CADTH Reimbursement Review
Lemborexant (Dayvigo)
Sponsor: Eisai Limited
Therapeutic area: Insomnia
This multi-part report includes:
Clinical Review
Pharmacoeconomic Review
Stakeholder Input
Clinical Review
Abbreviations
AE
adverse event
AHI
Apnea-Hypopnea Index
AUC
area under the curve
BAC
blood alcohol concentration
BAI
Beck Anxiety Inventory
BDI-2
Beck Depression Inventory
BZRA
benzodiazepine receptor agonist
C-SSRS
Columbia-Suicide Severity Rating Scale
CBT-I
cognitive behavioural therapy for insomnia
CCMV
complete case missing value
CCSSP
Canadian Consortium of Sleep and Sleep Interested Physicians
CDEC
CADTH Canadian Drug Expert Committee
CI
confidence interval
CINeMA
Confidence in Network Meta-Analysis
CPAB
Cognitive Performance Assessment Battery
CrI
credible interval
DB
double-blind
DORA
dual orexin receptor antagonist
DSM-5
Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition
EQ VAS
EQ Visual Analogue Scale
EQ-5D-3L
3-Level EQ-5D
FAS
full analysis set
FSS
Fatigue Severity Scale
HRQoL
health-related quality of life
ICC
intraclass correlation coefficient
IQR
interquartile range
ISI
Insomnia Severity Index
ISWRD
irregular sleep-wake rhythm disorder
ITC
indirect treatment comparison
LEM
lemborexant
LEM5
lemborexant 5 mg
LEM10
lemborexant 10 mg
LPS
latency to persistent sleep
LSEQ
Leeds Sleep Evaluation Questionnaire
LSM
least squares mean
MAR
missing at random
MDSC
Mood Disorders Society of Canada
MID
minimal important difference
MMRM
mixed model of repeated measures
MNAR
missing not at random
MVA
motor vehicle accident
NMA
network meta-analysis
OR
odds ratio
OX1R
orexin receptor 1
OX2R
orexin receptor 2
PBO
placebo
PGI-Insomnia
Patient Global Impression–Insomnia
PP
per-protocol
PSG
polysomnography
PSQI
Pittsburgh Sleep Quality Index
PSUR
periodic safety update report
RCT
randomized controlled trial
SAE
serious adverse event
SD
standard deviation
SDLP
standard deviation of lateral position
SE
standard error
SMD
standardized mean difference
sQUAL
subjective quality of sleep
sSOL
subjective sleep onset latency
sTST
subjective total sleep time
sWASO
subjective wake after sleep onset
T-BWSQ
Tyrer Benzodiazepine Withdrawal Symptom Questionnaire
TEAE
treatment-emergent adverse event
TST
total sleep time
WASO
wake after sleep onset
WASO2H
wake after sleep onset in the second half of the night
Z-drugs
zolpidem, eszopiclone, zaleplon, and zopiclone
ZOL
zolpidem tartrate
ZOL-ER
zolpidem tartrate extended-release
ZOL-IR
zolpidem tartrate immediate-release
Executive Summary
An overview of the submission details for the drug under review is provided in Table 1.
Item | Description |
|---|---|
Drug product | Lemborexant (Dayvigo), 5 mg per tablet and 10 mg per tablet, oral |
Indication | For the treatment of insomnia, characterized by difficulties with sleep onset and/or sleep maintenance |
Reimbursement request | As per indication |
Health Canada approval status | NOC |
Health Canada review pathway | Standard |
NOC date | November 4, 2020 |
Sponsor | Eisai Limited |
NOC = Notice of Compliance.
Source: Sponsor’s submission package for review of lemborexant.1
Introduction
Insomnia disorder is the most common sleep disorder and, according to the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5), is described as being dissatisfied with the quality or quantity of sleep and having difficulty initiating and/or maintaining sleep, and is associated with daytime impairment.2,3 The DSM-5 criteria include sleep disturbances occurring at least 3 nights per week for at least 3 months.3,4 In Canada, the prevalence is estimated to be between 12% and 24%5,6 and the incidence is estimated to be between 3.8% and 7.3% per year.7,8 Older age, female sex, comorbid medical or psychiatric conditions, and social and environmental factors have been identified as common risk factors for insomnia.2,3 Insomnia can be diagnosed as a disorder on its own or as a symptom associated with many other medical conditions and has been closely linked to reduced life expectancy and increased economic costs through lost productivity, workplace accidents and motor vehicle accidents (MVAs), and greater health care usage.2,3,7-10
Per the Alberta Medical Association’s 2015 Assessment to Management of Adult Insomnia clinical practice guideline, insomnia can be treated and managed in a primary care setting or by a specialist when the problem cannot be diagnosed or if the insomnia is resistant to treatment.3 Nonpharmacologic treatment options such as sleep hygiene education and cognitive behavioural therapy for insomnia (CBT-I) are recommended as an initial treatment.3,10,11 Pharmacologic treatments include benzodiazepine receptor agonists (BZRAs) — among them, benzodiazepines and Z-drugs (zolpidem tartrate [ZOL], eszopiclone, zaleplon, and zopiclone) — dual orexin receptor antagonists (DORAs), histamine receptor antagonists, and melatonin receptor agonists.12 Off-label medications that have sedating effects (e.g., antidepressants, antihistamines, anticonvulsants, antipsychotic drugs) may be used in specific situations but are generally not recommended as a first-line treatment due to the lack of efficacy and safety evidence in this population.3,12 Long-term use of hypnotics is discouraged as the studies supporting their approval were based on short-term use2 and are not recommended as a first-line treatment option.3,12
Lemborexant (LEM) is a DORA indicated for the treatment of insomnia, characterized by difficulties with sleep onset and/or sleep maintenance.1 The recommended dosage is 5 mg once per night and may be increased to the maximum recommended dose of 10 mg based on clinical response and tolerability.13 LEM is taken orally once per night within a few minutes before going to bed, with at least 7 hours before planned awakening time.
The objective of this report is to perform a systematic review of the beneficial and harmful effects of lemborexant 5 mg (LEM5) or lemborexant 10 mg (LEM10) tablets taken orally once daily at bedtime for the treatment of patients with insomnia, characterized by difficulties with sleep onset and/or sleep maintenance.
Following the issuance of the draft CADTH Canadian Drug Expert Committee (CDEC) recommendation for LEM in August 2022, the following additional information was provided to CADTH:
1 unpublished manuscript by Drake et al.14 that provided evidence for LEM’s efficacy as measured by the Patient Global Impression–Insomnia (PGI-Insomnia) tool in the SUNRISE 2 study
a periodic safety update report (PSUR)15 that included aggregate data from approximately 4,024 adult patients with insomnia disorder, irregular sleep-wake rhythm disorder (ISWRD), or healthy volunteers who were enrolled in the LEM clinical development program
a published network meta-analysis (NMA) by De Crescenzo et al. (2022)16 comparing LEM to other pharmacologic treatments for the acute and long-term treatment of adults with insomnia.
These data were not included in the submission to CADTH and provided more information on the clinical meaningfulness of the subjective PGI-Insomnia instrument, and on LEM’s safety and comparison to other drugs for the treatment of insomnia. The information has been summarized and critically appraised as an addendum to the CADTH report in Appendix 6.
Stakeholder Perspectives
The information in this section is a summary of input provided by the patient groups that responded to CADTH’s call for patient input, by clinician groups, and by a clinical expert consulted by CADTH for the purpose of this review.
Patient Input
CADTH received input from 3 patient groups: the Mood Disorders Society of Canada (MDSC), Migraine Canada, and Menopause Chicks. The 3 groups conducted surveys and interviews with patients and caregivers to inform their input. Respondents from all 3 patient groups indicated that sleep problems significantly impacted their quality of life, energy level, cognitive function, mood the next day, and daytime activities. Most respondents reported having tried various treatments for sleep problems (e.g., benzodiazepines, Z-drugs). Many reported being dissatisfied and discontinued treatment due to side effects such as next-day sedation and cognitive impairment, and fear of developing a substance use disorder. The groups indicated the following as key outcomes for patients and caregivers: uninterrupted and restorative sleep, greater access to treatment, more effective treatment options, long-term effectiveness, fewer side effects, less stress and anxiety, improved productivity, and improved relationships. MDSC input included 3 respondents who had experience with LEM and accessed the drug through private health insurance. They described being able to manage their sleep problems without becoming dependent on the medication or experiencing serious side effects, and without feeling lethargic and sleepy the next morning.
Clinician Input
Input From the Clinical Expert Consulted by CADTH
The clinical expert consulted for this review stated that the current goals of treatment are to improve sleep initiation, maintenance, and terminal insomnia, leading to restorative sleep. According to the clinical expert, CBT-I is the first-line treatment for insomnia, but many patients have limited access to and/or success with this option; thus, pharmacotherapy is often used in addition to or in place of CBT-I. Per the expert, when a medication is used for extended periods of time, a patient may have a waning response or no response. At this point, it can be difficult to withdraw the therapy if the patient has developed tolerance to the drug and the patient may experience rebound insomnia. Another concern raised by the clinical expert was the risk of cognitive and behavioural changes the next morning that can lead to falls and other dangers, particularly for older adult patients.
The clinical expert suggested that LEM may be a first-line pharmacologic treatment for insomnia and noted that it would be necessary to determine how to optimally transition from other currently available medications (e.g., Z-drugs) to LEM. The expert indicated that most patients with insomnia may be candidates for treatment with LEM except for those who are pregnant, are nursing, or have narcolepsy. According to the clinical expert, patients are asked general questions about their sleep rather than have measurements taken in clinics. The expert thought that this practice does not tend to vary among physicians. The clinical expert indicated that few clinics are performing sleep studies for insomnia (except where another sleep disorder is suspected) because access is limited across Canada.
The expert noted that chronic insomnia generally does not go away and tends to worsen with age, menopause, or as a result of other major negative life events. The expert suggested that a patient may wish to trial being off medication; they can be supported by additional sleep management tools such as CBT-I. When deprescribing a medication, the clinical expert would observe for a return of symptoms or rebound insomnia. Per the clinical expert, insomnia is typically treated by family physicians or psychiatrists.
Clinician Group Input
CADTH received input from 2 clinician groups: the Canadian Consortium of Sleep and Sleep Interested Physicians (CCSSP) and the National Advisory Board. The clinician group input was aligned with that given by the clinical expert consulted by CADTH.
Drug Program Input
Input was obtained from the drug programs that participate in the CADTH reimbursement review process. Key issues raised by the drug plans included concerns over the most appropriate comparator to LEM, the necessity for patients to fail a treatment for insomnia before accessing LEM, the exclusion of comorbid conditions, and the use of polysomnography (PSG) for measuring efficacy. The clinical expert indicated the uncertainty of ZOL being the most appropriate comparator and how it compared to zopiclone, the latter of which was noted as being more commonly used in Canadian practice. The expert also stated that it would not be reasonable for patients to have to fail a less expensive drug with greater risk of harms before accessing safer alternatives if the 2 drugs had similar efficacy. Further, the clinical expert noted that there is currently a lack of evidence supporting the use of LEM in patients with comorbid conditions that were excluded from the SUNRISE 1 and SUNRISE 2 studies (based on Beck Depression Inventory [BDI-2], Beck Anxiety Inventory [BAI], and Apnea-Hypopnea Index [AHI] scores), but given that insomnia is closely linked to anxiety and depression, it would be very difficult to exclude these comorbidities until trials could be performed. Lastly, the expert stated that PSG results should not be used as a marker for efficacy or a necessary criterion for accessing LEM.
Clinical Evidence
Pivotal Studies and Protocol Selected Studies
Description of Studies
Two double-blind (DB), phase III, randomized controlled trials (RCTs) — SUNRISE 1 and SUNRISE 2 — were included in the systematic review of LEM.
The SUNRISE 1 trial (N = 1,006) was designed to assess the safety and efficacy of LEM5 and LEM10 for 30 days in females who were 55 years or older and males who were 65 years or older, all of whom had insomnia disorder according to the DSM-5. Comparators included zolpidem tartrate extended-release (ZOL-ER) 6.25 mg and appearance-matched placebos (PBOs) for both active compounds. The primary outcome was latency to persistent sleep (LPS) and key secondary outcomes were wake after sleep onset (WASO), wake after sleep onset in the second half of the night (WASO2H), and sleep efficiency as measured by PSG. Other secondary and exploratory outcomes important to the CADTH review included patient-reported outcomes such as the 3-level EQ-5D (EQ-5D-3L), Insomnia Severity Index (ISI), Fatigue Severity Scale (FSS), PGI-Insomnia, and quality of sleep questionnaires. Patients had a mean age of 63.9 (standard deviation [SD] = 6.81) years and 86.4% were female. At baseline, mean LPS was approximately 45 minutes, mean WASO was around 114 minutes, mean WASO2H was 77 minutes, and mean sleep efficiency was 68%.
The SUNRISE 2 trial (N = 971) was designed to assess the long-term safety and efficacy of LEM5 and LEM10 for up to 12 months in adults 18 years or older who had insomnia disorder according to the DSM-5. The first 6 months of the SUNRISE 2 study consisted of 3 treatment groups: LEM5, LEM10, and PBO. For the next 6 months of the trial, patients who were randomized to PBO were rerandomized to active treatment (i.e., LEM5 or LEM10) for the remainder of the trial. The primary outcome was subjective sleep onset latency (sSOL) and key secondary outcomes were subjective wake after sleep onset (sWASO) and subjective sleep efficiency as recorded in the sleep diary. Other secondary and exploratory outcomes important to the CADTH review were the same as the patient-reported outcomes listed for SUNRISE 1. Patients had a mean age of 54.5 (SD = 13.80) years and 68.2% were female. At baseline, mean sSOL was approximately 64 minutes, sWASO was 134 minutes, and subjective sleep efficiency was 62%.
Efficacy Results
Statistical testing was conducted based on a gatekeeping procedure for both studies. In SUNRISE 1, the following outcomes were controlled for multiplicity: LPS, sleep efficiency, WASO, and WASO2H. In SUNRISE 2, the following outcomes were controlled for multiplicity: sSOL, subjective sleep efficiency, and sWASO. Efficacy data have been summarized in Table 2 for SUNRISE 1 and Table 3 for SUNRISE 2.
Table 2: Summary of Key Efficacy Results From the SUNRISE 1 Study, FAS
Result | PBO (N = 208) | ZOL (N = 263) | LEM5 (N = 266) | LEM10 (N = 269) |
|---|---|---|---|---|
LPS | ||||
Baseline, n | 208 | 262 | 266 | 269 |
Geometric mean (SD), minutes | 33.61 (NR) | 30.96 (NR) | 32.98 (NR) | 33.31 (NR) |
Median (Q1 to Q3), minutes | 33.63 (20.75 to 59.50) | 31.50 (17.50 to 61.25) | 33.13 (20.25 to 62.25) | 38.50 (17.75 to 62.00) |
Days 29 to 30, na | 200 | 250 | 260 | 260 |
Geometric mean (SD), minutes | 24.88 (NR) | 27.88 (NR) | 18.87 (NR) | 17.49 (NR) |
Median (Q1 to Q3), minutes | 27.25 (15.25 to 45.63) | 27.00 (15.00 to 41.00) | 21.63 (14.50 to 33.00) | 21.75 (13.25 to 33.00) |
Change from baseline, median (Q1 to Q3), minutes | –6.63 (–20.75 to 6.88) | –2.88 (–23.75 to 12.50) | –12.00 (–32.25 to –0.25) | –16.25 (–37.50 to –1.88) |
Geometric LSM treatment ratio, active vs. PBO (95% CI)b | Reference | 1.22 (1.06 to 1.40) | 0.77 (0.67 to 0.89) | 0.72 (0.63 to 0.83) |
P valueb,c | Reference | 0.0063 | 0.0003 | < 0.0001 |
WASO | ||||
Baseline, n | 208 | 262 | 266 | 269 |
Mean (SD), minutes | 111.75 (37.18) | 114.31 (39.92) | 113.44 (38.95) | 114.83 (40.00) |
Days 29 to 30, na | 200 | 250 | 260 | 260 |
Mean (SD), minutes | 92.09 (40.97) | 77.71 (39.93) | 69.10 (34.53) | 68.60 (35.20) |
Change from baseline, mean (SD), minutes | –18.58 (41.93) | –36.50 (43.41) | –43.89 (39.26) | –46.43 (39.60) |
LSM visit estimate (SE),d minutes | –21.43 (2.46) | –37.68 (2.22) | –45.40 (2.19) | –46.78 (2.19) |
LSM treatment difference (active minus PBO) (95% CI)d | Reference | –16.25 (–22.31 to –10.18) | –23.96 (–29.98 to –17.95) | –25.35 (–31.36 to –19.34) |
P valuec,d | Reference | < 0.0001 | < 0.0001 | < 0.0001 |
WASO2H | ||||
Baseline, n | 208 | 262 | 266 | 269 |
Mean (SD), minutes | 74.44 (30.11) | 78.04 (33.85) | 76.60 (32.90) | 76.88 (32.13) |
Days 29 to 30, na | 200 | 250 | 260 | 260 |
Mean (SD), minutes | 64.37 (32.45) | 56.74 (31.11) | 49.11 (28.18) | 48.15 (27.84) |
Change from baseline, mean (SD), minutes | –8.92 (31.91) | –21.42 (36.26) | –27.19 (33.05) | –28.84 (33.14) |
LSM visit estimate (SE),e minutes | –10.98 (1.97) | –20.74 (1.78) | –27.39 (1.75) | –28.74 (1.76) |
LSM treatment difference (active minus ZOL) (95% CI)e | NA | Reference | –6.65 (–11.15 to –2.15) | –8.00 (–12.53 to –3.47) |
P valuec, e | NA | Reference | 0.0038 | 0.0005 |
Sleep efficiency | ||||
Baseline, n | 208 | 262 | 266 | 269 |
Mean (SD), % | 68.89 (9.64) | 68.13 (11.42) | 68.36 (11.27) | 67.85 (10.85) |
Days 29 to 30, na | 200 | 250 | 260 | 260 |
Mean (SD), % | 74.49 (9.85) | 77.17 (10.19) | 81.29 (8.80) | 81.99 (8.80) |
Change from baseline, mean (SD), % | 5.35 (9.90) | 9.06 (11.23) | 12.93 (9.74) | 14.09 (10.51) |
LSM visit estimate (SE),f % | 6.34 (0.60) | 9.50 (0.55) | 13.42 (0.53) | 14.37 (0.54) |
LSM treatment difference (active minus PBO) (95% CI)f | Reference | 3.15 (1.67 to 4.63) | 7.07 (5.61 to 8.54) | 8.03 (6.57 to 9.49) |
P valuec,f | Reference | < 0.0001 | < 0.0001 | < 0.0001 |
Harms | ||||
Safety population, N | 209 | 263 | 266 | 268 |
TEAEs, n (%) | 53 (25.4) | 93 (35.4) | 74 (27.8) | 82 (30.6) |
SAEs, n (%) | 0 | 4 (1.5) | 2 (0.8) | 0 |
WDAEs from study treatment, n (%) | 2 (1.0) | 7 (2.7) | 2 (0.8) | 3 (1.1) |
Deaths, n (%) | 0 | 0 | 0 | 0 |
Notable harms | ||||
Somnolence, n (%) | 4 (1.9) | 4 (1.5) | 11 (4.1) | 19 (7.1) |
Impaired driving performance, n (%) | NR | NR | NR | NR |
Falls, n (%) | 0 | 0 | 4 (1.5) | 0 |
MVA (road traffic accident), n (%) | 0 | 1 (0.4) | 0 | 0 |
Workplace accidents, n (%) | NR | NR | NR | NR |
Hallucination: Tactile, n (%) | 0 | 0 | 0 | 1 (0.4) |
Drug misuse (intentional overdose), n (%) | 0 | 0 | 0 | 0 |
Postural instabilityg | NA | NA | NA | NA |
Baseline mean (SD) | 23.08 (17.51) | 26.01 (22.13) | 26.40 (20.78) | 23.69 (19.52) |
Days 2 to 3 change from baseline, mean (SD) | –2.02 (13.66) | 4.07 (18.92) | –0.82 (20.38) | 0.56 (17.08) |
Days 30 to 31 change from baseline, mean (SD) | 1.68 (16.58) | 2.12 (18.36) | –0.85 (16.20) | 0.48 (14.85) |
Impaired attention: Power of attentiong | NA | NA | NA | NA |
Baseline mean (SD), milliseconds | 1,421.0 (210.27) | 1,418.7 (195.95) | 1,452.9 (263.04) | 1,399.2 (192.47) |
Days 2 to 3 change from baseline, LSM (SE), milliseconds | –22.53 (10.48) | 27.46 (9.57) | 8.24 (9.47) | 17.14 (9.59) |
Days 30 to 31 change from baseline, LSM (SE), milliseconds | –5.97 (13.23) | 37.76 (12.02) | 37.29 (11.77) | 31.22 (11.89) |
Impaired attention: Continuity of attentiong | NA | NA | NA | NA |
Baseline mean (SD), units | 90.7 (4.77) | 90.6 (6.04) | 91.0 (5.15) | 91.3 (4.15) |
Days 2 to 3 change from baseline, LSM (SE), units | –0.09 (0.32) | –1.12 (0.30) | 0.26 (0.29) | –0.53 (0.30) |
Days 30 to 31 change from baseline, LSM (SE), units | –0.25 (0.37) | –0.32 (0.33) | –0.14 (0.32) | –0.57 (0.33) |
Rebound insomniag | NA | NA | NA | NA |
sSOL average first 7 nights, n (%) | 45 (23.3) | 66 (27.4) | 52 (20.7) | 44 (17.3) |
sSOL average last 7 nights, n (%) | 44 (23.3) | 63 (26.9) | 53 (21.8) | 60 (24.4) |
sWASO average first 7 nights, n (%) | 29 (14.9) | 52 (21.6) | 48 (19.4) | 41 (16.3) |
sWASO average last 7 nights, n (%) | 33 (17.5) | 41 (17.5) | 46 (19.1) | 43 (17.7) |
Withdrawal symptoms, n (%) | 28 (14.1) | 37 (14.7) | 30 (11.6) | 26 (10.0) |
C-SSR: Suicidal ideation at end of study, n (%) | 0 | 2 (0.8) | 0 | 0 |
C-SSRS = Columbia-Suicide Severity Rating Scale; CI = confidence interval; FAS = full analysis set; LEM5 = lemborexant 5 mg; LEM10 = lemborexant 10 mg; LPS = latency to persistent sleep; LSM = least squares mean; MMRM = mixed model of repeated measures; MVA = motor vehicle accident; NA = not applicable; NR = not reported; PBO = placebo; Q1 = first quartile; Q3 = third quartile; SAE = serious adverse event; SD = standard deviation; SE = standard error; sSOL = subjective sleep onset latency; sWASO = subjective wake after sleep onset; TEAE = treatment-emergent adverse event; vs. = versus; WASO = wake after sleep onset; WASO2H = wake after sleep onset in the second half of the night; WDAE = withdrawal due to adverse event; ZOL = zolpidem tartrate.
aThe number of patients analyzed for the change from baseline at this time point (not the number of patients who provided data at this time point).
bBased on an MMRM model with log transformation of LPS and factors of age group, region, treatment, visit (days 1 to 2, and days 29 to 30), and treatment-by-visit interaction as fixed effects, and the baseline LPS as a covariate. Missing values were imputed using multiple imputation and assumed to be missing not at random.
cP value has been adjusted for multiple testing (i.e., the type I error rate has been controlled).
dBased on an MMRM model with factors of age group, region, treatment, visit (days 1 to 2, and days 29 to 30), and treatment-by-visit interaction as fixed effects, and the baseline WASO as a covariate. Missing values were imputed using multiple imputation and assumed to be missing not at random.
eBased on an MMRM model with factors of age group, region, treatment, visit (days 1 to 2, and days 29 to 30), and treatment-by-visit interaction as fixed effects, and the baseline WASO2H as a covariate. Missing values were imputed using multiple imputation and assumed to be missing not at random.
fBased on an MMRM model with factors of age group, region, treatment, visit (days 1 to 2, and days 29 to 30), and treatment-by-visit interaction as fixed effects, and the baseline SE as a covariate. Missing values were imputed using multiple imputation and assumed to be missing not at random.
gSafety results were based on the FAS population.
Source: SUNRISE 1 Clinical Study Report.17
Table 3: Summary of Key Efficacy Results From the SUNRISE 2 Study, FAS
Outcome | PBO (N = 318) | LEM5 (N = 316) | LEM10 (N = 315) |
|---|---|---|---|
sSOL | |||
Baseline, n | 316 | 314 | 312 |
Geometric mean (SD), minutes | 44.99 (NR) | 42.97 (NR) | 45.05 (NR) |
Median (Q1 to Q3), minutes | 55.86 (34.14 to 78.93) | 53.57 (32.86 to 75.71) | 55.71 (33.57 to 85.07) |
Month 6, na | 249 | 245 | 229 |
Geometric mean (SD), minutes | 27.42 (NR) | 18.62 (NR) | 19.35 (NR) |
Median (Q1 to Q3), minutes | 50.71 (29.29 to 75.71) | 36.58 (21.50 to 57.36) | 35.71 (21.67 to 60.00) |
Change from study baseline, median (Q1 to Q3), minutes | –11.43 (–33.57 to 0.00) | –21.81 (–44.29 to –11.14) | –28.21 (–54.43 to –9.29) |
Geometric LSM treatment ratio, active vs. PBO (95% CI)a | Reference | 0.732 (0.64 to 0.84) | 0.701 (0.61 to 0.81) |
P valueb,c | Reference | < 0.0001 | < 0.0001 |
sWASO | |||
Baseline, n | 314 | 313 | 311 |
Mean (SD), minutes | 132.49 (80.20) | 132.77 (82.52) | 136.83 (87.39) |
Month 6, na | 248 | 244 | 227 |
Mean (SD), minutes | 103.15 (82.29) | 81.79 (76.80) | 86.38 (77.79) |
Change from study baseline, mean (SD), minutes | –32.14 (55.28) | –51.45 (67.30) | –48.12 (68.55) |
LSM visit estimate (95% CI),d minutes | –29.28 (–36.34 to –22.21) | –46.75 (–53.92 to –39.58) | –41.95 (–49.19 to –34.70) |
LSM treatment difference (active minus PBO) (95% CI),d minutes | Reference | –17.47 (–27.31 to –7.64) | –12.67 (–22.38 to –2.96) |
P valuec,d | Reference | 0.0005 | 0.0105 |
Subjective sleep efficiency | |||
Baseline, n | 307 | 302 | 299 |
Mean (SD), % | 61.34 (17.84) | 63.14 (18.23) | 62.03 (17.25) |
Month 6, na | 242 | 235 | 220 |
Mean (SD), % | 71.40 (18.31) | 78.55 (16.24) | 76.53 (17.99) |
Change from study baseline, mean (SD), % | 10.36 (13.80) | 15.34 (14.61) | 15.55 (15.62) |
LSM visit estimate (95% CI),e % | 9.64 (7.99 to 11.30) | 14.19 (12.50 to 15.88) | 14.31 (12.60 to 16.02) |
LSM treatment difference (active minus PBO) (95% CI),e % | Reference | 4.55 (2.24 to 6.86) | 4.67 (2.37 to 6.96) |
P valuec,e | Reference | 0.0001 | < 0.0001 |
Harms, safety population | |||
Safety population, N | 319 | 314 | 314 |
AEs, n (%) | 200 (62.7) | 192 (61.1) | 187 (59.6) |
SAEs, n (%) | 5 (1.6) | 7 (2.2) | 9 (2.9) |
WDAEs from study treatment, n (%) | 12 (3.8) | 13 (4.1) | 26 (8.3) |
Deaths, n (%) | 0 | 0 | 0 |
Notable harms | |||
Somnolence, n (%) | 5 (1.6) | 27 (8.6) | 41 (13.1) |
Impaired driving performance, n (%) | NR | NR | NR |
Falls, n (%) | 10 (3.1) | 5 (1.6) | 5 (1.6) |
MVA (road traffic accident), n (%) | 1 (0.3) | 0 | 1 (0.3) |
Workplace accidents, n (%) | NR | NR | NR |
Hallucination: Hypnagogic, n (%) | 0 | 1 (0.3) | 2 (0.6) |
Hallucination: Hypnopompic, n (%) | 0 | 0 | 1 (0.3) |
Drug misuse (intentional overdose), n (%) | 1 (0.3) | 2 (0.6) | 0 |
On-treatment FAS, N | NA | 444 | 437 |
Rebound insomnia | NA | NA | NA |
sSOL average first 7 nights, n (%) | NA | 53 (11.94) | 46 (10.53) |
sSOL average last 7 nights, n (%) | NA | 52 (11.71) | 41 (9.38) |
sWASO average first 7 nights, n (%) | NA | 55 (12.39) | 62 (14.19) |
sWASO average last 7 nights, n (%) | NA | 60 (13.51) | 52 (11.90) |
On-treatment safety analysis set, N | NA | 447 | 437 |
Withdrawal symptoms, n (%) | NA | 84 (20.7) | 65 (16.8) |
C-SSR: Suicidal ideation at 12 months, n (%) | NA | 1 (0.5) | 1 (0.5) |
AE = adverse event; C-SSR = Columbia-Suicide Severity Rating Scale; CCMV = complete case missing value; CI = confidence interval; FAS = full analysis set; LEM5 = lemborexant 5 mg; LEM10 = lemborexant 10 mg; LSM = least squares mean; MMRM = mixed model of repeated measures; MNAR = missing not at random; MVA = motor vehicle accident; NA = not applicable; NR = not reported; PBO = placebo; Q1 = first quartile; Q3 = third quartile; SAE = serious adverse event; SD = standard deviation; sSOL = subjective sleep onset latency; sWASO = subjective wake after sleep onset; vs. = versus; WDAE = withdrawal due to adverse event.
aThe number of patients analyzed for the change from baseline at this time point (not the number of patients who provided data at this time point).
bBased on an MMRM model with log transformation of sSOL and factors of age group, region, treatment, visit (first 7 nights, month 1, month 3, and month 6), and treatment-by-visit interaction as fixed effects, and the study baseline sSOL as a covariate. Missing values were imputed using multiple imputation and assumed to be MNAR or CCMV.
cP value has been adjusted for multiple testing (i.e., the type I error rate has been controlled).
dBased on an MMRM model with factors of age group, region, treatment, visit (first 7 nights, month 1, month 3, and month 6), and treatment-by-visit interaction as fixed effects, and the study baseline sWASO as a covariate. Missing values were imputed using multiple imputations and assumed to be MNAR or CCMV.
eBased on an MMRM model with factors of age group, region, treatment, visit (first 7 nights, month 1, month 3, and month 6), and treatment-by-visit interaction as fixed effects, and the study baseline subjective sleep efficiency as a covariate. Missing values were imputed using multiple imputation and assumed to be MNAR or CCMV.
Source: SUNRISE 2 Clinical Study Report.18
Health-Related Quality of Life and Severity of Symptoms
The clinical expert emphasized the importance of patient-reported outcomes such as the EQ-5D-3L, ISI, FSS, PGI-Insomnia, and quality of sleep questionnaires. For the EQ-5D-3L visual analogue scale in the SUNRISE 1 trial, the least squares mean (LSM) treatment difference for LEM10 versus PBO was 2.53 (95% confidence interval [CI], 0.69 to 4.38) and for LEM5 versus PBO was 0.52 (95% CI, –1.32 to 2.37). In the SUNRISE 2 trial, the LSM treatment difference for LEM10 versus PBO was 1.04 (95% CI, –1.36 to 3.43) and for LEM5 versus PBO was –0.96 (95% CI, –3.31 to 1.39). All patient-reported outcome questionnaires were other secondary or exploratory outcomes and were not adjusted for multiplicity; therefore, definitive conclusions could not be made from the results.
Sleep Latency (Sleep Onset): Latency to Persistent Sleep, Subjective Sleep Onset Latency
In SUNRISE 1, the geometric LSM treatment ratio for LPS for LEM10 compared to PBO was 0.72 (95% CI, 0.63 to 0.83; P < 0.0001) and for LEM5 compared to PBO was 0.77 (95% CI, 0.67 to 0.89; P = 0.0003).
In SUNRISE 2, the geometric LSM treatment ratio for LPS for LEM10 compared to PBO was 0.70 (95% CI, 0.61 to 0.81; P < 0.0001) and for LEM5 compared to PBO was 0.73 (95% CI, 0.64 to 0.84; P < 0.0001).
Waking After Sleep Onset (Sleep Maintenance): WASO, WASO2H, sWASO
In the SUNRISE 1 study, the LSM treatment differences for WASO for LEM10 versus PBO was –25.35 minutes (95% CI, –31.36 minutes to –19.34 minutes; P < 0.0001) and for LEM5 versus PBO was –23.96 minutes (95% CI, –29.98 minutes to –17.95 minutes; P < 0.0001). The LSM treatment differences for WASO2H for LEM10 versus ZOL was –8.00 minutes (95% CI, –12.53 minutes to –3.47 minutes; P = 0.0005) and for WASO2H for LEM5 versus ZOL was –6.65 minutes (95% CI, –11.15 minutes to –2.15 minutes; P = 0.0038).
In the SUNRISE 2 study, the LSM treatment differences for LEM10 versus PBO was –12.67 minutes (95% CI, –22.38 minutes to –2.96 minutes; P = 0.0105) and for LEM5 versus PBO was –17.47 minutes (95% CI, –27.31 minutes to –7.64 minutes; P = 0.0005).
Sleep Efficiency: Sleep Efficiency and Subjective Sleep Efficiency
In SUNRISE 1, the LSM treatment differences for LEM10 versus PBO was 8.03% (95% CI, 6.57% to 9.49%; P < 0.0001) and for LEM5 versus PBO was 7.07% (95% CI, 5.61% to 8.54%; P < 0.0001).
In SUNRISE 2, the LSM treatment differences for LEM10 versus PBO was 4.67% (95% CI, 2.37% to 6.96%; P < 0.0001) and for LEM5 versus PBO was 4.55% (95% CI, 2.24% to 6.86%; P = 0.0001).
Harms Results
Harms data have been summarized in Table 2 for SUNRISE 1 and Table 3 for SUNRISE 2.
Adverse Events
In the SUNRISE 1 study, approximately one-third of patients experienced a treatment-emergent adverse event (TEAE). Rates were relatively similar among all groups: 82 (30.6%) patients, 74 (27.8%) patients, 93 (35.4%) patients, and 53 (25.4%) patients in the LEM10, LEM5, ZOL, and PBO groups, respectively. In the SUNRISE 2 study, more than half of the patients experienced a TEAE and rates were similar among all groups: 187 (59.6%) patients, 192 (61.1%) patients, and 200 (62.7%) patients in the LEM10, LEM5, and PBO groups, respectively. The most common events in both studies were headache, somnolence, and nasopharyngitis.
Serious Adverse Events
Serious adverse events (SAEs) were rare in both studies. In SUNRISE 1, 2 (0.8%) patients and 4 (1.5%) patients in the LEM5 and ZOL groups, respectively, experienced at least 1 SAE. No patients in the LEM10 or PBO groups reported an SAE. In SUNRISE 2, 9 (2.9%) patients, 7 (2.2%) patients, and 5 (1.6%) patients in the LEM10, LEM5, and PBO groups, respectively, experienced at least 1 SAE. No SAEs occurred in more than 1 patient per treatment group.
Withdrawals Due to Adverse Events
In general, there were few withdrawals from treatment due to adverse events (AEs) in both studies. In SUNRISE 1, 3 (1.1%) patients, 2 (0.8%) patients, 7 (2.7%) patients, and 2 (1.0%) patients in the LEM10, LEM5, ZOL, and PBO groups, respectively, stopped treatment due to an AE. No events occurred in more than 1 patient in any treatment group. In SUNRISE 2, 26 (8.3%) patients, 13 (4.1%) patients, and 12 (3.8%) patients in the LEM10, LEM5, and PBO groups, respectively, stopped treatment due to an AE. The following events occurred in more than 1 patient in any group: headache, somnolence, nightmare, and palpitations.
Mortality
No deaths were reported in either the SUNRISE 1 or SUNRISE 2 trial.
Notable Harms
In both studies, rates of somnolence were numerically higher among patients who received LEM10 compared to LEM5 (7.1% versus 4.1% in the SUNRISE 1 study and 13.1% versus 8.6% in the SUNRISE 2 study) and were greater than rates in either the ZOL group (1.5%) or PBO group (1.9%) in SUNRISE 1 or the PBO group (1.6%) in SUNRISE 2.
Falls were rare in SUNRISE 1 (1.5% in the LEM5 group and 0% for all other groups) and in SUNRISE 2 (1.6% in each of the LEM10 and LEM5 groups and 3.1% for the PBO group).
A road traffic accident (MVA for the CADTH systematic review protocol) was described for 1 patient who received ZOL in SUNRISE 1; no other treatment groups reported an MVA. In SUNRISE 2, 1 patient each in the LEM10 and PBO groups reported an MVA and no MVAs were reported in the LEM5 group.
Reports of hallucinations were rare in both studies. In SUNRISE 1, tactile hallucination was reported for 1 patient who received LEM10 (0 patients for all other treatments). In SUNRISE 2, hypnagogic hallucination was reported for 3 patients (2 patients who received LEM10 and 1 patient who received LEM5) while hypnopompic hallucination was reported for 1 patient who received LEM10. The PBO group did not have any reports of hallucinations.
No intentional overdoses were reported in the SUNRISE 1 trial. Intentional overdoses were reported for 2 patients who received LEM5, 1 patient who received PBO, and 0 patients who received LEM10 in the SUNRISE 2 trial.
Neither trial reported impaired driving or workplace accidents.
Postural instability was assessed in SUNRISE 1. On days 2 to 3, the LSM treatment difference between the LEM10 group and the PBO group was 2.91 units (95% CI, –0.28 units to 6.10 units) and between LEM5 and PBO was 2.49 units (95% CI, –0.70 units to 5.67 units). The LSM treatment difference between the LEM10 group and the ZOL group was –4.29 units (95% CI, –7.32 units to –1.26 units) and between the LEM5 group and the ZOL group was –4.71 units (95% CI, –7.73 units to –1.70 units). On days 30 to 31, the LSM treatment difference between the LEM10 group and the PBO group was –0.58 units (95% CI, –3.68 units to 2.53 units) and between the LEM5 group and the PBO group was –0.71 units (95% CI, –3.80 units to 2.38 units). The LSM treatment difference between the LEM10 group and the ZOL group was –2.57 units (95% CI, –5.53 units to 0.39 units) and between the LEM5 group and the ZOL group was –2.70 units (95% CI, –5.64 units to 0.23 units). Since there was no adjustment for multiplicity, the results are uncertain.
Impaired attention was assessed in the SUNRISE 1 study using 2 components of the Cognitive Performance Assessment Battery (CPAB): power of attention and continuity of attention. On both days 2 to 3 and days 30 to 31, the mean change from baseline for power of attention decreased for the PBO group and increased for the LEM10, LEM5, and ZOL groups. On days 2 to 3, the mean change from baseline for continuity of attention increased for the LEM5 group and decreased for the LEM10, PBO, and ZOL groups. On days 30 to 31, the mean change from baseline for continuity of attention decreased for all groups. Since there was no adjustment for multiplicity for this outcome, conclusions based on the results cannot be drawn with certainty.
In SUNRISE 1, differences in reports of rebound insomnia during the follow-up period between the treatment groups were not tested statistically. The frequency of rebound insomnia appeared similar between the LEM10 and LEM5 groups based on sSOL measures (17% to 21% for the first 7 nights of follow-up and 22% to 24% for the last 7 nights of follow-up) and proportions were numerically higher for the ZOL and PBO groups (23% to 27% for the first 7 nights and 23% to 27% for the last 7 nights). The results using sWASO measures were similar for the LEM10 and LEM5 groups (16% to 19% for the first 7 nights and 18% to 19% for the last 7 nights) as well as the ZOL and PBO groups (15% to 22% for the first 7 nights and 18% for the last 7 nights). Rates of rebound insomnia were generally lower in SUNRISE 2 and similar between the LEM10 and LEM5 groups based on sSOL measures (11% to 12% for the first 7 nights and 9% to 12% for the last 7 nights) and sWASO measures (12% to 14% for both the first and last 7 nights).
Rates of withdrawal symptoms were similar among the LEM10, LEM5, ZOL, and PBO groups in SUNRISE 1 (10.0%, 11.6%, 14.7%, and 14.1%, respectively) and for the LEM10 and LEM5 groups in SUNRISE 2 (16.8% and 20.7%, respectively).
In both the SUNRISE 1 and SUNRISE 2 studies, suicidal ideation was reported in no more than 3 patients in any treatment group at any postbaseline time point.
Critical Appraisal
Both the SUNRISE 1 and SUNRISE 2 trials appeared to have appropriate methods for blinding to the assigned treatment, randomization with stratification, and adequate power for the primary and secondary outcomes. Adjustments for multiplicity were made for all primary and key secondary outcomes and the type I error was controlled for in both studies. All primary and key secondary outcomes were objective PSG measures (SUNRISE 1) or subjective measures based on sleep diary responses (SUNRISE 2). The sponsor noted the importance of having objective outcomes to assess the physiologic effect of the medication along with subjective outcomes to measure the patient’s perception of the medication’s effect. According to the clinical expert, PSG results may not always be interpreted meaningfully or consistently when compared side-by-side with subjective or patient-reported outcomes and consequently, may not be the most meaningful marker of efficacy. The expert further emphasized that insomnia is a subjective issue; therefore, patient-reported outcomes and perceptions of sleep changes may be more appropriate for assessing treatment effect. With all subjective measures, there is a risk of bias that cannot be measured and leads to uncertainty of how meaningful the results are. The direction of the treatment effect for objective and subjective measures aligned in the SUNRISE 1 study, which contributes to the certainty of the results. The numerically higher rates of discontinuations in the LEM10 group compared to the LEM5 group may bias the results, though the magnitude and direction of bias is unknown. There was some amount of missing data at postbaseline visits for all outcomes in both trials, particularly for long-term end points in the SUNRISE 2 study; this prevents strong conclusions from being made. Prespecified subgroup analyses by age were considered exploratory, may not have been powered to detect a treatment difference, and were not adjusted for multiplicity, and there was variability in the change from baseline results (noted by large SDs and interquartile ranges [IQRs]). For responder analyses, SUNRISE 1 was not powered to detect a treatment difference and neither trial was adjusted for multiplicity. As a result of these limitations, conclusions could not be drawn from either the subgroup or responder analysis results.
In general, the clinical expert consulted for this review confirmed that the populations of the SUNRISE 1 and SUNRISE 2 trials were similar to those of patients seen in Canadian clinics and that the trial results would be generalizable with some limitations. There was a large proportion of individuals screened out before randomization, thus producing a study population that may not adequately represent the broader Canadian population with insomnia who would otherwise be eligible for treatment with LEM. Eligibility for SUNRISE 1 was restricted to females 55 years or older and males 65 years or older and the clinical expert stated that the generalizability of the results would be limited to patients matching these demographics. Further, both SUNRISE 1 and SUNRISE 2 excluded a number of comorbid conditions (e.g., based on BDI-2 and BAI scores) and had AHI cut-offs that the clinical expert suggested may have captured individuals with insomnia related to mild sleep apnea rather than psychophysiological insomnia. It is uncertain how applicable the trial results would be to patients with the excluded comorbidities or different AHI scores. No dose changes were allowed during the studies and it is noted in the Health Canada product monograph that the recommended nightly dose for LEM is 5 mg, which may be increased to 10 mg based on clinical response and tolerability.19 ZOL was the active comparator in SUNRISE 1 and discussions with the clinical expert and a representative from the Canadian public drug plans indicated that ZOL is not publicly funded by any drug plans in Canada and is less commonly used for the treatment of insomnia; therefore, it is uncertain if it is the most appropriate comparator for a Canadian setting. Patients were required to maintain a sleep diary throughout the course of both studies, and the clinical expert stated that a sleep diary may not be required in clinical practice. Thus, screening out patients who could not comply with completing a daily sleep diary excluded patients who could be candidates for LEM. Most outcomes identified in the input received by CADTH from patient groups aligned with efficacy and harms outcomes in the studies, though there are still gaps in the evidence for the use of LEM in patients with comorbid conditions and alongside other medications.
Indirect Comparisons
Description of Studies
One sponsor-submitted indirect treatment comparison (ITC) (NMA 1) and a published NMA (NMA 2) were included. NMA1 is a systematic review with 11 studies, that evaluated the efficacy and safety of LEM in patients with insomnia by comparing it to relevant drugs in Canadian public formularies (e.g., zopiclone, temazepam, triazolam, flurazepam, nitrazepam) with respect to clinical end points evaluated objectively (by PSG) or subjectively (patient-reported). The clinical end points included LPS, WASO, sleep efficiency, and total sleep time (TST) with subjective assessment in these same end points. Harms related to the use of LEM were also evaluated in an ITC analysis, including treatment discontinuations, somnolence, dizziness, headache, and in a posthoc analysis, the risk of falls. NMA 2 is a published comparative efficacy analysis by McElroy et al. (2021) aimed at evaluating the efficacy and safety of LEM against other insomnia treatments through a systematic literature review and NMA.20 The ITC search strategy included RCTs of drugs used in adults with primary insomnia (not all reimbursed in Canada). The drugs of interest in NMA 2 were LEM, suvorexant, benzodiazepines, Z-drugs (zolpidem, eszopiclone, zaleplon, zopiclone), trazodone, and ramelteon. Of these, only zolpidem, zopiclone, eszopiclone, trazodone, triazolam, and temazepam were available in the body of evidence from NMA 2 and of interest to this CADTH reimbursement review.
Efficacy Results
Indirect evidence from the NMAs suggest that for the end point of LPS, LEM5 is superior to triazolam and PBO but no evidence of a difference between LEM5 and LEM10 was observed. With LEM5 as a reference, LPS was longer in the PBO group (mean difference = –19.1 minutes [95% CI, –3.20 minutes to –35.0 minutes], in which a negative value in the mean difference implies improvement in favour of LEM5). Patients treated with LEM5 had a reduction in LPS when compared to triazolam 0.5 mg (mean difference = –34.1 minutes; 95% CI, –5.47 minutes to –62.8 minutes). The results for LEM10 were consistent with LEM5. In NMA 2, LEM showed a reduction in LPS when compared to PBO (–18.6 minutes [95% credible interval or CrI, –29.0 minutes to –10.9 minutes]), ZOL-ER (–13.4 minutes [95% CrI, –24.4 minutes to –4.9 minutes)], and triazolam (–23.2 minutes [95% CrI, –38.8 minutes to –9.6 minutes]).
For the end point of WASO, the evidence suggests LEM5 and LEM10 were superior to PBO, but the evidence against triazolam was very imprecise in detecting a difference in PSG-assessed WASO between LEM5, LEM10, and triazolam 0.5 mg. In NMA 2, for WASO, LEM was superior to PBO and zolpidem tartrate immediate-release (ZOL-IR), with an average reduction of 21.3 minutes (95% CrI, –29.6 minutes to –10.1 minutes) and 19.6 minutes (–31.9 minutes to –0.3 minutes), respectively.
For the evaluation of objectively measured sleep efficiency, LEM5, LEM10, flurazepam 30 mg, and triazolam 0.5 mg could be compared in the NMA. The mean differences in sleep efficiency for LEM5 and LEM10 compared with PBO were 7.62% (95% CI, 5.93% to 9.31%) and 8.80% (95% CI, 7.06% to 10.5%), respectively, where higher values mean improvement in favour of LEM. The mean differences in sleep efficiency for LEM5 and LEM10 compared with triazolam were 9.62% (95% CI, 4.92% to 14.3%) and 10.8% (95% CI, 6.09% to 15.5%), respectively. Effect estimates for the comparisons between LEM5 and LEM10 and flurazepam were too imprecise to draw a conclusion.
TST data were only available for LEM5 and LEM10 against PBO. The NMA showed that effect estimates were imprecise in detecting a difference between LEM5 and LEM10 (mean difference = –4.65 minutes; 95% CI, –2.45 minutes to 11.8 minutes). Although relative to PBO, LEM5 and LEM10 were associated with an improvement of 34.8 minutes (95% CI, 27.4 minutes to 42.4 minutes) and 39.5 minutes (95% CI, 32.1 minutes to 46.9 minutes), respectively.
In the second NMA, for the subjective outcomes, LEM was superior to PBO in all end points evaluated but not against eszopiclone for the subjective quality of sleep (sQUAL) end point (mean difference = –0.6 [95% CrI, –0.9 to –0.2]). For the rest of the comparisons, no evidence of effect was observed.
Harms Results
The evidence from the ITC suggested that LEM10 had an increased risk of drug discontinuation when compared to LEM5 (odds ratio [OR] = 1.99; 95% CI, 1.06 to 3.74) and PBO, but not against the other comparators. The odds of discontinuations were less for PBO compared with LEM10 (OR = 0.48; 95% CI, 0.25 to 0.91). The effect estimates for all other comparisons with LEM10 were too imprecise to draw a conclusion.
For the end point of somnolence, when compared with LEM5, PBO had reduced odds of somnolence (OR = 0.25; 95% CI, 0.12 to 0.52); similarly, the odds were reduced in the triazolam 0.25 mg group (OR = 0.31; 95% CI, 0.14 to 0.69) and zopiclone group. Increased odds of somnolence for LEM10 were observed against PBO, triazolam 0.25 mg, and zopiclone 7.5 mg. For other comparisons (i.e., LEM5 and LEM10 versus flurazepam, temazepam, and triazolam 0.125 mg), the effect estimates were too imprecise to detect a difference.
For the end point of dizziness, the effect estimates were too imprecise to draw conclusions about the effect of LEM5 or LEM10 compared with PBO, flurazepam, triazolam, or zopiclone.
For the end point of headache, the results were also too imprecise to detect a difference in the odds of headache between LEM5 and each of the alternatives. This situation also occurred in the comparison of LEM10 to the other comparators.
In an additional posthoc analysis (Bucher ITCs) of studies reporting falls, using LEM5 as the reference, no evidence of any difference could be detected when comparing to patients receiving triazolam, flurazepam, lorazepam, trazodone, benzodiazepines, and Z-drugs due to the high imprecision of the results. When LEM10 was used as the reference, the odds of falls were higher with triazolam, flurazepam, and lorazepam when compared to LEM10. When the entire class of benzodiazepines and trazodone were compared to LEM10, the odds of falls were also higher with the former drugs. Even though these findings suggested that LEM10 is associated with a reduction in the odds of falls when compared to other drugs, the results were very imprecise with wide CIs, which made it difficult to draw conclusions.
In the second NMA evaluated in this CADTH report, there was no evidence of increased or decreased odds for presenting SAEs for patients receiving LEM when compared to relevant comparators, mainly due to wide CrIs. Similarly, no difference was observed in the odds of withdrawals due to AEs or in the odds of falls. LEM was associated with lower odds of dizziness compared with ZOL-IR, ZOL-ER, and eszopiclone. LEM, however, increased the odds of somnolence when compared to PBO, ZOL, and eszopiclone.
Critical Appraisal
The results from both NMAs have uncertainty due to the risk of bias in the individual studies (i.e., unclear randomization, allocation concealment, and baseline imbalances), heterogeneity in the pairwise comparisons, and suspected publication bias. Furthermore, the evidence is imprecise in most of the effect estimates from both NMAs, with wide CIs that could include an appreciable threshold of benefit or harm. In the NMAs, there were concerns of incomplete information and discrepancies in the included studies that could affect the plausibility of the transitivity assumption. Overall, the populations included in the individual studies of the network are generalizable to the Canadian population without comorbid conditions.
Other Relevant Evidence
Description of Studies
Study 312 was an open-label, phase IIIb, pilot, multicentre trial (N = 53) investigating next-dose transition from ZOL to LEM for the treatment of insomnia. The trial included adult patients with insomnia who were receiving ZOL as monotherapy, and who agreed to substitute it with LEM.
Efficacy Results
Overall, 81.1% of patients successfully transitioned to LEM at the end of the 2-week titration period and entered study 312’s extension phase. A total of 15 (48.4%) patients had an LEM dose increase from 5 mg to 10 mg while 5 (22.7%) patients had an LEM dose decrease from 10 mg to 5 mg at the end of the 2-week titration period.
At the end of the titration period, patients in both the LEM5 and LEM10 groups indicated that LEM had a positive effect on sleep, time to fall asleep, and TST. A large proportion of patients felt that the medication was “too weak.” In the overall trial population, the mean change in ISI total score was –4.6 (SD = 6.26) and the mean change in the quality of sleep score was –0.19 (SD = 0.92) at the end of the titration period.
In the overall trial population, at baseline and at the end of the titration period, the mean sleep efficiency scores were 79.03% (SD = 85.4%) and 80.17% (SD = 8.49%), respectively. The mean WASO scores were 80.90 (SD = 33.23) minutes and 83.92 (SD = 35.44) minutes, respectively, and the mean TST scores were 403.44 (SD = 62.07) minutes and 412.11 (SD = 60.17) minutes, respectively.
Harms Results
Of the 53 patients enrolled in the core study, 20 (37.7%) patients experienced at least 1 TEAE (5 patients from the LEM5 group and 15 patients from the LEM10 group). The most common TEAEs were abnormal dreams (7.5%) and somnolence (7.5%). In the overall trial population, 13% of patients withdrew from treatment due to an AE. No deaths or SAEs leading to study drug discontinuation were reported in the study.
Critical Appraisal
Study 312 had an open-label design, small sample size, short study duration, no formal statistical testing, subjective secondary end points, and 50% screening failures, and chose ZOL as the previous treatment to transition from (rather than other treatments that may have been more relevant to Canadian clinical practice); this prevented conclusions from being drawn and limited generalizability to the Canadian population with insomnia.
Conclusions
Both LEM10 and LEM5 demonstrated statistically significant improvements in sleep onset, sleep maintenance, and sleep efficiency among adults with insomnia relative to PBO in the SUNRISE 1 and SUNRISE 2 trials. In SUNRISE 1, all primary and key secondary outcomes were for objective PSG measures and were clinically meaningful based on suggested thresholds for a clinically important effect identified from the literature — except for WASO2H, which did not have a minimal important difference (MID) or threshold identified. In SUNRISE 2, all primary and key secondary outcomes were for subjective sleep diary measures, and none reached the suggested thresholds for a clinically important effect identified from the literature. Numerical differences in ISI item 4 to item 7 and FSS indicated a benefit from treatment with LEM over PBO, but due to the lack of adjustment for multiple comparisons and no established MID for ISI item 4 to item 7 and FSS, conclusions could not be drawn from these outcomes. Other patient-reported outcomes such as the EQ-5D-3L, PGI-Insomnia, and quality of sleep scale were exploratory, were not controlled for multiplicity, and did not have MIDs for populations with insomnia; therefore, no conclusions could be drawn regarding whether treatment with LEM conferred a benefit for these outcomes. The clinical expert consulted for this review emphasized the importance of subjective outcomes and how patients perceive changes in their sleep, and sponsor-submitted posthoc analyses of SUNRISE 2 data lent support to the meaningfulness of the PGI-Insomnia and ISI subjective outcomes. However, the sleep improvements based on PSG and sleep diary outcomes observed in the SUNRISE 1 and SUNRISE 2 studies did not appear to be reflected in the results from the patient-reported questionnaires (i.e., ISI, FSS, and perceived sleep quality).
It is uncertain if the differences in treatment effect observed in SUNRISE 1 and SUNRISE 2 would be experienced by and be meaningful to all patients who could be treated with LEM. There did not appear to be a clear difference in efficacy between LEM10 and LEM5, although differences in efficacy between the 2 doses were not tested statistically in the trials. The product monograph’s recommendation to start with LEM5 and the higher rates of somnolence and treatment discontinuations for LEM10 would be considerations when prescribing or increasing a patient’s dose. Overall, the clinical expert indicated that LEM demonstrated a minor harms profile with few SAEs, low rates of withdrawals from treatment due to AEs, and no deaths. Patients with specific comorbid conditions such as sleep apnea, anxiety, and depression were excluded from the studies based on the exclusion criteria for AHI, BAI, and BDI-2 scores. Further research showing adequate efficacy and safety is needed to inform broader treatment with LEM. Indirect evidence suggested LEM is superior to triazolam 0.5 mg for LPS and sleep efficiency, is superior to ZOL for WASO and LPS, and is inferior to eszopiclone in sleep quality; however, there is uncertainty in this conclusion due to limitations of the NMAs and differences in conclusions for some outcome comparisons across NMAs. Evidence was very uncertain or absent for the other comparisons and end points due to imprecision, risk of bias, and heterogeneity in the pairwise comparisons. Additionally, evidence for transitioning from ZOL to LEM from the pilot study 312 was limited by the study design, small sample size, and large proportion of screening failures, preventing conclusions from being drawn. Overall, LEM appears to be effective relative to PBO for important sleep-related outcomes, and long-term results from SUNRISE 2 supported those observed during the first 6 months of treatment. There were no serious safety concerns, but efficacy for health-related quality of life (HRQoL) and subjective appraisals of symptoms and sleep quality were less certain due to limitations of the trials. ZOL may not have been the most relevant comparator in Canadian practice, and comparisons with ZOL in the trial (except for WASO2H) were not controlled for multiplicity; therefore, there is uncertainty in the conclusions about the comparative efficacy. LEM appeared to be more effective than ZOL for the outcome of WASO2H, which was noted as being important for sleep maintenance, though there was no MID identified and there was uncertainty if the change observed in SUNRISE 1 was clinically meaningful. Moreover, there was no direct evidence for efficacy or harms relative to other relevant comparators that may be used in Canadian clinical practice, and the indirect evidence was uncertain. Owing to its superiority over PBO, LEM may be another treatment option for patients with insomnia.
Introduction
Disease Background
Insomnia disorder is the most common sleep disorder and, according to the DSM-5, is described as being dissatisfied with the quality or quantity of sleep as well as having difficulty initiating and/or maintaining sleep, and is associated with daytime impairment.2,3 The DSM-5 criteria include sleep disturbances occurring at least 3 nights per week for at least 3 months causing significant distress or impairment in daily functioning, having adequate opportunity for sleep, ruling out other sleep disorders, and excluding the possibility of being caused by coexisting mental disorders or medical conditions, or by a substance.4
According to the Alberta Medical Association’s 2015 Assessment to Management of Adult Insomnia clinical practice guideline, there are no validated questionnaires for the diagnosis of sleep disorders and a diagnosis should be made based on clinical judgment.3 There are instruments for assessing insomnia and related conditions that can support a diagnosis such as the Sleep Disorders Assessment Questionnaire, ISI, and screening tools for psychiatric and medical disorders that affect sleep. A sleep diary may be used in clinical practice to track a patient’s perception of their sleep outcomes, particularly when CBT-I is used to treat insomnia.
Estimates for the prevalence and incidence of insomnia vary based on the population studied and how insomnia has been defined.8 The prevalence of insomnia is estimated to be between 12% and 24% based on surveys of adults in Canada.5,6 There is additional uncertainty in the numbers, given that individuals with insomnia may not immediately seek advice from their primary care physicians until symptoms are bothersome; thus, many individuals are not diagnosed.2,21 A Canadian study (N = 3,073) investigating the incidence of insomnia found that 3.8%, 9.3%, and 13.9% of adults without insomnia at baseline developed an insomnia disorder at the 1-year, 3-year, and 5-year follow-up time points of the study, respectively.7 Another study of adults in Quebec found that 30.7% of survey respondents who reported no insomnia symptoms at baseline had developed symptoms within 1 year while 7.3% had developed an insomnia disorder in that time.8
Older age, female sex, comorbid medical or psychiatric conditions, and social and environmental factors have been identified as common risk factors for insomnia.2,3 It has been reported that adults aged between 30 years and 59 years are almost twice as likely to have insomnia compared to adults aged 18 years to 29 years.2,3 Furthermore, natural age-related changes and medical issues increase the risk of insomnia among older adults. It has been estimated that females are 1.2 to 1.5 times more likely to have insomnia than males.2,3 When compared to people without insomnia, patients with insomnia have consistently demonstrated impaired HRQoL on different generic health questionnaires — typically on multiple domains assessed by the instrument with some variability by age.22 This trend was also observed when comparing patients with different severity of symptoms where those with insomnia disorder scored lower than those with mild or occasional insomnia symptoms.22 Insomnia can be diagnosed as a disorder on its own or as a symptom associated with other conditions such as chronic pain, heart disease, respiratory disease, gastrointestinal problems, cancer, and diabetes.3,8 The negative impact insomnia has on HRQoL was found to have a compounding effect on poor sleep for patients with existing conditions such as multiple sclerosis, Parkinson disease, and cancer.22 Additionally, insomnia has been closely linked to increased risks of mental health, occupational, and medical issues; reduced life expectancy; and increased economic costs through lost productivity, workplace accidents and MVAs, and greater health care usage.2,3,7,9,10
Standards of Therapy
Per the Alberta Medical Association’s clinical practice guideline, insomnia can be treated and managed in a primary care setting.3 A patient may be referred to a physician or medical centre that specializes in treating sleep disorders when the problem cannot be diagnosed or treated in the primary setting or if the insomnia is resistant to treatment or worsens. Referrals may also depend on the availability of specialists, with the possibility of long wait times.
According to the clinical expert CADTH consulted for this review, the primary goals of treatment are to improve sleep initiation and maintenance and reduce terminal insomnia, and for sleep to be more restorative. These goals were consistent with those noted by the clinician groups that provided input for the review, with the addition of improved related daytime function. The group emphasized that simply treating nocturnal symptoms is inadequate if overall daytime function is not also improved.
Nonpharmacologic treatment options such as sleep hygiene education (e.g., changing sleep habits, relaxation techniques) and CBT-I are recommended as an initial treatment of insomnia.3,10,11,23 It is recommended that behavioural therapy be introduced before or concurrently with pharmacotherapy, and that the former be continued even if medication is stopped. The clinical expert consulted for this review described how CBT-I works to target the underlying mechanisms of insomnia while pharmacotherapy treats the symptoms. It has been noted that CBT-I may not be accessible to all patients due to cost or lack of availability in the patient’s region,10,23 although the clinical expert suggested that access to CBT-I is less of an issue now with the availability of CBT-I courses and treatment through online and book formats. Other issues with CBT-I are that patients may be unwilling or unable to participate, or patients may be unresponsive to treatment.10 When these barriers have been identified, pharmacologic treatment can be considered.
Pharmacologic treatments for insomnia can be categorized based on 4 different mechanisms of action: BZRAs, DORAs, histamine receptor antagonists, and melatonin receptor agonists.12 The BZRA group includes benzodiazepine hypnotics (e.g., flurazepam, temazepam, triazolam) and non-BZRAs, also known as Z-drugs (e.g., zopiclone, zolpidem); DORAs include suvorexant and LEM; histamine receptor antagonists include low-dose doxepin; and melatonin receptor agonists include ramelteon.12,23 Of the medications listed, suvorexant and ramelteon are not available in Canada. Off-label medications that have sedating effects (e.g., antidepressants, antihistamines, anticonvulsants, antipsychotic drugs) may also be used in specific situations but are generally not recommended as a first-line treatment due to the lack of efficacy and safety evidence in this population.3,12 This was also noted in the clinician group input submitted to CADTH. The Alberta Medical Association’s clinical practice guideline emphasizes a short initial treatment duration (i.e., limited prescription without refills) of the lowest possible dose with follow-up within 2 weeks to 4 weeks to assess adverse effects and whether there is a need for continued treatment. For sleep onset insomnia (trouble falling asleep, but not maintaining sleep), non-BZRAs or melatonin receptor agonists are recommended.12 For sleep maintenance or mixed insomnia (sleep onset and sleep maintenance), DORAs, non-BZRAs, and low-dose doxepin would be considered acceptable.12 Tapering medication may take weeks to months and is recommended to improve the transition to on-treatment or off-treatment, avoid rebound insomnia, and promote long-term success.3 Despite the fact that insomnia can be chronic and unremitting, long-term use of these medications, particularly hypnotic drugs, is discouraged as the studies supporting their approval were based on short-term use.2 Specifically with the older benzodiazepine hypnotics, their use as a first-line treatment option is not recommended due to their long half-life, their higher risk of tolerance and dependence, and the availability of safer options.3,12 Resistant insomnia and insomnia that occurs with other comorbidities may warrant the long-term use of medications.3 For the extended use of sedatives, it is recommended that follow-up visits occur every 3 months to 4 months until the insomnia is stable, after which reassessment can be made at 6 months. Over-the-counter medications with sedative effects such as those containing diphenhydramine or doxylamine and alcohol are not recommended for the treatment of insomnia.3,12 Studies of alternative therapies for treating insomnia were noted to have methodological limitations that have prevented the use of their findings.2 The clinical expert also noted that cannabinoids have gained widespread use — again, with little clinical trial data. The expert suggested that the widespread prevalence of over-the-counter medications, alcohol, and cannabinoids, as well as the off-label use of antidepressants and antipsychotic drugs, suggests that no single drug or mechanism of action can resolve the majority of problems with insomnia.
Drug
The key characteristics of LEM, Z-drugs, benzodiazepines, doxepin, antidepressants, and antipsychotic drugs are summarized in Table 4.
LEM (Dayvigo) is indicated for the treatment of insomnia, characterized by difficulties with sleep onset and/or sleep maintenance.1 The drug is available in 5 mg and 10 mg tablets to be taken orally once per night within a few minutes before going to bed, with at least 7 hours before planned awakening time.13 The recommended dose is 5 mg once per night, although the dose may be increased to the maximum recommended dose of 10 mg based on clinical response and tolerability. The drug is a competitive antagonist of both orexin receptor 1 (OX1R) and orexin receptor 2 (OX2R), with a higher affinity for OX2R. The orexin neuropeptide signalling system is a central promoter of wakefulness and blocking the binding of wake-promoting neuropeptides orexin A and orexin B to receptors OX1R and OX2R is thought to suppress wake drive.
LEM underwent a standard review at Health Canada and was issued a Notice of Compliance on November 4, 2020. The sponsor has requested reimbursement as per the approved Health Canada indication.1 LEM has not been previously reviewed by CADTH.
Table 4: Key Characteristics of Lemborexant, Z-Drugs, Benzodiazepines, Doxepin, Antidepressants, and Antipsychotic Drugs
Drug name | Mechanism of action | Indicationa | Route of administration | Recommended dosage | Serious adverse effects or safety issues | Other |
|---|---|---|---|---|---|---|
Lemborexant | Competitive antagonist of OX1R and OX2R. Blocking the binding of wake-promoting neuropeptides orexin A and orexin B to receptors (OX1R and OX2R) is thought to suppress wake drive. | For the treatment of insomnia, characterized by difficulties with sleep onset and/or sleep maintenance | Oral | 5 mg once per night within a few minutes before going to bed with at least 7 hours before planned awakening time. The dose may be increased to 10 mg based on response and tolerability |
| NA |
Z-drugs | GABA A receptor– positive modulator presumed to exert its therapeutic effects through binding the benzodiazepine site of alpha-1 subunit containing GABA A receptors, increasing the frequency of chloride channel opening resulting in the inhibition of neuronal excitation | For short-term use (usually not exceeding 7 to 10 days) for:
| Oral, sublingual | Varies by drug |
| Drugs: Zolpidem, zopiclone |
Benzodiazepines | Depressants of the CNS, believed to enhance or facilitate the effects of the inhibitory neurotransmitter GABA and act as agonists at the benzodiazepine receptor’s sites | Temazepam: For the symptomatic relief of transient and short-term insomnia characterized by difficulty in falling asleep, frequent nocturnal awakenings, and/or early morning awakenings. Treatment should usually not exceed 7 to 10 consecutive days. | Oral | Varies by drug |
| Drugs: Temazepam |
Doxepin | Doxepin binds with high affinity to the histamine H1 receptor where it functions as an antagonist. The exact mechanism by which doxepin exerts its sleep maintenance effect is unknown but is believed to be due to its antagonism of the H1 receptor. | For the treatment and symptomatic relief of insomnia characterized by frequent nocturnal awakenings, and/or early morning awakenings | Oral | 6 mg once daily, though 3 mg once daily may be appropriate for some patients For older adult patients, the recommended dosage is 3 mg once daily and can be increased to 6 mg, if clinically indicated |
| NA |
Antidepressants | Unclear in humans | None for insomnia | Oral | Varies by drug |
| Drugs: Trazodone |
Antipsychotic drugs | Interact with a broad range of neurotransmitter receptors with direct and indirect effects | None for insomnia | Oral | Varies by drug |
| Drugs: Quetiapine |
CNS = central nervous system; GABA = gamma-aminobutyric acid; MAOI = monoamine oxidase inhibitor; NA = not applicable; OX1R = orexin receptor 1; OX2R = orexin receptor 2; QTc = QT interval corrected for heart rate; Z-drugs = zolpidem, eszopiclone, zaleplon, and zopiclone.
aHealth Canada–approved indication.
Sources: Product monographs for Dayvigo,13 Sublinox,24,25 temazepam,24,26 Silenor,27 trazodone,28,29 and quetiapine.30,31
Stakeholder Perspectives
Patient Group Input
This section was prepared by CADTH staff based on the input provided by 3 patient groups. The full patient group submissions are included in the stakeholder input section at the end of this report.
The patient and caregiver input received for this review was collected by 3 groups: MDSC, Migraine Canada, and Menopause Chicks. The input provided by MDSC included 1,249 respondents and was sourced from a survey conducted from September 21 to October 7, 2021, interviews with 3 respondents with insomnia, several family members, 2 clinicians, and social media interactions. The input provided by Migraine Canada consisted of 1,385 respondents and was sourced from 2 online surveys conducted in the fall of 2021 and in March 2022. The input provided by Menopause Chicks consisted of 1,027 respondents and was sourced from an online survey conducted in the fall of 2021, and a focus group with 4 participants.
Respondents from all 3 patient groups indicated that sleep problems significantly impacted their quality of life, energy level, cognitive function, and mood the next day. More than 70% of respondents to the surveys reported sleep dissatisfaction and insufficient sleep duration, and more than 60% reported some degree of disruption of daytime activities. The daytime activities that were most commonly impacted included the ability to work, conduct household chores, exercise, fulfill family obligations, and spend time with family and friends. Moreover, due to the perceived stigma of insomnia, many reported delaying getting a diagnosis and seeking treatment for fear of what other people might think. According to the patient input received, most respondents have tried various treatments for sleep problems (e.g., benzodiazepines, Z-drugs), especially respondents with insomnia symptoms, mental illness, and pain. Many of them were dissatisfied and discontinued the treatment due to side effects, such as next-day sedation and cognitive impairment, and fear of developing a substance use disorder.
Respondents from all 3 groups reported that they would like a treatment to address the following key outcomes that are important to patients, family members, and caregivers: uninterrupted and restorative sleep, greater access to treatment, more effective treatment options, long-term treatment effectiveness, fewer side effects, less stress and anxiety, improved productivity, and improved relationships with family members and colleagues. The input received from MDSC included 3 respondents with experience with LEM for poor sleep and/or insomnia; all accessed the drug through private health insurance. They indicated that they were able to manage their sleep problems without becoming dependent on the medication or experiencing serious side effects, and without feeling lethargic and sleepy the next morning.
Clinician Input
Input From the Clinical Expert Consulted by CADTH
All CADTH review teams include at least 1 clinical specialist with expertise regarding the diagnosis and management of the condition for which the drug is indicated. Clinical experts are a critical part of the review team and are involved in all phases of the review process (e.g., providing guidance on the development of the review protocol, assisting in the critical appraisal of clinical evidence, interpreting the clinical relevance of the results, providing guidance on the potential place in therapy). The following input was provided by 1 clinical specialist with expertise in the diagnosis and management of insomnia.
Unmet Needs
The clinical expert consulted for this review stated that the current goals of treatment are to improve sleep initiation, maintenance, and terminal insomnia, leading to restorative sleep. First-line treatment for insomnia is CBT-I according to the clinical expert, yet many patients have limited access to and/or success with this option. As a result, pharmacotherapy is often used in addition to or in place of CBT-I. The clinical expert described that CBT-I targets the underlying mechanisms of insomnia, whereas medications tend to target the symptoms.
As per the clinical expert, patients may have no response or a waning response to medications when used for extended periods of time, at which point it can be difficult to withdraw the therapy if the patient has developed a tolerance to it and experiences rebound insomnia. Another concern raised by the clinical expert was the risk of cognitive and behavioural changes the next morning that can lead to falls and other dangers, particularly for older adult patients.
Place in Therapy
The clinical expert suggested that LEM may be a first-line pharmacologic treatment for insomnia and noted that it would be necessary to determine how to optimally transition from other currently available medications (e.g., Z-drugs) to LEM.
Patient Population
The expert indicated that most patients with insomnia may be candidates for treatment with LEM except for those who are pregnant, nursing, or have narcolepsy.
Assessing Response to Treatment
Per the clinical expert, patients are asked generally if they are sleeping better and longer, and feel refreshed, rather than performing tests and having measurements taken in clinics. The expert suspected that methods for the evaluation of treatment response do not vary among physicians. The clinical expert indicated that few clinics are performing sleep studies (except where another sleep disorder is suspected), particularly since access is limited in many clinics across Canada.
Discontinuing Treatment
The expert noted that chronic insomnia generally does not go away unless there is successful behavioural intervention or another major illness overtakes it. Furthermore, the clinical expert reported that insomnia tends to worsen with age, menopause, or major negative life events. It was suggested by the expert that a patient may wish to trial being off the medication and can be supported by additional sleep management tools such as CBT-I. When deprescribing a medication, the clinical expert would observe the patient for a return of symptoms or rebound insomnia.
Prescribing Conditions
Per the clinical expert, insomnia is typically treated by family physicians and few patients are referred to sleep specialists, for instance, if another comorbid sleep condition is suspected.
Clinician Group Input
This section was prepared by CADTH staff based on the input provided by 2 clinician groups. The full clinician group submissions are included in the stakeholder input section at the end of this report.
Clinician group input on the review of LEM for the treatment of insomnia was received from 2 clinician groups: the CCSSP and the National Advisory Board, comprising Canadian family physicians and psychiatrists with expertise in the management of insomnia.
The clinician groups identified that current pharmacotherapy options for treating insomnia disorder include benzodiazepines and Z-drugs, which can pose a significant risk of adverse effects such as delirium, falls, MVAs, cognitive impairment, dependance, and tolerance in some populations, including older adults and patients with comorbid conditions. Moreover, both clinician groups noted that due to a lack of safe on-label pharmacologic options and limited access to CBT-I for treating insomnia, physicians have resorted to prescribing off-label sedating drugs, including antipsychotic drugs, antidepressants, and anticonvulsants for long periods that are generally not supported by guidelines. The CCSSP noted that all current pharmacologic treatments should be considered symptomatic as they do not modify the underlying mechanisms of insomnia. Additionally, both groups noted the widespread use of over-the-counter medications by patients in combination with alcohol and cannabis to improve sleep, which can have harmful effects on their mental and physical health. Thus, new drugs with good evidence of improved efficacy, tolerability, and safety for the treatment of insomnia are critical.
According to the clinician groups, patients who are most likely to respond better to treatment with LEM are older adults with chronic insomnia as well as patients with comorbidities of major depressive disorder, anxiety, attention-deficit/hyperactivity disorder, post-traumatic stress disorder, obstructive sleep apnea, and fibromyalgia. Both groups agreed that responses to treatment are typically assessed by improvement in sleep onset, LPS, sleep efficiency, and TST, as well as daytime alertness, and functioning. Both groups noted that the ISI and Epworth Sleepiness Scale are the most frequently used patient-reported outcomes to document treatment response and remission from insomnia in clinical trials. The CCSSP also indicated that response should be assessed every 2 weeks to 4 weeks when treatment is initiated, and then every 3 months to 6 months if a patient remains stable.
Both groups agreed that the novel mechanisms of LEM would improve the evolving paradigm of insomnia medications with its high pharmacologic specificity, improved safety, tolerability, and efficacy profiles. The clinician groups indicated that LEM can be considered as first-line treatment for all patients with insomnia disorder who are offered pharmacotherapy and clinicians have felt that the clinical trial data generally aligned with their experiences with LEM in practice. The clinician groups stated that the prescription of LEM should not be limited to sleep specialists and that discontinuing treatment may be considered if there are concerning AEs, the risk of drug-drug interactions, or a lack of treatment response.
Drug Program Input
The drug programs provide input on each drug being reviewed through CADTH’s reimbursement review processes by identifying issues that may impact their ability to implement a recommendation. The implementation questions and corresponding responses from the clinical expert consulted by CADTH are summarized in Table 5.
Table 5: Summary of Drug Plan Input and Clinical Expert Response
Drug program implementation questions | Clinical expert response |
|---|---|
Comparators | |
Issues with the choice of comparator in the submitted trial(s):
Is the lower dose appropriate as a comparator and is ZOL an appropriate comparator for Canada? | ZOL is not publicly funded by any drug plans in Canada and, therefore, is infrequently used by the clinical expert for treating insomnia. The clinical expert was uncertain if ZOL would be the best comparator, and if so, at which dose. |
Other implementation issues regarding relevant comparators (e.g., access and/or funding, covered population):
How comparable are ZOL and zopiclone? | The clinical expert was uncertain if ZOL and zopiclone were comparable for the treatment of insomnia, and if so, at what doses, but suggested that zopiclone may be an appropriate comparator in place of zolpidem. |
Initiation criteria | |
With no prior therapies required for eligibility, patients on LEM, ZOL or other drugs could still enrol in the study as long as they had not used the drugs within a certain time frame, depending on the medication they were on. If a patient failed suvorexant (the same class of medication as LEM), they were not eligible for the study. Would patients need to fail less expensive alternatives (benzodiazepines or zopiclone) to qualify for treatment? | According to the clinical expert, most complaints about the drugs currently available for treating insomnia (e.g., benzodiazepines, Z-drugs) are related to the side effects rather than lack of efficacy. The clinical expert suggested that rather than trialling a patient on a less expensive treatment that has a higher risk of adverse events and having them fail on that drug to be able to access alternatives, it would be reasonable to start a patient on a drug that is associated with a lower risk of adverse events (i.e., LEM) and at least a similar efficacy first. |
Patients with other sleeping disorders were excluded from the trials — more specifically, those with narcolepsy or potential narcolepsy, sleep apnea, parasomnia, depression, anxiety, and/or nocturia. Is it reasonable to exclude patients with these conditions? Would it be acceptable for patients with these comorbidities to receive LEM? | The clinical expert noted that, currently, data are lacking that show what effect LEM would have in patients with these comorbidities, and excluding these patients from treatment with LEM would be reasonable until there is better evidence of efficacy and safety. The clinical expert further stated that if there is proof of safe and effective use in such patients, LEM may gain widespread use (e.g., among those with depression and/or anxiety), but not until then. The expert also added that since insomnia may precede, travel with, and follow episodes of anxiety and/or depression, it would be very difficult to exclude these comorbidities until trials could be completed. |
Renewal criteria | |
PSG was conducted the first 2 nights at baseline and the last 2 nights of treatment. Since PSG is not always available or covered in all jurisdictions, should PSG be considered a marker for efficacy, as it may be less important for funding criteria? | The clinical expert stated that PSG results cannot always be interpreted meaningfully in relation to insomnia complaints and should not be used as a marker for efficacy or a necessary criterion to access LEM. |
Discontinuation criteria | |
Insomnia medications have been known to be habit forming for many individuals. Acute insomnia guidelines generally recommend a short-term course of therapy for 1 week to 2 weeks along with best supportive care, which includes cognitive behavioural therapy and lifestyle modifications. In the SUNRISE 1 clinical trial, patients received 30 days of therapy. In the SUNRISE 2 trial, patients received LEM vs. placebo (for the first 6 months); in the last 6 months, all patients were on LEM. How will criteria be implemented to avoid long-term use of this medication? | For consideration by CDEC. |
Prescribing criteria | |
In keeping with clinical practice guidelines for insomnia, how will criteria align with the recommended initiation of the lowest possible dose on an as-needed basis with close monitoring by the prescriber? | For consideration by CDEC. |
There are concerns if used in combination with other hypnotics such as benzodiazepines and zopiclone due to additive effects. Also, there is a concern with the concomitant use of alcohol as patients with heavy alcohol use were excluded from the trials. | For consideration by CDEC. |
Care provision issues | |
A major concern is falls among older adults. | For consideration by CDEC. |
Pricing conditions | |
The list prices of the drug comparators for the BIA were taken from the Ontario Drug Benefit Formulary. The list prices of these medications are variable across jurisdictions. According to the sponsor's BIA, pan-Canadian direct costs over 3 years would be $76,394,909 with an incremental cost of $59,686,413. This is a significant expenditure for drug plans, considering this is an incremental cost for a drug that may have marginal improvements over ZOL, a drug that is not funded in any Canadian jurisdiction. | For consideration by CDEC. |
BIA = budget impact analysis; CDEC = CADTH Canadian Drug Expert Committee; LEM = lemborexant; PSG = polysomnography; vs. = versus; Z-drugs = zolpidem, eszopiclone, zaleplon, and zopiclone; ZOL = zolpidem tartrate.
Clinical Evidence
The clinical evidence included in the review of LEM (Dayvigo) is presented in 3 sections. The first section, the systematic review, includes pivotal studies provided in the sponsor’s submission to CADTH and Health Canada, as well as those studies that were selected according to an a priori protocol. The second section includes indirect evidence from the sponsor and indirect evidence selected from the literature that met the selection criteria specified in the review. The third section includes sponsor-submitted long-term extension studies and additional relevant studies that were considered to address important gaps in the evidence included in the systematic review.
Following the issuance of the draft CDEC recommendation for LEM in August 2022, the following additional information was provided to CADTH: 1 unpublished manuscript by Drake et al.14 that provided evidence for LEM’s efficacy by the PGI-Insomnia in the SUNRISE 2 study; a PSUR15 that included aggregate data from approximately 4,024 adult patients with insomnia disorder, ISWRD, or healthy volunteers who were enrolled in the LEM clinical development program; and a published NMA by De Crescenzo et al. (2022)16 comparing LEM to other pharmacologic treatments for the acute and long-term treatment of adults with insomnia. These data were not included in the submission to CADTH and provided more information on the clinical meaningfulness of the subjective PGI-Insomnia instrument, and on LEM’s safety and comparative evidence versus other drugs for the treatment of insomnia. The information has been summarized and critically appraised as an addendum to the CADTH report in Appendix 6.
Systematic Review (Pivotal and Protocol Selected Studies)
Objectives
To perform a systematic review of the beneficial and harmful effects of LEM5 or LEM10 tablets taken orally once daily at bedtime for the treatment of patients with insomnia, characterized by difficulties with sleep onset and/or sleep maintenance.
Methods
Studies selected for inclusion in the systematic review included pivotal studies provided in the sponsor’s submission to CADTH and Health Canada, as well as those meeting the selection criteria presented in Table 6. Outcomes included in the CADTH review protocol reflect outcomes considered to be important to patients, clinicians, and drug plans.
Table 6: Inclusion Criteria for the Systematic Review
Criteria | Description |
|---|---|
Population | Patients with insomnia, characterized by difficulties with sleep onset and/or sleep maintenance Subgroups:
|
Intervention | Lemborexant 5 mg or 10 mg tablet taken orally, once daily at bedtime |
Comparator |
|
Outcomes | Efficacy outcomes:
Harms outcomes:
|
Study designs | Published and unpublished phase III and phase IV RCTs |
AE = adverse event; ESS = Epworth Sleepiness Scale; FSS = Fatigue Severity Scale; HRQoL = health-related quality of life; ISI = Insomnia Severity Index; MVA = motor vehicle accident; RCT = randomized controlled trial; SAE = serious adverse event; SDLP = standard deviation of lateral position; vs. = versus; WDAE = withdrawal due to adverse event.
aOff-label use.
The literature search for clinical studies was performed by an information specialist using a peer-reviewed search strategy according to the PRESS Peer Review of Electronic Search Strategies checklist.32
Published literature was identified by searching the following bibliographic databases: MEDLINE All (1946–) via Ovid and Embase (1974–) via Ovid. All Ovid searches were run simultaneously as a multifile search. Duplicates were removed using Ovid deduplication for multifile searches, followed by manual deduplication in Endnote. The search strategy consisted of both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. The main search concept was lemborexant. Clinical trials registries were searched: the US National Institutes of Health’s ClinicalTrials.gov, the WHO’s International Clinical Trials Registry Platform search portal, Health Canada’s Clinical Trials Database, and the European Union Clinical Trials Register.
No filters were applied to limit the retrieval by study type. Retrieval was not limited by publication date or by language. Conference abstracts were excluded from the search results. Refer to Appendix 1 for the detailed search strategies.
The initial search was completed on March 24, 2022. Regular alerts updated the search until the meeting of CDEC on July 28, 2022.
Grey literature (literature that is not commercially published) was identified by searching relevant websites from the Grey Matters: A Practical Tool For Searching Health-Related Grey Literature checklist.33 Included in this search were the websites of regulatory agencies (US FDA and European Medicines Agency). Google was used to search for additional internet-based materials. Refer to Appendix 1 for more information on the grey literature search strategy.
These searches were supplemented by contacting the manufacturer of the drug for information regarding unpublished studies.
Two CADTH clinical reviewers independently selected studies for inclusion in the review based on titles and abstracts, according to the predetermined protocol. Full-text articles of all citations considered potentially relevant by at least 1 reviewer were acquired. Reviewers independently made the final selection of studies to be included in the review, and differences were resolved through discussion.
Findings From the Literature
A total of 6 reports of 2 studies34-39 were identified from the literature for inclusion in the systematic review (Figure 1). The included studies are summarized in Table 7. A list of excluded studies is presented in Appendix 2.
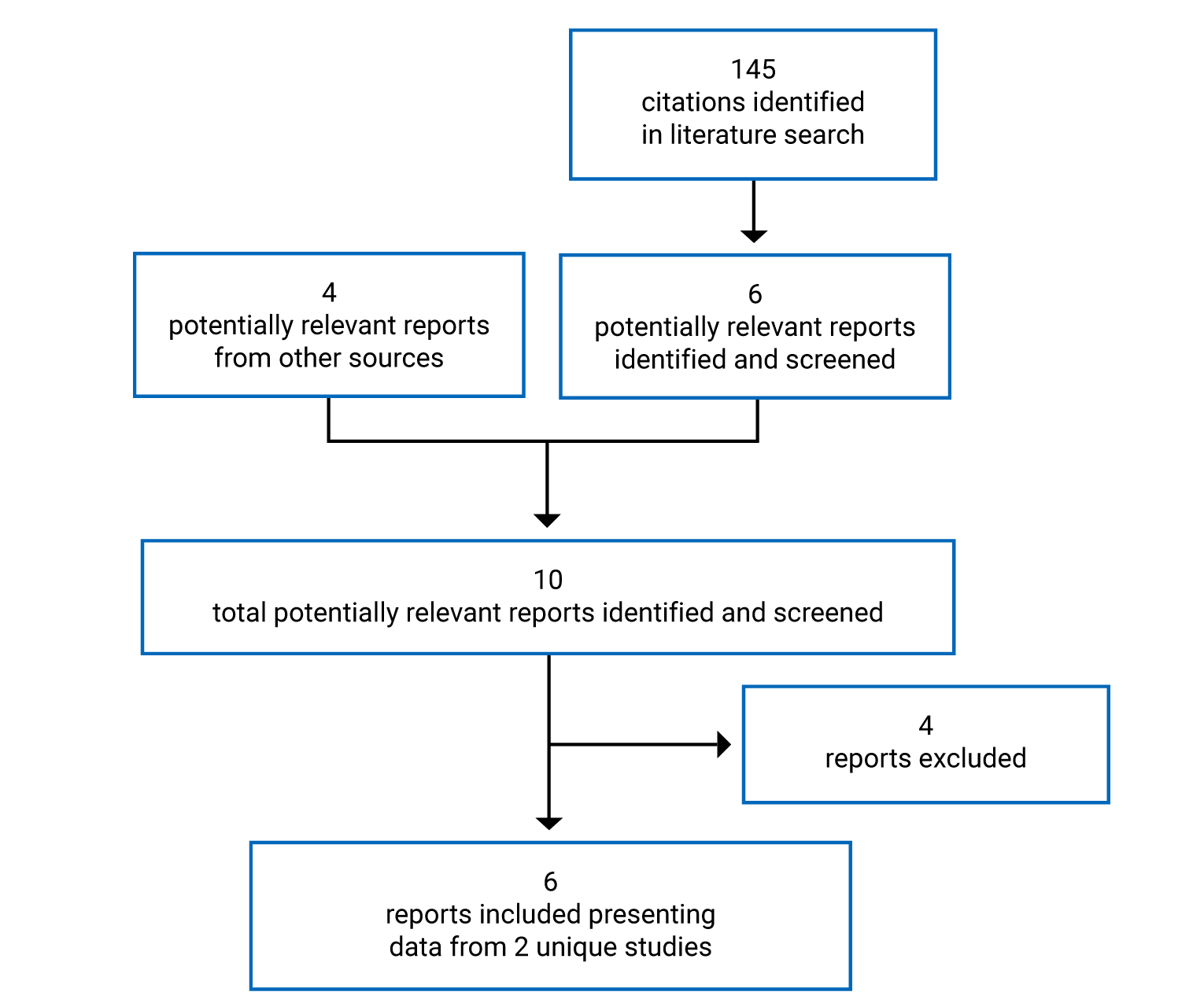
Table 7: Details of Included Studies — SUNRISE 1 AND SUNRISE 2
Detail | SUNRISE 1 study | SUNRISE 2 study |
|---|---|---|
Designs and populations | ||
Study design | Phase III, DB, RCT with PBO control and active comparator and parallel groups | Phase III, DB, RCT with PBO control and parallel groups |
Locations | 67 sites in North America (including 5 sites in Canada) and Europe | 101 sites in North America (including 4 sites in Canada), Asia, Europe, and Oceania |
Patient enrolment dates | May 31, 2016, to January 30, 2018 | November 15, 2016, to January 08, 2019 |
Randomized (N) | N = 1,006:
| Period 1 (PBO-controlled): N = 971:
Period 2 (all active treatment): 258 patients from the PBO group were rerandomized to LEM10 and LEM5:
|
Inclusion criteria |
|
|
Exclusion criteria |
| |
|
| |
Drugs | ||
Interventionc |
|
|
Comparator(s)c |
|
|
Duration | ||
Screening, run-in,d and baseline phase | Maximum 35 days | Maximum 35 days |
Double-blind phase | 30 days | Period 1: 6 months (PBO-controlled) Period 2: 6 months (all active treatment) |
Follow-up phase | 14 days | 14 days |
Outcomes | ||
Primary end point | Mean change from baseline LPS on days 29 to 30 for LEM10 and LEM5 vs. PBO | Mean change from baseline sSOL at month 6 |
Secondary and exploratory end points | Key secondary:
Other secondary:
Exploratory:
Other exploratory PSG end points:
| Key secondary:
Other secondary:
Exploratory:
|
Notes | ||
Publications | Rosenberg et al. (2019)37 | |
AHI = Apnea-Hypopnea Index; BAI = Beck Anxiety Inventory; BDI-2 = Beck Depression Inventory; CBT = cognitive behavioural therapy; DB = double-blind; DSM-5 = Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition; ECG = electrocardiogram; EQ-5D-3L = 3-level EQ-5D; ESS = Epworth Sleepiness Scale; FSS = Fatigue Severity Scale; IRLS = International Restless Legs Scale; ISI = Insomnia Severity Index; LEM = lemborexant; LEM5 = lemborexant 5 mg; LEM10 = lemborexant 10 mg; LPS = latency to persistent sleep; NREM = nonrapid eye movement; PBO = placebo; PD = pharmacodynamic; PGI-Insomnia = Patient Global Impression–Insomnia; PK = pharmacokinetic; PSG = polysomnography; QTcF = a prolonged corrected QT interval by Fridericia’s formula interval; RCT = randomized controlled trial; REM = rapid eye movement; SDSB = Sleep Disorders Screening Battery; sSOL = subjective sleep onset latency; STOP-Bang = Snoring, Tiredness, Observed apnea, blood Pressure, Body mass index, Age, Neck circumference, and Gender; sTST = subjective total sleep time; sWASO = subjective wake after sleep onset; T-BWSQ = Tyrer Benzodiazepine Withdrawal Symptom Questionnaire; TST = total sleep time; vs. = versus; WASO = wake after sleep onset; WASO1H = wake after sleep onset in the first half of the night; WASO2H = wake after sleep onset in the second half of the night; WPAI: GH = Work Productivity and Activity Impairment Questionnaire: General Health; ZOL = zolpidem tartrate.
aInsomnia disorder according to the DSM-5:4 “(1) Complained of dissatisfaction with night time sleep, in the form of difficulty staying asleep and/or awakening earlier in the morning than desired despite adequate opportunity for sleep (note that if the complaint was limited to difficulty initiating sleep, the patient was not eligible); (2) Frequency of complaint 3 or more times per week; (3) Duration of complaint greater than or equal to 3 months; (4) Associated with complaint of daytime impairment.”
bExclusionary score on SDSB as follows: (1) STOP-Bang Sleep Apnea Questionnaire score greater than or equal to 5; (2) IRLS score greater than or equal to 16; (3) ESS score greater than 15 (scores of 11 to 15 required excessive daytime sleepiness to be recorded in the patient's medical history).
cAll medications were taken orally, once daily at bedtime.
dDuring the placebo run-in phase of the SUNRISE 1 study, all patients received 1 LEM-matched PBO tablet and 1 ZOL-matched PBO tablet in a single blind manner. During the placebo run-in phase of the SUNRISE 2 study, all patients received 1 LEM-matched PBO tablet in a single blind manner.
eOutcome comparing LEM10 and LEM5 to ZOL. US-only outcome.
fResponders analysis in the SUNRISE 1 study: (1) objective sleep onset response was defined as LPS less than or equal to 20 minutes (provided mean baseline LPS was greater than 30 minutes); (2) subjective sleep onset response was defined as sSOL less than or equal to 20 minutes (provided mean baseline sSOL was greater than 30 minutes); (3) objective sleep maintenance response was defined as WASO less than or equal to 60 minutes (provided mean baseline WASO was greater than 60 minutes and was reduced by greater than 10 minutes compared to baseline); and (4) subjective sleep maintenance response was defined as sWASO less than or equal to 60 minutes (provided mean WASO was greater than 60 minutes and was reduced by greater than 10 minutes compared to baseline).
gRebound insomnia assessed using the sleep diary in the SUNRISE 1 study: (1) the change from baseline for sSOL on each of the first 3 nights, the mean sSOL of the first 3 nights, the mean sSOL of the first 7 nights, and the mean sSOL of the second 7 nights of the follow-up period; (2) the change from baseline for sWASO on each of the first 3 nights, the mean sWASO of the first 3 nights, the mean sWASO of the first 7 nights, and the mean sWASO of the second 7 nights of the follow-up period; (3) the proportion of patients whose sSOL was longer than at screening at the following time points during the follow-up period by at least 5 minutes: each of the first 3 nights, the mean of the first 3 nights, the mean of the first 7 nights, and the mean of the second 7 nights; and (4) the proportion of patients whose sWASO was higher than at screening at the following time points during the follow-up period by at least 5 minutes: each of the first 3 nights, the mean of the first 3 nights, the mean of the first 7 nights, and the mean of the second 7 nights.
hResponders analysis in the SUNRISE 2 study: (1) sleep onset responder defined as sSOL at baseline was greater than or equal to 30 minutes and mean sSOL at 6 months was less than or equal to 20 minutes; (2) sleep maintenance responder defined as sWASO at baseline was greater than or equal to 60 minutes and mean sWASO at 6 months was less than or equal to 60 minutes and showed a reduction of greater than 10 minutes compared to baseline.
iRebound insomnia assessed using the sleep diary in the SUNRISE 2 study: (1) the change from screening of sSOL on each of the first 3 nights, the mean sSOL of the first 7 nights, and the mean sSOL of the second 7 nights of the follow-up period; (2) the change from screening of sWASO on each of the first 3 nights, the mean sWASO of the first 7 nights, and the mean sWASO of the second 7 nights of the follow-up period; (3) the proportion of patients whose sSOL was longer than at screening for each of the first 3 nights, or whose mean sSOL was longer than at screening for the first 7 nights or the second 7 nights of the follow-up period; (4) the proportion of patients whose sWASO was higher than at screening for each of the first 3 nights, or whose mean sWASO was higher than at study baseline for the first 7 nights or the second 7 nights of the follow-up period.
jPersistence of effect assessment: (1) the mean change from study baseline of sSOL, of subjective sleep efficiency, of sWASO, and of sTST at month 3, month 6, month 9, and month 12 compared to month 1; (2) the mean change from period 2 baseline (month 6) of sSOL, of subjective sleep efficiency, of sWASO, and of sTST at month 9 and month 12 compared to month 7 (the first month of treatment in period 2); (3) the mean change from study baseline and period 2 baseline (as appropriate) of sSOL, subjective sleep efficiency, sWASO, and sTST at 3 months of exposure and 6 months of exposure compared to 1 month of exposure.
Sources: SUNRISE 1 Clinical Study Report17 and SUNRISE 2 Clinical Study Report.18
Description of Studies
Details of the 2 pivotal studies included are summarized in Table 7 and diagrams of the trial designs for SUNRISE 1 and SUNRISE 2 are depicted in Figure 2 and Figure 3, respectively.
Figure 2: SUNRISE 1 Study Design
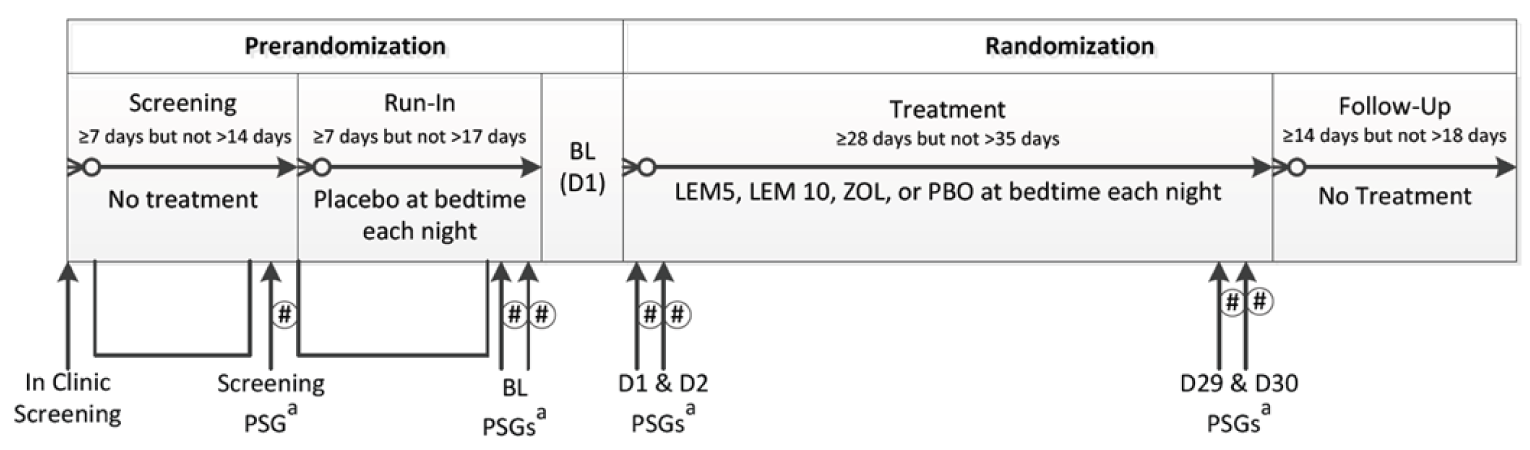
# = Cognitive Drug Research posture and Cognitive Performance Assessment Battery assessments in the morning following the polysomnography assessment; BL = baseline; D = day; LEM5 = lemborexant 5 mg; LEM10 = lemborexant 10 mg; PBO = placebo; PSG = polysomnography; ZOL = zolpidem tartrate.
a All PSG visits required an overnight stay in the clinic. At least 2 nights must have intervened between the second BL PSG and BL (D1).
Source: SUNRISE 1 Clinical Study Report.17
SUNRISE 1 Study
SUNRISE 1 (N = 1,006) was a DB, phase III, multicentre (including 5 sites in Canada) RCT designed to assess the safety and efficacy of LEM5 and LEM10 compared with PBO and ZOL for 30 days in females aged 55 years or older and males aged 65 years or older, all of whom had insomnia disorder.17,37 Patients were randomized in a 5:5:5:4 ratio to LEM5, LEM10, ZOL, or PBO. A computer-generated randomization scheme was used and randomization was performed centrally with an interactive voice and web response system. Randomization was stratified by country and age group (55 years to younger than 65 years versus 65 years and older). The trial end date was January 30, 2018.
A prespecified interim analysis was conducted by an independent statistician after 50% of patients had been randomized and either completed the day 31 evaluations or discontinued from the trial to assess if there was a statistically significant difference between LEM10 and ZOL on WASO2H at days 29 to 30. No other end points, treatment groups, or time points were analyzed, and it was expected that there was no impact on the type I error rate. The final Clinical Study Report was dated November 29, 2018.
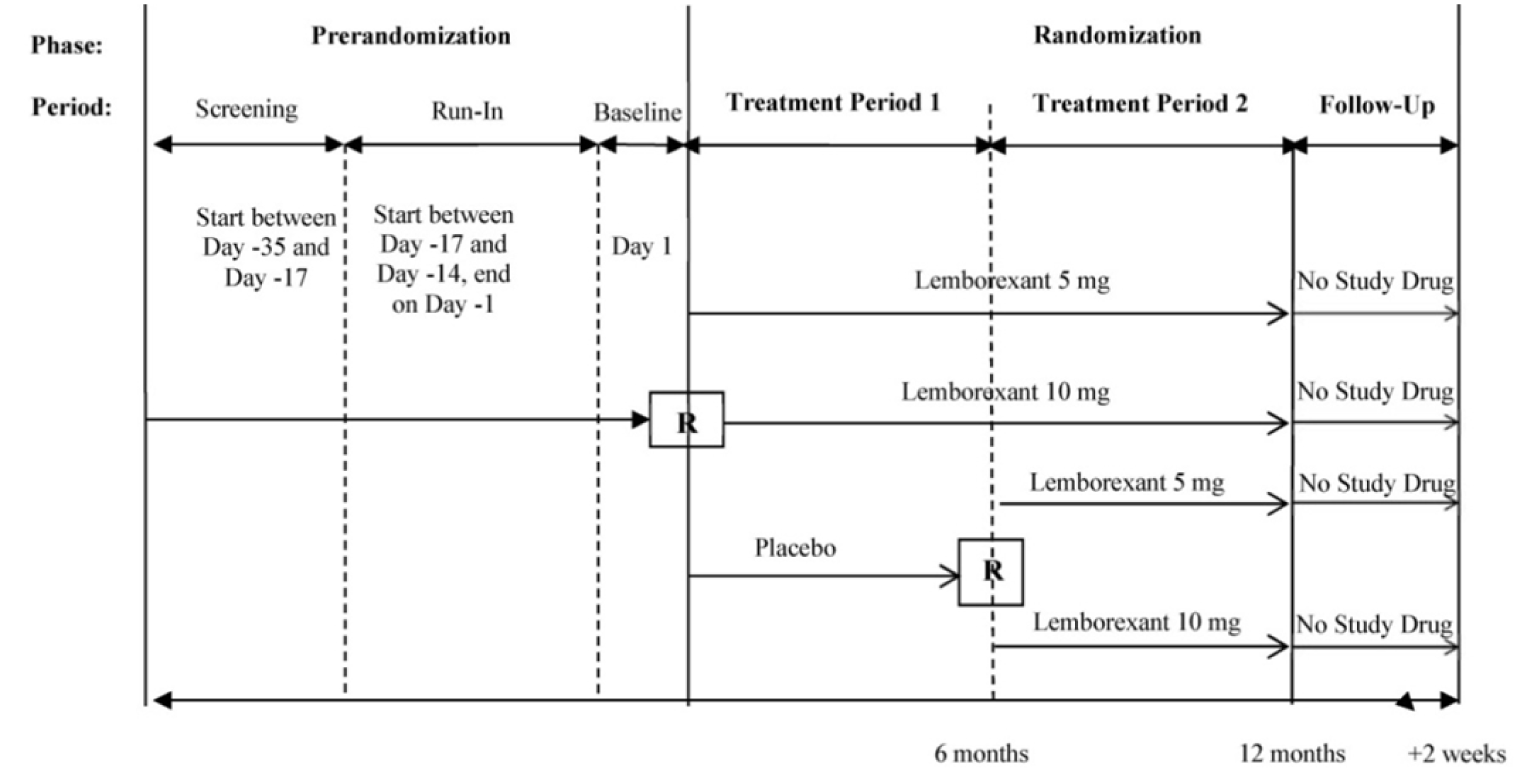
SUNRISE 2 Study
SUNRISE 2 (N = 971) was a DB, phase III, multicentre (including 4 sites in Canada) RCT designed to assess the long-term safety and efficacy of LEM5 and LEM10 compared with PBO for up to 12 months in adults 18 years or older who had insomnia disorder.18,35,39 Patients were randomized in an approximately 1:1:1 ratio to LEM5, LEM10, or PBO in period 1 (first 6 months). Patients randomized to PBO were rerandomized approximately 1:1 at the end of 6 months to either LEM5 or LEM10 in period 2 (second 6 months). A computer-generated randomization scheme was used and randomization was performed centrally with an interactive voice and web response system. Both randomization and rerandomization (for period 2) were stratified by country and age group (18 years to younger than 65 years versus 65 years and older). The PBO-controlled period 1 portion of the trial was completed on May 31, 2018, while the trial end date was January 8, 2019. The report containing the first 6 months of trial data was dated December 4, 2018, while the report containing data for 12 months was dated March 25, 2019.
Patients were made aware that they all would receive PBO at some point during the trial and active treatment for at least 6 months but were not told when either would take place.
SUNRISE 1 and SUNRISE 2 Studies
Both studies consisted of a prerandomization phase and randomization phase.
The prerandomization phase was a maximum of 35 days and included the screening, run-in, and baseline periods. During the screening period, participants had to have completed the electronic sleep diary within 1 hour of waking for at least 7 consecutive mornings as well as performed additional screening evaluations (e.g., postural stability, CPAB, PSG). During the run-in period, participants received PBO tablets that were taken once per night until baseline (day 1), completed the electronic sleep diary for at least 7 consecutive mornings, and did additional baseline evaluations. During the baseline period, participants completed patient-reported questionnaires (e.g., ISI, FSS, EQ-5D-3L, Columbia-Suicide Severity Rating Scale [C-SSRS]) before being randomized. Assessments and the administration of PBO during the prerandomization phase were to exclude patients who could not comply with study procedures (e.g., completing the sleep diary and other study restrictions) as well as exclude patients who demonstrated a PBO response.
The randomization phase included the treatment period (30 days in the SUNRISE 1 study and at least 6 months and up to 12 months in the SUNRISE 2 study) and follow-up period (a 14-day treatment-free interval before the end-of-study visit). In SUNRISE 1, patients completed the in-clinic assessments (i.e., postural stability, CPAB, and PSG) on day 2, day 3, day 29, and day 30. In SUNRISE 2, patients completed the ISI, FSS, C-SSRS, EQ-5D-3L, and PGI-Insomnia at month 1, month 3, month 6, month 9, and month 12. The sleep diary was completed each day during the treatment and follow-up periods in both studies. The Tyrer Benzodiazepine Withdrawal Symptom Questionnaire (T-BWSQ) and C-SSRS were completed at the end-of-study visit.
Populations
Inclusion and Exclusion Criteria
SUNRISE 1 and SUNRISE 2 Studies
To participate, patients in either trial must have been adults (aged 55 years or older for females and 65 years or older for males in the SUNRISE 1 study only) with a diagnosis of insomnia disorder according to the DSM-5. Patients in SUNRISE 1 must have had an ISI score of at least 13 while those in the SUNRISE 2 study must have had a score of at least 15 to participate. Key exclusion criteria included diagnosis of a sleep-related breathing disorder, periodic limb movement disorder, restless legs syndrome, circadian rhythm sleep disorder, narcolepsy, depression, anxiety, or the use of any prohibited over-the-counter concomitant medications or insomnia treatments within 1 week or 5 half-lives of beginning the trial. Additionally, patients in SUNRISE 1 must have had an AHI score greater than 15 whereas in SUNRISE 2, patients aged 18 years to 64 years must have had an AHI score of at least 10 and patients 65 years and older must have had an AHI score of at least 15.
Baseline Characteristics
Baseline characteristics are summarized in Table 8.
Table 8: Summary of Baseline Characteristics — SUNRISE 1 AND SUNRISE 2 Studies, FAS
Characteristic | SUNRISE 1 study | SUNRISE 2 study | |||||
|---|---|---|---|---|---|---|---|
PBO (N = 208) | ZOL (N = 263) | LEM5 (N = 266) | LEM10 (N = 269) | PBO (N = 318) | LEM5 (N = 316) | LEM10 (N = 315) | |
Demographics | |||||||
Age (years), mean (SD) | 63.4 (6.36) | 64.3 (7.12) | 63.7 (6.78) | 64.2 (6.88) | 54.5 (14.01) | 54.2 (13.74) | 54.8 (13.68) |
Median (range) | 62.0 (55 to 82) | 63.0 (55 to 83) | 63.0 (55 to 88) | 64.0 (55 to 85) | 56.0 (18 to 83) | 55.0 (20 to 85) | 55.0 (18 to 88) |
< 65 years,a mean (SD) | 115 (55.3) | 143 (54.4) | 148 (55.6) | 147 (54.6) | 229 (72.0) | 229 (72.5) | 229 (72.7) |
≥ 65 years, mean (SD) | 93 (44.7) | 120 (45.6) | 118 (44.4) | 122 (45.4) | 89 (28.0) | 87 (27.5) | 86 (27.3) |
Sex, n (%) | |||||||
Male | 24 (11.5) | 37 (14.1) | 37 (13.9) | 39 (14.5) | 102 (32.1) | 107 (33.9) | 93 (29.5) |
Female | 184 (88.5) | 226 (85.9) | 229 (86.1) | 230 (85.5) | 216 (67.9) | 209 (66.1) | 222 (70.5) |
Race, n (%) | |||||||
White | 153 (73.6) | 173 (65.8) | 199 (74.8) | 202 (75.1) | 232 (73.0) | 222 (70.3) | 225 (71.4) |
Black | 51 (24.5) | 80 (30.4) | 63 (23.7) | 62 (23.0) | 23 (7.2) | 27 (8.5) | 26 (8.3) |
Asian | 2 (1.0) | 5 (1.9) | 2 (0.8) | 5 (1.9) | 59 (18.6) | 61 (19.3) | 58 (18.4) |
Other | 2 (1.0) | 5 (1.9) | 2 (0.8) | 0 | 4 (1.3) | 6 (1.9) | 6 (1.9) |
Baseline disease characteristics and medical history | |||||||
LPS (minutes), mean (SD) | 43.89 (33.60) | 44.52 (38.35) | 44.86 (36.53) | 44.61 (32.99) | NA | NA | NA |
Median | 33.63 | 31.50 | 33.13 | 38.50 | NA | NA | NA |
Sleep efficiency (%), mean (SD) | 68.89 (9.64) | 68.13 (11.42) | 68.36 (11.27) | 67.85 (10.85) | NA | NA | NA |
WASO (minutes), mean (SD) | 111.75 (37.18) | 114.31 (39.92) | 113.44 (38.95) | 114.83 (40.00) | NA | NA | NA |
WASO2H (minutes), mean (SD) | 74.44 (30.11) | 78.04 (33.85) | 76.60 (32.90) | 76.88 (32.13) | NA | NA | NA |
TST (minutes), mean (SD) | 330.67 (46.27) | 326.99 (54.85) | 328.00 (54.22) | 325.07 (52.82) | NA | NA | NA |
sSOL (minutes),b mean (SD) | 55.90 (37.39) | 60.54 (36.35) | 65.79 (43.53) | 60.88 (42.51) | 64.03 (45.21) | 62.19 (45.67) | 64.97 (44.02) |
Median | 49.29 | 53.21 | 58.57 | 53.57 | 55.86 | 53.57 | 55.71 |
Subjective sleep efficiency (%),b mean (SD) | 56.08 (17.34) | 55.49 (15.80) | 56.05 (17.09) | 54.31 (18.32) | 61.34 (17.84) | 63.14 (18.23) | 62.03 (17.25) |
sWASO (minutes),b mean (SD) | 170.89 (80.68) | 173.06 (77.21) | 166.76 (82.05) | 173.35 (83.45) | 132.49 (80.20) | 132.77 (82.52) | 136.83 (87.39) |
sTST (minutes),b mean (SD) | 276.23 (87.65) | 273.07 (81.21) | 275.74 (83.65) | 266.10 (92.16) | 304.25 (91.46) | 315.52 (93.50) | 306.89 (88.03) |
Quality of sleep,b mean (SD) | 3.87 (1.43) | 3.87 (1.37) | 3.78 (1.35) | 3.70 (1.31) | 3.84 (1.44) | 3.94 (1.27) | 3.92 (1.35) |
ISI daytime functioning (item 4 to item 7), mean (SD) | 11.2 (2.44) | 11.1 (2.51) | 10.9 (2.42) | 10.8 (2.33) | 11.0 (2.10) | 11.4 (2.02) | 11.1 (2.15) |
FSS total score, mean (SD) | 37.5 (13.60) | 37.1 (13.79) | 37.5 (13.52) | 37.4 (13.11) | 35.1 (13.55) | 37.4 (12.74) | 36.0 (13.01) |
FSS average score, mean (SD) | 4.2 (1.51) | 4.1 (1.53) | 4.2 (1.50) | 4.2 (1.46) | 3.9 (1.51) | 4.2 (1.42) | 4.0 (1.45) |
BDI-2 total score, mean (SD) | 3.0 (3.53) | 2.8 (3.66) | 3.2 (3.87) | 3.0 (3.86) | 3.8 (4.23) | 3.9 (4.16) | 4.1 (4.32) |
BAI total score, mean (SD) | 1.7 (2.62) | 1.6 (2.51) | 1.7 (2.57) | 1.8 (2.67) | 2.3 (3.05) | 2.5 (3.05) | 2.6 (3.12) |
BAI = Beck Anxiety Inventory; BDI-2 = Beck Depression Inventory; FAS = full analysis set; FSS = Fatigue Severity Scale; ISI = Insomnia Severity Index; LEM5 = lemborexant 5 mg; LEM10 = lemborexant 10 mg; LPS = latency to persistent sleep; NA = not applicable; PBO = placebo; SD = standard deviation; sSOL = subjective sleep onset latency; sTST = subjective total sleep time; sWASO = subjective wake after sleep onset; TST = total sleep time; WASO = wake after sleep onset; WASO2H = wake after sleep onset in the second half of the night; ZOL = zolpidem tartrate.
aPatients in the SUNRISE 1 study were aged 55 years or older.
bBaseline sleep diary variables were analyzed with data handling rules applied.
Sources: SUNRISE 1 Clinical Study Report17 and SUNRISE 2 Clinical Study Report.18
SUNRISE 1 Study
The mean age of all randomized patients in SUNRISE 1 was 63.9 (SD = 6.81) years and most patients were female (83.6%) and white (72.3%). More patients were aged between 55 years and 64 years (55.0%) compared to 65 years and older (45.0%). Mean and median ages were similar among the treatment groups and the proportion of females was similar among the groups. There was a smaller proportion of patients who were white and a larger proportion of patients who were Black in the ZOL group compared to the other treatments. Overall, the mean and median LPS were 44.50 (SD = 35.47) minutes and 34.25 minutes, respectively, while the mean sleep efficiency was 68.27% (SD = 10.87%), and the mean WASO was 113.69 (SD = 39.09) minutes. Across treatment groups, most characteristics were balanced with a few exceptions. The baseline mean sSOL was longest in the LEM5 group at 65.79 (SD = 43.53) minutes and shortest in the PBO group at 55.90 (SD = 37.39) minutes. The baseline mean sWASO was longest in the LEM10 group at 173.35 (SD = 83.45) minutes and shortest in the LEM5 group at 166.76 (SD = 82.05) minutes. The baseline mean subjective total sleep time (sTST) was longest in the PBO group at 276.23 (SD = 87.65) minutes and shortest in the LEM10 group at 266.10 (SD = 92.16) minutes.
SUNRISE 2 Study
The mean age of all randomized patients in SUNRISE 2 was 54.5 (SD = 13.80) years and most patients were female (68.2%) and white (71.5%). More patients were younger than 65 years (72.4%) compared to those 65 years or older (27.6%). Mean and median ages were similar among the treatment groups and the proportion of females was similar among the groups. Overall, the mean and median sSOL were 63.73 (SD = 44.94) minutes and 55.21 minutes, respectively, while the mean subjective sleep efficiency was 62.17% (SD = 17.77%) and the mean sWASO was 134.02 (SD = 83.35) minutes. Across treatment groups, most characteristics were balanced, though the baseline mean sTST was longest in the LEM5 group at 315.52 (SD = 93.50) minutes and shortest in the PBO group at 304.25 (SD = 91.46) minutes.
Interventions
The doses used in both the SUNRISE 1 and SUNRISE 2 studies were LEM5 and LEM10. PBOs were matched in appearance to the active drugs. All study drugs were taken orally in tablet form immediately before bed (i.e., when the patient intended to sleep) for the entirety of the trial.
Patients were restricted to consuming no more than 4 cups of caffeinated beverages or 400 mg of caffeine per day. They were to avoid caffeine after 13:00 on days when a PSG reading took place (for SUNRISE 1) and after 18:00 during the rest of the trial. Alcohol was restricted to no more than 2 drinks per day, not within 3 hours of bedtime, and not on days when a PSG reading took place (for SUNRISE 1). Other prohibited therapeutics included strong and moderate CYP3A inhibitors and all CYP3A inducers, all treatments for insomnia, and any medications with the purposes of inducing sleep or wakefulness, or with known sedating or alerting effects.
SUNRISE 1 Study
ZOL was the active comparator in the trial. According to the sponsor, ZOL was available as both 6.25 mg and 12.5 mg doses for the trials, and the former was selected.17 The 6.25 mg dose is recommended for females and older adult patients.17 Health Canada product monographs exist for ZOL sublingual orally disintegrating tablets in 5 mg and 10 mg doses, with the lower dose being recommended for females and older adult patients.25
During the single blind run-in period, patients received 1 LEM-matched PBO tablet and 1 ZOL-matched PBO tablet. During the DB treatment period, all patients took 2 tablets each night based on the treatment group to which they were randomized:
LEM5 — 1 LEM 5 mg tablet and 1 ZOL-matched PBO tablet
LEM10 — 1 LEM 10 mg tablet and 1 ZOL-matched PBO tablet
ZOL — 1 ZOL 6.25 mg tablet and 1 LEM-matched PBO tablet
PBO — 1 LEM-matched PBO tablet and 1 ZOL-matched PBO tablet.
SUNRISE 2 Study
During the single blind run-in period, patients received 1 LEM-matched PBO. During the DB treatment period 1, all patients took 1 tablet each night based on the treatment group to which they were randomized:
LEM5 — 1 LEM 5 mg tablet
LEM10 — 1 LEM 10 mg tablet
PBO — 1 LEM-matched PBO tablet.
During the DB treatment period 2, all patients took 1 tablet each night based on the treatment group to which they were randomized at the beginning of the trial, with patients in the PBO group rerandomized to active treatment (i.e., LEM5 or LEM10).
Outcomes
A list of efficacy end points identified in the CADTH systematic review protocol that were assessed in the clinical trials included in this review are summarized in Table 9. A detailed discussion and critical appraisal of the outcome measures is provided in Appendix 4.
Table 9: Summary of Outcomes of Interest Identified in the CADTH Review Protocol
Outcome measure | SUNRISE 1 study | SUNRISE 2 study |
|---|---|---|
HRQoL | ||
EQ-5D-3L | Exploratory | Exploratory |
Severity of symptoms | ||
ISI (item 4 to item 7) | Other secondary | Other secondary |
FSS | Other secondary | Other secondary |
PGI-Insomnia | Exploratory | Exploratory |
Sleep latency | ||
LPSa | Primary, other secondary | NR |
sSOLa | Other secondary | Primary, other secondary, exploratory |
Sleep maintenance | ||
WASOa | Key secondary, other secondary | NR |
WASO2Ha | Key secondary, other secondary | NR |
sWASOa | Other secondary | Key secondary, other secondary, exploratory |
TST | ||
TST | Other secondary | NR |
sTST | Other secondary | Other secondary, exploratory |
Sleep efficiency | ||
Sleep efficiencya | Key secondary | NR |
Subjective sleep efficiencya | Other secondary | Key secondary, other secondary, exploratory |
Quality of sleep | Exploratory | Exploratory |
EQ-5D-3L = 3-level EQ-5D; FSS = Fatigue Severity Scale; HRQoL = health-related quality of life; ISI = Insomnia Severity Index; LPS = latency to persistent sleep; NR = not reported; PGI-Insomnia = Patient Global Impression–Insomnia; sSOL = subjective sleep onset latency; sTST = subjective total sleep time; sWASO = subjective wake after sleep onset; TST = total sleep time; WASO = wake after sleep onset; WASO2H = wake after sleep onset in the second half of the night.
aPrimary and key secondary outcomes were included in the multiple testing procedure.
Efficacy Outcomes
Health-Related Quality of Life
The EQ-5D-3L is a generic instrument and was used in both trials to measure HRQoL. The 5 domains include mobility, self-care, usual activities, pain/discomfort, and anxiety/depression along with a visual analogue scale where patients rate their health from 0 = worst imaginable health state to 100 = best imaginable health state.17,40,41 No information on the validity, reliability, responsiveness, or MID of the EQ-5D-3L for patients with insomnia was identified from the literature.
Severity of Symptoms
The ISI, FSS, and PGI-Insomnia were used in both trials to measure the severity of insomnia. The ISI is a 7-item patient-reported questionnaire that captures the nature, severity, and impact of insomnia.17,42 The 7 dimensions are severity of sleep onset, sleep maintenance, early morning awakening problems, sleep dissatisfaction, interference of sleep difficulties with daytime functioning, noticeability of the sleep problems by others, and distress caused by the sleep difficulties. Each item is answered based on a 5-point Likert scale, where 0 = no problem to 4 = very severe problem, for a total score ranging from 0 to 28, with a higher score indicating more acute symptoms of insomnia. Item 4 to item 7 were analyzed as a measure of daytime functioning.17 Strong convergent validity was demonstrated between the ISI items and subjective sleep measures as well as between the ISI total score and the Pittsburgh Sleep Quality Index (PSQI) total score and the 12-item Short Form (12) Health Survey mental component.42 There was weak to moderate correlation between the ISI total score and the Short Form (12) Health Survey physical component42 and PSG-derived sleep measures at baseline and posttreatment.43 Criterion validity was demonstrated with the ISI being able to identify insomnia among 183 patients evaluated for treatment.42 The ISI was found to have high internal consistency, with moderate to strong correlations between individual items and the total ISI score.42,44 Several studies found that the ISI is sensitive to detecting changes in perceived sleep difficulties with treatment.42-44 A 7-point reduction in the ISI total score corresponded to moderate improvements, a 9-point reduction corresponded to marked improvements,42 and a 6-point reduction was suggested to be a clinically meaningful improvement in patients with primary insomnia.45 There was a lack of evidence assessing the psychometric properties and MID for only item 4 to item 7.
The FSS is a 9-item patient-reported questionnaire that captures a patient’s agreement with each statement from 1 = strongly disagree to 7 = strongly agree.17 The FSS responses are summed for a total score and higher scores indicate greater fatigue. Construct validity was demonstrated with moderate to strong correlation between the FSS and fatigue as measured on a visual analogue scale as well as the Epworth Sleepiness Scale in patients with sleep-wake disorders.46 The FSS showed excellent internal consistency and strong test-retest reliability in patients with sleep-wake disorders.46 No information on the responsiveness or MID of the FSS for patients with insomnia was identified from the literature.
The PGI-Insomnia is a patient-reported questionnaire that evaluates the patient’s perception of how the study drug has impacted their sleep.17 Three items assess the drug’s effects (i.e., helped or worsened sleep, decreased or increased time to fall asleep, and increased or decreased TST) and 1 item assesses the patient’s perceived appropriateness of the drug strength. The former 3 items are rated on a 3-point scale, where 1 = positive effect, 2 = neutral effect, and 3 = negative effect, and the latter item involves rating the medication on a separate 3-point scale, where 1 = too strong, 2 = just right, and 3 = too weak. No information on the validity, reliability, responsiveness, or MID of the PGI-Insomnia for patients with insomnia was identified from the literature.
Objective Sleep Latency, Sleep Maintenance, Total Sleep Time, and Sleep Efficiency
PSG was used in the SUNRISE 1 trial to objectively measure aspects of sleep. PSG readings scored sleep parameters and sleep architecture in 30-second epochs using standard criteria performed by trained scorers. In SUNRISE 1, PSG parameters were averaged for pairs of consecutive days when readings took place. The parameters included LPS (a measure of sleep latency), WASO (a measure of sleep maintenance), WASO2H, TST, and sleep efficiency. Briefly, LPS was defined as the number of minutes from lights off to the first epoch of 20 consecutive epochs of nonwakefulness; WASO was the number of minutes spent awake from the onset of persistent sleep until lights on; WASO2H was the number of minutes spent awake during the interval from 240 minutes after lights off (i.e., second half of the night) until lights on; TST was the number of minutes of sleep from sleep onset until terminal awakening; and sleep efficiency was the proportion of time spent asleep per time in bed, calculated as TST divided by the interval from lights off until lights on. The sponsor suggested the following thresholds as clinically meaningful: a decrease in LPS of 15 minutes, a decrease in WASO of 20 minutes or a decrease of 10 minutes for each half of the night, and an increase in sleep efficiency by 5%.17 These thresholds were similar to those suggested in the literature.10
Evidence from the literature suggested that LPS derived from PSG does not accurately distinguish between primary insomnia and normal sleepers.47 There was strong test-retest reliability when comparing the mean of LPS measurements over 3 nights in patients with insomnia.48 No information on the responsiveness to change of LPS for patients with insomnia was identified from the literature. A mean change of at least a 10-minute difference between treatment versus PBO groups was suggested as a threshold for clinical importance.10
Construct validity was demonstrated between PSG-derived and actigraphy-derived measures of WASO,49 but it was found that PSG-derived measures do not accurately distinguish between primary insomnia and normal sleepers.47 There was adequate test-retest reliability when comparing the mean of WASO measurements over 3 nights in patients with insomnia.48 No information on the responsiveness of WASO for patients with insomnia was identified from the literature. A mean change of at least a 20-minute difference between treatment versus PBO groups was suggested as a threshold for clinical importance.10 No information on the validity, reliability, or responsiveness of WASO2H for patients with insomnia was identified from the literature.
Moderate construct validity was demonstrated between PSG-derived and self-reported measures of TST,50 but it was found that PSG-derived measures do not accurately distinguish between primary insomnia and normal sleepers.47 There was adequate test-retest reliability when comparing the mean of TST measurements over 3 nights in patients with insomnia.48 No information on the responsiveness of TST for patients with insomnia was identified from the literature. A mean change of at least a 20-minute difference between treatment versus PBO groups was suggested as a threshold for clinical importance.10
Strong construct validity was demonstrated between PSG-derived and actigraphy-derived sleep efficiency,51 but it was found that PSG-derived measures do not accurately distinguish between primary insomnia and normal sleepers.47 No information on the reliability or responsiveness of sleep efficiency for patients with insomnia was identified from the literature. A mean change of at least a 5% difference between treatment versus PBO groups was suggested as a threshold for clinical importance.10
Subjective Sleep Latency, Sleep Maintenance, Total Sleep Time, Sleep Efficiency, and Quality of Sleep
The patient-recorded electronic sleep diary was used to track subjective sleep measures in both the SUNRISE 1 and SUNRISE 2 studies. The diary was completed in the first hour upon waking throughout the trials and included sSOL (sleep latency), sWASO (sleep maintenance), sTST, subjective sleep efficiency, and quality of sleep. The parameters were defined as follows: sSOL was the estimated number of minutes from the time that the patient attempted to sleep until sleep onset; sWASO was the sum of the estimated minutes of wake during the night after initial sleep onset until when the patient stopped trying to sleep for the night, operationalized as the time the patient got out of bed for the day; sTST was the derived minutes of sleep from sleep onset until when the patient stopped trying to sleep for the night; and subjective sleep efficiency was the proportion of sTST per subjective time spent in bed, calculated as the interval from the time that a patient reported attempting to sleep until the time the patient stopped trying to sleep for the night, operationalized as the time the patient got out of bed for the day, and time spent asleep derived from subjective time spent in bed minus sWASO. Quality of sleep of the previous night was rated on a scale from 1 to 9, where 1 was extremely poor and 9 was extremely good.
Strong convergent validity was demonstrated between the sSOL and the “difficulty falling asleep” item of the ISI.42 Moderate convergent validity was demonstrated between the sSOL and the PSQI52 as well as the actigraphy-derived SOL.53 Discriminant validity has been demonstrated between patients with insomnia and controls.54 No information on the reliability or responsiveness of sSOL for patients with insomnia was identified from the literature. A mean change of at least a 20-minute difference between treatment versus PBO groups was suggested as a threshold for clinical importance.10
Strong convergent validity was demonstrated between the sWASO and the ISI “difficulty of staying asleep” item.42 Moderate convergent validity was demonstrated between the sWASO and the PSQI52 as well as the actigraphy-derived WASO.53 Discriminant validity has been demonstrated between patients with insomnia and controls.54 No information on the reliability or responsiveness of sWASO for patients with insomnia was identified from the literature. A mean change of at least a 30-minute difference between treatment versus PBO groups was suggested as a threshold for clinical importance.10
Moderate to strong convergent validity was demonstrated between the sTST and the total ISI score,42 actigraphy-derived TST,53 and PSG-derived TST.50 Discriminant validity has been demonstrated between patients with insomnia and controls.54 No information on the reliability or responsiveness of sTST for patients with insomnia was identified from the literature. A mean change of at least a 30-minute difference between treatment versus PBO groups was suggested as a threshold for clinical importance.10
Strong convergent validity was demonstrated between the subjective sleep efficiency and the total ISI score42 as well as the PSQI.52 Weak convergent validity was demonstrated between subjective sleep efficiency and actigraphy-derived sleep efficiency.53 Discriminant validity has been demonstrated between patients with insomnia and controls.54 No information on the reliability or responsiveness of subjective sleep efficiency for patients with insomnia was identified from the literature. A mean change of at least a 10% difference between treatment versus PBO groups was suggested as a threshold for clinical importance.10
Responder analyses were conducted on days 1 to 2 and days 29 to 30 using PSG (i.e., objective responders) and during the first 7 nights of treatment and last 7 nights of treatment using the sleep diary (i.e., subjective responders) for both sleep onset and sleep maintenance in the SUNRISE 1 study and at 6 months and 12 months using the sleep diary in the SUNRISE 2 study. Objective sleep onset response was defined as LPS being 20 minutes or less, provided the mean baseline LPS was greater than 30 minutes. Subjective sleep onset response was defined as sSOL being 20 minutes or less, provided the mean baseline sSOL was greater than 30 minutes. Objective sleep maintenance response was defined as WASO being 60 minutes or less, provided the mean baseline WASO was greater than 60 minutes and was reduced by more than 10 minutes compared to baseline. Subjective sleep maintenance response was defined as sWASO being 60 minutes or less, provided the mean baseline sWASO was greater than 60 minutes and was reduced by more than 10 minutes compared to baseline.
Harms Outcomes
The incidence and seriousness of AEs, withdrawals due to AEs, and deaths were reported for the safety population during the treatment and follow-up periods in both trials. AEs, SAEs, and protocol-defined notable harms were described based on preferred term and associated system organ class. Notable harms from the CADTH systematic review protocol included cognitive or psychomotor impairment (e.g., somnolence, impaired driving performance, postural instability or falls, impaired attention, MVA, workplace accidents), rebound insomnia, withdrawal symptoms or dependence, drug misuse, suicidal ideation, and hallucinations.
Postural stability was assessed using the Cognitive Drug Research posture device, which measures directional trunk movements or body sway through a cable attached to the patient’s waist and connected to an ataxiameter.17 Tests were performed within 5 minutes of waking and patients were instructed to stand as still as possible with their eyes closed for 1 minute. Body sway was measured in units of one-third degree of the angle of arc where a higher number indicated greater sway and less postural stability. The sponsor suggested that a 7-unit difference between LEM and PBO groups would be clinically meaningful.17 No information on the validity, reliability, or responsiveness of postural stability measures for patients with insomnia was identified by the CADTH review team from the literature. A 7-unit change in body sway from baseline (or a 35% increase) has been associated with an alcohol dose of 0.5 g per kilogram body mass,55 leading to impairment on tasks requiring postural stability.56
Impaired attention was captured using the CPAB, a study-specific battery of assessments.17 Tests were performed after the postural stability test (i.e., soon after waking). The entire CPAB consisted of 9 tasks: simple reaction time, choice reaction time, digit vigilance, immediate word recall, delayed word recall, word recognition, picture recognition, numeric working memory, and spatial working memory. Scores could be calculated for 4 domains, 2 of which were related to attention: power of attention and continuity of attention. For power of attention scores, a lower number is better, while for continuity of attention scores, a higher number is better. No information on the validity, reliability, responsiveness, or MID of the CPAB for patients with insomnia was identified from the literature.
Rebound insomnia was assessed based on sSOL and sWASO responses during the follow-up period. Rebound insomnia was suggested if the sSOL or sWASO was at least 5 minutes longer during the follow-up period compared to screening.17
Withdrawal symptoms or dependence was assessed using the T-BWSQ at the end of the study. Patients responded to each listed symptom as being present or absent and the severity, where 0 = no, 1 = yes (moderate), and 2 = yes (severe).17,57 The responses were summed for a total score. No information on the validity of the T-BWSQ for patients with insomnia was identified from the literature. High interitem associations were found for the scores of 3 perceptual items: sensitivity to smell, touch, and the perception of things moving when they were still; meanwhile, items such as sensitivity to noise, depression, and shaking were generally independent.57 The T-BWSQ scores during the period of withdrawal were greater in patients taking higher drug doses and for longer periods of time.57 A mean change of at least 3 points indicates a patient experienced withdrawal symptoms.57
Suicidal ideation was captured using the C-SSR, which assesses a patient’s degree of suicidality (suicidal ideation and behaviour).17,58 Four constructs are measured, including the severity of ideation rated on a 5-point ordinal scale, the intensity of ideation containing 5 items rated on a 5-point ordinal scale, behaviour rated on a nominal scale, and lethality rated on a 6-point ordinal scale for actual lethality or on a 3-point ordinal scale for potential lethality of attempts.58
Statistical Analysis
The statistical analysis of efficacy end points conducted in the SUNRISE 1 and SUNRISE 2 studies is summarized in Table 10.
Sleep diary data handling rules were applied to sleep diary data when responses were illogical. The 3 main errors were related to a.m. and p.m. and 24-hour clock use, incorrectly choosing the hour versus minutes, and reporting a final wake time that was later than the time the patient got out of bed for the day. The data presented in the CADTH review are with data handling rules applied.
Table 10: Statistical Analysis of Efficacy End Points — SUNRISE 1 AND SUNRISE 2 Studies
End point | Statistical model | Adjustment factors | Sensitivity analyses |
|---|---|---|---|
SUNRISE 1 study | |||
Mean change from baseline LPS on days 29 to 30 for LEM10 and LEM5 vs. PBO | MMRM For the model: UN matrix; AR(1) covariance matrix in the case of nonconvergence of UN | Age group, geographic region, treatment, visit, and treatment-by-visit interaction as fixed effects, and baseline LPS as a covariate based on the FAS |
|
Mean change from baseline sleep efficiency on days 29 to 30 for LEM10 and LEM5 vs. PBO | MMRM For the model: UN matrix; AR(1) covariance matrix in the case of nonconvergence of UN | Age group, geographic region, treatment, visit, and treatment-by-visit interaction as fixed effects, and baseline as covariate based on the FAS | Same as previously |
Mean change from baseline WASO on days 29 to 30 for LEM10 and LEM5 vs. PBO | MMRM For the model: UN matrix; AR(1) covariance matrix in the case of nonconvergence of UN | Age group, geographic region, treatment, visit, and treatment-by-visit interaction as fixed effects, and baseline as covariate based on the FAS | Same as previously |
Mean change from baseline WASO2H on days 29 to 30 for LEM10 and LEM5 vs. ZOL | MMRM For the model: UN matrix; AR(1) covariance matrix in the case of nonconvergence of UN | Age group, geographic region, treatment, visit, and treatment-by-visit interaction as fixed effects, and baseline as covariate based on the FAS | Same as previously |
Proportion of responders on days 1 to 2 and days 29 to 30 for LEM10 and LEM5 vs. ZOL and PBO | CMH test | Age group | None |
SUNRISE 2 study | |||
Mean change from baseline sSOL at month 6 | MMRM For the model: UN matrix; TOEP in the case of nonconvergence of UN; AR(1) covariance matrix in the case of nonconvergence of TOEP | The corresponding study baseline value, age group, region, treatment, time, and interaction of treatment by time |
|
Mean change from baseline subjective sleep efficiency at month 6 | MMRM For the model: UN matrix; TOEP in the case of nonconvergence of UN; AR(1) covariance matrix in the case of nonconvergence of TOEP | The corresponding study baseline value, region, age group, treatment, time, and interaction of treatment by time | Same as previously |
Mean change from baseline sWASO at month 6 | MMRM For the model: UN matrix; TOEP in the case of nonconvergence of UN; AR(1) covariance matrix in the case of nonconvergence of TOEP | The corresponding study baseline value, region, age group, treatment, time, and interaction of treatment by time | Same as previously |
Proportion of responders at month 6 and month 12 | CMH test | Age group, region | None |
AR(1) = autoregressive; CCMV = complete case missing value; CMH = Cochran-Mantel-Haenszel; FAS = full analysis set; LEM5 = lemborexant 5 mg; LEM10 = lemborexant 10 mg; LPS = latency to persistent sleep; MAR = missing at random; MMRM = mixed model of repeated measures; MNAR = missing not at random; PBO = placebo; PP = per-protocol; sSOL = subjective sleep onset latency; sWASO = subjective wake after sleep onset; TOEP = Toeplitz covariance matrix; UN = unstructured covariance; vs. = versus; WASO = wake after sleep onset; WASO2H = wake after sleep onset in the second half of the night; ZOL = zolpidem tartrate.
Primary Outcome
SUNRISE 1 Study
The primary end point was the change from baseline for mean LPS on days 29 to 30 for LEM10 and LEM5 compared to PBO. The null hypothesis was that there was no difference in the mean change from baseline for LPS on days 29 to 30 for LEM10 versus PBO, then LEM5 versus PBO, while the alternative hypothesis was that a treatment difference existed.
The geometric LSM treatment ratio of changes from baseline have been reported in the CADTH review for active treatment (i.e., LEM or ZOL) versus PBO of the visit per baseline ratio in each group (i.e., [visit per baseline ratio of LEM10] versus [visit per baseline ratio of PBO]).
SUNRISE 2 Study
The primary end point was the mean change from study baseline in sSOL at month 6. The null hypothesis was that there was no difference in the mean change from study baseline at month 6 for LEM10 versus PBO, then LEM5 versus PBO, while the alternative hypothesis was that a treatment difference existed.
Similar to SUNRISE 1, the geometric LSM treatment ratio of changes from baseline have been reported.
Power Calculation
SUNRISE 1 Study
The sample size was estimated for each comparison of LEM10 versus PBO and LEM5 versus PBO for the mean change from baseline for the primary end point (LPS) based on a 2-sided t test at the 0.05 alpha level for each comparison. Based on a previous dose-finding study of LEM,59 it was determined that a sample size of 250 patients for LEM5, 250 patients for LEM10, and 200 patients for PBO had at least 95% power for detecting estimated treatment differences of –1.15 between LEM10 and PBO, and –0.75 between LEM5 and PBO for log-transformed LPS values.
Power estimates were made for the key secondary end points (WASO, WASO2H, and sleep efficiency). It was determined that a sample size of 250 patients for each of the LEM5, LEM10, and ZOL groups and 200 patients for the PBO group had at least 95% power for detecting a statistically significant difference between LEM and PBO for change from baseline for sleep efficiency and at least 80% power for detecting a statistically significant difference between LEM10 and ZOL or PBO for change from baseline for WASO2H and WASO based on a 2-sided, 2-sample t test at a significance level of 5%. For sleep efficiency, the estimated treatment differences were 7% and 5% for LEM10 versus PBO and LEM5 versus PBO, respectively. For WASO2H, the estimated treatment difference was –11 minutes between LEM10 and ZOL while for WASO, the estimated treatment difference was –15 minutes between LEM10 and PBO.
SUNRISE 2 Study
Sample size calculations were conducted in a similar manner as in the SUNRISE 1 study. It was determined that a sample size of 300 patients per treatment group at a 5% (2-sided) level of significance had greater than 90% power for detecting an estimated treatment difference in sSOL of –8.7 minutes when comparing a dose of LEM to PBO.
For key secondary end points, a sample size of 300 patients in each group had more than 99% power for detecting an estimated treatment difference in subjective sleep efficiency of 5.5% and 90% power for detecting an estimated treatment difference in sWASO of –11.4 minutes when comparing LEM to PBO. A total of 900 patients provided greater than 99% power for detecting a treatment difference in sleep onset responder rates of 16% and sleep maintenance responder rates of 24.4% compared with PBO.
Statistical Testing
SUNRISE 1 Study
Statistical analyses were conducted after study completion and database locks. Continuous variables were reported using descriptive statistics (e.g., number of observations, mean, SD, median). Categorical variables were reported as numbers and percentages.
All statistical testing was performed at the 5% level of significance (2-sided). Where statistical comparisons were not defined, pairwise comparisons were tested. Efficacy end points were calculated as the average of the pairs of values (e.g., average of day 1 and day 2 [days 1 to 2]).
To control the overall type I error at the 0.05 significance level, a gatekeeping testing procedure was used where the first primary efficacy end point comparison (i.e., LPS for LEM10 versus PBO) was performed at the 0.05 significance level and subsequent testing proceeded only if the previous test was statistically significant. Tests were conducted in the following order:
LPS — LEM10 versus PBO
LPS — LEM5 versus PBO
sleep efficiency — LEM10 versus PBO
sleep efficiency — LEM5 versus PBO
WASO — LEM10 versus PBO
WASO2H — LEM10 versus ZOL
WASO — LEM5 versus PBO
WASO2H — LEM5 versus ZOL.
The primary outcome was analyzed using a mixed model of repeated measures (MMRM) analysis with factors of age (55 years to younger than 65 years and 65 years or older), geographic region (North America and Europe), treatment, visit (days 1 to 2 and days 29 to 30), and treatment-by-visit interaction as fixed effects, and baseline LPS as a covariate based on the full analysis set (FAS). The unstructured covariance matrix was used in the analysis, or the autoregressive covariance matrix was in the case of nonconvergence of the unstructured covariance matrix. The LPS data are nonnormally distributed, and a log transformation was performed. LSMs, 95% CIs for treatment differences, and P values were calculated.
SUNRISE 2 Study
Data reporting and statistical testing were conducted in a similar manner as SUNRISE 1. End points used different baselines and were specified as the baseline for period 1 (month 1 to month 6) or period 2 (month 7 to month 12). Efficacy end points were calculated as the average of 7-day sleep diary parameters (e.g., the average of the first 7 days of treatment). Exposure data for duration of exposure were grouped by treatment (i.e., LEM5 and LEM10). Each group included (1) period 1 patients in the on-treatment FAS using the change from study baseline and (2) period 2 patients who previously received PBO on the on-treatment FAS using the change from period 2 baseline for the respective doses. Hypothesis testing was not performed for efficacy end points beyond the month 6 visit or for other secondary or exploratory end points.
To control the overall type I error at the 0.05 significance level, a gatekeeping testing procedure was used where the first primary efficacy end point comparison (i.e., sSOL for LEM10 versus PBO) was performed at the 0.05 significance level and subsequent testing proceeded only if the previous test was statistically significant. Tests were conducted in the following order:
sSOL — LEM10 versus PBO
sSOL — LEM5 versus PBO
subjective sleep efficiency — LEM10 versus PBO
subjective sleep efficiency — LEM5 versus PBO
sWASO — LEM10 versus PBO
sWASO — LEM5 versus PBO.
The primary outcome was analyzed using an MMRM analysis with adjustments made for the corresponding study baseline value, region (North America, Europe, New Zealand, and Asia), age group (younger than 65 years, and 65 years or older), treatment, time (first 7 nights, month 1, month 2, month 3, month 4, month 5, and month 6), and the interaction of treatment by time. The unstructured covariance matrix was used in the analysis, the Toeplitz covariance matrix was used in the case of nonconvergence of the unstructured covariance matrix, and the autoregressive covariance matrix was used in the case of nonconvergence of Toeplitz covariance matrix. The sSOL data are nonnormally distributed, and a log transformation was performed. LSMs, 95% CIs for treatment differences, and P values were calculated.
Data Imputation
SUNRISE 1 Study
Missing data were imputed using a pattern-mixture model using multiple imputation assuming data were not missing at random (MAR) and using the complete case missing value (CCMV) pattern (i.e., patients who completed all primary efficacy assessments without missing values). Missing values were imputed using all available values.
SUNRISE 2 Study
The imputation of missing data was conducted in a similar manner as in SUNRISE 1.
Subgroup Analyses
SUNRISE 1 Study
Prespecified subgroups included age groups (aged 55 years to younger than 65 years, 65 years to younger than 75 years, and 75 years or older); alternative age groups (aged 55 years to younger than 65 years and 65 years or older); sex (male or female); race (white, Black, Asian, or other); geographic region (North America or Europe); and body mass index (less than 18.5 kg/m2, 18.5 kg/m2 to less than 25 kg/m2, 25 kg/m2 to 30 kg/m2, and greater than 30 kg/m2). No hypothesis testing was performed in the subgroup analyses. The CADTH review identified subgroups based on age and previous treatment as being relevant.
SUNRISE 2 Study
Prespecified subgroups were similar to those in SUNRISE 1 with the exception of age groups (younger than 65 years, 65 years to younger than 75 years, and 75 years or older); alternative age groups (younger than 65 years, and 65 years or older); and region (North America, Europe, New Zealand, and Asia). No hypothesis testing was performed in the subgroup analyses.
Sensitivity Analyses
SUNRISE 1 Study
Several sensitivity analyses were performed on the primary efficacy analyses:
the per-protocol (PP) analysis set with multiple imputations for missing data
a completer analysis for patients who completed all primary efficacy assessments and had no missing visits without imputations for missing data
an as-treated analysis based on the actual treatment received regardless of randomization with multiple imputations for missing data
an analysis assuming missing data were MAR without imputations for missing data
an analysis assuming missing data were missing not at random (MNAR) using CCMV-4, wherein up to 4 monotone missing patterns were used for missing value imputation
a tipping point analysis where a range of shifts was used in the multiple imputations of missing data, assuming MNAR to identify at what point the treatment effect would change the results from statistically significant to nonsignificant.
SUNRISE 2 Study
The following sensitivity analyses were performed on the primary efficacy analyses:
an analysis assuming missing data were MNAR using CCMV-7, wherein up to 7 monotone missing patterns were used for missing value imputation
a similar tipping point analysis as in SUNRISE 1
an analysis using nonlog-transformed data with multiple imputations for missing data
an analysis using CCMV-7 on nonlog-transformed data
a tipping point analysis on nonlog-transformed data.
Supplementary analyses were performed on the primary efficacy analyses and were similar to those in SUNRISE 1 for the PP analysis, the completer analysis, the MAR assumption analysis, and the MAR assumption analysis on nonlog-transformed data.
Secondary Outcomes
SUNRISE 1 Study
Key secondary end points included the change from baseline for mean sleep efficiency on days 29 to 30 for LEM10 and LEM5 compared to PBO, the change from baseline for mean WASO on days 29 to 30 for LEM10 and LEM5 compared to PBO, and the change from baseline for mean WASO2H on days 29 to 30 for LEM10 and LEM5 compared to ZOL.
The same MMRM model was used with factors of age group (aged 55 years to younger than 65 years, and 65 years or older), geographic region, treatment, visit (days 1 to 2 and days 29 to 30), and treatment-by-visit interaction as fixed effects, and baseline as a covariate based on the FAS. Similar to the primary outcomes, missing data were imputed using a pattern-mixture model with the same missing data assumptions and imputation methods.
Responder analyses were conducted using the Cochran-Mantel-Haenszel test and adjusted for age group. Missing data were considered nonresponders and no multiplicity adjustments were made.
SUNRISE 2 Study
Key secondary end points included the mean change from study baseline in subjective sleep efficiency at month 6 and the mean change from study baseline of sWASO at month 6.
As with SUNRISE 1, an MMRM model was used with similar adjustments made for the corresponding study baseline value, region, age group (younger than 65 years, and 65 years or older), treatment, time (first 7 nights, month 1, month 2, month 3, month 4, month 5, and month 6) and the interaction of treatment by time. Missing data were imputed in a similar manner as in SUNRISE 1.
Responder analyses were conducted in a similar manner as in SUNRISE 1 with adjustments made for age group and region.
Analysis Populations
SUNRISE 1 Study
The FAS (N = 1,006) consisted of all randomized patients who received at least 1 dose of study drug and had at least 1 postdose primary efficacy measurement. Unless otherwise specified, all efficacy end points were summarized and analyzed using the FAS. The summaries for the FAS and PP analysis set were based on patients “as randomized.”
The safety analysis set (N = 1,006) consisted of all randomized patients who received at least 1 dose of study drug and had at least 1 postdose safety assessment. The summary for the safety analysis set was based on patients “as treated.”
The PP analysis set (N = 992) consisted of all randomized patients who received a protocol-assigned study drug and did not have a major protocol deviation that was likely to affect the primary or key secondary efficacy end points. These included being randomized during the run-in period before randomization visit 5, and deviations of treatment assignment, treatment administration, and/or dispensing (e.g., patients who received the wrong dose or completed PSG assessment on visit 7 and visit 8 without being dosed). Most patients (more than 95%) were included in the PP analysis set and the most common reason for exclusion was due to the study drug not being administered or an incorrect study drug being dispensed (12 [1.2%] patients). One patient randomized to the LEM10 group received PBO and was included in the PBO group in the safety analysis set.
SUNRISE 2 Study
The FAS (N = 949) consisted of all randomized patients who received at least 1 dose of study drug and had at least 1 postdose primary efficacy measurement. Efficacy analyses for period 1 were performed on the FAS unless otherwise specified. The on-treatment FAS was made up of patients who received at least 1 dose of LEM and had at least 1 postdose primary efficacy measurement. The FAS and PP analysis set were based on patients “as randomized.”
The safety analysis set (N = 947) consisted of all randomized patients who received at least 1 dose of study drug and had at least 1 postdose safety assessment. The on-treatment safety analysis set was made up of patients who received at least 1 dose of LEM and had at least 1 postdose safety assessment. The safety analysis set was based on patients “as treated.”
The 6-month completer analysis set (N = 639) consisted of all randomized patients in the FAS who had all efficacy assessments up to and including month 6 (i.e., week 1 and month 1 to month 6 visits) without missing primary or key secondary efficacy assessments at any of these visits.
The PP analysis set (N = 921) consisted of all randomized patients who sufficiently complied with the protocol and included all patients in the FAS who sufficiently complied with the protocol during period 1. The criteria for exclusion in this analysis set were violated inclusion or exclusion criteria, duplicate randomization, a missing primary efficacy assessment, prohibited concomitant medication, a study drug not being administered, an incorrect study drug kit dispensed, and noncompliance with study medication. Most patients (more than 94%) were included in the PP analysis set and the most common reason for exclusion was due to less than 80% compliance (15 patients; 1.5%).
Results
Patient Disposition
Patient disposition is summarized in Table 11.
Table 11: Patient Disposition — SUNRISE 1 and SUNRISE 2 Studies
Patient disposition | SUNRISE 1 study | SUNRISE 2 study | |||||
|---|---|---|---|---|---|---|---|
PBO | ZOL | LEM5 | LEM10 | PBO | LEM5 | LEM10 | |
Screened, N | 3,537 | 2,059 | |||||
Randomized, N (%) | 1,006 (28.4) | 971 (47.2) | |||||
Randomized, n | 208 | 263 | 266 | 269 | 325 | 323 | 323 |
Not treated, n (%) | 0 | 0 | 0 | 0 | 4 (1.2) | 4 (1.2) | 4 (1.2) |
Completed study, n (%) | 198 (95.2) | 246 (93.5) | 258 (97.0) | 260 (96.7) | 257 (80.1) | 251 (78.7) | 226 (70.8) |
Discontinued from study,a n (%) | 10 (4.8) | 17 (6.5) | 8 (3.0) | 9 (3.3) | 58 (18.1) | 51 (16.0) | 80 (25.1) |
Primary reason(s) for discontinuation,b n (%) | 10 (4.8) | 17 (6.5) | 8 (3.0) | 9 (3.3) | 58 (18.1) | 51 (16.0) | 80 (25.1) |
Adverse eventc | 2 (1.0) | 6 (2.3) | 2 (0.8) | 3 (1.1) | 8 (2.5) | 7 (2.2) | 15 (4.7) |
Lost to follow-up | 2 (1.0) | 1 (0.4) | 1 (0.4) | 0 | 5 (1.6) | 3 (0.9) | 6 (1.9) |
Patient choice | 2 (1.0) | 1 (0.4) | 2 (0.8) | 1 (0.4) | 15 (4.7) | 11 (3.4) | 17 (5.3) |
Inadequate therapeutic effect | 1 (0.5) | 0 | 0 | 0 | 17 (5.3) | 9 (2.8) | 11 (3.4) |
Withdrawal of consent | 2 (1.0) | 3 (1.1) | 1 (0.4) | 2 (0.7) | 13 (4.0) | 10 (3.1) | 20 (6.3) |
Other | 1 (0.5) | 6 (2.3) | 2 (0.8) | 3 (1.1) | 0 | 11 (3.4) | 11 (3.4) |
Other reason(s) for discontinuation,b n (%) | 1 (0.5) | 3 (1.1) | 0 | 0 | 10 (3.1) | 6 (1.9) | 14 (4.4) |
Adverse eventc | 0 | 1 (0.4) | 0 | 0 | 0 | 0 | 0 |
Patient choice | 1 (0.5) | 1 (0.4) | 0 | 0 | 6 (1.9) | 2 (0.6) | 6 (1.9) |
Inadequate therapeutic effect | 0 | 0 | 0 | 0 | 3 (0.9) | 3 (0.9) | 5 (1.6) |
Other | 0 | 1 (0.4) | 0 | 0 | 2 (0.6) | 1 (0.3) | 4 (1.3) |
FAS, N (%) | 208 (100) | 263 (100) | 266 (100) | 269 (100) | 318 (97.8) | 316 (97.8) | 315 (97.5) |
PP, N (%) | 205 (98.6) | 261 (99.2) | 264 (99.2) | 262 (97.4) | 306 (94.2) | 309 (95.7) | 306 (94.7) |
Safety, N (%) | 209 (100.5)d | 263 (100) | 266 (100) | 268 (99.6) | 319 (98.2) | 314 (97.2) | 314 (97.2) |
6-month completer analysis set, N (%) | NA | NA | NA | NA | 217 (66.8) | 213 (65.9) | 209 (64.7) |
FAS = full analysis set; LEM5 = lemborexant 5 mg; LEM10 = lemborexant 10 mg; NA = not applicable; PBO = placebo; PP = per-protocol; ZOL = zolpidem tartrate.
aDiscontinued from period 1 in the SUNRISE 2 study.
bAs reported on the patient disposition case report form. Multiple “other” reasons for discontinuation may have been checked on the case report form; therefore, percentages may add up to more than the overall percentage of patients who discontinued.
cCorresponding adverse events leading to withdrawal from the study or study drug were reported on the adverse events case report form.
dOne patient who was randomized to LEM10 received PBO instead; therefore, this patient was counted in the PBO group rather than the LEM10 group.
Sources: SUNRISE 1 Clinical Study Report17 and SUNRISE 2 Clinical Study Report.18
SUNRISE 1 Study
In the SUNRISE 1 trial, 3,537 individuals were screened, of whom 2,531 (71.6%) were screening failures. The main reasons for screening failures were not meeting eligibility criteria (65.1%) and consent withdrawal (4.4%). Additional population-level data were not available to indicate which eligibility criteria were most commonly not met. In total, 1,006 patients were randomized in the treatment period. All patients who were randomized were treated with study medication. Overall, 962 (95.6%) patients completed the trial with similar completion rates across treatment groups ranging from 93% in the ZOL group to 97% in the LEM5 group.
SUNRISE 2 Study
In the SUNRISE 2 trial, 2,059 individuals were screened, of whom 1,088 (52.8%) were screening failures. The main reasons for screening failures were not meeting eligibility criteria (45.5%) and consent withdrawal (4.3%). Additional population-level data were not available to indicate which eligibility criteria were most commonly not met. In total, 971 patients were randomized in treatment period 1. All but 12 patients who were randomized were treated with study medication. In total, 734 (75.6%) patients completed period 1, with a higher proportion of discontinuations in the LEM10 group (25.1%) compared to either the LEM5 group (16.0%) or the PBO group (18.1%). The most common reasons for discontinuation were withdrawal of consent and patient choice.
Exposure to Study Treatments
Exposure to study medications is summarized in Table 12 and Table 13 for the SUNRISE 1 study and SUNRISE 2 study, respectively.
Table 12: Treatment Exposure — SUNRISE 1 Study, Safety Analysis Set
Treatment exposure | PBO (N = 209) | ZOL (N = 263) | LEM5 (N = 266) | LEM10 (N = 268) |
|---|---|---|---|---|
Exposure ≥ 4 weeks, n (%) | 195 (93.3) | 247 (93.9) | 255 (95.9) | 255 (95.1) |
Duration of exposure (days), mean (SD) | 29.5 (4.67) | 29.4 (4.59) | 29.9 (3.31) | 30.1 (3.98) |
LEM5 = lemborexant 5 mg; LEM10 = lemborexant 10 mg; PBO = placebo; SD = standard deviation; ZOL = zolpidem tartrate.
Source: SUNRISE 1 Clinical Study Report.17
Table 13: Treatment Exposure — SUNRISE 2 Study, On-Treatment Safety Analysis Set
Treatment exposure | LEM5 (N = 447) | LEM10 (N = 437) |
|---|---|---|
Exposure ≥ 1 month, n (%) | 434 (97.1) | 417 (95.4) |
Exposure ≥ 3 months, n (%) | 405 (90.6) | 380 (87.0) |
Exposure ≥ 6 months, n (%) | 374 (83.7) | 335 (76.7) |
Exposure ≥ 9 months, n (%) | 243 (54.4) | 213 (48.7) |
Exposure ≥ 12 months, n (%) | 230 (51.5) | 204 (46.7) |
Duration of exposure (days), mean (SD) | 260.5 (116.34) | 245.2 (122.09) |
LEM5 = lemborexant 5 mg; LEM10 = lemborexant 10 mg; SD = standard deviation.
Note: One month was defined as at least 23 days, 3 months was defined as at least 83 days, 6 months was defined as at least 173 days, 9 months was defined as at least 263 days, and 12 months was defined as at least 353 days in the SUNRISE 2 study. Data were reported for period 2 (i.e., after patients who received PBO in period 1 were rerandomized to either LEM5 or LEM10).
Source: SUNRISE 2 Clinical Study Report.18
Treatment compliance was assessed based on the amount of study drug returned at the end of the treatment periods and most patients (more than 95% of patients in SUNRISE 1 and more than 92% and 73% of patients in SUNRISE 2 period 1 and period 2, respectively) were between 80% and 100% compliant with the study medications during the trial, with similar compliance among treatment groups.
In SUNRISE 1, most patients (at least 93%) had completed at least 4 weeks of treatment in the trial and the mean duration of exposure for patients in the safety analysis set was similar among all treatment groups.
In SUNRISE 2, most patients (at least 76.7%) had completed at least 6 months of active treatment in the trial; the proportion of patients was lower among those in the LEM10 group (76.7% of patients) compared to the LEM5 group (83.7%). The mean duration of exposure for patients in the on-treatment safety analysis set was higher in the LEM5 group at 260.5 (SD = 116.34) days compared to the LEM10 group at 245.2 (SD = 122.09) days.
Protocol Deviations
Protocol deviations for both pivotal trials are summarized in Table 14.
SUNRISE 1 Study
Overall, 114 (11.3%) patients had at least 1 major protocol deviation. The most common protocol deviations were related to inclusion criteria (3.8%), study procedures or assessments (3.6%), study drug administration or dispensing (2.6%), and exclusion criteria (1.9%).
SUNRISE 2 Study
Overall, 27 (2.8%) patients had at least 1 major protocol deviation. The most common protocol deviations were related to prohibited concomitant medication (0.7%), study procedures or assessments (0.7%), and visit scheduling (0.5%).
Table 14: Protocol Deviations — SUNRISE 1 AND SUNRISE 2 Studies, FAS
Protocol deviations | SUNRISE 1 study | SUNRISE 2 study | |||||
|---|---|---|---|---|---|---|---|
PBO (N = 208) | ZOL (N = 263) | LEM5 (N = 266) | LEM10 (N = 269) | PBO (N = 318) | LEM5 (N = 316) | LEM10 (N = 315) | |
Patients with ≥ 1 major protocol deviation, n (%) | 26 (12.5) | 24 (9.1) | 32 (12.0) | 32 (11.9) | 13 (4.1) | 6 (1.9) | 8 (2.5) |
Concomitant medication | 0 | 1 (0.4) | 0 | 2 (0.7) | 3 (0.9) | 0 | 4 (1.3) |
Exclusion criteria | 2 (1.0) | 4 (1.5) | 4 (1.5) | 9 (3.3) | 0 | 0 | 0 |
Inclusion criteria | 6 (2.9) | 10 (3.8) | 13 (4.9) | 9 (3.3) | 0 | 0 | 0 |
Other protocol deviation | 0 | 0 | 1 (0.4) | 0 | 1 (0.3) | 1 (0.3) | 0 |
Safety reporting | 0 | 0 | 1 (0.4) | 0 | 0 | 0 | 0 |
Study procedures or assessments | 11 (5.3) | 7 (2.7) | 8 (3.0) | 10 (3.7) | 4 (1.3) | 2 (0.6) | 1 (0.3) |
Study treatment administration or dispensing | 9 (4.3) | 3 (1.1) | 7 (2.6) | 7 (2.6) | 3 (0.9) | 0 | 0 |
Study treatment compliance | 0 | 0 | 1 (0.4) | 0 | 1 (0.3) | 1 (0.3) | 1 (0.3) |
Visit scheduling | 0 | 0 | 0 | 2 (0.7) | 1 (0.3) | 2 (0.6) | 2 (0.6) |
FAS = full analysis set; LEM5 = lemborexant 5 mg; LEM10 = lemborexant 10 mg; PBO = placebo; ZOL = zolpidem tartrate.
Sources: SUNRISE 1 Clinical Study Report17 and SUNRISE 2 Clinical Study Report.18
Efficacy
Only those efficacy outcomes and analyses of subgroups identified in the CADTH systematic review protocol are reported as follows. Refer to Appendix 3 for additional detailed efficacy data.
Health-Related Quality of Life: EQ-5D-3L and Visual Analogue Scale
SUNRISE 1 Study
Most patients in the trial reported having “no problems” for any of the dimensions at either baseline or day 31 (Table 15). At most, there were 3 patients in any treatment group who reported “extreme problems” for a dimension at any time. For the EuroQol Visual Analogue Scale (EQ VAS) at day 31, the LSM treatment differences for LEM10 versus PBO and LEM5 versus PBO were 2.53 points (95% CI, 0.69 points to 4.38 points) and 0.52 points (95% CI, –1.32 points to 2.37 points), respectively, and for LEM10 versus ZOL and LEM5 versus ZOL were 3.10 points (95% CI, 1.35 points to 4.85 points) and 1.09 points (95% CI, –0.65 points to 2.83 points), respectively.
SUNRISE 2 Study
Similarly, most patients in the SUNRISE 2 trial reported having “no problems” for any of the dimensions at baseline, month 1, month 3, and month 6 (Table 16). At most, there were 9 patients in any treatment group who reported “extreme problems” for a dimension at any time. For the EQ VAS at month 1, the LSM treatment differences for LEM10 versus PBO and LEM5 versus PBO were 1.26 points (95% CI, –0.81 points to 3.32 points) and 0.62 points (95% CI, –1.43 points to 2.67 points), respectively, while at month 3 they were 0.86 points (95% CI, –1.42 points to 3.15 points) and 1.03 points (95% CI, –1.23 points to 3.29 points), respectively, and at month 6 they were 1.04 points (95% CI, –1.36 points to 3.43 points) and –0.96 points (95% CI, –3.31 points to 1.39 points), respectively.
Long-term EQ-5D results based on 3 months, 6 months, 9 months, and 12 months of exposure to LEM showed that most patients reported “no problems” for any of the dimensions (Table 62). In general, the long-term results for EQ VAS scores supported the results observed in the first 6 months.
Table 15: Change From Baseline EQ-5D-3L and Visual Analogue Scale (Exploratory Outcome) — SUNRISE 1 Study, FAS
Outcome | PBO (N = 208) | ZOL (N = 263) | LEM5 (N = 266) | LEM10 (N = 269) |
|---|---|---|---|---|
Mobility dimension | ||||
Baseline, n | 208 | 263 | 266 | 269 |
No problems, n (%) | 187 (89.9) | 245 (93.2) | 233 (87.6) | 251 (93.3) |
Some problems, n (%) | 21 (10.1) | 17 (6.5) | 32 (12.0) | 18 (6.7) |
Extreme problems, n (%) | 0 | 1 (0.4) | 1 (0.4) | 0 |
Day 31, n | 198 | 244 | 257 | 253 |
No problems, n (%) | 179 (90.4) | 224 (91.8) | 233 (90.7) | 238 (94.1) |
Some problems, n (%) | 19 (9.6) | 20 (8.2) | 23 (8.9) | 15 (5.9) |
Extreme problems, n (%) | 0 | 0 | 1 (0.4) | 0 |
Self-care dimension | ||||
Baseline, n | 208 | 263 | 266 | 269 |
No problems, n (%) | 204 (98.1) | 260 (98.9) | 260 (97.7) | 265 (98.5) |
Some problems, n (%) | 4 (1.9) | 2 (0.8) | 5 (1.9) | 4 (1.5) |
Extreme problems, n (%) | 0 | 1 (0.4) | 1 (0.4) | 0 |
Day 31, n | 198 | 244 | 257 | 253 |
No problems, n (%) | 194 (98.0) | 240 (98.4) | 254 (98.8) | 252 (99.6) |
Some problems, n (%) | 3 (1.5) | 4 (1.6) | 2 (0.8) | 1 (0.4) |
Extreme problems, n (%) | 1 (0.5) | 0 | 1 (0.4) | 0 |
Usual activities dimension | ||||
Baseline, n | 208 | 263 | 266 | 269 |
No problems, n (%) | 166 (79.8) | 210 (79.8) | 193 (72.6) | 219 (81.4) |
Some problems, n (%) | 42 (20.2) | 52 (19.8) | 72 (27.1) | 49 (18.2) |
Extreme problems, n (%) | 0 | 1 (0.4) | 1 (0.4) | 1 (0.4) |
Day 31, n | 198 | 244 | 257 | 253 |
No problems, n (%) | 166 (83.8) | 211 (86.5) | 217 (84.4) | 221 (87.4) |
Some problems, n (%) | 31 (15.7) | 32 (13.1) | 39 (15.2) | 31 (12.3) |
Extreme problems, n (%) | 1 (0.5) | 1 (0.4) | 1 (0.4) | 1 (0.4) |
Pain or discomfort dimension | ||||
Baseline, n | 208 | 263 | 266 | 269 |
No problems, n (%) | 153 (73.6) | 190 (72.2) | 188 (70.7) | 219 (81.4) |
Some problems, n (%) | 54 (26.0) | 70 (26.6) | 76 (28.6) | 47 (17.5) |
Extreme problems, n (%) | 1 (0.5) | 3 (1.1) | 2 (0.8) | 3 (1.1) |
Day 31, n | 198 | 244 | 257 | 253 |
No problems, n (%) | 153 (77.3) | 169 (69.3) | 185 (72.0) | 197 (77.9) |
Some problems, n (%) | 42 (21.2) | 72 (29.5) | 69 (26.8) | 54 (21.3) |
Extreme problems, n (%) | 3 (1.5) | 3 (1.2) | 3 (1.2) | 2 (0.8) |
Anxiety or depression dimension | ||||
Baseline, n | 208 | 263 | 266 | 269 |
No problems, n (%) | 185 (88.9) | 236 (89.7) | 229 (86.1) | 233 (86.6) |
Some problems, n (%) | 21 (10.1) | 25 (9.5) | 34 (12.8) | 35 (13.0) |
Extreme problems, n (%) | 2 (1.0) | 2 (0.8) | 3 (1.1) | 1 (0.4) |
Day 31, n | 198 | 244 | 257 | 253 |
No problems, n (%) | 180 (90.9) | 218 (89.3) | 227 (88.3) | 230 (90.9) |
Some problems, n (%) | 17 (8.6) | 23 (9.4) | 29 (11.3) | 22 (8.7) |
Extreme problems, n (%) | 1 (0.5) | 3 (1.2) | 1 (0.4) | 1 (0.4) |
VAS | ||||
Baseline, n | 208 | 263 | 266 | 269 |
Mean (SD) | 81.45 (13.15) | 79.88 (14.41) | 78.55 (15.03) | 81.09 (14.94) |
Day 31, na | 198 | 244 | 257 | 253 |
Mean (SD) | 83.89 (13.02) | 82.48 (13.31) | 82.79 (13.32) | 86.09 (10.20) |
Change from baseline, LSM visit estimate (SE)b | 1.64 (0.79) | 1.08 (0.72) | 2.16 (0.71) | 4.17 (0.71) |
LSM treatment difference (active minus PBO) (95% CI)b | Reference | –0.57 (–2.43 to 1.30) | 0.52 (–1.32 to 2.37) | 2.53 (0.69 to 4.38) |
P valueb,c | Reference | 0.5513 | 0.5792 | 0.0072 |
LSM treatment difference (active minus ZOL) (95% CI)b | NA | Reference | 1.09 (–0.65 to 2.83) | 3.10 (1.35 to 4.85) |
P valueb,c | NA | Reference | 0.2206 | 0.0005 |
ANCOVA = analysis of covariance; CI = confidence interval; EQ-5D-3L = 3-level EQ-5D; FAS = full analysis set; LEM5 = lemborexant 5 mg; LEM10 = lemborexant 10 mg; LSM = least squares mean; NA = not applicable; PBO = placebo; SD = standard deviation; SE = standard error; VAS = visual analogue scale; ZOL = zolpidem tartrate.
aThe number of patients analyzed for the change from baseline at this time point (not the number of patients who provided data at this time point).
bBased on an ANCOVA model with factors of age group, region, treatment, and the baseline VAS as covariates. Missing values were not imputed.
cP value was not adjusted for multiple testing (i.e., the type I error rate was not controlled).
Source: SUNRISE 1 Clinical Study Report.17
Table 16: Change From Baseline EQ-5D-3L and Visual Analogue Scale (Exploratory Outcome) — SUNRISE 2 Study, FAS
Outcome | PBO (N = 318) | LEM5 (N = 316) | LEM10 (N = 315) |
|---|---|---|---|
Mobility dimension | |||
Baseline, n | 318 | 316 | 315 |
No problems, n (%) | 284 (89.3) | 278 (88.0) | 287 (91.1) |
Some problems, n (%) | 34 (10.7) | 38 (12.0) | 28 (8.9) |
Extreme problems, n (%) | 0 | 0 | 0 |
Month 1, n | 299 | 300 | 290 |
No problems, n (%) | 272 (91.0) | 266 (88.7) | 270 (93.1) |
Some problems, n (%) | 27 (9.0) | 34 (11.3) | 20 (6.9) |
Extreme problems, n (%) | 0 | 0 | 0 |
Month 3, n | 283 | 275 | 262 |
No problems, n (%) | 254 (89.8) | 238 (86.5) | 246 (93.9) |
Some problems, n (%) | 29 (10.2) | 37 (13.5) | 16 (6.1) |
Extreme problems, n (%) | 0 | 0 | 0 |
Month 6, n | 258 | 257 | 234 |
No problems, n (%) | 223 (86.4) | 225 (87.5) | 213 (91.0) |
Some problems, n (%) | 35 (13.6) | 32 (12.5) | 21 (9.0) |
Extreme problems, n (%) | 0 | 0 | 0 |
Self-care dimension | |||
Baseline, n | 318 | 316 | 315 |
No problems, n (%) | 315 (99.1) | 310 (98.1) | 309 (98.1) |
Some problems, n (%) | 3 (0.9) | 6 (1.9) | 6 (1.9) |
Extreme problems, n (%) | 0 | 0 | 0 |
Month 1, n | 299 | 300 | 290 |
No problems, n (%) | 296 (99.0) | 294 (98.0) | 285 (98.3) |
Some problems, n (%) | 3 (1.0) | 6 (2.0) | 5 (1.7) |
Extreme problems, n (%) | 0 | 0 | 0 |
Month 3, n | 283 | 275 | 262 |
No problems, n (%) | 279 (98.6) | 266 (96.7) | 260 (99.2) |
Some problems, n (%) | 4 (1.4) | 9 (3.3) | 2 (0.8) |
Extreme problems, n (%) | 0 | 0 | 0 |
Month 6, n | 258 | 257 | 234 |
No problems, n (%) | 256 (99.2) | 252 (98.1) | 227 (97.0) |
Some problems, n (%) | 2 (0.8) | 5 (1.9) | 7 (3.0) |
Extreme problems, n (%) | 0 | 0 | 0 |
Usual activities dimension | |||
Baseline, n | 318 | 316 | 315 |
No problems, n (%) | 238 (74.8) | 238 (75.3) | 238 (75.6) |
Some problems, n (%) | 79 (24.8) | 75 (23.7) | 74 (23.5) |
Extreme problems, n (%) | 1 (0.3) | 3 (0.9) | 3 (1.0) |
Month 1, n | 299 | 300 | 290 |
No problems, n (%) | 245 (81.9) | 233 (77.7) | 238 (82.1) |
Some problems, n (%) | 53 (17.7) | 66 (22.0) | 51 (17.6) |
Extreme problems, n (%) | 1 (0.3) | 1 (0.3) | 1 (0.3) |
Month 3, n | 283 | 275 | 262 |
No problems, n (%) | 235 (83.0) | 217 (78.9) | 218 (83.2) |
Some problems, n (%) | 48 (17.0) | 55 (20.0) | 43 (16.4) |
Extreme problems, n (%) | 0 | 3 (1.1) | 1 (0.4) |
Month 6, n | 258 | 257 | 234 |
No problems, n (%) | 215 (83.3) | 208 (80.9) | 204 (87.2) |
Some problems, n (%) | 43 (16.7) | 45 (17.5) | 29 (12.4) |
Extreme problems, n (%) | 0 | 4 (1.6) | 1 (0.4) |
Pain or discomfort dimension | |||
Baseline, n | 318 | 316 | 315 |
No problems, n (%) | 213 (67.0) | 207 (65.5) | 225 (71.4) |
Some problems, n (%) | 103 (32.4) | 102 (32.3) | 81 (25.7) |
Extreme problems, n (%) | 2 (0.6) | 7 (2.2) | 9 (2.9) |
Month 1, n | 299 | 300 | 290 |
No problems, n (%) | 197 (65.9) | 203 (67.7) | 212 (73.1) |
Some problems, n (%) | 100 (33.4) | 92 (30.7) | 71 (24.5) |
Extreme problems, n (%) | 2 (0.7) | 5 (1.7) | 7 (2.4) |
Month 3, n | 283 | 275 | 262 |
No problems, n (%) | 176 (62.2) | 193 (70.2) | 187 (71.4) |
Some problems, n (%) | 107 (37.8) | 77 (28.0) | 73 (27.9) |
Extreme problems, n (%) | 0 | 5 (1.8) | 2 (0.8) |
Month 6, n | 258 | 257 | 234 |
No problems, n (%) | 164 (63.6) | 168 (65.4) | 165 (70.5) |
Some problems, n (%) | 90 (34.9) | 82 (31.9) | 65 (27.8) |
Extreme problems, n (%) | 4 (1.6) | 7 (2.7) | 4 (1.7) |
Anxiety or depression dimension | |||
Baseline, n | 318 | 316 | 315 |
No problems, n (%) | 267 (84.0) | 264 (83.5) | 277 (87.9) |
Some problems, n (%) | 50 (15.7) | 51 (16.1) | 34 (10.8) |
Extreme problems, n (%) | 1 (0.3) | 1 (0.3) | 4 (1.3) |
Month 1, n | 299 | 300 | 290 |
No problems, n (%) | 262 (87.6) | 250 (83.3) | 252 (86.9) |
Some problems, n (%) | 37 (12.4) | 46 (15.3) | 35 (12.1) |
Extreme problems, n (%) | 0 | 4 (1.3) | 3 (1.0) |
Month 3, n | 283 | 275 | 262 |
No problems, n (%) | 243 (85.9) | 232 (84.4) | 234 (89.3) |
Some problems, n (%) | 40 (14.1) | 41 (14.9) | 27 (10.3) |
Extreme problems, n (%) | 0 | 2 (0.7) | 1 (0.4) |
Month 6, n | 258 | 257 | 234 |
No problems, n (%) | 219 (84.9) | 221 (86.0) | 204 (87.2) |
Some problems, n (%) | 38 (14.7) | 36 (14.0) | 30 (12.8) |
Extreme problems, n (%) | 1 (0.4) | 0 | 0 |
VAS | |||
Baseline, n | 318 | 316 | 315 |
Mean (SD) | 72.8 (16.86) | 71.2 (17.77) | 73.0 (17.46) |
Month 1, na | 299 | 300 | 290 |
Mean (SD) | 74.6 (16.19) | 74.4 (17.82) | 76.2 (16.53) |
Change from baseline, mean (SD) | 1.8 (14.35) | 3.0 (14.85) | 2.8 (13.48) |
LSM treatment difference (active minus PBO) (95% CI)b | Reference | 0.62 (–1.43 to 2.67) | 1.26 (–0.81 to 3.32) |
P valueb,c | Reference | 0.5510 | 0.2334 |
Month 3, na | 283 | 275 | 262 |
Mean (SD) | 75.4 (16.32) | 76.2 (16.90) | 76.8 (17.04) |
Change from baseline, mean (SD) | 2.9 (15.09) | 4.3 (16.44) | 3.4 (15.17) |
LSM treatment difference (active minus PBO) (95% CI)b | Reference | 1.03 (–1.23 to 3.29) | 0.86 (–1.42 to 3.15) |
P valueb,c | Reference | 0.3716 | 0.4591 |
Month 6, na | 258 | 257 | 234 |
Mean (SD) | 75.6 (15.71) | 75.2 (17.65) | 78.0 (16.51) |
Change from baseline, mean (SD) | 4.0 (15.73) | 3.6 (16.91) | 4.8 (14.82) |
LSM treatment difference (active minus PBO) (95% CI)b | Reference | –0.96 (–3.31 to 1.39) | 1.04 (–1.36 to 3.43) |
P valueb,c | Reference | 0.4245 | 0.3960 |
CI = confidence interval; EQ-5D-3L = 3-level EQ-5D; FAS = full analysis set; LEM5 = lemborexant 5 mg; LEM10 = lemborexant 10 mg; LSM = least squares mean; MMRM = mixed model of repeated measures; PBO = placebo; SD = standard deviation; VAS = visual analogue scale.
aThe number of patients analyzed for the change from baseline at this time point (not the number of patients who provided data at this time point).
bBased on an MMRM model with factors of age group, region, treatment, visit (month 1, month 3, and month 6), and treatment-by-visit interaction as fixed effects, and study baseline VAS score as a covariate. Missing values were not imputed and assumed to be missing at random.
cP value was not adjusted for multiple testing (i.e., the type I error rate was not controlled).
Source: SUNRISE 2 Clinical Study Report.18
Severity of Symptoms: Insomnia Severity Index, Fatigue Severity Scale, and Patient Global Impression–Insomnia
SUNRISE 1 Study
For ISI item 4 to item 7 at day 31, the LSM treatment differences for LEM10 versus PBO and LEM5 versus PBO were –1.08 points (95% CI, –1.71 points to –0.46 points) and –1.10 points (95% CI, –1.73 points to –0.47 points), respectively, and for LEM10 versus ZOL and LEM5 versus ZOL were 0.33 points (95% CI, –0.26 points to 0.92 points) and 0.32 points (95% CI, –0.28 points to 0.91 points), respectively (Table 17).
Table 17: Change From Baseline ISI Item 4 to Item 7 and FSS Total Score (Other Secondary Outcomes) — SUNRISE 1 Study, FAS
Outcome | PBO (N = 208) | ZOL (N = 263) | LEM5 (N = 266) | LEM10 (N = 269) |
|---|---|---|---|---|
ISI (item 4 to item 7) | ||||
Baseline, n | 208 | 263 | 266 | 269 |
Mean (SD) | 11.21 (2.44) | 11.06 (2.51) | 10.91 (2.42) | 10.84 (2.33) |
Day 31, na | 198 | 244 | 257 | 253 |
Mean (SD) | 7.30 (3.56) | 5.87 (3.42) | 6.12 (3.49) | 6.10 (3.62) |
Change from baseline, LSM visit estimate (SE)b | –3.48 (0.27) | –4.90 (0.24) | –4.58 (0.24) | –4.57 (0.24) |
LSM treatment difference (active minus PBO) (95% CI)b | Reference | –1.42 (–2.05 to –0.78) | –1.10 (–1.73 to –0.47) | –1.08 (–1.71 to –0.46) |
P valueb,c | Reference | < 0.0001 | 0.0006 | 0.0007 |
LSM treatment difference (active minus ZOL) (95% CI)b | NA | Reference | 0.32 (–0.28 to 0.91) | 0.33 (–0.26 to 0.92) |
P valueb,c | NA | Reference | 0.2951 | 0.2744 |
FSS (total score) | ||||
Baseline, n | 208 | 263 | 266 | 269 |
Mean (SD) | 37.48 (13.60) | 37.15 (13.79) | 37.47 (13.52) | 37.42 (13.11) |
Day 31, na | 198 | 244 | 257 | 253 |
Mean (SD) | 30.57 (13.78) | 29.96 (12.59) | 29.53 (13.45) | 29.54 (13.03) |
Change from baseline, LSM visit estimate (SE)d | –5.76 (0.89) | –6.66 (0.81) | –7.03 (0.80) | –6.93 (0.80) |
LSM treatment difference (active minus PBO) (95% CI)d | Reference | –0.89 (–3.00 to 1.22) | –1.26 (–3.35 to 0.82) | –1.17 (–3.26 to 0.93) |
P valuec,d | Reference | 0.4074 | 0.2348 | 0.2745 |
LSM treatment difference (active minus ZOL) (95% CI)d | NA | Reference | –0.37 (–2.35 to 1.60) | –0.27 (–2.26 to 1.71) |
P valuec,d | NA | Reference | 0.7110 | 0.7854 |
ANCOVA = analysis of covariance; CI = confidence interval; FSS = Fatigue Severity Scale; ISI = Insomnia Severity Index; LEM5 = lemborexant 5 mg; LEM10 = lemborexant 10 mg; LSM = least squares mean; NA = not applicable; PBO = placebo; SD = standard deviation; SE = standard error; ZOL = zolpidem tartrate.
aThe number of patients analyzed for the change from baseline at this time point (not the number of patients who provided data at this time point).
bBased on an ANCOVA model with factors of age group, region, treatment, and the baseline ISI as covariates. Missing values were not imputed.
cP value was not adjusted for multiple testing (i.e., the type I error rate was not controlled).
dBased on an ANCOVA model with factors of age group, region, treatment, and the baseline FSS as covariates. Missing values were not imputed.
Source: SUNRISE 1 Clinical Study Report.17
For FSS total scores at day 31, the LSM treatment differences for LEM10 versus PBO and LEM5 versus PBO were –1.17 points (95% CI, –3.26 points to 0.93 points) and –1.26 points (95% CI, –3.35 points to 0.82 points), respectively, and for LEM10 versus ZOL and LEM5 versus ZOL were –0.27 points (95% CI, –2.26 points to 1.71 points) and –0.37 points (95% CI, –2.35 points to 1.60 points), respectively (Table 17).
According to the PGI-Insomnia, most patients among all treatment groups indicated that the treatment they received had a positive effect in helping them sleep (64% for each of LEM10 and LEM5, 72% for ZOL, and 42% for PBO), decreased the time to fall asleep (65% for LEM10, 60% for LEM5, 63% for ZOL, and 43% for PBO), and increased the TST (62% for each of LEM10 and LEM5, 71% for ZOL, and 44% for PBO) (Table 19). More than half of the patients in the active treatment groups responded that the medication strength was “just right” (56% for LEM10, 52% for LEM5, 52% for ZOL, and 39% for PBO) compared to patients who received PBO, where more responded that the treatment was “too weak.” Overall, it appeared that patients were more satisfied with the active treatments than PBO, though this outcome was not adjusted for multiplicity and conclusions cannot be drawn with certainty.
SUNRISE 2 Study
For ISI item 4 to item 7, the LSM treatment differences for LEM10 versus PBO and LEM5 versus PBO at month 1 were –0.94 points (95% CI, –1.51 points to –0.38 points) and –0.71 points (95% CI, –1.27 points to –0.15 points), respectively, while at month 3 were –1.36 points (95% CI, –1.96 points to –0.76 points) and –1.16 points (95% CI, –1.75 points to –0.57 points), respectively, and at month 6 were –1.32 points (95% CI, –1.92 points to –0.71 points) and –1.30 points (95% CI, –1.90 points to –0.71 points), respectively (Table 18).
For FSS total scores, the LSM treatment differences for LEM10 versus PBO and LEM5 versus PBO at month 1 were –2.04 points (95% CI, –3.83 points to –0.25 points) and –1.66 points (95% CI, –3.44 points to 0.12 points), respectively, while at month 3 were –3.04 points (95% CI, –4.91 points to –1.18 points) and –2.18 points (95% CI, –4.02 points to –0.34 points), respectively, and at month 6 were –2.56 points (95% CI, –4.57 points to –0.54 points) and –2.50 points (95% CI, –4.48 points to –0.52 points), respectively (Table 18).
For the PGI-Insomnia, most patients among all treatment groups indicated that the treatment they received had a positive effect in helping them sleep (more than 59%, 65%, and 67% of patients at month 1, month 3, and month 6 in the LEM groups, respectively, versus 34%, 41%, and 45% of patients for PBO at the same time points, respectively), decreased the time to fall asleep (more than 61%, 68%, and 72% of patients at month 1, month 3, and month 6 in the LEM groups, respectively, versus 40%, 42%, and 46% of patients for PBO at the same time points, respectively), and increased the TST (more than 53%, 55%, and 58% of patients at month 1, month 3, and month 6 in the LEM groups, respectively, versus 36%, 39%, and 40% of patients for PBO at the same time points, respectively) (Table 20). Around half of the patients in the LEM groups responded that the medication strength was “just right,” with more than 43% at month 1, 49% at month 3, and 53% at month 6 versus 29%, 34%, and 36% of patients in the PBO group at the same time points, respectively. Similarly, patients treated with LEM appeared to be more satisfied compared to patients treated with PBO, though the results are not adjusted for multiplicity.
Long-term ISI item 4 to item 7 and FSS total score results based on 3 months, 6 months, 9 months, and 12 months of exposure to LEM supported those observed during the first 6 months of treatment (Table 63).
The long-term PGI-Insomnia results based on 3 months, 6 months, 9 months, and 12 months of exposure to LEM were consistent with those during the main trial (Table 64).
Table 18: Change From Baseline ISI Item 4 to Item 7 and FSS Total Score (Other Secondary Outcomes) — SUNRISE 2 Study, FAS
Outcome | PBO (N = 318) | LEM5 (N = 316) | LEM10 (N = 315) |
|---|---|---|---|
ISI (item 4 to item 7) | |||
Baseline, n | 318 | 316 | 315 |
Mean (SD) | 11.0 (2.10) | 11.4 (2.02) | 11.0 (2.15) |
Month 1, na | 296 | 300 | 286 |
Mean (SD) | 7.8 (3.32) | 7.2 (3.78) | 7.0 (3.69) |
Change from baseline, mean (SD) | –3.1 (3.41) | –4.1 (3.66) | –4.2 (4.01) |
LSM treatment difference (active minus PBO) (95% CI)b | Reference | –0.71 (–1.27 to –0.15) | –0.94 (–1.51 to –0.38) |
P valueb,c | Reference | 0.0137 | 0.0011 |
Month 3, na | 283 | 274 | 259 |
Mean (SD) | 7.2 (3.51) | 6.2 (3.82) | 6.0 (3.67) |
Change from baseline, mean (SD) | –3.7 (3.55) | –5.2 (3.88) | –5.2 (4.05) |
LSM treatment difference (active minus PBO) (95% CI)b | Reference | –1.16 (–1.75 to –0.57) | –1.36 (–1.96 to –0.76) |
P valueb,c | Reference | 0.0001 | < 0.0001 |
Month 6, na | 257 | 258 | 234 |
Mean (SD) | 6.6 (3.45) | 5.4 (3.58) | 5.4 (3.54) |
Change from baseline, mean (SD) | –4.3 (3.66) | –6.0 (3.76) | –5.7 (4.00) |
LSM treatment difference (active minus PBO) (95% CI)b | Reference | –1.30 (–1.90 to –0.71) | –1.32 (–1.92 to –0.71) |
P valueb,c | Reference | < 0.0001 | < 0.0001 |
FSS (total score) | |||
Baseline, n | 318 | 316 | 315 |
Mean (SD) | 35.2 (13.55) | 37.4 (12.74) | 36.0 (13.01) |
Month 1, na | 296 | 300 | 286 |
Mean (SD) | 31.0 (12.88) | 30.6 (13.59) | 29.6 (13.50) |
Change from baseline, mean (SD) | –3.9 (11.62) | –6.6 (11.83) | –6.4 (13.68) |
LSM treatment difference (active minus PBO) (95% CI)d | Reference | –1.66 (–3.44 to 0.12) | –2.04 (–3.83 to –0.25) |
P valuec,d | Reference | 0.0670 | 0.0257 |
Month 3, na | 283 | 274 | 259 |
Mean (SD) | 30.6 (12.40) | 29.4 (13.91) | 27.8 (13.37) |
Change from baseline, mean (SD) | –4.3 (11.37) | –7.7 (12.97) | –7.9 (13.56) |
LSM treatment difference (active minus PBO) (95% CI)d | Reference | –2.18 (–4.02 to –0.34) | –3.04 (–4.91 to –1.18) |
P valuec,d | Reference | 0.0206 | 0.0014 |
Month 6, na | 257 | 258 | 234 |
Mean (SD) | 29.0 (12.95) | 27.0 (13.48) | 26.4 (13.29) |
Change from baseline, mean (SD) | –6.3 (12.07) | –10.1 (13.56) | –8.9 (14.91) |
LSM treatment difference (active minus PBO) (95% CI)d | Reference | –2.50 (–4.48 to –0.52) | –2.56 (–4.57 to –0.54) |
P valuec,d | Reference | 0.0134 | 0.0128 |
CI = confidence interval; FAS = full analysis set; FSS = Fatigue Severity Scale; ISI = Insomnia Severity Index; LEM5 = lemborexant 5 mg; LEM10 = lemborexant 10 mg; LSM = least squares mean; MMRM = mixed model of repeated measures; PBO = placebo; SD = standard deviation.
Note: Data were reported with sleep diary handling rules to address potential errors and illogical values.
aThe number of patients analyzed for the change from baseline at this time point (not the number of patients who provided data at this time point).
bBased on an MMRM model with factors of age group, region, treatment, visit (month 1, month 3, and month 6), and treatment-by-visit interaction as fixed effects, and study baseline ISI score as a covariate. Missing values were not imputed and assumed to be missing at random.
cP value was not adjusted for multiple testing (i.e., the type I error rate was not controlled).
dBased on an MMRM model with factors of age group, region, treatment, visit (month 1, month 3, and month 6), and treatment-by-visit interaction as fixed effects, and study baseline FSS score as a covariate. Missing values were not imputed and assumed to be missing at random.
Source: SUNRISE 2 Clinical Study Report.18
Table 19: PGI-Insomnia (Exploratory Outcome) — SUNRISE 1 Study, FAS
Outcome | PBO (N = 208) | ZOL (N = 263) | LEM5 (N = 266) | LEM10 (N = 269) |
|---|---|---|---|---|
Patients, n | 198 | 244 | 257 | 253 |
Study medication helped or worsened sleep | ||||
Positive medication effect, n (%) | 84 (42.4) | 176 (72.1) | 165 (64.2) | 161 (63.6) |
Neutral medication effect, n (%) | 49 (24.7) | 42 (17.2) | 52 (20.2) | 54 (21.3) |
Negative medication effect, n (%) | 65 (32.8) | 26 (10.7) | 40 (15.6) | 38 (15.0) |
P valuea,b (active vs. PBO) | Reference | < 0.0001 | < 0.0001 | < 0.0001 |
P valuea,b (active vs. ZOL) | NA | Reference | 0.0571 | 0.0427 |
Study medication decreased or increased time to fall asleep | ||||
Positive medication effect, n (%) | 85 (42.9) | 154 (63.1) | 154 (59.9) | 165 (65.2) |
Neutral medication effect, n (%) | 35 (17.7) | 35 (14.3) | 41 (16.0) | 33 (13.0) |
Negative medication effect, n (%) | 78 (39.4) | 55 (22.5) | 62 (24.1) | 55 (21.7) |
P valuea,b (active vs. PBO) | Reference | < 0.0001 | 0.0003 | < 0.0001 |
P valuea,b (active vs. ZOL) | NA | Reference | 0.4630 | 0.6250 |
Study medication increased or decreased total sleep time | ||||
Positive medication effect, n (%) | 88 (44.4) | 173 (70.9) | 159 (61.9) | 157 (62.1) |
Neutral medication effect, n (%) | 32 (16.2) | 33 (13.5) | 50 (19.5) | 48 (19.0) |
Negative medication effect, n (%) | 78 (39.4) | 38 (15.6) | 48 (18.7) | 48 (19.0) |
P valuea,b (active vs. PBO) | Reference | < 0.0001 | 0.0002 | 0.0002 |
P valuea,b (active vs. ZOL) | NA | Reference | 0.0325 | 0.0369 |
Appropriateness of medication strength | ||||
Just right, n (%) | 78 (39.4) | 127 (52.0) | 133 (51.8) | 141 (55.7) |
Too strong, n (%) | 2 (1.0) | 14 (5.7) | 11 (4.3) | 17 (6.7) |
Too weak, n (%) | 118 (59.6) | 103 (42.2) | 113 (44.0) | 95 (37.5) |
P valuea,b (active vs. PBO) | Reference | 0.0080 | 0.0088 | 0.0006 |
P valuea,b (active vs. ZOL) | NA | Reference | 0.9468 | 0.4104 |
FAS = full analysis set; LEM5 = lemborexant 5 mg; LEM10 = lemborexant 10 mg; NA = not applicable; PBO = placebo; PGI-Insomnia = Patient Global Impression–Insomnia; vs. = versus; ZOL = zolpidem tartrate.
aP value was based on chi-square test comparing “positive” to other categories combined. The same test comparison was done with “just right” to other categories combined.
bP value was not adjusted for multiple testing (i.e., the type I error rate was not controlled).
Source: SUNRISE 1 Clinical Study Report.17
Table 20: PGI-Insomnia (Exploratory Outcome) — SUNRISE 2 Study, FAS
Outcome | PBO (N = 318) | LEM5 (N = 316) | LEM10 (N = 315) |
|---|---|---|---|
Month 1, n | 299 | 300 | 290 |
Study medication helped or worsened sleep | |||
Positive medication effect, n (%) | 103 (34.4) | 179 (59.7) | 178 (61.4) |
Neutral medication effect, n (%) | 87 (29.1) | 74 (24.7) | 64 (22.1) |
Negative medication effect, n (%) | 109 (36.5) | 47 (15.7) | 48 (16.6) |
P valuea,b (active vs. PBO) | Reference | < 0.0001 | < 0.0001 |
Study medication decreased or increased time to fall asleep | |||
Positive medication effect, n (%) | 119 (39.8) | 184 (61.3) | 193 (66.6) |
Neutral medication effect, n (%) | 54 (18.1) | 44 (14.7) | 39 (13.4) |
Negative medication effect, n (%) | 126 (42.1) | 72 (24.0) | 58 (20.0) |
P valuea,b (active vs. PBO) | Reference | < 0.0001 | < 0.0001 |
Study medication increased or decreased total sleep time | |||
Positive medication effect, n (%) | 106 (35.5) | 159 (53.0) | 169 (58.3) |
Neutral medication effect, n (%) | 61 (20.4) | 47 (15.7) | 46 (15.9) |
Negative medication effect, n (%) | 132 (44.1) | 94 (31.3) | 75 (25.9) |
P valuea,b (active vs. PBO) | Reference | < 0.0001 | < 0.0001 |
Appropriateness of medication strength | |||
Just right, n (%) | 86 (28.8) | 131 (43.7) | 126 (43.4) |
Too strong, n (%) | 4 (1.3) | 17 (5.7) | 26 (9.0) |
Too weak, n (%) | 209 (69.9) | 152 (50.7) | 138 (47.6) |
P valuea,b (active vs. PBO) | Reference | 0.0040 | < 0.0001 |
Month 3, n | 283 | 275 | 262 |
Study medication helped or worsened sleep | |||
Positive medication effect, n (%) | 115 (40.6) | 179 (65.1) | 172 (65.6) |
Neutral medication effect, n (%) | 68 (24.0) | 46 (16.7) | 49 (18.7) |
Negative medication effect, n (%) | 100 (35.3) | 50 (18.2) | 41 (15.6) |
P valuea,b (active vs. PBO) | Reference | < 0.0001 | < 0.0001 |
Study medication decreased or increased time to fall asleep | |||
Positive medication effect, n (%) | 119 (42.0) | 188 (68.4) | 183 (69.8) |
Neutral medication effect, n (%) | 52 (18.4) | 31 (11.3) | 27 (10.3) |
Negative medication effect, n (%) | 112 (39.6) | 56 (20.4) | 52 (19.8) |
P valuea,b (active vs. PBO) | Reference | < 0.0001 | < 0.0001 |
Study medication increased or decreased total sleep time | |||
Positive medication effect, n (%) | 111 (39.2) | 152 (55.3) | 156 (59.5) |
Neutral medication effect, n (%) | 56 (19.8) | 47 (17.1) | 45 (17.2) |
Negative medication effect, n (%) | 116 (41.0) | 76 (27.6) | 61 (23.3) |
P valuea,b (active vs. PBO) | Reference | 0.0001 | < 0.0001 |
Appropriateness of medication strength | |||
Just right, n (%) | 97 (34.3) | 137 (49.8) | 135 (51.5) |
Too strong, n (%) | 0 | 13 (4.7) | 20 (7.6) |
Too weak, n (%) | 186 (65.7) | 125 (45.5) | 107 (40.8) |
P valuea,b (active vs. PBO) | Reference | 0.0002 | < 0.0001 |
Month 6, n | 258 | 257 | 234 |
Study medication helped or worsened sleep | |||
Positive medication effect, n (%) | 116 (45.0) | 173 (67.3) | 161 (68.8) |
Neutral medication effect, n (%) | 62 (24.0) | 49 (19.1) | 42 (17.9) |
Negative medication effect, n (%) | 80 (31.0) | 35 (13.6) | 31 (13.2) |
P valuea,b (active vs. PBO) | Reference | < 0.0001 | < 0.0001 |
Study medication decreased or increased time to fall asleep | |||
Positive medication effect, n (%) | 119 (46.1) | 187 (72.8) | 171 (73.1) |
Neutral medication effect, n (%) | 51 (19.8) | 31 (12.1) | 31 (13.2) |
Negative medication effect, n (%) | 88 (34.1) | 39 (15.2) | 32 (13.7) |
P valuea,b (active vs. PBO) | Reference | < 0.0001 | < 0.0001 |
Study medication increased or decreased total sleep time | |||
Positive medication effect, n (%) | 103 (39.9) | 149 (58.0) | 145 (62.0) |
Neutral medication effect, n (%) | 54 (20.9) | 39 (15.2) | 40 (17.1) |
Negative medication effect, n (%) | 101 (39.1) | 69 (26.8) | 49 (20.9) |
P valuea,b (active vs. PBO) | Reference | < 0.0001 | < 0.0001 |
Appropriateness of medication strength | |||
Just right, n (%) | 93 (36.0) | 143 (55.6) | 125 (53.4) |
Too strong, n (%) | 5 (1.9) | 11 (4.3) | 16 (6.8) |
Too weak, n (%) | 160 (62.0) | 103 (40.1) | 93 (39.7) |
P valuea,b (active vs. PBO) | Reference | 0.1256 | 0.0073 |
FAS = full analysis set; LEM5 = lemborexant 5 mg; LEM10 = lemborexant 10 mg; PBO = placebo; PGI-Insomnia = Patient Global Impression–Insomnia; vs. = versus.
aP value was based on chi-square test comparing “positive” to other categories combined. The same test comparison was done with “just right” to other categories combined.
bP value was not adjusted for multiple testing (i.e., the type I error rate was not controlled).
Source: SUNRISE 2 Clinical Study Report.18
Sleep Latency (Sleep Onset): Latency to Persistent Sleep, Subjective Sleep Onset Latency
SUNRISE 1 Study
Data for LPS are not normally distributed and were log transformed. Statistical comparisons were made using the geometric LSM treatment ratio.
The primary efficacy outcome was the mean change from baseline to days 29 to 30 for LPS comparing LEM10 to PBO, then LEM5 to PBO (Table 21). The median changes for the LEM10 and LEM5 groups were –16.25 minutes (IQR = –37.50 minutes to –1.88 minutes) and –12.00 minutes (IQR = –32.25 minutes to –0.25 minutes), respectively. The geometric LSM treatment ratio for the change from baseline for LEM10 compared to PBO was 0.72 (95% CI, 0.63 to 0.83; P < 0.0001) and for LEM5 compared to PBO was 0.77 (95% CI, 0.67 to 0.89; P = 0.0003).
Table 21: Sleep Onset, Change From Baseline LPS (Primary and Other Secondary Outcomes) — SUNRISE 1 Study, FAS
Outcome | PBO (N = 208) | ZOL (N = 263) | LEM5 (N = 266) | LEM10 (N = 269) |
|---|---|---|---|---|
Baseline, n | 208 | 262 | 266 | 269 |
Geometric mean (SD), minutes | 33.61 (NR) | 30.96 (NR) | 32.98 (NR) | 33.31 (NR) |
Median (Q1 to Q3), minutes | 33.63 (20.75 to 59.50) | 31.50 (17.50 to 61.25) | 33.13 (20.25 to 62.25) | 38.50 (17.75 to 62.00) |
Days 1 to 2, na | 208 | 262 | 266 | 269 |
Geometric mean (SD), minutes | 26.88 (NR) | 24.25 (NR) | 21.79 (NR) | 20.22 (NR) |
Median (Q1 to Q3), minutes | 27.25 (15.25 to 45.63) | 27.00 (15.00 to 41.00) | 21.63 (14.50 to 33.00) | 21.75 (13.25 to 33.00) |
Change from baseline, median (Q1 to Q3), minutes | –6.25 (–23.13 to 10.63) | –5.63 (–24.50 to 5.75) | –10.00 (–29.50 to 1.25) | –10.50 (–35.25 to –0.25) |
Geometric LSM treatment ratio, active vs. PBO (95% CI)b | Reference | 0.97 (0.86 to 1.1) | 0.85 (0.75 to 0.96) | 0.80 (0.70 to 0.90) |
P valueb,c | Reference | 0.6550 | 0.0092 | 0.0002 |
Geometric LSM treatment ratio, active vs. ZOL (95% CI)b | NA | Reference | 0.87 (0.78 to 0.98) | 0.82 (0.73 to 0.92) |
P valueb,c | NA | Reference | 0.0218 | 0.0006 |
Days 29 to 30, na | 200 | 250 | 260 | 260 |
Geometric mean (SD), minutes | 24.88 (NR) | 27.88 (NR) | 18.87 (NR) | 17.49 (NR) |
Median (Q1 to Q3), minutes | 25.75 (14.75 to 44.25) | 28.50 (17.00 to 52.25) | 18.75 (11.75 to 31.00) | 19.25 (11.25 to 29.25) |
Change from baseline, median (Q1 to Q3), minutes | –6.63 (–20.75 to 6.88) | –2.88 (–23.75 to 12.50) | –12.00 (–32.25 to –0.25) | –16.25 (–37.50 to –1.88) |
Geometric LSM treatment ratio, active vs. PBO (95% CI)b | Reference | 1.22 (1.06 to 1.40) | 0.77 (0.67 to 0.89) | 0.72 (0.63 to 0.83) |
P valueb,d | Reference | 0.0063 | 0.0003 | < 0.0001 |
Geometric LSM treatment ratio, active vs. ZOL (95% CI)b | NA | Reference | 0.63 (0.56 to 0.72) | 0.59 (0.52 to 0.68) |
P valueb,c | NA | Reference | < 0.0001 | < 0.0001 |
CI = confidence interval; FAS = full analysis set; LEM5 = lemborexant 5 mg; LEM10 = lemborexant 10 mg; LPS = latency to persistent sleep; LSM = least squares mean; MMRM = mixed model of repeated measures; NA = not applicable; NR = not reported; PBO = placebo; Q1 = first quartile; Q3 = third quartile; SD = standard deviation; vs. = versus; ZOL = zolpidem tartrate.
aThe number of patients analyzed for the change from baseline at this time point (not the number of patients who provided data at this time point).
bBased on an MMRM model with log transformation of LPS and factors of age group, region, treatment, visit (days 1 to 2, and days 29 to 30), and treatment-by-visit interaction as fixed effects, and the baseline LPS as a covariate. Missing values were imputed using multiple imputation and assumed to be missing not at random.
cP value was not adjusted for multiple testing (i.e., the type I error rate was not controlled).
dP value was adjusted for multiple testing (i.e., the type I error rate was controlled).
Source: SUNRISE 1 Clinical Study Report.17
Comparisons between LEM10 versus PBO and LEM5 versus PBO at days 1 to 2 and between LEM10 versus ZOL and LEM5 versus ZOL at days 1 to 2 and days 29 to 30 were other secondary outcomes (Table 21). The geometric LSM treatment ratio for the change from baseline for LEM10 versus PBO and LEM5 versus PBO at days 1 to 2 were 0.80 (95% CI, 0.70 to 0.90) and 0.85 (95% CI, 0.75 to 0.96), respectively. The geometric LSM treatment differences for LEM10 versus ZOL and LEM5 versus ZOL at days 1 to 2 were 0.82 (95% CI, 0.73 to 0.92) and 0.87 (95% CI, 0.78 to 0.98), respectively, and at days 29 to 30 were 0.59 (95% CI, 0.52 to 0.68) and 0.63 (95% CI, 0.56 to 0.72), respectively.
Results for sSOL for the first 7 nights and last 7 nights of the treatment period supported the LPS results comparing LEM10 and LEM5 versus PBO and ZOL (Table 65).
Sensitivity analyses for missing data imputation, tipping point analysis, PP, completer, and as-treated populations indicated that there were no changes to the conclusions for the primary efficacy outcomes. Analyses and conclusions for key secondary outcomes were consistent with those for the primary outcome.
Detailed data for subgroup analyses of the primary efficacy outcome are summarized in Table 60.
To be included in the sleep onset responder analyses, patients must have had an LPS greater than 30 minutes at baseline for objective response and an sSOL greater than 60 minutes at baseline for subjective response (Table 67). The LPS results from days 1 to 2 showed that 31.0% and 28.6% of patients receiving LEM10 and LEM5 were considered objective sleep onset responders compared to 19.3% and 27.1% of patients receiving ZOL and PBO, respectively. Based on results from days 29 to 30, 38.7% and 36.7% of patients receiving LEM10 and LEM5 were considered objective sleep onset responders compared to 21.4% and 28.0% of patients receiving ZOL and PBO, respectively. The sSOL results from the first 7 days of the treatment period showed that 14.4% and 12.3% of patients receiving LEM10 and LEM5 were considered subjective sleep onset responders compared to 9.9% and 4.0% of patients receiving ZOL and PBO, respectively. Based on results from the last 7 days of the treatment period, 20.1% and 21.3% of patients receiving LEM10 and LEM5 were considered subjective sleep onset responders compared to 11.3% and 10.0% of patients receiving ZOL and PBO, respectively.
SUNRISE 2 Study
Data for sSOL are not normally distributed and were log transformed. Statistical comparisons were made using the geometric LSM treatment ratio.
The primary efficacy outcome was the mean change from baseline to month 6 for sSOL comparing LEM10, then LEM5, to PBO (Table 22). The median changes for LEM10 and LEM5 groups were –28.21 minutes (IQR = –54.43 minutes to –9.29 minutes) and –21.81 minutes (IQR = –44.29 minutes to –11.14 minutes), respectively. The geometric LSM treatment ratio for the change from baseline for LEM10 versus PBO was 0.70 (95% CI, 0.61 to 0.81; P < 0.0001) and for LEM5 versus PBO was 0.73 (95% CI, 0.64 to 0.84; P < 0.0001).
Comparisons between LEM10 and LEM5 versus PBO for the first 7 nights of period 1, month 1, and month 3 were other secondary outcomes (Table 22). The geometric LSM treatment ratios for the change from baseline for LEM10 versus PBO and LEM5 versus PBO for the first 7 nights were 0.75 (95% CI, 0.70 to 0.81) and 0.78 (95% CI, 0.73 to 0.84), respectively, for month 1 were 0.77 (95% CI, 0.70 to 0.85) and 0.81 (95% CI, 0.74 to 0.89), respectively, and for month 3 were 0.77 (95% CI, 0.68 to 0.87) and 0.78 (95% CI, 0.69 to 0.88), respectively.
Long-term sSOL results based on 1 month, 3 months, 6 months, 9 months, and 12 months of exposure to LEM supported the results observed in the first 6 months (Table 66).
Sensitivity analyses with or without data handling rules applied, without log transformation of data, MMRM analysis assuming MAR, and MNAR using CCMV-7 did not change the conclusions for the primary efficacy outcome. Analyses and conclusions for key secondary outcomes were consistent with those for the primary outcome.
Detailed data for subgroup analyses of the primary efficacy outcome are summarized in Table 61.
To be included in the sleep onset responder analyses, patients must have had an sSOL greater than 30 minutes at baseline for subjective response (Table 68). The sSOL results from month 6 showed that 30.1%, 31.2%, and 17.7% of patients receiving LEM10, LEM5, and PBO, respectively, were considered subjective sleep onset responders. Based on results from month 12, and the rerandomization of PBO patients, 37.2% and 34.2% of patients receiving LEM10 and LEM5, respectively, were considered subjective sleep onset responders.
Table 22: Sleep Onset, Change From Baseline sSOL (Primary and Other Secondary Outcomes) — SUNRISE 2 Study, FAS
Outcome | PBO (N = 318) | LEM5 (N = 316) | LEM10 (N = 315) |
|---|---|---|---|
Baseline, n | 316 | 314 | 312 |
Geometric mean (SD), minutes | 44.99 (NR) | 42.97 (NR) | 45.05 (NR) |
Median (Q1 to Q3), minutes | 55.86 (34.14 to 78.93) | 53.57 (32.86 to 75.71) | 55.71 (33.57 to 85.07) |
First 7 nights of period 1, na | 314 | 310 | 310 |
Geometric mean (SD), minutes | 40.94 (NR) | 30.99 (NR) | 30.77 (NR) |
Median (Q1 to Q3), minutes | 50.71 (29.29 to 75.71) | 36.58 (21.50 to 57.36) | 35.71 (21.67 to 60.00) |
Change from study baseline, median (Q1 to Q3), minutes | –3.00 (–17.14 to 7.86) | –11.00 (–28.00 to 0.00) | –12.21 (–30.95 to –0.48) |
Geometric LSM treatment ratio, active vs. PBO (95% CI)b | Reference | 0.781 (0.725 to 0.842) | 0.752 (0.698 to 0.811) |
P valueb,c | Reference | < 0.0001 | < 0.0001 |
Month 1, na | 299 | 298 | 297 |
Geometric mean (SD), minutes | 34.61 (NR) | 26.98 (NR) | 27.14 (NR) |
Median (Q1 to Q3), minutes | 42.86 (23.33 to 67.14) | 32.50 (20.00 to 55.00) | 31.79 (17.14 to 58.81) |
Change from study baseline, median (Q1 to Q3), minutes | –7.14 (–25.71 to 3.57) | –13.71 (–35.00 to –1.00) | –19.86 (–36.43 to –3.57) |
Geometric LSM treatment ratio, active vs. PBO (95% CI)b | Reference | 0.810 (0.735 to 0.893) | 0.770 (0.698 to 0.848) |
P valueb,c | Reference | < 0.0001 | < 0.0001 |
Month 3, na | 279 | 268 | 264 |
Geometric mean (SD), minutes | 29.62 (NR) | 21.72 (NR) | 22.71 (NR) |
Median (Q1 to Q3), minutes | 37.14 (18.14 to 61.00) | 24.79 (14.71 to 40.71) | 26.43 (15.00 to 47.14) |
Change from study baseline, median (Q1 to Q3), minutes | –11.29 (–27.86 to 1.43) | –20.71 (–41.50 to –6.09) | –25.71 (–46.60 to –4.67) |
Geometric LSM treatment ratio, active vs. PBO (95% CI)b | Reference | 0.78 (0.69 to 0.88) | 0.77 (0.68 to 0.87) |
P valueb,c | Reference | < 0.0001 | < 0.0001 |
Month 6, na | 249 | 245 | 229 |
Geometric mean (SD), minutes | 27.42 (NR) | 18.62 (NR) | 19.35 (NR) |
Median (Q1 to Q3), minutes | 34.29 (16.43 to 60.00) | 22.29 (12.86 to 35.43) | 23.57 (12.86 to 40.71) |
Change from study baseline, median (Q1 to Q3), minutes | –11.43 (–33.57 to 0.00) | –21.81 (–44.29 to –11.14) | –28.21 (–54.43 to –9.29) |
Geometric LSM treatment ratio, active vs. PBO (95% CI)b | Reference | 0.73 (0.64 to 0.84) | 0.70 (0.61 to 0.81) |
P valueb,d | Reference | < 0.0001 | < 0.0001 |
CCMV = complete case missing value; CI = confidence interval; FAS = full analysis set; LEM5 = lemborexant 5 mg; LEM10 = lemborexant 10 mg; LSM = least squares mean; MMRM = mixed model of repeated measures; MNAR = missing not at random; NR = not reported; PBO = placebo; Q1 = first quartile; Q3 = third quartile; SD = standard deviation; sSOL = subjective sleep onset latency; vs. = versus.
Note: Data were reported with sleep diary handling rules to address potential errors and illogical values.
aThe number of patients analyzed for the change from baseline at this time point (not the number of patients who provided data at this time point).
bBased on an MMRM model with log transformation of sSOL and factors of age group, region, treatment, visit (first 7 nights, month 1, month 3, and month 6), and treatment-by-visit interaction as fixed effects, and the study baseline sSOL as a covariate. Missing values were imputed using multiple imputation and assumed to be MNAR or CCMV.
cP value was not adjusted for multiple testing (i.e., the type I error rate was not controlled).
dP value was adjusted for multiple testing (i.e., the type I error rate was controlled).
Source: SUNRISE 2 Clinical Study Report.18
Waking After Sleep Onset (Sleep Maintenance): WASO, WASO2H, sWASO
SUNRISE 1 Study
After sleep efficiency, the next key secondary efficacy outcomes in the statistical testing procedure were the mean change from baseline to days 29 to 30 for WASO comparing LEM10 to PBO, for WASO2H comparing LEM10 to ZOL, for WASO comparing LEM5 to PBO, and for WASO2H comparing LEM5 to ZOL (Table 23). The LSM treatment difference for WASO for LEM10 versus PBO was –25.35 minutes (95% CI, –31.36 minutes to –19.34 minutes; P < 0.0001). The LSM treatment difference for WASO2H for LEM10 versus ZOL was –8.00 minutes (95% CI, –12.53 minutes to –3.47 minutes; P = 0.0005). The LSM treatment difference for WASO for LEM5 versus PBO was –23.96 minutes (95% CI, –29.98 minutes to –17.95 minutes; P < 0.0001). The LSM treatment difference for WASO2H for LEM5 versus ZOL was –6.65 minutes (95% CI, –11.15 minutes to –2.15 minutes; P = 0.0038).
Comparisons for WASO between LEM10 versus PBO and LEM5 versus PBO at days 1 to 2 and LEM10 versus ZOL and LEM5 versus ZOL at days 1 to 2 and at days 29 to 30 were other secondary outcomes (Table 23). The LSM treatment differences for LEM10 versus PBO and LEM5 versus PBO at days 1 to 2 were –42.27 minutes (95% CI, –47.57 minutes to –36.97 minutes) and –33.40 minutes (95% CI, –38.71 minutes to –28.09 minutes), respectively. The LSM treatment differences for LEM10 versus ZOL and LEM5 versus ZOL at days 1 to 2 were –15.03 minutes (95% CI, –20.01 minutes to –10.05 minutes) and –6.16 minutes (95% CI, –11.15 minutes to –1.17 minutes), respectively, and at days 29 to 30 were –9.10 minutes (95% CI, –14.75 minutes to –3.45 minutes) and –7.72 minutes (95% CI, –13.36 minutes to –2.08 minutes), respectively.
Comparisons for WASO2H between LEM10 versus PBO and LEM5 versus PBO at days 1 to 2 and days 29 to 30 and LEM10 versus ZOL and LEM5 versus ZOL at days 1 to 2 were other secondary and exploratory outcomes (Table 23). The LSM treatment differences for LEM10 versus PBO and LEM5 versus PBO at days 1 to 2 were –28.33 minutes (95% CI, –32.68 minutes to –23.98 minutes) and –21.66 minutes (95% CI, –26.01 minutes to –17.30 minutes), respectively, and at days 29 to 30 were –17.76 minutes (95% CI, –22.57 minutes to –12.96 minutes) and –16.41 minutes (95% CI, –21.23 minutes to –11.60 minutes), respectively. The LSM treatment difference for LEM10 versus ZOL and LEM5 versus ZOL at days 1 to 2 were –13.13 minutes (95% CI, –17.21 minutes to –9.04 minutes) and –6.46 minutes (95% CI, –10.55 minutes to –2.36 minutes), respectively.
Table 23: Sleep Maintenance, Change From Baseline WASO and WASO2H (Key Secondary and Other Secondary Outcomes) — SUNRISE 1 Study, FAS
Outcome | PBO (N = 208) | ZOL (N = 263) | LEM5 (N = 266) | LEM10 (N = 269) |
|---|---|---|---|---|
WASO | ||||
Baseline, n | 208 | 262 | 266 | 269 |
Mean (SD), minutes | 111.75 (37.18) | 114.31 (39.92) | 113.44 (38.95) | 114.83 (40.00) |
Days 1 to 2, na | 208 | 262 | 266 | 269 |
Mean (SD), minutes | 96.67 (41.25) | 69.92 (33.52) | 63.48 (31.48) | 55.23 (30.49) |
Change from baseline, mean (SD), minutes | –15.07 (36.94) | –44.36 (38.07) | –49.96 (39.58) | –59.59 (37.75) |
LSM visit estimate (SE),b minutes | –18.03 (2.21) | –45.27 (1.99) | –51.43 (1.97) | –60.30 (1.97) |
LSM treatment difference (active minus PBO) (95% CI),b minutes | Reference | –27.24 (–32.57 to –21.91) | –33.40 (–38.71 to –28.09) | –42.27 (–47.57 to –36.97) |
P valueb,c | Reference | < 0.0001 | < 0.0001 | < 0.0001 |
LSM treatment difference (active minus ZOL) (95% CI)b | NA | Reference | –6.16 (–11.15 to –1.17) | –15.03 (–20.01 to –10.05) |
P valueb,c | NA | Reference | 0.0154 | < 0.0001 |
Days 29 to 30, na | 200 | 250 | 260 | 260 |
Mean (SD), minutes | 92.09 (40.97) | 77.71 (39.93) | 69.10 (34.53) | 68.60 (35.20) |
Change from baseline, mean (SD), minutes | –18.58 (41.93) | –36.50 (43.41) | –43.89 (39.26) | –46.43 (39.60) |
LSM visit estimate (SE),b minutes | –21.43 (2.46) | –37.68 (2.22) | –45.40 (2.19) | –46.78 (2.19) |
LSM treatment difference (active minus PBO) (95% CI),b,c minutes | Reference | –16.25 (–22.31 to –10.18) | –23.96 (–29.98 to –17.95) | –25.35 (–31.36 to –19.34) |
P valueb,d | Reference | < 0.0001 | < 0.0001 | < 0.0001 |
LSM treatment difference (active minus ZOL) (95% CI),b minutes | NA | Reference | –7.72 (–13.36 to –2.08) | –9.10 (–14.75 to –3.45) |
P valueb, c | NA | Reference | 0.0073 | 0.0016 |
WASO2H | ||||
Baseline, n | 208 | 262 | 266 | 269 |
Mean (SD), minutes | 74.44 (30.11) | 78.04 (33.85) | 76.60 (32.90) | 76.88 (32.13) |
Days 1 to 2, na | 208 | 262 | 266 | 269 |
Mean (SD), minutes | 67.38 (32.89) | 53.30 (27.71) | 46.32 (25.60) | 39.78 (23.71) |
Change from baseline, mean (SD), minutes | –7.06 (31.10) | –24.64 (33.35) | –30.28 (32.06) | –37.10 (30.82) |
LSM visit estimate (SE),e minutes | –8.83 (1.81) | –24.03 (1.63) | –30.48 (1.61) | –37.15 (1.61) |
LSM treatment difference (active minus PBO) (95% CI),e minutes | Reference | –15.20 (–19.57 to –10.83) | –21.66 (–26.01 to –17.30) | –28.33 (–32.68 to –23.98) |
P valuec,e | Reference | < 0.0001 | < 0.0001 | < 0.0001 |
LSM treatment difference (active minus ZOL) (95% CI),e minutes | NA | Reference | –6.46 (–10.55 to –2.36) | –13.13 (–17.21 to –9.04) |
P valuec,e | NA | Reference | 0.0020 | < 0.0001 |
Days 29 to 30, na | 200 | 250 | 260 | 260 |
Mean (SD), minutes | 64.37 (32.45) | 56.74 (31.11) | 49.11 (28.18) | 48.15 (27.84) |
Change from baseline, mean (SD), minutes | –8.92 (31.91) | –21.42 (36.26) | –27.19 (33.05) | –28.84 (33.14) |
LSM visit estimate (SE),e minutes | –10.98 (1.97) | –20.74 (1.78) | –27.39 (1.75) | –28.74 (1.76) |
LSM treatment difference (active minus PBO) (95% CI),e minutes | Reference | –9.76 (–14.60 to –4.93) | –16.41 (–21.23 to –11.60) | –17.76 (–22.57 to –12.96) |
P valuec,e | Reference | < 0.0001 | < 0.0001 | < 0.0001 |
LSM treatment difference (active minus ZOL) (95% CI),e minutes | NA | Reference | –6.65 (–11.15 to –2.15) | –8.00 (–12.53 to –3.47) |
P valued,e | NA | Reference | 0.0038 | 0.0005 |
CI = confidence interval; FAS = full analysis set; LEM5 = lemborexant 5 mg; LEM10 = lemborexant 10 mg; LSM = least squares mean; MMRM = mixed model of repeated measures; NA = not applicable; PBO = placebo; SD = standard deviation; SE = standard error; WASO = wake after sleep onset; WASO2H = wake after sleep onset in the second half of the night; ZOL = zolpidem tartrate.
aThe number of patients analyzed for the change from baseline at this time point (not the number of patients who provided data at this time point).
bBased on an MMRM model with factors of age group, region, treatment, visit (days 1 to 2, and days 29 to 30), and treatment-by-visit interaction as fixed effects, and the baseline WASO as a covariate. Missing values were imputed using multiple imputation and assumed to be missing not at random.
cP value was not adjusted for multiple testing (i.e., the type I error rate was not controlled).
dP value was adjusted for multiple testing (i.e., the type I error rate was controlled).
eBased on an MMRM model with factors of age group, region, treatment, visit (days 1 to 2, and days 29 to 30), and treatment-by-visit interaction as fixed effects, and the baseline WASO2H as a covariate. Missing values were imputed using multiple imputation and assumed to be missing not at random.
Source: SUNRISE 1 Clinical Study Report.17
Results for sWASO for the first 7 nights and last 7 nights of the treatment period supported the WASO results comparing LEM10 versus PBO and LEM5 versus PBO, but not compared to ZOL where the latter comparator appeared to show a similar treatment effect during the first 7 days of treatment and a numerically greater treatment effect during the last 7 days of treatment compared to LEM (Table 65).
To be included in the sleep maintenance responder analyses, patients must have had a WASO greater than 60 minutes at baseline for an objective response and a sWASO greater than 60 minutes at baseline for a subjective response (Table 67). The WASO results from days 1 to 2 showed that 65.0% and 51.1% of patients receiving LEM10 and LEM5, respectively, were considered objective sleep maintenance responders compared to 46.4% and 17.1% of patients receiving ZOL and PBO, respectively. Based on results from days 29 to 30, 46.6% and 44.4% of patients receiving LEM10 and LEM5, respectively, were considered objective sleep maintenance responders compared to 34.9% and 22.5% of patients receiving ZOL and PBO, respectively. The sWASO results from the first 7 days of the treatment period showed that 21.2% and 17.6% of patients receiving LEM10 and LEM5, respectively, were considered subjective sleep maintenance responders compared to 17.5% and 10.2% of patients receiving ZOL and PBO, respectively. Based on results from the last 7 days of the treatment period, 23.8% and 24.3% of patients receiving LEM10 and LEM5, respectively, were considered subjective sleep maintenance responders compared to 24.3% and 16.2% of patients receiving ZOL and PBO, respectively.
SUNRISE 2 Study
After subjective sleep efficiency, the next key secondary efficacy outcomes in the statistical testing procedure were the mean change from baseline to month 6 for sWASO comparing LEM10 to PBO, then LEM5 to PBO (Table 24). The LSM treatment ratio for LEM10 versus PBO was –12.67 (95% CI, –22.38 to –2.96; P = 0.0105) and for LEM5 versus PBO was –17.47 (95% CI, –27.31 to –7.64; P = 0.0005).
Comparisons between LEM10 versus PBO and LEM5 versus PBO for the first 7 nights of period 1, month 1, and month 3 were other secondary outcomes (Table 24). The LSM treatment ratios for LEM10 versus PBO and LEM5 versus PBO for the first 7 nights were –16.72 (95% CI, –23.81 to –9.63) and –14.33 (95% CI, –21.41 to –7.25), respectively, while for month 1 they were –7.01 (95% CI, –15.10 to 1.09) and –5.51 (95% CI, –13.57 to 2.54), respectively, and for month 3 they were –10.08 (95% CI, –19.05 to –1.10) and –13.42 (95% CI, –22.22 to –4.63), respectively.
Long-term sWASO results based on 1 month, 3 months, 6 months, 9 months, and 12 months of exposure to LEM supported the results observed in the first 6 months (Table 66).
To be included in the sleep maintenance responder analyses, patients must have had a WASO greater than 60 minutes at baseline for a subjective response (Table 68). The sWASO results from month 6 showed that 30.0%, 35.0%, and 20.4% of patients receiving LEM10, LEM5, and PBO, respectively, were considered subjective sleep maintenance responders. Based on the results of month 12 and the rerandomization of PBO patients, 39.6% and 35.0% of patients receiving LEM10 and LEM5, respectively, were considered subjective sleep maintenance responders.
Table 24: Sleep Maintenance, Change From Baseline sWASO (Key Secondary and Other Secondary Outcomes) — SUNRISE 2 Study, FAS
Outcome | PBO (N = 318) | LEM5 (N = 316) | LEM10 (N = 315) |
|---|---|---|---|
Baseline, n | 314 | 313 | 311 |
Mean (SD), minutes | 132.49 (80.20) | 132.77 (82.52) | 136.83 (87.39) |
First 7 nights of period 1, na | 312 | 308 | 309 |
Mean (SD), minutes | 127.79 (86.97) | 113.53 (85.72) | 113.77 (83.54) |
Change from study baseline, mean (SD), minutes | –6.12 (45.89) | –20.21 (46.02) | –23.30 (47.70) |
LSM visit estimate (95% CI),b minutes | –4.77 (–10.13 to 0.59) | –19.10 (–24.49 to –13.71) | –21.49 (–26.88 to –16.10) |
LSM treatment difference (active vs. PBO) (95% CI)b | Reference | –14.33 (–21.41 to –7.25) | –16.72 (–23.81 to –9.63) |
P valueb,c | Reference | < 0.0001 | < 0.0001 |
Month 1, na | 297 | 297 | 293 |
Mean (SD), minutes | 114.17 (81.34) | 107.07 (80.64) | 109.42 (79.99) |
Change from study baseline, mean (SD), minutes | –19.01 (50.28) | –23.42 (56.25) | –26.82 (56.99) |
LSM visit estimate (95% CI),b minutes | –17.18 (–23.25 to –11.12) | –22.69 (–28.73 to –16.66) | –24.18 (–30.20 to –18.17) |
LSM treatment difference (active vs. PBO) (95% CI)b | Reference | –5.51 (–13.57 to 2.54) | –7.01 (–15.10 to 1.09) |
P valueb,c | Reference | 0.1796 | 0.0898 |
Month 3, na | 278 | 267 | 262 |
Mean (SD), minutes | 104.87 (83.46) | 89.48 (79.26) | 95.66 (85.02) |
Change from study baseline, mean (SD), minutes | –27.08 (54.41) | –42.98 (60.06) | –39.42 (62.78) |
LSM visit estimate (95% CI),b minutes | –26.83 (–33.33 to –20.32) | –40.25 (–46.83 to –33.68) | –36.91 (–43.65 to –30.16) |
LSM treatment difference (active vs. PBO) (95% CI)b | Reference | –13.42 (–22.22 to –4.63) | –10.08 (–19.05 to –1.10) |
P valueb,c | Reference | 0.0028 | 0.0277 |
Month 6, na | 248 | 244 | 227 |
Mean (SD), minutes | 103.15 (82.29) | 81.79 (76.80) | 86.38 (77.79) |
Change from study baseline, mean (SD), minutes | –32.14 (55.28) | –51.45 (67.30) | –48.12 (68.55) |
LSM visit estimate (95% CI),b minutes | –29.28 (–36.34 to –22.21) | –46.75 (–53.92 to –39.58) | –41.95 (–49.19 to –34.70) |
LSM treatment difference (active vs. PBO) (95% CI)b | Reference | –17.47 (–27.31 to –7.64) | –12.67 (–22.38 to –2.96) |
P valueb, d | Reference | 0.0005 | 0.0105 |
CCMV = complete case missing value; CI = confidence interval; FAS = full analysis set; LEM5 = lemborexant 5 mg; LEM10 = lemborexant 10 mg; LSM = least squares mean; MMRM = mixed model of repeated measures; MNAR = missing not at random; PBO = placebo; SD = standard deviation; sWASO = subjective wake after sleep onset; vs. = versus.
Note: Data were reported with sleep diary handling rules to address potential errors and illogical values.
aThe number of patients analyzed for the change from baseline at this time point (not the number of patients who provided data at this time point).
bBased on an MMRM model with factors of age group, region, treatment, visit (first 7 nights, month 1, month 3, and month 6), and treatment-by-visit interaction as fixed effects, and the study baseline sWASO as a covariate. Missing values were imputed using multiple imputations and assumed to be MNAR or CCMV.
cP value was not adjusted for multiple testing (i.e., the type I error rate was not controlled).
dP value was adjusted for multiple testing (i.e., the type I error rate was controlled).
Source: SUNRISE 2 Clinical Study Report.18
Total Sleep Time: Total Sleep Time, Subjective Total Sleep Time
SUNRISE 1 Study
Comparisons between LEM10 versus PBO and LEM5 versus PBO and LEM10 versus ZOL and LEM5 versus ZOL for both days 1 to 2 and days 29 to 30 were other secondary outcomes (Table 25). The LSM treatment differences for LEM10 versus PBO and LEM5 versus PBO at days 1 to 2 were 56.90 minutes (95% CI, 50.46 minutes to 63.34 minutes) and 44.05 minutes (95% CI, 37.59 minutes to 50.51 minutes), respectively, and at days 29 to 30 were 38.85 minutes (95% CI, 31.64 minutes to 46.05 minutes) and 34.16 minutes (95% CI, 26.95 minutes to 41.36 minutes), respectively. The LSM treatment differences for LEM10 versus ZOL and LEM5 versus ZOL at days 1 to 2 were 23.10 minutes (95% CI, 17.04 minutes to 29.15 minutes) and 10.25 minutes (95% CI, 4.18 minutes to 16.32 minutes), respectively, and at days 29 to 30 were 24.10 minutes (95% CI, 17.32 minutes to 30.88 minutes) and 19.41 minutes (95% CI, 12.63 minutes to 26.20 minutes), respectively.
Results for sTST for the first 7 nights and last 7 nights of the treatment period supported the TST results comparing LEM10 versus PBO and LEM5 versus PBO, but not compared to ZOL where the latter comparator appeared to show a similar treatment effect during the first 7 days and last 7 days of treatment compared to LEM (Table 65).
Table 25: Change From Baseline Total Sleep Time (Other Secondary Outcome) — SUNRISE 1 Study, FAS
Outcome | PBO (N = 208) | ZOL (N = 263) | LEM5 (N = 266) | LEM10 (N = 269) |
|---|---|---|---|---|
Baseline, n | 208 | 262 | 266 | 269 |
Mean (SD), minutes | 330.67 (46.27) | 326.99 (54.85) | 328.00 (54.22) | 325.07 (52.82) |
Days 1 to 2, na | 208 | 262 | 266 | 269 |
Mean (SD), minutes | 350.11 (52.24) | 382.42 (41.53) | 393.22 (40.35) | 404.65 (36.59) |
Change from baseline, mean (SD), minutes | 19.44 (43.35) | 55.31 (48.14) | 65.22 (46.70) | 79.58 (47.35) |
LSM visit estimate (SE),b minutes | 23.59 (2.68) | 57.39 (2.43) | 67.64 (2.40) | 80.49 (2.40) |
LSM treatment difference (active minus PBO) (95% CI),b minutes | Reference | 33.80 (27.32 to 40.28) | 44.05 (37.59 to 50.51) | 56.90 (50.46 to 63.34) |
P valueb,c | Reference | < 0.0001 | < 0.0001 | < 0.0001 |
LSM treatment difference (active minus ZOL) (95% CI),b minutes | NA | Reference | 10.25 (4.18 to 16.32) | 23.10 (17.04 to 29.15) |
P valueb,c | NA | Reference | 0.0010 | < 0.0001 |
Days 29 to 30, na | 200 | 250 | 260 | 260 |
Mean (SD), minutes | 357.48 (47.33) | 370.25 (48.85) | 389.97 (42.44) | 393.16 (42.83) |
Change from baseline, mean (SD), minutes | 25.65 (47.59) | 43.34 (54.01) | 61.99 (46.82) | 67.86 (52.12) |
LSM visit estimate (SE),b minutes | 30.18 (2.95) | 44.92 (2.67) | 64.33 (2.63) | 69.02 (2.63) |
LSM treatment difference (active minus PBO) (95% CI),b minutes | Reference | 14.75 (7.48 to 22.01) | 34.16 (26.95 to 41.36) | 38.85 (31.64 to 46.05) |
P valueb,c | Reference | < 0.0001 | < 0.0001 | < 0.0001 |
LSM treatment difference (active minus ZOL) (95% CI),b minutes | NA | Reference | 19.41 (12.63 to 26.20) | 24.10 (17.32 to 30.88) |
P valueb,c | NA | Reference | < 0.0001 | < 0.0001 |
CI = confidence interval; FAS = full analysis set; LEM5 = lemborexant 5 mg; LEM10 = lemborexant 10 mg; LSM = least squares mean; MMRM = mixed model of repeated measures; NA = not applicable; PBO = placebo; SD = standard deviation; SE = standard error; TST = total sleep time; ZOL = zolpidem tartrate.
aThe number of patients analyzed for the change from baseline at this time point (not the number of patients who provided data at this time point).
bBased on an MMRM model with factors of age group, region, treatment, visit (days 1 to 2, and days 29 to 30), and treatment-by-visit interaction as fixed effects, and the baseline TST as a covariate. Missing values were not imputed and assumed to be missing at random.
cP value was not adjusted for multiple testing (i.e., the type I error rate was not controlled).
Source: SUNRISE 1 Clinical Study Report.17
SUNRISE 2 Study
Comparisons between LEM10 versus PBO and LEM5 versus PBO for the first 7 nights of period 1, month 1, month 3, and month 6 were other secondary outcomes (Table 26). The LSM treatment differences for LEM10 versus PBO and LEM5 versus PBO for the first 7 nights were 31.80 minutes (95% CI, 23.26 minutes to 40.33 minutes) and 22.03 minutes (95% CI, 13.49 minutes to 30.58 minutes), respectively, while at month 1 they were 22.13 minutes (95% CI, 11.76 minutes to 32.51 minutes) and 11.76 minutes (95% CI, 1.42 minutes to 22.10 minutes), respectively, at month 3 they were 21.69 minutes (95% CI, 10.01 minutes to 33.36 minutes) and 17.37 minutes (95% CI, 5.78 minutes to 28.97 minutes), respectively, and at month 6 they were 22.69 minutes (95% CI, 10.14 minutes to 35.23 minutes) and 18.56 minutes (95% CI, 6.14 minutes to 30.97 minutes), respectively.
Long-term sTST results based on 1 month, 3 months, 6 months, 9 months, and 12 months of exposure to LEM supported the results observed in the first 6 months (Table 66).
Table 26: Change From Baseline Subjective Total Sleep Time (Other Secondary Outcome) — SUNRISE 2 Study, FAS
Outcome | PBO (N = 318) | LEM5 (N = 316) | LEM10 (N = 315) |
|---|---|---|---|
Baseline, n | 307 | 302 | 299 |
Mean (SD), minutes | 304.25 (91.46) | 315.52 (93.50) | 306.89 (88.03) |
First 7 nights of period 1, na | 303 | 295 | 296 |
Mean (SD), minutes | 318.51 (96.30) | 350.80 (96.00) | 351.43 (91.65) |
Change from study baseline, mean (SD), minutes | 14.78 (55.00) | 34.29 (54.14) | 46.01 (55.11) |
LSM visit estimate (95% CI),b minutes | 11.42 (4.97 to 17.86) | 33.45 (26.93 to 39.96) | 43.21 (36.66 to 49.76) |
LSM treatment difference (active minus PBO) (95% CI),b minutes | Reference | 22.03 (13.49 to 30.58) | 31.80 (23.26 to 40.33) |
P valueb,c | Reference | < 0.0001 | < 0.0001 |
Month 1, na | 291 | 284 | 282 |
Mean (SD), minutes | 335.83 (95.38) | 357.14 (93.50) | 355.96 (92.73) |
Change from study baseline, mean (SD), minutes | 30.74 (70.69) | 39.32 (63.55) | 53.22 (67.91) |
LSM visit estimate (95% CI),b minutes | 27.46 (19.82 to 35.11) | 39.22 (31.51 to 46.94) | 49.60 (41.81 to 57.38) |
LSM treatment difference (active minus PBO) (95% CI),b minutes | Reference | 11.76 (1.42 to 22.10) | 22.13 (11.76 to 32.50) |
P valueb,c | Reference | 0.0259 | < 0.0001 |
Month 3, na | 269 | 256 | 251 |
Mean (SD), minutes | 353.84 (98.70) | 386.42 (82.55) | 374.99 (91.60) |
Change from study baseline, mean (SD), minutes | 48.16 (75.86) | 65.82 (71.33) | 70.95 (70.91) |
LSM visit estimate (95% CI),b minutes | 46.44 (37.98 to 54.91) | 63.82 (55.23 to 72.40) | 68.13 (59.41 to 76.85) |
LSM treatment difference (active minus PBO) (95% CI),b minutes | Reference | 17.37 (5.78 to 28.97) | 21.69 (10.01 to 33.36) |
P valueb,c | Reference | 0.0034 | 0.0003 |
Month 6, na | 242 | 235 | 220 |
Mean (SD), minutes | 356.03 (95.37) | 392.08 (86.95) | 379.25 (95.38) |
Change from study baseline, mean (SD), minutes | 53.53 (74.54) | 76.21 (77.71) | 78.32 (80.74) |
LSM visit estimate (95% CI),b minutes | 51.40 (42.38 to 60.42) | 69.95 (60.81 to 79.10) | 74.08 (64.73 to 83.43) |
LSM treatment difference (active minus PBO) (95% CI),b minutes | Reference | 18.56 (6.14 to 30.97) | 22.69 (10.14 to 35.23) |
P valueb,c | Reference | 0.0034 | 0.0004 |
CI = confidence interval; FAS = full analysis set; LEM5 = lemborexant 5 mg; LEM10 = lemborexant 10 mg; LSM = least squares mean; MMRM = mixed model of repeated measures; PBO = placebo; SD = standard deviation; sTST = subjective total sleep time.
Note: Data were reported with sleep diary handling rules to address potential errors and illogical values.
aThe number of patients analyzed for the change from baseline at this time point (not the number of patients who provided data at this time point).
bBased on an MMRM model with factors of age group, region, treatment, visit (first 7 nights, month 1, month 2, month 3, month 4, month 5, and month 6), and treatment-by-visit interaction as fixed effects, and the study baseline sTST as a covariate. Missing values were not imputed and assumed to be missing at random.
cP value was not adjusted for multiple testing (i.e., the type I error rate was not controlled).
Source: SUNRISE 2 Clinical Study Report.18
Sleep Efficiency: Sleep Efficiency and Subjective Sleep Efficiency
SUNRISE 1 Study
The first key secondary outcome in the statistical testing procedure was the mean change from baseline to days 29 to 30 for sleep efficiency comparing LEM10 to PBO, then LEM5 to PBO (Table 27). The LSM treatment difference for LEM10 versus PBO was 8.03% (95% CI, 6.57% to 9.49%; P < 0.0001) and for LEM5 versus PBO was 7.07% (95% CI, 5.61% to 8.54%; P < 0.0001).
Comparisons between LEM10 versus PBO and LEM5 versus PBO at days 1 to 2 were other secondary outcomes (Table 27). The LSM treatment difference for LEM10 versus PBO was 11.60% (95% CI, 10.30% to 12.90%) and for LEM5 versus PBO was 9.01% (95% CI, 7.70% to 10.31%).
Results for subjective sleep efficiency for the first 7 nights and last 7 nights of the treatment period supported the sleep efficiency results comparing LEM10 versus PBO and LEM5 versus PBO (Table 65).
SUNRISE 2 Study
The first key secondary outcome in the statistical testing procedure was the mean change from baseline to month 6 for subjective sleep efficiency comparing LEM10 to PBO, then LEM5 to PBO (Table 27). The LSM treatment difference for LEM10 versus PBO was 4.67% (95% CI, 2.37% to 6.96%; P < 0.0001) and for LEM5 versus PBO was 4.55% (95% CI, 2.24% to 6.86%; P = 0.0001).
Comparisons between LEM10 versus PBO and LEM5 versus PBO for the first 7 nights of period 1, month 1, and month 3 were other secondary outcomes (Table 28). The LSM treatment differences for LEM10 versus PBO and LEM5 versus PBO for the first 7 nights were 5.79% (95% CI, 4.13% to 7.45%) and 4.30% (95% CI, 2.64% to 5.96%), respectively, while for month 1 they were 3.62% (95% CI, 1.64% to 5.60%) and 2.23% (95% CI, 0.31% to 4.15%), respectively, and for month 3 they were 4.36% (95% CI, 2.22% to 6.50%) and 4.22% (95% CI, 2.07% to 6.38%), respectively.
Long-term subjective sleep efficiency results based on 1 month, 3 months, 6 months, 9 months, and 12 months of exposure to LEM supported the results observed in the first 6 months (Table 66).
Sleep Quality
SUNRISE 1 Study
Mean LSM treatment differences in quality of sleep for LEM10 versus PBO and LEM5 versus PBO for the first 7 days of the treatment period were 0.57 points (95% CI, 0.33 points to 0.80 points) and 0.49 points (95% CI, 0.25 points to 0.72 points), respectively, and for the last 7 days were 0.41 points (95% CI, 0.14 points to 0.69 points) and 0.53 points (95% CI, 0.26 points to 0.80 points), respectively (Table 29). The LSM treatment differences for LEM10 versus ZOL and LEM5 versus ZOL for the first 7 days of the treatment period were –0.12 points (95% CI, –0.34 points to 0.10 points) and –0.20 points (95% CI, –0.42 points to 0.02 points), respectively, and for the last 7 days were –0.13 points (95% CI, –0.38 points to 0.13 points) and –0.01 points (95% CI, –0.27 points to 0.24 points), respectively.
Table 27: Change From Baseline Sleep Efficiency (Key Secondary and Other Secondary Outcomes) — SUNRISE 1 Study, FAS
Outcome | PBO (N = 208) | ZOL (N = 263) | LEM5 (N = 266) | LEM10 (N = 269) |
|---|---|---|---|---|
Baseline, n | 208 | 262 | 266 | 269 |
Mean (SD), % | 68.89 (9.64) | 68.13 (11.42) | 68.36 (11.27) | 67.85 (10.85) |
Days 1 to 2, na | 208 | 262 | 266 | 269 |
Mean (SD), % | 73.11 (10.77) | 79.85 (8.46) | 81.96 (8.38) | 84.33 (7.61) |
Change from baseline, mean (SD), % | 4.22 (9.03) | 11.70 (9.73) | 13.60 (9.73) | 16.48 (9.62) |
LSM visit estimate (SE),b % | 5.16 (0.54) | 12.12 (0.49) | 14.16 (0.49) | 16.76 (0.49) |
LSM treatment difference (active minus PBO) (95% CI),b % | Reference | 6.96 (5.65 to 8.27) | 9.01 (7.70 to 10.31) | 11.60 (10.30 to 12.90) |
P valueb,c | Reference | < 0.0001 | < 0.0001 | < 0.0001 |
Days 29 to 30, na | 200 | 250 | 260 | 260 |
Mean (SD), % | 74.49 (9.85) | 77.17 (10.19) | 81.29 (8.80) | 81.99 (8.80) |
Change from baseline, mean (SD), % | 5.35 (9.90) | 9.06 (11.23) | 12.93 (9.74) | 14.09 (10.51) |
LSM visit estimate (SE),b % | 6.34 (0.60) | 9.50 (0.55) | 13.42 (0.53) | 14.37 (0.54) |
LSM treatment difference (active minus PBO) (95% CI),b % | Reference | 3.15 (1.67 to 4.63) | 7.07 (5.61 to 8.54) | 8.03 (6.57 to 9.49) |
P valueb,d | Reference | < 0.0001 | < 0.0001 | < 0.0001 |
CI = confidence interval; FAS = full analysis set; LEM5 = lemborexant 5 mg; LEM10 = lemborexant 10 mg; LSM = least squares mean; MMRM = mixed model of repeated measures; PBO = placebo; SD = standard deviation; SE = standard error; ZOL = zolpidem tartrate.
aThe number of patients analyzed for the change from baseline at this time point (not the number of patients who provided data at this time point).
bBased on an MMRM model with factors of age group, region, treatment, visit (days 1 to 2, and days 29 to 30), and treatment-by-visit interaction as fixed effects, and the baseline SE as a covariate. Missing values were imputed using multiple imputation and assumed to be missing not at random.
cP value was not adjusted for multiple testing (i.e., the type I error rate was not controlled).
dP value was adjusted for multiple testing (i.e., the type I error rate was controlled).
Source: SUNRISE 1 Clinical Study Report.17
Table 28: Change From Baseline Subjective Sleep Efficiency (Key Secondary and Other Secondary Outcomes) — SUNRISE 2 Study, FAS
Outcome | PBO (N = 318) | LEM5 (N = 316) | LEM10 (N = 315) |
|---|---|---|---|
Baseline, n | 307 | 302 | 299 |
Mean (SD), % | 61.34 (17.84) | 63.14 (18.23) | 62.03 (17.25) |
First 7 nights of period 1, na | 303 | 295 | 296 |
Mean (SD), % | 63.88 (18.85) | 69.97 (18.31) | 69.96 (17.43) |
Change from study baseline, mean (SD), % | 2.68 (10.77) | 6.61 (10.39) | 8.27 (10.57) |
LSM visit estimate (95% CI),b % | 2.10 (0.85 to 3.34) | 6.40 (5.14 to 7.66) | 7.89 (6.61 to 9.17) |
LSM treatment difference (active minus PBO) (95% CI)b | Reference | 4.30 (2.64 to 5.96) | 5.79 (4.13 to 7.45) |
P valueb,c | Reference | < 0.0001 | < 0.0001 |
Month 1, n | 291 | 284 | 282 |
Mean (SD), % | 67.53 (18.25) | 71.56 (18.30) | 71.04 (17.55) |
Change from study baseline, mean (SD), % | 6.11 (12.88) | 7.87 (12.26) | 9.92 (12.92) |
LSM visit estimate (95% CI),b % | 5.54 (4.11 to 6.97) | 7.76 (6.31 to 9.21) | 9.15 (7.67 to 10.64) |
LSM treatment difference (active minus PBO) (95% CI)b | Reference | 2.23 (0.31 to 4.15) | 3.62 (1.64 to 5.60) |
P valueb,c | Reference | 0.0230 | 0.0003 |
Month 3, n | 269 | 256 | 251 |
Mean (SD), % | 70.58 (18.54) | 77.29 (15.26) | 75.15 (17.21) |
Change from study baseline, mean (SD) | 9.16 (13.64) | 13.03 (13.52) | 13.61 (14.04) |
LSM visit estimate (95% CI),b % | 8.58 (7.00 to 10.15) | 12.80 (11.24 to 14.36) | 12.94 (11.37 to 14.50) |
LSM treatment difference (active minus PBO) (95% CI)b | Reference | 4.22 (2.07 to 6.38) | 4.36 (2.22 to 6.50) |
P valueb,c | Reference | 0.0001 | < 0.0001 |
Month 6, n | 242 | 235 | 220 |
Mean (SD), % | 71.40 (18.31) | 78.55 (16.24) | 76.53 (17.99) |
Change from study baseline, mean (SD), % | 10.36 (13.80) | 15.34 (14.61) | 15.55 (15.62) |
LSM visit estimate (95% CI),b % | 9.64 (7.99 to 11.30) | 14.19 (12.50 to 15.88) | 14.31 (12.60 to 16.02) |
LSM treatment difference (active minus PBO) (95% CI)b | Reference | 4.55 (2.24 to 6.86) | 4.67 (2.37 to 6.96) |
P valueb, d | Reference | 0.0001 | < 0.0001 |
CCMV = complete case missing value; CI = confidence interval; FAS = full analysis set; LEM5 = lemborexant 5 mg; LEM10 = lemborexant 10 mg; LSM = least squares mean; MMRM = mixed model of repeated measures; MNAR = missing not at random; PBO = placebo; SD = standard deviation; vs. = versus.
Note: Data were reported with sleep diary handling rules to address potential errors and illogical values.
aThe number of patients analyzed for the change from baseline at this time point (not the number of patients who provided data at this time point).
bBased on an MMRM model with factors of age group, region, treatment, visit (first 7 nights, month 1, month 3, and month 6), and treatment-by-visit interaction as fixed effects, and the study baseline subjective sleep efficiency as a covariate. Missing values were imputed using multiple imputation and assumed to be MNAR or CCMV.
cP value was not adjusted for multiple testing (i.e., the type I error rate was not controlled).
dP value was adjusted for multiple testing (i.e., the type I error rate was controlled).
Source: SUNRISE 2 Clinical Study Report.18
SUNRISE 2 Study
Mean LSM treatment differences in quality of sleep for LEM10 versus PBO and LEM5 versus PBO for the first 7 days of the treatment period were 0.48 points (95% CI, 0.31 points to 0.65 points) and 0.47 points (95% CI, 0.30 points to 0.64 points), respectively, while at month 1 they were 0.17 points (95% CI, –0.02 points to 0.36 points) and 0.19 points (95% CI, 0.00 points to 0.38 points), respectively, at month 3 they were 0.29 points (95% CI, 0.07 points to 0.52 points) and 0.24 points (95% CI, 0.02 points to 0.47 points), respectively, and at month 6 they were 0.32 points (95% CI, 0.08 points to 0.56 points) and 0.28 points (95% CI, 0.04 points to 0.52 points), respectively (Table 30).
Long-term quality of sleep results based on 1 month, 3 months, 6 months, 9 months, and 12 months of exposure to LEM supported the results observed in the first 6 months (Table 69).
Harms
Detailed harms data are summarized in Table 31. Only those harms identified in the CADTH systematic review protocol are reported as follows.
Table 29: Change From Baseline Quality of Sleep (Exploratory Outcome) — SUNRISE 1 Study, FAS
Outcome | PBO (N = 208) | ZOL (N = 263) | LEM5 (N = 266) | LEM10 (N = 269) |
|---|---|---|---|---|
Baseline, n | 206 | 262 | 264 | 269 |
Mean (SD) | 3.87 (1.43) | 3.87 (1.37) | 3.78 (1.35) | 3.70 (1.31) |
First 7 nights of treatment, na | 202 | 254 | 261 | 266 |
Mean (SD) | 4.48 (1.55) | 5.20 (1.52) | 4.93 (1.53) | 4.96 (1.58) |
Change from baseline, LSM visit estimate (SE)b | 0.60 (0.10) | 1.29 (0.09) | 1.09 (0.09) | 1.17 (0.09) |
LSM treatment difference (active minus PBO) (95% CI)b | Reference | 0.69 (0.45 to 0.93) | 0.49 (0.25 to 0.72) | 0.57 (0.33 to 0.80) |
P valueb,c | Reference | < 0.0001 | < 0.0001 | < 0.0001 |
LSM treatment difference (active minus ZOL) (95% CI)b | NA | Reference | –0.20 (–0.42 to 0.02) | –0.12 (–0.34 to 0.10) |
P valueb,c | NA | Reference | 0.0756 | 0.2885 |
Last 7 nights of treatment, na | 196 | 248 | 253 | 258 |
Mean (SD) | 4.82 (1.66) | 5.40 (1.59) | 5.31 (1.65) | 5.12 (1.63) |
Change from baseline, LSM (SE)b | 0.93 (0.11) | 1.47 (0.10) | 1.46 (0.10) | 1.35 (0.10) |
LSM treatment difference (active minus PBO) (95% CI)b | Reference | 0.54 (0.27 to 0.82) | 0.53 (0.26 to 0.80) | 0.41 (0.14 to 0.69) |
P valueb,c | Reference | 0.0001 | 0.0002 | 0.0029 |
LSM treatment difference (active minus ZOL) (95% CI)b | NA | Reference | –0.01 (–0.27 to 0.24) | –0.13 (–0.38 to 0.13) |
P valueb,c | NA | Reference | 0.9225 | 0.3333 |
CI = confidence interval; FAS = full analysis set; LEM5 = lemborexant 5 mg; LEM10 = lemborexant 10 mg; LSM = least squares mean; MMRM = mixed model of repeated measures; NA = not applicable; PBO = placebo; SD = standard deviation; SE = standard error; ZOL = zolpidem tartrate.
aThe number of patients analyzed for the change from baseline at this time point (not the number of patients who provided data at this time point).
bBased on an MMRM model with factors of age group, region, treatment, visit (first 7 nights and last 7 nights), and treatment-by-visit interaction as fixed effects, and the baseline quality of sleep rating as a covariate. Missing values were not imputed and assumed to be missing at random.
cP value was not adjusted for multiple testing (i.e., the type I error rate was not controlled).
Source: SUNRISE 1 Clinical Study Report.17
Table 30: Change From Baseline Quality of Sleep (Exploratory Outcome) — SUNRISE 2 Study, FAS
Outcome | PBO (N = 318) | LEM5 (N = 316) | LEM10 (N = 315) |
|---|---|---|---|
Baseline, n | 316 | 314 | 312 |
Mean (SD) | 3.8 (1.43) | 4.0 (1.27) | 4.0 (1.35) |
First 7 nights of period 1, na | 314 | 310 | 310 |
Mean (SD) | 4.0 (1.43) | 4.6 (1.49) | 4.6 (1.53) |
Change from study baseline, mean (SD) | 0.2 (1.12) | 0.6 (1.08) | 0.7 (1.15) |
LSM treatment difference (active minus PBO) (95% CI)b | Reference | 0.47 (0.30 to 0.64) | 0.48 (0.31 to 0.65) |
P valueb,c | Reference | < 0.0001 | < 0.0001 |
Month 1, n | 300 | 298 | 297 |
Mean (SD) | 4.4 (1.55) | 4.6 (1.41) | 4.6 (1.51) |
Change from study baseline, mean (SD) | 0.5 (1.28) | 0.7 (1.23) | 0.7 (1.37) |
LSM treatment difference (active minus PBO) (95% CI)b | Reference | 0.19 (0.00 to 0.38) | 0.17 (–0.02 to 0.36) |
P valueb,c | Reference | 0.0490 | 0.0879 |
Month 3, n | 280 | 268 | 264 |
Mean (SD) | 4.6 (1.59) | 5.0 (1.49) | 5.0 (1.64) |
Change from study baseline, mean (SD) | 0.8 (1.40) | 1.0 (1.41) | 1.0 (1.56) |
LSM treatment difference (active minus PBO) (95% CI)b | Reference | 0.24 (0.02 to 0.47) | 0.29 (0.07 to 0.52) |
P valueb,c | Reference | 0.0356 | 0.0110 |
Month 6, n | 249 | 245 | 229 |
Mean (SD) | 4.8 (1.65) | 5.2 (1.48) | 5.2 (1.65) |
Change from study baseline, mean (SD) | 1.0 (1.49) | 1.3 (1.50) | 1.3 (1.62) |
LSM treatment difference (active minus PBO) (95% CI)b | Reference | 0.28 (0.04 to 0.52) | 0.32 (0.08 to 0.56) |
P valueb,c | Reference | 0.0244 | 0.0103 |
CI = confidence interval; FAS = full analysis set; LEM5 = lemborexant 5 mg; LEM10 = lemborexant 10 mg; LSM = least squares mean; MMRM = mixed model of repeated measures; PBO = placebo; SD = standard deviation.
aThe number of patients analyzed for the change from baseline at this time point (not the number of patients who provided data at this time point).
bBased on an MMRM model with factors of age group, region, treatment, visit (first 7 mornings, month 1, month 2, month 3, month 4, month 5, and month 6), and treatment-by-visit interaction as fixed effects, and study baseline end point as a covariate. Missing values were not imputed and assumed to be missing at random.
cP value was not adjusted for multiple testing (i.e., the type I error rate was not controlled).
Source: SUNRISE 2 Clinical Study Report.18
Table 31: Summary of Harms — SUNRISE 1 and SUNRISE 2 Studies, Safety Analysis Set
Harm | SUNRISE 1 study | SUNRISE 2 study | |||||
|---|---|---|---|---|---|---|---|
PBO (N = 209) | ZOL (N = 263) | LEM5 (N = 266) | LEM10 (N = 268) | PBO (N = 319) | LEM5 (N = 314) | LEM10 (N = 314) | |
Patients with ≥ 1 TEAE by preferred term | |||||||
n (%) | 53 (25.4) | 93 (35.4) | 74 (27.8) | 82 (30.6) | 200 (62.7) | 192 (61.1) | 187 (59.6) |
Most common events,a n (%) | |||||||
Headache | 13 (6.2) | 14 (5.3) | 17 (6.4) | 13 (4.9) | 21 (6.6) | 28 (8.9) | 21 (6.7) |
Somnolence | 4 (1.9) | 4 (1.5) | 11 (4.1) | 19 (7.1) | 5 (1.6) | 27 (8.6) | 41 (13.1) |
Nasopharyngitis | 3 (1.4) | 1 (0.4) | 7 (2.6) | 1 (0.4) | 40 (12.5) | 30 (9.6) | 29 (9.2) |
Influenza | 2 (1.0) | 1 (0.4) | 0 | 0 | 15 (4.7) | 15 (4.8) | 16 (5.1) |
Patients with ≥ 1 SAE | |||||||
n (%) | 0 | 4 (1.5) | 2 (0.8) | 0 | 5 (1.6) | 7 (2.2) | 9 (2.9) |
Patients who stopped treatment due to AEs by preferred term | |||||||
n (%) | 2 (1.0) | 7 (2.7) | 2 (0.8) | 3 (1.1) | 12 (3.8) | 13 (4.1) | 26 (8.3) |
Most common events,b n (%) | |||||||
Headache | 0 | 0 | 1 (0.4) | 1 (0.4) | 2 (0.6) | 1 (0.3) | 0 |
Somnolence | 1 (0.5) | 1 (0.4) | 1 (0.4) | 0 | 2 (0.6) | 3 (1.0) | 9 (2.9) |
Nightmare | 0 | 0 | 1 (0.4) | 0 | 0 | 1 (0.3) | 4 (1.3) |
Palpitations | 0 | 0 | 0 | 0 | 0 | 0 | 2 (0.6) |
Deaths | |||||||
n (%) | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
Notable harms | |||||||
Somnolence, n (%) | 4 (1.9) | 4 (1.5) | 11 (4.1) | 19 (7.1) | 5 (1.6) | 27 (8.6) | 41 (13.1) |
Impaired driving performance, n (%) | NR | NR | NR | NR | NR | NR | NR |
Falls, n (%) | 0 | 0 | 4 (1.5) | 0 | 10 (3.1) | 5 (1.6) | 5 (1.6) |
MVA (road traffic accident), n (%) | 0 | 1 (0.4) | 0 | 0 | 1 (0.3) | 0 | 1 (0.3) |
Workplace accidents, n (%) | NR | NR | NR | NR | NR | NR | NR |
Hallucination, n (%) | NA | NA | NA | NA | NA | NA | NA |
Tactile | 0 | 0 | 0 | 1 (0.4) | NR | NR | NR |
Hypnagogic | NR | NR | NR | NR | 0 | 1 (0.3) | 2 (0.6) |
Hypnopompic | NR | NR | NR | NR | 0 | 0 | 1 (0.3) |
Drug misuse (intentional overdose), n (%) | 0 | 0 | 0 | 0 | 1 (0.3) | 2 (0.6) | 0 |
AE = adverse event; LEM5 = lemborexant 5 mg; LEM10 = lemborexant 10 mg; MVA = motor vehicle accident; NA = not applicable; NR = not reported; PBO = placebo; SAE = serious adverse event; TEAE = treatment-emergent adverse event; ZOL = zolpidem tartrate.
aFrequency of at least 5% of patients in any treatment group.
bFrequency of more than 1 patient in any treatment group.
Sources: SUNRISE 1 Clinical Study Report17 and SUNRISE 2 Clinical Study Report.18
Adverse Events
In the SUNRISE 1 study, 82 (30.6%) patients, 74 (27.8%) patients, 93 (35.4%) patients, and 53 (25.4%) patients in the LEM10, LEM5, ZOL, and PBO groups experienced at least 1 AE, respectively. The most common AEs occurring in at least 5% of patients in any group were headache (4.9%, 6.4%, 5.3%, and 6.2% in the LEM10, LEM5, ZOL, and PBO groups, respectively), somnolence (7.1%, 4.1%, 1.5%, and 1.9% in the LEM10, LEM5, ZOL, and PBO groups, respectively), and nasopharyngitis (0.4%, 2.6%, 0.4%, and 1.0% in the LEM10, LEM5, ZOL, and PBO groups, respectively).
In the SUNRISE 2 study, 187 (59.6%) patients, 192 (61.1%) patients, and 200 (62.7%) patients in the LEM10, LEM5, and PBO groups experienced at least 1 AE, respectively. The most common AEs occurring in at least 5% of patients in any group were headache (6.7%, 8.9%, and 6.6% in the LEM10, LEM5, and PBO groups, respectively), somnolence (13.1%, 8.6%, and 1.6% in the LEM10, LEM5, and PBO groups, respectively), nasopharyngitis (9.2%, 9.6%, and 12.5% in the LEM10, LEM5, and PBO groups, respectively), and influenza (5.1%, 4.8%, and 4.7% in the LEM10, LEM5, and PBO groups, respectively).
Serious Adverse Events
In the SUNRISE 1 study, 2 (0.8%) patients and 4 (1.5%) patients in the LEM5 and ZOL groups experienced at least 1 SAE, respectively. No patients in the LEM10 or PBO groups reported an SAE. No SAEs occurred in more than 1 patient per treatment group.
In the SUNRISE 2 study, 9 (2.9%) patients, 7 (2.2%) patients, and 5 (1.6%) patients in the LEM10, LEM5, and PBO groups experienced at least 1 SAE, respectively. No SAEs occurred in more than 1 patient per treatment group.
Withdrawals Due to Adverse Events
In the SUNRISE 1 study, 3 (1.1%) patients, 2 (0.8%) patients, 7 (2.7%) patients, and 2 (1.0%) patients in the LEM10, LEM5, ZOL, and PBO groups stopped treatment due to an AE, respectively. No events occurred in more than 1 patient in any treatment group.
In the SUNRISE 2 study, 26 (8.3%) patients, 13 (4.1%) patients, and 12 (3.8%) patients in the LEM10, LEM5, and PBO groups stopped treatment due to an AE, respectively. The following events occurred in more than 1 patient in any group: headache, somnolence, nightmare, and palpitations.
Mortality
No deaths were reported in either the SUNRISE 1 or SUNRISE 2 trial.
Notable Harms
In the SUNRISE 1 study, somnolence was reported for 19 (7.1%) patients, 11 (4.1%) patients, 4 (1.5%) patients, and 4 (1.9%) patients who received LEM10, LEM5, ZOL, and PBO, respectively. In the SUNRISE 2 study, somnolence was reported for 41 (13.1%) patients, 27 (8.6%) patients, and 5 (1.6%) patients who received LEM10, LEM5, and PBO, respectively.
In SUNRISE1, falls were reported for 4 (1.5%) patients in the LEM5 group and 0 patients in all other groups while in SUNRISE 2, falls were reported for 5 (1.6%) patients in each of the LEM10 and LEM5 groups and 10 (3.1%) patients in the PBO group.
A road traffic accident (MVA for the CADTH systematic review protocol) was described for 1 patient who received ZOL in SUNRISE 1; no other treatment groups reported an MVA. In SUNRISE 2, 1 patient each in the LEM10 and PBO groups reported an MVA and no MVAs were reported in the LEM5 group.
In the SUNRISE 1 study, tactile hallucination was reported for 1 patient who received LEM10 and was not reported for any other treatment groups. In the SUNRISE 2 study, hypnagogic hallucination was reported for 3 patients who received LEM10 (2 patients) and LEM5 (1 patient) and for 0 patients in the PBO group, while hypnopompic hallucination was reported for 1 patient who received LEM10 and for 0 patients in the LEM5 and PBO groups.
No intentional overdoses were reported in SUNRISE 1. In SUNRISE 2, intentional overdoses were reported for 2 patients who received LEM5, 1 patient who received PBO, and 0 patients who received LEM10.
Neither trial reported impaired driving or workplace accidents.
Postural instability was assessed in SUNRISE 1 (Table 32). On days 2 to 3, the LSM treatment difference for LEM10 versus PBO was 2.91 units (95% CI, –0.28 units to 6.10 units) and for LEM5 versus PBO was 2.49 units (95% CI, –0.70 units to 5.67 units). The LSM treatment difference for LEM10 versus ZOL was –4.29 units (95% CI, –7.32 units to –1.26 units) and for LEM5 versus ZOL was –4.71 units (95% CI, –7.73 units to –1.70 units). On days 30 to 31, the LSM treatment difference for LEM10 versus PBO was –0.58 units (95% CI, –3.68 units to 2.53 units) and for LEM5 versus PBO was –0.71 units (95% CI, –3.80 units to 2.38 units). The LSM treatment difference for LEM10 versus ZOL was –2.57 units (95% CI, –5.53 units to 0.39 units) and for LEM5 versus ZOL was –2.70 units (95% CI, –5.64 units to 0.23 units). Since there was no adjustment for multiplicity, the results are uncertain.
Table 32: Notable Harms, Postural Instability — SUNRISE 1 Study, FAS
Postural instability | PBO (N = 208) | ZOL (N = 263) | LEM5 (N = 266) | LEM10 (N = 269) |
|---|---|---|---|---|
Baseline, na | 199 | 238 | 245 | 242 |
Mean (SD), units | 23.08 (17.51) | 26.01 (22.13) | 26.40 (20.78) | 23.69 (19.52) |
Days 2 to 3, nb | 190 | 233 | 237 | 233 |
Mean (SD), units | 20.81 (14.59) | 29.86 (25.25) | 25.73 (23.42) | 24.36 (20.11) |
Change from baseline, mean (SD), units | –2.02 (13.66) | 4.07 (18.92) | –0.82 (20.38) | 0.56 (17.08) |
LSM treatment difference (active minus PBO) (95% CI),c units | Reference | 7.20 (4.00 to 10.40) | 2.49 (–0.70 to 5.67) | 2.91 (–0.2 to 6.10) |
P valuec | Reference | < 0.0001 | 0.1258 | 0.0741 |
LSM treatment difference (active minus ZOL) (95% CI),c units | NA | Reference | –4.71 (–7.73 to –1.70) | –4.29 (–7.32 to –1.26) |
P valuec | NA | Reference | 0.0022 | 0.0055 |
Days 30 to 31, nb | 160 | 192 | 208 | 201 |
Mean (SD), units | 22.19 (18.14) | 27.65 (21.85) | 25.10 (19.64) | 22.76 (20.05) |
Change from baseline, mean (SD), units | 1.68 (16.58) | 2.12 (18.36) | –0.85 (16.20) | 0.48 (14.85) |
LSM treatment difference (active minus PBO) (95% CI),c units | Reference | 1.99 (–1.15 to 5.14) | –0.71 (–3.80 to 2.38) | –0.58 (–3.68 to 2.53) |
P valuec | Reference | 0.2136 | 0.6528 | 0.7161 |
LSM treatment difference (active minus ZOL) (95% CI),c units | NA | Reference | –2.70 (–5.64 to 0.23) | –2.57 (–5.53 to 0.39) |
P valuec | NA | Reference | 0.0712 | 0.0890 |
CI = confidence interval; FAS = full analysis set; LEM5 = lemborexant 5 mg; LEM10 = lemborexant 10 mg; LSM = least squares mean; MMRM = mixed model of repeated measures; NA = not applicable; PBO = placebo; SD = standard deviation; ZOL = zolpidem tartrate.
aExtreme values from 2 patients were removed (patient 4057 to 1031 had values of 3,084, 856, and 853 and patient 4057 to 1035 had values of 253, 1,286, and 1,293 for baseline, days 2 to 3, and days 30 to 31, respectively). Both patients were from the same site with reported body sway values well out of physiologic range, which therefore skewed the mean body sway values.
bThe number of patients analyzed for the change from baseline at this time point (not the number of patients who provided data at this time point).
cBased on an MMRM model with factors of age group, region, treatment, visit (days 2 to 3, and days 30 to 31), and treatment-by-visit interaction as fixed effects, and the baseline posture stability of body sway as a covariate. Body sway was reported in units of one-third degree angle of arc (lower values are better). Missing values were not imputed and assumed to be missing at random.
Source: SUNRISE 1 Clinical Study Report.17
Table 33: Notable Harms, Impaired Attention — SUNRISE 1 Study, FAS
Impaired attention | PBO (N = 208) | ZOL (N = 263) | LEM5 (N = 266) | LEM10 (N = 269) | |
|---|---|---|---|---|---|
CPAB power of attention | |||||
Baseline, n | 195 | 239 | 249 | 246 | |
Mean (SD), milliseconds | 1,421.0 (210.27) | 1,418.7 (195.95) | 1,452.9 (263.04) | 1,399.2 (192.47) | |
Days 2 to 3, na | 186 | 233 | 240 | 236 | |
Mean (SD), milliseconds | 1,408.8 (180.12) | 1,457.5 (221.11) | 1,465.3 (223.32) | 1,438.3 (229.82) | |
Change from baseline, LSM (SE), milliseconds | –22.53 (10.48) | 27.46 (9.57) | 8.24 (9.47) | 17.14 (9.59) | |
P valueb (active vs. PBO) | Reference | < 0.0001 | 0.0141 | 0.0016 | |
P valueb (active vs. ZOL) | NA | Reference | 0.1031 | 0.3825 | |
Days 30 to 31, na | 156 | 194 | 206 | 202 | |
Mean (SD), milliseconds | 1,428.2 (191.33) | 1,471.7 (223.15) | 1,493.8 (302.21) | 1,435.2 (178.34) | |
Change from baseline, LSM (SE), milliseconds | –5.97 (13.23) | 37.76 (12.02) | 37.29 (11.77) | 31.22 (11.89) | |
P valueb (active vs. PBO) | Reference | 0.0086 | 0.0086 | 0.0244 | |
P valueb (active vs. ZOL) | NA | Reference | 0.9762 | 0.6744 | |
CPAB continuity of attention | |||||
Baseline, n | 195 | 239 | 249 | 246 | |
Mean (SD), units | 90.7 (4.77) | 90.6 (6.04) | 91.0 (5.15) | 91.3 (4.15) | |
Days 2 to 3, na | 186 | 233 | 240 | 236 | |
Mean (SD), units | 90.7 (4.53) | 89.5 (6.89) | 91.2 (3.36) | 90.5 (5.47) | |
Change from baseline, LSM (SE), units | –0.09 (0.32) | –1.12 (0.30) | 0.26 (0.29) | –0.53 (0.30) | |
P valueb (active vs. PBO) | Reference | 0.0088 | 0.3726 | 0.2579 | |
P valueb (active vs. ZOL) | NA | Reference | 0.0002 | 0.1120 | |
Days 30 to 31, na | 156 | 194 | 206 | 202 | |
Mean (SD), units | 90.5 (4.58) | 90.3 (4.91) | 90.8 (4.49) | 90.6 (4.68) | |
Change from baseline, LSM (SE), units | –0.25 (0.37) | –0.32 (0.33) | –0.14 (0.33) | –0.57 (0.33) | |
P valueb (active vs. PBO) | Reference | 0.8686 | 0.8194 | 0.4707 | |
P valueb (active vs. ZOL) | NA | Reference | 0.6745 | 0.5565 | |
CPAB = Cognitive Performance Assessment Battery; FAS = full analysis set; LEM5 = lemborexant 5 mg; LEM10 = lemborexant 10 mg; LSM = least squares mean; MMRM = mixed model of repeated measures; NA = not applicable; PBO = placebo; SD = standard deviation; SE = standard error; vs. = versus; ZOL = zolpidem tartrate.
aThe number of patients analyzed for the change from baseline at this time point (not the number of patients who provided data at this time point).
bBased on an MMRM model with factors of age group, region, treatment, visit (days 2 to 3 and days 30 to 31), and treatment-by-visit interaction as fixed effects, and the baseline CPAB domain as a covariate. Missing values were not imputed and assumed to be missing at random.
Source: SUNRISE 1 Clinical Study Report.17
Table 34: Notable Harms, Rebound Insomnia Assessed During Follow-Up — SUNRISE 1 and SUNRISE 2 Studies
Rebound insomnia | SUNRISE 1 studya | SUNRISE 2 studyb | ||||
|---|---|---|---|---|---|---|
PBO (N = 208) | ZOL (N = 263) | LEM5 (N = 266) | LEM10 (N = 269) | LEM5 (N = 444) | LEM10 (N = 437) | |
sSOL average of first 7 nights, n | 193 | 241 | 251 | 254 | 335 | 328 |
Rebound, n (%) | 45 (23.3) | 66 (27.4) | 52 (20.7) | 44 (17.3) | 53 (11.94) | 46 (10.53) |
sSOL average of last 7 nights, n | 189 | 234 | 243 | 246 | 327 | 312 |
Rebound, n (%) | 44 (23.3) | 63 (26.9) | 53 (21.8) | 60 (24.4) | 52 (11.71) | 41 (9.38) |
sWASO average of first 7 nights, n | 194 | 241 | 248 | 251 | 335 | 325 |
Rebound, n (%) | 29 (14.9) | 52 (21.6) | 48 (19.4) | 41 (16.3) | 55 (12.39) | 62 (14.19) |
sWASO average of last 7 nights, n | 189 | 234 | 241 | 243 | 327 | 311 |
Rebound, n (%) | 33 (17.5) | 41 (17.5) | 46 (19.1) | 43 (17.7) | 60 (13.51) | 52 (11.90) |
FAS = full analysis set; LEM5 = lemborexant 5 mg; LEM10 = lemborexant 10 mg; PBO = placebo; PSG = polysomnography; sSOL = subjective sleep onset latency; sWASO = subjective wake after sleep onset; ZOL = zolpidem tartrate.
Note: “Rebound” is defined as having an end point value at the specified time point that is 5 minutes higher than baseline (last 7 nights before screening PSG or run-in period for SUNRISE 1 or SUNRISE 2, respectively).
aData reported for FAS.
bData reported for on-treatment FAS.
Sources: SUNRISE 1 Clinical Study Report17 and SUNRISE 2 Clinical Study Report.18
Table 35: Notable Harms, Withdrawal Symptoms or Dependence From the T-BWSQ Assessed During Follow-Up — SUNRISE 1 and SUNRISE 2 Studies
T-BWSQ | SUNRISE 1 studya | SUNRISE 2 studyb | ||||
|---|---|---|---|---|---|---|
PBO (N = 209) | ZOL (N = 263) | LEM5 (N = 266) | LEM10 (N = 268) | LEM5 (N = 447) | LEM10 (N = 437) | |
End of study, nc | 198 | 252 | 259 | 259 | 406 | 388 |
Score ≥ 3,d n (%) | 28 (14.1) | 37 (14.7) | 30 (11.6) | 26 (10.0) | 84 (20.7) | 65 (16.8) |
LEM5 = lemborexant 5 mg; LEM10 = lemborexant 10 mg; PBO = placebo; T-BWSQ = Tyrer Benzodiazepine Withdrawal Symptom Questionnaire; ZOL = zolpidem tartrate.
aData reported for safety analysis set.
bData reported for on-treatment safety analysis set.
cThe number of patients analyzed for the change from baseline at this time point (not the number of patients who provided data at this time point).
dA score of 3 or greater indicated that there was evidence for withdrawal symptoms from the active treatment.
Sources: SUNRISE 1 Clinical Study Report17 and SUNRISE 2 Clinical Study Report.18
Table 36: Notable Harms, Suicidal Ideation From the C-SSRS — SUNRISE 1 and SUNRISE 2 Studies
Suicidal ideation | SUNRISE 1 studya | SUNRISE 2 studyb | ||||
|---|---|---|---|---|---|---|
PBO (N = 209) | ZOL (N = 263) | LEM5 (N = 266) | LEM10 (N = 268) | LEM5 (N = 447) | LEM10 (N = 437) | |
Baseline, n | 204 | 252 | 255 | 254 | 447 | 437 |
Suicidal ideation, n (%) | 0 | 3 (1.1) | 1 (0.4) | 2 (0.7) | 3 (0.7) | 5 (1.1) |
Day 3, nc | 192 | 245 | 239 | 248 | NA | NA |
Suicidal ideation, n (%) | 3 (1.4) | 0 | 2 (0.8) | 2 (0.7) | NA | NA |
Day 31, nc | 198 | 242 | 256 | 256 | NA | NA |
Suicidal ideation, n (%) | 1 (0.5) | 3 (1.1) | 1 (0.4) | 1 (0.4) | NA | NA |
6 months of exposure, nc | NA | NA | NA | NA | 367 | 350 |
Suicidal ideation, n (%) | NA | NA | NA | NA | 1 (0.3) | 2 (0.6) |
12 months of exposure, nc | NA | NA | NA | NA | 204 | 193 |
Suicidal ideation, n (%) | NA | NA | NA | NA | 1 (0.5) | 1 (0.5) |
End of study, nc | 193 | 242 | 249 | 252 | NR | NR |
Suicidal ideation, n (%) | 0 | 2 (0.8) | 0 | 0 | NR | NR |
C-SSRS = Columbia-Suicide Severity Rating Scale; LEM5 = lemborexant 5 mg; LEM10 = lemborexant 10 mg; NA = not applicable; NR = not reported; PBO = placebo; ZOL = zolpidem tartrate.
Note: Any suicidal ideation is positive if any of the following categories is endorsed: (1) wish to be dead, (2) nonspecific active suicidal thoughts, (3) active suicidal ideation with any method (not plan) without intent to act, (4) active suicidal ideation with some intent to act without specific plan, and/or (5) active suicidal ideation with specific plan and intent.
aData reported for safety analysis set.
bData reported for on-treatment safety analysis set.
cThe number of patients analyzed for the change from baseline at this time point (not the number of patients who provided data at this time point).
Sources: SUNRISE 1 Clinical Study Report17 and SUNRISE 2 Clinical Study Report.18
Impaired attention was assessed in SUNRISE 1 using 2 components of the CPAB: power of attention and continuity of attention (Table 33). For power of attention on days 2 to 3, the LSM change from baseline was 17.14 (standard error [SE] = 9.59) milliseconds, 8.24 (SE = 9.47) milliseconds, 27.46 (SE = 9.57) milliseconds, and –22.53 (SE = 10.48) milliseconds for the LEM10, LEM5, ZOL, and PBO groups, respectively. On days 30 to 31, the LSM change from baseline was 31.22 (SE = 11.89) milliseconds, 37.29 (SE = 11.77) milliseconds, 37.76 (SE = 12.02) milliseconds, and –5.97 (SE = 13.23) milliseconds for the LEM10, LEM5, ZOL, and PBO groups, respectively. For continuity of attention on days 2 to 3, the LSM change from baseline was –0.53 (SE = 0.30) units, 0.26 (SE = 0.29) units, –1.12 (SE = 0.30) units, and –0.09 (SE = 0.32) units for the LEM10, LEM5, ZOL, and PBO groups, respectively. On days 30 to 31, the LSM change from baseline was –0.57 (SE = 0.33) units, –0.14 (SE = 0.33) units, –0.32 (SE = 0.33) units, and –0.25 (SE = 0.37) units for the LEM10, LEM5, ZOL, and PBO groups, respectively.
Rebound insomnia was assessed using average values for sSOL and sWASO for the first 7 nights and last 7 nights of the follow-up period (Table 34). In SUNRISE 1, rebound insomnia was reported for 17.3%, 20.7%, 27.4%, and 23.3% of patients who received LEM10, LEM5, ZOL, and PBO, respectively, during the first 7 nights and 24.4%, 21.8%, 26.9%, and 23.3% for the respective groups during the last 7 nights based on sSOL data. Rebound insomnia was reported for 16.3%, 19.4%, 21.6%, and 14.9% of patients who received LEM10, LEM5, ZOL, and PBO, respectively, during the first 7 nights and 17.7%, 19.1%, 17.5%, and 17.5% for the respective groups during the last 7 nights based on sWASO data. In SUNRISE 2, rebound insomnia was reported for 10.5% and 11.9% of patients who received LEM10 and LEM5, respectively, during the first 7 nights and 9.4% and 11.7% of patients who received LEM10 and LEM5, respectively, during the last 7 nights based on sSOL data. Rebound insomnia was reported for 14.2% and 12.4% of patients who received LEM10 and LEM5, respectively, during the first 7 nights and 11.9% and 13.5% of patients who received LEM10 and LEM5, respectively, during the last 7 nights based on sWASO data.
Withdrawal was assessed using the T-BWSQ at the end-of-study visit (Table 35). In SUNRISE 1, 10.0%, 11.6%, 14.7%, and 14.1% of patients who received LEM10, LEM5, ZOL, and PBO, respectively, had a score of at least 3, indicating that they experienced withdrawal symptoms. In SUNRISE 2, 16.8% and 20.7% of patients who received LEM10 and LEM5, respectively, also had a score of at least 3.
Suicidal ideation was assessed using the C-SSRS in both pivotal trials (Table 36). In both SUNRISE 1 and SUNRISE 2, suicidal ideation was reported in no more than 3 patients who received any treatment at any postbaseline time point.
Critical Appraisal
Internal Validity
Both the SUNRISE 1 and SUNRISE 2 trials appeared to have appropriate methods for blinding (i.e., appearance-matched PBOs for all active drugs), allocation concealment, randomization with stratification, and adequate power for the primary and secondary outcomes. Adjustments for multiplicity were made for all primary and key secondary outcomes in both trials (i.e., LPS, sleep efficiency, WASO, and WASO2H in SUNRISE 1 and sSOL, subjective sleep efficiency, and sWASO in SUNRISE 2).
A prespecified interim analysis was conducted in SUNRISE 1 once half of the planned number of patients (n = 475) had completed the trial or discontinued. The data for WASO2H were unblinded and analyzed by an independent statistician external to the sponsor who assessed if the trial would have a significant treatment effect when comparing mean change from baseline to days 29 to 30 of LEM10 versus ZOL for WASO2H. The sponsor stated that other data remained blinded during the analysis and the results were disclosed to 2 prespecified individuals, 1 each at the sponsor and sponsor’s codevelopment partner. As a result, SUNRISE 1 was not terminated for futility or efficacy. The sponsor indicated that there was no expected impact on the type I error rate. The procedures for maintaining blinding and independent analysis appear to have been adequate and the prespecified interim analysis was unlikely to produce bias.
For both studies, a computer-generated randomization scheme was used and randomization was performed centrally, which typically has a low risk of bias. Baseline characteristics were generally well balanced among treatment groups and imbalances that were observed could have been due to chance. In SUNRISE 1, the largest difference among baseline disease characteristics was approximately 10 minutes for the mean sSOL between the PBO group (56 minutes) and the LEM5 group (66 minutes) as well as for the mean sTST between patients in the LEM10 group (266 minutes) and the PBO group (276 minutes). In SUNRISE 2, the largest difference was approximately 12 minutes for the mean sTST between the PBO group (304 minutes) and the LEM5 group (316 minutes). It is uncertain if these differences are large enough to bias the trial results and what impact they would have on treatment effect. Although there was information summarizing medication history, it was not clear if treatments were used specifically for insomnia, which is particularly important since some medications can be used off-label for insomnia (e.g., trazodone, quetiapine). Prior treatment for insomnia was identified as a subgroup of interest in the CADTH systematic review protocol.
In the SUNRISE 1 study, all primary and key secondary outcomes were objective (i.e., LPS, WASO, WASO2H, and sleep efficiency) and were supported by subjective other secondary and exploratory outcomes. In the SUNRISE 2 study, all outcomes were subjective (i.e., sSOL, sWASO, and subjective sleep efficiency). The sponsor noted the importance of having objective outcomes, which are less prone to bias, to assess the physiologic effect of the medication along with subjective outcomes to measure the patient’s perception of the medication’s effect. Per the clinical expert, PSG results may not always be interpreted meaningfully or consistently when compared side-by-side with subjective or patient-reported outcomes. For instance, a patient may feel as though they did not sleep well when their objective measures do not indicate any problems. For this reason, the expert suggested that PSG should not be used as a marker of efficacy or a requirement for accessing LEM. It was further emphasized by the clinical expert that insomnia is largely a subjective issue and that sleep complaints are very individualized; therefore, subjective outcomes and how a patient perceives changes in their sleep may be more appropriate for assessing a treatment effect in practice. With all subjective measures, there is a risk of bias that cannot be easily measured and leads to uncertainty of how meaningful the results are. In the trials, the risk of bias was likely low given that there was no indication of unblinding. Further, the use of both objective and subjective measures in SUNRISE 1 and the consistency between the outcomes could be a more reliable method that increases certainty of the trial results.
Evidence of adequate validity was available for all PSG and sleep diary outcomes except for WASO2H. Evidence for reliability was available for only LPS, WASO, and TST outcomes and no data on responsiveness to change were identified for these outcomes from the literature. Clinically important differences relative to PBO for all PSG and sleep diary outcomes, except WASO2H, were found in the literature, though it was not specified if these were estimated from patients with insomnia. Both the ISI and FSS had adequate validity and reliability and MIDs were identified. No information was found from the literature that validated the EQ-5D-3L or PGI-Insomnia or showed any MIDs for patients with insomnia.
Discontinuations were low in the SUNRISE 1 trial in the LEM10 group (3.3%) and LEM5 group (3.0%) where AEs and “other” were the most common reasons for stopping treatment. As such, the risk of attrition bias was low. In the SUNRISE 2 trial, discontinuations appeared imbalanced and higher in the LEM10 group (25.2%) compared to the LEM5 group (16.0%). Withdrawal of consent and AEs were the most common reasons for the disproportionate loss of patients from the LEM10 group. It is possible that the higher rates of discontinuations bias the results in SUNRISE 2, though the direction of bias is unknown.
For all trial outcomes, there was some amount of missing data at postbaseline visits and less than the entire trial population contributed to the analyses (i.e., between 3% and 5% missing data at days 29 to 30 for SUNRISE 1, and between 21% and 27% missing data at month 6 for SUNRISE 2). This was especially true for long-term end points in SUNRISE 2. Large amounts of missing data increase the uncertainty of the treatment estimates and prevent strong conclusions from being made from the trial results. For primary and key secondary outcomes, missing data were imputed via a pattern-mixture model using multiple imputation assuming data were MNAR and all available values were used to impute missing data. The results of the sensitivity analyses assessing missing data did not change the conclusions for the primary and key secondary outcomes. For responder analyses, missing data were considered nonresponders, which is a conservative approach. For the EQ-5D-3L, ISI, FSS, and quality of sleep outcomes, missing values were not imputed and assumed to be MAR.
Subgroup analyses by age groups were prespecified in both studies and considered exploratory. The analyses may not have been powered to detect a treatment difference and there were no adjustments made for multiplicity. The number of patients in each treatment group by subgroup age was small and there was variability in the change from baseline results (noted by large SDs and IQRs). As a result of these limitations, conclusions could not be drawn from the results.
The clinical expert agreed that the thresholds for objective and subjective sleep onset and maintenance response could be meaningful to patients but suggested it can be difficult to quantify an exact value for improved sleep that would be meaningful and patient-reported outcomes may better indicate whether a treatment is beneficial rather than a numerical value. In SUNRISE 1, study eligibility did not require patients to have complaints about sleep onset; therefore, the sleep onset responder analyses only included 53% to 58% and 72% to 79% of the treatment groups for objective sleep onset responders and subjective sleep onset responders, respectively, at the end of treatment. Conversely, patients were required to have complaints about sleep maintenance, and the sleep maintenance analyses included more than 99% and more than 95% of the randomized populations of the objective sleep onset responders and subjective sleep maintenance responders, respectively, at the end of treatment. In SUNRISE 2, it was not specified if patients must have had complaints about sleep onset and sleep maintenance and around 79% to 80% and 79% to 83% of the treatment groups contributed to the analyses for sleep onset and maintenance, respectively, at month 6. Although SUNRISE 2, not SUNRISE 1, was powered to detect a treatment difference from the responder analyses, neither trial adjusted for multiplicity and conclusions could not be drawn from the results.
Sleep diary data handling rules were applied when patients’ responses were illogical (e.g., errors related to a.m. or p.m. and 24-hour clock use, incorrectly choosing the hour versus minutes, reporting a final wake time that was later than the time the patient got out of bed for the day). In SUNRISE 1, there were 2 instances where applying the rules changed the P value and significance of the results. The first instance was the change from baseline sWASO for the first week of treatment without rules applied, which was significantly less for LEM5 compared to ZOL. When the rules were applied, the results were not significant. The second instance was the change from baseline sWASO for the last week of treatment without rules applied, which was not significantly less for LEM5 compared to PBO. When the rules were applied, the results were statistically significant. Neither of the instances was a primary or key secondary outcome and did not change the final conclusions of the trial. In SUNRISE 2, there were no cases where applying the rules changed the results from statistically significant to nonsignificant.
External Validity
In general, the clinical expert consulted for this review confirmed that the populations of the SUNRISE 1 study and the SUNRISE 2 study were similar to those of patients seen in Canadian clinics and the study results would be generalizable to patients with insomnia in Canada with some limitations.
The CADTH review team and clinical expert consulted for this review noted concern over the large proportion of individuals screened out before randomization — nearly 71.6% in SUNRISE 1 and 52.8% in SUNRISE 2. The major reasons for screening failures were individuals not meeting eligibility criteria (65.1% in SUNRISE 1 and 45.5% in SUNRISE 2) and withdrawal of consent (less than 5% in either trial). Additional population-level details were not available to determine if any specific inclusion or exclusion criteria were the main reasons for screening out patients. The screening process may have produced a study population that does not adequately represent the broader Canadian population with insomnia who may otherwise be eligible for treatment with LEM, which limits generalizability of the trial findings. Both trials had a similar prerandomization phase consisting of screening and PBO run-in periods used to exclude individuals who demonstrated a PBO response and exclude those who could not comply with study procedures (e.g., sleep diary completion, alcohol restriction). It is possible that the eligibility criteria resulted in enriched study populations and, consequently, treatment effects observed in the studies would be larger than what would be observed in clinical practice.
Eligibility for SUNRISE 1 was restricted to females 55 years or older and males 65 years or older and the clinical expert stated that the generalizability of the results would be limited to patients matching these demographics. The sponsor indicated that 65 years is physiologically meaningful since the incidence of insomnia increases with age and it was suggested that the younger age would include females experiencing menopause, another time when the incidence of insomnia increases. It is unclear if the different age cut-offs had an impact on the results, though the clinical expert did not expect them to be a major issue with generalizability. To be included, patients must have scored at least 13 or 15 on the ISI to participate in the SUNRISE 1 or SUNRISE 2 trial, respectively. Based on findings from the literature, subthreshold insomnia is from 8 to 14 while clinical insomnia of moderate severity is from 15 to 21.42 It is unclear what the reason is for the different ISI cut-offs in the studies and if this had any impact on the results.
The clinical expert noted the extensive list of comorbidities (e.g., depression and anxiety based on BDI-2 and BAI scores) likely excluded many individuals from participating who could have otherwise been potential candidates for treatment with LEM, and that this limits the generalizability to patients with these conditions. Furthermore, to participate in the studies, AHI scores must have been greater than 10 for patients aged 18 years to 64 years or greater than 15 for patients aged 65 years or older in SUNRISE 2 and for all patients in SUNRISE 1. The expert explained that patients with an AHI score of 5 to 15 could have sleep-disordered breathing (i.e., mild sleep apnea) that presents as insomnia and a lower cut-off would be more selective for patients with psychophysiological insomnia by excluding those with sleep apnea.
No dose changes for any medications were allowed during the trial and it was noted in the Health Canada product monograph that the recommended nightly dose for LEM is 5 mg and may be increased to 10 mg based on clinical response and tolerability.19 ZOL was the active comparator in SUNRISE 1 and, according to the sponsor, is available as both 6.25 mg and 12.5 mg doses, with the former dose being used in the trial. The sponsor noted that the lower dose is recommended for females and older adult patients. Health Canada product monographs exist for ZOL sublingual orally disintegrating tablets in 5 mg and 10 mg doses, with the lower dose being recommended for females and older adult patients.25 It is not clear what the reason is for the differences in available doses or what impact this would have on the treatment effects. Discussions with the clinical expert and a representative from the public drug plans indicated that ZOL is not publicly funded by any drug plans in Canada and, consequently, is less commonly used for the treatment of insomnia. As a result, it is uncertain if ZOL is the most appropriate comparator for a Canadian setting. It was suggested that ZOL and zopiclone, the latter of which is more commonly used in Canadian practices, may be comparable treatments, but clinical evidence does not confirm this or at what dose the drugs would be considered equivalent.
The clinical expert stated that PSG measures are uncommon in clinical practice for assessing insomnia and instead, patients are typically asked general questions about their sleep and how they feel. In SUNRISE 1, PSG measures were taken as the average of 2 nights, which the clinical expert indicated would be more accurate than a single reading, but still may not be completely accurate due to a “first night effect” that can be observed among many patients with insomnia. Many patients will have a PSG reading that is better than normal for the first night they are in the sleep lab and readings on subsequent nights in the sleep lab will revert closer to what the patient normally experiences at home. The clinical expert also explained that this improvement is typically not observed among normal sleepers who, instead, have a worse reading on their first night of the test. Patients were required to maintain a sleep diary throughout the course of the studies. The clinical expert stated that patients may not be required to do so in clinical practice, depending on the treatment, and screening out patients who could not comply with completing a daily sleep diary may have excluded patients who would be candidates for LEM.
Based on the input CADTH received from patient groups, patients are looking for treatments that are safe and tolerable, have long-term efficacy, and do not interfere with next-day activities such as cognitive function and work, school, and/or home responsibilities. The patient groups also had concerns with harms and how treatment can impact insomnia related to other comorbidities, as well as dependence and rebound insomnia that have been associated with other medications for insomnia. The outcomes assessed in the pivotal trials generally focused on efficacy for improving sleep, as measured by PSG and the sleep diary, as well as HRQoL assessed by both generic and disease-specific instruments. Notable harms, including the assessment of cognitive performance immediately after waking, withdrawal symptoms, and rebound insomnia, were addressed in the SUNRISE 1 study, and some were assessed in the SUNRISE 2 study. Per the clinical expert, medications other than benzodiazepines and nonbenzodiazepines, such as LEM, are not expected to produce rebound insomnia effects and although rates of rebound insomnia were low in the studies, there was an indication that it could occur in some patients. In general, rates of rebound insomnia appeared to have been lower in SUNRISE 2, which studied the long-term results of treatment with LEM, compared to SUNRISE 1, though it is worth reiterating that firm conclusions cannot be drawn when there are large amounts of missing data and where differences were not tested statistically. The clinical expert felt that while it is important and useful to assess this harm outcome after stopping LEM, the 2-week follow-up period may not have been long enough to observe the full duration of possible rebound insomnia. According to the clinical expert, this is particularly important since the problem can, for example, last for many weeks after stopping benzodiazepines and rebound insomnia symptoms can interfere with subsequent treatments. Of the notable harms identified in the CADTH systematic review protocol, the expert indicated that it would be important to inform patients about the possibility of next-day somnolence and rebound insomnia when discussing treatment with LEM, particularly when prescribing to older adults or using the 10 mg dose. Other notable harms, such as impaired driving performance and workplace accidents, were not reported on in either trial and it is uncertain if LEM had any impact on these outcomes. Additional gaps in the evidence include the safe and effective use of LEM in patients with comorbid conditions and alongside other medications, both of which were identified as being important issues to patients.
As is the case with clinical trials, patients tend to receive much closer attention and care during the studies compared to what is normal from their health care providers, which may bias the results and impact generalizability to typical Canadian practice.
Indirect Evidence
Objectives and Methods for the Summary of Indirect Evidence
The objective of this section is to summarize and appraise the evidence from ITCs for the relative efficacy and safety of LEM for the treatment of insomnia, characterized by difficulties with sleep onset and/or sleep maintenance. The aim is to fill a gap created by the absence of trials directly comparing LEM to comparators relevant in the Canadian landscape, as stated in the protocol of this CADTH report.
A focused literature search for NMAs dealing with orexin antagonists or insomnia was run in MEDLINE All (1946–) on March 24, 2022. Retrieval was not limited by publication date or by language.
No published ITCs were found in the literature search from CADTH specifically assessing and comparing LEM to comparators relevant to the Canadian practice and of interest based on inclusion criteria in this clinical report.
Description of Indirect Comparison(s)
The sponsor submitted 2 NMAs to CADTH for review, which are summarized and appraised in this report.
The first NMA60 (referred to as NMA 1) evaluated the treatment of adults with insomnia disorder with LEM. This work is a sponsor-submitted NMA to compare LEM to drugs currently available in the Canadian public drug plans to assess safety and efficacy data that can only be derived through the use of indirect techniques. Currently, the drugs that receive reimbursement within their Health Canada–approved labels are zopiclone, temazepam, triazolam, flurazepam, and nitrazepam.
The sponsor also submitted a published NMA20 (referred to as NMA 2) that was a comparative efficacy analysis aimed at evaluating the efficacy and safety of LEM against other insomnia treatments through a systematic literature review and NMA. The NMA search strategy included RCTs of drugs used in adults with primary insomnia — not all of which are reimbursed in Canada. The drugs of interest in NMA 2 were LEM, suvorexant, benzodiazepines, Z-drugs, trazodone, and ramelteon. Of these, only trazodone, the Z-drugs zolpidem, zopiclone, and eszopiclone, and benzodiazepines triazolam and temazepam were available in the body of evidence from NMA 2 and of interest to this CADTH reimbursement review.
Methods of NMA 1
Objectives
The objective of NMA 1 was to conduct a systematic literature review and NMA to indirectly assess the safety and efficacy of LEM compared with current formulary options within Canadian drug plans.
Study Selection Methods
A literature search of PubMed, the Cochrane Database of Systematic Reviews, and Google Scholar was conducted for randomized PBO-controlled trials evaluating LEM, zopiclone, temazepam, triazolam, flurazepam, and nitrazepam for the treatment of insomnia in adult patients. The search was limited to publication dates ranging from January 1990 to February 2021. Given the strong effects from PBO in insomnia trials, trial selection was limited to those randomized trials that included a PBO group.
Eligibility criteria were used to select relevant trials. Search terms consisted of insomnia, insomnia disorder, sleep initiation and maintenance disorders, lemborexant, zopiclone, temazepam, triazolam, flurazepam, nitrazepam, and PBO. As part of an exploratory posthoc analysis of drugs not approved by Health Canada for primary insomnia but most commonly used off-label, PBO-controlled randomized trials evaluating trazodone (an antidepressant), lorazepam (a benzodiazepine), and quetiapine (an antipsychotic drug) were also identified using the same aforementioned inclusion criteria. However, these trials were not included in the main analysis, and only included as an exploratory posthoc analysis to the main NMA.
Included studies must have met the following criteria:
must have been DB, parallel group, and PBO-controlled (crossover trials were excluded)
must have enrolled adult (aged at least 18 years) males and females with insomnia
must have enrolled at least 30 patients into each group
must have had treatment duration of at least 3 days
must have had trials groups that included LEM, zopiclone, temazepam, triazolam, flurazepam, nitrazepam, trazodone, lorazepam, quetiapine, and PBO in 1 of the study groups
must have had clinical end points that included reduction from baseline in objective LPS or sSOL, and WASO, and improvement in sleep efficiency and TST reported through PSG or by patient-reported sleep diaries.
The checklist for randomized trials developed by the National Institute for Health and Care Excellence61 was used to assess the risk of bias of all trials that met the inclusion criteria. Randomized trials were categorized with respect to their perceived risk of bias (low risk of bias, unclear risk of bias, high risk of bias).
These were the 4 main clinical end points of interest:
LPS, defined as the estimated time in minutes from the attempt to sleep until sleep onset, typically measured using PSG in most trials
an additional end point, sSOL, which is similar to LPS but measured via patient diaries, was added and used for the analysis of trials only reporting such patient-reported outcomes
WASO, defined as the estimated sum of time in minutes of wake during the night after initial sleep onset until the patient got out of bed
Sleep efficiency, defined as the percentage of time asleep relative to the total time in bed and was expressed as a percent
TST, the total time in minutes of sleep from sleep onset until terminal awakening.
The following data were extracted from each trial: the sample size, the year of publication, the region where the trial was conducted, the study duration, the mean patient age, how the end points were measured (PSG versus subjective patient diaries), the definition of primary and secondary end points, the measures of variance reported in the clinical end points (e.g., SD), the number of patient withdrawals due to adverse drug reactions, and the frequency of patient-reported somnolence, dizziness, and headache. Methods for data extraction were not reported. With these data, pooled estimates of treatment effects and safety end points for each drug relative to PBO were initially generated using standard meta-analysis data pooling techniques. The pooled effect size by study drug relative to PBO was presented in forest plots.
For these standard meta-analyses, statistical heterogeneity between studies was assessed by both the Q statistic and the I2 test statistic. P values associated with the Q statistic (chi-square with k-1 degrees of freedom, where k is the number of studies) were also reported. In situations where the Q statistic was statistically significant or the I2 statistic was greater than 25%, a random-effects model was used within drug data pooling as opposed to a fixed-effects model. Study heterogeneity was evaluated through L’Abbé plots, while publication bias was assessed through an evaluation of funnel plots and by the method proposed by Egger.62
ITC Analysis Methods
PBO-controlled trials evaluating LEM, zopiclone, temazepam, triazolam, flurazepam, and nitrazepam in at least 1 of the treatment groups were used to build the primary NMA diagram for an indirect comparison of drug efficacy and safety using the methodology that expresses NMA models through a network meta-regression framework.
To evaluate the impact on trial-level parameters such as treatment duration, patient age, mode of efficacy evaluation (i.e., PSG versus patient sleep diary), multivariate network meta-regression was also used with such parameters as independent variables, which generated an adjusted indirect comparison. Variables that were not statistically significant at the P less than 0.05 level were eliminated from the network meta-regression model. A second NMA diagram was built for the addition of trazodone, quetiapine, and lorazepam as part of the posthoc analysis.
Inconsistency for those networks with closed loops of direct and indirect evidence was evaluated through a chi-square statistic where possible.
The analyses comprised the comparative effectiveness analysis relative to LEM5 and LEM10 expressed as a weighted average of the estimated mean differences for PSG-measured LPS, WASO, sleep efficiency, and TST, if such data were available. A second NMA reported subjectively assessed efficacy outcomes (i.e., sSOL, sWASO, subjective sleep efficiency, and sTST).
The effect sizes for the mean change in LPS, WASO, sleep efficiency, and TST were expressed and reanalyzed as standardized mean differences (SMDs) using the Cohen’s D statistic. SMDs are calculated as the ratio of the treatment effect (the mean difference in the treatment group minus the difference in the PBO group) to the pooled SD of these differences. SMDs using the Cohen’s D statistic do not have units and the magnitude of benefit. The following criteria based on the European Guideline for the Diagnosis and Treatment of Insomnia63 were used: less than 0.4 = small effect size; 0.4 to less than 0.8 = good effect size; 0.8 or greater = very good effect size. Binary end points were expressed as ORs and 95% CIs.
All trials included in NMA 1 were assessed to determine if they were similar with respect to study characteristics that could transform the treatment effect so the transitivity assumption could be deemed plausible.
Drugs not approved by Health Canada for the treatment of insomnia but frequently reported as being used off-label in Canada (e.g., trazodone, quetiapine, lorazepam) were assessed in a separate scenario analysis added to the network diagram for an indirect comparison to LEM5 and LEM10, respectively, but are not depicted in this report.
Results of NMA 1
Summary of Included Studies
The sponsor-submitted systematic review resulted in a total of 4,557 citations that were initially identified. After deduplication and abstract selection, 56 full-text articles were retrieved and assessed for eligibility. Six additional studies were identified through hand searches for potential inclusion in the current synthesis. In total, 62 full-text articles were assessed for eligibility. Of the 62 published RCTs, 11 studies met the inclusion criteria and provided a total of 15 active drug groups that would contribute to NMA 1 (Table 37).
The included studies and characteristics are shown in Table 37. There were 3 trials for LEM5 and LEM10, 3 trials for flurazepam 30 mg, 1 trial for temazepam 15 mg, 1 trial for zopiclone 7.5 mg, 4 trials that evaluated triazolam at doses of 0.125 mg, 0.25 mg, and 0.50 mg, and 1 trial with trazodone 50 mg. There were no PBO-controlled randomized trials for nitrazepam, quetiapine, and lorazepam that met the inclusion criteria. In addition, the lone zopiclone trial did not provide suitable clinical efficacy end points that could be used for analysis. As a result, these drugs could not be added to the network diagram for an indirect efficacy analysis. Only 2 studies were conducted in Canada. Seven studies were conducted in the US and 2 studies were conducted in multiple countries.
Two of the trials enrolled patients older than 55 years while the remainder enrolled patients 18 years or older. The sleep outcomes in 5 trials were measured by PSG.
Five of the 11 studies were considered too difficult to assess because of limited data, leading to the conclusion that the risk of bias was high or unclear. Two studies had unclear randomization processes and 3 studies had unclear allocation concealment procedures. Six studies had imbalances in the baseline characteristics across groups. All studies had adequate blinding of participants and individuals administering care.
Table 37: Placebo-Controlled Insomnia Trials Meeting the Inclusion Criteria
Study | Region | Duration (days) | Patient age (years) | PSG | Patient sleep diary | Comparators | Sample size | Usable study outcomes |
|---|---|---|---|---|---|---|---|---|
Murphy (2017) | US | 15 | 19 to 80 | Yes | Yes | LEM5, LEM10 | Total = 126 (LEM5 = 38, LEM10 = 32 vs. PBO = 56) | LPS, sSOL, WASO, sleep efficiency, |
Rosenberg (2018) | EU and North America | 30 | ≥ 55 | Yes | Yes | LEM5, LEM10 | Total = 743 (LEM5 = 269, LEM10 = 266 vs. PBO = 208) | LPS, sSOL, WASO, sleep efficiency, TST, safety |
Kärppä et al. (2020) | Global | 180 | ≥ 18 | No | Yes | LEM5, LEM10 | Total = 949 (LEM5 = 316, LEM10 = 315 vs. PBO = 318) | sSOL, sWASO, sleep efficiency, sTST, harms |
Scharf (1990) | US | 7 | 21 to 65 | No | Yes | FLU 30 mg vs. PBO | Total = 163 (FLU = 83 vs. PBO = 80) | Harms |
Cohen (1990) | US | 7 | 18 to 65 | No | Yes | FLU 30 mg vs. PBO | Total = 112 (FLU = 56 vs. PBO = 56) | Harms |
Fleming (1995) | Canada | 3 | 21 to 60 | Yes | Yes | FLU 30 mg vs. PBO | Total = 71 (FLU = 36 vs. PBO = 35) | Sleep efficiency, harms |
Leppik (1997) | US | 28 | 59 to 85 | No | Yes | TEM 15 mg vs. TRIAZ 0.125 mg | Total = 253 (TEM 15 mg = 84 vs. TRIAZ 0.125 mg = 85 vs. PBO = 84) | sSOL, sTST, harms |
Hajak (1994) | Canada | 28 | 18 to 71 | No | Yes | ZOP 7.5 mg vs. TRIAZ 0.25 mg | Total = 1,217 (ZOP 7.5 mg = 612 vs. TRIAZ 0.25 mg = 307 vs. PBO = 298) | Harms |
Walsh (1998a) | US | 19 | 18 to 60 | Yes | Yes | TRIAZ 0.25 mg | Total = 65 (TRIAZ 0.25 mg = 31 vs. PBO = 34) | Harms |
Walsh (1998b) | US | 14 | 21 to 65 | No | Yes | TRAZ 50 mg vs. PBO | Total = 201 (TRAZ 50 mg = 98 vs. PBO = 103) | sSOL, sWASO, |
Ware (1997) | US | 28 | 21 to 55 | Yes | Yes | TRIAZ 0.50 mg vs. PBO | Total = 73 (TRIAZ 0.50 mg = 36 vs. PBO = 37) | LPS, WASO, sleep efficiency |
EU = European Union; FLU = flurazepam; LEM5 = lemborexant 5 mg; LEM10 = lemborexant 10 mg; LPS = latency to persistent sleep; PBO = placebo; PSG = polysomnography; sSOL = subjective sleep onset latency; sTST = subjective total sleep time; sWASO = subjective wake after sleep onset; TST = total sleep time; TEM = temazepam; TRIAZ = triazolam; TRAZ = trazodone; vs. = versus; WASO = wake after sleep onset; ZOP = zopiclone.
Source: Sponsor-submitted indirect treatment comparison report.60
Results
In Figure 4, the general network framework for the primary analysis of all outcomes that was built to compare treatment alternatives directly and indirectly for insomnia disorder is presented. All subsequent networks were simpler versions of this network diagram, driven by trial group availability.
Figure 4: Overall Network for All Outcomes
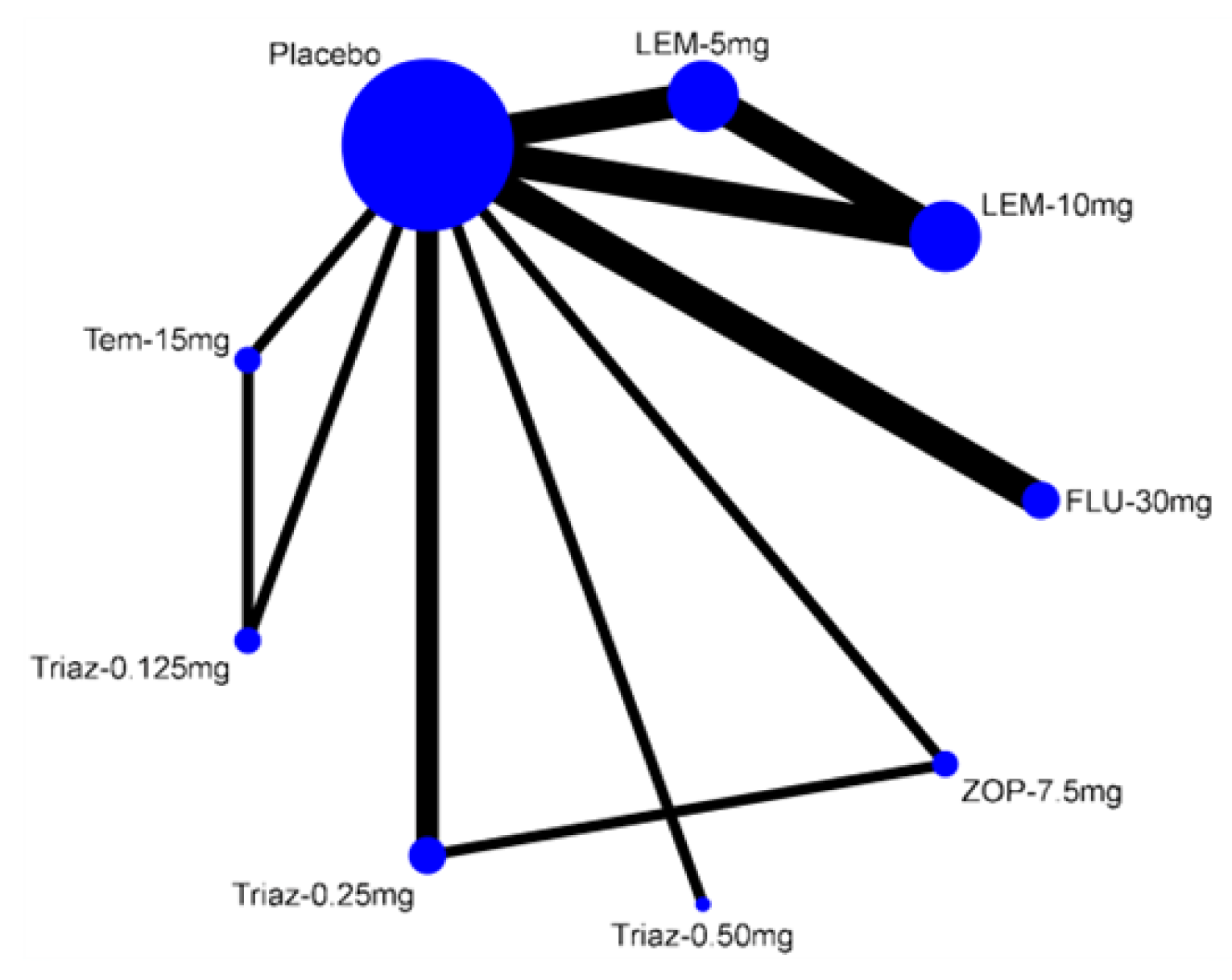
FLU = flurazepam; LEM = lemborexant; tem = temazepam; triaz = triazolam; ZOP = zopiclone.
Note: From the Canadian public drug plan perspective. The thickness of the lines represents the weight of the available evidence. Thicker lines indicate larger trials and more patients. Data for all safety and efficacy outcomes were not available for all comparators.
Source: Sponsor-submitted indirect treatment comparison report.60
The 5 trials reporting PSG-measured sleep outcomes consisted of the 3 LEM studies, 1 trial evaluating flurazepam 30 mg, and another study with triazolam 0.5 mg. From these trials, only the LEM studies reported complete efficacy data consisting of LPS, WASO, sleep efficiency, and TST.
Nitrazepam, zopiclone, lorazepam and quetiapine could not be added to the network evaluating drug efficacy because no PBO-controlled randomized trials meeting the inclusion criteria were identified. Furthermore, in some of the older trials, efficacy data in terms of LPS and sSOL, WASO, sleep efficiency, and TST were not consistently reported. As a result, revised network diagrams had to be built for each efficacy end point.
An evaluation of the I2 statistic among the forest plots evaluating safety and efficacy revealed a range between 0.0% for the WASO end point to 71.7% in the case of somnolence. An evaluation of heterogeneity using L’Abbé plots for drug discontinuation and somnolence suggested some heterogeneity, especially with the latter outcome. When evaluating publication bias, the Egger test failed to show statistical significance for publication bias (P = 0.14). However, asymmetry of the funnel plot for the LPS outcome suggested publication bias.
Objectively Measured Latency to Persistent Sleep
The network for this clinical end point is presented in Figure 5. The LPS was measured by PSG and expressed as the mean difference (SMDs using Cohen’s D were also used by the authors but not discussed in this text to avoid redundancy).
Figure 5: Network for Latency to Persistent Sleep Efficacy Outcome for Insomnia Treatments
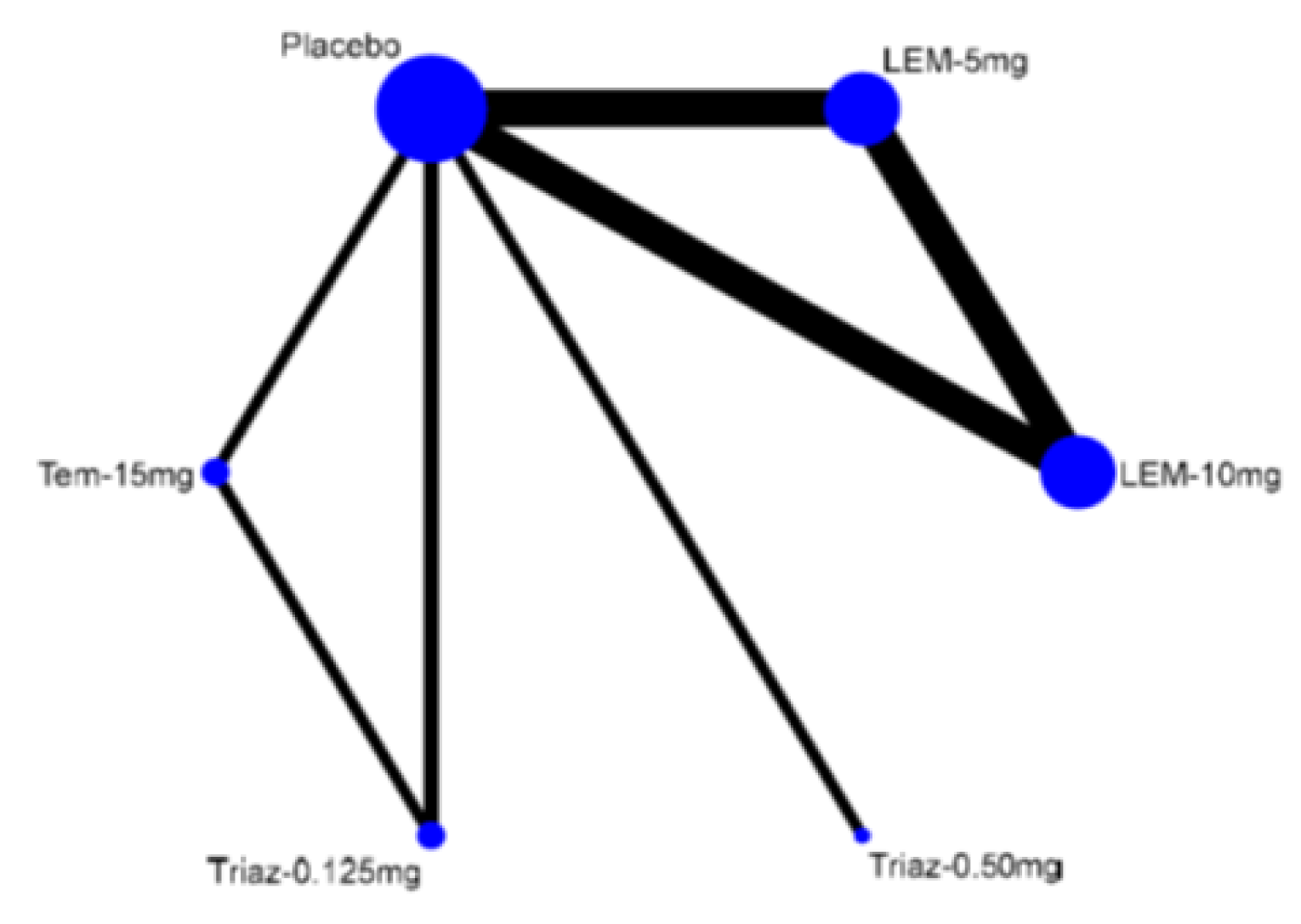
LEM = lemborexant; tem = temazepam; triaz = triazolam.
Note: From the Canadian public drug plan perspective.
Source: Sponsor-submitted indirect treatment comparison report.60
Using LEM5 as the reference, the findings suggested that LPS was longer in the PBO group (mean difference = –19.1 minutes; 95% CI, –3.20 minutes to –35.0 minutes), in which a negative value in the mean difference implies improvement in favour of LEM5 (Table 38). Furthermore, patients treated with LEM5 had a reduction in LPS when compared to triazolam 0.5 mg (mean difference = –34.1 minutes; 95% CI, –5.47 minutes to –62.8 minutes). The results for LEM10 were consistent with LEM5. NMA 1 also revealed that LEM5 and LEM10 were consistent with respect to PSG-measured LPS.
Table 38: Difference in Latency to Persistent Sleep With LEM5 and LEM10 Relative Comparators
Comparator | Mean differencea | 95% CI | P value |
|---|---|---|---|
Reference: LEM5 | Reference | Reference | Reference |
Placebo | –19.1 minutes | –3.20 minutes to –35.0 minutes | 0.019 |
LEM10 | 2.43 minutes | 18.9 minutes to –14.0 minutes | 0.77 |
Triazolam 0.50 mg | –34.1 minutes | –5.47 minutes to –62.8 minutes | 0.02 |
Reference: LEM10 | Reference | Reference | Reference |
Placebo | –21.6 minutes | –5.14 minutes to –38.0 minutes | 0.01 |
LEM5 | –2.43 minutes | 14.0 minutes to –18.9 minutes | 0.77 |
Triazolam 0.50 mg | –36.6 minutes | –7.62 minutes to –65.4 minutes | 0.013 |
CI = confidence interval; LEM = lemborexant; LEM5 = lemborexant 5 mg; LEM10 = lemborexant 10 mg.
Note: Statistically significant differences (95% CI excluding 0) are highlighted in bold.
aThis is the mean difference relative to LEM reported in minutes. A negative mean difference value implies improvement in favour of LEM relative to comparators, meaning that it took the patient longer to fall asleep with the comparator (as compared to LEM).
Source: Sponsor-submitted indirect treatment comparison report.60
Objectively Measured Wake After Sleep Onset
There were 3 LEM studies and only 1 trial that assessed triazolam 0.5 mg. There was no evidence of a difference in PSG-assessed WASO between LEM5, LEM10, and triazolam 0.5 mg (Table 39). The mean differences in WASO for LEM5 and LEM10 compared with PBO were –21.9 minutes (95% CI, –8.66 minutes to –35.1 minutes) and –22.5 minutes (95% CI, –8.59 minutes to –36.4 minutes), respectively, where a negative difference implied improvement in the WASO end point in favour of LEM.
Table 39: Difference in Wake After Sleep Onset of Comparative Drugs Relative to LEM5 and LEM10
Comparator | Mean differencea | 95% CI | P value |
|---|---|---|---|
Reference: LEM5 | Reference | Reference | Reference |
Placebo | –21.9 minutes | –8.66 minutes to –35.1 minutes | 0.001 |
LEM10 | 0.65 minutes | 13.2 minutes to –12.0 minutes | 0.92 |
Triazolam 0.50 mg | 0.13 minutes | 26.7 minutes to –26.4 minutes | 0.99 |
Reference: LEM10 | Reference | Reference | Reference |
Placebo | –22.5 minutes | –8.59 minutes to –36.4 minutes | 0.002 |
LEM5 | –0.65 minutes | 12.0 minutes to –13.3 minutes | 0.92 |
Triazolam 0.50 mg | –0.52 minutes | 26.4 minutes to –27.4 minutes | 0.97 |
CI = confidence interval; LEM = lemborexant; LEM5 = lemborexant 5 mg; LEM10 = lemborexant 10 mg.
Note: Statistically significant differences (95% CI excluding 0) are highlighted in bold.
aThis is the mean difference relative to LEM reported in minutes. A negative mean difference value signifies improvement for LEM relative to comparators, meaning that the patient was awake for a longer period of time after initial sleep onset compared to LEM.
Source: Sponsor-submitted indirect treatment comparison report.60
Objectively Measured Sleep Efficiency
Four active comparators with PSG data could be obtained for the evaluation of objectively measured sleep efficiency: LEM5, LEM10, flurazepam 30 mg, and triazolam 0.5 mg. The flurazepam 30 mg values were derived from only a 3-day treatment end point (Table 40). The mean differences in sleep efficiency for LEM5 and LEM10 compared with PBO were 7.62% (95% CI, 9.31% to 5.93%) and 8.80% (95% CI, 10.5% to 7.06%), respectively. The mean differences in sleep efficiency for LEM5 and LEM10 compared with triazolam were 9.62% (95% CI, 14.3% to 4.92%) and 10.8% (95% CI, 15.5% to 6.09%), respectively. Effect estimates for the comparisons between LEM5 and LEM10 and flurazepam were too imprecise to draw a conclusion.
Table 40: Difference in Sleep Efficiency With LEM5 and LEM10 Relative to Comparators
Comparator | Mean difference (%)a | 95% CI | P value |
|---|---|---|---|
Reference: LEM5 | Reference | Reference | Reference |
Placebo | 7.62% | 9.31% to 5.93% | < 0.001 |
LEM10 | –1.18% | 0.48% to –2.83% | 0.16 |
Triazolam 0.50 mg | 9.62% | 14.3% to 4.92% | < 0.001 |
Flurazepam 30 mg | 1.12% | 6.56% to –4.32% | 0.69 |
Reference: LEM10 | Reference | Reference | Reference |
Placebo | 8.80% | 10.5% to 7.06% | < 0.001 |
LEM5 | 1.18% | 2.84% to –0.48% | 0.16 |
Triazolam 0.50 mg | 10.8% | 15.5% to 6.09% | < 0.001 |
Flurazepam 30 mg | 3.00% | 7.76% to –3.16% | 0.41 |
CI = confidence interval; LEM5 = lemborexant 5 mg; LEM10 = lemborexant 10 mg.
Note: Statistically significant differences (95% CI excluding 0) are highlighted in bold.
aThis is the mean difference in sleep efficiency relative to lemborexant expressed as a percentage. A positive mean difference value signifies improvement for lemborexant relative to comparators.
Source: Sponsor-submitted indirect treatment comparison report.60
Objectively Measured Total Sleep Time
TST data were only available for LEM5 and LEM10. The NMA indicated that LEM10 provided additional minutes of TST when compared to LEM5, but the effect estimate was imprecise (mean difference = –4.65 minutes; 95% CI, –2.45 minutes to 11.8 minutes; Table 41). Relative to PBO, LEM5 and LEM10 were associated with an improvement of 34.8 minutes (95% CI, 27.4 minutes to 42.4 minutes) and 39.5 minutes (95% CI, 32.1 minutes to 46.9 minutes), respectively, in TST.
Table 41: Difference in Total Sleep Time With LEM5 and LEM10 Relative to Comparators
Comparator | Mean difference (%)a | 95% CI | P value |
|---|---|---|---|
Reference: LEM5 | Reference | Reference | Reference |
Placebo | 34.8 minutes | 27.4 minutes to 42.2 minutes | < 0.001 |
LEM10 | –4.65 minutes | –2.45 minutes to 11.8 minutes | 0.20 |
Reference: LEM10 | Reference | Reference | Reference |
Placebo | 39.5 minutes | 32.1 minutes to 46.9 minutes | < 0.001 |
LEM5 | 4.65 minutes | –2.45 minutes to 11.8 minutes | 0.20 |
CI = confidence interval; LEM5 = lemborexant 5 mg; LEM10 = lemborexant 10 mg.
Note: Statistically significant differences (95% CI excluding 0) are highlighted in bold.
aThis is the mean difference relative to lemborexant expressed in minutes. A positive mean difference value signifies improvement in TST for lemborexant relative to comparators.
Source: Sponsor-submitted indirect treatment comparison report.60
Clinical Outcomes Subjectively Measured
Different scenarios were evaluated to include end points measured not by PSG but by patient reporting. There were only 4 trials reporting subjective sleep outcomes data. These consisted of the 3 LEM studies and 1 study with temazepam 15 mg and triazolam 0.125 mg using a PBO control. From these trials, only the LEM studies reported complete efficacy data consisting of sSOL, sWASO, subjective sleep efficiency, and sTST. All results are presented in Table 42.
Comparative efficacy for sSOL between triazolam 0.125 mg, temazepam 15 mg, LEM5, and LEM10 was then formally evaluated in NMA 1. Using LEM5 as the reference, the finding suggested a 14.8-minute reduction (95% CI, 11.1-minute reduction to 18.5-minute reduction) in sSOL relative to the PBO group (Table 42). The finding for LEM10 compared with PBO was consistent with LEM5. The effect estimates for all other comparisons were too imprecise to draw conclusions about the comparative efficacy for sSOL.
Only the 3 LEM trials reported sWASO data. In this case, LEM5 and LEM10 were superior to PBO but no difference was detected between the 2 doses.
Similarly, only 3 LEM studies reported subjective sleep efficiency. LEM5 and LEM10 were superior to PBO in percentage subjective sleep efficiency improvement, but no evidence of difference between the 2 drugs was detected since the effect estimates were imprecise.
There were sTST data for LEM, temazepam 15 mg, and triazolam 0.125 mg. Effect estimates between LEM10 and LEM5 in the sTST end point were too imprecise to draw conclusions (Table 42). However, relative to PBO, LEM5 was associated with an sTST improvement of 22.8 minutes (95% CI, 12.8 minutes to 32.8 minutes). The effect for LEM10 compared with PBO was identical. Furthermore, no evidence of a difference in sTST between LEM5, LEM10, temazepam 15 mg, and triazolam 0.125 mg was observed due to the imprecision of the effect estimates.
Table 42: Summary of Efficacy Estimates of LEM5 and LEM10 Using Subjective End Points
Comparator | Mean difference (95% CI) | |||
|---|---|---|---|---|
sSOL (minutes)a | sWASO (minutes) | Sleep efficiency (%) | sTST (minutes) | |
Reference: LEM5 | ||||
Placebo | –14.8 (–11.1 to –18.5) | –12.5 (–3.22 to –21.7) | 4.67 (6.36 to 3.0) | 22.8 (32.8 to 12.8) |
LEM10 | 0.97 (4.79 to –2.85) | 6.84 (16.6 to –3.0) | –1.80 (0.08 to –3.67) | –7.89 (2.07 to –17.8) |
Triazolam 0.125 mg | 3.19 (17.0 to –10.6) | NA | NA | 1.90 (24.4 to –20.6) |
Temazepam 15 mg | 3.19 (16.6 to –10.2) | NA | NA | 12.8 (35.1 to –9.51) |
Reference: LEM10 | ||||
Placebo | –15.8 (–12.6 to –19.5) | –19.3 (–9.93 to –28.7) | 6.47 (8.30 to 4.64) | 22.8 (32.8 to 12.8) |
LEM5 | –0.97 (2.85 to –4.79) | –6.84 (2.96 to –16.6) | 1.80 (3.67 to –0.08) | 7.89 (17.8 to –2.07) |
Triazolam 0.125 mg | 2.22 (16.5 to –11.6) | NA | NA | 9.80 (32.4 to –12.8) |
Temazepam 15 mg | 2.22 (15.6 to –11.2) | NA | NA | 20.7 (43.1 to –1.69) |
CI = confidence interval; LEM5 = lemborexant 5 mg; LEM10 = lemborexant 10 mg; LPS = latency to persistent sleep; NA = not applicable; sSOL = subjective sleep onset latency; sTST = subjective total sleep time; sWASO = subjective wake time after sleep onset.
Notes: All values are mean difference (95% CI).
Statistically significant differences (95% CI excluding 0) are highlighted in bold.
aAlso referred to throughout the report as subjectively measured LPS.
Source: Sponsor-submitted indirect treatment comparison report.60
Harms
The analysis of harms in this ITC included treatment discontinuations, somnolence, dizziness, and headache.
The odds of discontinuations for LEM10 were greater compared with LEM5 (OR = 1.99; 95% CI, 1.06 to 3.74) (Table 43). No evidence of difference in effect estimates for all other comparisons with LEM5 was detected due to imprecision. The odds of discontinuations were less for PBO compared with LEM10 (OR = 0.48; 95% CI, 0.25 to 0.91). The effect estimates for all other comparisons with LEM10 were also too imprecise to draw a conclusion regarding comparative efficacy.
When compared with LEM5 (Table 44), there are reduced odds of somnolence for PBO, triazolam 0.25 mg, and zopiclone, and increased odds of somnolence for LEM10. The results for LEM10 were similar. For other comparisons (i.e., LEM5 and LEM10 versus flurazepam, temazepam, and triazolam 0.125 mg), there was no evidence of difference in effect estimates since these were too imprecise.
For the end point of dizziness (Table 45), the effect estimates were too imprecise to draw conclusions about the effect of LEM5 or LEM10 compared with PBO, flurazepam, triazolam, or zopiclone.
The final end point indirectly compared in NMA 1 was the development of headache from the respective drugs. Overall, no evidence of difference in the odds of headache between LEM5 and each of alternatives was found, likely due to the imprecision of the results (Table 46). This also was observed when LEM10 was the reference comparator.
Table 43: Drug Discontinuations Between Drugs for Insomnia When Compared to LEM5 and LEM10
Comparator | OR | 95% CI | P value |
|---|---|---|---|
Reference: LEM5 | |||
Placebo | 0.95 | 0.46 to 1.97 | 0.89 |
LEM10 | 1.99 | 1.06 to 3.74 | 0.033 |
Flurazepam 30 mg | 2.09 | 0.62 to 6.99 | 0.23 |
Temazepam 15 mg | 0.78 | 0.19 to 3.25 | 0.74 |
Triazolam 0.125 mg | 0.77 | 0.18 to 3.22 | 0.72 |
Triazolam 0.25 mg | 1.04 | 0.19 to 57.9 | 0.98 |
Reference: LEM10 | |||
Placebo | 0.48 | 0.25 to 0.91 | 0.025 |
LEM5 | 0.50 | 0.27 to 0.95 | 0.033 |
Flurazepam 30 mg | 1.05 | 0.33 to 3.35 | 0.93 |
Temazepam 15 mg | 0.39 | 0.10 to 1.57 | 0.19 |
Triazolam 0.125 mg | 0.39 | 0.10 to 1.55 | 0.18 |
Triazolam 0.25 mg | 0.54 | 0.01 to 28.7 | 0.75 |
CI = confidence interval; LEM5 = lemborexant 5 mg; LEM10 = lemborexant 10 mg; OR = odds ratio.
Note: Statistically significant differences (95% CI excluding 1) are highlighted in bold.
Source: Sponsor-submitted indirect treatment comparison report.60
Table 44: Risk of Somnolence Between Drugs for Insomnia When Compared to LEM5 and LEM10
Comparator | OR | 95% CI | P value |
|---|---|---|---|
Reference: LEM5 | |||
Placebo | 0.25 | 0.12 to 0.52 | < 0.001 |
LEM10 | 1.69 | 1.11 to 2.55 | 0.013 |
Flurazepam 30 mg | 1.17 | 0.44 to 3.10 | 0.74 |
Temazepam 15 mg | 0.92 | 0.20 to 4.15 | 0.71 |
Triazolam 0.125 mg | 0.61 | 0.13 to 2.91 | 0.54 |
Triazolam 0.25 mg | 0.31 | 0.14 to 0.69 | 0.04 |
Zopiclone 7.5 mg | 0.26 | 0.12 to 0.58 | 0.001 |
Reference: LEM10 | |||
Placebo | 0.15 | 0.074 to 0.30 | < 0.001 |
LEM5 | 0.59 | 0.39 to 0.90 | 0.013 |
Flurazepam 30 mg | 0.70 | 0.27 to 1.80 | 0.46 |
Temazepam 15 mg | 0.54 | 0.12 to 2.43 | 0.43 |
Triazolam 0.125 mg | 0.36 | 0.08 to 1.70 | 0.20 |
Triazolam 0.25 mg | 0.18 | 0.08 to 0.40 | < 0.001 |
Zopiclone 7.5 mg | 0.16 | 0.07 to 0.34 | < 0.001 |
CI = confidence interval; LEM5 = lemborexant 5 mg; LEM10 = lemborexant 10 mg; OR = odds ratio.
Note: Statistically significant differences (95% CI excluding 1) are highlighted in bold.
Source: Sponsor-submitted indirect treatment comparison report.60
Table 45: Risk of Dizziness Between Drugs for Insomnia When Compared to LEM5 and LEM10
Comparator | OR | 95% CI | P value |
|---|---|---|---|
Reference: LEM5 | |||
Placebo | 1.40 | 0.43 to 4.48 | 0.58 |
LEM10 | 0.52 | 0.11 to 2.43 | 0.40 |
Flurazepam 30 mg | 7.11 | 0.58 to 87.7 | 0.13 |
Triazolam 0.25 mg | 1.59 | 0.47 to 5.36 | 0.46 |
Zopiclone 7.5 mg | 1.42 | 0.42 to 4.75 | 0.57 |
Reference: LEM10 | |||
Placebo | 2.69 | 0.62 to 11.8 | 0.19 |
LEM5 | 1.93 | 0.41 to 9.03 | 0.40 |
Flurazepam 30 mg | 13.7 | 0.95 to 198 | 0.054 |
Triazolam 0.25 mg | 3.06 | 0.67 to 14.0 | 0.15 |
Zopiclone 7.5 mg | 2.73 | 0.61 to 12.4 | 0.19 |
CI = confidence interval; LEM5 = lemborexant 5 mg; LEM10 = lemborexant 10 mg; OR = odds ratio.
Source: Sponsor-submitted indirect treatment comparison report.60
Table 46: Indirect Comparison of Headache Between Alternative Drugs for Insomnia
Comparator | OR | 95% CI | P value |
|---|---|---|---|
Reference: LEM5 | |||
Placebo | 0.80 | 0.51 to 1.25 | 0.32 |
LEM10 | 0.77 | 0.49 to 1.19 | 0.24 |
Flurazepam 30 mg | 0.89 | 0.37 to 2.18 | 0.81 |
Temazepam 15 mg | 0.92 | 0.38 to 2.22 | 0.86 |
Triazolam 0.125 mg | 1.18 | 0.50 to 2.79 | 0.70 |
Triazolam 0.25 mg | 0.79 | 0.45 to 1.39 | 0.4 |
Zopiclone 7.5 mg | 0.80 | 0.46 to 1.37 | 0.41 |
Reference: LEM10 | |||
Placebo | 1.04 | 0.65 to 1.67 | 0.86 |
LEM5 | 1.30 | 0.84 to 2.04 | 1.18 |
Flurazepam 30 mg | 1.17 | 0.47 to 2.88 | 0.74 |
Temazepam 15 mg | 1.21 | 0.50 to 2.94 | 0.68 |
Triazolam 0.125 mg | 1.55 | 0.65 to 3.69 | 0.32 |
Triazolam 0.25 mg | 1.03 | 0.57 to 1.85 | 0.92 |
Zopiclone 7.5 mg | 1.04 | 0.59 to 1.82 | 0.90 |
CI = confidence interval; LEM5 = lemborexant 5 mg; LEM10 = lemborexant 10 mg; OR = odds ratio.
Source: Sponsor-submitted indirect treatment comparison report.60
An additional analysis of studies reporting falls was submitted by the sponsor to indirectly evaluate the risk of falls between LEM5 and LEM10 against a series of drugs currently used for the treatment of insomnia.
The authors first used 2 randomized LEM trials (the SUNRISE 1 and SUNRISE 2 trials) that reported falls data relative to PBO and ZOL. The first step in the analysis was to estimate the pooled risk of falls with LEM5 and LEM10 relative to PBO using these data. In the case of LEM5, the OR for the pooled risk of falls relative to PBO was estimated to be 1.32 (95% CI, 0.11 to 16.31). For LEM10, the OR for the pooled risk of falls relative to PBO was estimated to be 0.52 (95% CI, 0.18 to 1.47).
After these results were obtained, the authors included 6 studies (Table 47) to indirectly estimate the risk of falls between alternative drugs to LEM5 and LEM10. There were 4 studies that were patient-level cohort evaluations and 2 studies that were meta-analyses of clinical or observational trials. The univariate method by Bucher was used for the indirect analysis. Not all comparators reporting OR were against PBO.
Table 47: Indirect Comparison of Risk of Falls Among Patients Taking LEM5 and LEM10 Versus Available Comparators
Reference | Drug | Study type | Patient age (years) | Sample size (N) | Country |
|---|---|---|---|---|---|
Neutel et al. (1996) | Triazolam Flurazepam Lorazepam | Prospective cohort | ≥ 60 | 361 patients | Canada |
Woolcott (2009) | BZD | Meta-analysis | ≥ 60 | 22 studies | Global |
Treves (2018) | Z-drugs | Meta-analysis | Adults | 14 studies | Global |
Yu (2017) | BZD BZD short BZD long Z-drugs | Case-control | ≥ 65 | 2,238 patients | Taiwan |
Amari (2020a) | BZD | Retrospective cohort | ≥ 65 | 1,075,772 patients | US |
Amari (2020b) | BZD | Retrospective cohort | Adults | 154,010 patients | US |
BZD = benzodiazepine; LEM5 = lemborexant 5 mg; LEM10 = lemborexant 10 mg; Z-drugs = zolpidem, eszopiclone, zopiclone, and zaleplon.
Source: Sponsor-submitted indirect treatment comparison report.60
In the retrospective cohort studies, the control group was considered the PBO for the purposes of the ITC.
ORs were obtained in an ITC of the included studies (Table 48). Using LEM5 as the reference, no evidence of any difference could be detected when comparing to patients receiving triazolam, flurazepam, lorazepam, trazodone, benzodiazepines, and Z-drugs due to the high imprecision of the results. When LEM10 was used as the reference, the odds of falls were higher with triazolam, flurazepam, and lorazepam when compared to LEM10. When the entire class of benzodiazepines and trazodone were compared to LEM10, the odds of falls were also higher with the former drugs. Even though these findings suggested that LEM10 is associated with a reduction in the odds of falls when compared to other drugs, the results are very imprecise with wide CIs that could include a small increase or a big increase.
Table 48: Indirect Comparison of Risk of Falls Among Patients Taking LEM5 and LEM10 Versus Available Comparators
Reference | Drugs | Indirect OR (95% CI) (vs. LEM5)a | Indirect OR (95% CI) (vs. LEM10)b |
|---|---|---|---|
Neutel et al. (1996) | Triazolam Flurazepam Lorazepam | 2.04 (0.16 to 25.3) 2.58 (0.21 to 32.0) 1.52 (0.12 to 19.2) | 5.19 (1.74 to 15.5) 6.54 (2.18 to 19.6) 3.85 (1.23 to 12.0) |
Woolcott (2009) | BZD | 1.21 (0.10 to 14.9) | 3.08 (1.07 to 8.83) |
Treves (2018) | Z-drugs | Falls = 1.81 (0.12 to 26.4) Fractures = 1.25 (0.10 to 15.1) | Falls = 4.62 (1.11 to 19.1) Fractures = 3.14 (1.09 to 9.04) |
Yu (2017) | BZD BZD short BZD long Z-drugs | 1.0 (0.08 to 12.2) 1.08 (0.09 to 13.2) 1.07 (0.09 to 13.1) 0.94 (0.08 to 11.5) | 2.54 (0.88 to 7.31) 2.73 (0.94 to 7.9) 2.71 (0.93 to 7.9) 2.38 (0.82 to 6.91) |
Amari (2020a) | BZD Trazodone | 2.02 (0.17 to 24.6) 1.75 (0.14 to 21.0) | 5.14 (1.80 to 14.7) 4.44 (1.56 to 12.7) |
Amari (2020b) | BZD Trazodone | 1.74 (0.14 to 22.1) 2.17 (0.18 to 26.4) | 4.42 (1.50 to 12.7) 5.5 (1.9 to 15.7) |
BZD = benzodiazepine; CI = confidence interval; LEM5 = lemborexant 5 mg; LEM10 = lemborexant 10 mg; OR = odds ratio; vs. = versus; Z-drugs = zolpidem, eszopiclone, zopiclone, and zaleplon.
aPooled risk of falls with LEM5 vs. PBO = 1.32 (95% CI, 0.11 to 16.3).
bPooled risk of falls with LEM10 vs. PBO = 0.52 (95% CI, 0.18 to 1.47).
Source: Sponsor-submitted indirect treatment comparison report.60
When evaluating evidence from 3 studies (Neutel et al. [1996], Amari [2020a], and Amari [2020b]) in the indirect comparison within a sensitivity analysis including moderate to severe falls, the associated pooled ORs of moderate or severe falls were 0.50 (95% CI, 0.045 to 3.55) and 1.02 (95% CI, 0.19 to 5.51) for LEM5 compared to PBO and LEM10 compared to PBO, respectively. Both effect estimates were too imprecise to draw a conclusion about the odds of falling during treatment with LEM compared with PBO. The findings of the indirect analysis between LEM (5 mg or 10 mg) and triazolam, flurazepam, lorazepam, benzodiazepines, or trazodone were too imprecise to detect any difference in the effect estimates.
Critical Appraisal of NMA 1
The submitted systematic review and NMA was conducted to assess the effects and harms of LEM against relevant comparators. Overall, based on the methods detailed in the technical report, the ITC had an overall adequate search strategy, screening, and appraisal of the risk of bias of the included studies. It was not clear if the data extraction and selection of studies were performed by a single assessor or multiple assessors to address differences in judgment for including or excluding studies and the evaluation of the risk of bias.
Overall, the researchers did an appropriate identification and inclusion of the relevant trials for the specific population and comparators. However, several head-to-head trials were excluded due to the strict inclusion criteria, increasing the potential of missing information and selective reporting. It is not clear if networks were adequately constructed and how models were assessed (i.e., proper modelling and fitting of the models). It can be assumed that the authors performed a frequentist approach, but it was not defined in the technical report (i.e., based on this, it could not be judged if any priors or convergence were appropriate to address). As none of the nodes within the network was directly connected, it was not possible to assess the inconsistency of the network.
The body of evidence included in the network presents issues of risk of bias according to the judgments presented by the investigators, specifically in terms of unclear randomization and allocation concealment. There were some systematic differences in the included studies that could affect the transitivity assumption, such as treatment duration and patient age; although none of these potential modifiers were examined by the authors and accounted for in the sensitivity analyses, there is the potential for residual variables not fully included in the assessments. The plausibility of the transitivity assumption is, therefore, uncertain.
The body of evidence presented heterogeneity (inconsistencies) in the effect estimates for different end points according to the assessment performed by the authors. The cause of the heterogeneity is difficult to explain exactly, but it is likely due to the differences in populations and settings from individual studies, which can increase uncertainty in the results. Also, there were some concerns about publication bias. The additional data and ITC presented for the evaluation of falls were obtained from different study designs used for crafting pooled estimates. These include risk of bias and assumptions from the body of evidence that create further uncertainty and make it difficult to integrate into a single effect estimate.
Effect estimates in this body of evidence for all end points presented highly imprecise results, which made it difficult to draw definite conclusions.
Overall, the populations included in the individual studies of the network are generalizable to the Canadian population. More end points on HRQoL could have been included to address important values and patients’ preferences. The information on risk of falls was important for decision-making, but this reported end point was performed posthoc in the ITC and with results too highly imprecise to draw conclusions.
Methods of NMA 2
Objectives
The objective of the report published by McElroy et al. (2021)20 was to compare the efficacy and safety of LEM with specified other insomnia treatments through a systematic literature review and NMA.
Study Selection Methods
MEDLINE and Embase were searched from inception to February 2019 and updated with a search of clinical trial registries and a targeted search of PubMed for pivotal trials in March 2021. Included studies were RCTs in adults with primary insomnia if they reported results following at least 1 week of treatment.
Interventions of interest were specified by the authors as LEM, suvorexant, trazodone, ramelteon, benzodiazepines (alprazolam, lorazepam, brotizolam, flunitrazepam, etizolam, triazolam, estazolam, and temazepam), and Z-drugs (zolpidem, eszopiclone, zaleplon, and zopiclone). Of these, only zolpidem, zopiclone, eszopiclone, trazodone, triazolam, and temazepam were available in the body of evidence from NMA 2 and of interest to this CADTH reimbursement review.
Comparators considered in the review by McElroy et al. (2021) included other pharmacologic treatments or PBO, which allowed the study to be joined to the network. If the comparator could not be used as a common reference to an intervention of interest, the study was excluded.
The outcomes of interest included LPS (objective), sleep onset latency (subjective), sleep efficiency (objective and subjective), WASO (objective and subjective), TST (objective and subjective), ISI, sQUAL, SAEs, withdrawal due to AEs, somnolence, dizziness, and falls or accidental injury.
Only articles published in the English language were included. RCTs had to have a time frame of at least 1 week of treatment duration and include at least 50 patients in total (and at least 20 patients per treatment group). Crossover trials were excluded.
All identified references were initially screened by title and abstract. Methods for the selection of full texts were not reported. Data extraction and quality appraisals were undertaken by 2 independent reviewers, with differences resolved by consensus or the involvement of a third reviewer. The quality of evidence was assessed using the National Institute for Health and Care Excellence methodology checklist for RCTs.
Analysis Methods
A Bayesian NMA was performed at the time points of 4 weeks, 3 months, and 6 months, with PBO as the reference treatment as it was the most frequent comparator. A random-effects linear regression shared parameter model was fitted for the 4-week efficacy outcomes, and fixed-effects models were fitted for the 3-month and 6-month outcomes due to the sparseness of the networks.
Efficacy estimates were reported as mean difference. Safety outcomes were analyzed as binary variables (the number and percentage experiencing ≥ 1 event), without continuity correction, and estimates were reported as OR. Complementary log-log models using duration of treatment as an offset were also fitted as sensitivity analyses, with estimates reported as hazard ratios.
Effect estimates were summarized using the median with 95% CrI. Model parameters were assessed using the Markov chain Monte Carlo method in WinBUGS software version 1.4.3 (the Bayesian inference Using Gibbs Sampling — or BUGS — project). A run for 50,000 iterations was performed and discarded as “burn-in,” and then the model was run for 100,000 more iterations for inference. Convergence was assessed by visual inspection of the history plot and Gelman-Rubin diagnostics. Noninformative priors were used. The residual deviance was used to assess model fit, and tau is presented as a measure of heterogeneity for random-effects models. The authors reported testing for consistency between direct and indirect evidence in closed loops, but no specific method is referenced.
Analyses for subgroup effects were conducted. The subgroups included were based on the proportion of the study population defined as older (ranging from 0% for studies not containing older adults to 100% for studies only containing older adults). Older adults were generally defined as people aged at least 65 years, although definitions varied by study.
Results of NMA 2
Included Studies
In total, 45 studies were included. The interventions included LEM and 15 other insomnia treatments, of which the most commonly studied was ZOL. No studies of etizolam, alprazolam, or lorazepam met the inclusion criteria. The studies covered a period from 1984 to 2020, and most were PBO-controlled and DB. The duration of treatment ranged from 2 weeks to 8 months. The mean age from each study varied from 38.0 years to 79.0 years.
Most (36 out of 45) studies were judged by the authors to have an unclear randomization process and/or concealment of allocation. Most studies were balanced in the baseline prognostic factors and properly blinded participants and care providers. Unexpected imbalances in withdrawals between groups were uncommon. Also, most studies used an intention-to-treat analysis.
The network for the outcome of TST at 4 weeks is presented in Figure 6. Networks for other outcomes and time points also had few (or no) closed loops.
Figure 6: Network Diagram for NMA 2, Total Sleep Time (Polysomnography) at 4 Weeks
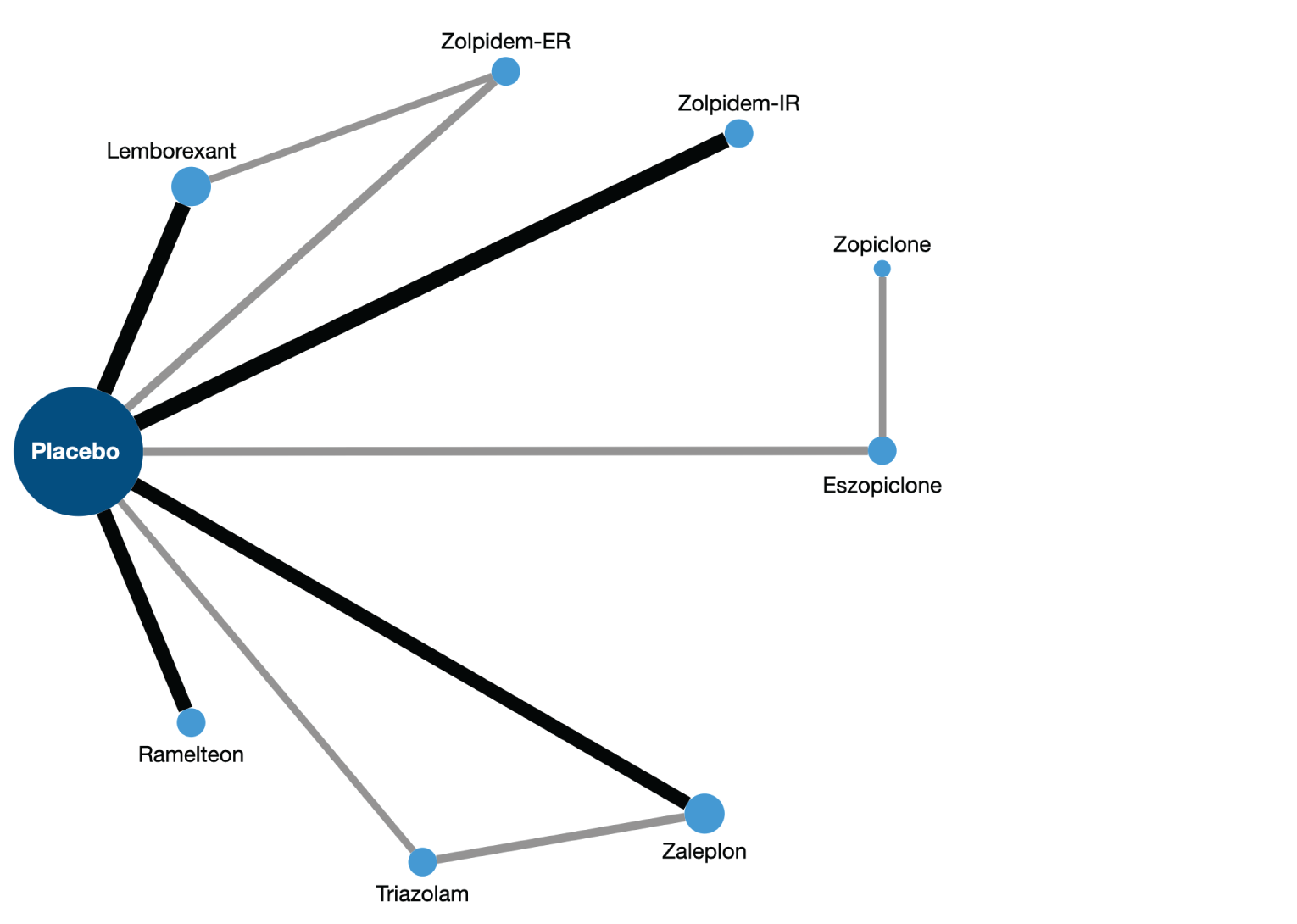
ER = extended-release; IR = immediate-release.
Note: Grey lines join treatment pairs that occur in 1 study, and black lines join treatment pairs that occur in 2 studies. The size of each circle is proportional to the number of treatment comparisons that involve that treatment.
Source: Adapted from McElroy et al. (2021).20
Efficacy Results
Objective sleep outcomes measured by PSG were analyzed at 4 weeks and subjective outcomes at 4 weeks, 3 months, and 6 months. The number of studies and interventions varied by outcome, with subjective outcomes more frequently reported.
On the objective efficacy outcome of TST, LEM showed prolonged sleep by a median of 38.1 minutes (95% CrI, 16.3 minutes to 60.7 minutes) compared with PBO (Table 49). For WASO, LEM was similarly superior to PBO and against ZOL-IR, with a median reduction of 21.3 minutes (95% CrI, –29.6 minutes to –10.1 minutes) and 19.6 minutes (95% CrI, –31.9 minutes to –0.3 minutes), respectively. LEM showed a reduction in LPS when compared to PBO (–18.6 minutes; 95% CrI, –29.0 minutes to –10.9 minutes), ZOL-ER (–13.4 minutes; 95% CrI, –24.4 minutes to –4.9 minutes), and triazolam (–23.2 minutes; 95% CrI, –38.8 minutes to –9.6 minutes). For the rest of the available comparisons, including zopiclone, the evidence was inconclusive due to wide CrIs that included the null effect. These results were inconsistent with results from NMA 1, which showed that LEM was superior to triazolam in LPS and sleep efficiency.
On the subjective outcomes (Table 49), LEM was superior to PBO in all end points evaluated but not against eszopiclone for the sQUAL end point (mean difference = –0.6; 95% CrI, –0.9 to –0.2). For the rest of the comparisons, including that for to zopiclone, no statistical difference in effect was observed. Similar to the objective outcomes, the evidence for many outcome comparisons was inconclusive due to wide CrIs that included the null effect.
Table 49: NMA 2, Comparisons of Lemborexant With Other Treatments for Insomnia, Efficacy Results at 4 Weeks
Outcomes | Objective (PSG) | Subjective (patient reported) | |||||||
|---|---|---|---|---|---|---|---|---|---|
TST, minutes (95% CrI) | WASO, minutes (95% CrI) | LPS, minutes (95% CrI) | SE, % (95% CrI) | sTST, minutes (95% CrI) | sWASO, minutes (95% CrI) | sSOL, minutes (95% CrI) | ISI (scale 0 to 28) (95% CrI) | sQUAL (scale 1 to 10) (95% CrI) | |
Lemborexant placebo | 38.1 (16.3 to 60.7) | –21.3 (–29.6 to –10.1) | –18.6 (–29.0 to –10.9) | 7.2 (3.4 to 10.8) | 22.5 (12.6 to 32.7) | –10.9 (–19.0 to –3.4) | –13.2 (–20.2 to –6.0) | –1.9 (–3.3 to –0.5) | 0.3 (0.1 to 0.6) |
Lemborexant vs. ZOL-IR | 21.1 (–13.0 to 50.2) | –19.6 (–31.9 to –0.3) | –6.3 (–19.7 to 3.8) | 3.3 (–1.8 to 9.0) | –5.3 (–17.2 to 6.3) | 3.1 (–7.4 to 13.3) | 0.2 (–8.0 to 8.9) | NA | –0.3 (–0.6 to 0.0) |
Lemborexant vs. ZOL-ER | 22.6 (–4.6 to 51.0) | –7.2 (–16.8 to 4.6) | –13.4 (–24.4 to –4.9) | 4.6 (–0.9 to 9.8) | –2.1 (–14.6 to 10.3) | 8.1 (–2.6 to 18.1) | –8.0 (–17.2 to 1.0) | 0.3 (–1.8 to 2.5) | –0.2 (–0.5 to 0.2) |
Lemborexant vs. Zopiclone | 24.2 (–21.7 to 73.1) | NA | –11.1 (–29.6 to 4.8) | 4.4 (–0.1 to 8.8) | NA | NA | NA | 0.9 (–2.4 to 4.0) | NA |
Lemborexant vs. Eszopiclone | 10.0 (–25.6 to 48.2) | –8.7 (–21.8 to 7.1) | –6.0 (–20.1 to 5.6) | 1.8 (–2.9 to 6.5) | –12.3 (–24.3 to 0.2) | 3.6 (–6.0 to 12.7) | 4.4 (–5.1 to 13.6) | 1.3 (–0.6 to 3.1) | –0.6 (–0.9 to –0.2) |
Lemborexant vs. Trazodone | NA | NA | NA | NA | 2.9 (–17.4 to 23.0) | –1.2 (–17.1 to 14.0) | –5.0 (–20.3 to 10.6) | NA | –0.2 (–0.8 to 0.4) |
Lemborexant vs. Triazolam | 22.1 (–16.4 to 62.1) | NA | –23.2 (–38.8 to –9.6) | 5.3 (–1.4 to 12.1) | –3.7 (–21.2 to 13.6) | NA | 2.0 (–14.4 to 18.5) | NA | –0.4 (–1.1 to 0.3) |
Lemborexant vs. Temazepam | NA | NA | NA | NA | 10.5 (–7.9 to 29.2) | 3.8 (–14.5 to 21.9) | 1.2 (not reported) | NA | NA |
Tau (measure of heterogeneity) | 11.0 (1.1 to 26.9) | 3.7 (0.2 to 14.1) | 4.2 (0.4 to 10.2) | 1.3 (0.1 to 8.0) | 4.7 (0.6 to 9.0) | 3.9 (0.3 to 9.8) | 5.3 (3.2 to 8.1) | 0.8 (0.2 to 2.2) | 0.1 (0.0 to 0.3) |
Dres (measure of model fit) vs. number of data points | 21.6 vs. 21 | 21.4 vs. 20 | 39.4 vs. 36 | 25.5 vs. 22 | 72.0 vs. 73 | 49.9 vs. 45 | 73.6 vs. 74 | 21.0 vs. 21 | 56.7 vs. 57 |
Number of studies | 10 | 11 | 18 | 11 | 34 | 22 | 34 | 10 | 27 |
Number of treatments | 9 | 7 | 10 | 8 | 12 | 10 | 11 | 6 | 11 |
Number of participants | 2,974 | 3,663 | 4,822 | 2,800 | 13,370 | 7,989 | 13,923 | 5,257 | 10,603 |
CrI = credible interval; Dres = residual deviance; ISI = Insomnia Severity Index; LPS = latency to persistent sleep; NA = not available; NMA = network meta-analysis; PSG = polysomnography; SE = sleep efficiency; sQUAL = subjective quality of sleep; sSOL = subjective sleep onset latency; sTST = subjective total sleep time; sWASO = subjective wake time after sleep onset; τ = tau; TST = total sleep time; vs. = versus; WASO = wake time after sleep onset; ZOL-ER = zolpidem tartrate extended-release; ZOL-IR = zolpidem tartrate immediate-release.
Note: Data were the mean difference between lemborexant and each comparator reported as median (95% CrI) from random-effects NMA. sQUAL was reported on a scale from 1 to 10, where a higher score indicated better quality of sleep. ISI was measured on a scale from 0 to 28, where lower scores indicated lower severity. Thus, for TST, SE, and sQUAL, positive differences indicated lemborexant performs better; for WASO, LPS or sSOL, and ISI, negative differences indicated lemborexant performs better. Statistically significant differences (95% CrI excluding 0) are highlighted in bold.
Source: Network meta-analysis 2, McElroy et al. (2021).20
No subgroup interactions between treatment effect and older subpopulation were found for any of the efficacy outcomes. When assessed in closed loops, no evidence of inconsistency was observed for TST, WASO, sTST, sWASO, sSOL, ISI, or sQUAL at 4 weeks (global test P > 0.20 for all). However, there was evidence of inconsistency for LPS (P = 0.002) and sleep efficiency (P = 0.011).
Harms
The evidence was inconclusive for the odds for presenting SAEs for patients receiving LEM when compared to relevant comparators, mainly due to wide CrIs or lack of evidence for some relevant comparators (Table 50). Similarly, the evidence was inconclusive for the odds of withdrawals due to AEs or in the odds of falls for all comparators investigated. LEM was associated with lower odds of dizziness compared with ZOL-IR, ZOL-ER, and eszopiclone. LEM, however, increased the odds of somnolence when compared to PBO, ZOL, and eszopiclone.
Table 50: NMA 2, Harms for Comparisons of Lemborexant With Other Treatments
Outcome | SAE | Withdrawal due to AE | Somnolence | Dizziness | Falls or injury |
|---|---|---|---|---|---|
Lemborexant vs. placebo, OR (95% CrI) | 1.38 (0.59 to 3.66) | 1.38 (0.69 to 2.95) | 7.73 (4.17 to 15.71) | 0.66 (0.32 to 1.35) | 0.68 (0.30 to 1.61) |
Lemborexant vs. ZOL-IR, OR (95% CrI) | NA | 0.60 (0.26 to 1.42) | 3.35 (1.50 to 7.85) | 0.34 (0.14 to 0.82) | NA |
Lemborexant vs. ZOL-ER, OR (95% CrI) | 0.32 (0.06 to 1.62) | 0.40 (0.15 to 1.06) | 2.91 (1.45 to 6.29) | 0.29 (0.12 to 0.64) | NA |
Lemborexant vs. zopiclone, OR (95% CrI) | NA | 0.44 (0.18 to 1.12) | NA | 0.37 (0.10 to 1.26) | NA |
Lemborexant vs. eszopiclone, OR (95% CrI) | 0.66 (0.17 to 2.47) | 0.86 (0.40 to 1.95) | 3.53 (1.48 to 8.61) | 0.19 (0.07 to 0.48) | 0.54 (0.20 to 1.50) |
Lemborexant vs. trazodone, OR (95% CrI) | NA | 0.57 (0.14 to 2.55) | 2.10 (0.81 to 5.69) | NA | NA |
Lemborexant vs. triazolam, OR (95% CrI) | NA | 0.75 (0.27 to 2.17) | 2.80 (0.69 to 11.89) | 0.31 (0.05 to 2.06) | NA |
Lemborexant vs. temazepam, OR (95% CrI) | NA | 0.72 (0.19 to 3.05) | NA | NA | NA |
Number of studies | 12 | 36 | 23 | 23 | 8 |
Number of treatments | 6 | 14 | 11 | 10 | 4 |
Number of patients | 6,456 | 15,398 | 10,328 | 9,363 | 4,800 |
AE = adverse event; CrI = credible interval; NA = not available; NMA = network meta-analysis; SAE = serious adverse event; vs. = versus; ZOL-ER = zolpidem tartrate extended-release; ZOL-IR = zolpidem tartrate immediate-release.
Notes: Data were median odds ratio of lemborexant vs. comparator with 95% CrI from fixed-effects NMA. Statistically significant differences (95% CrI excluding 1) are highlighted in bold.
Source: Network meta-analysis 2, McElroy et al. (2021).20
There was no evidence of inconsistency based on the global test (P > 0.05) for the safety outcomes assessed, although there was some evidence of inconsistency in the PBO–ZOL-IR–temazepam and PBO–ZOL-IR–triazolam loops for withdrawals due to AEs.
There was evidence of subgroup interaction for the somnolence and age group, implying that older people had higher odds of somnolence, but the authors state that separate analyses of studies in older adults (based on 17 of the 23 studies that reported somnolence; 7 studies for older adults and 10 studies for adults) indicated that the assumption was inconsistent and, hence, uncertain for drawing conclusions.
Critical Appraisal of NMA 2
NMA 2 assessed the efficacy and harms of LEM against other comparators, some of which were relevant to the Canadian landscape. This included zopiclone, which was not assessed in NMA 1. Overall, the described methods for the search strategy, screening of records, and data extraction were appropriate to identify relevant RCTs. However, the body of evidence from the included studies presented risk of bias, mainly in the randomization and allocation concealment domains, and some concerns of selective reporting bias due to some studies not reporting full results.
There were no obvious concerns of heterogeneity among the comparisons for the end points included (i.e., statistical heterogeneity), and a good fit for the models was observed in the NMA. However, some important clinical and methodological differences across included studies were identified. As noted by the authors, the studies included were published over a long period of time (1984 to 2020) with the possibility of including different undetected baseline prognostic factors. Few characteristics of the included studies and their patients were reported, precluding the ability to ascertain whether other important differences were present. Furthermore, not all trials included the same subjective and objective measurements, and some used different measures of the same outcome and/or measured the same outcomes at different time points (e.g., efficacy results for the NMAs of 4-week outcomes included those measured from 1 week to 6 weeks). These differences between studies create uncertainty in the plausibility of the transitivity assumption, which overall could not be fully assessed due to the small number of closed loops to measure consistency (as a statistical manifestation of transitivity). Some studies identified in the search failed to report numerical results when the results were not statistically significant, and therefore could not be included in the NMA, which may have led to publication bias.
The ITC had sparse networks, which limited the interaction models that could be fitted. As a result, although the subgroup analysis indicated that the results from the main NMA also apply to the older population, comparisons between different active treatments in older adults could not be made. Furthermore, as mentioned by the authors, different scales used to measure sleep quality were transformed to a common scale. This has some limitations, as the transformation does not guarantee comparability of the categories in the transformed scales.
Results in efficacy and harm estimates were imprecise in many comparisons and end points (i.e., wide CrIs that included the null effect and may have included an appreciable threshold for benefit or harm), which adds to the uncertainty in the effect estimates. As a result of this imprecision, no definitive conclusions can be drawn for many outcome comparisons.
The results of the relevant comparisons are overall generalizable, with trials including Canadian sites and populations. No results on HRQoL end points were evaluated, which was considered an important end point by patients for this CADTH review.
Other Relevant Evidence
This section includes a summary of a trial included in the sponsor’s submission to CADTH that did not meet the criteria for the systematic review but provided information on switching patients from ZOL to LEM.
Study 312
Description of the Study
The open-label, phase IIIb, pilot, multicentre trial (study 312)64 has been summarized to provide additional evidence regarding the next-dose transition from ZOL to LEM for the treatment of insomnia. The trial included adult patients with insomnia who were receiving ZOL as monotherapy, and who agreed to substitute it with LEM.
Methods
The primary objective of study 312 was the evaluation of the proportion of patients aged 18 years and older with insomnia disorder taking ZOL, who successfully transitioned to LEM5 or LEM10 after 2 weeks of receiving LEM. The secondary objectives were to evaluate the proportion of patients who increased from LEM5 to LEM10 or decreased from LEM10 to LEM5 during the 2-week titration period, to evaluate the patients’ impression of treatment using the PGI-Insomnia at the end of the 2-week titration period, and to evaluate the safety and tolerability of LEM in patients previously treated with ZOL.
Study 312 was divided into 3 phases (Figure 7):
the pretreatment phase, consisting of up to a 3-week screening period and a 1-day baseline period
the treatment phase, consisting of a 2-week titration period
the extension phase, consisting of the maintenance period of up to 12 weeks (for patients who did not enter the extension phase, a follow-up period started immediately after the end of the treatment phase and lasted for 4 weeks).
The results of the extension phase of study 312 were not provided by the sponsor; therefore, all results that are summarized in this report are from the core trial, consisting of the pretreatment and treatment phases.
During the pretreatment phase, including screening and baseline periods, patients were assessed for eligibility to participate in the trial. During the screening period, patients continued to take ZOL at the dose prescribed by their health care provider: ZOL-IR at 5 mg or 10 mg, or ZOL-ER at 6.25 mg or 12.5 mg. Patients were provided with an actigraph to wear continuously on their wrist, and an electronic data collection system was used to record the start and end times of nocturnal sleep periods. During the baseline period, all eligible patients were assigned to 1 of 2 cohorts based on the frequency of ZOL use during the screening period as follows.
Cohort 1 included patients with intermittent or mixed use of ZOL, including:
patients who received ZOL at least 3 nights per week but fewer than 5 nights per week, for the last 2 weeks of the screening period (cohort 1A)
patients who met both criteria for intermittent and frequent use of ZOL for 1 week each of the last 2 weeks (cohort 1B).
Cohort 2 included patients with frequent use of ZOL — namely, patients who received ZOL at least 5 nights per week for at least the last 2 weeks of the screening period.
During the 2-week treatment phase (the titration period of LEM), all eligible patients self-administered LEM at doses of 5 mg or 10 mg. Patients in cohort 1 all began treatment on LEM5, while those in cohort 2 were randomized in a 1:1 ratio to begin treatment on LEM5 (cohort 2A) or LEM10 (cohort 2B). After the end of the treatment phase, patients were eligible to enter the 12-week extension phase if they wished to continue receiving LEM at the dose that they took at the end of the titration period. For patients who did not enter the extension phase, the follow-up period started immediately after the end of the treatment phase and lasted for 4 weeks. The purpose of this period was to evaluate AEs and other safety parameters. During this period, it was recommended that patients continue their insomnia treatment with the health care provider who treated them before the study, if they so desired. The end of the trial was the date of the last study visit for the last patient in the core trial.
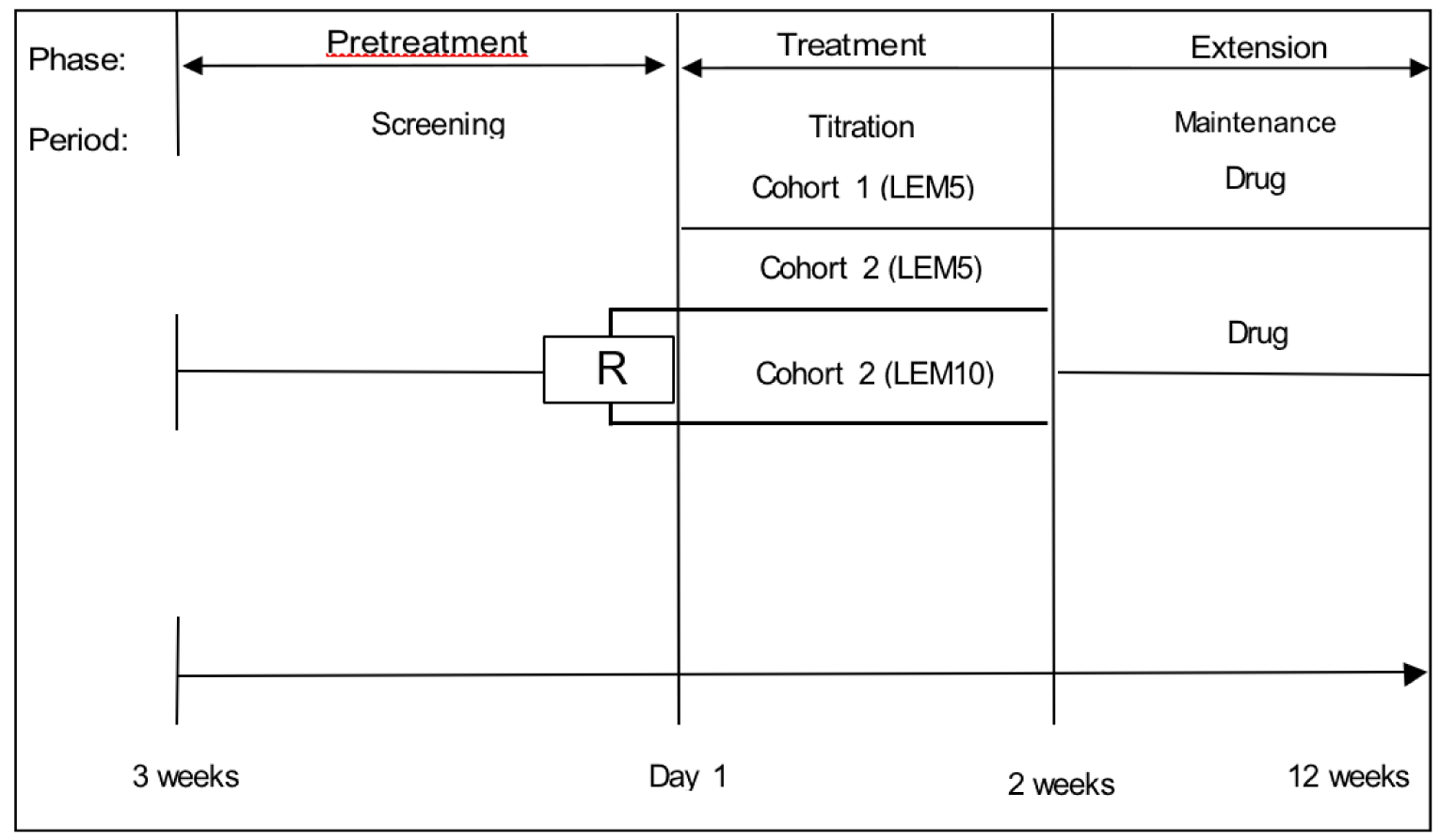
LEM5 = lemborexant 5 mg; LEM10 = lemborexant 10 mg; R = randomization.
Source: Study 312 Clinical Study Report.64
Every morning during the screening and treatment phases, patients entered their insomnia drug use data into the data collection system and recorded their sleep log data. Patients continued to wear an actigraph on their wrist throughout the screening and treatment phases. Data from the actigraph were collected at a sampling rate (epoch) of every 30 seconds and were scored as sleep or wake with a validated algorithm. Actigraphy data were used to evaluate the following sleep parameters:
TST — the total time spent in sleep according to the epoch-by-epoch wake or sleep categorization during time in bed
sleep efficiency — the total duration of sleep epochs during the defined nocturnal sleep periods divided by time in bed and multiplied by 100%
WASO — the total time spent awake according to the epoch-by-epoch wake or sleep categorization between sleep start (based on “lights out”) and “got up”
wake bouts — wake of at least 5 minutes that occurred during time in bed
sleep bouts — continuous sleep of at least 10 minutes that occurred during time out of bed.
The PGI-Insomnia and quality of sleep rating were completed each morning provided that LEM was taken the previous evening. The ISI was completed at each clinic visit except the follow-up visit. The PGI-Insomnia had 3 items related to study medication effects (helped or worsened sleep, decreased or increased time to fall asleep, and increased or decreased TST) that were answered on a 3-point scale (positive, neutral, or negative medication effect) and 1 item related to perceived appropriateness of medication strength that was answered on a different 3-point scale (too strong, just right, or too weak). The quality of sleep rating is a self-reported measure of sleep quality, where patients were asked to judge the quality of their sleep the night before on a scale from 1 to 9, where 1 = extremely poor, 5 = not good not poor, and 9 = extremely good. The ISI is a self-reported questionnaire, where patients were asked to report the nature, severity, and impact of insomnia across 7 items: sleep onset, sleep maintenance, early morning awakening, sleep dissatisfaction, interference of sleep difficulties with daytime functioning, noticeability of the sleep problems by others, and distress caused by the sleep difficulties. Each item was rated on a 5-point Likert scale ranging from “no problem” to “very severe problem,” for a total score of 0 to 28.
Populations
Patients were eligible to participate in study 312 if they met the following inclusion criteria:
were aged 18 years or older at the time of informed consent
met the DSM-5 criteria for insomnia disorder
reported spending at least 7 hours in bed per night
had confirmation of intermittent or frequent use of ZOL.
Patient were not eligible to participate in the trial if they met any of the following key exclusion criteria:
had any history of moderate or severe obstructive sleep apnea
had current evidence of bronchiectasis, emphysema, asthma, chronic obstructive pulmonary disease, diagnosis of periodic limb movement disorder, restless legs syndrome, circadian rhythm sleep disorder, or an exclusionary score on screening instruments to rule out individuals with symptoms of certain sleep disorders other than insomnia (e.g., International Restless Legs Scale score of 16)
habitually napped during the day more than 3 times per week
reported symptoms potentially related to narcolepsy, a history of sleep-related violent behaviour, or sleep-driving, or any other complex sleep-related behaviour (e.g., making phone calls or preparing and eating food while sleeping), whether spontaneous or associated with a pharmacologic sleep drug
had taken a dose of ZOL-IR greater than 10 mg per night, or ZOL-ER greater than 12.5 mg per night, or a dose of ZOL that was lower than what was prescribed
had used any pharmacologic modality of treatment for insomnia other than ZOL, including marijuana, within 1 week or 5 half-lives, whichever was longer, before the screening period
had a prolonged corrected QT interval by Fridericia’s formula interval that is greater than 450 milliseconds as demonstrated by a repeated electrocardiogram
had any suicidal ideation with intent, with or without a plan at screening or within 6 months of screening, or any lifetime suicidal behaviour
had evidence of clinically significant disease (e.g., cardiac disease, respiratory disease, gastrointestinal disease, renal disease)
was a patient for whom a sedating drug was contraindicated for safety reasons because of the patient’s occupation or activities
had psychotic disorder(s) or unstable recurrent affective disorder(s) evident by use of antipsychotic drugs or prior suicide attempt(s) within approximately the past 2 years
had a history of drug or alcohol dependency or abuse within approximately the past 2 years.
Patient baseline characteristics have been summarized in Table 51. There were no notable differences in baseline demographic characteristics across treatment groups (LEM5 and LEM10) or 2 cohorts (cohort 1 and cohort 2). The overall mean age of patients was 59.0 (SD = 12.21) years. More than half of patients were female (66.0%), and the majority was white (77.4%) and non-Hispanic or Latino (75.5%).
Of the 10 patients assigned to cohort 1, 3 (30.0%) patients had previously received ZOL at a dose of 5 mg and 7 (70.0%) patients had received ZOL at a dose of 10 mg. Of the 43 patients assigned to cohort 2, 13 (30.2%) patients had previously received ZOL at a dose of 5 mg, 29 (67.4%) patients had received ZOL at a dose of 10 mg, 1 (2.3%) patient had received ZOL at a dose of 6.25 mg, 5 (11.6%) patients had received ZOL at a dose of 12.5 mg, and 1 (2.3%) patient had been taking another ZOL dose. The mean duration of treatment with ZOL was 2,037.7 (SD = 1,043.89) days. All patients had previously used hypnotics and sedatives at screening, 4 (7.5%) patients had previously received anxiolytics (all in cohort 2), and 1 (1.9%) patient had previously received antidepressants (in cohort 2).
Table 51: Baseline Characteristics by Cohort and Dose of Lemborexant — Study 312, FAS
Characteristic | Cohort | Starting dose | ||
|---|---|---|---|---|
Cohort 1 N = 10 | Cohort 2 N = 43 | LEM5 N = 31 | LEM10 N = 22 | |
Sex, n (%) | ||||
Female | 7 (70.0) | 28 (65.1) | 21 (67.7) | 14 (63.6) |
Male | 3 (30.0) | 15 (34.9) | 10 (32.3) | 8 (36.4) |
Age (years), mean (SD) | 62.2 (6.65) | 58.3 (13.12) | 55.8 (12.51) | 63.5 (10.44) |
Age category, n (%) | ||||
18 years to 64 years | 5 (50.0) | 27 (62.8) | 21 (67.7) | 11 (50.0) |
≥ 65 years | 5 (50.0) | 16 (37.2) | 10 (32.3) | 11 (50.0) |
Race, n (%) | ||||
White | 8 (80.0) | 33 (76.7) | 23 (74.2) | 18 (81.8) |
Black | 2 (20.0) | 8 (18.6) | 7 (22.6) | 3 (13.6) |
Asian | 0 | 1 (2.3) | 0 | 1 (4.5) |
Japanese | 0 | 1 (2.3) | 0 | 1 (4.5) |
Other | 0 | 1 (2.3) | 0 | 0 |
Prior ZOL use, n (%) | ||||
ZOL-IR 5 mg | 3 (30.0) | 13 (30.2) | NR | NR |
ZOL-IR 10 mg | 7 (30.0) | 29 (67.4) | NR | NR |
ZOL-ER 6.25 mg | NA | 1 (2.3) | NR | NR |
ZOL-ER 12.5 mg | NA | 5 (11.6) | NR | NR |
Prior anxiolytic use, n (%) | 0 | 4 (9.3) | 3 (9.7) | 1 (4.5) |
Prior hypnotic and sedative use, n (%) | 10 (100.0) | 43 (100.0) | 31 (100.0) | 22 (100.0) |
Prior antidepressant use, n (%) | 0 | 1 (2.3) | 0 | 1 (4.5) |
FAS = full analysis set; LEM5 = lemborexant 5 mg; LEM10 = lemborexant 10 mg; NA = not applicable; NR = not reported; SD = standard deviation; ZOL = zolpidem tartrate; ZOL-ER = zolpidem tartrate extended-release; ZOL-IR = zolpidem tartrate immediate-release.
Source: Study 312 Clinical Study Report.64
Interventions
The initial treatment allocation has been shown in Figure 7. In the treatment phase (the titration period of LEM), all eligible patients self-administered LEM at doses of 5 mg or 10 mg orally once daily a few minutes before the patient intended to sleep. All patients in cohort 1 (intermittent or mixed use of ZOL) started the titration period on LEM5. Patients who met the criteria for intermittent use of ZOL for the last 2 weeks of the screening period and were assigned to receive LEM5 were categorized as cohort 1A. Patients who met the criteria for intermittent and frequent use of ZOL for the last 2 weeks of the screening period were assigned to receive LEM5 and were categorized as cohort 1B. Patients in cohort 2 were randomized in a ratio of 1:1 to receive either LEM5 or LEM10 and were categorized as cohort 2A and cohort 2B, respectively. Patients were allowed 1 LEM dose adjustment during the titration period. However, they were encouraged to remain on their assigned dose for 7 days to reflect common clinical practice. Patients were instructed about study restrictions regarding time spent in bed, alcohol consumption, and mealtimes.
The use of concomitant medication and procedures was monitored throughout the core trial. Patients were required to stop taking any prohibited or over-the-counter medications within 1 week or 5 half-lives before the treatment period, whichever was longer. Prohibited medications included strong and moderate CYP3A inhibitors, all CYP3A inducers, any medications for insomnia treatment (except ZOL use during the screening period), hypnotics, and sedatives.
Most patients who entered the core trial were taking at least 1 concomitant medication, including 80% of patients in cohort 1 and 83.7% of patients in cohort 2. The most frequently used concomitant medications during the trial were cardiovascular system drugs (70% in cohort 1 and 60.5% in cohort 2), alimentary tract and metabolism drugs (40% in cohort 1 and 34.9% in cohort 2), nervous system drugs (50% in cohort 1 and 34.9% in cohort 2), and antiinfective and antibacterial drugs (20.9% in cohort 2). Only 1 patient in cohort 2B received concomitant antidepressants during the treatment phase.
Outcomes
The primary outcome of the trial was the proportion of patients who successfully transitioned to LEM at the end of the 2-week titration period. The transition to LEM was defined as a patient who continued to receive LEM at the end of the 2-week titration period and either entered the extension phase or had chosen not to enter the extension phase for reasons not related to LEM (e.g., study-related travel expenses, preference to continue insomnia management with another health care provider).
Secondary outcomes included:
the proportion of patients who transitioned to LEM at the end of the 2-week titration period within each cohort
the proportion of patients in the LEM5 treatment groups with dose increased to LEM10 at the end of the titration period by cohort and overall
the proportion of patients in the LEM10 treatment group with dose decreased to LEM5 at the end of the titration period in cohort 2
the proportion of patients with positive medication effect rating on each PGI-Insomnia item at the end of the 2-week titration period by cohort and overall, using the value at the end of the titration period.
Exploratory outcomes included:
the change from baseline in mean ISI score at the end of the titration period by cohort and overall at the end of the titration period
the change from baseline in mean quality of sleep rating at the end of the titration period by cohort and overall at the end of the titration period
the mean TST, mean sleep efficiency, mean WASO, and number of wake bouts — sleep-related actigraphy variables that were discerned by comparing nights when an evening dose of LEM5 or LEM10 was taken to nights when an evening dose of ZOL was taken
the mean duration of sleep bouts — a wake-related actigraphy variable that was discerned by comparing the daytime after an evening dose of LEM5 or LEM10 was taken to the daytime after an evening dose of ZOL was taken.
Safety end points included the incidence of TEAEs, out-of-normal-range laboratory tests and vital signs, suicidality, and abnormal electrocardiogram findings.
Statistical Analysis
The FAS included all patients who received at least 1 dose of LEM, while the safety analysis set included patients who received at least 1 dose of LEM and had at least 1 postdose safety assessment. As a pilot trial, sample size estimates were not based on statistical calculations. Since this was a pilot study and open-label in nature, no formal statistical testing was conducted. The trial outcomes were summarized by treatment group (LEM5 and LEM10) and by cohort (cohort 1 and cohort 2) using descriptive statistics. No imputation was used to handle missing data.
Patient Disposition
A total of 99 patients were screened for entry into study 312. Of those, 53 (53.5%) patients were enrolled in the core trial, including 10 patients in cohort 1 and 43 patients in cohort 2 (Table 52). Of the 46 screening failures, 40 (87.0%) patients failed to meet inclusion criteria, 4 (8.7%) patients withdrew consent, and 2 (4.3%) patients were excluded for other reasons.
Most patients in cohort 1 (90.0%) and cohort 2 (79.1%) completed the core trial. The most common reason for withdrawal from the trial among patients in cohort 1 was an AE (10.0%). The most frequently reported reasons for trial withdrawal among patients in cohort 2 were AEs (14.0%) and withdrawal of consent (4.7%). Of the 53 patients, 43 (81.1%) patients transitioned from ZOL to LEM after 2 weeks of receiving LEM.
Table 52: Patient Disposition — Study 312
Patient disposition | Cohort | Starting dose | ||
|---|---|---|---|---|
Cohort 1 N = 10 | Cohort 2 N = 43 | LEM5 N = 31 | LEM10 N = 22 | |
Randomized, n (%) | 10 (100.0) | 43 (100.0) | 31 (100.0) | 22 (100.0) |
Completed study, n (%) | 9 (90.0) | 34 (79.1) | 26 (83.9) | 17 (77.3) |
Dose was changed by PI, n (%) | 4 (40.0) | 12 (27.9) | 13 (41.9) | 3 (13.6) |
Discontinued study, n (%) | 1 (10.0) | 9 (20.9) | 5 (16.1) | 5 (22.7) |
Dose was changed by PI, n (%) | 1 (10.0) | 2 (9.1) | 2 (6.5) | 2 (9.1) |
Patient attempted to maintain the dose, n (%) | 0 | 4 (9.3) | 2 (6.5) | 2 (9.1) |
Primary reasons for discontinuation, n (%) | ||||
Adverse event | 1 (10.0) | 6 (14.0) | 3 (9.7) | 4 (18.2) |
Withdrawal of consent | 0 | 2 (4.7) | 2 (6.5) | 0 |
Other | 0 | 1 (2.3) | 0 | 1 (4.5) |
Full analysis set, n | 10 | 43 | 31 | 22 |
Safety analysis set, n | 10 | 43 | 31 | 22 |
LEM5 = lemborexant 5 mg; LEM10 = lemborexant 10 mg; PI = principal investigator.
Source: Study 312 Clinical Study Report.64
Exposure to Study Treatments
All patients had at least 1 day of exposure to the study drug. A total of 53 patients were exposed to LEM during the core trial. The mean duration of exposure to LEM was 10.4 (SD = 5.8) weeks in cohort 1, 9.5 (SD = 6.07) weeks in cohort 2, 10.1 (SD = 5.75) weeks in the LEM5 group, and 8.9 (SD = 6.36) weeks in the LEM10 group.
Efficacy
Transition From ZOL to LEM at the End of the Titration Period
Overall, 81.1% of patients successfully transitioned to LEM at the end of the 2-week titration period and entered the extension phase. Of the 10 patients who were assigned to LEM5 in cohort 1, 9 (90.0%) patients transitioned to LEM at the end of the 2-week titration period. Of the 43 patients in cohort 2, including 21 patients assigned to LEM5 and 22 patients to LEM10, 34 (79.1%) patients transitioned to LEM at the end of the 2-week titration period (Table 53). A total of 9 (90.0%) patients in cohort 1 and 34 (79.1%) patients in cohort 2 entered the extension phase after a 2-week titration period.
Table 53: Patients Transitioning From ZOL to LEM at the End of the Titration Period — Study 312, FAS
Disposition | Cohort | Last dose | ||
|---|---|---|---|---|
Cohort 1 N = 10 | Cohort 2 N = 43 | LEM5 N = 21 | LEM10 N = 32 | |
Transition to lemborexant based on the last dose, n (%) | 9 (90.0) | 34 (79.1) | 16 (76.2) | 27 (84.4) |
Entered the extension phase,a n (%) | 9 (90.0) | 34 (79.1) | 16 (76.2) | 27 (84.4) |
FAS = full analysis set; LEM = lemborexant; LEM5 = lemborexant 5 mg; LEM10 = lemborexant 10 mg; ZOL = zolpidem tartrate.
aFor those patients who had completed the core trial and not yet started the extension, and for whom there was no indication that they would discontinue the trial, it is assumed that they entered the extension and hence successfully transitioned to lemborexant.
Source: Study 312 Clinical Study Report.64
Lemborexant Dose Adjustment at the End of the Titration Period
A total of 15 (48.4%) patients had an LEM dose increase from 5 mg to 10 mg at the end of the 2-week treatment phase, including 5 (50.0%) patients in cohort 1 and 10 (47.6%) patients in cohort 2A (Table 54). A total of 5 (22.7%) patients in cohort 2 had an LEM dose decrease from 10 mg to 5 mg at the end of the 2-week titration period. The dose change occurred in most patients on day 8 of the titration period.
Table 54: Patients With Lemborexant Dose Change at the End of the Titration Period — Study 312, FAS
Last dose | Cohort | Starting dose | ||
|---|---|---|---|---|
Cohort 1 N = 10 | Cohort 2 N = 43 | LEM5 N = 31 | LEM10 N = 22 | |
LEM5, n (%) | 5 (50.0) | 16 (37.2) | 16 (51.6) | 5 (22.7) |
LEM10, n (%) | 5 (50.0) | 27 (62.8) | 15 (48.4) | 17 (77.3) |
FAS = full analysis set; LEM5 = lemborexant 5 mg; LEM10 = lemborexant 10 mg.
Source: Study 312 Clinical Study Report.64
PGI-Insomnia Results
The summary of the patient’s impression of treatment using the PGI-Insomnia has been presented in Table 55. In the LEM5 group, 8 (38.1%) patients at baseline on ZOL and 9 (42.9%) patients at the end of the titration period of LEM reported a positive medication effect on sleep. In the LEM10 group, 15 (46.9%) patients reported a positive medication effect on sleep both at baseline and at the end of the titration period. At baseline and at the end of the titration period, a decrease in time to fall asleep was reported by 27 (50.9%) patients and 30 (58.2%) patients in the LEM5 group, respectively, and by 17 (53.1%) patients and 18 (56.3%) patients in the LEM10 group, respectively. At baseline and at the end of the titration period of LEM, 8 (38.1%) patients and 9 (42.9%) patients in the LEM5 group, respectively, and 13 (40.6%) patients and 12 (37.5%) patients in the LEM10 group, respectively, reported an increase in TST. At baseline on ZOL and at the end of the titration phase of LEM, 11 (52.4%) patients and 13 (40.6%) patients in the LEM5 group, respectively, and 13 (40.6%) patients and 16 (50.0%) patients in the LEM10 group, respectively, reported that the medication was “too weak.”
In cohort 1, 4 (40.0%) patients at baseline on ZOL and 5 (50.0%) patients at the end of the titration period of LEM reported a positive medication effect on sleep. In cohort 2, 19 (44.2%) patients reported a positive medication effect on sleep both at baseline and at the end of the titration period. At baseline and at the end of the titration period, a decrease in time to fall asleep was reported by 5 (50.0%) patients and 8 (80.0%) patients in cohort 1, respectively, and by 22 (51.2%) patients in cohort 2. At baseline and at the end of the titration period, 3 (30.0%) patients and 5 (50.0%) patients in cohort 1, respectively, and 18 (41.9%) patients and 16 (37.2%) patients in cohort 2, respectively, reported an increase in TST. At baseline on ZOL and at the end of the titration phase, 7 (70.0%) patients and 2 (20.0%) patients in cohort 1, respectively, and 17 (39.5%) patients and 21 (48.8%) patients in cohort 2, respectively, reported that the medication was “too weak.”
Table 55: Summary of PGI-Insomnia — Study 312, FAS
Parameter | Baseline on ZOL | End of titration of LEMa | ||
|---|---|---|---|---|
LEM5 | LEM10 | LEM5 | LEM10 | |
Cohort 1 | ||||
N | 5 | 5 | 5 | 5 |
Study medication helped or worsened sleep, n (%) | ||||
Positive effect | 2 (40) | 2 (40) | 3 (60) | 3 (60) |
Neutral effect | 2 (40) | 1 (20) | 1 (20) | 2 (40) |
Negative effect | 1 (20) | 2 (40) | 1 (20) | 0 |
Study medication decreased or increased time to fall asleep, n (%) | ||||
Positive effect | 3 (60) | 2 (40) | 4 (80) | 4 (80) |
Neutral effect | 2 (40) | 2 (40) | 0 | 1 (20) |
Negative effect | 0 | 1 (20) | 1 (20) | 0 |
Study medication increased or decreased total sleep time, n (%) | ||||
Positive effect | 2 (40) | 1 (20) | 2 (40) | 3 (60) |
Neutral effect | 2 (40) | 2 (40) | 1 (20) | 2 (40) |
Negative effect | 1 (20) | 2 (40) | 2 (40) | 0 |
Appropriateness of medication strength, n (%) | ||||
Just right | 2 (40) | 1 (20) | 4 (80) | 4 (80) |
Too strong | 0 | 0 | 0 | 0 |
Too weak | 3 (60) | 4 (80) | 1 (20) | 1 (20) |
Cohort 2 | ||||
N | 16 | 27 | 16 | 27 |
Study medication helped or worsened sleep, n (%) | ||||
Positive effect | 6 (37.5) | 13 (48.1) | 7 (43.7) | 12 (44.4) |
Neutral effect | 4 (25.0) | 8 (29.6) | 7 (43.7) | 9 (33.3) |
Negative effect | 6 (37.5) | 6 (22.3) | 2 (12.4) | 6 (22.3) |
Study medication decreased or increased time to fall asleep, n (%) | ||||
Positive effect | 7 (43.7) | 15 (55.6) | 8 (50.0) | 14 (51.8) |
Neutral effect | 3 (18.8) | 6 (22.2) | 4 (25.0) | 8 (29.6) |
Negative effect | 6 (37.5) | 6 (22.2) | 4 (25.0) | 5 (18.6) |
Study medication increased or decreased total sleep time, n (%) | ||||
Positive effect | 6 (37.4) | 12 (44.4) | 7 (43.7) | 9 (24.3) |
Neutral effect | 5 (31.2) | 8 (29.6) | 7 (43.7) | 12 (44.4) |
Negative effect | 5 (31.2) | 7 (26.0) | 2 (12.6) | 6 (31.3) |
Appropriateness of medication strength, n (%) | ||||
Just right | 8 (50.0) | 18 (66.7) | 9 (56.3) | 10 (37.0) |
Too strong | 0 | 0 | 1 (6.2) | 2 (7.5) |
Too weak | 8 (50.0) | 9 (33.3) | 6 (37.5) | 15 (55.5) |
FAS = full analysis set; LEM = lemborexant; LEM5 = lemborexant 5 mg; LEM10 = lemborexant 10 mg; PGI-Insomnia = Patient Global Impression–Insomnia; ZOL = zolpidem tartrate.
a“End of titration period” was defined as the last dose taken for the period.
Source: Study 312 Clinical Study Report.64
ISI Results
The summary of the ISI results has been presented in Table 56. In the overall trial population, the mean ISI total score was 14.1 (SD = 5.99) at baseline on ZOL and 9.5 (SD = 5.93) at the end of the titration period of LEM, with a mean change of –4.6 (SD = 6.26). In the LEM5 and LEM10 groups, the mean changes from baseline in the total ISI score were –4.8 (SD = 7.99) and –4.5 (SD = 4.96), respectively. In cohort 1 and cohort 2, the mean changes from baseline in the total ISI score were –7.1 (SD = 8.09) and –4.0 (SD = 5.72), respectively.
In the overall trial population, the mean quality of sleep score was 5.25 (SD = 1.49) at baseline and 5.07 (SD = 1.67) at the end of the titration period, for a mean change of –0.19 (SD = 0.92). In the LEM5 and LEM10 groups, the mean changes from baseline in quality of sleep score were 0.05 (SD = 2.20) and –0.34 (SD = 1.74), respectively. In cohort 1 and cohort 2, the mean changes from baseline in quality of sleep score were 0.22 (SD = 1.15) and –0.28 (SD = 2.06), respectively.
Actigraphy-Derived Sleep Measures
The summary of sleep measures, derived from actigraphy, has been summarized in Table 56. In the overall trial population, at baseline and at the end of the titration period, the mean sleep efficiency scores were 79.03% (SD = 85.4%) and 80.17% (SD = 8.49%), respectively; the mean WASO scores were 80.90 (SD = 33.23) minutes and 83.92 (SD = 35.44) minutes, respectively; and the mean TST scores were 403.44 (SD = 62.07) minutes and 412.11 (SD = 60.17) minutes, respectively. The mean number of wake bouts during sleep was 5.16 (SD = 2.43) at baseline in ZOL and 4.60 (SD = 2.42) at the end of the titration period of LEM, while the mean duration of sleep bouts was 17.09 (SD = 2.42) minutes at baseline and 17.11 (SD = 2.20) minutes at the end of the titration period.
At baseline and at the end of the titration period, the mean sleep efficiency scores for cohort 1 were 78.46% (SD = 6.37%) and 78.08% (SD = 6.82%), respectively, and for cohort 2 were 79.16% (SD = 9.02%) and 80.65% (SD = 8.83%), respectively, while the mean WASO scores for cohort 1 were 79.71 (SD = 23.32) minutes and 90.42 (SD = 24.10) minutes, respectively, and for cohort 2 were 81.16 (SD = 35.32) minutes and 82.42 (SD = 37.67) minutes, respectively. At baseline and at the end of the titration period, the mean TST for cohort 1 were 404.19 (SD = 47.56) minutes and 404.74 (SD = 65.07) minutes, respectively, and for cohort 2 were 403.27 (SD = 65.40) minutes and 413.81 (SD = 59.76) minutes, respectively. At baseline and at the end of the titration period, the mean number of wake bouts during sleep for cohort 1 were 5.80 (SD = 2.45) and 5.02 (SD = 2.43), respectively, and for cohort 2 were 5.22 (SD = 1.84) and 4.45 (SD = 2.53), respectively, while the mean duration of sleep bouts for cohort 1 were 16.95 (SD = 2.26) minutes and 17.12 (SD = 2.48) minutes, respectively, and for cohort 2 were 17.00 (SD = 1.51) minutes and 17.13 (SD = 2.35) minutes, respectively.
Table 56: Summary of Sleep Measures — Study 312, FAS
Parameter | Cohort | Last dose | ||
|---|---|---|---|---|
Cohort 1 N = 10 | Cohort 2 N = 43 | LEM5 N = 21 | LEM10 N = 22 | |
ISI (total score) | ||||
Baseline, mean (SD) | 18.0 (4.03) | 13.2 (6.05) | 14.3 (6.04) | 14.0 (6.06) |
End of titration, mean (SD) | 10.9 (6.67) | 9.2 (5.79) | 9.6 (6.81) | 9.5 (5.40) |
Change from baseline, mean (SD) | –7.1 (8.09) | –4.0 (5.72) | –4.8 (7.99) | –4.5 (4.96) |
Quality of sleep | ||||
Baseline, mean (SD) | 5.09 (1.02) | 5.29 (1.60) | 5.20 (1.58) | 5.25 (1.50) |
End of titration, mean (SD) | 5.31 (1.43) | 5.01 (1.73) | 5.39 (1.72) | 4.86 (1.62) |
Change from baseline, mean (SD) | 0.22 (1.15) | –0.28 (2.06) | 0.05 (2.20) | –0.34 (1.74) |
Actigraphy-derived sleep measures | ||||
Sleep efficiency (%) | ||||
Baseline, mean (SD) | 78.46 (6.37) | 79.16 (9.02) | 80.54 (6.85) | 78.08 (9.45) |
End of titration, mean (SD) | 78.08 (6.82) | 80.65 (8.83) | 81.58 (6.68) | 79.24 (9.49) |
WASO, minutes | ||||
Baseline, mean (SD) | 79.71 (23.32) | 81.16 (35.32) | 78.31 (29.86) | 82.53 (35.60) |
End of titration, mean (SD) | 90.42 (24.10) | 82.42 (37.67) | 79.80 (28.96) | 86.61 (39.37) |
TST, minutes | ||||
Baseline, mean (SD) | 404.19 (47.56) | 403.27 (65.40) | 416.125 (41.23) | 395.39 (71.75) |
End of titration, mean (SD) | 404.74 (65.07) | 413.81 (59.76) | 421.45 (55.74) | 405.99 (63.11) |
Number of wake bouts, n | ||||
Baseline, mean (SD) | 5.80 (2.45) | 5.02 (2.43) | 4.70 (2.16) | 5.45 (2.58) |
End of titration, mean (SD) | 5.22 (1.84) | 4.45 (2.53) | 3.91 (1.66) | 5.05 (2.74) |
Duration of sleep bouts, minutes | ||||
Baseline, mean (SD) | 16.95 (2.26) | 17.12 (2.48) | 17.31 (2.12) | 16.95 (2.62) |
End of titration, mean (SD) | 17.00 (1.51) | 17.13 (2.35) | 17.07 (2.10) | 17.13 (2.30) |
FAS = full analysis set; ISI = Insomnia Severity Index; LEM5 = lemborexant 5 mg; LEM10 = lemborexant 10 mg; SD = standard deviation; TST = total sleep time; WASO = wake after sleep onset.
Note: The “end of titration” period is defined as the last dose taken for the period.
Source: Study 312 Clinical Study Report.64
Harms
Safety results from study 312 have been summarized in Table 57. Of the 53 patients enrolled in the core trial, 20 (37.7%) patients experienced at least 1 TEAE, including 5 (13.9%) patients while taking LEM5 and 15 (40.5%) patients while taking LEM10. A total of 4 (40.0%) patients in cohort 1 and 16 (37.2%) patients in cohort 2 experienced at least 1 TEAE. In the overall trial population, the percentage of patients who withdrew from treatment due to an AE was 13%. TEAEs leading to LEM dose adjustment occurred in 1 (10%) patient in cohort 1 and 10 (23.3%) patients in cohort 2. The most common TEAEs (more than 5% of patients) were abnormal dreams (7.5%) and somnolence (7.5%). Of the 4 patients, 1 patient experienced treatment-emergent somnolence while taking LEM5, and 3 patients experienced treatment-emergent somnolence while taking LEM10. All 3 patients who experienced treatment-emergent abnormal dreams were taking LEM10. No deaths or severe AEs leading to study drug discontinuation were reported in the trial.
Table 57: Summary of Harms — Study 312
Parameter | Cohort | On-treatment dose | ||
|---|---|---|---|---|
Cohort 1 N = 10 | Cohort 2 N = 43 | LEM5 N = 36 | LEM10 N = 37 | |
TEAEs, n (%) | 4 (40.0) | 16 (37.2) | 5 (13.9) | 15 (40.5) |
TEAEs leading to study drug dose adjustment, n (%) | 1 (10.0) | 10 (23.3) | 2 (5.6) | 9 (24.3) |
TEAEs leading to study drug withdrawal, n (%) | 1 (10.0) | 6 (14.0) | 2 (5.6) | 5 (13.5) |
TEAEs leading to study drug dose reduction, n (%) | 0 | 5 (11.6) | 0 | 5 (13.5) |
Other TEAEs associated with special situations, n (%) | 2 (20.0) | 3 (7.0) | 3 (8.3) | 2 (5.4) |
Overdose, n (%) | 1 (10.0) | 3 (7.0) | 3 (8.3) | 1 (2.7) |
Misuse, n (%) | 1 (10.0) | 0 | 0 | 1 (2.7) |
Abuse, n (%) | 0 | 1 (2.3) | 1 (2.8) | 0 |
Medication error, n (%) | 0 | 1 (2.3) | 1 (2.8) | 0 |
TEAEs by MedDRA preferred term (> 5%) | ||||
Abnormal dreams, n (%) | 0 | 4 (9.3) | 0 | 4 (10.8) |
Somnolence, n (%) | 0 | 4 (9.3) | 1 (2.8) | 3 (8.1) |
Accidental overdose, n (%) | 0 | 2 (4.7) | 2 (5.6) | 0 |
LEM5 = lemborexant 5 mg; LEM10 = lemborexant 10 mg; MedDRA = Medical Dictionary for Regulatory Activities; TEAE = treatment-emergent adverse event.
Note: LEM5 and LEM10 are on-treatment doses (i.e., dose taken at the time of adverse event).
aA TEAE is defined as an adverse event that started on or after the date of the first dose of the study drug, up to 14 days after the last dose of the study drug. This includes TEAEs considered by the investigator to be related to the study drug or TEAEs with missing causality.
Source: Study 312 Clinical Study Report.64
Critical Appraisal
Internal Validity
The open-label administration of the study drug could introduce bias as knowledge of the treatment may lead patients and investigators to overestimate subjective benefits and harms. All efficacy end points were descriptive and there was no formal statistical testing, so it is not possible to draw definitive conclusions regarding changes from baseline, or for differences across cohorts or LEM doses. The transition to LEM was defined as patients who (1) continued to receive LEM at the end of the 2-week titration period; (2) had entered the extension phase or had chosen not to enter the extension phase for reasons not related to LEM; and (3) had not started the extension, but there was no indication of these patients having discontinued the trial. This may lead to an overestimation of the number of patients who transitioned to LEM from ZOL. The subjective nature of some trial end points, including the PGI-Insomnia and ISI, may have led to patients overestimating or underestimating sleep changes with a transition from ZOL to LEM. According to the clinical expert consulted by CADTH, data assessed during the titration period of LEM may underestimate the potential benefits and overestimate the potential AEs, since withdrawal symptoms and rebound insomnia can occur for 2 months to 3 months during the transition from ZOL to a new treatment, including LEM.
External Validity
Study 312 enrolled patients from US sites only, and they were predominantly white (approximately 77%). Since ZOL is not a publicly funded medication in Canada, the trial results cannot be fully generalized to the Canadian population. This trial did not provide information on transitioning to LEM from other drugs that may commonly be used for insomnia in Canada. Although the lower dose of ZOL (6.5 mg) is recommended for females and older adults, the majority of patients enrolled in the screening phase were prescribed ZOL at higher doses: 10 mg in cohort 1 and 12.5 mg in cohort 2. The small sample size further limits generalizability of this trial to the Canadian population. There were nearly 50% screening failures, which further reduces the generalizability of the results (i.e., patients enrolled in study 312 may not be reflective of the average patient transitioning from ZOL to LEM).
Discussion
Summary of Available Evidence
Two DB, phase III, PBO-controlled RCTs (SUNRISE 1 and SUNRISE 2) were pivotal trials and included in the systematic review. SUNRISE 1 (N = 1,006) was designed to assess the safety and efficacy of LEM5 and LEM10 for 30 days in females who were 55 years or older and males who were 65 years or older, all of whom had insomnia disorder according to the DSM-5 criteria. Patients had a mean age of 63.9 (SD = 6.81) years and 86.4% were female. Comparators included ZOL and appearance-matched PBOs for all active compounds. The primary outcome was LPS and key secondary outcomes were WASO, WASO2H, and sleep efficiency as measured by PSG. SUNRISE 2 (N = 971) was designed to assess the long-term safety and efficacy of LEM5 and LEM10 for up to 12 months in adults 18 years or older who had insomnia disorder according to the DSM-5 criteria. Patients had a mean age of 54.5 (SD = 13.80) years and 68.2% were female. The first 6 months of SUNRISE 2 consisted of 3 treatment groups: LEM5, LEM10, and PBO. For the next 6 months of the trial, patients who were randomized to the PBO were rerandomized to active treatment (i.e., LEM5 or LEM10) for the remainder of the trial. The primary outcome was sSOL and the key secondary outcomes were sWASO and subjective sleep efficiency as recorded in the sleep diary. Other secondary and exploratory outcomes in either study that were important to the CADTH review included patient-reported outcomes such as the EQ-5D-3L, ISI, FSS, PGI-Insomnia, and quality of sleep questionnaires. Harms and notable harms (identified in the CADTH systematic review protocol) were assessed.
Two NMAs were included in this CADTH report. NMA 1, the sponsor-submitted systematic review, evaluated the efficacy and safety of LEM in patients with insomnia by comparing it to relevant drugs in Canadian public formularies (zopiclone, temazepam, triazolam, flurazepam, and nitrazepam) with respect to clinical end points evaluated objectively (by PSG) or subjectively (patient-reported). The objective clinical end points included LPS, WASO, sleep efficiency, and TST, with subjective assessment in these same end points. Harms related to the use of LEM were also evaluated in an NMA, including treatment discontinuations, somnolence, dizziness, headache, and in a posthoc analysis, the risk of falls, which were assessed using Bucher ITCs. NMA 2, published by McElroy et al. (2021), was a comparative efficacy analysis aimed at evaluating the efficacy and safety of LEM against other insomnia treatments through a systematic literature review and NMA that included RCTs of drugs used in adults with primary insomnia; not all of these drugs are reimbursed in Canada. The drugs included in this NMA that were of interest to the CADTH review were LEM, benzodiazepines, Z-drugs, and trazodone.
Study 312 (N = 53) was an open-label, phase IIIb trial that provided information about the next-dose transition from ZOL to LEM and was summarized and critically appraised. Eligible patients were adults taking ZOL for insomnia who did not have obstructive sleep apnea or other sleep-related behaviours, or were taking ZOL-IR greater than 10 mg or ZOL-ER greater than 12.5 mg. Randomized patients had a mean age of 59 (SD = 12.21) years and 66.0% were female. The primary outcome was the proportion of patients who successfully transitioned from ZOL to LEM10 or LEM5 over a 2-week treatment phase (titration period). Patients who completed the treatment phase could continue in an extension phase for up to 12 weeks. Secondary outcomes included the proportion of patients who changed their LEM dose, PGI-Insomnia, and safety outcomes. Harms were also assessed.
Interpretation of Results
Efficacy
The SUNRISE 1 and SUNRISE 2 trials appeared to have appropriate methods for blinding (i.e., appearance-matched PBOs for all active drugs), allocation concealment, randomization with stratification to minimize bias, and adequate power for the primary and secondary outcomes. All primary and key secondary efficacy outcomes compared to PBO (except WASO2H) in SUNRISE 1 and SUNRISE 2 and WASO2H when compared to ZOL in SUNRISE 1 were controlled for type I error. Treatment differences for objective PSG outcomes (in SUNRISE 1) reached the suggested thresholds for clinically important differences relative to PBO identified from the literature. However, nearly all these outcomes had variability in the results (i.e., mean changes from baseline with large SDs and LSM treatment differences with wide CIs) and subjective sleep diary outcomes did not reach the suggested thresholds for clinically important differences compared to PBO, which contribute to the uncertainty of how clinically meaningful the results are. SUNRISE 1 used ZOL as an active comparator and the comparisons of LEM10 and LEM5 versus ZOL for WASO2H were the only outcomes adjusted for multiplicity with the active comparator. Definitive conclusions could not be drawn for other results comparing LEM to ZOL due to the lack of adjustment for multiplicity. Other key limitations of the pivotal studies include the large proportion of screening failures (more than 50% in either trial); missing data, particularly for long-term outcomes; the exclusion of many comorbid conditions (according to the exclusion criteria for BDI-2, BAI, and AHI scores); the use of ZOL as a comparator; and the subjective nature of most outcomes leading to uncertainty in the results. Thus, it is difficult to make strong conclusions and generalize to all patients with insomnia who may be treated in a Canadian setting.
The results from the indirect evidence from both NMAs have uncertainty due to the risk of bias (e.g., unclear randomization, allocation concealment, baseline imbalances within the included trials), heterogeneity in the pairwise comparisons (for NMA 1), and suspected publication bias. The network of NMA 1 was sparse without any direct evidence for active comparators; thus, consistency could not be ascertained. Similarly, in NMA 2, there were few closed loops; thus, there was little evidence for consistency. In both NMAs, the plausibility of the transitivity assumption was uncertain because the description of the methodological and clinical characteristics of the trials were limited. Conclusions could not be drawn for many outcome comparisons due to imprecision in both NMAs.
Study 312 had an open-label design, small sample size, short study duration, 50% screening failures, and subjective secondary end points, and chose ZOL as the previous treatment to transition from (rather than other treatments that may have been more relevant to Canadian clinical practice), which prevent firm conclusions from being drawn and limit generalizability to the Canadian population with insomnia.
Health-Related Quality of Life
For both the SUNRISE 1 and SUNRISE 2 studies, most patients reported no problems and few patients reported extreme problems on the 5 dimensions of the EQ-5D-3L at all time points of the studies. The EQ-5D-3L is an outcome that could be important to patients and their care providers, but since the analysis of HRQoL was not adjusted for multiple comparisons, there is uncertainty in conclusions about the effect of LEM on HRQoL versus relevant comparators. The clinical expert stated that it would be difficult to be sure if the changes were clinically meaningful, particularly with a generic HRQoL instrument and no MID identified for patients with insomnia. HRQoL was not assessed in the NMAs or in study 312.
Symptom Severity
Both LEM doses appeared to result in a larger improvement in ISI item 4 to item 7 and FSS compared with PBO, though there is uncertainty in this conclusion because the analysis was not adjusted for multiple comparisons. Input that CADTH received from patient groups described sleep problems negatively impacting next-day function; social and physical activities; work, school or home responsibilities; mental health; and quality of life as being major issues. These issues were mostly echoed by the input received from clinician groups and it was suggested that improved daytime function and patient perception of sleep changes were more important than sleep measures. In general, the uncertainty resulting from a lack of control for multiple comparisons and the unclear benefit of either dose of LEM over comparators indicates that the needs that are unmet by current treatments have not been adequately addressed by the patient-reported questionnaires used in the SUNRISE 1 and SUNRISE 2 studies.
In general, the proportion of positive responses on the PGI-Insomnia appeared similar between the LEM10, LEM5, and ZOL groups, and appeared to be greater than those from the PBO group. There were no adjustments for multiple comparisons and no MID was identified for this instrument, which makes it challenging to conclude if the differences observed between treatments were clinically meaningful. The clinical expert suggested that while it is likely that patients believed the medication was helping, they may also have had high expectations for sleep improvements that the medication was unable to provide. The expert further explained that sleep naturally degrades with age, which could be another factor that must be considered when setting expectations.
Sleep Latency and Sleep Onset
LEM10 and LEM5 were found to be superior to PBO in both trials and to ZOL in SUNRISE 1 for the primary outcomes (i.e., LPS and sSOL). Treatment differences at days 29 to 30 in SUNRISE 1 and at month 6 in SUNRISE 2 appeared similar between LEM10 and LEM5. Compared to PBO, both LEM groups had an LPS median change from baseline value greater than the suggested threshold for a clinically important effect of 10 minutes; however, there was substantial variability in the extent of the response for individual patients. Compared to PBO, neither LEM group sSOL median change from baseline reached the suggested threshold for a clinically important effect of 20 minutes at month 6 in SUNRISE 2. This suggested, on average, that patients’ perception of their improvement in sleep onset was not clinically meaningful. The SDs and IQRs were large for the mean and median changes in both studies, indicating variability in the responses, which should be taken into account when considering how meaningful the results are. The sSOL results of SUNRISE 1 were other secondary outcomes and supported the primary outcome. Long-term results in SUNRISE 2 suggested that the improvement was sustained up to month 12. Limitations with both subgroup and responder analyses, as described earlier, prevented firm conclusions from being drawn. Input CADTH received from clinician groups stated that the 2 main goals of treatment are improving sleep continuity (sleep onset, sleep maintenance, and TST) and daytime function. It was also emphasized that addressing only sleep outcomes is not sufficient and some clinicians stated that daytime functioning was a more important outcome to evaluate. Likewise, the clinical expert consulted by CADTH described insomnia as largely being a subjective and individualized issue and highlighted the importance of subjective measures that capture the patient’s opinion of a treatment effect. Moreover, the expert suggested objective PSG measures may be less clinically meaningful in practice, given that they are not commonly used for assessing insomnia in Canadian clinics and readings can be impacted by the first-night effect observed in sleep labs, as discussed earlier.
Indirect evidence from NMA 1 suggests that LEM5 is superior to triazolam 0.5 mg in LPS by objective measures, and superior to LEM10 only in sSOL end points. For the other comparisons, the evidence was uncertain or absent (i.e., compared with zopiclone, temazepam, flurazepam, and triazolam 0.125 mg). Indirect evidence for LEM10 suggests that it is superior to triazolam 0.5 mg for objectively measured LPS, but no different when compared to LEM5. For the other comparisons, the evidence was very uncertain or absent (i.e., against zopiclone, temazepam, flurazepam, triazolam 0.125 mg, and triazolam 0.25 mg). NMA 2, however, suggests that LEM is associated with better LPS against triazolam. These findings need to be interpreted in light of limitations of the NMAs, as previously described.
Sleep Maintenance
The key secondary outcomes for the SUNRISE 1 and SUNRISE 2 studies were WASO, WASO2H, and sWASO. LEM10 and LEM5 were favoured over PBO for WASO in SUNRISE 1 and sWASO in SUNRISE 2. Results favoured LEM10 and LEM5 over ZOL for WASO2H in SUNRISE 1, indicating LEM improved sleep maintenance in the second half of the night compared to ZOL, which the sponsor stated has a loss of effect on sleep maintenance.17 Treatment differences for sleep maintenance outcomes at days 29 to 30 in SUNRISE 1 and at month 6 in SUNRISE 2 were similar between LEM10 and LEM5. Compared to PBO, both LEM groups had mean change from baseline values greater than the suggested threshold for a clinically important effect of 20 minutes for WASO, indicating a clinically meaningful difference was observed. Compared to PBO, neither LEM group had mean changes from baseline that reached the suggested threshold for a clinically important effect of 30 minutes for sWASO at month 6 in SUNRISE 2. These results indicated that, on average, patients’ perception of their improvement in sleep maintenance may not be clinically meaningful. No MID or threshold for a clinically important difference was identified for WASO2H and it is uncertain how clinically meaningful the improvement in sleep for the second half of the night was. According to the clinical expert consulted by CADTH, treatments that help a patient maintain sleep in the second half of the night are particularly important since most hypnotics do not address this. The sWASO results of SUNRISE 1 were other secondary outcomes and supported the primary outcome. Long-term results in SUNRISE 2 suggested that the improvement was sustained. Limitations with responder analyses, as described earlier, prevent firm conclusions from being drawn.
The indirect comparison of WASO from NMA 1 had wide CrIs, suggesting a difference in effects between LEM and triazolam or PBO, while NMA 2 suggested that LEM was superior to PBO and ZOL in the WASO end point. No evidence was available for other relevant comparators.
Total Sleep Time
For both the SUNRISE 1 and SUNRISE 2 studies, on average, patients in the LEM10 group or LEM5 group appeared to experience greater improvements in TST and sTST compared to PBO, and when compared to ZOL in SUNRISE 1. The results for these outcomes are uncertain because the analyses were not adjusted for multiple comparisons, so there is an increased risk of false-positive conclusions. Treatment differences appeared to be similar between LEM10 and LEM5 versus comparators. The sTST results of SUNRISE 1 were other secondary outcomes and supported the primary outcome. Long-term results in SUNRISE 2 suggested that the improvement was sustained.
In NMA 1, LEM was only compared to PBO for TST, with no difference detected due to wide CrIs. In NMA 2, LEM was superior to PBO in TST, but no difference was detected against other comparators (including zopiclone, ZOL, or triazolam) due to imprecision in the effect estimates.
Sleep Efficiency
The key secondary outcomes for the SUNRISE 1 and SUNRISE 2 studies were sleep efficiency and subjective sleep efficiency, respectively. LEM10 and LEM5 were favoured over PBO in both trials. Treatment differences for sleep efficiency outcomes were similar between LEM10 and LEM5 compared to PBO at days 29 to 30 in SUNRISE 1 and at month 6 in SUNRISE 2. Compared to PBO, both LEM groups had mean change from baseline values greater than the suggested threshold for a clinically important effect of 5% for objectively measured sleep efficiency, suggesting a clinically meaningful difference was observed. Compared to PBO, neither LEM group mean change from baseline reached the suggested threshold for a clinically important effect of 10% for subjective sleep efficiency at month 6 in SUNRISE 2. This suggested, on average, that patients’ perception of the change in their time spent asleep per time spent in bed may not have been clinically meaningful. The clinical expert suggested that small improvements in efficiency, like those observed in the studies, may not be meaningful to patients until the difference is much larger. The subjective sleep efficiency results of SUNRISE 1 were other secondary outcomes and supported the primary outcome. Long-term results in SUNRISE 2 suggested that the improvement was sustained.
From the indirect evidence, NMA 1 suggested that LEM5 and LEM10 were superior to PBO and triazolam for sleep efficiency but with wide CrIs for the comparison against flurazepam. This was in contrast to NMA 2, which showed only superiority to PBO, but not against triazolam or other relevant comparators due to wide CrIs.
Quality of Sleep
For both the SUNRISE 1 and SUNRISE 2 studies, on average, patients in the LEM10 group or the LEM5 group appeared to rate their quality of sleep as more improved compared to PBO, but not when compared to ZOL in SUNRISE 1. Treatment differences appeared similar between LEM10 and LEM5. Long-term results in SUNRISE 2 suggested that the improvements were sustained. Sleep quality was an exploratory outcome in both trials and conclusions are limited because the analyses were not adjusted for multiple comparisons. Sleep improvements based on PSG and sleep diary outcomes that patients on LEM experienced did not appear to be reflected in the results from the patient-reported questionnaires. The CADTH review team and clinical expert agreed that the minimal change in patients’ perception of their overall sleep quality could impact the interpretation of the other objective and subjective outcomes if patients did not feel that their quality of sleep was greatly improved with treatment. The expert suggested the discrepancy could be due to patients having expectations for improvement that could not be fulfilled by the medication and that sleep improvement may be limited due to the natural deterioration of sleep that occurs with age. The expert also suggested that, in practice, a qualitative response (e.g., patients stating that their sleep has improved) is more meaningful than a numerical change or MID on a scale.
Input provided by clinician groups indicated that the clinical trial data generally aligned with their experiences with LEM in practice. Overall, the clinical expert believed LEM showed efficacy for some patients from their perspective, but it does not completely solve their insomnia issues or necessarily meet the expectations of all patients.
Regarding the indirect evidence, quality of sleep was evaluated only in NMA 2, which showed that LEM was superior to PBO and eszopiclone but not against the other relevant comparators.
Harms
In general, the AEs, SAEs, and most notable harms in the SUNRISE 1 and SUNRISE 2 studies were not considered to be major concerns, according to the clinical expert consulted for this review. The most frequently reported AEs (headache, somnolence, and nasopharyngitis) were the same between the studies and SAEs were rare. The CADTH review team noted the numerically larger proportion of withdrawals due to AEs from treatment in the LEM10 group compared to the others in SUNRISE 2, which raised concerns with the clinical expert when considering treatment of older adult patients and increasing a patient’s dose from 5 mg to 10 mg.
The harms identified as important by patient and clinician groups’ input were partially addressed in the pivotal studies, though there are limitations to the conclusions that can be drawn from the data. Per the clinical expert and input from clinician groups, benzodiazepines and nonbenzodiazepines are associated with the risk of falls and daytime impairment, which have subsequent consequences if patients have fractures, broken bones, or workplace and vehicular accidents. In the pivotal trials, the frequency of falls was generally low and postural instability did not appear to be greatly affected among patients who received LEM10 or LEM5 for 30 days. No treatment groups reached the 7-unit threshold considered clinically meaningful for increased body sway, but comparisons were not controlled for type I error; therefore, firm conclusions cannot be drawn from these data. In addition, no conclusions regarding long-term effects can be drawn from these data. Both the patient and clinician groups raised concerns of medications causing daytime impairment and next-day effects such as impaired attention. Although the results from the CPAB for attention did not raise concerns with the clinical expert, it was noted there may be extra consideration made regarding treatment for patients with preexisting cognitive impairment issues. According to the clinical expert and clinician groups, rebound insomnia associated with stopping treatment is a major concern with currently available medications. Although rates were generally low among patients receiving LEM10 or LEM5 in both studies (less than 25%), it did occur during the follow-up period. Furthermore, rebound insomnia was assessed for only 2 weeks after stopping treatment, which may not be enough follow-up time to capture the total duration of the issue, per the clinical expert. In addition, there was a notable amount of missing data for this outcome in the SUNRISE 2 trial, which raises uncertainty in the long term results for rebound insomnia. The expert indicated that the possibility of somnolence and rebound insomnia would be important to discuss with any patients taking LEM. Concerns over dependence on medication and withdrawal when stopping treatment were noted in both the patient and clinician group inputs. Patients reporting withdrawal symptoms during the follow-up period were generally low (less than 20% of patients), though there was some amount of missing data for all treatment groups, especially in SUNRISE 2.
The clinical expert and clinician group input emphasized the improved safety profile compared to current medications used for insomnia. Further, the clinical expert and clinician groups indicated that, after CBT-I, LEM could be used as a first-line pharmacotherapy due to its overall efficacy, unique mechanism of action, and generally low risk of AEs compared to other medications for insomnia. The clinical expert noted that its potential use as a first-line treatment may be limited by contraindications and significant side effects that individual patients may experience. According to the expert, if efficacy were comparable between LEM and currently available drug treatments, the low risk of AEs for the former is likely to make it the preferred treatment choice in practice, though currently, there is a lack of direct evidence for most relevant comparators and the indirect evidence has limitations. Gaps in the evidence include the safe use of LEM in patients with comorbid conditions who were excluded from the studies (e.g., sleep-related breathing disorder, depression, anxiety based on AHI, BDI-2, and BAI scores) as well as the use of LEM with other medications. Overall, the clinical expert indicated that LEM demonstrated a minor AE profile based on the data available to date and, considering the limitations discussed, there were no major issues with generalizing the safety results to the adult Canadian population with insomnia.
The sponsor-submitted NMA 1 suggested that LEM10 had an increased risk of drug discontinuation when compared to LEM5 and PBO, but not against the other comparators. In the end point of somnolence, LEM5 was superior to LEM10, but had higher odds of somnolence compared to triazolam 0.25 mg and zopiclone. There was no difference in the rest of the comparators. LEM10 had a higher risk of somnolence against LEM5, triazolam 0.25 mg, zopiclone, and PBO. For the end point of dizziness, there were no differences detected between any of the comparators of LEM5 or LEM10.
In an additional Bucher ITC of studies reporting falls, using LEM5 as the reference, no difference was detected when compared to triazolam, flurazepam, lorazepam, trazodone, benzodiazepines, and Z-drugs, though there is some uncertainty in the conclusions due to imprecision of the effects. When LEM10 was used as the reference, the risk of falls was likely higher with triazolam when compared to LEM10, but the size of the effect is uncertain due to serious limitations with the analysis. When benzodiazepines were compared to LEM10, the risk of falls was also likely higher with the former drugs, though it is difficult to draw conclusions due to substantial imprecision. When trazodone was compared to LEM10, the odds of falls were greater across all patient age groups. Due to the limitations with the ITCs, there is uncertainty with the findings from the indirect evidence.
In NMA 2, there was no conclusive evidence of increased or decreased odds for presenting SAEs for patients receiving LEM when compared to relevant comparators, mainly due to wide CrIs. Similarly, there was no conclusive evidence for the odds of withdrawals due to AEs or in the odds of falls. LEM was associated with lower odds of dizziness compared with ZOL-IR, ZOL-ER, and eszopiclone. LEM, however, increased the odds of somnolence when compared to PBO, ZOL, and eszopiclone. These findings should be interpreted with consideration for the limitations of the NMA, as previously described.
In study 312, TEAEs were reported with similar frequency between cohort 1 (previous intermittent or mixed use of ZOL) and cohort 2 (previous frequent use of ZOL). TEAEs leading to dose adjustment, withdrawal, and dose reduction were numerically higher in cohort 2. Based on the on-treatment dose, TEAEs were more frequently reported in the LEM10 group compared to the LEM5 group. Likewise, TEAEs leading to change in study drug dose were more frequent in the LEM10 group. The small sample size, short study duration, and allowance for a dose change between 5 mg and 10 mg make it difficult to draw meaningful conclusions about safety while transitioning from ZOL to LEM. There was no evidence for the safety of transitioning from other drugs that may be prescribed for insomnia.
Conclusions
Both LEM10 and LEM5 demonstrated statistically significant improvements in sleep onset, sleep maintenance, and sleep efficiency among adults with insomnia relative to PBO in the SUNRISE 1 and SUNRISE 2 trials. In SUNRISE 1, all primary and key secondary outcomes were for objective PSG measures and were clinically meaningful based on suggested thresholds for a clinically important effect identified from the literature, except for WASO2H, which did not have an MID or threshold identified. In SUNRISE 2, all primary and key secondary outcomes were for subjective sleep diary measures, and none reached the suggested thresholds for a clinically important effect identified from the literature. Numerical differences in ISI item 4 to item 7 and FSS indicated a benefit from treatment with LEM over PBO, but due to the lack of adjustment for multiple comparisons and no established MID for ISI item 4 to item 7 and FSS, conclusions could not be drawn from these outcomes. Other patient-reported outcomes such as the EQ-5D-3L, PGI-Insomnia, and quality of sleep scale were exploratory, were not controlled for multiplicity, and did not have MIDs for populations with insomnia; therefore, no conclusions could be drawn regarding whether treatment with LEM conferred a benefit for these outcomes. The clinical expert consulted for this review emphasized the importance of subjective outcomes and how patients perceive changes in their sleep. However, the sleep improvements based on PSG and sleep diary outcomes observed in the studies did not appear to be reflected in the results from the patient-reported questionnaires (i.e., ISI, FSS, and perceived sleep quality). It is uncertain if the differences in treatment effect observed in SUNRISE 1 and SUNRISE 2 would be experienced by and be meaningful to all patients who could be treated with LEM.
There did not appear to be a clear difference in efficacy between LEM10 and LEM5, although differences in efficacy between the 2 doses was not tested statistically in the trials. The product monograph’s recommendation to start with LEM5 and the higher rates of somnolence and treatment discontinuations for LEM10 would be considerations when prescribing or increasing a patient’s dose. Overall, the clinical expert indicated that LEM demonstrated a minor harms profile with few SAEs, low rates of withdrawals from treatment due to AEs, and no deaths. Patients with specific comorbid conditions such as sleep apnea, anxiety, and depression were excluded from the studies based on the exclusion criteria for AHI, BAI, and BDI-2 scores; further research showing adequate efficacy and safety is needed to inform broader treatment with LEM. Indirect evidence suggested LEM is superior to triazolam 0.5 mg for LPS and sleep efficiency and superior to ZOL for WASO and LPS, and inferior to eszopiclone in sleep quality; however, there is uncertainty in this conclusion due to limitations of the NMAs and differences in conclusions for some outcome comparisons across the NMAs. Evidence was very uncertain or absent for the other comparisons and end points due to imprecision, the risk of bias, and heterogeneity in the pairwise comparisons. Additionally, evidence for transitioning from ZOL to LEM from the pilot study 312 was limited by the study design, small sample size, and large proportion of screening failures preventing conclusions from being drawn. Overall, LEM appears to be effective relative to PBO for important sleep-related outcomes, and long-term results from SUNRISE 2 supported those observed during the first 6 months of treatment. There were no serious safety concerns, but efficacy for HRQoL and subjective appraisals of symptoms and sleep quality are less certain due to limitations of the trials. ZOL may not have been the most relevant comparator in Canadian practice, and comparisons with ZOL in the trial (except for WASO2H) were not controlled for multiplicity; therefore, there is uncertainty in the conclusions about the comparative efficacy. LEM appeared to be more effective than ZOL for the outcome of WASO2H, which was noted as being important for sleep maintenance, though there was no MID identified and there was uncertainty if the change observed in SUNRISE 1 was clinically meaningful. Moreover, there is no direct evidence for efficacy or harms relative to other relevant comparators that may be used in Canadian clinical practice, and the indirect evidence is uncertain. Owing to its superiority over PBO, LEM may be another treatment option for patients with insomnia.
References
1.Drug Reimbursement Review sponsor submission: Dayvigo (lemborexant), 5 mg and 10 mg oral tablets [internal sponsor's package]. Mississauga (ON): Eisai Limited; 2022.
2.Brasure M, MacDonald R, Fuchs E, et al. AHRQ Comparative Effectiveness Reviews. Management of Insomnia Disorder. Rockville (MD): Agency for Healthcare Research and Quality (US); 2015.
3.Clinical Practice Guideline: assessment to management of adult insomnia. Edmonton (AB): Toward Optimized Practice; 2015: https://top.albertadoctors.org/CPGs/Lists/CPGDocumentList/Adult-Insomnia-CPG.pdf. Accessed 2022 May 09.
4.American Psychiatric Association. Diagnostic and statistical manual of mental disorders. 5th ed. Washington (DC): American Psychiatric Publishing; 2013.
5.Chaput JP, Yau J, Rao DP, Morin CM. Prevalence of insomnia for Canadians aged 6 to 79. Health Rep. 2018;29(12):16-20. PubMed
6.Health Canada. Summary basis of decision (SBD) for Dayvigo. 2021; https://hpr-rps.hres.ca/reg-content/summary-basis-decision-detailTwo.php?lang=en&linkID=SBD00529. Accessed 2022 May 09.
7.Morin CM, Jarrin DC, Ivers H, Mérette C, LeBlanc M, Savard J. Incidence, persistence, and remission rates of insomnia over 5 years. JAMA Netw Open. 2020;3(11):e2018782. PubMed
8.LeBlanc M, Mérette C, Savard J, Ivers H, Baillargeon L, Morin CM. Incidence and risk factors of insomnia in a population-based sample. Sleep. 2009;32(8):1027-1037. PubMed
9.Daley M, Morin CM, LeBlanc M, Grégoire JP, Savard J. The economic burden of insomnia: direct and indirect costs for individuals with insomnia syndrome, insomnia symptoms, and good sleepers. Sleep. 2009;32(1):55-64. PubMed
10.Sateia MJ, Buysse DJ, Krystal AD, Neubauer DN, Heald JL. Clinical practice guideline for the pharmacologic treatment of chronic insomnia in adults: an American Academy of Sleep Medicine clinical practice guideline. J Clin Sleep Med. 2017;13(2):307-349. PubMed
11.Summary of reports: interventions for insomnia disorder. Ottawa (ON): CADTH; 2018: https://www.cadth.ca/sites/default/files/pdf/insomnia_summary_e.pdf. Accessed 2022 May 09.
12.Neubauer DN. Pharmacotherapy for insomnia in adults. In: Post TW, ed. UpToDate: UpToDate; 2022 Mar 4: http://www.uptodate.com. Accessed 2022 Mar 15.
13.Health Canada reviewer's report: Dayvigo (lemborexant) [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Dayvigo (lemborexant), 5 mg and 10 mg oral tablets. Mississauga (ON): Eisai Limited; 2020.
14.DRAKE CL, YARDLEY J, PINNER K, LENDERKING W, SAVVA Y, MOLINE M. Perception of Lemborexant Effectiveness as Assessed by the Patient Global Impression- Insomnia Questionnaire. (unpublished).
15.Periodic Safety Update Report for Lemborexant. Eisai Limited; 2022.
16.De Crescenzo F, D'Alò GL, Ostinelli EG, et al. Comparative effects of pharmacological interventions for the acute and long-term management of insomnia disorder in adults: a systematic review and network meta-analysis. Lancet. 2022;400(10347):170-184. PubMed
17.Clinical Study Report: E2006-G000-304. SUNRISE 1. A multicenter, randomized, double-blind, placebo-controlled, active comparator, parallel-group study of the efficacy and safety of lemborexant in subjects 55 years and older with insomnia disorder [internal sponsor's report]. Woodcliff Lake (NJ): Eisai Inc.; 2018.
18.Clinical Study Report: E2006-G000-303. SUNRISE 2. A long-term multicenter, randomized, double-blind, controlled, parallel-group study of the safety and efficacy of lemborexant in subjects with insomnia disorder [internal sponsor's report]. Woodcliff Lake (NJ): Eisai Inc.; 2018.
19.Dayvigo (lemborexant): 5 mg, 10 mg oral tablet [product monograph]. Mississsauga (ON): Eisai Limited; 2020 Nov 3.
20.McElroy H, O'Leary B, Adena M, Campbell R, Monfared AAT, Meier G. Comparative efficacy of lemborexant and other insomnia treatments: a network meta-analysis. J Manag Care Spec Pharm. 2021;27(9):1296-1308. PubMed
21.Morin CM, LeBlanc M, Bélanger L, Ivers H, Mérette C, Savard J. Prevalence of insomnia and its treatment in Canada. Can J Psychiatry. 2011;56(9):540-548. PubMed
22.Kyle SD, Morgan K, Espie CA. Insomnia and health-related quality of life. Sleep Med Rev. 2010;14(1):69-82. PubMed
23.Rios P, Cardoso R, Morra D, et al. Clinical evaluation of interventions for the management of insomnia: a review of reviews. (CADTH Technology review no. 10). Ottawa (ON): CADTH; 2020: https://www.cadth.ca/sites/default/files/pdf/op0527_insomnia_clinical-evaluation-corrected.pdf. Accessed 2022 May 09.
24.Fleming JAE. Chapter 8: Insomnia. Compendium of Therapeutic Choices. 7th ed. Ottawa (ON): Canadian Pharmacists Association; 2014: https://www.pharmacists.ca/cpha-ca/assets/File/CTC7_Sample%20Chapter_Insomnia.pdf. Accessed 2022 May 09.
25.Sublinox® (zolpidem tartrate): sublingual orally disintegrating tablets (ODT), 5 mg and 10 mg, oral [product monograph]. Laval (QC): Bausch Health, Canada Inc.; 2022: https://pdf.hres.ca/dpd_pm/00065109.PDF. Accessed 2022 May 09.
26.Temazepam (temazepam): 15 mg and 30 mg capsules USP [product monograph]. Toronto (ON): Apotex Inc.; 2020: https://pdf.hres.ca/dpd_pm/00059186.PDF. Accessed 2022 May 09.
27.Silenor® (doxepin): 3 and 6 mg doxepin as doxepin hydrochloride [product monograph]. Montreal (QC): Paladin Labs Inc.; 2012 Dec 7: https://pdf.hres.ca/dpd_pm/00018598.PDF. Accessed 2022 May 09.
28.Swinson RP. Chapter: Post-traumatic stress disorder. Compendium of Therapeutic Choices. 7th ed. Ottawa (ON): Canadian Pharmacists Association: https://www.pharmacists.ca/cpha-ca/assets/File/CTC_Sample%20Chapter_PTSD.pdf. Accessed 2022 May 09.
29.Trazodone-50, Trazodone-100 (trazodone hydrochloride tablets USP): 50 mg and 100 mg; Trazodone-150 D (trazodone hydrochloride tablets USP): 150 mg [product monograph]. Laval (QC): PRO DOC LTÉE; 2021 Oct 5: https://pdf.hres.ca/dpd_pm/00063106.PDF. Accessed 2022 May 09.
30.Swinson RP. Chapter 2: Anxiety disorders. Compendium of Therapeutic Choices. 7th ed. Ottawa (ON): Canadian Pharmacists Association; 2014: https://www.pharmacists.ca/cpha-ca/assets/File/CTC7_Sample%20Chapter_AnxietyDisordersChapter2.pdf. Accessed 2022 May 09.
31.Quetiapine fumarate XR (quetiapine fumarate extended-release tablets): extended-release oral tablets, 50 mg, 150 mg, 200 mg, 300 mg and 400 mg quetiapine (as quetiapine fumarate) [product monograph]. Brampton (ON): Sanis Health Inc.; 2022: https://pdf.hres.ca/dpd_pm/00065360.PDF. Accessed 2022 May 09.
32.McGowan J, Sampson M, Salzwedel DM, Cogo E, Foerster V, Lefebvre C. PRESS Peer Review of Electronic Search Strategies: 2015 guideline statement. J Clin Epidemiol. 2016;75:40-46. PubMed
33.Grey matters: a practical tool for searching health-related grey literature. Ottawa (ON): CADTH; 2019: https://www.cadth.ca/grey-matters. Accessed 2022 Mar 24.
34.Chepke C, Jain R, Rosenberg R, et al. Improvement in fatigue and sleep measures with the dual orexin receptor antagonist lemborexant in adults with insomnia disorder. Postgrad Med. 2022:1-10. PubMed
35.Karppa M, Yardley J, Pinner K, et al. Long-term efficacy and tolerability of lemborexant compared with placebo in adults with insomnia disorder: results from the phase 3 randomized clinical trial SUNRISE 2. Sleep. 2020;43(9):14. PubMed
36.Moline M, Zammit G, Cheng JY, Perdomo C, Kumar D, Mayleben D. Comparison of the effect of lemborexant with placebo and zolpidem tartrate extended release on sleep architecture in older adults with insomnia disorder. J Clin Sleep Med. 2021;17(6):1167-1174. PubMed
37.Rosenberg R, Murphy P, Zammit G, et al. Comparison of lemborexant with placebo and zolpidem tartrate extended release for the treatment of older adults with insomnia disorder: a phase 3 randomized clinical trial. JAMA Network Open. 2019;2(12):e1918254. PubMed
38.Roth T, Rosenberg R, Morin CM, et al. Impact of lemborexant treatment on insomnia severity: analyses from a 12-month study of adults with insomnia disorder. Sleep Med. 2022;90:249-257. PubMed
39.Yardley J, Karppa M, Inoue Y, et al. Long-term effectiveness and safety of lemborexant in adults with insomnia disorder: results from a phase 3 randomized clinical trial. Sleep Med. 2021;80:333-342. PubMed
40.EuroQol Group. EuroQol--a new facility for the measurement of health-related quality of life. Health Policy. 1990;16(3):199-208. PubMed
41.Brooks R. EuroQol: the current state of play. Health Policy. 1996;37(1):53-72. PubMed
42.Morin CM, Belleville G, Belanger L, Ivers H. The Insomnia Severity Index: psychometric indicators to detect insomnia cases and evaluate treatment response. Sleep. 2011;34(5):601-608. PubMed
43.Bastien CH, Vallières A, Morin CM. Validation of the Insomnia Severity Index as an outcome measure for insomnia research. Sleep Med. 2001;2(4):297-307. PubMed
44.Gagnon C, Belanger L, Ivers H, Morin CM. Validation of the Insomnia Severity Index in primary care. J Am Board Fam Med. 2013;26(6):701-710. PubMed
45.Yang M, Morin CM, Schaefer K, Wallenstein GV. Interpreting score differences in the Insomnia Severity Index: using health-related outcomes to define the minimally important difference. Curr Med Res Opin. 2009;25(10):2487-2494. PubMed
46.Valko PO, Bassetti CL, Bloch KE, Held U, Baumann CR. Validation of the fatigue severity scale in a Swiss cohort. Sleep. 2008;31(11):1601-1607. PubMed
47.Edinger JD, Ulmer CS, Means MK. Sensitivity and specificity of polysomnographic criteria for defining insomnia. J Clin Sleep Med. 2013;9(5):481-491. PubMed
48.Gaines J, Vgontzas AN, Fernandez-Mendoza J, et al. Short- and long-term sleep stability in insomniacs and healthy controls. Sleep. 2015;38(11):1727-1734. PubMed
49.Marino M, Li Y, Rueschman MN, et al. Measuring sleep: accuracy, sensitivity, and specificity of wrist actigraphy compared to polysomnography. Sleep. 2013;36(11):1747-1755. PubMed
50.Bianchi MT, Williams KL, McKinney S, Ellenbogen JM. The subjective-objective mismatch in sleep perception among those with insomnia and sleep apnea. J Sleep Res. 2013;22(5):557-568. PubMed
51.Khan CT, Woodward SH. Calibrating actigraphy to improve sleep efficiency estimates. J Sleep Res. 2018;27(4):e12613. PubMed
52.Dietch JR, Taylor DJ, Sethi K, Kelly K, Bramoweth AD, Roane BM. Psychometric evaluation of the PSQI in U.S. college students. J Clin Sleep Med. 2016;12(8):1121-1129. PubMed
53.Jungquist CR, Pender JJ, Klingman KJ, Mund J. Validation of capturing sleep diary data via a wrist-worn device. Sleep Disorders. 2015;2015:758937. PubMed
54.Levenson JC, Troxel WM, Begley A, et al. A quantitative approach to distinguishing older adults with insomnia from good sleeper controls. J Clin Sleep Med. 2013;9(2):125-131. PubMed
55.McClelland GR. Body sway and the effects of psychoactive drugs — a review. Human Psychopharmacology: Clinical and Experimental. 1989;4(1):3-14.
56.Jongen S, Vuurman E, Ramaekers J, Vermeeren A. Alcohol calibration of tests measuring skills related to car driving. Psychopharmacology (Berl). 2014;231(12):2435-2447. PubMed
57.Tyrer P, Murphy S, Riley P. The Benzodiazepine Withdrawal Symptom Questionnaire. J Affect Disord. 1990;19(1):53-61. PubMed
58.Posner K, Brown GK, Stanley B, et al. The Columbia-Suicide Severity Rating Scale: initial validity and internal consistency findings from three multisite studies with adolescents and adults. Am J Psychiatry. 2011;168(12):1266-1277. PubMed
59.Eisai Inc. NCT01995838: A multicenter, randomized, double-blind, placebo-controlled, parallel-group, Bayesian adaptive randomization design, dose response study of the efficacy of E2006 in adults and elderly subjects with chronic insomnia. ClinicalTrials.gov. Bethesda (MD): U.S. National Library of Medicine; 2020: https://clinicaltrials.gov/ct2/show/NCT01995838. Accessed 2022 May 09.
60.Lemborexant (Dayvigo) for the treatment of adults with insomnia disorder: a systematic review and network meta-analysis to indirectly compare safety and efficacy to agents available on Canadian public drug plans [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Dayvigo (lemborexant), 5 mg and 10 mg oral tablets. Mississauga (ON): Eisai Limited; 2020 Nov 3.
61.National Institute for Health and Care Excellence. The guidelines manual: appendices B–I: Appendix C: Methodology checklist: randomised controlled trials. (NICE Process and methods guideline PMG6) 2012; https://www.nice.org.uk/process/pmg6/resources/the-guidelines-manual-appendices-bi-2549703709/chapter/appendix-c-methodology-checklist-randomised-controlled-trials. Accessed 2022 May 1.
62.Egger M, Davey Smith G, Schneider M, Minder C. Bias in meta-analysis detected by a simple, graphical test. BMJ. 1997;315(7109):629-634. PubMed
63.Riemann D, Baglioni C, Bassetti C, et al. European guideline for the diagnosis and treatment of insomnia. J Sleep Res. 2017;26(6):675-700. PubMed
64.Clinical Study Report: E2006-A001-312. A multicenter, pilot study to evaluate next-dose transition from zolpidem to lemborexant for the treatment of insomnia [internal sponsor's report]. Woodcliff Lake (NJ): Eisai Inc.; 2021 Mar 30.
65.Mallinson DC, Kamenetsky ME, Hagen EW, Peppard PE. Subjective sleep measurement: comparing sleep diary to questionnaire. Nat Sci Sleep. 2019;11:197-206. PubMed
66.Sanchez-Ortuno MM, Edinger JD. Internight sleep variability: its clinical significance and responsiveness to treatment in primary and comorbid insomnia. J Sleep Res. 2012;21(5):527-534. PubMed
67.Feige B, Al-Shajlawi A, Nissen C, et al. Does REM sleep contribute to subjective wake time in primary insomnia? A comparison of polysomnographic and subjective sleep in 100 patients. J Sleep Res. 2008;17(2):180-190. PubMed
68.Shrivastava D, Jung S, Saadat M, Sirohi R, Crewson K. How to interpret the results of a sleep study. J Community Hosp Intern Med Perspect. 2014;4(5):24983-24983. PubMed
69.Dittner AJ, Wessely SC, Brown RG. The assessment of fatigue: a practical guide for clinicians and researchers. J Psychosom Res. 2004;56(2):157-170. PubMed
70.Sinnott PL, Joyce VR, Barnett PG. Guidebook: preference measurement in economic analysis. Menlo Park (CA): Health Economics Research Center; 2007: https://www.herc.research.va.gov/files/BOOK_419.pdf. Accessed 2022 Apr 9.
71.Lord SR, Sherrington C, Menz HB,Close JCT. Postural stability and falls. Falls in older people: risk factors and strategies for prevention. 2nd ed. Cambridge (GB): Cambridge University Press; 2007:26-49.
72.Wesnes KA, Garratt C, Wickens M, Gudgeon A, Oliver S. Effects of sibutramine alone and with alcohol on cognitive function in healthy volunteers. Br J Clin Pharmacol. 2000;49(2):110-117. PubMed
73.Carney CE, Buysse DJ, Ancoli-Israel S, et al. The consensus sleep diary: standardizing prospective sleep self-monitoring. Sleep. 2012;35(2):287-302. PubMed
74.Buysse DJ, Cheng Y, Germain A, et al. Night-to-night sleep variability in older adults with and without chronic insomnia. Sleep Med. 2010;11(1):56-64. PubMed
75.Vallieres A, Ivers H, Bastien CH, Beaulieu-Bonneau S, Morin CM. Variability and predictability in sleep patterns of chronic insomniacs. J Sleep Res. 2005;14(4):447-453. PubMed
76.Ballesio A, Aquino M, Feige B, et al. The effectiveness of behavioural and cognitive behavioural therapies for insomnia on depressive and fatigue symptoms: A systematic review and network meta-analysis. Sleep Med Rev. 2018;37:114-129. PubMed
77.Macdonald RR. Measurement, Design and Analysis: an Integrated Approach. by E. J. Pedhazur & L. P. Schmelkin. Br J Math Stat Psychol. 1992;45(1):163-163.
78.Wohlgemuth WK, Edinger JD, Fins AI, Sullivan RJ, Jr. How many nights are enough? The short-term stability of sleep parameters in elderly insomniacs and normal sleepers. Psychophysiology. 1999;36(2):233-244. PubMed
79.Dranitsaris G. Estimating the Risk of Motor Vehicle Accidents: Zopiclone/BZDs vs. Lemborexant [internal sponsor supplied]. Toronto (ON): Augmentium Pharma Consulting Inc.; 2021.
80.Vermeeren A, Jongen S, Murphy P, et al. On-the-road driving performance the morning after bedtime administration of lemborexant in healthy adult and elderly volunteers. Sleep. 2019;42(4):01.
81.Verster JC, Spence DW, Shahid A, Pandi-Perumal SR, Roth T. Zopiclone as positive control in studies examining the residual effects of hypnotic drugs on driving ability. Curr Drug Saf. 2011;6(4):209-218. PubMed
82.Taylor B, Rehm J. The relationship between alcohol consumption and fatal motor vehicle injury: high risk at low alcohol levels. Alcohol Clin Exp Res. 2012;36(10):1827-1834. PubMed
83.Taylor B, Irving HM, Kanteres F, et al. The more you drink, the harder you fall: a systematic review and meta-analysis of how acute alcohol consumption and injury or collision risk increase together. Drug Alcohol Depend. 2010;110(1-2):108-116. PubMed
84.Gustavsen I, Bramness JG, Skurtveit S, Engeland A, Neutel I, Mørland J. Road traffic accident risk related to prescriptions of the hypnotics zopiclone, zolpidem, flunitrazepam and nitrazepam. Sleep Med. 2008;9(8):818-822. PubMed
85.Higgins JP, Altman DG, Gøtzsche PC, et al. The Cochrane Collaboration's tool for assessing risk of bias in randomised trials. BMJ. 2011;343:d5928. PubMed
86.Nikolakopoulou A, Higgins JPT, Papakonstantinou T, et al. CINeMA: An approach for assessing confidence in the results of a network meta-analysis. PLoS Med. 2020;17(4):e1003082. PubMed
87.Buysse DJ, Reynolds CF, 3rd, Monk TH, Berman SR, Kupfer DJ. The Pittsburgh Sleep Quality Index: a new instrument for psychiatric practice and research. Psychiatry Res. 1989;28(2):193-213. PubMed
88.Parrott AC, Hindmarch I. Factor analysis of a sleep evaluation questionnaire. Psychol Med. 1978;8(2):325-329. PubMed
89.Zisapel N, Laudon M. Subjective assessment of the effects of CNS-active drugs on sleep by the Leeds sleep evaluation questionnaire: a review. Hum Psychopharmacol. 2003;18(1):1-20. PubMed
Appendix 1: Literature Search Strategy
Note that this appendix has not been copy-edited.
Clinical Literature Search
Overview
Interface: Ovid
Databases:
MEDLINE All (1946-present)
Embase (1974-present)
Note: Subject headings and search fields have been customized for each database. Duplicates between databases were removed in Ovid.
Date of search: March 24, 2022.
Alerts: Bi-weekly search updates until July 27, 2022.
Search filters applied: None.
Limits:
Conference abstracts: excluded
Syntax | Description |
|---|---|
/ | At the end of a phrase, searches the phrase as a subject heading |
* | Before a word, indicates that the marked subject heading is a primary topic; or, after a word, a truncation symbol (wildcard) to retrieve plurals or varying endings |
.ti | Title |
.ot | Original title |
.ab | Abstract |
.hw | Heading word; usually includes subject headings and controlled vocabulary |
.kf | Keyword heading word |
.dq | Candidate term word (Embase) |
.pt | Publication type |
.mp | Mapped term |
.rn | Registry number |
.nm | Name of substance word (MEDLINE) |
medall | Ovid database code: MEDLINE All, 1946 to present, updated daily |
oemezd | Ovid database code; Embase, 1974 to present, updated daily |
Multi-Database Strategy
(Dayvigo* or Lemborexant or E 2006 or E2006).ti,ab,kf,rn,nm,hw,ot.
0K5743G68X.rn,nm.
or/1-2
3 use medall
*Lemborexant/
(Dayvigo* or Lemborexant or E 2006 or E2006).ti,ab,kf,dq.
or/5-6
7 use oemezd
(conference abstract or conference review).pt.
8 not 9
or/4,10
remove duplicates from 11
Clinical Trials Registries
ClinicalTrials.gov
Produced by the U.S. National Library of Medicine. Targeted search used to capture registered clinical trials.
[Search -- Studies with results | Lemborexant, insomnia]
WHO ICTRP
International Clinical Trials Registry Platform, produced by the World Health Organization. Targeted search used to capture registered clinical trials.
[Search terms – Lemborexant, insomnia]
Health Canada’s Clinical Trials Database
Produced by Health Canada. Targeted search used to capture registered clinical trials.
[Search terms -- Lemborexant, insomnia]
EU Clinical Trials Register
European Union Clinical Trials Register, produced by the European Union. Targeted search used to capture registered clinical trials.
[Search terms -- Lemborexant, insomnia]
Grey Literature
Search dates: March 15, 2022 – March 16, 2022.
Keywords: [Lemborexant, Dayvigo, insomnia, sleep disorder*]
Limits: None.
Updated: Search updated prior to the completion of stakeholder feedback period
Relevant websites from the following sections of the CADTH grey literature checklist Grey Matters: A Practical Tool for Searching Health-Related Grey Literature were searched:
Health Technology Assessment Agencies
Health Economics
Clinical Practice Guidelines
Drug and Device Regulatory Approvals
Advisories and Warnings
Drug Class Reviews
Clinical Trials Registries
Databases (free)
Health Statistics
Internet Search
Open Access Journals
Appendix 2: Excluded Studies
Note that this appendix has not been copy-edited.
Reference | Reason for exclusion |
|---|---|
Chepke, C., et al. (2022). "Improvement in fatigue and sleep measures with the dual orexin receptor antagonist lemborexant in adults with insomnia disorder." Postgraduate Medicine: 1-10. | Posthoc analysis |
Moline, M., et al. (2021). "Comparison of the effect of lemborexant with placebo and zolpidem tartrate extended release on sleep architecture in older adults with insomnia disorder." Journal of Clinical Sleep Medicine 17(6): 1167-1174. | Posthoc analysis |
Roth, T., et al. (2022). "Impact of lemborexant treatment on insomnia severity: analyses from a 12-month study of adults with insomnia disorder." Sleep Medicine 90: 249-257. | Posthoc analysis |
Appendix 3: Detailed Outcome Data
Note that this appendix has not been copy-edited.
Table 60: Subgroup Analyses by Age, Change From Baseline LPS — SUNRISE 1 Study, FAS
Outcome | PBO (N = 208) | ZOL (N = 263) | LEM5 (N = 266) | LEM10 (N = 269) |
|---|---|---|---|---|
Age subgroup 1: 55 to < 65 years | ||||
Baseline, n | 115 | 142 | 148 | 147 |
Geometric mean, minutes | 33.04 | 32.33 | 32.19 | 34.24 |
Median (Q1 to Q3), minutes | 33.50 (21.25 to 55.50) | 34.50 (16.50 to 65.75) | 33.88 (19.00 to 66.75) | 42.25 (18.00 to 62.75) |
Days 1 to 2, na | 115 | 143 | 148 | 147 |
Geometric mean, minutes | 26.05 | 23.32 | 23.01 | 19.93 |
Median (Q1 to Q3), minutes | 26.00 (14.50 to 46.50) | 24.00 (14.00 to 41.50) | 22.75 (15.38 to 33.25) | 21.50 (13.25 to 34.00) |
Change from baseline, median (Q1 to Q3), minutes | –4.75 (–22.00 to 13.00) | –7.00 (–27.00 to 3.25) | –8.75 (–32.38 to 3.13) | –13.00 (–40.00 to –0.50) |
Geometric LSM treatment ratio, active vs. PBO (95% CI)b | Reference | 0.94 (0.79 to 1.11) | 0.93 (0.79 to 1.10) | 0.79 (0.67 to 0.93) |
P valueb,c | Reference | 0.4495 | 0.3967 | 0.0053 |
Geometric LSM treatment ratio, active vs. ZOL (95% CI)b | NA | Reference | 0.99 (0.85 to 1.16) | 0.84 (0.72 to 0.99) |
P valueb,c | NA | Reference | 0.9287 | 0.0317 |
Days 29 to 30, na | 111 | 134 | 145 | 143 |
Geometric mean, minutes | 24.45 | 26.97 | 17.69 | 16.43 |
Median (Q1 to Q3), minutes | 24.75 (15.25 to 46.50) | 28.75 (15.25 to 53.00) | 18.25 (11.50 to 28.00) | 18.00 (11.25 to 25.50) |
Change from baseline, median (Q1 to Q3), minutes | –6.75 (–18.25 to 8.25) | –4.00 (–28.75 to 11.25) | –12.50 (–34.75 to 0.50) | –17.25 (–42.50 to –2.75) |
Geometric LSM treatment ratio, active vs. PBO (95% CI)b | Reference | 1.14 (0.93 to 1.39) | 0.71 (0.59 to 0.87) | 0.67 (0.55 to 0.81) |
P valueb,c | Reference | 0.2017 | 0.0007 | < 0.0001 |
Geometric LSM treatment ratio, active vs. ZOL (95% CI)b | NA | Reference | 0.63 (0.52 to 0.75) | 0.59 (0.49 to 0.71) |
P valueb,c | NA | Reference | < 0.0001 | < 0.0001 |
Age subgroup 1: 65 to < 75 years | ||||
Baseline, n | 83 | 91 | 103 | 98 |
Geometric mean, minutes | 34.09 | 28.89 | 33.30 | 32.65 |
Median (Q1 to Q3), minutes | 34.50 (20.00 to 65.75) | 30.50 (17.50 to 55.00) | 32.75 (20.75 to 57.75) | 36.13 (17.75 to 62.75) |
Days 1 to 2, na | 83 | 91 | 103 | 98 |
Geometric mean, minutes | 28.75 | 24.33 | 19.84 | 20.33 |
Median (Q1 to Q3), minutes | 30.75 (17.50 to 47.00) | 27.25 (15.25 to 38.50) | 20.00 (13.00 to 32.25) | 22.88 (12.25 to 31.75) |
Change from baseline, median (Q1 to Q3), minutes | –5.50 (–23.25 to 8.00) | –3.00 (–23.25 to 7.50) | –12.25 (–27.50 to 0.75) | –8.50 (–32.00 to –1.50) |
Geometric LSM treatment ratio, active vs. PBO (95% CI)b | Reference | 1.00 (0.82 to 1.22) | 0.75 (0.61 to 0.90) | 0.78 (0.64 to 0.95) |
P valueb,c | Reference | 0.9738 | 0.0029 | 0.0127 |
Geometric LSM treatment ratio, active vs. ZOL (95% CI)b | NA | Reference | 0.75 (0.62 to 0.90) | 0.78 (0.65 to 0.95) |
P valueb,c | NA | Reference | 0.0026 | 0.0118 |
Days 29 to 30, na | 80 | 88 | 100 | 94 |
Geometric mean, minutes | 25.09 | 28.64 | 19.16 | 18.73 |
Median (Q1 to Q3), minutes | 27.88 (14.25 to 43.75) | 28.50 (17.88 to 52.38) | 18.13 (11.88 to 30.50) | 20.50 (11.25 to 32.00) |
Change from baseline, median (Q1 to Q3), minutes | –5.50 (–26.75 to 5.25) | –0.50 (–19.63 to 13.25) | –13.38 (–30.25 to –2.25) | –11.38 (–35.00 to 0.00) |
Geometric LSM treatment ratio, active vs. PBO (95% CI)b | Reference | 1.32 (1.06 to 1.64) | 0.81 (0.65 to 1.00) | 0.79 (0.64 to 0.99) |
P valueb,c | Reference | 0.0142 | 0.0467 | 0.0375 |
Geometric LSM treatment ratio, active vs. ZOL (95% CI)b | NA | Reference | 0.61 (0.50 to 0.75) | 0.60 (0.49 to 0.74) |
P valueb,c | NA | Reference | < 0.0001 | < 0.0001 |
Age subgroup 1: ≥ 75 years | ||||
Baseline, n | 10 | 29 | 15 | 24 |
Geometric mean, minutes | 36.37 | 31.12 | 39.17 | 30.53 |
Median (Q1 to Q3), minutes | 37.38 (26.75 to 66.75) | 28.25 (21.50 to 54.50) | 40.25 (25.00 to 48.75) | 38.13 (15.00 to 49.25) |
Days 1 to 2, na | 10 | 29 | 15 | 24 |
Geometric mean, minutes | 21.99 | 29.13 | 24.36 | 21.64 |
Median (Q1 to Q3), minutes | 23.00 (16.75 to 26.25) | 36.75 (22.00 to 46.75) | 23.50 (13.25 to 36.25) | 20.00 (15.00 to 28.75) |
Change from baseline, median (Q1 to Q3), minutes | –9.38 (–32.75 to –3.50) | 3.00 (–23.75 to 15.25) | –10.25 (–22.75 to –2.25) | –9.13 (–27.75 to 8.13) |
Geometric LSM treatment ratio, active vs. PBO (95% CI)b | Reference | 1.28 (0.75 to 2.16) | 1.07 (0.59 to 1.92) | 1.01 (0.59 to 1.75) |
P valueb,c | Reference | 0.3613 | 0.8229 | 0.9670 |
Geometric LSM treatment ratio, active vs. ZOL (95% CI)b | NA | Reference | 0.84 (0.53 to 1.33) | 0.79 (0.53 to 1.18) |
P valueb,c | NA | Reference | 0.4466 | 0.2527 |
Days 29 to 30, na | 9 | 28 | 15 | 23 |
Geometric mean, minutes | 28.59 | 30.04 | 31.78 | 19.50 |
Median (Q1 to Q3), minutes | 25.75 (18.75 to 56.00) | 29.25 (24.38 to 39.88) | 29.00 (21.75 to 43.25) | 20.50 (11.00 to 29.75) |
Change from baseline, median (Q1 to Q3), minutes | –10.25 (–23.50 to 6.75) | 1.13 (–17.63 to 18.00) | –5.25 (–18.00 to 3.50) | –16.50 (–29.00 to 4.00) |
Geometric LSM treatment ratio, active vs. PBO (95% CI)b | Reference | 1.31 (0.80 to 2.16) | 1.32 (0.76 to 2.29) | 0.83 (0.50 to 1.40) |
P valueb,c | Reference | 0.2807 | 0.3180 | 0.4778 |
Geometric LSM treatment ratio, active vs. ZOL (95% CI)b | NA | Reference | 1.01 (0.66 to 1.53) | 0.63 (0.44 to 0.92) |
P valueb,c | NA | Reference | 0.9791 | 0.0164 |
Age subgroup 2: 55 to < 65 years | ||||
Baseline, n | 115 | 142 | 148 | 147 |
Geometric mean, minutes | 33.04 | 32.33 | 32.19 | 34.24 |
Median (Q1 to Q3), minutes | 33.50 (21.25 to 55.50) | 34.50 (16.50 to 65.75) | 33.88 (19.00 to 66.75) | 42.25 (18.00 to 62.75) |
Days 1 to 2, na | 115 | 142 | 148 | 147 |
Geometric mean, minutes | 26.05 | 23.32 | 23.01 | 19.93 |
Median (Q1 to Q3), minutes | 26.00 (14.50 to 46.50) | 24.00 (14.00 to 41.50) | 22.75 (15.38 to 33.25) | 21.50 (13.25 to 34.00) |
Change from baseline, median (Q1 to Q3), minutes | –4.75 (–22.00 to 13.00) | –7.00 (–27.00 to 3.25) | –8.75 (–32.38 to 3.13) | –13.00 (–40.00 to –0.50) |
Geometric LSM treatment ratio, active vs. PBO (95% CI)b | Reference | 0.94 (0.79 to 1.11) | 0.93 (0.79 to 1.10) | 0.79 (0.67 to 0.93) |
P valueb,c | Reference | 0.4495 | 0.3967 | 0.0053 |
Geometric LSM treatment ratio, active vs. ZOL (95% CI)b | NA | Reference | 0.99 (0.85 to 1.16) | 0.84 (0.72 to 0.99) |
P valueb,c | NA | Reference | 0.9287 | 0.0317 |
Days 29 to 30, na | 111 | 134 | 145 | 143 |
Geometric mean, minutes | 24.45 | 26.97 | 17.69 | 16.43 |
Median (Q1 to Q3), minutes | 24.75 (15.25 to 46.50) | 28.75 (15.25 to 53.00) | 18.25 (11.50 to 28.00) | 18.00 (11.25 to 25.50) |
Change from baseline, median (Q1 to Q3), minutes | –6.75 (–18.25 to 8.25) | –4.00 (–28.75 to 11.25) | –12.50 (–34.75 to 0.50) | –17.25 (–42.50 to –2.75) |
Geometric LSM treatment ratio, active vs. PBO (95% CI)b | Reference | 1.14 (0.93 to 1.39) | 0.71 (0.59 to 0.87) | 0.67 (0.55 to 0.81) |
P valueb,c | Reference | 0.2017 | 0.0007 | < 0.0001 |
Geometric LSM treatment ratio, active vs. ZOL (95% CI)b | NA | Reference | 0.63 (0.52 to 0.75) | 0.59 (0.49 to 0.71) |
P valueb,c | NA | Reference | < 0.0001 | < 0.0001 |
Age subgroup 2: ≥ 65 years | ||||
Baseline, n | 93 | 120 | 118 | 122 |
Geometric mean, minutes | 34.33 | 29.42 | 33.99 | 32.23 |
Median (Q1 to Q3), minutes | 34.50 (20.50 to 65.75) | 30.25 (17.63 to 54.75) | 33.00 (23.75 to 55.75) | 36.38 (17.50 to 60.00) |
Days 1 to 2, na | 93 | 120 | 118 | 122 |
Geometric mean, minutes | 27.93 | 25.41 | 20.36 | 20.58 |
Median (Q1 to Q3), minutes | 27.75 (17.50 to 45.50) | 28.75 (15.25 to 40.88) | 20.13 (13.25 to 32.25) | 22.38 (13.25 to 31.25) |
Change from baseline, median (Q1 to Q3), minutes | –6.50 (–25.25 to 7.00) | –2.25 (–23.50 to 9.00) | –12.13 (–25.00 to –1.75) | –8.50 (–32.00 to 1.00) |
Geometric LSM treatment ratio, active vs. PBO (95% CI)b | Reference | 1.03 (0.86 to 1.24) | 0.78 (0.65 to 0.93) | 0.81 (0.67 to 0.97) |
P valueb,c | Reference | 0.7308 | 0.0066 | 0.0209 |
Geometric LSM treatment ratio, active vs. ZOL (95% CI)b | NA | Reference | 0.75 (0.63 to 0.89) | 0.78 (0.66 to 0.93) |
P valueb,c | NA | Reference | 0.0011 | 0.0046 |
Days 29 to 30, na | 89 | 116 | 115 | 117 |
Geometric mean, minutes | 25.43 | 28.97 | 20.46 | 18.88 |
Median (Q1 to Q3), minutes | 27.75 (14.50 to 44.00) | 28.50 (18.63 to 46.50) | 21.75 (12.25 to 32.25) | 20.50 (11.25 to 31.50) |
Change from baseline, median (Q1 to Q3), minutes | –6.25 (–23.75 to 5.75) | 0.13 (–19.63 to 13.88) | –11.50 (–27.75 to –1.25) | –14.00 (–32.50 to 0.75) |
Geometric LSM treatment ratio, active vs. PBO (95% CI)b | Reference | 1.32 (1.08 to 1.61) | 0.86 (0.70 to 1.05) | 0.80 (0.66 to 0.98) |
P valueb,c | Reference | 0.0060 | 0.1262 | 0.0290 |
Geometric LSM treatment ratio, active vs. ZOL (95% CI)b | NA | Reference | 0.65 (0.54 to 0.78) | 0.61 (0.51 to 0.73) |
P valueb,c | NA | Reference | < 0.0001 | < 0.0001 |
CI = confidence interval; FAS = full analysis set; LEM5 = lemborexant 5 mg; LEM10 = lemborexant 10 mg; LPS = latency to persistent sleep; LSM = least squares mean; MAR = missing at random; MMRM = mixed model of repeated measures; NA = not applicable; PBO = placebo; Q1 = first quartile; Q3 = third quartile; SD = standard deviation; vs. = versus; ZOL = zolpidem tartrate.
aThe number of patients analyzed for the change from baseline at this time point (not the number of patients who provided data at this time point).
bEstimates and 95% CI based on an MMRM model with log transformation of LPS and factors of age group, region, treatment, visit (days 1 to 2 and days 29 to 30), and treatment-by-visit interaction as fixed effects, and baseline LPS as a covariate. Each subgroup uses this model with only patients in that subgroup, removing the factors for age group and region when applied to those subgroups, respectively. Missing values were not imputed and assumed to be MAR.
cP value was not adjusted for multiple testing (i.e., the type I error rate was not controlled).
Source: SUNRISE 1 Clinical Study Report.17
Table 61: Subgroup Analyses by Age, Change From Baseline sSOL — SUNRISE 2 Study, FAS
Outcome | PBO (N = 318) | LEM5 (N = 316) | LEM10 (N = 315) |
|---|---|---|---|
Age subgroup 1: < 65 years | |||
Baseline, n | 228 | 228 | 226 |
Geometric mean, minutes | 44.72 | 44.52 | 46.99 |
Median (Q1 to Q3), minutes | 55.86 (33.93 to 78.21) | 53.57 (34.64 to 73.57) | 55.71 (35.71 to 85.86) |
First 7 nights of period 1, na | 226 | 224 | 225 |
Geometric mean, minutes | 40.03 | 32.77 | 31.48 |
Median (Q1 to Q3), minutes | 50.71 (28.57 to 70.00) | 37.14 (23.33 to 60.00) | 35.36 (22.07 to 61.50) |
Change from study baseline, median (Q1 to Q3), minutes | –2.86 (–19.29 to 7.71) | –9.29 (–25.06 to 0.00) | –13.57 (–31.57 to –1.43) |
Geometric LSM treatment ratio, active vs. PBO (95% CI)b | Reference | 0.81 (0.74 to 0.89) | 0.76 (0.70 to 0.84) |
P valueb,c | Reference | < 0.0001 | < 0.0001 |
Month 1, na | 212 | 217 | 218 |
Geometric mean, minutes | 34.00 | 28.65 | 26.99 |
Median (Q1 to Q3), minutes | 42.86 (23.33 to 64.29) | 33.07 (20.00 to 55.71) | 31.43 (16.43 to 55.71) |
Change from study baseline, median (Q1 to Q3), minutes | –8.00 (–25.71 to 3.57) | –11.43 (–33.57 to –0.71) | –20.36 (–36.43 to –4.29) |
Geometric LSM treatment ratio, active vs. PBO (95% CI)b | Reference | 0.84 (0.75 to 0.94) | 0.76 (0.68 to 0.86) |
P valueb,c | Reference | 0.0028 | < 0.0001 |
Month 3, na | 200 | 193 | 191 |
Geometric mean, minutes | 26.85 | 22.01 | 22.46 |
Median (Q1 to Q3), minutes | 35.00 (16.29 to 60.00) | 24.29 (14.71 to 40.71) | 26.50 (14.25 to 47.14) |
Change from study baseline, median (Q1 to Q3), minutes | –12.95 (–30.21 to 0.00) | –20.71 (–40.00 to –6.43) | –25.50 (–45.00 to –6.43) |
Geometric LSM treatment ratio, active vs. PBO (95% CI)b | Reference | 0.84 (0.73 to 0.97) | 0.81 (0.70 to 0.94) |
P valueb,c | Reference | 0.0175 | 0.0046 |
Month 6, na | 169 | 176 | 161 |
Geometric mean, minutes | 24.60 | 19.19 | 18.13 |
Median (Q1 to Q3), minutes | 30.43 (16.43 to 60.00) | 22.50 (13.00 to 35.71) | 22.64 (11.43 to 40.00) |
Change from study baseline, median (Q1 to Q3), minutes | –12.86 (–35.77 to 0.00) | –21.86 (–40.07 to –10.93) | –28.86 (–53.71 to –11.29) |
Geometric LSM treatment ratio, active vs. PBO (95% CI)b | Reference | 0.81 (0.67 to 0.96) | 0.71 (0.59 to 0.85) |
P valueb,c | Reference | 0.0177 | 0.0002 |
Age subgroup 1: 65 to < 75 years | |||
Baseline, n | 68 | 75 | 65 |
Geometric mean, minutes | 44.78 | 40.02 | 42.34 |
Median (Q1 to Q3), minutes | 49.64 (33.93 to 77.29) | 52.86 (30.71 to 82.86) | 60.00 (31.43 to 92.14) |
First 7 nights of period 1, na | 68 | 75 | 64 |
Geometric mean, minutes | 42.33 | 27.38 | 29.24 |
Median (Q1 to Q3), minutes | 48.71 (30.00 to 83.57) | 36.43 (17.32 to 53.69) | 36.43 (23.21 to 63.20) |
Change from study baseline, median (Q1 to Q3), minutes | –4.21 (–16.96 to 7.50) | –15.36 (–35.71 to –0.86) | –12.06 (–32.07 to –0.71) |
Geometric LSM treatment ratio, active vs. PBO (95% CI)b | Reference | 0.71 (0.61 to 0.83) | 0.72 (0.61 to 0.84) |
P valueb,c | Reference | < 0.0001 | < 0.0001 |
Month 1, na | 68 | 71 | 62 |
Geometric mean, minutes | 36.18 | 24.17 | 27.74 |
Median (Q1 to Q3), minutes | 45.00 (27.86 to 69.29) | 32.50 (20.00 to 49.70) | 32.14 (20.00 to 68.57) |
Change from study baseline, median (Q1 to Q3), minutes | –5.00 (–18.75 to 4.37) | –19.29 (–41.43 to –0.71) | –20.00 (–36.43 to –0.29) |
Geometric LSM treatment ratio, active vs. PBO (95% CI)b | Reference | 0.72 (0.59 to 0.89) | 0.76 (0.62 to 0.94) |
P valueb,c | Reference | 0.0021 | 0.0122 |
Month 3, na | 61 | 68 | 60 |
Geometric mean, minutes | 38.58 | 21.92 | 23.81 |
Median (Q1 to Q3), minutes | 46.79 (23.57 to 80.00) | 27.14 (16.71 to 42.86) | 25.00 (16.57 to 53.64) |
Change from study baseline, median (Q1 to Q3), minutes | –5.43 (–21.43 to 10.00) | –22.14 (–42.71 to –6.09) | –31.29 (–50.29 to –5.14) |
Geometric LSM treatment ratio, active vs. PBO (95% CI)b | Reference | 0.64 (0.50 to 0.83) | 0.67 (0.52 to 0.86) |
P valueb,c | Reference | 0.0006 | 0.0022 |
Month 6, na | 61 | 63 | 56 |
Geometric mean, minutes | 35.16 | 17.82 | 23.12 |
Median (Q1 to Q3), minutes | 42.14 (17.14 to 70.00) | 22.86 (12.68 to 34.86) | 25.00 (14.36 to 44.24) |
Change from study baseline, median (Q1 to Q3), minutes | –10.00 (–21.79 to 5.00) | –26.19 (–57.10 to –12.14) | –29.64 (–57.07 to –5.14) |
Geometric LSM treatment ratio, active vs. PBO (95% CI)b | Reference | 0.56 (0.43 to 0.72) | 0.69 (0.53 to 0.90) |
P valueb,c | Reference | < 0.0001 | 0.0060 |
Age subgroup 1: ≥ 75 years | |||
Baseline, n | 20 | 11 | 21 |
Geometric mean, minutes | 48.94 | 33.54 | 34.68 |
Median (Q1 to Q3), minutes | 59.64 (40.14 to 92.86) | 41.43 (19.29 to 75.14) | 34.00 (17.14 to 74.29) |
First 7 nights of period 1, na | 20 | 11 | 21 |
Geometric mean, minutes | 46.99 | 23.23 | 28.05 |
Median (Q1 to Q3), minutes | 67.43 (46.43 to 87.74) | 28.57 (18.71 to 50.00) | 30.00 (18.43 to 50.71) |
Change from study baseline, median (Q1 to Q3), minutes | –5.07 (–13.14 to 15.95) | –14.29 (–56.43 to 2.14) | –4.29 (–14.71 to 1.43) |
Geometric LSM treatment ratio, active vs. PBO (95% CI)b | Reference | 0.65 (0.49 to 0.88) | 0.79 (0.62 to 1.02) |
P valueb,c | Reference | 0.0051 | 0.0686 |
Month 1, na | 19 | 10 | 17 |
Geometric mean, minutes | 35.89 | 16.07 | 26.94 |
Median (Q1 to Q3), minutes | 32.86 (22.86 to 84.29) | 23.93 (17.86 to 24.57) | 30.00 (15.14 to 60.00) |
Change from study baseline, median (Q1 to Q3), minutes | –13.71 (–35.24 to 0.43) | –14.17 (–20.00 to –2.26) | –7.14 (–26.71 to –2.14) |
Geometric LSM treatment ratio, active vs. PBO (95% CI)b | Reference | 0.67 (0.43 to 1.03) | 0.88 (0.61 to 1.28) |
P valueb,c | Reference | 0.0676 | 0.5055 |
Month 3, na | 18 | 7 | 13 |
Geometric mean, minutes | 35.63 | 13.54 | 21.45 |
Median (Q1 to Q3), minutes | 40.07 (19.29 to 92.86) | 16.71 (7.86 to 40.71) | 18.00 (15.00 to 30.00) |
Change from study baseline, median (Q1 to Q3), minutes | –12.57 (–49.29 to 0.00) | –18.71 (–44.43 to –2.86) | –4.71 (–51.31 to –3.57) |
Geometric LSM treatment ratio, active vs. PBO (95% CI)b | Reference | 0.63 (0.35 to 1.12) | 0.74 (0.45 to 1.20) |
P valueb,c | Reference | 0.1120 | 0.2133 |
Month 6, na | 19 | 6 | 12 |
Geometric mean, minutes | 32.13 | 12.32 | 20.37 |
Median (Q1 to Q3), minutes | 36.43 (16.43 to 69.29) | 16.07 (5.00 to 20.00) | 23.14 (14.23 to 66.07) |
Change from study baseline, median (Q1 to Q3), minutes | –13.00 (–41.43 to –0.24) | –15.71 (–46.43 to –5.83) | –16.00 (–58.49 to 7.71) |
Geometric LSM treatment ratio, active vs. PBO (95% CI)b | Reference | 0.70 (0.29 to 1.69) | 0.71 (0.35 to 1.45) |
P valueb,c | Reference | 0.4156 | 0.3407 |
Age subgroup 2: < 65 years | |||
Baseline, n | 228 | 228 | 226 |
Geometric mean, minutes | 44.72 | 44.52 | 46.99 |
Median (Q1 to Q3), minutes | 55.86 (33.93 to 78.21) | 53.57 (34.64 to 73.57) | 55.71 (35.71 to 85.86) |
First 7 nights of period 1, na | 226 | 224 | 225 |
Geometric mean, minutes | 40.03 | 32.77 | 31.48 |
Median (Q1 to Q3), minutes | 50.71 (28.57 to 70.00) | 37.14 (23.33 to 60.00) | 35.36 (22.07 to 61.50) |
Change from study baseline, median (Q1 to Q3), minutes | –2.86 (–19.29 to 7.71) | –9.29 (–25.06 to 0.00) | –13.57 (–31.57 to –1.43) |
Geometric LSM treatment ratio, active vs. PBO (95% CI)b | Reference | 0.81 (0.74 to 0.89) | 0.76 (0.70 to 0.84) |
P valueb,c | Reference | < 0.0001 | < 0.0001 |
Month 1, na | 212 | 217 | 218 |
Geometric mean, minutes | 34.00 | 28.65 | 26.99 |
Median (Q1 to Q3), minutes | 42.86 (23.33 to 64.29) | 33.07 (20.00 to 55.71) | 31.43 (16.43 to 55.71) |
Change from study baseline, median (Q1 to Q3), minutes | –8.00 (–25.71 to 3.57) | –11.43 (–33.57 to –0.71) | –20.36 (–36.43 to –4.29) |
Geometric LSM treatment ratio, active vs. PBO (95% CI)b | Reference | 0.84 (0.75 to 0.94) | 0.76 (0.68 to 0.86) |
P valueb,c | Reference | 0.0028 | < 0.0001 |
Month 3, na | 200 | 193 | 191 |
Geometric mean, minutes | 26.85 | 22.01 | 22.46 |
Median (Q1 to Q3), minutes | 35.00 (16.29 to 60.00) | 24.29 (14.71 to 40.71) | 26.50 (14.25 to 47.14) |
Change from study baseline, median (Q1 to Q3), minutes | –12.95 (–30.21 to 0.00) | –20.71 (–40.00 to –6.43) | –25.50 (–45.00 to –6.43) |
Geometric LSM treatment ratio active/PBO (95% CI)b | Reference | 0.84 (0.73 to 0.97) | 0.81 (0.70 to 0.94) |
P valueb,c | Reference | 0.0175 | 0.0046 |
Month 6, na | 169 | 176 | 161 |
Geometric mean, minutes | 24.60 | 19.19 | 18.13 |
Median (Q1 to Q3), minutes | 30.43 (16.43 to 60.00) | 22.50 (13.00 to 35.71) | 22.64 (11.43 to 40.00) |
Change from study baseline, median (Q1 to Q3), minutes | –12.86 (–35.77 to 0.00) | –21.86 (–40.07 to –10.93) | –28.86 (–53.71 to –11.29) |
Geometric LSM treatment ratio, active vs. PBO (95% CI)b | Reference | 0.81 (0.67 to 0.96) | 0.71 (0.59 to 0.85) |
P valueb,c | Reference | 0.0177 | 0.0002 |
Age subgroup 2: ≥ 65 years | |||
Baseline, n | 88 | 86 | 86 |
Geometric mean, minutes | 45.69 | 39.12 | 40.32 |
Median (Q1 to Q3), minutes | 53.57 (34.64 to 80.36) | 52.71 (30.71 to 82.14) | 58.21 (29.29 to 84.29) |
First 7 nights of period 1, na | 88 | 86 | 85 |
Geometric mean, minutes | 43.34 | 26.82 | 28.94 |
Median (Q1 to Q3), minutes | 51.43 (30.57 to 85.71) | 36.29 (17.50 to 51.67) | 35.71 (20.00 to 60.00) |
Change from study baseline, median (Q1 to Q3), minutes | –4.21 (–16.54 to 9.36) | –15.30 (–36.00 to –0.83) | –9.29 (–27.50 to 0.00) |
Geometric LSM treatment ratio, active vs. PBO (95% CI)b | Reference | 0.70 (0.61 to 0.80) | 0.73 (0.64 to 0.83) |
P valueb,c | Reference | < 0.0001 | < 0.0001 |
Month 1, na | 87 | 81 | 79 |
Geometric mean, minutes | 36.12 | 22.99 | 27.56 |
Median (Q1 to Q3), minutes | 44.29 (23.74 to 71.61) | 28.57 (20.00 to 46.43) | 32.14 (20.00 to 64.29) |
Change from study baseline, median (Q1 to Q3), minutes | –5.57 (–25.00 to 2.00) | –16.32 (–40.71 to –1.71) | –17.14 (–35.71 to –0.29) |
Geometric LSM treatment ratio, active vs. PBO (95% CI)b | Reference | 0.72 (0.60 to 0.86) | 0.78 (0.65 to 0.94) |
P valueb,c | Reference | 0.0004 | 0.0083 |
Month 3, na | 79 | 75 | 73 |
Geometric mean, minutes | 37.90 | 20.97 | 23.37 |
Median (Q1 to Q3), minutes | 45.36 (22.86 to 81.79) | 26.71 (14.43 to 42.86) | 23.57 (16.00 to 46.00) |
Change from study baseline, median (Q1 to Q3), minutes | –6.43 (–27.43 to 8.57) | –20.71 (–42.86 to –5.86) | –27.14 (–51.31 to –3.57) |
Geometric LSM treatment ratio, active vs. PBO (95% CI)b | Reference | 0.65 (0.52 to 0.81) | 0.68 (0.55 to 0.85) |
P valueb,c | Reference | 0.0001 | 0.0007 |
Month 6, na | 80 | 69 | 68 |
Geometric mean, minutes | 34.42 | 17.26 | 22.61 |
Median (Q1 to Q3), minutes | 37.14 (17.14 to 69.29) | 20.36 (12.50 to 32.86) | 25.00 (14.36 to 44.24) |
Change from study baseline, median (Q1 to Q3), minutes | –10.77 (–32.64 to 2.43) | –21.67 (–56.07 to –11.43) | –26.00 (–58.21 to –2.21) |
Geometric LSM treatment ratio, active vs. PBO (95% CI)b | Reference | 0.58 (0.45 to 0.74) | 0.70 (0.55 to 0.89) |
P valueb,c | Reference | < 0.0001 | 0.0042 |
CCMV = complete case missing value; CI = confidence interval; FAS = full analysis set; LEM5 = lemborexant 5 mg; LEM10 = lemborexant 10 mg; LSM = least squares mean; MAR = missing at random; MMRM = mixed model of repeated measures; NR = not reported; PBO = placebo; Q1 = first quartile; Q3 = third quartile; SD = standard deviation; sSOL = subjective sleep onset latency; vs. = versus.
Note: Data reported with sleep diary handling rules to address potential errors and illogical values.
aThe number of patients analyzed for the change from baseline at this time point (not the number of patients who provided data at this time point).
bEstimates and 95% CI based on an MMRM model with log transformation of sSOL and factors of age group, region, visit (first 7 nights, month 1, month 2, month 3, month 4, month 5 and month 6), and treatment-by-visit interaction as fixed effects, and study baseline sSOL as a covariate. Each subgroup uses this model with only patients in that subgroup, removing the factors for age group and region when applied to those subgroups, respectively. Missing values were not imputed and assumed to be MAR.
cP value was not adjusted for multiple testing (i.e., the type I error rate was not controlled).
Source: SUNRISE 2 Clinical Study Report.18
Table 62: Long-Term Change From Baseline EQ-5D-3L and VAS Based on Months of Exposure to Lemborexant (Exploratory Outcome) — SUNRISE 2 Study, On-Treatment FAS
Outcome | LEM5 (N = 444) | LEM10 (N = 437) |
|---|---|---|
Baseline,a n | 444 | 437 |
Mobility dimension | ||
3-months exposure, nb | 398 | 380 |
No problems, n (%) | 347 (87.2) | 345 (90.8) |
Some problems, n (%) | 51 (12.8) | 35 (9.2) |
Extreme problems, n (%) | 0 | 0 |
6-months exposure, nb | 359 | 339 |
No problems, n (%) | 318 (88.6) | 300 (88.5) |
Some problems, n (%) | 41 (11.4) | 39 (11.5) |
Extreme problems, n (%) | 0 | 0 |
9-months exposure, nb | 241 | 215 |
No problems, n (%) | 218 (90.5) | 197 (91.6) |
Some problems, n (%) | 23 (9.5) | 18 (8.4) |
Extreme problems, n (%) | 0 | 0 |
12-months exposure, nb | 205 | 195 |
No problems, n (%) | 179 (87.3) | 180 (92.3) |
Some problems, n (%) | 26 (12.7) | 15 (7.7) |
Extreme problems, n (%) | 0 | 0 |
Self-care dimension | ||
3-months exposure, nb | 398 | 380 |
No problems, n (%) | 388 (97.5) | 374 (98.4) |
Some problems, n (%) | 10 (2.5) | 6 (1.6) |
Extreme problems, n (%) | 0 | 0 |
6-months exposure, nb | 359 | 339 |
No problems, n (%) | 350 (97.5) | 329 (97.1) |
Some problems, n (%) | 9 (2.5) | 10 (2.9) |
Extreme problems, n (%) | 0 | 0 |
9-months exposure, nb | 241 | 215 |
No problems, n (%) | 235 (97.5) | 212 (98.6) |
Some problems, n (%) | 6 (2.5) | 3 (1.4) |
Extreme problems, n (%) | 0 | 0 |
12-months exposure, nb | 205 | 195 |
No problems, n (%) | 200 (97.6) | 191 (97.9) |
Some problems, n (%) | 5 (2.4) | 4 (2.1) |
Extreme problems, n (%) | 0 | 0 |
Usual activities dimension | ||
3-months exposure, nb | 398 | 380 |
No problems, n (%) | 322 (80.9) | 318 (83.7) |
Some problems, n (%) | 72 (18.1) | 60 (15.8) |
Extreme problems, n (%) | 4 (1.0) | 2 (0.5) |
6-months exposure, nb | 359 | 339 |
No problems, n (%) | 298 (83.0) | 297 (87.6) |
Some problems, n (%) | 56 (15.6) | 41 (12.1) |
Extreme problems, n (%) | 5 (1.4) | 1 (0.3) |
9-months exposure, nb | 241 | 215 |
No problems, n (%) | 204 (84.6) | 188 (87.4) |
Some problems, n (%) | 35 (14.5) | 27 (12.6) |
Extreme problems, n (%) | 2 (0.8) | 0 |
12-months exposure, nb | 205 | 195 |
No problems, n (%) | 175 (85.4) | 170 (87.2) |
Some problems, n (%) | 28 (13.7) | 25 (12.8) |
Extreme problems, n (%) | 2 (1.0) | 0 |
Pain or discomfort dimension | ||
3-months exposure, nb | 398 | 380 |
No problems, n (%) | 270 (67.8) | 263 (69.2) |
Some problems, n (%) | 122 (30.7) | 115 (30.3) |
Extreme problems, n (%) | 6 (1.5) | 2 (0.5) |
6-months exposure, nb | 359 | 339 |
No problems, n (%) | 235 (65.5) | 228 (67.3) |
Some problems, n (%) | 116 (32.3) | 104 (30.7) |
Extreme problems, n (%) | 8 (2.2) | 7 (2.1) |
9-months exposure, nb | 241 | 215 |
No problems, n (%) | 169 (70.1) | 155 (72.1) |
Some problems, n (%) | 69 (28.6) | 58 (27.0) |
Extreme problems, n (%) | 3 (1.2) | 2 (0.9) |
12-months exposure, nb | 205 | 195 |
No problems, n (%) | 144 (70.2) | 134 (68.7) |
Some problems, n (%) | 53 (25.9) | 56 (28.7) |
Extreme problems, n (%) | 8 (3.9) | 5 (2.6) |
Anxiety or depression dimension | ||
3-months exposure, nb | 398 | 380 |
No problems, n (%) | 338 (84.9) | 333 (87.6) |
Some problems, n (%) | 57 (14.3) | 46 (12.1) |
Extreme problems, n (%) | 3 (0.8) | 1 (0.3) |
6-months exposure, nb | 359 | 339 |
No problems, n (%) | 308 (85.8) | 291 (85.8) |
Some problems, n (%) | 51 (14.2) | 48 (14.2) |
Extreme problems, n (%) | 0 | 0 |
9-months exposure, nb | 241 | 215 |
No problems, n (%) | 210 (87.1) | 192 (89.3) |
Some problems, n (%) | 31 (12.9) | 23 (10.7) |
Extreme problems, n (%) | 0 | 0 |
12-months exposure, nb | 205 | 195 |
No problems, n (%) | 177 (86.3) | 168 (86.2) |
Some problems, n (%) | 28 (13.7) | 27 (13.8) |
Extreme problems, n (%) | 0 | 0 |
VAS | ||
Baseline,a n | 444 | 437 |
Mean (SD) | 72.8 (17.26) | 73.7 (16.88) |
3-months exposure, nb | 398 | 380 |
Change from baseline, mean (SD) | 3.2 (16.00) | 2.9 (15.59) |
6-months exposure, nb | 359 | 339 |
Change from baseline, mean (SD) | 3.2 (16.76) | 4.3 (15.73) |
9-months exposure, nb | 241 | 215 |
Change from baseline, mean (SD) | 6.9 (16.17) | 5.9 (15.49) |
12-months exposure, nb | 205 | 195 |
Change from baseline, mean (SD) | 8.5 (17.10) | 6.8 (15.72) |
FAS = full analysis set; EQ-5D-3L = 3-level EQ-5D; LEM5 = lemborexant 5 mg; LEM10 = lemborexant 10 mg; SD = standard deviation; VAS = visual analogue scale.
aBaseline is a) Study Baseline for data for patients who received lemborexant in period 1 and b) Treatment Period 2 Baseline for patients rerandomized from placebo to lemborexant in period 2.
bThe number of patients analyzed for the change from baseline at this time point (not the number of patients who provided data at this time point).
Source: SUNRISE 2 Clinical Study Report.18
Table 63: Long-Term Change From Baseline ISI Item 4 to Item 7 and FSS Total Score Based on Months of Exposure to Lemborexant (Exploratory Outcomes) — SUNRISE 2 Study, On-Treatment FAS
Outcome | LEM5 (N = 444) | LEM10 (N = 437) |
|---|---|---|
ISI (items 4 to 7) | ||
Baseline,a n | 444 | 437 |
Mean (SD) | 10.0 (3.27) | 9.8 (3.28) |
3-months exposure, nb | 394 | 373 |
Change from baseline, mean (SD) | –4.2 (4.10) | –4.1 (4.18) |
6-months exposure, nb | 368 | 345 |
Change from baseline, mean (SD) | –4.8 (4.12) | –4.6 (4.12) |
9-months exposure, nb | 233 | 207 |
Change from baseline, mean (SD) | –6.7 (3.64) | –6.6 (4.02) |
12-months exposure, nb | 220 | 204 |
Change from baseline, mean (SD) | –7.0 (3.76) | –6.6 (3.97) |
FSS (total score) | ||
Baseline,a n | 444 | 437 |
Mean (SD) | 34.9 (13.30) | 34.3 (13.34) |
3-months exposure, nb | 394 | 373 |
Change from baseline, mean (SD) | –5.9 (12.67) | –6.2 (13.17) |
6-months exposure, nb | 368 | 345 |
Change from baseline, mean (SD) | –7.6 (13.73) | –7.5 (14.46) |
9-months exposure, nb | 233 | 207 |
Change from baseline, mean (SD) | –11.5 (13.29) | –10.7 (14.65) |
12-months exposure, nb | 220 | 204 |
Change from baseline, mean (SD) | –13.3 (14.40) | –11.0 (15.57) |
FAS = full analysis set; FSS = Fatigue Severity Scale; ISI = Insomnia Severity Index; LEM5 = lemborexant 5 mg; LEM10 = lemborexant 10 mg; SD = standard deviation.
aBaseline is a) Study Baseline for data for patients who received lemborexant in period 1 and b) Treatment Period 2 Baseline for patients rerandomized from placebo to lemborexant in period 2.
bThe number of patients analyzed for the change from baseline at this time point (not the number of patients who provided data at this time point).
Source: SUNRISE 2 Clinical Study Report.18
Table 64: Long-Term PGI-Insomnia Based on Months of Exposure to Lemborexant (Exploratory Outcome) — SUNRISE 2 Study, On-Treatment FAS
Outcome | LEM5 (N = 444) | LEM10 (N = 437) |
|---|---|---|
3-months exposure, na | 398 | 380 |
Study medication helped/worsened sleep | ||
Positive medication effect, n (%) | 264 (66.3) | 258 (67.9) |
Neutral medication effect, n (%) | 72 (18.1) | 71 (18.7) |
Negative medication effect, n (%) | 62 (15.6) | 51 (13.4) |
Study medication decreased/increased time to fall asleep | ||
Positive medication effect, n (%) | 274 (68.8) | 262 (68.9) |
Neutral medication effect, n (%) | 48 (12.1) | 46 (12.1) |
Negative medication effect, n (%) | 76 (19.1) | 72 (18.9) |
Study medication increased/decreased total sleep time | ||
Positive medication effect, n (%) | 227 (57.0) | 234 (61.6) |
Neutral medication effect, n (%) | 75 (18.8) | 65 (17.1) |
Negative medication effect, n (%) | 96 (24.1) | 81 (21.3) |
Appropriateness of medication strength | ||
Just right, n (%) | 210 (52.8) | 202 (53.2) |
Too strong, n (%) | 22 (5.5) | 26 (6.8) |
Too weak, n (%) | 166 (41.7) | 152 (40.0) |
6-months exposure, na | 359 | 339 |
Study medication helped/worsened sleep | ||
Positive medication effect, n (%) | 242 (67.4) | 238 (70.2) |
Neutral medication effect, n (%) | 71 (19.8) | 60 (17.7) |
Negative medication effect, n (%) | 46 (12.8) | 41 (12.1) |
Study medication decreased/increased time to fall asleep | ||
Positive medication effect, n (%) | 256 (71.3) | 247 (72.9) |
Neutral medication effect, n (%) | 46 (12.8) | 44 (13.0) |
Negative medication effect, n (%) | 57 (15.9) | 48 (14.2) |
Study medication increased/decreased total sleep time | ||
Positive medication effect, n (%) | 211 (58.8) | 218 (64.3) |
Neutral medication effect, n (%) | 59 (16.4) | 53 (15.6) |
Negative medication effect, n (%) | 89 (24.8) | 68 (20.1) |
Appropriateness of medication strength | ||
Just right, n (%) | 202 (56.3) | 195 (57.5) |
Too strong, n (%) | 18 (5.0) | 17 (5.0) |
Too weak, n (%) | 139 (38.7) | 127 (37.5) |
9-months exposure, na | 241 | 215 |
Study medication helped/worsened sleep | ||
Positive medication effect, n (%) | 177 (73.4) | 165 (76.7) |
Neutral medication effect, n (%) | 41 (17.0) | 33 (15.3) |
Negative medication effect, n (%) | 23 (9.5) | 17 (7.9) |
Study medication decreased/increased time to fall asleep | ||
Positive medication effect, n (%) | 191 (79.3) | 169 (78.6) |
Neutral medication effect, n (%) | 23 (9.5) | 23 (10.7) |
Negative medication effect, n (%) | 27 (11.2) | 23 (10.7) |
Study medication increased/decreased total sleep time | ||
Positive medication effect, n (%) | 150 (62.2) | 157 (73.0) |
Neutral medication effect, n (%) | 43 (17.8) | 29 (13.5) |
Negative medication effect, n (%) | 48 (19.9) | 29 (13.5) |
Appropriateness of medication strength | ||
Just right, n (%) | 146 (60.6) | 134 (62.3) |
Too strong, n (%) | 12 (5.0) | 16 (7.4) |
Too weak, n (%) | 83 (34.4) | 65 (30.2) |
12-months exposure, na | 205 | 195 |
Study medication helped/worsened sleep | ||
Positive medication effect, n (%) | 153 (74.6) | 152 (77.9) |
Neutral medication effect, n (%) | 30 (14.6) | 29 (14.9) |
Negative medication effect, n (%) | 22 (10.7) | 14 (7.2) |
Study medication decreased/increased time to fall asleep | ||
Positive medication effect, n (%) | 157 (76.6) | 156 (80.0) |
Neutral medication effect, n (%) | 24 (11.7) | 16 (8.2) |
Negative medication effect, n (%) | 24 (11.7) | 23 (11.8) |
Study medication increased/decreased total sleep time | ||
Positive medication effect, n (%) | 128 (62.4) | 127 (65.1) |
Neutral medication effect, n (%) | 35 (17.1) | 29 (14.9) |
Negative medication effect, n (%) | 42 (20.5) | 39 (20.0) |
Appropriateness of medication strength | ||
Just right, n (%) | 130 (63.4) | 118 (60.5) |
Too strong, n (%) | 5 (2.4) | 13 (6.7) |
Too weak, n (%) | 70 (34.1) | 64 (32.8) |
FAS = full analysis set; LEM5 = lemborexant 5 mg; LEM10 = lemborexant 10 mg; PGI-Insomnia = Patient Global Impression–Insomnia.
aThe number of patients analyzed for the change from baseline at this time point (not the number of patients who provided data at this time point).
Source: SUNRISE 2 Clinical Study Report.18
Table 65: Change From Baseline sSOL, sWASO, Sleep Efficiency, and sTST (Other Secondary Outcomes) — SUNRISE 1 Study, FAS
Outcome | PBO (N = 208) | ZOL (N = 263) | LEM5 (N = 266) | LEM10 (N = 269) |
|---|---|---|---|---|
sSOL | ||||
Baseline, n | 206 | 258 | 263 | 269 |
Mean (SD), minutes | 55.90 (37.39) | 60.54 (36.35) | 65.79 (43.53) | 60.88 (42.51) |
Median, minutes | 49.29 | 53.21 | 58.57 | 53.57 |
First 7 nights of treatment, na | 202 | 251 | 259 | 266 |
Mean (SD), minutes | 48.91 (31.64) | 44.61 (27.57) | 42.39 (28.08) | 38.64 (32.09) |
Median, minutes | 41.67 | 38.10 | 34.29 | 29.64 |
Change from baseline, mean (SD), minutes | –6.83 (23.04) | –16.23 (29.53) | –22.54 (32.81) | –21.88 (29.27) |
Change from baseline, median, minutes | –2.86 | –10.00 | –14.86 | –15.00 |
P valueb,c (active vs. PBO) | Reference | 0.0347 | < 0.0001 | < 0.0001 |
P valueb,c (active vs. ZOL) | NA | Reference | 0.0122 | < 0.0001 |
Last 7 nights of treatment, na | 196 | 246 | 252 | 258 |
Mean (SD), minutes | 47.60 (32.77) | 43.64 (30.65) | 38.80 (28.03) | 36.51 (31.06) |
Median, minutes | 38.57 | 37.50 | 30.36 | 27.50 |
Change from baseline, mean (SD), minutes | –8.10 (27.45) | –17.04 (30.68) | –25.20 (34.85) | –24.79 (34.07) |
Change from baseline, median, minutes | –4.00 | –10.71 | –18.54 | –17.14 |
P valueb,c (active vs. PBO) | Reference | 0.0039 | < 0.0001 | < 0.0001 |
P valueb,c (active vs. ZOL) | NA | Reference | 0.0176 | < 0.0001 |
sWASO | ||||
Baseline, n | 206 | 259 | 264 | 266 |
Mean (SD), minutes | 170.89 (80.68) | 173.06 (77.21) | 166.76 (82.05) | 175.35 (83.45) |
First 7 nights of treatment, na | 202 | 253 | 261 | 262 |
Mean (SD), minutes | 143.53 (80.57) | 124.83 (75.28) | 127.37 (78.30) | 119.78 (74.83) |
Model-adjusted change from baseline, mean, minutes | –27.56 | –48.09 | –39.97 | –53.90 |
P valueb,d (active vs. PBO) | Reference | < 0.0001 | 0.0093 | < 0.0001 |
P valueb,d (active vs. ZOL) | NA | Reference | 0.0706 | 0.1949 |
Last 7 nights of treatment, na | 196 | 247 | 253 | 253 |
Mean (SD), minutes | 135.85 (85.01) | 109.63 (72.58) | 119.30 (81.65) | 117.08 (83.75) |
Model-adjusted change from baseline, mean, minutes | –36.06 | –62.00 | –47.55 | –56.64 |
P valueb,d (active vs. PBO) | Reference | < 0.0001 | 0.0396 | 0.0002 |
P valueb,d (active vs. ZOL) | NA | Reference | 0.0059 | 0.3064 |
Subjective sleep efficiency | ||||
Baseline, n | 201 | 247 | 253 | 258 |
Mean (SD), % | 56.08 (17.34) | 55.49 (15.80) | 56.05 (17.09) | 54.31 (18.32) |
First 7 nights of treatment, na | 197 | 240 | 251 | 254 |
Mean (SD), % | 62.45 (17.58) | 66.45 (16.42) | 65.96 (18.20) | 68.10 (18.36) |
Model-adjusted change from baseline, mean, % | 6.97 | 12.11 | 10.74 | 13.81 |
P valueb,e (active vs. PBO) | Reference | < 0.0001 | 0.0008 | < 0.0001 |
P valueb,e (active vs. ZOL) | NA | Reference | 0.1963 | 0.1093 |
Last 7 nights of treatment, na | 190 | 235 | 245 | 244 |
Mean (SD), % | 63.96 (19.25) | 69.45 (16.93) | 68.19 (19.25) | 69.92 (19.10) |
Model-adjusted change from baseline, mean, % | 8.69 | 14.82 | 13.29 | 15.87 |
P valueb,e (active vs. PBO) | Reference | < 0.0001 | 0.0005 | < 0.0001 |
P valueb,e (active vs. ZOL) | NA | Reference | 0.2196 | 0.4013 |
sTST | ||||
Baseline, n | 201 | 247 | 253 | 258 |
Mean (SD), minutes | 276.23 (87.65) | 273.07 (81.21) | 275.74 (83.65) | 266.10 (92.16) |
First 7 nights of treatment, na | 197 | 240 | 251 | 254 |
Mean (SD), minutes | 305.35 (89.78) | 325.64 (81.85) | 322.66 (89.71) | 332.92 (91.54) |
Model-adjusted change from baseline, mean, minutes | 32.09 | 57.71 | 51.14 | 66.59 |
P valueb,f (active vs. PBO) | Reference | < 0.0001 | 0.0007 | < 0.0001 |
P valueb,f (active vs. ZOL) | NA | Reference | 0.2174 | 0.0949 |
Last 7 nights of treatment, na | 190 | 235 | 245 | 244 |
Mean (SD), minutes | 312.53 (95.87) | 340.20 (83.58) | 334.22 (94.34) | 343.68 (95.79) |
Model-adjusted change from baseline, mean, minutes | 40.65 | 71.04 | 64.22 | 78.47 |
P valueb,f (active vs. PBO) | Reference | < 0.0001 | 0.0003 | < 0.0001 |
P valueb,f (active vs. ZOL) | NA | Reference | 0.2718 | 0.2317 |
FAS = full analysis set; LEM5 = lemborexant 5 mg; LEM10 = lemborexant 10 mg; MMRM = mixed model of repeated measures; NA = not applicable; PBO = placebo; SD = standard deviation; sSOL = subjective sleep onset latency; sTST = subjective total sleep time; sWASO = subjective wake after sleep onset; vs. = versus; ZOL = zolpidem tartrate.
Note: Data reported with sleep diary handling rules to address potential errors and illogical values.
aThe number of patients analyzed for the change from baseline at this time point (not the number of patients who provided data at this time point).
bP value was not adjusted for multiple testing (i.e., the type I error rate was not controlled).
cBased on an MMRM model with log transformation of sSOL and factors of age group, region, treatment, visit (first 7 nights and last 7 nights), and treatment-by-visit interaction as fixed effects, and baseline sSOL as a covariate. Missing values were not imputed and assumed to be missing at random.
dBased on an MMRM model with factors of age group, region, treatment, visit (first 7 nights and last 7 nights), and treatment-by-visit interaction as fixed effects, and baseline sWASO as a covariate. Missing values were not imputed and assumed to be missing at random.
eBased on an MMRM model with factors of age group, region, treatment, visit (first 7 nights and last 7 nights), and treatment-by-visit interaction as fixed effects, and baseline subjective sleep efficiency as a covariate. Missing values were not imputed and assumed to be missing at random.
fBased on an MMRM model with factors of age group, region, treatment, visit (first 7 nights and last 7 nights), and treatment-by-visit interaction as fixed effects, and baseline sTST as a covariate. Missing values were not imputed and assumed to be missing at random.
Source: SUNRISE 1 Clinical Study Report.17
Table 66: Long-Term Change From Baseline sSOL, sWASO, Subjective Sleep Efficiency, and sTST Based on Months of Exposure to Lemborexant (Exploratory Outcomes) — SUNRISE 2 Study, On-Treatment FAS
Outcome | LEM5 (N = 444) | LEM10 (N = 437) |
|---|---|---|
sSOL | ||
Baseline,a n | 442 | 434 |
Geometric mean, minutes | 37.21 | 39.41 |
Median (Q1 to Q3), minutes | 48.10 (27.86 to 72.50) | 52.14 (30.00 to 77.14) |
1-month exposure, patients, nb | 415 | 412 |
Geometric mean, minutes | 24.70 | 25.19 |
Median (Q1 to Q3), minutes | 30.00 (17.14 to 52.50) | 30.00 (15.71 to 55.71) |
Change from study baseline, median (Q1 to Q3) | –10.00 (–30.00 to 0.00) | –14.00 (–34.29 to –0.71) |
3-months exposure, patients, nb | 386 | 375 |
Geometric mean, minutes | 20.72 | 21.87 |
Median (Q1 to Q3), minutes | 23.57 (13.88 to 40.71) | 24.29 (13.57 to 47.14) |
Change from study baseline, median (Q1 to Q3) | –14.64 (–35.12 to –2.14) | –17.31 (–42.14 to –1.50) |
6-months exposure, patients, nb | 352 | 331 |
Geometric mean, minutes | 18.24 | 19.05 |
Median (Q1 to Q3), minutes | 21.57 (12.14 to 35.71) | 22.86 (12.14 to 40.00) |
Change from study baseline, median (Q1 to Q3) | –17.14 (–38.21 to –2.86) | –20.00 (–47.14 to –2.14) |
9-months exposure, patients, nb | 233 | 213 |
Geometric mean, minutes | 16.79 | 17.08 |
Median (Q1 to Q3), minutes | 19.80 (11.43 to 35.00) | 20.61 (10.00 to 36.67) |
Change from study baseline, median (Q1 to Q3) | –26.29 (–46.43 to –10.71) | –32.86 (–58.57 to –12.86) |
12-months exposure, patients, nb | 216 | 204 |
Geometric mean, minutes | 16.85 | 17.33 |
Median (Q1 to Q3), minutes | 20.00 (11.33 to 34.29) | 21.20 (10.71 to 39.17) |
Change from study baseline, median (Q1 to Q3) | –25.71 (–46.58 to –10.32) | –32.86 (–55.68 to –13.00) |
sWASO | ||
Baseline,a patients, n | 441 | 433 |
Mean (SD), minutes | 124.75 (82.83) | 126.48 (88.09) |
1-month exposure, nb | 414 | 408 |
Change from baseline, mean (SD), minutes | –19.21 (54.74) | –20.87 (52.77) |
3-months exposure, nb | 385 | 373 |
Change from baseline, mean (SD), minutes | –33.70 (59.01) | –31.37 (60.52) |
6-months exposure, nb | 351 | 329 |
Change from baseline, mean (SD), minutes | –38.27 (65.34) | –36.16 (68.04) |
9-months exposure, nb | 232 | 212 |
Change from baseline, mean (SD), minutes | –52.54 (70.85) | –56.00 (73.36) |
12-months exposure, nb | 215 | 203 |
Change from baseline, mean (SD), minutes | –53.40 (61.50) | –56.76 (70.60) |
Subjective sleep efficiency | ||
Baseline,a patients, n | 430 | 421 |
Mean (SD), % | 65.34 (19.11) | 64.66 (17.91) |
1-month exposure, nb | 400 | 396 |
Change from baseline, mean (SD), % | 6.71 (12.33) | 8.08 (12.09) |
3-months exposure, nb | 373 | 361 |
Change from baseline, mean (SD), % | 10.39 (13.82) | 10.98 (13.81) |
6-months exposure, nb | 342 | 321 |
Change from baseline, mean (SD), % | 11.75 (15.25) | 12.05 (15.71) |
9-months exposure, nb | 222 | 205 |
Change from baseline, mean (SD), % | 15.54 (15.95) | 17.38 (16.29) |
12-months exposure, nb | 207 | 196 |
Change from baseline, mean (SD), % | 15.83 (14.33) | 17.55 (15.94) |
sTST | ||
Baseline,a patients, n | 430 | 421 |
Mean (SD), minutes | 326.42 (97.80) | 320.53 (92.28) |
1-month exposure, nb | 400 | 396 |
Change from baseline, mean (SD), minutes | 33.82 (64.31) | 42.47 (64.10) |
3-months exposure, nb | 373 | 361 |
Change from baseline, mean (SD), minutes | 51.46 (72.80) | 57.61 (70.31) |
6-months exposure, nb | 342 | 321 |
Change from baseline, mean (SD), minutes | 58.58 (80.17) | 60.97 (80.91) |
9-months exposure, nb | 222 | 205 |
Change from baseline, mean (SD), minutes | 72.99 (82.31) | 82.66 (82.81) |
12-months exposure, nb | 207 | 196 |
Change from baseline, mean (SD), minutes | 73.72 (76.15) | 85.45 (81.01) |
FAS = full analysis set; LEM5 = lemborexant 5 mg; LEM10 = lemborexant 10 mg; Q1 = first quartile; Q3 = third quartile; SD = standard deviation; sSOL = subjective sleep onset latency; sTST = subjective total sleep time; sWASO = subjective wake after sleep onset.
Note: Data reported with sleep diary handling rules to address potential errors and illogical values.
aBaseline is a) Study Baseline for data for patients who received lemborexant in period 1 and b) Treatment Period 2 Baseline for patients rerandomized from placebo to lemborexant in period 2.
bThe number of patients analyzed for the change from baseline at this time point (not the number of patients who provided data at this time point).
Source: SUNRISE 2 Clinical Study Report.18
Table 67: Objective and Subjective Sleep Onset and Sleep Maintenance Respondersa (Other Secondary Outcomes) — SUNRISE 1 Study, FAS
Outcome | PBO (N = 208) | ZOL (N = 263) | LEM5 (N = 266) | LEM10 (N = 269) |
|---|---|---|---|---|
LPS — Days 1 to 2 | ||||
Patients, na,b | 118 | 140 | 147 | 155 |
Responder, n (%)c | 32 (27.1) | 27 (19.3) | 42 (28.6) | 48 (31.0) |
Nonresponder, n (%) | 86 (72.9) | 113 (80.7) | 105 (71.4) | 107 (69.0) |
Missing, n (%)d | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
P value (active vs. PBO)e,f | Reference | 0.1346 | 0.8009 | 0.4906 |
P value (active vs. ZOL)e,f | NA | Reference | 0.0721 | 0.0218 |
LPS — Days 29 to 30 | ||||
Patients, na,b | 118 | 140 | 147 | 155 |
Responder, n (%)c | 33 (28.0) | 30 (21.4) | 54 (36.7) | 60 (38.7) |
Nonresponder, n (%) | 81 (68.6) | 102 (72.9) | 91 (61.9) | 89 (57.4) |
Missing, n (%)d | 4 (3.4) | 8 (5.7) | 2 (1.4) | 6 (3.9) |
P value (active vs. PBO)e,f | Reference | 0.2240 | 0.1211 | 0.0643 |
P value (active vs. ZOL)e,f | NA | Reference | 0.0040 | 0.0013 |
WASO — Days 1 to 2 | ||||
Patients, na,g | 205 | 261 | 266 | 266 |
Responder, n (%)h | 35 (17.1) | 121 (46.4) | 136 (51.1) | 173 (65.0) |
Nonresponder, n (%) | 170 (82.9) | 140 (53.6) | 130 (48.9) | 93 (35.0) |
Missing, n (%)d | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
P value (active vs. PBO)e,f | Reference | < 0.0001 | < 0.0001 | < 0.0001 |
P value (active vs. ZOL)e,f | NA | Reference | 0.2973 | < 0.0001 |
WASO — Days 29 to 30 | ||||
Patients, na,g | 205 | 261 | 266 | 266 |
Responder, n (%)h | 46 (22.4) | 91 (34.9) | 118 (44.4) | 124 (46.6) |
Nonresponder, n (%) | 151 (73.7) | 159 (60.9) | 142 (53.4) | 134 (50.4) |
Missing, n (%)d | 8 (3.9) | 11 (4.2) | 6 (2.3) | 8 (3.0) |
P value (active vs. PBO)e,f | Reference | 0.0023 | < 0.0001 | < 0.0001 |
P value (active vs. ZOL)e,f | NA | Reference | 0.0283 | 0.0048 |
sSOLi — First 7 nights of the treatment period | ||||
Patients, na,j | 150 | 203 | 211 | 194 |
Responder, n (%)k | 6 (4.0) | 20 (9.9) | 26 (12.3) | 28 (14.4) |
Nonresponder, n (%) | 141 (94.0) | 178 (87.7) | 181 (85.8) | 163 (84.0) |
Missing, n (%)d | 3 (2.0) | 5 (2.5) | 4 (1.9) | 3 (1.5) |
P value (active vs. PBO)e,f | Reference | 0.0424 | 0.0076 | 0.0021 |
P value (active vs. ZOL)e,f | NA | Reference | 0.4122 | 0.1674 |
sSOLi — Last 7 nights of the treatment period | ||||
Patients, na,j | 150 | 203 | 211 | 194 |
Responder, n (%)k | 15 (10.0) | 23 (11.3) | 45 (21.3) | 39 (20.1) |
Nonresponder, n (%) | 126 (84.0) | 171 (84.2) | 155 (73.5) | 149 (76.8) |
Missing, n (%)d | 9 (6.0) | 9 (4.4) | 11 (5.2) | 6 (3.1) |
P value (active vs. PBO)e,f | Reference | 0.6259 | 0.0036 | 0.0101 |
P value (active vs. ZOL)e,f | NA | Reference | 0.0063 | 0.0165 |
sWASOi — First 7 nights of the treatment period | ||||
Patients, na,l | 197 | 251 | 255 | 260 |
Responder, n (%)m | 20 (10.2) | 44 (17.5) | 45 (17.6) | 55 (21.2) |
Nonresponder, n (%) | 173 (87.8) | 201 (80.1) | 207 (81.2) | 201 (77.3) |
Missing, n (%)d | 4 (2.0) | 6 (2.4) | 3 (1.2) | 4 (1.5) |
P value (active vs. PBO)e,f | Reference | 0.0271 | 0.0249 | 0.0017 |
P value (active vs. ZOL)e,f | NA | Reference | 0.9681 | 0.2994 |
sWASOi — Last 7 nights of the treatment period | ||||
Patients, na,l | 197 | 251 | 255 | 260 |
Responder, n (%)m | 32 (16.2) | 61 (24.3) | 62 (24.3) | 62 (23.8) |
Nonresponder, n (%) | 155 (78.7) | 178 (70.9) | 182 (71.4) | 186 (71.5) |
Missing, n (%)d | 10 (5.1) | 12 (4.8) | 11 (4.3) | 12 (4.6) |
P value (active vs. PBO)e,f | Reference | 0.0365 | 0.0371 | 0.0468 |
P value (active vs. ZOL)e,f | NA | Reference | 0.9909 | 0.8994 |
FAS = full analysis set; NA = not applicable; LEM5 = lemborexant 5 mg; LEM10 = lemborexant 10 mg; LPS = latency to persistent sleep; PBO = placebo; sSOL = subjective sleep onset latency; sWASO = subjective wake after sleep onset; WASO = wake after sleep onset; vs. = versus; ZOL = zolpidem tartrate.
aThe number of patients analyzed for the change from baseline at this time point (not the number of patients who provided data at this time point).
bNumber of patients with LPS greater than 30 minutes at baseline.
cResponders are defined as LPS less than or equal to 20 minutes provided baseline LPS greater than 30 minutes.
dPatients with missing information due to early withdrawal or other reasons are considered as nonresponders in the analysis.
eP value is based on Cochran-Mantel-Haenszel test stratified by age group.
fP value was not adjusted for multiple testing (i.e., the type I error rate was not controlled).
gNumber of patients with WASO greater than 60 minutes at baseline.
hResponders are defined as WASO less than or equal to 60 minutes and a reduction from baseline of greater than 10 minutes, provided baseline WASO was greater than 60 minutes.
iWith diary handling rules applied.
jNumber of patients with sSOL greater than 60 minutes at baseline.
kResponders are defined as sSOL less than or equal to 20 minutes provided baseline sSOL was greater than 30 minutes.
lNumber of patients with sWASO greater than 60 minutes at baseline.
mResponders are defined as visit sWASO less than or equal to 60 minutes and a reduction from baseline of greater than 10 minutes, provided baseline sWASO was greater than 60 minutes.
Source: SUNRISE 1 Clinical Study Report.17
Table 68: Long-Term Subjective Sleep Onset and Sleep Maintenance Responders (Other Secondary Outcomes) — SUNRISE 2 Study, FAS
Outcome | PBO | LEM5 | LEM10 |
|---|---|---|---|
sSOL — Month 6 (FAS) | |||
Patients at baseline, N | 318 | 316 | 315 |
Patients, na,b | 254 | 250 | 249 |
Responder, n (%)c | 45 (17.7) | 78 (31.2) | 75 (30.1) |
Nonresponder, n (%) | 154 (60.6) | 123 (49.2) | 114 (45.8) |
Missing, n (%)d | 55 (21.7) | 49 (19.6) | 60 (24.1) |
Difference in proportion vs. PBO (P value)e,f | Reference | 13.67 (0.0004) | 12.53 (0.0009) |
sSOL — Month 12 (on-treatment FAS) | |||
Patients at baseline, N | NA | 444 | 437 |
Patients, na,b | NA | 310 | 285 |
Responder, n (%)c | NA | 106 (34.2) | 106 (37.2) |
Nonresponder, n (%) | NA | 151 (48.7) | 141 (49.5) |
Missing, n (%)d | NA | 53 (17.1) | 38 (13.3) |
95% CI for proportion of respondersg | NA | (28.9 to 39.5) | (31.6 to 42.8) |
sWASO — Month 6 (FAS) | |||
Patients at baseline, N | 318 | 316 | 315 |
Patients, na,b | 250 | 263 | 257 |
Responder, n (%)h | 51 (20.4) | 92 (35.0) | 77 (30.0) |
Nonresponder, n (%) | 147 (58.8) | 117 (44.5) | 111 (43.2) |
Missing, n (%)d | 52 (20.8) | 54 (20.5) | 69 (26.8) |
Difference in proportion vs. PBO (P value)e,f | Reference | 14.65 (0.0002) | 9.82 (0.0110) |
sWASO — Month 12 (on-treatment FAS) | |||
Patients at baseline, N | NA | 444 | 437 |
Patients, na,b | NA | 317 | 280 |
Responder, n (%)h | NA | 111 (35.0) | 111 (39.6) |
Nonresponder, n (%) | NA | 156 (49.2) | 138 (49.3) |
Missing, n (%)d | NA | 50 (15.8) | 31 (11.1) |
95% CI for proportion of respondersg | NA | (29.8 to 40.3) | (33.9 to 45.4) |
CI = confidence interval; FAS = full analysis set; LEM5 = lemborexant 5 mg; LEM10 = lemborexant 10 mg; NA = not applicable; PBO = placebo; sSOL = subjective sleep onset latency; sWASO = subjective wake after sleep onset; vs. = versus.
Note: Data reported with sleep diary handling rules to address potential errors and illogical values.
aThe number of patients analyzed for the change from baseline at this time point (not the number of patients who provided data at this time point).
bNumber of patients with sSOL greater than 30 minutes (for sSOL responders) or sWASO greater than 60 minutes (for sWASO responders) at study baseline.
cResponders are defined as visit sSOL less than or equal to 20 minutes provided study baseline sSOL greater than 30 minutes.
dPatients with missing information due to early withdrawal or other reasons were considered as nonresponders in the analysis. Missing responders did not have an sSOL or sWASO value for the visit due to missing data (i.e., early withdrawal from the study or incomplete diary data).
eP value is based on Cochran-Mantel-Haenszel test stratified by region and age group.
fP value was not adjusted for multiple testing (i.e., the type I error rate was not controlled).
gTwo-sided 95% CI based on normal approximation.
hResponders are defined as visit WASO less than or equal to 60 minutes, a reduction from study baseline by greater than 10 minutes, and study baseline WASO greater than 60 minutes.
Source: SUNRISE 2 Clinical Study Report.18
Table 69: Long-Term Change From Baseline Quality of Sleep Based on Months of Exposure to Lemborexant (Exploratory Outcome) — SUNRISE 2 Study, On-Treatment FAS
Outcome | LEM5 (N = 444) | LEM10 (N = 437) |
|---|---|---|
Baseline,a n | 442 | 434 |
Mean (SD) | 4.2 (1.46) | 4.2 (1.49) |
1-month exposure, nb | 415 | 412 |
Change from baseline, mean (SD) | 0.7 (1.20) | 0.6 (1.27) |
3-months exposure, nb | 386 | 375 |
Change from baseline, mean (SD) | 0.9 (1.39) | 0.8 (1.44) |
6-months exposure, nb | 352 | 331 |
Change from baseline, mean (SD) | 1.0 (1.50) | 1.0 (1.50) |
9-months exposure, nb | 233 | 213 |
Change from baseline, mean (SD) | 1.3 (1.47) | 1.4 (1.65) |
12-months exposure, nb | 216 | 204 |
Change from baseline, mean (SD) | 1.5 (1.44) | 1.6 (1.76) |
FAS = full analysis set; LEM5 = lemborexant 5 mg; LEM10 = lemborexant 10 mg; SD = standard deviation.
aBaseline is a) study baseline for data for patients who received lemborexant in period 1 and b) treatment period 2 baseline for patients rerandomized from placebo to lemborexant in period 2.
bThe number of patients analyzed for the change from baseline at this time point (not the number of patients who provided data at this time point).
Source: SUNRISE 2 Clinical Study Report.18
Appendix 4: Description and Appraisal of Outcome Measures
Note that this appendix has not been copy-edited.
Aim
To describe the following outcome measures and review their measurement properties (validity, reliability, responsiveness to change, and MID) presented in Table 70.
Measure | SUNRISE 1 study | SUNRISE 2 study |
|---|---|---|
LPS | Primary, other secondary | NA |
Sleep Efficiency | Key secondary | NA |
WASO | Key secondary, other secondary | NA |
WASO2H | Key secondary, other secondary | NA |
TST | Other secondary | NA |
sSOL | Other secondary | Primary, other secondary, exploratory |
Subjective Sleep Efficiency | Other secondary | Key secondary, other secondary, exploratory |
sWASO | Other secondary | Key secondary, other secondary, exploratory |
sTST | Other secondary | Other secondary, exploratory |
ISI | Other secondary | Other secondary |
FSS | Other secondary | Other secondary |
EQ-5D-3L and VAS | Exploratory | Exploratory |
PGI-Insomnia | Exploratory | Exploratory |
T-BWSQ | Safety | Safety |
Postural stability | Safety | NA |
EQ-5D-3L = 3-level EQ-5D; FSS = Fatigue Severity Scale; ISI = Insomnia Severity Index; LPS = latency to persistent sleep; NA = not applicable; PGI-Insomnia = Patient Global Impression–Insomnia; sSOL = subjective sleep onset latency; sTST = subjective total sleep time; sWASO = subjective wake after sleep onset; T-BWSQ = Tyrer Benzodiazepine Withdrawal Symptom Questionnaire; TST = total sleep time; VAS = visual analogue scale; WASO = wake after sleep onset; WASO2H = wake after sleep onset in the second half of the night.
Findings
Table 71: Summary of Outcome Measures and Their Measurement Properties
Outcome measure | Description | Conclusions about measurement properties | MID |
|---|---|---|---|
sSOL | It is a self-reported measure, derived from a sleep diary that estimates the length of time (in minutes) between turning off the lights when the patient attempts to sleep and the time the patient actually falls asleep.43,65,66 A shorter duration of sSOL is indicative of improved sleep. | Validity: Convergent validity was supported by a strong correlation between the ‘Difficulty falling asleep’ item of the ISI and sSOL (r = 0.56, P < 0.05).42 In another study, convergent validity was demonstrated through a moderate correlation between sSOL and the PSQI (r = 0.44).52 A moderate correlation was found between sSOL and actigraphy-derived SOL (r = 0.44, P < 0.01).53 Discriminant validity has been demonstrated between patients with insomnia and controls (AUC = 0.84; 95% CI, 0.77 to 0.92).54 Reliability and responsiveness to change: No data were found. | Suggested threshold for a clinically important difference relative to placebo: mean change ≥ 20 minutes.10 |
sWASO | It is a self-reported measure, derived from a sleep diary that refers to periods of wakefulness occurring after defined sleep onset. It measures time spent awake (in minutes) after initial sleep onset until last awakening.43,65,66 A shorter duration of sWASO is indicative of improved sleep. | Validity: Convergent validity was supported by a strong correlation between the ‘Difficulty of staying asleep’ item of the ISI and sWASO (r = 0.57, P < 0.05).42 Convergent validity was demonstrated through a moderate correlation between sWASO and the PSQI (r = 0.37).52 Another study found a moderate correlation between sWASO and actigraphy-derived WASO (r = 0.41, P < 0.05).53 Discriminant validity has been demonstrated between patients with insomnia and controls (AUC = 0.93; 95% CI, 0.88 to 0.98).54 Reliability and responsiveness to change: No data were found. | Suggested threshold for a clinically important difference relative to placebo: mean change ≥ 30 minutes.10 |
sTST | It is a self-reported measure, derived from a sleep diary that estimates the duration of sleep (in minutes) from sleep onset to sleep offset.43,65,66 Longer sTST indicates improved sleep. | Validity: Convergent validity was supported by a strong correlation between the total ISI score and sTST (r = –0.54, P < 0.05).42 Another study found a strong correlation between sTST and actigraphy-derived TST (r = 0.64, P < 0.01).53 sTST was found to moderately correlate with PSG-derived TST (r = 0.39, P < 0.01).50 Discriminant validity has been demonstrated between patients with insomnia and controls (AUC = 0.87; 95% CI, 0.80 to 0.93).54 Reliability and responsiveness to change: No data were found. | Suggested threshold for a clinically important difference relative to placebo: mean change ≥ 30 minutes.10 |
Subjective Sleep Efficiency | It is a self-reported measure, derived from a sleep diary that measures the percentage of total time in bed actually spent in sleep. It is calculated as the sTST divided by the total time spent asleep and multiplied by 100. Time spent asleep is derived from subjective time spent in bed after subtracting sWASO.43,65,66 A higher subjective sleep efficiency indicates improved sleep. | Validity: Convergent validity was supported by a strong correlation found between the total ISI score and subjective sleep efficiency (r = –0.59, P < 0.05).42 Convergent validity was also demonstrated through a strong correlation between subjective sleep efficiency and the PSQI (r = –0.52).52 Another study found a weak correlation between subjective sleep efficiency and actigraphy-derived sleep efficiency (r = 0.20, P > 0.05).53 Discriminant validity has been demonstrated between patients with insomnia and controls (AUC = 0.94; 95% CI, 0.89 to 0.99).54 Reliability and responsiveness to change: No data were found. | Suggested threshold for a clinically important difference relative to placebo: mean change ≥ 10%.10 |
LPS | It is a PSG-derived measure that estimates the time (in minutes) from lights off to the first epoch of 20 consecutive epochs of nonwakefulness.48,66,67 A shorter duration of LPS is indicative of improved sleep. | Validity: ROC analysis showed that LPS derived from PSG does not accurately distinguish between primary insomnia and normal sleepers (i.e., without insomnia) (AUC = 0.63).47 Reliability: In terms of test-retest reliability, the mean of multiple LPS measurements over 3 nights demonstrated substantial agreement (ICC = 0.80; 95% CI, 0.73 to 0.85) in patients with insomnia.48 Responsiveness to change: No data were found. | Suggested threshold for a clinically important difference relative to placebo: mean change ≥ 10 minutes.10 |
TST | It is a PSG-derived measure that estimates the time (in minutes) of sleep from sleep onset until terminal awakening.48,66,67 Longer TST indicates improved sleep. | Validity: A moderate correlation was found between PSG-derived and self-reported measures of TST (r = 0.39; P < 0.001).50 PSG-derived TST was found to moderately correlate with self-reported TST (r = 0.39, P < 0.01).50 ROC analysis showed that TST derived from PSG does not accurately distinguish between primary insomnia and normal sleepers (i.e., without insomnia) (AUC = 0.57).47 Reliability: In terms of test-retest reliability, the mean of multiple TST measurements over 3 nights demonstrated substantial agreement (ICC = 0.69; 95% CI, 0.59 to 0.77) in patients with insomnia.48 Responsiveness to change: No data were found. | Suggested threshold for a clinically important difference relative to placebo: mean change ≥ 20 minutes.10 |
Sleep Efficiency | It is a PSG-derived measure that estimates the proportion of time spent asleep per time in bed. It is calculated as the TST divided by the interval from lights off until lights on.48,66,67 A higher sleep efficiency indicates improved sleep. | Validity: Construct validity was demonstrated through a strong correlation between PSG-derived and actigraphy-derived sleep efficiency (r = 0.65, P < 0.005).51 ROC analysis showed that PSG-derived sleep efficiency does not accurately distinguish between primary insomnia and normal sleepers (i.e., without insomnia) (AUC = 0.64).47 Reliability and responsiveness to change: No data were found. | Suggested threshold for a clinically important difference relative to placebo: mean change ≥ 5%.10 |
WASO | It is a PSG-derived measure that refers to the time (in minutes) of wake from the onset of persistent sleep until lights on. 68 It measures wakefulness, excluding the wakefulness occurring before sleep onset; and is a better reflection of sleep fragmentation.48,66,67 A shorter duration of WASO is indicative of improved sleep. | Validity: Construct validity was supported by a strong correlation between PSG-derived and actigraphy-derived WASO (r = 0.61, P < 0.001).49 ROC analysis showed that PSG-derived WASO does not accurately distinguish between primary insomnia and normal sleepers (i.e., without insomnia) (AUC = 0.55).47 Reliability: In terms of test-retest reliability, the mean of multiple WASO measurements over 3 nights demonstrated substantial agreement (ICC = 0.69; 95% CI, 0.59 to 0.77) in patients with insomnia.48 Responsiveness to change: No data were found. | Suggested threshold for a clinically important difference relative to placebo: mean change ≥ 20 minutes.10 |
WASO2H | It is a PSG-derived measure that estimates the time of wake-up (in minutes) during the interval from 240 minutes after lights are turned off until lights are turned on.48,66,67 A shorter duration of WASO2H is indicative of improved sleep. | No data were found supporting the validity, reliability, or responsiveness to change for patients with insomnia. | No reported MID was identified for patients with insomnia. |
ISI | The ISI is a self-reported 7-item instrument that was designed to assess the severity of both nighttime and daytime components of insomnia.42 It comprises the following items: severity of sleep onset, sleep maintenance, early morning awakening problems, sleep dissatisfaction, interference of sleep difficulties with daytime functioning, noticeability of sleep problems by others, and distress caused by the sleep difficulties. A 5-point Likert scale is used to score each item (e.g., with anchors at 0 “no problem” and 4 “very severe problem” for rating severity of insomnia problems), yielding a total score ranging from 0 to 28. Higher ISI scores indicate more acute symptoms of insomnia as follows42:
| Validity: Convergent validity was demonstrated through strong correlations between the ISI items and subjective sleep measures as follows: between the ISI ‘Difficulty falling asleep’ item and sSOL (r = 0.56, P < 0.05), the ISI ‘Difficulty staying asleep’ item and sWASO (r = 0.57, P < 0.05), the total ISI score and sTST (r = –0.54, P < 0.05), and the total ISI score and subjective sleep efficiency (r = –0.59, P < 0.05).42 The ISI total score was found to strongly correlate with the PSQI total score (r = 0.80) and SF-12 mental component (r = –0.51), and moderately correlated with SF-12 physical component (r = –0.31).42 Construct validity was demonstrated through moderate to strong correlations between the ISI score and the corresponding sleep diary measures at baseline (r = 0.32 to 0.55) and moderate to strong correlations at posttreatment (r = 0.05 to 0.91).43 However, the ISI score was found to be weakly-to-moderately correlated with PSG-derived sleep measures at baseline (r = 0.07 to 0.045) and posttreatment (r = 0.23 to 0.45).43 Criterion validity was demonstrated by ability of the ISI to identify the presence or absence of insomnia in 183 patients evaluated for insomnia treatment.42 Reliability: The ISI was found to have a high internal consistency (Cronbach alpha = 0.90 to 0.92), with moderate to substantial correlations between individual items and total ISI score (r = 0.55 to 0.85).42,44 Responsiveness to change: Several studies found that the ISI is a sensitive measure to detect changes in perceived sleep difficulties with treatment.42-44 | A 7-point reduction in ISI score for moderate improvements and a 9-point reduction in ISI score for marked improvements.42 A 6-point reduction is recommended to represent a clinically meaningful improvement in individuals with primary insomnia.45 |
FSS | The FSS is a self-reported 9-item instrument designed to evaluate the severity of fatigue and its effect on a person’s activity and lifestyle in patients with insomnia disorders during the past week. A 7-point Likert scale is used to score each item with anchors at 1 “strong disagreement with the statement” and 7 “strong agreement with the statement,” yielding a total score ranging from 9 to 63, with a higher score indicating greater fatigue severity. The FSS total scores are more commonly reported as the mean score over the 9 items, ranging from 1 to 7.46,69 When using a score of ≥ 4 points to define fatigue, fatigue was found in 62% of patients with sleep disorders, including insomnia.46 | Validity: Construct validity was demonstrated through a strong correlation between the FSS and fatigue as indicated on the VAS (r = 0.71, P < 0.05).46 A moderate to strong correlation was found between the FSS and ESS in patients with sleep-wake disorders (r = 0.31 to 0.71).46 Reliability: The FSS showed excellent internal consistency (Cronbach alpha = 0.93), and substantial to almost perfect test-retest reliability in patients with sleep-wake disorders (Lin’s correlation coefficient of concordance, r = 0.61 to 0.83).46 Responsiveness to change: No data were found. | No reported MID was identified for patients with insomnia. |
EQ-5D-3L | The EQ-5D is a generic self-reported HRQoL instrument that may be applied to a wide range of health conditions and treatments.40,41 The first of 2 parts of the EQ-5D is a descriptive system that classifies respondents (aged ≥ 12 years) based on the following 5 dimensions: mobility, self-care, usual activities, pain/discomfort, and anxiety/depression. The EQ-5D-3L has 3 possible levels (1, 2, or 3) for each domain, representing ‘no problems,’ ‘some problems,’ and ‘extreme problems,’ respectively. Respondents are asked to choose the level that reflects their health state for each of the 5 dimensions, corresponding with 243 different health states.40,41 The second part is a 20 cm visual analogue scale (EQ VAS) that has end points labelled 0 and 100, with respective anchors of ‘worst imaginable health state’ and ‘best imaginable health state.’ Respondents are asked to rate their health by drawing a line from an anchor box to the point on the EQ VAS which best represents their health on that day. Hence, the EQ-5D produces 3 types of data for each respondent:
The EQ-5D index score is generated by applying a multiattribute utility function to the descriptive system. Scores less than 0 represent health states that are valued by society as being worse than dead, while scores of 0 and 1.00 are assigned to the health states ‘dead’ and ‘perfect health,’ respectively.40,41 | No data were found supporting the validity, reliability, or responsiveness to change for patients with insomnia. | No reported MID was identified for patients with insomnia. Overall reported MIDs for the EQ-5D-3L have ranged from 0.033 to 0.074 based on various studies in different countries with different populations.70 |
PGI-Insomnia | It is a self-reported instrument assessing a patient’s perception of the effects of a study drug on their sleep at the end of the study. The PGI-Insomnia consists of 4 items pertaining to the therapeutic effect of the study drug. The first 3 items refer to the effects of the study drug and are scored on a 3-point Likert scale as follows:
The last item refers to the perceived appropriateness of the study drug strength and is scored on a 3-point Likert scale as follows: (1) too strong, (2) just right, (3) too weak. Each item of the PGI-Insomnia is reported separately as number and percentage of patients at each time point. | No data were found supporting the validity, reliability, or responsiveness to change for patients with insomnia. | No reported MID was identified for patients with insomnia. |
T-BWSQ | The T-BWSQ is a self-reported 20-item questionnaire completed at the end of study that is used to assess the incidence of symptoms during withdrawal.57 Of the 20 items, 7 refer to somatic symptoms, 10 to disturbances of perception and sensation, and 3 are independent items that include depressed mood, loss of control of voluntary movement, and memory loss. Patients are asked about the presence or absence and severity of the symptoms listed in the questionnaire. A 3-point Likert scale is used to score each item as follows: 0 = “no,” 1 = “yes – moderate,” or 2 = “yes – severe,” yielding a total score from 0 to 40. A higher total T-BWSQ score indicates more withdrawal effects upon drug discontinuation.57 | Validity: No data were found. Reliability: High interitem associations were found for the scores of 3 perceptual items, sensitivity to smell, touch, and perception of things moving when they were still (Goldman and Kruskal’s λ ≥ 0.5), while items such as sensitivity to noise, depression, and shaking, were largely independent (Goldman and Kruskal’s λ < 0.5).57 Responsiveness to change: The T-BWSQ scores during the period of withdrawal were greater in patients taking higher drug dosages and for longer periods of time.57 | In a study of 68 patients who received benzodiazepines, a change in the mean total T-BWSQ score of 3 or greater was indicative of withdrawal symptoms.57 |
Postural stability | Postural stability is defined as the ability of a person to maintain the position of the body, or more precisely, its centre of mass, within certain boundaries of space.71 Postural stability is assessed using the Cognitive Drug Research posture device. Patients are asked to stand on a firm surface with feet comfortably apart, either barefoot or wearing socks, as still as possible with eyes closed for 1 minute. The Cognitive Drug Research posture device measures directional trunk movements - body sway, through the ataxiameter connected to a cable placed around the patient’s waist. The body sway data are then transferred to the laptop. The body sway is measured in arbitrary units, with a higher number indicating more body sway (less postural stability). One unit of body sway is defined as one-third degree angle of arc movement of the ataxiameter. | No data were found supporting the validity, reliability, or responsiveness to change for patients with insomnia. | A 7-unit change in body sway from baseline (or 35% increase)72 is associated with an alcohol dose of 0.5 g/kg body mass,55 leading to impairment on tasks requiring postural stability.56 |
AUC = area under the curve; CI = confidence interval; EQ-5D-3L = 3-level EQ-5D; ESS = Epworth Sleepiness Scale; FSS = Fatigue Severity Scale; HRQoL = health-related quality of life; ICC = intraclass correlation coefficient; ISI = Insomnia Severity Index; LPS = latency to persistent sleep; MID = minimal important difference; PGI-Insomnia = Patient Global Impression–Insomnia; PSG = polysomnography; PSQI = Pittsburgh Sleep Quality Index; ROC = receiver operating characteristic; SF-12 = Short Form (12) Health Survey; sSOL = subjective sleep onset latency; sTST = subjective total sleep time; sWASO = subjective wake after sleep onset; T-BWSQ = Tyrer Benzodiazepine Withdrawal Symptom Questionnaire; TST = total sleep time; VAS = visual analogue scale; WASO = wake after sleep onset; WASO2H = wake after sleep onset in the second half of the night.
Sleep Diary and Subjective Sleep Measures: sSOL, sWASO, sTST, and Subjective Sleep Efficiency
The sleep diary is the accepted standard for collecting data over time on self-reported sleep. The sleep diary consists of questions to assess the patient’s rating of sleep quality each night. It should be completed upon arising each morning. It is a valuable tool for recording various parameters and aspects of sleep, including temporal aspects (e.g., bedtime, lights-out time, attempts at sleep, wake-up time), and quantitative aspects (e.g., sleep onset latency, number and duration of awakenings, TST).73 Additionally, a sleep diary is also used to assess the patient’s perception of the quality of sleep scored on 9-point Likert scale with anchors at 1 “being extremely poor” and 9 “being extremely good.”
Sleep outcome measures derived from the sleep diary include sSOL, subjective sleep efficiency, sWASO, and sTST43,65 (Table 71):
Subjective sleep onset latency (sSOL): estimates the length of time (in minutes) between time from initial lights out and the time patient actually falls asleep.68 It is crucial that the “lights out” time is close to the patient’s routine bedtime at home as this can affect the estimation of the sSOL.
sWASO: refers to periods of wakefulness occurring after defined sleep onset. This parameter measures time spent awake (in minutes) after initial sleep onset until last awakening.
sTST: estimates the total amount of sleep time scored during the total recording time. It estimates the duration of sleep (in minutes) from sleep onset to sleep offset.
Subjective sleep efficiency: refers to percentage of total time in bed actually spent asleep. It is calculated as the sTST divided by the total time spent asleep and multiplied by 100. Time spent asleep is derived from subjective time spent in bed after subtracting sWASO.
Due to night-to-night sleep variability in patients with insomnia, a sleep diary should be completed for at least 1 to 2 weeks to establish a baseline level. Once a baseline sleep pattern is established, the patient and health care provider can use the sleep diary to monitor treatment progress and symptom recurrence.74,75
Psychometric Properties
In a study of 183 patients with insomnia and 62 controls, convergent validity was supported by strong correlations between subjective sleep measures and the ISI items as follows: between sSOL and the ISI item “Difficulty falling asleep” (r = 0.56; P < 0.05), between sWASO and the ISI item “Difficulty staying asleep” (r = 0.57, P < 0.05), as well as between the total ISI score and sTST (r = –0.54; P < 0.05) and subjective sleep efficiency (r = –0.59; P < 0.05).42 Jungquist et al.53 evaluated construct validity of the electronic diary measures by mapping them against actigraphy-derived objective sleep data. The study found a strong correlation between subjective and objective TST (r = 0.64; P < 0.01), moderate correlations between subjective and objective SOL (r = 0.44; P < 0.01) and WASO (r = 0.41; P < 0.05), and a weak correlation between subjective and objective SE (r = 0.20; P > 0.05).53 Another study by Mallinson et al.65 found a moderate correlation between sleep duration data derived from a sleep diary and self-reported questionnaire in a cohort of 1,516 adults (Spearman’s rank correlation coefficient, r = 0.48; 95% CI, 0.44 to 0.52). In a study of 92 patients with insomnia,50 self-reported TST was found to moderately correlate with PSG-derived TST (r = 0.39; P < 0.01). Convergent validity was demonstrated through moderate correlations of the PSQI with sSOL (r = 0.44) and sWASO (r = 0.37), and a strong correlation with subjective sleep efficiency (r = –0.52) in a study of 1,039 undergraduate students.52 Levenson et al.54 found that subjective measures, including sSOL, sWASO, subjective sleep efficiency, and sTST performed better at discriminating between the patients with insomnia and healthy sleepers (area under the curve [AUC] = 0.84 to 0.94), compared to actigraphy-derived measures (AUC = 0.58 to 0.61).54
Minimal Important Difference
The clinical significance thresholds relative to PBO for each subjective measure were determined using the nominal consensus of a task force composed of content experts in the field of insomnia, based on their expertise and familiarity with the literature and clinical practice (Table 71).10 The clinical significance threshold for sSOL was defined as a mean change at least 20 minutes, for sWASO and sTST as a mean change at least 30 minutes, and for subjective sleep efficiency as a mean change at least 10%, compared to PBO.10
Polysomnography and Objective Sleep Measures
PSG is a gold standard for measuring sleep objectively that includes including electrophysiological recordings of brain activity (EEG), muscle activity (EMG), and eye movements (EOG).51,76 However, its complexity and cost limit its use outside of medical sleep disorders.51 In addition, the screening PSG included channels for assessment of symptoms of sleep apnea and periodic limb movement disorder. The PSG recording is categorized into different sleep stages, including sleep stage I, sleep stage II, slow wave sleep, rapid eye movement sleep, and WASO.76
Sleep outcome measures derived from PSG include LPS, sleep efficiency, WASO, and WASO2H48,66,67 (Table 71):
LPS: refers to the time (in minutes) from lights off to the first epoch of 20 consecutive epochs of nonwakefulness.
TST: refers to the time (in minutes) of sleep from sleep onset until terminal awakening.
Sleep Efficiency: It refers to the proportion of time spent asleep per time in bed. It is calculated as the TST divided by the interval from lights off until lights on.
WASO: refers to the time (in minutes) of wake from the onset of persistent sleep until lights on.68 This parameter measures wakefulness, excluding the wakefulness occurring before sleep onset; and is a better reflection of sleep fragmentation.
WASO2H: refers to the time of wake-up (in minutes) during the interval from 240 minutes after lights are turned off until lights are turned on.
Psychometric Properties
Construct validity was demonstrated though a strong correlation between PSG-derived and actigraphy-derived sleep efficiency (r = 0.65, P < 0.005).51 In a study of 90 patients with insomnia, a strong correlation was found between PSG-derived and actigraphy-derived WASO (r = 0.61, P < 0.001).49 The same study found that actigraphy tended to underestimate minutes of WASO compared to PSG using the Bland-Altman plot.49 In another study, convergent validity was supported by a moderate correlation between PSG-derived and self-reported measures of TST (r = 0.39; P < 0.001).50 Edinge et al.,47 using receiver operating characteristic analyses, found that none of the PSG-derived measures accurately discriminated primary insomnia from normal sleep: AUC was 0.63 for LPS, 0.64 for sleep efficiency, 0.67 for WASO, and 0.57 for TST.47
Gaines et al.48 evaluated test-retest reliability of PSG-derived sleep measures in 150 patients with insomnia and 151 controls using 2-way random-effects intraclass correlation coefficients (ICCs) to compare single measurement or the mean of multiple measurements over 3 nights. In patients with insomnia, single-measure TST demonstrated moderate agreement (ICC = 0.43; 95% CI, 0.32 to 0.53), whereas the mean of multiple TST measurements over 3 nights demonstrated substantial agreement (ICC = 0.69; 95% CI, 0.59 to 0.77). Similarly, moderate agreement was found in single-measure LPS (ICC = 0.57; 95% CI, 0.48 to 0.65) and substantial agreement in the mean of multiple LPS measurements (ICC = 0.80; 95% CI, 0.73 to 0.85). Single-measure WASO demonstrated fair agreement (ICC = 0.59), whereas the mean of multiple WASO measurements demonstrated substantial agreement (ICC = 0.64; 95% CI, 0.52 to 0.73) in patients with insomnia.48
Minimal Important Difference
The clinical significance thresholds relative to PBO for each PSG-derived measure were determined using the nominal consensus of the task force composed of content experts in the field of insomnia, based on their expertise and familiarity with the literature and clinical practice (Table 71).10 The clinical significance threshold for LPS was defined as a mean change at least 10 minutes, for WASO and TST as a mean change at least 20 minutes, and for sleep efficiency as a mean change at least 5%.10
Other Considerations and Limitations
There are some challenges in evaluating reliability of sleep measures derived from sleep diaries, such as night-to-night sleep variability in patients with insomnia that may violate the constancy assumption of test-retest reliability. Thus, a valid test-retest reliability assessment will require many nights to overcome the variability issue in sleep itself.77,78 In terms of assessing internal consistency, the sleep diary items are not expected to correlate with one another, as the sleep diary is not intended to measure 1 specific construct, but multiple.77,78
The 2020 CADTH Technology Review23 highlighted that the clinical significance of symptomatic changes (MIDs) in insomnia disorder are poorly understood, and there are no standards to help investigators evaluate whether a statistically significant improvement in outcome translates into a clinically significant improvement.
Appendix 5: Additional Data on Motor Vehicle Accidents
Note that this appendix has not been copy-edited.
A sponsor-submitted report79 that aimed to explain assumptions regarding the risk of MVAs associated with treatment with LEM compared with zopiclone, which was used to inform the pharmacoeconomic model, has been summarized.
The sponsor-submitted report presented the results of a randomized, DB, 4-period, crossover controlled trial that aimed to evaluate the effect of LEM versus zopiclone on driving performance in 48 healthy volunteers.80 Participants were assigned to receive LEM at doses of 2.5 mg, 5 mg, or 10 mg, or zopiclone at a dose of 7.5 mg at bedtime. The primary end point of the trial was the standard deviation of lateral position (SDLP) on a standardized on-the-road driving test, which is an objective measure of road tracking errors (i.e., lane weaving).81 A clinically meaningful mean difference in SDLP was considered to be at least 2.4 cm, demonstrated in a systematic review to be equivalent to a person driving with a blood alcohol concentration (BAC) of 0.05%.82 Based on the reanalysis of the trial results presented in the sponsor-submitted report, the odds of having a SDLP greater than 2.4 cm were greater in participants who received zopiclone compared to those who received LEM at doses of 5 mg and 10 mg (OR = 3.57; 95% CI, 1.19 to 11.5, and OR = 4.33; 95% CI, 1.38 to 15.00, respectively).
The authors of the sponsor-submitted report concluded that the trial results suggested that the risk of a nonfatal MVA in patients who received zopiclone for insomnia would be at least equivalent to a risk of injury at a BAC of 0.05%. Per the authors of the sponsor-submitted report, Taylor et al. (2012)82 demonstrated via a systematic review that alcohol use is associated with an increased odds of a fatal MVA with an estimated OR of 1.74 (95% CI, 1.43 to 2.14) for every 0.02% increase in BAC, while the odds of fatal injury at a BAC of 0.05% would be approximately 3.57 (95% CI, 1.19 to 11.5). In another systematic review,83 the odds of a nonfatal MVA injury following 2 standard drinks were estimated at 2.20 (95% CI, 2.03 to 2.09). Based on these data, the authors of the sponsor-submitted report concluded that the odds of a nonfatal MVA in a patient receiving zopiclone instead of LEM5 or LEM10 for insomnia management would be at least equivalent to the odds of nonfatal MVA with alcohol impairment at the 0.05% level, which would be 2.20 (95% CI, 2.03 to 2.09).
The authors of the sponsor-submitted report concluded that their assumption was consistent with the results of a Norwegian prospective cohort study of 3.1 million people, who filled prescriptions for zopiclone, ZOL, nitrazepam, and flunitrazepam for 2 years.84 The study found that all 4 medications were associated with an increased risk of MVAs, as assessed by a standardized incidence ratio: the standardized incidence ratio for zopiclone was 2.3 (95% CI, 2.0 to 2.8), for ZOL was 2.2 (95% CI, 1.4 to 3.4), for nitrazepam was 2.7 (95% CI, 1.8 to 3.9), and for flunitrazepam was 4.0 (95% CI, 2.4 to 6.4).84
Critical Appraisal
Internal Validity
There were important limitations to the methods used to estimate the odds of MVAs in the sponsor-submitted report. The assumptions made by the authors to use SDLP and BAC data to estimate odds of MVAs after taking zopiclone or LEM are unlikely to be valid. There are likely differences in the effects of alcohol and the effects of medications used to treat insomnia (e.g., LEM, zopiclone) that would impact the odds of MVAs. The assumed odds of MVAs for patients taking zopiclone compared with those taking LEM, as extrapolated by the authors of the sponsor-submitted report, may be very different than the actual odds.
External Validity
The sponsor-submitted report on MVAs has limited external validity. The SDLP trial included only healthy volunteers (who explicitly had no sleep disorders and were described as “good sleepers”), which limits generalizability of the trial results to patients with insomnia. The small sample size further limits generalizability of this study to the Canadian population. Furthermore, the Norwegian prospective cohort study used to substantiate the conclusions did not include data on LEM.
Appendix 6: Additional Information Provided to CADTH for the Reconsideration Process
Note that this appendix has not been copy-edited.
Background
Following the issuance of the draft CDEC recommendation for LEM in August 2022, the following additional information was provided to CADTH:
1 unpublished manuscript by Drake et al.14 that provided evidence for LEM’s efficacy as measured by the PGI-Insomnia in SUNRISE 2;
A PSUR15 that included aggregate data from approximately 4,024 adult patients with insomnia disorder, ISWRD, or healthy volunteers who were enrolled in the LEM clinical development program; and
A published NMA by De Crescenzo et al. (2022)16 comparing LEM to other pharmacologic treatment for the acute and long-term treatment of adults with insomnia.
These data were not included in the submission to CADTH and provided more information on the clinical meaningfulness of the subjective PGI-Insomnia instrument, safety, and comparison to other drugs for the treatment of insomnia.
Other Sponsor-Submitted Evidence
This section includes sponsor-submitted evidence that was considered to address important gaps in the evidence included in the systematic review and CDEC initial recommendation decision.
Sponsor-Submitted Evidence: Drake et al. (unpublished)
One unpublished manuscript by Drake et al.14 was submitted by the sponsor to provide evidence for LEM’s efficacy by the PGI-Insomnia in SUNRISE 2. SUNRISE 2 has been described in the CADTH review of LEM and only the Drake et al. results and a critical appraisal of the submitted evidence will be summarized.
Posthoc analyses were conducted to examine the possible relationships between the PGI-Insomnia items and ISI items to assess patients’ perception of medication efficacy as well as between the PGI-Insomnia item 4 (appropriateness of medication strength) and TEAEs. The first analysis compared PGI-Insomnia items 2 and 3 (how the study medication increased or decreased the time to fall asleep and TST, respectively) to sSOL and sTST. The second analysis compared PGI-Insomnia item 4 (appropriateness of medication strength) to subjective sleep measures sSOL, sWASO, and sTST. The third analysis attempted to examine possible correlations between patients’ responses of PGI-Insomnia items 1 to 3 to a modified ISI scoring system (modified total score [item 5 removed], insomnia symptoms domain [items 1, 2, 3], and daytime functioning domain [items 4, 6, 7]). Using an anchor-based approach, the authors estimated the magnitude of change perceived by patients that was considered clinically meaningful. Finally, the authors examined safety data for a possible relationship between TEAEs and PGI-Insomnia item 4.
Confirmatory factor analysis was performed on the FAS (N = 949; patients who received at least 1 dose of study drug and had at least 1 postdose primary efficacy measurement). The analysis was used to assess the fit of a prespecified 2-factor solution model: factor 1 was the insomnia symptoms domain (items 1, 2, 3) and factor 2 was the daytime functioning domain (items 4, 6, 7). Item 5 was removed to achieve best model fit and it was found that item 5 was highly correlated with item 7. The model fit statistic was 0.956 for the comparative fit index and 0.075 for the root mean square error of approximation, which the authors deemed to be acceptable. Loadings were above 0.4.
Efficacy
Patients who reported a positive response on the PGI-Insomnia items 2 and 3 generally demonstrated larger magnitudes of improvement in sSOL (decrease time to sleep) and sTST (increased time spent sleeping), respectively, compared to those who reported neutral or negative responses on the PGI-Insomnia items.
Patients who responded to PGI-Insomnia item 4 that the strength of medication was “just right” had a numerically greater median change from baseline to month 6 compared to those who responded “too weak” for the sSOL. No clear trend was observed between results for medication strength that was “just right” compared to “too strong.” A similar trend was observed for sWASO and sTST comparing categories of “just right” to “too weak” and, likewise, no clear trend was observed between “just right” and “too strong.” None of the apparent differences in changes from baseline for sSOL, sWASO, or sTST across PGI-Insomnia item 4 categories were tested statistically. In nearly all categories of different responses to medication strength and results for sSOL, sWASO, and sTST, patients who received LEM10 or LEM5 showed a greater numerical change from baseline compared to PBO, though it is worth noting that most comparisons of either LEM10 or LEM5 versus PBO did not reach statistical significance.
The modified ISI score (item 5 removed from total score) had acceptable internal validity (Cronbach alpha = 0.70). Both the insomnia symptoms domain (items 1, 2, 3) and daytime functioning domain (items 4, 6, 7) demonstrated weaker internal consistency (Cronbach alpha = 0.47 and 0.68, respectively) than the modified ISI. Patients who indicated a positive response to the PGI-Insomnia items 1 to 3 had the greatest mean change from baseline for the modified ISI score (range from –9.90 to –10.5), which the authors indicated that a 10-point decrease for the modified ISI would be clinically meaningful. Patients who had neutral and negative responses had smaller mean changes from baseline (range from –4.92 to –6.31 and range from –2.42 to –3.59, respectively). None of the apparent differences in changes in the modified ISI score across PGI-Insomnia items 1 to 3 response options were tested statistically. Trends were similar for the insomnia symptoms and daytime functioning domains.
Safety
Patients who reported that medication strength was “too strong” also had a higher rate of any TEAE compared to those who reported medication strength to be either “just right” or “too weak” on PGI-Insomnia item 4: 77.8%, 58.6% and 62.8% of patients, respectively. Categories of “too strong,” “just right,” and “too weak” corresponded with rates of somnolence of 33.3%, 12.3% and 3.6%, respectively. None of the apparent differences in the rate of TEAEs across PGI-Insomnia item 4 categories were tested statistically.
Critical Appraisal
Since the data used in the Drake et al. study were the same as those from SUNRISE 2, the internal and external validity are largely similar. PGI-Insomnia and ISI were exploratory and secondary outcomes, respectively, in SUNRISE 2, and neither was controlled for increased risk of type I error. SUNRISE 2 was not designed to show relationships between the sleep measurements, and the confidence in posthoc analyses results are limited by this. No CIs were presented for the posthoc data, but variability in results was noted by wide ranges, large SDs, and wide quartile ranges. Internal consistency was assessed for modified ISI scores, though no other psychometric properties were assessed. An estimated clinically important difference of a decrease in 10 points on the ISI from baseline to 6 months has been suggested from the analyses in the Drake et al. manuscript, and it would be important to confirm this in other studies.
Sponsor-Submitted Evidence: Periodic Safety Update Report (2022)
The PSUR15 includes aggregate data from approximately 4,024 adult patients with insomnia disorder, ISWRD, or healthy volunteers have been enrolled in the LEM clinical development program to date. In total, 2,641 received LEM, 990 received PBO, and 393 received a BZRA (i.e., ZOL, eszopiclone, brotizolam, or flunitrazepam); patients may have received more than 1 medication. Most patients who received LEM were female (n = 1,666, 63%), aged between 18 years and 65 years (n = 1,968, 75%), and white (n = 1,779, 67%). It is estimated that there are more than 137 million patient days of exposure as of the date of the PSUR.
Key safety concerns were identified and reported for the total population treated (patients with insomnia, ISWRD, or healthy volunteers). Of those considered notable harms in the CADTH systematic review protocol for LEM, there was no “significant new information” identified for daytime impairment or somnolence. ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
The indication for LEM includes patients with insomnia and not ISWRD and the aggregated data in the PSUR make it difficult to attribute safety signals to only patients with insomnia.
Indirect Evidence
Description of Indirect Comparisons
One sponsor-submitted ITC (NMA 1) and 1 published NMA (NMA 2) were previously summarized and appraised.
An additional NMA published by De Crescenzo et al. (2022)16 has become available and will hereafter be referred to as NMA 3. The objective of this section is to summarize and appraise NMA 3 for the relative efficacy and safety of LEM for the treatment of insomnia, characterized by difficulties with sleep onset and/or sleep maintenance and compare the reliability of NMA 3 to the previously submitted NMAs.
Methods of NMA 3
Objectives
The objective of the study published by De Crescenzo et al. (2022)16 was to conduct a systematic review and NMA to inform clinical practice by comparing different pharmacologic treatments for the acute and long-term treatment of adults with insomnia.
Study Selection Methods
Databases searched included the Cochrane Central Register of Controlled Trials, MEDLINE, Embase, and PsycINFO from inception to November 25, 2021. PubMed was also searched for the current year (i.e., 2021) only. Searches were also conducted using the WHO International Clinical Trials Registry Platform, ClinicalTrials.gov, China National Knowledge Infrastructure, Baidu Scholar, and websites of regulatory agencies (British National Formulary [BNF], European Medicines Association, the US FDA, Pharmaceuticals and Medical Devices Agency, Therapeutic Goods Administration from inception to November 25, 2021. Investigators and relevant trial authors were also contact to obtain information about unpublished trials. Included studies were DB RCTs evaluating pharmacologic treatments as oral monotherapy, compared to PBO and/or to another active drug, in adults with a diagnosis of insomnia disorder according to specific, standardized diagnostic criteria.
Interventions of interests included antidepressants (amitriptyline, doxepin, trazodone), antihistaminergics (doxylamine, diphenhydramine, hydroxyzine, promethazine), antipsychotic drugs (quetiapine), short-acting benzodiazepines (brotizolam, midazolam, triazolam), intermediate-acting benzodiazepines (alprazolam, estazolam, loprazolam, lorazepam, lormetazepam, nimetazepam, rilmazafone, temazepam), long-acting benzodiazepines (diazepam, flunitrazepam, flurazepam, haloxaloam, nitrazepam, quazepam), benzodiazepine-like drugs (eszopiclone, zaleplon, ZOL, zopiclone), melatoninergic drugs (melatonin, ramelteon), and orexin receptor antagonists (daridorexant, LEM, seltorexant, suvorexant). Combination treatments, barbiturates, chloral hydrate, ethchlorvynol, triclofos sodium, and nonpharmacologic products were excluded.
Studies were selected, extracted, and assessed for risk of bias by 2 independent reviewers; any discrepancies were resolved with other members of the review team. Risk of bias was assessed using criteria outlined in the Cochrane Handbook for Systematic Reviews of Interventions (2011)85 and certainty of the indirect evidence was assessed using Confidence in Network Meta-Analysis (CINeMA).86 Sensitivity analyses were conducted evaluating the results including only studies with overall low risk of bias.
The primary outcomes included efficacy (quality or satisfaction with sleep as a continuous outcome, measured by self-rated validated scales such as the PSQI,87 ISI,43 or the Leeds Sleep Evaluation Questionnaire [LSEQ]88,89), all-cause discontinuation, discontinuation due to AEs, and the total number of patients experiencing at least 1 AE. Additional secondary outcomes included sleep onset latency, wake time after sleep onset, TST, and number of awakenings evaluated both by PSG and by sleep questionnaire or sleep diary (i.e., subjective), hangover (e.g., sedation, reduced alertness during the day) or increased alertness, rebound or withdrawal phenomena, the total number of patients with 1 specific AE, and the total number of patients with SAEs as defined by the FDA.
ITC Analysis Methods
Frequentist NMAs were conducted using a random-effects model. For rare events (i.e., studies with no events in some treatment groups), a fixed-effects Mantel-Haenszel approach was used and compared results with a random-effects inverse-variance model; if they were consistent, the random-effects model was used.
Each treatment represented a node in the network and was not disaggregated by treatment dose. Benzodiazepines were pooled into 3 treatment nodes, irrespective of dose: short-acting benzodiazepines (mean half-life of less than 6 hours), intermediate-acting benzodiazepines (6 to 24 hours), and long-acting benzodiazepines (greater than 24 hours).
Acute or “short-term” outcomes were assessed after 4 weeks of treatment where available, otherwise data from week 1 to 12 were used as closely to the 4-week time point as possible. For long-term outcomes, the longest time points after 3 months of treatment were used. It was assumed that missing dichotomous data were for patients who dropped out after randomization and had a negative outcome. For missing continuous data, the method used in the original trial were adopted (usually MMRM or the last observation carried forward). If neither the MMRM nor the last observation carried forward results were reported, data were analyzed for patients who completed the trial.
The following NMAs were conducted for the primary outcomes:
Efficacy – sleep quality in the short term
Efficacy – sleep quality in the long term
Acceptability – Dropouts due to any reason in the short term
Acceptability – Dropouts due to any reason in the long term
Tolerability – Dropouts due to AEs in the short term
Tolerability – Dropouts due to AEs in the long term
Safety – Patients with at least 1 AE during the trial as long as follow-up
The authors also conducted NMAs for the secondary outcomes previously listed, but the results were not reported in the publication or supplementary appendix. A hyperlink to results for the secondary outcomes on GitHub is provided by the authors.
Results for sleep quality were presented as SMD with 95% CIs, and all metrics of sleep quality were included in the analyses. The results of all other outcomes were presented as ORs with 95% CIs.
The authors evaluated the exchangeability assumption by comparing key study characteristics across studies using descriptive statistics, although the results were not reported. For the primary outcomes, the following subgroup or sensitivity analyses were conducted: aged older than 65 years versus 18 years to 65 years; studies with less versus more severe patients at baseline; sponsored trials versus nonsponsored trials; only studies deemed low risk of bias; only studies using standardized diagnostic criteria for insomnia; and trials without imputed SDs for continuous outcomes (i.e., efficacy).
Inconsistency was assessed using both global (design-by-treatment test) and local (back calculation and separate indirect from direct design evidence methods; comparing direct and indirect evidence for each pairwise treatment comparison) approaches. Heterogeneity for all direct pairwise comparisons was measured using tau (τ) and the magnitude of heterogeneity over the entire network was estimated using τ2 and I2 estimated from the NMA models.
Results of NMA 3
Summary of Included Studies
A total of 170 RCTs were included in the literature review, and 154 DB RCTs were eligible for inclusion in the NMAs. The publication dates spanned from May 1, 1977, to November 25, 2021. Across the included studies, 36 pharmacologic treatments were compared with each other or with PBO. The mean sample size was 265 (SD = 311) participants, mean age was 51.7 (SD = 12.2) years, and 62.8% of patients included in the network were women. Most studies (52.5%) included patients aged 18 to 65 years, 9.4% only included patients aged older than 65 years, and 38.1% did not have age limits. The median duration of treatment was 2 weeks for acute treatment (IQR = 2 weeks to 4 weeks) and 25 weeks (IQR = 19 weeks to 26 weeks) for long-term treatment. The authors determined that 48.3% of the included studies had a low risk of bias, 19.4% had an unclear risk of bias, and 32.4% had a high risk of bias.
Network diagrams are presented as follows for sleep quality in the short term (Figure 8) and long term (Figure 9), dropouts due to any reason in the short term (Figure 10) and long term (Figure 11), dropouts due to AEs in the short term (Figure 12) and long term (Figure 13), and patients with at least 1 AE during the trial as long as follow-up (Figure 14).
Figure 8: Efficacy — Sleep Quality in the Short Term
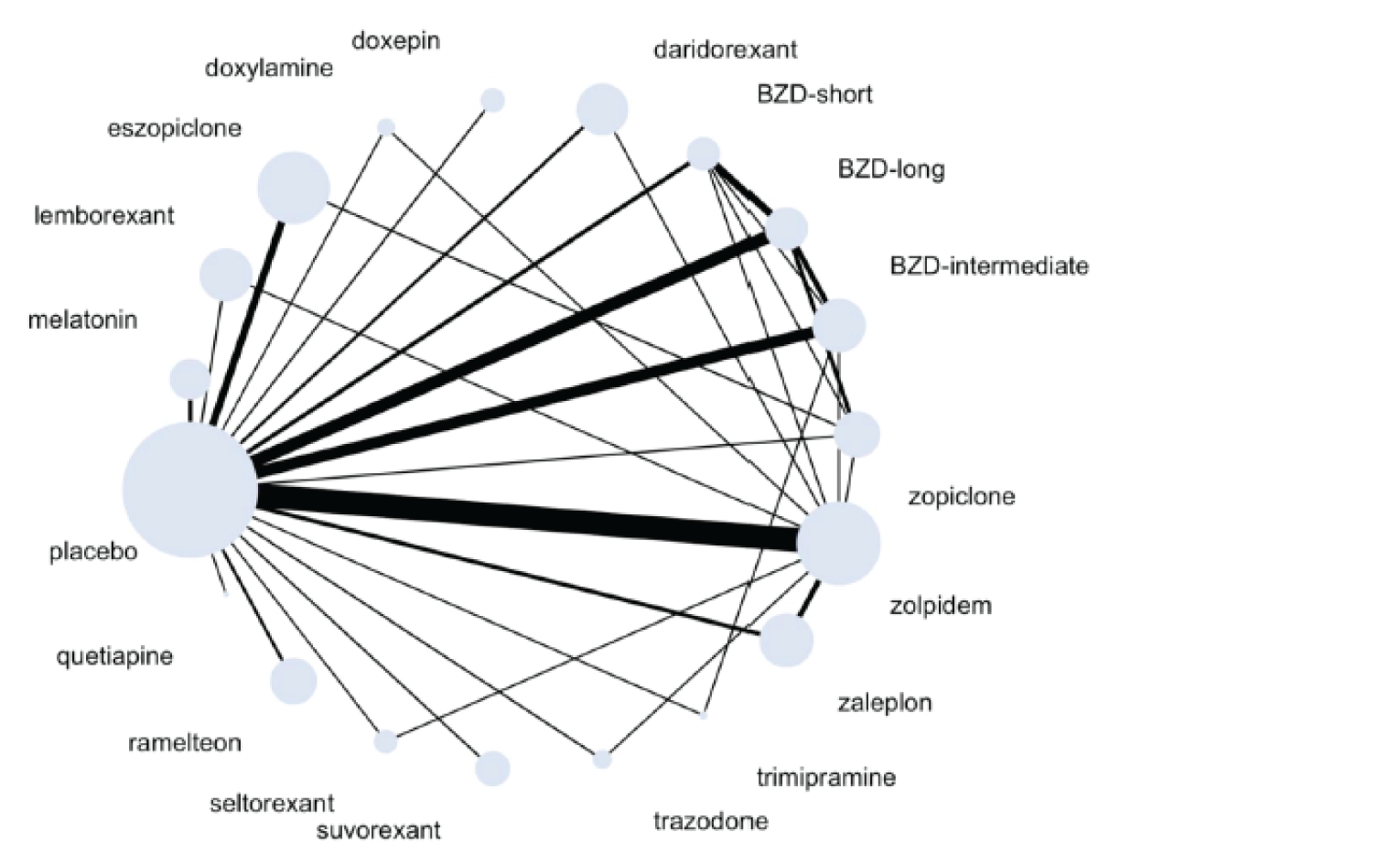
BZD = benzodiazepine.
Note: Number of studies = 86; number of treatments = 19; number of participants = 21,213.
Source: De Crescenzo et al. (2022).16
Figure 9: Efficacy — Sleep Quality in the Long Term
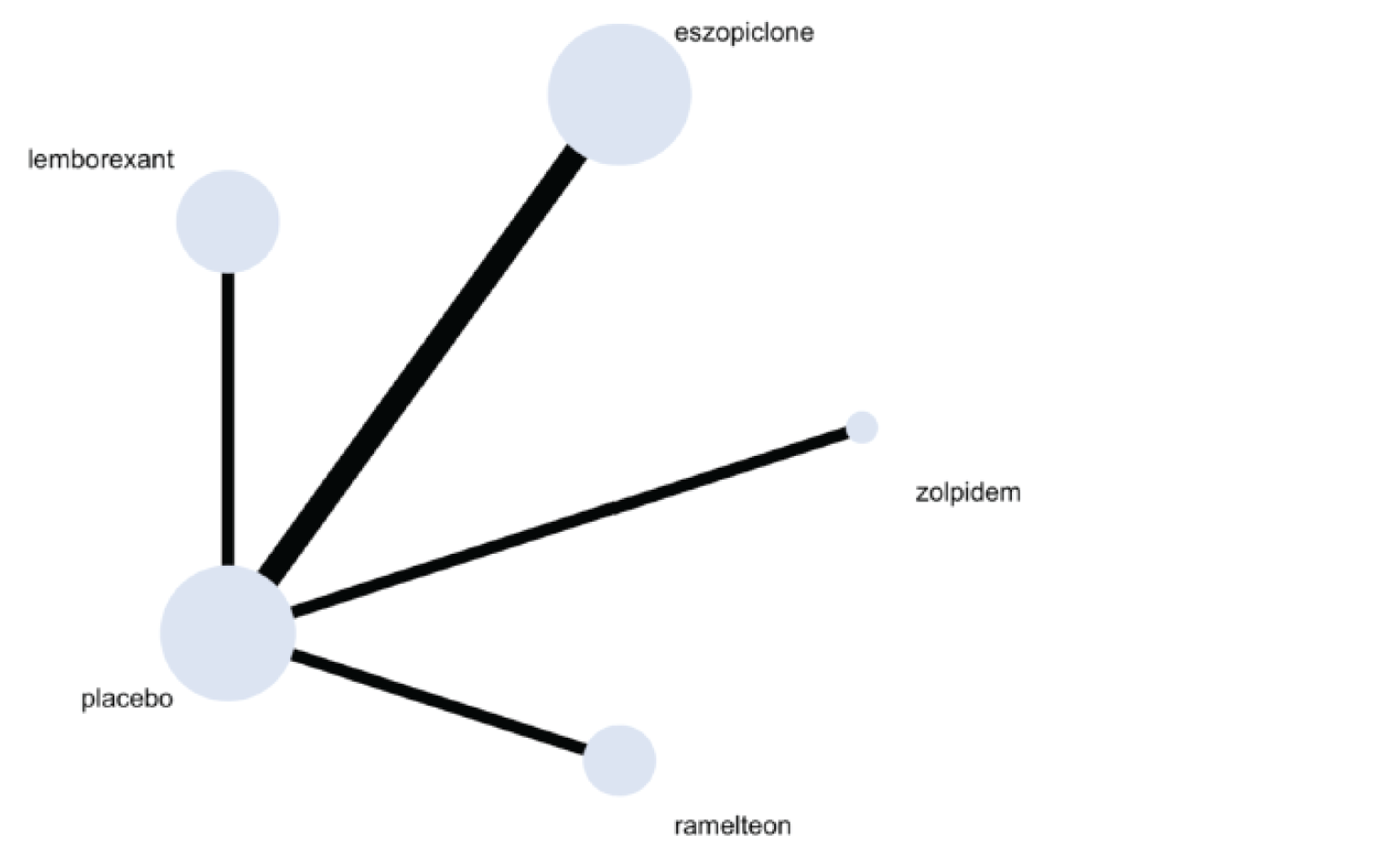
Note: Number of studies = 5; number of treatments = 5; number of participants = 2,560.
Source: De Crescenzo et al. (2022).16
Figure 10: Acceptability — Dropout Due to Any Reason in the Short Term
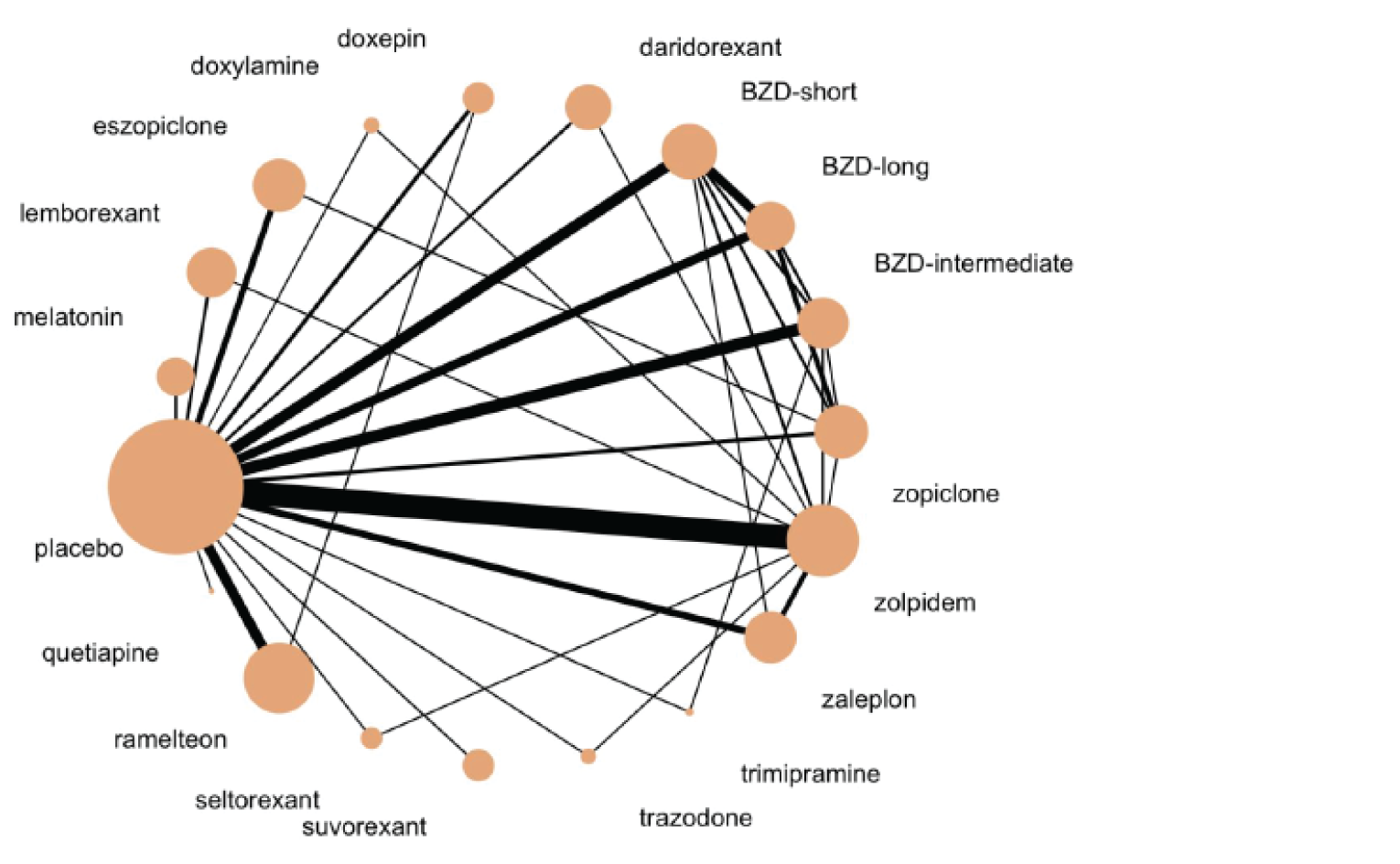
BZD = benzodiazepine.
Note: Number of studies = 100; number of treatments = 19; number of participants = 27,991.
Source: De Crescenzo et al. (2022).16
Figure 11: Acceptability — Dropout Due to Any Reason in the Long Term
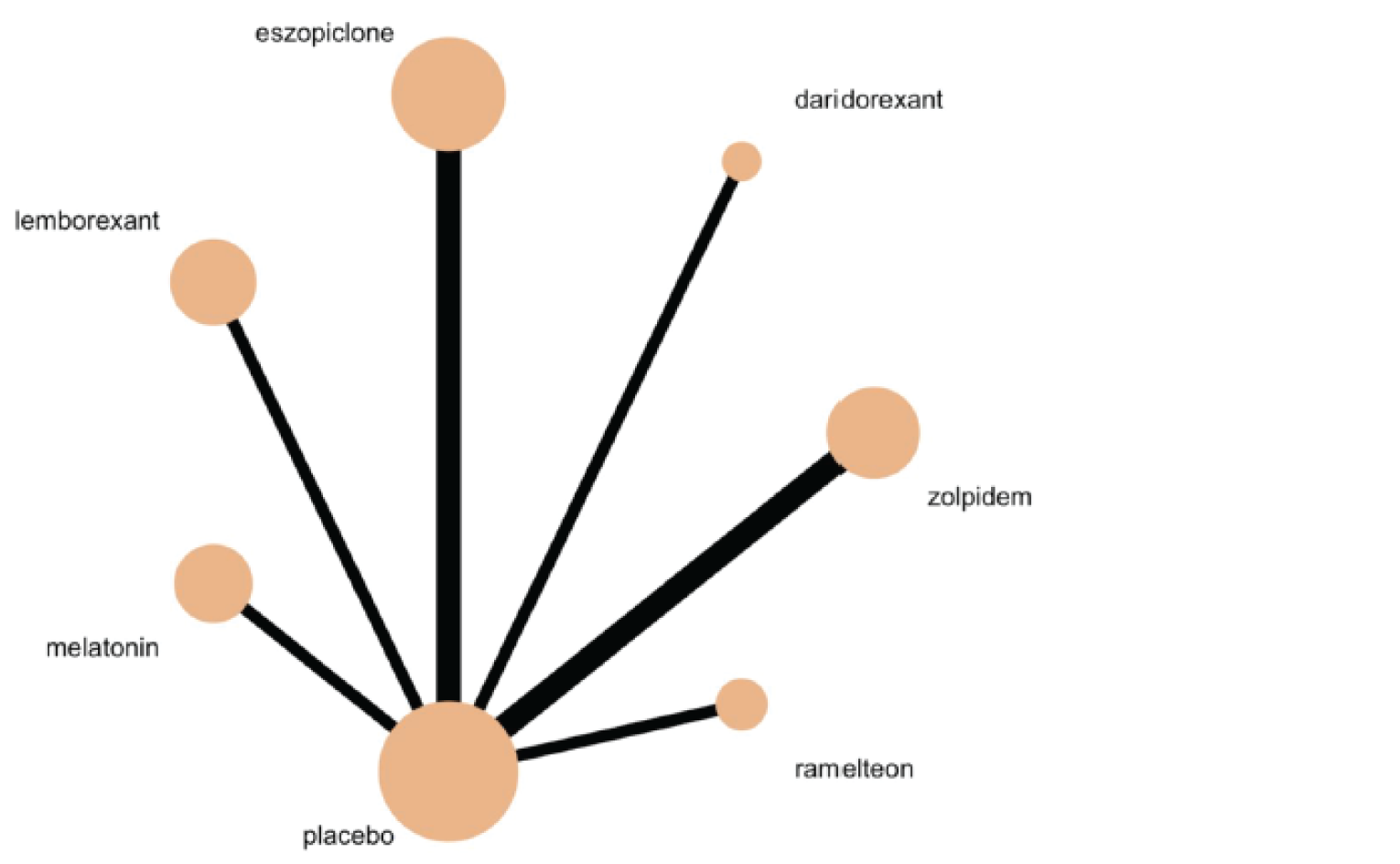
Note: Number of studies = 8; number of treatments = 7; number of participants = 5,152.
Source: De Crescenzo et al. (2022).16
Figure 12: Tolerability — Dropout Due to Adverse Events in the Short Term
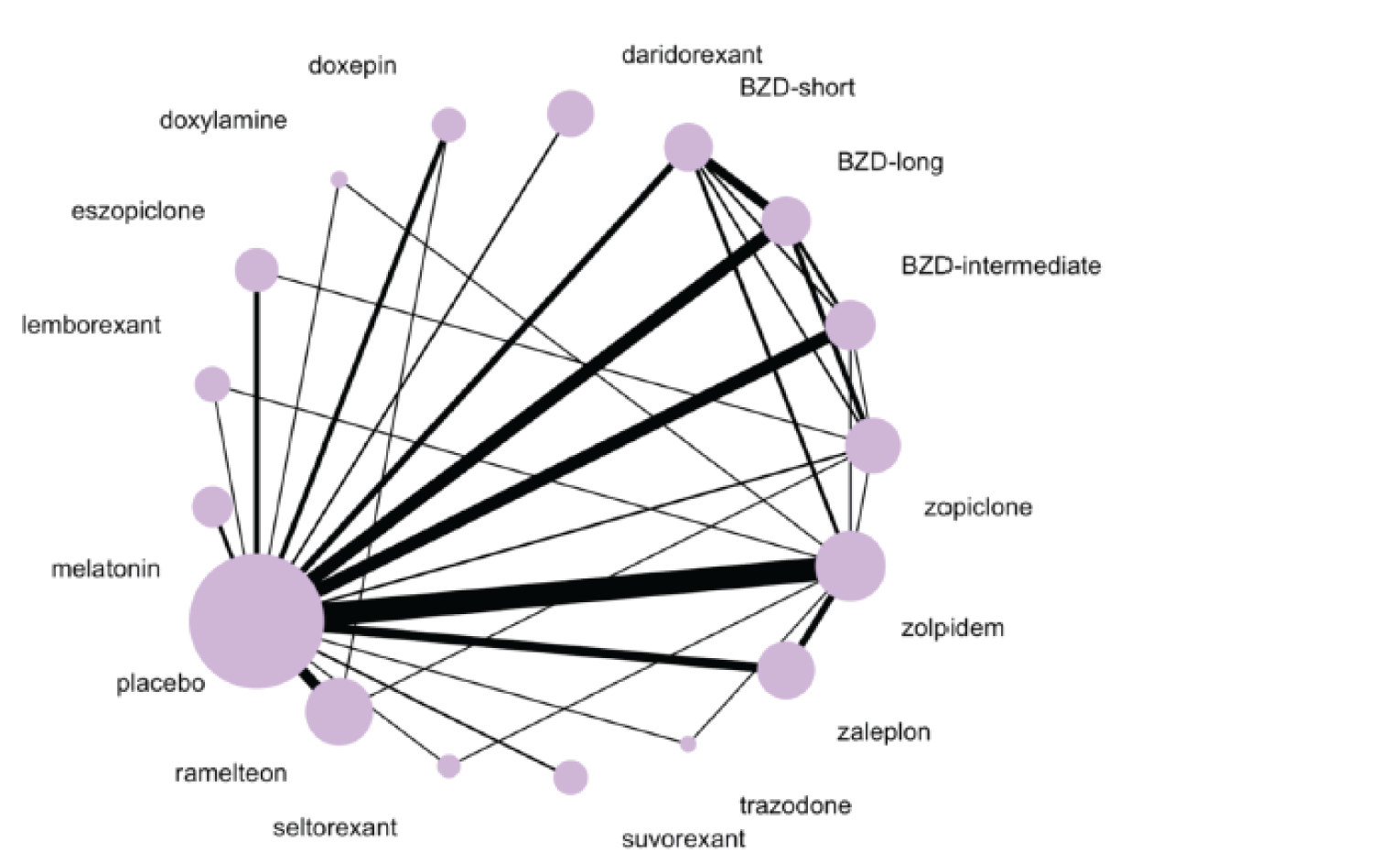
BZD = benzodiazepine.
Note: Number of studies = 76; number of treatments = 17; number of participants = 22,811.
Source: De Crescenzo et al. (2022).16
Figure 13: Tolerability — Dropout Due to Adverse Events in the Long Term
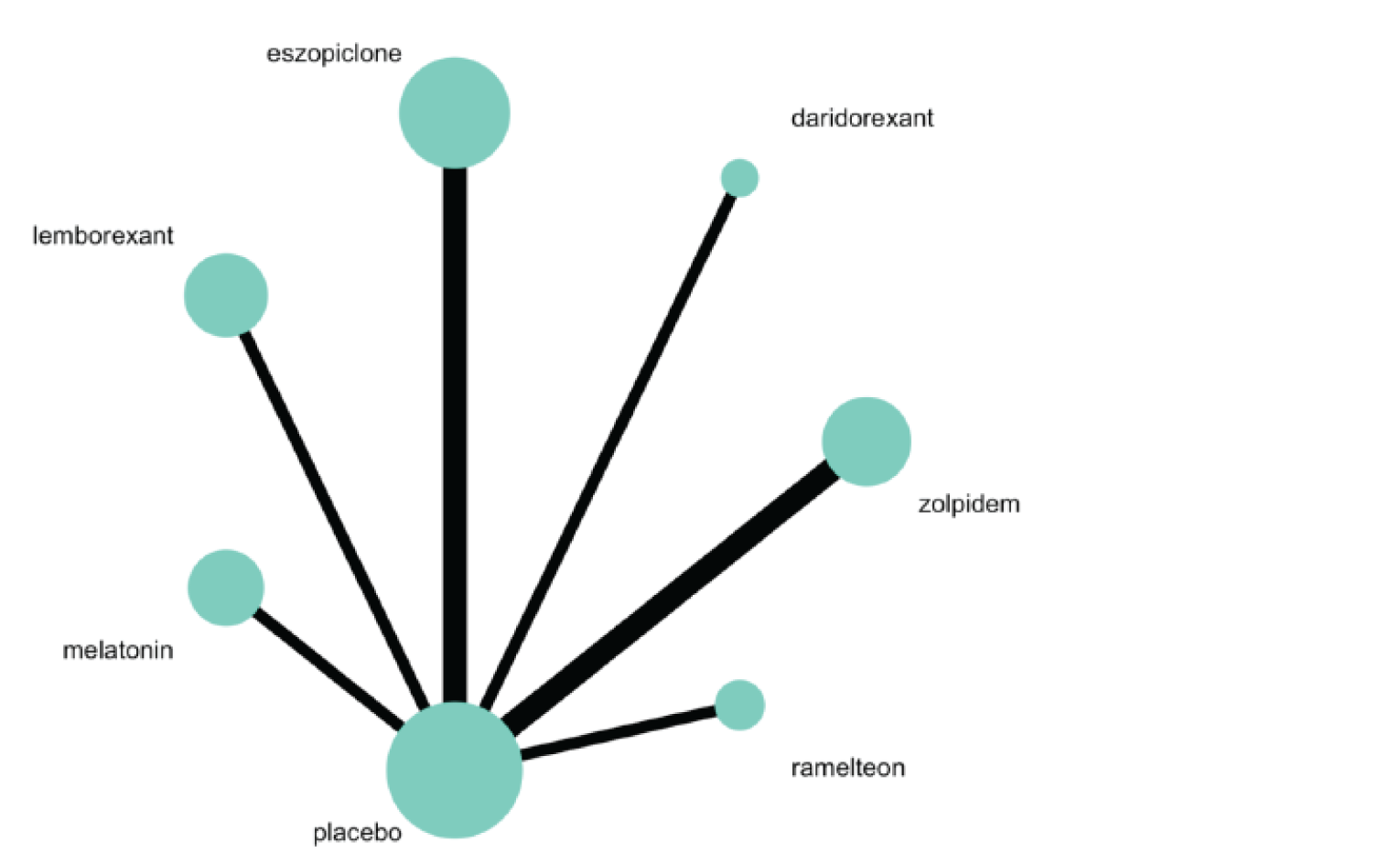
Note: Number of studies = 8; number of treatments = 7; number of participants = 5,152.
Source: De Crescenzo et al. (2022).16
Figure 14: Safety — Patients With At Least 1 Adverse Event During the Trial as Long as Follow-Up
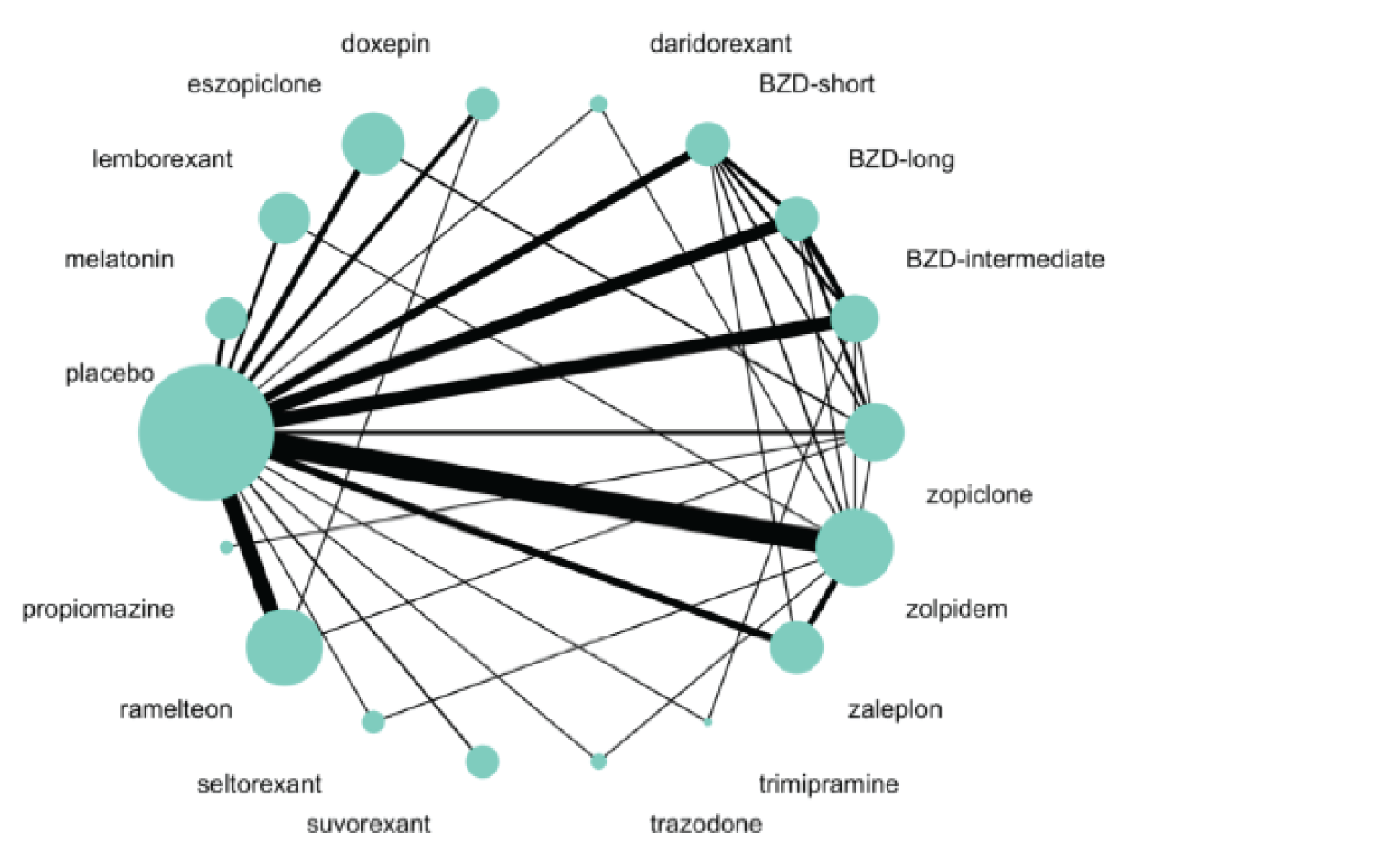
BZD = benzodiazepine.
Note: Number of studies = 86; number of treatments = 18; number of participants = 12,218.
Source: De Crescenzo et al. (2022).16
Primary Outcome Results
The number of studies and interventions varied by outcome, with short-term outcomes reported more frequently than long-term outcomes.
The primary efficacy outcome was sleep quality or satisfaction as measured by any self-reported scale such as PSQI, ISI, or LSEQ. Indirect evidence from the NMAs (Table 72) suggest that LEM was superior to PBO in both the short-term and long-term, but inferior to short-acting and intermediate-acting benzodiazepines, as a class, in the short-term analysis. All other comparisons with LEM were inconclusive due to wide 95% CIs that included the null effect. Based on CINeMA, the comparison of LEM versus PBO in short-term efficacy was associated with a “moderate” degree of certainty, and in long-term was associated with a “very low” degree of certainty. The comparisons between LEM and short- and intermediate-acting benzodiazepines were associated with “moderate” and “low” degrees of certainty, respectively.
The acceptability outcome (Table 72) was measured as dropouts for any reason, also described as all-cause discontinuation. All comparisons with LEM were inconclusive due to wide 95% CIs that included the null effect.
Indirect evidence from the NMAs for tolerability (i.e., dropouts due to AEs) and safety (i.e., patients who experienced at least 1 AE) are presented in Table 73. No results were conclusive for the outcome of tolerability. Results for the outcome of safety suggested that LEM was superior to short- and long-acting benzodiazepines, as a class, a “low” degree of certainty based on CINeMA. For the rest of the available comparisons, including zopiclone, the evidence was inconclusive due to wide 95% CIs that included the null effect.
The sensitivity and subgroup analyses were generally consistent with the base case for the comparison of LEM versus PBO, where possible to conduct. However, the results for LEM versus other active therapies were not reported in the sensitivity and subgroup analyses.
Table 72: Indirect Results for Efficacy and Acceptability
Comparison | Efficacy,a short-term SMD (95% CI) | Efficacy,a long-term SMD (95% CI) | Acceptability,b short-term OR (95% CI) | Acceptability,b long-term OR (95% CI) |
|---|---|---|---|---|
Comparator vs. LEM c | ||||
BZD-S | 0.47 (0.13 to 0.82) | — | 1.21 (0.79 to 1.85) | - |
BZD-I | 0.31 (0.00 to 0.63) | — | 0.97 (0.61 to 1.53) | - |
BZD-L | 0.22 (–0.09 to 0.54) | — | 0.94 (0.60 to 1.47) | - |
DARI | –0.12 (–0.49 to 0.25) | — | 1.13 (0.67 to 1.90) | 0.49 (0.20 to 1.22) |
DOXE | –0.06 (–0.50 to 0.39) | — | 1.05 (0.59 to 1.86) | - |
DOXY | 0.12 (–0.38 to 0.62) | — | 0.71 (0.27 to 1.84) | - |
ESZO | 0.16 (–0.16 to 0.48) | 0.22 (–0.24 to 0.68) | 0.96 (0.61 to 1.51) | 0.52 (0.26 to 1.05) |
LEM vs. Comparator d | ||||
MELA | 0.22 (–0.15 to 0.60) | — | 0.86 (0.52 to 1.40) | 1.57 (0.67 to 3.67) |
Placebo | 0.36 (0.08 to 0.63) | 0.41 (0.04 to 0.78) | 0.86 (0.59 to 1.25) | 1.31 (0.73 to 2.34) |
QUET | 0.30 (–0.89 to 1.50) | — | 2.01 (0.14 to 28.81) | - |
RAME | 0.24 (–0.14 to 0.62) | 0.41 (–0.12 to 0.94) | 0.74 (0.49 to 1.12) | 0.83 (0.35 to 1.98) |
SELT | –0.08 (–0.58 to 0.41) | — | 1.62 (0.58 to 4.52) | - |
SUVO | 0.04 (–0.37 to 0.46) | — | 0.95 (0.57 to 1.58) | - |
TRAZ | –0.17 (–0.62 to 0.29) | — | 0.74 (0.30 to 1.81) | - |
TRIM | –0.20 (–0.92 to 0.52) | — | 1.10 (0.33 to 3.67) | - |
ZALE | 0.17 (–0.16 to 0.50) | — | 0.79 (0.50 to 1.25) | - |
ZOL | –0.10 (–0.38 to 0.19) | 0.38 (–0.27 to 1.03) | 0.81 (0.55 to 1.21) | 1.95 (0.92 to 4.11) |
ZOPI | –0.5 (–0.49 to 0.19) | — | 0.84 (0.54 to 1.30) | - |
BZD-I = intermediate-acting benzodiazepine; BZD-L = long-acting benzodiazepine; BZD-S = short-acting benzodiazepine; CI = confidence interval; DARI = daridorexant; DOXE = doxepin; DOXY = doxylamine; ESZO = eszopiclone; LEMB = lemborexant; MELA = melatonin; OR = odds ratio; QUET = quetiapine; RAME = ramelteon; SELT = seltorexant; SMD = standardized mean difference; SUVO = suvorexant; TRAZ = trazodone; TRIM = trimipramine; vs. = versus; ZALE = zaleplon; ZOL = zolpidem tartrate; ZOPI = zopiclone.
aThe “efficacy” outcome includes sleep quality as measured by self-rated validated scales including but not limited to the Pittsburgh Sleep Quality Index (PSQI), the Insomnia Severity Index (ISI), and the Leeds Sleep Evaluation Questionnaire (LSEQ). “Short term” refers to outcomes at 4 weeks, or where not reported, at the closest time point between 1 week to 12 weeks of treatment. “Long term” refers to the longest-available data point for an outcome greater than 3 months.
bThe “acceptability” outcome includes dropouts for any reason. “Short term” refers to outcomes at 4 weeks, or where not reported, at the closest time point between 1 week to 12 weeks of treatment. “Long term” refers to the longest-available data point for an outcome greater than 3 months.
cFor efficacy (SMD) results below 0 favour LEM. For tolerability (OR) results above 1 favour LEM.
dFor efficacy (SMD) results above 0 favour LEM. For tolerability (OR) results below 1 favour LEM.
Source: Adapted from De Crescenzo et al. (2022).16
Table 73: Indirect Results for Tolerability and Safety
Comparison | Tolerability,a short term OR (95% CI) | Tolerability,a short term OR (95% CI) | Safetyb at study end point OR (95% CI) |
|---|---|---|---|
Comparator vs. LEM c | |||
BZD-S | 2.17 (0.65 to 7.17) | — | 1.54 (1.06 to 2.24) |
BZD-I | 1.79 (0.53 to 6.08) | — | 1.30 (0.89 to 1.90) |
BZD-L | 1.90 (0.56 to 6.45) | — | 1.79 (1.22 to 2.61) |
DARI | 0.87 (0.22 to 3.39) | 0.63 (0.15 to 2.68) | 1.15 (0.58 to 2.26) |
DOXE | 2.00 (0.47 to 8.50) | — | 0.89 (0.57 to 1.37) |
DOXY | 1.01 (0.15 to 6.87) | — | - |
ESZO | 1.62 (0.47 to 5.64) | 0.89 (0.35 to 2.27) | 1.45 (1.00 to 2.09) |
LEM vs. comparator d | |||
MELA | 0.95 (0.19 to 4.76) | 1.87 (0.60 to 5.85) | 1.05 (0.66 to 1.68) |
Placebo | 0.68 (0.22 to 2.11) | 1.60 (0.69 to 3.68) | 1.05 (0.78 to 1.40) |
PROP | — | — | 0.60 (0.25 to 1.41) |
RAME | 0.57 (0.17 to 1.93) | 2.04 (0.57 to 7.35) | 0.96 (0.69 to 1.33) |
SELT | 0.60 (0.11 to 3.39) | — | 1.56 (0.85 to 2.86) |
SUVO | 1.05 (0.29 to 3.77) | — | 1.05 (0.67 to 1.65) |
TRAZ | 0.33 (0.07 to 1.67) | — | 0.76 (0.38 to 1·51) |
TRIM | — | — | 0.37 (0.11 to 1·24) |
ZALE | 0.57 (0.17 to 1.84) | — | 1.23 (0.86 to 1·76) |
ZOL | 0.38 (0.13 to 1.16) | 0.79 (0.28 to 2.21) | 1.19 (0.91 to 1·55) |
ZOPI | 0.34 (0.10 to 1.11) | — | 0.94 (0.71 to 1·26) |
BZD-I = intermediate-acting benzodiazepine; BZD-L = long-acting benzodiazepine; BZD-S = short-acting benzodiazepine; CI = confidence interval; DARI = daridorexant; DOXE = doxepin; DOXY = doxylamine; ESZO = eszopiclone; LEMB = lemborexant; MELA = melatonin; OR = odds ratio; ROP = propiomazine.; RAME = ramelteon; SELT = seltorexant; SUVO = suvorexant; TRAZ = trazodone; TRIM = trimipramine; vs. = versus; ZALE = zaleplon; ZOL = zolpidem tartrate; ZOPI = zopiclone.
aThe “tolerability” outcome refers to dropouts due to adverse event. “Short term” refers to outcomes at 4 weeks, or where not reported, at the closest time point between 1 week to 12 weeks of treatment. “Long term” refers to the longest-available data point for an outcome greater than 3 months.
bThe “safety” outcome refers to patients with any adverse event.
cFor tolerability (OR) results above 1 favour LEM. For safety (OR) results above 1 favour LEM.
dFor tolerability (OR) results below 1 favour LEM. For safety (OR) below above 1 favour LEM.
Source: Adapted from De Crescenzo et al. (2022).16
Critical Appraisal of NMA 3
The published NMA by De Crescenzo et al. (2022) assessed the efficacy and harms of a comprehensive list of active pharmacologic treatments for adults with insomnia disorder as evaluated in DB RCTs. Some of the included pharmacologic treatments were relevant to the Canadian landscape, including zopiclone. The described systematic literature review was appropriately conducted with regard to the search strategy, screening of records, data extraction, and risk of bias assessment.
According to the Cochrane Risk of Bias Tool,85 the authors identified that approximately one-third (32.4%) of the included articles had a high risk of bias, while 19.4% were unclear and the remainder (48.3%) had a low risk of bias. The authors identified that many trials did not report adequate information about randomization and allocation concealment.
The authors assessed an extensive selection of outcomes, although most of them were not presented in the publication nor the supplementary appendix. For efficacy, only the primary efficacy outcome (i.e., sleep quality as defined by self-reported scales such as PSQI, ISI, LSEQ, and others) was reported in the main text of the publication and assessed by CADTH.
The authors thoroughly assessed heterogeneity and inconsistency in the NMAs. For short-term outcomes, there were some concerns of heterogeneity, within-study bias, and some major concerns with regard to imprecision in comparators informing the NMAs; for long-term outcomes, the networks were sparsely populated with no closed loops, and there were major concerns regarding suspected reporting bias, within-study bias, and imprecision. In the networks with no closed loops, incoherence could not be addressed.
The assumption of exchangeability was assessed by comparing key study characteristics using descriptive statistics, but these results were not reported, precluding the ability to confirm the assertion that there were no strong signals of this assumption being violated. The authors only identified age as a potentially important prognostic factor, which may be insufficient.
Aside from the limitations identified by the authors, there were some important methodological considerations identified. There may have been additional relevant trials that were excluded due to the requirements for trials to be DB, and the exclusion of crossover and cluster-randomized trials. These types of trials could have been included with appropriate adjustments and/or sensitivity analyses. The choice of a random-effects model for the NMAs (except for rare events) was appropriate. Different doses of the included therapies were pooled into 1 node, introducing heterogeneity and uncertainty into interpretation of the indirect evidence; moreover, benzodiazepines were pooled into 3 nodes based on their median half-life (short-acting, intermediate-acting, and long-acting), and not disaggregated by therapy, which may not have been appropriate. Short-term or acute outcomes were measured at 4 weeks where possible, but the closest available time point was used instead in the absence of a 4-week outcome; as the median duration of treatment for acute outcomes was 2 weeks (IQR = 2 weeks to 4 weeks), this also introduces heterogeneity in the networks. Similarly, long-term outcomes were assessed as the longest-available time point after 3 months, and the median duration of treatment for long-term outcomes was 25 weeks (IQR = 19 weeks to 26 weeks), introducing considerable heterogeneity in outcome assessment. The primary efficacy outcome included multiple metrics of sleep quality. Finally, multiple methods were used for imputation, but a sensitivity analysis without imputed values was consistent for the comparison of LEM versus PBO in short-term efficacy, so the risk of bias may be low. However, in the absence of sensitivity analyses for LEM versus the active comparators, the presence and direction of potential bias is unclear.
Overall, there is considerable uncertainty in the evidence base and as a result of some of the methodological assumptions detailed herein. For most comparisons, the results were inconclusive due to wide 95% CIs that included the null value.
Summary of NMA 3 in Comparison to NMA 1 and NMA 2
The key similarities and differences between NMA 1, 2, and 3 are summarized in Table 74. Overall, NMA 3 had a broader and more comprehensive scope than NMA 1 and NMA 2 and included more studies and more treatments. However, the additional treatments are not of interest for the purpose of this review.
The methodological approach of NMA 3 had some notable differences from the previously submitted NMAs. Like NMA 1, NMA 3 only included DB RCTs; however, NMA 1 was limited to PBO-controlled RCTs whereas NMA 3 did not require trials to be PBO-controlled for inclusion. While NMA 2 was conducted using a Bayesian framework and NMA 1 was unclear (but likely frequentist), NMA 3 was conducted using a frequentist framework. NMA 3 uniquely pooled (1) all licensed doses for any given therapy and (2) benzodiazepines into 3 nodes based on their median half-life. The selection of reported outcomes also differed; where NMA 1 and NMA 2 reported a suite of objective and subjective efficacy measures; NMA 3 did not report those same outcomes in the publication nor supplementary appendix but provided a hyperlink to GitHub, which was not included in the scope of CADTH’s review of this evidence.
In terms of results, NMA 3 was similar to the previously submitted NMAs in that most comparisons for all reported outcomes were inconclusive due to wide 95% CIs or 95% CrIs including the null value. In NMA 3, LEM was superior to PBO for short- and long-term efficacy, and superior to short- and long-acting benzodiazepines for the outcome of safety (i.e., patients with any AE) at study end point. Short- and intermediate-acting benzodiazepine were superior to LEM for the outcome of short-term efficacy. All other comparisons with LEM were inconclusive.
Overall, NMA 3 was more comprehensive but had similar methodological limitations to NMA 1 and NMA 2.
Table 74: Summary Comparison of NMA 1, NMA 2, and NMA 3
Comparison | NMA 1 | NMA 2 | NMA 3 |
|---|---|---|---|
Source | Sponsor-submitted NMA | McElroy et al. (2021) | De Crescenzo et al. (2022) |
Number of studies included | 11 | 45 | 154 |
Number of active therapies included | 15 | 16 | 36 |
Key eligibility criteria for study design |
|
|
|
NMA methodology |
|
|
|
Pooled nodes | No | No |
|
Main efficacy outcomes reported |
|
|
|
Safety/harms outcomes reported |
|
|
|
Summary of efficacy conclusions |
|
|
|
Summary of safety/harms conclusions |
|
|
|
Major sources of potential bias or uncertainty |
|
|
|
AE = adverse event; DB = double-blind; CI = confidence interval; CINeMA = Confidence in Network Meta-analysis; ISI = Insomnia Severity Index; LEM = lemborexant; LPS = latency to p[persistent sleep; LSEQ = Leeds Sleep Evaluation Questionnaire; NMA = network meta-analysis; PBO = placebo; PSQI = Pittsburgh Sleep Quality Index; RCT = randomized controlled trial; SAE = serious adverse event; SE = sleep efficiency; SOL = sleep onset latency; sQUAL = subjective quality of sleep; TST = total sleep time; vs. = versus; WASO = wake after sleep onset; ZOL = zolpidem tartrate; ZOL-ER = zolpidem tartrate extended-release; ZOL-IR = zolpidem tartrate immediate-release.
aHowever, sensitivity analysis including only studies at low risk of bias had similar results to base case.
Pharmacoeconomic Review
Abbreviations
BIA
budget impact analysis
CI
confidence interval
CUA
cost-utility analysis
ICER
incremental cost-effectiveness ratio
MVA
motor vehicle accident
NMA
network meta-analysis
QALY
quality-adjusted life-year
SDLP
standard deviation of lateral position
sSOL
subjective sleep onset latency
WPA
workplace accident
Z-drugs
zolpidem, eszopiclone, zaleplon, and zopiclone
Executive Summary
The executive summary comprises 2 tables (Table 1 and Table 2) and a conclusion.
Item | Description |
|---|---|
Drug product | Lemborexant (Dayvigo), oral tablet |
Submitted price | Lemborexant: 5 mg, 10 mg: $1.5198 per tablet |
Indication | For the treatment of insomnia, characterized by difficulties with sleep onset and/or sleep maintenance |
Health Canada approval status | NOC |
Health Canada review pathway | Standard |
NOC date | November 4, 2020 |
Reimbursement request | As per indication |
Sponsor | Eisai Limited |
Submission history | Previously reviewed: No |
NOC = Notice of Compliance.
Table 2: Summary of Economic Evaluation
Component | Description |
|---|---|
Type of economic evaluation | Cost-utility analysis Decision-tree model |
Target population | Patients with insomnia, characterized by difficulties with sleep onset and/or sleep maintenance |
Treatment | Lemborexant |
Comparators |
|
Perspective | Canadian publicly funded health care payer |
Outcome | QALYs |
Time horizon | 6 months |
Key data source |
|
Submitted results |
|
Key limitations |
|
CADTH reanalysis results |
|
ICER = incremental cost-effectiveness ratio; MVA = motor vehicle accident; QALY = quality-adjusted life-year; sSOL = subjective sleep onset latency; WPA = workplace accident.
Conclusions
The CADTH clinical review concluded lemborexant demonstrated improvements in sleep onset, sleep maintenance, and sleep efficiency among adults with insomnia relative to placebo. However, the sleep improvements based on polysomnography and sleep diary outcomes observed in the SUNRISE 1 and SUNRISE 2 studies did not appear to be reflected in the results from the patient-reported questionnaires. Considering the limitations with both objective and subjective outcomes, it is uncertain if the differences in response rates would be meaningful to all patients who could be treated with lemborexant. Any conclusions based on the indirect evidence are uncertain due to limitations of the network meta-analysis (NMA). Evidence was absent for some comparators or very uncertain for clinical efficacy and harms outcomes due to imprecision, risk of bias, and heterogeneity in the pairwise comparisons. Therefore, no firm conclusions could be made about the relative response rates and harms associated with lemborexant versus active comparators.
To address the identified limitations with the sponsor’s pharmacoeconomic evaluation, CADTH undertook a reanalysis with the following changes: it assumed no difference in the risk of falls, motor vehicle accidents (MVAs), workplace accidents (WPAs), and the number of physician visits among treatments, and it excluded disutilities associated with treatment. In the CADTH base case, trazodone was dominant over all other comparators besides lemborexant. Therefore, the resultant incremental cost-effectiveness ratio (ICER) for lemborexant compared to trazodone was $76,941 per quality-adjusted life-year (QALY) gained, where lemborexant had a 17% probability of being cost-effective at a $50,000 per QALY threshold.
The interpretation of the CADTH base case is limited by the comparative clinical data. There is a high degree of uncertainty in the estimates used to model treatment response among active comparators, which CADTH was unable to account for in the CADTH base case. Given the limitations of the clinical evidence and the small differences in QALYs between comparators in the CADTH base case, there is uncertainty as to whether there is adequate evidence to warrant a price premium for lemborexant over other active comparators. As such, CADTH conducted a cost comparison to understand the percentage price reduction required for lemborexant to be costed similarly to relevant comparators. Based on the CADTH reanalysis, the submitted price of lemborexant would need to be reduced by 76% to 82% to be equivalent to the cost of active comparators.
Stakeholder Input Relevant to the Economic Review
This section is a summary of the feedback received from the patient groups, registered clinicians, and drug plans that participated in the CADTH review process (specifically, information that pertains to the economic submission).
Patient input from caregivers, patients with poor sleep and migraines, and the general population was received from 3 groups: Migraine Canada, Menopause Chicks, and Mood Disorders Society of Canada. Their data were collected via online surveys, questionnaires, focus groups, and 1-on-1 interviews. Many respondents were Canadian females who had accessed health care services to discuss their sleep issues. Sleep issues or insomnia had a negative impact on quality of life, affecting one’s energy levels, cognitive functioning, mood, physical exercise, ability to perform household responsibilities, work performance or work attendance, relationships, ability to provide caregiving, and socializing. Current pharmacologic interventions included over-the-counter medications and prescription medications such as Z-drugs (zolpidem, eszopiclone, zaleplon, and zopiclone), benzodiazepines, trazodone, amitriptyline, mirtazapine, lemborexant, and antipsychotic drugs. Patients expressed a desire for improvement in uninterrupted sleep, waking up restful, ability to perform work and family responsibilities, reduced side effects (i.e., somnolence and cognitive impairment), and treatment effectiveness over longer terms. Patients expressed a need for new medications in Canada because treatment efficacy of many currently used drugs diminishes over time. Patients who had experience with lemborexant reported improvement in time to sleep, regularity in sleep patterns, long-term drug effectiveness, and reduced gastrointestinal-related adverse effects.
Clinical input was received from Mood Disorders Society of Canada and 2 registered clinician groups: Canadian Consortium of Sleep and Sleep Interested Physicians, and the National Advisory Board consisting of Canadian family physicians and psychiatrists with expertise in the management of insomnia. Although there are no Canadian guidelines or evidence-based recommendations on the management of insomnia, the current pathway of care is first-line treatment with cognitive behaviour therapy, followed by pharmacotherapy. Current pharmacologic treatments include benzodiazepines (triazolam, flurazepam, nitrazepam, and temazepam), Z-drugs (zopiclone, zolpidem, and eszopiclone) and doxepin, often prescribed for longer periods than recommended and in combination with inappropriate medications such as opioids. Side effects included cognitive and physical impairment, delirium, falls, MVAs, respiratory depression, memory issues, increased morbidity and mortality risk with the use of inappropriate medications, dependence, tolerance, and withdrawal symptoms with chronic use, especially in older adults or the medically ill. Off-label treatments include antidepressants (mirtazapine, amitriptyline), other benzodiazepines (lorazepam, clonazepam), alpha-2 delta ligand anticonvulsants (gabapentin and pregabalin) and low-dose antipsychotic drugs (quetiapine, olanzapine, risperidone). Some over-the-counter medication containing doxylamine, dimenhydrinate, and diphenhydramine are also frequently used in this patient population. Treatment goals include improved sleep continuity, daytime function, overall occupational function, and health-related quality of life. Other priorities include decrease in fatigue, impaired attention and/or concentration, disrupted mood, lack of motivation, and impaired social life. The clinicians noted lemborexant would be a first-line therapy for all patients with insomnia being offered pharmacotherapy, and would shift the current treatment paradigm such that other drugs are used later in therapy.
Drug plan input received for this review noted the comparator used in the SUNRISE trials is zolpidem, which is not publicly reimbursed and received a negative recommendation in September 2013 by the CADTH Canadian Drug Expert Committee.1 Further, additional populations outside the indication of interest may be treated with lemborexant, as patients with narcolepsy, parasomnia, sleep apnea, dementia, and comorbid depression are often treated with similar drugs as patients with insomnia.
Several of these concerns were addressed in the sponsor’s model:
The sponsor’s model evaluated some of the patient and clinically relevant outcomes (i.e., somnolence and dizziness).
CADTH also addressed some of these concerns as follows:
CADTH assessed the budget impact associated with the reimbursement of lemborexant as a first-line therapy.
CADTH was unable to address the following concerns raised from stakeholder input owing to structural or data limitations:
The comparative safety of insomnia treatments for some relevant outcomes such as MVAs, WPAs, falls, treatment dependence, tolerance, and withdrawal could not be assessed due to a lack of evidence.
The cost-effectiveness of lemborexant relative to some relevant comparators (e.g., doxepin, mirtazapine) could not be assessed.
Economic Review
The current review is for lemborexant (Dayvigo) for the treatment of insomnia, characterized by difficulties with sleep onset and/or sleep maintenance.2
Economic Evaluation
Summary of Sponsor’s Economic Evaluation
Overview
The sponsor submitted a cost-utility analysis (CUA) assessing lemborexant for the treatment of patients with insomnia, characterized by difficulties with sleep onset and/or sleep maintenance.2 The modelled population is consistent with the Health Canada indication and reimbursement request. Comparator treatments indicated for insomnia included benzodiazepines (flurazepam, nitrazepam, triazolam, and temazepam), a Z-drug (zopiclone), and no treatment. The sponsor’s analysis also considered some off-label treatments as comparators of interest, including another benzodiazepine (lorazepam), an antidepressant (trazodone), and an antipsychotic drug (quetiapine).2
Lemborexant is available as 5 mg or 10 mg oral tablets. The recommended dose is 5 mg taken once daily, but depending on clinical response and tolerability, the dose can be increased to a maximum recommended dose of 10 mg. At the submitted price of $1.5198 per 5 mg tablet or 10 mg tablet, the 30-day cost of lemborexant is $45.59. The 30-day cost of comparators ranges from $1.26 to $15.31, depending on the active comparator and its drug dosage. In the sponsor’s submitted model, no drug costs were accrued for patients receiving no treatment.
The submitted model reported QALYs over a time horizon of 180 days. The base-case analysis was conducted from the perspective of the Canadian public health care payer. Given the time horizon of less than 1 year, no discounting was applied to either costs or health outcomes.2
Model Structure
The sponsor submitted a decision-tree model to capture the efficacy, safety, and mortality impacts of insomnia and its associated treatments. Patients entered the model and either achieved response or no response. Response was defined by a subjective sleep onset latency (sSOL) of 20 minutes or less. The model further captured the occurrence of certain adverse events (i.e., falls, MVAs, and WPAs) and considered mortality separately as patients could remain alive or be dead by the end of the modelled time horizon. Patients were assigned to lemborexant or 1 of the comparators upon model entry and were assumed to continue to receive their assigned treatment over the modelled time horizon. The sponsor’s submitted model structure can be found in Appendix 3.
Model Inputs
The modelled patient characteristics for the sponsor’s submission were based on the SUNRISE 2 trial (patients aged 18 years and older; 68.2% female).2 The modelled population was divided into 2 subgroups: younger patients and older patients. Younger patients were assumed to comprise 72.4% of the cohort, and based on the SUNRISE 2 trial, the average age in the younger patients subgroup and the older patients subgroup was 55 years and 70 years, respectively.
Treatment efficacy was based on response rates, which were obtained from the SUNRISE 1 and SUNRISE 2 trials as well as a sponsor-commissioned NMA.2-4 The sponsor’s estimated response rates on placebo and lemborexant were pooled from the SUNRISE 1 and SUNRISE 2 trials, and it was assumed that 84% of patients were on the low dose (5 mg) and 16% of patients were on the high dose (10 mg), based on claims data.5 The response rates on temazepam and trazodone were based on standardized mean differences in sSOL relative to placebo, which were obtained from the sponsor’s submitted NMA.2 The sponsor assumed flurazepam, nitrazepam, zopiclone, triazolam, and lorazepam would have equivalent efficacy to temazepam while quetiapine would have equivalent efficacy to trazodone. The sponsor also assumed that both treatment efficacy and adherence would be maintained over the time horizon and would not vary by age.3
The modelled adverse events associated with insomnia and its treatment included falls, MVAs, and WPAs. The baseline rate of falls among older patients was based on published literature while the baseline rate of falls among younger patients was assumed to be 5% that of the older population.6,7 The baseline rate of fatal falls was a weighted average of fatality rates after nonfracture hospitalization, non–hip fracture hospitalization, and hip fracture hospital admissions.8 The sponsor also modelled an increased risk of recurrent falls for patients who had had a prior fall.6 Treatment increased the risk of falls compared to no treatment. The relative risk of falls with lemborexant was based on pooled data from the SUNRISE 1 and SUNRISE 2 trials,3,4 weighted by the sample size of each trial.3,4 Despite the sponsor conducting an indirect treatment comparison to derive the risk of falls for active comparators versus lemborexant, the sponsor populated this estimate using published literature that showed an increased risk of falls associated with active comparators, compared to no treatment.9,10 The data on falls was not available for all active comparators, so assumptions were made by the sponsor, such as assuming quetiapine had the same risk of falls as trazodone.
The baseline risk of fatal MVAs, nonfatal MVAs, fatal WPAs, and nonfatal WPAs was based on the incidence of accidents in the US population, which served as a proxy for Canada.11,12 The sponsor assumed that the risk of MVAs did not vary by age but that the rate of all WPAs among the older age group was 27% of the younger age group.13 The sponsor also assumed that lemborexant treatment did not impair driving. However, treatments with active comparators did increase the risk of MVAs based on a sponsor-conducted comparison that assumed that an intoxicated person is at the same risk of an MVA as a person with insomnia.2 The effect of insomnia treatments on WPAs was assumed to be the same as MVAs.
Responders were assumed to have an age-adjusted utility values as that of the general population,14 while nonresponders were assigned a disutility for insomnia.15 Disutilities associated with somnolence, dizziness, falls, MVAs, and WPAs were obtained from published literature.2,8,16,17
Costs included drug acquisition, physician visits, cognitive behaviour therapy sessions, and the management of adverse events. Drug costs for lemborexant were based on the sponsor’s submitted price while the cost of comparators were based on the Ontario Drug Benefit Formulary.2,18 For comparators with variable dosing, the sponsor calculated drug costs based on the average dose within the product monograph’s recommended dosing range. Drug acquisition costs and dosing were consistent with those reported in the overview section. The costs of physician visits and cognitive behaviour therapy sessions were obtained from the Ontario Schedule of Benefits: Physician Services Under the Health Insurance Act.19 The cost to manage falls, WPAs, and MVAs came from a variety of sources or assumptions.19-21 Relevant costs were inflated to 2021 dollars.
Summary of Sponsor’s Economic Evaluation Results
All analyses were run probabilistically (2,000 iterations for the base case and 1,000 iterations for the scenario analyses). The ICER for the deterministic results did not align with that of the probabilistic results; however, this was due to the small incremental difference in QALYs. The deterministic ICER was $196,546 per QALY for untreated patients compared to patients treated with lemborexant (incremental QALY = 0.003) whereas the probabilistic results estimated an ICER of $855,067 (incremental QALY = 0.001).
Base-Case Results
The sponsor conducted a sequential analysis and lemborexant was associated with the lowest expected total cost of $1,591. All active comparators were dominated (more costly and less effective) by lemborexant. The undominated, “no treatment,” was associated with incremental costs of $680 and incremental QALYs of 0.001 compared to lemborexant, for an ICER of $855,067 per QALY. Results from the sponsor’s probabilistic analysis revealed that there was a 68.5% chance that lemborexant would produce fewer QALYs than no treatment.
Table 3: Summary of the Sponsor’s Economic Evaluation Results
Drug | Total costs ($) | Total QALYs | Sequential ICER ($/QALY) |
|---|---|---|---|
Lemborexant | 1,591 | 0.3126 | Reference |
Lorazepam (0.5 mg to 2 mg) | 1,792 | 0.2810 | Dominateda |
Quetiapine (25 mg) | 1,817 | 0.2673 | Dominateda |
Trazodone (50 mg) | 1,818 | 0.2671 | Dominateda |
Nitrazepam (5 mg) | 1,871 | 0.2747 | Dominateda |
Temazepam (15 mg) | 1,878 | 0.2750 | Dominateda |
Zopiclone (7.5 mg) | 1,916 | 0.2769 | Dominateda |
Flurazepam (30 mg) | 1,962 | 0.2597 | Dominateda |
Triazolam (0.50 mg) | 1,966 | 0.2704 | Dominateda |
No treatment | 2,271 | 0.3134 | 855,067 |
ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year.
a“Dominated” refers to a treatment having higher total costs and lower total QALYs when compared to the previous less costly treatment.
Source: Sponsor’s pharmacoeconomic submission.2
Sensitivity and Scenario Analysis Results
The sponsor provided scenario analyses exploring the impact of defining the response rate based on the wake after sleep onset instrument, varying the costs to manage adverse events, applying different disutility values, varying the cost of physician visit, extending the time horizon to 1 year, and adopting a societal perspective. The results were sensitive to scenarios where a 1-year time horizon or a societal perspective was adopted, in which case lemborexant became the dominant therapy.
CADTH Appraisal of the Sponsor’s Economic Evaluation
CADTH identified several key limitations to the sponsor’s analysis that have notable implications on the economic analysis.
Relevant comparators were omitted from the analysis. The clinical expert consulted for this review noted that some pharmacologic treatments for insomnia were not included in the analysis. Doxepin and mirtazapine are commonly prescribed medications in Canadian clinical practice that are reimbursed by several of the public formularies. As these comparators were not included in the analysis, their cost-effectiveness compared to lemborexant is unknown; however, notably, their list price on the Ontario Drug Benefit Formulary is less costly than lemborexant (Appendix 1).
CADTH could not address this limitation.
The response rate with lemborexant use relative to active comparators is highly uncertain. The sponsor modelled a higher response rate on lemborexant relative to active comparators. The sponsor submitted an indirect treatment comparison of treatment response measured using sSOL; however, the comparative clinical evidence is only available for triazolam 0.125 mg and temazepam 15 mg. There is no comparative evidence available for the sponsor’s other active comparators: flurazepam, lorazepam, nitrazepam, zopiclone, trazodone, and quetiapine. Further, the indirect treatment comparison suggested that lemborexant is superior to triazolam 0.125 mg; however, the effect estimates are imprecise, which make it difficult to ascertain the magnitude and direction of comparative treatment response. Additional limitations of the NMA were also identified, and include risk of bias, heterogeneity in the pairwise comparisons, and uncertainty in the plausibility of the transitivity assumption. As such, no firm conclusions about the comparative efficacy of lemborexant can be drawn relative to active comparators that may be used in Canadian clinical practice.
In a scenario analysis, CADTH explored the uncertainty in comparative treatment response based on sSOL by assuming no difference in the response rates between lemborexant and active comparators.
There was insufficient evidence for the impact of insomnia treatment on the risk of MVAs or WPAs. In the sponsor’s submission, the impact of insomnia treatment on the risk of MVAs was based on the standard deviation of lateral position (SDLP) on a standardized on-the-road driving test (a measure of lane swerving). Specifically, the cut-off of those at increased risk of an MVA was assumed to be at least 2.4 cm, a value demonstrated in a systematic review to be equivalent to a person driving with a blood alcohol concentration of 0.05%.22 Using that threshold, the sponsor applied the SDLP cut-off to a study by Vermeeren et al. (2019) that aimed to evaluate the effect of lemborexant compared to zopiclone on driving performance in 48 healthy volunteers.23 Based on those findings, the sponsor assumed lemborexant would not have an increased risk of an MVA, while zopiclone and all other relevant comparators in the model would have a risk of an MVA equivalent to those driving with a blood alcohol concentration of 0.05%. There were important limitations to this approach, where primarily the assumption to naively use the SDLP cut-off for blood alcohol concentrations to estimate the odds of an MVA after taking zopiclone or lemborexant is unlikely to be valid. There are likely differences in the relationship between alcohol and MVAs, and between medications used to treat insomnia (e.g., lemborexant, zopiclone) and MVAs, that would impact the odds of MVAs. Therefore, both the direction and magnitude of difference between these relationships cannot be inferred, and are likely different from that used by the sponsor. According to the clinical expert consulted for this review by CADTH, there is no evidence to suggest there is a causal relationship between insomnia treatments and the risk of MVAs.
The sponsor-submitted report on MVAs also lacks external validity. The study by Vermeeren et al. included only healthy volunteers (who explicitly had no sleep disorders and were described as “good sleepers”), which limits generalizability of the trial results to patients with insomnia.23 The small sample size further limits generalizability of this study to the Canadian population. The clinical expert for this review also noted that any evidence of MVAs in patients with severe sleep apnea is not directly transferable to a patient population with insomnia.
The effect of insomnia treatments on WPAs was assumed to be the same as MVAs. As the evidence on MVAs is insufficient, and no causal evidence was provided between WPAs and insomnia treatments, the sponsor biased the results of its cost-effectiveness analysis in favour of lemborexant by assuming a difference in MVA and WPA risk for lemborexant versus relevant comparators.
In the CADTH reanalysis, it was assumed there would be no difference in the risk of MVAs and WPAs between lemborexant and all relevant comparators.
The impact of insomnia treatments on the risk of falls is highly uncertain. The sponsor assumed that lemborexant use is associated with an increased risk of falls compared to placebo, but at a reduced risk compared to other active comparators. However, the impact of insomnia treatments on the risk of falls is highly uncertain. The sponsor estimated the risk of falls with lemborexant use by pooling results from the SUNRISE 1 and SUNRISE 2 trials (for LEM5, odds ratio = 1.32; 95% confidence interval [CI], 0.11 to 16.31; for LEM10, odds ratio = 0.52; 95% CI, 0.18 to 1.47).3,4 As exhibited by the wide overlapping 95% CIs, no firm conclusions can be drawn due to serious imprecision.
The sponsor derived the risk of falls compared to other active comparators from the literature.9,10 The study that the sponsor used by Neutel et al. (1996) was conducted more than 25 years ago, and it is unclear whether all participants in the study were diagnosed with insomnia because the study selected a population based on claims data that did not provide the health indication for which treatment is prescribed.9 The odds of falls after benzodiazepine use in insomnia patients may be different than in a population with conditions other than insomnia, which limits the applicability of the results of this study to the indicated population considered in this review. Further, the study by Amari et al. (2020) compared the risk of falls among adult patients with insomnia treated with commonly used prescription medications relative to a matched control cohort without sleep disorders.10 The results of Amari et al. are prone to confounding; the comparator and control group were only matched on age and sex, and not on the presence of disease.10 The risk of falls associated with insomnia treatment may have also been overestimated by having a control group that is healthier than the intervention group. The study notes a higher Charlson Comorbidity Index score for the intervention group, indicating that the patients receiving insomnia treatment were sicker than those in the control group, which may have biased the results against the active comparators.
The sponsor-submitted supplementary indirect treatment comparison of lemborexant to active insomnia treatments produced estimates with wide 95% CIs that included the null value. The sponsor biased the results of its cost-effectiveness analysis in favour of lemborexant by modelling a reduced risk of falls for lemborexant compared to other active comparators. However, any conclusions regarding the relative risk of falls with lemborexant use compared to other active insomnia treatments is highly uncertain due to the lack of direct evidence and imprecision in the indirect estimates.
In the CADTH reanalysis, it was assumed there would be no difference in the risk of falls between lemborexant and all relevant comparators.
CADTH explored the impact of an increased risk of falls associated with benzodiazepines in a scenario analysis.
The disutilities associated with the impact of insomnia treatment is likely double counted. The sponsor adopted several disutilities in its model, including disutilities for having insomnia, for active treatment of insomnia and its common side effects (i.e., somnolence and dizziness), and for having events such as falls, MVA, or WPAs. There is likely double counting of the disutilities, as those who do not respond to treatment and suffer from insomnia are also given the disutility of somnolence and dizziness. Further, as disutilities were pulled from published sources, there was a risk of overlap in the estimates specified in the sponsor’s report. Where the sample population used to derive the disutility associated with someone with insomnia, may include patients currently on treatment and experiencing somnolence and dizziness. In these cases, the disutility associated with insomnia likely captures some or all of the disutility associated with somnolence and dizziness and avoids potential double counting.
In the CADTH reanalysis, treatment disutilities were excluded due to the risk of double counting. However, the impact of including treatment disutilities in the CADTH reanalysis was explored in a scenario analysis.
The number of additional primary care visits for patients with no treatment was overestimated. The sponsor assumed that untreated patients seek primary care 4 times more than patients on lemborexant. The clinical expert consulted for this review noted the sponsor overestimated the number of additional primary care visits sought for insomnia by untreated patients over the 6-month time horizon. The clinical expert also noted that the modelled differences in primary care visits between active comparators was not meaningful.
In the CADTH reanalysis, it was assumed there is no difference in the number of additional primary care visits for all relevant comparators.
The submitted model does not capture key aspects of the treatment paradigm. The sponsor’s submitted decision-tree model was based primarily on patient response and nonresponse captured by the sSOL scale. According to the clinical expert consulted by CADTH for this review, sleep treatment is often associated with depression or anxiety; however, mood disorders accompanying insomnia have not been considered in this analysis. Further, insomnia is often cyclic in nature where some patients continue their medication and obtain some benefit, while others discontinue and have rebound insomnia. The decision-tree framework and chosen time horizon do not capture all these possibilities and their associated costs and the impact on quality of life.
CADTH could not address this limitation.
There was inaccurate treatment cost and dosing of some active comparators. The lowest unit price in public drug plan formularies was not adopted for temazepam, triazolam, and zopiclone, and the dose adopted for temazepam and triazolam did not align with the recommended doses in their respective product monographs.
An additional minor limitation was identified; specifically, the sponsor’s results lacked face validity. The clinical expert consulted by CADTH for this review did not expect that untreated patients with insomnia, characterized by difficulties with sleep onset and/or sleep maintenance, would have the highest number of QALYs (i.e., treatment lowers net quality of life).
Additionally, the following key assumptions were made by the sponsor and have been appraised by CADTH (refer to Table 4).
Table 4: Key Assumptions of the Submitted Economic Evaluation (Not Noted as Limitations to the Submission)
Sponsor’s key assumption | CADTH comment |
|---|---|
Health state utility values were adopted from the literature. | Uncertain. To inform the pharmacoeconomic model, the sponsor adopted health state utility values from the literature.14,15 The clinical expert consulted for this review noted that patient-reported outcomes and perceptions of sleep changes are more appropriate for assessing treatment effect. However, sleep improvement measured using objective outcomes did not reflect the results from patient-reported questionnaires, adding uncertainty to whether health state utilities are reflective of the response observed in the SUNRISE trials. |
CADTH Reanalyses of the Economic Evaluation
Base-Case Results
Key limitations identified included methodical limitations in the sponsor-submitted direct and indirect comparisons informing the comparative response rates to insomnia treatments and the impact of insomnia treatments on the risk of falls. The comparative efficacy evidence was also absent for most active comparators. Additionally, there was no clinical evidence to support the impact of insomnia treatment response on the risk of MVAs and WPAs. CADTH also identified limitations with the model structure, which did not capture key aspects of the treatment paradigm, excluded comparators relevant in clinical practice, and double counted disutilities. The sponsor’s estimated incremental number of additional physician visits was also likely overestimated.
The CADTH base case was derived by making changes in model parameter values and assumptions, in consultation with the clinical expert. CADTH’s base case assumed there is no difference in the risk of falls, MVAs, WPAs, and the number of additional physician visits for insomnia between insomnia treatments and placebo.
Table 5: CADTH Revisions to the Submitted Economic Evaluation
Stepped analysis | Sponsor’s value or assumption | CADTH value or assumption |
|---|---|---|
Corrections to sponsor’s base case | ||
1. Dosing | Temazepam = 15 mg Triazolam = 0.5 mg | Temazepam = 30 mg Triazolam = 0.125 mg |
2. Unit prices | Temazepam = $0.2317 Triazolam = $0.2551 Zopiclone = $0.4685 | Temazepam = $0.0877 Triazolam = $0.1496 Zopiclone = $0.1350 |
Changes to derive the CADTH base case | ||
1. MVAs and WPAs | The sponsor assumed an increased risk of having an MVA and WPA (RR = 2.18) under treatment with flurazepam, nitrazepam, zopiclone, triazolam, temazepam, quetiapine, trazodone, or lorazepam compared with placebo. | CADTH assumed no difference in the relative risk of MVAs and WPAs (RR = 1). |
2. Falls | The sponsor assumed an increased risk of falls under treatment with lemborexant (RR = 1.18), flurazepam (RR = 3.05), nitrazepam (RR = 2.16), zopiclone (RR = 2.16), triazolam (RR = 2.50), temazepam (RR = 2.16), quetiapine (RR = 2.63), trazodone (RR = 2.63), or lorazepam (RR = 1.91) compared with placebo. | CADTH assumed no difference in the relative risk of falls (RR = 1). |
3. Treatment disutilities | Included | Excluded |
4. Additional primary care visits | The sponsor assumed primary care visits by untreated patients (n = 10) are 4 times more than patients on lemborexant (n = 2.5). The sponsor assumed primary care visits by patients on benzodiazepines was higher (n = 3.33) compared with patients on lemborexant (n = 2.5). | CADTH assumed no difference in the number of primary care visits for all relevant comparators. |
CADTH base case | Reanalysis 1 + 2 + 3 + 4 | |
MVA = motor vehicle accident; RR = relative risk; WPA = workplace accident.
In the CADTH base case, trazodone was dominant over all other comparators besides lemborexant. Compared to trazodone, lemborexant was associated with additional costs ($229) and QALYs (0.003), resulting in an ICER of $76,941 per QALY. At a willingness-to-pay threshold of $50,000 per QALY, lemborexant had a 19% probability of being cost-effective. Results of the CADTH reanalysis are presented in Table 6; of note, incremental QALY gains between comparators were marginal. The results of stepped analysis are presented in Table 13 in Appendix 4, while the disaggregated results are available in Table 14 and Table 15 of Appendix 4.
Table 6: Summary of CADTH’s Reanalysis Results
Drug | Total costs ($) | Incremental costs ($) | Total QALYs | Incremental QALYs | Sequential ICER ($/QALYs) |
|---|---|---|---|---|---|
Trazodonea (50 mg) | 1,307 | Reference | 0.3202 | Reference | Reference |
Quetiapine (25 mg) | 1,307 | 1.25 | 0.3202 | 0.000 | Dominatedb |
Lorazepam (0.5 mg to 2 mg) | 1,314 | 12.25 | 0.3165 | –0.001 | Dominatedb |
Temazepam (15 mg) | 1,322 | 20.45 | 0.3194 | –0.001 | Dominatedb |
No treatment | 1,325 | 23.41 | 0.3180 | –0.002 | Dominatedb |
Zopiclone (7.5 mg) | 1,330 | 28.95 | 0.3194 | –0.001 | Dominatedb |
Flurazepam (30 mg) | 1,331 | 29.20 | 0.3194 | –0.001 | Dominatedb |
Triazolam (0.50 mg) | 1,333 | 31.58 | 0.3194 | –0.001 | Dominatedb |
Nitrazepam (5 mg) | 1,337 | 35.57 | 0.3194 | –0.001 | Dominatedb |
Lemborexant | 1,532 | 228.84 | 0.3232 | 0.003 | 76,941 |
ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year.
aThe reference product is the least costly alternative that is not dominated.
b“Dominated” refers to a treatment having higher total costs and lower total QALYs when compared to the previous less costly treatment.
Scenario Analysis Results
To address uncertainty in the comparative harms and clinical efficacy evidence, CADTH conducted scenario analyses. In a scenario analysis, CADTH assumed the sponsor’s estimated increased risk of falls would apply specifically for the benzodiazepine comparators; however, this assumption had a marginal impact on the sequential ICER. In another scenario analysis, CADTH assumed no difference in treatment response (based on sSOL) between lemborexant and active comparators. This assumption removed all benefit for lemborexant versus active comparators, resulting in costs being the only differences between the treatments. Finally, a scenario including disutility associated with treatment was conducted; however, this had little impact on the sequential ICER. The full results from the scenario analysis are presented in Table 16.
Price Reduction Analyses
There is a high degree of uncertainty in the estimates used to model treatment response among active comparators, which CADTH was unable to account for in the CADTH base case. Given the limitations of the clinical evidence, and small differences in QALYs between comparators in the CADTH base case, there is uncertainty as to whether there is adequate evidence to warrant a price premium for lemborexant over other active comparators. As such, CADTH conducted a cost comparison to understand the percentage price reduction required for lemborexant to be costed similarly to relevant comparators.
Based on the CADTH reanalysis, when considering the cost associated with the least costly treatment (lorazepam, a benzodiazepine used off-label), the submitted price of lemborexant would need to be reduced by 79%. When considering the comparators from each drug class, the submitted price of lemborexant would need to be reduced by 76% to 82% to be equivalent to the least costly comparator in each class.
Table 7: CADTH Price Reduction Analysis
Scenario | Sponsor’s submitted price ($) | Reduction needed (%) | Reduced price ($) | Savingsa ($) |
|---|---|---|---|---|
Price reduction required to equal least costly treatment (lorazepam 0.5 mg) | 1.52 | 79% | 0.32 | 216 |
Price reduction required to equal least costly benzodiazepine (temazepam 15 mg) | 1.52 | 76% | 0.36 | 208 |
Price reduction required to equal cost of Z-drug (zopiclone 7.5 mg) | 1.52 | 73% | 0.41 | 199 |
Price reduction required to equal cost of antipsychotic drug (quetiapine 25 mg) | 1.52 | 83% | 0.27 | 225 |
Price reduction required to equal cost of antidepressant (trazodone 50 mg) | 1.52 | 82% | 0.28 | 224 |
aSavings account for drug costs and cognitive behaviour therapy costs over the 180-day time horizon. Savings are estimated from the deterministic analysis.
Issues for Consideration
The clinical expert noted that the use of over-the-counter products (e.g., cannabinoids) is frequent in the treatment of insomnia. If the introduction of lemborexant fit an unmet need for that patient population, the population size of insomnia patients seeking pharmacologic treatment may increase.
The clinical expert consulted for this review noted that insomnia is often associated with anxiety and/or depression. Further, drug plan input indicated that treatment for insomnia, narcolepsy, parasomnia, and sleep apnea are often treated with similar drugs. In the event lemborexant is used in a population outside the indication, the estimated budget impact may be significantly underestimated.
Overall Conclusions
The CADTH clinical review concluded that lemborexant demonstrated improvements in sleep onset, sleep maintenance, and sleep efficiency among adults with insomnia relative to placebo; however, the sleep improvements based on polysomnography and sleep diary outcomes observed in the SUNRISE 1 and SUNRISE 2 studies did not appear to be reflected in the results from the patient-reported questionnaires. Considering the limitations with both objective and subjective outcomes, it is uncertain if the differences in response rates would be meaningful to all patients who could be treated with lemborexant. Any conclusions based on the indirect evidence are uncertain due to limitations of the NMA. Evidence was absent for some comparators or very uncertain for clinical efficacy and harms outcomes due to imprecision, risk of bias, and heterogeneity in the pairwise comparisons. Therefore, no firm conclusions could be made on the relative response rates and harms associated with lemborexant versus active comparators.
To address the identified limitations with the sponsor’s pharmacoeconomic evaluation, CADTH undertook a reanalysis with the following changes: it assumed no difference in the risk of falls, MVAs, WPAs and the number of physician visits among treatments, and it excluded disutilities associated with treatment. In the CADTH base case, trazodone was dominant over all other comparators besides lemborexant. Therefore, the resultant ICER for lemborexant compared to trazodone was $76,941 per QALY gained, where lemborexant had a 17% probability of being cost-effective at a $50,000 per QALY threshold.
The interpretation of the CADTH base case is limited by the comparative clinical data. There is a high degree of uncertainty in the estimates used to model treatment response among active comparators, which CADTH was unable to account for in the CADTH base case. Given the limitations of the clinical evidence, and small differences in QALYs between comparators in the CADTH base case, there is uncertainty as to whether there is adequate evidence to warrant a price premium for lemborexant over other active comparators. As such, CADTH conducted a cost comparison to understand the percentage price reduction required for lemborexant to be costed similarly to relevant comparators. Based on the CADTH reanalysis, the submitted price of lemborexant would need to be reduced by 76% to 82% to be equivalent to the cost of active comparators.
References
1.Drug Reimbursement Review: Sublinox (zolpidem tartrate) for the short-term treatment of insomnia. Ottawa (ON): CADTH; 2013: https://www.cadth.ca/zolpidem-tartrate. Accessed 2022 May 30.
2.Pharmacoeconomic evaluation [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Dayvigo (lemborexant), 5 mg and 10 mg oral tablets. Mississauga (ON): Eisai Limited; 2020 Nov 3.
3.Karppa M, Yardley J, Pinner K, et al. Long-term efficacy and tolerability of lemborexant compared with placebo in adults with insomnia disorder: results from the phase 3 randomized clinical trial SUNRISE 2. Sleep. 2020;43(9). PubMed
4.Rosenberg R, Murphy P, Zammit G, et al. Comparison of lemborexant with placebo and zolpidem tartrate extended release for the treatment of older adults with insomnia disorder: a phase 3 randomized clinical Trial. JAMA Netw Open. 2019;2(12):e1918254. PubMed
5.PharmaStat. Ottawa (ON): IQVIA; 2021: https://www.iqvia.com/. Accessed 2022 May 20.
6.Manis DR, McArthur C, Costa AP. Associations with rates of falls among home care clients in Ontario, Canada: a population-based, cross-sectional study. BMC Geriatr. 2020;20(1):80. PubMed
7.Australian Institute of Health and Welfare. Hip fracture incidence and hospitalisation in Australia 2015–16 Data tables. Table S3.1: Hospitalisation for new hip fracture, by age and sex, 2015–16. 2019: https://www.aihw.gov.au/getmedia/d4236d00-0277-48a6-bb6d-b7c911ed7207/aihw-phe-226-data-tables.xlsx.aspx. Accessed 2022 May 20.
8.Tannenbaum C, Diaby V, Singh D, Perreault S, Luc M, Vasiliadis HM. Sedative-hypnotic medicines and falls in community-dwelling older adults: a cost-effectiveness (decision-tree) analysis from a US Medicare perspective. Drugs Aging. 2015;32(4):305-314. PubMed
9.Neutel CI, Hirdes JP, Maxwell CJ, Patten SB. New evidence on benzodiazepine use and falls: the time factor. Age Ageing. 1996;25(4):273-278. PubMed
10.Amari D FF, Juday T, Wang W, Gor D, Wickwire E. Risk of Falls Among Adult Patients on Commonly Used Insomnia Medications in the United States. . Academy of Managed Care Pharmacy (AMCP) Managed Care & Specialty Pharmacy Nexus 2020; Meeting 2020b. Alexandria (VA): Academy of Managed Care Pharmacy; 2020.
11.Blincoe LJ, Miller TR, Zaloshnja E, Lawrence BA. The economic and societal impact of motor vehicle crashes, 2010 (Revised). (Report No. DOT HS 812 013). Washington (DC): National Highway Traffic Safety Administration; 2015: https://crashstats.nhtsa.dot.gov/Api/Public/ViewPublication/812013. Accessed 2022 May 20.
12.Leigh JP. Economic burden of occupational injury and illness in the United States. Milbank Q. 2011;89(4):728-772. PubMed
13.U.S. Bureau of Labour Statistics. Labor force statistics from the current population survey, occupation: Employed persons by detailed occupation and age, including median age. 2019: https://www.bls.gov/cps/demographics.htm#age. Accessed 2022 May 20.
14.Ara R, Brazier JE. Populating an economic model with health state utility values: moving toward better practice. Value Health. 2010;13(5):509-518. PubMed
15.Olfson M, Wall M, Liu SM, Morin CM, Blanco C. Insomnia and impaired quality of life in the United States. J Clin Psychiatry. 2018;79(5). PubMed
16.Matza LS, Deger KA, Vo P, Maniyar F, Goadsby PJ. Health state utilities associated with attributes of migraine preventive treatments based on patient and general population preferences. Qual Life Res. 2019;28(9):2359-2372. PubMed
17.Spicer RS, Miller TR, Hendrie D, Blincoe LJ. Quality-adjusted life years lost to road crash injury: updating the injury impairment index. Ann Adv Automot Med. 2011;55:365-377. PubMed
18.Ontario Ministry of Health, Ontario Ministry of Long-Term Care. Ontario drug benefit formulary/comparative drug index. 2022; https://www.formulary.health.gov.on.ca/formulary/. Accessed 2022 Apr 15.
19.Schedule of benefits for physician services under the Health Insurance Act: effective October 1, 2021. Toronto (ON): Ontario Ministry of Health; 2021: https://www.health.gov.on.ca/en/pro/programs/ohip/sob/physserv/sob_master.pdf. Accessed 2022 May 20.
20.Patient cost estimator. 2022; https://www.cihi.ca/en/patient-cost-estimator. Accessed 2022 Feb 28.
21.Pincus D, Wasserstein D, Nathens AB, Bai YQ, Redelmeier DA, Wodchis WP. Direct medical costs of motorcycle crashes in Ontario. CMAJ. 2017;189(46):E1410-e1415. PubMed
22.Taylor B, Irving HM, Kanteres F, et al. The more you drink, the harder you fall: a systematic review and meta-analysis of how acute alcohol consumption and injury or collision risk increase together. Drug Alcohol Depend. 2010;110(1-2):108-116. PubMed
23.Vermeeren A, Jongen S, Murphy P, et al. On-the-road driving performance the morning after bedtime administration of lemborexant in healthy adult and elderly volunteers. Sleep. 2019;42(4). PubMed
24.Newfoundland and Labrador. The Newfoundland and Labrador Interchangeable Drug Products Formulary Vol 86. 2022; https://www.gov.nl.ca/hcs/files/nlpdp-formularyvol86.pdf. Accessed 2022 Apr 15.
25.B. C. Government. BC PharmaCare formulary search. 2022; https://pharmacareformularysearch.gov.bc.ca. Accessed 2022 Apr 15.
26.Triazolam (triazolam): 0.125 mg and 0.25 mg tablets [product monograph]. Vaughan (ON): AA Pharma Inc.; 2012: https://www.aapharma.ca/downloads/en/PIL/2016/Triazolam-PM.pdf. Accessed 2022 May 30.
27.Restoril (temazapam): 15 mg and 30 mg capsules [product monograph]. Vaughan (ON): AA Pharma Inc.; 2017: https://www.aapharma.ca/downloads/en/PIL/2017/Restoril%20PM_EN.pdf. Accessed 2022 May 30.
28.DeltaPA. [Ottawa (ON)]: IQVIA; 2021: https://www.iqvia.com/. Accessed April 15 2022.
29.Kamphuis J, Taxis K, Schuiling-Veninga CC, Bruggeman R, Lancel M. Off-label prescriptions of low-dose quetiapine and mirtazapine for insomnia in The Netherlands. J Clin Psychopharmacol. 2015;35(4):468-470. PubMed
30.Jaffer KY, Chang T, Vanle B, et al. Trazodone for insomnia: a systematic review. Innov Clin Neurosci. 2017;14(7-8):24-34. PubMed
31.Coe HV, Hong IS. Safety of low doses of quetiapine when used for insomnia. Ann Pharmacother. 2012;46(5):718-722. PubMed
32.Bonnet MH, Arand DL. The use of lorazepam TID for chronic insomnia. Int Clin Psychopharmacol. 1999;14(2):81-89. PubMed
33.Budget Impact Analysis [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Dayvigo (lemborexant), 5 mg and 10 mg oral tablets. Mississauga (ON): Eisai Limited; 2022 Feb 1.
34.Saskatchewan Drug Plan: search formulary. 2022; https://formulary.drugplan.ehealthsask.ca/SearchFormulary. Accessed 2022 Apr 15.
35.Alberta Blue Cross. Alberta Blue Cross Drug Benefit List. 2021; https://ab.bluecross.ca/dbl/idbl_main1.php. Accessed 2022 Apr 15.
36.Nova Scotia Pharmacare. Nova Scotia Pharmacare Formulary. 2021; https://novascotia.ca/dhw/pharmacare/documents/formulary.pdf. Accessed 2022 Apr 15.
37.RAMQ List of Medications. Quebec (QC): Regie de l'assurance maladie du Quebec; 2021: https://www.ramq.gouv.qc.ca/sites/default/files/documents/liste-med-2021-09-29-en_0.pdf. Accessed 2021 Oct 29.
38.Morin CM, LeBlanc M, Daley M, Gregoire JP, Mérette C. Epidemiology of insomnia: prevalence, self-help treatments, consultations, and determinants of help-seeking behaviors. Sleep Med. 2006;7(2):123-130. PubMed
39.Morin CM, LeBlanc M, Bélanger L, Ivers H, Mérette C, Savard J. Prevalence of insomnia and its treatment in Canada. Can J Psychiatry. 2011;56(9):540-548. PubMed
Appendix 1: Cost Comparison Table
Note that this appendix has not been copy-edited.
The comparators presented in the following table have been deemed to be appropriate based on feedback from the clinical expert and drug plan. Comparators may be recommended (appropriate) practice or actual practice. Existing Product Listing Agreements are not reflected in the table and as such, the table may not represent the actual costs to public drug plans.
Table 8: CADTH Cost Comparison Table for Insomnia
Treatment | Strength/ | Form | Price ($) | Recommended dosage | Daily cost ($) | Annual cost ($) |
|---|---|---|---|---|---|---|
Lemborexant (Dayvigo) | 5 mg 10 mg | Tablet | 1.5198a | 5 mg to 10 mg once daily | 1.52 | 555 |
Antidepressants | ||||||
Doxepin (Sinequan) | 3 mg 6 mg 10 mg 25 mg 50 mg 75 mg 100 mg 150 mg | Capsule | 0.652b 1.3047b 0.3877 0.3205c 0.8824 1.1648 1.5319 1.3101 | 3 mg to 6 mg once daily | 0.32 | 117 |
Benzodiazepines | ||||||
Flurazepam | 15 mg 30 mg | Capsule | 0.1166 0.1364 | 30 mg once daily | 0.14 | 50 |
Nitrazepam | 5 mg 10 mg | Tablet | 0.1737 0.2599 | 5 mg to 10 mg once daily | 0.17 to 0.26 | 63 to 94 |
Temazepam | 15 mg 30 mg | Capsule | 0.0725 c 0.0877 c | 30 mg once daily | 0.09 | 32 |
Triazolam | 0.125 mg 0.25 mg | Tablet | 0.1496 0.2551 | 0.125 mg once daily | 0.15 | 55 |
Z-drugs | ||||||
Zopiclone (generics) | 3.75 mg 5 mg 7.5 mg | Tablet | 0.0670 d 0.1069 d 0.1350 d | 3.75 mg to 7.5 mg once daily | 0.07 to 0.14 | 25 to 49 |
Note: All prices are from the Ontario Drug Benefit Formulary (accessed April 15, 2022), unless otherwise indicated, and do not include dispensing fees.
aSponsor’s submitted price.2
bIQVIA Delta PA database,28 accessed April 15, 2022.
cNewfoundland and Labrador formulary,24 accessed April 15, 2022.
dBritish Columbia formulary,25 accessed April 15, 2022.
Table 9: CADTH Cost Comparison Table for Insomnia (Not Indicated for Insomnia)
Treatment | Strength/ concentration | Form | Price ($) | Recommended dosage | Daily cost ($) | Annual cost ($) |
|---|---|---|---|---|---|---|
Antidepressants | ||||||
Mirtazapine (generics) | 15 mg 30 mg 45 mg | Orally Disintegrating Tablet | 0.4046 0.3100 1.2132 | 7.5 mg to 30 mg once daily | 0.31 | 113 |
Trazodone (generics) | 50 mg 100 mg 150 mg | Tablet | 0.0554 0.0989 0.1453 | 50 mg once daily | 0.06 | 20 |
Antipsychotic drugs | ||||||
Quetiapine (generics) | 25 mg 100 mg 200 mg 300 mg 50 mg 150 mg 200 mg 300 mg 400 mg | Tablet Extended-release tablet | 0.0494 0.1318 0.2647 0.3863 0.2501 0.4926 0.6661 0.9976 1.3270 | 25 mg to 200 mg once daily | 0.05 to 0.26 | 18 to 96 |
Benzodiazepines | ||||||
Lorazepam (generics) | 0.5 mg 1 mg 2 mg | Tablet | 0.0359 0.0447 0.0699 | 0.5 mg to 2 mg once daily | 0.04 to 0.07 | 13 to 26 |
Note: All prices are from the Ontario Drug Benefit Formulary (accessed April 15, 2022),18 unless otherwise indicated, and do not include dispensing fees. Recommended dosage was obtained from published literature.29-32
Appendix 2: Submission Quality
Note that this appendix has not been copy-edited.
Description | Yes/no | Comments |
|---|---|---|
Population is relevant, with no critical intervention missing, and no relevant outcome missing | No | Relevant comparators such as mirtazapine and doxepin were excluded from the analysis. Refer to CADTH appraisal section. |
Model has been adequately programmed and has sufficient face validity | No | The model has not been adequately programmed. The sponsor’s decision-tree modelled multiple outcomes as a compound probability (i.e., risk of fatal falls, nonfatal falls, fatal MVAs, nonfatal MVAs, fatal WPAs, and nonfatal WPAs at 1 chance node). Good modelling practice is to model 2 possible outcomes following a chance node in a decision-tree. The results generated by the model lack face validity. The clinical expert consulted for this review noted that the results do not meet their expectation; specifically, that untreated patients would not have a higher number of QALYs compared to patients treated with active therapy, including lemborexant. |
Model structure is adequate for decision problem | No | The submitted model structure was found to be inadequate in capturing clinically meaningful response and patient function. Refer to CADTH appraisal section. |
Data incorporation into the model has been done adequately (e.g., parameters for probabilistic analysis) | No | Refer to CADTH appraisal section. |
Parameter and structural uncertainty were adequately assessed; analyses were adequate to inform the decision problem | Yes | No comment. |
The submission was well organized and complete; the information was easy to locate (clear and transparent reporting; technical documentation available in enough details) | No | CADTH identified several limitations with the submission related to transparency. It was difficult to trace the model parameters used in the analysis. |
Appendix 3: Additional Information on the Submitted Economic Evaluation
Note that this appendix has not been copy-edited.
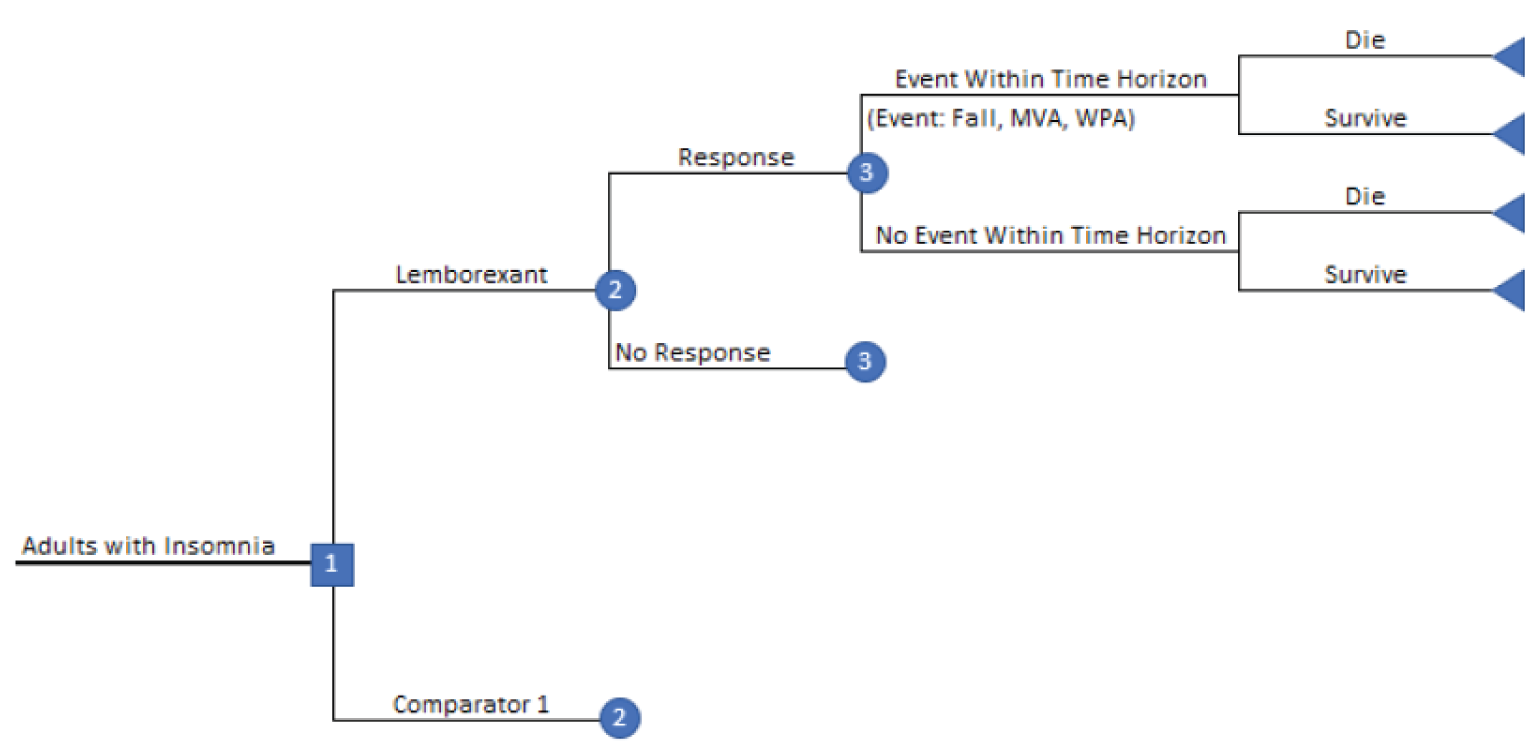
Detailed Results of the Sponsor’s Base Case
Table 11: Disaggregated Summary of the Sponsor’s Economic Evaluation Results for Insomnia — QALYs
Comparator | Treatment | Falls | MVAs | WPAs | Premature death | Total |
|---|---|---|---|---|---|---|
Lemborexant | 0.3699 | –0.0162 | –0.0003 | –0.0007 | –0.0400 | 0.3126 |
Lorazepam (0.5 mg to 2 mg) | 0.3659 | –0.0229 | –0.0010 | –0.0019 | –0.0591 | 0.2810 |
Quetiapine (25 mg) | 0.3667 | –0.0270 | –0.0010 | –0.0020 | –0.0695 | 0.2673 |
Trazodone (50 mg) | 0.3667 | –0.0270 | –0.0010 | –0.0020 | –0.0695 | 0.2671 |
Nitrazepam (5 mg) | 0.3660 | –0.0246 | –0.0011 | –0.0020 | –0.0636 | 0.2747 |
Temazepam (15 mg) | 0.3660 | –0.0246 | –0.0010 | –0.0020 | –0.0634 | 0.2750 |
Zopiclone (7.5 mg) | 0.3679 | –0.0246 | –0.0010 | –0.0019 | –0.0634 | 0.2769 |
Flurazepam (30 mg) | 0.3649 | –0.0286 | –0.0010 | –0.0019 | –0.0738 | 0.2597 |
Triazolam (0.50 mg) | 0.3676 | –0.0264 | –0.0010 | –0.0019 | –0.0679 | 0.2704 |
Untreated | 0.3677 | –0.0140 | –0.0010 | –0.0019 | –0.0374 | 0.3134 |
MVA = motor vehicle accident; QALY = quality-adjusted life-year; WPA = workplace accident.
Table 12: Disaggregated Summary of the Sponsor’s Economic Evaluation Results for Insomnia — Costs
Treatment | Drug | Other resource use | Events | Total |
|---|---|---|---|---|
Lemborexant | 273 | 801 | 517 | 1,591 |
Lorazepam (0.5 mg to 2 mg) | 8 | 932 | 852 | 1,792 |
Quetiapine (25 mg) | 9 | 843 | 965 | 1,817 |
Trazodone (50 mg) | 10 | 836 | 972 | 1,818 |
Nitrazepam (5 mg) | 31 | 930 | 910 | 1,871 |
Temazepam (15 mg) | 42 | 935 | 902 | 1,878 |
Zopiclone (7.5 mg) | 84 | 935 | 897 | 1,916 |
Flurazepam (30 mg) | 24 | 934 | 1,003 | 1,962 |
Triazolam (0.50 mg) | 92 | 929 | 946 | 1,966 |
Untreated | 0 | 1,654 | 616 | 2,271 |
Appendix 4: Additional Details on the CADTH Reanalyses and Sensitivity Analyses of the Economic Evaluation
Note that this appendix has not been copy-edited.
Table 13: Summary of the Stepped Analysis of the CADTH Reanalysis Results
Stepped analysis | Drug | Total costs ($) | Total QALYs | ICER ($/QALYs) |
|---|---|---|---|---|
Deterministic | ||||
Sponsor’s base case | Lemborexanta | 1,589 | 0.3120 | Reference |
Lorazepam (0.5 mg to 2 mg) | 1,737 | 0.2825 | Dominatedb | |
Quetiapine (25 mg) | 1,749 | 0.2688 | Dominatedb | |
Trazodone (50 mg) | 1,750 | 0.2688 | Dominatedb | |
Nitrazepam (5 mg) | 1,805 | 0.2766 | Dominatedb | |
Temazepam (15 mg) | 1,816 | 0.2766 | Dominatedb | |
Zopiclone (7.5 mg) | 1,859 | 0.2785 | Dominatedb | |
Flurazepam (30 mg) | 1,905 | 0.2611 | Dominatedb | |
Triazolam (0.50 mg) | 1,913 | 0.2719 | Dominatedb | |
Untreated | 2,209 | 0.3152 | 196,546 | |
Sponsor’s corrected base | Lemborexanta | 1,589 | 0.3125 | Reference |
Lorazepam (0.5 mg to 2 mg) | 1,737 | 0.2825 | Dominatedb | |
Quetiapine (25 mg) | 1,749 | 0.2688 | Dominatedb | |
Trazodone (50 mg) | 1,750 | 0.2688 | Dominatedb | |
Temazepam (15 mg) | 1,790 | 0.2766 | Dominatedb | |
Zopiclone (7.5 mg) | 1,799 | 0.2785 | Dominatedb | |
Nitrazepam (5 mg) | 1,805 | 0.2766 | Dominatedb | |
Triazolam (0.50 mg) | 1,849 | 0.2719 | Dominatedb | |
Flurazepam (30 mg) | 1,905 | 0.2611 | Dominatedb | |
Untreated | 2,209 | 0.3152 | 232,529 | |
CADTH reanalysis 1 | Lemborexanta | 1,589 | 0.3125 | Reference |
Lorazepam (0.5 mg to 2 mg) | $1,641 | 0.2852 | Dominatedb | |
Quetiapine (25 mg) | $1,653 | 0.2715 | Dominatedb | |
Trazodone (50 mg) | $1,654 | 0.2715 | Dominatedb | |
Temazepam (15 mg) | $1,695 | 0.2793 | Dominatedb | |
Zopiclone (7.5 mg) | $1,703 | 0.2812 | Dominatedb | |
Nitrazepam (5 mg) | $1,710 | 0.2793 | Dominatedb | |
Triazolam (0.50 mg) | $1,753 | 0.2747 | Dominatedb | |
Flurazepam (30 mg) | $1,809 | 0.2639 | Dominatedb | |
Untreated | 2,113 | 0.3179 | 96,667 | |
CADTH reanalysis 2 | Quetiapine (25 mg)a | $1,400 | 0.3145 | Reference |
Trazodone (50 mg) | $1,402 | 0.3145 | Dominatedb | |
Lorazepam (0.5 mg to 2 mg) | $1,497 | 0.3136 | Dominatedb | |
Temazepam (15 mg) | $1,505 | 0.3138 | Dominatedb | |
Zopiclone (7.5 mg) | $1,514 | 0.3157 | 96,691 | |
Flurazepam (30 mg) | $1,514 | 0.3129 | Dominatedb | |
Triazolam (0.50 mg) | $1,516 | 0.3155 | Dominatedb | |
Nitrazepam (5 mg) | $1,520 | 0.3138 | Dominatedb | |
Lemborexant | $1,530 | 0.3201 | 3,641 | |
Untreated | $2,209 | 0.3152 | Dominatedb | |
CADTH reanalysis 3 | Lemborexanta | 1,589 | 0.3155 | Reference |
Lorazepam (0.5 mg to 2 mg) | 1,737 | 0.2854 | Dominatedb | |
Quetiapine (25 mg) | 1,749 | 0.2716 | Dominatedb | |
Trazodone (50 mg) | 1,750 | 0.2716 | Dominatedb | |
Temazepam (15 mg) | 1,790 | 0.2794 | Dominatedb | |
Zopiclone (7.5 mg) | 1,799 | 0.2794 | Dominatedb | |
Nitrazepam (5 mg) | 1,805 | 0.2794 | Dominatedb | |
Triazolam (0.50 mg) | 1,849 | 0.2730 | Dominatedb | |
Flurazepam (30 mg) | 1,905 | 0.2648 | Dominatedb | |
Untreated | 2,209 | 0.3152 | Dominatedb | |
CADTH reanalysis 4 | Untreateda | 1,421 | 0.3152 | Reference |
Lemborexant | 1,589 | 0.3125 | Dominatedb | |
Lorazepam (0.5 mg to 2 mg) | $1,649 | 0.2825 | Dominatedb | |
Temazepam (15 mg) | $1,703 | 0.2766 | Dominatedb | |
Zopiclone (7.5 mg) | $1,711 | 0.2785 | Dominatedb | |
Nitrazepam (5 mg) | $1,718 | 0.2766 | Dominatedb | |
Quetiapine (25 mg) | $1,749 | 0.2688 | Dominatedb | |
Trazodone (50 mg) | $1,750 | 0.2688 | Dominatedb | |
Triazolam (0.50 mg) | $1,761 | 0.2719 | Dominatedb | |
Flurazepam (30 mg) | $1,818 | 0.2611 | Dominatedb | |
CADTH base case (1 + 2 + 3 + 4) | Quetiapine (25 mg)a | 1,305 | 0.3201 | Reference |
Trazodone (50 mg) | 1,306 | 0.3201 | Dominatedb | |
Lorazepam (0.5 mg to 2 mg) | 1,314 | 0.3193 | Dominatedb | |
Temazepam (15 mg) | 1,322 | 0.3193 | Dominatedb | |
Untreated | 1,325 | 0.3179 | Dominatedb | |
Zopiclone (7.5 mg) | 1,331 | 0.3193 | Dominatedb | |
Flurazepam (30 mg) | 1,331 | 0.3193 | Dominatedb | |
Triazolam (0.50 mg) | 1,333 | 0.3193 | Dominatedb | |
Nitrazepam (5 mg) | 1,337 | 0.3193 | Dominatedb | |
Lemborexant | 1,530 | 0.3231 | 75,907 | |
Probabilistic | ||||
Sponsor’s base case | Lemborexanta | 1,591 | 0.3126 | Reference |
Lorazepam (0.5 mg to 2 mg) | 1,792 | 0.2810 | Dominatedb | |
Quetiapine (25 mg) | 1,817 | 0.2673 | Dominatedb | |
Trazodone (50 mg) | 1,818 | 0.2671 | Dominatedb | |
Nitrazepam (5 mg) | 1,871 | 0.2747 | Dominatedb | |
Temazepam (15 mg) | 1,878 | 0.2750 | Dominatedb | |
Zopiclone (7.5 mg) | 1,916 | 0.2769 | Dominatedb | |
Flurazepam (30 mg) | 1,962 | 0.2597 | Dominatedb | |
Triazolam (0.50 mg) | 1,966 | 0.2704 | Dominatedb | |
Untreated | 2,271 | 0.3134 | 855,067 | |
Sponsor’s corrected base case | Lemborexanta | 1,585 | 0.3126 | Reference |
Lorazepam (0.5 mg to 2 mg) | 1,799 | 0.2808 | Dominatedb | |
Trazodone (50 mg) | 1,803 | 0.2673 | Dominatedb | |
Quetiapine (25 mg) | 1,811 | 0.2671 | Dominatedb | |
Zopiclone (7.5 mg) | 1,855 | 0.2769 | Dominatedb | |
Temazepam (15 mg) | 1,862 | 0.2748 | Dominatedb | |
Nitrazepam (5 mg) | 1,865 | 0.2750 | Dominatedb | |
Triazolam (0.50 mg) | 1,917 | 0.2702 | Dominatedb | |
Flurazepam (30 mg) | 1,973 | 0.2594 | Dominatedb | |
Untreated | 2,272 | 0.3133 | 938,176 | |
CADTH base case (1 + 2 + 3 + 4) | Trazodonea | 1,301 | 0.3202 | Reference |
Quetiapine (25 mg) | 1,303 | 0.3202 | Dominatedb | |
Lorazepam (0.5 mg to 2 mg) | 1,314 | 0.3194 | Dominatedb | |
Temazepam (15 mg) | 1,322 | 0.3194 | Dominatedb | |
Untreated | 1,325 | 0.3180 | Dominatedb | |
Zopiclone (7.5 mg) | 1,330 | 0.3194 | Dominatedb | |
Flurazepam (30 mg) | 1,331 | 0.3194 | Dominatedb | |
Triazolam (0.50 mg) | 1,333 | 0.3194 | Dominatedb | |
Nitrazepam (5 mg) | 1,337 | 0.3194 | Dominatedb | |
Lemborexant | 1,530 | 0.3231 | 76,941 | |
ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year.
aReference product is least costly alternative that is not dominated.
bDominated refers to a treatment having higher total costs and lower total QALYs when compared to the previous less costly treatment.
Table 14: Disaggregated Summary of CADTH’s Economic Evaluation Results — QALYs
Comparator | Treatment | Falls | MVAs | WPAs | Premature death | Total |
|---|---|---|---|---|---|---|
Trazodone | 0.3699 | –0.0140 | –0.0003 | –0.0007 | –0.0348 | 0.3202 |
Quetiapine (25 mg) | 0.3700 | –0.0140 | –0.0003 | –0.0007 | –0.0348 | 0.3202 |
Lorazepam (0.5 mg to 2 mg) | 0.3692 | –0.0140 | –0.0003 | –0.0007 | –0.0348 | 0.3194 |
Temazepam (15 mg) | 0.3692 | –0.0140 | –0.0003 | –0.0007 | –0.0348 | 0.3194 |
Untreated | 0.3677 | –0.0140 | –0.0003 | –0.0007 | –0.0348 | 0.3180 |
Zopiclone (7.5 mg) | 0.3692 | –0.0140 | –0.0003 | –0.0007 | –0.0348 | 0.3194 |
Flurazepam (30 mg) | 0.3692 | –0.0140 | –0.0003 | –0.0007 | –0.0348 | 0.3194 |
Triazolam (0.50 mg) | 0.3692 | –0.0140 | –0.0003 | –0.0007 | –0.0348 | 0.3194 |
Nitrazepam (5 mg) | 0.3692 | –0.0140 | –0.0003 | –0.0007 | –0.0348 | 0.3194 |
Lemborexant | 0.3729 | –0.0140 | –0.0003 | –0.0007 | –0.0348 | 0.3231 |
MVA = motor vehicle accident; QALY = quality-adjusted life-year; WPA = workplace accident.
Table 15: Disaggregated Summary of CADTH’s Economic Evaluation Results — Costs
Treatment | Drug | Other resource use | Events | Total ($) |
|---|---|---|---|---|
Trazodone | 10 | 839 | 459 | 1,307 |
Quetiapine (25 mg) | 9 | 840 | 459 | 1,307 |
Lorazepam (0.5 mg to 2 mg) | 8 | 847 | 459 | 1,314 |
Temazepam (15 mg) | 16 | 847 | 459 | 1,322 |
Untreated | 0 | 866 | 459 | 1,325 |
Zopiclone (7.5 mg) | 24 | 847 | 459 | 1,330 |
Flurazepam (30 mg) | 25 | 847 | 459 | 1,331 |
Triazolam (0.50 mg) | 27 | 847 | 459 | 1,333 |
Nitrazepam (5 mg) | 31 | 847 | 459 | 1,337 |
Lemborexant | 273 | 800 | 459 | 1,530 |
Table 16: Summary of CADTH’s Scenario Analysis
Scenario | Drug | Total costs ($) | Total QALYs | ICER ($/QALYs) |
|---|---|---|---|---|
Probabilistic | ||||
Assuming benzodiazepine use is associated with a higher risk of falls (flurazepam (30 mg): RR = 3.05; nitrazepam (5 mg), zopiclone (7.5 mg), temazepam (15 mg): RR = 2.16; triazolam (0.50 mg): RR = 2.50) | Trazodone (50 mg) | 1,305 | 0.3201 | Reference |
Quetiapine (25 mg) | 1,306 | 0.3202 | Dominateda | |
Untreated | 1,325 | 0.3179 | Dominateda | |
Lemborexant | 1,533 | 0.3231 | 76,171 | |
Lorazepam (0.5 mg to 2 mg) | 1,554 | 0.2882 | Dominateda | |
Temazepam (15 mg) | 1,607 | 0.2822 | Dominateda | |
Nitrazepam (5 mg) | 1,622 | 0.2822 | Dominateda | |
Triazolam (0.50 mg) | 1,665 | 0.2758 | Dominateda | |
Flurazepam (30 mg) | 1,722 | 0.2676 | Dominateda | |
Zopiclone (7.5 mg) | 2,494 | 0.2822 | Dominateda | |
Assuming no difference in the response rates between lemborexant and active comparators | Trazodone (50 mg) | $1,266 | 0.32324 | Reference |
Quetiapine (25 mg) | $1,269 | 0.32324 | Dominateda | |
Temazepam (15 mg) | $1,272 | 0.32324 | Dominateda | |
Zopiclone (7.5 mg) | $1,280 | 0.32324 | Dominateda | |
Flurazepam (30 mg) | $1,281 | 0.32324 | Dominateda | |
Triazolam (0.50 mg) | $1,283 | 0.32324 | Dominateda | |
Nitrazepam (5 mg) | $1,287 | 0.32324 | Dominateda | |
Lorazepam (0.5 mg to 2 mg) | $1,313 | 0.32324 | Dominateda | |
Untreated | $1,324 | 0.31808 | Dominateda | |
Lemborexant | $1,531 | 0.32324 | Dominateda | |
Including disutilities associated with treatment | Quetiapine (25 mg) | $1,300 | 0.3202 | Reference |
Trazodone (50 mg) | $1,307 | 0.3202 | Dominateda | |
Lorazepam (0.5 mg to 2 mg) | $1,314 | 0.3194 | Dominateda | |
Temazepam (15 mg) | $1,322 | 0.3194 | Dominateda | |
Untreated | $1,325 | 0.3180 | Dominateda | |
Zopiclone (7.5 mg) | $1,330 | 0.3194 | Dominateda | |
Flurazepam (30 mg) | $1,331 | 0.3194 | Dominateda | |
Triazolam (0.50 mg) | $1,333 | 0.3194 | Dominateda | |
Nitrazepam (5 mg) | $1,337 | 0.3194 | Dominateda | |
Lemborexant | $1,525 | 0.3231 | 75,846 | |
ICER = incremental cost per QALY gained; NA = not applicable; QALY = quality-adjusted life-year.
aDominated refers to a treatment having higher total costs and lower total QALYs when compared to the previous less costly treatment.
Appendix 5: Submitted Budget Impact Analysis and CADTH Appraisal
Note that this appendix has not been copy-edited.
Table 17: Summary of Key Take-Aways
Key take-aways of the budget impact analysis |
|---|
|
CUA = cost-utility analysis.
Summary of Sponsor’s Budget Impact Analysis
The sponsor submitted a budget impact analysis (BIA)33 estimating the incremental budget impact of reimbursing lemborexant for use by patients aged 18 years and older with treatment of insomnia, characterized by difficulties with sleep onset and/or sleep maintenance. The BIA was undertaken from the perspective of the Canadian public drug plans over a 3-year time horizon (2023 to 2026), with a baseline year of 2022-2023. The sponsor’s pan-Canadian estimates reflect the aggregated results from provincial budgets (excluding Quebec). Key inputs to the BIA are documented in Table 18.
The sponsor estimated the market size via a claims-based approach, using historical provincial public drug plan claims data from IQVIA PharmaStat (2015 to 2021) to calculate the number of claims and units for drugs currently reimbursed beyond 2022, assuming a linear or logarithmic trend.5 The sponsor assumed all claims for on-label comparators (zopiclone, flurazepam, nitrazepam, temazepam and triazolam) were for treatment of insomnia. The sponsor assumed 60% of claims for trazodone and 25% of claims for other off-label treatments are for insomnia. In a scenario with lemborexant entering the market, the sponsor assumed lemborexant would have a market share of 10.2% in year 1, 13.8% in year 2 and 16.6% in year 3.
The sponsor estimated average drug acquisition costs for comparators based on the proportion of claims of each strength and the unit price for each strength, standardized for 30-day claims. Unit prices of comparators were obtained from public formularies.18,25,34-37 Markups and dispensing fees for each jurisdiction were included. Then, results for each jurisdiction were aggregated for the pan-Canadian budget impact estimate.
Table 18: Summary of Key Model Parameters
Parameter | Sponsor’s estimate (year 1/year 2/year 3) |
|---|---|
Number of claims (3 years) | |
Total claims | 4,065,636 / 4,117,700 / 4,172,349 |
Z-drugs (zopiclone) | 712,683 / 709,194 / 705,995 |
Benzodiazepines (alprazolam, bromazepam, clonazepam, diazepam, flurazepam, lorazepam, nitrazepam, oxazepam, temazepam, triazolam, chlordiazepoxide, clobazam) | 930,865 / 897,850 / 866,894 |
Antidepressants (amitriptyline, mirtazapine, trazodone) | 1,877,093 / 1,948,871 / 2,020,884 |
Antipsychotic drugs (quetiapine) | 544,995 / 561,785 / 578,576 |
Market uptake (3 years) | |
Uptake (reference scenario) | |
Lemborexant | 0.0% / 0.0% / 0.0% |
Z-drugs (zopiclone) | 17.5% / 17.2% / 16.9% |
Benzodiazepines (alprazolam, bromazepam, clonazepam, diazepam, flurazepam, lorazepam, nitrazepam, oxazepam, temazepam, triazolam, chlordiazepoxide, clobazam) | 22.9% / 21.8% / 20.8% |
Antidepressants (amitriptyline, mirtazapine, trazodone) | 46.2% / 47.3% / 48.4% |
Antipsychotic drugs (quetiapine) | 13.4% / 13.6/% / 13.9% |
Uptake (new drug scenario) | |
Lemborexant | 10.2% / 13.8% / 16.6% |
Z-drugs (zopiclone) | 15.7% / 14.8% / 14.1% |
Benzodiazepines (alprazolam, bromazepam, clonazepam, diazepam, flurazepam, lorazepam, nitrazepam, oxazepam, temazepam, triazolam, chlordiazepoxide, clobazam) | 20.6% / 18.8% / 17.3% |
Antidepressants (amitriptyline, mirtazapine, trazodone) | 41.5% / 40.8% / 40.4% |
Antipsychotic drugs (quetiapine) | 12.0% / 11.8/% / 11.6% |
Cost of treatment | |
Cost of treatment over 30 days Lemborexant Zopiclone Alprazolam Bromazepam Clonazepam Diazepam Flurazepam Lorazepam Nitrazepam Oxazepam Temazepam Triazolam Chlordiazepoxide Clobazam Amitriptyline Mirtazapine Trazodone Quetiapine | $45.59 $20.63 $5.33 $2.23 $3.21 $4.29 $4.84 $2.18 $9.24 $2.46 $10.22 $11.14 $7.38 $15.76 $4.63 $13.91 $5.45 $14.44 |
Summary of the Sponsor’s Budget Impact Analysis Results
The sponsor estimated that funding lemborexant for the treatment of patients with insomnia would result in a budget impact of $14,784,357 in year 1, $20,243,541 in year 2, and $24,658,515 in year 3, for 3-year total budget impact of $59,686,413.
CADTH Appraisal of the Sponsor’s Budget Impact Analysis
CADTH identified several key limitations to the sponsor’s analysis that have notable implications on the results of the BIA:
The number of eligible patients is underestimated: Given the claims database does not indicate the corresponding health indication each distinct drug claim, and the proportion of claims pertaining to use for other health indications is unknown, using a claims-based approach to estimate market size introduces significant uncertainty in the proportion of claims used for insomnia. The clinical expert consulted for this review by CADTH noted insomnia is often left undiagnosed because patients do not seek treatment. Further, insomnia is diagnosed based on the DSM-5 criteria in clinical practice.38,39 However, there are aspects of insomnia that are not identified in this classification such as terminal insomnia, nonrestorative sleep, and wakefulness after sleep. Given the claims database does not provide information about the health indication, there is uncertainty in the estimated eligible population. The number of eligible patients is likely underestimated because insomnia is generally underdiagnosed.
The sponsor assumed 60% of claims for trazodone and 25% of claims for other off-label treatments are for insomnia. However, according to the clinical expert consulted for this review by CADTH, trazodone is rarely used as an antidepressant in clinical practice and it is likely that almost all claims are to be for treatment of insomnia. Further, some off-label treatments are used to treat insomnia more often than others in clinical practice. The clinical expert noted that it is more likely that 40% of claims for benzodiazepines used off-label, 10% of claims for antidepressants and 5% of claims for antipsychotic drugs are prescribed for insomnia.
In the CADTH reanalysis, 95% of claims for trazodone, 40% of claims for benzodiazepines used off-label, 10% of claims for antidepressants and 5% of claims for antipsychotic drugs were assumed to be prescribed for insomnia based on feedback from clinal expert.
The market share of lemborexant is underestimated: The clinical expert consulted by CADTH found the sponsor’s estimate that 16.6% of patients with insomnia would be prescribed lemborexant by year 3 was an underestimate, as lemborexant may be used as a first-line drug. The clinical expert noted uptake could be as high as 20% to 25%, depending on its long-term relative efficacy.
In the CADTH reanalysis, the market share of lemborexant was 10% in year 1, 15% in year 2, and 20.0% in year 3 based on feedback from clinal expert.
Treatment costs of comparators is underestimated: Treatment costs of comparators in the BIA are not aligned with the CUA, the sponsor’s approach has consistently overestimated the cost of flurazepam, lorazepam, nitrazepam, temazepam, zopiclone, trazodone, and quetiapine when compared with the costs used in the CUA. This may have underestimated the budget impact.
CADTH corrected the treatment costs of flurazepam, lorazepam, nitrazepam, temazepam, zopiclone, trazodone, and quetiapine by aligning the prices in the BIA with those adopted in the CUA.
CADTH Reanalyses of the Budget Impact Analysis
CADTH revised the sponsor’s base case by revising the proportion of claims of off-label treatments for insomnia based on a clinical expert consulted by CADTH, increasing market share of lemborexant and aligning treatment costs between the CUA and BIA.
Table 19: CADTH Revisions to the Submitted Budget Impact Analysis
Stepped analysis | Sponsor’s value or assumption | CADTH value or assumption |
|---|---|---|
Corrections to sponsor’s base case | ||
1. Treatment costs | The treatment costs of flurazepam, lorazepam, nitrazepam, temazepam, zopiclone, trazodone, and quetiapine are misaligned between BIA and CUA. | The treatment costs of flurazepam, lorazepam, nitrazepam, temazepam, zopiclone, trazodone, and quetiapine are aligned between BIA and CUA. |
Changes to derive the CADTH base case | ||
1. Proportion of claims for insomnia | Trazodone = 60% Other off-label treatments = 25% | Trazodone = 95% Benzodiazepines (alprazolam, bromazepam, clonazepam, diazepam, lorazepam, oxazepam, temazepam, chlordiazepoxide, clobazam) = 40% Antidepressants (amitriptyline, mirtazapine) = 10% Antipsychotic drugs (quetiapine) = 5% |
2. Market share of lemborexant (year 1 / year 2 / year 3) | 10.2% / 13.8% / 16.6% | 10% / 15% / 20.0% |
CADTH base case | Reanalysis 1 + 2 | |
In the CADTH reanalysis, the 3-year budget impact of reimbursing lemborexant from the public drug plan perspective for use by patients aged 18 years and older for treatment of insomnia was $89,782,016 (year 1: $20,602,763; year 2: $28,099,123; year 3: $41,080,131).
The results of the CADTH stepwise reanalysis are presented in summary format in Table 6 and a more detailed breakdown is presented in Table 20.
Table 20: Summary of the CADTH Reanalyses of the Budget Impact Analysis
Stepped analysis | 3-year total |
|---|---|
Submitted base case | $59,686,413 |
Submitted base case, corrected | $70,151,701 |
CADTH reanalysis 1 | $82,798,394 |
CADTH reanalysis 2 | $76,087,214 |
CADTH base case | $89,782,016 |
CADTH also conducted an additional scenario analysis to address uncertainty around the percentage of trazodone claims that were for insomnia, using the CADTH base case. Results are provided in Table 21.
Table 21: Detailed Breakdown of the CADTH Reanalyses of the Budget Impact Analysis
Stepped analysis | Scenario | Year 0 (current situation) | Year 1 | Year 2 | Year 3 | 3-year total |
|---|---|---|---|---|---|---|
Submitted base case | Reference | $39,809,273 | $40,423,913 | $41,050,097 | $41,688,817 | $123,162,828 |
New drug | $39,809,273 | $55,208,270 | $61,293,638 | $66,347,332 | $182,849,241 | |
Budget impact | $0 | $14,784,357 | $20,243,541 | $24,658,515 | $59,686,413 | |
CADTH base case | Reference | $13,582,985 | $13,717,252 | $13,855,514 | $14,002,907 | $41,575,672 |
New drug | $13,582,985 | $34,320,014 | $41,954,637 | $55,083,037 | $131,357,688 | |
Budget impact | $0 | $20,602,763 | $28,099,123 | $41,080,131 | $89,782,016 | |
CADTH scenario analysis: 82.5% of trazodone claims were for insomnia based on the Wong et al. (2017) study | Reference | $13,101,672 | $13,218,376 | $13,339,093 | $13,468,956 | $40,026,425 |
New drug | $13,101,672 | $32,476,077 | $39,554,427 | $51,726,278 | $123,756,782 | |
Budget impact | $0 | $19,257,701 | $26,215,334 | $38,257,323 | $83,730,357 |
Stakeholder Input
Patient Input
Migraine Canada
About Migraine Canada
Migraine Canada is a national federally registered charity, founded in late fall of 2018, with a mission to provide support and education as well as raise awareness about the impact of migraines. We advocate for optimal care for those living with migraines and support research to find a cure. With the help of dedicated physicians and contributors, Migraine Canada delivers evidence based, up-to-date disease and treatment information to Canadian living with migraine, including patients and caregivers, as well as healthcare professionals. We educate patients, caregivers, and healthcare professionals by researching, developing, and sharing electronic and print materials containing the most current migraine information. We drive awareness and education through our website, social media channels and forums. We have a growing community of over 2,000 individuals subscribing to our email list. We provide patient support through participation in regional on-line support groups, with more than 3,000 members on our Facebook page.
Website: www.migrainecanada.org
Information Gathering
The information provided in this submission was collected through a Quality-of-Life online survey that was launched by Migraine Canada in late fall of 2021. It was promoted across Canada through Migraine Canada’s digital and social media channels. In total, 1,165 Canadian adults with migraine and their caregivers responded to the online survey. Of our total respondents, 19% live with low frequency migraine, 28% live with 8-14 days / month with migraine and 52% live with chronic migraine 15 or mores days. The spectrum of representation was national with the majority (68%) participating between the age of 30-59.
Migraine Canada launched a second national online survey in March 2022 to gather additional insights to support our submission and seek input from patients with experience on Dayvigo (lemborexant). It was promoted across Canada through Migraine Canada’s digital and social media channels with promotion. In total, 220 Canadians with migraine responded to the survey related directly to insomnia. Of our total respondents, 91% were female and 9% male. Similar to the quality-of-life survey, the majority of patients were between the age of 30-59 (69%).
Disease Experience
Migraines are not just headaches but a neurological disease. Migraine impacts 1 billion people worldwide, or about 1 in 7 people. Migraine is most common between the ages of 25 and 55 but it can impact people of all ages including children (10%) but it affects three-times (25%) as many women as men (8%).
Migraines are classified according to their monthly frequency. Episodic Migraine is defined as impacting less than 15 days per month and 12% of adults living with migraine fall into this group; Chronic Migraine impacts more than 15 days per month and 2% of the adult migraine populations. Migraines often present with severe, throbbing, recurring pain, usually on one side of the head (or both sides or no pain at all). Nausea, vomiting, dizziness, extreme sensitivity to sound, light, touch, and smell, and tingling or numbness in the extremities or face are also common symptoms. About 25% of migraine sufferers also have a visual disturbance called an aura, which usually lasts less than an hour. Attacks usually last between 4 and 72 hours.
Migraine is usually categorized according to accompanying symptoms (aura, vestibular, hemiplegic) but also according to monthly frequency of attacks. Episodic migraine refers to attacks occurring 14 days or less and is now further separated in low-frequency (1-6 days) and high frequency (7-14 days). Chronic migraine is diagnosed when patients have 15 or more headache days per month. Chronic migraine is associated with increased disability and co-morbidities. It is also associated with medication overuse headache (MOH), a complication of frequent use of acute treatments that induce even more frequent and intractable headaches. The estimated prevalence of MOH varies according to countries but is usually between 0.5% and 2% of the global population (GBD 2015). Medication overuse feeds the headache cycle and patients are trapped in a vicious cycle, unable to get adequate pain relief.
There are two main states of life for a migraine patient: the active attack (ictal state) and in-between attacks (interictal state). During the attack itself, symptoms may prevent the person’s ability to accomplish their tasks, work and interact with others. The pain is at least moderate and often severe, throbbing and diffuse. The nausea and vomiting are obviously disruptive and may prevent oral medications efficiency. The sensory hypersensitivity forces many patients to isolate themselves in a dark room and stop all activities. Auras are neurological deficits that can accompany migraines (including loss of vision, speech, and sensation, even muscle strength) which can last for hours. Some migraines are also accompanied with dizziness, vertigo and loss of balance. People generally experience reduced cognition during a migraine, with slowed thinking, lack of focus, and difficulty reading and speaking. This typically disrupts most activities involving a computer or interacting with other people. A controlled migraine attack managed with effective treatment can be brief, but uncontrolled attacks may last multiple days in a row.
People living with migraine commonly live with several complications, including issues with sleep.
Impact on Sleep
Issues with sleep is significant ranging from only 7% having no issues with sleep to 38% always or regularly having sleep disrupted due to their migraine.
Sleep disruption reported by patients caused by migraine over the past month was significant for respondents. Close to 20% reported 16-30 days as always or very often disrupted, followed by 19% who reported 11-15 days of disrupted sleep.
Patients rated their quality of sleep as very poor (17%), often disrupted (37%) and sometimes disrupted (30%). Only 16% rated their sleep as “good”. When as specifically if migraine impacts sleep, 84% of patients attribute their migraine as having a negative impact.
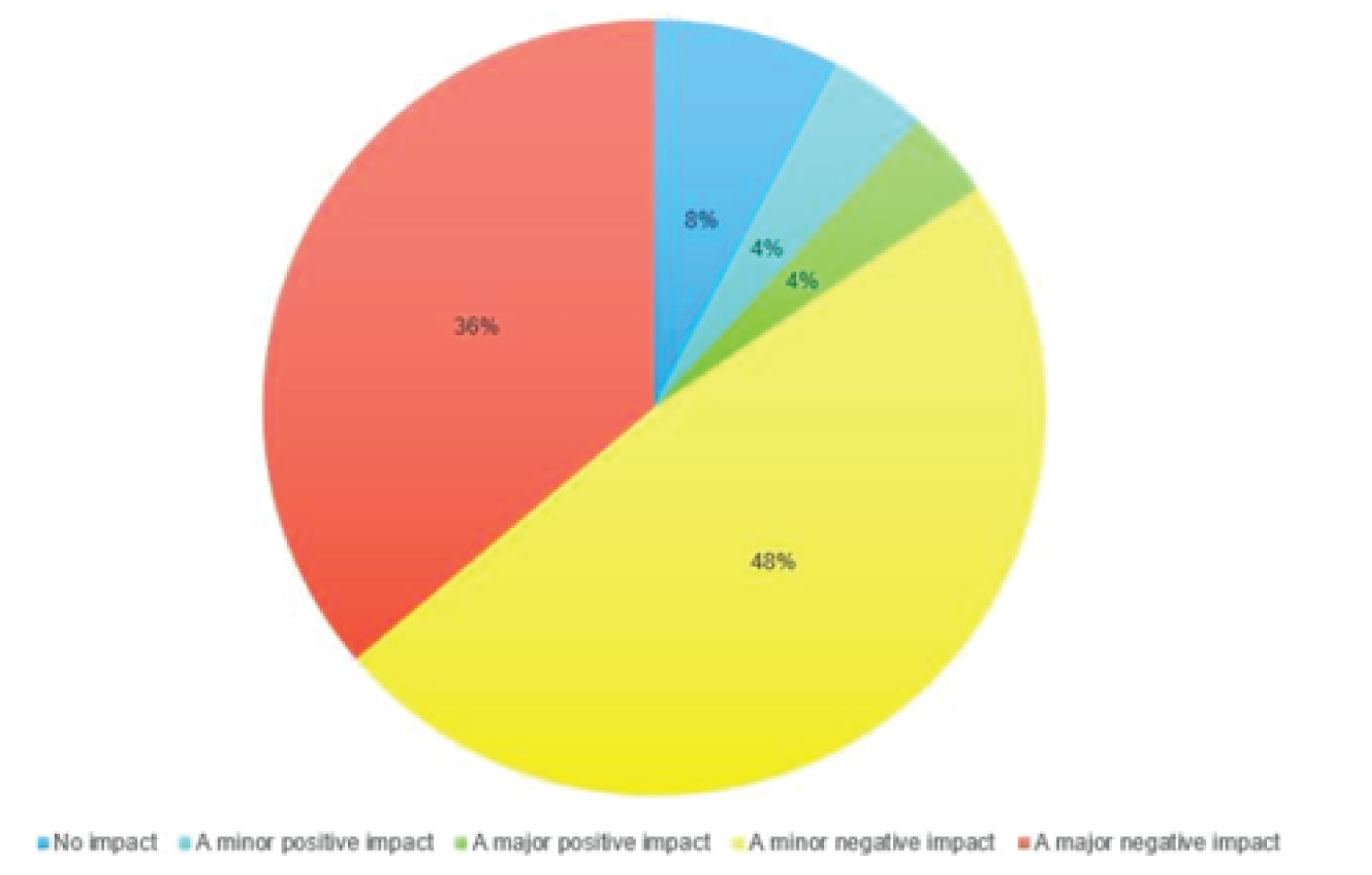
When asked how often patients experience poor sleep, close to 28% reported sleep issues nightly and close to 41% experience issues 3 or more nights each week.
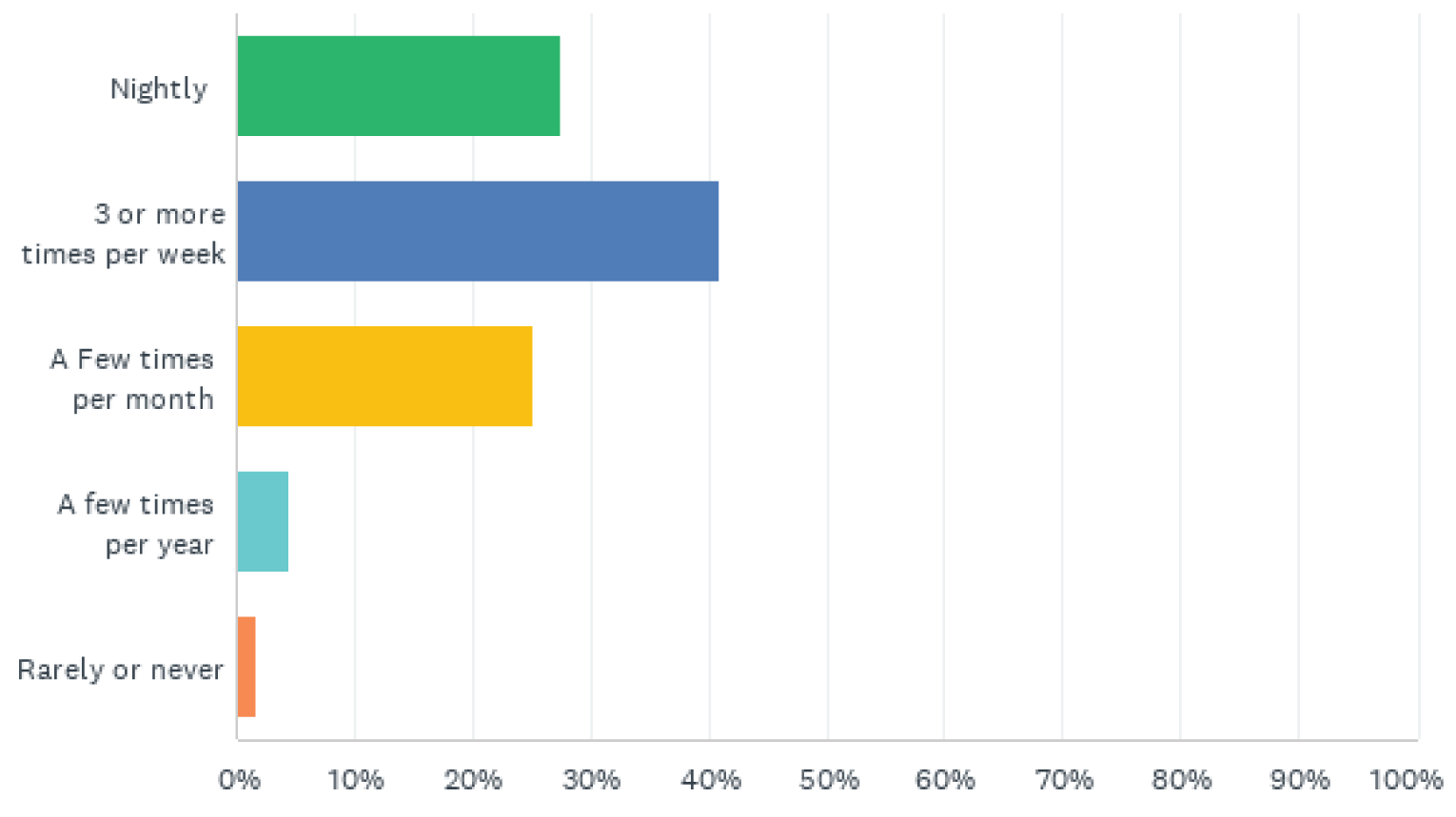
We asked respondents to rank a number on how often they had difficulty falling asleep, difficulty staying asleep, early morning ranking and difficulty functioning.
Criteria | Nightly | 3-6 times/week | 1-2 times/week | Rarely or never |
|---|---|---|---|---|
Difficulty falling asleep | 16% | 23% | 31% | 30% |
Difficulty staying asleep | 20% | 31% | 33% | 16% |
Early morning waking with inability to return to sleep | 10% | 30% | 32% | 29% |
Difficulty functioning the following day due to lack of sleep | 12% | 28% | 42% | 18% |
Over 90% of patients have had these symptoms lasting more than 3 months. Close to 20% have been diagnosed with insomnia by a healthcare provider. Close to 60% have informed/spoken with a healthcare professional about their sleep issues.
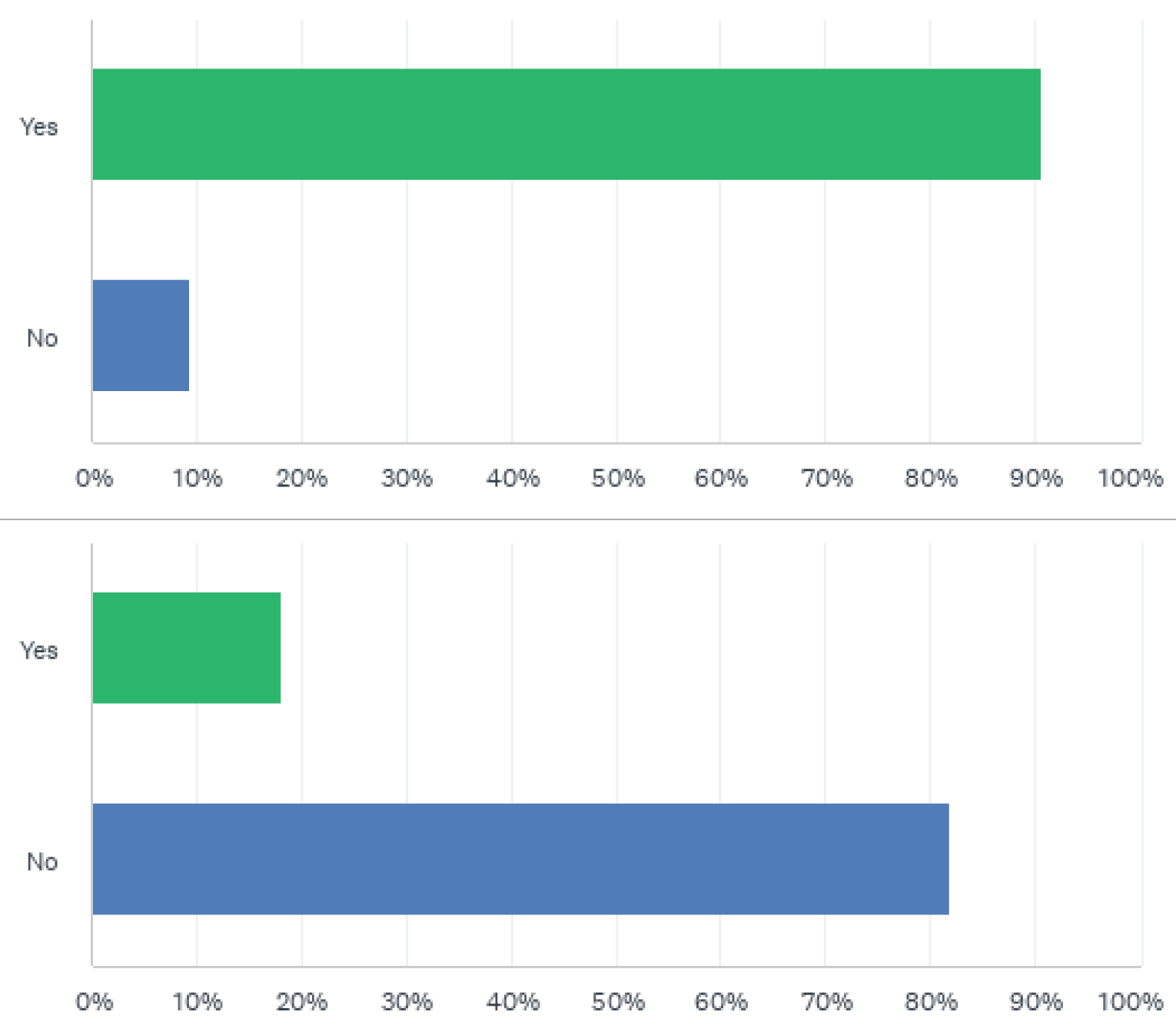
When asked what the outcome of the conversations, the majority of comments included being prescribed sleeping pills. Some other comments included:
“Talk about sleep hygiene/routine (which I already new/did), sleep apnea test. Trying different medications to see if it helps but so far no success”.
“Sleep is one of my triggers in my headache diary and when discussed I was offering sleeping pills which I declined as I am not keep on taking sleeping pills. The conversation ended there”.
“My doctor won’t prescribe sleeping pills. Medications are too addicting and I need to solve the issue with behavioural changes which I’ve tried and hasn’t helped”. “I was told to relax more”.
“Basically work on sleep hygiene and try medication which I was taken off by another Dr.”
“They blame migraine medication and its side effects. Regardless it’s a big issue”.
When asked how insomnia or sleep issues have negatively impacted quality of life, 86% indicated energy level was impacted, followed by 75% having cogitative functioning (ability to focus, pay attention and memory) impacted. Mood, engaging in physical exercise and ability to do household responsibilities were commonly affected and negatively impacting quality of life.
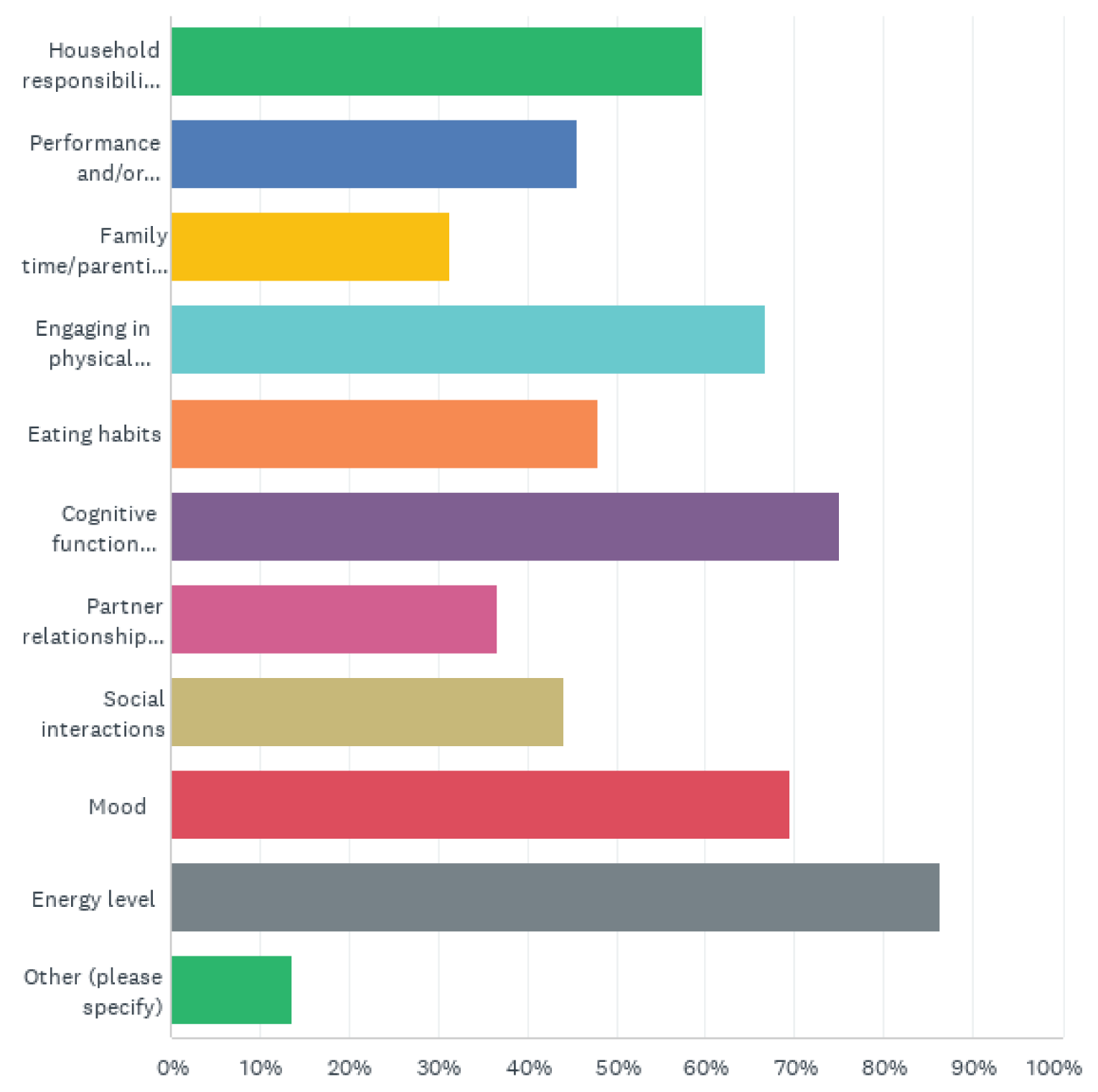
When asked specifically if patients feel their sleep negatively impacts their migraine (frequency and intensity), 66% said yes. Approximately 24% were not sure which impacted which.
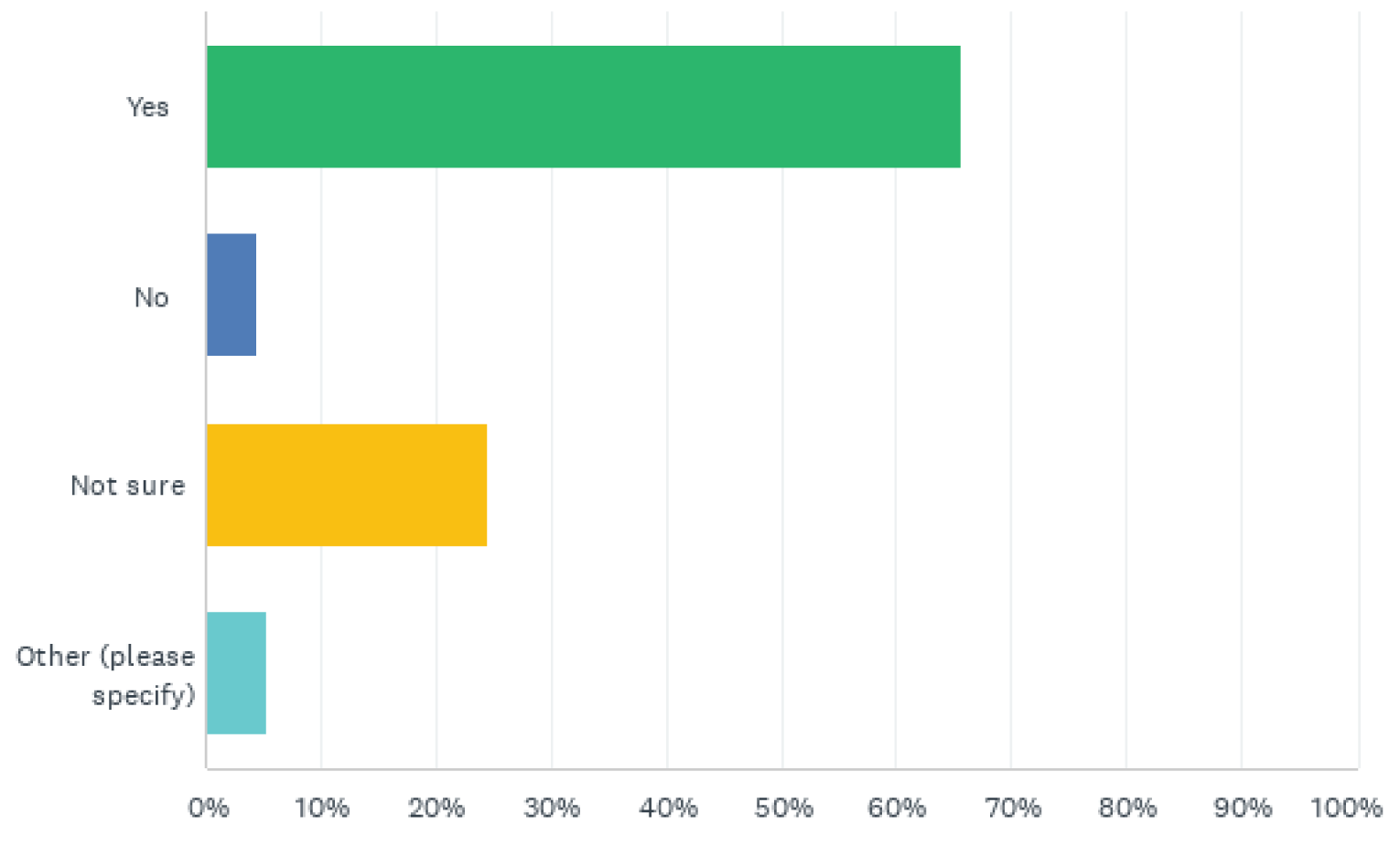
Some comments included:
“I haven’t been able to connect the two. My headaches are so frequent, and I rarely sleep well so I don’t know if one impact the other or if they exist independently”.
“My migraine starts during the night 90% of the time and I can’t get back to sleep”.
“Sleep is one of my triggers in my headache diary and when discussed I was offered a sleep aid which I declined as I am not keen on taking prescription pills. The conversation ended there”.
We also asked respondents if they feel their migraines are the cause of their sleep issues. 26% said yes, 25% said no and 34% weren’t sure.
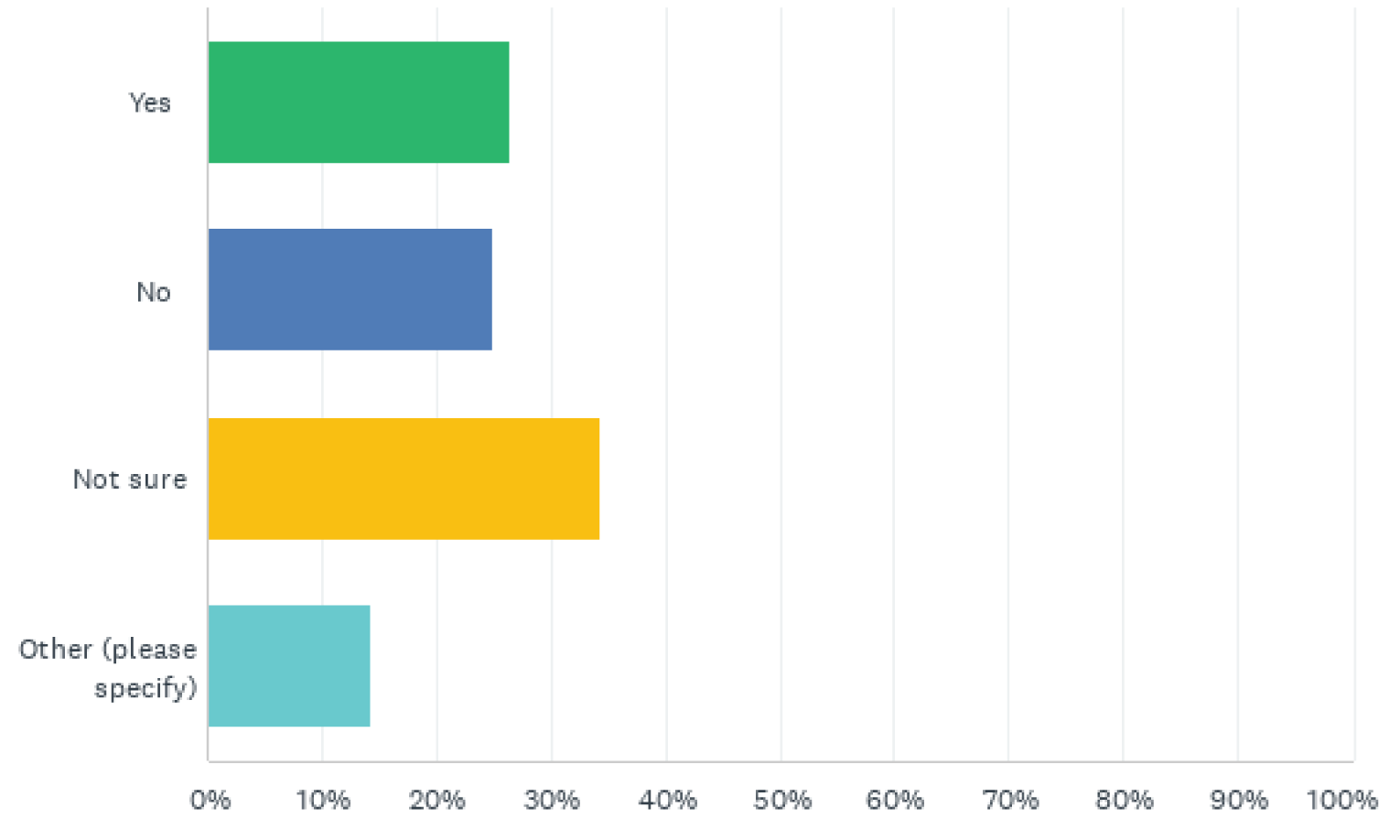
Patients commented:
“Not always but is a factor when insomnia persists daily for a long period”.
“Migraines are not the main cause for the sleep issues but they do sometimes play a role”.
“I think they each have a negative impact on the other. I believe if I could get rid of my migraines, my body could adjust and eventually have good sleep patterns”.
When asked to what extent sleep problems interfere with daily functioning (ie daytime fatigue, ability to function at work/daily chores, concentration, memory, mood), over 40% had much or very much interference. Only 20% reported a little impact.
In the past two weeks, to what extent did your insomnia/sleep issues interfere with your daily functioning (e.g., daytime fatigue, ability to function at work/daily chores, concentration, memory, mood, etc.)?
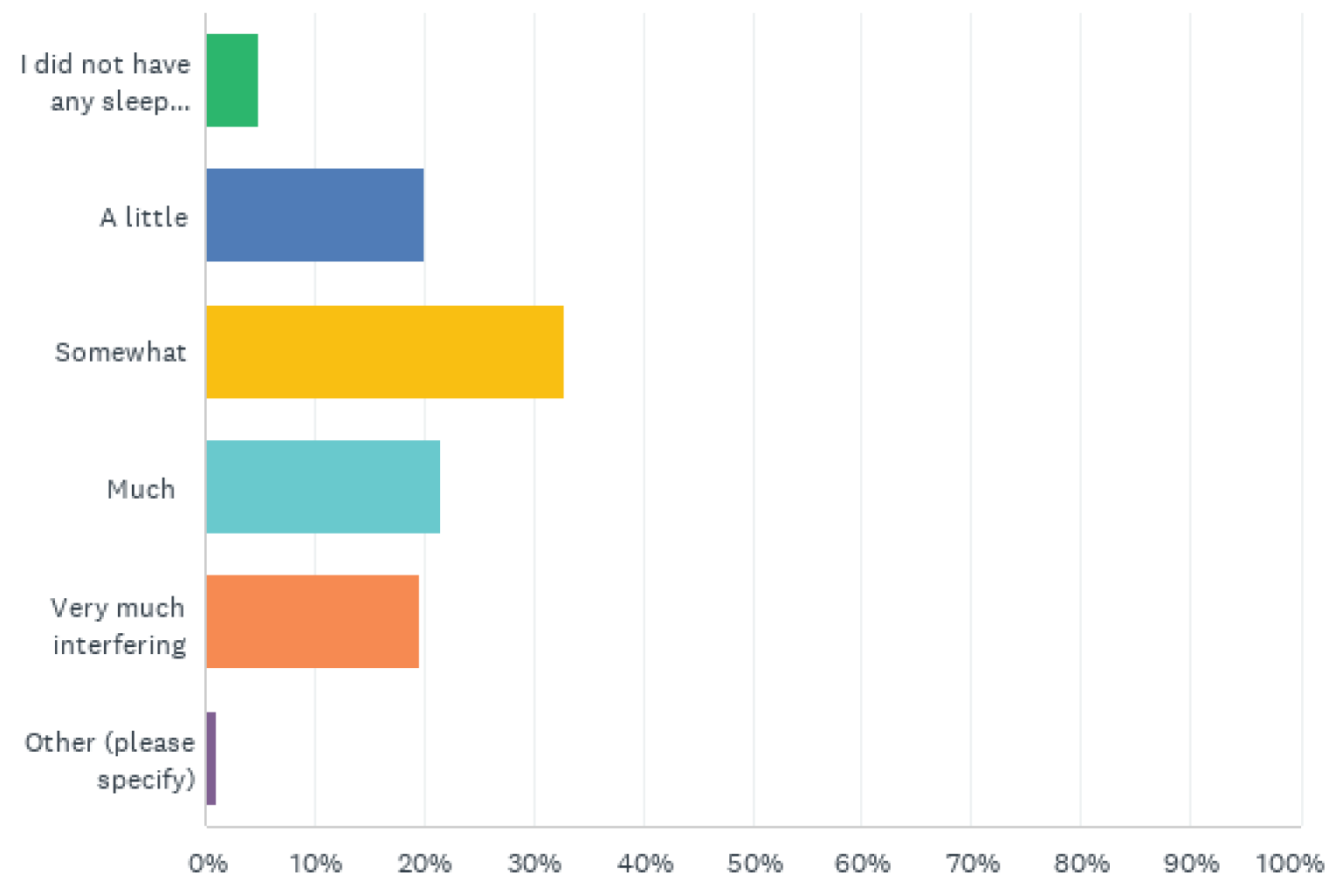
Experiences With Currently Available Treatments
Patients have tried a number of different treatments and remedies. Over 42% have tried sleep hygiene behavioural therapies, followed by relaxation and mindfulness. Following non pharmacologic intervention, close to 40% have tried over the counter and prescription medications.
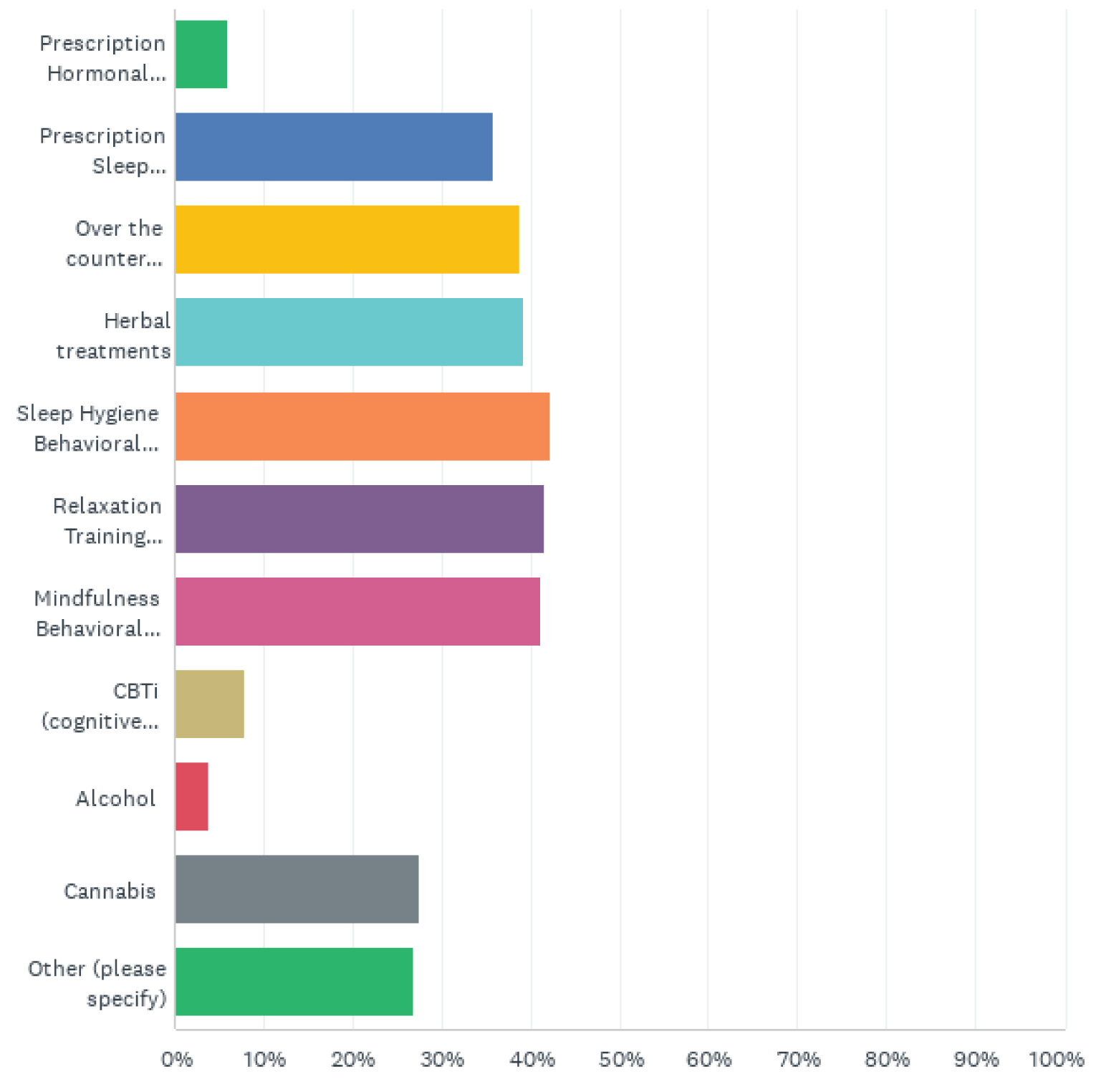
The majority (60%) of patients are not satisfied with how they currently manage their insomnia/sleep issues. Patient testimonials:
“Gabapentine prescription. Discontinued, too many side effects”. “Tried amitriptyline for two years, helped sleep but not the migraines”.
“Amytriptaline for 18 months helped but I gained quite a bit of weight. Beyond that nothing but the obvious – don’t drink caffeine, get fresh air, exercise, medication. Nothing helps”.
“Tried a few different medications but they made things worse”.
“I was prescribed medication but it left me feeling groggy so I stopped taking it”.
“My doctor won’t prescribe me anything because everything that works for people is addicting. So I suffer with no sleep and migraine”.
“A couple of the prescribed medications I’ve tried made feel so horrible the next day. Its like an out of body experience. Helped my sleep but side effects were to much. At least feeling absolutely exhausted is better than feeling spacey and out of it”.
“I take prescription sleeping pills nightly and take stimulant every morning”.
“Medication/meditation. Medication made me very groggy throughout the next day as I’m very sensitive”.
Improved Outcomes
Overall, patients have not found an over the counter or prescription medication that works. Many commented that the sides effects from medications currently available contribute to discontinuation. A priority for people living with migraine is to find a treatment that will decrease frequency and/or intensity of their migraines.
Sleep is an important piece of the puzzle in managing migraine. Physicians treating patients with migraine encourage and emphasize the importance of lifestyle changes. Commonly referred to as SEEDS (Sleep, Exercise, Eat, Diary, Stress). Lack of sleep significantly impacts many things including tolerance, mental health and overall cognitive functioning.
Patients have made the analogy relating migraine to being in a “washing machine”. Things are going around and around with all the puzzle pieces swirling around. If patients can get one or two pieces of the puzzle under control, it would be helpful. More sleep, better sleep can help lead to better mental health, ability to have energy to exercise, eat better, etc.
People living with migraine are desperate for options that will help improve their quality of life. If patients can control the complications they experience due to their disease (migraine), its one less thing causing stress and anxiety. Sleep is a significant contributor that can’t be ignored. A medication that can help to improve sleep quality and quantity and reduce daytime insomnia would be welcome.
Medications that are not addicting would be welcome. Many physicians are hesitant to prescribe current options for this reason and many patients do not want to take current medications for fear of becoming addicted. Additional desirable outcomes for patients include less side effects (ie. somnolence, cognitive impairment). An additional outcome for patients is effectiveness over longer-term drug therapy. Many products currently available stop working.
Patient comments related to improved outcomes include:
“Finding long term success with any prescription or combinations. I either don’t sleep enough, have interrupted sleep or sleep too much. Success to me would be 7-8 hours all the time”.
“Nothing works for me. I regularly go days and weeks without sleep. I think any new medication that might help would be welcome”.
“Getting enough exercise helps immeasurable; worry makes it all worse; success – fall asleep easily without anxiety about when I will wake up”.
“Success would be consistent quality rest. No real success except taking time off to just sleep as much as my body wants”.
“I don’t remember a time when I slept consistently. I’m on enough medications that give me side effects but they work. As exhausted as I am from lack of sleep, I can’t manage the additional side effects of the sleeping pills that I’ve tried. So I don’t sleep”.
“Finding long term success with any prescription or combinations. I either don’t sleep enough, have interrupted sleep, or sleep too much. Success would be 7-8 hours regularly”.
Experience With Drug Under Review
We did not have any patients with experience on Dayvigo participate in the second survey.
Companion Diagnostic Test
Not Applicable.
Anything Else?
Dayvigo is a first in class medication that offers a new mechanism of action to Canadian patients. There have not been new medications to help people manage insomnia in decades (since 1990’s) and the current medications that exist come with the risk of abuse, physical dependency and lack in tolerance over time.
Studies on Lemborexant support they are effective, safe and have greater benefit to risk. It meets the criteria patients have mentioned that are important to them in a new medication including fewer side effects, no rebound insomnia after discontinuation, no negative impact on cognitive functioning (ie. memory, attention) or impairment. Tolerance with Dayvigo in longer term use is also demonstrated.
Patient comments about need for new medications in Canada:
“It’s been over 3 years and I still don’t get a full night’s sleep or ever feel rested. It affects my relationships and my self-esteem greatly”.
“I’d welcome a medication that I don’t need to worry about becoming addicted to adding to my already to many health issues”.
“The medication’s I’ve tried end up not working after a while and then I tried something new and had to sort through different side effects”.
“My doctor won’t prescribe any sleeping pills because they are addicting and just tells me to manage it naturally which if that worked, I wouldn’t be telling him a literally don’t sleep. Ridiculous”.
“I just don’t manage to sleep, can’t fall asleep, can’t stay asleep. I like to find a medication that can help me sleep for 5-6 hours regularly”.
Patients in Canada deserves equitable access to all medications approved by Health Canada. There is no size fits all. Patients and clinicians need options.
Conflict of Interest Declaration — Migraine Canada
To maintain the objectivity and credibility of the CADTH reimbursement review process, all participants in the drug review processes must disclose any real, potential, or perceived conflicts of interest. This Patient Group Conflict of Interest Declaration is required for participation. Declarations made do not negate or preclude the use of the patient group input. CADTH may contact your group with further questions, as needed.
Did you receive help from outside your patient group to complete this submission? If yes, please detail the help and who provided it.
This submission was summarized and written solely by the staff at Migraine Canada, free from consultation, advice, influence or financial support from any outside individual, group or company.
Did you receive help from outside your patient group to collect or analyze data used in this submission? If yes, please detail the help and who provided it.
Migraine Canada worked with a third party to create the on-line Quality of Life survey. Analysis was completed internally.
Migraine Canada independently developed and analyzed the second survey circulated for feedback on Lemborexant.
List any companies or organizations that have provided your group with financial payment over the past 2 years AND who may have direct or indirect interest in the drug under review.
Table 2: Financial Disclosures for Migraine Canada
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
No COI | — | — | — | — |
Menopause Chicks
About Menopause Chicks
Menopause Chicks is an online learning community for women interested in being proactive with their own health. We teach hormone health, sleep, stress and sexual health and other topics as they relate to perimenopause, menopause and post-menopause. While our reach extends 100,000+, many of our members (40,000) engage via a private online facebook group.
Information Gathering
Menopause Chicks conducts ongoing research with its 40,000+ members. In Fall 2021, we asked members (via an online survey) to share their experiences with sleep/poor sleep. We followed up with a small online interview/focus group (November 10, 2021) honing in on specific lived experiences with poor sleep, treatments tried, treatments tried and stopped, and treatments still using. In March 22, in celebration of #WorldSleepDay, we hosted an all-day online learning event for our members with the goal of encouraging more women to have conversations with about sleep/poor sleep/the impact of poor sleep with their health team. Our group is based in Canada, the majority (50%+) of our members are Canadian. A copy of the Fall 2021 Menopause Chicks Research can be found here.
Survey responses: 1027 (68.49% Canadian), 100% female, 92% were 45+ (60% 45-54, 43% in perimenopause; 39% in postmenopause), 77% experience poor sleep more than once-per-week; the most common form of insomnia: waking up too early. 827 responders had tried prescription medication to address poor sleep.
Focus Group participants: 4 (100% Canadian).
#WorldSleepDay attendees: 500 (geography undetermined.)
Disease Experience
Our survey showed poor sleep significantly impacted energy level, cognitive function and mood the next day. Other impacts to quality of life included: ability to engage in physical exercise, eating habits, household responsibilities, performance or attendance at work, relationships with partner, time with family and friends, ability to parent or care for aging parents and socializing.
The majority of respondents had tried one or more over-the-counter, sleep hygiene/routine, or mindfulness/medication practice in an effort to manage their insomnia. Most indicated their level of current satisfaction with insomnia treatment as “overwhelmingly dissatisfyied.”
Example of open-ended responses:
“The most challenging part of trying to navigate insomnia has been having to give up working full-time.” “I’ve tried talking to my doctor about insomnia impacts my life, but he won’t listen to me.”
“It’s so frustrating—I feel it’s hit and miss. I find a routine that works for a while, but then it stops working. I need something that will help me sleep consistently!”
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| who have lived experience with insomnia:
Some time-stamps to note as the conversation relates to disease experience include:
“It took me down really bad” – ||||||||, Time: 5:05
“When you are unable to sleep, it is miserable. I thought I was going insane, I didn’t want to live anymore, I just couldn’t thrive.” – ||||||||, Time: 9:10-11:50
“It started with a burst of anxiety and sleeplessness…I was terrified I was never going to sleep again; fearful of going to bed!” – ||||||||, Time 13:40-15:06
Some time-stamps to note as the conversation relates how insomnia impacts quality of life include:
“Better sleep brings comfort back. Enjoying sleep again allows me to serve my family, be present for my family, do errands I want to do…be present for whatever I want to do in life.” – ||||||||, Time: 34:46-35:11
“Stress and lack of sleep led me to create Menopause Chicks…because sleep deprivation was turning me into the kind of mother I had no intention of being…it was impacting my relationship with my kids!” – |||||||| , Time: 39:41-40:50
Experiences With Currently Available Treatments
Table 3: Respondents’ Experience Addressing Insomnia
Options | Percentage (%) |
|---|---|
Prescription medication | 18% |
Hormone therapy | 24% |
Over the counter medications | 33% |
Herbal treatments | 48% |
Sleep hygiene | 42% |
Relaxation training | 37% |
Mindfulness | 37% |
CBTi (Cognitive Behaviour Therapy for Insomnia) | 4% |
Alcohol | 9% |
Cannabis | 24% |
861 respondents had tried one or more of the following: magnesium, melatonin, cannabis, antihistamines or anti-allergic medications to manage insomnia.
Of the respondents who had tried prescription medications for poor sleep, the majority had discontinued use due to dissatisfaction with how they felt the next day or fear of becoming addicted.
Example responses to open ended question: “What has been the most challenging in managing your insomnia?” “I define success if I feel rested in the morning. Nothing I have tried to-date seems to work consistently.”
“The biggest challenge is the snowball-effect on my body from sleep deprivation. I’m stressed so I don’t sleep. I don’t sleep so I become more stressed.”
“The most challenging is waking up at 3 a.m. and not being able to get back to sleep and not wanting to take anything in the middle of the night for fear of how it could impact the quality of my next day.”
Respondents had experience with Z –Drugs, Benzodiazepines, Desyrel/trazodone, Elavil/amitriptyline, Remeron/mirtazapine, Dayvigo/lemborexant, Antipsychotics/First generation, Antipsychotics/Second generation and Alpha Deta
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| who have lived experience with insomnia:
Some time-stamps to note as the conversation relates to experience with currently available treatments include:
“I bought a boatload of herbals” – ||||||||, Time: 22:43-24:50
“I tried many, many different things that did not help…I do not want to hate going to bed!” – ||||||||, Time: 27:21-28:00
Improved Outcomes
Respondents’ desired outcomes include: uninterrupted sleep, waking rested and feeling they can handle responsibilities of the day (work, family, etc.) They would like to see more emphasis/conversation on sleep as a key health indicator—in society and during their health appointments; many cite poor sleep as not being something their doctor ever brings up or something that never becomes personal priority (i.e. “I ‘should’ be able to handle this on my own.)
Over the years, anecdotal conversations in the Menopause Chicks community have pointed towards fear of prescription medications and how they can make women feel the following day, or they fear becoming reliant on a specific medication. There is a common understanding that sleep medications have traditionally been tested on men and often not prescribed properly for women. Members would appreciate getting updates on new developments in this area as a way of supporting their own health, but also to help shift the societal paradigm from “avoid sleeping pills at all costs” to “there are prescription options that are helpful and supportive for women.”
Experience With Drug Under Review
In our member survey, one respondent indicated they were currently taking lemborexant.
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||, we heard: (55:05 mark)
“I have had success using lemborexant in both male and female patients. One patient had been challenged with insomnia for 10 years and it was significantly impacting her quality of life, including her ability to parent and exercise. She mentioned lemborexant to me and after doing my own research, we decided to start her on the recommended dose. She called me two days later and she had slept through the night for the first time in 10 years.” ||||||||||||||||||||||||||||||||||||||||, NP.
The key values important to patients and caregivers, when it comes to the treatment of insomnia include: Does it relieve patient from the burden of “excessive awakeness”? Does it produce 7-8 hours of sleep? Is the sleep restorative that it positively influences quality of life for the patient the following day? Both patients and health professionals want more choice; more options when it comes to treating poor sleep/insomnia.
Companion Diagnostic Test
Not applicable.
Anything Else?
Thank you for considering this input from a demographic whose health concerns are often overlooked.
Over half of women said they felt dismissed or disappointed leaving their health appointment, that their physician. That number is even higher for Indigenous women and women of colour.
3-in-10 women reported challenges accessing the health care they needed. – InHerWords.ca, BC Women’s Health Foundation
Conflict of Interest Declaration — Menopause Chicks
To maintain the objectivity and credibility of the CADTH reimbursement review process, all participants in the drug review processes must disclose any real, potential, or perceived conflicts of interest. This Patient Group Conflict of Interest Declaration is required for participation. Declarations made do not negate or preclude the use of the patient group input. CADTH may contact your group with further questions, as needed.
Did you receive help from outside your patient group to complete this submission? If yes, please detail the help and who provided it.
No.
After learning about CADTH, I did meet with ||||||||||||||||||||||||||||||||||||||||||||||||||||||||, CADTH in January 2022.
Did you receive help from outside your patient group to collect or analyze data used in this submission? If yes, please detail the help and who provided it.
No.
List any companies or organizations that have provided your group with financial payment over the past 2 years AND who may have direct or indirect interest in the drug under review.
Table 4: Financial Disclosures for Menopause Chicks
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
Pure Pharmacy | — | — | — | X |
Eisai | X | — | — | — |
Mood Disorders Society of Canada
About Mood Disorders Society of Canada
Mood Disorders Society of Canada (MDSC) has evolved to become one of Canada’s best-connected mental health NGOs with a demonstrated track record for forging and maintaining meaningful and sustained partnerships with the public, private and non-profit sectors throughout Canada.
MDSC has grown out of the vision and drive of a number of mental health lived experienced leaders from across Canada who in 1995 saw the need for a broad-based structure to bring consumers of mental health services together and who believe that consumers have a key role to play with regard to education and advocacy at the national level.
It was formally launched and incorporated in 2001 with the overall objective of providing people with mood disorders with a strong, cohesive voice at the national level to improve access to treatment, inform research, and shape program development and government policies with the goal of improving the quality of life for people affected by mood disorders.
The MDSC’s overall objective is to provide people with mood disorders with a strong, cohesive voice at the national level by:
Raising awareness that mood disorders are treatable medical issues and working towards eliminating barriers to full community participation in reducing discrimination and stigma, involving members of the public, government and treatment/service providers.
Building a national clearinghouse of information and resources related to mood disorders.
Advocating for the creation of adequate and accessible stigma-free programs for Canadians living with or suffering from mental illness.
Ensuring that the voices of persons lived or living with mental illness and family members are accurately understood and communicated on issues of national importance by building on existing networks and alliances.
Website: https://mdsc.ca/
Information Gathering
Information used to compile this submission was gathered via the following: Mood Disorders Society of Canada (MDSC) conducted a national Sleep and Mental Health survey to understand sleep behaviours and how sleep problems such insomnia impact our mental health, and how mental health issues can also impact our sleep.
MDSC hired the independent research firm Narrative Research to conduct the survey and analyse the results, Our research objectives included:
Delineating the different profiles of sleep disturbances in people with/without symptoms of mental disorders.
Understanding the perceived impacts of sleep problems on mental health and daily functioning.
Characterizing levels of knowledge about sleep and what topics are of greatest interest.
Identifying the use and perceived effectiveness of various types of sleep treatments and therapies.
The online survey of the general population was conducted with a random sample of 1,200 respondents across Canada. In addition, MDSC shared a survey link through its network (notably on social media), resulting in 49 additional surveys being completed. Quotas were applied to the general population survey based on age, gender and region, while the survey results were also weighted on those characteristics. In addition to the questions included on the general population survey, the network survey included a few more questions, resulting in an average completion time of 22 minutes. The average survey length for the general population survey was 18 minutes. The survey was in field from September 21 to October 7, 2021.
Two in ten respondents mention having been formerly diagnosed by a health professional with a sleep disorder. Regardless of having been diagnosed with a sleep disorder, insomnia is prevalent among respondents, with more than half who say that they have experienced insomnia over the past year, specifically difficulty falling asleep or staying asleep, or waking up too early and not being able to get back to sleep. Again, those reportedly suffering from insomnia are more likely to be dissatisfied or neutral about their sleep pattern. They are also most likely to include females, and those with household incomes of less than $50k per year.
Some demographics of the 1,249 completed respondents.
Age:
16 to 29 = 13%
30 to 49 = 39%
50+ = 48%
Gender:
Girl/Woman = 54%
Boy/ Man = 45%
27% of respondents are retired, 44% employed, 9% employed part-time, 5% self-employed, 9% unemployed, with 3% currently identifying as students.
Income levels were:
Under $27,000 – 10%
$27,001 - $41,000 = 15%
$41,001 - $50,000 = 9%
$50,001- $100,000 = 36%
$101,000 or more = 22%
Prefer not to say = 8%
MDSC also gathered information for this submission through individual interviews with three patients who have been struggling living with insomnia, and who have tried a variety of treatments and therapies. We also interviewed several family members to gain further insight.
We spoke at great length with two clinicians. One a family physician and one a psychiatrist.
Additional experience and perspectives was garnered through our reviewing patient and family member input and comments/ shared experiences through our MDSC online Discussion Forum which is hosted on the MDSC website and is a portal for in-depth online discussions.
MDSC has very large number of dedicated followers and our organization has with more than 87,000 social media followers. We have extensive website visitors as well, along with our main mdsc.ca website, our depressionhurts.ca website alone has 500 visitors per day and is extremely active. Our national mental health campaign, Defeat Depression, holds mental health walks from coast to coast with over thousands of people taking part. We also have a national online discussion support chat line that has over 2,800 discussion threads and over 35,000 posts
It is through the above context and our 20+ years of ongoing collective efforts of direct engagement with patients and representing the lived experiences of the patient community that we bring to this submission. It is the goal of our organization to be their voice in this process.
Disease Experience
The impacts on a person with insomnia often have wide ranging consequences. According to the results of our national sleep and mental health survey, dealing with serious sleep problems causes distress for most respondents to varying degrees, most significantly for those with a formally diagnosed sleep or mental health disorder, and those reporting insomnia. The issues identified are mostly related to difficulties sleeping, such as having trouble falling asleep or staying asleep, with resulting consequences of feeling tired or having little energy. There is an across the board understanding that sleep has a direct and significant impact on most aspects related to a person’s overall health, including vitality, mental health, intellectual functions, productivity, and body pains/aches. The results of the national survey also clearly indicate sleep issues are seen as having important consequences on society, and there remains a need for increased public education.
One quarter of the survey respondents indicate that they snore loudly, that is loud enough to be heard through closed doors or resulting in their bed-partner elbowing them for snoring at night. This is most prevalent among those self- reporting insomnia, males, Atlantic Canadian respondents and non-white individuals. One in seven report that someone observed them stop breathing or chocking/gasping during their sleep.
Respondents with a formal sleep disorder diagnosis are more likely to report having insomnia, snore loudly and have stopped breathing or chocked/gasped during their sleep. In addition, a diagnosis of a sleep disorder, insomnia and snoring are more common among those who have been formerly diagnosed with mental illness. Also determined was that 60% of respondents stated there was a stigma associated with the illness. Stigma is very real and people can delay getting a diagnosis and seeking treatment due to a fear of what friends, family may think, in addition to their own self- stigma.
During one discussion, the individual informed me that stress and anxiety have a great influence on the quality of their sleep, and they felt that these two factors were the primary reason of their sleep problem. They also identified a drastic increase in their levels of both stress and anxiety since the covid-19 pandemic began.
Following this meeting, in a further discussion, a family member also detailed how they had seen a significant change in their partners’ ability to “turn off” the anxiety (primarily caused by news exposure and work pressures) and linked stressors that have had a profound negative affect on their sleep. The family member stated that the usual pattern seemed to be their partner would go 4-6 days with broken sleep consisting of roughly 4-6 hours of sleep on good nights, interspersed with periods of getting out of bed and moving to the living room, unable to turn off the thinking and unable to fall asleep. On occasion total sleep was even less. This in itself has caused the other partner to have broken sleep during most of these nights as well. During these periods it was mentioned that the family member was feeling stressed, temperamental and emotionally and physically drained.
Respondents in the survey who have a formal sleep disorder or mental health diagnosis, and those who experienced insomnia in the past year, expressed they feel much more likely that sleep impacts how they interact with their spouse/partner or their children. With those respondents between 16 and 49 years of age in a relationship are more likely to say that sleep impacts their relationships to some degree. The impact of sleep on someone’s relationship with their children is also considered more important among parents and guardians 16-49 years old than among those who are older.
It was indicated in the survey responses that 86% of respondents indicated some level of dissatisfaction in their sleep patterns. Of these, 77% stated the sleep problems had at least a little to very much interfering with their daily functions. Within this 7 per cent group, 42% identified their cognitive functions were impacted, 38% stated their household chores were affected, 38% identified with physical exercise being impacted and 28% stated with work was impacted.
One person being interviewed stated sleep is a major factor in mood disorders, and getting enough sleep is very important for wellness maintenance. There was a solid understanding on the connection between mental health and sleep. Our survey results show has an impact on most physical and mental functions.
Respondents were asked how much actual sleep time they got on a daily basis over the past two weeks. For respondents who identified as being unemployed, retired, on short or long-term disability, and those who did not disclose their occupational status reportedly slept an average of 7 hours per night. Respondents who are employed, a student, or volunteer full-time reported sleeping an average of 6 hours before days when they work/have class/volunteer, while they slept an average of 7 hours on other nights. Of the respondents who have identified as having experienced insomnia over the past year, or with a formal sleep disorder diagnosis, and those with a mental health diagnosis, slept an average of one hour less per night compared to other respondents.
As an additional indicator of the ramifications of sleep problems and insomnia, one-third of respondents who are working, studying or volunteering full time have missed time off work, school or volunteer activities due to sleep problems in the past year, and report an average of eight missed days. Those respondents who have a mental health diagnosis (11 days) or a sleep disorder diagnosis (10 days). Looking at the entire responses, the average lost productivity due to sleep issues averages three days in the past year.
Experiences With Currently Available Treatments
Survey respondents who identified as having experienced insomnia during the past year (n=673-676) were asked extra questions about sleep medication and treatments. One quarter of respondents are clearly dissatisfied. More than one quarter of respondents have used prescribed medication in the past to help with their sleep. Past usage of such medication is far more common among those who have been diagnosed with a sleep disorder (57%), people who have experienced insomnia (39%) and those with a mental health diagnosis (62%).
62% report having taken prescribed sleeping medication in the past two weeks, either at least three times a week (35%), once or twice a week (17%), or less than once a week (10%). Respondents who have received a sleep disorder diagnosis are more likely to have taken prescribed sleep medication in the past two weeks with 81% responding affirmative.
On average, the longest period of time that respondents have been using prescribed sleep medications at least three times a week was 59 months (nearly five years). Respondents who have taken prescribed sleep medication mostly saw a positive impact on their sleep from taking these medications and to a lesser extent, on their mental health.
In a separate MDSC national mental health survey conducted in September, 2021, 45% of respondents identified Improving Access to Medications and Treatment as their number 1 election issue for the Government of Canada, with 94% of them identifying it as important. It was the number one priority specified by respondents.
From the clinician in-person (Zoom) interviews:
Clinician #1 (Family physician, over 30 years’ practice, prior, pharmacist. Patient case load of 2,200)
This physician went into great detail on working with hundreds of patients with insomnia, and treated the full spectrum of patients, right from the newly presenting to those who have struggled with insomnia for decades. The challenge he expressed was trying to find the treatment which was safe, stable and tolerated.
During the interview this physician stated that in the years past there was a higher tendency to prescribe benzodiazepines or Z-drugs for insomnia, however there were several key areas of concern, from dependencies to next morning drowsiness.
Clinician #2 (Psychiatrist, over 25 years’ practice)
This Psychiatrist described his many years of working with patients who had among other mental health issues, comorbid issues of insomnia which was compounding recovery and their wellness. He described how sleep was one of the pillars of health and was a key area that needed to be balanced in order to move forward with the patients lives. He went into great details on a treatment pathway many had taken, again reiterating what I had heard previously by clinician #1 and two patients, seemed like there was earlier usage of medications such as trazodone and other benzodiazepines, but there was always the real concern of issuing opioids, dependencies and using these medications.
One instance involved a patient who was dealing with migraines and insomnia. This person was on trazodone daily and a further 15 mg of zopiclone to deal with the insomnia. The patient was always feeling sluggish and mornings were very challenging to get motivated and active. So, when the new treatment Lemborexant became available the patient was weaned off the previous medication and then tried Lemborexant. The result was the patient told the clinician “this is incredible”. The difference was quite profound to them, and they were then getting 7-8 hours of sleep a night.
Another patient who was living with PTSD and had insomnia as a symptom, this person was also finding it difficult to manage their insomnia and had tried for years to get in into a livable situation. Once they began using Lemborexant, they found it to be extremely helpful, and changed the way they were able to live.
It is important to also point out from both these clinicians I heard very aligned experiences, that there has been concern for working with patients who have multiple issues that they are trying to address. For instance, both described the caution needed when dealing with a patient who presented with pain, mental illness and symptoms of insomnia. That in the past there was less options for treatments, which led to more use of opioids as part of the treatments, and this was a concern. Both went into how much having Lemborexant as one of the new tools in their toolbox was extremely helpful
Also both were very aware of how when they are working with patients who have insomnia one of the predominate issues facing many patients is equitable access. While this treatment may not seem, for those who are either unemployed or underemployed, if they are not covered for the treatment regiment, there is a real barrier to access. While we are only talking about a couple dollars a day, if you are on social assistance, or have a wage job, this cost is a real obstacle.
Recently in particular, the pandemic and the economic havoc that has ensued (employment slowdowns, re-structuring, business closures etc.) there are people who are falling between the cracks for coverage. As seen in the demographics of survey participants,34% are earning under $50,000 per year. MDSC has heard directly from patients consistently throughout the years that if you are not employed in an occupation that has a solid benefits plan with sufficient drug coverage, often, covering these expenditures is a severe challenge. One person recently stated it clearly “... I was laid off in July but the company I worked for allowed us to prepay for benefits for 3 further months in an agreement with Manulife. I was on the CERB until it ended and then transitioned over to EI. I get the full amount on EI available, but with rent and basic living expenses it leaves very little for anything else. I have only a few weeks left of medication and the costs are very high...”
We need to realize that many lower income occupations do not come with drug coverage. Additionally, if you are unemployed, or under-employed, and if your medications are not covered within provincial health care plans, you must pay out of pocket. It is why we hear often from patients about not being able to afford the medication they need to recover and maintain their wellness. They either cannot afford the medication or if they do buy it, they will skip doses and try to stretch the prescription out to last two or more months at a time.
Improved Outcomes
MDSC strongly believes that it is crucial that patients are informed of, have access to and have choice of medications that work for them. Patients need to be able to decide on the medication that they feel works for their illness, with the side effects that are acceptable to their lives. What is very well known is that medications can affect one person differently then the way it may impact another person. That is why often, it takes a period of time, and trying different treatments for the patient to find the treatment that works for them. They need to be able to make informed decisions on which side effects they are best able to accept. The goal being to take the treatments that help them best manage the particular illness they are dealing with, in a manner which does not expose them to additional side effects that may cause other issues for them to then have to cope with.
Our position is the unwavering importance that treatment coverage must be available to everyone, regardless of their economic status. It should be a health related right, either through their employer and a quality drug plan, when available, or when a person is not covered through private coverage, due to reasons such as being unemployed or disabled, or any other similar situation, they need to be covered within provincial and territorial health care plans to have access to the treatments that work best for them. Anything less is barrier to equal access, a barrier to health, and detrimental to the success of Canadian society.
Patients, family members, and caregivers believe strongly that access to treatment should not be limited to only those with private drug plan coverage, while those who work for employers who do not have drug coverage do not get access to the medication for their individual illness. Our position is that accessing the medications to treat illness should be fully equitable for all those who are ill.
Experience With Drug Under Review
Of the three individuals who we interviewed and identified as having taken Lemborexant (Dayvigo) three stated they had private health coverage, with one stating as having some private coverage but relied on the provincial health care coverage mainly. None had detailed any experience in clinical trials.
We asked specifically what a meaningful, successful outcome for a good sleep medication would be. We were looking for what they felt was the key values and also asked if they felt they were receiving this now. All there stated what was important to them was to be able to trust that they could fix their sleep problems so that they would be able to enjoy their days again. Especially when it came to interacting with family members and work colleagues. They also all stated to be more productive at work. Minimizing any side effects are a prominent concern. Two identified their being able to not becoming anxious or stressed because they would worry about not being able to count on normal sleep.
Patient #1
“I am finding I am seeing the ability to be able to level off my irregular sleeping patterns, and trust that I will be able to feel rested when I go to work the next day”
“Not having to only rely on waiting until near midnight each night before I finally drift off to sleep, only to waken by 3”
Patient #2
Expressed their feelings of to not become dependent on the medication over the long term. They have been looking for a medication that was gentle on their stomach and not overpowering, which they claimed to feel with this medication.
They stated while it “was too soon to see any pronounced impact, they did not have the feeling of next morning dullness and drowsiness” which they have had in the past.
Patient #3
This patient stated she had tried several different medications in the past, and all seemed to lose their effectiveness after several weeks, leading to either having to take more dosage, which resulted in her feeling hung over the next day. She expressed she has tried Dayvigo, which was working for her without any major side effects.
“Less time laying there tossing and turning now”.
Of these three:
two had tried melatonin in the past
two had on occasion used Gravol
one had used Zopiclone for 8 months
one had used Quetiapine (50mg)
one had used Seroquel for sleeping (100mg) and they stated they found that dose left them feeling very tired
Clinician #1 (Family physician, over 30 years’ practice, prior pharmacist. Patient case load of 2,200)
The physician informed me that the introduction of Lemborexant has been a real game changer and that it was “something so totally different”. He stated he treats the full spectrum of patients, and in doing so there is always the goal of ensuring the cure is not worse than the disease. He has been prescribing Lemborexant over the past year and a half and he is fully impressed with the outcomes. He articulated that with this new treatment he is not worried about issues such as next day sedation. He went on to detail how while treating the full range of patients, he saw an across-the-board positive outcome throughout. Patients who respond well, respond very well. Another key benefit was the quickness of the medication, patients describe taking the medication 20 minutes before bed, they could take it while doing the dishes, or on the couch and get the result 20 minutes later while going to bed. He expressed no concern with attentiveness the next morning, there were no experiences of next day sedation which could impact things like driving, work attendance etc.
He went on to describe a patient who had not informed him that she had been quietly struggling with insomnia for 20 years. He prescribed Lemborexant, and received a call two days later from this patient who was completely thrilled with the fact she was able to now sleep, and stated there was no after effect of impact at all.
Another keynote was that this medication worked well even if the patient was on multiple medications. He indicated that he was able to wean a person off other higher doses of medications once they were able to use Lemborexant to address their insomnia.
Clinician #2 (Psychiatrist, over 25 years’ practice)
As described a little earlier in this submission, this clinician informed me of numerous patients that had been on other medications and he migrated some of them over to Lemborexant. He stated he had good success with this medication one patient went on to state how impressed they were with the treatment telling him…“this is incredible”. and they were then getting 7-8 hours of sleep a night.
One of the real noticeable things the psychiatrist told me about was how they felt confident when prescribing Lemborexant, in that there would not be a rebound in the insomnia, and they would be able to start and stop the treatment if/ when needed. They also went on to let me know that even if a patient missed a day, they would not see any negative issue. There was not experiences with next day sedation
Companion Diagnostic Test
Not applicable.
Anything Else?
Mood Disorders Society of Canada (MDSC) is proud to represent and speak on behalf of patients across Canada. Through the course of our business, we engage with patients, family members and caregivers every day on an on- going basis.
A significant component of recovery and wellness maintenance includes access to medications. Finding the right medication that works for the individual can take many months (if you are fortunate) or many years for the patient. During this phase, we need to recognize that the family members connected to the patient are also going through this process.
We know that getting good, consistent, quality sleep is a crucial part of your overall wellness. While many of us tend to delay addressing sleep problems, we often find ourselves reaching a point where it makes itself known to us as being a problem, usually in a manner which is quite noticeable.
Sleep is one of the foundational blocks of our wellness, and it affects all areas of our health and wellness. It eliminates toxins and repairs our bodies, regulates blood sugar, mood and stress, boosts immunity and energizes nerve cells and muscles. Without proper sleep, we quickly can see negative impacts such as drowsiness, daytime fatigue, irritability and headaches, difficulty focusing or paying attention, lack of the ability to complete intricate tasks, and invariably, leads to increased tendencies to make wrong decisions, such as poor unhealthy food choices.
As a society, we have become more pressured to over perform, to place business and success at the forefront of all of our priorities. Coupled with increased media exposure and the pandemic, we have seen a dramatic increase in sleep problems and insomnia. Over the past 18 months, many are re-evaluating priorities and are realizing they are experiencing some imbalances. Many Canadians are now eager to see normalcy return in to their daily realities. This is why finding the right treatment options will support patients return to a healthier life.
We must make sure medications are made available and they can access, their medications if they are not covered by private health care plans. This is crucial to enable patients the ability to maintain work, interact with their family and friends and feel like they are contributing to society.
From our discussions with both patients and clinician, it is vitally important to ensure coverage for this medication. While the cost is negligible, it is so important that barriers do not exist in accessing this new treatment.
Conflict of Interest Declaration — Mood Disorders Society of Canada
To maintain the objectivity and credibility of the CADTH reimbursement review process, all participants in the drug review processes must disclose any real, potential, or perceived conflicts of interest. This Patient Group Conflict of Interest Declaration is required for participation. Declarations made do not negate or preclude the use of the patient group input. CADTH may contact your group with further questions, as needed.
Did you receive help from outside your patient group to complete this submission? If yes, please detail the help and who provided it.
No.
Did you receive help from outside your patient group to collect or analyze data used in this submission? If yes, please detail the help and who provided it.
No.
List any companies or organizations that have provided your group with financial payment over the past 2 years AND who may have direct or indirect interest in the drug under review.
Table 5: Financial Disclosures for Mood Disorders Society of Canada
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
Janssen Inc | — | — | — | X |
Pfizer Canada | — | — | X | — |
Lundbeck Canada | — | — | — | X |
Viatris | — | — | X | — |
Abbvie Inc | — | — | X | — |
Eisai | — | — | X | — |
Clinician Input
National Advisory Board
About the National Advisory Board
National advisory board comprising Canadian physicians including family physicians and psychiatrists with interest and experience in the management of insomnia.
Information Gathering
Advisory board meetings, literature reviews, conferences, discussions with colleagues, clinical experience, patient testimonials.
Current treatments
Describe the current treatment paradigm for the disease.
According to the Public Health Agency of Canada, 1 in 2 adults have trouble falling asleep or staying asleep, while 1 in 3 have difficulty staying awake during the day. Approximately 13% of Canadians meet formal diagnostic criteria for insomnia disorder. The prevalence of insomnia in Canada is further increased in the presence of chronic conditions including hypertension (19%); asthma (21%); diabetes (22%), cancer (23%); back problems (23%); arthritis (24%) migraine (26%); heart disease (26%); peptic ulcer (28%); and stroke (29%). Up to 2/3 of patients with chronic pain conditions also experience sleep disorders. The prevalence of insomnia disorder and the incidence of new cases of insomnia disorder have increased worldwide since the beginning of the COVID-19 pandemic. Canada has one of the highest rates of insomnia disorder since the beginning of the COVID-19 pandemic, second only to the United States.
There has been a paradigm shift in the assessment and treatment of insomnia disorder beginning with the establishment of formal criteria in DSM-5 (2013); the recognition of sleep having a restorative function on multiple aspects of health; the changing focus of insomnia treatments from medications that increase sleepiness to those that reduce alertness; and the importance of CBTi and sleep hygiene in the treatment of insomnia disorder. However, there remain many barriers to the effective management of insomnia disorder including a lack of medical education at all levels concerning insomnia from neurobiology to comorbidities, limited access to services, poor availability of resources, misconceptions about sleep needs, misinformation about self-medication with cannabis, alcohol, and OTC medications as well as the widespread use of off- label and inappropriate medications. In fact, a Canadian study of OTC use has shown a trajectory of increasing use over time in more than I in 5 individuals, and suggested clinical intervention could pre-empt vulnerability to counter- productive self-medication.
Despite the high prevalence of insomnia disorder, there are no Canadian guidelines or evidence-based recommendations. Further, there is no mention of sleep health in any of the current Canadian guidelines for the management of hypertension, diabetes, dementia or obesity – all recognized comorbidities. In fact, ironically, the only guidance relates the the risks of existing treatment (Canadian Coalition for Seniors Mental Health Canadian Guidelines on Benzodiazepine Receptor Agonist Use Disorder Among Older Adults 2019; Pottie, K., et al., Deprescribing benzodiazepine receptor agonists: Evidence-based clinical practice guideline. Can Fam Physician, 2018. 64(5): p. 339-351; Choosing Wisely: https://choosingwiselycanada.org/geriatrics/).
The pharmacological management of insomnia disorder represents a significant challenge in current clinical practice in Canada. The two major classes of approved and reimbursed medications for short-term use are the benzodiazepines (BZPs) [triazolam, flurazepam, nitrazepam, temazepam] and Z- drugs [zopiclone, zolpidem, eszopiclone]. However, in reality these medications are used for much longer periods than recommended and in a potentially dangerous and harmful way e.g, in combination with inappropriate medications such as opioids (OTC and prescription), antihistaminic compounds including OTC cold and flu treatments, or substances such as alcohol and cannabis; and in an unsafe way e.g., driving or operating machinery within 12 hrs of ingestion.
It is well recognized that chronic use of BZPs and Z-drugs is physically and psychologically harmful, due to their addictive potential as well as the common side effects of cognitive and physical impairment. These drugs increase fall risk, especially in the elderly, as well as contributing to next day physical and cognitive impairment. In the opioid pandemic over the last few years, there has been a heightened awareness of the increased morbidity and mortality risk when these medication classes are prescribed in combination with opioids. This realization has significantly reduced prescribing of both of these medications, and led to situations where patients are denied treatment for treating their sleep disorder and pain disorder. According to Canadian Institute of Health Information and Canadian Centre on Substance Use and Addiction hospitalization due to opioid poisoning was most common to co-occur with use of BZPs (19% in 2014- 2015); fatal overdose with opioid was significantly increased with concurrent use of BZPs; and in Ontario for 2015, BZPs were present in post-mortem toxicology reports in half of all opioid related deaths.Compounded sedation and thus risk of death also occurs with other neuropathic pain medications e.g., gabapentin and pregabalin commonly used in conditions such as diabetes and peripheral vascular disease.
The BZPs and Z-drugs mode of action (MOA) is primarily through GABAA receptor agonism and their effect on sleep is through their sedative action. The third class of approved hypnotic is a tricyclic antidepressant that is also sedative due to is antihistaminic activity. Essentially due to their MOA, BZPs and Z-drugs lead to physical dependence, withdrawal and rebound insomnia concerns: 10 – 30% chronic BZD and Z-drug users are physically dependent; 50% BZD and Z- drug users suffer from withdrawal symptoms; 5 – 58% of BZD and Z-drug users develop rebound insomnia, after 2-4 weeks of treatment.
However, with the increasing understanding of the neurobiology of sleep there is a consequent changing focus of insomnia treatments from sedative medications to those that reduce wakefulness e.g., very recent data suggests that compared with healthy controls, patients with primary insomnia exhibited significantly decreased functional connectivity density (FCD) in the left medial frontal gyrus and increased FCD in the left supplementary motor area (JI B, et al.
Neuropsychiatric Disease and Treatment 2022:18 1–10). Consequently, the introduction of an agent with a novel MOA heralds a paradigm shift in the ability to address some of the fundamental dysfunctions in insomnia disorder.
Treatment Goals
What are the most important goals that an ideal treatment would address?
Insomnia increases the risks of physical (stroke, type 2 diabetes, hypertension, MI, cancer, CHF) and psychiatric comorbidity (depression, anxiety, dementia), as well as overall mortality (OR:1.93 – 2.14). Further, overall mortality risk increases with the number of insomnia symptoms. Insomnia has a debilitating impact on an individual’s health and functional ability on a functional basis.
The economic burden of insomnia in Canada is substantial e.g., $6.6 billion annually and $5010 per person annually in Quebec in 2009, and with 5 weeks of work lost per year due to presenteeism, 1 week lost per year lost due to absenteeism and double the accident rate (not including driving accidents).
Approximately, 74% of Canadians drive to work each day. In Motor Vehicle Accident (MVA) based deaths 11.2% drivers tested positive for sedative-hypnotic prescription drugs post-mortem, while MVA-related accident-based hospitalizations increased from 5.6 to 6.5x within 2 weeks after filling a BZD prescription. Further, 73% of Canadians with insomnia did not feel productive at work and 31% made an error at work with 12% actually falling asleep at work.
Concomitant disease burden and drug savings due to improved management of insomnia.
Treatment Gaps (Unmet Needs)
Considering the treatment goals in Section 4, please describe goals (needs) that are not being met by currently available treatments.
As a result of lack of safe on-label pharmacological options for treating insomnia disorder, physicians have resorted to off-label use of sedating drugs including antidepressants, antipsychotics, and anticonvulsant medications. These classes of medications however have their own inherent long list of harmful side effects. Most worrisome are daytime sedation, anticholinergic side effects, and significant weight gain leading to the many health consequences associated with obesity. The American Academy of Sleep Medicine and Choose Wisely Canada clearly state that these alternatives have potential harm that outweighs the benefit and strongly caution against the use of these medications for treating sleep disorders.
Because of the lack of safe and effective prescription treatment options, many patients have resorted to self-treatment with alcohol and cannabis not infrequently combined with OTCs (sedating antihistamines, diphenhydramine, cold medications). It cannot be overemphasized the harm that overuse of these products are causing to both mental and physical health of patients. This is causing yet another health care crisis in our society and the economic and social costs are quickly mounting.
Which patients have the greatest unmet need for an intervention such as the drug under review?
A CADTH review of interventions for the management of insomnia found the use of sedative drugs is frequently for longer durations than the evidence supports; important points summarized as follows:
Current provincial reimbursement for seniors serves counter to deprescribing initiatives
Lack of coverage options for safer alternatives results in off label trazodone use, with similar risk of falls in seniors
Seniors living in Long-Term Care (LTC) facilities are particularly vulnerable to inappropriate use of BZD & Z-drugs
Evaluating effectiveness/gaps in deprescribing initiatives
Impact of inappropriate use of BZD & Z-drugs on drug plan wastage, safety concerns and associated health care costs for Canadians with insomnia.
BZD/Z-drug & off-label medications use initiated at Canadian Hospitals
The elderly are extremely vulnerable to inappropriate prescribing with 20 -53% in LTC in Canada being prescribed antipsychotic medication without an underlying psychiatric diagnosis. BZPs are in the top 10 drug classes prescribed to seniors with BZP & Z-drugs rate of use increasing with age.
Several Canadian guidelines recommend to optimize the safety and quality of life of older adults through the appropriate use and prescribing of medications, and the deprescribing of inappropriate medications which includes prioritizing the reduction of sedative hypnotics and encouraging policy makers to reimburse alternative interventions (pharmacological & non-pharmacological) that are proven safe and effective. Yet in reality, safety is compromised by the current reimbursement plans e.g., reimbursement criteria in Ontario encourages trial of BZPs and off-label use of trazodone. The latter is the most common medication in the “Other antidepressants” drug class — used by 25.8% of seniors living in LTC. Trazodone, even at low-dose, has been shown to have the same fall risk as BZPs in nursing homes in Ontario. The increase in trazodone and quetiapine users has exceeded the decrease in BZPs users in LTC in Ontario, while in Quebec, 82.5% of trazodone prescriptions are for the off-label use of insomnia.
Of note, the effect of BZPs on postural stability is 3x worse than a person with blood alcohol legal limit for impaired driving and 52-90% increase risk of hip fractures due to BZD and Z-drug use, respectively. In 2015 the costs of hospitalization, emergency department and outpatient visit costs due to inappropriate BZP use in Canada were $3,076 per elderly patient per year.
Four of the top 5 drugs identified by deprescribing guidelines across Canada include BZPs, atypical antipsychotics, typical antipsychotics and zopiclone (with BZDs ranked 1st). These guidelines recommend to deprescribe BZPs and Z-drugs if used more than 4 weeks in adults and in elderly independent of duration of use and not to use BZPs or other sedative-hypnotics in older adults as first choice for insomnia. Yet 34% of family physicians prescribe sedative or hypnotic medications for more than a year.
An Alberta study in 2015 found that the overall prevalence of BZP and Z-drug use was 10% overall, increased with age and was consistently highest among females, and with 20% using both classes of drug and 10% having 3 or more prescribers. Days of consecutive use were highest among the elderly. Further, in Canada, drug plan cost wasted due to excessive dosing and excessive duration of use of BZPs and Z-drugs accounts for 9% and 59% respectively.
American and Canadian guidelines do not recommend trazodone or low-dose antipsychotics for sleep. However, in hospital settings antipsychotics and trazodone are used widely for insomnia even in vulnerable populations of children or elderly. An Ontario study found that 11.5% of children and adolescents in an inpatient treatment unit were being prescribed quetiapine, and in 81%% this was for either insomnia or insomnia and another reason (66% continued on quetiapine after discharge). A Nova Scotia study of hospitalized seniors in 16 different hospitals reported a point prevalence of 34.6%.
The above Canadian data highlight the urgent and dire need to pursue safe and effective interventions for the treatment of insomnia disorder. The wealth of clinical trial data coupled with the significant clinical experience of the group is consistent and emphasizes the place of lemborexant in the modern treatment algorithm for insomnia disorder.
Place in Therapy
How would the drug under review fit into the current treatment paradigm?
Lemborexant is a dual-acting orexin antagonist and representative of a new class of rationally developed medications for sleep disorders. The MOA is unique and novel compared to all existing treatments and involves modulation of an endogenous neurotransmitter system. The data reviewed indicate broad benefit that include a positive effect on sleep architecture, lack of hangover and cognitive effects as well as increased continuous positive airway pressure (CPAP) compliance reported in patients with obstructive sleep apnea (OSA) and likely downstream cost benefit associated with CPAP compliance.
Insomnia disorder frequently becomes a persistent condition thus earlier identification and intervention is key. In view of the positive efficacy: safety ratio of lemborexant compared with existing alternatives, this agent should be considered as part of first-line treatment. Earlier use of a safe and effective agent with a MOA that has the potential to ameliorate the course of the illness is therefore likely to shift the current treatment paradigm in terms of a focus on earlier use. If lemborexant is used early, there is the greatest potential for improving outcomes in the treatment of insomnia disorder in Canada. It is the opinion of the group that lemborexant that it works quickly, keeps working (no tolerance) and often continues to improve in its action.
Please indicate whether or not it would be appropriate to recommend that patients try other treatments before initiating treatment with the drug under review. Please provide a rationale from your perspective.
From a clinical perspective, it is important to choose the drug with the optimal risk: benefit [short and long-term] for the patient based on individual and disease characteristics. Existing therapies whether indicated or off-label comport unacceptable risk or are completely inappropriate (see response to 6.3 for further details). Therefore, it makes clinical sense to use the best agent as first-line treatment and avoid the harms associated with the drugs currently being used. It is the opinion of the group that lemborexant is the best and most effective agent now available in Canada.
How would this drug affect the sequencing of therapies for the target condition?
Current approved and non-approved therapies typically include Z-drugs, BZPs, antihistamines and antipsychotics. The risks of BZPs include habituation, tolerance and dependence and diversion to cognitive impairment, daytime sedation, memory and motor deficits, delirium, rebound insomnia. The risks of Z- drugs include habituation, tolerance and dependence, diversion, cognitive impairment, daytime sedation, rebound insomnia and complex sleep behaviors. Efficacy diminishes as early as in 4 weeks due to tolerance. In clinical practice not only are these drugs continued for much longer periods than indicated in the product monograph but doses are frequently escalated despite Health Canada alerts recommending reduction in dose to reduce next day impairment.
Antihistamines and antipsychotics are inappropriate and are associated with a multitude of physical health risks (cardiac, metabolic, neurological).
It is the opinion of the group that lemborexant should be offered as a first-line option to potentially prevent chronicity and refraction and reduce likelihood of physical and psychiatric comorbidities. See 7.1 for additional comments from the group.
Which patients would be best suited for treatment with the drug under review?
Given the prevalence of sleep disorders, it is probable that most patients presenting with these complaints in routine practice would benefit from treatment. Further, because of the high rates of comorbidity, both physical and psychiatric, insomnia disorder is a condition that requires assessment and treatment. See 7.1 for additional comments from the group.
How would patients best suited for treatment with the drug under review be identified?
Given the prevalence of s disorders patients are likely to present in routine clinical practice from family practice to specialist clinics. Appropriate clinical assessment is always required. In specialist and sleep clinics it is more likely that rating scales will be utilized but are not necessary for diagnosis. Identification of contributory/confounding factors is part of the clinical assessment. Pre- symptomatic does not really apply to this condition. The criteria for insomnia disorder are now formally defined in DSM-5. See 7.1 for additional comments from the group.
Which patients would be least suitable for treatment with the drug under review?
Patients that have a history of complex sleep behaviors; primary sleep disorders; genetic conditions such as Smith- Magenis syndrome; non-adherence; and treatment refraction. Patients unable or unwilling to implement sleep hygiene strategies. Lemborexant is contraindicated in patients with severe hepatic disease, and there are interactions with diltiazem and modafinil.
Is it possible to identify those patients who are most likely to exhibit a response to treatment with the drug under review?
It is likely that many patients with insomnia disorder would exhibit a positive response to lemborexant, and especially if medication naïve. Thus, the treatment should be a first-line pharmacotherapy choice before harmful alternatives such as Z-drugs and BZPs, to avoid risk of iatrogenic treatment refraction, physical harm including falls and dependence. Given the prevalence of insomnia disorder such patients presenting to physicians should be assessed for treatment.
What outcomes are used to determine whether a patient is responding to treatment in clinical practice?
Response in clinical practice is typically assessed by qualitative improvement in sleep (sleep diaries), day time alertness and functioning through self-report and collateral. Scales used in clinical practice include the with Insomnia Severity Index [ISI] and the Epworth Sleepiness Scale (ESS) which are both short questionnaires. Comorbidities are assessed with Patient Health Questionnaire [PHQ-9] and General Anxiety Disorder [GAD-7] as well as Clinically Useful Depression Outcome scale (CUDOS). The Sheehan Disability Scale (SDS) is used to assess functionality.
What would be considered a clinically meaningful response to treatment?
A clinically meaningful response to treatment would involve qualitative and quantitative improvement in sleep (sleep efficacy), daytime alertness and function, reduction in concomitant medications; improvement in associated relevant conditions, and patient satisfaction.
How often should treatment response be assessed?
Treatment response should be assessed at patient visits through self-report of sleep (supplemented by collateral where possible) and daytime functioning; supplemented with the use of rating scales in specialist clinics.
Side effects of treatment should also be assessed at patient visits. The frequency of adverse effects and side effect profile of lemborexant are both well established and favorable. It is not envisaged that there would be the need for any additional monitoring as it relates to this treatment (ie: blood tests or other interventions).
What factors should be considered when deciding to discontinue treatment?
Discontinuing or switching medications is something that should always be done cautiously and collaboratively taking into account previous treatment history and with a clear rationale. This may include poor or limited response, side effects, or drug-drug interactions. Alternative treatments should be carefully considered in terms of risk: benefit, cost and acceptability. Rebound insomnia is reported with almost all existing treatments but particularly GABA A agonists, and contributes to dependence and difficulty in switching from BZPs and Z-drugs. Lemborexant, given its MOA, is less likely to be associated with rebound insomnia and this is consistent with the clinical experience of the group. Guidance is also provided through the Canadian SwitchRx website.
What settings are appropriate for treatment with the drug under review?
Settings would include family practice, specialist community clinics (general psychiatric, sleep disorders, PTSD/veterans, addictions, women’s health, occupational medicine, neurology), hospital inpatients and outpatients.
For non-oncology drugs, is a specialist required to diagnose, treat, and monitor patients who might receive the drug under review?
Given that sleep disorders are prevalent and managed by many different specialities relevant reviewers should potentially include psychiatrists and family physicians, as well as pulmonologists and neurologists.
Additional information
Is there any additional information you feel is pertinent to this review?
The group have significant experience in dealing with sleep disorders and the management of complex patients. In discussions, clinicians have shared stories of lemborexant imparting life-changing outcomes for patients by improving cognition, minimizing polypharmacy, enabling significant weight loss, and reducing suicidal and homicidal ideation. Please see comments from the group as follows:
Dr. Walter Chow, a family physician from Victoria, BC, stated that the increasing prevalence of insomnia needs to be recognized, especially with the COVID-19 pandemic and its associated stressors.
Dr. Pierre Chue, a psychiatrist from Edmonton, AB, identified that safe and effective treatments for insomnia are lacking, specifically non-addictive medications.
Dr. Alain Sotto, a family physician from Toronto, ON, noted that many workplace accidents are caused by next-day impairment associated with use of benzodiazepines and Z-drugs—which is particularly important for patients who work as pilots, train engineers, etc. “I actually give a copy of the Health Canada warning to my patients, which states they should NOT drive for 12 hours after taking zopiclone 7.5 mg—all my patients are shocked that it’s actually written.”
Dr. Pieter Strauss, a psychiatrist from Abbotsford, BC, stated the need for insomnia to be viewed as a primary problem; moreover, clinicians should inquire about sleep at every patient visit.
Dr. Roger McIntyre, a psychiatrist from Toronto, ON, observed that, attitudinally, insomnia is often perceived as a diagnosis of later consideration rather than a diagnosis of priority consideration.
Dr. Tom Janzen, a family physician from London, ON, added that clinicians are taught that insomnia is a symptom of other conditions, yet a lack of healthy sleep can lead to other comorbidities.
Dr. Kaplan posited that treatments should be adjusted based on whether a patient is experiencing primary or comorbid insomnia.
Dr. McIntyre remarked that hypnotic medications are prescribed with impunity in Canada; therefore, safety index is a major unmet need in this space.
Dr. Chow emphasized that many clinicians are fearful of regulatory college oversight of benzodiazepines and Z-drugs prescribing practices; this can cause primary care clinicians to avoid prescribing these drugs entirely.
Dr. Alan Lowe, a psychiatrist from North York, ON, noted a lack of patient education; patients should better understand insomnia and the treatment options that are available beyond medications, such as cognitive behavioural therapy for insomnia (CBT-I). He added that patients who are educated about insomnia are less likely to self-medicate with substances such as alcohol and marijuana.
Dr. Kaplan noted that non-pharmacological therapies, such as CBT-I, generally lack availability and accessibility.
Dr. Michael Mak, a psychiatrist from Toronto, ON, acknowledged that patients with insomnia often require immediate treatment; consequently, clinicians need improved access to pharmacotherapy and CBT-I.
Dr. Ruzica Jokic, a psychiatrist from Kingston, ON, commented on the ambiguity of treatment duration recommendations in the presence of medical and psychiatric comorbidities.
Dr. Chue noted that patients often take concomitant medications and substances (e.g. alcohol, cannabis), which pose risks when combined with benzodiazepines and Z-drugs.
Dr. Boivin elaborated that understanding the safety of intermittent use of hypnotic medications is crucial, especially for shift work and atypical work schedules.
Dr. Jokic detailed concerns with long-term benzodiazepine and Z-drug use among the elderly due to comorbid conditions and negative effects on cognition, suggesting that clinicians move away from prescribing these drugs in this population.
Dr. Chow stated, “Elderly patients have that increased fall risk and are very sensitive to anticholinergic medications, especially in conjunction with the polypharmacy that they're already getting. So, in my experience, they do very well with lemborexant. And in some patients who still need their previous insomnia medication, I've been able to reduce doses drastically to a level where I'm more comfortable that I'm not adding more harm than good by trying to get them a good night's sleep.” Similarly, Dr. Chow identified increased fall risk and anticholinergic sensitivity—particularly with polypharmacy—as considerations specific to the elderly. Moreover, his elderly patients have fared well on lemborexant, as it has allowed for drastic reductions of other insomnia medications for a harm-reduction approach.
Dr. Boivin added that patients often use insomnia medications nightly for years, despite established recommendations for the shortest possible duration.
Dr. Kaplan commented that discontinuing benzodiazepines and Z-drugs is extremely difficult, as patients with tolerance experience withdrawal.
Dr. Janzen commented that the lemborexant MoA has unique properties compared to past substances.
Dr. Chue underscored that lemborexant may benefit from the current trend of emphasizing “natural” therapies (e.g. melatonin, marijuana) and that benzodiazepine and Z-drugs significantly impair cognition, emotion, and memory, which makes it difficult for patients to benefit from behavioural treatment and cognitive therapy. Conversely, lemborexant's lack of cognitive impairment allows for a combination of pharmacotherapy and an enhanced response to behavioural or cognitive therapy. “I see a lot of PTSD patients who are prescribed up to their ears with benzodiazepines and other Z-drugs to reduce some of that hypervigilance, arousal, and anxiety. Yet those very drugs actually impact negatively on the other interventions that we are trying to implement with this very difficult and damaged population.”
Dr. Kaplan highlighted that, unlike benzodiazepines and Z-drugs, lemborexant improves sleep architecture—including sleep stages 3, 4, and REM—which leads to improved recovery of both body and brain.
Dr. Jokic and Dr. Lowe emphasized that lemborexant improves daytime functioning and overall quality of life. Notably, patients with OSA are more compliant with their CPAP therapy since lemborexant helps with middle and late insomnia; this reduces downstream issues with CPAP non-compliance, such as increased risk of cardiovascular disease and/or psychiatric disorders.
From his occupational medicine practice, Dr. Sotto identified that business executives who travel extensively for work could benefit substantially from lemborexant. Currently, these patients use zopiclone 7.5 mg; however, they are often deterred by the associated 12-hour impairment after ingestion. Dr. Sotto highlighted the need for personalized therapy to meet the demands of each patient.
Dr. Boivin added that there is interest in lemborexant use to improve sleep-wake cycles in patients with circadian rhythm disorders—notably, shift workers, patients with psychiatric disorders, and patients with fibromyalgia.
Dr. Sotto highlighted that patients taking lemborexant 5 mg cannot drive for 7-9 hours compared to 12 hours with zopiclone; this is a significant difference that clinicians should balance against the needs of each patient’s lifestyle.
Dr. Strauss stated that many patients with insomnia are unaware of their degree of impairment from lack of sleep and fatigue. This may be due to comorbid anxiety and depression that prevents them from adequately addressing sleep or use of medications that cause severe daytime sedation. “I've seen with the patients that I've switched over or started treating de novo with lemborexant, how people say they are woken up and how they're suddenly finding themselves capable and that executive tasks take a shorter time. And I've already started seeing that self-confidence improves as a result of that.”
Dr. Lowe highlighted the uniqueness of lemborexant because, in addition to other sleep stages, it increases REM, which is important in many psychiatric conditions where REM and slow-wave sleep (SWS) are suppressed.
Dr. Lowe reported good results from lemborexant treatment—used in combination with other psychotropic agents—among his patients with chronic psychiatric conditions. Patients convey waking up more refreshed, which allows other psychotropic agents to be reduced.
Dr. Chue alluded to the link between insomnia and the development of significant inflammatory markers over time, including an increased risk of cancer. Therefore, insomnia is not only a disease process in and of itself, but also worsens other conditions and pathologies.
Dr. Boivin identified daytime functioning as the most important factor for successful insomnia management, rather than time-to-sleep onset and total sleep time. She acknowledged that patient reporting is subjective; however, patients' perception of their sleep is very important and a key goal of CBT-I.
Dr. Boivin further emphasized that the significance of overall patient functioning, which involves obtaining a history of their daily activities, asking how they feel about their sleep (e.g. are they anxious if they wake up in the night?), and asking how they function throughout the day.
Dr. Chow suggested that short- and long-term safety of a pharmacological treatment is important, particularly from a clinician's perspective.
Dr. Kaplan noted that successful insomnia management may improve other comorbid conditions in which insomnia is a secondary concern.
Dr. Sotto stated that the driving test data from the lemborexant safety study provided valuable information for patient use, as well as an indicator of next-day functioning.
Dr. Sotto identified the necessity of counselling for successful insomnia management, emphasizing that this is especially important for patients who have been taking benzodiazepines and Z-drugs. Patients require education that being “knocked out” by a GABA agonist does not equate to high quality sleep.
Dr. Jokic added that patients should be informed that they should observe improvements in thinking, attention, and concentration and, thus, work performance with better quality sleep.
Dr. Sotto stated, “The comment I wanted to bring to your list is I think we need to put patient counselling. Most people think that when you take a sleep drug, especially if they've been on benzos or Z-drugs, they think they're going to get hit on the head and knocked out. And that is a really bad misconception.
Lemborexant doesn't do that—it doesn’t block your GABA receptor. So you have to explain to the patient, you've been on Z-drugs for 10 years, I'm going to give you lemborexant, don't expect to get knocked out, it's not how it works. And once you educate them, I think that's really where the rubber meets the road.”
Dr. Jokic added that patients should be informed that they should observe improvements in thinking, attention, and concentration and, thus, work performance with better quality sleep.
Dr. Chue stated, “And if they're sleeping better then it's an opportunity to start looking at reduction in the medications that we've been utilizing to try and improve sleep or sedate. So, that can take some refining over time, depending on the number of medications and overall complexity.”
Dr. Mak responded that any pharmacologically-naïve patients or those who wish to move away from benzodiazepines or Z-drugs are ideal for lemborexant.
Dr. Kaplan emphasized that all patients with insomnia should be considered for lemborexant.
Dr. Sotto noted, “Perimenopausal women come in, they haven’t slept, they’re anxious, they’re flashing, they’re hot. They just come in as a disaster, and we do them a terrible disservice because we’re not treating their lack of sleep. So, I think they’re a prime example where lemborexant would be great.”
Dr. Lowe identified that patients with refractory insomnia and those with late insomnia should be considered for lemborexant.
In addition to patients who report sleep issues, Dr. Kaplan remarked that clinicians should also consider lemborexant for patients on long-term benzodiazepines or Z-drugs—oftentimes, these individuals do not recognize that they are impaired. To this end, Dr. Kaplan stated that he is proactively discussing lemborexant with all his patients on benzodiazepines or Z-drugs.
Dr. Mak added that patients waitlisted for CBT-I could be treated with lemborexant.
Dr. Lowe suggested that patients who are self-medicating with alcohol and/or marijuana would be good candidates for lemborexant.
Dr. Chow commented that he greets every patient in his clinical practice by asking them how they are managing through the COVID-19 pandemic and, if they are struggling, he asks them how they are sleeping. This simple introduction uncovers many patients with insomnia.
Dr. Kaplan underscored that all patients with chronic pain should be asked about their sleep quality, as poor sleep can worsen pain and vice versa. Additionally, many medications used for chronic pain are sedating, though that does not necessarily equate to high quality sleep. Moreover, combining benzodiazepines or Z-drugs with opioids for chronic pain treatment greatly increases the risk of overdose; he urged clinicians to balance pain severity against the risk of opioid misuse. Dr. Kaplan urged psychiatrists to consider a patient’s chronic pain medications when prescribing psychiatric medications, such as benzodiazepines or Z-drugs. Dr. Kaplan expressed excitement about lemborexant as it can help patients with chronic pain sleep without it being a sedative, which substantially decreases the risk of overdose. He recommends that this be a major point of emphasis for lemborexant use.
Dr. Kaplan expressed excitement about lemborexant as it can help patients with chronic pain sleep without it being a sedative, which substantially decreases the risk of overdose. He recommends that this be a major point of emphasis for lemborexant use.
Dr. Jokic concurred with Dr. Kaplan, noting that lemborexant can be combined safely with pregabalin for the treatment of fibromyalgia.
Dr. Sotto: given the effect improper sleep can have on other comorbidities, lemborexant is both life-sustaining and lifesaving and, therefore, should be covered.
Dr. Janzen commented that payors need to be informed of the population benefits of a successful insomnia medication to improve comorbidity burden (e.g. anxiety, depression, psychosis) and safety (e.g. preventing hip fractures). Additionally, it is necessary to outline to payors that by treating even a small percentage of people with insomnia, the risks associated with the current insomnia treatment options can be reduced significantly.
Dr. Lowe remarked that if payors wish to save costs, they need to fund medications that are safe, efficacious, and improve functional outcomes. In his practice, Dr. Lowe has begun observing improved CPAP compliance, which indirectly reduces costs (e.g. costs from cardiovascular events).
Dr. Sotto argued that, given the effect improper sleep can have on other comorbidities, lemborexant is both life-sustaining and lifesaving and, therefore, should be covered.
Dr. Kaplan noted a major benefit of lemborexant amongst his patients with chronic pain is that they now have a safe option for sleep that can be taken in combination with opioids; this is extremely important as sleep is necessary for pain management. “So, for me, lemborexant is revolutionary. Instead of using a medication with sleep as a side effect, we can use a medication that’s going to help their actual sleep.”
Dr. Jokic reported her patients with mood disorders feel less foggy, can think more clearly, are more active during the day, and can concentrate. However, it is difficult to objectively measure quality of life in clinical practice, so she relies on subjective patient-reported outcomes to assess daytime functioning and quality of life. “And for me, the biggest success is that people are actually re-engaging— going back to work, going back to school—and that is something that we can objectively measure with some scales that affect daytime function.”
Dr. Mak noted that he has had success switching long-term users of benzodiazepines and Z-drugs to lemborexant, particularly patients over 65 years or those with newly developed movement disorders.
Dr. Chow reported success with cross-titration. Patients who have been on high- dose benzodiazepines or Z-drugs for many years require a slower taper period. Furthermore, a broken sleep-and-wake switch justifies using reduced doses of sleep switch medications. Moreover, temporary co-administration of hypnotic medications and lemborexant during cross-titration has been proven by SwitchRx but should be individualized for each patient.
Dr. Jokic added that none of her patients taking lemborexant and benzodiazepines or Z-drugs in parallel have experienced any worsening of daytime functioning.
Dr. Chow stated, “I find with typical antipsychotics the taper is usually over a matter of weeks. With benzos and Z-drug hardcore users, it's a matter of months, sometimes taking down only by 10% every few weeks. I have been much more successful at harm reduction and getting them down on the doses of those less favourable medications, and lemborexant has really been able to help with that.”
Dr. Kaplan highlighted the issue of caffeine addiction in patients with insomnia, noting that lemborexant can help reduce this dependency. Many patients claim they need coffee to wake up; however, coffee carries health risks (e.g. atrial fibrillation).
Dr. Jokic reported that patients with treatment-resistant mood disorders describe improvements with lemborexant—they can read a book, can compose a sentence without losing their train of thought, and do not need reminders everywhere.
Dr. Kaplan added that patients who are sleeping better often report improved mood as measured by PHQ-9.
Dr. Kaplan added a personal story, stating that he travelled a lot prior to the pandemic. He has tried benzodiazepines and Z-drugs, which resulted in severe next-day sedation and impairment, so he is interested to see how lemborexant will improve travel.
Dr. Kaplan noted a major benefit of lemborexant amongst his patients with chronic pain is that they now have a safe option for sleep that can be taken in combination with opioids; this is extremely important as sleep is necessary for pain management. “So, for me, lemborexant is revolutionary. Instead of using a medication with sleep as a side effect, we can use a medication that’s going to help their actual sleep.”
Dr. Chow highlighted positive feedback from his patients, including that they fall asleep quicker, feel more refreshed and clear-headed in the morning, and do not need coffee to get rid of morning brain fog. Patients do not explicitly state that they fall less; however, Dr. Chow posits that this can be extrapolated.
Dr. Kaplan agreed that requiring less coffee is a subtle—but vital—indication of improvement.
Dr. Jokic reported her patients with mood disorders feel less foggy, can think more clearly, are more active during the day, and can concentrate. However, it is difficult to objectively measure quality of life in clinical practice, so she relies on subjective patient-reported outcomes to assess daytime functioning and quality of life. “And for me, the biggest success is that people are actually re-engaging— going back to work, going back to school—and that is something that we can objectively measure with some scales that affect daytime function.”
Dr. Mak noted that he has had success switching long-term users of benzodiazepines and Z-drugs to lemborexant, particularly patients over 65 years or those with newly developed movement disorders.
Dr. Strauss shared an anecdote of a patient who used trazodone for 20 years for sleep as part of her management for generalized anxiety disorder (GAD), social anxiety, PTSD, and major depressive disorder (MDD). Additionally, she had a history of comorbid alcohol dependence but had been abstinent for four years. The patient was morbidly obese with a poor quality of life. Dr. Strauss noted that initial attempts to switch this patient to lemborexant resulted in physical withdrawal (e.g. shivers, tremors, nausea). A second attempt was made with a more gradual trazodone taper. Lemborexant has been life-changing for this patient—she is social, feels more confident, is more cognitively capable, and lost 30 pounds from increased activity levels.
Dr. Chow shared a story of an elderly patient who previously used zopiclone nightly and lorazepam as needed. With oversight from the College of Physicians, the patient was gradually weaned from benzodiazepines and Z-drugs to amitriptyline, trazodone, and quetiapine as needed. The patient was also on tamsulosin and finasteride for urinary retention symptoms. The patient was cross-titrated off trazodone, quetiapine, and amitriptyline, in addition to stopping tamsulosin and finasteride due to urinary improvements. Dr. Chow commented that this highlights the anticholinergic side effects of many medications used in the elderly. With lemborexant, the patient went from five medications to one—a cost saving from the payor’s perspective.
Dr. Jokic recounted a high-functioning 60-year-old with severe depression with psychotic features requiring polypharmacy, including mirtazapine, olanzapine, and duloxetine. The patient encountered significant issues getting restorative sleep and experienced profound cognitive dysfunction. Dr. Jokic stopped mirtazapine, decreased the olanzapine dose, and added lemborexant. The patient’s functioning improved significantly; in addition to losing 20 pounds, they reported being able to exercise, read, and volunteer.
Dr. Lowe added that he sees patients with severe psychiatric disorders and OSA similar to Dr. Jokic's case. He has observed great success reducing symptoms of suicidal and homicidal ideation among this population with lemborexant treatment.
Dr. Chow commented that he provided lemborexant samples to his dentist; after three days of lemborexant use, they reported no impairments and felt clear-headed.
Dr. Boivin shared that she has provided lemborexant samples to her postmenopausal friends with sleep problems, and they have reported positive effects.
Conflict of Interest Declarations — National Advisory Board
To maintain the objectivity and credibility of the CADTH drug review programs, all participants in the drug review processes must disclose any real, potential, or perceived conflicts of interest. This conflict of interest declaration is required for participation. Declarations made do not negate or preclude the use of the clinician group input. CADTH may contact your group with further questions, as needed. Please see the Procedures for CADTH Drug Reimbursement Reviews (section 6.3) for further details.
Did you receive help from outside your clinician group to complete this submission? If yes, please detail the help and who provided it.
Eisai provided clinical trial data specific to lemborexant; organized the advisory panel with physicians nationwide and provided a summary of the discussions. Beyond the data provided, Eisai has not influenced the opinions provided in this submission, which remains entirely that of the contributory authors/advisory board members.
Did you receive help from outside your clinician group to collect or analyze any information used in this submission? If yes, please detail the help and who provided it.
See above.
List any companies or organizations that have provided your group with financial payment over the past two years AND who may have direct or indirect interest in the drug under review. Please note that this is required for each clinician that contributed to the input — please add more tables as needed (copy and paste). It is preferred for all declarations to be included in a single document.
Declaration for Clinician 1
Name: Dr. Pierre Chue
Position: Professor of Psychiatry, University of Alberta
Date: March 18, 2022
Table 6: COI Declaration for National Advisory Board — Clinician 1
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
Eisai | — | X | — | — |
Janssen | — | — | X | — |
Lundbeck | — | — | X | — |
Otsuka | — | — | X | — |
HLS | — | — | X | — |
Teva | X | — | — | — |
Declaration for Clinician 2
Name: Dr. Walter K. Chow
Position: B.Sc. (Pharmacy), MD. Family Physician
Date: March 2022
Table 7: COI Declaration for National Advisory Board — Clinician 2
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
Eisai | — | — | X | — |
Declaration for Clinician 3
Name: Dr. Kyle O. Lee
Position: Family Physician
Date: March 21, 2022
Table 8: COI Declaration for National Advisory Board — Clinician 3
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
Eisai Ltd. | — | X | — | — |
LiV CPD Network | X | — | — | — |
Ontario College of Family Physicians | X | — | — | — |
Elvium | X | — | — | — |
Janssen | X | — | — | — |
Bausch Health | X | — | — | — |
Touchstone Institute | X | — | — | — |
ICPDHM/CHRC | X | — | — | — |
Academy C.A.H.E. | X | — | — | — |
Declaration for Clinician 4
Name: Albert Ng
Position: Physician
Date: March 18, 2022
Table 9: COI Declaration for National Advisory Board — Clinician 4
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
AstraZeneca | — | X | — | — |
Boehringer | X | — | — | — |
Amgen | — | X | — | — |
Eisai | X | — | — | — |
Abbott | X | — | — | — |
Declaration for Clinician 5
Name: Tom Janzen, Parkwood Institute, London, Ontario
Position: Physician on Assessment Unit Mental Health and CMIO
Date: March 21, 2022
Table 10: COI Declaration for National Advisory Board — Clinician 5
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
Abbvie | — | X | — | — |
Otsuka | — | — | X | — |
Jannsen | — | X | — | — |
Takeda | — | — | X | — |
Eisai | — | X | — | — |
Lundbeck | — | — | X | — |
Declaration for Clinician 6
Name: Dr. Christine Palmay
Position: Consultant, Slide Deck – Sleep During Midlife Years and Beyond
Date: March 18, 2022
Table 11: COI Declaration for National Advisory Board — Clinician 6
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
Eisai | — | — | X | — |
Declaration for Clinician 7
Name: Lionel Noronha
Position: Family Physician
Date: March 18, 2022
Table 12: COI Declaration for National Advisory Board — Clinician 7
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
Astra Zeneca | X | — | — | — |
Takeda | X | — | — | — |
NovoNordisk | — | — | — | — |
ICI | X | — | — | — |
LivAgency | X | — | — | — |
Pfizer | X | — | — | — |
Amgen | — | X | — | — |
Merck | X | — | — | — |
Lily | — | — | X | — |
Abbott | X | — | — | — |
Janssen | X | — | — | — |
BMS | X | — | — | — |
CCRN | X | — | — | — |
Servier | X | — | — | — |
BI | X | — | — | — |
Otsuka | X | — | — | — |
Eisai | X | — | — | — |
Canadian Consortium of Sleep and Sleep Interested Physicians
About the Canadian Consortium of Sleep and Sleep interested Physicians
This clinician group is comprised of a network of senior clinicians across Canada who are specialists in or have a very strong interest in the treatment of sleep disorders. The group includes nationally and internationally known experts in sleep disorders, insomnia, mood, anxiety and attention deficit hyperactivity disorder (ADHD), who are extremely active in continuing medical education to public and professional audiences worldwide.
There are over 300 years of multi-disciplinary clinical experience among these clinicians that spans not only sleep medicine and insomnia, but general practice, psychology, psychiatry, neurology and respirology. All have significant experience with the evolution, strengths, and weaknesses of treatments in insomnia disorder with and without multiple comorbidities, as well as a keen awareness of the longstanding gaps in treatment options for our patients.
Clinicians in the group also represent a wide variety of treatment settings, including hospital, community, and private outpatient settings. All have academic appointments or university affiliations, and many are heavily involved in national and international research, clinical trials, as well as guideline development in insomnia and many of its major comorbid disorders. The group also includes feedback and research studies from the first recipient of the CIHR Distinguished Scientist Award for Insomnia Research. (CM)
Information Gathering
The information gathered for this submission was compiled from:
Significant group clinical experience with lemborexant in more than 1000 patients combined since its Health Canada indication and availability in December 2020.
A review of the pertinent research data on insomnia disorder, current treatments and lemborexant.
Please note that there are three separate document files with this submission:
The clinician input template
References
Financial disclosures
Current Treatments
Insomnia disorder has been shown to be an independent clinical entity with clear diagnostic criteria. (1) It has a very significant prevalence in Canada (over 13% with the disorder and 30-40% with symptoms) that is linked to medical and psychiatric illness as well as significant morbidity and health system costs. (2-4) Recent data put the estimated cost to the province of Quebec from insomnia alone at $6.6 billion yearly. (4) Insomnia disorder has also clearly shown to have a bidirectional relationship with multiple common comorbid medical and psychiatric comorbidities such as major depressive disorder (MDD) and chronic pain. (5) and the treatment of insomnia has been shown to improve these comorbid conditions. (6,7)
The first line therapy for insomnia disorder is cognitive behavior therapy (CBT-I), a short-term, sleep-focused, non-drug treatment. This includes sleep hygiene education, cognitive therapy, relaxation therapy, stimulus control and sleep restriction. The most critical parts of CBT-I appear to be the behavioral sleep scheduling procedures, including stimulus control and sleep restriction. (8,9) However, in the Canadian context delivering this treatment is severely limited by lack of publicly funded access and training, as well as the limited number of adequately trained health-care providers competent to deliver treatment. Although it is quite efficacious with few adverse effects, and great leaps have been made to deliver this service through telemedicine strategies and digital therapeutics, many patients cannot or choose not to do CBT-I as it takes significant effort and motivation. Up to 30% of patients also drop out of CBT-I therapy before finishing (10) and 30-35% of patients do not respond even after a full course of CBT-I treatment. (9,11) There may also be specific subtypes of insomnia that pharmacotherapy may be better suited for. (12, 13)
Hence, the current practical standard of care for community clinicians for the management of insomnia disorder in Canada is largely pharmacotherapy. Unfortunately, this currently consists of a small range of drugs with limited evidence of efficacy, effectiveness, safety warnings, or that are used off label. This leads to the lack of or inconsistent treatment of insomnia disorder. Thus newer, safer and well tolerated pharmacotherapeutic agents with good evidence are very necessary in the treatment paradigm for insomnia disorder.
Traditionally, the classes of drugs that are indicated by Health Canada for pharmacotherapy for insomnia have included the benzodiazepines and the benzodiazepine receptor agonists (BzRA) zopiclone, zolpidem, zaleplon and eszopiclone, which have a similar but more specific mechanism of action. Although there can be subtle differences between the BzRA in their subunit binding patterns, all the above drugs work as sleep promoters through the Gamma aminobutyric acid (GABA-A) receptor agonism. More recently, two agents that block wake promoting neurotransmitters have been indicated, doxepin, an antidepressant that selectively blocks histamine at very low doses, and the drug currently under review, the novel dual orexin receptor antagonist (DORA) lemborexant.
Though effective, there are significant challenges to treatment of insomnia disorder with the benzodiazepines and to a lesser degree the BzRA. They can confer a significant risk of adverse effects, such as delirium, falls, motor vehicle accidents, respiratory depression, cognitive impairment, memory issues as well as abuse, dependence, tolerance, and withdrawal symptoms with long-term use particularly in the elderly or medically ill. (14, 15) Insomnia disorder is also mostly a long-term chronic illness (16), yet treatment guidelines, as well as large groups such Choosing Wisely and deprescribing.org recommend against the use of these drugs in the long term. (8, 17-19)
And though the evidence does not completely support this, Health Canada monographs and regulatory colleges in many provinces have put punitive dispensing restrictions and excess monitoring on the benzodiazepines and BzRA, (20-25) making clinicians even more hesitant to treat insomnia disorder with them. Despite a better safety profile and promising data, low dose doxepin has not been proven to be widely successful in its clinical use and only has an indication for sleep maintenance. (26)
Because of these limitations, numerous drugs without Health Canada approval are routinely used in the treatment of insomnia and are often a first line treatment for many Canadian clinicians. Commonly used ones that have mixed recommendations include the hormone melatonin and the sedating antidepressant trazodone. (27,28) Many other off label agents are also utilized, and these include sedating antidepressants (mirtazapine, amitriptyline), other members of the benzodiazepine class (lorazepam, clonazepam), alpha-2 delta ligand anticonvulsants (gabapentin and pregabalin) and even the mostly inappropriate usage of low dose atypical antipsychotics (quetiapine, olanzapine, risperidone). Though guidelines indicate that these can be useful in insomnia disorder cases with significant comorbid illness or certain subpopulations, (27) evidence is scant and these are not recommended treatments. (8,17,18)
Poorly regulated over the counter (OTC) preparations containing doxylamine, dimenhydrinate and diphenhydramine are also used frequently in Canada (3) and can also lead to tolerance, dependence, falls and very deleterious cognitive side effects, especially in the elderly. (29-31) Surveys also indicate a high use of other substances such as alcohol and cannabis for insomnia. (32) Outside of very rare usage of cannabis for sleep difficulties associated with significant comorbidities, (33) the use of cannabis for insomnia disorder can be a dangerous practice, yet it is common and heavily promoted by the legalized retail and medical cannabis industry. All the above factors lead to a confusing landscape and at times mistreatment for Canadian patients suffering from insomnia disorder.
The underlying disease mechanisms of insomnia disorder are still being investigated and are complex and multifactorial. No pharmacological treatment appears to modify the disease mechanisms, and all medication treatment at this point should be considered symptomatic. However, early prompt treatment may reduce further chronicity and disability of insomnia disorder. (27) CBT-I directly targets the perpetuating factors contributing to the chronicity of the disorder and may thus be considered to partially modify the underlying mechanisms. (34) Other off label treatments may facilitate a reduction and improve insomnia symptoms by treating the underlying comorbidity and CBT-I has been shown to do this as well. (7, 35)
Treatment Goals
Current treatment guidelines for insomnia disorder are centered around 2 primary goals, to improve sleep continuity [i.e., nocturnal symptoms such as improving sleep onset, sleep maintenance by reducing awakenings and increasing the total sleep time (TST)] and to improve related daytime function through decreases in fatigue, impaired attention/concentration, disrupted mood, lack of motivation as well as impaired social and professional life impairments. (17).
By definition, treatment of insomnia disorder would not provoke adverse effects such as next day cognitive impairment, unsteadiness or behavioral abnormality occurring during sleep. Simply improving nocturnal symptoms is not adequate if not achieving an improvement overall daytime function. Normal sleep architecture should be preserved and restored as much as possible as well.
Insomnia is related to many adverse health consequences including depression, cardiovascular disease, hypertension, obesity, and neurodegenerative disease. (36-38) Optimal management of insomnia should also have a significant positive impact on burden on these diseases, overall occupational function, and health related quality of life.
Treatment Gaps (Unmet Needs)
Considering the treatment goals, please describe goals (needs) that are not being met by currently available treatments.
Insomnia is a multifactorial complex disease, and it is well known that not all patients respond to all treatments. Unfortunately given the currently indicated treatments, it has long been a “one size fits all” approach for the Canadian clinician which has not previously considered the variety of insomnia symptom types, mechanisms, and associated comorbidities.
As mentioned previously, CBT-I is an excellent first line treatment, but is often not accessible or acceptable to the patient and has a limited response rate even when used optimally. Hence pharmacotherapy will still be commonly used by Canadian clinicians either in tandem, after, or instead of this first line treatment. Many of the currently approved medications have potential side effects that limit their use in several populations. Long term efficacy is often undocumented and only 3 agents, lemborexant, eszopiclone and zolpidem have data of 6 months or more. (39-41)
Even when used properly as per the current evidence, current treatments such as benzodiazepines and to some extent the BzRA, commonly show a significant lack of response, tachyphylaxis and tolerance in clinical practice. Clinicians have not had a safe and endorsed treatment for chronic insomnia so prescribing scheduled drugs for lengths of time and at doses that guidelines and monographs mainly do not support, using off label agents or even trivializing and not treating insomnia occurs frequently. Given this and the wide use of OTC and substances by patients for sleep, it is quite clear outcomes are not being met in insomnia disorder. Treatments with better evidence on key outcomes with improved tolerability and safety are critical. Compliance with medication is typically not an issue, however both psychological and physical dependency with certain agents can be problematic.
Which patients have the greatest unmet need for an intervention such as the drug under review?
As noted above, could be argued that the majority of patients with insomnia disorder have an unmet need. Insomnia disorder is very common and presents frequently to the primary care physician. Almost one-third of visits to a family practice network were related to a sleep complaint and 11% met the criteria for insomnia disorder, (42) which is remarkably consistent with the Canadian population prevalence data of 30-35% for a sleep complaint and more than 13% for the disorder. (3) Equitable access to another accessible, tolerable, and efficacious approved treatment such as lemborexant is simply necessary to continue to give further options for the Canadian clinician to address this common and disabling complaint.
Particular groups of patients with a greater unmet need would include.
Groups at greater risk and prevalence of insomnia disorder. This includes women, shift workers, individuals with chronic pain, and patients with comorbid medical and psychiatric disorders such as depression, anxiety,
ADHD and bipolar disorder. (43-45) We have seen clinically favourable responses with lemborexant in all these groups.
The elderly and hospitalized patients. Older patients have a high rates of insomnia disorder that can lead to many deleterious outcomes such as falls, cognitive decline and dementia (46, 47). Only doxepin and lemborexant have shown safety and efficacy for insomnia disorder in this group. (48-50) Eszopiclone, a newer BzRA has some degree of efficacy and safety in the elderly, (51) but belongs to a class of medications that has proven troublesome in the past. There is also some thought that the mechanism of lemborexant would lead to more favourable response in the elderly as the insomnia disorder in this group may be more related to orexin dysfunction. (52) A trend towards increased efficacy has been seen in the clinical trial data (50) and this also fits the clinical experience of this group.
None of these agents are on public formulary in any Canadian province, which leads to suboptimal prescribing choices for insomnia disorder in the elderly. This is especially pertinent in hospital settings where many patients are given off label and even potentially dangerous agents for their insomnia. More equitable access to lemborexant and other medications with safety and efficacy data in the elderly would begin to address that for Canadian clinicians working with patients in acute and long term care facilities.
Patients with substance abuse, especially to alcohol or opiates: There are strong bidirectional relationships between substance abuse and insomnia (53) and sleep disturbances are a strong risk factor for relapse in substance use disorders. (54) Yet these patients have even more limited options as the benzodiazepines and BzRA drugs to a lesser degree can promote dependence and are usually not recommended for these groups of patients. Lemborexant has not been classified as a controlled substance by Health Canada and there is no evidence of potential or actual substance abuse issues with this drug, (55) hence it has become a natural option for these patients.
Patients on regularly prescribed opiate medications: The benzodiazepines (and BzRA drugs to a lesser degree) lead to potential increased risk for potentially lethal respiratory depression, mortality and severe respiratory events when used in conjunction with opiates. (56) Although there is no data yet in conjunction with opiates, lemborexant does not appear to have any impact on respiratory depression (57-59) and appears to have limited adverse effects at supratherapeutic doses consistent with potential overdose. (60) Lemborexant is often used clinically by this group as an option for treating insomnia in these patients.
Patients with chronic insomnia disorder requiring long term pharmacotherapy: As noted above, only three of the agents, zolpidem, eszopiclone and lemborexant have controlled trial data of greater than 6 months. (39-41). Lemborexant offers an additional option, as it has long term data up to 12 months. (61)
Patients under 18: There are no indicated treatments for insomnia disorder in this group.
Patients with comorbid insomnia and sleep apnea – Though the data does not always support this, especially for the BzRA drugs (62) Health Canada monographs indicate that both BzRA and benzodiazepines are relatively contraindicated in this group (20-23), limiting treatment options. The comorbidity of sleep apnea and insomnia (COMISA) is common and is likely a significant more indolent phenotype of the disease demonstrating higher rates of morbidity as well as risks of comorbid disorders such as depression and cardiovascular disease. (63-65) Although CBT-I is the first line treatment and has shown efficacy in this group, (66) clinically lemborexant has become a natural choice if pharmacotherapeutic treatment for COMISA is required because of the data showing no worsening of sleep apnea. (57-59)
Place in Therapy
How would the drug under review fit into the current treatment paradigm?
As noted above, lemborexant is a DORA (Dual Orexin Receptor Antagonist) which is a unique, novel, and more specific mechanism of action. It is part of a new evolving paradigm of medications with high pharmacological specificity to offer improved safety, efficacy, and more targeted symptom outcomes in insomnia disorder.
This competitive and transient dual orexin receptor antagonism targets a completely different cerebral network in comparison to other medications used both on and off label for insomnia. It directly and specifically targets the mechanism of high wakefulness and hyperarousal during the night which may be more related to the underlying disease process of insomnia disorder. It does this in a precise fashion without almost any other effect on other neurotransmitter areas. (67) This is in direct contrast to most other indicated agents that promote inhibitory neurotransmitters and/or crudely and non-specifically suppress indirect arousal mechanisms. It also appears to increase total sleep time in a more natural fashion by increasing REM sleep. (68) The clinical significance of this is unclear, but it may promote better memory and emotion regulation (69) and is direct contrast to the majority of commonly used sleep promoting drugs. (70)
Lemborexant is clearly a first line therapy for all patients with insomnia disorder that are offered pharmacotherapy. It has clinical trial data in comorbid and elderly populations demonstrating excellent efficacy/tolerability, a very low side effect profile, (39, 50, 71) no apparent tolerance, withdrawal, or dependence, (61) and limited overall next day effects even on driving. (72, 73) Lemborexant also demonstrates limited drug interactions and no change in dosing or adverse events is suggested in wide age and weight groups. (74, 75) Even though the FDA classified it as a schedule IV drug, there is no compelling evidence of abuse potential in theory (55) or seen in clinical trials. As noted earlier, Health Canada has not classified it as a controlled substance.
There is also clear response with lemborexant in severe insomnia, (76) and a reduction of next day fatigue. (77) Also, a recent meta-analysis evaluating a number of insomnia treatments indirectly indicated that lemborexant had the highest probability of being the best treatment for 3 of the 4 outcomes measured objectively by polysomnography. These were a measure of sleep onset, latency to persistent sleep (LPS), and two measures of overall sleep quality, the amount of time spent in bed in sleep, or sleep efficiency (SE) as well as total sleep time (TST). (78)
Our clinical experience has also mostly matched the above trial data and our group would also clearly consider lemborexant among one of the first agents to be used in insomnia disorder pharmacotherapy for all Canadian clinicians.
Although the unique mechanism of lemborexant would complement other insomnia pharmacotherapy, combination pharmacotherapy for insomnia disorder would be off label and saved for more resistant or comorbid patients. However, our group have found clinically that even though the other agent can’t often be discontinued, the dose can be lowered, lowering the risk profile. Pharmacotherapy can often complement CBT-I and may facilitate earlier insomnia remission (79,80). Extrapolation from other studies would the support concomitant use of lemborexant and CBT-I, given its unique mechanism of action and the lack of tolerance, rebound, and withdrawal. We have also seen clinically that the unique mechanism of lemborexant also complements other pharmacological treatments for common comorbid conditions such as depression and bipolar disorder by not interfering with the mechanism of action and not increasing side effects.
The availability and usage of lemborexant has already caused a shift towards better treatment of insomnia disorder in the current treatment paradigm. We have already seen fewer patients who are resorting to less proven riskier medications, cannabis, OTC medication and alcohol to help their symptoms. Lemborexant could also be considered benzodiazepine and BzRa “sparing” as previously clinicians would have no choice but to use these medications long term in an off-label fashion to treat the patient constantly having to weigh the risks of the agent versus treatment of the disorder.
Earlier, safer treatment of insomnia disorder has also been seen with the first line use of lemborexant which may reduce chronicity and the aforementioned consequences of the disease. More equitable access for lemborexant would further this paradigm shift. We also believe this is sustainable to the Canadian health care system because the agent is priced very competitively in this country for a new first in class agent with a unique mechanism, especially given the significant economic burden of insomnia. This group has had many patients who have had no qualms for paying out of pocket for lemborexant given the marked improvement in their functioning, cognition and limited next day side effects.
Please indicate whether or not it would be appropriate to recommend that patients try other treatments before initiating treatment with the drug under review. Please provide a rationale from your perspective.
Patients should always be offered or trialed on some form of CBT-I, or at the very least stimulus control and sleep restriction as a first line treatment, as this is an efficacious non-drug long term intervention with very few adverse effects. After this, given that major comorbidities have been assessed and treated, as noted above lemborexant would be a first choice pharmacotherapeutic treatment for all insomnia patients given the data on efficacy, tolerability, safety and potential unique mechanism of action that may be disease modifying.
The BzRA, especially eszopiclone, which has a wide variety of efficacy and safety data in multiple populations superior to the other insomnia medications (81,82) could be considered for short term/acute insomnia or second line treatment for chronic insomnia. Doxepin could be considered in the elderly if sleep maintenance is an issue. (49) Trazodone and melatonin have some guideline support and could be considered. (27,28) Other off label treatments could still be considered if there is a major comorbid condition to be treated (27), failure of the above treatments, or if financial access to newer agents is an issue.
How would this drug affect the sequencing of therapies for the target condition?
As mentioned above, lemborexant has allowed us to use treatments such as benzodiazepines, BzRa and off label treatments such as trazodone and mirtazapine later in therapy. The safety and tolerability profile of lemborexant and the DORA class clearly differs from those of more traditional sleep-promoting drugs. (83)
If lemborexant fails, the risk benefit ratio of other agents is more defensible for patients and clinicians. This drug could be used as a subsequent line of therapy if the patient is stable on current treatment and has been offered CBT-I initially or concomitantly. Off label combination use with other agents for sleep has proven to be useful clinically with lemborexant as well.
Which patients would be best suited for treatment with the drug under review?
Data formally identifying of subgroups that will preferably respond to lemborexant is still unclear. As this drug acts in a mechanism to “turn off the wake signal”, clinically it is hypothesized that it may work well for patients suffering states of hyperarousal, such as those with chronic pain, mood, anxiety, or trauma related conditions. The anxiety and trauma aspects may be particularly important due to the level of collective global societal traumas experienced during the COVID-19 pandemic and the significantly increased rates of insomnia disorder (more than 25% in one recent Quebec study) in Canada. (84)
Many of the other groups that would be clinically well suited to lemborexant have a great unmet need for treatments and have been outlined above in question 5.2. To reiterate this would include:
Patients who don’t respond, or are unable or unwilling to do CBT-I. – As noted above, this is a high percentage.
The elderly – Given the unsuitability of many other agents because of further cognitive impairment and fall risk. One entire study for Lemborexant was in patients aged 55+ (50) and there appears to be a trend towards a greater effect on sleep in the 65+ group in sub analyses of the clinical trials. This has matched our clinical experience.
Patients with comorbid neurodegenerative diseases – Orexin system dysfunction appears to be related to both Alzheimer’s disease and frontal temporal dementia. (85,86) Though this is a complex dynamic process that has yet to be fully clarified, it appears that transient competitive antagonism may help sleep in these patients as lemborexant has shown improvement in sleep disruption associated with Alzheimer’s disease. (87)
Individuals with comorbid substance abuse issues – There is emerging evidence linking orexin dysfunction with the biology of addiction (88, 89) and we have seen clinically that lemborexant uniquely helps some sleep issues in patients with comorbid substance abuse disorders that would have been excluded from clinical trial data sets.
Hospitalized or other patients at risk of falls – Recent data indicate very low rates of postural stability change in next day and middle of the of the night dosing with lemborexant. (90) It may even have an actual protective effect against falls in a hospitalized population (91) in direct contrast to almost any on and off label psychotropic medication used for sleep. (92) Increasing sleep time overall may also mitigate the fall risk seen with decreased sleep. (93)
Patients with untreated or potential obstructive sleep apnea (OSA) – As there is data for lemborexant not worsening or creating OSA regardless of severity (57-59).
Individuals who are on opiate painkillers – Because of this lack of worsening airway dynamics, lemborexant may also clinically suited to patients on opiate painkillers as noted in question 5.2.
Patients who have evidence of complex sleep related behaviours either de novo or from other agents. – This has been shown over 3% of patients on the BzRA zopiclone and zolpidem (94) and it is also outlined as a class effect warning in the monograph for the BzRA drugs. (20-23) Although vivid dreaming and nightmares have been reported with lemborexant, the agent has not shown any evidence of producing complex sleep related behaviours in the clinical trial data or in the clinical experience of this group.
Patients who wish to receive assistance in z-drug/benzodiazepine/sedative deprescribing due to emerging deleterious effects or lowering the potential risk of them. – A small clinical trial and our experience have noted that a significant number of patients can switch to lemborexant quite easily, (95) though slow cross titration can be necessary.
Actual disease characteristics that would indicate suitability for lemborexant treatment would be chronicity of disease given it is one of only two indicated sleep agents that has efficacy data for up to 12 months (40, 61). Given the reduction of hyperarousal by lemborexant, we have also found clinically that patients that have disorders of the arousal system (such as insomnia disorder comorbid with anxiety depression, bipolar disorders, ADHD, post-traumatic stress disorder (PTSD), and chronic pain syndromes appear to respond better.
How would patients best suited for treatment with the drug under review be identified?
The diagnosis of insomnia disorder is made with history taking, clinical examination and judgment. Although there are clear criteria, insomnia disorder is also a longitudinal illness often accompanied by many comorbid, sleep, medical and/or psychiatric disorders. (96, 97) The insomnia complaint can often be a risk factor, separate disorder or symptom of its major comorbidities as almost ¾ of patients have at least one major comorbidity. (1, 42) Patient reporting of subjective symptoms can be prone to selection and/or recall bias, hindering the diagnosis. Depending on training and experience there can be much variability in expert opinion on the interpretation of the contribution of insomnia disorder in a particular patient’s overall case. Subsequent over or under attribution to comorbid conditions often occurs.
There are no laboratory tests to diagnose insomnia disorder, however validated diagnostic tools have been developed such as the Insomnia Severity Index to assist diagnosis and treatment monitoring (98,99). There are also other scales to establish the likelihood of other sleep disorders that include the STOPBANG and Berlin questionnaire (sleep apnea), IRLS (restless legs syndrome) and the MEQ (circadian rhythm disorders). (100) Common comorbidities such as depression, anxiety, bipolar disorder, and ADHD need to be screened for as well and tools such as the PHQ-9, (depression) GAD-7, (anxiety), MDQ (bipolar disorder) and the ASRS (ADHD) can be used. (100) However, these are all subjective scales that lack specificity to create a diagnosis and there is variability in usage and stringent comorbidity screening. This does not preclude the treatment of insomnia, especially with CBT-I, but not assessing comorbidities can potentially greatly reduce the effectiveness of pharmacotherapy. Simple monitoring with sleep diaries and movement-based technologies is also popular clinically.
Often a polysomnogram or sleep study (PSG) is used to rule out other sleep disorders but is not recommended routinely for insomnia workup (97). Full PSG testing is superior in this facet, but not widely accessible in many parts of the country without cost or significant wait times. Home PSG testing is notoriously inaccurate in the setting of insomnia disorder and the overutilization of this can interfere with an insomnia workup and incorrectly judge the contribution of a breathing related sleep disorder, jeopardizing the order in which the insomnia disorder is treated.
Insomnia disorder is not challenging to diagnose properly in clinical practice, but a major issue is the lack of understanding of how its many medical, sleep and mental health comorbidities interact to ensure proper treatment. Misattribution often occurs in clinical practice, and it can take many years and the right consultations to clarify the correct diagnosis and comorbidities. System issues in diagnostic and treatment difficulties are related to a lack of primary care training, full PSG and insomnia specialist support in parts of Canada. The population of many provinces outside of Ontario often only have one or two centers that treat insomnia patients.
It is unclear if there is an insomnia prodrome, but early and prompt intervention with CBT-I or short-term medications in the acute phase intuitively can lessen disability in the future. (101)
Which patients would be least suitable for treatment with the drug under review?
Those who have not responded to multiple attempts with other agents (lemborexant may be tried, but expectations would be guarded) and who have not had formal behavioral sleep medicine interventions. Patients with a high degree of untreated comorbidity, pediatric patients as there are no data, or narcolepsy type illnesses that already lack orexin would not be suitable. Patients with nightmare disorder or REM sleep behaviour disorder may be less suitable, given that lemborexant has been seen to increase REM more than other classes of agents, (68) but clinically this has not always seen to be the case.
There is also no data for lemborexant in the transient insomnia patient that requires as needed sleep medication and the mechanism of action would likely be more suited to a chronic insomnia that requires regular pharmacotherapy.
Nonetheless, many of this group have found clinical success in off label as needed use, especially in shift workers.
Is it possible to identify those patients who are most likely to exhibit a response to treatment with the drug under review?
This sort of response specificity has remained elusive in insomnia disorder, although further work with more specific agents such as lemborexant as well as insomnia phenotypes may eventually change this. Since the mechanism of action of lemborexant is to transiently inhibit the wake and arousal system, intuitively patients who have this disruption may respond better. As previously noted, clinically this group has seen better responses in many areas where arousal is disrupted such as patients with insomnia and MDD, anxiety ADHD, PTSD, and fibromyalgia. The elderly may also have a type of insomnia that responds to the orexin blocking mechanism of action (52). The group has also seen that those without long term benzodiazepine or BzRA use may do somewhat better, indicating again the potential suitability of lemborexant as a first line therapy.
What outcomes are used to determine whether a patient is responding to treatment in clinical practice?
Outcomes used in clinical trials include objective measures of sleep on the PSG such as LPS, TST, wake after sleep onset (WASO) as well as similar variables calculated by subjective patient sleep diary measures. TST is thought to be most correlated to self-report next day function. (102)
The Insomnia Severity Index (ISI) is the most frequently used patient reported outcome to document treatment response and remission from insomnia in clinical trials. This scale correlates well with outcomes used in clinical practice which would be self-reports of improvement insomnia symptoms, sleep quality, nighttime wakening, amount of sleep, next day fatigue, and ultimately improvement in daytime functioning and quality of life. (99)
What would be considered a clinically meaningful response to treatment?
There has been significant lack of standardization of clinically meaningful outcome measures in insomnia clinical trials (103), and there may be a mismatch between subjective and objective definitions of response and remission. (104) However, when using the ISI, which is a 7-item patient-report scale with a maximum score of 28, a cutoff score above 8 or 10 have both been used insomnia disturbance, a score of below 8 is used to indicate absence of insomnia, and a score greater than 14 suggests moderate to severe insomnia (98, 99). In clinical trials of both CBT-I and pharmacologic agents, a change in the total ISI score of 7 or greater indicates a clinically meaningful improvement of insomnia symptom severity, whereas an absolute value on the total ISI score of below 8 points indicates a remission from insomnia. (99)
Although there can be great variability, commonly used definitions of objective response are a LPS or WASO of below 30 min, sleep efficiency over 80% as well as an increase of TST over 30 minutes. Lemborexant is equivalent or above clinically significant effect sizes for subjective and objective variables compared to other indicated pharmacotherapeutic agents for sleep (78, 105)
The magnitude of response to treatment can vary greatly by physician in insomnia disorder. Factors include recognition of insomnia disorder as a separate dimension that requires treatment, training in treatment modalities for insomnia, the ability to assess, screen and get major comorbidities treated, adherence to guideline-based therapy, therapeutic rapport with patient, as well as the availability of full PSG and CBT-I resources.
How often should treatment response be assessed?
This will depend on the severity. When treatment is initiated, response should be assessed every 2-4 weeks to monitor response, especially if concomitant CBT-I is being pursued or the medication is being tapered. If a patient remains stable, review every 3-6 months would be warranted. (27) Because of the lack of tolerance, long term side effects or apparent tachyphylaxis with lemborexant, assessment of treatment response in chronic insomnia may not need to be as frequent as it is with other agents such as benzodiazepines or BzRa drugs where the side effects and risks clearly worsen with age. (14)
What factors should be considered when deciding to discontinue treatment?
Factors to be considered include both level and stability of response and the key outcome how the sleep leads to improved next day function. Lack of response in this area would lead to discontinuing treatment. Conversely, a very positive response may also lead to consideration of discontinuing treatment if concomitant CBT-I has been used or if the response is longstanding and stable. Lemborexant has no evidence of physical withdrawal and can be stopped quickly making it much easier to discontinue treatment compared to the benzodiazepines and to a lesser extent BzRA. Stopping these drugs quickly can lead to numerous deleterious psychological effects and even seizures. (14) Other factors to consider in discontinuing lemborexant are uncommon adverse events such as excessive next day fatigue, disturbing dreams and rarely sleep paralysis. Off label additional treatment may be needed in resistant patients, but because of the unique mechanism of lemborexant that will be often in combination therapy with a traditional insomnia agent rather than instead of.
What settings are appropriate for treatment with the drug under review?
This is an oral tablet that does not need supervision. It can be taken in all settings (hospital inpatient/outpatient, community settings or at home by the patient)
For non-oncology drugs, is a specialist required to diagnose, treat, and monitor patients who might receive the drug under review?
No, as noted above, insomnia is an extremely common disorder. It presents in some fashion to most clinical specialties. Lemborexant is a safe, tolerable agent that is can easily be used by any physician that needs to treat insomnia with pharmacotherapy. Most commonly this would be the community family physician, psychiatrist, or sleep specialist. Given its favourable efficacy and safety in the elderly as well as evidence that it may help sleep in neurodegenerative conditions, geriatric physicians, hospitalists and internal medicine specialists may initiate treatment as well.
Additional Information
Lemborexant is a very safe, effective, and tolerable first line agent suitable for a wide age range of people years who suffer from insomnia, which is a serious and common condition that can lead to significant morbidity, mortality and health system costs if not adequately treated. This group strongly believes that the data for lemborexant accurately reflect our clinical experience and it has become a much needed and valuable 1st line pharmacotherapy for insomnia disorder in a wide variety of settings. It is easy to prescribe and is competitively priced for a first in class agent with this level of efficacy and safety.
Lemborexant has been found to be very helpful alone or in combination to treat those with severe chronic refractory insomnia associated with medical and psychiatric comorbidities. Patients often will report “the most natural sleep I have had,” “felt the most rested I have ever felt,” and “finally I have gotten the sleep I have been wanting for so long.” Significant improvements in function and return to work from disability has been seen a number of times. Clinicians themselves suffering with insomnia have also been started on this agent and reported similar benefits.
More equitable access to this agent will allow better and earlier treatment of insomnia disorder and help reduce the current byzantine pantheon of off label medication, OTC and chemical usage of treatments for insomnia disorder that has far more deleterious effects on the patient and the health care system both directly and indirectly.
Conflict of Interest Declarations — Canadian Consortium of Sleep and Sleep interested Physicians
To maintain the objectivity and credibility of the CADTH drug review programs, all participants in the drug review processes must disclose any real, potential, or perceived conflicts of interest. This conflict of interest declaration is required for participation. Declarations made do not negate or preclude the use of the clinician group input. CADTH may contact your group with further questions, as needed. Please see the Procedures for CADTH Drug Reimbursement Reviews (section 6.3) for further details.
No.
Did you receive help from outside your clinician group to complete this submission?
No.
Did you receive help from outside your clinician group to collect or analyze any information used in this submission.
Not applicable.
List any companies or organizations that have provided your group with financial payment over the past two years AND who may have direct or indirect interest in the drug under review. Please note that this is required for each clinician who contributed to the input — please add more tables as needed (copy and paste). It is preferred for all declarations to be included in a single document.
Declaration for Clinician 1
Name: Pierre Blier, MD, PhD
Position: Professor, Department of Psychiatry, University of Ottawa
Date: March 17, 2022
Table 13: COI Declaration for CCSSP — Clinician 1
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
Eisai | — | — | X | — |
Lundbeck/Otsuka | — | — | X | — |
Eisai | — | — | X | — |
Declaration for Clinician 2
Name: Thien Thanh Dang Vu
Position: Neurologist, Professor
Date: March 2, 2022
Table 14: COI Declaration for CCSSP — Clinician 2
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
Eisai | — | X | — | — |
Declaration for Clinician 3
Name: Alex Desautels
Position: Clinical assistant professor, University of Montreal; Medical Director, Center for Advanced Research in Sleep Medicine Hôpital du Sacré-Coeur de Montréal
Date: March 9, 2022
Table 15: COI Declaration for CCSSP — Clinician 3
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
Jazz Pharma | X | — | — | — |
Paladin Labs | X | — | — | — |
Sunovion | X | — | — | — |
UCB Pharma | X | — | — | — |
Eisai | X | — | — | — |
Biron | — | — | X | — |
Canopy Growth | — | — | X | — |
CIHR | — | — | — | X |
American Academy Sleep Medicine | — | — | — | X |
Canadian Heart and Stroke Foundation | — | — | — | X |
Declaration for Clinician 4
Name: Raymond Gottschalk
Position: Consultant
Date: March 24, 2022
Table 16: COI Declaration for CCSSP — Clinician 4
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
Eisai | — | X | — | — |
Paladin Labs. | — | X | — | — |
Jazz Pharmaceuticals | — | X | — | — |
Declaration for Clinician 5
Name: Jeffrey Habert, MD, CCFP, FCFP
Position: Assistant Professor, University of Toronto, Department of Family and Community Medicine
Date: 12/03/2022
Table 17: COI Declaration for CCSSP — Clinician 5
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
Sunovion, Novartis, Astra-Zeneca, HLS, Bayer, Lundbeck | X | — | — | — |
Eisai, Pfizer, Purdue, Lilly, Amgen, Abbvie | — | X | — | — |
Novo Nordisk, Otsuka | — | X | — | — |
Declaration for Clinician 6
Name: Martin Katzman
Position: Professor; Clinical Director
Date: March 25, 2022
Table 18: COI Declaration for CCSSP — Clinician 6
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
START Clinic for Mood and Anxiety Disorders | — | — | — | X |
Adler Graduate Professional School | — | — | X | — |
Northern Ontario School of Medicine | — | X | — | — |
University of Toronto | X | — | — | — |
Abbvie | — | — | X | — |
Biron | — | X | — | — |
Alefia Cannabis | X | — | — | — |
Allergan | — | — | X | — |
Bausch Health | — | X | — | — |
Canopy | X | X | — | — |
Eisai | — | — | X | — |
Elvium | — | X | — | — |
Empower Cannabis | X | — | — | — |
Lundbeck | — | — | X | — |
Janssen | — | — | X | — |
Eli Lilly | X | — | — | — |
Novartis | X | — | — | — |
Merck | X | — | — | — |
Otsuka | — | X | — | — |
Pfizer | X | — | — | — |
Purdue | X | — | — | — |
Sante Cannabis | X | — | — | — |
Shire | X | — | — | — |
Sunovion | — | X | — | — |
Takeda | — | X | — | — |
Tilray | — | X | — | — |
AstraZeneca | X | — | — | — |
Biotics | X | — | — | — |
Canadian Foundation for Innovation | — | — | X | — |
Lotte & Hecht Memorial Foundation | — | X | — | — |
One Datapoint patent pending | X | — | — | — |
Echo Touch patent pending | X | — | — | — |
Declaration for Clinician 7
Name: Atul Khullar, MD, MSc, FRCPC, DABPN, DABSM, DABOM
Position: Clinical Associate Professor, University of Alberta Dept of Psychiatry
Date: Feb 8, 2022
Table 19: COI Declaration for CCSSP — Clinician 7
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
Abbvie/Allergan | — | X | — | — |
Sunovion | — | — | X | — |
Otsuka | — | X | — | — |
Lundbeck | — | X | — | — |
Jazz Pharma | — | X | — | — |
Paladin Pharma | X | — | — | — |
Pfizer | X | — | — | — |
Takeda | X | — | — | — |
Bausch Health | — | — | X | — |
Eisai | — | X | — | — |
Elvium | — | — | X | — |
Declaration for Clinician 8
Name: Serge Lessard
Position: Medical director introspect research centre
Date: March 22, 2022
Table 20: COI Declaration for CCSSP — Clinician 8
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
Allergan - research | — | — | — | X |
Abbvie, eisai, elvium, Lundbeck, takeda | — | — | X | — |
Astra Zeneca, Bausch, Biron, Jazz, Otsuka,Sunovion | X | — | — | — |
Declaration for Clinician 9
Name: Alan Lowe
Position: Assistant Professor, University of Toronto; Psychiatry Staff, North York General Hospital
Date: March 2022
Table 21: COI Declaration for CCSSP — Clinician 9
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
Jazz Pharma | X | — | — | — |
Paladin Labs | X | — | — | — |
Eisai | — | — | X | — |
Sunovion | — | X | — | — |
Declaration for Clinician 10
Name: Michael Mak
Position: Psychiatrist
Date: March 19, 2022
Table 22: COI Declaration for CCSSP — Clinician 10
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
Eisai | — | X | — | — |
Sunovion | X | — | — | — |
Janssen | — | — | — | — |
Otsuka | — | X | — | — |
Paladin | X | — | — | — |
Declaration for Clinician 11
Name: Roger McIntyre
Position: Psychiatrist
Date: March 19, 2022
Table 23: COI Declaration for CCSSP — Clinician 11
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
Lundbeck, Janssen, Alkermes, Pfizer | — | X | — | — |
Mitsubishi Tanabe, Novo Nordish, Kris | — | X | — | — |
Purdue, Otsuka, Takeda, Neurocrine | — | X | — | — |
Sunovion, Bausch Health, Axsome, Sanofi | — | X | — | — |
Eisai, Intra-Cellular, Abbvie, Atai Life Sciences, NewBridge Pharmaceuticals | — | X | — | — |
Declaration for Clinician 12
Name: Charles Morin
Position: Professor of Psychology, Director, Sleep Research Center, and Canada Research; Chair in Behavioural Sleep Medicine, Université Laval
Date: March 22, 2022
Table 24: COI Declaration for CCSSP — Clinician 12
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
Lallemand Health (Research Contract) | — | — | — | X |
Eisai (Unrestricted Grant) | — | — | — | X |
Eisai, Idorsia, Pear Therapeutics | — | X | — | — |
Eisai, Idorsia | X | — | — | — |
Mapi Research Trust | — | — | X | — |
Declaration for Clinician 13
Name: Roumen Milev
Date: March 2, 2022
Table 25: COI Declaration for CCSSP — Clinician 13
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
AbbVie | X | — | — | — |
Allergan Canada | X | — | — | — |
Sunovion Canada | X | — | — | — |
Janssen Canada | X | — | — | — |
Nubiyota | — | — | — | X |
Lallemand Canada | — | — | — | X |
CAN-BIND/OBI | — | — | — | X |
CIHR | — | — | — | X |
Pfizer Canada | X | — | — | — |
Lundbeck Canada | X | — | — | — |
Neonmind | X | — | — | — |
Otsuka Canada | X | — | — | — |
KYE | X | — | — | — |
Declaration for Clinician 14
Name: Charles H. Samuels
Position: Medical Director, Centre for Sleep and Human Performance
Date: March 9, 2022
Table 26: COI Declaration for CCSSP — Clinician 14
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
Jazz Pharmaceuticals | X | — | — | — |
Paladin Pharmaceuticals | X | — | — | — |
Sunovion Pharmaceuticals | X | — | — | — |
Cerebra Health | X | — | — | — |
Eisai Pharmaceuticals | — | — | X | |
University of Calgary Faculty of Medicine | X | — | — | — |
Royal Canadian Mounted Police | X | — | — | — |
College of Physicians and Surgeons of Alberta | — | — | X | — |
Declaration for Clinician 15
Name: Jennifer Swainson
Position: Associate Clinical Professor Dept of Psychiatry University of Alberta; Psychiatrist, Misericordia Community Hospital
Date: Feb 15, 2022
Table 27: COI Declaration for CCSSP — Clinician 15
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
Otsuka | X | — | — | — |
Sunovion | X | — | — | — |
Eisai | X | — | — | — |
Janssen | — | — | X | — |
Lundbeck | — | X | — | — |
Allergan | X | — | — | — |
References Supporting CADTH Position Statement
1. Diagnostic and Statistical Manual of Mental Disorders: DSM-5. 5th Ed. American Psychiatric Association, 2013. DSM-V, doi-org.db29.linccweb.org/10.1176/appi.
2. Morin CM, LeBlanc M, Daley M, Grégoire JP, Mérette C. Epidemiology of insomnia: Prevalence, self-help treatments, consultations, and determinants of help-seeking behaviors. Sleep Med. 2006 Mar;7(2):123-130. doi:10.1016/j.sleep.2005.08.008.
3. Morin CM, LeBlanc M, Bélanger L, Ivers H, Mérette C, Savard J. Prevalence of Insomnia and its treatment in Canada. Can J Psychiatry. 2011 Sep;56(9):540-8. doi: 10.1177/070674371105600905.
4. Daley M, Morin CM, LeBlanc M, Grégoire JP, Savard J. The economic burden of insomnia: direct and indirect costs for individuals with insomnia syndrome, insomnia symptoms, and good sleepers. Sleep. 2009 Jan 1;32(1):55-64. PMID: 19189779.
5. Rosenberg RP. The bidirectional relationship between insomnia and comorbid disorders. J Clin Psychiatry. 2021 Mar 16;82(2):EI20008BR2C. doi: 10.4088/JCP.EI20008BR2.
6. Reddy MS, Chakrabarty A. "Comorbid" insomnia. Indian J Psychol Med. 2011 Jan;33(1):1-4. doi: 10.4103/0253-7176.85388.
7. Wu JQ, Appleman ER, Salazar RD, Ong JC. Cognitive behavioral therapy for insomnia comorbid with psychiatric and medical conditions: a meta-analysis. JAMA Intern Med. 2015 Sep;175(9):1461-72. doi: 10.1001/jamainternmed.2015.3006.
8. Riemann D, Baglioni C, Bassetti C, et al. European guideline for the diagnosis and treatment of insomnia. J Sleep Res. 2017 Dec;26(6):675-700. doi:10.1111/jsr.12594.
9. Edinger JD, Arnedt JT, Bertisch SM, Carney CE, Harrington JJ, Lichstein KL, Sateia MJ, Troxel WM, Zhou ES, Kazmi U, Heald JL, Martin JL. Behavioral and psychological treatments for chronic insomnia disorder in adults: an American Academy of Sleep Medicine systematic review, meta- analysis, and GRADE assessment. J Clin Sleep Med. 2021 Feb 1;17(2):263-298. doi: 10.5664/jcsm.8988.
10. Harvey AG, Tang KY. Cognitive behaviour therapy for primary insomnia: can we rest yet. Sleep Med Rev 2003;7(3):237-62. doi: 10.1053/smrv.2002.0266.
11. Morin CM, Vallières A, Guay B, et al. Cognitive behavioral therapy, singly and combined with medication, for persistent insomnia: a randomized controlled trial. JAMA. 2009 May 20;301(19):2005-2015. doi:10.1001/jama.2009.682.
12. Vgontzas AN, Fernandez-Mendoza J. Insomnia with short sleep duration: nosological, diagnostic, and treatment implications. Sleep Med Clinics. 2013 Sep 1;8(3):309-322. doi:10.1016/j.jsmc.2013.04.009.
13. Vgontzas AN, Fernandez-Mendoza J, Liao D, Bixler EO. Insomnia with objective short sleep duration: the most biologically severe phenotype of the disorder. Sleep Med Rev. 2013 Aug;17(4):241-254. doi:10.1016/j.smrv.2012.09.005.
14. Brandt J, Leong C. Benzodiazepines and Z-drugs: an updated review of major adverse outcomes reported on in epidemiologic research. Drugs R D 2017 Dec;17(4):493-507. doi: 10.1007/s40268-017-0207-7.
15. Canadian guidelines on benzodiazepine receptor agonist use disorder among older adults. Toronto, ON: Canadian Coalition for Seniors’ Mental Health; 2019. 26 p. Available from: http://ccsmh.ca/wp-content/uploads/2019/11/Benzodiazepine_ Receptor_Agonist_Use_Disorder_ENG.pdf
16. Morin CM, Jarrin DC, Ivers H, Mérette C, LeBlanc M, Savard J. Incidence, persistence, and remission rates of insomnia over 5 Years. JAMA Netw Open. 2020;Nov 2;3(11):e2018782. doi:10.1001/jamanetworkopen.2020.18782.
17. Sateia MJ, Buysse D, Krystal AD, Neubauer DN, Heald JL. Clinical practice guideline for the pharmacologic treatment of chronic insomnia in adults: an American Academy of Sleep Medicine clinical practice guideline. J Clin Sleep Med. 2017;13(2):307-49. doi:10.5664/jcsm.6470
18. Choosing Wisely Canada. Canadian Deprescribing Network. Drowsy without feeling lousy: a toolkit for reducing inappropriate use of benzodiazepines and sedative-hypnotics among older adults in primary care. 2019. Version 1.1. [Internet]. https://choosingwiselycanada.org/wp- content/uploads/2017/12/CWC-Toolkit-BenzoPrimaryCare-V3.pdf
19. Deprescribing.org. Is a benzodiazepine or Z-drug still needed for sleep? 2018. [Internet]. https://deprescribing.org/wp-content/uploads/2018/08/benzodiazepine-deprescribing- information-pamphlet.pdf
20. Health Canada. Health Canada Advisories: Benzodiazepines (CPhA Monograph). https://www.psychdb.com/_media/meds/benzos/benzodiazepines_cpha_monograph_.pdf
21. Health Canada. Drug Product Database. [Internet]. Imovane (zopiclone). https://pdf.hres.ca/dpd_pm/00058189.pdf
22. Health Canada. Drug Product Database. [Internet]. Sublinox (zolpidem). https://pdf.hres.ca/dpd_pm/00052044.pdf
23. Health Canada. Drug Product Database. [Internet]. Lunesta (eszopiclone). https://pdf.hres.ca/dpd_pm/00055610.pdf
24. College of Physicians and Surgeons of British Columbia. Practice Standards. 2022. Safe Prescribing of Opioids and Sedatives. Version 4.6. [Internet]. https://www.cpsbc.ca/files/pdf/PSG-Safe-Prescribing.pdf
25. College of Physicians & Surgeons of Manitoba. Standard of Practice. 2020. Prescribing Benzodiazepines & Z-Drugs (including Zopiclone & other drugs). [Internet]. https://cpsm.mb.ca/assets/Standards%20of%20Practice/Standard%20of%20Practice%20Pres cribing%20Benzodiazepines%20and%20Z-Drugs.pdf
26. Health Canada. Drug Product Database. [Internet]. Silenor (doxepin). https://pdf.hres.ca/dpd_pm/00018598.pdf
27. Toward Optimized Practice. Clinical Practice Guideline. Assessment to management of adult insomnia. December 2015. Available from: www.topalbertadoctors.org/download/1920/Adult%20Insomnia%20CPG.pdf?_2016052707210 6.
28. Wilson SJ, Anderson K, Baldwin D et al. British Association for the Psychopharmacology consensus statement on evidence-based treatment of insomnia, parasomnias and circadian rhythm disorders: an update. J Psychopharmacol 2019;33(8):923–47. doi: 10.1177/0269881119855343.
29. Bahji A, Kasurak E, Sterling M, et al. Misuse and dependence of dimenhydrinate: A mixed studies systematic review. J Psychiat Res. 2020 Oct 30:S0022-3956(20)31035-9. doi: 10.1016/j.jpsychires.2020.10.032.
30. Abraham O, Schleiden L, Albert SM. Over-the-counter medications containing diphenhydramine and doxylamine used by older adults to improve sleep. Int J Clin Pharm 2017 Aug;39(4):808-17. doi: 10.1007/s11096-017-0467-x.
31. Albert SM, Roth T, Toscani M, Vitiello MV, Zee P. Sleep health and appropriate use of OTC sleep aids in older adults-recommendations of a Gerontological Society of America workgroup. Gerontologist. 2017 Apr 1;57(2):163-170. doi: 10.1093/geront/gnv139.
32. Goodhines PA, Gellis LA, Ansell EB, Park A. Cannabis and alcohol use for sleep aid: A daily diary investigation. Health Psychol. 2019 Nov;38(11):1036-1047. doi: 10.1037/hea0000765.
33. Health Canada. 2018. Cannabis (marihuana, marijuana) and the cannabinoids (dried or fresh plant and oil administration by ingestion or other means; psychoactive agent). [Internet]. https://www.canada.ca/content/dam/hc-sc/documents/services/drugs- medication/cannabis/information-medical-practitioners/information-health-care-professionals- cannabis-cannabinoids-eng.pdf
34. Morin CM, Drake CL, Harvey AG, et al. Insomnia disorder. Nat Rev Dis Primers. 2015;1:1-18. doi:10.1038/nrdp.2015.26.
35. Geiger-Brown JM, Rogers VE, Liu W, Ludeman EM, Downton KD, Diaz-Abad M. Cognitive behavioral therapy in persons with comorbid insomnia: a meta-analysis. Sleep Med Rev. 2015 Oct;23:54-67. doi:10.1016/j.smrv.2014.11.007.
36. Buysse DJ. Insomnia. JAMA. 2013 Feb 20;309(7):706-16. doi: 10.1001/jama.2013.193.
37. Daley M, Morin CM, LeBlanc M, Gregoire JP, Savard J, Baillargeon L. Insomnia and its relationship to health-care utilization, work absenteeism, productivity and accidents. Sleep Med. 2009 Apr;10(4):427-438. doi:10.1016/j.sleep.2008.04.005.
38. Sivertsen B, Overland S, Neckelmann D, et al. The long-term effect of insomnia on work disability: the HUNT-2 historical cohort study. Am J Epidemiol 2006;163:1018-24. doi: 10.1093/aje/kwj145.
39. Kärppä M, Yardley J, Pinner K, et al. Long-term efficacy and tolerability of lemborexant compared with placebo in adults with insomnia disorder: results from the phase 3 randomized clinical trial SUNRISE 2. Sleep. 2020 Sep 14;43(9):zsaa123. doi: 10.1093/sleep/zsaa123.
40. Roth T, Walsh JK, Krystal A et al. An evaluation of the efficacy and safety of eszopiclone over 12 months in patients with chronic primary insomnia. Sleep Med. 2005 Nov;6(6):487-95. doi: 10.1016/j.sleep.2005.06.004.
41. Roehrs TA, Randall S, Harris E, et al. Twelve months of nightly zolpidem does not lead to rebound insomnia or withdrawal symptoms: a prospective placebo-controlled study. J Psychopharmacol 2012 Aug;26(8):1088-95. doi: 10.1177/0269881111424455.
42. Maire M, Linder S, Dvořák C, Merlo C, Essig S, Tal K, Del Giovane C, Syrogiannouli L, Duss SB, Heinzer R, Nissen C, Bassetti CLA, Auer R. Prevalence and management of chronic insomnia in Swiss primary care: Cross-sectional data from the "Sentinella" practice-based research network. J Sleep Res. 2020 Oct;29(5):e13121. doi: 10.1111/jsr.13121.
43. Singareddy R, Vgontzas AN, Fernandez-Mendoza J, Liao D, Calhoun S, Shaffer ML, Bixler EO. Risk factors for incident chronic insomnia: a general population prospective study. Sleep Med. 2012 Apr;13(4):346-53. doi: 10.1016/j.sleep.2011.10.033.
44. LeBlanc M, Mérette C, Savard J, Ivers H, Baillargeon L, Morin CM. Incidence and risk factors of insomnia in a population-based sample. Sleep. 2009 Aug;32(8):1027-37. doi: 10.1093/sleep/32.8.1027.
45. Roth T. Insomnia: definition, prevalence, etiology, and consequences. J Clin Sleep Med. 2007 Aug 15;3(5 Suppl):S7-10. PMID: 17824495.
46. Avidan AY, Fries BE, James ML, Szafara KL, Wright GT, Chervin RD. Insomnia and hypnotic use, recorded in the minimum data set, as predictors of falls and hip fractures in Michigan nursing homes. J Am Geriatr Soc. 2005 Jun;53(6):955-62. doi: 10.1111/j.1532-5415.2005.53304.x.
47. Cross NE, Carrier J, Postuma RB, Gosselin N, Kakinami L, Thompson C, Chouchou F, Dang-Vu TT. Association between insomnia disorder and cognitive function in middle-aged and older adults: a cross-sectional analysis of the Canadian Longitudinal Study on Aging. Sleep. 2019 Aug 1;42(8):zsz114. doi: 10.1093/sleep/zsz114.
48. Yeung W-F, Chung K-F, Yung K-P, et al. Doxepin for insomnia: a systematic review of randomized placebo-controlled trials. Sleep Med Rev. 2015 Feb;19:75-83. doi: 10.1016/j.smrv.2014.06.001.
49. Rojas-Fernandez CH, Chen Y. Use of ultra-low-dose (≤6 mg) doxepin for treatment of insomnia in older people. Can Pharm J (Ott). 2014 Sep;147(5):281-9. doi: 10.1177/1715163514543856.
50. Rosenberg R, Murphy P, Zammit G, et al. Comparison of lemborexant with placebo and zolpidem tartrate extended release for the treatment of older adults with insomnia disorder. JAMA Netw Open 2019 Dec 27;2(12):e1918254. doi: 10.1001/jamanetworkopen.2019.18254.
51. Ancoli-lsrael S, Krystal AD, McCall WV, et al. A 12-week, randomized, double-blind, placebo-controlled study evaluating the effect of eszopiclone 2 mg on sleep/wake function in older adults with primary and comorbid insomnia. Sleep 2010 Feb;33(2):225-34. doi: 10.1093/sleep/33.2.225.
52. Nixon JP, Mavanji V, Butterick TA, Billington CJ, Kotz CM, Teske JA. Sleep disorders, obesity, and aging: the role of orexin. Ageing Res Rev. 2015 Mar;20:63-73. doi: 10.1016/j.arr.2014.11.001.
53. Pasman JA, Smit DJA, Kingma L, Vink JM, Treur JL, Verweij KJH. Causal relationships between substance use and insomnia. Drug Alcohol Depend. 2020 Sep 1;214:108151. doi: 10.1016/j.drugalcdep.2020.108151.
54. Fortuna LR, Cook B, Porche MV, Wang Y, Amaris AM, Alegria M. Sleep disturbance as a predictor of time to drug and alcohol use treatment in primary care. Sleep Med. 2018 Feb;42:31-37. doi: 10.1016/j.sleep.2017.12.009.
55. Asakura S, Shiotani M, Gauvin DV, Fujiwara A, Ueno T, Bower N, Beuckmann CT, Moline M. Nonclinical evaluation of abuse liability of the dual orexin receptor antagonist lemborexant. Regul Toxicol Pharmacol. 2021 Dec;127:105053. doi: 10.1016/j.yrtph.2021.105053.
56. Boon M, van Dorp E, Broens S, Overdyk F. Combining opioids and benzodiazepines: effects on mortality and severe adverse respiratory events. Ann Palliat Med. 2020 Mar;9(2):542-557. doi: 10.21037/apm.2019.12.09.
57. Cheng JY, Moline M, Zammit GK, Filippov G, Bsharat M, Hall N. Respiratory safety of lemborexant in healthy subjects: a single-dose, randomized, double-blind, placebo-controlled, crossover study. Clin Drug Investig. 2021 May;41(5):449-57. doi: 10.1007/s40261-021-01018-5.
58. Cheng JY, Filippov G, Moline M, Zammit GK, Bsharat M, Hall N. Respiratory safety of lemborexant in healthy adult and elderly subjects with mild obstructive sleep apnea: a randomized, double‐ blind, placebo‐controlled, crossover study. J Sleep Res. 2020 Aug;29(4): e13021. doi: 10.1111/jsr.13021.
59. Moline M, Cheng JY, Lorch D, Hall N, Shah D. (2021, December 5-8). Respiratory safety of lemborexant in adult and elderly subjects with moderate to severe sleep apnea. American College of Neuropsychopharmacology (ACNP) Congress, San Juan, Puerto Rico.
60. Landry I, Nakai K, Ferry J, Aluri J, Hall N, Lalovic B, et al. Pharmacokinetics, pharmacodynamics, and safety of the dual orexin receptor antagonist lemborexant: findings from single‐dose and multiple‐ascending‐dose phase 1 studies in healthy adults. Clin Pharmacol Drug Dev. 2021 Feb;10(2):153-65. doi: 10.1002/cpdd.817.
61. Yardley J, Kärppä M, Inoue Y, Pinner K, Perdomo C, Ishikawa K, et al. Long-term effectiveness and safety of lemborexant in adults with insomnia disorder: results from a phase 3 randomized clinical trial. Sleep Med. 2021 Apr;80:333-42. doi: 10.1016/j.sleep.2021.01.048.
62. Nigam G, Camacho M, Riaz M. The effect of nonbenzodiazepines sedative hypnotics on apnea- hypopnea index: A meta-analysis. Ann Thorac Med. 2019 Jan-Mar;14(1):49-55. doi: 10.4103/atm.ATM_198_18.
63. Sweetman A, Lack L, Bastien C. Co-Morbid Insomnia and Sleep Apnea (COMISA): prevalence, consequences, methodological considerations, and recent randomized controlled trials. Brain Sci. 2019 Dec 12;9(12):371. doi: 10.3390/brainsci9120371.
64. Lang CJ, Appleton SL, Vakulin A, McEvoy RD, Wittert GA, Martin SA, Catcheside PG, Antic NA, Lack L, Adams RJ. Co-morbid OSA and insomnia increases depression prevalence and severity in men. Respirology. 2017 Oct;22(7):1407-1415. doi: 10.1111/resp.13064.
65. Hein M, Lanquart JP, Mungo A, Loas G. Cardiovascular risk associated with co-morbid insomnia and sleep apnoea (COMISA) in type 2 diabetics. Sleep Sci. 2022 Jan-Mar;15(Spec 1):184-194. doi: 10.5935/1984-0063.20220018.
66. Sweetman A, Melaku YA, Lack L, Reynolds A, Gill TK, Adams R, Appleton S. Prevalence and associations of co-morbid insomnia and sleep apnoea in an Australian population-based sample. Sleep Med. 2021 Jun;82:9-17. doi: 10.1016/j.sleep.2021.03.023.
67. Kishi T, Nishida M, Koebis M, Taninaga T, Muramoto K, Kubota N, et al. Evidence‐based insomnia treatment strategy using novel orexin antagonists: A review. Neuropsychopharm Rep. 2021 Dec;41(4):450-8. doi: 10.1002/npr2.12205.
68. Clark JW, Brian ML, Drummond SPA, Hoyer D, Jacobson LH. Effects of orexin receptor antagonism on human sleep architecture: A systematic review. Sleep Med Rev. 2020 Oct;53:101332. doi: 10.1016/j.smrv.2020.101332.
69. Perogamvros L, Dang-Vu TT, Desseilles M, Schwartz S. Sleep and dreaming are for important matters. Front Psychol. 2013 Jul 25;4:474. doi: 10.3389/fpsyg.2013.00474.
70. Moline M, Zammit G, Cheng JY, Perdomo C, Kumar D, Mayleben D. Comparison of the effect of lemborexant with placebo and zolpidem tartrate extended release on sleep architecture in older adults with insomnia disorder. Journal of Clinical Sleep Medicine. 2021 Jun;17(6):1167-74. doi: 10.5664/jcsm.9150.
71. Waters K. Review of the efficacy and safety of lemborexant, a Dual Receptor Orexin Antagonist (DORA), in the treatment of adults with insomnia disorder. Ann Pharmacother. 2022 Feb;56(2):213-21. doi: 10.1177/10600280211008492.
72. Moline M, Zammit G, Yardley J, Pinner K, Kumar D, Perdomo C, et al. Lack of residual morning effects of lemborexant treatment for insomnia: summary of findings across 9 clinical trials. Postgrad Med. 2021 Jan 2;133(1):71-81. doi: 10.1080/00325481.2020.1823724.
73. Vermeeren A, Jongen S, Murphy P, Moline M, Filippov G, Pinner K, et al. On-the-road driving performance the morning after bedtime administration of lemborexant in healthy adult and elderly volunteers. Sleep. 2019 Apr 1;42(4): zsy260. doi: 10.1093/sleep/zsy260.
74. Landry I, Aluri J, Nakai K, Hall N, Miyajima Y, Ueno T, Dayal S, Filippov G, Lalovic B, Moline M, Reyderman L. Evaluation of the CYP3A and CYP2B6 Drug-Drug Interaction Potential of Lemborexant. Clin Pharmacol Drug Dev. 2021 Jun;10(6):681-690. doi: 10.1002/cpdd.915.
75. Lalovic B, Majid O, Aluri J, Landry I, Moline M, Hussein Z. Population pharmacokinetics and exposure‐response analyses for the most frequent adverse events following treatment with lemborexant, an orexin receptor antagonist, in subjects with insomnia disorder. J Clin Pharmacol 2020 Dec;60(12):1642-54. doi: 10.1002/jcph.1683.
76. Roth T, Rosenberg R, Morin CM, Yardley J, Pinner K, Perdomo C, et al. Impact of lemborexant treatment on insomnia severity: analyses from a 12-month study of adults with insomnia disorder. Sleep Med. 2022 Feb;90:249-57. doi: 10.1016/j.sleep.2022.01.024.
77. Chepke C, Jain R, Rosenberg R, Moline M, Yardley J, Pinner K, et al. Improvement in fatigue and sleep measures with the dual orexin receptor antagonist lemborexant in adults with insomnia disorder. Postgraduate Medicine. 2022 Mar 20:1-10. doi: 10.1080/00325481.2022.2049553.
78. McElroy H, O’Leary B, Adena M, Campbell R, Monfared AAT, Meier G. Comparative efficacy of lemborexant and other insomnia treatments: a network meta-analysis. JMCP. 2021 Sep;27(9):1296-308. doi: 10.18553/jmcp.2021.21011.
79. Morin CM, Edinger JD, Beaulieu-Bonneau S, et al. Effectiveness of sequential psychological and medication therapies for insomnia disorder: a randomized clinical trial. JAMA Psychiatry. 2020;77(11):1-9. doi: 10.1001/jamapsychiatry.2020.1767.
80. Qaseem A, Kansagara D, Forciea MA, Cooke M, Denberg TD. Management of chronic insomnia disorder in adults: a clinical practice guideline from the American College of Physicians. Ann Intern Med. 2016 May 3;165:125-133. doi:10.7326/M15-2175.
81. Rösner S, Englbrecht C, Wehrle R, Hajak G, Soyka M. Eszopiclone for insomnia. Cochrane Database Syst Rev. 2018 Oct 10;10(10):CD010703. doi: 10.1002/14651858.CD010703.pub2.
82. Zheng X, He Y, Yin F, Liu H, Li Y, Zheng Q, Li L. Pharmacological interventions for the treatment of insomnia: quantitative comparison of drug efficacy. Sleep Med. 2020 Aug;72:41-49. doi: 10.1016/j.sleep.2020.03.022.
83. Muehlan C, Vaillant C, Zenklusen I, Kraehenbuehl S, Dingemanse J. Clinical pharmacology, efficacy, and safety of orexin receptor antagonists for the treatment of insomnia disorders. Exp Opin Drug Metab Toxicol. 2020 Nov 1;16(11):1063-78. doi: 10.1080/17425255.2020.1817380.
84. Morin CM, Vézina-Im LA, Ivers H, Micoulaud-Franchi JA, Philip P, Lamy M, Savard J. Prevalent, incident, and persistent insomnia in a population-based cohort tested before (2018) and during the first-wave of COVID-19 pandemic (2020). Sleep. 2022 Jan 11;45(1):zsab258. doi: 10.1093/sleep/zsab258.
85. Um YH, Lim HK. Orexin and Alzheimer's Disease: A New Perspective. Psychiatry Investig. 2020 Jul;17(7):621-626. doi: 10.30773/pi.2020.0136. Epub 2020 Jun 11. PMID: 32517419; PMCID: PMC7385219.
86. Hwang YT, Piguet O, Hodges JR, Grunstein R, Burrell JR. Sleep and orexin: A new paradigm for understanding behavioural-variant frontotemporal dementia? Sleep Med Rev. 2020 Dec;54:101361. doi: 10.1016/j.smrv.2020.101361.
87. Moline M, Thein S, Bsharat M, Rabbee N, Kemethofer-Waliczky M, Filippov G, Kubota N, Dhadda S. Safety and Efficacy of Lemborexant in Patients With Irregular Sleep-Wake Rhythm Disorder and Alzheimer's Disease Dementia: Results From a Phase 2 Randomized Clinical Trial. J Prev Alzheimers Dis. 2021;8(1):7-18. doi: 10.14283/jpad.2020.69.
88. Mehr JB, Bilotti MM, James MH. Orexin (hypocretin) and addiction. Trends Neurosci. 2021 Nov;44(11):852-855. doi: 10.1016/j.tins.2021.09.002.
89. James MH, Mahler SV, Moorman DE, Aston-Jones G. A Decade of Orexin/Hypocretin and Addiction: Where Are We Now? Curr Top Behav Neurosci. 2017;33:247-281. doi: 10.1007/7854_2016_57. PMID: 28012090; PMCID: PMC5799809.
90. Murphy P, Kumar D, Zammit G, Rosenberg R, Moline M. Safety of lemborexant versus placebo and zolpidem: effects on auditory awakening threshold, postural stability, and cognitive performance in healthy older participants in the middle of the night and upon morning awakening. J Clin Sleep Med. 2020 May 15;16(5):765-73. doi: 10.5664/jcsm.8294.
91. Sogawa R, Emoto A, Monji A, Miyamoto Y, Yukawa M, Murakawa‐Hirachi T, et al. Association of orexin receptor antagonists with falls during hospitalization. Clinical Pharmacy Therapeu. 2022 Mar; online ahead of print. doi: 10.1111/jcpt.13619.
92. Andrade C. Sedative Hypnotics and the Risk of Falls and Fractures in the Elderly. J Clin Psychiatry. 2018 May/Jun;79(3):18f12340. doi: 10.4088/JCP.18f12340.
93. Stone KL, Ensrud KE, Ancoli-Israel S. Sleep, insomnia and falls in elderly patients. Sleep Med. 2008 Sep;9 Suppl 1:S18-22. doi: 10.1016/S1389-9457(08)70012-1.
94. Chen LF, Lin CE, Chou YC, Mao WC, Chen YC, Tzeng NS. A comparison of complex sleep behaviors with two short-acting Z-hypnosedative drugs in nonpsychotic patients. Neuropsychiatr Dis Treat. 2013;9:1159-62. doi: 10.2147/NDT.S48152.
95. Rosenberg R, Amchin J, Kumar D, Perdomo C, Moline M, Malhotra M. A multicenter open-label pilot study evaluation next-dose transition from zolpidem to Lemborexant: subgroup analysis of older adults (Poster Number NR-19). Am J Geriatr Psychiatry. 2021;29(4S): S123.
96. Baglioni C, Battagliese G, Feige B, et al. Insomnia as a predictor of depression: a meta-analytic evaluation of longitudinal epidemiological studies. J Affect Dis. 2011 Dec;135(1-3):10-19. doi:10.1016/j.jad.2011.01.011.
97. Schutte-Rodin S, Broch L, Buysse D, Dorsey C, Sateia M. Clinical guideline for the evaluation and management of chronic insomnia in adults. J Clin Sleep Med. 2008 Oct 15;4(5):487-504. PMID: 18853708.
98. Bastien CH, Vallières A, Morin CM. Validation of the Insomnia Severity Index as an outcome measure for insomnia research. Sleep Med. 2001;2(4):297-307. doi: 10.1016/S1389- 9457(00)00065-4.
99. Morin CM, Belleville G, Belanger L, Ivers H. The Insomnia Severity Index: psychometric indicators to detect insomnia cases and evaluate treatment response. Sleep. 2011 May;34(5):601-608. doi:10.1093/sleep/34.5.601.
100. Khullar A. Igwe O. CPS: Therapeutic Choices. Ottawa (ON): Canadian Pharmacists Association; 2021. Chapter 104, Insomnia; p. 1687-1710.
101. Christensen H, Batterham PJ, Gosling JA, et al. Effectiveness of an online insomnia program (SHUTi) for prevention of depressive episodes (the GoodNight Study): a randomised controlled trial. Lancet Psychiatry. 2016 Apr;3(4):333-341. doi:10.1016/S2215-0366(15)00536-2.
102. Cudney LE, Frey BN, McCabe RE, Green SM. Investigating the relationship between objective measures of sleep and self-report sleep quality in healthy adults: a review. J Clin Sleep Med. 2022 Mar 1;18(3):927-936. doi: 10.5664/jcsm.9708.
103. Morin CM. Measuring outcomes in randomized clinical trials of insomnia treatments. Sleep Med Rev. 2003 Jun;7(3):263-79. doi: 10.1053/smrv.2002.0274.
104. Pillai V, Roth T, Drake CL. Towards quantitative cutoffs for insomnia: how current diagnostic criteria mischaracterize remission. Sleep Med. 2016 Oct;26:62-68. doi: 10.1016/j.sleep.2016.01.013.
105. Winkler A, Auer C, Doering BK, Rief W. Drug treatment of primary insomnia: a meta-analysis of polysomnographic randomized controlled trials. CNS Drugs. 2014 Sep;28(9):799-816. doi: 10.1007/s40263-014-0198-7.
PubMed References
Suzuki H, Hibino H. Characteristics of patients who were able to switch from benzodiazepine hypnotics to lemborexant. SAGE Open Medicine. 2021 Jan;9:205031212110379. doi: 10.1177/20503121211037903.
Murphy P, Moline M, Mayleben D, Rosenberg R, Zammit G, Pinner K, et al. Lemborexant, A Dual Orexin Receptor Antagonist (DORA) for the treatment of insomnia disorder: results from a Bayesian, adaptive, randomized, double-blind, placebo-controlled study. J ClinSleep Med. 2017 Nov 15;13(11):1289-99. doi: 10.5664/jcsm.6800.
Leftover
Vgontzas AN, Fernandez-Mendoza J, Lenker KP, Basta M, Bixler EO, Chrousos GP. Hypothalamic- pituitary-adrenal (HPA) axis response to exogenous corticotropin-releasing hormone (CRH) is attenuated in men with chronic insomnia. J Sleep Res. 2021 Nov 25:e13526. doi:10.1111/jsr.13526
Glass J, Lanctot KL, Herrmann N, Sproule BA, Busto UE. Sedative hypnotics in older people with insomnia: meta-analysis of risks and benefits. BMJ. 2005 Nov 19;331(7526):1169. doi:10.1136/bmj.38623.768588.47
Canadian Coalition for Seniors’ Mental Health. Canadian Guidelines on Benzodiazepine Receptor Agonist Use Disorder Among Older Adults. 2019. [Internet]. https://ccsmh.ca/wp- content/uploads/2019/11/Benzodiazepine_Receptor_Agonist_Use_Disorder_ENG.pdf
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up-to-date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
Redactions: Confidential information in this document may be redacted at the request of the sponsor in accordance with the CADTH Drug Reimbursement Review Confidentiality Guidelines
Stakeholder Input: The views expressed in each submission are those of the submitting organization or individual; not necessarily the views of CADTH or of other organizations. As such, they are independent of CADTH and do not necessarily represent or reflect the view of CADTH. No endorsement by CADTH is intended or should be inferred. By filing with CADTH, the submitting organization or individual agrees to the full disclosure of the information. CADTH does not edit the content of the submissions.
CADTH does use reasonable care to prevent disclosure of personal information in posted material; however, it is ultimately the submitter’s responsibility to ensure no identifying personal information or personal health information is included in the submission. The name of the submitting organization or individual and all conflict of interest information are included in the submission; however, the name of the author, including the name of an individual patient or caregiver submitting the patient input, are not posted.
Accessibility: CADTH is committed to treating people with disabilities in a way that respects their dignity and independence, supports them in accessing material in a timely manner, and provides a robust feedback process to support continuous improvement. All materials prepared by CADTH are available in an accessible format. Where materials provided to CADTH by a submitting organization or individual are not available in an accessible format, CADTH will provide a summary document upon request. More details on CADTH’s accessibility policies can be found here.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.