CADTH Reimbursement Review
Cariprazine (Vraylar)
Sponsor: Allergan (an AbbVie Inc. company)
Therapeutic area: Bipolar disorder
This multi-part report includes:
Clinical Review
Pharmacoeconomic Review
Stakeholder Input
Clinical Review
Abbreviations
AE
adverse event
ANCOVA
analysis of covariance
CANMAT
Canadian Network for Mood and Anxiety Treatments
CGI-BP
Clinical Global Impression–Bipolar Disorder
CGI-I
Clinical Global Impression–Improvement
CGI-S
Clinical Global Impression–Severity of Illness
CI
confidence interval
CINeMA
Confidence in Network Meta-Analysis
Crl
credible interval
C-SSRS
Columbia–Suicide Severity Rating Scale
DSM-IV
Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition
DSM-IV-TR
Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition, Text Revision
DSM-5
Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition
EPS
extrapyramidal symptom
FAST
Functioning Assessment Short Test
GAF
Global Assessment of Functioning
GRADE
Grading of Recommendations Assessment, Development, and Evaluation
HAM-A
Hamilton Anxiety Rating Scale
HAM-D
Hamilton Depression Rating Scale
HRQoL
health-related quality of life
IAM
Institute for Advancements in Mental Health
ITC
indirect treatment comparison
ITT
intention-to-treat
LOCF
last observation carried forward
LSM
least squares mean
MADRS
Montgomery–Åsberg Depression Rating Scale
MDSC
Mood Disorders Society of Canada
MID
minimal important difference
mITT
modified intention-to-treat
MMRM
mixed model of repeated measures
NICE
National Institute for Health and Care Excellence
NMA
network meta-analysis
NR
not reported
OR
odds ratio
PANSS
Positive and Negative Syndrome Scale
QIDS-SR
Quick Inventory of Depressive Symptomatology–Self-Rated
RCT
randomized controlled trial
RE
random effects
SAE
serious adverse event
SD
standard deviation
SE
standard error
TEAE
treatment-emergent adverse event
WC-CAN
Western Canadian Clinical Advisory Network
WDAE
withdrawal due to adverse event
YMRS
Young Mania Rating Scale
Executive Summary
An overview of the submission details for the drug under review is provided in Table 1.
Item | Description |
|---|---|
Drug product | Cariprazine (Vraylar), 1.5 mg, 3 mg, 4.5 mg, and 6 mg oral capsules |
Indication | Cariprazine is indicated as monotherapy for:
|
Reimbursement request | As per indication. |
Health Canada approval status | Approved |
Health Canada review pathway | Standard |
NOC date | April 22, 2022 |
Sponsor | Allergan (an AbbVie Inc. company) |
NOC = Notice of Compliance.
Introduction
Living with bipolar disorder is associated with a substantial burden of illness that people experience for approximately half of their lives.1 The estimated average age of onset in Canada is 22.5 years2 and the estimated lifetime prevalence of bipolar I disorder in Canada is 0.87%, affecting males and females equally.1 Quality of life and psychosocial functioning, including the ability to maintain proper work, are severely impacted by bipolar disorder and more pronounced in those living with depressive symptoms, with multiple previous episodes or a longer duration of illness, and in those with cognitive decline.1 In addition, suicide risk is substantially higher for patients living with bipolar disorder relative to the general population (10.7 deaths due to suicide per 100,000 people per year).1
Bipolar I disorder is a mood disorder characterized by episodes of mania, hypomania, and major depression.3 Episodes of mania and depression present with significant changes in mood, energy, behaviour, sleep, and cognition. Mania also presents with change in activity. The Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5) includes specifiers that describe characteristics of bipolar disorder and can be used to guide treatment decisions for acute mania and depression. The presence of mixed features is a specifier for patients experiencing at least 3 nonoverlapping symptoms from the opposing pole (mania or depression) during the majority of the days of the current episode.4
There are no disease-modifying treatments for bipolar disorder. Bipolar disorder is treated with the combination of pharmacologic, nonpharmacologic (e.g., electroconvulsive therapy), and psychosocial (e.g., psychotherapy) treatments. The clinical experts stated that the primary goal of current treatments is to improve acute symptoms and, by doing so, restore functioning. The prevention of recurrent mood episodes was described as the secondary goal. Long-term treatment efficacy is more uncertain as high-quality longitudinal studies of longer duration are limited. In Canada, pharmacologic treatments are usually managed by family physicians in milder to moderate cases or by psychiatrists in more severe cases, although this varies regionally. Medications include mood stabilizers (which include drugs from a variety of classes, such as second-generation antipsychotic drugs, anticonvulsants, and lithium), and antidepressants. The clinical experts stated that overall, there are many different pharmacologic options, and the choice of treatment is usually guided by evidence of efficacy and tolerability, characteristics of the patient (age, income, individual preferences), characteristics of the disorder (including, but not limited to, predominant symptomatology or polarity [mania, depression, or mixed features], medical and psychiatric comorbidities, and resistance to treatment) and characteristics of the treatments (safety and tolerability issues, availability, cost). The clinical experts indicated that the use of off-label drugs for mania is uncommon as there are several drugs available in Canada with adequate efficacy. In contrast, the experts indicated fewer treatments are available for the management of depressive episodes, and they are associated with relatively high rates of treatment failure due to nonresponse or poor tolerability. As a result, the use of drugs without approval, such as antidepressants, is common for bipolar depression.
Cariprazine is a second-generation antipsychotic drug that is approved by Health Canada for use in adults as monotherapy for the acute management of manic or mixed episodes associated with bipolar I disorder (bipolar mania) and the acute management of depressive episodes associated with bipolar I disorder (bipolar depression).5 The mechanism of action for cariprazine is unknown.5 The sponsor has requested reimbursement as per the indication.6 As such, the objective of this review is to perform a systematic review of the beneficial and harmful effects of cariprazine 1.5 mg, 3 mg, 4.5 mg, and 6 mg for use as monotherapy in adults for the acute management of manic or mixed episodes associated with bipolar I disorder (bipolar mania) and for the acute management of depressive episodes associated with bipolar I disorder (bipolar depression). Cariprazine has been previously reviewed by CADTH for the treatment of schizophrenia in adults and is approved by Health Canada for the acute and long-term maintenance treatment of schizophrenia in adults as well.
Stakeholder Perspectives
The information in this section is a summary of input provided by the patient groups that responded to CADTH’s call for patient input and from clinical experts consulted by CADTH for the purpose of this review.
Patient Input
This section was prepared by CADTH staff based on the input provided by patient groups.
Two responses to CADTH’s call for patient input were received for this review: a submission from the Institute for Advancements in Mental Health (IAM) and a submission from the Mood Disorders Society of Canada (MDSC). IAM and MDSC are organizations that support individuals living with mental illness such as bipolar disorder, including patients, their families, and service providers.
The information used to inform the IAM submission was based on 2 online surveys conducted in 2018 and in February 2022. Potential respondents to these online surveys included members of the IAM and Hope and Me — Mood Disorders Association of Ontario client networks. Among the respondents of the 2018 survey, 12% self-described as personally diagnosed, 50% were caregivers, 63% were family members or friends of someone diagnosed, and 18% worked in social services. Among the respondents of the 2022 survey, 33% identified as an individual living with symptoms of bipolar disorder, 58% were relatives, 8% were caregivers of someone with lived experience, and 1% did not specify. MDSC drew information from interviews with patients and family members, 2 national mental health surveys conducted in 2018 and in September 2021, and shared experiences that had been posted on the MDSC online discussion forum. The interviews were conducted with 5 patients with bipolar disorder, including semi-structured phone interviews with adults living with bipolar disorder in January 2021, and 3 family members.
Respondents indicated that living with bipolar disorder had impacted their mental health, social relationships, and day-to-day functioning at work and school. Patients can also experience a lack of insight into their illness, which impacts their ability and motivation to seek treatment and causes significant strain in relationships. Survey respondents described the advantages of taking medications for bipolar disorder, which include managing symptoms of bipolar disorder, experiencing fewer episodes of mental illness, and avoiding visits to the hospital. They also described disadvantages of taking medications for bipolar disorder; these include requiring frequent follow-ups with health care providers, needing to take the medication daily, and dealing with the symptoms — including bipolar depression, which was not being well controlled. Further, respondents described the benefits of an injectable formulation, which include convenience and not needing to remember to take it daily, while the difficulties were pain at injection site and frequent travel to clinics. The most common side effects of medications for bipolar disorder identified by respondents were drowsiness, dry mouth, restlessness, and weight gain. Respondents also identified the cost of medications as a significant barrier to access.
Survey respondents reported that treatment of bipolar disorder is individualized, as not every patient will respond to 1 medication. To find the right medication that enables the highest degree of functioning while minimizing side effects, patients with bipolar disorder often have to go through a trial-and-error process. This process involves taking a number of different medications and at different dosages until their goals of therapy have been achieved. This process can make it challenging for patients to adhere to their prescribed regimen and can be exacerbated by additional challenges, such as waiting to be approved for coverage by public drug programs and experiencing relapse. As a result, patients feel that outcomes can be improved by increasing equitable access to, and the selection of, medications that are reimbursable. According to respondents, antipsychotic medications could be improved by increasing their ability to control the symptoms of bipolar disorder, improving the side effect profile, and providing a greater range of strengths and dosages to lower the frequency of administration.
A copy of the patient input from IAM and MDSC is presented in Appendix 5.
Clinician Input
Input From Clinical Experts Consulted by CADTH
The clinical experts consulted by CADTH indicated numerous challenges with addressing treatment goals for patients living with bipolar I disorder using currently available treatments. Insufficient response to treatment was noted as being very common, particularly in bipolar depression. There are no disease-modifying treatments and the long-term effectiveness of current treatments is unclear. Bipolar disorder is typically a lifelong, persistent, and/or highly recurrent condition. Some key outcomes are not adequately addressed by current treatments. For example, the extent to which current treatments address cognition directly, instead of indirectly through mood symptoms, is unclear. Tolerability is a problem, particularly in bipolar depression, where the most effective drugs, like quetiapine and olanzapine, have well-known metabolic side effects; this is particularly concerning given the elevated, and independent, risk of metabolic and cardiovascular conditions in this population. Finally, adherence is also an issue — poor compliance is very common in real-world settings.
Based on the currently available clinical evidence, the clinical experts felt it was very unlikely that cariprazine would cause a shift in treatment paradigm, despite having a somewhat distinct pharmacologic profile. Mechanistically, cariprazine was described as very similar to currently available treatments and, therefore, very much within the current paradigm of symptomatic management. However, the experts noted that the combination of efficacy for both acute mania and depression, as well as an acceptable tolerability profile, may eventually result in cariprazine as a first-line treatment. The experts did not identify any reason to recommend that patients try other treatments before cariprazine. The clinical experts suggested cariprazine will probably be used in monotherapy and in combination with either lithium or anticonvulsants, which is a standard approach with second-generation antipsychotic drugs in bipolar disorder.
The experts indicated that it is challenging to identify and diagnose patients with bipolar disorder, and that misdiagnosis and/or delayed diagnosis are relatively common. Relatedly, they stated there are no diagnostic tools or tests that are useful, and the diagnosis is based on clinical assessment.
At this time, the clinical experts stated that it is not possible to identify patients who are most likely to exhibit a response to treatment with cariprazine. They noted that the reliable prediction of response has not been achieved even with sophisticated research methods (e.g., genomics, neuroimaging), and certainly cannot be done reliably with the most widely available clinical tools. Other than polarity of mood episode, there are no other validated indices to predict response to any given drug, according to the clinical experts. The clinical experts stated that presymptomatic patients should not be treated with cariprazine, or any other drug, mostly due to the low predictive power of current assessment tools. The clinical experts did not identify any patients who would be least suited for treatment with cariprazine, noting that within the population of adults with bipolar I disorder, there were no major contraindications unique to cariprazine.
The clinical experts identified the Young Mania Rating Scale (YMRS), the Montgomery–Åsberg Depression Rating Scale (MADRS), and the Hamilton Depression Rating Scale (HAM-D) as the most commonly used outcomes to assess response to treatment in research settings, but in the real world, patient-rated questionnaires such as the Patient Health Questionnaire and the Beck Depression Inventory are more common. The experts also noted that all of these outcomes, however, have very good concurrent validity. A reduction in the frequency or severity of symptoms, an improvement in symptoms, the stabilization (no deterioration) of symptoms, the ability to perform activities of daily living, and improved survival were all clinically meaningful according to the clinical experts. They described a reduction in the severity of symptoms (e.g., controlling physical agitation) and frequency of symptoms as the usual first goal of treatment. Subsequently, the experts stated that treatment aims to restore functioning — including improving cognitive functioning and coping skills — with a return to work, school, and/or daily activities being an important benchmark. The experts identified long-term goals, such as the prevention of relapses and recurrences, as well as the onset and progression of psychiatric comorbidities (e.g., anxiety disorders, substance abuse) and medical comorbidities (e.g., obesity, diabetes).
Regarding how often treatment response should be assessed, the clinical experts suggested that in the acute phase, response is usually assessed between 2 weeks to 4 weeks, depending on the severity. In the maintenance phase, it is recommended that patients be assessed at least every 2 months to 3 months. The clinical experts indicated that treatment discontinuation is determined by either lack of response or poor tolerability, noting that most guidelines recommend discontinuing a treatment if there is no response to very poor response within 4 weeks to 6 weeks. Further, they indicated that discontinuation due to tolerability depends on the severity and progression of specific side effects, particularly extrapyramidal symptom (EPS) and akathisia, which are the most common side effects of cariprazine and similar drugs. These side effects can be time-dependent; they tend to be worse during initial titration phases but improve with time. If side effects are moderate to severe and/or do not meaningfully improve in 1 weeks to 2 weeks, treatment should be discontinued.
The clinical experts reported that family physicians can and frequently do diagnose bipolar disorder and regularly prescribe similar drugs. The experts also noted that there are no special tests required for the diagnosis of bipolar disorder, nor for the prescription and monitoring of cariprazine. The clinical experts noted that given the high prevalence of bipolar disorder and the relative lack of psychiatrists across Canada, a significant proportion of patients is treated by family physicians; therefore, the experts recommended that requiring the involvement of specialists would significantly restrict the use of this medication.
Clinician Group Input
Two clinician groups provided input to this review: Canadian Network for Mood and Anxiety Treatments (CANMAT), a network of academic and clinical experts that produces treatment guidelines and educational material for health professionals and information for patients and families, and Western Canadian Clinical Advisory Network (WC-CAN), a network of senior psychiatrists across Alberta and British Columbia. One clinician on behalf of CANMAT and 6 clinicians with the WC-CAN contributed to these submissions. Both clinician groups recognized the unmet need for a medication that is effective in multiple phases of bipolar disorder, including bipolar depression, with low rates of adverse events (AEs) to minimize polypharmacy and improve adherence. The clinical experts consulted by CADTH identified additional unmet needs, which include the absence of disease-modifying drugs, the uncertainty regarding the long-term effectiveness and direct effects on cognition of currently available treatments, and the lack of depot alternatives for commonly used first-line pharmacologic options. Both clinician groups advocated for cariprazine as a first-line treatment option for patients with bipolar disorder in the treatment of acute mania and depression and for cariprazine to be used as monotherapy and possibly as combination therapy with other mood stabilizers.
Drug Program Input
Input was obtained from the drug programs that participate in the CADTH reimbursement review process. The following were identified as key factors that could potentially impact the implementation of a CADTH recommendation for cariprazine:
considerations for the initiation of therapy
considerations for generalizability.
Detailed drug program input is found in Table 6.
Clinical Evidence
Pivotal Studies and Protocol Selected Studies
Description of Studies
The systematic review of cariprazine included a total of 6 multi-centre, randomized, double-blind, placebo-controlled, parallel-group studies in adults with a primary diagnosis of bipolar I disorder. Of the 6 included randomized controlled trials (RCTs), 3 evaluated cariprazine 3 mg to 12 mg (flexible dose) for the treatment of acute manic or mixed episodes (study RGH-MD-31 [N = 238], study RGH-MD-32 [N = 312], and study RGH-MD-33 [N = 497] — frequently referred to as the bipolar mania studies in this report) and 3 evaluated cariprazine 1.5 mg and 3.0 mg (fixed dose) for the treatment of acute depressive episodes (study RGH-MD-56 [N = 578], study RGH-MD-53 [N = 493], and study RGH-MD-54 [N = 488] — frequently referred to as the bipolar depression studies in this report). The flexible-dosing regimen in the bipolar mania studies involved dose adjustments based on treatment response assessed by the investigator (study RGH-MD-31) or using the YMRS (study RGH-MD-32 and study RGH-MD-33) and tolerability, determined at the discretion of the investigator. The objective of each of the studies was similar: to evaluate the efficacy, safety, and tolerability of cariprazine monotherapy versus placebo for the treatment of acute manic or mixed episodes or acute depressive episodes associated with bipolar I disorder. The primary end point in all studies was the change in symptoms, measured using the YMRS total score in the studies of acute manic or mixed episodes and the MADRS total score in the studies of acute depressive episodes. The secondary end point was the change in the Clinical Global Impression–Severity of Illness (CGI-S) score; this was consistent across studies. Primary and secondary outcomes were assessed at week 3 in the acute mania studies and at week 6 in the acute depression studies. Other measures of changes in symptom severity (Clinical Global Impression–Improvement [CGI-I], Positive and Negative Syndrome Scale [PANSS], HAM-D, Hamilton Anxiety Rating Scale [HAM-A], and Quick Inventory of Depressive Symptomatology–Self-Rated [QIDS-SR]), functioning (Functioning Assessment Short Test [FAST]), suicidal ideation (Columbia–Suicide Severity Rating Scale [C-SSRS]), response rate, and remission rate were also reported.
The mean age of patients enrolled in the included studies ranged between 36 (standard deviation [SD] = 11) years and 44 (SD = 13) years and the mean weight of patients ranged from 70 (SD = 20) kg to 87 (SD = 25) kg. The population in the acute mania studies was slightly younger and had a lower body weight than patients in the acute depression studies. More patients in the acute mania studies were male (ranging from 54% to 68% across studies) and more patients in the acute depression studies were female (ranging from 57% to 65% across studies). The duration of bipolar I disorder was a mean of 10 (SD = 9) years to 16 (SD = 10) years and the age of onset ranged from 23 (SD = 8) years to 28 (SD = 11) years. The duration of and age of onset of bipolar I disorder was not reported in study RGH-MD-53 or study RGH-MD-54. During the trials for acute mania or mixed episodes, between 81% and |||||| of patients were currently experiencing a manic episode and between and 20% were experiencing a mixed episode. Between |||||| and |||||| of patients were diagnosed with a moderate episode, |||||| to |||||| with a severe episode without psychotic features, and |||||| to |||||| with a severe episode with psychotic features. During study RGH-MD-53 and study RGH-MD-54, between |||||| and |||||| of patients were currently experiencing a severe depressive episode and between |||||| and |||||| were experiencing a moderate depressive episode, and the duration of the current episode was a mean of 3.3 (SD = 2.3) months to 3.8 (SD = 2.5) months. Similar statistics were not reported in study RGH-MD-56.
Efficacy Results
A summary of key efficacy results for the studies in patients with acute manic or mixed episodes of bipolar disorder is presented in Table 2; in Table 3, a similar summary is presented for the studies in patients with acute depressive episodes of bipolar disorder. Of note, the bipolar studies used a flexible-dose regimen for cariprazine. The overall mean daily dose in study RGH-MD-31 and study RGH-MD-32 was 8.8 (SD = ||||||) mg and 7.5 (SD = ||||||) mg per day, respectively. The overall mean daily dose in study RGH-MD-33 was 4.8 (SD = ||||||) mg. The overall mean daily dose was not reported in the bipolar depression studies.
All 3 studies of acute mania demonstrated that treatment with flexible dosing of cariprazine was associated with a greater reduction of symptoms of acute mania relative to placebo, based on the YMRS total score at week 3. This was based on a difference in score between cariprazine 3 mg to 12 mg and placebo of –6.1 (95% confidence interval [CI], –8.9 to –3.3; P < 0.0001) in study RGH-MD-31, and –4.3 (95% CI, –6.7 to –1.9; P = 0.0004) in study RGH-MD-32. In study RGH-MD-33, the difference in score between cariprazine 3 mg to 6 mg and placebo was –6.1 (95% CI, –8.4 to –3.8; P < 0.001). The within-group change in the YMRS score was clinically meaningful for both the cariprazine and placebo treatment groups, based on a within-group minimal important difference (MID) of 6.6 points.7 All sensitivity analyses supported the results of the primary efficacy analyses. Subgroup analyses based on the pivotal trials did not suggest a difference in efficacy between patients experiencing a manic episode and patients experiencing a mixed episode. In the studies of acute bipolar depression, treatment with cariprazine 1.5 mg was associated with a greater reduction of symptoms of depression relative to placebo, based on a least squares mean (LSM) difference in the MADRS total score at week 6 of –2.5 (95% CI, –4.6 to –0.4; P = 0.0417) in study RGH-MD-53, –2.5 (95% CI, –4.6 to –0.4; P = 0.0331) in study RGH-MD-54, and –4.0 (95% CI, –6.3 to –1.6; P = 0.0030) in study RGH-MD-56. The comparison of cariprazine 3.0 mg to placebo did not consistently demonstrate a benefit with treatment. In study RGH-MD-54, the LSM difference was in favour of cariprazine 3.0 mg relative to placebo (LSM difference = –3.0; 95% CI, –5.1 to –0.9; P = 0.0103). The LSM difference in study RGH-MD-53 and study RGH-MD-56 was –1.8 (95% CI, –3.9 to 0.4; P = 0.1051) and –2.5 (95% CI, –4.9 to –0.1; P = 0.1122), respectively. A between-group MID of at least 2 points was identified for the MADRS total score.8,9 Comparisons that were statistically significant were also clinically meaningful as per the MID, with the exception of cariprazine 3.0 mg in study RGH-MD-56, which was not statistically significant.
The secondary end point in all studies was the change in CGI-S, which is an outcome based on a global assessment of symptom severity relative to other patients that the assessor has observed. The CGI-S was validated through a comparison to the PANSS in patients with schizophrenia, but evidence of reliability and responsiveness were not identified. In the acute mania studies, the cariprazine treatment groups exhibited a greater change in overall severity based on the CGI-S at week 3 than the placebo treatment groups, which is consistent with the primary analysis. This was based on a difference in score between cariprazine 3 mg to 12 mg and placebo of –0.6 (95% CI, –1.0 to –0.3; P = 0.0001) in study RGH-MD-31, and –0.4 (95% CI, –0.7 to –0.1; P = 0.0027) in study RGH-MD-32. In study RGH-MD-33, the difference in score between cariprazine 3 mg to 6 mg and placebo was –0.6 (95% CI, –0.9 to –0.4; P < 0.001). In the acute depression studies, a benefit in terms of the change from baseline to week 6 in the CGI-S was demonstrated for comparisons of cariprazine 1.5 mg to placebo in study RGH-MD-53 (LSM difference = –0.3; 95% CI, –0.6 to –0.1; P = 0.0417) and study RGH-MD-56 (LSM difference = –0.4; 95% CI, –0.6 to –0.1; P = 0.0132). The LSM difference of the change from baseline in CGI-S at week 6 was –0.2 (95% CI, –0.4 to 0.1; P = 0.1370), –0.3 (95% CI, –0.5 to –0.0; P = 0.0662), and –0.3 (95% CI, –0.5 to –0.0; P = 0.1122) for study RGH-MD-53, study RGH-MD-54, and study RGH-MD-56, respectively. Similar to the primary analysis, cariprazine 3.0 mg did not demonstrate a benefit relative to placebo, nor did the 1.5 mg treatment group in study RGH-MD-54 (LSM difference = –0.2; 95% CI, –0.5 to 0.0; P = 0.0714). The suggested MID for the CGI-S is a difference of 1 point for both within-group and between-group analyses. Based on this threshold, a clinically meaningful within-group difference was observed for all treatment groups (except placebo in study RGH-MD-31); however, the between-group differences were not clinically meaningful.
Other assessments of the change in symptoms were reported in the included studies. A lack of control for multiplicity of testing, however, rendered additional efficacy outcomes as supportive only.
In the studies of acute mania, the overall improvement of symptoms using the CGI-I, the change in symptoms of depression using the MADRS total score, and the change in severity of psychotic symptoms using the PANSS were assessed. The results of the CGI-I at week 3 were supportive of the primary and secondary analyses. The LSM difference of the change from baseline in CGI-I at week 3 for cariprazine compared to placebo was –0.8 (95% CI, –1.2 to –0.5; P < 0.0001), –0.5 (95% CI, –0.7 to –0.2; P = 0.0004), and –0.7 (95% CI, –0.9 to –0.4; P < 0.001) in study RGH-MD-31, study RGH-MD-32, and study RGH-MD-33, respectively. An MID was not identified for the CGI-I, which made it difficult to interpret this outcome further. The results of the change in MADRS total score at week 3 were consistent with a small reduction of depressive symptoms, with no apparent difference between cariprazine and placebo. The clinical experts consulted by CADTH did not expect to see a change in depressive symptoms for patients experiencing an acute manic episode, but also suggested that not observing an increase in symptoms of depression is notable. A numerical reduction in the PANSS total score was observed at week 3 in all treatment groups (cariprazine and placebo) in the bipolar mania studies; however, limitations of the PANSS outcome led to difficulty with the interpretation of the results in the context of short-term treatment for acute mania associated with bipolar disorder.
The bipolar depression studies also assessed changes in severity of symptoms of depression using the HAM-D and QIDS-SR tools and symptoms of anxiety using the HAM-A tool. A clinically significant difference of 2 points or 3 points in the HAM-D has been suggested in the literature, although justification for this threshold was unclear and likely opinion-based.8,10 The difference in the change in depressive symptoms based on the HAM-D at week 6 was inconsistent across studies, although a numerical decrease in HAM-D score (reduction of symptoms) was observed for all treatment groups. Also, study RGH-MD-56 reported similar results at week 6 and week 8. Neither cariprazine 1.5 mg nor 3.0 mg demonstrated a benefit relative to placebo based on the change in depressive symptoms at week 6 as per the QIDS-SR. A numerical reduction in the HAM-A score at week 6 indicating an improvement of symptoms of anxiety was observed in all treatment groups, with no difference observed between cariprazine 3.0 mg and placebo. The clinical relevance of these changes is unknown. Overall, the evidence in support of changes in the severity of symptoms associated with a depressive episode of bipolar disorder were inconsistent with respect to the difference between cariprazine 1.5 mg and placebo and did not support a benefit with cariprazine 3.0 mg relative to placebo.
The incidence of most severe suicidal ideation and most severe suicidal behaviour per the C-SSRS was reported in all studies except study RGH-MD-31. In all treatment groups of the bipolar mania studies, suicidal ideation was reported in 1% to 3% of patients. In the bipolar depression studies, suicidal ideation was reported in 3% to 11% of patients. The incidence by dose of cariprazine varied between studies. Suicidal behaviour was not reported for any patients in any of the included studies.
Daily functioning was also identified as an outcome of interest to patients and by clinicians. |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||. Functioning was not assessed in any of the other included studies.
Response rates and remission rates based on reductions in the YMRS total score (acute mania studies) and MADRS total score (depressive studies) were also reported. These outcomes were also not controlled for multiplicity and, therefore, were considered supportive only. In the acute mania studies, a response was observed in 48% to 61% of patients receiving cariprazine and 25% to 44% of patients receiving placebo. Remission was observed in 42% to 52% of patients receiving cariprazine and 23% to 35% of patients receiving placebo. The clinical experts indicated that a trial duration of 3 weeks is likely too short to observe full remission, which may take up to 4 weeks to 6 weeks for an acute manic or mixed episode. In the acute depressive studies, 41% to 50% of patients and 43% to 52% of patients receiving cariprazine 1.5 mg and 3.0 mg, respectively, were considered responders as per the MADRS definition. The response rate among patients receiving placebo ranged from 32% to 40% across the trials. The benefit of treatment with cariprazine (1.5 mg and 3.0 mg) was inconsistently demonstrated across the studies based on this outcome. Similar results were reported for the analysis of MADRS remitters, where 26% to 37% of patients and 26% to 32% of patients receiving cariprazine 1.5 mg and 3.0 mg, respectively, and 20% to 23% of patients receiving placebo were considered to have a remission of depressive symptoms.
Outcomes related to health-related quality of life (HRQoL), hospitalization, cognitive impairment, and persistence with therapy were included in the CADTH systematic review protocol but not identified in the included studies.
Harms Results
In the bipolar mania studies, the percentage of patients who reported a treatment-emergent adverse event (TEAE) ranged from 78% to 86% for patients randomized to cariprazine (3 mg to 12 mg or 3 mg to 6 mg) and 61% to 79% for patients randomized to placebo. In the bipolar depression studies, the percentage of patients who reported an AE ranged from 50% to 62% for patients randomized to cariprazine 1.5 mg, 49% to 62% for patients randomized to cariprazine 3.0 mg, and 46% to 55% for patients randomized to placebo. The overall rate of AEs was higher in the acute mania trials than the acute depression trials, despite a shorter duration of treatment. This may be due to the use of a higher dose of cariprazine. Whether AEs were more likely to be detected in an inpatient setting or the result of the higher dose of cariprazine in the acute mania trials, or both, is unknown.
In all included studies, serious adverse events (SAEs) were infrequently reported and 1 death was reported in all of the included trials. In the bipolar mania studies, SAEs were reported by 3.2% to 4.2% of patients randomized to cariprazine (3 mg to 12 mg or 3 mg to 6 mg) and 1.9% to 4.2% of patients randomized to placebo. In the bipolar depression studies, the percentage of patients who reported at least 1 SAE in the cariprazine 1.5 mg and cariprazine 3 mg treatment groups ranged from 0.6% to 1.4% and 0 to 1.4%, respectively. In the placebo treatment groups, the percentage of patients who reported at least 1 SAE ranged from 1.3% to 3.4%. In the bipolar mania studies, patients who stopped treatment due to AEs (withdrawal due to adverse event [WDAE]) ranged from 9% to 14% of patients randomized to cariprazine and 5% to 10% of patients randomized to placebo. In the bipolar depression studies, WDAEs were reported by 3% to 8% of patients randomized to cariprazine 1.5 mg, 6% to 12% of patients randomized to cariprazine 3.0 mg, and 3% to 10% of patients randomized to placebo. The most common reasons for WDAEs were mania, akathisia, restlessness, and agitation. WDAEs tended to be slightly more frequent among patients randomized to cariprazine compared to placebo, but this was inconsistent across studies.
Of the notable harms identified in the CADTH systematic review protocol, hyperglycemia, weight gain, sexual dysfunction, tardive dyskinesia, and neuroleptic malignant syndrome were infrequently reported in all trials. Additionally, vomiting and EPS were infrequently reported in the bipolar depression studies. In the acute mania studies, the following notable harms were reported more frequently with cariprazine versus placebo: EPS (10% to 25% versus 2% to 10%), akathisia (17% to 22% versus 4% to 6%), vomiting (8% to 10% versus 3% to 5%), and restlessness (6% to 8% versus 1% to 5%). Similarly in the bipolar depression studies, akathisia (5% to 14% versus 1% to 3%) and restlessness (2% to 7% versus 3% to 4%) were more common in the cariprazine groups versus the placebo group and occurred more frequently with cariprazine 3.0 mg than cariprazine 1.5 mg (akathisia was 5% to 6% versus 6% to 14% and restlessness was 1% to 3% versus 6% to 7% for the 1.5 mg dose group versus the 3.0 mg dose group, respectively). The frequency of AEs during a short treatment period of 3 weeks in the acute mania studies and up to 8 weeks in the acute depression studies, and with the high discontinuation rates in the studies, is notable, although comparable to other treatments for bipolar disorder as indicated by the clinical experts consulted by CADTH.
Weight gain (an increase in body weight of at least 7%) was captured in the safety assessment of vital signs. While the duration of the trials may not have been long enough to sufficiently assess the impact of the treatment of cariprazine on weight gain, this outcome was still observed in the trials. However, there was only a slight difference in weight gain between the cariprazine and placebo treatment groups.
Table 2: Summary of Key Results From Pivotal and Protocol Selected Studies — Bipolar Mania
Event | RGH-MD-31 study | RGH-MD-32 study | RGH-MD-33 study | |||
|---|---|---|---|---|---|---|
CAR 3 mg to 12 mg N = 118 | Placebo N = 117 | CAR 3 mg to 12 mg N = 158 | Placebo N = 152 | CAR 3 mg to 6 mg N = 167 | Placebo N = 161 | |
Change from baseline to week 3 in YMRS total score (mITT population)a | ||||||
N (%) | 118 (100) | 117 (100) | 158 (100) | 152 (100) | 165 (98.8) | 160 (99.4) |
Baseline, mean (SD) | NA | NA | 32.3 (5.8) | 32.1 (5.6) | 33.2 (5.6) | 32.6 (5.8) |
Baseline, mean (SEM) | 30.6 (0.5) | 30.2 (0.5) | NA | NA | NA | NA |
Change from baseline, LSM (SE) | –13.3 (||||||) | –7.2 (||||||) | –19.6 (0.9) | –15.3 (0.9) | –18.6 (0.8) | –12.5 (0.8) |
LSM difference vs. placebo (95% CI) | –6.1 (–8.9 to –3.3) | Reference | –4.3 (–6.7 to –1.9) | Reference | –6.1 (–8.4 to –3.8) | Reference |
P value | < 0.0001 | Reference | 0.0004 | Reference | < 0.001 | Reference |
Change from baseline to week 3 in CGI-S total score (mITT population)a | ||||||
N (%) | 118 (100) | 117 (100) | 158 (100) | 152 (100) | 165 (98.8) | 160 (99.4) |
Baseline, mean (SD) | 4.7 (||||||) | 4.6 (||||||) | 4.6 (0.6) | 4.6 (0.6) | 4.8 (0.6) | 4.8 (0.7) |
Change from baseline, LSM (SE) | –1.4 (0.1) | –0.8 (0.1) | –1.9 (0.1) | –1.5 (0.1) | –1.9 (0.1) | –1.3 (0.1) |
LSM difference vs. placebo (95% CI) | –0.6 (–1.0 to –0.3) | Reference | –0.4 (–0.7 to –0.1) | Reference | –0.6 (–0.9 to –0.4) | Reference |
P value | 0.0001 | Reference | 0.0027 | Reference | < 0.001 | Reference |
YMRS response (≥ 50% reduction from baseline in YMRS total score) (mITT population)b | ||||||
n/N (%) | 57/118 (48.3) | 29/117 | 93/158 (58.9) | 67/152 | 100/165 (60.6) | 60/160 |
P valuec | 0.0002 | NA | 0.0097 | NA | < 0.001 | NA |
YMRS remission (YMRS total score ≤ 12) (mITT population)b | ||||||
n/N (%) | 49/118 (41.5) | 27/117 | 82/158 (51.9) | 53/152 | 74/165 | 47/160 |
P valuec | 0.0023 | Reference | 0.0025 | Reference | 0.003 | Reference |
Harms, n (%) (safety population) | ||||||
N (safety population) | 118 | 118 | 158 | 154 | 167 | 161 |
AEs | 101 (85.6) | 93 (78.8) | 127 (80.4) | 97 (63.0) | 131 (78.4) | 98 (60.9) |
SAEs | 4 (3.4) | 5 (4.2) | 5 (3.2) | 3 (1.9) | 7 (4.2) | 3 (1.9) |
WDAEs (from study treatment) | 17 (14.4) | 12 (10.2) | 15 (9.5) | 11 (7.1) | 15 (9.0) | 8 (5.0) |
Deaths | 0 | 0 | 0 | 0 | 1 (0.6) | 0 |
Notable harms, n (%) (safety population) | ||||||
Suicidal ideation | 0 | 1 (0.8) | 2 (1.3) | 2 (1.3) | 0 | 1 (0.6) |
EPS | 29 (24.6) | 11 (9.3) | 24 (15.2) | 3 (1.9) | 16 (9.6) | 8 (5.0) |
Akathisia | 22 (18.6) | 7 (5.9) | 35 (22.2) | 7 (4.5) | 29 (17.4) | 6 (3.7) |
Insomnia | 10 (8.5) | 3 (2.5) | 9 (5.7) | 8 (5.2) | 15 (9.0) | 15 (9.3) |
Sedation | 7 (5.9) | 1 (0.8) | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
Metabolic effects (metabolism and nutrition disorders) | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
Hyperglycemia (blood glucose increased) | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
Weight gain | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
Restlessness | 7 (5.9) | 1 (0.8) | 9 (5.7) | 1 (0.6) | 14 (8.4) | 8 (5.0) |
Vomiting | 10 (8.5) | 4 (3.4) | 16 (10.1) | 6 (3.9) | 14 (8.4) | 8 (5.0) |
Sexual dysfunction (libido decreased) | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
Tardive dyskinesia | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
Neuroleptic malignant syndrome | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
AE = adverse event; ANCOVA = analysis of covariance; CAR = cariprazine; CGI-S = Clinical Global Impression–Severity of Illness; CI = confidence interval; EPS = extrapyramidal symptom; LSM = least squares mean; mITT = modified intention-to-treat; NA = not applicable; SAE = serious adverse event; SD = standard deviation; SE = standard error; SEM = standard error of the mean; WDAE = withdrawal due to adverse event; vs. = versus; YMRS = Young Mania Rating Scale.
aAnalysis was based on an ANCOVA model for change from baseline, with treatment group and study centre as factors and baseline value for the outcome as a covariate.
bThe percentage of responders and of remitters was analyzed using logistic regression, with treatment group and baseline YMRS total score as explanatory variables.
cThe P value was not adjusted for multiple testing (i.e., the type I error rate was not controlled).
Source: Clinical Study Reports for study RGH-MD-31, study RGH-MD-32, and study RGH-MD-33.11-13
Table 3: Summary of Key Results From Pivotal and Protocol Selected Studies — Bipolar Depression
Event | RGH-MD-53 study | RGH-MD-54 study | RGH-MD-56 study | ||||||
|---|---|---|---|---|---|---|---|---|---|
CAR 1.5 mg N = 162 | CAR 3 mg N = 153 | Placebo N = 163 | CAR 1.5 mg N = 154 | CAR 3 mg N = 164 | Placebo N = 156 | CAR 1.5 mg N = 145 | CAR 3 mg N = 145 | Placebo N = 145 | |
Change from baseline to week 6 in MADRS total score (mITT population)a | |||||||||
N (%) | 162 (100) | 153 (100) | 163 | 154 (100) | 164 (100) | 156 | 145 (100) | 145 (100) | 141 |
Baseline, mean (SD) | 31.5 (4.3) | 31.4 (4.7) | 31.3 | 30.7 (4.3) | 31.0 (4.9) | 30.2 | 30.3 (4.4) | 30.6 (4.7) | 30.4 |
Change from baseline, LSM (SE) | –14.8 (0.76) | –14.1 (0.78) | –12.4 (0.75) | –15.1 (0.77) | –15.6 (0.76) | –12.6 (0.76) | –15.1 (0.8) | –13.7 (0.9) | –11.1 |
LSM difference vs. placebo (95% CI) | –2.5 | –1.8 | Reference | –2.5 | –3.0 | Reference | –4.0 | –2.5 | Reference |
P value | 0.0417 | 0.1051 | Reference | 0.0331 | 0.0103 | Reference | 0.003 | 0.1122 | Reference |
Change from baseline to week 6 in CGI-S total score (mITT population)a | |||||||||
N (%) | 162 (100) | 153 (100) | 163 | 154 (100) | 164 (100) | 156 | 145 (100) | 145 (100) | 141 |
Baseline, mean (SD) | 4.5 (0.6) | 4.5 | 4.5 | 4.5 | 4.5 | 4.5 | 4.4 | 4.4 | 4.4 |
Change from baseline, LSM (SE) | –1.5 (0.09) | –1.4 (0.09) | –1.2 | –1.6 (0.10) | –1.6 (0.09) | –1.3 | –1.4 (0.1) | –1.3 (0.1) | –1.0 |
LSM difference vs. placebo (95% CI) | –0.3 | –0.2 | Reference | –0.2 | –0.3 | Reference | –0.4 | –0.3 | Reference |
P value | 0.0417 | 0.1370b | Reference | 0.0714 | 0.0662 | Reference | 0.0132 | 0.1122b | Reference |
MADRS responders (≥ 50% reduction from baseline in MADRS total score) (mITT population)c | |||||||||
n (%) | 66 (40.7) | 65 (42.5) | 58 | 74 (48.1) | 85 (51.8) | 62 | 72 (49.7) | 65 | 45 |
OR (95% CI) | 1.2 | 1.3 | Reference | 1.4 (0.9 to 2.2) | 1.7 (1.1 to 2.6) | Reference | 2.10 (1.30 to 3.41) | 1.74 (1.07 to 2.82) | Reference |
P valued | 0.3383 | 0.2088 | Reference | 0.1300 | 0.0243 | Reference | 0.0024 | 0.0243 | Reference |
MADRS remitters (MADRS total score ≤ 10) (mITT population)c | |||||||||
n (%) | 42 (25.9) | 40 (26.1) | 32 | 51 (33.1) | 53 (32.3) | 36 | 53 (36.6) | 40 | 28 |
OR (95% CI) | 1.5 | 1.5 | Reference | 1.7 | 1.7 | Reference | 2.38 (1.38 to 4.09) | 1.59 (0.91 to 2.78) | Reference |
P valued | 0.1648 | 0.1625 | Reference | 0.0374 | 0.0391 | Reference | 0.0017 | 0.1048 | Reference |
Harms, n (%) (safety population) | |||||||||
N (safety population) | 167 | 158 | 165 | 157 | 165 | 158 | 146 | 146 | 145 |
AEs | 82 (49.1) | 78 (49.4) | 75 | 89 (56.7) | 102 (61.8) | 83 | 91 (62.3) | 91 | 79 |
SAEs | 1 (0.6) | 0 | 5 (3.0) | 2 (1.3) | 2 (1.2) | 2 (1.3) | 2 (1.4) | 2 (1.4) | 5 (3.4) |
WDAEs (from study treatment) | 5 (3.0) | 11 (7.0) | 5 (3.0) | 7 (4.5) | 9 (5.5) | 4 (2.5) | 12 (8.2) | 17 (11.6) | 15 (10.3) |
Deaths | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
Notable harms, n (%) (safety population) | |||||||||
Suicidal ideation | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
EPS | ||||||||| | ||||||||| | ||||||||| | 0 | 1 (0.6) | 1 (0.6) | ||||||||| | ||||||||| | ||||||||| |
Akathisia | 9 (5.4) | 15 (9.5) | 3 (1.8) | 10 (6.4) | 9 (5.5) | 5 (3.2) | 7 (4.8) | 21 (14.4) | 2 (1.4) |
Insomnia | ||||||||| | ||||||||| | ||||||||| | 7 (4.5) | 12 (7.3) | 11 (7.0) | 10 (6.8) | 17 (11.6) | 12 (8.3) |
Sedation | ||||||||| | ||||||||| | ||||||||| | 8 (5.1) | 5 (3.0) | 2 (1.3) | ||||||||| | ||||||||| | ||||||||| |
Metabolic effects (metabolism and nutrition disorders) | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
Hyperglycemia (blood glucose increased) | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
Weight gain | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
Restlessness | 4 (2.4) | 11 (7.0) | 5 (3.0) | 2 (1.3) | 12 (7.3) | 6 (3.8) | 4 (2.7) | 9 (6.2) | 5 (3.4) |
Vomiting | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
Sexual dysfunction (libido decreased) | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
Tardive dyskinesia | ||||||||| | ||||||||| | ||||||||| | 0 | 1 (0.6) | 0 | ||||||||| | ||||||||| | ||||||||| |
Neuroleptic malignant syndrome | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
AE = adverse event; CAR = cariprazine; CGI-S = Clinical Global Impression–Severity of Illness; CI = confidence interval; EPS = extrapyramidal symptom; LOCF = last observation carried forward; LSM = least squares mean; MADRS = Montgomery–Åsberg Depression Rating Scale; mITT = modified intention-to-treat; MMRM = mixed model of repeated measures; OR = odds ratio; SAE = serious adverse event; SD = standard deviation; SE = standard error; vs. = versus; WDAE = withdrawal due to adverse event.
aEstimates were derived from an MMRM with fixed factors (treatment group, pooled study centre, and visit), a covariate (baseline), and interactions (treatment group by visit and baseline by visit).
bThe P value tested after a failed prior test could not be interpreted for inference.
cThe P value for a between-treatment comparison at each visit was based on a logistic regression model, which included treatment group and the baseline MADRS total score value. The P value was from a z test. LOCF was used for imputation.
dThe P value was not adjusted for multiple testing (i.e., the type I error rate was not controlled).
Source: Clinical Study Reports for study RGH-MD-53, study RGH-MD-54, and study RGH-MD-56.14-16
Critical Appraisal
Appropriate methods of randomization were used, although there was the potential for unblinding or knowledge of treatment received due to AEs — most notably EPS and akathisia, which were more common in the cariprazine treatment groups relative to placebo. Treatment groups were well balanced in terms of baseline characteristics. Discontinuation rates were high in all included studies, but generally aligned with expectations for clinical trials for acute episodes of bipolar disorder. Overall discontinuation rates were balanced between treatment groups in most studies, except study RGH-MD-54 and study RGH-MD-56 where discontinuation was notably higher among the cariprazine 3.0 mg group. Discontinuation was also higher for patients in the placebo treatment group compared to cariprazine 1.5 mg in study RGH-MD-56. The imbalance in discontinuation rates in study RGH-MD-56 appears to be driven by discontinuation due to AEs and withdrawal of consent. In the bipolar mania studies, there was an imbalance in the reason for discontinuation due to AEs (more frequent with cariprazine) and insufficient therapeutic response (more frequent with placebo), which may have biased the safety and efficacy results in favour of cariprazine. Missing data were handled using the last observation carried forward (LOCF) approach (study RGH-MD-31) and the mixed model of repeated measures (MMRM) approach (all other studies). Both methods rely on the assumption that data are missing at random, which is likely not the case given the imbalance in reasons for discontinuation that have been described. However, the sponsor conducted a pattern-mixture model analysis that relies on the assumption that data are not missing at random. The results of the pattern-mixture model analysis were consistent with the results of the primary analysis. All studies implemented methods to control for multiplicity up to the secondary end point, which was the change from baseline in the CGI-S at week 3 (bipolar mania studies) and week 6 (bipolar depression studies). Study RGH-MD-31 and study RGH-MD-32 used a closed testing procedure to control for the type I error rate; study RGH-MD-33 and the 3 bipolar depression studies used a matched parallel gatekeeping procedure. The analyses of the primary and secondary outcomes were the only outcomes controlled for multiplicity. Therefore, all other efficacy outcomes are at risk of type I error and viewed as supportive evidence only.
The clinical experts described the patient population included in the trials for cariprazine as typical for clinical trials, but lacking characteristics that are often seen in clinical practice such as the presence of comorbidities, rapid cycling, other diagnoses, comorbid substance use disorder, and elevated risk of suicide. The exclusion criteria can lead to a less severe and less complex sample relative to clinical practice. The clinical experts indicated that the baseline characteristics were suggestive of a patient population with bipolar I disorder of moderate severity. Overall, clinical experts did not have any major issues with the generalizability of the study populations to Canadian patients experiencing acute episodes associated with bipolar I disorder based on the baseline characteristics considered as a whole. In study RGH-MD-31 and study RGH-MD-32, the permitted dose of cariprazine ranged from 3 mg to 12 mg daily, which extends beyond the Health Canada–approved dose of up to 6 mg cariprazine daily. As such, specific conclusions regarding the effects of the Health Canada–approved dosing cannot be drawn based on these 2 studies. However, study RGH-MD-33 provided evidence for cariprazine at a dose that was consistent with the Health Canada indication (3 mg to 6 mg treatment group), which demonstrated a similar treatment effect to the higher doses used in study RGH-MD-31 and study RGH-MD-32. Dosing was consistent with the approved indication in all other studies included in this review. The studies for bipolar mania involved rapid titration that is inconsistent with how this drug is expected to be used by most patients treated in an outpatient setting. Generalizing the efficacy, safety, and tolerability outcomes observed in the trials to an outpatient setting for the treatment of acute mania is associated with some uncertainty. Another consideration for the intervention is that the clinical experts indicated it is unlikely for cariprazine to be used only for the acute management of episodes associated with bipolar I disorder. While the duration of the trials was considered adequate to observe a treatment effect on an acute episode, they were too short to properly assess safety and tolerability or efficacy beyond 3 weeks (bipolar mania studies) and 6 weeks to 8 weeks (bipolar depression studies). Lastly, all of the outcomes used in the studies are commonly used in clinical trials or research settings for bipolar I disorder. None of the included outcomes are designed for or typically used in clinical practice as per feedback from the clinical experts.
Indirect Comparisons
Description of Studies
One network meta-analysis (NMA) submitted by the sponsor17 and 2 published NMAs18,19 that examined the comparative efficacy, safety, and tolerability of acute treatments for bipolar I disorder were included in this report. All of the NMAs conducted a systematic review of RCTs in adults either with acute bipolar mania (Kishi et al. [2021]),18 acute bipolar depression (Kadakia et al. [2021]),19 or both populations (sponsor-submitted NMA).17 The sponsor-submitted NMA performed separate analyses for the bipolar mania and depression populations. All of the included NMAs specified treatments for acute episodes of bipolar I disorder |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||. Note that Kadakia et al. was limited to atypical antipsychotic drugs and recent publications (since May 2015). The sponsor-submitted NMA was conducted using a |||||||||||||||||||||||||||, the publication by Kishi et al. performed both pairwise and frequentist NMAs using a random effects (RE) model, and Kadakia et al. performed an NMA with a Bayesian approach where the base case was based on an RE model.
Efficacy Results
A total of ||||||||| studies were included in the sponsor-submitted NMA: ||||||||| studies in the manic or mixed bipolar I disorder patient population and ||||||||| studies in the depressive bipolar I disorder patient population. |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||.
For the acute mania NMAs, ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||. The analysis of change from baseline in the YMRS score ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| but this network was associated with evidence of inconsistency, statistical heterogeneity, and imprecision of the results, and, therefore, uncertainty about any conclusions that could be drawn.
For the acute depression NMAs, MADRS response |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||. Further, the relative treatment effect in terms of |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||. The analysis of MADRS remission ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||. Of note, the presence of inconsistency for this network is unknown as inconsistency was not formally assessed. Additionally, it is unknown whether variability in the baseline MADRS score influenced the results of the NMA. The analysis of change from baseline in MADRS |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||.
The results suggest weight gain (greater than 7%) |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||. However, these results were considered highly uncertain due to potential heterogeneity, a lack of precision (mania NMA), and bias resulting from a small number of events. Therefore, there is uncertainty about the conclusion of ||||||||||||||||||||||||||| in terms of weight gain.
Overall, the sponsor-submitted NMA |||||||||||||||||||||||||||||||||||| for treatment with cariprazine relative to other comparators of interest for the treatment of acute manic or mixed episodes or acute depressive episodes.
Harms Results
In the bipolar mania NMAs, the analysis of the rate of EPS as well as sedation or somnolence |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||. In the bipolar depression NMAs, ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||. This comparison was limited to aripiprazole and lurasidone as comparators. The analysis of the rate of sedation or somnolence suggested ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| in the rate of sedation or somnolence was reported for other comparisons of cariprazine 1.5 mg or cariprazine 3.0 mg and other treatments.
In the bipolar mania NMAs, all-cause discontinuation and discontinuation due to AEs were limited by evidence of inconsistency and substantial statistical heterogeneity. The results of the analysis suggest cariprazine ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||.
Critical Appraisal
Studies that included patients with a dual diagnosis of substance use disorder, or that investigated an intervention not used as monotherapy, were excluded from the systematic review, which may have resulted in missing potentially relevant patients and interventions. The study design was limited to double-blind RCTs and the quality of the studies was assessed using the National Institute for Health and Care Excellence (NICE) checklist and the Jadad rubric. It is unclear how the quality assessment was used and the Jadad rubric is not considered to be a reliable tool for assessing study quality. An insufficient quality assessment may have resulted in the inclusion of low-quality trials. Additionally, a sensitivity analysis for the quality of data was not performed.
Variation in the health care setting — particularly among the studies for manic or mixed episodes and publication year, which ranged from 1991 to 2019 — are potential sources of heterogeneity among the included studies. Baseline patient characteristics, including age, sex, race, HAM-D score, MADRS score, YMRS score, CGI-S score, and time since diagnosis, lacked important details and were subject to a large amount of missing data, hindering the ability to conduct a robust assessment of heterogeneity in the study populations. As a result, no studies were excluded based on outliers in the baseline characteristics and it is unknown if the NMA was impacted by heterogeneity among the included patient populations. Inconsistency was assessed using a node-splitting approach, which is an appropriate statistical assessment of inconsistency, although it does not incorporate information from the entire network in the analysis. Evidence of inconsistency was identified in the following networks of the manic or mixed episodes studies: change from baseline in YMRS, all-cause discontinuation, and discontinuation due to AEs. For the NMAs of outcomes in depressive studies, the author of the sponsor-submitted report stated that inconsistency could not be assessed for the following networks: MADRS remission, weight gain, EPS, and all-cause discontinuation. The author reported that evidence of inconsistency was not identified for the remaining outcomes in the networks. However, very wide 95% CIs for the inconsistency factor of comparisons in the NMA for the following outcomes may suggest otherwise: sedation or somnolence (manic or mixed and depressive), all-cause discontinuation (manic or mixed), and discontinuations due to AEs (manic or mixed and depressive).
Missing data were an issue for certain outcomes, in part due to a small number of studies in the NMAs. This issue was compounded by the fact that there were few events per study for some outcomes, which was the case for the analysis of EPS (both the manic or mixed network and the depressive network) and weight gain (the depressive network). |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||.
The 2 published NMAs summarized for this review18,19 were limited by insufficiently reported data and details about the methodology used, as well as the low quality of evidence informing the networks. As a result, this summary has focused on the sponsor-submitted NMA. Briefly, the results of the published NMAs were generally consistent with the sponsor-submitted NMA, although subject to similar and additional limitations.
Other Relevant Evidence
Two studies were included as other relevant evidence for the review of cariprazine. One was study RGH-MD-36,20 a long-term, open-label study that examined the long-term safety and tolerability of cariprazine 3 mg to 12 mg daily in patients with bipolar mania, and 1 was a post hoc analysis (McIntyre et al. [2019])21 that provided additional efficacy data on cariprazine in the subpopulation of patients with bipolar mania with mixed features.
Study RGH-MD-36
Description of Study
Patients were eligible to enrol in study RGH-MD-36 if they were not currently taking any treatment or had a documented history of intolerance or inadequate response to their current therapy. They were treated with a flexible dose of cariprazine for up to 16 weeks of treatment. During the screening period and for the first 2 weeks and up to 3 weeks of open-label treatment, all patients were hospitalized. At the end of week 3, all patients were discharged and followed as outpatients. Patients were discontinued from the study if they presented with clinical instability (by the end of week 3), with tolerability concerns, with worsening of symptoms, or with inadequate response, or if the investigator deemed it appropriate at any time to discontinue a patient.
All patients were required to have a total score of 18 or more on the YMRS and a total score of less than 18 on the MADRS. Further, a body mass index between ||||||||| kg/m2 and ||||||||| kg/m2, inclusive, was required. In comparison to the inclusion criterion regarding YMRS total score, the pivotal trials in bipolar mania (study RGH-MD-31,11 study RGH-MD-32,12 and study RGH-MD-3313) used a YMRS total score of 20 or more, and a score of 4 or more on 2 of the 4 following YMRS items: irritability, speech, content, and disruptive/aggressive behaviour.
Of the 403 patients who enrolled in the long term open-label study, a total of 402 patients received at least 1 dose of open-label cariprazine (safety population). The mean age of patients in the study was 41.4 (SD = 10.5) years. The majority of patients was male (57.2%) and White (51.2%). At baseline, the mean weight and body mass index was 86.5 (SD = 17.8) kg and 29.2 (SD = 5.3) kg/m2, respectively. The mean age at onset and the known duration of bipolar I disorder was 27.9 (SD = 11.3) years and ||||||||| (SD = |||||||||) months, respectively. The duration of the current manic episode for the majority of patients (53.2%) was greater than 21 days.
Efficacy Results
A total of 132 (32.8%) patients completed the study and ||||||||| patients entered safety follow-up. The most frequently reported reason for discontinuation during the open-label treatment period was withdrawal of consent (19.7%), followed by AE (16.4%), and protocol violation (13.7%).
The mean change from baseline to week 16 in YMRS total score was –15.2 (SD = 9.2) and the mean change from baseline to week 16 in MADRS total score was –1.6 (SD = 7.5). At week 16, YMRS response criteria (≥ 50% reduction from baseline) was met by 64.2% of patients and YMRS remission criteria (total score ≤ 12) was met by 63.4% of patients.
Harms Results
TEAEs were reported in 335 (83.3%) patients during the open-label treatment. The most commonly reported AEs (frequency ≥ 10%) were akathisia (32.6%), headache (16.7%), constipation (10.7%), and nausea (10.4%). SAEs were reported in 30 (7.5%) patients. The following SAEs were reported in more than 1 patient: the worsening of mania in 9 (2.2%) patients, depression in 5 (1.2%) patients, akathisia in 3 (0.7%) patients, suicidal ideation in 2 (0.5%) patients, and suicide attempt in 2 (0.5%) patients. The most severe suicidal ideation and suicidal behaviour per the C-SSRS was reported in 35 (8.8%) patients and 3 (0.8%) patients, respectively. No deaths were reported in the safety population. Premature discontinuation due to at least 1 AE was reported in 66 (16.4%) patients during the open-label treatment. The most frequently cited reason was akathisia in 19 (4.7%) patients and depression in 6 (1.5%) patients.
The most commonly reported notable harms (frequency ≥ 5%) included akathisia in 131 (32.6%) patients, insomnia in 28 (7.0%) patients, EPS in 27 (6.7%) patients, restlessness in 26 (6.5%) patients, vomiting in 24 (6.0%) patients, sedation in 23 (5.7%) patients, and increase in weight in 23 (5.7%) patients. A total of ||||||||| patients with at least 1 AE was related to extrapyramidal symptoms during open-label treatment. During the open-label treatment, 129 (32.1%) patients required treatment for extrapyramidal symptoms, of which 74 (18.4%) patients used a beta-blocking drug (propranolol or propranolol hydrochloride), 64 (15.9%) patients used an anti-Parkinson drug (benztropine mesylate or biperiden), and ||||||||| patients used a psycholeptic drug (diphenhydramine hydrochloride, diphenhydramine, or zolpidem tartrate).
Critical Appraisal
In the absence of an active comparator or placebo group, the interpretation of the efficacy results from the long-term open-label study RGH-MD-36 is limited. This is compounded by the use of descriptive statistics only. The use of the LOCF approach could overestimate or underestimate the overall long-term treatment benefits, particularly given the very high rates of discontinuation in the open-labelled study. Patients were discontinued from the study if they presented with clinical instability by the end of week 3, with any tolerability concerns, with worsening of symptoms, or with inadequate response, or if the investigator deemed it appropriate at any time to discontinue a patient. Consequently, the resultant population may be more tolerant of cariprazine, which could potentially lead to an underreporting of AEs and a response bias as patients with an inadequate response (defined as an increase in the YMRS or MADRS total score by 30% or more at the end of week 2 or thereafter) were prematurely discontinued from the study.
The clinical experts consulted by CADTH stated that the exclusion of patients with, for example, rapid cycling and active substance use disorder can lead to patients with complex cases who are seen in clinical practice being missed in the study. However, the clinical experts recognized that clinical trials will typically use said exclusion criteria to avoid confounding variables. There was a notable discontinuation rate of greater than 50%, which decreases the certainty and generalizability of the efficacy and safety results. According to the clinical experts, a discontinuation rate of approximately 35% is typically anticipated for clinical trials in bipolar mania. Further, some patients in the study received a dose higher than the Health Canada–recommended daily dose of cariprazine, which is up to 6 mg per day.
Post Hoc Analysis
Description of Study
Data from 3 pivotal trials of cariprazine in adult patients with acute manic or mixed episodes associated with bipolar I disorder were pooled and used for the post hoc analysis. The objective of the post hoc analysis was to determine the effect of cariprazine on manic and depressive symptoms versus placebo in the subpopulation of patients with mania and subsyndromal depressive features.
A total of 1,037 patients were pooled from the pivotal trials. The number of patients who met the DSM-5 criteria for mixed state (≥ 3 depressive symptoms) and the 2 proxy definitions for mixed episode (≥ 2 depressive symptoms and a MADRS total score ≥ 10) was 141 (13.6%), 269 (25.9%), and 453 (43.7%), respectively.
Results
The pooled placebo and active treatment groups showed an improvement in the mean YMRS total score at week 3 relative to baseline. The difference between cariprazine and placebo in change in mean YMRS total score was –3.79 (standard error [SE] = not reported [NR]; P = 0.0248), –2.91 (SE = NR; P = 0.0207), and –5.49 (SE = NR; P < 0.0001) in patients with mixed features as defined by 3 or more depressive symptoms, 2 or more depressive symptoms, and a MADRS total score of 10 or more, respectively, in favour of cariprazine.
The results of the change in mean MADRS total score at week 3 relative to baseline were inconsistent based on the definition used for patients with mixed features. There was a benefit with cariprazine based on the MADRS total score of 10 or more and no difference was observed using the other 2 definitions. The difference between cariprazine and placebo in change in mean MADRS total score was –1.59 (SE = NR; P < 0.0082) in patients with mixed features as defined by a MADRS total score of 10 or more, in favour of cariprazine.
The proportion of responders (≥ 50% improvement from baseline in the YMRS total score) was higher for cariprazine in the 2 or more depressive symptoms group (47%; P = 0.0483) and the MADRS total score of 10 or more group (57%; P = < 0.0001) than in the placebo group (34% and 31%, respectively). There was no difference between the cariprazine and placebo treatment groups (P = 0.2608), based on the 3 or more depressive symptoms definition for patients with mixed features.
The proportion of remitters (YMRS total score ≤ 12) was higher for cariprazine in the 2 or more depressive symptoms group (39%; P = 0.0462) and the MADRS total score of 10 or more group (44%; P = < 0.0001) than in the placebo group (27% and 23%, respectively). There was no difference between the cariprazine and placebo treatment groups (P = 0.1224) based on the 3 or more depressive symptoms definition for patients with mixed features.
Critical Appraisal
The pooled, post hoc analysis was summarized to supplement the evidence for patients experiencing mixed episodes associated with bipolar I disorder. The pooled analysis is subject to the same limitations of the bipolar mania studies included in the systematic review, in addition to a small sample size and a lack of power to detect a difference between treatment groups. Moreover, given the subgroups of interest were not included as stratification variables at randomization, differences in baseline characteristics between the groups would be expected to introduce bias into the results observed. Overall, the results of this analysis should be considered exploratory.
Conclusions
Six RCTs informed the systematic review of cariprazine. These included the 3 pivotal trials for the acute treatment of mania or mixed episodes of bipolar I disorder (study RGH-MD-31, study RGH-MD-32, and study RGH-MD-33) and 3 pivotal trials for the acute treatment of depressive episodes of bipolar I disorder (study RGH-MD-53, study RGH-MD-54, and study RGH-MD-56). The studies of acute mania or mixed episodes evaluated a flexible dose of cariprazine ranging from 3 mg to 12 mg once daily, and the studies of acute depressive episodes evaluated a fixed dose of cariprazine 1.5 mg and 3.0 mg once daily.
All 3 studies of acute mania demonstrated that treatment with cariprazine was associated with a statistically significant and clinically meaningful greater reduction in symptoms of acute mania relative to placebo, based on the YMRS total score after 3 weeks of treatment. This was supported by the results of the secondary end point, which demonstrated a greater reduction in overall disease severity after 3 weeks based on the CGI-S. The studies of acute bipolar depression demonstrated that treatment with cariprazine 1.5 mg was associated with a statistically significant and clinically meaningful greater reduction in symptoms of depression relative to placebo, based on the change in the MADRS total score at week 6. A dose response was not observed as cariprazine 3.0 mg did not consistently demonstrate a benefit relative to placebo, since the primary end point was not met in 2 of the 3 pivotal trials. The results of the secondary end point — change from baseline to week 6 in the CGI-S — were consistent with the primary analysis, except for 1 study (study RGH-MD-54) that did not demonstrate a benefit with cariprazine 1.5 mg relative to placebo. Additional efficacy outcomes were not controlled for multiplicity and should only be considered as supportive evidence. Additional outcomes were generally consistent with the primary and secondary analyses.
The frequency of AEs due to EPS, akathisia, vomiting, and restlessness were considered relevant safety concerns, although consistent with the safety profile of similar treatments. Both safety and efficacy outcomes may have been impacted by the high discontinuation rates across studies due to AEs, insufficient therapeutic response, and withdrawal of consent, which may have overestimated the reported results. Additionally, the short duration of the trials limited the ability to sufficiently evaluate certain outcomes such as weight gain. Direct comparisons to other available treatments were not identified, but uncertain evidence from 3 NMAs suggests that treatment with cariprazine offers ||||||||| relative to other second-generation antipsychotic drugs and relevant treatments as per YMRS and MADRS outcomes. Cariprazine may exhibit a different tolerability profile, but a conclusion about this cannot be drawn due to the uncertainty of the available evidence.
Introduction
Disease Background
Living with bipolar disorder is associated with a substantial burden of illness that people experience for approximately half of their lives.1 Bipolar disorder frequently manifests in late adolescence and young adulthood, with an overall average age of onset of 25 years.1 The typical age of onset differs geographically; it tends to be earlier in the US (18 years to 20 years) and Canada (22.5 years) and later in European countries (29 years).1-3 The estimated lifetime prevalence of bipolar I disorder in Canada is 0.87%, affecting males and females equally.1 Quality of life and psychosocial functioning (e.g., the ability to maintain proper work) are severely impacted by bipolar disorder and more pronounced in those living with depressive symptoms, in those with multiple previous episodes or a longer duration of illness, and in those with cognitive impairment.1 In addition, suicide risk is substantially higher for patients living with bipolar disorder relative to the general population (10.7 deaths due to suicide per 100,000 per year).1
Bipolar disorder is a mood disorder characterized by episodes of mania, hypomania, and major depression,3 and can be divided into 2 main diagnostic subtypes — namely, bipolar I disorder and bipolar II disorder. Bipolar I disorder involves the presence of at least 1 full manic episode, with features that include inflated self-esteem, the decreased need for sleep, pressured speech, racing thoughts, distractibility, psychomotor agitation, and risky behaviour.1 Bipolar II disorder involves a hypomanic episode, in which manic symptoms are brief or less severe and do not significantly impact functional impairment, hospitalization, or psychosis.
Episodes of mania and depression present with significant changes in mood, energy, behaviour, sleep, and cognition. Mania also presents with change in activity. To diagnose mania as per the DSM-5 criteria, abnormal and persistent elevated, expansive, or irritable mood, and abnormal and persistent increased activity or energy must present for most of the day, every day for 1 week minimum. In addition, the episode must have at least 3 of the symptoms of mania listed in Table 4. Also, the mood disturbance must lead to marked impairment in functioning, require hospitalization, or be accompanied by psychotic features.1,22 Episodes of bipolar depression are characterized by a minimum of 2 weeks of depressed mood and/or the inability to feel pleasure, and at least 4 of the symptoms listed in Table 4, as per the DSM-5.1,22 The DSM-5 includes specifiers that describe characteristics of bipolar disorder and can be used to guide treatment decisions for acute mania and depression. The presence of mixed features is a specifier, which describes a complex presentation of bipolar disorder.1 To qualify for the mixed features specifier, a patient must be experiencing at least 3 nonoverlapping symptoms from the opposing pole (mania or depression) during the majority of the days of the current episode.4
Table 4: Symptoms of Bipolar Mania and Depression
Symptoms of mania | Symptoms of depression |
|---|---|
| Changes in:
|
The diagnosis of bipolar disorder is challenging for many reasons, including a lack of insight from the individual into the psychopathology and functional impairment they are experiencing, the frequent onset of depressive states, and high rates of comorbidity, which all can lead to variation in help-seeking behaviour for hypomanic or manic periods.1,22 Misdiagnosis and delayed diagnosis are relatively common. Often, patients are not accurately diagnosed and may be treated for other disorders, especially unipolar depression, for up to 10 years from the onset of symptoms.1 It is very common for patients diagnosed with bipolar disorder to have comorbid psychiatric diagnoses, which increases the complexity of the illness and difficulty of making an accurate diagnosis. Common comorbidities include disorders of substance use, impulse control, anxiety, and personality.1 The clinical experts consulted by CADTH noted there are no diagnostic tools or tests that are useful, and the diagnosis is based on a clinical assessment centred on the criteria that has been described.
Standards of Therapy
There are no disease-modifying treatments for bipolar disorder. The clinical experts stated that the primary goal of current treatments is to improve acute symptoms and, by doing so, restore functioning. The prevention of recurrent mood episodes was described as the secondary goal, which can be achieved over the short-term to medium term (e.g., 6 months to 12 months) with current treatments, although more often for manic episodes than depressive episodes. Long-term efficacy is more unknown as high-quality longitudinal studies of longer duration are limited.
Bipolar disorder is treated with the combination of pharmacologic, nonpharmacologic (e.g., electroconvulsive therapy), and psychosocial (e.g., psychotherapy) treatments. In Canada, pharmacologic treatments are usually managed by family physicians in milder to moderate cases (which tend to be predominantly chronically depressed patients), or by psychiatrists in more severe cases (more presentations of mania or rapid cycling). However, the experts noted that there is a lot of regional variability as psychiatrists tend to be concentrated in urban settings.
Medications include mood stabilizers (which include drugs from a variety of classes, such as second-generation antipsychotic drugs, anticonvulsants, and lithium) and antidepressants. The 2018 CANMAT and ISBD guidelines list recommendations for the treatment of mania with considerations for safety and tolerability concerns, as efficacy is comparable among first-line options.1 For example, lithium is recommended unless there is a reason not to, such as mixed features, comorbid substance use, or previous nonresponse to lithium.1 The guidelines do not indicate a preference for monotherapy, noting that about 20% more patients respond to combination therapy based on clinical trial data than with monotherapy. The clinical experts described the use of lithium with other drugs as common in clinical practice. The 2018 CANMAT guidelines provide more guidance for the optimization of therapy for patients experiencing bipolar depression. The guidance takes into consideration current and prior medication use and response, personal preference, safety and tolerability, and clinical features that may influence prognosis. The clinical experts stated that overall, there are many different options of medications, with no consensual first or best option in clinical practice. The choice is usually guided by characteristics of the patient, including, but not limited to, predominant symptomatology or polarity (mania, depression, or mixed features), age, income, and medical and psychiatric comorbidities. Of note, the 2018 CANMAT guidelines list cariprazine as the last or second-last option for first-line monotherapy treatment of acute mania and acute depression, while also noting that safety concerns have a limited impact and tolerability concerns have a minor impact on the selection of cariprazine for treatment. The clinical experts suggested that the lack of evidence for the use of cariprazine as maintenance therapy is a limitation of its use. However, they also noted that a benefit of cariprazine is the potential to treat both acute mania and acute depression. Additionally, while the 2021 CANMAT guidelines specific to bipolar disorder with mixed presentations do not include any first-line treatment options due to insufficient evidence in this population, cariprazine is recommended as a second-line treatment option for acute mania with mixed features.4
The clinical experts indicated that the use of off-label drugs for mania is less common as there are several drugs approved for use in Canada with level 1 evidence of efficacy for the treatment of mania. For reference, the 2018 CANMAT guidelines define level 1 data as evidence based on a meta-analysis with a narrow CI or replicated, double-blind RCT that includes a placebo or active control comparison with at least 30 participants in each active treatment arm.1 In contrast, the experts indicated that there are only a few drugs with Health Canada approval and/or level 1 evidence of efficacy for the management of depressive episodes, and they are associated with relatively high rates of treatment failure due to insufficient response or poor tolerability. As a result, the use of drugs without approval for bipolar depression is common. For example, the experts noted that antidepressants are widely used in the real world, despite limited evidence of their efficacy and the fact that most treatment guidelines only recommend them as second-line or third-line options. Given the overall low response and remission rates of pharmacologic therapy in bipolar disorder, most patients use combinations of 2 to 3 different drugs — usually of mechanistically distinct drugs (e.g., an antipsychotic, lithium, and an antidepressant). Monotherapy is preferred, but harder to sustain in the real world.
Drug
Cariprazine is an atypical antipsychotic drug that has been approved by Health Canada for use in adults as monotherapy for the acute management of manic or mixed episodes associated with bipolar I disorder (bipolar mania) and the acute management of depressive episodes associated with bipolar I disorder (bipolar depression).5 The mechanism of action for cariprazine is unknown; however, it may be mediated through partial agonist activity at the central dopamine D3 and D2 receptors, and serotonin 5-HT1A receptors. Cariprazine also has antagonist activity at serotonin 5-HT2A receptors.5 Cariprazine forms 2 major metabolites, desmethyl cariprazine and didesmethyl cariprazine, that have in vitro receptor binding profiles similar to the parent drug. The drug and its active metabolites have an extended half-life of 2 days to 4 days for cariprazine, 1 day to 2 days for desmethyl cariprazine and 1 week to 3 weeks for didesmethyl cariprazine.5
Cariprazine is available as 1.5 mg, 3 mg, 4.5 mg, and 6 mg oral capsules administered once daily.5 The recommended dosage of cariprazine depends on the type of bipolar disorder — bipolar mania or bipolar depression. For bipolar mania, the suggested initial dosage is 1.5 mg to 6 mg once daily. Depending on clinical response and tolerability, subsequent dose increases may be made in 1.5 mg increments to a maximum of 6 mg daily for bipolar mania, although the lowest effective dose should be used.5 For bipolar depression, the recommended dosage is 1.5 mg once daily, which may be increased to 3 mg daily on day 15 depending on clinical response and tolerability. The lowest effective dose should be used and the maximum recommended dosage for bipolar depression is 3 mg daily.5 Due to the long half-life of the drug and its active metabolites, changes in dosage will not be fully reflected in the plasma for several weeks; thus, treatment response and the occurrence of adverse effects may be delayed following initiation and after a dosage change.5
The sponsor has requested reimbursement as per the indication.6 Cariprazine has been previously reviewed by CADTH for the treatment of schizophrenia in adults. Cariprazine is also approved by Health Canada for the treatment of schizophrenia in adults.
Table 5: Key Characteristics of Treatments for Bipolar I Disorder
Drug | Bipolar disorder indicationa | Oral recommended dosage in adults (as monotherapy) | Other |
|---|---|---|---|
Second-generation antipsychotic drugs | |||
Cariprazine | Acute management of manic or mixed episodes and depressive episodes associated with BD1 in adults | Manic episodes: Flexible dosing, 1.5 mg to 6 mg once daily Depressive episodes: 1.5 mg per day (maximum 3.0 mg per day) | — |
Aripiprazole | The treatment of manic or mixed episodes in BD1 in adults | 15 mg once daily (maximum 30 mg per day) | May be used as acute monotherapy or co-therapy with lithium or divalproex sodium |
Asenapine | The treatment of manic or mixed episodes in BD1 in adults | 5 mg twice daily (maximum 10 mg twice daily) | Sublingual tablet May be used as acute monotherapy or co-therapy with lithium or divalproex sodium |
Lurasidone | For the acute management of depressive episodes associated with BD1 | 20 mg once daily (maximum 60 mg per day) | As monotherapy or as adjunctive therapy with lithium or valproate |
Olanzapine | For the acute treatment of manic or mixed episodes in BD1. Demonstrated efficacy as maintenance treatment | 15 mg once daily; can be adjusted to 5 mg to 20 mg per day | Olanzapine may be used as monotherapy or co-therapy with drugs commonly used in the treatment of acute BD (e.g., lithium, divalproex sodium). |
Paliperidone | For the treatment of schizophrenia and related psychotic disorders | 3 mg to 6 mg; recommended dosage is 6 mg per day. Maximum of 12 mg per day | — |
Quetiapine | As monotherapy for the acute management of:
| Bipolar mania: 400 mg to 800 mg per day, administered in 2 divided doses Bipolar depression: 300 mg to 600 mg per day; recommended dosage is 300 mg per day | May be used as acute monotherapy or co-therapy with lithium or divalproex sodium |
Risperidone | As monotherapy for the acute management of manic episodes associated with BD1 | 1 mg to 6 mg per day | — |
Ziprasidone | For the treatment of acute manic or mixed episodes associated with BD | 40 mg to 80 mg twice daily, taken with food | — |
Other mood stabilizers | |||
Lithium | Treatment of mania episodes of manic-depressive illness. Maintenance therapy preventing or diminishing the frequency of subsequent relapses in bipolar manic-depressive patients (with a history of mania) | Acute mania: 600 mg to 1,800 mg per day in 3 divided doses | For acute mania, dose is individualized to the patient to obtain serum concentrations of between 0.8 mmol/L and 1.2 mmol/L The clinical experts indicated that lithium may also be administered as a single dose to reduce the risk of adverse renal outcomes. |
Divalproex | Treatment of the manic episodes associated with BD (DSM-III-R) | 1,000 mg per day to 2,500 mg per day, administered in 3 divided doses (maximum of 60 mg/kg per day) | — |
Other | |||
Carbamazepine | Monotherapy or as an adjunct to lithium in the treatment of acute mania or prophylaxis of bipolar (manic-depressive) disorders in patients who are resistant to or are intolerant of conventional antimanic drugs | 400 mg per day to 1,200 mg per day, administered in divided doses. Maximum dosage of 1,600 mg per day | A dosage higher than 800 mg per day is rarely required when given in combination with lithium or other treatments. |
Haloperidol | Management of manifestations of acute and chronic psychosis, including schizophrenia and manic states | 1 mg to 2 mg twice daily or 3 times per day up to 4 mg to 6 mg 3 times per day | A dosage of 30 mg to 40 mg daily may be required in severely disturbed patients who remain inadequately controlled. |
Clonazepam | Indication not specific to BD | Recommended dosage of 8 mg per day to 10 mg per day divided into 3 doses. Maximum dosage of 20 mg per day | — |
Chlorpromazine | Management of psychotic disorders such as schizophrenia | 25 mg to 75 mg daily in 2 to 4 divided doses or one 75 mg evening dosage (before sleep). The maximum daily dose is 1 g. | — |
BD = bipolar disorder; BD1 = bipolar I disorder; DSM-III-R = Diagnostic and Statistical Manual of Mental Disorders, Third Edition, Revised.
aHealth Canada–approved indication for acute treatment.
Source: Product monographs for cariprazine,5 aripiprazole,23 asenapine,24 lurasidone,25 olanzapine,26 paliperidone,27 quetiapine,28 risperidone,29 ziprasidone,30 lithium,31 divalproex,32 carbamazepine,33 haloperidol,34 clonazepam,35 and chlorpromazine.36
Stakeholder Perspectives
The information in this section is a summary of input provided by the patient groups and clinician groups that responded to CADTH’s call for patient input and from clinical experts consulted by CADTH for the purpose of this review.
Patient Group Input
This section was prepared by CADTH staff based on the input provided by patient groups.
Two responses to CADTH’s call for patient input were received for this review: a submission from IAM and a submission from MDSC. IAM and MDSC are organizations that support individuals living with mental illness such as bipolar disorder, including patients, their families, and service providers.
The information used to inform the IAM submission was based on 2 online surveys conducted in 2018 and February 2022. Potential respondents to these online surveys included members of the IAM and Hope and Me – Mood Disorders Association of Ontario client networks. Among the respondents of the 2018 survey, 12% self-described as personally diagnosed, 50% were caregivers, 63% were family members or friends of someone diagnosed, and 18% worked in social services. Among the respondents of the 2022 survey, 33% identified as an individual living with symptoms of bipolar disorder, 58% were relatives, 8% were caregivers of someone with lived experience, and 1% did not specify. MDSC drew information from interviews with patients and family members, 2 national mental health surveys conducted in 2018 and September 2021, and shared experiences that have been posted on the MDSC online discussion forum. The interviews were conducted with 5 patients with bipolar disorder, including semi-structured phone interviews with adults living with bipolar disorder in January 2021, and 3 family members.
Respondents indicated that living with bipolar disorder has impacted their mental health, social relationships, and day-to-day functioning at work and school. Patients can also experience a lack of insight into their illness, which impacts their ability and motivation to seek treatment and causes significant strain in relationships. Survey respondents described the advantages of taking medications for bipolar disorder, which include managing symptoms of bipolar disorder, experiencing fewer episodes of mental illness, and avoiding visits to the hospital. They also described disadvantages of taking medications for bipolar disorder; these include requiring frequent follow-ups with health care providers, needing to take the medication daily, and dealing with the symptoms — including bipolar depression, which was not being well controlled. Further, respondents described the benefits of an injectable formulation, which include convenience and not needing to remember to take it daily, while the difficulties were pain at injection site and frequent travel to clinics. The most common side effects of medications for bipolar disorder identified by respondents were drowsiness, dry mouth, restlessness, and weight gain. Respondents also identified the cost of medications as a significant barrier to access.
Survey respondents reported that treatment of bipolar disorder is individualized, as not every patient will respond to 1 medication. To find the right medication that enables the highest degree of functioning while minimizing side effects, patients with bipolar disorder often have to go through a trial-and-error process. This process involves taking a number of different medications and at different dosages until their goals of therapy have been achieved. This process can make it challenging for patients to adhere to their prescribed regimen and can be exacerbated by additional challenges such as waiting to be approved for coverage by public drug programs and experiencing relapse. As a result, patients feel that outcomes can be improved by increasing equitable access to, and the selection of, medications that are reimbursable. According to respondents, antipsychotic medications can be improved by increasing their ability to control the symptoms of bipolar disorder, improving the side effect profile, and providing a greater range of strengths and dosages to lower the frequency of administration.
A copy of the patient input from IAM and MDSC are presented in Appendix 5.
Clinician Input
Input From Clinical Experts Consulted by CADTH
All CADTH review teams include at least 1 clinical specialist with expertise regarding the diagnosis and management of the condition for which the drug is indicated. Clinical experts are a critical part of the review team and are involved in all phases of the review process (e.g., providing guidance on the development of the review protocol, assisting in the critical appraisal of clinical evidence, interpreting the clinical relevance of the results, providing guidance on the potential place in therapy). The following input was provided by 2 clinical specialists with expertise in the diagnosis and management of bipolar I disorder.
Unmet Needs
The clinical experts indicated that there are a number of challenges with addressing treatment goals for patients living with bipolar I disorder using currently available treatments. Insufficient response to treatment was noted as being very common, particularly in bipolar depression. Estimates vary, but around 50% of patients do not respond sufficiently well to the first option, and about 30% to 40% of patients will go on to develop treatment resistance (e.g., failure to respond to at least 3 drugs). As mentioned earlier, there are no disease-modifying treatments for bipolar disorder and the long-term effectiveness of current treatments is unclear. More often than not, bipolar disorder is a lifelong, persistent and/or highly recurrent condition. There are key outcomes that are not adequately addressed by current treatments. For example, the extent to which current treatments address cognition directly, instead of indirectly through mood symptoms, is unclear. Tolerability is a problem, particularly in bipolar depression, where the most effective drugs, like quetiapine and olanzapine, have well-known metabolic side effects, which are particularly concerning given the elevated, and independent, risk of metabolic and cardiovascular conditions in this population. Finally, adherence is also an issue; poor compliance is very common in real-world settings. All common first-line options for bipolar depression (e.g., quetiapine, lurasidone, lithium, lamotrigine) are daily oral medications, with no depot alternatives.
Place in Therapy
Based on the currently available clinical evidence, the clinical experts felt it was very unlikely that cariprazine would cause a shift in treatment paradigm, despite having a somewhat distinct pharmacologic profile. The experts indicated that the overall effect sizes, response and remission rates, and frequency of side effects of cariprazine are broadly similar to currently available treatments. Nonetheless, the experts noted that given the combination of efficacy for both acute mania and depression, as well as an acceptable tolerability profile, it is expected that cariprazine will eventually be used as a first-line treatment. Additionally, the experts did not identify any reason to recommend that patients try other treatments before cariprazine. The clinical experts suggested cariprazine will probably be used in monotherapy and in combination with either lithium or anticonvulsants, which is a standard approach with the use of second-generation antipsychotic drugs in bipolar disorder. In addition, the clinical experts noted that cariprazine was not developed based on a model of the pathophysiology of bipolar disorder; it is mechanistically very similar to currently available treatment and, therefore, very much within the current paradigm of symptomatic management.
Patient Population
At this time, the clinical experts stated that it is not possible to identify patients who are most likely to exhibit a response to treatment with cariprazine. They noted that reliable prediction of response has not been achieved even with sophisticated research methods (e.g., genomics, neuroimaging), and certainly cannot be done reliably with the most widely available clinical tools. Other than polarity of mood episode, there are no other validated indices to predict response to any given drug, according to the clinical experts. They also referred to several studies that have assessed potential clinical and biologic predictors of response to pharmacologic treatment, but noted the findings are mostly inconsistent and nonspecific. Further, the experts indicated that even the presence of psychotic symptoms is not a reliable predictor, as patients with no history of psychosis are known to potentially respond to antipsychotic drugs. In practice, the experts stated that the choice of treatment is guided by patients’ characteristics and preference but is fundamentally a trial-and-error approach. Overall, the experts had not identified anything that would indicate specific subpopulations are more or less likely to respond to cariprazine based on the currently available clinical data.
The experts indicated that it is challenging to identify and diagnose patients with bipolar disorder, and that misdiagnosis and/or delayed diagnosis are relatively common. Further, the experts noted that it is well-documented that most patients are initially treated as patients with unipolar depression — even for years, in some situations — before receiving the diagnosis of bipolar disorder. Relatedly, they stated there are no diagnostic tools or tests that are useful, and the diagnosis is based on clinical assessment.
The clinical experts stated that presymptomatic patients should not be treated with cariprazine, or any other drug, mostly due to the low predictive power of current assessment tools (i.e., it is not possible to predict the development of bipolar disorder with a high degree of confidence — even in a person with a confluence of well-known risk factors, such as first-degree family history, early onset of symptoms, or history of trauma).
The clinical experts did not identify any patients who would be least suited for treatment with cariprazine, noting that within the population of adults with bipolar I disorder, there were no major contraindications (other than the usual for this population) for cariprazine.
Assessing Response to Treatment
The clinical experts identified YMRS, MADRS, and HAM-D as the most commonly used outcomes to assess response to treatment in research settings, largely due to the fact that they are clinician-administered. They also reported that in the real world, patient-rated questionnaires like the Patient Health Questionnaire and the Beck Depression Inventory are more common. The experts noted that all of these outcomes, however, have very good concurrent validity.
A reduction in the frequency or severity of symptoms, improvement in symptoms, stabilization (no deterioration) of symptoms, ability to perform activities of daily living, and improved survival were all clinically meaningful according to the clinical experts. They described a reduction in the severity of symptoms (e.g., controlling physical agitation) and frequency of symptoms as the usual first goal of treatment. The experts described research studies that typically use a threshold of improvement of 25% to 50%, but noted that most clinicians rely on subjective reports; therefore, the magnitude that is considered meaningful does vary a lot across physicians. Subsequently, the experts stated that treatment aims to restore functioning — including improving cognitive functioning and coping skills — with a return to work, school, and/or daily activities being an important benchmark. The experts described long-term goals, such as the prevention of relapses and recurrences, as well as the onset and progression of psychiatric comorbidities (e.g., anxiety disorders, substance abuse) and medical comorbidities (e.g., obesity, diabetes).
Regarding how often treatment response should be assessed, the clinical experts suggested that in the acute phase, response is usually assessed between 2 weeks and 4 weeks, depending on the severity. In the maintenance phase, it is recommended that patients be assessed at least every 2 months to 3 months.
Discontinuing Treatment
The clinical experts indicated that treatment discontinuation is determined by either a lack of response or poor tolerability, noting that most guidelines recommend discontinuing a treatment if there is no response to very poor response within 4 weeks to 6 weeks. Further, they indicated that discontinuation due to tolerability depends on the severity and progression of specific side effects — particularly EPS and akathisia, which are the most common side effects of cariprazine and similar drugs. These side effects can be time-dependent; they tend to be worse during initial titration phases but improve with time. If side effects are moderate to severe and/or do not meaningfully improve in 1 week to 2 weeks, treatment should be discontinued.
Prescribing Conditions
The clinical experts reported that family physicians can and frequently do diagnose bipolar disorder and regularly prescribe similar drugs. The experts also noted that there are no special tests required for the diagnosis of bipolar disorder, nor for the prescription and monitoring of cariprazine. Given the high prevalence of bipolar disorder and the relative lack of psychiatrists in Canada, a significant proportion of patients are treated by family physicians; therefore, requiring the involvement of specialists would significantly restrict the use of this medication.
Clinician Group Input
This section was prepared by CADTH staff based on the input provided by patient groups.
Two clinician groups provided input to this review: CANMAT and WC-CAN. One clinician on behalf of CANMAT and 6 clinicians with the WC-CAN contributed to these submissions. Both clinician groups recognized the unmet need for a medication that is effective in multiple phases of bipolar disorder, including bipolar depression, with low rates of AEs to minimize polypharmacy and improve adherence. Both clinician groups advocated for cariprazine as a first-line treatment option for patients with bipolar disorder in the treatment of acute mania and depression and to be used as monotherapy and possibly as combination therapy with other mood stabilizers.
Drug Program Input
The drug programs provide input on each drug being reviewed through CADTH’s reimbursement review processes by identifying issues that may impact their ability to implement a recommendation. The implementation questions and corresponding responses from the clinical experts consulted by CADTH are summarized in Table 6.
Table 6: Summary of Drug Plan Input and Clinical Expert Response
Drug program implementation questions | Clinical expert response |
|---|---|
Initiation of therapy | |
Are the YMRS, MADRS, and HAM-D scoring systems used in clinical practice and, if not, will these pose a challenge if included in eligibility criteria? Participants in the bipolar mania studies had a baseline YMRS of ≥ 20 (with a score of ≥ 4 on at least 2 of these items: irritability, speech, content, and disruptive/aggressive behaviour) and a MADRS of < 18. The participants in the bipolar depression studies had a HAM-D ≥ 20 with a HAM-D item 1 score ≥ 2. Assuming these scores are not applicable to eligibility criteria, it would be helpful for CDEC to outline what will be acceptable documentation of diagnosis. An example is a statement of confirmed diagnosis from a family physician or from a psychiatrist. | The clinical experts indicated that the YMRS, MADRS, and HAM-D are mostly used in research settings, largely due to the fact that they are clinician-administered. In the real world, patient-rated questionnaires like the Patient Health Questionnaire and the Beck Depression Inventory are more common. These all, however, have very good concurrent validity. Regarding confirmation of a diagnosis of bipolar I disorder, the clinical experts indicated that there are no diagnostic tools or tests that are useful and, therefore, the diagnosis is based on clinical assessment. The clinical experts indicated that due to the high prevalence of bipolar disorder and insufficient number of psychiatrists in Canada, it is appropriate for a family physician or a psychiatrist to confirm a diagnosis. Additionally, the experts noted that this is consistent with current clinical practice, where family physicians frequently diagnose patients with bipolar disorder and prescribe similar drugs to cariprazine. |
Will this be considered for use as first-line treatment or for use upon the failure of traditional, less expensive first-line drugs? | The clinical experts felt that the evidence for cariprazine suggests that it is broadly similar to currently available treatments. However, given the combination of efficacy for both acute mania and depression, as well as the acceptable tolerability profile of cariprazine, it is expected to eventually be used as a first-line treatment. |
Generalizability | |
As the anticipated indication is for the treatment of patients in the acute setting, would patients who are currently stable on established therapy but who are having tolerability/safety concerns be eligible to switch to a trial of cariprazine? | The clinical experts indicated that this will depend on the severity and impact of the tolerability/safety concerns. There is always risk in switching treatments given that response to 1 drug does not guarantee response to another, even for those very mechanistically similar. Nonetheless, there are situations where the side effects from established drugs (e.g., weight gain from quetiapine, which can drastically impact health-related quality of life over the long-term, or akathisia from lurasidone, which patients often experience as a very distressful phenomenon) should justify a switch to cariprazine. |
It is not uncommon to see requests for patients with schizoaffective disorder, bipolar subtype. It would be helpful to know if these populations would be included or excluded from coverage or if treatment would be restricted to the subtypes as described in the indication? | One of the clinical experts reported they were unable to identify a reason why patients with schizoaffective disorder would respond to or tolerate cariprazine any differently than patients with bipolar disorder, noting the caveat that schizoaffective disorder is less common and, therefore, less studied than bipolar disorder. The clinical experts also reported that the treatment of schizoaffective disorders is more similar to the treatment of schizophrenia than to the treatment of bipolar disorder, noting that some studies with schizophrenia select a broad population that includes schizoaffective disorder (e.g., schizophrenia spectrum disorder). |
CDEC = CADTH Canadian Drug Expert Committee; HAM-D = Hamilton Depression Rating Scale; MADRS = Montgomery–Åsberg Depression Rating Scale; YMRS = Young Mania Rating Scale.
Clinical Evidence
The clinical evidence included in the review of cariprazine is presented in 3 sections. The first section, the systematic review, includes pivotal studies provided in the sponsor’s submission to CADTH and Health Canada, as well as those studies that were selected according to an a priori protocol. The second section includes indirect evidence from the sponsor and indirect evidence selected from the literature that met the selection criteria specified in the review. The third section includes sponsor-submitted long-term extension studies and additional relevant studies that were considered to address important gaps in the evidence included in the systematic review.
Systematic Review (Pivotal and Protocol Selected Studies)
Objectives
To perform a systematic review of the beneficial and harmful effects of cariprazine 1.5 mg, 3 mg, 4.5 mg, and 6 mg for use as monotherapy in adults for the acute management of manic or mixed episodes associated with bipolar I disorder (bipolar mania) and for the acute management of depressive episodes associated with bipolar I disorder (bipolar depression)
Methods
Studies selected for inclusion in the systematic review included pivotal studies provided in the sponsor’s submission to CADTH and Health Canada, as well as those meeting the selection criteria presented in Table 7. Outcomes included in the CADTH review protocol reflect outcomes considered to be important to patients, clinicians, and drug plans.
Of note, the systematic review protocol presented as follows was established before the granting of a Notice of Compliance from Health Canada.
Table 7: Inclusion Criteria for the Systematic Review
Criteria | Description |
|---|---|
Population |
Subgroups:
|
Intervention | Cariprazine (oral) as monotherapy, 1.5 mg, 3 mg, 4.5 mg, and 6 mg daily |
Comparator | Bipolar mania First-line treatment:
Second-line treatment:
Third-line treatment:
Bipolar depression First-line treatment:
Second-line treatment:
Third-line treatment:
|
Outcomes | Efficacy outcomes:
Harms outcomes:
|
Study designs | Published and unpublished phase III and phase IV RCTs |
AE = adverse event; HRQoL = health-related quality of life; RCT = randomized controlled trial; SAE = serious adverse event; WDAE = withdrawal due to adverse event.
aMay be used alone or in combination with other treatments (e.g., lithium, divalproex).
The literature search for clinical studies was performed by an information specialist using a peer-reviewed search strategy according to the PRESS Peer Review of Electronic Search Strategies checklist.37
Published literature was identified by searching the following bibliographic databases: MEDLINE All (1946–) via Ovid, Embase (1974–) via Ovid, and APA [American Psychological Association] PyscINFO (1806‒) via Ovid. All Ovid searches were run simultaneously as a multifile search. Duplicates were removed using Ovid deduplication for multifile searches, followed by manual deduplication in Endnote. The search strategy consisted of both controlled vocabulary, such as the US National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. The main search concept was Vraylar (cariprazine). Clinical trials registries were searched: the US National Institutes of Health’s ClinicalTrials.gov, the WHO’s International Clinical Trials Registry Platform search portal, Health Canada’s Clinical Trials Database, and the European Union Clinical Trials Register.
No filters were applied to limit the retrieval by study type. Retrieval was not limited by publication date or by language. Conference abstracts were excluded from the search results. Refer to Appendix 1 for the detailed search strategies.
The initial search was completed on March 8, 2022. Regular alerts updated the search until the meeting of the CADTH Canadian Drug Expert Committee on June 22, 2022.
Grey literature (literature that is not commercially published) was identified by searching relevant websites from the Grey Matters: A Practical Tool For Searching Health-Related Grey Literature checklist.38 Included in this search were the websites of regulatory agencies (US FDA and European Medicines Agency). Google was used to search for additional internet-based materials. Refer to Appendix 1 for more information on the grey literature search strategy.
These searches were supplemented by contacting the sponsor of the drug for information regarding unpublished studies.
Two CADTH clinical reviewers independently selected studies for inclusion in the review based on titles and abstracts, according to the predetermined protocol. Full-text articles of all citations considered potentially relevant by at least 1 reviewer were acquired. Reviewers independently made the final selection of studies to be included in the review, and differences were resolved through discussion.
Findings From the Literature
A total of 388 studies were identified from the literature for inclusion in the systematic review (Figure 1). The included studies are summarized in Table 8. No studies were excluded (Appendix 2).
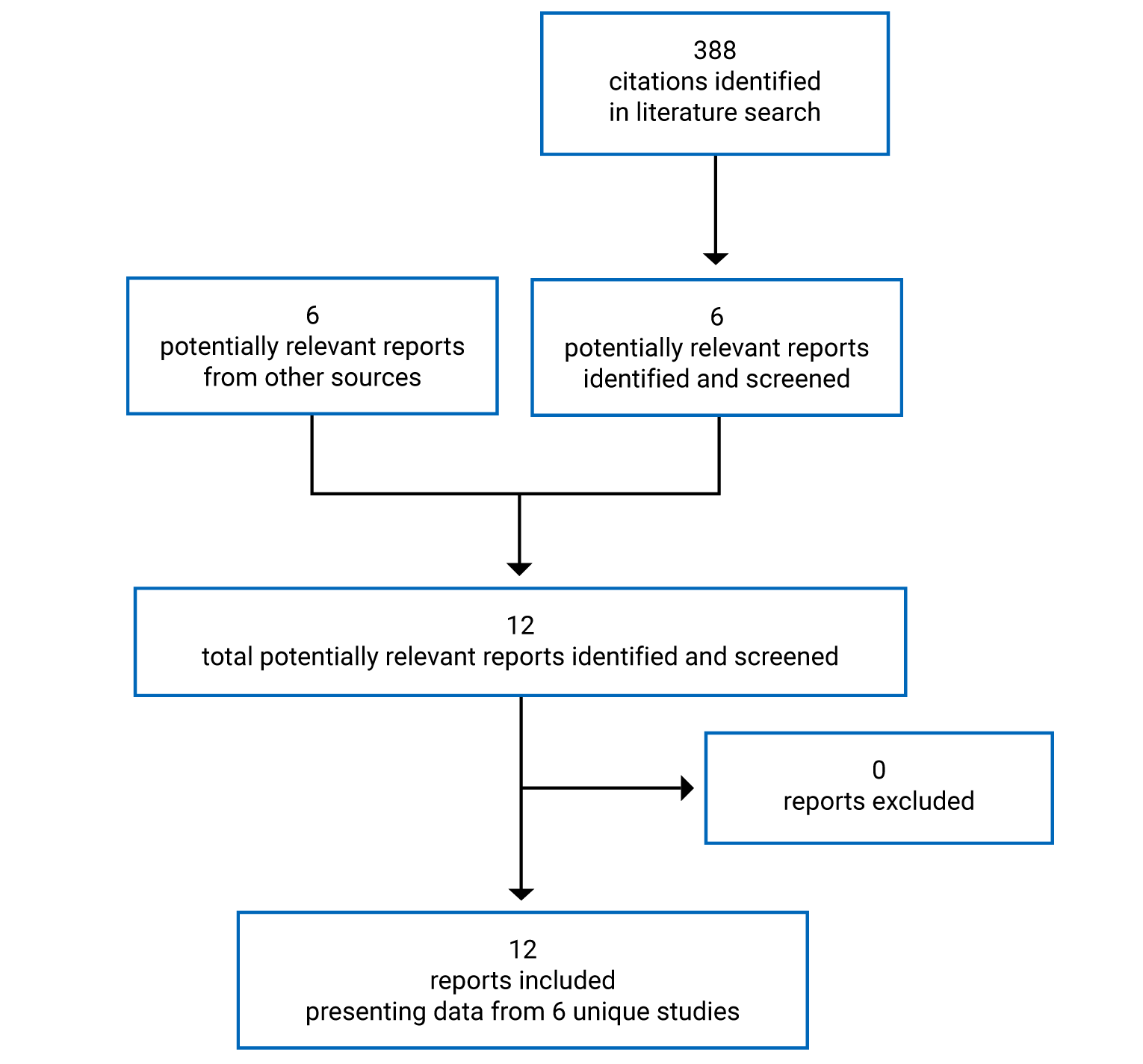
Table 8: Details of Included Studies for Bipolar Mania
Detail | RGH-MD-31 study | RGH-MD-32 study | RGH-MD-33 study |
|---|---|---|---|
Designs and populations | |||
Study design | Phase II, DB, parallel-group, flexible-dose RCT | Phase III, DB, parallel-group, flexible-dose RCT | Phase III, DB, parallel-group, flexible-dose RCT |
Locations | 32a centres in the US, India, and Russia | 28 centres in the US and India | 65 centres in the US and Eastern Europe (Ukraine, Romania, Russia, Serbia, and Croatia) |
Patient enrolment dates | Start date: June 2007 End date: July 2008 | Start date: February 2010 End date: July 2011 | Start date: February 2010 End date: December 2011 |
Randomized (N) | 238 | 312 | 497 |
Inclusion criteria |
| ||
Exclusion criteria |
| ||
Drugs | |||
Intervention | Cariprazine 3 mg to 12 mg (flexible dosing), oral administration, once daily | Cariprazine 3 mg to 12 mg (flexible dosing), oral administration, once daily | Cariprazine 3 mg to 6 mg (flexible dosing), oral administration, once daily Cariprazine 6 mg to 12 mg (flexible dosing), oral administration, once daily |
Comparator(s) | Placebo, oral administration, once daily | Placebo, oral administration, once daily | Placebo, oral administration, once daily |
Duration | |||
Phase | |||
Washout | Up to 4 days | 4 days to 7 days | 4 days to 7 days |
Double-blind | 3 weeks | 3 weeks | 3 weeks |
Follow-up | 2 weeks | 2 weeks | 2 weeks |
Outcomes | |||
Primary end point | YMRS total score, change from baseline to week 3 | ||
Secondary and exploratory end points | Secondary:
Exploratory:
Change from baseline to week 3:
| ||
Notes | |||
Publications | Durgam et al. (2015)39 | Sachs et al. (2015)40 | Calabrese et al. (2015)41 |
CGI-I = Clinical Global Impression–Improvement; CGI-S = Clinical Global Impression–Severity of Illness; DB = double-blind; DSM-IV-TR = Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition, Text Revision; ECT = electroconvulsive therapy; EPS = extrapyramidal symptom; MADRS = Montgomery–Åsberg Depression Rating Scale; NMS = neuroleptic malignant syndrome; PANSS = Positive and Negative Syndrome Scale; RCT = randomized controlled trial; TSH = thyroid-stimulating hormone; UDS = urine drug screen; YMRS = Young Mania Rating Scale.
Note: Three additional reports were included — Durgam et al. (2015),39 Sachs et al. (2015),40 and Calabrese et al. (2015).41
a3 of the study centres were discontinued before any patients had been consented and screened; 29 centres participated in the study.
bDSM-IV-TR Axis I diagnoses include delirium, dementia, amnestic disorder, and other cognitive disorders, as well as schizophrenia, schizoaffective disorder, and other psychotic disorders.
Source: Clinical Study Reports for study RGH-MD-31, study RGH-MD-32, and study RGH-MD-33.11-13
Table 9: Details of Included Studies for Bipolar Depression
Detail | RGH-MD-53 study | RGH-MD-54 study | RGH-MD-56 study |
|---|---|---|---|
Designs and populations | |||
Study design | Phase III, multi-centre, randomized, double-blind, placebo-controlled, parallel-group, fixed-dose study | Phase III, multi-centre, randomized, double-blind, placebo-controlled, parallel-group, fixed-dose study | Phase IIb, multi-centre, randomized, double-blind, placebo-controlled, parallel-group, fixed-dose study |
Locations | 85 study centres in the US and non-US (not specified) | 85 study centres in the US and non-US (not specified) | 86 study centres located in the US (41 centres), Canada (3 centres), Bulgaria (11 centres), Russia (17 centres), Ukraine (11 centres), and Colombia (3 centres) |
Patient enrolment dates | Start date: March 31, 2016 End date: March 18, 2018 | Start date: March 17, 2016 End date: July 19, 2017 | Start date: July 26, 2011 End date: January 10, 2014 |
Randomized (N) | 493 | 488 | 578 |
Inclusion criteria |
| Same as RGH-MD-53 |
|
Exclusion criteria |
| Same as RGH-MD-53 |
|
Drugs | |||
Intervention | Cariprazine 1.5 mg per day and 3.0 mg per day capsules, oral administration | Cariprazine 1.5 mg per day and 3.0 mg per day capsules, oral administration | Cariprazine 0.75 mg per day,a 1.5 mg per day, and 3.0 mg per day capsules, oral administration |
Comparator(s) | Matching placebo capsules, oral administration | Matching placebo capsules, oral administration | Matching placebo capsules, oral administration |
Duration | |||
Phase | |||
Run-in | 2 weeks | 2 weeks | 2 weeks |
Double-blind | 6 weeks | 6 weeks | 8 weeks |
Follow-up | 1 week | 1 week | 1 week |
Outcomes | |||
Primary end point | Change from baseline to week 6 in MADRS total score | Change from baseline to week 6 in MADRS total score | Change from baseline to week 6 in MADRS total score |
Secondary and exploratory end points | Secondary Change from baseline in:
Exploratory Change from baseline in:
| Same as RGH-MD-53 | Secondary Change from baseline in:
Exploratory Change from baseline in:
|
Notes | |||
Publications | Earley et al. (2020)42 | Earley et al. (2019)43 | Durgam et al. (2016)44 |
BMI = body mass index; BD = bipolar disorder; CGI-S = Clinical Global Impression–Severity of Illness; DSM-IV-TR = Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition, Text Revision; DSM-5 = Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition; ECT = electroconvulsive therapy; FAST = Functioning Assessment Short Test; HAM-A = Hamilton Anxiety Rating Scale; HAM-D = Hamilton Depression Rating Scale; MADRS = Montgomery–Åsberg Depression Rating Scale; MINI = Mini International Neuropsychiatric Interview; QIDS-SR = Quick Inventory of Depressive Symptomatology–Self-Rated; YMRS = Young Mania Rating Scale.
Note: Three additional reports were included — Earley et al. (2020),42 Earley et al. (2019),43 and Durgam et al. (2016).44
aExcluded from report.
Source: Clinical Study Reports for study RGH-MD-53, study RGH-MD-54, and study RGH-MD-56.14-16
Description of Studies
A summary of the details of included studies for bipolar mania and bipolar depression is available in Table 8 and Table 9, respectively.
Three pivotal trials for the treatment of acute manic or mixed episodes were identified for this review. These included 1 phase II study (study RGH-MD-31 [N = 238]) and 2 phase III studies (study RGH-MD-32 [N = 312] and study RGH-MD-33 [N = 497]). The objective of each of the 3 bipolar mania studies was to evaluate the efficacy, safety, and tolerability of cariprazine monotherapy versus placebo for the treatment of acute manic or mixed episodes associated with bipolar I disorder. Each of the studies was a multi-centre, randomized, double-blind, placebo-controlled, parallel-group, flexible-dose study in adults with a primary diagnosis of bipolar I disorder. Patients were enrolled in study RGH-MD-31 between 2007 and 2008, and in study RGH-MD-32 and study RGH-MD-33 between 2010 and 2011. None of the pivotal trials included study centres located in Canada.
Patients were randomized at a 1:1 ratio to 1 of 2 treatment groups in study RGH-MD-31 and study RGH-MD-32 — cariprazine 3 mg to 12 mg (flexible dose) or placebo. In study RGH-MD-33, patients were randomized at a 1:1:1 ratio to 1 of 3 treatment groups — cariprazine 3 mg to 6 mg, cariprazine 6 mg to 12 mg, or placebo. Randomization was not stratified in any of the studies. Data have not been presented for the cariprazine 6 mg to 12 mg group of study RGH-MD-33 as the dosage above 6 mg per day is not aligned with the Health Canada–approved indication.5
Each of the studies included a no-drug washout period during the screening phase (up to 4 days to 7 days) followed by a 3-week double-blind treatment period and a 2-week follow-up period. All patients started hospitalization during the screening phase and remained hospitalized for a minimum of 2 weeks (14 days) following the start of the double-blind treatment period. After 2 weeks, patients were permitted to be discharged and followed as outpatients if the following criteria were met: the severity of illness was mild or less (based on a score of 3 or less on the CGI-S), there was no significant risk of suicide or violent behaviour (based on investigator clinical judgment), and the patient was ready for discharge (based on investigator opinion). Patients who were not eligible for discharge could be re-evaluated any time after day 14 and before day 21. Additionally, following transitioning to an outpatient setting, patients could be re-hospitalized or placed in a day treatment program if necessary.
Three pivotal trials for the treatment of acute depressive episodes were identified for this review. These included 1 phase IIb study (study RGH-MD-56 [N = 578]) and 2 phase III studies (study RGH-MD-53 [N = 493] and study RGH-MD-54 [N = 488]). The objective of each of the 3 bipolar depression studies was to evaluate the efficacy, safety, and tolerability of cariprazine 1.5 mg per day and 3 mg per day versus placebo in patients with bipolar I depression. Each of the studies was a multi-centre, randomized, double-blind, placebo-controlled, parallel-group, fixed-dose study in adults with a primary diagnosis of bipolar I disorder. Patients were enrolled in study RGH-MD-31 between 2007 and 2008, and in study RGH-MD-32 and study RGH-MD-33 between 2010 and 2011. None of the study centres in study RGH-MD-53 or study RGH-MD-54 were located in Canada, while 3 centres in study RGH-MD-56 were located in Canada.
Patients were randomized at a 1:1:1 ratio to 1 of 3 treatment groups in study RGH-MD-53 and study RGH-MD-54 — cariprazine 1.5 mg per day, cariprazine 3.0 mg per day, or placebo. In study RGH-MD-56, patients were randomized at a 1:1:1:1 ratio to 1 of 4 treatment groups — cariprazine 0.75 mg per day, cariprazine 1.5 mg per day, cariprazine 3.0 mg per day, or placebo. Randomization was not stratified in any of the studies. Data have not been presented for the cariprazine 0.75 mg group of study RGH-MD-56 as the dosage is not aligned with the Health Canada–approved indication.5
Each of the studies included a 2-week no-drug washout period during the screening phase, followed by a 6-week or, in the case of study RGH-MD-56 only, 8-week double-blind treatment period and a 1-week follow-up period. In study RGH-MD-53 and study RGH-MD-54, patients may have been hospitalized for up to 7 days during the screening period or during the first week of the double-blind treatment period. In study RGH-MD-56, patients may have been hospitalized for up to 2 weeks following the start of the double-blind treatment period.
Populations
Inclusion and Exclusion Criteria
A list of inclusion and exclusion criteria for bipolar mania and bipolar depression is available in Table 8 and Table 9, respectively.
All studies enrolled adult patients (18 to 65 years of age) with bipolar I disorder with or without psychotic symptoms as per the criteria of the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition, Text Revision (DSM-IV-TR) (studies for bipolar mania) or without psychotic features as per the DSM-5 (studies for bipolar depression). Diagnosis was confirmed by the administration of either the Structured Clinical Interview for DSM [Diagnostic and Statistical Manual of Mental Disorders] or the Mini International Neuropsychiatric Interview. In the bipolar mania studies, patients with comorbid diagnoses such as conduct disorder, obsessive-compulsive disorder, anxiety disorders, and substance abuse were eligible for enrolment.
In the bipolar mania studies, patients were required to have a YMRS total score of at least 20, a score of at least 4 on 2 of the 4 YMRS items (irritability, speech, content, and disruptive/aggressive behaviour), and a MADRS total score of less than 18. Patients were also required to be voluntarily hospitalized with a primary diagnosis of mania. In the bipolar depression studies, patients were required to have a HAM-D total score of at least 20, a HAM-D item 1 score of at least 2, and a CGI-S score of at least 4. Patients also needed to have had a previous manic or mixed episode, verified by either treatment with an antipsychotic medication with an approved indication for mania, hospital or medical records, or a patient report corroborated by a caretaker or a previous or current treating clinician. Additionally, patients had be in the process of being treated as an outpatient, with a current major depressive episode of at least 4 weeks and not exceeding 12 months in duration.
All studies excluded patients if they had had another DSM-IV-TR or DSM-5 Axis I diagnosis or Axis II diagnosis severe enough to interfere with participation, or alcohol or substance abuse or dependence within the prior 3 months (studies for bipolar mania) or prior 6 months (studies for bipolar depression), suicide risk, or significant medical conditions that could interfere with the study or endanger the patient’s well-being. Additionally, patients who had received electroconvulsive therapy within 3 months of screening or a depot neuroleptic within 3 months of screening (studies for bipolar mania) or 6 months of screening (studies for bipolar depression) were excluded.
In the bipolar mania studies, patients were excluded if they were experiencing their first manic episode or met the criteria for rapid cycling. In the bipolar depression studies, patients were excluded if they had a YMRS total score of greater than 12 (or greater than 10 in study RGH-MD-56), 4 or more episodes of a mood disturbance (depression, mania, hypomania, or mixed state) within 12 months, or a history of nonresponse to 2 or more antidepressant trials of adequate dose and treatment duration with or without mood stabilizers in the current depressive episode. Additionally, patients were excluded from study RGH-MD-53 and study RGH-MD-54 if they experienced treatment failure of quetiapine, lurasidone, or Symbyax (fluoxetine and olanzapine) in the treatment of bipolar depression during the current depressive episode. Patients were excluded from study RGH-MD-56 if they had a history of nonresponse in the current depressive episode to 2 or more adequate treatment trials with Symbyax (fluoxetine and olanzapine), quetiapine (including monotherapy), lithium (including monotherapy), or a mood stabilizer (lithium, valproate, lamotrigine, carbamazepine, or oxcarbazepine) in combination with an antidepressant.
Baseline Characteristics
A summary of baseline characteristics in the bipolar mania studies is provided in Table 10.
In the bipolar mania studies, the mean age of patients was between 36 (SD = 11) years and 43 (SD = 12) years, between 54% and 68% of patients were male, and the mean weight of patients ranged from 70 (SD = 20) kg to 82 (SD = 16) kg. The distribution of patients by race varied between the 3 studies. In study RGH-MD-31, 40% to 47% of patients were White, 26% to 31% of patients were Black, and 24% to 25% of patients were Asian. In study RGH-MD-32, 57% to 58% of patients were Asian, and in study RGH-MD-33, 70% to 71% of patients were White. Patients with ongoing metabolic disorders ranged from 9% to 18% in the bipolar mania studies. In study RGH-MD-33, ongoing metabolic disorders were reported in 18% of patients randomized to cariprazine and 10% of patients randomized to placebo. The duration of bipolar I disorder was a mean of 10 (SD = 9) years to 15 (SD = 10) years and the age of onset ranged from 23 (SD = 8) years to 28 (SD = 10) years. During the trials, between 81% and 91% of patients were currently experiencing a manic episode and between 10% and 20% of patients were experiencing a mixed episode. The mean baseline efficacy scores are presented in Table 11. At baseline, the mean YMRS total score ranged from 30 (standard error of the mean = 0.5) to 33 (SD = 6), and the mean CGI-S score ranged from 4.6 (SD = 0.6) to 4.8 (SD = 0.7). Additionally, the mean MADRS total score at baseline ranged from 8.2 (SD = 4.1) to 9.6 (SD = 3.7) and the PANSS mean score at baseline ranged from 60.2 (standard error of the mean = 1.3) to 63.0 (SD = 14.9).
A summary of baseline characteristics in the bipolar depression studies is provided in Table 12. In the bipolar depression studies, the mean age of patients was between 41 (SD = 11) years and 44 (SD = 13) years, between 57% and 65% of patients were female, the mean weight of patients ranged from 80 (SD = 17) kg to 87 (SD = 25) kg, and 72% to 78% of patients were White. Between ||||||||| and ||||||||| of patients had a history of metabolic disorders. The duration of and age of onset of bipolar I disorder was not reported in study RGH-MD-53 or study RGH-MD-54. In study RGH-MD-56, the duration of bipolar I disorder ranged from 14.6 (SD = 9.5) years to 15.5 (SD = 10.3) years and the age of onset ranged from 25.4 (SD = 10.2) years to 28.4 (SD = 11.4) years. During study RGH-MD-53 and study RGH-MD-54, between 11% and 28% of patients were currently experiencing a severe depressive episode and between 71% and 89% were experiencing a moderate depressive episode, and the duration of the current episode was a mean of 3.5 (SD = 2.5) months to 3.9 (SD = 2.6) months. The proportion of patients with mild, moderate, or severe depressive episode (current or most recent) were not reported in study RGH-MD-56. The mean efficacy scores at baseline are presented in Table 13. At baseline, the mean MADRS total score ranged from 30.3 (SD = 4.4) to 31.5 (SD = 4.8), the mean CGI-S score ranged from 4.4 (SD = 0.5) to 4.5 (SD = 0.6), and the mean HAM-D score at baseline ranged from 23.9 (SD = 3.2) to 24.9 (SD = 2.9). Where available, the HAM-A score, QIDS-SR score, and FAST total score were also summarized (Table 13).
A summary of relevant prior medications used by patients in the bipolar mania studies and bipolar depression studies is available in Table 14 and Table 15, respectively.
Table 10: Summary of Baseline Characteristics — Bipolar Mania, Safety Population
Characteristic | RGH-MD-31 study | RGH-MD-32 study | RGH-MD-33 study | |||
|---|---|---|---|---|---|---|
CAR 3 mg to 12 mg N = 118 | Placebo N = 118 | CAR 3 mg to 12 mg N = 158 | Placebo N = 154 | CAR 3 mg to 6 mg N = 167 | Placebo N = 161 | |
Demographics | ||||||
Age, mean (SD) | 38.0 (10.3) | 38.7 (11.0) | 35.8 (11.4) | 36.7 (11.8) | 43.1 (12.2) | 41.5 (11.4) |
Sex, n (%) | ||||||
Female | 38 (32.2) | 41 (34.7) | 53 (33.5) | 59 (38.3) | 77 (46.1) | 72 (44.7) |
Male | 80 (67.8) | 77 (65.3) | 105 (66.5) | 95 (61.7) | 90 (53.9) | 89 (55.3) |
Race, n (%) | ||||||
White | 47 (39.8) | 55 (46.6) | 33 (20.9) | 33 (21.4) | 117 (70.1) | 114 (70.8) |
Black | 36 (30.5) | 31 (26.3) | 33 (20.9) | 29 (18.8) | ||||||||| | ||||||||| |
Asian | 30 (25.4) | 28 (23.7) | 91 (57.6) | 88 (57.1) | ||||||||| | ||||||||| |
Other | 5 (4.2) | 4 (3.4) | 1 (0.6) | 4 (2.6) | ||||||||| | ||||||||| |
Weight (kg), mean (SD) | 75.0 | 79.3 | 69.55 (20.1) | 71.86 (20.3) | 82.42 (16.2) | 81.70 (16.0) |
BMI (kg/m2), mean (SD) | 25.8 (5.9) | 27.2 (5.8) | 25.24 (6.0) | 25.73 (6.0) | 28.22 (5.3) | 27.99 (5.2) |
Medical history, n (%) | ||||||
Patients with ongoing abnormalities, n (%) | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
Cardiac disorders | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
Metabolic disorders | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
Diabetes mellitusa | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
Hypercholesterolemia | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
Obesity/overweight | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
Nervous system disorders | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
Psychiatric disorders | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
Psychiatric history | ||||||
Duration of bipolar I disorder (years), mean (SD) | 14.6 (9.1) | 14.8 (9.7) | 10.0 (9.1) | 10.9 (8.2) | 15.2 (10.5) | 13.5 (8.8) |
Age at onset (years), mean (SD) | 23.4 (8.1) | 23.9 (10.2) | 25.9 (10.4) | 25.8 (10.1) | 27.9 (11.3) | 28.0 (10.4) |
Duration of current episode, n (%) | ||||||
≤ 7 days | — | — | 18 (11.4) | 25 (16.2) | 20 (12.0) | 18 (11.2) |
> 7 days to ≤ 14 days | — | — | 77 (48.7) | 67 (43.5) | 68 (40.7) | 72 (44.7) |
> 14 days to ≤ 21 days | — | — | 18 (11.4) | 22 (14.3) | 25 (15.0) | 24 (14.9) |
> 21 days | — | — | 45 (28.5) | 40 (26.0) | 54 (32.3) | 47 (29.2) |
≤ 1 month | 71 (60.2) | 78 (66.1) | — | — | — | — |
> 1 month to 6 months | 45 (38.1) | 36 (30.5) | — | — | — | — |
> 6 months | 2 (1.7) | 4 (3.4) | — | — | — | — |
Duration of hospitalization for current episode (days), n (%) | ||||||
0 | ||||||||| | ||||||||| | — | — | — | — |
1 day to 7 days | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
8 days to 14 days | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
More than 14 days | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
Duration of hospitalization for current episode (days), mean (SD) | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
DSM-IV-TR diagnosis, n (%) | ||||||
Most recent episode, manic | 96 (81.4) | 95 (80.5) | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
Hypomanic/unspecified | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
Mild | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
Moderate | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
Severe without psychotic features | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
Severe with psychotic features | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
Most recent episode, mixed | 22 (18.6) | 23 (19.5) | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
Unspecified | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
Mild | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
Moderate | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
Severe without psychotic features | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
Severe with psychotic features | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
Pattern of episode, n (%) | ||||||
With full interepisode recovery | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
Without full interepisode recovery | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
Number of previous psychiatric hospitalizations, mean (SD) | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
Number of manic/mixed episodes during lifetime, mean (SD) | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
Number of depressed episodes during lifetime, n (%) | ||||||
0 | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
1 | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
2 | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
3 | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
4 | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
5 to 10 | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
> 10 | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
Number of patients with previous suicide attempts, n (%) | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
BMI = body mass index; CAR = cariprazine; DSM-IV-TR = Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition, Text Revision; SD = standard deviation.
aDiabetes mellitus: type 1 diabetes mellitus and type 2 diabetes mellitus.
bReported as 7 or fewer days (includes 0 days).
Source: Clinical Study Reports for study RGH-MD-31, study RGH-MD-32, and study RGH-MD-33.11-13
Table 11: Mean Baseline Efficacy Score — Bipolar Mania, Modified Intention-to-Treat Population
Efficacy parameter | RGH-MD-31 study | RGH-MD-32 study | RGH-MD-33 study | |||
|---|---|---|---|---|---|---|
CAR 3 mg to 12 mg N = 118 | Placebo N = 117 | CAR 3 mg to 12 mg N = 158 | Placebo N = 152 | CAR 3 mg to 6 mg N = 158 | Placebo N = 154 | |
YMRS total score, mean (SD)a | 30.6 (0.5) | 30.2 (0.5) | 32.3 (5.8) | 32.1 (5.6) | 33.2 (5.6) | 32.6 (5.8) |
CGI-S score, mean (SD)a | 4.7 (0.1) | 4.6 (0.1) | 4.6 (0.6) | 4.6 (0.6) | 4.8 (0.6) | 4.8 (0.7) |
MADRS total score, mean (SD)a | 9.0 (0.4) | 8.8 (0.4) | 8.3 (4.0) | 8.2 (4.1) | ||||||||| | ||||||||| |
PANSS, mean (SD)a | 60.2 (1.3) | 60.5 (1.5) | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
CAR = cariprazine; CGI-S = Clinical Global Impression–Severity of Illness; MADRS = Montgomery–Åsberg Depression Rating Scale; PANSS = Positive and Negative Syndrome Scale; SD = standard deviation; SEM = standard error of the mean; YMRS = Young Mania Rating Scale.
aFor study RGH-MD-31 only, SEM was reported instead of SD.
Source: Clinical Study Reports for study RGH-MD-31, study RGH-MD-32, and study RGH-MD-33.11-13
Table 12: Summary of Baseline Characteristics — Bipolar Depression, Safety Population
Characteristic | RGH-MD-53 study | RGH-MD-54 study | RGH-MD-56 study | ||||||
|---|---|---|---|---|---|---|---|---|---|
CAR 1.5 mg N = 167 | CAR 3 mg N = 158 | PBO N = 165 | CAR 1.5 mg N = 158 | CAR 3 mg N = 157 | PBO N = 165 | CAR 1.5 mg N = 146 | CAR 3 mg N = 146 | PBO N = 145 | |
Demographics | |||||||||
Age, mean (SD) | 42.2 (12.0) | 43.9 (11.8) | 44.6 (11.5) | 42.7 (12.1) | 41.9 (11.6) | 43.8 (12.6) | 40.9 (11.4) | 42.8 (10.8) | 43.6 (12.0) |
Sex, n (%) | |||||||||
Female | 107 (64.1) | 103 (65.2) | 97 (58.8) | 98 (62.4) | 94 (57.0) | 92 (58.2) | 92 (63.0) | 88 (60.3) | 89 (61.4) |
Male | 60 (35.9) | 55 (34.8) | 68 (41.2) | 59 (37.6) | 71 (43.0) | 66 (41.8) | 54 (37.0) | 58 (39.7) | 56 (38.6) |
Race, n (%) | |||||||||
White | 120 (71.9) | 117 (74.1) | 120 (72.7) | 123 (78.3) | 126 (76.4) | 115 (72.8) | 109 (74.7) | 113 (77.4) | 110 (75.9) |
Black | 41 (24.6) | 39 (24.7) | 45 (27.3) | 29 (18.5) | 37 (22.4) | 37 (23.4) | 30 (20.5) | 26 (17.8) | 30 (20.7) |
Asian | 3 (1.8) | 2 (1.3) | 0 | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
Other | 3 (1.8) | 0 | 0 | 3 (1.9) | 2 (1.3) | 3 (1.9) | 5 (3.4) | 7 (4.8) | 4 (2.8) |
Weight (kg), mean (SD) | 85.9 (21.5) | 83.5 (20.6) | 85.0 (20.3) | 86.8 (25.1) | 86.1 (20.0) | 86.6 (21.1) | 81.4 (16.8) | 81.5 (17.9) | 80.0 (17.1) |
BMI (kg/m2), mean (SD) | 29.8 (7.3) | 29.4 (7.4) | 29.7 (7.4) | 30.1 (8.3) | 29.8 (7.0) | 30.2 (6.9) | 28.4 (5.4) | 28.3 (5.6) | 27.8 (5.3) |
Medical history | |||||||||
System organ class or preferred term, n (%) | |||||||||
Cardiac disorders | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
Metabolic disorders, n (%) | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
Diabetes mellitusa | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
Hypercholesterolemia | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
Obesity/overweight | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
Nervous system disordersb | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
Psychiatric disordersc | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
Psychiatric history | |||||||||
Duration of bipolar I disorder (years), mean (SD) | NR | NR | NR | NR | NR | NR | 15.5 (10.3) | 14.6 (9.5) | 15.3 (10.2) |
Age at onset (years), mean (SD) | NR | NR | NR | NR | NR | NR | 25.4 (10.2) | 28.1 (11.0) | 28.4 (11.4) |
Bipolar I disorder, current or most recent episode depressed, n (%) | |||||||||
Mild | 3 (1.8) | 1 (0.6) | 0 | 0 | 1 (0.6) | 0 | NR | NR | NR |
Moderate | 118 (70.7) | 117 (74.1) | 130 (78.8) | 132 (84.1) | 143 (86.7) | 141 (89.2) | NR | NR | NR |
Severe | 46 (27.5) | 39 (24.7) | 33 (20.0) | 25 (15.9) | 21 (12.7) | 17 (10.8) | NR | NR | NR |
Duration of current episode of bipolar I disorder (months), n (%) | |||||||||
≤ 3.0 | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
> 3 to 6 | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
> 6 to 12 | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
> 12 | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
Mean (SD) | 3.6 (2.5) | 3.5 (2.5) | 3.7 (2.8) | 3.9 (2.6) | 3.6 (2.2) | 3.8 (2.5) | 3.7 (2.7) | 3.5 (2.4) | 3.3 (2.3) |
Number of manic/mixed episodes, mean (SD) | 3.8 (3.3) | 3.9 (5.0) | 4.5 (4.2) | 4.3 (4.7) | 4.6 (5.0) | 4.6 (6.7) | ||||||||| | ||||||||| | ||||||||| |
Number of depressive episodes, mean (SD) | 6.8 (7.2) | 6.7 (9.3) | 7.2 (8.2) | 7.0 (5.7) | 6.8 (8.9) | 7.3 (7.4) | 7.2 (8.0) | 6.8 (7.0) | 6.2 (5.8) |
Number of mood episodes (manic, mixed, hypomanic depressive) during past year, mean (SD) | 1.6 (0.7) | 1.5 (0.7) | 1.5 (0.6) | 1.5 (0.7) | 1.5 (0.7) | 1.5 (0.7) | ||||||||| | ||||||||| | ||||||||| |
BMI = body mass index; CAR = cariprazine; NR = not reported; PBO = placebo; SD = standard deviation.
aDiabetes mellitus: type 1 diabetes mellitus and type 2 diabetes mellitus.
bBased on medical and surgical history.
cRelevant medical history, recovered (study RGH-MD-53); relevant medical history, recovered and ongoing (study RGH-MD-54); medical and surgical history (study RGH-MD-56).
Source: Clinical Study Reports for study RGH-MD-53, study RGH-MD-54, and study RGH-MD-56.14-16
Table 13: Mean Baseline Efficacy Score — Bipolar Depression, Modified Intention-to-Treat Population
Efficacy parameter | RGH-MD-53 study | RGH-MD-54 study | RGH-MD-56 study | ||||||
|---|---|---|---|---|---|---|---|---|---|
CAR 1.5 mg N = 162 | CAR 3 mg N = 153 | Placebo N = 163 | CAR 1.5 mg N = 154 | CAR 3 mg N = 164 | Placebo N = 156 | CAR 1.5 mg N = 146 | CAR 3 mg N = 146 | Placebo N = 145 | |
MADRS total score, mean (SD) | 31.5 (4.3) | 31.4 (4.7) | 31.3 (4.1) | 30.6 (4.2) | 31.1 (4.8) | 30.3 (4.5) | 30.3 (4.4) | 30.6 (4.7) | 30.4 (4.6) |
CGI-S score, mean (SD) | 4.5 (0.6) | 4.5 (0.6) | 4.5 (0.5) | 4.5 (0.5) | 4.5 (0.5) | 4.5 (0.5) | 4.4 (0.5) | 4.4 (0.5) | 4.4 (0.5) |
HAM-D score, mean (SD) | 24.7 (3.5) | 24.5 (3.1) | 24.7 (3.0) | 24.9 (2.9) | 24.6 (3.2) | 24.4 (2.3) | 23.9 (3.2) | 24.0 (3.1) | 24.1 (2.8) |
HAM-A score, mean (SD) | 18.9 (6.2) | 18.7 (6.0) | 18.7 (5.6) | 18.4 (4.8) | 18.4 (6.0) | 18.5 (5.8) | NA | NA | NA |
QIDS-SR score, mean (SD) | 15.6 (3.7) | 15.6 (3.8) | 15.3 (3.5) | 15.3 (3.4) | 15.4 (4.1) | 15.2 (3.9) | NA | NA | NA |
FAST total score | NA | NA | NA | NA | NA | NA | ||||||||| | ||||||||| | ||||||||| |
CAR = cariprazine; CGI-S = Clinical Global Impression–Severity of Illness; FAST = Functioning Assessment Short Test; HAM-A = Hamilton Anxiety Rating Scale; HAM-D = Hamilton Depression Rating Scale; MADRS = Montgomery–Åsberg Depression Rating Scale; NA = not available; QIDS-SR = Quick Inventory of Depressive Symptomatology–Self-Rated; SD = standard deviation.
Source: Clinical Study Reports for study RGH-MD-53, study RGH-MD-54, and study RGH-MD-56.14-16
Table 14: Prior Medications — Bipolar Mania, Safety Population
Preferred term | RGH-MD-31 study | RGH-MD-32 study | RGH-MD-33 study | |||
|---|---|---|---|---|---|---|
CAR 3 mg to 12 mg N = 118 | Placebo N = 118 | CAR 3 mg to 12 mg N = 158 | Placebo N = 154 | CAR 3 mg to 6 mg N = 167 | Placebo N = 161 | |
Prior medications, n (%) | ||||||
Valproate semisodium | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
Valproate sodium/valproic acid | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
Lamotrigine | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
Risperidone | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
Quetiapine | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
Quetiapine fumarate | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
Olanzapine | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
Lithium | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
Haloperidol | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
Aripiprazole | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
Ziprasidone | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
Paliperidone | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
CAR = cariprazine.
Source: Clinical Study Reports for study RGH-MD-31, study RGH-MD-32, and study RGH-MD-33.11-13
Table 15: Prior Medications — Bipolar Depression, Safety Population
Preferred term or ATC classa | RGH-MD-53 study | RGH-MD-54 study | RGH-MD-56 study | ||||||
|---|---|---|---|---|---|---|---|---|---|
CAR 1.5 mg N = 167 | CAR 3 mg N = 158 | Placebo N = 165 | CAR 1.5 mg N = 157 | CAR 3 mg N = 165 | Placebo N = 158 | CAR 1.5 mg N = 146 | CAR 3 mg N = 146 | Placebo N = 145 | |
Prior medications, n (%) | |||||||||
Aripiprazole | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
Risperidone | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
Paliperiodone | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
Quetiapine | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
Quetiapine fumarate | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
Olanzapine | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
Clozapine | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
Asenapine/ asenapine maleate | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
Valproate sodium/valproic acid | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
Valproate semisodium | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
Ziprasidone | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
Lurasidone/lurasidone HCl | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
Lithium | ||||||||| | ||||||||| | ||||||||| | 14 | 20 (12.1) | 16 | ||||||||| | ||||||||| | ||||||||| |
Lamotrigine | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
SSRIsa | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
Other antidepressantsa | ||||||||| | ||||||||| | ||||||||| | 30 | 42 (25.5) | 47 | ||||||||| | ||||||||| | ||||||||| |
ATC = Anatomic Therapeutic Chemical; CAR = cariprazine; HCl = hydrochloride; SSRI = selective serotonin reuptake inhibitor.
aPrior medications reported by ATC 2nd level in study RGH-MD-56; 58% of patients reported psychoanaleptics as prior medications.
Source: Clinical Study Reports for study RGH-MD-53, study RGH-MD-54, and study RGH-MD-56.14-16
Interventions
Study interventions cariprazine and placebo were administered orally, as a single dose, once daily at approximately the same time in all studies. As the studies were double-blind, cariprazine and placebo were available as capsules identical in appearance. Patients received treatment for 3 weeks in the bipolar mania studies, for 6 weeks in study RGH-MD-53 and study RGH-MD-54, and for 8 weeks in study RGH-MD-56. All investigational products were dispensed in blister packs, with 1 provided for each week of the treatment period. All blister packs included enough capsules for 7 days of treatment plus 3 extra days (up to 10 days of treatment). In the bipolar mania studies, blister packs were dispensed on day 0, day 7, and day 14. In the bipolar depression studies, 1 to 2 blister packs were dispensed at day 0, and at the end of week 1, week 2, and week 4. In the 8-week RGH-MD-56 study, 2 blister packs were also dispensed at week 6. In all studies, patients were instructed to return all unused study drugs at each study visit.
Bipolar Mania Studies
In study RGH-MD-31 and study RGH-MD-32, patients were randomized to 1 of 2 treatment groups: cariprazine 3 mg to 12 mg or placebo. In study RGH-MD-33, patients were randomized to 1 of 3 treatment groups: cariprazine 3 mg to 6 mg, cariprazine 6 mg to 12 mg, or placebo. All products (cariprazine and placebo) were identical in appearance to maintain blinding. The daily dose for each patient ranged from 1 capsule to 4 capsules in study RGH-MD-31 and study RGH-MD-32 or 1 capsule to 3 capsules in study RGH-MD-33. In all studies, treatment was administered to patients by hospital staff while the patients were hospitalized. For patients who were discharged early, the patient or a caregiver was responsible for ensuring the study drug was taken as directed.
In the bipolar mania studies, the intervention was based on a flexible-dose regimen. Patients in the cariprazine treatment groups received cariprazine 1.5 mg per day on day 0 and cariprazine 3 mg per day on day 1, each provided as 1 capsule. The dose could be increased to 2 3 mg capsules (a total of 6.0 mg per day) on day 2 if the patients were experiencing an inadequate response without tolerability problems, based on the judgment of the investigator. Dose increases differed slightly between study RGH-MD-31 and study RGH-MD-32 beginning on day 3. In study RGH-MD-31, the dose could be increased by 1 capsule to 3 3 mg capsules (9.0 mg per day) on day 3, and starting on day 4, the dose could be increased by 1 capsule to a maximum of 4 3 mg capsules (12.0 mg per day), depending on response and tolerability. In study RGH-MD-32 (Figure 22), the dose could be increased to 6.0 mg per day on day 2 due to inadequate response without tolerability problems, based on investigator judgment. Patients remained on the dose administered at day 2 for 2 days (day 2 and day 3). On day 4, inadequate responders were identified using the YMRS (less than 50% improvement in YMRS from day 2 to day 4). The dose was increased to 9.0 mg per day on day 4 for 3 days (day 4 to day 6) for patients with an inadequate response without tolerability issues. Additional increases at increments of 3 mg per day were determined using the YMRS assessment of improvement to a maximum of 12 mg per day. In study RGH-MD-33 (Figure 23), all patients randomized to receive cariprazine were administered cariprazine 1.5 mg per day on day 0 and cariprazine 3 mg per day on day 1. Those in the 3 mg per day to 6 mg per day group remained on the 3 mg per day dosage on day 2, while patients in the 6 mg to 12 mg per day treatment group received 6.0 mg on day 2. Beginning on day 3, the approach to dosing titration was similar to study RGH-MD-32 in that dose increases were made based on an assessment of inadequate response as per the YMRS and in the absence of tolerability issues. Dose increases were considered at day 5, day 7, and day 10. Dose increases were made at increments of 1.5 mg per day in the cariprazine 3 mg per day to 6 mg per day group (up to 1 or 2 additional 1.5 mg capsules, corresponding to a total of 4.5 mg or 6.0 mg per day, respectively), and 3 mg per day in the cariprazine 6 mg per day to 12 mg per day group (up to 1 or 2 additional 3 mg capsules, corresponding to a total of 9 mg per day or 12 mg per day, respectively).
In all studies, dose increases or decreases were made in increments of 1 capsule as described. A decrease in the dose was considered if there were tolerability problems. Alternatively, patients could skip the dose for 1 day to 2 days (study RGH-MD-31) or 1 day to 3 days (study RGH-MD-32 and study RGH-MD-33). In study RGH-MD-32 and study RGH-MD-33, dose adjustments (an increase or decrease except for a temporary drug discontinuation for 1 day to 3 days) were not permitted after day 14. Each of the studies indicated that frequent switching was not allowed; additional detail was not provided. Of note, adjustments to the number of capsules administered (dose adjustments) were assessed and implemented for patients in the placebo groups in a similar manner to the cariprazine groups.
Bipolar Depression Studies
In study RGH-MD-53 and study RGH-MD-54, patients were randomized to 1 of 3 treatment groups: cariprazine 1.5 mg, cariprazine 3.0 mg, or placebo. In study RGH-MD-56, patients were randomized to 1 of 4 treatment groups: cariprazine 0.75 mg (not shown), cariprazine 1.5 mg, cariprazine 3.0 mg, or placebo.
In study RGH-MD-53 and study RGH-MD-54, all patients randomized to cariprazine dose groups received cariprazine 1.5 mg per day for 2 weeks, from day 1 through day 14. For patients randomized to the cariprazine 3 mg per day group, the dose was increased to 3 mg per day on day 15. In study RGH-MD-56, all patients randomized to cariprazine treatment groups received cariprazine 0.5 mg per day on day 1 and day 2. The dose was increased to 0.75 mg per day on day 3, then 1.0 mg per day on day 5, and 1.5 mg per day on day 8. Patients randomized to the cariprazine 3 mg treatment group had another dose increase to 3 mg on day 15 of treatment.
If there were tolerability issues, temporary discontinuation of treatment for up to 3 consecutive days was permitted at the discretion of the investigator. Patients unable to tolerate the fixed dose of treatment or patients off drug for 4 or more consecutive days were prematurely discontinued from the study.
Concomitant Therapy and Rescue Medications
Concomitant therapy and rescue medications that were permitted for use in the included studies are described in Table 16. Additional psychotropic medications, including psychostimulants, were not allowed — with some exceptions. Patients were permitted to use the following for insomnia: zolpidem, zolpidem extended release, zaleplon, chloral hydrate, and eszopiclone. For EPS that emerged or worsened during the study, patients could be treated with diphenhydramine, benztropine or equivalent, or propranolol for the treatment of akathisia. For agitation, restlessness, irritability, and hostility, patients could be treated with lorazepam, oxazepam, or diazepam.
Outcomes
A list of efficacy end points identified in the CADTH review protocol that were assessed in the clinical trials included in this review is provided and further summarized in Table 17. A detailed discussion and critical appraisal of the outcome measures is provided in Appendix 4.
Table 16: Concomitant and Rescue Medications Permitted During the Trials
Medication and dosing | Notes | |
|---|---|---|
Mania/mixed trials | Depression trials | |
For insomnia | ||
| Same as mania/mixed trials, in addition to zopiclone (maximum of 7.5 mg per day) | The medication was documented as concomitant therapy. No such medication was permitted within 8 hours of psychiatric or neurologic assessments. In the mania/mixed trials, insomnia was documented as an AE. |
For EPS that emerged or worsened during the study | ||
| Same as mania/mixed trials | Three EPS scales (AIMS, BARS, and SAS) were performed to support the decision to use rescue medication (except in cases of a medical urgency such as dystonia or severe akathisia). The need for continued use was assessed by the investigator at least once a week. EPS was documented as an AE and the medication was documented as concomitant therapy. |
For agitation, restlessness, irritability, and hostility | ||
|
|
|
AE = adverse event; AIMS = Abnormal Involuntary Movement Scale; BARS = Barnes Akathisia Rating Scale; EPS = extrapyramidal symptom; SAS = Simpson-Angus Scale.
aMaximum of 2 mg per day in study RGH-MD-31 and maximum of 3 mg per day in study RGH-MD-32 and study RGH-MD-33.
Source: Clinical Study Reports for study RGH-MD-31, study RGH-MD-32, study RGH-MD-33, study RGH-MD-53, study RGH-MD-54, and study RGH-MD-56.11-16
Table 17: Summary of Outcomes of Interest Identified in the CADTH Review Protocol
Outcome measure | RGH-MD-31 study | RGH-MD-32 study | RGH-MD-33 study | RGH-MD-53 study | RGH-MD-54 study | RGH-MD-56 study |
|---|---|---|---|---|---|---|
YMRS total score | Primary | Primary | Primary | NA | NA | NA |
CGI-S | Secondary | Secondary | Secondary | Secondary | Secondary | Secondary |
CGI-I | Exploratory | Exploratory | Exploratory | NA | NA | NA |
MADRS total score | Exploratory | Exploratory | Exploratory | Primary | Primary | Primary |
PANSS total score | Exploratory | Exploratory | Exploratory | NA | NA | NA |
HAM-D total score | NA | NA | NA | Exploratory | Exploratory | Exploratory |
HAM-A total score | NA | NA | NA | Exploratory | Exploratory | NA |
QIDS-SR | NA | NA | NA | Exploratory | Exploratory | NA |
FAST | NA | NA | NA | NA | NA | ||||||||| |
CGI-I = Clinical Global Impression–Improvement; CGI-S = Clinical Global Impression–Severity of Illness; FAST = Functioning Assessment Short Test; HAM-A = Hamilton Anxiety Rating Scale; HAM-D = Hamilton Depression Rating Scale; MADRS = Montgomery–Åsberg Depression Rating Scale; NA = not applicable; PANSS = Positive and Negative Syndrome Scale; QIDS-SR = Quick Inventory of Depressive Symptomatology–Self-Rated; YMRS = Young Mania Rating Scale.
Source: Clinical Study Reports for study RGH-MD-31, study RGH-MD-32, study RGH-MD-33, study RGH-MD-53, study RGH-MD-54, and study RGH-MD-56.11-16
Young Mania Rating Scale (Change in Symptom Severity, Response Rate, and Remission Rate)
The YMRS is an 11-item, clinician-administered rating scale used to assess the severity of manic symptoms.45 A severity rating is assigned to each item, based on the patient’s subjective report of his or her condition over the past 48 hours and the clinician’s assessment of the patient’s behaviour. Item 5, item 6, item 8, and item 9 (irritability, speech, content, and disruptive/aggressive behaviour) are graded on a 0 to 8 scale while the remaining 7 items (elevated mood, increased motor activity-energy, sexual interest, sleep, language-thought disorder, appearance, and insight) are graded on a 0 to 4 scale, based on increasing severity. The YMRS total score ranges from 0 to 60 where higher scores indicate more severe mania; thus, a negative change (or decrease) from baseline indicates a reduction (or improvement) in manic symptoms.45
In the bipolar mania studies, the YMRS was administered by an experienced and trained rater using the YMRS Scripted Interview Guide developed by Concordant Rater Systems. Assessments and ratings were to have been made by the same rater at approximately the same time of day. The YMRS total score was used to inform multiple outcomes in the bipolar mania studies — namely, the change from baseline to week 3 in the YMRS total score, the remission rate at week 3, and the response rate at week 3. The response rate was defined by the proportion of patients with an improvement in the YMRS total score of at least 50%. The remission rate was defined by the proportion of patients with a YMRS total score of 12 or less.
In patients with acute manic or mixed bipolar disorder, the minimal clinically significant difference was 6.6 points.7 Also, there is evidence to support a 50% reduction on the YMRS score as a clinically meaningful definition of response in acute treatment of manic or mixed episodes in pediatric patients with bipolar I disorder.46
Montgomery–Åsberg Depression Rating Scale (Change in Symptom Severity, Response Rate, Remission Rate)
The MADRS is a 10-item, clinician-rated scale used to assess the severity of depressive symptoms during the past week.47,48 Each item is rated on a scale of 0 (item not present or normal) to 6 (severe or continuous presence of the symptoms), resulting in a maximum total score of 60 points, in which higher scores indicate greater depressive symptomology.47
Similar to the YMRS, the MADRS was used to inform multiple outcomes in the bipolar depression studies. This included the change from baseline to week 6 in MADRS total score, MADRS response, and MADRS remission where response was defined as at least a 50% reduction from baseline in the MADRS total score and remission was defined as a MADRS total score of 10 or less. The MADRS response, remission, and total score were reported by visit. In the bipolar mania studies, the MADRS total score was evaluated as the change from baseline to week 3.
The psychometric properties of MADRS are based on studies in major depressive disorder. There is evidence to support an improvement of at least 2 points on the MADRS as clinically relevant.8,9 Response to treatment is usually defined as at least a 50% reduction on the MADRS total score from baseline.49 No consensus was reached for a cut-off score on the MADRS for defining remission in clinical trials.50 The criterion score to identify remission has ranged from 4 through 12 in various trials in depression.49,51,52 In bipolar disorder, a cut-off score of 5 and 10 has been associated with remission and a softer definition of remission, respectively.53
Clinical Global Impression–Severity of Illness and Clinical Global Impression–Improvement (Change in Symptom Severity)
The CGI-S is a 7-point scale that measures the overall severity of the illness in comparison with the severity of other patients the physician has observed. CGI-S assesses the overall severity of mental disorders at the time of the assessment on a 7-point scale ranging from 1 (normal, not at all ill) to 7 (extremely ill).54
The CGI-I is a 7-point scale that measures the change in the overall severity of illness for the individual patient. The 7-point scale of the CGI-I ranges from 1 (very much improved) to 7 (very much worse).54
The bipolar mania studies indicated that both the CGI-S and the CGI-I were assessed by a psychiatrist. The bipolar depression studies indicated that the CGI-S was administered by the investigator or a sub-investigator with extensive professional training and experience in assessing mental illness. In the bipolar mania studies, the CGI-S and CGI-I were evaluated as a change from baseline to week 3. In the bipolar depression studies, the CGI-S was evaluated as a change from baseline to week 6 (study RGH-MD-53 and study RGH-MD-54) or week 7 (study RGH-MD-56). The CGI-S score by visit was also reported in study RGH-MD-53.
A 1-point improvement has been considered as a clinical improvement in clinical studies in schizophrenia and based on expert opinion for within-group differences.55,56, 57,58 Evidence for an MID in the CGI-I scale was not found.
Positive and Negative Syndrome Scale (Change in Symptom Severity)
The PANSS is a 30-item rating scale that was developed to assess the severity of positive and negative symptoms within the past week in patients with schizophrenia. The PANSS is administered as a standardized Structured Clinical Interview. It was reported that information is obtained from the patient and supporting clinical information from family, hospital staff, and other reliable informants. It consists of 3 subscales — namely, positive symptoms, negative symptoms, and general psychopathology. The PANSS total score is informed by 30 items: 7 positive symptoms, 7 negative symptoms, and 16 general psychopathology symptoms, each rated on a 7-point scale from 1 (absent) to 7 (extreme). The total score ranges from 30 to 210 and higher scores indicate more severe symptoms or psychopathology.59,60 The PANSS total score was reported as the change from baseline to week 3 in the bipolar mania studies. Evidence of an MID for the PANSS in patients with bipolar disorder was not identified. Evidence of an MID for the PANSS in patients with schizophrenia that was identified is opinion-based and associated with uncertainty.
Hamilton Depression Rating Scale (Change in Symptom Severity, Remission Rate)
The 17-item HAM-D is a clinician-rated scale used to assess the severity of symptoms and address both somatic and psychological symptoms of depression.61-63 The items are either rated on a 5-point scale (a 0 to 4 spectrum) or a 3-point scale (a 0 to 2 spectrum), where increasing scores represent increasing severity of symptoms.64,65 Scores are summed to obtain a total score out of 52 or 53.10,66 The psychometric properties of HAM-D are based on studies of patients with major depressive disorder. NICE recommended a 3-point difference between the drug and placebo groups as a criterion for clinical significance.10 A separate report suggested a 2-point difference between an antidepressant and placebo might be clinically relevant.8 Remission was defined as a score of 7 or less on the HAM-D total score by a consensus panel in 1991.62,67 Suggestions for an optimal cut-off score to define remission has ranged from 2 to 7.62 The generalizability of the psychometric assessment of the HAM-D to patients with bipolar disorder is unclear.
Hamilton Anxiety Rating Scale (Change in Symptom Severity)
The HAM-A is a 14-item, clinician-rated scale used to assess somatic and psychic anxiety symptoms.68,69 The items are rated on a 5-point scale (a 0 to 4 spectrum), where increasing scores indicate higher levels of symptom severity, and are summed to yield a total score.15 Evidence for the MID of HAM-A was not found. The use of the HAM-A as an indicator of the severity of anxiety states in depressive disorders has been criticized70; however, there is some controversy regarding this conclusion, since the HAM-A is commonly used as an outcome measure in trials with patients with depression. The generalizability of the HAM-A to patients with bipolar disorder is unknown.
Quick Inventory of Depressive Symptomatology–Self-Rated (Change in Symptom Severity)
The QIDS-SR is a 16-item, self-reported tool that measures depressive symptom severity.66 Items included assess Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition (DSM-IV) diagnostic symptoms for major depressive disorder. The recall period is 7 days as patients are asked to rate their symptoms during this period. The responses are converted from the 16 items into 9 DSM-IV symptom criterion domains: sleep, weight, psychomotor changes, depressed mood, decreased interest, fatigue, guilt, concentration, and suicidal ideation. The items are used to characterize a major depressive episode. Each item is scored on a scale of 0 to 3, with higher scores representing greater symptom severity. The total score ranges from 0 to 27.66 Evidence for an MID in the QIDS-SR scale was not identified.
Functioning Assessment Short Test (Functioning)
The FAST is a 24-item, clinician-rated scale used to assess functional impairment in patients with mental disorders. The items are divided into 6 areas of functioning: autonomy, occupational functioning, cognitive functioning, financial issues, interpersonal relationships, and leisure time. Items are rated on a 4-point scale (0 = no difficulty; 3 = severe difficulty). The total score is the sum of all 24 items, with higher scores indicating greater difficulty.71 There is evidence to suggest the minimum clinically important difference ranges from an 8-point to 9-point change from baseline.72
Columbia–Suicide Severity Rating Scale
The C-SSRS is a clinician-rated instrument that reports the severity of both suicidal ideation and behaviour. Suicidal ideation is rated using a 5-item scale ranging from 1 (wish to be dead) to 5 (active suicidal ideation with specific plan and intent). The C-SSRS also captures information about the intensity of ideation — specifically, the frequency, duration, controllability, deterrents, and reasons for the most severe types of ideation. Suicidal behaviour is also rated using a 5-item scale, ranging from 0 (no suicidal behaviour) to 4 (actual attempt). The C-SSRS was reported in all studies except study RGH-MD-31 and an assessment was completed at all study visits by the investigator or designee with extensive professional training and experience in assessing mental illness.5
Statistical Analysis
Primary Outcome of the Studies
The primary outcome in the bipolar mania studies was the change from baseline to week 3 in the YMRS total score. The primary outcome in the bipolar depression studies was the change from baseline to week 6 in the MADRS total score.
Power Calculation
Power calculations for the primary end points are described as follows. Power calculations did not account for secondary end points.
In study RGH-MD-31, a sample size of approximately 120 patients in each treatment group would have provided at least 80% power to detect an effect size (treatment group difference relative to pooled SD) of 0.363 at a 2-sided significance level of 0.05.
In study RGH-MD-32, a sample size of 160 randomized patients in each of the 2 treatment groups provided 90% power to detect effect sizes (treatment group difference relative to pooled SD) of 0.40 between the placebo group and the cariprazine treatment group in the primary efficacy parameter, based on an MMRM using simulations. The simulation assumed a correlation of 0.7 between the repeated measures and effect sizes of 0.16, 0.17, 0.27, 0.32, 0.36, and 0.40 for the cariprazine treatment group for the planned postbaseline visits.
In study RGH-MD-33, adjustments were made for multiple comparisons involving the 2 efficacy end points and 2 cariprazine flexible-dose groups by using the matched parallel gatekeeping procedure. A sample size of 165 randomized patients in each of the 3 treatment groups provided 92% power to detect effect sizes (treatment group difference relative to pooled SD) of 0.430 between the placebo and cariprazine groups (6 mg per day to 12 mg per day and 3 mg per day to 6 mg per day) for the primary efficacy parameter, respectively, based on an MMRM model using simulations. The simulation assumed a correlation of 0.7 between the repeated measures and effect sizes of 0.43 for both the cariprazine 6 mg per day to 12 mg per day treatment group and the 3 mg per day to 6 mg per day treatment group for the primary and secondary parameters.
The power calculation for study RGH-MD-31 did not account for loss to follow-up. The power calculations for study RGH-MD-32 and study RGH-MD-33 assumed a 35% dropout rate.
The power calculations used in study RGH-MD-53 and study RGH-MD-54were identical. For the comparison of the primary end point in RGH-MD-53 and RGH-MD-54, the sample size of 160 patients per arm provided approximately 82% statistical power to show a statistically significantly higher effect in each dose of cariprazine versus placebo. The study had statistical power of 90% to show that at least 1 of the 2 cariprazine doses was statistically significantly more efficacious than placebo in the primary end point. These calculations assumed an effect size of 0.36 (treatment group difference relative to SD). All statistical powers presented in this section were calculated adjusting for multiple comparisons using a matched parallel gatekeeping procedure, with the familywise type I error rate being controlled at a 0.05 level (2-sided). The dropout rate was assumed to be 22% at week 6. The within-person correlation for both the primary and secondary end points was assumed to be 0.6, as was correlation between the 2 end points (primary and secondary). Assumptions of effect sizes, correlation coefficients, and dropout rate were based on the RGH-MD-56 study.
In study RGH-MD-56, a sample size of 150 randomized patients in each of the 4 treatment groups provided approximately 90% power to detect at least 1 of the 3 effect sizes at a 2-sided significance level of 0.05 at week 6 for the primary efficacy parameter, adjusted for multiple comparisons. This was based on assumed effect sizes (treatment group difference relative to pooled SD) of at least 0.30, 0.36, and 0.4 for the 3 cariprazine dosage groups (0.75 mg per day, 1.5 mg per day, and 3 mg per day) at week 6, a correlation coefficient of 0.66 for within-patient assessments for both the primary and secondary efficacy parameters, a correlation coefficient of 0.60 between the primary and secondary efficacy parameters, and a 25% patient dropout rate at week 6, for the primary efficacy parameter, adjusted for multiple comparisons. The correlation coefficients for within-patient assessments and the dropout rate were based on study RGH-MD-52.
Statistical Test or Model
In study RGH-MD-31, the primary analyses were performed using the LOCF approach. The comparison between cariprazine and placebo was performed by means of an analysis of covariance (ANCOVA) model, with treatment group and study centre as factors and baseline YMRS total score as a covariate. The normality assumption in the primary efficacy analysis model was checked by examining the normal probability plot of the residuals from the ANCOVA model. In study RGH-MD-32 and study RGH-MD-33, the primary analysis was performed using an MMRM with treatment group, study centre, visit, and treatment-group-by-visit interaction as fixed effects and the baseline value and baseline-by-visit interaction as the covariates. An unstructured covariance matrix was used to model the covariance of within-patient scores. The Kenward-Roger approximation was used to estimate denominator degrees of freedom.
The analysis of the primary end point in the bipolar depression studies was similar to that which was described for study RGH-MD-32 and study RGH-MD-33. In study RGH-MD-56, pairwise tests of no difference of the change from baseline between the 3 cariprazine dose groups and placebo were conducted; the LSM difference with 95% CI is reported for each comparison. In addition, for each treatment group, the fitted mean change (least squares) is provided. The study was considered positive if at least 1 dose group of cariprazine was statistically superior to placebo at week 6.
In the bipolar mania studies, the primary efficacy analysis was based on the intention-to-treat (ITT) population. All statistical tests were 2-sided hypothesis tests performed at the 5% level of significance for main effects. All CIs were 2-sided 95% CIs, unless stated otherwise. The baseline for efficacy was defined as the values recorded at visit 2 before the first dose of the double-blind study drug.
Descriptive statistics were presented by visit and treatment group for all efficacy parameters based on the LOCF and the observed cases approaches in study RGH-MD-31. In study RGH-MD-32, study RGH-MD-33, and study RGH-MD-56, by-visit analyses based on an MMRM for all continuous efficacy parameters using observed cases were also performed.
All efficacy analyses were based on the ITT population, unless stated otherwise. The baseline for each specific efficacy end point was defined as the value recorded at visit 2 (week 0). If this value was not available, the last available value before the first dose was to be used as the baseline value. Efficacy results were considered to be statistically significant after considering control for multiplicity, described under the summary of secondary outcomes of the studies as follows. All statistical hypothesis tests were performed at the 2-sided 5% significance level for main effects. All CIs were 2-sided 95% CIs, unless stated otherwise. By-visit analyses, which were done using the LOCF approach, were presented for all efficacy parameters.
Data Imputation Methods
In study RGH-MD-31, data were imputed using the LOCF approach for missing postbaseline total scores. Data were only imputed if at least 1 nonmissing postbaseline total score was available for that patient. Individual item scores were not carried forward (not imputed).
In study RGH-MD-32, study RGH-MD-33, study RGH-MD-53, study RGH-MD-54, and study RGH-MD-56, the primary analysis was performed based on all postbaseline scores using only the observed cases without imputation of missing values.
Additionally, in the depression studies, the baseline value was carried forward only for the intermittent missing values immediately after baseline. If all the postbaseline values were missing, the baseline value was not carried forward.
Subgroup Analyses
Subgroup analyses by demographic factors and baseline bipolar mania were performed for the primary analysis in the bipolar mania studies — the change from baseline at week 3 in the YMRS total score. The following subgroups were explored: age group (< 55 years, ≥ 55 years), sex (male, female), race group (White, all other races), geographic region (US, non-US), and baseline bipolar I type (mania, mixed). All subgroup analyses were reported descriptively by treatment group.
Sensitivity Analyses
In study RGH-MD-31, 2 sensitivity analyses were performed on the primary efficacy parameter (change from baseline to week 3 in the YMRS total score). Between-treatment group comparisons at week 3 were performed on the observed cases, using the ANCOVA model described for the primary analysis, and using an MMRM with treatment group, study centre, visit, and treatment-group-by-visit interaction as fixed effects and baseline YMRS total score as a covariate. An unstructured covariance matrix was used to model the covariance of within-patient measurements. This analysis was performed on the changes from baseline at all postbaseline time points during the double-blind treatment phase using only the observed cases.
In study RGH-MD-32 and study RGH-MD-33, a sensitivity analysis using a pattern-mixture model based on nonfuture dependent missing value restrictions was performed to assess the robustness of the primary MMRM results to the possible violation of the missing-at-random assumption.
The analysis of the primary end point in the depression studies was similar to that which was described for study RGH-MD-32 and study RGH-MD-33.
Secondary Outcomes of the Studies
In the bipolar mania studies, the secondary efficacy outcome was the change from baseline to week 3 in the CGI-S score. In the bipolar depression studies, the secondary efficacy outcome was the change from baseline to week 6 in the CGI-S score. In each study, the secondary outcome was analyzed using a similar approach to the primary analysis (ANCOVA model or MMRM model).
In study RGH-MD-31 and study RGH-MD-32, the analysis of the secondary end point was carried out inferentially at a 2-sided 5% significance level only if the result of the primary efficacy end point was significant at the 0.05 level. This is a closed testing procedure that controls the studywise type I error rate.
In study RGH-MD-33, a matched parallel gatekeeping procedure was used to control the overall type I error rate for multiple comparisons of the 2 active doses versus placebo across the primary and secondary hypotheses. The primary hypotheses consisted of 2 null hypotheses, corresponding to the comparisons of cariprazine 3 mg to 6 mg and cariprazine 6 mg to 12 mg, respectively, with placebo in regard to the primary efficacy parameter. Similarly, the secondary hypotheses include comparisons of cariprazine 3 mg to 6 mg and cariprazine 6 mg to 12 mg, respectively, with placebo in regard to the secondary efficacy parameter. Rejection of at least 1 of the primary hypotheses was required to examine the secondary hypotheses; significance in the secondary end point for a dose level could only be claimed if the corresponding primary hypothesis was found to be significant.
Similar to study RGH-MD-33, study RGH-MD-53 and study RGH-MD-54 implemented a parallel gatekeeping procedure to control the overall type I error rate for multiple comparisons. The primary hypotheses consisted of 4 null hypotheses, corresponding to comparisons of cariprazine 1.5 mg and cariprazine 3.0 mg to placebo for the primary efficacy analysis (MADRS total score) and the same comparisons for the secondary efficacy analysis (CGI-S score). The hypotheses corresponding to the primary efficacy analyses served as a parallel gatekeeper for the secondary efficacy analyses.
Table 18: Statistical Analysis of Efficacy End Points
End point | Statistical model | Adjustment factor | Sensitivity analysis |
|---|---|---|---|
Bipolar mania studies (study RGH-MD-31, study RGH-MD-32, and study RGH-MD-33) | |||
Primary: Change from baseline to week 3 in YMRS total score |
|
|
|
Secondary: Change from baseline to week 3 in the CGI-S score | Similar to primary end point | Similar to primary end point | None |
Bipolar depression studies (study RGH-MD-53, study RGH-MD-54, and study RGH-MD-56) | |||
Primary: Change from baseline to week 6 in MADRS total score | MMRM |
| PMM |
Secondary: Change from baseline to week 6 in the CGI-S score | Similar to primary end point | Similar to primary end point | None |
ANCOVA = analysis of covariance; CGI-S = Clinical Global Impression–Severity of Illness; MADRS = Montgomery–Åsberg Depression Rating Scale; MMRM = mixed model of repeated measures; OC = observed case; PMM = pattern-mixture model, YMRS = Young Mania Rating Scale.
Source: Clinical Study Reports for study RGH-MD-31, study RGH-MD-32, study RGH-MD-33, study RGH-MD-53, study RGH-MD-54, and study RGH-MD-56.11-16
Analysis Populations
Three analysis sets were described for all included studies, which comprised the randomized population, the safety population, and the ITT population.
The randomized population was defined as consisting of all patients who were screened and randomized, which is consistent with the definition of an ITT population.
The safety population was defined as consisting of all patients who were randomized and who received at least 1 dose of the double-blind investigational product.
The ITT population defined by the sponsor consisted of all patients in the safety population who had at least 1 postbaseline assessment of the YMRS total score (mania studies) or MADRS total score (depression studies). As this is not a true definition of an ITT population, it has been referred to as a modified intention-to-treat (mITT) population herein.
Results
Patient Disposition
A summary of the patient disposition in the bipolar mania studies and bipolar depression studies is provided in Table 19 and Table 20, respectively.
In the bipolar mania studies, 68%, 66%, and 64% of screened patients were randomized to study RGH-MD-31, study RGH-MD-32, and study RGH-MD-33, respectively. Discontinuation rates were similar between treatment groups and ranged from 23% to 38% across studies. The most common reasons for discontinuation across studies were AEs (5% to 14%), insufficient therapeutic response (1% to 26%), and withdrawal of consent (9% to 17%). In general, more patients randomized to placebo discontinued due to insufficient therapeutic response compared to patients randomized to cariprazine. Discontinuation due to AEs was more common among patients randomized to cariprazine relative to placebo. Discontinuation due to withdrawal of consent was similar between treatment groups, with the exception of study RGH-MD-32 (16.5% versus 11.0% for cariprazine versus placebo).
In the bipolar depression studies, 57%, 62%, and 58% of screened patients were randomized to study RGH-MD-53, study RGH-MD-54, and study RGH-MD-56, respectively. The proportion of patients who discontinued from study ranged from 15% to 36% across the studies, and an imbalance in discontinuation rates between treatment groups was observed in study RGH-MD-54 and study RGH-MD-56. In both studies, the proportion of patients who discontinued was higher in the cariprazine 3 mg treatment group relative to cariprazine 1.5 mg or placebo. The most common reasons for discontinuation included AEs (3% to 12%), lost to follow-up (3% to 7%), and withdrawal of consent (2% to 10%), and were generally similar between treatment groups with the exception of AEs in study RGH-MD-53 (7% for cariprazine 3 mg versus 3% for each of cariprazine 1.5 mg and placebo) and withdrawal of consent in study RGH-MD-56 (3%, 10%, and 8% for cariprazine 1.5 mg, cariprazine 3 mg, and placebo, respectively).
Exposure to Study Treatments
A summary of exposure to study treatments for the bipolar mania studies and bipolar depression studies is provided in Table 21 and Table 22. Overall, the mean duration of treatment was similar between treatment groups in all studies. Of note, the bipolar studies used a flexible-dose regimen for cariprazine. The overall mean daily dose in study RGH-MD-31 and study RGH-MD-32 was 8.8 (SD = |||||||||) mg and 7.5 (SD = |||||||||) mg per day, respectively. The overall mean daily dose in study RGH-MD-33 was 4.8 (SD = |||||||||) mg. The overall mean daily dose was not reported in the bipolar depression studies.
Table 19: Patient Disposition — Bipolar Mania
Characteristic | RGH-MD-31 study | RGH-MD-32 study | RGH-MD-33 study | |||
|---|---|---|---|---|---|---|
CAR 3 mg to 12 mg | Placebo | CAR 3 mg to 12 mg | Placebo | CAR 3 mg to 6 mg | Placebo | |
Screened, N | 348 | 472 | 782a | |||
Randomized, N (%)b | 118 (33.9) | 120 (34.5) | 158 (33.5) | 154 (32.6) | 167 (21.4) | 161 (20.6) |
Discontinued from study, N (%) | 43 (36.4) | 45 (38.1) | 50 (31.6) | 48 (31.2) | 38 (22.8) | 39 (24.2) |
Reason for discontinuation, N (%) | ||||||
Adverse events | 17 (14.4) | 12 (10.2) | 15 (9.5) | 11 (7.1) | 15 (9.0) | 8 (5.0) |
Insufficient therapeutic response | 11 (9.3) | 18 (15.3) | 7 (4.4) | 16 (10.4) | 2 (1.2) | 15 (9.3) |
Protocol violation | 2 (1.7) | 0 | 1 (0.6) | 2 (1.3) | 1 (0.6) | 1 (0.6) |
Withdrawal of consent | 13 (11.0) | 14 (11.9) | 26 (16.5) | 17 (11.0) | 18 (10.8) | 14 (8.7) |
Lost to follow-up | 0 | 1 (0.8) | 1 (0.6) | 0 | 1 (0.6) | 0 |
Other | 0 | 0 | 0 | 2 (1.3) | 1 (0.6) | 1 (0.6) |
Randomized (ITT) | 118 | 120 | 158 | 154 | 167 | 161 |
mITT, N | 118 | 117 | 158 | 152 | 167 | 161 |
Safety, N | 118 | 118 | 158 | 154 | 167 | 161 |
CAR = cariprazine; ITT = intention-to-treat; mITT = modified intention-to-treat.
aIn total, 169 patients were randomized to receive 6 mg to 12 mg per day CAR; this treatment group was excluded from this report.
bNumber of randomized patients per number of screened patients.
Source: Clinical Study Reports for study RGH-MD-31, study RGH-MD-32, and study RGH-MD-33.11-13
Table 20: Patient Disposition — Bipolar Depression
Characteristic | RGH-MD-53 study | RGH-MD-54 study | RGH-MD-56 study | ||||||
|---|---|---|---|---|---|---|---|---|---|
CAR 1.5 mg | CAR 3 mg | Placebo | CAR 1.5 mg | CAR 3 mg | Placebo | CAR 1.5 mg | CAR 3 mg | Placebo | |
Screened, N | 866 | 782 | 1,013a | ||||||
Randomized, N (%)b | 168 (19.4) | 158 (18.2) | 167 (19.3) | 160 (20.5) | 165 (21.1) | 163 (20.8) | 147 (14.5) | 146 (14.4) | 148 (14.6) |
Discontinued from study, n (%) | 31 (18.6) | 30 (19) | 30 (18.2) | 23 (14.6) | 31 (18.8) | 23 (14.6) | 29 (19.9) | 52 (35.6) | 40 (27.6) |
Reason for discontinuation, n (%) | |||||||||
Adverse events | 5 (3) | 11 (7) | 5 (3) | 7 (4.5) | 9 (5.5) | 4 (2.5) | 12 (8.2) | 17 (11.6) | 15 (10.3) |
Lost to follow-up | 11 (6.6) | 7 (4.4) | 7 (4.2) | 7 (4.5) | 6 (3.6) | 5 (3.2) | 7 (4.8) | 9 (6.2) | 4 (2.8) |
Withdrawal of consent | 6 (3.6) | 5 (3.2) | 7 (4.2) | 3 (1.9) | 8 (4.8) | 6 (3.8) | 4 (2.7) | 15 (10.3) | 11 (7.6) |
Lack of efficacy | 1 (0.6) | 2 (1.3) | 7 (4.2) | 0 | 3 (1.8) | 2 (1.3) | 2 (1.4) | 4 (2.7) | 5 (3.4) |
Protocol violation | 4 (2.4) | 1 (0.6) | 3 (1.8) | 0 | 0 | 1 (0.6) | 3 (2.1) | 7 (4.8) | 5 (3.4) |
Noncompliance with study drug | 3 (1.8) | 2 (1.3) | 1 (0.6) | 3 (1.9) | 2 (1.2) | 3 (1.9) | NA | NA | NA |
Other | 1 (0.6) | 2 (1.3) | 0 | 3 (1.9) | 3 (1.8) | 2 (1.3) | 1 (0.7) | 0 | 0 |
Randomized (ITT), N | 168 | 158 | 167 | 160 | 165 | 163 | 147 | 146 | 148 |
mITT, N | 162 | 153 | 163 | 154 | 164 | 156 | 145 | 145 | 141 |
Safety, N | 167 | 158 | 165 | 157 | 165 | 158 | 146 | 146 | 145 |
CAR = cariprazine; ITT = intention-to-treat; mITT = modified intention-to-treat; NA = not available.
aIn total, 143 patients were randomized to receive 0.75 mg per day CAR; this treatment group was excluded from this report.
bNumber of randomized patients per number of screened patients.
Source: Clinical Study Reports for study RGH-MD-53, study RGH-MD-54, and study RGH-MD-56.14-16
Table 21: Exposure — Bipolar Mania, Safety Set
Measure of exposure | RGH-MD-31 study | RGH-MD-32 study | RGH-MD-33 study | |||
|---|---|---|---|---|---|---|
CAR 3 mg to 12 mg N = 118 | Placebo N = 118 | CAR 3 mg to 12 mg N = 158 | Placebo N = 154 | CAR 3 mg to 6 mg N = 167 | Placebo N = 161 | |
Duration of treatment in days,a mean (SD) | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
Distribution of treatment duration, n (%) | ||||||
1 day | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
2 days to 7 days | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
8 days to 14 days | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
15 days to 21 days | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
More than 21 days | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
Overall mean daily dose, mean (SD) | ||||||
Mg per day | 8.8 (|||||) | NA | 7.5 (|||||) | NA | 4.8 (|||||) | NA |
Capsules per day | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
Final dose (capsules per day), n (%) | ||||||
1 | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
2 | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
3 | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
4 | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
CAR = cariprazine; NA = not applicable; SD = standard deviation.
aDuration of treatment = date of the last dose of double-blind study drug – date of the first dose of double-blind study drug + 1.
Source: Clinical Study Reports for study RGH-MD-31, study RGH-MD-32, and study RGH-MD-33.11-13
Table 22: Exposure — Bipolar Depression, Safety Set
Treatment duration | RGH-MD-53 study | RGH-MD-54 study | RGH-MD-56 study | ||||||
|---|---|---|---|---|---|---|---|---|---|
CAR 1.5 mg N = 167 | CAR 3 mg N = 158 | Placebo N = 165 | CAR 1.5 mg N = 158 | CAR 3 mg N = 157 | Placebo N = 165 | CAR 1.5 mg N = 146 | CAR 3 mg N = 146 | Placebo N = 145 | |
Duration of treatment in days,a mean (SD) | 37.5 (11.3) | 37.6 (10.6) | 39.1 (8.9) | 38.6 (9.1) | 38.5 (9.0) | 39.3 (8.7) | 49.3 (14.7) | 46.0 (16.5) | 46.2 (18.2) |
Distribution of treatment duration, n (%) | |||||||||
1 day | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
2 days to 7 days | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
8 days to 14 days | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
15 days to 28 days | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
29 days to 42 days | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
> 42 days | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
Overall mean daily dose, mean (SD) | NR | NR | NR | NR | NR | NR | NR | NR | NR |
CAR = cariprazine; NR = not reported; SD = standard deviation.
aDuration of treatment = (study treatment end date – study treatment start date) + 1.
Source: Clinical Study Reports for study RGH-MD-53, study RGH-MD-54, and study RGH-MD-56.14-16
Concomitant Medications
In the bipolar mania studies, the mean daily dose of lorazepam used as a rescue medication to control agitation, restlessness, irritability, and hostility was similar between treatment groups by study week and overall. In study RGH-MD-31, 78% of patients used lorazepam. In study RGH-MD-32, 78% of patients used lorazepam and 1 patient used diazepam. In study RGH-MD-33, 54% of patients used lorazepam, 8% used diazepam, and 0.6% used oxazepam. Each of the studies noted that the rescue use of benzodiazepines decreased over time in accordance with the study protocol.
In study RGH-MD-53, patients in the placebo, cariprazine 1.5 mg, and cariprazine 3 mg groups, |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| was reported during the double-blind treatment period.
In study RGH-MD-54, |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| as rescue medication for the control of symptoms of agitation, restlessness, or hostility during the double-blind treatment period. The proportion of patients and the doses administered were generally similar among treatment groups.
In study RGH-MD-56, 6.9% of patients used lorazepam and 2.4% of patients used diazepam as rescue medication to control symptoms of agitation, restlessness, or hostility during the double-blind treatment period. The proportion of patients and the doses administered were generally similar among treatment groups.
Efficacy
Only those efficacy outcomes and analyses of subgroups identified in the review protocol are reported as follows. Refer to Appendix 3 for detailed efficacy data.
Bipolar Mania
Change in Symptom Severity
In the bipolar mania studies, symptoms of mania were evaluated using the YMRS, symptoms of depression were evaluated using the MADRS, and positive and negative symptoms were evaluated using the PANSS. A global assessment of severity and improvement of symptoms were evaluated using the CGI-S and CGI-I, respectively. The results are summarized in the following sections.
Symptoms of Mania: The change from baseline to week 3 in YMRS total score was the primary end point in all of the bipolar mania studies (Table 23). The treatment group difference was in favour of cariprazine for all doses assessed in each of the 3 studies. This was based on a difference in score (LSM difference) between cariprazine 3 mg to 12 mg and placebo of –6.1 (95% CI, –8.9 to –3.3; P < 0.0001) in study RGH-MD-31, and –4.3 (95% CI, –6.7 to –1.9; P = 0.0004) in study RGH-MD-32. In study RGH-MD-33, the difference in score between cariprazine 3 mg to 6 mg and placebo was –6.1 (95% CI, –8.4 to –3.8; P < 0.001).
Sensitivity analyses on the primary outcome were conducted in all 3 studies (data not shown). In study RGH-MD-31, the sensitivity analysis using observed cases corresponded to an LSM difference of –5.5 (95% CI, –7.9 to –3.1; P < 0.0001) and the sensitivity analysis using an MMRM corresponded to an LSM difference of –7.0 (95% CI, –10.0 to –4.0; P < 0.0001). In study RGH-MD-32 and study RGH-MD-33, the sensitivity analysis was performed using a pattern-mixture model based on nonfuture dependent missing value restrictions (data not shown). All sensitivity analyses supported the results of the primary efficacy analyses.
The change from baseline to week 3 in YMRS total score was also analyzed by subgroup — by patients with mania and by patients with mixed mania. Results were reported as descriptive statistics, presented in Table 24. The changes from baseline to week 3 in YMRS total score based on the subgroups were consistent with the primary analyses, except for the mixed mania subgroup in study RGH-MD-32. However, the mixed mania subgroups were associated with very small sample sizes, which limits the interpretability of the results.
Global Assessment of Symptoms: The change from baseline to week 3 in CGI-S total score was the secondary end point in all of the bipolar mania studies (Table 25). In each of the 3 studies, the treatment group difference in CGI-S total score was in favour of cariprazine for all doses assessed. This was based on a difference in score between cariprazine 3 mg to 12 mg and placebo of –0.6 (95% CI, –1.0 to –0.3; P = 0.0001) in study RGH-MD-31, and –0.4 (95% CI, –0.7 to –0.1; P = 0.0027) in study RGH-MD-32. In study RGH-MD-33, the difference in score between cariprazine 3 mg to 6 mg and placebo was –0.6 (95% CI, –0.9 to –0.4; P < 0.001).
The CGI-I outcome is defined by an assessment of the change in overall severity of illness. The CGI-I was an exploratory outcome in all of the bipolar mania studies. The score at week 3 and the LSM difference of cariprazine compared to placebo are presented in Table 26. The LSM difference of the change from baseline in CGI-I at week 3 for cariprazine compared to placebo was –0.8 (95% CI, –1.2 to –0.5; P < 0.0001), –0.5 (95% CI, –0.7 to –0.2; P = 0.0004), and –0.7 (95% CI, –0.9 to –0.4; P < 0.001) in study RGH-MD-31, study RGH-MD-32, and study RGH-MD-33, respectively.
Depressive Symptoms: In all of the bipolar mania studies, the change in depressive symptoms was evaluated using the MADRS and assessed as the change from baseline to week 3 in the MADRS total score (Table 27). This outcome was considered exploratory in all studies. Briefly, the LSM difference for cariprazine 3 mg to 12 mg compared to placebo indicated no difference between treatments in study RGH-MD-31 and study RGH-MD-32. The LSM difference in score in study RGH-MD-33 was –1.5 (95% CI, –2.5 to –0.6; P = 0.002) for cariprazine 3 mg to 6 mg compared to placebo.
Positive and Negative Symptoms: Patients were assessed using the PANSS to evaluate positive and negative symptoms in the bipolar mania studies. The PANSS was an exploratory outcome reported as the change from baseline to week 3 in the PANSS total score (Table 28). In study RGH-MD-31, the LSM difference in PANSS total score was –3.6 (95% CI, –6.7 to –0.4; P = 0.0269) for cariprazine 3 mg to 12 mg compared to placebo. In study RGH-MD-32, the LSM difference in PANSS total score was –3.3 (95% CI, –5.5 to –1.1; P = 0.0035). In study RGH-MD-33, the LSM difference in total score was –7.4 (95% CI, –9.7 to –5.0; P < 0.001) for cariprazine 3 mg to 6 mg compared to placebo.
Suicidal Ideation
A summary of the incidence of most severe suicidal ideation and most severe suicidal behaviour per the C-SSRS is summarized in Table 29. This outcome was not reported in study RGH-MD-31. In all treatment groups, suicidal ideation was reported in 1% to 3% of patients. Suicidal behaviour was not reported for any patients.
Response Rate and Remission Rate
Response rate and remission rate based on the YMRS were assessed in all bipolar mania studies. The results for response rate and remission rate at week 3 are summarized in Table 30. The response rate, defined as a reduction of at least 50% from baseline in the YMRS total score, was 48.3%, 58.9%, and 60.6% for the cariprazine treatment groups, and 24.8%, 44.1%, and 37.5% for the placebo treatment groups, in study RGH-MD-31, study RGH-MD-32, and study RGH-MD-33, respectively. The remission rate, defined as a YMRS total score of 12 or less, was 41.5%, 51.9%, and 44.8% in the cariprazine treatment groups, and 23.1%, 34.9%, and 29.4% for the placebo treatment groups, in study RGH-MD-31, study RGH-MD-32, and study RGH-MD-33, respectively.
Functioning
Functioning (e.g., psychosocial, occupational) was not reported in the bipolar mania studies.
Table 23: Change From Baseline to Week 3 in YMRS Total Score — Modified Intention-to-Treat Population
Study/treatment group | N included in analysis | Baseline score, mean (SD)a | Change at week 3, LSM (SE) | LSM difference vs. placebo (95% CI) | P value vs. placebo |
|---|---|---|---|---|---|
RGH-MD-31 studyb | |||||
CAR 3 mg to 12 mg | 118 | 30.6 (0.5) | –13.3 (|||||) | –6.1 (–8.9 to –3.3) | < 0.0001 |
Placebo | 117 | 30.2 (0.5) | –7.2 (|||||) | Reference | Reference |
RGH-MD-32 studyc | |||||
CAR 3 mg to 12 mg | 158 | 32.3 (5.8) | –19.6 (0.9) | –4.3 (–6.7 to –1.9) | 0.0004 |
Placebo | 152 | 32.1 (5.6) | –15.3 (0.9) | Reference | Reference |
RGH-MD-33 studyc | |||||
CAR 3 mg to 6 mg | 165 | 33.2 (5.6) | –18.6 (0.8) | –6.1 (–8.4 to –3.8) | < 0.001 |
Placebo | 160 | 32.6 (5.8) | –12.5 (0.8) | Reference | Reference |
ANCOVA = analysis of covariance; CAR = cariprazine; CI = confidence interval; LSM = least squares mean; MMRM = mixed model of repeated measures; OC = observed case; SD = standard deviation; SE = standard error; SEM = standard error of the mean; vs. = versus; YMRS = Young Mania Rating Scale.
aFor study RGH-MD-31 only, SEM was reported instead of SD.
bAnalysis was based on an ANCOVA model for change from baseline, with treatment group and study centre as factors and the baseline YMRS value as a covariate.
cMMRM analysis is based on an MMRM using the OC data, with treatment group, pooled study centre, visit, and treatment-group-by-visit interaction as factors, baseline value and baseline-by-visit interaction as covariates, and an unstructured covariance matrix.
Source: Clinical Study Reports for study RGH-MD-31, study RGH-MD-32, and study RGH-MD-33.11-13
Table 24: Subgroup Analysis, Change From Baseline to Week 3 in YMRS Total Score — Modified Intention-to-Treat Population
Subgroup | RGH-MD-31 study | RGH-MD-32 study | RGH-MD-33 study | |||
|---|---|---|---|---|---|---|
CAR 3 mg to 12 mg N = 118 | Placebo N = 117 | CAR 3 mg to 12 mg N = 158 | Placebo N = 152 | CAR 3 mg to 6 mg N = 165 | Placebo N = 160 | |
Patients with mania | ||||||
n | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
Baseline, mean (SD) | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
Change from baseline, mean (SD) | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
Difference in change, mean (SE) | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
Patients with mixed mania | ||||||
n | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
Baseline, mean (SD) | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
Change from baseline, mean (SD) | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
Difference in change, mean (SE) | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
CAR = cariprazine; SD = standard deviation; SE = standard error; YMRS = Young Mania Rating Scale.
Source: Common Technical Document (Sponsor submission).73
Table 25: Change From Baseline to Week 3 in CGI-S Total Score — Modified Intention-to-Treat Population
Study/treatment group | N included in analysis | Baseline score, mean (SD)a | Change at week 3, LSM (SE) | LSM difference vs. placebo (95% CI) | P value vs. placebo |
|---|---|---|---|---|---|
RGH-MD-31 studyb | |||||
CAR 3 mg to 12 mg | 118 | 4.7 (0.1) | –1.4 (|||||) | –0.6 (–1.0 to –0.3) | 0.0001 |
Placebo | 117 | 4.6 (0.1) | –0.8 (|||||) | Reference | Reference |
RGH-MD-32 studyc | |||||
CAR 3 mg to 12 mg | 158 | 4.6 (0.6) | –1.9 (0.1) | –0.4 (–0.7 to –0.1) | 0.0027 |
Placebo | 152 | 4.6 (0.6) | –1.5 (0.1) | Reference | Reference |
RGH-MD-33 studyc | |||||
CAR 3 mg to 6 mg | 165 | 4.8 (0.6) | –1.9 (0.1) | –0.6 (–0.9 to –0.4) | < 0.001 |
Placebo | 160 | 4.8 (0.7) | –1.3 (0.1) | Reference | Reference |
ANCOVA = analysis of covariance; CAR = cariprazine; CGI-S = Clinical Global Impression–Severity of Illness; CI = confidence interval; LSM = least squares mean; MMRM = mixed model of repeated measures; OC = observed case; SD = standard deviation; SE = standard error; SEM = standard error of the mean; vs. = versus.
aFor study RGH-MD-31 only, SEM was reported instead of SD.
bAnalysis was based on an ANCOVA model for change from baseline, with treatment group and study centre as factors and baseline CGI-S score as a covariate.
cMMRM analysis was based on an MMRM using the OC data, with treatment group, pooled study centre, visit, and treatment-group-by-visit interaction as factors, baseline value and baseline-by-visit interaction as covariates, and an unstructured covariance matrix.
Source: Clinical Study Reports for study RGH-MD-31, study RGH-MD-32, and study RGH-MD-33.11-13
Table 26: Score at Week 3 in CGI-I Total Score — Modified Intention-to-Treat Population
Study/treatment group | N included in analysis | Baseline score, mean (SD) | Score at week 3, LSM (SE) | LSM difference vs. placebo (95% CI) | P value vs. placebo |
|---|---|---|---|---|---|
RGH-MD-31 studya | |||||
CAR 3 mg to 12 mg | 118 | NA | ||||||||| | –0.8 (–1.2 to –0.5) | < 0.0001b |
Placebo | 117 | NA | ||||||||| | Reference | Reference |
RGH-MD-32 studyc | |||||
CAR 3 mg to 12 mg | 158 | NA | 2.0 (0.1) | –0.5 (–0.7 to –0.2) | 0.0004b |
Placebo | 152 | NA | 2.5 (0.1) | Reference | Reference |
RGH-MD-33 studyc | |||||
CAR 3 mg to 6 mg | 165 | NA | 2.2 (0.1) | –0.7 (–0.9 to –0.4) | < 0.001b |
Placebo | 160 | NA | 2.9 (0.1) | Reference | Reference |
CAR = cariprazine; CGI-I = Clinical Global Impression–Improvement; CI = confidence interval; LSM = least squares mean; MMRM = mixed model of repeated measures; NA = not applicable; OC = observed case; SD = standard deviation; SE = standard error; vs. = versus.
aAnalysis was based on an analysis-of-variance model for change from baseline, with treatment group and study centre as factors.
bThe P value was not adjusted for multiple testing (i.e., the type I error rate was not controlled).
cMMRM analysis was based on an MMRM using the OC data, with treatment group, pooled study centre, visit, and treatment-group-by-visit as factors, baseline value and baseline-by-visit interaction as covariates, and an unstructured covariance matrix.
Source: Clinical Study Reports for study RGH-MD-31, study RGH-MD-32, and study RGH-MD-33.11-13
Table 27: Change From Baseline to Week 3 in MADRS Total Score — Modified Intention-to-Treat Population
Study/treatment group | N included in analysis | Baseline score, mean (SD)a | Change at week 3, LSM (SE) | LSM difference vs. placebo (95% CI) | P value vs. placebo |
|---|---|---|---|---|---|
RGH-MD-31 studyb | |||||
CAR 3 mg to 12 mg | 118 | 9.0 (0.4) | ||||||||| | –0.6 (–2.1 to 0.9) | 0.4052c |
Placebo | 117 | 8.8 (0.4) | ||||||||| | Reference | Reference |
RGH-MD-32 studyd | |||||
CAR 3 mg to 12 mg | 158 | 8.3 (4.0) | –3.7 (0.4) | –0.3 (–1.5 to 0.8) | 0.5626c |
Placebo | 152 | 8.2 (4.1) | –3.3 (0.4) | Reference | Reference |
RGH-MD-33 studyd | |||||
CAR 3 mg to 6 mg | 165 | ||||||||| | –4.0 (0.4) | –1.5 (–2.5 to –0.6) | 0.002c |
Placebo | 160 | ||||||||| | –2.4 (0.4) | Reference | Reference |
ANCOVA = analysis of covariance; CAR = cariprazine; CI = confidence interval; LSM = least squares mean; MADRS = Montgomery–Åsberg Depression Rating Scale; MMRM = mixed model of repeated measures; OC = observed case; SD = standard deviation; SE = standard error; SEM = standard error of the mean; vs. = versus.
aFor study RGH-MD-31 only, SEM was reported instead of SD.
bAnalysis was based on an ANCOVA model for change from baseline, with treatment group and study centre as factors and respective baseline value as a covariate.
cThe P value was not adjusted for multiple testing (i.e., the type I error rate was not controlled).
dMMRM analysis was based on an MMRM using the OC data, with treatment group, pooled study centre, visit, and treatment-group-by-visit interaction as factors, baseline value and baseline-by-visit interaction as covariates, and an unstructured covariance matrix.
Source: Clinical Study Reports for study RGH-MD-31, study RGH-MD-32, and study RGH-MD-33.11-13
Table 28: Change From Baseline to Week 3 in PANSS Total Score — Modified Intention-to-Treat Population
Study/treatment group | N included in analysis | Baseline score, mean (SD)a | Change at week 3, LSM (SE) | LSM difference vs. placebo (95% CI) | P value vs. placebo |
|---|---|---|---|---|---|
RGH-MD-31 studyb | |||||
CAR 3 mg to 12 mg | 118 | 60.2 (1.3) | ||||||||| | –3.6 (–6.7 to –0.4) | 0.0269c |
Placebo | 117 | 60.5 (1.5) | ||||||||| | Reference | Reference |
RGH-MD-32 studyd | |||||
CAR 3 mg to 12 mg | 158 | ||||||||| | –16.5 (0.8) | –3.3 (–5.5 to –1.1) | 0.0035c |
Placebo | 152 | ||||||||| | –13.2 (0.8) | Reference | Reference |
RGH-MD-33 studyd | |||||
CAR 3 mg to 6 mg | 165 | ||||||||| | –14.3 (0.8) | –7.4 (–9.7 to –5.0) | < 0.001c |
Placebo | 160 | ||||||||| | –6.9 (0.9) | Reference | Reference |
CAR = cariprazine; CI = confidence interval; LSM = least squares mean; MMRM = mixed model of repeated measures; OC = observed case; PANSS = Positive and Negative Syndrome Scale; SD = standard deviation; SE = standard error; SEM = standard error of the mean; vs. = versus.
aFor study RGH-MD-31 only, SEM was reported instead of SD.
bAnalysis was based on an analysis of covariance model for change from baseline, with treatment group and study centre as factors and respective baseline value as a covariate.
cThe P value was not adjusted for multiple testing (i.e., the type I error rate was not controlled).
dMMRM analysis was based on an MMRM using the OC data, with treatment group, pooled study centre, visit, and treatment-group-by-visit interaction as factors, baseline value and baseline-by-visit interaction as covariates, and an unstructured covariance matrix.
Source: Clinical Study Reports for study RGH-MD-31, study RGH-MD-32, and study RGH-MD-33.11-13
Table 29: Suicidal Ideation per Columbia–Suicide Severity Rating Scale — Safety Population
Factor | RGH-MD-31 study | RGH-MD-32 study | RGH-MD-33 study | |||
|---|---|---|---|---|---|---|
CAR 3 mg to 12 mg N = 118 | Placebo N = 118 | CAR 3 mg to 12 mg N = 158 | Placebo N = 154 | CAR 3 mg to 6 mg N = 167 | Placebo N = 161 | |
Suicidal ideation, n (%) | NR | NR | 4 (2.5) | 3 (2.0) | 2 (1.2) | 3 (1.9) |
Suicidal behaviour, n (%) | NR | NR | 0 | 0 | 0 | 0 |
CAR = cariprazine; NR = not reported.
Source: Clinical Study Reports for study RGH-MD-31, study RGH-MD-32, and study RGH-MD-33.11-13
Table 30: YMRS Response and Remission Rates at Week 3 — Modified Intention-to-Treat Population
Factor | RGH-MD-31 study | RGH-MD-32 study | RGH-MD-33 study | |||
|---|---|---|---|---|---|---|
CAR 3 mg to 12 mg N = 118 | Placebo N = 118 | CAR 3 mg to 12 mg N = 158 | Placebo N = 154 | CAR 3 mg to 6 mg N = 167 | Placebo N = 161 | |
YMRS response (≥ 50% reduction from baseline in YMRS total score)a | ||||||
n/N (%) | 57/118 (48.3) | 29/117 (24.8) | 93/158 (58.9) | 67/152 (44.1) | 100/165 (60.6) | 60/160 (37.5) |
P valueb | 0.0002 | — | 0.0097 | — | < 0.001 | — |
YMRS remission (YMRS total score ≤ 12)a | ||||||
n/N (%) | 49/118 (41.5) | 27/117 (23.1) | 82/158 (51.9) | 53/152 (34.9) | 74/165 (44.8) | 47/160 (29.4) |
P valueb | 0.0023 | — | 0.0025 | — | 0.003 | — |
CAR = cariprazine; YMRS = Young Mania Rating Scale.
aThe percentage of responders and of remitters was analyzed using logistic regression, with treatment group and baseline YMRS total score as explanatory variables.
bThe P value was not adjusted for multiple testing (i.e., the type I error rate was not controlled).
Source: Clinical Study Reports for study RGH-MD-31, study RGH-MD-32, and study RGH-MD-33.11-13
Health-Related Quality of Life, Hospitalization, Cognitive Impairment, and Persistence With Therapy
Outcomes related to HRQoL, hospitalization, cognitive impairment, and persistence with therapy were not reported in the bipolar mania studies.
Bipolar Depression
Change in Symptom Severity
Symptoms of Depression: The change from baseline to week 6 in the MADRS total score was the primary end point in all of the bipolar depression studies (Table 31). The LSM difference of the change from baseline in the MADRS total score at week 6 was in favour of cariprazine 1.5 mg when compared to placebo in all studies. This was based on an LSM difference of –2.5 (95% CI, –4.6 to –0.4; P = 0.0417) in study RGH-MD-53, –2.5 (95% CI, –4.6 to –0.4; P = 0.0331) in study RGH-MD-54, and –4.0 (95% CI, –6.3 to –1.6; P = 0.0030) in study RGH-MD-56. The comparison of cariprazine 3.0 mg to placebo in study RGH-MD-53 and study RGH-MD-56 did not demonstrate a difference between treatment groups. In study RGH-MD-54, the LSM difference was in favour of cariprazine 3.0 mg relative to placebo (LSM difference = –3.0 [95% CI, –5.1 to –0.9; P = 0.0103]).
In the bipolar depression studies, sensitivity analyses of the primary efficacy outcomes were performed using a pattern-mixture model for missing data imputation (data not shown). The sensitivity analyses performed in study RGH-MD-53 and study RGH-MD-54 were supportive of the primary analyses. In study RGH-MD-56, sensitivity analysis of the comparison between cariprazine 1.5 mg and placebo were consistent with the primary analysis. The analysis of cariprazine 3.0 mg compared to placebo provided mixed results. More specially, the LSM difference for cariprazine compared to placebo was statistically significant for the cariprazine 3 mg group when the shift parameter ranged from 0 to 2 units, but when it ranged from 3 units to 6 units, the comparison was not statistically significant (P value > 0.05).
The change from baseline in the HAM-D score and QIDS-SR score were additional outcomes (exploratory) used to assess depressive symptoms in the bipolar depression studies. Exploratory outcomes were not controlled for multiplicity and as such, the statistical significance of any difference cannot be inferred with certainty.
Table 31: Change From Baseline to Week 6 in MADRS Total Score — Modified Intention-to-Treat Population
Study/treatment group | N included in analysis | Baseline score, mean (SD) | Change at week 6, LSM (SE) | LSM difference vs. placebo (95% CI) | P value vs. placeboa |
|---|---|---|---|---|---|
RGH-MD-53 studyb | |||||
CAR 1.5 mg | 162 | 31.5 (4.3) | –14.8 (0.76) | –2.5 (–4.6 to –0.4) | 0.0417 |
CAR 3.0 mg | 153 | 31.4 (4.7) | –14.1 (0.78) | –1.8 (–3.9 to 0.4) | 0.1051 |
Placebo | 163 | 31.3 (4.1) | –12.4 (0.75) | Reference | Reference |
RGH-MD-54 studyb | |||||
CAR 1.5 mg | 154 | 30.7 (4.3) | –15.1 (0.77) | –2.5 (–4.6 to –0.4) | 0.0331 |
CAR 3.0 mg | 164 | 31.0 (4.9) | –15.6 (0.76) | –3.0 (–5.1 to –0.9) | 0.0103 |
Placebo | 156 | 30.2 (4.4) | –12.6 (0.76) | Reference | Reference |
RGH-MD-56 studyb | |||||
CAR 1.5 mg | 145 | 30.3 (4.4) | –15.1 (0.8) | –4.0 (–6.3 to –1.6) | 0.0030 |
CAR 3.0 mg | 145 | 30.6 (4.7) | –13.7 (0.9) | –2.5 (–4.9 to –0.1) | 0.1122 |
Placebo | 141 | 30.4 (4.6) | –11.1 (0.9) | Reference | Reference |
CAR = cariprazine; CI = confidence interval; LSM = least squares mean; MADRS = Montgomery–Åsberg Depression Rating Scale; MMRM = mixed model of repeated measures; SD = standard deviation; SE = standard error; vs. = versus.
aAdjusted P values: Adjustment was performed using a matched parallel gatekeeping procedure to control the overall type I error rate for multiple comparisons of 2 active doses vs. placebo at week 6 for the primary and secondary efficacy parameters.
bEstimates were derived from an MMRM with fixed factors (treatment group, pooled study centre, and visit), a covariate (baseline), and interactions (treatment group by visit and baseline by visit).
Source: Clinical Study Reports for study RGH-MD-53, study RGH-MD-54, and study RGH-MD-56.14-16
The results of the change in HAM-D score from baseline to week 6 and week 8 (study RGH-MD-56 only) are presented in Table 32. The analysis of change in HAM-D did not demonstrate a treatment group difference for cariprazine 1.5 mg or cariprazine 3.0 mg relative to placebo in study RGH-MD-53. The difference in HAM-D total score for the comparison of cariprazine 1.5 mg to placebo corresponded to an LSM difference of –2.4 (95% CI, –4.0 to –0.8; P = 0.0042) and –2.7 (95% CI, –4.4 to –1.0; P = 0.018) in study RGH-MD-53 and study RGH-MD-56, respectively. The analysis of the cariprazine 3.0 mg compared to placebo did not demonstrate a treatment group difference in study RGH-MD-54. In study RGH-MD-56, an LSM difference of –2.2 (95% CI, –3.9 to –0.5; P = 0.0133) was reported. Study RGH-MD-56 also assessed the change from baseline in the HAM-D score at week 8, which was consistent with the results at week 6 (Table 32).
The change in QIDS-SR score from baseline to week 6 was only assessed in study RGH-MD-53 and study RGH-MD-54. The results did not correspond to a treatment group difference between either cariprazine 1.5 mg or cariprazine 3.0 mg and placebo (Table 33).
Table 32: Change From Baseline to Week 6 and Week 8 in HAM-D Score — Modified Intention-to-Treat Population
Study/treatment group | N included in analysis | Baseline score, mean (SD) | Change at week 6, LSM (SE) | LSM difference vs. placebo (95% CI) | P value vs. placeboa |
|---|---|---|---|---|---|
RGH-MD-53 studyb | |||||
CAR 1.5 mg | 162 | 24.7 (3.5) | –12.2 (0.60) | –1.6 (–3.2 to 0.1) | 0.0590 |
CAR 3.0 mg | 153 | 24.5 (3.1) | –11.1 (0.60) | –0.5 (–2.1 to 1.2) | 0.5599 |
Placebo | 163 | 24.7 (3.0) | –10.6 (0.59) | Reference | Reference |
RGH-MD-54 studyb | |||||
CAR 1.5 mg | 154 | 24.9 (2.9) | –12.6 (0.60) | –2.4 (–4.0 to –0.8) | 0.0042 |
CAR 3.0 mg | 164 | 24.6 (3.2) | –11.5 (0.58) | –1.3 (–3.0 to 0.3) | 0.0996 |
Placebo | 156 | 24.4 (2.3) | –10.2 (0.59) | Reference | Reference |
RGH-MD-56 studyc | |||||
Change at week 6 | |||||
CAR 1.5 mg | 145 | 23.9 (3.2) | –11.8 (0.6) | –2.7 (–4.4 to –1.0) | 0.0018 |
CAR 3.0 mg | 145 | 24.0 (3.1) | –11.3 (0.6) | –2.2 (–3.9 to –0.5) | 0.0133 |
Placebo | 141 | 24.1 (2.8) | –9.1 (0.6) | Reference | Reference |
Change at week 8 | |||||
CAR 1.5 mg | 145 | 23.9 (3.2) | –12.7 (0.6) | –2.3 (–4.1 to –0.6) | 0.0104 |
CAR 3.0 mg | 145 | 24.0 (3.1) | –12.6 (0.7) | –2.2 (–4.0 to –0.4) | 0.0193 |
Placebo | 141 | 24.1 (2.8) | –10.4 (0.7) | Reference | Reference |
CAR = cariprazine; CI = confidence interval; HAM-D = Hamilton Depression Rating Scale; LSM = least squares mean; MMRM = mixed model of repeated measures; SD = standard deviation; SE = standard error; vs. = versus.
aThe P value was not adjusted for multiple testing (i.e., the type I error rate was not controlled).
bThis was based on a linear model for each visit, controlling for fixed factors (treatment group and pooled study centre) and a covariate (baseline).
cP values were from an MMRM, with treatment group, pooled study centre, visit, and treatment-group-by-visit interaction as fixed effects and the baseline value and baseline-value-by-visit interaction as covariates. An unstructured covariance matrix was used to model the covariance of within-patient scores.
Source: Clinical Study Reports for study RGH-MD-53, study RGH-MD-54, and study RGH-MD-56.14-16
Table 33: Change From Baseline to Week 6 in QIDS-SR Score — Modified Intention-to-Treat Population
Study/treatment group | N included in analysis | Baseline score, mean (SD) | Change at week 3, LSM (SE) | LSM difference vs. placebo (95% CI) | P value vs. placeboa |
|---|---|---|---|---|---|
RGH-MD-53 studyb | |||||
CAR 1.5 mg | 162 | 15.6 (3.7) | –7.0 (0.42) | –1.1 (–2.2 to 0.1) | 0.0752 |
CAR 3.0 mg | 153 | 15.6 (3.8) | –7.0 (0.43) | –1.1 (–2.2 to 0.1) | 0.0787 |
Placebo | 163 | 15.3 (3.5) | –6.0 (0.42) | Reference | Reference |
RGH-MD-54 studyb | |||||
CAR 1.5 mg | 154 | 15.3 (3.4) | –6.9 (0.39) | –0.8 (–1.9 to 0.3) | 0.1348 |
CAR 3.0 mg | 164 | 15.4 (4.1) | –6.8 (0.39) | –0.7 (–1.8 to 0.4) | 0.2117 |
Placebo | 156 | 15.2 (3.9) | –6.1 (0.39) | Reference | Reference |
CAR = cariprazine; CI = confidence interval; LSM = least squares mean; MMRM = mixed model of repeated measures; QIDS-SR = Quick Inventory of Depressive Symptomatology–Self-Rated; SD = standard deviation; SE = standard error; vs. = versus.
aThe P value was not adjusted for multiple testing (i.e., the type I error rate was not controlled).
bEstimates were derived from an MMRM with fixed factors (treatment group, pooled study centre, and visit), a covariate (baseline), and interactions (treatment group by visit and baseline by visit).
Source: Clinical Study Reports for study RGH-MD-53 and study RGH-MD-54.14,15
Global Assessment of Symptoms: The change in the CGI-S total score from baseline to week 6 was assessed as the secondary efficacy analysis in all included studies for bipolar depression (Table 34). The comparison of cariprazine 1.5 mg to placebo corresponded to an LSM difference of –0.3 (95% CI, –0.6 to –0.1; P = 0.0417) and –0.4 (95% CI, –0.6 to –0.1; P = 0.0132) in study RGH-MD-53 and study RGH-MD-56, respectively. A treatment group difference was not observed for the comparison of cariprazine 1.5 mg to placebo or any of the comparisons of cariprazine 3.0 mg to placebo.
Symptoms of Anxiety: In study RGH-MD-53 and study RGH-MD-54, the change in symptoms of anxiety at week 6 was an exploratory outcome assessed using the HAM-A score (Table 35). The treatment group difference for cariprazine 1.5 mg compared to placebo corresponded to an LSM difference of –1.5 (95% CI, –2.9 to –0.1; P = 0.0393) in study RGH-MD-53 and –1.6 (95% CI, –2.9 to –0.3; P = 0.0144) in study RGH-MD-54. A treatment group difference was not observed for the comparisons of cariprazine 3.0 mg to placebo in the 2 studies.
Functioning (e.g., Psychosocial, Occupational)
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||.
Suicidal Ideation
A summary of the incidence of most severe suicidal ideation and most severe suicidal behaviour per the C-SSRS in all included studies for bipolar depression is summarized in Table 37. Suicidal ideation was reported in 3% to 11% of patients. The incidence of suicidal ideation by dose of cariprazine varied between studies. Suicidal behaviour was not reported for any patients in any of the included studies.
Response Rate and Remission Rate
Response rate at week 6 was assessed using the MADRS (at least 50% reduction from baseline in the MADRS total score) as an exploratory outcome in the bipolar depression studies (Table 38). In study RGH-MD-53, treatment with cariprazine (1.5 mg or 3.0 mg) was not associated with being a responder when compared to placebo. In study RGH-MD-54, the comparison of cariprazine 3.0 mg to placebo corresponded to an odds ratio (OR) of 1.7 (95% CI, 1.1 to 2.6; P = 0.0243); cariprazine 1.5 mg was not associated with being a responder when compared to placebo. In study RGH-MD-56, the comparison of cariprazine 1.5 mg and 3.0 mg to placebo corresponded to an OR of 2.10 (95% CI, 1.30 to 3.41; P = 0.0024) and 1.74 (95% CI, 1.07 to 2.82; P = 0.0243), respectively.
Table 34: Change From Baseline to Week 6 in CGI-S Total Score — Modified Intention-to-Treat Population
Study/treatment group | N included in analysis | Baseline score, mean (SD) | Change at week 6, LSM (SE) | LSM difference vs. placebo (95% CI) | P value vs. placeboa |
|---|---|---|---|---|---|
RGH-MD-53 studyb | |||||
CAR 1.5 mg | 162 | 4.5 (0.6) | –1.5 (0.09) | –0.3 (–0.6 to –0.1) | 0.0417 |
CAR 3.0 mg | 153 | 4.5 (0.6) | –1.4 (0.09) | –0.2 (–0.4 to 0.1) | 0.1370c |
Placebo | 163 | 4.5 (0.5) | –1.2 (0.09) | Reference | Reference |
RGH-MD-54 studyb | |||||
CAR 1.5 mg | 154 | 4.5 (0.5) | –1.6 (0.10) | –0.2 (–0.5 to 0.0) | 0.0714 |
CAR 3.0 mg | 164 | 4.5 (0.5) | –1.6 (0.09) | –0.3 (–0.5 to –0.0) | 0.0662 |
Placebo | 156 | 4.5 (0.5) | –1.3 (0.09) | Reference | Reference |
RGH-MD-56 studyb | |||||
CAR 1.5 mg | 145 | 4.4 (0.5) | –1.4 (0.1) | –0.4 (–0.6 to –0.1) | 0.0132 |
CAR 3.0 mg | 145 | 4.4 (0.5) | –1.3 (0.1) | –0.3 (–0.5 to –0.0) | 0.1122c |
Placebo | 141 | 4.4 (0.5) | –1.0 (0.1) | Reference | Reference |
CAR = cariprazine; CGI-S = Clinical Global Impression–Severity of Illness; CI = confidence interval; LSM = least squares mean; MMRM = mixed model of repeated measures; SD = standard deviation; SE = standard error; vs. = versus.
aAdjusted P values: Adjustment was performed using a matched parallel gatekeeping procedure to control the overall type I error rate for multiple comparisons of 2 active doses vs. placebo at week 6 for the primary and secondary efficacy parameters.
bEstimates were derived from an MMRM with fixed factors (treatment group, pooled study centre, and visit), a covariate (baseline), and interactions (treatment group by visit and baseline by visit).
cP value tested after a failed prior test cannot be interpreted for inference.
Source: Clinical Study Reports for study RGH-MD-53, study RGH-MD-54, and study RGH-MD-56.14-16
The remission rate at week 6 was assessed using the MADRS (MADRS total score of 10 or less) and the HAM-D (HAM-D total score of 7 or less), both as exploratory outcomes in the bipolar depression studies (Table 38). In study RGH-MD-53, treatment with cariprazine (1.5 mg or 3.0 mg) was not associated with being a remitter when compared to placebo based on the MADRS definition. In study RGH-MD-54, the comparison of cariprazine 1.5 mg and 3.0 mg to placebo corresponded to an OR of 1.7 (95% CI, 1.0 to 2.8; P = 0.0374) and an OR of 1.7 (95% CI, 1.0 to 2.8; P = 0.0391), respectively. In study RGH-MD-56, the comparison of cariprazine 1.5 mg and 3.0 mg to placebo corresponded to an OR of 2.38 (95% CI, 1.38 to 4.09; P = 0.0017) and an OR of 1.59 (95% CI, 0.91 to 2.78; P = 0.1048), respectively.
Regarding remission based on the HAM-D tool, the comparison of cariprazine 1.5 mg to placebo corresponded to an OR of 2.2 (95% CI, 1.3 to 3.9; P = 0.0051) in study RGH-MD-53, an OR of 1.8 (95% CI, 1.0 to 3.0; P = 0.0356) in study RGH-MD-54, and an OR of 2.34 (95% CI, 1.31 to 4.18; P = 0.0042) in study RGH-MD-56. There was no difference in the odds of being a remitter as per the HAM-D definition for the comparison of cariprazine 3.0 mg to placebo in any of the studies.
Response rate and remission rate were also assessed at week 8 in study RGH-MD-56 (Table 39). The results at week 8 were consistent with the results at week 6, with the exception of the comparison of cariprazine 3.0 mg to placebo for HAM-D remitters, which corresponded to an OR of 1.74 (95% CI, 1.01 to 2.99; P = 0.0453).
Table 35: Change From Baseline to Week 6 in HAM-A Score — Modified Intention-to-Treat Population
Study/treatment group | N included in analysis | Baseline score, mean (SD) | Change at week 6, LSM (SE) | LSM difference vs. placebo (95% CI) | P value vs. placeboa |
|---|---|---|---|---|---|
RGH-MD-53 studyb | |||||
CAR 1.5 mg | 162 | 18.9 (6.2) | –8.6 (0.51) | –1.5 (–2.9 to –0.1) | 0.0393 |
CAR 3.0 mg | 153 | 18.7 (6.0) | –7.8 (0.53) | –0.7 (–2.1 to 0.8) | 0.3527 |
Placebo | 163 | 18.7 (5.6) | –7.1 (0.51) | Reference | Reference |
RGH-MD-54 studyb | |||||
CAR 1.5 mg | 154 | 18.4 (4.8) | –8.8 (0.47) | –1.6 (–2.9 to –0.3) | 0.0144 |
CAR 3.0 mg | 164 | 18.4 (6.0) | –8.2 (0.47) | –1.1 (–2.4 to 0.2) | 0.1116 |
Placebo | 156 | 18.5 (5.8) | –7.2 (0.47) | Reference | Reference |
CAR = cariprazine; CI = confidence interval; HAM-A = Hamilton Anxiety Rating Scale; LSM = least squares mean; MMRM = mixed model of repeated measures; SD = standard deviation; SE = standard error; vs. = versus.
aThe P value was not adjusted for multiple testing (i.e., the type I error rate was not controlled).
bEstimates were derived from an MMRM with fixed factors (treatment group, pooled study centre, and visit), a covariate (baseline), and interactions (treatment group by visit and baseline by visit).
Source: Clinical Study Reports for study RGH-MD-53 and study RGH-MD-54.14,15
Table 36: Change From Baseline to Week 8 in FAST Score — Modified Intention-to-Treat Population
Study/treatment group | N included in analysis | Baseline score, mean (SD) | Change at week 8, LSM (SE) | LSM difference vs. placebo (95% CI) | P value vs. placeboa |
|---|---|---|---|---|---|
RGH-MD-56 studyb | |||||
CAR 1.5 mg | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
CAR 3.0 mg | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
Placebo | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
ANCOVA = analysis of covariance; CAR = cariprazine; CI = confidence interval; FAST = Functioning Assessment Short Test; LSM = least squares mean; SD = standard deviation; SE = standard error; vs. = versus.
aThe P value was not adjusted for multiple testing (i.e., the type I error rate was not controlled).
bP values were from an ANCOVA model for change from baseline at a given visit, with treatment group and pooled study centre as factors and the baseline value as a covariate.
Source: Clinical Study Report for study RGH-MD-56.16
Table 37: Suicidal Ideation per Columbia–Suicide Severity Rating Scale — Safety Population
Factor | RGH-MD-53 study | RGH-MD-54 study | RGH-MD-56 study | ||||||
|---|---|---|---|---|---|---|---|---|---|
CAR 1.5 mg N = 167 | CAR 3 mg N = 158 | Placebo N = 165 | CAR 1.5 mg N = 154 | CAR 3 mg N = 164 | Placebo N = 156 | CAR 1.5 mg N = 145 | CAR 3 mg N = 145 | Placebo N = 141 | |
Suicidal ideation, n (%) | ||||||| | ||||||| | ||||||| | ||||(10.8) | ||||(7.9) | ||||(8.2) | 8 (5.5) | 13 (9.0) | 15 (10.6) |
Suicidal behaviour, n (%) | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
CAR = cariprazine.
Source: Clinical Study Reports for RGH-MD-53, RGH-MD-54, and RGH-MD-56.14-16
Table 38: MADRS Response and Remission Rate and HAM-D Remission Rate at Week 6 — Modified Intention-to-Treat Population
Factor | RGH-MD-53 study | RGH-MD-54 study | RGH-MD-56 study | ||||||
|---|---|---|---|---|---|---|---|---|---|
CAR 1.5 mg N = 162 | CAR 3 mg N = 153 | Placebo N = 163 | CAR 1.5 mg N = 154 | CAR 3 mg N = 164 | Placebo N = 156 | CAR 1.5 mg N = 145 | CAR 3 mg N = 145 | Placebo N = 141 | |
MADRS responders (≥ 50% reduction from baseline in MADRS total score)a | |||||||||
n (%) | 66 (40.7) | 65 (42.5) | 58 (35.6) | 74 (48.1) | 85 (51.8) | 62 (39.7) | 72 (49.7) | 65 (44.8) | 45 (31.9) |
OR (95% CI) | 1.2 | 1.3 | Reference | 1.4 (0.9 to 2.2) | 1.7 (1.1 to 2.6) | Reference | 2.10 (1.30 to 3.41) | 1.74 (1.07 to 2.82) | Reference |
P valueb | 0.3383 | 0.2088 | Reference | 0.1300 | 0.0243 | Reference | 0.0024 | 0.0243 | Reference |
MADRS remitters (MADRS total score ≤ 10)a | |||||||||
n (%) | 42 (25.9) | 40 (26.1) | 32 (19.6) | 51 (33.1) | 53 (32.3) | 36 (23.1) | 53 (36.6) | 40 (27.6) | 28 (19.9) |
OR (95% CI) | 1.5 | 1.5 | Reference | 1.7 | 1.7 | Reference | 2.38 (1.38 to 4.09) | 1.59 (0.91 to 2.78) | Reference |
P valueb | 0.1648 | 0.1625 | Reference | 0.0374 | 0.0391 | Reference | 0.0017 | 0.1048 | Reference |
HAM-D remitters (HAM-D total score ≤ 7)a | |||||||||
n (%) | 44 (30.6) | 32 (22.7) | 32 (16.4) | 45 (32.4) | 35 (23.8) | 32 (22.1) | 44 (30.3) | 31 (21.4) | 22 (15.6) |
OR (95% CI) | 2.2 | 1.5 | Reference | 1.8 (1.0 to 3.0) | 1.1 (0.6 to 1.9) | Reference | 2.34 (1.31 to 4.18) | 1.46 (0.80 to 2.69) | Reference |
P valueb | 0.0051 | 0.1797 | Reference | 0.0356 | 0.7172 | Reference | 0.0042 | 0.2186 | Reference |
CAR = cariprazine; CI = confidence interval; HAM-D = Hamilton Depression Rating Scale; LOCF = last observation carried forward; MADRS = Montgomery–Åsberg Depression Rating Scale; OR = odds ratio.
aThe P value for a between-treatment comparison at each visit was based on a logistic regression model that included treatment group and the baseline MADRS or HAM-D total score value, based on the outcome. The P value was from a z test. LOCF was used for imputation.
bThe P value was not adjusted for multiple testing (i.e., the type I error rate was not controlled).
Source: Clinical Study Reports for study RGH-MD-53, study RGH-MD-54, and study RGH-MD-56.14-16
Health-Related Quality of Life, Hospitalization, Cognitive Impairment, and Persistence With Therapy
Outcomes related to HRQoL, hospitalization, cognitive impairment, and persistence with therapy were not reported in the bipolar mania studies.
Harms
Only those harms identified in the review protocol are reported as follows. Refer to Table 40 and Table 41 for detailed harms data from the bipolar mania studies and bipolar depression studies, respectively.
Table 39: MADRS Response and Remission Rate and HAM-D Remission Rate at Week 8 — Intention-to-Treat Population
Factor | RGH-MD-56 study | ||
|---|---|---|---|
Cariprazine 1.5 mg (N = 145) | Cariprazine 3 mg (N = 145) | Placebo (N = 141) | |
MADRS responders (≥ 50% reduction from baseline in MADRS total score)a | |||
n (%) | ||||||||| | ||||||||| | ||||||||| |
OR (95% CI) | ||||||||| | ||||||||| | ||||||||| |
P valueb | ||||||||| | ||||||||| | ||||||||| |
MADRS remitters (MADRS total score ≤ 10)a | |||
n (%) | ||||||||| | ||||||||| | ||||||||| |
OR (95% CI) | ||||||||| | ||||||||| | ||||||||| |
P valueb | ||||||||| | ||||||||| | ||||||||| |
HAM-D remitters (HAM-D total score ≤ 7)a | |||
n (%) | ||||||||| | ||||||||| | ||||||||| |
OR (95% CI) | ||||||||| | ||||||||| | ||||||||| |
P valueb | ||||||||| | ||||||||| | ||||||||| |
CI = confidence interval; HAM-D = Hamilton Depression Rating Scale; MADRS = Montgomery–Åsberg Depression Rating Scale;; OR = odds ratio;.
aAnalyses were based on a logistic regression model for the probability of response. The model included treatment group and corresponding baseline value as explanatory variables.b The P value was not adjusted for multiple testing (i.e., the type I error rate was not controlled).
Source: Clinical Study Report for study RGH-MD-56.16
Adverse Events
In the bipolar mania studies, the percentage of patients who reported an AE ranged from 78% to 86% for patients randomized to cariprazine (3 mg to 12 mg or 3 mg to 6 mg) and 61% to 79% for patients randomized to placebo. In all bipolar mania studies, overall AEs were reported more frequently by patients in the cariprazine treatment group than the placebo treatment group. The most common AEs reported more frequently by patients randomized to cariprazine compared to placebo, respectively, were extrapyramidal disorder (10% to 25% versus 2% to 9%), headache (11% to 20% versus 10% to 20%), akathisia (17% to 22% versus 4% to 6%), restlessness (6% to 8% versus 1% to 5%), constipation (5% to 15% versus 6% to 10%), dyspepsia (4% to 13% versus 3% to 7%), and vomiting (8% to 10% versus 3% to 5%). Of these, extrapyramidal disorder, akathisia, dyspepsia, and nausea were reported more frequently by patients randomized to cariprazine compared to placebo in the 3 studies.
In the bipolar depression studies, the percentage of patients who reported an AE ranged from 50% to 62% for patients randomized to cariprazine 1.5 mg, 49% to 62% for patients randomized to cariprazine 3.0 mg, and 46% to 55% for patients randomized to placebo. In all bipolar depression studies, overall AEs were reported more frequently by patients in the cariprazine treatment groups than the placebo groups. The most common AEs reported more frequently by patients randomized to cariprazine compared to placebo, respectively, were akathisia (5% to 14% versus 1% to 3%), nausea (4% to 9% versus 1% to 5%), and somnolence (2% to 7% versus 2% to 4%).
Serious Adverse Events
In all included studies, SAEs were infrequently reported. In the bipolar mania studies, SAEs were reported by 3.2% to 4.2% of patients randomized to cariprazine (3 mg to 12 mg or 3 mg to 6 mg) and 1.9% to 4.2% of patients randomized to placebo. Mania was 1 of the most common SAEs reported in the bipolar mania studies and was similar between treatment groups. Other SAEs in the included studies were reported in fewer than 1% of patients. In the bipolar depression studies, the percentage of patients who reported at least 1 SAE in the cariprazine 1.5 mg and cariprazine 3 mg treatment groups ranged from 0.6% to 1.4% and 0 to 1.4%, respectively. In the placebo treatment groups, the percentage of patients who reported at least 1 SAE ranged from 1.3% to 3.4%.
Withdrawals Due to Adverse Events
In the bipolar mania studies, WDAEs ranged from 9% to 14% of patients randomized to cariprazine and 5% to 10% of patients randomized to placebo. In the bipolar depression studies, WDAEs were reported by 3% to 8% of patients randomized to cariprazine 1.5 mg, 6% to 12% of patients randomized to cariprazine 3.0 mg, and 3% to 10% of patients randomized to placebo. The most common reasons for WDAEs were mania, akathisia, restlessness, and agitation.
Mortality
Among the 6 included studies, 1 death was reported in the cariprazine treatment group of study RGH-MD-33.
Notable Harms
Notable harms are AEs that are prespecified in the CADTH systematic review protocol, which are reported in Table 40 and Table 41.
As previously reported for the bipolar mania studies, EPS, akathisia, restlessness, and vomiting were reported more frequently by patients randomized to cariprazine than placebo. In the cariprazine and placebo treatment groups, respectively, insomnia was reported by 5.7% to 9.0% of patients and 2.5% to 9.3% of patients and sedation was reported by 1.8% to 5.9% of patients and 0.6% to 2.5% of patients. Metabolic effects (metabolism and nutrition disorders) were reported by |||||||||||||||||||||||||||||||||||| of patients and weight gain was reported by ||||||||||||||||||||||||||| of patients randomized to cariprazine and placebo, respectively. Hyperglycemia (blood glucose increased) and sexual dysfunction (libido decreased) were infrequently reported (less than 2 patients in any treatment group) and tardive dyskinesia or neuroleptic malignant syndrome were not reported by any patients.
As previously reported for the bipolar depression studies, akathisia was reported more frequently by patients randomized to cariprazine 1.5 mg and 3.0 mg than placebo. Akathisia was also more common in the cariprazine 3.0 mg group than in the cariprazine 1.5 mg group in study RGH-MD-53 and study RGH-MD-56 (9.5% versus 5.4% and 14.4% versus 4.8% in study RGH-MD-53 and study RGH-MD-56, respectively). The following notable harms were reported in the cariprazine 1.5 mg, cariprazine 3.0 mg, and placebo treatment groups, respectively: |||||||||||||||||||||||||||||||||||||||||||||, insomnia (||||||||| to 6.8% versus ||||||||| to 11.6% versus ||||||||| to 8.3%), |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||, restlessness (1.3% to 2.7% versus 6.2% to 7.3% versus 3.0% to 3.8%), and |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||. Other notable harms such as ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||, respectively, among all the bipolar depression studies. Lastly, ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| were not reported by any patients.
Table 40: Summary of Harms — Bipolar Mania, Safety Population
Harm | RGH-MD-31 study | RGH-MD-32 study | RGH-MD-33 study | |||
|---|---|---|---|---|---|---|
CAR 3 mg to 12 mg N = 118 | Placebo N = 118 | CAR 3 mg to 12 mg N = 158 | Placebo N = 154 | CAR 3 mg to 6 mg N = 167 | Placebo N = 161 | |
Patients with ≥ 1 TEAE during the double-blind treatment phase | ||||||
n (%) | 101 (85.6) | 93 (78.8) | 127 (80.4) | 97 (63.0) | 131 (78.4) | 98 (60.9) |
Most common events,a n (%) | ||||||
Extrapyramidal disorder | 29 (24.6) | 11 (9.3) | 24 (15.2) | 3 (1.9) | 16 (9.6) | 8 (5.0) |
Headache | 23 (19.5) | 24 (20.3) | 18 (11.4) | 16 (10.4) | 18 (10.8) | 15 (9.3) |
Akathisia | 22 (18.6) | 7 (5.9) | 35 (22.2) | 7 (4.5) | 29 (17.4) | 6 (3.7) |
Constipation | 18 (15.3) | 10 (8.5) | 13 (8.2) | 10 (6.5) | 8 (4.8) | 4 (2.5) |
Nausea | 18 (15.3) | 12 (10.2) | 16 (10.1) | 10 (6.5) | 16 (9.6) | 9 (5.6) |
Dyspepsia | 15 (12.7) | 8 (6.8) | 17 (10.8) | 5 (3.2) | ||||||||| | ||||||||| |
Dizziness | 11 (9.3) | 8 (6.8) | 13 (8.2) | 6 (3.9) | ||||||||| | ||||||||| |
Insomnia | 10 (8.5) | 3 (2.5) | 9 (5.7) | 8 (5.2) | 15 (9.0) | 15 (9.3) |
Vomiting | 10 (8.5) | 4 (3.4) | 16 (10.1) | 6 (3.9) | 14 (8.4) | 8 (5.0) |
Diarrhea | 7 (5.9) | 8 (6.8) | 11 (7.0) | 2 (1.3) | 4 (2.4) | 11 (6.8) |
Restlessness | 7 (5.9) | 1 (0.8) | 9 (5.7) | 1 (0.6) | 14 (8.4) | 8 (5.0) |
Sedation | 7 (5.9) | 1 (0.8) | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
Somnolence | ||||||||| | ||||||||| | 9 (5.7) | 2 (1.3) | ||||||||| | ||||||||| |
Vision blurred | 7 (5.9) | 1 (0.8) | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
Mania | 6 (5.1) | 8 (6.8) | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
Pain in extremity | 6 (5.1) | 3 (2.5) | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
Pyrexia | 6 (5.1) | 5 (4.2) | 8 (5.1) | 3 (1.9) | 0 | 0 |
Tremor | 6 (5.1) | 5 (4.2) | 18 (11.4) | 6 (3.9) | 4 (2.4) | 3 (1.9) |
Agitation | 5 (4.2) | 8 (6.8) | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
Abdominal discomfort | ||||||||| | ||||||||| | 8 (5.1) | 6 (3.9) | ||||||||| | ||||||||| |
Toothache | 3 (2.5) | 7 (5.9) | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
Patients with ≥ 1 SAE | ||||||
n (%) | 4 (3.4) | 5 (4.2) | 5 (3.2) | 3 (1.9) | 7 (4.2) | 3 (1.9) |
Most common events,b n (%) | ||||||
Mania | 2 (1.7) | 4 (3.4) | 2 (1.3) | 1 (0.6) | 2 (1.2) | 1 (0.6) |
Patients who stopped treatment due to AEs | ||||||
n (%) | 17 (14.4) | 12 (10.2) | 15 (9.5) | 11 (7.1) | 15 (9.0) | 8 (5.0) |
Most common events,a n (%) | ||||||
Mania | 3 (2.5) | 6 (5.1) | 2 (1.3) | 5 (3.2) | 3 (1.8) | 3 (1.9) |
Akathisia | ||||||||| | ||||||||| | 5 (3.2) | 0 | 3 (1.8) | 0 |
Restlessness | ||||||||| | ||||||||| | NA | NA | NA | NA |
Agitation | ||||||||| | ||||||||| | NA | NA | ||||||||| | ||||||||| |
Deaths | ||||||
n (%) | 0 | 0 | 0 | 0 | 1 (0.6) | 0 |
Pulmonary embolism, n (%) | 0 | 0 | 0 | 0 | 1 (0.6) | 0 |
Notable harms, n (%) | ||||||
Extrapyramidal symptoms | 29 (24.6) | 11 (9.3) | 24 (15.2) | 3 (1.9) | 16 (9.6) | 8 (5.0) |
Akathisia | 22 (18.6) | 7 (5.9) | 35 (22.2) | 7 (4.5) | 29 (17.4) | 6 (3.7) |
Insomnia | 10 (8.5) | 3 (2.5) | 9 (5.7) | 8 (5.2) | 15 (9.0) | 15 (9.3) |
Sedation | 7 (5.9) | 1 (0.8) | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
Metabolic effects (metabolism and nutrition disorders) | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
Hyperglycemia (blood glucose increased) | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
Weight gain | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
Restlessness | 7 (5.9) | 1 (0.8) | 9 (5.7) | 1 (0.6) | 14 (8.4) | 8 (5.0) |
Vomiting | 10 (8.5) | 4 (3.4) | 16 (10.1) | 6 (3.9) | 14 (8.4) | 8 (5.0) |
Sexual dysfunction (libido decreased) | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
Tardive dyskinesia | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
Neuroleptic malignant syndrome | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
AE = adverse event; CAR = cariprazine; NA = not applicable; SAE = serious adverse event; TEAE = treatment-emergent adverse event.
aFrequency of greater than 5% in any treatment group.
bFrequency of greater than 1% in any treatment group.
Source: Clinical Study Reports for study RGH-MD-31, study RGH-MD-32, and study RGH-MD-33.11-13
Table 41: Summary of Harms — Bipolar Depression, Safety Population
Harm | RGH-MD-53 study | RGH-MD-54 study | RGH-MD-56 study | ||||||
|---|---|---|---|---|---|---|---|---|---|
CAR 1.5 mg N = 167 | CAR 3 mg N = 158 | Placebo N = 165 | CAR 1.5 mg N = 157 | CAR 3 mg N = 165 | Placebo N = 158 | CAR 1.5 mg N = 146 | CAR 3 mg N = 146 | Placebo N = 145 | |
Patients with ≥ 1 TEAE | |||||||||
n (%) | 82 (49.1) | 78 (49.4) | 75 (45.5) | 89 (56.7) | 102 (61.8) | 83 (52.5) | 91 (62.3) | 91 (62.3) | 79 (54.5) |
Most common events,a n (%) | |||||||||
Akathisia | 9 (5.4) | 15 (9.5) | 3 (1.8) | 10 (6.4) | 9 (5.5) | 5 (3.2) | 7 (4.8) | 21 (14.4) | 2 (1.4) |
Headache | ||||||||| | ||||||||| | ||||||||| | 7 (4.5) | 12 (7.3) | 13 (8.2) | 10 (6.8) | 10 (6.8) | 16 (11.0) |
Insomnia | ||||||||| | ||||||||| | ||||||||| | 7 (4.5) | 12 (7.3) | 11 (7.0) | 10 (6.8) | 17 (11.6) | 12 (8.3) |
Restlessness | 4 (2.4) | 11 (7.0) | 5 (3.0) | 2 (1.3) | 12 (7.3) | 6 (3.8) | 4 (2.7) | 9 (6.2) | 5 (3.4) |
Nausea | 13 (7.8) | 8 (5.1) | 5 (3.0) | 6 (3.8) | 15 (9.1) | 1 (0.6) | 12 (8.2) | 12 (8.2) | 7 (4.8) |
Agitation | 3 (1.8) | 7 (4.4) | 10 (6.1) | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
Dizziness | ||||||||| | ||||||||| | ||||||||| | 8 (5.1) | 6 (3.6) | 3 (1.9) | ||||||||| | ||||||||| | ||||||||| |
Fatigue | 9 (5.4) | 5 (3.2) | 2 (1.2) | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
Somnolence | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | 9 (6.2) | 10 (6.8) | 6 (4.1) |
Diarrhea | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | 9 (6.2) | 3 (2.1) | 8 (5.5) |
Dry mouth | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
Patients with ≥ 1 SAE | |||||||||
n (%) | 1 (0.6) | 0 | 5 (3.0) | 2 (1.3) | 2 (1.2) | 2 (1.3) | 2 (1.4) | 2 (1.4) | 5 (3.4) |
Patients who stopped treatment due to AEs | |||||||||
n (%) | 5 (3.0) | 11 (7.0) | 5 (3.0) | 7 (4.5) | 9 (5.5) | 4 (2.5) | 12 (8.2) | 17 (11.6) | 15 (10.3) |
Most common events,b n (%) | |||||||||
Akathisia | ||||||||| | ||||||||| | ||||||||| | 3 (1.9) | 1 (0.6) | 0 | ||||||||| | ||||||||| | ||||||||| |
Deaths | |||||||||
n (%) | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
Notable harms, n (%) | |||||||||
Extrapyramidal symptoms | ||||||||| | ||||||||| | ||||||||| | 0 | 1 (0.6) | 1 (0.6) | ||||||||| | ||||||||| | ||||||||| |
Akathisia | ||||||||| | ||||||||| | ||||||||| | 10 (6.4) | 9 (5.5) | 5 (3.2) | 7 (4.8) | 21 (14.4) | 2 (1.4) |
Insomnia | ||||||||| | ||||||||| | ||||||||| | 7 (4.5) | 12 (7.3) | 11 (7.0) | 10 (6.8) | 17 (11.6) | 12 (8.3) |
Sedation | ||||||||| | ||||||||| | ||||||||| | 5 (3.0) | 8 (5.1) | 2 (1.3) | ||||||||| | ||||||||| | ||||||||| |
Metabolic effects (metabolism and nutrition disorders) | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
Hyperglycemia (blood glucose increased) | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
Weight gain | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
Restlessness | 4 (2.4) | 11 (7.0) | 5 (3.0) | 2 (1.3) | 12 (7.3) | 6 (3.8) | 4 (2.7) | 9 (6.2) | 5 (3.4) |
Vomiting | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
Sexual dysfunction (libido decreased) | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
Tardive dyskinesia | ||||||||| | ||||||||| | ||||||||| | 0 | 1 (0.6) | 0 | ||||||||| | ||||||||| | ||||||||| |
Neuroleptic malignant syndrome | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
AE = adverse event; CAR = cariprazine; SAE = serious adverse event; TEAE = treatment-emergent adverse event.
aFrequency of greater than 5% in any treatment group.
bFrequency of greater than 1% in any treatment group.
Note: Study RGH-MD-53 and study RGH-MD-54 included SAEs that occurred during the double-blind treatment period and within 30 days of the date of the last dose of the double-blind investigational product. For patients who did not participate in the safety follow-up period, events that occurred within 30 days of the last dose of the double-blind investigational product were also included.
Source: Clinical Study Reports for study RGH-MD-53, study RGH-MD-54, and study RGH-MD-56.14-16
Weight gain was captured in the safety assessment of vital signs as a potentially clinically significant vital sign. In study RGH-MD-31, study RGH-MD-32, and study RGH-MD-33, an increase in body weight of at least 7% was reported in ||||||||||||||||||||||||||| of patients in the cariprazine treatment groups, respectively, and ||||||||||||||||||||||||||| of patients in the placebo treatment groups, respectively. In study RGH-MD-53, study RGH-MD-54, and study RGH-MD-56, an increase in body weight of at least 7% was reported in ||||||||| and 6.9% of patients in the cariprazine 1.5 mg treatment groups, respectively, ||||||||| and 4.8% of patients in the cariprazine 3.0 mg treatment groups, respectively, and ||||||||| and 3.5% of patients in the placebo treatment groups, respectively.
Critical Appraisal
Internal Validity
All of the included studies were randomized, double-blind, placebo-controlled studies. A drug washout period of 4 days to 7 days was included in the studies for bipolar mania and up to 2 weeks for the studies for bipolar depression. This was considered an appropriate duration of time for treatments for bipolar I disorder. Appropriate methods of randomization were used, although there was the potential for unblinding or knowledge of treatment received due to AEs — most notably, EPS and akathisia, which were more common in the cariprazine treatment groups relative to placebo. This may have affected many of the end points assessed in the trials as they are based on a subjective assessment of symptom severity or clinical assessment. Treatment groups were well balanced in terms of baseline characteristics. Some imbalances in the severity of the current or most recent episode were observed, as the proportion of patients in the cariprazine treatment groups who were experiencing a severe episode as per the DSM-5 was higher relative to placebo in study RGH-MD-53 (27.5%, 24.7%, and 20.0% for cariprazine 1.5 mg, cariprazine 3.0 mg, and placebo, respectively) and study RGH-MD-54 (15.9%, 12.7%, and 10.8% for cariprazine 1.5 mg, cariprazine 3.0 mg, and placebo, respectively). These data were not available for study RGH-MD-56. The direction of potential bias is unclear. In all studies, the mean baseline efficacy scores were comparable between treatment groups and indicative of patients experiencing a bipolar mania and depression in the corresponding studies, as per feedback from the clinical experts.
Discontinuation rates were high, ranging from ||||||||| across bipolar mania studies and ||||||||| across the bipolar depression studies. While the clinical experts consulted by CADTH indicated that high discontinuation rates are typical of clinical trials for bipolar disorder, this may be a concern depending on the causes for discontinuation. Moreover, expected discontinuation rates for bipolar mania and bipolar depression are 25% and 35%, respectively, as per feedback from the experts. Overall discontinuation rates were balanced between treatment groups in most studies, except study RGH-MD-54 and study RGH-MD-56 for bipolar depression where discontinuation was notably higher among the cariprazine 3.0 mg group. Discontinuation was also higher for patients in the placebo treatment group compared to cariprazine 1.5 mg in study RGH-MD-56. The imbalance in discontinuation rates in study RGH-MD-56 appears to be driven by discontinuation due to AEs and withdrawal of consent. In the bipolar mania studies, there was an imbalance in the reason for discontinuation due to AEs (more frequent with cariprazine) and insufficient therapeutic response (more frequent with placebo), which may have biased the safety and efficacy results in favour of cariprazine. Missing data were handled using the LOCF approach (study RGH-MD-31) and MMRM approach (all other studies). Both methods rely on the assumption that data are missing at random, which is likely not the case given the imbalance in reasons for discontinuation that have been described. However, the sponsor conducted a pattern-mixture model analysis that relies on the assumption that data are not missing at random. The results of the pattern-mixture model analysis were consistent with the results of the primary analysis. The power calculations for study RGH-MD-31 did not account for loss to follow-up. End points that failed to reach statistical significance may have been underpowered given the high discontinuation rate. The power calculations for study RGH-MD-32 and study RGH-MD-33 assumed a 35% dropout rate, and the dropout rate was assumed to be 22% by week 6 for study RGH-MD-53 and study RGH-MD-54, and 25% by week 6 for study RGH-MD-56. Discontinuations may have been an issue for end points that failed to reach statistical significance in study RGH-MD-56 as well, as they also might have been underpowered.
All studies implemented methods to control for multiplicity up to the secondary end point, which was the change from baseline in the CGI-S at week 3 (bipolar mania studies) and week 6 (bipolar depression studies). Study RGH-MD-31 and study RGH-MD-32 used a closed testing procedure to control for the type I error rate; study RGH-MD-33 and the 3 bipolar depression studies used a matched parallel gatekeeping procedure. The analyses of the primary and secondary outcomes were the only outcomes controlled for multiplicity; therefore, all other efficacy outcomes should be considered supportive due to the risk of type I error.
The YMRS and MADRS are well-validated outcomes. The YMRS was developed to assess mania severity in patients with bipolar disorder whereas the MADRS was developed to assess the severity of depressive symptoms in patients with major depressive disorder. However, both outcomes are commonly used in research related to bipolar disorder. Both have an established MID: 6 points for YMRS and 2 points for MADRS. Both of these outcomes are administered by a trained clinician or investigator and based on the patient’s input and the rater’s judgment. Given that experiencing a bipolar episode may impact the patient’s perception of their current state, the reliability of the assessment may decrease. Further, the YMRS is based on a 48-hour recall period and the MADRS is based on a 1-week recall period, which may further contribute to the patient’s report of symptoms.
Evidence supporting an assessment of the psychometric properties of the CGI scale is based on studies in patients with schizophrenia rather than bipolar disorder (those studies were not identified in this review). Validity of the CGI scale is weak, and evidence of reliability and responsiveness were not identified. A 20% reduction in the PANSS total score, which has been found to correspond to a 1-point improvement on the CGI-S, has been used both as a predefined measure of clinical improvement and as criteria for response to antipsychotic treatment in a number of clinical trials in schizophrenia.56-58
Evidence of a psychometric property assessment of the PANSS, HAM-D, HAM-A, and QIDS-SR that was identified for this review was based on patients with schizophrenia or major depressive disorder; no evidence in patients with bipolar disorder was identified. An MID was not identified for the HAM-A or QIDS-SR and consensus about an MID for the PANSS and HAM-D was unclear. The FAST demonstrated evidence of validity and reliability, but responsiveness was not assessed. Additionally, an MID that ranges from an 8-point to 9-point change relative to baseline was identified.72
External Validity
The clinical experts described the patient population included in the trials for cariprazine as typical for clinical trials, but lacking characteristics that are often seen in clinical practice. This includes the presence of comorbidities, rapid cycling, other diagnoses, substance use disorder, and the elevated risk of suicide — all of which were exclusion criteria in the trials. The exclusion criteria can lead to a less severe and less complex sample relative to clinical practice. The clinical experts indicated that the baseline characteristics were suggestive of a patient population with bipolar I disorder of moderate severity. Patients who required pharmacologic treatment to control EPS or who had a history of tardive dyskinesia or neuroleptic malignant syndrome were excluded from the bipolar mania studies. This may result in an underestimation of the occurrence of these symptoms in the trial population and, in turn, impact the generalizability of the safety results to the broader population of patients with bipolar mania seen in clinical practice. No study centres located in Canada were included in the bipolar mania studies, 3 Canadian centres were included in study RGH-MD-56, and it was unclear whether Canadian sites were included in study RGH-MD-53 and study RGH-MD-54. The clinical experts consulted by CADTH stated that the population of patients in Canada who had bipolar disorder is not expected to differ significantly from patients in the study locations included in the trials. Further, the acute treatment of bipolar disorder is expected to be standardized across countries. Overall, clinical experts did not have any major issues with the generalizability of the study populations to patients in Canada experiencing acute episodes associated with bipolar I disorder based on the baseline characteristics considered as a whole.
The intervention used in the bipolar mania studies followed a flexible-dosing regimen for cariprazine. The permitted dose ranged from 3 mg to 12 mg daily in study RGH-MD-31 and study RGH-MD-32, which extends beyond the Health Canada–approved dose of up to 6 mg cariprazine daily. Further, the overall mean daily dosage in these trials was greater than 6 mg per day (between 7.5 mg per day and 8.8 mg per day). As a result, specific conclusions regarding the effects of the Health Canada–approved dosing cannot be drawn based on these 2 studies. However, study RGH-MD-33 provided evidence for cariprazine at a dose that was consistent with the Health Canada indication (3 mg to 6 mg treatment group), which demonstrated a similar treatment effect to the higher doses used in study RGH-MD-31 and study RGH-MD-32. Dosing was consistent with the approved indication in all other studies included in this review. The studies for bipolar mania involved a complicated titration of cariprazine based on an assessment of treatment response and tolerability of cariprazine. Feedback from the clinical experts indicated that while treatment response and tolerability are important considerations, the rapid titration schedule used in the trials is not how this drug is expected to be used for most patients treated in an outpatient setting. The clinical experts suggested that physicians will likely initiate treatment with cariprazine at 1.5 mg per day, then increase to 3 mg per day after 1 week, in contrast to the trials where the dose was increased to 3.0 mg per day after 1 day of treatment with 1.5 mg per day, and up to 6.0 mg per day as early as the third day of treatment. Generalizing the efficacy, safety, and tolerability outcomes observed in the trials to an outpatient setting for the treatment of acute mania is associated with some uncertainty. Another consideration for the intervention is that the clinical experts indicated it is unlikely for cariprazine to be used only for acute treatment of episodes associated with bipolar I disorder. While the duration of the trials was considered adequate to observe a treatment effect on an acute episode, they were too short to properly assess safety and tolerability or efficacy beyond 3 weeks (bipolar mania studies) and 6 weeks to 8 weeks (bipolar depression studies). Co-interventions and rescue therapy for the treatment of insomnia, emerging EPS symptoms, agitation, restlessness, irritability, and hostility were permitted in the trials. The clinical experts confirmed that the use of these interventions was considered appropriate and consistent with clinical practice and other clinical trials.
All of the outcomes used in the studies are commonly used in clinical trials or research settings for bipolar I disorder. None of the included outcomes are designed for or typically used in clinical practice, as per feedback from the clinical experts. The bipolar mania studies were primarily conducted in an inpatient setting, which is a well-controlled treatment setting. The clinical experts indicated that cariprazine could be used for the treatment of acute episodes of bipolar I disorder in an outpatient setting, as a patient does not always need to be hospitalized to initiate therapy, as long as they are not at risk of self-harm and/or harming others or will not be considered certifiable for an involuntary admission according to each province’s or territory’s Mental Health Act. The generalizability of the study results of the bipolar mania studies should be taken into account when considering cariprazine for the outpatient treatment of acute manic episodes. The bipolar depression studies were conducted in an outpatient setting, which was considered appropriate by the clinical experts consulted by CADTH. The assessment of patients in the trials occurred more frequently compared to clinical practice. In the bipolar mania studies, patient visits occurred every 2 days to 7 days and in the bipolar depression studies, patient visits occurred every 1 week to 2 weeks. The clinical experts indicated that in a clinical practice (an outpatient setting), follow-up typically occurs 1 month after the initiation of treatment. More frequent assessments are more likely to detect and adjust treatment for safety and tolerability issues or issues with response to treatment, thereby potentially inflating the efficacy, tolerability, and safety profile of cariprazine based on the clinical trials.
Indirect Evidence
Objectives and Methods for the Summary of Indirect Evidence
The aim of this section was to appraise the indirect evidence used to inform the pharmacoeconomic model, and to identify indirect comparisons that fill gaps in the evidence from the systematic review. Although direct evidence is available on the efficacy and safety of cariprazine versus placebo, comparative efficacy studies versus other treatments for acute episodes of bipolar I disorder that were of interest to this review were not identified in the systematic literature search.
A focused literature search for NMAs dealing with bipolar disorder was run in MEDLINE All (1946–) on March 8, 2022. No filters were applied to limit the retrieval by study type.
Three potentially relevant NMAs were identified in the literature, in addition to the sponsor-submitted NMA. The indirect treatment comparison (ITC) published by Bahji et al. (2020) was excluded because the results were limited to a ranking of comparisons to placebo (pairwise comparisons between cariprazine and other active treatments were not available). Therefore, the sponsor-submitted NMA and 2 published NMAs, Kishi et al. (2021) and Kadakia et al. (2021), were appraised and summarized for this review.18,19,74
This section will appraise the sponsor-submitted NMA, and the following section will appraise the 2 published ITCs.
Description of Network Meta-Analyses
One NMA submitted by the sponsor17 and 2 published NMAs18,19 that examined the comparative efficacy, safety, and tolerability of acute treatments for bipolar I disorder were included in this report. All of the NMAs conducted a systematic review of RCTs in adults either with acute bipolar mania (Kishi et al. [2021]),18 acute bipolar depression (Kadakia et al. [2021]),19 or both populations (sponsor-submitted NMA).17 The sponsor-submitted NMA performed separate analyses for the bipolar mania and depression populations. All included NMAs specified treatments for acute episodes of bipolar I disorder that were administered orally or sublingually as monotherapy. This included second-generation antipsychotic drugs and other treatments, such as lithium, divalproex, and carbamazepine. Note that Kadakia et al. was limited to second-generation antipsychotic drugs and recent publications (since May 2015). The sponsor-submitted NMA was conducted using a Bayesian approach, the publication by Kishi et al. performed both pairwise and frequentist NMAs using an RE model, and Kadakia et al. performed an NMA with a Bayesian approach where the base case was based on an RE model.
Methods of Sponsor-Submitted Network Meta-Analysis
Objectives
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Study Selection Methods
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Table 42: Study Selection Criteria for Sponsor-Submitted Network Meta-Analysis
Category | Inclusion criteria | Exclusion criteria |
|---|---|---|
Population | ||||||||||||||||||||||||||||||||||||||| | ||||||||||||||||||||||||||||||||||||||| |
Intervention | ||||||||||||||||||||||||||||||||||||||| | ||||||||||||||||||||||||||||||||||||||| |
Comparator | ||||||||||||||||||||||||||||||||||||||| | ||||||||||||||||||||||||||||||||||||||| |
Outcome | ||||||||||||||||||||||||||||||||||||||| | ||||||||||||||||||||||||||||||||||||||| |
Study design | ||||||||||||||||||||||||||||||||||||||| | ||||||||||||||||||||||||||||||||||||||| |
Publication characteristics | ||||||||||||||||||||||||||||||||||||||| | ||||||||||||||||||||||||||||||||||||||| |
Databases searched | ||||||||||||||||||||||||||||||||||||||| | |
Manual searches | ||||||||||||||||||||||||||||||||||||||| | |
Selection process | ||||||||||||||||||||||||||||||||||||||| | |
Data extraction process | ||||||||||||||||||||||||||||||||||||||| | |
Quality assessment | ||||||||||||||||||||||||||||||||||||||| | |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Source: Sponsor-submitted network meta-analysis.17
Indirect Treatment Comparison Analysis Methods
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Table 43: Indirect Treatment Comparison Analysis Methods
Characteristic | Sponsor-submitted network meta-analysis |
|---|---|
ITC methods | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |
Priors | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |
Assessment of model fit | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |
Assessment of consistency | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |
Assessment of convergence | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |
Outcomes | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |
Follow-up time points | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |
Construction of nodes | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |
Sensitivity analyses | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |
Subgroup analysis | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |
Methods for pairwise meta-analysis | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Source: Sponsor-submitted network meta-analysis.17
Results of Sponsor-Submitted Network Meta-Analysis
Summary of Included Studies
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Table 44: Assessment of Homogeneity for Sponsor-Submitted Network Meta-Analysis
Category | Description and handling of potential effect modifiers |
|---|---|
Patient demographics | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |
Patient population | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |
Disease severity | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |
Treatment history | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |
Clinical trial eligibility criteria | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |
Dosing of comparators | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |
Placebo response | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |
Definitions of end points | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |
Timing of end point evaluation or trial duration | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |
Withdrawal frequency | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |
Clinical trial setting | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |
Study design | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |
Study date | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |
Source: Sponsor-submitted network meta-analysis.17
Results for Bipolar Mania/Mixed Studies
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Figure 2: Network Diagram for |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| Manic or Mixed Studies

This figure has been redacted.
Source: Sponsor-submitted network meta-analysis.17
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Figure 3: Network Diagram for |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| Manic or Mixed Studies

This figure has been redacted.
Source: Sponsor-submitted network meta-analysis.17
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Figure 4: Network Diagram for |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| Manic or Mixed Studies

This figure has been redacted.
Source: Sponsor-submitted network meta-analysis.17
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Figure 5: Network Diagram for |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| Manic or Mixed Studies

This figure has been redacted.
Source: Sponsor-submitted network meta-analysis.17
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Figure 6: Network Diagram for |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| Manic or Mixed Studies

This figure has been redacted.
Source: Sponsor-submitted network meta-analysis.17
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Figure 7: Network Diagram for |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| Manic or Mixed Studies

This figure has been redacted.
Source: Sponsor-submitted network meta-analysis.17
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Figure 8: Network Diagram for |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| Manic or Mixed Studies

This figure has been redacted.
Source: Sponsor-submitted network meta-analysis.17
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Figure 9: Network Diagram for |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| Manic or Mixed Studies

This figure has been redacted.
Source: Sponsor-submitted network meta-analysis.17
Table 45: Key Efficacy Results for Manic or Mixed Episodes — Network Meta-Analysis
Outcome | ||||||||||||||||||||||||| | ||||||||||||||||||||||||| | ||||||||||||||||||||||||| |
|---|---|---|---|
||||||||||||||||||||||||| | ||||||||||||||||||||||||| | ||||||||||||||||||||||||| | |
Number of studies (patients), model | ||||||||||||||||||||||||| | ||||||||||||||||||||||||| | ||||||||||||||||||||||||| |
||||||| | ||||||||||||||||||||||||| | ||||||||||||||||||||||||| | ||||||||||||||||||||||||| |
|||||||||||| | ||||||||||||||||||||||||| | ||||||||||||||||||||||||| | ||||||||||||||||||||||||| |
||||||||| | ||||||||||||||||||||||||| | ||||||||||||||||||||||||| | ||||||||||||||||||||||||| |
||||||||||||| | ||||||||||||||||||||||||| | ||||||||||||||||||||||||| | ||||||||||||||||||||||||| |
|||||||||| | ||||||||||||||||||||||||| | ||||||||||||||||||||||||| | ||||||||||||||||||||||||| |
||||||| | ||||||||||||||||||||||||| | ||||||||||||||||||||||||| | ||||||||||||||||||||||||| |
|||||||||| | ||||||||||||||||||||||||| | ||||||||||||||||||||||||| | ||||||||||||||||||||||||| |
|||||||||| | ||||||||||||||||||||||||| | ||||||||||||||||||||||||| | ||||||||||||||||||||||||| |
||||||||||| | ||||||||||||||||||||||||| | ||||||||||||||||||||||||| | ||||||||||||||||||||||||| |
||||||||||| | ||||||||||||||||||||||||| | ||||||||||||||||||||||||| | ||||||||||||||||||||||||| |
|||||||||||| | ||||||||||||||||||||||||| | ||||||||||||||||||||||||| | ||||||||||||||||||||||||| |
Comment | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Source: Sponsor-submitted network meta-analysis.17
Table 46: Key Safety Results for Manic or Mixed Episodes — Network Meta-Analysis
Outcome | |||||||||||||||||||||||| | |||||||||||||||||||||||| | |||||||||||||||||||||||| | |||||||||||||||||||||||| | |||||||||||||||||||||||| |
|---|---|---|---|---|---|
|||||||||||||||||||||||| | |||||||||||||||||||||||| | |||||||||||||||||||||||| | |||||||||||||||||||||||| | |||||||||||||||||||||||| | |
Number of studies (patients), model | |||||||||||||||||||||||| | |||||||||||||||||||||||| | |||||||||||||||||||||||| | |||||||||||||||||||||||| | |||||||||||||||||||||||| |
|||||||||||||||||||||||| | |||||||||||||||||||||||| | |||||||||||||||||||||||| | |||||||||||||||||||||||| | |||||||||||||||||||||||| | |||||||||||||||||||||||| |
|||||||||||||||||||||||| | |||||||||||||||||||||||| | |||||||||||||||||||||||| | |||||||||||||||||||||||| | |||||||||||||||||||||||| | |||||||||||||||||||||||| |
|||||||||||||||||||||||| | |||||||||||||||||||||||| | |||||||||||||||||||||||| | |||||||||||||||||||||||| | |||||||||||||||||||||||| | |||||||||||||||||||||||| |
|||||||||||||||||||||||| | |||||||||||||||||||||||| | |||||||||||||||||||||||| | |||||||||||||||||||||||| | |||||||||||||||||||||||| | |||||||||||||||||||||||| |
|||||||||||||||||||||||| | |||||||||||||||||||||||| | |||||||||||||||||||||||| | |||||||||||||||||||||||| | |||||||||||||||||||||||| | |||||||||||||||||||||||| |
|||||||||||||||||||||||| | |||||||||||||||||||||||| | |||||||||||||||||||||||| | |||||||||||||||||||||||| | |||||||||||||||||||||||| | |||||||||||||||||||||||| |
|||||||||||||||||||||||| | |||||||||||||||||||||||| | |||||||||||||||||||||||| | |||||||||||||||||||||||| | |||||||||||||||||||||||| | |||||||||||||||||||||||| |
|||||||||||||||||||||||| | |||||||||||||||||||||||| | |||||||||||||||||||||||| | |||||||||||||||||||||||| | |||||||||||||||||||||||| | |||||||||||||||||||||||| |
|||||||||||||||||||||||| | |||||||||||||||||||||||| | |||||||||||||||||||||||| | |||||||||||||||||||||||| | |||||||||||||||||||||||| | |||||||||||||||||||||||| |
|||||||||||||||||||||||| | |||||||||||||||||||||||| | |||||||||||||||||||||||| | |||||||||||||||||||||||| | |||||||||||||||||||||||| | |||||||||||||||||||||||| |
|||||||||||||||||||||||| | |||||||||||||||||||||||| | |||||||||||||||||||||||| | |||||||||||||||||||||||| | |||||||||||||||||||||||| | |||||||||||||||||||||||| |
|||||||||||||||||||||||| | |||||||||||||||||||||||| | |||||||||||||||||||||||| | |||||||||||||||||||||||| | |||||||||||||||||||||||| | |||||||||||||||||||||||| |
Comment | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Source: Sponsor-submitted network meta-analysis.17
Results for Bipolar Depression Studies
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Figure 10: Network Diagram for |||||||||||||||||||||||||||||||||||||||||||||||| Depressive Studies

This figure has been redacted.
Source: Sponsor-submitted network meta-analysis.17
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Figure 11: Network Diagram for |||||||||||||||||||||||||||||||||||||||||||||||| Manic or Mixed Studies

This figure has been redacted.
Source: Sponsor-submitted network meta-analysis.17
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Figure 12: Network Diagram for |||||||||||||||||||||||||||||||||||||||||||||||| Depressive Studies

This figure has been redacted.
Source: Sponsor-submitted network meta-analysis.17
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Figure 13: Network Diagram for |||||||||||||||||||||||||||||||||||||||||||||||| Depressive Studies

This figure has been redacted.
Source: Sponsor-submitted network meta-analysis.17
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Figure 14: Network Diagram for |||||||||||||||||||||||||||||||||||||||||||||||| Depressive Studies

This figure has been redacted.
Source: Sponsor-submitted network meta-analysis.17
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Figure 15: Network Diagram for |||||||||||||||||||||||||||||||||||||||||||||||| Depressive Studies

This figure has been redacted.
Source: Sponsor-submitted network meta-analysis.17
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Figure 16: Network Diagram for |||||||||||||||||||||||||||||||||||||||||||||||| Depressive Studies

This figure has been redacted.
Source: Sponsor-submitted network meta-analysis.17
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Figure 17: Network Diagram for |||||||||||||||||||||||||||||||||||||||||||||||| Depressive Studies

This figure has been redacted.
Source: Sponsor-submitted network meta-analysis.17
Table 47: Key Efficacy Results for Depressive Episodes — Network Meta-Analysis
Outcome | ||||||||||||||||||||||||||| | ||||||||||||||||||||||||||| | ||||||||||||||||||||||||||| | |||
|---|---|---|---|---|---|---|
|||||||||||| | ||||||||||||||||||||||||||| | ||||||||||||||||||||||||||| | ||||||||||||||||||||||||||| | |||
Treatment | |||||||||||||||||||||| | ||||||||||||||||||||||||||| | ||||||||||||||||||||||||||| | |||||||||||||||||||||||| | |||||||||||||||||||||| | |||||||||||||||||||||| |
Number of studies (patients), model | ||||||||||||||||||||||||||| | ||||||||||||||||||||||||||| | ||||||||||||||||||||||||||| | |||
||||||||||||||||||||||||||| | |||||||||||||||||||||| | ||||||||||||||||||||||||||| | ||||||||||||||||||||||||||| | |||||||||||||||||||||||| | |||||||||||||||||||||| | ||||||||||||||||||||||||||| |
||||||||||||||||||||||||||| | |||||||||||||||||||||| | ||||||||||||||||||||||||||| | ||||||||||||||||||||||||||| | |||||||||||||||||||||||| | |||||||||||||||||||||| | ||||||||||||||||||||||||||| |
||||||||||||||||||||||||||| | |||||||||||||||||||||| | ||||||||||||||||||||||||||| | ||||||||||||||||||||||||||| | |||||||||||||||||||||||| | |||||||||||||||||||||| | ||||||||||||||||||||||||||| |
||||||||||||||||||||||||||| | |||||||||||||||||||||| | ||||||||||||||||||||||||||| | ||||||||||||||||||||||||||| | |||||||||||||||||||||||| | |||||||||||||||||||||| | ||||||||||||||||||||||||||| |
||||||||||||||||||||||||||| | |||||||||||||||||||||| | ||||||||||||||||||||||||||| | ||||||||||||||||||||||||||| | |||||||||||||||||||||||| | |||||||||||||||||||||| | ||||||||||||||||||||||||||| |
||||||||||||||||||||||||||| | |||||||||||||||||||||| | ||||||||||||||||||||||||||| | ||||||||||||||||||||||||||| | |||||||||||||||||||||||| | |||||||||||||||||||||| | ||||||||||||||||||||||||||| |
||||||||||||||||||||||||||| | |||||||||||||||||||||| | ||||||||||||||||||||||||||| | ||||||||||||||||||||||||||| | |||||||||||||||||||||||| | |||||||||||||||||||||| | ||||||||||||||||||||||||||| |
||||||||||||||||||||||||||| | |||||||||||||||||||||| | ||||||||||||||||||||||||||| | ||||||||||||||||||||||||||| | |||||||||||||||||||||||| | |||||||||||||||||||||| | ||||||||||||||||||||||||||| |
||||||||||||||||||||||||||| | |||||||||||||||||||||| | ||||||||||||||||||||||||||| | ||||||||||||||||||||||||||| | |||||||||||||||||||||||| | |||||||||||||||||||||| | ||||||||||||||||||||||||||| |
||||||||||||||||||||||||||| | |||||||||||||||||||||| | ||||||||||||||||||||||||||| | ||||||||||||||||||||||||||| | |||||||||||||||||||||||| | |||||||||||||||||||||| | ||||||||||||||||||||||||||| |
||||||||||||||||||||||||||| | |||||||||||||||||||||| | ||||||||||||||||||||||||||| | ||||||||||||||||||||||||||| | |||||||||||||||||||||||| | |||||||||||||||||||||| | ||||||||||||||||||||||||||| |
Comment | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| | |||
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Source: Sponsor-submitted network meta-analysis.17
Table 48: Key Safety Results for Depressive Episodes — Network Meta-Analysis
Outcome | ||||||||||||||||||| | ||||||||||||||||||| | ||||||||||||||||||| | ||||||||||||||||||| | ||||||||||||||||||| | |||||
|---|---|---|---|---|---|---|---|---|---|---|
||||||||||||||||||| | ||||||||||||||||||| | ||||||||||||||||||| | ||||||||||||||||||| | ||||||||||||||||||| | ||||||
||||||||||||||| | ||||||||||||||| | ||||||||||||| | ||||||||||||||| | ||||||||||||| | ||||||||||||||| | ||||||||||||||| | ||||||||||||||| | ||||||||||||| | |||||||||||| | |
Number of studies (patients), model | ||||||||||||||||||| | ||||||||||||||||||| | ||||||||||||||||||| | ||||||||||||||||||| | ||||||||||||||||||| | |||||
||||||||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| | ||||||||||| |
||||||||||||||||||| | ||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| | ||||||||||| |
||||||||||||||||||| | ||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| | ||||||||||| |
||||||||||||||||||| | ||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| | ||||||||||| |
||||||||||||||||||| | ||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| | ||||||||||| |
||||||||||||||||||| | ||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| | ||||||||||| |
||||||||||||||||||| | ||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| | ||||||||||| |
||||||||||||||||||| | ||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| | ||||||||||| |
||||||||||||||||||| | ||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| | ||||||||||| |
||||||||||||||||||| | ||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| | ||||||||||| |
||||||||||||||||||| | ||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| | ||||||||||| |
Comment | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| | |||||
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Source: Sponsor-submitted network meta-analysis.17
Critical Appraisal of Sponsor-Submitted Network Meta-Analysis
Overall, the prespecified study selection criteria for the systematic review used to inform the sponsor-submitted NMA was considered appropriate, although not without limitations. Studies that included patients with a dual diagnosis of substance use disorder, that investigated a nonoral intervention, or that investigated an intervention that was not used as monotherapy were excluded from the systematic review. These exclusion criteria would result in missing potentially relevant patients and interventions. HRQoL was not included as an outcome of interest; this was an outcome of importance to patients and clinicians. The study design was limited to double-blind RCTs and the quality of the studies was assessed using the NICE checklist and Jadad rubric. It is unclear how the quality assessment was used in the systematic review and NMA as poor quality was not reported as a reason for exclusion of any study. Further, the Jadad rubric is not considered to be a reliable tool for assessing study quality.75 An insufficient quality assessment may have resulted in the inclusion of low-quality trials.
Information about the patient population type (by bipolar episode description), health care setting, study phase, blinding, duration of study, study country, and publication year were reported for the included studies. Variation in the health care setting — particularly among the studies for manic or mixed episodes and publication year, which ranged from 1991 to 2019 — are potential sources of heterogeneity among the included studies that may bias the results. Additionally, approximately 33% of included studies (overall) were conducted in the US and details about studies conducted in Canada were not available. Baseline patient characteristics, including age, sex, race, HAM-D score, MADRS score, YMRS score, CGI-S score, and time since diagnosis, were summarized, although poorly reported (they were only presented graphically). Sex, race, and age were not expected to influence relative treatment effect. The sponsor-submitted NMA reported that heterogeneity due to characteristics other than age, sex, and race could not be assessed robustly because of a large amount of missing data for the baseline patient characteristics identified. No studies were excluded based on outliers in the baseline characteristics and it is unknown if the NMA was impacted by heterogeneity among the included patient populations. Moreover, transitivity was insufficiently assessed and, therefore, may by an issue for the validity of the indirect comparison. An assessment of statistical heterogeneity using I2 was also performed, but only for NMAs of studies for manic or mixed episodes for the following outcomes: change from baseline in YMRS, all-cause discontinuation, and discontinuation due to AEs. Evidence of statistical heterogeneity rated as moderate (I2 = 25% to 50%), high (I2 = 50% to 75%), and very high (I2 > 75%) was identified for some of the comparisons included in the 3 networks. It should be noted that a sensitivity analysis was performed on the NMA of YMRS-related outcomes and discontinuation outcomes in the manic or mixed episode studies. The sensitivity analysis excluded studies that only assessed patients experiencing manic episodes (i.e., no patients experienced mixed episodes). The results of the sensitivity analyses were consistent with the base-case analyses. Subgroup analyses or a meta-regression analysis were not conducted.
Inconsistency was assessed in closed loops of the networks using a node-splitting approach and summarized as an inconsistency plot. This is considered an appropriate statistical assessment of inconsistency, although it does not incorporate information from the entire network in the analysis. Evidence of inconsistency was identified using this approach in the following networks of the manic or mixed episode studies: change from baseline in YMRS, all-cause discontinuation, and discontinuation due to AEs. For the NMAs of outcomes in depressive studies, the sponsor-submitted NMA reported that inconsistency could not be assessed for the following networks: MADRS remission, weight gain, EPS, and all-cause discontinuation. The author reported that evidence of inconsistency was not identified for the remaining outcomes in the networks. However, very wide 95% CIs for the inconsistency factor for comparisons in the NMA for the following outcomes may suggest inconsistency: sedation or somnolence (manic or mixed and depressive), all-cause discontinuation (manic or mixed), discontinuations due to AEs (manic or mixed and depressive).
Different doses for comparator treatments were not accounted for in the network, which may represent a notable source of heterogeneity in the network. As there was potential for heterogeneity based on the feasibility assessment, an RE model was used for all base-case analyses, which was appropriate in this situation. Missing data was an issue identified by the sponsor-submitted NMA, resulting from a small number of studies. This issue was compounded by the fact that there were few events per study for some outcomes, which was the case for the analysis of EPS (both the manic or mixed network and depressive network) and weight gain (depressive network). The use of an RE model with noninformative priors for the base-case analysis and having insufficient data resulted in point estimates with wide credible intervals (Crls) and, therefore, high uncertainty in the results. Relative treatment effects were also reported for analyses using the alternative models that were fitted, including the fixed effect model. In general, the other analyses were consistent with the base-case analysis (with a few exceptions), and the fixed effect model improved precision.
There was some variability in the definitions used for outcomes, as described in the Results section. For example, the author opted to include more data rather than exclude studies based on varying thresholds used to define response and remission rates, which could have increased the estimated uncertainty in relative effect estimates. For the other outcomes (weight gain, EPS, sedation or somnolence), the study definition was used to maximize the amount of data used in the analysis. There was variability in the time points of assessment as well. The time of assessment for outcomes in manic or mixed studies ranged from 3 weeks to 4 weeks, and in depressive studies ranged from 6 weeks to 8 weeks; however, this was not expected to have a significant impact on the comparability of the results as per feedback from the clinical expert consulted by CADTH.
Methods of Published Network Meta-Analyses
Objectives
The objective of the ITC published by Kishi et al. (2021) was to conduct a systematic review and RE model NMA to compare the efficacy, acceptability, tolerability, and safety of pharmacologic interventions for adults with acute bipolar mania.
The objective of the ITC published by Kadakia et al. (2021) was to conduct a Bayesian NMA to compare the relative efficacy and tolerability of atypical antipsychotic monotherapy in adults with bipolar depression.
Study Selection Methods
A summary of the eligibility criteria for the published ITCs is provided in Table 49.
Kishi et al. (2021) included patients with acute bipolar mania and Kadakia et al. (2021) included patients with bipolar depression. Both ITCs included monotherapies for the treatment of bipolar disorder as relevant interventions; Kishi et al. was limited to oral treatments lasting at least 10 days and Kadakia et al. was limited to second-generation antipsychotic drugs, as described in Table 49. Both ITCs included efficacy outcomes related to treatment response and improvement in symptoms, metabolic outcomes, and safety outcomes related to discontinuation. Studies that were included were RCTs published before March 14, 2021 (Kishi et al.), or between May 2015 and May 4, 2020 (Kadakia et al.). Kishi et al. excluded RCTs that were open label, and allowed antipsychotic drugs as rescue medication or studies that terminated early without efficacy analysis; Kadakia et al. did not specify exclusion criteria related to the study design other than studies that were not RCTs. Kishi et al. also excluded studies that were at high risk of selection bias according to the Cochrane RoB criteria. Kadakia et al. used the Cochrane RoB 2 tool to assess risk of bias. Additionally, both studies assessed publication bias using funnel plots.
Table 49: Study Selection Criteria and Methods for Published Indirect Treatment Comparisons
Factor | Kishi et al. (2021) | Kadakia et al. (2021) |
|---|---|---|
Population | Adults with acute bipolar mania Excluded: Studies including children/adolescents | Adults (> 18 years) with bipolar depression, where at least 50% of the population was diagnosed with bipolar I disorder |
Intervention | Oral medication monotherapy lasting ≥ 10 days | Second-generation antipsychotic monotherapy:
|
Comparator | Oral medication monotherapy lasting ≥ 10 days Placebo | Any of the interventions listed previously or placebo |
Outcome | The primary outcomes were response to treatment (efficacy) and all-cause discontinuation (acceptability). The secondary outcomes were the improvement of mania symptoms and discontinuation due to inefficacy (withdrawal of consent, depression, and individual adverse events). | Studies reporting at least 1 of the following outcomes:
|
Study design | Double-blind and single-blinda RCTs Excluded: Open-label studies, studies that allowed antipsychotic drugs as a rescue medication during a trial, and studies that terminated early without efficacy analysis | RCTs |
Publication characteristics | Studies published before March 14, 2021 | Studies published between May 2015 and May 4, 2020 |
Databases searched | PubMed, the Cochrane Library, and Embase databases |
|
Selection process | Not reported | Title and abstract screening, followed by full-text review for all references/publications by 2 independent reviewers. Discrepancies were resolved by a third reviewer. |
Data extraction process | Not reported | Data extraction by 2 independent researchers, cross-checked for accuracy |
Quality assessment | Cochrane RoB criteria Funnel plots will be used to explore potential publication bias. Excluded: Studies with selection bias evaluated as high risk, according to the Cochrane RoB criteria | Cochrane RoB 2 criteria Publication bias was assessed by comparison-adjusted funnel plots, with tests for asymmetry applied to cases with ≥ 10 studies. |
APA = American Psychological Association; CGI-BP-S = Clinical Global Impression–Bipolar Disorder–Severity; LDL = low-density lipoprotein; MADRS = Montgomery–Åsberg Depression Rating Scale; RCT = randomized controlled trial; RoB = risk of bias; RoB 2 = risk of bias 2.
aSingle-blind studies were considered for objective outcomes.
Source: Kishi et al. (2021)18 and Kadakia et al. (2021).19
Indirect Treatment Comparison Analysis Methods
Analysis methods of the published ITCs are summarized in Table 50. The publication by Kishi et al. (2021) performed both pairwise and frequentist NMAs using an RE model. Kadakia et al. (2021) performed an NMA with a Bayesian approach where the base case was based on an RE model. Justification for the selection of methods used in the Kishi et al. NMA was unclear, as well as in the Kadakia et al. NMA (the referenced RE estimated additional variance parameters that are associated with study heterogeneity). A description of the prior distribution, assessment of model fit, and convergence diagnostics was not provided for either study.
Both of the published NMAs reported that transitivity was evaluated by comparing the distribution of potential effect modifiers across comparisons in the network. Potential effect modifiers reported by Kishi et al. included sample size, the duration of the study, and mean age. Potential effect modifiers reported by Kadakia et al. included the following baseline characteristics: age, gender, body weight, body mass index, percentage of patients with bipolar I disorder, baseline MADRS, baseline Clinical Global Impression–Bipolar Disorder–Severity depression score, and age of bipolar onset. Both published NMAs reported that common heterogeneity across all comparisons was assumed and estimated in each network using tau-squared statistics. In the NMA published by Kishi et al., a meta-regression analysis was performed to examine whether some potentially confounding factors (e.g., publication year, mean age, number of total patients, percentage of male patients) would be associated with the extent of effect on primary outcome. Kadakia et al. reported that a meta-regression was not performed because it was not feasible due to an insufficient number of trials required to perform a meta-regression analysis.
In the NMA by Kishi et al., inconsistency was assessed by a statistical evaluation that was performed using the design-by-treatment test (globally) and the Separate Direct from Indirect Evidence test (locally). Kadakia et al. reported that an assessment of incoherence was not applicable because there were no closed loops in the NMA.
The indirect evidence from the publication by Kishi et al. assessed the credibility of the findings of each NMA using the Confidence in Network Meta-Analysis (CINeMA) application based on the Grading of Recommendations Assessment, Development and Evaluation (GRADE) approach.
Table 50: Analysis Methods of Published Indirect Treatment Comparisons
Factor | Kishi et al. (2021) | Kadakia et al. (2021) |
|---|---|---|
ITC methods | Both pairwise and frequentist NMAs were performed using the RE model | Bayesian NMA; base-case models were fit with RE models |
Priors | Not reported | Not reported |
Assessment of model fit | Not reported | Not reported |
Assessment of consistency | For the NMA, common heterogeneity across all comparisons were assumed and estimated in each network. Network heterogeneity was assessed using tau-squared statistics. Statistical evaluation of incoherence was performed using the design-by-treatment test (globally) and the SIDE test (locally). | A common heterogeneity parameter across the various treatment comparisons was assumed, and heterogeneity was assessed by the between-study variance tau-squared for each outcome, and further characterized by comparing with its predictive distribution. Confidence of evidence, which included an assessment of inconsistency, was evaluated based on the GRADE approach. |
Assessment of convergence | Not reported | Not reported |
Outcomes |
|
|
Follow-up time points | Outcome assessments were targeted at 3 weeks or 4 weeks. For studies without 3-week or 4-week data, data were used at the points closest to 3 weeks over 10 days to 12 weeks. | 6 weeks or 8 weeks |
Construction of nodes | For studies involving 2 or more treatment groups of the same drug with different doses, data from the treatment arms were pooled for analysis, provided that they were administered within a therapeutic dose range. | For trials with multiple fixed-dose arms, the results were pooled across dose. |
Sensitivity analyses | Analyses were for primary outcomes in which only half the weight was given to studies:
| Examined the impact of pooled vs. stratified doses of each second-generation antipsychotic drug as well as restricted the data at the 6-week time point (i.e., data reported at other time points were removed) |
Subgroup analysis | None | None |
Methods for pairwise meta-analysis | For pairwise meta-analyses, heterogeneity was assessed using I2 statistics. | Not reported |
AE = adverse event; CGI-BP-S = Clinical Global Impression–Bipolar Disorder–Severity; EPS = extrapyramidal symptom; GRADE = Grading of Recommendation, Assessment, Development aclinicand Evaluation; ITC = indirect treatment comparison; MADRS = Montgomery–Åsberg Depression Rating Scale; NMA = network meta-analysis; RE = random effect; SIDE = Separate Direct from Indirect Evidence; tau = Kendall tau rank correlation; vs. = versus.
Source: Kishi et al. (2021)18 and Kadakia et al. (2021).19
Results of NMAs
Summary of Included Studies
The NMA published by Kishi et al. (2021) included 72 double-blind RCTs (n = 16,442) of 23 drugs and placebo. The mean study duration was 3.96 (SD = 2.39) weeks, the mean age was 39.55 years, and 50.93% of patients were male. Some of the included studies comprised patients with rapid cycling (14 studies), or patients experiencing a mixed state or episode (38 studies). Additionally, 21 (29.2%) studies had a low overall risk of bias and other studies (70.8%) were evaluated as moderate overall risk of bias. The 3 pivotal trials for cariprazine were included in this NMA.39-41
A total of 18 trials (n = 7,969) that were multisite, randomized, double-blind, placebo-controlled trials were included in the NMA published by Kadakia et al. (2021). Among the included studies, the mean age ranged from 29.2 years to 43.6 years, between 34.3% and 48.1% of patients were male, the mean baseline MADRS score ranged from 26.9 to 32.0, and the mean baseline Clinical Global Impression–Bipolar Disorder–Severity overall score ranged from 4.2 to 4.5 and depression ranged from 4.3 to 4.9. Where reported (11 studies), baseline body weight ranged from 63.9 kg to 88.8 kg, and the age of onset was a mean of 25.4 years to 28.4 years (reported in 3 studies). The overall risk of bias was low for 12 studies (67%) and there were some concerns (driven by the randomization process) for 6 studies (33%) as per the Cochrane risk of bias 2. The 3 pivotal trials for cariprazine were included in this NMA.42-44
Results for Published Network Meta-Analyses
The results of the primary outcomes of the Kishi et al. NMA are presented in Table 51. Mania rating scale scores, discontinuation due to inefficacy, clinical remission and psychotic symptoms, and tolerability and safety outcomes were also reported for this NMA; however, definitions of these outcomes were not provided. Therefore, this review focuses on the primary outcomes of the Kishi et al. NMA.
The network diagram for response to treatment and all-cause discontinuation is available in Appendix 3 (Figure 24 and Figure 25, respectively). Response to treatment was defined as at least 50% improvement in YMRS score or a similar outcome. No difference between treatments in terms of response to treatment was identified in the NMA published by Kishi et al. Regarding all-cause discontinuation, cariprazine did not outperform any of the comparators. In addition, olanzapine was associated with a lower rate of all-cause discontinuation relative to cariprazine (relative risk = 1.556; 95% CI, 1.134 to 2.135). Of note, the comparison of cariprazine to olanzapine was associated with a CINeMA confidence rating of very low.
The results of the Kadakia et al. (2021) NMA are presented in Table 52 and Table 53. A network diagram was not available. Efficacy and metabolic outcomes summarized for this review include the change from baseline in MADRS score, response based on the MADRS score (defined as ≥ 50% improvement in MADRS), remission based on the MADRS score (MADRS ≤ 10), change from baseline in weight (kg), and weight gain of at least 7% (Table 52). Cariprazine did not demonstrate a benefit relative to active comparators in terms of outcomes related to MADRS. Further, quetiapine outperformed cariprazine in terms of the change from baseline in MADRS (mean difference = −2.52; 95% CrI, −4.11 to −0.92) and response in MADRS (OR = 1.44; 95% CrI, 1.08 to 1.91), olanzapine outperformed cariprazine in terms of the change from baseline in MADRS (mean difference = −2.29; 95% CrI, −4.09 to −0.46), and lurasidone outperformed cariprazine in terms of the response in MADRS (OR = 1.78; 95% CrI, 1.08 to 2.77). Regarding the metabolic outcomes, cariprazine demonstrated a benefit relative to olanzapine (mean difference = 2.24; 95% CrI, 1.66 to 2.80) and quetiapine (mean difference = 0.52; 95% CrI, 0.07 to 0.96) based on the change in weight (kg) and relative to olanzapine based on weight gain of at least 7% (OR = 24.93; 95% CrI, 3.35 to 95.57).
A summary of safety and tolerability outcomes from the Kadakia et al. NMA includes the rate of EPS, somnolence, akathisia, all-cause discontinuation, and discontinuation due to AE (Table 53). There was no difference between cariprazine and active comparators for any of these outcomes, except quetiapine for the rate of somnolence, which was higher for quetiapine relative to cariprazine (OR = 3.03; 95% CrI, 1.13 to 6.47).
Table 51: Key Results for Kishi et al. (2021) Network Meta-Analysis, Pairwise Comparisons With Cariprazine
Comparator | Response to treatment | All-cause discontinuation |
|---|---|---|
RR (95% CI) | RR (95% CI) | |
Number of studies (patients), model | 56 studies (14,503 patients), RE model | 70 studies (16,324 patients), RE model |
Placebo | 1.558 (1.262 to 1.924) | 1.007 (0.766 to 1.324) |
Quetiapine | 1.004 (0.768 to 1.312) | 1.327 (0.918 to 1.919) |
Aripiprazolea | 0.981 (0.761 to 1.265) | 0.834 (0.609 to 1.142) |
Asenapinea | 0.822 (0.615 to 1.099) | 0.991 (0.684 to 1.436) |
Paliperidone | 1.118 (0.816 to 1.533) | 1.323 (0.873 to 2.004) |
Risperidone | 0.923 (0.699 to 1.218) | 1.288 (0.892 to 1.859) |
Lithium | 1.074 (0.838 to 1.375) | 0.978 (0.710 to 1.348) |
Divalproex | NR | NR |
Olanzapine | 0.981 (0.768 to 1.253) | 1.556 (1.134 to 2.135) |
Carbamazepinea | 1.221 (0.846 to 1.762) | 0.840 (0.572 to 1.233) |
Ziprasidone | 1.153 (0.836 to 1.590) | 1.164 (0.811 to 1.672) |
Clonazepam | NR | NR |
Chlorpromazine | NR | 0.379 (0.017 to 8.585) |
Comment | No information about priors used CINeMA confidence rating was very low for all comparisons of cariprazine to other treatments | No information about priors used CINeMA confidence rating was very low for all comparisons of cariprazine to other treatments |
CI = confidence interval; CINeMA = Confidence in Network Meta-Analysis; NR = not reported; RE = random effect; RR = relative risk.
aResults were based on a comparison where the comparator was the reference value (i.e., cariprazine vs. comparator). All other results corresponded to a comparison where cariprazine was the reference value (i.e., comparator vs. cariprazine).
Source: Kishi et al. (2021).18
Table 52: Key Efficacy and Metabolic Results for Kadakia et al. (2021) Network Meta-Analysis, Pairwise Comparisons With Cariprazine
Factor | Change from baseline in MADRS | Response in MADRS (≥ 50% improvement in MADRS) | Remission (MADRS ≤ 10) | Change from baseline in weight (kg) | Weight gain ≥ 7% |
|---|---|---|---|---|---|
Mean (95% Crl) | OR (95% CrI) | OR (95% CrI) | Mean (95% CrI) | OR (95% CrI) | |
Number of studies (patients), model | 18 studies (NR), RE model | 18 studies (NR), RE model | 4 studies (NR), RE model | 15 studies (NR), RE model | 15 studies (NR), RE model |
Placeboa | −2.29 (−3.47 to −1.09) | 1.47 (1.17 to 1.82) | 1.61 (1.12 to 2.23) | 0.65 (0.34 to 0.96) | 3.50 (1.26 to 8.65) |
Aripiprazolea | −1.21 (−3.70 to 1.29) | 1.35 (0.90 to 1.95) | NA | 0.44 (−0.42 to 1.30) | 2.67 (0.56 to 8.41) |
Olanzapine | −2.29 (−4.09 to − 0.46) | 1.08 (0.76 to 1.51) | NA | 2.24 (1.66 to 2.80) | 24.93 (3.35 to 95.57) |
Quetiapine | −2.52 (−4.11 to − 0.92) | 1.44 (1.08 to 1.91) | NA | 0.52 (0.07 to 0.96) | 1.26 (0.34 to 3.13) |
Ziprasidone | 0.94 (−1.34 to 3.27) | 0.74 (0.50 to 1.08) | NA | NA | NA |
Lurasidone | −2.42 (−5.01 to 0.14) | 1.78 (1.08 to 2.77) | 1.39 (0.66 to 2.60) | −0.31 (−0.95 to 0.33) | 6.85 (0.16 to 39.89) |
Quality of evidence based on GRADE assessment by authors (active comparisons only) | Quality of evidence was very low or low | Quality of evidence was very low to moderate | Quality of evidence was very low | Quality of evidence was very low or low, except for comparison relative to olanzapine (moderate) | Quality of evidence was low, except for comparison relative to olanzapine (moderate) |
CI = confidence interval; CrI = credible interval; MADRS = Montgomery–Åsberg Depression Rating Scale; NR = not reported; OR = odds ratio; RE = random effect; NA = not applicable.
aResults were based on a comparison where the comparator was the reference value (i.e., cariprazine vs. comparator). All other results corresponded to a comparison where cariprazine was the reference value (i.e., comparator vs. cariprazine).
Source: Kadakia et al. (2021).19
Table 53: Key Safety Results for Kadakia et al. (2021) Indirect Treatment Comparison, Pairwise Comparisons With Cariprazine
Factor | EPS | Somnolence | Akathisia | All-cause discontinuation | Discontinuation due to AE |
|---|---|---|---|---|---|
OR (95% CrI) | OR (95% CrI) | OR (95% CrI) | OR (95% CrI) | OR (95% CrI) | |
Number of studies (patients), model | 11 studies (NR), RE model | 15 studies (NR), RE model | 7 studies (NR), RE model | 18 studies (NR), RE model | 18 studies (NR), RE model |
Placeboa | 2.26 (1.26 to 3.83) | 1.90 (0.81 to 4.05) | 3.79 (1.19 to 9.27) | 1.05 (0.77 to 1.41) | 1.50 (0.82 to 2.64) |
Aripiprazolea | 1.28 (0.49 to 2.77) | 1.04 (0.32 to 2.61) | 0.57 (0.06 to 2.23) | 0.66 (0.38 to 1.06) | 0.70 (0.25 to 1.64) |
Olanzapine | NA | 1.79 (0.64 to 3.85) | NA | 0.68 (0.42 to 1.06) | 1.04 (0.37 to 2.23) |
Quetiapine | 1.33 (0.58 to 2.66) | 3.03 (1.13 to 6.47) | NA | 0.96 (0.64 to 1.37) | 1.79 (0.80 to 3.42) |
Ziprasidone | NA | 3.12 (0.99 to 7.67) | NA | 1.34 (0.79 to 2.11) | 1.12 (0.41 to 2.37) |
Lurasidone | 1.98 (0.43 to 6.51) | 0.93 (0.23 to 2.52) | 6.61 (0.15 to 13.84) | 1.07 (0.54 to 1.90) | 0.81 (0.21 to 2.23) |
Quality of evidence based on GRADE assessment by authors (active comparisons only) | Quality of evidence was low | Quality of evidence was very low or low, except for comparison relative to quetiapine (moderate) | Quality of evidence was low | Quality of evidence was very low or low | Quality of evidence was low |
AE = adverse event; CrI = credible interval; EPS = extrapyramidal symptom; GRADE = Grading of Recommendation, Assessment, Development and Evaluation; NA = not applicable; NR = not reported; OR = odds ratio; RE = random effect.
aResults were based on a comparison where the comparator was the reference value (i.e., cariprazine vs. comparator). All other results corresponded to a comparison where cariprazine was the reference value (i.e., comparator vs. cariprazine).
Source: Kadakia et al. (2021).19
Critical Appraisal of Published Network Meta-Analyses
Kishi et al. (2021) was limited to oral treatments and excluded open-label studies, studies that allowed antipsychotic drugs as a rescue medication during a trial, and studies that terminated early without an efficacy analysis. While this likely increased the quality of the evidence included in the NMA, it also may have missed relevant studies. Kadakia et al. (2021) limited relevant interventions and/or comparators to second-generation antipsychotic drugs, therefore excluding relevant comparators such as lithium and divalproex. Additionally, this NMA was considered an update that focused on trials published in May 2015 or later, thereby excluding older relevant publications. In the Kishi et al. published NMA, 70.8% of included studies were evaluated as having a moderate overall risk of bias. In the Kadakia et al. NMA, the risk of bias of included studies was less concerning, as 12 studies (67%) were rated as having a low risk of bias, and 6 studies (33%) were rated as having some concerns (driven by the randomization process) with the risk of bias. Both of the published NMAs listed potential effect modifiers that had been identified. The Kishi et al. NMA performed a meta-regression analysis with placebo as the control to assess its effect on the primary outcome. Older studies identified by publication year and studies that included a higher proportion of male individuals were associated with a higher relative risk of response to treatment and studies with more patients with psychotic features had a lower relative risk of all-cause discontinuation. Kadakia et al. noted that a meta-regression, which can potentially adjust for effect modifiers, was not feasible.
Both published NMAs assessed heterogeneity using tau-squared statistics and common heterogeneity across all comparisons was assumed. The NMA published by Kishi et al. evaluated inconsistency both globally and locally using the design-by-treatment test and the SIDE test, respectively. The NMA published by Kadakia et al. reported that the confidence of evidence was based on the GRADE approach; however, there were no closed loops in the network and, therefore, inconsistency was not considered to be a concern. Both published NMAs used an RE model for the analyses; this was considered appropriate, although a rationale for doing so was not clear. Additionally, an assessment of model fit, information about priors, and an assessment of convergence was not reported.
A network diagram for each outcome was provided for the Kishi et al. NMA, but none were available for the Kadakia et al. NMA. Direct and indirect evidence were provided for both NMAs.
Kishi et al. used CINeMA to assess the confidence of the evidence within the network. Kadakia et al. used GRADE to assess the quality of evidence for comparisons. Overall, the quality of the evidence and confidence in the evidence was rated as low.
Other Relevant Evidence
This section includes submitted long-term studies and additional relevant studies included in the sponsor’s submission to CADTH that were considered to address important gaps in the evidence included in the systematic review.
Long-Term Study
One long-term open-label study, study RGH-MD-36,20 is summarized as follows. It examined the long-term safety and tolerability of cariprazine in patients with bipolar mania.
Methods
Study RGH-MD-36,20 a phase III, open-label study, was conducted to evaluate the long-term safety and tolerability of flexibly dosed cariprazine (3 mg to 12 mg daily) in adult patients with manic or mixed episodes associated with bipolar I disorder for up to 16 weeks of treatment. Patients were eligible to enrol in study RGH-MD-36 if they were not currently taking any treatment or had a documented history of intolerance or inadequate response to their current therapy. The study included a washout period of up to 4 days to 7 days. During the screening period and for the first 2 weeks and up to 3 weeks of open-label treatment, all patients were hospitalized. At the end of week 3, all patients were discharged and followed as outpatients. Patients were discontinued from the study if they presented with clinical instability (by the end of week 3), with tolerability concerns, with worsening of symptoms, or with inadequate response, or if the investigator deemed it appropriate at any time to discontinue a patient. An inadequate therapeutic response was defined as an increase in the YMRS or MADRS total score by 30% or more at the end of week 2 or thereafter relative to baseline. Patients were evaluated every week during the first 4 weeks of open-label treatment, then every 2 weeks for the remainder of the study. After completing 16 weeks of treatment or prematurely discontinuing, patients were evaluated for an additional 3 weeks for safety follow-up. During the safety follow-up period, patients could be cross-titrated to and stabilized on an appropriate medication at the discretion of the investigator.
The open-label study was conducted between 2010 and 2012 in the US, Germany, Hungary, Poland, and Spain. There were no Canadian study sites in the study.
Populations
The eligibility criteria for enrolment at screening are briefly summarized as follows: adults 18 to 65 years of age, inclusive, with a diagnosis of bipolar I disorder (per the DSM-IV-TR criteria and confirmed by the Structured Clinical Interview) and who had had a manic or mixed episode (with or without psychotic symptoms) for which treatment was indicated within 12 months of the study. All patients were required to have a total score of 18 or more on the YMRS and a total score of less than 18 on the MADRS. Further, a body mass index between ||||||||| kg/m2 and ||||||||| kg/m2, inclusive, was required. In comparison to the inclusion criterion regarding the YMRS total score, the pivotal trials in bipolar mania (study RGH-MD-31,11 study RGH-MD-32,12 and study RGH-MD-3313) used a YMRS total score of 20 or more and a score of 4 or more on 2 of the 4 following YMRS items: irritability, speech, content, and disruptive/aggressive behaviour.
Patients who presented with a principal Axis I diagnosis other than bipolar I disorder, any other DSM-IV-TR Axis II disorder that would interfere with study participation, rapid cycling, any personality or cognitive or psychotic disorders, alcohol or substance dependence or abuse (aside from nicotine and caffeine) within the past 3 months of the study, a substance-induced manic or hypomanic episode, or were pregnant or breastfeeding were excluded from the study. Notably, patients who presented with their first manic episode and patients who had received treatment with any investigational product, including cariprazine, within the past 3 months or 5 half-lives (whichever was longer) before visit 1 were excluded from the study. Additionally, patients with a history of suicide attempt in the past year, who had scored 5 or more on MADRS item 10, or who were determined to have a significant suicide risk according to the C-SSRS or investigator judgment were excluded from the study. Patients with a history of tardive dyskinesia or neuroleptic malignant syndrome or requiring pharmacologic therapy for extrapyramidal symptoms were also excluded. Overall, the exclusion criteria were similar to the exclusion criteria used in the pivotal trials in bipolar mania.
Of the 403 patients who enrolled in the long term open-label study, a total of 402 patients received at least 1 dose of open-label cariprazine (safety population). The mean age of patients in the study was 41.4 (SD = 10.5) years. The majority of patients were male (57.2%) and White (51.2%). At baseline, the mean weight and body mass index was 86.5 (SD = 17.8) kg and 29.2 (SD = 5.3) kg/m2, respectively. The mean age at onset and the known duration of bipolar I disorder was 27.9 (SD = 11.3) years and ||||||||| (SD = |||||||||) months, respectively. The duration of the current manic episode for the majority of patients (53.2%) was greater than 21 days. Refer to Table 54 for a summary of baseline characteristics of patients enrolled in study RGH-MD-36.
Table 54: Summary of Baseline Characteristics in Study RGH-MD-36 — Safety Population
Characteristic | Cariprazine 3 mg to 12 mg (N = 402) |
|---|---|
Demographics | |
Age, mean (SD) | 41.4 (10.5) |
Sex, n (%) | |
Female | 172 (42.8) |
Male | 230 (57.2) |
Race, n (%) | |
White | 206 (51.2) |
Black or African American | 182 (45.3) |
American Indian or Alaska Native | ||||||||| |
Asian | ||||||||| |
Other | ||||||||| |
Weight (kg), mean (SD) | 86.5 (17.8) |
BMI (kg/m2), mean (SD) | 29.2 (5.3) |
Medical history (ongoing) | |
Patients with ongoing abnormalities, n (%) | ||||||||| |
Cardiac disorders | ||||||||| |
Metabolic and nutrition disorders | ||||||||| |
Obesity | ||||||||| |
Hypercholesterolemia | ||||||||| |
Hyperlipidemia | ||||||||| |
Type 2 diabetes mellitus | ||||||||| |
Nervous system disorders | ||||||||| |
Psychiatric disorders | ||||||||| |
Psychiatric history | |
Duration of bipolar I disorder (months), mean (SD) | ||||||||| |
Age at onset (years), mean (SD) | 27.9 (11.3) |
Duration of current episode, n (%) | |
≤ 7 days | 19 (4.7) |
> 7 days to ≤ 14 days | 102 (25.4) |
> 14 days to ≤ 21 days | 67 (16.7) |
> 21 days | 214 (53.2) |
DSM-IV-TR diagnosis (code), n (%) | |
Most recent episode, manic | |
Hypomanic/unspecified (296.40) | ||||||||| |
Mild (296.41) | ||||||||| |
Moderate (296.42) | ||||||||| |
Severe without psychotic features (296.43) | ||||||||| |
Severe with psychotic features (296.44) | ||||||||| |
Most recent episode, mixed | |
Unspecified (296.60) | ||||||||| |
Mild (296.61) | ||||||||| |
Moderate (296.62) | ||||||||| |
Severe without psychotic features (296.63) | ||||||||| |
Severe with psychotic features (296.64) | ||||||||| |
Number of previous psychiatric hospitalizations, mean (SD)a | ||||||||| |
Number of manic/mixed episodes during lifetime, mean (SD)a | ||||||||| |
Number of depressed episodes during lifetime, n (%) | |
0 | ||||||||| |
1 | ||||||||| |
2 | ||||||||| |
3 | ||||||||| |
4 | ||||||||| |
5 to 10 | ||||||||| |
> 10 | ||||||||| |
Number of patients with previous suicide attempts, n (%) | ||||||||| |
BMI = body mass index; DSM-IV-TR = Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition, Text Revision; SD = standard deviation.
aThe total number of patients was 400.
Source: Clinical Study Report of study RGH-MD-36.20
Interventions
The open-label treatment period was 16 weeks in duration. On day 0, patients received cariprazine 1.5 mg daily. On day 1 and day 2, patients received cariprazine 3 mg daily. On day 3, the dose of cariprazine could be increased in increments of 3 mg per day depending on patient response and tolerability to cariprazine as well as investigator judgment. The maximum daily dose was 6 mg on day 3 and day 4, 9 mg on day 5 and day 6, and 12 mg on day 7 and onwards. In the event of a dose-related AE, the dose of cariprazine could be lowered to what was previously prescribed in decrements of 1 capsule per day. A drug holiday for up to 3 days was permitted if there were any tolerability concerns or AEs and it was deemed appropriate by the investigator. Capsules containing cariprazine 1.5 mg or 3.0 mg were provided for oral administration as a single dose each evening unless tolerability concerns required switching to morning administration.
Psychotropic medications were prohibited during the open-label study with the following notable exceptions at prespecified daily doses or maximum daily doses: lorazepam for agitation; eszopiclone, zolpidem, zolpidem extended release, chloral hydrate, or zaleplon for insomnia; and diphenhydramine, benztropine, or propranolol for extrapyramidal symptoms.
Outcomes
The safety outcomes included AEs, clinical laboratory tests, vital signs, physical examinations, electrocardiograms, and ophthalmologic exams. Suicidal ideation and behaviour were assessed using the C-SSRS. Treatment-emergent extrapyramidal symptoms were assessed by the Barnes Akathisia Rating Scale, Abnormal Involuntary Movement Scale, and the Simpson-Angus Scale.
The efficacy outcomes included the change from baseline in the YMRS and MADRS total score, and YMRS response and remission rates at week 3, which were defined as a 50% or greater reduction from baseline and a total score of 12 or less, respectively.
Statistical Analysis
The open-label treatment period began on the day when the first dose of cariprazine was administered and ended when the last scheduled evaluation was completed on week 16 or earlier if the patient had prematurely discontinued. Baseline values were defined as the last value documented before the first dose of open-label cariprazine was taken by the patient.
Safety analyses were conducted on the safety population, which included all patients who received at least 1 dose of open-label cariprazine in study RGH-MD-36. Descriptive statistics were performed to summarize the safety parameters for the safety population. Inferential analyses were not performed.
Efficacy analyses were conducted on the mITT population, which included patients from the safety population who had completed a YMRS assessment at baseline and at least once more during the postbaseline period in study RGH-MD-36. Descriptive statistics were performed to summarize the efficacy parameters for the mITT population, with missing postbaseline data imputed using the LOCF approach and without missing data imputed using the observed cases approach. Inferential analyses were not performed.
Patient Disposition
Of the 672 patients screened, a total of 403 patients were enrolled. A total of 402 patients received at least 1 dose of open-label cariprazine (safety population) and 399 patients from the safety population completed a YMRS assessment at baseline and at least once during the postbaseline period (mITT population). A total of 132 (32.8%) patients completed the study and 285 (70.9%) patients entered safety follow-up. The most frequently reported reason for discontinuation during the open-label treatment period was withdrawal of consent (19.7%), followed by AE (16.4%), and protocol violation (13.7%). Refer to Table 55 for a summary of patient disposition in study RGH-MD-36.
Table 55: Summary of Patient Disposition in Study RGH-MD-36
Characteristic | Cariprazine 3 mg to 12 mg |
|---|---|
Screened, Na | 672 |
Enrolled, N (%)b | 403 |
Discontinued from study, N (%) | 270 (67.2) |
Reason for discontinuation, N (%) | |
Withdrawal of consent | 79 (19.7) |
Adverse event | 66 (16.4) |
Protocol violationc | 55 (13.7) |
Lost to follow-up | 42 (10.4) |
Insufficient therapeutic response | 26 (6.5) |
Did not meet inclusion/exclusion criteria | 0 |
Otherd | 2 (0.5) |
mITT, N | 399 |
Safety, N | 402 |
mITT = modified intention-to-treat.
aOf the 269 screen failures, 229 were due to the fact that they did not meet inclusion or exclusion criteria, 30 were due to withdrawal of consent, 3 were due to adverse events, 2 were due to lost to follow-up, and 5 were due to other reasons not specified.
bOne patient withdrew consent.
cThe majority of protocol violations (32 out of 55) were due to a positive urine drug screen for cocaine, cannabinoids, amphetamines, or other unspecified drugs.
dOther reasons included 1 patient who relocated and 1 patient who was deemed noncompliant according to investigator judgment.
Source: Clinical Study Report of study RGH-MD-36.20
Exposure to Study Treatments
The mean duration of treatment exposure was 57.7 (SD = 43.6) days, and the median duration of treatment exposure was 42.0 (range = 1 to 127) days. The total time at risk was ||||||| patient-years.
The overall mean daily dose was cariprazine 6.2 (SD = 2.6) mg. The overall modal daily dose for 1.0%, 29.1%, 28.1%, 25.9%, and 15.9% of patients was 1.5 mg, 3 mg, 6 mg, 9 mg, and 12 mg, respectively. The final daily dose for 1%, 27.1%, 30.3%, 24.4%, and 17.2% of patients was 1.5 mg, 3 mg, 6 mg, 9 mg, and 12 mg, respectively.
The overall mean patient compliance with cariprazine was ||||||| (SD = |||||||). The overall median patient compliance was ||||||| (range = ||||||| to |||||||) in the safety population.
Efficacy
Only those efficacy outcomes identified in the review protocol are reported as follows.
The mean change from baseline in the YMRS and MADRS total score for the mITT population in study RGH-MD-36 was provided up to week 16 as shown in Table 56. The mean YMRS total score at baseline was 26.1 (SD = 5.0). The mean change from baseline to week 16 in the YMRS total score was –15.2 (SD = 9.2) per LOCF and –20.7 (SD = 6.0) per observed case. The mean MADRS total score at baseline was 9.9 (SD = 3.5). The mean change from baseline to week 16 in the MADRS total score was –1.6 (SD = 7.5) per LOCF and –4.3 (SD = 7.0) per observed case.
The YMRS response and remission rates for the mITT population in study RGH-MD-36 were provided up to week 16 as shown in Table 57. YMRS response criteria (≥ 50% reduction from baseline) was met by 64.2% (LOCF) of patients by week 16 and ||||||||| (observed cases). YMRS remission criteria (total score ≤ 12) was met by 63.4% (LOCF) of patients at week 16 and ||||||||| (observed cases).
Table 56: Change From Baseline to Week 3 and Week 16 in YMRS and MADRS Total Scores in Study RGH-MD-36 — Modified Intention-to-Treat Population
Efficacy measure | Cariprazine 3 mg to 12 mg | |||||
|---|---|---|---|---|---|---|
LOCF analysis | OC analysis | |||||
n included in analysis (%) | Baseline score, mean (SD) | Mean (SD) change from baseline | n included in analysis (%) | Baseline score, mean (SD) | Mean (SD) change from baseline | |
Change at week 3 | ||||||
YMRS total score | 399 (100.0) | 26.1 (5.0) | |||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| |
MADRS total score | 399 (100.0) | 9.9 (3.5) | |||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| |
Change at week 16 | ||||||
YMRS total score | 399 (100.0) | 26.1 (5.0) | –15.2 (9.2) | |||||||||||||| | |||||||||||||| | –20.7 (6.0) |
MADRS total score | 399 (100.0) | 9.9 (3.5) | –1.6 (7.5) | |||||||||||||| | |||||||||||||| | –4.3 (7.0) |
LOCF = last observation carried forward; MADRS = Montgomery–Åsberg Depression Rating Scale; OC = observed case; SD = standard deviation; YMRS = Young Mania Rating Scale.
Source: Clinical Study Report of study RGH-MD-36.20
Table 57: YMRS Response and Remission Rates at Week 3 and Week 16 in Study RGH-MD-36 — Modified Intention-to-Treat Population
Factor | Cariprazine 3 mg to 12 mg | |
|---|---|---|
LOCF analysis | OC analysis | |
Rate at week 3 | — | — |
YMRS response (≥ 50% reduction from baseline in YMRS total score) | ||
n/N (%) | 230/399 (57.6) | |||||||||||||| |
YMRS remission (YMRS total score ≤ 12) | ||
n/N (%) | 229/399 (57.4) | |||||||||||||| |
Rate at week 16 | — | — |
YMRS response (≥ 50% reduction from baseline in YMRS total score) | ||
n/N (%) | 256/399 (64.2) | |||||||||||||| |
YMRS remission (YMRS total score ≤ 12) | ||
n/N (%) | 253/399 (63.4) | |||||||||||||| |
LOCF = last observation carried forward; OC = observed case; YMRS = Young Mania Rating Scale.
Source: Clinical Study Report of study RGH-MD-36.20
Harms
Only those harms identified in the review protocol are reported as follows. Refer to Table 58 for detailed harms data.
AEs were reported in 335 (83.3%) patients in the safety population during the open-label treatment. The most commonly reported TEAEs (frequency ≥ 10%) were akathisia (32.6%), headache (16.7%), constipation (10.7%), and nausea (10.4%). The most frequently reported TEAEs that were considered severe were akathisia, extrapyramidal disorder, and anxiety, with each event reported in 3 (0.7%) patients.
SAEs were reported in 30 (7.5%) patients during open-label treatment. The following SAEs were reported in more than 1 patient: worsening of mania in 9 (2.2%) patients, depression in 5 (1.2%) patients, akathisia in 3 (0.7%) patients, suicidal ideation in 2 (0.5%) patients, and suicide attempt in |||||||||||||| patients.
No deaths were reported in the safety population. The most severe suicidal ideation and suicidal behaviour per the C-SSRS were reported in 35 (8.8%) patients and 3 (0.8%) patients, respectively, during the open-label treatment.
Premature discontinuation due to at least 1 AE was reported in 66 (16.4%) patients during the open-label treatment. The most frequently reported AEs that led to premature discontinuation of the study were akathisia in 19 (4.7%) patients and depression in 6 (1.5%) patients. Notably, 2 (0.5%) patients and 1 (0.2%) patient discontinued the study due to suicide attempt and suicidal ideation, respectively.
The most commonly reported notable harms (frequency ≥ 5%) included akathisia in 131 (32.6%) patients, insomnia in 28 (7.0%) patients, extrapyramidal symptoms in 27 (6.7%) patients, restlessness in 26 (6.5%) patients, vomiting in 24 (6.0%) patients, sedation in 23 (5.7%) patients, and an increase in weight in 23 (5.7%) patients. A total of |||||||||||||| patients with at least 1 TEAE was related to extrapyramidal symptoms during open-label treatment. The most commonly reported TEAEs (frequency ≥ 5%) related to extrapyramidal symptoms were the following: akathisia in 131 (32.6%) patients, tremor in 31 (7.7%) patients, extrapyramidal disorder in 27 (6.7%) patients, and restlessness in 26 (6.5%) patients. During the open-label treatment, 129 (32.1%) patients required treatment for extrapyramidal symptoms, of which 74 (18.4%) patients used a beta-blocking drug (propranolol or propranolol hydrochloride), 64 (15.9%) patients used an anti-Parkinson drug (benztropine mesylate or biperiden), and |||||||||||||| patients used a psycholeptic drug (diphenhydramine hydrochloride, diphenhydramine, or zolpidem tartrate).
Table 58: Summary of Harms in Study RGH-MD-36 — Safety Population
Harm | Cariprazine 3 mg to 12 mg (N = 402) |
|---|---|
Patients with ≥ 1 TEAE during open-label treatment period | |
n (%) | 335 (83.3) |
Most common events,a n (%) | |
Akathisia | 131 (32.6) |
Headache | 67 (16.7) |
Constipation | 43 (10.7) |
Nausea | 42 (10.4) |
Dyspepsia | 38 (9.5) |
Toothache | 35 (8.7) |
Back pain | 32 (8.0) |
Tremor | 31 (7.7) |
Insomnia | 28 (7.0) |
Extrapyramidal disorder | 27 (6.7) |
Restlessness | 26 (6.5) |
Vomiting | 24 (6.0) |
Sedation | 23 (5.7) |
Weight increase | 23 (5.7) |
Diarrhea | 20 (5.0) |
Patients with ≥ 1 SAE during open-label treatment period | |
n (%) | 30 (7.5) |
Most common events,b n (%) | |
Mania | 9 (2.2) |
Depression | 5 (1.2) |
Akathisia | 3 (0.7) |
Suicidal ideation | 2 (0.5) |
Suicidal attempt | |||||||||||||| |
Patients who stopped treatment due to AEs during open-label treatment period | |
n (%) | 66 (16.4) |
Most common events,b n (%) | |
Akathisia | 19 (4.7) |
Depression | 6 (1.5) |
Extrapyramidal disorder | |||||||||||||| |
Mania | |||||||||||||| |
Alanine aminotransferase, increased | |||||||||||||| |
Anxiety | |||||||||||||| |
Aspartate aminotransferase, increased | |||||||||||||| |
Bipolar I disorder | |||||||||||||| |
Dystonia | |||||||||||||| |
Hypertension | |||||||||||||| |
Insomnia | |||||||||||||| |
Sedation | |||||||||||||| |
Suicide attempt | |||||||||||||| |
Toothache | |||||||||||||| |
Deaths | |
n (%) | 0 |
Notable harms, n (%) during open-label treatment period | |
Akathisia | 131 (32.6) |
Insomnia | 28 (7.0) |
Extrapyramidal disorder | 27 (6.7) |
Restlessness | 26 (6.5) |
Vomiting | 24 (6.0) |
Sedation | 23 (5.7) |
Weight, increased | 23 (5.7) |
Metabolic effects (metabolism and nutrition disorders) | |||||||||||||| |
Suicide ideation | 4 (1.0) |
Suicide attempt | |||||||||||||| |
Blood glucose, increased | |||||||||||||| |
Sexual dysfunction (decreased libido) | |||||||||||||| |
Tardive dyskinesia | |||||||||||||| |
Neuroleptic malignant syndrome | |||||||||||||| |
AE = adverse event; NR = not reported; SAE = serious adverse event; TEAE = treatment-emergent adverse event.
aFrequency of 5% or more.
bFrequency of more than 1 patient.
Source: Clinical Study Report of study RGH-MD-36.20
Critical Appraisal
In the absence of an active comparator or placebo group, the interpretation of the efficacy results from the long-term open-label study RGH-MD-36 is limited. This is compounded by the use of descriptive statistics only. The use of an LOCF approach could underestimate the overall long-term treatment benefits. Although the expectation is that patients who receive the study drug would improve over time with respect to the efficacy parameters, the results can remain difficult to interpret given the aforementioned limitations. The open-label study design can bias the reporting of end points, particularly any subjective measures included in the efficacy and safety parameters due to the unblinding of the study drug during the treatment period. Patients were discontinued from the study if they presented with clinical instability by the end of week 3, with any tolerability concerns, with worsening of symptoms, or with inadequate response, or if the investigator deemed it appropriate at any time to discontinue a patient. Because of that, the resultant population may be more tolerant and responsive of cariprazine. This could potentially lead to an underreporting of AEs and a response bias, as patients with an inadequate response (defined as an increase in the YMRS or MADRS total score of 30% or more at the end of week 2 or thereafter) were prematurely discontinued from the study.
The clinical experts consulted by CADTH stated that the exclusion of patients with, for example, rapid cycling and active substance use disorder can lead to patients with complex cases who are seen in clinical practice being missed in the study. However, the clinical experts recognized that clinical trials will typically use said exclusion criteria to avoid confounding variables. There was a notable discontinuation rate of greater than 50%, which decreases the certainty and generalizability of the efficacy and safety results. According to the clinical experts, a discontinuation rate of approximately 35% is typically anticipated for clinical trials in bipolar mania. Further, some patients in the study received a dose higher than the Health Canada–recommended daily dose of cariprazine, which is up to 6 mg per day.
Post Hoc Analysis
A post hoc analysis by McIntyre et al. (2019)21 is briefly summarized here to provide additional efficacy data on cariprazine in the subpopulation of patients with bipolar mania with mixed features.
Data from 3 pivotal trials of cariprazine in adult patients with bipolar I disorder were pooled. The objective of the post hoc analysis was to determine the effect of cariprazine on manic and depressive symptoms versus placebo in the subpopulation of patients with mania and subsyndromal depressive features. Further, the post hoc analysis sought to determine the frequency of patients who met the DSM-5 criteria for a mixed state (≥ 3 nonoverlapping depressive symptoms) and 2 other definitions for a mixed episode (≥ 2 depressive symptoms and a MADRS total score ≥ 10). The depressive symptoms used in the definitions were each linked to an item on the MADRS and/or the PANSS. Depressive mood, fatigue and loss of energy, diminished interest or pleasure, psychomotor retardation, worthlessness and feelings of guilt, and suicidal thoughts were linked to MADRS item 1 or item 2, MADRS item 7, MADRS item 8, PANSS item G7, MADRS item 9, and MADRS item 10, respectively. A MADRS total score of 1 or more or PANSS score of 2 or more on any of the aforementioned items would indicate the presence of that symptom.
Refer to the systematic review section for detailed descriptions of study design and patient population in study RGH-MD-31,11 study RGH-MD-32,12 and study RGH-MD-33.13
Results
A total of 1,037 patients were pooled from the pivotal trials. Refer to Figure 18 for a summary of baseline characteristics of the patients included. The number of patients who met the DSM-5 criteria for a mixed state (≥ 3 depressive symptoms) and the 2 proxy definitions for a mixed episode (≥ 2 depressive symptoms and a MADRS total score ≥ 10) were 141 (13.6%), 269 (25.9%), and 453 (43.7%), respectively.
Figure 18: Summary of Baseline Characteristics in the McIntyre et al. (2019) Study — Bipolar Mania With Mixed Features
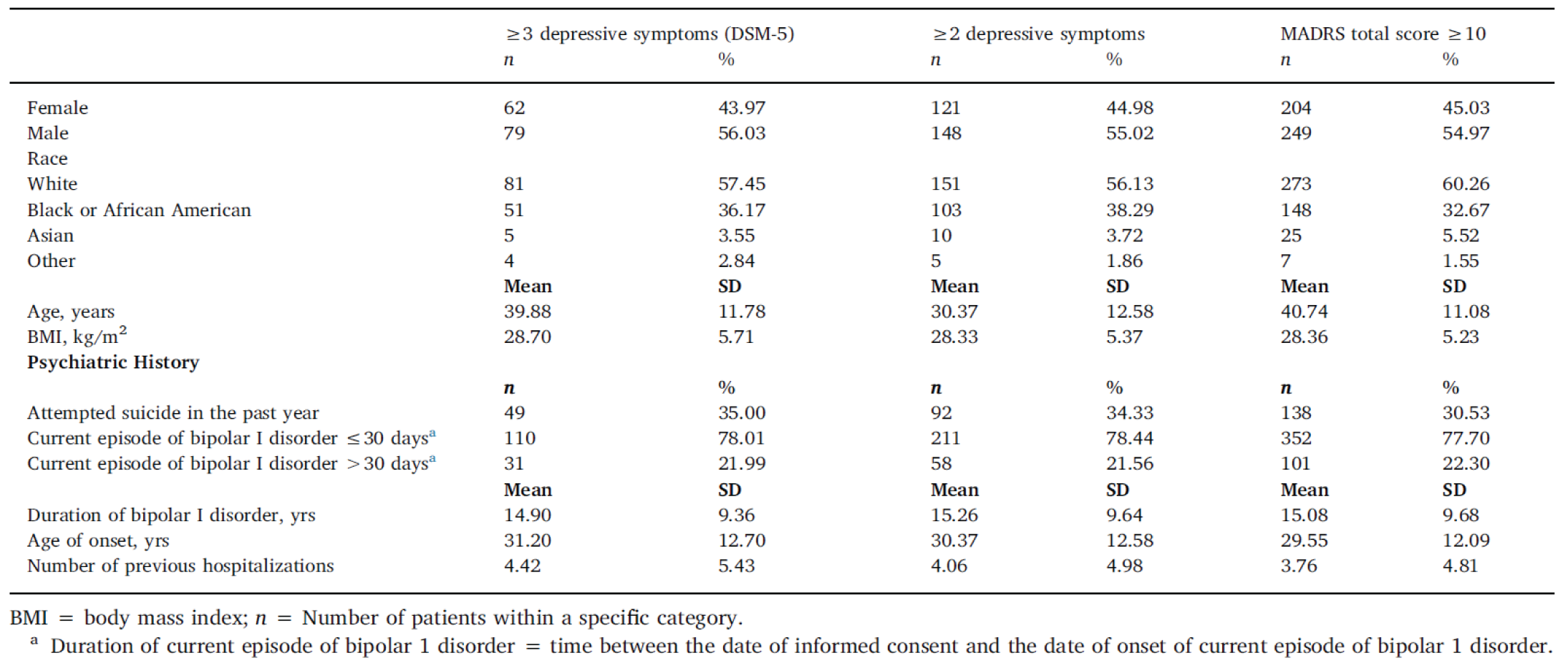
DSM-5 = Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition; MADRS = Montgomery–Åsberg Depression Rating Scale; SD = standard deviation; yrs = years.Source: McIntyre RS, et al., Copyright 2019. This work is licensed under the CC BY-NC-ND 4.0 (Attribution-NonCommercial-NoDerivatives 4.0) International License. Full text available here: https://www.sciencedirect.com/science/article/pii/S0165032718322092?via%3Dihub.21
The pooled placebo and active treatment groups showed an improvement in the mean YMRS total score at week 3 relative to baseline, as shown in Figure 19. The difference between cariprazine and placebo in change in mean YMRS total score was –3.79 (SE = NR; P = 0.0248), –2.91 (SE = NR; P = 0.0207), and –5.49 (SE = NR; P < 0.0001) in patients with mixed features as defined by 3 or more depressive symptoms, 2 or more depressive symptoms, and a MADRS total score of 10 or more, respectively, in favour of cariprazine.
Figure 19: Change in Mean YMRS Total Score at Week 3 in the McIntyre et al. (2019) Study — Bipolar Mania With Mixed Features
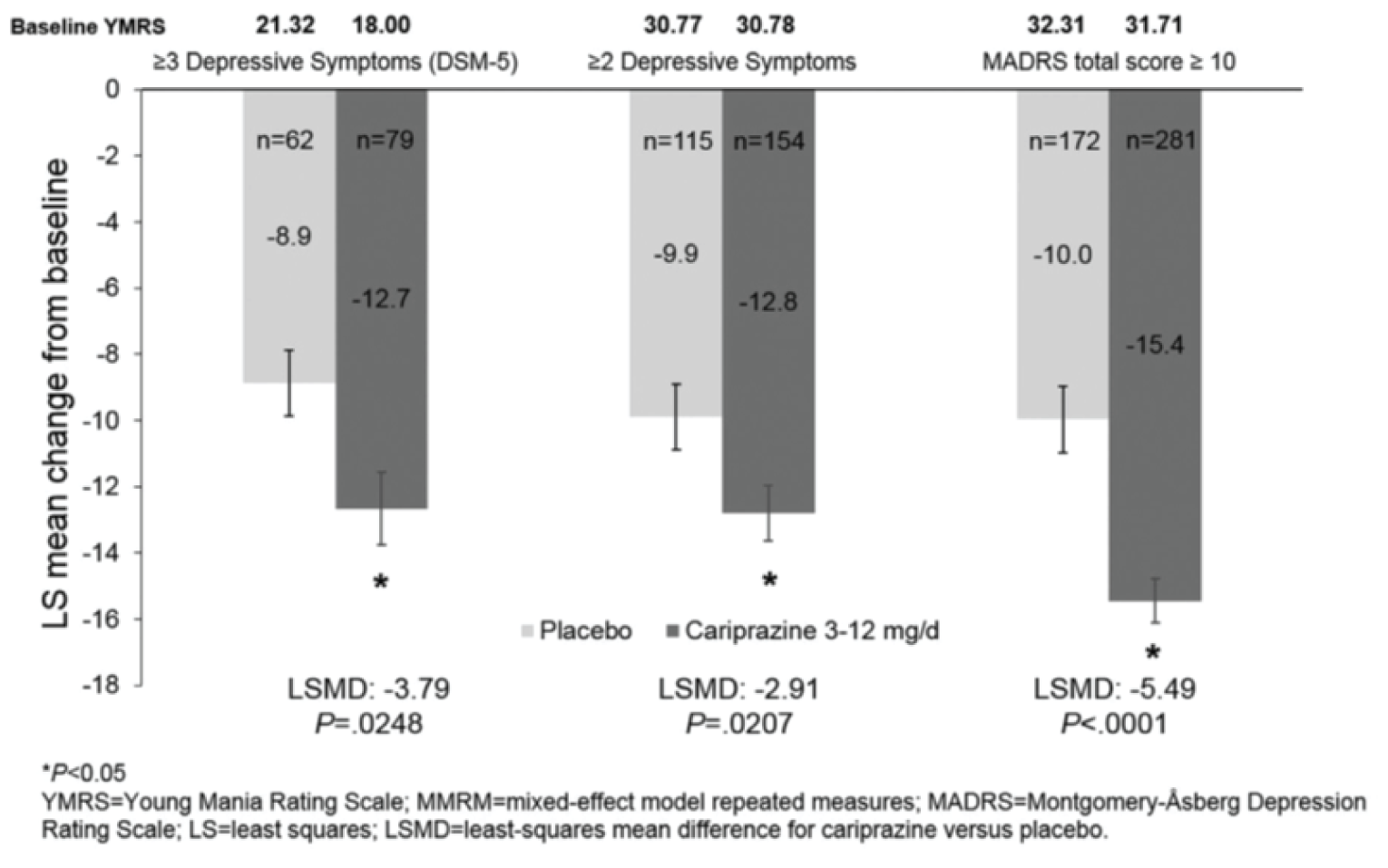
DSM-5 = Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition
Source: McIntyre RS, et al., Copyright 2019. This work is licensed under the CC BY-NC-ND 4.0 (Attribution-NonCommercial-NoDerivatives 4.0) International License. Full text available here: https://www.sciencedirect.com/science/article/pii/S0165032718322092?via%3Dihub.21
The change in mean MADRS total score at week 3 relative to baseline is shown in Figure 20. The results were inconsistent based on the definition used for patients with mixed features. There was a benefit with cariprazine based on the MADRS total score of 10 or more and no difference was observed using the other 2 definitions (3 or more depressive symptoms and 2 or more depressive symptoms). The difference between cariprazine and placebo in change in mean MADRS total score was –1.59 (SE = NR; P < 0.0082) in patients with mixed features as defined by a MADRS total score of 10 or more, in favour of cariprazine.
Figure 20: Change in Mean MADRS Total Score at Week 3 in the McIntyre et al. (2019) Study — Bipolar Mania With Mixed Features
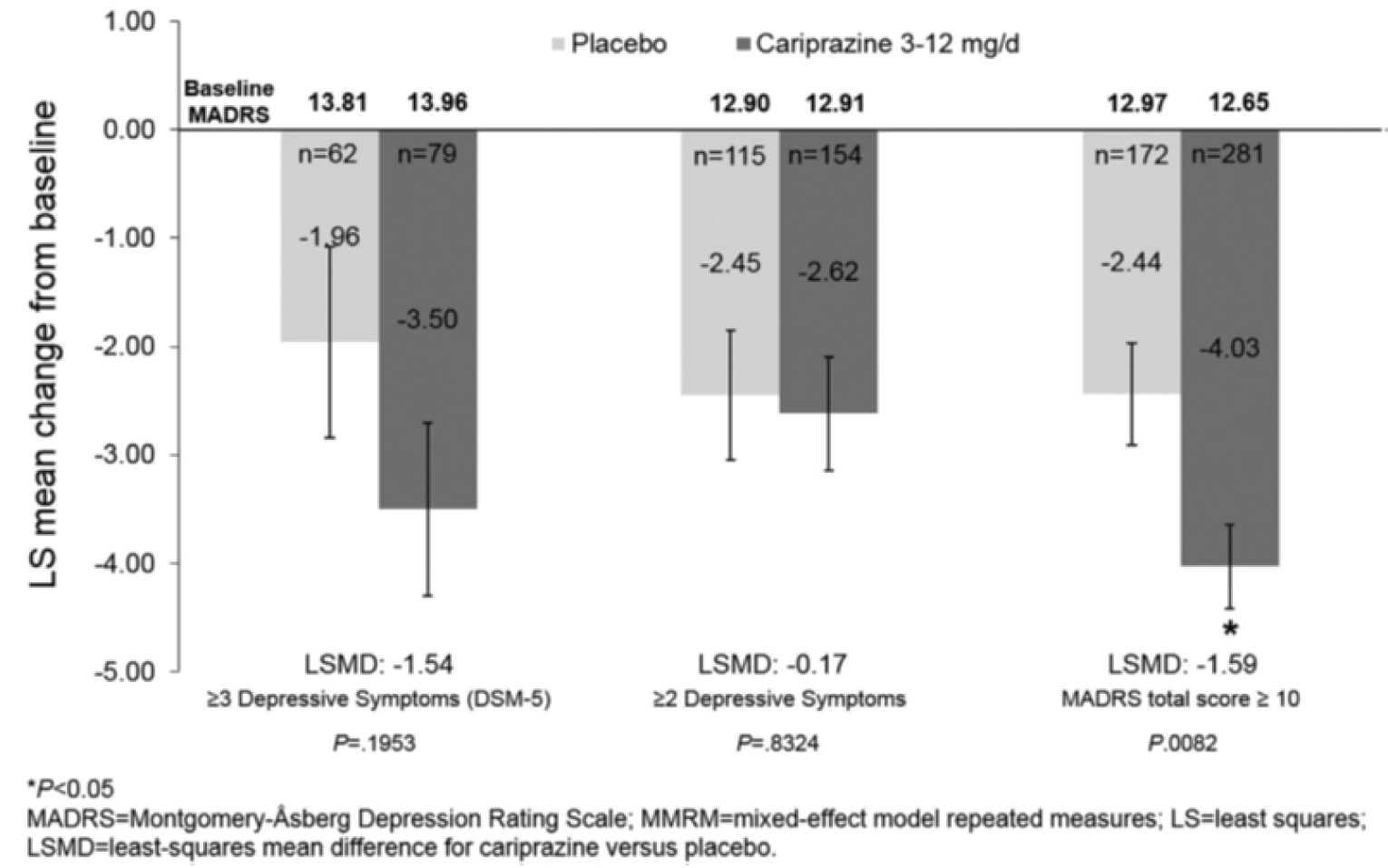
Source: McIntyre RS, et al., Copyright 2019. This work is licensed under the CC BY-NC-ND 4.0 (Attribution-NonCommercial-NoDerivatives 4.0) International License. Full text available here: https://www.sciencedirect.com/science/article/pii/S0165032718322092?via%3Dihub.21
The proportion of responders (≥ 50% improvement from baseline in the YMRS total score) was higher for cariprazine in the 2 or more depressive symptoms group (47%; P = 0.0483) and MADRS total score of 10 or more group (57%; P = < 0.0001) than for placebo (34% and 31%, respectively), as shown in Figure 21. There was no difference between the cariprazine and placebo treatment groups (P = 0.2608) based on the 3 or more depressive symptoms definition for patients with mixed features.
The proportion of remitters (YMRS total score ≤ 12) was higher for cariprazine in the 2 or more depressive symptoms group (39%; P = 0.0462) and MADRS total score of 10 or more group (44%; P = < 0.0001) than for placebo (27% and 23%, respectively), as shown in Figure 21. There was no difference between the cariprazine and placebo treatment groups (P = 0.1224) based on the 3 or more depressive symptoms definition for patients with mixed features.
Figure 21: Responder and Remission Rates at Week 3 in the McIntyre et al. (2019) Study — Bipolar Mania With Mixed Features
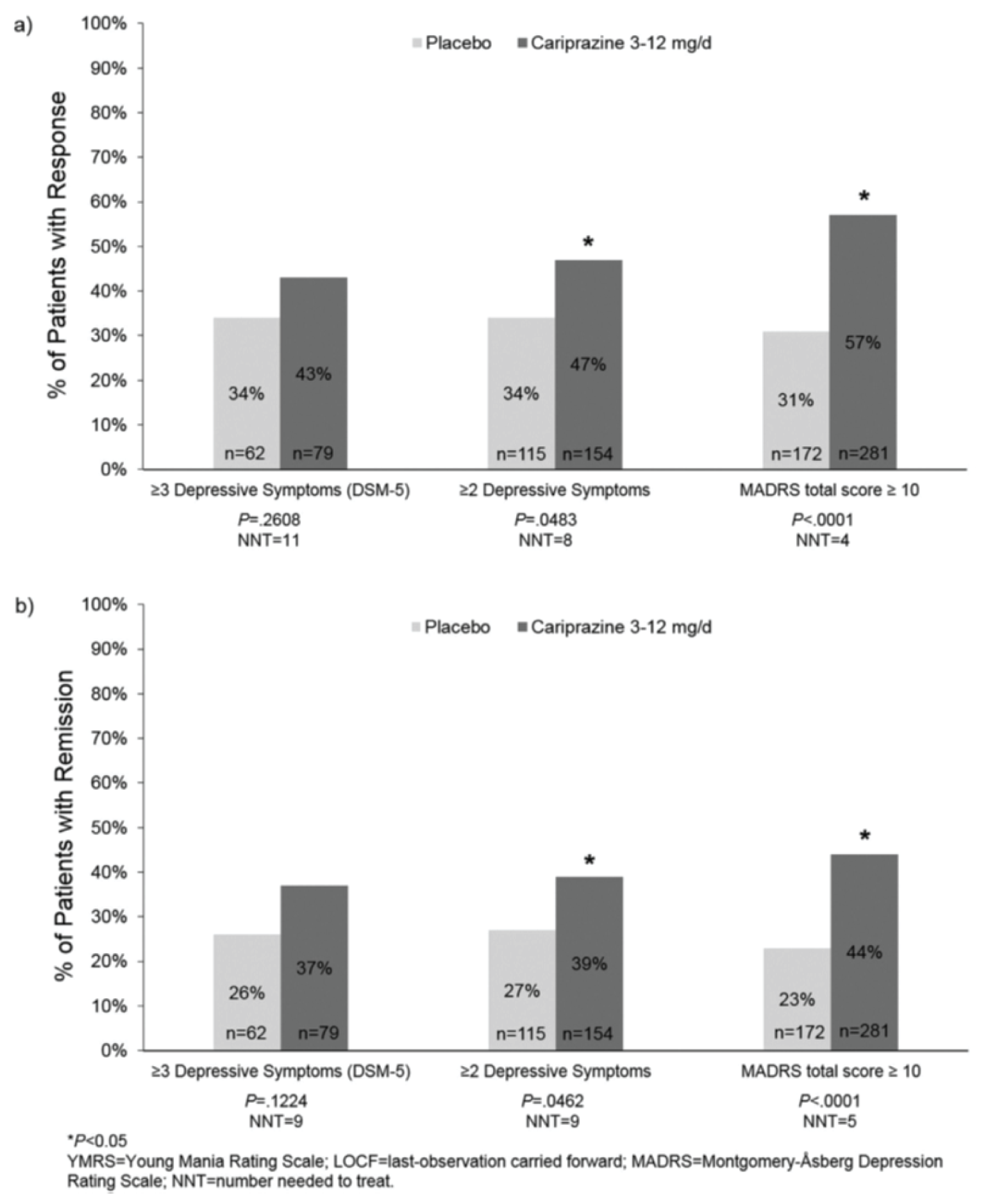
Source: McIntyre RS, et al., copyright 2019. This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 International (CC BY-NC-ND 4.0) licence. Full text available here: https://www.sciencedirect.com/science/article/pii/S0165032718322092?via%3Dihub.21
The results of the sensitivity analyses were consistent with the primary analyses using the MMRM approach. Missing data were imputed using the LOCF approach.
Critical Appraisal
None of the P values were adjusted for multiplicity and the post hoc nature of the pooled analyses can be considered hypothesis-generating, inflating the probability of type I error in favour of the treatment group. Further, missing data were imputed using the LOCF approach, which could potentially underestimate the overall treatment benefits. Finally, unbalanced comparisons were likely made, including that the total number of patients in the MADRS total score of 10 or more group was numerically higher than the 2 other definitions of mixed episode.
Discussion
Summary of Available Evidence
The systematic review of cariprazine included a total of 6 multi-centre, randomized, double-blind, placebo-controlled, parallel-group studies in adults with a primary diagnosis of bipolar I disorder. Of the 6 included RCTs, 3 evaluated cariprazine 3 mg to 12 mg (flexible dose) for the treatment of acute manic or mixed episodes (study RGH-MD-31 [N = 238], study RGH-MD-32 [N = 312], and study RGH-MD-33 [N = 497]) and 3 evaluated cariprazine 1.5 mg and 3.0 mg (fixed dose) for the treatment of acute depressive episodes (study RGH-MD-56 [N = 578], study RGH-MD-53 [N = 493], and study RGH-MD-54 [N = 488]). The objective of each of the studies was similar: to evaluate the efficacy, safety, and tolerability of cariprazine monotherapy versus placebo for the treatment of acute manic or mixed episodes or acute depressive episodes associated with bipolar I disorder. The primary end point in all studies was the change in symptoms severity, measured using the YMRS total score in the studies of acute manic or mixed episodes and the MADRS total score in the studies of acute depressive episodes. The secondary end point was the change in CGI-S scores and was consistent across studies. Primary and secondary outcomes were assessed at week 3 in the acute mania studies and at week 6 in the acute depression studies. Other measures of changes in symptom severity (CGI-I, PANSS, HAM-D, HAM-A, QIDS-SR), functioning (FAST), suicidal ideation (C-SSRS), response rate, and remission rate were also reported.
There was also indirect evidence from 3 NMAs (1 sponsor-submitted NMA and 2 published NMAs) that evaluated the effectiveness, safety, and tolerability of cariprazine relative to second-generation antipsychotic drugs and other therapies used as monotherapy for the treatment of acute episodes associated with bipolar I disorder.17-19 Two additional studies were also summarized to address gaps in the evidence. This included 1 long-term open-label study (study RGH-MD-36 [N = 402]) that examined the long-term safety and tolerability of cariprazine 3 mg to 12 mg (flexible dose) in patients with bipolar mania, and 1 post hoc analysis by McIntyre et al. (2019)21 that provided additional efficacy data on cariprazine in the subpopulation of patients with bipolar mania with mixed features based on pooled data from the pivotal trials (N = 1,037).
Interpretation of Results
Efficacy
Input received from both patient groups and clinicians for the review of cariprazine indicated that second-generation antipsychotic medications can be improved by increasing the ability to mitigate the symptoms of bipolar disorder. The primary end point in all studies was based on outcomes assessing the change in symptom severity. More specifically, the primary end point in the bipolar mania studies was the change in the YMRS total score at week 3 and the primary end point in the bipolar depression studies was the change in the MADRS total score at week 6. All 3 studies of acute mania demonstrated that treatment with flexible dosing of cariprazine was associated with a greater reduction of symptoms of acute mania relative to placebo, based on the YMRS total score at week 3. The within-group change in the YMRS score was clinically meaningful for both the cariprazine and placebo treatment groups, based on a within-group MID of 6.6 points.7 The placebo response may reflect care received in the inpatient treatment setting; however, the between-group difference indicated an added benefit in favour of cariprazine. Although it is common for clinical trials for bipolar mania or mixed episodes to be conducted in an inpatient setting, whether a clinically meaningful change in symptoms of mania would have been observed in an outpatient treatment setting is unknown. In the studies of acute bipolar depression, treatment with cariprazine 1.5 mg was associated with a greater reduction of symptoms of depression relative to placebo, based on the MADRS total score at week 6, whereas the comparison of cariprazine 3.0 mg to placebo did not consistently demonstrate a benefit with treatment. This is consistent with expectations of the clinical experts consulted by CADTH, who indicated that insufficient response to treatment was very common for bipolar depression. Based on a between-groups MID of at least 2 points that was identified for the MADRS total score,8,9 the between-group differences for cariprazine 1.5 mg and 3.0 mg compared to placebo were clinically meaningful.
A subgroup analysis of the primary outcome by patients with mania and patients with mixed mania was reported as descriptive results. The sample size of patients with mixed mania was very small in all bipolar mania studies, ranging from 15 patients to 23 patients per treatment group. Overall, the subgroup analysis of patients with mania was consistent with the primary analysis and the subgroup analysis of patients with mixed mania was also consistent for study RGH-MD-31 and study RGH-MD-33. Additionally, a post hoc pooled analysis of data from study RGH-MD-31, study RGH-MD-32, and study RGH-MD-33 was summarized as other relevant evidence for this review. The objective of the post hoc analysis was to determine the effect of cariprazine on manic and depressive symptoms versus placebo. The post hoc analysis was performed in the subpopulation of patients with mania and subsyndromal depressive features, based on the DSM-5 criteria for mixed features, and 2 other definitions for a mixed episode (at least 2 depressive symptoms and a MADRS total score of at least 10). Briefly, all 3 definitions of patients experiencing a mixed presentation were associated with a greater change in YMRS total score at week 3 relative to placebo, which is consistent with the primary analysis of the individual trials. However, the post hoc analysis and subgroup analysis were performed on subgroups that were not included as stratification variables at randomization, which may bias the results. Additionally, the post hoc analysis was limited by a lack of control for multiplicity.
The secondary end point in all studies was the change in CGI-S, which is an outcome based on a global assessment of symptom severity relative to other patients that the assessor has observed. The CGI-S has been validated through a comparison to the PANSS in patients with schizophrenia, but evidence of reliability and responsiveness were not identified. In the acute mania studies, the cariprazine treatment groups exhibited a greater change in overall severity based on the CGI-S at week 3 than the placebo treatment groups did, which is consistent with the primary analysis. In the acute depression studies, a benefit in terms of the change from baseline to week 6 in the CGI-S was demonstrated for comparisons of cariprazine 1.5 mg to placebo in study RGH-MD-53 and study RGH-MD-56. Similar to the primary analysis, cariprazine 3.0 mg did not demonstrate a benefit relative to placebo, nor did the 1.5 mg treatment group in study RGH-MD-54. The suggested MID for the CGI-S is a difference of 1 point for both within-group and between-group analyses. Based on this threshold, a clinically meaningful within-group difference was observed for all treatment groups (except placebo in study RGH-MD-31). However, the between-group differences were not clinically meaningful.
Other assessments of the change in symptoms were reported in the included studies; however, a lack of control for multiplicity renders additional efficacy outcomes as supportive only. In the studies of acute mania, the overall improvement of symptoms using the CGI-I, the change in symptoms of depression using the MADRS total score, and the change in psychopathology using the PANSS were assessed. The results of the CGI-I at week 3 were supportive of the primary and secondary analyses. At baseline, the mean MADRS total score ranged from approximately 8 to 10, which is suggestive of mild depression.76 A small reduction in symptoms of depression assessed at week 3 using the MADRS total score was observed, with no difference between cariprazine and placebo. The clinical experts consulted by CADTH did not expect to see a change in depressive symptoms for patients experiencing an acute manic episode, but also suggested that not observing an increase in symptoms of depression is notable. In addition, the clinical experts indicated that an assessment at 3 weeks is typically too short to identify a meaningful difference in depression severity. A numerical reduction in the PANSS total score was observed at week 3 in all of the bipolar mania studies. Although the clinical experts consulted by CADTH noted that PANSS was commonly used to assess symptoms of psychosis in patients with bipolar disorder, it was designed to evaluate patients with schizophrenia. Further, evidence of validity, reliability, and an MID of the PANSS is based on short-term trials for schizophrenia, defined as 6 weeks in duration.77 In summary, it is difficult to interpret the results of the PANSS analysis in the context of short-term treatment for acute mania associated with bipolar disorder.
In the bipolar depression studies, changes in symptoms of depression were also assessed using the HAM-D and QIDS-SR and symptoms of anxiety was assessed using the HAM-A. A numerical change in depressive symptoms based on the HAM-D at week 6 consistent with a reduction of symptoms was observed in all treatment groups. Study RGH-MD-56 reported similar results for the HAM-D at week 6 and week 8. The QIDS-SR was only reported in study RGH-MD-53 and study RGH-MD-54 and neither dose of cariprazine (1.5 mg or 3.0 mg) demonstrated a benefit relative to placebo based on the change in depressive symptoms at week 6, as per the QIDS-SR measured in these studies. A numerical reduction in the HAM-A score at week 6 indicating an improvement of symptoms of anxiety was seen in all treatment groups, with no difference being observed between cariprazine 3.0 mg and placebo. The HAM-A has been criticized for its use in depressive disorders70; therefore, clinical relevance of these changes is unknown. Overall, the evidence in support of changes in the severity of symptoms associated with a depressive episode of bipolar disorder were inconsistent with respect to the difference between cariprazine 1.5 mg and placebo, and did not support a benefit with cariprazine 3.0 mg relative to placebo. Dose response was not observed in the depression trials. It is unclear why a lower dose of cariprazine appears to work better than a higher dose in this patient population.
Daily functioning was also identified as an outcome of interest to patients and by clinicians. ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Response rate and remission rate based on reductions in the YMRS total score (acute mania studies) and MADRS total score (depressive studies) were also reported. These outcomes were also not controlled for multiplicity and, therefore, were considered supportive only. The definitions of response and remission are supported by published evidence and are commonly used in research settings, as per feedback from the clinical experts. In the acute mania studies, the results for response rate were consistent with the primary end point. A response was observed in 48% to 61% of patients receiving cariprazine and 25% to 44% of patients receiving placebo. Remission was observed in 42% to 52% of patients receiving cariprazine and in 23% to 35% of patients receiving placebo. Both of these outcomes are consistent with a high placebo response observed with other assessments of symptom severity. Additionally, the clinical experts indicated that a trial duration of 3 weeks is likely too short to observe full remission, which may take up to 4 weeks to 6 weeks for an acute manic or mixed episode. In the acute depressive studies, 41% to 50% of patients receiving cariprazine 1.5 mg and 43% to 52% of patients receiving cariprazine 3.0 mg were considered responders as per the MADRS definition. The response rate among patients receiving placebo ranged from 32% to 40% across the trials. The benefit of treatment with cariprazine (1.5 mg and 3.0 mg) was inconsistently demonstrated across the studies based on this outcome. Similar results were reported for the analysis of MADRS remitters, where 26% to 37% of patients and 26% to 32% of patients receiving cariprazine 1.5 mg and cariprazine 3.0 mg, respectively, and 20% to 23% of patients receiving placebo were considered to have a remission of depressive symptoms. The CANMAT guidelines for the management of patients with bipolar disorder reported that “across several different medications for bipolar depression, early improvement (after 2 weeks) has been found to be a reasonable predictor of overall response, whereas lack of early improvement is a more robust predictor of nonresponse.”1 Feedback from the clinical experts indicated that a response should be observed in trials of up to 6 weeks’ duration.
HRQoL, hospitalizations, and daily functioning — including while at work and school — were important outcomes identified by patient groups. An assessment of functioning was included as an exploratory outcome in 1 out of the 6 included trials, which limits conclusions that can be drawn about this outcome. Hospitalizations and HRQoL, as well as cognitive impairment and persistence with therapy, were not included as outcomes in any of the trials.
The studies that have been discussed so far are limited to placebo-controlled trials. Given the availability of other treatments for the acute treatment of manic and depressive episodes associated with bipolar I disorder, the absence of a direct head-to-head trial is a limitation. A comparison of cariprazine to other treatments for the treatment of acute episodes of bipolar disorder was only available through indirect evidence, which has been summarized to address this gap in the evidence. The sponsor-submitted NMA was the most comprehensive analysis. It reported the following outcomes: YMRS or MADRS response, YMRS or MADRS remission, change from baseline in YMRS or MADRS, weight gain, EPS, sedation or somnolence, all-cause discontinuation, and discontinuation due to AEs. Separate NMAs were conducted for treatments for manic or mixed episodes and depressive episodes. The results of the NMA of weight gain greater than 7% ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||. Therefore, a conclusion about benefit in terms of weight gain cannot be made with confidence. Further, the sponsor-submitted NMA ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||. This was based on the following outcomes: YMRS response, YMRS remission, and change from baseline in the YMRS. In general, the sponsor-submitted NMA also |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| based on the following outcomes: MADRS response, MADRS remission, and change form baseline in the MADRS. ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||. The 2 published NMAs summarized for this review18,19 were insufficiently reported and therefore limited by concerns with the methodology as well as with low-quality evidence informing the networks. ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||.
An additional consideration for the interpretation of the evidence is that the clinical experts consulted by CADTH suggested that physicians will likely initiate treatment with cariprazine at 1.5 mg per day, then increase to 3 mg per day after 1 week, in contrast to the trials where the dose was increased to 3.0 mg per day after 1 day of treatment with 1.5 mg per day, and up to 6.0 mg per day as early as the third day of treatment. Also, the mean daily dose of cariprazine used in 2 of the 3 trials for bipolar mania was greater than the maximum dose approved by Health Canada (6.0 mg per day).5 Generalizing the efficacy as well as the safety and tolerability outcomes observed in the trials to an outpatient setting for the treatment of acute mania is uncertain. Although tolerability and safety outcomes may be less of an issue in this treatment setting, the impact on efficacy outcomes is uncertain based on the evidence of the trials, given the flexible-dose study design.
Harms
AEs were reported more frequently in patients randomized to cariprazine than placebo in all trials for acute mania and acute depression. The overall rate of AEs was higher in the acute mania trials than the acute depression trials, despite a shorter duration of treatment, although higher dosage for mania may be a factor. Whether AEs were more likely to be detected in an inpatient setting or the result of the higher dose of cariprazine in the acute mania trials, or both, is unknown. SAEs were reported infrequently, and 1 death was reported in all of the included trials. Withdrawal from treatment due to AEs tended to be slightly more frequent among patients randomized to cariprazine compared to placebo, but this was inconsistent across studies.
Of the notable harms identified in the CADTH systematic review protocol, hyperglycemia, weight gain, sexual dysfunction, tardive dyskinesia, and neuroleptic malignant syndrome were infrequently reported in all trials. Additionally, vomiting and EPS were infrequently reported in the bipolar depression studies. In the acute mania studies, EPS, akathisia, vomiting, and restlessness were reported more frequently with cariprazine compared to placebo. They have also been identified as common adverse reactions (at least 5% and at least twice the rate of placebo) in the product monograph, along with dyspepsia and somnolence.5 Of note, patients who required pharmacologic treatment to control EPS were excluded from the bipolar mania studies. As such, the impact of EPS on treatment with cariprazine may have been underestimated in the trials. Similarly in the bipolar depression studies, akathisia and restlessness were more common in the cariprazine treatment groups than in the placebo treatment groups and occurred more frequently with cariprazine 3.0 mg than with cariprazine 1.5 mg. They were also included as common adverse reactions in the product monograph in addition to nausea and EPS.5 The frequency of AEs during a short treatment period of 3 weeks in the acute mania studies and up to 8 weeks in the acute depression studies, and with the high discontinuation rates in the studies, is notable, although comparable to other treatments for bipolar disorder as indicated by the clinical experts consulted by CADTH. One long-term (16 weeks), open-label, single-arm study, study RGH-MD-36, examined the safety and tolerability of cariprazine in patients experiencing bipolar mania. The frequency of AEs was similar to the pivotal trials, although this may be underestimated due to the high discontinuation rate (67%) and is limited by the single-arm study design.
Weight gain, measured as an increase in body weight of at least 7%, was captured in the safety assessment of vital signs. While the duration of the trials may not have been long enough to sufficiently assess the impact of treatment of cariprazine on weight gain, this outcome was still observed in the trials. However, there was only a slight difference in weight gain between the cariprazine and placebo treatment groups, which was also stated in the product monograph.5
The sponsor-submitted NMA included an analysis of EPS, sedation or somnolence, and discontinuations.17 There was |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| although highly uncertain due to the poor quality of the evidence. From the available evidence, cariprazine appears to have a similar safety profile to other atypical psychotics for bipolar I disorder; however, the results of the NMAs on safety and tolerability outcomes should be viewed with caution due to the limitations of the ITCs.
Conclusions
Six RCTs informed the systematic review of cariprazine. These RCTs included 3 pivotal trials for the acute treatment of mania or mixed episodes (study RGH-MD-31, study RGH-MD-32, and study RGH-MD-33) and 3 pivotal trials for the acute treatment of depressive episodes (study RGH-MD-53, study RGH-MD-54, and study RGH-MD-56) of bipolar I disorder. The studies of acute mania or mixed episodes evaluated a flexible dosage of cariprazine ranging from 3 mg to 12 mg once daily, and the studies of acute depressive episodes evaluated a fixed dosage of cariprazine of 1.5 mg and 3.0 mg once daily.
All 3 studies of acute mania demonstrated that treatment with cariprazine was associated with a statistically significant and clinically meaningful greater reduction in symptoms of acute mania relative to placebo, based on the YMRS total score after 3 weeks of treatment. This was supported by the results of the secondary end point, which demonstrated a greater reduction in overall disease severity after 3 weeks based on the CGI-S. The studies of acute bipolar depression demonstrated that treatment with cariprazine 1.5 mg was associated with a statistically significant and clinically meaningful greater reduction in symptoms of depression relative to placebo, based on the change in the MADRS total score at week 6. A dose response was not observed as cariprazine 3.0 mg did not consistently demonstrate a benefit relative to placebo, since the primary end point was not met in 2 of the 3 pivotal trials. The results of the secondary end point — the change from baseline to week 6 in the CGI-S — were consistent with the primary analysis, except for 1 study that did not demonstrate a benefit with cariprazine 1.5 mg relative to placebo (study RGH-MD-54). Additional efficacy outcomes were not controlled for multiplicity and should only be considered as supportive evidence. Additional outcomes were generally consistent with the primary and secondary analyses.
The frequency of AEs due to EPS, akathisia, vomiting, and restlessness were considered relevant safety concerns, although consistent with the safety profile of similar treatments. Both safety and efficacy outcomes may have been impacted by the high discontinuation rates across studies due to AEs, insufficient therapeutic response, and withdrawal of consent, which may have overestimated the reported results. Additionally, the short duration of the trials limited the ability to sufficiently evaluate certain outcomes such as weight gain. Direct comparisons to other available treatments were not identified, but uncertain evidence from 3 NMAs suggests that treatment with cariprazine ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||. Cariprazine may exhibit a different tolerability profile, but a conclusion about this cannot be drawn due to the uncertainty of the available evidence.
References
1.Yatham LN, Kennedy SH, Parikh SV, et al. Canadian Network for Mood and Anxiety Treatments (CANMAT) and International Society for Bipolar Disorders (ISBD) 2018 guidelines for the management of patients with bipolar disorder. Bipolar Disord. 2018;20(2):97-170. PubMed
2.Schaffer A, Cairney J, Cheung A, Veldhuizen S, Levitt A. Community survey of bipolar disorder in Canada: lifetime prevalence and illness characteristics. Can J Psychiatry. 2006;51(1):9-16. PubMed
3.Stovall J. Bipolar disorder in adults: epidemiology and pathogenesis. In: Post TW, ed. UpToDate. Waltham (MA): UpToDate; 2022: http://www.uptodate.com. Accessed 2022 Feb 16.
4.Yatham LN, Chakrabarty T, Bond DJ, et al. Canadian Network for Mood and Anxiety Treatments (CANMAT) and International Society for Bipolar Disorders (ISBD) recommendations for the management of patients with bipolar disorder with mixed presentations. Bipolar Disord. 2021;23(8):767-788. PubMed
5.Vraylar (cariprazine as hydrochloride): capsules, 1.5 mg, 3 mg, 4.5 mg and 6 mg, oral [product monograph]. Markham (ON): Allergan Inc.; 2022 Apr 22.
6.Drug Reimbursement Review sponsor submission: Vraylar (cariprazine as hydrochloride), 1.5 mg, 3 mg, 4.5 mg and 6 mg oral capsules [internal sponsor's package]. Markham (ON): Allergan Inc.; 2021 Nov 15.
7.Lukasiewicz M, Gerard S, Besnard A, et al. Young Mania Rating Scale: how to interpret the numbers? Determination of a severity threshold and of the minimal clinically significant difference in the EMBLEM cohort. Int J Methods Psychiatr Res. 2013;22(1):46-58. PubMed
8.Montgomery SA, Moller HJ. Is the significant superiority of escitalopram compared with other antidepressants clinically relevant? Int Clin Psychopharmacol. 2009;24(3):111-118. PubMed
9.Thase ME, Mahableshwarkar AR, Dragheim M, Loft H, Vieta E. A meta-analysis of randomized, placebo-controlled trials of vortioxetine for the treatment of major depressive disorder in adults. Eur Neuropsychopharmacol. 2016;26(6):979-993. PubMed
10.Moncrieff J, Kirsch I. Efficacy of antidepressants in adults. BMJ. 2005;331(7509):155-157. PubMed
11.Clinical Study Report: RGH-MD-31. A double-blind, placebo-controlled evaluation of the safety and efficacy of RGH-188 in patients with acute mania associated with bipolar I disorder [internal sponsor's report]. Jersey City (NJ): Forest Research Institute, Inc.; 2009 Mar 12.
12.Clinical Study Report: RGH-MD-32. A double-blind, placebo-controlled evaluation of the safety and efficacy of cariprazine in patients with acute mania associated with bipolar I disorder [internal sponsor's report]. Jersey City (NJ): Forest Research Institute, Inc.; 2012 Jul 31.
13.Clinical Study Report: RGH-MD-33. A double-blind, placebo-controlled evaluation of the safety and efficacy of cariprazine in patients with acute mania associated with bipolar I disorder [internal sponsor's report]. Jersey City (NJ): Forest Research Institute, Inc.; 2012 Jul 31.
14.Clinical Study Report: RGH-MD-53. A phase 3, randomized, double-blind, placebo-controlled, parallel-group, multicenter, fixed-dose clinical trial evaluating the efficacy, safety and tolerability of cariprazine in patients with bipolar I depression [internal sponsor's report]. Madison (NJ): Forest Laboratories, LLC; 2018 May 29.
15.Clinical Study Report: RGH-MD-54. A phase 3, randomized, double-blind, placebo-controlled, parallel-group, multicenter, fixed-dose clinical trial evaluating the efficacy, safety and tolerability of cariprazine in patients with bipolar I depression [internal sponsor's report]. Madison (NJ): Forest Laboratories, LLC; 2018 May 29.
16.Clinical Study Report: RGH-MD-56. A double-blind, placebo-controlled evaluation of the safety and efficacy of cariprazine in patients with bipolar depression [internal sponsor's report]. Jersey City (NJ): Forest Research Institute, Inc.; 2014 Oct 9.
17.3524: Indirect treatment comparisons of cariprazine for the treatment of bipolar I disorder: network meta-analysis report [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Vraylar (cariprazine as hydrochloride) capsules, 1.5 mg, 3 mg, 4.5 mg and 6 mg cariprazine, oral. Markham (ON): Allergan Inc.; 2022 Jan 25.
18.Kishi T, Ikuta T, Matsuda Y, et al. Pharmacological treatment for bipolar mania: a systematic review and network meta-analysis of double-blind randomized controlled trials. Mol Psychiatry. 2021;27(2):1136-1144. PubMed
19.Kadakia A, Dembek C, Heller V, et al. Efficacy and tolerability of atypical antipsychotics for acute bipolar depression: a network meta-analysis. BMC Psychiatry. 2021;21(1):249. PubMed
20.Clinical Study Report: RGH-MD-36. A long-term open-label study of the safety and tolerability of cariprazine in patients with bipolar I disorder [internal sponsor's report]. Jersey City (NJ): Forest Research Institute, Inc.; 2012 Sep 27.
21.McIntyre RS, Masand PS, Earley W, Patel M. Cariprazine for the treatment of bipolar mania with mixed features: A post hoc pooled analysis of 3 trials. J Affect Disord. 2019;257:600-606. PubMed
22.Suppes T. Bipolar disorder in adults: clinical features. In: Post TW, ed. UpToDate. Waltham (MA): UpToDate; 2022: http://www.uptodate.com. Accessed 2022 Feb 16.
23.Abilify (aripiprazole): 2 mg, 5 mg, 10 mg, 15 mg and 20 mg and 30 mg oral tablets [product monograph]. Saint-Laurent (QC): Otsuka Canada Pharmaceutical Inc.; 2021 Feb 11: https://pdf.hres.ca/dpd_pm/00060025.PDF. Accessed 2022 Jan 6.
24.Saphris (asenapine as asenapine maleate): 5 mg and 10 mg sublingual tablets [product monograph]. Kirkland (QC): Organon Canada Inc.; 2021 Apr 27: https://pdf.hres.ca/dpd_pm/00060860.PDF. Accessed 2022 Jan 6.
25.Latuda (lurasidone hydrochloride): 20 mg, 40 mg, 60 mg, 80 mg and 120 mg film-coated oral tablets [product monograph]. Mississauga (ON): Sunovion Pharmaceuticals Canada Inc.; 2020 Mar 18: https://pdf.hres.ca/dpd_pm/00055478.PDF. Accessed 2022 Jan 6.
26.Zyprexa (olanzapine): 2.5 mg, 5 mg, 7.5 mg, 10 mg, 15 mg, 20 mg oral tablets [product monograph]; or Zyprexa Zydis (olanzapine): 5 mg, 10 mg, 15 mg, 20 mg orally disintegrating tablets [product monograph]; or Zyprexa IntraMuscular (olanzapine tartrate): 10 mg / vial for intramuscular injection [product monograph]. Toronto (ON): Eli Lilly Canada Inc.; 2020 Jan 29: https://pdf.hres.ca/dpd_pm/00057094.PDF. Accessed 2022 Jan 6.
27.Invega (paliperidone): 3 mg, 6 mg, 9 mg oral extended-release tablets [product monograph]. Toronto (ON): Janssen Inc; 2020 Dec 17: https://pdf.hres.ca/dpd_pm/00059282.PDF. Accessed 2022 Jan 6.
28.Seroquel (quetiapine fumarate): 25, 100, 200 and 300 mg, oral use immediate-release tablets [product monograph]. Mississauga (ON): AstraZeneca Canada Inc.; 2021 Nov 29: https://pdf.hres.ca/dpd_pm/00063750.PDF. Accessed 2022 Jan 6.
29.Apo-Risperidol (risperidone): 0.25 mg, 0.5 mg, 1 mg, 2 mg, 3 mg and 4 mg oral tablets [product monograph]; or Apo-risperidol (risperidone): 1 mg / mL oral solution [product monograph]. Toronto (ON): APOTEX INC; 2021 Sep 23: https://pdf.hres.ca/dpd_pm/00063055.PDF. Accessed 2022 Jan 6.
30.Zeldox (ziprasidone): 20, 40, 60, and 80 mg oral capsules [product monograph]. Kirkland (QC): Upjohn Canada ULC; 2020 May 6: https://pdf.hres.ca/dpd_pm/00056273.PDF. Accessed 2022 Jan 6.
31.Apo-Lithium Carbonate (lithium carbonate): 150 and 300 mg capsules [product monograph]. Toronto (ON): Apotex Inc.; 2013 Dec 5: https://pdf.hres.ca/dpd_pm/00023004.PDF. Accessed 2022 Apr 23.
32.Apo-Divalproex (valproic acid as divalproex sodium): 125 mg, 250 mg and 500 mg enteric-coated tablets [product monograph]. Toronto (ON): Apotex Inc.; 2021 Dec 15: https://pdf.hres.ca/dpd_pm/00064132.PDF. Accessed 2021 Dec 15.
33.Apo-Carbamazepine (carbamazepine): 200 mg tablets; Apo-Carbamazepine CR (carbamazepine): 200 mg and 400 mg controlled release tablets [product monograph]. Toronto (ON): Apotex Inc.; 2018 Aug 17: https://pdf.hres.ca/dpd_pm/00047110.PDF. Accessed 2022 Apr 23.
34.Teva-haloperidol (haloperidol): 0.5, 1, 2, 5, 10 and 20 mg tablets [product monograph]. Toronto (ON): Teva Canada Limited; 2016 Aug 26: https://pdf.hres.ca/dpd_pm/00036413.PDF. Accessed 2022 Jan 6.
35.Apo-Clonazepam (clonazepam): 0.5 mg and 2 mg tablets [product monograph]. Toronto (ON): Apotex Inc.; 2021 Jun 9: https://pdf.hres.ca/dpd_pm/00061752.PDF. Accessed 2022 Apr 23.
36.Teva-Chlorpromazine (chlorpromazine hydrochloride) 25 mg, 50 mg and 100 mg tablets [product monograph]. Toronto (ON): Teva Canada Limited; 2012 Dec 11: https://pdf.hres.ca/dpd_pm/00018580.PDF. Accessed 2022 Apr 23.
37.McGowan J, Sampson M, Salzwedel DM, Cogo E, Foerster V, Lefebvre C. PRESS Peer Review of Electronic Search Strategies: 2015 guideline statement. J Clin Epidemiol. 2016;75:40-46. PubMed
38.Grey matters: a practical tool for searching health-related grey literature. Ottawa (ON): CADTH; 2019: https://www.cadth.ca/grey-matters. Accessed 2022 Feb 16.
39.Durgam S, Starace A, Li D, et al. The efficacy and tolerability of cariprazine in acute mania associated with bipolar I disorder: a phase II trial. Bipolar Disord. 2015;17(1):63-75. PubMed
40.Sachs GS, Greenberg WM, Starace A, et al. Cariprazine in the treatment of acute mania in bipolar I disorder: a double-blind, placebo-controlled, phase III trial. J Affect Disord. 2015;174:296-302. PubMed
41.Calabrese JR, Keck PE, Jr., Starace A, et al. Efficacy and safety of low- and high-dose cariprazine in acute and mixed mania associated with bipolar I disorder: a double-blind, placebo-controlled study. J Clin Psychiatry. 2015;76(3):284-292. PubMed
42.Earley WR, Burgess MV, Khan B, et al. Efficacy and safety of cariprazine in bipolar I depression: A double-blind, placebo-controlled phase 3 study. Bipolar Disord. 2020;22(4):372-384. PubMed
43.Earley W, Burgess MV, Rekeda L, et al. Cariprazine treatment of bipolar depression: a randomized double-blind placebo-controlled phase 3 study. Am J Psychiatry. 2019;176(6):439-448. PubMed
44.Durgam S, Earley W, Lipschitz A, et al. An 8-week randomized, double-blind, placebo-controlled evaluation of the safety and efficacy of cariprazine in patients with bipolar I depression. Am J Psychiatry. 2016;173(3):271-281. PubMed
45.Young RC, Biggs JT, Ziegler VE, Meyer DA. A rating scale for mania: reliability, validity and sensitivity. Br J Psychiatry. 1978;133:429-435. PubMed
46.Youngstrom E, Zhao J, Mankoski R, et al. Clinical significance of treatment effects with aripiprazole versus placebo in a study of manic or mixed episodes associated with pediatric bipolar I disorder. J Child Adolesc Psychopharmacol. 2013;23(2):72-79. PubMed
47.Montgomery S, Åsberg M. A new depression scale designed to be sensitive to change. Br J Psychiatry. 1979;134(4):382-389. PubMed
48.Duru G, Fantino B. The clinical relevance of changes in the Montgomery-Asberg Depression Rating Scale using the minimum clinically important difference approach. Curr Med Res Opin. 2008;24(5):1329-1335. PubMed
49.Leucht S, Fennema H, Engel RR, Kaspers-Janssen M, Lepping P, Szegedi A. What does the MADRS mean? Equipercentile linking with the CGI using a company database of mirtazapine studies. J Affect Disord. 2017;210:287-293. PubMed
50.Zimmerman M, Posternak MA, Chelminski I. Defining remission on the Montgomery-Asberg depression rating scale. J Clin Psychiatry. 2004;65(2):163-168. PubMed
51.Zimmerman M, Chelminski I, Posternak M. A review of studies of the Montgomery-Asberg Depression Rating Scale in controls: implications for the definition of remission in treatment studies of depression. Int Clin Psychopharmacol. 2004;19(1):1-7. PubMed
52.Hawley CJ, Gale TM, Sivakumaran T. Defining remission by cut off score on the MADRS: selecting the optimal value. J Affect Disord. 2002;72(2):177-184. PubMed
53.Berk M, Ng F, Wang WV, et al. The empirical redefinition of the psychometric criteria for remission in bipolar disorder. J Affect Disord. 2008;106(1-2):153-158. PubMed
54.Guy W. ECDEU assessment manual for psychopharmacology. Revised 1976 ed. Rockville (MD): U.S. Department of Health, Education and Welfare, Public Health Service, Alcohol, Drug Abuse, and Mental Health Administration, National Institute of Mental Health, Psychopharmacology Research Branch, Division of Extramural Research Programs; 1976: https://archive.org/stream/ecdeuassessmentm1933guyw#page/218/mode/2up. Accessed 2022 May 27.
55.Leucht S, Kane JM, Etschel E, Kissling W, Hamann J, Engel RR. Linking the PANSS, BPRS, and CGI: clinical implications. Neuropsychopharmacology. 2006;31(10):2318-2325. PubMed
56.Rabinowitz J, Mehnert A, Eerdekens M. To what extent do the PANSS and CGI-S overlap? J Clin Psychopharmacol. 2006;26(3):303-307. PubMed
57.Nasrallah H, Morosini P, Gagnon DD. Reliability, validity and ability to detect change of the Personal and Social Performance scale in patients with stable schizophrenia. Psychiatry Res. 2008;161(2):213-224. PubMed
58.Patrick DL, Burns T, Morosini P, et al. Reliability, validity and ability to detect change of the clinician-rated Personal and Social Performance scale in patients with acute symptoms of schizophrenia. Curr Med Res Opin. 2009;25(2):325-338. PubMed
59.Kay SR, Opler LA, Lindenmayer JP. Reliability and validity of the positive and negative syndrome scale for schizophrenics. Psychiatry Res. 1988;23(1):99-110. PubMed
60.Kay SR, Fiszbein A, Opler LA. The positive and negative syndrome scale (PANSS) for schizophrenia. Schizophr Bull. 1987;13(2):261-276. PubMed
61.Heo M, Murphy CF, Meyers BS. Relationship between the Hamilton Depression Rating Scale and the Montgomery-Asberg Depression Rating Scale in depressed elderly: a meta-analysis. Am J Geriatr Psychiatry. 2007;15(10):899-905. PubMed
62.Zimmerman M, Posternak MA, Chelminski I. Is the cutoff to define remission on the Hamilton Rating Scale for Depression too high? J Nerv Ment Dis. 2005;193(3):170-175. PubMed
63.Lam RW, Michalak EE, Swinson RP. Assessment scales in depression, mania and anxiety. London (GB): Taylor and Francis; 2005.
64.Bagby RM, Ryder AG, Schuller DR, Marshall MB. The Hamilton Depression Rating Scale: has the gold standard become a lead weight? Am J Psychiatry. 2004;161(12):2163-2177. PubMed
65.O'Sullivan RL, Fava M, Agustin C, Baer L, Rosenbaum JF. Sensitivity of the six-item Hamilton Depression Rating Scale. Acta Psychiatr Scand. 1997;95(5):379-384. PubMed
66.Rush AJ, Trivedi MH, Ibrahim HM, et al. The 16-Item Quick Inventory of Depressive Symptomatology (QIDS), clinician rating (QIDS-C), and self-report (QIDS-SR): a psychometric evaluation in patients with chronic major depression. Biol Psychiatry. 2003;54(5):573-583. PubMed
67.Frank E, Prien RF, Jarrett RB, et al. Conceptualization and rationale for consensus definitions of terms in major depressive disorder. Remission, recovery, relapse, and recurrence. Arch Gen Psychiatry. 1991;48(9):851-855. PubMed
68.Hamilton M. A rating scale for depression. J Neurol Neurosurg Psychiatry. 1960;23(1):56-62. PubMed
69.Shear MK, Vander Bilt J, Rucci P, et al. Reliability and validity of a structured interview guide for the Hamilton Anxiety Rating Scale (SIGH-A). Depress Anxiety. 2001;13(4):166-178. PubMed
70.Maier W, Buller R, Philipp M, Heuser I. The Hamilton Anxiety Scale: reliability, validity and sensitivity to change in anxiety and depressive disorders. J Affect Disord. 1988;14(1):61-68. PubMed
71.Rosa AR, Sanchez-Moreno J, Martinez-Aran A, et al. Validity and reliability of the Functioning Assessment Short Test (FAST) in bipolar disorder. Clin Pract Epidemol Ment Health. 2007;3:5. PubMed
72.Roux P, Brunet-Gouet E, Ehrminger M, et al. Minimum clinically important differences for the Functioning Assessment Short Test and a battery of neuropsychological tests in bipolar disorders: results from the FACE-BD cohort. Epidemiol Psychiatr Sci. 2020;29:e144. PubMed
73.Drug Reimbursement Review sponsor submission: Vraylar (cariprazine as hydrochloride), 1.5 mg, 3 mg, 4.5 mg and 6 mg oral capsules [internal sponsor's package]. Markham (ON): Allergan Inc.; 2022 Jan 28.
74.Bahji A, Ermacora D, Stephenson C, Hawken ER, Vazquez G. Comparative efficacy and tolerability of pharmacological treatments for the treatment of acute bipolar depression: A systematic review and network meta-analysis. J Affect Disord. 2020;269:154-184. PubMed
75.Cochrane. 8.3.3 Quality scales and Cochrane reviews. In: Higgins JPT, Green S, eds. Cochrane handbook for systematic reviews of interventions. London (GB): The Cochrane Collaboration; 2011: https://handbook-5-1.cochrane.org/chapter_8/8_3_3_quality_scales_and_cochrane_reviews.htm. Accessed 2022 Mar 28.
76.Muller MJ, Himmerich H, Kienzle B, Szegedi A. Differentiating moderate and severe depression using the Montgomery-Asberg depression rating scale (MADRS). J Affect Disord. 2003;77(3):255-260. PubMed
77.Committee for Medicinal Products for Human Use. Guideline on clinical investigation of medicinal products, including depot preparations in the treatment of schizophrenia London (GB): European Medicines Agency; 2012: https://www.ema.europa.eu/en/documents/scientific-guideline/guideline-clinical-investigation-medicinal-products-including-depot-preparations-treatment_en.pdf. Accessed 2022 Jan 10.
78.Carmody TJ, Rush AJ, Bernstein I, et al. The Montgomery Asberg and the Hamilton ratings of depression: a comparison of measures. Eur Neuropsychopharmacol. 2006;16(8):601-611. PubMed
79.Davidson J, Turnbull CD, Strickland R, Miller R, Graves K. The Montgomery-Asberg Depression Scale: reliability and validity. Acta Psychiatr Scand. 1986;73(5):544-548. PubMed
80.Senra C. Evaluation and monitoring of symptom severity and change in depressed outpatients. J Clin Psychol. 1996;52(3):317-324. PubMed
81.Mulder RT, Joyce PR, Frampton C. Relationships among measures of treatment outcome in depressed patients. J Affect Disord. 2003;76(1-3):127-135. PubMed
82.Maier W, Philipp M, Heuser I, Schlegel S, Buller R, Wetzel H. Improving depression severity assessment--I. Reliability, internal validity and sensitivity to change of three observer depression scales. J Psychiatr Res. 1988;22(1):3-12. PubMed
83.Peralta V, Cuesta MJ. Psychometric properties of the positive and negative syndrome scale (PANSS) in schizophrenia. Psychiatry Res. 1994;53(1):31-40. PubMed
84.Edwards BC, Lambert MJ, Moran PW, McCully T, Smith KC, Ellingson AG. A meta-analytic comparison of the Beck Depression Inventory and the Hamilton Rating Scale for Depression as measures of treatment outcome. Br J Clin Psychol. 1984;23(Pt 2):93-99. PubMed
85.Lambert MJ, Hatch DR, Kingston MD, Edwards BC. Zung, Beck, and Hamilton Rating Scales as measures of treatment outcome: a meta-analytic comparison. J Consult Clin Psychol. 1986;54(1):54-59. PubMed
86.Faries D, Herrera J, Rayamajhi J, DeBrota D, Demitrack M, Potter WZ. The responsiveness of the Hamilton Depression Rating Scale. J Psychiatr Res. 2000;34(1):3-10. PubMed
87.Hamilton M. The assessment of anxiety states by rating. Br J Med Psychol. 1959;32(1):50-55. PubMed
88.Altman EG, Hedeker DR, Janicak PG, Peterson JL, Davis JM. The Clinician-Administered Rating Scale for Mania (CARS-M): development, reliability, and validity. Biol Psychiatry. 1994;36(2):124-134. PubMed
89.Haro JM, Kamath SA, Ochoa S, et al. The Clinical Global Impression-Schizophrenia scale: a simple instrument to measure the diversity of symptoms present in schizophrenia. Acta Psychiatr Scand Suppl. 2003(416):16-23. PubMed
90.Thase ME, Harrington A, Calabrese J, Montgomery S, Niu X, Patel MD. Evaluation of MADRS severity thresholds in patients with bipolar depression. J Affect Disord. 2021;286:58-63. PubMed
91.Zimmerman M, Posternak MA, Chelminski I. Derivation of a definition of remission on the Montgomery-Asberg depression rating scale corresponding to the definition of remission on the Hamilton rating scale for depression. J Psychiatr Res. 2004;38(6):577-582. PubMed
92.Iannuzzo RW, Jaeger J, Goldberg JF, Kafantaris V, Sublette ME. Development and reliability of the HAM-D/MADRS interview: an integrated depression symptom rating scale. Psychiatry Res. 2006;145(1):21-37. PubMed
93.Andreasen NC, Carpenter WT, Jr., Kane JM, Lasser RA, Marder SR, Weinberger DR. Remission in schizophrenia: proposed criteria and rationale for consensus. Am J Psychiatry. 2005;162(3):441-449. PubMed
94.van Os J, Burns T, Cavallaro R, et al. Standardized remission criteria in schizophrenia. Acta Psychiatr Scand. 2006;113(2):91-95. PubMed
95.National Institute for Health Care and Excellence. Depression: the treatment and management of depression in adults. (Clinical guideline 90) 2014; https://www.nice.org.uk/guidance/cg90. Accessed 2022 May 27.
96.Bonnin CM, Martinez-Aran A, Reinares M, et al. Thresholds for severity, remission and recovery using the functioning assessment short test (FAST) in bipolar disorder. J Affect Disord. 2018;240:57-62. PubMed
97.Posner K, Brown GK, Stanley B, et al. The Columbia-Suicide Severity Rating Scale: initial validity and internal consistency findings from three multisite studies with adolescents and adults. Am J Psychiatry. 2011;168(12):1266-1277. PubMed
98.Mundt JC, Greist JH, Jefferson JW, Federico M, Mann JJ, Posner K. Prediction of suicidal behavior in clinical research by lifetime suicidal ideation and behavior ascertained by the electronic Columbia-Suicide Severity Rating Scale. J Clin Psychiatry. 2013;74(9):887-893. PubMed
Appendix 1: Literature Search Strategy
Note that this appendix has not been copy-edited.
Clinical Literature Search
Overview
Interface: Ovid
Databases
MEDLINE All (1946-present)
Embase (1974-present)
APA PsycINFO (1806-present)
Note: Subject headings and search fields have been customized for each database. Duplicates between databases were removed in Ovid.
Date of search: March 8, 2022
Alerts: Bi-weekly search updates until project completion
Search filters applied: No filters were applied to limit the retrieval by study type
Limits
Publication date limit: none
Language limit: none
Conference abstracts: excluded
Syntax | Description |
|---|---|
/ | At the end of a phrase, searches the phrase as a subject heading |
* | Before a word, indicates that the marked subject heading is a primary topic; or, after a word, a truncation symbol (wildcard) to retrieve plurals or varying endings |
.ti | Title |
.ot | Original title |
.ab | Abstract |
.hw | Heading word; usually includes subject headings and controlled vocabulary |
.kf | Author keyword heading word |
.dq | Candidate term word (Embase) |
.pt | Publication type |
.rn | Registry number |
.nm | Name of substance word (MEDLINE) |
.id | Key concept (PsycINFO) |
medall | Ovid database code: MEDLINE All, 1946 to present, updated daily |
oemezd | Ovid database code; Embase, 1974 to present, updated daily |
psyh | Ovid database code; APA PyscINFO, 1806 to present, updated weekly |
Multidatabase Strategy
(cariprazine* or vraylar* or reagila* or mp 214 or mp214 or rgh 188 or rgh188 or F6RJL8B278 or KQD7C255YG).ti,ab,kf,ot,hw,rn,nm.
1 use medall
*cariprazine/
(cariprazine* or vraylar* or reagila* or mp 214 or mp214 or rgh 188 or rgh188).ti,ab,kf,dq.
or/3-4
5 not (conference review or conference abstract).pt.
6 use oemezd
(cariprazine* or vraylar* or reagila* or mp 214 or mp214 or rgh 188 or rgh188).ti,ab,id.
8 use psyh
2 or 7 or 9
remove duplicates from 10
Clinical Trials Registries
ClinicalTrials.gov
Produced by the US National Library of Medicine. Targeted search used to capture registered clinical trials.
[Search -- (cariprazine* OR vraylar* OR reagila* OR "mp 214" OR mp214 OR "rgh 188" OR rgh188)]
WHO ICTRP
International Clinical Trials Registry Platform, produced by the World Health Organization. Targeted search used to capture registered clinical trials.
[Search terms -- (cariprazine* OR vraylar* OR reagila* OR "mp 214" OR mp214 OR "rgh 188" OR rgh188)]
Health Canada’s Clinical Trials Database
Produced by Health Canada. Targeted search used to capture registered clinical trials.
[Search terms -- cariprazine, vraylar, reagila, MP 214, MP214, RGH 188, RGH188]
EU Clinical Trials Register
European Union Clinical Trials Register, produced by the European Union. Targeted search used to capture registered clinical trials.
[Search terms -- (cariprazine* OR vraylar* OR reagila* OR "mp 214" OR mp214 OR "rgh 188" OR rgh188)]
Grey Literature
Search dates: February 16 - March 9, 2022
Keywords: cariprazine, Vraylar, Reagila, MP 214, MP214, RGH 188, RGH188
Limits: Publication years: none
Updated: Search updated prior to the meeting of the CADTH Canadian Drug Expert Committee (CDEC)
Relevant websites from the following sections of the CADTH grey literature checklist Grey Matters: A Practical Tool for Searching Health-Related Grey Literature were searched:
Health Technology Assessment Agencies
Health Economics
Clinical Practice Guidelines
Drug and Device Regulatory Approvals
Advisories and Warnings
Drug Class Reviews
Clinical Trials Registries
Databases (free)
Internet Search.
Appendix 2: Excluded Studies
No studies were excluded.
Appendix 3: Detailed Outcome Data
Note that this appendix has not been copy-edited.
Figure 22: Dosing Titration at Visit 3 to Visit 6 — Study RGH-MD-32
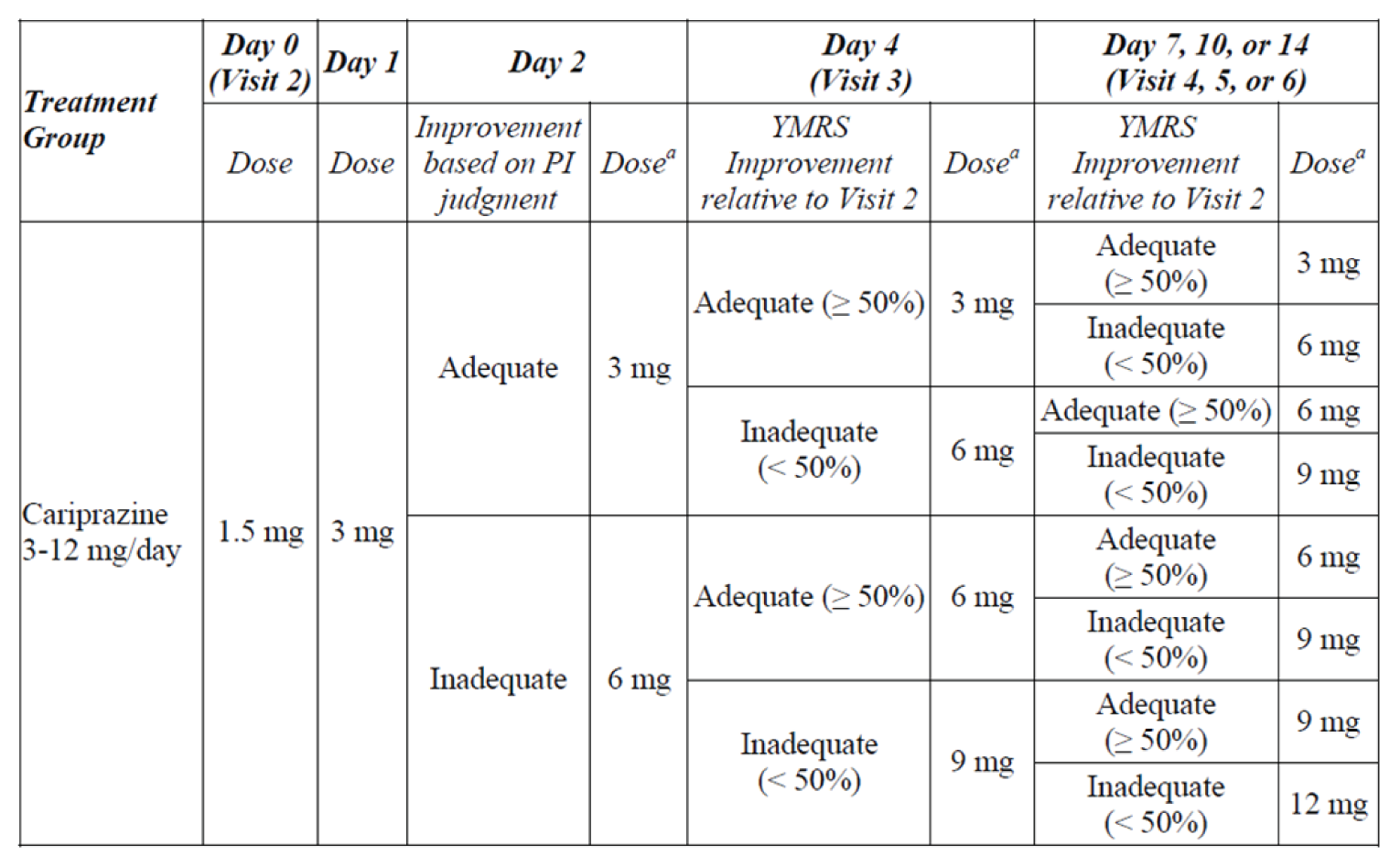
PI = principal investigator; YMRS = Young Mania Rating Scale.
a Patients with an inadequate response who did not have tolerability issues as judged by the investigator could have their dose increased by 1 capsule.
Source: Clinical Study Report for Study RGH-MD-32.12
Figure 23: Dosing Titration at Visit 3 to Visit 6 — RGH-MD-33

YMRS = Young Mania Rating Scale.
a Patients with an inadequate response who did not have tolerability issues as judged by the principal investigator could have had their dose increased by 1 capsule.
Source: Clinical Study Report for Study RGH-MD-33.13
Figure 24: Network Diagram for Response to Treatment — Kishi et al. (2021) Network Meta‑Analysis
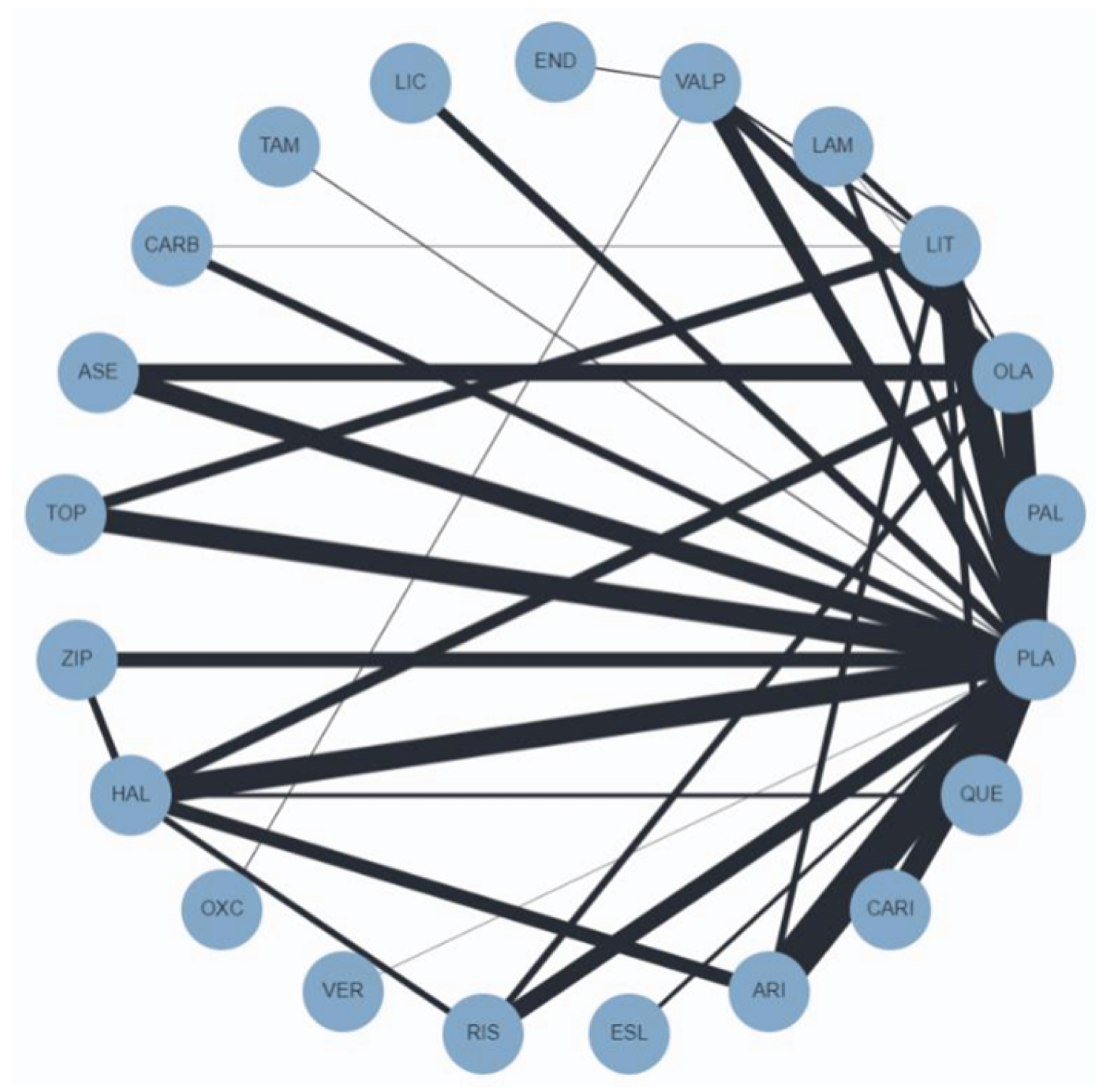
Source: Kishi T, et al., Copyright 2021. This work is licensed under the CC BY 4.0 (Attribution 4.0) International License. Full text available here: https://www.nature.com/articles/s41380-021-01334-4.18
Figure 25: Network Diagram for All-Cause Discontinuation — Kishi et al. (2021) Network Meta‑Analysis
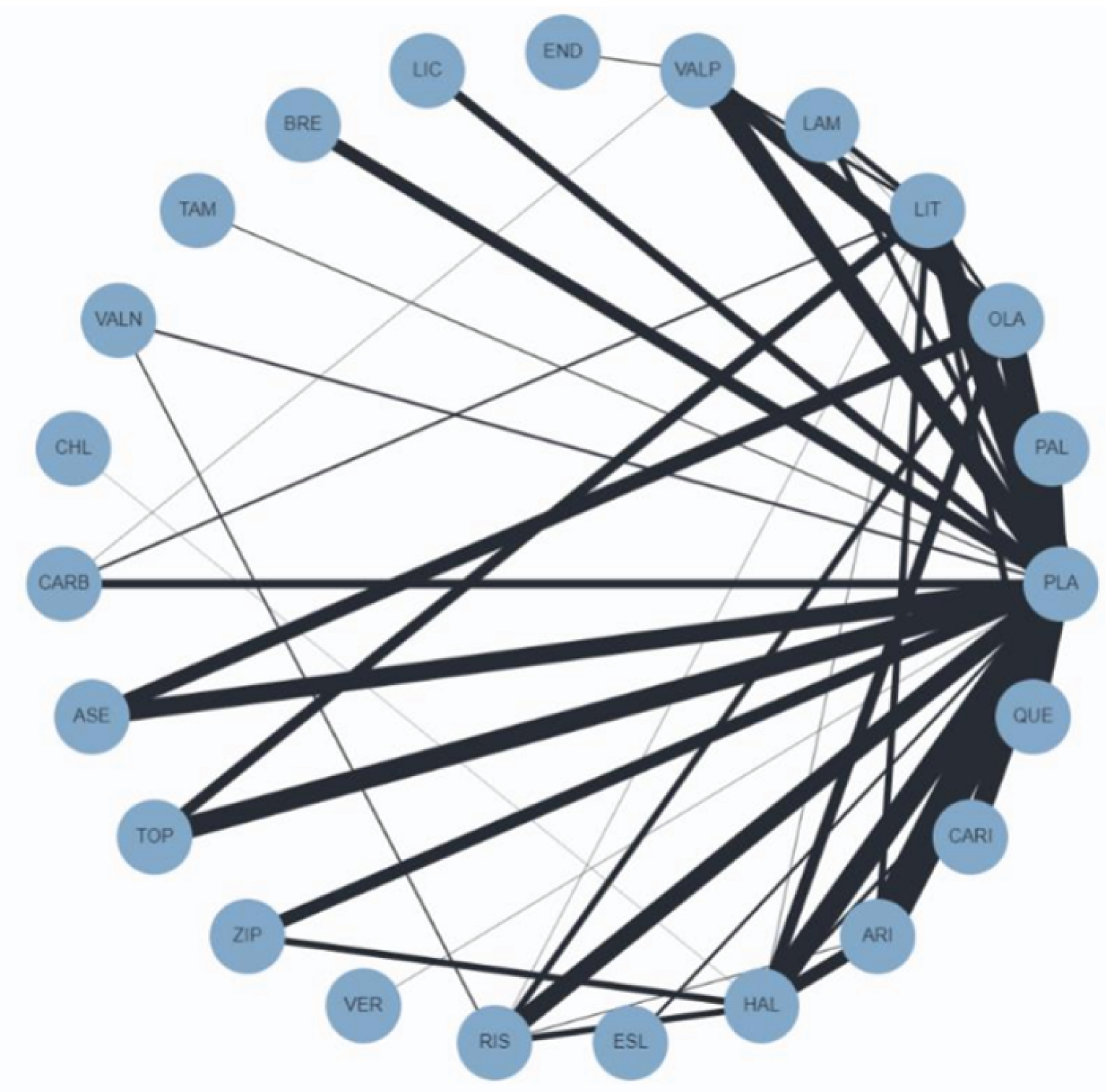
Source: Kishi T, et al., Copyright 2021. This work is licensed under the CC BY 4.0 (Attribution 4.0) International License. Full text available here: https://www.nature.com/articles/s41380-021-01334-4.18
Appendix 4: Description and Appraisal of Outcome Measures
Note that this appendix has not been copy-edited.
Aim
To describe the outcome measures summarized in Table 60, and review their measurement properties including validity, reliability, responsiveness to change, and the MID.
Table 60: Outcome Measures Included in Each Study
Outcome measure | RGH-MD-31 | RGH-MD-32 | RGH-MD-33 | RGH-MD-53 | RGH-MD-54 | RGH-MD-56 |
|---|---|---|---|---|---|---|
YMRS total score | Primary | Primary | Primary | NA | NA | NA |
CGI-S | Secondary | Secondary | Secondary | Secondary | Secondary | Secondary |
CGI-I | Exploratory | Exploratory | Exploratory | NA | NA | NA |
MADRS total score | Exploratory | Exploratory | Exploratory | Primary | Primary | Primary |
PANSS total score | Exploratory | Exploratory | Exploratory | NA | NA | NA |
HAM-D total score | NA | NA | NA | Exploratory | Exploratory | Exploratory |
HAM-A total score | NA | NA | NA | Exploratory | Exploratory | NA |
QIDS-SR | NA | NA | NA | Exploratory | Exploratory | NA |
FAST | NA | NA | NA | NA | NA | ||||||||||| |
CGI-I = Clinical Global Impression–Improvement; CGI-S = Clinical Global Impression–Severity of Illness; FAST = Functioning Assessment Short Test; HAM-A = Hamilton Anxiety Rating Scale; HAM-D = Hamilton Depression Rating Scale; MADRS = Montgomery–Åsberg Depression Rating Scale; NA = not applicable; PANSS = Positive and Negative Syndrome Scale; QIDS-SR = Quick Inventory of Depressive Symptomatology–Self-Rated; YMRS = Young Mania Rating Scale.
Source: Clinical Study Report for Study RGH-MD-31,11 RGH-MD-32,12 RGH-MD-33,13 RGH-MD-53,14 RGH-MD-54,15 RGH-MD-56.16
Findings
The validity, reliability, responsiveness, and the MID of each outcome measure were summarized and evaluated in Table 61.
Table 61: Summary of Outcome Measures and Their Measurement Properties
Outcome measure | Type | Conclusions about measurement properties | MID |
|---|---|---|---|
YMRS total score | An 11-item, clinician-administered rating scale used to assess the severity of manic symptoms.45 A severity rating is assigned to each item based on the patient’s subjective report of his or her condition over the past 48 hours and the clinician’s assessment of the patient’s behaviour. Items 5, 6, 8 and 9 are graded on a 0 to 8 scale while the remaining 7 are graded on a 0 to 4 scale, based on increasing severity. The YMRS total score ranges from 0 to 60.45 | Validity: For convergent validity, YMRS was statistically significantly correlated with the Beigel Mania Rating Scale, Petterson Mania Scale, and an 8-point global rating scale (Spearman coefficients: 0.71, 0.89, and 0.88, respectively; P < 0.001).45 Reliability: YMRS showed good interrater reliability (Spearman correlation) on the total score (0.93) and the individual item scores (0.66 to 0.92).45 Responsiveness: Differences in the YMRS scores between treated patients with bipolar mania and patients before treatment were statistically significant.45 | In patients with acute manic/mixed bipolar disorder, the minimal clinically significant difference was 6.6 points.7 There is evidence to support a 50% reduction on YMRS as a clinically meaningful definition of response in acute treatment of manic/mixed episode in pediatric patients with bipolar I disorder.46 A YMRS score ≤ 12 indicates remission of manic symptoms.45 A cut-off score of 4 and 7 has been associated with remission and a softer definition of remission, respectively.53 |
CGI-S | CGI-S assesses the overall severity of mental disorders at the time of the assessment on a 7-point scale (1 = normal; 7 = extremely ill).54 | There is little information regarding the validity of CGI-S in patients with schizophrenia and no evidence for its reliability and responsiveness was found.56 | A 1-point improvement has been considered as clinical improvement in clinical studies in schizophrenia and based on expert opinion for within-group differences.55,56,57,58 |
CGI-I | CGI-I assesses improvement in mental disorders relative to baseline on a 7-point scale (1 = very much improved; 7 = very much worse).54 | Evidence for the validity, reliability, and responsiveness of CGI-I was not found. | Evidence for an MID in the CGI-I scale was not found. |
MADRS total score | A 10-item, clinician-rated scale used to assess the severity of depression.47,48 Each item is rated on a 0 (item not present or normal) to 6 (severe or continuous presence of the symptoms) scale, resulting in a maximum total score of 60 points, in which higher scores indicate greater depressive symptomology.47,90 | The psychometric properties of MADRS summarized as follows are based on studies in major depressive disorder. Validity: For content validity, MADRS does not adequately define the severity of depression or remission because not all core symptoms used as diagnostic criteria in the DSM-IV are assessed.78 MADRS has good convergent validity (high degree of correlation with scores on other depression scales).78,61,79 Reliability: MADRS has high internal consistency.78 The clinician interrater reliability of MADRS was acceptable on individual items and the total score.79 Responsiveness: Studies have repeatedly found the MADRS to have greater sensitivity to treatment-related change compared to the HAM-D79-81; however, at least 1 study involving patients with major depressive disorder found its sensitivity to be lower than that of the HAM-D.82 | The psychometric properties of MADRS summarized as follows are based on studies in major depressive disorder. There is evidence to support an improvement of ≥ 2 points on the MADRS as clinically relevant.8,9 Response to treatment is usually defined as ≥ 50% reduction on the MADRS total score from baseline.49 No consensus reached for a cut-off score on the MADRS for defining remission in clinical trials.50 The criterion score to identify remission has ranged from 4 through 12 in various trials in depression.49,51,52 In bipolar disorder, a cut-off score of 5 and 10 has been associated with remission and a softer definition of remission, respectively.53 |
PANSS total score | A 30-item rating scale that assesses the presence and severity of psychopathology. It consists of 3 subscales (positive symptoms, negative symptoms, and general psychopathology), as well as a total score. The total score ranges from 30 to 210, with higher scores indicating more severe symptoms or psychopathology.59,60 | The psychometric properties of PANSS summarized as follows are based on studies in schizophrenia. Validity: Scores on all subscales were reported to exhibit a normal distribution, suggesting suitability for parametric statistical analysis. The range of scores was less than the potential range suggesting a lack of ceiling effect.60 Reliability: Internal consistency was demonstrated for the positive (alpha = 0.73), negative (alpha = 0.83), and general psychopathology (alpha = 0.79) subscales. Test-retest reliability was assessed 3 to 6 months later; the Pearson correlation coefficients were 0.80, 0.68, and 0.60 for the positive, negative, and general psychopathology subscales, respectively.60 The positive and negative subscales showed good interrater reliability; interclass correlation coefficients were 0.72 and 0.80, respectively. The general psychopathology subscale demonstrated moderate interrater reliability; interclass correlation was 0.56.83 Responsiveness: Evidence was not found. | The psychometric properties of PANSS summarized as follows are based on studies in schizophrenia. Clinical trials in schizophrenia have used a 20% reduction in the PANSS total score as a predefined measure of clinical improvement or criterion for response to antipsychotic treatment.56-58 According to the European Medicines Agency, a responder threshold of 30% reduction on the total PANSS score from baseline is considered clinically relevant in short-term clinical trials in patients with acute symptoms of schizophrenia.77 |
HAM-D | A 17-item, clinician-rated scale used to assess the severity of symptoms and address both somatic and psychological symptoms of depression.61,68,62,63 The items are either rated on a 5-point scale (0 to 4 spectrum) or a 3-point scale (0 to 2 spectrum), where increasing scores represent increasing severity of symptoms.64,65 Scores are summed to obtain a total score out of 52 or 53.10,66 | The psychometric properties of HAM-D summarized as follows are based on studies in major depressive disorder. Validity: Since there is only a partial overlap between the content of the HAM-D and DSM-IV symptom inclusion diagnostic criteria for major depressive disorder, the content validity of the HAM-D has been found to be poor.62,64 The convergent validity of the HAM-D was adequate, as this scale has demonstrated moderate to high correlation with many other depression scales.64 The discriminant validity was also adequate.64 Reliability: Reliability coefficients for internal consistency, interrater reliability, and test-retest reliability are good for the overall scale, as are the internal reliability estimates for the individual items of the scale. Although numerous items have weak interrater and retest reliability at the item level, the use of a structured interview guide may help to increase the item and total scale reliability.64 Responsiveness: HAM-D has been found to be more sensitive to change in patients’ conditions compared to other depression scales such as the Beck Depression Inventory.84,85 However, the multidimensional nature of the HAM-D may reduce its sensitivity to detect changes in the severity of depression over time.78 For instance, the full HAM-D scale has been shown to be less sensitive than unidimensional subscales of its items.86 | The psychometric properties of HAM-D summarized as follows are based on studies in major depressive disorder. The National Institute for Health and Clinical Excellence recommended a 3-point difference between drug and placebo arms as a criterion for clinical significance,10 A separate report suggested a 2-point difference between antidepressant and placebo might be clinically relevant.8 Remission was defined as a score ≤ 7 on the HAM-D total score by a consensus panel in 1991.62,67 Suggestions for an optimal cut-off score to define remission has ranged from 2 to 7.62 |
HAM-A | A 14-item, clinician-rated scale used to assess somatic and psychic anxiety symptoms. The items are rated on a 5-point scale (0 to 4 spectrum), where increasing scores indicate higher levels of symptom severity, and are summed to yield a total score.69,87 | The psychometric properties of HAM-A summarized as follows are based on studies in major depressive disorder. Validity: Concurrent validity of both the HAM-A total score and its subscales was adequate.70 Reliability: Interrater reliability of both the HAM-A total score and its subscales was adequate.70 Responsiveness: HAM-A has good sensitivity to change during anxiolytic treatment.70 | Evidence for an MID in the HAM-A scale was not found. |
QIDS-SR | A 16-item, self-reported tool that measures depressive symptom severity.66 Items included assess DSM-IV criterion diagnostic symptoms for major depressive disorder. The recall period is 7 days as patients are asked to rate their symptoms during this period. The responses are converted from the 16 items into 9 DSM-IV symptom criterion domains. Each item is scored on a scale of 0 to 3, with higher scores representing greater symptom severity. The total score ranges from 0 to 27.66 | The psychometric properties of QIDS-SR summarized as follows are based on studies in major depressive disorder. Validity: QIDS-SR scores were highly correlated with the 30-Item Inventory Depressive Symptomatology – Self-Report (Cronbach alpha = 0.96) and 24-Item HAM-D (0.86) total scores.66 Reliability: QIDS-SR was found to have high internal consistency (Cronbach alpha = 0.86).66 Responsiveness: Evidence was not found. | Evidence for an MID in the QIDS-SR scale was not found. |
FAST | A 24-item, clinician-rated scale used to assess functional impairment in patients with mental disorders. The items are divided into 6 areas of functioning: (1) autonomy, (2) occupational functioning, (3) cognitive functioning, (4) financial issues, (5) interpersonal relationships, and (6) leisure time. Items are rated on a 4-point scale (0 = no difficulty; 3 = severe difficulty). The total score is the sum of all 24 items, with higher scores indicating greater difficulty.71 | Validity: For concurrent validity, the Pearson correlation coefficient between GAF (higher scores on GAF indicate better psychosocial functioning) and FAST was –0.90 (P < 0.001).71 FAST was found to be sensitive to change in severity of symptoms in bipolar disorder.71 Reliability: For internal consistency, the Cronbach alpha was 0.91 and high (coefficient not reported) for the total scale and each domain, respectively.71 For test-retest reliability in 1 week, the intraclass correlation coefficient was 0.98 (P < 0.01).71 Responsiveness: Evidence not found. | There is evidence to suggest the minimum clinically important difference ranges from an 8- to 9-point change from baseline.72 |
C-SSRS | An interview-based measure of suicidal ideation and behaviour with 4 subscales (ideation severity, ideation intensity, behaviour, and lethality). The items on each subscale are rated on 3-point to 6-point ordinal scales or a nominal scale. A higher total score indicates a higher level of suicidality. | The validity of this scale has been demonstrated in adolescents with MDD. | Unspecified |
CGI-I = Clinical Global Impression–Improvement; CGI-S = Clinical Global Impression–Severity of Illness; DSM-IV = Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition; FAST = Functioning Assessment Short Test; GAF = Global Assessment of Functioning; HAM-A = Hamilton Anxiety Rating Scale; HAM-D = Hamilton Depression Rating Scale; MADRS = Montgomery–Åsberg Depression Rating Scale; MDD = major depressive disorder; MID = minimal important difference; PANSS = Positive and Negative Syndrome Scale; QIDS-SR = Quick Inventory of Depressive Symptomatology–Self-Rated; YMRS = Young Mania Rating Scale.
Young Mania Rating Scale
The YMRS is an 11-item rating scale used to assess the severity of manic symptoms.45 The 11 items are: (1) elevated mood; (2) increased motor activity-energy; (3) sexual interest; (4) sleep; (5) irritability; (6) speech (rate and amount); (7) language-thought disorder; (8) content; (9) disruptive-aggressive behaviour; (10) appearance; and (11) insight. Each item consists of 5 explicitly defined grades of severity meant to reflect the core symptoms of the manic phase of bipolar disorder. The scale is administered by a trained clinician during a 15-to-30-minute interview. A severity rating is assigned to each item based on the patient’s subjective report of his or her condition over the previous 48 hours and the clinician’s assessment of the patient’s behaviour, with emphasis on the latter. Items 5, 6, 8 and 9 are graded on a 0 to 8 scale while the remaining 7 are graded on a 0 to 4 scale, based on increasing severity. The former items are given twice the weight of the others to compensate for and in anticipation of poor cooperation from patients who are severely ill. The YMRS total score ranges from 0 to 60.45 The YMRS does not assess concomitant depressive symptoms and should therefore be administered concurrently with a depression rating scale in patients with symptoms of depression or those experiencing a mixed episode.
Validity
For concurrent validity, the YMRS was compared to 3 other mania rating scales (Beigel Mania Rating Scale, Petterson Mania Scale, and an 8-point global rating scale) and was shown to be statistically significantly correlated with all 3 rating scales (Spearman coefficients: 0.71, 0.89, and 0.88, respectively; P < 0.001).45
Reliability
The YMRS has demonstrated good interrater reliability (Spearman rank-order correlation) on the total score (0.93) and the individual item scores (0.66 to 0.92).45
Responsiveness
The YMRS has been shown to be sensitive to change. Differences in the YMRS scores between treated patients with bipolar mania and patients before treatment have been found to be statistically significant.45
Clinical Relevance
In a cohort of adult patients (n = 3,255) with bipolar disorder who experienced an acute manic/mixed episode, the minimal clinically significant difference was determined to be 6.6 points on the YMRS with reference to a 1-point difference on the Clinical Global Impression–Bipolar Disorder (CGI-BP) mania scale.7 There is evidence to support a 50% reduction from baseline on the YMRS total score as a clinically meaningful definition of response in the acute treatment of manic/mixed episode in pediatric patients with bipolar I disorder based on a CGI-BP Overall Improvement score of 1 or 2.46 A YMRS score that is 12 or less indicates remission of manic symptoms.45 It has also been proposed that a YMRS cut-off score of 4 and 7 corresponds to a severity score of 1 (“normal, not at all ill”) and 2 (“borderline mentally ill”) on the CGI-BP scale in patients with bipolar disorder with mania or mixed episodes, respectively.53 The authors stated that “normal, not at all ill” appears to approximate clinical remission from acute episodes, while “borderline mentally ill” appears to be a softer approximation of remission with mild residual symptoms.
Limitations
The following limitations have been identified in the YMRS: (1) differences in weighting of symptoms might suggest those assigned a greater weight are more important, thereby inflating the total score; (2) administration of the scale is vague and contains no standardized format or questions to systematically elicit symptoms; (3) the scale was normed on 20 manic patients and it is unclear whether mean scores among bipolar manic patients would differ significantly from other diagnostic groups; (4) the score is partly based on patient self-report at a time when thought may be highly disordered, which may decrease the reliability of the assessment; and (5) the scale includes some symptoms (appearance and insight) that are less central to mania, while at the same time combining distinct symptoms into one (decreased need for sleep with insomnia).88
Clinical Global Impression Scale
The CGI is a 3-item scale used to assess overall severity and response to treatment of mental disorders.54 The usual CGI scale items include severity of illness (CGI-S) at the time of assessment on a 7-point scale (1 = normal; 7 = extremely ill), global improvement (CGI-I) relative to baseline on a 7-point scale (1 = very much improved; 7 = very much worse), and an efficacy index which incorporates the clinician’s assessment of therapeutic effect in relation to adverse effects in a 4 point x 4 point grid rating scale. More specifically, the efficacy index is calculated by dividing the therapeutic score by the side effect score. The therapeutic score ranges from 1 (“unchanged or worse”) to 4 (“marked”) and the side effect score ranges from 1 (“none”) to 4 (“outweighs”).54 The difficulty of combining the 2 concepts of efficacy and AEs has led to criticism of the efficacy index.89 There is no total score for the CGI scale but rather, scores on the individual items are considered separately.
Studies determining the psychometric properties of the CGI scale in patients with bipolar disorder were not found. Instead, evidence for the psychometric properties of the CGI scale in patients with schizophrenia are summarized as follows.
Validity
There is little information regarding the validity of the CGI scale. Rabinowitz et al.56 sought to validate the CGI-S scale by comparing the PANSS total and CGI-S scores using data from 7 trials of risperidone in patients with schizophrenia. The CGI-S scores from the pooled trials corresponded to the following mean PANSS scores: 1 (normal) = PANSS 55.5, 2 (borderline ill) = PANSS 67.0, 3 (mildly ill) = PANSS 79.6, 4 (moderately ill) = PANSS 92.4, and 5 (markedly ill) = PANSS 99.7. The predefined measures of clinical improvement were a 20% reduction in the PANSS score and a 1-point decrease on the CGI-S scale. The sensitivities and specificities for the CGI-S to detect this level of improvement in the 7 trials ranged from 64.5% to 89.6% and 65.7% to 82.8%, respectively. From this assessment, it appears that the CGI-S and PANSS are correlated and exhibit substantial agreement in detecting change in patients with schizophrenia.
Reliability
Evidence for the reliability of the CGI scale was not found.
Responsiveness
Evidence for the responsiveness of the CGI scale was not found.
Clinical Relevance
A 1-point improvement on the CGI-S has been linked to a 20% reduction in the PANSS total score. Both of which have been used as predefined measures of clinical improvement and anchors for within-group differences based on expert opinion in a number of clinical trials and validity studies in schizophrenia, respectively.56-58
Montgomery–Åsberg Depression Rating Scale
The MADRS is a 10-item, clinician-rated scale used to assess the severity of depression in the past week and detect changes due to antidepressant treatment.47,48,90 The scale is commonly used in antidepressant efficacy trials.91 The 10 items are47: (1) apparent sadness; (2) reported sadness; (3) inner tension; (4) reduced sleep; (5) reduced appetite; (6) concentration difficulties; (7) lassitude; (8) inability to feel; (9) pessimistic thoughts; and (10) suicidal thoughts. Each item is rated on a 0 (item not present or normal) to 6 (severe or continuous presence of the symptoms) scale, resulting in a maximum total score of 60 points, in which higher scores indicate greater depressive symptomology.47,90 The scoring instructions for major depressive disorder indicate that a total score ranging from 0 to 6 indicates “no depression,” 7 to 19 indicates “mild depression,” 20 to 34 indicates “moderate depression,” and 35 or more indicates “severe depression.”76 In contrast, the severity thresholds for adult patients with bipolar I depression with reference to the CGI-S scale were found to be the following: a total score of 0 to 6 indicates “normal, not at all ill,” 7 to 12 indicates “borderline mentally ill,” 13 to 18 indicates “mildly ill,” 19 to 23 indicates “moderately ill,” 24 to 36 indicates “markedly ill,” 37 to 39 indicates “severely ill,” and 40 or more indicates “extremely ill.”90
Studies determining the psychometric properties (with the exception of clinical relevance) of the MADRS scale in patients with bipolar disorder were not found. Instead, evidence for the psychometric properties of the MADRS scale in patients with major depressive disorder are summarized as follows.
Validity
For content validity, most of the items are highly related to the core concept of depression. However, the scale does not adequately define the severity of depression or remission because not all of the core symptoms used as diagnostic criteria in the DSM-IV are assessed by the MADRS.78 The MADRS has demonstrated good convergent validity as indicated by its high degree of correlation with scores on other measures such as the 17-item HAM-D and the 6-item HAM-D.78,61,79 Further, the MADRS has been shown to be able to discriminate between different levels of severity in depression.78
Reliability
The MADRS has demonstrated high internal consistency, slightly higher than the HAM-D.78 The clinician interrater reliability of MADRS was also found to be acceptable on individual items as well as the total score.79
Responsiveness
Studies have repeatedly found the MADRS to have greater sensitivity to treatment-related change compared to the HAM-D,79-81 however at least 1 study involving patients with major depressive disorder found its sensitivity to be lower than that of the HAM-D.82 This high capability of the MADRS to detect change in patients’ conditions over time may be related to its more uniform structure compared to the HAM-D.92
Clinical Relevance
There is evidence to support that an improvement of 2 points or more on the MADRS is considered clinically relevant.8,9 Response to treatment is usually defined as at least 50% reduction of the MADRS total score from baseline.49 No consensus has emerged regarding a cut-off value on the MADRS for defining remission in clinical trials.50 The criterion score to identify a patient who has experienced remission has ranged from 6 through 12 in various trials.49,51 According to 1 study that set out to establish an empirically based cut-off value for remission, a narrow definition for remission is a MADRS cut-off value of 4 points or less. On the basis of a less conservative definition of remission, the recommended cut-off value was 9 points or less.50 There is also evidence to support that a MADRS score of less than 10 is a valid cut point for remission.52
It has been proposed that a MADRS cut-off score of 5 and 10 corresponds to a severity score of 1 (“normal, not at all ill”) and 2 (“borderline mentally ill”) on the CGI-BP scale in patients with bipolar depression, respectively.53 The authors stated that “normal, not at all ill” appears to approximate clinical remission from acute episodes, while “borderline mentally ill” appears to be a softer approximation of remission with mild residual symptoms.
Positive and Negative Syndrome Scale
The PANSS is a 30-item rating scale that requires a 30- to 40-minute patient interview to gather information on which to assess the patient with regard to the presence and severity of psychopathology in the previous week. The PANSS instrument provides a complete definition for each item as well as detailed anchoring criteria for each of the 7 rating points (1 = absence of symptoms; 7 = extremely severe symptoms). Of the 30 items, 7 items are related to positive symptoms (i.e., delusions, conceptual disorganization, hallucinatory behaviour, excitement, grandiosity, suspiciousness and hostility), 7 items to negative symptoms (i.e., blunted affect, emotional withdrawal, poor rapport, passive/apathetic social withdrawal, difficulty in abstract thinking, lack of spontaneity and flow of conversation, and stereotyped thinking), and 16 items to general psychopathology (i.e., somatic concern, anxiety, guilt feelings, tension, mannerisms and posturing, depression, motor retardation, uncooperativeness, unusual thought content, disorientation, poor attention, lack of judgment and insight, disturbance of volition, poor impulse control, preoccupation, and active social avoidance).59,60 The PANSS total score ranges from 30 to 210.
Studies determining the psychometric properties of the PANSS in patients with bipolar disorder were not found. Instead, evidence for the psychometric properties of the PANSS in patients with schizophrenia are summarized as follows.
Validity
Kay et al.60 reported on the psychometric properties of the PANSS in 101 inpatients with schizophrenia. Scores on all subscales were reported to exhibit a normal distribution, suggesting suitability for parametric statistical analysis. Further, the range of scores was less than the potential range suggesting a lack of ceiling effect.
Reliability
Internal consistency was demonstrated for the positive (alpha = 0.73), negative (alpha = 0.83), and general psychopathology (alpha = 0.79) subscales. Test-retest reliability was assessed 3 to 6 months later on a cohort of 15 patients who remained hospitalized; the Pearson correlation coefficients were 0.80, 0.68, and 0.60 for the positive, negative, and general psychopathology subscales, respectively.60 Peralta and Cuesta reported on the interrater reliability of the PANSS from a sample of 100 consecutively admitted patients with schizophrenia.83 The positive and negative subscales showed good interrater reliability; interclass correlation coefficients were 0.72 and 0.80, respectively. The general psychopathology subscale demonstrated moderate interrater reliability; interclass correlation was 0.56.
Responsiveness
Evidence for the responsiveness of the PANSS was not found.
Clinical Relevance
A number of clinical trials in schizophrenia have used a 20% reduction in the PANSS total score, which has been found to correspond to a 1-point decrease on the CGI-S, as predefined measures of clinical improvement or criterion for response to antipsychotic treatment.56-58 According to the European Medicines Agency, a responder threshold of 30% reduction on the total PANSS score from baseline is considered clinically relevant in short-term clinical trials conducted to determine the efficacy and safety of a drug product in patients with acute symptoms of schizophrenia.77 In a comparison of PANSS to the CGI scale, it was suggested that an absolute reduction of 15 points in the PANSS total score corresponds to “minimally improved” on the CGI-Improvement score, and a reduction of the CGI–Severity of Illness score by 1 severity step.55 In comparison, a reduction of 33 points in the PANSS total score corresponds to “much improved” on the CGI-Improvement score. However, the aforementioned estimates were sensitive to the baseline severity of illness to the extent that patients with a lower baseline severity of illness required smaller reductions in the PANSS to produce a particular improvement in the CGI. For this reason, it has been suggested that change in the PANSS score has limited usefulness as a primary outcome due to variability in baseline symptom intensity.93,94 A score of 3 or less on 8 PANSS items (P1, P2, P3, N1, N4, N6, G5 and G9) for a period of at least 6 months has been considered to represent remission of disease.93,94
17-Item Hamilton Depression Rating Scale
The 17-item HAM-D is a clinician-rated scale that requires a patient interview and family report to gather information on which to assess the severity of symptoms and address both somatic and psychological symptoms of depression.61,68,62,63 The items are either rated on a 5-point scale (0 to 4 spectrum) or a 3-point scale (0 to 2 spectrum), where increasing scores represent increasing severity of symptoms.64,65 Scores are summed to obtain a total score out of 52 or 53.10,66 The scoring instructions indicate that a total score ranging from 0 to 7 indicates “no depression,” 8 to 13 indicates “mild depression,” 14 to 18 indicates “moderate depression,” 19 to 22 indicates “severe depression,” and a total score of 23 or greater indicates “very severe depression.”62
Studies determining the psychometric properties of the HAM-D in patients with bipolar disorder were not found. Instead, evidence for the psychometric properties of the HAM-D in patients with major depressive disorder are summarized as follows.
Validity
Since there is only partial overlap between the content of the HAM-D and DSM-IV symptom inclusion diagnostic criteria for major depressive disorder, the content validity of the HAM-D has been found to be poor.62,64 The convergent validity of the HAM-D has been shown to be adequate, as this scale has demonstrated moderate to high correlation with many other depression scales.64 Similarly, the discriminant validity of this scale has been shown to be adequate.64
Reliability
Reliability coefficients for internal consistency, interrater reliability, and test-retest reliability are generally good for the overall scale, as are the internal reliability estimates for the individual items of the scale. Although numerous items have weak interrater and retest reliability at the item level, the use of a structured interview guide may help to increase the item and total scale reliability.64
Responsiveness
Several meta-analyses have found the HAM-D to be more sensitive to change in patients’ conditions compared to other depression scales such as the Beck Depression Inventory.84,85 However, the multidimensional nature of the HAM-D may reduce its sensitivity to detect changes in the severity of depression over time.78 For instance, the full HAM-D scale has been shown to be less sensitive than unidimensional subscales of its items.86
Clinical Relevance
For clinical trials, NICE recommends a 3-point difference between drug and placebo arms as a criterion for clinical significance, though no justification for this figure was provided.10 In the updated NICE guidelines,95 there was no mention of what constituted a clinically significant difference. A separate report by Montgomery et al. suggested a difference of 2-points between antidepressant and placebo might be clinically relevant,8 though similar to the NICE guidelines, it appears that this figure was opinion-based. Therefore, neither a formally derived minimal clinically important difference nor an evidence-based, clinically significant difference for the HAM-D was identified. Response is defined as a 50% reduction from the baseline HAM-D total score.62 Remission was defined as a score of 7 or less on the HAM-D total score by a consensus panel in 1991,67 and since then, this level has been widely adopted in clinical research.62 However, more recent evidence has suggested that, based on a narrow definition of DSM-IV remission, which requires an absence of clinically significant symptoms of depression, the optimal cut-off should be 2 or lower on the HAM-D total score.62 A score of 7 or less was found to be an appropriate level when a broader definition of remission is used.62
Hamilton Anxiety Rating Scale (HAM-A)
The HAM-A is a 14-item, clinician-rated scale used to assess somatic and psychic anxiety symptoms.69,87 Although this scale was developed to assess anxiety neurosis, it has also been applied in depression.69,70 The items are rated on a 5-point scale (0 to 4 spectrum), where increasing scores indicate higher levels of symptom severity, and are summed to yield a total score. The total score ranged from 0 (absence of anxiety) to 56 (most severe form of anxiety).15
Studies determining the psychometric properties of the HAM-A in patients with bipolar disorder were not found. Instead, evidence for the psychometric properties of the HAM-A in patients with depressive disorders are summarized as follows.
Validity
The concurrent validity of both the HAM-A total score and its subscales was found to be adequate.70 However, a disadvantage of the HAM-A is its inability to distinguish between anxiolytic and antidepressant effects. In a sample of patients with depression, 1 study found that both the HAM-A total score and its subscale scores were unable to discriminate between patients with depression with and without additional symptoms of anxiety.70 This low specificity may be due, in part, to the inclusion of an item which measures severity of depressive states. The authors concluded that this scale should not be used as an indicator of the severity of anxiety states in depressive disorders.70 However, there is some controversy regarding this conclusion, since the HAM-A is commonly used as an outcome measure in trials with patients with depression.
Reliability
The interrater reliability of both the HAM-A total score and its subscales was found to be adequate.70
Responsiveness
HAM-A has demonstrated good sensitivity to change during anxiolytic treatment.70
Clinical Relevance
Evidence for the MID of HAM-A was not found.
16-item Quick Inventory of Depressive Symptomatology–Self-Rated
The QIDS-SR is a 16-item, self-reported tool that measures depressive symptom severity.66 Items included assess DSM-IV criterion diagnostic symptoms for major depressive disorder. The recall period is 7 days as patients are asked to rate their symptoms during this period. The responses are converted from the 16 items into 9 DSM-IV symptom criterion domains: 1) sad mood; 2) concentration; 3) self-criticism; 4) suicidal ideation; 5) interest; 6) energy/fatigue; 7) sleep disturbance (initial, middle, and late insomnia or hypersomnia); 8) decrease/increase in appetite/weight; and 9) psychomotor agitation/retardation. Each item is scored on a scale of 0 to 3, with higher scores representing greater symptom severity. The total score ranges from 0 to 27. The scoring instructions indicate that a total score ranging from 0 to 5 indicates “no depression,” 6 to 10 indicates “mild depression,” 11 to 15 indicates “moderate depression,” 16 to 20 indicates “severe depression,” and a total score of 21 or greater indicates “very severe depression.”66
Studies determining the psychometric properties of the QIDS-SR in patients with bipolar disorder were not found. Instead, evidence for the psychometric properties of the QIDS-SR in patients with major depressive disorder are summarized as follows.
Validity
The QIDS-SR scores were highly correlated with the 30-Item Inventory Depressive Symptomatology – Self-Report (Cronbach alpha = 0.96) and the 24-Item HAM-D (0.86) total scores.66
Reliability
The QIDS-SR was found to have high internal consistency (Cronbach alpha = 0.86).66
Responsiveness
Evidence for the responsiveness of the QIDS-SR was not found.
Clinical Relevance
Evidence for the MID of the QIDS-SR was not found.
Functioning Assessment Short Test
The FAST is a 24-item, clinician-rated scale used to assess functional impairment in patients with mental disorders including bipolar disorder.71 The items are divided into 6 areas of functioning: (1) autonomy, (2) occupational functioning, (3) cognitive functioning, (4) financial issues, (5) interpersonal relationships, and (6) leisure time. Items are rated on a 4-point scale (0 = no difficulty, 1 = mild difficulty, 2 = moderate difficulty, and 3 = severe difficulty). The total score is the sum of all 24 items, with higher scores indicating greater difficulty in functioning. A score of 0 to 11 has been associated with “nonimpaired,” 12 to 20 with “mild impairment,” 21 to 40 with “moderate impairment,” and greater than 40 with “severe impairment.”96 However, the aforementioned severity thresholds of FAST were based on severity thresholds on the Global Assessment of Functioning (GAF) tool that were derived from expert opinion.
The psychometric properties of the FAST in adult patients with bipolar disorder have been summarized as follows.
Validity
For concurrent validity, the Pearson correlation coefficient between GAF (higher scores on GAF indicates better psychosocial functioning) and FAST was –0.90 (P < 0.001).71 FAST was sensitive to changes in the severity of symptoms in bipolar disorder as indicated by statistically significantly lower FAST scores in euthymic patients compared to patients with bipolar mania or bipolar depression.71
Reliability
For internal consistency, the Cronbach alpha was 0.91 and high (coefficient not reported) for the total scale and each domain, respectively.71 For test-retest reliability in 1 week, the intraclass correlation coefficient (n = 15) was 0.98 (P < 0.01).71
Responsiveness
Evidence for the responsiveness to change of the FAST was not found.
Clinical Relevance
There is evidence to suggest the minimum clinically important difference on the FAST ranges from an 8- to 9-point change relative to baseline based on the expert-derived minimum clinically important difference of 1 on the CGI-S scale and 10 on the GAF as anchors.72
Columbia–Suicide Severity Rating Scale
The C-SSRS is an interview-based assessment tool for evaluating suicidal ideation and behaviour.97 It was developed to monitor changes in suicidality over time by incorporating assessments of lifetime suicidal ideation and behaviour as well as between-visit changes. The C-SSRS has 4 subscales: severity of ideation (e.g., specificity of suicidal thoughts or intent with methods or plans), intensity of ideation (e.g., frequency and duration of suicidal thoughts), behaviour (e.g., preparatory actions, suicide attempts, nonsuicidal injurious behaviour), and lethality (assessment of actual suicide attempts; actual lethality is rated on a 6-point ordinal scale, and if actual lethality is 0, potential lethality of attempts is rated on a 3-point ordinal scale). The items on the ideation and lethality subscales are rated on 3-point to 6-point ordinal scales, and the behaviour subscale uses a nominal scale. A higher total score indicates a higher level of suicidality.
The psychometric properties of the C-SSRS were assessed in 3 studies that were presented in 1 publication. Study 1 included adolescents who had previously attempted suicide, Study 2 involved adolescents with a diagnosis of major depressive disorder (MDD), and Study 3 was conducted in adult patients who presented to the emergency department for psychiatric reasons.97 The intensity of ideation subscale demonstrated moderate to high internal consistency in all 3 studies. In support of convergent validity, the suicidal ideation and behaviour subscales on the C-SSRS correlated moderately to strongly with the corresponding suicide-related items on the MADRS and Beck Depression Inventory, as well as with the Scale for Suicide Ideation and the Columbia Suicide History Form in Study 1 and Study 3. Further analysis in Study 1 and Study 2 showed that the change in the severity and intensity of ideation subscale scores over time significantly corresponded with Scale for Suicide Ideation or Suicidal Ideation Questionnaire–Junior score changes. Similarly, the classification of suicidal behaviours on the C-SSRS over time in Study 1 demonstrated moderate to full agreement with the classification of the same behaviour using the Columbia Suicide History Form. The divergent validity of the C-SSRS severity and intensity of ideation subscales was analyzed in Study 1, and a weak to moderate correlation between these subscales and somatic depression items on the Beck Depression Inventory and the MADRS was observed; however, this study population did not include adults with MDD.97
A minimal clinically important difference was not reported for the C-SSRS; however, predictive validity was examined in 2 studies. For each increase in C-SSRS level of lifetime suicide ideation by 1 SD in an adolescent population, the odds of attempting suicide during the 24-week study increased by 45%.97 A validation study of the electronic version of the C-SSRS evaluated an existing set of assessments extracted from multiple studies in which the majority (91%) of total patients had MDD, and demonstrated that patients who reported severe lifetime suicidal ideation or a history of suicidal behaviour at baseline were up to 9 times more likely to report suicidal behaviour during their study participation.98
Pharmacoeconomic Review
Abbreviations
AE
adverse event
BIA
budget impact analysis
CANMAT
Canadian Network for Mood and Anxiety Treatments
EPS
extrapyramidal symptom
IAM
Institute for Advancements in Mental Health
MADRS
Montgomery–Åsberg Depression Rating Scale
NMA
network meta-analysis
QALY
quality-adjusted life-year
Executive Summary
The executive summary comprises 2 tables (Table 1 and Table 2) and a conclusion.
Item | Description |
|---|---|
Drug product | Cariprazine (Vraylar), oral capsules |
Submitted price | Cariprazine, 1.5 mg, 3.0 mg, 4.5 mg, and 6.0 mg: $4.90 per capsule |
Indication | As monotherapy for:
|
Health Canada approval status | NOC |
Health Canada review pathway | Standard review |
NOC date | April 22, 2022 |
Reimbursement request | As per indication |
Sponsor | Allergan (an AbbVie Inc. company) |
Submission history | Previously reviewed: In progress Indication: Schizophrenia Recommendation: TBD |
NOC = Notice of Compliance; TBD = to be determined.
Table 2: Summary of Economic Evaluation
Component | Description |
|---|---|
Type of economic evaluation | Cost-utility analysis Decision tree + Markov model |
Target populations | Adults with manic or mixed episodes and depressive episodes associated with bipolar I disorder |
Treatment | Cariprazine |
Comparators | Manic or mixed episodes:
Depressive episodes:
|
Perspective | Canadian publicly funded health care payer |
Outcomes | QALYs, LYs |
Time horizon | 5 years |
Key data source | Comparative clinical efficacy data were derived from a sponsor-submitted NMA that was used to determine transition probabilities, discontinuation rates, and rates of AEs. |
Submitted results |
|
Key limitations |
|
CADTH reanalysis results |
|
AE = adverse event; LY = life-year; NMA = network meta-analysis; QALY = quality-adjusted life-year.
Conclusions
The CADTH clinical review noted that the results of the network meta-analysis (NMA) ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||. Thus, there is no evidence to warrant a price premium for cariprazine.
Additional limitations were identified in the sponsor’s pharmacoeconomic analysis that have notable implications for the results. First, the model structure does not accurately characterize the disease pathway of bipolar I disorder or the expected use of cariprazine in clinical practice. In addition, cariprazine was modelled as monotherapy, though experts noted it may be used in combination with an anticonvulsant or mood stabilizer. The sponsor also included haloperidol, clonazepam, and chlorpromazine as subsequent therapies; however, these were determined not to be relevant comparators in any setting.
Based on the results of the NMA, the CADTH base-case reanalysis took the form of a cost-minimization analysis. For the CADTH base case, haloperidol, clonazepam, and chlorpromazine were excluded as subsequent line therapies. As well, CADTH fixed a programming error in the sponsor’s calculation of drug acquisition costs. In the CADTH base case, cariprazine was associated with total costs of $3,947 per patient in the manic or mixed phase over 5 years — greater than all comparators except paliperidone ($3,992). In the absence of data to support a price premium, a price reduction of 83% would be required to ensure similar treatment costs when compared with the least costly comparator in this setting, risperidone ($3,738). In the depressive phase, cariprazine was associated with greater total costs of $7,935 per patient over 5 years compared to the least costly comparator, quetiapine ($7,395). A price reduction of 75% would be required to ensure similar treatment costs with quetiapine.
The results are associated with uncertainty as the clinical experts asserted that cariprazine would continue to be used as maintenance therapy after the acute symptoms (mania or mixed, or depressive) had resolved, and the models considered only a single episode of mania or mixed symptoms or depressive symptoms. A unique benefit of cariprazine in this regard is its long half-life; however, this feature could also require additional monitoring for adverse events (AEs), which could be challenging for patients located in remote centres. In addition, experts noted that the daily dose of cariprazine could be increased to 12 mg in some patients as was done in the clinical trials. The increased dose, flat pricing and initial dose escalation, and additional monitoring will result in increased costs to the health care system. Additional price reductions may be warranted to ensure cariprazine does not lead to any increased costs.
Stakeholder Input Relevant to the Economic Review
This section is a summary of the feedback received from the patient groups, registered clinicians, and drug plans that participated in the CADTH review process.
CADTH received patient input from 2 patient groups as part of this review, the Institute for Advancements in Mental Health (IAM) and the Mood Disorders Society of Canada. IAM provides 1-to-1 and group counselling to people with serious mental illness as well as training for frontline workers and community education. IAM conducted a survey of its client network, 63% of whom described themselves as a family member or friend of someone who had been diagnosed, and 77% of whom were born in Canada. The Mood Disorders Society of Canada conducted individual interviews with 4 patients, 3 family members, and 1 long-term care colleague. Patients reported being currently treated for their mental symptoms using long-acting injectable medications and oral medications. Within the IAM survey, 70% of respondents reported that current medications control symptoms well and 80% reported being able to avoid hospital visits. The most common side effects of medications, occurring in greater than 50% of patients, were drowsiness, dry mouth, and restlessness. Weight gain was the most commonly cited AE associated with medication and was identified as a contributing factor to general medical comorbidity and reduced quality of life. No patients reported experience with cariprazine.
CADTH received clinician input from 2 clinician groups — the Western Canadian Clinical Advisory Network, a network of senior psychiatrists across Alberta and British Columbia, and the Canadian Network for Mood and Anxiety Treatments (CANMAT), a network of academic and clinical experts that produces treatment guidelines and educational material for health professionals and information for patients and families. Clinician experts noted 3 distinct phases of treatment for bipolar disorder: acute mania or mixed episodes, acute depressive episodes, and long-term maintenance aimed at preventing the recurrence of future episodes. Current treatments consist of atypical antipsychotic drugs and anticonvulsants. It was noted that only quetiapine is effective in treating both manic and depressive episodes. Both clinician groups indicated that cariprazine would be a first-line treatment for mania and depression given its efficacy and favourable metabolic profile with lower sedation and weight gain. The groups suggested that it would be most commonly used as monotherapy but may be combined with mood stabilizers in some cases.
Drug plan feedback noted the long effective half-life of cariprazine, which may require additional monitoring for adverse effects. The plans noted challenges with access to psychiatric and follow-up care in rural settings, making the initiation of cariprazine difficult in these areas. The drug plans noted concerns related to the combination usage of cariprazine with other currently approved medications. Plans also commented on whether patients currently stable on established therapy would switch to cariprazine to alleviate tolerability and safety concerns with their current therapy.
Several of these concerns were addressed in the sponsor’s model:
The sponsor included risk ratios for weight gain and comorbidities associated with such weight gain.
CADTH was unable to address the following concerns raised from stakeholder input:
The sponsor’s model was focused on acute episodes of bipolar disorder specifically and did not consider the possibility of maintenance treatment with cariprazine.
The sponsor’s model considered monotherapy only, while clinician and drug plan input highlighted the potential for combination usage with other therapies.
The sponsor’s model did not consider the impact of requiring greater monitoring with cariprazine or the potential costs this may be associated with for patients living in remote areas.
Economic Review
The current review is for cariprazine (Vraylar) for the acute treatment of manic or mixed episodes and depressive episodes associated with bipolar I disorder in adults.
Economic Evaluation
Summary of Sponsor’s Economic Evaluation
Overview
The sponsor submitted 2 cost-utility analyses assessing cariprazine compared with other first-line treatments for bipolar I disorder. The model population was adults with manic or mixed episodes and depressive episodes associated with bipolar I disorder, which aligns with the Health Canada indication and reimbursement request.1
Cariprazine is indicated as monotherapy for the acute treatment of manic or mixed episodes and depressive episodes associated with bipolar I disorder. The recommended dosage for manic or mixed episodes is 1.5 mg to 6 mg once daily. The starting dose of cariprazine is 1.5 mg and can be increased thereafter by 1.5 mg increments, based on clinical response and tolerability. The recommended dosage for depressive episodes is 1.5 mg once daily but can be increased to 3 mg once daily on day 15.1 Cariprazine is available in oral capsules of various sizes (1.5 mg, 3 mg, 4.5 mg, and 6 mg), each at a cost of $4.90 per capsule. The cost used in the sponsor’s model was $137.29 per 28 days.
The sponsor included different comparators for manic or mixed episodes and depressive episodes. For manic or mixed episodes, the primary comparators were quetiapine, asenapine, aripiprazole, paliperidone, and risperidone. The sponsor also included olanzapine, carbamazepine, haloperidol, and ziprasidone as second-line therapies, and clonazepam and chlorpromazine as third-line therapies. These therapies were assumed to be used equally regardless of first-line therapy to avoid biasing the results in favour of any 1 comparator. For the primary comparators, the 28-day costs ranged from $22.71 for risperidone to $162.04 for paliperidone.2 For the second-line therapies, the 28-day costs ranged from $22.99 for carbamazepine to $82.85 for ziprasidone.2 The 28-day costs for the third-line therapies were $10.91 for clonazepam and $23.60 for chlorpromazine.2 For the depressive episodes, the primary comparators were quetiapine and lurasidone, with divalproex and olanzapine included as second-line and third-line comparators, respectively. As with the manic or mixed episodes model, subsequent therapies were considered equally for all primary comparators so as not to bias the results in favour of any 1 comparator. For the primary comparators, the 28-day costs were $34.94 for quetiapine and $137.29 for lurasidone.2 For divalproex and olanzapine, the 28-day costs were $17.11 and $29.79, respectively.2
Outcomes of the models included quality-adjusted life-years (QALYs) and life-years over a time horizon of 5 years. Discounting (1.5% per annum) was applied to both costs and outcomes. For the manic or mixed episodes model, a 4-week cycle length was used while an 8-week cycle was used for the depressive episodes model, with a half-cycle correction applied.
Model Structure
The sponsor included separate models for manic or mixed episodes and depressive episodes. The model structures for both were identical and consisted of an initial decision tree followed by a Markov model. In each model, patients began in an active episode and received 1 of the first-line therapies; they were then categorized into responders and nonresponders. Patients with a response continued on the same treatment in the Markov respond-and-continue-monotherapy portion of the model. Those without a response discontinued and switched treatment; these patients entered the Markov model in the second-line therapy health state. In the manic or mixed episodes model, the initial assessment period defined response as a 50% improvement in the Young Mania Rating Scale. For the depressive episodes model, response was defined as a 50% improvement in the Montgomery–Åsberg Depression Rating Scale. Once in the Markov model, at the end of each model cycle, patients may either remain in their current health state, discontinue to second-line or third-line treatments (i.e., nonresponse, which is effectively best supportive care), or die. Progression to third-line treatment may be due to any reason, including lack of efficacy, AEs, patient preference, or physician preference. A figure depicting the sponsor’s model structure is available in Appendix 3 (Figure 1).
Model Inputs
The modelled populations were based on pooled baseline characteristics from 6 phase II and phase III placebo-controlled trials of cariprazine — 3 studies for mania or mixed symptoms of the disorder and 3 studies for depressive symptoms of the disorder.2
In the sponsor’s analysis, it was assumed that patients entered the model while experiencing a manic or mania episode or a depressive episode and were treated with first-line therapy: quetiapine, asenapine, aripiprazole, paliperidone, risperidone, or cariprazine for manic or mixed episodes, and quetiapine, lurasidone, or cariprazine for depressive episodes. After the initial assessment phase (4 weeks in manic or mixed and 8 weeks in depressive), patients were responders or nonresponders, and progressed further into the Markov model. Transition probabilities between the health states were derived from a sponsor-commissioned NMA for the first cycle.3 Discontinuation rates for the first cycle were also included as determined in the NMA, with the discontinuation rate beyond the first cycle based on placebo data. Death was based on Canadian life table data. An additional mortality multiplier was applied for patients experiencing a stroke event.2 Given a lack of evidence in the second-line therapy, no treatment effect was assumed for olanzapine, carbamazepine, haloperidol, and ziprasidone.
The dose of cariprazine used in the model was as described earlier, resulting in a cost of $137.29 per 28 days.2 Dosages for comparators were derived from the 2018 CANMAT and ISBD guidelines and respective product monographs.2 Costs were represented as a weighted average by various drug strengths based on historical public claims data.
Treatment-related AEs were included in the sponsor’s model for the first cycle and consisted of extrapyramidal symptoms (EPS) and sedation. Rates of AEs were taken from the NMA; where data were unavailable for comparators, the rate was taken from the placebo group. In the manic or mixed episode phase, rates of EPS ranged from 4.6% for quetiapine to 17.4% for cariprazine while rates for sedation ranged from 11.9% for paliperidone to 37.2% for cariprazine. In the depressive phase, rates of EPS ranged from 5.5% for quetiapine to 17.3% for lurasidone and rates for sedation ranged from 7.4% for cariprazine to 30.7% for quetiapine. The impact of treatment-related weight gain on comorbidities was also considered. Base rates for various comorbidity events (diabetes, hypertension, coronary heart disease, and stroke) were derived from a 2021 PHAC report.4 The increased relative risk for such events with significant weight gain was derived from the published literature.4 And the relative risk of weight gain with the comparators was derived from the sponsor’s NMA.3 The relative risk of weight gain with a given comparator was then multiplied by the increased rate of a comorbidity associated with significant weight gain, to get per cycle rates of comorbidities for each comparator.2
Health-related utilities were included for treatment response, AEs, and comorbidities. The baseline health state utility value for patients with bipolar I disorder was 0.80, derived from Revicki et al. (2005), and was applied to patients in the respond and continue state and the second-line treatment state.5 Patients in the nonresponse states experienced a utility of 0.55 for a manic episode and 0.57 for a depressive episode.5 Utility decrements were also applied for weight gain, EPS, sedation, and all metabolic comorbidities.2
All costs used in the model were reported in 2022 Canadian dollars. The drug acquisition costs for cariprazine and comparators have been previously described. In addition to drug costs, patients were assumed to require regular monitoring tests and physician follow-up. Patients could also require emergency room visits and hospitalizations in the nonresponse state (i.e., third-line setting). Blood test costs were derived from the Ontario Schedule of Benefits for Laboratory Services.6 Medical visit costs associated with psychiatrists and general practitioners were derived from the Ontario Schedule of Benefits for Physician Services.7 Costs for subsequent medications were included and were equal, regardless of the initial monotherapy. All comparators in each specific line and type of episode were assumed to receive equal market share (e.g., clonazepam and chlorpromazine each have a 50% share in third-line mania). The cost for AEs such as EPS and sedation was assumed to be 1 additional physician visit, quantified at $112.2 Costs per 28 days that ranged from $52 for hypertension to $350 for diabetes were included in both models.4
Summary of Sponsor’s Economic Evaluation Results
All analyses were run probabilistically (1,000 iterations for base-case and scenario analyses). The deterministic and probabilistic results were similar. The probabilistic findings are presented as follows.
Base-Case Results
The results of the sponsor’s analysis demonstrated that, for manic or mixed episodes only, aripiprazole and risperidone remained on the cost-effectiveness frontier (Table 3). All other comparators, including cariprazine, were dominated by aripiprazole as they produced fewer QALYs at a higher cost. In the manic or mixed episode phase, the probability of cost-effectiveness of cariprazine at a $50,000 per QALY willingness-to-pay threshold was approximately 9%.
For depressive episodes, quetiapine and lurasidone comprised the efficacy frontier (Table 4). Cariprazine was dominated by quetiapine as it produced fewer QALYs at a higher cost. The probability of cost-effectiveness of cariprazine at a $50,000 per QALY threshold was approximately 15%.
Full disaggregated results of the sponsor’s submitted economic evaluation are available in Appendix 3.
Sensitivity and Scenario Analysis Results
The sponsor conducted several scenario analyses pertaining to the discount rate, time horizon, utility values, and transition probabilities. Results of the sensitivity and scenario analyses demonstrated that the incremental cost-effectiveness ratio is predicated upon very small incremental QALYs. As such, even marginal differences in QALYs can have large effects on the incremental cost-effectiveness ratio.
Table 3: Summary of the Sponsor’s Economic Evaluation Results for Manic or Mixed Episodes
Drug | Total costs ($) | Total QALYs | Sequential ICER ($/QALY) |
|---|---|---|---|
Aripiprazole | 4,738.70 | 2.6900 | Reference |
Cariprazine | 4,984.84 | 2.6883 | Dominated by aripiprazole |
Risperidone | 5,024.31 | 2.6935 | 79,887 vs. aripiprazole |
ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year; vs. = versus.
Note: The submitted analyses are based on publicly available prices of comparators and may not reflect confidential negotiated prices. Only treatments on the cost-effectiveness frontier are reported in this table, with the exception of cariprazine as it is the drug under review.
Source: Sponsor’s pharmacoeconomic submission.2
Table 4: Summary of the Sponsor’s Economic Evaluation Results for Depressive Episodes
Drug | Total costs ($) | Total QALYs | Sequential ICER ($/QALY) |
|---|---|---|---|
Quetiapine | 7,421.76 | 2.8053 | Reference |
Cariprazine | 7,921.93 | 2.7990 | Dominated by quetiapine |
Lurasidone | 8,032.32 | 2.8335 | 21,672 vs. quetiapine |
ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year; vs. = versus.
Note: The submitted analyses are based on publicly available prices of comparators and may not reflect confidential negotiated prices. Only treatments on the cost-effectiveness frontier are reported in this table, with the exception of cariprazine as it is the drug under review.
Source: Sponsor’s pharmacoeconomic submission.2
CADTH Appraisal of the Sponsor’s Economic Evaluation
CADTH identified several key limitations to the sponsor’s analysis that have notable implications for the economic analysis.
The model structure does not accurately characterize the disease pathway and expected use of cariprazine. The sponsor submitted 2 economic models as part of this review, each pertaining to a single episode of either bipolar mania or bipolar depression. Patients entering the models were assumed to be experiencing an episode and receiving first-line therapy, from which they could: respond and continue treatment; or move to second-line and third-line therapy, after which the treatment and its benefits were assumed to cease. This characterization of the disease course and expected use of cariprazine did not align with clinical expert opinion.
The experts emphasized that patients with bipolar I disorder typically require lifelong pharmacologic treatment (i.e., maintenance treatment) and that treatment would not stop after resolving 1 acute episode. In addition, it was stated that this requirement for maintenance therapy would influence the choice of treatment used for the acute episode to enable continuation of 1 medication (avoiding switching between treatments). As such, the clinical experts anticipated continuing cariprazine treatment into the maintenance phase in patients for whom it is effective with acceptable tolerability. The experts noted that cariprazine is mechanistically and pharmacologically similar to other currently available antipsychotic drugs and would expect it to be similarly effective in the maintenance phase. Furthermore, experts noted that the long half-life of cariprazine makes it a desirable drug for use in maintenance therapy, because the overall effectiveness is not expected to diminish due to an occasional missed dose. Based on this feedback, treatment with cariprazine is expected to continue well beyond the acute episode for which it is initiated. This aspect of treatment was not modelled by the sponsor and could not be addressed without substantial revisions to the submitted models. In addition, the occurrence of subsequent episodes of mania or depression was not considered and, as such, the model only provides information on the treatment of a first episode.
CADTH was unable to address this in reanalysis.
There is uncertainty in the clinical inputs used to parameterize the model. The sponsor submitted an NMA to inform many of the clinical parameters used in the model, including rates of response, discontinuation, AEs, and weight gain. This NMA was appraised as part of the CADTH clinical review, which noted that cariprazine ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||. The assessment of discontinuation was limited by evidence of inconsistency and substantial heterogeneity, ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||. Overall, the data from the NMA |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| modelled for any model input. Furthermore, the clinical review noted issues with criteria for study inclusion and quality assessment, missing data, heterogeneity, and outcome definition, all of which contribute uncertainty to the analysis.
As part of the base case, given the findings from the CADTH clinical review, CADTH converted the sponsor’s cost-utility analysis into a cost-minimization analysis, in which no difference in clinical parameters was assumed. The total costs were calculated for each comparator over the time horizon. CADTH noted that in the sponsor’s base case, QALY differences were minimal (< 0.01).
Cariprazine could be used in combination with other therapies. The sponsor modelled cariprazine as monotherapy, with the possibility of second-line or subsequent therapies to be used upon discontinuation. However, the clinical experts noted that, especially for the more moderate or severe patients, the expectation is that cariprazine would eventually be used in combination with an anticonvulsant or mood stabilizer such as lamotrigine, lithium, or valproic acid. The expert cited the high rates of treatment failure with all drugs as rationale for this treatment practice.
CADTH was unable to address this in reanalysis due to a lack of clinical information.
The model contained programming inconsistencies and errors. CADTH notes that the sponsor’s model contained programming inconsistencies and errors pertaining to the incorporation of drug acquisition costs into the Markov trace. Specifically, the wrong cell names were referenced, leading to incorrect costs for aripiprazole and risperidone in the sponsor’s base case.
As part of the base case, CADTH corrected these errors.
Several included comparators were deemed not appropriate in the manic or mixed episode setting. The sponsor included haloperidol, clonazepam, and chlorpromazine in the second-line and third-line treatment settings, which was deemed not appropriate. The clinical experts noted that haloperidol is mainly used for agitation control but rarely for bipolar disorder. Similarly, clonazepam and chlorpromazine were noted to be used very infrequently and again, only for agitation control.
As part of the base case, CADTH removed haloperidol, clonazepam, and chlorpromazine from the manic or mixed episode treatment regimen. In the second-line setting, market share was redistributed to olanzapine, carbamazepine, and ziprasidone, while patients were not assumed to receive any active therapy in the third-line setting.
Flat pricing and dose titrations may lead to increased costs with cariprazine. The recommended daily dose of cariprazine is 1.5 mg to 6 mg for manic or mixed episodes and 1.5 mg to 3 mg for depressive episodes. For manic or mixed episodes, the dose can be increased by 1.5 mg increments, based on clinical response and tolerability. For initial treatment with cariprazine, the experts noted that it is likely that they would prescribe 1.5 mg capsules to allow patients to titrate to an effective dose. As such, in the first few months of treatment, the cost of cariprazine may be much more costly than anticipated (i.e., patients would take 2 1.5 mg capsules to achieve a daily dose of 3 mg, or 3 1.5 mg capsules to achieve a daily dose of 4.5 mg, or 4 1.5 mg capsules to achieve a daily dose of 6 mg). The experts noted that patients treated in the community setting are often assessed monthly, meaning a patient could maintain this dosing schedule for at least that long. Because of the flat pricing for cariprazine ($4.90 per capsule), this will result in increased treatment costs to the health care system that are not reflected in the CADTH base case. In addition, experts noted that some patients may continue to take 1.5 mg twice daily in maintenance to manage akathisia symptoms, which will further increase drug costs to the system.
Table 5: Key Assumptions of the Submitted Economic Evaluation — Not Noted as Limitations to the Submission
Sponsor’s key assumption | CADTH comment |
|---|---|
Treatment response in the manic/mixed setting was defined as a 50% improvement in the YMRS from baseline and a 50% improvement in the MADRS from baseline in the depressive setting. | Appropriate, according to clinical experts. |
After the acute episode and initial response, patients discontinue cariprazine according to the rates seen in the placebo arm of the NMA. | Not appropriate. Clinical experts did not feel that the assumption that patients would discontinue treatment after the initial acute episode was valid. Experts indicated that treatment with cariprazine would continue into maintenance therapy. |
MADRS = Montgomery–Åsberg Depression Rating Scale; NMA = network meta-analysis; YMRS = Young Mania Rating Scale.
CADTH Reanalyses of the Economic Evaluation
Base-Case Results
CADTH converted the sponsor’s cost-utility analysis to a cost-minimization analysis as part of the base case, in light of the available comparative clinical information and issues identified with the sponsor’s model structure. This involved setting all clinical parameters, including response rates, discontinuation rates, weight gain rate ratios, and rates of AEs equal to that of cariprazine. In addition, CADTH corrected a programming error and excluded the comparators haloperidol, clonazepam, and chlorpromazine (Table 6).
In the CADTH base case for manic or mixed episodes, cariprazine was associated with estimated total costs of $3,947 over the 5-year time horizon (Table 7). This was more than all other comparators except paliperidone, which was associated with treatment costs of $3,992. The least expensive comparator was risperidone, which was associated with costs of $3,738. As noted in Table 7, the costs attributed to the initial treatment are small, with the majority of patients off treatment by week 20.
In the CADTH base case for depressive episodes, cariprazine was associated with estimated total costs of $7,935 over the 5-year time horizon (Table 8). This was equal to lurasidone, but more expensive than quetiapine, which had total costs of $7,395. While similar across comparators, subsequent therapy and comorbidity costs were higher for the treatment of depressive episodes than for manic or mixed episodes, given the nature of the subsequent therapies included (after first-line treatment).
Scenario Analysis Results
CADTH undertook price reduction analyses based on the cost-minimization analysis. As the only costs expected to differ by treatment are the drug acquisition costs (given that all other resource use is assumed equal), these are the only costs reported (Table 9).
Cariprazine was compared to the least costly alternative for manic or mixed episodes (risperidone) and for depressive episodes (quetiapine). The CADTH base case suggested price reductions of 83% and 75% would be required to ensure cost parity with the least costly comparator in the manic or mixed setting and depressive setting, respectively.
Table 6: CADTH Revisions to the Submitted Economic Evaluation — Cost-Minimization Analysis
Stepped analysis | Sponsor’s value or assumption | CADTH value or assumption |
|---|---|---|
Corrections to sponsor’s base case | ||
1. type of evaluation | Cost-utility analysis | Cost-minimization analysis |
2. Programming error |
| Corrected in-text formulas to refer to the appropriate acquisition cost |
Changes to derive the CADTH base case | ||
1. Response rates (transition probabilities) | Based on NMA | All comparators equal to cariprazine |
2. Discontinuation rates | Based on NMA | All comparators equal to cariprazine |
3. Weight gain risk ratio | Based on NMA | All comparators equal to cariprazine |
4. Rates of AEs | Based on NMA | All comparators equal to cariprazine |
5. Inappropriate comparators | Included haloperidol, clonazepam, chlorpromazine | Excluded costs and effectiveness of these comparators |
CADTH base case | NA | Reanalysis 1 + 2 + 3 + 4 + 5 |
AE = adverse event; NA = not applicable; NMA = network meta-analysis.
Table 7: Cost Summary of the CADTH Base Case for Manic or Mixed Episodes — Cost-Minimization Analysis
Parameter | Cariprazine | Quetiapine | Asenapine | Aripiprazole | Paliperidone | Risperidone |
|---|---|---|---|---|---|---|
Discounted costs ($) | ||||||
Total cost | 3,947 | 3,792 | 3,859 | 3,754 | 3,992 | 3,738 |
Drug acquisition | 250 | 96 | 162 | 57 | 295 | 41 |
Subsequent therapy | 63 | 63 | 63 | 63 | 63 | 63 |
Tests and medical visits | 3,503 | 3,503 | 3,503 | 3,503 | 3,503 | 3,503 |
Comorbidity costs | 69 | 69 | 69 | 69 | 69 | 69 |
Adverse events | 61 | 61 | 61 | 61 | 61 | 61 |
Table 8: Cost Summary of the CADTH Base Case for Depressive Episodes — Cost-Minimization Analysis
Parameter | Cariprazine | Quetiapine | Lurasidone |
|---|---|---|---|
Discounted costs ($) | |||
Total cost | 7,935 | 7,395 | 7,935 |
Drug acquisition | 724 | 184 | 724 |
Subsequent therapy | 1,714 | 1,714 | 1,714 |
Tests and medical visits | 3,417 | 3,417 | 3,417 |
Comorbidity costs | 2,060 | 2,060 | 2,060 |
Adverse events | 19 | 19 | 19 |
Table 9: CADTH Price Reduction Analyses on the Cost-Minimization Analysis — 5-Year Horizon
Analysis | Drug acquisition costs ($) for cariprazine | |
|---|---|---|
Price reduction | Manic/mixed episodes vs. risperidone ($41) | Depressive episodes vs. quetiapine ($184) |
No price reduction | 250 | 724 |
10% | 225 | 652 |
20% | 200 | 579 |
30% | 175 | 507 |
40% | 150 | 434 |
50% | 125 | 362 |
60% | 100 | 290 |
70% | 75 | 217 |
75% | 62 | 184 |
80% | 50 | NA |
83% | 41 | NA |
NA = not applicable; vs. = versus.
Issues for Consideration
CADTH notes that in the studies for bipolar mania (study RGH-MD-31, study RGH-MD-32, and study RGH-MD-33), cariprazine could be administered at a daily dose of up to 12 mg, which is higher than the Health Canada indication.1 Though this would be considered off-label use, clinical experts indicated that some patients in clinical practice would receive 12 mg daily, which would further increase costs to the health care system.
Feedback from the drug plans highlighted the long effective half-life of cariprazine, which may require additional monitoring for AEs.
Overall Conclusions
In its review of the sponsor’s NMA, the CADTH clinical review noted that results of the analysis did not suggest a benefit with cariprazine compared to any other first-line comparators in terms of response rate, weight gain, AEs such as EPS and sedation, or all-cause discontinuation in either the manic or mixed setting or depressive setting. In some cases, placebo or comparators demonstrated better effects for outcomes. Thus, there is no evidence to warrant a price premium for cariprazine.
Key limitations were with the sponsor’s approach to its economic model. First, the model structure does not accurately characterize the disease pathway of bipolar I disorder or the expected use of cariprazine in clinical practice. In addition, cariprazine was modelled as monotherapy, though experts noted it may be used in combination with an anticonvulsant or mood stabilizer. The sponsor also included haloperidol, clonazepam, and chlorpromazine, which were determined not to be relevant comparators in any setting.
Based on the results of the NMA, the CADTH base-case reanalysis took the form of a cost-minimization analysis. For the CADTH base case, haloperidol, clonazepam, and chlorpromazine were excluded as subsequent line therapies; as well, CADTH fixed a programming error in the sponsor’s calculation of drug acquisition costs. In the CADTH base case, cariprazine was associated with total costs of $3,947 per patient in the manic or mixed episode phase over 5 years — greater than all comparators except paliperidone ($3,992). In the absence of data to support a price premium, a price reduction of 83% would be required to ensure similar costs with the least costly comparator in this setting, risperidone ($3,738). In the depressive phase, cariprazine was associated with total costs of $7,935 per patient over 5 years compared to the least costly comparator, quetiapine ($7,395). In the absence of data to support a price premium, a price reduction of 75% would be required to ensure costs similar to quetiapine.
Uncertainty remains in the results as the clinical experts asserted that cariprazine would continue to be used as maintenance therapy after the acute symptoms had resolved, and the models considered only a single episode of mania or mixed symptoms or depressive symptoms. A unique benefit of cariprazine in this regard is its long half-life; however, this feature could also require additional monitoring for AEs. In addition, experts noted that the daily dose of cariprazine could be increased to 12 mg in some patients, as was done in the clinical trials. The increased dose, flat pricing and initial dose escalation, and additional monitoring will result in increased costs to the health care system. Additional price reductions may be warranted to ensure cariprazine does not lead to any increased costs. CADTH performed a scenario analysis in which the drug acquisition costs for cariprazine were doubled based on the likelihood of extensive dose titrations described earlier. Results of this analysis suggested a price reduction of 92% would be required to ensure similar costs to risperidone.
References
1.Inc. A. Vraylar product monograph. 2021.
2.Pharmacoeconomic evaluation [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: VRAYLARTM (Cariprazine) (as hydrochloride) capsules, 1.5 mg, 3 mg, 4.5 mg and 6 mg cariprazine, oral. Markham (ON): Allergan Inc.; 2022 Jan 28.
3.BresMed. 3524: indirect treatment comparisons of cariprazine for the treatment of bipolar I disorder: network meta-analysis report. 2022.
4.Lachaine J, Beauchemin C, Mathurin K. Cost-effectiveness of asenapine in the treatment of bipolar disorder in Canada. BMC Psychiatry. 2014;14. PubMed
5.Revicki D, Hanlon J, Martin S, et al. Patient-based utilities for bipolar disorder-related health states. 87. 2005(2-3):203-210.
6.Schedule of benefits for laboratory services: effective July 1, 2020. Toronto (ON): Ontario Ministry of Health; 2020: https://www.health.gov.on.ca/en/pro/programs/ohip/sob/lab/lab_mn2020.pdf. Accessed 1800 Jan 1.
7.Schedule of benefits for physician services under the Health Insurance Act: effective October 1, 2021. Toronto (ON): Ontario Ministry of Health; 2021: https://www.health.gov.on.ca/en/pro/programs/ohip/sob/physserv/sob_master.pdf. Accessed 1800 Jan 1.
8.Ontario Ministry of H, Ontario Ministry of Long-Term C. Ontario drug benefit formulary/comparative drug index. 2021; https://www.formulary.health.gov.on.ca/formulary/. Accessed March 15, 2022.
9.Inc. OC. Saphris asenapine sublingual tablets product monograph. 2021; https://pdf.hres.ca/dpd_pm/00060860.PDF. Accessed March 14, 2022.
10.Inc. AP. AG-Quetiapine Product Monograph. 2020; https://pdf.hres.ca/dpd_pm/00056588.PDF. Accessed March 14, 2022.
11.Inc. MP. Ipg-risperidone product monograph. 2022; https://pdf.hres.ca/dpd_pm/00065018.PDF. Accessed March 15, 2022.
12.Inc. A. Apo-Lithium Carbonate product monograph. 2013; https://pdf.hres.ca/dpd_pm/00023004.PDF. Accessed March 15, 2022.
13.Inc. A. Apo-divalproex product monograph. 2021; https://pdf.hres.ca/dpd_pm/00064132.PDF. Accessed March 15, 2022.
14.Inc. AP. Ziprasidone capsules. 2019; https://pdf.hres.ca/dpd_pm/00053524.PDF. Accessed March 23, 2022.
15.Inc A. Carbamazepine Product Monograph. 2018; https://pdf.hres.ca/dpd_pm/00047110.PDF. Accessed March 23, 2022.
16.Limited TC. Chlorpromazine product monograph. 2012; https://pdf.hres.ca/dpd_pm/00018580.PDF. Accessed March 23, 2022.
17.Inc. A. Clonazepam product monograph. 2021; https://pdf.hres.ca/dpd_pm/00061752.PDF. Accessed March 23, 2022.
18.Findling R, Nyilas M, Forbes R. Acute treatment of pediatric bipolar i disorder, manic or mixed episode, with aripiprazole: a randomized, double-blind, placebo-controlled study. J Clin Psychiatry. 2009;70:1441-1451. PubMed
19.Yatham L, Kennedy S, Parikh S, et al. Canadian Network for Mood and Anxiety Treatments (CANMAT) and International Society for Bipolar Disorders (ISBD) 2018 guidelines for the management of patients with bipolar disorder. Bipolar Disorders. 2018;20:97-170. PubMed
20.Inc. MP. Mar-Paliperidone Product Monograph. 2021; https://pdf.hres.ca/dpd_pm/00061732.PDF. Accessed March 14, 2022.
21.Inc. SPC. Latuda lurasidone hydrochloride. 2020; https://pdf.hres.ca/dpd_pm/00055478.PDF. Accessed March 15, 2022.
22.Statistics Canada. Table 17-10-0057-01 Projected population, by projection scenario, age and sex, as of July 1 (x 1,000). 2022; https://www150.statcan.gc.ca/t1/tbl1/en/tv.action?pid=1710005701. Accessed April 21, 2022.
23.McDonald K, Bulloch A, Duffy A, et al. Prevalence of Bipolar I and II Disorder in Canada. Can J Psychiatry. 2015;60(3):151-156. PubMed
24.Care CAfSH. Understanding the Gap: a pan-canadian analysis of prescription drug insurance coverage. 2017; http://innovativemedicines.ca/wp-content/uploads/2017/12/20170712-understanding-the-gap.pdf. Accessed April 21, 2022.
25.Dinh T. Understanding the Gap. Paper presented at: The Conference Board of Canada 2018.
Appendix 1: Cost Comparison Table
Note that this appendix has not been copy-edited.
The comparators presented in the following table have been deemed to be appropriate based on feedback from clinical experts. Comparators may be recommended (appropriate) practice or actual practice. Existing Product Listing Agreements are not reflected in the table and as such, the table may not represent the actual costs to public drug plans.
Table 10: CADTH Cost Comparison Table for Manic or Mixed Episodes Associated With Bipolar Disorder
Treatment | Strength / concentration | Form | Price | Recommended dosagea | Daily cost | 28-day cost | Annual cost |
|---|---|---|---|---|---|---|---|
Cariprazine | 1.5 mg 3.0 mg 4.5 mg 6.0 mg | Capsule | $4.9000b | 1.5 mg to 6 mg daily | $4.90 | $137 | $1,790 |
First-line treatment | |||||||
Aripiprazole | 2 mg 5 mg 10 mg 15 mg 20 mg 30 mg | Tablet | $0.8092 $0.9046 $1.0754 $1.2692 $1.0017 $1.0017 | 10 mg to 30 mg dailyc | $1.00 to $1.27 | $28 to $36 | $366 to $464 |
Asenapine | 5 mg 10 mg | Tablet | $1.5910 $1.5910 | 5 mg to 10 mg twice daily | $3.18 | $89 | $1,162 |
Divalproex | 125 mg 250 mg 500 mg | Tablet Tablet Tablet | $0.1539 $0.2767 $0.5537 | 250 mg 3 times daily | $0.83 | $23 | $303 |
Lithium | 150 mg 300 mg | Capsule Capsule | $0.0667 $0.0657 | 900 mg to 1,800 mg daily | $0.20 to $0.39 | $6 to $11 | $72 to $144 |
Paliperidone | 3 mg 6 mg 9 mg | ER Tablet | $3.9820 $5.9560 $7.9390 | 6 mg dailyd | $5.96 | $167 | $2,175 |
Quetiapine | 50 mg 150 mg 200 mg 300 mg 400 mg 25 mg 100 mg 200 mg 300 mg | ER Tablet ER Tablet ER Tablet ER Tablet ER Tablet Tablet Tablet Tablet Tablet | $0.2501 $0.4926 $0.6661 $0.9776 $1.3270 $0.0494 $0.1318 $0.2647 $0.3863 | 400 mg to 800 mg daily | $0.53 to $2.65 | $15 to $74 | $193 to $969 |
Risperidone | 0.25 mg 0.5 mg 1 mg 2 mg 3 mg 4 mg | Tablet Tablet Tablet Tablet Tablet Tablet | $0.1036 $0.1735 $0.2397 $0.4795 $0.7180 $0.9574 | 1 mg to 4 mg daily | $0.24 to $0.96 | $7 to $27 | $88 to $350 |
Second-line treatment | |||||||
Carbamazepine | 200 mg | Tablet | $0.1540 | 400 mg to 1,200 mg daily | $0.31 to $0.92 | $9 to $26 | $112 to $337 |
Olanzapine | 2.5 mg 5 mg 7.5 mg 10 mg 15 mg | Tablet Tablet Tablet Tablet Tablet | $0.1772 $0.3544 $0.5316 $0.7088 $1.0631 | 5 mg to 20 mg daily | $0.35 to $1.42 | $10 to $40 | $129 to $518 |
Ziprasidone | 20 mg 40 mg 60 mg 80 mg | Capsule Capsule Capsule Capsule | $1.3784 $1.5786 $1.5786 $1.5786 | 40 mg to 80 mg twice daily | $1.58 | $88 | $1,153 |
Third-line treatment | |||||||
Chlorpromazine | 25 mg 50 mg 100 mg | Tablets | $0.2454 $0.2808 $0.7475 | 150 mg daily | $1.03 | $29 | $376 |
Clonazepam | 0.5 mg 2 mg | Tablets | $0.0418 $0.0721 | 8 mg to 10 mg daily | $0.29 to $0.36 | $8 to $10 | $105 to $132 |
ER = extended release.
Note: All prices are from the Ontario Drug Benefit Formulary (accessed March 2022),8 unless otherwise indicated, and do not include dispensing fees. Annual costs are based on 365.25 days per year.
aUnless otherwise indicated, recommended doses are from the respective product monographs.9-17
bSponsor-submitted price.2
cDose from published clinical trial, Findling et al. 2009,18 referenced in the CANMAT and ISBD guidelines.19
dDose for schizophrenia, aligns with CANMAT and ISBD guidelines.19,20
Table 11: CADTH Cost Comparison Table for Depressive Episodes Associated With Bipolar Disorder
Treatment | Strength/ | Form | Price | Recommended dosagea | Daily cost | 28-day cost | Annual cost |
|---|---|---|---|---|---|---|---|
Cariprazine | 1.5 mg 3.0 mg 4.5 mg 6.0 mg | Capsule | $4.9000b | 1.5 mg to 3 mg daily | $4.90 | $137 | $1,790 |
First-line treatment | |||||||
Lamotrigine | 25 mg 100 mg 150 mg | Tablet | $0.0698 $0.2787 $0.4107 | 50 to 100 mg twice daily | $0.28 to $0.56 | $8 to $16 | $102 to $204 |
Lithium | 150 mg 300 mg | Capsule Capsule | $0.0667 $0.0657 | 900 mg to 1,800 mg daily | $0.20 to $0.39 | $6 to $11 | $72 to $144 |
Lurasidone | 20 mg 40 mg 60 mg 80 mg 120 mg | Tablet Tablet Tablet Tablet Tablet | $4.9000 | 20 mg to 60 mg daily | $4.90 | $137 | $1,790 |
Quetiapine | 50 mg 150 mg 200 mg 300 mg 400 mg 25 mg 100 mg 200 mg 300 mg | ER Tablet ER Tablet ER Tablet ER Tablet ER Tablet Tablet Tablet Tablet Tablet | $0.2501 $0.4926 $0.6661 $0.9776 $1.3270 $0.0494 $0.1318 $0.2647 $0.3863 | 300 mg daily | $0.39 | $11 | $141 |
Second-line treatment | |||||||
Olanzapine | 2.5 mg 5 mg 7.5 mg 10 mg 15 mg | Tablet Tablet Tablet Tablet Tablet | $0.1772 $0.3544 $0.5316 $0.7088 $1.0631 | 5 mg to 20 mg daily | $0.35 to $1.42 | $10 to $40 | $129 to $518 |
Third-line treatment | |||||||
Divalproex | 125 mg 250 mg 500 mg | Tablet Tablet Tablet | $0.1539 $0.2767 $0.5537 | 250 mg 3 times daily | $0.83 | $23 | $303 |
ER = extended release.
Note: All prices are from the Ontario Drug Benefit Formulary (accessed March 2022),8 unless otherwise indicated, and do not include dispensing fees. Annual costs are based on 365.25 days per year.
aUnless otherwise indicated, recommended doses are from the respective product monographs.10,13,21
bSponsor-submitted price.2
Appendix 2: Submission Quality
Note that this appendix has not been copy-edited.
Description | Yes/no | Comments |
|---|---|---|
Population is relevant, with no critical intervention missing, and no relevant outcome missing | Yes | No comment. |
Model has been adequately programmed and has sufficient face validity | No | CADTH identified errors regarding the calculation of drug acquisition costs for various comparators. |
Model structure is adequate for decision problem | No | The sponsor’s models only considered a single episode of bipolar disorder, either manic/mixed or depressive. This does not reflect the anticipated use of cariprazine in clinical practice. Clinical experts indicated that cariprazine would certainly be used in maintenance therapy. |
Data incorporation into the model has been done adequately (e.g., parameters for probabilistic analysis) | Yes | No comment. |
Parameter and structural uncertainty were adequately assessed; analyses were adequate to inform the decision problem | No | Given the results of the NMA suggesting no difference between cariprazine and other comparators, a cost-minimization analysis would have been more appropriate. |
The submission was well organized and complete; the information was easy to locate (clear and transparent reporting; technical documentation available in enough details) | No | Details regarding the calculation of transition probabilities and discontinuation rates from the NMA were lacking. Little to no information on the methodology used to calculate comparator drug costs using a weighted average. Technical report contained grammatical errors and references were missing. |
NMA = network meta-analysis.
Appendix 3: Additional Information on the Submitted Economic Evaluation
Note that this appendix has not been copy-edited.
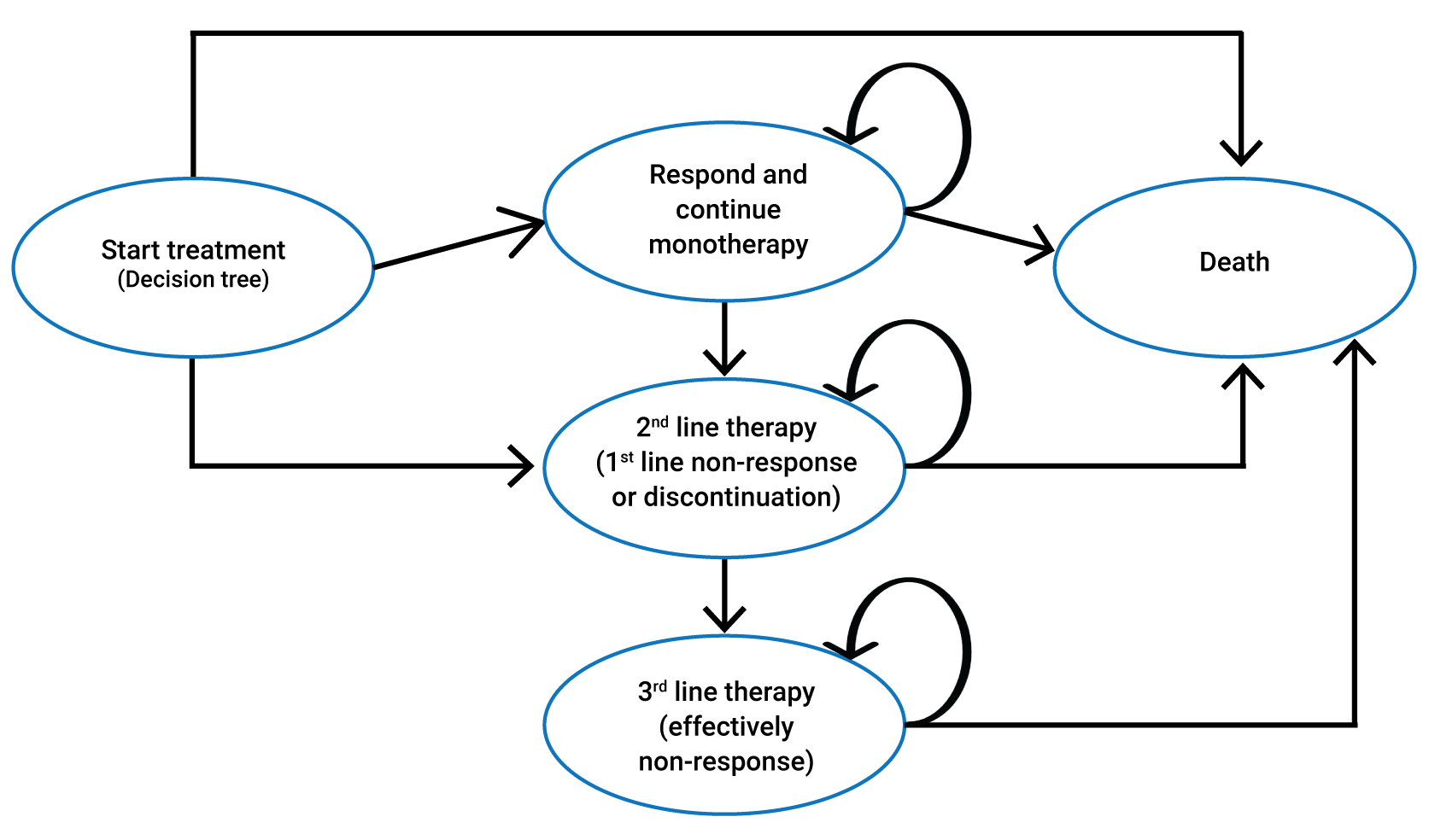
Detailed Results of the Sponsor’s Base Case
Table 13: Disaggregated Results of the Sponsor’s Base Case — Manic or Mixed
Parameter | Cariprazine | Quetiapine | Asenapine | Aripiprazole | Paliperidone | Risperidone |
|---|---|---|---|---|---|---|
Discounted LYs | ||||||
Total | 4.83 | 4.83 | 4.83 | 4.83 | 4.83 | 4.83 |
Respond and continue | 0.07 | 0.05 | 0.04 | 0.07 | 0.05 | 0.08 |
Second-line | 0.08 | 0.08 | 0.08 | 0.08 | 0.08 | 0.09 |
Third-line | 4.68 | 4.69 | 4.71 | 4.68 | 4.70 | 4.66 |
Discounted QALYs | ||||||
Total | 2.69 | 2.69 | 2.68 | 2.69 | 2.69 | 2.69 |
Respond and continue | 0.05 | 0.04 | 0.03 | 0.05 | 0.04 | 0.06 |
Second-line | 0.07 | 0.07 | 0.06 | 0.07 | 0.06 | 0.07 |
Third-line | 2.57 | 2.58 | 2.59 | 2.57 | 2.59 | 2.56 |
Discounted costs ($) | ||||||
Total | 4,985 | 4,806 | 4,868 | 4,739 | 4,969 | 5,024 |
Drug acquisition | 235 | 82 | 123 | 16 | 242 | 301 |
Subsequent therapy | 1,114 | 1,118 | 1,123 | 1,113 | 1,120 | 1,110 |
Tests and medical visits | 3,507 | 3,507 | 3,508 | 3,507 | 3,508 | 3,506 |
Comorbidity costs | 68 | 69 | 69 | 68 | 69 | 69 |
Adverse events | 61 | 30 | 45 | 35 | 32 | 38 |
LY = life-year; QALY = quality-adjusted life-year.
Table 14: Probabilistic Cost-Effectiveness Sequential Analysis From Sponsor’s Base Case — Manic or Mixed
Treatment | Cost | QALYs | ICER ($/QALY) |
|---|---|---|---|
Aripiprazole | $4,738.70 | 2.6900 | Reference |
Quetiapine | $4,805.87 | 2.6857 | Dominated by aripiprazole |
Asenapine | $4,867.88 | 2.6800 | Dominated by aripiprazole |
Paliperidone | $4,969.30 | 2.6865 | Dominated by aripiprazole |
Cariprazine | $4,984.84 | 2.6883 | Dominated by aripiprazole |
Risperidone | $5,024.31 | 2.6935 | $79,887 vs. aripiprazole |
ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year; vs. = versus.
Table 15: Disaggregated Results of the Sponsor’s Base Case — Depressive
Parameter | Cariprazine | Quetiapine | Lurasidone |
|---|---|---|---|
Discounted LYs | |||
Total | 4.75 | 4.75 | 4.75 |
Respond and continue | 0.28 | 0.32 | 0.42 |
Second-line | 0.25 | 0.26 | 0.27 |
Third-line | 4.22 | 4.18 | 4.07 |
Discounted QALYs | |||
Total | 2.80 | 2.81 | 2.83 |
Respond and continue | 0.23 | 0.26 | 0.34 |
Second-line | 0.20 | 0.20 | 0.21 |
Third-line | 2.40 | 2.38 | 2.32 |
Discounted costs ($) | |||
Total | 7,922 | 7,422 | 8,032 |
Drug acquisition | 728 | 199 | 945 |
Subsequent therapy | 1,713 | 1,697 | 1,651 |
Tests and medical visits | 3,412 | 3,411 | 3,409 |
Comorbidity costs | 2,051 | 2,074 | 2,000 |
Adverse events | 19 | 40 | 28 |
LY = life-year; QALY = quality-adjusted life-year.
Table 16: Probabilistic Cost-Effectiveness Sequential Analysis From Sponsor’s Base Case — Depressive
Treatment | Cost | QALYs | ICER ($/QALY) |
|---|---|---|---|
Quetiapine | $7,421.76 | 2.81 | Reference |
Cariprazine | $7,921.93 | 2.80 | Dominated by quetiapine |
Lurasidone | $8,032.32 | 2.83 | $21,672 vs. quetiapine |
ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year; vs. = versus.
Appendix 4: Additional Details on the CADTH Reanalyses and Sensitivity Analyses of the Economic Evaluation
Note that this appendix has not been copy-edited.
Scenario Analyses
CADTH conducted a scenario analysis in which drug acquisition costs for cariprazine were doubled for manic/mixed episodes (Table 17). Clinical experts indicated that extensive dose titration may be required to achieve a stable dose, which would likely result in a higher use of the 1.5 mg tablets. In addition, the experts noted that some patients may continue with a 1.5 mg twice daily dose to manage side effects which would further increase cariprazine costs long term.
Table 17: Scenario Analysis, Manic or Mixed — Doubled Cariprazine Costs
Parameter | Cariprazine | Quetiapine | Asenapine | Aripiprazole | Paliperidone | Risperidone |
|---|---|---|---|---|---|---|
Discounted costs ($) | ||||||
Total cost | 3,947 | 3,792 | 3,859 | 3,754 | 3,992 | 3,738 |
Drug acquisition | 500 | 96 | 162 | 57 | 295 | 41 |
Subsequent therapy | 63 | 63 | 63 | 63 | 63 | 63 |
Test and medical visits | 3,503 | 3,503 | 3,503 | 3,503 | 3,503 | 3,503 |
Comorbidity costs | 69 | 69 | 69 | 69 | 69 | 69 |
Adverse events | 61 | 61 | 61 | 61 | 61 | 61 |
Note: In this scenario, cariprazine would require a 92% price reduction to ensure similar costs to risperidone.
Appendix 5: Submitted Budget Impact Analysis and CADTH Appraisal
Note that this appendix has not been copy-edited.
Table 18: Summary of Key Take-Aways
Key take-aways of the budget impact analysis |
|---|
|
BIA = budget impact analysis.
Summary of Sponsor’s Budget Impact Analysis
The submitted budget impact analysis (BIA) assessed the introduction of cariprazine for the treatment of acute episodes of bipolar disorder. The analysis was taken from the perspective of the Canadian public drug plans using a claims-based approach, with drug acquisition costs included in the base case. A 3-year time horizon was used, from quarter 2 of 2023 to quarter 1 of 2026, with quarter 2 of 2022 as a base year. Approximately 5 years of historical claims data were obtained from the IQVIA Pharmastat database and were used to project claims into the time horizon of the BIA. Claims data from the IQVIA RxDynamics database were used to estimate the proportion of Pharmastat claims that were related to bipolar disorder. These data were used to estimate the number of claims per comparator for each year of the BIA.
The reference case scenario included all comparators used in the pharmacoeconomic analysis along with some additional products. The scenario consisted of aripiprazole, asenapine, divalproex, lamotrigine, lithium, lurasidone, paliperidone, quetiapine, and risperidone. The new drug scenario included cariprazine along with these other comparators.
Table 19: Summary of Key Model Parameters
Parameter | Sponsor’s estimate (Reported as year 1/ year 2/ year 3 if appropriate) |
|---|---|
Target population | |
Total claims for bipolar drugs | 3,253,578 / 3,291,539 / 3,325,556 |
Market uptake (3 years) | |
Uptake (reference scenario) Aripiprazole Asenapine Divalproex Lamotrigine Lithium Lurasidone Paliperidone Quetiapine Risperidone | ||||||%/|||||%/|||||% ||||||%/|||||%/|||||% ||||||%/|||||%/|||||% ||||||%/|||||%/|||||% ||||||%/|||||%/|||||% ||||||%/|||||%/|||||% ||||||%/|||||%/|||||% ||||||%/|||||%/|||||% ||||||%/|||||%/|||||% |
Uptake (new drug scenario) Cariprazine Aripiprazole Asenapine Divalproex Lamotrigine Lithium Lurasidone Paliperidone Quetiapine Risperidone | ||||||%/|||||%/|||||% ||||||%/|||||%/|||||% ||||||%/|||||%/|||||% ||||||%/|||||%/|||||% ||||||%/|||||%/|||||% ||||||%/|||||%/|||||% ||||||%/|||||%/|||||% ||||||%/|||||%/|||||% ||||||%/|||||%/|||||% ||||||%/|||||%/|||||% |
Cost of treatment (per patient) | |
Cost of treatment per day in Ontario Cariprazine Aripiprazole Asenapine Divalproex Lamotrigine Lithium Lurasidone Paliperidone Quetiapine Risperidone | $4.90 $1.13 $3.18 $1.29 $0.56 $0.26 $4.90 $5.96 $0.93 $0.81 |
Note: Drug prices are based on the Ontario Drug Benefit Formulary but may differ by jurisdiction.
Summary of the Sponsor’s Budget Impact Analysis Results
The estimated budget impact of funding cariprazine for the treatment of people with bipolar I disorder was $5,138,234, $16,296,787, and $23,441,313 for years 1 through 3, respectively, for a cumulative incremental impact of $44,876,334 over the 3-year time horizon.
CADTH Appraisal of the Sponsor’s Budget Impact Analysis
CADTH identified several key limitations to the sponsor’s analysis that have notable implications on the results of the BIA:
Use of a claims-based approach to estimate market size introduces uncertainty with the anticipated budget impact of cariprazine. Claims-based BIAs are limited in that claims are not indication-specific, and include all claims for comparator drugs that may be used for other conditions (e.g., depression). The sponsor attempted to account for this by applying indication-specific adjustment factors derived from Ontario data from the IQVIA RxDynamics database. While this approach is more thorough than one in which Pharmastat data alone are used, the derivation of market size using claims data is still associated with uncertainty. For instance, no information or source was provided for the RxDynamics database from which the claims by indication data were derived, making validation difficult. Furthermore, it is unclear whether the claims by indication data for Ontario would be generalizable to the other jurisdictions, as is assumed in the sponsor’s base case. In addition, the sponsor did not convert the claims data into the number of users; instead, the sponsor assumed unit to unit and claim to claim displacement between cariprazine and comparators. This methodology is uncertain given the large number of comparators and various unit sizes available for each product. For transparency and completeness, claims data-based models should provide an estimate of the number of active beneficiaries converted from the number of claims.
In addition, there is uncertainty regarding the duration of treatment given the discrepancy between the Health Canada indication and anticipated use of cariprazine. In the sponsor’s base case, each claim was standardized to ||||||||||||||||||; that is the period for which costs are incurred. This assumption is uncertain, given that cariprazine and other comparators are dispensed in bottles containing 30 capsules, suggesting the duration of claims could be longer.
Given these limitations, CADTH conducted a de novo BIA using an epidemiology-based approach. CADTH maintained the sponsor’s original market shares and daily cost estimates for cariprazine and comparators. This approach assumes all comparators will be used long-term for maintenance therapy and does not impose a maximum length of treatment.
CADTH Calculation of the Budget Impact Analysis
Due to the limitations outlined previously, CADTH conducted a de novo BIA using an epidemiology-based approach, the assumptions for which are outlined in Table 20. These assumptions were derived from published literature and clinical expert opinion. Importantly, the BIA assumed that patients would be treated continuously on these products throughout the time horizon of the BIA, to reflect clinicians’ expectations for maintenance therapy with cariprazine. Market uptake and daily costs for all products were borrowed from the sponsor’s original analysis.
Due to the uncertainty around public coverage rates and the proportion of patients treated pharmacologically, CADTH performed scenario analyses around these values.
Table 20: Summary of Key Model Parameters of the CADTH Budget Impact Analysis
Parameter | CADTH estimate (Reported as year 1/ year 2/ year 3 if appropriate) | Notes/sources |
|---|---|---|
Target population | ||
Canadian population (aged 15 and older) | 25,530,700 / 25,861,100 / 26,189,300 | Statistics Canada, Table 17-10-0057-0122 Population aged 15 and older to align with prevalence estimate from CCHS |
Lifetime prevalence of bipolar I disorder | 0.87% | Data from CCHS 2012 for a population aged 15 and older23 |
Proportion of patients treated pharmacologically | 50% (alternate value tested in scenario analysis) | Clinical expert opinion |
Proportion of patients with public coverage | 70.9% (alternate value tested in scenario analysis) | Proportion of Canadians eligible for coverage based on the Understanding the Gap report and conference proceedings24,25 |
Number of patients eligible for cariprazine | 78,741 / 79,760 / 80,772 | Calculation |
CCHS = Canadian Community Health Survey.
A detailed breakdown of the results from CADTH’s BIA is presented in Table 21. Based on the CADTH BIA, the estimated budget impact of funding cariprazine for the treatment of bipolar I disorder is expected to be $3,270,933 in year 1, $10,386,918 in year 2, and $14,974,693 in year 3, for a 3-year total of $28,632,545.
A scenario analysis was conducted in which the price reduction of 83% recommended from the pharmacoeconomic report for manic/mixed episodes was used. Results of this analysis estimated a 3-year costs savings of $2,108,298 with funding cariprazine.
Table 21: Detailed Breakdown of the CADTH Reanalyses of the Budget Impact Analysis
Stepped analysis | Scenario | Year 1 | Year 2 | Year 3 | 3-year total |
|---|---|---|---|---|---|
Submitted base case | Reference | $45,863,672 | $46,583,317 | $47,228,105 | $139,675,094 |
New drug | $51,001,906 | $62,880,104 | $70,669,418 | $184,551,429 | |
Budget impact | $5,138,234 | $16,296,787 | $23,441,313 | $44,876,334 | |
CADTH epidemiologic BIA | Reference | $28,250,703 | $28,735,854 | $29,207,410 | $86,193,967 |
New drug | $31,521,636 | $39,122,772 | $44,182,104 | $114,826,512 | |
Budget impact | $3,270,933 | $10,386,918 | $14,974,693 | $28,632,545 | |
CADTH scenario analysis 1: 100% public coverage | Reference | $39,845,843 | $40,530,119 | $41,195,219 | $121,571,180 |
New drug | $44,459,289 | $55,180,215 | $62,316,084 | $161,955,588 | |
Budget impact | $4,613,446 | $14,650,096 | $21,120,865 | $40,384,408 | |
CADTH scenario analysis 2: 60% of patients treated pharmacologically | Reference | $33,900,843 | $34,483,025 | $35,048,892 | $103,432,760 |
New drug | $37,825,963 | $46,947,327 | $53,018,525 | $137,791,815 | |
Budget impact | $3,925,120 | $12,464,302 | $17,969,632 | $34,359,054 | |
CADTH scenario analysis 3: 83% price reduction from PE model | Reference | $28,250,703 | $28,735,854 | $29,207,410 | $86,193,967 |
New drug | $28,015,037 | $27,975,280 | $28,095,352 | $84,085,669 | |
Budget impact | –$235,666 | –$760,574 | –$1,112,058 | –$2,108,298 |
BIA = budget impact analysis; PE = pharmacoeconomic.
Stakeholder Input
Patient Input
Institute for Advancements in Mental Health
About the Institute for Advancements in Mental Health
The Institute for Advancements in Mental Health (IAM) is a connector, collaborator, thought leader and solution-driven organization supporting, innovating and driving change for better mental health. IAM innovates in mental health with a focus on returning solutions back to communities, through partnership and collaboration. Historically serving those impacted by psychotic illnesses such as schizophrenia and psychosis, including bipolar disorder, IAM serves anyone impacted by serious mental illness and their families, caregivers/supports and communities. Our direct services include one-to-one and group counselling utilizing cognitive behavioural therapy-based interventions, information and system navigation, training for frontline workers, community education and more.
Website: https://www.iamentalhealth.ca
Information Gathering
This submission is based on our 40-year history of serving adults with schizophrenia and other chronic mental illnesses, their families, service providers and communities. Much of our learning comes directly from our work with clients and the expertise of our frontline staff. We also draw on knowledge gained from a survey of our client network, which was conducted by Ipsos in 2018 as well as a recent survey (February 2022) conducted of both our client network and that of Hope and Me – Mood Disorders Association of Ontario’s – whose network primarily consists of persons with lived experience of bipolar disorder.
As cariprazine is not yet available in the Canadian market, our (recent) survey addresses individuals’ experience with antipsychotics in general.
Our clients are primarily adults from the southern and central regions of Ontario though we do serve a number of clients virtually from northern regions of Ontario. They comprise individuals who experience symptoms of schizophrenia or psychosis (not all of our clients have a formal diagnosis), as well as the family members, friends and community members who interact with those individuals. Our clients also include health service providers and social service providers who work with individuals with psychotic illnesses, including schizophrenia and bipolar disorder though to a lesser extent.
Clients and survey respondents range in age, gender, educational background, income, and employment status.
Within our Ipsos survey, respondents self-described as:
12% “personally diagnosed”
50% “caregiver”
63% “family member/friend of someone diagnosed”
18% “work in social services”
77% of survey respondents were born in Canada with 83% self-describing as “white”. 55% of respondents came from the GTA, while 20% came from southwestern Ontario, 14% came from Eastern Ontario, 5% from Central Ontario and 4% from Northern Ontario. An additional 2% came from outside Ontario.
Within our 2022 CADTH cariprazine survey, respondents identified as:
33% “individual with lived experience (living with symptoms of bipolar disorder)”
58% “relative of someone with lived experience”
0% “friend of someone with lived experience”
8% “caregiver of someone with lived experience”
IAM has received funding from HLS Therapeutics, Inc., Janssen Inc., Otsuka Pharmaceutical Co. Ltd., Sunovion and AbbVie ranging from $5,000.00 to $50,000.00 in the last two years. IAMdeclared no conflict of interest in the preparation of this submission.
Disease Experience
Our patient group includes individuals with schizophrenia and other related illnesses with psychosis as a main feature. Many of our clients experience symptoms of psychosis without having a formal diagnosis. Often, their symptoms have a significant impact on day-to-day functioning. Our client’s experiences vary widely but typically involve some level of cognitive impairment, delusions and hallucinations. The cognitive impairment can range from mild to severe but is typically strongest in the cognitive domains of working and episodic memory, attention, processing speed, problem solving, and social cognition. A large number of clients also experience anosognosia, a lack of insight into their illness, which often impacts their ability and motivation to access treatment and supports. This symptom can cause significant strain in relationships, including those with caregivers, family members, and friends ultimately leading to social isolation and a lack of supports for the individual with the illness.
Experiences with Currently Available Treatments
In our 2018 (Ipsos) study of our network, 55% of respondents were taking long-acting injectable medications or had taken them before, while 98% were taking or had taken oral medications to manage their schizophrenia/psychosis symptoms. The most common side effects they reported were drowsiness (58%), dry mouth (50%), restlessness (50%), dizziness (45%), muscle stiffness (45%), constipation (43%) and anxiety (43%).
In our recent survey of our network: 45% of respondents are taking injectable medications, while 54% are taking oral medications to manage their symptoms of bipolar disorder. 36% of respondents find injectable medication to be the best, while 45% find pill form to be the best.
In our 2018 study, of those taking long-acting injectable medications, the most common stated benefits were convenience and not needing to remember to take it every day. The difficulties were most frequently stated to be pain at the injection site and frequent travel to clinics.
In our 2022 study, 70% of respondents reported the advantage of taking antipsychotic medications is they control symptoms well and they experience fewer episodes of mental illness; 80% reported being able to avoid visits to the hospital. Among the disadvantages of taking antipsychotic medication, 33% stated the need to visit a healthcare professional often for monitoring and that they don’t control their symptoms well and that the medication needs to be taken every day. 44% of respondents stated that after taking antipsychotic medications they were “highly likely” to manage the manic and depressive symptoms of bipolar disorder (e.g., exaggerated self-esteem/feelings of grandeur, decreased need for sleep; depressed mood) with 33% responding they were “very likely” to manage these symptoms.
While in 2018, 63% of our respondents paid for their medications with government insurance, 23% paid out of pocket for their medications. 23% of respondents identified the cost of medications as a significant challenge to access. Other challenges identified included: preferred medication not being covered by public drug programs (20%), and wait times for approvals of certain medications under the Ontario Public Drug Program Special Access Programs and Exceptional Access Programs (13%). 63% of respondents in 2018 agreed that it is difficult to pay for health care bills including medication, visits to specialists, counselling, etc.
In our 2022 study, 44% of respondents believe antipsychotic medication can be improved by increasing its ability to control symptoms and reducing the side effects; 33% said it can be improved by having to visit a doctor or psychiatrist less often and reducing the cost. Finally, 22% said providing a greater range of strengths and dosages, making it easier to access at the pharmacy and having to take it less frequently.
33% of respondents believe that pharmacological treatments are most effective when provided in conjunction with psychosocial ones. However, 57% of respondents find it too difficult to access psychosocial supports (e.g., individual counselling, case management from a community mental health agency, etc.) and 42% said they’re too expensive.
Improved Outcomes
For our patient group, treatment and recovery is a nonlinear, individual process. For many, the process of finding the right medication that allows for the highest level of daily functioning, while managing side effects, is often achieved through a “trial and error” process of trying several different medications and dosages to find what works best. This process can make it difficult for clients to adhere to treatment and is exacerbated by additional challenges such as difficulty accessing psychiatrists, obtaining prescriptions, understanding medication options, cost of medications, and wait times to access medications through public drug programs. When the right combination of therapy and medication is determined, individuals may still experience relapse and may require extensive supports to adhere to the treatment plan. This “trial and error” practice of finding the right medication for each individual would be improved by having quick, simple and affordable access to a wide range of treatments and medications to suit unique needs.
Experience with Drug under Review
We do not have knowledge of our client’s use of cariprazine.
Companion Diagnostic Test
We are unable to provide this information for our patient group.
Anything Else?
The greater the variety and affordability of medications on the market, the more treatment adherence we are likely to see among individuals with bipolar and other psychotic disorders, and by extension, greater levels of recovery. IAM advocates for a wide selection of reimbursable medications in the Canadian marketplace
Conflict of Interest Declaration — Institute for Advancements in Mental Health
Did you receive help from outside your patient group to complete this submission? If yes, please detail the help and who provided it.
Yes. Hope & Me (Mood Disorders Association of Ontario) helped distribute our (2022) survey to its network of persons with lived experience of bipolar disorder. https://mooddisorders.ca/
Did you receive help from outside your patient group to collect or analyze data used in this submission? If yes, please detail the help and who provided it.
This submission is partially informed by data previously gathered by Ipsos for a 2018 survey of our network. The purpose of the survey was to: better understand the perceptions of our organization; assess the familiarity, use and helpfulness of our services; determine what advocacy issues to focus on; and to understand the experience of those personally diagnosed with schizophrenia or psychosis and their caregivers, including their rating of access and wait times for various services or treatments, and the financial burden of living with schizophrenia or psychosis.
List any companies or organizations that have provided your group with financial payment over the past 2 years AND who may have direct or indirect interest in the drug under review.
Table 1: Financial Disclosures for the Institute for Advancements in Mental Health
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
HLS Therapeutics, Inc. | — | X | — | — |
Janssen Inc. | — | — | — | X |
Otsuka Pharmaceutical Co. Ltd. | — | — | — | X |
Sunovian | X | — | — | — |
AbbVie | — | — | X | — |
Mood Disorders Society of Canada
About Mood Disorders Society of Canada
Mood Disorders Society of Canada (MDSC) has evolved to become one of Canada’s best-connected mental health NGOs with a demonstrated track record for forging and maintaining meaningful and sustained partnerships with the public, private and non-profit sectors throughout Canada.
MDSC has grown out of the vision and drive of a number of mental health lived experienced leaders from across Canada who in 1995 saw the need for a broad-based structure to bring consumers of mental health services together and who believe that consumers have a key role to play with regard to education and advocacy at the national level.
It was formally launched and incorporated in 2001 with the overall objective of providing people with mood disorders with a strong, cohesive voice at the national level to improve access to treatment, inform research, and shape program development and government policies with the goal of improving the quality of life for people affected by mood disorders.
The MDSC’s overall objective is to provide people with mood disorders with a strong, cohesive voice at the national level by:
Raising awareness that mood disorders are treatable medical issues and working towards eliminating barriers to full community participation in reducing discrimination and stigma, involving members of the public, government and treatment/service providers.
Building a national clearinghouse of information and resources related to mood disorders.
Advocating for the creation of adequate and accessible stigma-free programs for Canadians living with or suffering from mental illness.
Ensuring that the voices of persons lived or living with mental illness and family members are accurately understood and communicated on issues of national importance by building on existing networks and alliances.
Website: https://mdsc.ca/
Information Gathering
Information used to compile this submission was gathered via the following:
MDSC information represented in this submission was obtained through discussions MDSC conducted directly through individual interviews with four patients who were diagnosed with bipolar disorder (two more than fifteen years ago) and who have extensive experience and knowledge with living with the illness, and journeys with treatments and therapies. We also had interviews with three family members to gain further insight in to the experiences of the person living with bipolar disorder. The summary of patient perspectives submitted here were gathered in January 2021 through semi-structured phone interviews with adults living with bipolar disorder. We also relay the direct experience of a long-term colleague who worked with our organization for 10 years and lives with the illness.
Additional experience and perspectives was garnered through our extensive patient and family member input and comments/ shared experiences through our MDSC online Discussion Forum which is linked through the MDSC website and has included in-depth online discussions.
MDSC has very large number of dedicated followers and our organization has with more than 63,000 social media followers. We have extensive website visitors as well, along with our main mdsc.ca website, our depressionhurts.ca website alone has 500 visitors per day and is extremely active. Our national mental health campaign, Defeat Depression, holds mental health walks from coast to coast with over 10,000 people taking part. We also have a national online discussion support chat line that has over 2,800 discussion threads and over 35,000 posts. The section on bipolar disorder contains 762 topics and over 13,000 posts.
It is through the above context and our 20+ years of ongoing collective efforts representing the lived experiences of the patient community that we bring to this submission. It is the goal of our organization to be their voice in this process.
Disease Experience
The psychosocial impacts on a person with bipolar disorder often has widespread consequences, which can be very serious and devastating to the individual themselves, as well as their families. Every single day we hear from patients or family members who are reaching out, often during times of semi-crisis and stress. When it comes to contacts regarding bipolar disorder, percentage wise, we are looking at a little over half the calls we receive are from concerned and basically burnt out family members who are trying to help their loved ones, but are at a loss of where to turn to next. When you are on the phone with a person who is truly struggling, basically they are trying to make their way through the day, minute by minute, hour through hour. As they are relaying their deepest raw feelings, fears and challenges, you cannot have any doubt in your mind that within these homes, there is no greater priority then trying to help their loved one recover.
Bipolar disorder usually begins in early adulthood, with the average age of onset around 18-24 years, although it can sometimes start in childhood or as late as the 40s or 50s. The younger a person is when they develop bipolar disorder, the more likely it is to have a genetic component. Bipolar disorder affects approximately 2.2% of the adult population some time in their lives. Men and women are equally affected. On average, people with bipolar disorder will see three to four physicians and spend over eight years seeking help before they receive a correct diagnosis. Early diagnosis, proper treatment and finding the right medication are important as they lessen the effects of the disorder on individuals and families.
Stigma is very real and people can delay getting a diagnosis and seeking treatment for bipolar disorder due to a fear of what friends, family and employers might think.
Bipolar disorder is a serious medical condition that involves changes in brain function leading to dramatic mood swings. These mood swings can be so severe that they impair normal functioning at work, at school and in relationships. As detailed within our What is Bipolar Disorder resource guide, Symptoms can include:
Mania: often begins with a sense of heightened energy, creativity and social ease - feelings which can quickly progress to an extreme, continuous elevated mood involving an exaggerated sense of self-esteem, and an expansive or irritable mood. When manic, people become more physically active, talkative and distractible and show a reduced need for sleep. They may not be aware that anything is wrong and may also enjoy the feeling mania brings. Judgment becomes impaired resulting in greater risk-taking behaviour including overspending and sexual activity. In severe cases, the person may also experience psychotic symptoms such as hallucinations (hearing or seeing things that are not there) or delusions (believing things that are not true). A few people have a different experience of mania where, instead of feeling euphoric, they are angry and belligerent.
Hypomania: This is a milder form of mania that has similar but less severe symptoms and causes less impairment. During a hypomanic episode, the person may have an elevated mood, feel better than usual and be more productive. However, hypomania can rarely be maintained and is often followed by an escalation to mania or a crash to depression.
Depression: Depression can take many forms. Unlike normal sadness, depressive symptoms are intense, pervasive, persistent feelings of despair, hopelessness, and frustration. Some people feel angry and irritable or are consumed by feelings of worthlessness or guilt. There is a loss of energy, limited interest in normal activities, changes in weight and difficulties with sleep. Thinking is slowed, concentration impaired and decision-making becomes a challenge. At its extreme, depression can involve hallucinations and delusions. Suicide is a serious risk. Depression can cause considerable interruption in all aspects of life.
We hear from parents who they themselves are becoming ill while caring for a family member with BPD due to the stress and anxiety that they are often faced with on an extended basis. This is affecting many of the family caregivers well-being. We also know that treatments, therapies and wellness maintenance is individualized. What works for one person may not work for the person down the road and vice versa, so new treatment options must be provided.
It is very important to understand the long-term or re-occurring severe impact that takes place when a person goes into mania. One person articulated very succinctly:
“People with bipolar disorder can have a serious problem in controlling their self-confidence. They reach the point where they need to stop being so confident of themselves. They need to stop but they just can't. They become overconfident & cross redlines. They only stop after crashing into something. They only stop after doing something stupid or saying something stupid……something that ruins everything good they did before. Something terrible that makes them lose friends & they suddenly fall from being in the top to being in bottom. Then their hypo mania turns into severe depression….. feeling terrible & guilty, and it might take them weeks before recovering….. and slowly they rise up, gain self confidence & become happy…... and again. they don't stop until they make another stupid mistake & fall in depression again. ..and so on …Being aware of this is good .. but being aware but helpless feels so terrible…”
People who live with bipolar disorder, and their family members (and often their close friends) know what this all about. A person will be doing well, and really living a fairly balanced day-to-day existence. In some cases, the person may begin to feel like they are all better now, and they may think OK, I don’t need my medication anymore. If this happens, or if mania begins to come back to the forefront, they may face a situation where their mania leads them into unwanted feelings and/or behaviours. All the positive steps forward and they have achieved, can feel lost. We have heard from some who detail to us that, after the period of feeling extremes and never ending energy, when something happens that feels like a cement truck just crushes their world, they can end up feeling ashamed or embarrassed. Then this feeling of desperation and “why can I not be normal like everyone else” then takes them the opposite way to feelings of extreme despondence and depression. Controlling this massive swing is so hard, but so important.
Experiences With Currently Available Treatments
In our MDSC national mental health survey conducted in September, 2021, 45% of respondents identified Improving Access to Medications and Treatment as their number1 election issue for the Government of Canada, with 94% of them identifying it as important. It was the number one priority specified by respondents.
In an international survey of Internet-based initiative Understanding needs, interactions, treatment, and expectations among individuals affected by bipolar disorder or schizophrenia: the UNITE global survey (McIntyre RS. Understanding needs, interactions, treatment, and expectations among individuals affected by bipolar disorder or schizophrenia: the UNITE global survey. J Clin Psychiatry. 2009;70 Suppl 3:5-11. doi: 10.4088/JCP.7075su1c.02. PMID: 19570496), which recruited patients and caregivers from 11 countries (Australia, Brazil, France, Greece, Germany, Italy, Spain, South Korea, Sweden, the United States, and the United Kingdom) of 5,074 respondents taking part in the survey from this total sample, 1,155 individuals with schizophrenia and 1,300 with bipolar disorder self-identified. The majority of respondents had been receiving medication for more than 5 years. Weight gain was the most commonly cited adverse event associated with medication use. Moreover, weight gain was identified as a contributing factor to general medical comorbidity and as a detractor to quality of life. Most respondents identified weight gain and general physical health as areas of deficiency in their perceived knowledge and interactions with health care providers. Overall, respondents expressed general dissatisfaction when interacting with mental health care providers.
With the bipolar subgroup, the percentage of patients who had a discussion with their health care providers about the impact of medication on weight gain was 56%, the long-term effect of health risks due to that weight gain was 42%, and the impact of psychiatric medications on general medical conditions was 40%.
A challenge that has been experienced by patients is equitable access. Recently in particular, the pandemic and the economic havoc that has ensued (employment slowdowns, re-structuring, business closures etc.) there are people who are falling between the cracks for coverage. Here are 2 statements from patients.
“Cover the costs of my medications during the pandemic. I was laid off in July but the company I worked for allowed us to prepay for benefits for 3 further months in an agreement with Manulife. I was on the CERB until it ended and then transitioned over to EI. I get the full amount on EI available, but with rent and basic living expenses it leaves very little for anything else. I have only a few weeks left of medication and the costs are very high…... The blue cross plan in Alberta is almost $70 a month in premiums alone.”
“I guess when I was told that things will never be the 'same' going forward, I found it hard to accept. I haven't been 'stable' in over four years and I just think it has to be better than this, especially when my brain is whacked out (either doomed or flying around - sometimes both at the same time). Each time an 'episode' happens, I lose hope. I'm sick of all the different drugs, so many didn't work and others side effects were horrible, even after giving them some time. Sometimes I almost like heading into mania, I feel (albeit false sense) happy, excited, energized, creative, productive. If only it didn't come with being an ***hole, short temper, irritable, edgy, and racing thoughts. Someone I love pointed me to this site/forum to find similar people and how/what they do to not only cope, but make their life better.”
It is important to note the impact depression has on a person with bipolar disorder. Our 2018 MDSC national survey showed 69% of respondents have been dealing with their depression for more than 11 years. With an incredible 49% of the respondents indicated they were not doing well with their symptoms.
Respondents were asked to indicate the frequency with which they experienced nine (9) problems over the last two weeks.
At the time of the survey, feeling tired/having little energy, sleeping problems (either falling/staying asleep or oversleeping), and feeling bad about oneself were problems being experienced by at least one-half of respondents most of the time (i.e., daily or more than half the days), while slightly fewer were bothered to this same frequency due to having little interest/pleasure in doing things, poor appetite/overeating, feeling down/depressed/hopeless and trouble concentrating.
Thoughts of suicide/self-harm and noticeable slowing of movement/speech were notably less common; however, more than one in ten reported experiencing each of these problems most of the time, while a notable minority experienced each of these problems several days during a two-week time period.
Overall, nearly all respondents strongly agree that all Canadians living with depression should be offered free access to innovative medication, while a similar portion offer the same level of agreement that all medications approved as safe and effective treatments for depression should be fully covered by public funding. Levels of agreement for both statements were generally consistent across audience segments. MDSC feels strongly this reflects Canadians views accurately in regards to mediations for depression and or bipolar disorder.
Improved Outcomes
Medication is a foundational necessity in treating bipolar disorder. It is a recurrent illness, often requiring long-term treatment. Many people will need a number of medications to manage their symptoms and maintain wellness. Finding the right combination of these treatments will rely on monitoring and discussion with their doctor or psychiatrist. While frustrating, the reality is that it can take long periods of experimentation to get the most effective treatment(s).
This is why it is crucial to increase patient access to and choice of medications. What has been very apparent is that medications affect one person differently then how it may affect the next. That is why often, it takes a period of time, and trying different treatments for the patient to find the treatment that works for them. They need to be able to see what they can mange and which side effects they are best able to accept. The goal being to take the treatments that help them live manageable lives with Bipolar Disorder, and not get exposed to additional side effects that may cause other issues for them to then need to cope with.
MDSC is familiar with private health care coverage for mental illness medications, we are aware some private plans cover new treatments – it is our position that this coverage leads to quicker recovery and wellness maintenance for the patient. This of course leads to other significant benefits, such as quicker return to work for the patient (a great benefit to the employer), lower negative long-term impact on the families of the patient.
The most significant challenge to accessing this treatment is that unless a person has, through their employer, a quality drug plan, they will not have access to the new treatments that could work best for them. This barrier to equal access is detrimental to the wellbeing of Canadians.
Patients, families and caregivers believe strongly that access to treatment should not be limited to those only with private drug plan coverage, while those who work for employers who do not have drug coverage do not get access to the best medication for their individual illness. Our position is that accessing the best medications to treat mental illness should be fully equitable for all those who suffer. With one in five people suffering from a mental illness, patients need choice. Choice offers hope.
When you speak with a person who has bipolar disorder, and you go into details of how it has been like for them to struggle through trying to find the right combinations of psychotherapies and medications to enable them to mitigate the onset of mania or depression, and when I come how to lessen the symptoms and negative affects, it is nothing short of incredible how serious this illness is. Then look at the broader impact of this illness, how it has laid havoc into the lives of family members and caregivers. There is no real comparison when we ask ourselves how important is it for these people to have a treatment that helps them. What would then trade off, or what would they give for help? Pretty well everything, it is simply that devastating on the families. If by approving access to this medication we can help some people impacted by bipolar, why would we not? Obviously there are many people who have not found the medication that works for them. If they had, we wouldn’t be getting the number of calls for help that we are.
According to Depression and Bipolar Alliance (DBSA) in the U.S, the organization features resources and aid, including more than 600 peer-led support groups. As reported in the BD International Journal of Psychiatry and Neurosciences, in their Patient Perspectives on the Diagnosis, Treatment, and Management of Bipolar Disorder (https://onlinelibrary.wiley.com/doi/10.1111/j.1399-5618.2005.00192.x#:~:text=Patient%20perspectives%20on%20the%20diagnosis%2C%20treatment%2C%20and%20management%20of%20bipolar%20disorder) DBSA A US-based consensus panel categorized unmet needs according to their relevance to patients, providers, or health systems to ensure a balanced view of unmet needs were presented. They found patients need medications that are quicker acting, have less troublesome side-effects, are more effective, and are significantly less expensive, and they need access to medications most likely to help them by not being at the mercy of restricted formularies. Patients gave a high priority to making treatment decisions jointly with their physicians and being partners in their wellness plan. Peer support can also be extremely helpful to people who have bipolar disorder.
Experience With Drug Under Review
In a phase 3 study conducted from March 2016 to July 2017: Cariprazine Treatment of Bipolar Depression: A Randomized Double-Blind Placebo-Controlled Phase 3 Study (Earley W, Burgess MV, Rekeda L, Dickinson R, Szatmári B, Németh G, McIntyre RS, Sachs GS, Yatham LN. Cariprazine Treatment of Bipolar Depression: A Randomized Double-Blind Placebo-Controlled Phase 3 Study. Am J Psychiatry. 2019 Jun 1;176(6):439-448. doi: 10.1176/appi.ajp.2018.18070824. Epub 2019 Mar 8. PMID: 30845817), participants were screened and recruited from 41 study centers in the United States and 31 centers in Europe. The study was approved by institutional review boards for U.S. sites or ethics committees and government agencies for European sites.
In a double-blind placebo-controlled study, adult participants (18-65 years old) who met DSM-5 criteria for bipolar I disorder and a current depressive episode were randomly assigned to receive placebo (N=158) or cariprazine at 1.5 mg/day (N=157) or 3.0 mg/day (N=165). The primary and secondary efficacy parameters were changes from baseline to week 6 in Montgomery-Åsberg Depression Rating Scale (MADRS) score and Clinical Global Impressions severity (CGI-S) score, respectively.
Both dosages of cariprazine were significantly more effective than placebo in improving depressive symptoms (reducing MADRS total score); the least squares mean differences were -2.5 (95% CI=-4.6, -0.4) for cariprazine at 1.5 mg/day and -3.0 (95% CI=-5.1, -0.9) for cariprazine at 3.0 mg/day. Both cariprazine dosages were associated with lower CGI-S scores compared with placebo, but the differences did not reach statistical significance after adjustment for multiplicity (least squares mean difference, -0.2 [95% CI=-0.5, 0.0] for the 1.5 mg/day group and -0.3 [95% CI=-0.5, 0.0] for the 3.0 mg/day group).
Results show Cariprazine, at both 1.5 mg/day and 3.0 mg/day, was effective, generally well tolerated, and relatively safe in reducing depressive symptoms in adults with bipolar I depression.
In a February 2020 research review, Cariprazine as a treatment across the bipolar I spectrum from depression to mania: mechanism of action and review of clinical data (Stahl, Stephen & Laredo, Sarah & Morrissette, Debbi. (2020). Cariprazine as a treatment across the bipolar I spectrum from depression to mania: mechanism of action and review of clinical data. Therapeutic Advances in Psychopharmacology. 10. 204512532090575. 10.1177/2045125320905752), which included looking at the efficacy and safety data of cariprazine in bipolar I disorder. Cariprazine was approved by the United States Food and Drug Administration (FDA) for the acute treatment of schizophrenia (1.5–6 mg/day) and acute mania/mixed mania in BPI disorder (3–6 mg/day) in September 2015.
The review articulated on several short-term (3 week) double-blind, placebo-controlled, randomized phase II/III clinical trials which investigated cariprazine at doses of 3–12 mg/day for the treatment of acute mania or DSM-IV mixed episodes in the context of BPI (i.e. meeting full diagnostic criteria for both a manic and a depressed episode) All of these trials showed that change from baseline to week 3 on the Young Mania Rating Scale (YMRS) was significantly greater in cariprazine-treated patients compared with placebo-treated patients. Additionally, a greater percentage of cariprazine-treated individuals met response (⩾50% improvement on YMRS score from baseline) and remission (YMRS score ⩽12) criteria at the end of 3 weeks compared with placebo-treated individuals. Furthermore, a 16-week, open label trial of cariprazine for BPI mania or DSM IV mixed episodes showed that cariprazine efficacy was extended over the longer-term. Since there was no greater efficacy in the high dose groups (6–12 mg/day), but greater side effects, cariprazine was approved for the treatment of bipolar mania at doses from 3 to 6 mg/day.
The review summarized that with cariprazine now approved across the bipolar I mood spectrum, from mania with or without depressive symptoms to depression with or without manic symptoms. The entry of this new agent into the therapeutic armamentarium for treating bipolar disorder validates the clinical utility of the newer concept of bipolar disorder as a spectrum of disorders rather than discrete disorders at each end of the spectrum, and also demonstrates the wisdom of naming psychotropic drugs such as cariprazine for their pharmacologic actions, and not for one of their clinical indications.
Companion Diagnostic Test
Not applicable.
Anything Else?
It takes years for the patient (as well as their families and carers) to go through many experiences to fully understand this complex mental illness, and the challenges in researching and trying various treatments and therapies on their way through, places such an incredible burden and on the health and wellbeing of full family unit, that it often leads to significant negative impacts within their lives. Bipolar disorder very rarely only affects the patient. It hits the full family. The right medication for maintenance is so very important for people with bipolar disorder. We must make sure new medications are made available. We also need to recognize that people may take their medications in an inconsistent manner. If they do not have access, if their medications are not covered, or if they discontinue medication once they are feeling better, it very well can lead to triggering a relapse. It is a hard fact, but there is no cure for bipolar. However, people with bipolar disorder can recover and do lead productive lives. A critical ingredient in their well-being is managing their medication effectively for the long-term. Recovery is not always tied to a full cure, it’s about living a meaningful, healthy and hearty life - despite the challenges of living with a mental illness.
Conflict of Interest Declaration — Mood Disorders Society of Canada
To maintain the objectivity and credibility of the CADTH reimbursement review process, all participants in the drug review processes must disclose any real, potential, or perceived conflicts of interest. This Patient Group Conflict of Interest Declaration is required for participation. Declarations made do not negate or preclude the use of the patient group input. CADTH may contact your group with further questions, as needed.
Did you receive help from outside your patient group to complete this submission? If yes, please detail the help and who provided it.
No.
Did you receive help from outside your patient group to collect or analyze data used in this submission? If yes, please detail the help and who provided it.
No.
List any companies or organizations that have provided your group with financial payment over the past 2 years AND who may have direct or indirect interest in the drug under review.
Table 2: Financial Disclosures for Mood Disorders Society of Canada
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
Janssen Inc | — | — | — | X |
Pfizer Canada | — | — | — | X |
Lundbeck Canada | — | — | — | X |
Abbvie Inc | — | — | X | — |
Eisai | — | — | X | — |
Clinician Input
Canadian Network for Mood and Anxiety Treatments
About the Canadian Network for Mood and Anxiety Treatments
Canadian Network for Mood and Anxiety Treatments (CANMAT) is a network of academic and clinical experts dedicated to improving clinical care for people with mood and anxiety disorders, with over 25 years of existence. We provide up-to-date scientific information, treatment guidelines and educational activities for health professionals, and clear and useful information about symptoms and treatments for patients and families. Specific to the area of Bipolar Disorder, CANMAT has been at the forefront of producing the most widely cited treatment guidelines in the world, and is the leading national group involved in the production and dissemination of clinical research in bipolar disorder.
Webiste: https://www.canmat.org/
Information Gathering
CANMAT represents many of top clinical, research, and educational experts in bipolar disorder across the country, and we are aware of the most up to date literature on current and new treatments, and we have clinical experience in use of all the currently available treatments.
Current Treatments
Bipolar Disorder is a lifetime recurrent condition characterized by manic and depressive episodes. It is the 4th leading cause of disability in young adults and is often associated with a high risk of suicide. Bipolar depression presents particular challenges, as use of conventional unimodal antidepressants usually worsens the course of the disorder and can induce a switch to a manic episode.
While several treatments are available for treating manic episodes, only lurasidone and quetiapine are approved by health Canada for treating depression in bipolar disorder. Of these two, only quetiapine is effective in treating both manic and depressive episodes that are inherent part of bipolar disorder. Thus, more treatments that are effective for treating both phases of the illness are urgently needed for use in clinical practice.
Psychosocial treatments are primarily used as adjunct to pharmacotherapy in reducing the risk of recurrence of mood episodes in bipolar disorder.
There are no other treatments that are available through special access for bipolar disorder.
Treatment Goals
The main goals of treatment of bipolar disorder include achieving symptomatic remission from manic and depressive episodes and preventing recurrence of mood episodes without causing any significant adverse event burden. Ultimately, improvement in functioning, cognition, quality of life, and reduced mortality are the goals of treatment.
Treatment Gaps (Unmet Needs)
Considering the treatment goals, please describe goals (needs) that are not being met by currently available treatments.
While remission from mania is possible with current treatments, symptomatic remission from depression is often challenging as many patients do not respond to or tolerate quetiapine or lurasidone. Further, while quetiapine has been shown to reduce recurrence of mood episodes, treatment adherence is poor given its significant adverse event burden. The efficacy of lurasidone in preventing mood episodes has not been demonstrated. There have not been any treatments that have been demonstrated yet in randomized controlled trials to show significant benefit in improving functioning, quality of life or cognitive functioning as primary outcome measures.
Which patients have the greatest unmet need for an intervention such as the drug under review?
Nearly all patients with bipolar disorder experience depressive episodes, which contribute to the greatest disease burden. Given this and given that only quetiapine has shown efficacy in treating depression in addition to mania, other treatments such as cariprazine which are effective in treating depression in addition to mania are urgently needed for all bipolar patients.
Place in Therapy
How would the drug under review fit into the current treatment paradigm?
This is the first treatment that targets both D3 and D2 receptors with a preferential affinity to D3 receptors. The medication can be used as a monotherapy to treat both mania and depression as it has demonstrated efficacy for both phases of the disorder. Given its benign profile related to metabolic issues, it will be used as a first line treatment for both mania and depression. This medication has shown efficacy for both treating mania and depression, and hence, it will likely be used more commonly as monotherapy, although combination with mood stabilizers may be an option in some cases.
Please indicate whether or not it would be appropriate to recommend that patients try other treatments before initiating treatment with the drug under review. Please provide a rationale from your perspective.
Given that it has a significantly better adverse event profile compared with quetiapine, there is no scientific or clinical rationale for trying quetiapine first before cariprazine.
How would this drug affect the sequencing of therapies for the target condition?
If cariprazine is effective, it will be used as a monotherapy in many situations. If cariprazine is partially effective, mood stabilizers such as lithium or valproate may be added. If it is ineffective, other atypical antipsychotics or mood stabilizers could be tried for treating and preventing mania while for depression, quetiapine or lurasidone could be considered.
Which patients would be best suited for treatment with the drug under review?
The drug appears to have a broader spectrum of efficacy based on post-hoc analyses of pivotal trials and given that it has a better adverse event profile, should be available as first option for all patients with bipolar disorder.
How would patients best suited for treatment with the drug under review be identified?
It is appropriate for all patients with bipolar disorder as it has a broader spectrum of efficacy as stated above.
Which patients would be least suitable for treatment with the drug under review?
It can cause extrapyramidal symptoms particularly at higher doses; hence, those with a history of such adverse events to other psychotropic medications are least suitable.
Is it possible to identify those patients who are most likely to exhibit a response to treatment with the drug under review?
There do not appear to be any specific predictors of response as it has efficacy across the spectrum.
What outcomes are used to determine whether a patient is responding to treatment in clinical practice?
Most clinicians use their clinical judgement after a thorough assessment of symptoms while others use rating scales such as the Young Mania Rating Scale or Montgomery-Asberg Depression Rating Scale to assess improvement and complement their evaluation. These are also the standard scales used in the research studies on Cariprazine.
What would be considered a clinically meaningful response to treatment?
In clinical research, > 50% reduction in severity of symptoms is considered a good response, while in clinical practice, clinicians assess symptoms of depression and mania and determine if there has been a resolution or reduction in severity of symptoms.
How often should treatment response be assessed?
Assessment of treatment depends on the severity of symptoms. If symptoms are severe, more frequent assessment may be required such as daily or every other day in hospitalized patients. In out-patient settings, assessment once a week or every two weeks would be appropriate.
What factors should be considered when deciding to discontinue treatment?
If a patient is experiencing adverse events that are intolerable, then treatment should be discontinued. Similarly, if there is no improvement in symptoms after a trial of up to 4 weeks, or if there is a recurrence while on medication despite being adherent, might call for discontinuation.
What settings are appropriate for treatment with the drug under review?
In patient, out-patient, office practice as well as specialty clinics.
For non-oncology drugs, is a specialist required to diagnose, treat, and monitor patients who might receive the drug under review?
Psychiatrists are often involved in establishing the diagnosis of bipolar disorder and outlining a management plan. Psychiatrists often work closely with family physicians to implement these plans, and when access to a psychiatrist is not readily available (as is the case in many jurisdictions), family physicians can also take the lead in diagnosing, treating and monitoring patients with bipolar disorder.
Conflict of Interest Declarations — Canadian Network for Mood and Anxiety Treatments
To maintain the objectivity and credibility of the CADTH drug review programs, all participants in the drug review processes must disclose any real, potential, or perceived conflicts of interest. This conflict of interest declaration is required for participation.
Declarations made do not negate or preclude the use of the clinician group input. CADTH may contact your group with further questions, as needed. Please see the Procedures for CADTH Drug Reimbursement Reviews (section 6.3) for further details.
Did you receive help from outside your clinician group to complete this submission? If yes, please detail the help and who provided it.
No outside help was received to complete the submission.
Did you receive help from outside your clinician group to collect or analyze any information used in this submission? If yes, please detail the help and who provided it.
No outside help was received to complete the submission.
List any companies or organizations that have provided your group with financial payment over the past two years AND who may have direct or indirect interest in the drug under review. Please note that this is required for each clinician who contributed to the input — please add more tables as needed (copy and paste). It is preferred for all declarations to be included in a single document.
Declaration for Clinician 1
Name: Roumen Milev
Position: Chair, Canadian Network for Mood and Anxiety Treatment
Date: February 6, 2022
Table 3: Conflict of Interest Declaration for Canadian Network for Mood and Anxiety Treatments — Clinician 1
Company | $0 to $5,000 | $5,001 to $10,000 | $10,001 to $50,000 | In excess of $50,000 |
|---|---|---|---|---|
AbbVie | X | — | — | — |
Allergan Canada | X | — | — | — |
Sunovion Canada | X | — | — | — |
Janssen Canada | X | — | — | — |
Nubiyota | — | — | — | X |
Lallemand Canada | — | — | — | X |
CAN-BIND/OBI | — | — | — | X |
CIHR | — | — | — | X |
Pfizer Canada | X | — | — | — |
Lundbeck Canada | X | — | — | — |
Neonmind | X | — | — | — |
Otsuka Canada | X | — | — | — |
KYE | X | — | — | — |
Western Canadian Clinical Advisory Network
About the Western Canadian Clinical Advisory Network
This clinician group is comprised of a network of senior psychiatrists across Alberta and British Columbia, who are specialists in or have a very strong interest in the treatment of bipolar disorder. The group includes nationally and internationally known mood disorders experts who are extremely active in continuing medical education to public and professional audiences worldwide. There is over 100 years of combined clinical experience among these clinicians and all have significant experience with the evolution, strengths, and weaknesses of treatments in bipolar disorder, as well as a keen awareness of the longstanding gaps in treatment options for our patients.
Clinicians in the group also represent a wide variety of treatment settings, including hospital, inpatient, community mental health clinic and private outpatient settings, as well as shared care with family physicians. Subspecialties including addiction, sleep, women’s health, emerging psychedelic treatments and obesity are also covered by this group. All have academic appointments or university affiliations, and many are heavily involved in research, clinical trials, and national guideline development in bipolar disorder.
Information Gathering
The information gathered for this submission was compiled from a combination of clinical experience and a review of the pertinent research data on bipolar illness. This includes current treatments as well as a review of data on cariprazine data.
Please note that there are three separate document files with this submission:
The clinician input template
References
Financial disclosures
Current Treatments
The current treatment paradigm for bipolar disorder is centered around 3 phases: acute mania/mixed states, acute bipolar depression, and long-term maintenance treatment aimed at preventing recurrence of further episodes of mania and depression. Although the goal of treatment is to return of the patient to full functionality, bipolar disorder is a chronic relapsing and remitting illness that requires elements of the Chronic Disease Management Model (1). Initial treatment in bipolar disorder ideally begins with an agent that can remit the current episode and support relapse prevention long term in all phases. This is necessary, as a large meta-analysis demonstrated a 1-year episode relapse rate of 44% (2) and the 5-year relapse rate of over 70% (3).
A number of drug agents currently in use for bipolar disorder. The drugs used primarily in clinical practice are the atypical antipsychotics, (of which the drug under review, cariprazine, falls in this class), the anticonvulsants (Valproic Acid, Carbamazepine, Lamotrigine) and the traditional salt Lithium. Many of these agents do not have a Health Canada indication for more than one of the above illness phases. However, off label use of these medications alone or in combination is common practice to control other phases (especially in bipolar depression) and maintain response/prevent relapse with varying degrees of evidence. Though now 4 years old, 2018 Canadian clinical practice guidelines for bipolar disorder (1) provides recommendations for which current treatment options may be most suitable for each phase of the illness. Much of the evidence for the cariprazine is newer and not reflected in these guidelines, yet it is still a recommended treatment for all the acute phases of bipolar disorder in this document.
Non-drug physical treatments include modalities of neurostimulation such as electroconvulsive therapy (ECT) (1) and repetitive transcranial magnetic stimulation (rTMS) (4) for the depressed phase of bipolar disorder. Though a useful adjunct, these are also off-label and have limited accessiblity in most parts of Canada.
Non-drug psychological treatments are useful supplementary in bipolar disorder. Canadian clinical practice guidelines (1) recommend first line psychoeducation in the maintenance phase to prevent recurrence as well as cognitive behavioral therapy (CBT), family focused therapy (FFT), as well as interpersonal social rhythms therapy (IPSRT) for both the maintenance and depressed phases. Again, there are well known significant accessibility issues similar to most psychological treatments in the Canadian health care system. Patients with bipolar disorder generally require long term pharmacotherapy.
Current treatments are primarily known to improve target symptoms of acute illness phases, maintain response/prevent relapse of bipolar disorder, but early prompt recognition and treatment appears to modify the underlying disease mechanism by reducing the risk of further episodes and subsequent progression of the disease (5,6).
Treatment Goals
The most important goals of the ideal treatment for bipolar disorder would be:
Symptomatic remission from acute manic, mixed, and depressive symptoms to return to full psychosocial functioning.
Relapse prevention – maintain mood stability and support functional recovery in the maintenance phase.
Treatment efficacy without induction of switches or rapid cycling between episodes
Demonstrate tolerability with a low side effect burden, most notably low rates of sedation, weight gain and corresponding metabolic disease.
An ideal treatment would address all illness phases; manic, mixed, and depressed mood states, as well as carry efficacy in maintenance treatment
Early treatment to significantly reduce the progression of the disease to restore or at least reduce cognitive function, chronic illness, and disability.
Prolong life by reducing suicidal behavior and other comorbidities (i.e. metabolic and cardiac) known to shorten life in bipolar disorder.
Reduce level of disease morbidity including reduction/prevention in health care system utilization such as emergency room usage and psychiatric hospitalization.
Reduce disability including level of caregiver burden, and increase the ability to maintain employment, independence, and health related quality of life. It has been estimated that 30% of patients do not return to their previous work role function after a bipolar diagnosis (7).
Treatment Gaps (Unmet Needs)
Considering the treatment goals, please describe goals (needs) that are not being met by currently available treatments.
As noted above, bipolar disorder is a heterogenous long term illness with multiple phases, and not all patients in each phase respond to available treatments. Since treatment is long term and the disease can be progressive, patients also often become refractory to pharmaceutical treatment. As many different options as possible with unique mechanisms of action are needed to reach the treatment goals and key outcomes mentioned in question 4.
Improved/increased options for treatment are clearly needed as bipolar disorder remains one of the top causes of disability in the world (8) and both the disability burden as well as the mortality gap between bipolar disorder patients relative to the general population are increasing (9,10).
Although there are many medications with a Health Canada indication for mania and mixed states of bipolar disorder, there is a paucity of approved treatments for both mania and depression (Quetiapine) as well as the key outcome of bipolar depression, (Lurasidone and Quetiapine) the predominant and more functionally impairing phase of the illness (11-13). Lithium is also used on label for mania and off label for depression, but the evidence in acute bipolar depression is only in combination (14). The agent also has weight gain, cognitive side effects, poor patient compliance, requires cumbersome blood work, and long-term treatment can lead to thyroid/renal difficulties (15, 16).
The most significant unmet need during the maintenance phase of bipolar is medication without adverse effects (17). Traditionally bipolar treatments have had significant tolerability issues. leading to over two thirds of patients showing of suboptimal adherence and 30-50% outright non-compliance (18,19). Non-compliance with treatment is the strongest factor that leads to recurrence (20) that has been shown to lead to a more resistant course of disease (21) and increased health care costs (21, 22).
A large patient survey and our clinical experience indicates that weight gain and sedation are two major dimensions that lead to lack of compliance (23). Metabolic consequences are the most concerning feature of drug treatment for many patients, leading to morbidity, a decrease of the quality of life, and decreased satisfaction with the treatment (24). This is critical to consider as patients with bipolar disorder are known independent of medication to have higher rates of obesity, diabetes, and cardiovascular disease (25,26). More tolerable treatments are needed that minimize iatrogenic morbidity from the medication itself, especially in the dimensions of weight gain and sedation. This will serve to improve compliance and theoretically reduce health care utilization for mental health relapse (21) and limit the potential future health care costs originating from weight gain, obesity, metabolic and cardiac disease.
More options for drugs that work in multiple phases of the illness are also important. Currently, over 70% of bipolar patients are seen to require treatment with more than one agent (27) and 30-40% of patients are seen to need more than 3 medications, especially in the depressive phase (28-30). This polypharmacy needed for efficacy and stability also increases side effect burden and jeopardizes patient compliance with the medications (30).
A medication with efficacy in multiple phases of bipolar disorder with low rates of metabolic side effects, such as cariprazine, is needed as an option to potentially minimize the need for treatment with multiple medications and increase compliance.
Other formulations are also needed to improve compliance/convenience, especially with newer medications for bipolar disorder. There are only two other Health Canada-approved non-oral formulations for bipolar disorder (Risperidone Consta and Aripiprazole extended release injectables). However, this type of formulation is not pertinent at this point for cariprazine.
Which patients have the greatest unmet need for an intervention such as the drug under review?
As noted above, the patients with the depressed phase of the bipolar illness (31). This is not a sub or niche population, but a predominant phase of the illness that would include almost all patients. A recent survey indicated that 1/3 of patients themselves felt that this was their biggest unmet need (32).
Patients with current weight problems, metabolic or cardiac comorbidity.
Patients who are excessively sedated with current treatments. Sedation has been linked to reduced physical activity and weight gain, impaired motor performance and risk of accidents, impairment in numerous psychosocial domains, reduced cognition, quality of life and stigma (33).
Patients on numerous agents for the disorder
Younger patients who have both a higher risk of non-compliance and weight gain with medications used in bipolar (21, 34).
Patients with suicidal behaviour, as the risk of death from suicide is 10-30 times greater than in the general population and 20-60% attempt suicide at least once in their lifetime (35).
Cariprazine would help to address all these needs in many bipolar patients by addressing all phases, especially bipolar depression, in a predominantly metabolically neutral, non-sedating fashion.
Place in Therapy
How would the drug under review fit into the current treatment paradigm?
Cariprazine has a novel and unique mechanism of action that is different from both other treatments and atypical antipsychotics used for bipolar disorder. More specifically, it has very distinctive effects on dopamine with both partial dopamine agonism and high potency D3 blockade. This blockade is very specific to cariprazine and this, as well as effects on serotonin and glutamate receptor subtypes, may contribute to improved clinical benefits compared to other agents (36, 37).
There is only one other indicated partial dopamine agonist for bipolar disorder (Aripiprazole) and this agent is widely used clinically as a tolerable treatment to improve outcomes in bipolar disorder. However, it has minimal bipolar depression data (1) and another agent of this class with a much different effect on dopamine would be very welcomed by clinicians.
Cariprazine would be a clear first line treatment in bipolar disorder because of the demonstrated acute efficacy against all phases (manic, mixed, depressed) of the illness (38-42) and favourable metabolic profile with much lower sedation/weight gain than other indicated or clinically used treatments for bipolar disorder (43).
Though not studied directly, cariprazine could be used in combination with other traditional mood stabilizers such as Lithium and Valproic Acid, as is done with other atypical antipsychotics currently. Cariprazine data for the maintenance phase is pending at this point, however extrapolating from the other atypical antipsychotics, as well as cariprazine’s demonstrated efficacy in manic, mixed and depressed states, it is likely to be positive. Many atypical antipsychotics with bipolar indications they are in maintenance treatment clinically.
With favourable access status, this drug would cause a significant shift in the evolving treatment paradigm to offer patients with all phases of bipolar disorder safer and more tolerable agents. Given the broad-spectrum efficacy of cariprazine in bipolar disorder, it will also likely reduce the frequent utilization of polypharmacy and the subsequent cumulative burden of side effects and drug interactions. Though we do not have clinical experience yet in Canada, this has occurred in the United States.
Similarly, clinicians are often forced to treat the polarity of the current episode (e.g. mania) with an agent that may not protect from or treat the patient for other phases. This leads to polypharmacy, further relapses, and inadequate mood control, all of which are negative long term prognostic factors. The availability of cariprazine should intuitively reduce that.
Please indicate whether or not it would be appropriate to recommend that patients try other treatments before initiating treatment with the drug under review. Please provide a rationale from your perspective.
Response redacted.
How would this drug affect the sequencing of therapies for the target condition?
If there is failure, other treatments described above such as Lithium, Aripiprazole, Quetiapine, Lurasidone or Lamotrigine would continue to be initiated depending on the predominant phase of illness. The treatment sequence would not significantly change for most current practice, except that with cariprazine the clinician would have another valuable first line broad spectrum option for multiple phases of bipolar disorder with few of the side effects that commonly lead to non-compliance.
One could also treat patients with this Cariprazine in subsequent lines of therapy as well depending again on phase of illness and response. However, as noted above, changing the sequence of therapy by selecting cariprazine as one of the first-choice options seems likely to ultimately reduce utilization of drugs with improved quality of life and reduced side effects that would impair compliance.
Which patients would be best suited for treatment with the drug under review?
Again, cariprazine is a broadspectrum agent with efficacy for most patients with bipolar disorder in either the depressed, manic or mixed phases. Hence almost any patient with bipolar disorder would be suited for cariprazine. A defining disease characteristic of potential response to this agent would be fatigued and tired patients as the incidence of sedation is low (43). This is a common symptom dimension that is seen clinically in bipolar disorder and has been shown to impair quality of life (47,48). Patients who develop weight gain or metabolic issues on other agents would also be a natural fit for the favourable metabolic profile of cariprazine.
As mentioned earlier, a group of patients in need of intervention are in acute bipolar depression, given the dearth of options in this area. The rapid efficacy of cariprazine across all the symptoms of bipolar depression (49), different subtypes of patients (50,51), and improvement in functional outcomes (52) indicate it would be well suited for almost all bipolar I patients in the acute phase of depression.
In particular, hospitalized and/or suicidal patients with bipolar depression would be good candidates for cariprazine. There is only one current Health Canada-approved treatment for acute bipolar depression (Lurasidone) that can be used without high rates of weight gain and sedation. As noted above, other first line treatment options with potential for a treatment response within the first few weeks (quetiapine, lithium) carry a significant potential side effect burden. Lamotrigine, while also a first line off-label option for bipolar depression with a favorable side effect profile, is not useful when response is needed quickly. For safety reasons, lamotrigine must be titrated over 6-8 weeks, and can take some time to reach a target dose and response. Cariprazine, however, could offer another tolerable option for acute response in the order of days to weeks.
Another area with great need of intervention are patients with bipolar disorder and comorbid substance abuse disorders (SUD). Patients with Bipolar disorder have up to 8 times the incidence of SUD compared to the general population and it is associated with worse outcomes (53,54). Cariprazine’s unique partial dopamine agonism may be well suited in treating patients with substance abuse issues (55).
How would patients best suited for treatment with the drug under review be identified?
The diagnosis of bipolar disorder is made with history taking, clinical examination and judgement. Although there are clear criteria, there can be much variability in expert opinion on their interpretation. Bipolar disorder is also a longitudinal illness often accompanied by many co-morbid psychiatric conditions and patient reporting of subjective symptoms can be prone to selection and/or recall bias, further hindering the diagnosis.
There are no laboratory tests to diagnose bipolar disorder, but validated diagnostic tools have been developed such as the mood disorders questionnaire (MDQ), bipolar spectrum diagnostic scale (BSDS) or the simple rapid mood screener (RMS) to assist diagnosis (56-58). However, these are subjective scales that lack specificity to create a diagnosis using them alone. Simple monitoring with structured mood charts is also popular clinically.
Bipolar disorder is challenging to diagnose properly in clinical practice and is often misdiagnosed as depression, or one of its major comorbidities such as disorders of anxiety, sleep, substance abuse/dependence or personality. Misdiagnosis often occurs in clinical practice, and it can take a number of years and the right medical consultation to clarify the correct diagnosis (59). System issues in diagnostic difficulties are related to a lack of primary care training and psychiatry specialist support, as well as variability in expert opinion.
Although there is potential developing criterion for a bipolar disorder prodrome and subsequent staging (60) there is not much data indicating that people who are presymptomatic should be treated (61). Early prompt intervention once diagnosed however does reduce episode number, morbidity and even potentially mortality (62, 63). Another new broad spectrum treatment such as cariprazine could increase awareness and education of bipolar disorder, leading to more prompt diagnosis and treatment of, further lessening the disability and stigma from this illness.
Which patients would be least suitable for treatment with the drug under review?
Since the clinical trial data notes potential high rates of akathisia, restlessness and EPS with higher doses (42), patients who have had previous difficulties with this side effect would be less suitable. There is no data in bipolar II (a type of bipolar that is predominantly depression and mood shifts) patients, but by convention in clinical practice many agents with efficacy in bipolar I phases (especially depression) are used off label in bipolar II disorder, as there is only one Health Canada indicated treatment for bipolar II depression (quetiapine) (1). This would likely be similar for the use of cariprazine.
Is it possible to identify those patients who are most likely to exhibit a response to treatment with the drug under review?
Response redacted.
What outcomes are used to determine whether a patient is responding to treatment in clinical practice?
Improvement in clinician assessed symptoms of mania and depression such as mood, sleep, energy, irritability, psychosis, concentration, and attention are some of the major outcomes used to determine response. More qualitative factors such as insight, judgment, participation in activities and a global assessment of daily function are also factored into the determination of response.
There is some overlap between outcomes in clinical trials and those used by clinicians. However, shorter self-rating scales or individual questions for depression or manic symptoms are more likely to be used in practice than standard clinical trial scales such as the Montgomery Asberg Depression Rating Scale (MADRS) or the Young Mania Rating Scale (YMRS). Formal functional outcome scales are not used widely in clinical practice, but the individual items on these scales do capture the range of outcomes that clinicians use to qualitatively determine patient response.
What would be considered a clinically meaningful response to treatment?
Clinically meaningful outcomes in bipolar have been defined as response as a 50% reduction in a score from a standard rating scale of symptomatology from an appropriate baseline, regardless of index episode type (manic, depressed, or mixed). In addition, the opposite pole cannot be significantly worsened during response (i.e., no worsening of depression when treating mania). Remission was defined as absence or minimal symptoms of both mania and depression for at least 1 week. Sustained remission requires at least eight consecutive weeks of remission, and perhaps as many as 12 weeks (64).
Clinically significant definitions of remission can vary. For mania it is a score below 13 or 9 on the YMRS and in depression a score below 11 on the MADRS. Additionally, definitions of composite remission (both YMRS and MADRS total score below 13) and worsening/switch to depression and mania (MADRS total score >14 and YMRS>12) have been used (64).
A more global measure, the seven-point Clinical Global Impression Scale (CGI), has also been commonly used in mental health disorders research. A score of 1 (not mentally ill) or 2 (borderline mentally ill) on the severity scale (CGI-S) or 1 (very much improved with treatment) or 2 (much improved with treatment) on the improvement scale (CGI-I) is considered clinically significant (65).
Clinically significant functional outcome measures are less clearly elucidated. The Sheehan Disability Scale (SDS) is often used, with scores >5 in any of the three sections (home, work/school, social) considered clinically significant. In bipolar disorder clinical trials, the Functioning Assessment Short Test (FAST) is gaining traction as a standard measurement (66). The FAST is a 24-item scale with a maximum score of 72 and scores of 12, 20 and 40 represent clinically meaningful cut-offs for mild, moderate, and severe functional impairment. A score below 12 indicates full functional recovery (67).
Most clinicians look for improvement over time, recognizing that functional recovery tends to lag, sometimes significantly, behind symptom improvement (68). Ability to perform basic and independent activities of daily living, though not formally measured, are also taken into account.
For more severe patients with multiple episodes, stabilization and the ability to live independently becomes an outcome measure, although return to full function is the aim in the first episodes.
The magnitude of response to treatment can vary greatly by physician greatly in bipolar disorder. Factors include recognition of illness, adherence to guideline-based therapy, therapeutic rapport with patient, specialist and intensive treatment program availability, as well as psychosocial treatment support.
How often should treatment response be assessed?
Acute manic, mixed or severely depressed phase – this would be daily in the hospital setting or partial hospitalization program
Less severe manic, mixed or depressed phases in the community– initially this could be from every 2-8 weeks depending on medication adjustments
Once treatment is stable – patients are reviewed every 3-6 months as indicated for emergence of symptoms.
What factors should be considered when deciding to discontinue treatment?
Further episodes or the lack of response to manic, depressive and mixed symptoms
Lack of functional improvement in the domains of work, school and home.
Adverse events that should be considered in discontinuing treatment are significant and daily anxiety, agitation, akathisia or restlessness and in very occasional cases with this drug metabolic issues such as weight gain of more than 7% of body weight.
What settings are appropriate for treatment with the drug under review?
Response redacted.
For non-oncology drugs, is a specialist required to diagnose, treat, and monitor patients who might receive the drug under review?
Response redacted.
Given the new nature of cariprazine and the indication of bipolar disorder, initially it would be mostly psychiatrists who would diagnose, treat and monitor patients with this drug. Eventually, with education and training, family practice physicians in the models above would potentially diagnose, treat, but most likely monitor this agent.
List any companies or organizations that have provided your group with financial payment over the past two years AND who may have direct or indirect interest in the drug under review. Please note that this is required for each clinician who contributed to the input — please add more tables as needed (copy and paste). It is preferred for all declarations to be included in a single document.
Declaration for Clinician 1
Name: Dr. Pratap Chokka
Position: Clinical Professor, University of Alberta Dept of Psychiatry
Date: February 15, 2022
Table 4: Conflict of Interest Declaration for Western Canadian Clinical Advisory Network — Clinician 1
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
Lundbeck | — | — | X | — |
Otsuka | — | X | — | — |
Janssen | X | — | — | — |
Declaration for Clinician 2
Name: Atul Khullar
Position: Clinical Associate Professor, University of Alberta Dept of Psychiatry
Date: February 8, 2022
Table 5: Conflict of Interest Declaration for Western Canadian Clinical Advisory Network — Clinician 2
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
Abbvie/Allergan | — | X | — | — |
Sunovion | — | — | X | — |
Otsuka | — | X | — | — |
Lundbeck | — | X | — | — |
Jazz Pharma | — | X | — | — |
Paladin Pharma | X | — | — | — |
Pfizer | X | — | — | — |
Takeda | X | — | — | — |
Bausch Health | — | — | X | — |
Eisai | — | X | — | — |
Elvium | — | — | X | — |
Declaration for Clinician 3
Name: Diane McIntosh
Position: Psychiatrist
Date: February 17, 2022
Table 6: Conflict of Interest Declaration for Western Canadian Clinical Advisory Network — Clinician 3
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
Janssen Ortho | — | — | X | — |
AbbVie/ Allergan | — | — | X | — |
Bausch Health | — | X | — | — |
Eisai | — | X | X | — |
Takeda | — | X | — | — |
Lundbeck/Otsuka | — | X | — | — |
Declaration for Clinician 4
Name: Margaret Oakander
Position: Clinical Associate Professor Dept of Psychiatry University of Calgary, Clinical Medical Director Southern Alberta Shared Mental Health Care Program, Clinical Medical Director Primary Care Liaison Calgary zone, Staff Psychiatrist CAMHC-NE Sunridge, Consulting Psychiatrist Eastside Community Mental Health Clinic
Date: February 8, 2022
Table 7: Conflict of Interest Declaration for Western Canadian Clinical Advisory Network — Clinician 4
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
Otsuka | — | — | X | — |
Sunovion | X | — | — | — |
Allergan/AbbVie | — | X | — | — |
Declaration for Clinician 5
Name: Dorothy Reddy
Position: Medical Director, Neurogenesis Clinics
Date: February 3, 2022
Table 8: Conflict of Interest Declaration for Western Canadian Clinical Advisory Network — Clinician 5
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
Shire Canada | X | — | — | — |
Sunovion | X | — | — | — |
Takeda | X | — | — | — |
Declaration for Clinician 6
Name: Jennifer Swainson
Position: Associate Clinical Professor Dept of Psychiatry University of Alberta; Psychiatrist, Misericordia Community Hospital
Date: February 15, 2022
Table 9: Conflict of Interest Declaration for Western Canadian Clinical Advisory Network — Clinician 6
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
Otsuka | X | — | — | — |
Sunovion | X | — | — | — |
Eisai | X | — | — | — |
Janssen | — | — | X | — |
Lundbeck | — | X | — | — |
Allergan | X | — | — | — |
Declaration for Clinician 7
Name: Rejish Thomas
Position: Psychiatrist
Date: February 6, 2022
Table 10: Conflict of Interest Declaration for Western Canadian Clinical Advisory Network — Clinician 7
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
Abbvie | X | — | — | — |
Lundbeck | X | — | — | — |
Janssen | X | — | — | — |
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up-to-date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
Redactions: Confidential information in this document may be redacted at the request of the sponsor in accordance with the CADTH Drug Reimbursement Review Confidentiality Guidelines
Stakeholder Input: The views expressed in each submission are those of the submitting organization or individual; not necessarily the views of CADTH or of other organizations. As such, they are independent of CADTH and do not necessarily represent or reflect the view of CADTH. No endorsement by CADTH is intended or should be inferred. By filing with CADTH, the submitting organization or individual agrees to the full disclosure of the information. CADTH does not edit the content of the submissions.
CADTH does use reasonable care to prevent disclosure of personal information in posted material; however, it is ultimately the submitter’s responsibility to ensure no identifying personal information or personal health information is included in the submission. The name of the submitting organization or individual and all conflict of interest information are included in the submission; however, the name of the author, including the name of an individual patient or caregiver submitting the patient input, are not posted.
Accessibility: CADTH is committed to treating people with disabilities in a way that respects their dignity and independence, supports them in accessing material in a timely manner, and provides a robust feedback process to support continuous improvement. All materials prepared by CADTH are available in an accessible format. Where materials provided to CADTH by a submitting organization or individual are not available in an accessible format, CADTH will provide a summary document upon request. More details on CADTH’s accessibility policies can be found here.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.