CADTH Reimbursement Review
Berotralstat (Orladeyo)
Sponsor: BioCryst Pharmaceuticals Inc.
Therapeutic area: Hereditary angioedema (HAE)
This multi-part report includes:
Clinical Review
Pharmacoeconomic Review
Stakeholder Input
Clinical Review
Abbreviations
AE-QoL
Angioedema Quality of Life
C1-INH
complement 1 esterase inhibitor
C4
complement 4
CI
confidence interval
EQ-5D-5L
5-Level EQ-5D
EQ VAS
EQ visual analogue scale
HAE
hereditary angioedema
HAEC
Hereditary Angioedema Canada
HRQoL
health-related quality of life
ITC
indirect treatment comparison
ITT
intention-to-treat population
LS
least squares
LTP
long-term prophylactic
MCS
mental component summary
MID
minimal important difference
PCS
physical component summary
RCT
randomized controlled trial
SC
subcutaneous
SD
standard deviation
SE
standard error
SF-36
Short Form (36) Health Survey
Executive Summary
An overview of the submission details for the drug under review is provided in Table 1.
Item | Description |
|---|---|
Drug product | Berotralstat (Orladeyo), 150 mg oral capsule |
Indication | For routine prevention of episodes of hereditary angioedema in adults and pediatric patients aged 12 years and older |
Reimbursement request | As per indication |
Health Canada approval status | NOC |
Health Canada review pathway | Standard |
NOC date | June 2, 2022 |
Sponsor | BioCryst Pharmaceuticals Inc. |
NOC = Notice of Compliance.
Introduction
Hereditary angioedema (HAE) is a rare autosomal-dominant disorder characterized by recurrent episodes of nonpruritic subcutaneous or submucosal edema, most commonly affecting the skin (cutaneous attacks), gastrointestinal tract (abdominal attacks), and respiratory tract (laryngeal attacks).1 The reported prevalence of HAE ranges from 1 in 93,000 to 1 in 50,000.1-3 There are 3 types of HAE: type 1 (85% of patients) is caused by decreased secretion of complement 1 esterase inhibitor (C1-INH); type 2 (15% of patients) is characterized by normal or elevated production of functionally impaired C1-INH; and a third type, known as HAE with normal C1-INH (formerly referred to as type 3 HAE), is characterized by normal C1-INH levels and function (prevalence is uncertain).1 Therapeutic options available in Canada for long-term prophylactic (LTP) treatment include C1-INHs, lanadelumab, oral attenuated androgens (e.g., danazol), and antifibrinolytics (e.g., tranexamic acid).1 The most commonly used treatments in Canada are C1-INHs, which replace missing or malfunctioning C1-INH proteins, but all are derived from human plasma and are administered by IV or subcutaneous (SC) injection. Lanadelumab also requires SC administration. Oral danazol and tranexamic acid are not approved to treat HAE and are limited by frequent and potentially serious adverse effects or poor efficacy.
Berotralstat is a plasma kallikrein inhibitor that decreases plasma kallikrein activity and controls excess bradykinin generation in patients with HAE.4 The Health Canada indication is for the routine prevention of HAE attacks in adults and pediatric patients aged 12 years and older.4 Berotralstat is available as a 150 mg oral capsule and the recommended dose is 150 mg once daily.4 Health Canada states that berotralstat should not be used for the treatment of acute HAE attacks, as the safety and efficacy for this use has not been established.
The objective of this report is to perform a systematic review of the beneficial and harmful effects of berotralstat for the routine prevention of recurrent episodes of HAE in adults and pediatric patients aged 12 years and older.
Stakeholder Perspectives
The information in this section is a summary of input provided by a patient group who responded to CADTH’s call for patient input and from a clinical expert consulted by CADTH for the purpose of this review.
Patient Input
One patient group, Hereditary Angioedema Canada (HAEC), submitted patient input for this review. HAEC is dedicated to creating awareness about HAE and related angioedemas, helping speed the diagnosis of patients, improving access to treatments, and enabling patients to become champions of their own quality of life. The input was based on data collected from surveys in 2019 (n = 66) and 2021 (n = 138), qualitative interviews with 11 patients with a mix of either type 1 or type 2 HAE, and comments from 3 patients who had experience with the treatment under investigation in a clinical trial.
Respondents rated on a scale of 1 (not at all) to 5 (significant) the impacts HAE had on their day-to-day activities, with weighted averages ranging from 2.20 for impacts on their ability to conduct household chores to 2.94 for affecting their ability to travel. The majority had to miss time from work due to HAE. Approximately 20% of patients reported that HAE required out-of-pocket expenditures for medical care, or that they were either very dissatisfied or dissatisfied with their current treatments. Among the 3 patients who had experience with berotralstat, 1 patient described the treatment as extremely effective in preventing episodes of HAE and the adverse effects as easy to tolerate. Two patients did not find the treatment effective in the prevention of episodes of HAE.
According to the patient input received, a majority of patients are seeking treatments with an easier mode of delivery, and some prefer a product that is not derived from plasma. Patients continue to seek treatments that better control attacks while offering greater convenience and ease of use. Treatments that eliminate or substantially reduce attacks compared to existing treatments are of critical importance to patients, as each angioedema attack can be severely debilitating, and in many cases life-threatening. Greater control of attacks would also reduce the anxiety and fear many patients experience due to unpredictable attacks and reduce the negative impact on a patient’s ability to work, pursue education, travel, exercise, do household chores, and socialize with family and friends.
Clinician Input
Input From Clinical Expert Consulted by CADTH
According to the clinical expert consulted by CADTH, the treatment burden of the injectable products used for LTP therapy can be substantial, particularly for those who have difficulty with self-administration by IV or SC injection, and considering the frequency of administration of C1-INH. Although androgens are administered orally, they are associated with significant adverse effects, and are contraindicated in certain patient populations. The expert noted that berotralstat could be considered a first-line option for LTP therapy, although it may not be the preferred option for use in women who are pregnant or in patients aged younger than 12 years due to limited clinical data.
The expert indicated that patients could be considered good candidates for treatment with berotralstat if they experience frequent HAE attacks that require acute treatment. The oral route of administration may be preferred for some patients and could be useful for patients who have to travel, for whom an LTP with C1-INH may be impractical. Patients who may not be appropriate candidates for treatment with berotralstat include those who were misdiagnosed as having HAE, but actually have histaminergic chronic urticaria or histaminergic idiopathic angioedema; those with HAE but who only have mild and intermittent symptoms (i.e., patients for whom on-demand therapy is sufficient); those who are currently well controlled and satisfied with their existing LTP therapy; and those who have a significant adverse reaction to berotralstat.
The ability to prescribe berotralstat should be limited to specialists with an expertise in the diagnosis and management of patients with angioedema, including immunologists, allergists, and hematologists. This will help ensure that the correct diagnosis has been made before initiating treatment with berotralstat and that the response to treatment is appropriately monitored. Response to treatment would be assessed based on a reduction in the frequency, severity, and duration of attacks. Patients and clinicians would also be seeking an increase in the ability to perform activities of daily living during attacks if these were previously affected. The expert noted that response to treatment with an LTP such as berotralstat would be initially assessed after 3 months, with subsequent follow-ups occurring every 6 or 12 months. The following were identified as situations in which discontinuing treatment with berotralstat could be appropriate: pregnancy, as adverse effects during pregnancy are unknown and C1-INH is the preferred option; intolerable adverse effects with berotralstat; or an inadequate response or loss of response (e.g., increase in attacks requiring rescue medication).
Clinician Group Input
Ten clinicians representing the Canadian Hereditary Angioedema Network provided input for this review. The input noted a need for a treatment to prevent attacks, improve the acute management of HAE, and provide convenient methods of self-administration. Patients with HAE are at risk of experiencing a life-threatening laryngeal attack, which can have a considerable impact on their health-related quality of life (HRQoL). Furthermore, IV treatments may have the effect of requiring patients to spend much time travelling to treatment and undergoing treatment if they are unable to self-administer. Current off-label oral prophylaxis options for Canadians include androgen therapy such as danazol. Androgens are associated with a range of severe adverse effects, such as headaches, hypertension, weight gain, masculinizing effects for women, hepatocellular carcinoma, dyslipidemia, and cardiac disease. The input suggests the treatment under review may provide a safe and effective oral prophylactic that may be preferred to the current standard of care by some patients, particularly those averse to long-term injections. The input recommends that the treatment be considered for all patients who are candidates for long-term prophylaxis.
Drug Program Input
The drug programs asked several questions regarding the place in therapy of berotralstat, potential for use in combination with other LTP treatments, and use in patients with HAE and normal C1-INH or children less than 12 years of age. The expert stated that the place in therapy of berotralstat would be similar to that of lanadelumab (Takhzyro), and that alignment with lanadelumab initiation, renewal, and discontinuation criteria were reasonable. No specific number of attacks is used as a threshold to initiate LTP therapy in clinical practice, but the criteria used in the clinical trials are often used as a guide. Patients with infrequent but severe HAE attacks may also benefit from LTP therapy. The clinical expert stated that no efficacy or safety data currently support the use of berotralstat in patients with HAE with normal C1-INH levels or in pediatric patients younger than 12. Data are lacking on the efficacy of berotralstat as add-on LTP therapy, although concurrent use with short-term prophylaxis or rescue treatment of acute attacks was allowed during the trials. The expert noted that patients may switch between different LTPs, although establishing response criteria for reimbursement in these patients may be difficult as the baseline (untreated) attack rate may not be known.
Clinical Evidence
Pivotal Studies and Protocol-Selected Studies
Description of Studies
The systematic review included 2 double-blind randomized controlled trials (RCTs) that evaluated the efficacy and safety of berotralstat versus placebo in patients aged 12 years and older with type 1 or 2 HAE who experienced at least 2 investigator-confirmed HAE attacks during the run-in period. The APeX-2 and APeX-J studies randomized patients to placebo, berotralstat 110 mg daily, or berotralstat 150 mg daily for 24 weeks (part 1), after which all patients in the placebo group were randomized to berotralstat 110 mg or 150 mg daily, and those on the active drug continued with the same dose for part 2 (double-blind, up to week 48 in the APeX-2 study or week 52 in APeX-J). In the subsequent part 3 of the trials, all patients were switched to open-label berotralstat 150 mg daily (up to week 240 in the APeX-2 study or week 104 in APeX-J). During the trials, all patients had access to standard-of-care treatments for acute HAE attacks (e.g., C1-INH or icatibant acetate). The primary outcome in both studies was the rate of investigator-confirmed HAE attacks over 24 weeks (part 1). All patient-reported HAE attacks were confirmed by the investigator if they included symptoms of swelling, which could be visible swelling or symptoms in the oropharyngeal or abdominal regions that are indicative of internal swelling. This review focused on a comparison of berotralstat 150 mg and placebo at 24 weeks that included 80 patients from the APeX-2 study and 13 patients from the APeX-J trial. Data from the berotralstat 110 mg group are not summarized in this report.
The APeX-2 study was conducted in 11 countries, including Canada (3 sites), the US, and Europe. The mean ages of patients enrolled were 40.0 years (standard deviation [SD] = 14.0) and 44.5 years (SD = 14.1) in the berotralstat 150 mg and placebo groups, respectively. Patients were predominantly female (58% and 68%, respectively), and white (95% and 93%, respectively), with mean baseline rates of 3.1 (SD = 1.6) and 2.9 (SD = 1.1) investigator-confirmed HAE attacks per month in the berotralstat 150 mg and placebo groups, respectively.
The APeX-J study was conducted at multiple centres in Japan. The enrolled patients had a mean age of 37.3 years (SD = 9.1) in the berotralstat 150 mg group and 42.3 years (SD = 13.5) in the placebo group. Most patients were female (86% and 83%, respectively) and Asian (86% and 100% in the berotralstat and placebo groups, respectively). At baseline, the mean expert-confirmed attacks per month was 2.0 (SD = 1.1) in the berotralstat 150 mg group and 2.5 (SD = 1.5) in the placebo group.
Efficacy Results
In the APeX-2 study, the rate of investigator-confirmed HAE attacks per month was 1.31 for the berotralstat 150 mg group and 2.35 for the placebo group, during the 24-week double-blind treatment period. The relative rate reduction was 44.2% (95% confidence interval [CI], 23.0% to 59.5%; P < 0.001) for berotralstat 150 mg versus placebo (Table 2). The results of the primary outcome were similar in the APeX-J study, which reported 1.11 and 2.18 expert-confirmed HAE attacks per month in the berotralstat 150 mg and placebo groups, respectively, with a rate reduction of 49.1% (95% CI, 20.4% to 67.5%; P = 0.003).
In the APeX-2 study, 58% of patients in the berotralstat 150 mg group and 25% in the placebo group achieved at least a 50% relative reduction in the rate of investigator-confirmed HAE attacks compared to baseline (odds ratio = 3.91, 95% CI, 1.51 to 10.16; P = 0.005) (Table 2). However, these analyses were not adjusted for multiple testing and should be interpreted with caution because of the potential for inflated type I error rate.
█ ██ █ ███ █ ███ in the berotralstat 150 mg group (██) of the APeX-2 study, and 1 patient in the placebo group (2.6%) had no investigator-confirmed HAE attacks during the 24-week treatment period. ████ █ █ ██ █ ████ the APeX-J study reported ██ █ █ █ █ ██ █ ██████ █ █ during the first 24 weeks of treatment.
The number and proportion of days with HAE symptoms during the first 24 weeks was a secondary outcome in the APeX-2 study. Patients in the berotralstat 150 mg group reported a mean of 19.4 days (SD = 21.5) with HAE symptoms compared with 29.2 days (SD = 24.3) for patients in the placebo group. The least squares (LS) mean difference in the proportion of days with symptoms was −0.078 (95% CI, −0.133 to −0.023), which translates to approximately 13 fewer symptom-days in the berotralstat versus placebo group (out of a total of 169 treatment days). Although the proportion of days with HAE symptoms favoured berotralstat over placebo, these data should be interpreted as indeterminate due to failure of a prior outcome in the statistical analysis hierarchy. In the APeX-J study, no statistically significant difference was detected between groups in the proportion of days with HAE symptoms (LS mean difference = −0.122; 95% CI, −0.280 to 0.036; P = 0.12).
HRQoL was measured using the Angioedema Quality of Life (AE-QoL) questionnaire. While both the berotralstat 150 mg and placebo groups of the APeX-2 study reported improvements in AE-QoL total scores at week 24 relative to baseline, no statistically significant difference was detected between groups in the LS mean difference (−4.9 points; 95% CI, −12.2 to 2.4; P = 0.19). In the APeX-J study, the LS mean difference for the change from baseline in the AE-QoL total score was −19.0 (95% CI, −39.0 to 1.0).
New information supplied by the sponsor as part of its Request for Reconsideration showed that, during part 2 of the APeX-2 study (week 24 to 48), the mean investigator-confirmed attack rates per month in the berotralstat 150 mg group were 1.7 (SD = ███) at 24 weeks (N = ██), and 1.1 (SD = ███) at week 48 (N = ██). The mean number of days with angioedema symptoms during part 2 was ████ days (SD = ████), and the proportion of days with symptoms was █████ (SD = █████) for patients in the berotralstat 150 mg group. Among the patients who switched from placebo to berotralstat 150 mg at week 24 (N = 17), the mean attack rate per month was ███ events (SD = ███) at 24 weeks (i.e., start of active treatment), and 0.6 events (SD = ███; N = 14) at 48 weeks. The proportion of days with angioedema symptoms was █████ █ ████ █ ███ for patients who switched to berotralstat 150 mg. Overall 83% of patients completed part 2 of the study, with 7 patients (13%) stopping therapy due to adverse events or lack of efficacy, and 2 others (4%) stopping for other reasons.
Among the ██ patients who entered part 3 of the APeX-2 study and received open-label berotralstat 150 mg daily, the overall adjusted patient-reported HAE attack rate was ███ events per month (SD = ███) while patients remained on treatment. The mean number of days with angioedema symptoms was ████ days (SD = ████), which corresponds to a proportion of days of ███ █ █ (SD = █████). During part 3, ██ patients (███) stopped treatment for the following reasons: █ █ ████ █ █ █ ███ █ ██ █ █ █ █ █ █ █ █ ██████ █ █████ █ ███████████████ █ ███████████ █ ████████ █ ███ █ ████ █ █████████ █ █ █ █ █ █ █ █ █ ██████ █ █████ █ ██████ █ ███████████ █ █ ██ █ ███████ █ ███████ █ █████████████ █ ███
Harms Results
Adverse events were reported by 85% of patients in the berotralstat 150 mg group and 77% of those in the placebo group during the first 24 weeks of the APeX-2 study. The most frequently reported events in the berotralstat group were nasopharyngitis (23%), nausea (15%), vomiting (15%), and diarrhea (13%). Gastrointestinal adverse events were reported more frequently by patients who received berotralstat 150 mg compared with those who received placebo (50% versus 36%).
No patients in the berotralstat group experienced a serious adverse event during the first 24 weeks of the APeX-2 study, whereas 3 patients in the placebo group experienced 4 serious adverse events (uterine leiomyoma, diverticulum intestinal hemorrhage, pneumonia, and transient ischemic attack). One patient in the berotralstat 150 mg group stopped treatment due to abnormal liver function test results, and 1 patient in the placebo group stopped the study drug due to a depressive episode. No deaths were reported, and no new safety signals were identified in part 2 ██ █ ████ of the APeX-2 trial among patients who received berotralstat 150 mg ██ █ ████ █ █ █ █████
All patients in the APeX-J study experienced 1 or more adverse events in the first 24 weeks. Gastrointestinal adverse events were reported by 43% of patients in the berotralstat 150 mg group compared with 17% of patients in the placebo group. One placebo-treated patient stopped treatment due to urticaria and no patients stopped treatment in the berotralstat 150 mg group. No serious adverse events were reported.
Table 2: Summary of Key Results From Pivotal and Protocol-Selected Studies
Outcome | APeX-2 (24 weeks) | APeX-J (24 weeks) | ||
|---|---|---|---|---|
Berotralstat 150 mg N = 40 | Placebo N = 40 | Berotralstat 150 mg N = 7 | Placebo N = 6 | |
Investigator-confirmed HAE attacksa | N = 40 | N = 40 | N = 7 | N = 6 |
Total number of attacks | 357 | 508 | ██ | ██ |
Number of patients with ≥ 1 attack, n (%) | 37 (92.5) | 38 (95.0) | ██████ | ██████ |
Attack rate per 28 days | 1.31 | 2.35 | 1.11 | 2.18 |
Rate reduction (%) vs. placebo (95% CI) | 44.2 (23.0 to 59.5) | Reference | 49.1 (20.4 to 67.5) | Reference |
P value | < 0.001 | Reference | 0.003 | Reference |
Proportion of patients with ≥ 50% relative reduction in adjusted investigator-confirmed HAE attack rateb | N = 40 | N = 40 | N = 7 | N = 6 |
Patients contributing to the analysis, n | 40 | 39 | 7 | 6 |
Number of responders, n (%) | 23 (58) | 10 (25) | 4 (57) | 0 |
Odds ratio (95% CI) vs. placebo | 3.91 (1.51 to 10.16) | Reference | ██ | ██████ |
P value | 0.005c | Reference | ██ | ██████ |
Harms, n (%)e | N = 40 | N = 39 | N = 7 | N = 6 |
Adverse events | 34 (85) | 30 (77) | 7 (100) | 6 (100) |
Serious adverse events | 0 | 3 (8) | 0 | 0 |
Stopped treatment due to adverse events | 1 (3) | 1 (3) | 0 | 1 (17) |
Deaths | 0 | 0 | 0 | 0 |
Any gastrointestinal adverse events | 20 (50) | 14 (36) | 3 (43) | 1 (17) |
CI = confidence interval; HAE = hereditary angioedema.
aNegative binomial model, with covariate for baseline HAE attack rate (< 2 or ≥ 2 attacks per month) and log of treatment duration as offset for the intention-to-treat population.
bFor the APeX-2 study the analysis was based on logistic regression model with covariate for baseline HAE attack rate for the intention-to-treat population.
cP value has not been adjusted for multiple testing (i.e., the type I error rate has not been controlled).
dFisher’s exact test.
eSafety population.
Source: Clinical Study Report for APeX-2 and6 Clinical Study Report for APeX-J.7
Critical Appraisal
Both RCTs were conducted using a similar 3-part study design and comparable statistical methods. Patients were allocated to treatment groups using appropriate methodology, with randomization stratified by a relevant prognostic factor (i.e., baseline HAE attack rate). Due to the small sample size of the trials (40 or 7 patients per treatment group), randomization may not have ensured the groups were balanced for all measured or unmeasured prognostic factors or confounders, and imbalances between treatment groups were observed at baseline for some patient characteristics. In addition, more patients in the placebo group of the APeX-2 study stopped treatment or withdrew before 24 weeks, which may also contribute to imbalances between groups. However, the impact of these differences on the study’s findings is unclear, and sensitivity analyses that explored different missing data assumptions were generally supportive of the primary analyses. There was ███ █ █ █ █ ██ of rescue C1-INHs in the berotralstat group compared with placebo in the APeX-2 study, which may have biased the results in favour of berotralstat, as C1-INH may provide a protective effect in the days after administration.
The primary outcome (investigator-confirmed HAE attack rate over 24 weeks) was considered clinically relevant by the expert consulted by CADTH. Other outcomes of interest to this review (e.g., laryngeal, treated or severe attack rate, and responder analyses) were either exploratory or ad hoc outcomes, and these analyses were not included in the hierarchical statistical analysis. Any analyses with P < 0.05 should be interpreted with caution because of the potential for an inflated type I error rate. Although the AE-QoL has been used in clinical trials of other HAE treatments, the instrument contains domains that are not specific to HAE. Neither study was designed to test for differences in the need for hospitalization or emergency visits, or mortality. As with most clinical trials, the studies were not powered to detect infrequent adverse effects or those with a lag time.
Although the data from part 2 and part 3 of the APeX-2 study suggest that patients who continued on berotralstat 150 mg may maintain a reduction in HAE attacks, these data were limited by potential selection and reporting bias and the lack of a comparator group. Investigators and patients were aware that patients were receiving active treatment, and their expectations of treatment could therefore affect reporting of subjective outcomes, such as symptoms of swelling or adverse effects. Moreover, HAE attacks in part 3 were not adjudicated by the investigator but based instead on patient-reported events. Attack events analyzed in part 3 therefore may not be comparable to the investigator-confirmed events in part 1 and 2. In both parts 2 and 3, the efficacy analyses were reported descriptively based on observed data with no imputation for missing data, and with no sensitivity analyses to assess the robustness of the results. Given the attrition observed, these results may overestimate treatment effects and under-report adverse effects, as patients who were tolerant of therapy and showed adequate response were more likely to continue in the trial. Finally, part 2 and part 3 were uncontrolled, which makes the change in the HAE attack rate difficult to interpret, particularly as HAE attacks are sporadic and can fluctuate through the year due to exposure to seasonal triggers, hormonal changes, or other factors.
With regard to external validity, the findings of the pivotal APeX-2 study were reflective of those enrolled, who were patients with type 1 or 2 HAE with an average of 3 HAE attacks per month, most of whom had experienced a prior laryngeal attack. The trial included patients who were medically appropriate for on-demand treatment as the sole management of HAE, and therefore may have excluded patients with more severe HAE who could not tolerate discontinuation of current LTP therapy. Compared to the Canadian population, the racial diversity in the APeX-2 trial was limited as most patients were white (94%). In addition, patients were predominantly female (63%) and between 18 and 65 years of age. Because only 4 adolescents and 4 patients over 65 years of age were enrolled in the berotralstat 150 mg and placebo groups, the ability to extrapolate to younger and older age groups is limited. The APeX-J study provided additional data from 13 patients from Japan. These patients were generally similar to those in the pivotal study, although patient weight and body mass index (BMI) were lower, as was the mean baseline HAE attack rate. Overall, the clinical expert consulted described the characteristics of the patient population enrolled in the trials as a good representation of the target population and the expert did not identify any issues that could substantially limit the generalizability of the findings.
There is no direct evidence comparing berotralstat to other LTP therapies. The comparative evidence was limited to 2 24-week randomized, placebo-controlled trials in which a total of 47 patients received berotralstat 150 mg daily.
Indirect Comparisons
No indirect evidence was available.
Other Relevant Evidence
Data from 1 open-label, long-term study was summarized in this report.
Description of Studies
APeX-S is an uncontrolled, phase II study that was conducted to evaluate the safety and efficacy of berotralstat in adults and pediatric patients aged 12 years and older with type 1 or 2 HAE. In this study, 127 patients were enrolled from either a prior berotralstat trial or recruited from the community, and all received open-label berotralstat 150 mg once daily for up to 48 weeks (interim analysis). At baseline the median age was 44.0 years (range = 12 to 72) and the majority of patients were female (61%), white (87%), and had a family history of HAE (80%).
Efficacy Results
Through to week 48, a total of █ ██ █ █ adjusted HAE attacks were reported among patients who received berotralstat 150 mg daily. The mean attack rate was 1.36 (SD = 1.51) attacks per month and the median attack rate was 0.93 attacks per month (range = 0 to 7.6).
Harms Results
During the 48-week period, 91% of patients in the berotralstat 150 mg group reported 1 or more adverse events, the most common being nasopharyngitis (34%), headache (15%), and diarrhea (14%). Overall, 41% of patients experienced gastrointestinal adverse events. A total of 9% of patients experienced a serious adverse event, with ███ █ ████ █ ███ experiencing an HAE attack requiring hospitalization. No deaths were reported.
Critical Appraisal
This study was limited by the open-label design and lack of randomization or control group. Moreover, there is potential selection and attrition bias. A total of 26% of patients treated with berotralstat 150 mg discontinued the long-term study, mainly due to adverse events or a lack of perceived efficacy. This attrition could have resulted in a population of patients more tolerant of and responsive to berotralstat, which may have biased the estimates in favour of efficacy and safety.
Conclusions
In patients with type 1 or 2 HAE, treatment with berotralstat 150 mg daily reduced the rate of investigator-confirmed HAE attacks, relative to placebo, based on 24-week data from the APeX-2 and APeX-J studies. The impact of berotralstat on HRQoL was uncertain; although improvement in the AE-QoL total score was observed, the difference versus placebo was not statistically significant. Longer-term, uncontrolled studies suggest that a reduction in HAE attacks may be maintained in patients who continued on therapy up to 48 weeks; however, due to the limitations associated with these data, the longer-term safety and efficacy of berotralstat are uncertain. No evidence was available regarding the impact of berotralstat on hospitalization, emergency visits, or mortality. Also, because no direct or indirect evidence comparing berotralstat to other LTP therapies was available, the relative efficacy and safety of berotralstat compared to other LTP treatments are unknown. Gastrointestinal adverse events were reported more frequently among patients who received berotralstat compared with those who received placebo. Due to the limited sample size and duration of the trials, the studies were not designed to detect infrequent adverse effects or those with a lag time.
Introduction
Disease Background
HAE is a rare autosomal-dominant disorder characterized by recurrent episodes of nonpruritic subcutaneous or submucosal edema, most commonly affecting the skin (cutaneous attacks), gastrointestinal tract (abdominal attacks), and respiratory tract (laryngeal attacks).1 The estimated prevalence of HAE is typically cited as 1 in 50,000,1,2 while estimates from Europe range from 1 in 93,000 to 1 in 64,000.3 HAE is caused by a deficiency or dysfunction of the C1-INH enzyme, a protease inhibitor that is a key regulator of the complement and contact systems, which leads to the activation of kallikrein and subsequent overproduction of the nanopeptide bradykinin.1,2 Bradykinin binds to bradykinin type 2 receptors on endothelial cells, causing increased vascular permeability, which may lead to angioedema if present in excessive amounts.1,2
There are 3 types of HAE: type 1 (85% of patients) is caused by decreased secretion of C1-INH; type 2 (15% of patients) is characterized by normal or elevated production of functionally impaired C1-INH; and a third type, known as HAE with normal C1-INH (formerly referred to as type 3 HAE), characterized by normal C1-INH levels and function (prevalence is uncertain).1 Mutations in the SERPING1 gene, which codes for C1-INH, are inherited in approximately 75% of patients with HAE, but de novo mutations may appear in 25% of patients.2 Although the age of onset in patients with HAE varies, the majority of patients experience their first attack in childhood or adolescence, with 12 years being the median age of onset.2
The diagnosis of type 1 and type 2 HAE is based on a detailed history and physical examination, along with confirmatory laboratory diagnostic tests (Table 3). Clinical practice guidelines from the World Allergy Organization and the European Academy of Allergy and Clinical Immunology recommend that all patients suspected of having type 1 or type 2 HAE should be assessed for blood levels of complement 4 (C4) and C1-INH proteins and C1-INH function.2 Other forms of angioedema that should be ruled out include acquired angioedema, angiotensin-converting-enzyme inhibitor–induced angioedema, mast cell–medicated angioedema, and idiopathic angioedema.2 The clinical presentation of these other forms of angioedema may be similar to HAE but the pathology and management are different.2
Cutaneous and abdominal attacks are the most frequent type of HAE attacks, reported in more than 90% of patients with HAE.8 Cutaneous attacks may involve areas of the face, extremities, and genitals. Facial swelling may involve the lips, tongue, oropharynx, and periorbital tissues, while extremity swelling can progress to affect large areas of the arms or legs. Abdominal attacks involve the gastrointestinal tract and can be extremely painful, accompanied by nausea, vomiting, and diarrhea. Laryngeal attacks are the least frequent type of attack, but 50% of patients may experience 1 or more episodes in their lifetime.9 Laryngeal attacks are the primary cause of mortality in patients with HAE due to the risk of asphyxiation.10
The onset of an HAE attack is often unpredictable and can occur without a clear precipitating factor or trigger.2 Known or suspected triggers for HAE attacks include accidental trauma, dental and medical procedures, psychological stress, fatigue, febrile illness, and the menstrual cycle.2 Exposure to some drugs, including estrogen-containing contraceptives, hormone replacement therapy, and angiotensin-converting-enzyme inhibitors, may also trigger HAE attacks.2 The frequency of attacks in patients who are symptomatic but untreated can range from weekly to less than yearly. Without treatment, each attack can last several days.11
Table 3: Types of Hereditary Angioedema
Type of HAE | Type 1 | Type 2 | HAE with normal C1-INH |
|---|---|---|---|
Proportion of HAE cases | 85% | 15% | Uncertain (rare) |
C1-INH level | Low | Normal or elevated | Normal |
C1-INH function | Low | Low | Normal |
Complement 4 level | Low | Low | Normal |
C1-INH = complement 1 esterase inhibitor; HAE = hereditary angioedema.
Source: Maurer et al. (2018).2
Standards of Therapy
The clinical management of HAE can be categorized as follows:
LTP treatment: ongoing long-term treatment to reduce the frequency and severity of HAE attacks and improve patient HRQoL)
short-term prophylactic treatment to reduce the risk of an attack when exposure to a trigger is anticipated (e.g., before dental or medical procedures)
acute treatment of HAE attacks to reduce the severity and alleviate the symptoms of an attack, minimize the functional impact of an attack, and reduce morbidity and potential mortality.1
Therapeutic options available in Canada for LTP treatment include plasma-derived C1-INHs, lanadelumab, oral attenuated androgens (e.g., danazol), and antifibrinolytics (e.g., tranexamic acid).1 The most commonly used treatments in Canada are C1-INHs, which replace missing or malfunctioning C1-INH proteins in patients with HAE. Three C1-INHs products are used in Canada for the treatment of HAE: Cinryze and Haegarda, which are indicated for LTP therapy, and Berinert, which is indicated for the acute treatment of HAE attacks. In addition to its use in the acute management of HAE attacks, Berinert is also routinely administered as an LTP treatment option, although this is beyond the indication approved by Health Canada. All 3 C1-INH products are derived from human plasma and are administered by IV or SC injection. Berinert is approved for IV administration; however, the clinical expert consulted by CADTH indicated that Berinert 1,500 IU is commonly administered by SC injection, in accordance with the dosages recommended in the product monograph for Haegarda (Table 4). Lanadelumab is a plasma kallikrein inhibitor that is approved for use as an LTP. This recombinant monoclonal antibody is administered by SC injection every 2 to 4 weeks.
The Canadian Hereditary Angioedema Guideline Committee recommends the use of C1-INH or lanadelumab as a first-line option for patients who require LTP treatment to manage their condition.1 These guidelines state that attenuated androgens may be effective for some patients who require LTP treatment but are not recommended as first-line treatments.1 Androgens or antifibrinolytics may be considered for LTP treatment of patients who have already demonstrated a benefit from these treatments or for those who have problems accessing first-line options, but the Canadian guidelines state that patients should not have to fail androgens or antifibrinolytics before using C1-INHs or lanadelumab as an LTP.1 The evidence of effectiveness of antifibrinolytics for LTP is limited, and androgens are associated with frequent and potentially serious adverse effects.1,2
Drug
Berotralstat is a plasma kallikrein inhibitor that decreases plasma kallikrein activity and controls excess bradykinin generation in patients with HAE.4 Plasma kallikrein is a protease that cleaves high-molecular-weight kininogen to generate cleaved high-molecular-weight kininogen and bradykinin, a potent vasodilator that increases vascular permeability, resulting in the swelling and pain associated the HAE. In patients with HAE due to C1-inhibitor deficiency or dysfunction, uncontrolled increases in plasma kallikrein activity result in angioedema attacks. Berotralstat is indicated for the routine prevention of episodes of HAE in adults and pediatric patients aged 12 years and older.4 It is available as a 150 mg oral capsule and the recommended dosage is 150 mg once daily.4 Dosages greater than 150 mg once daily are not recommended due to the potential for QT prolongation.4 Health Canada states that the safety and efficacy of berotralstat for the treatment of acute attacks have not been established, and the drug should not be used for acute attacks.4
Berotralstat was approved by Health Canada through the standard review process. The sponsor has requested reimbursement according to the indication. This drug has not been reviewed by CADTH previously. Berotralstat is approved for use in Australia, Europe, and the US.1
Table 4: Key Characteristics of Preventive Treatments for HAE
Characteristic | Berotralstat | Lanadelumab | Berinert | Cinryze | Haegarda |
|---|---|---|---|---|---|
Mechanism of action | Plasma kallikrein inhibition | Plasma kallikrein inhibition | Replace missing or malfunctioning C1-INH protein in patients with HAE | Replace missing or malfunctioning C1-INH protein in patients with HAE | Replace missing or malfunctioning C1-INH protein in patients with HAE |
Indicationa | Routine prevention of episodes of HAE in adult and pediatric patients aged 12 years and older | Routine prevention of episodes of HAE in adolescents and adults | Treatment of acute abdominal, facial, or laryngeal episodes of HAE of moderate to severe intensity in pediatric and adult patients | Routine prevention of angioedema attacks in adults and adolescents with HAE | Routine prevention of HAE attacks in adolescent and adult patients |
Route of administration | Oral | SC | IV (approved) SC (not approved) | IV | SC |
Recommended dosage | 150 mg once daily | 300 mg q.2.w. 300 mg q.4.w. can be considered if the patient is well controlled (e.g., attack-free) for more than 6 months | 20 IU per kg (IV) for acute attack 20 IU per kg IV or 60 IU per kg SC every 3 to 4 days for prophylaxis (off-label) | 1,000 IU every 3 or 4 days The dosing interval may need to be adjusted according to individual response | 60 IU/kg body weight twice-weekly (every 3 to 4 days) |
Dosage forms and strengths | 150 mg capsule | 300 mg/vial | 500 IU/vial 1,500 IU/vial | 500 IU/vial | 2,000 IU/vial 3,000 IU/vial |
Monitoring requirements | No additional monitoring required over and above usual clinical practice | No additional monitoring required over and above usual clinical practice | Patients with known risk factors for thrombotic events should be monitored closely | Patients with known risk factors for thrombotic events should be monitored closely | Risk of thrombotic events is noted, but no specific statements regarding monitoring |
Other | Non–plasma-derived | Non–plasma-derived, recombinant monoclonal antibody | Derived from human plasma | Derived from human plasma | Derived from human plasma |
C1-INH = complement 1 esterase inhibitor; HAE = hereditary angioedema; q.2.w. = every 2 weeks; q.4.w. = every 4 weeks; SC = subcutaneous.
aHealth Canada–approved indication.
Source: Product monographs for Orladeyo,4 Takhzyro,12 Berinert,13 Cinryze,14 and Haegarda15 and CADTH Technology Review.16
Stakeholder Perspectives
Patient Group Input
This section was prepared by CADTH staff based on the input provided by patient groups.
One patient group, HAEC, submitted patient input for this review. HAEC is dedicated to creating awareness about HAE and related angioedemas, speeding the diagnosis of patients, improving access to treatments, and helping patients become champions of their own quality of life. The input was based on data collected from surveys in 2019 (n = 66) and 2021 (n = 138), qualitative interviews with 11 patients with a mix of either type 1 or type 2 HAE, and comments from 3 patients who had experience with the treatment under investigation in a clinical trial.
Respondents rated the impacts HAE had on their day-to-day activities on a scale of 1 (not at all) to 5 (significant), with weighted averages ranging from 2.20 for impacts on their ability to conduct household chores to 2.94 for affecting their ability to travel. Some patients reported that HAE required out-of-pocket expenditures for medical care and some patients indicated that they were either very dissatisfied or dissatisfied with their current treatments. Among the 3 patients who had experience with the treatment under review, 1 patient described the treatment as extremely effective in prevention of episodes of HAE and the adverse effects as easy to tolerate. Two patients did not find the treatment effective in the prevention of episodes of HAE.
According to the patient input received, a majority of patients are seeking treatments with an easier mode of delivery, and some prefer a product that is not derived from plasma. Patients continue to seek treatments that better control attacks while offering greater convenience and ease of use. Treatments that eliminate or substantially reduce attacks compared to existing treatments are of critical importance to patients as each edema attack can be severely debilitating, and in many cases life-threatening. Greater control of attacks would also reduce the anxiety and fear many patients experience due to unpredictable attacks and reduce the negative impact on a patient’s ability to work, pursue education, travel, exercise, do household chores, and socialize with family and friends. A copy of the patient input is presented at the end of this report.
Clinician Input
Input From Clinical Experts Consulted by CADTH
All CADTH review teams include at least 1 clinical specialist with expertise in the diagnosis and management of the condition for which the drug is indicated. Clinical experts are a critical part of the review team and are involved in all phases of the review process (e.g., providing guidance on the development of the review protocol, assisting in the critical appraisal of clinical evidence, interpreting the clinical relevance of the results, and providing guidance on the potential place in therapy). The following input was provided by 1 clinical specialist with expertise in the diagnosis and management of HAE.
Description of the Current Treatment Paradigm for the Disease
Current LTP treatments for HAE include C1-INH replacement therapy, which restores C1-INH in the contact activation system pathway, reducing HAE attacks. It also restores C1-INH in the complement system pathway and restores C4 levels, which may be important in fighting infection and destroying autoreactive and malignant cells. C1-INH also acts in the coagulation pathway and normalizes the D-dimer, which is often elevated in HAE without any clinical consequence. Lanadelumab is a fully human monoclonal antibody that binds plasma kallikrein and inhibits its proteolytic activity. In patients with HAE due to C1-INH deficiency or dysfunction (i.e., type 1 or type 2), an uncontrolled increase in plasma kallikrein activity leads to an increase in bradykinin and results in angioedema attacks. Lanadelumab controls bradykinin generation by decreasing plasma kallikrein activity in patients with HAE.
Additional treatment options include anabolic steroids and tranexamic acid. Anabolic steroids (e.g., danazol) increase the production of endogenous C1-INH from the liver, but their use is limited by masculinizing effects and an increased risk of hepatic tumours. Tranexamic acid reduces the symptoms of HAE attacks, but its mechanism of action is unknown, it increases the risk of thrombosis, and it may not be tolerated due to gastrointestinal side effects.
Treatment Goals
An ideal treatment for HAE would:
prolong life by reducing or eliminating life-threatening HAE attacks (e.g., laryngeal attacks)
reduce the frequency, severity, and duration of HAE attacks
be associated with minimal or no adverse effects
improve HRQoL for those living with HAE and reduce the burden on their caregivers
help maintain independence, increasing the ability to maintain employment and attend school
reduce other health care utilization (e.g., emergency room visits and hospital admissions)
offer more convenient administration than existing options.
Unmet Needs
Many patients living with HAE find it inconvenient or impossible to self-administer C1-INH intravenously twice-weekly (e.g., because it is difficult to find a vein), and some do not like administering 3 times the dose of C1-INH by SC injection twice-weekly (Haegarda). Because C1-INHs currently approved in Canada are derived from human plasma, there is a remote risk of transmitting viral infections, and some patients may not wish to use these products. Lanadelumab, which requires only a single SC injection once every 2 weeks may be more convenient to administer and is not plasma-derived, but still requires injections. As previously noted, the other available LTP treatments are less effective (e.g., tranexamic acid) or have significant side effects (e.g., danazol).
Place in Therapy
Berotralstat, an oral therapy, may offer advantages over existing treatments for ease of administration and has the potential to shift the current treatment paradigm. It could be considered a first-line option for LTP treatment, although it may not be the preferred option for people who are pregnant or younger than 12 years of age, given the limited clinical data for these groups. Patients who experience breakthrough symptoms while using berotralstat could administer C1-INH IV or icatibant SC to manage attacks.
Although not specifically indicated for combination usage in Canada, berotralstat could be added to C1-INH (IV or SC twice-weekly prophylaxis), danazol, or lanadelumab if patients wanted extra assurance that they would not have an attack. However, patients would most likely start this medication and then withdraw their existing LTP therapies completely.
Berotralstat is a plasma kallikrein inhibitor that decreases plasma kallikrein activity and controls excess bradykinin generation in patients with HAE. It does not address the underlying disease process, as it does not replace the deficient or dysfunctional C1-INH protein in patients with type 1 or 2 HAE, respectively.
Patient Population
HAE can be challenging to diagnose, as patients with chronic urticaria may also develop swelling. Accurate diagnosis of type 1 and 2 HAE typically requires testing C1-INH levels, C1-INH function, and C4 levels. It may be challenging in some areas of Canada to access testing for C1-INH levels and function in a timely manner. Diagnosis of HAE with normal C1-INH can require genetic testing that is only available in some specialized centres and out-of-pocket expenditures may be required. Acquired angioedema may pose additional challenges for clinicians, as this condition can have many of the same biochemical abnormalities as type 1 HAE. Although acquired C1-INH deficiency can be differentiated from type 1 HAE by the presence of low C1q levels, this testing is not generally available in Canada.
Patients could be considered good candidates for treatment with berotralstat if they experience frequent HAE attacks that require acute treatment. The oral route of administration would be beneficial for patients who are unable to self-administer C1-INH by IV (e.g., because of arthritis or problems finding veins) or SC injection and do not have a caregiver to assist. Berotralstat may also be useful for patients who must travel, for whom LTP treatment with C1-INH may be impractical. In addition, many patients may prefer the convenience offered by berotralstat over that of existing treatment options.
Based on the available clinical evidence, patients with type 1 or 2 HAE are the most likely to respond to treatment with berotralstat (as other forms of HAE have not been studied). The patients who could benefit most (i.e., those in greatest need of an additional intervention) are those who experience frequent and severe attacks, those who have an inadequate response to LTP with C1-INH or lanadelumab, and those who require larger amounts of C1-INH to control their attacks. This would be true for patients with any form of bradykinin-mediated angioedema, including patients who have HAE with normal levels of C1-INH or acquired angioedema. The clinical expert noted that it would not be necessary to try another LTP treatment before initiating treatment with berotralstat.
The following patients may not be appropriate candidates for treatment with berotralstat:
those who are misdiagnosed as having HAE but actually have histaminergic chronic urticaria or histaminergic idiopathic angioedema
those with HAE who have only mild and intermittent symptoms (i.e., for whom on-demand therapy is sufficient)
those whose HAE is currently well controlled and who are satisfied with their existing LTP therapy
those who have a significant adverse reaction to berotralstat.
Assessing Response to Treatment
Assessing a response to LTP treatment in clinical practice is similar to the evaluations conducted in clinical trials. Patients and clinicians are seeking a reduction in the frequency, severity, and duration of attacks, which, in turn, can result in a reduced need for rescue medications, emergency department visits, and hospital admissions. There should be an increase in the ability to perform activities of daily living during attacks, if these were previously affected. Assessments can vary across individual patients, as a certain level of symptoms may be acceptable to some patients living with the condition but not to others. Initial response to treatment would typically be assessed at 3 months. Patients would subsequently visit a clinic once every 6 months, and those with very well-controlled HAE would often be seen only once per year.
Discontinuing Treatment
The following were identified as situations in which discontinuing treatment with berotralstat could be appropriate:
pregnancy — adverse effects during pregnancy are unknown, and C1-INH is the preferred option
allergic reaction or any significant adverse event to berotralstat
inadequate response or loss of response (e.g., increase in attacks requiring rescue medication).
Prescribing Conditions
Prescribing authority should be limited to specialists with an expertise in the diagnosis and management of patients with angioedema, including immunologists, allergists, and hematologists. This will help ensure that the correct diagnosis has been made before initiating treatment with berotralstat and that the response to treatment is appropriately monitored.
Clinician Group Input
This section was prepared by CADTH staff based on the input provided by a clinician group. A copy of the clinician group input received is available at the end of this report.
Input was received from 1 clinician group, the Canadian Hereditary Angioedema Network, a not-for-profit organization of physicians who treat, or are interested in HAE. Its members contribute to the knowledge of HAE and its treatments by participating in clinical trials, conducting observational research, developing clinical practice guidelines, and assessing health technologies.
Unmet Needs
Patients with HAE require a variety of treatment options to address a range of unmet needs, including improvement in prevention of attacks, improvement in the acute management of HAE, and more convenient methods of administration that do not require injections or carry the risk of transmitting an infectious agent. No oral prophylactic treatments for HAE are currently licensed in Canada. Attenuated androgens have been used off-label, but are associated with severe adverse effects, require regular monitoring, and cannot be used during pregnancy. Tranexamic acid is a popular option for children but has an incomplete evidence base and poor efficacy.
Different treatment options are vital to ensure patients have options when they are faced with drug shortages, which is currently a reality and potentially will continue to be in the future. Ensuring the availability of optional treatments is particularly important when dealing with a potentially life-threatening condition.
Place in Therapy
Berotralstat, which is administered orally, may be associated with a lower treatment burden for some patients compared to injectable prophylactics such as lanadelumab or a plasma-derived C1-INH. A safe and effective oral prophylactic may be preferred to the current standard of care by some patients, particularly those who are averse to a long-term injection regimen, have difficulty with injections due to disability or phobias, are on anticoagulants or may bruise easily, or will not use blood products. While most recent guidelines recommend berotralstat as a first-line option, this (and any therapy) should be the subject of shared decision-making between the patient and the HAE specialist.
The issue of combining prophylactic therapies has not been addressed in studies available at this time. All patients should be equipped to treat angioedema attacks, and patients and physicians should agree on an acute treatment plan.
Patient Population
As stated in The International/Canadian Hereditary Angioedema Guideline, all effective treatments for long-term prophylaxis should be offered to patients, and all available treatments should be the subject of shared decision-making between the patient and the HAE specialist. Like any LTP, if 1 treatment is not effective, or if a patient has adverse effects from a therapy or has technical difficulties administering a therapy, the patient should be able to try another. Additionally, some patients will prefer less-frequent dosing of an LTP, such as with lanadelumab, which is self-administered every 2 weeks, over daily oral medication.
There are no specific predictors as to who would preferentially respond to berotralstat. LTP is considered at every follow-up visit for patients with HAE. Those already on LTP would also have a review at each follow-up visit, to determine if a switch in treatment would be beneficial for that patient.
Those least suitable for treatment with berotralstat are patients who are pregnant or lactating and patients younger than 12 years of age.
Diagnosis and treatment of HAE may be a problem in some patients given how rare it is, which is why HAE should be treated and managed by an HAE specialist.
Assessing Response to Treatment
The opinion of the patient on their response to treatment is a key consideration. But more objectively meaningful response is assessed by decreased frequency of HAE attacks, need for rescue treatments, decreased severity of attacks, decrease in emergency room visits, ability to work, increased quality of life, and adverse effects profile.
Response should be assessed at every follow-up visit. Follow-up frequency varies according to the nature and severity of the patient’s disease but can occur every 3, 6, or 12 months.
Discontinuing Treatment
Considerations leading to treatment discontinuation include ineffectiveness (poor control of HAE with increased or continued attack frequency and severity) and adverse effects.
Prescribing Conditions
A large majority of HAE patients will be under the care of an HAE specialist, such as an allergist or immunologist, hematologist, dermatologist, or possibly a pediatrician or internist.
Drug Program Input
The drug programs provide input on each drug being reviewed through CADTH’s reimbursement review processes by identifying issues that may affect their ability to implement a recommendation. The implementation questions and corresponding responses from the clinical experts consulted by CADTH are summarized in Table 5.
Table 5: Summary of Drug Plan Input and Clinical Expert Response
Drug program implementation questions | Clinical expert response |
|---|---|
Relevant comparators | |
The APeX-2 study was placebo-controlled. Placebo may not be an appropriate comparator given the number of available therapies for prophylaxis of HAE. Approved LTP therapies for HAE include plasma-derived C1-INHs. Lanadelumab (Takhzyro) is the only drug therapy approved for prophylaxis of HAE. Berinert IV (approved for treatment of acute attacks) has also been used off-label for LTP of HAE. | For CDEC consideration. |
Plasma-derived C1-INHs such as Cinryze IV and Haegarda SC are not funded by drug programs as they are plasma-derived products. | For CDEC consideration. |
Considerations for initiation of therapy | |
Berotralstat is not indicated by specific HAE type (i.e., type 1, 2, or HAE with normal C1-INH function). APeX-2 and APeX-S enrolled patients with type 1 and 2 HAE. Patients with HAE with normal C1-INH were not represented in either clinical trial; however, the Health Canada indication does not specify HAE type for berotralstat. Would berotralstat be used in patients with HAE with normal C1-INH? Are results from the trials generalizable for patients with HAE with normal C1-INH? Lanadelumab is also indicated for prophylaxis of HAE (type not specified); However, the reimbursement recommendation for lanadelumab was specific for type 1 and type 2 HAE. There is no consensus among clinical experts managing HAE on the specific number of attacks that corresponds to a threshold for initiation of LTP therapy. Is there a specific number of attacks that corresponds to a threshold for initiation of LTP therapy? APeX-2 enrolled patients with baseline attack rates of greater than or equal to 2 or less than 2 attacks per month. Lanadelumab recommendation: Initiation criteria requires patients to have experienced at least 3 HAE attacks within any 4-week period before initiating lanadelumab therapy that required the use of an acute injectable treatment. | Berotralstat may theoretically be of benefit to HAE patients with normal C1-INH function, but there is currently no evidence to support use in this population. Other available treatments may be more suitable for patients with HAE and normal C1-INH. No specific number of attacks is used as a threshold to initiate LTP, but often the criteria used in the clinical trials are used as a guide. Patients who experience less-frequent but severe or disabling attacks may also be benefit from long-term therapy. |
Indicated for patients 12 years and older. In an international survey, patients with type 1 and 2 HAE had a mean age of onset of 11.5 years with a wide range from 0 to 58 years. There is therefore potential for requests for patients younger than what is specified by the indication. Should patients who are younger than 12 years of age be treated with berotralstat? | Data are lacking on the safety and efficacy of berotralstat in children less than 12 years of age. Until safety data become available, it is unlikely the drug will be used in this population. |
No curative treatments are available for HAE. What is the treatment duration of LTP agents? Is treatment indefinite? Patients receiving berotralstat may receive a greater reduction in the number of attacks the longer therapy is maintained. An open-label trial for berotralstat up to 240 weeks has been completed. Is it expected that a greater reduction in number of attacks would be achieved if patients maintained longer-term therapy? | LTP treatment is indefinite until a more effective treatment becomes available or patients experience adverse effects with therapy. The longer-term berotralstat data are limited. Dropouts in whom berotralstat was ineffective may have led to a greater reduction in attacks over time in the open-label studies. Further evidence is required on the longer-term effectiveness of berotralstat. Berotralstat is not replacing missing or dysfunctional C1-INH, which is the underlying pathology of the disease. There is a risk that, over time, patients on berotralstat may develop acquired angioedema or auto-antibodies to C1-INH, which would lead to an increase in attacks. Additional trial data are required to determine if berotralstat may lose its effectiveness with longer-term use. |
Should patients who do not respond to lanadelumab (no reduction from baseline number of attacks) be eligible for treatment with berotralstat? Are there data for switching between products for LTP of HAE? Can CDEC comment on patients switching? How should response to therapy be evaluated for patients who switch from injectable LTPs? Drug plans may not have baseline information for these patients before treatment being administered. | Patients not responding to lanadelumab may be switched to berotralstat, although clinical trial data demonstrating efficacy in this patient population are lacking. For patients switching between LTP therapies it is difficult to know the true (i.e., untreated) baseline rate of attacks. Renewal criteria that include a specific response threshold that must be met may be difficult to implement in practice. |
Alignment with lanadelumab may be considered if CDEC determines that both drugs are first-line therapies for LTP for HAE. The initiation criteria for lanadelumab are as follows:
Should the initiation criteria for berotralstat be aligned with that of lanadelumab? If the recommendation for berotralstat is aligned by type of HAE (1 and 2), there will be a treatment gap for patients with HAE with normal C1-INH. Should a reimbursement recommendation for patients with HAE with normal C1-INH be considered? If considered for berotralstat, should it also be considered for lanadelumab? Both products have the Health Canada indication for prevention of HAE (not differentiated by type). Clinical trials have included only patients with type 1 and type 2 HAE. Type 1 HAE makes up 85% of HAE patients. Type 2 HAE makes up 15% of patients. The prevalence of HAE with normal C1-INH (previously referred to as type 3 HAE) is unknown, and there are unlikely to be clinical trials for this specific type. | Patients who have experienced severe attacks (e.g., laryngeal) should not be required to meet a minimum number of attacks to qualify for LTP. According to the clinical expert, berotralstat may theoretically be of benefit to HAE patients with normal C1-INH function, but there is currently no evidence to support use in this population. |
Considerations for continuation or renewal of therapy | |
Not all drug plans reimburse icatibant acetate (Firazyr), nor do all patients receive icatibant acetate for acute treatment. It may be difficult for drug plans to determine if patients are accessing acute injectable treatments such as plasma-derived agents through CBS. Drug plans may have to rely on physician reporting of such cases when assessing requests. Can CDEC include a discussion point regarding what reduction of HAE attacks would be indicative of a response? Alignment with lanadelumab for response to therapy with respect to reduction of HAE attacks indicative of response would be appropriate. Lanadelumab criteria vary across jurisdictions. Listing criteria in at least 2 jurisdictions stipulate a 50% reduction in HAE attacks within 3 months from baseline for renewal, and continued response is defined as maintenance of reduction of at HAE episodes of at least 50% from baseline. Other jurisdictions do not specify a reduction in attacks for response. However, if a patient experiences and maintains a 30% reduction from baseline, should that be deemed a treatment failure that warrants discontinuation of therapy? It may not be cost-effective if a 50% reduction is HAE attacks is achieved. | A 20% reduction in attack frequency is considered a mild improvement, 50% reduction is moderate, and 70% is considered marked improvement. For patients switching between LTP therapies it is difficult to know the true (i.e., untreated) baseline rate of attacks. Renewal criteria that include a specific response threshold that must be met may be difficult to implement in practice. |
Renewal criteria for lanadelumab should be considered when considering renewal criteria for berotralstat. The renewal criteria for lanadelumab is as follows:
Should the renewal criteria for berotralstat be aligned with that of lanadelumab? Should a specific reduction in HAE attacks that is indicative of response be considered for inclusion in the recommendation? In general, it is helpful for assessments if the baseline time frame aligns with the renewal assessment time frame, i.e., the baseline is the number of attacks in 3 months. Renewal assessed at 3 months evaluates the number of attacks on treatment within 3 months. | Aligning the renewal criteria for berotralstat with those used for lanadelumab would be reasonable. Defining a specific response criteria in cases where the untreated baseline attack rate was unclear is difficult. |
Considerations for discontinuation of therapy | |
Consistency with discontinuation criteria for lanadelumab may be considered. However, it may be helpful for jurisdictions to have additional clarification around inadequate response or loss of response as a discussion point. Treatment with lanadelumab should be discontinued in patients who either respond inadequately or exhibit a loss of response, defined as follows:
Should the discontinuation criteria for berotralstat be aligned with that of lanadelumab? Are these definitions of an inadequate response or loss of response appropriate? | Aligning the discontinuation criteria for berotralstat with those used for lanadelumab would be reasonable. |
Considerations for prescribing of therapy | |
The berotralstat recommended dose is 150 mg orally once daily with food. There may be less potential risk of dose escalation with berotralstat than lanadelumab. | For CDEC consideration. |
Berotralstat is administered orally. Other options for prophylaxis of HAE are either IV or SC. | For CDEC consideration. |
Limited numbers of allergists and immunologists are available in some regions, and if restricted, access may be an issue. With previous comparators, specialized general practitioners or internists with experience in prescribing have been identified as having expertise in management of HAE. Lanadelumab recommendation specifies specialist physicians with experience in the diagnosis of HAE. Would this be appropriate for berotralstat as well? | Prescribing authority should be limited to specialists with an expertise in the diagnosis and management of patients with angioedema, including immunologists, allergists, and hematologists. |
Berotralstat is the first oral plasma kallikrein inhibitor. There may be a risk of combination therapy with lanadelumab, as it has a different mechanism of action. In practice, will berotralstat be used in combination with other prophylactic treatments for HAE such as lanadelumab? In addition, there is a risk that berotralstat may be used in combination with plasma-derived proteins. This would be difficult for drug plans to determine if patients are using plasma-based products as they are funded through a different mechanism. Berotralstat may also be used in combination with icatibant acetate if attacks do occur despite prophylaxis. Can short-term prophylaxis be used in combination with LTP therapy? The aim of short-term prophylaxis is to minimize the risk of attacks when exposure to a potential or known trigger is anticipated. | Combination LTP therapy is possible, although data supporting add-on therapy are limited. Short-term prophylaxis may be used in combination with LTP therapy. All patients require access to treatments to manage acute attacks. |
What is the place in therapy for berotralstat vs. lanadelumab? | Berotralstat and lanadelumab have a similar place in therapy. |
Generalizability | |
If the recommendation excludes HAE patients with normal C1-INH, this would deviate from the Health Canada indication and may create a need to consider requests outside of criteria. | For CDEC consideration. |
How should patients who want to switch from lanadelumab to berotralstat be assessed, as a baseline number of attacks is assessed before starting therapy? If they are attack-free for a period of time, should switching be considered? Patients may desire to be switched to an oral therapy. | When switching patients between LTP therapies, response should be based on the attack rate before starting any prophylaxis. Some patients may prefer an oral treatment vs. an injectable option, even if berotralstat was not as effective as other options. |
Care provision issues | |
Injection-site reactions from alternative products may be a rationale for switching to berotralstat. Adverse events from berotralstat did not result in discontinuations in clinical trials,. | For CDEC consideration. |
System and economic issues | |
The budget impact is difficult to interpret or validate, as it includes products provided through both CBS and drug plans. | For CDEC consideration. |
The plasma-derived products (C1-INHs) are reimbursed through CBS and Héma-Québec. The non–plasma-derived products, icatibant acetate (for treatment of acute attacks) and lanadelumab (for prophylaxis), are reimbursed through drug plans. When lanadelumab was implemented, it was anticipated that use of the plasma-derived products may be reduced with increasing uptake of lanadelumab. This was an increased cost to drug plans, but cost offsets elsewhere may have been realized through the reduction of blood products funded through CBS. Berotralstat, if listed, may have a similar effect of shifting costs from blood products to drug programs, perhaps to a lesser extent as it is a second entry product. | For CDEC consideration. |
Lanadelumab has successfully completed pCPA negotiations. Icatibant acetate has also successfully completed pCPA negotiations. Plasma-derived products are procured through purchase agreements through CBS. | For CDEC consideration. |
It may be easier for some patients to access products through CBS vs. products reimbursed through drug plans with strict reimbursement criteria (e.g., lanadelumab). | For CDEC consideration. |
Having berotralstat available may reduce the potential risk of drug shortages of plasma-derived products. An oral product may reduce health system costs of administration and increase accessibility for patients. Patients accessing products through CBS may have no co-pay associated with therapy. Listed drug products may be subject to a patient co-pay or deductible; the cost to the patient may therefore increase when switching from a product available through CBS to a product available through a drug plan. | For CDEC consideration. |
C1-INH = complement 1 esterase inhibitor; CBS = Canadian Blood Services; CDEC = CADTH Canadian Drug Expert Committee; HAE = hereditary angioedema; LTP = long-term prophylactic; pCPA = pan-Canadian Pharmaceutical Alliance; SC = subcutaneous.
Clinical Evidence
The clinical evidence included in the review of berotralstat is presented in 3 sections. The first section, the systematic review, includes pivotal studies provided in the sponsor’s submission to CADTH and Health Canada, as well as those studies that were selected according to an a priori protocol. The second section includes indirect evidence selected from the literature that met the selection criteria specified in the review. The third section includes sponsor-submitted long-term extension studies and additional relevant studies that were considered to address important gaps in the evidence included in the systematic review.
Systematic Review (Pivotal and Protocol-Selected Studies)
Objectives
To perform a systematic review of the beneficial and harmful effects of berotralstat 150 mg oral capsules for the routine prevention of recurrent episodes of HAE in adults and pediatric patients aged 12 years and older.
Methods
Studies selected for inclusion in the systematic review included pivotal studies provided in the sponsor’s submission to CADTH and Health Canada, as well as those meeting the selection criteria presented in Table 6. Outcomes included in the CADTH review protocol reflect outcomes considered to be important to patients, clinicians, and drug plans.
Table 6: Inclusion Criteria for the Systematic Review
Criteria | Description |
|---|---|
Population | Adult and pediatric patients with HAE who are 12 years of age and older Subgroups:
|
Intervention | Berotralstat 150 mg oral capsule once daily |
Comparator |
|
Outcomes | Efficacy outcomes:
Harms outcomes: AEs, SAEs, WDAEs, mortality, gastrointestinal adverse events |
Study designs | Published and unpublished phase III and IV randomized controlled trials |
AE = adverse event; HAE = hereditary angioedema; SAE = serious adverse event; WDAE = withdrawal due to adverse event.
The literature search for clinical studies was performed by an information specialist using a peer-reviewed search strategy according to the PRESS Peer Review of Electronic Search Strategies checklist.1
Published literature was identified by searching the following bibliographic databases: MEDLINE All (1946–) via Ovid and Embase (1974–) via Ovid. All Ovid searches were run simultaneously as a multifile search. Duplicates were removed using Ovid deduplication for multifile searches, followed by manual deduplication in EndNote. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. The main search concept was Orladeyo (berotralstat). Clinical trials registries searched included the US National Institutes of Health’s clinicaltrials.gov, WHO’s International Clinical Trials Registry Platform search portal, Health Canada’s Clinical Trials Database, and the European Union Clinical Trials Register.
No filters were applied to limit the retrieval by study type. Retrieval was not limited by publication date or by language. Conference abstracts were excluded from the search results. Appendix 1 provides detailed search strategies.
The initial search was completed on March 14, 2022. Regular alerts updated the search until the meeting of the CADTH Canadian Drug Expert Committee on July 27, 2022.
Grey literature (literature that is not commercially published) was identified by searching relevant websites from the Grey Matters: A Practical Tool For Searching Health-Related Grey Literature checklist.2 Included in this search were the websites of regulatory agencies (US FDA and European Medicines Agency). Google was used to search for additional internet-based materials. Appendix provides more information on the grey literature search strategy.
In addition, the sponsor was contacted for information regarding unpublished studies.
Two CADTH clinical reviewers independently selected studies for inclusion in the review based on titles and abstracts, according to the predetermined protocol. Full-text articles of all citations considered potentially relevant by at least 1 reviewer were acquired. Reviewers independently made the final selection of studies to be included in the review, and differences were resolved through discussion.
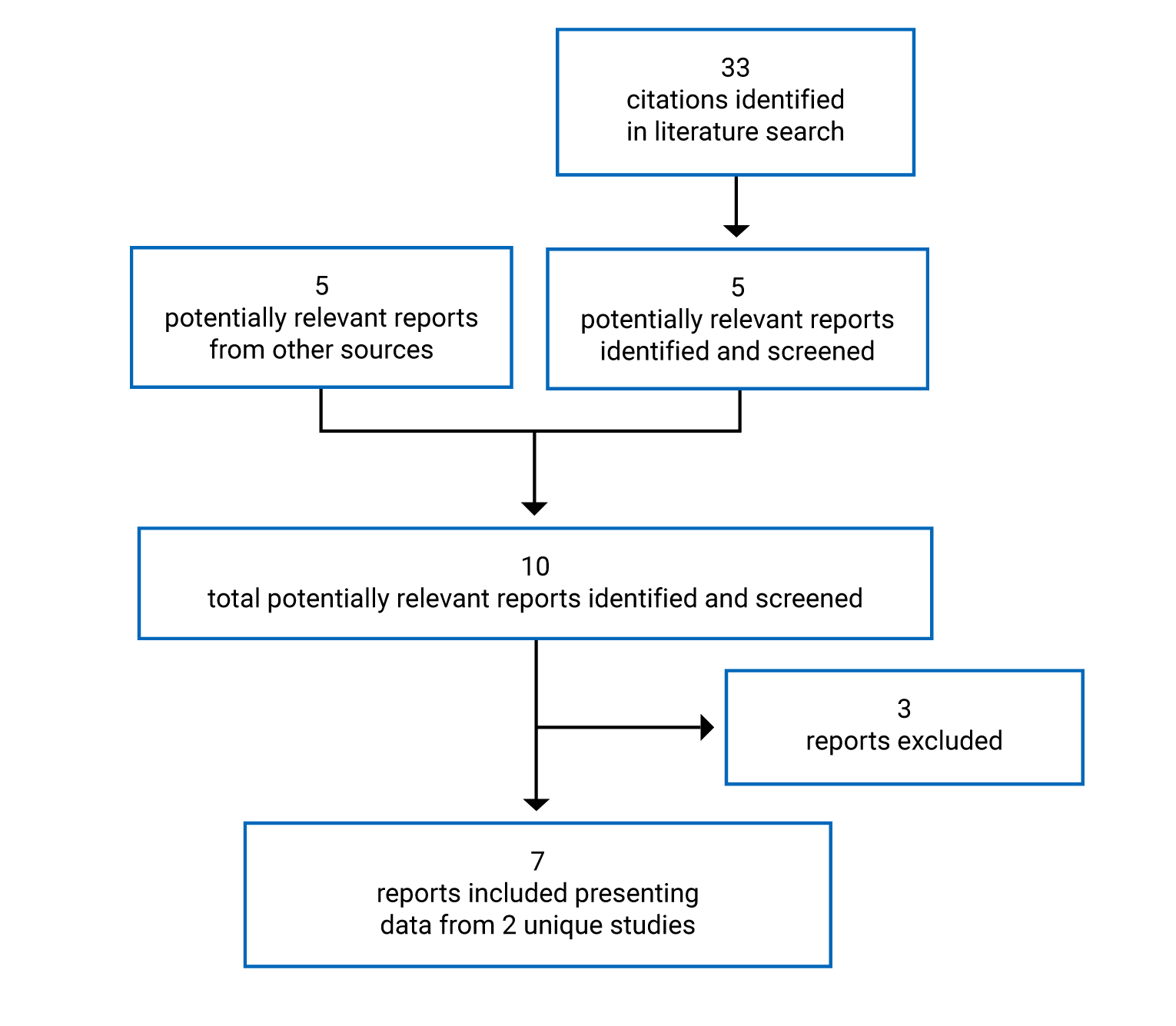
Findings From the Literature
A total of 2 studies were identified from the literature for inclusion in the systematic review (Figure 1). The included studies are summarized in Table 7. A list of excluded studies is presented in Appendix 2.
Description of Studies
Two double-blind, placebo-controlled RCTs met the inclusion criteria for the systematic review (APeX-2, APeX-J) (Table 7).
The objective of the APeX-2 study was to determine the efficacy, safety, and tolerability of prophylactic berotralstat compared with placebo in patients with type 1 or 2 HAE. The study included a run-in phase and 3 treatment phases (Figure 2). The patients enrolled underwent a 14- to 56-day run-in period to determine the baseline rate of HAE attacks, and those with 2 or more qualifying attacks during the run-in were eligible for randomization. A total of 121 patients were randomized 1:1:1 to placebo, berotralstat 110 mg, or berotralstat 150 mg daily for 24 weeks via an interactive web or voice response system (part 1). Randomization was stratified by the investigator-confirmed HAE attack rate during the screening period (≥ 2 attacks or < 2 attacks per 28 days). After 24 weeks, patients in the placebo group were rerandomized 1:1 to double-blind berotralstat 110 mg or 150 mg daily. Patients initially randomized to a berotralstat group continued the same double-blind dose from week 24 to week 48 (part 2). After 48 weeks, all patients continued on open-label berotralstat, and those receiving the 110 mg dose were transitioned to 150 mg daily for week 48 to 96 (part 3). The primary outcome was the rate of investigator-confirmed HAE attacks during the first 24 weeks of treatment. The study was conducted in 11 countries including Canada (3 sites), the US, and Europe.
The objective of the APeX-J study was to evaluate the efficacy and safety of berotralstat 110 mg and 150 mg daily for the suppression of events in patients with type 1 or 2 HAE. The trial used a design similar to that shown in Figure 2 and included a 56-day run-in period and 3 treatment phases: part 1, week 0 to week 24 (double-blind, placebo-controlled); part 2, week 24 to week 52 (double-blind, uncontrolled); and part 3, week 52 to week 104 (open-label, uncontrolled). Patients were eligible for randomization if they reported at least 2 qualifying angioedema events during the run-in phase. The randomization methods, treatment groups, and dosages used in APeX-J were the same as those reported for the APeX-2 study. The primary outcome was the rate of expert-confirmed HAE attacks during the first 24 weeks of treatment for berotralstat versus placebo. A total of 19 patients were randomized from 10 study sites in Japan.
Both trials were ongoing at the time this report was drafted, with limited or no information available for parts 2 or 3. The interim clinical study reports provided data from part 1 of the APeX-2 study (up to April 10, 2019) and the APeX-J study (up to November 15, 2019). This report focuses on the results of the berotralstat 150 mg daily dosage group, as this dosage was consistent with Health Canada recommendations. The results of the berotralstat 110 mg dose are not summarized in this report.
Table 7: Details of Included Studies
Study detail | APeX-2 | APeX-J |
|---|---|---|
Designs and populations | ||
Study design | Double-blind RCT | Double-blind RCT |
Locations | North America, Europe | Japan |
Patient enrolment dates | March 14, 2018, to April 10, 2019 (part 1) | December 27, 2018, to November 15, 2019 (part 1) |
Randomized (N) | 121 | 19 |
Inclusion criteria | Adults and adolescents ≥ 12 years of age with confirmed diagnosis of HAE type 1 or type 2a:
| Adults and adolescents ≥ 12 years of age with confirmed diagnosis of HAE type 1 or type 2a:
|
Exclusion criteria |
| Same as APeX-2 |
Drugs | ||
Interventionc | Berotralstat 150 mg orally per day Berotralstat 110 mg orally per dayd | Berotralstat 150 mg orally per day Berotralstat 110 mg orally per dayd |
Comparator(s) | Placebo (switched to berotralstat at 24 weeks)e | Placebo (switched to berotralstat at 24 weeks)e |
Duration | ||
Phase | ||
Run-in | 14 to 56 days | 56 days |
Double-blind part 1 | 24 weeks | 24 weeks |
Double-blind part 2 | 24 weeks | 28 weeks |
Open-label part 3 | Up to 48 weeks | Up to 52 weeks |
Follow-up | 3 weeks | 3 weeks |
Outcomes | ||
Primary end point | Rate of investigator-confirmed HAE attacks over 24 weeks (part 1) | Rate of expert-confirmed HAE attacks over 24 weeks (part 1) |
Secondary and exploratory end points | Secondary:
Exploratory:
| Secondary:
Exploratory:
|
Notes | ||
Publications | Ohsawa et al. (2021)18 | |
ACE = angiotensin-converting enzyme; AE-QoL = Angioedema Quality of Life questionnaire; C1-INH = complement 1 esterase inhibitor; C4 = complement 4; CFB = change from baseline; CrCl = creatinine clearance; CV = cardiovascular; ECG = electrocardiogram; HAE = hereditary angioedema; LLN = lower limit of normal; RCT = randomized controlled trial; SOC = standard of care.
Note: Five additional reports were included (FDA Multidiscipline Review,19 European Public Assessment Report for Orladeyo,20 Zuraw et al. [2021],17 Wedner et al. [2021],5 Ohsawa et al. [2021]18) in the original systematic review. One additional unpublished report was supplied by the sponsor as part of the Request for Reconsideration, and this report is summarized in Appendix 5.21
aDefined as having a C1-INH functional level below 50% and a C4 level below the LLN reference range, as assessed during the screening period. In the absence of a low C4 value drawn during the intercritical period (i.e., patient was not having an HAE attack), 1 of the following was acceptable to confirm the diagnosis of HAE: SERPING1 gene mutation known or likely to be associated with type 1 or type 2 HAE assessed during the screening period; confirmed family history of C1-INH deficiency; or C4 redrawn and retested during an attack in the screening period with the results below the LLN reference range. For patients with a C1-INH function of 50% or greater but less than the assay LLN (74%), a SERPING1 gene mutation known or likely to be associated with type 1 or type 2 HAE, as assessed during the screening period or a repeat C1-INH functional level below 50%, was considered acceptable for enrolment.
bDuring the run-in period, HAE attacks had to meet all the following criteria: the attacks were unique, which was defined as an attack that did not begin within 48 hours of the end of a previous attack; the attacks must have either been treated, required medical attention, or been documented to cause functional impairment based on patient entry in an electronic diary, with functional impairment defined as the patient being unable to perform daily activities without restriction (i.e., patients recorded that they were at least slightly restricted in their daily activities during their HAE attack); the attacks included symptoms of swelling, and symptoms of swelling, in addition to visible swelling, and may also have included symptoms in the oropharyngeal or abdominal regions that were indicative of internal swelling; and the attacks were confirmed by the investigator in the APeX-2 study or the independent expert in the APeX-J study to be HAE attacks. Patients were contacted within 2 business days of the attack to discuss the attack and any queries on the data entered in the electronic diary, as applicable.
cDosage for berotralstat during part 1 and part 2 of the study. During part 3 of the study, all patients received open-label berotralstat. Those receiving berotralstat 110 mg daily were switched to 150 mg daily.
dNot a Health Canada–recommended dosage.
eAt 24 weeks, patients in the placebo group were randomized to receive either double-blind berotralstat 110 mg or 150 mg daily. During part 3 all patients were switched to berotralstat 150 mg daily.
Source: Clinical Study Report for APeX-26 and Clinical Study Report for APeX-J.7
Figure 2: Study Schematic for APeX-2
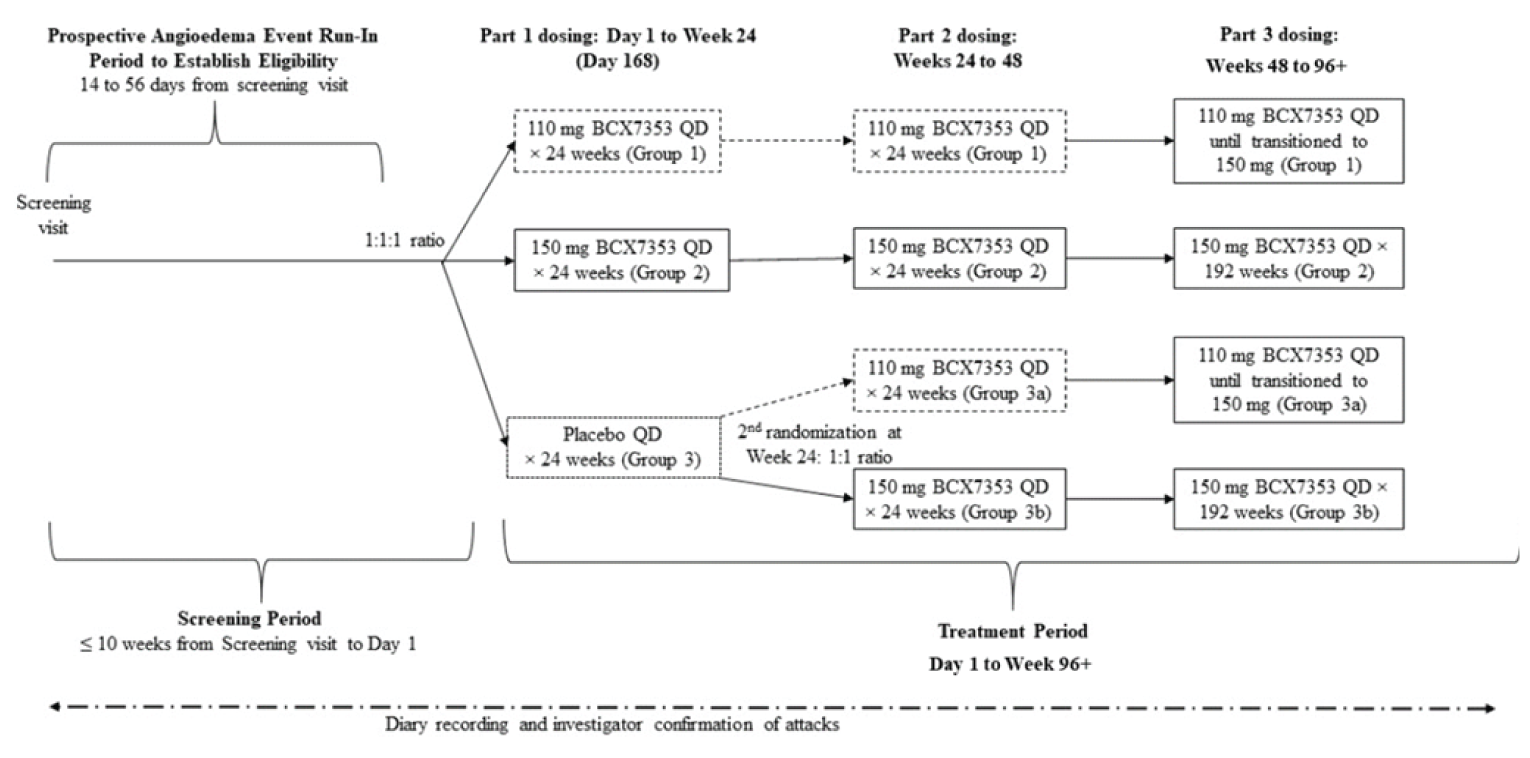
BCX7353 = berotralstat; QD = once daily.
Note: In the APeX-2 study, the run-in phase ranged from 14 to 56 days. Once a patient had recorded 2 attacks that met the criteria, they could be randomized on or after day 28. Patients who experienced 3 or more attacks could be randomized on or after day 14. In the APeX-J study, the run-in phase was 56 days for all patients and patients had to report at least 2 eligible attacks to qualify for randomization.
Source: Clinical Study Report for APeX-2.6
Populations
Inclusion and Exclusion Criteria
Both studies enrolled patients aged 12 years and older with a confirmed diagnosis of type 1 or 2 HAE, who experienced at least 2 qualifying HAE attacks during the run-in phase. In addition, the patients had to have access to standard-of-care treatments for acute attacks and be medically appropriate for on-demand treatment as the sole medical management of their HAE (Table 7).
Patients were excluded if they had been diagnosed with another form of recurrent angioedema, had suspected C1-INH resistance, or had a preplanned procedure for which short-term prophylaxis was required. Patients were required to stop prophylactic use of C1-INH, androgens, or tranexamic acid, 14 or 28 days before screening.
Baseline Characteristics
The mean ages of patients enrolled in the APeX-2 study were 40.0 years (SD = 14.0) and 44.5 years (SD = 14.1) in the berotralstat 150 mg and placebo groups, respectively (Table 8). Two patients per group (5%) were adolescents 12 to 17 years of age. Patients were predominantly female (58% and 68%), and white (95% and 93%), and most had a family history of HAE (█ █ ██ █ ████ in the berotralstat and placebo groups, respectively). Most patients had at least 2 attacks per month at baseline (75% and 68%) and the mean baseline rates were 3.1 (SD = 1.6) and 2.9 (SD = 1.1) investigator-confirmed HAE attacks per month in the berotralstat 150 mg and placebo groups, respectively. Approximately 75% of patients enrolled had received prior prophylactic treatments for HAE, with a similar frequency between treatment groups (Table 9).
In the APeX-J study, the mean ages of patients enrolled were 37.3 years (SD = 9.1) in the berotralstat 150 mg group and 42.3 years (SD = 13.5) in the placebo group (Table 8). █ █ ███ █ ██ █ ███ █ ████ █ █████ █ █████ █ ███. Most patients were female (86% and 83%) and Asian (86% and 100%) in the berotralstat and placebo groups, respectively. The mean baseline attack rates were 2.0 (SD = 1.1) and 2.5 (SD = 1.5) per month for the berotralstat and placebo groups, respectively. In the berotralstat group, 86% had received prior prophylactic treatment for HAE, compared with 67% of patients in the placebo group (Table 9).
There were imbalances between groups within the trials in the mean age, proportion of females, weight, prior laryngeal attack, and prior emergency visit in past year (Table 8). Differences were also noted between the studies in the mean weight, race, baseline attack rate, family history of HAE, emergency visit for HAE in the past year, and type of prior prophylactic therapy for HAE.
Interventions
In both the APeX-2 and APeX-J studies, eligible patients were randomized to receive double-blind placebo, berotralstat 110 mg, or berotralstat 150 mg daily for the first 24 weeks (part 1). The study drug was supplied as identical-looking capsules containing either placebo, berotralstat 55 mg, or berotralstat 75 mg. Patients were instructed to take 2 capsules daily with food.
During part 2 of the trials, patients in the berotralstat groups continued on the same dose of study drug, and those in the placebo group were rerandomized to berotralstat 110 mg or berotralstat 150 mg daily for 24 weeks in APeX-2 study, or for 28 weeks in the APeX-J study. Patients were informed they were receiving the active drug during part 2 but were not aware of the dose of berotralstat. During part 3 of the studies, patients received open-label berotralstat, with those who previously received the 110 mg dose switched to 150 mg daily.
Table 8: Summary of Baseline Characteristics
Characteristic | APeX-2 | APeX-J | ||
|---|---|---|---|---|
Berotralstat 150 mg N = 40 | Placebo N = 40 | Berotralstat 150 mg N = 7 | Placebo N = 6 | |
Age (years), mean (SD) | 40.0 (14.0) | 44.5 (14.1) | 37.3 (9.1) | 42.3 (13.5) |
Age (years), median (range) | 39 (12 to 69) | 43.5 (14 to 72) | ██████████ | █████ |
Age 12 to 17 years, n (%) | 2 (5) | 2 (5) | █ | █ |
Female, n (%) | 23 (58) | 27 (68) | 6 (86) | 5 (83) |
Race, n (%) | ||||
White | 38 (95) | 37 (93) | 0 | 0 |
Black or African American | 1 (3) | 2 (5) | 0 | 0 |
Asian | 0 | 0 | 6 (86) | 6 (100) |
Other | 1 (3) | 1 (3) | 1 (14) | 0 |
Weight (kg), median (range) | 82.1 (57.5 to 149.7) | 77.0 (57.3 to 134.7) | ████████████ | █████████ |
BMI (kg/m2), median (range) | 28.6 (21.0 to 54.1) | 27.8 (19.9 to 51.0) | ████████████ | █████████ |
Baseline investigator-confirmed HAE attack rate per month, mean (SD)a | 3.1 (1.6) | 2.9 (1.1) (N = 39) | 2.0 (1.1) | 2.5 (1.5) |
Baseline investigator-confirmed HAE attack rate per month, median (range)a | 2.7 (0.9 to 6.7) | 3.0 (1.3 to 6.2) | 2.2 (0.8 to 3.9) | 2.2 (0.9 to 5.3) |
Baseline investigator-confirmed attack rate, n (%) | ||||
≥ 2 attacks per month | 30 (75) | 27 (68) | 4 (57) | 3 (50) |
< 2 attacks per month | 10 (25) | 12 (30) | 3 (43) | 3 (50) |
Prior laryngeal attack (lifetime), n (%) | 26 (65) | 34 (85) | █████ | █████ |
Laryngeal attack in past year, n (%) | 9 (23) | 17 (43) | 0 | 3 (50) |
Emergency visit in past year, n (%) | ██████ | ██████ | █████ | ██████ |
Hospitalization in past year, n (%) | █████ | ████ | █ | █████ |
Diagnosis of HAE, n (%) | ||||
C4 < LLN and C1-INH function < 50% | 35 (88) | 38 (95) | ██████ | ██████ |
C4 < LLN and C1-INH function 50% to 74% and SERPING1 mutation | 1 (3) | 0 | █ | █ |
C4 ≥ LLN and C1-INH function < 50% and family history | 3 (8) | 1 (3) | █ | █ |
C4 ≥ LLN and C1-INH function < 50% and SERPING-1 mutation | 0 | 1 (3) | █ | █ |
C4 ≥ LLN and C1-INH function 50% to 74% and SERPING1 mutation | 1 (3) | 0 | █ | █ |
Age at diagnosis of HAE (years), median (range) | ██████████ | █████████ | █████████ | ████████ |
Age at first symptom onset of HAE (years), median (range) | ███████████ | ███████████ | ██████████ | ████████ |
Family history of type 1 or 2 HAE, n (%) | ██████ | ██████ | █████ | █████ |
BMI = body mass index; C4 = complement 4; C1-INH = complement 1 esterase inhibitor; HAE = hereditary angioedema; LLN = lower limit of normal; SD = standard deviation.
aThe baseline attack rate in the APeX-2 study was based on the investigator-confirmed events between screening and the first dose of the study drug. The median number of days was 36.5 (range = 15 to 72 days) in the berotralstat 150 mg group and 36 days (range = 20 to 66 days) in the placebo group.
Source: Clinical Study Report for APeX-26 and Clinical Study Report for APeX-J.7
Table 9: Summary of Prior Long-Term Prophylactic Treatments for Hereditary Angioedema
Medication | APeX-2 | APeX-J | ||
|---|---|---|---|---|
Berotralstat 150 mg N = 40 | Placebo N = 40 | Berotralstat 150 mg N = 7 | Placebo N = 6 | |
Any past prophylactic treatment for HAE, n (%) | 30 (75) | 29 (73) | 6 (86) | 4 (67) |
Berinert | █████ | █████ | █ | █████ |
Cinryze | ██████ | ██████ | █████ | █ |
Haegarda | █████ | █████ | ██ | ██ |
Tranexamic acid | █████ | ████ | 3 (43) | 3 (50) |
Other a | ████ | █ | ████ | █ |
Any androgen use, b n (%) | 21 (53) | 25 (63) | 2 (29) | 1 (17) |
Any C1-INH,c n (%) | 21 (53) | 16 (40) | 1 (14) | 1 (17) |
C1-INH = complement 1 esterase inhibitor; HAE = hereditary angioedema; NR = not reported.
aOther medications included desogestrel (APeX-2) and goreisan (APeX-J).
bIncludes androgens (unspecified), oxandrolone, methyl-testosterone, danazol, and stanozolol.
cIncludes plasma-derived C1-INH (Cinryze, Berinert, Haegarda), recombinant C1-INH (Ruconest) and fresh frozen plasma.
Source: Clinical Study Report for APeX-26 and Clinical Study Report for APeX-J.7
All patients were required to have access to acute treatments for angioedema events and to administer these treatments for an attack following the medical management plan advised by their physician. Use of C1-INH for short-term prophylaxis of unplanned procedures was allowed.
Patients were prohibited from using androgens or tranexamic acid for prophylaxis within 28 days before screening and during the trial. C1-INH used for prophylaxis of HAE was prohibited within 14 days before screening and during the study. Use of an angiotensin-converting-enzyme inhibitor within 7 days, or initiation of estrogen-containing contraceptives within 56 days before screening was not permitted as these drugs may exacerbate HAE. Other prohibited treatments included concurrent use of drugs metabolized by cytochrome P450 enzyme (CYP) 2D6, CYP2C9, CYP2C19, or CYP3A4 that have a narrow therapeutic index or are known to prolong the QT interval, as well as drugs with a narrow therapeutic index that are transported by the P-glycoprotein efflux pump.
Outcomes
A list of efficacy end points identified in the CADTH review protocol that were assessed in the clinical trials included in this review is provided in Table 10. These end points are further summarized in the following section. A detailed discussion and critical appraisal of the outcome measures are provided in Appendix 4.
Table 10: Summary of Outcomes of Interest Identified in the CADTH Review Protocol
Outcome measure | APeX-2 | APeX-J |
|---|---|---|
Part 1 (week 0 to 24) | ||
Investigator (or expert) confirmed HAE attack rate; day 1 to 24 weeks | Primary | Primary |
Change from baseline to week 24 in AE-QoL total score | Secondary | Secondary |
Number and proportion of days with angioedema symptoms through 24 weeks | Secondary | Secondary |
Investigator-confirmed HAE attack rate; day 8 to 24 weeks | Secondary | Secondary |
Proportion of patients with no attacks over 24 weeks | Exploratory | Exploratory |
Use of HAE medications to treat attacks over 24 weeks | Exploratory | Exploratory |
Proportion of responders (≥ 50%, ≥ 70%, or ≥ 90% relative reduction in adjusted investigator-confirmed HAE attack rate) | Exploratorya | Exploratory |
Change from baseline to week 24 in EQ-5D-5L and EQ VAS | Exploratory | Exploratory |
Laryngeal attack rate | Exploratory (ad hoc) | Exploratory (ad hoc) |
Moderate or severe HAE attack rate | Exploratory (ad hoc) | Exploratory (ad hoc) |
Attack-free months | Exploratory (ad hoc) | NR |
AE-QoL = Angioedema Quality of Life questionnaire; EQ-5D-5L = 5-Level EQ-5D questionnaire; EQ VAS = EQ visual analogue scale; HAE = hereditary angioedema, NR = not reported.
aThe proportion of responders defined as a 70% or greater or a 90% or greater reduction in HAE attack rate were ad hoc analyses in the APeX-2 study.
Source: Clinical Study Report for APeX-26 and Clinical Study Report for APeX-J.7
The primary outcome of part 1 in both studies was the investigator-confirmed attack rate from day 1 to 24 weeks. Patients were required to document the presence or absence of symptoms of an HAE attack daily using an electronic diary. If an attack was reported, details regarding the location, severity, symptoms, and duration of attack were required to be recorded, along with the timing of any treatments administered and whether additional medical care was sought for the attack. Administration of the study drug was also recorded daily using the diary. All patients were required to complete the diary symptom data during the run-in period to determine the baseline rate of HAE attacks, and then daily throughout the treatment period until the study was completed or the patient discontinued the trial. Adherence was monitored electronically and if at any time the diary completion was less than 90%, then additional training was provided or patients were reminded via phone. Patients who stopped the study drug continued to record HAE attacks until their last study visit. Investigators could view electronic diary entries in real time and contacted patients within 2 business days of the end of an attack to review the attack details and gather additional data if needed to confirm the event as an HAE attack. Attacks reported verbally to the investigator, but not recorded using the diary, were also counted. In APeX-2, only investigator-confirmed events were included in the primary outcome analysis. In the APeX-J study, all HAE events were adjudicated by an independent expert selected by the sponsor.
During the run-in phase, HAE attacks had to meet all 4 criteria to qualify as an event, but during the treatment period only criteria 3 and 4 were required. The criteria were:
The attacks were unique, which was defined as an attack that did not begin within 48 hours of the end of a previous attack.
The attacks must have either been treated, required medical attention, or been documented to cause functional impairment based on patient entry in the electronic diary. Functional impairment was defined as the patient being unable to perform daily activities without restriction (i.e., patients recorded that they were at least slightly restricted in their daily activities during their HAE attack).
The attacks included symptoms of swelling. In addition to visible swelling, these may also have included symptoms in the oropharyngeal or abdominal regions that were indicative of internal swelling.
The attacks were confirmed by the investigator to be HAE attacks in the APeX-2 study, or by the independent expert in the APeX-J study.
The baseline attack rate was calculated as the number of attacks that met the criteria from the screening visit to the first dose date multiplied by 28 and divided by the date of the first study drug dose minus the screening date plus 1. After randomization, the investigator-confirmed attack rate was based on the entire dosing period, from day 1 (first dose in part 1) to the first dose of the study drug in part 2 of the study (primary outcome) or the effective treatment period (once drug concentration reached a steady state), which was day 8 to the administration of the first dose in part 2 (secondary outcome). For any patients who stopped treatment early, an attack that began within 24 hours of stopping therapy was included in the calculation of the attack rate; otherwise, any attacks that occurred after treatment was stopped were not included.
For the responder analyses, the on-treatment investigator-confirmed attack rate had to meet the same criteria as attacks in the run-in period and were reported as adjusted investigator-confirmed events. Two additional criteria were applied: the attacks had to be unique (> 48 hours between attacks), and the attacks had to be treated, require medical attention, or cause functional impairment. In the APeX-2 study the preplanned responder analysis was defined as a 50% or greater relative reduction in the attack rate versus baseline. Post hoc analyses based on 70% or greater and 90% or greater thresholds were also conducted. In the APeX-J study, all 3 analyses (≥ 50%, ≥ 70%, and ≥ 90%) were preplanned. According to the clinical expert consulted for this review, a 20% improvement in the attack rate is considered a mild effect, 50% is considered moderate, and 70% is considered a marked effect.
The number and proportion of days with HAE symptoms were calculated from day 1 to week 24. In both studies, an ad hoc analysis was conducted for laryngeal attacks (defined as visible swelling in the mouth, tongue, or lips, lump in throat [tightness], difficulty swallowing, change in voice, or difficulty breathing), and investigator-confirmed events that were rated as moderate to severe by the patient. Ad hoc data were reported in the APeX-2 study for attack-free months, based on the number of patients with no investigator-confirmed attacks in each 28-day period. For this outcome, patients who discontinued the study drug in a given month were not considered attack-free in that month.
The AE-QoL score was a secondary outcome in both studies. The AE-QoL is a patient-reported angioedema-specific HRQoL measure that consists of 17 questions in 4 domains (functioning, fatigue or mood, fears or shame, and food).22 Each item has 5 responses from 1 (never) to 5 (very often) that is scored from 0 to 4 over a 4-week recall period. A total score and individual domain scores are generated and converted to a linear scale of 1 to 100, with higher scores representing higher impairment. The evidence to support the validity, reliability, and responsiveness of the AE-QoL in patients with recurrent angioedema is summarized in Appendix 4. A minimal important difference (MID) of 6 points has been reported for patients with angioedema in the literature.23
Other HRQoL measures were reported as exploratory outcomes. The 5-Level EQ-5D (EQ-5D-5L) questionnaire includes 2 parts: a descriptive system and a visual analogue scale (EQ VAS). The descriptive system has 5 dimensions (mobility, self-care, usual activities, pain or discomfort, and anxiety or depression), each of which has 5 levels (no problems, slight problems, moderate problems, severe problems, and extreme problems). In both berotralstat studies, the descriptive system was converted to an index score using the US value set.24 The EQ VAS records the patient’s self-rated health on a vertical scale, with anchors labelled “the worst health you can imagine” and “the best health you can imagine” (scored from 0 to 100, respectively). The EQ-5D-5L has not been validated in patients with HAE.
Adverse events were any untoward medical occurrence, which may or may not be related to the study drug. HAE attacks and their symptoms were not defined as adverse events unless they met the criteria for a serious adverse event. The criteria for serious adverse events included death; events that were life-threatening, required hospitalization or prolongation of hospitalization; those resulting in a persistent or significant disability or incapacity; a congenital anomaly or birth defect; or an event that may have required medical or surgical intervention to prevent 1 of the other outcomes listed.
The primary outcomes for parts 2 and 3 of the trials were safety-related, and the secondary efficacy outcomes were the frequency of angioedema events, HRQoL, and durability of treatment response.
Statistical Analysis
The rate of confirmed HAE events was analyzed using a negative binomial regression model that included the treatment, the stratification variable (< 2 or ≥ 2 confirmed attacks per month at baseline), and the log of treatment duration as the offset. The primary analysis was based on the intention-to-treat (ITT) population for patients who were on treatment and did not include any data after treatment discontinuation. A negative binomial model was selected for the primary analysis because the Poisson model showed evidence of overdispersion (i.e., the variance in the data was greater than the mean). Similar methods were used to analyze secondary or exploratory attack-rate outcomes in both trials (Table 11). The change from baseline in the HRQoL measures was analyzed using a mixed model of repeated measures that included the baseline attack rate, baseline score, visit, and visit by treatment interaction terms as covariates. The proportion of days with HAE symptoms through 24 weeks was analyzed using an analysis of covariance model, and the responder analysis used a logistic regression model, both of which included the baseline attack rate as a covariate.
There was no imputation for missing data for any outcomes reported in either study. For the primary outcome in the APeX-2 study, 3 sensitivity analyses were to explore the impact of missing data. One analysis included event data reported after the patient stopped treatment, and a second analysis included post–treatment-cessation data (where available) plus multiple imputation methods to impute data for patients who stopped treatment but did not continue to report attacks. The APeX-2 study also conducted a tipping-point analysis, which estimated the magnitude of effect required among patients with missing data in the active treatment group to change the result to nonstatistically significant. Other sensitivity analyses were conducted using the per-protocol population and only patients who completed the study. Similar sensitivity analyses were conducted in the APeX-J study (Table 11).
In both the APeX-2 and the APeX-J studies, the type I error rate was controlled for the primary and 3 secondary outcomes, and for the 2 dosage groups versus placebo using hierarchical testing and the Hochberg procedure. Both the 110 mg and 150 mg berotralstat groups were tested for the primary outcome at an alpha level of 0.05, and if both showed a P value of less than 0.05, then testing continued for both groups at the alpha 0.05 level. If the highest P value was greater than 0.05 and the lowest was less than 0.025, then testing for the statistically significant dosage group continued at the 0.025 level. If the primary outcome null hypothesis was not rejected for both dosage groups, then testing stopped. The order of testing in the APeX-2 study was the rate of confirmed HAE attacks during the entire 24-week treatment period (primary), the change from baseline in AE-QoL, the proportion of symptom-days, and the rate of HAE attacks in the effective treatment period (day 8 to 24 weeks). For the APeX-J study, the order of testing was the rate of confirmed attacks during the entire 24-week treatment period (primary), the proportion of symptom-days, the rate of HAE attacks (day 8 to 24 weeks), and the change from baseline in AE-QoL. There was no control of the type I error rate for the exploratory or other outcomes tested. Both trials were ongoing at the time this report was written. The analysis of the efficacy outcomes for part 1 (an interim analysis) was conducted once the last patient had completed part 1.
In the APeX-J study, the primary analysis was based on the ITT population, but a pooled analysis was also planned that combined patients from the APeX-J study with those from the APeX-2 study. The same hierarchical and Hochberg procedure was applied to the testing of outcomes for the combined analysis; however, this testing was conducted independently of the primary ITT analysis (which failed to reject the null hypothesis on the second outcome tested for the berotralstat 150 mg group).
Of the subgroups of interest to this review, the APeX-2 study conducted preplanned analyses based on the baseline attack rate (≥ 2 versus < 2 per month) and age group (< 18 years, 18 to 65 years, > 65 years). An ad hoc analysis was conducted based on subgroups with or without prior use of androgens. The same 3 subgroups of interest were preplanned for analyses in the APeX-J study, but due to the small sample size, the analyses were not conducted. Instead, subgroup data were reported for the combined APeX-2 and APeX-J population.
With 40 patients per group, the APeX-2 study had a 94% power to detect a 50% attack-rate reduction (treatment difference of 0.5 attacks per week) between berotralstat and placebo (2-sided test, significance level of 0.05). The power calculations assumed a normalized placebo attack rate of 1 with a common SD of 0.55, and a 20% dropout rate. Data from the phase II Study 203 (APeX-1) were used to support these assumptions.
Study APeX-J had limited statistical power and did not meet its target enrolment of 8 patients per group. Assuming a weekly angioedema event rate of 0.9 for placebo and a common SD of 0.5, with 8 patients per group, the study had a 61% power to detect an event-rate reduction of 67% or greater (i.e., a treatment difference of 0.6 events per week) for each dose of berotralstat versus placebo. Due to the sample size limitations, a supplemental statistical analysis was conducted that combined the patients enrolled in the APeX-J trial with those in APeX-2. A combined sample size of 48 patients per group would have better than a 99% power to detect an event rate reduction of 67% or greater between each dose of berotralstat and placebo (2-sided alpha 0.05).
Table 11: Statistical Analysis of Efficacy End points
Study/end point | Statistical model | Adjustment factors | Sensitivity analyses |
|---|---|---|---|
APeX-2 | |||
Investigator-confirmed HAE attack rate from day 1 to week 24 | Negative binomial model (no imputation for missing data) |
|
|
Investigator-confirmed HAE attack rate from day 8 to week 24 Treated HAE attack rate Laryngeal attack rateb Moderate or severe HAE attack rateb | Same as above | Same as above | NR |
Change from baseline to week 24 in the AE-QoL total score, EQ-5D-5L index score, and EQ VAS | MMRM | Baseline attack rate, baseline score, visit, visit by treatment interaction | NR |
Proportion of days with HAE symptoms through 24 weeks | ANCOVA | Baseline attack rate | NR |
Proportion of patients with no attacks | Chi-square test | NR | NR |
Proportion of responders | Logistic regression | Baseline attack rate | NR |
Attack-free months | Descriptive data (completer population) | NR | NR |
APeX-Jc | |||
Expert-confirmed HAE attack rate from day 1 to week 24 | Negative binomial model (no imputation for missing data) |
|
|
Expert-confirmed HAE attack rate from day 8 to week 24 Treated HAE attack rate Laryngeal attack rateb Moderate or severe HAE attack rateb | Same as above | Same as above | NR |
Proportion of days with HAE symptoms through 24 weeks | ANCOVA | Baseline attack rate | NR |
Change from baseline to week 24 in the AE-QoL total score, EQ-5D-5L index score and EQ VAS | MMRM | Baseline attack rate, baseline score, visit, visit by treatment interaction | NR |
Proportion of patients with no attacks | Chi-square test | NR | NR |
Proportion of responders | Logistic regression | NR | NR |
AE-QoL = Angioedema Quality of Life questionnaire; ANCOVA = analysis of covariance; EQ-5D-5L = 5-Level EQ-5D questionnaire; EQ VAS = EQ visual analogue scale; HAE = hereditary angioedema; MMRM = mixed model for repeated measures; NR = not reported.
aIncluded data recorded after the study drug was stopped until patient started a new prophylactic treatment.
bAd hoc analysis.
cThe combined analyses that pooled data from the APeX-2 and APeX-J studies also included a covariate for the statistical models.
Source: Clinical Study Report for APeX-26 and Clinical Study Report for APeX-J.7
Analysis Populations
In both studies the ITT population included all randomized patients, regardless of whether the study drug was administered. The safety population included all patients who received at least 1 dose of the study drug according to the drug received at first dose.
Results
Patient Disposition
In part 1 of the APeX-2 study, 160 patients were screened for entry, of whom 121 (76%) were randomized. The most common reasons for excluding patients were: █ █ █ █ ████ █ ████████ █ █████████ █ ██████████ █ █ █ ███ █ ████ █ ██ █ █ █ █ █ █ █ ███ █ ███ █ █████ █ ██ █ ███ █ █████ █ ██████████ █ █████████████ █ █ █ █████ █ ██ █ ███ █ ██ █ █ █ █ █ █ █ █ █████ █ ████ In the berotralstat 150 mg group, ██ █ █ █ ███ patients (██) randomized discontinued the study early (withdrawal of consent) compared with █████ patients (███) in the placebo group (due to withdrawal of consent, increased frequency of attacks, or other reasons). Three patients (8%) in the berotralstat 150 mg group stopped the study drug early compared with 5 patients (13%) in the placebo group. One patient treated with placebo never received any study drug (Table 12).
In the berotralstat 150 mg group, 37 patients (93%) completed part 1 of APeX-2 and entered part 2. Six patients discontinued early (16%).5 Reasons for discontinuation were adverse events for 2 patients, lack of efficacy for 3 patients, and other reasons for 1 patient. Among patients initially randomized to placebo, 34 patients (85%) completed part 1 and 17 patients were randomized to berotralstat 150 mg daily. Two of these patients (18%) discontinued early due to lack of efficacy and 1 patient withdrew consent.5
In the APeX-J study, 25 patients were screened for entry, 19 of whom (76%) were randomized to 1 of 3 treatment groups. None of the patients in the berotralstat 150 mg and placebo groups withdrew from part 1 of the study, and only 1 patient in the placebo group (17%) stopped treatment early due to an adverse event (Table 12).
Table 12: Patient Disposition (Part 1)
Disposition | APeX-2 | APeX-J | ||
|---|---|---|---|---|
Berotralstat 150 mg | Placebo | Berotralstat 150 mg | Placebo | |
Screened, N | 160a | 25b | ||
Randomized total, N (%) | 121 (76)c | 19 (76)d | ||
Randomized, N | 40 | 40e | 7 | 6 |
Discontinued from study, N (%) | ████ | █████ | 0 | 0 |
Reason for discontinuation, N (%) | ||||
Withdrew consent | ████ | ████ | 0 | 0 |
Increased frequency of attacks | █ | ████ | 0 | 0 |
Other | █ | ████ | 0 | 0 |
Discontinued study drug, N (%) | 3 (8) | 5 (13) | 0 | 1 (17) |
Reason for discontinuation, N (%) | ||||
Adverse events | 1 (3) | 1 (3) | 0 | 1 (17) |
Lack of efficacy | 1 (3) | 2 (5) | 0 | 0 |
Withdrew consent | 1 (3) | 1 (3) | 0 | 0 |
Other | 0 | 1 (3) | 0 | 0 |
Intention-to-treat population, N (%) | 40 (100) | 40 (100) | 7 (100) | 6 (100) |
Safety population, N (%) | 40 (100) | 39 (98) | 7 (100) | 6 (100) |
aIn the APeX-2 study, of the 39 patients who failed screening, 36 did not meet inclusion criteria (most common: 15 patients did not meet HAE diagnostic criteria, 7 patients did not record 2 or more HAE attacks during run-in), and 3 patients withdrew consent.
bIn the APeX-J study 6 patients failed screening including 3 patients who did not record 2 or more HAE attacks during run-in, 2 patients who did not meet other inclusion criteria, and 1 patient who withdrew consent.
cIncludes 41 patients who were randomized to the berotralstat 110 mg dose group.
dIncludes 6 patients who were randomized to the berotralstat 110 mg dose group.
eOne patient did not receive treatment.
Source: Clinical Study Report for APeX-26 and Clinical Study Report for APeX-J.7
Exposure to Study Treatments
The median treatment duration was 168 days in the berotralstat 150 mg and placebo groups in both the APeX-2 and APeX-J studies (Table 13). All patients had access to treatments to manage acute HAE attacks, and the most commonly reported options were C1-INH or icatibant acetate. The proportions of acute events that were treated were generally similar in the berotralstat 150 and placebo groups of the APeX-2 study (87% and 88%) and the APeX-J study (███ and ███, respectively), although there were differences between groups in the specific medications administered (Table 13). More attacks were treated with a C1-INH in in the berotralstat group than in the placebo group in the APeX 2 study (55% versus 36%, respectively), but the ██ █ ██ █ ███ █ █ █ ██ in the APeX-J study (███ versus ███).
Table 13: Extent of Exposure (Part 1 Safety Population)
Outcome | APeX-2 (24 weeks) | APeX-J (24 weeks) | ||
|---|---|---|---|---|
Berotralstat 150 mg N = 40 | Placebo N = 39 | Berotralstat 150 mg N = 7 | Placebo N = 6 | |
Study drug | ||||
Duration of exposure, days | ||||
Mean (SD) | 156.7 (40.3) | 154.8 (36.5) | ██████████ | ██████ |
Median (range) | 168 (14 to 170) | 168 (23 to 168) | ████████████ | ██████ |
Patient-years of exposure | ████ | ████ | ███ | ███ |
Concomitant medications available | ||||
Any medication for acute HAE treatment, n (%) | ██████ | ██████ | ██████ | ██████ |
Complement C1-INHa | ██████ | ██████ | ██████ | ██████ |
Conestat alfa (Ruconest) | ██████ | ██████ | ██████ | ██████ |
Ecallantide (Kalbitor) | ██████ | ██████ | ██████ | ██████ |
Icatibant acetate (Firazyr) | ██████ | ██████ | ██████ | ██████ |
Tranexamic acid | ██████ | ██████ | ██████ | ██████ |
Any C1-INH,b n (%) | ██████ | ██████ | ██████ | ██████ |
Acute HAE treatments administered | ||||
Investigator-confirmed HAE events, n | 357 | 508 | ██████ | ██████ |
Investigator-confirmed acute HAE events that were treated, n (%) | 310 (87) | 446 (88) | ██████ | ██████ |
Berinert | 150 (42) | 91 (18) | ██████ | ██████ |
Cinryze | 27 (8) | 69 (14) | ██████ | ██████ |
Ecallantide (Kalbitor) | 0 | 0 | ██████ | ██████ |
Icatibant acetate (Firazyr) | 135 (38) | 299 (59) | ██████ | ██████ |
Conestat alfa (Ruconest) | 20 (6) | 26 (5) | ██████ | ██████ |
Tranexamic acid | NR | NR | ██████ | ██████ |
Any C1-INHb | 196 (55) | 185 (36) | ██████ | ██████ |
C1-INH = complement 1 esterase inhibitor; HAE = hereditary angioedema; NR = not reported; SD = standard deviation.
aIncludes plasma-derived C1-INH (Cinryze, Berinert, Haegarda).
bIncludes Cinryze, Berinert, Haegarda, recombinant C1-INH (Ruconest) and fresh frozen plasma.
Source: Clinical Study Report for APeX-26 and Clinical Study Report for APeX-J.7
Efficacy
Only those efficacy outcomes and analyses of subgroups identified in the review protocol are reported. Appendix 3 provides detailed efficacy data.
Hereditary Angioedema Attacks
In the APeX-2 study, the mean number of attacks per month at baseline was 3.1 (SD = 1.6) in the berotralstat 150 mg group and 2.9 (SD = 1.1) in the placebo group (The attack criteria used to determine the baseline rate were different than the criteria used during the on-treatment period.) During part 1, there were 402 and 601 HAE attacks reported by patients in the berotralstat 150 mg and placebo groups, of which 357 (89%) and 508 (85%) were confirmed by the investigator in the berotralstat 150 mg and placebo groups, respectively. During treatment, the rate of confirmed attacks per month was 1.31 for the berotralstat 150 mg group and 2.35 for the placebo group, with a relative rate reduction of 44.2% (95% CI, 23.0% to 59.5%; P < 0.001) (Table 14). The mean investigator-confirmed attack rate by month is shown in Appendix 3, Figure 3 and Table 26.
The results of the sensitivity analyses for the rate of investigator-confirmed HAE attacks were generally supportive of the results of the primary analysis, although the magnitude of the treatment effects was reduced for the analysis that included imputed or observed HAE attack data after the patient stopped the study drug (rate reduction = 35%; 95% CI, 9.2% to 52.9%; P = 0.011) for berotralstat 150 mg versus placebo). The tipping-point analysis showed that a doubling of the attack rate in the berotralstat 150 mg group would be required for the missing data to alter the results of the analysis.
The relative rate reduction in investigator-confirmed HAE attacks during the effective treatment period (day 8 to start of part 2) for the berotralstat 150 mg group versus placebo was 46.5% (95% CI, 25.6% to 61.5%). No conclusions can be drawn with regard to the statistical significance of this difference, as testing was stopped due to failure of a prior outcome in the testing hierarchy.
During the 24-week treatment period, █ █ ██████ in the berotralstat 150 mg group ██ █ █ and ██ █ █ █ ██ in the placebo group █ █ ██ █ █ experienced no investigator-confirmed HAE attacks, with ███ █ ████ █ █ detected between groups in the APeX-2 study █ █ █ ████.
For investigator-confirmed attacks that received acute treatment, the APeX-2 study reported an attack rate of 1.04 events per month in the berotralstat 150 mg group, compared with 2.05 events per month in the placebo group (Table 14). The rate reduction was 49.2% (95% CI, 25.5 to 65.4; P < 0.001). These data should be interpreted with caution because there was no control of the type I error rate.
Ad hoc, exploratory analyses reported a rate reduction of 62.6% (95% CI, 9.6% to 84.6%; ████████) for laryngeal HAE attacks, and a rate reduction of 39.5% (95% CI, ████ to █████; ███████) for investigator-confirmed moderate-to-severe HAE attacks (Table 14). These data should be interpreted with caution as they were not controlled for the type I error rate.
During part 2 of the APeX-2 study, the mean investigator-confirmed attack rate per month in the berotralstat 150 mg group was 1.7 (standard error [SE] = 0.32) at 24 weeks (N = 37), 1.3 (SE = 0.26) at week 28, and 1.1 (SE = 0.25) at week 48. The number of patients contributing data to the week 28 and week 48 results was not reported (31 of 37 patients [84%] completed part 2).5 Among the patients switched from placebo to berotralstat 150 mg (n = 17), the mean attack rate per month was 2.6 events (SE = 0.61) at 24 weeks, 1.3 events (SE = 0.41) at 28 weeks and 0.6 events (SE = 0.23) at 48 weeks (number of patient not reported; 14 of 17 patients [82%] completed part 2).5 Additional unpublished data supplied by the sponsor for part 2 and part 3 of the APeX-2 study are summarized in Appendix 5.
In the APeX-J study, a total of ██ angioedema events were reported by patients in the berotralstat 150 mg group compared with █ ██ events among patients who received placebo during the first 24 weeks of the study. Overall, ███ of events were confirmed by the expert (██ events in the berotralstat group and ██ in the placebo group). █ ██ █ ████ █ ██ █ ███████ █ ████ █ ██ █ █ █ █ █ ████ █ ████ █ ███ █ ██. During part 1, the rate of expert-confirmed HAE events was 1.11 attacks per month and 2.18 per month in the berotralstat 150 mg and placebo groups, respectively (Table 14). The relative rate reduction was 49.1% (95% CI, 20.4% to 67.5%; P = 0.003) for ber otralstat 150 mg versus placebo. ██ █ ████████ █ █ █ █ █████ █ ██████ █ █████ █ █ █ ███████ █ █████████ █ ███████ █ ██████, as did the expert-confirmed event rate for the effective treatment period (day 8 to start of part 2) (rate reduction = 47.6%; 95% CI, 17.7% to 66.6%; P value not reported as statistical testing was stopped due to failure of a prior outcome). Exploratory analysis of the treated attack rate and ad hoc analyses on the rate of laryngeal, or moderate-to-severe HAE attacks are shown in Table 14.
█ █ █ ████████ █ ████████████ █ ███ █ ████ █ █████ █ ██ █ █ ██████ █ ███████ █ ██ █ █████ █ █████ █ █ █ █ █ █ ███ █ ██ █ █ █ ███ █ █████ █ ████████ █ ███████ █ █ █. This analysis reported a confirmed HAE attack rate of █ █ ██ events per months in the berotralstat 150 mg group (N = ██) and █ █ ██ events per month in the placebo group (N = ██), with a relative rate reduction of █ █ ███ (95% CI, ██ █ ██ to █ ████; P < █ █ ███) which should be interpreted as supportive evidence only.
Subgroup analyses for the APeX-2 study and the combined results for APeX-2 and APeX-J studies are reported in Appendix 3, Table 27. The direction of treatment effects was generally consistent across subgroups based on baseline attack rate, and prior androgen use. The subgroup of adolescents was too small to draw any meaningful inferences from the data.
Table 14: Investigator-Confirmed HAE Attack Rate (Part 1 Intention-to-Treat Population)
Outcome | APeX-2 (24 weeks) | APeX-J (24 weeks) | ||
|---|---|---|---|---|
Berotralstat 150 mg N = 40 | Placebo N = 40 | Berotralstat 150 mg N = 7 | Placebo N = 6 | |
Investigator-confirmed HAE attacksa | ||||
Number of patients contributing to the analysis | 40 | 40 | 7 | 6 |
Total number of attacks | 357 | 508 | 46 | 94 |
Number of patients with ≥ 1 attacks, n (%) | 37 (92.5) | 38 (95.0) | ██████ | ██████ |
Attack rate per 28 days | 1.31 | 2.35 | 1.11 | 2.18 |
Rate reduction vs. placebo, % (95% CI) | 44.2 (23.0 to 59.5) | Reference | 49.1 (20.4 to 67.5) | Reference |
P value | < 0.001 | Reference | 0.003 | Reference |
Treated investigator-confirmed HAE attacksa | ||||
Patients contributing to the analysis, n | 40 | 40 | 7 | 6 |
Total number of treated attacks | 311 | 449 | ██ | ██ |
Number of patients with ≥ 1 attacks, n (%) | 32 (80.0) | 37 (92.5) | ██████ | ██████ |
Attack rate per 28 days | ████ | ████ | ████ | ████ |
Rate reduction vs. placebo, % (95% CI) | ████████████ | Reference | ███████████ | Reference |
P value | ████████████ | Reference | ████████████ | Reference |
Investigator-confirmed laryngeal HAE attacks (ad hoc)a | ||||
Patients contributing to the analysis, n | 40 | 40 | █ | █ |
Total number of laryngeal attacks | ██ | ██ | █ | █ |
Number of patients with ≥ 1 attacks, n (%) | ████████ | ████████ | █████ | █████ |
Attack rate per 28 days | 0.06 | 0.17 | ████ | ████ |
Rate reduction vs. placebo, % (95% CI) | 62.6 (9.6 to 84.6) | Reference | ████████████ | Reference |
P value | 0.029b | Reference | ████████████ | Reference |
Moderate or severe investigator-confirmed HAE attacks (ad hoc)a | ||||
Number of patients contributing to the analysis | 40 | 40 | █ | █ |
Total number of attacks rated as moderatec | ███ | ███ | ██ | ██ |
Total number of attacks rated as severec | ██ | ██ | █ | █ |
Number of patients with ≥ 1 attacks, n (%) | ██ | ██ | ██ | ██ |
Attack rate per 28 days | ████ | ████ | ████ | ████ |
Rate reduction vs. placebo, % (95% CI) | 39.5 ████████ | reference | ████████████ | Reference |
P value | ████████████ | reference | ████████████ | Reference |
CI = confidence interval; HAE = hereditary angioedema; NR = not reported.
aNegative binomial model, with covariate for baseline HAE attack rate and log of treatment duration as offset for the intention-to-treat population.
bP value has not been adjusted for multiple testing (i.e., the type I error rate has not been controlled).
cSeverity rating according to the patient electronic diary.
Source: Clinical Study Report for APeX-26 and Clinical Study Report for APeX-J.7
During part 1 of the APeX-2 study, patients in the berotralstat 150 mg group reported a mean of 19.4 (SD = 21.5) days with HAE symptoms compared with 29.2 days (SD = 24.3) for patients in the placebo group (Table 15). The LS mean difference in the proportion of days with symptoms was −0.078 (95% CI, −0.133 to −0.023), which translates to approximately 13 fewer symptom-days in the berotralstat versus placebo group (out of a total of 169 treatment days). No conclusions can be drawn with regard to statistical significance of this difference, as testing was stopped due to failure of a prior outcome in the statistical testing hierarchy.
In the APeX-J study, no difference between groups was detected in the proportion of days with HAE symptoms (LS mean difference −0.122; 95% CI, −0.280 to 0.036; P = 0.12) (Table 15).
In the APeX-2 study, █████ █ ██████ of patients in the berotralstat 150 mg versus placebo groups, respectively, reported 1 or more attack-free months during the 24-week treatment period (Appendix 3, Table 28). Attack-free months were not reported in the APeX-J study.
Table 15: Days With Angioedema Symptoms (Part 1 Intention-to-Treat Population)
Outcome | APeX-2 (24 weeks) | APeX-J (24 weeks) | ||
|---|---|---|---|---|
Berotralstat 150 mg N = 40 | Placebo N = 40 | Berotralstat 150 mg N = 7 | Placebo N = 6 | |
Days with angioedema symptoms from investigator-confirmed attacksa | ||||
Patients contributing to the analysis, n | 40 | 39b | 7 | 6 |
Number of days with symptoms, mean (SD) | 19.4 (21.5) | 29.2 (24.3) | ██████████ | ███████ |
Number of days with symptoms, median (range) | ███████████ | ████████ | ████████ | ███████ |
Proportion of days with symptoms, LS mean (SE) | 0.119 (0.019) | 0.197 (0.020) | 0.118 (0.050) | 0.240 (0.054) |
LS mean difference in proportion of days vs. placebo (95% CI) | −0.078 (−0.133 to −0.023) | Reference | −0.122 (−0.280 to 0.036) | Reference |
P value | NRc | Reference | 0.12 | Reference |
CI = confidence interval; LS = least squares; NR = not reported; SD = standard deviation; SE = standard error.
aAnalysis of covariance model with baseline attack rate as covariate for the intention-to-treat population.
bOne patient from the placebo group who did not receive any study drug was missing from the analysis because this patient had no on-treatment days.
cStatistical testing stopped due to failure of prior outcome in the statistical testing hierarchy.
Source: Clinical Study Report for APeX-26 and Clinical Study Report for APeX-J.7
The responder analyses were exploratory end points in both studies. As these analyses have not been controlled for type I error rate, they should be interpreted with caution because of the potential for inflated type I error rate.
More patients in the berotralstat 150 mg group than the placebo group achieved at least a 50% relative reduction in the rate of investigator-confirmed HAE attacks compared to baseline (58% versus 25%; odds ratio = 3.91; 95% CI, 1.51 to 10.16; P = 0.005). The differences favoured berotralstat versus placebo for the proportion of patients with at least a 70% relative reduction, but not for the proportion with at least a 90% relative reduction (both analyses were conducted an ad hoc) (Table 16).
Similar trends were observed for the APeX-J study (Table 16).
Table 16: Responder Analysis (Part 1 Intention-to-Treat Population)
Outcome | APeX-2 (24 weeks) | APeX-J (24 weeks) | ||
|---|---|---|---|---|
Berotralstat 150 mg N = 40 | Placebo N = 40 | Berotralstat 150 mg N = 7 | Placebo N = 6 | |
Proportion of patients with ≥ 50% relative reduction in adjusted investigator-confirmed HAE attack ratea | ||||
Patients contributing to the analysis, n | 40 | 39 | 7 | 6 |
Responders, n (%) | 23 (58) | 10 (25) | 4 (57) | 0 |
Odds ratio (95% CI) vs. placebo | 3.91 (1.51 to 10.16) | Reference | NE | Reference |
P value | 0.005b | Reference | 0.07b,c | Reference |
Proportion of patients with ≥ 70% relative reduction in adjusted investigator-confirmed HAE attack ratea,d | ||||
Patients contributing to the analysis, n | 40 | 39 | 7 | 6 |
Responders, n (%) | 20 (50) | 6 (15) | 2 (29) | 0 |
Odds ratio (95% CI) vs. placebo | 5.63 (1.93 to 16.46) | Reference | NE | Reference |
P value | 0.002b | Reference | 0.46b,c | Reference |
Proportion of patients with ≥ 90% relative reduction in adjusted investigator-confirmed HAE attack ratea,d | ||||
Patients contributing to the analysis, n | 40 | 39 | 7 | 6 |
Responders, n (%) | 9 (23) | 3 (8) | 0 | 0 |
Odds ratio (95% CI) vs. placebo | 3.61 (0.89 to 14.66) | Reference | NE | Reference |
P value | 0.073b | Reference | NE | Reference |
CI = confidence interval; HAE = hereditary angioedema; NE = not estimable.
aFor the APeX-2 study, the analysis was based on logistic regression model with covariate for baseline HAE attack rate for the intention-to-treat population.
bP value has not been adjusted for multiple testing (i.e., the type I error rate has not been controlled).
cFisher’s exact test.
dAd hoc analysis in the APeX-2 study.
Source: Clinical Study Report for APeX-26 and Clinical Study Report for APeX-J.7
Health-Related Quality of Life
HRQoL was measured using the AE-QoL (secondary outcome) and EQ-5D-5L (exploratory outcome) instruments. While both the berotralstat 150 mg and placebo groups of the APeX-2 study reported improvements in the AE-QoL total scores at week 24, no statistically significant difference was detected between groups in the LS mean difference (−4.9 points; 95% CI, −12.2 to 2.4; P = 0.19) (Table 17). In the APeX-J study, the LS mean difference for the change from baseline in the AE-QoL total score was −19.0 (95% CI, −39.0 to 1.0).
In the APeX-2 study, no differences were detected between the berotralstat 150 mg and placebo groups for the change from baseline to week 24 in the EQ-5D-5L index score (█████ █ ███ █ ████ █ ███ █ █ █ █ ████ █ ██████████ █ ██████ █ █ █ ██ or the EQ VAS (█ █ ██ █ ████ █ █ ██ █ ████ █ █ ██ █ ████ █ ██ █ ██ █ █████). In the APeX-J study the LS mean difference for the change from baseline in the EQ VAS was █ █ █ █ █ █ █ █ ██ █ ███ █ ██████ █ █████; not controlled for type I error rate) and the EQ-5D-5L index score was ███ █ ████ █ █████ █ ████ █ █ ████ █ █ █ ███ for the berotralstat 150 mg group versus placebo groups.
Table 17: Change From Baseline in AE-QoL Total Score (Part 1 Intention-to-Treat Population)
Outcome | APeX-2 24 weeks) | APeX-J (24 weeks) | ||
|---|---|---|---|---|
Berotralstat 150 mg N = 40 | Placebo N = 40 | Berotralstat 150 mg N = 7 | Placebo N = 6 | |
Change from baseline to week 24 in AE-QoL total scorea | ||||
Number of patients contributing to the analysis | 38 | 36 | 7 | 6 |
Baseline score, mean (SD) | ██████████ | ██████ | █████████ | ███████ |
Change from baseline to week 24, LS mean (SE) | −14.6 (2.6) | −9.7 (2.6) | −15.8 (6.4) | 3.2 (6.8) |
LS mean difference vs. placebo (95% CI) | −4.9 (−12.2 to 2.4) | Reference | −19.0 (−39.0 to 1.0) | Reference |
P value | 0.19 | Reference | NRb | Reference |
AE-QoL = Angioedema Quality of Life questionnaire; CI = confidence interval; LS = least squares; NR = not reported; SD = standard deviation; SE = standard error.
Note: AE-QoL scores range from 0 to 100, with a negative change in score indicating an improvement in health-related quality of life.
aMixed model for repeated measures analysis with baseline attack rate, baseline AE-QoL value, visit, and visit by treatment interaction as covariates based on the intention-to-treat population (includes patients who stopped the study drug but remained in the study).
bStatistical testing stopped due to failure of prior outcome in the statistical testing hierarchy.
Source: Clinical Study Report for APeX-26 and Clinical Study Report for APeX-J.7
Mortality
No deaths were reported in the first 48 weeks of the APeX-2 study or the first 24 weeks of the APeX-J study.
Hospitalization or Emergency Visits
Professional care was sought for █ █ █████ █ █████ investigator-confirmed HAE attacks reported by patients in the berotralstat 150 mg group during the first 24 weeks of the APeX-2 study. Of these attacks, █ █ ██████ █ ██ █ █ █ █ █ ███ █ █ █████ █ █ █ █ █ ██visit and █ █ ██ █ ████ █ █ █ ███████ █ ██████. In the placebo group, patients sought care for ████ █ ████ █ ███ attacks, including ██ █ ██████ █ █████ █ ███ █ ███ and █ ███ █ █████ █ ██. ██████ █ ████ █ █ █ ████████ █ ██ █ █ █ █ █ █ █ ██ █ ██████████ █ █ █████████████████ █ █████ █ ██████ █ ███ █ ██.
In the APeX-J study, professional care was sought for ████ █ ██ █ █████ expert-confirmed attacks in patients who received berotralstat 150 mg, and in ██ █ ████ █ █████ █ █████ reported among those who received placebo. Of these events, █ █ █ █ █ █ ██ in the berotralstat group and █ █ ████ █ ██ in the placebo group required an emergency visit. █████ █ ███████ █ ██ █ █ ██ █ ███ █ ██████████ █ █████.
Harms
Only those harms identified in the review protocol are reported. Table 18 provides detailed harms data for part 1 of the trials (first 24 weeks).
Adverse Events
Adverse events were reported by 85% of patients in the berotralstat 150 mg group and 77% of those in the placebo group during the first 24 weeks of the APeX-2 study. The most frequently reported events in the berotralstat group was █ ███ █ ███ █ ███ █ █ █ █ █ ███, nausea (15%), vomiting (15%) and diarrhea (15%). The most common events in the placebo group were ██ █ ███████ █ █ ███ █ ████ and nausea (18%) (Table 18). One patient in the berotralstat 150 mg group reported a grade 3 or 4 adverse event of back pain. Four patients in the placebo group reported grade 3 or 4 adverse events of diverticular hemorrhage, uterine leiomyoma, pneumonia, increased gamma-glutamyl transferase, and transient ischemic attack.
All patients in the APeX-J study reported 1 of more adverse events during part 1, with nasopharyngitis reported most frequently in the berotralstat 150 mg and placebo groups (Table 18). One grade 3 or 4 adverse event was reported in the APeX-J study in a patient treated with placebo who reported decreased platelet count.
Serious Adverse Events
No patients in the berotralstat group of the APeX-2 study experienced a serious adverse event during the 24-week study period. Three patients in the placebo group experienced 4 serious adverse events of uterine leiomyoma, diverticulum intestinal hemorrhage, pneumonia, and transient ischemic attack.
No serious adverse events were reported in the first 24 weeks of the APeX-J study.
Withdrawal Due to Adverse Events
In the APeX-2 study, 1 patient in the berotralstat 150 mg group stopped treatment due to abnormal liver function test results, and 1 patient in the placebo group stopped the study drug due to a depressive episode. One placebo-treated patient in the APeX-J study stopped treatment due to urticaria.
Mortality
No deaths were reported during the first 48 weeks of the APeX-2 study or the first 24 weeks of the APeX-J study.
Notable Harms
Gastrointestinal adverse events were reported more frequently among patients who received berotralstat 150 mg compared with placebo in the APeX-2 study (50% versus 36%, respectively), and in the APeX-J study (43% versus 17%, respectively). No patients stopped treatment due to gastrointestinal adverse events in the first 24 weeks of either study. The product monograph states that gastrointestinal adverse effects generally occur early after therapy begins, become less frequent over time, and typically self-resolve.4
Table 18: Summary of Harms (Part 1 Safety Population)
Adverse event | APeX-2 (24 weeks) | APeX-J (24 weeks) | ||
|---|---|---|---|---|
Berotralstat 150 mg N = 40 | Placebo N = 39 | Berotralstat 150 mg N = 7 | Placebo N = 6 | |
Patients with ≥ 1 adverse event | ||||
n (%) | 34 (85) | 30 (77) | 7 (100) | 6 (100) |
Most common events,a n (%) | ||||
Nausea | 6 (15) | 7 (18) | 0 | 0 |
Vomiting | 6 (15) | 1 (3) | NR | NR |
Diarrhea | 5 (13)6 (15) | 0 | 1 (14) | 0 |
Abdominal pain | 9 (23) | 4 (10) | 1 (14) | 0 |
Nasopharyngitis | █████ | █████ | 2 (29) | 4 (67) |
Back pain | 4 (10) | 1 (3) | 1 (14) | 0 |
Headache | 4 (10) | 2 (5) | 0 | 1 (17) |
Patients with ≥ 1 serious adverse event | ||||
n (%) | 0 | 3 (8) | 0 | 0 |
Patients with ≥ 1 grade 3 or 4 treatment-emergent adverse event | ||||
n (%) | 1 (3) | 4 (10) | 0 | 1 (17) |
Patients who stopped treatment due to adverse events | ||||
n (%) | 1 (3) | 1 (3) | 0 | 1 (17) |
Deaths | ||||
n (%) | 0 | 0 | 0 | 0 |
Notable harms | ||||
Any GI abdominal adverse event, n (%) | 20 (50) | 14 (36) | 3 (43) | 1 (17) |
Any GI abdominal adverse event leading to treatment discontinuation, n (%) | 0 | 0 | 0 | 0 |
GI = gastrointestinal; NR = not reported.
aFrequency higher than 10% in any treatment group in the APeX-2 study.
Source: Clinical Study Report for ApeX-2 study6 and Clinical Study Report for ApeX-J study.7
ApeX-2 Study – Part 2 (Week 24 to Week 48)
Wedner et al. (2021)5 provided a summary of adverse events for patients who received berotralstat for up to 48 weeks (N = 40) in the APeX-2 study. Most patients (95%) reported at least 1 adverse event, including 1 serious adverse event in a patient who was hospitalized for a routine screening procedure. The most common adverse events were upper respiratory tract infection (53%), abdominal pain (30%), nausea (20%), and diarrhea (18%). In part 2 of the study, 2 patients who received the 150 mg dose (8%) stopped treatment due to adverse events; 1 due to gastrointestinal events (anal incontinence), and 1 due to palpitations and tachycardia. Among patients who switched from placebo to berotralstat 150 mg (N = 17), no new serious adverse events were reported and no patients stopped treatment due to adverse events.5 No new safety signals were detected based on data up to 48 weeks treatment.5
Critical Appraisal
Internal Validity
APeX-2 and APeX-J Part 1
Both RCTs were conducted using a similar 3-part study design and comparable statistical methods. Patients were allocated to treatment groups using appropriate methodology (i.e., interactive web or voice response technology), with randomization stratified by a relevant prognostic factor (i.e., investigator-confirmed HAE attack rate during the screening period [≥ 2 attacks or < 2 attacks per 28 days]). Due to the small sample size of the trials, randomization may not have ensured the groups were balanced for all measured or unmeasured prognostic factors or confounders, and imbalances between treatment groups were observed for some of the baseline patient characteristics. Differences were noted in the mean age and weight, proportion of females, history of laryngeal attacks, and HAE-related emergency visits in past year. However, the clinical expert consulted for this review noted that these baseline differences were unlikely to bias the results. Four patients in the placebo group (10%) withdrew from the APeX-2 study during the first 24 weeks, compared with 2 patients in the berotralstat group (5%). In addition, efficacy outcomes were analyzed using the on-treatment time only, which meant that 1 patient in the placebo group who did not receive any study drug did not contribute any data to the analyses. There were more patients who stopped treatment early in the placebo group than in the berotralstat 150 mg group (13% versus 8%, respectively). It is possible the differences in losses or exclusions could contribute to imbalances between groups, although the potential impact on the study’s results is unclear.
Both studies were double-blind during part 1, with the active study drug and placebo supplied as identical-looking capsules. Gastrointestinal adverse effects were reported more frequently among patients who received berotralstat compared with placebo, but it is unclear if this contributed to unblinding, given that these adverse effects are similar to gastrointestinal symptoms associated with HAE attacks.
The primary efficacy outcome was based on the rate of investigator-confirmed HAE attacks, which was considered to be appropriate and clinically relevant by the clinical expert consulted and by regulators.19,20 All patient-reported events were reviewed by the investigator to ensure they met the predefined criteria for an attack. Given the subjective nature of the events, patients may over-report the frequency of attacks. Moreover, the clinical expert noted that patients may have difficulty distinguishing gastrointestinal adverse effects associated with berotralstat from gastrointestinal symptoms of an HAE attack. The FDA stated that investigator confirmation of attacks may help ensure that only swelling attacks, and not prodromal symptoms or pre-emptive rescue medication use, were counted as events.19 According to the clinical expert consulted for this review, a 20% improvement in the attack rate is generally considered a mild effect, 50% is considered moderate, and 70% is considered a marked effect.
The sample size of the pivotal APeX-2 trial was small, but due to the rarity of HAE, it was considered acceptable by regulators.19,20 Both studies reported power calculations, and despite the low power of the APeX-J study, it did detect a statistically significant difference between the berotralstat 150 mg and placebo group for the primary outcome. Due to the anticipated small sample size in the APeX-J study (which was conducted in Japan only), the study protocol described a pooled analysis that combined the patients from APeX-J and APeX-2. However, because the study’s protocol specified the primary analysis would be based on patients enrolled in APeX-J only, the pooled analysis was considered supplementary data by CADTH.
The rate of HAE attacks was analyzed using a negative binomial model, which, according to the APeX-2 statistical analysis plan, was selected as the primary analysis because overdispersion was detected with the Poisson model. Analyses were based on the on-treatment time, with no imputation for missing data. Three sensitivity analyses were conducted in APeX-2 to explore the impact of missing data. The sensitivity analyses included data for attacks reported after stopping therapy with or without imputation for patients with no outcome data reported after stopping study drug, and a tipping-point analysis that estimated the response level at which the missing data in the berotralstat groups would change the results. The results of the sensitivity analyses were supportive of the primary analysis in general, but the magnitude of the effect for berotralstat 150 mg was not as strong in the analysis that used observed data post–treatment discontinuation and also imputed missing data post–treatment discontinuation. Subgroup analyses by baseline attack rate of prior androgen use were generally consistent with the overall treatment population. Too few adolescents were enrolled to allow for meaningful interpretation of this subgroup.
There were differences between groups in the type of acute treatments administered for HAE attacks. In the APeX-2 study, a greater proportion of attacks were treated with any C1-INH in the berotralstat group compared with the placebo group (55% versus 36%, respectively), and fewer attacks were treated with icatibant acetate (38% versus 59%, respectively). The clinical expert noted that the C1-INHs have a longer duration of action (3 days) compared with icatibant acetate (which may be administered every 6 hours). In addition to alleviating symptoms of the acute attack, C1-INHs may provide a protective effect for patients and reduce the risk of subsequent attacks for days after administration. The █ █ ███ █ ███ of C1-INH in the berotralstat group may therefore potentially favour active treatment versus placebo in the APeX-2 study. Possible bias favouring placebo was noted for the APeX-J study, as fewer patients in the active group were treated with C1-INHs.
Both trials used hierarchical testing and the Hochberg procedure to control the type I error rate for the primary outcome and 3 secondary outcomes as well as the 2 berotralstat dosage groups. Other outcomes that were of interest to this review (e.g., the responder analysis) were not controlled for multiplicity of testing. Moreover, the rate of laryngeal, moderate or severe attacks, and the 70% or greater and 90% or greater responder threshold analyses (in the APeX-2 study) were conducted post hoc. Both trials used a relatively short run-in period to determine the baseline rate of attacks (14 to 56 days in the APeX-2 study; 56 days in APeX-J). Given the unpredictable nature of HAE attacks, this limited observation time could add uncertainty to the baseline rate. Variability in the baseline attack rate would not affect the interpretation of the primary outcome (which was based on on-treatment attack rate), but it could affect the interpretation of the responder analyses (which was based on the change from the baseline rate).
Neither study was designed to test for differences in the need for hospitalization or emergency visits. HRQoL was measured using the AE-QoL as a secondary outcome, and the EQ-5D-5L as an exploratory outcome. The AE-QoL has evidence to support the validity, reliability, and responsiveness in patients with recurrent angioedema, which included patients with histamine- or bradykinin-mediated angioedema. However, the FDA did not consider the AE-QoL a well-defined or reliable assessment of HAE-related quality of life for the purpose of labelling, noting that the nutrition and mood domains of the AE-QoL are not specific to HAE, the clinically meaningful within-person change has not been established, and the 4-week recall period was long.19
As both trials included a placebo control group, there is no direct evidence comparing berotralstat to other LTP therapies. As with most clinical trials, the studies were not powered to detect infrequent adverse effects or those with a lag time.
APeX-2 Parts 2 and 3
Several limitations were identified for parts 2 and 3 of the APeX-2 study. First, the investigators and patients were aware that patients were receiving active treatment, and their expectations of treatment could affect reporting of subjective outcomes such as symptoms or adverse effects. In addition, there was potential selection bias, as patients who respond to berotralstat and are able to tolerate treatment are more likely to continue therapy compared to patients with less favourable outcomes. The efficacy analyses were based on observed data with no imputation for missing data, and with no sensitivity analyses to assess the robustness of the results. Given the attrition observed, the reported results may overestimate the treatment effects and under-report adverse effects. Finally, part 2 and 3 were uncontrolled, which makes the change in HAE attack rate difficult to interpret, particularly because HAE attacks are sporadic and may fluctuate through the year due to exposure to seasonal triggers, hormonal changes, or other factors.
A full-text report of part 3 of the APeX-2 study was not available at the time of the initial systematic review, and the sponsor-submitted posters and data tables did not allow CADTH to fully appraise the potential for bias.25-28 As part of the Request for Reconsideration, the final Clinical Study Report that contained data from part 2 and part 3 of APeX-2 study was supplied by the sponsor, and additional appraisal points are included in Appendix 5.
External Validity
The findings of the pivotal APeX-2 study were reflective of those enrolled: patients with type 1 or 2 HAE who had on average 3 HAE attacks per month, most of whom had experienced a prior laryngeal attack. Although the proportion of patients with type 1 versus type 2 HAE were not reported in either study, most patients (88% to 100%) had their diagnosis confirmed by low C4 levels plus a functional level of C1-INH of less than 50%, which is consistent with clinical practice. Approximately a third of patients had a baseline attack rate of less than 2 attacks per month, which the clinical expert stated may be lower than the typical frequency at which an LTP is initiated in clinical practice. Although the expert acknowledged that patients with infrequent but more severe attacks may also be considered for an LTP. The trial included patients who were medically appropriate for on-demand treatment as the sole management of HAE, and therefore may have excluded patients with more severe HAE who could not tolerate discontinuation of current LTP therapy.
Compared to the Canadian population, racial diversity in the APeX-2 trial was limited as most patients were white (94%). In addition, patients were predominantly female (63%) and aged between 18 and 65 years. Because only 4 adolescents and 4 patients over 65 were enrolled in the berotralstat 150 mg and placebo groups in the APeX-2 study, there are limited data to extrapolate to younger and older age groups. In total, 10 of the randomized patients (8%) were from Canada. The study reported that 24% of patients screened were excluded from the study, with most patients eliminated because they did not meet the diagnostic or baseline attack-rate criteria for the trial. The APeX-J study provided additional data from 13 patients from Japan. These patients were generally similar to those in the pivotal study, although patient weight and BMI were lower, as was their mean baseline HAE attack rate. Overall, the clinical expert consulted for this review considered the characteristics of the patient population enrolled in the trials to be a good representation of the target population and the expert did not identify any issues with the use of concurrent treatments or conduct of the trials that could substantially affect the generalizability of the findings.
The duration of the controlled portion of the trials was limited to 24 weeks, which may be considered short, given that LTP treatment is potentially life-long therapy. Due to the limitations of the longer-term data, the efficacy and safety of berotralstat beyond 24 weeks are uncertain.
Indirect Evidence
Objectives and Methods for the Summary of Indirect Evidence
As no direct comparative data for the use of berotralstat for the routine prevention of recurrent episodes of HAE were identified in the systematic review, a search for indirect evidence was conducted.
A focused literature search for indirect treatment comparisons (ITCs) dealing with Orladeyo (berotralstat) and HAE was run in MEDLINE All (1946–) on March 14, 2022. No limits were applied. The search results for ITCs that met the patient, intervention, comparator, and outcome criteria in the review protocol (Table 6) were screened by 1 researcher. Although no ITC was submitted by the sponsor, an indirect comparison feasibility assessment included in the sponsor’s submission was reviewed.28
No relevant ITCs were found in the literature search. CADTH’s review of the sponsor’s feasibility assessment is provided in the following section.
Appraisal of the Feasibility Assessment
The sponsor conducted a feasibility assessment28 to determine if the clinical trials for treatments used for routine prevention of HAE attacks were sufficiently similar to permit valid comparison in an ITC. Five studies were evaluated: APeX-217 and APeX-J18 (berotralstat), HELP−0329 (lanadelumab), COMPACT30 (C1-INH SC), and CHANGE31 (C1-INH IV).
The authors of the feasibility assessment identified a number of important differences in the study designs and patient characteristics of the trials and concluded that it was not possible to generate robust estimates of the comparative treatment effects due to between-study heterogeneity. The sponsor cited reviews by other health technology assessment agencies that support their conclusions; however, none of these reports included both lanadelumab and berotralstat. Three reports32-34 compared lanadelumab to C1-INH, and 1 compared berotralstat to C1-INH.35 Similarly, a recent National Institute for Health and Care Excellence review did not consider lanadelumab a relevant comparator, based on the treatment patterns of HAE in the UK at the time of the review.36 The Scottish Medicines Consortium stated that lanadelumab, C1-INH, androgens, and tranexamic acid were all considered relevant comparators to berotralstat, but in its review, comparative data were not provided and the sponsor’s economic model was based on a no-treatment comparator.37
Based on the information presented in the sponsor’s feasibility assessment,28 the clinical expert consulted for this review agreed that the heterogeneity between the berotralstat and C1-INH trials is significant and that any ITC is unlikely to produce robust estimates of comparative efficacy or safety. However, because fewer differences exist between berotralstat and lanadelumab trials, such an ITC may have been possible. The APeX and HELP−03 RCTs were both parallel, double-blind design trials, with a run-in period to establish the baseline attack rate and a treatment duration of 24 and 26 weeks. There were some differences in the enrolment criteria related to the baseline attack rate, with the lanadelumab trial enrolling patients with 1 or more attacks per 4 weeks, whereas the berotralstat studies enrolled those with 2 or more events during the run-in period (14 to 56 days). However, the mean baseline attack rate was generally similar for the berotralstat (2.9 to 3.1 attacks per month) and lanadelumab trials (3.5 to 4.0 attacks per month), as was the on-treatment attack rate in the placebo groups (APeX: 2.35 and 2.18 attacks per 4 weeks; HELP−03: 1.97 attacks per 4 weeks). The mean age, BMI, sex, and racial distribution were comparable between trials. The treatments used for acute attacks were similar, and both studies prohibited the concurrent use of other prophylactic treatments for HAE. There was a difference in the reporting of events, with the berotralstat studies requiring patients to record attack-related data every 24 hours, compared with 72 hours in the lanadelumab study, but in both studies, all attack events had to be confirmed by the investigator or clinical expert. The sample size of the trials was limited (19 and 80 patients in the APeX studies, and 125 patients for HELP−03), which may contribute to uncertainty in an ITC, and may limit the ability to use methods such as a matching adjusted indirect comparison.
Lanadelumab was listed as a comparator of interest in the protocol to CADTH’s systematic review. While an ITC that included all relevant treatments for the prevention of HAE attacks was likely not feasible, a focused ITC comparing berotralstat to lanadelumab may have been possible and would have been of interest to CADTH.
Other Relevant Evidence
This section includes submitted long-term extension studies and additional relevant studies included in the sponsor’s submission to CADTH that were considered to address important gaps in the evidence included in the systematic review.
The open-label study, APeX-S, provides longer-term safety and efficacy data that supplement the evidence from the RCTs in the systematic review.
Long-Term Studies
APeX-S is an ongoing phase II study conducted to evaluate the safety and efficacy of berotralstat in adults and pediatric patients aged 12 years and older with type 1 or 2 HAE.
Methods
Approximately █ █ ████ █ ███ who participated in a previous study of berotralstat or who were expected to benefit from treatment were to be manually allocated to receive an oral dose of berotralstat (110 mg or 150 mg) once daily. Results for the berotralstat 110 mg group are not described in this report given that it is not a Health Canada–recommended dose. A total of 127 patients were enrolled into the 150 mg group and results were presented through to week 48 in the interim report.
Efficacy results related to HAE attacks (i.e., frequency, severity, and disease activity over time) were evaluated as a secondary end point. Safety assessments consisted of all adverse events including treatment-emergent adverse events, serious adverse events, as well as adverse events of special interest.
Populations
In APeX-S, the inclusion and exclusion criteria were generally aligned with those in the pivotal trials,6,7 with a distinction being that APeX-S patients did not have to meet a minimum number of HAE attacks to qualify for inclusion. A total of 227 of 254 screened patients were allocated to either the berotralstat 110 mg (n = 100) or 150 mg (n = 127) groups at 49 sites in 22 countries in North America, Europe, Asia, and Africa. Baseline demographics were generally consistent with those in the APeX-26 pivotal trial. In the 150 mg group the median age was 44.0 years (range = 12 to 72) and the majority of patients were female (60.6%), white (86.6%), and had a fmily history of HAE (79.5%). No baseline attack rate data were provided for the following reasons: baseline measures for some patients were not collected due to rollover from a previous berotr alstat study (██ █ █████ █ ███████ █ █ █ ██ █ █ █ █ █ █ █ █ ██ █ ███ █ ████ █ ████████ █ ███ █ ████), some patients were on prophylactic HAE medications at study entry ( █ █ █ █ █ of patients in the 150 mg group at screening), and some patients had recently discontinued androgens used as HAE prophylaxis (██ █ ██ of patients discontinued < 2 weeks before berotralstat initiation). Patients enrolled from a previous berotralstat study had to have demonstrated a minimum HAE attack rate for entry into those prior studies. Of the ██ patients who had not previously participated in a berotralstat study, █ ██ █ ██ █ ██ had their HAE diagnosis confirmed by a C4 level below the lower limit of normal plus a C1-INH function of less than 50%.
Table 19: Summary of Baseline Characteristics for APeX-S Study (Safety Population)
Characteristic | Berotralstat 150 mg (N = 127) |
|---|---|
Age (years), median (range) | 44.0 (12 to 72) |
12 to 17 years, n (%) | 5 (3.9) |
18 to 64 years, n (%) | 119 (93.7) |
≥ 65 years, n (%) | 3 (2.4) |
Females, n (%) | 77 (60.6) |
Ethnicity, n (%) | |
Hispanic or Latino | 2 (1.6) |
Not Hispanic or Latino | 115 (90.6) |
Unknown | 1 (0.8) |
Not reported | 9 (7.1) |
Race, n (%) | |
American Indian or Alaskan Native | █ |
Asian | 10 (7.9) |
Black or African American | 2 (1.6) |
White | 110 (86.6) |
Other | 5 (3.9) |
Weight (kg), median (range) | ████████████████ |
Body mass index, (kg/m2), median (range) | ███████████████ |
Age at onset of first symptoms of HAE (years), median (range) | ██████████████ |
Age at diagnosis of HAE (years), median (range) | ████████████ |
Family history of diagnosed type 1 or 2 HAE, n (%) | ████████ |
Prior laryngeal attack (lifetime), n (%) | ███████ |
Prior laryngeal attack in past year, n (%) | 35 (27.6) |
Emergency visit in past year due to HAE, n (%) | ███████ |
Hospitalization in past year due to HAE, n (%) | ███████ |
Past prophylactic medications targeted and/or approved for HAE | |
Any androgena | 81 (63.8) |
Any C1-INHb | 32 (25.2) |
Tranexamic acid | ████████ |
Berinert | ████████ |
Cinryze | ██████ |
Complement C1-INHc | ██████ |
Conestat alfa | █████ |
Other | ██████ |
Participated in a previous berotralstat study, n (%) | ████████ |
C1-INH = complement 1 esterase inhibitor; HAE = hereditary angioedema.
aThe summary of any androgens includes androgens (unspecified), oxandrolone, methyl-testosterone, danazol (Danocrine), and stanozolol.
bThe summary of any C1-INH would include plasma-derived C1-INH replacement (Cinryze, Berinert, Haegarda), recombinant C1-INH replacement (Ruconest), and fresh frozen plasma.
cComplement C1-INH is the WHO coded term for plasma-derived C1-INH (Cinryze, Berinert, Haegarda).
Source: Clinical Study Report for APeX-S.38
Outcomes
The relevant efficacy end points for this study included HAE attack and laryngeal attack frequency, attack severity, number of attacks requiring acute treatment, number and proportion of days with angioedema symptoms, and number of patients who were HAE attack-free. Relevant patient-reported outcomes during long-term administration of berotralstat were evaluated using the AE-QoL. All patient-reported HAE attacks were recorded in a paper diary. These patient-reported HAE attacks were reviewed and confirmed or rejected programmatically according to a set of predefined rules before inclusion to be considered an “adjusted attack.” The prespecified rules for an adjusted attack were: 1 or more symptoms of swelling; no alternative explanation for the attack (i.e., allergic reaction); attack began more than 24 hours from the end of the prior attack (any attack that began within 24 hours from the end of a prior attack was combined with the prior attack); and the attack lasted for longer than 24 hours if untreated. Relevant safety outcomes included treatment-emergent adverse events, serious adverse events, and adverse events of special interest.
Statistical Analysis
All efficacy and safety analyses were descriptive in nature and were conducted using the safety population, which included all patients who received 1 or more doses of the study drug. There was no imputation for missing data.
Patient Disposition
Patient disposition of the APeX-S study is summarized in Table 20. A total of 254 patients were screened and 127 patients were allocated to the berotralstat 150 mg group. A total of 26.0% of patients in this group discontinued the study drug by week 48, mainly due to adverse events (10.2%) or perceived lack of efficacy (8.7%), with 94 patients still in the study as of the data cut-off. All 127 allocated patients were included in the safety population.
Table 20: Patient Disposition in APeX-S Study Through Week 48
Disposition | Berotralstat 150 mg (N = 127) |
|---|---|
Screened, n | 254 |
Allocated, n | 127 |
Discontinued study drug, n (%) | 33 (26.0) |
Reason for discontinuation of study drug, n (%) | |
Laboratory abnormality or adverse event | 13 (10.2) |
Intercurrent illness or emergence of new illness, medical condition, or pregnancy | 1 (0.8) |
Investigator judgment | 1 (0.8) |
Perceived lack of efficacy | 11 (8.7) |
Patient withdrew consent | 5 (3.9) |
Other | 2 (1.6) |
Safety population, n | 127 |
Source: Clinical Study Report for ApeX-S.38
Exposure to Study Treatments
In the APeX-S study, through to week 48, the total number of patient-years of exposure was 106.6 for the berotralstat 150 mg group, with a median of 342.0 days (range = 11 to 540). In terms of concomitant medications, most patients (81.9%) had received C1-INH in the period between the first dose through 30 days after the last dose of berotralstat; 63.8% of patients took a plasma-derived C1-INH (i.e., Cinryze, Berinert, and Haegarda). Other concomitant HAE medications included icatibant acetate (Firazyr) (45.8%), icatibant (16.3%), and fresh frozen plasma (16.3%).
Table 21: Extent of Exposure in APeX-S Study Through Week 48 (Safety Population)
Outcome | Berotralstat 150 mg (N = 127) |
|---|---|
Duration of exposure, daysa | |
Mean (SD) | 306.5 (143.3) |
Median (range) | 342.0 (11 to 540) |
Patient-years of exposureb | 106.6 |
Concomitant medications taken for HAE, n (%) | |
Any concomitant medication for HAE | ████████ |
Any C1-INHc | ████████ |
Complement C1-INHd | ███████ |
Conestat alfa | ███████ |
Plasma | ███████ |
C1-inhibitor, plasma-derived | ██████ |
Any icatibant | ████████ |
Icatibant acetate | ████████ |
Icatibant | ████████ |
Tranexamic acid | ███████ |
Danazol | ██████ |
C1 = complement 1; C1-INH = complement 1 esterase inhibitor; HAE = hereditary angioedema; SD = standard deviation.
aThe duration of exposure was calculated as last dose date − first dose date + 1.
bPatient-years of exposure was calculated for each patient as (last dose date − first dose date + 1)/365.25 and then summed across all patients in a given dose group.
cThe summary of any C1-INH includes plasma-derived C1-INH replacement (Cinryze, Berinert, Haegarda), recombinant C1-INH replacement (Ruconest), and fresh frozen plasma.
dComplement C1-INH is the WHO coded term for plasma-derived C1-INH (Cinryze, Berinert, Haegarda).
Source: Clinical Study Report for APeX-S.38
Efficacy
Adjusted Hereditary Angioedema Attacks
Through to week 48, in the 150 mg dose group, there were a total of █████ adjusted HAE attacks. A total of █████ of patients had 1 or more attacks, and █████ of attacks were treated with any medication. The mean attack rate was 1.36 (SD = 1.51) attacks per month and the median attack rate was 0.93 (range = 0 to 7.6) attacks per month.
Adjusted Laryngeal Hereditary Angioedema Attacks
Through to week 48, in the 150 mg dose group, there were a total of ███ adjusted laryngeal HAE attacks. A total of █ █ █ █ █ of patients had 1 or more attacks, and █████ of attacks were treated with any medication.
Adjusted Hereditary Angioedema Attacks Among Subgroups
The trial was not designed to investigate the effectiveness of the treatment by subgroups; all of which had small sample sizes. Among subgroups in the 150 mg group, the median adjusted attack rates per month were ███ █ ██ █ ████ among patients 12 to 17 years of age (n = 5); ██ █ █ █ ██ █ ███ among patients aged 65 years or older (n = 3); and ████ █ ████ among patients aged 18 to 64 years (n = 119).
Patient-Assessed Severity of Adjusted Attacks
Of the █ █ ███ adjusted attacks assessed by patients, (█████) were assessed as moderate in severity, followed by mild (█████), severe (█████), and negligible (████).
Adjusted Attacks Requiring Acute Treatment
Of the █████ adjusted attacks that occurred during the study in the 150 mg dose group, 82% were treated with a standard-of-care acute attack medication, the most common being Berinert (44.6%) and icatibant acetate (Firazyr) (37.6%).
Number and Proportion of Days with Reported Angioedema Symptoms
Through to week 48, the median number of days and proportion of days with reported angioedema symptoms among all patients in the 150 mg dose group was ██ █ █ █ ███ █ ██ and 0.07 (range = 0 to 0.7), respectively.
Number of Patients Who Were Adjusted Hereditary Angioedema Attack–Free
A patient who completed dosing in the period of interest and reported no attacks during this same period was considered attack-free. A total of ██ █ ████ patients (█████) in the 150 mg dose group remained attack-free through to week 24 and █ █ █ █ ██ patients (█ █ ██) remained attack-free from baseline through to week 48.
Health-Related Quality of Life
The AE-QoL total score ranges from 0 points (best) to 100 points (worst). The mean AE-QoL total score among patients in the 150 mg group was 37.8 (SD = 17.9) at baseline (n = 118); with a mean change from baseline of −14.7 (SD = 17.8) points through to week 48 (n = 73).
Table 22: Efficacy Outcomes in APeX-S Study Through Week 48 (Safety Population)
Outcome | Berotralstat 150 mg (N = 127) |
|---|---|
Adjusted HAE attacksa,b | |
Total number of attacks | █████ |
Number of patients with ≥ 1 attack, n (%) | █████████ |
Total number of treated attacks | ████ |
Number of patients with ≥ 1 treated attack, n (%) | █████████ |
Attacks per month, median (range) | 0.93 (0 to 7.6) |
Attack-level duration (hours), median (range) | ██████████████████ |
Adjusted laryngeal HAE attacksb,c | |
Total number of attacks | ███ |
Number of patients with ≥ 1 attack, n (%) | ████████ |
Total number of treated attacks | 119 |
Number of patients with ≥ 1 treated attack, n (%) | ████████ |
Adjusted HAE attacks per month among subgroups | |
Age 12 to 17, n | 5 |
Median (range) | █████████████ |
Age 18 to 64, n | 119 |
Median (range) | ███████████ |
Age ≥ 65, n | 3 |
Median (range) | ████████ |
Number of adjusted HAE attacks with severity as assessed by patient, n (%) | |
Negligible | ████████ |
Mild | █████████ |
Moderate | ████████ |
Severe | ████████ |
Acute medications for adjusted HAE attacks | |
Number of attacks, n | █████ |
Number of attacks treated with acute attack medication,d n (%) | ███████████ |
Berinert | █████████ |
Icatibant acetate | █████████ |
Cinryze | ███████ |
Conestat alfa | ███████ |
Fresh frozen plasma | ██████ |
Any C1-INH,e n (%) | █████████ |
Number of days with reported angioedema symptoms, median (range) | ██████████ |
Patients who were adjusted HAE attack-free, n (%)f | |
0 to 24 weeks | ████████████ |
0 to 48 weeks | ██████████ |
AE-QoL total score | |
Baseline, n | 118 |
Baseline score, mean (SD) | 37.8 (17.9) |
Week 48, n | 73 |
Change from baseline to week 48, mean (SD) | −14.7 (17.8) |
AE-QoL = Angioedema Quality of Life questionnaire; C1-INH = complement 1 esterase inhibitor; HAE = hereditary angioedema; SD = standard deviation.
aThe attack rate was based on reported attacks up to the time of data cut-off with no distinction between diaries remaining with patients until their next visit (up to 12 weeks of data lag) and diaries with no attacks. Attack rates reported at later study time points may therefore underestimate the number of attacks. The 150 mg dose group has 3 of 673 months of diary data remaining with the patient for months 1 to 6, and it is estimated that approximately 6% of diaries are remaining with patients for months 7 to 12.
bThese adjusted attacks were determined programmatically and needed to have: 1 or more symptoms of swelling; no alternative explanation for the attack (i.e., allergic reaction); begun more than 24 hours from the end of the prior attack (any attack that began within 24 hours from the end of a prior attack was combined with the prior attack); had a duration of longer than 24 hours if untreated.
cLaryngeal attacks were attacks that involve visible swelling in the mouth, tongue, and/or lips or any of the following internal swelling symptoms: lump in throat (tightness), difficulty swallowing, change in voice, or difficulty breathing. Laryngeal attack symptoms were a subset of peripheral attack symptoms.
dMedications were as recorded in the patient diary for each attack. The percentages provided were based on the number of adjusted attacks.
eThe summary of any C1-INH includes plasma-derived C1-INH replacement (Cinryze, Berinert, Haegarda), recombinant C1-INH replacement (Ruconest), and fresh frozen plasma.
fA patient who completed dosing in the period of interest and reported no attacks during this same period was considered attack-free. Patients who reported no attacks and discontinued before the end of the planned treatment period or who experienced attacks in the period were not considered attack-free. Denominators were the numbers of patients who completed dosing or discontinued in the period of interest.
Source: Clinical Study Report for APeX-S.38
Harms
A summary of treatment-emergent adverse events at the interim analysis is presented in Table 23. During the 48-week period, 90.6% of patients in the berotralstat 150 mg group reported 1 or more adverse events, the most common being nasopharyngitis (33.9%), headache (15.0%), and diarrhea (14.2%). A total of 9.4% of patients experienced 1 or more serious adverse events, with █ █ █ █ ███████ █ ███ experiencing an HAE attack requiring hospitalization. Adverse events of special interest included a group of gastrointestinal abdominal events consisting of gastrointestinal signs and symptoms or motility and defecation conditions, which occurred in █████ of patients. No deaths were reported in the berotralstat 150 mg group.
Table 23: Summary of TEAEs in APeX-S Study Through Week 48 (Safety Population)
Adverse event | Berotralstat 150 mg (N = 127) |
|---|---|
Any TEAEs, n (%) | 115 (90.6) |
Common TEAEs,a n (%) | |
Nasopharyngitis | 43 (33.9) |
Upper respiratory tract infection | 13 (10.2) |
Urinary tract infection | ███████ |
Influenza | ██████ |
Gastroenteritis | ██████ |
Bronchitis | █████ |
Abdominal pain | ████████ |
Diarrhea | 18 (14.2) |
Nausea | ███████ |
Abdominal pain upper | ██████ |
Abdominal distension | ██████ |
Vomiting | ██████ |
Flatulence | ██████ |
Headache | 19 (15.0) |
Arthralgia | ███████ |
Back pain | ██████ |
Increased alanine transaminase | ██████ |
Oropharyngeal pain | ██████ |
Patients with drug-related TEAE, n (%) | 57 (44.9) |
Patients with ≥ 1 SAE, n (%) | 12 (9.4) |
Common SAEsb, n (%) | |
HAE attack requiring hospitalization | ██████ |
Patients who discontinued study drug due to adverse events, n (%) | 13 (10.2) |
AESIs, n (%) | |
Gastrointestinal abdominalc | ████████ |
AESI = adverse event of special interest; HAE = hereditary angioedema; SAE = serious adverse event; TEAE = treatment-emergent adverse event.
aObserved in 5% or more of patients.
bSAEs affecting 2 or more patients.
cA gastrointestinal abdominal TEAE was any TEAE with a preferred term within the Medial Dictionary for Regulatory Activities 19.1 hierarchy under the high-level group terms of 1) gastrointestinal signs and symptoms or 2) gastrointestinal motility and defecation conditions.
Source: Clinical Study Report for APeX-S.38
Critical Appraisal
Internal Validity
This phase II study is an ongoing, open-label, long-term study that evaluated the safety and efficacy of berotralstat for up to 48 weeks of treatment. As there was no active comparator and all outcomes were descriptive in nature, it is difficult to make any inferences regarding the results. The baseline attack rates were not calculated and it was therefore not possible to determine changes in attack rates over time from baseline. An additional limitation is the open-label nature of treatment, which can bias the reporting of subjective end points (i.e., harms). The interpretation of efficacy outcomes is limited by the large amount of missing data due to attrition. A total of 26% of patients in the berotralstat 150 mg group discontinued the study, mainly due to adverse events or a lack of perceived efficacy. This attrition could have resulted in a population of patients who were more tolerant of berotralstat, as those not responding to treatment or experiencing adverse events may be less likely to continue participating in the APeX-S study. Including patients more tolerant of berotralstat can also lead to biased estimates of efficacy and adverse events, potentially overestimating efficacy and underestimating the frequency of the adverse events being reported. The use of concomitant HAE drugs among patients throughout the APeX-S study may have increased the risk of observing additional side effects not attributable to berotralstat alone. HRQoL data are difficult to interpret as available scores continued to diminish over time, with 57.5% of patients reporting an AE-QoL total score at week 48.
External Validity
The APeX-S trial used inclusion and exclusion criteria similar to those of the pivotal trials6,7 and enrolled predominantly middle-aged white females. The expert consulted for this review considered the patients enrolled in the pivotal trials to be representative of patients with type 1 or 2 HAE in Canada. Nevertheless, the high dropout rate of 26% in the APeX-S study may have led to patients who are less representative of the recruited population, decreasing the generalizability of the results of the study.
Discussion
Summary of Available Evidence
The systematic review included 2 double-blind RCTs that evaluated the efficacy and safety of berotralstat versus placebo in patients with HAE type 1 or 2. The APeX-2 and APeX-J studies randomized patients to placebo, berotralstat 110 mg, or berotralstat 150 mg daily for 24 weeks (part 1), after which all placebo patients were randomized to berotralstat 110 mg or 150 mg daily, and those on active drug continued with the same dose for part 2 (double-blind, up to 52 weeks). In the subsequent part 3 of the trials, all patients were switched to open-label berotralstat 150 mg daily (up to 104 weeks). The primary outcome in both studies was the rate of investigator-confirmed HAE attacks over the first 24 weeks (part 1). This review focused on a comparison between berotralstat 150 mg and placebo, which included 80 patients from the APeX-2 study and 13 patients from the APeX-J trial.
One open-label, long-term study was also summarized in this report. The APeX-S trial provided supplemental safety and efficacy data for patients who received berotralstat 150 mg daily for up to 48 weeks (N = 127). No indirect evidence comparing berotralstat to other prophylactic treatments for HAE were submitted by the sponsor and none were found in the literature.
Interpretation of Results
Efficacy
During the first 24 weeks of the APeX-2 study, treatment with berotralstat 150 mg daily reduced the rate of investigator-confirmed attacks by 44% relative to placebo. Patients experienced, on average, 1.3 attacks per month when receiving berotralstat as LTP therapy, compared with 2.4 attacks per month for those receiving placebo. Only █ █ █████ █ █ in the berotralstat group reported no confirmed HAE attacks, and overall, patients reported 13 fewer symptom-days while on berotralstat versus placebo. Other exploratory or ad hoc analyses of the treated, laryngeal, and moderate or severe attack rates were generally supportive of the results of the primary outcome. However, as these outcomes were either not defined a priori or were not controlled for type I errors, any results with a P value of less than 0.05 should be interpreted with caution due to the potentially inflated type I error rate. Similarly, the exploratory and ad hoc responder analyses were not controlled for the type I error rate. These analyses suggest that more patients in the berotralstat group achieved at least a 50% or a 70% reduction (but not a 90% reduction) in the rate of HAE attacks compared with the placebo group. According to the clinical expert consulted, the treatment effects observed were considered modest improvements, given that a 20% reduction in attacks is generally considered a mild effect, and a 50% reduction is considered a moderate effect. Both the European Medicines Agency and FDA evaluations of berotralstat stated that the clinical relevance of the effect size for the primary end point was modest.19,20
The subgroup analyses based on baseline attack rate, and prior androgen use were generally consistent with the overall results, but due to the small sample size of the groups and the lack of statistical analysis, the subgroup data should be interpreted with caution. Because only 2 adolescents received berotralstat 150 mg, the efficacy and safety data for this population were limited.
Additional supportive data from the APeX-J study showed a 49% reduction in the expert-confirmed HAE attack rate with berotralstat 150 mg versus placebo over 24 weeks of therapy.
While the patient group input indicated that reducing the frequency of attacks was important, improving HRQoL was also a concern. Neither study detected a difference between groups in HRQoL, measured using the AE-QoL or EQ-5D, and the impact of berotralstat on HRQoL is therefore uncertain.
The key limitations of the studies were the small sample size and the short duration of the comparative treatment period (24 weeks). Due to the limited sample size (80 patients in the APeX-2 trial and 13 patients in APeX-J), randomization may not ensure the groups were balanced for all measured or unmeasured prognostic factors or confounders. At baseline, there were imbalances between groups in the mean age, proportion of females, weight, proportion with 2 or more attacks per month, prior laryngeal attacks, and prior emergency visits in the past year, but it is unclear what impact these differences may have had on the findings. In addition, more patients discontinued from the placebo group than from the berotralstat group, which may also lead to bias. However, the results of sensitivity analyses that assessed the impact of missing data were generally supportive of the primary analysis. The clinical expert noted the ██ █ ██████ of C1-INH versus other rescue therapies may have biased the results in favour of the berotralstat group in APeX-2, due to the long duration of action and potential protective effect of C1-INH. The extent to which this may have affected the HAE attack rate results is unclear.
With regard to the duration of the trials, the comparative treatment period was only 24 weeks. Longer-term noncomparative data were available, but had limitations. Wedner et al. (2021)5 reported 48-week data of the APeX-2 study, and the sponsor submitted posters and data-output tables that supplied select 96-week results as part of the initial submission to CADTH.25-28 (In the Request for Reconsideration, new data for parts 2 and 3 of APeX-2 were supplied by the sponsor and these data are summarized in Appendix 5.) Additional 48-week data were available from the uncontrolled, open-label, long-term study (APeX-S). The 48-week results suggest a reduction in HAE attacks may be maintained in patients who continued on therapy. Of the 40 patients initially randomized to berotralstat 150 mg in the APeX-2 study, 31 (78%) completed 48 weeks. █ ███ █ ████ █ ███ █ ████ stopped treatment due to adverse events or lack of efficacy and ██ █ ███ █ █ █ █ ██ stopped for other reasons. As patients who responded to therapy and showed adequate tolerance were more likely to continue treatment, the efficacy results likely overestimated the effects of berotralstat. In addition to the potential selection bias, the lack of a control group limits the ability to draw causal inferences from the findings. Moreover, patients’ awareness that they were receiving active therapy may have biased reporting of subjective outcomes (such as HAE attack symptoms or adverse events) based on patients’ expectations of treatment. The durability of treatment effects of berotralstat beyond 24 weeks therefore remains uncertain.
With regard to external validity, the clinical expert consulted for this review described the characteristics of the patient population enrolled in the trials as representative of the target population and the expert did not identify any issues that could substantially affect the generalizability of the findings. The trials are representative of patients with type 1 and 2 HAE who were suitable for management using on-demand HAE therapy only, and on average, had a baseline rate of 3 HAE attacks per month.
Because limited information were reported in the RCTs on the impact of berotralstat on hospitalization or emergency visits, the impact of treatment on health care resource use or mortality are unknown. There were no head-to-head studies, and the sponsor did not conduct an ITC, and the comparative efficacy and safety of berotralstat relative to other LTP therapies are also unknown.
Harms
Most patients reported 1 or more adverse events during the RCTs, with gastrointestinal adverse events reported more frequently among patients who received berotralstat 150 mg versus placebo. However, no patients stopped treatment due to gastrointestinal adverse events during the first 24 weeks of the studies. The expert noted that the symptoms of an abdominal HAE attack may be difficult to distinguish from gastrointestinal-related adverse events. According to the product monograph, gastrointestinal adverse effects generally occur early, become less frequent over time and usually self-resolve.4
Withdrawals due to adverse effects in the first 48 weeks of the APeX-2 study were similar to those in the open-label, long-term study (APeX-S). In the berotralstat 150 mg group, 3 patients (8%) in the APeX-2 study and 13 patients (10%) in the APeX-S study stopped treatment due to adverse effects. Comparative safety data were limited to 24 weeks; however, no new safety signals were identified among patients who received berotralstat 150 mg for up to 48 weeks in part 2 of the APeX-2 trial (N = 37) or in the APeX-S study (N = 127). While serious adverse events were rare, their frequency should be interpreted cautiously considering the small sample size and relatively limited follow-up time. As with most clinical trials, the studies were not powered to detect infrequent adverse effects or those with a lag time.
The sponsor indicated that berotralstat will be available in Canada through a dedicated patient support program that will “connect the patient with both a nurse and a pharmacist qualified to review the patient’s medication history and to educate patients on how to best manage adverse effects and provide adherence strategies.”39
Conclusions
In patients with type 1 or 2 HAE, treatment with berotralstat 150 mg daily reduced the rate of investigator-confirmed HAE attacks, relative to placebo, based on 24-week data from the APeX-2 and APeX-J studies. The impact of berotralstat on HRQoL was uncertain; although improvement in the AE-QoL total score was observed, the difference versus placebo was not statistically significant. Longer-term, uncontrolled studies suggest that a reduction in HAE attacks may be maintained in patients who continued on therapy up to 48 weeks; however, due to the limitations associated with these data, the longer-term safety and efficacy of berotralstat are uncertain. No evidence was available regarding the impact of berotralstat on hospitalization, emergency visits, or mortality. Also, because no direct or indirect evidence comparing berotralstat to other LTP therapies was available, the relative efficacy and safety of berotralstat compared to other LTP treatments are unknown. Gastrointestinal adverse events were reported more frequently among patients who received berotralstat compared with those who received placebo. Due to the limited sample size and duration of the trials, the studies were not designed to detect infrequent adverse effects or those with a lag time.
References
1.Betschel S, Badiou J, Binkley K, et al. The International/Canadian Hereditary Angioedema Guideline. Allergy Asthma Clin Immunol. 2019;15(1):72. PubMed
2.Maurer M, Magerl M, Ansotegui I, et al. The international WAO/EAACI guideline for the management of hereditary angioedema-the 2017 revision and update. Allergy. 2018;73(8):1575-1596. PubMed
3.Aygören-Pürsün E, Magerl M, Maetzel A, Maurer M. Epidemiology of Bradykinin-mediated angioedema: a systematic investigation of epidemiological studies. Orphanet J Rare Dis. 2018;13(1):73-73. PubMed
4.Orladeyo (berotralstat): 150 mg oral capsules [product monograph]. Oakville (ON): Innomar Strategies; 2022 Jun 2.
5.Wedner HJ, Aygoren-Pursun E, Bernstein J, et al. Randomized trial of the efficacy and safety of berotralstat (BCX7353) as an oral prophylactic therapy for hereditary angioedema: results of APeX-2 through 48 weeks (part 2). J Allergy Clin Immunol Pract. 2021;9(6):2305-2314.e2304. PubMed
6.Interim Clinical Study Report: BCX7353-302. Part 1. A phase 3, randomized, double-blind, placebo-controlled, parallel group study to evaluate the efficacy and safety of two dose levels of BCX7353 as an oral treatment for the prevention of attacks in subjects with hereditary angioedema [internal sponsor's report]. Durham (NC): BioCryst Pharmaceuticals, Inc; 2019 Oct 31.
7.Interim Clinical Study Report: BCX7353-301. Part 1. A phase 3, randomized, double-blind, placebo-controlled, parallel-group study to evaluate the efficacy and safety of two dose levels of BCX7353 as an oral treatment for the supression of events in subjects with hereditary angioedema [internal sponsor's report]. Durham (NC): BioCryst Pharmaceuticals, Inc; 2019 Dec 26.
8.Bork K, Meng G, Staubach P, Hardt J. Hereditary angioedema: new findings concerning symptoms, affected organs, and course. Am J Med. 2006;119(3):267-274. PubMed
9.Lumry WR. Overview of epidemiology, pathophysiology, and disease progression in hereditary angioedema. Am J Manag Care. 2013;19(7 Suppl):s103-110. PubMed
10.Bork K, Hardt J, Witzke G. Fatal laryngeal attacks and mortality in hereditary angioedema due to C1-INH deficiency. J Allergy Clin Immunol. 2012;130(3):692-697. PubMed
11.Busse PJ, Christiansen SC, Riedl MA, et al. US HAEA Medical Advisory Board 2020 guidelines for the management of hereditary angioedema. J Allergy Clin Immunol Pract. 2021;9(1):132-150.e133. PubMed
12.Takhzyro (lanadelumab injection): prefilled syringes and vials; 300 mg/2 mL solution for subcutaneous injection [product monograph]. Toronto (ON): Takeda Canada Inc; 2021 Mar 22: https://pdf.hres.ca/dpd_pm/00060484.PDF. Accessed 2022 Apr 20.
13.Berinert 500 / Berinert 1500 (C1 esterase inhibitor, human): powder and diluent for solution for injection; for intravenous administration; 500 IU/vial, reconstituted with 10 mL of diluent; 1500 IU/vial, reconstituted with 3 mL of diluent [product monograph]. Ottawa (ON): CSL Behring Canada, Inc; 2020 Feb 14: https://pdf.hres.ca/dpd_pm/00055050.PDF. Accessed 2022 Apr 20.
14.Cinryze (C1 esterase inhibitor (human)): 500 IU powder for solution/vial reconstituted with 5 mL of diluent for intravenous injection [product monograph]. Toronto (ON): Takeda Canada Inc; 2021 Feb 22: https://pdf.hres.ca/dpd_pm/00060070.PDF. Accessed 2022 Apr 20.
15.Haegarda (C1 esteraase inhibitor subcutanous (human)): powder and iluent for solution for injection for subcutaneous administration; 2000 IU/vial, reconstituted with 4 mL of diluent, 3000 IU/vial, reconstituted with 5.6 mL of diluent [product monograph]. Ottawa (ON): CSL Behring Canada, Inc; 2022 Apr 13: https://pdf.hres.ca/dpd_pm/00065454.PDF. Accessed 2022 Apr 20.
16.Drug therapies for the long-term prophylaxis of hereditary angioedema attacks. (CADTH technology review no. 25). Ottawa (ON): CADTH; 2019: https://www.cadth.ca/sites/default/files/hta-he/ob0007-hae-prophylaxis-redacted.pdf. Accessed 2022 Apr 29.
17.Zuraw B, Lumry WR, Johnston DT, et al. Oral once-daily berotralstat for the prevention of hereditary angioedema attacks: a randomized, double-blind, placebo-controlled phase 3 trial. J Allergy Clin Immunol. 2021;148(1):164-172.e169. PubMed
18.Ohsawa I, Honda D, Suzuki Y, et al. Oral berotralstat for the prophylaxis of hereditary angioedema attacks in patients in Japan: a phase 3 randomized trial. Allergy. 2021;76(6):1789-1799. PubMed
19.Center for Drug Evaluation Research. Multi-discipline review(s). Orladayo (berotralstat) 150 mg oral capsules. Company: BioCryst Pharmaceuticals, Inc. Application No.: 214094. Approval date: 12/3/2020 (FDA approval package). Silver Spring (MD): U.S. Food and Drug Administration (FDA); 2020 Dec 3: https://www.accessdata.fda.gov/drugsatfda_docs/nda/2020/214094Orig1s000TOC.cfm Accessed 2022 Mar 11.
20.Committee for Medicinal Products for Human Use. Assessment report: Orladeyo (berotralstat). (European public assessment report). Amsterdam (NL): European Medicines Agency; 2021 Feb 25: https://www.ema.europa.eu/en/documents/assessment-report/orladeyo-epar-public-assessment-report_en.pdf. Accessed 2022 Apr 4.
21.Clinical Study Report: BCX7353-302 [APeX-2]. A phase 3, randomized, double-blind, placebo-controlled, parallel group study to evaluate the efficacy and safety of two dose levels of BCX7353 as an oral treatment for the prevention of attacks in subjects with hereditary angioedema [internal sponsor's report]. Durham (NC): BioCryst Pharmaceuticals, Inc; 2022 Sep 29.
22.Weller K, Groffik A, Magerl M, et al. Development and construct validation of the angioedema quality of life questionnaire. Allergy. 2012;67(10):1289-1298. PubMed
23.Weller K, Magerl M, Peveling-Oberhag A, Martus P, Staubach P, Maurer M. The Angioedema Quality of Life Questionnaire (AE-QoL) - assessment of sensitivity to change and minimal clinically important difference. Allergy. 2016;71(8):1203-1209. PubMed
24.van Hout B, Janssen MF, Feng YS, et al. Interim scoring for the EQ-5D-5L: mapping the EQ-5D-5L to EQ-5D-3L value sets. Value Health. 2012;15(5):708-715. PubMed
25.Aygoren-Pursun E, McNeil D, Collis PJ, Desai B, Tomita DK, Johnston DT. Oral berotralstat treatment for 96 weeks consistently reduces hereditary angioedema (HAE) attack rates regardless of baseline attack rate [poster] [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Orladeyo (berotralstat), 150 mg capsule. Durham (NC): BioCyst Pharmaceuticals Inc; 2022 Feb 22.
26.Gower RG, Banerji A, Collis PJ, Desai B, Tomita DK, Lumry WR. Sustained improvement observed in patient-reported quality of life (QoL) with 96 weeks of oral berotralstat treatment [poster] [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Orladeyo (berotralstat), 150 mg capsule. Durham (NC): BioCyst Pharmaceuticals Inc; 2022 Feb 22.
27.Wedner HJ, Tachdjian R, Craig T, et al. Sustained reductions in hereditary angioedema (HAE) attack rates observed over 96 weeks of oral berotralstat treatment regardless of initial response [poster] [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Orladeyo (berotralstat), 150 mg capsule. Durham (NC): BioCyst Pharmaceuticals Inc; 2022 Feb 22.
28.Drug Reimbursement Review sponsor submission: Orladeyo (berotralstat), 150 mg capsule [internal sponsor's package]. Durham (NC): BioCyst Pharmaceuticals Inc; 2022 Feb 22.
29.Banerji A, Riedl MA, Bernstein JA, et al. Effect of lanadelumab compared with placebo on prevention of hereditary angioedema attacks: a randomized clinical trial. JAMA. 2018;320(20):2108-2121. PubMed
30.Craig T, Zuraw B, Longhurst H, et al. Long-term outcomes with subcutaneous C1-inhibitor replacement therapy for prevention of hereditary angioedema attacks. J Allergy Clin Immunol Pract. 2019;7(6):1793-1802.e1792.
31.Zuraw BL, Busse PJ, White M, et al. Nanofiltered C1 inhibitor concentrate for treatment of hereditary angioedema. N Engl J Med. 2010;363(6):513-522. PubMed
32.Prophylaxis for hereditary angioedema with lanadelumab and C1 inhibitors: effectiveness and value. (Final evidence report). Boston (MA): Institute for Clinical and Economic Review; 2018 Feb 15: https://icer.org/wp-content/uploads/2020/10/ICER_HAE_Final_Evidence_Report_111518-1.pdf. Accessed 2022 Apr 12.
33.Drug Reimbursement Review clinical report: lanadelumab (Takhzyro) for routine prevention of attacks of hereditary angioedema in adolescents and adults. Ottawa (ON): CADTH; 2020 Jan: https://www.cadth.ca/sites/default/files/cdr/clinical/sr0618-takhzyro-clinical-review-report.pdf. Accessed 2022 Apr 12.
34.Reevaluation of Takhzyro (lanadelumab injection) ereditary angioedema. Montreal (QC): INESSS; 2020: https://www.inesss.qc.ca/fileadmin/doc/INESSS/Produits_sanguins/Aout_2020/INESSS_Takhzyro_english_summary.pdf. Accessed 2022 Apr 12.
35.Berotralstat (hereditary angioedema) – Benefit assessment according to §35a Social Code Book V1. Koln (DE): Institute for Quality and Efficiency in Health Care; 2021 Sep 13: https://www.iqwig.de/download/a21-80_berotralstat_extract-of-dossier-assessment_v1−0.pdf. Accessed 2022 Apr 12.
36.Berotralstat for preventing recurrent attacks of hereditary angioedema. (Technology appraisal guidance TA738). London (GB): National Institute for Health and Care Excellence; 2021 Oct 20: https://www.nice.org.uk/guidance/ta738/resources/berotralstat-for-preventing-recurrent-attacks-of-hereditary-angioedema-pdf-82611261223621. Accessed 2022 Apr 12.
37.Berotralstat 150 mg hard capsules (Orladeyo). (SMC2405). Glasgow (GB): Scottish Medicines Consortium; 2022 Mar 7: https://www.scottishmedicines.org.uk/media/6734/berotralstat-orladeyo-final-feb-2022-amended-220222-for-website.pdf. Accessed 2022 Apr 12.
38.Interim Clinical Study Report: BCX7353-204. An open-label study to evaluate the long-term safety of daily oral BCX7353 in subjects with type 1 and 2 hereditary angioedema (Interim clinical study report) [internal sponsor's report]. Durkam (NC): BioCryst Pharmaceuticals, Inc; 2019 Oct 30.
39.BioCyst Pharmaceuticals Inc comments to Orladeyo (berotralstat) clinical report [internal additional sponsor's information]. Durham (NC): BioCyst Pharmaceuticals Inc; 2022 Jun 2.
40.Aygoren-Pursun E, Bygum A, Grivcheva-Panovska V, et al. Oral plasma kallikrein inhibitor for prophylaxis in hereditary angioedema. N Engl J Med. 2018;379(4):352-362. PubMed
41.Farkas H, Stobiecki M, Peter J, et al. Long-term safety and effectiveness of berotralstat for hereditary angioedema: the open-label APeX-S study. Clin Transl Allergy. 2021;11(4):e12035. PubMed
42.van Reenen M, Janssen B. EQ-5D-5L User Guide. Basic information on how to use the EQ-5D-5L instrument. Rotterdam (NL): EuroQol Research Foundation; 2015.
43.Reeve BB, Wyrwich KW, Wu AW, et al. ISOQOL recommends minimum standards for patient-reported outcome measures used in patient-centered outcomes and comparative effectiveness research. Qual Life Res. 2013;22(8):1889-1905. PubMed
44.McClure N, Sayah F, Xie F, Luo N, Johnson J. Instrument-defined estimates of the minimally important difference for EQ-5D-5L index scores. Value Health. 2017;20(4):644-650. PubMed
Appendix 1: Literature Search Strategy
Note that this appendix has not been copy-edited.
Clinical Literature Search
Overview
Interface: Ovid
Databases:
MEDLINE All (1946-present)
Embase (1974-present)
Note: Subject headings and search fields have been customized for each database. Duplicates between databases were removed in Ovid.
Date of search: March 14, 2022
Alerts: Weekly search updates until project completion
Search filters applied: No filters were applied to limit the retrieval by study type.
Limits:
Publication date limit: none
Language limit: none
Conference abstracts: excluded
Syntax | Description |
|---|---|
/ | At the end of a phrase, searches the phrase as a subject heading |
MeSH | Medical Subject Heading |
exp | Explode a subject heading |
* | Before a word, indicates that the marked subject heading is a primary topic; or, after a word, a truncation symbol (wildcard) to retrieve plurals or varying endings |
.ti | Title |
.ot | Original title |
.ab | Abstract |
.hw | Heading word; usually includes subject headings and controlled vocabulary |
.kf | Keyword heading word |
.dq | Candidate term word (Embase) |
.pt | Publication type |
.rn | Registry number |
.nm | Name of substance word (MEDLINE) |
medall | Ovid database code: MEDLINE All, 1946 to present, updated daily |
oemezd | Ovid database code; Embase, 1974 to present, updated daily |
Multi-Database Strategy
(Orladeyo* or berotralstat* or bcx-7353 or bcx7353 or who 10907 or 88SH1NBL2B or XZA0KB1BDQ).ti,ab,kf,ot,hw,nm,rn.
1 use medall
*berotralstat/ or (Orladeyo* or berotralstat* or bcx-7353 or bcx7353 or who 10907 or 88SH1NBL2B).ti,ab,kf,dq.
3 use oemezd
4 not (conference review or conference abstract).pt.
2 or 5
remove duplicates from 6
Clinical Trials Registries
ClinicalTrials.gov
Produced by the US National Library of Medicine. Targeted search used to capture registered clinical trials.
Search – Orladeyo (berotralstat); hereditary angioedema
WHO ICTRP
International Clinical Trials Registry Platform, produced by the World Health Organization. Targeted search used to capture registered clinical trials.
Search – Orladeyo (berotralstat); hereditary angioedema
Health Canada’s Clinical Trials Database
Produced by Health Canada. Targeted search used to capture registered clinical trials.
Search – Orladeyo (berotralstat); hereditary angioedema
EU Clinical Trials Register
European Union Clinical Trials Register, produced by the European Union. Targeted search used to capture registered clinical trials.
Search – Orladeyo (berotralstat); hereditary angioedema
Grey Literature
Search dates: March 10 to 14, 2022
Keywords: Orladeyo (berotralstat); hereditary angioedema
Limits: Publication years: none
Updated: Search updated prior to the completion of stakeholder feedback period
Relevant websites from the following sections of the CADTH grey literature checklist Grey Matters: A Practical Tool for Searching Health-Related Grey Literature were searched:
Health Technology Assessment Agencies
Health Economics
Clinical Practice Guidelines
Drug and Device Regulatory Approvals
Advisories and Warnings
Drug Class Reviews
Clinical Trials Registries
Databases (free)
Internet Search
Open Access Journals.
Appendix 2: Excluded Studies
Note that this appendix has not been copy-edited.
Reference | Reason for exclusion |
|---|---|
Aygoren-Pursun E, Bygum A, Grivcheva-Panovska V, et al. Oral Plasma Kallikrein Inhibitor for Prophylaxis in Hereditary Angioedema. N Engl J Med. 2018;379(4):352-362. | Study design40 |
Farkas H, Stobiecki M, Peter J, et al. Long-term safety and effectiveness of berotralstat for hereditary angioedema: The open-label APeX-S study. Clin Transl Allergy. 2021;11(4):e12035. Interim Clinical Study Report: BCX7353-204. An open-label study to evaluate the long-term safety of daily oral BCX7353 in subjects with type 1 and 2 hereditary angioedema (Interim Clinical Study Report) [internal sponsor's report]. Durkam (NC): BioCryst Pharmaceuticals, Inc; 2019 Oct 30 |
Appendix 3: Detailed Outcome Data
Note that this appendix has not been copy-edited.
Figure 3: Plot of Mean Investigator-Confirmed HAE Attack Rate by Month — APeX-2 (Part 1 ITT Population)
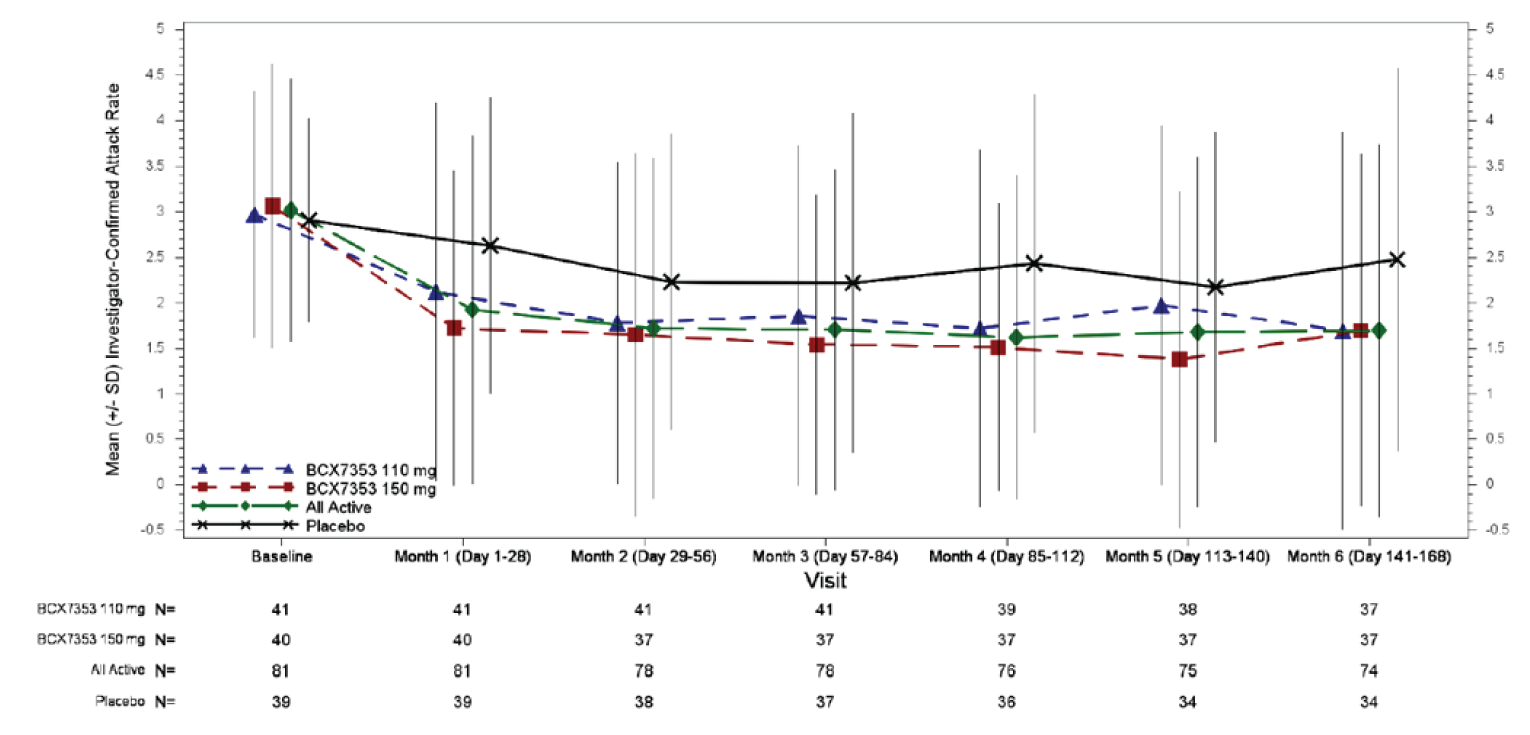
BCX7353 = berotralstat; HAE = hereditary angioedema; ITT = intention-to-treat; SD = standard deviation.
Source: Clinical Study Report for APeX-2.6
Table 26: Investigator-Confirmed Attacks by Month— APeX-2 Study (Part 1 ITT Population)
Time point | Berotralstat 150 mg N = 40 | Placebo N = 40 |
|---|---|---|
Baseline attack rate, N | 40 | 39 |
Baseline attack rate, mean (SD) | 3.1 (1.6) | 2.9 (1.1) |
Month 1 attack rate, N | 40 | 39 |
Month 1 attack rate, mean (SD) | 1.7 (1.7) | 2.6 (1.6) |
Month 2 attack rate, N | 37 | 38 |
Month 2 attack rate, mean (SD) | 1.7 (2.0) | 2.2 (1.6) |
Month 3 attack rate, N | 37 | 37 |
Month 3 attack rate, mean (SD) | 1.5 (1.6) | 2.2 (1.9) |
Month 4 attack rate, N | 37 | 36 |
Month 4 attack rate, mean (SD) | 1.5 (1.6) | 2.4 (1.9) |
Month 5 attack rate, N | 37 | 34 |
Month 5 attack rate, mean (SD) | 1.4 (1.9) | 2.2 (1.7) |
Month 6 attack rate, N | 37 | 34 |
Month 6 attack rate, mean (SD) | 1.7 (1.9) | 2.5 (2.1) |
ITT = intention-to-treat; SD = standard deviation
Source: Clinical Study Report for APeX-2.6
Table 27: Subgroup Analyses for Investigator-Confirmed HAE Attacks (Part 1 ITT Population)
Investigator-confirmed HAE attacksa | APeX-2 (24 weeks) | Combined APeX-2 and APeX-J | ||
|---|---|---|---|---|
Subgroup/outcome | Berotralstat 150 mg N = 40 | Placebo N = 40 | Berotralstat 150 mg N = 47 | Placebo N = 46 |
Baseline attack rate ≥ 2 per month | ||||
Number of patients contributing to the analysis | █████ | █████ | 34 | 30 |
Attack rate per 28 days | █████ | █████ | 1.79 | 2.94 |
Rate reduction (%) versus placebo (95% CI) | 39.9 (14.4 to 57.8) | reference | 39.0 (16.1 to 55.7) | reference |
P value | █████ | reference | 0.002b | reference |
Baseline attack rate < 2 per month | ||||
Number of patients contributing to the analysis | █████ | █████ | 13 | 15 |
Attack rate per 28 days | █████ | █████ | 0.47 | 1.44 |
Rate reduction (%) versus placebo (95% CI) | 65.7 (23.8 to 84.5) | reference | 67.4 (35.9 to 83.5) | reference |
P value | █████ | reference | 0.001b | reference |
Age 12 to 17 years | ||||
Number of patients contributing to the analysis | 2 | 2 | █████ | █████ |
Attack rate per 28 days | 0.11 | 0.03 | █████ | █████ |
Rate reduction (%) versus placebo (95% CI) | -289.5 (-10119 to 85.2) | reference | -289.5 (-10119 to 85.2)c | reference |
P value | 0.42b | reference | █████ | reference |
Age 18 to 64 years | ||||
Number of patients contributing to the analysis | 37 | 35 | █████ | █████ |
Attack rate per 28 days | 1.44 | 2.59 | █████ | █████ |
Rate reduction (%) versus placebo (95% CI) | 44.4 (24.6 to 59.0) | reference | 45.9 (29.2 to 58.7) | reference |
P value | <0.001b | reference | █████ | reference |
Age ≥ 65 years | ||||
Number of patients contributing to the analysis | 1 | 3 | █████ | █████ |
Attack rate per 28 days | 0.62 | 1.56 | █████ | █████ |
Rate reduction (%) versus placebo (95% CI) | 60.2 (-90.2 to 91.7) | reference | 62.0 (-79.3 to 91.9) | reference |
P value | 0.25b | reference | █████ | reference |
Prior androgen used | ||||
Number of patients contributing to the analysis | █████ | █████ | █████ | █████ |
Attack rate per 28 days | █████ | █████ | █████ | █████ |
Rate reduction (%) versus placebo (95% CI) | 48.1 (23.7 to 64.7) | reference | 46.8 (23.3 to 63.1) | reference |
P value | █████ | reference | █████ | reference |
No prior androgen used | ||||
Number of patients contributing to the analysis | █████ | █████ | █████ | █████ |
Attack rate per 28 days | █████ | █████ | █████ | █████ |
Rate reduction (%) versus placebo (95% CI) | 34.3 (-14.5 to 62.3) | reference | 42.1 (9.7 to 62.9) | reference |
P value | █████ | reference | █████ | reference |
CI = confidence interval; HAE = hereditary angioedema; ITT = intention-to-treat.
aNegative binomial model, with covariate for baseline HAE attack rate and log of treatment duration as offset for ITT population.
bP value has not been adjusted for multiple testing (i.e., the type I error rate has not been controlled).
cModel fit was questionable.
dPost hoc subgroup analysis in the APeX-2 study.
Source: Clinical Study Report for APeX-26 and Clinical Study Report for APeX-J.7
Table 28: Ad Hoc Analysis of Attack-Free Months— APeX-2 Study (Part 1 Completer Population)
Outcome | Berotralstat 150 mg (N = 40) | Placebo (N = 40) |
|---|---|---|
Attack-free months (24 weeks)a | ||
Number of patients contributing to the analysis | █████ | █████ |
Number of attack-free months, mean (SD) | █████ | █████ |
Number (%) of patients with a total number of attack-free months of: | ||
0 | █████ | █████ |
1 | █████ | █████ |
2 | █████ | █████ |
3 | █████ | █████ |
4 | █████ | █████ |
5 | █████ | █████ |
6 | █████ | █████ |
NR = not reported; SD = standard deviation.
aPatients were considered attack-free for a given month if they did not experience any investigator-confirmed attacks in that 28 day period. Patients who discontinued study drug in a given month were not considered attack-free in that month. The analysis excluded any patient who withdrew from the study before 24 weeks.
Source: Clinical Study Report for APeX-2.6
Appendix 4: Description and Appraisal of Outcome Measures
Note that this appendix has not been copy-edited.
Aim
To describe the following outcome measures and their measurement properties (validity, reliability, responsiveness to change, and MID):
Angioedema Quality of Life questionnaire (AE-QoL)
5-Level EQ-5D questionnaire (EQ-5D-5L)
Findings
A focused literature search was conducted to identify the psychometric properties and the MID of each of the stated outcome measures. The findings on reliability, validity, responsiveness, and the MID of each outcome measure are summarized in Table 29.
Table 29: Summary of Outcome Measures and Their Measurement Properties
Outcome measure | Type | Conclusions about measurement properties | MID |
|---|---|---|---|
AE-QoL | The AE-QoL questionnaire is an angioedema-specific, patient-reported, HR-QoL measure which consists of 17 questions in 4 domains, functioning, fatigue/mood, fears/shame and food.22 Each item has a total of 5 answers, 1 = never to 5 = very often, with each scored 0 to a maximum of 4 points, respectively. A total score, and individual domain scores are generated, and converted on to a linear scale of 0 to 100, with higher scores representing higher impairment. | Validity: Content validity was assessed through a data acquisition, item generation, and item reduction phase. Construct validity was assessed using a known groups approach and demonstrated a linear relationship between self-rated disease and QoL burden with the total AE-QoL score. Strong correlations were observed between the AE-QoL and DLQI total scores, and between the domain scores, supporting convergent validity of AE-QoL in recurrent angioedema.22 Reliability: Reliability of the AE-QoL instrument was demonstrated through internal consistency and test-retest assessments in one study.22 The AE-QoL was found to have excellent internal consistency for the whole instrument as well as across each domain (Cronbach alpha > 0.80). The AE-QoL was shown to have acceptable test-retest reliability for the total score and individual domains (Pearson’s coefficient > 0.70). Responsiveness: One study investigated responsiveness of the AE-QoL measure to change in a sample of 278 patients with recurrent angioedema by correlating changes in its scores over time with changes in the applied anchors (self-rated angioedema disease and QoL burden and SF-12).23 The AE-QoL total score changes over time correlated moderately with changes in the self-rated angioedema activity and strongly with angioedema-specific quality of life impairment. The functional domain was observed to be the most sensitive to change. AE-QoL total score changes correlated weakly with changes in the SF-12 PCS and MCS scores. | The MID was estimated to be 6.0 points for the total AE-QoL score, based on an anchored-based approach in a sample population of 278 patients with recurrent angioedema.23 No MID has been determined for domain-specific scores. |
EQ-5D-5L | The EQ-5D-5L questionnaire is a generic, preference-based, HRQoL measure consisting of descriptive questions and a VAS.42 The descriptive questions comprise of 5 dimensions, mobility, self-care, usual activities, pain/discomfort, and anxiety/depression. Each dimension is divided into 5 levels of perceived problems ranging from “no problems” to “extreme problems.” The VAS records the patient’s self-rated health on a 20 cm scale with end points 0 to 100 labelled “the worst health you can imagine” and the best health you can imagine,” respectively. | The EQ-5D-5L questionnaire was not validated in the patients with HAE. | The MID was not determined in the patients with HAE. |
AE-QoL = Angioedema Quality of Life questionnaire; DLQI = Dermatology Life Quality Index; EQ-5D-5L = 5-Level EQ-5D questionnaire; HRQoL = health-related quality of life; MID = minimal important difference; MCS = Mental Component Summary; PCS = Physical Component Summary; QoL = quality of life; SF-12 = Short Form (12) Health Survey; VAS = visual analogue scale.
Angioedema Quality of Life Questionnaire
The AE-QoL questionnaire is an angioedema-specific, patient-reported, HRQoL measure.22 It was developed and validated as the first instrument to measure HRQoL impairment in patients with any type of recurrent angioedema. It is a short, self-administered questionnaire that consists of 17 questions with 5 possible answers each (1 = never to 5 = very often). A recall period of 4 weeks was chosen, based on the heterogeneity in frequency of attacks in recurrent angioedema patients. Each item answered by the respondent is scored between 0 and 4 points, depending on the answer chosen (i.e., never = 0 points, very often = 4 points). The questions address 4 domains, functioning (impairment of work, physical activity and spare time activities); fatigue/mood (difficulties falling asleep, waking up during the night, feeling tired during the day, difficulties concentrating, feeling downhearted); fears/shame (feeling burdened from swellings, fear and embarrassment of new swellings, ashamed to visit public places, fear of long-term negative drug effects); food (limitations in eating and in the selection of foods and beverages).22 A total score, and individual domain scores can be generated, based on the sum of all completed items divided by the maximum sum of all possible items. The raw scores are converted onto a linear scale ranging from 0 to 100, with higher scores representing higher HRQoL impairment.
Validity
The development and content validity of the AE-QoL instrument consisted of data acquisition, item generation and item reduction phases, and final instrument validation in a sample of 120 adult patients with recurring angioedema (n = 10, item generation; n = 110, instrument validation).22 The validation population included 73 (66.4%) females, adults aged 18 years and older, and 3 diagnosis categories: 1) type 1 or 2 HAE, 2) chronic spontaneous urticaria (patients with wheals and angioedema), or 3) other (recurrent angioedema without C1-INH deficiency and without wheals or recurrent angioedema with no clear allocation to either category).
Validation of the AE-QoL consisted of construct and convergent validity assessments.22 Construct validity was assessed using a known groups approach; patients received a self-administered questionnaire which included sociodemographic questions, as well as self-rating of angioedema-specific questions based on a 5-point scale for disease activity (response options: “none,””1–2,” “3–4,” “more than 4 attacks,” and “attacks almost every day”) and quality of life impairment (response options: “none,” “mild,” “moderate,” “severe,” and “very severe”). A linear correlation was demonstrated between increasing AE-QoL total scores and increasing levels of self-rated angioedema activity (P < 0.001) and quality of life impairment (P < 0.001).22 Of note, no correlation coefficients were provided in the study results. Convergent validity was assessed by testing the strength of correlation of the AE-QoL with other instruments that measured similar constructs, the Dermatology Life Quality Index (DLQI) and the generic Short Form (36) Health Survey (SF-36). A strong correlation (Pearson coefficient r > 0.50) was observed between the AE-QoL and DLQI total scores, supporting convergent validity of AE-QoL in recurrent angioedema. The individual domain scores were poorly correlated with the DLQI scores (r = 0.44 for functioning, 0.38 for fatigue/mood, 0.40 for fears/shame, and 0.31 for food). The correlation of the AE-QoL total score and the SF-36 Mental Component Summary (MCS) score was strong (r = −0.68), while the correlation with the SF-36 Physical Component Summary (PCS) was found to be weak (r = −0.24).22 With respect to the individual domains, only the functioning domain correlated with the PCS score (r = −0.47), while the fatigue/mood, and fears/shame correlated strongly with the MCS score (r = −0.59 and −0.525, respectively).
Reliability
Reliability of the AE-QoL instrument was demonstrated through internal consistency and test-retest assessments.22 The AE-QoL was found to have excellent internal consistency for the whole instrument (Cronbach alpha 0.89) as well as across each domain (Cronbach alpha between 0.83 to 0.90). To assess test-retest reliability, a subsample of 46 patients (including 15 patients with HAE) were asked to complete the AE-QoL twice in 3-week intervals. The AE-QoL was shown to have acceptable test-retest reliability (Pearson’s coefficient for the total score was 0.83, and ranging from 0.68 to 0.90 for individual domains) based on the generally-accepted threshold for patient-reported outcome measures.22,43 The domain with the lowest reproducibility was the fatigue/mood domain.
Responsiveness to Change
A subsequent study by Weller and colleagues sought to assess both responsiveness to change and the MID for the AE-QoL instrument.23 Responsiveness of the AE-QoL measure to change was assessed in a sample of 278 patients with recurrent angioedema by correlating changes in its scores over time with changes in the applied anchors. The chosen anchors were self-rated angioedema specific disease activity and quality of life impairment as described in the initial validation study, as well as the Short Form (12) Health Survey.22,23 AE-QoL total score changes over time correlated moderately with changes in the self-rated angioedema activity (Spearman’s rho r = 0.39) and strongly with changes in the self-rated angioedema-specific quality of life impairment (r = 0.5). Furthermore, a strong correlation was observed with changes in the AE-QoL functioning domain (r = 0.59), and moderate correlations were observed in the other 3 domains, indicating that the functioning domain is the most sensitive to change. AE-QoL total score changes correlated weakly with changes in the Short Form (12) Health Survey PCS (r = −0.26) and MCS (r = −0.29), and correlations were consistently weak across each AE-QoL domain.
Minimal Important Difference
The MID of the AE-QoL was evaluated by anchor-based and distributional criterion approaches.23 For the anchor-based approach, the magnitude (mean ± SD) of the total AE-QoL score changes during improved (n = 26), unchanged (n = 60), or worsening (n = 18) self-rated angioedema-related quality of life impairment were –12.5 ± 16.5 (median: –12.5), –0.3 ± 12.6 (median: 0), and 6.3 ± 12.4 (median: 6.5) points, respectively. A change was defined as a 1-step change (e.g., from moderate to severe, or moderate to mild). In a second approach, a receiver operating characteristic curve analysis of the self-rated quality of life impairment ratings identified the best cut-off point for clinically meaningful changes in the AE-QoL total score to be -5.5 points for quality of life improvement and 5.5 points for quality of life worsening, based on a desired balance of sensitivity and specificity.23 The distributional criterion approach (one-half of the SD of the baseline AE-QoL total score values), estimated a MID of 10.5 points. Given that the anchor-based approach is a more direct and patient-centred method over the distributional criterion approach, the results of the anchor-based approach were favoured by the authors, and a MID of 6 points was chosen as a meaningful change in quality of life to the patient.23 This MID of 6 points was used in the pivotal trials.6,7
5-Levels EQ-5D Questionnaire
The EQ-5D-5L questionnaire is a generic, preference-based, HRQoL measure consisting of descriptive questions and the EQ VAS.42 The descriptive questions comprise of 5 dimensions, mobility, self-care, usual activities, pain/discomfort, and anxiety/depression. Each dimension is divided into 5 levels (1, 2, 3, 4, 5) representing “no problems,” “slight problems,” “moderate problems,” “severe problems,” and “extreme problems,” respectively. Respondents are asked to choose one level that reflects their own health state for each of the 5 dimensions. The 5 questions are scored and together contribute to the EQ-5D index (utility) score between 0 and 1, where 0 represents death, and 1 represents perfect health. Different utility functions are available that reflect the preferences of specific populations (e.g., US, UK). The second part of the tool records the patient’s self-rated health on a 20 cm scale with end points 0 and 100, with respective anchors of “the worst health you can imagine” and “the best health you can imagine,” respectively.
The EQ-5D-5L measure has not been validated in patients with recurrent angioedema or type 1 or type 2 HAE specifically. Therefore, its validity, reliability, and responsiveness to change has not been evaluated in the patients with HAE. No estimate of the MID for the EQ-5D-5L index score was found in patients with HAE but in the general Canadian population a summarized mean of 0.056 ± a SD of 0.011 (interquartile range = 0.049 to 0.063) has been reported.44 Overall, the EQ-5D-5L is not considered to be a validated outcome in the study population.
Appendix 5: Long-term Extension Data Used to Inform the Request for Reconsideration
Note that this appendix has not been copy-edited.
Long-Term Extension Studies
The following summary was prepared based on new information on the longer-term extension phases (part 2 and 3) of the APeX-2 study using data from the September 29, 2022 CSR submitted by the sponsor as part of the Request for Reconsideration.21 Only data for the Health Canada approved berotralstat dose of 150 mg daily has been summarized.
Methods
The primary objective of part 2 and 3 of the APeX-2 study was to evaluate the long-term safety and tolerability of berotralstat in patients with HAE type 1 or 2. The secondary objectives were to assess the HAE attack rate and impact on HRQoL. The extension phases of APeX-2 trial did not have a control group and all patients received either berotralstat 110 mg or 150 mg daily. In part 2 (week 24 to 48), patients and investigators were blinded to the berotralstat dose, but in part 3 (week 48 up to week 240), all patients received unblinded berotralstat 150 mg daily. The flow of patients through APeX-2 phases is shown in Figure 4. A total of 54 patients in part 2 and 81 patients in part 3 received berotralstat 150 mg daily. The CSR states that due to attrition of patients between week 144 and 240, the focus of the final CSR was on data through to week 144.
Figure 4: APeX-2 Study Schematic
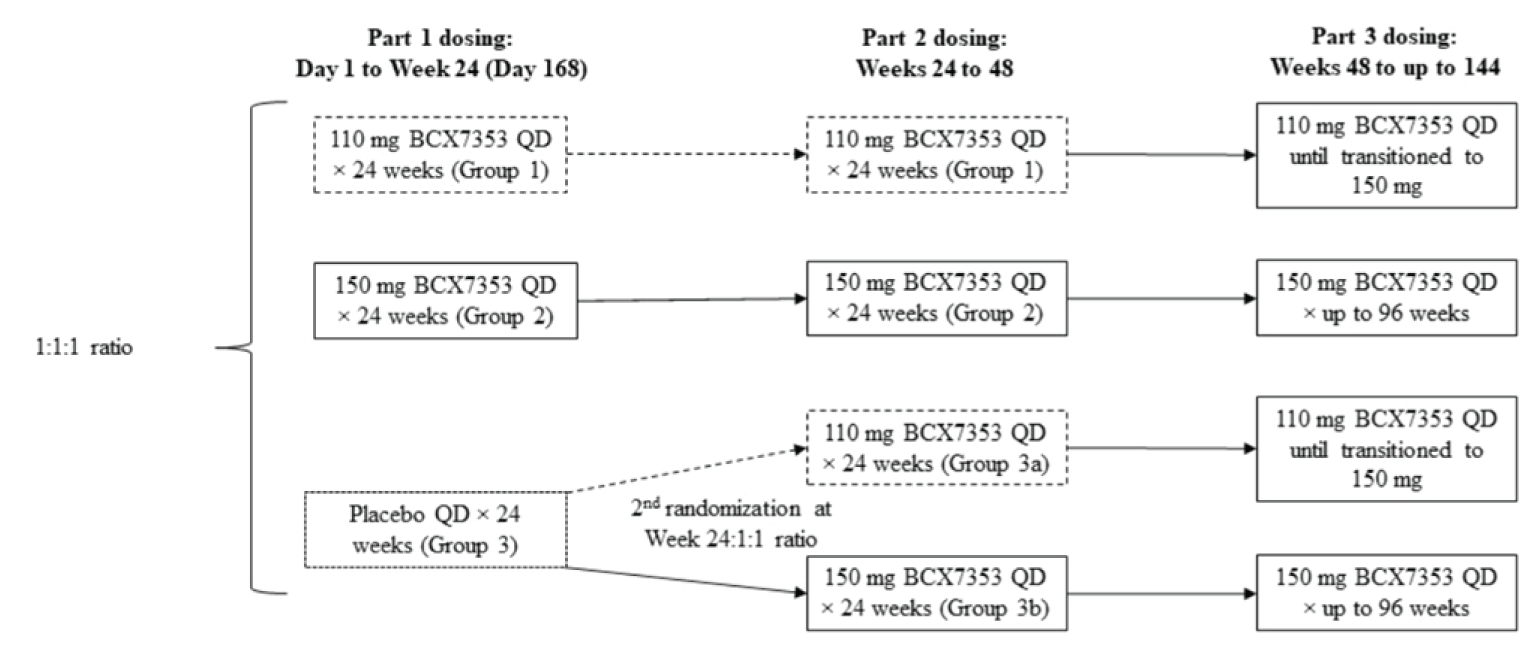
BCS7353 = berotralstat; QD = once daily.
Source: Clinical Study Report for APeX-2 Parts 2 and 3.21
Populations
The APeX-2 study enrolled patients ≥ 12 years of age with a confirmed diagnosis of HAE type 1 or 2, who experienced at least 2 qualifying HAE attacks during the run-in phase. In addition, the patients had to have access to standard-of-care treatments for acute attacks and be medically appropriate for on-demand treatment as the sole medical management of their HAE.
The mean age of patients who received berotralstat 150 mg in part 2 █████ of APeX-2 ranged from 40.7 years (SD = 14.2) to 45.7 years (14.8), 60% to 77% were women and 24% to 41% were men, and most patients were white (88% to 95%) (Table 30).
Table 30: Patient Demographics for Extension Phase of APeX-2
Characteristic | Part 2 | Part 3 | |
|---|---|---|---|
Berotralstat 150 mg N = 37 | Placebo then berotralstat 150 mg N = 17 | All berotralstat 150 mg █████ | |
Age, years, mean (SD) | 40.7 (14.2) | 45.7 (14.8) | █████ |
Age 12-17, n (%) | 2 (5) | 1 (6) | █████ |
Female, n (%) | 22 (60) | 13 (77) | █████ |
Male, n (%) | 15 (41) | 4 (24) | █████ |
Race, n (%) | |||
Asian | 0 | 0 | █████ |
Black or African American | 1 (3) | 1 (6) | █████ |
White | 35 (95) | 15 (88) | █████ |
Other | 1 (3) | 1 (6) | █████ |
BMI, kg/m2, median (range) | 30.8 (6.8) | 30.8 (7.2) | █████ |
BMI = body mass index; SD = standard deviation.
Source: Clinical Study Report for APeX-2 parts 2 and 3.21
Interventions
Patients initially randomized to berotralstat 150 mg daily in part 1 (week 0 to 24), continued to receive double-blind berotralstat 150 mg in part 2 (week 24 to 48). At week 24, patients initially randomized to placebo were rerandomized to receive double-blind berotralstat 150 mg or 110 mg daily during part 2. All patients who entered part 3 (week 48 to 144) received open-label berotralstat 150 mg daily.
Outcomes
Efficacy outcomes that were of interest to this review included the rate of HAE attacks, proportion of days with angioedema symptoms, and durability of AE-QoL and EQ-5D-5L scores.
Patients reported HAE attacks using an electronic diary, and in part 2, all attacks were confirmed by the investigator. During part 3, no investigator confirmation was required, but all patient-reported attacks underwent a computer-based review were confirmed or rejected based on the following criteria:
Attack must include at least 1 symptom of swelling
Patient response the diary question, “In retrospect, could there be an alternative explanation for your symptoms other than an HAE attack (i.e., allergic reaction, viral cold etc)?” must have been “no”
Attack must have been unique (attack began >24 hours from end of the prior attack) otherwise the attack was combined with and treated as a continuation of the preceding attack
If untreated, attack must have a duration of > 24 hours.
In part 3, the adjusted patient-reported attack rate were reported as events per 28 days, and for the entire dosing period of part 3. The investigator-confirmed attack rate was reported by month (every 28 days) for part 1 and 2, and over the entire dosing period for part 1 and 2. The entire dosing period began on day 1 of part 1 for those randomized to berotralstat, and the day 1 for part 2 on those switched from placebo to berotralstat at week 24 (labelled as the adjusted day 1). For patients who stopped treatment early, any events that started within 24 hours of the last dose of berotralstat were included in the attack rate calculations. The follow-up period ended 24 hours after the last dose of study drug for patients who stopped treatment.
The number and proportion of days with angioedema symptoms were calculated based on diary data for patients who received at least 1 dose of berotralstat in either part 2 or part 3. HRQoL was assessed using the AE-QoL questionnaire and the EQ-5D-5L instrument.
Data were collected on the number and proportion of patients who reported treatment-emergent adverse events, serious adverse events or who stopped treatment due to adverse events.
Statistical Analysis
There was no statistical testing for part 2 or 3. All results were reported descriptively with no imputation for missing data.
Patient Disposition
Of the 40 patients randomized to berotralstat 150 mg daily, 37 patients (93%) continued in part 2. Six patients (16%) discontinued during part 2 due to lack of efficacy (8%), adverse events (5%) or other reasons (3%). Another 5 patients (14%) stopped treatment at the 48 week visit, including 2 patients (5%) due to lack of efficacy. Among patients randomized to placebo at the start of the study, 34 patients (87%) completed part 1 and 17 were rerandomized to receive berotralstat 150 mg daily. Three of these patients (18%) discontinued during part 2 due to lack of efficacy (12%) or withdrawal of consent (6%) (Table 30).
Overall, █ █ █ █ ██████ █ █ █ ██████ █ ██ █ ██ and received at least 1 dose of berotralstat 150 mg during this period. This group consisted of █ █ ███████ █ ██████████████ █ ███ █ ██ █ ███ randomized in APeX-2, including 26 patients initially ██ █ ███ █ ██████ █ ████ █ ████████ █ █ █ ███████ █ ████ █ █████ █ ██ █ ████ randomized to berotralstat 150 mg, then berotralstat 150 mg, and █ █ ████ █ ██████████████████████████████████ █ ██ █ ██ █ █████ in part 1 and 2. During █ █ ██ █ ███ █ █ █ ████, █████ █ ████ █ █ █ ████████ █ ███ █ ████ █ █ ███ █ ███ █ ███ █ █ █ █ ███ █ █ █ █ █ ██ █ ████ █ ██████ █ ██████.
Table 31: Patient Disposition for Part 2 of APeX-2
Detail | Berotralstat 150 mg (N = 40) | Placebo (N = 39) |
|---|---|---|
Completed Part 1, n (%) | 37 (93) | 34 (87) |
Part 2 | Berotralstat 150 mg | Placebo then berotralstat 150 mg |
Continued in Part 2 | 37 | 17 |
Discontinued drug in Part 2, n (%)a | 6 (16) | 3 (18) |
Adverse event | 2 (5) | 0 |
Lack of efficacy | 3 (8) | 2 (12) |
Withdrawal of consent | 0 | 1 (6) |
Other | 1 (3) | 0 |
Continued in Part 3, n (%)a | 26 (70) b | █████ |
aPercentage calculated based on the patients who continued in part 2.
█ ███████████████████████████████████ █ ███████████████████████████████████████████████ █ █ █ █ █ █ █ █ █ ██ █ ████ █ ███████ █ ██████
Source: Clinical Study Report for APeX-2 parts 2 and 321
Exposure to Study Treatments
The mean duration of exposure for the 40 patients initially randomized to berotralstat 150 mg was ████ days (SD = ████), including 21 patients who were exposed for greater than ████ days (████ weeks). The total patient-years of exposure was ████ for this group.
The mean duration of exposure was 639 days (SD = 341) for patients in the placebo then berotralstat 150 mg group for a total of ████ person-years of exposure.
Efficacy
During part 2 of the APeX-2 study, a total ████ investigator-confirmed HAE attacks were reported in berotralstat 150 mg group and ████ events in the placebo then berotralstat 150 mg group, of which ████ and ████ were treated with acute therapies. Among patients who continued on berotralstat 150 mg in part 2, the mean baseline rate of investigator-confirmed attacks was 3.2 (SD = 1.6) events per month (N = 37). In this group at 6 months, the mean attack rate was 1.7 (SD = 1.9) with a mean change of −1.5 (SD = 1.8) events per month, and at 12 months the mean attack rate was 1.1 (SD = 1.4) with a mean change in rate of −1.9 (SD = 1.5, N = 32) (Table 32). Among patients who switched from placebo to berotralstat 150 mg (N = 17), the mean baseline attack rate was 2.8 (SD = 1.4), and at 6 months it was 0.6 (SD = 0.9), with a mean change from baseline of −1.9 (SD = 1.4, N = 14).
The mean overall attack rate was ████ events per month (SD = 1.6) during part 1 and 2 for patients randomized to receive berotralstat 150 mg and who remained on treatment. During part 2, the overall attack rate was ████ events per month (SD = ████) among patients switched from placebo to berotralstat 150 mg.
mean number of days with angioedema symptoms was ████ days (SD = ████) and ████ days (SD = ████), and the proportion of days with symptoms was ████ (SD = ████) and ████ (SD = ████) in the berotralstat 150 mg, and the placebo then berotralstat 150 mg groups, respectively.
For patients who continued berotralstat 150 mg in part 2, the mean AE-QoL total scores were as follows: baseline 44.1 (SD = 16.8, N = 37); week 48, 27.1 (SD = 21.2, N = ████); and change from baseline −15.2 (SD = 14.1). Among patients switched from placebo to berotralstat 150 mg, the baseline mean AE-QoL score was 35.1 (SD = 15.1, N = ████); week 48 was 25.0 (SD = 19.7, N = ████) and change from baseline was −10.0 (SD = 20.9). The AE-QoL and EQ-5D data for part 2 are shown in Table 32.
Table 32: Efficacy Outcomes for Part 2 of APeX-2
Outcome | Berotralstat 150 mg N = 37 | Placebo then berotralstat 150 mg N = 17 |
|---|---|---|
Investigator-confirmed attack rate | ||
Baseline | N = 37 | N = 17 |
Mean (SD) | 3.2 (1.6) | 2.8 (1.4) |
6 Months | N = 37 | N = 14 |
Mean (SD) | 1.7 (1.9) | 0.6 (0.9) |
Change from baseline, mean (SD) | −1.5 (1.8) | −1.9 (1.4) |
12 Months | N = 32 | NA |
Mean (SD) | 1.1 (1.4) | NA |
Change from baseline, mean (SD) | −1.9 (1.5) | NA |
AE-QoL total scorea | ||
Baseline | N = 37 | N = 17 |
Mean (SD) | 44.1 (16.8) | 35.1 (15.1) |
Week 48 | N = 34 | N = 13 |
Mean (SD) | 27.1 (21.2) | 25.0 (19.7) |
Change from baseline, mean (SD) | −15.2 (14.1) | −10.0 (20.9) |
████████████████████████████ | ||
████████████████████████ | █████████████ | █████████████ |
█████████████████ | █████████████ | █████████████ |
████████████████████████ | █████████████ | █████████████ |
█████████████████ | █████████████ | █████████████ |
████████████████████████ | █████████████ | █████████████ |
████████████████████████████ | ||
████████████████████████ | █████████████ | █████████████ |
█████████████████ | █████████████ | █████████████ |
████████████████████████ | █████████████ | █████████████ |
█████████████████ | █████████████ | █████████████ |
████████████████████████ | █████████████ | █████████████ |
AE-QoL = Angioedema Quality of Life; NA = not applicable; SD = standard deviation; VAS = visual analogue scale.
aAE-QoL score range from 0 (best) to 100 (worst).
bEQ-5D VAS scores range from 0 (worst health state you can imagine) to 100 (the best health state you can imagine). The index score falls between −1 and 1, where 1 is full health.
Source: Clinical Study Report for APeX-2 Part 2 and 3.21
During part 3 of APeX-2, the overall adjusted patient-reported HAE attack rate was ████ █ ███ █ ████ █ ████ █ ███ █ ██ █ █ while patients remained on treatment. The mean attack rate over time for the █ ███ █ ██ █ ███████ █ ███ █ ███ is shown in Table 33. ██ █ ████ █ ███ █ ███ █ ████ █ ██ █ ████ █ ██ █ █████ █ ██████████████ █ ██████ █ ████ █ ██ █ ███ █ ██████ █ █ █ █ █ █ █ ████████████ █ ████████████████ █ █ █ ███████ █ ███
The mean baseline AE-QoL score was █ █ ██ █ ███████ █ █████████ █ █████████ █ ██████ █ █ █ ██ █ ███ who entered part 3, and █ █ ████ █ █████ █ █████ █ ██ █ ████ █ ████ █ █ ████ █ ███ █ █████ █ █ █ ████ █ ████ █ ██ █ █ █ █ █ █ █ ██ █ ███ █ ███ █ ████ █ ██████ █ █ █ ██ █ ████████ █ ████████ █ ██████ █ ██████ █ ██ █ ██ █ █ ██ █ ██████ █ █ █ ██ █ █████ █ ██████ █ ██████ █ █ ███████ █ █████ █ ██ █ ███.
Table 33: Adjusted Patient-Reported HAE Attack Rate per Month for Part 3 of APeX-2
Time point | N (%) | Attack rate per month, mean (SD)a |
|---|---|---|
████████████████ | ████████████████ | ████████████████ |
████████████████ | ████████████████ | ████████████████ |
████████████████ | ████████████████ | ████████████████ |
████████████████ | ████████████████ | ████████████████ |
████████████████ | ████████████████ | ████████████████ |
████████████████ | ████████████████ | ████████████████ |
████████████████ | ████████████████ | ████████████████ |
HAE = hereditary angioedema; SD = standard deviation.
aMonthly attack rate was defined as the total number of adjusted patient-reported HAE attacks experienced during the treatment period adjusted for the length of a month (defined as 28 days) and the number of days the patient was on treatment during that month. The end of month 6 was defined as the start of part 2 treatment or the end of part 1 treatment if the patient did not continue to part 2. Month 7 was defined as beginning on the day after the end of month 6 and continuing through day 196. Remaining months (8 and up) were defined as 28 day intervals. For patients who switched from placebo to berotralstat, visits were adjusted according to the date of the first dose of active treatment.
bEnd of part 1 for patients initially randomized to berotralstat 110 mg or 150 mg daily. For patients who were switched from placebo to berotralstat, this represents the first 6 months of active therapy during part 2.
Source: Clinical Study Report for APeX-2 Part 2 and 3.21
Harms
During part 2, 72% of patients who received berotralstat 150 mg experienced at least one adverse event, including 2 patients who reported a serious adverse event (uterine leiomyoma, patient kept for observation after a radioactive iodine test). Gastrointestinal abdominal-related adverse events were reported by ████ patients (████). Four patients (7%) stopped treatment due to adverse events; 2 of which stopped due to gastrointestinal-related events. In part 2, the most common adverse events reported among all treated patients were nasopharyngitis (18%), nausea (8%), upper respiratory tract infection (8%), abdominal pain (6%), and dyspepsia (5%) (Table 34).
During █ █ ███ █ ██, ██ █ █████ experienced at least 1 adverse event, of which the most frequently reported adverse events were ██ █ █ █ ███ █ ████ █ █████ █ █ ████ █ █ █ █████ █ ██ █ █████ █ ██ █ █████████ █ ████ █ ████ █ ████ █ █ █ ██ █ █████ █ █ █ ███ █ █████████████████ █ █ █ ██ █ ████████████████████████████ █ ██ █ █ █ █ ██ █ █ █ █ █ █ █████ █ █████ █ █ █ █ █ █ ███ █ ████████ █ ██████ █ ████ █ ████ █ █ ███ █ █ ██ █ ███ █ ████ █ ███████ █ ███ █ ██ █ ██████ █ ███ █ █████████ █ ██████ █ ██ █ ███.
No deaths occurred during part 2 or 3 of the APeX-2 study.
Table 34: Summary of Harms in Part 2 and 3 of APeX-2
Adverse event | Part 2 | ████████ | |
|---|---|---|---|
Berotralstat 150 mg N = 37 | Placebo then berotralstat 150 mg N = 17 | ████████ | |
Patients with ≥ 1 adverse events, n (%) | 27 (73) | 12 (71) | ████████ |
SAE, n (%) | 1 (3) | 1 (6) | ████████ |
Death, n (%) | 0 | 0 | ████████ |
Stopped therapy due to adverse events, n (%) | 2 (5) | 2 (12) | ████████ |
Gastrointestinal-related adverse events, n (%) | 10 (27) | 9 (53) | ████████ |
Gastrointestinal-related adverse event leading to treatment discontinuation, n (%) | 1 (3) | 1 (6) | ████████ |
SAE = serious adverse event.
Source: Clinical Study Report for APeX-2 Part 2 and 3.21
Critical Appraisal
Internal Validity
Several limitations were identified for part 2 and 3 of the APeX-2 study. First of all, the investigators and patients were aware that patients were receiving active treatment, and thus their expectations of treatment could affect reporting of subjective outcomes such as symptoms or adverse effects. In addition, there was potential selection bias, as patients who respond to berotralstat and are able to tolerate treatment are more likely to continue therapy than patients with less favourable outcomes. By the end of week 48, 8 of 40 patients (20%) initially randomized to berotralstat 150 mg had stopped treatment, and █ █ ██████ █ ████████ █ ██████. No information was available on the completeness of patient diary data during part 2 or 3, thus the extent of missing diary data is unknown. There was no statistical testing for part 2 and 3. The efficacy analyses were reported descriptively based on observed data with no imputation for missing data, and with no sensitivity analyses to assess the robustness of the results. Given the attrition observed, the results reported may overestimate the treatment effects, and under-report adverse effects.
The HAE attack rate data in part 3 were based on patient-reported events and were not confirmed by an investigator as in part 1 and 2, thus these events may not be comparable.
In addition, part 2 and 3 were uncontrolled which makes the change in HAE attack rate difficult to interpret, particularly since HAE attacks are sporadic and may fluctuate through the year owing to exposure to seasonal triggers, hormonal changes or other factors.
External Validity
Part 2 and 3 of the APeX-2 study share the same potential limitations to external validity as the controlled part of the study. Due to the potential selection bias, the results likely reflect a subset of patients who are able to tolerate berotralstat and have perceived a benefit with treatment and may not truly reflect the longer effects in an unselected HAE population.
Pharmacoeconomic Review
Abbreviations
AE
adverse event
BIA
budget impact analysis
C1-INH
complement 1 esterase inhibitor
CBS
Canadian Blood Services
HAE
hereditary angioedema
HAEC
Hereditary Angioedema Canada
ICER
incremental cost-effectiveness ratio
ITC
indirect treatment comparison
LTP
long-term prophylactic
QALY
quality-adjusted life-year
RDI
relative dose intensity
SC
subcutaneous
Executive Summary
The executive summary comprises 2 tables (Table 1 and Table 2) and a conclusion.
Item | Description |
|---|---|
Drug product | Berotralstat (Orladeyo), 150 mg oral capsule |
Submitted price | Berotralstat, 150 mg, oral capsule: $850.00 per capsule |
Indication | Proposed: for routine prevention of episodes of hereditary angioedema in adults and pediatric patients aged 12 years and older |
Health Canada approval status | NOC |
Health Canada review pathway | Standard |
NOC date | June 2, 2022 |
Reimbursement request | As per indication |
Sponsor | BioCryst Pharmaceuticals Inc. |
Submission history | No |
NOC = Notice of Compliance.
Table 2: Summary of Economic Evaluation
Component | Description |
|---|---|
Type of economic evaluation | Cost-utility analysis Markov model |
Target population | Adults and pediatric patients aged 12 years and older |
Treatment | Berotralstat plus acute treatment of HAE attacks as they occur |
Comparators |
|
Perspective | Canadian publicly funded health care payer |
Outcomes | QALYs, LYs |
Time horizon | Lifetime (58 years) |
Key data source | Clinical efficacy for patients receiving berotralstat and no LTP was modelled based on patient-reported HAE attack rates from the APeX-2 clinical trial |
Submitted results | ICER = $4,710,158 per QALY for berotralstat vs. no LTP (incremental costs: $6,940,661; incremental QALYs: 1.47) |
Key limitations |
|
CADTH reanalysis results |
|
C1-INHs = complement 1 esterase inhibitors; HAE = hereditary angioedema; ICER = incremental cost-effectiveness ratio; LY = life-year; LTP = long-term prophylactic; QALY = quality-adjusted life-year; RDI = relative dose intensity; ITC = indirect treatment comparison.
Conclusions
The CADTH clinical review concluded that fewer investigator-confirmed hereditary angioedema (HAE) attacks occurred in patients treated with berotralstat compared to placebo in a pivotal trial assessed up to 24 weeks. No significant differences in health-related quality of life were detected as measured by the Angioedema Quality of Life or EQ-5D questionnaire. However, limited sample size, unbalanced treatment groups, and greater numbers of patients discontinuing from the placebo group compared to the berotralstat group may have biased the results. Due to limited data on hospitalization or emergency visits, the impact of berotralstat on health care resource use or mortality is unknown. An open-label extension study assessing patients receiving berotralstat for up to 48 weeks suggested a sustained reduction in investigator-reported HAE attacks, but was limited by potential selection, attrition, and reporting bias. Furthermore, gastrointestinal adverse events (AEs) were reported more frequently among patients receiving berotralstat compared with placebo. Notably, no direct or indirect comparative efficacy and safety data were available comparing berotralstat to other long-term prophylactic (LTP) treatments, and the relative efficacy and safety of berotralstat is therefore unknown.
To address the identified limitations with the sponsor’s pharmacoeconomic evaluation, CADTH undertook a reanalysis that replaced patient-reported attack rates for berotralstat and placebo with investigator-confirmed attack rates, adjusted subsequent rescue therapy use to reflect clinical practice, and adjusted the relative dose intensity (RDI) of berotralstat to 100% and included drug wastage. CADTH results were similar to those of the sponsor in that berotralstat was not considered cost-effective based on conventionally accepted incremental cost-effectiveness ratio (ICER) thresholds, with an ICER exceeding $4 million per quality-adjusted life-year (QALY) when compared to no LTP. In the CADTH base case, berotralstat was associated with an ICER of $14,559,490 per QALY gained, and a price reduction of approximately 93% is required to achieve a mean cost-effective estimate at a willingness-to-pay threshold of $50,000 per QALY.
The key limitation with the sponsor’s submission is the absence of comparative clinical information for berotralstat. As such, the cost-effectiveness of berotralstat in comparison to other LTP treatments is unknown. Therefore, there is no evidence to support a price premium for berotralstat in comparison to other LTP treatments.
Stakeholder Input Relevant to the Economic Review
This section is a summary of the feedback received from the patient groups, registered clinicians, and drug plans that participated in the CADTH review process.
CADTH received patient input from Hereditary Angioedema Canada (HAEC), an organization dedicated to creating awareness about HAE and related angioedemas. HAEC conducted surveys of Canadian patients with HAE and caregivers. Patients reported that HAE interfered with their daily lives and resulted in anxiety and fear, along with impacts on ability to work, travel, exercise, and perform daily activities. For patients currently receiving treatment, approximately 66% expressed being satisfied or extremely satisfied with the effectiveness of their current HAE treatment for preventing attacks. The remaining proportion of patients highlighted concerns with treatment administration with preference for oral administration, supply issues with plasma-derived HAE treatments, and lack of efficacy. HAEC received comments from 3 Canadian patients treated with berotralstat. Two out of the 3 respondents did not find berotralstat to be effective in preventing HAE attacks. Patients noted side effects such as abdominal pain and diarrhea, and 1 respondent reported that berotralstat was less tolerable than other treatments such as Berinert and Haegarda. Most patients noted the importance of treatments with an easier mode of delivery and were concerned about vein damage following repeated IV administration of plasma-derived HAE treatments. Notably, berotralstat is administered orally in capsule form and would address this gap in available treatments for HAE.
CADTH received registered clinician input from the Canadian Hereditary Angioedema Network, an organization of physicians who treat HAE and contribute to the knowledge of HAE and its treatments. Continuous regular treatments currently available in Canada aimed at minimizing the number, frequency, and severity of HAE attacks were identified as the complement 1 esterase inhibitor (C1-INH) concentrates Cinryze and Haegarda, and lanadelumab, with the latter 2 administered by subcutaneous (SC) injection. Historically, attenuated androgens such as danazol have been used off-label as oral prophylactics. Canadian Hereditary Angioedema Network input stated that a safe oral prophylactic would be preferable to a long-term injection regimen and that berotralstat would be similarly considered for first-line treatment. The clinician input noted that there are no known specific predictors for those who would preferentially respond to berotralstat.
Feedback from the drug plans highlighted concerns with the pivotal clinical trial being placebo-controlled, which is inappropriate given the number of available therapies for HAE. Drug plans also stated that plasma-derived C1-INH treatments are not funded by drug programs because they are plasma-derived products, which poses challenges for drug plans in determining patient access through Canadian Blood Services (CBS). There is currently no consensus among clinical experts managing HAE on the specific number of attacks that corresponds to a threshold for initiation of LTP. Drug plans also noted uncertainty surrounding treatment duration for patients on LTPs as discontinuation criteria and stopping rules were unclear, but patients receiving berotralstat may have received greater reductions in attacks the longer therapy was maintained. Drug plans stated that alignment between lanadelumab and berotralstat may be considered for discontinuation criteria. Furthermore, uncertainty surrounding treatment switching and eligibility between berotralstat and lanadelumab for LTPs was highlighted, where alignment of initiation criteria and reimbursement recommendations for lanadelumab and berotralstat may also be considered. There also may be use of combination therapy due to its different mechanism of action, which would pose another challenge for drug plans as plasma-based products are funded through a different mechanism. However, the availability of berotralstat may reduce the potential risk of drug shortages of plasma-derived products.
Several of these concerns were addressed in the sponsor’s model:
The sponsor’s model compared berotralstat to no LTP for the routine prevention of HAE.
In addition, CADTH addressed some of these concerns:
CADTH adjusted the market shares of berotralstat in the budget impact analysis to reflect clinical expert feedback on the anticipated use of berotralstat.
CADTH was unable to address the following concerns raised from stakeholder input:
Uncertainty in analyses due to lack of direct comparative clinical evidence comparing berotralstat to other HAE treatments could not be addressed.
Exploration of the impact of adverse events was not possible due to their exclusion from the economic model.
Economic Review
The current review is for berotralstat (Orladeyo) for the routine prevention of episodes of HAE in adults and pediatric patients aged 12 years and older.
Economic Evaluation
Summary of Sponsor’s Economic Evaluation
Overview
The sponsor submitted a cost-utility analysis of berotralstat compared with no LTP in adults and pediatric patients aged 12 years and older with HAE. Both patients receiving berotralstat and those receiving no LTP additionally received acute treatment for HAE attacks as they occurred. The target population was aligned with the Health Canada indication and the sponsor’s reimbursement request. The sponsor’s submission also included a scenario analysis comparing berotralstat with C1-INHs and lanadelumab in the target population.
Berotralstat is available as a 150 mg oral capsule in 28-capsule cartons. The recommended dosage of berotralstat is 150 mg once daily.1 At the submitted price of $850.00 per capsule ($23,800.00 per 28-capsule carton), the annual cost of berotralstat is $310,463.2 The no LTP comparator consisted of avoidance of known triggers plus acute treatment of HAE attacks as they occur. Costs of acute maintenance of HAE attacks were applied to all patients. The sponsor included 3 brands of C1-INHs (Cinryze, Haegarda, and Berinert IV or SC) and lanadelumab in its scenario analysis as comparator treatments. The cost of lanadelumab is $20,538 per 300 mg dose, with patients requiring an SC injection every 2 weeks with the potential for a reduction to an SC injection every 4 weeks if the patient is considered well controlled for more than 6 months.3 The annual cost of lanadelumab is $535,822 per patient, with the potential of falling to $267,911 once a patient is well controlled for 6 months. The cost of Cinryze is █ █ ██ per 1,000 IU, given through IV administration and divided into 2 500 IU doses per week, resulting in an annual cost of ██ ██ ███.4 The cost of Haegarda is $██ ███ per 2,000 IU and $██ ███ per 3,000 IU at dosages of 60 IU per kilogram of body weight twice weekly, resulting in an annual cost of $███ ███ ██4 The cost of Berinert IV is $███ ██ per 500 IU and $██ ██ ██ █ per 1,500 IU at dosages of 20 IU per kilogram of body weight twice weekly, resulting in an annual cost of $█ ███ ███.4 The cost per 500 IU and 1,500 IU of Berinert SC is identical to that of Berinert IV, with a recommended dosage of 60 IU per kg twice weekly, resulting in an annual cost of $██ ███ ██.4 Costs for C1-INHs were calculated using an average body weight of 75 kg with consideration for drug wastage (Appendix 1).
Modelled outcomes included QALYs and life-years over a time horizon of 58 years. A base-case analysis was conducted from the perspective of the Canadian public health care system, with costs and outcomes discounted at 1.5% per year. The cycle length of the model was 28 days with a half-cycle correction applied.
Model Structure
A Markov model developed to capture costs and outcomes associated with the prevention of HAE attacks comprised 2 primary health states (alive and dead), with 2 substates within the alive health state (attack and attack-free).2 Patients in the attack substate are those who are currently experiencing an HAE attack, and those in the attack-free substate are those currently attack-free. Patients entered the model in the attack-free health state, corresponding with the pivotal clinical trial.5 Patients receiving berotralstat and no LTP could then remain attack-free or transition to the attack state based on treatment-specific patient-reported attack rates and duration of attack as observed in the APeX-2 clinical trial.5 The primary efficacy measure to characterize the clinical benefit of berotralstat was the reduction in patient-reported attack rate from baseline. Patients could transition to the death state from any of the other health states, as dictated by general population mortality rates. The model assumed no discontinuation of any LTP and no HAE-specific mortality. AEs from the clinical trial data were not expected to affect costs or health-related quality of life within the economic evaluation, and modelling of grade 3 and 4 AEs was therefore excluded. The sponsor’s submitted model structure can be found in Appendix 3.
Model Inputs
The modelled patient characteristics for the sponsor’s submission were based on the APeX-2 clinical trial (mean age: 41.6; 66.1% female; mean weight: 83.7 kg).5
Treatment response for patients receiving berotralstat and no LTP was based on a reduction from baseline in the patient-reported HAE attack rate per month across 96 weeks.5 The baseline attack rate for patients receiving berotralstat and no LTP was derived from the APeX-2 clinical trial, and clinical improvement was characterized by the percent reduction in mean number of patient-reported attacks from baseline, assessed monthly.5 Time spent in the attack state was calculated using the monthly patient-reported HAE attack rate and mean duration of attack specific to berotralstat (████ ███) or no LTP (█ █████ █), derived from the APeX-2 trial.5 Patient-reported attack rates beyond 24 months for berotralstat and 6 months for patients receiving no LTP were not available in the observed data and were assumed to remain constant for the remainder of the time horizon following the last observation recorded in the APeX-2 trial. Background mortality was informed by the general population matched for age and gender in the APeX-2 trial.6
Utility values were sourced from Nordenfelt et al. (2014), a retrospective survey of patients from a Swedish registry providing 5-Level EQ-5D data for time spent attack-free as well as time spent experiencing an HAE attack.7 The sponsor provided an option to use attack location proportions from the APeX-2 trial as a proxy for attack severity to calculate the utility of those in the attack state. However, the base-case utility value was based on average attack severity irrespective of attack location. An average attack severity disutility value of −0.313 was calculated based on the difference in utility values between those in the attack and attack-free states.7 Disutility associated with the attack state was applied for the total duration of time (hours) that each patient spent in the attack state per cycle. For patients who were attack-free, a regression analysis was performed to quantify the impact of age and frequency of prior HAE attacks on HAE patients, with an additional disutility applied to the Nordenfelt et al. (2014) attack-free utility of 0.825 based on 0.02205 per 10 years of age and −0.0043 for each attack in the previous cycle.7
Costs included drug acquisition costs for LTP and acute treatment, administration costs, and health care resource utilization. Relevant costs were inflated to 2021 Canadian dollars. Drug acquisition costs for berotralstat were sourced from the sponsor and no drug costs were associated with no LTP.2 Costs for acute treatment following HAE attacks were calculated based on the clinical expert’s opinion of the total proportion of patients requiring acute therapy, further specified by treatment received (Berinert, Cinryze, or icatibant).2,3 No administration costs were included for berotralstat as it was orally self-administered. Health care resource costs were only applied to patients in the attack state and included costs for emergency room visits, hospitalization, inpatient stays, intubations, CT scans, and specialist visits, depending on attack location.8,9 Drug wastage was not considered in the base-case analysis for LTP or acute treatment following HAE attacks. All health care resource costs were sourced from the Ontario Schedule of Benefits for Physician Services and the Ontario Case Costing Initiative.8,9
Costs in the scenario analysis assessing other LTP treatments available in Canada similarly included costs for LTP and acute treatment, administration costs, and health care resource utilization, with relevant costs inflated to 2021 Canadian dollars.8,9 Drug acquisition costs for lanadelumab in the scenario analysis were sourced from the Ontario Exceptional Access Program and costs for C1-INHs were derived from the sponsor’s submission and could not be verified by CADTH.2,3 Administration costs in the scenario analysis evaluating C1-INHs and lanadelumab as comparators were determined based on dose per administration multiplied by cost of treatment.8 For treatments using weight-dependent dosing, the average patient weight from APeX-2 was used to calculate dose per administration. Drug wastage per administration was considered in the scenario analysis assessing other LTP treatments in Canada.
Summary of Sponsor’s Economic Evaluation Results
All analyses were run probabilistically (1,500 iterations for the base-case and scenario analyses). The deterministic and probabilistic results were similar. The probabilistic findings are presented in the following section.
Base-Case Results
Berotralstat was associated with incremental costs of $6,940,611 and 1.47 incremental QALYs in comparison to no LTP, resulting in an ICER of $4,710,158 per QALY gained (Table 3).
Sensitivity and Scenario Analysis Results
In a key sensitivity analysis, berotralstat was compared to no LTP and naively compared to C1-INHs (Cinryze, Berinert, and Haegarda) and lanadelumab. The sponsor was unable to conduct an indirect treatment comparison (ITC) due to heterogeneity and noncomparability between clinical trials. A naive sequential analysis was conducted, and probabilistic results estimated that berotralstat was associated with incremental costs of $6,231,906 and incremental QALYs of 0.26 in comparison to Cinryze, resulting in an ICER of $24,240,136 (Table 10, Appendix 3). Due to higher list prices, costs associated with Takhzyro, Haegarda, and Berinert were estimated to be higher than those of berotralstat.
The sponsor conducted further scenario analyses involving the inclusion of LTP discontinuation, a single attack-free utility estimate irrespective of age and prior attacks, utility estimates based on attack location, caregiver disutilities, and an RDI of 100% and drug wastage. The ICER was most sensitive to the application of utility estimates that did not incorporate age or prior HAE attack history, increasing to $5,661,538.
Table 3: Summary of the Sponsor’s Economic Evaluation Results
Drug | Total costs ($) | Incremental costs ($) | Total QALYs | Incremental QALYs | ICER vs. no LTP ($ per QALY) |
|---|---|---|---|---|---|
No LTP | 2,924,654 | Reference | 22.86 | Reference | Reference |
Berotralstat | 9,865,264 | 6,940,611 | 24.34 | 1.47 | 4,710,158 |
ICER = incremental cost-effectiveness ratio; LTP = long-term prophylactic; QALY = quality-adjusted life-year.
Note: The submitted analysis is based on the publicly available prices of the comparator treatments.
Source: Sponsor’s pharmacoeconomic submission.2
Additional results from the sponsor’s submitted economic evaluation base case are presented in Appendix 3.
CADTH Appraisal of the Sponsor’s Economic Evaluation
CADTH identified several key limitations to the sponsor’s analysis that have notable implications for the economic analysis:
The comparative clinical efficacy and safety of berotralstat in comparison with LTP treatments is highly uncertain: The sponsor submitted an indirect comparison feasibility assessment indicating that differences in the study design and patient characteristics of the clinical trials for treatments used for routine prevention of HAE attacks led to an inability to generate robust estimates of comparative treatment effects due to between-study heterogeneity. The CADTH clinical review concluded that the heterogeneity between the berotralstat and C1-INH trials is significant, and that any ITC is unlikely to provide robust estimates of comparative efficacy or safety. However, the CADTH clinical review indicated that there are fewer differences between the berotralstat and lanadelumab trials (APeX and HELP-03 RCTs) and that a focused ITC may have been possible and of interest to CADTH. Based on the results of the indirect comparison feasibility assessment submitted by the sponsor, the CADTH clinical review could not reach any conclusions regarding the treatment effect of berotralstat compared to lanadelumab or C1-INHs (Cinryze, Berinert, and Haegarda). The incremental cost-effectiveness of berotralstat compared to lanadelumab and C1-INHs is therefore unknown. Given this considerable uncertainty, there is no justification for berotralstat to have a price premium over other LTP treatments available in Canada.
The sponsor provided a naive comparison of berotralstat to other LTP treatments in a key scenario analysis using unadjusted comparative efficacy data from the following clinical trials: APeX-2 and APeX-J (berotralstat), HELP-03 (lanadelumab), COMPACT (C1-INH SC), and CHANGE (C1-INH IV).5,10-12 The interpretability of the results from these naive comparisons is highly limited and there is no clinical evidence available to indicate that berotralstat results in a similar treatment benefit (i.e., no difference in total QALYs) or safety outcomes when compared to lanadelumab and C1-INHs (Cinryze, Berinert, and Haegarda). Limitations with the available clinical data affect the interpretability of the sponsor’s naive scenario analysis comparing berotralstat to other LTP treatments.
Furthermore, the clinical expert consulted by CADTH noted that other treatments such as danazol and tranexamic acid were excluded from the key scenario analysis assessing all comparators despite being currently used in practice as LTP treatments. According to the CADTH Guidelines for Economic Evaluations, the base case must include all relevant comparators (i.e., treatments currently reimbursed by at least 1 participating drug plan for the indication under review or treatments that are currently used off-label in Canadian practice) to reflect all components of the decision problem.13 Consequently, the cost-effectiveness of berotralstat relative to all appropriate treatment comparators is also unknown.
CADTH was unable to address this limitation in reanalysis but maintains that the base-case analysis compares berotralstat to no LTP. There is no evidence to suggest that berotralstat is equally as effective or worse than other LTP treatments available in Canada for HAE.
No treatment is an infrequently used comparator in comparison to active treatment: Given the availability of various approved LTP treatments for HAE in Canada, no treatment is a less frequently used comparator for berotralstat. The clinical expert consulted by CADTH noted that various treatment options are available for patients diagnosed with HAE, allowing patients to switch treatments upon treatment failure or discontinue due to other reasons. The placebo comparator used in the pivotal trial has limited clinical relevance and would not be used in practice for patients seeking treatment, which limits its relevance as a primary comparator. The sponsor’s inclusion of no treatment as the primary comparator for berotralstat may affect the interpretability of the sponsor’s cost-effectiveness analysis.
CADTH could not address this limitation in reanalysis.
Attack rates were patient-reported and assumed to remain constant beyond the duration of the pivotal trial: The attack rates used by the sponsor were patient-reported attack rates from the APeX-2 trial (Appendix 3). The CADTH clinical review and clinical experts consulted by CADTH noted that investigator-confirmed attack rates are preferred over patient-reported attack rates to reduce potential bias and mitigate the likelihood of patient errors in reporting attacks. For example, clinical experts noted that gastrointestinal AEs could be misreported as HAE attacks by patients without formal confirmation based on clinical criteria. Investigator-confirmed attack rates are available from the APeX-2 trial; however, attack rates after 6 months of follow-up were limited by poor data quality and could not be used due to missing data, the lack of a control arm after 6 months of follow-up, and missing information regarding patient attrition at each data-collection time point. The CADTH clinical review concluded that patient dropout is most likely to occur due to a lack of response or drug intolerance, and the continuous reduction in attack rates observed in patients remaining in the trial after 6 months likely overestimates the efficacy of berotralstat. Consequently, the cost-effectiveness of berotralstat compared to no LTP is likely biased in favour of berotralstat.
Furthermore, reductions in patient-reported attack rates were available up to 24 months for berotralstat and 6 months for no LTP. The sponsor assumed that the last observation in the APeX-2 trial would hold constant for the remainder of the model’s lifetime time horizon of 58 years. There is no available evidence to suggest that a sustained treatment benefit would occur for the patient’s lifetime and the base case does not incorporate discontinuation rates or treatment switching upon lack of efficacy. The clinical expert consulted by CADTH did not expect this sustained treatment effect given berotralstat’s mechanism of action and the lack of long-term efficacy data. The expert also noted that patients receiving berotralstat long-term may be at higher risk for developing autoimmune conditions, which would further affect costs and health-related quality of life. The assumption that reductions in attack rate will remain constant beyond 24 months biases the cost-effectiveness estimates in favour of berotralstat. In consideration of the modelling of attack rates, the cost-effectiveness of berotralstat is unknown due to high uncertainty in long-term efficacy and the inappropriateness of the modelled patient-reported attack rates.
CADTH used investigator-confirmed attack rates from the APeX-2 trial up to 6 months for berotralstat and no LTP, after which reanalysis assumed the last observed attack rate was carried forward for the remainder of the time horizon due to limitations in the available data after 6 months of follow-up.
The sponsor’s model does not fully capture key aspects of disease most relevant to the patient population: The sponsor’s submitted model structure was based primarily on experiencing attacks or remaining attack-free, as captured by patient-reported attack rates. However, the clinical expert consulted by CADTH pointed out that critical aspects of disease management that affect patient outcomes, such as side effects from treatment related to severe, chronic abdominal symptoms, were not modelled. All grade 3 or 4 treatment-emergent AEs were excluded from the economic model despite a lack of evidence that safety profiles across berotralstat and other available LTP treatments do not differ. The clinical expert consulted by CADTH noted that berotralstat reportedly results in increased gastrointestinal side effects, which aligns with patient input received. The clinical expert also noted that the sponsor’s estimated frequency of rescue medication use did not accurately reflect clinical practice. The sponsor assumed that 100% of patients receiving berotralstat who require subsequent rescue medication would be treated with icatibant, whereas 50% of patients receiving no LTP are treated with icatibant, with the remaining 50% receiving Berinert IV. Based on clinical expert feedback, 50% of all patients requiring rescue medication would be treated with icatibant with the remainder receiving Berinert IV, irrespective of the LTP treatment received. Last, the clinical expert consulted by CADTH expressed concern with the exclusion of tracheotomy from the economic evaluation as it is an important outcome, particularly for those experiencing laryngeal attacks that affect hospitalization costs as well as health-related quality of life. The exclusion of tracheotomy contributes to the model’s inability to capture attack severity across different attack locations, and consequently reduces the model’s interpretability and generalizability to patients with HAE. As a result, the cost-effectiveness of berotralstat is uncertain.
CADTH adjusted the proportions of icatibant and Berinert IV rescue medication use for patients receiving berotralstat to reflect clinical expert feedback. CADTH could not address the remaining limitations surrounding the exclusion of severe, chronic abdominal symptoms and tracheotomy from the economic evaluation.
The sponsor’s derivation of utility values is uncertain: The literature source used to derive utility values used a formula for attack-free utility from Nordenfelt et al. (2014) to estimate the burden of HAE and subsequent health utility of HAE patients in Sweden using 5-Level EQ-5D data.7 The study demonstrated that attack frequency and older age were associated with lower health-utility scores, which the sponsor applied in its calculation of utility values. However, the study also demonstrated that the number of days since the last HAE attack was associated with increased health-utility scores, which were excluded from the formula used by the sponsor without justification. The effect of this exclusion on the incremental cost-effectiveness of berotralstat is unknown. Additionally, the applicability of utility values derived from a Swedish population to represent Canadians is unknown. Last, the utility values used in the model do not consider attack severity, which the clinical expert noted differed by location. The sponsor applied utilities irrespective of attack location using an average disutility across all patients with HAE in the model. CADTH notes that the sponsor provided alternate time trade-off–based utilities by attack location, but there was limited value in applying them in reanalysis due to limitations in the derivation of utilities using direct methods such as time trade-off. The CADTH Guidelines for the Economic Evaluation of Health Technologies in Canada recommend that utilities from an indirect method of measurement based on a generic classification can be used in economic modelling due to ease of access, comparability, and interpretability.13 Consequently, it is uncertain if the sponsor’s utility values are applicable to Canadian patients with HAE and the sponsor’s estimates of cost-effectiveness are further limited by uncertainty.
CADTH could not address this limitation in reanalysis.
Additional limitations were identified, but were not considered to be key limitations:
The application of relative dose intensity and drug wastage likely underestimates drug costs: The sponsor incorporated a RDI of 98% for berotralstat, which was multiplied by drug acquisition costs. However, the sponsor’s approach to estimating drug acquisition costs does not consider other factors that influence dosing, such as dose delays, reductions, or escalation. The exclusion of such factors introduces uncertainty into the derivation of drug acquisition costs for berotralstat. Furthermore, a decreased RDI was disproportionately applied for berotralstat and not for other LTP comparators in the key scenario analysis comparing berotralstat with C1-INHs and lanadelumab. Similarly, drug wastage for IV and SC comparator treatments was excluded from the sponsor’s base-case analysis. Because vial sharing is not anticipated, exclusion of drug wastage is inappropriate. The sponsor’s assumption likely biases estimates of cost-effectiveness in favour of berotralstat.
In reanalysis, CADTH assumed an RDI of 100% for berotralstat and included drug wastage for IV and SC LTP treatments.
Additional risk of mortality due to HAE was not modelled: The sponsor did not consider HAE-specific mortality in its economic evaluation. Existing evidence shows that laryngeal attacks would lead to a reported mortality rate of 40% if left untreated.14 This was supported by the clinical expert consulted by CADTH, who noted that laryngeal attacks are more severe than attacks occurring in other locations and result in an additional risk of mortality. The sponsor’s exclusion of HAE-specific mortality may overestimate the life expectancy of HAE patients, but this is unlikely to affect the estimated ICER, given that no deaths due to HAE attacks were reported in the APeX-2 trial up to 48 weeks of follow-up.
CADTH could not address this limitation in reanalysis.
Additionally, key assumptions made by the sponsor were appraised by CADTH (Table 4).
CADTH Reanalyses of the Economic Evaluation
Base-Case Results
The CADTH base case was derived by making changes in model parameter values and assumptions, in consultation with the clinical expert. Changes to the sponsor’s analyses are summarized in Table 5 and include alterations to the modelled attack rates, frequency of subsequent rescue therapy use, and a revised RDI and inclusion of drug wastage.
In the CADTH base case, berotralstat was associated with a total cost of $11,386,931 and 23.26 QALYs compared to $2,535,765 and 22.65 QALYs for patients receiving no LTP. The ICER for berotralstat compared to no LTP was $14,559,490 per QALY with a 0% probability of being cost-effective at a willingness-to-pay threshold of $50,000. Detailed information and disaggregated results are presented in Table 13 in Appendix 4.
Table 4: Key Assumptions of the Submitted Economic Evaluation (Not Noted as Limitations to the Submission)
Sponsor’s key assumption | CADTH comment |
|---|---|
Patients will continue treatment with berotralstat for the remainder of their lifetime. | Inappropriate. Switching to another LTP treatment is expected to occur in the event of a lack of treatment efficacy with berotralstat, according to the clinical expert consulted by CADTH. Given the number of other available LTP treatments in Canada, patients would likely switch based on preference and discussion with their physicians, according to patient input received by CADTH. |
Distribution of attack severity of berotralstat from the APeX-2 trial applies to all other LTP treatment comparators. | Unknown. Clinical data informing severity distribution data for lanadelumab and C1-INHs was not available. Given that the base-case analysis uses utilities that do not incorporate attack severity by location, the impact on the ICER is expected to be minimal. |
In the key scenario analysis in which a naive comparison between berotralstat and other LTP treatments was conducted, the sponsor assumed that 55% of patients receiving lanadelumab would switch from receiving the recommended 300 mg dose administered subcutaneously every 2 weeks to receiving it every 4 weeks after 12 months. | Unknown. Although the product monograph indicates that a dosing interval of 300 mg every 4 weeks may be considered if the patient is well controlled or attack-free for more than 6 months, there is high uncertainty regarding the clinical data available to inform optimal dosing for well-controlled patients. |
ICER = incremental cost-effectiveness ratio; LTP = long-term prophylactic.
Table 5: CADTH Revisions to the Submitted Economic Evaluation
Stepped analysis | Sponsor’s value or assumption | CADTH value or assumption |
|---|---|---|
Corrections to sponsor’s base case | ||
None | — | — |
Changes to derive the CADTH base case | ||
1. Attack rates | Patient-reported attack rates up to 24 months were applied for those receiving berotralstat and 6 months for no LTP. The last available observation was carried forward for the remainder of the model time horizon. | Investigator-confirmed attack rates were used in place of patient-reported attack rates with up to 6 months of available data for those receiving berotralstat and no LTP. The last observation was carried forward for the remainder of the model time horizon. |
2. Subsequent rescue therapy use | For patients receiving berotralstat that require subsequent rescue therapy, 100% were assumed to be treated with icatibant based on clinical expert opinion. | 50% of patients receiving berotralstat requiring subsequent rescue therapy were assumed to use icatibant, with the remaining 50% using Berinert as informed by the clinical expert consulted by CADTH. |
3. RDI and wastage | An RDI of 98% was applied and no drug wastage was assumed. | Adjusted RDI of 100% was applied and drug wastage was assumed to occur. |
CADTH base case | Reanalysis 1 + 2 + 3 | |
LTP = long-term prophylactic; RDI = relative dose intensity.
Table 6: Summary of the Stepped Analysis of the CADTH Reanalysis Results
Stepped analysis | Drug | Total costs ($) | Total QALYs | ICER ($/QALY) |
|---|---|---|---|---|
Sponsor’s base case (probabilistic) | No LTP | $2,924,654 | 22.86 | Reference |
Berotralstat | $9,865,264 | 24.34 | $4,710,158 | |
Sponsor’s base case (deterministic) | No LTP | $3,080,475 | 22.86 | Reference |
Berotralstat | $9,853,746 | 24.33 | $4,598,309 | |
CADTH reanalysis 1 — investigator-confirmed attack rates | No LTP | $3,422,271 | 22.67 | Reference |
Berotralstat | $11,737,898 | 23.27 | $13,945,580 | |
CADTH reanalysis 2 — subsequent rescue therapy use | No LTP | $2,924,654 | 22.86 | Reference |
Berotralstat | $9,865,264 | 24.33 | $4,710,158 | |
CADTH reanalysis 3 — RDI and drug wastage | No LTP | $3,439,704 | 22.86 | Reference |
Berotralstat | $10,046,463 | 24.33 | $4,485,266 | |
CADTH base case (reanalysis 1 + 2 + 3, deterministic) | No LTP | $2,798,041 | 22.67 | Reference |
Berotralstat | $11,574,128 | 23.26 | $14,717,788 | |
CADTH base case (reanalysis 1 + 2 + 3, probabilistic) | No LTP | $2,535,765 | 22.65 | Reference |
Berotralstat | $11,386,931 | 23.26 | $14,559,490 |
ICER = incremental cost-effectiveness ratio; LTP = long-term prophylactic; QALY = quality-adjusted life-year; RDI = relative dose intensity.
Scenario Analysis Results
CADTH performed price-reduction analyses based on the sponsor’s base case and the CADTH base-case reanalysis. Based on the CADTH base case, a price reduction of approximately 93% would be required to achieve a mean cost-effective estimate at a willingness-to-pay threshold of $50,000 per QALY.
Table 7: CADTH Price-Reduction Analyses
Analysis | Incremental cost-effectiveness ratios for berotralstat vs. no LTP ($ per QALY) | |
|---|---|---|
Price reduction | Sponsor base case | CADTH reanalysis |
No price reduction | 4,710,158 | 14,559,490 |
10% | 4,068,562 | 13,000,100 |
20% | 3,426,965 | 11,440,710 |
30% | 2,785,369 | 9,881,320 |
40% | 2,143,773 | 8,321,929 |
50% | 1,502,176 | 6,762,539 |
60% | 860,580 | 5,203,149 |
70% | 218,983 | 3,643,759 |
80% | NA | 2,084,369 |
90% | NA | 524,979 |
93% | NA | 57,162 |
LTP = long-term prophylactic; NA = not applicable; QALY = quality-adjusted life-year.
Note: Based on the sponsor’s base case, a price reduction of approximately 73% would be required to achieve a mean cost-effective estimate at a willingness-to-pay threshold of $50,000 per QALY.
CADTH performed a scenario analysis to determine the impact of alternative attack rates on the cost-effectiveness of berotralstat. Noncomparative investigator-confirmed attack rates were included from 6 months up to 12 months for patients receiving berotralstat, with the last observation carried forward for the remainder of the time horizon, to align with the sponsor’s methodology. The results of these analyses are presented in Table 14 in Appendix 4. The scenario analysis using attack rates up to 12 months resulted in an ICER of $7,848,146 per QALY comparing berotralstat against no LTP.
Issues for Consideration
Given that no public list prices were available for plasma-derived agents, the prices for these treatments were submitted by the sponsor as part of its pharmacoeconomic submission; CADTH was unable to confirm their accuracy. It was noted that drug plans do not cover the costs of plasma-derived agents and that these treatments are available through CBS. Consequently, the cost estimates are highly uncertain and there is further uncertainty surrounding the cost-effectiveness of berotralstat in comparison to C1-INHs.
The clinical expert emphasized the uncertainty surrounding dosing for the off-label use of Berinert SC as an LTP treatment. Dosing may vary by patient, with the clinical expert recommending an initial dose 40 IU/kg, which was increased to 60 IU/kg.
The clinical expert also noted the potential for berotralstat to be used in combination with existing LTP treatments such as danazol or C1-INHs. The cost-effectiveness of berotralstat used in combination with existing drugs for HAE is unknown.
Overall Conclusions
The CADTH clinical review concluded that fewer investigator-confirmed HAE attacks occurred in patients treated with berotralstat compared to placebo in the pivotal trial assessed up to 24 weeks. No significant differences in health-related quality of life were detected using the Angioedema Quality of Life or EQ-5D questionnaire. However, limited sample size, unbalanced treatment groups, and a greater rate of patients discontinuing from the placebo group compared to the berotralstat group may have biased the results. Due to limited data on hospitalization or emergency visits, the impact of berotralstat on health care resource use or mortality is unknown. The open-label extension study assessing patients receiving berotralstat up to 48 weeks suggested a sustained reduction in investigator-reported HAE attacks but was limited by potential bias in selection, attrition, and reporting. Furthermore, gastrointestinal AEs were reported more frequently among patients receiving berotralstat compared with placebo. Notably, no direct or indirect comparative efficacy and safety data were available comparing berotralstat to other LTP treatments, and the relative efficacy and safety of berotralstat is therefore unknown.
To address the identified limitations with the sponsor’s pharmacoeconomic evaluation, CADTH undertook a reanalysis that replaced patient-reported attack rates for berotralstat and placebo with investigator-confirmed attack rates, adjusted subsequent rescue therapy use to reflect clinical practice, and adjusted the RDI of berotralstat to 100% and included drug wastage. CADTH results were similar to those of the sponsor in that berotralstat is not considered cost-effective based on conventionally accepted ICER thresholds, with an ICER exceeding $4 million per QALY when compared to no LTP. In the CADTH base case, berotralstat was associated with an ICER of $14,559,490 per QALY gained, and a price reduction of approximately 93% is required to achieve a mean cost-effective estimate at a threshold of $50,000 per QALY.
The key limitation with the sponsor’s submission is the absence of comparative clinical information for berotralstat. As such, the cost-effectiveness of berotralstat in comparison to other LTP treatments is unknown. Therefore, there is no evidence to support a price premium of berotralstat in comparison to other LTP treatments.
References
1.Orladeyo (berotralstat): 150 mg oral capsules [product monograph]. Oakville (ON): Innomar Strategies; 2022 Jun 2.
2.Pharmacoeconomic evaluation [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Orladeyo (berotralstat), 150 mg capsule [internal sponsor's package]. Durham (NC): BioCyst Pharmaceuticals Inc; 2022 Feb 22.
3.Exceptional Access Program (EAP). Toronto (ON): Ontario Ministry of Health; Ontario Ministry of Long-Term Care; 2022: https://www.health.gov.on.ca/en/pro/programs/drugs/odbf/odbf_except_access.aspx. Accessed 2022 May 30.
4.Drug Reimbursement Review sponsor submission: Orladeyo (berotralstat), 150 mg capsule [internal sponsor's package]. Durham (NC): BioCyst Pharmaceuticals Inc; 2022 Feb 22.
5.Interim Clinical Study Report: BCX7353-302. Part 1. A phase 3, randomized, double-blind, placebo-controlled, parallel group study to evaluate the efficacy and safety of two dose levels of BCX7353 as an oral treatment for the prevention of attacks in subjects with hereditary angioedema [internal sponsor's report]. Durham (NC): BioCryst Pharmaceuticals, Inc; 2019 Oct 31.
6.Statistics Canada. Life expectancy and other elements of the life table, Canada, all provinces except Prince Edward Island. Table: 13-10-0114-01. 2022; https://www150.statcan.gc.ca/t1/tbl1/en/tv.action?pid=1310011401. Accessed 2022 May 30.
7.Nordenfelt P, Dawson S, Wahlgren CF, Lindfors A, Mallbris L, Bjorkander J. Quantifying the burden of disease and perceived health state in patients with hereditary angioedema in Sweden. Allergy Asthma Proc. 2014;35(2):185-190. PubMed
8.Schedule of benefits for physician services under the Health Insurance Act: effective October 1, 2021). Toronto (ON): Ontario Ministry of Health; 2021: https://www.health.gov.on.ca/en/pro/programs/ohip/sob/physserv/sob_master.pdf. Accessed 2022 May 30.
9.Ontario Case Costing Initiative (OCCI). Toronto (ON): Ontario Health and Long-Term Care; 2017: https://data.ontario.ca/dataset/ontario-case-costing-initiative-occi. Accessed 2022 May 30.
10.Interim Clinical Study Report: BCX7353-204. An open-label study to evaluate the long-term safety of daily oral BCX7353 in subjects with type 1 and 2 hereditary angioedema (Interim clinical study report) [internal sponsor's report]. Durkam (NC): BioCryst Pharmaceuticals, Inc; 2019 Oct 30.
11.Sutherland G, Dinh T. Understanding the gap: a pan-Canadian analysis of prescription drug insurance coverage. Ottawa (ON): Conference Board of Canada; 2017: http://innovativemedicines.ca/wp-content/uploads/2017/12/20170712-understanding-the-gap.pdf. Accessed 2022 May 30.
12.Lumry WR, Zuraw B, Cicardi M, et al. Long-term health-related quality of life in patients treated with subcutaneous C1-inhibitor replacement therapy for the prevention of hereditary angioedema attacks: findings from the COMPACT open-label extension study. Orphanet J Rare Dis. 2021;16(1):86. PubMed
13.Guidelines for the economic evaluation of health technologies: Canada. 4th ed. Ottawa (ON): CADTH; 2017: https://www.cadth.ca/guidelines-economic-evaluation-health-technologies-canada-4th-edition. Accessed 2022 May 30.
14.Bork K, Hardt J, Witzke G. Fatal laryngeal attacks and mortality in hereditary angioedema due to C1-INH deficiency. J Allergy Clin Immunol. 2012;130(3):692-697. PubMed
15.Budget Impact Analysis [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Orladeyo (berotralstat), 150 mg capsule. Durham (NC): BioCyst Pharmaceuticals Inc; 2022 Feb 22.
16.Lumry WR, Settipane RA. Hereditary angioedema: epidemiology and burden of disease. Allergy Asthma Proc. 2020;41(Suppl 1):S08-S13. PubMed
17.Drug therapies for the long-term prophylaxis of hereditary angioedema attacks. (CADTH technology review no. 25). Ottawa (ON): CADTH; 2019: https://www.cadth.ca/sites/default/files/hta-he/ob0007-hae-prophylaxis-redacted.pdf. Accessed 2022 May 30.
18.Proceedings of the Canadian Society of Allergy and Clinical Immunology Annual Scientific Meeting 2019. Allergy Asthma Clin Immunol. 2020;16(S1):47.
19.Betschel S, Badiou J, Binkley K, et al. The International/Canadian Hereditary Angioedema Guideline. Allergy Asthma Clin Immunol. 2019;15:72. PubMed
Appendix 1: Cost-Comparison Table
Note that this appendix has not been copy-edited.
The comparators presented in the Table 8 have been deemed to be appropriate based on feedback from clinical experts. Comparators may be recommended (appropriate) practice or actual practice. Existing product listing agreements are not reflected in the table and as such, the table may not represent the actual costs to public drug plans.
Table 8: CADTH Cost-Comparison for the Routine Prevention of HAE Attacks
Treatment | Strength / concentration | Form | Price ($) | Recommended dosage | Daily cost ($) | Annual cost ($) |
|---|---|---|---|---|---|---|
Berotralstat (Orladeyo) | 150 mg | Oral capsule | 850.0000a | 150 mg once daily | 850.00 | 310,463 |
Plasma-derived agents | ||||||
Lanadelumab (Takhzyro) | 300 mg / 2 mL | Solution for SC injection | 20,538.0000b | 300 mg every 2 weeks 300 mg every 4 weeks may be considered if the patient is well controlled for more than 6 months | 1,467.00 733.50 once well controlled for 6 months | 535,822 267,911 once well controlled for 6 months |
C1 esterase inhibitor (Cinryze) | 500 IU | Powder for solution with diluent for IV injection | ███████ per 1,000 IUc | 1,000 IU every 3 or 4 days | ███████ | ███████ |
C1 esterase inhibitor (Haegarda) | 2,000 IU 3,000 IU | Powder for solution with diluent for SC injection | ███████c ███████c | 60 IU / kg every 3 or 4 days | ███████ | ███████ |
Plasma-derived agents not indicated for prophylactic use in HAE | ||||||
C1 esterase inhibitor (Berinert) | 500 IU 1,500 IU | Powder for solution with diluent for IV injection | ███████c ███████c | 20 IU / kg Prophylactic use is not indicated, although clinical trials and guidelines specify a dose every 3 to 4 days | ███████ | ███████ |
Powder for solution with diluent for SC injection | 60 IU / kg Prophylactic use is not indicated, although clinical trials and guidelines specify a dose every 3 to 4 days | ███████ | ███████ | |||
HAE = hereditary angioedema; SC = subcutaneous.
All annual costs were determined by multiplying daily costs by 365.25. Costs assume a body weight of 75 kg and include wastage of unused medication in vials. Costs do not include administration or dispensing fees.
aSponsor’s submitted price.2
bCost sourced from the Ontario Ministry of Health and Long-Term Care Exceptional Access Program (accessed March 2022).3
cNo public price available. Price listed was submitted by sponsor as part of submitted model; CADTH was unable to confirm accuracy.2
Appendix 2: Submission Quality
Note that this appendix has not been copy-edited.
Description | Yes/No | Comments |
|---|---|---|
Population is relevant, with no critical intervention missing, and no relevant outcome missing | No | CADTH identified limitations with the available clinical data comparing berotralstat to other LTP treatments (lanadelumab, Berinert, Haegarda, and Cinryze). While these treatments were excluded from the base case due to a lack of comparative efficacy data, the submitted base case requires all critical interventions to be modelled. Refer to the CADTH appraisal section. |
Model has been adequately programmed and has sufficient face validity | No | The model contained several IFERROR statements and an issue in which the cost of Firazyr rescue medication reduces to $0, specifically for those receiving no LTP once drug wastage is incorporated into the model. |
Model structure is adequate for decision problem | No | The submitted model structure was found to be inadequate in capturing key outcomes related to patient health-related quality of life such as tracheotomy, chronic GI symptoms, and frequency of rescue medication use. Refer to the CADTH appraisal section. |
Data incorporation into the model has been done adequately (e.g., parameters for probabilistic analysis) | Yes | No comment. |
Parameter and structural uncertainty were adequately assessed; analyses were adequate to inform the decision problem | Yes | No comment. |
The submission was well organized and complete; the information was easy to locate (clear and transparent reporting; technical documentation available in enough details) | No | Reporting lacked transparency and technical documentation of the modelling methods in the accompanying pharmacoeconomic report were not sufficient in detail. There is information missing regarding the calculation of several parameters, including the methodology for acute treatment costs and utilities. |
LTP = long-term prophylactic.
Appendix 3: Additional Information on the Submitted Economic Evaluation
Detailed Results of the Sponsor’s Base Case
Table 10: Disaggregated Summary of the Sponsor’s Economic Evaluation Results
Parameter | Berotralstat | No LTP | Incremental |
|---|---|---|---|
Discounted LYs | |||
Total | 31.04 | 31.04 | 0.00 |
Attack-free | NA | NA | NA |
Attack | NA | NA | NA |
Discounted QALYs | |||
Total | 24.34 | 22.86 | 1.47 |
Attack-free | 24.16 | 21.56 | 2.60 |
Attack | 0.18 | 1.31 | -1.13 |
Discounted costs ($) | |||
Total | 9,865,264 | 2,924,654 | 6,940,611 |
Prophylactic treatments costs | 9,443,342 | 0 | 9,443,342 |
Attack costs | 421,923 | 2,924,654 | -2,502,731 |
ICER ($/QALY) | 4,710,158 | ||
ICER = incremental cost-effectiveness ratio; LTP = long-term prophylactic; LY= life-year; NA = not applicable; QALY= quality-adjusted life-year.
Table 11: Disaggregated Summary of Sponsor’s Sensitivity Analysis Including LTP Comparators
Treatment | Component | Value | Incremental (versus reference) | Incremental (sequential) |
|---|---|---|---|---|
Discounted QALYs | ||||
No LTP | Attack-free | 21.56 | NA | NA |
Attack | 1.31 | NA | NA | |
Total | 22.86 | NA | NA | |
Berotralstat | Attack-free | 24.16 | 2.603 | NA |
Attack | 0.18 | −1.13 | NA | |
Total | 24.34 | 1.47 | NA | |
Cinryze | Attack-free | 23.49 | 1.935 | −0.67 |
Attack | 0.59 | −0.72 | 0.41 | |
Total | 24.08 | 1.22 | −0.26 | |
Berinert | Attack-free | 23.81 | 2.249 | 0.31 |
Attack | 0.42 | −0.89 | −0.17 | |
Total | 24.22 | 1.36 | 0.14 | |
Lanadelumab | Attack-free | 24.29 | 2.73 | 0.48 |
Attack | -0.16 | −1.46 | −0.57 | |
Total | 24.13 | 1.27 | −0.09 | |
Haegarda | Attack-free | 23.91 | 2.36 | −0.38 |
Attack | 0.36 | −0.95 | 0.52 | |
Total | 24.27 | 1.41 | 0.14 | |
Discounted costs ($) | ||||
No LTP | Prophylactic treatments costs | 0 | NA | NA |
Administration costs | 0 | NA | NA | |
Attack costs | 2,924,654 | NA | NA | |
Total | 2,924,654 | NA | NA | |
Berotralstat | Prophylactic treatments costs | 9,443,342 | 9,443,342 | NA |
Administration costs | 0 | 0 | NA | |
Attack costs | 421,923 | −2,502,731 | NA | |
Total | 9,865,264 | 6,940,611 | NA | |
Cinryze | Prophylactic treatments costs | 2,949,055 | 2,949,055 | 2,949,055 |
Administration costs | 54 | 54 | 54 | |
Attack costs | 684,249 | −2,240,404 | 262,327 | |
Total | 3,633,359 | 708,705 | −6,231,906 | |
Berinert | Prophylactic treatments costs | 17,729,074 | 17,729,074 | 14,780,019 |
Administration costs | 19 | 19 | −36 | |
Attack costs | 481,731 | −2,442,922 | −202,518 | |
Total | 18,210,824 | 15,286,171 | 14,577,466 | |
Lanadelumab | Prophylactic treatments costs | 12,735,966 | 12,735,966 | −4,993,108 |
Administration costs | 7 | 7 | −12 | |
Attack costs | 286,242 | −2,638,411 | −195,489 | |
Total | 13,022,215 | 10,097,562 | −5,188,609 | |
Haegarda | Prophylactic treatments costs | 13,039,764 | 13,039,764 | 303,797 |
Administration costs | 7 | 7 | 0 | |
Attack costs | 414,366 | −2,510,288 | 128,124 | |
Total | 13,454,136 | 10,529,483 | 431,921 | |
Treatment | ICER versus reference ($) | Sequential ICER ($) | ||
No LTP | Reference | Reference | ||
Cinryze | 582,601 | 582,601 | ||
Berotralstat | 4,710,158 | 24,240,136 | ||
Berinert | 11,229,965 | Dominated | ||
Lanadelumab | 7,946,706 | Dominated | ||
Haegarda | 7,469,637 | Dominated | ||
ICER = incremental cost-effectiveness ratio; LTP = long-term prophylactic; LY= life-year; NA = not applicable; QALY= quality-adjusted life-year.
Note: All LYs were identical across all treatments included in the economic evaluation and disaggregated results were not available from the sponsor (LYs = 31.04, refer to Table 10).
Table 12: Patient-Reported and Investigator-Confirmed HAE Attack Rates (Monthly)
Month | Mean number of attacks (patient-reported) | Mean number of attacks (investigator-confirmed) | ||
|---|---|---|---|---|
Berotralstat | No LTP | Berotralstat | No LTP | |
1 | ███████ | ███████ | ███████ | ███████ |
2 | ███████ | ███████ | ███████ | ███████ |
3 | ███████ | ███████ | ███████ | ███████ |
4 | ███████ | ███████ | ███████ | ███████ |
5 | ███████ | ███████ | ███████ | ███████ |
6 | ███████ | ███████ | ███████ | ███████ |
7 | ███████ | ███████ | ███████ | ███████ |
8 | ███████ | ███████ | ███████ | ███████ |
9 | ███████ | ███████ | ███████ | ███████ |
10 | ███████ | ███████ | ███████ | ███████ |
11 | ███████ | ███████ | ███████ | ███████ |
12 | ███████ | ███████ | ███████ | ███████ |
13 | ███████ | ███████ | ███████ | ███████ |
14 | ███████ | ███████ | ███████ | ███████ |
15 | ███████ | ███████ | ███████ | ███████ |
16 | ███████ | ███████ | ███████ | ███████ |
17 | ███████ | ███████ | ███████ | ███████ |
18 | ███████ | ███████ | ███████ | ███████ |
19 | ███████ | ███████ | ███████ | ███████ |
20 | ███████ | ███████ | ███████ | ███████ |
21 | ███████ | ███████ | ███████ | ███████ |
22 | ███████ | ███████ | ███████ | ███████ |
23 | ███████ | ███████ | ███████ | ███████ |
24 | ███████ | ███████ | ███████ | ███████ |
HAE = hereditary angioedema; LTP = long-term prophylactic; NA = not available.
aInvestigator-confirmed attack rates were unavailable after 6 months for patients receiving berotralstat and placebo. However, attack rates were assessed at month 7 and 12 in a smaller cohort of patients due to attrition. Estimates following 6 months of data could not be used in the CADTH base-case analysis due to missing information but were assessed in a scenario analysis.
Appendix 4: Additional Details on the CADTH Reanalyses and Sensitivity Analyses of the Economic Evaluation
Note that this appendix has not been copy-edited.
Detailed Results of CADTH Base Case
Table 13: Disaggregated Summary of CADTH’s Economic Evaluation Results
Parameter | Berotralstat | No LTP | Incremental |
|---|---|---|---|
Discounted LYs | |||
Total | 31.04 | 31.04 | 0.00 |
Attack-free | NA | NA | NA |
Attack | NA | NA | NA |
Discounted QALYs | |||
Total | 23.26 | 22.65 | 0.61 |
Attack-free | 22.31 | 21.22 | 1.09 |
Attack | 0.95 | 1.43 | −0.48 |
Discounted costs ($) | |||
Total | 11,386,931 | 2,535,765 | 8,851,166 |
Prophylactic treatments costs | 9,636,442 | 0 | 9,636,442 |
Attack costs | 1,750,489 | 2,535,765 | −785,276 |
ICER ($ per QALY) | 14,559,490 | ||
ICER = incremental cost-effectiveness ratio; LTP = long-term prophylactic; LY= life-year; QALY = quality-adjusted life-year.
Scenario Analyses
CADTH performed a scenario analysis to determine the impact of alternate attack rates on the cost-effectiveness of berotralstat. Noncomparative investigator-confirmed attack rates were included from 6-months up to 12-months for patients receiving berotralstat with the last observation carried forward for the remainder of the time horizon, aligned with the sponsor’s methodology.
Table 14: Disaggregated Summary of CADTH’s Scenario Analysis
Stepped analysis | Intervention | Total costs ($) | Total QALYs | ICER ($ per QALY) |
|---|---|---|---|---|
CADTH base case | No LTP | 2,535,765 | 22.65 | Reference |
Berotralstat | 11,386,931 | 23.26 | 14,559,490 | |
Included noncomparative investigator-confirmed attack rates extended from 6-months up to 12-months for patients receiving berotralstat with the last observation carried forward | No LTP | 2,527,460 | 22.69 | Reference |
Berotralstat | 10,769,715 | 23.74 | 7,848,146 |
ICER = incremental cost-effectiveness ratio; LTP = long-term prophylactic; QALY = quality-adjusted life-year.
Appendix 5: Submitted Budget Impact Analysis and CADTH Appraisal
Note that this appendix has not been copy-edited.
Table 15: Summary of Key Takeaways
Key takeaways of the budget impact analysis |
|---|
|
Summary of Sponsor’s Budget Impact Analysis
The submitted BIA estimated the introduction of berotralstat for the treatment of HAE in adults and pediatric patients 12 years or older.15 The analysis took the perspective of CADTH-participating Canadian public drug plans using a top-down epidemiological approach and incorporated drug acquisition costs. A time horizon of 3 years was taken. The target population’s size was estimated using the prevalence of HAE.16 Further specification of population size included an estimation of a 67% diagnosis rate, increasing to 70% in Year 1, 73% in Year 2, and 75% in Year 3.17 The proportion of diagnosed patients receiving prescribed treatment was 92%,18 and 66% of treated patients were identified to require LTP. The proportion of patients requiring LTP increased to 68% in Year 1, 70% in Year 2 and 72% in Year 3. The base-case analysis examines patients eligible for CBS-covered treatments, for which costs were excluded. The reference case scenario included lanadelumab, Haegarda, Cinryze, Berinert, and no LTP for all provinces except for PEI, where lanadelumab is not publicly funded. The new drug scenario included berotralstat, lanadelumab, Haegarda, Cinryze, Berinert, and no LTP. Key inputs to the BIA and the sponsor’s methodology in calculating target population are documented in Table 17.
Table 16: Summary of Key Model Parameters
Parameter | Sponsor’s estimate (reported as Year 1 / Year 2 / Year 3 if appropriate) |
|---|---|
Target population | |
CADTH-participating pan-Canadian population | 29,641,613 |
Prevalence of HAE16 | 0.00149% |
Proportion of HAE patients diagnosed17 | 70% / 73% / 75% |
Proportion of patients receiving prescribed treatment18 | 92% |
Proportion of treated patients requiring LTP | 68% / 70% / 72% |
Proportion of patients eligible for public coverage | 75% |
Number of patients eligible for drug under review | 195 / 210 / 222 |
Market uptake (3 years) | |
Uptake (reference scenario) for all provinces except PEI Lanadelumab Haegarda Cinryze Berinert No LTP | ██████████████ ██████████████ ██████████████ ██████████████ ██████████████ |
Uptake (reference scenario) for PEI Lanadelumab Haegarda Cinryze Berinert No LTP | ██████████████ ██████████████ ██████████████ ██████████████ ██████████████ |
Uptake (new drug scenario) Berotralstat Lanadelumab Haegarda Cinryze Berinert No LTP | ██████████████ ██████████████ ██████████████ ██████████████ ██████████████ ██████████████ |
Uptake (reference scenario) for PEI Berotralstat Lanadelumab Haegarda Cinryze Berinert No LTP | ██████████████ ██████████████ ██████████████ ██████████████ ██████████████ ██████████████ |
Cost of treatment (per patient)a | |
Cost of treatment over 28 days Berotralstat Lanadelumab Haegarda Cinryze Berinert No LTP | $23,800 $31,218 $0 $0 $0 $0 |
HAE = hereditary angioedema; LTP = long-term prophylactic; PEI = Prince Edward Island.
aCost of complement 1 esterase inhibitors were excluded from the base case as they are not covered by drug plans and are accessed through Canadian Blood Services. Inclusion of these costs were assessed in a scenario analysis conducted by the sponsor.
Summary of the Sponsor’s Budget Impact Analysis Results
The sponsor’s estimated budget impact of funding berotralstat for the treatment of HAE in adults and pediatric patients over 12 years of age was $1,682,075 in Year 1, $4,939,478 in Year 2, and $7,542,738 in Year 3, for a 3-year total of $14,164,290.
The sponsor also conducted a scenario analysis that estimated the budget impact for funding berotralstat when a broader health system perspective was accounted for, which included the costs to CBS and the provincial drug plans. In this scenario analysis, the reimbursement of berotralstat led to cost savings of $10,149,307 to the Canadian health system over the 3-year time horizon.
CADTH Appraisal of the Sponsor’s Budget Impact Analysis
CADTH identified several key limitations to the sponsor’s analysis that have notable implications on the results of the BIA:
Market shares for berotralstat are likely underestimated: The sponsor anticipated a gradual uptake of berotralstat from █ █ █ to ██ ██ in years 1 to 3 in the new drug scenario. Given that there are no orally administered LTPs available for patients with HAE, clinical experts noted that the market share estimates for berotralstat were likely underestimated and patients would opt for treatment with berotralstat given overall preference for oral administration over IV or SC administration. Clinical experts indicated that uptake would be rapid if it were to be made available, taking up 50% of the market by year 1 and reaching 67% by year 3.
CADTH increased the market shares of berotralstat in the base case to reach 50% by year 1 and 67% by year 3, as anticipated by clinical experts. The comparator treatments were proportionately decreased to reflect uptake of berotralstat.
Market shares for comparator products are highly uncertain: As lanadelumab is only funded under restricted access, the true market shares of lanadelumab are uncertain given the variation in eligibility criteria in each jurisdiction offering funding. Upon consultation with provincial drug plans, CADTH received feedback that the base year estimate of lanadelumab usage may align with the sponsor’s estimate of ████ of patients. However, it was expressed that there is likely a disparity between authorized approval requests and true utilization data, with uncertainty remaining in these estimates. According to data accessed from several plans, the growth in lanadelumab access requests did not support the sponsor’s predicted uptake of lanadelumab reaching ██ ██ in the reference scenario and ██ ██ in the uptake scenario by year 3; these market shares are therefore likely overestimated. Notably, the market shares for the other comparator products (Berinert, Haegarda, and Cinryze) are also associated with considerable uncertainty due to their coverage outside drug plans.
CADTH maintained the sponsor’s base year market share of lanadelumab of ███ █ but adjusted it proportionately to reflect the uptake of berotralstat in the new drug scenario to reach 5% by year 3. There remains considerable uncertainty in the estimated market shares, and to test some of that uncertainty, an additional scenario analysis was conducted estimating a higher initial market share of lanadelumab.
Uncertainty in deriving target population: The sponsor’s prevalence of 1 in 67,000 is not representative of the Canadian population. As per the updated International and Canadian Hereditary Angioedema Guidelines 2019, Type I and II HAE prevalence is estimated to occur in approximately 1 in 50,000.19 Clinical experts consulted by CADTH also supported that 1 in 50,000 is a more reasonable estimation of prevalence in Canada. An increase or decrease in target population will lead to large fluctuations in the anticipated budget impact for berotralstat and an underestimated prevalence led to an underestimation of target population.
CADTH adjusted the prevalence rate to 1 in 50,000 to reflect Canadian HAE guidelines in reanalysis.
Target population is underestimated by excluding those not covered by drug plans: The sponsor assumed that 75% of patients would be eligible for public coverage by drug plans with berotralstat and lanadelumab. Given that the sponsor’s assumption was not based on provincial coverage data, CADTH explored the impact of public drug coverage in a scenario analysis.
CADTH increased public coverage to 100% in a scenario analysis.
Lack of clarity regarding treatment discontinuation: Drug plan and clinician input indicated uncertainty in stopping rules due to lack of efficacy or other reasons following treatment with berotralstat. Although there are no clear discontinuation criteria for berotralstat, increases in discontinuation rates would affect the budget impact of berotralstat.
CADTH could not address this concern in reanalysis.
CADTH Reanalyses of the Budget Impact Analysis
Table 17: CADTH Revisions to the Submitted Budget Impact Analysis
Stepped analysis | Sponsor’s value or assumption | CADTH value or assumption |
|---|---|---|
Corrections to sponsor’s base case | ||
1. NIHB total costs for CBS scenario analysis was miscalculated | Total incremental costs to public payer were miscalculated and did not include CBS for only the NIHB calculation. | CADTH corrected the total costs to reflect the sum of costs in year 1 through 3 that reflect inclusion of CBS into the drug plan perspective. |
Changes to derive the CADTH base case | ||
1. Market shares underestimated in the uptake scenario | ████████████ | 50% / 59% / 67% |
2. Prevalence underestimated | 1 in 67,000 | 1 in 50,000 |
CADTH base case | Reanalysis 1 + 2 | |
The results of the CADTH step-wise reanalysis are presented in summary format in Table 18 and a more detailed breakdown is presented in Table 19. Based on the CADTH base case, the budget impact of the reimbursement of berotralstat for the treatment of HAE in adults and pediatric patients over 12 years of age is expected to be $24,529,115 in year 1, $31,074,770 in year 2, and $37,288,339 in year 3. The 3-year total budget impact for berotralstat is $92,892,224.
A scenario analysis assessing the budget impact when the percentage of the population covered by public plans was increased to 100% led to a 3-year budget impact of $123,856,298. A scenario analysis assessing the budget impact if the price of berotralstat is discounted to the WTP threshold of $50,000 per QALY resulted in a 3-year budget impact of $14,516,287 in cost savings. An additional scenario analysis assessing the budget impact if CBS were to be included in the provincial drug plan perspective resulted in a 3-year cost savings of $26,327,191 to the Canadian health system. A scenario analysis increasing market shares of lanadelumab to 30% in the base year resulted in a 3-year budget impact of $70,291,426.
Table 18: Summary of the CADTH Reanalyses of the Budget Impact Analysis
Stepped analysis | Three-year total |
|---|---|
Submitted base case | $14,164,290 |
CADTH reanalysis 1 | $69,322,555 |
CADTH reanalysis 2 | $18,980,149 |
CADTH base case | $92,892,224 |
Table 19: Detailed Breakdown of the CADTH Reanalyses of the Budget Impact Analysis
Stepped analysis | Scenario | Year 0 (current situation) | Year 1 | Year 2 | Year 3 | Three-year total |
|---|---|---|---|---|---|---|
Submitted base case (corrected) | Reference | $8,206,695 | $11,876,496 | $15,938,623 | $20,209,877 | $48,024,996 |
New drug | $8,206,695 | $13,558,571 | $20,878,100 | $27,752,614 | $62,189,286 | |
Budget impact | $0 | $1,682,075 | $4,939,478 | $7,542,738 | $14,164,290 | |
CADTH base case | Reference | $10,996,971 | $11,935,879 | $12,814,653 | $13,540,617 | $38,291,149 |
New drug | $10,996,971 | $36,464,994 | $43,889,422 | $50,828,956 | $131,183,372 | |
Budget impact | $0 | $24,529,115 | $31,074,770 | $37,288,339 | $92,892,224 | |
CADTH scenario analysis: CBS and drug plans perspective | Reference | $69,037,094 | $74,931,785 | $80,447,248 | $85,006,500 | $240,385,533 |
New drug | $69,037,094 | $67,962,947 | $71,618,787 | $74,412,697 | $213,994,431 | |
Budget impact | $0 | -$6,968,838 | -$8,828,461 | −$10,593,803 | −$26,391,102 | |
CADTH scenario analysis: 93% price reduction | Reference | $10,996,971 | $11,935,879 | $12,814,653 | $13,540,617 | $38,291,149 |
New drug | $10,996,971 | $8,102,733 | $7,958,487 | $7,713,642 | $23,774,862 | |
Budget impact | $0 | −$3,833,146 | -$4,856,166 | −$5,826,975 | −$14,516,287 | |
CADTH sensitivity analysis (100% public coverage) | Reference | $14,662,628 | $15,914,505 | $17,086,203 | $18,054,156 | $51,054,865 |
New drug | $14,662,628 | $48,619,992 | $58,519,230 | $67,771,941 | $174,911,163 | |
Budget impact | $0 | $32,705,487 | $41,433,027 | $49,717,785 | $123,856,298 | |
CADTH sensitivity analysis (increased lanadelumab market shares) | Reference | $21,993,942 | $23,871,758 | $25,629,305 | $27,081,235 | $76,582,297 |
New drug | $21,993,942 | $42,432,933 | $49,143,430 | $55,297,360 | $146,873,723 | |
Budget impact | $0 | $18,561,176 | $23,514,125 | $28,216,125 | $70,291,426 |
Note: the submitted analysis is based on the publicly available prices of the comparator treatments.
Stakeholder Input
Patient Input
HAE Canada
About HAE Canada
HAE Canada (haecanada.org) is dedicated to creating awareness about HAE and other related angioedema, to help speed the diagnosis of patients, and to enable them to become champions for their own quality of life. We equip patients, caregivers, family members and health care providers with the information, tools and resources they need to ensure that those with HAE and other related angioedema can live healthy and productive lives. Additionally, HAE Canada is committed to improving patient access to Health Canada approved treatments for hereditary angioedema.
Information Gathering
In February and March 2022, HAE Canada (HAEC) attempted to contact patients who had experience with Berotralstat (Orladeyo). HAEC emailed our membership and contacted three Canadian physician investigators who had patients enrolled in the APeX-2 Study and asked that they connect these patients with HAEC so that we could get their insights regarding their challenges with hereditary angioedema and experiences with berotralstat for the routine prevention of recurrent attacks of hereditary angioedema. Three patients provided comments to HAEC about their experience with berotralstat. (Note: The APeX-2 study had very few Canadian participants with 3 of 47 study sites in Canada, with a total of 121 patients enrolled globally. Identifying and contacting patients with experience with berotralstat is extremely difficult).
Also, in 2021 HAE Canada conducted our 2nd National Report Card survey, offered in English and French, of patients and caregivers to better understand the needs and experiences of patients with HAE and to inform HAE Canada’s policy and advocacy activities related to improving access to safe and effective treatments.
Additionally, in 2020, qualitative interviews, using a semi-structured interview guide, were conducted by HAE Canada with eleven (11) patients with a mix of either type 1 or type 2 HAE to better understand and characterize patient patterns of use for treatments for HAE. The interviews included questions and discussion on patients experience with HAE attacks, their experiences with HAE treatment, the needs and challenges of living with HAE and their experiences with services related to treatment use and supply.
And, in 2019 HAE Canada conducted two surveys to gain insight into patient experience and expectation with therapies used to treat hereditary angioedema. The surveys were in support of the HAEC patient submission to CADTH with respect to lanadelumab (Takhzyro) and to the HAE Forum organized by Canadian Blood Services with respect to C1 Esterase Inhibitor Subcutaneous [Human] (Haegarda).
This report reflects the results of our surveys regarding patient experience with HAE treatments, and patient commentary specific to the use of berotralstat, as well as insights HAE Canada has garnered from more than a decade of experience in patient support and advocacy related to hereditary angioedema.
Disease Experience
Hereditary angioedema (HAE) is a severely debilitating and life-threatening disease. It manifests as unpredictable, recurrent/intermittent edema attacks in different parts of the body including the gastrointestinal tract, upper respiratory tract, extremities and face. Gastrointestinal (GI) attacks are common in HAE, with severe abdominal pain and other GI symptoms. Untreated laryngeal attacks may result in asphyxiation and death. Swelling in other body parts can also significantly interfere with patients’ daily pursuits, resulting in severely impaired quality of life.
Patients may still be affected by HAE even after the physical symptoms of an attack abate. For many, the expectation of HAE attacks imposes harsh limits on activities and plans. Due to the unpredictable nature of the disease, many patients experience high levels of distress and anxiety in everyday life, often attributed to: restricted or disrupted social life, anxiety due to fear of future attacks, the concern of HAE being passed to their children, and disruption/interference in educational and career pursuits. Many patients report that they do not pursue higher education due to HAE, and that they deliberately elect to not seek out certain jobs, and job advancements, due to expected recurrent edema attacks.
We asked in our 2019 survey: On a scale of 1 - 5 please rate how Hereditary Angioedema impacts or limits your life and day-to-day activities. 1 is "not at all" and 5 is "significant impact". We had 6 categories as follows.
Table 1: Hereditary Angioedema Impacts or Limits on Day-to-Day Activities
1 (not at all) | 2 | 3 | 4 | 5 (significant impact) | Not applicable | Weighted average (WA) | |
|---|---|---|---|---|---|---|---|
Ability to Travel N=66 | |||||||
10pts (15%) | 20pts (30%) | 11pts (17%) | 6pts (9%) | 15pts (23%) | 4pts (6%) | 2.94 | |
Ability to Exercise N=66 | |||||||
18pts (27%) | 13pts (20%) | 9pts (14%) | 11pts (17%) | 13pts (20%) | 2pts (3%) | 2.81 | |
Ability to Work N=66 | |||||||
14pts (21%) | 16pts (24%) | 10pts (15%) | 8pts (12%) | 12pts (18%) | 6pts (9%) | 2.80 | |
Financial Situation N=66 | |||||||
26pts (39%) | 16pts (24%) | 3pts (4.5%) | 9pts (14%) | 8pts (12%) | 4pts (6%) | 2.31 | |
Ability to spend time with family and friends N=66 | |||||||
23pts (35%) | 18pts (27%) | 14pts (21%) | 6pts (9%) | 4pts (6%) | 1pt (1.5%) | 2.23 | |
Ability to Conduct Household Chores N=66 | |||||||
24pts (36%) | 18pts (27%) | 12pts (18%) | 5pts (8%) | 5pts (8%) | 2pts (3%) | 2.20 | |
Patients had an option to add free-form commentary to the question re: impacts on day-to-day activities. These are a selection of their comments:
“… From the ages of 20-50 I had attacks weekly and it did affect my life adversely. A preventative medicine would have been fantastic when I was younger.”
“The veil of anxiety coloured my life every day.”
We asked: How has hereditary angioedema affected you psychologically/emotionally?
Patients said:
“I nearly died from a laryngeal HAE attack which has profoundly changed all levels of my life.”
“When I was undiagnosed, I experienced a lot of pain (abdominal attacks) and with no diagnosis — no one believed me”
“Depending on the location of the attack I have not wanted to go out in public.”
“Unrelenting source of stress.”
“Chronic anxiety over the unpredictability of this disease.”
“Depression, anxiety, feature of future attacks, embarrassment and shame”
We asked: How has hereditary angioedema impacted you financially? (n=65)
61.54% (n=40) reported HAE caused them to miss time at work or be less productive at work
21.54% (n=14) reported HAE required them to spend out-of-pocket for medical care
9.23% (n=6) reported that HAE has prevented them from securing a job
6.15% (n=4) reported hereditary angioedema has impeded their ability to advance in the workplace
Some patients expounded:
“Reluctant to advance further due to fear of additional work stressors having a negative impact on my health.”
“Retired now but it was very challenging to meet the demands of work before I stopped.”
“My inability to pay for the medication while being a student has left me on welfare.”
“Caused me to be absent from my job.”
Conclusion: The impact of Hereditary angioedema (HAE) goes well beyond its immediate debilitating and life-threatening manifestations. The majority of our recently surveyed patients/caregivers report having regular fear of unpredictable attacks. These patients experience generalized anxiety and stress along with many other emotional and cognitive impacts. HAE also interferes with patients’ daily activities, with the disease having substantial negative impact on many patients’ ability to work, travel, exercise, do household chores, and socialize with family and friends. HAE inhibits many patients’ ability to pursue higher education or job advancements, and negatively affects their personal finances due to sub-optimal employment, interference with employment and costs due to treatment for HAE.
Experiences With Currently Available Treatments
Areas of Unmet Need
Recognizing the burden to patients associated with HAE, including the ever-present risk of experiencing a life-threatening laryngeal attack, improved preventative treatments are urgently needed. Patients that may have the greatest unmet need for an intervention such as oral, once-daily berotralstat are:
Patients who find current prophylactic treatments to be ineffective
There is no current way to predict who will respond best to any current treatment for HAE, and while some patients respond extremely well to certain treatments, others do not. This heterogeneity in response to treatment drives an urgent need for treatment options for Long-term Prophylaxis (LTP).
Patients who experience damage to their veins or worry about future damage to their veins
For instance, one patient reported during a one-on-one patient interview in 2020: “I took Berinert IV as prophylaxis twice per week until my veins got so bad …then I was lucky enough to get on the Haegarda drug trial, which is effectively Berinert SubQ. This gave my veins a rest.” Another patient interviewed in 2020 reported: “I moved from IV to SubQ because of issues with my veins. I didn’t know SubQ was an option. When I found out I moved to it. I was using the same veins too often, which was causing damage…”
Patients who find it difficult and uncomfortable to self-administer intravenous or subcutaneous prophylactic treatments for HAE
Many patients have reported that they have difficulty self-administering treatment for HAE. This can be a function of a patient having damaged veins, or having difficulty finding a vein for intravenous infusion, or simply having great discomfort or general difficulty with the self-administration of an IV treatment. With respect to the administration of either subcutaneous or intravenous treatment for HAE, some patients have strong needle-aversion which makes an effective oral medication highly attractive to this subset of patients.
Patients who live far away from hospital care
IV HAE treatments have the effect of requiring patients to expend much time traveling to treatment and undergoing treatment; especially if they have difficulty doing home infusions.
Patients concerned about risk of infectious agent transmission and supply interruptions/shortages from plasma-derived HAE treatments
Even though multiple critical steps are taken to minimize the risk of infection from transfusion of blood products, the risk of infectious agent transmission from plasma-derived products, in some cases, drives patient preference for non-plasma derived treatments.
Of importance, Canadian Blood Services (CBS) recognizes that the use and demand for plasma-derived therapies continue to rise globally, while the percentage of plasma-derived products produced from plasma collected at Canadian donor centers is decreasing. While CBS is working to develop capacity to collect more plasma domestically to address plasma supply issues, an important strategy to lessen demand of these therapies is to also offer patients non-plasma derived therapies when such therapies offer the required efficacy, safety and convenience for patients.
Satisfaction with Current Treatments
In our (2021) National Report Card survey, we asked patients: Please rate how satisfied/dissatisfied you are with the effectiveness of your current HAE treatment to prevent attacks. (138 patients responded to this question).
Table 2: Effectiveness of Current HAE Treatment to Prevent Attacks
Very dissatisfied | Dissatisfied | Neither satisfied nor dissatisfied | Satisfied | Very satisfied | Not applicable | Total | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
3.6% | N=5 | 13.0% | N=18 | 10.9% | N=15 | 25.4% | N=35 | 29% | N=40 | 18% | N=25 | N=138 |
When adjusting the results to remove the 25 patients for which this question was “Not Applicable” (changing the denominator to 113 respondents) we find that over 20% of patients are currently very dissatisfied or dissatisfied with the effectiveness of their current treatment used to prevent attacks. Numerous patients provided comments about their satisfaction with the effectiveness of current treatments including:
“Effective oral treatment would be best.”
“A better way of administering medication would help.”
“New, non-blood sourced medication would be preferable -an oral rather than injected medication would be preferred”
“I had been on danazol for 30 years, when without warning, there was no supply left in the country - this was EXTREMELY stressful - no drug, no alternative - and had to try to track down my immunologist who was out of the country to figure out what to do. It leaves us on edge. If only this could be given orally, we would be happy.”
“Hate having to do prophylaxis treatment every second day, would love a pill!”
“I am SO sorry to have to say that I am dissatisfied because I appreciate the improvement that Berinert and Firazyr have made to my quality of life overall. However, because my life revolves around needles, my injection schedule and dealing with pain on a daily basis, I have to be honest and say that I am "dissatisfied".”
“The injections twice a week around the belly are causing soreness”
“Berinert works excellent while I'm having an attack, but I don't find subcutaneous super effective at preventing the attacks.”
“Although my medication is all working, I do have to do 3 infusions per week in addition to my other treatments so that's a lot of needles! Travelling with so much medication is so difficult as well.”
“Would be a lot easier to not have to have my wife give me IV prophylaxis twice a week - hard on my veins.”
“Would like other treatment options.”
“Would like easier admin. Not IV”
“IV starts every 2 days can be exhausting.”
“I would prefer pills to sub-cutaneous injections; however, I am happy that I have access to the medication.”
“Please encourage research to develop an oral medication (pill) that is effective in preventing attacks, so that we can stop sticking ourselves with needles.”
“Really, I just want my life back. A pill would make things so much easier than sticking myself with a needle except when I’m having a throat or neck swell. My anxiety is sometimes out of control and if I overthink this disease, I can end up with a swell which I turn gives me a panic attack. It’s just super frustrating. Things have definitely got better but I’m still infusing an average of 10 times a month which in my opinion is too much. The cluster swells are exhausting.”
“I have been so fortunate that I have had excellent care and treatment. My daughters have just been diagnosed (no symptoms yet) and the only thing I would love to see for them is a pill rather than needles. I have one daughter with an extreme phobia of needles which will present a real problem if/when she requires treatment. I guess the other thing would be more knowledgeable of HAE among the medical professionals as well.”
Conclusion: HAE patients, (and CBS) urgently require prophylactic treatments that are more convenient and easier to administer at home, such as oral once-daily berotralstat.
Improved Outcomes
Patients continue to seek treatments that better control attacks while offering greater convenience and ease of use. Treatments that eliminate or substantially reduce attacks compared to existing treatments are of critical importance to patients as each edema attack can be severely debilitating, and in many cases life-threatening.
Greater control of attacks would also ameliorate the ever-present anxiety and fear many patients experience due to unpredictable attacks and reduce the negative impact on a patient’s ability to work, pursue education, travel, exercise, do household chores, and socialize with family and friends.
We asked, in our 2019 survey to support patient input to CADTH (re: lanadelumab): If you were to consider taking a new therapy for your hereditary angioedema, please rate the following on a scale of 1 - 5. 1 is "not important" and 5 is "extremely important". We had various categories.
Table 3: Rating of Considerations for New Therapy
1 (not important) | 2 | 3 | 4 | 5 (significantly important) | Not applicable | Weighted average (WA) |
|---|---|---|---|---|---|---|
Improved management/reduction in attacks of edema (swelling) n=57 | ||||||
1pt (1.75%) | 0pts (0%) | 2pts (3.5%) | 7pts (12.3%) | 47pts (82.5%) | 0pts (0%) | 4.74 |
No direct cost to user/patient n=58 | ||||||
2pts (3.5%) | 1pt (1.7%) | 1pt (1.7%) | 2pts (3.5%) | 52pts (90%) | 0pt (0%) | 4.74 |
Easier mode of delivery as a subcutaneous option (vs. IV) n=58 | ||||||
2pts (3.5%) | 1pt (1.7%) | 3pts (5%) | 7pts (12%) | 44pts (76%) | 1pts (1.7%) | 4.58 |
A more convenient dosing interval/less frequent dosing n=58 | ||||||
5pts (8.6%) | 2pts (3.5%) | 5pts (8.6%) | 8pts (13.8%) | 38pts (65.5%) | 0pts (0%) | 4.24 |
Patients (76%) overwhelmingly are seeking treatments with an easier mode of delivery.
The addition of subcutaneously administered lanadelumab (Takhzyro) to the treatment armamentarium for HAE was extremely important. Many patients who had the opportunity to switch to lanadelumab, or try lanadelumab during clinical trials, experienced substantial or total reduction in attack frequency while also benefiting from an easier to use therapy. However, some patients who tried this treatment saw little or no benefit from this treatment, and still require a treatment that offers a more convenient method of preventing HAE attacks.
Conclusion: Of critical importance to patients are therapies with an easier mode of delivery that are effective in preventing attacks and have fewer side effects.
Experience With Drug Under Review
In February and March 2022, HAE Canada (HAEC) attempted to contact patients who had experience with berotralstat (Orladeyo). Three patients provided comments to HAEC about their experience with berotralstat. (Note: The APeX-2 study had very few Canadian participants with 3 of 47 study sites in Canada, with a total of 121 patients enrolled globally. Identifying and contacting patients with experience with berotralstat is extremely difficult).
Patient 1: A female patient with HAE who was enrolled in the Apex-2 study, who was on treatment for between 1 and 2 years.
This patient reported having HAE attacks, before starting berotralstat, approximately once per week focused primarily in her extremities (limbs/hands/feet) and in her gastrointestinal system.
Based on this patient’s personal experience with berotralstat, she found this treatment to be extremely effective in prevention of attacks of HAE and she also found the side-effects to be easy to tolerate. She reported only noticing one treatment-related side effect “abdominal pain” which she rated as being “very tolerable”.
We asked her: On a scale of 1-5 how would you rate your quality of life (QoL) while taking berotralstat? 1 is "low/seriously impacted", and 5 is "high/normal living". She selected “5” suggesting that this treatment afforded her the opportunity to live a normal life. When we asked her “How has berotralstat changed, or how is it expected to change, your long-term health and well-being?” She replied: “No more crises with this treatment” She added: It’s so easy to add it in daily routine.”
Patient 2: A female patient with HAE who was enrolled in the in the Apex-2 study who was on treatment for between 1 and 2 years.
This patient reported having 1-2 HAE attacks per month, before starting berotralstat, and having approximately 3-4 attacks per month (focused primarily on her gastrointestinal system) while taking berotralstat. Consequently, she found this treatment to not be effective in the prevention of attacks of HAE.
We asked this patient, if 1 is "completely intolerable" and 5 is "very tolerable" how would you rate berotralstat’s side effects? This patient rated the tolerability of side effect to be a “3” (neither completely intolerable or very tolerable). We asked to identify specific side effects that she experienced with berotralstat and to rate them on a scale of 1 – 5 with 1 "completely intolerable" and 5 "very tolerable". She listed “abdominal pain” as a treatment related side-effect and rated its tolerability a “3”. She also listed “diarrhea” as a treatment related side-effect and rated its tolerability a “3”.
She added: “Orladeyo (berotralstat) was not really effective on me, however, worked very well for my daughter.”
When we asked her “Can you tell us about your story and why access to berotralstat and future therapies are so important to you? She replied: “It is important mostly for the next generations (my kids and grandkids).”
Patient 3: A male patient with HAE who was enrolled in the Apex-2 study, who was on treatment for between 1 and 2 years.
On the issue of treatment choice, this patient reported that he found it extremely important, in the context of shared decision-making with his physician, to be able to make a choice of treatment based upon each different drug’s known side effects. He also reported that the mode of delivery for a drug (eg. IV, subcutaneous, oral) was a key factor when making a choice of treatment (with his physician) for his HAE.
Based on this patient’s personal experience with berotralstat, he did not find this treatment to be effective in prevention of attacks of HAE as he experienced break through attacks every four to five days. He also found the side-effects to be difficult to tolerate.
The patient reported that he experiences other treatments prior to the berotralstat trial. When comparing berotralstat to his previous experience with the treatments Berinert (C1 Esterase Inhibitor [human]) and Haegarda (c1 esterase inhibitor subcutaneous [human] injection) he reports that berotralstat was much harder to tolerate than both Berinert and Haegarda. The side effects he reported experiencing while on berotralstat that he found difficult to tolerate were abdominal pain and diarrhea. Presently he is on a new clinical trial with no serious side effects to report.
We asked this patient: On a scale of 1-5 how would you rate your quality of life (QoL) while taking Orladeyo? 1 is "low/seriously impacted", and 5 is "high/normal living". This patient selected “3” suggesting that this treatment, while not negatively impacting his QoL, also did not afford him any improvement in QoL.
Companion Diagnostic Test
The identification biomarkers and development of accompanying bioassays are urgently needed to accompany clinical trials and enable personalized medicine for HAE. Biomarkers are sought because they can be utilized to diagnose, guide therapies, or make predictions regarding the clinical course of HAE.
HAE Canada encourages ongoing research to identify and validate biomarkers for HAE, and to monitor these biomarkers longitudinally to determine their clinical utility and predictive value.
Anything Else?
HAE is a heterogeneous disease with complex pathophysiology. Current knowledge cannot provide convincing explanations for the clinical variability of the disease, and despite detailed research and identification of novel defects, a proportion of patients with HAE are still labeled as HAE-Unidentified (HAE-UI) wherein the genetic defect has not yet been identified. More research work is required to uncover different disease endotypes to identify specified targets for therapeutic intervention with the goal of more effective, individualized management of the disease.
These advances may bring new therapeutic modalities for the management of HAE.
Conflict of Interest Declaration — HAE Canada
To maintain the objectivity and credibility of the CADTH reimbursement review process, all participants in the drug review processes must disclose any real, potential, or perceived conflicts of interest. This Patient Group Conflict of Interest Declaration is required for participation. Declarations made do not negate or preclude the use of the patient group input. CADTH may contact your group with further questions, as needed.
Did you receive help from outside your patient group to complete this submission? If yes, please detail the help and who provided it.
HAE Canada used regular and contracted employee assistance to conduct research and complete this submission.
Did you receive help from outside your patient group to collect or analyze data used in this submission? If yes, please detail the help and who provided it.
The collection and analysis of data was accomplished exclusively through the use of HAE Canada resources and tools. Both regular and contracted staff participated in data collection and analysis efforts.
List any companies or organizations that have provided your group with financial payment over the past 2 years AND who may have direct or indirect interest in the drug under review.
Table 4: Financial Disclosures for HAE Canada
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
BioCryst | — | — | — | X |
BioMarin | — | — | X | — |
CSL Behring Canada | — | — | — | X |
KalVista | — | — | X | — |
Pharvaris | — | — | X | — |
Takeda Canada | — | — | — | X |
Clinician Input
Canadian Hereditary Angioedema Network
About the Canadian Hereditary Angioedema Network
The Canadian Hereditary Angioedema Network (CHAEN) is an organization of physicians who treat and/or are interested in Hereditary Angioedema, and who contribute to the knowledge of HAE and its treatments, including participating in clinical trials, conducting observational research, and involvement in local/provincial and national clinical guideline development and health technology assessment. Our vision is to enable HAE patients in Canada to receive appropriate support and care so that they are able to live full lives. CHAEN is incorporated under the Canada Not-For-Profit Corporations Act.
Information Gathering
Information was gathered through personal experience in treating patients with hereditary angioedema, literature review, and virtual discussion among experts. Some of the contributors to this submission were investigators in the APeX-2 study, a Phase 3, Randomized, Double-blind, Placebo-controlled, Parallel Group Study to Evaluate the Efficacy and Safety of Two Dose Levels of BCX7353 (Berotralstat) as an Oral Treatment for the Prevention of Attacks in Subjects With Hereditary Angioedema.
Current Treatments
HAE can be categorized into 3 different types including HAE with deficient C1-inhibitor levels (HAE-1), HAE with dysfunctional C1-inhibitor (HAE-2), and HAE with normal C1-inhibitor function (HAE nC1-INH) previously referred to as type 3. For the purposes of this submission, we are focusing on currently available treatments in Canada for HAE-1 and HAE-2 that are for long-term prophylaxis (LTP), which involves initiating continuous regular treatment aimed at minimizing the number, frequency, and severity of attacks.
For the Long-Term Prophylaxis of HAE Attacks, the treatments available in Canada are:
C1-INH concentrate - human (Cinryze), which is a plasma-derived treatment administered intravenously.
C1-INH concentrate - human (Haegarda) which is a plasma-derived treatment administered subcutaneously.
Lanadelumab (Takhzyro) - Human monoclonal antibody which is administered subcutaneously.
Treatment Goals
The ultimate goal for an HAE treatment is to achieve no angioedema attacks, and to achieve total control of the disease and normalize the patient's life. Recognizing the burden to patients associated with HAE, including the ever-present risk of experiencing a life-threatening laryngeal attack, the impact of HAE on a person’s health-related quality of life (HRQoL) can be considerable. Thus, improved preventative treatments are urgently needed. Patients continue to seek treatments that better control attacks while offering greater convenience and ease of use.
Further, IV treatments have the effect of requiring patients to spend much time traveling to treatment and undergoing treatment; especially if they have difficulty doing home infusions. Of note, certain patients have trouble with self-cannulation. Also, subcutaneous treatments, while offering convenience to many patients, are not ideal or effective for all patients. Additionally, certain patients have an aversion to needles, driving the need for treatments with an oral method of administration.
Canadian Blood Services (CBS) has identified the decrease in the percentage of plasma-derived products delivered to Canadian patients that are produced from plasma collected at Canadian donor centres as a material risk needing mitigation. CBS further identifies that globally, the use and demand for plasma-derived therapies continue to rise.
The standard -of-care treatment for HAE is plasma derived C1 esterase inhibitor concentrate, which is prepared from large pools of human plasma. While CBS has the goal of collecting more plasma domestically to help mitigate plasma supply issues, an important strategy to mitigate demand of plasma-derived therapies is to also offer patients non-plasma derived therapies when such therapies offer required efficacy, safety and convenience.
Further, product safety as it relates to risk of infectious agent transmission from plasma-derived products, remains a concern with some patients. Although multiple critical steps are taken to minimize the risk of infection from transfusion of blood products, this remains top-of-mind for certain patients driving their preference for non-plasma derived treatments.
Treatment Gaps (Unmet Needs)
Considering the treatment goals, please describe goals (needs) that are not being met by currently available treatments.
HAE patients require a variety of treatment options to address a range of unmet needs including:
improvement in prevention of attacks
improvement in the acute management of HAE
More convenient methods/modalities of self-administration (vs. Intravenous self-administration or Subcutaneous self-administration)
Different treatment options are vital also to ensure patients have options when they are faced with drug shortages, which is currently a reality and potentially will continue to be in the future. Ensuring the availability of optional treatments is particularly important when dealing with a potentially life-threatening condition.
Which patients have the greatest unmet need for an intervention such as the drug under review?
There are currently no effective licensed oral prophylactic treatments for HAE in Canada. However, berotralstat is currently under review by Health Canada.
Historically, many patients in Canada have used attenuated androgens (androgen therapy) such as danazol, and stanozolol as (off-label) oral prophylaxis. These medications are associated with a range of severe side effects, such as headaches, hypertension, weight gain, masculinizing effects for women, hepatocellular carcinoma, dyslipidemia and cardiac disease. These drugs require regular monitoring and can’t be used in pregnancy. Androgen therapy is no longer recommended in guidelines for HAE as first line LTP. In the few patients who elect to stay on this treatment, they need to be made aware of side effects and monitoring requirements. Stanozolol has been discontinued in Canada.
Tranexamic acid (cyklokapron) is a popular option for children but has an incomplete evidence base and poor efficacy.
HAE patients need prophylactic treatments that can safely be taken regularly for years or even decades. Berotralstat may provide that option.
Patients that may have the greatest unmet need for an intervention such as berotralstat are:
Patients who find current prophylactic treatments to be ineffective
Patients who experience damage to their veins or worry about future damage to their veins.
Patients who find it difficult and uncomfortable to self-administer intravenous or subcutaneous prophylactic treatments for HAE.
Patients who live far away from hospital care
Patients concerned about risk of infectious agent transmission and supply interruptions / shortages from plasma-derived HAE treatments.
Patients who travel frequently, and require a treatment that is easy to transport, does not require refrigeration or complicated reconstitution, and is easy to administer.
HAE patients urgently require prophylactic treatments that are more convenient and easier to administer at home, such as oral once-daily berotralstat.
Place in Therapy
How would the drug under review fit into the current treatment paradigm?
To improve patient quality of life, reducing the treatment burden of HAE prophylaxis is an important consideration. A safe and effective oral prophylactic may be preferred to the current standard of care by some patients, particularly those who are averse to a long-term injection regimen.
For instance, some patients are needle phobic, have difficulty with injections, or have arthritis or are otherwise disabled making self-injecting difficult or impossible. Some patients may be on anticoagulation/ASA who experience easy bruising due to current HAE treatments and there may be patients who won’t use blood products. Younger patients who meet the age indication for berotralstat may see an effective oral agent to be ideal given the difficulties and aversions associated with injectable therapy for this demographic. While most recent guidelines recommend this drug as a first line, this (and any therapy) should be the subject of shared decision-making between the patient and the HAE specialist.
Because berotralstat is given orally, it may be associated with a lower treatment burden compared to injectable prophylactics such as lanadelumab or plasma derived C1 inhibitor for some patients.
The aim of long-term prophylaxis is to reduce the frequency and/or severity of attacks of HAE and minimize the impact of HAE on QoL, thereby enabling patients to live normal lives. Patients who are candidates for long-term therapy with berotralstat should explore with their treating physician the benefits and risks associated with berotralstat to optimize patient care.
The issue of combining therapies has so far not been addressed in studies.
It is important to remember that no prophylactic regimen has been associated with the complete elimination of angioedema. Therefore, despite being on prophylaxis, all patients should be equipped to treat angioedema attacks and an acute treatment plan should be agreed to between patient and physician.
Please indicate whether or not it would be appropriate to recommend that patients try other treatments before initiating treatment with the drug under review. Please provide a rationale from your perspective.
As stated in The International/Canadian Hereditary Angioedema Guideline all effective treatments for long-term prophylaxis should be offered to patients, and all available treatments should be the subject of shared decision-making between the patient and the HAE specialist.
For patients who are pregnant and/or breastfeeding, berotralstat would not be used.
How would this drug affect the sequencing of therapies for the target condition?
Like any LTP, if one is not effective, or if a patient has side effects from a therapy or has technical difficulties administering a therapy, the patient should be able to try another. The decision as to which treatment to try first should be the subject of shared decision-making between the patient and the HAE specialist.
Which patients would be best suited for treatment with the drug under review?
There are no specific predictors as to who would preferentially respond to berotralstat. This treatment should be considered along with other currently available treatments for long-term prophylaxis with patient preference contributing to the ultimate treatment choice. All patients who are candidates for LTP should be made aware of this new treatment option. There are those where an oral therapy would be clearly preferred.
Additionally, for patients who travel frequently, this treatment offers tremendous convenience as it is easy to administer (by mouth), does not require refrigeration, and is easy to transport.
How would patients best suited for treatment with the drug under review be identified?
Long term prophylaxis (LTP) is considered at every follow up visit for HAE patients. Shared decision making between patient and clinician occurs and once the patient is ready for LTP- all LTP options are discussed, and again shared decision-making occurs to find the best treatment option for that patient. Those patients already on LTP, would also have a review at each follow up visit, to see if a switch in treatment would be potentially beneficial for that patient.
Diagnosis and treatment of HAE may be a problem in some patients given how rare it is, which is why HAE should be treated and managed by an HAE specialist.
Pre-symptomatic patients are not generally candidates for LTP.
Which patients would be least suitable for treatment with the drug under review?
Patients least suitable for treatment with the drug under review are pregnant and lactating women and pediatric patients < 12 years of age.
Is it possible to identify those patients who are most likely to exhibit a response to treatment with the drug under review?
At this time, we have no way to predict who will respond best to this (or any) treatment for HAE.
What outcomes are used to determine whether a patient is responding to treatment in clinical practice?
Yes, the outcomes used in clinical practice do align with the outcomes used in clinical trials. Clinical follow-up includes a review of number and severity of attacks, and also a review of side effects and response to acute and prophylactic treatment. Some clinics will use angioedema control scores and health related QoL scores.
What would be considered a clinically meaningful response to treatment?
The opinion of the patient on their response to treatment is a key consideration. But more objectively meaningful response is assessed by decreased frequency of HAE attacks, need for rescue treatments, decreased severity of attacks, decrease in emergency room visits, ability to work, increased QOL, and side effects profile.
How often should treatment response be assessed?
Response should be assessed at every follow up visit. Follow-up frequency is variable based on the nature/severity of the patient’s disease but can occur every 3, 6 or 12 months.
What factors should be considered when deciding to discontinue treatment?
Considerations leading to treatment discontinuation include:
ineffectiveness (poor control of HAE with increased or continued attack frequency and severity)
side effects.
Additionally, there will be some patients who prefer less frequent dosing for LTP such as with lanadelumab which is self-administered every 2 weeks vs daily oral medication.
What settings are appropriate for treatment with the drug under review?
As the treatment under review (berotralstat) is a once-a-day oral treatment, administration at home is an appropriate setting.
For non-oncology drugs, is a specialist required to diagnose, treat, and monitor patients who might receive the drug under review?
The large majority of HAE patients will be under an HAE specialists care including allergist/immunologist, hematologist, dermatologist, possibly pediatrician or Internist.
Additional Information
No.
Conflict of Interest Declarations — Canadian Hereditary Angioedema Network
To maintain the objectivity and credibility of the CADTH drug review programs, all participants in the drug review processes must disclose any real, potential, or perceived conflicts of interest. This conflict of interest declaration is required for participation. Declarations made do not negate or preclude the use of the clinician group input. CADTH may contact your group with further questions, as needed. Please refer to the Procedures for CADTH Drug Reimbursement Reviews (section 6.3) for further details.
Did you receive help from outside your clinician group to complete this submission? If yes, please detail the help and who provided it.
This clinician group submission by CHAEN was completed with our own resources.
Did you receive help from outside your clinician group to collect or analyze any information used in this submission? If yes, please detail the help and who provided it.
No.
List any companies or organizations that have provided your group with financial payment over the past two years AND who may have direct or indirect interest in the drug under review. Please note that this is required for each clinician who contributed to the input.
Declaration for Clinician 1
Name: Amin Kanani
Position: Head, Division of Allergy and Clinical Immunology St. Paul’s Hospital and the University of British Columbia
Date: March 2022
Table 5: COI Declarations for Canadian Hereditary Angioedema Network — Clinician 1
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
CSL Behring | — | X | — | — |
Takeda | — | X | — | — |
Biocryst | X | — | — | — |
KalVista | X | — | — | — |
Declaration for Clinician 2
Name: Stephen Betschel
Position: Clinical Immunologist and Allergist, Unity Health — St. Michael's Hospital.
Date: 14-03-2022
Table 6: COI Declarations for Canadian Hereditary Angioedema Network — Clinician 2
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
CSL Behring | — | X | — | — |
Takeda | — | — | X | — |
Declaration for Clinician 3
Name: Dr. Chrystyna Kalicinsky
Position: Physician – adult Clinical Immunology and Allergy
Date: 15 / 03 / 2022
Table 7: COI Declarations for Canadian Hereditary Angioedema Network — Clinician 3
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
CSL Behring | X | — | — | — |
Takeda | X | — | — | — |
Declaration for Clinician 4
Name: Dr. William Yang
Position: Clinical Assistant Professor — Faculty of Medicine, University of Ottawa; Chair, Red Maple Trials Inc.
Date: 14-03-2022
Table 8: COI Declarations for Canadian Hereditary Angioedema Network — Clinician 4
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
CSL Behring | — | — | — | X |
Takeda/Shire | — | — | — | X |
Biocryst | — | — | — | X |
Pharming | — | — | — | X |
Pharvaris | — | — | X | — |
Dermira | X | — | — | — |
Ionis | — | — | X | — |
Declaration for Clinician 5
Name: Dr. Gina Lacuesta
Position: Physician, Assistant Professor, Faculty of Medicine, Department of Medicine, Dalhousie University
Date: March 9, 2022
Table 9: COI Declarations for Canadian Hereditary Angioedema Network — Clinician 5
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
CSL Behring | X | — | — | — |
Takeda | X | — | — | — |
Declaration for Clinician 6
Name: Hugo Chapdelaine
Position: Clinical Immunologist, Montreal Clinical research Institute
Date: 14-03-2022
Table 10: COI Declarations for Canadian Hereditary Angioedema Network — Clinician 6
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
Takeda | X | — | — | — |
CSL-Behring | X | — | — | — |
Pharvaris | X | — | — | — |
Declaration for Clinician 7
Name: Dr Susan Waserman
Position: Allergist/Clinical Immunologist McMaster University
Date: March 9, 2022
Table 11: COI Declarations for Canadian Hereditary Angioedema Network — Clinician 7
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
Takeda | — | X | — | — |
CSL-Behring | X | — | — | — |
BOD CHAEN | X | — | — | — |
Declaration for Clinician 8
Name: Paul Kevin Keith
Position: Professor of Medicine, McMaster University
Date: March 17, 2022
Table 12: COI Declarations for Canadian Hereditary Angioedema Network — Clinician 8
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
ALK | X | — | — | — |
Astra Zeneca | X | — | — | — |
Bausch | X | — | — | — |
CSL Behring | X | — | — | — |
GSK | X | — | — | — |
Medexus | X | — | — | — |
Novartis | X | — | — | — |
Sanofi | X | — | — | — |
Takeda | X | — | — | — |
Valeo | X | — | — | — |
Declaration for Clinician 9
Name: R. Borici-Mazi
Position: Allergy Immunology
Date: March 17, 2022
Table 13: COI Declarations for Canadian Hereditary Angioedema Network — Clinician 9
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
CSL Behring | X | — | — | — |
Takeda | X | — | — | — |
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up-to-date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
Redactions: Confidential information in this document may be redacted at the request of the sponsor in accordance with the CADTH Drug Reimbursement Review Confidentiality Guidelines
Stakeholder Input: The views expressed in each submission are those of the submitting organization or individual; not necessarily the views of CADTH or of other organizations. As such, they are independent of CADTH and do not necessarily represent or reflect the view of CADTH. No endorsement by CADTH is intended or should be inferred. By filing with CADTH, the submitting organization or individual agrees to the full disclosure of the information. CADTH does not edit the content of the submissions.
CADTH does use reasonable care to prevent disclosure of personal information in posted material; however, it is ultimately the submitter’s responsibility to ensure no identifying personal information or personal health information is included in the submission. The name of the submitting organization or individual and all conflict of interest information are included in the submission; however, the name of the author, including the name of an individual patient or caregiver submitting the patient input, are not posted.
Accessibility: CADTH is committed to treating people with disabilities in a way that respects their dignity and independence, supports them in accessing material in a timely manner, and provides a robust feedback process to support continuous improvement. All materials prepared by CADTH are available in an accessible format. Where materials provided to CADTH by a submitting organization or individual are not available in an accessible format, CADTH will provide a summary document upon request. More details on CADTH’s accessibility policies can be found here.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.