present experience with prescription medications for obesity management, with 57% reporting experience specifically with semaglutide. Diabetes Canada is a national health charity representing the millions of Canadians who are affected by diabetes and leads the fight against diabetes by helping people live healthy lives, preventing the onset and consequences of diabetes, and discovering a cure. Its submission contains patient input from an online survey conducted in March 2022. A total of 29 people in Canada participated in the survey; 3 identified as living with prediabetes and 26 identified as living with type 2 diabetes. Among those who answered the question (n = 21), 19 (90%) respondents said they identify as living with overweight or obesity. Two people said they have experience with the drug under review. Obesity Matters is a group of people with common experiences and concerns. The goal of Obesity Matters is to provide an opportunity for communities across Canada to share personal feelings, experiences, and coping strategies, and offer support so they can take action and seek the help they deserve. The input from Obesity Matters was based on a survey conducted from March 2 to 15, 2022, with 104 respondents. A video was also provided in Obesity Matters’ input.
The 4 patient group inputs reported that overweight and obesity affect many areas of life and patients usually present with various comorbid conditions, such as arthritis, hypertension, sleep apnea, gastroesophageal reflux disease, irritable bowel syndrome, high cholesterol, diabetes, fatty liver disease, asthma, osteoarthritis, infertility, cancers, and mental health issues. Overweight and obesity lead to a multitude of negative impacts, including pain and impacts on mobility, regular activities, self image, and patients’ families and relationships. A common theme in the submissions was the stigma associated with the disease, with patients experiencing discrimination from physicians and employers. Regarding current management options, there are very few medication options, and those that are available do not have public or full private coverage. In addition, patients indicated that these drugs have side effects that include nausea, diarrhea, constipation, and headaches. Patients considered it important for them to have a medication for weight management with long-term effectiveness and fewer side effects that is also affordable and easy to administer. Key outcomes identified by the patient advocacy groups as important to patients with overweight or obesity were weight loss, reducing weight-related comorbidity, and improving HRQoL.
In the input by the GI Society, those who had tried semaglutide found it easier to adhere to lifestyle modifications while taking that medication. In the input by Diabetes Canada, both patients said their ability to maintain or lose weight and meet target blood sugar levels was “much better” on semaglutide injection 2.4 mg than before, though 1 patient indicated improved GI side effects on semaglutide injection while the other patient indicated “much worse” GI side effects. One patient from the Obesity Canada and the Canadian Liver Foundation input stated that semaglutide had been very effective and described increased energy and reduction in medication needed to control blood pressure and cholesterol.
Clinician Input
Input From Clinical Experts Consulted by CADTH
All CADTH review teams include at least 1 clinical specialist with expertise regarding the diagnosis and management of the condition for which the drug is indicated. Clinical experts are a critical part of the review team and are involved in all phases of the review process (e.g., providing guidance on the development of the review protocol, assisting in the critical appraisal of clinical evidence, interpreting the clinical relevance of the results, providing guidance on the potential place in therapy). The following input was provided by a clinical specialist with expertise in weight management.
Unmet Needs
There are 4 approved drugs for weight loss in Canada. However, access to these drugs is limited as none is covered by provincial drug plans. Access to bariatric surgery is very limited and differs depending on where the patient resides; there are also patients who are unwilling to undergo this invasive procedure. Access to lifestyle programs is also limited and, in many cases, patients have to pay out of pocket for weight-loss programs that are not always evidence-based or even to access the services of a registered dietitian.
Those patients who pursue lifestyle changes in their effort to lose weight can expect to lose 3% to 5% of their total body weight; however, there is a high risk of regaining the weight after 1 year to 2 years. This regaining of weight is also observed when drugs that are used as a means for weight loss are discontinued. Bariatric surgery remains the only intervention that induces a significant and consistent weight loss that is typically maintained for 8 years to 10 years post surgery.
Current therapies do not fully address the multifaceted nature of obesity as they are only able to target a few of the known pathways involved in managing weight.
Place in Therapy
There are a variety of stages of a patient’s weight-loss journey where semaglutide could be used, including first-line treatment, in combination with structured lifestyle changes. It may also be used in patients who have undergone bariatric surgery, where it would be third-line treatment, behind lifestyle changes (required before being considered for bariatric surgery) and surgery. Given the significant efficacy advantage of semaglutide over liraglutide, the clinical expert saw semaglutide replacing liraglutide completely. The clinical expert also noted that they are more comfortable prescribing GLP-1 agonists than naltrexone-bupropion as the latter has more drug interactions and side effects, and because a cardiovascular safety study was never completed for this combination.
The clinical expert also noted that given that weight reductions of 20% or greater are not uncommon with semaglutide, they are increasingly seeing bariatric surgeons recommending patients try semaglutide first as a potential alternative to bariatric surgery. This was not something that was ever considered with the other weight-loss drugs on the market.
Patient Population
The majority of patients who can tolerate semaglutide would be expected to have at least some weight loss from taking the drug, and according to the clinical expert, patients who report significant hunger and difficulty reducing portion sizes tend to be the patients who respond the most to the drug, although some weight loss is also seen in patients who do not report significant hunger or overeating. The clinical expert, therefore, believes that any patient living with obesity would be a potential candidate for semaglutide, although they avoid using it in patients with a history of certain types of pancreatitis and in the rare patient who has a personal history or family history of medullary thyroid carcinoma.
The patients most in need of intervention with weight-loss drugs are those who are experiencing weight-related comorbidities such as hypertension, type 2 diabetes or prediabetes, nonalcoholic fatty liver disease, polycystic ovary disease, infertility, osteoarthritis, and so forth. There are also patients who do not suffer from any of these comorbidities but who still feel very distressed and limited by higher body weight who may benefit from drug therapy.
Patients who have no weight-related comorbidities and who remain active and living a full life despite a BMI of more than 30 kg/m2 may be less likely to benefit from semaglutide. Using the Edmonton Obesity Staging System, a patient who is stage I to stage III would be most likely to benefit from drug therapy.
Diagnosis of obesity is not that difficult and can be performed in the primary care setting, as primary care physicians are very well versed in evaluating and screening for weight-related comorbidities.
There is no reliable way to predict which patients would respond best to semaglutide or other weight-loss drugs. With weight-loss medications, there is typically a trial period of 12 weeks to 16 weeks at the maximum tolerated dose of the medication, and if the patient’s weight is unchanged or does not reduce by at least 5% of total body weight, that is the generally accepted definition of a nonresponse.
Assessing Response to Treatment
There are numerous weight-related comorbidities and improvement in any of these comorbidities should be assessed. Important outcomes that the clinical expert considers clinically meaningful for their patients include the following:
improved survival
improved hemoglobin A1C by at least 0.5%
improved blood pressure
improvement/normalization of liver enzymes
improvement in lipid profile (reduced triglycerides and low-density lipoprotein, in particular)
the patient reporting reduced hunger or reduced food cravings and feeling more in control of their food intake
reduced risk of weight-related cancers (e.g., endometrial, breast)
the patient reporting improved mobility or ability to perform daily activities
the resolution of prediabetes with glucose parameters returning to the “normal” range
a total body weight loss of 5% or greater
a plateau in weight regain or reversal of weight regain in a patient who has undergone bariatric surgery.
Discontinuing Treatment
The clinical expert identified the development of gallstones as 1 situation where they have had to discontinue GLP-1 agonists, although they noted that GLP-1 agonists could be re-initiated after surgical removal of the gallbladder (cholecystectomy). The GLP-1 agonists would also likely be stopped in patients who develop acute pancreatitis or in those who are unable to tolerate the drug (due to nausea, for example), although most patients can tolerate a lower dose and still obtain some weight-loss benefit. Patients with more severe GI side effects can also often tolerate the medication better when it is uptitrated more slowly than the typical titration protocol.
The drug would also likely be stopped in patients who continue to gain weight or in those who are not experiencing any weight loss on the drug.
The issue of whether to continue or stop semaglutide immediately after bariatric surgery has not been well studied and there is likely a difference in practice between different surgical centres. It is common to use semaglutide in the context of weight regain after bariatric surgery.
Prescribing Conditions
The clinical expert believed that specialist intervention would only be required for more complex cases where patients have undergone bariatric surgery and are experiencing weight regain; otherwise, primary care physicians should easily be able to manage patients on semaglutide. Monitoring factors would include weight as well as other metabolic parameters that are relevant to the patient’s pre-existing comorbidities, such as lipid profile, blood pressure, and glucose parameters. In addition, patients should be encouraged to engage in lifestyle modifications and the prescribing clinician should periodically assess patient engagement in these behaviours and provide support to patients to engage in further changes.
Clinician Group Input
This section was prepared by CADTH staff based on the input provided by clinician groups. The full clinician group submissions are included in the Stakeholder Input section at the end of this report.
Four clinician groups provided input. These groups were the Calgary Weight Management Centre, Centre de Médecine Métabolique de Lanaudière, Obesity Canada and the Canadian Association of Bariatric Physicians and Surgeons Surgeons — the latter 2 of which provided a joint input. The input from the clinician groups was consistent with that provided by the clinical expert consulted by CADTH on this review. The clinician groups believed that semaglutide is likely to replace liraglutide and naltrexone-bupropion for many patients.
Drug Program Input
The drug programs provide input on each drug being reviewed through CADTH’s reimbursement review processes by identifying issues that may impact their ability to implement a recommendation. The implementation questions and corresponding responses from the clinical expert consulted by CADTH are summarized in Table 4.
Table 4: Summary of Drug Plan Input and Clinical Expert Response
Drug program implementation questions | Clinical expert response |
|---|---|
Considerations for initiation of therapy | |
The requested indication differs from the Health Canada indication. How is prediabetes established? Is there evidence to support this criterion? The requested indication is as an adjunct to a reduced-calorie diet and physical activity. How is adherence to diet and exercise monitored? | The clinical expert noted that although there is an established definition of prediabetes, the definitions differ slightly between the DC and ADA. The DC defines prediabetes as a hemoglobin A1C of 6.0% to 6.4% (ADA uses 5.7% to 6.4%), or an FPG of 6.1 mmol/L to 6.9 mmol/L (also called impaired fasting glucose), or a 2-hour plasma glucose result after a 75 g oral glucose challenge of 7.8 mmol/L to 11.0 mmol/L (also called impaired glucose tolerance). Adherence to diet and exercise is not reliably monitored in Canada unless the patient is part of a structured weight management program, and relatively few of those exist in this country. |
How would treatment failure be determined? Would patients who drop below a BMI of 35 kg/m2 be eligible to continue treatment? Would patients be eligible for re-treatment? | Patients who are not able to lose at least 5% of their body weight or cannot tolerate the drug would typically be seen as treatment failures. The clinical expert believed that patients who drop below a BMI of 35 kg/m2 should definitely be continued on treatment, as they are highly likely to regain the weight they lost if they were to discontinue therapy. There are examples where patients would be re-treated. For example, a patient may have been disappointed with the results in a previous trial of semaglutide but would benefit from better instruction on how to use the drug. There may be patients who develop gallstones while on semaglutide and have the drug restarted once their gallbladder has been removed. |
Considerations for continuation or renewal of therapy | |
How is response to therapy assessed? | Weight is easily monitored. A number of other metabolic parameters/biomarkers that are associated with the comorbidities of overweight/obesity would also be monitored, including glycemic status, blood pressure, lipids, and so forth. |
Considerations for discontinuation of therapy | |
What parameters would be used to define loss of response to therapy? | If the patient begins to gain weight, that would indicate loss of response. |
Generalizability | |
As mentioned previously, studies include patients with comorbid weight-related illness (such as hypertension and diabetes); however, the requested indication is prediabetes. What is the impact? | The STEP trials did not conduct any preplanned subgroup analyses that would specifically address the population they identified in their listing request; however, a post hoc subgroup analysis was provided for the STEP 1 trial. There were patients in the STEP trials who could be categorized as prediabetic. The ADA definition of prediabetes, which allows for a wider range of hemoglobin A1C and is used in the STEP trials, likely includes a significantly larger number of patients than the DC definition of prediabetes. |
Care provision issues | |
There may be challenges with monitoring the adherence to and impact of diet and exercise changes. | For CDEC consideration. |
System and economic issues | |
The projected patient populations for semaglutide in the base case were as follows:
This base-case budget impact analysis predicts that adding semaglutide to the pan-Canadian public drug plans for chronic weight management will result in incremental costs of $164 million, $350 million, and $550 million in year 1, year 2, and year 3, respectively, for a total 3-year cost of $1,064 million in the indicated population and incremental costs of $27 million, $57 million, and $90 million in year 1, year 2, and year 3, respectively, for a total 3-year cost of $174 million in the requested reimbursement criteria population. | For CDEC consideration. |
ADA = American Diabetes Association; BMI = body mass index; CDEC = CADTH Canadian Drug Expert Committee; DC = Diabetes Canada; FPG = fasting plasma glucose.
Clinical Evidence
The clinical evidence included in the review of semaglutide is presented in 3 sections. The first section, the systematic review, includes pivotal studies provided in the sponsor’s submission to CADTH and Health Canada, as well as those studies that were selected according to an a priori protocol. The second section includes indirect evidence from the sponsor and indirect evidence selected from the literature that met the selection criteria specified in the review. The third section includes sponsor-submitted long-term extension studies and additional relevant studies that were considered to address important gaps in the evidence included in the systematic review.
Systematic Review (Pivotal and Protocol Selected Studies)
Objectives
To perform a systematic review of the beneficial and harmful effects of semaglutide 2.4 mg for SC injection as an adjunct to a reduced caloric diet and increased physical activity for chronic weight management in adult patients
Methods
Studies selected for inclusion in the systematic review included pivotal studies provided in the sponsor’s submission to CADTH and Health Canada, as well as those meeting the selection criteria presented in Table 5. Outcomes included in the CADTH review protocol reflect outcomes considered to be important to patients, clinicians, and drug plans.
Table 5: Inclusion Criteria for the Systematic Review
Criteria | Description |
|---|---|
Patient population | Adults with an initial BMI of 30 kg/m2 or greater (obesity), or 27 kg/m2 or greater (overweight) in the presence of at least 1 weight-related comorbidity such as hypertension, T2DM, dyslipidemia, or OSA Subgroups:
|
Intervention | Semaglutide 2.4 mg SC injection once weekly. Patients begin with a 16-week dose escalation, beginning with 0.25 mg weekly, then 0.5 mg weekly, 1 mg weekly, and 1.7 mg weekly, for 4 weeks each, before reaching the maintenance dosage of 2.4 mg once weekly. |
Comparators | A reduced-calorie diet and increased physical activity with any of the following:
|
Outcomes | Efficacy outcomes
Harms outcomes
|
Study design | Published and unpublished phase III and phase IV RCTs |
AE = adverse event; BMI = body mass index; CV = cardiovascular; GERD = gastroesophageal reflux disease; GI = gastrointestinal; HRQoL = health-related quality of life; NAFLD = nonalcoholic fatty liver disease; OA = osteoarthritis; OSA = obstructive sleep apnea; PCOS = polycystic ovary syndrome; RCT = randomized controlled trial; SAE = serious adverse event; SC = subcutaneous; T2DM = type 2 diabetes mellitus; TIA = transient ischemic attack; vs. = vs.; WDAE = withdrawal due to adverse event.
The literature search was performed by an information specialist using a peer-reviewed search strategy according to the PRESS Peer Review of Electronic Search Strategies checklist.14
Published literature was identified by searching the following bibliographic databases: MEDLINE All (1946—) via Ovid and Embase (1974—) via Ovid. All Ovid searches were run simultaneously as a multi-file search. Duplicates were removed using Ovid deduplication for multi-file searches, followed by manual deduplication in Endnote. The search strategy comprised both controlled vocabulary, such as the US National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. The main search concepts were Wegovy (semaglutide) and weight management. Clinical trials registries were searched: the US National Institutes of Health’s ClinicalTrials.gov, the WHO’s International Clinical Trials Registry Platform search portal, Health Canada’s Clinical Trials Database, and the European Union Clinical Trials Register.
No filters were applied to limit the retrieval by study type. Retrieval was not limited by publication date or by language. Conference abstracts were excluded from the search results. Refer to Appendix 1 for the detailed search strategies.
The initial search was completed on April 5, 2022. Regular alerts updated the search until the meeting of the CADTH Canadian Drug Expert Committee on July 27, 2022.
Grey literature (literature that is not commercially published) was identified by searching relevant websites from the Grey Matters: A Practical Tool For Searching Health-Related Grey Literature checklist.15 Included in this search were the websites of regulatory agencies (the US FDA and European Medicines Agency). Google was used to search for additional internet-based materials. Refer to Appendix 1 for more information on the grey literature search strategy.
These searches were supplemented through contacts with appropriate experts. In addition, the sponsor of the drug was contacted for information regarding unpublished studies.
Two CADTH clinical reviewers independently selected studies for inclusion in the review based on titles and abstracts, according to the predetermined protocol. Full-text articles of all citations considered potentially relevant by at least 1 reviewer were acquired. Reviewers independently made the final selection of studies to be included in the review, and differences were resolved through discussion.
Findings From the Literature
A total of 5 studies were identified from the literature for inclusion in the systematic review (Figure 1). The included studies are summarized in Table 6. A list of excluded studies is presented in Appendix 2.
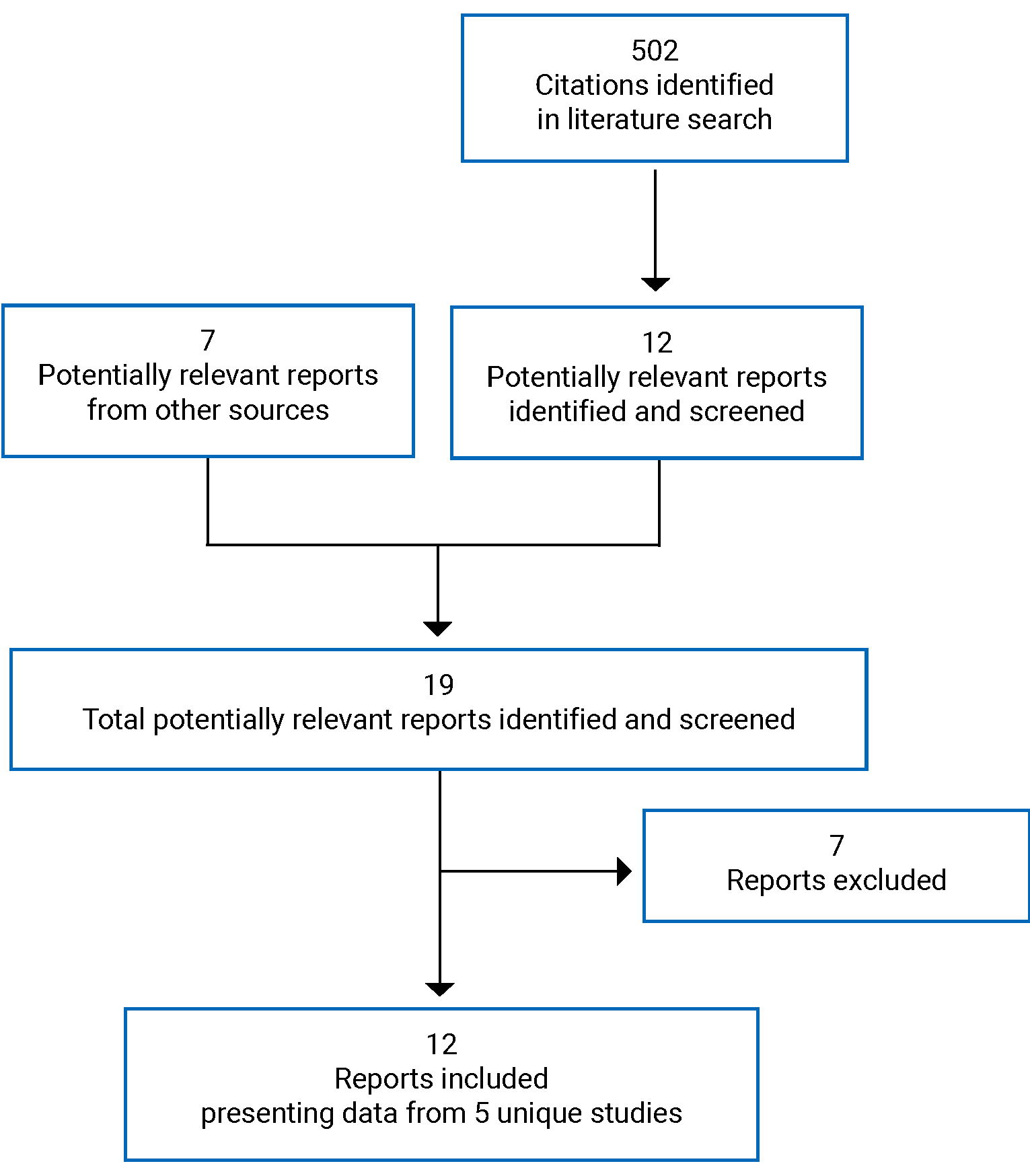
Table 6: Details of the STEP 1 Study (Any Weight-Related Comorbidity)
Factor | STEP 1 study | |
|---|---|---|
Design and populations | ||
Study design | Double-blind RCT, phase IIIa | |
Locations | 129 sites, 16 countries (Canada, the US, the European Union, Mexico, South America, India, Japan, and Taiwan) | |
Study period | June 4, 2018, to April 19, 2020 | |
Randomized (N) | N = 1,961 | |
Inclusion criteria |
Randomization criteria:
| |
Exclusion criteria |
| |
Drugs | ||
Intervention | Semaglutide 2.4 mg SC injection once weekly as an adjunct to a reduced-calorie diet and increased physical activity | |
Comparator(s) | Placebo once weekly as an adjunct to a reduced-calorie diet and increased physical activity | |
Phase | ||
Duration | ||
Screening | 1 week | |
Double-blind | 68 weeks | |
Follow-up | 7 weeks | |
Outcomes | ||
Primary end point | Co-primary:
| |
Other end points | Confirmatorya and supportive secondary end points
Supportive secondary end points: Safety end points
| |
Notes | ||
Publications | Wilding et al. (2021)16 | |
BMI = body mass index; C-SSRS = Columbia–Suicide Severity Rating Scale; DEXA = dual energy X-ray absorptiometry; FPG = fasting plasma glucose; ICIQ-UI SF = International Consultation on Incontinence Questionnaire-Urinary Incontinence Short Form; IWQOL-Lite-CT = Impact of Weight on Quality of Life–Lite Clinical Trials Version; PHQ-9 = Patient Health Questionnaire-9; RCT = randomized controlled trial; SAE = serious adverse event; SC = subcutaneous; SF-36 = Short Form (36) Health Survey; SPS-6 = Stanford Presenteeism Scale-6; TEAE = treatment-emergent adverse event.
aConfirmatory end points were controlled for multiplicity.
Source: Clinical Study Report for STEP 1 (2020),17 Health Canada reviewer’s report (2022),18 and sponsor’s submission (2022).19
Table 7: Details of the STEP 2 Study (Type 2 Diabetes)
Factor | STEP 2 study |
|---|---|
Designs and populations | |
Study design | Double-blind RCT, phase IIIa |
Locations | 149 sites, 12 countries (Canada, the US, European Union, South America, India, Japan, South Africa, and the United Arab Emirates) |
Study period | June 4, 2018, to May 1, 2020 |
Randomized (N) | N = 1,210 |
Inclusion criteria |
Randomization criteria:
|
Exclusion criteria |
|
Drugs | |
Intervention | Semaglutide 2.4 mg SC injection once weekly as an adjunct to a reduced-calorie diet and increased physical activity |
Comparator(s) | Placebo once weekly as an adjunct to a reduced-calorie diet and increased physical activity |
Phase | |
Duration | |
Screening | 1 week |
Double-blind | 68 weeks |
Follow-up | 7 weeks |
Outcomes | |
Primary end point | Co-primary:
|
Other end points | Confirmatorya and supportive secondary end points
Exploratory
Change from baseline at week 0 to week 68 in:
Patients who, after 68 weeks, achieve (yes/no) the following in:
Supportive secondary end points: Safety end points
|
Notes | |
Publications | Davies et al. (2021)20 |
6MWT = six-minute walk test; BMI = body mass index; CKD-EPI = Chronic Kidney Disease Epidemiology Collaboration; C-SSRS = Columbia–Suicide Severity Rating Scale; FPG = fasting plasma glucose; IWQOL-Lite-CT = Impact of Weight on Quality of Life–Lite Clinical Trials Version; KDIGO = Kidney Disease: Improving Global Outcomes; OAD = oral antidiabetic drug; PHQ-9 = Patient Health Questionnaire-9; RCT = randomized controlled trial; SAE = serious adverse event; SC = subcutaneous; SF-36 = Short Form (36) Health Survey; SU = sulfonylurea; TEAE = treatment-emergent adverse event; WPAI:SHP = Work Productivity and Activity Impairment Questionnaire: Specific Health Problem V2.0; UACR = urine albumin to creatinine ratio.
aConfirmatory end points were controlled for multiplicity.
Source: Clinical Study Report for STEP 2 (2020),21 Health Canada reviewer’s report (2022),18 and sponsor’s submission (2022).19
Table 8: Details of the STEP 3 Study (Concomitant Intensive Behavioural Therapy)
Factor | STEP 3 study | |
|---|---|---|
Designs and populations | ||
Study design | Double-blind RCT, phase IIIa | |
Locations | 41 sites in the US | |
Study period | August 1, 2018, to April 28, 2020 | |
Randomized (N) | N = 611 | |
Inclusion criteria |
Randomization criteria:
| |
Exclusion criteria |
| |
Drugs | ||
Intervention | Semaglutide 2.4 mg SC injection once weekly as an adjunct to intensive behavioural therapy and an initial 8-week low-calorie diet | |
Comparator(s) | Placebo once weekly as an adjunct to intensive behavioural therapy and an initial 8-week low-calorie diet | |
Phase | ||
Duration | ||
Screening | 1 week | |
Double-blind | 68 weeks | |
Follow-up | 7 weeks | |
Outcomes | ||
Primary end point | Co-primary:
| |
Other end points | Confirmatorya and supportive secondary end points
| |
Notes | ||
Publications | Wadden et al. (2021)22 | |
BMI = body mass index; C-SSRS = Columbia–Suicide Severity Rating Scale; FPG = fasting plasma glucose; IWQOL-Lite-CT = Impact of Weight on Quality of Life–Lite Clinical Trials Version; PHQ-9 = Patient Health Questionnaire-9; RCT = randomized controlled trial; SAE = serious adverse event; SC = subcutaneous; SF-36 = Short Form (36) Health Survey; TEAE = treatment-emergent adverse event; WPAI:SHP = Workplace Productivity and Impairment Questionnaire: Specific Health Problem; WRSSM = Weight-Related Sign and Symptom Measure.
aConfirmatory end points were controlled for multiplicity.
Source: Clinical Study Report for STEP 3 (2020),23 Health Canada reviewer’s report (2022),18 and sponsor’s submission (2022).19
Table 9: Details of the STEP 4 Study (Dose Escalation and Randomized Withdrawal)
Factor | STEP 4 study |
|---|---|
Designs and populations | |
Study design | Double-blind RCT, phase IIIa |
Locations | 73 sites, 10 countries (the US, Europe, South Africa, and Israel) |
Study period | June 4, 2018, to March 20, 2020 |
Randomized (N) | N = 902 |
Inclusion criteria |
Run-in criteria:
Randomization criteria:
|
Exclusion criteria |
|
Drugs | |
Intervention | Semaglutide 2.4 mg SC injection once weekly as an adjunct to a reduced-calorie diet and increased physical activity |
Comparator(s) | Placebo once weekly as an adjunct to a reduced-calorie diet and increased physical activity |
Phase | |
Duration | |
Screening | 1 week |
Run-in | 20 weeks (including 16 weeks dose escalation) |
Double-blind | 48 weeks |
Follow-up | 7 weeks |
Outcomes | |
Primary end point | Percentage change from randomization (week 20) to week 68 in body weight |
Other end points | Confirmatorya and supportive secondary end points
Exploratory
Supportive secondary end points: Safety end points
|
Notes | |
Publications | Rubino et al. (2021)24 |
BMI = body mass index; C-SSRS = Columbia–Suicide Severity Rating Scale; FPG = fasting plasma glucose; PHQ-9 = Patient Health Questionnaire-9; RCT = randomized controlled trial; SAE = serious adverse event; SC = subcutaneous; SF-36 = Short Form (36) Health Survey; SPS-6 = Stanford Presenteeism Scale-6; TEAE = treatment-emergent adverse event; WRSSM = weight-related sign and symptom measure.
aConfirmatory end points were controlled for multiplicity.
Source: Clinical Study Report for STEP 4 (2020),25 Health Canada reviewer’s report (2022),18 and sponsor’s submission (2022).19
Table 10: Details of the STEP 8 Study (Comparison With Liraglutide)
Factor | STEP 8 study |
|---|---|
Designs and populations | |
Study design | OL RCT, phase IIIb |
Locations | 19 sites in the US |
Study period | September 11, 2019, to May 11, 2021 |
Randomized (N) | N = 338 |
Inclusion criteria |
|
Exclusion criteria |
|
Drugs | |
Intervention | Semaglutide 2.4 mg SC injection once weekly as an adjunct to a reduced-calorie diet and increased physical activity |
Comparator(s) | Liraglutide 3.0 mg SC injection once daily as an adjunct to a reduced-calorie diet and increased physical activity Placebo matched to either semaglutide or liraglutide as an adjunct to a reduced-calorie diet and increased physical activity |
Phase | |
Duration | |
Screening | 1 week |
Double-blind | 68 weeks |
Follow-up | 7 weeks |
Outcomes | |
Primary end point |
|
Other end points | Confirmatory secondary Proportion of patients with body weight reduction from baseline to week 68 of:
Supportive secondary
Exploratory
|
Notes | |
Publications | Rubino et al. (2022)26 |
BMI = body mass index; FPG = fasting plasma glucose; OL = open-label; RCT = randomized controlled trial; SAE = serious adverse event; SC = subcutaneous; TEAE = treatment-emergent adverse event; vs. = versus.
Source: Clinical Study Report for STEP 8 (2021),27 Health Canada reviewer’s report (2022),18 and sponsor’s submission (2022).19
Description of Studies
Four pivotal multinational sponsor-funded DB RCTs and 1 open-label RCT were included in this review. The open-label RCT, STEP 8, compared semaglutide to liraglutide while the remaining studies, STEP 1 to STEP 4, compared semaglutide to placebo. All studies were 68 weeks in duration. Randomization was conducted centrally using an interactive web response system in all studies.
The objective of the STEP 1 study was to compare the effect of a semaglutide SC 2.4 mg injection once weekly versus placebo as an adjunct to a reduced-calorie diet and increased physical activity in patients with overweight or obesity on body weight (primary objective), and cardiovascular risk factors, clinical outcome assessment, glucose metabolism, and other factors related to body weight (secondary objectives). This was a DB RCT that randomized 1,961 patients with overweight or obesity, 2:1, to semaglutide 2.4 mg or placebo. No stratification was mentioned. Enrolment occurred at 129 sites in 16 countries, including Canada. The study began with a screening visit where inclusion and exclusion criteria were assessed and patient mental health was evaluated, followed by a randomization visit; then, visit 3 to visit 24 during the treatment period were clinical or phone visits. Visits occurred every 2 weeks during the dose escalation period up to week 20, then every 4 weeks during the maintenance period until week 68. Some assessments, such as assessment of diet and physical activity and body weight, occurred every second visit while other assessments, such as HRQoL, occurred less frequently. A final follow-up visit was conducted at week 75. Patients who withdrew consent during the study were asked if they were willing to undergo a final “end of treatment” visit, where final assessments were performed. Patients who discontinued the trial product were asked to continue with scheduled visits and assessments. The data cut-off date was May 11, 2020, and the date of publication of the Clinical Study Report was August 17, 2020.
The objectives of the STEP 2 study were to compare the effect of a semaglutide SC 2.4 mg injection once weekly versus placebo as an adjunct to a reduced-calorie diet and increased physical activity in patients with overweight or obesity and type 2 diabetes on body weight (primary objective) and cardiovascular risk factors, clinical outcome assessment, and glycemic control (secondary objectives). This DB RCT randomized 1,210 patients with overweight or obesity and type 2 diabetes, 1:1:1, to either semaglutide 1.0 mg, semaglutide 2.4 mg, or placebo, once weekly. Randomization was stratified according to background diabetes treatment: diet and physical activity only, or treatment with metformin or SGLT-2 inhibitor monotherapy, or sulfonylurea or glitazone monotherapy or combination therapy with up to 3 oral antidiabetic drugs (OADs) (metformin, sulfonylureas, SGLT-2 inhibitors, or glitazone). After stratification for background diabetes treatment, patients were further stratified by hemoglobin A1C at screening (lower than 8.5% or 8.5% and higher). It is only the semaglutide 2.4 mg weekly dosage that is of interest for this review, as it is the Health Canada–approved dose for this indication. Enrolment occurred at 149 sites in 12 countries, including Canada. Visits and assessments occurred at the same intervals as in STEP 1. Patients who withdrew consent or discontinued treatment were handled in a similar manner to the STEP 1 study. The data cut-off date was May 20, 2020, and the date of publication of the Clinical Study Report was August 28, 2020.
The objectives of the STEP 3 study were to compare the effect of a semaglutide SC 2.4 mg injection once weekly versus placebo as an adjunct to intensive behavioural therapy (IBT) in patients with overweight or obesity on body weight (primary objective), and cardiovascular risk factors, clinical outcome assessment, and glucose metabolism (secondary objectives). This DB RCT randomized 611 patients with overweight or obesity, 2:1, to either semaglutide 2.4 mg weekly or matched placebo. No stratification was mentioned. Enrolment occurred at 41 sites in the US. STEP 3 had more frequent study visits — weekly during the 16-week dose escalation period, every 2 weeks through week 24, then every 4 weeks until the end of the maintenance period. Assessment of body weight occurred at every visit, while assessment of other outcomes like HRQoL occurred 7 times over the course of the study. Patients who withdrew consent or discontinued treatment were handled in a similar manner to the STEP 1 and STEP 2 studies. The data cut-off date was May 19, 2020, and the date of publication of the Clinical Study Report was August 20, 2020.
The STEP 4 study had a different design feature in that it had a 20-week run-in period where all patients were titrated to the target dosage of semaglutide 2.4 mg once weekly. All patients started on semaglutide 0.25 mg once weekly, then increased their dose every 4 weeks to the maintenance dosage of 2.4 mg once weekly by week 16 (as per the Health Canada–approved dosage regimen), and they continued on this dosage until randomization occurred at week 20. Of the 902 patients who entered the run-in, 99 (11%) patients did not end up being randomized into the study, with the most common reason being an AE (5%). The primary objective of STEP 4 was to compare the effect of a semaglutide SC 2.4 mg injection once weekly versus placebo as an adjunct to a reduced-calorie diet and increased physical activity in patients with overweight or obesity who have reached the target dosage of semaglutide during the run-in period on body weight. There were multiple secondary objectives, divided up with respect to whether they were efficacy-related from randomization (week 20) to week 68 (cardiovascular risk factors, clinical outcome assessment, and glucose metabolism), efficacy-related from week 0 to week 68 (effects on body weight in patients who achieved the target dose during the run-in period), and safety and tolerability from week 0 to week 20 and from week 20 to week 75. This DB RCT randomized 803 patients in a 1:1 manner to either semaglutide 2.4 mg or placebo, and patients were enrolled at 73 sites across the US, Europe, South Africa, and Israel. No Canadian sites were identified. No stratification was mentioned. After the 20-week run-in, visits were conducted every 4 weeks from week 20 until end of treatment (week 68), followed by an end-of-trial visit at week 75. Body weight and waist circumference were assessed at every second visit while other outcomes like HRQoL were assessed 3 times during the run-in and 4 times during the treatment period. Patients who withdrew consent or discontinued treatment were handled in a similar manner to STEP 1 and STEP 2. The data cut-off date was April 16, 2020, and the date of publication of the Clinical Study Report was July 16, 2020.
STEP 8 was the only study that featured an active control. The primary objective of STEP 8 was to demonstrate the superiority of semaglutide 2.4 mg SC injection weekly versus liraglutide 3.0 mg SC injection daily as an adjunct to a reduced-calorie diet and increased physical activity in patients with obesity, or with overweight and at least 1 weight-related comorbidity on body weight. The trial also contained a placebo group, and the semaglutide and liraglutide groups were blinded versus placebo but not versus each other, as semaglutide is administered once weekly and liraglutide is administered daily. Patients were randomized 3:1:3:1 to semaglutide, matched placebo, liraglutide, matched placebo, and the study enrolled patients at 19 sites in the US. No stratification was described. After randomization, study visits occurred every 2 weeks for the first 20 weeks, then every 4 weeks until week 44, then every 6 weeks until the end of treatment (week 68), followed by an end-of-trial follow-up visit at week 75. Body weight was assessed every visit from week 0 to week 4, then every second visit through week 44, then every visit until end of study, while waist circumference was assessed every second visit throughout. The data cut-off date was May 31, 2021, and the date of publication of the Clinical Study Report was September 1, 2021.
Populations
Inclusion and Exclusion Criteria
All studies except STEP 2 included patients with a BMI of 30.0 kg/ m2 or greater, or 27.0 kg/m2 or greater with the presence of at least 1 of the following weight-related comorbidities (treated or untreated): hypertension, dyslipidemia, obstructive sleep apnea, or cardiovascular disease (Table 6, Table 8, Table 9, and Table 10). In STEP 2, all patients had to have type 2 diabetes to be enrolled, so the BMI cut-off for everyone was 27 kg/m2 (Table 7). Patients in all studies also had to have a history of at least 1 unsuccessful effort to lose weight through diet. Additionally, there were randomization criteria that needed to be met, including having the ability to keep a food diary, having a PHQ-9 score of less than 15 at randomization, and having no suicidal behaviour or ideation. Other than in STEP 2, which enrolled patients with type 2 diabetes, patients with a hemoglobin A1C of 6.5% or greater were excluded, as were patients who had a self-reported change in body weight of greater than 5 kg within 90 days of screening. STEP 8 also excluded patients with a history of type 1 or type 2 diabetes. Additionally, STEP 2 excluded patients with renal impairment (an estimated glomerular filtration rate less than 30 mL per minute per 1.73 m2, or an estimated glomerular filtration rate less than 60 mL per minute per 1.73 m2 in those treated with SGLT-2 inhibitors). STEP 2 also excluded patients with uncontrolled and potentially unstable diabetic retinopathy or maculopathy.
Baseline Characteristics
Across the studies (Table 11, Table 12, and Table 13), the mean age of patients was 46 years to 49 years with the exception of STEP 2, where the mean age was 55 years. The majority of patients (75% to 80%) was female, with the exception of STEP 2 where there was a roughly equal percentage of females and males in the study. The vast majority of patients was White across the studies (75% to 93%), with the exception of STEP 2, where about 60% of patients were White and 27% were Asian. Baseline body weight in STEP 1, STEP 3, and STEP 8 was approximately 105 kg, and slightly lower (approximately 100 kg) in STEP 2, which focused on patients with type 2 diabetes and even lower in STEP 4 (approximately 96 kg), which featured a 20-week run-in where all patients received semaglutide before randomization. Baseline hemoglobin A1C was around 5.7% in STEP 1 and STEP 3, 5.5% in STEP 8, and 5.4% in STEP 4, which featured the run-in, and much higher in STEP 2 (8.1%), which enrolled patients with type 2 diabetes.
In the STEP 1 and STEP 4 studies, baseline characteristics were well balanced between groups. In the STEP 2 study, there were greater proportions of females in the semaglutide group versus placebo (55% versus 47%) and patients who had never smoked (61% in the semaglutide group versus 55% in the placebo group). In STEP 3, there were fewer females in the semaglutide group than in the placebo group (77% versus 88%); otherwise, there were no other clear numerical differences between groups. In the STEP 8 study, there were more females in the semaglutide group versus the liraglutide or placebo groups (81% versus 76% versus 78%, respectively) and baseline body weight was lower with semaglutide and liraglutide when compared to placebo (103 kg versus 104 kg versus 109 kg, respectively). As well, the percentage of patients who had never smoked was different between groups |||| || ||| || ||| ||| ||||||||||| || ||||||||||| || ||||||||.
Table 11: Summary of Baseline Characteristics for STEP 1 and STEP 2 Studies — Full Analysis Set
Characteristic | STEP 1 study | STEP 2 study | ||
|---|---|---|---|---|
Semaglutide N = 1,306 | Placebo N = 655 | Semaglutide N = 404 | Placebo N = 403 | |
Mean (SD) age, years | 46 (13) | 47 (12) | 55 (11) | 55 (11) |
Age group (years), n (%) | ||||
18 to < 65 | 1,198 (92) | 607 (93) | 316 (78) | 317 (79) |
≥ 65 to < 75 | 99 (8) | 46 (7) | 78 (19) | 78 (19) |
≥ 75 to < 85 | 8 (1) | 2 (0.3) | 10 (3) | 8 (2) |
≥ 85 | 1 (< 0.1) | 0 | 0 | 0 |
Female, n (%) | 955 (73) | 498 (76) | 223 (55) | 190 (47) |
Race | ||||
White | 973 (75) | 499 (76) | 237 (59) | 242 (60) |
Asian | 181 (14) | 80 (12) | 112 (28) | 108 (27) |
Black/African descent | 72 (6) | 39 (6) | 35 (9) | 37 (9) |
Not applicable | 38 (3) | 17 (3) | 0 | 0 |
Other | 25 (2) | 8 (1) | 16 (4) | 13 (3) |
American Indian or Alaska Native | 17 (1) | 10 (2) | 4 (1) | 2 (1) |
Native Hawaiian/other Pacific Islander | 0 | 2 (0.3) | 0 | 1 (< 1) |
BMI (kg/m2), mean (SD) | 37.8 (6.7) | 38.0 (6.5) | 35.9 (6.4) | 35.9 (6.5) |
BMI (kg/m2) | ||||
< 30 | 81 (6) | 36 (6) | 68 (17) | 77 (19) |
30 to ≤ 35 | 436 (33) | 207 (32) | 140 (35) | 135 (34) |
35 to ≤ 40 | 406 (31) | 208 (32) | 103 (26) | 97 (24) |
≥ 40 | 383 (29) | 204 (31) | 93 (23) | 94 (23) |
Waist circumference, cm, mean (SD) | 114.6 (14.8) | 114.8 (14.4) | 114.5 (14.3) | 115.5 (13.9) |
Body weight, kg, mean (SD) | 105.4 (22.1) | 105.2 (21.5) | 99.9 (22.5) | 100.5 (20.9) |
Hemoglobin A1C, %, mean (SD) | 5.7 (0.3) | 5.7 (0.3) | 8.1 (0.8) | 8.1 (0.8) |
FPG, mmol/L, mean (SD) | 5.3 (0.6) | 5.3 (0.6) | 8.5 (2.3) | 8.8 (2.3) |
Smoking habits, n (%) | ||||
Never smoked | 828 (63) | 409 (62) | 247 (61.1) | 222 (55.1) |
Previous smoker | 318 (24) | 178 (27) | 108 (26.7) | 119 (29.5) |
Current smoker | 160 (12) | 68 (10) | 49 (12.1) | 62 (15.4) |
Comorbidities, n (%) | ||||
Coronary artery disease | ||||
No | 1,268 (97) | 636 (97) | 375 (93) | 367 (91) |
Yes | 32 (3) | 17 (3) | 26 (6) | 33 (8) |
Unknown | 6 (1) | 2 (0.3) | 3 (1) | 3 (1) |
Cerebrovascular disease | ||||
No | 1,289 (99) | 648 (99) | 390 (97) | 385 (96) |
Yes | 13 (1) | 6 (1) | 12 (3) | 14 (4) |
Unknown | 4 (0.3) | 1 (0.2) | 2 (1) | 4 (1) |
Impaired glucose tolerance | ||||
No | 1,171 (90) | 593 (91) | NA | NA |
Yes | 47 (4) | 20 (3) | NA | NA |
Unknown | 88 (7) | 42 (6) | NA | NA |
Impaired fasting glucose | ||||
No | 1,133 (87) | 577 (88) | NA | NA |
Yes | 109 (8) | 42 (6) | NA | NA |
Unknown | 64 (5) | 36 (6) | NA | NA |
Elevated hemoglobin A1C | ||||
No | 976 (75) | 492 (75) | NA | NA |
Yes | 235 (18) | 116 (18) | NA | NA |
Unknown | 95 (7) | 47 (7) | NA | NA |
BMI = body mass index; FPG = fasting plasma glucose; NA = not applicable; SD = standard deviation.
Source: Clinical Study Reports for STEP 1 (2020)17 and STEP 2 (2020).21
Table 12: Summary of Baseline Characteristics for STEP 3 and STEP 4 Studies — Full Analysis Set
Characteristic | STEP 3 study | STEP 4 study | ||
|---|---|---|---|---|
Semaglutide N = 407 | Placebo N = 204 | Semaglutide N = 535 | Placebo N = 268 | |
Mean (SD) age, years | 46 (13) | 46 (13) | 47 (12) | 46 (12) |
Age group (years), n (%) | ||||
18 to < 65 | 379 (93) | 186 (91) | 503 (94) | 252 (94) |
≥ 65 to < 75 | 27 (7) | 16 (8) | 29 (5) | 15 (6) |
≥ 75 to < 85 | 1 (0.2) | 2 (1) | 3 (1) | 1 (0.4) |
≥ 85+ | 0 | 0 | 0 | 0 |
Female, n (%) | 315 (77) | 180 (88) | 429 (80) | 205 (77) |
Race, n (%) | ||||
White | 307 (75) | 158 (78) | 446 (83) | 226 (84) |
Asian | 5 (1) | 6 (3) | 15 (3) | 4 (2) |
Black/African descent | 80 (20) | 36 (18) | 69 (13) | 35 (13) |
Not applicable | 0 | 0 | 0 | 0 |
Other | 11 (3) | 4 (2) | 5 (1) | 3 (1) |
American Indian or Alaska Native | 1 (0.2) | 0 | 0 | 0 |
Native Hawaiian or other Pacific Islander | 3 (1) | 0 | 0 | 0 |
BMI (kg/m2), mean (SD) | 38.1 (6.7) | 37.8 (6.9) | 34.5 (6.9) | 34.1 (7.1) |
BMI (kg/m2), patients, n (%) | ||||
< 25 | NA | NA | 7 (1) | 9 (3) |
25 to < 30 | NA | NA | 153 (29) | 69 (26) |
< 30 | 23 (6) | 15 (7) | NA | NA |
30 to ≤ 35 | 126 (31) | 58 (28) | 166 (31) | 97 (36) |
35 to ≤ 40 | 136 (33) | 76 (37) | 116 (22) | 52 (19) |
≥ 40 | 122 (30) | 55 (27) | 93 (17) | 41 (15) |
Waist circumference, cm, mean (SD) | 113.6 (15.1) | 111.8 (16.2) | 105.5 (15.9) | 104.7 (16.9) |
Body weight, kg, mean (SD) | 106.9 (22.8) | 103.7 (22.9) | 96.5 (22.5) | 95.4 (22.7) |
Hemoglobin A1C, %, mean (SD) | 5.7 (0.3) | 5.8 (0.3) | 5.4 (0.3) | 5.4 (0.3) |
FPG, mmol/L, mean (SD) | 5.2 (0.5) | 5.2 (0.5) | 4.9 (0.4) | 4.8 (0.4) |
Smoking habits, n (%) | ||||
Never smoked | 298 (73) | 144 (71) | 351 (66) | 174 (65) |
Previous smoker | 88 (22) | 47 (23) | 143 (27) | 62 (23) |
Current smoker | 21 (5) | 13 (6) | 41 (8) | 32 (12) |
Comorbidities, n (%) | ||||
Coronary artery disease | ||||
No | 396 (97) | 198 (97) | 530 (99) | 265 (99) |
Yes | 6 (2) | 4 (2) | 4 (1) | 3 (1) |
Unknown | 5 (1) | 2 (1) | 1 (0.2) | 0 |
Cerebrovascular disease | ||||
No | 395 (97) | 201 (99) | 522 (97.6) | 264 (98.5) |
Yes | 5 (1) | 1 (1) | 13 (2.4) | 4 (1.5) |
Unknown | 7 (2) | 2 (1) | 0 | 0 |
Impaired glucose tolerance | ||||
No | 348 (86) | 171 (84) | 469 (88) | 243 (91) |
Yes | 18 (4) | 12 (6) | 31 (6) | 11 (4) |
Unknown | 41 (10) | 21 (10) | 35 (7) | 14 (5) |
Impaired fasting glucose | ||||
No | 350 (86) | 171 (84) | 466 (87) | 242 (90) |
Yes | 42 (10) | 23 (11) | 43 (8) | 18 (7) |
Unknown | 15 (4) | 10 (5) | 26 (5) | 8 (3) |
Elevated hemoglobin A1C | ||||
No | 291 (72) | 139 (68) | NR | NR |
Yes | 97 (24) | 58 (28) | NR | NR |
Unknown | 19 (5) | 7 (3) | NR | NR |
BMI = body mass index; FPG = fasting plasma glucose; NA = not applicable; NR = not reported; SD = standard deviation.
Source: Clinical Study Reports for STEP 3 (2020)23 and STEP 4 (2020).25
Table 13: Summary of Baseline Characteristics, Full Analysis Set — STEP 8 Study
Characteristic | STEP 8 study | ||
|---|---|---|---|
Semaglutide N = 126 | Liraglutide N = 127 | Placebo N = 85 | |
Mean (SD) age, years | 48 (14) | 49 (13) | 51 (12) |
Age group, years, n (%) | |||
18 to < 65 | ||| |||| | ||| |||| | || |||| |
≥ 65 to < 75 | || |||| | || |||| | | |||| |
≥ 75 to < 85 | | ||| | | ||| | ||||| |
≥ 85 | ||||| | ||||| | ||||| |
Female, n (%) | 102 (81) | 97 (76) | 66 (78) |
Race, n (%) | |||
White | 94 (75) | 95 (75) | 60 (71) |
Asian | 4 (3) | 6 (5) | 3 (4) |
Black/African descent | 25 (20) | 20 (16) | 19 (22) |
Not applicable | |||
Other | 2 (2) | 3 (2) | 2 (2) |
American Indian or Alaska Native | 0 | 0 | 0 |
Native Hawaiian or other Pacific Islander | 1 (1) | 3 (2) | 1 (1) |
BMI (kg/m2), mean (SD) | 37.0 (7.4) | 37.2 (6.4) | 38.8 (6.5) |
BMI (kg/m2), patient, n (%) | |||
< 30 | 9 (7) | 11 (9) | 4 (5) |
30 to ≤ 35 | 51 (41) | 42 (33) | 20 (24) |
35 to ≤ 40 | 37 (29) | 38 (30) | 31 (37) |
≥ 40 | 29 (23) | 36 (28) | 30 (35) |
Waist circumference, cm, mean (SD) | 111.8 (16.3) | 113.5 (15.0) | 115.4 (15.1) |
Body weight, kg, mean (SD) | 102.5 (25.3) | 103.7 (22.5) | 108.8 (23.1) |
Hemoglobin A1C, %, mean (SD) | 5.5 (0.3) | 5.5 (0.3) | 5.6 (0.4) |
FPG, mmol/L, mean (SD) | 5.3 (0.6) | 5.3 (0.5) | 5.4 (0.7) |
Smoking habits, patients, n (%) | |||
Never smoked | || |||| | || |||| | || |||| |
Previous smoker | || |||| | || |||| | || |||| |
Current smoker | | ||| | || ||| | | ||| |
Comorbidities, patients, n (%) | |||
Coronary artery disease | |||
No | 120 (95) | 123 (97) | 81 (95) |
Yes | 4 (3) | 3 (2) | 4 (5) |
Unknown | | ||| | | ||| | ||||| |
Cerebrovascular disease | |||
No | 126 (100) | 127 (100) | 85 (100) |
Yes | 0 | 0 | 0 |
Unknown | 0 | 0 | 0 |
Impaired glucose tolerance | |||
No | ||| |||| | ||| |||| | || |||| |
Yes | ||||| | | ||| | | ||| |
Unknown | || ||| | | ||| | | |||| |
Impaired fasting glucose | |||
No | ||| |||| | ||| |||| | || |||| |
Yes | || |||| | || ||| | || |||| |
Unknown | ||||| | | ||| | | ||| |
Elevated hemoglobin A1C | |||
No | || |||| | ||| |||| | || |||| |
Yes | || |||| | || |||| | || |||| |
Unknown | | ||| | | ||| | | ||| |
BMI = body mass index; FPG = fasting plasma glucose; SD = standard deviation.
Source: Clinical Study Report for STEP 8 (2021).27
Interventions
In all the STEP trials, semaglutide and placebo injection devices were identical in appearance to facilitate blinding. Trial product was administered using a PDS290 pre-filled pen-injector with a 3 mL cartridge containing semaglutide 1.0 mg/mL or 3.0 mg/mL (depending on dose level) or placebo. To mitigate GI side effects with GLP-1 agonist treatment, dose escalation to the maintenance dose was required. Patients were initiated at a once weekly dose of 0.25 mg and followed a fixed-dose escalation regimen, with dose increases every 4 weeks (to dose levels of 0.5 mg, 1.0 mg, 1.7 mg, and 2.4 mg per week), aiming at reaching the maintenance dose of 2.4 mg (or the corresponding volume of placebo) after 16 weeks. If a patient did not tolerate the maintenance dose of 2.4 mg, they could stay at a lower dose of 1.7 mg semaglutide once weekly. This was only allowed if the patient would otherwise discontinue trial product completely and only if considered safe. It was recommended that the patient make at least 1 attempt to re-escalate to the recommended maintenance dosage of 2.4 mg once weekly, as per the investigator’s discretion. STEP 4 had a 20-week run-in period that included 16 weeks of dose escalation, where all patients received semaglutide, and patients were randomized at the conclusion of this 20-week period.
If a single dose of trial product was missed, it was to be administered as soon as noticed, provided the time to the next scheduled dose was at least 2 days (48 hours) away. If a dose was missed and the next scheduled dose was less than 2 days (48 hours) away, the patient was not to administer a dose until the next scheduled dose. A missed dose was not to affect the scheduled dosing day of the week. If 2 or more consecutive doses of trial product were missed, the patient was encouraged to recommence the treatment if considered safe, as per the investigator’s discretion, and if the patient did not meet any of the discontinuation criteria. Recommencement of treatment was then to occur as early as the situation allowed.
All patients in STEP 2 had type 2 diabetes and were continued on their existing regimens for diabetes. To minimize risk of hypoglycemia, patients who were on sulfonylureas had their doses reduced by 50% at the discretion of the investigator, from randomization. Patients could switch their OAD within the same class, and if intensification of treatment was required outside of provisions for rescue therapy (fasting plasma glucose [FPG] greater than 15 mmol/L), this change in regimen was to follow the American Diabetes Association/European Association for the Study of Diabetes guidelines (excluding GLP-1 receptor agonists, dipeptidyl-peptidase IV inhibitors, and amylin analogues). If any drugs were added, they were to be weight-neutral as much as possible, and were to be first based on intensification of existing background therapy or addition of new background OADs. If insulin was required for rescue, it was to be used for as short a duration as possible.
All patients in the STEP trials received counselling regarding diet (typically, 500 kcal deficit per day relative to the estimated total energy expenditure calculated once at randomization) and physical activity (100 minutes to 150 minutes of physical activity per week, depending on the study). Counselling was done by a dietitian or a similar qualified health care professional (according to local requirements) every fourth week via visits or phone contacts. Patients were instructed to record their food intake and physical activity daily (via paper diary, digital app or similar tool) to assist and evaluate their lifestyle intervention. In STEP 3, the first 8 weeks of the study consisted of a 1,000 kcal per day to 1,200 kcal per day liquid calorie diet at the discretion of the investigator, provided as meal replacements and portion-controlled meals. After 8 weeks, patients were gradually transitioned to a less strict hypocaloric diet consisting of conventional foods. From week 8 to end of treatment, the daily caloric target was calculated based on body weight at randomization. For example, patients weighing under 200 pounds were restricted to 1,200 kcal per day, patients weighing more than 300 pounds were restricted to 1,800 kcal per day, and for patients between 200 pounds and 300 pounds, body weight (in pounds) was multiplied by 6 to arrive at the daily caloric restriction. The calculated caloric target was kept for the remainder of the trial except if a patient achieved a BMI of 22.5 kg/m2 or lower, in which case the recommended energy intake was recalculated with no caloric deficit for the remainder of the trial. STEP 3 also focused on interventions to influence patient behaviour, referred to as IBT. Patients were given a guide, which had a dietitian section, as well as a handout. Each IBT session covered a specific topic, such as advice on diet or physical activity, as well as lifestyle modification (challenging negative thoughts, obtaining social support). Initially, intensive behavioural support occurred weekly, delivered by a dietitian or similarly trained health care professional. Progress was discussed with reviews of the food diary, addressing any compliance or other issues, and patients were prepared for the next stage, the structured diet. Most topics were accompanied by a homework assignment from the handout that was to be completed for the next visit.
During the trials, patients were not to initiate any anti-obesity treatment (e.g., medication) that was not part of the trial procedures. If such treatment was initiated, patients were instructed to stop the treatment.
Outcomes
A list of efficacy end points identified in the CADTH review protocol that were assessed in the clinical trials included in this review is provided in Table 14.
Table 14: Summary of Outcomes of Interest Identified in the CADTH Review Protocol
Outcome measure | STEP 1 study | STEP 2 study | STEP 3 study | STEP 4 study | STEP 8 study |
|---|---|---|---|---|---|
Mortality | Reported in harms | Reported in harms | Reported in harms | Reported in harms | Reported in harms |
Body weight | Co-primary: Percentage change from baseline in body weight (1) | ||||
–5% | Co-primary (2) | Co-primary (2) | Co-primary (2) | Supportive secondary | Exploratory |
–10% | Confirmatory secondary (3) | Confirmatory secondary (3) | Confirmatory secondary (3) | Supportive secondary | Confirmatory secondary (2) |
–15% | Confirmatory secondary (4) | Confirmatory secondary (4) | Confirmatory secondary (4) | Supportive secondary | Confirmatory secondary (3) |
–20% | Supportive secondary | Supportive secondary | Supportive secondary | Supportive secondary | Confirmatory secondary (4) |
Body weight: Waist circumference | Confirmatory secondary (5) | Confirmatory secondary (5) | Confirmatory secondary (5) | Confirmatory secondary (2) | Supportive secondary |
BMI | Supportive secondary | Supportive secondary | Supportive secondary | Supportive secondary | NR |
HRQoL: SF-36 version 2.0 acute, physical function | Confirmatory secondary (7) | Confirmatory secondary (10) | Confirmatory secondary (7) | Confirmatory secondary (4) | NR |
HRQoL: SF-36 version 2.0 acute, other domains | Supportive secondary | Supportive secondary | Supportive secondary | Supportive secondary | NR |
HRQoL: IWQOL-Lite-CT, physical function | Confirmatory secondary (8) | Confirmatory secondary (11) | NR | NR | NR |
Normalization of blood glucose: Change in glycemic status | Supportive secondary | Supportive secondary | Exploratory | Exploratory | Supportive secondary |
Weight-related comorbidity | NR | NR | NR | NR | NR |
Non-fatal CV event | Reported in harms | Reported in harms | Reported in harms | Reported in harms | Reported in harms |
HCRU | NR | NR | NR | NR | NR |
Use of concomitant meds | Supportive secondary | Exploratory | Exploratory | Exploratory | NR |
Physical function: 6MWT | NR | Exploratory (BMI ≥ 35 kg/m2) | NR | NR | NR |
Outcomes in the statistical hierarchy but not in our protocol | CFB in SBP (6) | CFB in:
| CFB in SBP (6) | CFB in SBP (3) | None |
6MWT = six-minute walk test; BMI = body mass index; CFB = change from baseline; CV = cardiovascular; HCRU = health care resource utilization; HRQoL = health-related quality of life; IWQOL-Lite-CT = Impact of Weight on Quality of Life–Lite Clinical Trials Version; NR = not reported; SBP = systolic blood pressure; SF-36 = Short Form (36) Health Survey.
Note: Numbers in parentheses indicate ranking in the hierarchy.
Body Weight
The percentage change from baseline to week 68 in body weight was the primary outcome (or a co-primary outcome) in all the included studies. Patients achieving at least a 5% reduction from baseline to week 68 in body weight was a co-primary outcome in the STEP 1 to STEP 4 studies, and patients achieving at least 10%, 15%, or 20% reductions were confirmatory secondary outcomes in some studies and supportive secondary outcomes in others (Table 14). Body weight was measured without shoes, on an empty bladder, and in light clothing. Measurements were to be recorded on a digital scale in kilograms or pounds (to 1 decimal place) using the same scale throughout the trial, calibrated yearly as a minimum.
The change from baseline to week 68 in waist circumference was a confirmatory secondary outcome in the STEP 1 to STEP 4 studies. Waist circumference was defined as the abdominal circumference located midway between the lower rib margin and the iliac crest and obtained in standing position with a non-stretchable measuring tape and to the nearest cm or inch. The tape had to touch the skin but not compress soft tissue and twists in the tape were to be avoided. The subject was asked to breathe normally. The same measuring tape was to be used throughout the trial. The measuring tape was provided by Novo Nordisk to ensure standardization.
Assessment of Glycemic Status
Investigators periodically assessed glycemic status using medical records, concomitant medications, blood glucose parameters (hemoglobin A1C, FPG), and AEs. Patients were categorized as having normoglycemia or prediabetes, or were diagnosed with type 2 diabetes according to the American Diabetes Association definitions.
Physical Function: Six-Minute Walk Test
Physical function was assessed in STEP 2, using the 6MWT, in a subgroup of patients with BMI of 35 kg/m2 or greater. Patients were asked to walk as far as possible in 6 minutes, without running, along a marked walkway of 20 m, and the distance walked was reported.
Health-Related Quality of Life
Questionnaires were used for measurements of HRQoL and patients completed the questionnaires themselves. HRQoL was assessed using the SF-36 in the STEP 1 to STEP 4 studies, and the physical function dimension was assessed as a confirmatory secondary outcome in each of these studies. The SF-36 is a generic HRQoL instrument that measures scores for 8 different health domains: physical function, role physical, bodily pain, general health, vitality, social functioning, and role emotional. In addition, mental and physical and component summaries can be calculated (mental component summary [MCS] and physical component summary [PCS], respectively; refer to Appendix 4 for detailed summary). Scores on the domains and MCS and PCS range from 0 to 100, with higher scores indicating better health status, and the MID is 2 points for each of the PCS and MCS. MID estimates range from 2 points to 4 points for the individual domains, and for the physical function domain the MID is 3 points.28 There is some evidence for the validity of the SF-36 in overweight and obesity; however, no specific MID has been described for these conditions. In addition to change from baseline, the sponsor also reported results for binary data (“responders”) on the physical function component of the SF-36, using a cut-off for response of 4.3 — a cut-off that was determined in consultation with the FDA and is intended to represent patient perception of a meaningful improvement.
HRQoL was also assessed using the IWQOL-Lite-CT questionnaire, as a confirmatory secondary outcome in the STEP 1 and STEP 2 studies. The IWQOL-Lite-CT is a shorter version of the 74-item Impact of Weight on Quality of Life (IWQOL), an instrument that was developed to assess HRQoL specifically in patients living with moderate to severe obesity. The IWQOL-Lite-CT has 20 self-administered items, with 2 domains: physical (7 items) and psychosocial (13 items). The total score is simply the sum of all items, and higher scores indicate poorer HRQoL. There was no MID found for the IWQOL-Lite-CT. Total scores and scale scores on the Impact of Weight on Quality of Life–Lite (IWQOL-Lite) questionnaire are transformed to a range from 0 to 100, with 100 being the best quality of life and 0 being the poorest.29
Statistical Analysis
Primary Outcomes of the Studies
Power Calculation
For the STEP 1 to STEP 4 trials, the power calculations were based on the randomization ratio, the 5% significance level, the statistical tests chosen for continuous outcomes (t-test on the mean differences assuming equal variances) and binary outcomes (Pearson chi-square test for 2 independent proportions), and permanent discontinuations of 20% (5% for STEP 4), with 60% of those retrieved at week 68 (based on study NN9536 to 4153). Patients in the placebo group who discontinue are assumed to have the same effect as patients who complete the trial in the placebo group, retrieved patients in the semaglutide group are assumed to have an effect corresponding to half the treatment difference (compared to placebo) of patients who complete the trial in the semaglutide group, and non-retrieved patients in the semaglutide group are assumed to have an effect corresponding to placebo. Further assumptions made to calculate power were based on findings from other projects conducted by the sponsor, including the SCALE, SUSTAIN, and PIONEER studies. Specific differences between groups were provided for each outcome in the hierarchy. Given these assumptions, the sample size of 1,950 (semaglutide = 1,300; placebo = 650) was to provide an effective power of 99% for the first 7 outcomes in the hierarchy. For STEP 2, the sample of 1,200 (400 in each group) provided an effective power of 94% for the first 9 outcomes in the hierarchy. For STEP 3, the planned sample of 600 patients (semaglutide = 400; placebo = 200) provided a power of 86% for the 7 efficacy outcomes in the hierarchy. For STEP 4, the sample of 750 (semaglutide = 500; placebo = 250) provided an effective power of 95% for the first 4 outcomes in the hierarchy. STEP 4 also had an additional assumption that at least 80% of patients would be eligible for randomization after the 20-week run-in, meaning that 900 patients would be started on trial product.
For STEP 8, the study was designed with an effective power of ||| to detect differences on all outcomes in the hierarchy at a 1-sided alpha of 0.025 (equivalent to a 2-sided alpha of 0.05). The power calculations were based on the same statistical tests described earlier, and assumptions were based on the SCALE study and the NN9536 to 4153 trial. Once again, the sponsor reported expected differences for each of the first 4 outcomes in the hierarchy.
Statistical Tests and Models
Analysis of covariance was used for all continuous outcomes using randomized treatment as factor and baseline value for the outcome being tested as covariate. For binary outcomes, binary logistic regression was used using randomized treatment as factor and baseline value for the outcome being tested as covariate (Table 15).
For the STEP 1 to STEP 4 trials, semaglutide was compared to placebo, and a hierarchical design was used to control for multiplicity. The outcomes identified in the hierarchy and their place in the hierarchy was fairly consistent between trials. In STEP 8, the primary comparison was between semaglutide and liraglutide, and multiplicity was also controlled for by use of a hierarchy; the outcomes in the hierarchy were generally consistent with those found in the placebo-controlled trials. It was not clear whether both co-primary outcomes had to be superior for overall superiority to be claimed.
The treatment policy or strategy estimand is used for confirmatory, multiplicity-controlled statistical evaluations. It estimates the population level treatment effect of semaglutide regardless of treatment adherence and/or other anti-obesity therapies and does not exclude data collected after discontinuation of treatment (e.g., due to tolerability issues) or after initiation of alternative treatment (e.g., due to lack of efficacy). The treatment policy estimand, according to the FDA guidance E9(R1) Statistical Principles for Clinical Trials: Addendum: Estimands and Sensitivity Analysis in Clinical Trials, is therefore relevant for those such as regulatory authorities evaluating the actual impact of an overall treatment strategy or policy for the indicated patient population.
Data Imputation Methods
A number of imputation methods were used across trials to account for missing data, including multiple imputation using retrieved patients, jump to reference multiple imputation, and single imputation as done by Sacks. The multiple imputation using retrieved patients was the primary method of imputation for the primary estimand, and this is where missing body weight measurement at week 68 for non-retrieved patients is imputed using data from retrieved patients in each treatment group. This is done according to the timing of the last available observation of body weight. Missing body weight at week 68 for patients on randomized treatment were imputed by sampling from available measurements at week 68 from patients on randomized treatment in the relevant randomized treatment group. The approach of jump to reference multiple imputation assumes that patients instantly lose any effect from randomized treatment after discontinuation beyond what could be expected from placebo as an adjunct to diet and exercise.
To account for missing baseline data, if no eligible observation was available at or before randomization, the mean of baseline values across all patients in the study was used as the baseline value.
Subgroup Analyses
No preplanned subgroups of relevance to the systematic review protocol were described in any of the included studies.
Sensitivity Analyses
The imputation methods described earlier were the sensitivity analyses performed during the STEP trials.
Secondary Outcomes of the Studies
Statistical tests used for secondary outcomes were the same as those used for primary outcomes (refer to Table 15). The order of outcomes in the testing hierarchy is reported in the summary of outcomes table (refer to Table 14).
Table 15: Statistical Analysis of Efficacy End Points
End point | Statistical model | Adjustment factors | Sensitivity analyses |
|---|---|---|---|
STEP 1 to STEP 4 studies, and STEP 8 study | |||
Change from baseline in:
| ANCOVA |
|
|
Binary outcomes:
| Binary logistic regression |
|
|
ANCOVA = analysis of covariance; IWQOL-Lite-CT = Impact of Weight on Quality of Life–Lite Clinical Trials Version; J2R-MI = jump to reference multiple imputation; LAO = last available observation; MMRM = mixed model of repeated measures; NR = not reported; SF-36 = Short Form (36) Health Survey.
aJ2R-MI: Missing observations were multiple (1,000x), imputed from placebo patients based on a jump to reference approach.
bS1-SI: Missing observations were imputed by adding a body weight regain rate of 0.3 kg per month to the LAO until baseline is reached.
cS2-SI: Missing observations were imputed by adding a body weight regain rate of 0.3 kg per month to the LAO until baseline is reached for semaglutide 2.4 mg only.
dMMRM: All responses were included in a MMRM with randomized treatment as factor and baseline body weight as covariate, all nested within visit. For binary outcomes, the MMRM was performed on body weight (kg) and individual missing week 68 responses were predicted from the MMRM; each subject was then classified for body weight loss of 5% or more and analyzed using a binary logistic regression model.
eNR: Patients with missing week 68 response were considered as nonresponders.
Analysis Populations
The full analysis set included all randomized patients, according to the intention-to-treat principle. These patients were to contribute to the evaluation as randomized. The safety analysis set included all randomized patients exposed to at least 1 dose of study drug, and were analyzed as treated.
Results
Patient Disposition
Study withdrawals were typically low across trials (7% or less) and there were no clear or consistent differences between groups within studies (Table 16 and Table 17). Treatment discontinuations were higher, ranging from 12% to 17% of patients with semaglutide and 14% to 22% of patients with placebo, except in the STEP 4 study, which featured the 20-week run-in and where treatment discontinuations were 6% with semaglutide and 12% with placebo. In the STEP 8 study, treatment discontinuations were ||| in the liraglutide group; the most common reason was AEs, which occurred in 2% of semaglutide patients and 12% of liraglutide patients. AEs were the most common reason for treatment discontinuations across the STEP trials.
Exposure to Study Treatments
Mean treatment duration was similar between groups within studies. It was generally between 57 weeks and 61 weeks in the STEP 1 to STEP 3 studies and the STEP 8 study, and around 65 weeks in the STEP 4 study, which had a 20-week run-in period.
Table 16: Patient Disposition for STEP 1, STEP 2, and STEP 3 Studies
Factor | STEP 1 study | STEP 2 study | STEP 3 study | |||
|---|---|---|---|---|---|---|
Semaglutide | Placebo | Semaglutide | Placebo | Semaglutide | Placebo | |
Screened, N | 2,303 | 1,595 | 742 | |||
Screen failures, N | 305 | 361 | 129 | |||
Withdrawn before randomization, N | 37 | 24 | 2 | |||
Randomized, N | 1,306 | 655 | 404 | 403 | 407 | 204 |
Randomized in violation of inclusion, exclusion, and/or randomization criteria, n (%) | 17 (1) | 9 (1) | 11 (3) | 17 (4) | 0 | 1 (1) |
Treatment discontinuations, n (%) | 223 (17) | 147 (22) | 47 (12) | 56 (14) | 68 (17) | 38 (19) |
Primary reason | ||||||
Adverse event | 91 (7) | 21 (3) | 26 (6) | 13 (3) | 26 (6) | 6 (1) |
Protocol violation | 3 (0.2) | 5 (1) | 1 (0.2) | 7 (2) | 0 | 1 (1) |
Pregnancy | 7 (1) | 3 (1) | 0 | 0 | 1 (0.2) | 2 (1) |
Lack of efficacy | 1 (< 0.1) | 16 (2) | 0 | 0 | 0 | 0 |
At the discretion of the investigator | 4 (0.3) | 1 (0.2) | 0 | 1 (0.2) | 0 | 1 (1) |
Safety concern as judged by the investigator | 15 (1) | 0 | 1 (0.2) | 0 | 1 (0.2) | 2 (1) |
Withdrawal of consent | 9 (1) | 10 (2) | 2 (1) | 7 (2) | 4 (1) | 3 (2) |
Lost to follow-up | 26 (2) | 25 (4) | 5 (1) | 3 (1) | 18 (4) | 7 (3) |
Other | 67 (5) | 66 (10) | 12 (3) | 25 (6) | 17 (4) | 16 (8) |
Study discontinuations, n (%) | 66 (5) | 46 (7) | 13 (3) | 20 (5) | 31 (8) | 13 (6) |
Primary reason | ||||||
Withdrawal by subject | 26 (2) | 17 (3) | 5 (1) | 12 (3) | 7 (2) | 3 (12) |
Lost to follow-up | 39 (3) | 28 (4) | 7 (2) | 7 (2) | 24 (6) | 10 (5) |
Death | 1 (< 0.1) | 1 (0.2) | 1 (0.2) | 1 (0.2) | 0 | 0 |
Full analysis set, n (%) | 1,306 (100) | 655 (100) | 404 (100) | 403 (100) | 407 (100) | 204 (100) |
Safety set, n (%) | 1,306 (100) | 655 (100) | 403 (99.8) | 402 (99.8) | 407 (100) | 204 (100) |
Source: Clinical Study Reports for STEP 1 (2020),17 STEP 2 (2020),21 and STEP 3 (2020).23
Table 17: Patient Disposition for STEP 4 and STEP 8 Studies
Factor | STEP 4 study | STEP 8 study | |||
|---|---|---|---|---|---|
Semaglutide | Placebo | Semaglutide | Liraglutide | Placebo | |
Screened, N | 1,051 | 387 | |||
Screen failures, N | 139 | 47 | |||
Withdrawn before randomization, N | 10 | 2 | |||
Included in run-in period, N | 902 | NA | |||
Included in run-in in violation of inclusion, exclusion, and/or run-in criteria, n (%) | 14 (2) | NA | |||
Received treatment in run-in period, N | 902 | NA | |||
Study treatment permanently discontinued before randomization, n (%) | 99 (11) | NA | |||
Primary reason | NA | ||||
Adverse event | 48 (5) | NA | |||
Protocol violation | 1 (0.1) | NA | |||
Pregnancy | 1 (0.1) | NA | |||
Run-in failure | 19 (2) | NA | |||
Safety concern as judged by the investigator | 2 (0.2) | NA | |||
Withdrawal of consent | 11 (1) | NA | |||
Lost to follow-up | 8 (1) | NA | |||
Other | 9 (1) | NA | |||
Withdrawn before randomization, n (%) | 99 (11) | NA | |||
Randomized, N | 535 | 268 | 126 | 127 | 85 |
Treatment discontinued, n (%) | 31 (6) | 31 (12) | 17 (14) | 35 (28) | 15 (18) |
Primary reason | |||||
Adverse event | 13 (2) | 6 (2) | | ||| | || |||| | | ||| |
Protocol violation | 1 (0.2) | 0 | | ||| | | ||| | |||| |
Pregnancy | 2 (0.4) | 0 | | ||| | | ||| | |||| |
Lack of efficacy | 0 | 0 | |||| | |||| | | ||| |
Safety concern as judged by the investigator | 0 | 0 | |||| | | ||| | |||| |
Withdrawal of consent | 1 (0.2) | 1 (0.4) | | ||| | | ||| | | ||| |
Lost to follow-up | 2 (0.4) | 1 (0.4) | | ||| | | ||| | | ||| |
Other | 12 (2) | 23 (9) | | ||| | | ||| | | ||| |
Study discontinuation, n (%) | 8 (2) | 8 (3) | 6 (5) | 9 (7) | 4 (5) |
Primary reason | |||||
Withdrawal by subject | 2 (0.4) | 4 (2) | 2 (2) | 4 (3) | 1 (1) |
Lost to follow-up | 5 (1) | 3 (1) | 4 (3) | 5 (4) | 3 (4) |
Death | 1 (0.2) | 1 (0.4) | 0 | 0 | 0 |
Full analysis set, n (%) | 535 (100) | 268 (100) | 126 (100) | 127 (100) | 85 (100) |
Safety set, n (%) | 535 (100) | 268 (100) | 126 (100) | 127 (100) | 85 (100) |
NA = not applicable.
Source: Clinical Study Reports for STEP 4 (2020)25 and STEP 8 (2021).27
Table 18: Treatment Exposure for STEP 1, STEP 2, and STEP 3 Studies — Full Analysis Set
Factor | STEP 1 study | STEP 2 study | STEP 3 study | |||
|---|---|---|---|---|---|---|
Semaglutide N = 1,306 | Placebo N = 655 | Semaglutide N = 404 | Placebo N = 403 | Semaglutide N = 407 | Placebo N = 204 | |
Treatment duration (from first dose to discontinuation of trial product) | ||||||
Mean treatment duration, weeks (SD) | 59.2 (20.2) | 57.4 (20.6) | 60.3 (20.1) | 61.0 (18.8) | 57.8 (21.3) | 58.1 (20.6) |
In trial observation (from date of randomization to date of last contact with study site) | ||||||
Mean (SD) weeks | 74.1 (8.5) | 73.1 (10.6) | 73.9 (9.3) | 73.5 (10.0) | 72.2 (12.2) | 72.4 (11.9) |
SD = standard deviation.
Source: Clinical Study Reports for STEP 1 (2020),17 STEP 2 (2020),21 and STEP 3 (2020).23
Table 19: Treatment Exposure for STEP 4 and STEP 8 Studies — Full Analysis Set
Factor | STEP 4 study | STEP 8 study | |||
|---|---|---|---|---|---|
Semaglutide N = 535 | Placebo N = 268 | Semaglutide N = 126 | Liraglutide N = 127 | Placebo N = 85 | |
Treatment duration (from first dose to discontinuation of trial product) | |||||
Mean treatment duration, weeks (SD) | 66.3 (10.7) | 64.9 (11.7) | |||| |||||| | |||| |||||| | |||| |||||| |
In trial observation (from date of randomization to date of last contact with study site) | |||||
Mean (SD) weeks | 75.2 (3.6) | 74.7 (4.9) | |||| ||||| | |||| |||||| | |||| ||||| |
SD = standard deviation.
Source: Clinical Study Reports for STEP 4 (2020)25 and STEP 8 (2021).27
Efficacy
Only those efficacy outcomes and analyses of subgroups identified in the review protocol are reported as follows. Refer to Appendix 3 for detailed efficacy data.
Mortality
This outcome was not reported as an efficacy outcome but was captured under the category of harms (Table 36 and Table 37). There was no more than 1 death in any treatment group in any of the included studies.
Body Weight
Changes in body weight were reported both as continuous outcomes (mean change from baseline) and binary outcomes. The results for percentage change in body weight are presented in Table 20 and Table 21 and the results for the binary body weight outcomes are presented in Table 22 and Table 23.
Percentage change from baseline to week 68 in body weight versus placebo was a co-primary outcome of the STEP 1 to STEP 3 studies, and the primary outcome of the STEP 4 and STEP 8 studies. There was a statistically significant difference in percentage reduction in body weight for semaglutide versus placebo in each of STEP 1 (difference between groups of –12.44% [95% CI, –13.37 to –11.51; P < 0.0001]), STEP 2 (difference between groups of –6.21% [95% CI, –7.28 to –5.15; P < 0.0001]), STEP 3 (difference between groups of –10.27% [95% CI, –11.97 to –8.57; P < 0.0001]), and STEP 4 (difference between groups of –14.75% [95% CI, – 16.00 to –13.50; P < 0.0001]), and a statistically significant difference in percentage reduction in body weight for semaglutide versus liraglutide in STEP 8 (difference between groups of ||||| |||| ||| |||||||||||||| |||||||||. Graphical representations of percentage change from baseline in body weight over time can be found in Appendix 3 (Figure 3, Figure 4, Figure 5, Figure 6, and Figure 7). Several sensitivity analyses were conducted, and results for these analyses were consistent with the findings of the primary analysis. For example, for STEP 1, the findings for the difference for semaglutide versus placebo for percentage reduction in weight ranged from –11.94% to –12.83%, consistent with the magnitude of difference in the primary analysis, –12.44%.
The proportion of patients achieving a 5% reduction from baseline in body weight was a co-primary outcome in the STEP 1 to STEP 3 studies, and there were greater percentages of patients in the semaglutide group than in the placebo group who achieved a 5% weight loss by week 68 in each of STEP 1 (OR = 11.22 [95% CI, 8.88 to 14.19; P < 0.0001]), STEP 2 (OR = 4.88 [95% CI, 3.58 to 6.64; P < 0.0001]), and STEP 3 (OR = 6.11 [95% CI, 4.04 to 9.26; P < 0.0001]). In STEP 4, where it was a supportive secondary outcome, the OR was 8.52 (95% CI, 5.93 to 12.24) for semaglutide versus placebo (Table 23). Patients achieving a reduction from baseline of at least 10%, 15%, and 20% were confirmatory secondary outcomes in the STEP 1 to STEP 3 studies, and the differences between semaglutide and placebo were statistically significant at each of these thresholds, across all of the studies (Table 23).
Patients achieving a weight reduction from baseline of at least 10%, 15%, and 20% were confirmatory secondary outcomes in the STEP 8 trial, and greater percentages of patients in the semaglutide group than the liraglutide group achieved at least a 10% reduction (OR = |||| |||| ||| ||||| ||||||| |||||||), at least a 15% reduction (OR = |||| |||| ||| ||||||||||| ||||||||), and at least a 20% reduction (OR = |||| |||| ||| ||||| ||||||| ||||||||) (Table 23). Similarly, there were statistically significant differences in favour of semaglutide for percentages of patients with at least a 10%, 15%, and 20% reduction in the STEP 1 to 3 studies.
Table 20: Percentage Change From Baseline to Week 68 in Body Weight for STEP 8 Study — Primary Analysis, In Trial, Full Analysis Set
Study | Semaglutide | Liraglutide | Placebo | Treatment difference vs. liraglutide (95% CI) | |||
|---|---|---|---|---|---|---|---|
Baseline, kg | Mean (SD) change | Baseline, kg | Mean (SD) change | Baseline, kg | Mean (SD) change | ||
STEP 8 | 102.5 (25.3) N = 126 | –16.4 (10.5) N = 117 | 103.7 (22.5) N = 127 | –6.4 (7.7) N = 117 | 108.8 (23.1) N = 85 | –1.6 (8.6) N = 78 | |||| |||||||||||||| |||||||| |
CI = confidence interval; FAS = full analysis set; SD = standard deviation; vs. = versus.
Note: Baseline sample sizes correspond to the FAS population. Week 68 responses were analyzed using an analysis of covariance model with randomized treatment as factor and baseline body weight as covariate.
Source: Clinical Study Report for STEP 8 (2021).27
Table 21: Percentage Change From Baseline to Week 68 in Body Weight for STEP 1 to STEP 4 Studies — Primary Analysis, In Trial, Full Analysis Set
Study | Semaglutide | Placebo | Treatment difference vs. placebo (95% CI) | ||
|---|---|---|---|---|---|
Baseline, kg | Mean (SD) change | Baseline, kg | Mean (SD) change | ||
STEP 1 | 105.4 (22.1) N = 1,306 | –15.6 (10.1) N = 1,212 | 105.2 (21.5) N = 655 | –2.8 (6.5) N = 577 | –12.44 (–13.37 to –11.51; |
STEP 2 | 99.9 (22.5) N = 404 | –9.9 (8.5) N = 388 | 100.5 (20.9) N = 403 | –3.4 (6.2) N = 376 | –6.21 (–7.28 to –5.15; |
STEP 3 | 106.9 (22.8) N = 407 | –16.5 (10.1) N = 373 | 103.7 (22.9) N = 204 | –5.8 (7.7) N = 189 | –10.27 (–11.97 to –8.57; |
STEP 4 | 96.5 (22.5) N = 535 | –8.3 (8.1) N = 520 | 95.4 (22.7) N = 268 | 6.5 (7.7) N = 250 | –14.75 (–16.00 to –13.50; |
CI = confidence interval; FAS = full analysis set; SD = standard deviation; vs. = versus.
Note: Baseline sample sizes correspond to the FAS population. For STEP 4, the initial baseline value is the week 20 (randomization) value and change is from week 20 to week 68. Week 68 responses were analyzed using an analysis of covariance model with randomized treatment as factor and baseline body weight as covariate.
Source: Clinical Study Reports for STEP 1 (2020),17 STEP 2 (2020),21 STEP 3 (2020),23 and STEP 4 (2020).25
Table 22: Patients With Reduction in Body Weight of 5% or More, 10% or More, 15% or More, and 20% or More for STEP 8 Study — In Trial, Full Analysis Set
Factor | Semaglutide Patients, n/N (%) | Liraglutide Patients, n/N (%) | Placebo Patients, n/N (%) | OR for semaglutide vs. liraglutide (95% CI) |
|---|---|---|---|---|
STEP 8 | N = 126 (FAS) | N = 127 (FAS) | N = 85 (FAS) | — |
≥ 5% | 102/117 (87) | 68/117 (58) | 23/78 (30) | Not reported |
≥ 10% | 83/117 (71) | 30/117 (26) | 12/78 (15) | |||| | ||||| |||||| |||||||| |
≥ 15% | 65/117 (56) | 14/117 (12) | 5/78 (6) | |||| | ||||||||||| |||||||| |
≥ 20% | 45/117 (39) | 7/117 (6) | 2/78 (3) | |||| | ||||||||||| |||||||| |
CI = confidence interval; FAS = full analysis set; OR = odds ratio; vs. = versus.
Note: Week 68 responses were analyzed using a binary logistic regression model with randomized treatment as factor and baseline body weight as covariate.
Source: Clinical Study Report for STEP 8 (2021).27
Table 23: Patients With Reduction in Body Weight of 5% or More, 10% or More, 15% or More, and 20% or More for STEP 1 to STEP 4 Studies — In Trial, Full Analysis Set
Factor | Semaglutide Patients, n/N (%) | Placebo Patients, n/N (%) | OR for semaglutide vs. placebo (95% CI) |
|---|---|---|---|
Reduction in body weight ≥ 5%, patients, n (%) | |||
STEP 1 | N = 1,306 (FAS) | N = 655 (FAS) | |
1,047/1,212 (86) | 182/577 (32) | 11.22 (8.88 to 14.19; P < 0.0001) | |
STEP 2 | N = 404 (FAS) | N = 403 (FAS) | |
267/388 (69) | 107/376 (29) | 4.88 (3.58 to 6.64; P < 0.0001) | |
STEP 3 | N = 407 (FAS) | N = 204 (FAS) | |
323/373 (87) | 90/189 (48) | 6.11 (4.04 to 9.26; P < 0.0001) | |
STEP 4 | N = 535 (FAS) | N = 268 (FAS) | |
461/520 (89) | 119/250 (48) | 8.52 (5.93 to 12.24; P < 0.0001)a | |
Reduction in body weight ≥ 10%, patients, n (%) | |||
STEP 1 | 838/1,212 (69) | 69/577 (12) | 14.68 (11.08 to 19.44; P < 0.0001) |
STEP 2 | 177/388 (46) | 31/376 (8) | 9.63 (6.34 to 14.64; P < 0.0001) |
STEP 3 | 281/373 (75) | 51/189 (27) | 6.87 (4.68 to 10.09; P < 0.0001) |
STEP 4 | 411/520 (79) | 51/250 (20) | 14.99 (10.30 to 21.80) |
Reduction in body weight ≥ 15%, patients, n (%) | |||
STEP 1 | 612/1,212 (51) | 28/577 (5) | 19.26 (12.89 to 28.76; P < 0.0001) |
STEP 2 | 100/388 (26) | 12/376 (3) | 7.65 (4.11 to 14.22; P < 0.0001) |
STEP 3 | 208/373 (56) | 25/189 (13) | 7.87 (4.90 to 12.63; P < 0.0001) |
STEP 4 | 331/520 (64) | 23/250 (9) | 19.07 (11.91 to 30.53) |
Reduction in body weight ≥ 20%, patients, n (%) | |||
STEP 1 | 388/1,212 (32) | 10/577 (2) | 26.89 (14.18 to 50.96; P < 0.0001) |
STEP 2 | 51/388 (13) | 6/376 (2) | 6.84 (2.86 to 16.33; P < 0.0001) |
STEP 3 | 133/373 (36) | 7/189 (4) | 13.73 (6.23 to 30.29; P < 0.0001) |
STEP 4 | 206/520 (40) | 12/250 (5) | 14.29 (7.77 to 26.28) |
CI = confidence interval; OR = odds ratio; vs. = versus.
Note: Week 68 responses were analyzed using a binary logistic regression model with randomized treatment as factor and baseline body weight as covariate. The denominator N values represent the number of observations at the relevant time point (68 weeks).
aThe P value was not controlled for multiplicity.
Source: Clinical Study Reports for STEP 1 (2020),17 STEP 2 (2020),21 STEP 3 (2020),23 and STEP 4 (2020).25
Change from baseline in waist circumference was also a confirmatory secondary outcome in the STEP 1 to STEP 4 studies (Table 25). The reduction in mean waist circumference was greater for semaglutide versus placebo in each of STEP 1 (treatment difference of – 9.42 cm [95% CI, –10.30 to –8.53; P < 0.0001]), STEP 2 (treatment difference of –4.88 cm [95% CI, –5.97 to –3.79; P < 0.0001]), STEP 3 (treatment difference of –8.34 cm [95% CI, –10.08 to –6.59; P < 0.0001]), and STEP 4 (treatment difference of –9.74 cm [95% CI, –10.94 to –8.54; P < 0.0001]). The change from baseline to week 68 was a supportive secondary outcome in the STEP 8 study, and the difference between semaglutide and liraglutide ||| ||||| || |||| ||| ||||||||||||(Table 24).
Body Mass Index
The mean change from baseline to week 68 in BMI was reported as a supportive secondary outcome in the STEP 1 to STEP 4 studies, and thus was not part of the statistical hierarchy (Table 26). The difference between groups with respect to mean change in BMI in STEP 1 was –4.61 kg/m2 (95% CI, –4.96 to –4.27), in STEP 2 was –2.26 kg/m2 (95% CI, –2.63 to –1.88), in STEP 3 was –3.77 kg/m2 (95% CI, –4.44 to –3.10), and in STEP 4 was –4.74 kg/m2 (95% CI, –5.16 to –4.32).
Table 24: Change From Baseline to Week 68 in Waist Circumference for STEP 8 Study — In Trial, Full Analysis Set
Study | Semaglutide | Liraglutide | Placebo | Treatment difference vs. liraglutide (95% CI) | |||
|---|---|---|---|---|---|---|---|
Baseline, cm | Mean (SD) change | Baseline, cm | Mean (SD) change | Baseline, cm | Mean (SD) change | ||
STEP 8 | 111.8 (16.3) | –13.6 (10.0) N = 114 | 113.5 (15.0) N = 127 | –6.8 (8.4) | 115.4 (15.1) N = 85 | –2.0 (7.2) | ||||| ||||||||||||| ||||||||| |
CI = confidence interval; FAS = full analysis set; SD = standard deviation; vs. = versus.
Note: Baseline sample sizes correspond to the FAS population. Week 68 responses were analyzed using an analysis of covariance model with randomized treatment as factor and baseline waist circumference as covariate.
aThe P value was not adjusted for multiplicity.
Source: Clinical Study Report for STEP 8 (2021).27
Table 25: Change From Baseline to Week 68 in Waist Circumference for STEP 1 to STEP 4 Studies — In Trial, Full Analysis Set
Study | Semaglutide | Placebo | Treatment difference vs. placebo (95% CI) | ||
|---|---|---|---|---|---|
Baseline, cm | Mean (SD) change | Baseline, cm | Mean (SD) change | ||
STEP 1 | 114.6 (14.8) | –14.1 (9.6) N = 1,210 | 114.8 (14.4) N = 655 | –4.4 (6.9) N = 575 | –9.42 (–10.30 to –8.53; P < 0.0001) |
STEP 2 | 114.5 (14.3) N = 404 | –9.7 (8.1) N = 387 | 115.5 (13.9) N = 403 | –4.3 (6.5) N = 375 | –4.88 (–5.97 to –3.79; |
STEP 3 | 113.6 (15.1) N = 407 | –15.2 (10.2) N = 371 | 111.8 (16.2) N = 204 | –6.1 (8.6) N = 189 | –8.34 (–10.08 to –6.59; P < 0.0001) |
STEP 4 | 105.5 (15.9) N = 535 | –6.9 (7.5) N = 518 | 104.7 (16.9) N = 268 | 3.2 (7.0) N = 248 | –9.74 (–10.94 to –8.54; P < 0.0001) |
CI = confidence interval; FAS = full analysis set; SD = standard deviation; vs. = versus.
Note: Baseline sample sizes correspond to the FAS population. For STEP 4, the initial baseline value is the week 20 (randomization) value and change is from week 20 to week 68. Week 68 responses were analyzed using an analysis of covariance model with randomized treatment as factor and baseline waist circumference as covariate.
Source: Clinical Study Reports for STEP 1 (2020),17 STEP 2 (2020),21 STEP 3 (2020),23 and STEP 4 (2020).25
Table 26: Mean Change From Baseline to Week 68 in Body Mass Index for STEP 1 to STEP 4 Studies — Full Analysis Set Population
Study | Semaglutide | Placebo | Treatment difference vs. placebo (95% CI) | ||
|---|---|---|---|---|---|
Mean (SD) baseline | Mean (SD) change | Mean (SD) baseline | Mean (SD) change | ||
STEP 1 | 37.8 (6.7) N = 1,306 | –5.8 (3.8) N = 1,212 | 38.0 (6.5) N = 655 | –1.0 (2.5) N = 577 | –4.61 (–4.96 to –4.27; P < 0.0001) |
STEP 2 | 35.9 (6.4) N = 404 | –3.6 (3.1) N = 388 | 35.9 (6.5) N = 403 | –1.2 (2.1) N = 376 | –2.26 (–2.63 to –1.88; P < 0.0001) |
STEP 3 | 38.1 (6.7) N = 407 | –6.2 (4.0) N = 373 | 37.8 (6.9) N = 204 | –2.2 (3.1) N = 189 | –3.77 (–4.44 to –3.10; P < 0.0001) |
STEP 4 | 34.5 (6.9) N = 535 | –2.7 (2.7) N = 520 | 34.1 (7.1) N = 268 | 2.0 (2.4) N = 250 | –4.74 (–5.16 to –4.32; P < 0.0001) |
CI = confidence interval; FAS = full analysis set; SD = standard deviation; vs. = versus.
Note: Baseline sample sizes correspond to the FAS population. For STEP 4, the initial baseline value is the week 20 (randomization) value and change is from week 20 to week 68. Week 68 responses were analyzed using an analysis of covariance model with randomized treatment as factor and baseline BMI as covariate. P values were not adjusted for multiple comparisons.
Source: Clinical Study Reports for STEP 1 (2020),17 STEP 2 (2020),21 STEP 3 (2020),23 and STEP 4 (2020).25
Health-Related Quality of Life
HRQoL was studied using the SF-36 in the STEP 1 to STEP 4 studies, and the mean change from baseline in physical functioning on the SF-36 was a confirmatory secondary outcome in each of these studies (Table 27). There was a statistically significant improvement in change in physical functioning score for semaglutide versus placebo in STEP 1 (1.80 [95% CI, 1.18 to 2.42; P < 0.0001]), STEP 2 (1.52 [95% CI, 0.44 to 2.61; P = 0.0061]), and STEP 4 (2.45 [95% CI, 1.59 to 3.32; P < 0.0001]). In STEP 3, the difference between groups was not statistically significant (0.84 [95% CI, –0.23 to 1.92; P = 0.1249]).
The proportion of patients achieving at least a 4.3-point increase from baseline in physical function, semaglutide versus placebo, was reported for STEP 1 (OR = 2.11 [95% CI, 1.53 to 2.91]), STEP 2 (OR = 1.72 [95% CI, 1.16 to 2.55]), STEP 3 (OR = 1.40 [95% CI, 0.80 to 2.44]), and STEP 4 (OR = 2.72 [95% CI, 1.18 to 6.29]) (Table 28).
Other domains of the SF-36 were reported descriptively for each group (refer to Appendix 4, Table 38).
Responses on the IWQOL-Lite-CT physical function score were reported as confirmatory secondary outcomes in the STEP 1 and STEP 2 studies. The difference between semaglutide and placebo in the mean change from baseline to week 68 in scores in STEP 1 was 9.43 (95% CI, 7.50 to 11.35; P < 0.0001) and in STEP 2 was 4.83 (95% CI, 1.79 to 7.86; P = 0.0018) (Table 29). Patients achieving at least a 20-point increase from baseline to week 68 were also reported; however, this outcome was not controlled for multiplicity. In STEP 1, 40% of semaglutide patients and 26% of placebo patients achieved this threshold (OR = 2.46 [95% CI, 1.90 to 3.18]) and in STEP 2, 35% of semaglutide patients and 23% of placebo patients achieved this threshold (OR = 1.73 [95% CI, 1.20 to 2.49]).
Table 27: Mean Change From Baseline to Week 68 in SF-36 Physical Functioning Score for STEP 1 to STEP 4 Studies — In Trial, Full Analysis Set
Study | Semaglutide | Placebo | Treatment difference vs. placebo (95% CI) | ||
|---|---|---|---|---|---|
Mean (SD) baseline | Mean (SD) change | Mean (SD) baseline | Mean (SD) change | ||
STEP 1 | N = 1,306 (FAS) | — | N = 655 (FAS) | — | — |
51.0 (6.9) N = 1,296 | 2.3 (6.6) N = 1,195 | 50.8 (7.9) N = 650 | 0.4 (7.4) N = 566 | 1.80 (1.18 to 2.42; P < 0.0001) | |
STEP 2 | N = 404 (FAS) | — | N = 403 (FAS) | — | — |
49.2 (8.8) N = 397 | 2.8 (7.7) N = 376 | 49.6 (8.3) N = 394 | 0.8 (7.0) N = 365 | 1.52 (0.44 to 2.61; P = 0.0061) | |
STEP 3 | N = 407 (FAS) | — | N = 204 (FAS) | — | — |
51.9 (6.7) N = 402 | 2.5 (5.7) N = 364 | 52.1 (6.8) N = 203 | 1.7 (5.7) N = 181 | 0.84 (–0.23 to 1.92; P = 0.1249) | |
STEP 4 | N = 535 (FAS) | — | N = 268 (FAS) | — | — |
53.8 (5.7) N = 534 | 1.0 (3.8) N = 515 | 54.1 (5.0) N = 268 | –1.2 (4.5) N = 245 | 2.45 (1.59 to 3.32; P < 0.0001) | |
CI = confidence interval; FAS = full analysis set; SD = standard deviation; SF-36 = Short Form (36) Health Survey; vs. = versus.
Note: For STEP 4, the initial baseline value is the week 20 (randomization) value and change is from week 20 to week 68. Week 68 responses were analyzed using an analysis of covariance model with randomized treatment as factor and baseline SF-36 physical function score as covariate. The N values (aside from those for the FAS) represent the number of observations at the relevant time point (68 weeks).
Source: Clinical Study Reports for STEP 1 (2020),17 STEP 2 (2020),21 STEP 3 (2020),23 and STEP 4 (2020).25
Table 28: Patients Achieving At Least a 4.3-Point Increase in SF-36 Physical Functioning Score From Baseline for STEP 1 to STEP 4 Studies — In Trial, Full Analysis Set
Study | Semaglutide Patients, n/N (%) | Placebo Patients, n/N (%) | Odds ratio for semaglutide vs. placebo (95% CI) |
|---|---|---|---|
STEP 1 | N = 1,306 (FAS) | N = 655 (FAS) | — |
318/1,195 (27) | 97/566 (17) | 2.11 (1.53 to 2.91; P < 0.0001) | |
STEP 2 | N = 404 (FAS) | N = 403 (FAS) | — |
111/376 (30) | 68/365 (19) | 1.72 (1.16 to 2.55; P = 0.0071) | |
STEP 3 | N = 407 (FAS) | N = 204 (FAS) | — |
86/364 (24) | 36/181 (20) | 1.40 (0.80 to 2.44; P = 0.2339) | |
STEP 4 | N = 535 (FAS) | N = 268 (FAS) | — |
58/515 (11) | 11/245 (5) | 2.72 (1.18 to 6.29; P = 0.0190) |
CI = confidence interval; FAS = full analysis set; SF-36 = Short Form (36) Health Survey; vs. = versus.
Note: Week 68 responses were analyzed using a binary logistic regression model with randomized treatment as factor and baseline SF-36 physical functioning score as covariate. The denominator N values represent the number of observations at the relevant time point (68 weeks). P values were not adjusted for multiple comparisons.
Source: Clinical Study Reports for STEP 1 (2020),17 STEP 2 (2020),21 STEP 3 (2020),23 and STEP 4 (2020).25
Table 29: Mean Change From Baseline to Week 68 in IWQOL-Lite-CT Physical Function Score for STEP 1 and STEP 2 Studies — In Trial, Full Analysis Set
Study | Semaglutide | Placebo | Treatment difference vs. placebo (95% CI) | ||
|---|---|---|---|---|---|
Mean (SD) baseline | Mean (SD) change | Mean (SD) baseline | Mean (SD) change | ||
STEP 1 | N = 1,306 (FAS) | — | N = 655 (FAS) | — | — |
65.4 (24.0) N = 1,296 | 15.0 (21.6) N = 1,193 | 64.0 (24.4) N = 649 | 6.0 (21.1) N = 566 | 9.43 (7.50 to 11.35; P < 0.0001) | |
STEP 2 | N = 404 (FAS) | — | N = 403 (FAS) | — | — |
67.1 (25.2) N = 397 | 11.4 (20.8) N = 376 | 69.2 (24.0) N = 394 | 4.9 (20.4) N = 365 | 4.83 (1.79 to 7.86; P = 0.0018) | |
CI = confidence interval; FAS = full analysis set; IWQOL-Lite-CT = Impact of Weight on Quality of Life–Lite Clinical Trials Version; SD = standard deviation; vs. = versus.
Note: Week 68 responses were analyzed using an analysis of covariance model with randomized treatment as factor and baseline IWQOL-Lite-CT as covariate. The N values (aside from those for the FAS) represent the number of observations at the relevant time point (68 weeks).
Source: Clinical Study Reports for STEP 1 (2020)17 and STEP 2 (2020).21
Table 30: Patients Achieving At Least a 20-Point Increase From Baseline to Week 68 for STEP 1 and STEP 2 Studies — In Trial, Full Analysis Set Population
Study | Semaglutide | Placebo | Odds ratio for semaglutide vs. placebo (95% CI) |
|---|---|---|---|
Patients, n/N (%) | Patients, n/N (%) | ||
STEP 1 | N = 1,306 (FAS) | N = 655 (FAS) | — |
473/1,193 (40) | 145/566 (26) | 2.46 (1.90 to 3.18; P < 0.0001) | |
STEP 2 | N = 404 (FAS) | N = 403 (FAS) | — |
131/376 (35) | 83/365 (23) | 1.73 (1.20 to 2.49; P = 0.0030) |
CI = confidence interval; FAS = full analysis set; IWQOL-Lite-CT = Impact of Weight on Quality of Life–Lite Clinical Trials Version; vs. = versus.
Note: Week 68 responses were analyzed using a binary logistic regression model with randomized treatment as factor and baseline IWQOL-Lite-CT score as covariate. The aforementioned P values were not adjusted for multiple comparisons. The denominator N values represent the number of observations at the relevant time point (68 weeks).
Source: Clinical Study Reports for STEP 1 (2020)17 and STEP 2 (2020).21
Normalization of Blood Glucose
Glycemic status (normoglycemic, prediabetes, diabetes) was assessed in all studies except STEP 2, which enrolled patients who already had type 2 diabetes.
In the STEP 8 study, in patients who were normoglycemic at baseline, the percentage of patients transitioning to prediabetes was ||| |||| ||| ||| for semaglutide, liraglutide, and placebo, respectively (Table 31). || |||||||| |||||||||| || ||||||||| In the STEP 1, STEP 3, and STEP 4 studies, 3% of semaglutide patients in each study progressed to prediabetes, while 6% to 13% of patients progressed to prediabetes in the placebo group.
In patients who were considered to have prediabetes at baseline, in the STEP 8 study, ||| of semaglutide patients became normoglycemic by end of study, compared to ||| of liraglutide patients and ||| of placebo patients, while for those progressing to diabetes, the results for semaglutide patients, liraglutide patients, and placebo patients were 3%, 3%, and 10%, respectively. In the STEP 1, STEP 3, and STEP 4 trials, 83% to 90% of semaglutide patients became normoglycemic compared to 48% to 68% of placebo patients. In the semaglutide group, no patients in STEP 3 or STEP 4 and 1% of patients in STEP 1 progressed to diabetes while in the placebo group, no patients in STEP 4, 1% of patients in STEP 3, and 3% of patients in STEP 1 progressed to diabetes.
Table 31: End-of-Study Status in Patients With Prediabetes or Normoglycemia at Baseline for STEP 8 Study
Study | Semaglutide | Liraglutide | Placebo | ||||||
|---|---|---|---|---|---|---|---|---|---|
Normoglycemic | Prediabetes | Diabetes | Normoglycemic | Prediabetes | Diabetes | Normoglycemic | Prediabetes | Diabetes | |
End-of-study status in patients with normoglycemia at baseline, n (%) | |||||||||
STEP 8 | || ||||||||| | | ||| | ||||| | || ||||||||| | | |||| | ||||| | || ||||||||| | || |||| | ||||| |
End-of-study status in patients with prediabetes at baseline, n (%) | |||||||||
STEP 8 | || ||||||||| | | ||| | | ||| | || ||||||||| | || |||| | | ||| | | ||||||||| | || |||| | | |||| |
Note: The N values in Table 31 represent the number of observations at the relevant time point (68 weeks).
Source: Clinical Study Reports for STEP 1 (2020),17 STEP 2 (2020),21 STEP 3 (2020),23 STEP 4 (2020),25 and STEP 8 (2021).27
Table 32: End-of-Study Status in Patients With Prediabetes or Normoglycemia at Baseline for STEP 1 to STEP 4 Studies
Study | Semaglutide | Placebo | ||||
|---|---|---|---|---|---|---|
Normoglycemic | Prediabetes | Diabetes | Normoglycemic | Prediabetes | Diabetes | |
End-of-study status in patients with normoglycemia at baseline, n (%) | ||||||
STEP 1 | 639 (97) N = 658 | 19 (3) | 0 | 303 (89) N = 340 | 37 (11) | 0 |
STEP 2 | NR | NR | NR | NR | NR | NR |
STEP 3 | 182 (97) N = 189 | 6 (3) | 0 | 81 (94) N = 87 | 5 (6) | 0 |
STEP 4 | 424 (97) N = 439 | 15 (3) | 0 | 185 (87) N = 213 | 27 (13) | 1 (1) |
End-of-study status in patients with prediabetes at baseline, n (%) | ||||||
STEP 1 | 466 (84) N = 554 | 85 (15) | 3 (1) | 110 (48) N = 230 | 113 (49) | 7 (3) |
STEP 2 | NR | NR | NR | NR | NR | NR |
STEP 3 | 162 (90) N = 181 | 19 (11) | 0 | 55 (55) N = 100 | 44 (44) | 1 (1) |
STEP 4 | 67 (83) N = 81 | 14 (17) | 0 | 23 (68) N = 34 | 11 (32) | 0 |
NR = not reported.
Note: The N values in Table 32 represent the number of observations at the relevant time point (68 weeks).
Source: Clinical Study Reports for STEP 1 (2020),17 STEP 2 (2020),21 STEP 3 (2020),23 and STEP 4 (2020).25
Table 33: Patients With Increase, Decrease, or No Change in Dose for Antihypertensive and Lipid-Lowering Medications for STEP 8 Study
Factor | Semaglutide, N = 117 | Liraglutide, N = 117 | Placebo, N = 79 | ||||||
|---|---|---|---|---|---|---|---|---|---|
Decrease, n (%) | No change, n (%) | Increase, n (%) | Decrease, n (%) | No change, n (%) | Increase, n (%) | Decrease, n (%) | No change, n (%) | Increase, n (%) | |
Antihypertensives | |||||||||
STEP 8 | | ||| | || |||| | || ||| | | ||| | || |||| | || ||| | | ||| | || |||| | | ||| |
Lipid-lowering medications | |||||||||
STEP 8 | | ||| | || |||| | | ||| | | ||| | || |||| | | ||| | ||||| | || |||| | | |||| |
Source: Clinical Study Report for STEP 8 (2021).27
Weight-Related Comorbidity
This outcome was not specifically studied in any of the included trials.
Non-Fatal Cardiovascular Event
This outcome was not reported as an efficacy outcome; however, these events were captured under the category of harms (Table 36 and Table 37). There were few non-fatal cardiovascular events across the studies and no clear differences in event rates between groups in any study.
Health Resource Utilization
This outcome was not specifically reported on in the included studies.
Dose Reduction or Complete Withdrawal of Concomitant Medications for Weight-Related Comorbidities
The percentage of patients who had a dose increase or decrease, or no change, from their baseline dosing of antihypertensive medication or lipid-lowering medication was an exploratory outcome of all the STEP trials. For the STEP 8 study, |||| of patients in the semaglutide group reduced their dose of antihypertensive medication versus |||| in each of the liraglutide and placebo groups, and |||| of patients in each of the semaglutide, liraglutide, and placebo groups increased their dose of antihypertensive medication (Table 33). In the STEP 1 to STEP 4 studies, dose decreases occurred in between 3% and 9% of semaglutide patients and between 2% and 4% of placebo patients, and dose increases occurred in between 4% and 7% of semaglutide patients and between 4% and 9% of placebo patients (Table 34).
Dose changes were also assessed for lipid-lowering medication. In the STEP 8 trial, |||| of semaglutide and liraglutide patients were able to reduce their dose versus no patients in the placebo group, and |||| of semaglutide patients, |||| of liraglutide patients, and |||| of placebo patients had a dose increase. In the STEP 1 to STEP 4 studies, 1% to 2% of semaglutide patients reduced their dose of lipid-lowering medication versus 0 to 1% with placebo, and 1% to 4% of patients in the semaglutide group had a dose increase versus 2% to 5% of placebo patients.
Physical Function
Physical function was assessed in the STEP 2 study using the 6MWT in patients with a BMI of 35 kg/m2 or greater (Table 35). The mean change (standard deviation [SD]) from baseline was 92.7 m (SD = 574.6) with semaglutide and 18.4 m (SD = 112.6) with placebo.
Table 34: Patients With Increase, Decrease, or No Change in Dose for Antihypertensive and Lipid-Lowering Medications for STEP 1 to STEP 4 Studies
Factor | Semaglutide | Placebo | ||||
|---|---|---|---|---|---|---|
Decrease, n (%) | No change, n (%) | Increase, n (%) | Decrease, n (%) | No change, n (%) | Increase, n (%) | |
Antihypertensives | ||||||
STEP 1 | 56 (5) | 216 (18) | 49 (4) | 10 (2) | 127 (22) | 45 (8) |
STEP 2 | 36 (9) | 160 (41) | 28 (7) | 14 (4) | 193 (51) | 34 (9) |
STEP 3 | 19 (5) | 68 (18) | 8 (2) | 4 (2) | 41 (22) | 10 (5) |
STEP 4 | 18 (3) | 97 (19) | 14 (3) | 5 (2) | 48 (19) | 11 (4) |
Lipid-lowering medications | ||||||
STEP 1 | 10 (1) | 155 (13) | 22 (2) | 6 (1) | 74 (13) | 23 (4) |
STEP 2 | 8 (2) | 178 (46) | 16 (4) | 3 (1) | 194 (51) | 19 (5) |
STEP 3 | 3 (1) | 49 (13) | 7 (2) | 1 (1) | 26 (14) | 5 (3) |
STEP 4 | 3 (1) | 59 (11) | 3 (1) | 0 | 27 (11) | 5 (2) |
Source: Clinical Study Reports for STEP 1 (2020),17 STEP 2 (2020),21 STEP 3 (2020),23 and STEP 4 (2020).25
Table 35: Change From Baseline to Week 68 in Six-Minute Walk Test for STEP 2 Study Subgroup
Study | Semaglutide | Placebo | ||
|---|---|---|---|---|
Mean (SD) baseline | Mean (SD) change | Mean (SD) baseline | Mean (SD) change | |
STEP 2 | 380.0 (132.3) N = 131 | 92.7 (574.6) N = 113 | 407.6 (106.9) N = 132 | 18.4 (112.6) N = 112 |
SD = standard deviation.
Source: Clinical Study Report for STEP 2 (2020).21
Harms
Only those harms identified in the review protocol are reported as follows. Refer to Table 36 for detailed harms data.
Adverse Events
In the STEP 8 study, 95% of patients in the semaglutide and placebo groups and 96% of patients in the liraglutide group reported at least 1 AE while on treatment during the study (Table 37). The most common AEs were GI-related, such as nausea (61% of semaglutide patients versus 59% of liraglutide patients versus 22% of placebo patients) and constipation (39% of semaglutide patients versus 32% of liraglutide patients versus 24% of placebo patients).
Table 36: Summary of Harms for STEP 1, STEP 2, and STEP 3 Studies — Safety Analysis Set
Harm | STEP 1 | STEP 2 | STEP 3 | |||
|---|---|---|---|---|---|---|
Semaglutide N = 1,306 | Placebo N = 655 | Semaglutide N = 404 | Placebo N = 403 | Semaglutide N = 407 | Placebo N = 204 | |
Patients with ≥ 1 AE, OTa | ||||||
n (%) | 1,171 (90) | 566 (86) | 353 (88) | 309 (77) | 390 (96) | 196 (96) |
AEs reported in ≥ 10% of patients (excluding notable harms) | ||||||
Nasopharyngitis | 281 (22) | 133 (20) | 68 (17) | 59 (15) | 90 (22) | 49 (24) |
Upper respiratory tract infection | 114 (9) | 80 (12) | 42 (10) | 38 (10) | 85 (21) | 44 (22) |
Headache | 198 (15) | 80 (12) | 31 (8) | 20 (5) | 78 (19) | 20 (10) |
Patients with ≥ 1 SAE, OTa | ||||||
n (%) | 128 (10) | 42 (6) | 40 (10) | 37 (9) | 37 (9) | 6 (3) |
Infections and infestations | 27 (2) | 10 (2) | 9 (2) | 9 (2) | 8 (2) | 0 |
Appendicitis | 5 (0.4) | 1 (0.2) | 1 (0.2) | 1 (0.2) | 3 (1) | 0 |
GI disorders | 18 (1) | 0 | 6 (2) | 3 (1) | 0 | 0 |
Hepatobiliary disorders | 17 (1) | 1 (0.2) | 2 (1) | 1 (0.2) | 10 (3) | 0 |
Cholelithiasis | 12 (1) | 1 (0.2) | 1 (0.2) | 0 | 7 (2) | 0 |
Musculoskeletal and connective tissue | 11 (1) | 5 (1) | 2 (1) | 2 (1) | 5 (1) | 0 |
Osteoarthritis | 3 (0.2) | 2 (0.3) | 1 (0.2) | 0 | 3 (1) | 0 |
Patients who stopped treatment due to AEs | ||||||
n (%) | 92 (7) | 20 (3) | 25 (6) | 14 (4) | 24 (6) | 6 (3) |
GI disorders | 59 (5) | 5 (1) | 17 (4) | 4 (1) | 14 (3) | 0 |
Fatal events, IT,b n (%) | 1 (0.1) | 1 (0.2) | 1 (0.2) | 1 (0.2) | 0 | 0 |
Causes | Sudden cardiac death | Glioblastoma | Myocardial infarction | Hepatocellular carcinoma | NA | NA |
Notable harms | ||||||
GI disorders, OT,a n (%) | 969 (74) | 314 (48) | 256 (64) | 138 (34) | 337 (83) | 129 (63) |
Nausea | 577 (44) | 114 (17) | 136 (34) | 37 (9) | 237 (58) | 45 (22) |
Diarrhea | 412 (32) | 104 (16) | 86 (21) | 48 (12) | 147 (36) | 45 (22) |
Vomiting | 324 (25) | 43 (7) | 88 (22) | 11 (3) | 111 (27) | 22 (11) |
Constipation | 306 (23) | 62 (10) | 70 (17) | 22 (6) | 150 (37) | 50 (25) |
Dyspepsia | 135 (10) | 23 (4) | 25 (6) | 5 (1) | 36 (9) | 10 (5) |
Abdominal pain | 130 (10) | 36 (6) | 13 (3) | 5 (1) | 54 (13) | 10 (5) |
Gallbladder-related disorders, OT,a n (%) | 34 (3) | 8 (1) | 1 (0.2) | 3 (1) | 20 (5) | 3 (2) |
Cholelithiasis | 23 (2) | 4 (1) | 1 (0.2) | 3 (1) | 13 (3) | 2 (1) |
Acute pancreatitis, OT,a n (%) | 3 (0.2) | 0 | 1 (0.2) | 1 (0.2) | 0 | 0 |
CV disorders, IT,b n (%) | 107 (8) | 75 (12) | 50 (12) | 39 (10) | 40 (10) | 22 (11) |
EAC-confirmed CV events | 6 (0.5) | 4 (0.6) | 6 (1.5) | 5 (1.2) | 2 (0.5) | 0 |
ACS | 4 (0.3) | 3 (0.5) | 2 (0.5) | 1 (0.2) | 0 | 0 |
Stroke | 1 (< 0.1) | 1 (0.2) | 3 (0.7) | 2 (0.5) | 1 (0.2) | 0 |
Coronary artery revascularization | 3 (0.2) | 0 | 0 | 1 (0.2) | 0 | 0 |
Hypoglycemia, OT,a n (%) | 8 (1) | 5 (1) | 23 (6) | 12 (3) | 2 (1) | 0 |
Severe | 0 | 0 | 1 (0.2) | 0 | 0 | 0 |
Injection site reactions, OT,a n (%) | 65 (5) | 44 (7) | 12 (3) | 10 (3) | 22 (5) | 12 (6) |
Psychiatric disorders, OT,a n (%) | 124 (10) | 83 (13) | 24 (6) | 15 (4) | 60 (15) | 24 (12) |
Anxiety | 32 (3) | 20 (3) | 3 (1) | 4 (1) | 18 (4) | 8 (4) |
Insomnia | 28 (2) | 18 (3) | 7 (2) | 4 (1) | 19 (5) | 10 (5) |
Depression | 15 (1) | 14 (2) | 2 (1) | 5 (1) | 16 (4) | 3 (2) |
Neoplasms — benign, malignant, and unspecified, n (%) | 46 (4) | 26 (4) | 10 (3) | 13 (3) | 43 (11) | 15 (7) |
ACS = acute coronary syndrome; AE = adverse event; CV = cardiovascular; EAC = event adjudication committee; GI = gastrointestinal; IT = in trial; NA = not applicable; OT = on treatment; SAE = serious adverse event.
aOT is defined as the time from first to last study drug administration plus 7 weeks’ follow-up.
bIT is defined as the interval from randomization to last contact with study site.
Source: Clinical Study Reports for STEP 1 (2020),17 STEP 2 (2020),21 and STEP 3 (2020).23
In the placebo-controlled studies, STEP 1 to STEP 4, AEs occurred in 88% to 96% of semaglutide patients and between 75% and 96% of placebo patients (Table 36 and Table 37). GI disorders were the most common AEs in the semaglutide groups in these studies, including nausea (14% to 58% in the semaglutide groups versus 5% to 22% in the placebo groups) and diarrhea (14% to 36% in the semaglutide groups versus 7% to 22% in the placebo groups).
Serious Adverse Events
In the STEP 8 study, SAEs occurred in 8% of semaglutide-treated patients, 11% of liraglutide patients, and 7% of placebo patients (Table 37). The most common SAEs were in the category of neoplasms — benign, malignant, and unspecified, occurring in 2% of patients in each of the semaglutide and liraglutide groups, and 1% of patients in the placebo group.
In the placebo-controlled studies, STEP 1 to STEP 4, SAEs occurred in 8% to 10% of patients in the semaglutide group and 3% to 9% of patients in the placebo group (Table 36 and Table 37).
Withdrawal Due to Adverse Events
In the STEP 8 study, permanent discontinuation of trial treatment due to AEs occurred in 3% of semaglutide patients, 13% of liraglutide patients, and 4% of placebo patients (Table 37). The most common reason for discontinuation of trial treatment was GI disorder, occurring in 1% in each of semaglutide and placebo patients, and 6% of liraglutide patients.
Permanent discontinuation of trial treatment due to AEs occurred in 6% to 7% of semaglutide patients and 3% to 4% of placebo patients in the STEP 1 to STEP 3 studies, and in 2% of semaglutide patients and 3% of placebo patients in the STEP 4 study, where patients had a 20-week run-in period (Table 36 and Table 37).
Table 37: Summary of Harms for STEP 4 and STEP 8 Studies — Safety Analysis Set
Harm | STEP 4 | STEP 8 | |||
|---|---|---|---|---|---|
Semaglutide N = 535 | Placebo N = 268 | Semaglutide N = 126 | Liraglutide N = 127 | Placebo N = 85 | |
Patients with ≥ 1 AE, OTa | |||||
n (%) | 434 (81) | 201 (75) | 120 (95.2) | 122 (96.1) | 81 (95.3) |
AEs reported in ≥ 10% of patients (excluding notable harms) | |||||
Nasopharyngitis | 58 (11) | 39 (15) | 10 (8) | 11 (9) | 9 (11) |
Upper respiratory tract infection | 23 (4) | 14 (5) | 9 (7) | 19 (15) | 18 (21) |
Headache | 41 (8) | 11 (4) | 20 (16) | 18 (14) | 10 (12) |
Arthralgia | 25 (5) | 15 (6) | 8 (6) | 14 (11) | 7 (8) |
Patients with ≥ 1 SAE, OTa | |||||
n (%) | 41 (8) | 15 (6) | 10 (8) | 14 (11) | 6 (7) |
Infections and infestations | 6 (1) | 4 (2) | 1 (1) | 4 (3) | 0 |
GI disorders | 1 (0.2) | 4 (2) | 0 | 0 | 0 |
Hepatobiliary disorders | 6 (1) | 2 (1) | 1 (1) | 2 (2) | 1 (1) |
Neoplasms — benign, malignant, and unspecified | 8 (2) | 1 (0.4) | 3 (2) | 2 (2) | 1 (1) |
Patients who stopped treatment due to AEs | |||||
n (%) | 8 (2) | 7 (3) | 4 (3) | 16 (13) | 3 (4) |
GI disorders | 2 (0.4) | 4 (2) | 1 (1) | 8 (6) | 1 (1) |
Fatal events, IT,b n (%) | 1 (0.2) | 1 (0.4) | 0 | 0 | 0 |
Cause | Unknown | Lung cancer | NA | NA | NA |
Notable harms, n (%) | |||||
GI disorders, OTa | 224 (42) | 70 (26) | 106 (84) | 105 (83) | 47 (55) |
Nausea | 75 (14) | 13 (5) | 77 (61) | 75 (59) | 19 (22) |
Diarrhea | 77 (14) | 19 (7) | 35 (28) | 23 (18) | 22 (26) |
Vomiting | 55 (10) | 8 (3) | 32 (25) | 26 (21) | 5 (6) |
Constipation | 62 (12) | 17 (6) | 49 (39) | 40 (32) | 20 (24) |
Dyspepsia | 9 (2) | 2 (1) | 11 (9) | 15 (12) | 5 (6) |
Abdominal pain | 35 (7) | 8 (3) | 8 (6) | 5 (4) | 1 (1) |
Gallbladder-related disorders, OTa | 8 (2) | 8 (3) | 1 (1) | 3 (2) | 1 (1) |
Cholelithiasis | 8 (2) | 7 (3) | 1 (1) | 2 (2) | 1 (1) |
Acute pancreatitis, OTa | 0 | 0 | 0 | 1 | 0 |
CV disorders, ITb | 26 (5) | 30 (11) | 16 (13) | 18 (14) | 9 (11) |
EAC-confirmed CV events | 1 (0.2) | 2 (1) | NR | NR | NR |
ACS | 0 | 1 (0.4) | NR | NR | NR |
TIA | 1 (0.2) | 0 | NR | NR | NR |
Coronary artery revascularization | 0 | 2 (1) | NR | NR | NR |
Hypoglycemia, OTa | 3 (1) | 3 (1) | 0 | 1 (1) | 0 |
Severe | 0 | 0 | 0 | ||
Injection site reactions, OTa | 14 (3) | 6 (2) | 0 | 14 (11) | 5 (6) |
Psychiatric disorders, OTa | 46 (9) | 35 (13) | 7 (6) | 19 (15) | 9 (11) |
Anxiety | 11 (2) | 8 (3) | | ||| | | ||| | | ||| |
Insomnia | 9 (2) | 7 (3) | 3 (2) | 7 (6) | 2 (2) |
Depression | 8 (2) | 8 (3) | | ||| | | ||| | | ||| |
Neoplasms — benign, malignant, and unspecified | 20 (4) | 6 (2) | | ||| | || ||| | | ||| |
ACS = acute coronary syndrome; AE = adverse event; CV = cardiovascular; EAC = event adjudication committee; GI = gastrointestinal; IT = in trial; NA = not applicable; NR = not reported; OT = on treatment; SAE = serious adverse event; TIA = transient ischemic attack.
aOT is defined as the time from first to last study drug administration plus 7 weeks’ follow-up.
bIT is defined as the interval from randomization to last contact with study site.
Source: Clinical Study Reports for STEP 4 (2020)25 and STEP 8 (2021).27
Mortality
There was no more than 1 death in any group in any of the included trials (Table 36 and Table 37).
Notable Harms
GI disorders were the most common of all the notable harms, as noted previously.
In the STEP 8 study, other notable harms included gallbladder-related disorders in 1% of each of the semaglutide and placebo groups, and 3% of liraglutide patients (Table 37). There were no cases of acute pancreatitis or hypoglycemia in the semaglutide or placebo groups, and 1 case of acute pancreatitis and 1 case of hypoglycemia in the liraglutide group. Cardiovascular disorders occurred in 13% of semaglutide patients, 14% of liraglutide patients, and 11% of placebo patients. There were no injection site reactions in the semaglutide group, and injection site reactions in 11% of liraglutide patients and 6% of placebo patients. Psychiatric disorders occurred in 6% of semaglutide patients, 15% of liraglutide patients, and 11% of placebo patients. The most common psychiatric disorders were anxiety (in 2% of semaglutide patients versus 3% of liraglutide patients versus 2% of placebo patients), insomnia (in 2% of semaglutide patients versus 6% of liraglutide patients versus 2% of placebo patients), and depression (in 2% of semaglutide patients versus 2% of liraglutide patients versus 1% of placebo patients). There were no reported cases of thyroid carcinoma.
In the placebo-controlled studies, STEP 1 to 4, gallbladder-related disorders occurred in between 0.2% and 4.9% of semaglutide patients and 0.7% and 3.0% of placebo patients, with the most common event being cholelithiasis, occurring in 0.2% to 3.2% of semaglutide patients and 0.6% to 2.6% of placebo patients. Very few patients had acute pancreatitis — between 0 and 0.2% of semaglutide patients and between 0 and 0.2% of placebo patients. Cardiovascular disorders occurred in 5% to 12% of semaglutide patients and between 10% to 12% of placebo patients and adjudicated cardiovascular events occurred in 0.2% to 1.5% of semaglutide patients and 0 to 1.2% of placebo patients.
Hypoglycemia occurred in 0.5% to 0.6% of semaglutide patients and 0 to 1.1% of placebo patients in the STEP 1, STEP 3, and STEP 4 studies, while in the STEP 2 study, where patients also had type 2 diabetes, they occurred in 6% of semaglutide patients and 3% of placebo patients. Injection site reactions occurred in 3% to 5% of semaglutide patients and 2% to 7% of placebo patients. Psychiatric disorders occurred in 6% to 15% of semaglutide patients and 4% to 13% of placebo patients. The most common psychiatric disorders were anxiety (in 0.7% to 4.4% of semaglutide patients versus 1.0% to 3.9% of placebo patients), insomnia (in 1.7% to 4.7% of semaglutide patients versus 1.0% to 4.9% of placebo patients), and depression (in 0.5% to 3.9% of semaglutide patients versus 1.2% to 3.0% of placebo patients).
Critical Appraisal
Internal Validity
Withdrawals from study were less than 10% in all groups across all studies, and in many groups were less than 5%, with no clear and consistent differences in study withdrawals between groups. Treatment discontinuations were more common in the placebo group in the STEP 1 study (17% versus 22% for semaglutide versus placebo) and STEP 4 study (6% versus 12% for semaglutide versus placebo). The large number of treatment withdrawals in STEP 1, the largest of the included studies, does potentially compromise the quality of the trial and data from the trial. There were no clear or consistent imbalances between comparison groups within studies with respect to key baseline characteristics such as weight, and the relatively low number of withdrawals from the studies should have helped to maintain these balances between comparison groups. There was missing data for week 68 assessments of all outcomes, including the primary outcome of percentage change from baseline in weight. The amount of missing data was often slightly larger than the reported number of study withdrawals, and it is not clear why this was the case. For example, in STEP 1 in the placebo group, the sample reported for the week 68 percentage change from baseline in weight was 577 patients, which is 12% less than the original baseline sample of 655, despite the fact that 7% of patients were reported as having withdrawn from the study in this group, and 22% were reported as having stopped treatment. A number of sensitivity analyses were performed to account for missing data, and their results were consistent with that of the primary analysis. Even though the overall conclusions may remain unaffected, the exact estimates of weight change could have been biased.
In all trials, patients were blinded to whether they received placebo or the active drug, and this was facilitated by the use of injector devices that were similar in appearance. Weight is an easily perceivable or measured indicator of treatment success, and it is possible that patients who are experiencing significant weight loss may begin to modify their behaviour to further enhance their weight loss. This compromises our ability to delineate weight loss directly to actual drug effect. Another source of potential unblinding in the placebo-controlled studies is the well-known and frequently observed GI side effects associated with this class — namely, nausea, vomiting, and diarrhea. These were far more common in the semaglutide group than in the placebo group in each of the studies, and this may have led some patients to guess which group they were assigned to.
HRQoL was assessed using the SF-36, a well-established generic scale, and the IWQOL-Lite-CT, a newer instrument developed for patients with overweight or obesity. A detailed review of the validity of both instruments can be found in Appendix 4. There is some evidence for the validity of the SF-36 for patients with overweight or obesity for the PCS and MCS; however, the validity of the subscales for this population has not been confirmed. No MID has been established for this instrument in this specific population. The IWQOL-Lite-CT is a shorter version of the IWQOL instrument, and although there is an MID for the longer instrument, there is no MID yet for the IWQOL-Lite-CT; this is a limitation when trying to interpret data from this instrument.
The STEP 4 study began with a 20-week run-in period where all patients received semaglutide and had their doses titrated to the eventual target dosage of 2.4 weekly by week 16. Aside from the fact that this is now a selected population that has demonstrated that they are able to tolerate the drug, patients who were randomized to placebo had their semaglutide discontinued. This type of design does help to reduce the number of study withdrawals and also provides information about potential withdrawal and/or rebound from removal of the drug. However, due to the potential for rebound upon drug withdrawal, this approach may also exaggerate the treatment effect, biasing results in favour of the study drug. Indeed, the largest treatment effect was seen in STEP 4, and this was the only trial where patients in the placebo group gained weight.
External Validity
The co-intervention that was employed in all the included trials was a diet and exercise regime. This is an issue when it comes to generalizability of findings from the STEP trials to how the drug may be used in clinical practice in Canada. Semaglutide is indicated as an adjunct to a reduced-calorie diet and physical activity. However, whether diet and exercise will be employed in a structured manner in real-world use and to the same extent that it was in the STEP trials is unclear. According to the clinical expert consulted by CADTH on this review, there is a lack of structured weight management programs that are financially accessible to patients in Canada. Therefore, it is not clear whether the weight loss achieved by semaglutide in the STEP trials will be of the same magnitude if these programs are not available to patients.
None of the trials included in this review were of sufficient size or duration to assess key clinical outcomes related to weight management — most notably, the risk of various weight-associated morbidities such as onset of type 2 diabetes and the risk of cardiovascular events. None of the morbidity-related outcomes in our review protocol were assessed as efficacy outcomes in the trials included in this review. The transition from normoglycemia to prediabetes, and the reverse, were assessed as exploratory outcomes; however, no conclusions can be drawn from this data. Cardiovascular events were not assessed as efficacy outcomes and when reported as harms, were uncommon. Therefore, although semaglutide clearly induces a statistically significant weight loss, the clinical significance of this weight loss, with respect to reducing the risk of various weight-related comorbidities, is uncertain and we do not know the long-term efficacy, or harms, of semaglutide.
HRQoL was assessed in the placebo-controlled trials but not versus liraglutide. Weight clearly has a significant impact on HRQoL and the impact on the physical function component of the SF-36 was formally assessed. However, other components, such as those related to mental health, were not, thus limiting any conclusions that can be drawn about this data. Given the impact that overweight and obesity have on mental health, the inability to draw conclusions about the impact of semaglutide on mental health is a limitation of the STEP trials.
There was 1 study, STEP 8, that compared semaglutide to an active comparator, liraglutide; the rest of the included trials were placebo-controlled. STEP 8 was, however, the smallest of the included trials, with only 125 patients in each of the 2 active groups. Therefore, there is limited direct evidence of the efficacy and harms of semaglutide compared to other drugs used for overweight or obesity.
In STEP 2, the clinical expert consulted by CADTH on this review noted that the inclusion criteria would not be generalizable to patients with type 2 diabetes who are receiving insulin, which could be a significant number of patients. They also noted that semaglutide is now approved as a 2.0 mg weekly dosage for type 2 diabetes and in the STEP 2 study, semaglutide was used at dosages of 1.0 mg weekly (previously the only dosage approved for type 2 diabetes) and 2.4 mg weekly. The clinical expert also noted that, other than in STEP 2, the populations were generally White females, which is not necessarily reflective of the general Canadian population with overweight and obesity but does tend to reflect the patients they see in their practice. The clinical expert also noted the fact that other than in STEP 2, patients were generally relatively free of comorbidities at baseline whereas patients with weight-related comorbidities are in greater need of an effective intervention.
Indirect Evidence
Objectives and Methods for the Summary of Indirect Evidence
The objective of this section is to summarize and appraise the evidence from ITCs for semaglutide versus relevant comparators for chronic weight management. Although semaglutide was compared with liraglutide in the STEP 8 trial, the sample size of the trial was small. Also, no direct evidence for semaglutide versus other relevant comparators was found. Therefore, evidence of efficacy and safety of semaglutide relative to active comparators is limited.
The sponsor submitted a systematic literature review and NMA to demonstrate the comparative effect of weekly semaglutide 2.4 mg when compared to relevant pharmacological comparators for weight management in patients with overweight or obesity.30 This ITC is summarized and appraised in this section.
A focused literature search for NMAs dealing with Wegovy (semaglutide) and weight management was run in MEDLINE All (1946-) on April 6, 2022. No limits were applied. One NMA comparing GLP-1 agents (dulaglutide, exenatide, efpeglenatide, liraglutide, lixisenatide, semaglutide, and taspoglutide) in terms of change in weight and AEs in adults with obesity or overweight was found31 and the results for semaglutide versus liraglutide 3.0 mg were consistent with the results for the sponsor-submitted NMA. Given the more comprehensive nature of the sponsor-submitted NMA, the published ITC is not described in this section.
Description of Sponsor-Submitted Indirect Treatment Comparison
The ITC included randomized trials of participants with a BMI of 27 kg/m2 or greater and 1 weight-related comorbidity, ||| || ||| ||||| || ||||||| |||| |||||||||||||| ||||||||||||||, or BMI of 30 kg/m2 or greater without weight-related comorbidities. The following interventions were of interest for the network: semaglutide 2.4 mg, || ||||||||| |||||||||| |||| ||| ||||||||| ||||||||||| ||| ||| |||||||| |||| |||||| |||||||||| ||| ||||||||| |||| |||||| ||||||||||| ||| |||||||||| |||| |||||| ||| |||||||||||||| |||||||| || ||||| ||||||||| Efficacy and safety outcomes were captured. Further details are reported in Table 38.
Table 38: Study Selection Criteria and Methods for Indirect Treatment Comparison
Characteristic | Indirect treatment comparison |
|---|---|
Population | Adults with:
Proposed populations of interest for the meta-analysis include:
|
Intervention |
|
Comparator | Any of the interventions listed previously |
Outcome | Efficacy outcomes |||||||||| || |||||||| |||||| || ||||| || || ||| ||| || |||||||| ||||||| |||| |||||||||| |||||| |||||| || |||||| |||||| |||||| || | |||| ||| || |||| |||| ||||| ||||||||||| || ||||| |||||||||||||||| ||||| || ||| ||| |||| ||||||| |||| ||| || ||||| |||||||||||||||| ||||| || ||| ||| |||| ||||||||||| ||||| || | |||||||||| || |||||||| ||||||||| |||| ||||||||||| || Safety outcomes
|
Study design |
|
Exclusion criteria | • |||||||||| |||||||||||||||||| ||||| |||||| ||||||||| ||||||||||||||||||||||||||| ||||||||||||||||||||||| ||||||| ||||||||||| |||| |||||||| |||||||||| |||||||||| ||||||||||||||||||||| ||||| |||||||||||| ||||||||||| ||||| | |||||||||| |||||||| |||| ||| |||| |||||||||| || | |||| ||||||| ||||||| ||| |||| |||| ||| |||||| ||| |
Databases searched | • |||||||||||||| |||||||||| ||||||| |||| ||||| || |||||| ||||||| |||||||||| | ||||| ||||||||||| ||||||||| ||| ||||||| |||||| |||| ||||||| |||||||||| ||| ||| ||||||||| ||| |||||||| |||||| ||||||| |||||||| |||||||||| ||||||||| |||||||| ||||||| |||||||| || |||||||||| |||||| |||||||||| ||||||||| || ||||||||| || ||||||| || ||||||| |||||| |
Selection process | Articles were screened independently by 2 analysts |
Data extraction process | Data were extracted by 1 analyst and checked by another |
Quality assessment | |||||||| ||||||||| ||| |||||| ||| |||| |||||||||| |||||| |||||||||||||| |||||||||| |
BMI = body mass index.
a|||||||||| ||||| |||||| ||| ||||||||||||| ||||||||||| |||||||||| |||| | ||||||||||||| |||||| ||||||| ||||||||| ||||||| ||| ||| ||||||||||| ||| |||| |||||||| |||||||| |||| |||| ||||||||| ||| ||| |||||||||| || |||||||| |||||||| ||||||| |||||||| ||||||
Source: Sponsor-submitted indirect treatment comparison (2022).30
Methods of Sponsor-Submitted Indirect Treatment Comparison
Objectives
To determine the efficacy and safety of weekly semaglutide 2.4 mg when compared to relevant pharmacological comparators for weight management in patients with overweight or obesity
Study Selection Methods
This systematic literature review involved searches from |||| |||||||||| ||||||||| ||| ||| |||| ||||||||| ||||||| ||||||| |||||||||| ||||||| |||| ||||| || |||||| ||||||| |||||||||| | ||||| ||||||||||| ||||||||| ||| ||||||| |||||| ||| ||| ||||||| |||||||||| ||| ||| ||||||||| ||| |||||||| |||||| ||||||| |||||||| |||||||||| ||||||||| |||||||| ||||||| |||||||| || |||||||||| |||||| |||||||||| |||||||| || ||||||||| || ||||||| || ||||||| |||||| ||| ||| |||||||| |||||||| || |||||||||| |||||||| The retrieved articles were reviewed by a single analyst and verified by a second in 2 stages (titles and abstracts, then full text) based on pre-specified inclusion criteria. Risk of bias was assessed using ||| |||||||| ||||||||| ||| |||||| ||| |||| |||||||||| |||||| |||||||||| ||||||||| |||| |||||||| |||||||||| || |||||||||||||| |||||||||| |||||||||||| |||||||| |||||||||||||||| ||||||||| ||||||||| || ||||||||| ||||||||| || ||||||| ||||||||| ||| |||||||||
Indirect Treatment Comparison Analysis Methods
Prior to conducting the ITC, a feasibility assessment was conducted. This included an assessment of trial comparability and generation of outcome-specific networks. The efficacy outcomes of interest were |||||||||| || |||||||| |||||| || ||||| ||| |||| ||| ||| || |||||||| ||||||| |||| ||||||| |||||| |||| |||||||| || |||||| || ||| ||||||| |||||| |||| |||||||| ||||||| |||||| |||| |||||||| || |||||||| ||||| |||||||| ||||| || ||||| |||||| |||| |||||||| || ||||| ||||||||||| || ||||| |||||||||||||||| ||||| || ||| ||| |||| |||||||| |||||| |||| |||||||| || |||| ||||||| ||||||||||| ||||| || ||||| |||||||||||||||| ||||| || ||| ||| |||| |||||||| |||||| |||| |||||||| || ||||| || || ||||||||| || |||||||| ||||||||| |||| ||||||||||| || |||||| ||||||| |||||||||| ||||||||| || |||||||| |||||||| |||||||||||||||| |||||||||| ||||||||| || |||||||| |||||||| ||||||| |||||||| |||||| ||| |||||| |||| |||||||| || ||||| ||||||||||||| || ||| ||| |||||| |||||||| || |||||||| |||| ||||||||| || |||||||||||||| ||||||||| || ||||| ||| ||||||||| |||||||||||||||| ||| || ||||
ITCs were conducted using a |||||||| ||||||||| ||| ||||||||||| |||||| ||||||||| |||||||| |||| | |||||| |||||||||| |||||||| |||| ||||| ||| |||||||||| |||||||| ||| ||| |||||||| |||||||||| ||||| |||| ||||| ||| |||||| ||||||||| |||| |||||| ||||||| |||| ||| ||||| ||||||| |||| |||||| |||| |||| ||| ||||| ||| ||| |||||||| || ||||||||| ||| |||||||| || ||||||| ||||| |||||||| ||||||||| || ||| || ||||| ||| || ||||||||| ||| |||||||| ||||||||||| ||||||||| |||||| ||||||||||| || | || | |||||| || ||| |||||||||| |||||||||| ||| ||| ||||| |||||||| ||||||||| Presented models were selected based on model fit.
The selection of priors, burn-in period, and number of iterations was not described.
Interstudy heterogeneity ||| |||||||| ||||||||||||| ||| ||||| ||||||| ||||||| |||||||||||||||| ||| ||||||| |||||||||||
Sensitivity analyses were conducted by excluding trials of ||||||||| ||||||||||| ||||||| ||||| ||||||| || ||||| ||||| ||||||||||||| |||||||| ||| |||||||| |||||| ||||||||||||| ||| ||||||||| || ||| ||| | ||||||| |||||| ||| ||||||||| |||||||| ||||||||| ||||||| ||||||| |||||||| |||| || ||||| |||||| |||||| |||| ||||||| ||||
Subgroup analyses were conducted for patients |||| |||| | |||||||| ||||||||| |||||||| ||||||| |||| | |||||||| ||||||||| |||||||| |||| |||||| ||||||| |||||||||| ||| |||||||| |||| ||||||||||||
||||||||||| ||| ||| ||||||||| ||| || | |||| || |||||| ||||| ||||| |||| ||||| |||||| || ||||||||| ||||||| No pairwise meta-analyses were presented.
Results of Sponsor-Submitted Indirect Treatment Comparison
Summary of Included Studies
|| |||||| ||| ||||||||||||| of pharmaceutical interventions were eligible. ||||| |||||| |||| ||||||| |||| ||| ||||||||||| |||||||||| ||||||| |||| |||| | |||||| |||||| || |||||||| |||||||||||| ||| ||| | ||| ||||||||| || ||||||| |||| ||||||| ||||||| || ||||||| ||||| |||||| ||| |||| | ||| | ||||||| |||| ||||| || |||| || ||||||||The main sources of ||||||||||| |||| |||| ||||||| || ||| ||||||||| ||||||||| || ||||||| |||| |||| || || ||||||| ||| ||||||||| || ||| || | ||||||||| |||||||||||| || |||| ||||||| ||||||| ||||| |||| |||| ||||||| |||||||||||| ||||| |||||| ||||| ||||||||| ||| ||||||||| || ||||| |||| ||| ||||| ||| ||| |||| ||| ||||| ||| |||||||| | |||||||||| |||| | |||||| |||| ||| || |||||||| |||||||| |||| ||| ||||| |||||||||| ||||| ||||| |||||||| |||||||| |||| ||| ||||| ||||||||| ||||| ||||||||| ||| ||||||||| |||||||| | |||||| |||| ||| || ||| |||||||| |||||||| |||| ||| ||||| |||||||There were insufficient data to permit the exploration of |||||||||| ||||||||||| || ||||| || |||| ||||||| |||||| ||| ||| ||||| |||||||| ||||||||| However, the impact of these factors across the trials (in addition to unknown patient characteristics) could be assessed via meta-regression based on the baseline risk in the control arms.
A summary of the heterogeneity among trials for key baseline characteristics and study design features are shown in Table 39.
Table 39: Assessment of Homogeneity for Sponsor-Submitted Indirect Treatment Comparison
Characteristic | Description and handling of potential effect modifiers |
|---|---|
Age at baseline | Mean age at baseline ranged from ||||| |||||| |||| ||||| ||||| |||||||| |||| ||| |||||| || |||| || ||||||||| ||| ||||||||| || ||||| |||| ||| ||||| ||| ||| |||| ||| ||||| ||| |||||||| | |||||||||| |||| | |||||| |||| ||| || ||||||||| |
Gender | The percentage of enrolled males ranged from || || ||| |
Weight | Mean weight ranged from |||| || |||||| |
BMI | |||| ||| |||||| |||| ||||||| || |||||||||| ||| ||||| ||||| |||||||| |||||||| |||| ||| ||||| ||||||||| ||||| ||||||||| ||| ||||||||| |||||||| | |||||| |||| ||| || ||| |||||||| |||||||| |||| ||| ||||| ||||||| |
Hemoglobin A1C | The mean hemoglobin A1C ranged from |||| || ||||| |
Clinical trial eligibility criteria | || |||||| ||||||||||| |||||||| |||||||| |||| |||| || | |||||||||| || |||||||| |||| |||| |
Study design | || |||||| |||||||| ||||||| || | |||||| |||||| ||||| |||||||| |||| ||||||||| |||||||||| || |||||| | ||||| ||| |||||||||||||| |||||||| ||||||| ||| || || | |||||| || | || ||| ||||||| |||| ||||| |||||||| |||| |||||||||||| |||||||||| |||||| ||| |||||| |||||| |||||||||| |||| ||||||||||| |||| |||||||||| || |||||||||| |
Co-interventions | Five trials specified ||| || |||| || ||| ||||||||| |||||||||||||| The components of ||| were inconsistently reported across the trials, but comprised |||||||||||| ||||||| |||||| ||| ||||||||| |||||||| |||||||| |
Dosing of comparators | |||||||||||| ||| |||||| |||||||||| |||||||| || ||||||||||| ||| || |||| ||||| ||| |||||||| || |||||||||| |||||| || | ||||| ||||| ||||||||||| ||| |||||||||||| || | |||| || ||| || ||| ||||||||| || |||||| |||||||||| || ||||| ||| ||||| ||||||||||||||| ||| |||||| |||||||||| |||||||| || |||||||| ||| || ||||| ||||| ||||| |||| |||||| ||| |||||| |||| |||||||| || |||||||| || || ||||| ||||| ||||| |||||||||||||||| ||| |||||| |||||||||| |||||||| || |||||||||| || |||||| ||| ||||||||| ||| |||||| ||| |||||||| || |||||||||| |||||| || | ||||| ||||| ||||| |||| ||| ||||||||| || | ||||||| || ||| ||||| ||||||||||| |||| ||| ||||||||| |||||| ||| ||| ||||| | ||||||||||||||||||| ||| |||||| |||||||||| |||||||| || ||||||||||| || |||||| ||| |||||||||| || |||||| ||| |||||||| || |||||||||| |||||| || | ||||| ||||| ||||| |||| ||| ||||||||| || | ||||||| || ||| ||||| ||||||||||| |||| ||| ||||||||| |||||| ||| ||| ||||| | ||||||||||||||||||| ||| |||||| |||||||||| |||||||| || ||||||||||| ||| || |||| || ||||||| ||||||| ||||||||||||||| |||||| |||||| ||||| ||| |||| ||| ||||||||| ||||||||| ||||| | ||||| ||| ||||| || |||| |||| ||| ||| ||| |||||||| || ||| ||||||||||| |||| || ||| |||||||| ||||| ||| ||||||||| ||| || |||||||||| || |||||| |
Timing of end point evaluation or trial duration | All trial end points were between ||||| ||||| |
BMI = body mass index; T2DM = type 2 diabetes mellitus; |||| ||||||||| |||||||||| |||||||.
Results
A graphical depiction of the evidence network for the total population without consideration for availability of outcome data are shown in Figure 2.
Figure 2: Evidence Network for the Total Population — Non–Outcome Specific — Redacted

This figure has been redacted as per the sponsor’s request.
||| | ||||| ||||| | |||.
Source: Sponsor-submitted indirect treatment comparison (2022).30
||||| |||||||| |||| ||||||||| |||||| ||||||||| |||| | |||||||| ||||||||||||||||||| ||||.
The models with the best fit (base-case models) are reported as follows:
Semaglutide was associated with ||||||| |||| || |||||||| ||||||||| || ||||| || |||||| |||| ||||| || ||||| || ||| |||| ||||||||||| |||||| |||||||| |||| ||||||||||| ||| || ||| |||||||| || || ||||| ||||| ||||| ||| |||||||
Semaglutide was associated with a ||||||| ||||||| ||||||||| |||| |||||||| || |||||| |||||||| |||| ||||||||||| ||| ||| |||||||||| || || ||| ||||||||| ||| ||| |||||||||| || || ||| ||||||||| ||| ||| |||||||| ||| || ||||| ||||| |||||| ||| |||||||| || || ||||| ||||| ||||| ||| ||||||||There was no evidence for a |||||||||| || |||| || |||| ||||||| ||||||||||| ||| ||||||||||| ||| ||| |||| ||||||| || |||||||||| ||| ||||||||||| ||| |||||||| ||| || ||||| ||||| ||||| ||| |||||||The treatment effects for semaglutide versus relevant comparators were ||||||||| ||||||| ||| |||| |||||||| || ||| |||| |||||||| |||||| |||||||||| |||||||| |||| ||| ||||| ||||||||||| || ||| |||||||| || |||||||| |||| ||||| ||||| ||| || |||||||| || | |||||||||| ||||||| ||||||||||| ||| ||||||||||| || |||||||||||||||||||| ||| |||||| |||||
Sensitivity analyses excluding trials of ||| were largely consistent with the main analyses.
The results of the main analyses are summarized in Table 40.
Table 40: Base-Case Analysis for Total Population of Semaglutide Versus Comparator — Redacted
|||||||||| | |||||||||| | ||||||||||| ||| || | |||||||||| || ||| ||||||||| ||||| | |||||||||| || ||| ||||||||| ||||| | |||||||| ||| || ||| | |||||||| || || ||| |
|---|---|---|---|---|---|---|
| || ||||||||| |||| |||||||| || |||| |||||| ||||| || ||||| || |||| ||||||||||| ||||||| || |||| |||| | ||||| |||||||||| | |||| ||||||| ||||| | |||||| | |||||| | |||||| | |||| ||||||| |||||| |
|||||| | |||| ||||||| |||||| | |||||| | |||||| | |||||| | |||||| | |
||||||| ||| || ||||||| |||| |||||||||| |||| |||| | ||||| |||||||||| | ||||| |||||||| |||||| | ||||| ||||||||| |||||| | ||||| ||||||||| |||||| | |||||||||||||| |||||| | ||||| ||||||||| |||||| |
|||||| | ||||| |||||||| ||||| | |||||| | ||||| ||||||| ||||| | |||||| | |||||| | |
|||||||||| || |||||||| |||| || |||| || |||| |||| | ||||| |||||||||| | |||| ||||||| ||||| | |||| ||||||| ||||| | |||| ||||||| ||||| | |||| ||||||| ||||| | |||||| |
|||||| | |||| ||||||| ||||| | |||||| | |||| ||||||| ||||| | |||||| | |||||| |
CFB = change from baseline; CrI = credible interval; |||||| |||||||| ||||||||||| |||||| |||| |||||||||||| ||||||||||| NA = not applicable; |||| | |||| | |||||||| ||||||||.
Note: Results that exclude the null value (1 for OR and 0 for mean difference) are indicated in bold.
||||| |||||| ||||||| |||||| |||| |||| ||| |||| ||||||||
Table redacted as per sponsor’s request.
Critical Appraisal of Sponsor-Submitted Indirect Treatment Comparison
The reported ITC was based on a broad systematic literature review, with study inclusion criteria reported transparently. A study protocol was finalized between Novo Nordisk and Mtech Access before conducting the review. Data were extracted in duplicate. The analyses were appropriately conducted and reported. The patients in the included studies match the people who would use this intervention in the real world. Key efficacy and safety outcomes were reported. Follow-up duration ||| |||||||||| |||||| ||||||. There was some ||||||||||| |||||||| ||||||||||||| |||| ||||||| || ||| |||||||||||| || |||| ||||||| ||||||| |||| ||| ||| || ||||||| |||||||| ||| ||| |||||||||||||||| in some trials. Further, it is unclear how the ||||||||| |||||||||| || |||||||| ||||||| |||| |||||| |||||| ||||| |||| |||||||| ||| |||||||| || ||||||||||| ||||||||||||| ||| ||||||||| || ||| ||||| ||||| ||| ||||||||||||| ||| || ||||||| ||||||| |||||||||||||||| |||||||| |||||||| |||| |||||||||| A sensitivity analysis was also conducted to assess the impact of including studies |||| ||| ||||||||||||| ||||| ||| |||| || | ||||||| ||||||| || ||||||||||||||| ||| |||||||||| |||||||| ||||||||| |||| ||||||||| ||||| |||||| ||| || ||| ||| || |||||| ||||||| ||||||| Reporting of methods was ||| ||||||||||||| || ||||||| || ||| |||||||| ||||||| ||| ||| ||||||||| |||||| || ||||||||||| || |||||| ||| |||||| || |||| || ||||| ||||||||||| |||||||| || ||||||| ||| |||||| || ||||||| ||||||| |||| ||| ||||||||||
Other Relevant Evidence
This section includes submitted long-term extension studies and additional relevant studies included in the sponsor’s submission to CADTH that were considered to address important gaps in the evidence included in the systematic review.
Long-Term Study (STEP 5 Study)
STEP 5 was the only 2-year (104-week) study in the STEP series of studies, and the reviewers believed that this additional follow-up might be useful when assessing efficacy and harms associated with semaglutide treatment. Like the STEP 1 to STEP 4 studies, STEP 5 was a placebo-controlled trial, although it was not pivotal and thus did not meet the inclusion criteria for the systematic review.
Methods
STEP 5 was a DB RCT conducted at 41 sites in Canada, the US and Europe, and randomized 304 patients with overweight or obesity, 1:1, to either semaglutide or placebo. Outcomes were similar to the other STEP trials, with the co-primary outcomes being percentage change from baseline in body weight and the percentage of patients achieving a 5% or greater weight reduction. Confirmatory secondary outcomes included the percentage of patients who achieved a 10% or greater reduction in weight by week 104, a 15% or greater reduction in weight by week 104, and change from baseline to week 104 in waist circumference, systolic blood pressure, and SF-36 (physical functioning).
Populations
Inclusion and exclusion criteria were similar to the STEP 1, STEP 3, STEP 4, and STEP 8 studies. Included were adults with a BMI of 30.0 kg/m2 or greater, or 27.0 kg/m2 or greater with at least 1 weight-related comorbidity and a history of at least 1 unsuccessful attempt at losing weight. To be randomized, patients also had to have kept a food diary, have a PHQ-9 score of less than 15 at randomization, and have no suicidal behaviour or ideation before randomization.
Interventions
Patients received a semaglutide SC 2.4 mg injection once weekly as an adjunct to a reduced-calorie diet and increased physical activity, versus matching placebo. The main co-intervention was diet and exercise, and these followed a protocol similar to those in the other STEP studies.
Outcomes
The efficacy outcomes were as described earlier and assessed as described previously for the STEP studies in the systematic review section of this report.
Statistical Analysis
||||||||||| |||||||| |||| ||| |||| || ||||| ||||||||| ||||| ||| ||| |||| |||||| |||| |||| |||||||| || ||| |||||||||| ||||||| | |||||||||||| ||||||| ||||||||| ||| |||| || ||||||| ||| |||| | |||||| ||| ||| |||||||| |||| |||||||| || ||| ||||||||| ||| ||| ||||| |||| |||||||| |||| ||||||| || ||| |||| |||||| |||||||| || ||| |||||||||| ||||||| |||| ||| ||||||||||| ||||||||| ||| |||| |||||||| ||| |||||||| ||| |||||||||| ||||||||| ||| ||| |||||| |||||||| ||| |||||||| ||| |||||||||| |||||||| ||| |||||||| || ||||| | |||| || ||||| ||||| ||| ||||||||||| ||||||| |||| |||||||| ||| ||| |||||| |||||| ||| ||| |||| |||| ||||||||||||| || |||| ||||||| |||| ||| ||||| ||||| ||| ||| |||||||||||| |||||| ||| ||| |||||| |||| ||||| || |||| ||||||| ||||||||||||||| |||| | ||||| |||| ||||||||| |||| ||| |||||||| |||||| ||| ||| ||||||| |||| ||| |||| ||| |||||||||||| |||||||| |||| ||| |||||| || |||| | ||||| ||||| ||| ||||||| ||||||| |||||| ||| ||||||||||| ||||||||
Patient Disposition
Trial product was permanently discontinued in ||| of patients in the semaglutide group and ||| of patients in the placebo group. The most common reason for ||||||||||||| ||||| ||||||| || ||| ||||||||||| ||||| ||| ||||||| ||||| ||| ||| || ||| ||||||||||| ||| |||||||| |||||||||||||| while “lost to follow-up” ||| ||| |||| |||||| |||||| || ||| ||||||| ||||| ||| ||| |||| Withdrawals from trial occurred with || || ||||||||||| |||||||| and ||| || ||||||| ||||||||, and “lost to follow-up” was the |||| |||||| |||||| |||| ||||||||||| |||| ||| |||| ||||||| |||||
Factor | STEP 5 study | |
|---|---|---|
Semaglutide | Placebo | |
Screened | |||||| | |
Screen failures | |||||| | |
Withdrawn before randomization | |||||| | |
Randomized | 152 (100) | 152 (100) |
Randomized in violation of inclusion, exclusion, and/or randomization criteria | | ||||| | | ||||| |
Trial product permanently discontinued, n (%) | || |||||| | || |||||| |
Adverse event | || ||||| | | ||||| |
Protocol violation | |||||| | | ||||| |
Pregnancy | | ||||| | |||||| |
Lack of efficacy | | ||||| | | ||||| |
Safety concern as judged by the investigator | | ||||| | | ||||| |
Withdrawal of consent | |||||| | | ||||| |
Lost to follow-up | | ||||| | || ||||| |
Other | | ||||| | | ||||| |
Withdrawn from trial, n (%) | | ||||| | || |||||| |
Withdrawal by subject | 0 | 4 (2.6) |
Lost to follow-up | 3 (2.0) | 14 (9.2) |
Death | 1 (0.7) | 0 |
Full analysis set, N | 152 (100) | 152 (100) |
Safety set, N | 152 (100) | 152 (100) |
Source: Clinical Study Report for STEP 5 (2021).32
Exposure to Study Treatments
The mean exposure to semaglutide was |||| ||||| || |||| ||||| for placebo, and the mean observation time was 110.5 weeks for semaglutide and 103.4 weeks for placebo.
Efficacy
Semaglutide evoked a statistically significantly greater percentage reduction in weight versus placebo, with a treatment difference between groups of –12.55% (95% CI, –15.33 to –9.77; P < 0.0001); this was the co-primary outcome of STEP 5. Figure 8 The other co-primary outcome was patients achieving a 5% or greater reduction in weight from baseline to week 104. This was achieved by 77% of semaglutide patients and 34% of placebo patients, a statistically significant difference between groups.
In patients who were normoglycemic at baseline| || || ||||||||||| |||||||| ||| ||| || ||||||| |||||||| were prediabetic by the end of trial, and in patients with prediabetes at baseline ||| || ||| ||||||||||| ||||| ||| ||| || ||| ||||||| ||||| |||||| ||||||||||||| || |||| |||, and || |||||||| || ||| ||||||||||| ||||| ||| || || |||||||| || ||| ||||||| ||||| |||| || || ||||||| |||||||| || ||| || |||||.
Harms
AEs were experienced by ||| of semaglutide patients and ||| of patients in the placebo group, while || of semaglutide patients and ||| in the placebo group had an SAE. As was the case with the STEP trials included in the systematic review, the most common AEs, semaglutide versus placebo, were || ||||||||| |||| || |||||| |||| || |||| and |||||||| |||| || ||||. Among other notable harms, semaglutide versus placebo, ||||||||||| ||||||||| |||||||| || || || ||| || ||||||||| || ||| || |||| |||||||||||| || || || ||||| ||||||||| |||| ||||||||| || || || |||| ||| ||||||||||| ||||||||| || ||| || |||| ||||| |||| || ||||| || ||||| |||||||||||||
Table 42: Efficacy Results for STEP 5 Study — Full Analysis Set
Outcome | STEP 5 | |
|---|---|---|
Semaglutide N = 152 | Placebo N = 152 | |
Mean change in body weight | ||
Baseline, kg (SD) | 105.6 (20.8) N = 152 | 106.5 (23.1) N = 152 |
Percentage change from baseline to week 104, kg (SD) | –15.9 (12.3) | –1.9 (8.9) |
Difference, semaglutide vs. placebo (95% CI) | –12.55% (–15.33 to –9.77; P < 0.0001) | |
Patients with reduction in body weight, n/N (%) | ||
≥ 5% | 111/144 (77.1) | 44/128 (34.4) |
OR (95% CI) | 4.99 (2.95 to 8.42; < 0.0001) | |
≥ 10% | 89/144 (61.8) | 17/128 (13.3) |
OR (95% CI) | |||| | ||||||||||| ||||||| | |
≥ 15% | 75/144 (52.1) | 9/128 (7.0) |
OR (95% CI) | |||| | ||||||||||| ||||||| | |
≥ 20% | 52/144 (36.1) | 3/128 (2.3) |
OR (95% CI) | ||||| | ||||||||||| ||||||| | |
Mean change in BMI, kg/m2 | ||
Baseline (SD) | 38.6 (6.7) N = 152 | 38.5 (7.2) N = 152 |
Mean change from baseline to week 104 (SD) | –6.2 (5.3) N = 144 | –0.7 (3.5) N = 128 |
Difference, semaglutide vs. placebo (95% CI) | ||||| ||||||||||||| ||||||||| | |
End-of-trial glycemic status of patients normoglycemic at baseline | ||
Normoglycemic | |||||||| | ||| ||||| |
Prediabetic | |||||||| | ||||||||| |
Diabetic | ||||||| | |||||||| |
End-of-trial glycemic status of patients prediabetic at baseline | ||
Normoglycemic | |||||||| | |||||||| |
Prediabetic | ||||||| | ||||||| |
Diabetic | ||||||| | |||||||| |
Change in dose for antihypertensive medications | ||
Decreased | | ||||| | | ||||| |
No change | || |||||| | || |||||| |
Increased | | ||||| | || |||||| |
Change in dose for lipid-lowering medications | ||
Decreased | | ||||| | | ||||| |
No change | || |||||| | || |||||| |
Increased | | ||||| | | ||||| |
BMI = body mass index; CI = confidence interval; OR = odds ratio; SD = standard deviation; SF-36 = Short Form (36) Health Survey; vs. = versus.
Note: Week 68 responses were analyzed using an analysis of covariance model with randomized treatment as factor and baseline body weight as covariate. Missing observations were multiple (1,000x), imputed from retrieved patients of the same randomized treatment arm. Week 68 responses were also analyzed using a binary logistic regression model with randomized treatment as factor and baseline SF-36 physical functioning score as covariate. Missing observations were multiple (1,000x), imputed from retrieved patients of the same randomized treatment arm.
Source: Clinical Study Report for STEP 5 (2021).32
Table 43: Harms in STEP 5 Study — Safety Analysis Set
Harm | STEP 5 study | |
|---|---|---|
Semaglutide N = 152 | Placebo N = 152 | |
Patients with ≥ 1 AE, OT | ||
n (%) | ||| |||| | ||| |||| |
Specific AE, ≥ 10% of patients, not mentioned elsewhere | ||
Nasopharyngitis | 24 (16) | 23 (15) |
Upper respiratory tract infection | 20 (13) | 23 (15) |
Gastroenteritis | 20 (13) | 4 (3) |
Headache | 16 (11) | 16 (11) |
Patients with ≥ 1 SAE, OT | ||
n (%) | || ||| | || |||| |
Infections and infestations | | ||| | | ||| |
GI disorders | | ||| | | ||| |
Hepatobiliary disorders | | ||| | ||||| |
Cholelithiasis | | ||| | ||||| |
Neoplasms — benign, malignant. and unspecified | | ||| | | ||| |
Patients who stopped treatment due to AEs | ||
n (%) | | ||| | | ||| |
GI disorders | | ||| | | ||| |
Fatal events, IT, n (%) | | ||| | ||||| |
Cause | ||||| |||||||||| |||||||||| | ||||| |
Notable harms, n (%) | ||
GI disorders, OT | ||| |||| | || |||| |
Nausea | 81 (53) | 33 (22) |
Diarrhea | 53 (35) | 36 (24) |
Vomiting | 46 (30) | 7 (5) |
Constipation | 47 (31) | 17 (11) |
Dyspepsia | 20 (13) | 7 (5) |
Abdominal pain | 20 (13) | 4 (3) |
Gallbladder-related disorders, OT | | ||| | | ||| |
Cholelithiasis | | ||| | | ||| |
Acute pancreatitis, OT | 0 | 0 |
CV disorders, IT | || |||| | || |||| |
EAC-confirmed CV events | ||
ACS | |||||| | |||||| |
TIA/stroke | |||||| | |||||| |
Coronary artery revascularization | ||
Hypoglycemia, OT | | ||| | |||||| |
Severe | 0 | 0 |
Injection site reactions, OT | || ||| | || |||| |
Psychiatric disorders, OT | || |||| | || |||| |
Anxiety | | ||| | || ||| |
Insomnia | | ||| | | ||| |
Depression | | ||| | | ||| |
Neoplasms — benign, malignant, and unspecified | || ||| | || ||| |
Thyroid-related | |||||| | |||||| |
ACS = acute coronary syndrome; AE = adverse event; CV = cardiovascular; EAC = event adjudication committee; GI = gastrointestinal; IT = in trial; OT = on treatment; SAE = serious adverse event; TIA = transient ischemic attack.
Source: Clinical Study Report for STEP 5 (2021).32
Critical Appraisal
Internal Validity
STEP 5 was reasonably well conducted, with proper procedures for randomization, blinding, and control for multiplicity. The limitations of this study were similar to those seen with the other STEP trials, such as the potential for unblinding to occur due to notable harms like GI AE that occur much more frequently with semaglutide than placebo. There were numerically more study withdrawals in the placebo group than with semaglutide, and a relatively large number of patients |||| || ||||||||| |||| || ||| ||||||| |||||, which may bias interpretation of both efficacy and harms outcomes.
External Validity
The generalizability issues with STEP 5 mirror those of the other STEP trials — notably, the structured weight management regime that patients followed in the trial, which is unlikely to be available to patients in most areas of Canada. Despite the longer follow-up in STEP 5 (104 weeks versus 68 weeks in the other STEP trials), STEP 5 was again not designed or powered to assess the impact of semaglutide on the development of weight-related comorbidities such as cardiovascular disease.
Discussion
Summary of Available Evidence
Five pivotal, multinational, sponsor-funded, 68-week RCTs were included in the systematic review. Four of those trials were double-blinded and placebo-controlled: STEP 1 (N = 1,950, randomized 2:1, semaglutide to placebo), STEP 2 (N = 1,210, randomized 1:1:1 to semaglutide 1.0 mg, semaglutide 2.4 mg, or placebo weekly), STEP 3 (N = 611, randomized 2:1, semaglutide to placebo), and STEP 4 (N = 803, randomized 1:1, semaglutide to placebo). STEP 2 included patients who were in the overweight category with comorbid type 2 diabetes. The STEP 1, STEP 3, and STEP 4 studies included patients with overweight (BMI of at least 27 kg/m2) or obesity (BMI of at least 30 kg/m2); patients who were overweight had to have at least 1 weight-related comorbidity other than type 2 diabetes. STEP 8 (N = 338, randomized 1:1:1) was the only trial that included an active comparator, liraglutide, as well as corresponding placebo controls for each of the active treatment groups. Across the trials, the primary outcomes were typically the percentage reduction from baseline in body weight and the number of patients achieving at least a 5% weight loss from baseline. Secondary outcomes that were controlled for multiplicity included patients achieving weight loss of at least 10% or 15% from baseline, as well as changes from baseline in patient-reported outcomes such as the physical function component of the SF-36, as well as the IWQOL-Lite-CT. All trials were well conducted, with methods to maintain adequate blinding, allocation concealment during randomization, and control for multiplicity, among others. Additional evidence included in this review were from a longer-term placebo-controlled trial that was non-pivotal (STEP 5, 104 weeks) as well as a sponsor-submitted ITC.
Across the studies, the mean age of patients was 46 years to 49 years, with the exception of STEP 2, where the mean age was 55 years. The majority of patients (75% to 80%) was female, with the exception of STEP 2 where there was a roughly equal percentage of females and males in the study. The vast majority of patients across the studies was White (75% to 93%), with the exception of STEP 2, where about 60% of patients were White and 27% were Asian. Baseline body weight was typically around 105 kg, and slightly lower (approximately 100 kg) in STEP 2, which focused on patients with type 2 diabetes, and even lower in STEP 4 (approximately 96 kg), which featured a 20-week run-in where all patients received semaglutide before randomization. Baseline hemoglobin A1C was around 5.7% in the STEP 1 and STEP 3 studies, 5.5% in the STEP 8 study, and 5.4% in the STEP 4 study, and much higher (8.1%) in the STEP 2 study, which enrolled patients with type 2 diabetes.
Interpretation of Results
Efficacy
There is clear and consistent evidence from 4 placebo-controlled DB RCTs that semaglutide evokes a statistically significant weight loss that is also clinically significant according to the clinical expert consulted by CADTH on this review. Semaglutide also resulted in a statistically and clinically significant weight loss versus liraglutide in a smaller study, STEP 8, where patients were not blinded with respect to their assigned active therapy, although they were blinded to their corresponding placebo group. However, none of these trials was designed to demonstrate a benefit for semaglutide over liraglutide or placebo with respect to key clinical outcomes such as reducing the number of patients developing weight-related comorbidity or cardiovascular events. While the included trials often measured changes in markers for comorbidities such as hypertension (blood pressure) or diabetes (hemoglobin A1C, FPG), these measurements were performed across the entire study population and thus do not provide any information about improvement in these parameters in patients who have these conditions, or, more importantly, whether treatment with semaglutide helps to reduce the risk of developing hypertension or diabetes. The only outcome that did report on this type of information looked at the number of patients who went from normoglycemia to prediabetes or from a prediabetic state to normoglycemia. These were not formal analyses, though, so although differences can be seen between groups, 1 cannot comment on the statistical significance of these differences. It is a well-established fact that patients with overweight or obesity are at a higher risk for a number of comorbidities; however, the impact of weight loss and, more notably, what constitutes a clinically significant weight loss is less clear. Guidelines produced by the UK and the FDA suggest that a weight loss of between 5% and 10% should be considered clinically meaningful33-35 (refer to Appendix 4 for a detailed review) and a 5% reduction from baseline was a co-primary outcome in 3 of the STEP trials. A retrospective observational study by Haase et al. (2021) found that for patients with a BMI of 40 kg/m2 or greater, a median 13% weight loss reduced their risk of type 2 diabetes by 41% and sleep apnea by 40% and reduced the risk of developing other conditions like hypertension, dyslipidemia, and asthma (refer to Appendix 4 for a detailed review).36 There do not appear to be other studies of this size or duration that attempt to demonstrate the benefits of weight loss, and the authors of Haase et al. (2021) noted that the lack of causative data limits any conclusions that can be drawn from their data. Overall, although guidelines and regulatory bodies appear to endorse a weight loss of 5% as clinically meaningful, the rigour with which this number was arrived at is unclear. The SELECT study is an ongoing trial with the objective of determining the superiority of semaglutide to placebo with respect to the prevention of major adverse cardiovascular events in patients with overweight or obesity who have established cardiovascular disease, but do not have diabetes. This event-driven trial is expected to past 5 years, and with an enrolment of 17,500 patients, this is the type of trial that would be needed to answer the types of questions that the STEP trials do not address.
From the input of patients to CADTH, it is clear that overweight and obesity have a significant impact on a patient’s HRQoL. Semaglutide did improve the physical function component of the SF-36 versus placebo in 3 of 4 STEP trials, suggesting that it may improve this component of HRQoL. However, the improvement over placebo did not meet the MID of 3 for this component of the SF-36, suggesting that these differences were of questionable clinical significance. Semaglutide also improved physical function scores on the physical function components of the IWQOL-Lite-CT in the 2 trials where it was assessed (STEP 1 and 2); however, there is no known MID for this scale and the clinical significance of this improvement cannot be determined. The remaining components of the SF-36 were not formally assessed and there was no assessment of HRQoL in STEP 8, the only trial that compared semaglutide to liraglutide. Although the lack of blinding between the semaglutide and liraglutide groups would have been a limitation of any analyses, the lack of HRQoL data comparing semaglutide to liraglutide is a limitation of this review.
The proposed listing criteria from the sponsor Is for use in patients with a BMI of 35 kg/m2 or greater and who are prediabetic.19 There were no preplanned subgroup analyses from any of the included studies that focused on this subgroup; however, the sponsor provided a post hoc subgroup analysis from |||| | in support of its proposed listing criteria.19 The mean percentage change from baseline body weight in this subgroup, over placebo, was |||||| |||| ||| |||||| |||||, compared to the weight loss of –12.4% (95% CI, –13.4 to –11.5), over placebo, reported for the overall population in |||| |. There were ||| of semaglutide-treated patients (||| with placebo) in this subgroup who achieved a 5% or greater reduction in weight compared to ||| (||| placebo) in the overall study population. Thus, the results in this subgroup appeared consistent with those reported for the entire population in |||| |. The fact that this was a post hoc analysis is a significant limitation; however, and it is not clear why only data from |||| | was presented. An additional complication with the proposed listing criteria is that there is not a single universal definition of prediabetes, and the American Diabetes Association definition differs from the Diabetes Canada definition. The clinical expert consulted by CADTH on this review was clear that the term prediabetes, using the Diabetes Canada definition, is widely accepted in their field of practice in the Canadian context.
Findings from the STEP 4 study suggest that patients who discontinue treatment with semaglutide are likely to regain a large portion of the weight they lost. In STEP 4, all patients were originally on semaglutide during a 20-week run-in period, and reached the target dosage of semaglutide 2.4 mg weekly by week 16. Randomization occurred at week 20, and after this time patients who were randomized to placebo began to gain weight. At week 68, the average increase in weight from week 20 in the placebo group was 6.5%, whereas patients in the placebo group in the other studies experienced weight losses of between 2% and 6%, depending on the study. Further evidence that discontinuing semaglutide results in weight regain was found in the extension to the STEP 1 study. In STEP 1, all patients were required to discontinue all interventions at week 68, including diet and lifestyle measures that were part of the study intervention. In the extension, a subset of 327 patients from sites in Canada, Germany, the UK, the US, and Japan were followed to week 120.37 Patients in the semaglutide group regained a mean (SD) of 11.6% (SD = 7.7%) of their body weight versus 1.9% (SD = 4.8%) in the placebo group from week 68 to week 120. Overall, it appears that the effects of semaglutide do not persist after the drug has been discontinued. It is not surprising that the pharmacological effects of semaglutide would not persist after drug discontinuation; however, any impact that semaglutide may have on patient behaviour does not appear to persist either. Given that the effects of semaglutide appear to plateau after around 60 weeks, patients will need to remain motivated to continue with therapy despite the fact that they may feel frustrated that weight loss has plateaued. This raises the concern that the use of semaglutide may result in significant fluctuations in weight for those patients who stop therapy, regain weight, then go back to taking semaglutide. There is evidence that these weight fluctuations can have a negative impact on a patient’s health, and might actually be worse than simply maintaining a consistently high BMI.38 The lack of data beyond 104 weeks, the long-term efficacy of semaglutide, and whether patients begin to gain weight at some point after that plateau at 60 weeks is also unknown.
The only drug that semaglutide has been directly compared to is liraglutide, another GLP-1 agonist. In the STEP 8 trial, semaglutide proved superior to liraglutide with respect to reducing weight; however, once again this trial was not designed to assess key clinically relevant outcomes such as the number of patients developing various comorbidities. One sponsor-submitted ITC compared semaglutide 2.4 mg to other pharmacological interventions, including ||||||||||| ||| ||| |||||||||| ||| ||||||||| |||| ||||||||| ||| |||||||| |||| |||||||| ||| ||||||| ||||||||| ||||||||| |||||| |||| ||| ||||| While the analysis appears robust, some pieces of information about the analyses (||||||||| ||||||| |||||||||| ||||||| || |||||||||| |||||||| ||||||| ||| ||||||||||| |||||||||||||) were not reported. There was some unaddressed |||||||| ||||||||||||| |||| ||||||| || ||| |||||||||||| || |||| ||||||| ||||||| |||| ||| ||||| |||||| and this contributes some uncertainty to the results. Consistency could not be assessed between |||||| ||| |||||||| |||||||| due to the structure of the evidence network. The results are || |||||| || ||||||||||| |||||| ||||||||||| ||| |||||||| ||| ||| |||||||||| || |||||||| ||||||||| || ||||| || |||||| |||| || || ||||| || |||| ||||||||||| |||||| ||| || |||||| || ||||||||||| |||||| |||||||||||| |||||||||| ||| |||||||||| ||| |||||||| ||| ||| ||||||| || ||||||| |||||| |||| |||||||| || ||||||. There was no evidence of a difference between ||||||||||| ||| ||||||||||| || |||||||||| ||| ||||||||| || ||| |||||||| || |||||||| |||| ||||. The consistency of the main results with the results of the sensitivity analyses excluding trials that included ||| increases confidence in the results.
Harms
GI AEs are the most common type of AE associated with the use of GLP-1 agonists and these were the most common AEs reported in all the STEP trials. These included both upper GI events (nausea, vomiting) and lower GI events (diarrhea, constipation), and are closely linked with the mechanism of the drug. These events lead to tolerability issues, with a numerically higher number of patients treated with semaglutide who withdrew from therapy due to a GI AE compared to placebo in each of the STEP trials. These withdrawals from treatment were typically in fewer than 5% of those treated with semaglutide, and in the STEP 8 trial, treatment discontinuations due to GI AEs were numerically lower in the semaglutide group |||||| than in the liraglutide group |||||||. In STEP 8, overall GI AEs were similar between the semaglutide and liraglutide groups (95% versus 96%, respectively); thus, it is not clear why discontinuations due to AEs may have been lower with semaglutide. The clinical expert consulted by CADTH on this review did note that, in their experience, if patients are seeing a benefit from drug therapy, they are more likely to put up with the GI side effects and that GI side effects do tend to improve with time or can be managed with a more gradual dose escalation than that stated in the product monograph. Additionally, a published pooled analysis of the STEP 1 to STEP 3 trials suggests that GI-related AEs appear to plateau beginning at around week 20, the end of the dose escalation phase.39 In their input to CADTH, patients highlighted the tolerability issues with current anti-obesity drugs as a limitation of this therapeutic area.
A number of the other safety and tolerability issues associated with the GLP-1 agonists either occurred in too few patients to see numerical differences in risk between semaglutide and placebo (such as acute pancreatitis) or are events that would likely require much longer follow-up to determine risk (such as medullary thyroid cancer). The product monograph for semaglutide, as is the case with other GLP-1 agonists, cautions against use in populations at higher risk of these disorders. Data from the 104-week STEP 5 trial did not suggest an increased risk of these longer-term safety issues with the additional follow-up; however, the difference in treatment duration was relatively modest (104 weeks versus 68 weeks) and unlikely to be of sufficient duration to add valuable information about the long-term safety of semaglutide.
In the sponsor-submitted ITC, there was || |||||||| ||| | |||||||||| || |||| || |||| ||||||| ||||||||||| ||| ||||||||||| ||| ||| |||| ||||||| || |||||||||| ||| ||||||||||| ||| |||||||| ||| || ||||| ||||| ||||||
Conclusions
Data from 4 placebo-controlled DB RCTs (the STEP 1, STEP 2, STEP 3, and STEP 4 trials) and 1 open-label RCT comparison to liraglutide (the STEP 8 trial) suggest that treatment with semaglutide injection 2.4 mg for 68 weeks produces a statistically significant weight loss compared to liraglutide and to placebo in patients with overweight or obesity, including patients with comorbid type 2 diabetes. Although the weight loss is considered clinically significant according to the clinical expert consulted by CADTH on this review, there is no clear evidence that this weight loss reduces the number of patients who may develop various weight-related comorbidities, including type 2 diabetes, cardiovascular disease, and osteoarthritis. There is some evidence of a statistically significant improvement in the physical component of HRQoL versus placebo; however, the clinical significance of this improvement is less clear because it did not meet the MID for 1 instrument and the MID is not known for the other. Longer-term evidence from the STEP 5 trial suggests that the weight loss observed at 104 weeks is consistent with that seen in the other trials at 68 weeks; however, it appears from all the STEP trials that weight loss with semaglutide plateaus before the end of 68 weeks of treatment, and that once patients stop semaglutide treatment, they may regain the majority of the weight lost. The most common tolerability issues with semaglutide are GI-related; these are common with this drug class. Evidence from a sponsor-submitted indirect comparison suggests that ||||||||||| ||| |||||| | ||||||| |||||| |||| |||| ||||||| ||||| |||||| |||| |||||| ||||||||| |||||||||||| ||||||||| ||| ||||||||||| ||| |||||||||
References
1.World Health Organization. Obesity. 2022; https://www.who.int/health-topics/obesity#tab=tab_1. Accessed 2022 May 2.
2.Statistics Canada. Overweight and obesity based on measured body mass index, by age group and sex. Table 13-10-0373-01. 2020; https://www150.statcan.gc.ca/t1/tbl1/en/tv.action?pid=1310037301. Accessed 2022 May 2.
3.Canadian Task Force on Preventive Health Care. CTFPHC recommendation for the prevention and management of adult obesity. 2015: https://canadiantaskforce.ca/wp-content/uploads/2016/06/2015-obesity-adults-clinician-summary-en-1.pdf. Accessed 2022 May 2.
4.Wegovy (semaglutide injection): solution for subcutaneous injection in a pre-filled pen; single-use pre-filled pen delivering doses of 0.25 mg, 0.5 mg, 1 mg, 1.7 mg or 2.4 mg: 0.25 mg/pen (0.25 mg/0.5 mL), 0.5 mg/pen (0.5 mg/0.5 mL), 1 mg/pen (1 mg/0.5 mL), 1.7 mg/pen (1.7 mg/0.75 mL), 2.4 mg/pen (2.4 mg/0.75 mL) and multi-use pre-filled pen (FlexTouch) delivering doses of 0.25 mg, 0.5 mg, 1 mg, 1.7 mg or 2.4 mg: 1 mg/pen (0.68 mg/mL), 2 mg/pen (1.34 mg/mL), 4 mg/pen (1.34 mg/mL), 6.8 mg/pen (2.27 mg/mL), 9.6 mg/pen (3.2 mgmL) [product monograph]. Mississauga (ON): Novo Nordisk Canada Inc; 2022 Jun 30.
5.Petry NM, Barry D, Pietrzak RH, Wagner JA. Overweight and obesity are associated with psychiatric disorders: results from the National Epidemiologic Survey on Alcohol and Related Conditions. Psychosom Med. 2008;70(3):288-297. PubMed
6.Hargens TA, Kaleth AS, Edwards ES, KL. B. Association between sleep disorders, obesity, and exercise: a review. Nat Sci Sleep.5:27-35. PubMed
7.Avenell A, Broom J, Brown TJ, et al. Systematic review of the long-term effects and economic consequences of treatments for obesity and implications for health improvement. Health Technol Assess. 2004;8(21):1-182. PubMed
8.Wharton S, Lau DC, Vallis M, et al. Obesity in adults: a clinical practice guideline. CMAJ. 2020;192(31):E875-E891. PubMed
9.CADTH Canadian Drug Expert Committee (CDEC) final recommendation: semaglutide (Ozempic - Novo Nordisk Canada Inc.). Ottawa (ON): CADTH; 2019 Apr 10: https://www.cadth.ca/sites/default/files/cdr/complete/SR0594%20Ozempic%20-%20CDEC%20Final%20Recommendation%20May%2017%2C%202019%20%28redacted%29_For%20posting.pdf. Accessed 2022 May 2.
10.CADTH reimbursement recommendation: semaglutide (Rybelsus) indicated as an adjunct to diet and exercise to improve glycemic control in adults with T2DM. Can J Health Technol. 2021;1(6). https://www.cadth.ca/sites/default/files/attachments/2021-06/CADTH_reimbursement_recommendation_semaglutide_%28rybelsus%29.pdf. Accessed 2022 May 2.
11.Saxenda (liraglutide) 6 mg/mL solution for injection in a pre-filled pen Human Glucagon Like Peptide-1 (GLP-1) [product monograph]. Mississauga (ON): Novo Nordisk Canada Inc.; 2021 Feb 25.
12.Contrave (naltrexone hydrochloride 8 mg and bupropion hydrochloride 90mg): extended-release tablets [product monograph]. Laval (QC): Valeant Canada LP; 2018 Feb 12: https://pdf.hres.ca/dpd_pm/00043849.PDF. Accessed 2022 May 2.
13.Xenical (orlistat): 120 mg capsules [product monograph]. Mesekenhagen (DE): CHEPLAPHARM Arzneimittel GmbH; 2017 Sep 27: https://pdf.hres.ca/dpd_pm/00041463.PDF. Accessed 2022 May 2.
14.McGowan J, Sampson M, Salzwedel DM, Cogo E, Foerster V, Lefebvre C. PRESS Peer Review of Electronic Search Strategies: 2015 guideline statement. J Clin Epidemiol. 2016;75:40-46. PubMed
15.Grey matters: a practical tool for searching health-related grey literature. Ottawa (ON): CADTH; 2019: https://www.cadth.ca/grey-matters. Accessed 2022 Apr 2.
16.Wilding JPH, Batterham RL, Calanna S, et al. Once-weekly semaglutide in adults with overweight or obesity. N Engl J Med. 2021;384(11):989-1002. PubMed
17.Clinical Study Report: NN9536-4373 (STEP 1). Effect and safety of semaglutide 2.4 mg once-weekly in subjects with overweight or obesity [internal sponsor's report]. Bagsvaerd (DK): Novo Nordisk; 2020 Aug 17.
18.Health Canada reviewer's report: Wegovy (semaglutide) [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Wegovy (semaglutide), 2.4 mg, solution for subcutaneous injection, single-dose pre-filled pen delivering doses of 0.25 mg, 0.5 mg, 1 mg, 1.7 mg, 2.4 mg Mississauga (ON): Novo Nordisk Canada Inc; 2022 Mar 10.
19.Drug Reimbursement Review sponsor submission: Wegovy (semaglutide), 2.4 mg, solution for subcutaneous injection, single-dose pre-filled pen delivering doses of 0.25 mg, 0.5 mg, 1 mg, 1.7 mg, 2.4 mg [internal sponsor's package]. Mississauga (ON): Novo Nordisk Canada Inc; 2022 Mar 10.
20.Davies M, Færch L, Jeppesen OK, et al. Semaglutide 2.4 mg once a week in adults with overweight or obesity, and type 2 diabetes (STEP 2): a randomised, double-blind, double-dummy, placebo-controlled, phase 3 trial. Lancet. 2021;397(10278):971-984. PubMed
21.Clinical Study Report: NN9536-4374 (STEP 2). Effect and safety of semaglutide 2.4 mg once-weekly in subjects with overweight or obesity and type 2 diabetes [internal sponsor's report]. Bagsvaerd (DK): Novo Nordisk; 2020 Aug 28.
22.Wadden TA, Bailey TS, Billings LK, et al. Effect of subcutaneous semaglutide vs placebo as an adjunct to intensive behavioral therapy on body weight in adults with overweight or obesity: the STEP 3 randomized clinical trial. JAMA.325(14):1403-1413. PubMed
23.Clinical Study Report: NN9536-4375 (STEP 3). Effect and safety of semaglutide 2.4 mg once-weekly as adjunct to intensive behavioural therapy in subjects with overweight or obesity [internal sponsor's report]. Bagsvaerd (DK): Novo Nordisk; 2020 Aug 20.
24.Rubino D, Abrahamsson N, Davies M, et al. Effect of continued weekly subcutaneous semaglutide vs placebo on weight loss maintenance in adults with overweight or obesity: the STEP 4 randomized clinical trial. JAMA. 2021;325(14):1414-1425. PubMed
25.Clinical Study Report: NN9536-4376 (STEP 4). Effect and safety of semaglutide 2.4 mg once-weekly in subjects with overweight or obesity who have reached target dose during run-in period [internal sponsor's report]. Bagsvaerd (DK): Novo Nordisk; 2020 Jul 16.
26.Rubino DM, Greenway FL, Khalid U, et al. Effect of weekly subcutaneous semaglutide vs daily liraglutide on body weight in adults with overweight or obesity without diabetes. the STEP 8 randomized clinical trial. JAMA. 2022;327(2):138-150. PubMed
27.Clinical Study Report: NN9536-4576 (STEP 8). Effect and safety of subcutaneous semaglutide 2.4 mg once weekly compared to liraglutide 3.0 mg once daily on weight management in subjects with overweight or obesity [internal sponsor's report]. Bagsvaerd (DK): Novo Nordisk; 2021 Sep 1.
28.Maruish M, Kosinski M, Bjorner J, et al. User's manual for the SF-36v2 health survey. 3rd ed. Loncoln (RI): QualityMetric Inccorporated; 2011.
29.Kolotkin RL, Crosby RD. Psychometric evaluation of the impact of weight on quality of life-lite questionnaire (IWQOL-lite) in a community sample. Qual Life Res. 2002;11(2):157-171. PubMed
30.Semaglutide 2.4 mg for management of obesity: systematic review, meta-analysis feasibility assessment and network meta-analysis report [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Wegovy (semaglutide), 2.4 mg, solution for subcutaneous injection, single-dose pre-filled pen delivering doses of 0.25 mg, 0.5 mg, 1 mg, 1.7 mg, 2.4 mg. Mississauga (ON): Novo Nordisk Canada Inc 2022 Mar 10.
31.Vosoughi K, Atieh J, Khanna L, et al. Association of glucagon-like peptide 1 analogs and agonists administered for obesity with weight loss and adverse events: a systematic review and network meta-analysis. EClinicalMedicine. 2021;42:101213. PubMed
32.Clinical Study Report: NN9536-4378 (STEP 5). Two-year effect and safety of semaglutide 2.4 mg once weekly in subjects with overweight or obesity [internal sponsor's report]. Bagsvaerd (DK): Novo Nordisk; 2021 Aug 17.
33.Obesity: guidance on the prevention, identification, assessment and management of overweight and obesity in adults and children (Clinical guideline 43). National Insitute for Health and Clinical Excellence: London (GB); 2006: https://www.nice.org.uk/guidance/cg189/evidence/obesity-update-appendix-p-pdf-6960327450. Accessed 2022 May 2.
34.Jensen MD, Ryan DH, Apovian CM, et al. 2013 AHA/ACC/TOS guideline for the management of overweight and obesity in adults: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines and The Obesity Society. J Am Coll Cardiol. 2014;63(25 Pt B):2985-3023. PubMed
35.Williamson DA, Bray GA, Ryan DH. Is 5% weight loss a satisfactory criterion to define clinically significant weight loss? Obesity (Silver Spring). 2015;23(12):19-20. PubMed
36.Haase CL, Lopes S, Olsen AH, Satylganova A, Schnecke V, McEwan P. Weight loss and risk reduction of obesity-related outcomes in 0.5 million people: evidence from a UK primary care database. Int J Obes (Lond). 2021;45(6):1249-1258. PubMed
37.Wilding JPH, Batterham RL, Davies M, et al. Weight regain and cardiometabolic effects after withdrawal of semaglutide: the STEP 1 trial extension. Diabetes Obes Metab. 2022. PubMed
38.Bangalore S, Fayyad R, Laskey R, DeMicco DA, Messerli FH, Waters DD. Body-weight fluctuations and outcomes in coronary disease. N Engl J Med. 2017;376(14):1332-1340. PubMed
39.Wharton S, Calanna S, Davies M, et al. Gastrointestinal tolerability of once-weekly semaglutide 2.4 mg in adults with overweight or obesity, and the relationship between gastrointestinal adverse events and weight loss. Diabetes Obes Metab. 2022;24(1):94-105. PubMed
40.Kadowaki T, Isendahl J, Khalid U, et al. Semaglutide once a week in adults with overweight or obesity, with or without type 2 diabetes in an east Asian population (STEP 6): a randomised, double-blind, double-dummy, placebo-controlled, phase 3a trial. Lancet Diabetes Endocrinol. 2022;10(3):193-206. PubMed
41.Enebo LB, Berthelsen KK, Kankam M, et al. Safety, tolerability, pharmacokinetics, and pharmacodynamics of concomitant administration of multiple doses of cagrilintide with semaglutide 2.4 mg for weight management: a randomised, controlled, phase 1b trial. Lancet. 2021;397(10286):1736-1748. PubMed
42.Friedrichsen M, Breitschaft A, Tadayon S, Wizert A, Skovgaard D. The effect of semaglutide 2.4 mg once weekly on energy intake, appetite, control of eating, and gastric emptying in adults with obesity. Diabetes Obes Metab. 2021;23(3):754-762. PubMed
43.Crabtree TSJ, Adamson K, Reid H, et al. Injectable semaglutide and reductions in HbA1c and weight in the real-world in people switched from alternative glucagon-like peptide 1 receptor agonists. Diabetes Obes Metab. 2022;24(7):1398-1401. PubMed
44.Masaki T, Ozeki Y, Yoshida Y, et al. Glucagon-like peptide-1 receptor agonist semaglutide improves eating behavior and glycemic control in Japanese obese type 2 diabetic patients. Metabolites. 2022;12(2):147. PubMed
45.Nauck MA, Petrie JR, Sesti G, et al. A phase 2, randomized, dose-finding study of the novel once-weekly human GLP-1 analog, semaglutide, compared with placebo and open-label liraglutide in patients with type 2 diabetes. 2016 Feb;39(2):231-241. PubMed: PM26358288. Diabetes Care. 2016;39(2):231-241. PubMed
46.O'Neil PM, Birkenfeld AL, McGowan B, et al. Efficacy and safety of semaglutide compared with liraglutide and placebo for weight loss in patients with obesity: a randomised, double-blind, placebo and active controlled, dose-ranging, phase 2 trial. Lancet. 2018;392(10148):637-649. PubMed
47.Kolotkin RL, Head S, Brookhart A. Construct validity of the Impact of Weight on Quality of Life Questionnaire. Obes Res. 1997;5(5):434-441. PubMed
48.Kolotkin RL, Williams VSL, Ervin CM, et al. Validation of a new measure of quality of life in obesity trials: Impact of Weight on Quality of Life-Lite Clinical Trials Version. Clin Obes. 2019;9(3):e12310. PubMed
49.Kolotkin RL, Head S, Hamilton M, Tse CK. Assessing impact of weight on quality of life. Obes Res. 1995;3(1):49-56. PubMed
50.Kolotkin RL, Ervin CM, Meincke HH, Højbjerre L, Fehnel SE. Development of a clinical trials version of the Impact of Weight on Quality of Life-Lite questionnaire (IWQOL-Lite Clinical Trials Version): results from two qualitative studies. Clin Obes. 2017;7(5):290-299. PubMed
51.J. C. A power primer. Psychol Bull. 1992;112(1):155-159. PubMed
52.Reeve BB, Wyrwich KW, Wu AW, et al. ISOQOL recommends minimum standards for patient-reported outcome measures used in patient-centered outcomes and comparative effectiveness research. Qual Life Res. 2013;22(8):1889-1905. PubMed
53.Tessier A, Mayo NE, Cieza A. Content identification of the IWQOL-Lite with the International Classification of Functioning, Disability and Health. Qual Life Res. 2011;20(4):467-477. PubMed
54.Kolotkin RL, Crosby RD, Williams GR. Assessing weight-related quality of life in obese persons with type 2 diabetes. Diabetes Res Clin Pract. 2003;61(2):125-132. PubMed
55.Crosby RD, Kolotkin RL, Williams GR. An integrated method to determine meaningful changes in health-related quality of life. J Clin Epidemiol. 2004;57(11):1153-1160. PubMed
56.Kolotkin RL, Williams VSL, von Huth Smith L, et al. Confirmatory psychometric evaluations of the Impact of Weight on Quality of Life-Lite Clinical Trials Version (IWQOL-Lite-CT). Clinical Obesity. 2021;11(5):e12477. PubMed
57.Ware JE Jr, Sherbourne CD. The MOS 36-item short-form health survey (SF-36). I. Conceptual framework and item selection. Med Care. 1992;30(6):473-483. PubMed
58.Amer RA, Khalifa KA, Alajlan SA, Ansari AA. Analyzing the psychometric properties of the Short Form-36 Quality of Life Questionnaire in patients with obesity. Obes Surg. 2018;28(8):2521-2527. PubMed
59.Koopman C, Pelletier KR, Murray JF, et al. Stanford presenteeism scale: health status and employee productivity. J Occup Environ Med. 2002;44(1):14-20. PubMed
60.Avery K, Donovan J, Peters TJ, Shaw C, Gotoh M, Abrams P. ICIQ: a brief and robust measure for evaluating the symptoms and impact of urinary incontinence. Neurourol Urodyn. 2004;23(4):322-330. PubMed
61.Corica F, Corsonello A, Apolone G, et al. Construct validity of the Short Form-36 health survey and its relationship with BMI in obese outpatients. Obesity (Silver Spring). 2006;14(8):1429-1437. PubMed
62.Karlsen TI, Tveita EK, Natvig GK, Tonstad S, Hjelmesaeth J. Validity of the SF-36 in patients with morbid obesity. Obes Facts. 2011;4(5):346-351. PubMed
63.Hirsch A, Bartholomae C, Volmer T. Dimensions of quality of life in people with non-insulin-dependent diabetes. Qual Life Res. 2000;9(2):207-218. PubMed
64.ATS Committee on Proficiency Standards for Clinical Pulmonary Function Laboratories. ATS statement: guidelines for the six-minute walk test. Am J Respir Crit Care Med. 2002;166(1):111-117. PubMed
65.Larsson UE, Reynisdottir S. The six-minute walk test in outpatients with obesity: reproducibility and known group validity. Physiother Res Int. 2008;13(2):84-93. PubMed
66.Elmahgoub SS, Van de Velde A, Peersman W, Cambier D, Calders P. Reproducibility, validity and predictors of six-minute walk test in overweight and obese adolescents with intellectual disability. Disabil Rehabil. 2012;34(10):846-851. PubMed
67.Morinder G, Mattsson E, Sollander C, Marcus C, Larsson UE. Six-minute walk test in obese children and adolescents: reproducibility and validity. Physiother Res Int. 2009;14(2):91-104. PubMed
68.Vanhelst J, Fardy PS, Salleron J, Beghin L. The six-minute walk test in obese youth: reproducibility, validity, and prediction equation to assess aerobic power. Disabil Rehabil. 2013;35(6):479-482. PubMed
69.Beriault K, Carpentier AC, Gagnon C, et al. Reproducibility of the 6-minute walk test in obese adults. Int J Sports Med. 2009;30(10):725-727. PubMed
70.Guyatt GH, Pugsley SO, Sullivan MJ, et al. Effect of encouragement on walking test performance. Thorax. 1984;39(11):818-822. PubMed
71.Priesnitz CV, Rodrigues GH, Stumpf CS, et al. Reference values for the 6-min walk test in healthy children aged 6-12 years. Pediatr Pulmonol. 2009;44(12):1174-1179. PubMed
72.Saad HB, Prefaut C, Missaoui R, Mohamed IH, Tabka Z, Hayot M. Reference equation for 6-min walk distance in healthy North African children 6-16 years old. Pediatr Pulmonol. 2009;44(4):316-324. PubMed
73.Center for Drug Evaluation Research. Guidance for industry developing products for weight management. Draft guidance. Rockville (MD): U.S. Food and Drug Administration; 2007: https://www.fda.gov/regulatory-information/search-fda-guidance-documents/developing-products-weight-management-revision-1. Accessed 2022 May 2.
74.Ryan DH, Yockey SR. Weight loss and improvement in comorbidity: differences at 5%, 10%, 15%, and over. Curr Obes Rep. 2017;6:187-194. PubMed
75.Clinical Practice Research Datalink. Primary care data for public health research. 2022; https://cprd.com/primary-care-data-public-health-research. Accessed 2022 May 2.
Appendix 1: Literature Search Strategy
Note that this appendix has not been copy-edited.
Clinical Literature Search
Overview
Interface: Ovid
Databases:
MEDLINE All (1946-present)
Embase (1974-present)
Note: Subject headings and search fields have been customized for each database. Duplicates between databases were removed in Ovid.
Date of search: April 5, 2022
Alerts: Weekly search updates until project completion
Search filters applied: No filters were applied to limit the retrieval by study type
Limits:
Publication date limit: none
Language limit: none
Conference abstracts: excluded
Syntax | Description |
|---|---|
/ | At the end of a phrase, searches the phrase as a subject heading |
MeSH | Medical Subject Heading |
exp | Explode a subject heading |
* | Before a word, indicates that the marked subject heading is a primary topic; or, after a word, a truncation symbol (wildcard) to retrieve plurals or varying endings |
# | Truncation symbol for 1 character |
adj# | Requires terms to be adjacent to each other within # number of words (in any order) |
.ti | Title |
.ot | Original title |
.ab | Abstract |
.hw | Heading word; usually includes subject headings and controlled vocabulary |
.kf | Keyword heading word |
.dq | Candidate term word (Embase) |
.pt | Publication type |
.mp | Mapped term |
.rn | Registry number |
.nm | Name of substance word (MEDLINE) |
medall | Ovid database code: MEDLINE All, 1946 to present, updated daily |
oemezd | Ovid database code; Embase, 1974 to present, updated daily |
Multi-Database Strategy
Wegovy*.ti,ab,kf,ot,hw,nm,rn.
(semaglutide* or Ozempic* or Rybelsus* or nn 9535 or nn9535 or NNC 0113-0217 or NNC01130217 or “NNC 01130217” or “NNC0113 0217” or 53AXN4NNHX).ti,ab,kf,ot,hw,nm,rn.
Weight loss/ or body mass index/ or exp overweight/ or exp anti-obesity agents/ or exp weight gain/ or adiposity/ or obesity management/
((weight* or fat) adj4 (loss* or losing or lost or reduc* or decreas* or gain* or increas* or excess* or manag* or chang* or watch*)).ti,ab,kf.
(obese or obesity or superobese or superobesity or morbidobese or morbidlyobese or antiobes* or overweight* or over weight* or adiposit* or corpulen* or body fat).ti,ab,kf.
(Quetelet* adj2 Index).ti,ab,kf.
((body mass index or BMI) adj3 (reduc* or lower* or great* or higher* or increase*)).ti,ab,kf.
(appetite* adj4 (supress* or depress*)).ti,ab,kf.
(eat* adj4 control*).ti,ab,kf.
or/3-9
2 and 10
1 or 11
12 use medall
Wegovy*.ti,ab,kf,dq.
*semaglutide/ or (semaglutide* or Ozempic* or Rybelsus* or nn 9535 or nn9535 or NNC 0113-0217 or NNC01130217 or “NNC 01130217” or “NNC0113 0217”).ti,ab,kf,dq.
Body weight loss/ or body mass/ or exp obesity/ or exp body weight gain/ or obesity management/ or antiobesity agent/ or antiobesity activity/
((weight* or fat) adj4 (loss* or losing or lost or reduc* or decreas* or gain* or increas* or excess* or manag* or chang* or watch*)).ti,ab,kf,dq.
(obese or obesity or superobese or superobesity or morbidobese or morbidlyobese or antiobes* or overweight* or over weight* or adiposit* or corpulen* or body fat).ti,ab,kf,dq.
(Quetelet* adj2 Index).ti,ab,kf,dq.
((body mass index or BMI) adj3 (reduc* or lower* or great* or higher* or increase*)).ti,ab,kf,dq.
(appetite* adj4 (supress* or depress*)).ti,ab,kf,dq
(eat* adj4 control*).ti,ab,kf,dq
or/16-22
15 and 23
14 or 24
25 use oemezd
26 not (conference review or conference abstract).pt.
13 or 27
remove duplicates from 28
Clinical Trials Registries
ClinicalTrials.gov
Produced by the US National Library of Medicine. Targeted search used to capture registered clinical trials.
Search: Wegovy (semaglutide), weight management
WHO ICTRP
International Clinical Trials Registry Platform, produced by the WHO. Targeted search used to capture registered clinical trials.
Search: Wegovy (semaglutide), weight management
Health Canada’s Clinical Trials Database
Produced by Health Canada. Targeted search used to capture registered clinical trials.
Search: Wegovy (semaglutide), weight management
EU Clinical Trials Register
European Union Clinical Trials Register, produced by the European Union. Targeted search used to capture registered clinical trials.
Grey Literature
Search dates: March 25-April 1, 2022
Keywords: Wegovy (semaglutide), weight management
Limits: Publication years: none
Updated: Search updated before the completion of stakeholder feedback period
Relevant websites from the following sections of the CADTH grey literature checklist Grey Matters: A Practical Tool for Searching Health-Related Grey Literature were searched:
Health Technology Assessment Agencies
Health Economics
Clinical Practice Guidelines
Drug and Device Regulatory Approvals
Advisories and Warnings
Drug Class Reviews
Clinical Trials Registries
Databases (free)
Internet Search
Open Access Journals
Appendix 2: Excluded Studies
Note that this appendix has not been copy-edited.
Reference | Reason for exclusion |
|---|---|
Kadowaki et al. (2022)40 Enebo et al. (2021)41 Friedrichsen et al. (2021)42 | Comparator (placebo control) |
Crabtree et al. (2022)43 Masaki et al. (2022)44 | Study design (non-RCT) |
Nauck et al. (2016)45 O'Neil et al. (2018)46 | Intervention |
Appendix 3: Detailed Outcome Data
Note that this appendix has not been copy-edited.
Table 46: Change From Baseline to Week 68 in SF-36, Other Domains, for STEP 1 to STEP 4
Factor | Semaglutide | Placebo | ||
|---|---|---|---|---|
Mean (SD) baseline | Mean (SD) change | Mean (SD) baseline | Mean (SD) change | |
Role physical | ||||
STEP 1 | 52.0 (6.6) N = 1,296 | 1.1 (7.2) N = 1,195 | 51.8 (7.1) N = 650 | –0.2 (7.2) N = 566 |
STEP 2 | 51.4 (7.5) N = 397 | 0.8 (7.4) N = 376 | 51.4 (6.9) N = 394 | 0.0 (7.1) N = 365 |
STEP 3 | 52.9 (6.5) N = 402 | 1.6 (6.5) N = 364 | 52.7 (6.6) N = 203 | 1.5 (6.7) N = 181 |
STEP 4 | 54.3 (5.3) N = 534 | 0.3 (5.0) N = 515 | 54.1 (4.9) N = 268 | –0.9 (5.3) N = 245 |
Bodily pain | ||||
STEP 1 | 52.8 (8.1) | 0.5 (8.2) | 52.6 (8.4) | –1.3 (8.9) |
STEP 2 | 52.4 (8.7) | 0.3 (9.0) | 52.8 (8.6) | –0.4 (8.6) |
STEP 3 | 53.1 (7.5) | 1.3 (7.1) | 53.1 (7.8) | 0.6 (8.3) |
STEP 4 | 54.2 (7.6) | 0.5 (7.0) | 54.2 (7.8) | –1.5 (7.7) |
General health | ||||
STEP 1 | 52.9 (7.9) | 2.0 (7.2) | 53.6 (7.8) | –0.6 (7.1) |
STEP 2 | 51.2 (7.6) | 2.2 (7.3) | 51.2 (7.8) | 0.6 (7.5) |
STEP 3 | 53.2 (7.9) | 3.4 (6.6) | 53.3 (8.6) | 1.9 (6.4) |
STEP 4 | 56.5 (7.0) | 0.3 (5.2) | 56.3 (6.9) | –1.8 (5.8) |
Vitality | ||||
STEP 1 | 55.3 (7.7) | 0.7 (8.0) | 55.5 (7.7) | –1.3 (7.9) |
STEP 2 | 55.6 (7.9) | 0.8 (7.9) | 56.5 (7.9) | –0.9 (7.9) |
STEP 3 | 54.6 (8.3) | 2.0 (8.2) | 54.7 (8.6) | 0.9 (7.8) |
STEP 4 | 56.8 (7.8) | 1.1 (7.1) | 56.4 (7.6) | –2.1 (7.6) |
Social functioning | ||||
STEP 1 | 54.1 (5.3) | –0.3 (6.6) | 53.9 (5.7) | –1.4 (7.4) |
STEP 2 | 53.7 (5.7) | 0.2 (6.6) | 54.1 (5.4) | –0.7 (7.4) |
STEP 3 | 54.3 (5.4) | 0.1 (6.6) | 53.9 (6.2) | –1.2 (8.0) |
STEP 4 | 54.5 (5.3) | 0.1 (6.2) | 54.4 (4.9) | –1.8 (6.9) |
Role emotional | ||||
STEP 1 | 53.4 (5.4) | –0.9 (7.3) | 53.2 (5.7) | –1.5 (7.6) |
STEP 2 | 52.7 (6.5) | –0.4 (7.7) | 53.3 (5.5) | –1.1 (7.8) |
STEP 3 | 54.2 (4.9) | –0.6 (5.6) | 53.6 (5.3) | –1.5 (7.7) |
STEP 4 | 53.7 (4.9) | 0.0 (5.5) | 53.9 (4.7) | –2.2 (7.0) |
Mental health | ||||
STEP 1 | 55.0 (5.7) | –0.8 (7.0) | 55.1 (5.8) | –1.7 (7.4) |
STEP 2 | 54.9 (6.4) | –0.4 (6.9) | 55.2 (5.7) | –1.6 (7.5) |
STEP 3 | 55.7 (5.5) | –0.5 (6.0) | 55.8 (5.8) | –1.5 (7.1) |
STEP 4 | 55.2 (6.3) | 0.2 (6.2) | 55.0 (6.3) | –2.2 (7.6) |
Physical component summary | ||||
STEP 1 | 51.1 (7.3) | 2.4 (6.7) | 51.1 (7.9) | 0.2 (7.1) |
STEP 2 | 49.8 (8.2) | 2.3 (7.2) | 49.9 (8.0) | 0.9 (6.6) |
STEP 3 | 51.6 (6.9) | 3.2 (7.0) | 51.7 (7.3) | 2.1 (6.0) |
STEP 4 | 54.3 (6.4) | 0.8 (4.9) | 54.4 (6.1) | –0.9 (5.6) |
Mental component summary | ||||
STEP 1 | 55.4 (5.7) | –1.5 (7.1) | 55.5 (5.9) | –2.1 (7.7) |
STEP 2 | 55.6 (6.1) | –0.9 (6.9) | 56.2 (5.5) | –1.8 (7.6) |
STEP 3 | 55.7 (5.3) | –0.9 (6.0) | 55.4 (6.1) | –2.2 (8.0) |
STEP 4 | 55.0 (6.2) | 0.0 (6.2) | 54.9 (6.2) | –2.4 (8.5) |
CI = confidence interval; SD = standard deviation.
Source: Clinical Study Reports for STEP 1 (2020),17 STEP 2 (2020),21 STEP 3 (2020),23 and STEP 4 (2020).25
Table 47: Change From Baseline to Week 68 in IWQOL-Lite-CT, Other Domains,
for STEP 1 and STEP 2
Factor | Semaglutide | Placebo | ||
|---|---|---|---|---|
Mean (SD) baseline | Mean (SD) change | Mean (SD) baseline | Mean (SD) change | |
Physical | ||||
STEP 1 | 64.5 (23.2) N = 1,296 | 14.0 (20.0) N = 376 | 64.0 (23.1) N = 649 | 5.0 (19.5) N = 365 |
STEP 2 | 66.4 (24.2) N = 397 | 11.0 (19.6) N = 381 | 69.0 (22.6) N = 394 | 4.4 (19.1) N = 374 |
Psychosocial | ||||
STEP 1 | 63.1 (23.0) | 17.4 (19.2) | 62.9 (22.7) | 6.9 (17.8) |
STEP 2 | 74.8 (21.6) | 9.6 (16.7) | 77.0 (19.8) | 5.6 (16.5) |
Total | ||||
STEP 1 | 63.6 (21.2) | 16.2 (17.8) | 63.3 (20.9) | 6.3 (16.8) |
STEP 2 | 71.9 (20.9) | 10.1 (15.9) | 74.2 (19.2) | 5.2 (15.5) |
CI = confidence interval; SD = standard deviation.
Source: Clinical Study Reports for STEP 1 (2020)17 and STEP 2 (2020).21
Figure 3: Percentage Change From Baseline in Body Weight Over Time for STEP 1
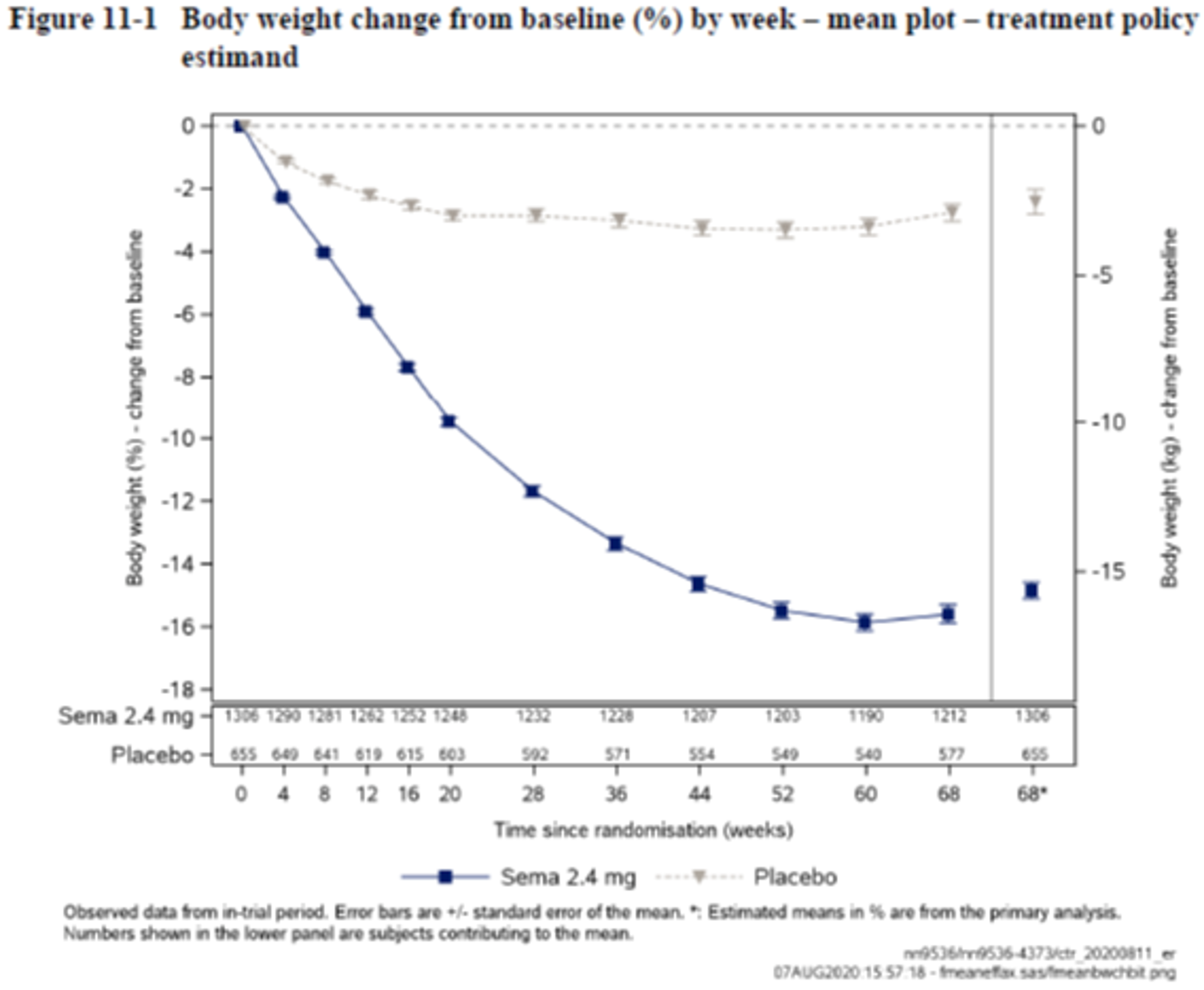
Source: Clinical Study Report for STEP 1 (2020).17
Figure 4: Percentage Change From Baseline in Body Weight Over Time for STEP 2
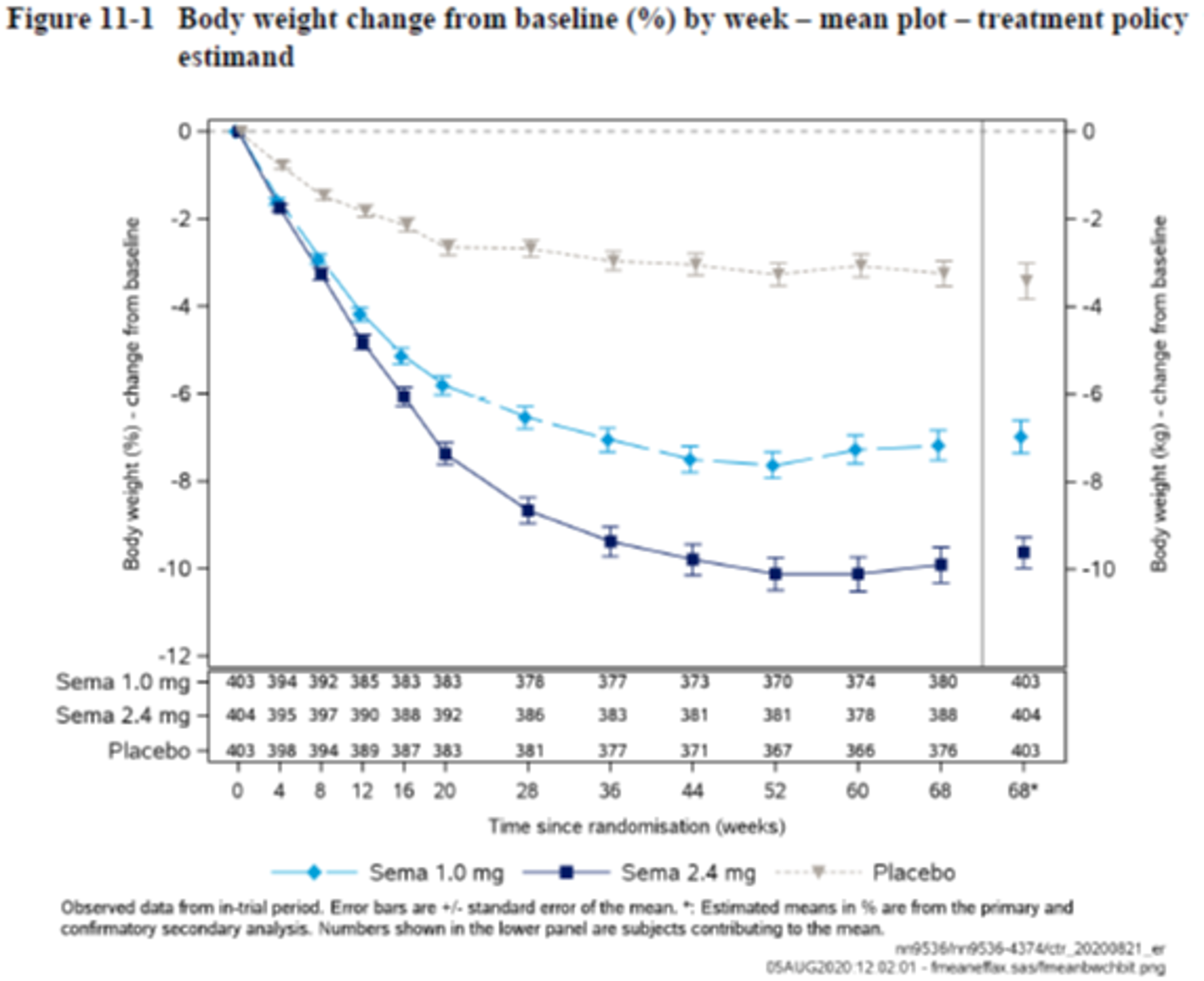
Source: Clinical Study Report for STEP 2 (2020).21
Figure 5: Percentage Change From Baseline in Body Weight Over Time for STEP 3
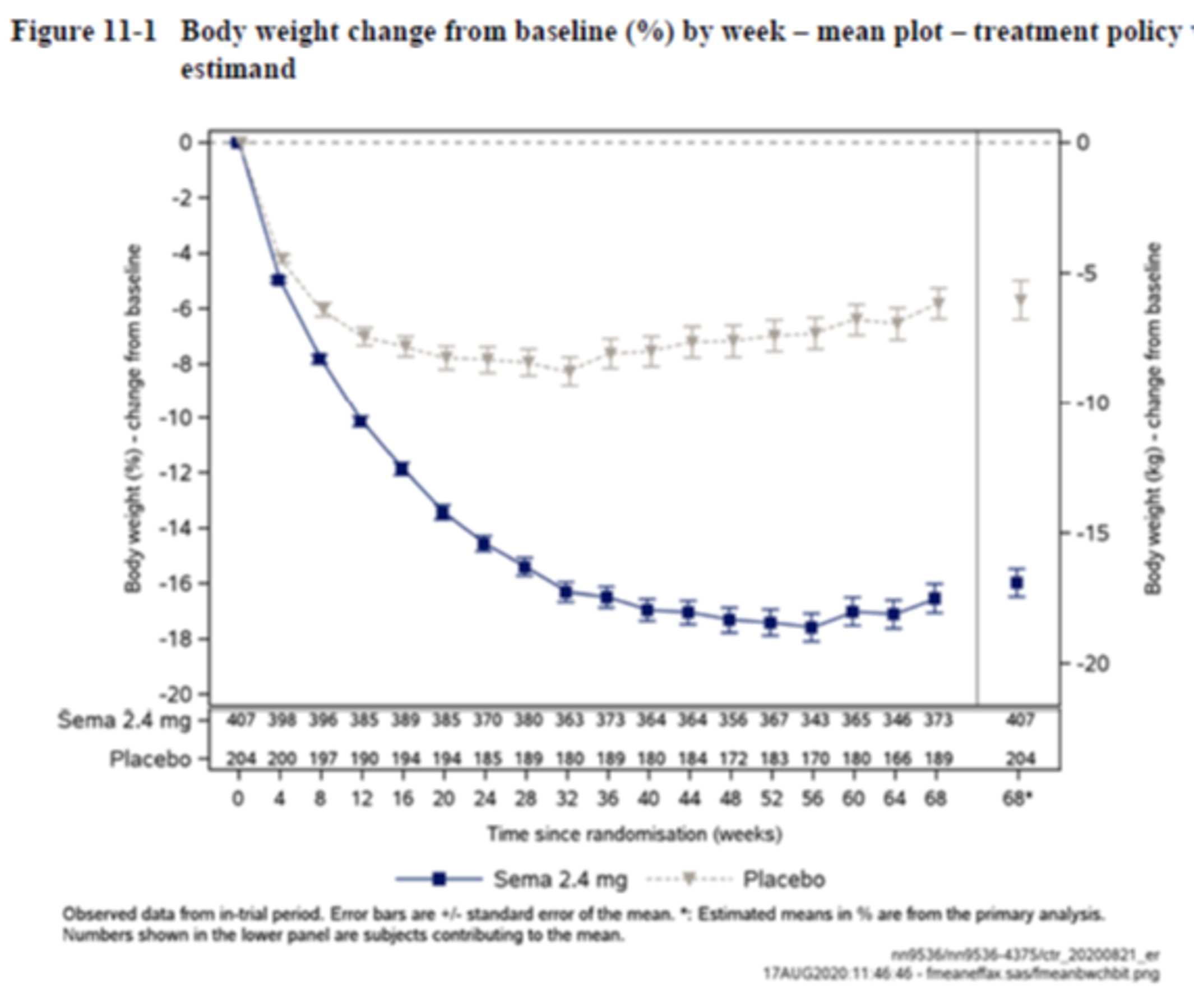
Source: Clinical Study Report for STEP 3 (2020).23
Figure 6: Percentage Change From Baseline in Body Weight Over Time for STEP 4
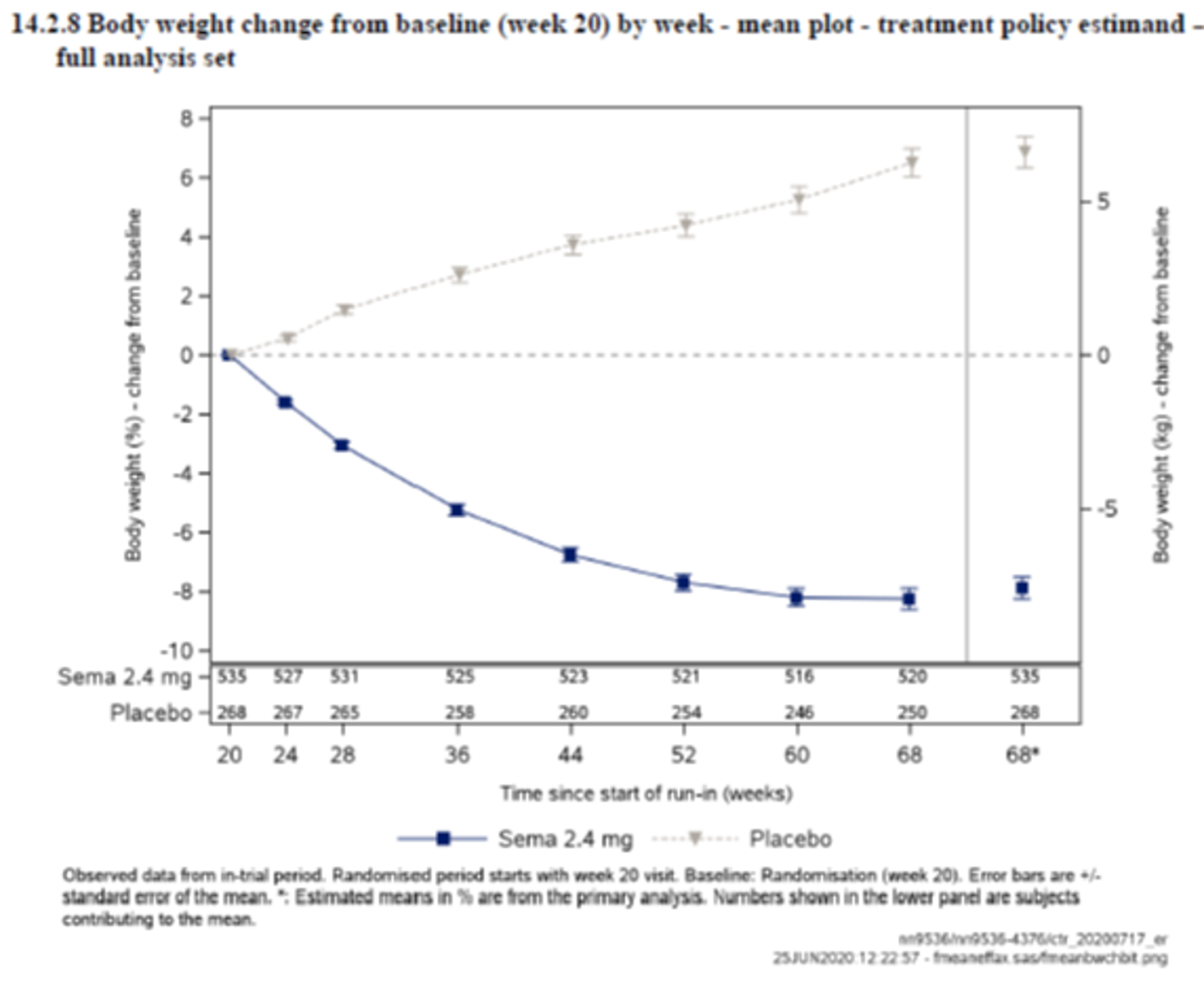
Source: Clinical Study Report for STEP 4 (2020).25


This figure has been redacted as per the sponsor’s request.
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Source: Clinical Study Report for STEP 5 (2021).32
Appendix 4: Description and Appraisal of Outcome Measures
Note that this appendix has not been copy-edited.
Aim
To describe the outcome measures in Table 48 and review their measurement properties (validity, reliability, responsiveness to change, and MID).
Table 48: Outcomes Reported in the Included Studies
Outcome measure | STEP 1 | STEP 2 | STEP 3 | STEP 4 | STEP 8 |
|---|---|---|---|---|---|
IWQOL-Lite-CT | Confirmatory secondary | Confirmatory secondary | NR | NR | NR |
SF-36 | Physical function: Confirmatory secondary Other domains: supportive secondary end points | Physical function: Confirmatory secondary Other domains: supportive secondary end points | Physical function: Confirmatory secondary Other domains: supportive secondary end points | Physical function: Confirmatory secondary Other domains: supportive secondary end points | NR |
6MWT | NR | Exploratory (for BMI ≥ 35 kg/m2 only) | NR | NR | NR |
6MWT = six-minute walk test; IWQOL = Impact of Weight on Quality of Life; IWQOL-Lite-CT = Impact of Weight on Quality of Life–Lite Clinical Trials Version; SF-36 = Short Form (36) Health Survey.
Findings
Table 49: Summary of Outcome Measures and Their Measurement Properties
Outcome measure | Type | Conclusions about measurement properties | MID |
|---|---|---|---|
IWQOL-Lite, total and individual item scores | Disease-specific measure of HRQoL 31-item self-administered 5-point Likert scale Higher scores indicate a poorer quality of life | Acceptable internal consistency has been demonstrated in adult patients who are living with overweight or obesity seeking treatment and with diabetes, as well as individuals in the community. Acceptable test-retest reliability has been demonstrated in the community population. There is evidence of convergent validity of total score and the physical function and work subscale scores with BMI and other quality of life scales. There is little evidence of responsiveness to change. | MID for improvement ranges from 7.7 to 12, depending on baseline score. |
IWQOL-Lite-CT, total and individual item scores | Disease-specific measure of HRQoL 20-item self-administered 5-point Likert scale Higher scores indicate a poorer quality of life | Satisfactory internal consistency, test-test reliability, and some evidence for validity was identified for adult patients who are living with overweight or obesity. | An MID was not identified for adult patients who are living with overweight or obesity. |
36-Item Short Form Survey | Generic measure of HRQoL 36 item self-administered Likert scale Higher scores indicating better health status. | For adult patients who are living with overweight or obesity in the community, there is some evidence of validity. For the PCS and MCS, however, the validity of the subscales in this patient population has not been confirmed. | General (non–disease-specific) MID: 2 points in PCS; 3 points in MCS; 2 to 4 points for individual dimensions. An MID was not identified for adult patients who are living with overweight or obesity. |
Six-minute walk test (6MWT) | The 6MWT is a supervised test that measures the distance a patient can walk on a hard flat surface over a 6-minute period. Walk tests aim to evaluate global function of organ systems involved in exercise, namely the heart, lungs, peripheral circulation, blood, nervous system, muscles, bones, and joints, during walking, a self-paced activity. Longer distance indicates better function | For patients who are living with overweight, There is some validity evidence. | No MID has been identified or proposed in patients with overweight. |
HRQoL = health-related quality of life; IWQOL-Lite = Impact of Weight on Quality of Life–Lite; IWQOL-Lite-CT = Impact of Weight on Quality of Life–Lite Clinical Trials Version; MCS = mental component summary; MID = minimal important difference; PCS = physical component summary; 6MWT = six-minute walk test; SF-36 = Short Form (36) Health Survey.
Impact of Weight on Quality of Life–Lite Questionnaire
The IWQOL-Lite questionnaire is a disease-specific questionnaire that was designed to assess the effect of obesity on quality of life in 8 key areas.47 The IWQOL-Lite-CT was developed in response to the limitations of the IWQOL-Lite version use among patients in clinical trials.48
The IWQOL-Lite is the shorter version of the full 74-item IWQOL questionnaire.47,49 The original 74-item IWQOL measures areas of quality of life identified by adult patients living with moderate to severe obesity as those of greatest concern to them (health, social/interpersonal, work, mobility, self-esteem, sexual life, activities of daily living, and comfort with food).47,49 The IWQOL-Lite has 31 self-administered items with 5 scales: self-esteem (7 items), sexual life (4 items), physical function (11 items), public distress (5 items), and work (4 items).29 The scale score consists of the sum of all the item scores, and all scale scores are added to create the total score.29 Total scores and scale scores on the IWQOL-Lite are transformed to a range from 0 to 100; on this scale, higher scores indicate a poorer quality of life.29 The IWQOL-Lite-CT is an even shorter version of the original IWQOL, with 20 self-administered items derived from the IWQOL-Lite in 2 domains (physical – 7 items and psychosocial – 13 items) scored in the same way as the IWQOL-Lite.48,50,48
In 1 of the studies that assessed the psychometric properties of the IWQOL-Lite questionnaire, a community-based sample of 492 individuals who are living with overweight or obesity (mean BMI 27.4 kg/m2) who were not undergoing weight-loss treatment completed the IWQOL-Lite.29 Convergent validity of the total score and subscale scores was assessed in individuals with a BMI of at least 25 kg/m2 using BMI, the SF-36 (including the MCS and PCS scores and each subscale score), the Rosenberg self-esteem scale, the Marlowe-Crowne social desirability scale, and ad hoc sexual life and public distress scales using items from the obesity quality of life instrument (OBQOL).29 The IWQOL-Lite total score demonstrated strong correlations (Pearson correlation coefficient R with a magnitude of more than 0.50)51 in the expected direction with BMI, the general health, vitality, and PCS scores of the SF-36, as well as the Rosenberg self-esteem score and the OBQOL-based measures.29 The IWQOL-Lite total score was weakly correlated (magnitude of R between 0.10 and 0.30) with the Marlowe-Crowne social desirability score and SF-36 role emotional score and moderately correlated (magnitude of R between 0.30 and 0.50) with the rest of the measures.29 The IWQOL-Lite physical function score was strongly correlated with the SF-36 physical functioning, role physical, bodily pain, general health, PCS scores, moderately correlated with the SF-36 vitality and social functioning scores, the OBQOL-based measures, and weakly correlated with the SF-36 MCS and role emotional scores.29 The IWQOL-Lite work score was weakly correlated with the SF-36 role emotional score and the Marlowe-Crowne score and moderately correlated with the rest of the measures.29 Internal consistency, as assessed with Cronbach’s alpha, was acceptable for the IWQOL-Lite subscale and total scores. Test-retest reliability was evaluated an average of 14 days apart (SD = 0.7 days) in 112 individuals. Intraclass correlation coefficients (ICCs) for test-retest reliability ranged from 0.81 (public distress) to 0.88 (physical function) for the subscale scores, and 0.94 for the total score.29 These measures of reliability are acceptable relative to the generally accepted threshold of 0.70 or higher.52
The content validity of the IWQOL-Lite was assessed through a study that compared it to the International Classification of Functioning, Disability and Health using the Delphi technique with 21 raters; this study found that content was compatible and had good content validity in English and French.53
In another validation study, IWQOL-Lite data were collected from 1,197 individuals (225 had type 2 diabetes) living with obesity who were seeking weight-loss treatment and gastric-bypass surgery in a clinical trial, to determine the impact of weight on quality of life and the psychometric properties of the IWQOL-Lite instrument.54 This study found that internal consistency was acceptable52 for the IWQOL-Lite total score and subscale scores in patients with and without diabetes.54 To test the scale structure and construct validity, confirmatory factor analysis was performed as part of the same study.54 These results found that there was comparable factor structure for patients with and without diabetes.54 Moderate to strong correlations51 were found between BMI and IWQOL-Lite for both patients with and without diabetes, which suggested the construct validity.54 The correlation coefficient ranged from –0.545 (sexual life) to –0.737 (public distress) for IWQOL-Lite subscale scores and BMI and was 0.705 for IWQOL-Lite total score and BMI among patients with diabetes.54 The correlation coefficient ranged from –0.458 (sexual life) to –0.749 (public distress) for IWQOL-Lite subscale scores and BMI and was 0.683 for IWQOL-Lite total score and BMI among patients without diabetes.54
An MID range was estimated for the IWQOL-Lite total score in patients living with obesity.55 This study used both anchor and distribution-based methods in a study of 1,476 patients in weight-loss trials and compared IWQOL-Lite total scores at baseline and 6 months.55 Patients were categorized according to baseline IWQOL-Lite total score using a normative mean (calculated from a sample of 534 individuals with a BMI of 18 to 29.9 kg/m2 not enrolled in any weight-loss treatment program) for comparison.55 The categories of baseline impairment were: none (less than 1 SD below the normative mean), mild (greater than or equal to 1 but less than 2 SDs from the normative mean), moderate (greater than or equal to 2 but less than 3 SDs from the normative mean), and severe (greater than 3 SDs from normative mean).55 Standard error of measurement corrected for regression to the mean was used to evaluate the precision of the IWQOL-Lite using the Edwards-Nunnally method for the distribution-based method.55 The anchor-based method considered a 5% to 9.9% decrease in weight to represent improvement and anything below this cut-off to represent no change.55 Discrepancies in the change in IWQOL-Lite score corresponding to improvement between the distribution-based and anchor-based methods were resolved by selecting the greater of the 2 cut-offs for a given category of baseline impairment.55 Greater quality of life change was observed with greater weight loss and more severe baseline quality of life impairments.55 The MIDs for improvement were 7.7 to 7.8 for patients with no impairment at baseline (depending on exact baseline score), 7.9 to 8.1 for patients with mild impairment, 8.1 to 8.4 for patients with moderate impairment, and 12.0 for patients with severe impairment.55 The MIDs for deterioration determined using the distribution-based method ranged from –7.8 to –4.4, depending on baseline severity of impairment.55
In terms of the IWQOL-Lite-CT, internal consistency reliability was found to be satisfactory. Kolotkin et al.48,56 evaluated the measurement properties of the IWQOL-Lite-CT using 2 different RCTs with semaglutide, 1 using a population of individuals living with obesity and 1 using a population of individuals with type 2 diabetes. It was reported that the Cronbach’s alpha values for total score at baseline and end of trial ranged from 0.93 and 0.96.48 The item and composite-level test-retest reliabilities were found to be satisfactory in both studies, with ICCs of 0.80 or more for all composite scores.48 For validity, the authors reported strong correlations with the SF-36 scales for physical and physical function scores, role physical, and vitality subscale score in both studies.48 Both studies also revealed positive construct validity of the composite scores through longitudinal analyses in comparison to changes in the SF-36 scale.48 The author reported that IWQOL-Lite-CT was able to discriminate between known groups. Effect sizes comparing baseline and week 68 IWQOL-Lite-CT scores were statistically significant for all composites (P < 0.0001). Anchor-based analyses indicated responder thresholds ranging from 13.5 to 16.6 in composite scores. The author concluded that the IWQOL-Lite-CT was an appropriate scale for clinical trials assessing the efficacy of new treatments for weight management.56
No MID was reported for IWQOL-Lite-CT version.
36-Item Short Form Survey
The 36-Item Short Form Survey (SF-36) is an instrument that measures general health that has been used extensively in clinical trials in a variety of population groups.57 There are 8 health domains in the SF-36 and for each of these a subscale score can be determined: physical functioning, role physical, bodily pain, general health, vitality, social functioning, role emotional, and mental health.57,58 There are 2 component summaries of the SF-36, the PCS and the MCS, that are derived with a scoring algorithm from the 8 domains.57,59,60 Scores on the PCS and MCS range from 0 to 100, with higher scores indicating better health status.57 Scoring for the summary scales uses norm-based methods; the general US population is used to derive the regression weights and constants. The PCS and MCS scales are transformed to have a mean of 50 and an SD of 10 in the general US population.28
The SF-36 version 2 (SF-36v2) was a modified version. It was made available in 1996; it contains minor changes to the original survey. Changes included: reduced ambiguity in instructions, better layout, increased item-level response choices, increased cultural/language comparability, and elimination of a response option from the items in the mental health and vitality dimensions.28
The original version of the SF-36 has some evidence of validity among patients living with obesity. In a study of outpatients living with obesity (N = 475) seeking treatment, the construct validity of the SF-36 was explored through main component analysis.61 This study found that BMI was associated with most factors, but not the mental health, vitality, and social functioning-based factors.61 In a study of patients living with morbid obesity (mean BMI of 41.7 kg/m2) with a referral to a rehabilitation centre, a factor analysis suggested that the 2 summary scales (PCS and MCS) had adequate factor loading, but that the validity of the original 8 subscales was not confirmed in this population.62
The construct validity and reliability of the original version of the SF-36 among patients living with obesity scheduled for bariatric surgery (N = 365) was evaluated in another study.58 Principal component analysis revealed 6 factors with an estimated Eigen value of greater than 1, ensuring that 6 factors were obtained.58 The identified 6-factor model was tested for fit using confirmatory factor analysis, which exhibited a good fit.58 Using Pearson’s correlation, the authors found that the correlations were satisfactory, with all factors showing a correlation below 0.70.58 The overall internal consistency reliability was found to be greater than 0.70 (Cronbach’s alpha = 0.717).58 Overall, the authors found that the main components closely related to increased BMI were physical activity, general health and body pain, physical role, emotional role, and mental health,58 which was in agreement with previous studies.
One study found evidence of validity for the original version of the SF-36 scale score in a group of people with type 2 diabetes,63 although it is important to note that these findings may not be applicable to patients living with obesity that do not have type 2 diabetes. A Cronbach’s alpha consistency value greater than 0.80 was attained for 6 of the individual scales on the SF-36, the physical functioning, role physical, bodily pain, vitality, role emotional, and mental health scales.63 The authors assessed the external validity of the SF-36 by comparing the scale scores at the start of diabetes therapy and education and 4 weeks after completion with the Well-Being Questionnaire, the Diabetes Treatment Satisfaction Questionnaire, the Diabetes, and the Quality of Life with Diabetes questionnaire.63 They found that there were significant differences in treatment satisfaction, role physical, general health, vitality, and social functioning scores before and 4 weeks after education and diabetes therapy on the SF-36 scale score.63 The authors did note that the SF-36 has a positive bias, as the positive answers receive higher scores.63
In the general population, clinically meaningful improvement is generally indicated by a change of 2 points in the SF-36 PCS and 3 points in the SF-36 MCS.28 Based on anchor data, following minimal mean group differences, in terms of t score points are described for SF-36 individual dimension scores: physical functioning, 3; role functioning, 3; bodily pain, 3; general health, 2; vitality, 2; social functioning, 3; role emotional, 4; and mental health, 3.28 These MID values were determined as appropriate for groups with mean t score ranges of 30 to 40.28 For higher t score ranges, MID values may be higher.28 No information about the MID of the SF-36 in the population living with obesity was identified.
6MWT
The 6MWT is a supervised test that measures the distance a patient can walk on a hard flat surface over a 6-minute period.64 The American Thoracic Society provides guidelines for standardization of this test to maximize reliability.64 Walk tests aim to evaluate global function of organ systems involved in exercise, namely the heart, lungs, peripheral circulation, blood, nervous system, muscles, bones, and joints, during walking, a self-paced activity.64 Walk tests were originally developed to primarily evaluate cardiopulmonary function in cardiac and pulmonary conditions (e.g., chronic obstructive pulmonary disease, heart failure, pulmonary hypertension), but studies have been performed to validate these tests in musculoskeletal conditions such as fibromyalgia.64
The reproducibility and validity of 6MWT in overweight or obese has been assessed in several studies.65-68 In a prospective repeated-measure validity study, Beriault et al. (2009) found that 6MWT was highly reproducible in obese adults.69 In 1 study, Elmahgoub et al. (2012)66 assessed the reproducibility and validity of the 6MWT in adolescent participants with overweight (N = 39). The adolescent participants performed the 6MWT twice with an interval of 1 week. The results showed a good reliability (intraclass correlation coefficient: 0.82). The smallest real difference was 82.6 m. The validity of 6MWT was demonstrated by the 6MWT distance was well correlated with relative peak oxygen uptake (beta = 0.69). The author concluded that 6MWT was a reliable and valid test in adolescents with overweight or obesity.66
The key limitations of the 6MWT, especially in pediatric patients, include: a learning effect with repeated testing; confounding effect of patient motivation, encouragement and cooperation; and impact of age, height, and weight on walk distance.64 The learning effect could result in performance and detection bias (i.e., false-positive apparent benefits) when evaluating an intervention using these walk tests in a non-blinded, uncontrolled study. Additionally, differences in patient motivation, encouragement and cooperation between assessments can impact walking distance by a similar magnitude as the effect of interventions,70 which can produce substantial variability and be a source of performance bias in a non-blinded, uncontrolled study. Finally, previous studies have identified that age, height and weight impact distance travelled in 6 minutes,71,72 which may affect 6MWT results obtained from trials of longer duration.
No MID has been identified or proposed in patient with overweight. MIDs for distances were reported for other conditions such as chronic obstructive pulmonary disease (43 m) and heart failure (54 m).
Long-Term Impact of Body Weight Reduction on Weight-Related Comorbidities
Obesity is a chronic disease associated with several health-related complications. The Canadian Adult Obesity Clinical Practice Guidelines released in 2020 indicated that obesity increases the risk of developing cardiovascular disease and certain types of cancers, which are some of the leading causes of early death in these patients.8 In addition, obesity is considered a risk factor for other serious conditions including type 2 diabetes, hypertension, dyslipidemia, obstructive sleep apnea, knee osteoarthritis, urinary incontinence, asthma, nonalcoholic steatohepatitis, and heart failure.19 Guidelines from the UK33 and the US34 suggest that minimal weight loss of between 5 and 10% is sufficient to have a clinical impact on outcomes. A 5% for body weight reduction is generally considered “clinically meaningful.”35 One of the criteria for approval medications for management of obesity In The US FDA Draft Guidance is that the medication achieve an average weight loss of 5% or greater than a placebo.73,74
To describe the impact of body weight reduction on long-term weight-related comorbidities, a brief summary of a study by Haase et al. (2021)36 is presented in the following section.
Overall Study Description
Haase et al.36 conducted a retrospective study to assess the impact of the body weight reduction on 10 clinical outcomes. The data sources used in this analysis were from UK Clinical Practice Research Datalink (CPRD) GOLD database75 and merged with Hospital Episode Statistics linkage information and death registry data from the Office for National Statistics.75
Study design: The study included a 4-year “baseline period” (year 1 to year 4) and a subsequent follow-up period. Index date for each included participant was defined as the date of the earliest BMI assessment and indicated the beginning of year 1 of the study. BMI assessments were made during the baseline period (after index date, years 1 to 4). The incidence of weight-related comorbidities was assessed during the follow-up period. Follow-up period ended at the date of the first event, death, transfer-out, or the last data collection.36
Inclusion and exclusion criteria: To be included in the study, participants had to be older than 18 years at index date and 70 years or younger at start of follow-up, have 1 or more BMI assessments during the “baseline period” (year 1 and year 4), and a have mean BMI between 25 and 50 kg/m2 during year 4 after the index date. Based on the change in those participants’ mean BMI during the “baseline period,” participants were categorized into 2 cohorts: 1 was the stable-weight cohort (defined as −5% to +5% BMI change). The other was the weight-loss cohort (defined as −25% to −10% BMI change). In order to confirm the intention to lose weight, it was required that participants in the weight loss cohort had a Read code in CPRD GOLD database indicating either a weight-loss diet, weight-loss drug prescription, or referral to a dietitian or for bariatric surgery during the baseline period. Participants with BMI change outside the ranges for these cohorts, participants with malignant cancer or thyroid disorder before the start of follow-up, and those with a record of pregnancy or limb amputation during the baseline period were excluded to ensure no unintentional weight loss.
Outcomes: Risk before and after weight loss for the following weight-related comorbidities was assessed: type 2 diabetes, sleep apnea, hip or knee osteoarthritis, hypertension, dyslipidemia, unstable angina or myocardial infarction, asthma, atrial fibrillation, heart failure, and chronic kidney disease.
Statistical analyses: Cox proportional hazard models with calendar time as the underlying time variable were used to estimate the difference in risk between the stable-weight and weight-loss cohorts. Participants with a baseline history of the weight- related comorbidity were excluded from the risk analysis only for that outcome. All statistical analyses were performed using the R environment for statistical computing and visualization (R Foundation for Statistical Computing; version 3.6.2).
Findings
Baseline and demographic characteristics: A total of 571,961 participants was included in this analysis. Among them, 523,138 were in the stable-weight cohort and 48,823 were in the weight-loss cohort. A total of 49.2% of the population were men. The median age at the start of the follow-up period was 55 years and the median follow-up time was 6.3 years. In the stable-weight cohort, the median BMI was 29.9 kg/m2 during year 1 and 30.0 kg/m2 during year 4. The median BMIs in the weight-loss cohort were 35.3 kg/m2 during year 1 and 30.4 kg/m2 during year 4, respectively, which represented a median weight loss of 13%. In the weight-loss cohort, 57.6% of participants were given dietary advice at some time point during the 4-year baseline period, 52.7% reported that they initiated a weight-loss diet, 27.0% received a weight-loss medication and 1.1% were referred for bariatric surgery (CPRD GOLD) or underwent bariatric surgery (Hospital Episode Statistics).36
Risk reduction following weight loss: the detail of results of risk reduction in weight-loss group is presented in Table 50. It was reported that, for the group with index BMI 40 kg/m2, the relative risk reductions with median 13% weight loss were observed for type 2 diabetes (41%), and sleep apnea (40%), hypertension (22%), dyslipidemia (19%), and asthma (18%). Similar results were observed in the sensitive analysis by excluding participants who had received sibutramine.
Limitations: The author indicated that this was the first study to assess, in a single real-world population, the differential impact of intentional weight loss on a range of weight-related comorbidities, for different BMI profiles. As the author acknowledged, the findings observed in this study was unable to provide conclusive evidence of the causative nature of the observations because of the retrospective and observational nature of this analysis.
Table 50: Outcome Risk Before and After Median 13% Weight Loss Starting at BMI of 35.0 kg/m2, 40.0 kg/m2, and 45.0 kg/m2 Relative to a Stable BMI of 30 kg/m2
Outcome | BMI before weight loss (kg/m2) | BMI after weight loss (kg/m2) | HRs relative to a stable BMI of 30 kg/m2 a | Relative risk reduction (%) | |
|---|---|---|---|---|---|
Risk before weight loss, HR (95% CI) | Risk after weight loss, HR (95% CI) | ||||
T2D | 35 | 30.5 | 1.97 (1.95 to 2.00) | 1.20 (1.14 to 1.26) | 39.3 |
40 | 34.8 | 3.05 (2.99 to 3.12) | 1.80 (1.71 to 1.90) | 41.0 | |
45 | 39.2 | 3.70 (3.56 to 3.86) | 2.26 (2.10 to 2.43) | 39.1 | |
Asthma | 35 | 30.5 | 1.22 (1.19 to 1.25) | 0.96 (0.89 to 1.04) | 21.2 |
40 | 34.8 | 1.36 (1.30 to 1.42) | 1.11 (1.02 to 1.22) | 17.8 | |
45 | 39.2 | 1.38 (1.26 to 1.50) | 1.21 (1.06 to 1.37) | 12.4 | |
Sleep apnea | 35 | 30.5 | 2.29 (2.23 to 2.36) | 1.32 (1.19 to 1.46) | 42.6 |
40 | 34.8 | 4.37 (4.18 to 4.57) | 2.64 (2.42 to 2.88) | 39.6 | |
45 | 39.2 | 6.93 (6.48 to 7.41) | 4.61 (4.18 to 5.08) | 33.5 | |
Hip/knee osteoarthritis | 35 | 30.5 | 1.42 (1.40 to 1.44) | 1.23 (1.17 to 1.30) | 13.1 |
40 | 34.8 | 1.80 (1.75 to 1.85) | 1.64 (1.55 to 1.73) | 8.9 | |
45 | 39.2 | 2.04 (1.93 to 2.16) | 2.00 (1.86 to 2.16) | 1.9 | |
Heart failure | 35 | 30.5 | 1.43 (1.40 to 1.47) | 1.55 (1.45 to 1.66) | –8.0 |
40 | 34.8 | 2.00 (1.92 to 2.08) | 1.99 (1.85 to 2.13) | 0.6 | |
45 | 39.2 | 2.70 (2.50 to 2.92) | 2.49 (2.26 to 2.75) | 7.9 | |
CKD | 35 | 30.5 | 1.10 (1.09 to 1.12) | 0.99 (0.94 to 1.03) | 10.6 |
40 | 34.8 | 1.19 (1.16 to 1.23) | 1.04 (0.99 to 1.09) | 13.1 | |
45 | 39.2 | 1.27 (1.20 to 1.34) | 1.08 (1.00 to 1.15) | 15.0 | |
Hypertension | 35 | 30.5 | 1.30 (1.29 to 1.32) | 1.01 (0.97 to 1.04) | 22.7 |
40 | 34.8 | 1.56 (1.53 to 1.59) | 1.23 (1.18 to 1.28) | 21.5 | |
45 | 39.2 | 1.72 (1.65 to 1.79) | 1.40 (1.32 to 1.49) | 18.5 | |
Dyslipidemia | 35 | 30.5 | 1.16 (1.15 to 1.17) | 0.95 (0.92 to 0.98) | 18.7 |
40 | 34.8 | 1.26 (1.24 to 1.28) | 1.02 (0.98 to 1.06) | 19.0 | |
45 | 39.2 | 1.27 (1.22 to 1.31) | 1.04 (0.98 to 1.10) | 17.9 | |
Atrial fibrillation | 35 | 30.5 | 1.42 (1.39 to 1.45) | 1.51 (1.42 to 1.60) | –6.1 |
40 | 34.8 | 2.01 (1.95 to 2.08) | 1.98 (1.86 to 2.10) | 1.6 | |
45 | 39.2 | 2.84 (2.67 to 3.03) | 2.60 (2.39 to 2.82) | 8.7 | |
Unstable angina/MI | 35 | 30.5 | 1.07 (1.05 to 1.10) | 1.00 (0.93 to 1.08) | 6.8 |
40 | 34.8 | 1.11 (1.06 to 1.16) | 1.13 (1.04 to 1.22) | –2.1 | |
45 | 39.2 | 1.10 (1.00 to 1.21) | 1.24 (1.10 to 1.39) | –12.9 | |
BMI = body mass index; CI = confidence interval; CKD = chronic kidney disease; HR = hazard ratio; MI = myocardial infarction; T2D = type 2 diabetes.
aHRs are presented relative to the outcome risk for an individual with stable BMI of 30.0 kg/m2.
Source: Haase et al. (2021). Copyright 2021 Lundegaard Haase et al. Reprinted in accordance with Creative Commons Attribution 4.0 International License (CC BY 4.0): https://creativecommons.org/licenses/by/4.0/.36
Pharmacoeconomic Review
Abbreviations
BIA
budget impact analysis
BMI
body mass index
CPAP
continuous positive airway pressure
CVD
cardiovascular disease
ICER
incremental cost-effectiveness ratio
OSA
obstructive sleep apnea
QALY
quality-adjusted life-year
T2DM
type 2 diabetes
TIA
transient ischemic attack
Executive Summary
The executive summary comprises 2 tables (Table 1 and Table 2) and a conclusion.
Item | Description |
|---|---|
Drug product | Semaglutide (Wegovy), subcutaneous injection |
Submitted price | Semaglutide (Wegovy): $363.51 per carton of 4 pre-filled, single-dose pens, regardless of strength (0.25 mg, 0.5 mg, 1 mg, 1.7 mg, or 2.4 mg) |
Indication | Indicated as an adjunct to a reduced-calorie diet and increased physical activity for chronic weight management in adult patients with an initial BMI of:
|
Health Canada approval status | NOC |
Health Canada review pathway | Standard |
NOC date | November 23, 2021 |
Reimbursement request | As an adjunct to a reduced-calorie diet and increased physical activity for chronic weight management in adult patients with an initial BMI of: • 35 kg/m2 or greater and prediabetes |
Sponsor | Novo Nordisk Canada Inc. |
Submission history | Previously reviewed: No, Semaglutide 2.4 mg (Wegovy) has not been previously reviewed |
BMI = body mass index; NOC = Notice of Compliance.
Table 2: Summary of Economic Evaluation
Component | Description |
|---|---|
Type of economic evaluation | Cost-utility analysis Markov model |
Target populations | Health Canada indication: As an adjunct to a reduced-calorie diet and increased physical activity for chronic weight management in adult patients with an initial BMI of 30 kg/m2 or greater (obesity), or 27 kg/m2 or greater (overweight) in the presence of at least 1 weight-related comorbidity such as hypertension, T2DM, dyslipidemia, or obstructive sleep apnea Reimbursement request: As an adjunct to a reduced-calorie diet and increased physical activity for chronic weight management in adult patients with an initial BMI of 35 kg/m2 or greater and prediabetes |
Treatment | Semaglutide 2.4 mg weekly for no more than 2 years as an adjunct to a reduced-calorie diet and increased physical activity |
Comparator | Standard care: Reduced-calorie diet and increased physical activity (defined as 500 kcal per day deficit + 150 minutes per week of physical activity) |
Perspective | Canadian publicly funded health care payer |
Outcomes | QALYs, LYs |
Time horizon | 40 years |
Key data source | STEP clinical trials |
Submitted results | Health Canada indication: ICER = $35,789 per QALY (incremental costs = $5,885; incremental QALYs = 0.164) Reimbursement request: ICER = $27,671 per QALY (incremental costs = $5,601; incremental QALYs = 0.202) |
Key limitations |
|
CADTH reanalysis results |
|
BMI = body mass index; ICER = incremental cost-effectiveness ratio; LY = life-year; QALY = quality-adjusted life-year; SF-36 = Short Form (36) Health Survey; T2DM = type 2 diabetes mellitus.
Conclusions
Based on the clinical review, data from placebo-controlled, double-blind randomized controlled trials suggest that semaglutide produces a statistically and clinically significant weight loss in patients with overweight or obesity compared to diet and exercise alone. Although the weight loss is considered clinically significant, there is no clear evidence regarding whether this weight loss reduces the number of patients who may develop various weight-related comorbidities, including type 2 diabetes, cardiovascular disease (CVD), and osteoarthritis. There is some evidence of an improvement in the physical component of health-related quality of life; however, the clinical significance of this improvement is less clear.
CADTH undertook reanalyses to address limitations in the sponsor’s economic evaluation. These included assuming no additional benefit once weight had been regained, removing comorbidities other than diabetes from the analysis, removing body mass index (BMI) as an independent risk factor for mortality, using a different value set for BMI-related utility, using data from the STEP 1 extension trial to determine weight regain post–treatment discontinuation, assuming 3 years of treatment use, and explicitly linking treatment discontinuation to average weight of the cohort.
Based on the reimbursement request population, in the CADTH base case, the incremental cost-effectiveness ratio (ICER) for semaglutide compared with standard care is $204,928 per quality-adjusted life-year (QALY) (incremental costs = $9,385; incremental QALYs = 0.046). CADTH notes the majority of incremental costs is from the cost of semaglutide ($10,074), with cost savings due to delay of type 2 diabetes onset (–$484) and less time spent being prediabetic (–$207). The degree of cost savings associated with prediabetes is highly uncertain. The removal of these cost savings increases the ICER to $209,449 per QALY. The majority of QALY gains (88%) are derived from the direct impact that weight loss has on patient utility — through improved physical functioning, for example. The remaining QALY gains (12%) are derived through delaying the onset of type 2 diabetes. Although no statistically significant conclusions from the clinical data could be concluded regarding delay in type 2 diabetes onset, the evidence is suggestive of improvements in glycemic control given the number of patients who return to “normal glycemic control.” As such, a delay in onset of type 2 diabetes delay is plausible. If semaglutide use leads to no delay in type 2 diabetes onset, the ICER increases to $241,914 per QALY.
To achieve cost-effectiveness at a $50,000 per QALY threshold, the price of semaglutide would need to decrease by 71%. If there are no savings to the health care system from temporary reversal of prediabetes and there is no delay in type 2 diabetes onset, then a price reduction of 80% would be required. These results assume that semaglutide is only given for a maximum of 3 years and there are no negative impacts associated with weight cycling, the process of losing and then regaining weight. The cost-effectiveness of semaglutide use beyond 3 years is highly uncertain as the sponsor’s model precluded an assessment of this. If long-term sustained semaglutide use does not translate into sustained weight loss and the prevention of weight-related comorbidities, then long-term use would likely be less cost-effective than in the CADTH base case. If weight loss is sustained, then the likelihood of preventing weight-related comorbidities would increase. Should this occur, then this could improve the cost-effectiveness of semaglutide relative to the CADTH base case. With regard to weight cycling, the impact of this is not explored in the sponsor’s analysis. Evidence regarding the impact of weight cycling is mixed and highlights the nuances with linking weight loss to impacts on weight-related comorbidities. Some evidence is suggestive of increased cardiac risk in some groups of patients. Should this occur, this would reduce the cost-effectiveness of semaglutide use relative to the CADTH base case.
Finally, the CADTH base case only applies to the restricted reimbursement request population of patients with a BMI greater than 35 kg/m2 with prediabetes. CADTH notes that only 6% of patients in the STEP 1 trial were overweight with a BMI under 30 kg/m2; therefore, assessing the magnitude of benefit in this subgroup is highly uncertain. As shown in the sponsor’s budget impact analysis (BIA), this group represents 32% of the Health Canada indication, equating to a budget impact of more than $300 million. As a scenario analysis, CADTH assessed cost-effectiveness using the sponsor’s assumptions and found the ICER increased to $223,572 per QALY. Overall, cost-effectiveness in the full Health Canada indication is highly uncertain. CADTH notes it will be less cost-effective in the full indication than the reimbursement request, given the reimbursement request identifies those most likely to benefit from therapy.
Stakeholder Input Relevant to the Economic Review
This section is a summary of the feedback received from the patient groups, registered clinicians, and drug plans that participated in the CADTH review process (specifically, information that pertains to the economic submission).
Input from caregivers and patients who are overweight and/or living with obesity, diabetes, or prediabetes was received from 5 Canadian organizations: the Gastrointestinal Society, Diabetes Canada, Obesity Canada, the Canadian Liver Foundation, and Obesity Matters. Input was collected via interviews and surveys. Patients living with obesity reported experiencing limited mobility, chronic pain, difficulty with daily tasks, physical limitations, stigma, depression, anxiety, negative impact on relationships, mental health issues, and decreased overall quality of life. The most common obesity-related comorbidities included arthritis, hypertension, sleep apnea, gastroesophageal reflux disease, irritable bowel syndrome, high cholesterol, and diabetes. Patients reported that the treatment of these concurrent health conditions complicate the management of obesity. Current treatments included psychological and behavioural therapy (including exercise and restrictive diet), pharmacotherapy (Contrave, Saxenda, orlistat, and over-the-counter weight-loss supplements), and bariatric surgery. Treatment goals included improvement in long-term weight loss, ability to perform daily tasks, quality of life, and obesity-related health complications. Patients with experience with semaglutide reported weight loss, a reduced appetite, and good management of blood sugar levels. Some patients reported nausea and gastrointestinal issues.
Clinician input was received from 4 groups: the Calgary Weight Management Centre, Centre de Médecine Métabolique de Lanaudière, and a joint input from Obesity Canada–Obésité Canada and the Canadian Association of Bariatric Physicians and Surgeons. The clinician input noted that current pharmacological interventions that are approved and commercially available in Canada for use as an adjunct to health behaviour interventions include orlistat (Xenical), liraglutide 3.0 (Saxenda), and naltrexone-bupropion (Contrave). The clinicians noted that Wegovy is not currently available in Canada and Ozempic is used off-label in the management of obesity. Some clinicians opined that psychological and behavioural therapy would remain the cornerstone treatment for chronic obesity and it would be the responsibility of clinicians to educate patients on the use of semaglutide in conjunction with other therapies. The reimbursement of semaglutide is expected to replace liraglutide and naltrexone-bupropion and may shift treatment to exclusively pharmacotherapy in community clinics, specialty clinics, and surgical centres. The clinician input noted that the current criteria of clinical success, defined as a weight loss of 5% or more after 12 weeks, may not adequately capture response. Treatment goals include improving or resolving obesity-related complications, including type 2 diabetes, hypertension, obstructive sleep apnea (OSA), and osteoarthritis. Lack of improvement in health-related issues such as improvement in general well-being, social life, diabetes control, blood pressure control, joint pain, and walking distance may signal nonresponsiveness and require consideration of treatment discontinuation.
The drug plans noted comparator drugs are not funded in most jurisdictions. The public drug plans requested clarification regarding diagnosis of prediabetes, adherence to adjunct therapy (reduced-calorie diet and physical activity), and re-treatment in patients who regain weight or in patients whose BMI dropped below 35 kg/m2.
Several of these concerns were addressed in the sponsor’s model:
Only diet and exercise were included as a relevant comparator given the lack of public funding for other weight-loss medications.
Quality of life associated with weight loss was included in the sponsor’s model.
Adverse events associated with semaglutide use were included.
CADTH was unable to address the following concerns raised from stakeholder input:
Re-treatment with semaglutide was not possible given the model structure.
Economic Review
The current review is for semaglutide (Wegovy) as an adjunct to a reduced-calorie diet and increased physical activity for chronic weight management in adult patients.
Economic Evaluation
Summary of Sponsor’s Economic Evaluation
Overview
The sponsor submitted an economic model that estimates outcomes in terms of long-term costs and QALYs, assessing the cost-effectiveness of semaglutide as an adjunct to a reduced-calorie diet and increased physical activity for chronic weight management in adult patients. Analysis relates to 2 patient populations.1
Health Canada indication: Adult patients with an initial BMI of 30 kg/m2 or greater (obesity), or 27 kg/m2 or greater (overweight) in the presence of at least 1 weight-related comorbidity such as hypertension, type 2 diabetes, dyslipidemia, or OSA.
Reimbursement request: Adult patients with an initial BMI of 35 kg/m2 or greater and prediabetes.
Analysis was conducted from the perspective of a provincial ministry of health with a time horizon of 40 years. A discount rate of 1.5% per annum was applied.
Semaglutide is delivered weekly as a 2.4 mg subcutaneous injection once maintenance dose is achieved (2.4 mg). Semaglutide is initiated at a dose of 0.25 mg weekly, which is increased every 4 weeks to doses of 0.5 mg (week 5 to week 8), 1.0 mg (week 9 to week 12), 1.7 mg (week 13 to week 16), and 2.4 mg weekly thereafter. After 12 weeks of receiving the full maintenance dose (28 weeks post–treatment initiation), if a patient has not lost at least 5% of their body weight, this is a proposed stopping rule for discontinuing treatment. Semaglutide is provided in a pack of 4 pre-filled pens. The unit cost for the pack of 4 pens is $363.51 ($90.88 per pen). The 28-day cost is $363.51 as the cost of pens is the same for all doses.
Within the economic evaluation, a semaglutide adjunct to diet and exercise is compared to diet and exercise alone (standard care). Comparison to other weight-loss medications was considered inappropriate due to the lack of publicly funded weight-loss pharmacotherapies. As semaglutide is an adjunct to diet and exercise, no treatment costs for the comparator therapy are included.
Model Structure
A cohort multi-state Markov model was developed in Microsoft Excel to simulate the progression of adult patients either receiving semaglutide as an adjunct therapy to diet and exercise versus diet and exercise alone.
The model estimates the impact of treatments on long-term costs and QALYs. To do this, the model assesses temporal changes on a range of risk factors (BMI, glycemic status, and cardiometabolic risk factors) associated with weight-related complications and events (acute coronary syndrome, stroke, cancer, sleep apnea, and knee replacement). The probability of patients developing these complications and events was derived from risk prediction models — other than the probability of temporary reversal of prediabetes, which was derived from the STEP 1 trial.2 The risk of death throughout the model is related to the risk of fatal events, the increased risk post weight-related events, the BMI of the patient, and the underlying age-gender specific population mortality.3-10 The model also applies an additional mortality multiplier to every mortality probability in the model, which accounts for an individual’s BMI. Treatment effectiveness is modelled indirectly through changes on BMI and cardiometabolic risk factors and directly through the effect on the temporary reversal of prediabetes.
For the first year, the model cycle length is 3 months with a subsequent cycle length of 1 year. Treatment is assumed to be discontinued after 7 months if 5% weight loss is not achieved. Likewise, at any point patients can discontinue therapy based on treatment discontinuation rates derived from the trial. Treatment is assumed to be discontinued for all patients at 2 years. After 2 years, patients are assumed to return to their baseline weight and pre-treatment glycemic status (should they not develop type 2 diabetes) over a period of 3 years. For nonresponders with semaglutide, the patient pathway is assumed to be consistent with that of patients who do not respond on diet and exercise alone.
Model Inputs
The Health Canada indication comprises 3 distinct subgroups, based on glycemic control: normal glycemic control, prediabetic (defined as hemoglobin A1C of 5.7% to 6.4% [39 mmol/mol to 46 mmol/mol]), and type 2 diabetes. Baseline patient characteristics are derived from the STEP 1 and STEP 2 trials weighted according to the proportion of patients falling into each of the 3 categories, based on prevalence in the Canadian population. For the reimbursement request indication, baseline patient characteristics are derived from a subgroup of the STEP 1 trial that only includes those with prediabetes and a BMI greater or equal to 35 kg/m2.
Treatment effectiveness for semaglutide was derived from the STEP trials and relates to treatment response (as measured by 5% weight loss at 12 weeks), temporary prediabetes reversal, change in systolic blood pressure, change on total cholesterol, and change in high-density lipoprotein cholesterol.
Treatment effectiveness for the full Health Canada indication for the first year on-treatment is based on a subgroup analysis of the STEP 1 trial, which looks at patients who have normal glucose tolerance or are prediabetic at baseline. Evidence from the STEP 2 trial is used to inform treatment effectiveness for patients who have type 2 diabetes for the first year on treatment. The STEP 5 trial was used to inform treatment effectiveness for year 1 to year 2. The STEP 5 trial does not include type 2 diabetes patients; therefore, effectiveness estimates for year 1 to year 2 are based on a trial population that is not reflective of the Health Canada indication.
Treatment effectiveness for the reimbursement request for the first year on treatment is based on a subgroup of the STEP 1 study that only includes those patients with a BMI of 35 kg/m2 or greater as well as being prediabetic. For year 1 to year 2, on-treatment effectiveness is based on evidence from the STEP 5 trial, which was conducted over a longer (2-year) time frame. No subgroup analysis was conducted to account for differences between the reimbursement request and trial inclusion criteria in the STEP 5 trial. Therefore, effectiveness estimates for year 1 to year 2 are based on a trial population that is not reflective of the reimbursement request.
Risk equations are used to estimate transition probabilities to complications (type 2 diabetes, cancer, CVD, sleep apnea) and events (stroke, myocardial infarction, knee replacement, bariatric surgery, angina, transient ischemic attack [TIA]). Mortality is based on literature-based estimates of event-related and complication-related mortality and general population mortality, sourced from Statistics Canada Life Tables. An additional mortality multiplier is also applied to non–disease-specific mortality probabilities based on a patient’s BMI.
Health state utilities in the model were based on a regression analysis that mapped Short Form (36) Health Survey responses from the STEP 1 study to the EQ-5D instrument. Analysis allowed estimation of utility values by age, presence of heart or circulatory disease, presence of hypertension, smoking status, prediabetes status, and BMI (linear, quadratic, and cubic effects). This allowed estimation of the utility scores by BMI. Additional decrements in utility were sourced from literature and related to diabetes, acute coronary syndrome, sleep apnea, cancer, stroke, bariatric surgery knee replacement, and TIAs. Health state utility values for combined states were based on an additive model.
Costs included in the model related to obesity treatment costs, long-term costs of the management of obesity-related complications, and acute costs of events related to obesity complications. Treatment costs related to the costs of semaglutide only, as described earlier. Other costs included in the model relate to the incidence of diabetes complications or acute events related to complications, and the long-term management of complications. These costs were sourced from the literature. The model did not include a cost of management of patients who either always had normal glucose levels or who had temporary reversal of diabetes.
Summary of Sponsor’s Economic Evaluation Results
The sponsor submitted results for both the Health Canada indication and the reimbursement request based on probabilistic analyses with 1,000 iterations. Several probabilistic scenario analyses were presented.
Base-Case Results
For the reimbursement requested indication, semaglutide was associated with increased obesity treatment and monitoring costs of $7,468 but reduced costs of obesity complications of –$1,728 ($44,716 versus $46,444) and reduced costs of obesity events of –$139 ($8,979 versus $8,840), leading to total incremental costs of $5,601 ($66,652 versus $61,051). The reduced costs of obesity complications were primarily due to type 2 diabetes. Semaglutide was associated with increased QALYs of 0.202 (17.15 versus 16.95). Thus, the estimated ICER was $27,671 per QALY.
For the Health Canada indication, semaglutide was associated with increased obesity treatment costs of $6,891 but reduced costs of obesity complications of –$891 ($49,682 versus $50,573) and reduced costs of obesity events of –$115 ($9,987 versus $10,102), leading to incremental costs of $5,885 ($72,271 versus $66,387). The reduced costs of obesity complications were due to type 2 diabetes and cancer. Semaglutide was associated with increased QALYs of 0.164 (17.94 versus 17.78). Thus, the estimated ICER was $35,789 per QALY.
Table 3: Summary of the Sponsor’s Economic Evaluation Results
Intervention | Total costs ($) | Incremental costs vs. standard care ($) | Total QALYs | Incremental QALYs vs. standard care | ICER vs. standard care ($/QALY) |
|---|---|---|---|---|---|
Health Canada indication | |||||
Standard care | 66,387 | Reference | 17.78 | Reference | Reference |
Semaglutide + standard care | 72,271 | 5,885 | 17.94 | 0.164 | 35,789 |
Reimbursement request | |||||
Standard care | 61,051 | Reference | 16.95 | Reference | Reference |
Semaglutide + standard care | 66,652 | 5,601 | 17.15 | 0.202 | 27,671 |
ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year; vs. = versus.
Source: Revised sponsor’s pharmacoeconomic model sent on May 13, 2022.11
The probability that semaglutide is optimal based on a threshold of $50,000 per incremental QALY was greater than 95% for the Health Canada indication and the reimbursement request.
Sensitivity and Scenario Analysis Results
Various scenario analyses were conducted, though the ICER remained below $50,000 per QALY across both the reimbursement request and full Health Canada indication. The largest impact came from using a shorter time horizon and choosing an alternative set of utility estimates to estimate the impact of weight loss.
CADTH Appraisal of the Sponsor’s Economic Evaluation
CADTH identified several key limitations to the sponsor’s analysis that have notable implications for the economic analysis.
The clinical impact associated with weight loss. In the sponsor’s model, there are 2 health impacts associated with weight loss. First, there is a direct utility benefit that patients experience through reduced weight. This is derived from improved physical functioning as well as improvements in mental well-being. The second is the impact on weight-related comorbidities. The sponsor’s model looks at 8 weight-related comorbidities that will be influenced by weight loss: type 2 diabetes, acute coronary syndrome, stroke (including TIA), sleep apnea, knee replacement, colon cancer, endometrial cancer, and breast cancer. In the STEP trials, no evidence is presented that shows a direct impact on any of these comorbidities, except type 2 diabetes onset. CADTH considered each comorbidity in turn and assessed whether short-term weight loss, followed by rapid weight regain, would impact any of these comorbidities.
Type 2 diabetes: In the sponsor’s analysis, the risk of developing type 2 diabetes is derived from the QDiabetes risk equation tool, with the option to use the Framingham Offspring risk equation tool as an alternative. Both equation sets include BMI as a risk factor to estimate type 2 diabetes onset in a cohort that loses weight. One limitation with this approach is that neither risk equation is validated for dramatic short-term shifts in weight. In the sponsor’s base case, an individual loses weight over a period of 2 years while on treatment, then regains all weight lost over the next 3 years. Using the risk equations, this approach results in a permanent reduction in the proportion of patients who develop type 2 diabetes. This is shown in Figure 2 (Appendix 3), which outlines what proportion of patients develops type 2 diabetes over time in the sponsor’s analysis, dependent on whether they receive semaglutide or diet and exercise alone. As the 2 curves never merge, this means fewer patients develop type 2 diabetes with semaglutide than they do with diet and exercise alone (approximately a 1.7% absolute permanent reduction in type 2 diabetes onset). The CADTH clinical expert noted that for patients who discontinue semaglutide and regain weight, the onset of type 2 diabetes will only be delayed, not prevented, and that any delay would be short lived once a patient discontinued therapy. This was confirmed in a study by Wilding et al. (2022), who looked at changes in hemoglobin A1C following discontinuation with semaglutide and found that treatment discontinuation had a large impact on glycemic control.12 Finally, there is likely a treatment effect associated with semaglutide that influences the likelihood of developing type 2 diabetes, which the risk equations do not account for. Therefore, delay in type 2 diabetes onset will be much shorter than predicted by the risk equation once treatment is discontinued.
CVD: The sponsor used the QRisk3 risk equation to predict CVD in patients who do not have type 2 diabetes. Although the risk equation is validated to predict CVD outcomes for a given a set of parameters, the model does not account for prior weight. For example, using the risk equation, an individual with a BMI of 30 kg/m2 has the same risk of developing CVD as an individual whose BMI goes from 35 kg/m2 to 30 kg/m2. It assumes that prior weight is not a predictor of future outcomes. A study by Haase et al. (2021) looks at the risk of obesity-related outcomes with intentional weight loss, in comparison with maintaining baseline weight.13 The study observes a cohort that has sustained weight loss (on average, 13% of body weight) over at least a 4-year period and then looks at the impact on obesity-related outcomes. The study found that a 13% weight loss, regardless of starting weight, had no benefit on atrial fibrillation, heart failure, or unstable angina and/or myocardial infarction rates. That is not to say weight does not correlate with these factors, but that weight loss may not mitigate the increased risk associated with obesity, at least in the short run. As weight loss improves CVD risk factors, the longer weight loss is sustained the more likely reductions in cardiovascular events will be seen. As the weight loss associated with semaglutide is close to 13% (approximately 15% in the STEP 1 trial full cohort and 13.28% in the subgroup of prediabetics with a BMI > 35 kg/m2) and is not maintained for 4 years in the sponsor’s model, there is insufficient evidence to suggest it will lead to a reduction in cardiovascular events. CADTH does note that in patients with type 2 diabetes who are at high risk of CVD, there is evidence to suggest that semaglutide (albeit at a lower dose than is used for weight loss) is associated with lower rates of cardiovascular events.14 This suggests in this patient subgroup there may be a treatment effect on cardiac outcomes, perhaps outside of weight loss. However, patients in this trial were over 50 years of age with type 2 diabetes and established CVD and therefore represent a different cohort than those mainly covered by the Health Canada indication and reimbursement request.
OSA: There is data to show that reductions in weight lead to benefits in sleep apnea. The study by Haase et al. showed benefits to sleep apnea associated with weight reduction; likewise, the likelihood of developing sleep apnea is strongly associated with obesity.13 A study by Blackman et al. (2016) also showed that weight loss obtained through pharmacotherapy reduced disease severity as measured through the apnea–hypopnea index.15 However, the sponsor assumed that reduction in weight leads to immediate and total alleviation of both sleep apnea–related health impacts and costs, such as discontinuation of continuous positive airway pressure (CPAP) use. Figure 5 shows the percentage of the cohort that has OSA over time as modelled in the CADTH base-case analysis. After 1 year, OSA prevalence decreases from 52% at baseline to 29% for a cohort that receives semaglutide. That assumes total alleviation of symptoms and costs. The CADTH clinical expert noted that it is unlikely weight loss would be associated with immediate changes to sleep apnea management. Many of these patients will have seen a sleep specialist to develop a treatment plan and for many patients, their symptoms will be already well controlled. A self-initiated change in management without specialist consultation may be dangerous to the patient, especially if they regain weight. Short-term weight reduction may delay the development of sleep apnea or improve symptoms in those who do not use CPAP, but this aspect was not considered by the sponsor. Finally, CADTH notes that the sponsor assumed that the utility associated with sleep apnea was the same as that of a patient with asthma. No justification was provided for this assumption.
Knee replacements: Knee replacements are an associated impact of weight, with data showing that knee replacements are more commonly performed in patients with a higher BMI.16 However, the CADTH clinical expert noted it was unlikely that someone who required a knee replacement would not require 1 after 2 years of weight loss. Likewise, short-term weight loss was unlikely going to mitigate the risk of ever needing a knee replacement. Conversely for some patients, weight loss is required for a knee replacement surgery to go ahead. Therefore, a reduction in weight may lead to an increase in the number of knee replacements. This procedure will likely lead to improved physical functioning, which is not considered by the sponsor. In the sponsor’s model, a knee replacement only leads to a cost and the potential of a fatal surgery.
Cancer: The sponsor included 3 cancers in the model — endometrial, breast, and colon cancer. With a reduction in weight, the sponsor assumed an immediate reduction in cancer risk. Table 10 in Appendix 3 shows the relative risk reduction in developing cancer by time since treatment initiation. The risk of developing colorectal cancer is assumed to decrease starting 3 months post–treatment initiation. Although studies show a correlation between weight and cancer, the mechanisms by which this association occurs is still uncertain. For breast and endometrial cancers, there is evidence to show that sustained weight loss may lead to a risk reduction in cancer onset.17,18 However, this weight reduction was sustained and was in patients over the age of 60. Finally, there have been several studies that have investigated the long-term impacts of bariatric surgery on cancer risk. As bariatric surgery leads to a high degree of sustained weight loss, this provides some insight into how weight loss relates to cancer risk. A review by Bruno and Berger (2020) found that in studies that noted a difference in cancer rates between those who underwent bariatric surgery versus those who did not, it was unclear whether reduction in cancer was due to weight loss or another treatment effect related to the surgery itself.19 Conversely, some studies show that bariatric surgery may be associated with an increased risk of colorectal cancer, for example. Finally, a recent study by Aminian et al. (2022) that looked at cancer incidence in those who received bariatric surgery versus a matched cohort that did not found that substantial weight loss (> 24%) was required to observe a meaningful reduction in cancer risk and differences in cancer incidence were mainly observed 6 years after surgery.20 Given the assumption of no sustained weight loss, there is insufficient evidence to suggest semaglutide will reduce cancer risk.
Overall, for each weight-related comorbidity, evidence shows that the study of obesity is complex and forming simple linear relationships between BMI and risk ignores confounders and complexities.
CADTH only included type 2 diabetes onset in the base-case analysis as a weight-related comorbidity that will be impacted by semaglutide use. CADTH felt, based on current evidence, it is unlikely that persistent effects on type 2 diabetes after weight regain post–treatment discontinuation would be observed. As the sponsor’s model did not allow for this modification, a shortened time horizon of 7 years was used. This includes 3 years on treatment and then 4 years off treatment, at which point all weight loss is regained. After this period, there would be no expected additional cost or health differences between those who received semaglutide and those who did not.
A scenario analysis was conducted that included the sponsor’s functionality of OSA benefit. CADTH notes this likely represents the most optimistic benefits associated with potential sleep apnea reduction.
Utility associated with weight loss. To model the direct impact of weight loss on utility, the sponsor mapped the Short Form (36) Health Survey from the STEP 1 trial to EQ-5D using a UK tariff. This introduced uncertainty into the analysis as EQ-5D data were not directly gathered from the trial. As noted in the CADTH economic guidelines, mapping as a means of deriving health utilities is not recommended unless there are no alternative approaches.21 In this submission, mapping is used to derive a relationship between BMI and utility. This was done before using direct methods. An alternative relationship between BMI and utility was provided by the sponsor using data from Søltoft et al. (2009) that explored the relationship between BMI and health-related quality of life in adults (n = 14,416) who were 18 years or older, using EQ-5D with a UK tariff.22 Given the larger sample size and the absence of mapping, the study by Søltoft likely provides a more robust estimate of the relationship between BMI and EQ-5D. CADTH notes that the sponsor also provided utility estimates employing a similar mapping exercise to patients from the SCALE obesity trial.23 Despite employing similar methods, different results were generated, further highlighting the uncertainty with the mapping approach. CADTH notes that utility estimates from the SCALE trial provide the most conservative utility estimates with regard to weight loss whereas utility estimates from the STEP 1 trial provide the most optimistic estimates.
CADTH used estimates from Søltoft et al., as provided by the sponsor, to determine utility benefits associated with weight loss.
Cost-effectiveness in the full Health Canada indication. The full Health Canada indication includes all patients with a BMI over 30 kg/m2 as well as those with a BMI over 27 kg/m2 with a weight-related comorbidity. A single trial was not conducted that included all these patients. The STEP 1 trial excluded type 2 diabetes, which was analyzed separately in the STEP 2 trial. The full Health Canada indication is very heterogenous, with the benefit of semaglutide likely varying significantly across separate groups. In STEP 1, overweight patients represent only 6% of the cohort, further adding uncertainty as to the benefit received by these patients. No preplanned subgroup analyses were performed by the sponsor, making any conclusions regarding very heterogenous populations difficult to form. The sponsor’s analysis largely assumed equivalent efficacy across many subgroups that may have different magnitudes of benefit.
CADTH presents the full Health Canada indication population as a scenario analysis.
Mortality associated with short-term weight loss. The sponsor assumes that every 1-point decrease in BMI is associated with a reduction in mortality risk, starting 3 months after treatment initiation. This mortality risk reduction is on top of the mortality risk reduction associated with preventing weight-related comorbidities. This estimate is derived from a study by Bhaskaran et al. (2018) that looks at a large prospective cohort of patients, noting the association between an individual’s baseline weight and their associated mortality risk across several comorbidities as well as all-cause mortality.10 Although the study may derive a robust estimate of the relationship between BMI and mortality, at a given point in time, this does not apply directly to weight loss as assumed by the sponsor.
First, the sponsor assumes that weight loss has an instantaneous impact on mortality. According to the CADTH clinical expert, any weight loss would need to be sustained for the benefit of weight loss to be realized. Studies by Sjöström et al. (2007, 2012) did find a reduction in deaths for those who underwent bariatric surgery.24,25 However, differences in deaths were not seen until after approximately 5 years to 6 years of follow-up, of which weight loss between 20% and 35% was sustained. The sponsor’s analysis looks at approximately 13% additional weight loss, relative to diet and exercise alone, over 2 years followed by full weight regain after 3 years. Another study by Doumouras et al. (2020), which looked at mortality outcomes in Canadian patients in Ontario undergoing bariatric surgery, found mortality differences post-surgery were seen after approximately 1.5 years.26 However, the study also found no difference in mortality for those with a BMI under 40 kg/m2 (hazard ratio = 1 [95% confidence interval, 0.67 to 1.53]) or those under the age of 55. This contradicts the sponsor’s assumption that weight loss leads to a mortality benefit across all ages and BMI levels. The average BMI of patients in this study was 47 kg/m2, with 27% having type 2 diabetes. This compares to 41 kg/m2 and 7% having type 2 diabetes in the study by Sjöström et al. This likely explains why a mortality benefit was seen sooner in the study by Doumouras as it represented a sicker cohort that is also not representative of those most likely to receive semaglutide. Overall, evidence concerning bariatric surgery likely represents the upper limit of potential mortality benefits derived through weight loss, given the degree of weight loss that is sustained, the selection bias associated with those eligible and receiving the procedure, and the mortality benefits it likely provides outside of weight loss. Given that weight loss with semaglutide is not as significant as bariatric surgery and is not sustained in the sponsor’s analysis, it is unlikely that semaglutide would be associated with a reduction in mortality.
Second, baseline weight before weight loss is not accounted for. A study by Xu et al. (2018), for example, found that the mortality rates of “normal weight” patients who were formerly overweight or obese were higher than patients who never exceeded “normal weight.”27 Due to confounding, a direct relationship between weight loss and mortality is highly uncertain when analyzing observational databases.
Overall, outside of the prevention of known comorbidities associated with elevated mortality risk, there is a high degree of uncertainty associated with weight loss and the impact on mortality. To exacerbate this uncertainty, when analyzing the mortality impact associated with weight loss, 1 would also need to tease out the treatment effects associated with different types of weight loss. For example, bariatric surgery may influence type 2 diabetes remission beyond the impact of weight loss, which may confer additional survival benefit.28
CADTH only included mortality associated with the prevention of weight-related comorbidities given the short period of time during which weight is lost.
Weight regain after treatment discontinuation. The sponsor assumes that after treatment discontinuation, weight is regained such that 3 years post–treatment discontinuation, all weight loss has been regained. The sponsor cites a paper by Ara et al. (2012) to inform the rate of weight regain.29 However, this study is a meta-analysis of pharmacotherapies used to treat obesity, which at the time did not include glucagon-like peptide 1 analogues. Therefore, it is uncertain how weight regain from prior weight-loss drugs, with different mechanisms of actions, would compare to semaglutide.
A study by Wilding et al. (2022), which is an extension of the STEP 1 trial, showed that after 1 year, patients who discontinued semaglutide had regained most of the weight they lost.12 After 68 weeks on semaglutide, weight loss was 17.3%; however, 52 weeks off treatment, patients regained 11.6 percentage points of weight. This would indicate that after an additional year, nearly all weight lost likely will have been regained. The sponsor used the data to fit an exponential distribution to this data to predict weight regain post-discontinuation.
CADTH assumed weight regain in line with the trial data, as estimated by the sponsor. This estimate better aligns with direct evidence from semaglutide discontinuations. A scenario analysis was conducted that assumed all weight would be regained after 2 years post–treatment discontinuation.
Time on treatment. The sponsor assumes patients will only be treated with semaglutide for 2 years, at which point 100% of patients discontinue. This is not a discontinuation criterion stated in the product monograph. Likewise, the clinical expert consulted by CADTH noted there would be no desire to suspend therapy if the patient wished to remain on the therapy given the known weight regain associated with treatment discontinuation. Due to the inflexibility with the sponsor’s model, CADTH was unable to assess a scenario where patients remained on therapy for longer than 3 years. If patients remain on therapy for longer than 2 years, then that weight loss may be sustained. In the absence of long-term evidence, it is unknown whether there would be a treatment waning effect over time whereby the patient remains on therapy but starts to regain weight.
CADTH used functionality within the sponsor’s model to increase treatment duration up to 3 years. No waning was assumed for those who remain on therapy.
Correlating weight and treatment discontinuation. The sponsor assumes that the impact of treatment discontinuation on weight loss, outside of those who do not respond, has been fully captured in the trial estimates. Therefore, discontinuation rates are used only in the model to calculate estimates of drug cost. This means the sponsor’s model includes health states with patients both on and off treatment. Good modelling practices should ensure there is minimal heterogeneity across model states; given that treatment discontinuation is associated with weight regain, not separating out these patients would increase heterogeneity across health states.30 Without correlating treatment effect and discontinuation rates, this also presents an issue for the probabilistic analysis as probabilistic runs will be created where discontinuation rates are high yet average weight loss is not affected. This would go against evidence presented for this submission.12 The sponsor also assumes that the impact of treatment discontinuation on average cohort weight loss has been fully captured within the trial. First, evidence shows that weight regain occurs over several years.12 For example, if patients discontinued therapy after 6 months, 1 would not expect the impact of weight regain to impact the average weight of the cohort for another year. Second, according to data provided by the sponsor, fewer than 5% of those who responded to therapy discontinued before 1 year. As more patients discontinue, the impact on the average weight of the cohort will become more pronounced as the trial shows weight loss plateauing in those who remain on therapy around 68 weeks.2 Therefore, the full impact of treatment discontinuation on the average weight of the cohort is unlikely to be fully captured in the weight loss estimates presented in the STEP 1 trial, which is used to estimate weight loss in the model.
The model does allow the functionality to disaggregate the cohort into those on and off treatment. This, in turn, allows weight to be correlated with the proportion of patients remaining on treatment, ensuring states are more homogenous and probabilistic runs hold more validity. With regard to the reimbursement request, CADTH notes the sponsor only provides the treatment policy estimand for those who respond to therapy, assuming the total impact of treatment discontinuation is accounted for in the weight-loss estimates. When disaggregating the cohort into those on and off treatment, the trial product estimand should be used as this is estimated only using data from those who remained on treatment, preventing the potential double counting associated with treatment discontinuation. Although the difference in treatment policy and trial product estimand is quite pronounced in the STEP 1 trial (–14.9% weight loss versus –16.9% weight loss, respectively), this applies to the whole cohort whereas the sponsor’s model estimates only apply to those who respond to therapy. In the STEP 1 trial, the majority of patients who discontinued therapy was those who did not respond. Therefore, the difference in the treatment policy and trial product estimand for those who respond will likely not be as pronounced.
Figure 4 in Appendix 4 shows the impact of assuming treatment discontinuation has a further impact on weight loss than what is assumed by the sponsor, using various assumptions. For the sponsor’s results to hold face validity (no weight regain at 3 years), patients who remain on therapy would need to continue to lose weight from year 2 to year 3 to compensate for those who discontinue and regain weight. Given the plateau in weight loss seen in the STEP 1 trial at 68 weeks and the substantial impact of weight regain, it is unlikely the sponsor’s assumptions of continuing weight loss after year 2 holds.
CADTH used functionality within the model to link discontinuation and weight regain. CADTH calibrated the model by increasing weight loss in those who remain on therapy such that the average weight of the cohort is unchanged at 2 years, as per the sponsor’s base case.
Prediabetes reversal cost. In the sponsor’s analysis, an individual who is prediabetic, defined as having hemoglobin A1C less or equal to 5.8%, will incur $189 of costs each year to the health service. This value was calculated by comparing health care costs between patients who are insulin resistant without type 2 diabetes versus those with no type 2 diabetes and who are not insulin resistant. Although this analysis may show those with prediabetes have higher costs than those who do not, it does not mean that upon achieving normal glycemic control, management and care for these patients will instantly shift. According to the clinical expert consulted by CADTH, a patient who is prediabetic and then reverts to having normal glycemic control will still be followed up frequently and will likely not have an instant shift in care. In the analysis, those who are prediabetic have an elevated risk of developing type 2 diabetes; therefore, additional costs are incurred for those who are prediabetic and then develop type 2 diabetes.
CADTH notes no functionality within the sponsor’s model to apply a cost to those who revert to having “normal glycemic control.” A scenario analysis was conducted that removed all cost savings associated with prediabetes.
Impact of weight cycling. There is uncertainty in the literature regarding the impact of weight cycling, the process of losing and then regaining weight. Given that weight regain is likely after treatment discontinuation if treatment is given for a short period of time, semaglutide would lead to rapid weight loss followed by rapid weight regain. A recent study by Bangalore et al. (2017) found that for patients with coronary artery disease, fluctuation in body weight was associated with higher mortality.31 An older study from Lissner et al. (1991) found associations between fluctuations in body weight and mortality and coronary heart disease.32 However, there is evidence that does not support this.33 There is some degree of uncertainty regarding whether weight fluctuations would lead to harm and no studies provide conclusive evidence. This is not explored in the sponsor’s model.
CADTH was unable to explore any negative consequences that may be associated with weight fluctuations. CADTH notes that this further highlights the complexities associated with predicting benefit from short-term weight loss.
Errors within the modelling approach. CADTH identified an error within the sponsor’s analysis that produced negative probabilities. Given this is not plausible, the sponsor was requested to fix this error. The sponsor provided a revised analysis on May 13, 2022, that fixed this error.
CADTH used the revised model in the base-case analysis.
Additionally, the following key assumptions were made by the sponsor and have been appraised by CADTH (refer to Table 4).
Table 4: Key Assumptions of the Submitted Economic Evaluation (Not Noted as Limitations to the Submission)
Sponsor’s key assumption | CADTH comment |
|---|---|
Additive model for combining utility effects within hybrid states | Likely inappropriate. Analysis adopts an additive assumption for utility values for hybrid states. This approach leads to the largest assumed utility effect of avoiding complications and is therefore likely to overestimate QALY benefits and underestimate the ICER. |
ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year.
CADTH Reanalyses of the Economic Evaluation
Base-Case Results
Table 5: CADTH Revisions to the Submitted Economic Evaluation
Stepped analysis | Sponsor’s value or assumption | CADTH value or assumption |
|---|---|---|
Corrections to sponsor’s submitted base case | ||
1. Corrected inconsistent formula | — | — |
Changes to derive the CADTH base case | ||
1. Inclusion of obesity-related complications | The sponsor included the following obesity-related comorbidities that will be impacted by semaglutide use:
The impact continues for the remainder of the patient’s life, even after full weight regain. | CADTH included the following obesity-related comorbidities that will be impacted by semaglutide use:
This was based on evidence available from the STEP trials, clinical expert opinion, and a review of the literature. As evidence shows that there is little difference in glycemic control post–treatment discontinuation, CADTH assumed that once weight was regained, there would be no further cost and health outcome differences between those who received semaglutide vs. those who did not. |
2. Additional mortality benefit applied to weight loss outside of comorbidities | The sponsor assumed that patients who lose weight will have a lower risk of dying relative to those who do not lose weight starting 3 months after treatment initiation. This mortality risk is independent of whether obesity-related comorbidities are developed. | CADTH assumed that elevated mortality risk would only be related to weight-related comorbidities. |
3. Time on treatment and correlation between treatment discontinuation and weight | The sponsor assumed patients would only be on treatment for a maximum of 2 years and that weight is unimpacted by the proportion of patients who discontinue outside of nonresponders. | CADTH assumed some patients would remain on treatment for 3 years. This was the maximum period allowed by the sponsor’s analysis. CADTH used the functionality provided in the sponsor’s model to explicitly link weight and treatment discontinuation. |
4. Utility associated with BMI | The sponsor mapped SF-36 scores from the STEP 1 trial onto EQ-5D using a validated mapping algorithm. This was used to determine the utility associated with different BMI levels. | CADTH used a large cohort study from the literature that directly measured EQ-5D in patients to determine the utility associated with different BMI levels. |
5. Weight catch-up post–treatment discontinuation | The sponsor assumed weight would be regained at a rate of 33% annually over 3 years. | CADTH used evidence from the STEP extension trial that looked at weight regain post–semaglutide discontinuation, finding 64% weight regain after 1 year. CADTH used the sponsor’s extrapolation of this data. Furter details are provided in Figure 3 in Appendix 4. |
CADTH base case (reimbursement request) | 1 + 2 + 3 + 4 + 5 | |
BMI = body mass index; SF-36 = Short Form (36) Health Survey; T2DM = type 2 diabetes mellitus.
In the CADTH base-case analysis, semaglutide was associated with more QALYs (5.95 versus 5.91) and higher costs ($14,647 versus $5,263) than standard care, leading to an ICER of $204,928 per QALY. The incremental treatment costs associated with semaglutide of $10,074 were partially offset by a reduction in the costs of complications from obesity of $691.
At a threshold of $50,000 per QALY, the probability that semaglutide was optimal was 0%. Figure 6 further outlines the uncertainty associated across probabilistic runs.
Table 6: Summary of the Stepped Analysis of the CADTH Reanalysis Results
Stepped analysis | Drug | Total costs ($) | Total QALYs | ICER ($/QALYs) |
|---|---|---|---|---|
Sponsor’s submitted base case (reimbursement request) | Standard care | $60,798 | 16.96 | Reference |
Semaglutide | $66,652 | 17.15 | 30,000 | |
Sponsor’s revised base case (reimbursement request) | Standard care | $61,051 | 16.951 | Reference |
Semaglutide | $66,652 | 17.153 | 27,671 | |
CADTH reanalysis 1 | Standard care | $5,130 | 5.743 | Reference |
Semaglutide | $11,941 | 5.831 | 96,484 | |
CADTH reanalysis 2 | Standard care | $75,225 | 18.805 | Reference |
Semaglutide | $80,515 | 18.982 | 30,031 | |
CADTH reanalysis 3 | Standard care | $58,475 | 16.746 | Reference |
Semaglutide | $64,236 | 16.939 | 29,810 | |
CADTH reanalysis 4 | Standard care | $58,475 | 17.024 | Reference |
Semaglutide | $64,126 | 17.211 | 30,151 | |
CADTH reanalysis 5 | Standard care | $58,403 | 16.798 | Reference |
Semaglutide | $64,122 | 16.958 | 35,644 | |
CADTH base case (1 + 2 + 3 + 4 + 5) — deterministic | Standard care | $5,079 | 5.911 | Reference |
Semaglutide | $14,482 | 5.957 | 204,965 | |
CADTH base case (1 + 2 + 3 + 4 + 5) — probabilistic | Standard care | $5,262 | 5.91 | Reference |
Semaglutide | $14,647 | 5.95 | 204,928 |
ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year.
Scenario Analysis Results
In the scenario analysis that considered further benefits associated with reduction in sleep apnea cases, the ICER decreased to $178,937 per QALY. CADTH notes this likely represents an overestimation of the benefits associated with sleep apnea prevention as it assumes that some patients with OSA experience total alleviation of symptoms and discontinuation of CPAP without consulting a sleep specialist. In the scenario analysis that removed prediabetic cost savings and assumed no delay in type 2 diabetes onset, the ICER increased to $247,859. Although delay in type 2 diabetes is plausible, it is uncertain to what extent this will occur. The true ICER may fall between the CADTH base case and this analysis. When weight was regained over 2 years, the ICER increased to $222,845, with estimated incremental QALYs associated with semaglutide decreasing from 0.046 to 0.043. Finally, an analysis was conducted that did not use a stopping rule; in this analysis, the ICER increased to $240,915.
In the scenario analysis that looked at the full Health Canada population, the ICER increased to $223,572 per QALY. CADTH notes that this analysis is highly uncertain as there is limited evidence to derive an accurate estimate of benefit for those who are overweight with weight-related comorbidity, for example.
With the sponsor’s submitted analysis, semaglutide is cost-effective at a $50,000 per QALY threshold for the reimbursement request without any price reductions. With the CADTH base-case analysis, the necessary price reduction for semaglutide to be cost-effective at a threshold of $50,000 per QALY is 71%. However, this increases to 80% if there is limited benefit associated with delays in type 2 diabetes diagnoses.
Table 7: CADTH Price Reduction Analyses
Analysis | ICERs for semaglutide vs. diet and exercise ($/QALY) | |
|---|---|---|
Price reduction | Corrected sponsor base case | CADTH reanalysis (reimbursement request) |
No price reduction | 27,671 | 204,916 |
10% | 23,998 | 182,917 |
20% | 20,324 | 160,919 |
30% | 16,650 | 138,921 |
40% | 12,976 | 116,923 |
50% | 9,303 | 94,924 |
60% | 5,629 | 72,926 |
70% | 1,955 | 50,928 |
71% | 853 | 48,728 |
80% | Dominant | 28,929 |
90% | Dominant | 6,931 |
100% | Dominant | Dominant |
ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year; vs. = versus.
Overall Conclusions
Based on the clinical review, data from placebo-controlled, double-blind randomized controlled trials suggest that semaglutide produces a statistically and clinically significant weight loss in patients with overweight or obesity compared to diet and exercise alone. Although the weight loss is considered clinically significant, there is no clear evidence regarding whether this weight loss reduces the number of patients who may develop various weight-related comorbidities, including type 2 diabetes, CVD, and osteoarthritis. There is some evidence of an improvement in the physical component of health-related quality of life; however, the clinical significance of this improvement is less clear.
CADTH undertook reanalyses to address limitations in the sponsor’s economic evaluation. These included assuming no additional benefit once weight had been regained, removing comorbidities other than diabetes from the analysis, removing BMI as an independent risk factor for mortality, using a different value set for BMI-related utility, using data from the STEP 1 extension trial to determine weight regain post–treatment discontinuation, assuming 3 years of treatment use, and explicitly linking treatment discontinuation to the average weight of the cohort.
Based on the reimbursement request population, in the CADTH base case, the ICER for semaglutide compared with standard care is $204,928 per QALY (incremental costs = $9,385; incremental QALYs = 0.046). CADTH notes the majority of incremental cost is from the cost of semaglutide ($10,074), with cost savings due to delay of type 2 diabetes onset ($484) and less time spent being prediabetic ($207). The degree of cost savings associated with prediabetes is highly uncertain. The removal of these cost savings increases the ICER to $209,449 per QALY. The majority of QALY gains (88%) is derived from the direct impact that weight loss has on patient utility — through improved physical functioning, for example. The remaining QALY gains (12%) are derived through delaying onset of type 2 diabetes. Although no statistically significant conclusions from the clinical data could be concluded regarding delay in type 2 diabetes onset, the evidence is suggestive of improvements in glycemic control given the number of patients who return to “normal glycemic control.” As such, a delay in onset of type 2 diabetes delay is plausible. If semaglutide use leads to no delay in type 2 diabetes onset, the ICER increases to $241,914 per QALY.
To achieve cost-effectiveness at a $50,000 per QALY threshold, the price of semaglutide would need to decrease by 71%. If there are no savings to the health care system from the temporary reversal of prediabetes and there is no delay in type 2 diabetes onset, then a price reduction of 80% would be required. These results assume that semaglutide is only given for a maximum of 3 years and there are no negative impacts associated with weight cycling. The cost-effectiveness of semaglutide use beyond 3 years is highly uncertain as the sponsor’s model precluded an assessment of this. If long-term sustained semaglutide use does not translate into sustained weight loss and the prevention of weight-related comorbidities, then long-term use would likely be less cost-effective than estimated in the CADTH base case. If weight loss is sustained, then the likelihood of preventing weight-related comorbidities would increase. Should this occur, then this could improve the cost-effectiveness of semaglutide relative to the CADTH base case. Regarding weight cycling, its impact is not explored in the sponsor’s analysis. Evidence regarding the impact of weight cycling is mixed and highlights the nuances with linking weight loss to impacts on weight-related comorbidities. Some evidence is suggestive of increased cardiac risk in some groups of patients. Should this occur, this would reduce the cost-effectiveness of semaglutide use relative to the CADTH base case.
Finally, the CADTH base case only applies to the restricted reimbursement request population of patients with a BMI greater than 35 kg/m2 with prediabetes. CADTH notes that only 6% of patients in the STEP 1 trial were overweight with a BMI under 30 kg/m2; therefore, assessing the magnitude of benefit in this subgroup is highly uncertain. As shown in the sponsor’s BIA, this group represents 32% of the Health Canada indication, equating to a budget impact of more than $300 million. As a scenario analysis, CADTH assessed cost-effectiveness using the sponsor’s assumptions and found the ICER increased to $223,572 per QALY. Overall, the cost-effectiveness in the full Health Canada indication is highly uncertain. CADTH notes it will be less cost-effective in the full indication than the reimbursement request given the reimbursement request identifies those most likely to benefit from therapy.
References
1.Pharmacoeconomic evaluation [internal sponsor's report]. In: Wegovy (semaglutide), 2.4 mg, solution for subcutaneous injection, single-dose pre-filled pen delivering doses of 0.25 mg, 0.5 mg, 1 mg, 1.7 mg, 2.4 mg [internal sponsor's package]. Mississauga (ON): Novo Nordisk Canada Inc; 2022 Mar 10.
2.Clinical Study Report: NN9536-4373 (STEP 1). Effect and safety of semaglutide 2.4 mg once-weekly in subjects with overweight or obesity [internal sponsor's report]. Bagsvaerd (DK): Novo Nordisk; 2020 Aug 17.
3.Statistics Canada. Life expectancy and other elements of the life table, Canada, all provinces except Prince Edward Island, 2019. Table: 13-10-0837-01. 2022; https://www150.statcan.gc.ca/t1/tbl1/en/cv.action?pid=1310083701. Accessed 2022 Jul 4.
4.Statistics Canada. Deaths and age-specific mortality rates, by selected grouped causes 2019. Table: 13-10-0392.01. 2022: https://www150.statcan.gc.ca/t1/tbl1/en/tv.action?pid=1310039201. Accessed 2022 Jul 4.
5.Singh JA, Jensen MR, Harmsen WS, Gabriel SE, Lewallen DG. Cardiac and thromboembolic complications and mortality in patients undergoing total hip and total knee arthroplasty. Ann Rheum Dis. 2011;70(20):2082-2088. PubMed
6.Johansson S, Rosengren A, Young K, Jennings E. Mortality and morbidity trends after the first year in survivors of acute myocardial infarction: a systematic review. BMC Cardiovasc Disord. 2017;17(1):53. PubMed
7.Brammås A, Jakobsson S, Ulvenstam A, Moore T. Mortality after ischemic stroke in patients with acute myocardial infarction: predictors and trends over time in Sweden. Stroke. 2013;44(11):3050-3055. PubMed
8.Cancer Research UK. Cancer survival statistics. 2011; http://www.cancerresearchuk.org/cancer-info/cancerstats/survival/. Accessed 2022 Jul 4.
9.Alam M, Bhanderi S, Matthews JH, et al. Mortality related to primary bariatric surgery in England. BJS open. 2017;1(4):122-127. PubMed
10.Bhaskaran K, Dos-Santos-Silva I, Leon DA, Douglas IJ, Smeeth L. Association of BMI with overall and cause-specific mortality: a population-based cohort study of 3·6 million adults in the UK. Lancet Diabetes Endocrinol. 2018;6(12):944-953. PubMed
11.Novo Nordisk Canada Inc. response to May 10, 2022 DRR request for additional information regarding Wegovy (semaglutide) DRR review: request to provide updated model with valid transition probabilities [internal additional sponsor's information]. Mississauga (ON): Novo Nordisk Canada Inc; 2022 May 13.
12.Wilding JPH, Batterham RL, Davies M, et al. Weight regain and cardiometabolic effects after withdrawal of semaglutide: The STEP 1 trial extension. Diabetes Obes Metab. 2022. PubMed
13.Haase CL, Lopes S, Olsen AH, Satylganova A, Schnecke V, McEwan P. Weight loss and risk reduction of obesity-related outcomes in 0.5 million people: evidence from a UK primary care database. Int J Obes. 2021;45(6):1249-1258. PubMed
14.Marso SP, Bain SC, Consoli A, et al. Semaglutide and cardiovascular outcomes in patients with type 2 diabetes. N Engl J Med. 2016;375(19):1834-1844. PubMed
15.Blackman A, Foster GD, Zammit G, et al. Effect of liraglutide 3.0 mg in individuals with obesity and moderate or severe obstructive sleep apnea: the SCALE Sleep Apnea randomized clinical trial. Int J Obes. 2016;40(8):1310-1319. PubMed
16.Wendelboe AM, Hegmann KT, Biggs JJ, et al. Relationships between body mass indices and surgical replacements of knee and hip joints. Am J Prev Med. 2003;25(4):290-295. PubMed
17.Luo J, Chlebowski RT, Hendryx M, et al. Intentional weight loss and endometrial cancer risk. J Clin Oncol. 2017;35(11):1189-1193. PubMed
18.Teras LR, Patel AV, Wang M, et al. Sustained weight loss and risk of breast cancer in women 50 years and older: a pooled analysis of prospective data. J Natl Cancer Inst. 2020;112(9):929-937. PubMed
19.Bruno DS, Berger NA. Impact of bariatric surgery on cancer risk reduction. Ann Transl Med. 2020;8(Suppl 1):S13. PubMed
20.Aminian A, Wilson R, Al-Kurd A, et al. Association of bariatric surgery with cancer risk and mortality in adults with obesity. JAMA. 2022;327(24):2323-2433. PubMed
21.Guidelines for the economic evaluation of health technologies: Canada. 4th ed. Ottawa (ON): CADTH; 2017: https://www.cadth.ca/guidelines-economic-evaluation-health-technologies-canada-4th-edition. Accessed 2022 Jul 4.
22.Søltoft F, Hammer M, Kragh N. The association of body mass index and health-related quality of life in the general population: data from the 2003 Health Survey of England. Qual Life Res. 2009;18(10):1293-1299. PubMed
23.Drug Reimbursement Review sponsor submission: Wegovy (semaglutide), 2.4 mg, solution for subcutaneous injection, single-dose pre-filled pen delivering doses of 0.25 mg, 0.5 mg, 1 mg, 1.7 mg, 2.4 mg [internal sponsor's package]. Mississauga (ON): Novo Nordisk Canada Inc; 2022 Mar 10.
24.Sjöström L, Narbro K, Sjöström CD, et al. Effects of bariatric surgery on mortality in swedish obese subjects. N Engl J Med. 2007;357(8):741-752. PubMed
25.Sjöström L, Peltonen M, Jacobson P, et al. Bariatric surgery and long-term cardiovascular events. JAMA. 2012;307(1):56-65. PubMed
26.Doumouras AG, Hong D, Lee Y, Tarride JE, Paterson JM, Anvari M. Association between bariatric surgery and all-cause mortality: a population-based matched cohort study in a universal health care system. Ann Intern Med. 2020;173(9):694-703. PubMed
27.Xu H, Cupples LA, Stokes A, Liu C-T. Association of obesity with mortality over 24 years of weight history: findings from the Framingham Heart Study. JAMA Network Open. 2018;1(7):e184587. PubMed
28.Singh AK, Singh R, Kota SK. Bariatric surgery and diabetes remission: who would have thought it? Indian J Endocrinol Metab. 2015;19(5):563-576. PubMed
29.Ara R, Blake L, Gray L, et al. What is the clinical effectiveness and cost-effectiveness of using drugs in treating obese patients in primary care? A systematic review. Health Technol Assess. 2012;16(5):iii-xiv, 1-195. PubMed
30.Zaric GS. The impact of ignoring population heterogeneity when Markov models are used in cost-effectiveness analysis. Med Decis Making. 2003;23(5):379-396. PubMed
31.Bangalore S, Fayyad R, Laskey R, DeMicco DA, Messerli FH, Waters DD. Body-weight fluctuations and outcomes in coronary disease. N Engl J Med. 2017;376(14):1332-1340. PubMed
32.Lissner L, Odell PM, D'Agostino RB, et al. Variability of body weight and health outcomes in the Framingham population. N Engl J Med. 1991;324(26):1839-1844. PubMed
33.Taylor CB, Jatulis DE, Fortmann SP, Kraemer HC. Weight variability effects: a prospective analysis from the Stanford Five-City Project. Am J Epidemiol. 1995;141(5):461-465. PubMed
34.Budget Impact Analysis [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Wegovy (semaglutide), 2.4 mg, solution for subcutaneous injection, single-dose pre-filled pen delivering doses of 0.25 mg, 0.5 mg, 1 mg, 1.7 mg, 2.4 mg [internal sponsor's package]. Mississauga (ON): Novo Nordisk Canada Inc; 2022 Mar 10.
35.Exceptional Access Program (EAP). Toronto (ON): Ontario Ministry of Health; Ontario Ministry of Long-Term Care; 2022: https://www.health.gov.on.ca/en/pro/programs/drugs/odbf/odbf_except_access.aspx. Accessed 2022 Jul 4.
36.DeltaPA. Ottawa (ON): IQVIA; 2021: https://www.iqvia.com/. Accessed 2022 April 13.
37.Wegovy (semaglutide injection): solution for subcutaneous injection in a pre-filled pen; single-use pre-filled pen delivering doses of 0.25 mg, 0.5 mg, 1 mg, 1.7 mg or 2.4 mg: 0.25 mg/pen (0.25 mg/0.5 mL), 0.5 mg/pen (0.5 mg/0.5 mL), 1 mg/pen (1 mg/0.5 mL), 1.7 mg/pen (1.7 mg/0.75 mL), 2.4 mg/pen (2.4 mg/0.75 mL) and multi-use pre-filled pen (FlexTouch) delivering doses of 0.25 mg, 0.5 mg, 1 mg, 1.7 mg or 2.4 mg: 1 mg/pen (0.68 mg/mL), 2 mg/pen (1.34 mg/mL), 4 mg/pen (1.34 mg/mL), 6.8 mg/pen (2.27 mg/mL), 9.6 mg/pen (3.2 mgmL) [product monograph]. Mississauga (ON): Novo Nordisk Canada Inc; 2022 Jun 30.
38.Statistics Canada. Projected population, by projection scenario, age and sex, as of July 1 (x 1,000). Table: Table 17-10-0057-01. 2019; https://www150.statcan.gc.ca/t1/tbl1/en/tv.action?pid=1710005701. Accessed 2022 Jul 4.
39.Indigenous Services Canada. Non-insured health benefits program: annual report 2019 to 2020. 2021; https://www.sac-isc.gc.ca/eng/1624462613080/1624462663098. Accessed 2022 Jul 4.
40.Statistics Canada. Health characteristics, annual estimates. Table: 13-10-0096-01. 2021; https://www150.statcan.gc.ca/t1/tbl1/en/tv.action?pid=1310009601. Accessed 2022 Jul 4.
41.Janssen I. The public health burden of obesity in Canada. Can J Diabetes. 2013;37(2):90-96. PubMed
42.Public Health Agency of Canada. Obesity in Canada. Ottawa (ON): Public Health Agency of Canada; 2011: http://www.phac-aspc.gc.ca/hp-ps/hl-mvs/oic-oac/assets/pdf/oic-oac-eng.pdf. Accessed 2022 Jul 4.
43.Twells LK, Janssen I, Kuk JL. Canadian adult obesity clinical practice guidelines: epidemiology of adult obesity. Edmonton (AB): Obesity Canada; 2020: https://obesitycanada.ca/wp-content/uploads/2021/05/2-Epidemiology-of-Adult-Obesity-5-with-links.pdf. Accessed 2022 Jul 4.
44.Sharma AM, Belanger A, Carson V, et al. Perceptions of barriers to effective obesity management in Canada: results from the ACTION study. Clin Obes. 2019;9(5):e12329. PubMed
45.Statistics Canada. Contact with a medical doctor in the last 12 months, by age group. Table: 13-10-0096-17. 2021; https://www150.statcan.gc.ca/t1/tbl1/en/tv.action?pid=1310009617. Accessed 2022 Jul 4.
46.Sutherland G, Dinh T. Understanding the gap: a pan-Canadian analysis of prescription drug insurance coverage. Ottawa (ON): Conference Board of Canada; 2017: http://innovativemedicines.ca/wp-content/uploads/2017/12/20170712-understanding-the-gap.pdf. Accessed 2022 Jul 4.
47.Statistics Canada. Older adults and population aging: statistics. 2022; https://www.statcan.gc.ca/en/subjects-start/older_adults_and_population_aging. Accessed 2022 Jul 4.
48.Gill LE, Bartels SJ, Batsis JA. Weight management in older adults. Curr Obes Rep. 2015;4(3):379-388. PubMed
49.Frank C, Molnar F, Holroyd-Leduc J. Weight loss in older patients. Can Fam Physician. 2019;65(10):723-723. PubMed
50.Pantalone KM, Hobbs TM, Chagin KM, et al. Prevalence and recognition of obesity and its associated comorbidities: cross-sectional analysis of electronic health record data from a large US integrated health system. BMJ Open. 2017;7(11):e017583. PubMed
51.Alkhawam H, Nguyen J, Sayanlar J, et al. Coronary artery disease in patients with body mass index ≥30 kg/m(2): a retrospective chart analysis. J Community Hosp Intern Med Perspect. 2016;6(3):31483. PubMed
Appendix 1: Cost Comparison Table
Note that this appendix has not been copy-edited.
The comparators presented in the following table have been deemed to be appropriate based on feedback from clinical expert. Comparators may be recommended (appropriate) practice or actual practice. Existing Product Listing Agreements are not reflected in the table and as such, the table may not represent the actual costs to public drug plans.
Table 8: CADTH Cost Comparison Table for Obesity
Treatment | Strength / concentration | Form | Price | Recommended dosage | Daily cost | Annual cost |
|---|---|---|---|---|---|---|
Semaglutide (Wegovy) | 0.25 mg/0.5 mL 0.5 mg/0.5 mL 1 mg/0.5 mL 1.7 mg/0.75mL 2.4 mg/0.75mL | 0.5 mL pre-filled pen for injection | $363.5100 per carton of 4 pens regardless of strength ($90.8775 per pen)a | First year: Week 1 to week 4: 0.25 mg once per week Week 5 to week 8: 0.5 mg once per week Week 9 to week 12: 1 mg once per week Week 13 to week 16: 1.7 mg once per week Week 17 and onwards: 2.4 mg once per week Second year: 2.4 mg once per week | $12.98 | $4,726 |
Pharmaceutical comparators | ||||||
Liraglutide (Saxenda) | 6 mg/mL | 3 mL pre-filled pen | $77.8959 | Initial dose 0.6 mg once daily, increasing by 0.6 mg daily per week until 3.0 mg daily dose is reached | $2.60, initial week $12.98, once full dose is reached | First year: $4,544 Subsequent years: $4,726 |
Naltrexone hydrochloride- bupropion (Contrave) | 8 mg/90 mg | Tablet | $2.2393 | Week 1: 1 tablet per day Week 2: 2 tablets per day Week 3: 3 tablets per day Week 4+: 2 tablets twice daily | First year: $8.67 Subsequent years: $8.93 | First year: $3,166 Subsequent years: $3,260 |
Orlistat (Xenical) | 120 mg | Capsule | $1.6574b | 120 mg 3 times daily with meals | 4.97 | 1,815 |
Note: All prices are from the IQVIA Delta PA wholesale price (accessed April 13, 2022),36 unless otherwise indicated, and do not include dispensing fees.
aSponsor’s submission (2022).34
bExceptional Access Program (2022), accessed April 27, 2022.35
Appendix 2: Submission Quality
Note that this appendix has not been copy-edited.
Description | Yes/No | Commentsa |
|---|---|---|
Population is relevant, with no critical intervention missing, and no relevant outcome missing | Yes | No comment |
Model has been adequately programmed and has sufficient face validity | Yes | No comment |
Model structure is adequate for decision problem | Yes | No comment |
Data incorporation into the model has been done adequately (e.g., parameters for probabilistic analysis) | No | The model allows for patients who discontinue treatment to enter a separate health state ensuring the probabilistic analysis correlates weight loss with treatment discontinuation. Though CADTH notes a trial product estimand for various efficacy estimates (weight loss) were not provided. This precluded a robust assessment. |
Parameter and structural uncertainty were adequately assessed; analyses were adequate to inform the decision problem | No | The inability to assign a cost to the temporary reversal of prediabetes is a limitation. The model does not allow consideration of treatment continuation beyond 3 years. |
The submission was well organized and complete; the information was easy to locate (clear and transparent reporting; technical documentation available in enough details) | Yes | No comment |
Appendix 3: Additional Information on the Submitted Economic Evaluation
Note that this appendix has not been copy-edited.
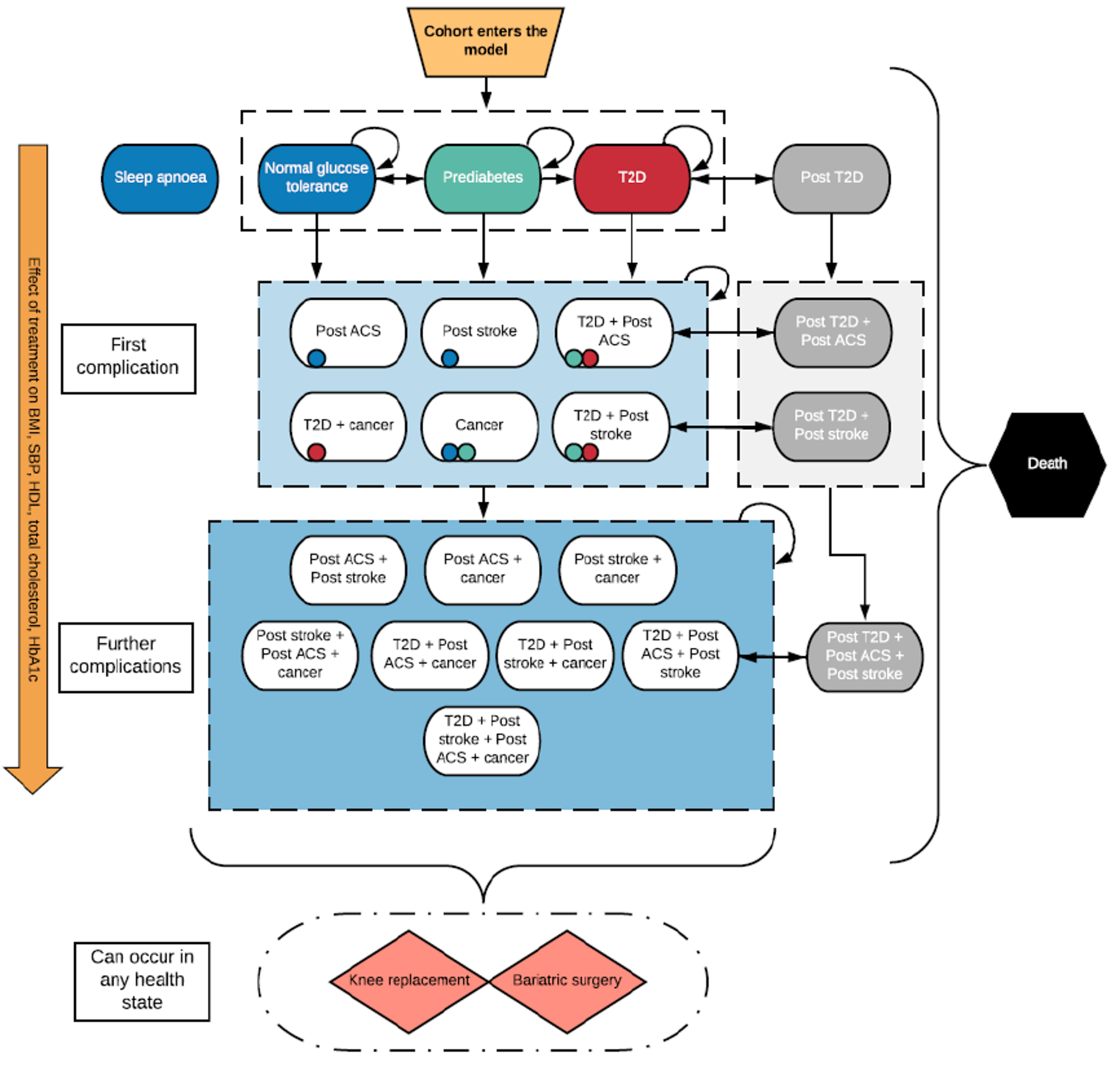
Figure 2: Reduction in type 2 Diabetes Mellitus Onset
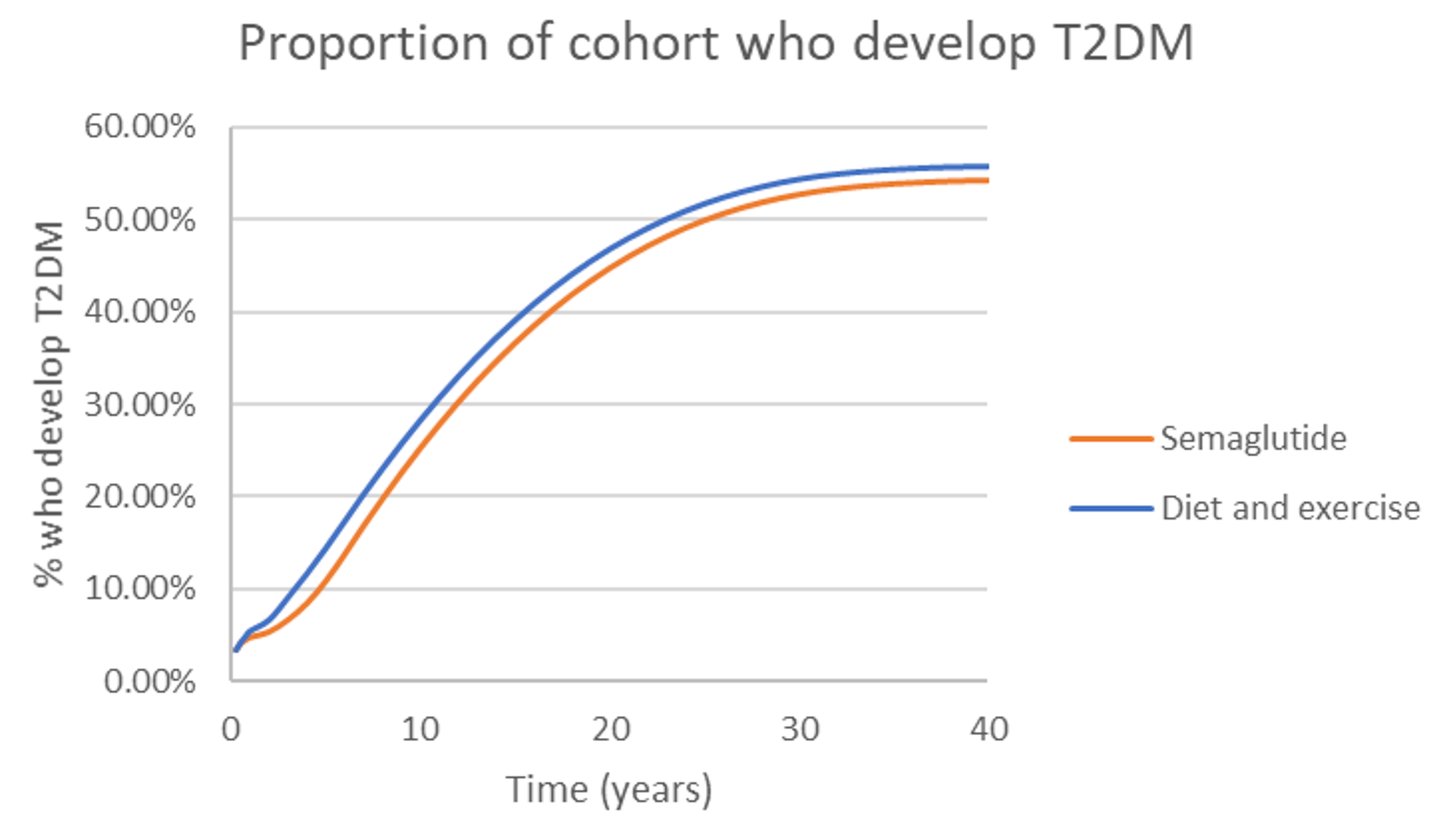
T2DM = type 2 diabetes mellitus.
Source: Sponsor’s submission (2022).1
Table 10: Relative Risk Reduction of Cancer Onset (Semaglutide Versus Diet and Exercise)
Relative risk Type of cancer | Time since treatment initiation | |||||
|---|---|---|---|---|---|---|
3 months | 6 months | 9 months | 12 months | 2 years | 3 years | |
Colorectal cancer | 0.94 | 0.92 | 0.89 | 0.88 | 0.92 | 0.97 |
Postmenopausal breast cancera | NA | NA | NA | NA | 0.94 | 0.98 |
Postmenopausal endometrial cancera | NA | NA | NA | NA | 0.42 | 0.75 |
NA = not applicable.
aAverage age of cohort is 48 and sponsor assumes an age of 50 for menopause, meaning no risk impact is assumed before menopause being reached for breast and endometrial cancer.
Source: Sponsor’s submission (2022).1
Detailed Results of the Sponsor’s Base Case
Table 11: Disaggregated Summary of Sponsor’s Base Case, Reimbursement Request — Revised Model
Item | Semaglutide | Standard care |
|---|---|---|
Total discounted costs ($) | 66,652 | 61,051 |
Obesity treatment costs ($) | 7,436 | 0 |
Obesity monitoring costs ($) | 5,432 | 5,401 |
Blood pressure treatment costs ($) | 229 | 228 |
T2DM pharmacy costs ($) | 0 | 0 |
Obesity complications: State costs ($) | 44,716 | 46,444 |
OSA | 2,031 | 2,087 |
Pre-T2DM | 1,981 | 2,101 |
T2DM | 19,726 | 21,019 |
Post-ACS | 3,191 | 3,221 |
Cancer | 12,407 | 12,606 |
Post-stroke | 5,383 | 5,412 |
Obesity complications: Events costs ($) | 8,840 | 8,979 |
Stroke (non-fatal) | 2,100 | 2,135 |
Fatal stroke | 601 | 610 |
TIA | 141 | 144 |
MI (non-fatal) | 1,040 | 1,057 |
Fatal MI | 461 | 468 |
Unstable angina (non-fatal) | 627 | 637 |
Fatal unstable angina | 268 | 272 |
Bariatric surgery (non-fatal) | 222 | 233 |
Fatal bariatric surgery | 0 | 0 |
Knee replacement (non-fatal) | 3,370 | 3,412 |
Fatal knee replacement | 10 | 10 |
Total QALYs (undiscounted) | 20.873 | 20.628 |
Total QALYs (discounted) | 17.153 | 16.951 |
No complication | 0.0 | 0.0 |
NGT (after being prediabetic) | 1.917 | 0.844 |
Pre-T2DM | 8.978 | 9.531 |
T2DM | 3.525 | 3.828 |
Post-ACS | 0.055 | 0.027 |
Post-ACS + T2DM | 0.950 | 0.976 |
Post-stroke | 0.032 | 0.016 |
Post-stroke + T2DM | 0.517 | 0.532 |
Post-ACS + post-stroke | 0.009 | 0.005 |
Post-ACS + post-stroke + T2DM | 0.208 | 0.220 |
Cancer | 0.735 | 0.728 |
Cancer + T2DM | 0.291 | 0.314 |
Cancer + post-ACS | 0.032 | 0.030 |
Cancer + post-stroke | 0.016 | 0.015 |
Cancer + post-ACS + post-stroke | 0.002 | 0.002 |
Cancer + post-ACS + T2DM | 0.077 | 0.081 |
Cancer + post-stroke + T2DM | 0.034 | 0.035 |
Cancer + post-ACS + post-stroke + T2DM | 0.019 | 0.020 |
OSA | –0.146 | –0.151 |
Stroke (non-fatal) | –0.020 | –0.021 |
Fatal stroke | –0.006 | –0.007 |
TIA | –0.001 | –0.001 |
MI (non-fatal) | –0.015 | –0.015 |
Fatal MI | –0.010 | –0.010 |
Unstable angina (non-fatal) | –0.013 | –0.013 |
Fatal unstable angina | –0.009 | –0.009 |
Bariatric surgery (non-fatal) | –0.003 | –0.003 |
Fatal bariatric surgery | 0.0 | 0.0 |
Knee replacement (non-fatal) | –0.021 | –0.022 |
Fatal knee replacement | 0.0 | 0.0 |
Total LYs (undiscounted) | 25.245 | 25.049 |
Total LYs (discounted) | 20.635 | 20.485 |
Source: Sponsor’s submission (2022).1
Appendix 4: Additional Details on the CADTH Reanalyses and Sensitivity Analyses of the Economic Evaluation
Note that this appendix has not been copy-edited.
Figure 3: Change in BMI Over Time in the Reimbursement Request Population — Prediabetes With a BMI > 35 kg/m2
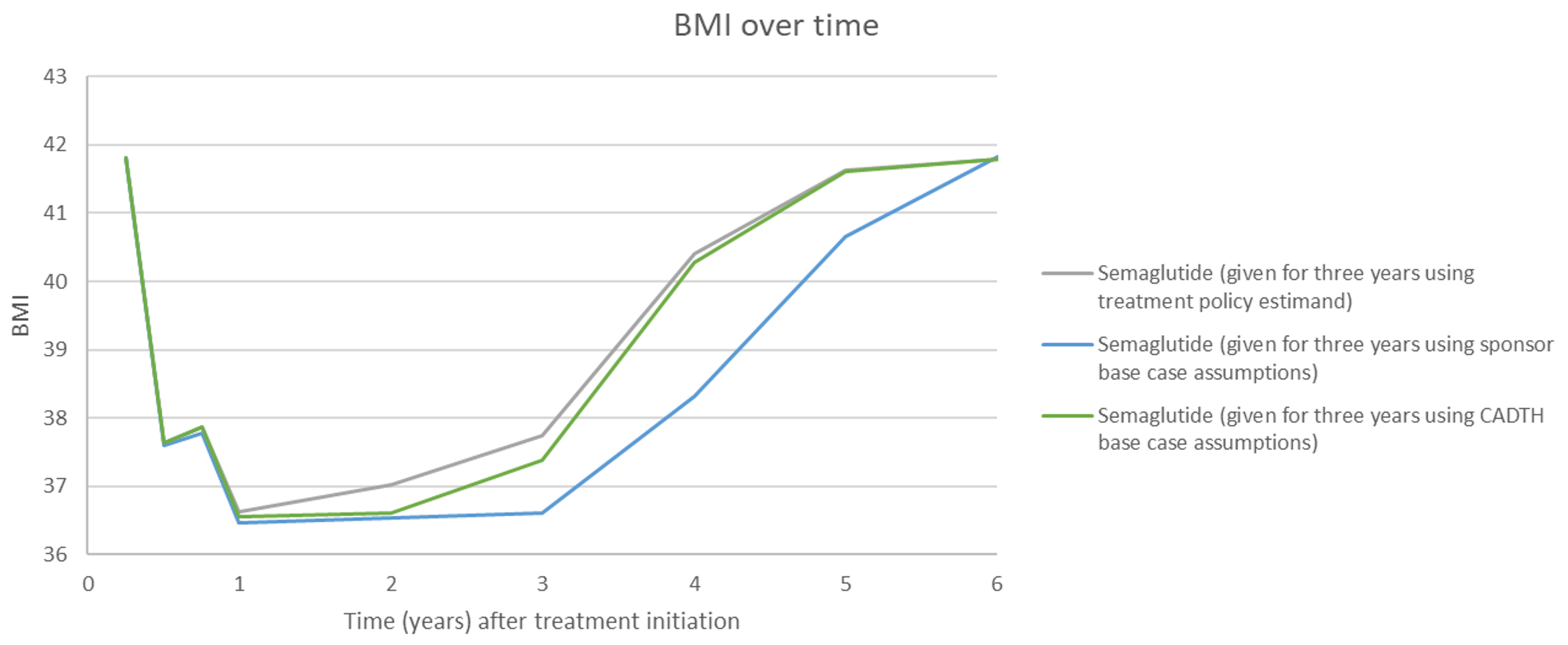
BMI = body mass index.
Source: CADTH calculations derived from sponsor’s submission (2022).1
Figure 4: Weight Regain Post–Treatment Discontinuation
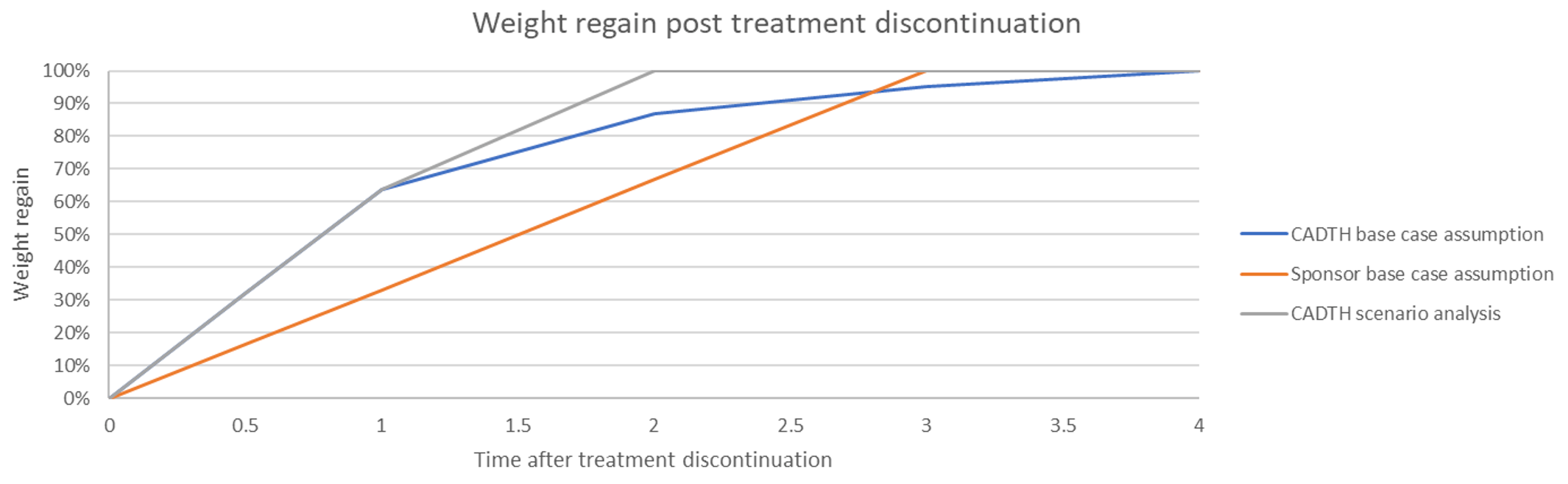
Source: CADTH calculations derived from sponsor’s submission (2022).1
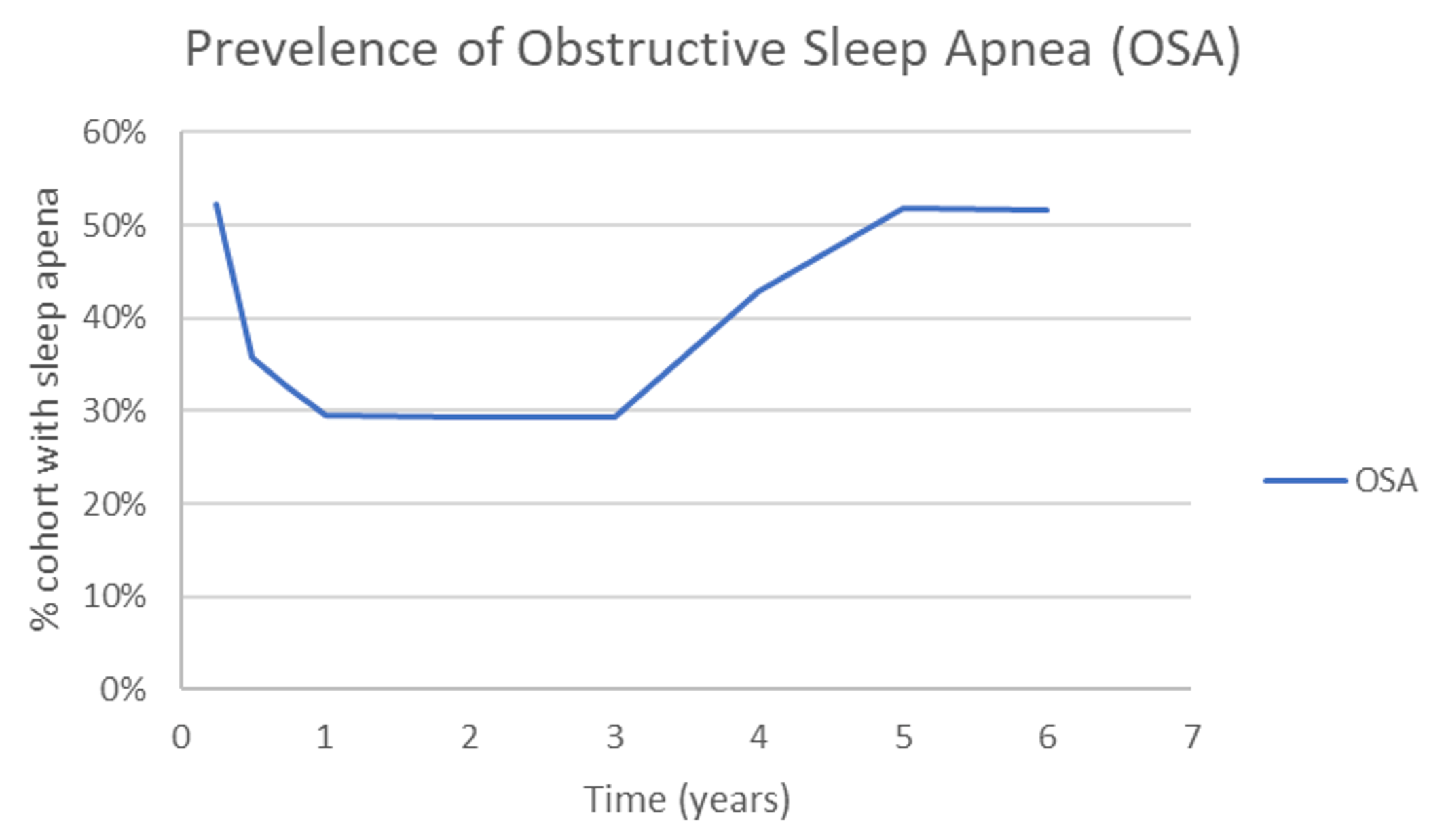
Detailed Results of CADTH Base Case
Table 12: Disaggregated Summary of CADTH’s Economic Evaluation Results (Reimbursement Request)
Item | Semaglutide | Standard Care |
|---|---|---|
Total discounted costs ($) | 14,647 | 5,263 |
Obesity treatment costs ($) | 10,074 | 0 |
Obesity monitoring costs ($) | 1,425 | 1,410 |
Blood pressure treatment costs ($) | 73 | 73 |
T2DM pharmacy costs ($) | 0 | 0 |
Obesity complications: State costs ($) | 2,999 | 3,690 |
OSA | 0 | 0 |
Pre-T2DM | 679 | 886 |
T2DM | 1,651 | 2,135 |
Post-ACS | 265 | 265 |
Cancer | 0 | 0 |
Post-stroke | 404 | 404 |
Obesity complications: Events costs ($) | 76 | 90 |
Stroke (non-fatal) | 0 | 0 |
Fatal stroke | 0 | 0 |
TIA | 0 | 0 |
MI (non-fatal) | 0 | 0 |
Fatal MI | 0 | 0 |
Unstable angina (non-fatal) | 0 | 0 |
Fatal unstable angina | 0 | 0 |
Bariatric surgery (non-fatal) | 76 | 90 |
Fatal bariatric surgery | 0 | 0 |
Knee replacement (non-fatal) | 0 | 0 |
Fatal knee replacement | 0 | 0 |
Total QALYs (undiscounted) | 6.220 | 6.173 |
Total QALYs (discounted) | 5.953 | 5.908 |
No complication | 0.0 | 0.0 |
NGT (after being prediabetic) | 2.236 | 1.069 |
Pre-T2DM | 3.201 | 4.173 |
T2DM | 0.330 | 0.481 |
Post-ACS | 0.0 | 0.0 |
Post-ACS + T2DM | 0.118 | 0.117 |
Post-stroke | 0.0 | 0.0 |
Post-stroke + T2DM | 0.070 | 0.069 |
Post-ACS + post-stroke | 0.0 | 0.0 |
Post-ACS + post-stroke + T2DM | 0.0 | 0.0 |
Cancer | 0.0 | 0.0 |
Cancer + T2DM | 0.0 | 0.0 |
Cancer + post-ACS | 0.0 | 0.0 |
Cancer + post-stroke | 0.0 | 0.0 |
Cancer + post-ACS + post-stroke | 0.0 | 0.0 |
Cancer + post-ACS + T2DM | 0.0 | 0.0 |
Cancer + post-stroke + T2DM | 0.0 | 0.0 |
Cancer + post-ACS + post-stroke + T2DM | 0.0 | 0.0 |
OSA | 0.0 | 0.0 |
Stroke (non-fatal) | 0.0 | 0.0 |
Fatal stroke | 0.0 | 0.0 |
TIA | 0.0 | 0.0 |
MI (non-fatal) | 0.0 | 0.0 |
Fatal MI | 0.0 | 0.0 |
Unstable angina (non-fatal) | 0.0 | 0.0 |
Fatal unstable angina | 0.0 | 0.0 |
Bariatric surgery (non-fatal) | –0.001 | –0.001 |
Fatal bariatric surgery | 0.0 | 0.0 |
Knee replacement (non-fatal) | 0.0 | 0.0 |
Fatal knee replacement | 0.0 | 0.0 |
Total LYs (undiscounted) | 6.957 | 6.957 |
Total LYs (discounted) | 6.657 | 6.657 |
Source: CADTH base-case estimates derived from sponsor’s submission (2022).1
Figure 6: Cost-Effectiveness Plane
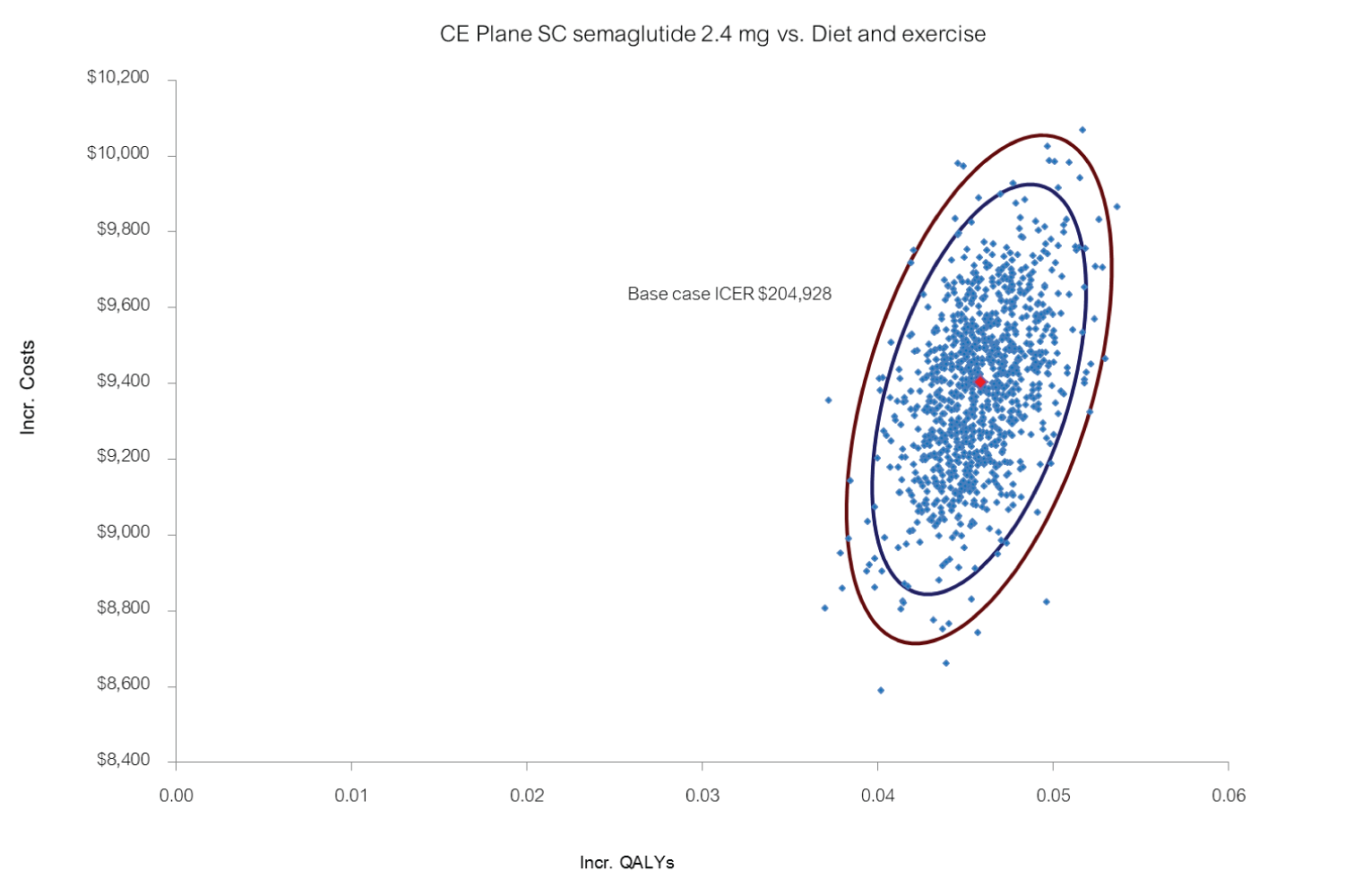
Source: CADTH base-case estimates derived from sponsor’s submission (2022).1
Scenario Analyses
Table 13: Summary of CADTH Scenario Analyses
Scenario analysis | Incremental costs: Semaglutide vs. standard care ($) | Incremental QALYs: Semaglutide vs. standard care | ICER ($/QALY): Semaglutide vs. standard care ($/QALY) | Price reduction to achieve $50,000 per QALY |
|---|---|---|---|---|
CADTH base case | 9,403 | 0.046 | 204,965 | 71% |
SA1: Inclusion of obstructive sleep apnea, assuming full alleviation of symptoms and costs for 30% of patients who receive semaglutide | 9,317 | 0.052 | 178,937 | 67% |
SA2: Health Canada indication | 8,811 | 0.039 | 223,572 | 75% |
SA3: Removal of prediabetes cost savings and no T2DM benefit | 10,096 | 0.041 | 247,859 | 80% |
SA4: no stopping rulea | 10,511 | 0.044 | 240,915 | 75% |
SA5: 2-year weight regain post–treatment discontinuation | 9,590 | 0.043 | 222,845 | 74% |
vs. = versus.
aIn this analysis the treatment efficacy was calibrated such that average weight loss of the cohort was 13.28% which matched the weight loss seen in the subgroup analysis (individuals with BMI > 35 kg/m2 and prediabetes) provided by the sponsor.
Appendix 5: Submitted Budget Impact Analysis and CADTH Appraisal
Note that this appendix has not been copy-edited.
Table 14: Summary of Key Take-Aways
Key take-aways of the budget impact analysis |
|---|
|
Summary of Sponsor’s Budget Impact Analysis
The sponsor submitted an prevalence-based BIA,34 assessing the expected budgetary impact of the reimbursement of semaglutide as an adjunct to a reduced-calorie diet and increased physical activity (standard therapy) for chronic weight management from the perspective of a Canadian public drug plan payer over a 3-year time horizon. Two populations were considered:
The full Health Canada indication population, consisting of adult patients with an initial BMI of 30 kg/m2 or greater or 27kg/m2 or greater in the presence of at least 1 weight-related comorbidity.37
The reimbursement request population, consisting of adults who have been diagnosed with obesity (BMI ≥ 35 kg/m2) and prediabetes.
Data for the model were obtained from various sources, including: Statistics Canada,38-40 archived data from the Canadian Health Measures Survey,41 and the Public Health Agency of Canada.42 Drug acquisition costs were included, with results presented both with and without dispensing fees and markups. The reference scenario only included standard therapy, which included behavioural therapy, medical nutrition, and physical activity, all of which incur no drug costs. Therefore, in the reference scenario no costs are incurred from a drug plan payer perspective. In this analysis all incremental costs are associated with semaglutide.
Key inputs to the BIA are documented in Table 15. Other assumptions made by the sponsor include:
As standard therapy consists of behavioural therapy, medical nutrition, and physical activity, no costs were assumed for public drug plans.
All patients begin therapy at the start of the year.
BMI is an adequate measure to determine who is overweight and obese.
Table 15: Summary of Key Model Parameters
Parameter | Sponsor’s estimate (full indication population) | Sponsor’s estimate (reimbursement request population) |
|---|---|---|
Target population, pan-Canadian analysis | BMI ≥ 30 kg/m2 OR BMI ≥ 27 kg/m2 with ≥ 1 weight-related comorbidity | BMI ≥ 35 kg/m2 with prediabetes |
Canadian population ≥ 18 years (excl. Quebec) | 24,541,119a | |
Proportion by gender (male/female) | 49.29%/50.71%a | |
Prevalence of obesity by gender and class (M/F) Overweight (BMI 27 kg/m2 to 29.9 kg/m2) Obesity class I (BMI 30 kg/m2 to 34.9 kg/m2) Obesity class II (BMI 35 kg/m2 to 39.9 mg/m2) Obesity class III (BMI ≥ 40 kg/m2) | 37.6%/27.4%b 18.8%/12.3% b 5.3%/6.9% b 2.1%/4.8% b | |
Prevalence of eligible comorbidities (M/F) Prediabetes | 46.36% overweight patientsc | 46.36% all patientsc |
Percentage patients who see their doctor | 76.3%d | |
Percentage evaluated and diagnosed with obesity Overweight (BMI 27 kg/m2 to 29.9 kg/m2) Obesity class I (BMI 30 kg/m2 to 34.9 kg/m2) Obesity class II (BMI 35 kg/m2 to 39.9 mg/m2) Obesity class III (BMI ≥ 40 kg/m2) | 35% 35%c 51%c 73%c | |
Annual growth rate of weight category Overweight (BMI 27 kg/m2 to 29.9 kg/m2) Obesity class I (BMI 30 kg/m2 to 34.9 kg/m2) Obesity class II (BMI 35 kg/m2 to 39.9 mg/m2) Obesity class III (BMI ≥ 40 kg/m2) | 0.91% 2.15% 2.15% 2.15% | |
Number of eligible patients who see their doctor and evaluated and diagnosed with obesity | 3,153,509 / 3,249,419 / 3,347,993 | 508,133 / 525,623 / 543,655 |
Overweight (BMI 27 kg/m2 to 29.9 kg/m2) | 1,007,563 / 1,029,600 / 1,052,006 | 0/0/0 |
Obesity class I (BMI 30 kg/m2 to 34.9 kg/m2) | 1,050,831 / 1,087,011 / 1,124,316 | 0/0/0 |
Obesity class II (BMI 35 kg/m2 to 39.9 mg/m2) | 604,035 / 624,827 / 646,265 | 280,272 / 289,920 / 299,867 |
Obesity class III (BMI ≥ 40 kg/m2) | 491,080 / 507,981 / 525,406 | 227,861 / 235,703 / 243,788 |
Proportion eligible for public coverage | 40.65%e | |
Total number of patients eligible for drug under review and public coverage | 1,281,425 / 1,319,993 / 1,359,635 | 206,493 / 213,536 / 220,797 |
Market uptake (3 years) | ||
Uptake (reference scenario) Standard therapy | 100%/100%/100% | |
Uptake (new drug scenario) Semaglutide + standard therapy Standard therapy | 3%/6%/9% 97%/94%/91% | |
Discontinuation | ||
Proportion nonresponders34 Discontinuation time point, for nonresponders (those who fail to lose 5% of their weight) | 21.4% 28 weeks (12 weeks after maintenance dose is reached) | 18.4% 28 weeks (12 weeks after maintenance dose is reached) |
Discontinuation rate First year Year 1 to year 2 Year 2 to year 3 | Only nonresponders discontinue 8.29% of responders 15.89% of responders | Only nonresponders discontinue 11.54% of responders 21.75% of responders |
Cost of treatment (per patient) | ||
Cost of treatment over first year of therapy Semaglutide + standard therapy (first year) Semaglutide + standard therapy (other years) Standard therapy | Nonresponders $2,545; Responders $4,725 Responders $4,725 $0 | |
BMI = body mass index; M/F = Male/female
aStatistics Canada.40
bCanadian Health Measure Survey data.40,42
dStatistics Canada, proportion patients age 18 to 64 who had contact with a medical doctor in past 12 months, 2016.45
eWeighted average of jurisdictional public drug plan eligibility estimates for those aged 25 to 64 and 65+ as reported by the Conference Board of Canada 2017.46
Summary of the Sponsor’s Budget Impact Analysis Results
The sponsor estimated the net 3-year budget impact associated with the reimbursement of semaglutide added to standard therapy in the full Health Canada indicated population of adult patients with an initial BMI of 30 kg/m3 or greater, or 27 kg/m3 or greater in the presence of at least 1 weight-related comorbidity, were estimated to be $163,723,233 in year 1, $350,235,914 in year 2, and $550,332,376 in year 3, for a 3-year cumulative budget impact of $1,064,291,523.
For the population included in the sponsor’s reimbursement request of adult patients who have been diagnosed with obesity (BMI ≥ 35 kg/m2) and prediabetes, the sponsor estimated the yearly incremental expenditures associated with semaglutide in addition to standard therapy, excluding dispensing fees and markup, would be $26,788,241 in year 1, $57,198,284 in year 2, and $89,935,204 in year 3, for a total 3-year cumulative budget impact of $173,921,729.
CADTH Appraisal of the Sponsor’s Budget Impact Analysis
CADTH identified several key limitations to the sponsor’s analysis that have notable implications on the results of the BIA:
Market share of semaglutide may be underestimated: The clinical expert consulted for this review by CADTH anticipated a potential higher uptake of semaglutide, expressing many patients are motivated to lose weight regardless of BMI category (overweight, obesity class I, II and III) or diabetes status. There are currently no treatments for chronic weight loss covered under public drug plans. As such, there is a potential willingness of patients to try pharmacotherapy, especially if clinical evidence supports its effectiveness, because lifestyle changes are difficult to implement. Having prediabetes is even more of a motivating factor, and the market share of semaglutide may be higher in the requested reimbursement population. The clinical expert noted the market share of semaglutide may increase to the range of 30% because many patients seeking treatment are interested in pharmacotherapy. Should market uptake of semaglutide be higher than estimated, the budget impact may be underestimated in the sponsor’s analysis.
As there are no widely used publicly funded weight-loss medications used in Canada, predicting market uptake in a population eligible for public reimbursement is very challenging given the lack of a reference product. Given the large eligible population, slight differences in market uptake could have a profound impact on the budget impact. CADTH estimates a series of budget impact estimates that cover the likely ranges of market uptake.
The proportion of patients covered by public drug plans is uncertain: The sponsor estimated that 40.65% of the eligible pan-Canadian population are enrolled under a public drug plan. This estimate was derived using values from a report by Sutherland and Dinh (2017).46 The report outlines the number of patients who are enrolled in a public plan by province. To estimate the proportion of patients eligible for public coverage, the sponsor considered the proportion of individuals enrolled in a public plan in the population over the age of 25 years, as the drug is not indicated for pediatric patients. For example, in Alberta, the sponsor estimated that 2,927,100 individuals are over the age of 25 years and of those, 683,400 individuals are enrolled in a public plan (683,400/2,929,100 = 23%). For this estimate to hold in the budget impact estimate for semaglutide, however, uptake in the population over 65 years would need to be identical to that in population under 65 years. As more patients over the age of 65 years are covered by public plans, the average estimate of public coverage is higher in this age group. Using Alberta as an example, from the Sutherland et al. study, the population size for individuals between the ages of 25 and 64 years is 2,419,400 and of these, 175,700 are enrolled in the public plans. This indicates that only 7% of this age group are covered by a public plan.
According to the clinical expert consulted by CADTH, those over 65 years would represent a minority of patients who would receive semaglutide, if funded. The proportion of individuals aged 65 years and above represent just over 18% of the total Canadian population and this age group represents less than 10% of patients enrolled in the STEP trials.47,37 As such, there may be less willingness to prescribe semaglutide in individuals over 65 years given the smaller evidence base. Further, weight management in geriatrics is different than that of younger adults as considerations need to be made regarding comorbidities such as sarcopenia and hip fractures. Older patients with these conditions may have negative consequences associated with weight loss, which may discourage the use of semaglutide in this population.48,49 Therefore, most individuals who would receive semaglutide would fall under 65 years of age. Removing individuals over 65 years, CADTH estimates roughly 24% public coverage rate for participating drug plans, excluding Quebec, with Non-Insured Health Benefits remaining at 100%. If 10% of individuals who receive semaglutide are assumed to be over 65 years of age, and of those, 90% are enrolled in a public plan, then the average public coverage increases to 31%.
Finally, CADTH notes the estimate of those enrolled in a public plan under the age of 65 is uncertain because the eligibility criteria are not the same for all jurisdictions. The report by Sutherland et al. considered average enrolment across all diseases and medications.46 Enrolment in a public plan will be contingent on costs borne by the patient. Many patients pay at least some portion of their income out of pocket for prescription drugs as it is required to be part of a public plan. When balancing enrolment in a public plan, patients are likely to consider the severity of the condition and their income in deciding whether to enrol in a public plan. Therefore, the average estimates of public enrolment presented by Sutherland et al. may overrepresent severe and life-threatening conditions as well as those that impact patients in higher income brackets.46 This may not represent the average patient who would benefit from semaglutide.
In a scenario analysis, CADTH explored the impact of the public drug plan coverage rates on the estimated budget impact.
Using prediabetes as a proxy for weight-related comorbidities is not be appropriate: The sponsor’s approach to use the estimate for prediabetes as a proxy for other weight-related comorbidities would exclude patients who may not have prediabetes but have other weight-related comorbidities such as hypertension, high cholesterol, coronary artery disease, and reduced kidney function.50 For example, 1 study reported that diabetes is present in only 15% of obese participants with evidence of coronary artery disease.51 Using prediabetes as a proxy for coronary artery disease would not be appropriate in this case as it would exclude 85% of obese individuals who have coronary artery disease, a weight-related comorbidity other than prediabetes.
CADTH could not address this limitation due to lack of data.
CADTH Reanalyses of the Budget Impact Analysis
CADTH did not undertake a base-case reanalysis. Instead, CADTH conducted several scenario analyses to explore uncertainties in market share of semaglutide and public reimbursement rates. Table 16 and Table 17 present the estimated cumulative 3-year total budget impact assuming the market share of semaglutide increases linearly at public coverage rates. CADTH notes that public coverage between 20 and 30% may represent a more likely estimate than the sponsor’s base case of 41%.
Table 16: Summary of the CADTH Scenario Analyses of the Budget Impact Analysis — Health Canada Indication
Market share of semaglutideb | 3-year total ($) | |||
|---|---|---|---|---|
Percentage eligible and enrolled in public planc | ||||
10% | 20% | 30% | 41% | |
9% | 325,165,752 | 580,169,925 | 835,174,097 | 1,064,291,523a |
10% | 361,295,280 | 644,633,250 | 927,971,219 | 1,182,546,137 |
15% | 541,942,920 | 966,949,875 | 1,391,956,829 | 1,773,819,205 |
20% | 722,590,561 | 1,289,266,499 | 1,855,942,438 | 2,365,092,273 |
25% | 903,238,201 | 1,611,583,124 | 2,319,928,048 | 2,956,365,342 |
30% | 1,083,885,841 | 1,933,899,749 | 2,783,913,657 | 3,547,638,410 |
aThis represents the sponsor’s base-case estimate.
bThis represents market share at 3 years assuming a linear increase up to this value. For example, 9% would be 3% in year 1, 6% in year 2, and 9% in year 3.
cPublic coverage for Non-Insured Health Benefits is assumed to be 100% in all analyses.
Table 17: Summary of the CADTH Scenario Analyses of the Budget Impact Analysis — Reimbursement Request
Market share of semaglutideb | Three-year total ($) | |||
|---|---|---|---|---|
Percentage eligible and enrolled in public planc | ||||
10% | 20% | 30% | 41% | |
9% | 53,167,206 | 94,832,250 | 136,497,295 | 173,921,729a |
10% | 59,074,673 | 105,369,167 | 151,663,661 | 193,246,366 |
15% | 88,612,010 | 158,053,751 | 227,495,491 | 289,869,548 |
20% | 118,149,347 | 210,738,334 | 303,327,322 | 386,492,731 |
25% | 147,686,683 | 263,422,918 | 379,159,152 | 483,115,914 |
30% | 177,224,020 | 316,107,501 | 454,990,983 | 579,739,097 |
aThis represents the sponsor’s base-case estimate.
bThis represents market share at 3 years assuming a linear increase up to this value. For example, 9% would be 3% in year 1, 6% in year 2, and 9% in year 3.
cPublic coverage for Non-Insured Health Benefits is assumed to be 100% in all analyses.
The total 3-year budget impact of reimbursing semaglutide population is estimated to be as high as $4,138,911,478, for the full indication population and as high as $676,362,279 for the reimbursement request, assuming market share of semaglutide is 35% and proportion of patients eligible for public coverage is 41%. CADTH notes that it is unlikely this range will be reached given the high value used for public coverage. A more reasonable range likely falls within the 20 to 30% estimates used for public coverage. With regard to market uptake the degree of uptake is highly uncertain given the absence of publicly funded weight-loss medications in Canada. CADTH notes in the full Health Canada population, more than 30% of the budget impact is attributed to overweight patients with weight-related comorbidities.
CADTH also conducted additional scenario analyses on the sponsor’s base case, which assumed 9% uptake at 3-years and 41% public coverage, to explore remaining uncertainties (Table 18).:
A. Markups and dispensing fees are included.
B. The price of semaglutide was reduced by 71%, the price reduction at which semaglutide would be considered cost-effective at a willingness to pay of $50,000 per QALY in the CADTH base-case reanalysis of the cost-utility analysis (refer to Table 7).
Table 18: Detailed Breakdown of the CADTH Reanalyses of the Budget Impact Analysis
Scenario analyses | Year 0 (current situation) | Year 1 | Year 2 | Year 3 | 3-year total |
|---|---|---|---|---|---|
Full indication population | |||||
Submitted base case | $0 | $163,723,233 | $350,235,914 | $550,332,376 | $1,064,291,523 |
CADTH scenario A: Fees and markups | $0 | $182,301,419 | $389,980,771 | $612,788,239 | $1,185,070,429 |
CADTH scenario B: Semaglutide price reduction of 71% | $0 | $474,797,37 | $101,568,415 | $159,596,389 | $308,644,541 |
Reimbursement request population (BMI > 35 kg/m2 and prediabetes) | |||||
Submitted base case | $0 | $26,788,241 | $57,198,284 | $89,935,204 | $173,921,729 |
CADTH scenario A: Fees and markups | $0 | $29,827,597 | $63,688,326 | $100,140,413 | $193,656,336 |
CADTH scenario B: Semaglutide price reduction of 71% | $0 | $7,768,589 | $16,587,502 | $26,081,209 | $50,437,301 |
BMI = body mass index.
Stakeholder Input
Patient Input
Gastrointestinal Society
About the Gastrointestinal Society
As the Canadian leader in providing trusted, evidence-based information on all areas of the gastrointestinal tract, the GI (Gastrointestinal) Society is committed to improving the lives of people with GI and liver condition, supporting research, advocating for appropriate patient access to healthcare, and promoting gastrointestinal and liver health. We have been covering obesity-related issues for many years, a summary can be found here https://badgut.org/?s=obesity.
The GI Society is a national charity formed in 2008 on the groundwork of its partner organization, the Canadian Society of Intestinal Research (CSIR), which was founded in Vancouver in 1976. We receive national and international attention, simply because we have earned the respect of both the gastrointestinal medical community and Canadians who battle GI and liver issues daily. During 2021, our English (www.badgut.org) and French (www.mauxdeventre.org) websites had 7.8 million page views by 5.8 million unique users.
All our programs and services focus on providing Canadians with trusted, commercial-free, medically-sound information on gut and liver diseases and disorders, including obesity, in both official languages. Our BadGut® lectures (currently on hiatus due to the pandemic), quarterly Inside Tract® newsletter, pamphlets, and educational videos arm Canadians with the information they require to better understand and manage their specific needs. We also work closely with healthcare professionals and governments at all levels toward system-wide improvements in care and treatment.
Information Gathering
Data for this submission came from a variety of sources, including contact with patients and patient caregivers, the results of published studies, and a survey we conducted from October 6, 2020 to January 10, 2021, open to individuals who had experienced obesity. The survey was open internationally, but the majority (96%) of respondents were from Canada. In total, we had 2,050 respondents answer many questions and, of those, 1,550 individuals completed the survey. 88 respondents had used liraglutide in the past or currently use it.
Disease Experience
Obesity is a multi-factorial, chronic, relapsing disease that occurs when a person has an excessive amount of body fat (adipose tissue) that might increase health complications. Obesity is defined as having a BMI of 30 kg/m2 or greater. Over the past few decades, obesity has become common in Canada and other developed nations. Several health organizations, including the Canadian Medical Association and the World Health Organization, classify obesity as a chronic disease. The European Union Commission has listed obesity as one of the high-risk groups who are “medically vulnerable”. We have a recent animated video available on our website regarding obesity https://badgut.org/obesity-video/.

Many health complications can arise from obesity, especially in individuals who have the disease for a long time or those living with class III obesity (BMI of 40 kg/m2 or greater). Excess weight influences biology in diverse ways, which can range from excess pressure in the abdominal region to hormonal effects, since adipose tissue can lead to certain hormone levels increasing. This can lead to many serious conditions, including type 2 diabetes, high blood pressure, heart disease, sleep apnea, endocrine conditions, mental health problems, and osteoarthritis. While these conditions can occur in individuals of any weight, they are more common in those living with obesity. Obesity can increase healing time and the chance of infection after surgeries and obesity in women can lead to increased risks during pregnancy. Obesity has also emerged as a factor that causes worse outcomes in those who develop COVID-19.
When presented with a list of comorbid conditions, only 9% of respondents said that they did not have any of them. The most common comorbidities were arthritis (51%), hypertension (33%), sleep apnea (30%), gastroesophageal reflux disease (29%), irritable bowel syndrome (29%), high cholesterol (25%), and diabetes (24%). These conditions come with their own symptoms, risks, and treatments, which can further complicate the management of obesity. In addition, when asked how much of an effect obesity has on their mental health, 64% chose between 7 and 10 on a ten-point scale, with ten being completely affects them and one being does not affect their mental health at all. Only 2% said that obesity does not affect their mental health.
On top of this, obesity itself can affect many areas of life. There is a strong stigma against individuals living with obesity, which can lead to mistreatment in many areas of life, including feeling ignored by physicians and being seen as lazy by potential employers. In fact, 72% of our survey respondents experienced social stigma as a result of their obesity. Many of our survey respondents said that they avoid getting medical care as they feel that their physician shames them for being fat, which can lead to more health problems because they don’t get timely treatment for any conditions they might develop, whether or not it is related to obesity. In the words of one survey respondent, “I don't go to the doctor as often as I should because I feel like a failure and that all my medical issues are caused by my obesity.” According to another respondent, “I've received the most shame about my weight from doctors to the point I'm scared to go. They should help, not shame.” One other person shared, “Obesity affects all of my life – family, social, and work.”
Experiences With Currently Available Treatments
Diet and Exercise
The most common treatment for obesity is lifestyle modifications. This involves reducing the amount of food an individual eats and/or increasing the amount of exercise in which an individual participates. It is a complex treatment that involves persistent effort. Telling patients that the only way to cure their disease is to constantly monitor their food intake and eat at a deficit puts a lot of pressure on individuals to cure their own disease, and increases stigma that obesity is easily fixed by diet alone. In reality, weight loss is much more difficult and complex. The body has hormonal influences and metabolic adaptations that fight hard to keep a person from losing weight long-term. In one American study, three years after participants concluded a weight loss program, only 12% had kept off at least 75% of the weight they had lost, while 40% had gained back more weight than they had originally lost. Many individuals with obesity are constantly yo-yoing in weight, often successfully losing hundreds of pounds over and over in an endless cycle. When this is the only option, patients often feel hopeless.
Medications
For a disease that affects 26.8% of Canadians, there are very few medication options, and those that are available do not have public or full private coverage. As each individual reacts differently to medications, and might have different root causes to their obesity, having a wide variety of medications accessible is extremely important. Available medications include:
Naltrexone and bupropion (Contrave®): supresses appetite by affecting two areas of the brain involved in the regulation of food intake. It is available in pill form, starting with a once-daily dosage and increasing gradually to two pills twice daily. Side effects can include nausea, constipation, and headaches.
Liraglutide (Saxenda® for weight management or Victoza® for type 2 diabetes treatment): regulates appetite level. Patients self-administered it subcutaneously daily, starting at a low initial dose and slowly increasing to the maintenance dose. Side effects most commonly include digestive symptoms such as nausea and diarrhea, which usually disappear after a few days or weeks. It can also cause low blood sugar, headaches, and dizziness.
Semaglutide (Wegovy™ for weight management or Ozempic® for type 2 diabetes treatment): regulates appetite level. Patients self-administer it subcutaneously weekly, starting at a low initial dose and slowly increasing to the maintenance dose. Side effects most often include digestive symptoms such as diarrhea and nausea, along with headaches.
Orlistat (Xenical®): inhibits the enzyme that breaks down dietary fat into absorbable components (lipase). Individuals who take this medication are unable to absorb all the calories from the fats they eat, so these fats are instead eliminated with bowel movements. Side effects can include diarrhea, oily stools, oily discharge when passing gas, and bowel urgency.
However, many respondents expressed concerns over both obtaining prescriptions for medications and paying for the often exorbitant costs of these drugs.
“Obesity has been classed as a chronic disease yet there is no funding for medications in the same manner as other chronic diseases.”
“I have a good benefits plan but they do not cover the cost of weight loss medication.”
“Most of us who could benefit from the medication do not have coverage to use the medication that could actually be beneficial.”
“I would be more than willing to try weight loss medications but they are so cost prohibitive.”
“I’ve asked my doctor for weight loss medication and she says no.”
“I have tried going on weight loss medication but unfortunately it has never gone past the discussion point. I have been eagerly looking forward to trying any sort of medication for my weight loss.”
“My doctor refused to try any weight loss drugs for me.”
Bariatric Surgery
Surgery is typically quite effective, but many patients and physicians prefer to leave it as a last resort because it can have serious side effects. There are four types of surgery currently available in Canada:
Gastric Sleeve: a surgeon will remove part of your stomach, leaving just a thin sleeve, approximately the size of a small banana, behind. This method simply reduces the amount of food you can eat during a window of time.
Gastric Bypass: a surgeon removes part of the stomach, leaving just a small pouch, and then connects the small pouch to the middle of the small intestine. Roux-en-Y is another name for this process. This surgery works in two ways: you can’t eat as much because the stomach is smaller, and your body won’t absorb as many calories because of the small intestine bypass.
Gastric Band: a surgeon will place a band around the upper part of the stomach to create a smaller pouch. The surgeon can adjust the band to make the available stomach area smaller or larger, as needed. However, surgeons do not often recommend it anymore, due to poor results.
Intragastric Balloons: this is a newer and less common form of surgery at this time. It is a temporary measure that involves placing a fluid-filled balloon into the stomach that delays the rate of gastric emptying. It is different from other methods of surgery as it does not involve modifying the structure of the digestive tract and it is reversible, but it still has risks.
Bariatric surgery often leads to significant weight loss and reversal of several obesity-related diseases, such as type 2 diabetes and high blood pressure. However, it can cause severe side effects; of those who have bariatric surgery, 5% experienced complications while in hospital and 6% needed hospital readmission within a month of release due to complications. The mortality rate for bariatric surgeries is between 0.1-2%. Severe nutritional deficiencies and gastrointestinal symptoms can also occur. Many individuals would prefer not to have surgery; in our survey 33% indicated that they would never consider bariatric surgery to treat their obesity. For the persons who do want bariatric surgery, the wait lists are often very long and it can be out of reach financially for many individuals. Additionally, this is not a absolute cure for obesity as several individuals identified significant weight gain following their bariatric surgery.
Improved Outcomes
The primary goal for treating obesity is weight loss. This weight loss then leads to improvements in other symptoms and conditions. However, most treatments for obesity are not effective in the long-term. Even in individuals who lose a significant amount of weight, many of them gain the weight back within five years. A medication that can be taken for chronic management of obesity will be extremely beneficial for the population, as part of a larger management program that includes lifestyle modifications. Those living with obesity who have tried semaglutide found it easier to adhere to lifestyle modifications while taking that medication.
Experience With Drug Under Review
Patients have had access to semaglutide under the name Ozempic® to treat type 2 diabetes since 2018. In addition to good management of blood sugar levels, many of these individuals experienced reduced appetite and weight loss, and some physicians prescribed Ozempic® off label to treat obesity. Then, in November 2021, Health Canada approved Wegovy™ for weight management. Wegovy™ differs from other weight management drugs because it only requires a single injection per week, which makes it easier for patients to manage than medications that they need to take daily. However, it is not an inexpensive medication, so drug coverage is important to those who take it. One respondent to our 2020 survey said, “Ozempic was working for me but they took it off the drugs payment scheme and I couldn't afford it anymore”.
Companion Diagnostic Test
If the drug in review has a companion diagnostic, please comment. Companion diagnostics are laboratory tests that provide information essential for the safe and effective use of particular therapeutic drugs. They work by detecting specific biomarkers that predict more favourable responses to certain drugs. In practice, companion diagnostics can identify patients who are likely to benefit or experience harms from particular therapies or monitor clinical responses to optimally guide treatment adjustments.
What are patient and caregiver experiences with the biomarker testing (companion diagnostic) associated with regarding the drug under review?
It is fairly easy to monitor whether a drug is positively affecting a person living with obesity, as they lose weight, which is easy to measure. However, the true benefit comes for the effect of this weight loss on other health conditions, requiring a wide range of tests, depending on the condition.
Anything Else?
Obesity is a complex condition and we had a wide range of comments from our survey. This woman from Ontario said, “I feel that there are way less resources allocated in our current healthcare system towards the prevention and treatment of this disease. Obesity is becoming a pandemic now and I have seen first hand how it had destroyed the health of so many near and dear ones in the family; it’s still so hard to get the healthier food because most of the healthier food is just way too expensive to be afforded by an average Joe. Also, a lot of effort is needed to pinpoint what causes one child to be obese and the other to be skinny in the same family - what genetic factors predispose someone to gain weight or not being able to lose it like others can? Or what resources are there to psychologically help obese people because often times, the dependency on food is there to mask other personal traumas that are mentally linked! Then there is this whole thing about some meds being insured by govt and some not. What if there is no private health coverage in place? There’s a lot of work needed in this field if we want our next generations to be less obese and more healthy. Having this survey is a positive step towards getting answers in this regard.”
Another person responding to our survey said, “I feel strongly that Pharmacare should cover the cost of Ozempic which is $191.00 per month.”
Patient Group Conflict of Interest Declaration — Gastrointestinal Society
To maintain the objectivity and credibility of the CADTH CDR and pCODR programs, all participants in the drug review processes must disclose any real, potential, or perceived conflicts of interest. This Patient Group Conflict of Interest Declaration is required for participation. Declarations made do not negate or preclude the use of the patient group input. CADTH may contact your group with further questions, as needed.
Did you receive help from outside your patient group to complete this submission? If yes, please detail the help and who provided it.
No. Furthermore, we did not receive any funding from any pharma company to conduct our survey or to complete this submission. The Canadian Society of Intestinal Research, our partner registered charity, which does not receive any funding from pharma, provided support for the survey.
Did you receive help from outside your patient group to collect or analyze data used in this submission? If yes, please detail the help and who provided it.
No.
List any companies or organizations that have provided your group with financial payment over the past two years AND who may have direct or indirect interest in the drug under review.
Table 1: Conflict of Interest Declaration for the Gastrointestinal Society
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
Novo Nordisk Canada Inc. for 2021 support of our Inside Tract® newsletter, pamphlet on Obesity, and partial support of Obesity video. | — | — | — | X |
Novo Nordisk Canada Inc. for 2022 support of our Inside Tract® newsletter, pamphlet on Obesity, and partial support of Obesity video. | — | — | — | X |
Obesity Canada and the Canadian Liver Foundation
About Obesity Canada and the Canadian Liver Foundation
Obesity Canada-Obésité Canada, previously known as the Canadian Obesity Network-Réseau canadien en obésité, is Canada’s leading obesity registered charity association for health professionals, researchers, trainees, students, policy makers and Canadians living with obesity. Currently, Obesity Canada-Obésité Canada has more than 20,000 professional members and over 25,000 public supporters.
Our mission: To improve the lives of Canadians through obesity research, education, and advocacy.
Our Vision: A day when people affected by the disease of obesity are understood, respected, and living healthy lives.
Website: https://obesitycanada.ca/
Founded in 1969, the Canadian Liver Foundation (CLF) was the first organization in the world dedicated to supporting education and research into all forms of liver disease. Today, the CLF continues to be the only national health charity committed to reducing the incidence and impact for Canadians of all ages living with or at risk for liver disease. The CLF is the only registered charity in Canada directing funds specifically for liver disease research in all its forms and has invested nearly $40 million in the scientific search for causes, preventative measures, and potential treatments for liver disease. The CLF reaches millions of Canadians through our public and professional education programs, patient support programs and other awareness, fundraising and outreach efforts.
Website: www.liver.ca
Information Gathering
Obesity Canada engaged individuals living with obesity through an online survey that was conducted between February and March 2022. The survey was distributed throughout our network of social media, newsletter mailing lists as well as within our online patient support community OC-Connect. The survey was also distributed to patients, caregivers and health professionals from across Canada by the Canadian Liver Foundation through the CLF website, social media, newsletter and patient databases. Recruitment by CLF was targeted specifically to liver disease patients and caregivers living with obesity. There were a total of 109 responses from Canadians living with obesity. The majority of responses came from Ontario (34%), British Columbia (21%), and Alberta (19%), with other responses coming from Saskatchewan, Manitoba, Quebec, New Brunswick and Nova Scotia. The majority of respondents were female (94%) and between the ages of 45-64 (67%). 107 (98%) respondents identified as patients or individuals living with obesity while 2 were caregivers. Over half of respondents (66%) of respondents indicated past or present experience with prescription medications for obesity management with 57% reporting experience specifically with Semaglutide.
Disease Experience
Obesity is a prevalent, complex, progressive and relapsing chronic disease, characterized by abnormal or excessive body fat (adiposity), that impairs health.
Population health studies measure the prevalence of obesity using a crude measure called the Body Mass Index (BMI). Although this measure is helpful for population health surveillance, it is not a tool that can be used to clinically diagnose people with obesity. At the individual level, obesity complications occur because of excess adiposity, location and distribution of adiposity and many other factors, including environmental, genetic, biologic and socioeconomic factors. Based on existing population surveillance studies, the prevalence of obesity in Canada has increased significantly over the past three decades.
In Canada, the prevalence of obesity (BMI > 30 kg/m2) in adults rose dramatically, increasing three-fold since 1985 and affecting 26.4% or 8.3 million Canadians in 2016. Severe obesity (BMI ≥ 35kg/m2 ), the fastest growing obesity subgroup, increased disproportionately over this same period. Since 1985, severe obesity increased 455% and affected an estimated 1.9 million Canadian adults in 2016. Between 25-30% of children and youth live with overweight and obesity; 3% live with severe obesity.
Adipose tissue not only influences the central regulation of energy homeostasis, but excessive adiposity can also become dysfunctional and predispose the individual to the development of many medical complications, such as type 2 diabetes, non-alcoholic fatty liver disease, high blood pressure, heart disease, stroke, arthritis, many forms of cancer, and other important health problems. Obesity can have serious impacts on those who live with it. Most concerning, it increases the risk of developing cardio- vascular disease and cancer, two primary causes of premature mortality in Canada, resulting in a reduction of life expectancy by six to 14 years. It is estimated that 20% of all cancers can be attributed to obesity, independent of diet.
Obesity is associated with a spectrum of liver abnormalities, known as non-alcoholic fatty liver disease (NAFLD), characterized by an excess fat buildup inside the liver. Due to an increase in the prevalence of obesity, NAFLD, the most common liver disease in Canada, is also rapidly becoming the most common cause of chronic liver disease among Canadians. NAFLD can range from simple fat buildup in the liver to inflammation and/or liver cell death. The development of non-alcoholic steatohepatitis (NASH), the more serious form of NAFLD, can lead to scarring (cirrhosis), liver cancer, liver failure, as well as the need for a liver transplant.
NAFLD has become an important public health issue because of its high prevalence, potential progression to severe liver disease, and association with serious cardiometabolic abnormalities, including type 2 diabetes, high blood cholesterol and high triglycerides, high blood pressure, and coronary heart disease. The underlying mechanism for fat build-up in the liver is believed to be insulin resistance, often a consequence of obesity and excess belly fat.
Lifestyle modification is considered the first line of treatment for patients with NAFLD, which includes diet modification, sustained weight loss, and increase in exercise. There are no approved pharmacological treatment agents for NAFLD and NASH currently. Due to its complex pathophysiology, different pathways are being studied for new drug development and treatments with the focus on metabolic pathways, reducing inflammation, and slowing or reversing fibrosis.
GLP-1 agonists are one of the various classes of drugs that are currently being investigated for the treatment of NASH. GLP-1 agonists can improve body weight, glucose and lipid metabolism and may help those living with NASH by aiding in reducing overall inflammation in the liver. Due to the increase in global prevalence of NAFLD/NASH and lack of approved pharmacological agents, there is a surge for emerging clinical trials with agents targeting via different pathways.
There is a growing disease burden associated with NAFLD, following the trajectory of increasing obesity in Canada and globally. It is estimated that between 2019 and 2030, the number of NAFLD cases in Canada would increase by 20%. Increasing rates of obesity translate into increasing NAFLD-related cases of cirrhosis (scarring) and liver cancer and related mortality. Prevention efforts should be aimed at reducing the incidence of NAFLD and slowing fibrosis progression among those already affected.
Obesity affects individuals, families and society. The economic cost is significant. In 2014, the global economic impact of obesity was estimated to be US $2.0 trillion or 2.8% of the global gross domestic product (GDP). In Canada, obesity and its related illnesses result in a large cost to society due to increases in direct (i.e., physician, hospital, emergency room use) and indirect costs (i.e., lost productivity, absenteeism, disability), estimated to be $7.1 billion in 2010.
Beyond its effects on overall health and well-being, obesity also affects people's’ overall social and economic well-being due to the pervasive social stigma associated with it.5 As common as other forms of discrimination — including racism — weight bias and stigma can increase morbidity and mortality.6 Obesity stigma translates into significant inequities in access to employment, healthcare and education, often due to widespread negative stereotypes that persons with obesity are lazy, unmotivated, or lacking in self-discipline.7,8
Obesity has long been misunderstood, trivialized, and stigmatized as a simple “lifestyle” issue that can be effectively addressed by the mantra of “eat-less-move-more”. This simplistic view of obesity disregards both the lived experience of persons with obesity as well as the vast body of scientific evidence showing that, like other chronic diseases, obesity is a rather heterogeneous condition resulting from the complex interaction of a multitude of socio-psycho-biological factors that promote excessive weight gain, and ultimately impairs health.
A better understanding of the biological underpinnings of this disease has emerged in recent years. The brain plays a central role in energy homeostasis by regulating food intake and energy expenditure. Importantly, research indicates that powerful neuro-hormonal factors effectively defend our bodies against weight loss, thereby often making obesity a life-long problem, where weight regain (or relapse) is the rule rather than the exception.
Obesity is a chronic disease, not simply a risk factor for other diseases. The World Health Organization, the Canadian Medical Association, and seven provincial and territorial medical associations as well as several international professional and scientific organizations recognize obesity as a chronic disease. In Canada, specifically, the lack of recognition of obesity as a chronic disease by provincial and territorial governments has a significant impact for Canadians. Obesity is more prevalent than diabetes, hypertension or virtually any other chronic diseases and also carries with it a more significant economic burden when left untreated To date no provincial or territorial government has taken serious steps to treat and manage this disease. Only a few provincial governments have focused their attention on health promotion among children and families and most have not implemented obesity treatment programs for Canadians living with obesity. This approach by itself is not evidence-based and ignores the more than 8 million Canadian adults currently living with obesity, condemning them to ineffective self management of a complex chronic disease.
The Canadian Clinical Practice Guidelines for the Treatment of Obesity, outline the current evidence and best practices for obesity management. However, pervasive weight bias in our society is a major barrier to access to obesity care.
Obesity Canada’s report card on access to obesity treatments shows that:
There is a profound lack of interdisciplinary teams for obesity prevention and management at the primary care level in Canada;
Anti-obesity medications are not covered by provincial public drug benefit programs or any of the Federal public drug benefit programs, and that
There are significant disparities in the access to bariatric surgery, with only 1 in 171 (0.58%) adults living with severe obesity having access to surgery every year. In many provinces and territories, wait times for bariatric surgery can go up to 5 years.
Due to lack of availability of evidence-based treatments in the health system, Canadians affected by obesity are left to navigate a complex landscape of unregulated weight-loss products and services, many of which lack a scientific rationale and openly promote unrealistic and unsustainable weight-loss goals.
Living with obesity is challenging on a day-to-day basis. Many experience limited mobility, chronic pain, difficulty with daily tasks and other physical limitations. Further, the environments we are expected to navigate for work, school, healthcare and even at home, are not typically designed to accommodate larger bodies and thus accessibility becomes a major obstacle. The societal bias and stigma associated with obesity is also a significant barrier to quality of life. There is an overwhelming incorrect perception that obesity is a self-inflicted condition that simply requires more willpower on behalf of the individual. This perception is amplified by the lack of recognition of obesity as a chronic disease by provincial health authorities and the severe lack of access to effective, evidence-based treatments. Living in a world that poorly misunderstands the chronic disease you live with and leaving the management of a complex chronic disease up to the individual using ineffective methods creates a cycle of failure and disease progression. This all can lead to further healthcare avoidance, lowered quality of life and increases in mental health issues.
Obesity increases the risk of serious chronic illnesses such as heart disease, cancer, stroke, diabetes and non-alcoholic fatty liver disease, among others. In our survey, 97% of respondents indicated that in addition to living with obesity they also have at least one obesity-related comorbidity. This speaks to the complex nature of obesity and the potential for effective obesity management to have far reaching impacts on health and wellbeing. Living with obesity often includes mobility issues and pain that limit daily life activities.
“The biggest impact is on mobility and keeping up. It is increasingly harder to do the activities I enjoy. I have heel, knee, and back pain that interferes with regular activities I enjoy. There is also an impact on my mood at times because I often feel defeated with efforts to lose weight.”
Many individuals who face these issues of physical pain and lack of mobility are denied care for these ailments such as orthopedic surgery, that would improve quality of life based on their obesity status, yet are not offered any meaningful treatment plan to get them to a weight where they would qualify for such interventions.
“I have experienced discrimination (from doctors and employers). Not physically “fitting” in - to chairs, clothes, etc. Now it’s mostly my mobility - I require double knee replacement and am denied surgery because of my weight”
Beyond issues of comorbidities, pain and mobility, living with obesity also has a significant impact on an individual’s social and psychological health. From depression and anxiety to avoiding public settings to missing out on important life experiences with friends and family, living with obesity is debilitating in many ways.
“Living with obesity, despite regular exercise, constant dietary vigilance and work with dietitians, exercise physiologists, psychologists has been unrelenting. Recurrent weight related injuries (i.e. back and hip problems) have caused years of chronic and acute pain and have limited participation in many leisure and physical activities. Missed life and missed quality of life due to misdiagnosis and delayed diagnoses and pursuing doctor-prescribed but no-evidence/harmful diet-related management interventions. Weight related stigma and discrimination have caused severe depression, trauma, and anxiety, social isolation and limited my work opportunities. Extensive out of pocket rehabilitation costs and costs associated with access to general life (i.e. extra plane tickets, special foods, doctor-prescribed but unproven weight management plans).”
“I try to stay out of the limelight - no pictures, never participate in events with family and tried to hide behind a variety of masks”
“It sucks. I wish my body could do all the things my mind wants to. It changes what you can do and changes your belief in what you can do. It robs you of possibilities.”
“It is debilitating. Constant chronic pain. Not living life to my full potential. Afraid to step out of the box.”
Experiences With Currently Available Treatments
Like many other chronic diseases, obesity is a manageable disease. In 2020, The Canadian Adult Obesity Clinical Practice Guidelines were published, marking a much-needed significant update in the evidence-based best practices. The guidelines describe three pillars of obesity treatment that improve obesity outcomes and support successful behavioral interventions. These pillars include psychological and behavioural therapy, anti-obesity medications (currently 3 approved in Canada) and bariatric surgery.
Despite the comprehensive evidence covered in the Clinical Practice Guidelines, there remains a gap in access to obesity care in Canada.13 While we have evidence that the three pillars of treatment are effective and AVAILABLE in Canada, none of them are appropriately ACCESSIBLE.
“It is so frustrating and demoralizing that the things that work for me are unattainable, I cannot afford the medications or to see a therapist regularly and the wait time for surgery is several years. I am left to try and manage on my own and it is just not possible”
“It is difficult enough as it is to afford life with a limited income and disability, it is out of the question to try to buy medications that cost hundreds of dollars a month. It is something I need and my doctor believes will help and it is sitting right there in front of me but I cannot use it.”
Obesity has not received official recognition as a chronic disease by the federal government or any of the provincial/territorial governments, despite the Canadian Medical Association and the World Health Organization’s declarations. 14,15 The lack of recognition of obesity as a chronic disease by public and private payers, health systems, the public, and media has a trickle-down effect on access to treatment. Obesity continues to be treated as a self-inflicted risk factor, which affects the type of interventions and approaches that are implemented by governments or covered by health benefit plans.16
All 109 respondents to our survey indicated that they have attempted to “self manage” obesity through typical health behaviour modification such as diet and exercise. Almost half (46%) indicated more than 20 separate attempts to self-manage obesity as an adult. Almost all respondents, (98%) reported utilizing restrictive dieting while 85% reported exercise as a method of weight management. Shockingly, 57% of survey respondents indicated the use of over-the-counter weight loss supplements which are not effective and not regulated in the same manner that medications are. This speaks to the desperation that individuals living with obesity have in trying to manage their disease with limited access to effective, evidence-based treatment options. An additional 37% indicated the use of popular commercial weight management programs. These self-directed obesity management methodologies resulted in only 5% of respondents indicating long term effectiveness. This is not an isolated finding as we know from research that although healthy eating and physical activity interventions alone are important for overall health and wellbeing, they are not effective treatments for any chronic disease, including obesity. Although medical nutrition therapy and physical activity interventions are the backbone of any chronic disease management program, to effectively treat a chronic disease, these interventions need to be provided in conjunction with evidence-based treatments such as behavioural and psychological therapies, pharmacotherapy, and bariatric surgery. Although self-management is also a core aspect of any chronic disease management, it is also recognized that treating a chronic disease requires additional medical support. In obesity, however, most patients are expected to simply self-manage their disease. The majority of survey respondents reported that self-directed obesity management strategies were not sustainable, with 86% indicating that self-management of obesity is not enough to manage obesity in the long-term.
In our survey, 72% of respondents indicated past or present experience with at least one of the previously available obesity medications in Canada (Contrave, Saxenda, Orlistat). Experience with these treatments varied in effectiveness with many reporting clinically significant (>5%) weight loss. While 67% reported experiencing side effects from the medication, 62% indicated these were manageable.
Cost associated with prescription medications is the single biggest barrier to access for individuals trying to manage their obesity. Less than half of our survey respondents had coverage for obesity medications through their drug plans and further still, of those that did, coverage was limited to 50% of the cost and often capped at a total which makes the medications inaccessible for even the ones lucky enough to have coverage.
“cost, I don't have any medical insurance to cover anything so it all comes out of pocket. Along with my physio I just can't afford it”
“For me the barriers to treatment are mainly cost. The latest and greatest are way outside my budget in retirement.”
While our current health system theoretically allows for most people with obesity to receive health care in a structured and systematic way, compelling evidence indicates that obesity is not effectively managed within our current health system.13,18 Canadian health professionals feel ill-equipped to support patients with obesity. 19-21 In addition, despite the important role health professionals can play in obesity management, they are an underutilized resource; most Canadians do not look to them for advice. A startling 89% of Canadians with obesity have never asked any licensed healthcare professional (family doctor, dietitian, pharmacist, etc.) about obesity. 23 Rather, consumers turn to a multi-billion-dollar commercial weight-loss industry. Many products and services offered in this space are unregulated and untested, but entice consumers with promises of significant and easy weight loss. While some approaches may actually achieve significant weight loss, more than 95% of diets and other approaches fail and result in weight regain, often to an even higher weight. An inability to lose and/or maintain weight loss perpetuates a vicious cycle of “yo-yo dieting,” which too often results in frustration, depression, poor self-esteem, and further weight gain.23
“I cannot tell you how many times I have lost 20 or 30 lbs on some new diet. The weight flies off fairly quickly, but it never lasts. It is almost impossible to diet forever and the weight always comes back with a vengeance. I just feel like giving up.”
Many patients report a great deal of success through bariatric surgery which is considered the current gold standard for obesity treatment, however, surgical intervention is not appropriate for all individuals living with obesity and it is not scalable for the population that could benefit from it, which is evident by the multi-year wait from time of referral across the country. This is a gap in care that effective anti-obesity medications can help fill.
There are very limited treatment options for those living with NAFLD or NASH. The current treatments have primarily aimed at improving those with biopsy-proven NASH and some degree of fibrosis. For instance, thiazolidinediones and vitamin E have been used for the treatment of NASH as they have shown mild improvement in NAFLD patients. Nonetheless, possible adverse effects of these compounds and the recommended short-term use of vitamin E have made the need for the development of alternative agents urgent.
Improved Outcomes
With outcomes for obesity treatment, patients look for a number of outcomes but many go beyond simple weight loss . Many patients are looking for quality of life improvements such as being able to participate in activities of daily living or being able to do things that they have been unable to do due to their obesity. Outcomes related to improvement in related comorbidities (diabetes, hypertension, sleep apnea) as well as outcomes related to everyday life such as productivity, energy levels, sleep, activity and mental health. While weight loss is typically the primary outcome measure for the efficacy of an anti-obesity therapy, from a patients’ viewpoint it goes much deeper and the weight loss is viewed as a needed step to the more meaningful quality of life outcomes.
“I need to lose weight so I can have the energy and mobility to play with my kids/grandkids” or “I am so preoccupied with worrying about my weight that my productivity and mental health suffer, if I can lose some weight, everything else will get better.”
Hence, from a patient’s view, the actual weight loss is less important than the impacts on the other outcomes.
If new treatments provide a positive impact on these outcomes, the quality of life of patients, caregivers and families would be drastically different. Obesity is a disease that impacts virtually all aspects of an individual’s daily life. Improvement in sleep, productivity, energy levels, reduced stress of other conditions, improved mental status would all make a significant difference. These outcomes will also positively impact social aspects of life where individuals living with obesity would be better equipped and more comfortable engaging in social situations.
“If I had access to effective obesity management, I would stop losing countless days each year in preventable physical and mental pain, use healthcare less, would have a higher salary, lose less time on disability and pay more taxes, I could contribute better as a citizen, I would stop bleeding my long-term savings into paraprofessionals and other uninsured treatments”
“I would be happier and feel better about myself. I would have more energy to be active and get more done around the house. I would feel more confident.”
Typically, when considering a therapy for obesity, patients tend to assess the trade-offs between the desired outcomes mentioned above and the potential side-effects of the therapy, the ease of use of the therapy, and the cost of the therapy. In many cases, the potential for moderate benefits of a therapy will outweigh many manageable side effects. Cost seems to be the most significant determining factor in choosing a therapy for obesity with over 80% of respondents indicating cost of treatment as the most important trade-off to consider.
Left untreated, chronic diseases such as obesity continue to progress, contributing to more comorbidity and mortality. In Canada, severe obesity has increased by 455% over the last three decades. This is in part due to the lack of treatments available for people who are affected by obesity. If we do not provide access to evidence-based treatments to patients living with obesity, their disease may continue to progress, which will impact their health and quality of life.
Experience With Drug Under Review
In our survey, 57% of individuals reported having past or present experience using Semaglutide. In general, experience with this medication was positive with an average reported weight loss of 12%. More than half of respondents (61%) reported experiencing side effects while using the medication however the vast majority indicated that the side effects were manageable. Only 13 individuals indicated that side effects were not manageable. Generally side effects include nausea and many reported that the nausea subsided over time as they titrated up to a full dose.
Since obesity is a heterogenous chronic disease (i.e. causes of obesity vary from person to person), treatments need to be tailored to meet patients’ needs and preferences. (This is not unlike any other chronic disease.) Although semaglutide may work for some patients, it may not work for all patients. Just like bariatric surgery may not work for all patients living with obesity. This is why Obesity Canada continues to advocate for more research to find new obesity treatments that can be tailored to patients’ needs and address root drivers of obesity. It is clear that current obesity treatments such as behavioural and psychological treatments, medications, and bariatric surgery can help many patients and should be available through the healthcare system. Our survey demonstrates that semaglutide can be an effective treatment for some patients living with obesity, but due to prohibited costs, the impact of this treatment for patients is difficult to assess.
“Using Semaglutide has been so effective for me! I have more energy, so more of the things I wish to do for my family occur. My blood pressure has dropped dramatically, along with my cholesterol numbers. So my overall medication load is reduced!”
“I started to have relief from hunger and had a modest weight loss of about 10% of starting weight. No side effects. Health improvement was pretty much limited to reducing to high normal blood pressure. But starting at nearly 400 pounds, the impact on quality of life was minimal. Because of the cost I had to quit before it had a long-term positive effect.”
“Total game changer. Hunger managed, all blood work improved, I have lost over 30% of my body weight. I have energy and want to move.”
“It is such a blessing (when I'm taking it) not to be hungry ALL THE TIME! However, it is far too expensive, and I don't take a high enough dose at regular enough intervals for any long-term benefits. I expect I would actually lose some weight and be much healthier if I could take the full 2.4 mg dose that was used in the studies and to do so on a consistent basis.”
Semaglutide has been reported to reduce liver enzyme (alanine aminotransferase) levels and other markers of liver inflammation.
Companion Diagnostic Test
Anything Else?
While Canada is viewed as a leader on the global stage when it comes to obesity science and expertise, we continue to lag behind in policy and access to treatment for obesity. We currently do not have any of the obesity medications included in public formularies. In 2021 another medication (Liraglutide) was submitted to CADTH for review and was subsequently NOT recommended for coverage. One rationale for the recommendation by CADTH was that while Liraglutide was shown to have clinically significant weight loss of 5%-10%, and that clinically significant weight loss is associated with improvements to comorbid conditions like type 2 diabetes and improved quality of life, Liraglutide clinical studies produced weight loss results on the lower end of this clinically significant range and therefore brought into question the true impact on comorbid conditions. The current medication (Semaglutide) which is under consideration has much more significant weight loss efficacy compared to Liraglutide (in the range of 16%) which would eliminate this point of contention that was seen in the Liraglutide submission to CADTH. This is far more weight loss than the clinically significant range (5%-10%) and is also approaching the efficacy of the current gold standard obesity treatment of bariatric surgery.
CADTH noted in the decision for Liraglutide, that obesity medications are most effective when combined with lifestyle and behavioural changes and that there were concerns determining the appropriate lifestyle changes in conjunction with pharmacotherapy. However, since the release of the Canadian Obesity Clinical Practice Guidelines, Canadian healthcare providers have access to the most current and up to date, evidence-based recommendations on obesity treatment including medical nutrition therapy and physical activity which addresses this concern for all obesity therapies including Semaglutide. Obesity Canada would also like to point out that supplementing pharmacologic interventions with lifestyle modifications to improve outcomes is not specific to obesity treatments. In fact, chronic disease management for a number of conditions including type 2 diabetes, hypertension and heart disease often include pharmacologic intervention supplemented by adjunct behavioural modification, yet this is NOT used as justification for not recommending coverage for these therapies.
Furthermore, one rationale from the CADTH experts for the Liraglutide submission indicated that patients would ‘regain the weight they had lost if pharmacologic treatment for weight management was discontinued…” Obesity Canada and our patient community expects that this flawed rationale is not used in this current review for Semaglutide. Like any chronic disease, discontinuation of treatment can lead to the disease returning, and the hypothetical relapse due to not using the treatment anymore should not play a role in the decisions regarding coverage for those who could benefit from using the medication. An individual taking medication to control hypertension would potentially see a relapse if they discontinued pharmacologic treatment, yet is this a consideration in CADTH’s decision to recommend coverage for hypertension medications? The same can be said about any other treatment for chronic disease. Obesity Canada expects that CADTH approaches this submission for Semaglutide and any future submission with the same chronic disease lens applied to other conditions and that recommendations are based on evidence, not hypotheticals.
Other jurisdictions have recognized the complexity of obesity as a chronic disease and the negative impact lack of treatment has on populations. The United States, the UK and Ireland for example have taken the lead globally and have begun to improve access to effective, evidence-based obesity treatments by including coverage for obesity medications. The U.S. government notes:
“Obesity has long been recognized as a disease in the US that impacts children and adults. Obesity is a complex, multifactorial, common, serious, relapsing, and costly chronic disease that serves as a major risk factor for developing conditions such as heart disease, stroke, type 2 diabetes, renal disease, non-alcoholic steatohepatitis, and certain types of cancer.”
And has recently provided guidance on federal benefit plan providers, indicating that they are not allowed to exclude obesity medications from coverage and that plan providers must have adequate coverage of FDA approved obesity medications on the formulary to meet patient needs. This is an example of governments recognizing the need to effectively treat obesity, a position we hope CADTH will also recognize.
Patient Group Conflict of Interest Declaration — Obesity Canada & Canadian Liver Foundation
To maintain the objectivity and credibility of the CADTH reimbursement review process, all participants in the drug review processes must disclose any real, potential, or perceived conflicts of interest. This Patient Group Conflict of Interest Declaration is required for participation. Declarations made do not negate or preclude the use of the patient group input. CADTH may contact your group with further questions, as needed.
Did you receive help from outside your patient group to complete this submission? If yes, please detail the help and who provided it.
This submission was completed by the staff and volunteers of OC and CLF. Outside input for this submission came from the patients and caregivers who participated in the online survey.
Did you receive help from outside your patient group to collect or analyze data used in this submission? If yes, please detail the help and who provided it.
No
List any companies or organizations that have provided your group with financial payment over the past 2 years AND who may have direct or indirect interest in the drug under review.
The Canadian Liver Foundation (CLF) is committed to bringing liver research to life for all Canadians through liver research, education, patient support and advocacy. The CLF receives funding from a variety of sources with the majority coming from donations from individuals across the country. We use these funds to support CLF liver awareness, education, patient support and research grant programs.
The CLF receives some program funding in the form of unrestricted educational grants from pharmaceutical companies. Grant agreements are established in support of activities initiated by the CLF and prohibit the funder from having any input or influence in program objectives or deliverables.
Table 2: Conflict of Interest Declaration for Obesity Canada and the Canadian Liver Foundation
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
Novo Nordisk | — | — | — | X |
Diabetes Canada
About Diabetes Canada
Diabetes Canada (www.diabetes.ca) is a national health charity representing the millions of Canadians who are affected by diabetes. Diabetes Canada leads the fight against diabetes by helping people live healthy lives, preventing the onset and consequences of diabetes, and discovering a cure. It has a heritage of excellence and leadership, and its co-founder, Dr. Charles Best, along with Dr. Frederick Banting, is credited with the co-discovery of insulin. Diabetes Canada is supported in its efforts by a community-based network of volunteers, employees, health care professionals, researchers, and partners. By providing education and services, advocating on behalf of people living with diabetes, supporting research and translating it into practical applications, Diabetes Canada is delivering on its mission. Diabetes Canada will continue to change the world for those affected by diabetes through healthier communities, exceptional care, and high-impact research.
Information Gathering
This submission contains patient input from an online survey conducted in March 2022. It was open for two weeks (from March 10 to March 24) to people across Canada with prediabetes or type 2 diabetes living with overweight or obesity, and their caregivers. It consisted of a self-administered questionnaire of closed- and open-ended questions about respondents’ lived experience with weight management, prediabetes or diabetes, medications (with specific questions about the drug under review, Wegovy [semaglutide injection] 2.4 mg) and expectations for new drug therapies in this country. Participation in the survey was solicited through Diabetes Canada’s social media channels (Facebook, Twitter, Instagram and LinkedIn).
Wegovy (semaglutide injection) 2.4 mg is a weight management medication indicated and currently available for people living with overweight or obesity who may or may not have prediabetes or diabetes. Consideration is being requested by the manufacturer for reimbursement of this medication for adult patients with an initial body mass index of 35 kg/m2 (Health Canada health risk classification: obese class II) or more and prediabetes. As such, this submission features input from people living with overweight or obesity, as well as from people with prediabetes or type 2 diabetes, to which prediabetes can progress.
A total of 29 people participated in the survey – 3 identified as living with prediabetes and 26 identified as living with type 2 diabetes. There were no caregiver respondents. Respondents resided in Newfoundland, Quebec, Ontario, Manitoba, Saskatchewan, Alberta and British Columbia, with the most representation from Ontario (n=12) and Alberta (n=6). Respondents’ ages ranged from 25-84 years, with the biggest concentration of respondents (n=8) falling in the 45-54 year grouping. About 76% (n=22) reported living with diabetes for 10 years or less (with 3 having had it for less than 1 year). There were 4 respondents who have been living with diabetes for 11-20 years and 3 for more than 20 years.
Among those who answered the question (n=21), 19 respondents (90%) said they identify as living with overweight or obesity and 15 respondents (71%) said they have been formally diagnosed with overweight or obesity by a health care provider. The amount of time respondents said they have been living with overweight or obesity ranged from 4-6 years to 30 years plus; people shared that their experience with overweight or obesity has lasted “most of my life”, “since my childhood years” and was present “even in adolescence”.
Of those who responded to the question, 2 people said they have experience with the drug under review, Wegovy (semaglutide injection) 2.4 mg. In total, 1 person reported currently take Wegovy (semaglutide injection) 2.4 mg along with other diabetes medications, while 1 person reported having taken Wegovy (semaglutide injection) 2.4 mg in the past, but not anymore.
Disease Experience
Wegovy (semaglutide injection) 2.4 mg is a GLP-1 receptor agonist medication that is indicated as an adjunct to a reduced calorie diet and increased physical activity for chronic weight management in adult patients living with overweight or obesity. Reimbursement is being requested specifically for people within this grouping who are also living with prediabetes. Prediabetes is often a precursor to type 2 diabetes.
Obesity is a chronic, often progressive condition with complex, multifactorial etiology. It is characterized by excess or abnormal body fat that can impair health. Its effects are numerous and far-reaching, impacting mental, mechanical, metabolic and monetary health. Overweight and obesity are associated with a higher risk for several other chronic diseases, including type 2 diabetes. Having diabetes can also increase risk for overweight or obesity for different reasons. It is estimated that 80-90% of people with type 2 diabetes live with overweight or obesity. Overweight and obesity can be challenging to treat and managing the condition is usually a life-long process. Management is multipronged and should be individualized to a person’s circumstances and needs. It may include behavioural interventions, emotional and mental health supports, nutrition, physical activity and, in some cases, medications and/or bariatric surgery. A big part of treating obesity is addressing the weight stigma, discrimination and bias that people experience in their daily lives.
Prediabetes is a term used to describe the condition of elevated blood sugar that, while abnormal, is not sufficiently high to constitute a diagnosis of diabetes. Prediabetes may refer to impaired fasting glucose and/or impaired glucose tolerance and/or a higher-than-normal hemoglobin A1c. With behavioural modifications, including attention to nutrition and physical activity, and pharmacotherapy for some, people with prediabetes can revert to normoglycemia. However, prediabetes significantly increases the risk for type 2 diabetes. In fact, Public Health Agency of Canada data suggest that more than half of the people with prediabetes will develop type 2 diabetes within eight to 10 years. For people living with overweight or obesity and prediabetes, various weight management approaches can help reduce likelihood of progression to diabetes.
Diabetes is a disease characterized by elevated levels of glucose in the blood. Common symptoms of diabetes include extreme fatigue, unusual thirst, frequent urination and weight gain or loss. Diabetes necessitates considerable daily self-management. Treatment regimens differ between individuals, but most include eating in a balanced manner, engaging in regular physical activity, taking medications (oral and/or injectable) as prescribed, monitoring blood glucose and managing stress.
About 90 to 95 percent of those diagnosed with diabetes live with type 2. Type 2 diabetes occurs when the pancreas does not produce enough insulin, or the body does not effectively use the insulin that is produced. Among other things, treatment may include exogenous insulin, in addition to other therapies, like oral and/or other injectable medications. Typically, type 1 diabetes presents in children and adolescents, while type 2 develops in adulthood, though either type of diabetes can be diagnosed at any age. Those of advancing age, with a genetic predisposition, who are part of a high-risk population (African, Arab, Asian, Hispanic, Indigenous or South Asian descent, low socioeconomic status) and/or who are living with comorbid conditions, including obesity, are at increased risk of type 2 diabetes.
It can be quite serious and problematic for people with diabetes when blood glucose levels are not at target. Low blood sugar can precipitate an acute crisis, such as confusion, coma, and/or seizure that, in addition to being dangerous, may also contribute to a motor vehicle, school/workplace or other type of accident, causing harm. High blood glucose can cause weakness, nausea, vomiting, abdominal pain and other symptoms. Over time, glucose levels above target can irreversibly damage blood vessels and nerves, resulting in issues like blindness, heart disease, kidney dysfunction, foot ulcers and lower limb amputations. One of the goals of diabetes management is to keep glucose levels within a target range to minimize symptoms and decrease the risk of complications and consequences.
Most respondents indicated that living with prediabetes or type 2 diabetes is preoccupying, inconvenient and burdensome. Management is constant, with the condition requiring a great deal of foresight and planning to deal with. While some suggested the impact to everyday life is minimal, the vast majority of respondents spoke negatively of their experience with prediabetes or diabetes and expressed feelings of guilt, shame, frustration and discouragement associated with their condition.
Survey respondents shared the ways in which prediabetes and type 2 diabetes impacts their daily life and overall quality of life. They provided the following insights:
“Slows me down. No energy.”
“I have to watch my diet so that takes all the pleasure out of food and going out to dinner. My doc keeps preaching doom and gloom.”
“Need for exercise and mindful eating, medical appointments and prescriptions.”
“Guilt, mental exhaustion.”
“Experience extreme fatigue. Not able to do intensive exercise, or exercise properly due to body weight. Sugar fluctuation causing blurred vision sometimes. Not able to reduce weight in spite of dieting. Unable to participate in outdoor activities.”
“I feel awful most of the time and I feel very trapped by what food I must eat.”
“I’ve essentially been living my entire adult life as diabetic. Chronic stress, fatigue and shame. Daily injections, medications and carb counting. Diabetes is involved in every activity of my day.”
“It restricts so many things I used to do. Now I get fatigued and headaches especially when my blood sugar is high (it’s always on the higher side). It’s frustrating!”
“Feel sluggish when my blood sugar is not balance [sic], feel insecure.”
“Affects my overall health.”
When asked specific questions about medical history, respondents (n=21) disclosed the following (in addition to prediabetes or type 2 diabetes):
52% have high blood pressure (n=11)
33% have abnormal cholesterol levels (n=7)
5% have a heart condition or heart disease (n=1)
10% have kidney issues or kidney disease (n=2)
48% have mental health concerns (n=10)
76% have weight management issues (n=16)
19% have eye problems (n=4)
5% have foot problems (n=1)
Additional conditions people experience include fatty liver, Sjogren's syndrome, asthma, osteoarthritis, brain inflammation, gall bladder issues, psoriasis, food sensitivities, environmental sensitivities, medication allergies and polycystic ovary syndrome.
Respondents also shared the ways in which overweight or obesity has impacted their daily life and overall quality of life. A few people commented that weight doesn’t significantly affect their day-to-day activities or general way of living, but many respondents felt otherwise. They said:
“I find it hard to do anything.”
“[I am] less active than before overweight. Lower self esteem. Want to avoid doctor because always reminded I need to lose weight.”
“Makes it harder to be physically active, I feel less attractive, more tired.”
“Weight affects everything I do, walking, housework, sitting, exercise.”
“[I experience] insecurities, discomfort, fatigue.”
“It causes joint pain and makes me feel depressed.”
“These days it affects my self worth and mental health more than my activity level. But it’s taken a lot to get there. Causes increased stress and increased likelihood for other health concerns.”
“[I experience] terrible self esteem, [it is] hard to navigate a size 0 world in a size 20 body. The world is not made for those suffering with obesity.”
“[I have been] getting tired easily. Panting when walking, and weight prevents me from using staircase as my legs pain. Feel that I am getting left out from get-togethers. Need to buy clothes often. Not able to stand for long hours and do housework including cooking. Overweight has caused knee problems. Quality of life has been affected. I feel body shamed. Doctors don't feel comfortable in treating obese person. Obesity has caused sleep apnea for me. In short, being overweight has caused me whole lot of problems mentally, physically and financially.”
“Obesity is a terrible disease both physically [and] mentally. Buying plus sized clothing is more expensive, fitting in vehicles, furniture… there are so many negative factors. The stereotype is that fat people can/should just diet or quit eating ‘bad’ food. Obesity is so much more than fat.”
These comments provide a glimpse at the lived reality of people experiencing overweight and obesity, demonstrate that the condition challenges physical and mental health, and illustrate the bias, stigma and discrimination people regularly face as they navigate the healthcare system and the world more generally.
Experiences With Currently Available Treatments
Of those who responded to the question (n=21), 3 people (14%) reported taking or having taken medication for weight management. When asked about likes and dislikes associated with these medications, one respondent said “I feel like it helps me towards my goals”. Another said “[I] love being off insulin. The swings still happen but I don’t feel panicky with them”.
The following criteria were considered to be “very important” or “important” in selecting a medication for weight management:
minimizes other side effects (100% of respondents)
affordability (94% of respondents)
ease – can be obtained without having to apply for special access authorization (88% of respondents)
long-term effectiveness – helps maintain weight loss (88% of respondents)
minimizes gastrointestinal side effects, e.g., diarrhea, nausea, vomiting, abdominal pain (88% of respondents)
timeliness – can be obtained immediately (82% of respondents)
short-term effectiveness – helps promote weight loss (76% of respondents)
medication can be taken in pill form by mouth rather than injection (71% of respondents)
Respondents also said that physician support, local availability, information about long-term side effects of the medication and the damage they may cause, effectiveness and limited interaction with other medications are also important considerations in choosing a weight management medication.
Other weight management methods previously tried or currently engaged in were reported by respondents as follows:
95% are eating healthy (n=18)
74% are engaging in physical activity (n=14)
16% are taking herbal remedies or over-the-counter supplements (n=3)
11% are using a commercial weight loss program (e.g., WW, Jenny Craig, Herbal Magic, etc.) (n=2)
11% are following a medically-supervised obesity management program (n=2)
11% are considering or have undergone bariatric surgery (n=2)
Respondents provided feedback on how manageable and successful they feel these approaches are:
“Not successful. They require extreme organization, dedication, and a strong mental mind. Motivation is moot as it can't overcome the other mental and physical barriers.”
“They have worked in past but I need to be determined.”
“I try to eat healthy but crave sweets.”
“I’ve been a consistently active person and have sometimes struggled with eating but mostly normally. In combination with medication I believe they are key. In my case adding medication helped me know what full felt like for the first time.”
“I can only succeed when I have the mental mindset to do so.”
“Successful but always end up gaining the weight back.”
“It’s a struggle.”
“Non sustainable [sic], on will power alone.”
Some respondents felt these strategies were effective (to varying degrees and under specific circumstances), but others expressed significant challenges with weight management. Of those who provided feedback on this question (n=7), 43% of people (n=3) said they were “very satisfied” or “satisfied” with the medications they take for weight management, while 29% (n=2) said they were “dissatisfied”; 29% (n=2) said they were neither “satisfied nor dissatisfied”.
With respect to antihyperglycemic treatment, 91% (n=19) of all respondents to this question (n=21) reported taking medication for their prediabetes or diabetes. Those being taken at the time of survey completion included insulin (glargine U300/other long-acting, short-acting, rapid-acting and premixed), GLP-1 receptor agonists, DPP-4 inhibitors, DPP-4 inhibitor/metformin combination, SGLT2 inhibitors and metformin. Additionally, respondents reported experience with insulin glargine, intermediate-acting insulin, TZDs and sulfonylureas. Of the 18 people who answered this question, 61% (n=11) said they were “very satisfied” or “satisfied” with their medication. Another 17% of people (n=3) expressed being “dissatisfied” or “very dissatisfied” with their medication, while 22% (n=4) were “neither satisfied nor dissatisfied”. Reported side effects of the medications included nausea, loss of appetite, atopic dyshidrasis, eczema, cheiropompholyx, constipation, diarrhea, bloating, fatigue, increased urination and yeast infections and weight gain.
Over 50% of respondents commented that their current medications were “much better” or “better” than previous treatments at meeting target fasting blood glucose levels, target levels upon waking, after meal targets and target hemoglobin A1c. The majority of respondents (50% or more) said their current medications were neither better nor worse when it came to gastrointestinal side effects (diarrhea, nausea, vomiting, abdominal pain), incidence of extreme thirst/dehydration, incidence/severity of yeast infections and incidence/severity of urinary tract infections. When it comes to weight management, 39% of respondents (n=7) said their current medications were “much better” or “better” at helping them to maintain or lose weight than previous therapies, 44% (n=8) said they were “about the same” and 17% (n=3) said they were “worse” or “much worse”.
When choosing a prediabetes or diabetes medication, respondents said it was important that the medication be affordable, discreet, without any major side effects, that it help meet hemoglobin A1c targets and prevent complications, and that it be immediately available.
People shared the following comments about what they like and dislike about their medications for prediabetes or diabetes:
“Controls appetite, hard on the stomach.”
“Helps blood sugar levels, sometimes tastes fishy.”
“I don't like medicines because I get bowel problems.”
“Doesn’t make much difference to me. It seems to regulate my sugars slightly.”
“Adding [an SGLT2] and [a GLP-1] decreased the required insulin. And helped me feel full and like my body was healing faster. When I added those meds it honestly felt like my body was functioning again for the first time in a long time. The increased urination and the increased yeast infections not great but worth it.”
“It’s affordable.”
“It’s convenient. Easy to remember.”
“I don’t like or dislike.”
Some respondents said they don’t experience any issues or barriers to accessing their medications, but others shared that they find it difficult to procure medications and adhere to their prescribed regimen because their treatments are expensive, they don’t have insurance coverage to offset the cost, they don’t have a regular doctor to manage their care, they need a specific brand of medication, they are confused by the number of medications they are taking and they have to get special authorization for coverage, which was described as a “struggle”.
Improved Outcomes
Here is input from respondents on what they desire in new treatments for prediabetes, diabetes and weight management, and improvements they’d like to see to current therapies:
“Lower cost.”
“Reversing diabetes and reversing fatty liver disease, reversing high blood pressure, reversing gastrointestinal issues.”
“Make it accessible to all obese persons.”
“Better universal screening.”
“No needles – there has to be an easier way.”
“Less injections and more oral meds. Something that doesn’t increase damage to other organs. AFFORDABILITY!!!”
“Coverage, seeing extra weight as a chronic health condition, which, when controlled prevents other health issues, saving healthcare money.”
“A cure.”
If new treatments provided the desired improvements, respondents shared how daily life and overall quality of life would be improved:
“It would have a great effect.”
“Improved overall health, physically and mentally. Prevention of potential future health issues.”
“Weight reduction helps in overall quality of life – ability to walk and exercise, easing joint problems, heart is not over burdened [sic], fatty liver can be reverses. Confidence to move in social circles.”
“Overall quality of life is improved because your body feels like it’s functioning again. Losing weights [sic] biggest impact is the social and mental well being [sic] it improves.”
“More energy and more feeling better.”
Experience With Drug Under Review
Of those who responded to the question (n=18), 1 person reported currently taking Wegovy (semaglutide injection) 2.4 mg, along with other medications. There was also 1 person who used to take it before, but not anymore. The medication was obtained through manufacturer’s sample for 2 respondents. Both people who reported experience with the drug under review said their ability to maintain or lose weight, meet target hemoglobin A1c levels and meet target blood sugar levels was “much better” on Wegovy (semaglutide injection) 2.4 mg than before. There was 1 respondent who said gastrointestinal issues (diarrhea, nausea, vomiting, abdominal pain) were “much better” on Wegovy (semaglutide injection) 2.4 mg compared to before and 1 respondent who said they were “much worse”. The respondents shared that Wegovy (semaglutide injection) 2.4 mg generally “helped a lot”, caused fewer cravings, resulted in weight loss (which was highly valued) and removed the need for insulin. One respondent said “not being on insulin is huge for me as I don’t feel like I’m on a roller coaster”.
Companion Diagnostic Test
Wegovy (semaglutide injection) 2.4 mg does not have a companion diagnostic.
Anything Else?
Overweight, obesity, prediabetes and diabetes are conditions that require intensive management. Diabetes Canada’s 2018 Clinical Practice Guidelines for the Prevention and Management of Diabetes in Canada highlight the importance of personalized care when it comes to treatment. Survey responses reinforce the message that different people require different modalities to help effectively manage their diseases. Their unique clinical profile, preferences and tolerance of therapy should direct prescribers to the most appropriate choice and combination of treatments for disease management. Health care providers must be supported in prescribing evidence-based therapies and, through public and private drug plans, patients should have access to a range of treatments that will allow them to optimize their health outcomes. For those paying out-of-pocket, costs should not be so high as to prohibit medication procurement.
While current therapies have generally led to improvement for many people, respondents hope for additional affordable agents that they can access in a timely manner and with good result to help them lead a normal life. Wegovy (semaglutide injection) 2.4 mg may help people to better manage their weight, which could potentially delay or prevent the progression of prediabetes to type 2 diabetes, improve lives and save millions in direct health care costs. For this reason, Wegovy (semaglutide injection) 2.4 mg should be an option for people living with obesity and prediabetes.
Below are some final thoughts from respondents on overweight, obesity, prediabetes and diabetes:
“There should be more help with the cost of drugs.”
“[There ought to be increased] funding for a cure or a more sustainable treatment.”
“[It is] frustrating that [treatments for other medication conditions are] covered, but not the newest and most effective medical [sic] for diabetes.”
Patient Group Conflict of Interest Declaration — Diabetes Canada
To maintain the objectivity and credibility of the CADTH reimbursement review process, all participants in the drug review processes must disclose any real, potential, or perceived conflicts of interest. This Patient Group Conflict of Interest Declaration is required for participation. Declarations made do not negate or preclude the use of the patient group input. CADTH may contact your group with further questions, as needed.
Did you receive help from outside your patient group to complete this submission? If yes, please detail the help and who provided it.
Diabetes Canada had no outside assistance to complete this submission.
Did you receive help from outside your patient group to collect or analyze data used in this submission? If yes, please detail the help and who provided it.
Diabetes Canada had no outside assistance to collect or analyze data used in this submission.
List any companies or organizations that have provided your group with financial payment over the past 2 years AND who may have direct or indirect interest in the drug under review.
Diabetes Canada receives unrestricted educational grants from, among others, manufacturers/vendors of medications, supplies, and devices for diabetes and its complications. These funds help the organization support community programs and services for people living with diabetes and contribute to research and advocacy efforts across Canada. No sponsor was involved in soliciting input for or developing the content of this submission.

Obesity Matters
"Wegovy™ Reimbursement Recommendation Review: Belief in a Brighter Future"
“It would mean the difference between being able to keep up with my children and not being able to do anything with them” (Canadian patient, March 2022).
“It would mean I could live life instead of watch it pass by” (Canadian patient, March 2022).
When you read quotes like these from people living with obesity, it is impossible not to feel the deep sense of helplessness this disease can inflict. It is impossible not to sympathize and understand that people have exhausted all options just to experience a quality of life attributed by positive health outcomes that so many take for granted every day.
These are responses to a survey conducted by Obesity Matters from March 2 to 15, 2022, where we asked our community members what it would mean to achieve sustained weight loss of at least 5 per cent, and up to the average of 15 per cent as demonstrated in Wegovy™ clinical trials.
The feedback and call to action was overwhelming from our 104 respondents, and the message from them was clear: Canadians living with obesity and overweight need evidence-based help, and CADTH should step up to ensure patients managing overweight and obesity are served by provincial drug programs in this regard by recommending that Wegovy be reimbursed. Failure to recommend reimbursement would be failure to see, hear and recognize obesity as a disease and Wegovy as offering clinically significant and socially impactful weight loss of at least 5 per cent to appropriate patients.
To reiterate, Wegovy can provide the healthy weight management – in conjunction with a reduced calorie diet and increased physical activity – to help patients who are seeking support and have been denied equitable access to health care on public health plans in Canada to-date. Now is the time that CADTH and regional governments through their drug programs in Canada stepped up and joined other countries who have made positive HTA decisions about treatments for obesity and recommend to drug plans that they should reimburse eligible patients who use this potentially life-saving medicine.
The evidence of need and treatment gap is clear with roughly 63 per cent of Canadians living with increased health risks due to excess weight and no treatments indicated for overweight or obesity currently recommended for reimbursement on regional drug plans. About 27 per cent of Canadians are classified as living with obesity, and we know the problems this disease presents to many segments of society1. We also know that obesity increases with age, calling into question why CADTH and the regional drug plans have yet to provide evidence-based obesity treatment options to the older impacted demographic that governments are mandated to help protect from a health and safety perspective.
From a health perspective, the consequences of obesity are well recognized and include increases in blood pressure, fatty liver disease, the onset of type 2 diabetes, sleep apnea, asthma, osteoarthritis, infertility, at least 13 different cancers3 and is associated with more than 200 other possible health complications4.
Obesity also puts an immense strain on Canada’s mental health crisis with studies showing significant increases in major depression, bipolar disorder and panic disorder among people who are living with obesity5,6. Anxiety, low self-esteem, body dissatisfaction and disordered eating are other mental-health related consequences of this disease7,8
And these mental and physical conditions associated with obesity do not only affect the people living with the disease, but they also end up as burdens on families as well as education, employment, economic and healthcare systems that affect everyone. 101 of 104 of our survey respondents said obesity has affected their family or relationships.
With so many severe societal ramifications, does it not make sense to do everything in our power to break this circuit at its source? Medication for diabetes, hypertension and many other obesity-related conditions are already either subsidized or covered by provincial health care plans. Funding treatments that address the co-morbidities of obesity and not funding obesity treatments is illogical, non-evidence-based, fiscally irresponsible and adds further burden to patients managing obesity. Bariatric surgery and other surgical options to address healthy weight are covered in Canada, further calling into question why evidence-based pharmacological treatments funded by regional drug plans have not yet been made available to doctors and patients in Canada.
The CADTH and Canadian government are woefully behind in this area compared to other countries as the lack of affordable treatment options compared to the number of people living with the disease has left a massive gap in treatment. Sticking with the status quo is not acceptable and further perpetuates the inequity of access to care for this patient population.
Reimbursement of obesity medications are rising across the globe with eight of the 15 countries with restricted reimbursement for obesity treatment Saxenda coming in the last two years.
Columbia, Israel and the United Kingdom in particular have progressed toward reimbursement of Saxenda9.
Wegovy is not far behind and is well on its way to public reimbursements in the UK. In fact, the National Institute for Health and Care Excellence (NICE) in the UK recently completed their HTA review of Wegovy issued draft guidance recommending semaglutide10. And yet, Canada is a laggard in its understanding of obesity and failure to reimburse evidence-based treatments.
88.46 per cent of Obesity Matters’ survey respondents listed drug costs as the number one barrier to their ability to manage a healthy weight. Drug costs were a bigger barrier for respondents than the cost of healthy food, the cost of exercise or trainers, the costs of dietitians, lack of healthcare practitioner support or even weight stigma.
Contrary to stereotypes and stigma related to people managing overweight and obesity, this patient population is not composed of people who are looking for a quick fix for aesthetic reasons – we know there are no quick fixes when it comes to managing a healthy weight and obesity. Instead, this population is seeking to maintain a healthy weight based on current science that has proven at least 5 per cent weight loss has health benefits11. In fact, 48 per cent of our survey respondents have already taken other prescription medication for obesity and are seeking evidence-based support for health purposes: these are people with real health problems, both mental and physical, who need help. These are people who want to live longer, healthier lives, reducing the chances of obesity-related comorbidities and complications.
These are people who want to participate in society, watch their children and grandchildren grow up and be able to function normally without stigma or pain.
“I want my life back. Obesity has robbed me of this. I am not a lazy slob sitting on my butt eating crap. I do not deserve to have obesity,” wrote one survey respondent. “Canada has a publicly funded healthcare system … and yet good health in Canada is treated as a privilege instead of a right for those with obesity.”
89 per cent of our survey respondents said they have had to change social or recreational plans due to managing obesity. 97 per cent said obesity has impacted their health, and 97 per cent have tried restrictive diets, exercise programs, obesity treatments, diet supplements or some other weight management solution and are still searching for a solution.
Treating obesity properly with evidence-based approaches outlined in the Canadian Obesity Guidelines, where pharmacotherapies are referenced as a first line treatment pillar, can have a significant positive impact on the quality of a patient’s life, and surely the clinical benefit and safety profile justify public payers reimbursing the product as a medically necessary treatment.
Losing weight for people living with obesity is not a simple matter of willpower because obesity is not a choice. Obesity is a chronic disease and is finally being treated as such more and more by the global medical community including the Centre for Disease Control (CDC).
With no Health Canada approved treatments covered by government drug programs in Canada, the current policies continue to perpetuate weight stigma and discrimination for people managing overweight and obesity in Canada. A similar finding related to CADTH’s positive work on exploring ways to increase its cultural competency when seeking to better address diversity and inclusion in drug decisions can be applied to the Wegovy review: Canadians managing overweight and obesity are one of the communities that have been overlooked in relation to securing supports to manage healthy weight with evidence-based treatments: “when CADTH makes recommendations without explicit consideration of these communities, CADTH may contribute to health inequalities.”12
Will the CADTH and Canadian government step up and join the rest of the world in recognizing obesity as a chronic disease and allow people to access proper health care? Or will they force millions to sit on the sideline, continue to perpetuate non-evidence-based messages about the positive long-term benefits of statistically meaningful maintained weight loss with the “eat less, move more” campaigns targeting all Canadians regardless of obesity disease state and watch life pass by?
Obesity Matters has cultivated a passionate community whose feelings can be summed up on the matter by this survey respondent:
“I fight every day for my health. I need more support. Getting COVID knocked me on my butt for two months and meant that I lost all of the exercise progress I had made and the weight gain that resulted meant my knees are making me nearly disabled again,” one community member shared with us to bring to the CADTH committee’s attention: “One bump in my journey and the fight back is almost impossible. Every moment of my life is dedicated to getting better, I can't give more than that, stop the bias and give us the safety nets/options we deserve as humans. The Obesity epidemic is most definitely a result of government choices, it's time to clean up this mess or pay a huge healthcare price in the future.”
Obesity Matters appreciates the CADTH committee’s review of our submission and video and looks forward to reviewing how Wegovy’s value to patients is addressed, ideally positively to the benefit of the currently underserved obesity patient population.
Sincerely,
Obesity Matters
Patient Point of View
It is a pleasure to present to the CADTH Submission Review Team on my perspective as a person actively managing my weight and as a patient advocate with Obesity Matters.
For most of my life, starting in my pre-teen years, I firmly believed the only way to manage my weight was to “eat less and move more”. I started dieting in my teens and took on the ideal that my weight determined my worth. If I couldn’t stick with a restrictive diet and a demanding fitness routine, then I was lazy or simply didn’t have the willpower. Sadly, as anyone who has ever gone on a diet knows, you may be able to white-knuckle your way through our obesogenic environment for a period of time but, eventually life happens and you gain back the weight… and, usually a few extra pounds too. You feel like a failure, you may turn to highly processed, highly palatable food to make you feel better and so begins the vicious cycle of yo-yo dieting.
Add to these other physical changes that happen to our body as a natural part of ageing, like hormonal changes, and the feat of reaching a healthy weight feels even more impossible.
One has to seriously question how they end up with a successful career, numerous healthy relationships with family and friends, a functioning home they like spending time in and, maybe even a happy pet they care for… yet, they can’t seem to manage their weight. Thanks to science, we now know our weight is not necessarily our fault. Your weight is highly heritable and life events, your health and your current environment play a big role in how much you weigh. It’s only when we acknowledge these facts that we can free ourselves of the diet culture shackles and take action to improve our health.
Weight management is not about arriving at some magical number on a scale. We now know carrying extra weight can predispose us to other chronic diseases like cardiovascular disease, diabetes and even some types of cancer. Sadly, we have also seen the consequences can be worse for those living in a larger body if you get COVID. Now more than ever, we, as a society, need to rise above the epidemic of Obesity and we must have a variety of evidence-based treatment options to help us get there. We know “eating less and moving more” is simply not enough.
No matter where you live in Canada or what your socio-economic status may be, you deserve these treatment options for the disease of Obesity. And, these options should be accessible and affordable.
After a lifetime of undervaluing my worth because of the weight bias and stigma that’s ramped in our culture, even in our medical care systems, I was fortunate and privileged to find the science and community I needed to reclaim my worth. I’m asking you, as the CADTH Submission review team for Wegovy, to be the catalyst for others struggling with their weight to find their path to reclaiming their health and their worth. You can do this by making evidence-based treatment options like Wegovy reimbursable and accessible for all Canadians.
Thank you for letting me share some of my story and speak on behalf of the Obesity Matters community.
Patient Group Conflict of Interest Declaration — Obesity Matters
To maintain the objectivity and credibility of the CADTH reimbursement review process, all participants in the drug review processes must disclose any real, potential, or perceived conflicts of interest. This Patient Group Conflict of Interest Declaration is required for participation. Declarations made do not negate or preclude the use of the patient group input. CADTH may contact your group with further questions, as needed.
Did you receive help from outside your patient group to complete this submission? If yes, please detail the help and who provided it.
There was no assistance from outside Obesity Matters to complete this submission.
Did you receive help from outside your patient group to collect or analyze data used in this submission? If yes, please detail the help and who provided it.
There was no help from outside Obesity Matters to collect or analyze data used in this submission.
List any companies or organizations that have provided your group with financial payment over the past 2 years AND who may have direct or indirect interest in the drug under review.
Table 3: Conflict of Interest Declaration for Obesity Matters
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
AAA Clinical Research | — | — | X | — |
Danone Canada | — | X | — | — |
Nestle Health Science | — | — | X | — |
Novo Nordisk | X | — | — | — |
Clinician Input
Centre de Médecine Métabolique de Lanaudière
About Centre de Médecine Métabolique de Lanaudière
Medical clinic, specialized in metabolic medicine, including, but not limited to, HBP, dyslipidemia, diabetes, thyroid disease, and obesity
Information Gathering
The author is specialized in the domain of obesity, member of many committees to progress the cause of obesity in Canada, diplomate of the ABOM and attends 2-3 international meetings yearly. He is well aware of the disease, its treatments, and what is coming up in the future. He also attends many advisory committees, so is aware of the publications regarding new drugs on the market, their indications and their approval by Health Canada
Current Treatments and Treatment Goals
We currently know that at least 40% of Canadian people suffer from overweight or obesity. This disease is related to many well- known complications, such as diabetes, hyperlipidemia, obstructive sleep apnea, etc., but also raises the risk of suffering of many cancers, infertility, arthrosis, etc.
We also know that even after dieting and exercising, less than 10% of patients keep a weight loss of over 10% after only a year. It is really difficult to lose and maintain weight. Also, it is well known that a minimal loss of 10% is required to help reduce the risk of many of the complications related to obesity. People suffering from obesity get caught in a vicious circle of weight loss and regain, making future weight losses even harder to achieve. They so expose themselves to an increased risk of many related diseases that have an impact on QoL, but also life expectancy. These non-pharmacological treatments are therefore very limited in their power to achieve sustainable weight losses and need to be supported by other therapies, such as drugs.
We already have an experience with other drugs such as liraglutide and naltrexone/bupropion and we see in a clinical practice how these drugs impact changes in the weight of our patients, but also help them modify their behavior, and in such, also help get better results from behavioral therapies.
Data gathered from bariatric surgery studies also show that sustained weight loss brings many advantages, such as prolonged life expectancy, better QoL, remission of certain diseases such as T2DM, obstructive sleep apnea, etc. There’s no reason to believe that results would be different from a medically obtained weight loss than from a surgically obtained weight loss.
Treatment Gaps (Unmet Needs)
Considering the treatment goals, please describe goals (needs) that are not being met by currently available treatments.
Presently, medical therapy without drugs (nutritional therapy and physical activity) gives weight loss around 5-8%, usually without any sustained result.
On the other side, bariatric surgery gives weight losses ranging 25-50%, depending on type of surgery, it is sustained in around 60% of patients, 40% of them regaining weight in the subsequent years. These results come at the expense of a surgical procedure with its related complications, both on the short and the long term (hernias, ulcers, leaks, malabsorption, malnutrition, drug and alcohol dependency, depression, suicidal risk, etc.).
Drugs clearly can fill this huge gap, many patients in the need of more than 8% weight loss, and can’t afford the risk, even minimal, of surgical complications, as out of proportion regarding their needs in weight loss. With semaglutide, we expect weight loss results in the lower range of those seen with bariatric surgeries without the risks associated to the surgery.
There’s also more and more literature regarding use of drugs after a bariatric surgery to prevent weight regain, which is another treatment gap. Often, these patients need to undergo another surgery, thus raising the risk of other complications.
Place in Therapy
How would the drug under review fit into the current treatment paradigm?
Semaglutide, being so far the most powerful drug for weight loss and with a well renowned security profile for patients, will clearly fit into the treatment algorithm and is called to replace liraglutide and naltrexone/bupropion in many patients, when its power is required. At our clinic, combining drugs (liraglutide or naltrexone/bupropion) to nutrition therapy and physical activity gives a mean of 12-15% weight loss, more than the 5-6% usually reported with the drugs in phase 3 trials. So, by comparison, with a good complete treatment, I expect (hope) to be able to reach and hopefully maintain something around 20% weight loss in a majority of patients, by using semaglutide instead of the other drugs.
Of course, to reach these goals, semaglutide will have to be used in conjunction with other therapies, such as behavioral therapy, medical nutrition therapy and physical activity.
I’m clearly aware that there’s a risk of a shift, or drift, from the patients to start to rely on the drug exclusively, without applying other therapies, as it will get easier. It will be our role, as expert leaders in the field, to make sure that both patients and the medical community will get educated on the proper use of the drug, i.e. in conjunction with other therapies. Relying only on the medication poses the risk of a weight regain after the initial weight loss, as can be seen in bariatric patients who rely only on the surgery to lose their weight.
Which patients would be best suited for treatment with the drug under review? Which patients would be least suitable for treatment with the drug under review?
Even if we are trying hard to shift the definition of obesity from a weight-centered definition to a definition more focused on the complications associated to the excess adiposity, BMI is still a practical way to help identify patients.
For my part, any patient suffering from excess adiposity with health-related complications (be it social, psychological or biological) should be considered as a potential candidate for drug therapy, in addition to the other recognized therapies. Certainly, any candidate with a BMI at or over 30 should become a candidate, but the decision shouldn’t be based only on this focus, as many patients with BMIs under 30 have obesity-related complications.
Outside BMI or the presence of obesity-related complications, there is no way to make this diagnosis, as it is made on clinical grounds only. There is an underdiagnosis, not based on the criteria, but mostly based on the fact that many clinicians don’t recognize obesity as a disease.
What outcomes are used to determine whether a patient is responding to treatment in clinical practice? How often should treatment response be assessed?
Even if so far, the definition of a clinical success is defined as a weight loss of 5% or more after 12 weeks, I think that improvement in any obesity-related disease, coupled to any weight loss, can be used as a definition of significant response, so the definition shouldn’t be restricted to numbers only. Studies have shown that weight reduction, starting at this famous 5%, leads to an improvement in many health conditions, this improvement increasing with the magnitude of weight loss. We need to consider that a majority of patients showing improvement in their health condition show weight losses consistently over 5%. Defining success based on clinical grounds rather than a % weight loss should be a good way of monitoring the response.
What factors should be considered when deciding to discontinue treatment with the drug under review?
A lack of significant improvement in health-related issues (well-being, social impacts, improvement in DM control, BP control, joint pain, walking distance (e.g. 6-minutes walk test), etc.) should be seen as a signal of non-responsiveness and the treatment should be re-evaluated to see where it fails. Given the multifaceted treatment of obesity, it will be extremely difficult to identify a single culprit to treatment failure and base the decision to discontinue the drug on it. However, if there is no response in terms of weight loss or complication improvement and the patient doesn’t follow the rest of the treatment (beside drug therapy), then drug discontinuation should be seriously considered.
What settings are appropriate for treatment with [drug under review]? Is a specialist required to diagnose, treat, and monitor patients who might receive [drug under review]?
Obesity as a disease should certainly be taken care of in a community setting and by primary care providers. Specialty clinics, such as the Centre de Médecine Métabolique de Lanaudière, will take part in this, both as care providers, but also as leaders in their region, by educating PCPs, and help them in all the learnings, identification of patients, give opinions, see patients in consultation, and help build a network of providers interested and involved in the care of patients suffering obesity. Usually, endocrinologists or internal medicine specialists are the specialists most often involved into this.
Additional Information
Nil
Conflict of Interest Declarations
To maintain the objectivity and credibility of the CADTH drug review programs, all participants in the drug review processes must disclose any real, potential, or perceived conflicts of interest. This conflict of interest declaration is required for participation.
Declarations made do not negate or preclude the use of the clinician group input. CADTH may contact your group with further questions, as needed. Please see the Procedures for CADTH Drug Reimbursement Reviews (section 6.3) for further details.
Did you receive help from outside your clinician group to complete this submission? If yes, please detail the help and who provided it.
No
Did you receive help from outside your clinician group to collect or analyze any information used in this submission? If yes, please detail the help and who provided it.
No
List any companies or organizations that have provided your group with financial payment over the past two years AND who may have direct or indirect interest in the drug under review. Please note that this is required for each clinician who contributed to the input — please add more tables as needed (copy and paste). It is preferred for all declarations to be included in a single document.
Declaration for Clinician 1
Name: Yves Robitaille
Position: Internal Medicine Specialist
Date: 18-03-2022
Table 4: Conflict of Interest Declaration for Centre de Médecine Métabolique de Lanaudière Clinician 1
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
NovoNordisk | — | — | X | — |
Bausch Health | X | — | — | — |
Declaration for Clinician 2
Name: Silvia Raluca Netedu
Position: Endocrinologist
Date: 18-03-2022
Table 5: Conflict of Interest Declaration for Centre de Médecine Métabolique de Lanaudière Clinician 2
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
NovoNordisk | X | — | — | — |
Calgary Weight Management Centre
About the Calgary Weight Management Centre
Founded in 2008, Calgary Weight Management Centre (CWMC) is a community-based organization that serves individuals living with overweight and obesity in Calgary and surrounding areas. At the time of inception, there were very few resources available that provided trusted and evidence-based support for this population. Many of these individuals have lived for many years with weight related metabolic and mental health comorbidity and poor quality of lives.
The team at CWMC consists of a variety of clinicians, including physicians, nutrition experts, psychologists and nurses. Most patients that attend the centre are referred either from their primary care provider or from their specialist provider, reflecting trust by the healthcare community in the region.
One of the foundational objectives at CWMC has been to provide a safe, non-judgemental and trustworthy environment where individuals living with obesity can receive credible, thorough and evidence-based assessments and advice. The overarching goal is to enhance the physical health and quality of life of people who are trying to manage their weight through the provision of an assortment of services.
Calgary Weight Management Centre website: www.cwmc.ca
Information Gathering
Information was gathered through a combination of discussion with expert colleagues and with patients, as well as a review of up-to-date literature. This includes a review of:
Canadian Adult Obesity Clinical Practice Guidelines https://obesitycanada.ca/guidelines/chapters/.
Once-Weekly Semaglutide in Adults with Overweight or Obesity. N Engl J Med 2021; 384:989-1002. DOI: 10.1056/NEJMoa2032183
Semaglutide 2·4 mg once a week in adults with overweight or obesity, and type 2 diabetes (STEP 2): a randomised, double-blind, double-dummy, placebo-controlled, phase 3 trial. The Lancet (British edition), 2021-03-13, Vol.397 (10278), p.971. https://doi.org/10.1016/S0140-6736(21)00213-0
Semaglutide 2.4 mg for the Treatment of Obesity: Key Elements of the STEP Trials 1 to 5. Obesity | VOLUME 28 | NUMBER 6 | JUNE 2020
Current Treatments
According to the new 2020 Canadian Adult Obesity Guidelines, health behaviour modification is fundamental in the treatment of obesity, as it is with other chronic diseases. This includes optimization of eating patterns, regular physical activity, and support with stress and time management as well as with sleep hygiene. Unfortunately, health behaviour modification produces only modest weight reduction after 1 year, and even this is difficult to maintain in the long term.
Like other chronic diseases, these health behaviours should be supported with concurrent interventions such as medications and, in some cases, surgery. This type of strategy encourages early intervention to slow down the progression of obesity.
Pharmacological interventions that are currently approved in Canada and commercially available for use as an adjunct to health behaviour interventions include Xenical (orlistat), liraglutide 3.0 (Saxenda), and naltrexone/bupropion (Contrave). The latter of these two medications target the brain regions involved in appetite, cravings and weight regulation. Bariatric surgery is an excellent too, but access to this treatment is very limited.
Treatment Goals
Clinical trials have demonstrated that semaglutide 2.4 mg weekly (ie. Wegovy) is a safe and effective adjunct to health behaviour modification in the treatment of obesity. It has been shown to reduce baseline body weight by about 17% after 1 year of treatment. It has also been shown to improve glycemic control and lipid profile, as well as health related quality of life. It has also been shown to reduce blood pressure. At 1.0 mg weekly, semaglutide is associated with cardiovascular benefit in individuals with T2DM.
Treatment Gaps (Unmet Needs)
Considering the treatment goals, please describe goals (needs) that are not being met by currently available treatments.
In 2016 the prevalence of obesity (BMI >=30) in the adult population was around 26%. An additional 34% of the adult population were in the overweight category (BMI>=25). The World Obesity Atlas 2022 (re: https://www.worldobesity.org/resources/resource-library/world-obesity-atlas-2022), published by the World Obesity Federation, predicts that by 2022, the prevalence of obesity in Canadian adults will be closer to 39%.
Currently approved and available obesity pharmacotherapy (Xenical, Saxenda, Contrave) produce on average 8-10% weight reduction at 1 year. Many patients do not respond to these medications or are unable to tolerate them due to side effects. Xenical is to be taken 3 times daily, and it is associated with significant side GI effects, making long term compliance difficult. Contrave can be associated with elevated blood pressure in some individuals, so it is not an appropriate option for several people with obesity. Saxenda is a once daily injectable, which can be a barrier to some individuals with needle phobia.
In 2020, less than 1% of Canadian adults living with obesity were receiving obesity pharmacotherapy, in part due to limited access to these medications. This reflects a significant unmet need. Wegovy offers a safe and very effective option to support physicians and patients in the management of obesity. It appears to be better tolerated that the other obesity pharmacotherapy that are available. It is also a once weekly injectable medication, making compliance easier.
Which patients have the greatest unmet need for an intervention such as the drug under review?
Severe mental health comorbidities
Lower socioeconomic status
Place in Therapy
How would the drug under review fit into the current treatment paradigm?
Wegovy produces weight reduction through its activity in the arcuate nucleus of hypothalamus. This is the part of the brain that is involved in appetite control and weight regulation. As a GLP-1 receptor agonist, Wegovy produces a feeling of early and prolonged satiety, thereby reducing food intake and ultimately reducing weight. Because it works on the underlying biology involved in appetite, it should be used early on as an adjunct to health behaviour modification in the treatment paradigm for anyone with overweight and obesity.
The results from the clinical trials have been profound in terms of weight loss, and therefore it has a great potential a first line option for early intervention to slow down the progression of obesity and its comorbidities.
Please indicate whether or not it would be appropriate to recommend that patients try other treatments before initiating treatment with the drug under review. Please provide a rationale from your perspective.
Like type 2 diabetes, the natural history of obesity is to worsen/progress over time. Therefore, our recommendation that this medication be offered to patients early to slow down progression. Of all approved pharmacotherapies, it offers the most profound effect on weight.
How would this drug affect the sequencing of therapies for the target condition?
It is our recommendation that this medication be offered as a first line pharmacotherapy in the management of obesity. Of all approved options, it has the greatest potential to slow down the progression of obesity and weight related comorbidities.
Which patients would be best suited for treatment with the drug under review?
Patients who would be best suited for treatment with Wegovy include those with a BMI:
30 kg/m2 or greater (obesity), or
27 kg/m2 or greater (overweight) in the presence of at least one weight-related comorbidity such as hypertension, type 2 diabetes mellitus, dyslipidemia, or obstructive sleep apnea
How would patients best suited for treatment with the drug under review be identified?
Patients would be identified by a measurement of their BMI, which is a simple calculation of an individual’s weight relative to their height. It would also be prudent to identify any weight related comorbidities as this would further support intervention with Wegovy.
Which patients would be least suitable for treatment with the drug under review?
Patients not eligible for this medication include those who:
Have a personal history or family history (1st degree relative) of medullary thyroid carcinoma or multiple endocrine neoplasia type 2
Are pregnancy or breastfeeding
Are currently struggling with anorexia nervosa or bulimia nervosa
Is it possible to identify those patients who are most likely to exhibit a response to treatment with the drug under review?
At this time, we are unable to predict which patients will respond to any intervention for the management of obesity, or to what degree.
That said, in the STEP 1 trial, which was a study of semaglutide 2.4 mg SC weekly in individuals with a BMI >=27 with a weight related comorbidity or >=30, roughly 9/10 participants achieved at least 5% of their baseline body weight. This is clinically meaningful weight loss as it is associated with health benefit.
What outcomes are used to determine whether a patient is responding to treatment in clinical practice?
The outcomes used in clinical practice to determine whether a patient is responding to treatment are aligned with those used in clinical trials.
Weight
Blood Pressure
Glycemic Control
Lipids
Quality of Life
Weight related comorbidity
What would be considered a clinically meaningful response to treatment?
The following would be considered a clinically meaningful response to treatment.
At least 5% weight reduction
Improvement in health-related quality of life, physical functioning, sexual health
Reduction in WC (visceral adiposity)
Reduction in BP, discontinuation of BP medications
Improvement in glycemic control – reduction of medications needed to control blood sugars
Slowdown in progression of prediabetes to T2DM
Improvement in lipid profile
Improvement in CV risk
Slowdown of obesity progression
How often should treatment response be assessed?
Clinical judgement is important here. Initially as the patient is titrating up to the highest effective and tolerated dose, treatment response could be monitored more frequently to assess tolerability. Once the desired dose has been achieved, surveillance can occur every 3 months or as dictated by other factors in the patient profile.
What factors should be considered when deciding to discontinue treatment?
The circumstances under which this medication should be discontinued include the following:
Patient is unable to tolerate Wegovy
Lack of response to the Wegovy: ie. has not achieved clinically meaningful weight loss or weight maintenance after 3 months on maximum tolerated dose
Patient continues to gain weight on Wegovy at the same rate as when off the medication.
Patient becomes pregnant
Patient develops pancreatitis
What settings are appropriate for treatment with the drug under review?
Community setting and specialty clinics (endocrinology, internal medicine, etc)
For non-oncology drugs, is a specialist required to diagnose, treat, and monitor patients who might receive the drug under review?
Obesity is a chronic disease that requires long term treatment. As such, it can be managed at the level of primary care. A specialist is not required to diagnose, treat or monitor patients who might receive semaglutide. Diagnosis, treatment and surveillance can be done at the level of primary care.
Additional Information
Please review STEP 1 trial results for further information on health benefits.
Conflict of Interest Declarations
To maintain the objectivity and credibility of the CADTH drug review programs, all participants in the drug review processes must disclose any real, potential, or perceived conflicts of interest. This conflict of interest declaration is required for participation. Declarations made do not negate or preclude the use of the clinician group input. CADTH may contact your group with further questions, as needed. Please see the Procedures for CADTH Drug Reimbursement Reviews (section 6.3) for further details.
Did you receive help from outside your clinician group to complete this submission? If yes, please detail the help and who provided it.
No assistance received
Did you receive help from outside your clinician group to collect or analyze any information used in this submission? If yes, please detail the help and who provided it.
No assistance received
List any companies or organizations that have provided your group with financial payment over the past two years AND who may have direct or indirect interest in the drug under review. Please note that this is required for each clinician who contributed to the input — please add more tables as needed (copy and paste). It is preferred for all declarations to be included in a single document.
Declaration for Clinician 1
Name: Dr. Shahebina Walji
Position: MD, CCFP, Diplomate American Board of Obesity Medicine; Assistant Clinical Professor, University of Calgary, Department of Family Medicine; Medical Director, Calgary Weight Management Centre
Date: 12-March-2022
Table 6: Conflict of Interest Declaration for Calgary Weight Management Centre Clinician 1
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
Bausch Health | — | — | X | — |
Novo Nordis | — | — | X | — |
Takeda | — | X | — | — |
Declaration for Clinician 2
Name: Dr. Clinton Logan
Position: MD
Date: 12-March-2022
Table 7: Conflict of Interest Declaration for Calgary Weight Management Centre Clinician 2
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
N/A | — | — | — | — |
Obesity Canada — Obésité Canada and the Canadian Association of Bariatric Physicians and Surgeons
About Obesity Canada — Obésité Canada and the Canadian Association of Bariatric Physicians and Surgeons
Obesity Canada — Obésité Canada (OC), a national registered charity association for healthcare professionals, researchers and policy makers working in obesity prevention and treatment and for Canadians living with obesity, coordinated the group clinician response. Obesity Canada’s mission is to improve the lives of Canadians living with obesity through research, education and advocacy. This includes improving access to all evidence-based obesity treatments.
For more information about Obesity Canada, please visit obesitycanada.ca
The Canadian Association of Bariatric Physicians and Surgeons (CABPS) represents Canadian specialists interested in the treatment of obesity and severe obesity for the purposes of professional development as well as coordination and promotion of common goals.
For more information about the Canadian Association of Bariatric Physicians and Surgeons, please visit cabps.ca
Information Gathering
Obesity Canada engaged clinicians through direct email requests and an open call for clinician contributors through OC Connect Pro, an online professional community. (obesity.timedright.ca/)
Clinicians provided responses to the templated questions in the submissions based on research results, clinical experience and their understanding of patient needs and challenges.
Current Treatments and Treatment Goals
Obesity is now recognized as a chronic disease by the Canadian Medical Association, and most medical organizations globally, including the WHO. In 2020, the updated evidence-informed Canadian Adult Obesity Clinical Practice Guidelines define obesity as “a chronic relapsing disease characterized by abnormal and/or excessive adipose tissue that impairs health”. Currently, more than 8.3 million adults and about 25-30% of Canadian children and youth live with obesity and may require medical support to manage their disease. Approximately (26.4%) 8 million Canadians have a body mass index (BMI) ≥30 kg/m2 or 1 in 3 Canadians. While obesity is recognized as a chronic disease, obesity management is not included in any provincial, territorial or federal chronic disease strategies. As outlined in the 2020 Canadian Adult Obesity Clinical Practice Guidelines, lifestyle interventions through healthy calorie-reduced diets and increased physical activity remain as the cornerstone of obesity management. It requires long-term support by the three pillars of evidence-based obesity management including: 1) Psychological & Behavioral therapy 2) Pharmacotherapy 3) Surgery. Many individuals living with obesity, who rely on diet and exercise only, have difficulty sustaining their efforts and finding a program that suits their needs, which can lead to yo-yo dieting. The weight regain is due mainly to hormonal and metabolic adaptation following weight loss, but nonetheless, it can lead to disappointment and a feeling of hopelessness, worsening obesity, and obesity related complications. Importantly, a meta-analysis of weight-loss clinical trials using calorie-reduced diets, exercise, or both, showed only modest ~3 kg body weight loss (Peirson L, et al. CMAJ Open 2014;2:E306-317 (DOI:10.9778/cmajo.20140012), which is often inadequate to improve obesity-related medical complications, such as type 2 diabetes and non-alcoholic fatty liver disease. This underscores the importance of the three pillars of obesity management, and especially pharmacotherapy. Managing obesity in our patients requires a multimodal chronic disease approach and access to appropriate existing pharmacotherapy. Unmanaged overweight and obesity leads to obesity related complications, such as type II diabetes, hypertension, osteoarthritis, cancer, and NAFLD. These complications do not only apply a significant burden to our healthcare system, the personal toll and quality of life is significantly affected in persons with obesity. Canadians are currently presented with “weight loss” programs that unfortunately are not rooted in the current available evidence-based approach. Many feel trapped in an endless cycle of multiple restrictive diet programs that ultimately are unsustainable. Even though we know that obesity is a neuroendocrine pathology that results in complex multisystemic disease, the main treatment modality that seems to be advocated for is “Eat less, Move more.” The evidence clearly does not support this as being an effective management. Unfortunately, this treatment advice often unfairly assumes or stereotypes people with obesity to be lazy, unmotivated, lacking willpower and contributes to the stigma of obesity.
The current treatment paradigm for the chronic disease of obesity consists of:
Hospital based Bariatric Centers
Bariatric Centers of Excellence/Regional Assessment & Treatment Centres (BCOE/RATC)
Adult Bariatric Specialty Clinics
Pediatric Bariatric/Obesity Programs
All offer: multidisciplinary support, medical nutrition therapy, activity prescription, psychological and behavioural, pharmacotherapy and surgical interventions
Private Bariatric Medicine Centers
Offer various support from multidisciplinary support, MNT, activity, psychological support and pharmacotherapy interventions.
Private Pay
Nonmedical Weight Loss clinics
These types of clinics may or may not be commercial weight-loss/ diet programs and typically do not have multidisciplinary or regulated health professional support and may or may not provide evidence-based care
Community Obesity management Clinics / Bariatric Medicine Centers
A systematic review of obesity management in primary care showed that improvements in clinically relevant health outcomes could be achieved by multi-component interventions that are delivered over the longer term by an interdisciplinary health team. The substantial impact of treating obesity in controlling and, in some cases, improving a wide range of clinical conditions including osteoarthritis, diabetes, sleep apnea, hypertension, urinary incontinence and even infertility has also been well demonstrated in recent research.
Health Canada has approved four medications for the treatment of obesity in adults in Canada – orlistat 120 mg (Xenical®), liraglutide 3.0 mg (Saxenda®), naltrexone-bupropion (Contrave), and Semaglutide (Wegovy). Of these medications, Saxenda, Wegovy and Contrave target the neuro endocrine pathology associated with obesity and have become a mainstay in the medical management of obesity. Semaglutide (Wegovy) has been approved by Health Canada in November of 2021 for obesity management. Unfortunately, the product Wegovy is not currently available in Canada and Ozempic is being used off-label in the management of obesity. Canadians obtain prescription drug coverage through a patchwork of public insurance, private benefit plans, and out-of-pocket payments. Based on CADTH prior review of Saxenda and Contrave, most provinces and public insurance policies do not cover anti-obesity medications, leaving a significant treatment gap in vulnerable populations that are at high risk of morbidity and mortality from the disease of obesity.
Treatment Goals
As one of the leading causes of type 2 diabetes, hypertension, arthritis, cancer and other important health problems, obesity can have serious impacts on those who live with it. An estimated 1 in 10 premature deaths among Canadian adults aged 20 to 64 is directly attributable to obesity.
Ideal treatment (with early diagnosis) would:
Improve or resolve obesity related complications including type 2 diabetes, hypertension, obstructive sleep apnea and osteoarthritis.
Provide an evidence-based option/adjuvant for effective treatment along with medical nutrition, behavioral management, thus reducing the need for surgical interventions.
Reduce the burden of increasing chronic disease on the Canadian health care system
Treatment Gaps (Unmet Needs)
Considering the treatment goals, please describe goals (needs) that are not being met by currently available treatments.
In Canada, accessibility of evidence-based effective obesity treatments is abysmal. Wait times for bariatric surgery are extremely poor (according to the 2019 Obesity Canada Report Card on Access to Obesity Treatment for Adults in Canada, surgery times can vary pre-covid from 8 months to 106 months. Individuals living with obesity have limited access to multidisciplinary health teams - healthcare professionals with training in obesity management or who are obesity focused, cognitive behavioral therapy, medical nutrition therapy and psychotherapy are also very limited. When it comes to the few obesity medications available in Canada, very few Canadians have coverage through either public or private drug plans. Current evidence suggests that the effectiveness of Wegovy is getting close to the effectiveness seen with bariatric surgery (the categorical weight loss of ⅓ of study participants reached above 20% weight loss.)
Which patients have the greatest unmet need for an intervention such as the drug under review?
Patients who have the greatest need for this medication would be those who have established obesity and obesity-related complications. Also, patients who are denied access to medical or surgical procedures due to their obesity, such as surgical management for certain orthopedic procedures and certain fertility related treatments. Over a quarter of the Canadian population including children have overweight or obesity and that number continues to increase, therefore this is not considered a niche population. On the contrary, this medication would have a mainstream use in the Canadian population. This would also be an effective option early treatment and prevention for patients who have overweight and a family history of obesity and obesity related complications
Place in Therapy
How would the drug under review fit into the current treatment paradigm?
Health Canada has approved four three medications for the treatment of obesity in adults in Canada: orlistat 120 mg (Xenical®), liraglutide 3.0 mg (Saxenda®), naltrexone-bupropion (Contrave), and semaglutide (Wegovy). Of these medications, Saxenda, Wegovy and Contrave target the neuroendocrine pathology associated with obesity and have become a mainstay in the medical management of obesity in the bariatric medicine clinics. Semaglutide (Wegovy) has been approved by Health Canada in November of 2021 for obesity management. Unfortunately, the product Wegovy is not currently available in Canada and Ozempic is currently being used for obesity management by bariatric medical and surgical specialists off-label in the management of obesity.
Is the drug under review the first treatment approved that will address the underlying disease process rather than being a symptomatic management therapy?
Semaglutide is the third treatment approved that addresses the underlying disease process, however it would be the first once weekly dosing available for patients who prefer this convenience or for those who are needle averse. Evidence also suggests that comparatively Semaglutide would have improved outcomes. The once weekly dose may increase compliance.
Would the drug under review be used as a first-line treatment, in combination with other treatments, or as a later (or last) line of treatment?
The medication could be used as both a first line treatment, and in combination with other treatments such as medical nutritional management, behavioral therapy, and surgical management.
Semaglutide can be used at any point including following surgical management. After surgery Semaglutide would be considered in the setting of weight regain (also known as weight recidivism, can include various definitions here as there are many) and appetite resurgence related to the chronic nature of the neuroendocrine pathology.
Would the drug under review be reserved for patients who are intolerant to other treatments or in whom other treatments are contraindicated?
Semaglutide could be used as a first line treatment as well as an integral part of a multimodal treatment plan, where Semaglutide is added to previously implemented nutritional and behavioral management. It could also be implemented pre or post bariatric surgical implementation. In terms of “failure” of the medication: if a patient has an intolerance to the medication or the medication has not been effective then this would be discontinued. At this point any other medications available could potentially be trialed, along with further nutritional and behavioral management, and/or surgical intervention.
Is the drug under review expected to cause a shift in the current treatment paradigm?
Semaglutide is expected to shift the current treatment paradigm as the current studies (would need to add a link here) show that it would be the most efficacious pharmacological treatment available at the moment, leading to double-digit percentage body weight loss, approaching that achieved by bariatric surgery. It may potentially reduce the number of patients that would require surgical bariatric interventions and may also help prevent weight regain post bariatric surgery.
Please indicate whether or not it would be appropriate to recommend that patients try other treatments before initiating treatment with drug under review. Please provide a rationale for your perspective.
This medication could be started as a first line in addition to medical nutritional and behavioral therapy. However, since obesity is a complex neuroendocrine disease, nutritional and behavioral management alone often may not be sufficient interventions in management. Therefore, initiating semaglutide would not be bound to a success or failure of recommended interventions and could be used as a stand-alone first line treatment.
Which patients would be best suited for treatment with the drug under review? Which patients would be least suitable for treatment with the drug under review?
Is it possible to identify those patients who are most likely to exhibit a response to treatment with drug under review?
Patients best suited to this medication would have been diagnosed with overweight or obesity, with or without the complications. Patients who are in most need for intervention are those that have established obesity and disease related complications that are affecting quality of life and would benefit from reduction in weight. Patients who have established disease and have not yet developed complications from obesity would also greatly benefit from intervention at this stage as this will prevent obesity related complications that generally would be chronic in nature. Please refer to Edmonton Obesity Staging System for information on disease staging.
Patients best suited for this treatment intervention would be identified primarily through visits to their physicians/ allied health professionals or via self identification. Diagnostic tools are available for objective diagnosis including body mass index (BMI), waist circumference, and where appropriate disease-staging systems such as the Edmonton Obesity Staging system.
The Edmonton Obesity Staging system is a validated tool to assess the disease of obesity allowing a clinician to not only classify a patient based on their body mass index but also the degree of associated conditions such as type 2 diabetes, impaired mobility, or psychologic distress.
Issues related to diagnosis and underdiagnosis include:
Weight bias (both from the health care professional and the patients themselves),
Inadequate professional training in diagnosing and managing obesity at all stages (undergraduate, post-graduate and continuing professional education),
Access to bariatric medical and surgical specialist physicians
Lack of available medical treatment options
Patients who are pre symptomatic (Patients who do not have diagnosed obesity currently but do have overweight and a consistent weight increase or are at high risk for obesity related complications) could consider this treatment.
Early and strong responders exist to all antiobesity medications, including semaglutide. To date there are no methods of identifying the patients that will most likely respond or respond most strongly. Stopping rules apply to both liraglutide 3.0 mg (Saxenda) and naltrexone-bupropion (Contrave) to assist primary care providers to discontinue medications due to lack of efficacy. There is no stopping rule for semaglutide as a majority of individuals respond to semaglutide treatment. With semaglutide treatment approximately 92% of patients will lose 5% or great of their total body weight at 12 months, 75% of patients will lose 10% or more of their total body weight at 12 months. In a two-year trial, 2 out 3 patients lost greater than or equal to 10% total body weight loss.
Which patients would be least suitable for treatment with the drug under review?
Patients that would be least suited to this medication would be those who have had adverse responses to previous attempts of trialing semaglutide.
Patients who have needle phobia
Patients who are not able to self administer medication (due to any cause), or whose caregivers are not able to administer the medication
Patients who have absolute contraindications to the medication
What outcomes are used to determine whether a patient is responding to treatment in clinical practice? How often should treatment response be assessed?
Currently, clinical outcomes that are considered positive or successful in clinical practice are aligned with the outcomes used in clinical trials. Clinical trials use percentage weight loss and categorical weight loss as a primary outcome. Secondary outcomes include cardiometabolic parameters, such as the resolution of prediabetes and the improvement in lipids and blood pressure.
Treatment response should be assessed periodically after initiation of medication. This could vary from clinician to clinician and patient to patient. Response can be measured every four to 6 weeks initially and then shift to every 3 months. These numbers will vary depending on patient and clinician preference.
A clinically meaningful response to treatment would include
5% reduction in total body weight in 3 months on the maximum therapeutic dose of 2.4 mg weekly
Improvements in laboratory markers of obesity related complications such as fasting glucose, hemoglobin A1c, and elevated triglycerides.
Reduction in pain scores for osteoarthritis
Improvement in general quality of life
Improvement in mobility
Reduction in obesity associated conditions such as sleep apnea, high blood pressure, and fatty liver.
Weight stability in those patients who would otherwise have continued upward weight trajectory
Ability to move forward with greater safety for a procedure such as a hip replacement.
What factors should be considered when deciding to discontinue treatment with the drug under review?
The decision to discontinue treatment would be considered if
There has not been a meaningful response to the treatment as described above IN POINT 6.10
The patient has an intolerance to the medications of has experienced side effects that are intolerable that are not improving over time with appropriate countermeasures
There is a more effective treatment available in the future that required the discontinuation of current medication
The medication becomes unaffordable for the patient to continue.
What settings are appropriate for treatment with [drug under review]? Is a specialist required to diagnose, treat, and monitor patients who might receive [drug under review]?
It would be appropriate you use this treatment while under review in the following settings
Community based obesity management programs or bariatric medicine clinics
Family medicine or primary care clinics
Hospital based bariatric medical and surgical centers
A physician who has training in obesity management in any specialty should be comfortable in the diagnosis, treatment, and monitoring of obesity.
Additional Information
Obesity is a chronic relapsing disease just like hypertension or diabetes and should be treated as such. This means that patients who achieved weight loss with semaglutide treatment should continue with its treatment, similar to that of diabetes management. Patients with diabetes who have achieved desirable, or goal glycemic control are advised to continue with pharmacotherapy. A similar paradigm should also apply to treatment of obesity as it is a chronic relapsing disease.
Conflict of Interest Declarations
To maintain the objectivity and credibility of the CADTH drug review programs, all participants in the drug review processes must disclose any real, potential, or perceived conflicts of interest. This conflict of interest declaration is required for participation. Declarations made do not negate or preclude the use of the clinician group input. CADTH may contact your group with further questions, as needed. Please see the Procedures for CADTH Drug Reimbursement Reviews (section 6.3) for further details.
Did you receive help from outside your clinician group to complete this submission? If yes, please detail the help and who provided it.
No.
Did you receive help from outside your clinician group to collect or analyze any information used in this submission? If yes, please detail the help and who provided it.
No.
List any companies or organizations that have provided your group with financial payment over the past two years AND who may have direct or indirect interest in the drug under review. Please note that this is required for each clinician who contributed to the input — please add more tables as needed (copy and paste). It is preferred for all declarations to be included in a single document.
Declaration for Clinician 1
Name: Dr. Tasneem Sajwani
Position: Family Medicine Physician
Date: February 21, 2022
Table 8: Conflict of Interest Declaration for Obesity Canada — Obésité Canada and the Canadian Association of Bariatric Physicians and Surgeons Clinician 1
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
Novo Nordisk (speaking fees) | X | — | — | — |
Bausch | X | — | — | — |
Declaration for Clinician 2
Name: David C W Lau, MD, PhD, FRCPC
Position: Professor of Medicine, University of Calgary Cumming School of Medicine
Table 9: Conflict of Interest Declaration for Obesity Canada — Obésité Canada and the Canadian Association of Bariatric Physicians and Surgeons Clinician 2
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
Novo Nordisk | X | — | — | — |
Bayer | X | — | — | — |
HLS Therapeutics | X | — | — | — |
BI | X | — | — | — |
CCRN | X | — | — | — |
CME at Sea | X | — | — | — |
Eli Lilly | X | — | — | — |
Novartis | X | — | — | — |
Pfizer | X | — | — | — |
Viatris | X | — | — | — |
Pfizer | X | — | — | — |
Declaration for Clinician 3
Name: Stephen Glazer
Position: Physician
Date: 20/02/2022
Table 10: Conflict of Interest Declaration for Obesity Canada — Obésité Canada and the Canadian Association of Bariatric Physicians and Surgeons Clinician 3
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
Novo Nordisk | X | — | — | — |
Bausch | X | — | — | — |
Declaration for Clinician 4
Name: David Macklin
Position: Medical Director Medcan weight management program/Lecturer U of T
Date: 18th February 2022
Table 11: Conflict of Interest Declaration for Obesity Canada — Obésité Canada and the Canadian Association of Bariatric Physicians and Surgeons Clinician 4
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
Novo Nordisk | — | — | — | X |
Declaration for Clinician 5
Name: Mary Forhan
Position: Scientific Director, Obesity Canada
Date: 22/02/2022
Table 12: Conflict of Interest Declaration for Obesity Canada — Obésité Canada and the Canadian Association of Bariatric Physicians and Surgeons Clinician 5
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
Novo Nordisk | X | — | — | — |
Declaration for Clinician 6
Name: Yvonne B. Kangong
Position: Family / Obesity Dr.
Date: March 27, 2022
Table 13: Conflict of Interest Declaration for Obesity Canada — Obésité Canada and the Canadian Association of Bariatric Physicians and Surgeons Clinician 6
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
Novo Nordisk | X | — | — | — |
Bausch | X | — | — | — |
Declaration for Clinician 7
Name: Sabrina Kwon
Position: Physician - Diplomate ABOM, Assistant Clinical Professor U of A
Date: March 30, 2022
Table 14: Conflict of Interest Declaration for Obesity Canada — Obésité Canada and the Canadian Association of Bariatric Physicians and Surgeons Clinician 7
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
Novo Nordisk | — | X | — | — |
Bausch | X | — | — | — |
Declaration for Clinician 8
Name: Rachel Capron
Position: Registered Dietitian, CDE CBE
Date: March 30, 2022
Table 15: Conflict of Interest Declaration for Obesity Canada — Obésité Canada and the Canadian Association of Bariatric Physicians and Surgeons Clinician 8
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
Novo Nordisk | X | — | — | — |
Bausch | — | — | — | — |
Declaration for Clinician 9
Name: Ryan Oughtred
Position: Licensed Naturopathic Doctor in BC, CNPBC#00466
Date: March 30, 2022
Table 16: Conflict of Interest Declaration for Obesity Canada — Obésité Canada and the Canadian Association of Bariatric Physicians and Surgeons Clinician 9
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
No COI | — | — | — | — |
Declaration for Clinician 10
Name: Sean Wharton
Position: Internal Medicine Physician at Hamilton Health Sciences, Medical Director Wharton Medical Clinic - Obesity and Diabetes Management Clinic
Date: March 30, 2022
Table 17: Conflict of Interest Declaration for Obesity Canada — Obésité Canada and the Canadian Association of Bariatric Physicians and Surgeons Clinician 10
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
Novo Nordisk | — | — | X | — |
Bausch | — | — | X | — |
Eli Lilly | — | X | — | — |
Declaration for Clinician 11
Name: Andrea Milne-Epp
Position: Family Physician, CCFP, ABOM, Clinical Associate Professor University of Alberta
Date: March 31, 2022
Table 18: Conflict of Interest Declaration for Obesity Canada — Obésité Canada and the Canadian Association of Bariatric Physicians and Surgeons Clinician 11
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
No COI | — | — | — | — |
Declaration for Clinician 12
Name: Michael Mindrum, MD, FRCPC
Position: Internal Medicine Physician
Date: March 31, 2022
Table 19: Conflict of Interest Declaration for Obesity Canada — Obésité Canada and the Canadian Association of Bariatric Physicians and Surgeons Clinician 12
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
Novo Nordisk | — | — | X | — |
Declaration 13
Name: Obesity Canada
Position: n/a
Date: March 31, 2022
Table 20: Conflict of Interest Declaration for Obesity Canada — Obésité Canada
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
Novo Nordisk | — | — | — | X |
Bausch | — | — | X | — |
Nestle Health Science | — | — | X | — |
TOPS | — | — | X | — |
Craving Change | X | — | — | — |
WW | — | — | X | — |
Desjardins Insurance | — | — | X | — |
Johnson & Johnson | — | — | X | — |
Medtronic | — | — | — | X |
International Medical Press | — | — | X | — |
Declaration 14
Name: Canadian Association for Bariatric Physicians & Surgeons
Position: n/a
Date: March 31, 2022
Table 21: Conflict of Interest Declaration for Canadian Association for Bariatric Physicians and Surgeons
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
Novo Nordisk | — | — | X | — |
Bausch | — | — | X | — |
Nestle Health Science | — | — | X | — |
Pfizer | X | — | — | |
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up-to-date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
Redactions: Confidential information in this document may be redacted at the request of the sponsor in accordance with the CADTH Drug Reimbursement Review Confidentiality Guidelines
Stakeholder Input: The views expressed in each submission are those of the submitting organization or individual; not necessarily the views of CADTH or of other organizations. As such, they are independent of CADTH and do not necessarily represent or reflect the view of CADTH. No endorsement by CADTH is intended or should be inferred. By filing with CADTH, the submitting organization or individual agrees to the full disclosure of the information. CADTH does not edit the content of the submissions.
CADTH does use reasonable care to prevent disclosure of personal information in posted material; however, it is ultimately the submitter’s responsibility to ensure no identifying personal information or personal health information is included in the submission. The name of the submitting organization or individual and all conflict of interest information are included in the submission; however, the name of the author, including the name of an individual patient or caregiver submitting the patient input, are not posted.
Accessibility: CADTH is committed to treating people with disabilities in a way that respects their dignity and independence, supports them in accessing material in a timely manner, and provides a robust feedback process to support continuous improvement. All materials prepared by CADTH are available in an accessible format. Where materials provided to CADTH by a submitting organization or individual are not available in an accessible format, CADTH will provide a summary document upon request. More details on CADTH’s accessibility policies can be found here.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.