CADTH Reimbursement Review
Maribavir (Livtencity)
Sponsor: Takeda Canada Inc.
Therapeutic area: Post-transplant cytomegalovirus infection
This multi-part report includes:
Clinical Review
Pharmacoeconomic Review
Stakeholder Input
Clinical Review
Abbreviations
ANC
absolute neutrophil count
AE
adverse event
CLF
Canadian Liver Foundation
CTTC
Cell Therapy Transplant Canada
CNS
central nervous system
CSR
clinical study report
CEM
cost-effectiveness model
CI
confidence interval
CMH
Cochran-Mantel-Haenszel
CMV
cytomegalovirus
DMC
Data Monitoring Committee
dGTP
deoxyguanosine triphosphate
EAC
Endpoint Adjudication Committee
eCRF
electronic case report form
eGFR
estimated glomerular filtration rate
EMA
European Medicines Agency
FAS
full analysis set
GI
gastrointestinal
GVHD
graft-versus-host disease
HRQoL
health-related quality of life
HUJ
health utility index
HSUV
health state utility value
HSCT
hematopoietic stem-cell transplant
HSV
herpes simplex virus
HLA
human leukocyte antigen
IRR
incidence rate ratio
ITC
indirect treatment comparison
IPD
individual patient data
ITT
intention to treat
IRT
interactive response technology
IAT
investigator-assigned anti-CMV treatment
IgG
immunoglobulin G
KF
Kidney Foundation of Canada
LLOQ
lower limit of quantitation
LOS
length of stay
mTOR
mammalian target of rapamycin
MRS
maribavir-resistance set
MCID
minimal clinically important difference
MID
minimally important difference
NE
not estimable
NOC
Notice of Compliance
NAT
nucleic acid test
PCR
polymerase chain reaction
PP
per protocol
PBL
peripheral blood leukocyte
PRS
primary resistance set
qPCR
quantitative PCR
RCT
randomized controlled trial
RASs
resistance-associated amino acid substitution
RMST
restricted mean survival time
RNA
ribonucleic acid
SF-36
Short Form 36
SAE
serious adverse event
SOT
solid organ transplant
SE
standard error
SD
standard deviation
TUDD
time until definitive deterioration
TBD
to be determined
TEAE
treatment-emergent adverse event
ULN
upper limit of normal
VAS
visual analogue scale
WBC
white blood cell
WDAE
withdrawal due to adverse event
Executive Summary
An overview of the submission details for the drug under review is provided in Table 1.
Item | Description |
|---|---|
Drug product | Maribavir (Livtencity) 400 mg (2 tablets of 200 mg) twice daily resulting in a daily dose of 800 mg |
Indication | Treatment of adults with post-transplant cytomegalovirus (CMV) infection or disease who are refractory (with or without genotypic resistance) to one or more prior antiviral therapies |
Reimbursement request | As per Health Canada indication |
Health Canada approval status | NOC |
Health Canada review pathway | Priority Review |
NOC date | September 15, 2022 |
Sponsor | Takeda Canada Inc. |
CMV = cytomegalovirus; NOC = Notice of Compliance; TBD = to be determined.
Introduction
Cytomegalovirus (CMV) infection may occur in post-transplant patients for a variety of factors — including due to the immunosuppression required for transplantation procedures and when transplant donors’ or recipients’ serostatus is positive depending on the type of transplant (HSCT/SOT). CMV infection may be asymptomatic and only detectable by viral replication; however, when symptoms are present (i.e., in the case of CMV infection manifesting into CMV disease or CMV syndrome) patients may experience fever, low white blood cell counts (leukopenia), muscle weakness, fatigue, shortness of breath, blurry vision or loss of vision and abdominal pain, blood in stools, nausea, vomiting or diarrhea.1 The possible complications of CMV in transplant patients include transplant failure, liver and digestive disease (i.e., hepatitis or colitis) and infections in different organs (i.e., pneumonia, pancreatitis, meningitis, myocarditis) or the blood (i.e., bacteremia).1 Although national data for CMV infections in solid organ transplant (SOT) and hematopoietic stem-cell transplant (HSCT) patients in Canada is limited, adult CMV seroprevalence of organ donors in Canada is estimated to be approximately 53%.2
Current approaches for the management of post-transplant CMV infection can be categorized into 3 groups: primary prophylaxis (involves the administration of antiviral drugs to prevent primary infection in patients at increased risk), secondary prophylaxis or maintenance (involves the administration of prophylactic doses of antiviral drugs to prevent CMV infection following primary infection), and pre-emptive therapy involves initiation of antiviral therapy based on serial screening with a sensitive polymerase chain reaction (PCR) assay in attempt to detect early infection mitigating the occurrence of CMV disease.3 Managing post-transplant CMV infection either through prophylaxis or for treatment rely on therapies such as foscarnet, valganciclovir, ganciclovir, letermovir, and cidofovir. However, treatment with these therapies is prone to resistance, toxicity, and hospitalization.
Patients who are refractory or resistant to 1 or more lines of antivirals have limited treatment options that typically require hospitalization for administration. The toxic side effects of some existing therapies also present challenges. For example, foscarnet has considerable nephrotoxicity and can interfere with the ability to deliver other important drugs, such as immune suppressors. Similarly, ganciclovir and/or valganciclovir may result in cytopenia that predisposes patients to graft failure and infection and also interferes with ability to deliver other important drugs. When patients are resistant to ganciclovir, foscarnet may be an option; however, when patients are resistant to both ganciclovir and foscarnet, clinical experts described subsequent therapies as limited.
Maribavir (Livtencity) is an oral tablet with a Health Canada indication for treatment of adults with post-transplant CMV infection or disease who are refractory (with or without genotypic resistance) to 1 or more prior antiviral therapies. The recommended dose is 400 mg (2 tablets of 200 mg) twice daily, resulting in a daily dose of 800 mg. Maribavir received Notice of Compliance (NOC) on September 15, 2022.
The objective of this review is to perform a systematic review of the beneficial and harmful effects of maribavir for the treatment of adults with post-transplant CMV infection or disease who are refractory (with or without genotypic resistance) to 1 or more prior antiviral therapies.
Stakeholder Perspectives
The information in this section is a summary of input provided by the patient groups who responded to CADTH’s call for patient input and from clinical expert(s) consulted by CADTH for the purpose of this review.
Patient Input
A total of 9 patient advocacy groups provided input on maribavir for the treatment of adults with post-transplant CMV infection or disease who are refractory and/or resistant to 1 or more prior antiviral therapies. The groups conducted a total of 3 surveys to capture input. The patients were predominantly those with myeloma and/or auto HSCT, noted by clinical experts to be a group for which CMV infection is not a concern, rather than patients who are allogenic-HSCT recipients at risk for CMV infection. Patients reported on the negative impact of staying in the hospital and away from home for weeks to months for treatment. CMV infection also affected patients’ ability to work and perform in school, mental health (i.e., stress and anxiety), ability to care for and spend time with families and friends, sexual life (i.e., intimacy concerns due to spreading CMV to their partners), and finances. Patients value effective medications with fewer side effects (i.e., taste disturbance, nausea, or vomiting, feeling weak or tired, urinary changes), no contraindications and interactions with immunosuppressants, that are simple to administer and covered by the drug plans. Patients also value an improvement to their quality of life, relieving CMV infection, eliminating overnight stays at a hospital, and reducing the severity of side effects (most commonly anxiety, weight loss, pain in the back, joints, or muscles, and diarrhea) caused by currently available treatments.
Clinician Input
Input From Clinical Experts Consulted by CADTH
The clinical experts identified that based on the limitations of existing therapies, the goals of anti-CMV treatment are to control the virus and its symptoms until a patient’s immune system is strong enough to fight the virus rather than eradicating it. As such, the goals of existing treatments are to improve symptoms (if the patient has end-organ disease), reduce mortality, improve graft function and/or reduce graft loss, minimize adverse effects, and improve quality of life.
The clinical experts indicated that challenges with existing treatments include high rates of hospitalizations for treatment administration and toxic side effects. The clinical experts also described concerns around patients becoming resistant to current treatment options, though they likely expect patients using maribavir to develop resistance as well. Clinical experts stressed the importance of treating patients with the least toxic and most effective drug early, citing that some of the outcomes from delayed treatment are irreversible (e.g., if graft loss due to ganciclovir or valganciclovir causing myelosuppression that cannot be reversed).
According to the clinical experts, resistance and refractory definitions are important to identify patients most suitable for treatment with maribavir. Patients most likely to respond to maribavir include those who have intolerances or life-threatening side effects to other drugs, those who can have their immunosuppression reduced and/or those that can have their immune function improve.
In routine clinical practice, the clinical experts indicated that anti-CMV treatment is given until CMV is either negative or low level; however, the definition of low level is unclear and treatment duration must be individualized based on multiple patient characteristics, for example, graft-versus-host disease (GVHD) or toxicity.
Per the clinical experts, complete response to maribavir would be defined as resolution of symptoms of end-organ disease and eradication of CMV viremia.
Clinician Group Input
The input provided by clinician groups generally aligned with the input provided by the clinical experts consulted by CADTH. Cell Therapy Transplant Canada (CTTC) submitted input. Pertaining to the patient population, the clinician group added that patients post-transplant often struggle with a lack of appetite and/or poor oral intake, therefore, the patients with difficulties of eating might be less suitable for maribavir, which is associated with dysgeusia but emphasized that toxicity profile of conventional salvage therapies is much more concerning. Furthermore, the clinician group emphasized that it is particularly challenging to treat CMV infection in patients with GVHD since GVHD therapies are immunosuppressive (i.e., increase the risk of CMV infection), myelosuppressive, and nephrotoxic (i.e., exacerbate the toxicities caused by valganciclovir or foscarnet, respectively).
Drug Program Input
Input was obtained from the drug programs that participate in the CADTH reimbursement review process. The following were identified as key factors that could potentially impact the implementation of a CADTH recommendation for maribavir:
considerations for initiation of therapy
considerations for discontinuation of therapy
considerations for prescribing of therapy
care provision issues
system and economic issues.
The clinical experts consulted by CADTH provided advice on the potential implementation issues raised by the drug programs.
Clinical Evidence
Pivotal Studies and Protocol Selected Studies
Description of Studies
One open-label randomized (2:1), double-arm phase III trial (SOLSTICE, N = 352) was included in the CADTH systematic review. The primary objective of the SOLSTICE study was to compare the efficacy and safety of maribavir versus IAT for treatment of refractory CMV infection (with or without resistance) in SOT and HSCT recipients. The trial included adult patients with documented CMV infection that is refractory to the most recent treatment or resistant to it (only if patients also met refractory criteria). Patients received 400 mg oral maribavir twice daily or another IAT (foscarnet, ganciclovir, valganciclovir, or cidofovir) for up to 8 weeks. The primary end point was confirmed CMV viremia clearance at the end of week 8 (regardless of premature treatment discontinuation). The key secondary end point was a composite of confirmed CMV viremia clearance and symptom control at the end of week 8, maintained through week 16 (8 weeks beyond the treatment phase) after receiving exclusively study-assigned treatment. Other secondary end points included recurrence, all-cause mortality, resistance to maribavir or IAT, health care resource utilization, and health-related quality of life (HRQoL). Harms outcomes were also examined. In the SOLSTICE study, both treatment groups were generally balanced but notable differences were observed in characteristics such as age, type of preparative conditioning regimen, presence of CMV RASs, and CMV serostatus for HSCT Donor/Recipient, CMV DNA level, and net immunosuppression use changed before initiation of study treatment.
The mean age of enrolled patients was 53.0 years (SD: 13.22 years). Most patients were White (75.6%) and male (60.5%). Most patients underwent a SOT (59.9%), with the kidney (50.2% of SOT patients), lung (29.4% of SOT patients), and heart (10.9% of SOT patients) being the most transplanted solid organs. Patients who underwent HSCT predominantly underwent allogenic transplant procedures (99.3%). Most patients who underwent SOT and HSCT had functioning graft status (89.1% and 85.1%, respectively). Most patients did not have confirmed acute or chronic GVHD, 91.2% and 96.9%, respectively, and did not use antilymphocyte treatment (57.7%). Majority of patients had some renal impairment (32.1% with mild and 23.3% with moderate), but no hepatic impairment (92.3%).
Efficacy Results
Results for the key efficacy outcomes in the SOLSTICE study are summarized in Table 2.
CMV Viremia Clearance
The primary end point was confirmed CMV viremia clearance at the end of week 8 (regardless of premature treatment discontinuation) as measured by CMV DNA levels. The adjusted difference in proportion of responders between maribavir and IAT was 32.8% (95% CI, 22.80% to 42.74%; P < 0.001), in favour of maribavir.
The key secondary end point was a composite of confirmed CMV viremia clearance and symptom control at the end of week 8, maintained through week 16. The adjusted difference in proportion of responders between maribavir and IAT is 9.5% (95% CI, 2.02% to 16.88%; P = 0.013), in favour of maribavir.
Time to CMV Viremia Clearance
The median observed time to CMV viremia clearance was 17.0 days (minimum: 5.0 days, maximum: 114.0 days) in the maribavir group and 20.0 days (minimum: 6.0 days, maximum: 111.0 days) in the IAT group. The Kaplan–Meier estimate for median days to CMV viremia clearance was 22.0 days (95% CI, 21.0 to 23.0 days) for the maribavir group and 29.0 days (95% CI, 22.0 days to 35.0 days) for the IAT group.
Recurrence
Of patients who responded to treatment, 33 (17.9%) in the maribavir group and 8 (12.3%) in the IAT group had CMV viremia recurrence during the first 8 weeks of the study. Comparative recurrence data cannot be interpreted because clearance is a prerequisite for recurrence.
All-Cause Mortality
The number of patients who died in the maribavir group was 27 (11.5%) and 13 (11.1%) in the IAT group. The median observed event time for those that died was 55.0 days (minimum: 3.0 days, maximum:182.0 days) in the maribavir group and 73.0 days (minimum: 13.0 days, maximum: 186.0 days) in the IAT group. The hazard ratio was 1.14 (95% CI, 0.549 to 2.357). Conclusions for all-cause mortality could not be drawn because the 95% confidence interval around the hazard ratio was wide, including the possibility of both appreciable benefit and harm for maribavir compared with IAT.
Resistance to Maribavir
In the maribavir group, 42 (19.6%) patients had new maribavir treatment-emergent known resistance-associated amino acid substitution (RASs) in pUL97 or pUL27. Of the patients in the maribavir group, 12.9% had new treatment-emergent RASs known to confer resistance to IAT detected in their genotype and 4.9% of patients in the IAT group had new treatment-emergent RASs known to confer resistance to IAT detected in their genotype.
Health Care Resource Utilization
The adjusted difference in rates ratio of hospital admissions between the maribavir and IAT groups during the on-treatment phase was 0.65 (95% CI, 0.45 to 0.94), favouring maribavir. The adjusted difference IRR of length of stay between the maribavir and IAT groups during the on-treatment phase was 0.46 (95% CI, 0.23 to 0.92), favouring maribavir.
HRQoL
Although HRQoL data were collected, it was only reported descriptively. Generally, patients reported an improvement in the HRQoL scores (i.e., EQ-5D utility score, SF-36) over time and across both treatment groups. No definitive conclusions can be made between the treatment groups due to a lack of statistical testing and missing data.
Harms Results
Overall, 228 (97.4%) patients in the maribavir group and 106 (91.4%) patients in the IAT group experienced at least 1 treatment-emergent adverse event (AE). Ninety (38.5%) patients in the maribavir group and 43 (37.1%) in the IAT group experienced at least 1 severe AE (SAE). Thirty-one (13.2%) patients in the maribavir group and 37 (31.9%) in the IAT group permanently discontinued treatment with study drugs due to AEs.
Table 2: Summary of Key Results from SOLSTICE
Detail | Maribavir N = 235 | IAT N = 117 |
|---|---|---|
CMV viremia clearance at week 8 (primary end point, randomized set) | ||
Overall responders, n (%) | 131 (55.7) | 28 (23.9) |
Adjusted difference in proportion of responders, % (95% CI) | 32.8 (22.80 to 42.74) | Reference |
Adjusted P value | < 0.001 | Reference |
CMV viremia clearance and symptom control at week 8 and maintenance through week 16 (key secondary end point, randomized set) | ||
Overall responders, n (%) | 44 (18.7) | 12 (10.3) |
Adjusted difference in proportion of responders, % (95% CI) | 9.5 (2.02 to 16.88) | Reference |
Adjusted P value | 0.013 | Reference |
Time to first CMV Viremia clearance at any time on study (randomized set) | ||
Number of patients with first CMV viremia clearance at any time on study, n (%) | 184 (78.3) | 65 (55.6) |
Number of patients censored, n (%) | 51 (21.7) | 52 (44.4) |
Observed event time for those who had CMV viremia clearance, median days (minimum, maximum) | 17.0 (5.0, 114.0) | 20.0 (6.0, 111.0) |
Kaplan–Meier estimates of time to first CMV viremia clearance, days (95% CI) | ||
|||||||||||||||||||||||||||||| | |||||||||||| | |||||||||||| |
50th (median) | 22.0 (21.0 to 23.0) | 29.0 (22.0 to 35.0) |
|||||||||||||||||||||||||||||| | |||||||||||| | |||||||||||| |
P valueb | 0.030 | Reference |
All-cause mortality | ||
Number of patients who died, n (%) | 27 (11.5) | 13 (11.1) |
|||||||||||||||||||||||||||||| | |||||||||||| | |||||||||||| |
Observed event time for those who died, median days (min, max) | 55.0 (3.0 to 182.0) | 73.0 (13.0 to 186.0) |
|||||||||||||||||||||||||||||| | ||
|||||||||||||||||||||||||||||| | |||||||||||| | |||||||||||| |
|||||||||||||||||||||||||||||| | |||||||||||| | |||||||||||| |
|||||||||||||||||||||||||||||| | |||||||||||| | |||||||||||| |
Hazard ratio (95% CI)b | ||
Treatment group: Maribavir vs. IAT | 1.14 (0.549, 2.357) | Reference |
Health care resource utilization | ||
Patients with ≥ 1 admission during on-treatment phase, n (%) | 75 (31.9) | 43 (36.8) |
Adjusted difference in rates of hospital admissions, incidence rate ratio (95% CI) | 0.65 (0.45, 0.94) | Reference |
LOS per patient during on-treatment phase, mean days (SD) | 3.1 (7.1) | 3.5 (7.6) |
Adjusted difference in LOS, incidence rate ratio (95% CI) | 0.46 (0.23, 0.92) | Reference |
Resistance to maribavir (maribavir-resistance set and primary resistance set) | ||
Patients in MRS and non-MRS | 214 | 100 |
Patients in MRS and non-MRS with post-baseline genotype, n (%) | 80 (37.4) | 38 (38.0) |
New maribavir RASs in pUL97 or pUL27, n (%) | 42 (19.6) | 0 |
Patients in PRS and non-PRS | 217 | 103 |
Patients in PRS and non-PRS with post-baseline genotype, n (%) | 80 (36.9) | 38 (36.9) |
New IAT RASs in pUL97 or pUL54a, n (%) | 28 (12.9) | 5 (4.9) |
Harms, n (%) (safety set) | ||
AEs (treatment-emergent) | 228 (97.4) | 106 (91.4) |
SAEs (treatment-emergent) | 90 (38.5) | 43 (37.1) |
WDAE (from study treatment) | 31 (13.2) | 37 (31.9) |
Deaths | 26 (11) | 12 (10) |
Notable harms, n (%) (Safety Set) | ||
Graft rejection (acute, chronic) or graft failure | 8 (3.4) | 3 (2.6) |
GVHD | 21 (9.0) | 5 (4.3) |
Immunosuppressant drug concentration level increased | 21 (9.0) | 1 (0.9) |
Invasive fungal or bacterial or viral infections | 55 (23.5) | 22 (19.0) |
Nausea | 50 (21.4) | 25 (21.6) |
Vomiting | 33 (14.1) | 19 (16.4) |
Diarrhea | 44 (18.8) | 24 (20.7) |
Neutropenia | 22 (9.4) | 26 (22.4) |
Taste disturbance (dysgeusia) | 87 (37.2) | 4 (3.4) |
Tissue-invasive CMV disease/syndrome | 8 (3.4) | 4 (3.4) |
AE = adverse event; CMV = cytomegalovirus; CI = confidence interval; GVHD = graft-vs.-host disease; IAT = investigator-assigned anti-CMV treatment; LOS = length of stay; MRS = maribavir-resistance set; NE = not estimable; PRS = primary resistance set; RASs = resistance-associated amino acid substitution; SAE = severe adverse event; SD = standard deviation; WDAE = withdrawal due to adverse event.
aSpecify model, covariates, analysis population and time point for each outcome. Includes maribavir RASs with cross-resistance to IAT.
bP value has not been adjusted for multiple testing.
SOLSTICE Clinical Study Report4
Critical Appraisal
There are limited concerns for internal validity. SOLSTICE was an open-label study. Stratified randomization was conducted using interactive response technology (IRT), suggesting allocation concealment. For the primary end point and multiple secondary end points, a central lab and an End point Adjudication Committee (EAC) was appropriately used to reduce the risk of detection bias. The study population in SOLSTICE study was adequately defined and the clinical experts consulted by CADTH indicated the eligibility criteria were overall appropriate. Both treatment groups were relatively balanced, with some notable differences in characteristics such as age, type of preparative conditioning regimen, presence of CMV RASs, and CMV serostatus for HSCT Donor/Recipient, CMV DNA level, and net immunosuppression use changed before initiation of study treatment. The analysis populations used in the SOLSTICE trial were appropriate for measuring the effect of the assignment to the interventions and all analyses were pre-specified. The comparators used were identified by the clinical experts as appropriate. Statistical testing was performed for the primary and key secondary outcome. However, the open-label design can increase the risk of performance and detection bias, particularly for outcomes that are subjective in measurement and interpretation (e.g., CMV symptom controls, subjective AEs). There were some outcomes in the study for which results may be biased due missing outcome data, notably, HRQoL.
There are some implications of the trial on external validity. One stark difference between how the treatment was administered in SOLSTICE and what would be expected in routine clinical practice was the 8-week fixed duration. As identified by the clinical experts consulted by CADTH for this review, clinicians treat patients until CMV DNA levels are low enough or negative, not for a fixed duration. The clinical experts indicated that the baseline characteristics of patients enrolled in SOLSTICE were generally representative of the post-transplant CMV patient population in Canada, although they noted that the SOLSTICE study patients would represent the most fit patients in this population, which is common in clinical trials. Furthermore, the clinical experts noted that although the comparators (i.e., IAT) used are reflective of routine clinical practice, the distribution of each IAT in SOLSTICE is not reflective of Canadian clinical practice. It may be difficult to design a trial with IAT distributions that reflect the diversity of Canadian clinical practice. As a result, generalizability of results to the Canadian setting is uncertain. Moreover, conclusions on comparative efficacy for each antiviral cannot be drawn.
Indirect Comparisons
No indirect treatment comparisons were appraised for this review.
Other Relevant Evidence
The sponsor provided a series of additional exploratory analyses of individual patient data (IPD) from SOLSTICE. The results of the IPD analyses were used as direct inputs into the base case and scenarios of the cost-effectiveness model. Details are presented in Appendix 5.
Conclusions
One open-label, randomized, double-arm phase III trial (SOLSTICE, N = 352) was included in the CADTH systematic review. The primary objective of the SOLSTICE study was to compare the efficacy and safety of maribavir versus IAT for treatment of refractory CMV infection (with or without resistance) in SOT and HSCT recipients. There is evidence of maribavir being more efficacious when compared to the IAT on achieving CMV viremia clearance and symptom control. However, disease control with maribavir is time-limited, in line with other antivirals. Conclusions for all-cause mortality could not be drawn because the 95% confidence interval around the hazard ratio was wide, including the possibility of both appreciable benefit and harm for maribavir compared with IAT. The proportion of patients experiencing taste disturbance, increased immunosuppressant concentration levels, and infections and infestations was higher with maribavir, but these events were manageable. The lower rates of hematologic and renal toxicities with maribavir fill a gap in the treatment landscape whereby other drugs have known toxicities limiting their use. Fewer patients in the maribavir group discontinued treatment due to AEs. There remains uncertainty on interpreting data for outcomes related to CMV recurrence, antiviral resistance, HRQoL, health care resource utilization, and subgroup analyses given the various methodological limitations.
Introduction
Disease Background
Transplantation is used as a therapy across many conditions, often with curative intent. SOT procedures using donor-provided solid organs such as hearts, kidneys, and lungs involves specialized surgery to treat end-organ dysfunction. HSCT procedures using donor-provided (allogeneic) hematopoietic stem cells involves IV infusion of stem cells to re-establish hematopoietic function and can be a potentially curative therapy for malignancies, severe aplastic anemia, and rare inborn errors of metabolism or primary immunodeficiencies.5-11
Patients having undergone any type of transplantation are at risk of developing life-threatening infections. Despite good donor-to-recipient matching, HSCT patients typically still require immunosuppressive medications to mitigate GVHD and reduce the risk of transplant rejection.6,12 The immunosuppression associated with transplantation also commonly allows micro-organisms to cause infection more easily, even those with limited pathogenicity.6,12 Important viruses to consider in transplant recipients include CMV which is a beta-herpes virus that remains dormant in the human body after primary infection for life. Although benign in patients with adequate immune function (patients remain asymptomatic despite CMV infection), patients with already compromised immune systems, immune suppression in preparation for transplantation, and post-transplant maintenance immunosuppression, are at significantly increased risk of CMV infection, which can manifest into clinical complications, including CMV disease.13,14
CMV infection may be asymptomatic and characterized by viral replication; however, CMV disease is likely to be symptomatic.1 CMV disease is characterized by symptoms such as fever, malaise, leukopenia, thrombocytopenia, and elevated liver enzymes.1 The possible complications of CMV in transplant patients include transplant failure, liver, and digestive disease (i.e., hepatitis or colitis) and infections in different organs (i.e., pneumonia, pancreatitis, meningitis, myocarditis) or the blood (i.e., bacteremia).1
Generally, risk factors for CMV infection after transplantation include CMV seropositivity of the transplant (i.e., seropositive donor and/or recipient), immune status and degree of immunosuppression, transplant type and organ type, advanced age, HLA-mismatch, acute rejection, and GVHD.1 However, the most important risk factor post-HSCT is CMV seropositivity of the transplant recipient.15-18 In post-SOT patients, the clinical experts consulted by CADTH indicated that the most important risk factor is mismatch CMV serostatus between the donor and recipient, precisely Donor+/Recipient-. Due to the impaired cellular immunity as a result of the induction and conditioning regimen, viral reactivation is the dominant mechanism of infection in HSCT patients. Furthermore, patients with a history of CMV disease (e.g., pneumonitis, gastrointestinal disease, and retinitis) 6 months before HSCT, which is reported to be rare by the clinical experts consulted by CADTH, are at a very high risk for infection and death.17,19
Definitions of common CMV infection and disease terms can be found in Table 3.
Table 3: Definitions of CMV Infection and Disease in Transplant Patients
Term | Definition |
|---|---|
CMV infection | Isolation or detection of CMV viral protein or nucleic acid in body fluid or tissue. |
Primary CMV infection | First detection of CMV infection in a patient with no evidence of prior CMV exposure. Severely immunocompromised patients might not develop CMV-specific antibodies. |
Recurrent CMV infection | New CMV infection with previous evidence of CMV infection. Patient typically has not had virus detected for an interval of at least 4 weeks during active surveillance. Recurrent infection may result from reactivation (endogenous) or re-infection (exogenous). CMV-specific antibodies can be passively transferred by blood products or immune globulin administration. |
CMV re-infection | Detection of a new CMV strain that is distinct from the strain that caused initial infection. |
CMV reactivation | The 2 viral strains (prior and current strain) are indistinguishable either by sequencing specific regions of the viral genome or by using a variety of molecular techniques. |
Viremia | Isolation of CMV in the blood or blood fraction through standard or rapid culture techniques. |
DNAemia (or RNAemia) | Detection of CMV DNA (or RNA) in plasma, serum, whole blood, or isolated PBLs, or in buffy-coat specimen samples. RNAemia is not commonly used to monitor transplant patients. |
CMV Syndrome | Only used in SOT recipients, probable CMV syndrome requires detection of CMV in blood, rapid culture, antigenemia, or NAT together with at least 2 of the following: 1. Fever ≥ 38°C for at least 2 days. 2. New or increased malaise (toxicity grade 2) or new or increased fatigue (toxicity grade 3)20 3. Leukopenia or neutropenia on 2 separate measurements at least 24 hours apart, defined as a WBC count of < 3,500 cells/µL, if the WBC count before the development of clinical symptoms was ≥ 4,000 cells/µL, or a WBC decrease of > 20%, if the WBC count before the development of clinical symptoms was < 4,000 cells/µL. The corresponding neutrophil counts are < 1,500 cells/µL or a decrease of > 20% if the neutrophil count before the onset of symptoms was < 1,500 cells/µL. 4. Atypical lymphocytes ≥ 5% 5. Thrombocytopenia (i.e., platelet count of < 100,000 cells/µL if the platelet count before the development of clinical symptoms was ≥ 115,000 cells/µL or a decrease of > 20% if the platelet count before the development of clinical symptoms was < 115,000 cells/µL) 6. Elevated hepatic aminotransferases (alanine aminotransferase or aspartate aminotransferase) to 2 times the upper limit of normal (applicable to non–liver transplant recipients). |
CMV = cytomegalovirus; dGTP = deoxyguanosine triphosphate; HSCT = hematopoietic stem-cell transplant; NAT = nucleic acid test; PBL = peripheral blood leukocyte; RNA = ribonucleic acid; WBC = white blood cell.
Source: Ljungman et al., 201721
Disease Prevalence and Incidence
The number of patients undergoing transplants in Canada has been rising over the past decades. The Canadian Institute for Health Information reported that the number of SOT procedures in Canada (excluding Quebec) increased from 1,036 in 2011 to 2,594 in 2020, where kidneys, livers, lungs, and hearts were the most transplanted organs (e.g., 1,459 kidneys were transplanted in 2020).22 Similarly, the Canadian Institute for Health Information reported that the number of autologous and allogeneic HSCT procedures in Canada increased steadily from 1,236 in 2010 to 1,605 in 2014.22,23 Globally, approximately 47% of HSCTs were allogeneic HSCTs.
National data for CMV infections in SOT and HSCT patients are limited. Adult CMV seroprevalence of organ donors in Canada is estimated to be approximately 53%.2 Per the sponsor’s submission, a sponsor-led systematic review of European and US studies found that CMV infection may occur in approximately 34% (ranging from 16% to 73%), and CMV disease occurs in approximately 8% (ranging from 3% to 16%), of SOT recipients.24 The Center for International Blood and Marrow Transplant Research reported that among the 9,469 allogeneic HSCTs performed between 2003 and 2010 (including sites in Canada), approximately 62% were performed in CMV-seropositive recipients (i.e., considered at high risk for CMV infection).15,18,23,25-27 Per the sponsor-led systematic review, CMV infection occurs in approximately 48% (ranging from 17% to 82%), and CMV disease occurs in about 7% (ranging from 2% to 18%), of HSCT patients.
Despite the limited data on refractory and resistant CMV infections in the Canadian context, the sponsor-submitted systematic review found that between 19% and 21% of SOT and 9% and 47% of HSCT patients experienced refractory CMV infection in Europe and the US.24 The majority of studies (4 studies) identified in the sponsor’s systematic review reported resistant CMV infection in 1% to 8% of SOT recipients, with 1 study from the Netherlands reporting that as many as 37% of SOT recipients had mutations conferring CMV resistance.24 In HSCT patients, 2% to 3% had resistant infection.24 Furthermore, a single-centre analysis of 735 lung transplant patients in Canada reported the incidence of drug-resistant CMV to be 1.98% in Donor+ and/or Recipient+ CMV patients and 4.7% in Donor+/Recipient- patients.28
Standards of Therapy
Current approaches for the management of CMV infection can be categorized into 3 groups: primary prophylaxis (involves the administration of antiviral drugs to prevent primary infection in patients at increased risk), secondary prophylaxis or maintenance (involves the administration of prophylactic doses of antiviral drugs to prevent CMV infection following primary infection) and pre-emptive therapy (involves initiation of antiviral therapy based on serial screening with a sensitive PCR assay in attempt to detect early infection and prevent the occurrence of CMV disease).3 According to the clinical experts consulted by CADTH, existing therapies do not eradicate CMV and therefore, the treatment goals are to improve symptoms (if end-organ CMV disease), reduce mortality, improve graft function and/or reduce graft loss, minimize adverse effects, and improve patients’ quality of life.
The most widely used antivirals for first-line pre-emptive therapy are IV ganciclovir, valganciclovir (oral prodrug of ganciclovir), and foscarnet. For post-HSCT patients, either IV ganciclovir or foscarnet may be used in the first-line setting.29 Generally, monitoring for CMV infection in a pre-emptive therapy setting using PCR should be performed weekly in CMV-seropositive recipients of an HSCT, until at least 100 days post-transplant.9 In post-SOT patients, valganciclovir or IV ganciclovir would be used for pre-emptive therapy. Oral valganciclovir is also used as a first-line therapy in non–severe CMV disease.30 Testing is often performed once a week, where 2 consecutive negative samples (1 week apart) would indicate clearance.31
In patients at higher risk of CMV infection (e.g., recipients of a transplant from CMV-seropositive donors who received T-cell-depleted allografts, HLA-mismatched allograft, an umbilical cord blood graft or those who are significantly immunosuppressed), PCR monitoring can be performed twice weekly to ensure timely treatment.32
Before approval of maribavir, no treatments were approved by Health Canada for patients with refractory or resistant CMV. Patients who are refractory to valganciclovir can be treated with high-dose IV ganciclovir and/or foscarnet; however, foscarnet is associated with considerable nephrotoxicity.32 If patients who are non–responsive to valganciclovir demonstrate life-threatening CMV disease, the clinical experts suggest that the typical subsequent treatment would be foscarnet. In the instance that patients who are non–responsive to valganciclovir have non–life-threatening disease, subsequent treatment would be high-dose IV ganciclovir. In either scenario, clinical experts described often considering maribavir if the patient meets the Health Canada criteria for Special Access. Additionally, the experts identified CMV immunoglobulin (Cytogam) as also used in SOT patients as an adjunctive drug. IV immunoglobulin G (IVIgG) is also used for replacement therapy in HSCT patients who have both low IgG, and infection in general (not only CMV, but also other bacterial and fungal infections), and is administered monthly until the IgG recovers.
Given that all currently available antivirals are DNA polymerase inhibitors, resistance to ganciclovir and valganciclovir can occur from mutations in the UL97 subunit protein, while mutations in UL54 can confer multi-drug resistance affecting foscarnet and cidofovir.33,34 According to the clinical experts consulted by CADTH, treating post-SOT patients with treatment-resistant CMV infection on valganciclovir would consist of reducing immunosuppression if possible. The clinical experts maintain that when reducing immunosuppression is not possible, they may switch to immunosuppressive drugs with better antiviral effect, for example, mammalian target of rapamycin (mTOR) inhibitors. In post-HSCT patients, the clinical experts indicated that it is more difficult to reduce immunosuppression due to patients often having GVHD.
When patients have multi-drug resistance (e.g., ganciclovir and/or valganciclovir and foscarnet), the clinical experts described subsequent therapy options to be limited. If the patient has multi-drug resistance or resistance and life-threatening intolerances to alternative drugs (ganciclovir and foscarnet), maribavir was accessed through Health Canada’s Special Access Program before regulatory approval. However, if maribavir was not available, combination therapy with ganciclovir and foscarnet was used. Cidofovir, another antiviral is typically considered a third-line drug and is associated with both myelotoxicity and nephrotoxicity.32 The clinical experts further noted that cidofovir has ocular toxicity and does not work well in clinical practice. Both foscarnet and cidofovir are available in Canada. Clinical experts also indicated using leflunomide in these scenarios, although to limited success. As per the clinical experts consulted for this review, there are also a growing number of discussions about whether letermovir would be an option although access to this for treatment (i.e., off-label indication) is limited and there is uncertainty about the dosing and benefit due to only case series and case report-level data being available. Viral specific T-cells are in the experimental phase across Canada.
Drug
Maribavir (Livtencity) is an oral tablet with a Health Canada indication for the treatment of adults with post-transplant CMV infection or disease who are refractory (with or without genotypic resistance) to 1 or more prior antiviral therapies. The recommended dose is 400 mg (2 tablets of 200 mg) twice daily, resulting in a daily dose of 800 mg. The sponsor is seeking reimbursement in accordance with the Health Canada indication. Maribavir has not previously been reviewed by CADTH for any indication.
Maribavir was approved by the FDA in November 2021 and is under review at the EMA.35,36 The FDA indication is for the treatment of adults and pediatric patients 12 years of age and older and weighing at least 35 kg with post-transplant CMV infection or disease that is refractory to treatment (with or without genotypic resistance) with ganciclovir, valganciclovir, cidofovir, or foscarnet.37 Maribavir does not appear to be under review at the Australian Therapeutic Goods Administration.38
Maribavir’s mechanism of action is through the inhibition of the UL97 protein kinase and the phosphorylation of its natural substrates. The drug under review exerts its effect by attaching to the UL97 encoded kinase at the adenosine triphosphate binding site, abolishing phosphorylation needed in processes including DNA replication, encapsidation, and the egress of viral capsules from the nuclei of infected cells.39-42 Key characteristics of maribavir and relevant comparator antiviral therapies are described in Table 4.
Table 4: Key Characteristics of Maribavir, Foscarnet, Cidofovir, Ganciclovir, and Valganciclovir
Detail | Maribavir | Foscarnet | Cidofovir | Ganciclovir | Valganciclovir |
|---|---|---|---|---|---|
Mechanism of action | Competitively inhibiting the CMV pUL97 viral protein kinase. | Inhibiting CMV UL54-encoded DNA polymerases. | Inhibiting CMV DNA polymerases. | Competitively inhibiting dGTP incorporation into DNA by DNA polymerase and by incorporating into viral DNA subsequently causing termination or very limited viral DNA elongation. | |
Indicationa | For adults with post-transplant CMV infection/disease who are refractory (with or without genotypic resistance) to one or more prior antiviral therapies. | For CMV retinitis in patients with AIDS and acyclovir-resistant mucocutaneous herpes simplex virus infections in immunocompromised patients. Not indicated for condition under review. | For CMV retinitis in adult patients with AIDS Not indicated for condition under review. | For treatment of CMV retinitis in immunocompromised patients, including patients with AIDS, iatrogenic suppression secondary to organ transplantation or those administered chemotherapy for neoplasia and 2). For the prevention of CMV disease in transplant recipients at risk for CMV disease Not indicated for condition under review. | For adult patients for:
|
Route of administration | Oral | IV | IV | IV | Oral |
Recommended dose | 400 mg (2 tablets of 200 mg) twice daily resulting in a daily dose of 800 mg. | Induction regimen: 90 mg/kg (1 to 1/2 to 2-hour infusion) every 12 hours or 60 mg/kg (minimum 1 hour infusion) every 8 hours over 2 to 3 weeks depending on clinical response. Maintenance regimen: 90 mg/kg/day to 120 mg/kg/day given as an IV infusion over 2 hours. | Induction regimen: 5 mg/kg infusion at a constant rate over 1 hour, to be administered once weekly for 2 consecutive weeks. Maintenance regimen: 3 to 5 mg/kg infusion depending on renal function at a constant rate over 1 hour, to be administered once every 2 weeks. | Initial dose: 5 mg/kg every 12 hours for seven to 14 days, followed by either 5 mg/kg once per day if on a seven-day weekly regimen, or 6 mg/kg once per day if on a five-day weekly regimen given as a constant IV infusion over one hour. The duration of treatment depends on the duration and degree of immunosuppression, typically 100 to 120 days post-transplantation. | 900 mg once daily (with food) starting within 10 days of transplantation and continuing until 100 days post-transplantation. |
Serious side effects / safety issues | Warnings and precautions: Expected to poorly penetrate across the blood-brain barrier so it is not expected to be effective in treating CMV CNS infections (e.g., meningoencephalitis); risk of adverse reactions or reduced therapeutic effect due to medicinal product interactions (i.e., dose adjustments listed in product monograph); potential to increase the drug concentrations of immunosuppressant drugs that are cytochrome P450 3A and/or P-gp substrates with narrow therapeutic ranges (including tacrolimus, cyclosporine, sirolimus and everolimus). | Warnings and precautions: Renal toxicity, QT prolongation, electrolyte disturbances, and seizures. | Serious warnings and precautions: Renal impairment is a major toxicity. Contraindicated in patients receiving other nephrotoxic drugs. Neutropenia associated with cidofovir. Potential carcinogen and teratogen. Ocular toxicity (decreased ocular pressure and potential for decreased visual acuity). | Serious warnings and precautions: Leukopenia, neutropenia, anemia, thrombocytopenia, pancytopenia, bone marrow failure, and aplastic anemia. Potential teratogen and carcinogen. | |
AIDS = Acquired Immune Deficiency Syndrome; CMV = cytomegalovirus; CNS = central nervous system; dGTP = deoxyguanosine triphosphate; SOT = solid organ transplant.
aHealth Canada–approved indication.
Source: maribavir product monograph,24 foscarnet product monograph,43 cidofovir product monograph,44 ganciclovir product monograph,45 valganciclovir product monograph.46
Stakeholder Perspectives
Patient Group Input
This section was prepared by CADTH staff based on the input provided by patient groups.
A total of 9 patient advocacy groups provided input on maribavir for the treatment of adults with post-transplant CMV infection or disease who are refractory and/or resistant to 1 or more prior antiviral therapies. Groups included the Kidney Foundation of Canada (KF), the Canadian Liver Foundation (CLF), Leukemia and Lymphoma Society of Canada, Myeloma Canada, Aplastic Anemia and Myelodysplasia Association of Canada, Lymphoma Canada, Myeloproliferative Neoplasm Canadian Research Foundation, Canadian Myeloproliferative Neoplasm Network, Canadian Chronic Myelogenous Leukemia Network, and Chronic Lymphocytic Leukemia Canada. These organizations are involved in advocacy and empowerment activities such as education, funding research, dissemination of information, and increasing awareness of diseases to support patients, their families and caregivers.
The groups designed and administered a total of 3 surveys to capture input. The KF survey, which was a self-administered questionnaire and distributed through KF social media channels, website, and e-newsletter between February and March 2022, had 9 respondents (8 kidney transplant recipients, 1 donor; unspecified number of patients with post-transplant CMV) from across Canada. The CLF survey, an online survey which was promoted on the organization’s website and social media channels from February 22 to March 25, 2022, was completed by 2 health professionals from Ontario and Alberta. The 7 blood cancer organizations co-administered a survey with multiple choice, open-ended and rating questions, which was distributed through social media networks and e-mail between February 1 and March 14, 2022, in English and French. One hundred respondents (97 from Canada, 3 from the UK and Belgium) completed the survey. Out of 100 responders, 93 received a HSCT, and 13 had a post-transplant CMV.
Patients described the impact of CMV and its treatment on their quality of life. One patient with a kidney transplant reported that their CMV got better after 8-week IV antiviral therapy; however, experienced relapse 3 weeks after viremia clearance. Patients reported that they had to stay in hospital away from home for weeks to months for treatment, and CMV infection affected their ability to work and perform in school, their mental health (i.e., stress and anxiety), their ability to care for and spend time with families and friends, their sexual life (i.e., intimacy concerns due to spreading CMV to their partners), and their finances.
Patients described their expectations for new CMV treatments. Patients value effective medications with fewer side effects (i.e., taste disturbance, nausea, or vomiting, feeling weak or tired, urinary changes), no contraindications and interactions with immunosuppressants, that are simple to administer and covered by the drug plans. Patients with blood cancer value an improvement to their quality of life, relieving CMV infection, eliminating overnight stays at a hospital, and reducing the severity of side effects (most commonly anxiety, weight loss, back/joint/muscle pain, and diarrhea) caused by currently available treatments.
The patients were predominantly those with myeloma and/or autologous-HSCT, noted by clinical experts to be a group for which risk of CMV infection is much lower than recipients of allogenic-HSCT. One respondent had reported experience taking maribavir.
Clinician Input
Input From Clinical Experts Consulted by CADTH
All CADTH review teams include at least 1 clinical specialist with expertise regarding the diagnosis and management of the condition for which the drug is indicated. Clinical experts are a critical part of the review team and are involved in all phases of the review process (e.g., providing guidance on the development of the review protocol; assisting in the critical appraisal of clinical evidence; interpreting the clinical relevance of the results; and providing guidance on the potential place in therapy). The following input was provided by 2 clinical specialists with expertise in the diagnosis and management of post-transplant CMV infection and/or disease in adults.
Unmet Needs
Per the clinical experts, given the limitations of existing anti-CMV therapies, treatment goals are to control the virus and its symptoms until a patient’s immune system is strong enough to fight the virus itself, rather than eradicating it. As such, the goals of existing treatments are to improve symptoms (if the patient has end-organ disease), reduce mortality, improve graft function and/or reduce graft loss, minimize adverse effects, and improve quality of life.
Challenges with existing treatments may include high rates of hospitalizations for treatment administration and toxic side effects. The clinical experts described that the current treatment options require hospitalization for IV therapy, which are inconvenient, expensive, and toxic (e.g., mucosal toxicity from foscarnet, renal toxicity from foscarnet and cidofovir, myelosuppression from high-dose ganciclovir). Drug toxicity was described to have subsequent downstream impacts, for example, lower blood counts with ganciclovir requires growth factor which increases risk of infection and potential for graft loss while renal toxicity from foscarnet requires adjusting other drug doses (i.e., calcineurin inhibitors) which are important for immune suppression and prescribing other antibiotics with potentially negative effects on other patient outcomes.
The clinical experts also described concerns around patients becoming resistant to current treatment options, though they likely expect patients using maribavir to develop resistance as well.
Place in Therapy
Clinical experts underscored the importance of treating patients with the least toxic and most effective drug early, citing that some of the outcomes from delayed treatment are irreversible (e.g., if graft loss due to ganciclovir or valganciclovir causes myelosuppression that cannot be reversed in post-HSCT patients and foscarnet causes graft loss in kidney transplant patients). The clinical experts indicated there is uncertainty about whether it would be better to combine therapies, especially if the patient has a high viral load, or to use it as a monotherapy. Per the clinical experts, if maribavir is used as part of combination therapy, it should not be combined with ganciclovir due to antagonistic mechanism of action. Determining which patients are likely to benefit from immediate maribavir and which patients may need combination therapy was identified as a potential area that would require further evidence generation. Per the experts, maribavir could be a combination therapy with foscarnet for patients who may be at risk of failing maribavir alone (e.g., very high viral loads at the time of therapy initiation) but there is no data on how best to do this.
If maribavir is reimbursed and available, the experts suggested it is expected to shift the treatment paradigm for refractory and/or resistant CMV infection, such that foscarnet would be shifted further down the lines of therapy from its current first-line as administering foscarnet requires hospital admission and toxicity management.
The clinical experts indicated that it would be inappropriate to recommend that patients try other treatments before initiating maribavir, noting the exception of an appropriate first-line therapy such as a trial of valganciclovir or ganciclovir. In the context of HSCT, a trial of foscarnet would be considered appropriate if cytopenia is an issue.
Patient Population
According to the clinical experts, resistance and refractory definitions are important to identify patients most suitable for treatment with maribavir. Patients most likely to respond to maribavir include those who have intolerances or life-threatening side effects to other drugs, those who can have their immunosuppression reduced and/or those that can have their immune function improve. The clinical experts indicated that in most cases, patients who are responding to ganciclovir or valganciclovir would not be appropriate recipients for maribavir; however, maribavir may be appropriate for those responding to ganciclovir or valganciclovir if intolerances exist (e.g., cytopenia). The patient populations currently most in need of an intervention are patients with lung transplant and bone marrow transplant.
The clinical experts indicated that patients best suited for maribavir would be identified by either a lack of change in CMV viral load or increase in CMV viral load after at least 2 weeks of appropriately dosed valganciclovir or ganciclovir. The CMV PCR test result at the third week would be needed to determine eligibility. If patients switch too early from the prior anti-CMV therapy to maribavir, then overdiagnosis of refractory and/or resistant infection can occur. Formal resistance testing should ideally be conducted before starting patients on maribavir; however, given the turnaround time for receiving results (i.e.,10 calendar days to 2 weeks), the experts suggested it may not be necessary to have results before initiating treatment.
The clinical experts emphasized that since maribavir has not been studied in some disease sites (e.g., central nervous system or retina) and penetration is unknown, those patients would be better suited to alternative drugs.
Assessing Response to Treatment
In routine clinical practice, the clinical experts indicated that anti-CMV treatment is given until CMV is either negative or low level; however, the definition of low level is unclear and treatment duration must be individualized based on multiple patient characteristics (e.g., GVHD, toxicity). The clinical experts clarified that treatment may be given for as little as 2 weeks but can be months of therapy. Clinically meaningful response to therapy would be resolution of any symptoms or resolution of end-organ disease. Patients would ideally have no evidence of CMV replication and no symptoms of CMV, however, this is not always feasible so if patients have either low level CMV without any evidence of CMV end-organ disease or symptoms, this is satisfactory for clinical experts. The experts added that highly sensitive assays make it challenging to identify the ideal end point for CMV negativity and there is a lack of literature around this.
According to the clinical experts, monitoring weekly CMV DNA level from plasma is the standard of care in Canada and transplant physicians follow-up with patients weekly or twice a month to regularly monitor CMV DNA levels.
Discontinuing Treatment
Per the clinical experts, complete response to maribavir would be defined as resolution of symptoms of end-organ disease and eradication of CMV viremia. Complete response would indicate that maribavir could be discontinued. On the contrary, lack of response to maribavir would generally be defined as rising viral loads despite therapy, resistance documented by genotyping, and progression of end-organ disease or symptoms. Lack of response would indicate that additional or alternative therapy might be necessary.
The experts added that clinicians would adhere to standard guidelines if maribavir was reimbursed and available. Per the Kotton et al. (2018)30 post-SOT guidelines identified by the experts, if highly sensitive assays (lower limit of quantification [LLOQ] < 200 IU/mL) are being used, therapy should be discontinued after 1 result is less than the LLOQ followed by confirmatory testing 1 week after discontinuation. In routine clinical practice, the experts described that the LLOQ of a highly sensitive assay may currently be a grey area. If the assay is not highly sensitive, the guidelines recommend that 2 consecutive undetectable (negative) results are needed to discontinue therapy.30 Per the Ljungman et al. (2019)29 post-HSCT guidelines, the clinicians may aim for 2 weeks of treatment and at least 1 negative CMV test. In both post-SOT and post-HSCT cases, if there is end-organ disease, there should be resolution of signs and symptoms before treatment is discontinued. The clinical experts also added that if CMV levels are good, falling and low, especially if there is toxicity with low blood cell counts or increase serum creatinine then therapy may be stopped before 2 negative tests, but the patient would be watched closely for rebound viremia.
Prescribing Conditions
According to the clinical experts, the appropriate setting for treatment with maribavir would be the community and/or outpatient setting. Specialists in transplant infectious disease or infectious diseases, if available, combined with the patients' primary transplant provider, are required to diagnose, treat, and monitor patients who might receive maribavir. The clinical experts also emphasized that the appropriate setting may depend on the availability of experts in a given province or region, suggesting that, for example, transplant infectious disease may not be available in some provinces so infectious disease or internal medicine may fulfill that role. Though, clinical experts maintained that clinicians with expertise both in the transplant type (SOT or HSCT) and in infections must be involved.
Additional Considerations
Per the clinical experts, clinicians are more concerned with resistance than refractory disease in routine clinical practice. The experts added that in trials, refractory CMV is defined as a 1 log10 rise in CMV viral load after 2 weeks of appropriately dosed antiviral therapy, probable refractory CMV is a CMV viral load that does not decrease in the same time frame, and resistant CMV refers to the viral genotyping that has mutations associated with reduced response to antiviral therapy. As per the experts, in routine practice, viral loads may not be reported in log numbers and stable or rising CMV viral loads on the third week post-transplant despite appropriate therapy are usually taken as an indication of refractory or resistant CMV which would trigger resistance testing. Providers are often concerned with any numerical rise but sometimes these do not fit the log definition and if testing is repeated too frequently or early, viral loads can fluctuate as much of the CMV in plasma is fragmented and does not represent whole genomes.
The clinical experts indicated that developing resistance to therapies is an important consideration. Per the experts, resistance is common in those who experience relapse after maribavir therapy and cross-resistance to ganciclovir is possible.47
Clinician Group Input
This section was prepared by CADTH staff based on the input provided by 1 clinician group.
The input provided by the clinician group generally aligned with the input provided by the clinical experts consulted by CADTH. CTTC, a multidisciplinary organization engaged in patient care, research, education in the field of HSCT and cell therapy, submitted input. A total of 6 clinicians and 2 CTTC committees (board of directors and standing committee of program directors) contributed to the input. Pertaining to the patient population, the clinician group also added that patients post-transplant often struggle with a lack of appetite and/or poor oral intake; therefore, the patients with difficulties of eating might be less suitable for maribavir, which is associated with dysgeusia but emphasized that toxicity profile of conventional salvage therapies is much more concerning. Furthermore, the clinician group emphasized that it is particularly challenging to treat CMV infection in patients with GVHD since GVHD therapies are immunosuppressive (i.e., increase the risk of CMV infection), myelosuppressive, and nephrotoxic (i.e., exacerbate the toxicities caused by valganciclovir or foscarnet, respectively). The group suggested that maribavir would be the new standard of care of these patients, if funded and available.
There was no input provided on the use of maribavir for post-SOT patients.
Drug Program Input
The drug programs provide input on each drug being reviewed through CADTH’s reimbursement review processes by identifying issues that may impact their ability to implement a recommendation. The implementation questions and corresponding responses from the clinical experts consulted by CADTH are summarized in Table 5.
Table 5: Summary of Drug Plan Input and Clinical Expert Response
Drug program implementation questions | Clinical expert response |
|---|---|
What is the definition of refractory and resistant CMV in clinical practice? What parameters are used? | Per the clinical experts, refractory CMV in trials is a 1 log10 rise in CMV viral load after 2 weeks of appropriately dosed antiviral therapy, probable refractory CMV is a CMV viral load that does not decrease in the same time frame, and resistant CMV refers to the viral genotyping that has mutations associated with reduced response to antiviral therapy. In routine clinical practice, the experts expressed that viral load may not be reported in log numbers, and therefore stable or rising CMV viral loads on the week 3 viral load assessment despite appropriate therapy are usually taken as an indication of refractory or resistant CMV. Clinicians are concerned with any numerical rise in CMV viral loads, but sometimes these do not fit the log definition and if testing is repeated too frequently or early, viral loads can fluctuate as much of the CMV in plasma is fragmented and does not represent whole genomes. The experts added that resistance testing is normally administered in this setting. |
Will prior antiviral therapies be limited to ganciclovir, valganciclovir, foscarnet, and cidofovir? Would it also include letermovir (Prevymis)? | According to the clinical experts, prior antiviral therapies typically include ganciclovir and/or valganciclovir or foscarnet unless there are extenuating circumstances. In SOT, ganciclovir and/or valganciclovir are the first-line, per the experts. In certain cases, cidofovir may be used; however, the experts indicated that it is a weak antiviral with renal and ocular toxicity. The experts also highlighted that resistance to ganciclovir in the UL54 gene often comes with cidofovir resistance, so the drug may be ineffective. Per the experts, letermovir is generally not included in prior antiviral therapies as it only has case report-level data on use as treatment for refractory or resistant CMV and appropriate dosing levels for routine clinical practice have not been identified. |
Should therapy end after a certain number of doses or period of time or other defined parameter? | Per the Kotton et al. (2018)30 post-SOT guidelines identified by the experts, if highly sensitive assays (LLOQ < 200 IU/mL) are being used, therapy should be discontinued after 1 result is less than the LLOQ followed by confirmatory testing 1 week after discontinuation. In routine clinical practice, the experts described that the LLOQ of a highly sensitive assay may currently be a grey area. If the assay is not highly sensitive, the guidelines recommend that 2 consecutive undetectable (negative) results are needed to discontinue therapy.30 Per the Ljungman et al. (2019)29 post-HSCT guidelines, the clinicians may aim for 2 weeks of treatment and at least 1 negative CMV test. In both post-SOT and post-HSCT cases, if there is end-organ disease, there should be resolution of signs and symptoms before treatment is discontinued. The clinical experts also added that if CMV levels are good, falling and low, especially if there is toxicity with low blood cell counts or increase serum creatinine then therapy may be stopped before 2 negative tests, but the patient would be watched closely for rebound viremia. If this is less than 8 weeks, there would be no need to extend therapy for this indication. |
Can maribavir be used in combination with other antivirals used for CMV prevention and treatment in transplant recipients? | The clinical experts expressed that maribavir has failed in trials of prevention in the HSCT population so it should not be used for this purpose. To treat CMV, the clinical experts noted that maribavir could possibly be used in combination therapy with foscarnet for patients who may be at risk of failing maribavir alone (e.g., patients with very high viral loads at the time of therapy initiation), however there is no data on how best to do this (i.e., which patient population would best benefit from combination therapy and/or duration of combination therapy). Per the experts, combinations with cidofovir, letermovir (off-label) and rapamycin/sirolimus may be possible as well. The clinical experts emphasized that maribavir cannot be combined with ganciclovir and/or valganciclovir because it has an antagonistic mechanism of action. |
Should maribavir be limited to infectious disease specialists and/or clinicians with expertise in the management of transplant patients? | Per the clinical experts, specialists in transplant infectious disease or infectious diseases, if available, combined with the patients' primary transplant provider, are required to diagnose, treat, and monitor patients who might receive maribavir. The clinical experts also emphasized that the appropriate setting may depend on the availability of experts in a given province or region, suggesting that for example transplant infectious disease may not be available in some provinces so infectious disease or internal medicine may fulfill that role. Though, clinical experts maintained that clinicians with expertise in the transplant type (SOT or HSCT) and in infections must be involved. |
No data available to Health Canada for pediatrics (< 18 years); therefore, Health Canada has not authorized an indication for pediatric use. Could the clinical expert provide input for pediatric use? | The clinical experts declined to make any comments pertaining to maribavir for pediatric use, citing that their primary area of practice is in the adult population. |
Will the diagnosis of resistant CMV infection include laboratory testing and if so, is it readily available in clinical practice? | As per the clinical experts, the diagnosis of resistant CMV infection requires laboratory testing, typically done at the National Microbiology Laboratory and there are no concerns about availability. However, the experts noted that turnaround time is at least 10 calendar days and can exceed 2 weeks. |
CMV = cytomegalovirus; HSCT = hematopoietic stem-cell transplant; PCR = polymerase chain reaction; SOT = solid organ transplant.
Clinical Evidence
The clinical evidence included in the review of maribavir is presented in 3 sections. The first section, the Systematic Review, includes pivotal studies provided in the sponsor’s submission to CADTH and Health Canada, as well as those studies that were selected according to an a priori protocol. The second section includes indirect evidence selected from the literature that met the selection criteria specified in the review. The third section includes sponsor-submitted long-term extension studies and additional relevant studies that were considered to address important gaps in the evidence included in the systematic review.
Systematic Review (Pivotal and Protocol Selected Studies)
Objectives
To perform a systematic review of the beneficial and harmful effects of maribavir 400 mg (2 tablets of 200 mg) twice daily (resulting in a daily dose of 800 mg) for the treatment adults with post-transplant cytomegalovirus (CMV) infection/disease who are refractory and/or resistant to 1 or more prior antiviral therapies.
Methods
Studies selected for inclusion in the systematic review included pivotal studies provided in the sponsor’s submission to CADTH and Health Canada, as well as those meeting the selection criteria presented in Table 6. Outcomes included in the CADTH review protocol reflect outcomes considered to be important to patients, clinicians, and drug plans.
Of note, the systematic review protocol presented below was established before the granting of a NOC from Health Canada.
Table 6: Inclusion Criteria for the Systematic Review
Criteria | Description |
|---|---|
Population | Adults with post-transplant CMV infection or disease who are refractory (with or without genotypic resistance) to one or more prior antiviral therapies. Subgroups:
|
Intervention | Maribavir 400 mg (2 tablets of 200 mg) administered twice daily orally resulting in a daily dose of 800 mg |
Comparator | Anti-CMV drugs, including:
|
Outcomes | Efficacy outcomes:
Harms outcomes:
|
Study designs | Published and unpublished phase III and IV RCTs |
AE = adverse event; CMV = cytomegalovirus; D = donor; GVHD = graft vs. host disease; HLA = human leukocyte antigen; HSCT = hematopoietic stem-cell transplant; R = recipient; RCT = randomized controlled trial; SAE = serious adverse event; SCr = serum creatinine; SOT = solid organ transplant; WDAE = withdrawal due to adverse event.
The literature search was performed by an information specialist using a peer-reviewed search strategy. The literature search for clinical studies was performed by an information specialist using a peer-reviewed search strategy according to the PRESS Peer Review of Electronic Search Strategies checklist.48
Published literature was identified by searching the following bibliographic databases: MEDLINE All (1946–) via Ovid and Embase (1974–) via Ovid. All Ovid searches were run simultaneously as a multi-file search. Duplicates were removed using Ovid deduplication for multi-file searches, followed by manual deduplication in Endnote. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Patient Headings), and keywords. The main search concept was maribavir. Clinical trials registries were searched: the US National Institutes of Health’s clinicaltrials.gov, WHO’s International Clinical Trials Registry Platform (ICTRP) search portal, Health Canada’s Clinical Trials Database, and the European Union Clinical Trials Register.
No filters were applied to limit the retrieval by study type. Retrieval was not limited by publication date or by language. Conference abstracts were excluded from the search results. Refer to Appendix 1 for the detailed search strategies.
The initial search was completed on April 29, 2022. Regular alerts updated the search until the meeting of the CADTH Canadian Drug Expert Committee (CDEC) on August 24, 2022.
Grey literature (literature that is not commercially published) was identified by searching relevant websites from the Grey Matters: A Practical Tool For Searching Health-Related Grey Literature checklist.49 Included in this search were the websites of regulatory agencies (US FDA and EMA). Google was used to search for additional internet-based materials. Refer to Appendix 1 for more information on the grey literature search strategy.
These searches were supplemented by reviewing bibliographies of key papers and through contacts with appropriate experts. In addition, the manufacturer of the drug was contacted for information regarding unpublished studies.
Two CADTH clinical reviewers independently selected studies for inclusion in the review based on titles and abstracts, according to the predetermined protocol. Full-text articles of all citations considered potentially relevant by at least 1 reviewer were acquired. Reviewers independently made the final selection of studies to be included in the review, and differences were resolved through discussion.
Findings From the Literature
A total of 1 study was identified from the literature for inclusion in the systematic review (Figure 1). The included study is summarized in Table 7. A list of excluded studies is presented in Appendix 2.
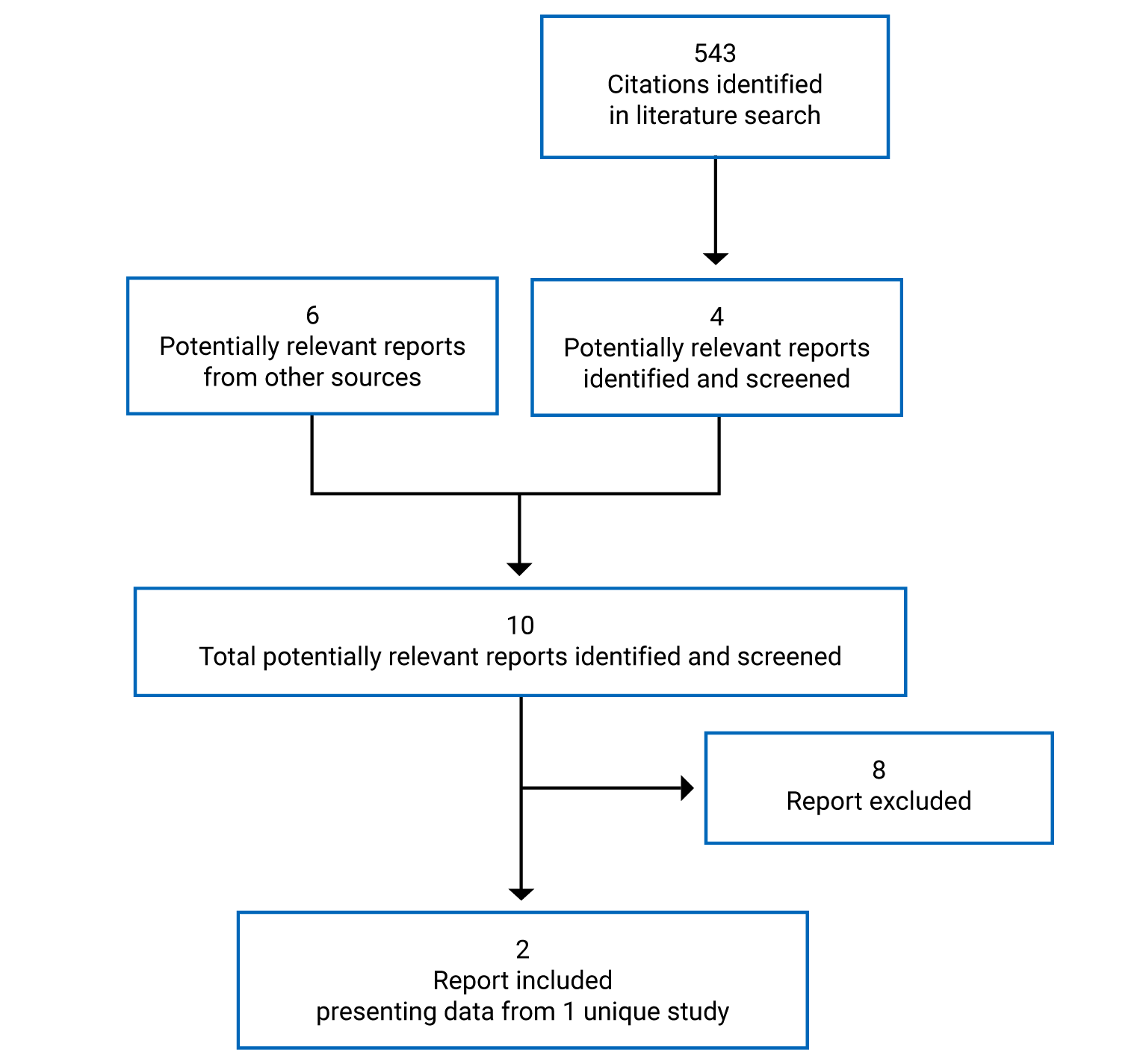
Table 7: Details of Included Study
Detail | SOLSTICE |
|---|---|
Study design | Phase III, multicenter, open-label, randomized controlled trial |
Locations | US, France, Belgium, Spain, Germany, Australia, UK, Canada, Croatia, Denmark, Italy, and Singapore |
Patient enrollment dates | December 22, 2016, to August 17, 2020 |
Randomized (N) | 352; Maribavir = 235; IAT = 117 |
Inclusion criteria |
|
Exclusion criteria |
|
Intervention | Maribavir 200 mg tablets were orally administered at 400 mg twice daily for 8 weeks for a total of 800 mg per day |
Comparator(s) | IAT for the 8 weeks of the study treatment phase. One or a pre-specified combination of 2 of the available anti-CMV drugs from the following were used: IV ganciclovir, oral valganciclovir, IV foscarnet, or IV cidofovir. Dose and dose regimen of the IAT were at the discretion of the investigator following best clinical practice for each patient based on the specific situation |
Phase | |
Screening | Up to 2 weeks before the treatment phase |
Treatment | Patients were randomized at week 0 and study treatment phase lasted from weeks 1 to 8. |
Rescue arm | Option to receive maribavir for participants randomized to IAT and in whom, despite a minimum of 3 weeks of therapy with IAT (week 3), the patient met criteria for lack of improvement or worsening of CMV infection. |
Follow-up | 12 weeks (weeks 9 to 20) (weekly first 4 weeks, every 2 weeks in the last 8 weeks) |
Primary end point | Confirmed CMV viremia clearance at the end of study week 8, defined as plasma CMV DNA concentration < LLOQ (i.e., < 137 IU/mL) per central laboratory result in 2 consecutive post-baseline samples, separated by at least 5 days. |
Secondary and exploratory end points | Key secondary:
Other secondary:
Exploratory:
|
Publications | Avery et al. (2021)50 |
CNS = central nervous system; CMV = cytomegalovirus; GI = gastrointestinal; HIV = HIV; HSCT = hematopoietic stem-cell transplant; IAT = investigator-assigned treatment; LLOQ = lower limit of quantitation; qPCR = quantitative polymerase chain reaction; SOT = solid organ transplant; ULN = upper limit of normal; Wk = week.
Source: SOLSTICE Clinical Study Report.4
Description of Studies
One trial met the inclusion criteria for this review.4,50 Study-specific details are listed in Table 7, and schematics of the trial design are included in Figure 2.
SOLSTICE (N = 352) was a randomized, multicenter, parallel assignment (2:1), open-label, active-controlled phase III trial comparing 8 weeks of treatment with either maribavir or investigator-assigned choice of comparator antiviral therapies (ganciclovir, valganciclovir, foscarnet, or cidofovir) in adult HSCT and SOT patients with CMV infections that are refractory (with or without resistance) to 1 or a combination of the antivirals.4 Patients were enrolled from 135 sites in 12 countries across North America, Europe, and Asia Pacific. The primary objective of the study was to compare the efficacy of maribavir to IAT in CMV viremia clearance at the end of study, week 8. Patients received 400 mg of oral maribavir (N = 235) twice daily (800 mg/day) or investigator-assigned treatment (N = 117) for at least 8 weeks, and up to 29 weeks. For drug administration as outpatients, a study diary for tracking adherence to study treatment dosing was dispensed for home use. A proportion of patients randomized to the IAT were entered into the maribavir rescue arm upon discretion of the investigator, after a minimum of 3 weeks of IAT. Patients visited the study site up to 19 times for up to 22-week period. The SOLSTICE study consisted of 3 phases: a screening phase of up to 2 weeks; an 8-week study treatment phase; and a 12-week follow-up phase. The screening phase consisted of collecting informed consent, checking the inclusion and exclusion criteria, and other clinical assessments. The screening phase was followed by stratification of patients based on 2 factors: transplant type (SOT or HSCT) and the most recent screening of whole blood or plasma CMV DNA viral load (categorized as per the 3 categories in Table 8). Following stratification, patients were randomized in a 2:1 allocation ratio using IRT. In the 12-week follow-up phase, study-specific evaluations, including CMV tests and safety assessments, occurred weekly for the first 4 weeks, then every 2 weeks for the final 8 weeks. Patients who entered the maribavir rescue arm participated in the study for up to 29 weeks. Patients in the IAT group who had an ineffective response to IAT could be evaluated to receive rescue treatment with maribavir for 8 weeks. The eligibility of patients who had to discontinue IAT for lack of antiviral activity and/or intolerance was assessed at week 3 up to week 7 for entry into the rescue arm of treatment with maribavir 400 mg twice daily for up to 8 weeks. No washout phase was reported, however, the minimum washout period before the first dose of study treatment for letermovir was changed from 14 days to 3 days to facilitate enrollment.
Figure 2: SOLSTICE Study Design
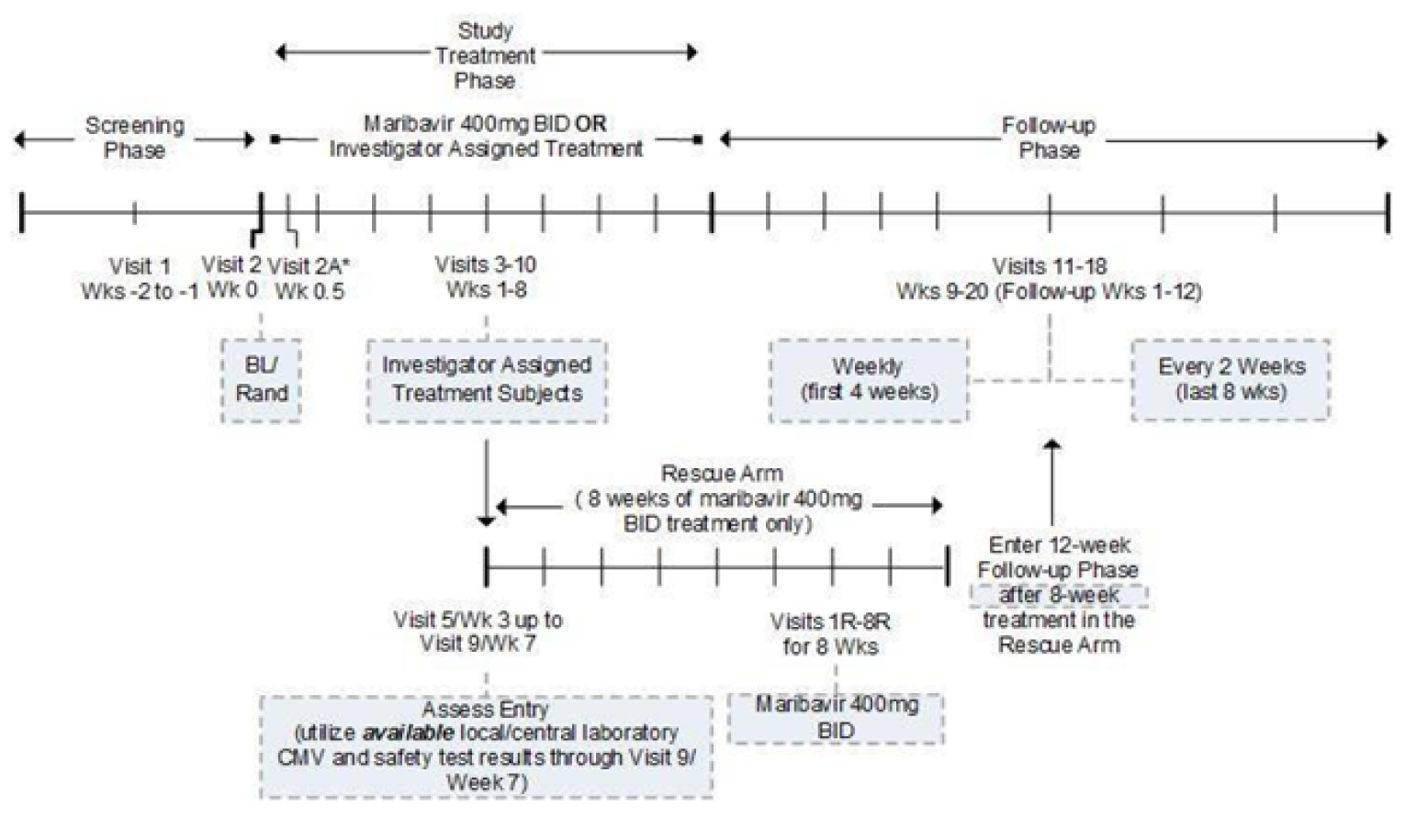
BID = twice daily; BL = baseline; CMV = cytomegalovirus; R = rescue; Rand = randomized; Wk = week.
Source: SOLSTICE Clinical Study Report.4
Table 8: Stratification of Patients by CMV DNA Viral Load Category
CMV DNA viral load category | Viral load (IU/mL) | |
|---|---|---|
Whole blood | Plasma | |
High | ≥ 273,000 | ≥ 91,000 |
Intermediate | ≥ 27,300 and < 273,000 | ≥ 9,100 and < 91,000 |
Low | ≥ 2,730 and < 27,300 | ≥ 910 and < 9,100 |
CMV = cytomegalovirus.
Source: SOLSTICE Clinical Study Report.4
Populations
Inclusion and Exclusion Criteria
Patients (≥ 12 years) were eligible for the SOLSTICE study if they underwent a SOT or HSCT and were diagnosed with CMV infection that was refractory to the most recently administered of the 4 anti-CMV treatment drugs. Specifically, refractory was defined as documented failure to achieve a greater than 1 log 10 decrease in CMV DNA level in whole blood or plasma after a 14-day or longer treatment period with IV ganciclovir, oral valganciclovir, IV foscarnet, or IV cidofovir. Eligible patients were also required to have an absolute neutrophil count (ANC) of at least 1,000/mm3 (1.0 × 109/L), platelet count of at least 2,5000/mm3 (25 × 109/L), hemoglobin of at least 8 g/dL, estimated glomerular filtration rate (eGFR) greater than 30 mL/min/1.73 m2, and a life expectancy of ≥ 8 weeks. Patients were excluded if they had vomiting, diarrhea, or other severe GI illness within 24 hours before the first dose of study treatment. Patients were also excluded if they had a current CMV infection that was considered refractory or resistant due to inadequate adherence to prior anti-CMV treatment and had tissue-invasive CMV disease with central nervous system involvement (including the retina). Patients with known positive results for HIV and undergoing treatment for acute or chronic hepatitis C were also considered ineligible. Additional detail regarding inclusion and exclusion criteria in the SOLSTICE study are provided in Table 7.
Baseline Characteristics
Baseline characteristics of all patients enrolled in the SOLSTICE study are presented in Table 9 and Table 10.
The mean age of enrolled patients was 53.0 years (SD: 13.22 years). Most patients were White (75.6%) and male (60.5%). Most patients underwent a SOT (59.9%), with the kidney (50.2% of SOT patients), lung (29.4% of SOT patients), and heart (10.9% of SOT patients) being the most transplanted solid organs. Patients who underwent HSCT predominantly underwent allogeneic transplant procedures (99.3%). Most patients who underwent SOT and HSCT had functioning graft status (89.1% in SOT patients versus 85.1% in HSCT patients). Most patients did not have confirmed acute or chronic GVHD (91.2% in acute GVHD versus 96.9% in chronic GVHD), and did not use antilymphocyte treatment (57.7%). Most patients had some renal impairment (32.1% with mild, 23.3% with moderate, and 3.1% with severe), but no hepatic impairment (92.3%).
For most patients, the current CMV infection is the first episode post-transplant (68.2%), there was no prior use of CMV prophylaxis (58.8%), and the current CMV infection was asymptomatic (86.4%). The CMV serostatus for patients who underwent SOT was mostly Donor +/Recipient- (83.4%), while for patients who underwent HSCT it was mostly either Donor +/Recipient + or Donor -/Recipient + (41.8% and 46.1%, respectively). The CMV DNA levels of most patients as assessed by central laboratory was low (67.6%). Most of the patients had a presence of CMV RASs known to confer resistance to ganciclovir, foscarnet, and/or cidofovir (54.3%), but did not have RASs known to confer resistance to maribavir (88.6%). The Karnofsky Scale Performance Status scores for most patients was 80 or above (60.2%).
Overall, both the maribavir and IAT treatment groups were relatively balanced in terms of baseline demographic and clinical characteristics. Some notable differences between the groups were observed in following characteristics: age, type of preparative conditioning regimen, presence of CMV RASs, and CMV serostatus for HSCT Donor/Recipient, CMV DNA level, and net immunosuppression use changed before initiation of study treatment. The differences were as follows: patients aged 65+ years (maribavir: 23.0% versus IAT: 13.7%), CMV serostatus for HSCT Donor+/Recipient+ (maribavir: 45.2% versus IAT: 35.4%), HSCT Donor-/Recipient+ (maribavir: 41.9% versus IAT: 54.2%).
There was a difference between the groups in CMV DNA level low category (maribavir: 65.1% versus IAT: 72.6%) and intermediate category (maribavir: 28.9% versus IAT: 21.4%). Net immunosuppression use changed before initiation of study-assigned treatment was also imbalanced (maribavir: 23.0% versus IAT: 30.8%).
Table 9: Summary of Baseline Characteristics (Randomized Set, N = 352)
Characteristic | Maribavir (N = 235) | IAT (N = 117) |
|---|---|---|
Age, mean (SD) | 53.8 (13.39) | 51.5 (12.80) |
Sex, n (%) | ||
Male | 148 (63.0) | 65 (55.6) |
Female | 87 (37.0) | 52 (44.4) |
Race, n (%) | ||
White | 179 (76.2) | 87 (74.4) |
Black or African American | 29 (12.3) | 18 (15.4) |
Asian | 9 (3.8) | 7 (6.0) |
Othera | 16 (6.8) | 5 (4.3) |
Missing | 2 (0.9) | 0 |
Current transplant type | ||
SOT,b n (%) | 142 (60.4) | 69 (59.0) |
Heart | 14 (9.9) | 9 (13.0) |
Lung | 40 (28.2) | 22 (31.9) |
Liver | 6 (4.2) | 1 (1.4) |
Pancreas | 2 (1.4) | 0 |
Intestine | 1 (0.7) | 0 |
Kidney | 74 (52.1) | 32 (46.4) |
Multiple | 5 (3.5) | 5 (7.2) |
Hematopoietic stem-cell transplant,b n (%) | 93 (39.6) | 48 (41.0) |
Autologous | 1 (1.1) | 0 |
Allogeneic | 92 (98.9) | 48 (100.0) |
Current graft status at baseline | ||
SOT,b n (%) | ||
Functioning with complications | 12 (8.5) | 8 (11.6) |
Functioning | 127 (89.4) | 61 (88.4) |
Othera | 3 (2.1) | 0 |
Hematopoietic stem-cell transplant,b n (%) | ||
Partially engrafted | 4 (4.3) | 1 (2.1) |
Functioning with complications | 11 (11.8) | 5 (10.4) |
Functioning | 78 (83.9) | 42 (87.5) |
Acute GVHD confirmed, n (%) | ||
No | 212 (90.2) | 109 (93.2) |
Yes | 23 (9.8) | 8 (6.8) |
Chronic GVHD confirmed, n (%) | ||
No | 229 (97.4) | 112 (95.7) |
Yes | 6 (2.6) | 5 (4.3) |
Type of preparative conditioning regimen, n (%) | ||
Myeloablative | 47 (51.1) | 16 (33.3) |
Non–myeloablative | 17 (18.5) | 12 (25.0) |
Reduced intensity conditioning regimen | 28 (30.4) | 17 (35.4) |
NA | 0 | 1 (2.1) |
Missing | 0 | 2 (4.2) |
Net immunosuppression use changed before the study, n (%) | ||
No | 181 (77.0) | 80 (68.4) |
Yes | 54 (23.0) | 36 (30.8) |
Missing | 0 | 1 (0.9) |
Antilymphocyte use, n (%) | ||
No | 135 (57.4) | 68 (58.1) |
Yes | 100 (42.6) | 49 (41.9) |
Renal impairment, n (%) | ||
No impairment | 81 (34.5) | 39 (33.3) |
Mild | 71 (30.2) | 42 (35.9) |
Moderate | 60 (25.5) | 22 (18.8) |
Severe | 8 (3.4) | 3 (2.6) |
Missing | 15 (6.4) | 11 (9.4) |
Hepatic impairment, n (%) | ||
No impairment | 218 (92.8) | 107 (91.5) |
Grade 1 | 9 (3.8) | 3 (2.6) |
Grade 2 | 4 (1.7) | 3 (2.6) |
Grade 3 or 4 | 0 | 0 |
Missing | 4 (1.7) | 4 (3.4) |
Karnofsky Performance Status Scale, n (%) | 213 | 108 |
100 | 37 (15.7) | 22 (18.8) |
90 | 65 (27.7) | 20 (17.1) |
80 | 39 (16.6) | 29 (24.8) |
70 | 43 (18.3) | 26 (22.2) |
60 | 15 (6.4) | 5 (4.3) |
50 | 5 (2.1) | 1 (0.9) |
40 | 6 (2.6) | 3 (2.6) |
30 | 1 (0.4) | 2 (1.7) |
20 | 2 (0.9) | 0 |
10 | 0 | 0 |
0 | 0 | 0 |
Missing | 22 (9.4) | 9 (7.7) |
Baseline CMV DNA levels from plasma by central laboratory (IU/mL),b mean n (SD) | 52921.6 (335894.69) | 88171.8 (595022.17) |
CMV DNA levels category as reported by central laboratory, n (%) | ||
Low | 153 (65.1) | 85 (72.6) |
Intermediate | 68 (28.9) | 25 (21.4) |
High | 14 (6.0) | 7 (6.0) |
Category of current CMV infection based on investigator assessment, n (%) | ||
CMV syndrome (SOT only) | 16 (6.8) | 10 (8.5) |
CMV tissue-invasive disease | 18 (7.7) | 4 (3.4) |
Asymptomatic CMV infection | 201 (85.5) | 103 (88.0) |
CMV serostatus for SOT,b n (%) | ||
Donor +/Recipient + | 11 (7.7) | 8 (11.6) |
Donor -/Recipient + | 3 (2.1) | 1 (1.4) |
Donor +/Recipient - | 120 (84.5) | 56 (81.2) |
Donor -/Recipient - | 7 (4.9) | 3 (4.3) |
Missing | 1 (0.7) | 1 (1.4) |
CMV serostatus for HSCT,b n (%) | ||
Donor +/Recipient + | 42 (45.2) | 17 (35.4) |
Donor -/Recipient + | 39 (41.9) | 26 (54.2) |
Donor +/Recipient - | 6 (6.5) | 3 (6.3) |
Donor -/Recipient - | 5 (5.4) | 1 (2.1) |
Missing | 1 (1.1) | 1 (2.1) |
Prior use of CMV prophylaxis, n (%) | ||
No | 135 (57.4) | 72 (61.5) |
Yes | 100 (42.6) | 45 (38.5) |
Current CMV infection is the first episode post-transplant, n (%) | ||
No | 73 (31.1) | 39 (33.3) |
Yes | 162 (68.9) | 78 (66.7) |
CMV = cytomegalovirus; GVHD = graft vs.-host disease; HSCT = hematopoietic stem-cell transplant; IU = international units; IAT = investigator-assigned treatment; NA = not applicable; SD = standard deviation; SOT = solid organ transplant.
aOther category includes Native Hawaiian or other Pacific Islander, American Indian or Alaska Native, and multiple races. The number of patients in each of those categories was 0.
bPercentages are based on the number of patients within the category.
Source: SOLSTICE Clinical Study Report.4
Table 10: Summary of Baseline Resistance Profile (Modified Randomized Set)
Characteristic | Maribavir (N = 234) | IAT (N = 116) |
|---|---|---|
Presence of CMV RASs known to confer resistance to ganciclovir, foscarnet, and/or cidofovir per central laboratory results, n (%) | ||
No | 96 (41.0) | 34 (29.3) |
Yes | 121 (51.7) | 69 (59.5) |
Unable to genotype | 17 (7.3) | 13 (11.2) |
Presence of CMV RASs known to confer resistance to maribavir per central laboratory results, n (%) | ||
No | 213 (91.0) | 97 (83.6) |
Yes | 1 (0.4) | 3 (2.6) |
Unable to genotype | 20 (8.5) | 16 (13.8) |
CMV = cytomegalovirus; IAT = investigator-assigned treatment; RASs = resistance-associated amino acid substitutions.
Source: SOLSTICE Clinical Study Report.4
Interventions
Randomized patients received either maribavir (N = 235) or IAT (N = 117). The IATs were chosen and prescribed by the investigator and were either administered at the hospital or other facilities used to administer IV products or were prescribed by the investigator and typically purchased by the patients at a commercial or hospital pharmacy.
Maribavir was administered every 12 hours. When it was not feasible to dose every 12 hours, the doses were separated by a minimum of 8 hours. If the timing of the first dose of maribavir on day 0 did not allow for a minimum of 8 hours between doses, only 1 dose of maribavir was administered on day 0. The strength of tablets was 200 mg, and patients were required to take 2 tablets of 200 mg maribavir every 12 hours (200 mg × 2 tablets in the morning and 200 mg times 2 tablets in the evening totalling to 800 mg/day). Maribavir was administered without regard to food and could have been crushed and/or dispersed in water via orogastric or nasogastric tube for a short period of time during the study treatment phase to avoid interruption or discontinuation of treatment. Interruption of therapy for a maximum of 7 consecutive days, or up to 2 study treatment interruptions for a total of up to 7 days was permitted at the investigator’s discretion if the end of the maribavir administration period remained fixed at a maximum of 8 weeks after the date of the start of treatment. Dose adjustments and dose interruptions were to be recorded on the electronic case report form (eCRF).
IAT drug type and the dose was at the direction of the investigator. Dual therapy with 2 IATs was permitted. Dose adjustment for safety or efficacy were allowed but had to be documented in the eCRF. During treatment with IAT, the investigator could interrupt therapy without permanent study treatment discontinuation as long as the interruption was for a maximum of 7 consecutive days, or up to 2 study treatment interruptions for a total of up to 7 days and the end of the IAT administration period remained fixed at a maximum of 8 weeks after the date of the start of treatment. After randomization, switching between valganciclovir and ganciclovir was permitted, but changing IAT to another anti-CMV drug or adding another anti-CMV drug during the treatment period was not permitted.
Concomitant Medications
Patients were permitted to use concomitant medications to complement the use of the anti-CMV drugs in the study (e.g., immunosuppressant drug or hemopoietic growth factors as needed for neutropenia) and prevent or treat viral infections (i.e., acyclovir, valacyclovir, or famciclovir). Antifungal and antibacterial drugs were also permitted. Maribavir was administered cautiously with drugs that are substrates of CYP2C19 and P-glycoprotein (P-gp), as inhibition of these enzymes by maribavir could increase concentrations of the substrates, particularly for tacrolimus and other narrow therapeutic index immunosuppressants.
Irrespective of the study group, patients were not permitted concomitant use of any unapproved drug or device, any investigational anti-CMV drug (e.g., receipt of CMV vaccine), and infusion of T-cells specific for CMV or regulatory T-cells for the control of transplant tolerance. In the maribavir group, patients were not permitted concomitant use of CYP3A inducers (e.g., avasimibe, carbamazepine, phenytoin, rifampin, rifabutin, St. John’s wort), herbal medications known to have potential toxicities or drug interactions (e.g., Ginkgo biloba or Piper methysticum) and select systemic anti-CMV therapies (i.e., ganciclovir, valganciclovir, foscarnet, cidofovir, leflunomide, artesunate, and letermovir) unless administration was unintentional for no longer than 1 day. In the IAT group, patients were not permitted concomitant use of leflunomide, artesunate, or letermovir while they were receiving IAT (except unintentional administration for no longer than 1 day).
Patients in the IAT group were eligible to transition into the maribavir rescue arm if after a minimum of 3 weeks of therapy with IAT (week 3) if they met protocol-defined criteria for lack of improvement or worsening of CMV infection. Criteria included increased whole blood or plasma CMV viremia levels of at least 1 log10 from baseline, tissue-invasive CMV disease that did not improve or worsened, and/or patient who did not achieve CMV viremia clearance (requiring continued anti-CMV treatment), and intolerance to the IAT.
Outcomes
A list of efficacy end points identified in the CADTH review protocol that were assessed in the clinical trial included in this review is provided in Table 11. These end points are further summarized below. A detailed discussion and critical appraisal of the outcome measures is provided in Appendix 4.
Table 11: Summary of Outcomes of Interest Identified in the CADTH Review Protocol
Outcome in CADTH Review protocol | Outcome measure in SOLSTICE | Outcome type in SOLSTICE |
|---|---|---|
Clinically significant CMV infection | Response assessed using confirmed CMV viremia clearance at the end of the 8-week treatment phase. | Primary |
Response assessed using CMV viremia clearance and symptom control achieved the end of 8-week treatment phase, with maintenance through week 16. Symptom control was defined as resolution or improvement of tissue-invasive CMV disease or CMV syndrome for patients symptomatic at baseline or no new symptoms of tissue-invasive CMV disease or CMV syndrome for patients asymptomatic at baseline. | Key secondary | |
Response assessed using achievement of the confirmed CMV viremia clearance after 8 weeks of receiving study-assigned treatment. Confirmed CMV viremia clearance at week 12, 16, or 20 was based on responders at week 8 who maintained CMV viremia clearance (defined as not having 2 consecutive viral load values > LLOQ) through week 12, 16, or 20. | Secondary | |
The maintenance of the CMV viremia clearance and CMV infection symptom control achieved at the end of study week 8 through weeks 12 to 20 | Secondary | |
Time to first CMV viremia clearance. | Exploratory | |
CMV viral load over time. | Exploratory | |
New CMV event | New CMV disease onset (CMV syndrome and tissue-invasive disease) by investigator assessment and confirmed by independent End point Adjudication Committee. | Secondary |
Recurrence of CMV viremia, defined as plasma CMV DNA concentrations ≥ LLOQ, when assessed by central specialty laboratory, in 2 consecutive plasma samples separated by at least 5 days after achieving confirmed viremia clearance. Recurrence of CMV viremia during and off study-assigned treatment. | Secondary | |
Time from first CMV viremia clearance to CMV viremia recurrence. | Exploratory | |
All-cause mortality | Death from any cause and time to all-cause mortality. | Secondary |
|||||||||||||||||||||||| | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| | ||||||||||||||||||||||| |
|||||||||||||||||||||||| | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| | ||||||||||||||||||||||| |
|||||||||||||||||||||||| | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| | ||||||||||||||||||||||| |
AE = adverse event; CMV = cytomegalovirus; GVHD = graft vs. host disease; IAT = investigator-assigned treatment; LLOQ = lower limit of quantification; RAS = resistance-associated amino acid substitution; SAE = serious adverse event; SF-36v2 = Short Form Health Survey 36 item Version 2; WDAE = withdrawal due to adverse event.
Source: SOLSTICE Clinical Study Report.4
Efficacy Assessments
Disease response assessments were made according to CMV DNA concentrations using PCR assay (COBAS AmpliPrep/COBAS TaqMan CMV Test) at a central virology laboratory. The first DNA sample was taken during the screening phase and then subsequent samples were taken weekly during the treatment phase. To note, blood samples were taken at all study visits (processed to obtain plasma) for all CMV DNA tests (quantitation, genotyping) and were tested in a central specialty laboratory; however, during the screening period local specialty laboratory results for CMV DNA quantitation could have been used only for eligibility assessment. Time points for evaluation of viral load for the primary end point were weeks 7 and 8. The permissible assessment windows were as follows: Week 0.5 (day 4) ± 1 day; week 1 (day 7) plus 2 days; weeks 2 to 4 ± 2 days; and weeks 5 to 8 ± 3 days.
Secondary evaluation of efficacy assessed the status of tissue-invasive disease and CMV syndrome in addition to CMV viremia clearance using results that were adjudicated by an independent EAC.
End Point Definitions
The primary end point was response confirmed by plasma CMV DNA clearance at the end of study week 8. This end point was defined as proportion of patients with plasma CMV DNA concentration of less than LLOQ (i.e., < 137 IU/mL) per central laboratory result in 2 consecutive post-baseline samples, separated by at least 5 days. Patients who initiated alternative (non–study) anti-CMV therapy or rescue treatment before week 8 were considered non–responders.
The key secondary end point was response defined as proportion of patients with confirmed CMV viremia clearance and symptom control at the end of study week 8, followed by maintenance of this treatment effect for an additional 8 weeks off treatment (i.e., follow-up week 16). Symptom control was defined as resolution or improvement of tissue-invasive CMV disease or CMV syndrome for patients who were symptomatic at baseline. For patients who were asymptomatic at baseline, symptom control was defined as no new symptoms of tissue-invasive CMV disease or CMV syndrome. Patients who initiated alternative (non–study) anti-CMV therapy before week 16 were counted as non–responders. Both the primary and secondary end points were assessed regardless of whether patients completed the 8 weeks of study-assigned treatment.
Three additional secondary end points, similar to the primary and key secondary end points, also captured response. The secondary end points were 1) achievement of the confirmed CMV viremia clearance after 8 weeks of receiving study-assigned treatment, 2) achievement of the confirmed CMV viremia clearance and CMV infection symptom control after 8 weeks of receiving study-assigned treatment, and 3) maintenance of the CMV viremia clearance and CMV infection symptom control achieved at the end of study week 8 through weeks 12 to 20. Achievement of the confirmed CMV viremia clearance after 8 weeks of receiving study-assigned treatment was defined the same as the primary end point except patients were required to complete 8 weeks of study treatment. Achievement of the confirmed CMV viremia clearance and CMV infection symptom control after 8 weeks of receiving study-assigned treatment was defined as proportion of patients who qualified for achievement of confirmed CMV viremia clearance after 8 weeks of study treatment and had resolution or improvement of tissue-invasive disease or CMV syndrome at week 8 and at the time point of interest or did not develop new symptoms at week 8 or time points of interest. Maintenance of the CMV viremia clearance and CMV infection symptom control achieved at the end of study week 8 through weeks 12 to 20 was defined the same as the key secondary end point, but maintenance was evaluated at week 12 and week 20 instead of week 16.
Recurrence of CMV viremia, recurrence of CMV viremia during and off study-assigned treatment, all-cause mortality and resistance to study drugs were additional secondary end points. Recurrence of CMV viremia was defined as proportion of patients with plasma CMV DNA concentrations of at least LLOQ, when assessed by central specialty laboratory, in 2 consecutive plasma samples separated by at least 5 days after achieving confirmed viremia clearance. All-cause mortality was defined by time to all-cause mortality. Resistance profile was defined as the proportion of patients with RASs, RASs to IAT were assessed on the UL97 (ganciclovir/valganciclovir) and UL54 (ganciclovir/valganciclovir, foscarnet, and cidofovir) genes, while RASs to maribavir were assessed on the UL97 and UL27 genes.
The exploratory end points included CMV viral load over time, time to first CMV viremia clearance, time from first CMV viremia clearance to viremia recurrence, |||||||||||||||||||||||, and |||||||||||||||||||||||. The CMV viral load over time was defined as change from baseline in log10 plasma CMV DNA viral load, reported for week 8 and week 16. The time to first CMV viremia clearance was defined as time (days) to first CMV viremia clearance (i.e., time to first of 2 consecutive CMV DNA values < LLOQ). Time from first CMV viremia clearance to viremia recurrence was assessed as presence of CMV DNA after the patient achieved confirmed CMV viremia clearance at any point in the study. ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||.
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||. The EQ-5D is a generic HRQoL instrument that can be applied to a wide range of health conditions and treatments to capture the net effect of treatment benefits and harms.51 The EQ-5D consists of 5 dimensions of health (mobility, self-care, usual activities, pain/discomfort, anxiety/depression) rated on a scale of 5 levels, ranging from 1 (“no problems”) to 5 (“extreme problems” or “unable to perform”). The EQ-5D index score is generated by applying a multi-attribute utility function to the descriptive system.52 The EQ-5D also has a visual analogue scale (VAS), by which overall health is self-rated on a scale ranging from 0 (“the worst health you can imagine”) to 100 (“the best health you can imagine”).51 |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||. The SF-36v2 is a 36-item, generic, self-reported health assessment questionnaire with 8 domains: physical functioning, role limitations due to physical health problems, bodily pain, general health, vitality, social functioning, role limitations due to emotional health problems, and mental health.53 For each of the 8 categories, a subscale score can be calculated. The SF-36v2 also provides 2 component summaries: the Physical Component Summary (PCS) and the Mental Component Summary (MCS), derived from aggregating the 8 domains according to a scoring algorithm.53
The incidence and severity of AEs were part of the safety evaluation in the study. AEs were Medical Dictionary for Regulatory Activities (MedDRA) Version 23 to show the incidence of all AEs by system organ class, preferred term, relationship to treatment, severity and seriousness.
Statistical Analysis
Data for the primary, key secondary, and other secondary end points for response (i.e., CMV viremia clearance and maintenance of response) were analyzed using statistical testing. For time-to-event data, some end points were summarized descriptively (i.e., Kaplan–Meier plots only) while others were analyzed statistically (i.e., hazard ratios, P values). Data for recurrence of CMV viremia, HRQoL and resistance to study treatment were summarized descriptively. For continuous variables, the number of non–missing observations, mean, SD, minimum and maximum values, median and interquartile range were presented. For categorical variables, the number of non–missing observations, number of missing and non–missing observations, and frequencies were reported. If not defined otherwise, the percentage denominator was the number of patients with non–missing information. In case of subgroups, the relative frequencies were calculated based on the patients in the respective category.
Sample Size Determination and Power Calculation
According to the SOLSTICE Statistical Analysis Plan, 90% power in hypothesis testing at an alpha level of 0.05 with a 2-sided test for the primary outcome required 315 patients with post-transplant CMV infection in the ratio of 2:1 (210 patients in the maribavir arm and 105 patients in the control arm).
To determine the sample size, the investigators assumed that at least 60% of maribavir-treated patients would have achieved undetectable plasma CMV DNA at Week 7 and Week 8 based on evidence from the sponsor’s previous phase II studies.40,41
The investigators considered 40% as an approximately reasonable estimate of the proportion of patients with confirmed undetectable plasma CMV DNA at Week 7 and Week 8 in a control arm. A treatment difference of 20% between the maribavir and control arms was considered a clinically meaningful difference. Applying a 2-arm continuity corrected Chi-square test of equal proportions and considering 10% dropouts, the investigators planned to enroll and randomize 351 patients (234 patients in maribavir arm and 117 patients in the control arm).
Primary and Key Secondary End Points
Confirmed plasma CMV DNA clearance at the end of study week 8 was defined as the proportion of patients with plasma CMV DNA concentration < LLOQ (i.e., < 137 IU/mL) per central laboratory result in 2 consecutive post-baseline samples, separated by at least 5 days. The difference in proportion of responders between treatment groups was obtained using Cochran-Mantel-Haenszel (CMH) weighted average across all strata, and tested using CMH method, with transplant type and baseline plasma CMV DNA concentration as 2 stratification factors. The 95% confidence limits of the weighted average of difference across strata were provided using the normal approximation. If the minimum expected number of patients in a response category in a treatment group, was less than 5, the groups were collapsed into 1 stratum level. Homogeneity across strata was tested using the Breslow-Day test. If the test was significant at alpha = 0.05 level, stratum-specific difference in proportion was also reported and the adjusted difference and 95% CI in proportion of responders between treatment groups was obtained and tested using minimum risk weight method of Mehrotra and Railkar (2000)54 instead of the CMH method. In efficacy analyses, the primary method to handle missing data due to early dropouts was to treat it as a non–responder. Time points for evaluation of viral load for the primary end point were weeks 7 and 8, but data from adjacent weeks may have been used to impute missing data. When adjacent data was not available as per the pre-specified imputation requirements, patients were counted as non–responders.55
For the key secondary end point, the difference in proportion of responders between treatment groups was obtained and tested using the same method as described for the primary end point.
Subgroup Analyses
The primary end point was reported for the following subgroups identified in the CADTH systematic review: CMV DNA viral load at baseline (low, intermediate, or high), prior antilymphocyte use (yes versus no), type of transplant (i.e., SOT versus HSCT, organ transplanted), and presence of CMV mutation resistant to ganciclovir, foscarnet, and/or cidofovir per central laboratory results (yes versus no). Not all subgroups identified in the protocol were analyzed in SOLSTICE.
Subgroup analysis was only conducted for the key secondary end point using the same subgroups as those for the primary end point: CMV DNA viral load at baseline (low, intermediate, or high), prior antilymphocyte use (yes versus no), type of transplant (i.e., SOT versus HSCT, organ transplanted), and presence of CMV mutation resistant to ganciclovir, foscarnet, and/or cidofovir per central laboratory results (yes versus no). Not all subgroups identified in the protocol were analyzed in SOLSTICE. Subgroup analyses were not conducted for any other end points.
Sensitivity Analyses
Sensitivity analyses were conducted based on CMV DNA concentration values, using the randomized set. The following sensitivity analyses for the primary end point were conducted:
considering patients with viremia clearance at premature discontinuation as responders
analyzing primary end point of response using multivariable logistic regression model with a pre-specified list of characteristics
repeating analyses by excluding patients who discontinue early from the analysis set
including clearance at any time during the first 8 weeks as response
including IAT patients who initiated alternative treatment before week 8 as responders if they met the criteria for clearance at week 8
limiting the sample to patients who completed 8 weeks of assigned therapy
excluding patients who discontinued treatment early
using stratification factors assigned at randomization.
Prior use of CMV prophylaxis and CMV serostatus were not included in the multivariable logistic regression model, with the investigators citing the biologic meaning and moderate to strong correlation with transplant type, which was 1 of the fixed variables. If at least 5% of patients had missing CMV DNA data to confirm response at week 8 due to the COVID-19 pandemic, missing CMV DNA levels were imputed using a multiple imputation method.
The sensitivity analyses conducted for the key secondary end point were similar to those conducted for the primary end point.
Multiplicity Testing
The hypothesis testing of the primary and key secondary end point was adjusted for multiple comparisons using a fixed-sequence testing procedure to control the family-wise type 1 error rate at 5% level. If the proportion of response for the primary efficacy end point was higher in the maribavir group and the test of adjusted difference in proportion of responders between treatment groups was statistically significant, and the proportion of response for the key secondary efficacy end point was higher in the maribavir group and the test was significant at the 0.05 level, it was concluded that the treatment effect was more durable for maribavir as compared to the IAT group. No adjustments were made for multiple comparisons for any of the other end points.
Other Secondary and Exploratory End Points
For other secondary end points for response, statistical analyses were conducted following the same method as described for the primary end point, at alpha = 0.05 (2-sided) without adjustment for multiple comparisons.
Recurrence of CMV viremia were summarized descriptively.
For all-cause mortality, mortality status for all patients was summarized descriptively. Additionally, Kaplan–Meier estimates of the minimum, median, maximum were reported. This end point was compared between the 2 groups using the log-rank test. The treatment difference (hazard ratio, and its 95% CI) between maribavir and IAT treatment groups was estimated using the stratified Cox’s regression model with transplant type and baseline plasma CMV DNA level as 2 stratification factors.
Data for resistance to study drugs were summarized descriptively.
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||.
All other time-to-event end points (i.e., time to viremia clearance and recurrence events and |||||||||||||||||||||||) were summarized either using Kaplan–Meier method or descriptive statistics (minimum, median, and maximum).
An AE summary table was used to present the number of events, number of patients and the percentage of patients having treatment-emergent AEs, SAEs, and treatment-emergent AEs that led to study discontinuation.
Censoring
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||. For all-cause mortality, patients who were alive at last contact were censored in the analysis.
Analysis Populations
The enrolled set consisted of all patients who had signed informed consent and some study procedures had begun (e.g., dispensed study-assigned treatment, current drug had been withdrawn).
The randomized set was used as the primary population for the analyses of most efficacy end points. The randomized set consisted of patients in the enrolled set who have been randomized to the study. Patients were analyzed in the group to which they were randomized. For all primary and secondary end points other than those assessing recurrence, efficacy evaluations during the treatment phase and follow-up phase included data before patients received alternative anti-CMV treatment or maribavir rescue therapy.
The modified randomized set was used for the analyses of some efficacy end points. This set consisted of all patients in the enrolled set who had been randomized to the study and had taken any dose of study-assigned treatment. Patients were analyzed in the treatment group to which they had been randomized.
The safety set was used to conduct safety analyses. The safety set included all patients who took any dose of the assigned treatment. Patients were analyzed according to the treatment that they received.-Safety data were reported separately for patients in the rescue arm.
The per protocol set consisted of all patients in the randomized set who did not have relevant major protocol deviations that could have affected the primary efficacy assessment. Prior to database lock, the sponsor reviewed the protocol deviations collected throughout the study and determined which of those were relevant major protocol deviations.
The maribavir-resistance set includes patients with pre-existing known (confirmed) maribavir-resistance mutations in UL97 and/or UL27 genes. The non–maribavir-resistance set includes all patients excluded from the maribavir-resistance set (i.e., those patients with evaluable genotyping data but without pre-existing confirmed maribavir-resistance mutations in UL97 and/or UL27 genes). The primary resistance (PRS) set included patients with pre-existing confirmed ganciclovir/valganciclovir, foscarnet, or cidofovir resistance mutations in UL97 and/or UL54 genes. The non–primary resistance set included all patients who were excluded from the PRS (i.e., those patient with evaluable genotyping data but without pre-existing known confirmed ganciclovir/valganciclovir, foscarnet, or cidofovir resistance mutations in UL97 and/or UL54 genes).
Protocol Amendments and Deviations
A summary of key protocol amendments implemented in the SOLSTICE study is presented in Table 12. In the original protocol the assessment of invasive bacterial and fungal infection was not part of the safety end point; however, it was added before patient enrollment began.
Table 12: Summary of Key Protocol Amendments in SOLSTICE
Amendment (date) | Key changes |
|---|---|
Amendment 1 (July 08, 2016) |
|
Amendment 2 (December 01, 2016) |
|
Amendment 3 (March 01, 2017) |
|
Amendment 4 (March 26, 2018) |
|
Amendment 5 (August 20, 2018) |
|
Amendment 6 (December 07, 2018) |
|
DMC = Data Monitoring Committee.
Source: SOLSTICE Clinical Study Report.4
Almost all patients (96.9%) had at least 1 protocol deviation or good clinical practice deviation during the study, with similar proportions in both groups (maribavir: 96.6% versus IAT: 97.4%). At least 1 major deviation was reported for 229 (65.1%) patients, with the distribution of major deviations being similar between treatment groups (maribavir: 66.0% versus IAT: 63.2%, respectively). |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||.
Results
Patient Disposition
Patient disposition in the SOLSTICE study is summarized in Table 13. In total, 415 patients were screened, of which 63 (15.2%) were screen failures. The most frequently reported reasons for screen failure were failure to demonstrate confirmed minimum CMV viral load ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| and failure to demonstrate that current CMV infection was refractory to the most recent CMV treatment ||||||||||||||||||||||||||||||||||||||||||||||. A total of 352 patients were randomized, 235 to the maribavir group and 117 to the IAT group. One randomized patient from each group was not dosed, leaving a total of 350 patients for the modified randomized and safety sets. Overall, 183 (77.9%) and 37 (31.6%) of patients in the maribavir and IAT groups, respectively, completed the 8-week study-assigned treatment. In total, 51 (21.7%) and 79 (67.5%) patients in the maribavir and IAT groups, respectively, discontinued from the study before the 8-week study treatment period; the primary reasons were due to AEs (maribavir: 6.4% versus IAT: 30.8%), lack of efficacy (maribavir: 8.9% versus IAT: 13.7%), and other reasons for discontinuation (maribavir: 1.7% versus IAT: 13.7%). Death led to treatment discontinuation for 3.0% for maribavir-treated patients and 0.9% of IAT-treated patients. Additional details on the reasons for study treatment discontinuation are presented in Table 13.
Table 13: Patient Disposition (Enrolled Set)
Detail | SOLSTICE | |
|---|---|---|
Maribavir | IAT | |
Screened, N | 415 | |
Screened failure, N (%) | 63 (15.2) | |
Randomized, N (%) | 235 | 117 |
Randomized but not dosed, n (%) | 1 (0.4) | 1 (0.9) |
Completed 8-week study-assigned treatment, n (%) | 183 (77.9) | 37 (31.6) |
Discontinued from study early, N (%) | 51 (21.7) | 79 (67.5) |
Primary reason for treatment discontinuation, N (%) | ||
Withdrawal of consent | 2 (0.9) | 8 (6.8) |
Death | 7 (3.0) | 1 (0.9) |
Non–Compliance | 2 (0.9) | 1 (0.9) |
Lack of efficacy | 21 (8.9) | 16 (13.7) |
Adverse events | 15 (6.4) | 36 (30.8) |
Lost to follow-up | 0 | 1 (0.9) |
Other | 4 (1.7) | 16 (13.7) |
Final status for patients in the randomized set with study-assigned treatment who did not switch to rescue treatment, n (%) | 235 (100.0) | 95 (81.2) |
Study completed | 199 (84.7) | 58 (49.6) |
Discontinued early | 36 (15.3) | 37 (31.6) |
Primary reason for discontinuation, N (%) | ||
Death | 24 (10.2) | 8 (6.8) |
Adverse event | 1 (0.4) | 5 (4.3) |
Noncompliance | 0 | 6 (5.1) |
Withdrawal of consent | 8 (3.4) | 16 (13.7) |
Lost to follow-up | 2 (0.9) | 1 (0.9) |
Other | 1 (0.4) | 1 (0.9) |
Rescue arm, N (%) | NA | 22 (18.8) |
Modified randomized, N (%) | 234 (99.6) | 116 (99.1) |
PP, N (%) | 223 (94.9) | 108 (92.3) |
Safety, N (%) | 234 (99.6) | 116 (99.1) |
Treatment type for IAT | ||
Foscarnet | NA | 47 (40.5) |
Ganciclovir | NA | 28 (24.1) |
Valganciclovir | NA | 28 (24.1) |
Cidofovir | NA | 6 (5.2) |
Foscarnet/valganciclovir | NA | 4 (3.4) |
Foscarnet/ganciclovir | NA | 3 (2.6) |
IAT = investigator-assigned treatment; NA = not applicable; PP = per protocol.
Source: SOLSTICE Clinical Study Report.4
Exposure to Study Treatments
Exposure to study treatment in SOLSTICE is summarized in Table 14. The 350 patients received at least 1 dose of a study drug; 234 patients in the maribavir group and 116 patients in the IAT group. For patients dosed with maribavir, the mean duration of exposure (i.e., days between the date of first exposure to the date of last exposure) was 52.5 days (SD: 11.81 days). The mean number of days in which at least 1 dose of study-assigned treatment was taken or administered was 48.6 days (SD: 13.82 days). For patients dosed with IAT, the mean duration of exposure was 36.0 days (SD: 18.06 days). The mean number of days in which at least 1 dose of study-assigned treatment was taken or administered was 31.2 days (SD: 16.91 days).
Concomitant medications in SOLSTICE were defined as any medication with a start date before the date of the first dose of study-assigned treatment and continuing after the first dose of study-assigned treatment or with a start date on or after the study-assigned treatment initiation and before the end of the on-treatment period. The most frequently reported concomitant medications (≥ 20%) were immunosuppressants (maribavir: 92.3% versus IAT: 94.0%), |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| corticosteroids for systemic use (maribavir: 75.6% versus IAT: 72.4%), |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||.
Table 14: Investigational Product Exposure (Safety Set)
Exposure detail | Maribavir (N = 234) | IAT (N = 116) |
|---|---|---|
Exposure duration (days)a | ||
nb | 230 | 114 |
Mean (SD) | 52.5 (11.81) | 36.0 (18.06) |
Actual exposure to study-assigned treatment (days)c | ||
nb | 230 | 114 |
Mean (SD) | 48.6 (13.82) | 31.2 (16.91) |
||||||||||||||||||||||| | ||
||||||||||||||||||||||| | ||||||||||||||||||||||| | ||||||||||||||||||||||| |
||||||||||||||||||||||| | ||||||||||||||||||||||| | ||||||||||||||||||||||| |
IAT = investigator-assigned anti-CMV treatment; N = number of subjects; SD = standard deviation.
aExposure duration is the number of days between the date of the first exposure and the date of last exposure of the drug administered.
bTwo patients in the IAT group (valganciclovir) and 4 patients in the maribavir group did not have any eDiary data collected for administration of oral study-assigned treatment. These patients are not included in this table.
Source: SOLSTICE Clinical Study Report.4
Dose Interruptions and Reductions
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Table 15: Change in Investigational Product Exposure (Safety Set)
||||||||||||||||||||||| | Maribavir (N = 234) | IAT (N = 116) |
|---|---|---|
||||||||||||||||||||||| | ||||||||||||||||||||||| | ||||||||||||||||||||||| |
||||||||||||||||||||||| | ||
||||||||||||||||||||||| | ||||||||||||||||||||||| | ||||||||||||||||||||||| |
||||||||||||||||||||||| | ||||||||||||||||||||||| | ||||||||||||||||||||||| |
||||||||||||||||||||||| | ||||||||||||||||||||||| | ||||||||||||||||||||||| |
||||||||||||||||||||||| | ||||||||||||||||||||||| | ||||||||||||||||||||||| |
||||||||||||||||||||||| | ||||||||||||||||||||||| | ||||||||||||||||||||||| |
||||||||||||||||||||||| | ||
||||||||||||||||||||||| | ||||||||||||||||||||||| | ||||||||||||||||||||||| |
||||||||||||||||||||||| | ||||||||||||||||||||||| | ||||||||||||||||||||||| |
||||||||||||||||||||||| | ||||||||||||||||||||||| | ||||||||||||||||||||||| |
||||||||||||||||||||||| | ||||||||||||||||||||||| | ||||||||||||||||||||||| |
||||||||||||||||||||||| | ||||||||||||||||||||||| | ||||||||||||||||||||||| |
||||||||||||||||||||||| | ||||||||||||||||||||||| | ||||||||||||||||||||||| |
AE = adverse events; IAT = investigator-assigned treatment; n = number of subjects experiencing the event at least once; m = number of events.
aChange from the previous entry for the medication was collected.
bPercentages are based on those who had reported a change from the previous entry for the medication. Some patients could have multiple changes throughout the treatment.
Source: SOLSTICE Clinical Study Report.4
Adherence
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Efficacy
Only those efficacy outcomes and analyses of subgroups identified in the review protocol are reported below. Refer to Appendix 3 for detailed efficacy data.
Clinically Significant CMV Infection
Confirmed CMV Viremia Clearance Response at Week 8 (Primary End Point)
Confirmed CMV viremia clearance results from the SOLISTICE study at week 8 are summarized in Table 16. For overall response, the adjusted difference in proportion of responders between maribavir and IAT was 32.8% (95% CI, 22.80% to 42.74%; P < 0.001), in favour of maribavir. Sensitivity analyses were mainly consistent with the main analysis with the notable exception of 1 analysis, where only patients on-treatment for 8 weeks were included, that failed to reach statistical significance.
In the maribavir group, of the 104 non–responders in the maribavir group, more than half (60, 57.7% patients) were confirmed non–responders for the primary end point.
These patients had CMV DNA measurements through week 8 but did not meet the response criteria at week 8. For 26 of 104 (25.0%) non–responders in the maribavir group, the reason for not achieving the primary end point was due to initiation of alternative (non–study) anti-CMV therapy before week 8. Seventeen (16.3%) maribavir-treated non–responders did not have CMV DNA measurement to evaluate response at week 8, predominantly due to early discontinuation (16 of the 17 patients with missing CMV DNA at week 8). In the IAT group, approximately 1-fifth of the non–responders (18 of 89, 20.2% patients) were confirmed non–responders. The common reasons for failure to achieve the primary end point in the IAT group were evenly distributed across initiation of alternative anti-CMV therapy before week 8 (24 of 89, 27.0% patients), missing CMV measurement (24 of 89, 27.0% patients), and meeting the criteria to switch to maribavir rescue therapy (22 of 89, 24.7% patients).
Results of the subgroup analyses for the primary end point (confirmed CMV viremia clearance response at week 8) are reported in Table 17.
Table 16: Summary of Confirmed CMV Viremia Clearance Response at Week 8 Results (Randomized Set)
Detail | Maribavir (N = 235) | IAT (N = 117) |
|---|---|---|
Overall responders, n (%) | 131 (55.7) | 28 (23.9) |
Overall non–responders, n (%) | 104 (44.3) | 89 (76.1) |
Unadjusted difference in proportion of responders, % (95% CI)a | 31.8 (21.81 to 41.82) | Reference |
Adjusted difference in proportion of responders, % (95% CI)b | 32.8 (22.80 to 42.74) | Reference |
P value: adjustedb | < 0.001 | Reference |
P value: Homogeneity across stratac | 0.598 | Reference |
CI = confidence interval; IAT = investigator-assigned treatment.
aUnadjusted difference in proportion (Maribavir to IAT) and the corresponding 95% CI is computed by the normal approximation method.
bCMH weighted average approach is used for the adjusted difference in proportion (Maribavir – IAT), the corresponding 95% CI, and the P value after adjusting for the transplant type and baseline plasma CMV DNA concentration if homogeneity is met. The minimum risk weight method is used if the homogeneity is not met. Only those with both stratification factors are included in the computation.
cBreslow-Day test was used for testing the homogeneity across strata. The stratum-specific difference in proportion was reported only if the P value for homogeneity across strata was significant.
Source: SOLSTICE Clinical Study Report.4
Table 17: Subgroup Analyses of Confirmed CMV Viremia Clearance Response at Week 8 (Randomized Set)
Subgroup | Maribavir (N = 235) | IAT (N = 117) | Adjusted difference in proportion of responders | |||
|---|---|---|---|---|---|---|
n/N | % (95% CI) | n/N | % (95% CI) | % (95% CI)a | P valueb | |
IAT type | ||||||
Ganciclovir/ Valganciclovir | 131/235 | 55.7 (49.39 to 62.10) | 15/56 | 26.8 (15.19 to 38.38) | 31.7 (18.63 to 44.78) | < 0.001 |
Foscarnet | 131/235 | 55.7 (49.39 to 62.10) | 9/47 | 19.1 (7.90 to 30.40) | 36.4 (23.37 to 49.40) | < 0.001 |
Cidofovir | 131/235 | 55.7 (49.39 to 62.10) | 0/6 | 0 (NA to NA) | NA | NA |
> 1 IAT | 131/235 | 55.7 (49.39 to 62.10) | 4/7 | 57.1 (20.48 to 93.80) | –3.2 (–40.31 to 33.96) | 0.867 |
Transplant type | ||||||
SOT | 79/142 | 55.6 (47.46 to 63.81) | 18/69 | 26.1 (15.73 to 36.45) | 30.5 (17.31 43.61) | < 0.001 |
HSCT | 52/93 | 55.9 (45.82 to 66.00) | 10/48 | 20.8 (9.34 to 32.32) | 36.1 (20.92 to 51.37) | < 0.001 |
||||||||||||||||||||||| | ||||||
||||||||||||||||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
||||||||||||||||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
||||||||||||||||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
||||||||||||||||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
||||||||||||||||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
||||||||||||||||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
||||||||||||||||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
CMV DNA Viral Load | ||||||
Low | 95/153 | 62.1 (54.40 to 69.78) | 21/85 | 24.7 (15.54 to 33.87) | 37.4 (25.41 to 49.37) | < 0.001 |
Intermediate/High | 36/82 | 43.9 (33.16 to 54.64) | 7/32 | 21.9 (7.55 to 36.20) | 21.8 (3.93 to 39.67) | 0.017 |
Antilymphocyte Use | ||||||
Yes | 53/100 | 53.0 (43.22 to 62.78) | 12/49 | 24.5 (12.45 to 36.53) | 29.9 (14.30 to 45.46) | < 0.001 |
No | 78/135 | 57.8 (49.45 to 66.11) | 16/68 | 23.5 (13.45 to 33.61) | 35.0 (21.94 to 48.01) | < 0.001 |
Resistance Status | ||||||
Yes | 76/121 | 62.8 (54.20 to 71.42) | 14/69 | 20.3 (10.80 to 29.78) | 44.1 (31.33 to 56.94) | < 0.001 |
No | 42/96 | 43.8 (33.83 to 53.67) | 11/34 | 32.4 (16.63 to 48.08) | 12.6 (–6.24 to 31.43) | 0.190 |
CI = confidence interval; CMV = cytomegalovirus; HSCT = hematopoietic stem-cell transplant; IAT = investigator-assigned treatment NA = not applicable; SOT = solid organ transplant.
aCMH weighted average approach was used for the adjusted difference in proportion (maribavir – IAT) and the corresponding 95% confidence interval adjusting for the transplant type and baseline plasma CMV DNA concentration that remained applicable. Kidney transplant included subjects with a most recent SOT type of kidney or kidney and other organ(s).
bP value has not been adjusted for multiple testing.
Source: SOLSTICE Clinical Study Report.4
Confirmed CMV Viremia Clearance and CMV Infection Symptom Control at Week 8 Followed by Maintenance Through Week 16 (Key Secondary End Point)
A summary of the confirmed CMV viremia clearance response and CMV symptom control from the SOLISTICE study at week 8 and maintained through week 16 is summarized in Table 18. For overall response, the adjusted difference in proportion of responders between maribavir and IAT is 9.5% (95% CI, 2.02% to 16.88%; P = 0.013), in favour of maribavir. Sensitivity analyses of the key secondary end point were consistent with the main analysis.
Maintenance of CMV Viremia Clearance and CMV Infection Symptom Control Achieved at the End of Week 8 Through Weeks 12 to 20 (Secondary End Point)
A summary of the confirmed CMV viremia clearance response and CMV symptom control from the SOLISTICE study at week 8 and maintained through week 12 to week 20 is summarized in Table 19. For overall response, the adjusted differences in proportion of responders between maribavir and IAT at weeks 12 to 20 was 13.5% (95% CI, 5.84% to 21.17%) and 9.8% (95% CI, 2.58% to 17.06%), respectively, in favour of maribavir.
Confirmed CMV Viremia Clearance Response at Study Week 8, 12, 16 and 20 After Receiving 8 Weeks of Study Treatment (Secondary End Point)
A summary of the confirmed CMV viremia clearance response from the SOLISTICE study at weeks 8, 12, 16, and 20, after receiving 8 weeks of treatment, is presented in Table 20. At week 8, the adjusted difference in proportion of responders was 36.8% (95% CI, 27.26 to 46.40). At week 12, the adjusted difference in proportion of responders was 17.8% (95% CI, 10.89 to 24.77) in favour of maribavir. At week 16, the adjusted difference in proportion of responders was 13.9% (95% CI, 7.21 to 20.56) in favour of maribavir. At week 20, the adjusted difference in proportion of responders was 14.2% (95% CI, 7.70 to 20.75) in favour of maribavir.
Table 18: Summary of Confirmed CMV Viremia Clearance and CMV Infection Symptom Control at Week 8 Followed by Maintenance Through Week 16 (Randomized Set)
Detail | Maribavir (N = 235) | IAT (N = 117) |
|---|---|---|
Overall Responders, n (%) | 44 (18.7) | 12 (10.3) |
Overall non–responders, n (%) | 191 (81.3) | 105 (89.7) |
Unadjusted difference in proportion of responders, % (95% CI)a | 8.5 (1.04 to 15.89) | Reference |
Adjusted difference in proportion of responders, % (95% CI)b | 9.5 (2.02 to 16.88) | Reference |
P value: adjustedb | 0.013 | Reference |
P value: Homogeneity across stratac | 0.312 | Reference |
CI = confidence interval; IAT = investigator-assigned treatment.
aUnadjusted difference in proportion (maribavir to IAT) and the corresponding 95% CI were computed by the normal approximation method.
bCMH weighted average approach was used for the adjusted difference in proportion (maribavir to IAT), the corresponding 95% CI, and the P value after adjusting for the transplant type and baseline plasma CMV DNA concentration if homogeneity was met. The minimum risk weight method was used if the homogeneity was not met. Only those with both stratification factors were included in the computation.
cBreslow-Day test was used for testing the homogeneity across strata. The stratum-specific difference in proportion was reported only if the P value for homogeneity across strata was significant.
Source: SOLSTICE Clinical Study Report.4
Table 19: Summary of Confirmed CMV Viremia Clearance and CMV Infection Symptom Control Response at Study Week 8, Maintenance Through Week 12 and Week 20 (Randomized Set)
Detail | Maribavir (N = 235) | IAT (N = 117) |
|---|---|---|
At study week 8 | ||
Responders, n (%) | 131 (55.7) | 28 (23.9) |
Non–responders, n (%) | 104 (44.3) | 89 (76.1) |
Unadjusted difference in proportion of responders, % (95% CI)a | 31.8 (21.81 to 41.82) | Reference |
Adjusted difference in proportion of responders, % (95% CI)b | 32.8 (22.80 to 42.74) | Reference |
P value: Adjustedb,c | < 0.001 | Reference |
P value: Homogeneity across stratab, c | 0.598 | Reference |
Maintenance through study week 12 | ||
Responders, n (%) | 53 (22.6) | 12 (10.3) |
Non–responders, n (%) | 182 (77.4) | 105 (89.7) |
Unadjusted difference in proportion of responders, % (95% CI)a | 12.3 (4.63 to 19.96) | Reference |
Adjusted difference in proportion of responders, % (95% CI)b,c | 13.5 (5.84 to 21.17) | Reference |
P value: Adjustedb,c | < 0.001 | Reference |
P value: Homogeneity across stratab,c | 0.236 | Reference |
Maintenance through study week 20 | ||
Responders, n (%) | 43 (18.3) | 11 (9.4) |
Non–responders, n (%) | 192 (81.7) | 106 (90.6) |
Unadjusted difference in proportion of responders, % (95% CI)a | 8.9 (1.66 to 16.14) | Reference |
Adjusted difference in proportion of responders, % (95% CI)b, c | 9.8 (2.58 to 17.06) | Reference |
P value: Adjustedb, c | 0.008 | Reference |
P value: Homogeneity across stratac | 0.435 | Reference |
CI = confidence interval; IAT = investigator-assigned anti-CMV treatment.
aUnadjusted difference in proportion (maribavir to IAT) and the corresponding 95% CI were computed by the normal approximation method.
bCMH weighted average approach was used for the adjusted difference in proportion (maribavir to IAT), the corresponding 95% CI, and the P value after adjusting for the transplant type and baseline plasma CMV DNA concentration if homogeneity was met. The minimum risk weight method was used if the homogeneity was not met. Only those with both stratification factors were included in the computation. Breslow-Day test was used for testing the homogeneity across strata. The stratum-specific difference in proportion was reported only if the p value for homogeneity across strata was significant.
cP value has not been adjusted for multiple comparisons.
Source: SOLSTICE Clinical Study Report4
Table 20: Summary of Confirmed CMV Viremia Clearance Response at Study Week 8, 12, 16 and 20 After Receiving 8 Weeks of Study Treatment (Randomized Set)
Detail | Maribavir (N = 235) | IAT (N = 1 17) |
|---|---|---|
Number of patients who had received study treatment | 183 | 37 |
At study week 8 | ||
Responders, n (%) | 129 (54.9) | 22 (18.8) |
Non–responders, n (%) | 106 (45.1) | 95 (81.2) |
Unadjusted difference in proportion of responders, % (95% CI)a | 36.1 (26.57 to 45.61) | Reference |
Adjusted difference in proportion of responders, % (95% CI)b | 36.8 (27.26 to 46.40) | Reference |
P value: Adjustedb,d | < 0.001 | Reference |
P value: Homogeneity across stratac,d | 0.201 | Reference |
Maintenance through study week 12 | ||
Responders, n (%) | 53 (22.6) | 6 (5.1) |
Non–responders, n (%) | 182 (77.4) | 111 (94.9) |
Unadjusted difference in proportion of responders, % (95% CI)a | 17.4 (10.75 to 24.10) | Reference |
Adjusted difference in proportion of responders, % (95% CI)b | 17.8 (10.89 to 24.77) | Reference |
P value: Adjustedb,d | < 0.001 | Reference |
P value: Homogeneity across stratac,d | 0.013 | Reference |
Maintenance through study week 16 | ||
Responders, n (%) | 44 (18.7) | 6 (5.1) |
Non–responders, n (%) | 191 (81.3) | 111 (94.9) |
Unadjusted difference in proportion of responders, % (95% CI)a | 13.6 (7.20 to 19.99) | Reference |
Adjusted difference in proportion of responders, % (95% CI)b | 13.9 (7.21 to 20.56) | Reference |
P value: Adjustedb,d | < 0.001 | Reference |
P value: Homogeneity across stratac,d | 0.023 | Reference |
Maintenance through study week 20 | ||
Responders, n (%) | 43 (18.3) | 5 (4.3) |
Non–responders, n (%) | 192 (81.7) | 112 (95.7) |
Unadjusted difference in proportion of responders, % (95% CI)a | 14.0 (7.87 to 20.18) | Reference |
Adjusted difference in proportion of responders, % (95% CI)b | 14.2 (7.70 to 20.75) | Reference |
P value: Adjustedb,d | < 0.001 | Reference |
P value: Homogeneity across stratac,d | 0.032 | Reference |
CI = confidence interval; CMV = cytomegalovirus.
aUnadjusted difference in proportion (maribavir to IAT) and the corresponding 95% CI were computed by the normal approximation method.
bCMH weighted average approach was used for the adjusted difference in proportion (maribavir to IAT), the corresponding 95% CI, and the P value after adjusting for the transplant type and baseline plasma CMV DNA concentration if homogeneity was met.
cThe minimum risk weight method was used if the homogeneity was not met. Only those with both stratification factors were included in the computation.
dP value has not been adjusted for multiple comparisons.
Source: SOLSTICE Clinical Study Report.4
Time to CMV Viremia Clearance
The median observed event time for patients who had CMV viremia clearance was 17.0 days (minimum: 5.0 days, maximum: 114.0 days) in the maribavir group and 20.0 days (minimum: 6.0, maximum: 111.0) in the IAT group. The Kaplan–Meier plot of CMV viremia clearance is depicted in Figure 3. The Kaplan–Meier estimate for median days to CMV viremia clearance was 22.0 days (95% CI, 21.0 to 23.0 days) for the maribavir group and 29.0 days (95% CI, 22.0 days to 35.0 days) for the IAT group. The sensitivity analysis was consistent with the main analysis.
New CMV Events
Post-Baseline New Onset of Symptomatic CMV Infection
Results for the new onset of symptomatic CMV infection post-baseline are summarized in Table 22. There were 14 (6.0%) patients in the maribavir group and 7 (6.0%) patients in the IAT group who had a confirmed new onset of CMV disease post-baseline by the EAC.
Figure 3: Cumulative Probability of Achieving First CMV Viremia Clearance at Any Time During the Study (Randomized Set)

Confidential figure redacted at the request of the sponsor.
Table 21: Time to First CMV Viremia Clearance at Any Time on Study (Randomized Set)
CMV viremia clearance response | Maribavir (N = 235) | IAT (N = 117) |
|---|---|---|
Number of patients with first CMV viremia clearance at any time on study, n (%) | 184 (78.3) | 65 (55.6) |
|||||||||||||||||||||||||||||||||||| | ||||||||| | ||||||||| |
Observed event time for those who had CMV viremia clearance, median days (min, max) | 17.0 (5.0 to 114.0) | 20.0 (6.0 to 111.0) |
Kaplan–Meier Estimates of time to first CMV viremia clearance, days (95% CI) | ||
||||||||| | ||||||||| | ||||||||| |
50th (Median) | 22.0 (21.0 to 23.0) | 29.0 (22.0 to 35.0) |
||||||||| | ||||||||| | ||||||||| |
P valuea | 0.030 | Reference |
CI = confidence interval; CMV = cytomegalovirus; IAT = investigator-assigned treatment.
aTwo-sided P value comparing treatment groups is from the log-rank test by Kaplan–Meier method. P value was not adjusted for multiple comparisons.
Source: SOLSTICE Clinical Study Report.4
Table 22: Summary of Post-Baseline New Onset of Symptomatic CMV Infection (Randomized Set)
Characteristic | Maribavir (N = 235) | IAT (N = 117) |
|---|---|---|
EAC confirmed new onset CMV disease post-baseline, n (%) | 14 (6.0) | 7 (6.0)a |
Week 8 | 7 (3.0) | 5 (4.3) |
Week 12 | 5 (2.1) | 1 (0.9) |
Week 16 | 1 (0.4) | 2 (1.7) |
Week 20 | 1 (0.4) | 0 (0.0) |
CMV = cytomegalovirus; EAC = End point Adjudication Committee; IAT = investigator-assigned treatment.
aOne patient in the IAT group had new onset of symptomatic CMV infection at both week 12 and week 16.
Source: SOLSTICE Clinical Study Report.4
Recurrence of CMV Viremia
Results for the recurrence of CMV viremia are summarized in Table 23, Table 24, and Table 25. There were 33 (17.9%) patients in the maribavir group and 8 (12.3%) patients in the IAT group who had CMV viremia recurrence during the first 8 weeks. During the follow-up weeks (i.e., week 9 through the end of study), there were 71 (38.6%) patients in the maribavir group and 14 (21.5%) patients in the IAT group who had CMV viremia recurrence.
Table 23: Summary of Recurrence of CMV Viremia During the First 8 weeks, the Follow-up Period, and Any Time on Study (Randomized Set)
Characteristic | Maribavir N = 235 | IAT N = 117 |
|---|---|---|
Number of patients who had CMV viremia clearance after study-assigned treatment at any time on study, n, (%) | 184 (78.3) | 65 (55.6) |
Patient with CMV viremia recurrencea, n (%) | ||
During the first 8 weeksb | 33 (17.9) | 8 (12.3) |
During the follow-up weeks (week 9 through end of study, including rescue visits if applicable) | 71 (38.6) | 14 (21.5) |
Any time on study | 104 (56.5) | 22 (33.8) |
CMV = cytomegalovirus; IAT = investigator-assigned anti-CMV treatment.
aPercentages are based on the number of patients in the Randomized Set who had CMV viremia clearance at any time on study.
bDuring first 8 weeks regardless of whether the study-assigned treatment was discontinued before the end of the stipulated 8 weeks of therapy.
Source: SOLSTICE Clinical Study Report.4
Table 24: Summary of Recurrence of CMV Viremia While On and Off Study-Assigned Treatment (Randomized Set)
Characteristic | Maribavir N = 235 | IAT N = 117 |
|---|---|---|
Number of patients who had CMV viremia clearance after study-assigned treatment at any time on study, n, (%) | 184 (78.3) | 65 (55.6) |
Patient with CMV viremia recurrencea, n (%) | ||
While on study-assigned treatment | 3 (4.6) | 29 (15.8) |
While off study-assigned treatmentc | 19 (29.2) | 75 (40.8) |
CMV = cytomegalovirus; IAT = investigator-assigned anti-CMV treatment.
aPercentages are based on the number of patients in the Randomized Set who had CMV viremia clearance at any time on study, including rescue visits.
Source: SOLSTICE Clinical Study Report.4
Table 25: Summary of Recurrence of CMV Viremia During the First 8 weeks, the Follow-up Period and Any Time on Study Restricted to Those Received 8-week Study-Assigned Treatment (Randomized Set)
Characteristic | Maribavir N = 183 | IAT N = 37 |
|---|---|---|
|||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| |
|||||||||||||||||||||||||||||||||||| | ||
While on study-assigned treatment | 25 (15.2) | 3 (9.7) |
|||||||||||||||||||||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| |
|||||||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Source: SOLSTICE Clinical Study Report.4
Time to CMV Viremia Recurrence
Results for the time from first CMV viremia clearance to CMV viremia recurrence are summarized in Table 26. The median observed time from first CMV viremia clearance to CMV viremia recurrence was 42.0 days (minimum: 14.0 days; maximum: 123.0 days) in the maribavir group and 45.5 days (minimum: 16.0; maximum: 89.0) in the IAT group. The Kaplan–Meier plot of time to CMV viremia recurrence in patients who achieved viremia clearance is depicted in Figure 4. The Kaplan–Meier estimate for median days from first CMV viremia clearance to CMV viremia recurrence was 71.0 days (95% CI, 57.0 to 92.0 days) for the maribavir group and NE (95% CI, 58.0 to NE) for the IAT group.
Results for the time from CMV viremia clearance at week 8 to CMV viremia recurrence requiring alternative treatment are summarized in Table 27. The median observed event time for those who had first CMV viremia clearance at study week 8 to CMV Viremia recurrence requiring alternative treatment was 20.5 days (minimum: 13.0 days; maximum: 80.0 days) in the maribavir group and 22.0 days (minimum: 14.0 days; maximum: 36.0 days) in the IAT group. The Kaplan–Meier plot of first CMV viremia clearance at week 8 to CMV viremia recurrence requiring alternative treatment is depicted in Figure 5. The Kaplan–Meier estimate for median days from first CMV viremia clearance at study week 8 to CMV viremia recurrence requiring alternative treatment was NE (95% CI, NE to NE) for the maribavir group and NE (95% CI, 30.0 to NE) for the IAT group.
Figure 4: Cumulative Probability of CMV Viremia Recurrence in Patients Who Achieved Viremia Clearance

Confidential figure redacted at the request of the sponsor.
CMV = cytomegalovirus; IAT = investigator-assigned treatment.
Confidential figure redacted at the request of the sponsor.
Source: SOLSTICE Clinical Study Report.4
Figure 5: Cumulative Probability of First CMV Viremia Clearance at Study Week 8 to CMV Viremia Recurrence Requiring Alternative Treatment (Randomized Set)

Confidential figure redacted at the request of the sponsor.
Source: SOLSTICE Clinical Study Report.4
Table 26: Time from First CMV Viremia Clearance to CMV Viremia Recurrence (Randomized Set)
Detail | Maribavir (N = 235) | IAT (N = 117) |
|---|---|---|
Number of patients with first CMV viremia clearance from study assigned treatment any time on study | 184 | 65 |
Number of patients with CMV viremia recurrence, n (%) | 104 (56.5) | 22 (33.8) |
||||||||||||||||||||||||||||||||||||||||||||| | ||||||||| | ||||||||| |
Observed event time for those who had CMV viremia recurrence, median days (min, max) | 42.0 (14.0 to 123.0) | 45.5 (16.0 to 89.0) |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| | ||
||||||||| | ||||||||| | ||||||||| |
||||||||| | ||||||||| | ||||||||| |
||||||||| | ||||||||| | ||||||||| |
||||||||| | ||||||||| | ||||||||| |
CMV = cytomegalovirus; CI = confidence interval; IAT = investigator-assigned treatment; NE = not estimable.
aTwo-sided P value comparing treatment groups is from the log-rank test by Kaplan–Meier method. P value was not adjusted for multiple comparisons.
Source: SOLSTICE Clinical Study Report.4
Table 27: Time from CMV Viremia Clearance at Week 8 to CMV Viremia Recurrence Requiring Alternative Treatment (Randomized Set)
Detail | Maribavir (N = 235) | IAT (N = 117) |
|---|---|---|
Number of patients with first CMV viremia clearance at week 8 | 131 | 28 |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| | ||||||||| | ||||||||| |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| | ||||||||| | ||||||||| |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| | ||||||||| | ||||||||| |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| | ||
||||||||| | ||||||||| | ||||||||| |
||||||||| | ||||||||| | ||||||||| |
||||||||| | ||||||||| | ||||||||| |
||||||||| | ||||||||| | ||||||||| |
CI = confidence interval; CMV = cytomegalovirus; IAT = investigator-assigned treatment; NE = not estimable.
aTwo-sided P value comparing treatment groups is from the log-rank test by Kaplan–Meier method. P value was not adjusted for multiple comparisons.
Source: SOLSTICE Clinical Study Report.4
All-Cause Mortality
Results for the all-cause mortality are summarized in Table 28. The number of patients who died in the maribavir group was 27 (11.5%) and 13 (11.1%) in the IAT group.
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Figure 6: Cumulative Probability of All-Cause Mortality (Randomized Set)

Confidential figure redacted at the request of the sponsor.
Table 28: Time to All-Cause Mortality (Randomized Set)
Detail | Maribavir (N = 235) | IAT (N = 117) |
|---|---|---|
Number of patients who died, n (%) | 27 (11.5) | 13 (11.1) |
|||||||||||||||||||||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| |
|||||||||||||||||||||||||||||||||||| | |||| ||||| |||||| | |||||||||||||||||| |
|||||||||||||||||||||||||||||||||||| | ||
|||||||||||||||||||||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| |
|||||||||||||||||||||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| |
|||||||||||||||||||||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| |
|||||||||||||||||||||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| |
|||||||||||||||||||||||||||||||||||| | ||
|||||||||||||||||||||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| |
CI = confidence interval; IAT = investigator-assigned treatment.
aTwo-sided P value comparing treatment groups is from the log-rank test by Kaplan–Meier method. P value was not adjusted for multiple comparisons.
bStratified Cox regression model using transplant type and baseline plasma CMV DNA level as stratification factors.
Source: SOLSTICE Clinical Study Report.4
Health Care Resource Utilization
Results from the health care resource utilization data are summarized in Table 29.
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Antiviral Resistance
Results from the treatment-emergent known RASs is summarized in Table 30. In the maribavir group, 42 (19.6%) patients had new maribavir treatment-emergent known RASs in pUL97 or pUL27. For RASs known to confer resistance to IAT (i.e., pUL97 and pUL54), 12.9% of patients in the maribavir group and 4.9% of patients in the IAT group had new treatment-emergent RASs.
HRQoL
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Table 29: Summary of Health Care Resource Utilization
Dimension | On-treatment phase | Full study period | ||
|---|---|---|---|---|
Maribavir (N = 235) | IAT (N = 117) | Maribavir (N = 235) | IAT (N = 117) | |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| | ||||
|||||||||||||||||||||||||||||||| | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| |
|||||||||||||||||||||||||||||||| | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| |
|||||||||||||||||||||||||||||||| | |||||||||||||||| | |||||||||||||||| | ||
|||||||||||||||||||||||||||||||| | |||||||||||||||| | |||||||||||||||| | ||
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| | ||||
|||||||||||||||||||||||||||||||| | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| |
|||||||||||||||||||||||||||||||| | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| |
|||||||||||||||||||||||||||||||| | |||||||||||||||| | |||||||||||||||| | ||
|||||||||||||||||||||||||||||||| | |||||||||||||||| | |||||||||||||||| | ||
|||||||||||||||||||||||||||||||| | |||||||||||||||| | |||||||||||||||| | ||
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Table 30: Summary of Treatment-Emergent Known Resistance-Associated Amino Acid Substitutions (Modified Randomized Set)
Detail | Maribavir (N = 234) | IAT (N = 116) |
|---|---|---|
Maribavir | ||
Patients in MRS + non-MRS, n | 214 | 100 |
Patients in MRS + non-MRS with post-baseline genotype, n (%) | 80 (37.4) | 38 (38.0) |
New maribavir RASs in pUL97 or pUL27 | 42 (19.6) | 0 |
pUL97 only | 42 (19.6) | 0 |
pUL27 only | 0 | 0 |
pUL97 and pUL27 | 0 | 0 |
IAT | ||
Patients in PRS + non-PRS, n | 217 | 103 |
Patients in PRS + non-PRS with post-baseline genotype, n (%) | 80 (36.9) | 38 (36.9) |
New IAT RASs in pUL97 or pUL54a | 28 (12.9) | 5 (4.9) |
pUL97 only | 19 (8.8) | 3 (2.9) |
pUL54 only | 8 (3.7) | 1 (1.0) |
pUL97 and pUL54 | 1 (0.5) | 1 (1.0) |
CMV = cytomegalovirus; IAT = investigator-assigned anti-CMV treatment; MRS = maribavir-resistance set; PRS = primary resistance set; RAS = resistance-associated amino acid substitution.
aIncludes maribavir RASs with cross-resistance to IAT.
Source: SOLSTICE Clinical Study Report.4
Table 31: Summary of SF-36v2 (Randomized Set)
Dimension | Maribavir (N = 235) | IAT (N = 117) | ||
|---|---|---|---|---|
Observed | Change from baseline | Observed | Change from baseline | |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| | ||||
|||||||||||||||| | ||||
|||||||||||||||| | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| |
|||||||||||||||| | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| |
|||||||||||||||| | ||||
|||||||||||||||| | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| |
|||||||||||||||| | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| |
|||||||||||||||| | ||||
|||||||||||||||| | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| |
|||||||||||||||| | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| | ||||
|||||||||||||||| | ||||
|||||||||||||||| | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| |
|||||||||||||||| | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| |
|||||||||||||||| | ||||
|||||||||||||||| | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| |
|||||||||||||||| | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| |
|||||||||||||||| | ||||
|||||||||||||||| | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| |
|||||||||||||||| | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Note: Some redacted rows have been deleted.
Source: SOLSTICE Clinical Study Report.4
Table 32: Summary of EQ-5D (Randomized Set)
Dimension | Maribavir (N = 235) | IAT (N = 117) | ||
|---|---|---|---|---|
Observed | Change from baseline | Observed | Change from baseline | |
|||||||||||||||||||||||||||||||||||||||||||||||| | ||||
|||||||||||||||| | ||||
|||||||||||||||| | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| |
|||||||||||||||| | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| |
|||||||||||||||| | ||||
|||||||||||||||| | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| |
|||||||||||||||| | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| |
|||||||||||||||| | ||||
|||||||||||||||| | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| |
|||||||||||||||| | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| |
|||||||||||||||||||||||||||||||||||||||||||||||||| | ||||
|||||||||||||||| | ||||
|||||||||||||||| | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| |
|||||||||||||||| | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| |
|||||||||||||||| | ||||
|||||||||||||||| | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| |
|||||||||||||||| | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Note: Some redacted rows have been deleted.
Harms
Only those harms identified in the review protocol are reported below. Refer to Table 33 for detailed harms data for the safety analysis set.
Adverse Events
Overall, 228 (97.4%) patients in the maribavir group and 106 (91.4%) patients in the IAT group experienced ≥ 1 treatment-emergent adverse event. The most common AEs were dysgeusia (maribavir: 37.2% versus IAT: 3.4%), nausea (maribavir: 21.4% versus IAT: 21.6%), and diarrhea (maribavir: n = 44, IAT: n = 31).
Serious Adverse Events
Overall, 90 (38.5%) patients in the maribavir group and 43 (37.1%) in the IAT group experienced at least 1 SAE (i.e., treatment-emergent). The most common SAEs were infections and infestations (maribavir: 22.6% versus IAT: 14.7%).
Withdrawal Due to Adverse Events
Overall, 31 (13.2%) patients in the maribavir group and 37 (31.9%) in the IAT group permanently discontinued treatment with study drugs due to treatment-emergent AEs. In the maribavir group, infections and infestations led to the discontinuation of 17 (7.3%) patients. In the IAT group, blood and lymphatic system disorders and renal and urinary disorders led to the discontinuation of 13 (11.2%) and 11 (9.5%) of patients, respectively.
Mortality
In SOLSTICE, a total of 27 (11.5%) patients in the maribavir group and 13 (11.2%) patients in the IAT group died.
Notable Harms
Overall, 55 (23.5%) patients in the maribavir group and 22 (19.0%) patients in the IAT group enrolled in SOLSTICE experienced invasive fungal or bacterial or viral infections. The most common types of infections were pneumonia (maribavir: 3.4% versus IAT: 1.7% patients), BK virus infection (maribavir: 2.1% versus IAT: 3.4% patients) and enterococcal infection and herpes zoster (maribavir: 2.1% versus IAT: 0.0% patients). Increase in immunosuppressant drug concentration levels was experienced by 21 (9.0%) patients in the maribavir group and 1 (0.9%) patient in the IAT group. Taste disturbance was experienced by 87 (37.2%) patient in the maribavir group and 4 (3.4%) patients in the IAT group.
Table 33: Summary of Harms (Safety Set)
Detail | Maribavir (N = 234) | IAT (N = 116) |
|---|---|---|
Patients with ≥ 1 treatment-emergent AEa | ||
n (%) | 228 (97.4) | 106 (91.4) |
Most common eventsa, n (%) | ||
Dysgeusia | 87 (37.2) | 4 (3.4) |
Nausea | 50 (21.4) | 25 (21.6) |
Diarrhea | 44 (18.8) | 24 (20.7) |
Vomiting | 33 (14.1) | 19 (16.4) |
Anemia | 29 (12.4) | 14 (12.1) |
Fatigue | 28 (12.0) | 10 (8.6) |
Pyrexia | 24 (10.3) | 17 (14.7) |
CMV viraemia | 24 (10.3) | 6 (5.2) |
Neutropenia | 22 (9.4) | 26 (22.4) |
Immunosuppressant drug level increased | 21 (9.0) | 1 (0.9) |
Taste disorder | 21 (9.0) | 1 (0.9) |
Acute kidney injury | 20 (8.5) | 11 (9.5) |
Headache | 19 (8.1) | 15 (12.9) |
Abdominal pain | 18 (7.7) | 3 (2.6) |
Decreased appetite | 18 (7.7) | 9 (7.8) |
Dizziness | 17 (7.3) | 5 (4.3) |
Edema peripheral | 17 (7.3) | 9 (7.8) |
Blood creatinine increased | 13 (5.6) | 5 (4.3) |
Dyspnea | 13 (5.6) | 8 (6.9) |
Arthralgia | 13 (5.6) | 3 (2.6) |
Cough | 13 (5.6) | 7 (6.0) |
CMV infection reactivation | 12 (5.1) | 3 (2.6) |
Thrombocytopenia | 11 (4.7) | 7 (6.0) |
Hypomagnesaemia | 9 (3.8) | 10 (8.6) |
Constipation | 9 (3.8) | 7 (6.0) |
Hypertension | 9 (3.8) | 8 (6.9) |
Hypokalemia | 8 (3.4) | 11 (9.5) |
Abdominal pain upper | 8 (3.4) | 6 (5.2) |
Leukopenia | 7 (3.0) | 8 (6.9) |
Pain in extremity | 5 (2.1) | 6 (5.2) |
Patients with ≥ 1 treatment-emergent SAEa | ||
n (%) | 90 (38.5) | 43 (37.1) |
Blood and lymphatic system disorders | 9 (3.8) | 7 (6.0) |
Gastrointestinal disorders | 13 (5.6) | 6 (5.2) |
General disorders and administration site conditions | 12 (5.1) | 3 (2.6) |
Infections and infestations | 53 (22.6) | 17 (14.7) |
Renal and urinary disorders | 9 (3.8) | 6 (5.2) |
Patients who stopped treatment due to treatment-emergent AEsa | ||
n (%) | 31 (13.2) | 37 (31.9) |
Blood and lymphatic system disorders | 0 | 13 (11.2) |
Neutropenia | 0 | 11 (9.5) |
Infections and infestations | 17 (7.3) | 8 (6.9) |
Renal and urinary disorders | 0 | 11 (9.5) |
Acute kidney injury | 0 | 6 (5.2) |
Deaths | ||
n (%) | 26 (11.1) | 12 (10.3) |
Blood and lymphatic system disorders | 0 (0.0) | 1 (0.9) |
Cardiac disorders | 2 (0.9) | 0 (0.0) |
General disorders and administration site conditions | 5 (2.1) | 0 (0.0) |
Immune system disorders | 1 (0.4) | 0 (0.0) |
Infections and infestations | 8 (3.4) | 6 (5.2) |
Neoplasms benign, malignant and unspecified (including cysts and polyps) | 4 (1.7) | 3 (2.6) |
Respiratory, thoracic and mediastinal disorders | 5 (2.1) | 3 (2.6) |
Vascular disorders | 2 (0.9) | 0 (0.0) |
Notable harmsa | ||
Graft rejection (acute, chronic) or graft failure | 8 (3.4) | 3 (2.6) |
GVHD | 21 (9.0) | 5 (4.3) |
Immunosuppressant drug concentration level increased | 21 (9.0) | 1 (0.9) |
Invasive fungal or bacterial or viral infections | 55 (23.5) | 22 (19.0) |
Nausea | 50 (21.4) | 25 (21.6) |
Vomiting | 33 (14.1) | 19 (16.4) |
Diarrhea | 44 (18.8) | 24 (20.7) |
Neutropenia | 22 (9.4) | 26 (22.4) |
Taste disturbance (dysgeusia) | 87 (37.2) | 4 (3.4) |
Tissue-invasive CMV disease/syndrome | 8 (3.4) | 4 (3.4) |
AE = adverse event; CMV = cytomegalovirus; GVHD = graft vs. host disease; SAE = serious adverse event.
aFrequency of greater than 5% in at least one arm.
Source: SOLSTICE Clinical Study Report4
Graft Outcomes
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||.
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Table 34: Summary of Graft Outcomes (Randomized Set)
Dimension | Maribavir (N = 235) | IAT (N = 117) |
|---|---|---|
|||||||||||||||||||||||||||||||| | ||
|||||||||||||||| | |||||||||||||||| | |||||||||||||||| |
|||||||||||||||| | |||||||||||||||| | |||||||||||||||| |
|||||||||||||||||||||||||||||||| | ||
|||||||||||||||||||||||||||||||||||||||||||||||| | ||
|||||||||||||||| | |||||||||||||||| | |||||||||||||||| |
|||||||||||||||| | |||||||||||||||| | |||||||||||||||| |
|||||||||||||||| | |||||||||||||||| | |||||||||||||||| |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| | |||||||||||||||| | |||||||||||||||| |
|||||||||||||||||||||||||||||||| | |||||||||||||||| | |||||||||||||||| |
|||||||||||||||||||||||||||||||||||||||||||||||| | ||
|||||||||||||||| | |||||||||||||||| | |||||||||||||||| |
|||||||||||||||| | |||||||||||||||| | |||||||||||||||| |
|||||||||||||||| | |||||||||||||||| | |||||||||||||||| |
|||||||||||||||| | ||
|||||||||||||||| | ||
|||||||||||||||| | |||||||||||||||| | |||||||||||||||| |
|||||||||||||||| | |||||||||||||||| | |||||||||||||||| |
|||||||||||||||| | |||||||||||||||| | |||||||||||||||| |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Note: Some redacted rows have been deleted.
Critical Appraisal
Internal Validity
SOLSTICE was an open-label trial, whereby the open-label design can increase the risk for of performance and detection bias, particularly for outcomes that are subjective in measurement and interpretation (e.g., symptoms, HRQoL, subjective AEs). However, the clinical experts noted that the need to individualize IAT, and the route of administration and side effects unique to maribavir would make blinding unfeasible. Given that the primary end point and multiple secondary end points were objective measures relying on a central lab and an EAC, the risk of detection bias is probably low. The end point used to assess response, CMV viremia clearance at the end of 8-week treatment phase, was a validated surrogate end point.58,59
Patients in SOLSTICE were assigned numbers according to the sequence of presentation for study participation and following stratification (for transplant type and CMV DNA viral load category), patients were randomized to either group using IRT, likely adequate allocation concealment. Both the treatment groups were relatively balanced, with some notable differences in characteristics such as age, type of preparative conditioning regimen, presence of CMV RASs, and CMV serostatus for HSCT Donor/Recipient, CMV DNA level, and net immunosuppression use changed before initiation of study treatment. ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||. It is uncertain whether the baseline differences between the IAT and maribavir groups are attributable to chance; however, the risk of bias due to the randomization process is probably low.
The analysis populations used in the SOLSTICE trial were appropriate for measuring the effect of assignment to the interventions. The randomized set was used for most analyses. For the primary and key secondary analysis in SOLSTICE, patients who received non–study treatment or were included in the rescue arm before week 8 were counted as non–responders. Safety outcomes were assessed in all patients that were treated with a study drug, which excluded 2 patients from the randomized set (patients in the rescue arm were reported separately). The sample size of 352 patients was adequate to estimate the primary end point of treatment response to detect a statistically significant difference at 90% power. All analyses were pre-specified. Only the primary and key secondary outcomes were adjusted for multiple comparisons, so there is uncertainty in the conclusions for other outcomes.
The comparators used in SOLSTICE were identified by the clinical experts as appropriate. Statistical testing was performed for the primary and key secondary outcomes and results were adjusted for transplant type and baseline plasma CMV DNA concentration levels if homogeneity across strata were not met.
Most of the subgroup analyses for response (primary end point) were pre-specified. Although statistical testing was conducted, the sample sizes for the subgroup analyses were small and the CIs reflected imprecision, and there was no control for type I error due to multiple testing. As a result, no conclusions can be drawn by the CADTH review team based on the subgroup analyses.
Multiple protocol amendments were implemented while the SOLSTICE study was being conducted, which included a minor change to the study eligibility criteria (i.e., ability to swallow pills). It was noted by the clinical experts consulted by CADTH that analyzing those who discontinued early in the primary efficacy analysis as responders seemed appropriate.
A high rate of protocol deviations occurred in SOLSTICE, similar in both groups, which creates some uncertainty in the data. Key protocol deviations were related to investigator patient medical care (i.e., laboratory reports or safety information not reviewed or followed up in a timely manner by the investigator), investigator safety reporting (regulatory or sponsor), visit scheduling, investigator safety reporting eCRF, and study treatment compliance. |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| (per the sponsor, if ≥ 5% of patients had missing CMV DNA data to confirm response at week 8 due to the COVID-19 pandemic, missing CMV DNA levels were to be imputed using a multiple imputation method). Although deviations in study drug and treatment could confound results, given that the rate of protocol deviations was similar between the 2 study groups, this is not likely to be of concern.
External Validity
The SOLSTICE trial was an international, multicenter study that included sites in Europe, US, and Canada. One stark difference between how the treatment was administered in SOLSTICE and what would be expected in routine clinical practice was the 8-week fixed duration. As identified by the clinical experts, clinicians treat patients until CMV DNA levels are low enough or negative, not for a fixed duration. Although the comparators used in the trial are reflective of clinical practice, the distribution of selected IAT treatments was noted as inconsistent with Canadian clinical practice. It may be difficult to design a trial with IAT distributions that reflect the diversity of Canadian clinical practice. Given these limitations of the trial, generalizability of results to the Canadian setting is uncertain. Furthermore, because of pooling of effects in the IAT group, no conclusions can be made about maribavir versus any particular antiviral.
The clinical experts consulted by CADTH reported that standard of care for assessing treatment response would be PCR testing every week. In the SOLSTICE study, after 8 weeks the treatment response was assessed by PCR testing weekly until week 12, then every 2 weeks through to week 20. The experts highlighted that turnaround time from testing to results for resistance may be longer than what is required for immediate care (irreversible outcomes such as death can occur in patients), often necessitating a treatment switch before the results are available and using the results for decision to continue with the new therapy.
The clinical experts indicated that the baseline characteristics of patients enrolled in SOLSTICE were generally representative of the post-transplant CMV patient population in Canada, although they noted that the SOLSTICE study patients would represent the healthiest patients in this population, which is common in clinical trials. Particularly, the post-transplant patients were assessed for performance using the Karnofsky scores, and clinical experts highlighted those patients in routine clinical practice would not be performing as well (i.e., scores would rarely be 100). Furthermore, the clinical experts noted that healthier patients with lower baseline viral load are less likely to develop resistance.
Overall, the clinical experts thought that the eligibility criteria used in the SOLSTICE study were appropriate and allowed enrollment of patients with post-transplant CMV infection that were generally representative of the Canadian patient population. The experts also noted that excluding CMV central nervous system and CMV retinitis, which is uncommon in patients with HSCT, is appropriate as maribavir may not penetrate the brain and/or eyes. A small proportion of patients screened (15.2%) were screen failures. The most frequently reported reasons for screen failure were failure to demonstrate confirmed minimum CMV viral load and failure to demonstrate that current CMV infection was refractory to the most recent CMV treatment, which are appropriate reasons given the study objectives and drug indication. Discontinuation rates of 79 (67.5%) patients in the IAT arm and 51 (21.7%) patients in the maribavir arm were as expected by the clinical experts. It was noted that most early discontinuations were due to lack of efficacy or clinical reasons (i.e., adverse events or toxicities), which was expected by the clinical experts because for AEs such as myelosuppression or renal toxicity, clinicians strive to get patients off drugs with known toxicities to avoid irreversible outcomes such as transplant failure or death.
In SOLSTICE, health care resource utilization (i.e., hospitalization rates and length of stay) was lower in the maribavir population. However, the clinical experts noted that these findings may not be generalizable given the variation in available health care resources across provinces and territories.
The primary outcome of response confirmed by CMV clearance and the key secondary outcome that also includes CMV symptom control is relevant to clinical practice and clinically meaningful to patients, as noted by the clinical experts and patient groups. Better HRQoL and fewer side effects compared to current therapies were also important considerations for patients.
Indirect Evidence
Objectives and Methods for the Summary of Indirect Evidence
A focused literature search for ITCs dealing with cytomegalovirus infections was run in MEDLINE All (1946-) on April 29, 2022. No limits were applied to the search.
No reports were found.
Other Relevant Evidence
This section includes additional relevant data included in the sponsor’s submission to CADTH that were considered to address important gaps in the evidence included in the systematic review.
IPD Analyses of SOLSTICE
The sponsor-provided IPD analysis conducted on data from SOLSTICE as additional explorations to the analyses already reported in the CSR. Description and results of the IPD analyses can be found in Appendix 5.
The sponsor’s rationale for undertaking the IPD analysis was that in some cases evidence from SOLSTICE was not reported in a format that could be readily incorporated into the maribavir global cost-effectiveness model (CEM) version 2. The results of the IPD analyses were used as direct inputs into the base case and scenarios of the CEM. These analyses were mostly exploratory and descriptive. Analyses with statistical testing were not pre-defined in a statistical analysis plan and were performed in a post-hoc manner. Therefore, definitive conclusion regarding efficacy and safety of maribavir cannot be drawn based on this evidence. As the sponsor has noted, the IPD analyses are exploratory and intended to be used as input for the CEM.
Discussion
Summary of Available Evidence
One open-label, randomized, double-arm phase III trial (SOLSTICE, N = 352) was included in the CADTH systematic review. The primary objective of the SOLSTICE study was to compare the efficacy and safety of maribavir versus IAT for treatment of refractory CMV infection (with or without resistance) in SOT and HSCT recipients. The trial included adult patients with documented CMV infection that is refractory to the most recent treatment or resistant (only if patients also met refractory criteria). Patients received 400 mg oral maribavir twice daily for up to 8 weeks. The primary end point was confirmed CMV viremia clearance at the end of week 8 (regardless of premature treatment discontinuation). The key secondary end point was a composite of confirmed CMV viremia clearance and symptom control at the end of week 8, maintained through week 16 (8 weeks beyond the treatment phase) after receiving exclusively study-assigned treatment. Other secondary end points included recurrence, all-cause mortality, health care resource utilization, and HRQoL. Harms outcomes were also examined. In the SOLSTICE study, both treatment groups were mostly balanced across characteristics, but there were notable differences across characteristics across age, type of preparative conditioning regimen, presence of CMV RASs, and CMV serostatus for HSCT Donor/Recipient, CMV DNA level, and net immunosuppression use changed before initiation of study treatment.
Interpretation of Results
Efficacy
Patients with post-transplant CMV infection that is refractory or resistant to first-line treatments have limited treatment options and poor outcomes. Current therapies have known toxicities and often require IV administration, resistance being a concern in SOT patients, whereby Donor+/Recipient- and lung transplant patients are more likely to develop resistance. Both the clinical experts and patient groups indicated that there is significant unmet need in this patient population, especially in older patients with immunosenescence and renal issues and patients with CMV infection that is resistant to therapies such as ganciclovir and/or valganciclovir and foscarnet.
The SOLSTICE trial investigated maribavir compared with IAT in adult patients with refractory CMV infection with or without resistance. The primary end point of the study was met since the adjusted difference in proportion of responders at week 8 between maribavir and IAT was 32.8% (95% CI, 22.80 to 42.74; P < 0.001), in favour of maribavir. More than 3/4 (78%) of patients completed the assigned 8-week treatment course of maribavir, as opposed to about 1/3 (32%) for IAT. This may be a function of lower efficacy and higher toxicity of the latter treatment, as illustrated by the higher early discontinuation rate and discontinuation due to AEs. The study included multiple sensitivity analyses of the primary and key secondary end points to address the potential for bias due higher rates of discontinuation in the IAT group.
The key secondary end point in SOLSTICE was supportive of the primary end point, as the adjusted proportion of responders at week 8 and maintenance at week 16 was 9.5% (95 CI, 2.02 to 16.88, P = 0.013). The results for other secondary outcomes related to confirmed CMV clearance and CMV symptom control maintenance at different time points was generally supportive of the findings for the primary end point; however, these outcomes were not adjusted for multiplicity and definitive conclusions cannot be drawn.
Comparative recurrence data were difficult to interpret because clearance is prerequisite for recurrence. Recurrence of CMV viremia during the first 8 weeks of the study occurred for 17.9% of maribavir-treated patients and 12.3% of IAT-treated patients. Recurrence occurred more frequently in the maribavir group than in the IAT group during the follow-up after week 8 (maribavir: 38.6% versus IAT: 21.5%). The sponsor indicated that there were a disproportionately higher proportion of patients with virologic clearance in the maribavir arm compared with IAT (maribavir: 78.3% versus IAT: 55.6%), which may have contributed to the higher recurrence rate for maribavir-treated patients compared with IAT in the follow-up period. Though recurrence was more frequent in the maribavir group, recurrence requiring treatment was lower in the maribavir group (maribavir: 26.0% versus IAT: 35.7%). The clinical experts consulted by CADTH indicated that recurrence is expected in this population because of the concomitant use of immunosuppression in some patients and is largely a function of underlying patient factors. Of note, the time to viremia recurrence appears to be similar or shorter for maribavir, which may mean that maribavir does not offer a longer disease-free interval in responders (Table 26 and Table 27). While response was higher with maribavir, it was not maintained and decreased steadily at later time points for both treatments (Table 21). Kinetics of viremia clearance (Figure 3 and Table 22) seem to slightly favour maribavir, but the absence of formal statistical testing precludes drawing definitive conclusions.
Resistance is a concern in this patient population, including developing resistance to maribavir, which would render the drug less efficacious, as noted by the clinical experts. In the maribavir group, 19.6% of patients who received maribavir had new treatment-emergent RASs known to confer resistance to maribavir detected in their genotype. Similarly, 12.9% of patients in the maribavir group had new treatment-emergent RASs known to confer resistance to IAT detected in their genotype and 4.9% of patients in the IAT group had new treatment-emergent RASs known to confer resistance to IAT detected in their genotype.
The findings for all-cause mortality between the treatment groups in the analysis based on all patients and in the analysis censoring patients at the start of alternative anti-CMV treatment or maribavir rescue therapy was inconclusive due to imprecision indicated by the wide confidence intervals. As noted by the clinical experts consulted by CADTH, these patient population has several patient-specific factors that may impact mortality.
Health care resource utilization between the treatment groups demonstrated a slight difference, favouring slightly lower hospitalization rate and length of stay for patients in the maribavir group (during the on-treatment study period). However, as values were not adjusted for multiple comparisons, limited conclusions can be drawn. Furthermore, the clinical experts noted that findings may not be generalizable given the variation in available health care resources across provinces and territories.
HRQoL was identified as an important outcome to patients. Reported HRQoL data seemed to indicate that EQ-5D and SF-36 scores generally improved during the study period, across both treatment groups. Although data were reported, differences between treatment groups were not tested statistically and there are concerns for missing data. Given the lack of literature assessing the EQ-5D or SF-36 for MID, validity, reliability, or responsiveness in patients with post-transplant CMV infection, no definitive conclusions can be drawn by the CADTH review team.
Multiple subgroup analyses that aligned with subgroups of interest in the CADTH review protocol were conducted in the SOLSTICE study. Most of the subgroups were pre-specified in the SOLSTICE study protocol. Results were broadly numerically consistent across various subgroups of interest. However, due to the small sample sizes, wide CIs, and absence of control for type I error, no definitive conclusions can be drawn by the CADTH review team.
Harms
SOLSTICE data related to harms indicated that maribavir is generally a safe option for patients, though there are some concerns with TEAEs such as dysgeusia, bacterial and fungal infections, and increased immunosuppressant drug concentrations.
Although a greater proportion of maribavir-treated patients had at least 1 TEAEs (maribavir: 97.4% versus IAT: 91.4%), the higher AEs in the maribavir group appeared to be driven by dysgeusia (maribavir: 37.2% versus IAT: 3.4%), which only led to discontinuation in 2 (0.9%) patients. Although maribavir may eliminate hospital visits needed for drug administration, which is an unmet need of patients, the side effect of dysgeusia – albeit manageable – still may be a concern for patients.
The rate of infections and infestations was also higher in patients treated with maribavir (maribavir: 22.6% versus IAT: 14.7%). ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
In SOLSTICE, 9.0% of patients in the maribavir group had TEAEs of increased immunosuppressant drug levels compared to 0.9% of patients in the IAT group, which was expected by the clinical experts given this had been explored in prior studies and is listed in the product monograph as a concern. The experts indicated this may be managed by reducing doses of concomitant immunosuppressant drugs.
Known hematologic and renal toxicities of existing drugs indicate a gap in the treatment landscape for post-transplant patients with CMV infection. Maribavir had a lower incidence of overall treatment-emergent SAEs associated with blood and lymphatic system (maribavir: 7.3% versus IAT: 18.1%) and renal and urinary treatment-emergent SAEs (maribavir: 3.8% versus 5.2%). There were no patients in the maribavir group who discontinued treatment for treatment-emergent hematologic disorders or renal and urinary disorders (SAEs).
Conclusions
One open-label, randomized, double-arm phase III trial (SOLSTICE, N = 352) was included in the CADTH systematic review. The primary objective of the SOLSTICE study was to compare the efficacy and safety of maribavir versus IAT for treatment of refractory CMV infection (with or without resistance) in SOT and HSCT recipients. There is evidence of maribavir being more efficacious when compared to the IAT on achieving CMV viremia clearance and symptom control. However, disease control with maribavir is time-limited, in line with other antivirals. Conclusions for all-cause mortality could not be drawn because the 95% confidence interval around the hazard ratio was wide, including the possibility of both appreciable benefit and harm for maribavir compared with IAT. The proportion of patients experiencing taste disturbance, increased immunosuppressant concentration levels, and infections and infestations was higher with maribavir, but these events were manageable. The lower rates of hematologic and renal toxicities with maribavir fill a gap in the treatment landscape whereby other drugs have known toxicities limiting their use. Fewer patients in the maribavir group discontinued treatment due to AEs. There remains uncertainty on interpreting data for outcomes related to CMV recurrence, antiviral resistance, HRQoL, health care resource utilization, and subgroup analyses given the various methodological limitations.
References
1.Azevedo LS, Pierrotti LC, Abdala E, et al. Cytomegalovirus infection in transplant recipients. Clinics (Sao Paulo). 2015;70(7):515-523. PubMed
2.Mabilangan C, Burton C, O’Brien S, Plitt S, Eurich D, Preiksaitis J. Using blood donors and solid organ transplant donors and recipients to estimate the seroprevalence of cytomegalovirus and Epstein–Barr virus in Canada: A cross-sectional study. Official Journal of the Association of Medical Microbiology and Infectious Disease Canada. 2020;5(3):158-176. PubMed
3.Tan BH. Cytomegalovirus Treatment. Curr. 2014;6(3):256-270. PubMed
4.Clinical Study Report: 303. A Phase 3, Multicenter, Randomized,Open-label, Active-controlled Study to Assess the Efficacy and Safety of Maribavir Treatment Compared to Investigator-assigned Treatment in Transplant Recipients with Cytomegalovirus (CMV) Infections that are Refractory or Resistant to Treatment with Ganciclovir, Valganciclovir, Foscarnet, or Cidofovir. In: Toronto (ON): Takeda Canada Inc.; 2021.
5.Al-Bar MA, Chamsi-Pasha H. Organ Transplantation. In: Al-Bar MA, Chamsi-Pasha H, eds. Contemporary Bioethics: Islamic Perspective. Cham: Springer International Publishing; 2015:209-225.
6.Fuji S, Kapp M, Einsele H. Challenges to preventing infectious complications, decreasing re-hospitalizations, and reducing cost burden in long-term survivors after allogeneic hematopoietic stem cell transplantation. Semin Hematol. 2012;49(1):10-14. PubMed
7.Peters C, Steward CG. Hematopoietic cell transplantation for inherited metabolic diseases: an overview of outcomes and practice guidelines. Bone Marrow Transplant. 2003;31(4):229-239. PubMed
8.Ringdén O. Allogeneic bone marrow transplantation for hematological malignancies--controversies and recent advances. Acta Oncol. 1997;36(6):549-564. PubMed
9.Storb R, Doney KC, Thomas ED, et al. Marrow transplantation with or without donor buffy coat cells for 65 transfused aplastic anemia patients. Blood. 1982;59(2):236-246. PubMed
10.Thomas ED, Buckner CD, Banaji M, et al. One hundred patients with acute leukemia treated by chemotherapy, total body irradiation, and allogeneic marrow transplantation. Blood. 1977;49(4):511-533. PubMed
11.Khaddour K HC, Mewawalla P. Hematopoietic Stem Cell Transplantation. Treasure Island (FL): StatPearls Publishing; 2022.
12.Bjorklund A, Aschan J, Labopin M, et al. Risk factors for fatal infectious complications developing late after allogeneic stem cell transplantation. Bone Marrow Transplant. 2007;40(11):1055-1062. PubMed
13.Frange P, Leruez-Ville M. Nouvelles perspectives thérapeutiques dans l’infection à cytomégalovirus. Revue d'Oncologie Hématologie Pédiatrique. 2017;5(2):56-66.
14.Angarone M, Ison MG. Prevention and early treatment of opportunistic viral infections in patients with leukemia and allogeneic stem cell transplantation recipients. J. 2008;6(2):191-201.
15.Ariza-Heredia EJ, Nesher L, Chemaly RF. Cytomegalovirus diseases after hematopoietic stem cell transplantation: a mini-review. Cancer Lett. 2014;342(1):1-8. PubMed
16.Bhutani D, Dyson G, Manasa R, et al. Incidence, risk factors, and outcome of cytomegalovirus viremia and gastroenteritis in patients with gastrointestinal graft-versus-host disease. Biol Blood Marrow Transplant. 2015;21(1):159-164. PubMed
17.Ljungman P, Hakki M, Boeckh M. Cytomegalovirus in hematopoietic stem cell transplant recipients. Hematol Oncol Clin North Am. 2011;25(1):151-169. PubMed
18.Walker CM, van Burik JA, De For TE, Weisdorf DJ. Cytomegalovirus infection after allogeneic transplantation: comparison of cord blood with peripheral blood and marrow graft sources. Biol Blood Marrow Transplant. 2007;13(9):1106-1115. PubMed
19.Ljungman P. The role of cytomegalovirus serostatus on outcome of hematopoietic stem cell transplantation. Curr Opin Hematol. 2014;21(6):466-469. PubMed
20.Institute NC. NCI Common Terminology Criteria for Adverse Events (CTCAE). https://ctep.cancer.gov/protocoldevelopment/electronic_applications/ctc.htm#ctc_40. Published 2009. Accessed.
21.Ljungman P, Boeckh M, Hirsch HH, et al. Definitions of Cytomegalovirus Infection and Disease in Transplant Patients for Use in Clinical Trials. Clinical Infectious Diseases. 2017;64(1):87-91. PubMed
22.Information CIfH. Data Quality Documentation for Users: Canadian Organ Replacement Register, 2011 to 2020 Data. 2021.
23.Niederwieser D, Baldomero H, Szer J, et al. Hematopoietic stem cell transplantation activity worldwide in 2012 and a SWOT analysis of the Worldwide Network for Blood and Marrow Transplantation Group including the global survey. Bone Marrow Transplant. 2016;51(6):778-785. PubMed
24.Drug Reimbursement Review sponsor submission: Livtencity (maribavir), 200mg tablets [internal sponsor's package]. In: Toronto (ON): Takeda Canada Inc.; 2022 Mar 14.
25.Humar A, Lipton J, Messner H, McGeer A, Mazzulli T. A cross-Canada survey of cytomegalovirus prevention and treatment practices in bone marrow transplant recipients. Can J Infect Dis. 1999;10(6):410-414. PubMed
26.Su SH, Martel-Laferriere V, Labbe AC, et al. High incidence of herpes zoster in nonmyeloablative hematopoietic stem cell transplantation. Biol Blood Marrow Transplant. 2011;17(7):1012-1017. PubMed
27.Young J-AH, Logan BR, Wu J, et al. Infections after Transplantation of Bone Marrow or Peripheral Blood Stem Cells from Unrelated Donors. Biology of blood and marrow transplantation: journal of the American Society for Blood and Marrow Transplantation. 2016;22(2):359-370.
28.Heliövaara E, Husain S, Martinu T, et al. Drug-resistant cytomegalovirus infection after lung transplantation: Incidence, characteristics, and clinical outcomes. J Heart Lung Transplant. 2019;38(12):1268-1274. PubMed
29.Ljungman P, de la Camara R, Robin C, et al. Guidelines for the management of cytomegalovirus infection in patients with haematological malignancies and after stem cell transplantation from the 2017 European Conference on Infections in Leukaemia (ECIL 7). Lancet Infect Dis. 2019;19(8):e260-e272. PubMed
30.Kotton CN, Kumar D, Caliendo AM, et al. The Third International Consensus Guidelines on the Management of Cytomegalovirus in Solid-organ Transplantation. Transplantation. 2018;102(6). PubMed
31.Kotton CN. Updates on antiviral drugs for cytomegalovirus prevention and treatment. Current Opinion in Organ Transplantation. 2019;24(4):469-475. PubMed
32.Caliendo AM. Approach to the diagnosis of cytomegalovirus infection. https://www.uptodate.com/contents/approach-to-the-diagnosis-of-cytomegalovirus-infection. Published 2022. Accessed.
33.Camargo JF, Komanduri KV. Emerging concepts in cytomegalovirus infection following hematopoietic stem cell transplantation. Hematol Oncol Stem Cell Ther. 2017;10(4):233-238. PubMed
34.Campos AB, Ribeiro J, Boutolleau D, Sousa H. Human cytomegalovirus antiviral drug resistance in hematopoietic stem cell transplantation: current state of the art. Rev Med Virol. 2016;26(3):161-182. PubMed
35.Mullard A. FDA approves decades-old maribavir for CMV infection. Nat Rev Drug Discov. 2022;21(1):9. PubMed
36.EMA. EMEA-000353-PIP02-16-M01. 2021.
37.FDA. LIVTENCITY FDA product label In:2021.
38.Adminstration TG. Prescription medicines: applications under evaluation. Australian Government. https://www.tga.gov.au/prescription-medicines-applications-under-evaluation?search_api_views_fulltext=livtencity&field_ws_pm_eval_apptype=All&sort_by=search_api_aggregation_2&sort_order=DESC&items_per_page=25. Published 2022. Updated 21 June 2022. Accessed June 27, 2022.
39.Prichard MN. Function of human cytomegalovirus UL97 kinase in viral infection and its inhibition by maribavir. Rev Med Virol. 2009;19(4):215-229. PubMed
40.Papanicolaou GA, Silveira FP, Langston AA, et al. Maribavir for Refractory or Resistant Cytomegalovirus Infections in Hematopoietic-cell or Solid-organ Transplant Recipients: A Randomized, Dose-ranging, Double-blind, Phase 2 Study. Clinical Infectious Diseases. 2019;68(8):1255-1264. PubMed
41.Maertens J, Cordonnier C, Jaksch P, et al. Maribavir for Preemptive Treatment of Cytomegalovirus Reactivation. N Engl J Med. 2019;381(12):1136-1147. PubMed
42.Krosky PM, Baek MC, Coen DM. The human cytomegalovirus UL97 protein kinase, an antiviral drug target, is required at the stage of nuclear egress. Journal of Virology. 2003;77(2):905-914. PubMed
43.Inc S. Foscarnet product monograph. 2020.
44.Inc. MP. Cidofovir product monograph. 2018.
45.Inc. AP. Ganciclovir product monograph. 2018.
46.Limited H-LR. Valganciclovir product monograph. 2002.
47.Chou S, Song K, Wu J, Bo T, Crumpacker C. Drug resistance mutations and associated phenotypes detected in clinical trials of maribavir for treatment of cytomegalovirus infection. J Infect Dis. 2020;29:29. PubMed
48.McGowan J, Sampson M, Salzwedel DM, Cogo E, Foerster V, Lefebvre C. PRESS Peer Review of Electronic Search Strategies: 2015 Guideline Statement. Journal of clinical epidemiology. 2016;75:40-46. PubMed
49.Grey matters: a practical tool for searching health-related grey literature. In: Ottawa (ON): CADTH; 2019: https://www.cadth.ca/grey-matters. Accessed 2022 Apr 29.
50.Avery RK, Alain S, Alexander BD, et al. Maribavir for Refractory Cytomegalovirus Infections With or Without Resistance Post-Transplant: Results from a Phase 3 Randomized Clinical Trial. Clinical Infectious Diseases. 2021;02:02.
51.van Reenen M JB. EQ-5D-5L User Guide. Basic information on how to use the EQ-5D-5L instrument. Rotterdam (NL): EuroQol Research Foundation. 2015.
52.Herdman M, Gudex C, Lloyd A, et al. Development and preliminary testing of the new five-level version of EQ-5D (EQ-5D-5L). Qual Life Res. 2011;20(10):1727-1736. PubMed
53.Ware JE, Jr., Sherbourne CD. The MOS 36-item short-form health survey (SF-36). I. Conceptual framework and item selection. Med Care. 1992;30(6):473-483. PubMed
54.Mehrotra DV, Railkar R. Minimum risk weights for comparing treatments in stratified binomial trials. Stat Med. 2000;19(6):811-825. PubMed
55.Statistical Analysis Plan for Clinical Study Report: 303. A Phase 3, Multicenter, Randomized,Open-label, Active-controlled Study to Assess the Efficacy and Safety of Maribavir Treatment Compared to Investigator-assigned Treatment in Transplant Recipients with Cytomegalovirus (CMV) Infections that are Refractory or Resistant to Treatment with Ganciclovir, Valganciclovir, Foscarnet, or Cidofovir. In: Toronto (ON): Takeda Canada Inc.; 2021.
56.Simons CL, Rivero-Arias O, Yu LM, Simon J. Multiple imputation to deal with missing EQ-5D-3L data: Should we impute individual domains or the actual index? Qual Life Res. 2015;24(4):805-815. PubMed
57.Ware JE, Jr., Kosinski, M., Bjorner, J. B., Turner-Bowker, D. M. Gandeck, B., & Marush, M. E. SF36 User Guide, 2016 F-36v2® Health Survey: Administration guide for clinical trial investigators. Lincoln, RI2008.
58.Duke ER, Williamson BD, Borate B, et al. CMV viral load kinetics as surrogate endpoints after allogeneic transplantation. The Journal of Clinical Investigation. 2021;131(1). PubMed
59.Natori Y, Alghamdi A, Tazari M, et al. Use of Viral Load as a Surrogate Marker in Clinical Studies of Cytomegalovirus in Solid Organ Transplantation: A Systematic Review and Meta-analysis. Clinical Infectious Diseases. 2017;66(4):617-631. PubMed
60.McClure NS, Sayah FA, Xie F, Luo N, Johnson JA. Instrument-defined estimates of the minimally important difference for EQ-5D-5L index scores. Value Health. 2017;20(4):644-650. PubMed
61.M Maruish MK, J Bjorner, ME Maruish, M Kosinski, JB Bjorner, B Gandek, DM Turner-Bowker, JE Ware. User’s manual for the SF36v2 Health Survey. Quality Metric Incorporated. 2011.
62.HQCo. A. 2014 Alberta population norms for EQ-5D-5L 2014.
63.Mandy van Reenen BJ, Elly Stolk, Kristina Secnik Boye, Mike Herdman, atthew Kennedy-Martin, Tessa Kennedy-Martin, Bernhard Slaap. EQ-5D-5L User Guide: Basic information on how to use the EQ-5D-5L instrument. EuroQol Research Foundation 2021. 2019.
64.van Hout B, Janssen MF, Feng YS, et al. Interim scoring for the EQ-5D-5L: mapping the EQ-5D-5L to EQ-5D-3L value sets. Value Health. 2012;15(5):708-715. PubMed
Appendix 1: Literature Search Strategy
Note that this appendix has not been copy-edited.
Systematic Review Search
Date of final search (as run): April 29, 2022
Limits: conference abstracts excluded
Filters suggested: None
Filters used: None
Databases: MEDLINE, Embase
MEDLINE
(maribavir* or livtencity* or benzimidavir* or benzimidazole riboside* or 1263w or 1263w94 or 1263 w 94 or bw1263 or bw1263w94 or gr 257406 or gr257406 or gw 1263 or gw1263 or GW 257406X or GW257406X or PTB4X93HE1).ti,ab,kf,ot,hw,rn,nm.
Embase
*Benzimidavir/ (maribavir* or livtencity* or benzimidavir* or benzimidazole riboside* or 1263w or 1263w94 or 1263 w 94 or bw1263 or bw1263w94 or gr 257406 or gr257406 or gw 1263 or gw1263 or GW 257406X or GW257406X).ti,ab,kf,dq.
Record search here, final “as run”:
Database(s): Embase 1974 to 2022 April 28, Ovid MEDLINE(R) ALL 1946 to April 28, 2022
Table 35: Systematic Review Search on Embase and MEDLINE Databases
# | Searches | Results |
|---|---|---|
1 | (maribavir* or livtencity* or benzimidavir* or benzimidazole riboside* or 1263w or 1263w94 or 1263 w 94 or bw1263 or bw1263w94 or gr 257406 or gr257406 or gw 1263 or gw1263 or GW 257406X or GW257406X or PTB4X93HE1).ti,ab,kf,ot,hw,rn,nm. | 744 |
2 | 1 use medall | 205 |
3 | *Benzimidavir/ | 120 |
4 | (maribavir* or livtencity* or benzimidavir* or benzimidazole riboside* or 1263w or 1263w94 or 1263 w 94 or bw1263 or bw1263w94 or gr 257406 or gr257406 or gw 1263 or gw1263 or GW 257406X or GW257406X).ti,ab,kf,dq. | 475 |
5 | 3 or 4 | 484 |
6 | 5 not (conference abstract or conference review).pt. | 437 |
7 | 6 use oemezd | 241 |
8 | 2 or 7 | 446 |
9 | remove duplicates from 8 | 267 |
ITC Search
MEDLINE
Run on April 29, 2022
Cytomegalovirus/ or exp Cytomegalovirus Infections/ (Cytomegalovirus or Cytomegalic or Inclusion Disease* or Inclusion body Disease* or Cytomegaloviruses or CMV or cytomegalia or cytomegalo or cytomegalus or cytomegalusvirus or Cytomegaly or salivary gland virus or cytomegaloinfection or cytomegaloviral).ti,ab,kf
Database(s): Ovid MEDLINE(R) ALL 1946 to April 28, 2022
Table 36: ITC Search on MEDLINE Database
# | Searches | Results |
|---|---|---|
1 | Cytomegalovirus/ or exp Cytomegalovirus Infections/ | 37465 |
2 | (Cytomegalovirus or Cytomegalic or Inclusion Disease* or Inclusion body Disease* or Cytomegaloviruses or CMV or cytomegalia or cytomegalo or cytomegalus or cytomegalusvirus or Cytomegaly or salivary gland virus or cytomegaloinfection or cytomegaloviral).ti,ab,kf. | 56224 |
3 | 1 or 2 | 61224 |
4 | network meta-analysis/ | 3694 |
5 | (meta-analysis/ or meta-analysis as topic/ or "meta analysis (topic)"/) and network.ti,ab,kf. | 6358 |
6 | ((indirect or indirect treatment or mixed treatment or bayesian) adj3 comparison*).ti,ab,kf. | 3919 |
7 | (network* adj3 (meta-analy* or metaanaly*)).ti,ab,kf. | 7207 |
8 | (multi* adj3 treatment adj3 comparison*).ti,ab,kf. | 271 |
9 | (mixed adj3 treatment adj3 (meta-analy* or metaanaly*)).ti,ab,kf. | 174 |
10 | umbrella review*.ti,ab,kf. | 932 |
11 | nma.ti,ab,kf. | 2972 |
12 | (Multi* adj2 paramet* adj2 evidence adj2 synthesis).ti,ab,kf. | 13 |
13 | (Multiparamet* adj2 evidence adj2 synthesis).ti,ab,kf. | 17 |
14 | (multi-paramet* adj2 evidence adj2 synthesis).ti,ab,kf. | 11 |
15 | MPES.ti,ab,kf. | 326 |
16 | or/4-15 | 15289 |
17 | 3 and 16 | 40 |
Appendix 2: Excluded Studies
Note that this appendix has not been copy-edited.
Reference | Reason for exclusion |
|---|---|
GAGELMANN, N., et al. (2018) Comparative Efficacy and Safety of Different Antiviral Agents for Cytomegalovirus Prophylaxis in Allogeneic Hematopoietic Cell Transplantation: A Systematic Review and Meta-Analysis. Biology of Blood & Marrow Transplantation 2018 24(10):2101-2109. | Systematic review was searched for additional studies eligible for inclusion in the CADTH protocol, none found. |
WINSTON, D. J., et al. (2012) Efficacy and safety of maribavir dosed at 100 mg orally twice daily for the prevention of cytomegalovirus disease in liver transplant recipients: a randomized, double-blind, multicenter controlled trial. American Journal of Transplantation 2012 12(11):3021-30 | Treatment strategy is prophylaxis, does not meet treatment indication specified in the CADTH protocol. |
MARTY, F. M., et al. (2011) Maribavir prophylaxis for prevention of cytomegalovirus disease in recipients of allogeneic stem-cell transplants: a phase 3, double-blind, placebo-controlled, randomised trial. The Lancet Infectious Diseases 11(4):284-92 | Treatment approach is prophylaxis, does not meet treatment indication specified in the CADTH protocol. |
AVERY, R. K., et al. (2010) Oral maribavir for treatment of refractory or resistant cytomegalovirus infections in transplant recipients. Transplant Infectious Disease 12(6):489-96 | Phase II study design, does not meet study design specified in the CADTH protocol. |
MAERTENS, J., et al. (2019) Maribavir for Preemptive Treatment of Cytomegalovirus Reactivation. New England Journal of Medicine 381(12):1136-1147 | Phase II study design, does not meet study design specified in the CADTH protocol. |
PAPANICOLAOU, G. A., et al. (2019) Maribavir for Refractory or Resistant Cytomegalovirus Infections in Hematopoietic-cell or Solid-organ Transplant Recipients: A Randomized, Dose-ranging, Double-blind, Phase 2 Study. Clinical Infectious Diseases. 68(8):1255-1264 | Phase II study design, does not meet study design specified in the CADTH protocol. |
Clinical Study 202 (TAK-620-202): Maribavir for Refractory or Resistant Cytomegalovirus Infections in Hematopoietic-cell or Solid-organ Transplant Recipients: A Randomized, Dose-ranging, Double-blind, Phase 2 Study | Phase II study design, does not meet study design specified in the CADTH protocol. |
Clinical Study 203 (TAK-620-203): Maribavir for Preemptive Treatment of Cytomegalovirus Reactivation | Phase II study design, does not meet study design specified in the CADTH protocol. |
Appendix 3: Detailed Outcome Data
Note that this appendix has not been copy-edited.
Change From Baseline in Log10 Plasma CMV Viral Load
Results for the log10 plasma CMV viral load changes from baseline are summarized in Table 39.
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||. The mean change from baseline in log10 plasma CMV DNA viral load at week 8 was -1.30 (SD: 0.994) in the maribavir group (N = 211) and -1.32 (SD: 1.152) in the IAT group (N = 65). The mean change from baseline in log10 plasma CMV DNA viral load at week 16 of the follow-up period was -1.49 (SD: 0.912) in the maribavir group (N = 196) and -1.39 (SD: 1.071) in the IAT group (N = 55).
Table 38: Subgroup Analyses of Confirmed CMV Viremia Clearance Response and Achieving Confirmed CMV Viremia Clearance and CMV Infection Symptom Control Followed by Maintenance through Week 16
Characteristic | Responders IAT (N = 117) | Responders Maribavir (N = 235) | ||
|---|---|---|---|---|
n/N | % (95% CI) | n/N | % (95% CI) | |
|||||||||||||||| | ||||
|||||||||||||||| | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| |
|||||||||||||||| | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| |
|||||||||||||||| | ||||
|||||||||||||||| | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| |
|||||||||||||||| | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| |
|||||||||||||||| | ||||
|||||||||||||||| | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| |
|||||||||||||||| | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| |
|||||||||||||||| | ||||
|||||||||||||||| | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| |
|||||||||||||||| | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Table 39: Summary and Analysis of Change from Baseline in Log10 Plasma CMV Viral Load (Randomized Set)
Log10 (Plasma CMV Viral Load) | Maribavir (N = 235) | IAT (N = 117) | ||
|---|---|---|---|---|
Observed | Change from Baseline | Observed | Change from Baseline | |
|||||||||||||||| | ||||
|||||||||||||||| | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| |
|||||||||||||||| | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| |
|||||||||||||||| | ||||
|||||||||||||||| | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| |
|||||||||||||||| | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| |
|||||||||||||||| | ||||
|||||||||||||||| | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| |
|||||||||||||||| | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| |
|||||||||||||||| | ||||
|||||||||||||||| | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| |
|||||||||||||||| | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| |
|||||||||||||||| | ||||
|||||||||||||||| | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| |
|||||||||||||||| | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| |
|||||||||||||||| | ||||
|||||||||||||||| | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| |
|||||||||||||||| | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Note: Some redacted rows have been deleted.
Appendix 4: Description and Appraisal of Outcome Measures
Note that this appendix has not been copy-edited.
Aim
To describe the following outcome measures and review their measurement properties (validity, reliability, responsiveness to change, and MID):
EQ-5D to measure HRQoL changes over time was one of the exploratory efficacy endpoints in SOLSTICE trial.
SF-36v2 to measure HRQoL changes over time was one of the exploratory efficacy endpoints in SOLSTICE trial.
Findings
Table 40: Summary of outcome measures and their measurement properties
Outcome measure | Type | Conclusions about measurement properties | MID |
|---|---|---|---|
EQ-5D | A generic, preference-based, HRQoL measure consisting of descriptive questions and a VAS. The descriptive questions cover 5 dimensions, while each dimension is divided into 5 levels of perceived problems. Higher scores indicate worse quality of life in individual scores and better quality of life in population index (HUI) scores. The VAS records the patient’s self-rated health on a 10 cm scale with end points 0 to 100 labelled “the worst health you can imagine” and “the best health you can imagine”, respectively.51 | No studies about reliability, validity, and responsiveness in population with post-transplant CMV infection were identified. | General (non–disease specific) population: An estimate between 0.037 and 0.06960 |
SF-36 | A 36-item, generic, self-reported, Likert scale questionnaire consisting of 8 domains. Individual domain score and 2 component summaries, PCS and MCS, are possible. Possible scores range from 0 to 100 with higher scores indicating better health status.53,61 | No studies about reliability, validity, and responsiveness in population with post-transplant CMV infection were identified. | General (non–disease specific) population: PCS: 2 points61 MCS: 3 points61 Individual dimensions: 2 to 4 points61 |
EQ-5D = EuroQoL-5 dimensions-5 levels questionnaire; HRQoL = health-related quality of life; HUI = health utility index; MCS = Mental Component Summary; MID = minimal important difference; PCS = physical component summary; SF-35 = Short Form-36 survey; VAS = visual analogue scale.
EQ-5D
The EQ-5D questionnaire is a generic, preference-based, HRQoL measure consisting of descriptive questions and a VAS.51 EQ-5D has been validated in terms of feasibility, convergent validity, discriminatory power, and ceiling effects in a diverse patient population from 6 countries with chronic conditions.51 Questions were answered based on how the patient felt that day.
The EQ-5D was developed by the EuroQol Group as an improvement to the EQ-5D 3 level (EQ-5D-3L), to improve sensitivity (measuring small and medium health changes) and reduce ceiling effects.60,52 The instrument is comprised of 5 dimensions: mobility, self-care, usual activities, pain/discomfort, and anxiety/depression.60,52 The instrument is comprised of 5 dimensions: mobility, self-care, usual activities, pain/discomfort, and anxiety/depression. Each dimension is rated on 5 levels: level 1 “no problems,” level 2 “slight problems,” level 3 “moderate problems,” level 4 “severe problems,” and level 5 “extreme problems” or “unable to perform.” Respondents are asked to choose the level that reflects their health state for each of the 5 dimensions. The numerical values assigned to levels 1 to 5 for each dimension reflect rank order categories of function. Data are not used to produce an individual dimension score. A total of 3,125 unique health states are possible, with 55555 representing the worst health state and 11111 representing the best state.
Results from the EQ-5D descriptive system can be converted into a single, country-specific index score using a scoring algorithm taking the local patient and population preferences into account.62 Therefore, the index score is a country-specific value and the lowest EQ-5D index (utility) score varies depending on the scoring algorithm used.51 Even though the range of index scores differs according the scoring algorithm used, in all scoring algorithms of the EQ-5D, a score of 0 represents the health state ‘dead’ and 1.0 reflects ‘perfect health’. Also, negative values are possible to represent health states that a society, not the patient, considers worse than death. Different utility functions are available that reflect the preferences of specific populations, e.g., US, UK. As an example, a Canadian scoring algorithm results in a score of -0.148 for health state 55555 (worst health state).
Another component of the EQ-5D is a visual analogue scale (EQ-VAS), which is 10 cm, continuous scale anchored by 2 verbal descriptors: 0 (worst health imaginable) to 100 (best health imaginable). The respondents are asked to mark an X on the scale that best represents their health on that day.62,51
In summary, the EQ-5D produces 3 types of data for each respondent62,51:
A profile indicating the extent of problems on each of the 5 dimensions represented by a 5-digit descriptor, such as 11121 or 21143.
A population preference-weighted health utility index (HUI) score based on the descriptive system.
A self-reported assessment of health status based on the EQ-VAS.
Even though EQ-5D has been validated in a diverse patient population in 6 countries,63 no literature was identified that assessed the EQ-5D for validity, reliability, or responsiveness in population with post-transplant CMV infection.
MID
An estimated MID for the general population was based off scoring algorithms for 6 countries (Canada, China, Spain, Japan, England, and Uruguay) to be between 0.037 and 0.069.60 The MCID estimates for the index score in the Canadian population have a summarized mean (SD) of 0.056 (0.011), and a summarized median of 0.056 (interquartile range 0.049 to 0.063).60 No MID was estimated in a population with post-transplant CMV infection.
Short Form – 36 version 2
The SF-36 is a 36-item, generic, self-reported health assessment questionnaire that has been used in clinical trials to study the impact of chronic disease on HRQoL.53 The original version (SF-36v1) was released in 1992 and a revised version (SF-36v2) was released in 1996 with minor changes to the original survey. Changes included: reduced ambiguity in instructions, better layout, increased item-level response choices, increased cultural/language comparability, and elimination of a response option from the items in the mental health and vitality dimensions.61 SF-36v2 is used more commonly.
The SF-36 consists of 8 domains: physical functioning, role limitations due to physical health problems, bodily pain, general health, vitality, social functioning, role limitations due to emotional health problems, and mental health.53 For each of the 8 categories, a subscale score can be calculated. The SF-36 also provides 2 component summaries: the PCS and the Mental Component Summary (MCS), derived from aggregating the 8 domains according to a scoring algorithm.53 The SF-36 PCS and MCS and individual domains are each measured on a scale of 0 to 100, with an increase in score indicating improvement in health status.53 The summary scales are scored using norm-based methods, with regression weights and constants derived from the general US population. Both the PCS and MCS scales are transformed to have a mean of 50 and a standard deviation (SD) of 10 in the general US population.61 Therefore, all scores above/below 50 are considered above/below average for the general US population.
No studies assessing psychometric properties of SF-36v2 in patient population with post-transplant CMV infection have been found.
MID
In the general population, clinically meaningful improvement is generally indicated by a change of 2 points in the SF-36 PCS and 3 points in the SF-36 version 2 MCS.61 Based on anchor data, following minimal mean group differences, in terms of t score points are described for SF-36 version 2 individual dimension scores: physical functioning, 3; role functioning, 3; bodily pain, 3; general health, 2; vitality, 2; social functioning, 3; role-emotional, 4; and mental health, 3.61 These MID values were determined as appropriate for groups with mean t score ranges of 30 to 40.61 For higher t score ranges, MID values may be higher.60,61 In the general population, clinically meaningful improvement is generally indicated by a change of 2 points in the SF-36 PCS and 3 points in the SF-36 version 2 MCS.61 Based on anchor data, following minimal mean group differences, in terms of t score points are described for SF-36 version 2 individual dimension scores: physical functioning, 3; role functioning, 3; bodily pain, 3; general health, 2; vitality, 2; social functioning, 3; role-emotional, 4; and mental health, 3.61 These MID values were determined as appropriate for groups with mean t score ranges of 30 to 40.61 For higher t score ranges, MID values may be higher.60,61
No information about the MID of the SF-36v2 in the population living with post-transplant CMV infection was found.
Appendix 5: IPD Analyses
Note that this appendix has not been copy-edited.
Populations
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Interventions
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Outcomes
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Table 41: IPD Analyses Used in the Sponsor-Provided Global CEM and CADTH Health Economics Report
IPD analysis | Use in model | Table used in base case | Table used in scenario | Scenario definition |
|---|---|---|---|---|
||||||||||||||||||||||||||||||||||||||||||||||||||| | ||||
||||||||||||||||||||||||||||||||||||||||||||||||||| | ||||||||||||||||||||||||||||||||||||||||||||||||||| | — | — | |||||||||||||||| |
||||||||||||||||||||||||||||||||||||||||||||||||||| | ||||||||||||||||||||||||||||||||||||||||||||||||||| | — | — | |
||||||||||||||||||||||||||||||||||||||||||||||||||| | ||||||||||||||||||||||||||||||||||||||||||||||||||| | — | |||||||||||||||| | |
||||||||||||||||||||||||||||||||||||||||||||||||||| | ||||
||||||||||||||||||||||||||||||||||||||||||||||||||| | ||||
||||||||||||||||||||||||||||||||||||||||||||||||||| | ||||
||||||||||||||||||||||||||||||||||||||||||||||||||| | ||||||||||||||||||||||||||||||||||||||||||||||||||| | — | |||||||||||||||| | |
||||||||||||||||||||||||||||||||||||||||||||||||||| | — | |||
||||||||||||||||||||||||||||||||||||||||||||||||||| | ||||
||||||||||||||||||||||||||||||||||||||||||||||||||| | ||||||||||||||||||||||||||||||||||||||||||||||||||| | — | — | |||||||||||||||| |
||||||||||||||||||||||||||||||||||||||||||||||||||| | ||||
||||||||||||||||||||||||||||||||||||||||||||||||||| | ||||||||||||||||||||||||||||||||||||||||||||||||||| | — | — | ||||||||||||||| |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Table 42: Additional IPD Analyses Used in CADTH Health Economics Report
Parameter | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| | ||||||
|---|---|---|---|---|---|---|---|
By treatment arm | By transplant type | By treatment arm and transplant type | Additional stratification factors | By individual IAT type | By individual IAT type and transplant type | Other analyses | |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| | |||||||
||||||||||||||| | ||||||||||||||| | ||||||||||||||| | ||||||||||||||| | ||||||||||||||| | ||||||||||||||| | ||||||||||||||| | ||||||||||||||| |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| | |||||||
||||||||||||||| | ||||||||||||||| | ||||||||||||||| | ||||||||||||||| | ||||||||||||||| | ||||||||||||||| | ||||||||||||||| | ||||||||||||||| |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| | |||||||
||||||||||||||| | ||||||||||||||| | ||||||||||||||| | ||||||||||||||| | ||||||||||||||| | ||||||||||||||| | ||||||||||||||| | ||||||||||||||| |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Statistical Analysis
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Efficacy
Treatment Response (Clearance) and Recurrence
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Utility
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Adverse Events
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
All-Cause Mortality
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Table 43: Week 0 No Response to Week 4 or Week 8 Response Status
Detail | Maribavir (N = 235) | IAT (N = 117) |
|---|---|---|
|||||||||||||||||||||||||||||||||||||||||| | ||
|||||||||||||||||||||||||||||||||||||||||| | |||||||||||||||||||||||||||||||||||||||||| | |||||||||||||||||||||||||||||||||||||||||| |
|||||||||||||||||||||||||||||||||||||||||| | |||||||||||||||||||||||||||||||||||||||||| | |||||||||||||||||||||||||||||||||||||||||| |
|||||||||||||||||||||||||||||||||||||||||| | ||
|||||||||||||||||||||||||||||||||||||||||| | |||||||||||||||||||||||||||||||||||||||||| | |||||||||||||||||||||||||||||||||||||||||| |
|||||||||||||||||||||||||||||||||||||||||| | |||||||||||||||||||||||||||||||||||||||||| | |||||||||||||||||||||||||||||||||||||||||| |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Table 44: Week 4 Response Status to Week 8 Response Status
Detail | Response at week 8 | No response at week 8 | ||
|---|---|---|---|---|
Maribavir | IAT | Maribavir | IAT | |
|||||||||||||||||||||||||||||||||| | |||||||||||||||||||||||||||||||||| | |||||||||||||||||||||||||||||||||| | |||||||||||||||||||||||||||||||||| | |||||||||||||||||||||||||||||||||| |
|||||||||||||||||||||||||||||||||| | |||||||||||||||||||||||||||||||||| | |||||||||||||||||||||||||||||||||| | |||||||||||||||||||||||||||||||||| | |||||||||||||||||||||||||||||||||| |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Table 45: Week 4 Response to Recurrence Requiring Treatment with an Anti-CMV Drug at Week 8
Detail | Recurrence at week 8 | No recurrence at week 8 | Death before meeting recurrence criteriaa | |||
|---|---|---|---|---|---|---|
Maribavir | IAT | Maribavir | IAT | Maribavir | IAT | |
|||||||||||||||||||||||||||||||||| | ||||||
||||||||||||||||||| | ||||||||||||||||||| | ||||||||||||||||||| | ||||||||||||||||||| | ||||||||||||||||||| | ||||||||||||||||||| | ||||||||||||||||||| |
||||||||||||||||||| | ||||||||||||||||||| | ||||||||||||||||||| | ||||||||||||||||||| | ||||||||||||||||||| | ||||||||||||||||||| | ||||||||||||||||||| |
|||||||||||||||||||||||||||||||||||||| | ||||||
||||||||||||||||||| | ||||||||||||||||||| | ||||||||||||||||||| | ||||||||||||||||||| | ||||||||||||||||||| | ||||||||||||||||||| | ||||||||||||||||||| |
||||||||||||||||||| | ||||||||||||||||||| | ||||||||||||||||||| | ||||||||||||||||||| | ||||||||||||||||||| | ||||||||||||||||||| | ||||||||||||||||||| |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Table 46: Confirmed CMV Viremia Clearance at Study Week 4 to Confirmed CMV Viremia Clearance Status at Week 8
||||||||||||||||||||||||||||||||||||||||||||||||||||||||| | Maribavir (Total = 235) | IAT (Total = 117) |
|---|---|---|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||| | ||
||||||||||||||||||| | ||||||||||||||||||| | ||||||||||||||||||| |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||| | ||
||||||||||||||||||| | ||||||||||||||||||| | ||||||||||||||||||| |
||||||||||||||||||| | ||||||||||||||||||| | ||||||||||||||||||| |
||||||||||||||||||| | ||||||||||||||||||| | ||||||||||||||||||| |
||||||||||||||||||| | ||||||||||||||||||| | ||||||||||||||||||| |
||||||||||||||||||| | ||||||||||||||||||| | ||||||||||||||||||| |
||||||||||||||||||| | ||||||||||||||||||| | ||||||||||||||||||| |
||||||||||||||||||| | ||||||||||||||||||| | ||||||||||||||||||| |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Table 47: EQ-5D UK Crosswalk HSUVs
Detail | Maribavir | IAT | |||||
|---|---|---|---|---|---|---|---|
m/n | Mean | SE | m/n | Mean | SE | ||
|||||||||||||||||||||||||||||||||||||| | |||||||
|||||||||||||||| | |||||||||||||||| | |||||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||||| | |||||||||||||| | |||||||||||||| |
|||||||||||||||| | |||||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||||| | |||||||||||||| | |||||||||||||| | |
|||||||||||||||| | |||||||||||||||| | |||||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||||| | |||||||||||||| | |||||||||||||| |
|||||||||||||||| | |||||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||||| | |||||||||||||| | |||||||||||||| | |
||||||||||||||||||||||||||||||||||||||||| | |||||||
|||||||||||||||| | |||||||||||||||| | |||||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||||| | |||||||||||||| | |||||||||||||| |
|||||||||||||||| | |||||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||||| | |||||||||||||| | |||||||||||||| | |
|||||||||||||||| | |||||||||||||||| | |||||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||||| | |||||||||||||| | |||||||||||||| |
|||||||||||||||| | |||||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||||| | |||||||||||||| | |||||||||||||| | |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Table 48: Restricted Mean Survival Time Difference: TUDD in Overall Health - Sensitivity Analysis
RMSTa difference (Maribavir to IAT) | Lower 95% CI | Upper 95% CI | P valueb |
|---|---|---|---|
|||||||||||||||| | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Table 49: Clinically Important AEs
AE Term | Maribavir (Total = 234) | IAT (Total = 116) | ||||
|---|---|---|---|---|---|---|
n (%) | m | Duration, mean (SD) | n (%) | m | Duration, mean (SD) | |
|||||||||||||||| | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||||| |
|||||||||||||||| | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||||| |
|||||||||||||||| | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||||| |
|||||||||||||||| | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||||| |
|||||||||||||||| | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||||| |
|||||||||||||||| | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||||| |
|||||||||||||||| | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| | |||||||||||||| | ||||||||||||||| | |||||||||||||||| |
|||||||||||||||| | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| | |||||||||||||| | ||||||||||||||| | |||||||||||||||| |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Table 50: Time to All-Cause Mortality From Week 8 to 20
Detail | Response at week 8 (Total = 159) | No -response at week 8 (Total = 193) |
|---|---|---|
|||||||||||||||| | |||||||||||||||| | |||||||||||||||| |
|||||||||||||||| | |||||||||||||||| | |||||||||||||||| |
||||||||||||||||||||||||||||
Source: Individual Patient Data Analysis of Study 303 - Maribavir
Table 51: All-Cause Mortality Regardless of Rescue or Anti-CMV Between Week 0 to 4 and Week 4 to 8
Detail | HSCT (Total = 141) | SOT (Total = 211) |
|---|---|---|
|||||||||||||||||||||||||||||||||||||||||||||||| | ||
|||||||||||||||| | |||||||||||||||| | |||||||||||||||| |
|||||||||||||||| | |||||||||||||||| | |||||||||||||||| |
|||||||||||||||||||||||||||||||||||||||||||||||| | ||
|||||||||||||||| | |||||||||||||||| | |||||||||||||||| |
|||||||||||||||| | |||||||||||||||| | |||||||||||||||| |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Critical Appraisal
These analyses were mostly exploratory and descriptive. Analyses with statistical testing were not pre-defined in a statistical analysis plan and were performed in a post-hoc manner. Therefore, definitive conclusion regarding efficacy and safety of maribavir cannot be drawn based on this evidence. As the sponsor have noted, the IPD analyses are exploratory and purported to be used as input for the CEM.
Pharmacoeconomic Review
Abbreviations
AE
adverse event
BIA
budget impact analysis
CMV
cytomegalovirus
csCMV
clinically significant cytomegalovirus
CUA
cost-utility analysis
EQ-5D
European Quality of Life 5 Dimension scale
HSCT
hematopoietic stem cell transplant
HRQoL
health-related quality of life
ICER
incremental cost-effectiveness ratio
LY
life-year
n-csCMV
non-clinically significant cytomegalovirus
QALY
quality-adjusted life-year
SOT
solid organ transplant
Executive Summary
The executive summary comprises 2 tables (Table 1 and Table 2) and a conclusion.
Item | Description |
|---|---|
Drug product | Maribavir (Livtencity), tablets |
Submitted price | Maribavir, 200mg, oral tablets: $276.7857 per tablet |
Indication | For the treatment of adults with post-transplant cytomegalovirus (CMV) infection/disease who are refractory (with or without genotypic resistance) to one or more prior antiviral therapies. |
Health Canada approval status | NOC |
Health Canada review pathway | Priority review |
NOC date | September 15, 2022 |
Reimbursement request | As per indication |
Sponsor | Takeda Canada Inc. |
Submission history | Previously reviewed: No |
CMV = cytomegalovirus; NOC = Notice of Compliance.
Table 2: Summary of Economic Evaluation
Component | Description |
|---|---|
Type of economic evaluation | Cost-utility analysis |
Target population | Adult solid organ transplant (SOT) or hematopoietic stem cell transplant (HSCT) recipients with refractory and/or resistant cytomegalovirus (CMV) infection/disease |
Treatment | Maribavir |
Comparator | Investigator assigned treatment (IAT) comprising of IV (IV) ganciclovir, oral valganciclovir, IV foscarnet and IV cidofovir |
Perspective | Canadian publicly funded health care payer |
Outcomes | Quality-adjusted life-years (QALYs), life-years (LYs) |
Time horizon | Lifetime (47 years) |
Key data source | Treatment efficacy of the treatment and comparators were derived from the Clinical Study Report and an individual patient-level data (IPD) analysis from the TAK-620 to 303 (SOLSTICE) trial |
Submitted results | Maribavir dominated IAT, providing more QALYs at a lower cost (incremental cost = -$496; incremental QALY = 0.17) |
Key limitations |
|
CADTH reanalysis results |
|
CMV = cytomegalovirus; HSCT = hematopoietic stem cell transplant; IAT = investigator assigned treatment; ICER = incremental cost-effectiveness ratio; IPD = individual patient-level data; LY = life-year; SOT = solid organ transplant; PSM = partitioned survival model; QALY = quality-adjusted life-year.
Conclusions
Evidence from the pivotal trial (SOLSTICE; Study 303) suggest that there is evidence of maribavir improving CMV viremia clearance and symptom control when compared to IAT over 16 weeks. However, disease control with maribavir is time-limited, like other antivirals, and evidence of maintained clearance (i.e., there was no clinically significant CMV recurrence) is less certain. Within the trial, no clinically meaningful difference in mortality between treatment options was demonstrated. The clinical experts consulted by CADTH noted that the distribution of each IAT in SOLSTICE is not reflective of Canadian clinical practice. As a result, generalizability of results to the Canadian setting is uncertain, and conclusions on comparative efficacy and cost-effectiveness for each antiviral cannot be drawn.
To address limitations with the sponsor’s submitted pharmacoeconomic evaluation, CADTH undertook a reanalysis with the following changes: removed the mortality difference between maribavir and IAT from week 8 onwards; assumed equivalent clinical efficacies for both treatments from week 8 for CMV clearance and week 20 for recurrence; and assumed that retreatment would occur using the same drug that was used initially. In the CADTH base case, the ICER of maribavir compared to IAT was $403,089 per QALY. A price reduction of approximately 4.5% is required for maribavir to be cost-effective at a $50,000 per QALY threshold.
The submitted price of maribavir and the cost savings from administration were 2 key drivers of overall costs and of the ICER within the model. Uncertainty remains as to whether such savings with respect to drug administration (~$71,000) would be realized. Further, there were limitations that CADTH was unable to address in the model, including the impact of treatment duration. Treatment duration was modelled as a fixed amount of time for each treatment; however, based on consultation with CADTH clinical experts, the practice would be highly variable and based on clinical judgment. As the cost of maribavir is an influential parameter, variation in treatment duration could significantly alter maribavir’s cost-effectiveness.
Considerable uncertainty further remains due to limited long-term clinical data. Other key drivers in the model included the clinical efficacy following initial treatment, as the true efficacy of maribavir and IAT for retreatment is not known and may be highly variable across patient groups (e.g., transplant type) and underlying patient characteristics. The long-term effects of maribavir on maintaining CMV clearance compared to other treatments further remains unknown. Given the limitations that were unable to be addressed in the model, further price reductions may be required to ensure cost-effectiveness.
Stakeholder Input Relevant to the Economic Review
This section is a summary of the feedback received from the patient groups, registered clinicians, and drug plans that participated in the CADTH review process.
CADTH received patient input from the Leukemia and Lymphoma Society of Canada on behalf of several Canadian charities, the Canadian Liver Foundation, and the Kidney Foundation of Canada (KF). All organizations collected input from Canadian patient and caregivers regarding post-transplant CMV experiences through online surveys. Patients indicated that symptoms of CMV interfered with their daily lives, including impacts on ability to work, travel, concentrate, exercise, and perform daily activities. For patients currently receiving treatment, the majority of respondents treated for established CMV infection received ganciclovir or valganciclovir as first-line treatment, followed by potential second-line treatment with foscarnet or cidofovir. Side effects of current treatments include vomiting, diarrhea, nausea, anxiety, loss of appetite, and depression. Respondents expressed the need for improved therapies and identified key aspects of treatment such as improved quality of life, improved length of survival, minimal travel required, minimized cost and length of treatment, oral route of drug administration, minimal interactions with other medications, and reduced side effects of treatment. Of all respondents, KF received input from 1 Canadian patient treated with maribavir. This respondent found that maribavir did not result in improved side effects (diarrhea, appetite, vomiting, urinary changes, fever, and unexplained bruises) and led to worse tiredness.
CADTH received registered clinician input from Cell Therapy Transplant Canada (CTC), a national multidisciplinary organization promoting research and excellence inpatient care in the field of HSCT and cell therapy. There are currently no Health Canada–approved therapies for resistant and/or refractory CMV infection and therefore no single standard approach, although letermovir may be administered as preventative therapy. Valganciclovir is most commonly used as first-line treatment in practice, followed by ganciclovir, cidofovir, or foscarnet. CTC stated that a safe, orally administered treatment that is well-tolerated and results in high response rates would be preferable to current treatments, where toxicity due to AEs associated with current treatments is noted to impact health-related quality of life. Maribavir is expected to become the preferred second-line therapy for patients who do not respond or tolerate first-line therapy (generally valganciclovir).
Feedback from the drug plans highlighted implementation concerns with the off-label use of comparator treatments as there are no approved drugs in Canada for the treatment of refractory and/or resistant CMV infection in transplant recipients. Furthermore, drug plans noted that there is a lack of a standard definition for refractory and/or resistant CMV. Regarding eligibility, it is also unclear whether prior antiviral therapy use would include letermovir, a preventative therapy. Drug plans also expressed uncertainty surrounding treatment duration and discontinuation of therapy. Additionally, the use of maribavir in combination with other antivirals for CMV prevention and treatment is unclear. Drug plans also noted the impacts of IV administration costs for comparator drugs and the potential cost savings associated with the oral mode of administration for maribavir.
Several of these concerns were addressed in the sponsor’s model:
the impact of IV administration costs could be explored in the model
treatment related AEs were considered in the model, including quality of life and cost considerations.
CADTH was unable to address the following concerns raised from stakeholder input:
variable treatment duration and discontinuation of therapy was not accounted for in the model
the model did not account for the use of maribavir in combination with other antivirals.
Economic Review
The current review is for maribavir (Livtencity) for adult solid organ transplant (SOT) or hematopoietic stem cell transplant (HSCT) patients with cytomegalovirus (CMV) infection or disease that is refractory and/or resistant to 1 or more prior antiviral therapies.
Economic Evaluation
Summary of Sponsor’s Economic Evaluation
Overview
The sponsor submitted a cost-utility analysis (CUA) of maribavir compared with a weighted investigator assigned treatment (IAT) comprising IV ganciclovir, oral valganciclovir, IV foscarnet, or IV cidofovir. The model population comprised adult SOT or HSCT recipients with CMV infection/disease that is refractory and/or resistant to 1 or more prior antiviral therapies. This population aligns with the Health Canada-indicated population and the reimbursement request.
Maribavir is self-administered as an oral tablet that contains 200 mg of maribavir per tablet. The recommended dosing for maribavir is 2 tablets twice daily for a total of 800 mg per day. The SOLSTICE trial had a mean treatment duration of 7.5 weeks; however, the length of treatment may vary significantly and would be decided using clinical judgment. Each tablet costs $276.80 and a 7.5-week course of treatment (52.5 days) costs $58,128.
The comparator, IAT, consisted of 4 comparator treatments (i.e., ganciclovir, valganciclovir, foscarnet, and cidofovir) with the distribution of comparators being informed by the pivotal trial. The cost of IAT was based on the weighted mean of treatment duration for each treatment and the unit cost, resulting in a drug acquisition cost of $17,791 for 1 course of IAT.
The clinical outcomes modelled are life-years (LYs) and quality-adjusted life-years (QALYs). The reference perspective is the public health care perspective. The time horizon is lifetime with a maximum age of 100 years, and the discount rate is 1.5%.
Model Structure
The sponsor submitted a 2-stage Markov state transition cohort model. In the first stage, from 0 to 52 weeks, there were 3 health states: clinically significant CMV infection (csCMV), non-clinically significant CMV infection (n-csCMV) and dead. In the second stage, beginning at 52 weeks, there were 2 health states: alive and dead. The model structure is shown in Figure 1, Appendix 3. The model uses a 4-week cycle length for the first 3 years, followed by a 1-year cycle length for the remainder of the time horizon. For the purpose of transitions, CMV viremia clearance is defined as plasma CMV DNA concentration that is less than the lower limit of quantification (LLOQ; 137 IU/mL) in 2 consecutive readings at least 5 days apart, and clinically significant recurrence is defined as a CMV viral load greater than LLOQ requiring treatment with an anti-CMV agent.
All patients begin in the csCMV health state from which they can transition to n-csCMV if CMV viremia clearance is achieved or remain if it is not achieved, beginning after the first cycle. From the n-csCMV health state, if a patient experiences a clinically significant recurrence of CMV, they can transition to the csCMV health state, or remain if clearance is maintained. Patients can transition to ‘dead’ from any health state, the rate of which is assumed to be related to CMV status (clinically significant or non-clinically significant) in the first 52 weeks of the model. In the second stage of the model CMV status is no longer tracked (i.e., the sponsor assumes that no further recurrences take place and that all CMV infections are resolved). In this stage, patients can remain in the ‘alive’ health state until they transition to the ‘dead’ health state based on transplant-specific mortality rates and the Canadian general population mortality.
Model Inputs
The baseline cohort is a population of adult HSCT and SOT patients with refractory or resistant CMV infection/disease. The cohort has a starting age of 53 years, and the proportion of males is 61%, based on the population included in the SOLSTICE trial.1 While HSCT and SOT patients are tracked separately in the model, a weighted average cost-effectiveness is derived based on the patient distribution (59.9% SOT) in the SOLSTICE trial. The sponsor assumed that all patients entered the model 1-year after their transplant.
The clinical pathway was informed by the clinical trial, literature, and clinical opinions via the sponsor’s UK advisory board and Canadian key opinion leaders.2 Patient mortality rates for weeks 0 to 4 and 4 to 8 are transplant-specific mortality rates as observed in the trial,3 and the health-state specific 12-week mortality rate from the trial from weeks 8 to 20 (the end of the trial) were converted into a 4-week probability that was applied from weeks 8 to 52.3 In the second stage of the model (week 52 onward), mortality was estimated based on transplant-specific mortality rates and Canadian age-based general population all-cause mortality. The transplant-specific mortality was based on data taken from the UK National Health Service (NHS)4 and the UK Haematological Malignancy Research Network.5
In the sponsor’s base case, the comparator treatment is an investigator assigned treatment (IAT) comprising the following drug distributions for both SOT and HSCT patients: ganciclovir (25.4%), valganciclovir (25.9%), foscarnet (43.5%), and cidofovir (5.2%). The drug distribution in the IAT was derived from the SOLSTICE trial.1 Comparative efficacy (i.e., CMV clearance and CMV recurrence) was derived for maribavir and IAT from the SOLSTICE trial and an individual patient data (IPD) analysis of the trial. The IPD analysis was used to directly estimate transition probabilities between weeks 0 and 8. The trial only collected data for 20 weeks, and so the sponsor used the IPD analysis to convert probabilities to 4-week transition probabilities that were applied from weeks 8 to 52. For CMV clearance, the sponsor used the IPD analysis probability for week 0 to 8, and for CMV recurrence the 12-week probability from week 8 to 20. The sponsor assumed that if a patient experienced clinically significant recurrence of CMV infection/disease that retreatment would use IAT regardless of the initial treatment, and the per-cycle probability of recurrence was based on the most recent treatment that the patient received.
Adverse events (AEs) for maribavir and IAT were applied in the model using the 20-week incidence rate reported in the SOLSTICE trial. The sponsor included only AEs with an incidence of over 10% and AEs relating to renal disorders and blood/immune dysfunction based on Canadian clinical feedback.6 In the base case, the sponsor also included a risk of graft loss based on published literature suggesting that graft loss occurred more frequently in patients with CMV infection within 3 months of an SOT than those without.7
Health-related quality of life (HRQoL) of patients from baseline to week 20 were collected using the EQ-5D-5L during the SOLSTICE trial, and health state utilities were derived from this using the EQ-5D-3L crosswalk algorithm described by van Hout et al.8 The transplant and health state specific utility values at week 8 were included in the first stage of the model. In the second stage of the model, the sponsor first calculated the difference between the Canadian general population utility score9 at age 53 and the transplant-specific (SOT or HSCT) utility score collected at week 20 in the SOLSTICE trial. Then, the age-based utility score applied in the model was calculated by subtracting those differences from the age-based general population utility. Utility decrements were applied for each AE based on the mean duration of the adverse event and the disutility mean as found in published literature about a UK population.10-14
The sponsor included direct medical costs associated with treatment. Dosing of maribavir in the model was applied as described in the overview section: 2 tablets at 200 mg, twice daily, for a total of 800 mg per day. For IAT, the sponsor used a weighted average cost for the 4 treatments included in the IAT based on the Health Canada–approved product monographs and unit costs for the drugs. Treatment duration for maribavir and IAT in the model was based on the mean time on treatment in weeks from the SOLSTICE trial. Unit costs were obtained from the Ontario Drug Benefit (ganciclovir and valganciclovir),15 Canadian wholesale price from IQVIA (foscarnet),16 and from a converted UK price (cidofovir).17 The sponsor assumed that administration of IV anti-CMV drugs (ganciclovir, foscarnet, and cidofovir) occurred exclusively in outpatient clinics. The sponsor used the cost per-hour of chemotherapy infusion as a proxy for the cost of infusion of anti-CMV medications that was estimated at a Toronto hospital.18
Health care resource utilization costs were also included in the model including inpatient visits, outpatient visits, monitoring costs (e.g., for drug toxicities), and costs associated with AEs and disease complications. The sponsor obtained costs from the Ontario Schedule of Benefits,19 the Ontario Laboratory Schedule of Benefits,20 and the Ontario Case Costing Initiative21 where possible. Costs associated with graft loss and potential retransplantation and dialysis were sourced from Canadian published literature.22,23
Summary of Sponsor’s Economic Evaluation Results
All analyses were run probabilistically using 5,000 iterations. The deterministic and probabilistic results were similar. The probabilistic findings are presented below. Comparator costs are based on publicly available list prices and may not reflect actual costs paid by public drug plans.
Base-Case Results
The sponsor’s economic evaluation finds that over a lifetime time horizon, maribavir accrues 10.53 LYs compared to 10.33 for IAT (incremental LYs = 0.20). The sponsor’s base-case analysis reports that maribavir dominates IAT (i.e., maribavir is less costly and provides more QALYs than IAT). Compared to IAT, maribavir provided an additional 0.17 QALYs and costs $496 less than IAT. The higher cost of initial treatment with maribavir (maribavir incurred $20,792 more than IAT) was offset by cost savings arising from administration (IAT was associated with $19,489 in administration costs) and lower retreatment costs (as maribavir was associated with lower recurrence rates).
Table 3: Summary of the Sponsor’s Economic Evaluation Results
Drug | Total costs ($) | Incremental costs ($) | Total QALYs | Incremental QALYs | ICER vs. maribavir ($/QALY) |
|---|---|---|---|---|---|
Maribavir | $139,314 | Ref. | 8.35 | Ref. | Ref. |
IAT | $139,810 | –$496 | 8.18 | 0.17 | Dominated |
IAT = investigator assigned treatment; ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year; Ref. = reference; vs. = versus.
Source: Sponsor’s pharmacoeconomic submission.6
Sensitivity and Scenario Analysis Results
One-way sensitivity analyses found that the results were most sensitive to the cost of maribavir, IV administration costs, IAT drug acquisition costs, followed by maribavir clearance and recurrence probabilities. The sponsor submitted several scenario analyses including reduced IAT and IV administration cost, retreatment with maribavir, IAT treatment distribution, multiple time horizons (1, 5, 10, and 20 years), and inpatient administration of IV IAT treatments. When the cost of IAT and IV administration costs were reduced by 25%, maribavir costs more (incremental cost = $13,772) and provided more QALYs (incremental QALYs = 0.17) than IAT, resulting in an ICER of $79,873. Additionally, when the IAT treatment distribution for SOT and HSCT changed from that in the SOLSTICE trial to the market share distribution estimated based on the sponsor’s internal estimates, the ICER for maribavir compared to IAT was $50,063 (incremental cost = $8,632; incremental QALY = 0.17). In most other scenario analyses, maribavir remained dominant.
CADTH Appraisal of the Sponsor’s Economic Evaluation
CADTH identified several key limitations to the sponsor’s analysis that have notable implications on the economic analysis:
Inappropriate implementation of comparator: In the sponsor’s economic evaluation, they used a combined comparator (IAT comprising ganciclovir, valganciclovir, foscarnet and cidofovir). When multiple comparators are relevant to a funding decision, treatments should be considered on their own and all comparators should be assessed in a sequential analysis. Several alternative antiviral treatments exist that are cheaper with respect to daily drug costs than maribavir based on its submitted price (refer to Appendix 1). As such, the interpretation of the economic value of maribavir was restricted to a comparison with a pooled comparator and the cost-effectiveness of maribavir relative to individual antiviral drugs is unknown.
For IAT, the distribution of the treatments and the treatment duration was based on the SOLSTICE trial. The sponsor assumed that the distribution of IAT drugs was the same for SOT and HSCT patients with the following distribution: ganciclovir – 25.4%; valganciclovir – 25.9%; foscarnet – 43.5%; and cidofovir – 5.2%. The clinical experts consulted by CADTH agreed that the distribution assumed by the sponsor is not reflective of Canadian practice for the modelled population. The clinical experts provided an estimated distribution that better reflects Canadian practice and that differs for SOT and HSCT as follows: ganciclovir – 15% (SOT) and 34% (HSCT); valganciclovir – 5% (SOT and HSCT); foscarnet – 79% (SOT) and 60% (HSCT); and cidofovir – 1% (SOT and HSCT). Notably, the proportion of patients receiving valganciclovir differed from the sponsor’s distribution because valganciclovir is used regularly as a first-line treatment for CMV and thus is not typically repeated for patients who have refractory and/or resistant CMV infections/disease. The different IAT distribution is likely to influence the IAT treatment and retreatment costs due to differing drug prices and a shift toward a higher proportion of patients being treated with IV drugs that have administration-related costs.
Further, the treatment durations that were used in the sponsor’s economic evaluation were based on what was observed in the SOLSTICE trial, however, the clinical experts consulted by CADTH suggested that the treatment durations were not reflective of Canadian practice. Treatment duration is decided clinically based on viral clearance and not a set duration, and may vary significantly by patient characteristic and transplant type. Acknowledging this structural limitation, the clinical experts consulted by CADTH suggested it would be more appropriate to assume a mean treatment duration of 5 to 6 weeks for all treatments.
The sponsor’s economic model was coded such that there was a single efficacy measure for IAT (i.e., not as a weighted measure of each treatment’s efficacy) and thus changes to the IAT distribution would only impact the costs and not treatment efficacy. As a result, CADTH was unable to adequately incorporate an IAT distribution that would be more reflective of Canadian practice within the submitted model.
Further, CADTH is unable to incorporate treatment duration that reflects Canadian treatment practice based on viral clearance due to the structure of the sponsor’s model and the lack of clinical data (i.e., time to viral clearance) collected in the SOLSTICE trial.
Uncertain long-term survival benefit: The sponsor assumed that mortality would differ by health state, from weeks 8 to 52 in the economic model. In the model, time spent in each health state (csCMV and n-csCMV) was linked to treatment efficacy and thus survival benefits were implicitly assumed between treatments. However, the trial results found no clinically meaningful difference in mortality between treatment arms (maribavir and IAT) because the trial was not adequately powered to detect this difference. Further, clinical experts consulted by CADTH suggested that differences in mortality are unlikely to be a result of which treatment the patient was given, but rather related to underlying patient characteristics. Patients with CMV infections requiring treatment often have underlying health problems which resulted in the CMV infection. At present, treatments do not address these underlying concerns and it is difficult to establish their impacts on mortality.
CADTH assumed that, from week 8 to 52, there would be no difference in mortality based on health state.
Approach to extrapolating long-term treatment efficacy likely overestimates clinical benefits (QALYs): The sponsor assumed that treatment efficacy (i.e., CMV clearance and recurrence) for both treatment arms would remain constant from week 8 to 52. For CMV clearance, the sponsor converted the CMV clearance probability from week 0 to 8 (i.e., the clearance found during initial treatment in the trial) and assumed this probability would apply in the model from week 8 to 52. In doing this, the sponsor assumed that the clinical efficacy for CMV clearance for those that require retreatment or who were non-responders and continue taking maribavir after 8 weeks, would be equivalent to those who experienced treatment success during their initial treatment. The clinical experts consulted by CADTH agreed that long-term retreatment efficacy was unlikely to remain constant or prove to be as efficacious as initial treatment. The trial did not include retreatment efficacy data for maribavir or IAT. For CMV recurrence, the sponsor converted treatment efficacy from weeks 8 to 20 in the trial to a 4-week probability and applied it as a constant probability from weeks 8 to 52. However, the clinical experts consulted by CADTH suggested that the treatment effects would not likely remain constant over this time period.
Applying the constant rate over time is potentially an overestimate of treatment efficacy as both maribavir and IAT are likely to have declining clearance rates over time. Similarly, recurrence rates may decline for both treatments. The model structure introduces additional uncertainty in the appropriateness to extrapolate treatment efficacy data from the trial due to the lack of differentiation between non-responders (i.e., those who do not achieve CMV clearance after 8 weeks) and recurrence (i.e., those who achieve clearance and later have a CMV recurrence). These groups of patients are expected to have differing treatment efficacy; however, this cannot be accounted for in the model as they all belong within the same health state (csCMV). The number of patients requiring retreatment during weeks 8 to 52 has important implications on the economic conclusions of the model due to the high costs of retreatment. Therefore, the lack of clinical data during that time period makes the results of the economic evaluation uncertain beyond the 8 weeks.
For weeks 8 to 52, CADTH assumed no additional CMV clearance benefit for maribavir over IAT, because after 8 weeks any patient receiving treatment would be considered a retreatment in the model and thus it would be inappropriate to use initial treatment clearance probabilities. For weeks 20 to 52, CADTH assumed no additional treatment benefit for maribavir over IAT for CMV recurrence.
CADTH conducted a scenario analysis assuming that CMV clearance probabilities for maribavir remained constant from weeks 8 to 20 (as in the sponsor base case), and then were equivalent to IAT from weeks 20 to 52.
Underestimated retreatment costs for maribavir: The sponsor assumed that all patients who have CMV recurrence or are non-responders would receive IAT. However, the approach to clinical management differs between these 2 distinct groups. Clinical experts consulted by CADTH suggested that, if a patient requires retreatment due to a recurrence, it is likely that they would be retreated with the initial treatment used (i.e., maribavir would be retreated with maribavir, and IAT with IAT). If patients are non-responders, clinical experts noted that these patients would be treated by a different antiviral drug; however, in clinical practice treatment may be extended beyond 8 weeks (e.g., to 12 weeks) before changing antivirals. While it is possible that some patients would receive retreatment with an alternative therapy (i.e., maribavir retreated with IAT, and IAT retreated with maribavir) it is unclear what proportion of patients this might be, and the sponsor’s submitted economic model does not allow for a combination of maribavir and IAT use for retreatment. As noted above, the structure of the sponsor’s model does not separately consider patients who have a treatment failure (i.e., CMV clearance was not achieved) or those who achieved clearance then later recurred. As the retreatment approach is likely to differ between these 2 distinct groups, there would be cost implications that are not currently captured in the submitted model.
CADTH assumed that maribavir was used to retreat patients who initially received maribavir, and that IAT was used to retreat patients who initially received IAT. This assumption does not address the need to differentiate between non-responders and those who achieve clearance and later recur. Therefore, this change may overestimate maribavir retreatment costs for non-responders (who would likely be retreated with an antiviral included in the IAT), however, a higher proportion of patients achieved CMV clearance following initial treatment with maribavir than IAT, and so retreatment with maribavir is likely appropriate for most retreatments taking place over 52 weeks.
Uncertain administration costs for IV drugs: The sponsor’s economic evaluation assumed that all IV treatments (ganciclovir, foscarnet, and cidofovir) were administered in an outpatient setting. As noted by the sponsor, and by the clinical experts consulted by CADTH, IV administration may take place in an inpatient setting. Where patients treated with foscarnet would be treated as inpatients, and some patients receiving ganciclovir and cidofovir may receive treatment in an inpatient setting. As maribavir is an oral tablet, it could be administered at patient’s homes (depending on patient severity), thus not accruing additional costs for both administration and inpatient care like IAT. Of note, transitioning from antivirals administered by IV to maribavir may be complicated by increased costs for some budget holders (e.g., public drug plans) while the associated savings are seen by others (e.g., hospital budgets). However, these savings may not be realized as some of the resources associated with IV administration are inelastic.
CADTH conducted a scenario analysis in which 100% of patients receiving foscarnet and cidofovir, and 50% of patients receiving ganciclovir receive treatment in an inpatient setting, using the same methods described by the sponsor in their scenario analysis.
To explore the sensitivity of the model to administration costs, using the same scenario described by the sponsor, CADTH conducted a scenario analysis exploring a 25% decrease in IV administration costs.
Additional limitations were identified but were not considered to be key limitations. These limitations are outlined subsequently.
Uncertainty in HRQoL data: Several limitations regarding utility values used in the sponsor’s economic evaluation were identified. The sponsor converted the HRQoL collected during the SOLSTICE trial using the EQ-5D-5L to EQ-5D-3L utilities using the crosswalk algorithm described by van Hout et al. (2012),8 thus increasing imprecision. It is not clear from the sponsor’s submission why the trial results were converted, and additionally, the sponsor used an outdated algorithm rather than the official EQ-5D-5L crosswalk index valuation calculator released by EQ-5D in 2019.24 Further, the documentation of HRQoL used in the approach to calculate utilities from week 52 onward presents additional limitations. The general population utility score used in the model was derived from a study conducted in Quebec,9 rather than using Canadian-wide population utility norms that are available.25 While the Quebec-specific study assesses HRQoL using the EQ-5D-5L measure (which aligns with the measure used in the SOLSTICE trial), the authors of the Quebec study state that “Quebec’s population is different from other Canadian provinces” and that Canadian population values may not reflect Quebec utilities.9 Finally, the utility values obtained from published literature (e.g., disutilities associated with AEs) were largely based on a UK population rather than Canadian.
CADTH notes that there are several sources of uncertainty regarding HRQoL used in the sponsor’s economic evaluation; however, the impact on conclusions regarding maribavir’s cost-effectiveness is likely limited.
Simplified recurrence assumptions: The sponsor assumed that after 52 weeks patients’ CMV status would no longer be tracked, thus no further CMV recurrence was included after this time. Clinical experts consulted by CADTH indicated that there may be a subpopulation of patients (e.g., lung transplant patients, typically resistant rather than refractory) that are likely to experience recurrence beyond 52 weeks. The subgroup of patients who remain at risk of CMV related outcomes and require long-term monitoring may result in considerable health care resource utilization.
CADTH notes that there may be considerable costs associated with longer-term CMV outcomes, however, this is likely only for a small subset of patients, and this could not be accounted for in the submitted model
Additionally, the following key assumptions were made by the sponsor and have been appraised by CADTH (See Table 4).
CADTH Re-analyses of the Economic Evaluation
Base-Case Results
The CADTH base case was derived by making changes in model parameter values and assumptions, in consultation with clinical experts. A summary of the re-analyses that are incorporated in the CADTH base case reanalysis are shown in Table 5.
The CADTH base case resulted in an ICER of $403,089 per QALY (incremental cost = $7,429; incremental QALYs = 0.02) with a 35.5% probability of being cost-effective at a $50,000 per QALY threshold. Cost-effectiveness was driven by the small and uncertain incremental QALY benefits. The small incremental QALY over a lifetime time horizon is because the main driver of QALY differences takes place in the first 8 to 20 weeks, with equivalent mortality for the remainder of the time horizon. Initial treatment costs of maribavir are a key component of the cost-effectiveness results as the drug acquisition costs are considerably higher than that of IAT (disaggregated results are presented in Table 12). The results of the stepped analysis are presented in Table 6.
Table 4: Key Assumptions of the Submitted Economic Evaluation (Not Noted as Limitations to the Submission)
Sponsor’s key assumption | CADTH comment |
|---|---|
IV drug administration has a similar cost as chemotherapy drugs at a Canadian hospital | This is considered an acceptable assumption. |
Risk of graft loss is only associated with CMV status | Clinical experts consulted by CADTH suggested that graft loss may also be associated with treatment itself for some types of transplant patients and is tied to time on treatment. No graft loss events occurred in the SOLSTICE trial for maribavir or IAT, however, this may be because graft loss events may need a longer study period for assessment (i.e., longer than the 20-week trial). |
The cost of foscarnet and cidofovir were not from the Canadian Drug Benefit; foscarnet wholesale price was provided by IQVIA, and the cost of cidofovir was converted from a UK price that was originally an estimate of the United States price | Ideally, Canadian Drug Benefit prices would be used for all comparator drugs. |
CMV = cytomegalovirus; IAT = investigator assigned treatment.
Table 5: CADTH Revisions to the Submitted Economic Evaluation
Stepped analysis | Sponsor’s value or assumption | CADTH value or assumption |
|---|---|---|
Corrections to sponsor’s base case | ||
None. | — | — |
Changes to derive the CADTH base case | ||
1. Survival benefit | Applied health state specific mortality rates from week 8 to 52 | Mortality risk equivalent in both health states from week 8 to 52 |
2. Treatment efficacy extrapolation | Assumed constant treatment efficacy (clearance and recurrence) from 8 to 52 weeks, extrapolated from trial results | CMV clearance probabilities from week 8 onwards are equivalent for maribavir and IAT; CMV recurrence probabilities from week 20 onwards are equivalent for maribavir and IAT |
3. Retreatment | Retreatment is done with IAT regardless of initial treatment (i.e., maribavir and IAT are both retreated with IAT) | Retreatment is the same as the initial treatment (i.e., retreat maribavir with maribavir, and IAT with IAT) |
CADTH base case | Re-analyses 1 + 2 + 3 | |
IAT = investigator assigned treatment.
Table 6: Summary of the Stepped Analysis of the CADTH Reanalysis Results
Stepped analysis | Drug | Total costs ($) | Total QALYs | ICER ($/QALYs) |
|---|---|---|---|---|
Sponsor’s base case (probabilistic) | Maribavir | $139,314 | 8.35 | Ref. |
IAT | $139,810 | 8.18 | Dominated | |
Sponsor’s base case (deterministic) | Maribavir | $139,693 | 8.33 | Ref. |
IAT | $140,511 | 8.15 | Dominated | |
CADTH reanalysis 1 – survival benefit | Maribavir | $143,661 | 8.81 | Ref. |
IAT | $146,053 | 8.79 | Dominated | |
CADTH reanalysis 2 – treatment efficacy extrapolation | IAT | $140,511 | 8.15 | Ref. |
Maribavir | $149,204 | 8.30 | $58,534 | |
CADTH reanalysis 3 – retreatment | Maribavir | $107,739 | 8.57 | Ref. |
IAT | $140,511 | 8.15 | Dominated | |
CADTH base case (re-analyses 1, 2 and 3, deterministic) | IAT | $146,034 | 8.79 | Ref. |
Maribavir | $153,516 | 8.80 | $404,415 | |
CADTH base case (re-analyses 1, 2 and 3, probabilistic) | IAT | $145,292 | 8.81 | Ref. |
Maribavir | $152,721 | 8.83 | $403,089 |
IAT = investigator assigned treatment; ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year; Ref. = reference.
Note: Comparator costs are based on publicly available list prices and may not reflect actual costs paid by public drug plans.
Scenario Analysis Results
CADTH also conducted scenario analyses on the exploratory reanalysis to assess the impact of alternative assumptions. A scenario analysis assuming maribavir CMV clearance probabilities from weeks 0 to 8 in the trial are constant from weeks 8 to 20 was conducted and found that with this assumption, maribavir dominates IAT (incremental cost = -$6,521; incremental QALY = 0.03). Another scenario analysis explored the impact of a 25% reduction in IV administration costs, which resulted in an ICER of $1,380,138 per QALY (inc. costs: $25,436; inc QALYs: 0.02). Finally, a scenario analysis where 100% of patients receiving foscarnet and cidofovir and 50% of patients receiving ganciclovir would receive treatment in hospital, found that maribavir dominated IAT (incremental cost = -$58,560; incremental QALY = 0.02).
A price-reduction analysis based on the CADTH re-analyses (Table 7) indicated that, at a willingness-to-pay threshold of $50,000 per QALY, maribavir would be considered cost-effective compared to IAT with a 4.5% price reduction.
Table 7: CADTH Price Reduction Analyses
Analysis | ICERs for Maribavir vs. IAT | |
|---|---|---|
Price reduction | Sponsor base case | CADTH reanalysis |
No price reduction | Dominant | $403,089 |
4.4% | Dominant | $52,219 |
4.5% | Dominant | $44,244 |
5% | Dominant | $4,373 |
IAT = investigator assigned treatment; ICER = incremental cost-effectiveness ratio; vs. = versus.
Issues for Consideration
Results from a phase 3 trial for the use of maribavir to treat CMV in HSCT patients as first-line therapy are pending (NCT02927067).26 If maribavir becomes indicated for use as first-line treatment, it may change the way it is used for refractory/resistant CMV in the future.
Overall Conclusions
Evidence from the pivotal trial (SOLSTICE; Study 303) suggest that there is evidence of maribavir improving CMV viremia clearance and symptom control when compared to IAT over 16 weeks. However, disease control with maribavir is time-limited, like other antivirals, and evidence of maintained clearance (i.e., there was no clinically significant CMV recurrence) is less certain. Within the trial, no clinically meaningful difference in mortality between treatment options was demonstrated. The clinical experts consulted by CADTH noted that the distribution of each IAT in SOLSTICE is not reflective of Canadian clinical practice. As a result, generalizability of results to the Canadian setting is uncertain, and conclusions on comparative efficacy and cost-effectiveness for each antiviral cannot be drawn.
To address limitations with the sponsor’s submitted pharmacoeconomic evaluation, CADTH undertook a reanalysis with the following changes: removed the mortality difference between maribavir and IAT from week 8 onwards; assumed equivalent clinical efficacies for both treatments from week 8 for CMV clearance and week 20 for recurrence; and assumed that retreatment would occur using the same drug that was used initially. In the CADTH base case, the ICER of maribavir compared to IAT was $403,089 per QALY. A price reduction of approximately 4.5% is required for maribavir to be cost-effective at a $50,000 per QALY threshold.
The submitted price of maribavir and the cost savings from administration were 2 key drivers of overall costs and of the ICER within the model. Uncertainty remains as to whether such savings with respect to drug administration (~$71,000) would be realized. Further, there were limitations that CADTH was unable to address in the model, including the impact of treatment duration. Treatment duration was modelled as a fixed amount of time for each treatment; however, based on consultation with CADTH clinical experts, the practice would be highly variable and based on clinical judgment. As the cost of maribavir is an influential parameter, variation in treatment duration could significantly alter maribavir’s cost-effectiveness.
Considerable uncertainty further remains due to limited long-term clinical data. Other key drivers in the model included the clinical efficacy following initial treatment, as the true efficacy of maribavir and IAT for retreatment is not known and may be highly variable across patient groups (e.g., transplant type) and underlying patient characteristics. The long-term effects of maribavir on maintaining CMV clearance compared to other treatments further remains unknown. Given the limitations that were unable to be addressed in the model, further price reductions may be required to ensure cost-effectiveness.
References
1.Clinical Study Report: 303. A Phase 3, Multicenter, Randomized,Open-label, Active-controlled Study to Assess the Efficacy and Safety of Maribavir Treatment Compared to Investigator-assigned Treatment in Transplant Recipients with Cytomegalovirus (CMV) Infections that are Refractory or Resistant to Treatment with Ganciclovir, Valganciclovir, Foscarnet, or Cidofovir [internal sponsor's report]. Toronto (ON): Takeda Canada Inc.; 2021.
2.Takeda Canada. Maribavir Canada HTA Key Opinion Leader Meeting. 2021 Dec.
3.Takeda Canada. IPD Analysis of 623-303 Data: Final Statistical Report. Version 4.1. 2021.
4.NHS Blood and Transplant. Organ and Tissue Donation and Transplantation Activity Report 2020/21. 2021.
5.National Institute for Health and Care Excellence. Technology appraisal guidance [TA591]. Letermovir for preventing cytomegalovirus disease after a stem cell transplant. 2019; https://www.nice.org.uk/guidance/ta591. Accessed 2022 Feb 4.
6.Pharmacoeconomic evaluation [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Livtencity (maribavir), 200mg tablets [internal sponsor's package]. Toronto (ON): Takeda Canada Inc.; 2022 Mar 14.
7.Hakimi Z, Aballea S, Ferchichi S, et al. Burden of cytomegalovirus disease in solid organ transplant recipients: a national matched cohort study in an inpatient setting. Transpl Infect Dis. 2017;19(5). PubMed
8.van Hout B, Janssen MF, Feng YS, et al. Interim scoring for the EQ-5D-5L: mapping the EQ-5D-5L to EQ-5D-3L value sets. Value Health. 2012;15(5):708-715. PubMed
9.Poder TG, Carrier N, Kouakou CRC. Quebec Health-Related Quality-of-Life Population Norms Using the EQ-5D-5L: Decomposition by Sociodemographic Data and Health Problems. Value Health. 2020;23(2):251-259. PubMed
10.Sullivan PW, Slejko JF, Sculpher MJ, Ghushchyan V. Catalogue of EQ-5D scores for the United Kingdom. Med Decis Making. 2011;31(6):800-804. PubMed
11.Ossa DF, Briggs A, McIntosh E, Cowell W, Littlewood T, Sculpher M. Recombinant erythropoietin for chemotherapy-related anaemia: economic value and health-related quality-of-life assessment using direct utility elicitation and discrete choice experiment methods. Pharmacoeconomics. 2007;25(3):223-237. PubMed
12.Bullement A, Nathan P, Willis A, et al. Cost Effectiveness of Avelumab for Metastatic Merkel Cell Carcinoma. Pharmacoecon Open. 2019;3(3):377-390. PubMed
13.Nafees B, Stafford M, Gavriel S, Bhalla S, Watkins J. Health state utilities for non small cell lung cancer. Health Qual Life Outcomes. 2008;6:84. PubMed
14.Tolley K, Goad C, Yi Y, Maroudas P, Haiderali A, Thompson G. Utility elicitation study in the UK general public for late-stage chronic lymphocytic leukaemia. Eur J Health Econ. 2013;14(5):749-759. PubMed
15.Ontario Ministry of Health, Ontario Ministry of Long-Term Care. Ontario drug benefit formulary/comparative drug index. 2022; https://www.formulary.health.gov.on.ca/formulary/. Accessed 2022 Feb 4.
16.DeltaPA. [Ottawa (ON)]: IQVIA; 2022: https://www.iqvia.com/. Accessed 2022 Feb 4.
17.Wolters Kluwer. Medi-Span: Drug Data Solutions for Healthcare. 2021; https://pricerx.medispan.com/Refresh/Login. Accessed 2022 Jun 30.
18.Tam VC, Ko YJ, Mittmann N, et al. Cost-effectiveness of systemic therapies for metastatic pancreatic cancer. Curr Oncol. 2013;20(2):e90-e106. PubMed
19.Schedule of benefits for physician services under the Health Insurance Act: effective October 1, 2021. Toronto (ON): Ontario Ministry of Health; 2022: https://www.health.gov.on.ca/en/pro/programs/ohip/sob/physserv/sob_master.pdf. Accessed 2022 Feb 4.
20.Schedule of benefits for laboratory services: effective July 1, 2020. Toronto (ON): Ontario Ministry of Health; 2020: https://www.health.gov.on.ca/en/pro/programs/ohip/sob/lab/lab_mn2020.pdf. Accessed 2022 Feb 4.
21.Ontario Case Costing Initiative (OCCI). Toronto (ON): Ontario Health and Long-Term Care; 2017: https://data.ontario.ca/dataset/ontario-case-costing-initiative-occi. Accessed 2022 Feb 4.
22.Levy AR, Sobolev B, James D, et al. The costs of change: direct medical costs of solid organ transplantation in British Columbia, Canada, 1995-2003. Value Health. 2009;12(2):282-292. PubMed
23.Ferguson TW, Whitlock RH, Bamforth RJ, et al. Cost-Utility of Dialysis in Canada: Hemodialysis, Peritoneal Dialysis, and Nondialysis Treatment of Kidney Failure. Kidney Med. 2021;3(1):20-30 e21. PubMed
24.EuroQol Research Foundation. EQ-5D-5L Crosswalk Index Value Calculator. 2019; https://euroqol.org/eq-5d-instruments/eq-5d-5l-about/valuation-standard-value-sets/crosswalk-index-value-calculator/. Accessed 2022 Jun 15.
25.Guertin JR, Feeny D, Tarride JE. Age- and sex-specific Canadian utility norms, based on the 2013-2014 Canadian Community Health Survey. CMAJ. 2018;190(6):E155-E161. PubMed
26.Takeda Development Center Americas I, Shire. A Study of Maribavir Compared to Valganciclovir to Treat Cytomegalovirus Infections in People Who Have Received Stem Cell Transplants (NCT02927067). National Institutes of Health U.S. National Library of Medicine ClinicalTrials.gov; 2016: https://clinicaltrials.gov/ct2/show/NCT02927067?term=NCT02927067&draw=2&rank=1. Accessed 2022 Jun 30.
27.Cell Therapy Transplant Canada. Research Netowrk. General Information. 2019; https://www.cttcanada.org/page/CTTCResearchNetwork?&hhsearchterms=%22number+and+transplant%22. Accessed 2022 Feb 4.
28.Canadian Institute for Health Information. Organ replacement in Canada: CORR annual statistics, 2020. 2020; https://www.cihi.ca/en/organ-replacement-in-canada-corr-annual-statistics-2020. Accessed 2021 Aug 27.
29.Dinh T, Sutherland G. Understanding the gap: a pan-Canadian analysis of prescription drug insurance coverage. Ottawa (ON): The Conference Board of Canada; 2017: https://www.conferenceboard.ca/e-library/abstract.aspx?did=9326. Accessed 2022 Feb 1.
Appendix 1: Cost Comparison Table
Note that this appendix has not been copy-edited.
The comparators presented in the following table have been deemed to be appropriate based on feedback from clinical experts. Comparators may be recommended (appropriate) practice or actual practice. Existing Product Listing Agreements are not reflected in the table and as such, the table may not represent the actual costs to public drug plans.
Table 8: CADTH Cost Comparison Table for Post-Transplant Cytomegalovirus Infection
Treatment | Strength / concentration | Form | Price ($) | Recommended dosage | Daily cost ($) | Estimated course cost (8 weeks) |
|---|---|---|---|---|---|---|
Maribavir (Livtencity) | 200 mg | Oral tablet | 276.7857a | 400 mg twice daily | 1,107.14 | 62,000 |
Antiviral drugs | ||||||
Cidofovir (Vistide) | 375 mg per vial | Solution for IV injection | 1302.0000b | Induction: 5 mg/kg once weekly for 2 weeks Maintenance: 3 to 5 mg/kg given once every 2 weeks | Induction: 186.00 Maintenance: 55.80 to 93.00 | 4,948 to 6,510 |
Foscarnet (Vocarvi) | 24 mg/mL | Solution for IV injection | 1.8913c | Induction: 90 mg/kg every 12 hours or 60 mg/kg every 8 hours for 2 to 3 weeks Maintenance: 90 to 120 mg/kg once daily | Induction: 1,063.87 Maintenance: 531.94 to 709.25 | 37,236 to 49,647 |
Ganciclovir (Cytovene) | 500 mg per vial | Powder for IV injection | 44.5480 | Induction: 5 mg/kg every 12 hours for 7 to 14 days Maintenance: 5 mg/kg once daily for 7 days each week or 6 mg/kg once daily for 5 days per week | Induction: 66.82 Maintenance: 33.41 to 40.09 | 1,871 to 2,339 |
Valganciclovir (Valcyte and generics) | 450 mg | Oral tablet | 5.8553 | Induction: 900 mg twice daily for 21 days Maintenance: 900 mg once daily | Induction: 23.42 Maintenance: 11.71 | 902 |
50 mg/mL | Powder for oral solution | 2.7452 | Induction: 98.83 Maintenance: 49.41 | 3,805 | ||
Note: All prices are from the Ontario Drug Benefit Formulary (accessed May 2022), unless otherwise indicated, and do not include dispensing fees. Recommended dosages are derived from respective product monographs unless otherwise indicated. Costs assume a body weight of 75 kg and do not include administration or dispensing fees. Course costs vary based on individual patient disease experience but is estimated by clinical experts to be a minimum of 8 to 12 weeks.
aManufacturer submitted price.6
bNo public price available. Price listed was submitted by sponsor as part of submitted model; CADTH was unable to confirm accuracy.6
cCost sourced from the IQVIA Delta PA database (accessed May 2022).16
Appendix 2: Submission Quality
Note that this appendix has not been copy-edited.
Description | Yes/No | Comments |
|---|---|---|
Population is relevant, with no critical intervention missing, and no relevant outcome missing | Yes | No comment |
Model has been adequately programmed and has sufficient face validity | Yes | No comment |
Model structure is adequate for decision problem | No | The model does not differentiate between patients who do not respond to initial treatment and those who respond and later experience a CMV recurrence. Additionally, while the structure of the model allows for changes to the IAT distribution and duration, any changes in IAT distribution would not result in efficacy data being revised accordingly. |
Data incorporation into the model has been done adequately (e.g., parameters for probabilistic analysis) | Yes | No comment |
Parameter and structural uncertainty were adequately assessed; analyses were adequate to inform the decision problem | Yes | No comment |
The submission was well organized and complete; the information was easy to locate (clear and transparent reporting; technical documentation available in enough details) | No | Difficult to identify appropriate results in IPD analysis and the Clinical Study Report; some incorrect table references |
Appendix 3: Additional Information on the Submitted Economic Evaluation
Note that this appendix has not been copy-edited.
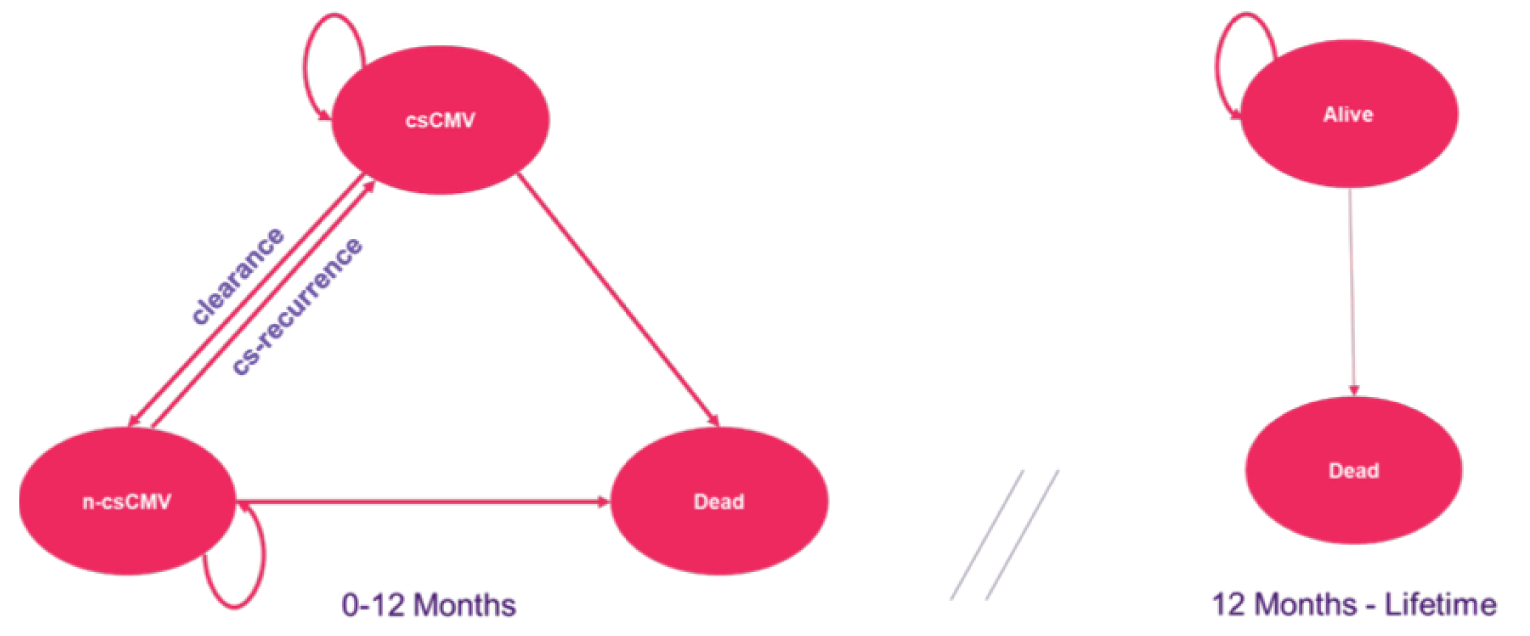
CMV = cytomegalovirus; csCMV = clinically significant CMV; n-csCMV = non-clinically significant CMV
Source: Sponsor submission6
Detailed Results of the Sponsor’s Base Case
Table 10: Disaggregated Summary of Sponsor’s Economic Evaluation Results
Parameter | Maribavir | IAT | Incremental |
|---|---|---|---|
Discounted LYs | |||
Total | 10.53 | 10.33 | 0.20 |
Discounted QALYs | |||
Total | 8.3533 | 8.1817 | 0.1724 |
By health state | |||
Clinically significant CMV (0-52 weeks) | 0.2719 | 0.3583 | -0.0864 |
Non-clinically significant CMV (0-52 weeks) | 0.3989 | 0.2939 | 0.1051 |
Alive (52 weeks+) | 7.6843 | 7.5312 | 0.1531 |
Disutilities | |||
Adverse events | -0.0016 | -0.0023 | -0.0006 |
Graft Loss | -0.0002 | -0.0002 | 0.0000 |
Discounted costs ($) | |||
Total | $139,314 | $139,810 | -$496 |
Treatment 1 costs (initial treatment) | $58,604 | $37,812 | $20,792 |
Acquisition | $58,138 | $17,782 | $40,356 |
Administration | $0 | $19,489 | -$19,489 |
Monitoring | $466 | $540 | -$75 |
Retreatment costs | $76,580 | $96,666 | -$20,087 |
Acquisition | $36,029 | $45,477 | -$9,448 |
Administration | $39,474 | $49,831 | -$10,357 |
Monitoring | $1,077 | $1,359 | -$282 |
Total health resource utilization | $1,017 | $1,242 | -$225 |
Emergency visits | $0 | $0 | $0 |
Outpatients | $1,017 | $1,242 | -$225 |
Hospitalizations | $0 | $0 | $0 |
Total adverse events | $1,304 | $1,800 | -$496 |
Total graft loss | $1,810 | $2,290 | -$481 |
CMV = cytomegalovirus; IAT = investigator assigned treatment; ICER = incremental cost-effectiveness ratio; LY= life-year; QALY = quality-adjusted life-year.
Appendix 4: Additional Details on the CADTH Re-Analyses and Sensitivity Analyses of the Economic Evaluation
Note that this appendix has not been copy-edited.
Table 11: Disaggregated Summary of CADTH’s Economic Evaluation Results
Parameter | Maribavir | IAT | Incremental |
|---|---|---|---|
Discounted LYs | |||
Total | 11.13 | 11.12 | 0.01 |
Discounted QALYs | |||
Total | 8.83 | 8.81 | 0.02 |
By health state | |||
Clinically significant CMV (0-52 weeks) | 0.29 | 0.37 | -0.08 |
Non-clinically significant CMV (0-52 weeks) | 0.39 | 0.30 | 0.08 |
Alive (52 weeks+) | 8.14 | 8.13 | 0.01 |
Disutilities | |||
Adverse events | -0.0014 | -0.0024 | 0.0010 |
Graft Loss | -0.0002 | -0.0002 | 0.0000 |
Discounted costs ($) | |||
Total | $152,721 | $145,292 | $7,429 |
Treatment 1 costs (initial treatment) | $58,604 | $37,812 | $20,792 |
Acquisition | $58,138 | $17,782 | $40,356 |
Administration | $0 | $19,489 | -$19,489 |
Monitoring | $466 | $540 | -$75 |
Retreatment costs | $90,013 | $101,921 | -$11,908 |
Acquisition | $88,830 | $47,948 | $40,882 |
Administration | $0 | $52,540 | -$52,540 |
Monitoring | $1,183 | $1,433 | -$250 |
Total health resource utilization | $1,083 | $1,293 | -$210 |
Emergency visits | $0 | $0 | $0 |
Outpatients | $1,083 | $1,293 | -$210 |
Hospitalizations | $0 | $0 | $0 |
Total adverse events | $1,083 | $1,878 | -$795 |
Total graft loss | $1,939 | $2,389 | -$450 |
ICER ($/QALY) | $403,089 | ||
CMV = cytomegalovirus; IAT = investigator assigned treatment; ICER = incremental cost-effectiveness ratio; LY= life-year; QALY = quality-adjusted life-year.
Scenario Analyses
Table 12: Summary of CADTH’s Scenario Analysis
Scenario analysis | Drug | Total costs ($) | Total QALYs | ICER ($/QALYs) |
|---|---|---|---|---|
CADTH base case | IAT | $145,292 | 8.81 | Ref. |
Maribavir | $152,721 | 8.83 | $403,089 | |
Maribavir efficacy maintained until week 20 | IAT | $145,292 | 8.81 | Ref. |
Maribavir | $138,772 | 8.83 | Dominant | |
25% reduction in IV administration costs | IAT | $127,285 | 8.81 | Ref. |
Maribavir | $152,721 | 8.83 | $1,380,138 | |
In hospital administration of IAT for some patients | IAT | $211,281 | 8.81 | Ref. |
Maribavir | $152,721 | 8.83 | Dominant |
CMV = cytomegalovirus; IAT = investigator assigned treatment; ICER = incremental cost-effectiveness ratio; LY= life-year; QALY = quality-adjusted life-year.
Appendix 5: Submitted Budget Impact Analysis (BIA) and CADTH Appraisal
Note that this appendix has not been copy-edited.
Table 13: Summary of Key Take-Aways
Key Take-aways of the BIA |
|---|
|
Summary of Sponsor’s BIA
The submitted budget impact analysis (BIA) estimated the introduction of maribavir for the treatment of adults with post-transplant cytomegalovirus (CMV) infection/disease who are resistant and/or refractory to one or more prior antiviral therapies. The analysis took the perspective of the CADTH-participating drug plans using a top-down epidemiological approach and incorporated drug acquisition costs. A time horizon of 3 years between 2023 to 2025 was taken, with 2022 being the base year of the model. The target population was estimated using the number of patients with HSCT or SOT, followed by further specifications for CMV infection and refractory and/or resistant (R/R) CMV. The reference case scenario included ganciclovir, valganciclovir, foscarnet, and cidofovir. The new drug scenario included maribavir in addition to the reference case comparators. Key inputs to the BIA and the sponsor’s methodology in calculating the target population are documented in Table 15.
Table 14: Summary of Key Model Parameters
Parameter | Sponsor’s estimate (reported as year 1 / year 2 / year 3) if appropriate |
|---|---|
Target population | |
Number of patients with HSCT27 | 34.4 per million Canadians |
Proportion of HSCT patients with CMV | 47% |
Proportion of R/R HSCT patients | 35% |
Number of patients with SOT28 | 79.7 per million Canadians |
Proportion of SOT patients with CMV | 37% |
Proportion of R/R SOT patients | 19% |
Total R/R population | 352 / 356 / 360 |
Proportion of patients covered by public drug plans29 | 63% |
Number of patients eligible for drug under review | 222 / 225 / 227 |
Market uptake (3 years) | |
Uptake for HSCT patients (reference scenario) | |
Maribavir | 0% / 0% / 0% |
Ganciclovir | 25% / 25% / 25% |
Valganciclovir | 20% / 20% / 20% |
Foscarnet | 50% / 50% / 50% |
Cidofovir | 5% / 5% / 5% |
Uptake for SOT patients (reference scenario) | |
Maribavir | 0% / 0% / 0% |
Ganciclovir | 40% / 40% / 40% |
Valganciclovir | 30% / 30% / 30% |
Foscarnet | 25% / 25% / 25% |
Cidofovir | 5% / 5% / 5% |
Uptake for HSCT patients (new drug scenario) | |
Maribavir | 50% / 70% / 80% |
Ganciclovir | 5% / 5% / 3% |
Valganciclovir | 10% / 9% / 6% |
Foscarnet | 32% / 15% / 10% |
Cidofovir | 3% / 1% / 1% |
Uptake for SOT patients (new drug scenario) | |
Maribavir | 50% / 65% / 80% |
Ganciclovir | 15% / 10% / 5% |
Valganciclovir | 20% / 15% / 10% |
Foscarnet | 12% / 9% / 4% |
Cidofovir | 3% / 1% / 1% |
Cost of treatment (per patient) | |
Cost of treatment per treatment course | |
Maribavir | $58,125 |
Ganciclovir | $2,612 |
Valganciclovir | $925 |
Foscarnet | $34,388 |
Cidofovir | $4,882 |
CMV = cytomegalovirus; HSCT = hematopoietic stem cell transplant; R/R = refractory and/or resistant; SOT = solid organ transplant.
Note: Costs of treatment are standardized to 8-week treatment course lengths for maribavir and each comparator.
Summary of the Sponsor’s BIA Results
The sponsor’s estimated budget impact of funding maribavir for the treatment of adults with post-transplant cytomegalovirus (CMV) infection/disease who are resistant and/or refractory to one or more prior antiviral therapies was $5,088,034 in year 1, $6,409,498 in year 2, and $7,614,829 in year 3, for a three-year total of $19,112,360.
CADTH Appraisal of the Sponsor’s BIA
CADTH identified several key limitations to the sponsor’s analysis that have notable implications on the results of the BIA:
Market shares for maribavir are likely overestimated in HSCT patients: The sponsor anticipated uptake of maribavir would reach 80% by year 3 in the new drug scenario. However, clinical experts consulted by CADTH noted that this estimate appears higher than expected. Clinical experts consulted by CADTH noted that there will be a slightly lower market shares for HSCT maribavir utilization than SOT in the R/R patient population due to comorbidity of CMV with GVHD (graft-versus-host disease). The majority of GVHD are gut-related, where absorption is of concern. Since there is no IV formulation for maribavir, it is likely that utilization of foscarnet and/or IV ganciclovir would occur for these HSCT patients with GVHD.
CADTH adjusted the market shares for maribavir in HSCT patients to reach 65% by year 3 in the new drug scenario.
Uncertainty in deriving target population: According to clinical experts consulted by CADTH, several of the sponsor’s parameters used to derive the target population did not meet face validity. For example, the incidence of CMV viremia in HSCT patients is highly uncertain and can vary depending on several factors (e.g., matched sibling donor, immunosuppression due to GvHD, older age, or other donor factors). Proportion of R/R HSCT patients was also overestimated at 35% and clinical experts suggested 25% to be a more reasonable estimate. Similarly, incidence of CMV viremia in SOT patients was underestimated at 37%, which was suggested by clinical experts to be closer to 55%. Lastly, the proportion of R/R SOT patients was underestimated by the sponsor to be 19%, which clinical experts suggested was closer to 30%. An increase or decrease in the target population leads to large fluctuations in the anticipated budget impact for maribavir. Therefore, by underestimating the incidence and proportion of patients with R/R CMV led to the budget impact being underestimated. CADTH could not address the uncertainty in parameter estimates such as incidence of CMV viremia in HSCT patients and therefore uncertainty remains in the target population estimate.
CADTH adjusted the target population parameters to reflect the previously mentioned clinical expert input.
Lack of clarity regarding treatment duration: Drug plan input indicated uncertainty in treatment duration and discontinuation of therapy due to lack of efficacy or other reasons following treatment with maribavir. Clinical experts consulted by CADTH noted that duration of treatment course can be highly variable and dependent on factors such as genotypic resistance. Genotypically resistant patients are likely to require longer treatment durations than refractory patients, such as a minimum of 8 to 12 weeks. CADTH notes that changes in discontinuation rates or treatment duration are expected to affect the budget impact of maribavir and therefore tested alternative treatment duration of 12 weeks in a scenario analysis.
CADTH assessed the impact of increasing treatment duration to 12 weeks for maribavir and all comparators in a scenario analysis.
Target population is potentially underestimated by excluding those not covered by drug plans: The sponsor assumed that 63% of patients would be eligible for public coverage by drug plans according to a 2017 analysis by the Canadian Alliance for Sustainable Health Care.29 Given that the target population is a key driver in budget impact estimates, CADTH explored the impact of increased public drug coverage in a scenario analysis.
CADTH increased public coverage to 100% in a scenario analysis.
Additional limitations were identified but were not considered to be key limitations. These limitations include the inclusion of intravenous immunoglobulin (IVIG) used as an adjunct treatment alongside therapies for R/R CMV patients, which would impact total costs. However, this utilization is not expected to be differential upon the introduction of maribavir, and is therefore unlikely to impact the budget impact.
CADTH Re-Analyses of the BIA
Table 15: CADTH Revisions to the Submitted BIA
Stepped analysis | Sponsor’s value or assumption | CADTH value or assumption |
|---|---|---|
Corrections to sponsor’s base case | ||
None. | — | — |
Changes to derive the CADTH base case | ||
1. Market shares overestimated for HSCT patients in the uptake scenario | HSCT patients: 50% / 70% / 80% | HSCT patients: 50% / 60% / 65% |
2. Estimation of target population did not meet face validitya | Proportion of R/R HSCT patients: 35% Incidence of CMV viremia in SOT patients: 37% Proportion of R/R SOT patients: 19% | Proportion of R/R HSCT patients: 25% Incidence of CMV viremia in SOT patients: 55% Proportion of R/R SOT patients: 30% |
CADTH base case | Reanalysis 1 + 2 | |
CMV = cytomegalovirus; HSCT = hematopoietic stem cell transplant; R/R = refractory and/or resistant; SOT = solid organ transplant.
aSponsor and CADTH population estimates are based on clinician opinion.
The results of the CADTH step-wise reanalysis are presented in summary format in Table 16 and a more detailed breakdown is presented in Table 17. Based on the CADTH base case, the budget impact of the reimbursement of maribavir for the treatment of adults with post-transplant cytomegalovirus (CMV) infection/disease who are resistant and/or refractory to one or more prior antiviral therapies is expected to be $7,811,026 in year 1, $10,073,188 in year 2, and $12,108,445 in year 3, for a three-year total of $29,992,660.
A scenario analysis assessing the budget impact when the percentage of the population covered by public plans was increased to 100% led to a three-year budget impact of $47,457,831. A scenario analysis assessing the budget impact if treatment duration of maribavir and all comparators was 12 weeks resulted in a three-year budget impact of $40,361,660.
Table 16: Summary of the CADTH Re-Analyses of the BIA
Stepped analysis | Three-year total |
|---|---|
Submitted base case | $19,112,360 |
CADTH reanalysis 1 | $18,859,468 |
CADTH reanalysis 2 | $30,173,297 |
CADTH base case | $29,992,660 |
BIA = budget impact analysis.
Table 17: Detailed Breakdown of the CADTH Re-Analyses of the BIA
Stepped analysis | Scenario | Year 0 (current situation) | Year 1 | Year 2 | Year 3 | Three-year total |
|---|---|---|---|---|---|---|
Submitted base case | Reference | $4,250,963 | $4,297,724 | $4,344,999 | $4,392,794 | $17,286,480 |
New drug | $4,250,963 | $9,385,757 | $10,754,497 | $12,007,623 | $36,398,840 | |
Budget impact | $0 | $5,088,033 | $6,409,498 | $7,614,829 | $19,112,360 | |
CADTH base case | Reference | $5,502,195 | $5,562,720 | $5,623,909 | $5,685,772 | $22,374,597 |
New drug | $5,502,195 | $13,373,746 | $15,697,097 | $17,794,218 | $52,367,256 | |
Budget impact | $0 | $7,811,026 | $10,073,188 | $12,108,445 | $29,992,660 | |
CADTH sensitivity analysis: public coverage 100% | Reference | $8,706,205 | $8,801,974 | $8,898,795 | $8,996,682 | $35,403,657 |
New drug | $8,706,205 | $21,161,477 | $24,837,750 | $28,156,055 | $82,861,487 | |
Budget impact | $0 | $12,359,503 | $15,938,955 | $19,159,373 | $47,457,831 | |
CADTH sensitivity analysis: treatment duration | Reference | $14,078,172 | $14,233,032 | $14,389,596 | $14,547,881 | $57,248,681 |
New drug | $14,078,172 | $24,798,689 | $27,967,990 | $30,765,491 | $97,610,341 | |
Budget impact | $0 | $10,565,656 | $13,578,394 | $16,217,610 | $40,361,660 |
BIA = budget impact analysis.
Note: the submitted analysis is based on the publicly available prices of the comparator treatments.
Stakeholder Input
Patient Input
Canadian Liver Foundation
About the Canadian Liver Foundation
Founded in 1969, the Canadian Liver Foundation (CLF) was the first organization in the world dedicated to supporting education and research into all forms of liver disease. Today, the CLF continues to be the only national health charity committed to reducing the incidence and impact for Canadians of all ages living with or at risk for liver disease. The CLF is the only registered charity in Canada directing funds specifically for liver disease research in all its forms and has invested nearly $40 million in the scientific search for causes, preventative measures, and potential treatments for liver disease. The CLF reaches millions of Canadians through our public and professional education programs, patient support programs and other awareness, fundraising and outreach efforts. Website: www.liver.ca
Information Gathering
Recruitment: The CLF invited patients, caregivers, and health care professionals from across Canada to fill out an online survey modelled on the CADTH, CDR and pCODR Programs submission template. The online survey was open f rom February 22nd to March 25th, 2022, and promoted on the CLF website, via CLF social media channels and to CLF patient, caregiver, and health care professional contacts across the country. Recruitment for the survey was targeted specifically to patients and caregivers affected by CMV post-liver transplant by the CLF through patient databases and social media.
Responses: The CLF online survey generated 2 responses in total from 2 health professionals. Among the 2 respondents, the reported home provinces were Ontario and Alberta, respectively. The input from health professionals is very helpful as we strongly believe that health professionals can be the voice for the patients who have either dealt with or a currently dealing with a CMV infection post-liver transplant. Due to the limited number of patients who specifically meet the criteria for the drug (i.e., post-transplant infection with CMV, patients who are refractory and/or resistance to one or more prior antiviral therapies, and the very limited number of patients who have had experience with the drug under review), securing patient and caregiver input for this submission was expectedly difficult.
The responses received have been used to compile the feedback for this submission. Demographic information of the CLF online survey respondents was requested in the survey, but response was not mandatory. Quotes from CLF questionnaire respondents are included in various sections of this submission.
Disease Experience
CMV is the most common infection in liver transplant patients. Transplant recipients are at a much greater risk for complications and death when faced with a CMV infection. The medication patients take following a liver transplant can help prevent damage to the donated organ, however they can have other effects on the immune system. The medications thus make it harder to fight off CMV and other infections. Most liver transplant patients who develop problems from a CMV infection have activated the CMV that has been dormant in their body for many years. It is also possible for a transplant patient to get CMV from the transplanted organ.
Respondents of the CLF survey of health professionals helped to paint a picture of how symptoms associated with post- liver transplant treatments impacted or limited their patients' day-to-day lives, indicating that this has seriously impacted their:
Ability to work
Ability to travel
Ability exercise
Ability to conduct household chores
Ability to spend time with family and friends
Ability to fulfill family obligations
Experiences With Currently Available Treatments
The risk of CMV infections is highest within the first three months after liver transplantation when the immunosuppressive therapy is kept at high intensity, requiring preventive strategies in order to avoid the development of CMV-related complications. Due to its direct and indirect effects, CMV infection prevention is a major strategy in post liver transplant patients.
With the use of prophylaxis against CMV, there has been a reported reduction of CMV infection up to 80% during the first 90 days after transplant. For established CMV infection and disease, intravenous ganciclovir (5mg/kg twice a day) is recommended for severe disease. For mild to moderate disease, oral valganciclovir (900mg twice a day) has shown to be equally effective to ganciclovir. Foscarnet and cidofovir are considered second line drugs. Therapy should be given for at least 2 weeks and discontinuation is based upon virological clearance and symptom resolution. Persistent virus in the blood stream after therapy and extensive involvement of the gastrointestinal tract have been identified as risk factors for CMV relapse.
CMV resistance to antiviral drugs is an emerging problem. Resistance happens through mutations of the viral DNA. The incidence of CMV resistance in liver transplant patients is not well defined, however it is believed that in solid organ transplants in general it is around 7% in high-risk patients. When ganciclovir and valganciclovir are shown to be ineffective due to resistance, patients should be treated with combination therapy, foscarnet and cidofovir or experimental treatments.
There is an unmet need for more durably effective treatments with minimal side effects to clear CMV in patients following liver transplantation. Health professionals who responded to the CLF online survey indicated that they have used the following treatment options to treat patients with for CMV infection post-liver transplantation:
Table 1: Treatment Options for Patients with CMV Infection Post-Liver Transplantation
Type of Treatment | Percentage of HCP respondents |
|---|---|
Ganciclovir (Cytovene) | 100% |
Valganciclovir (Valcyte) | 100% |
Foscarnet | 50% |
Health professionals who responded to the CLF online survey reported the following "somewhat intolerable" side effects that their patients experienced during treatment with current or previous therapies:
Vomiting
Diarrhea
Nausea
Anxiety
Loss of appetite
Depression
Improved Outcomes
Responses on the effectiveness, side effectiveness, and value of available therapies point to the need for improved therapies and indeed improved outcomes. The health professionals that responded to the CLF survey felt that it was "very important" that patients and their physicians have access to new treatments for CMV infection post-transplant.
“Most treatments for CMV have intolerable side effects: kidney failure, hematologic abnormalities, febrile neutropenia When treating resistant CMV, these side effects lead to severe limitations in treatment, leading to life-threatening situations. New drugs with proved efficacy and optimal profile of side effects are urgently needed.” – Health Care Professional
“Oral medication would allow freedom from IV and freedom from hospitalization. A less toxic medication that treats resistant CMV would allow patients to be free of toxicity from usual treatments that can cause renal failure.” – Health Care Professional.
Experience With Drug Under Review
Maribavir is an antiviral medication that is used to treat post-transplant CMV. Maribavir is administered orally and works by preventing the activity of the human CMV enzyme, thus blocking virus replication. This treatment has the potential to treat adult and pediatric patients (12 years of age and older) successfully and safely for CMV infections/disease who have failed all other available anti-viral therapies. Maribavir is a member of a new class of drugs called benzimidazole ribosides. Maribavir was approved for medical use in the United States in November 2021.
Companion Diagnostic Test
Not applicable – this drug does not require a companion diagnostic test.
Anything Else?
The Canadian Liver Foundation believes that patients and their physicians should have access to a broad range of treatment options regardless of geographic location, financial status, treatment status or disease severity in order t o ensure the best possible outcomes. It is up to the physicians to make individual treatment recommendations based on the needs of their patients.
“I think maribavir is a significant advance for transplant patients. We often see patients that have side effects from standard CMV medications. It would be great to avoid these side effects.” – Health Care Professional
“It is important to understand how complicated it is treating patients with CMV infection Side effects commonly lead to hospital readmissions and life-threatening complications. Just to prevent hematologic side effects related to valganciclovir, many times we need to administer granulocyte colony stimulating factor, which has significant costs.
When using foscarnet, most patients will develop kidney failure and it is not uncommon to see patients needing dialysis. Therefore, having maribavir availability is urgent.” – Health Care Professionals
Conflict of Interest Declaration — Canadian Liver Foundation
To maintain the objectivity and credibility of the CADTH reimbursement review process, all participants in the drug review pr ocesses must disclose any real, potential, or perceived conflicts of interest. This Patient Group Conflict of Interest Declaration is required for participation. Declarations made do not negate or preclude the use of the patient group input. CADTH may contact your group w ith further questions, as needed.
Did you receive help from outside your patient group to complete this submission? If yes, please detail the help and who provided it.
No outside assistance was utilized to complete this submission. This submission was completed by CLF staff and volunteers. Th e only outside input for this submission came from the patients, caregivers and health care professionals who responded to the CLF’s online survey.
Did you receive help from outside your patient group to collect or analyze data used in this submission? If yes, please detail the help and who provided it.
No outside assistance was utilized to collect or analyze data used in this submission. This submission was completed by CLF staff and volunteers. The only outside input for this submission came from the patients, caregi vers and health care professionals who responded to the CLF’s online survey.
List any companies or organizations that have provided your group with financial payment over the past 2 years AND who may have direct or indirect interest in the drug under review.
Table 2: Financial Disclosures for the Canadian Liver Foundation
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
Hoffmann-La Roche | — | — | — | X (not related to liver transplant) |
The Leukemia & Lymphoma Society of Canada, Myeloma Canada, CLL Canada, Aplastic Anemia & Myelodysplasia Association of Canada, Lymphoma Canada, MPN Canadian Research Foundation, Canadian MPN Network, Canadian CML Network
About The Leukemia & Lymphoma Society of Canada, Myeloma Canada, CLL Canada, Aplastic Anemia & Myelodysplasia Association of Canada, Lymphoma Canada, MPN Canadian Research Foundation, Canadian MPN Network, Canadian CML Network
The organizations involved in this submission are registered Canadian charities that provide support, education, and advocacy for their respective patient constituencies. The Leukemia and Lymphoma Society of Canada—the author of this submission is a national charitable status organization dedicated to finding a cure for blood cancers and its ability to improve the quality of life of people affected by blood cancers and their families by funding life-enhancing research and providing educational resources, services and support. The Leukemia and Lymphoma Society of Canada is the largest charitable organization in Canada dedicated to blood cancer, our focus includes:
Funding research from bench to bedside.
Rethinking how a person navigates their blood cancer experience
Providing targeted blood cancer information
Offering tools for psychological and emotional support
Empowering Canadians to take charge of their blood cancer experience through practical support and advocacy
To learn more about the organizations involved in this submission, you can visit their respective websites:
Leukemia & Lymphoma Society of Canada (LLSC) — bloodcancers.ca
Myeloma Canada — myelomacanada.ca
Aplastic Anemia & Myelodysplasia Association of Canada (AAMAC) — aamac.ca
Lymphoma Canada — lymphoma.ca
MPN Canadian Research Foundation — cmpnrf.ca
Canadian MPN Network — canadianmpnnetwork.ca
Canadian CML Network — cmlnetwork.ca
CLL Canada — cllcanada.org
Information Gathering
The aforementioned patient organizations collaborated to create an online survey, that was distributed through social media networks [Facebook, Twitter, Instagram] and by email, between February 1 and March 14, 2022, in English and French. Collaborating organizations also connected with clinicians across the country to share the survey with their patients. The survey uses multiple choice, open-ended and rating questions, and uses skipping logic to allow respondents to pass on questions not relevant to them.
There were 100 respondents to the survey, with three (3) respondents from outside Canada (United Kingdom, Belgium). All provinces were represented in the survey, however there were no respondents from Nunavut or the Yukon. The majority of respondents were from Ontario (41%, 41 ppl), followed by Québec (18%, 18 ppl), Alberta (14%, 14 ppl) and British Columbia (12%, 12 ppl). (Manitoba [1], New Brunswick [2], Newfoundland and Labrador [2], Nova Scotia [3], Northwest Territories [1], Prince Edward Island [1], Saskatchewan [1].)
All respondents were 35+ years old, with the majority between 65-74 (53%, 53 ppl) and 55–64 (32%, 32 ppl). (35–44 [2], 45–54 [5], 75+ [7]). Fifty-eight percent (58%) were biologically female.
The majority of respondents were diagnosed with multiple myeloma (87%, 87 ppl), followed by Chronic Lymphocytic Leukemia (4%, 4 ppl), Acute Myeloid Leukemia (2%, 2 ppl), Myelodysplasia (2%, 2 ppl), Acute Lymphoblastic Leukemia (1%, 1 per), and non-Hodgkin lymphoma (1%, 1 per).
Ninety-three (93) participants responded ‘yes’ to having had a hematopoietic stem cell transplant (bone marrow transplant) and 13 respondents indicated they have had a post-transplant cytomegalovirus infection (CMV).
Disease Experience
Patients with blood cancer often present with relapsed or refractory disease. The majority of patients must undergo multiple lines of treatment, which include chemotherapy, stem cell transplant (SCT), chimeric antigen receptor T-cell therapy (CAR T-cell) and others. These lines of treatment come with a range of side effects. Patients with acute disease, must often wait until their cancer progresses, while patients with chronic disease, often will be on treatment for life.
Respondents were asked how many lines of treatment they received prior to stem cell transplant, the majority had received two (2) prior lines of treatment before stem cell transplant (41) followed by one (1) prior line of treatment (26), four (4) people received three (3) lines of treatment prior to STC, three (3) people received four (4) prior lines of therapy, two (2) people received five (5) prior lines of therapy and three (3) received 10 or more prior lines of therapy prior to SCT.
Of the 93 respondents who did undergo stem cell transplant, 13 responded ‘yes’ when asked if they had ever been diagnosed with post-transplant cytomegalovirus infection (CMV).
Of the 13 patients with CMV infection, six (6) had multiple myeloma, two (2) had acute myeloid leukemia (AML), two (2) had chronic lymphocytic leukemia (CLL), two (2) had myelodysplasia and one (1) had myelofibrosis. Eight (8) were women and five (5) were men. Seven (7) were aged between 65-74, three (3) were aged 55–64, two (2) were aged 75+ and one (1) was 45–54. Six (6) patients had a stem cell transplant using their own stem cells and six (6) had a stem cell transplant using donor bone marrow, peripheral blood, umbilical cord blood and one (1) person did not say.
When asked how many lines of therapy they had received prior to their SCT, three (3) patients had at least one prior line of therapy, five (5) have had two prior lines of therapy prior to SCT, two (2) had four previous lines of therapy, one (1) had five previous lines of therapy and one (1) had ten or more lines of therapy prior to SCT.
Two (2) patients were diagnosed within the first 30 days following SCT, three (3) patients were diagnosed with CMV 31–60 days post-transplant, one (1) was diagnosed 91–120 days post-transplant, and one (1) 121–180 days post-transplant. Six (6) respondents skipped this question.
When asked how long patients had active symptoms of CMV, the majority reported 1–6 months (5) and three (3) people reported having active symptoms for less than one month. Five (5) respondents skipped this question. Two (2) of the respondents with active CMV infections lasting less than one month had longer than expected stays in the transplant centre and additional visits to the transplant centre (2). Three (3) respondents were readmitted to the hospital/transplant centre after going home and five (5) patients had additional visits at the hospital/transplant centre to treat or monitor the CMV infection, including two (2) who had a longer stay than expected at the transplant/hospital centre.
Four (4) patients spent less than one week away from home either due to in-hospital treatments or appointments to treat CMV infection symptoms, two (2) patients had to spend one to four weeks away from home to treat symptoms of CMV and two (2) patients had to spend one to three months away from home to manage and treat symptoms caused by CMV. Five (5) patients did not respond.
In addition to CMV infection following SCT, five (5) patients presented with other infections (bacterial, fungal or viral), three (3) patients presented with graft versus host disease (GvHD) and one (1) patient presented with GvHD also had lung problems, heart problems, and B cell immunodeficiency, bilateral cataracts.
Patients with CMV infection (13 respondents) were asked to rate, on a scale from 1 to 5, with 1 being no impact and 5 being an extremely significant impact, how CMV infection impacted their quality of life- seven (7) patients answered the following questions.
Patients were asked to rate on a scale of 1–5, how the symptoms of CMV impacted their day-to-day life, including ability to work, ability to travel, ability to exercise, personal image, ability to spend time with family and friends, intimate relationships, ability to continue daily activities, ability to concentrate, and mental health.
When asked how CMV infection impacted their ability to work–three respondents (3) reported ‘significant impact - 4’ to their ability to work due to CMV, two (2) reported ‘no impact - 1’, one (1) reported ‘moderate impact - 3’, and one (1) reported ‘extremely significant impact - 5’.
When asked how CMV affected their ability to concentrate, three (3) patients reported ‘‘no impact - 1’’, two (2) reported ‘extremely significant impact - 5’, one (1) reported a ‘moderate impact - 3’on their ability to concentrate, and one (1) reported a ‘mild impact - 2’.
When asked about the mental health impact, two (2) reported ‘moderate impact - 3’, two (2) reported ‘no impact - 1’, one (1) reported an ‘extremely significant impact - 5’, one (1) reported a ‘significant impact—4’, and one reported a ‘moderate impact—3’ and on their mental health.
When asked about how CMV infection impacted their ability to spend time with family and friends on a scale from 1 to 5, three (3) respondents said it had ‘no impact - 1’, one (1) said it had an ‘extremely significant impact—5’, one said it had a ‘significant impact—4’ one (1) said it had a ‘mild impact - 2’.
When asked about their ability to continue daily activities, four (4) patients said it had ‘no impact - 1’, two (2) said it had an ‘extremely significant impact - 5’, and one (1) said it had a ‘moderate impact - 3’.
Patients were asked about the psychosocial impact on quality of life of a CMV infection. Respondents (7) were asked to rate on a scale from 1 to 5, where 1 is no impact and 5 is extremely significant impact, how a CMV infection affected stress/anxiety, depression, sleep, feelings of isolation, support, friends and family relationships, concentration, sexual desire, life goals, financial impact and appetite. The psychosocial impacts most affected were sexual desire, interruption of life goals, and loss of appetite.
When asked about loss of sexual desire, three (3) said it had a ‘significant impact - 4’, two (2) said it had ‘no impact - 1’, one (1) respondent said it had an ‘extremely significant impact - 5’, and one (1) said it had a ‘moderate impact - 3’.
When asked about the interruption of life goals/accomplishments (career/school, etc.), two (2) said it had an ‘extremely significant impact - 5’, two (2) said it had a ‘significant impact - 4’, and three (3) said it had ‘no impact - 1’.
When asked about stress and anxiety, two (2) reported a ‘moderate impact - 3’, two (2) reported a ‘mild impact - 2’, one (1) patient reported an ‘extremely significant impact - 5’, one (1) patient reported a ‘significant impact - 4’ and one (1) reported ‘no impact - 1’.
When asked about problems concentrating, three (3) said it had ‘no impact - 1’, two (2) said it had an ‘extremely significant impact - 5’, one (1) said it had a ‘moderate impact - 3’and one (1) said it had a ‘mild impact - 2’.
When asked about how far patients had to travel to receive treatment for CMV infection, six (6) patients responded, five (5) had to travel less than 100kms and one (1) patient had to travel 100–200 kms to receive treatment. One (1) of the patients who had to travel less than 100kms felt this had a ‘significant impact - 4’ on their care because treatment was not available locally. Two (2) patients reported ‘mild impact—2’ or ‘moderate impact—3’ on their finances related to travel for care. Being away from support systems had a ‘moderate impact - 3’ on two (2) patients and two patients (2) reported a ‘moderate impact - 3’ on their ability to care for family/family commitments.
Experiences With Currently Available Treatments
Patients were asked a series of questions regarding treatment, six (6) patients responded to the following questions. When asked if they were given prophylaxis to prevent post-transplant CMV, all respondents said ‘No’ (1) or ‘I’m not sure’ (5). When asked what treatment they received following a CMV diagnosis, three (3) respondents answered they were given Ganciclovir intravenously, two (2) received Valganciclovir (Oral Tablets) and three (3) did not remember. One patient (1) received both Ganciclovir and Valganciclovir.
Patients were asked to rate about the side effects from the treatment they received (diarrhea, nausea, vomiting, pain, tenderness or swelling of the abdomen, eye pain, constipation, headache, weight loss, back, joint or muscle pain, mouth ulcers, depression, anxiety, vision problems [seeing specks, flashes of light, darkness, etc.], decreased urination, swelling or numbness of limbs, hives or rashes, itching, yellowing of skin, loss of appetite, unintentional trembling or shaking, seizures, other) on a scale of 1–5 with 1 being no impact and 5 being an extremely significant impact. Anxiety, weight loss, back, joint or muscle pain and diarrhea were more commonly reported followed by nausea, pain, tenderness or swelling of the abdomen, swelling or numbness of the limbs (hands, arms, feet, ankles or lower legs), and loss of appetite.
Two (2) patients reported a ‘mild impact - 2’ on anxiety, one (1) reported an ‘extremely significant impact - 5’ and one (1) reported a ‘moderate impact - 3’.
Three (3) patients reported a ‘moderate impact - 3’on back, joint or muscle pain, and one (1) reported a ‘mild impact - 2’.
Two (2) patients reported ‘significant - 4’ weight loss, two (2) patients reported ‘moderate - 3’ weight loss.
One (1) patient reported ‘extremely significant - 5’ diarrhea, one (1) patient reported ‘significant - 4’ diarrhea, one (1) patient reported ‘moderate - 3’ diarrhea and one (1) patient reported ‘mild - 2’ diarrhea.
Two (2) of the six (6) respondents indicated they had experienced difficulty accessing treatment.
Improved Outcomes
When asked to rate on a scale of 1–5, with 1 being not important and 5 being extremely important, which factors are most important to them when deciding upon a treatment for their CMV infection; five (5) patients who responded to the question, responded overwhelmingly that it was ‘extremely important–5’ for the treatment to improve quality of life, that it is recommended by the healthcare team (5). Similarly four (4) patients felt it was ‘extremely important–5’ that there was a degree of certainty that the treatment would relieve their CMV infection, while one (1) patient said this was ‘‘important - 4’. Four (4) patients felt it was, ‘extremely important–5’ that a treatment improved their length of survival, one (1) patient said it was ‘important - 4’. Three (3) patients felt that the impact on the caregiver was ‘extremely important - 5’ and two (2) patients said it was ‘important - 4’. Three (3) patients felt that the least amount of travel required to receive treatment was ‘extremely important - 5’, one (1) patient said it was ‘important - 4’, and one (1) patient said it was ‘somewhat important - 3’. Three (3) patients felt coverage of the by insurance/drug plan was ‘extremely important - 5’, one (1) patient said it was ‘somewhat important - 3’ and one (1) patient said it was not at all important (1). Other important treatment considerations included that it requires no overnight stay at a hospital, and the severity of a treatment’s accompanying side effects.
Experience With Drug Under Review
When asked what treatment patients had received to treat their CMV infection, no patient reported any experience with maribavir.
Companion Diagnostic Test
No companion Diagnostic Test is required.
Anything Else?
Patients were asked to provide additional information about their experience with CMV, a few relevant comments are as follows:
“I was diagnosed twice with high levels, one level of treatment required outpatient intravenous treatment twice a day, I was suffering from many side effects from the BMT so the 2 trips a day to the hospital were emotionally and physically draining for my care giver and myself. It was an overwhelming experience, my care giver and I were so thankful the CMV infection was over. I provide peer support and I always afraid the patients will develop a CMV infection that requires treatment.”
“The first time I was in hospital for 4 weeks that was before my transplant I had two other infections so we thought it might happen again after my SCT.”
“I had to wait for approval to be able to get the medication.”
“I had the infusion at home my daughter was trained at the Royal Free hospital pharmacist to do the infusion at home it was very good.
Conflict of Interest Declaration — The Leukemia & Lymphoma Society of Canada
To maintain the objectivity and credibility of the CADTH reimbursement review process, all participants in the drug review processes must disclose any real, potential, or perceived conflicts of interest. This Patient Group Conflict of Interest Declaration is required for participation. Declarations made do not negate or preclude the use of the patient group input. CADTH may contact your group with further questions, as needed.
Did you receive help from outside your patient group to complete this submission? If yes, please detail the help and who provided it.
No.
Did you receive help from outside your patient group to collect or analyze data used in this submission? If yes, please detail the help and who provided it.
No.
List any companies or organizations that have provided your group with financial payment over the past 2 years AND who may have direct or indirect interest in the drug under review.
Table 3: Financial Disclosures for The Leukemia & Lymphoma Society of Canada
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
Takeda | X | — | — | — |
The Kidney Foundation of Canada
About the Kidney Foundation of Canada
The Kidney Foundation of Canada is committed to achieving excellent kidney health, optimal quality of life, and a cure for kidney disease.
The Kidney Foundation of Canada is the leading charity committed to eliminating the burden of kidney disease through:
Funding and stimulating innovative research for better prevention, treatments and a cure;
Providing education and support to prevent kidney disease in those at risk and empower those with kidney disease to optimize their health status;
Advocating for improved access to high quality healthcare;
Increasing public awareness and commitment to advancing kidney health and organ donation.
For more information, please visit: www.kidney.ca
Information Gathering
CADTH is interested in hearing from a wide range of patients and caregivers in this patient input submission. Describe how you gathered the perspectives: for example, by interviews, focus groups, or survey; personal experience; or a combination of these. Where possible, include when the data were gathered; if data were gathered in Canada or elsewhere; demographics of the respondents; and how many patients, caregivers, and individuals with experience with the drug in review contributed insights. We will use this background to better understand the context of the perspectives shared.
Patient input was collected in February and March 2022 by the Kidney Foundation of Canada in both official languages via a self-administered questionnaire from people across Canada. The survey was directed at people living with a kidney transplant and their caregivers and inquired about respondents’ lived experience with a kidney transplant and medications and expectations for new drug therapies in Canada. The survey posed a number of questions specifically about the drug under review, maribavir. Awareness about the surveys was generated through the Kidney Foundation’s social media channels (Twitter and Facebook). It was also promoted on the Kidney Foundation’s website and e-newsletter.
A total of 9 people responded to the survey with 7 completed and 2 partially completed surveys. 6 respondents identified as kidney transplant recipients and 1 identified as a donor and caregiver. Of the 7 people that responded to the question about their current age or the current age of the person they care for, 2 were 25 to 39 years old, 2 were 40 to 54 years old, and 3 were 55-69 years old. 7 respondents answered the question about how long they had lived with a transplant. 1 respondent reported living with a transplant for under 1 year, 1 for 3 to 5 years, 3 for 6 to 10 years, 1 for 11 to 20 years and 1 respondent reported more than 20 years with the disease.
Disease Experience
CADTH involves clinical experts in every review to explain disease progression and treatment goals. Here we are interested in understanding the illness from a patient’s perspective. Describe how the disease impacts patients’ and caregivers’ day-to-day life and quality of life. Are there any aspects of the illness that are more important to control than others?
Kidney disease describes a variety of diseases and disorders that affect the kidneys. Most diseases of the kidney attack the nephrons and damage their ability to eliminate waste and excess fluids. Often, kidney disease is associated with other medical conditions such as diabetes, high blood pressure and heart disease.
Chronic kidney disease (CKD) is the presence of kidney damage, or a decreased level of kidney function, for a period of three months or more. Kidney disease can range from mild to severe and in some cases, lead to kidney failure (sometimes referred to as end-stage kidney disease, or ESKD). There are usually no specific symptoms of kidney disease until the damage is severe. When kidneys fail, waste accumulates in the body and dialysis treatments or a kidney transplant become crucial for survival.
A kidney transplant is generally considered the best treatment for most people with kidney failure. However, not everyone is a candidate for a transplant. People may not be eligible, for example, if they have other serious health issues in addition to kidney disease. Even if they are eligible for a transplant, a kidney donor may not be immediately available. Most people start dialysis while they wait for a kidney donor.
The advantages of a transplant include better quality of life with fewer limitations than dialysis. For example, a transplant won’t take hours of treatment time out of a person’s week, and they may feel physically stronger, able to work, travel and stay more active.
The main disadvantage of a transplant, in addition to the general risks of surgery, is that they will have to take medications every day, which may increase their risk of infection and have other side effects. A transplant is considered a treatment and not a cure since recipients will have to take medication for the rest of their lives to prevent their bodies from rejecting the new kidney.
Before being considered for a kidney transplant, all potential recipients must undergo a rigorous evaluation to determine if they are suitable transplant candidates. This is a detailed medical assessment that could include doctors’ evaluations of the heart, lung, stomach, bladder and blood vessels. Many tests and procedures may be needed to make sure they are healthy enough for the transplant surgery and the medications needed to prevent rejection of the kidney. They may also need to see a psychologist or psychiatrist before the transplant surgery to explore their feelings about this treatment. The transplant work-up can take up to a year to complete.
Most respondents who participated in the survey spoke about how a transplant changed their lives. Some respondents talked about the positive effects such as returning to work, the ability to have a family and resuming their studies and travels. They said “my kidney transplant was fabulous!” while others were more guarded, “I have resumed a normal rhythm of life but with more worries and precautions”.
Other respondents talked about their tiredness both prior to and following the transplant. “I have more energy than when I was on dialysis, but I still burn out faster than a healthy person.” Others spoke of the effects of long-term chronic kidney disease, “I'm retired and have been beating (sic) kidney disease for 40 years. As a result, I have weak bones, try to exercise every day (sic). Some days are good others I need to take it easy”.
Others spoke of side effects following the transplant “…but I have many side effects following the transplant and taking anti-rejections and cortisone: diarrhoea, abundant hair loss, diabetes... It's not always a pleasure”.
Caregivers spoke of how it effects both the person with the condition and themselves “our life has forever changed. He was diagnosed with CKD (untreated high blood pressure). It was hard for both of us. He was always tired, felt sick, discouraged and no life (as he always say)”. (sic)
Respondents also talked about their particular challenges of living with both a kidney transplant and cytomegalovirus (CMV).“…Still enjoy being intimate with my wife, but that all changed when we were told I had CMV. It is spread through blood, semen and saliva great (sic) my wife is scared of catching CMV”.
Experiences With Currently Available Treatments
CADTH examines the clinical benefit and cost-effectiveness of new drugs compared with currently available treatments. We can use this information to evaluate how well the drug under review might address gaps if current therapies fall short for patients and caregivers.
Describe how well patients and caregivers are managing their illnesses with currently available treatments (please specify treatments). Consider benefits seen, and side effects experienced and their management. Also consider any difficulties accessing treatment (cost, travel to clinic, time off work) and receiving treatment (swallowing pills, infusion lines).
57% of respondents have taken medication for CMV. Of those taking medication for CMV, 50% had taken ganciclovir, 75% had taken valganciclovir and 1 (25%) reported taking maribavir.
2 people reported being “very satisfied”, 1 person indicated that they were “satisfied” with the medication they are currently taking for high CMV, and 1 was “neither satisfied nor unsatisfied”. From those who responded about what they liked or didn’t like about the medications they took for CMV, their effectiveness in treating CMV and eliminating symptoms of the virus.1 respondent said “they were effective in curing me of the disease fairly quickly. The cost of going ahead was a negative as was the IV administration while working.” Another said, “My CMV numbers dropped like a rock. Did eight weeks and CMV was undetectable. So happy !! (sic) On no (sic) three weeks later it was back.”
Respondents also reported changes they had experienced as a result of current medication compared to previous therapies. 25% reported about the same change in taste, diarrhea, nausea or vomiting, feeling weak or tired and urinary changes while 75% didn’t know. 100% of respondents didn’t know if there were changes to fever, chills or sore throats or unexplained bruising or bleeding.
When asked about what factors were “very important” or “important” in choosing transplant medications in general, the following factors were identified as “very important” or “important” by the majority of respondents: tiredness, interference with sleep, foot edema, effect on mood, interference with other medications, changes in appetite, cost and length of time on the medication. One respondent stated that edema was neither important or unimportant, two respondents stated change in appetite was neither important or unimportant, one respondent also stated that cost was unimportant.
Additionally, patients were asked what else was important to them when taking transplant medications. A number of responses included side effects, impact on health, effectiveness and interactions with other medications and cost. A respondent stated “Ensure that it is compatible with the rest of the medication and that it is available at a reasonable cost to the patient” while another said, “We live in Saskatchewan and all my husband's meds are covered (because he's a kidney transplant). This is most important to us, and it should be to any transplant recipients”.
Patients also spoke of lowered immunity following a transplant and its effects, especially with COVID-19 in mind, “with Covid (sic) in mind protecting myself and still being able to see family and friends. Being on dialysis ties you down. Getting that kidney should allow you some freedom but the lowered immune (sic) makes it difficult”.
Improved Outcomes
CADTH is interested in patients’ views on what outcomes we should consider when evaluating new therapies. What improvements would patients and caregivers like to see in a new treatment that is not achieved in currently available treatments? How might daily life and quality of life for patients, caregivers, and families be different if the new treatment provided those desired improvements? What trade-offs do patients, families, and caregivers consider when choosing therapy?
Most respondents spoke about medication side effects when asked about their expectations when choosing a drug therapy. They also spoke about cost and having a better quality of life. Patients said, “that they are effective, simple to administer, and do not interfere with other medicines” and “no contraindications and no interaction with immunosuppressants. Side effects that are minimal or easily managed”. They also spoke about quality of life, “that these medicines have fewer side-effects for a better quality of life” and about medication costs “all meds (sic) are covered by the government, and it should be the same nationwide”.
Experience With Drug Under Review
1 respondent reported taking or having taken maribavir, while one person did not know if they had taken maribavir. One of the respondents had switched from another medication and accessed it through a clinical trial. 3 people responded to the question about how their health changed on maribavir compared to before, although 2 of those responses answered with “I don’t know” to all the questions. The one respondent said that changes in tastes, diarrhea, upset stomach or vomiting, urinary changes, fever, chills or sore throat had, or unexplained bruising, had remained the same and that feeling tired or weak was worse.
Companion Diagnostic Test
This question is not applicable to this submission.
Anything Else?
Every year, thousands of Canadians wait for a life-saving transplant and of those, hundreds will die while on the transplant waiting list. For those patients who receive a new organ, many will experience challenges navigating through the complex Canadian health care system and will need to learn to live with the difficulties of being an organ transplant recipient.
Tens of thousands of Canadians currently live with an organ transplant and many experience challenges with mental health, financial strain, and the uncertainty of how long this new organ will last. For all the benefits of transplantation, the reality for someone receiving an organ transplant is that they are a transplant patient for life. To live with a transplant means a lifetime of immune suppressing medication, managing the side effects of these medications, and a lifetime of check-ups, medical tests and concerns that they may one day lose their transplant and begin the journey all over again.
In many instances, transplantation is the only life-saving option available for patients with end-stage organ failure. For others, transplantation leads to better outcomes than alternative and more conservative treatments and offer significant savings to the health system. For example, kidney transplantation is widely considered the best treatment for people with kidney failure. A transplant enables people who would otherwise be on dialysis at least three times a week for four to five hours at a time, to live a relatively normal, healthy, and productive life, while providing a less costly option for the health care system compared to dialysis. The total annual cost of dialysis ranges from $56,000 to $107,000 per patient. The cost of a transplant is $66,000 in the first year, then $23,000 in subsequent years. For each kidney transplant patient, the health care system saves up to $84,000 annually.
Those living with a kidney transplant experience additional health and financial challenges. Many would benefit from effective, affordable treatments that they can access equitably and in a timely manner.
Maribavir may help people to achieve better health outcomes and improve their quality of life. For this reason, it should be available as an option for people living with a transplant and CMV.
Conflict of Interest Declaration — The Kidney Foundation of Canada
To maintain the objectivity and credibility of the CADTH drug reimbursement review process, all participants in the drug review processes must disclose any real, potential, or perceived conflicts of interest. This Patient Group Conflict of Interest Declaration is required for participation. Declarations made do not negate or preclude the use of the patient group input. CADTH may contact your group with further questions, as needed.
Did you receive help from outside your patient group to complete this submission? If yes, please detail the help and who provided it.
There was no external assistance from outside our patient group for this submission.
Did you receive help from outside your patient group to collect or analyze data used in this submission? If yes, please detail the help and who provided it.
There was no external assistance with data collection or analysis used for this submission.
List any companies or organizations that have provided your group with financial payment over the past two years AND who may have direct or indirect interest in the drug under review.
Table 4: Conflict of Interest Declaration for the Kidney Foundation of Canada
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
Alexion Pharma Canada Corp | — | X | — | — |
Amgen Canada Inc. | — | — | — | X |
Astellas Pharma Canada Inc. | — | — | X | |
AstraZeneca Canada Inc. | — | — | X | — |
Horizon Pharma Inc. | — | — | X | — |
Janssen Pharmaceutical Companies | — | — | — | X |
Otsuka Canada Pharmaceutical Inc. | — | — | — | X |
Paladin | X | — | — | — |
Sanofi | — | X | — | |
Clinician Input
Cell Therapy Transplant Canada
About Cell Therapy Transplant Canada
Cell Therapy Transplant Canada (CTTC) is a member-led, national, multidisciplinary organization providing leadership and promoting excellence in patient care, research and education in the field of hematopoietic stem cell transplant and cell therapy.
We are the professional society representing the stem cell transplant community in Canada, including physician, nursing, laboratory, and allied health professionals, along with an active family and caregiver group.
Information Gathering
The proposed submission was discussed by two CTTC committees – our Board of Directors, and our standing committee of program directors, representing the allogeneic stem cell transplant programs across Canada. These two committees were provided an opportunity to review this report and provide input.
Current Treatments
Response: There are no Health Canada approved therapies for this indication. There are a number of therapies that are used off label, most of which were included in the SOLSTICE trial. There is no single standard approach to the treatment of CMV in recipients of allogeneic stem cell transplant (AlloSCT). It is well recognized that CMV is a significant source of morbidity and mortality in AlloSCT. The most common approach is monitoring of CMV DNA in plasma, and pre-emptive therapy for patients with rising viral levels, with the aim of preventing CMV infection. Some patients at high risk receive letermovir as preventative therapy (previously reviewed by CADTH in 2017), but practice does vary, and low risk patients (CMV seronegative recipients, well matched transplants, no use of anti-thymocyte globulin or alemtuzumab) may not receive letermovir. For patients with rising CMV DNA in plasma, valganciclovir is the most commonly used first line therapy. Valganciclovir is associated with significant myelosuppression, a very concerning adverse event for patients post AlloSCT who often have some degree of baseline pancytopenia in the months following transplant.
For patients that do not respond to or do not tolerate valganciclovir, there is no single standard salvage therapy. Therapies commonly used in Canada are ganciclovir, cidofovir, or foscarnet, similar to the standard therapies used in the SOLSTICE trial. All of these agents have significant challenges (myelosuppression and need for inpatient admission with ganciclovir, renal toxicity with foscarnet).
Treatment Goals
What are the most important goals that an ideal treatment would address?
Response: The ideal treatment for refractory CMV infection would be oral, would be well tolerated in fragile post transplant patients, and would offer high response rates. Relapsed/refractory CMV remains a significant challenge in recipients of AlloSCT, with current therapies offering poor overall response rates and high toxicity. Higher response rates and lower rates of toxicity would reduce symptom burden and reduce requirements for inpatient care. This would result in improved health-related quality of life.
Treatment Gaps (Unmet Needs)
Considering the treatment goals, please describe goals (needs) that are not being met by currently available treatments.
Response: Current available treatment options are far from ideal. Overall response rates are low, resulting in a higher burden of symptoms due to CMV, associated with morbidity and mortality. All available therapies are associated with significant toxicity (myelosuppression with valganciclovir and ganciclovir, renal toxicities with foscarnet, need for IV administration of ganciclovir, foscarnet and cidofovir).
Which patients have the greatest unmet need for an intervention such as the drug under review?
Response: The population defined in the SOLSTICE trial mirrors that of the population with an unmet need – patients that do not adequately respond to first line therapy for CMV (usually valganciclovir). In addition, patients that do not tolerate first line therapies would benefit from this therapy as well. First line therapy in Canada is usually valganciclovir, which causes significant myelosuppression, which is a significant challenge in AlloSCT recipients.
Place in Therapy
How would the drug under review fit into the current treatment paradigm?
Response: Given that this therapy was shown to be superior to current standard of care options, it would become the dominant first line therapy for relapsed/refractory CMV infection. It is likely that the current treatment paradigm for initial management of CMV will not change significantly (letermovir prophylaxis for high-risk patients, weekly CMV monitoring and pre-emptive therapy with valganciclovir for all patients). For patients that do not respond to initial therapy (usually valganciclovir) or have side effects such as low cell counts or increased creatinine, maribavir is superior to all existing salvage options.
An important consideration will be the management of patients who do not tolerate existing therapies, even if CMV levels are declining. In the SOLSTICE trial, 31.9% of patients receiving standard of care therapies (most commonly valganciclovir, ganciclovir or foscarnet) had to discontinue treatment due to adverse events. We believe that this accurately represents the toxicity associated with these therapies, and maribavir would be an important option for these patients, given the superior toxicity profile.
Please indicate whether or not it would be appropriate to recommend that patients try other treatments before initiating treatment with the drug under review. Please provide a rationale from your perspective.
Response: This therapy will be used as second line therapy. It would not be appropriate to require patients to try other therapies as salvage prior to maribavir, given that these therapies have been shown by the SOLSTICE trial to both be inferior and more toxic than maribavir.
How would this drug affect the sequencing of therapies for the target condition?
Response: This therapy would become the preferred second line therapy for patients who do not respond to or do not tolerate first line therapy (usually with valganciclovir). Maribavir would displace foscarnet, which is nephrotoxic, to third line.
Which patients would be best suited for treatment with the drug under review?
Response: All patients who do not respond appropriately to first line therapy would be well suited for this therapy.
How would patients best suited for treatment with the drug under review be identified?
Response: Patients undergoing alloSCT are managed in highly specialized stem cell transplant clinics, at a limited number of tertiary care centres across Canada. These centres have physicians and clinical teams that are experienced at managing and monitoring CMV, and we do not expect misdiagnosis to be a significant issue. Patients that are eligible for this therapy will be identified by these teams.
Which patients would be least suitable for treatment with the drug under review?
Response: It’s challenging to identify a subset of patients with relapsed/refractory CMV who would be least suitable for this therapy. The only notable toxicity that was strongly associated with maribavir was dysgeusia. It is not uncommon for patients post-transplant to struggle with lack of appetite and poor oral intake, so potentially patients already experiencing difficulties eating might be less well suited. However, the overall toxicity profile of conventional salvage therapies was much more concerning.
Is it possible to identify those patients who are most likely to exhibit a response to treatment with the drug under review?
Response: All patients with relapsed or refractory CMV infection would be good candidates for this therapy. Predictors of response to maribavir are unknown so all refractory patients would be treated.
What outcomes are used to determine whether a patient is responding to treatment in clinical practice?
Response: The outcomes that were used in the clinical trial are used in clinical practice (overall response rate, rate of symptomatic CMV infection, toxicity profile).
What would be considered a clinically meaningful response to treatment?
Response: We support the monitoring criteria used in the trial (weekly CMV DNA levels from plasma). This is standard of care in Canada. Previous clinical experience and evidence shows that rising CMV levels will eventually lead to symptomatic CMV disease, which is associated with significant morbidity and mortality. This clinical practice is not likely to vary across physicians.
How often should treatment response be assessed?
Response: These patients are followed quite closely by transplant physicians (often weekly or biweekly visits), with regular monitoring of CMV DNA levels.
What factors should be considered when deciding to discontinue treatment?
Response: In general, the criteria used in the clinical trial to determine lack of response are those used in clinical practice (Lack of CMV viremia clearance by week 8 of therapy), and also Severe Treatment emergent adverse events.
What settings are appropriate for treatment with the drug under review?
Response: This therapy should only be prescribed for this indication by specialists working in a clinic associated with an allogeneic stem cell transplant program. In general, these are located in cancer centres associated with tertiary care hospitals in Canada.
For non-oncology drugs, is a specialist required to diagnose, treat, and monitor patients who might receive the drug under review?
Response: See previous statement – this therapy should be only available to specialists (hematologists or infectious disease clinicians) working in one of the limited number of allogeneic stem cell transplant programs in Canada. These programs are all located in tertiary care academic hospitals/cancer centres.
Additional information
Is there any additional information you feel is pertinent to this review?
Response: The availability of a Health Canada approved and provincially funded therapy for relapsed or refractory CMV would be an important step forward for our community. There is a significant unmet need for this indication, with existing therapies offering low response rates and high rates of toxicity. The completion of a randomized control trial for this indication is a large step forward for our community and our patients. Despite several improvements in CMV care over the past decade (the widespread adoption of CMV monitoring and pre-emptive therapy, the use of letermovir prophylaxis for high-risk patients), CMV remains a significant challenge for our patients. In particular, patients with chronic graft versus host disease (GVHD) and CMV infection are very challenging to manage. Almost universally, GVHD therapies are immunosuppressive, and increase the risk of CMV infection. GVHD therapies are also commonly myelosuppressive, and can be nephrotoxic, and the toxicity of existing therapies like valganciclovir or foscarnet poses significant challenges. The availability of an oral, well tolerated therapy with much higher response rates will be an important step forward for these patients, and if funded and available, will become the new standard of care.
Conflict of Interest Declarations — Cell Therapy Transplant Canada
To maintain the objectivity and credibility of the CADTH drug review programs, all participants in the drug review processes must disclose any real, potential, or perceived conflicts of interest. This conflict of interest declaration is required for participation. Declarations made do not negate or preclude the use of the clinician group input. CADTH may contact your group with further questions, as needed. Please see the Procedures for CADTH Drug Reimbursement Reviews (section 6.3) for further details.
Did you receive help from outside your clinician group to complete this submission? If yes, please detail the help and who provided it.
No help from outside the clinician group was obtained.
Did you receive help from outside your clinician group to collect or analyze any information used in this submission? If yes, please detail the help and who provided it.
No help from outside the clinician group was obtained.
List any companies or organizations that have provided your group with financial payment over the past two years AND who may have direct or indirect interest in the drug under review. Please note that this is required for each clinician that contributed to the input — please add more tables as needed (copy and paste). It is preferred for all declarations to be included in a single document.
Declaration for Clinician 1
Name: Dr. C. Kristjan Paulson
Position: President, Cell Therapy Transplant Canada (CTTC); Assistant Professor, University of Manitoba
Date: 16-03-2022
Table 5: Conflict of Interest Declaration for Cell Therapy Transplant Canada — Clinician 1
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
Takeda, Advisory Board | X | — | — | — |
Declaration for Clinician 2
Name: Dr. Mohamed Elemary
Position: Secretary, CTTC; Hematologist, Saskatoon Cancer Center; Professor, University of Saskatchewan
Date: 16-03-2022
Table 6: Conflict of Interest Declaration for Cell Therapy Transplant Canada — Clinician 2
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
Jazz Pharmaceuticals | X | — | — | — |
AbbVie pharmaceuticals | X | — | — | — |
Bristol Myers Squibb | X | — | — | — |
Paladin Labs Inc. | X | — | — | — |
AstraZeneca | X | — | — | — |
Pfizer | X | — | — | — |
Novartis | X | — | — | — |
Declaration for Clinician 3
Name: Dr. Jonas Mattsson
Position: Director, Messner Allogeneic Transplant Program; Professor, University of Toronto
Date: 16-03-2022
Table 7: Conflict of Interest Declaration for Cell Therapy Transplant Canada — Clinician 3
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
ITB-Med Biopharmaceuticals | — | X | — | — |
Takeda Canada, Inc | — | X | — | — |
Jazz Pharmaceuticals Canada | X | — | — | — |
Mallinckrodt (Therakos) | — | X | — | — |
Merck Canada Inc | X | — | — | — |
Sanofi Canada | X | — | — | — |
Declaration for Clinician 4
Name: Dr. Mona Shafey
Position: Director, Alberta Blood & Marrow Transplant Program
Date: 23-03-2022
Table 8: Conflict of Interest Declaration for Cell Therapy Transplant Canada — Clinician 4
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
No COI | — | — | — | — |
Declaration for Clinician 5
Name: Dr. Jean-Sébastien Delisle
Position: Director-at-Large (Research), CTTC; Associate Professor, Université de Montréal
Date: 24-03-2022
Table 9: Conflict of Interest Declaration for Cell Therapy Transplant Canada — Clinician 5
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
No COI | — | — | — | — |
Declaration for Clinician 6
Name: Dr. Wilson Lam
Position: Director-at-Large (Education), CTTC; Assistant Professor, University of Toronto
Date: 29-03-2022
Table 10: Conflict of Interest Declaration for Cell Therapy Transplant Canada — Clinician 6
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
Jazz Pharmaceuticals | X | — | — | — |
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up-to-date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third-party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
Redactions: Confidential information in this document may be redacted at the request of the sponsor in accordance with the CADTH Drug Reimbursement Review Confidentiality Guidelines
Stakeholder Input: The views expressed in each submission are those of the submitting organization or individual; not necessarily the views of CADTH or of other organizations. As such, they are independent of CADTH and do not necessarily represent or reflect the view of CADTH. No endorsement by CADTH is intended or should be inferred. By filing with CADTH, the submitting organization or individual agrees to the full disclosure of the information. CADTH does not edit the content of the submissions.
CADTH does use reasonable care to prevent disclosure of personal information in posted material; however, it is ultimately the submitter’s responsibility to ensure no identifying personal information or personal health information is included in the submission. The name of the submitting organization or individual and all conflict-of-interest information are included in the submission; however, the name of the author, including the name of an individual patient or caregiver submitting the patient input, are not posted.
Accessibility: CADTH is committed to treating people with disabilities in a way that respects their dignity and independence, supports them in accessing material in a timely manner, and provides a robust feedback process to support continuous improvement. All materials prepared by CADTH are available in an accessible format. Where materials provided to CADTH by a submitting organization or individual are not available in an accessible format, CADTH will provide a summary document upon request. More details on CADTH’s accessibility policies can be found here.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.