CADTH Reimbursement Review
Ozanimod (Zeposia)
Sponsor: Celgene Inc., a Bristol Myers Squibb Company
Therapeutic area: Ulcerative colitis
This multi-part report includes:
Clinical Review
Pharmacoeconomic Review
Stakeholder Input
Clinical Review
Abbreviations
5-ASA
5-aminosalicylate
AE
adverse event
CI
confidence interval
CRP
C-reactive protein
CYP2C8
cytochrome P450 2C8
EQ VAS
EuroQol Visual Analogue Scale
EQ-5D-5L
5-level EQ-5D
IBD
inflammatory bowel disease
ITC
indirect treatment comparison
ITT
intention to treat
HRQoL
health-related quality of life
MCID
minimal clinically important difference
MCS
SF-36 Mental Component Summary
NMA
network meta-analysis
NRI
nonresponder imputation
OLE
open-label extension
OLP
open-label period
OR
odds ratio
PCS
SF-36 Physical Component Summary
PP
per protocol
RBS
rectal bleeding subscore
RCT
randomized controlled trial
S1P
sphingosine 1-phosphate
SAE
serious adverse event
SCCAI
Simple Clinical Colitis Activity Index
SD
standard deviation
SF-36
Short Form (36) Health Survey
SFS
stool frequency subscore
TNF
tumour necrosis factor
UC
ulcerative colitis
WPAI-UC
Work Productivity and Activity Impairment Questionnaire – Ulcerative Colitis
Executive Summary
An overview of the submission details for the drug under review is provided in Table 1.
Item | Description |
|---|---|
Drug product | Ozanimod (Zeposia), capsules, 0.23 mg, 0.46 mg, and 0.92 mg, oral administration |
Indication | For the treatment of adult patients with moderately to severely active UC who have had an inadequate response, loss of response, or were intolerant to either conventional therapy or a biologic agent |
Reimbursement request | As per indication |
Health Canada approval status | NOC |
Health Canada review pathway | Standard |
NOC date | April 8, 2022 |
Sponsor | Celgene Inc., a Bristol Myers Squibb company |
NOC = Notice of Compliance; UC = ulcerative colitis.
Introduction
Inflammatory bowel disease (IBD) is a term used to describe disorders that involve chronic inflammation of the digestive tract. There are 2 main types of IBD: Crohn disease and ulcerative colitis (UC). Crohn disease is characterized by inflammation of the lining of the digestive tract, often involving the deep layers of the digestive tract. UC causes inflammation and ulcers in the digestive tract, affecting the innermost lining of the large intestine (colon) and rectum.1,2 While both diseases are characterized by diarrhea, abdominal pain, rectal bleeding, and weight loss, UC is characterized by blood in the stool with mucus, frequent diarrhea, loss of appetite, and tenesmus (strong urge to use the bathroom without necessarily having a bowel movement).3,4 The incidence rate for UC in Canada ranges from a low of 8.4 per 100,000 people in Alberta to a high of 21.4 per 100,000 people in Nova Scotia.5-7 There are an additional 15,000 individuals living with IBD in Canada that are not clearly classified (Crohn disease versus UC).5-8
Anti-inflammatory drugs are typically used as first-line therapy for mild to moderate UC and include 5-aminosalicylates (5-ASAs) (mesalamine, balsalazide, and olsalazine), sulfasalazine, and corticosteroids. For patients who do not have an adequate response on a 5-ASA or corticosteroid, conventional immunosuppressants such as azathioprine, mercaptopurine, and methotrexate are treatment options. Biologic therapies are the mainstay treatment for patients with moderate to severe UC and are used for induction and maintenance when other treatments have been unsuccessful, or in those who cannot tolerate other treatments. Approximately 5% to 10% of patients with UC may require surgery.9 UC surgery typically involves removing the entire colon and rectum and, in most cases, an ileoanal anastomosis procedure is performed. Colectomy is generally reserved for 3 scenarios: development of colorectal dysplasia, complications (e.g., toxic megacolon and/or perforation), and failure of medical therapy.
Ozanimod is an immune modulator that targets the sphingosine 1-phosphate (S1P) 1 receptor (S1P1) and the S1P 5 receptors (S1P5) on immune cells. S1P receptors are a specific part of the immune cell that plays an important role in inflammatory conditions such as UC. By binding to the S1P receptors on immune cells, ozanimod is thought to act as a gatekeeper, keeping these cells from moving out of the lymph node and into the circulation, thereby preventing UC inflammation. Ozanimod is administered as an oral capsule, with an initial dosage of 0.23 mg once daily from day 1 to day 4 followed by 0.46 mg once daily from day 5 to day 7. Following the 7-day dose escalation, a stable dose of 0.92 mg once daily is taken orally beginning on day 8.
The objective of this review is to evaluate the beneficial and harmful effects of ozanimod 0.92 mg daily for the treatment of adult patients with moderately to severely active UC who have had an inadequate response, a loss of response, or were intolerant to either conventional therapy or a biologic agent.
Stakeholder Perspectives
The information in this section is a summary of input provided by the patient groups that responded to CADTH’s call for patient input and from the clinical expert consulted by CADTH for the purpose of this review.
Patient Input
The patient input received for this review was collected by the Gastrointestinal (GI) Society and Crohn’s and Colitis Canada (CCC). The input provided by the GI Society included more than 1,500 respondents and was sourced from 4 online surveys (2015, 2018, and 2 surveys in 2020) of respondents with IBD, including UC, one-on-one conversations, and phone, email, and social media interactions. The input provided by the CCC came from more than 3,900 respondents with IBD and came from multiple sources, including multiple surveys (late 2017 to early 2018 and 2021) and a phone interview. The CCC input included 8 respondents with experience using Zeposia for UC; all accessed ozanimod through a clinical trial.
Respondents from both the GI Society and the CCC reported that UC has a profound effect on all aspects of life — physically, emotionally, and socially — regardless of whether they are at home, school, or in the workplace. Symptoms associated with UC (such as diarrhea, rectal bleeding, abdominal pain, bloating, cramping, anemia due to blood loss, frequent and urgent bowel movements, and fatigue) not only affect day-to-day living, they also cause anxiety and stress. Respondents from both groups experienced constant concerns about future flare-ups, which can be disrupting. Respondents reported decreased quality of life during periods of active disease, with patients spending a lot of time in the bathroom. Even during periods of remission, respondents reported the need to stay close to a bathroom, thereby limiting their activities. Moreover, due to the perceived stigma of UC, many report hiding their disease from work colleagues, friends, and family. In extreme cases, based on patient input received from the CCC, thoughts of suicide were reported due to the inability to control and cope with the impacts of UC on their personal and social lives, as well as reports of consequences to their career or schooling. Based on the patient input received from the GI Society, only 24% of respondents with IBD reported that the currently available medications are adequate to control their disease. Patient groups indicated that available treatments initially may have helped relieve some of the symptoms, but the treatments were unsuccessful in controlling their symptoms. Respondents reported the need for new and effective treatment options to achieve mucosal healing and reduce or eliminate the debilitating symptoms of UC. Moreover, respondents stressed that sustained remission or treatment response is more important than relieving any 1 symptom.
Clinician Input
Input From the Clinical Experts Consulted by CADTH
The clinical expert consulted by CADTH detailed 4 unmet needs related to therapies for the treatment of UC. First, while currently available therapies are effective, most patients with UC are unable to achieve complete endoscopic remission. As such, better UC therapies are needed to break through the “therapeutic ceiling” of current treatments. Second, it is unknown what the best treatment strategies are for patients with moderate to severe UC. Currently, there are no tools that can predict which patients will respond to which therapy. Third, there is still uncertainty about the ideal long-term therapeutic target and the overall benefits of targeting clinical, endoscopic, and/or histologic remission. Finally, access to coverage for UC treatments presents a major burden to both patients and care providers. Many jurisdictions require the patient’s UC to fail conventional immunosuppressants before biologics are approved.
The clinical expert consulted by CADTH indicated that the novel mechanism of ozanimod would be a valuable addition to the treatment paradigm, since the current therapies for moderate to severe UC are limited. According to the clinical expert, ozanimod may become a first-line advanced therapy among patients whose condition failed to respond to 5-ASAs, given ozanimod’s oral route of administration and efficacy in treating moderate UC. The clinical expert indicated that ozanimod may be considered among patients whose UC has failed other biologic therapies, although the data for its effectiveness after failure of anti–tumour necrosis factor (anti-TNF) therapy are less promising.
Clinician Group Input
No clinician group input was received for this review.
Drug Program Input
Input was obtained from the drug programs that participate in the CADTH reimbursement review process. The following were identified as key factors that could potentially impact the implementation of a CADTH recommendation for ozanimod:
considerations for initiation of therapy
considerations for continuation or renewal of therapy
considerations for discontinuation of therapy
considerations for prescribing of therapy
generalizability of trial populations to the broader populations in the jurisdictions
care provision issues
The clinical expert consulted by CADTH provided advice on the potential implementation issues raised by the drug programs.
Clinical Evidence
Pivotal Studies and Protocol-Selected Studies
Description of Study
One sponsor-conducted study that met the CADTH review protocol criteria was included in this systematic review. The TRUE NORTH study was a phase III, multicentre, randomized, double-blind, placebo-controlled trial of oral ozanimod as induction and maintenance therapy for adult patients with moderate to severe UC. A total of 645 patients were enrolled across 250 sites from 29 countries in North America (including 8 sites in Canada), Europe, Asia Pacific, South America, and South Africa. The trial consisted of a 10-week induction period followed by a 42-week maintenance period. The induction period was composed of 2 cohorts: cohort 1, in which patients were randomized in a 2:1 ratio to receive either ozanimod 0.92 mg daily (N = 429) or matching placebo (N = 216) in a double-blind fashion, and cohort 2, in which patients received open-label ozanimod 0.92 mg once daily. Patients were evaluated for clinical response and remission at week 10 of the induction period. Patients who had a clinical response to ozanimod at the end of the induction period proceeded to the maintenance period and were re-randomized in a 1:1 ratio to receive either ozanimod 0.92 mg daily (N = 230) or matching placebo (N = 227) in a double-blind fashion. Patients who were randomized to placebo in the induction period and had a clinical response at week 10 continued to receive placebo in the maintenance period.
The primary outcome of the study was clinical remission as measured by the Mayo score, a disease-specific instrument that assesses disease severity and response to treatment in patients with UC. The Mayo scoring system is a combined endoscopic and clinical assessment composed of 4 components: rectal bleeding, stool frequency, Physician’s Global Assessment, and endoscopy findings. Each part is rated from 0 to 3, yielding a total score of 0 to 12. The primary and key secondary end points that relied on the Mayo score were assessed using the 3-component Mayo score, which excludes the Physician’s Global Assessment. The key secondary end points were controlled for multiplicity using a statistical testing hierarchy and each study period was considered an independent study. The primary end point and the following key secondary end points were assessed in both the induction and maintenance periods: clinical response, endoscopic improvement, and mucosal healing. The key secondary end points assessed only in the maintenance period were clinical remission in patients who were in remission at week 10, corticosteroid-free remission, and durability of clinical remission. Other efficacy outcomes included health-related quality of life (HRQoL) outcomes, as assessed by the 5-level EQ-5D (EQ-5D-5L) and the Short Form (36) Health Survey (SF-36), and work productivity, as assessed by the Work Productivity and Activity Impairment Questionnaire – Ulcerative Colitis (WPAI-UC).
Patients who completed the induction period and did not have a clinical response were invited to participate in an optional open-label extension (OLE) study. Patients who completed the maintenance period or those who experienced disease relapse during the maintenance period were also given the opportunity to enter the OLE study.
Nearly 90% of the study patients were white, more than half were male, and the mean age was 42 years. The mean 3-component Mayo score and 4-component Mayo score ranged from 6.6 (standard deviation [SD] = 1.15) to 6.7 (SD = 1.31) and 8.6 (SD = 1.42) to 9.1 (SD = 9.0), respectively, across treatment groups in both study periods. Disease severity as assessed by mucosal appearance at endoscopy was classified as severe in approximately 60% and 50% of patients in the induction period and maintenance period, respectively. All patients had been previously treated with other UC medications. Excluding patients who received placebo during both the induction period and the maintenance period, patients in each treatment group at the start of the induction and maintenance period had previously received the following UC medications: corticosteroids (range, 70% to 78%), oral aminosalicylic acids (97% to 99%), immunomodulators (37% to 46%), azathioprine (30% to 38%), mercaptopurine (less than 10%), methotrexate (less than 6%), anti-TNF biologics (28% to 33%, aside from 44% in the open-label ozanimod group), and non–anti-TNF biologics (14% to 29%).
Efficacy Results
Key efficacy results are presented in Table 2.
Clinical Remission
Clinical remission was measured at week 10 and week 52 using a 7-day scoring algorithm and was defined as a rectal bleeding subscore (RBS) of 0, a stool frequency subscore (SFS) of 0 or 1 (and a decrease of at least 1 point from the baseline SFS), and an endoscopy subscore of 0 or 1 point without friability. The proportion of patients in clinical remission was significantly higher among patients in cohort 1 of the induction period who received ozanimod compared with those who received placebo (18.4% versus 6.0%; difference in proportions of 12.4%; 95% confidence interval [CI], 7.5% to 17.2%; P < 0.0001) at week 10 and among patients who continued to receive ozanimod in the maintenance period compared with those who were re-randomized to placebo (37.0% versus 18.5%; difference in proportions of 18.6%; 95% CI, 10.8% to 26.4%; P < 0.0001).
Clinical Response
Clinical response was measured using a 7-day scoring algorithm and was defined as a reduction from baseline in the 3-component Mayo score of at least 2 points and at least 35%, and a reduction from baseline in the RBS of at least 1 point or an absolute RBS of 0 or 1. The proportion of patients with clinical response was significantly higher with ozanimod compared with placebo during both the induction period (47.8% versus 25.9%; difference in proportions of 21.9%; 95% CI, 14.4% to 29.3%; P < 0.0001) and the maintenance period (60.0% versus 41.0%; difference in proportions of 19.2%; 95% CI, 10.4% to 28.0%; P < 0.0001).
Durable Clinical Remission
The proportion of patients with durable clinical remission, defined as patients in clinical remission at week 10 and at week 52 in all patients who entered the maintenance period, was significantly greater in patients who remained on ozanimod compared with patients re-randomized to placebo (17.8% versus 9.7%; difference in proportions of 8.2%; 95% CI, 2.8% to 13.6%; P = 0.003).
Maintenance of Clinical Remission
The proportion of patients who maintained clinical remission at week 52 in a subset of patients who were in clinical remission at week 10 was greater among those who remained on ozanimod compared with patients re-randomized to placebo in the maintenance period (51.9% versus 29.3%; difference in proportions of 23.9%; 95% CI, 9.1% to 38.6%; P = 0.0025).
Endoscopic Improvement
Endoscopic improvement was defined as an endoscopy subscore of 0 or 1 without friability. A greater proportion of patients randomized to ozanimod had endoscopic improvement compared with patients randomized to placebo at week 10 (27.3% versus 11.6%; difference in proportions of 15.7%; 95% CI, 9.7% to 21.7%; P < 0.0001). At week 52, the proportion of patients with endoscopic improvement was greater in patients who continued on ozanimod compared with those re-randomized to placebo (45.7% versus 26.4%; difference in proportions of 19.4%; 95% CI, 11.0% to 27.7%, P < 0.001).
Mucosal Healing
Mucosal healing was defined as an endoscopy subscore of 0 or 1 without friability and a Geboes score of less than 2. A greater proportion of patients randomized to ozanimod had mucosal healing compared with patients randomized to placebo at week 10 of the induction period (12.6% versus 3.7%; difference in proportions of 8.9%; 95% CI, 4.9% to 12.9%; P < 0. 001). At week 42 of the maintenance period (week 52 of the study), the proportion of patients with mucosal healing was greater in patients who continued on ozanimod compared with those re-randomized to placebo (29.6% versus 14.1%; difference in proportions of 15.6%; 95% CI, 8.2% to 22.9%; P < 0.001).
Corticosteroid-Free Remission
The proportion of patients with corticosteroid-free remission at week 52 (clinical remission while off corticosteroids for at least 12 weeks) was greater among patients who remained on ozanimod compared with those re-randomized to placebo (31.7% versus 16.7%; difference in proportions of 15.2%; 95% CI, 7.8% to 22.6%; P < 0.001).
Harms Results
Key harms results are presented in Table 2.
Table 2: Summary of Key Results From the TRUE NORTH Trial
Outcome measure | Induction perioda (ITT, week 10) | Maintenance periodb (ITT, week 52) | ||||
|---|---|---|---|---|---|---|
Cohort 1 | Cohort 2 | PL to PL (N = 69) | Re-randomized patients | |||
OZ (N = 429) | PL (N = 216) | OZ (N = 367) | OZ to PL (N = 227) | OZ to OZ (N = 230) | ||
Clinical remission (3-component Mayo score) | ||||||
Patients in clinical remission,c n (%) | 79 (18.4) | 13 (6.0) | 77 (21.0) | 17 (24.6) | 42 (18.5) | 85 (37.0) |
Odds ratio (95% CI)d | 3.59 (1.94 to 6.64) | — | — | 2.78 (1.77 to 4.29) | ||
Difference in proportions, % (95% CI)d | 12.4 (7.5 to 17.2) | — | — | 18.6 (10.8 to 26.4) | ||
P value | < 0.0001 | Reference | — | — | Reference | < 0.0001 |
Clinical response (3-component Mayo score) | ||||||
Patients with clinical response,e n (%) | 205 (47.8) | 56 (25.9) | 193 (52.6) | 27 (39.1) | 93 (41.0) | 138 (60.0) |
Odds ratio (95% CI)d | 2.67 (1.86 to 3.84) | — | — | 2.27 (1.54 to 3.33) | ||
Difference in proportions, % (95% CI)d | 21.9 (14.4 to 29.3) | — | — | 19.2 (10.4 to 28.0) | ||
P value | < 0.0001 | Reference | — | — | Reference | < 0.0001 |
Endoscopic improvement | ||||||
Patients in endoscopic improvement, n (%) | 117 (27.3) | 25 (11.6) | 100 (27.2) | 20 (29.0) | 60 (26.4) | 105 (45.7) |
Odds ratio (95% CI)d | 2.876 (1.80 to 4.59) | — | — | 2.476 (1.65 to 3.71) | ||
Difference in proportions, % (95% CI)d | 15.7 (9.7 to 21.7) | — | — | 19.4 (11.0 to 27.7) | ||
P value | < 0.0001 | Reference | — | — | Reference | < 0.001 |
Mucosal healing | ||||||
Patients in mucosal healing, n (%) | 54 (12.6) | 8 (3.7) | 42 (11.4) | 7 (10.1) | 32 (14.1) | 68 (29.6) |
Odds ratio (95% CI)d | 3.77 (1.76 to 8.07) | — | — | 2.64 (1.64 to 4.26) | ||
Difference in proportions, % (95% CI)d | 8.9 (4.9 to 12.9) | — | — | 15.6 (8.2 to 22.9) | ||
P value | < 0.001 | Reference | — | — | Reference | < 0.001 |
Corticosteroid-free remission | ||||||
Patients in corticosteroid-free remission, n (%) | — | — | — | 17 (24.6) | 38 (16.7) | 73 (31.7) |
Odds ratio (95% CI)c | — | — | — | — | 2.56 (1.60 to 4.09) | |
Difference in proportions, % (95% CI)c | — | — | — | — | 15.2 (7.8 to 22.6) | |
P value | — | — | — | — | Reference | < 0.001 |
Durable clinical remission | ||||||
Patients in durable remission, n (%) | — | — | — | 5 (7.2) | 22 (9.7) | 41 (17.8) |
Odds ratio (95% CI)c | — | — | — | — | 2.65 (1.38 to 5.06) | |
Difference in proportions, % (95% CI)c | — | — | — | — | 8.2 (2.8 to 13.6) | |
P value | — | — | — | — | Reference | 0.003 |
Summary of harms (safety) | ||||||
Patients with ≥ 1 TEAE, n (%) | 172 (40.1) | 82 (38.0) | 146 (39.8) | 27 (39.1) | 83 (36.6) | 113 (49.1) |
Patients with ≥ 1 serious TEAE, n (%) | 17 (4.0) | 7 (3.2) | 23 (6.3) | 4 (5.8) | 18 (7.9) | 12 (5.2) |
Patients who discontinued treatment due to TEAE, n (%) | 14 (3.3) | 7 (3.2) | 14 (3.8) | 0 | 6 (2.6) | 3 (1.3) |
Deaths, n (%) | 0 | 0 | 1 (0.3) | 0 | 0 | 0 |
CI = confidence interval; CMH = Cochran-Mantel-Haenszel; ITT = intention to treat; OZ = ozanimod; PL = placebo; RBS = rectal bleeding subscore; SD = standard deviation; SFS = stool frequency subscore; TEAE = treatment-emergent adverse event; TNF = tumour necrosis factor.
aProportion of participants in clinical remission at week 10 week of the induction period (ITT population, nonresponder imputation).
bProportion of participants in clinical remission at week 52 of the total treatment maintenance period (ITT population, nonresponder imputation).
cClinical remission was measured using the 3-component Mayo score definition using a 7-day scoring algorithm and defined as an RBS of 0 and an SFS of ≤ 1 point (and a decrease of ≥ 1 point from the baseline SFS) and an endoscopy subscore of ≤ 1 point without friability.
dOdds ratio (active vs. PL), treatment difference, and 2-sided 95% Wald CI and P value for comparison between the cohort 1 OZ group and PL groups are based on the CMH test, stratified by corticosteroid use at screening and prior anti-TNF use (yes or no). For the maintenance period analysis, the comparison between the OZ 1 mg to OZ 1 mg group vs. the OZ 1 mg to PL group is based on the CMH test, stratified by remission status at week 10 and corticosteroid use at week 10 (yes or no).
eClinical response was measured using the 3-component Mayo score definition using a 7-day scoring algorithm and defined as a reduction from baseline in the 3-component Mayo score of ≥ 2 points and ≥ 35%, and a reduction from baseline in the RBS of ≥ 1 point or an absolute RBS of ≤ 1 point.
Source: Clinical Study Report for the TRUE NORTH study.10
Adverse Events
During the induction period, at least 1 treatment-emergent adverse event (TEAE) was reported by 40.1% and 38.0% of patients in the cohort 1 ozanimod group and cohort 1 placebo group, respectively. Among patients re-randomized to placebo and those who continued on ozanimod during the maintenance period, 36.6% and 49.1% of patients reported at least 1 TEAE, respectively.
The TEAEs reported by at least 2% of patients in any treatment group during the induction period were anemia, nasopharyngitis, headache, nausea, alanine aminotransferase increase, pyrexia, arthralgia, colitis ulcerative, and upper respiratory tract infection. Of these, anemia, nausea, and pyrexia were not reported by any patients during the maintenance period; the remaining TEAEs were reported by patients in a proportion similar to the induction period. Apart from anemia, which was reported in 4.2% to 5.6% of patients, these TEAEs were reported in less than 4% of any treatment group. The following commonly reported TEAEs were exclusive to re-randomized patients in the maintenance period: gamma-glutamyl transferase increased (0.4% to 3.0%), edema peripheral (2.6%), and herpes zoster (0.4% to 2.2%).
Serious Adverse Events
During the induction period, serious TEAEs were reported by 4.0% and 3.2% of patients in the cohort 1 ozanimod group and cohort 1 placebo group, respectively. The most common serious TEAE reported in the induction period was colitis ulcerative in both treatment groups (approximately 1.4%). Additional serious TEAEs reported in the cohort 1 ozanimod group were anemia (0.9%) and appendicitis (0.2%).
During the maintenance period, 7.9% of the patients re-randomized to placebo and 5.2% of the patients who continued ozanimod reported at least 1 serious TEAE. The serious TEAEs reported in at least 2 patients in the re-randomized placebo group included colitis ulcerative (4% in the re-randomized placebo group and 0.4% in the ozanimod group) and complicated appendicitis (0.9% in the re-randomized placebo group).
Withdrawals Due to Adverse Events
Withdrawal from the study due to TEAEs during the induction period was similar across the treatment groups at approximately 3%. The most common reason for withdrawal due to TEAEs was colitis ulcerative (0.7% in the cohort 1 ozanimod group and 1.9% on the cohort 1 placebo group). Two patients (0.5%) in the cohort 2 ozanimod group discontinued from the study due to bradycardia.
The percentage of patients who withdrew from the study due to TEAEs during the maintenance period was 2.6% among those re-randomized to placebo and 1.3% in patients who remained on ozanimod. Four (1.8%) patients in the group re-randomized to placebo withdrew from the study due to colitis ulcerative.
Mortality
During the study period, only 1 death was reported, which was recorded in the induction period cohort 2 ozanimod group.
Notable Harms
Of the serious or opportunistic infections reported, the only infection reported in at least 2 patients in any treatment group was herpes zoster (0.5% in the induction period cohort 1 ozanimod group; 0.3% in the induction period cohort 2 ozanimod group; 1.7% in the maintenance period ozanimod group). Each of the following infections was reported in 1 patient over all treatment groups and periods: pyelonephritis, vestibular neuronitis, pneumonia influenza, respiratory syncytial virus test positive, urinary tract infection, Clostridium difficile infection, complicated appendicitis, gastroenteritis norovirus, large intestine infection, measles, and yersinia infection.
Macular edema was reported by 1 patient in both the induction period cohort 1 ozanimod group and the maintenance period ozanimod group.
During the induction period, only the cohort 1 ozanimod group reported hepatic effects (0.5% or less of the group), including alanine aminotransferase increased, hepatic enzyme increased, aspartate aminotransferase increased, liver function test increased, and transaminases increased. In the maintenance period, blood bilirubin increase was reported in 1 patient re-randomized to placebo. Among patients who remained on ozanimod, alanine aminotransferase increase, and liver function test increase were each reported in 1 patient.
Lymphopenia was reported in 2 (0.9%) patients in the maintenance period ozanimod group.
Critical Appraisal
The TRUE NORTH trial was limited by differential dropout between treatment groups in the maintenance period and a study design that resulted in an enriched patient population entering the maintenance period. Although approximately 90% of randomized patients completed the induction period, only approximately 50% had a clinical response and continued into the maintenance period. As selection into the maintenance period was based on clinical response, this likely created an enriched patient population that was more likely to benefit from ozanimod treatment compared with the indicated population as a whole. According to the clinical expert consulted by CADTH, this is a common trial design used in UC programs, as it is challenging to keep nonresponders in a long-term study. Furthermore, of those who continued into the maintenance period, the proportion of patients who completed the trial among the patients re-randomized to receive placebo versus those who continued to receive ozanimod was 54.6% and 80%, respectively. Following disease relapse, a greater proportion of patients in the re-randomized placebo group compared with the ozanimod group discontinued the maintenance period to enter the OLE study (35.7% versus 14.8%, respectively). Although the direction of any bias is unclear, it is possible that the differential dropout rate between the 2 treatment groups may have introduced attrition bias in favour of ozanimod.
Patients had the opportunity to enrol in the OLE study where they would receive open-label ozanimod. There was significant study discontinuation due to disease relapse and entry into the OLE study (34% of patients re-randomized from ozanimod to placebo and 14% of patients re-randomized from ozanimod to ozanimod). Additionally, there may be a subset of patients who experience a delayed response to induction therapy, and they would not have been eligible to continue in the maintenance period. All of these factors contribute to the difficulty in assessing the generalizability of the efficacy results.
Indirect Comparisons
Description of Studies
Two indirect treatment comparison (ITC) studies were reviewed. The sponsor-submitted ITC was a systematic review and network meta-analysis (NMA) comparing ozanimod with currently existing medications for the treatment of moderate to severe UC.11 One NMA study (Lasa et al.)12 that included ozanimod for patients with moderate to severe UC was included from the CADTH literature search.
In the sponsor-submitted ITC, ozanimod was compared with ustekinumab, infliximab, certolizumab, adalimumab, vedolizumab, tofacitinib, golimumab, filgotinib, etrasimod or the biosimilar versions of these therapies, and placebo. Phase II or III randomized controlled trials (RCTs) were included. Clinical response, clinical remission, endoscopic improvement, and safety were evaluated. In the Lasa et al. study, ozanimod was compared with infliximab, adalimumab, golimumab, vedolizumab, ustekinumab, tofacitinib, etrolizumab, upadacitinib, filgotinib, etrasimod, TD-1473, and placebo. Phase III RCTs were included in this report. In the Lasa et al. report, clinical remission and endoscopic improvement were evaluated. Safety outcomes were examined in the 2 ITCs.
In the sponsor-submitted ITC, 22 RCTs were included in the analyses. Bayesian NMAs were performed using random-effects or fixed-effects models in all analyses. Due to the significant heterogeneity observed across the included trials, especially the study designs that are common in UC, adjustments were made to the data in older treat-through trials to more closely resemble modern re-randomized trials in the maintenance phase. The mean age of patients in the induction phase ranged from 34.1 to 44.8 years, and the mean Mayo score ranged from 8.0 to 9.1. The sponsor report noted differences between trials with respect to the percentage of males (range, 42% to 100%), mean C-reactive protein (CRP) level at baseline (range, 7 mg/L to 35.8 mg/L), years since UC diagnosis (range, 3.8 to 14.6 years), extent of disease (left-sided: range, 15% to 63%; extensive: range, 6.6% to 80.8%; other: range, 0 to 63.4%), and use of concomitant steroids (range, 25% to 100%). In the maintenance phase, baseline characteristics were reported only for the re-randomized arms of the re-randomized trials. Patients in maintenance phase trials were mostly similar in terms of age and sex. The mean Mayo score was similar for most trials. In the Lasa et al. report, NMAs were conducted using the multivariate frequentist approach on 23 RCTs. The mean age of patients in the induction phase ranged from 34.4 to 43 years, and females comprised 33.7% to 45.5% of the study populations. Eleven trials required patients to be naive to anti-TNF biologics at study entry. Among studies that allowed but did not require prior therapy with anti-TNF biologics, there was variation in the percentage of patients who did have prior therapy with these drugs (15% to 58%). Reporting of disease duration varied across studies but appear comparable among studies (mean = 3.8 to 14.6 years). Of the 22 studies evaluating maintenance therapy, 10 were done using a treat-straight-through strategy and 12 followed a randomized responders design. Patients in the maintenance phase ranged in mean age from 34.4 to 43 years, and females comprised 33.7% to 47.7% of the study populations.
Efficacy Results
In the sponsor’s report, results from the NMA suggested that for the induction phase, in the overall population, no treatment was favoured when ozanimod was compared with other active treatments for clinical response. Similar results were found for the biologic-naive patients. Among biologic-exposed patients, there was no evidence for a difference between ozanimod and other relevant active treatments, except that ozanimod was favoured over adalimumab (odds ratio [OR] = 3.13; 95% credible interval [CrI], 1.42 to 7.31). For the maintenance phase, in the overall population, results of the NMA showed no evidence for a difference between ozanimod and other active treatments, except that ozanimod had a less favourable clinical response compared with vedolizumab 300 mg every 8 weeks (OR = 0.55; 95% CrI, 0.34 to 0.92), tofacitinib 5 mg (OR = 0.57; 95% CrI, 0.33 to 0.97), and tofacitinib 10 mg (OR = 0.40; 95% CrI, 0.23 to 0.69). For the biologic-naive population, ozanimod had a less favourable clinical response compared with vedolizumab 300 mg every 8 weeks (OR = 0.47; 95% CrI, 0.24 to 0.87), tofacitinib 5 mg (OR = 0.45; 95% CrI, 0.22 to 0.89), and tofacitinib 10 mg (OR = 0.36; 95% CrI, 0.18 to 0.72). For biologic-exposed patients, there was no evidence for a difference between ozanimod and any of the active comparators.
In the sponsor’s report, for the outcome of clinical remission, for the induction phase, no treatment was favoured when ozanimod was compared with other active treatments in the overall population. Similar results were found for the biologic-naive patients. Among biologic-exposed patients, there was no evidence for a difference between ozanimod and other active treatments, except that ozanimod was favoured over adalimumab (OR = 4.19; 95% CrI, 1.56 to 11.49). For the maintenance phase, there was no evidence for a difference between ozanimod and other active treatments, except that ozanimod had a less favourable rate of clinical remission compared with vedolizumab 300 mg every 8 weeks (OR = 0.56; 95% CrI, 0.34 to 0.92), tofacitinib 5 mg (OR = 0.57; 95% CrI, 0.34 to 0.97), and tofacitinib 10 mg (OR = 0.40; 95% CrI, 0.24 to 0.69). For the biologic-naive population, ozanimod had a less favourable rate of clinical remission compared with vedolizumab 300 mg every 8 weeks (OR = 0.47; 95% CrI, 0.25 to 0.88), tofacitinib 5 mg (OR = 0.45; 95% CrI, 0.23 to 0.89) and tofacitinib 10 mg (OR = 0.37; 95% CrI, 0.19 to 0.72). For biologic-exposed patients, there was no evidence for a difference between ozanimod and any of the active comparators. In the Lasa et al. report, no treatment was favoured when ozanimod was compared with other active treatments for induction of clinical remission in the overall population, in biologic-naive patients, and in biologic-exposed patients.
In the sponsor’s report, for the outcome of endoscopic improvement, for the induction phase, the NMA results found there was no evidence for a difference between ozanimod and other active comparators, except that ozanimod was favoured over adalimumab in the overall population (OR = 2.04; 95% CrI, 1.16 to 3.76) and in biologic-naive patients (OR = 2.04; 95% CrI, 1.16 to 3.76). Among biologic-exposed patients, no active treatments were favoured over others for endoscopic improvement. For the maintenance phase, there was no evidence for a difference between ozanimod and other active comparators, except that ozanimod had a less favourable rate of endoscopic improvement compared with vedolizumab 300 mg every 4 weeks (OR = 0.46; 95% CrI, 0.24 to 0.88) and tofacitinib 10 mg (OR = 0.42; 95% CrI, 0.22 to 0.79). For the biologic-naive population, ozanimod had a less favourable rate of endoscopic improvement compared with tofacitinib 10 mg (OR = 0.34; 95% CrI, 0.15 to 0.77). For biologic-exposed patients, there was no evidence for a difference between ozanimod and any of the active comparators. In the Lasa et al. report, the endoscopic improvement results of the ITC suggested that ozanimod was favoured over adalimumab for the overall population (OR = 1.79; 95% CI, 1.07 to 3.01) and in biologic-naive patients (OR = 2.07; 95% CI, 1.14 to 3.74). In biologic-exposed patients, no treatment was favoured over another for induction of endoscopic improvement.
Harms Results
The NMA results showed there was no evidence for a difference between ozanimod and other relevant active treatments in the incidence of any adverse events (AEs), SAEs, and AEs leading to discontinuation for either the induction or maintenance phases. For incidence of serious infections at induction, there was no evidence for a difference between ozanimod and any of the active comparators, except that golimumab was favoured over ozanimod (OR = 0.04; 95% CrI, 0 to 0.79). At maintenance, there was no evidence for a difference between ozanimod and other active treatments in the incidence of serious infections.
Critical Appraisal
A significant concern with the ITCs presented is that the studies included in the analyses were highly heterogeneous in terms of both study design and patient characteristics. One of the major concerns with design heterogeneity in UC trials is how trials transition from the induction to the maintenance phase. In the sponsor-submitted ITC, adjustments were made to the data in older treat-through trials to more closely resemble modern re-randomized trials in the maintenance phase to alleviate the impact of heterogeneity in study design on result interpretation. Different approaches have been adopted to address this heterogeneity, for example, using recalculated data from treat-through studies to mimic a re-randomized trial, or including only re-randomized trials. Results of this sensitivity analysis suggested that exclusion of the recalculated treat-through data did not alter the results from the base-case analyses.
Other significant heterogeneities can be found in the definition of clinical outcomes, timing of study end point evaluation, subgroup definitions, and patients’ baseline characteristics. In the sponsor’s ITC, a number of trial and patient characteristics were considered treatment-effect modifiers. Despite various statistical techniques being employed to lessen the impact of potential clinical heterogeneity on the estimated treatment effect of ozanimod, there is still significant uncertainty in the ITC results. In the Lasa et al. report, patients’ baseline characteristics were not reported in detail; therefore, limited data are available to examine the treatment effect and safety of ozanimod in the study population, particularly in the subgroups of patients who were biologic-naive and biologic-exposed. In addition, there was insufficient analysis conducted to account for trial and clinical heterogeneity, thus limiting the utility and robustness of the results.
In both ITCs, safety data were sparse and available for the overall population only. In addition, wider CrIs are observed due to the low event rate for some of the safety outcomes, such as AEs leading to discontinuation and serious infections; thus, the interpretation of the results is challenging.
Other Relevant Evidence
Description of Studies
The phase III OLE study was summarized to provide additional evidence regarding the long-term safety and efficacy of ozanimod for the treatment of patients with moderately or severely active UC at the time points beyond the TRUE NORTH parent study. The OLE study included patients who completed at least 10 weeks of the induction period without experiencing a clinical response or completed the maintenance period to week 52, or those who experienced disease relapse during the maintenance period of the TRUE NORTH trial.13 Of the 824 patients who entered the OLE study from the TRUE NORTH trial, 43.4% were enrolled after completing the induction period, 39.9% entered after completing the maintenance period, and 16.6% entered after discontinuing from the maintenance period.
Efficacy Results
The long-term efficacy of ozanimod as measured in the OLE study found that at week 46, ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||. However, by week 142, the treatment response rates decreased markedly. The results from the OLE study; however, were limited by the relatively small number of patients evaluated at each assessment point. Additionally, there was a high rate of treatment discontinuations (38.6%) during the OLE study, mostly due to lack of response, patient decision, and AEs.
Harms Results
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Critical Appraisal
The OLE was a single-group study that did not include an active or placebo comparison group; without a comparison group, it is not possible to know the true benefit of treatment and it is difficult to interpret results. All efficacy end points were descriptive, as there was no formal statistical testing. Although certain procedures have been performed to maintain blinding to the treatment assignment from the parent trial, the open-label administration of the drug could introduce bias, as knowledge of the treatment may lead patients and investigators to overestimate its potential benefits and harms. The treatment response rates were higher in the patients who were re-randomized to placebo in the TRUE NORTH study. This may be explained by the longer follow-up period for these patients, as they were more likely to discontinue treatment earlier in the original study. The eligibility criteria of the OLE study specified that patients had to complete the induction or maintenance periods of the parent TRUE NORTH study, or discontinue the maintenance period due to disease relapse, which potentially allowed for selection bias. Patients who did not have a treatment response at study entry could discontinue the study treatment if no clinical improvement was observed from the baseline visit of the TRUE NORTH study by week 10. Additionally, there was a high rate of treatment discontinuations |||||||||| during the OLE study, mostly due to lack of response, patient decision, and AEs. This may have resulted in the enrolment of more patients who were better able to tolerate ozanimod and, as a result, there were fewer reports of AEs. The inclusion of patients with no initial response to ozanimod during the TRUE NORTH parent trial (68.2%) is likely to underestimate the benefit observed during this extension study compared with the maintenance period of the parent study. Given that this was an ongoing study, the results were limited to the interim analysis as of March 31, 2020, and there were small numbers of evaluable patients, especially at weeks 96 and 142.
Conclusions
Based on the TRUE NORTH trial, ozanimod was efficacious in achieving induction and maintenance of clinical remission and clinical response in patients with moderately or severely active UC. Moreover, ozanimod was also found to be efficacious in achieving endoscopic improvement, mucosal healing, corticosteroid-free remission, durable clinical remission, and maintenance of clinical remission. However, the generalizability of the results to the real-world setting is limited due to the re-randomization study design and the option for enrolment into an open-label trial during the maintenance period. Based on the available ITCs, it remains uncertain how ozanimod compares with other advanced treatments for moderate to severe UC in efficacy and safety.
Introduction
Disease Background
IBD is a term used to describe disorders that involve chronic inflammation of the digestive tract. There are 2 main types of IBD: Crohn disease and UC. Crohn disease is characterized by inflammation of the lining of the digestive tract, often involving the deep layers of the digestive tract. UC causes inflammation and ulcers in the digestive tract, affecting the innermost lining of the large intestine (colon) and rectum.1,2 While both diseases are characterized by diarrhea, abdominal pain, rectal bleeding, and weight loss, UC is characterized by blood in the stool with mucus, frequent diarrhea, loss of appetite, and tenesmus (strong urge to use the bathroom without necessarily having a bowel movement).3,4 While the etiology of UC is not completely understood, there is growing evidence to suggest that genetic and environmental factors may contribute to the irregular immune response that aberrantly recruits activated immune cells to the colon,3 which results in chronic inflammation that damages the colon and causes the UC symptoms. UC generally develops in young adulthood5-7 and persists throughout life, marked by periods of spontaneous remission and relapse.14 The most common initial manifestation of UC is bloody diarrhea with or without mucus. In addition to frequent evacuations with blood and mucus, other symptoms include urgency or tenesmus of evacuations, fever, abdominal pain, and weight loss.3,4
While endoscopic procedures with tissue biopsy are the only way to definitively diagnose UC, the path to a UC diagnosis also includes a review of medical history, a physical exam, and a series of medical tests. Part of the diagnosis process involves laboratory testing of blood and fecal matter to eliminate the possibility that symptoms are being caused by enteric infections from bacteria, viruses, or parasites. In addition, tests to rule out other forms of IBD, such as Crohn disease, are performed.
UC has a worldwide annual incidence rate of 1.2 to 20.3 cases per 100,000 people and a prevalence of 7.6 to 246.0 cases per 100,000 people.3 The highest age-standardized prevalence rate of IBD in 2017 occurred in high-income countries in North America,15 with Canada having 1 of the highest rates in the world.5 Estimated annual incidence rates for UC in Canada range from a low of 8.4 per 100,000 people in Alberta to a high of 21.4 per 100,000 people in Nova Scotia.5-7 There are an additional 15,000 individuals living with IBD in Canada who do not have a confirmed diagnosis of Crohn disease or UC (termed indeterminate colitis).8
The majority of individuals living with UC have a mild to moderate disease course; generally with active disease at diagnosis followed by alternating exacerbations and longer periods of remission.16 However, an aggressive disease course is experienced in 10% to 15% of patients, with a cumulative risk of relapse of between 70% and 80% at 10 years postdiagnosis.16 Regardless of severity, UC is associated with high rates of fatigue and sleep difficulties.16 According to patient input received for this review, the need to be near and the time spent in bathrooms is disruptive to work and social obligations, which in turn has negative physical, emotional, and social impacts. Approximately half of all patients required UC-related hospitalization at some point during the disease course. Moreover, approximately 1.5% of patients with UC are diagnosed with colorectal cancer, typically after prolonged active inflammation. While UC is not associated with an increased risk of all-cause mortality after the first year after diagnosis,17 gastrointestinal-specific mortality may be increased.16,17
UC has a tremendous economic and societal burden due to its impact on school, work, and social interaction. In Canada, approximately $1.2 billion is spent on health care utilization costs in patients with IBD, and an estimated indirect cost of $1.5 billion is borne due to loss of work and productivity, disability coverage, and premature retirement or death.18,19 In fact, the annual cost due to medical absenteeism is approximately $88 million,9 while the estimated lifetime lost wages due to premature retirement due to UC is $994,760 per person.9 Furthermore, 56% to 74% of people living with IBD in Canada have reported paying out of pocket for complementary and alternative medicines,20-22 with no difference between patients with Crohn disease and those with UC.20
Standards of Therapy
According to the clinical expert consulted by CADTH for the purpose of this review, the immediate goal of UC treatment is improvement in symptoms (i.e., induction of clinical remission), as patients can be severely affected by rectal bleeding, urgency, and diarrhea. Reduction in biomarkers of inflammation, such as fecal calprotectin, is an intermediate-term goal. Long-term treatment goals, as indicated by the clinical expert, are to induce and maintain endoscopic remission and, possibly, to achieve mucosal healing (a composite of both endoscopic and histologic healing), alter the normal course of the disease (i.e., avoidance of colectomy and hospitalization), and normalize quality of life. These goals are consistent with the recently published Selecting Therapeutic Targets in Inflammatory Bowel Disease (STRIDE)-II consensus guidelines. However, as described by the clinical expert, many patients with UC are left with residual symptoms (most frequently, abnormal stool frequency) even after achieving long-term resolution of rectal bleeding or endoscopic remission.
Anti-inflammatory drugs are typically used as first-line therapy for mild to moderate UC and include 5-ASAs (mesalamine, balsalazide, and olsalazine), sulfasalazine, and corticosteroids. The clinical expert indicated that patients with UC are initially treated with a 5-ASA, with corticosteroids added for induction therapy in patients with more severely active disease. The choice of 5-ASA and its route of administration (e.g., oral or as an enema or suppository) depends on the extent of the colon that is affected. Patients with acute severe UC in hospital typically receive IV corticosteroids. Due to the side effects associated with corticosteroids, they should be reserved for induction therapy and not considered for long-term maintenance therapy.
For patients who do not have an adequate response on a 5-ASA or corticosteroid, conventional immunosuppressants, such as azathioprine, mercaptopurine, and methotrexate, are treatment options. The clinical expert noted that many public drug plans require that, to be eligible for an advanced therapy such as a biologic, the patient’s condition must have failed to respond to conventional immunosuppressants; however, conventional immunosuppressants are generally ineffective as induction therapy and have considerable toxicities.
Biologic therapies are the mainstay treatment for patients with moderate to severe UC. They are used for induction and maintenance when other treatments have been unsuccessful or when patients cannot tolerate other treatments. There are 3 main classes of biologics used to treat UC: anti-TNF drugs (infliximab, adalimumab, and golimumab), anti-integrin drugs (vedolizumab), and anti–interleukin-12 and -23 drugs (ustekinumab). Tofacitinib, a Janus kinase inhibitor, is a small-molecule drug that is also considered an advanced therapy, along with biologics. According to the clinical expert, all of these drugs are effective, and each has its own advantages and disadvantages with respect to safety, convenience, and efficacy. The clinical expert indicated that infliximab is generally used for patients who have acute severe UC in the hospitalized setting. While tofacitinib has excellent efficacy, its safety profile is potentially concerning. Accordingly, tofacitinib has largely been relegated to second-line therapy. Patients who do not have a response to, lose response to, or are intolerant to 1 advanced therapy can move to a different advanced therapy, with consideration for the reason for treatment failure as an important determinant of the choice of second-line drug.
Patients with UC may also be prescribed other medications to manage specific symptoms, which may include antidiarrheal medications, pain relievers, antispasmodics, and iron supplements. The clinical expert consulted by CADTH indicated that while some patients with UC will seek out complementary or alternative medicines, these therapies are generally not effective for the long-term management of moderately to severely active UC.
Approximately 5% to 10% of patients with UC may require surgery.9 UC surgery typically involves removing the entire colon and rectum (proctocolectomy) and in most cases, an ileoanal anastomosis (J-pouch) procedure is performed. The procedure involves the construction of a pouch from the end of the small intestine which is then attached directly to the anus to allow for relatively normal evacuation. According to the clinical expert consulted by CADTH, colectomy is generally reserved for 3 scenarios: development of colorectal dysplasia; complications (e.g., toxic megacolon and/or perforation); and failure of medical therapy.
Drug
Ozanimod is an immune modulator that targets the S1P1 and S1P5 receptors on immune cells. S1P receptors are a specific part of the immune cell that plays an important role in inflammatory conditions such as UC. By binding to the S1P receptors on immune cells, ozanimod is thought to act as a gatekeeper, keeping these cells from moving out of the lymph nodes and into the circulation.
On April 8, 2022, ozanimod received a Notice of Compliance from Health Canada for the treatment of adult patients with moderately to severely active UC who have had an inadequate response, a loss of response, or were intolerant to either conventional therapy or a biologic drug. Ozanimod has been previously approved by Health Canada for the treatment of adult patients with relapsing-remitting multiple sclerosis to decrease the frequency of clinical exacerbation and has been previously reviewed by CADTH for this indication.
Ozanimod received approval from the FDA in May 2021 for the treatment of moderately to severely active UC in adults.23 Ozanimod received approval from the European Medicines Agency in May 2020 for the treatment of adult patients with moderately to severely active UC who have had an inadequate response, lost response, or were intolerant to either conventional therapy or a biologic drug.24
Ozanimod is administered as an oral capsule at a dosage of 0.23 mg once daily from day 1 to day 3, 0.46 mg once daily from day 5 to day 7, and 0.92 mg once daily from day 8 onward.
Key characteristics of commonly used medical treatments for UC are presented in Table 3.
Table 3: Key Characteristics of Ozanimod and Main Comparators
Detail | Ozanimod | Vedolizumab | Ustekinumab | Infliximab | Golimumab | Tofacitinib | Adalimumab |
|---|---|---|---|---|---|---|---|
Mechanism of action | S1P receptor modulator that binds to the S1P1 receptors on lymphocytes, preventing egress from lymph nodes. The mechanism by which ozanimod and its active metabolites exert their therapeutic effects in MS and UC is unknown, but may involve reduction in lymphocyte migration into the CNS and intestine. | IgG1 monoclonal antibody. Binds to the human alpha 4 beta 7 integrin, acting as a gut-selective anti-inflammatory biologic. | Human IgG1 monoclonal antibody. Neutralizes cellular responses mediated by IL-12 and IL-23. | Anti-TNF. IgG1k monoclonal antibody that neutralizes the biological activity of TNF alpha by specifically binding to its receptors. | Anti-TNF. Human monoclonal antibody that binds with p55 or p75 human TNF receptors. | Selective JAK inhibitor. Blocks several cytokine pathways and lymphocyte activation. | Anti-TNF. Human IgG1 monoclonal antibody. Binds and blocks TNF alpha and its interactions with p55 and p75 cell-surface TNF receptors. |
Indicationa | Treatment of adult patients with moderately to severely active UC who had an inadequate response, a loss of response, or were intolerant to either conventional therapy or biologic agent. | Treatment of adult patients with moderately to severely active UC who have had an inadequate response to, loss of response to, or were intolerant to either conventional therapy or infliximab, a TNF-alpha antagonist. | Treatment of adult patients with moderately to severely active UC who have failed or were intolerant to treatment with immunomodulators or corticosteroids, but never failed treatment with a biologic, or have failed or were intolerant to treatment with a biologic. | Induction and maintenance of clinical remission and mucosal healing, and reduction or elimination of corticosteroid use in adult patients with moderately to severely active UC who have had an inadequate response to conventional therapy. | Induction and maintenance of clinical response in adults with moderately to severely active UC who have had an inadequate response to or have medical contraindications for conventional therapy, including corticosteroids, aminosalicylates, azathioprine, or 6-MP. | For the treatment of adult patients with moderately to severely active UC with an inadequate response to, loss of response to, or intolerance to either conventional UC therapy or a TNF-alpha inhibitor. | For the treatment of adult patients with moderately to severely active UC who have had an inadequate response to conventional therapy, including corticosteroids and/or azathioprine or 6-MP or who are intolerant to such therapies. |
Route of administration | Oral | IV induction followed by SC injection for maintenance | IV induction followed by SC injection for maintenance | IV | SC | Oral | SC |
Recommended dose |
| 30 mg administered by IV infusion at 0, 2, and 6 weeks and then every 8 weeks thereafter. The SC maintenance dose is 108 mg every 8 weeks. |
| Induction dose of 5 mg/kg at 0, 2, and 6 weeks followed by 5 mg/kg every 8 weeks thereafter. | 200 mg initial dose by SC injection at week 0 followed by 100 mg at week 2, and then 50 mg every 4 weeks thereafter. | 10 mg (as tofacitinib citrate) twice daily. | 160 mg at week 0 followed by 80 mg at week 2 administered by SC injection. |
Serious adverse effects or safety issues | Malignancies, particularly of the skin, have been reported in patients taking ozanimod in clinical trials. Initiation of ozanimod may result in transient reductions in heart rate and atrioventricular delays. | Infections and malignancies have been reported in patients taking vedolizumab, but no clinically significant differences have been found. | Immunomodulating drugs have the potential to increase the risk of infections and malignancy. No clinically significant differences have been found in terms of malignancies. | Infections and malignancies have been observed in patients receiving infliximab. | Upper respiratory infections and reactions at the site injection, but no clinically significant differences compared with placebo. | A Health Canada warning indicated an increased risk of thromboses (pulmonary and deep vein thrombosis) and death, and increased risk of serious infection, including herpes zoster infections. | Serious infections (pneumonia), malignancies, and neurologic events have been reported more frequently in patients taking adalimumab. |
Other | — | — | — | — | — | Not recommended in combination with biological UC therapies or with potent immunosuppressants such as azathioprine and cyclosporine. | — |
6-MP = mercaptopurine; CNS = central nervous system; Ig = immunoglobulin; IL = interleukin; JAK = Janus kinase; MS = multiple sclerosis; S1P = sphingosine 1-phosphate; S1P1 = S1P 1 receptor; S1P5 = S1P 5 receptor; SC = subcutaneous; TNF = tumour necrosis factor; UC = ulcerative colitis.
aHealth Canada–approved indication.
Source: Product monographs for ozanimod (Zeposia),25 ustekinumab (Stelara),26 infliximab (Remicade),27 vedolizumab (Entyvio),28 golimumab (Simponi),29 tofacitinib (Xeljanz)30 and adalimumab (Humira).31
Stakeholder Perspectives
Patient Group Input
This section was prepared by CADTH staff based on the input provided by patient groups. The full patient group submissions are included in the Stakeholder Input section at the end of this report.
The patient input received for this review was collected by the GI Society and the CCC. The input provided by the GI Society included more than 1,500 respondents with IBD, including UC, and was sourced from 4 online surveys (conducted in 2015, 2018, and 2 conducted in 2020), one-to-one conversations, and phone, email, and social media interactions. The input provided by the CCC consisted of more than 3,900 respondents with IBD and was sourced from multiple surveys (conducted from late 2017 to early 2018 and in 2021) and a phone interview. The CCC input included 8 respondents with experience using ozanimod for UC; all accessed ozanimod through a clinical trial.
Respondents from both groups reported that UC has had a profound effect on all aspects of their life — physically, emotionally, and socially — regardless of whether they are at home, at school, or in the workplace. Symptoms associated with UC such as diarrhea, rectal bleeding, abdominal pain, bloating, cramping, anemia due to blood loss, frequent and urgent bowel movements, and fatigue not only affect day-to-day living, but also cause anxiety, stress, and isolation. Respondents from both groups experienced constant concerns about future flare-ups, which can be disruptive. Respondents reported decreased quality of life during periods of active disease, with patients spending a lot of time in the bathroom. Even during periods of remission, respondents reported the need to stay close to a bathroom, thereby limiting their activities. Moreover, due to the perceived stigma of UC, many report hiding their disease from work colleagues, friends, and family. In extreme cases, based on patient input received from the CCC, thoughts of suicide were reported due to the inability to control and cope with the impacts of UC on their personal and social lives, as well as consequences on their career or schooling. Based on the patient input received from the GI Society, only 24% of respondents with IBD reported that the currently available medications are adequate to control their disease. Patient groups indicated that available treatments may have helped initially to relieve some of the symptoms, but the treatments were unsuccessful in controlling their symptoms. Respondents reported the need for new and effective treatment options to achieve mucosal healing and reduce or eliminate the debilitating symptoms of UC. Moreover, respondents stressed that sustained remission or treatment response is more important than relieving any 1 symptom.
Six of the 8 respondents who were prescribed ozanimod reported treatment benefits, such as ease of use and improved symptoms and quality of life, with a general sense of feeling healthier and happier. One respondent discontinued use of ozanimod due to multiple side effects, including headache, serious infection, joint pain, and nasopharyngitis. Half of the respondents indicated the ozanimod capsules were difficult to swallow.
Clinician Input
Input From the Clinical Experts Consulted by CADTH
All CADTH review teams include at least 1 clinical specialist with expertise regarding the diagnosis and management of the condition for which the drug is indicated. Clinical experts are a critical part of the review team and are involved in all phases of the review process (e.g., providing guidance on the development of the review protocol, assisting in the critical appraisal of clinical evidence, interpreting the clinical relevance of the results, and providing guidance on the potential place in therapy). The following input was provided by 1 clinical specialist with expertise in the diagnosis and management of UC.
Unmet Needs
The clinical expert consulted by CADTH detailed 4 unmet needs related to therapies for the treatment of UC. First, while currently available therapies are effective, most patients with UC are unable to achieve complete endoscopic remission. As such, better UC therapies are needed to break through the “therapeutic ceiling” of current treatments. Second, it is unknown what the best treatment strategies are for patients with moderate to severe UC. Currently, there is no way to predict which patients will respond to which therapy; as a result, the appropriate sequencing of advanced therapies is unclear. Third, there is still uncertainty about the ideal long-term therapeutic target and the overall benefits of targeting clinical, endoscopic, and/or histologic remission. Finally, although access to advanced therapies is generally excellent in Canada compared with other countries, access to coverage for UC treatments continues to present a major burden to both patients and care providers. Many jurisdictions require the failure of treatment with conventional immunosuppressants before biologics are approved for patients with UC. The clinical expert noted that the current criteria for reimbursement requiring the failure of ineffective conventional immunosuppressants or corticosteroids, which carry a high risk of AEs, create a situation where clinicians are forced to make decisions that may be harmful to their patients to satisfy reimbursement requirements.
Place in Therapy
The clinical expert consulted by CADTH indicated that the novel mechanism of ozanimod would be a valuable addition to the treatment paradigm, since the current therapies for moderate to severe UC are limited. According to the clinical expert, ozanimod may become a first-line advanced therapy among patients whose condition has failed to respond to 5-ASAs, given ozanimod’s oral route of administration and efficacy in treating moderate UC. The clinical expert indicated that ozanimod may be considered among patients whose condition has failed to respond to other biologic therapies, although the data for ozanimod’s effectiveness after anti-TNF failure is less promising.
The clinical expert noted that while the treatment under review addresses the underlying disease process in terms of lymphocyte trafficking, the mechanism of inflammation in UC is extremely complex. Current strategies for using biologic monotherapy in UC only allow targeting of 1 pathway of inflammation, although there are likely dozens contributing to UC inflammation, and preliminary trials suggest combination strategies may potentially be more effective than current treatment options. However, they would come at considerably greater cost and patients may be at higher risk for drug-related AEs.
Patient Population
The drug under review targets patients with UC. The diagnosis of UC is based on clinical, endoscopic, and histopathologic features. Overall, most patients have a distinctive clinical history of bloody diarrhea, urgency, and tenesmus, and the endoscopic appearance of contiguous inflammation from the rectum upward is characteristic. Histopathologic features of chronic mucosal inflammation confirm the diagnosis. The likelihood of misdiagnosis or under-diagnosis is relatively low due to its distinctive clinical features (e.g., fecal urgency, tenesmus, and rectal bleeding), although there may be delays to diagnosis for patients due to delays in endoscopy access.
According to the clinical expert, treatment with ozanimod would be suitable for patients with moderate to severe UC. There may be potentially greater uptake in patients with more moderate UC whose condition has failed to respond to a 5-ASA but who have not initiated treatment with other biologic therapies, or who have active disease as determined by endoscopy. Currently, there are no predictive tools to identify the ideal candidate for the medication under review. The identification of patients best suited for treatment with ozanimod would primarily be based on clinical judgment. Ozanimod may also be used in patients with moderately to severely active UC that has failed to respond to other biologic therapies, although the data are less promising for induction of remission among patients who have experienced treatment failure with an anti-TNF therapy.
The clinical expert did stress that patients with presymptomatic UC should not be treated with any UC medications due to a measurable AE rate, and that there are no tools to determine who will go on to develop UC. In addition, patients with conduction abnormalities, significant liver disease, potential for drug–drug interactions, and ocular disease or diabetes may not be suitable for treatment with ozanimod.
Assessing Response to Treatment
Treatment response is determined through symptomatic assessment, evaluation of stool and blood biomarkers, and endoscopy (with or without histopathology). Response to UC treatment may be indicated by a reduction in symptom severity (e.g., resolution of rectal bleeding, normalization or near normalization of stool frequency, and resolution of fecal urgency), reduction in UC biomarkers such as CRP and fecal calprotectin, and improvement in endoscopy features (e.g., endoscopic improvement within the first 4 to 6 months and complete or near endoscopic remission by 12 months).
The clinical expert acknowledged that other outcomes concerning quality of life, activities of daily living, and work productivity may be important outcomes for patients, but these outcomes have not been historically considered markers of true therapeutic efficacy. While histopathology is also important, it is not currently recommended as a therapeutic target.
According to the clinical expert, symptom response should be assessed within 4 to 12 weeks of initiating treatment, biomarker response assessed within 6 months, and endoscopic response assessed within 1 year (ideally by 6 months). The clinical expert indicated that treatment should be discontinued in patients with no endoscopic response to treatment, and that the decision would not be based on symptoms alone due to discordance between symptoms and endoscopic assessment. Treatment would also be expected to be discontinued if the criteria for a drug-related AE were met. Temporary holds on treatment may be required in extenuating circumstances (e.g., need for surgery, development of infection) but, overall, most patients would continue treatment if a positive response was achieved.
Prescribing Conditions
The clinical expert consulted stressed that among patients with UC, ozanimod should be prescribed by a gastroenterologist.
Clinician Group Input
No clinician group input was received for this review.
Drug Program Input
The drug programs provide input on each drug being reviewed through CADTH’s reimbursement review processes by identifying issues that may impact their ability to implement a recommendation. The implementation questions and corresponding responses from the clinical experts consulted by CADTH are summarized in Table 4.
Table 4: Summary of Drug Plan Input and Clinical Expert Response
Drug program implementation questions | Clinical expert response |
|---|---|
Considerations for initiation of therapy | |
Consider alignment with criteria for tofacitinib (oral, small-molecule therapy). | For CDEC consideration. |
Consideration for continuation or renewal of therapy | |
Consider alignment with criteria for tofacitinib. | The CADTH reimbursement recommendation for tofacitinib for UC specifies that patients be assessed after 8 weeks of therapy and discontinued if a clinical response has not been achieved. The clinical expert highlighted that some patients may not have a clinical response until after the first 8 weeks of treatment and that constraints on how frequently patients can be assessed mean that almost no patients will receive a second endoscopy at 8 weeks. |
Consideration for discontinuation of therapy | |
Consider alignment with criteria for tofacitinib. | For CDEC consideration. |
Consideration for prescribing of therapy | |
The requested reimbursement criteria include use in patients who were intolerant to either conventional therapy or a biologic drug. Would clinicians prescribe ozanimod along with a TNF-alpha inhibitor? | Typically, advanced therapies are prescribed as monotherapy and are prescribed sequentially. Combination therapy with another advanced UC treatment (i.e., a biologic or JAK inhibitor) is the exception and occurs only in very rare cases where the patient’s condition fails to respond to all available treatments and requires an off-label option. |
Generalizability | |
The generalizability of results is limited for a subset of patients, as patients younger than 18 years and older than 75 years of age were not studied. | There are other options that would be potentially better suited for patients older than 75 years of age. There are several reasons why it would be rarer to use ozanimod in older patients. First, UC is less common in older patients. Second, vedolizumab or ustekinumab is typically used in this population, given the favourable side effect profiles of these drugs. Finally, this population is much more likely to be on other drugs or have cardiac or ocular comorbidities that would potentially be considered as relative contraindications to ozanimod. |
Care provision issues | |
Bradycardia can occur after the first dose; the product monograph does not suggest starting in hospital to monitor. This may present as a potential issue in care provision. | Bradycardia is a result of a dosing effect, and it is not necessary to initiate ozanimod in hospital. In prescribing the medication, the dosing is escalated during the first week of treatment, which addresses the bradycardia. In the trials, this first-dose effect is generally very mild, and a baseline ECG to rule out significant cardiac conduction abnormalities would occur (for which ozanimod would be contraindicated). When used for the multiple sclerosis indication, hospitalization for the first dose is unnecessary. Also, a recent integrated safety analysis demonstrated that the risk of clinically significant cardiac adverse events from ozanimod is very low. |
CDEC = CADTH Canadian Drug Expert Committee; ECG = electrocardiogram; JAK = Janus kinase; UC = ulcerative colitis.
Clinical Evidence
The clinical evidence included in the review of ozanimod is presented in 3 sections. The first section, the systematic review, includes pivotal studies provided in the sponsor’s submission to CADTH and Health Canada, as well as those studies that were selected according to an a priori protocol. The second section includes indirect evidence from the sponsor and indirect evidence selected from the literature that met the selection criteria specified in the review. The third section includes sponsor-submitted long-term extension studies and additional relevant studies that were considered to address important gaps in the evidence included in the systematic review.
Systematic Review (Pivotal and Protocol-Selected Studies)
Objectives
To perform a systematic review of the beneficial and harmful effects of ozanimod 1.0 mg per day for the treatment of moderately to severely active UC in adult patients who had an inadequate response, a loss of response, or were intolerant to either conventional therapy or biologic drug.
Methods
Studies selected for inclusion in the systematic review included pivotal studies provided in the sponsor’s submission to CADTH and Health Canada, as well as those meeting the selection criteria presented in Table 5. Outcomes included in the CADTH review protocol reflect outcomes considered to be important to patients, clinicians, and drug plans.
Of note, the systematic review protocol presented subsequently was established before the granting of a Notice of Compliance by Health Canada.
Table 5: Inclusion Criteria for the Systematic Review
Criteria | Description |
|---|---|
Population | Adult patients between the ages of 18 to 75 years with moderately to severely active UC who had an inadequate response, a loss of response, or were intolerant to either conventional therapy or a biologic agent. Subgroups:
|
Intervention | Ozanimod, oral capsule. Dosage:
|
Comparator |
|
Outcomes | Efficacy outcomes:
Harms outcomes: Incidence and type of AEs, SAEs, WDAEs, notable harms (e.g., serious or opportunistic infection, bradycardia, heart conduction abnormalities, macula edema, blood pressure increase, liver enzyme increase, lymphopenia) |
Study designs | Published and unpublished phase III and IV RCTs |
AE = adverse event; HRQoL = health-related quality of life; RCT = randomized controlled trial; SAE = serious adverse event; UC = ulcerative colitis; WDAE = withdrawal due to adverse event.
aThese outcomes were identified as being of particular importance to patients in the input received by CADTH from patient groups.
The literature search for clinical studies was performed by an information specialist using a peer-reviewed search strategy according to the PRESS Peer Review of Electronic Search Strategies checklist.32
Published literature was identified by searching the following bibliographic databases: MEDLINE All (1946–) through Ovid and Embase (1974–) through Ovid. All Ovid searches were run simultaneously as a multifile search. Duplicates were removed using Ovid deduplication for multifile searches, followed by manual deduplication in Endnote. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. The main search concepts were Zeposia (ozanimod). Clinical trial registries were searched: the US National Institutes of Health’s clinicaltrials.gov, the WHO’s International Clinical Trials Registry Platform (ICTRP) search portal, Health Canada’s Clinical Trials Database, and the European Union Clinical Trials Register.
No filters were applied to limit the retrieval by study type. Retrieval was not limited by publication date or by language. Conference abstracts were excluded from the search results. Refer to Appendix 1 for the detailed search strategies.
The initial search was completed on February 2, 2022. Regular alerts updated the search until the meeting of the CADTH Canadian Drug Expert Committee (CDEC) on May 25, 2022.
Grey literature (literature that is not commercially published) was identified by searching relevant websites from the Grey Matters: A Practical Tool For Searching Health-Related Grey Literature checklist.33 Included in this search were the websites of regulatory agencies (FDA and European Medicines Agency). Google was used to search for additional internet-based materials. Refer to Appendix 1 for more information on the grey literature search strategy.
These searches were supplemented by reviewing bibliographies of key papers and through contacts with appropriate experts. In addition, the sponsor of the drug was contacted for information regarding unpublished studies.
A focused literature search for NMAs dealing with UC was run in MEDLINE All (1946–) on February 2, 2022. No limits were applied to the search.
Two CADTH clinical reviewers independently selected studies for inclusion in the review based on titles and abstracts, according to the predetermined protocol. Full-text articles of all citations considered potentially relevant by at least 1 reviewer were acquired. Reviewers independently made the final selection of studies to be included in the review, and differences were resolved through discussion.
Findings From the Literature
One study was identified from the literature for inclusion in the systematic review (Figure 1). The included study is summarized in Table 6. A list of excluded studies is presented in Appendix 2.
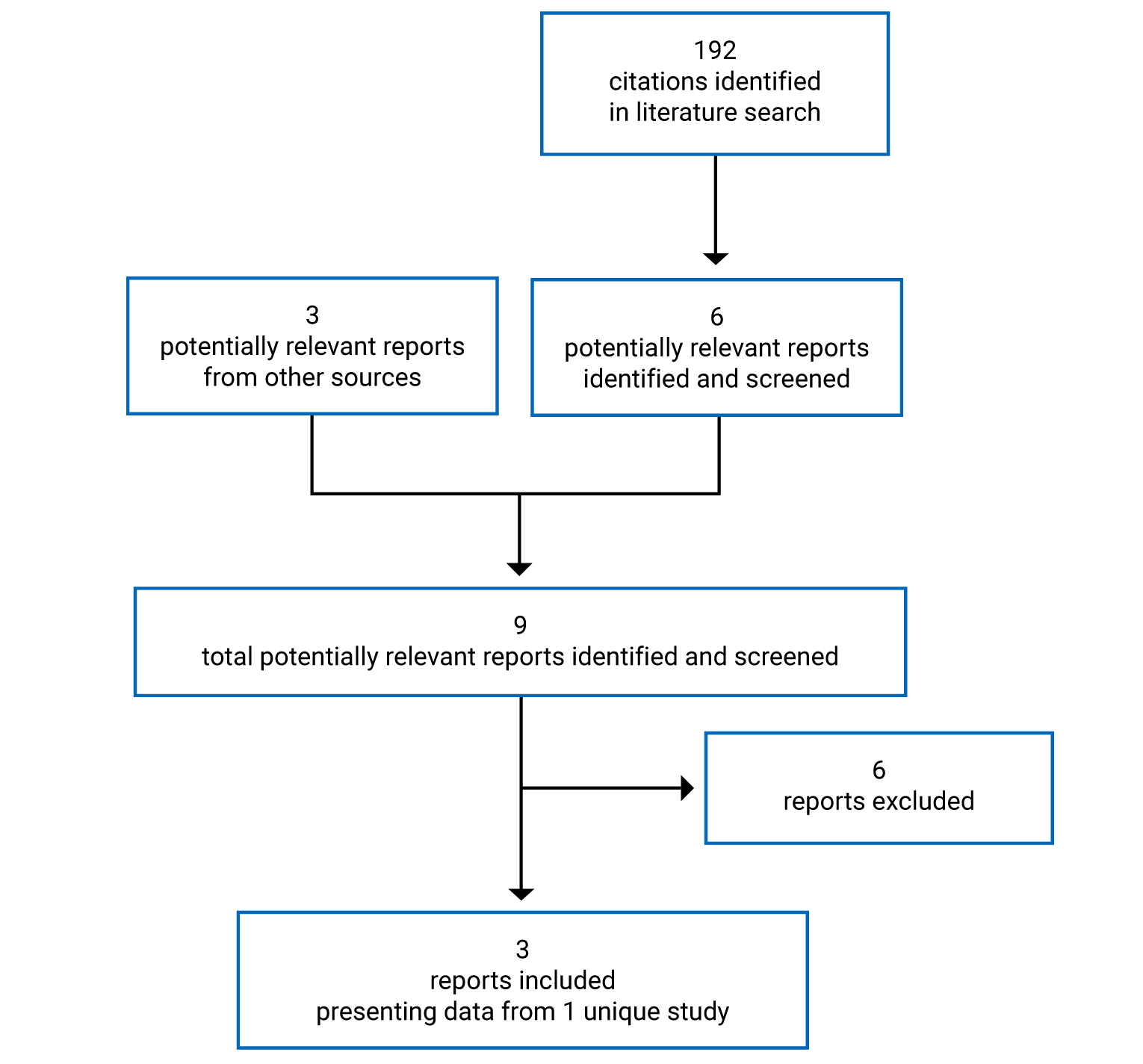
Table 6: Details of Included Studies
Detail | TRUE NORTH |
|---|---|
Designs and populations | |
Study design | Phase III, multicentre, randomized, DB, placebo-controlled trial |
Locations | Patients enrolled across 250 sites in 29 countries (Sites in North America, Europe, Asia, South America, and South Africa) |
Patient enrolment dates | First patients enrolled on August 12, 2015 |
Randomized (N) |
|
Inclusion criteria |
|
Exclusion criteria |
|
Drugs | |
Intervention |
|
Comparator(s) |
|
Duration | |
Phase | |
Screening | Up to 5 weeks |
Induction | 10 weeks |
Maintenance | 42 weeks |
Safety follow-up | 3 months |
Outcomes | |
Primary end point | Clinical remission based on the 3-component Mayo score at week 10 (end of induction period) and at week 52 (end of 42-week maintenance period) |
Secondary and exploratory end points | Key secondary (assessed at week 52):
Other efficacy end points:
Exploratory end point (post hoc):
Safety:
Pharmacokinetic and pharmacodynamic:
|
Notes | |
Publications | |
ADR = adverse drug reaction; ALC = absolute lymphocyte count; bpm = beats per minute; CRP = C-reactive protein; DB = double blind; ECG = electrocardiogram; EMA = European Medicines Agency; EQ-5D-5L = 5-level EQ-5D; Hgb = hemoglobin; HR = heart rate; HRQoL = health-related quality of life; IgG = immunoglobulin G; PK = pharmacokinetic; SAE = serious adverse event; SF-36 = Short Form (36) Health Survey; TEAE = treatment-emergent adverse event; TNF = tumour necrosis factor; UC = ulcerative colitis; ULN = upper limit of normal; VZV = varicella-zoster virus; WPAI-UC = Work Productivity and Activity Impairment Questionnaire – Ulcerative Colitis.
Note: Two additional reports were included.23,24
aOutcome was also assessed at week 10.
Source: Clinical Study Report for the TRUE NORTH study10 and supplement to Sandborn et al.34
Description of Studies
One sponsor-conducted study which met the CADTH review protocol criteria was included in this systematic review. The TRUE NORTH study was a phase III, multicentre, randomized, double-blind, placebo-controlled trial of oral ozanimod as induction and maintenance therapy for adult patients with moderate to severe UC. A total of 645 patients were enrolled across 250 sites from 29 countries in North America (including 8 sites in Canada), Europe, Asia Pacific, South America, and South Africa. The trial consisted of a 10-week induction period followed by a 42-week maintenance period. The induction period was composed of 2 cohorts: cohort 1, in which patients were randomized in a 2:1 ratio to receive either ozanimod 0.92 mg daily (N = 429) or matching placebo (N = 216) In a double-blind fashion, and cohort 2, in which patients received open-label ozanimod 0.92 mg once daily. Patients were evaluated for clinical response and remission at week 10 of the induction period. Patients who had a clinical response to ozanimod at the end of the induction period proceeded to the maintenance period and were re-randomized in a 1:1 ratio to receive either ozanimod 0.92 mg daily (N = 230) or matching placebo (N = 227) in a double-blind fashion. Patients who were randomized to placebo in the induction period and had a clinical response at week 10 continued to receive placebo in the maintenance period. A schematic of the TRUE NORTH trial is presented in Figure 2.
The primary outcome of the study was clinical remission as measured by the Mayo score, a disease-specific instrument that assesses disease severity and response to treatment in patients with UC. The Mayo scoring system is a combined endoscopic and clinical assessment composed of 4 components: rectal bleeding, stool frequency, Physician’s Global Assessment, and endoscopy findings. Each part is rated from 0 to 3, yielding a total score of 0 to 12. The primary and key secondary end points that relied on the Mayo score were assessed using the 3-component Mayo score, which excludes the Physician’s Global Assessment. The key secondary end points were controlled for multiplicity using a statistical testing hierarchy, and each study period was considered an independent study. The primary end point and the following key secondary end points were assessed in both the induction and maintenance periods: clinical response, endoscopic improvement, and mucosal healing. The key secondary end points assessed only in the maintenance period were clinical remission in patients who were in remission at week 10, corticosteroid-free remission, and durability of clinical remission. Other efficacy outcomes included HRQoL outcomes, as assessed by the EQ-5D-5L and the SF-36, and work productivity, as assessed by the WPAI-UC.
Of note, the study included patients who had received anti-TNF therapy and those who had not. The proportion of patients who had previously received anti-TNF therapy was limited to approximately 30% in cohort 1. Patients who had previously received anti-TNF therapy could begin enrolling into cohort 2 once the proportion of patients in cohort 1 who were experienced with anti-TNF therapy hit the randomization limit of approximately 30%. Those patients who were naive to anti-TNF therapy continued to enrol into cohort 1 and could enrol into cohort 2 only after cohort 1 had been closed to enrolment. The proportion of patients who had previously received anti-TNF therapy was limited to approximately 50% in cohort 2.
Patients who completed the induction period and did not have a clinical response were invited to participate in an optional OLE study (RPC01-3102).13 Patients who completed the maintenance period or who experienced disease relapse during the maintenance period were also given the opportunity to enter the OLE study. Disease relapse was defined as having met all of the following criteria: an increase in partial Mayo score of at least 2 points from week 10 and a partial Mayo score of at least 4 points, an endoscopy subscore of at least 2 points, and the exclusion of other potential reasons for an increase in disease activity, such as infection or change in medication.
Randomization at the beginning of both the induction and maintenance periods was stratified. Randomization of patients in cohort 1 of the induction period was stratified by corticosteroid use at screening (yes or no) and prior anti-TNF therapy (yes or no). Re-randomization in the maintenance period was stratified by clinical remission status (as defined by either the 3-component or 4-component Mayo score) at week 10 (yes or no) and corticosteroid use at week 10 (yes or no). Treatment allocation and randomization stratification was centrally allocated across all centres using an interactive voice- and/or web-activated response system.
The first patient visit occurred on August 12, 2015, and the last patient visit occurred on March 27, 2020. Database locks were performed after the completion of blinded treatment for the induction and maintenance periods. The first database lock was executed on June 27, 2019, after all patients in cohort 1 had completed the induction period (week 10). Another database lock was executed on June 15, 2020, after all patients had completed the maintenance period.
There was 1 notable departure from Good Clinical Practice policies and procedures: The paper source documents for 9 patients from a single site were lost after the monitor completed the site close-out visit. All patients who were enrolled at the site were allocated to induction cohort 2 of the open-label study and did not contribute to the induction period efficacy results. Sensitivity analyses of the primary and secondary end points of the maintenance period excluding the 9 patients for which the original source documents were lost were consistent with the primary analyses for the intention-to-treat (ITT) population.
Figure 2: Study Schema for the TRUE NORTH Trial
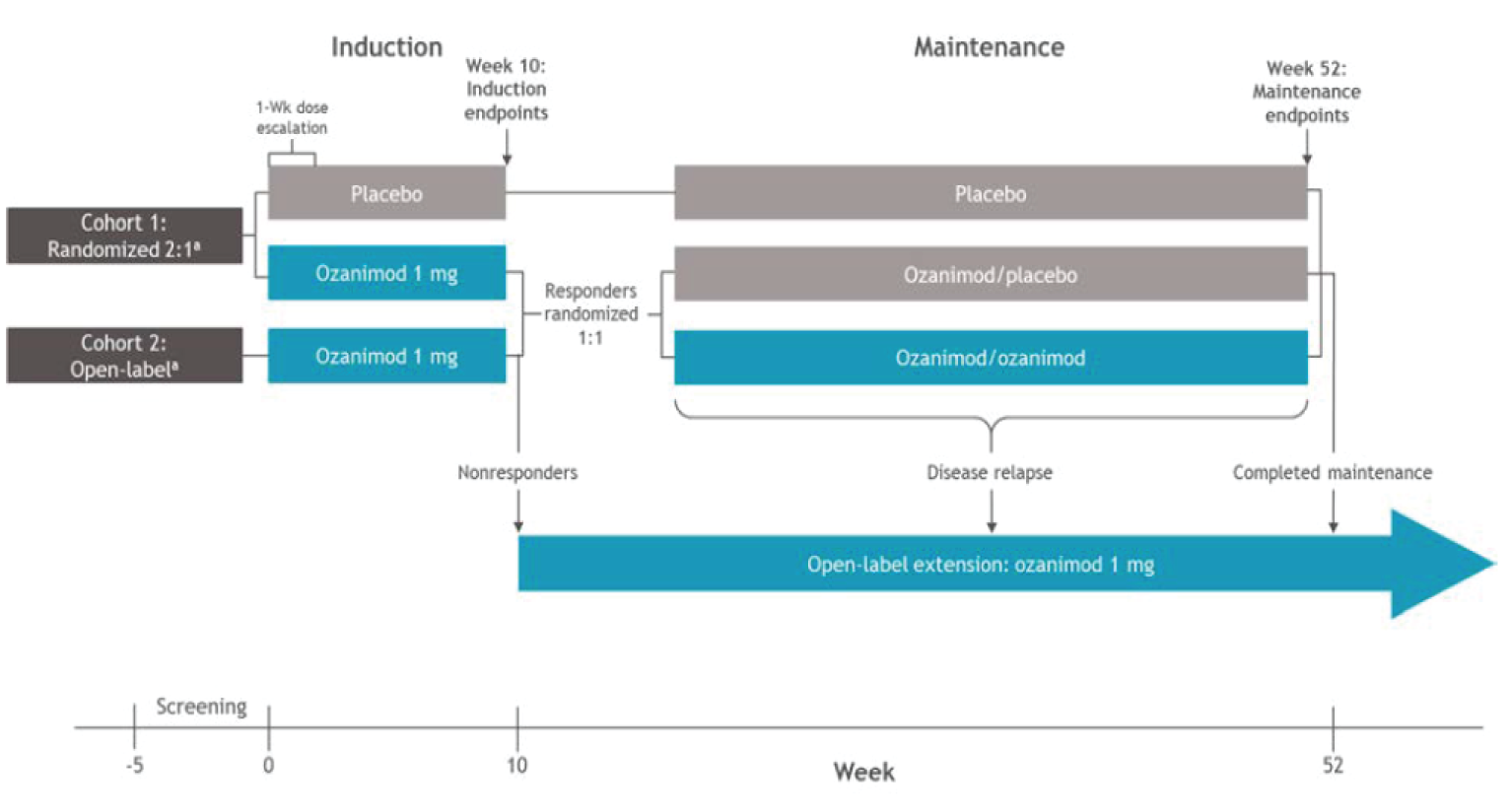
TNF = tumour necrosis factor.
a Patients were stratified by prior anti-TNF exposure (yes or no) and corticosteroid use (yes or no) at screening. The randomization in the maintenance period was stratified by clinical remission at week 10 (yes or no) and corticosteroid use at week 10 (yes or no).
Source: Clinical Study Report for TRUE NORTH study.10
Populations
Inclusion and Exclusion Criteria
The key inclusion and exclusion criteria applied to the TRUE NORTH trial are summarized in Table 6. Briefly, patients eligible for enrolment were adults 18 to 75 years of age with moderately to severely active UC, which was defined as a total Mayo score of 6 to 12, with an endoscopy subscore of 2 or higher, an RBS of 1 or higher, and an SFS of 1 or higher. Patients were required to have received stable dosages of oral aminosalicylates and/or glucocorticoids (prednisone at a dosage of ≤ 20 mg per day or budesonide) for at least 2 weeks before screening endoscopy and to continue receiving the same dosage for the duration of the induction period; the glucocorticoid dose had to be tapered once the patient entered the maintenance period. A documented presence of varicella-zoster virus immunoglobulin G antibody or completed varicella-zoster virus vaccination at least 30 days before randomization was also required. Patients were excluded from the trial if they had a diagnosis of Crohn disease or indeterminate colitis, presence or history of a fistula consistent with Crohn disease, a clinically relevant cardiac condition, or a history of uveitis or macular edema.
Baseline Characteristics
The baseline characteristics of the patients enrolled in the induction period and of those who entered the maintenance period are summarized in Table 7.
Most patients were male. The average age of the patients randomized to receive ozanimod and placebo was 42 and 43 years in the induction and maintenance periods, respectively. Among the patients randomized to receive ozanimod and placebo in both periods, 86% to 89% of patients were white and the mean age at UC diagnosis was 34.4 to 36.0 years.
Table 7: Summary of Baseline Characteristics of Participants in the TRUE NORTH Trial
Characteristic | Induction period (ITT population) | Maintenance period (ITT population) | ||||
|---|---|---|---|---|---|---|
Cohort 1 | Cohort 2 | PL to PL (N = 69) | Re-randomized patients | |||
OZ (N = 429) | PL (N = 216) | OZ (N = 367) | OZ to PL (N = 227) | OZ to OZ (N = 230) | ||
Demographics | ||||||
Sex, n (%) | ||||||
Male | 245 (57.1) | 143 (66.2) | 214 (58.3) | 46 (66.7) | 122 (53.7) | 117 (50.9) |
Female | 184 (42.9) | 73 (33.8) | 153 (41.7) | 23 (33.3) | 105 (46.3) | 113 (49.1) |
Mean age, years (SD) | 41.4 (13.54) | 41.9 (13.64) | 42.1 (13.72) | 44.1 (14.72) | 43.0 (13.71) | 42.4 (13.53) |
Race, n (%) | ||||||
White | 370 (86.2) | 192 (88.9) | 336 (91.6) | 62 (89.9) | 202 (89.0) | 205 (89.1) |
Black or African American | 14 (3.3) | 4 (1.9) | 10 (2.7) | 3 (4.3) | 9 (4.0) | 9 (3.9) |
Asian | 36 (8.4) | 17 (7.9) | 12 (3.3) | 4 (5.8) | 12 (5.3) | 13 (5.7) |
Other | 9 (2.1) | 3 (1.4) | 9 (2.5) | 0 | 4 (1.8) | 3 (1.3) |
Mean weight, kg (SD) | 74.4 (18.25) | 75.0 (16.28) | 76.4 (18.59) | 76.3 (17.02) | 75.4 (17.76) | 74.8 (19.38) |
Mean body mass index, kg/m3 (SD) | 25.40 (5.49) | 25.11 (4.48) | 25.88 (5.80) | 25.45 (4.87) | 25.83 (5.41) | 25.65 (5.80) |
Region, n (%) | ||||||
North America | 107 (24.9) | 60 (27.8) | 80 (21.8) | 13 (18.8) | 49 (21.6) | 56 (24.3) |
Eastern Europea | 215 (50.1) | 112 (51.9) | 200 (54.5) | 49 (71.0) | 136 (59.9) | 121 (52.6) |
Western Europeb | 62 (14.5) | 21 (9.7) | 60 (16.3) | 3 (4.3) | 26 (11.5) | 31 (13.5) |
Asia Pacific | 36 (8.4) | 20 (9.3) | 27 (7.4) | 4 (5.8) | 13 (5.7) | 20 (8.7) |
South America | 3 (0.7) | 0 | 0 | 0 | 1 (0.4) | 1 (0.4) |
South Africa | 6 (1.4) | 3 (1.4) | 0 | 0 | 2 (0.9) | 1 (0.4) |
UC disease characteristics | ||||||
Mean age at UC symptom onset, years (SD) | 33.7 (13.04) | 34.6 (13.52) | 33.7 (13.51) | 35.8 (13.29) | 35.1 (13.48) | 33.4 (13.02) |
Mean age at UC diagnosis, years (SD) | 34.6 (13.22) | 35.3 (13.60) | 34.5 (13.43) | 36.5 (13.69) | 36.0 (13.44) | 34.4 (13.01) |
Mean duration since symptom onset, years (SD) | 7.9 (7.17) | 7.6 (7.08) | 8.65 (7.76) | 8.47 (8.42) | 8.21 (7.79) | 9.24 (7.88) |
Mean duration since diagnosis, years (SD) | 6.9 (6.6) | 6.8 (7.0) | 7.91 (7.4) | 7.75 (8.0) | 7.23 (7.2) | 8.36 (7.3) |
Extent of disease, n (%) | ||||||
Limited to left side of colon | 268 (62.5) | 134 (62.0) | 237 (64.6) | 41 (59.4) | 157 (69.2) | 152 (66.1) |
Extensive | 161 (37.5) | 82 (38.0) | 130 (35.4) | 28 (40.6) | 70 (30.8) | 78 (33.9) |
3-component Mayo scorec (centrally read) at baseline | ||||||
Mean (SD) | 6.6 (1.21) | 6.6 (1.15) | 6.8 (1.26) | 6.4 (1.17) | 6.4 (1.24) | 6.7 (1.31) |
Median | 7.0 | 7.0 | 7.0 | 7.0 | 7.0 | 7.0 |
Minimum, maximum | 3, 9 | 4, 9 | 4, 9 | 4, 9 | 3, 9 | 4, 9 |
4-component Mayo scored (centrally read) at baseline | ||||||
Mean (SD) | 8.9 (1.47) | 8.9 (1.35) | 9.1 (1.49) | 8.6 (1.37) | 8.6 (1.42) | 8.9 (1.57) |
Median | 9.0 | 9.0 | 9.0 | 9.0 | 9.0 | 9.0 |
Minimum, maximum | 6, 12 | 6, 12 | 6, 12 | 6, 11 | 6, 12 | 6, 12 |
4-component Mayo scored (centrally read) at baseline, n (%) | ||||||
≤ 9 | 280 (65.3) | 140 (64.8) | 205 (55.9) | 52 (75.4) | 164 (72.2) | 135 (58.7) |
> 9 | 149 (34.7) | 76 (35.2) | 162 (44.1) | 17 (24.6) | 63 (27.8) | 95 (41.3) |
Mucosal appearance at endoscopy (centrally read),e n (%) | ||||||
Moderate disease | 179 (41.7) | 86 (39.8) | 138 (37.6) | 33 (47.8) | 111 (48.9) | 98 (42.6) |
Severe disease | 250 (58.3) | 130 (60.2) | 229 (62.4) | 36 (52.2) | 116 (51.1) | 132 (57.4) |
Mean fecal calprotectin, mg/kg (SD) | 2,508.96 (4,526.2) | 3,440.42 (6,351.6) | 2,970.56 (5,558.1) | 2,481.47 (5,436.4) | 2,987.32 (5,832.4) | 2,284.32 (3,911.8) |
Mean C-reactive protein, mg/L (SD) | 8.0 (13.42) | 11.1 (18.09) | 9.4 (13.62) | 7.2 (12.08) | 6.8 (10.15) | 6.8 (10.67) |
Prior UC medication and response category (safety population) | ||||||
n | 429 | 216 | 367 | 69 | 227 | 230 |
Corticosteroids | 322 (75.1) | 162 (75.0) | 286 (77.9) | 49 (71.0) | 168 (74.0) | 163 (70.9) |
Failed to respond | 200 (46.6) | 96 (44.4) | 168 (45.8) | 26 (37.7) | 97 (42.7) | 93 (40.4) |
Intolerant | 50 (11.7) | 28 (13.0) | 28 (7.6) | 9 (13.0) | 19 (8.4) | 19 (8.3) |
Corticosteroid dependent | 106 (24.7) | 56 (25.9) | 104 (28.3) | 14 (20.3) | 46 (20.3) | 56 (24.3) |
Oral aminosalicylic acids | 418 (97.4) | 210 (97.2) | 362 (98.6) | 68 (98.6) | 221 (97.4) | 227 (98.7) |
Failed to respond | 313 (73.0) | 162 (75.0) | 269 (73.3) | 55 (79.7) | 165 (72.7) | 169 (73.5) |
Intolerant | 36 (8.4) | 22 (10.2) | 29 (7.9) | 8 (11.6) | 18 (7.9) | 24 (10.4) |
Immunomodulators | 174 (40.6) | 93 (43.1) | 166 (45.2) | 23 (33.3) | 85 (37.4) | 89 (38.7) |
Failed to respond | 118 (27.5) | 70 (32.4) | 121 (33.0) | 15 (21.7) | 58 (25.6) | 63 (27.4) |
Intolerant | 58 (13.5) | 34 (15.7) | 55 (15.0) | 9 (13.0) | 24 (10.6) | 33 (14.3) |
Azathioprine | 145 (33.8) | 74 (34.3) | 136 (37.1) | 18 (26.1) | 70 (30.8) | 72 (31.3) |
Failed to respond | 94 (21.9) | 50 (23.1) | 95 (25.9) | 9 (13.0) | 44 (19.4) | 49 (21.3) |
Intolerant | 50 (11.7) | 24 (11.1) | 46 (12.5) | 7 (10.1) | 20 (8.8) | 27 (11.7) |
Mercaptopurine | 33 (7.7) | 22 (10.2) | 28 (7.6) | 6 (8.7) | 13 (5.7) | 19 (8.3) |
Failed to respond | 23 (5.4) | 16 (7.4) | 23 (6.3) | 4 (5.8) | 12 (5.3) | 15 (6.5) |
Intolerant | 12 (2.8) | 10 (4.6) | 9 (2.5) | 2 (2.9) | 2 (0.9) | 8 (3.5) |
Methotrexate | 10 (2.3) | 11 (5.1) | 13 (3.5) | 5 (7.2) | 5 (2.2) | 2 (0.9) |
Failed to respond | 8 (1.9) | 8 (3.7) | 11 (3.0) | 3 (4.3) | 5 (2.2) | 2 (0.9) |
Intolerant | 1 (0.2) | 3 (1.4) | 2 (0.5) | 2 (2.9) | 1 (0.4) | 0 |
Anti-TNF | 130 | 65 | 159 | 15 (21.7) | 65 (28.6) | 76 (33.0) |
Primary nonresponderf | 49 (37.7) | 21 (32.3) | 60 (37.7) | 3 (4.3) | 22 (9.7) | 30 (13.0) |
Secondary nonresponderg | 84 (64.6) | 42 (64.6) | 109 (68.6) | 10 (14.5) | 46 (20.3) | 47 (20.4) |
Intolerantg | 27 (20.8) | 17 (26.2) | 26 (16.4) | 3 (4.3) | 12 (5.3) | 18 (7.8) |
Non–anti-TNF biologics | 80 (18.6) | 44 (20.4) | 106 (28.9) | 11 (15.9) | 33 (14.5) | 42 (18.3) |
Primary nonresponder | 24 (5.6) | 9 (4.2) | 25 (6.8) | 3 (4.3) | 6 (2.6) | 7 (3.0) |
Secondary nonresponder | 49 (11.4) | 33 (15.3) | 75 (20.4) | 8 (11.6) | 21 (9.3) | 30 (13.0) |
Intolerant | 10 (2.3) | 4 (1.9) | 12 (3.3) | 1 (1.4) | 5 (2.2) | 8 (3.5) |
ITT = intention to treat; OZ = ozanimod; PL = placebo; SD = standard deviation; TNF = tumour necrosis factor; UC = ulcerative colitis.
aEastern European countries include Belarus, Bulgaria, Croatia, Czech Republic, Georgia, Greece, Hungary, Latvia, Republic of Moldova, Poland, Romania, Russian Federation, Serbia, Slovakia, and Ukraine.
bWestern European countries include Austria, Belgium, Germany, Italy, the Netherlands, and the UK.
cThree-component Mayo score is the sum of the rectal bleeding subscore, stool frequency subscore, and the endoscopy subscore.
dFour-component Mayo Score is the sum of the rectal bleeding subscore, stool frequency subscore, Physician’s Global Assessment subscore, and the endoscopy subscore.
eDerived from Robarts data.
fPercentages for patients who were intolerant to or whose condition did not respond to anti-TNF treatment were calculated as a percentage of the number of patients who received prior anti-TNF treatment rather than the total safety population for each treatment group. Primary nonresponse was defined as signs and symptoms of persistently active disease despite an adequate trial of induction treatment with an anti-TNF drug (per the country’s approved label).
gSecondary nonresponse was defined as recurrence of symptoms during maintenance dosing following prior clinical benefit. Intolerance included inability to achieve doses, dose levels, or treatment durations because of treatment-related side effects and/or laboratory abnormalities. Patients could be classified under more than 1 response category if they received more than 1 prior anti-TNF and experienced a different response to each therapy.
Source: Clinical Study Report for the TRUE NORTH study.10
The extent of disease was limited to the left side of the colon in approximately 60% of patients in both the induction and maintenance periods. The mean 3-component Mayo score and 4-component Mayo score ranged from 6.6 (SD = 1.15) to 6.7 (SD = 1.31) and 8.6 (SD = 1.42) to 9.1 (SD = 9.0), respectively, across treatment groups in both study periods. Finally, disease severity, as assessed by mucosal appearance at endoscopy, was classified as severe disease in approximately 60% of patients across treatment groups in the induction period, and in approximately 50% of patients across treatment groups in the maintenance period.
All patients were previously treated with other UC medications. Excluding those patients who received placebo during both the induction and maintenance periods, patients in each treatment group at the start of the induction and maintenance periods had previously received the following UC medications: corticosteroids (range, 70% to 78%), oral aminosalicylic acids (range, 97% to 99%), immunomodulators (range, 37% to 46%), azathioprine (range, 30% to 38%), mercaptopurine (less than 10%), methotrexate (less than 6%), anti-TNF biologics (range, 28% to 33%, aside from 44% in the open-label ozanimod group), and non–anti-TNF biologics (14% to 29%).
Interventions
Patients were randomized to receive 1 of 2 interventions: ozanimod or placebo. The ozanimod and placebo capsules were identical in physical appearance. Dose escalation was implemented due to the results of prior phase I and phase II studies that suggested dose escalation resulted in a less profound decrease in heart rate or blood pressure.
On day 1 of the induction period, patients initiated their assigned intervention in accordance with a 7-day dose escalation regimen. From day 1 to day 4, patients received ozanimod 0.23 mg or matching placebo once daily as 1 capsule. From day 5 to day 7, patients received ozanimod 0.46 mg or matching placebo once daily as 2 capsules. From day 8 onward, patients received ozanimod 0.92 mg or matching placebo once daily for 9 weeks as 1 capsule. Patients who received ozanimod in the induction period and continued in the maintenance period were re-randomized to receive ozanimod 0.92 mg once daily for 42 weeks as one 0.92 mg capsule or matching placebo as a single capsule once daily for 42 weeks. Patients from cohort 1 of the induction period who had been randomized to receive placebo and showed a clinical response at week 10 continued to received placebo in the maintenance period in a double-blind manner.
Concomitant Therapy
All treatments, other than ozanimod, taken by the patients on entry into the trial or any time during the study period, including the safety follow-up visit, were regarded as concomitant medications and were documented as such.
Patients who were receiving a 5-ASA or oral corticosteroid at screening were to keep their prescribed dose steady through to week 10. Oral 5-ASA or corticosteroids were not started in patients who were not receiving them at screening. Patients receiving 5-ASA were to maintain a stable dose through week 52 of the maintenance period. For patients who were receiving an oral corticosteroid, steroid tapering was introduced after week 10. Upon entering the maintenance period, tapering proceeded as follows:
Prednisone greater than 10 mg per day or equivalent: Reduced at a rate of 5 mg per week until a dosage of 10 mg per day (or equivalent) was achieved.
Prednisone 10 mg per day or equivalent (or once a dosage of 10 mg per day or equivalent was achieved by tapering): Reduced at a rate of 2.5 mg per week until discontinuation.
Budesonide MMX greater than 9 mg every day: Reduced to 9 mg every other day for 2 weeks and then discontinued.
For patients who were unable to tolerate corticosteroid tapering, the corticosteroid dose was increased and tapering was recommenced within 2 weeks.
Concomitant medications that were prohibited during the induction or maintenance periods and during the observational 30-day safety follow-up visit included:
treatment during the study with Class Ia or Class III antiarrhythmic drugs or treatment with 2 or more drugs in a combination known to prolong PR interval (e.g., combination of a beta-blocker and verapamil) unless approved by the sponsor’s representative
biologic therapies, such as abatacept, infliximab, etanercept, adalimumab, anakinra, rituximab, vedolizumab, and golimumab immunosuppressive drugs (e.g., azathioprine, mercaptopurine, cyclosporine, methotrexate)
any per-rectum therapy, including enemas (e.g., 5-ASA, corticosteroid), other than that required for endoscopy preparation
antimotility medications
oral cyclosporine, tacrolimus, sirolimus, or mycophenolate mofetil
any investigational drug other than the investigational drug specified in this study
chronic use of nonsteroidal anti-inflammatory drugs (NSAIDs) (occasional use [for headache, arthritis, myalgias, or menstrual cramps, for example] of acetaminophen, NSAIDs, acetaminophen, and ASA up to 325 mg per day was permitted)
live vaccines or live attenuated vaccines (also not allowed within 4 weeks before randomization)
IV immunoglobulin or plasmapheresis (also not allowed within 3 months before randomization)
treatment with D-penicillamine, leflunomide, or thalidomide
treatment with natalizumab, fingolimod, etrasimod, or tofacitinib
immunosuppressive drugs that deplete lymphocytes
breast cancer resistance protein inhibitors (e.g., cyclosporine, eltrombopag)
monoamine oxidase inhibitors (e.g., selegiline, phenelzine)
cytochrome P450 2C8 (CYP2C8) inducers (e.g., rifampicin) or inhibitors (e.g., gemfibrozil and clopidogrel)
The following medications were not permitted for use between the 30-day safety follow-up visit and the 90-day safety follow-up visit:
Class Ia or Class III antiarrhythmic drugs or treatment with 2 or more drugs in a combination known to prolong PR interval (e.g., combination of a beta-blocker and verapamil) were prohibited during the study unless approved by the sponsor’s representative
natalizumab, fingolimod, and etrasimod
immunosuppressive drugs that deplete lymphocytes
monoamine oxidase inhibitors (e.g., selegiline, phenelzine)
CYP2C8 inducers (e.g., rifampicin) and inhibitors (e.g., gemfibrozil, clopidogrel)
live vaccines or live attenuated vaccines
Outcomes
A list of efficacy end points identified in the CADTH review protocol that were assessed in the clinical trials included in this review is provided in Table 8. These end points are further summarized subsequently. A detailed discussion and critical appraisal of the clinical instruments and HRQoL measures used in the trial is provided in Appendix 4.
Table 8: Summary of Outcomes of Interest in the TRUE NORTH Trial Identified in the CADTH Review Protocol
Outcome measure | Induction period | Maintenance period |
|---|---|---|
Clinical remission using the 3-component Mayo score | Primary | Primary |
Clinical remission using the 4-component Mayo score | Other efficacy end point | Other efficacy end point |
Clinical response using the 3-component Mayo score | Key secondary | Key secondary |
Clinical response using the 4-component Mayo score | Other efficacy end point | Other efficacy end point |
Rectal bleeding | Exploratory (post hoc) | NR |
Endoscopic improvement | Key secondary | Key secondary |
Corticosteroid-free remission | NR | Key secondary |
Mucosal healing | Key secondary | Key secondary |
Durable clinical remission | NR | Key secondary |
Maintenance of clinical remission | NR | Key secondary |
Histologic remission | Other efficacy end point | Other efficacy end point |
HRQoL:
| Other efficacy end point | Other efficacy end point |
Work productivity:
| Other efficacy end point | Other efficacy end point |
EQ-5D-5L = 5-level EQ-5D; HRQoL = health-related quality of life; NR = not reported; SF-36 = Short Form (36) Health Survey; WPAI-UC = Work Productivity and Activity Impairment Questionnaire – Ulcerative Colitis.
Source: Clinical Study Report for the TRUE NORTH study.10
Clinical Remission
Clinical remission was the primary efficacy end point in the TRUE NORTH study and was expressed as the proportion of patients who were in clinical remission. Clinical remission was defined according to the 3- and 4-component Mayo score based on a 7-day scoring algorithm.1,35
The Mayo score is a disease-specific, physician-measured instrument that assesses disease severity and response to treatment in patients with UC. The Mayo scoring system is a combined endoscopic and clinical scale used to assess the severity of UC.1,35 In its complete form, the Mayo score is composed of 4 components: rectal bleeding, stool frequency, Physician’s Global Assessment, and endoscopy findings. Each part is rated from 0 to 3, yielding a total score of 0 to 12.
Clinical remission was measured at the conclusion of the induction period at week 10 and at the conclusion of the maintenance period at week 52. The definitions of clinical remission were as follows:
Clinical remission based on the 3-component Mayo score was defined as an RBS of 0 and an SFS of 1 or less with a decrease of 1 or more points from the baseline SFS and an endoscopy subscore of 1 or less.
Clinical remission based on the 4-component Mayo score was defined as a score of 2 or less with no individual subscore of greater than 1 point.
To determine the endoscopy subscore for the Mayo score, endoscopy recordings were centrally read by a gastroenterologist blinded to treatment assignment.
Clinical Response
Clinical response was a key secondary efficacy end point of the TRUE NORTH study and was expressed as the proportion of patients who had a clinical response. Clinical response was also defined according to 3- and 4-component Mayo scores based on a 7-day scoring algorithm. Clinical response was assessed at the conclusion of the induction period at week 10 and at the conclusion of the maintenance period at week 52. The definitions of clinical response were as follows:
Clinical response based on the 3-component Mayo score was defined as a reduction from baseline in the 3-component score of 2 or more points and 35% or greater, and a reduction in RBS of 1 or more points from baseline or an absolute RBS of less than 1 point.
Clinical response in the 4-component Mayo score was defined as a reduction from baseline in the 4-component score of 3 or more points and more than 30%, and a reduction in RBS of more than 1 point from baseline or an absolute RBS of 1 point or less.
Rectal Bleeding
RBS was a post hoc exploratory end point in the TRUE NORTH study and was expressed as the change from baseline in the RBS of the Mayo score. RBS was reported for baseline, week 2, week 4, week 5, week 6, week 8, and week 10 of the induction period.
Endoscopic Improvement
Endoscopic improvement was a key secondary outcome in the TRUE NORTH study and was expressed as the proportion of patients with endoscopic improvement. Endoscopic improvement was defined as an endoscopy subscore of 1 or less without friability. Endoscopic improvement was assessed at the conclusion of the induction period at week 10 and at the conclusion of the maintenance period at week 52.
Corticosteroid-Free Remission
Corticosteroid-free remission was a key secondary outcome of the maintenance period in the TRUE NORTH study and expressed as the proportion of patients with corticosteroid-free remission. Corticosteroid-free remission was defined as being in clinical remission at 52 weeks while off corticosteroids for at least 12 weeks.
Mucosal Healing
Mucosal healing was a key secondary outcome in the TRUE NORTH study and expressed as the proportion of patients with mucosal healing. Mucosal healing was assessed using the endoscopy subscore of the Mayo score and the Geboes index score.36,37
The Geboes score is a 6-item instrument that classifies histological changes into 1 of 6 grades (grade 0 to grade 5). Each grade is assessed on a 4-point scale and given equal weight, as follows: “no abnormality,” “mild abnormality,” “mild/moderate diffuse or multifocal abnormalities,” and “severe diffuse or multifocal abnormalities.” The higher the score, the greater the inflammation.
Mucosal healing was defined as an endoscopy subscore of 1 point or less without friability and a Geboes index score of less than 2 (no neutrophils in the epithelial crypts or lamina propria and no increase in eosinophils, no crypt destruction, and no erosion ulcerations of granulation tissue). Mucosal healing was assessed at week 10 of the induction period and at week 42 of the maintenance period (week 52 of the study).
Durable Clinical Remission
Durable clinical remission was a key secondary outcome of the maintenance period in the TRUE NORTH study and expressed as the proportion of patients in clinical remission at week 10 and at week 52 in all patients who entered the maintenance period.
Maintenance of Remission
The maintenance of remission was a key secondary outcome of the maintenance period in the TRUE NORTH study and expressed as the proportion of patients with clinical remission at week 52 in a subset of patients in remission at week 10.
Histologic Remission
Histologic remission was classified as an “other efficacy end point” in the TRUE NORTH study. Histologic remission was assessed using the Geboes index score and was expressed as the proportion of patients with histologic remission. Histologic remission was defined as a Geboes index score of less than 2 (no neutrophils in the epithelial crypts or lamina propria and no increase in eosinophils, no crypt destruction, and no erosion ulcerations of granulation tissue). Histologic remission was assessed at the conclusion of the induction period at week 10 and at the conclusion of the maintenance period at week 52.
HRQoL
HRQoL in the TRUE NORTH study was classified as an “other efficacy end point” and was assessed using 2 instruments: the SF-36 and the EQ-5D-5L. HRQoL outcomes were expressed as the change from baseline to week 10, and from baseline to week 52.
The SF-36 is a generic self-reported health assessment questionnaire that has been used in clinical trials to study the impact of chronic disease on HRQoL. The SF-36 consists of 8 domains: physical functioning, role limitations due to physical health problems, bodily pain, general health, vitality, social functioning, role limitations due to emotional health problems, and mental health. The SF-36 also provides 2 component summaries: the Physical Component Summary (PCS) and the Mental Component Summary (MCS), which are scores created by aggregating the 8 domains.38 The PCS and MCS and individual domains are each measured on a scale of 0 to 100, with increasing score indicating improvement in health status.38
The EQ-5D-5L is a generic self-reported HRQoL outcome measure that may be applied to a variety of health conditions and treatments.39 The first component of the EQ-5D-5L assesses 5 dimensions: mobility, self-care, usual activities, pain/discomfort, and anxiety/depression.39 It is a descriptive system that classifies respondents (aged ≥ 12 years) based on these 5 dimensions. Each dimension has 5 levels: no problems, slight problems, moderate problems, severe problems, and extreme problems. The EQ-5D-5L has 5 possible levels for each dimension and respondents are asked to choose the level that reflects their health state for each of the 5 dimensions.39 The second component of the EQ-5D-5L is a 20 cm visual analogue scale (EQ VAS) that has end points labelled 0 and 100, with respective anchors of “worst imaginable health state” and “best imaginable health state.” Respondents are asked to rate their health by drawing a line from an anchor box to the point on the EQ VAS that best represents their health on that day. The EQ-5D-5L index score is generated by applying a multiattribute utility function to the descriptive system.40 Different utility functions are available that reflect the preferences of specific populations (e.g., US or UK). Scores less than 0 represent health states that are valued by society as being worse than dead, while scores of 0 and 1.00 are assigned to the health states “dead” and “perfect health,” respectively.
Work Productivity
Work productivity was classified as an “other efficacy end point” in the TRUE NORTH study and was assessed using the WPAI-UC.41,42 Work productivity was measured at week 10 and week 52.
The WPAI-UC is a self-administered 6-item questionnaire with a 7-day recall period that measures the impact of health problems on absenteeism (percentage of work time missed due to UC), presenteeism (percentage of impairment due to UC while working), percentage of overall work impairment due to UC (combined absenteeism and presenteeism), and percentage of daily activity impairment.41,42 The WPAI-UC scores from all domains are expressed as percentages (0% to 100%) of impairment, with lower values indicating less impairment due to the health problem.41
Safety
The primary safety outcomes assessed in TRUE NORTH were:
TEAEs
serious adverse events (SAEs)
TEAEs leading to discontinuation of the investigational drug
TEAEs of special interests, including bradycardia and heart conduction abnormalities, pulmonary effects, hepatic effects, macular edema, malignancies, and serious or opportunistic infections
changes from baseline for clinical laboratory measures, vital signs, and ECG and pulmonary function tests.
Statistical Analysis
Efficacy Analysis
For the purpose of statistical analyses, the induction period and the maintenance period were treated as 2 independent studies. For the induction period, the efficacy end points were formally examined with statistical hypothesis tests conducted on the efficacy results obtained from the patients randomized and dosed in cohort 1. Cohort 2 was open-label and did not contain a control group; therefore, all cohort 2 efficacy end points were summarized and described without statical hypothesis testing. For the maintenance period, patients (in either cohort 1 or cohort 2 and with a clinical response based on either the 3-component or 4-component Mayo score at week 10) who were re-randomized to either ozanimod or placebo contributed to the ITT population.
The statistical analysis of efficacy end points conducted in the TRUE NORTH trial is summarized in Table 9.
Table 9: Statistical Analysis of Efficacy End Points
End point | Statistical model | Adjustment factors | Sensitivity analyses |
|---|---|---|---|
Proportion of patients at week 10 and week 52 who:
| Cochran-Mantel-Haenszel |
|
|
Change in baseline rectal bleeding subscore during the induction period |
| Stratified by corticosteroid use at screening (yes or no) and prior anti-TNF use (yes or no) | None performed |
Proportion of patients:
| Cochran-Mantel-Haenszel | Stratified by corticosteroid use at screening (yes or no), prior anti-TNF use (yes or no), remission status at week 10 and corticosteroid use at week 10 |
|
Change in SF-36 from baseline to week 10 | ANCOVA | Stratified by corticosteroid use at screening (yes or no) and prior anti-TNF use (yes or no) | None performed |
Change in EQ-5D-5L from baseline to week 10 and from baseline to week 52 | ANCOVA |
| None performed |
WPAI-UC at week 10, week 40, and at week 52 | NR | NR | None performed |
ANCOVA = analysis of covariance; EQ-5D-5L = 5-level EQ-5D; MI = multiple imputation; NR = not reported; NRI = nonresponder imputation; SF-36 = Short Form (36) Health Survey; TNF = tumour necrosis factor; WPAI-UC = Work Productivity and Activity Impairment Questionnaire – Ulcerative Colitis.
Source: Clinical Study Report for the TRUE NORTH study.10
Sample Size Determination
For cohort 1 of the induction period, a sample size of approximately 600 patients randomized in a 2:1 ratio (400 received ozanimod 1 mg and 200 received placebo) was planned. The sample size was determined to provide at least 90% power to detect a difference of 10% between groups in the proportion of patients with clinical remission based on a 2-sided Fisher exact test at an alpha of 0.05. Sample size determination was based on the results from a previous study of ozanimod 1 mg (RPC01 to 201) that anticipated that at least 16% of patients in the ozanimod group and approximately 6% of patients in the placebo group would be in clinical remission at the end of the induction period.
The sample size for cohort 2 of the induction period was also based on the same phase II study cited previously, which anticipated that at least 60% of patients treated with ozanimod would have a clinical response at the end of the induction period. Assuming a 5% dropout rate, enrolment of approximately 900 patients into the induction period, of which 700 would receive ozanimod, was planned. This was to ensure approximately 420 patients would have a clinical response to ozanimod so that approximately 400 patients could potentially be enrolled into the maintenance period. Therefore, an addition of approximately 300 patients receiving ozanimod 1 mg was planned for enrolment into cohort 2.
For the maintenance period, a placebo remission rate of 16% at week 52 was assumed based on a prior study.43 A sample size of 400 patients (200 patients per treatment group) was determined, based on a 2-sided Fisher exact test at alpha = 0.05, to provide 90% power to detect a statistically significant improvement in a remission rate of 14% or higher. To account for a 5% rate of patients who had a clinical response to induction therapy with ozanimod not entering the maintenance period, approximately 420 patients with a clinical response to ozanimod were required at the end of the induction period.
Primary Efficacy Analysis
The primary analysis of the proportion of patients in clinical remission at week 10 and week 52 was carried out on the ITT population using a 2-sided Cochran-Mantel-Haenszel test at the 5% level of significant, stratified by corticosteroid use at screening (yes or no) and prior anti-TNF use (yes or no). Patients who met the criteria for treatment failure were imputed using nonresponder imputation (NRI).
Treatment of patients was considered to have failed if any of the following occurred:
a protocol-prohibited change in medications, including:
postbaseline initiation of or an increase in the total daily dose level higher than the maximum dose taken between the screening and baseline visit of the following:
corticosteroids or 5-ASA dose to treat UC
a prolonged course of system corticosteroids of longer than 14 days for treatment of disease other than UC
immune-suppressing therapy, including initiation of mercaptopurine, azathioprine, anti-TNF drugs, vedolizumab, or tofacitinib
a colectomy (partial or total) or ostomy
discontinuation of ozanimod or placebo due to lack of therapeutic effect before the week 10 or week 52 efficacy evaluation.
The primary analysis was repeated on the per-protocol (PP) population and on key subgroups of the ITT population. These were considered sensitivity (supportive) analyses and were not subject to familywise type I error control.
Secondary and Other Efficacy Analysis
The secondary end points were tested in order using a hierarchical testing procedure to control the overall type I error rate for multiple end points. If the primary end point was statistically significant, the proportion of patients with a clinical response at week 10 and week 52 was tested at the 5% significance level. This testing procedure continued through each of the key secondary end points until the end point failed to reach statistical significance, after which subsequent key secondary end points were considered exploratory. The end points listed as other efficacy end points were tested in a nonhierarchical fashion without adjustments for multiplicity.
All key secondary and other efficacy end points expressed as proportions of patients were tested using the same type of Cochran-Mantel-Haenszel test as specified for the primary end point, with treatment failures imputed as nonresponders (refer to Table 9). All efficacy end points expressed as changes from baseline were analyzed with an analysis of covariance (ANCOVA) model adjusted for the baseline response parameter of interest, corticosteroid use at screening, and prior anti-TNF use.
Safety Analyses
All safety analyses were carried out on the safety population.
Sensitivity Analysis
A sensitivity analysis of the primary efficacy end point (clinical remission) based on a 14-day scoring algorithm was performed to support the primary analysis. Sensitivity analyses were conducted for the primary end point and the secondary end point of clinical response, with the use of observed-cases analysis (assumption of data missing completely at random) and with the use of multiple imputation (assumption of data missing at random).
Subgroup Analyses
Predefined subgroup analyses were performed for the primary and key secondary end points. The relevant subgroup analyses were conducted for the induction and maintenance periods: corticosteroid use at screening (yes or no), prior anti-TNF use (yes or no), extent of colitis (left-sided versus extensive), and moderate UC status at baseline (4-component Mayo score 6 to 10, yes or no).
Missing Data
For the proportion-based primary and key secondary efficacy end points, patients with missing week 10 and/or missing week 52 efficacy data were considered nonresponders using NRI. Sensitivity analyses around missing data could include tipping-point analysis, missing data imputed using multiple imputation, and analysis of observed cases with no imputation. For continuous efficacy end points, analyses were performed using observed cases with no imputation.
Analysis Populations
All patient populations were defined and documented before database lock. The following analysis populations were used in the statistical analysis: ITT population, PP population, and safety population.
The ITT populations were used as the primary population for all efficacy parameters. Patients were analyzed according to their randomized group. For each treatment group in the induction period, the ITT population included all randomized (cohort 1) or enrolled (cohort 2) patients who received at least 1 dose of the study drug. For the maintenance period, the ITT population included all randomized patients who received at least 1 dose of the study drug in the maintenance period.
The PP populations consisted of all patients in the ITT population who adhered to the protocol. Patients were excluded from the PP populations if they violated the eligibility criteria or significantly deviated from the study plan. Specific reasons for exclusion from these populations were documented before database lock and included, but were not limited to, investigational drug noncompliance greater than 20%, receiving an incorrect investigational drug for more than 1 week in the induction period or more than 1 month in the maintenance period, and missing more than 2 visits while still on the study.
The safety populations consisted of all patients who received at least 1 dose of the investigational drug. The safety populations were used for all summaries of safety data. Patients randomized to receive any amount of ozanimod were summarized in the ozanimod group; otherwise, they were to be summarized in the placebo group.
Results
Patient Disposition
Details of patient disposition in the induction period and maintenance period are summarized in Table 10.
A total of 1,831 patients were screened for entry into the study’s induction period. Of those, 1,012 were enrolled into the TRUE NORTH study, including 645 patients in cohort 1 (429 randomized to ozanimod and 216 to placebo) and 367 patients in cohort 2 (all treated with ozanimod). Most ozanimod-treated patients in cohort 1 (93.5%) and cohort 2 (88.3%) completed the induction period, with 54.3% and 61.0% continuing to the maintenance period, and 37.1% and 21.5% enrolled in the OLE study, respectively. Among the placebo-treated patients in cohort 1, 88.9% completed the induction period, 55.6% enrolled in the OLE following the induction period, and 31.9% continued into the maintenance period.
The most frequently reported reason for withdrawal from the induction period among patients in cohort 1 in descending order were AEs and withdrawal by patients in the ozanimod treatment group and lack of efficacy, withdrawal by patients, and AEs in the placebo treatment group. The most frequently reported reasons for study withdrawal among patients in cohort 2 of the induction period were withdrawal by patient, AEs, and lack of efficacy. A total of 526 patients were treated during the maintenance period of the study, including 230 patients who were randomized to ozanimod 1 mg, 227 who were re-randomized from ozanimod 1 mg to placebo, and 69 who continued on placebo. The completion rate for the maintenance period was 80% for the patients continuously treated with ozanimod, approximately 55% for those re-randomized from ozanimod 1 mg to placebo, and approximately 65% for the patients continuously treated with placebo. Most patients who completed the maintenance period enrolled in the OLE study.
The most frequently reported reason for discontinuing from the trial during the maintenance period was disease relapse. Disease relapse was reported in 13.5% of patients continuously treated with ozanimod, approximately 33.9% in those re-randomized from ozanimod to placebo, and approximately 29% among the patients continuously treated with placebo.
In total, 824 of the 1,012 patients who entered TRUE NORTH went on to enrol in the OLE study.13
Protocol Deviations
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Characteristics | Induction period | Maintenance period | ||||
|---|---|---|---|---|---|---|
Cohort 1 | Cohort 2 | PL to PL | Re-randomized patients | |||
OZ | PL | OZ | OZ to PL | OZ to OZ | ||
Randomized, N | 429 | 216 | 367 | 69 | 227 | 230 |
Patients dosed,a N (%) | 429 (100) | 216 (100) | 367 (100) | 69 (100) | 227 (100) | 230 (100) |
Completion of induction periodb | 401 (93.5) | 192 (88.9) | 324 (88.3) | NA | NA | NA |
Completed induction week 10 and continued into maintenance periodb,c | 233 (54.5) | 69 (31.9) | 224 (61.0) | NA | NA | NA |
Completed induction week 10 and enrolled into OLE studyb | 159 (37.1) | 120 (55.6) | 79 (21.5) | NA | NA | NA |
Completed induction week 10 but discontinued study participation and did not enrol in OLE studyb | 9 (2.1) | 3 (1.4) | 21 (5.7) | NA | NA | NA |
Patients who completed maintenance periodb | NA | NA | NA | 45 (65.2) | 124 (54.6) | 184 (80.0) |
Completed maintenance week 42 (week 52 of study) and enrolled into OLE studyb | NA | NA | NA | 42 (60.9) | 116 (51.1) | 171 (74.3) |
Completed maintenance week 42 (week 52 of study) but discontinued study participation and did not enrol in OLE studyb | NA | NA | NA | 3 (4.3) | 8 (3.5) | 13 (5.7) |
Discontinued from study,b,d N (%) | 28 (6.5) | 24 (11.1) | 43 (11.7) | 24 (34.8) | 103 (45.4) | 46 (20.0) |
Did not complete maintenance period and enrolled in OLE study | — | — | — | 22 (31.9) | 81 (35.7) | 34 (14.8) |
Reason for discontinuation,b N (%) | ||||||
Adverse events | 12 (2.8) | 6 (2.8) | 12 (3.3) | 0 | 5 (2.2) | 2 (0.9) |
Lost to follow-up | 10 (2.3) | 8 (3.7) | 20 (5.4) | 1 (1.4) | 13 (5.7) | 7 (3.0) |
Lack of efficacy | 4 (0.9) | 10 (4.6) | 9 (2.5) | 0 | 3 (1.3) | 2 (0.9) |
Noncompliance with protocol or protocol deviation | 2 (0.5) | 0 | 1 (0.3) | 0 | 0 | 1 (0.4) |
Othere | 1 (0.2) | 0 | 0 | 1 (1.4) | 2 (0.9) | 0 |
Withdrawal by patients | 1 (1.4) | 13 (5.7) | 7 (3.0) | |||
Physician decision | 0 | 0 | 1 (0.3) | 0 | 0 | 0 |
Maintenance disease relapse | NA | NA | NA | 20 (29.0) | 77 (33.9) | 31 (13.5) |
Enrolled in OLE study | 0 | 0 | 0 | 2 (2.9) | 3 (1.3) | 3 (1.3) |
ITT, N | 429 (100) | 216 (100) | 367 (100) | 69 (100) | 227 (100) | 230 (100) |
PP, N | 429 (100) | 216 (100) | 367 (100) | 69 (100) | 227 (100) | 230 (100) |
Safety, N | 422 (98.4) | 214 (99.1) | 361 (98.4) | 67 (97.1) | 221 (97.4) | 224 (97.4) |
ITT = intention to treat; NA = not applicable; OLE = open-label extension; OZ = ozanimod; PL = placebo; PP = per protocol.
aPercentages are based on the number of patients in the randomized population (cohort 1) divided by the enrolled population (cohort 2 and maintenance period).
bPercentages are based on the number of patients dosed.
cTo continue into the maintenance period, patients were required to be in clinical response as assessed by the 3- or 4-component Mayo.
dPatients who discontinued from the induction period were withdrawn from the study.
eOther reasons include leaving the country; lost to follow-up; sponsor withdrew patients due to prolonged breast cancer chemotherapy; early term visit was 90 days after last dose, so a 90-day follow-up visit was not needed; and wife wanted to get pregnant.
Source: Clinical Study Report for the TRUE NORTH study.10
||||||||||||||| | |||||||||||||||||||||||||||||| | |||||
|---|---|---|---|---|---|---|
|||||||||||||||||||||||||||||| | |||||||||||||||||||||||||||||| | |||||
||||||||||||||| | ||||||||||||||| | ||||||||||||||| | ||||||||||||||| | |||
||||||||||||||| | ||||||||||||||| | ||||||||||||||| | ||||||||||||||| | ||||||||||||||| | ||||||||||||||| | |
||||||||||||||||||||||||||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| |
|||||||||||||||||||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| |
|||||||||||||||||||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| |
|||||||||||||||||||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| |
|||||||||||||||||||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| |
|||||||||||||||||||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| |
|||||||||||||||||||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| |
|||||||||||||||||||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| |
|||||||||||||||||||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| |
|||||||||||||||||||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| |
|||||||||||||||||||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| |
Note: This table has been redacted as per the sponsor’s request.
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Exposure to Study Treatments
Extent of Exposure
In the induction period, the mean duration of exposure to ozanimod and placebo in cohort 1 was 10.4 (SD = 1.7) weeks and 10.3 (SD = 2.2) weeks, respectively. In the maintenance period, the mean duration of exposure to the investigational drug was 37.6 (SD = 11.3) weeks in patients re-randomized to ozanimod and 30.8 (SD = 14.8) weeks to patients re-randomized to placebo.
Concomitant Medications
Common concomitant medications for patients in both the induction and maintenance periods included medications used for endoscopies, such as propofol, midazolam, and macrogol 4000.
All patients enrolled in the trial were required to be treated with other concomitant therapies, including aminosalicylates. Indeed, mesalazine and sulfasalazine were taken by a total of 71% and 13% of patients, respectively.
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
In total, corticosteroids for systemic use were used in approximately 31% of patients in the induction period and in 31.7% of patients re-randomized in the maintenance period. Prednisone was the most commonly used corticosteroid and its use across the treatment periods was as follows:
Induction period: 18.1% of patients in the cohort 1 ozanimod group, 16.1% of patients in the placebo group, and 17.6% in the cohort 2 ozanimod group.
Maintenance period: 15.9% of patients who remained on placebo, 14.1% of patients who were re-randomized to placebo, and 17.0% who remained on ozanimod.
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
||||||||||||||| | |||||||||||||||||||||||||||||| | |||||
|---|---|---|---|---|---|---|
|||||||||||||||||||||||||||||| | ||||||||||| |||||| | |||||
||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | |||
||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | |
|||||||||||||||||||| | ||||||
||||||||||||||||||||||||||||||||||||||||| | ||||||
||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| |
||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| |
||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| |
||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| |
||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| |
||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| |
||||||||||||||||||||||||||||||||||||||||| | ||||||
||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| |
||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| |
||||||||||||||||||||||||||||||||||||||||| | ||||||
||||||||||||||||||||||||||||||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| |
||||||||||||||||||||||||||||||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| |
||||||||||||||||||||||||||||||||||||||||| | ||||||
||||||||||||||||||||||||||||||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| |
||||||||||||||||||||||||||||||||||||||||| | ||||||
||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| |
||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| |
||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| |
Note: This table has been redacted as per the sponsor’s request.
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Efficacy
Only those efficacy outcomes and analyses of subgroups identified in the review protocol are reported subsequently. Refer to Appendix 3 for detailed efficacy data.
For the induction period, only cohort 1 data (double-blind ozanimod once daily or placebo) was used to assess the efficacy end points. As cohort 2 did not have a placebo control, no inferential statistics were conducted; instead, descriptive statistics are provided in the tables.
Clinical Remission
Clinical remission, as defined by the 3-component and 4-component Mayo in both the induction and maintenance periods, is summarized in Table 13.
Table 13: Proportion of Patients With Clinical Remission as Measured by the Mayo Score in the TRUE NORTH Trial
Outcome measure | Induction perioda | Maintenanceb | ||||
|---|---|---|---|---|---|---|
Cohort 1 | Cohort 2 | PL to PL (N = 69) | Re-randomized patients | |||
OZ (N = 429) | PL (N = 216) | OZ (N = 367) | OZ to PL (N = 227) | OZ to OZ (N = 230) | ||
3-component Mayoc | ||||||
Patients in clinical remission, n (%) | 79 (18.4) | 13 (6.0) | 77 (21.0) | 17 (24.6) | 42 (18.5) | 85 (37.0) |
Odds ratio (95% CI)d | 3.59 (1.94 to 6.64) | — | — | 2.76 (1.77 to 4.29) | ||
Difference in proportions, % (95% CI)d | 12.4 (7.5 to 17.2) | — | — | 18.6 (10.8 to 26.4) | ||
P value | < 0.0001 | Reference | — | — | Reference | < 0.0001 |
||||||||||||||||||||||||||||||||||||||| | ||||||
|||||||||||||||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| |
|||||||||||||||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||
|||||||||||||||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||
|||||||||||||||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| |
CI = confidence interval; CMH = Cochran-Mantel-Haenszel; DBL = database lock; ITT = intention to treat; OZ = ozanimod; PL = placebo; RBS = rectal bleeding subscore; SFS = stool frequency subscore; TNF = tumour necrosis factor.
Note: Patients with any RBS, SFS, or endoscopy subscores missing at week 10 and week 52 were classified as not being in clinical remission.
aProportion of patients in clinical remission at week 10 of the induction period (ITT population, nonresponder imputation).
bProportion of patients in clinical remission at week 42 of the treatment maintenance period (week 52 of the study) (ITT population, nonresponder imputation).
cClinical remission was measured using the 3-component Mayo score using a 7-day scoring algorithm and defined as an RBS of 0 and an SFS of ≤ 1 point (and a decrease of ≥ 1 point from the baseline SFS) and an endoscopy subscore ≤ 1 point without friability.
dOdds ratio (active vs. PL), treatment difference, and 2-sided 95% Wald CI and P value for comparison between the cohort 1 OZ group and PL group are based on the CMH test, stratified by corticosteroid use at screening and prior anti-TNF use (yes or no). For the maintenance period analysis, the comparison between the OZ 1 mg to OZ 1 mg group vs. the OZ 1 mg to PL group is based on the CMH test, stratified by remission status at week 10 and corticosteroid use at week 10 (yes or no).
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Source: Clinical Study Report for the TRUE NORTH study.10
Three-Component Mayo Score
The proportion of patients in clinical remission in the cohort 1 ozanimod group versus the cohort 1 placebo group at week 10 of the induction period, based on the 3-component Mayo definition using a 7-day scoring algorithm, was 18.4% and 6.0%, respectively; this represents a statistically significant difference in proportion between the groups of 12.4% (95% CI, 7.5% to 17.2%; P < 0.001). The odds of being in clinical remission at week 10 of the induction period among patients in cohort 1 were greater in patients who received ozanimod compared with those who received placebo (OR = 3.59; 95% CI, 1.94 to 6.64).
The proportion of patients in clinical remission based on the 3-component Mayo definition using a 7-day scoring algorithm in the patients who were re-randomized to placebo and in those who remained on ozanimod at week 52 of the maintenance period was 18.5% and 37.0%, respectively; representing a statistically significant difference in proportion between the groups of 18.6% (95% CI, 10.8% to 26.4%; P < 0.001). The odds of achieving clinical remission at week 52 of the induction period were greater in patients who remained on ozanimod compared with those re-randomized to placebo (OR = 2.76; 95% CI, 1.77 to 4.29).
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Sensitivity Analysis
In both the induction and maintenance periods, the results of the sensitivity analyses for the primary end point (using observed cases only, multiple imputation, and PP analysis) were consistent with the main results. At week 10, a statistically significantly higher proportion of patients in the cohort 1 ozanimod group were in clinical remission compared with the placebo group when sensitivity analyses were performed using observed cases (21.2% versus 7.6%; difference in proportion of 13.7%; 95% CI, 8.0 to 19.4; P < 0.0001), multiple imputation (20% versus 7.4%; difference in proportion of 12.6%; 95% CI, 7.4% to 17.8%, P < 0.0001) and the PP population (18.2% versus 6.1%; difference in proportion of 12.1%; 95% CI, 7.3% to 17.0%; P < 0.0001).
At week 52, a statistically significantly higher proportion of patients in the re-randomized ozanimod group were in clinical remission compared with the re-randomized placebo group when sensitivity analyses were performed using observed cases (54.1% versus 38.2%; difference in proportion of 17.2%; 95% CI, 5.5 to 28.8; P < 0.005), multiple imputation (44.0% versus 26.1%; difference in proportion of 17.9%; 95% CI, 7.7% to 28.2%, P = 0.0009) and the PP population (37.9% versus 18.6%; difference in proportion of 19.1%; 95% CI, 11.2% to 27.1%; P < 0.0001).
Subgroup Analysis
The subgroup analyses of the proportion of patients in clinical remission at week 10 and week 52 as defined by the 3-component Mayo score based on prior use of anti-TNF, disease severity, and disease extent are summarized in Table 14.
In the induction period, treatment effect was greater in patients with no prior use of anti-TNF, moderate UC, and left-sided disease.
Durable Clinical Remission
Results pertaining to the proportion of patients with durable clinical remission (patients in clinical remission at week 10 and at week 52 among all patients who entered the maintenance period) are summarized in Table 15.
At week 42 of the maintenance period (week 52 of the study), the proportion of patients with durable remission in the patients re-randomized to placebo versus those who remained on ozanimod was 9.7% and 17.8%, respectively; this represents a statistically significant difference in proportion between the groups of 8.2% (95% CI, 2.8% to 13.6%; P = 0.003). The odds of durable remission at week 52 among patients who remained on ozanimod were greater compared with those who were re-randomized to placebo (OR = 2.65; 95% CI, 1.38 to 5.06).
Table 14: Proportion of Patients in Clinical Remissiona Based on Prior Use of Anti-TNF, Disease Severity, and Disease Extent in the TRUE NORTH Trial
Subgroup | Ozanimod 1 mg | Placebo | Treatment comparisonb | ||
|---|---|---|---|---|---|
Difference in proportion, % (95% CI)a | ||||||||||||| | Nominal P valueb,c | |||
Outcomes at 10 weeks (induction period) | |||||
Prior use of anti-TNF therapy, n (%) | |||||
No prior anti-TNF | n = 299 66 (22.1) | n = 151 10 (6.6) | 15.4 (9.2 to 21.5) | ||||||||||||| | < 0.0001 |
Prior anti-TNF | n = 130 13 (10.0) | n = 65 3 (4.6) | 5.4 (−1.8 to 12.6) | ||||||||||||| | 0.1947 |
Disease severity (moderate UC,d yes or no), n (%) | |||||
Yes | n = 362 74 (20.4) | n = 191 13 (6.8) | 13.3 (7.9 to 18.7) | ||||||||||||| | < 0.0001 |
No | n = 67 5 (7.5) | n = 25 0 | 6.9 (0.60 to 13.2) | ||||||||||||| | 0.1827 |
Disease extent, n (%) | |||||
Extensive | n = 161 24 (14.9) | n = 82 5 (6.1) | 9.0 (1.5 to 16.6) | ||||||||||||| | 0.0387 |
Left-sided | n = 268 55 (20.5%) | n = 134 8 (6.0) | 14.5 (8.3 to 20.8) | ||||||||||||| | 0.0001 |
Outcomes at 52 weeks (maintenance period) | |||||
Prior use of anti-TNF therapy, n (%) | |||||
No prior anti-TNF | n = 154 63 (40.9) | n = 158 35 (22.2) | 18.5 (8.6 to 28.3) | ||||||||||||| | 0.0003 |
Prior anti-TNF | n = 76 22 (28.9) | n = 69 7 (10.1) | 18.4 (6.2 to 30.6) | ||||||||||||| | 0.0053 |
Disease severity (moderate UC,d yes or no), n (%) | |||||
Yes | n = 192 75 (39.1) | n = 206 40 (19.4) | 19.7 (11.1 to 28.2) | ||||||||||||| | < 0.0001 |
No | n = 38 10 (26.3) | n = 21 2 (9.5) | 13.3 (–5.9 to 32.5) | ||||||||||||| | 0.2256 |
Disease extent, n (%) | |||||
Extensive | n = 78 28 (35.9) | n = 70 13 (18.6) | 19.5 (6.0 to 33.0) | ||||||||||||| | 0.0074 |
Left-sided | N = 152 57 (37.5) | n = 157 29 (18.5) | 18.5 (8.9 to 28.1) | ||||||||||||| | 0.0002 |
CI = confidence interval; CMH = Cochran-Mantel-Haenszel; ITT = intention to treat; RBS = rectal bleeding subscore; SFS = stool frequency subscore. TNF = tumour necrosis factor; UC = ulcerative colitis.
aClinical remission is defined as an RBS of 0 and an SFS of ≤ 1 point (and a decrease of ≥ 1 point from the baseline SFS) and an endoscopy subscore of ≤ 1 point without friability.
bOdds ratio (active vs. placebo), treatment difference, 2-sided 95% Wald CI and P value for comparison between the active and placebo groups are based on the CMH test, stratified by corticosteroid use at screening and prior anti-TNF use (yes or no).
cP values < 0.05 are considered nominally significant because no multiplicity adjustment was applied.
dModerate UC was defined as a 4-component Mayo score of 6 to 10.
Source: Clinical Study Report for the TRUE NORTH study.10
Table 15: Proportion of Patients With Durable Clinical Remissiona in the Maintenance Period of the TRUE NORTH Trial
Outcome measure | Placebo to placebo (N = 69) | Re-randomized patients | |
|---|---|---|---|
Ozanimod 1 mg to placebo (N = 227) | Ozanimod 1 mg to ozanimod 1 mg (N = 230) | ||
Patients in durable remission, n (%) | 5 (7.2) | 22 (9.7) | 41 (17.8) |
Odds ratio (95% CI)c | — | 2.65 (1.38 to 5.06) | |
Difference in proportions, % (95% CI)c | — | 8.2 (2.8 to 13.6) | |
P valuec | — | Reference | 0.003 |
CI = confidence interval; CMH = Cochran-Mantel-Haenszel; ITT = intention to treat; RBS = rectal bleeding subscore; SFS = stool frequency subscore; TNF = tumour necrosis factor.
Note: Patients with any RBS, SFS, or endoscopy subscores missing at week 10 or week 52 are classified as not having durable clinical remission.
aDurable clinical remission was defined as an RBS of 0 and an SFS of ≤ 1 point (and a decrease of ≥ 1 point from the baseline SFS) and an endoscopy subscore of ≤ 1 point without friability at weeks 10 and 52.
bProportion of patients in clinical remission at week 42 of the treatment maintenance period (week 52 of the study) (ITT population, nonresponder imputation).
cOdds ratio (active vs. placebo), treatment difference, and 2-sided 95% Wald CI and P value for comparison between the cohort 1 ozanimod group and placebo group are based on the CMH test, stratified by corticosteroid use at screening and prior anti-TNF use (yes or no). For the maintenance period analysis, the comparison between the ozanimod 1 mg to ozanimod 1 mg group vs. the ozanimod 1 mg to placebo group is based on the CMH test, stratified by remission status at week 10 and corticosteroid use at week 10 (yes or no).
Source: Clinical Study Report for the TRUE NORTH study.10
The subgroup analysis of the proportion of patients who had durable remission at week 52 based on prior use of anti-TNF, disease severity, and disease extent is summarized in Appendix 3.
Maintenance of Clinical Remission
Results pertaining to the proportion of patients who maintained remission at week 52 in the subset of patients who were in remission at week 10 are summarized in Table 16.
At week 42 of the maintenance period (week 52 of the study) in the subset of patients who were in remission at week 10, the proportion of patients who were in remission among those re-randomized to placebo versus those who remained on ozanimod was 29.3% and 51.9%, respectively, representing a statistically significant difference in proportion between the groups of 23.9% (95% CI, 9.1% to 38.6%; P = 0.0025). The odds of maintaining remission at week 52 among patients who remained on ozanimod were greater compared with those who were re-randomized to placebo (OR = 2.88; 95% CI, 1.45 to 5.74).
There was no difference in the proportion of patients in clinical remission at week 52 in the subset of patients in clinical remission at week 52 between those re-randomized to placebo compared with those re-randomized to ozanimod when using observed cases only. The other sensitivity analyses for maintenance of clinical remission were consistent with the main analysis.
Table 16: Proportion of Patients With Maintenance of Remissiona During the Maintenance Period of the TRUE NORTH Trial
Outcome measure | Placebo to placebo (N = 69) | Re-randomized patients | |
|---|---|---|---|
Ozanimod 1 mg to placebo (N = 227) | Ozanimod 1 mg to ozanimod 1 mg (N = 230) | ||
Patients in durable remission, n (%) | 5 (41.7) | 22 (29.3) | 41 (51.9) |
Odds ratio (95% CI)b | — | 2.88 (1.45 to 5.74) | |
Difference in proportions, % (95% CI)b | — | 23.9 (9.1 to 38.6) | |
P value | — | Reference | 0.0025 |
CI = confidence interval; CMH = Cochran-Mantel-Haenszel; ITT = intention to treat; RBS = rectal bleeding subscore; SFS = stool frequency subscore; TNF = tumour necrosis factor.
Note: Patients with any RBS, SFS, or endoscopy subscores missing at week 52 are classified as not maintaining remission.
aClinical remission at week 10 and week 52 was defined as an RBS of 0 and an SFS of ≤ 1 point (and a decrease of ≥ 1 point from the baseline SFS) and an endoscopy subscore of ≤ 1 point without friability.
bOdds ratio (active vs. placebo), treatment difference, and 2-sided 95% Wald CI and P value for comparison between the cohort 1 ozanimod group and placebo group are based on the CMH test, stratified by corticosteroid use at screening and prior anti-TNF use (yes or no). For the maintenance period analysis, the comparison between the ozanimod 1 mg to ozanimod 1 mg group vs. the ozanimod 1 mg to placebo group is based on the CMH test, stratified by remission status at week 10 and corticosteroid use at week 10 (yes or no).
Source: Clinical Study Report for the TRUE NORTH study.10
The subgroup analysis of the proportion of patients who had maintained remission at week 52 based on prior use of anti-TNF, disease severity, and disease extent is summarized in Appendix 3.
Clinical Response
Clinical response, as defined by the 3-component and 4-component Mayo, in both the induction and maintenance periods is summarized in Table 17.
Three-Component Mayo Score
The proportion of patients with a clinical response based on the 3-component Mayo definition using a 7-day scoring algorithm in the cohort 1 ozanimod group versus the cohort 1 placebo group at week 10 of the induction period was 47.8% and 25.9%, respectively, representing a statistically significant difference in proportion between the groups of 21.9% (95% CI, 14.4% to 29.3%; P < 0.0001). The odds of being in clinical response at week 10 of the induction period among patients in cohort 1 were greater in patients who received ozanimod compared with those who received placebo (OR = 2.67; 95% CI, 1.86 to 3.84).
The proportion of patients with a clinical remission based on the 3-component Mayo definition using a 7-day scoring algorithm in patients who were re-randomized to placebo versus those who remained on ozanimod at week 42 of the maintenance period (week 52 of the study) was 41.0% and 60.0%, respectively, representing a statistically significant difference in proportion between the groups of 19.2% (95% CI, 10.4% to 28.0%). The odds of achieving clinical remission at week 52 were 2.3 times greater in patients who remained on ozanimod compared with those re-randomized to placebo (OR = 2.27; 95% CI, 1.54 to 3.33).
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Table 17: Proportion of Patients in Clinical Response as Measured by the Mayo Score in the TRUE NORTH Trial
Mayo score | Induction perioda | Maintenance periodb | ||||
|---|---|---|---|---|---|---|
Cohort 1 | Cohort 2 | PL to PL (N = 69) | Re-randomized patients | |||
OZ (N = 429) | PL (N = 216) | OZ (N = 367) | OZ to PL (N = 227) | OZ to OZ (N = 230) | ||
3-component Mayo score | ||||||
Patients in clinical response, n (%) | 205 (47.8) | 56 (25.9) | 193 (52.6) | 27 (39.1) | 93 (41.0) | 138 (60.0) |
Odds ratio (95% CI)c | 2.67 (1.86 to 3.84) | — | — | 2.27 (1.54 to 3.33) | ||
Difference in proportions, % (95% CI)c | 21.9 (14.4 to 29.3) | — | — | 19.2 (10.4 to 28.0) | ||
P value | < 0.0001 | Reference | — | — | Reference | < 0.0001 |
||||||||||||||||||||||||||||||||||||||| | ||||||
|||||||||||||||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| |
|||||||||||||||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||
|||||||||||||||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||
|||||||||||||||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| |
CI = confidence interval; CMH = Cochran-Mantel-Haenszel; DBL = database lock; ITT = intention to treat; OZ = ozanimod; PL = placebo; RBS = rectal bleeding subscore; SFS = stool frequency subscore; TNF = tumour necrosis factor.
Note: P values < 0.05 are considered nominally significant because no multiplicity adjustment was applied.
aProportion of patients in clinical response at week 10 of the induction period (ITT population, nonresponder imputation).
bProportion of patients in clinical response at week 42 of the treatment maintenance period (week 52 of the study) (ITT population, nonresponder imputation).
cOdds ratio (active vs. PL), treatment difference, and 2-sided 95% Wald CI and P value for comparison between the cohort 1 OZ group and PL group are based on the CMH test, stratified by corticosteroid use at screening and prior anti-TNF use (yes or no). For the maintenance period analysis, the comparison between the OZ 1 mg to OZ 1 mg group vs. the OZ 1 mg to PL group is based on the CMH test, stratified by remission status at week 10 and corticosteroid use at week 10 (yes or no).
Source: Clinical Study Report for the TRUE NORTH study.10
The subgroup analyses of the proportion of patients who experienced clinical response at week 10 and week 52, as defined by the 3-component Mayo score based on prior use of anti-TNF, disease severity, and disease extent, are summarized in Appendix 3.
Rectal Bleeding
Rectal bleeding was an exploratory outcome assessed only in the induction period. Change in RBS from baseline over the induction period is illustrated in Figure 3. Symptomatic improvement in RBS was observed 1 week after completing the required 7-day dose escalation at week 2 in the cohort 1 ozanimod group, and continued to improve, with increasing separation from placebo through to week 10. Compared with the cohort 1 placebo group, a greater reduction from baseline in the least squares mean for the RBS was observed in the cohort 1 ozanimod group at all postbaseline time points.
||||||||||||||||||||||||||||||||||||||||||||||||||||
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Figure 3: Plot of Least Squares Mean Estimate of Change in RBS From Baselinea
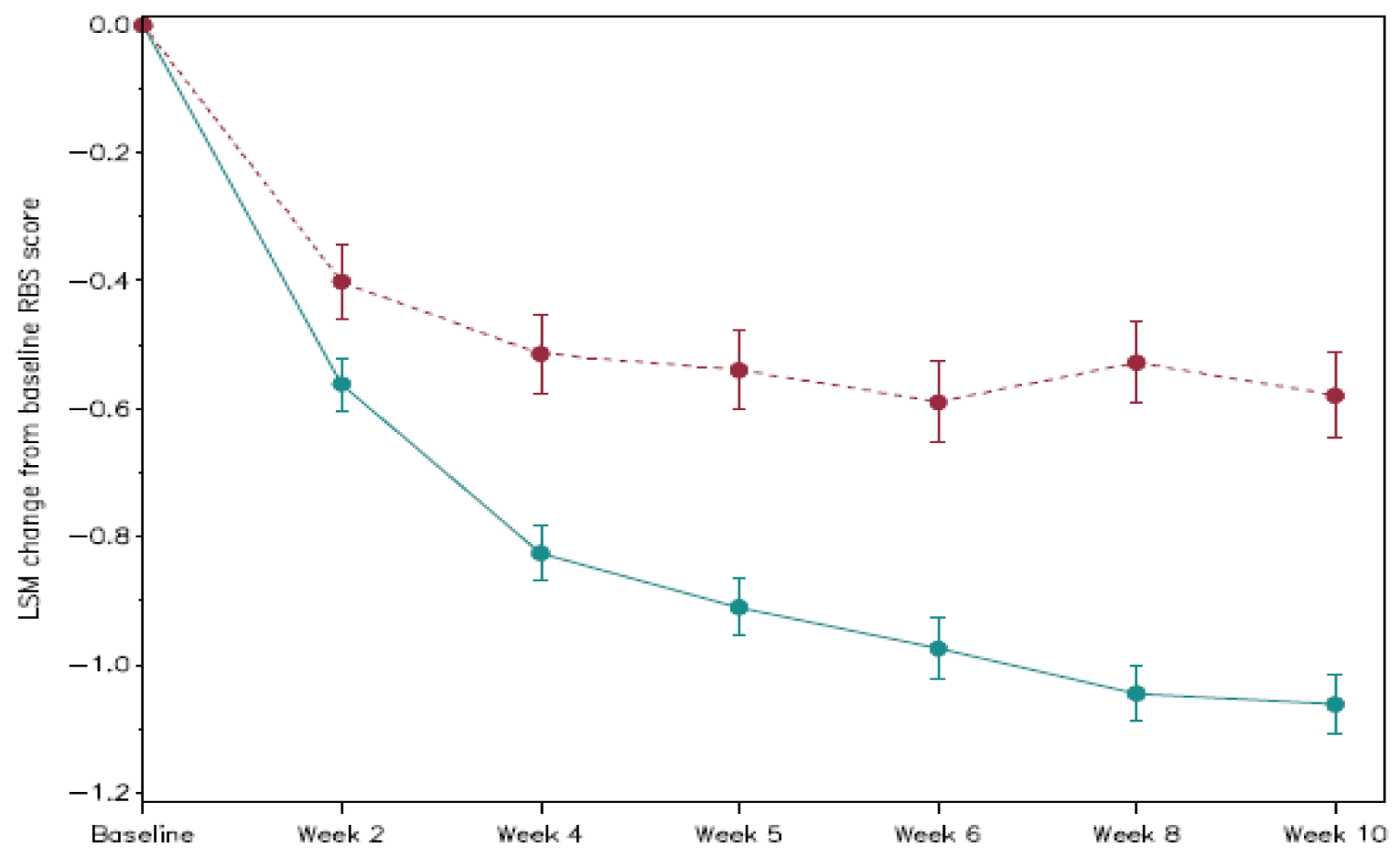
ITT = intention to treat; LSM = least squares mean; RBS = rectal bleeding score; RPC1063 = ozanimod.
Note: Ozanimod change is indicated by a solid line and change score in the placebo group is indicated by the dotted line. Error bars denote standard error.
a Cohort 1 induction period, ITT population, observed data.
Source: Clinical Study Report for TRUE NORTH.10
|||||||||||||||||||||||||| | ||||||||||||| | |||||
|---|---|---|---|---|---|---|
||||||||||||| | ||||||||||||| | |||||
||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | |||
||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | |
||||||||||||||||||||||||||||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| |
|||||||||||||||||||||||||| | ||||||
||||||||||||||||||||||||||||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| |
||||||||||||||||||||||||||||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| |
|||||||||||||||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| |
||||||||||||||||||||||||||||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| |
||||||||||||||||||||||||||||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| |
|||||||||||||||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| |
||||||||||||||||||||||||||||||||||||||| | ||||||
||||||||||||||||||||||||||||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| |
|||||||||||||||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| |
||||||||||||||||||||||||||||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| |
||||||||||||||||||||||||||||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| |
|||||||||||||||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| |
||||||||||||||||||||||||||||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| |
||||||||||||||||||||||||||||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| |
|||||||||||||||||||||||||| | ||||||
||||||||||||||||||||||||||||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| |
||||||||||||||||||||||||||||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| |
|||||||||||||||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| |
||||||||||||||||||||||||||||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| |
||||||||||||||||||||||||||||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| |
|||||||||||||||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| |
||||||||||||||||||||||||||||||||||||||| | ||||||
||||||||||||||||||||||||||||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| |
|||||||||||||||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| |
||||||||||||||||||||||||||||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| |
||||||||||||||||||||||||||||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| |
|||||||||||||||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| |
||||||||||||||||||||||||||||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| |
Note: This table has been redacted as per the sponsor’s request.
Endoscopic Remission
Endoscopic remission was not measured in this study.
Endoscopic Improvement
Results pertaining to the proportion of patients who achieved endoscopic improvement at week 10 of the induction period and week 42 of the maintenance period (week 52 of the study) are summarized in Table 19. Endoscopic remission was defined as an endoscopy subscore for the Mayo score of 1 or less without friability.
The proportion of patients with endoscopic improvement at week 10 of the induction period was 27.3% and 11.6%, respectively; representing a statistically significant difference in proportion between the groups of 15.7% (95% CI, 9.7% to 21.7%; P < 0.0001). The odds of endoscopic improvement at week 10 of the induction period among patients in cohort 1 were greater in patients who received ozanimod compared with those who received placebo (OR = 2.88; 95% CI, 1.80 to 4.59).
At week 42 of the maintenance period (week 52 of the study), the proportion of patients with endoscopic improvement in the group re-randomized to placebo versus the group that remained on ozanimod was 26.4% and 45.7%, respectively; representing a statistically significant difference in proportion between the groups of 19.4% (95% CI, 11.0% to 27.7%; P < 0.001). The odds of endoscopic improvement at week 52 among patients who remained on ozanimod were greater compared with those who were re-randomized to placebo (OR = 2.48; 95% CI, 1.65 to 3.72).
Table 19: Proportion of Patients With Endoscopic Improvementa in the TRUE NORTH Trial
Detail | Induction periodb | Maintenance periodc | ||||
|---|---|---|---|---|---|---|
Cohort 1 | Cohort 2 | PL to PL (N = 69) | Re-randomized patients | |||
OZ (N = 429) | PL (N = 216) | OZ (N = 367) | OZ to PL (N = 227) | OZ to OZ (N = 230) | ||
Patients with endoscopic improvement, n (%) | 117 (27.3) | 25 (11.6) | 100 (27.2) | 20 (29.0) | 60 (26.4) | 105 (45.7) |
Odds ratio (95% CI)d | 2.88 (1.80 to 4.59) | — | — | 2.48 (1.65 to 3.72) | ||
Difference in proportions, % (95% CI)d | 15.7 (9.7 to 21.7) | — | — | 19.4 (11.0 to 27.7) | ||
P value | < 0.0001 | Reference | — | — | Reference | < 0.001 |
CI = confidence interval; CMH = Cochran-Mantel-Haenszel; ITT = intention to treat; OZ = ozanimod; PL = placebo; RBS = rectal bleeding subscore; SFS = stool frequency subscore; TNF = tumour necrosis factor.
Note: Patients with missing endoscopy subscores at week 10 and week 52 were classified as not having endoscopic improvement.
aEndoscopic improvement is defined as an endoscopy subscore of ≤ 1 point without friability.
bProportion of patients in endoscopic remission at week 10 of the induction period (ITT population, nonresponder imputation).
cProportion of patients in endoscopic remission at week 52 of the total treatment maintenance period (ITT population, nonresponder imputation).
dOdds ratio (active vs. placebo), treatment difference, and 2-sided 95% Wald CI and P value for comparison between the cohort 1 OZ group and PL group are based on the CMH test, stratified by corticosteroid use at screening and prior anti-TNF use (yes or no). For the maintenance period analysis, the comparison between the OZ 1 mg to OZ 1 mg group vs. the OZ 1 mg to PL group is based on the CMH test, stratified by remission status at week 10 and corticosteroid use at week 10 (yes or no).
Source: Clinical Study Report for the TRUE NORTH study.10
The subgroup analysis of the proportion of patients who experienced endoscopic improvement at week 10 and week 52 based on prior use of anti-TNF, disease severity, and disease extent is summarized in Appendix 3.
Mucosal Healing
Results pertaining to the proportion of patients with mucosal healing at week 10 of the induction period and week 42 of the maintenance period (week 52 of the study) are summarized Table 20. Mucosal healing was defined as a Mayo score endoscopy subscore of 1 or less without friability and a Geboes index score of 2 or less.
The proportion of patients with mucosal healing in the cohort 1 ozanimod group versus the cohort 1 placebo group at week 10 of the induction period was 12.6% and 3.7%, respectively; representing a statistically significant difference in proportion between the groups of 8.9% (95% CI, 4.9% to 12.9%; P < 0.001). The odds of mucosal healing at week 10 of the induction period among patients in cohort 1 were greater in patients who received ozanimod compared with those who received placebo (OR = 3.77; 95% CI, 1.76 to 8.07).
At week 42 of the maintenance period (week 52 of the study), the proportion of patients with mucosal healing in the group re-randomized to placebo versus the group that remained on ozanimod was 14.1% and 29.6%, respectively; representing a statistically significant difference in proportion between the groups of 15.6% (95% CI, 8.2% to 22.9%; P < 0.001). The odds of mucosal healing at week 52 among patients who remained on ozanimod were greater compared with those who were re-randomized to placebo (OR = 2.64; 95% CI, 1.64 to 4.26).
The subgroup analysis of the proportion of patients who experienced mucosal healing at week 10 and week 52 based on prior use of anti-TNF, disease severity, and disease extent is summarized in Appendix 3.
Need for Colectomy
Need for colectomy was not measured in this study.
Histologic Remission
Results pertaining to the proportion of patients who achieved histologic remission at week 10 of the induction period and week 42 of the maintenance period (week 52 of the study) are summarized in Table 21. Histologic remission was based on a Geboes index score of 2.0 or less.
The proportion of patients in histologic remission in the cohort 1 ozanimod group versus the cohort 1 placebo group at week 10 of the induction period was 18.2% and 7.4%, respectively, representing a difference in proportion between the groups of 10.8% (95% CI, 5.8% to 15.8%). The odds of histologic remission at week 10 of the induction period among patients in cohort 1 were greater in patients who received ozanimod compared with those who received placebo (OR = 2.80; 95% CI, 1.59 to 4.93).
At week 42 of the maintenance period (week 52 of the study), the proportion of patients in histologic remission among those re-randomized to placebo versus those who remained on ozanimod was 16.3% and 33.5%, respectively, representing a difference in proportion between the groups of 17.3% (95% CI, 9.6% to 24.9%). The odds of being in histologic remission at week 52 among patients who remained on ozanimod was higher by more than twofold compared with those who were re-randomized to placebo (OR = 2.68; 95% CI, 1.70 to 4.23).
Corticosteroid-Free Remission
Results pertaining to corticosteroid-free remission, which was only assessed at week 42 of the maintenance period (week 52 of the study), are summarized in Table 22. Corticosteroid-free remission was defined as clinical remission while off corticosteroids for at least 12 weeks.
At week 52, the proportion of patients with corticosteroid-free remission in the group re-randomized to placebo versus the group that remained on ozanimod was 16.7% and 31.7%, respectively; representing a statistically significant difference in proportion between the groups of 15.2% (95% CI, 7.8% to 22.6%; P < 0.001). The odds of being in corticosteroid-free remission at week 42 of the maintenance period (week 52 of the study) among patients who remained on ozanimod were greater compared with those who were re-randomized to placebo (OR = 2.56; 95% CI, 1.60 to 4.09).
Table 20: Proportion of Patients With Mucosal Healinga in the TRUE NORTH Trial
Detail | Induction periodb | Maintenance periodc | ||||
|---|---|---|---|---|---|---|
Cohort 1 | Cohort 2 | PL to PL (N = 69) | Re-randomized patients | |||
OZ (N = 429) | PL (N = 216) | OZ (N = 367) | OZ to PL (N = 227) | OZ to OZ (N = 230) | ||
Patients in mucosal healing, n (%) | 54 (12.6) | 8 (3.7) | 42 (11.4) | 7 (10.1) | 32 (14.1) | 68 (29.6) |
Odds ratio (95% CI)d | 3.77 (1.76 to 8.07) | — | — | 2.64 (1.64 to 4.26) | ||
Difference in proportions, % (95% CI)d | 8.9 (4.9 to 12.9) | — | — | 15.6 (8.2 to 22.9) | ||
P valued | < 0.001 | — | — | — | Reference | < 0.001 |
CI = confidence interval; CMH = Cochran-Mantel-Haenszel; ITT = intention to treat; OZ = ozanimod; PL = placebo; RBS = rectal bleeding subscore; SFS = stool frequency subscore; TNF = tumour necrosis factor.
Note: Patients with a missing endoscopy subscore or missing Geboes index score at week 10 and week 52 were classified as not having mucosal healing.
aMucosal healing is defined as an endoscopy subscore of ≤ 1 point without friability and a Geboes index score of < 2.0 (no neutrophils in the epithelial crypts or lamina propria and no increase in eosinophils, no crypt destruction, and no erosions, ulcerations, or granulation tissue).
bProportion of patients in mucosal healing at week 10 of the induction period (ITT population, nonresponder imputation).
cProportion of patients in mucosal healing at week 42 of the treatment maintenance period (week 52 of the study) (ITT population, nonresponder imputation).
dOdds ratio (active vs. PL), treatment difference, and 2-sided 95% Wald CI and P value for comparison between the cohort 1 OZ group and PL group are based on the CMH test, stratified by corticosteroid use at screening and prior anti-TNF use (yes or no). For the maintenance period analysis, the comparison between the OZ 1 mg to OZ 1 mg group vs. the OZ 1 mg to PL group is based on the CMH test, stratified by remission status at week 10 (yes or no) and corticosteroid use at week 10 (yes or no).
Source: Clinical Study Report for the TRUE NORTH study.10
Table 21: Proportion of Patients in Histologic Remissiona in the TRUE NORTH Trial
Detail | Induction periodb | Maintenance periodc | ||||
|---|---|---|---|---|---|---|
Cohort 1 | Cohort 2 | PL to PL (N = 69) | Re-randomized patients | |||
OZ (N = 429) | PL (N = 216) | OZ (N = 367) | OZ to PL (N = 227) | OZ to OZ (N = 230) | ||
Patients in histologic remission, n (%) | 78 (18.2) | 16 (7.4) | 64 (17.4) | 10 (14.5) | 37 (16.3) | 77 (33.5) |
Odds ratio (95% CI)d | 2.80 (1.59 to 4.93) | — | — | 2.68 (1.70 to 4.23) | ||
Difference in proportions, % (95% CI)d | 10.8 (5.8 to 15.8) | — | — | 17.3 (9.6 to 24.9) | ||
P value | < 0.001 | Reference | — | — | Reference | < 0.001 |
CI = confidence interval; CMH = Cochran-Mantel-Haenszel; ITT = intention to treat; OZ = ozanimod; PL = placebo; RBS = rectal bleeding subscore; SFS = stool frequency subscore; TNF = tumour necrosis factor.
Note: Patients with a missing Geboes index score at week 10 and week 52 were classified as not being in histologic remission.
aHistologic remission is defined as a Geboes index score of < 2.0 (no neutrophils in the epithelial crypts or lamina propria and no increase in eosinophils, no crypt destruction, and no erosions, ulcerations, or granulation tissue).
bProportion of patients in clinical remission at week 10 of the induction period (ITT population, nonresponder imputation).
cProportion of patients in clinical remission at week 42 of the maintenance period (week 52 of the study) (ITT population, nonresponder imputation).
dOdds ratio (active vs. PL), treatment difference, and 2-sided 95% Wald CI and P value for comparison between the cohort 1 OZ and PL group are based on the CMH test, stratified by corticosteroid use at screening and prior anti-TNF use (yes or no). For the maintenance period analysis, the comparison between the OZ 1 mg to OZ 1 mg group vs. the OZ 1 mg to PL group is based on the CMH test, stratified by remission status at week 10 (yes or no) and corticosteroid use at week 10 (yes or no).
Source: Clinical Study Report for the TRUE NORTH study.10
Table 22: Proportion of Patients in Corticosteroid-Free Remissiona During the Maintenance Period in the TRUE NORTH Trial
Detail | Placebo to placebo (N = 69) | Re-randomized patients | |
|---|---|---|---|
Ozanimod to placebo (N = 227) | Ozanimod to ozanimod (N = 230) | ||
Patients in corticosteroid-free remission, n (%) | 17 (24.6) | 38 (16.7) | 73 (31.7) |
Odds ratio (95% CI)c | — | 2.56 (1.60 to 4.09) | |
Difference in proportions, % (95% CI)c | — | 15.2 (7.8 to 22.6) | |
P valuec | — | Reference | < 0.001 |
CI = confidence interval; CMH = Cochran-Mantel-Haenszel; ITT = intention to treat; RBS = rectal bleeding subscore; SFS = stool frequency subscore; TNF = tumour necrosis factor.
Note: Patients with any of RBS, SFS, and endoscopy subscores missing at week 52 were classified as not being in corticosteroid-free remission.
aCorticosteroid-free remission is defined as clinical remission (which is defined as an RBS of 0 and an SFS of ≤ 1 point (and a decrease of ≥ 1 point from the baseline SFS) and an endoscopy subscore of ≤ 1 point) at week 52 while off corticosteroids for ≥ 12 weeks.
bProportion of patients in clinical remission at week 42 of the maintenance period (week 52 of the study) (ITT population, nonresponder imputation).
cOdds ratio (active vs. placebo), treatment difference, and 2-sided 95% Wald CI and P value for comparison between the cohort 1 ozanimod group and placebo groups are based on the CMH test, stratified by corticosteroid use at screening and prior anti-TNF use (yes or no). For the maintenance period analysis, the comparison between the ozanimod 1 mg to ozanimod 1 mg group vs. the ozanimod 1 mg to placebo group is based on the CMH test, stratified by remission status at week 10 (yes or no) and corticosteroid use at week 10 (yes or no).
Source: Clinical Study Report for the TRUE NORTH study.10
The subgroup analysis of the proportion of patients who achieved corticosteroid-free remission at week 52 based on prior use of anti-TNF, disease severity, and disease extent is summarized in Appendix 3.
Depression and Anxiety
Depression and anxiety were not directly measured in the TRUE NORTH trial.
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Harms
Only those harms identified in the review protocol are reported subsequently. Refer to Table 23 for detailed harms data.
Table 23: Summary of Harms in the TRUE NORTH Trial
Harm | Induction period | Maintenance period | ||||
|---|---|---|---|---|---|---|
Cohort 1 | Cohort 2 | PL to PL (N = 69) | Re-randomized patients | |||
OZ (N = 429) | PL (N = 216) | OZ (N = 367) | OZ to PL (N = 227) | OZ to OZ (N = 230) | ||
Patients with ≥ 1 TEAE, n (%) | 172 (40.1) | 82 (38.0) | 146 (39.8) | 27 (39.1) | 83 (36.6) | 113 (49.1) |
TEAEs reported in ≥ 2% of patients in any treatment group | ||||||
Anemia | 18 (4.2) | 12 (5.6) | 16 (4.4) | 0 | 0 | 0 |
Nasopharyngitis | 15 (3.5) | 3 (1.4) | 10 (2.7) | 3 (4.3) | 4 (1.8) | 7 (3.0) |
Headache | 14 (3.3) | 4 (1.9) | 10 (2.7) | 0 | 1 (0.4) | 8 (3.5) |
Nausea | 12 (2.8) | 3 (1.4) | 3 (0.8) | 0 | 0 | 0 |
Alanine aminotransferase increased | 11 (2.6) | 0 | 6 (1.6) | 0 | 1 (0.4) | 11 (4.8) |
Pyrexia | 11 (2.6) | 3 (1.4) | 2 (0.5) | 0 | 0 | 0 |
Arthralgia | 10 (2.3) | 3 (1.4) | 5 (1.4) | 2 (2.9) | 6 (2.6) | 7 (3.0) |
Colitis ulcerative | 6 (1.4) | 5 (2.3) | 9 (2.5) | 1 (1.4) | 10 (4.4) | 1 (0.4) |
Upper respiratory tract infection | 5 (1.2) | 1 (0.5) | 8 (2.2) | 3 (4.3) | 4 (1.8) | 2 (0.9) |
Gamma-glutamyl transferase increased | 0 | 0 | 0 | 0 | 1 (0.4) | 7 (3.0) |
Edema, peripheral | 0 | 0 | 0 | 0 | 0 | 6 (2.6) |
Herpes zoster | 0 | 0 | 0 | 0 | 1 (0.4) | 5 (2.2) |
Vomiting | 0 | 0 | 0 | 2 (2.9) | 2 (0.9) | 2 (0.9) |
Abdominal pain | 0 | 0 | 0 | 2 (2.9) | 1 (0.4) | 1 (0.4) |
Constipation | 0 | 0 | 0 | 3 (4.3) | 1 (0.4) | 1 (0.4) |
Patients with ≥ 1 serious TEAEs, n (%) | 17 (4.0) | 7 (3.2) | 23 (6.3) | 4 (5.8) | 18 (7.9) | 12 (5.2) |
Serious TEAEs reported in ≥ 2 patients in any treatment group, n (%) | ||||||
Colitis ulcerative | 6 (1.4) | 4 (1.9) | 9 (2.5) | 1 (1.4) | 9 (4.0) | 1 (0.4) |
Anemia | 4 (0.9) | 0 | 1 (0.3) | 0 | 0 | 0 |
Appendicitis | 1 (0.2) | 0 | 2 (0.5) | 0 | 0 | 0 |
Gastroenteritis | 0 | 0 | 2 (0.5) | 0 | 0 | 0 |
Complicated appendicitis | 0 | 0 | 0 | 0 | 2 (0.9) | 0 |
Patients who discontinued treatment due to a TEAE, n (%) | 14 (3.3) | 7 (3.2) | 14 (3.8) | 0 | 6 (2.6) | 3 (1.3) |
Reason for discontinuation reported in ≥ 2 patients in any treatment group, n (%) | ||||||
Colitis ulcerative | 3 (0.7) | 4 (1.9) | 4 (1.1) | 0 | 4 (1.8) | 0 |
Bradycardia | 0 | 0 | 2 (0.5) | 0 | 0 | 0 |
Patients who experienced an interruption of the study drug due to a TEAE, n (%) | 6 (1.4) | 3 (1.4) | 5 (1.4) | 0 | 7 (3.1) | 8 (3.5) |
Reasons for discontinuation reported in ≥ 2 patients in any treatment group, n (%) | ||||||
Complicated appendicitis | — | — | — | 0 | 2 (0.9) | 0 |
Deaths, n (%) | 0 | 0 | 1 (0.3) | 0 | 0 | 0 |
Notable harms, n (%) | ||||||
Serious or opportunistic infection | ||||||
Herpes zoster | 2 (0.5) | 0 | 1 (0.3) | 0 | 0 | 4 (1.7) |
Pyelonephritis | 1 (0.2) | 0 | 0 | 0 | 0 | 0 |
Vestibular neuronitis | 1 (0.2) | 0 | 0 | 0 | 0 | 0 |
Pneumonia influenza | 0 | 0 | 1 (0.3) | 0 | 0 | 0 |
Respiratory syncytial virus test positive | 0 | 0 | 1 (0.3) | 0 | 0 | 0 |
Urinary tract infection | 0 | 0 | 1 (0.3) | 0 | 0 | 0 |
Clostridium difficile infection | 0 | 0 | 0 | 0 | 0 | 1 (0.4) |
Complicated appendicitis | 0 | 0 | 0 | 0 | 1 (0.4) | 0 |
Gastroenteritis norovirus | 0 | 0 | 0 | 0 | 0 | 1 (0.4) |
Large intestine infection | 0 | 0 | 0 | 1 (1.4) | 0 | 0 |
Measles | 0 | 0 | 0 | 0 | 1 (0.4) | 0 |
Yersinia infection | 0 | 0 | 0 | 0 | 1 (0.4) | 0 |
Macular edema | 1 (0.2) | 0 | 1 (0.3) | 0 | 0 | 1 (0.4) |
Bradycardia and heart conduction abnormalities | ||||||
Bradycardia | 0 | 0 | 3 (0.8) | 0 | 0 | 0 |
Sinus bradycardia | 0 | 0 | 1 (0.3) | 0 | 0 | 0 |
Second degree and higher atrioventricular block | 0 | 0 | 0 | 0 | 0 | 0 |
Hepatic effects | ||||||
Alanine aminotransferase increased | 2 (0.5) | 0 | 1 (0.3) | 0 | 0 | 1 (0.4) |
Hepatic enzyme increased | 2 (0.5) | 0 | 0 | 0 | 0 | 0 |
Aspartate aminotransferase increased | 1 (0.2) | 0 | 0 | 0 | 0 | 0 |
Liver function test increased | 1 (0.2) | 0 | 0 | 0 | 0 | 1 (0.4) |
Transaminases increased | 1 (0.2) | 0 | 0 | 0 | 0 | 0 |
Blood bilirubin increased | 0 | 0 | 0 | 0 | 1 (0.4) | 0 |
Lymphopenia | 0 | 0 | 0 | 0 | 0 | 2 (0.9) |
AE = adverse event; AESI = adverse effect of special interest; MedDRA = Medical Dictionary for Regulatory Activities; NR = not reported; OZ = ozanimod; PL = placebo; TEAE = treatment-emergent adverse event.
Note: A TEAE is defined as any AE with a date of first onset or date of worsening in severity on or after the date of the first induction period dose, excluding those with onset after the date of the first maintenance period dose. Patients with multiple events reported for the same summary level are counted only once. Percentages are based on the number of patients in the safety population.
TEAEs were coded using MedDRA version 22.1.
Source: Clinical Study Report for the TRUE NORTH study.10
Adverse Events
During the induction period, at least 1 TEAE was reported by 40.1% and 38.0% of patients in the cohort 1 ozanimod group and cohort 1 placebo group, respectively. Among patients re-randomized to placebo versus those who continued on ozanimod during the maintenance period, 36.6% and 49.1% of patients reported at least 1 TEAE, respectively.
The TEAEs reported by at least 2% of patients in any treatment group during the induction period were: anemia, nasopharyngitis, headache, nausea, alanine aminotransferase increase, pyrexia, arthralgia, colitis ulcerative, and upper respiratory tract infection. Of these, anemia, nausea, and pyrexia were not reported by any re-randomized patients during the maintenance period, with the remaining TEAEs reported by a similar proportion of patients as in the induction period. Apart from anemia, which was reported in 4.2% to 5.6% of patients, these TEAEs were reported in less than 4% of any treatment group. The following commonly reported TEAEs were exclusive to re-randomized patients in the maintenance period: gamma-glutamyl transferase increased (0.4% to 3.0%), edema peripheral (2.6%), and herpes zoster (0.4% to 2.2%).
Serious Adverse Events
During the induction period, serious TEAEs were reported by 4.0% and 3.2% of patients in the cohort 1 ozanimod group versus the cohort 1 placebo group, respectively. The most common serious TEAE reported in the induction period was colitis ulcerative in both treatment groups (approximately 1.4%). Additional serious TEAEs reported in the cohort 1 ozanimod group were anemia (0.9%) and appendicitis (0.2%).
During the maintenance period, 7.9% of patients re-randomized to placebo and 5.2% of patients who continued ozanimod reported at least 1 serious TEAE. The serious TEAEs reported in at least 2 patients in the re-randomized placebo group included colitis ulcerative (4% in the re-randomized placebo group and 0.4% in the ozanimod group) and complicated appendicitis (0.9% in the re-randomized placebo group).
Withdrawals Due to Adverse Events
Withdrawal from the study due to TEAEs during the induction period was similar across the treatment groups at approximately 3%. The most common reason for withdrawal due to TEAEs was colitis ulcerative (cohort 1 ozanimod: 0.7%; cohort 1 placebo: 1.9%). Two (0.5%) patients in the cohort 2 ozanimod group discontinued from the study due to bradycardia.
The percentage of patients who withdrew from the study due to TEAEs during the maintenance period was 2.6% among those re-randomized to ozanimod versus 1.3% in patients who remained on ozanimod. Four (1.8%) patients in the group re-randomized to placebo withdrew from the study due to colitis ulcerative.
Mortality
During the study period, only 1 death was reported, which was recorded in the induction period cohort 2 ozanimod group.
Notable Harms
Of the serious or opportunistic infections reported, the only 1 reported in at least 2 patients in any treatment group was herpes zoster (induction period cohort 1 ozanimod: 0.5%; induction period cohort 2 ozanimod: 0.3%; maintenance period ozanimod: 1.7%). Each of the following infections were reported in 1 patient over all treatment groups and periods: pyelonephritis, vestibular neuronitis, pneumonia influenza, positive respiratory syncytial virus test, urinary tract infection, Clostridioides difficile infection, complicated appendicitis, gastroenteritis norovirus, large intestine infection, measles, and yersinia infection.
Macular edema was reported by 1 patient in each of the induction period cohort 1 ozanimod group and the maintenance period ozanimod group.
During the induction period, only the cohort 1 ozanimod group reported hepatic effects (0.5% or less of the group), including alanine aminotransferase increased, hepatic enzyme increased, aspartate aminotransferase, liver function test increased, and transaminases increased. In the maintenance period, an increase in blood bilirubin was reported in 1 patient re-randomized to placebo. Among the patients who remained on ozanimod, alanine aminotransferase increase and liver function test increase were each reported in 1 patient.
Lymphopenia was reported in 2 patients (0.9%) in the maintenance period ozanimod group.
Critical Appraisal
Internal Validity
The TRUE NORTH trial employed appropriate methods for blinding, treatment allocation, and randomization. The treatment groups were well balanced during both study periods. The use of separate induction and maintenance studies was consistent with European Medicines Agency guidelines and similar to other studies assessing other medications for the treatment of UC.
Outcomes were objectively obtained with validated instruments that have been similarly used in other UC trials, and the process to carry out outcome measurements was well described and assessed in blinded fashion. There appears to be a low risk of bias due to the selection of the reported results, and the results presented followed the prespecified analysis plan. As described earlier, the study protocol underwent several amendments, which were all well addressed and unlikely to affect the end results or imply bias due to patient selection.
The TRUE NORTH trial was limited by several study design issues. Although approximately 90% of randomized patients completed the induction period, only approximately 50% had a clinical response and continued into the maintenance period. Furthermore, of those who continued into the maintenance period, the proportion of patients who completed the trial among patients re-randomized to receive placebo versus those who continued to receive ozanimod was 54.6% and 80%, respectively. Moreover, a greater proportion of patients in the re-randomized placebo group discontinued the maintenance period of the trial to enter the OLE study compared with the ozanimod group (35.7% versus 14.8%). Study withdrawal due to disease relapse was based on a prespecified definition of disease relapse that included an objective, blinded, centrally read endoscopic assessment. These patients would have been considered nonresponders in the efficacy analyses. Although the direction of any bias is unclear, it is possible that the differential dropout rate between the 2 treatment groups may have introduced attrition bias in favour of ozanimod.
Regarding the statistical analysis, the study was powered to assess the outcome of clinical remission and clinical response. All analyses were performed using the ITT method, ensuring that the prognostic balance created from randomization was maintained. Patients who stopped or deviated from the intervention were properly accounted for in the ITT approach. The key secondary efficacy end points were addressed using the multiplicity hierarchical testing procedure which controlled for type I error. Missing data pertaining to the primary and secondary outcomes were addressed using NRI. While the NRI approach may be considered appropriate, as patients who discontinue treatment are assigned no treatment benefit, it may cause a biased estimation in certain situations. Sensitivity analyses were conducted around missing data using tipping-point analysis, multiple imputation, and analysis of observed cases with no imputation to confirm study results. Results were generally found to be consistent. Since missing data for continuous end points were not imputed and there were large proportions of discontinuations in each period, results for the HRQoL outcomes and the WPAI-UC were at considerable risk of bias, potentially in favour of ozanimod.
Several subgroup analyses were performed to examine the consistency of the treatment effect observed for the primary and key secondary efficacy end points. However, proper interpretation of all subgroups was not possible due to the lack of sample size considerations for these subgroups and their absence from the statistical testing hierarchy. The subgroups were underpowered to detect significant effect modification by subgroups of interest according to the CADTH review protocol, such as prior anti-TNF use and disease severity, though the results suggested (as shown by inconsistency in statistical significance between the subgroups) a differential treatment effect for these subgroups, particularly for the primary end point.
External Validity
The demographic and disease characteristics of the study population were considered by the clinical expert to be generally reflective of the relevant population with UC in Canada.
Disease Extent and Severity
While the disease extent favoured left-sided colitis, the disease severity was considered high, with most patients having an endoscopy subscore of 3, which is reflective of moderate to severe disease activity and typical of the relevant patient population in Canada, as noted by the clinical expert consulted by CADTH.
Race
Approximately 90% of enrolled patients were white. This proportion of white patients in IBD clinical trials is commonplace, mainly due to heavy recruitment from North American and European centres.44 While there may be some genetic polymorphisms that influence treatment response by race, none are routinely used in clinical practice nor related to ozanimod, according to the clinical expert.
Age
The lack of representation of patients over the age of 65 has little impact on the generalizability of the trial. According to the clinical expert consulted by CADTH, patients with IBD are generally younger in age, which is evident, given that the mean age at UC diagnosis among study patients was approximately 35 years. In addition, other treatments with a more favourable side effect profile are typically used among older patients with UC. Finally, older patients are more likely to be on other medications or have cardiac and/or ocular comorbidities that would be contraindications for ozanimod. It should also be noted that the product monograph for Zeposia states, “Health Canada has not authorized Zeposia for maintenance treatment of UC in patients ≥ 65 years of age.”25
Enriched Patient Population
The trial criterion that directed entry into the maintenance period, clinical response, likely created an enriched patient population. Consequently, the patients who entered the maintenance period may be more likely to benefit from treatment with ozanimod than the general population in the real-world setting. According to the clinical expert consulted by CADTH, this is the common trial design used in UC programs, as it is challenging to keep nonresponders in a long-term study. Additionally, there may be a subset of patients who experience a delayed response to induction therapy. Indeed, a recent phase III upadacitinib program found that approximately half of the patients with UC who did not respond during an initial 8-week induction did respond with an extended 16-week induction period. This added another layer of difficulty to assess the generalizability of efficacy results from this 2-stage, enrichment design trial.
Availability of Open-Label Ozanimod Upon Relapse
Patients had the opportunity to enrol in the OLE study, where they would receive ozanimod upon disease relapse during the maintenance period. Indeed, there was significant study discontinuation due to disease relapse and entry into the OLE study (34% of patients re-randomized from ozanimod to placebo and 14% of patients re-randomized from ozanimod to ozanimod); these patients were imputed as nonresponders for the primary and key secondary end points. It is possible that the proportions of patients discontinuing double-blind treatment from the main trial who then receive open-label ozanimod upon disease relapse may not reflect the proportions of discontinuations of ozanimod treatment in the real world, where patients are not blinded to their treatment.
Response to Prior UC Treatment
The observed failure rate of prior UC treatment at baseline was a function of the clinical trial design. For example, compared with the general population with UC, 75% of patients with UC do not experience treatment failure with steroids. According to the clinical expert consulted by CADTH, in the confines of the inclusion and exclusion criteria for clinical trials in moderate to severe UC that require the failure of conventional treatment, the failure rates observed in TRUE NORTH are expected. Similarly, the failure rate for biologic treatment was capped by the trial design.
Prohibited Concomitant Medications
According to the clinical expert consulted by CADTH, the concomitant medications prohibited during the study period and/or during the observations follow-up period through the 30-day safety follow-up visit would not limit the trial results to be generalized to the UC patient population in practice. This is mainly because the general population with UC tends to be otherwise young, healthy individuals whose condition has failed to respond to biologic therapies before treatment with ozanimod, or who would be using biologic therapies after the failure of treatment with ozanimod rather than concomitantly.
Treatment Regimen
The study protocol did not include rectal therapy and required corticosteroid tapering during the study period, creating a treatment regimen that is harsher than in clinical practice. Therefore, the treatment regimen in the TRUE NORTH trial may not be representative of clinical practice, where patients may be kept on the drug longer by using rectal therapy or corticosteroids to ameliorate symptoms while waiting for a response. Of note, patients who could not taper corticosteroids were not considered to have experienced treatment failure; rather, tapering was reset or paused.
Indirect Evidence
Objectives and Methods for the Summary of Indirect Evidence
As there was no direct evidence comparing ozanimod with other active therapies for the treatment of moderate to severe UC in adult patients, a review of indirect evidence was undertaken.
The sponsor submitted an ITC in patients with moderate to severe UC.11 CADTH also conducted a literature search to identify potentially relevant ITCs in this patient population. A focused literature search for NMAs dealing with UC was run in MEDLINE All (1946–) on February 2, 2022. No limits were applied to the search. Titles, abstracts, and full-text articles were screened for inclusion by 1 reviewer based on the population, intervention, comparator, and outcome criteria outlined in Table 5. Two studies (Lasa et al. [2022]12 and Burr et al. [2021]45) describing NMAs of the efficacy and safety of biologics and small-molecule drugs, including ozanimod, for patients with moderate to severe UC were identified. The 2 published ITCs assessed the same biologic drugs and small-molecule drugs, except that in the Lasa et al. ITC, etrasimod and TD-1473 were also included. Both ITCs used the same statistical methods in data analyses and the findings were similar. Therefore, the Lasa et al. ITC has been summarized and appraised in this review.
The objective of this section is to summarize and critically appraise the sponsor-submitted ITC and the Lasa et al. report.
Description of Indirect Comparison
Both ITCs included a systematic review of the literature to identify trials investigating ozanimod or comparator interventions in patients with moderate to severe UC, and an NMA that compared ozanimod with other active treatments.
In the sponsor-submitted ITC, ozanimod was compared with ustekinumab, infliximab, certolizumab, adalimumab, vedolizumab, tofacitinib, golimumab, filgotinib, etrasimod, or the biosimilar versions of these therapies, and placebo. Phase II or III RCTs were included. Clinical response, clinical remission, and endoscopic improvement were evaluated based on subgroups of patients who were biologic-naive or biologic-exposed, and also in the induction and maintenance phases of drug administration.
In the Lasa et al. report, ozanimod was compared with infliximab, adalimumab, golimumab, vedolizumab, ustekinumab, tofacitinib, etrolizumab, upadacitinib, filgotinib, etrasimod, TD-1473, and placebo. Only phase III RCTs were included in this report. In the Lasa et al. report, clinical remission, endoscopic improvement, and steroid-free remission were evaluated (“clinical response” was withdrawn as an outcome of interest in an amendment to the protocol in 2021). Results of clinical remission and endoscopic improvement were reported separately for the subgroups of biologic-naive and biologic-exposed patients during the induction phase and the maintenance phase.
Safety outcomes were examined in the 2 ITCs.
Table 24: Study Selection Criteria and Methods for ITCs
Detail | Sponsor-submitted ITC | Lasa et al. (2022) |
|---|---|---|
Population | Adult (≥ 18 years) patients with moderate to severe UC who were either biologic-naive or biologic-exposed | |
Intervention and comparators |
|
|
Outcome |
|
|
Study design | Phase II, phase III, and phase II and III RCTs | Phase III RCTs |
Publication characteristics | English-language only:
| Articles published between January 1, 1990, and July 1, 2021 (no language restrictions) |
Exclusion criteria |
| Phase II trials |
Databases searched | Search conducted in October 2020. Ovid platform, Ovid MEDLINE including Epub Ahead of Print, In-Process and Other Non-Indexed Citations, Embase, Cochrane Central Register of Controlled Trials, and the Database of Abstracts of Reviews of Effects were searched. Separate searches were performed for trials and systematic reviews/meta-analyses. Grey literature search of ClinicalTrials.gov, hand searches of identified conferences of interest from 2019 to 2020 and bibliographies of relevant SLRs identified via the original database search. | MEDLINE, Embase, and the Cochrane Central Register of Controlled Trials. Major congresses’ databases were also reviewed manually from January 1, 2018, to July 3, 2021 |
Selection process | Conducted by 2 independent reviewers | |
Data extraction process | Performed by 1 reviewer and validated by a second reviewer | Performed by 2 reviewers |
Quality assessment |
|
|
AE = adverse event; ITC = indirect treatment comparison; RCT = randomized controlled trial; SAE = serious adverse event; SLR = systematic literature review; UC = ulcerative colitis.
Source: Sponsor-submitted ITC11 and Lasa et al. (2022).12
In both ITCs, the methods and results have been described as outlined by the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement and the corresponding extension statement for NMAs.46
The patient population, intervention, and comparators and outcome measures for study selection in the 2 ITCs are presented in Table 24.
Methods of Sponsor-Submitted ITC
Objectives
The objective of this ITC was to compare the treatment efficacy and safety of ozanimod relative to currently existing medications for the treatment of moderate to severe UC.
Study Selection Methods
Phase II or III RCTs that were used to inform the ITC were identified through a systematic literature search conducted by the ITC authors. Multiple databases were searched to identify clinical trials (published between 2000 and 2020) that evaluated the efficacy of drug therapies for moderate to severe UC. Study selection was conducted independently by 2 reviewers. Data extraction was performed by 1 reviewer, with extraction verified by a second reviewer. The quality of the included studies was assessed using the University of York Centre for Reviews and Dissemination criteria for assessment of risk of bias in RCTs.47
ITC Analysis Methods
Bayesian NMAs were performed using random-effects or fixed-effects models in all analyses. Placebo was chosen as the reference treatment for all analyses. The primary analyses focused on clinical response, clinical remission, and endoscopic improvement. Supplemental safety analyses were also performed. Due to the significant heterogeneity observed across the included trials, especially a study design that is common in UC, adjustments were made to the data in older treat-through trials (involves a single randomization step at baseline) to more closely resemble modern re-randomized trials in the maintenance phase (involves an additional re-randomization step for patients who are responders during the induction phase). For example, when data were unavailable for sustained clinical responders in 1 particular study to impute the sustained clinical responder data at maintenance, the ratio of biologic-naive responders to sustained responders available in the biologic-naive placebo arm in a second study was applied to the number of clinical responders at maintenance in the first study to obtain the number of patients who were sustained clinical responders. The report described a conservative approach to trial and data inclusion to reduce the influence of the heterogeneity. Model fits were assessed, and the best model was selected using methods outlined in the National Institute for Health and Care Excellence (NICE) Technical Support Documents. An ordinal model with a probit link was used to assess clinical response and clinical remission, given these outcomes approximately represented ordered categories of the underlying Mayo score. For endoscopic improvement, a standard binomial model with a logit link was used, as this outcome was described by a single dichotomous variable. Authors of this ITC indicated that in all cases, outcomes were transformed to ORs (associated 95% CrIs were reported, as well) to facilitate clinical interpretation of findings consistent with the standard outcome reporting method used by clinical trials in UC as well as previous NMAs conducted by evidence review groups. Sensitivity analyses were conducted to test the robustness of the primary outcome analyses by various factors, such as removing Asian trials, pooling doses, restricting maintenance analyses to re-randomized data, and adjusting for placebo response.
Analyses were conducted for 3 patient populations: those who had been exposed to or experienced failure with prior biologic therapy (biologic-experienced), those who had not been exposed to or had not experienced failure with prior biologic therapy (biologic-naive), and an overall analysis that combined data from the previous populations. In addition, separate analyses were performed for studies reporting data at the end of the induction (6 to 14 weeks) and maintenance (52 to 60 weeks) phases.
Detailed statistical methods of ITC are provided in Table 25.
Table 25: ITC Analysis Methods
Detail | Sponsor-submitted ITC |
|---|---|
ITC methods | All NMAs were performed using a Bayesian framework. |
Priors | Default vague prior distributions that take the conservative approach of assuming no pre-existing information were assigned for the treatment effects, trial baselines, common regression terms (beta), and between-study variance in all primary analyses for both the unadjusted and baseline risk-adjusted models. A sensitivity analysis that explores a half-normal prior on the between-trial heterogeneity parameter in the random effects leveraged by the previous ustekinumab and TNF inhibitor submissions to NICE in UC was also performed. |
Assessment of model fit | The preferred model was chosen based on a combination of statistical and clinical considerations. From a statistical standpoint, lower deviance information criteria and residual deviance were favoured. From a clinical perspective, random-effects models likely have better clinical validity relative to fixed-effects models due to the potential clinical heterogeneity described in the report and were therefore favoured by default, where a fixed-effects model only was chosen when the authors were confident that models were not generating conclusions contrary to the direct evidence observed in the clinical trials informing the network. |
Assessment of consistency | Inconsistency assessments for key primary outcomes (clinical response, clinical remission, endoscopic improvement) were performed, showing similar posterior mean deviances between consistency and inconsistency models across all outcomes through deviance plots. In addition, across all outcomes, there was significant overlap of the pairwise conclusions as well as the model fit statistics derived from the consistency and inconsistency models. Therefore, no evidence of significant inconsistency was observed. |
Assessment of convergence | All analyses were performed using 4 unique sets of starting values and were based on burn-in and sampling durations of 20,000 iterations or more, with additional samples taken to achieve convergence when necessary. Convergence was monitored quantitatively using the latest implementation Gelman-Rubin diagnostic (Rhat) based on 4 chains. Samples were considered to have converged if Rhat was equal to or less than 1.05. After convergence has been reached, concerns turn to whether there were sufficient independent samples for stable estimates. The newest version of ESS and MCSE estimation was used to ensure sufficient postconvergence samples were taken to support inference. If the rank-normalized ESS was greater than 400 (i.e., 100 per chain), then samples were taken to ensure the MCSE was small enough to allow for stable estimates to at least 1 decimal place. All assessments of ESS and MCSE were made for each parameter that was reported. |
Outcomes | Clinical remission, clinical response, endoscopic improvement, and safety outcomes. |
Follow-up time points | Separate analyses were performed for studies reporting data at the induction (6 to 14 weeks) and maintenance (52 to 60 weeks) periods. |
Construction of nodes | NR |
Sensitivity analyses |
|
Subgroup analysis | Separate analyses were performed for 3 populations (overall, biologic-naive, and biologic-experienced), given expected differences in clinical efficacy associated with prior treatment and precedence from previous NMA publications in UC. |
Methods for pairwise meta-analysis | Pairwise comparisons of interventions estimated from NMAs were presented through forest plots that report ORs with 95% CrIs, the Bayesian analogue to confidence intervals that represent the interval for which there is a 95% probability that the estimated parameter will fall within. League tables summarizing efficacy vs. all treatments were provided throughout the appendix for a complete summary of all pairwise estimates within each analysis. Statements regarding treatment differences are primarily informed by pairwise differences in effect estimates, with “statistically nonsignificant” conclusions derived from the overlap of pairwise CrIs with unity (i.e., no difference). All NMAs were performed using R and JAGS based on the code outlined in the NICE evidence synthesis Decision Support Unit Technical Support Document series. |
CrI = credible interval; ESS = effective sample size; ITC = indirect treatment comparison; JAGS = Just Another Gibbs Sampler; MCSE = Monte Carlo standard error; NICE = National Institute for Health and Care Excellence; NMA = network meta-analysis; NR = not reported; OR = odds ratio; TNF = tumour necrosis factor; UC = ulcerative colitis.
Source: Sponsor-submitted ITC.11
Results of Sponsor-Submitted ITC
Summary of Included Studies
In total, 26 RCTs were identified from the systematic review. Among them, 9 were induction-only, 2 were maintenance-only, and 15 had both induction and maintenance periods. Of the 17 trials with maintenance periods, 9 had a treat-through maintenance design and 8 had a re-randomized maintenance design. Four trials were excluded due to heterogeneity associated with trial design and/or outcome definitions. Twenty-two RCTs were included in the NMA. The included RCTs evaluated the efficacy and safety of the following therapies: 1 S1P inhibitor (ozanimod), 3 TNF-alpha inhibitors (adalimumab, golimumab, infliximab), 1 alpha 4 beta 7 integrin inhibitor (vedolizumab), 1 IL-12 and -23 inhibitor (ustekinumab), and 1 Janus kinase inhibitor (tofacitinib).
Patients in the induction phase ranged in mean age from 34.1 to 44.8 years and a mean Mayo score of 8.0 to 9.1. The sponsor report noted differences between trials with respect to the percentage of males (range, 42% to 100%), mean CRP level at baseline (range, 7 mg/L to 35.8 mg/L), years since UC diagnosis (ranged from 3.8 years to 14.6 years), extent of disease (left-sided: range, 15% to 63%; extensive: range, 6.6% to 80.8%; other: range, 0% to 63.4%), and use of concomitant steroids (ranged from 25.0% to 100.0%). Trials differed in their eligibility criteria regarding prior anti-TNF biologics. Nine trials required patients to be naive to anti-TNF biologics at study entry. Among studies that allowed but did not require prior therapy with anti-TNF biologics, there was variation in the percentage of patients who had received prior therapy with these drugs (ranged from 15% to 58.0%).
In the maintenance phase, baseline characteristics were reported only for the re-randomized arms of re-randomized trials. Patients in maintenance phase trials were mostly similar in terms of age (mean age ranged from 38.6 to 43.4 years) and sex (percentage of males ranged from 48.1% to 61.1%). The mean Mayo score was similar for most trials (range, 7.9 to 8.9) with the exception of the OCTAVE SUSTAIN trial, which showed lower mean Mayo scores. Where reported, the sponsor noted differences among trials in terms of mean CRP level at baseline (ranged from 0.7 mg/L to 9.6 mg/L), years since UC diagnosis (range, 5.4 to 8.7 years), extent of disease (left-sided: range, 30.6% to 69.2%; extensive: ranged, 11.2% to 68.3%; other: range, 10.6% to 52.8%) and use of concomitant steroids (range, 28% to 58%).
The sponsor reported that most trials provided evidence of appropriate randomization sequence generation (N = 23 trials) and appropriate allocation concealment (N = 21 trials). It was not explicitly stated in 20 trials whether care providers, participants, and outcome assessor groups were all blind to treatment allocation. Nineteen trials included an ITT analysis with appropriate methods used to account for missing data. A description of important differences across trials for key characteristics is provided in Table 26.
Figure 4 to Figure 15 present the networks of evidence for base-case analysis of clinical response, clinical remission, and endoscopic improvement during induction or maintenance in the overall patient population.
Table 26: Assessment of Homogeneity for Sponsor-Submitted ITC
Detail | Description and handling of potential effect modifiers |
|---|---|
Treatment history | Differences in eligibility criteria were noted regarding whether the eligible patient population was either naive to or intolerant to biologic therapies, or whose condition had an inadequate response to biologic therapies. As a result, separate subgroup analyses were performed that stratified patients by biologic exposure status within the NMAs. |
Patient characteristics | Baseline mean CRP levels, years since UC diagnosis, extent of disease, and use of concomitant steroids was found to vary across trials. Results of univariate treatment-effect modifier assessments indicated that concomitant steroid use at baseline, CRP level at baseline, duration of disease, extent of colitis, and previous treatment with an anti-TNF (which was considered the most important potential effect modifier) were potential effect modifiers. However, due to the inconsistencies in how some variables (steroid use, CRP levels, and duration of disease) were reported and defined, adjustment for their potential modification of treatment effect was not feasible. |
Placebo response | Placebo response varied across trials with certain outcomes being more variable (e.g., response and remission during the maintenance phase). In response to heterogeneity across placebo arms and a potential relationship observed with treatment effects (the sponsors report that an overall negative relationship was observed where trials with a higher placebo response often had a worse treatment effect), the sponsors explored placebo-adjusted, network meta-regression NMA models as sensitivity analyses for the primary outcomes of clinical response, remission, and endoscopic improvement, when feasible, based on network structure. |
Definitions of outcomes | Outcome definition in TRUE NORTH trial: Clinical response was based on either the 3-component or 4-component Mayo score. Sponsors report that the majority of the trials used outcome definitions that were similar to those used in the TRUE NORTH trial, with some exceptions:
|
Timing of end point evaluation or trial duration | The primary induction period assessment varied from 2 to 14 weeks across trials, while the maintenance period varied from 22 to 50 weeks after the induction period. Total trial duration varied from 8 to 60 weeks, excluding any open-label safety extension periods. The sponsors restricted the time point of assessment eligible for the NMA to 6 to 14 weeks for induction, and 52 to 60 weeks for maintenance to limit heterogeneity. |
Clinical trial setting | Five trials (Suzuki [2014], Motoya [2019], Jiang [2015], Kobayashi [2016], and PURSUIT-J) restricted recruitment to an entirely Asian population. The sponsors explored the influence of these trials on NMA findings by excluding them in a sensitivity analysis. |
Study design | Some trials used a treat-through design while others used a re-randomized design, and the patients who were re-randomized to maintenance in re-randomized trials varied. To address this, the sponsors used 1 of 3 approaches:
|
CRP = C-reactive protein; ITC = indirect treatment comparison; NMA = network meta-analysis; TNF = tumour necrosis factor; UC = ulcerative colitis.
Source: Sponsor-submitted ITC.11
Figure 4: Network Diagram for Clinical Response and Clinical Remission — Induction Phase, Overall Population
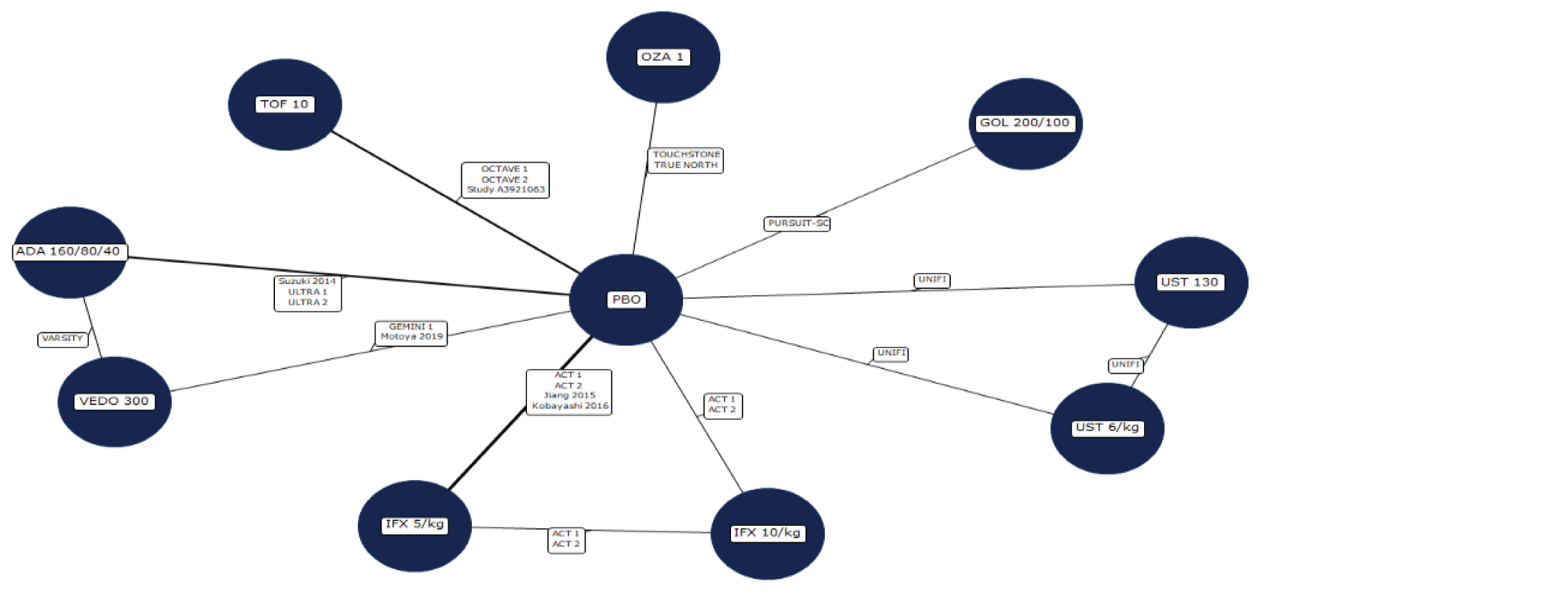
ADA = adalimumab; GOL = golimumab; IFX = infliximab; OZA = ozanimod; PBO = placebo; TOF = tofacitinib; UST = ustekinumab; VEDO = vedolizumab.
Source: Sponsor-submitted indirect treatment comparison.11
Figure 5: Network Diagram for Endoscopic Improvement — Induction Phase, Overall Population
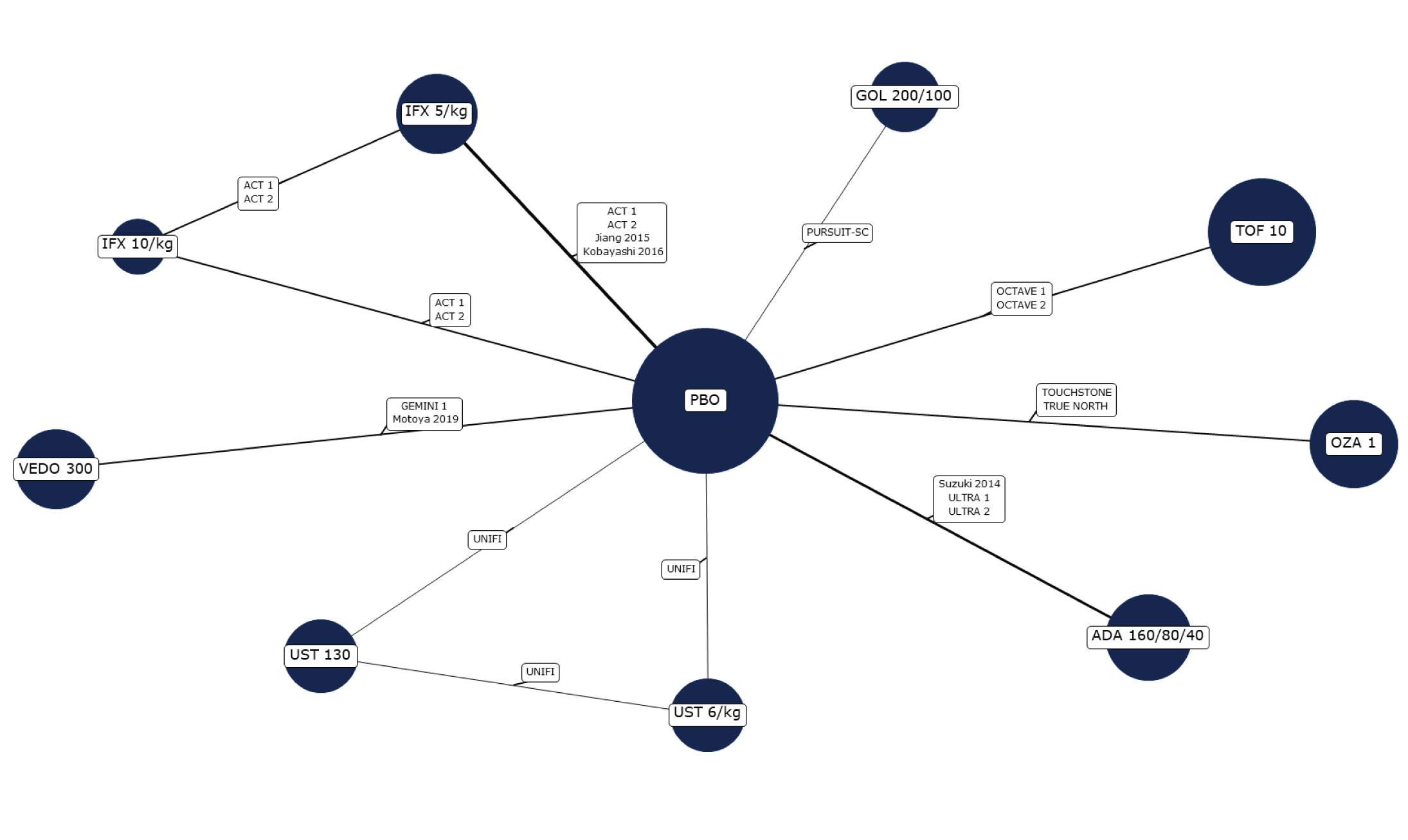
ADA = adalimumab; GOL = golimumab; IFX = infliximab; OZA = ozanimod; PBO = placebo; TOF = tofacitinib; UST = ustekinumab; VEDO = vedolizumab.
Source: Sponsor-submitted indirect treatment comparison.11
Figure 6: Network Diagram for Clinical Response and Clinical Remission — Maintenance Phase, Overall Population
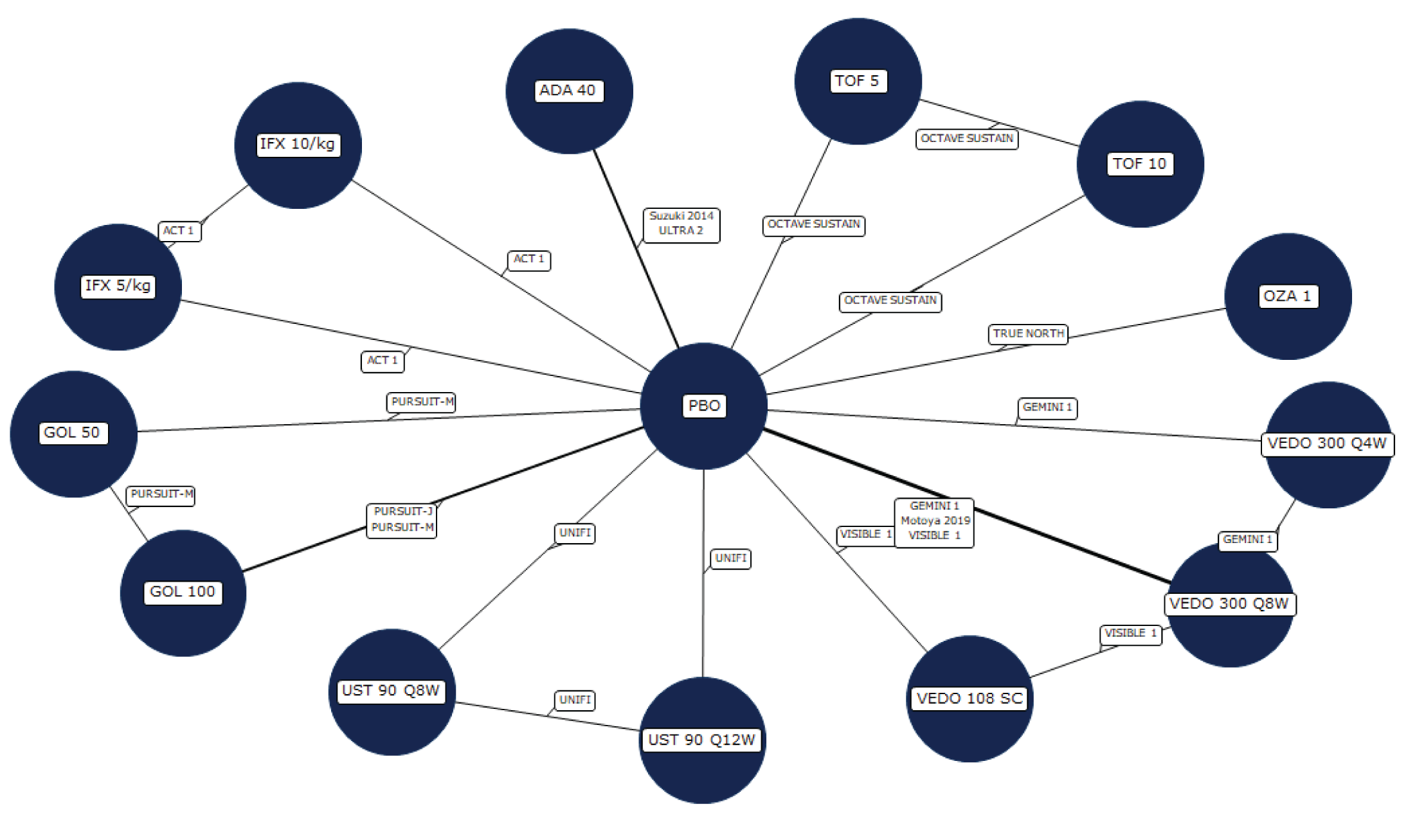
ADA = adalimumab; GOL = golimumab; IFX = infliximab; OZA = ozanimod; PBO = placebo; Q4W = every 4 weeks; Q8W = every 8 weeks; Q12W = every 12 weeks; SC = subcutaneous; TOF = tofacitinib; UST = ustekinumab; VEDO = vedolizumab.
Source: Sponsor-submitted indirect treatment comparison.11
Figure 7: Network Diagram for Endoscopic Improvement — Maintenance Phase, Overall Population
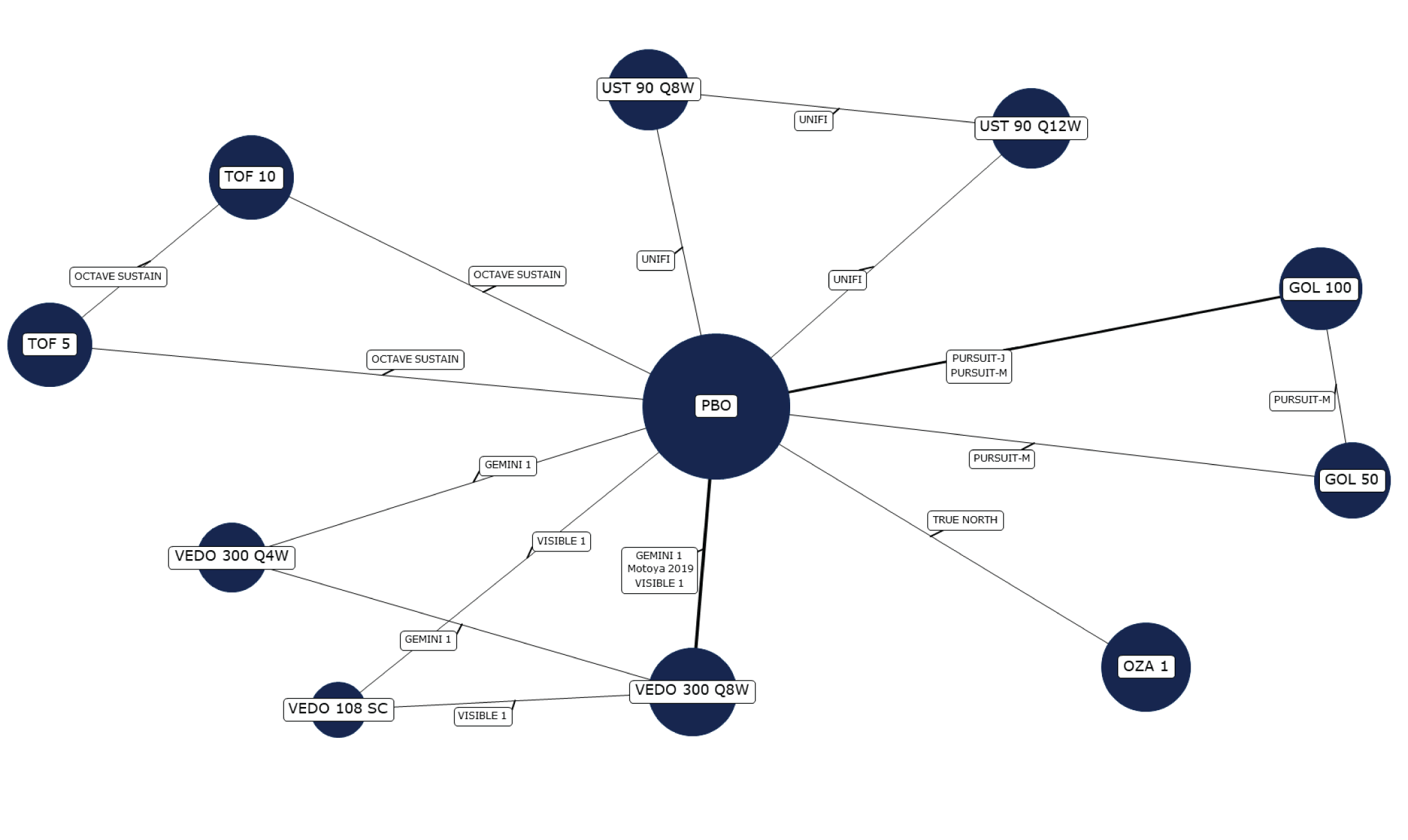
ADA = adalimumab; GOL = golimumab; IFX = infliximab; OZA = ozanimod; PBO = placebo; Q4W = every 4 weeks; Q8W = every 8 weeks; Q12W = every 12 weeks; SC = subcutaneous; TOF = tofacitinib; UST = ustekinumab; VEDO = vedolizumab.
Source: Sponsor-submitted indirect treatment comparison.11
Figure 8: Network Diagram for Adverse Events — Induction Phase, Overall Population
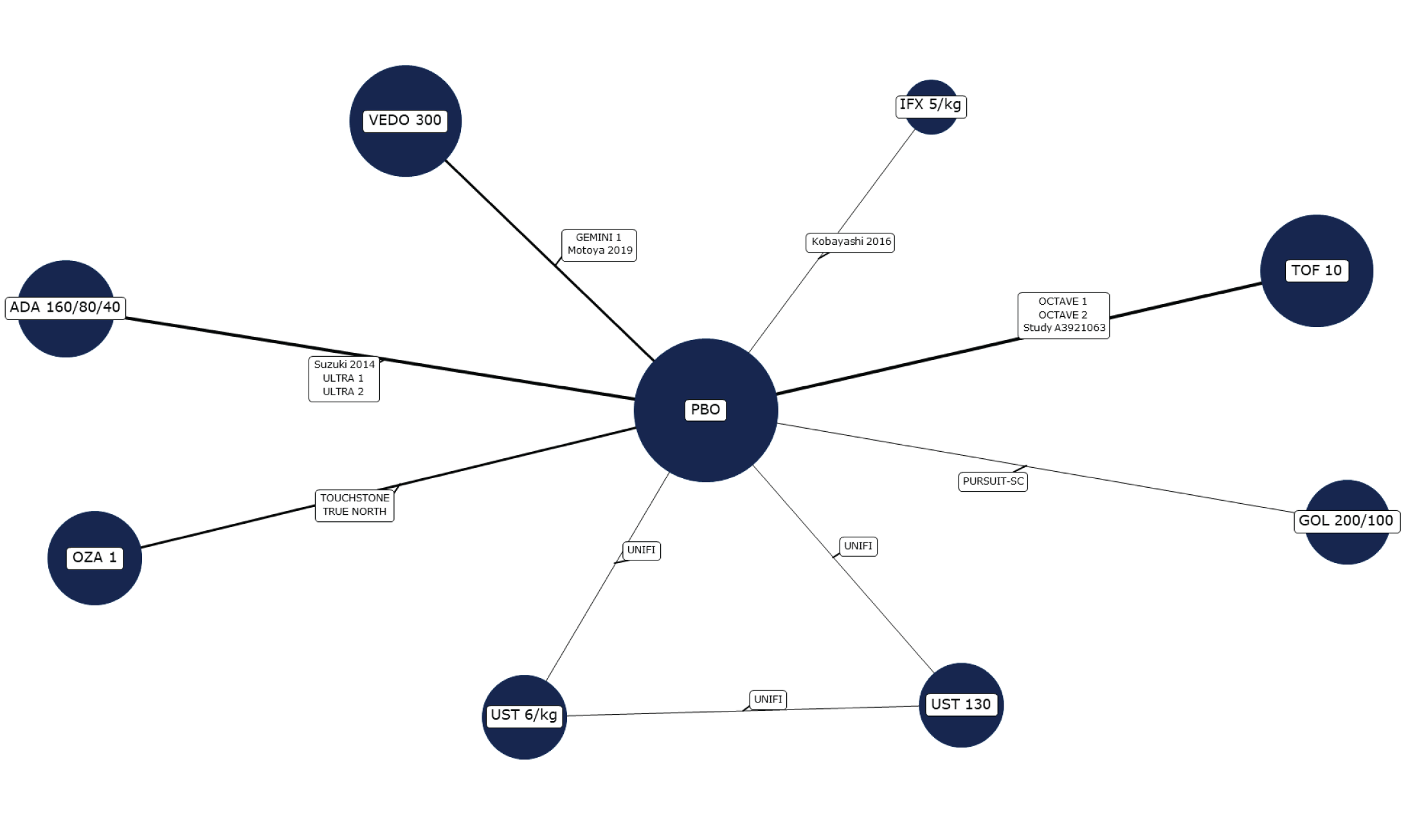
ADA = adalimumab; GOL = golimumab; IFX = infliximab; OZA = ozanimod; PBO = placebo; SC = subcutaneous; TOF = tofacitinib; UST = ustekinumab; VEDO = vedolizumab.
Source: Sponsor-submitted indirect treatment comparison.11
Figure 9: Network Diagram for Adverse Events — Maintenance Phase, Overall Population
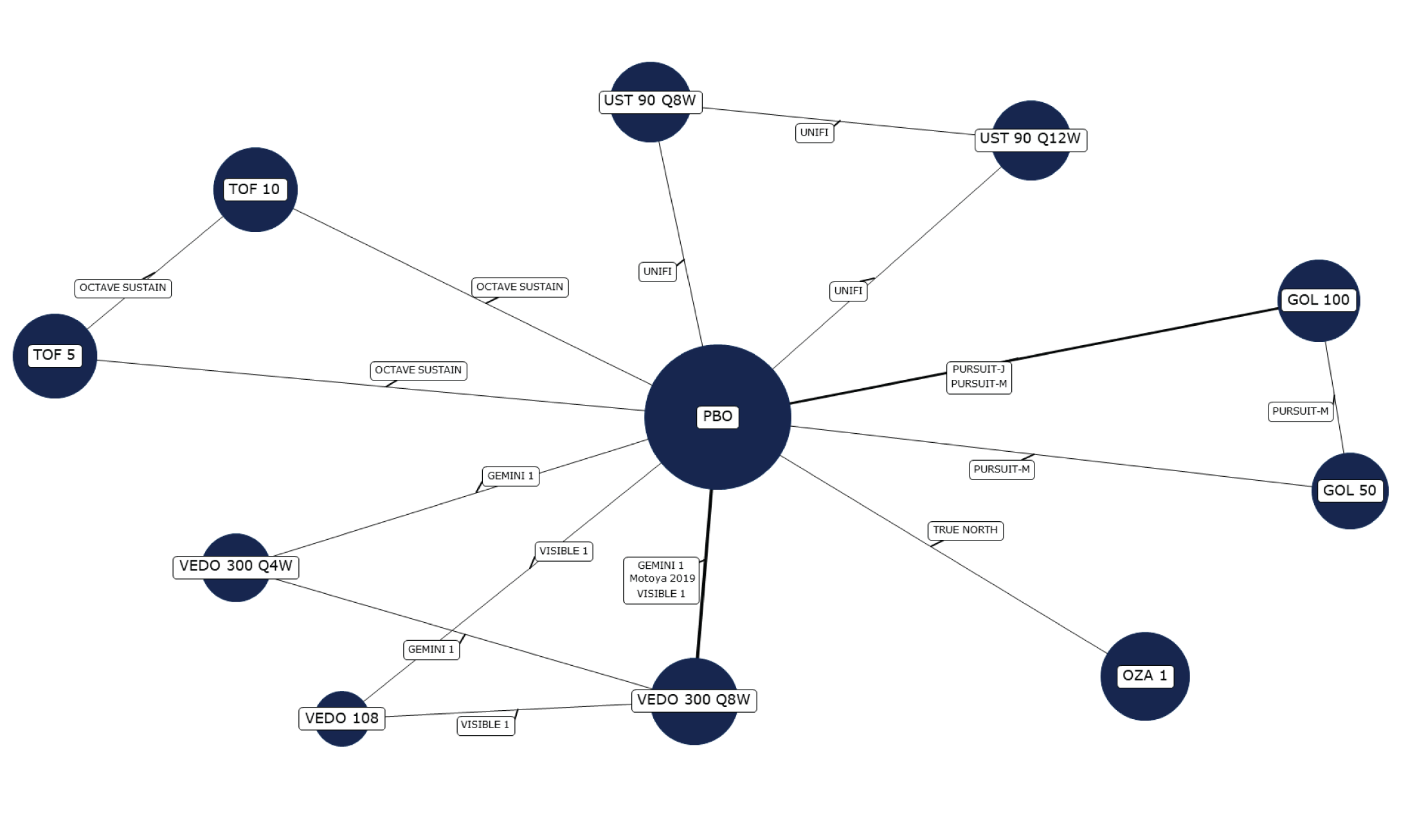
ADA = adalimumab; GOL = golimumab; IFX = infliximab; OZA = ozanimod; PBO = placebo; Q4W = every 4 weeks; Q8W = every 8 weeks; Q12W = every 12 weeks; TOF = tofacitinib; UST = ustekinumab; VEDO = vedolizumab.
Note: Safety maintenance analyses were limited to re-randomized trials.
Source: Sponsor-submitted indirect treatment comparison.11
Figure 10: Network Diagram for Serious Adverse Events — Induction Phase, Overall Population
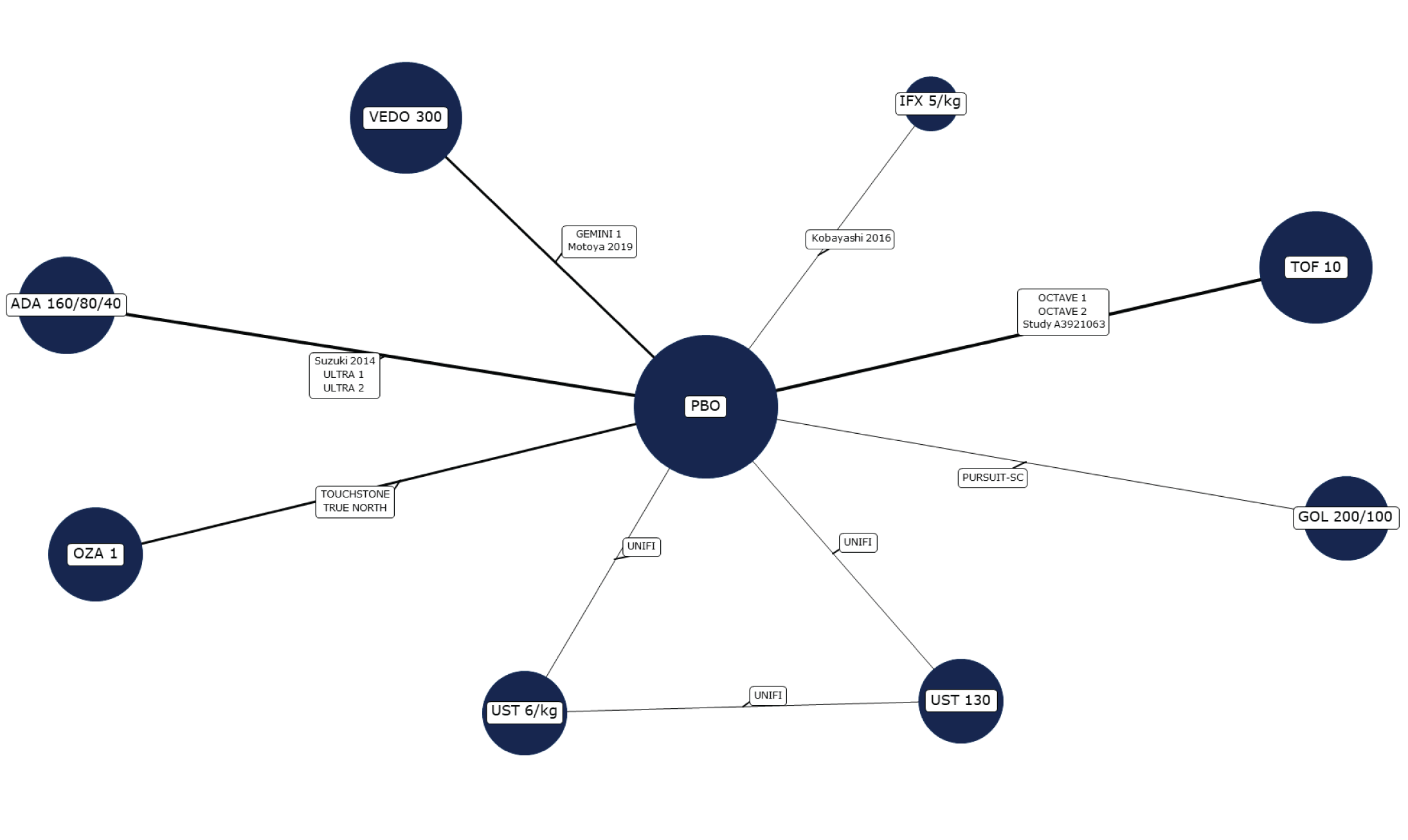
ADA = adalimumab; GOL = golimumab; IFX = infliximab; OZA = ozanimod; PBO = placebo; SC = subcutaneous; TOF = tofacitinib; UST = ustekinumab; VEDO = vedolizumab.
Source: Sponsor-submitted indirect treatment comparison.11
Figure 11: Network Diagram for Serious Adverse Events — Maintenance Phase, Overall Population
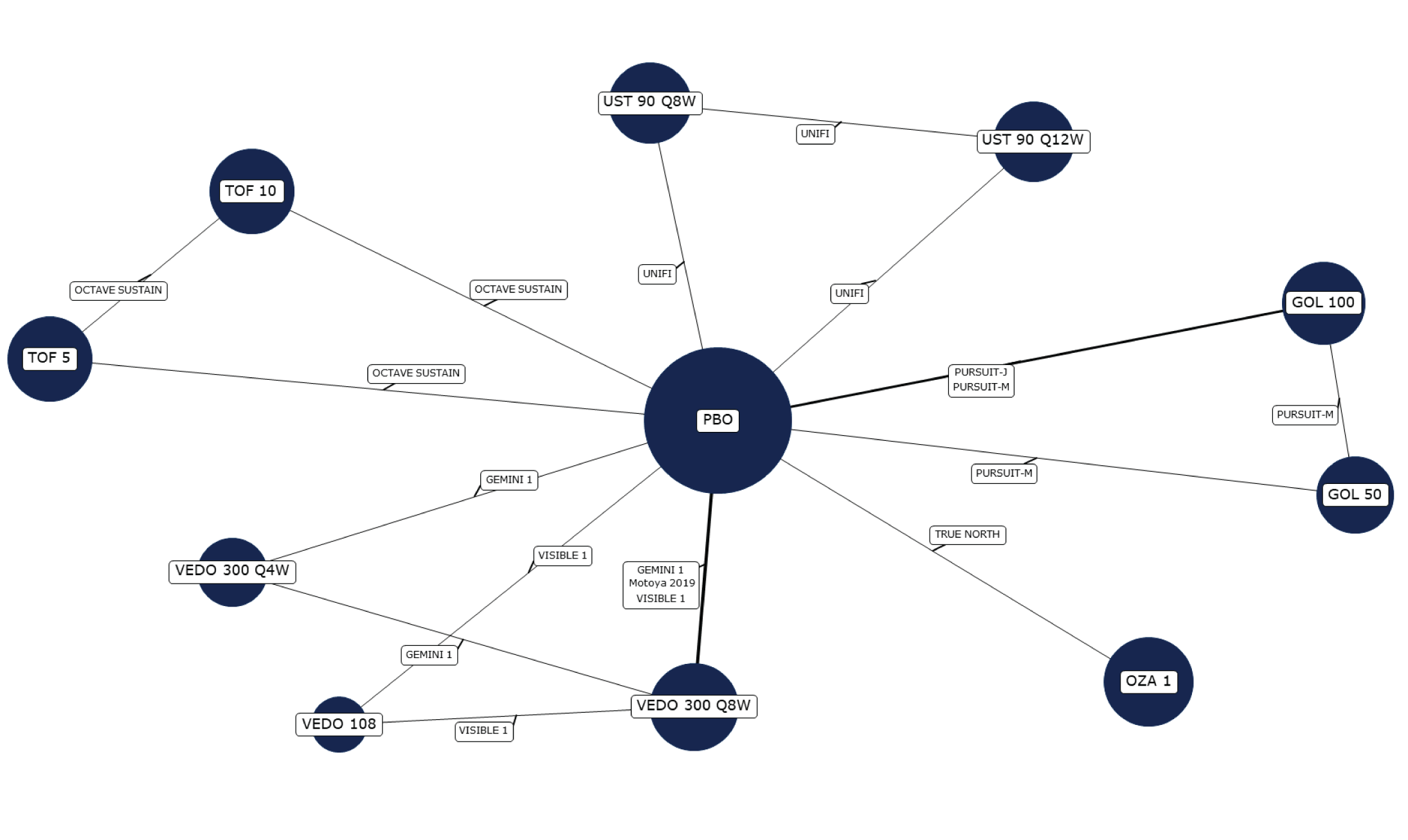
Safety maintenance analyses were limited to re-randomized trials.
ADA = adalimumab; GOL = golimumab; IFX = infliximab; OZA = ozanimod; PBO = placebo; Q4W = every 4 weeks; Q8W = every 8 weeks; Q12W = every 12 weeks; TOF = tofacitinib; UST = ustekinumab; VEDO = vedolizumab.
Source: Sponsor-submitted indirect treatment comparison.11
Figure 12: Network Diagram for Adverse Events Leading to Discontinuation — Induction Phase, Overall Population
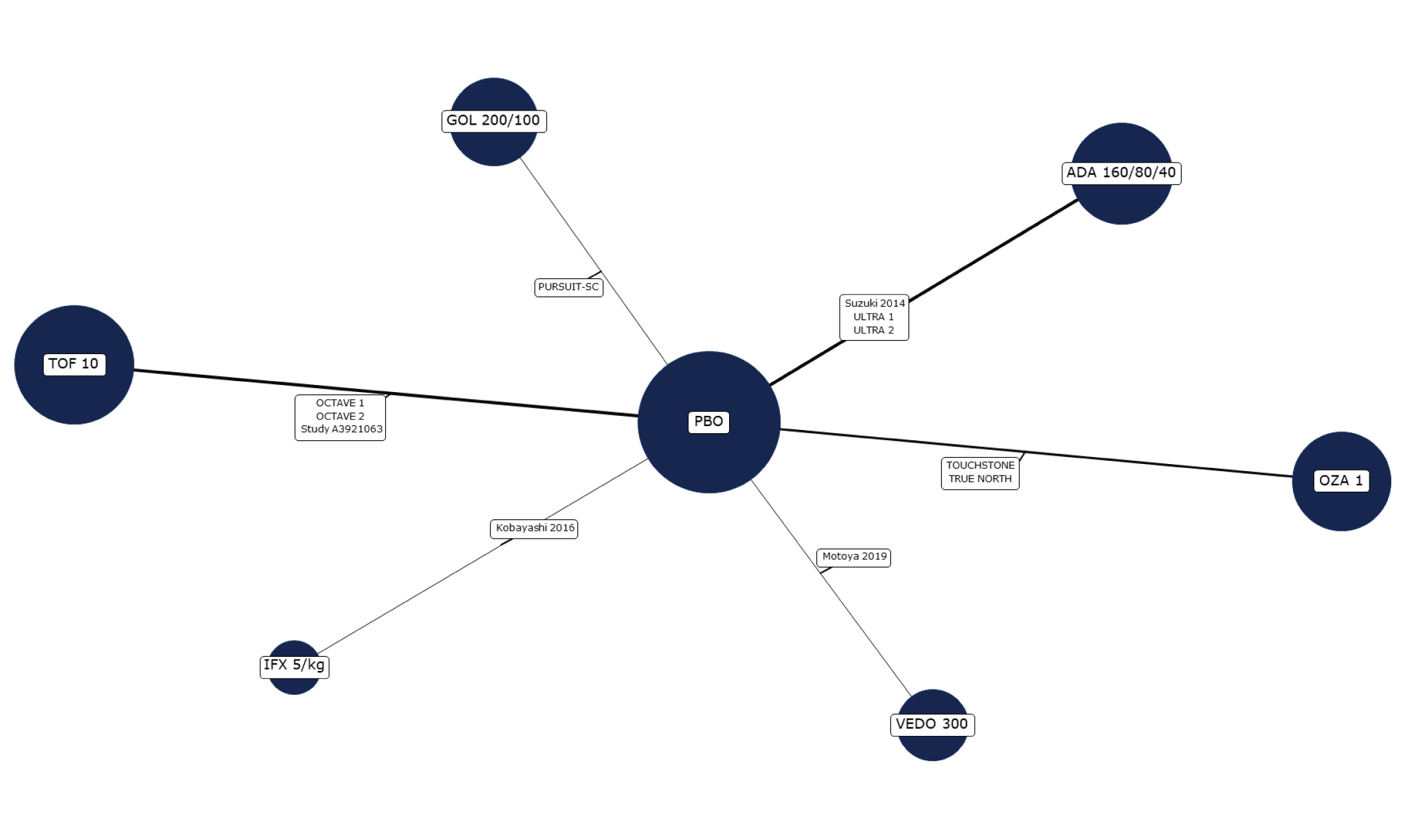
ADA = adalimumab; GOL = golimumab; IFX = infliximab; OZA = ozanimod; PBO = placebo; SC = subcutaneous; TOF = tofacitinib; UST = ustekinumab; VEDO = vedolizumab.
Source: Sponsor-submitted indirect treatment comparison.11
Figure 13: Network Diagram for Adverse Events Leading to Discontinuation — Maintenance Phase, Overall Population
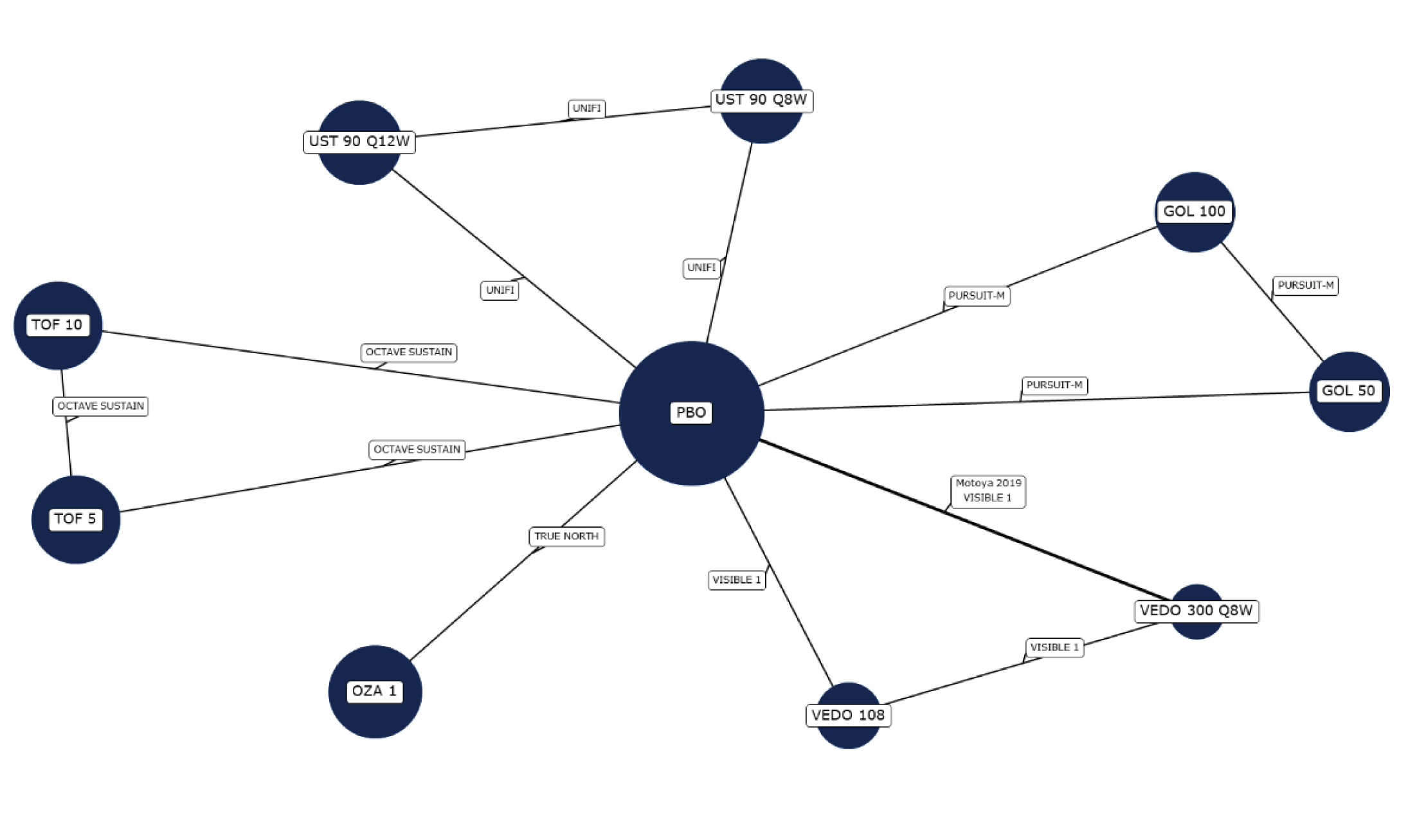
ADA = adalimumab; GOL = golimumab; IFX = infliximab; OZA = ozanimod; PBO = placebo; Q8W = every 8 weeks; Q12W = every 12 weeks; TOF = tofacitinib; UST = ustekinumab; VEDO = vedolizumab.
Note: Safety maintenance analyses were limited to re-randomized trials.
Source: Sponsor-submitted indirect treatment comparison.11
Figure 14: Network Diagram for Serious Infections — Induction Phase, Overall Population
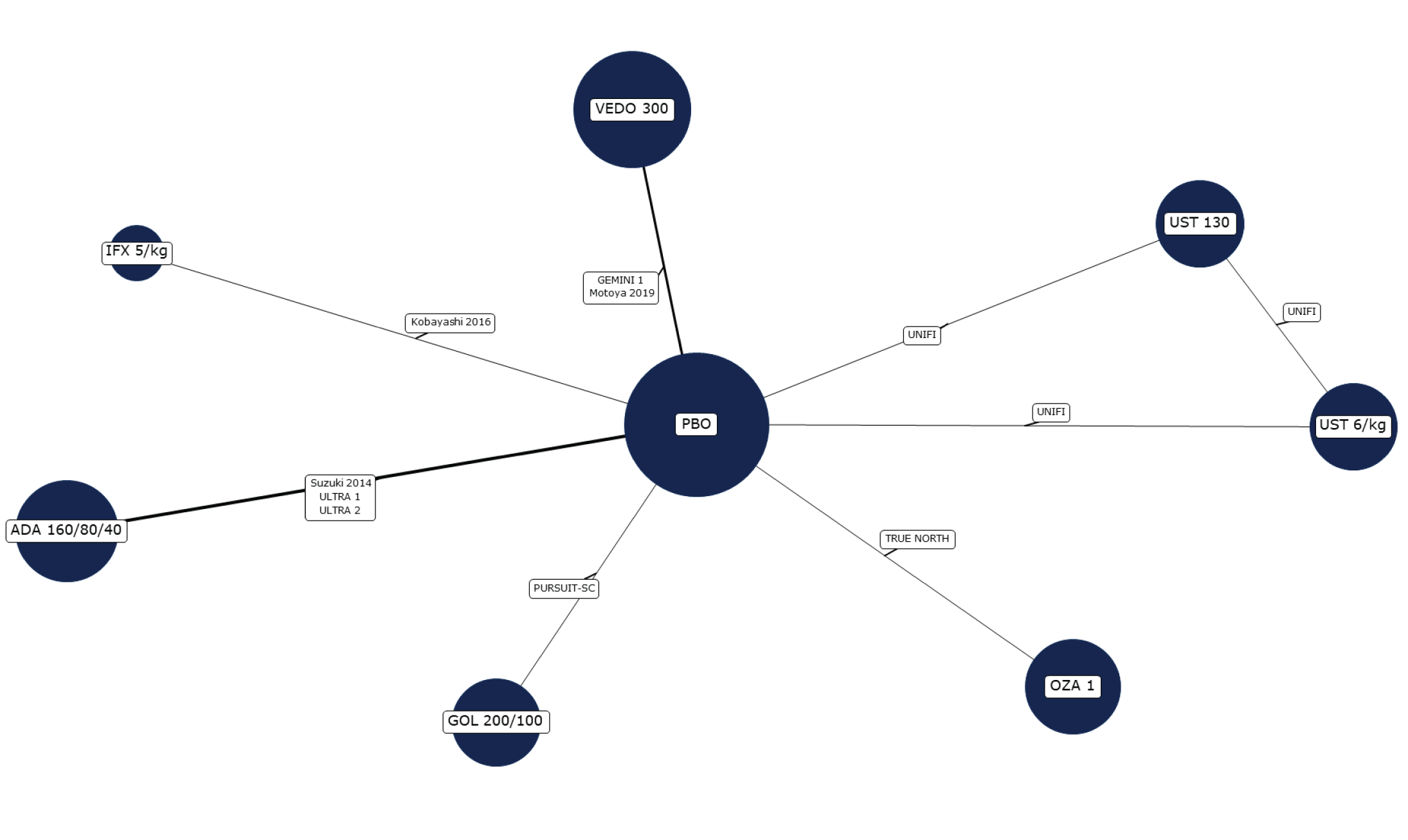
ADA = adalimumab; GOL = golimumab; IFX = infliximab; OZA = ozanimod; PBO = placebo; SC = subcutaneous; TOF = tofacitinib; UST = ustekinumab; VEDO = vedolizumab.
Note: Doses of tofacitinib were excluded from the network, as there were zero placebo events reported across the OCTAVE trials.
Source: Sponsor-submitted indirect treatment comparison.11
Figure 15: Network Diagram for Serious Infections — Maintenance Phase, Overall Population
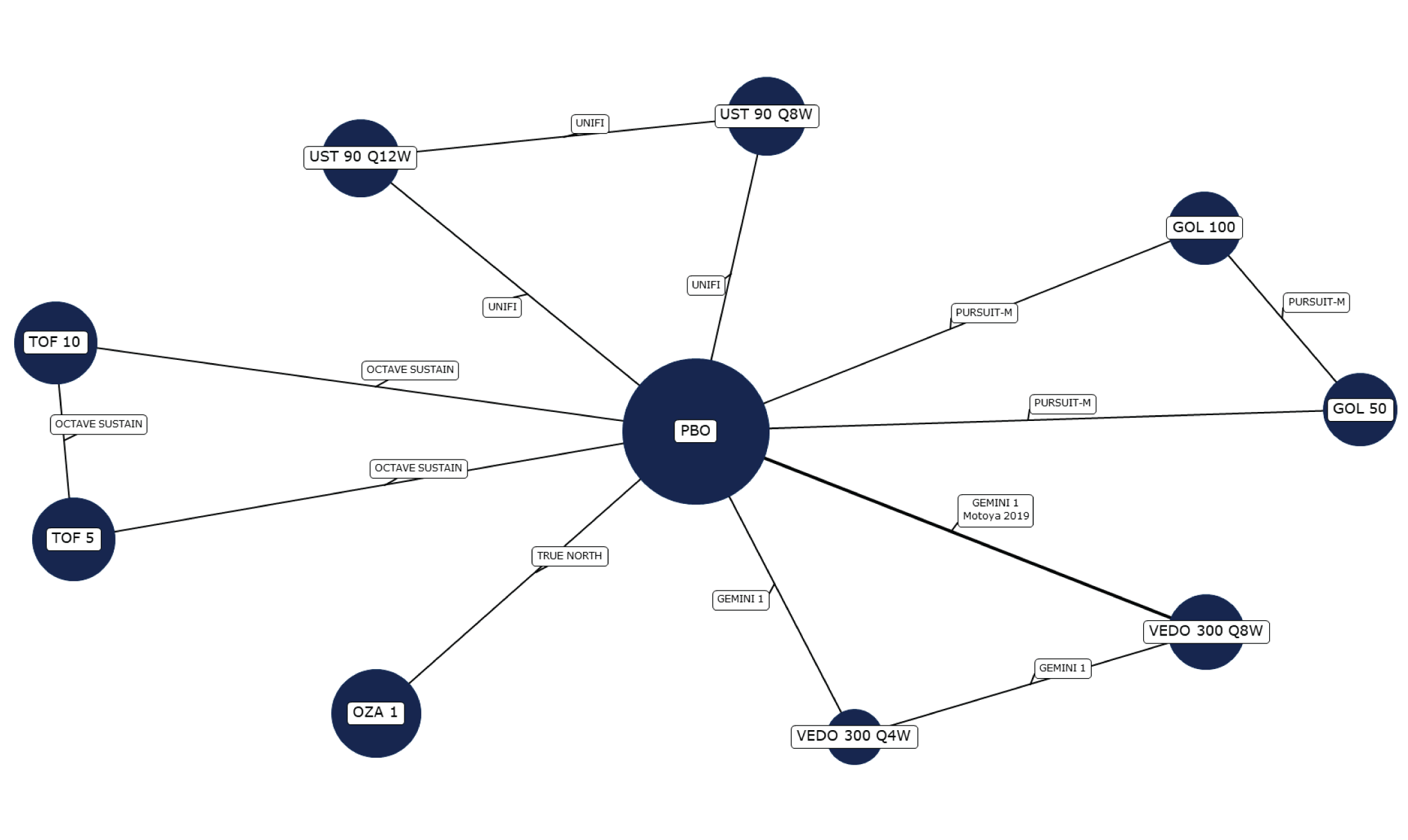
ADA = adalimumab; GOL = golimumab; IFX = infliximab; OZA = ozanimod; PBO = placebo; Q4W = every 4 weeks; Q8W = every 8 weeks; Q12W = every 12 weeks; TOF = tofacitinib; UST = ustekinumab; VEDO = vedolizumab.
Note: Safety maintenance analyses were limited to re-randomized trials.
Source: Sponsor-submitted indirect treatment comparison.11
Results
Detailed efficacy results are presented in Table 27. Only the results for ozanimod versus relevant comparators are summarized in this section.
Clinical Response
For the induction phase, results from random-effects and fixed-effects models found that all active treatments were superior to placebo for clinical response in the overall population and biologic-naive population. For the biologic-exposed population, results from both random-effects and fixed-effects models suggested that all active treatments were favoured over placebo; however, the 95% CrIs of clinical response from random-effects models did not exclude the null for all the comparisons between active treatments and placebo. In the overall population, no treatment was favoured when ozanimod was compared for clinical response with other active treatments for adult patients with moderate to severe UC. Similar results were found for the biologic-naive patients; no treatment was favoured over others for clinical response among patients with moderate to severe UC. Among biologic-exposed patients, results from fixed-effects models showed no evidence for a difference between ozanimod and any of the comparators, except that ozanimod was favoured over adalimumab (OR = 3.13; 95% CrI, 1.42 to 7.31).
For the maintenance phase, results from fixed-effects models found that all active treatments were superior to placebo for clinical response in the overall population, biologic-naive population, and biologic-exposed population. Results from random-effects models showed that 95% CrIs of clinical response did not exclude the null for some comparisons between active treatments and placebo. Based on the fixed-effects models, for the overall population, ozanimod had a less favourable clinical response compared with vedolizumab 300 mg every 8 weeks (OR = 0.55; 95% CrI, 0.34 to 0.92), tofacitinib 5 mg (OR = 0.57; 95% CrI, 0.33 to 0.97), and tofacitinib 10 mg (OR = 0.40; 95% CrI, 0.23 to 0.69). ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||. For biologic-exposed patients |||||||||||||||||||||||||||||||||||||||||||| showed no evidence for a difference between ozanimod and any of the comparators (Table 28) ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Clinical Remission
For the induction phase, results from random-effects and fixed-effects models found that all active treatments were superior to placebo for clinical remission in the overall population and biologic-naive population. For the biologic-exposed population, results from both random-effects and fixed-effects models suggested that all active treatments were favoured over placebo; however, the 95% CrIs of clinical remission from random-effects models did not exclude the null for all the comparisons between active treatments and placebo. In the overall population, no treatment was favoured when ozanimod was compared with other active treatments for clinical remission among adult patients with moderate to severe UC. Similar results were found for the biologic-naive patients; no treatment was favoured between ozanimod and its comparators for clinical remission among patients with moderate to severe UC. Among the biologic-exposed patients, the results from fixed-effects models showed no evidence for a difference between ozanimod and other active comparators, except that ozanimod was favoured over adalimumab (OR = 4.19; 95% CrI, 1.56 to 11.49). Results from random-effects models suggested that no treatment was favoured when ozanimod was compared with other active treatments.
For the maintenance phase, results from random-effects models and fixed-effects models found that all active treatments were superior to placebo for clinical remission in the overall population, biologic-naive population, and biologic-exposed population; however, results from random-effects models showed the 95% CrIs of clinical remission did not exclude the null for some comparisons between active treatments and placebo. For the overall population, results from fixed-effects models showed no evidence for a difference between ozanimod and other active treatments, except that ozanimod had less favourable results for clinical remission compared with vedolizumab 300 mg every 8 weeks (OR = 0.56; 95% CrI, 0.34 to 0.92), tofacitinib 5 mg (OR = 0.57; 95% CrI, 0.34 to 0.97), and tofacitinib 10 mg (OR = 0.40; 95% CrI, 0.24 to 0.69). ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||. For biologic-exposed patients, no treatment was favoured when ozanimod was compared with other active treatments (Table 28). Results from random-effects models suggested that no treatment was favoured when ozanimod was compared with other active treatments.
Endoscopic Improvement
For the induction phase, results from random-effects and fixed-effects models found that all active treatments were superior to placebo for endoscopic improvement in the overall population, biologic-naive population, and biologic-exposed |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| population. However, the 95% CrIs of estimates of endoscopic improvement from random-effects models did not exclude the null for all comparisons between active treatments and placebo in the biologic-exposed population. In the overall population, there was no evidence for a difference between ozanimod and other active comparators, except that ozanimod was favoured over adalimumab (OR = 2.04; 95% CrI, 1.16 to 3.76). Similar results were found for biologic-naive patients; ozanimod was favoured over adalimumab ||||||||||||||||||||||||||||||||||||||||||||||||||||||||| for endoscopic improvement. Among biologic-exposed patients, no active treatments were favoured over others for endoscopic improvement (Table 27). Results from random-effects models suggested that no treatment was favoured when ozanimod was compared with other active treatments.
For the maintenance phase, results from random-effects and fixed-effects models found that all active treatments were superior to placebo for endoscopic improvement in the overall population, biologic-naive population, and biologic-population. However, the 95% CrIs of estimates of endoscopic improvement from random-effects models did not exclude the null for some of the comparisons between active treatments and placebo. For the overall population, there was no evidence for a difference between ozanimod and other active comparators, except that ozanimod had less favourable endoscopic improvement compared with vedolizumab 300 mg every 4 weeks (OR = 0.46; 95% CrI, 0.24 to 0.88) and tofacitinib 10 mg (OR = 0.42; 95% CrI, 0.22 to 0.79). For the biologic-naive population, ozanimod had less favourable endoscopic improvement compared with tofacitinib 10 mg (OR = 0.34; 95% CrI, 0.15 to 0.77). For biologic-exposed patients, there was no evidence for a difference between ozanimod and other active comparators (Table 28). Similarly, results from random-effects models suggested that no treatment was favoured when ozanimod was compared with other active treatments.
In general, results of the sensitivity analyses were consistent with the base-case analyses.
Table 27: Summary of NMA Results for Efficacy Outcomes at Induction (Ozanimod Versus Comparator)
Population | Treatment | Clinical response, median OR (95% Crl) | Clinical remission, median OR (95% Crl) | Endoscopic improvement, median OR (95% Crl) |
|---|---|---|---|---|
Overall | Infliximab 5 mg/kg | |||||||||||||||||||||| | |||||||||||||||||||||| | |||||||||||||||||||||| |
Infliximab 10 mg/kg | |||||||||||||||||||||| | |||||||||||||||||||||| | |||||||||||||||||||||| | |
Adalimumab 160 mg, 80 mg, 40 mg | |||||||||||||||||||||| | |||||||||||||||||||||| | 2.04 (1.16 to 3.76) | |
Golimumab 200 mg, 100 mg | |||||||||||||||||||||| | |||||||||||||||||||||| | |||||||||||||||||||||| | |
Vedolizumab 300 mg | |||||||||||||||||||||| | |||||||||||||||||||||| | |||||||||||||||||||||| | |
Tofacitinib 10 mg | |||||||||||||||||||||| | |||||||||||||||||||||| | |||||||||||||||||||||| | |
Ustekinumab 6 mg/kg | |||||||||||||||||||||| | |||||||||||||||||||||| | |||||||||||||||||||||| | |
Ustekinumab 130 mg | |||||||||||||||||||||| | |||||||||||||||||||||| | |||||||||||||||||||||| | |
Biologic-naive | Infliximab 5 mg/kg | |||||||||||||||||||||| | |||||||||||||||||||||| | |||||||||||||||||||||| |
Infliximab 10 mg/kg | |||||||||||||||||||||| | |||||||||||||||||||||| | |||||||||||||||||||||| | |
Adalimumab 160 mg, 80 mg, 40 mg | |||||||||||||||||||||| | |||||||||||||||||||||| | |||||||||||||||||||||| | |
Golimumab 200 mg, 100 mg | |||||||||||||||||||||| | |||||||||||||||||||||| | |||||||||||||||||||||| | |
Vedolizumab 300 mg | |||||||||||||||||||||| | |||||||||||||||||||||| | |||||||||||||||||||||| | |
Tofacitinib 10 mg | |||||||||||||||||||||| | |||||||||||||||||||||| | |||||||||||||||||||||| | |
Ustekinumab 6 mg/kg | |||||||||||||||||||||| | |||||||||||||||||||||| | |||||||||||||||||||||| | |
Ustekinumab 130 mg | |||||||||||||||||||||| | |||||||||||||||||||||| | |||||||||||||||||||||| | |
Biologic-exposeda | Adalimumab 160 mg, 80 mg, 40 mg | 3.13 (1.42 to 7.31) | 4.19 (1.56 to 11.49) | |||||||||||||||||||||| |
Vedolizumab 300 mg | |||||||||||||||||||||| | |||||||||||||||||||||| | |||||||||||||||||||||| | |
Tofacitinib 10 mg | |||||||||||||||||||||| | |||||||||||||||||||||| | |||||||||||||||||||||| | |
Ustekinumab 6 mg/kg | |||||||||||||||||||||| | |||||||||||||||||||||| | |||||||||||||||||||||| | |
Ustekinumab 130 mg | |||||||||||||||||||||| | |||||||||||||||||||||| | |||||||||||||||||||||| |
CrI = credible interval; NMA = network meta-analysis; OR = odds ratio.
Note: OR > 1 indicates results favouring ozanimod; bold values indicate statistical significance.
aResults are from fixed-effects models; otherwise, results were from random-effects models.
Source: Sponsor-submitted indirect treatment comparison.11
Table 28: Summary of NMA Results for Efficacy Outcomes at Maintenance (Ozanimod Versus Comparator)
Population | Treatment | Clinical response, median OR (95% Crl) | Clinical remission, median OR (95% Crl) | Endoscopic improvement, median OR (95% Crl) |
|---|---|---|---|---|
Overalla | Infliximab 5 mg/kg | |||||||||||||||||||||| | |||||||||||||||||||||| | |||||||||||||||||||||| |
Infliximab 10 mg/kg | |||||||||||||||||||||| | |||||||||||||||||||||| | |||||||||||||||||||||| | |
Adalimumab 40 mg | |||||||||||||||||||||| | |||||||||||||||||||||| | |||||||||||||||||||||| | |
Golimumab 50 mg | |||||||||||||||||||||| | |||||||||||||||||||||| | |||||||||||||||||||||| | |
Golimumab 100 mg | |||||||||||||||||||||| | |||||||||||||||||||||| | |||||||||||||||||||||| | |
Vedolizumab 300 mg q.4.w. | |||||||||||||||||||||| | |||||||||||||||||||||| | 0.46 (0.24 to 0.88) | |
Vedolizumab 300 mg q.8.w. | 0.55 (0.34 to 0.92) | 0.56 (0.34 to 0.92) | |||||||||||||||||||||| | |
Vedolizumab 108 mg SC | |||||||||||||||||||||| | |||||||||||||||||||||| | |||||||||||||||||||||| | |
Tofacitinib 5 mg | 0.57 (0.33 to 0.97) | 0.57 (0.34 to 0.97) | |||||||||||||||||||||| | |
Tofacitinib 10 mg | 0.40 (0.23 to 0.69) | 0.40 (0.24 to 0.69) | 0.42 (0.22 to 0.79) | |
Ustekinumab 90 mg q.8.w. | |||||||||||||||||||||| | |||||||||||||||||||||| | |||||||||||||||||||||| | |
Ustekinumab 90 mg q.12.w. | |||||||||||||||||||||| | |||||||||||||||||||||| | |||||||||||||||||||||| | |
Biologic-naivea | Infliximab 5 mg/kg | |||||||||||||||||||||| | |||||||||||||||||||||| | |||||||||||||||||||||| |
Infliximab 10 mg/kg | |||||||||||||||||||||| | |||||||||||||||||||||| | |||||||||||||||||||||| | |
Adalimumab 40 mg | |||||||||||||||||||||| | |||||||||||||||||||||| | |||||||||||||||||||||| | |
Golimumab 50 mg | |||||||||||||||||||||| | |||||||||||||||||||||| | |||||||||||||||||||||| | |
Golimumab 100 mg | |||||||||||||||||||||| | |||||||||||||||||||||| | |||||||||||||||||||||| | |
Vedolizumab 300 mg q.4.w. | |||||||||||||||||||||| | |||||||||||||||||||||| | |||||||||||||||||||||| | |
Vedolizumab 300 mg q.8.w. | |||||||||||||||||||||| | |||||||||||||||||||||| | |||||||||||||||||||||| | |
Vedolizumab 108 mg SC | |||||||||||||||||||||| | |||||||||||||||||||||| | |||||||||||||||||||||| | |
Tofacitinib 5 mg | |||||||||||||||||||||| | |||||||||||||||||||||| | |||||||||||||||||||||| | |
Tofacitinib 10 mg | |||||||||||||||||||||| | |||||||||||||||||||||| | 0.34 (0.15 to 0.77) | |
Ustekinumab 90 mg q.8.w. | |||||||||||||||||||||| | |||||||||||||||||||||| | |||||||||||||||||||||| | |
Ustekinumab 90 mg q.12.w. | |||||||||||||||||||||| | |||||||||||||||||||||| | |||||||||||||||||||||| | |
Biologic-exposeda | Infliximab 5 mg/kg | |||||||||||||||||||||| | |||||||||||||||||||||| | |||||||||||||||||||||| |
Infliximab 10 mg/kg | |||||||||||||||||||||| | |||||||||||||||||||||| | |||||||||||||||||||||| | |
Adalimumab 40 mg | |||||||||||||||||||||| | |||||||||||||||||||||| | |||||||||||||||||||||| | |
Golimumab 50 mg | |||||||||||||||||||||| | |||||||||||||||||||||| | |||||||||||||||||||||| | |
Golimumab 100 mg | |||||||||||||||||||||| | |||||||||||||||||||||| | |||||||||||||||||||||| | |
Vedolizumab 300 mg q.4.w. | |||||||||||||||||||||| | |||||||||||||||||||||| | |||||||||||||||||||||| | |
Vedolizumab 300 mg q.8.w. | |||||||||||||||||||||| | |||||||||||||||||||||| | |||||||||||||||||||||| | |
Vedolizumab 108 mg SC | |||||||||||||||||||||| | |||||||||||||||||||||| | |||||||||||||||||||||| | |
Tofacitinib 5 mg | |||||||||||||||||||||| | |||||||||||||||||||||| | |||||||||||||||||||||| | |
Tofacitinib 10 mg | |||||||||||||||||||||| | |||||||||||||||||||||| | |||||||||||||||||||||| | |
Ustekinumab 90 mg q.8.w. | |||||||||||||||||||||| | |||||||||||||||||||||| | |||||||||||||||||||||| | |
Ustekinumab 90 mg q.12.w. | |||||||||||||||||||||| | |||||||||||||||||||||| | |||||||||||||||||||||| |
CrI = credible interval; NA = not applicable; NMA = network meta-analysis; OR = odds ratio; q.2.w. = every 2 weeks; q.4.w. = every 4 weeks; q.8.w. = every 8 weeks; q.12.w. = every 12 weeks; SC = subcutaneous.
Note: OR > 1 indicates results favouring ozanimod; bold values indicate statistical significance.
aFrom fixed-effects models.
Source: Sponsor-submitted indirect treatment comparison.11
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Serious Infections
At induction, results |||||||||||||||||||||||||||||||||||||||||||| showed no evidence for a difference between ozanimod and other active treatments in the incidence of serious infections, except that golimumab was favoured over ozanimod (OR 0.04; 95% CrI, 0 to 0.79).
At maintenance, results |||||||||||||||||||||||||||||||||||||||||||| showed no evidence for a difference between ozanimod and other active treatments in the incidence of serious infections.
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Methods of the Lasa et al. ITC
Objectives
The objective of the ITC by Lasa et al.12 was to compare the relative efficacy and safety of biologics and small-molecule drugs for the treatment of patients with moderate to severe UC.
Study Selection Methods
The phase III RCTs that were used to inform the ITC were identified through a systematic literature search. Multiple databases were searched (between January 1, 1990, and July 1, 2021) for trials that evaluated the efficacy of drug therapies for moderate to severe UC, without language restrictions. Study selection and data extraction were conducted independently by 2 reviewers. The quality of the included studies was assessed using the Cochrane risk-of-bias tool.
ITC Analysis Methods
The Lasa report analyzed both induction therapy and maintenance therapy for patients with UC. The primary outcome was the induction of clinical remission. Secondary outcomes were endoscopic improvement, steroid-free remission, AEs, and SAEs. Random-effects models were used for estimating the effect of individual therapies. NMA was conducted using the multivariate frequentist approach described by Rücker and Schwarzer, using R software. Additional prespecified, exploratory pairwise and NMAs were done to evaluate clinical remission and endoscopic improvement for induction therapy in biologic-naive and biologic-exposed populations, including studies with available data on previous biologic exposure.
Direct comparisons were performed by use of RevMan software. Outcome measures were reported as ORs and associated 95% CIs.
Results of the Lasa ITC
Summary of Included Studies
The authors identified 29 studies (4 being head-to-head RCTs) that fulfilled the inclusion criteria from Table 24. Of these, 23 studies assessed induction therapy with either a biologic or a small-molecule drug, comprising a total of 10,061 patients with UC. There were 5 studies of IV infliximab, 3 studies of adalimumab, 1 study of golimumab, 3 studies of IV vedolizumab, 1 study of tofacitinib, 1 study of ustekinumab, 1 study of ozanimod, 1 study of filgotinib, 4 studies of etrolizumab, and 2 studies of upadacitinib.
The mean age of patients in the induction phase ranged from 34.4 to 43 years, and females comprised 33.7% to 45.5% of the study populations. Eleven trials required patients to be naive to anti-TNF biologics at study entry. Among studies that allowed but did not require prior therapy with anti-TNF biologics, there was variation in the percentage of patients who did have prior therapy with these drugs (range of 15% to 58%). Disease duration varied across studies (mean with SDs or median years with range) (mean 3.8 to 14.6 years) but appears comparable among studies.
Of the 22 studies evaluating maintenance therapy, 10 used a treat-through strategy (2,528 patients) and 12 followed a randomized responders design (3,484 patients). Patients in the maintenance phase ranged in mean age from 34.4 to 43 years, and females comprised 33.7% to 47.7% of the study populations. The authors analyzed steroid-free remission in maintenance trials only, as corticosteroid tapering was not allowed in induction trials.
The authors noted that across all studies, all outcomes were assessed uniformly on the basis of the standard definition of the Mayo score, with follow-up durations of 6 to 14 weeks for induction therapy and 26 to 66 weeks for maintenance therapy, and all studies were sponsored by industry. Only 7 studies evaluated histological remission. In addition, not all clinical trials reported on steroid-free remission, particularly the older trials.
The authors conducted a risk-of-bias assessment that showed a low risk of bias for most of the included studies. Details on sources of heterogeneity are provided in Table 29.
Table 29: Assessment of Homogeneity for Lasa et al. Report
Detail | Description and handling of potential effect modifiers |
|---|---|
Treatment history | The induction of clinical remission and endoscopic improvement was evaluated in biologic-naive and biologic-exposed populations in prespecified analyses. Data for upadacitinib according to previous biologic exposure were not available and so the authors did not include it in their analysis. |
Definitions of end points | The authors reported 2 major differences in outcome definitions:
|
Trial duration | Follow-up durations were 6 to 14 weeks for induction therapy and 26 to 66 weeks for maintenance therapy. |
Study design | Thorough comparisons between all of the included studies could be done only for induction outcomes, as the different trial designs for maintenance studies (treat straight through vs. randomized responders) could only be analyzed in 2 different meta-analyses. |
Source: Lasa et al. (2022).12
Results
Induction of Clinical Remission
No treatment was favoured when ozanimod was compared with other active treatments (shown in Table 24) for induction of clinical remission in the overall population, biologic-naive patients, and biologic-exposed patients.
Endoscopic Improvement
In the overall population, results of the ITC suggested that ozanimod was favoured over adalimumab (OR = 1.79; 95% CI, 1.07 to 3.01) for induction of endoscopic improvement. In biologic-naive patients, ozanimod was favoured over adalimumab for endoscopic improvement (OR = 2.07; 95% CI, 1.14 to 3.74). In biologic-exposed patients, no treatment was favoured over another for induction of endoscopic improvement.
Adverse Events
Results of the ITC suggested there was no evidence for a difference between ozanimod and other active comparators (refer to Table 24 for the list of comparators) in the incidence of AEs in the overall population during induction.
Serious Adverse Events
Results of the ITC suggested there was no evidence for a difference between ozanimod and other active comparators (refer to Table 24 for the list of comparators) in the incidence of SAEs in the overall population during induction.
Critical Appraisal of ITCs
In the 2 ITCs, studies were identified by searching multiple databases based on prespecified inclusion and exclusion criteria. Both the methods and results have been described as outlined by the PRISMA statement and the corresponding extension statement for NMAs. The reviewers of these 2 ITCs used appropriate methods for study selection and data extraction. The quality of the included studies was assessed using validated tools. However, there was no discussion on how any potential biases in the trials could have an impact on the data analyses in the ITCs and there was no description of sensitivity analyses being conducted to assess the impact of studies with poor quality.
A significant concern with the ITCs presented is that the studies included in the analyses were highly heterogeneous in terms of both study design and patient characteristics. One of the major concerns with design heterogeneity in UC trials is how trials transition from the induction to the maintenance phase. In addition, in a study using the re-randomized design, the patient population at the start of the maintenance period was enriched according to their response in the induction period; therefore, this could be a different population compared with the original population. In the sponsor-submitted ITC, adjustments were made to the data in older treat-through trials to more closely resemble modern re-randomized trials in the maintenance phase. Different approaches have been adopted to address this heterogeneity, for example, using recalculated data from treat-through studies to mimic a re-randomized trial or including only re-randomized trials. Results of this sensitivity analysis suggested that exclusion of the recalculated treat-through data did not alter the results from the base-case analyses.
Other significant heterogeneities can be found in the definitions of clinical outcomes, timing of study end point evaluation, subgroup definitions, and patients’ baseline characteristics. In the sponsor’s ITC, baseline mean CRP levels, years since UC diagnosis, extent of disease, use of concomitant steroids, and prior treatment with anti-TNFs or other biologics were considered important treatment-effect modifiers. However, due to the inconsistencies in how some variables (steroid use, CRP levels, and duration of disease) were reported and defined, adjustment for their potential modification of treatment effect was not feasible. According to the clinical expert consulted by CADTH, severity of disease should be considered a treatment-effect modifier as well. Despite various statistical techniques being employed to lessen the impact of potential clinical heterogeneity on the estimated treatment effect of ozanimod, there is still significant uncertainty in the ITC results. Furthermore, in the sponsor’s ITC, inconsistency assessments for the main outcomes (clinical response, clinical remission, and endoscopic improvement) were conducted. However, inconsistency analyses require closed loops of evidence to compare direct and indirect estimates. Given the lack of closed loops, an interpretation of the results of inconsistency assessments is difficult. In the Lasa et al. report, patients’ baseline characteristics were not reported in detail; therefore, limited data are available to examine the treatment effect and safety of ozanimod in the study population, in particular in the subgroups of patients who were biologic-naive and biologic-exposed. In addition, there was insufficient analysis conducted to account for trial and clinical heterogeneity, thus limiting the utility and robustness of the results.
In the sponsor’s report, results were derived from random-effects or fixed-effects models. Reasons for model selection were justified by the authors and based on statistical and clinical considerations.
In both ITCs, safety data were sparse and available for the overall population only. In addition, wider CrIs are observed due to the low event rate for some of the safety outcomes, such as AEs leading to discontinuation and serious infections; thus, the interpretation of the results is challenging.
Other Relevant Evidence
This section includes sponsor-submitted long-term extension studies and additional relevant studies that were considered to address important gaps in the evidence included in the systematic review.
Long-Term Extension Study
The phase III, OLE13 study has been summarized to provide additional evidence regarding the long-term safety and efficacy of ozanimod for the treatment of patients with moderately or severely active UC for time points beyond the TRUE NORTH parent study.10 At the time of this review, the OLE study was ongoing, and the sponsor provided data from the interim analysis conducted on data from the March 31, 2020, data cut-off. All patients included in the OLE study continued to receive ozanimod until the end of 2021, or until marketing authorization was obtained in the country of the clinical site, whichever happened first.
Methods
To be eligible for inclusion in the OLE study, patients needed to complete at least 10 weeks of the induction period in the TRUE NORTH study or at least 1 year of treatment with ozanimod in the open-label period (OLP) of the phase II, multicentre, randomized, double-blind, placebo-controlled TOUCHSTONE study.48 Patients in this extension study received 0.92 mg of open-label ozanimod once daily. Although this was an open-label trial, certain procedures were performed for patients who were enrolled from cohort 1 of the TRUE NORTH parent study to maintain blinding to treatment assignment in the parent study. These procedures included dose escalation, cardiac monitoring, and certain laboratory tests. Efficacy results for the 54 patients who enrolled from the OLP of the TOUCHSTONE study were not included in the sponsor’s clinical study report due to insufficient follow-up. Safety results from the patients in the OLP of the TOUCHSTONE study were provided; since the TOUCHSTONE parent study is not summarized in this report and the sample size is limited, the safety results for these patients are not summarized in this report. Therefore, all results that are summarized in this report are from the patients enrolled in the OLE of the TRUE NORTH study.
Populations
Patients were eligible to participate in the OLE study if they met any of the following:
completed the induction period in the TRUE NORTH study and did not have a clinical response
completed the maintenance period or experienced disease relapse during the maintenance period in the TRUE NORTH study
completed at least 1 year of the OLP of the TOUCHSTONE study.
Patients were not eligible to participate in the OLE study if they met any of the following exclusion criteria:
Exclusion related to medications:
Patients who had received any of the following therapies since the first dose of the investigational drug in the prior ozanimod study: A biologic drug; an investigational drug other than ozanimod; D-penicillamine, leflunomide, thalidomide, natalizumab, fingolimod, etrasimod, or tofacitinib; lymphocyte-depleting therapies; or a live vaccine or live attenuated vaccine within 4 weeks before visit 1 of this study.
Patients who were currently receiving or required initiation of any of the following therapies: Corticosteroids at a dose that exceeds the prednisone equivalent of 40 mg, immunosuppressive drugs (e.g., azathioprine, mercaptopurine, or methotrexate); chronic use of NSAIDs; Class Ia or Class III antiarrhythmic drugs or treatment with 2 or more drugs in a combination known to prolong PR interval.
Patients who were receiving treatment with CYP2C8 inhibitors or inducers at day 1 of the OLE or monoamine oxidase inhibitors in the 2 weeks before day 1.
Patients who were receiving treatment with breast cancer resistance protein inhibitors.
Exclusions related to general health:
Patients with clinically relevant hepatic, neurologic, pulmonary, ophthalmological, endocrine, psychiatric, or other major systemic disease.
Patients with clinically relevant cardiovascular conditions, including a history or presence of recent myocardial infarction, unstable angina, stroke, transient ischemic attack, decompensated heart failure requiring hospitalization, Class III or IV heart failure, sick sinus syndrome, or severe untreated sleep apnea.
Exclusions related to laboratory results:
Patients with liver function impairment or persisting elevations of aspartate aminotransferase or alanine aminotransferase greater than 5 times the upper limit of normal (ULN), or direct bilirubin greater than 3 times the ULN.
Patients with a forced expiratory volume at 1 second or forced vital capacity of less than 50% of predicted values.
Patient baseline characteristics have been summarized in Table 30. Baseline value was defined as the last measurement collected on or before the date of the first dose of ozanimod in the parent studies. There were no notable differences in baseline demographic characteristics across treatment groups in the parent study for patients who entered the OLE study. The mean age of patients in the TRUE NORTH total group was 41.7 (SD = 13.65). Just more than half of patients were male (59.2%); the majority were white (89.0%), non-Hispanic or Latino (95.6%), and from Eastern Europe (56.5%). A total of 31.9% of patients had used tobacco or nicotine. The majority of patients (97.7%) in the TRUE NORTH total group had previously received 5-ASA drugs. A total of 33.7% and 31.9% of patients, respectively, indicated prior use of anti-TNF drugs and systemic corticosteroids at screening.
Table 30: Baseline Characteristics of the OLE Study (ITT Population)
Characteristic | Treatment group in TRUE NORTH | |||
|---|---|---|---|---|
Placebo to placebo N = 184 | Ozanimod to placebo N = 196 | Ozanimod to ozanimod N = 441 | Total N = 821 | |
Sex, n (%) | ||||
Female | 60 (32.6) | 91 (46.4) | 184 (41.7) | 335 (40.8) |
Male | 124 (67.4) | 105 (53.6) | 257 (58.3) | 257 (58.3) |
Age (years), mean (SD) | 41.9 (13.64) | 43.0 (13.64) | 41.0 (13.64) | 41.7 (13.65) |
Age category, n (%) | ||||
18 to 64 years | 171 (92.9) | 188 (95.9) | 418 (94.8) | 777 (94.6) |
≥ 65 years | 13 (7.1) | 8 (4.1) | 23 (5.2) | 44 (5.4) |
Race, n (%) | ||||
White | 165 (89.7) | 174 (88.8) | 392 (88.9) | 731 (89.0) |
Black | 4 (2.2) | 9 (4.6) | 11 (2.5) | 24 (2.9) |
Asian | 13 (7.1) | 10 (5.1) | 31 (7.0) | 54 (6.6) |
Other | 2 (1.1) | 3 (1.5) | 7 (1.6) | 12 (1.5) |
Region, n (%) | ||||
North America | 47.5 (25.5) | 42 (21.4) | 108 (24.5) | 197 (24.0) |
Eastern Europe | 104 (56.5) | 120 (61.2) | 240 (54.4) | 464 (56.5) |
Western Europe | 17 (9.2) | 23 (11.7) | 63 (14.3) | 103 (12.5) |
Asia Pacific | 13 (7.1) | 9 (4.6) | 25 (5.7) | 47 (5.7) |
South America | 0 | 1 (0.5) | 2 (0.5) | 3 (0.4) |
South Africa | 3 (1.6) | 1 (0.5) | 3 (0.7) | 7 (0.9) |
Tobacco or nicotine usage, n (%) | ||||
Never | 118 (64.1) | 135 (68.9) | 306 (69.4) | 559 (68.1) |
Former | 54 (29.3) | 52 (26.5) | 110 (24.9) | 216 (26.3) |
Current | 12 (6.5) | 9 (4.6) | 25 (5.7) | 46 (5.6) |
Prior anti-TNF use, n (%) | ||||
Yes | 56 (30.4) | 56 (28.6) | 165 (37.4) | 277 (33.7) |
No | 128 (69.6) | 140 (71.4) | 276 (62.6) | 544 (66.3) |
Prior corticosteroid use, n (%) | ||||
Yes | 64 (34.8) | 53 (27.0) | 145 (32.9) | 262 (31.9) |
No | 120 (65.2) | 143 (73.0) | 296 (67.1) | 559 (68.1) |
Prior oral 5-ASA use, n (%) | ||||
Yes | 179 (97.3) | 191 (97.4) | 432 (98.0) | 802 (97.7) |
No | 5 (2.7) | 5 (2.6) | 9 (2.0) | 19 (2.3) |
5-ASA = 5-aminosalicylate; ITT = intention to treat; OLE = open-label extension; SD = standard deviation; TNF = tumour necrosis factor.
Note: Baseline demographics are taken from the parent study. Baseline value was defined as the last measurement collected on or before the date of the first dose of ozanimod in the parent study.
Source: OLE interim Clinical Study Report.13
Interventions
All patients self-administered ozanimod at a dosage of 0.92 mg orally once daily. Given the open-label nature of the study, all patients, investigators, and staff members were aware of the treatment assignment. Patients who entered the OLE study from cohort 2 of the TRUE NORTH study did not undergo dose escalation and continued to receive ozanimod at a dosage of 0.92 mg daily. However, all patients who entered the OLE study from cohort 1 of the TRUE NORTH study received ozanimod at a dosage of 0.92 mg once daily after a 7-day dose escalation regimen consisting of 4 days of treatment with ozanimod at a dose of 0.23 mg, followed by 3 days of treatment with ozanimod at a dose of 0.46 mg, and followed by ozanimod at a dosage of 0.92 mg daily starting on day 8.
The use of concomitant medication and procedures was monitored throughout the OLE study and was generally similar to that of the parent TRUE NORTH study. The majority of patients (98.2%) who entered the OLE study received at least 1 concomitant medication. The most frequently used concomitant medications (≥ 5% of patients) were mesalazine (71.0%), sulfasalazine (13.5%), and budesonide (7.3%) among antidiarrheal and intestinal anti-inflammatory and anti-infective drugs; propofol (14.9%) and fentanyl (7.6%) among anesthetics; and prednisone (21.0%) and methylprednisolone (8.8%) among corticosteroids.
Outcomes
Several primary and secondary end points assessed in the primary evaluation period of the parent TRUE NORTH study were also assessed during the OLE study. Efficacy end points included:
proportion of patients in clinical remission, measured using the 3-component Mayo score definition using a 7-day scoring algorithm and defined as an RBS of 0 and an SFS of 1 or less, and an endoscopy subscore of 1 or less.
proportion of patients with clinical response, measured using the 3-component Mayo score definition using a 7-day scoring algorithm and defined as a reduction from baseline in the 3-component Mayo score of 2 points or greater and 35% or greater, and a reduction from baseline in RBS of 1 point or greater or an absolute RBS of 1 point or less.
proportion of patients with endoscopic improvement (endoscopy subscore of ≤ 1 point).
proportion of patients with corticosteroid-free remission (clinical remission while off corticosteroids for ≥ 12 weeks).
The proportions of patients with mucosal healing and histologic remission were not evaluated for the interim OLE report.
Safety end points included the incidence, severity, and relationship of TEAEs, SAEs, TEAEs leading to treatment discontinuation, and TEAEs leading to drug interruptions.
Statistical Analysis
Due to the lack of a comparison group and the open-label nature of the OLE study, there was no formal statistical testing conducted. As such, all results presented are for the full analysis set of patients who entered the OLE from the parent study. As this extension study was for patients who previously participated in the TRUE NORTH parent study, there was no statistical basis for the sample size. NRI was used to handle missing data across all efficacy end points, in which any patient with missing information was considered a nonresponder.
Patient Disposition
Of the 824 patients who entered the OLE study from the parent TRUE NORTH study, 358 patients were enrolled after completing the induction period, 329 patients were enrolled after completing the maintenance period, and 137 patients were enrolled after discontinuing from the maintenance period (Table 31). One patient consented to but did not receive treatment. Two patients were included in the category “consented but never treated” in error in this interim report and were not included in the ITT population. Out of 821 patients, 441 patients were in the placebo to placebo group, where patients received placebo in the induction period of the TRUE NORTH study before entering the OLE study; 196 patients were in the ozanimod to ozanimod group, where patients were treated with ozanimod 1 mg in cohort 1 or 2 during the induction period; and 196 patients were in the ozanimod to placebo group, which consisted of patients re-randomized to receive placebo during the maintenance period in the TRUE NORTH study (Table 32).
Of the 821 patients, 430 patients (52.4%) completed 46 weeks in the OLE study; 618 patients (38.7%) withdrew from the study as of the data cut-off date. The 3 most commonly reported reasons for treatment discontinuation in this group were lack of efficacy (18.9%), withdrawal by patient (11.9%), and AEs (3.4%). The proportions of reasons for discontinuation are presented in Table 32. The treatment discontinuation rate was lower in the ozanimod to placebo group. Patients who did not have a clinical response or remission at OLE study entry were advised to withdraw from the study if no clinical improvement from the baseline visit was observed by week 10.
Table 31: Patients Enrolling in the OLE Study From the TRUE NORTH Trial
Characteristics | Cohort 1 | Cohort 2 | |
|---|---|---|---|
Placebo N = 216 | Ozanimod N = 429 | Ozanimod N = 367 | |
Induction period | |||
N | 216 | 429 | 367 |
Completed induction period, n | 401 | 192 | 324 |
Enrolled in OLE study following induction period (nonresponders only), n | 159 | 120 | 79 |
Maintenance period | |||
N | 69 | 227 | 367 |
Completed maintenance period, n | 45 | 124 | 184 |
Enrolled in OLE study after completing maintenance period, n | 42 | 116 | 171 |
Discontinued from maintenance period, n | 24 | 103 | 46 |
Enrolled in OLE study after discontinuing from maintenance period (disease relapse), n | 22 | 81 | 34 |
OLE = open-label extension.
Source: Clinical Study Report for the TRUE NORTH study.10
Table 32: Patient Disposition Within the OLE Study by Treatment Group
Characteristics | Placebo to placebo N = 184 | Ozanimod to placebo N = 197 | Ozanimod to ozanimod N = 443 | Total N = 824 |
|---|---|---|---|---|
Consented, n (%) | 184 | 197 | 443 | 824 |
Consented but never treated, n (%) | 0 | 1 (0.5) | 2 (0.5) | 3 (0.4)a |
Included in the ITT (safety) population, n (%) | 184 (100.0) | 196 (99.5) | 441 (99.5) | 821 (99.6) |
Number of patients, n (%)b | ||||
Completed week 22 | 142 (77.2) | 145 (74.0) | 300 (68.0) | 587 (71.5) |
Completed week 46 | 121 (65.8) | 93 (47.4) | 216 (49.0) | 430 (52.4) |
Completed week 94 | 65 (35.3) | 39 (19.9) | 82 (18.6) | 186 (22.7) |
Completed week 142 | 21 (11.4) | 10 (5.1) | 40 (9.1) | 71 (8.6) |
Withdrew from OLE treatment, n (%)b | 93 (50.5) | 43 (21.9) | 182 (41.3) | 618 (38.7) |
Primary reason for treatment discontinuation, n (%)b | ||||
Physician decision | 5 (2.7) | 0 | 21 (4.8) | 26 (3.2) |
Noncompliance with drug | 1 (0.5) | 0 | 0 | 1 (0.1) |
Noncompliance with protocol (protocol deviation) | 2 (1.1) | 0 | 2 (0.5) | 4 (0.5) |
Adverse events | 9 (4.9) | 4 (2.0) | 15 (3.4) | 28 (3.4) |
Lack of efficacy | 45 (24.5) | 22 (11.2) | 88 (20.0) | 155 (18.9) |
Withdrawal by patient | 28 (15.2) | 15 (7.7) | 55 (12.5) | 98 (11.9) |
Pregnancy | 1 (0.5) | 1 (0.5) | 1 (0.2) | 3 (0.4) |
Otherc | 2 (1.1) | 1 (0.5) | 0 | 3 (0.4) |
ITT = intention to treat; OLE = open-label extension; UC = ulcerative colitis.
aTwo patients were included in the category “consented but never treated” in error in this interim report: 1 patient consented and was treated with the study drug; the other patient consented but was never dosed, and that patient subsequently withdrew consent.
bDenominators for percentages are the number of patients in the ITT population. All patients who received at least 1 dose of the investigational drug in this study comprised both the ITT population and the safety population.
cOther reasons include lost to follow-up and UC progression or flare.
Source: Open-label extension interim Clinical Study Report.13
Exposure to Study Treatments
In the OLE study, the mean duration of exposure to study treatment in the TRUE NORTH total group was 1.17 years (SD = 0.94), while the mean overall duration of exposure, including the parent study, was 1.75 years (SD = 1.60). The number of patients treated with ozanimod for more than 1 year was 389 (47.4%) in the total group.
The treatment compliance rate was calculated as the ratio of the total number of actual capsules taken divided by the total number of expected capsules during the treatment period, multiplied by 100%. In the TRUE NORTH total group, the mean treatment compliance rate was 92.34% (SD = 27.36), and the number of patients with any drug interruption was 62 (7.6%).
Efficacy
Efficacy results have been summarized in Table 33. Only those efficacy outcomes and analyses of subgroups identified in the review protocol are reported subsequently. At the time of the interim analysis for the OLE, the efficacy results included data for patients who had completed at least 10 weeks of the induction period in the TRUE NORTH study.
|||||||||||||||||||||||||||||||||||||||||||| | |||||||||||||||||||||| | |||
|---|---|---|---|---|
|||||||||||||||||||||| | |||||||||||||||||||||| | |||||||||||||||||||||| | |||||||||||||||||||||| | |
|||||||||||||||||||||| | ||||
|||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| |
|||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| |
|||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| |
|||||||||||||||||||||| | ||||
|||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| |
|||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| |
|||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| |
|||||||||||||||||||||| | ||||
|||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| |
|||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| |
|||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| |
|||||||||||||||||||||| | ||||
|||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| |
|||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| |
|||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| |
ITT = intention to treat (nonresponder imputation); OLE = open-label extension; RBS = rectal bleeding subscore; SFS = stool frequency subscore.
Note: This table has been redacted as per sponsor’s request.
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||13
The majority of patients (68.2%) enrolled from the TRUE NORTH parent study had not achieved a clinical response when they entered the OLE study (nonresponders). The available efficacy results were limited by the relatively small number of evaluable patients; of the 821 patients in the total group, only 384 patients at week 46 had completed all the assessments required for assessing efficacy end points (RBS, SFS, and endoscopy score), 158 patients at week 94 had completed all the assessments, and only 53 patients at week 142 had completed all the assessments.
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Harms
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|||||||||||||||||||||||||||||||||||||||||||||||||||||||| | |||||||||||||| | |||
|---|---|---|---|---|
|||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| | |
|||||||||||||||||||||||||||||||||||||||||| | ||||
|||||||||||||||||||||||||||||||||||||||||| | ||||
|||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| |
|||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| |
|||||||||||||||||||||||||||||||||||||||||| | ||||
|||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| |
|||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| |
|||||||||||||||||||||||||||||||||||||||||| | ||||
|||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| |
|||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| |
|||||||||||||||||||||||||||||||||||||||||| | ||||
|||||||||||||||||||||||||||||||||||||||||| | ||||
|||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| |
|||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| |
|||||||||||||||||||||||||||||||||||||||||| | ||||
|||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| |
|||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| |
|||||||||||||||||||||||||||||||||||||||||| | ||||
|||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| |
|||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| |
|||||||||||||||||||||||||||||||||||||||||| | ||||
|||||||||||||||||||||||||||||||||||||||||| | ||||
|||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| |
|||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| |
|||||||||||||||||||||||||||||||||||||||||| | ||||
|||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| |
|||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| |
|||||||||||||||||||||||||||||||||||||||||| | ||||
|||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| |
|||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| |
Note: This table has been redacted as per sponsor’s request.
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| | |||||||||||||||||||| | |||
|---|---|---|---|---|
|||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| | |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| | ||||
|||||||||||||||||||||||||||||||||||||||||| | ||||
|||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| |
|||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| |
|||||||||||||||||||||||||||||||||||||||||| | ||||
|||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| |
|||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| |
|||||||||||||||||||||||||||||||||||||||||| | ||||
|||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| |
|||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| | ||||
|||||||||||||||||||||||||||||||||||||||||| | ||||
|||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| |
|||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| |
|||||||||||||||||||||||||||||||||||||||||| | ||||
|||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| |
|||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| |
|||||||||||||||||||||||||||||||||||||||||| | ||||
|||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| |
|||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| | ||||
|||||||||||||||||||||||||||||||||||||||||| | ||||
|||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| |
|||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| |
|||||||||||||||||||||||||||||||||||||||||| | ||||
|||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| |
|||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| |
|||||||||||||||||||||||||||||||||||||||||| | ||||
|||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| |
|||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| |
Note: This table has been redacted as per sponsor’s request.
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| | |||||||||||||||||||| | |||
|---|---|---|---|---|
|||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| | ||||||||||| | |
||||||||||||||||||||||||||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| | ||||||||||| |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| | ||||
||||||||||||||||||||||||||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| | ||||||||||| |
|||||||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| | ||||||||||| |
||||||||||||||||||||||||||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| | ||||||||||| |
|||||||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| | ||||||||||| |
||||||||||||||||||||||||||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| | ||||||||||| |
|||||||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| | ||||||||||| |
||||||||||||||||||||||||||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| | ||||||||||| |
|||||||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| | ||||||||||| |
||||||||||||||||||||||||||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| | ||||||||||| |
|||||||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| | ||||||||||| |
||||||||||||||||||||||||||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| | ||||||||||| |
|||||||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| | ||||||||||| |
||||||||||||||||||||||||||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| | ||||||||||| |
|||||||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| | ||||||||||| |
||||||||||||||||||||||||||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| | ||||||||||| |
|||||||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| | ||||||||||| |
||||||||||||||||||||||||||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| | ||||||||||| |
|||||||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| | ||||||||||| |
||||||||||||||||||||||||||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| | ||||||||||| |
|||||||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| | ||||||||||| |
||||||||||||||||||||||||||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| | ||||||||||| |
|||||||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| | ||||||||||| |
||||||||||||||||||||||||||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| | ||||||||||| |
|||||||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| | ||||||||||| |
||||||||||||||||||||||||||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| | ||||||||||| |
|||||||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| | ||||||||||| |
||||||||||||||||||||||||||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| | ||||||||||| |
|||||||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| | ||||||||||| |
||||||||||||||||||||||||||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| | ||||||||||| |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| | ||||
||||||||||||||||||||||||||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| | ||||||||||| |
|||||||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| | ||||||||||| |
||||||||||||||||||||||||||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| | ||||||||||| |
|||||||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| | ||||||||||| |
||||||||||||||||||||||||||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| | ||||||||||| |
|||||||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| | ||||||||||| |
||||||||||||||||||||||||||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| | ||||||||||| |
|||||||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| | ||||||||||| |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| | ||||
||||||||||||||||||||||||||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| | ||||||||||| |
|||||||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| | ||||||||||| |
||||||||||||||||||||||||||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| | ||||||||||| |
|||||||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| | ||||||||||| |
||||||||||||||||||||||||||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| | ||||||||||| |
|||||||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| | ||||||||||| |
Note: This table has been redacted as per sponsor’s request.
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Critical Appraisal
Internal Validity
The OLE was a single-group study that did not include an active or placebo comparison group; without a comparison group, it is not possible to know the true benefit of treatment and it is difficult to interpret results. All efficacy end points were descriptive, as there was no formal statistical testing. Although certain procedures have been performed to maintain blinding to treatment assignment from the parent trial, the open-label administration of the drug could introduce bias, as knowledge of the treatment may lead patients and investigators to overestimate its potential benefits and harms. The treatment response rates were higher in patients who were in the placebo to placebo TRUE NORTH group. This may be explained by the longer follow-up period for these patients, as they were more likely to discontinue treatment earlier in the original study.
The eligibility criteria for the OLE study specified that patients had to complete the induction or maintenance periods of the parent TRUE NORTH study or discontinue the maintenance period due to disease relapse, which potentially allowed for selection bias. Patients who did not have a treatment response at study entry could discontinue the study treatment if no clinical improvement was observed from the baseline visit of the TRUE NORTH study by week 10. Additionally, there was a high rate of treatment discontinuations (38.6%) during the OLE study, mostly due to lack of response, patient decision, and AEs. This may have resulted in the enrolment of more patients who were better able to tolerate ozanimod and, as a result, fewer AE reports. The inclusion of patients with no initial response to ozanimod during the TRUE NORTH parent trial (68.2%) is likely to underestimate the benefit observed during this extension study compared with the maintenance period of the parent study. Given that this was an ongoing study, the results were limited to the interim analysis as of March 31, 2020, and there were small numbers of evaluable patients, especially at weeks 96 and 142. The results of the long-term extension study should be interpreted with caution, as there is a high risk that the study results are strongly biased for the aforementioned reasons.
Outcomes related to HRQoL and work productivity assessed in the TRUE NORTH study using instruments such as the EQ-5D, SF-36, and WPAI-UC, were not assessed in the OLE study. Thus, the long-term benefit of ozanimod on HRQoL and work productivity remains unknown.
External Validity
Since the patients who took part in the OLE study were originally from the parent TRUE NORTH trial and the eligibility criteria remained the same, it is reasonable to expect that the same limitations to generalizability are relevant to this long-term extension study.
Discussion
Summary of Available Evidence
The current CADTH systemic review included 1 phase III, multicentre, stratified, randomized, double-blind, placebo-controlled dose escalation induction and maintenance trial: the TRUE NORTH study. The TRUE NORTH study evaluated the efficacy of ozanimod for the treatment of moderately to severely active UC among adult patients who had an inadequate response, a loss of response, or were intolerant to either conventional therapy or biologic drugs. While the trial consisted of 3 treatment groups in both the induction and maintenance periods, the current CADTH review focused on the efficacy end points between the randomized treatment groups in each study period. All patients initiated the investigational drug in accordance with a 7-day dose escalation schedule. On day 8, patients commenced the full dose of the investigational drug until the end of the induction period at week 10. At the end of the induction period, patients who had a clinical response based on the 3-component Mayo score continued to the maintenance period of the trial. Patients were re-randomized to receive either ozanimod or matching placebo and continued with the investigational drug until the end of the maintenance period at week 52. The primary efficacy outcome of TRUE NORTH was clinical remission. Key secondary efficacy end point were clinical response, endoscopic improvement, mucosal healing, corticosteroid-free remission, durable clinical remission, and maintenance of remission. Exploratory and other end points included rectal bleeding, histologic remission, HRQoL, and work productivity.
At the induction period baseline, 429 and 216 patients in cohort 1 were randomized to ozanimod and placebo, respectively. At the maintenance period baseline, 230 and 227 patients were re-randomized to ozanimod and placebo, respectively. At baseline, the average age of patients was approximately 41.9 years (SD = 13.6 years); approximately 86% to 89% of patients were identified as being white, the average age at UC diagnosis was approximately 33.7 (SD = 13.04) years, the extent of disease was limited to the left side of the colon in approximately 60% of patients, and approximately 60% of patients across treatment groups were classified as having severe disease. At baseline, the 3-component Mayo and 4-component Mayo scores were similar across all treatment groups, ranging from 6.6 (SD = 1.21) to 6.8 (SD = 1.26) and 8.6 (SD = 1.42) to 9.1 (SD = 1.49), respectively. According to the clinical expert, responses to prior UC medication, namely the treatment failure rates, were a function of the clinical trial inclusion and exclusion criteria for moderate to severe UC in which failure of conventional treatment is required.
The TRUE NORTH trial is limited due to only 50% of patients completing the maintenance period and the rate of differential dropout between the treatment groups during the maintenance period, which potentially may have introduced attrition bias in favour of ozanimod.
The long-term safety and efficacy of ozanimod in patients with moderate the severe UC was further evaluated in the OLE study — an OLE study of patients who completed at least 10 weeks of the induction period without experiencing a clinical response, or who completed the maintenance period to week 52, or who experienced disease relapse during the maintenance period of the TRUE NORTH trial.13 Of the 824 patients who entered the OLE study from the TRUE NORTH trial, 43.4% were enrolled after completing the induction period, 39.9% entered after completing the maintenance period, and 16.6% entered after discontinuing from the maintenance period.
Two relevant Bayesian NMA reports were included: 1 sponsor-submitted report and 1 publication. In the sponsor-submitted ITC, ozanimod was compared with ustekinumab, infliximab, certolizumab, adalimumab, vedolizumab, tofacitinib, golimumab, filgotinib, etrasimod, or the biosimilar versions of these therapies, and placebo. Phase II or III RCTs were included. Clinical response, clinical remission, endoscopic improvement, and safety were evaluated. In the Lasa report, ozanimod was compared with infliximab, adalimumab, golimumab, vedolizumab, ustekinumab, tofacitinib, etrolizumab, upadacitinib, filgotinib, etrasimod, TD-1473, and placebo. Phase III RCTs were included in this report. In the Lasa report, clinical remission and endoscopic improvement were evaluated. Safety outcomes were examined in the 2 ITCs.
Interpretation of Results
Efficacy
In the TRUE NORTH trial, the difference in the proportion of patients in clinical remission was statistically significant, favouring patients who were randomized to ozanimod compared with those randomized to placebo at the end of the induction period (difference in proportions of 12.4%; 95% CI, 7.5% to 17.5%) and maintenance period (difference in proportion of 18.6%; 95% CI, 10.8% to 26.4%) as measured by the 3-component Mayo score. Similarly, the differences in proportion of patients with clinical response, endoscopic improvement, mucosal healing, corticosteroid-free remission, durable clinical remission, and maintenance of clinical remission at the end of the induction period and maintenance period were statistically significant, favouring patients who were randomized to ozanimod compared with those randomized to placebo. Subgroup analysis pointed toward a trend of better efficacy among patients without prior anti-TNF therapy, and those with moderate disease.
The differences in proportions across the efficacy outcomes were relatively modest, ranging from 8.2% (durable clinical remission at the end of the maintenance period) to 12.4% (clinical remission at the end of the induction period) to 26.7% (clinical response at the end of the induction period). According to the clinical expert consulted by CADTH, the observed effect sizes are consistent with other approved therapies for moderately to severely active UC. Regarding the small absolute difference in patients with durable clinical remission, the clinical expert consulted noted that durable clinical remission is a more stringent outcome to measure maintenance therapy because week 52 alone captures a heterogeneous group of initial responders who go into remission, and those responders and remitters who may have briefly lost but recaptured remission by week 52.
The main efficacy outcome (clinical remission) and key secondary outcome (clinical response) that selected which patients moved into the maintenance period were based on the Mayo score. The decision to base conclusions of efficacy on the 3-component Mayo score is based on FDA recommendations,49 which found that the 4-component scoring system is subject to bias due to the Physician’s Global Assessment component of the score, and that it is poorly correlated to disease activity. Accordingly, the TRUE NORTH trial definition for clinical remission and clinical response conforms to the definitions laid out by the FDA.
There are several factors that make it difficult to generalize the trial results to the treatment of the indicated population in clinical practice. Extrapolating the results to the indicated population as a whole, ozanimod would not induce a treatment response in almost half of the patients who initially take the drug; in those who do respond, clinical remission would be achieved in approximately 1-third of patients. Of note, the treatment regimen employed in the TRUE NORTH study did not include rectal therapy and required corticosteroid tapering during the study period, creating a treatment regimen that is harsher than in clinical practice and possibly less favourable for ozanimod.
The trial criterion that directed entry into the maintenance period likely created an enriched patient population in which patients who entered the maintenance period were more likely to benefit from treatment with ozanimod compared with the general UC population in the real-world setting. Moreover, the trial design excluded patients who may have had a delayed induction response from entering the maintenance period. Despite this study design being a common trial design for therapeutics for UC (as it is challenging to retain nonresponders in a long-term study), the 2-stage enrichment design may have overestimated the treatment effect, making it difficult to assess the generalizability of efficacy and safety.
The interpretability of the efficacy results may also be limited by differential dropout rates between the treatment groups, with a greater proportion of patients in the re-randomized placebo group discontinuing the maintenance period trial to enter the OLE study compared with the ozanimod group |||||||||||||||||||||||. The clinical expert noted it is common for studies in UC to allow patients who lose response to enter an OLE study. Patients who discontinued the maintenance period to enter the OLE study were imputed as nonresponders and it is not possible to determine the likely direction of bias from these discontinuations. Moreover, it is possible that the proportions of discontinuations upon disease relapse to receive open-label ozanimod were higher than they would be in clinical practice where patients are not blinded to their treatment.
Input from patient groups highlighted HRQoL as an important outcome and an important treatment goal for patients. Reliable and valid IBD-specific instruments, such as the 32-item Inflammatory Bowel Disease Questionnaire, Short Inflammatory Bowel Disease Questionnaire, and IMPACT-III,50,51 were not included and generic measures were used instead. Moreover, as multiplicity was not controlled for the analysis of the HRQoL end points, interpretation of its significance must be made with caution.
Conclusions could not be drawn from the OLE study due to the lack of a control group, the relatively small number of patients evaluated at each assessment point, and the high rate of treatment discontinuations due to lack of response, patient decision, and AEs.
Two ITCs were summarized, 1 that was submitted by the sponsor, and 1 published ITC by Lasa et al. Both ITCs evaluated the relative efficacy and safety of active treatments for patients with moderate to severe UC. Based on the results of the sponsor-submitted ITC, no treatment was favoured when ozanimod was compared with other currently available active treatments for achieving clinical response, clinical remission and endoscopic improvement, ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||. Based on the findings from the Lasa ITC, no treatment was favoured when ozanimod was compared with other active treatments for clinical remission and endoscopic improvement, except that it was favoured over adalimumab for clinical remission and endoscopic improvement. Conclusions could not be established for the efficacy of ozanimod compared with other relevant active treatments in achieving clinical response, clinical remission, and endoscopic improvement. The applicability of the ITCs is impacted by the heterogeneity in study design and patient populations across trials and the inability to comprehensively assess its impact on the study results.
Harms
In the context of the TRUE NORTH trial, among all patients who received ozanimod in the induction period, 2.9% withdrew from the study due to an AE. In the maintenance period, 0.9% withdrew from the study due to an AE. Accordingly, there were no notable safety concerns leading to discontinuation.
The percentage of patients reporting at least 1 TEAE was consistent between treatment groups during the induction period (approximately 40%). In the maintenance period, a higher percentage of patients who remained on ozanimod reported at least 1 TEAE compared with those re-randomized to placebo (49.1% versus 36.6%). Likewise, the proportion of patients with at least 1 serious TEAE was consistent across the treatment groups.
Of the notable harms of interest — serious or opportunistic infections, bradycardia, heart conduction abnormality, macular edema, blood pressure increase, liver enzyme increase, and lymphopenia — none exceeded 1% in any treatment group. However, in the OLE study, a greater percentage of patients reported lymphopenia than during the TRUE NORTH study.
The ITC safety results did not show evidence for a difference between ozanimod and other active comparators in the incidence of AEs, SAEs, and AEs leading to discontinuation in either the induction or maintenance phase. In both ITCs, safety data were sparse and available for the overall population only. In addition, wider CrIs were observed due to the low event rate for some of the safety outcomes, such as AEs leading to discontinuation and serious infections. As with the efficacy results, conclusions could not be drawn regarding the safety of ozanimod versus relevant comparators.
Conclusions
Based on the TRUE NORTH trial, ozanimod was efficacious in achieving induction and maintenance of clinical remission and clinical response in patients with moderately or severely active UC. Moreover, ozanimod was also found to be efficacious in achieving endoscopic improvement, mucosal healing, corticosteroid-free remission, durable clinical remission, and maintenance of clinical remission. However, the generalizability of the results to the real-world setting is limited due to the re-randomization study design and the option for enrolment into an open-label trial during the maintenance period. Based on the available ITCs, it remains uncertain how ozanimod compares with other advanced treatments for moderate to severe UC in efficacy and safety.
References
1.Schroeder KW, Tremaine WJ, Ilstrup DM. Coated oral 5-aminosalicylic acid therapy for mildly to moderately active ulcerative colitis. A randomized study. N Engl J Med. 1987;317(26):1625-1629. PubMed
2.Stenson W. Inflammatory bowel diseaes. In: Goldman I BJ, ed. Cecil Textbook of Medicine, 21st ed. Philadephia (PA): WB Saunders Co; 2000:722-729.
3.Danese S, Fiocchi C. Ulcerative colitis. N Engl J Med. 2011;365(18):1713-1725. PubMed
4.Travis SP, Stange EF, Lémann M, et al. European evidence-based consensus on the management of ulcerative colitis: current management. J Crohns Colitis. 2008;2(1):24-62. PubMed
5.Ng SC, Shi HY, Hamidi N, et al. Worldwide incidence and prevalence of inflammatory bowel disease in the 21st century: a systematic review of population-based studies. Lancet. 2017;390(10114):2769-2778. PubMed
6.Molodecky NA, Soon IS, Rabi DM, et al. Increasing incidence and prevalence of the inflammatory bowel diseases with time, based on systematic review. Gastroenterology. 2012;142(1):46-54.e42; quiz e30. PubMed
7.Benchimol EI, Fortinsky KJ, Gozdyra P, Van den Heuvel M, Van Limbergen J, Griffiths AM. Epidemiology of pediatric inflammatory bowel disease: a systematic review of international trends. Inflamm Bowel Dis. 2011;17(1):423-439. PubMed
8.Coward S, Clement F, I BE, al e. The rising prevalence of inflammatory bowel disease in Canada: analyzing the past to predict the future. Gastroenterol. 2018;1:2.
9.Kuenzig ME, Lee L, El-Matary W, et al. The impact of inflammatory bowel disease in Canada 2018: indirect costs of IBD care. J Can Assoc Gastroenterol. 2019;2(Suppl 1):S34-S41. PubMed
10.Clinical Study Report: RPC01-3101. A phase 3, multicenter, randomized, double-blind, placebo-controlled trial of oral RPC1063 as induction and maintenace therapy for moderate to severe ulcerative colitis [internal sponsor's report]. Couvet (CH): Celgene International II Sarl; 2020 Oct 29.
11.Ozanimod (ZEPOSIA) for the treatment of moderate-to-severe ulcerative colitis technical report: systematic literature review and network meta-analysis of clinical evidence [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Zeposia (ozanimod), 0.23 mg, 0.46 mg and 0.92 mg capsules. Saint-Laurent (QC): Bristol-Myers Squibb Canada; 2021 Apr 30.
12.Lasa JS, Olivera PA, Danese S, Peyrin-Biroulet L. Efficacy and safety of biologics and small molecule drugs for patients with moderate-to-severe ulcerative colitis: a systematic review and network meta-analysis. Lancet Gastroenterol Hepatol. 2022;7(2):161-170. PubMed
13.Clinical Study Report: RPC01-3102. A phase 3, multicentre, open-label extension trial of oral PRC1063 as therapy for moderate to severe ulcerative colitis [internal sponsor's report]. Couvet (CH): Celgene International II Sarl; 2020 Oct 28.
14.Cosnes J, Gower-Rousseau C, Seksik P, Cortot A. Epidemiology and natural history of inflammatory bowel diseases. Gastroenterology. 2011;140(6):1785-1794. PubMed
15.Alatab S, Sepanlou SG, Ikuta K, et al. The global, regional, and national burden of inflammatory bowel disease in 195 countries and territories, 1990–2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet Gastroenterol Hepatol. 2020;5(1):17-30. PubMed
16.Fumery M, Singh S, Dulai PS, Gower-Rousseau C, Peyrin-Biroulet L, Sandborn WJ. Natural history of adult ulcerative colitis in population-based cohorts: a systematic review. Clin Gastroenterol Hepatol. 2018;16(3):343-356.e343. PubMed
17.Bernstein CN, Nugent Z, Targownik LE, Singh H, Lix LM. Predictors and risks for death in a population-based study of persons with IBD in Manitoba. Gut. 2015;64(9):1403-1411. PubMed
18.Kawalec P, Malinowski KP. Indirect health costs in ulcerative colitis and Crohn's disease: a systematic review and meta-analysis. Expert Rev Pharmacoecon Outcomes Res. 2015;15(2):253-266. PubMed
19.Longobardi T, Jacobs P, Wu L, Bernstein CN. Work losses related to inflammatory bowel disease in Canada: results from a National Population Health Survey. Am J Gastroenterol. 2003;98(4):844-849. PubMed
20.Rawsthorne P, Clara I, Graff LA, et al. The Manitoba Inflammatory Bowel Disease Cohort study: a prospective longitudinal evaluation of the use of complementary and alternative medicine services and products. Gut. 2012;61(4):521-527. PubMed
21.Nguyen GC, Croitoru K, Silverberg MS, Steinhart AH, Weizman AV. Use of complementary and alternative medicine for inflammatory bowel disease is associated with worse adherence to conventional therapy: the COMPLIANT study. Inflamm Bowel Dis. 2016;22(6):1412-1417. PubMed
22.Weizman AV, Ahn E, Thanabalan R, et al. Characterisation of complementary and alternative medicine use and its impact on medication adherence in inflammatory bowel disease. Aliment Pharmacol Ther. 2012;35(3):342-349. PubMed
23.Celgene Corporation. Prescribing information: Zeposia (ozanimod) for oral use. Silver Spring (MD): U.S. Food and Drug Administration; 2021: https://www.accessdata.fda.gov/drugsatfda_docs/label/2021/209899s003lbl.pdf. Accessed 2022 Feb 4.
24.European Public Assessment Report (EPAR): Zeposia (ozanimod). Amsterdam (NL): European Medicines Agency; 2021: https://www.ema.europa.eu/en/medicines/human/EPAR/zeposia#authorisation-details-section. Accessed 2022 Feb 4.
25.Zeposia (ozanimod): 0.23 mg, 0.46 mg and 0.92 mg capsules [product monograph]. Saint-Laurent (QC): Celgene Inc; 2022 Apr 7: https://pdf.hres.ca/dpd_pm/00065373.PDF. Accessed 2022 Apr 29.
26.Stelara (ustekinumab): 45 mg/0.5 mL, 90 mg/1.0 mL solution for subcutaneous injection; 130 mg/26 mL (5mg/ML) solution for intravenous infusion [product monograph]. Toronto (ON): Janssen Inc; 2020 Jan 23: https://pdf.hres.ca/dpd_pm/00054738.PDF. Accessed 2022 Mar 29.
27.Remicade (infliximab): 100 mg/vial powder for solution, sterile, lyophilized [product monograph]. Toronto (ON): Janssen Inc; 2019 Jun 06: https://pdf.hres.ca/dpd_pm/00051606.PDF. Accessed 2022 Mar 29.
28.Entyvio (vedolizumab): 300 mg / vial powder for concentrate for solution for intravenous injection; 108 mg/0.68 mL prefilled syringe or pen solution for subcutaneous injection [product monograph]. Toronto (ON): Takeda Canada Inc; 2015 Jan 29: https://pdf.hres.ca/dpd_pm/00058905.PDF. Accessed 2022 Mar 29.
29.Simponi (golimumab): 50 mg/0.5 mL, 100 mg/1.0 mL solution for subcutaneous injection; 50 50 mg/4.0 mL solution for intravenous infusion [product monograph]. Toronto (ON): Janssen Inc; 2019 Jun 20: https://pdf.hres.ca/dpd_pm/00052895.PDF. Accessed 2022 Mar 29.
30.Xeljanz (tofacitinib): 5 mg, 10 mg oral tablets; 11 mg extended-release oral tablets [product monograph]. Kirkland (QC) Pfizer Canada ULC; 2019 Oct 24: https://pdf.hres.ca/dpd_pm/00053735.PDF. Accessed 2022 Mar 29.
31.Humira (adalimumab injection): 40 mg in 0.8 mL sterile solution (50 mg/mL) subcutaneous injection, 10 mg in 0.1 mL sterile solution (100 mg/mL) subcutaneous injection, 20 mg in 0.2 mL sterile solution (100 mg/mL) subcutaneous injection, 40 mg in 0.4 mL sterile solution (100 mg/mL) subcutaneous injection, 80 mg in 0.8 mL sterile solution (100 mg/mL) subcutaneous injection [product monograph]. St-Laurent (QC): AbbVie Corporation; 2021 Apr 21: https://pdf.hres.ca/dpd_pm/00061690.PDF. Accessed 2022 May 2.
32.McGowan J, Sampson M, Salzwedel DM, Cogo E, Foerster V, Lefebvre C. PRESS Peer Review of Electronic Search Strategies: 2015 guideline statement. J Clin Epidemiol. 2016;75:40-46. PubMed
33.Grey matters: a practical tool for searching health-related grey literature. Ottawa (ON): CADTH; 2019: https://www.cadth.ca/grey-matters. Accessed 2022 Feb 8.
34.Sandborn WJ, Feagan BG, D'Haens G, et al. Ozanimod as induction and maintenance therapy for ulcerative colitis. N Engl J Med. 2021;385(14):1280-1291. PubMed
35.Lewis JD, Chuai S, Nessel L, Lichtenstein GR, Aberra FN, Ellenberg JH. Use of the noninvasive components of the Mayo score to assess clinical response in ulcerative colitis. Inflamm Bowel Dis. 2008;14(12):1660-1666. PubMed
36.Geboes K, Riddell R, Ost A, Jensfelt B, Persson T, Löfberg R. A reproducible grading scale for histological assessment of inflammation in ulcerative colitis. Gut. 2000;47(3):404-409. PubMed
37.Bryant RV, Winer S, Travis SP, Riddell RH. Systematic review: histological remission in inflammatory bowel disease. Is 'complete' remission the new treatment paradigm? An IOIBD initiative. J Crohns Colitis. 2014;8(12):1582-1597. PubMed
38.Bernklev T, Jahnsen J, Lygren I, Henriksen M, Vatn M, Moum B. Health-related quality of life in patients with inflammatory bowel disease measured with the short form-36: psychometric assessments and a comparison with general population norms. Inflamm Bowel Dis. 2005;11(10):909-918. PubMed
39.Brooks R. The EuroQol Group after 25 years. New York (NY): Springer; 2013.
40.Sinnott PL, Joyce VR, Barnett P. Preference measurement in economic analysis. Guidebook. Menlo Park (CA): Health Economics Resource Center 2007.
41.Yarlas A, Bayliss M, Cappelleri JC, et al. Psychometric validation of the SF-36(®) Health Survey in ulcerative colitis: results from a systematic literature review. Qual Life Res. 2018;27(2):273-290. PubMed
42.Reilly MC, Zbrozek AS, Dukes EM. The validity and reproducibility of a work productivity and activity impairment instrument. Pharmacoeconomics. 1993;4(5):353-365. PubMed
43.Feagan BG, Rutgeerts P, Sands BE, et al. Vedolizumab as induction and maintenance therapy for ulcerative colitis. N Engl J Med. 2013;369(8):699-710. PubMed
44.Sedano R, Hogan M, McDonald C, Aswani-Omprakash T, Ma C, Jairath V. Underrepresentation of minorities and underreporting of race and ethnicity in Crohn's disease clinical trials. Gastroenterology. 2022;162(1):338-340.e332. PubMed
45.Burr NE, Gracie DJ, Black CJ, Ford AC. Efficacy of biological therapies and small molecules in moderate to severe ulcerative colitis: systematic review and network meta-analysis. Gut. 2021;22:22. PubMed
46.Hutton B, Salanti G, Caldwell DM, et al. The PRISMA extension statement for reporting of systematic reviews incorporating network meta-analyses of health care interventions: checklist and explanations. Ann Intern Med. 2015;162(11):777-784. PubMed
47.Systematic reviews: CRD's guidance for undertaking reviews in health care. York (GB): University of York Centre for Reviews and Dissemination; 2009.
48.Clinical Study Report: RPC01-202. A phase 2, multi-center, randomized, double-blind, placebo controlled parallel-group study to evaluate the clinical efficacy and saftely of induction therapy with RPC1063 in patients with moderately to severely active ulcerative colitis. The TOUCHSTONE trial [internal sponsor's report]. San Diego (CA): Receptos; 2015 Nov 4.
49.Center for Drug Evaluation and Research. Ulcerative colitis: clinical trial end points guidance for industry: draft guidance. Rockville (MD): U.S. Food and Drug Administration; 2016: https://www.fda.gov/downloads/Drugs/GuidanceComplianceRegulatoryInformation/Guidances/UCM515143.pdf. Accessed 2019 Oct 10.
50.Yarlas A, Maher S, Bayliss M, et al. The inflammatory bowel disease questionnaire in randomized controlled trials of treatment for ulcerative colitis: systematic review and meta-analysis. J Patient Cent Res Rev. 2020;7(2):189-205. PubMed
51.Chen XL, Zhong LH, Wen Y, et al. Inflammatory bowel disease-specific health-related quality of life instruments: a systematic review of measurement properties. Health Qual Life Outcomes. 2017;15(1):177. PubMed
52.Choi D, Stewart AP, Bhat S. Ozanimod: a first-in-class sphingosine 1-phosphate receptor modulator for the treatment of ulcerative colitis. Ann Pharmacother. 2021:10600280211041907. PubMed
53.Colombel JF, D'Haens G, Irving P, et al. P037. Effect of ozanimod treatment and discontinuation on absolute lymphocyte count in moderate-to-severe ulcerative colitis: results from a phase 3 trial. Am J Gastroenterol. 2021;116(Suppl 1):S9.
54.Hudesman D, Long M, Wolf D, et al. P035. Ozanimod for moderate-to-severe ulcerative colitis: North American population results during induction and maintenance in the phase 3 True North study. Am J Gastroenterol. 2021;116(Suppl 1):S9.
55.Long M, Cross R, Calkwood J, et al. P038. Ozanimod first-dose cardiac effects in patients with moderately to severely active ulcerative colitis and relapsing multiple sclerosis. Am J Gastroenterol. 2021;116(Suppl 1):S9-S10.
56.Sandborn WJ, Feagan BG, Hanauer S, et al. Long-term efficacy and safety of ozanimod in moderately to severely active ulcerative colitis: results from the open-label extension of the randomized, phase 2 TOUCHSTONE study. J Crohns Colitis. 2021;15(7):1120-1129. PubMed
57.Sands B, Pondel M, Silver M, et al. P031. Impact of prior biologic exposure on response to ozanimod for moderate-to-severe ulcerative colitis in the phase 3 True North study. Am J Gastroenterol. 2021;116(Suppl 1):S8.
58.Dhanda AD, Creed TJ, Greenwood R, Sands BE, Probert CS. Can endoscopy be avoided in the assessment of ulcerative colitis in clinical trials? Inflamm Bowel Dis. 2012;18(11):2056-2062. PubMed
59.Mohammed Vashist N, Samaan M, Mosli MH, et al. Endoscopic scoring indices for evaluation of disease activity in ulcerative colitis. Cochrane Database Syst Rev. 2018;1:CD011450. PubMed
60.Levesque B, Pola S, King D, et al. Responsiveness of central endoscopic assessment of disease activity using the Modified Mayo Clinic score in ulcerative colitis. Gastroenterology. 2013;144:S-767.
61.Walsh AJ, Ghosh A, Brain AO, et al. Comparing disease activity indices in ulcerative colitis. J Crohns Colitis. 2014;8(4):318-325. PubMed
62.Higgins PD, Schwartz M, Mapili J, Zimmermann EM. Is endoscopy necessary for the measurement of disease activity in ulcerative colitis? Am J Gastroenterol. 2005;100(2):355-361. PubMed
63.Mosli MH, Feagan BG, Zou G, et al. Reproducibility of histological assessments of disease activity in UC. Gut. 2015;64(11):1765-1773. PubMed
64.Lemmens B, Arijs I, Van Assche G, et al. Correlation between the endoscopic and histologic score in assessing the activity of ulcerative colitis. Inflamm Bowel Dis. 2013;19(6):1194-1201. PubMed
65.Kim DB, Lee K-M, Lee JM, et al. Correlation between histological activity and endoscopic, clinical, and serologic activities in patients with ulcerative colitis. Gastroenterol Res Pract. 2016;2016:5832051-5832051. PubMed
66.Mosli MH, Feagan BG, Zou G, et al. Development and validation of a histological index for UC. Gut. 2017;66(1):50-58. PubMed
67.Irvine EJ. Quality of life of patients with ulcerative colitis: past, present, and future. Inflamm Bowel Dis. 2008;14(4):554-565. PubMed
68.Gibson PR, Vaizey C, Black CM, et al. Relationship between disease severity and quality of life and assessment of health care utilization and cost for ulcerative colitis in Australia: a cross-sectional, observational study. J Crohns Colitis. 2014;8(7):598-606. PubMed
69.Panés J, Domènech E, Aguas Peris M, et al. Association between disease activity and quality of life in ulcerative colitis: results from the CRONICA-UC study. J Gastroenterol Hepatol. 2017;32(11):1818-1824. PubMed
70.Stark RG, Reitmeir P, Leidl R, Konig HH. Validity, reliability, and responsiveness of the EQ-5D in inflammatory bowel disease in Germany. Inflamm Bowel Dis. 2010;16(1):42-51. PubMed
71.Yarlas A, Maher SM, Bayliss MS, Lovley A, Cappelleri JC, DiBonaventura MD. Psychometric validation of the work productivity and activity impairment questionnaire in ulcerative colitis: results from a systematic literature review. J Patient Rep Outcomes. 2018;2(1):62. PubMed
72.Rubin D, Keyashian K, Bunnag A, et al. Correlation between clinical, endoscopic, and histologic disease activity in ulcerative colitis: 1712. Am J Gastroenterol. 2012;107:S694.
73.Iacucci M, Cannatelli R, Gui X, et al. Assessment of endoscopic healing by using advanced technologies reflects histological healing in ulcerative colitis. J Crohns Colitis. 2020;14(9):1282-1289. PubMed
74.Samaan MA, Mosli MH, Sandborn WJ, et al. A systematic review of the measurement of endoscopic healing in ulcerative colitis clinical trials: recommendations and implications for future research. Inflamm Bowel Dis. 2014;20(8):1465-1471. PubMed
75.Cooney RM, Warren BF, Altman DG, Abreu MT, Travis SP. Outcome measurement in clinical trials for ulcerative colitis: towards standardisation. Trials. 2007;8:17. PubMed
76.Magro F, Lopes J, Borralho P, et al. Comparison of the Nancy index with continuous Geboes score: histological remission and response in ulcerative colitis. J Crohns Colitis. 2020;14(7):1021-1025. PubMed
77.Lobatón T, Bessissow T, Ruiz-Cerulla A, et al. Prognostic value of histological activity in patients with ulcerative colitis in deep remission: a prospective multicenter study. United European Gastroenterol. 2018;6(5):765-772. PubMed
78.Feng YS, Kohlmann T, Janssen MF, Buchholz I. Psychometric properties of the EQ-5D-5L: a systematic review of the literature. Qual Life Res. 2021;30(3):647-673. PubMed
79.Buchholz I, Janssen MF, Kohlmann T, Feng YS. A systematic review of studies comparing the measurement properties of the three-level and five-level versions of the EQ-5D. Pharmacoeconomics. 2018;36(6):645-661. PubMed
80.Herdman M, Gudex C, Lloyd A, et al. Development and preliminary testing of the new five-level version of EQ-5D (EQ-5D-5L). Qual Life Res. 2011;20(10):1727-1736. PubMed
81.Yarlas A, D'Haens G, Willshire D, Teynor M. Remission status predicts work-related outcomes for patients with mild-to-moderate ulcerative colitis receiving short-term and long-term daily therapy with multimatrix mesalamine: 1935. Am J Gastroenterol. 2015;110.
82.Reilly M, Brown M, Brabant YM. Minimally important differences for WPAI:CD scores: defining relevant impact on work productivity in active Chron’s disease: 962 Am J Gastroenterol. 2007;102:S472.
Appendix 1: Literature Search Strategy
Note that this appendix has not been copy-edited.
Clinical Literature Search
Overview
Interface: Ovid
Databases:
MEDLINE All (1946 to present)
Embase (1974 to present)
Note: Subject headings and search fields have been customized for each database. Duplicates between databases were removed in Ovid.
Date of search: February 2, 2022
Alerts: Bi-weekly search updates until project completion
Search filters applied: No filters were applied to limit the retrieval by study type.
Limits:
No date or language limits were used
Conference abstracts: excluded
Syntax | Description |
|---|---|
/ | At the end of a phrase, searches the phrase as a subject heading |
MeSH | Medical Subject Heading |
.fs | Floating subheading |
exp | Explode a subject heading |
* | Before a word, indicates that the marked subject heading is a primary topic; or, after a word, a truncation symbol (wildcard) to retrieve plurals or varying endings |
.ti | Title |
.ot | Original title |
.ab | Abstract |
.hw | Heading word; usually includes subject headings and controlled vocabulary |
.kf | Author keyword heading word (MEDLINE) |
.dq | Candidate term word (Embase) |
.rn | Registry number |
.nm | Name of substance word (MEDLINE) |
medall | Ovid database code: MEDLINE All, 1946 to present, updated daily |
oemezd | Ovid database code; Embase, 1974 to present, updated daily |
Multi-Database Strategy
(Zeposia* or ozanimod* or RPC1063 or RPC 1063 or 3UPR33JAAM or Z80293URPV).ti,ab,kf,ot,hw,rn,nm.
1 use medall
*ozanimod/
(Zeposia* or ozanimod* or RPC1063 or RPC 1063).ti,ab,kf,dq.
3 or 4
5 use oemezd
6 not (conference review or conference abstract).pt.
2 or 7
remove duplicates from 8
Clinical Trials Registries
ClinicalTrials.gov
Produced by the US National Library of Medicine. Targeted search used to capture registered clinical trials.
[Search -- Studies with results | Zeposia or ozanimod]
WHO ICTRP
International Clinical Trials Registry Platform, produced by the World Health Organization. Targeted search used to capture registered clinical trials.
[Search terms -- Zeposia or ozanimod]
Health Canada’s Clinical Trials Database
Produced by Health Canada. Targeted search used to capture registered clinical trials.
[Search terms -- Zeposia or ozanimod]
EU Clinical Trials Register
European Union Clinical Trials Register, produced by the European Union. Targeted search used to capture registered clinical trials.
[Search terms -- Zeposia or ozanimod]
Grey Literature
Search dates: January 21, 2022 to January 27, 2022
Keywords: Zeposia, ozanimod, ulcerative colitis
Limits: None
Updated: Search updated prior to the completion of stakeholder feedback period
Relevant websites from the following sections of the CADTH grey literature checklist Grey Matters: A Practical Tool for Searching Health-Related Grey Literature were searched:
Health Technology Assessment Agencies
Health Economics
Clinical Practice Guidelines
Drug and Device Regulatory Approvals
Advisories and Warnings
Drug Class Reviews
Clinical Trials Registries
Databases (free)
Health Statistics
Internet Search
Appendix 2: Excluded Studies
Note that this appendix has not been copy-edited.
Reference | Reason for exclusion |
|---|---|
Choi et al.52 | Review article |
Colombel et al.53 | Abstracts related to the pivotal study |
Hudesman et al.54 | Abstracts related to the pivotal study |
Long et al.55 | Study population |
Sandborn et al.56 | Open-label extension study of the pivotal trial |
Sands et al.57 | Abstracts related to the pivotal study |
Appendix 3: Detailed Outcome Data
Note that this appendix has not been copy-edited.
Table 39: Proportion of Patients in Clinical Responsea Based on Prior Use of Anti-TNF, Disease Severity, and Disease Extent in TRUE NORTH
End point | Patients, n (%) | Treatment comparisonb | |||
|---|---|---|---|---|---|
Ozanimod 1 mg | Placebo | Difference in proportion (95% CI)b | Odds ratio (95% CI)b | Nominal P valueb,c | |
Outcomes at 10 weeks (induction period) | |||||
Prior use of anti-TNF therapy | |||||
No prior anti-TNF | n = 299 157 (52.5) | n = 151 44 (29.1) | 0.23 (0.14 to 0.33) | 2.69 (1.77 to 4.08) | < 0.0001 |
Prior anti-TNF | n = 130 48 (36.9) | n = 65 12 (18.5) | 0.19 (0.06 to 0.31) | 2.62 (1.27 to 5.41) | 0.0084 |
Disease severity (moderate UC,d yes/no) | |||||
Yes | n = 362 175 (48.3) | n = 191 51 (26.7) | 0.21 (0.13 to 0.29) | 2.59 (1.76 to 3.81) | < 0.0001 |
No | n = 67 30 (44.8) | n = 25 5 (20.0%) | 0.22 (0.02 to 0.42) | 2.96 (0.97 to 9.03) | 0.0539 |
Disease Extent | |||||
Extensive | n = 161 67 (41.6) | n = 82 20 (24.4) | 0.18 (0.06 to 0.30) | 2.28 (1.25 to 4.15) | 0.0066 |
Left-sided | n = 268 138 (51.5) | n = 134 36 (26.9) | 0.24 (0.15 to 0.34) | 2.95 (1.87 to 4.66) | < 0.0001 |
Outcomes at 52 weeks (maintenance period) | |||||
Prior use of anti-TNF therapy | |||||
No prior anti-TNF | n= 154 96 (62.3) | n = 158 76 (48.1) | 0.14 (0.03 to 0.25) | 1.80 (1.14 to 2.85) | 0.0119 |
Prior anti-TNF | n = 76 42 (55.3) | n = 69 17 (24.6) | 0.30 (0.16 to 0.45) | 4.148 (1.96 to 8.78) | 0.0002 |
Disease severity (moderate UC,d yes/no) | |||||
Yes | n = 192 119 (62.0) | n = 206 85 (41.3) | 0.21 (0.11 to 0.30) | 2.41 (1.59 to 3.64) | < 0.0001 |
No | n = 38 19 (50.0) | n = 21 8 (38.1) | 0.11 (−0.17 to 0.38) | 1.57 (0.50 to 4.60) | 0.4568 |
Disease extent | |||||
Extensive | n = 78 43 (55.1) | n = 70 28 (40) | 0.16 (0.003 to 0.32) | 1.97 (1.00 to 3.91) | 0.0513 |
Left-sided | n = 152 95 (62.5) | n = 157 65 (41.4) | 0.20 (0.10 to 0.31) | 2.39 (1.50 to 3.82) | 0.0003 |
CI = confidence interval; CMH = Cochran-Mantel-Haenszel; ITT = intention to treat; RBS = rectal bleeding subscore; SFS = stool frequency subscore. TNF = tumour necrosis factor.
aClinical response is defined as a reduction from baseline in the 9-point Mayo score of ≥ 2 points and ≥ 35%, and a reduction from baseline in the RBS of ≥ 1 point or an absolute RBS of ≤ 1 point.
bOdds ratio (active/placebo), treatment difference, 2-sided 95% Wald CI and P value for comparison between the active and placebo groups are based on the CMH test, stratified by corticosteroid use at screening and prior anti-TNF use (yes or no).
cP values < 0.05 are considered nominally significant because no multiplicity adjustment was applied.
dModerate UC was defined as a 4-component Mayo score of 6 to 10.
Source: Clinical Study Report for the TRUE NORTH study.10
Table 40: Proportion of Patients in Endoscopic Improvementa Based on Prior Use of Anti-TNF, Disease Severity, and Disease Extent in TRUE NORTH
End point | Patients, n (%) | Treatment comparisonb | |||
|---|---|---|---|---|---|
Ozanimod 1 mg | Placebo | Difference in proportion (95% CI)b | Odds ratio (95% CI)b | Nominal P valueb,c | |
Outcomes at 10 weeks (induction period) | |||||
Prior use of anti-TNF | |||||
No prior anti-TNF | n = 299 97 (32.4) | n = 151 18 (11.9) | 0.21 (0.13 to 0.30) | 3.54 (2.05 to 6.12) | < 0.001 |
Prior anti-TNF | n = 130 20 (15.4) | n = 65 7 (10.8) | 0.05 (−0.05 to 0.14) | 1.51 (0.60 to 3.79) | 0.378 |
Disease severity (moderate UCd yes/no) | |||||
Yes | N = 362 109 (30.1) | N = 191 25 (13.1) | 0.17 (0.10 to 0.24) | 2.84 (1.76 to 4.56) | < 0.001 |
No | N = 67 8 (11.9) | N = 25 1 (4.0) | 0.08 (−0.04 to 0.19) | 3.13 (0.36 to 27.27) | 0.291 |
Disease extent | |||||
Extensive | n = 161 34 (21.1) | n = 82 8 (9.8) | 0.12 (0.03 to 0.21) | 2.51 (1.10 to 5.70) | 0.024 |
Left-sided | n = 268 83 (31.0) | n = 134 18 (13.4) | 0.18 (0.09 to 0.26) | 2.86 (1.64 to 5.00) | < 0.001 |
Outcomes at 52 weeks (induction period) | |||||
Prior use of anti-TNF | |||||
No prior anti-TNF | n = 154 77 (50.0) | n = 158 48 (30.4) | 0.19 (0.09 to 0.30) | 2.35 (1.46 to 3.77) | < 0.001 |
Prior anti-TNF | n = 76 28 (36.8) | n = 69 12 (17.4) | 0.19 (0.05 to 0.32) | 2.933 (1.30 to 6.61) | 0.009 |
Disease severity (moderate UCd yes/no) | |||||
Yes | n = 63 19 (30.2) | n = 206 57 (27.7) | 0.20 (0.11 to 0.29) | 2.46 (1.60 to 3.78) | < 0.001 |
No | n = 36 14 (16.7) | n = 21 3 (14.3) | 0.21 (−0.01 to 0.42) | 3.46 (0.79 to 15.08) | 0.091 |
Disease extent | |||||
Extensive | n = 28 7 (25.0) | n = 70 15 (21.4) | 0.204 (0.06 to 0.35) | 2.84 (1.32 to 6.12) | 0.007 |
Left-sided | n = 152 13 (31.7) | n = 157 45 (28.7) | 0.19 (0.09 to 0.30) | 2.40 (1.48 to 3.89) | < 0.001 |
CI = confidence interval; CMH = Cochran-Mantel-Haenszel; ITT = intention to treat; RBS = rectal bleeding subscore; SFS = stool frequency subscore. TNF = tumour necrosis factor.
aEndoscopic improvement is defined as a Mayo endoscopic score ≤ 1 without friability.
bOdds ratio (active/placebo), treatment difference, 2-sided 95% Wald CI and P value for comparison between the active and placebo groups are based on the CMH test, stratified by corticosteroid use at screening and prior anti-TNF use (yes or no).
cP values < 0.05 are considered nominally significant because no multiplicity adjustment was applied.
dModerate UC was defined as a 4-component Mayo score of 6 to 10.
Source: Clinical Study Report for the TRUE NORTH study.10
Table 41: Proportion of Patients in Mucosal Healinga Based on Prior Use of Anti-TNF, Disease Severity, and Disease Extent in TRUE NORTH
End point | n (%) patients | Treatment comparisonb | |||
|---|---|---|---|---|---|
Ozanimod 1 mg | Placebo | Difference in proportion (95% CI)b | Odds ratio (95% CI)b | Nominal P valueb,c | |
Outcomes at 10 weeks (induction period) | |||||
Prior use of anti-TNF | |||||
No prior anti-TNF | n = 299 47 (15.7) | n = 151 6 (4.0) | 0.12 (0.07 to 0.17) | 4.49 (1.87 to 10.74) | < 0.001 |
Prior anti-TNF | n = 130 7 (5.4) | n = 65 2 (3.1) | 0.023 (−0.03 to 0.08) | 1.81 (0.36 to 9.08) | 0.465 |
Disease severity (moderate UCd yes/no) | |||||
Yes | n = 62 50 (13.8) | n = 191 8 (4.2) | 0.10 (0.05 to 0.14) | 3.61 (1.68 to 7.77) | < 0.001 |
No | n = 67 4 (6.) | n = 25 0 | 0.06 (−0.001 to 0.11) | 1.42 (0.211 to 9.54) | 0.241 |
Disease extent | |||||
Extensive | n = 62 16 (9.9) | n = 82 4 (4.9) | 0.05 (−0.02 to 0.12) | 2.14 (0.70 to 6.54) | 0.167 |
Left-sided | n = 268 38 (14.2) | n = 134 4 (3.0) | 0.11 (0.061 to 0.16) | 5.30 (1.87 to 5.42) | < 0.001 |
Outcomes at 52 weeks (maintenance period) | |||||
Prior use of anti-TNF | |||||
No prior anti-TNF | n = 154 51 (33.1) | n = 158 28 (17.7) | 0.15 (0.06 to 0.25) | 2.32 (1.36 to 3.96) | 0.002 |
Prior anti-TNF | n = 76 17 (22.4) | n = 69 4 (5.8) | 0.16 (0.06 to 0.27) | 4.78 (1.48 to 15.44) | 0.005 |
Disease severity (moderate UCd yes/no) | |||||
Yes | n = 192 61 (31.8) | n = 206 31 (15.0) | 0.17 (0.087 to 0.25) | 2.71 (1.65 to 4.45) | < 0.001 |
No | n = 38 7 (18.4) | n = 21 1 (4.8) | 0.16 (−0.01 to 0.33) | 4.80 (0.56 to 40.94) | 0.120 |
Disease extent | |||||
Extensive | n = 78 21 (26.9) | n = 70 7 (10.0) | 0.19 (0.06 to 0.31) | 3.61 (1.41 to 9.28) | 0.004 |
Left-sided | n = 152 47 (30.9) | n = 152 25 (15.9) | 0.15 (0.05 to 0.24) | 2.36 (1.35 to 4.12) | 0.002 |
CI = confidence interval; CMH = Cochran-Mantel-Haenszel; ITT = intention to treat; RBS = rectal bleeding subscore; SFS = stool frequency subscore. TNF = tumour necrosis factor.
aMucosal healing is defined as a Mayo endoscopic score ≤ 1 point without friability and Geboes index score < 2.0 (no neutrophils in the epithelial crypts or lamina propria and no increase in eosinophils, no crypt destruction, and no erosions, ulcerations, or granulation tissue) in the same subject.
bOdds ratio (active/placebo), treatment difference, 2-sided 95% Wald CI and P value for comparison between the active and placebo groups are based on the CMH test, stratified by corticosteroid use at screening and prior anti-TNF use (yes or no).
cP values < 0.05 are considered nominally significant because no multiplicity adjustment was applied.
dModerate UC was defined as a 4-component Mayo score of 6 to 10.
Source: Clinical Study Report for the TRUE NORTH study.10
Table 42: Proportion of Corticosteroid-Free Remissiona Based on Prior Use of Anti-TNF, Disease Severity, and Disease Extent at Week 52 in TRUE NORTH
End point | n (%) patients | Treatment comparisonb | |||
|---|---|---|---|---|---|
Ozanimod 1 mg | Placebo | Difference in proportion (95% CI)b | Odds ratio (95% CI)b | Nominal P valueb,c | |
Prior use of anti-TNF | |||||
No prior anti-TNF | n = 154 55 (35.7) | N = 158 31 (19.6) | 0.16 (0.07 to 0.26) | 2.46 (1.44 to 4.22) | < 0.001 |
Prior anti-TNF | N = 76 18 (23.7) | N = 69 7 (10.1) | 0.16 (0.02 to 0.24) | 2.89 (1.08 to 7.75) | 0.033 |
Disease severity (Moderate UCd yes/no) | |||||
Yes | n = 192 68 (35.4) | n = 206 37 (18.0) | 0.17 (0.10 to 0.26) | 2.72 (1.67 to 4.43) | < 0.001 |
No | n = 38 5 (13.2) | n = 21 1 (4.8) | 0.09 (−0.05 to 0.22) | 3.61 (0.33 to 40.01) | 0.294 |
Disease extent | |||||
Extensive | n = 78 26 (33.3) | n = 70 11 (15.7) | 0.21 (0.08 to 0.34) | 3.90 (1.59 to 9.56) | 0.002 |
Left-sided | n = 152 47 (30.9) | n = 157 27 (17.2) | 0.13 (0.04 to 0.22) | 2.19 (1.25 to 3.84) | 0.006 |
CI = confidence interval; CMH = Cochran-Mantel-Haenszel; ITT = intention to treat; RBS = rectal bleeding subscore; SFS = stool frequency subscore. TNF = tumour necrosis factor.
aCorticosteroid-free remission is defined as clinical remission while off corticosteroids for at least 12 weeks.
bOdds ratio (active/placebo), treatment difference, 2-sided 95% Wald CI and P value for comparison between the active and placebo groups are based on the CMH test, stratified by corticosteroid use at screening and prior anti-TNF use (yes or no).
cP values < 0.05 are considered nominally significant because no multiplicity adjustment was applied.
dModerate UC was defined as a 4-component Mayo score of 6 to 10.
Source: Clinical Study Report for the TRUE NORTH study.10
Table 43: Proportion of Patients With Durable Remissiona Based on Prior Use of Anti-TNF, Disease Severity, and Disease Extent at Week 52 in TRUE NORTH
End point | n (%) patients | Treatment comparisonb | |||
|---|---|---|---|---|---|
Ozanimod 1 mg | Placebo | Difference in proportion (95% CI)b | Odds ratio (95% CI)b | Nominal P valueb,c | |
Prior use of anti-TNF | |||||
No prior anti-TNF | n = 154 37 (24.0) | n = 158 19 (12.0) | 0.12 (0.04 to 0.19) | 3.20 (1.55 to 6.61) | 0.002 |
Prior anti-TNF | n = 76 4 (5.3) | n = 69 3 (4.3) | 0.005 (−0.06 to 0.07) | 1.13 (0.21 to 5.60) | 0.888 |
Disease severity (moderate UCd yes/no) | |||||
Yes | n = 192 37 (19.3) | n = 206 22 (10.7) | 0.09 (0.03 to 0.15) | 2.68 (1.38 to 5.22) | 0.004 |
No | n = 38 4 (10.5) | n = 21 0 | 0.03 (−0.03 to 0.09) | 2.33 (0.07 to 76.67) | 0.439 |
Disease extent | |||||
Extensive | n = 78 12 (15.4) | n = 70 7 (10.0) | 0.08 (−0.02 to 0.17) | 2.71 (0.80 to 9.14) | 0.104 |
Left-sided | n = 152 29 (19.1) | n = 157 15 (9.6) | 0.09 (0.02 to 0.15) | 2.60 (1.21 to 5.60) | 0.013 |
CI = confidence interval; CMH = Cochran-Mantel-Haenszel; ITT = intention to treat; RBS = rectal bleeding subscore; SFS = stool frequency subscore; TNF = tumour necrosis factor.
aDurable remission is defined as clinical remission at week 10 and week 52 in patients who entered the maintenance period.
bOdds ratio (active/placebo), treatment difference, 2-sided 95% Wald CI and P value for comparison between the active and placebo groups are based on the CMH test, stratified by corticosteroid use at screening and prior anti-TNF use (yes or no).
cP values < 0.05 are considered nominally significant because no multiplicity adjustment was applied.
dModerate UC was defined as a 4-component Mayo score of 6 to 10.
Source: Clinical Study Report for the TRUE NORTH study.10
Table 44: Proportion of Patients With Clinical Remission in a Subset of Patients in Remission at Week 10a Based on Prior Anti-TNF Use of Anti-TNF, Disease Severity, and Disease Extent at Week 52 in TRUE NORTH
End point | n (%) patients | Treatment comparisonb | |||
|---|---|---|---|---|---|
Ozanimod 1 mg | Placebo | Difference in proportion (95% CI)b | Odds ratio (95% CI)b | Nominal P valueb,c | |
Prior use of anti-TNF | |||||
No prior anti-TNF | n = 154 37 (57.8) | n =158 19 (32.8) | 0.250 (0.08 to 0.42) | 2.89 (1.36 to 6.14) | 0.0055 |
Prior anti-TNF | n = 76 4 (26.7) | n = 69 3 (17.6) | 0.11 (−0.15 to 0.37) | 2.33 (0.31 to 17.80) | 0.4349 |
Disease severity (moderate UCd yes/no) | |||||
Yes | n = 69 37 (53.6) | n = 74 22 (29.7) | 0.25 (0.10 to 0.40) | 2.99 (1.47 to 6.09) | 0.0024 |
No | n = 10 4 (40.0) | n = 1 0 | NA | NA | NA |
Disease extent | |||||
Extensive | n =22 12 (54.5) | n = 22 7 (31.8) | 0.26 (−0.04 to 0.55) | 2.87 (0.79 to 0.35) | 0.1031 |
Left-sided | n = 53 29 (50.9) | n = 57 15 (28.3) | 0.24 (0.06 to 0.42) | 2.85 (1.26 to 6.46) | 0.0112 |
CI = confidence interval; CMH = Cochran-Mantel-Haenszel; ITT = intention to treat; RBS = rectal bleeding subscore; SFS = stool frequency subscore. TNF = tumour necrosis factor.
Note: For subgroups that are less than 5% of the ITT population, “NA” is displayed for comparison statistics.
aPercentage based on number of patients in clinical remission at week 10 (as shown).
bOdds ratio (active/placebo), treatment difference, 2-sided 95% Wald CI and P value for comparison between the active and placebo groups are based on the CMH test, stratified by corticosteroid use at screening and prior anti-TNF use (yes or no).
cP values < 0.05 are considered nominally significant because no multiplicity adjustment was applied.
dModerate UC was defined as a 4-component Mayo score of 6 to 10.
Source: Clinical Study Report for the TRUE NORTH study.10
Appendix 4: Description and Appraisal of Outcome Measures
Note that this appendix has not been copy-edited.
Aim
To describe the following outcome measures and review their measurement properties (validity, reliability, responsiveness to change, and minimal important difference [MID]):
Primary outcome:
Mayo score
Other outcomes:
Geboes score
SF-36
EQ-5D-5L
WPAI-UC
Findings
Table 45: Summary of Outcome Measures and Their Measurement Properties
Outcome measure | Type | Conclusions about measurement properties | MID |
|---|---|---|---|
Mayo score | A disease-specific physician-measured score that included the following components: rectal bleeding, stool frequency, PGA, and endoscopy findings. | Validity: Construct validity of the full Mayo score was demonstrated by a strong correlation with the patient’s assessment of disease activity (rho = 0.71 at week 12).35 A strong correlation was found between the partial and total Mayo scores (rho = 0.97 at weeks 4 and 8).58 Construct validity of the Mayo endoscopic subscore was supported by a strong correlation with the total Mayo score (Spearman’s rho = 0.97), the Riley histologic score (r = 0.55) and the Rubin histologic score (r = 0.60).59 Reliability and responsiveness: The endoscopic subscore was found to have moderate-to-substantial inter-rater agreement (r, 0.45 to 0.75). It was also found to be responsive to change over time with treatment.35,59-61 | Clinical response: Clinical response is indicated by a reduction in total Mayo score of at least 3 points.35 Clinical remission: Clinical remission is indicated by a total Mayo score of ≤ 2 points, with or without an individual subscore of < 1.35,62 |
Geboes Scale | The Geboes score is a commonly used histologic index in UC for assessing disease severity and/or activity.36,37 It is a classification system consisting of 6 grades, with 4 subgrades each, that are meant to be progressive. | Validity: Criterion validity of the Geboes score was supported by a strong correlation between the Geboes score and a global disease activity, assessed using VAS (r = 0.66; 95% CI, 0.57 to 0.72).63 Construct validity was supported by strong correlations between the Geboes score and the Mayo endoscopic subscore, endoscopic activity index, and clinical activity index (Spearman rank correlation range, 0.54 to 0.80).64,65 Reliability and responsiveness: The Geboes score was found to have substantial to almost perfect intra-rater agreement (ICC range, 0.77 to 0.84) and moderate inter-rater agreement (ICC range, 0.51 to 0.60).63 The Geboes score was found to be responsive to treatment-related changes (SES = 1.87; 95% CI, 1.54 to 2.20).66 | Histological healing: Histological healing was empirically defined in specimens of endoscopically uninflamed tissue as the average Geboes score below 2.36 |
SF-36 | A generic self-reported questionnaire consisting of 8 domains: physical functioning, role physical, bodily pain, general health, vitality, social functioning, role emotional, and mental health. | Validity: Construct validity was demonstrated through moderate to strong correlations (r > 0.4) between the 8 subscales of the SF-36 and corresponding domains of 5 patient-reported clinical constructs. The scale showed evidence of discriminant validity (against disease activity/symptom status).41 Reliability and responsiveness: The SF-36 was found to have good internal consistency for all 8 subscales (Cronbach alpha > 0.7) and good test–retest assessments for 6 of the 8 subscales (ICC > 0.7).41 The scale and its subscores were found to be responsive to treatment-related changes.41 | An absolute score increase of 3 to 5 points for PCS, MCS, and individual subscores.67 |
EQ-5D-5L | A generic preference-based HRQoL instrument consisting of a VAS and a composite index score of 5 dimensions: mobility, self-care, usual activities, pain/discomfort, and anxiety/depression. | Validity: Construct validity was supported by a moderate to strong correlation of the EQ-5D-5L with the IBDQ (r = 0.69), physician-completed SCCAI (r= −0.53), and patient-completed SCCAI (r = −0.49).68,69 Reliability and responsiveness: Test–retest reliability was generally moderate for all domains of the EQ-5D-5L (kappa, 0.41 to 0.58), except for the “anxiety/depression” domain (kappa = 0.28).69 | An EQ-5D-3L index score of 0.05 and VAS of 10.9 were estimated for improved health; VAS of 14.4 and the EQ-5D-3L index of 0.067 for deteriorated health in patients with UC.70 |
WPAI-UC | A self-reported disease-specific questionnaire consisting of 6 items divided into 4 domains: absenteeism, presenteeism, percentage of overall work impairment, and regular activities impairment. | Validity: Convergent validity was demonstrated for all WPAI domains between the SIBDQ bowel symptoms (Spearman rank-order coefficient of 0.47 to 0.68) and SF-12v2 bodily pain (0.52 to 0.55) subscores, and between the WPAI and measures of disease activity (median = 0.45).71 Known-group validity, a form of construct validity demonstrated that patients with worse health outcomes scored worse on the WPAI than patients with better health outcomes, based on partial Mayo, SCCAI, UC-DAI, and FACIT-Fatigue disease severity measures.71 Reliability and responsiveness: Patients with active UC disease who achieved remission at week 8 reported a 25% to 30% decrease in presenteeism, OWI, and activity impairment, and a 9% decrease in absenteeism. Responsiveness to effective treatment was demonstrated with an approximate 20% decrease in presenteeism, OWI, and activity impairment, and an 8% decrease in absenteeism.71 | Evidence of an MID was not identified. |
MID = minimal important difference; UC = ulcerative colitis; PGA = Physician’s Global Assessment; CAI = Clinical Activity Index; FACIT-Fatigue = Functional Assessment of Chronic Illness Therapy Fatigue scale; IBD = inflammatory bowel disease; ICC = intraclass correlation; SF-36 = Short Form (36) Health Survey; PCS = Physical Component Summary, MCS = Mental Component Summary, OWI = overall work impairment; SCCAI = Simple Clinical Colitis Activity Index; IBDQ = Inflammatory Bowel Disease Questionnaire; VAS = Visual Analogue Scale; WPAI-UC = Work Productivity and Activity Impairment Questionnaire – Ulcerative Colitis.
Mayo Score
The Mayo scoring system is a combined endoscopic and clinical scale used to assess the severity of UC. It was first developed by Dr. Schroeder in 1987 and is now one of the most commonly used disease activity indices in UC.1,35 In its complete form, the Mayo score is composed of 4 components: rectal bleeding, stool frequency, PGA, and endoscopy findings. Each part is rated from 0 to 3, yielding a total score of 0 to 12. A score of 3 to 5 points indicates mildly active disease, while a score of 6 to 10 points indicates moderately active disease, and a score of 11 to 12 points indicates severe disease. Two abridged versions of the Mayo score have been developed and validated: the partial Mayo score that excludes the endoscopy subscore, resulting in a composite of the rectal bleeding, stool frequency, and PGA, and the noninvasive 6-point score comprising only the bleeding and stool frequency subscores.35,59 Mucosal healing has been defined as a Mayo endoscopic subscore of 0 or 1 in major trials of biological therapies in UC. The grading of each component is defined in Table 46.
Table 46: Components and Grading of the Mayo Score in Ulcerative Colitis
Component | Grading |
|---|---|
Stool frequency | 0 = Normal 1 = 1 to 2 stools per day more than normal 2 = 3 to 4 stools per day more than normal 3 = More than 4 stools per day more than normal |
Rectal bleeding | 0 = None 1 = Streaks of blood with stool less than half the time 2 = Obvious blood with stool half of the time or more 3 = Passing blood alone |
Findings on endoscopy | 0 = Normal or inactive disease 1 = Mild disease (erythema, decreased vascular pattern, mild friability) 2 = Moderate disease (marked erythema, absent vascular pattern, friability, erosions) 3 = Severe disease (spontaneous bleeding, ulceration) |
Physician rating of disease activity | 0 = Normal 1 = Mild disease 2 = Moderate disease 3 = Severe disease |
Psychometric Properties
A recent Cochrane systematic review, consisting of 20 primary studies, assessed the validity, reliability, and responsiveness of endoscopic-scoring indices for evaluation of disease activity in UC.59 Content validity was not assessed in any of the included studies.59 The review identified 2 studies that assessed construct validity of the Mayo endoscopic subscore which found a strong correlation between the Mayo endoscopic subscore and 2 histologic indices, including the Riley index score (r = 0.55) and Rubin histologic index score (r = 0.60).58,72 However, the endoscopic subscore failed to discriminate between patients who achieved remission and response compared with those who did not.59 In terms of intra- and inter-rater reliability, the systematic review conducted reported a moderate-to-substantial agreement in the inter-rater reliability estimates (r = 0.45 to 0.75) and a substantial agreement in the intra-rater reliability estimates (r = 0.75) for the endoscopic subscore.59 A Canadian study consisting of 82 patients with UC (mean age = 49.9; SD = 14.8) demonstrated that the threshold of the Mayo endoscopic subscore for predicting histological healing was equal to 0, with sensitivity of 81.4% (95% CI, 25.4 to 90.9), specificity of 95.7% (95% CI, 67.0 to 100), and accuracy of 85.4% (95% CI, 77.0 to 86.6).73 Another study consisting of 149 subjects with moderate to severe UC demonstrated a strong correlation between the partial and total Mayo scores (Spearman rho = 0.97 at weeks 4 and 8).58
An evaluation of the construct validity of the total and partial Mayo scores was conducted in 75 patients with UC.35 Both the total and partial Mayo scores were strongly correlated with patient assessment of disease activity (rho = 0.71 and rho = 0.70, respectively).35 Moreover, the Mayo score was found to correlated with patient assessment of change in UC activity,35 and with improvement in quality-of-life measures.74 A study evaluating the comparative inter-rater variation for 3 UC disease activity indices (n = 100) found that the inter-rater agreement for the total Mayo score was high (kappa = 0.72); however, the agreement was lower for the relatively subjective PGA and endoscopic subscores with kappa scores of 0.56 and 0.38, respectively.61 An evaluation of the reliability and responsiveness of the Mayo endoscopic subscore was assessed in a placebo-controlled trial evaluating change in UC disease activity after treatment with mesalamine.60 The authors reported both excellent inter- and intraobserver reliability with intraclass correlation [ICC] of 0.79 and 0.89, respectively. In addition, the Mayo endoscopic subscore was found to be responsive to change over time with treatment.60 Rubin et al. also reported a strong correlation between the Mayo Clinic Endoscopic subscore and the Simple Clinical Colitis Activity Index (SCCAI) (r = 0.53, P < 0.001).72
Minimal Important Difference
In a study of 105 patients with UC, the optimal cut point of change in the total Mayo score to identify a clinical improvement or response was 2.5 with sensitivity of 88%, specificity of 80%, using patient’s rating of the improvement as an anchor.35 What is considered the optimal cut point for clinical remission, however, varies. While Lewis et al. reported a cut point of change of 4.5 with sensitivity of 88% and specificity of 78%, cut points determined from other clinical trials ranged from a Mayo score of 0.6 to 2.4,35,62, As with remission, different definitions of response have been used, most commonly a reduction of the baseline total Mayo score of either 2 or 3 points.62 The FDA, on the other hand, defines clinical remission as a Mayo score of 2 or less with no individual subscore greater than 1 (stool frequency subscore of 0 or 1, endoscopy subscore of 0 or 1, and rectal bleeding subscore of 0).49 Also, the FDA defines clinical response as a reduction in the total Mayo score of 30% or more from baseline with a decrease in rectal bleeding subscore greater than or equal to 1 point or absolute rectal bleeding subscore of less than or equal to 1.{US Food and Drug Administration.49
Limitations
Although the Mayo score is a widely recognized UC activity index and is accepted by Canadian and American regulatory bodies, the instrument has limitations. Cooney et al. argued that the PGA and the endoscopy subscore components of the Mayo score are subjective and, consequently, introduces variability and lack of precision into the index. The PGA also includes a sigmoidoscopy score, which introduces double counts of some elements.75 Additionally, a single general item in the PGA is not sensitive to adequately capture benefits in all or some of the important signs and symptoms of UC. As a result, the FDA does not recommend using the PGA subscore or the full Mayo score to support a marketing decision; however, it does recommend the endoscopy, stool frequency, and rectal bleeding subscores as outcome measures for clinical trials until a well-defined and reliable instrument if available.49
Geboes Score
The Geboes score is a commonly used histologic index in UC for assessing disease severity and/or activity.36,37 It is a classification system consisting of 6 grades, with 4 subgrades each, that are meant to be progressive. Grading is performed on hematoxylin-eosin stained sections from biopsies obtained in the colonic mucosa. The grades and subgrades are defined as follows:
Grade 0 (structural change only): No abnormality (0.0), mild abnormality (0.1), mild/moderate diffuse (0.2), and severe diffuse or multifocal abnormalities (0.3).
Grade 1 (chronic inflammation): No abnormality (0.0), mild abnormality (0.1), mild/moderate diffuse (0.2), and severe diffuse or multifocal abnormalities (0.3).
Grade 2 (2A: lamina propria neutrophils; 2B: lamina propria eosinophils) : No abnormality (0.0), mild abnormality (0.1), mild/moderate diffuse (0.2), and severe diffuse or multifocal abnormalities (0.3).
Grade 3 (neutrophils in the epithelium): No abnormality (0.0), mild abnormality (0.1), mild/moderate diffuse (0.2), and severe diffuse or multifocal abnormalities (0.3).
Grade 4 (crypt destruction): No abnormality (0.0), mild abnormality (0.1), mild/moderate diffuse (0.2), and severe diffuse or multifocal abnormalities (0.3).
Grade 5 (erosions or ulcers): No abnormality (0.0), mild abnormality (0.1), mild/moderate diffuse (0.2), and severe diffuse or multifocal abnormalities (0.3).36
Subgrades are assessed based on the worst area of the biopsy. The higher the grade or subgrade, the greater the inflammation. The Geboes score may also be converted into a continuous scale with each subgrade being assigned an ordinal value, yielding values between 0 and 22.36
Psychometric Properties
An evaluation of the construct validity of the Geboes score in a cohort of 442 patients with UC previously enrolled in other studies found that the score was strongly correlated with the Nancy index score (r = 0.88, P < 0.001).76 Another study that evaluated the construct validity of the Geboes score in 131 patients with UC found that it was strongly correlated with the Mayo endoscopic subscore (r = 0.54, R < 0.001).64 Finally, in a study of 82 patients with UC (mean age = 47.5 years; SD = 15.9 years, the Geboes score was found to be strongly correlated with the endoscopic activity index (r = 0.77, P < 0.001) and weakly correlated with the clinical activity index (r = 0.40, P < 0.001) and C-reactive protein level (r = 0.42, P < 0.001).65 In a study of 49 patients with UC (mean age = 40.2 years; SD = 2.9 years), the criterion validity of the Geboes score was evaluated against a 100 mm global disease activity VAS (the most severe activity was scored as 1 and no disease activity was scored as 0).63 The Geboes scale, when used a continuous scale, was found to be strongly correlated with the VAS (r = 0.66; 95% CI, 0.57 to 0.72). The Geboes and the VAS were moderately correlated when the Geboes score was used as a 6-grade ordinal scale (r = 0.61; 95% CI, 0.50 to 0.67), and weakly correlated when used as a categorical scale (inactive = grade 0 or 1, mildly active = grade 2 or 3, severely active = grade 4 or 5) (r = 0.58; 95% CI, 0.48 to 0.64).63
Mosli et al. also evaluated intra-rater and inter-rater reliability of the Geboes score by having 5 pathologists independently reviewed 50 digital slide images 3 times, approximately 2 weeks apart.63 When used as a 6-grade ordinal scale, the Geboes score was found to have almost perfect intrarater agreement (ICC: 0.82; 95% CI, 0.73 to 0.88), and moderate inter-rater agreement (ICC: 0.56; 95% CI, 0.39 to 0.67). When used as a continuous scale, the Geboes score demonstrated almost perfect intra-rater agreement (ICC = 0.84; 95% CI, 0.80 to 0.89) and moderate inter-rater agreement (ICC = 0.60; 95% CI, 0.46 to 0.71).63 Intra-rater reliability of the individual items of the Geboes found strong agreement for the detection of erosions and ulcerations (ICC = 0.81; 95% CI, 0.72 to 0.86), substantial agreement for the detection of neutrophils in the epithelium (ICC = 0.71; 95% CI, 0.64 to 0.78), and erosion or ulceration (ICC = 0.78; 95% CI, 0.71 to 0.84), and moderate agreement for the detection of crypt destruction (ICC = 0.61; 95% CI, 0.53 to 0.68) and lamina propria eosinophils (ICC = 0.59; 95% CI, 0.50 to 0.67).63 Inter-rater reliability of the individual items of the Geboes scale ranged from weak (detection of lamina propria eosinophils: ICC = 0.26; 95% CI, 0.15 to 0.45; and detection of neutrophils in the epithelium: ICC = 0.48; 95% CI, 0.37 to 0.58) to moderate (erosions or ulcerations (ICC = 0.56; 95% CI, 0.43 to 0.67); and detection of chronic inflammatory infiltrate: ICC = 0.64; 95% CI, 0.50 to 0.74).63
In a later Mosil et al. study consisting of 155 patients with UC (mean age, 41.7 ± 14.1 years), the Geboes scoring system was found to have almost perfect intra-rater agreement (ICC = 0.88; 95% CI, 0.79 to 0.93) and substantial inter-rater agreement (ICC = 0.79; 95% CI, 0.63 to 0.87).66 In the same study, the responsiveness of the Geboes scoring system was evaluated using an analysis of standardized effect size (SES) and Guyatt’s responsiveness statistics (GRS).66 The responsiveness to change was moderate to large based on SES and GRS of 1.87 (95% CI, 1.54 to 2.20) and 1.23 (95% CI, 0.97 to 1.50), respectively for the Geboes score based on treatment assignment, and 1.05 (95% CI, 0.78 to 1.31) and 0.84 (95% CI, 0.59 to 1.09), respectively based on the Mayo clinical subscore of at least 2 points.66 Histological activity, defined as Geboes score ≥ 3.1, was found to be an independent risk factor for clinical relapse in patients with UC (OR = 4.31; 95% CI, 1.52–12.21; P = 0.006).77
Minimal Important Difference
Histological healing was empirically defined in specimens of endoscopically uninflamed tissue as the average Geboes score below 2.36
Short Form (36) Health Survey
The SF-36 is a generic self-reported health assessment questionnaire that has been used in clinical trials to study the impact of chronic disease on HRQoL. The original version (SF-36v1) was released in 1992; however, a revised version (SF-36v2), released in 1996, is used more commonly. The SF-36 consists of 8 domains: physical functioning, role limitations due to physical health problems, bodily pain, general health, vitality, social functioning, role limitations due to emotional health problems, and mental health. The SF-36 also provides 2 component summaries: the PCS and the MCS, which are scores created by aggregating the 8 domains. The SF-36 PCS and MCS and individual domains are each measured on a scale of 0 to 100, with an increase in score indicating improvement in health status.38
Psychometric Properties
The construct validity, reliability, and responsiveness of the SF-36v2 among patients with UC was recently assessed in a systematic review that consisted of 43 studies.41 Construct validity of the SF-36 subscales was supported by a moderate-to-high correlation with the corresponding domains of 5 patient-reported tools, including the IBD Quality of Life Questionnaire, Brief Pain Inventory, Short Health Scale, and Rating Form of IBD Patient Concerns (r ≥ 0.4).41 The SF-36 was found to discriminative between subgroups of patients classified by disease activity, symptom status, and comorbidity status. In terms of reliability and responsiveness, 1 included study found that the SF-36 had high internal consistency for all 8 subscales (Cronbach alpha > 0.7) and high test–retest reliability for 6 of the 8 subscales (ICC > 0.7); the 2 subscales that had lower test–retest reliability were the role physical and role emotional subscales with ICCs of 0.64 and 0.63, respectively. The possibility of high floor and ceiling effects may explain the lower test–retest reliability for the role physical and role emotional subscale.41 Finally, the systematic review found that the SF-36 scale and its subscores were responsive to treatment-related changes following effective treatment in noncomparative trials or among treated patients relative to controls in RCTs.41
Minimal Important Difference
An absolute score increase of 3 to 5 points for both the PCS and MCS, as well as the individual scores in the SF-36, was shown to capture MID across various conditions, including colitis.67
Five-Level EQ-5D
The EQ-5D-5L is a generic self-reported HRQoL outcome measure that may be applied to a variety of health conditions and treatments.39 The first 2 components of the EQ-5D-5L assesses 5 domains: mobility, self-care, usual activities, pain/discomfort and anxiety/depression.39 Each domain has 5 levels: no problem; slight problems; moderate problems; severe problems; and extreme problems. A descriptive system that classifies respondents (aged ≥ 12 years) based on the following 5 dimensions: mobility, self-care, usual activities, pain/discomfort, and anxiety/depression. The EQ-5D-5L has 5 possible levels for each domain and respondents are asked to choose the level that reflects their health state for each of the 5 domains resulting in 3,125 possible health states.39 The second component of the EQ-5D-5L is a 20 cm visual analogue scale (EQ VAS) that has end points labelled 0 and 100, with respective anchors of “worst imaginable health state” and “best imaginable health state.” Respondents are asked to rate their health by drawing a line from an anchor box to the point on the EQ VAS which best represents their health on that day. Thus, the EQ-5D-5L produces 3 types of data for each respondent:
a profile indicating the extent of problems on each of the 5 dimensions represented by a 5-digit descriptor (e.g., 15121, 33211)
a population preference-weighted health index score based on the descriptive system
a self-reported assessment of health status based on the EQ VAS.
The EQ-5D-5L tool have been applied to a wide range of health conditions and treatments, including IBD.78,79 The EQ-5D-5L index score is generated by applying a multi-attribute utility function to the descriptive system.40 Different utility functions are available that reflect the preferences of specific populations (e.g., US or UK). Scores less than 0 represent health states that are valued by society as being worse than dead, while scores of 0 and 1.00 are assigned to the health states “dead” and “perfect health,” respectively.
Psychometric Properties
The face and content validity of the EQ-5D-5L index score was investigated by Herdman et al. using focus groups.80 An Australian study of 175 patients with UC (mean age, 42 ± 15 years) that examined the construct validity of the EQ-5D-5L found that it was strongly correlated with the disease-specific Inflammatory Bowel Disease Questionnaire (IBDQ) (r = 0.69, P < 0.001).68 Mean EQ-5D-5L scores were found to be significantly greater for patients with UC in remission (mean = 0.81, SD = 0.18) than for patients who had active disease (mean = 0.72, SD = 0.19). Likewise, among patients with active UC, lower scores were observed in patients with mild disease (mean = 0.78, SD = 0.18) than in those with moderate to severe disease (mean = 0.68, SD = 0.19).68 A similar pattern was observed for EQ VAS scores.
A prospective, noninterventional study conducted at 37 hospital centres in Spain found a consistent and linear relationship between the EQ-5D-5L and the SCCAI among a group of 199 patients with UC (mean age, 39 ± 11 years).69 In this study, patients with UC completed both the EQ-5D-5L and SCCAI at 3 and 6 months. The SCCAI was also completed by treating gastroenterologists who were blinded to patient responses. The construct validity of the EQ-5D-5L was then evaluated by mapping its index scores to those of patient- and physician-completed SCCAIs. The study found a moderate correlation between EQ-5D-5L index scores and patient-completed SCCAI (r = –0.49, P < 0.001), and a strong correlation between EQ-5D-5L index scores and physician-completed SCCAI (r = –0.53, P < 0.001).69 In particular, a moderate to strong correlation was observed between the “general well-being” item on the patient-completed and physician-completed SCCAIs to the “pain/discomfort” (r = 0.52 to 0.54) and “usual activities” items (r = 0.38 to 0.40) on the EQ-5D-5L scores at month 3; and for “general well-being” and “pain/discomfort” (r = 0.64 to 0.66) and “usual activities” items (r = 0.57 to 0.61) at month 6.69 In addition, decline in HRQoL was observed during disease flare. Indeed, the difference in EQ-5D-5L index scores from 3 to 6 months was lower in patients who experienced worsening disease (mean, –0.069 ± 0.07) compared with patients in stable condition (mean, 0.022 ± 0.11) or improving disease state (mean, 0.035 ± 0.13).69 In terms of reliability, a moderate agreement was observed across all domains of patient-completed and physician-completes SCCAIs (kappa range, 0.41 to 0.58), except for fair agreement between the “anxiety/depression” domain and patient-completed SCCAI (kappa = 0.28).69 Finally, agreement between the EQ-5D-5L and patient-completed and physician-completed SCCAIs index scores was 74.2% and 68.8%, respectively.69 To date, there is no literature evaluating the responsiveness of the EQ-5D-5L among patients with UC over time. However, in the general population and across multiple other conditions (e.g., musculoskeletal/orthopedic, lung/respiratory, cancer) pooled from 32 countries, the EQ-5D-5L index score was observed to be responsive in detecting improved health with a standardized response means ranging (SRM) between 0.31 and 0.86; stable health with SRM ranging between −0.09 and 0.31; and deteriorated health with SRM ranging between −0.47 and 0.44.78
Minimal Important Difference
A literature search was conducted to identify the minimal clinically important difference (MCID) of the EQ-5D-5L in patients with UC and none were identified. However, Stark et al. estimated a disease-specific MCID of the EQ-5D-3L using a regression model; the MCIDs for improved health were reported to be 10.9 for the VAS, and 0.050 (European Union) and 0.076 (UK) for the EQ-5D-3L index score.70 This is within the range of other reported MCIDs for the EQ-5D-3L index score of 0.033 to 0.074.40
Work Productivity and Activity Impairment Questionnaire – Ulcerative Colitis
The WPAI is one of the most frequently used patient-reported, work-related outcome measures.42,71 The WPAI measures the impact of general health problems (WPAI – General Health) or the impact of a specific disease, such as UC (WPAI-UC) on 4 domains: absenteeism (work time missed due to a patient’s UC), Presenteeism (impairment while working due to a patient’s UC), presenteeism (impaired productivity at work), overall work impairment (overall productivity loss, accounting for both absenteeism and presenteeism, due to a patient’s UC), and nonwork activities (activity impairment). The WPAI-UC is a self-administered 6-item questionnaire with a 7-day recall period.42 The items include employment status (employed or not employed); hours at work missed because of UC; hours at work missed because of other reasons; hours actually worked; overall impairment in productivity while working (VAS from 0 to 10) and overall impairment in regular activities (VAS from 0 to 10) due to UC. Scores from all 4 domains are expressed as percentages (0% to 100%) of impairment, with higher values indicating greater impairment due to the health problem and less productivity.41
Psychometric Properties
The psychometric properties of the WPAI in patients with UC were evaluated in a systematic review consisting of 8 articles and 5 posters.41 One included study that assessed the convergent validity between the WPAI domains and other HRQoL measures, including the Short Inflammatory Bowel Disease Questionnaire and the SF-12v2 found that the strongest evidence for convergent validity was reported between all WPAI domains and the Short Inflammatory Bowel Disease Questionnaire bowel symptoms (Spearman rank-order coefficient r = 0.47 to 0.68) and SF-12v2 bodily pain (r = 0.52 to 0.55) subscores.71 With the exception of absenteeism, the WPAI domains also converged with the Short Inflammatory Bowel Disease Questionnaire social function, and SF-12v2 role physical and role emotional subscores.41 Convergent validity was also assessed between the WPAI and the SCCAI, the UC Disease Activity Index (UC-DAI), and the partial Mayo score in 3 individual studies.71 Inter-scale correlations between the WPAI domains and disease - activity measures ranged from 0.32 to 0.85 (median = 0.45). Across the 3 studies, convergence with disease activity was supported for presenteeism, overall work impairment (OWI) and activity impairment (r = 0.43 to 0.60); the median correlation for absenteeism was not far behind (0.39).41 Furthermore, a known-group validity assessment demonstrated that patients with worse health outcomes scored worse on the WPAI than patients with better health outcomes based on partial Mayo, SCCAI, UC-DAI, and the Functional Assessment of Chronic Illness Therapy Fatigue scale (FACIT-Fatigue) disease severity measures.71 In terms of responsiveness, data from 3 RCTs investigating either multi-matrix mesalamine treatment or adalimumab in patients with UC found that the WPAI was responsive to treatment effect, as patients reported an approximate 20% decrease in presenteeism, OWI and activity impairment, and an 8% decrease in absenteeism.71 In another study included in the review, the ability of WPAI domains to detect changes was evaluated by assessing the magnitude of change among patients demonstrating changes in disease states (i.e., change from active disease to remission, or vice versa).71 The study demonstrated that patients with active UC disease who achieved remission at week 8 reported a 25% to 30% decrease in presenteeism, OWI, and activity impairment, and a 9% decrease in absenteeism. The inverse was found in patients with disease relapse.71 Test–retest reliability of the WPAI domains was assessed in 1 of the studies included in the review81 that compared scores at the start and end of an open-label maintenance treatment period in patients whose remission status was unchanged (as determined by the UC-DAI).71
Minimal Important Difference
There is currently no defined MID for the WPAI for patients with UC. Among patients with Crohn disease, an MID is estimated as a decrease of 7 points.82
Pharmacoeconomic Review
Abbreviations
AE
adverse event
CEF
cost-effectiveness frontier
CT
conventional therapy
ITC
indirect treatment comparison
NMA
network meta-analysis
QALY
quality-adjusted life-year
TNF
tumour necrosis factor
UC
ulcerative colitis
Executive Summary
The executive summary comprises 2 tables (Table 1 and Table 2) and a conclusion.
Item | Description |
|---|---|
Drug product | Ozanimod (Zeposia), 0.23 mg (0.25 mg ozanimod HCl), 0.46 mg (0.50 mg ozanimod HCl), 0.92 mg (1.0 mg ozanimod HCl) capsules |
Submitted price | Ozanimod, 0.23 mg: $68.4929 per capsulea Ozanimod, 0.46 mg: $68.4929 per capsulea Ozanimod, 0.92 mg: $68.4932 per capsuleb |
Indication | For the treatment of adult patients with moderately to severely active ulcerative colitis (UC) who have had an inadequate response, loss of response, or were intolerant to either conventional therapy or a biologic agent |
Health Canada approval status | NOC |
Health Canada review pathway | Standard |
NOC date | April 8, 2022 |
Reimbursement request | As per indication |
Sponsor | Celgene Inc., a Bristol Myers Squibb Company |
Submission history | Previously reviewed: Yes Indication: Multiple sclerosis, relapsing-remitting Recommendation date: June 23, 2021 Recommendation: Do not reimburse |
HCl = hydrochloride; NOC = Notice of Compliance.
a$479.45 per multiple strengths 7-unit starter pack, available for days 1 to 7 only.
b$1,917.81 per 28-unit pack.
Table 2: Summary of Economic Evaluation
Component | Description |
|---|---|
Type of economic evaluation | Cost-utility analysis Decision tree followed by a Markov cohort model |
Target populations | Adult patients (≥ 18 years of age) with moderately to severely active UC with or without prior exposure to biologica drugs (i.e., biologic-experienced or biologic-naive) |
Treatment | Ozanimod |
Comparatorsb |
|
Perspective | Canadian publicly funded health care payer |
Outcomes | QALYs and LYs |
Time horizon | Lifetime (58 years) |
Key data source | The TRUE NORTH (NCT02435992) trial informed treatment efficacy and safety for ozanimod vs. placebo; an unpublished sponsor-commissioned NMA informed comparative treatment efficacy between ozanimod and biologic comparators |
Submitted results | Biologic-naive population:
Biologic-experienced population:
|
Key limitations |
|
CADTH reanalysis results |
|
CT = conventional therapy; IL = interleukin; JAK = Janus kinase; LY = life-year; NMA = network meta-analysis; QALY = quality-adjusted life-year; SC = subcutaneous; TNF = tumour necrosis factor; UC = ulcerative colitis.
aBiologic refers to anti-TNF therapies (infliximab, adalimumab, and golimumab), and small-molecule drugs (tofacitinib, ustekinumab, and vedolizumab).
bAll comparators are included in the biologic-naive and biologic-experienced population analyses.
Conclusions
Based on an appraisal of the TRUE NORTH trial, the CADTH clinical reviewers found that ozanimod was efficacious in inducing and maintaining clinical remission and clinical response, as well as in achieving mucosal healing, durable clinical response, and histologic remission when compared with placebo in patients with moderately to severely active ulcerative colitis (UC). However, CADTH noted that the generalizability of the trial data to the Canadian setting was limited due to the re-randomization study design and the option for enrolment into an open-label trial during the maintenance period. Since there are no trials comparing ozanimod with the advanced therapies of interest (i.e., biologics and small-molecule drugs), comparisons among treatments were based on the sponsor-commissioned network meta-analysis (NMA). The CADTH Clinical Review determined that the applicability of the indirect treatment comparison (ITC) is impacted by the heterogeneity of study designs and patient populations across trials; the impact on the results of the NMA could not be assessed. An additional published ITC was identified, although similar limitations were noted in terms of the heterogeneity of the study design and patient populations. CADTH concluded there is a high degree of uncertainty with respect to the comparative clinical efficacy and safety of ozanimod versus advanced treatments for moderate to severe UC.
In its base case, CADTH attempted to address the limitations identified with the economic analysis submitted by the sponsor by making the following changes in model parameter values and assumptions, in consultation with clinical expert feedback: excluding ustekinumab as a comparator, assuming the clinical efficacy and safety of all biologic treatments (note that biologic refers to anti–tumour necrosis factor [anti-TNF] therapies and small-molecule drugs) to be equal to that of ozanimod; applying alternate utility values for non-surgical health states, assuming the proportion of patients receiving an escalated dose to be 0% across biologic therapies, adjusting the proportion of patients receiving concomitant conventional therapy (CT) across biologic therapies to reflect Canadian clinical practice, and aligning disease management resource use to published literature. However, these reanalyses need to be considered in the context of the submitted model, as concerns regarding the transparency and validity of the model output were noted.
Results from the CADTH base case were similar to the sponsor’s base case in that ozanimod was not among the optimal treatments (i.e., not on the cost-effectiveness frontier [CEF]) in either population (biologic-naive or biologic-experienced). Ozanimod was strictly dominated (more costly and less effective) when compared with infliximab biosimilar in both the biologic-naive and biologic-experienced populations. A price reduction of between 43% and 73% is necessary for ozanimod to be considered an optimal therapy at a $50,000 per quality-adjusted life-year (QALY) willingness-to-pay threshold, depending on the patient population and comparative data assumptions.
Stakeholder Input Relevant to the Economic Review
This section is a summary of the feedback received from the patient groups, clinician groups, and drug plans that participated in the CADTH review process.
Two patient groups provided input for the ozanimod submission for UC: Crohn and Colitis Canada and the Gastrointestinal Society. The input was based on patient surveys, published literature, and interviews. Some of the surveys incorporated patients with experience with ozanimod, while most of the feedback included patients who received conventional and biologic therapies. The most important outcome for patients with moderate to severe UC is sustained remission and treatment response. Currently available first-line treatments include anti-inflammatory drugs together with corticosteroids, as well as second-line treatments typically consisting of immunomodulators or immunosuppressants and biologics, which tend to be prescribed concomitantly with corticosteroids. While patients with mild to moderate levels of UC may experience improvements in their overall condition with initial treatments, patients with moderately to severely active UC often experience loss of response and/or remission under various treatment options and, as such, continual treatment switching is required to achieve an adequate response until all therapeutic options are exhausted. Crohn and Colitis Canada included input from 7 patients who had experience with the drug under review through a clinical trial. The majority of these patients identified benefits with ozanimod, including ease of administration, being able to resume productive and social lives, as well as achieving improvements with chronic pain, exhaustion, and depression. Patients want treatments to be safe, improve quality of life, and allow them to perform daily activities with ease, as well as increase the duration of remission, improve symptoms, and decrease side effects.
No clinician input was received for this review.
CADTH-participating drug plans provided feedback centred on health resource use regarding the first-dose administration of ozanimod. As studies have indicated a non-negligible increased risk of bradycardia during the first-dose administration of ozanimod, the drug plan input noted the potential need to initiate treatment in a hospital or clinical setting to monitor detrimental cardiac outcomes.
Several of these concerns were addressed in the sponsor’s model:
The most important outcome for patients with moderately to severely active UC is sustained clinical remission and/or response, which are the primary health states in the maintenance phase of the sponsor’s model.
The model incorporates serious adverse events (AEs) and quality of life measures.
A proportion of patients are prescribed a mix of aminosalicylates, corticosteroids, and conventional immunomodulators as concomitant therapy while receiving biologics.
In addition, CADTH addressed some of these concerns as follows:
Although there are no published data on loss of response and remission from the maintenance clinical trials to inform how they vary over the patients’ lifetimes, CADTH considered input from patient groups and clinical expert feedback regarding the challenges of sustaining therapeutic targets indefinitely. To address this issue, CADTH conducted scenario analyses with the aim of illustrating the possible impact of a declining loss of response risk, whereby a 1-time 30% reduction in treatment efficacy was applied to the maintenance phase of all treatments.
CADTH was unable to address the following concerns raised from stakeholder input:
Input from patient groups and clinical expert feedback confirmed that the disease management journey for the population with moderate to severe UC is characterized by continual treatment switching until all therapeutic options are exhausted. However, CADTH was not able to consider multiple lines of treatment, as this would require currently unavailable efficacy data from populations whose condition has failed to respond to 2 biologics.
Economic Review
The current review is for ozanimod (Zeposia) for adult patients (≥ 18 years of age) with moderately to severely active UC who have had an inadequate response, a loss of response, or were intolerant to either CT or a biologic drug.
Economic Evaluation
Summary of Sponsor’s Economic Evaluation
Overview
The sponsor submitted a cost-utility analysis of ozanimod compared with other biologic agents and CT. The term biologic agent was used as a catch-all term for anti-TNF and small-molecule therapies. Aligned with Health Canada’s indicated population, the modelled population comprised adults in Canada between the ages of 18 and 75 years with moderately to severely active UC (defined as a Mayo score of 6 to 12 accompanied by a Mayo rectal bleeding subscore ≥ 2)1 who experienced an inadequate response, a loss of response, or were intolerant to either CT or biologic drugs. The cost-utility analysis is conducted separately for the biologic-naive and -experienced populations.
Ozanimod is a once-daily, orally administered novel modulator of sphingosine 1-phosphate receptor pathways.2 Treatment with ozanimod is initiated with a 7-day dose-escalation regimen to mitigate cardiac effects (days 1 to 4: 0.23 mg daily capsule; days 5 to 7: 0.46 mg daily capsule), followed by a maintenance dosage of 0.92 mg daily from day 8 onward.3 The ozanimod regimen captured in the economic model reflects the Health Canada dosing regimen. At the sponsor’s reported price of $68.49 per capsule (multiple strengths: 0.23 mg, 0.46 mg, and 0.92 mg),1 the annual cost of ozanimod is $25,000.
The comparators for this analysis include TNF inhibitors (i.e., adalimumab, adalimumab biosimilar, infliximab, infliximab biosimilar, golimumab), 1 Janus kinase inhibitor (i.e., tofacitinib), 3 cell adhesion molecule inhibitors (i.e., ustekinumab, vedolizumab IV, vedolizumab subcutaneous (SC), and CT (i.e., mix of 5-aminosalicylates, corticosteroids, and immunomodulators). These comparators are the same for both the biologic-naive and biologic-experienced populations. The recommended dosing regimen for comparators is sourced from product monographs and their costs sourced from the Ontario Drug Benefit Formulary. These are summarized in Table 9. The annual maintenance costs for the comparators ranged from $12,253 for an adalimumab biosimilar to $32,152 for ustekinumab, based on the recommended doses.
The economic evaluation was conducted over a lifetime time horizon (approximately 58 years), from the perspective of the Canadian public health care payer. Costs and clinical outcomes (life-years and QALYs) are discounted at 1.5% per annum.
Model Structure
The sponsor submitted a hybrid model structure that considers a short-term induction phase (decision tree) and a longer-term maintenance phase (Markov model) to evaluate clinical outcomes and costs.1 The same model structure was used for both biologic-naive and -experienced patient populations. Patients entered the model in the induction phase with active UC and initiated treatment. Patients who entered the model on a biologic drug could experience 1 of the following outcomes: remission, response without remission, discontinuation of treatment due to treatment-related AEs, or failure to achieve response. Patients who achieved remission or response without remission at the end of the induction phase entered the maintenance phase of the Markov model in their corresponding health states, while nonresponders and those who discontinued biologic therapy due to AEs moved to the CT induction branch of the decision tree. For patients who entered the model in the induction phase on CT, as well as for those who re-entered the induction phase on CT following failure of a biologic drug (i.e., the biologic-experienced population), it was possible to achieve remission, achieve response without remission, or fail to achieve response. Those who responded to CT entered the maintenance phase in their corresponding health states, while those who experienced treatment failure entered the maintenance phase in active UC.
The maintenance phase was composed of 9 Markov health states: remission, response without remission, active UC, surgery, post-surgery remission, post-surgery complications, revision surgery, post-revision surgery remission, and death.1 During the maintenance phase, patients in the remission and response without remission health states received treatment until they experienced loss of response, upon which patients who entered the model on ozanimod or biologics or CT transitioned to the active UC health state, discontinued treatment, and moved to the CT induction phase. Patients treated with ozanimod or other biologic drugs could experience treatment-related AEs during the maintenance phase, whereupon they were assumed to discontinue treatment and re-enter the decision tree, undergoing the induction phase on the CT branch. Based on their response status at the end of the induction phase on CT, these patients were distributed across the active UC, remission, and response without remission health states, capturing the probability that some patients could respond to CT after experiencing the failure of their primary biologic therapy.
Patients for whom CT was a second-line treatment in the maintenance phase could lose response and transition from the remission or response without remission health states to active UC. These patients stayed in the active UC health state until they underwent colectomy, died, or reached the end of the model’s time horizon. Following the first colectomy, patients discontinued treatment for the remainder of their lifetime and remained in the surgery health state for 6 months.1 This is aligned with clinical practice, as colectomy-specific surgical procedures tend to be completed in stages. After surgery, patients could experience complications or achieve remission. The former could transition to the post-surgery complications health state or remain in remission, whereas the latter could remain in post-surgery complications or transition to the revision surgery health state, upon which patients entered the post-revision surgery remission health state for the remainder of the model’s time horizon. Finally, patients could transition to death from any of the maintenance model health states at any time.
In addition to direct comparison, the sponsor’s model allowed for a treatment sequence option (Figure 1) that allowed biologic-naive patients to receive 2 lines of biologic drugs and a third line of CT.1
Model Inputs
Baseline patient characteristics were derived from the TRUE NORTH clinical trial4 and informed the drug dosage regimens, the age- and gender-specific distribution of the general mortality risk, and the length of the lifetime horizon. The average patient in the cohort was 41.4 years old, weighed 74.4 kg, and was more likely to be male (57.1%).1 The sponsor submitted an NMA5 in the absence of head-to-head trial data comparing ozanimod with its biologic comparators. Bayesian NMAs were performed using random- or fixed-effects models, with a focus on the clinical response and clinical remission outcomes in the primary analyses.5 These were conducted for 3 patient populations: biologic-naive, biologic-experienced, and mixed. CT efficacy was represented by the placebo arm of the clinical trials included in the NMA.
The mean absolute probabilities of achieving remission, response, and neither response nor remission that were used in the induction and maintenance phases of the model were derived from the NMA’s induction- and maintenance-specific phases of the clinical trials (Table 11, Table 12, Table 13, and Table 14; Appendix 3). Due to the lack of long-term efficacy data for UC treatments beyond the typical trial duration of 1 year, a key assumption in the sponsor’s approach was that of constant treatment effect and corresponding loss of response over the lifetime time horizon. Discontinuation due to treatment-emergent AEs derived from the systematic literature review conducted by the sponsor was applied at a constant rate each cycle to the cohort on ozanimod or biologic therapy and differed by treatment, patient population, and phase (i.e., induction or maintenance).
Probabilities for transitioning from the active UC to surgery health state, as well as from the post-surgery complications to the revision surgery health state, were derived from the estimate by Targownik et al. (2012) of a 20-year risk of colectomy based on data from the University of Manitoba Inflammatory Bowel Disease Epidemiology Database.6 The rate informing the proportion of patients that experienced complications post surgery originated from a US-based study of patients with UC who underwent colectomy between 2005 and 2008,7 while the probability of experiencing complications after post-surgery remission was informed by the estimate by Suzuki et al. (2012) of the long-term cumulative risk of pouchitis for patients in Japan with UC who underwent a total proctocolectomy between 1986 and 2009.8
Patients accrued health state–specific QALYs, as well as treatment-related and health state–specific costs as they transitioned through changes in disease activity. Utility values for non-surgical health states were sourced from Woehl et al. (2008),9 while values for surgical states were obtained from Arseneau et al. (2006).10 These were applied to all patients alive in each health state using an age- and sex-adjusted utility approach.11 In addition, the model applied a disutility multiplier to patients experiencing serious infections in each 2-week cycle to partially account for the impact that treatment-emergent AEs could have on quality of life. The model applied age- and sex-specific annual probabilities of mortality derived from general population life tables from Statistics Canada.12 The base case assumed a higher risk of dying for patients with moderately to severely active UC who underwent surgery (standardized mortality ratio = 1.3) based on findings from a meta-analysis of overall and cause-specific mortality in UC.13
Resource use by health state was informed mostly by a study from Tsai et al. (2008).14 Based on the advice of a Canadian clinical expert, the sponsor downwardly adjusted resource use for consultant visits and blood tests for 4 specific health states, namely: response without remission, active UC, surgery, and revision surgery.1 Unit dose and dosing frequency during the model’s induction and maintenance phase, for both normal and escalated doses, were derived from the respective product monographs for ozanimod and biologic therapies.1 The model assumed that 30% of patients would receive escalated doses during the maintenance phase.1 The proportions of patients with escalated doses treated with ozanimod and vedolizumab (SC) were set to 0 in the sponsor’s model, providing that dose escalation had not been evaluated in the respective clinical trials.15,16
Drug acquisition costs for ozanimod were based on the sponsor’s submitted price; the unit cost for ustekinumab IV was derived from the Saskatchewan Formulary, while costs for every other biologic and non-biologic comparator were obtained from the Ontario Drug Benefit Formulary. Wastage costs for IV drugs with weight-based dosing were considered by assuming 1-time vial usage.
Summary of Sponsor’s Economic Evaluation Results
The sponsor conducted the reference case for the biologic-naive and biologic-experienced population of patients with moderate to severe UC through a probabilistic sensitivity analysis with 5,000 simulations.1 The deterministic and probabilistic results were similar. The probabilistic findings are presented subsequently.
Base-Case Results
The sequential multiple comparisons of cost-utility findings for each population are presented in Table 3 and Table 4. For the biologic-naive population, the CEF was represented by CT and tofacitinib, while for the biologic-experienced population, the CEF was represented by CT, infliximab biosimilar, and tofacitinib. All other treatments were either strictly or extendedly dominated. Ozanimod was strictly dominated by infliximab biosimilar in the biologic-naive population, signifying that the intervention represented higher costs and worse health outcomes than infliximab biosimilar.
Table 3: Summary of the Sponsor’s Economic Evaluation Results, Biologic-Naive
Drug | Total costs | Total QALYs | Sequential ICER ($/QALY) |
|---|---|---|---|
Conventional therapy | $130,018 | 12.039 | Reference |
Tofacitinib | $172,339 | 12.692 | $64,809 |
ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year.
Note: The submitted analysis is based on the publicly available prices of the comparator treatments. Only treatments on the cost-effectiveness frontier are reported in this table.
Source: Sponsor’s pharmacoeconomic submission.1
Table 4: Summary of the Sponsor’s Economic Evaluation Results, Biologic-Experienced
Drug | Total costs | Total QALYs | Sequential ICER ($/QALY) |
|---|---|---|---|
Conventional therapy | $131,218 | 11.913 | Reference |
Infliximab biosimilar | $151,408 | 12.206 | $68,904 |
Tofacitinib | $157,454 | 12.282 | $79,495 |
ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year.
Note: The submitted analysis is based on the publicly available prices of the comparator treatments. Only treatments on the cost-effectiveness frontier are reported in this table.
Source: Sponsor’s pharmacoeconomic submission.1
Moreover, ozanimod was extendedly dominated by a combination of CT and infliximab biosimilar in the biologic-experienced population, signifying that ozanimod was not on the CEF and was not as cost-effective as other alternatives. Table 17 and Table 18 present the results from the sponsor’s sequential analysis, which include dominated treatments for the biologic-naive and biologic-experienced populations, respectively (Appendix 3).
Sensitivity and Scenario Analysis Results
The sponsor conducted sensitivity and scenario analyses. Pairwise 1-way sensitivity analyses were conducted using the deterministic model to assess the impact of specific parameters on the incremental cost-effectiveness ratio, incremental QALYs, and incremental costs for the biologic-naive and biologic-experienced populations. The parameters that had the largest impact on the model’s findings were the clinical remission rates as well as the utility values assigned to clinical remission and active UC.
The sponsor’s economic submission considered 13 alternative scenarios for further analysis. These were pairwise comparisons that evaluated each comparator treatment relative to ozanimod; hence, they do not provide relevant information when assessing the cost-effectiveness of ozanimod in the current setting. The sponsor conducted a treatment sequence analysis that compared multiple treatment lines for the biologic-naive population only. The treatment sequence containing ozanimod (i.e., ozanimod to vedolizumab IV to CT) was strictly dominated.
CADTH Appraisal of the Sponsor’s Economic Evaluation
CADTH identified several key limitations to the sponsor’s analysis that have notable implications for the economic analysis:
High degree of uncertainty in the comparative efficacy of ozanimod and comparators: Although the sponsor performed statistical adjustments to the maintenance treat-through data that were intended to better align with what would be observed in a re-randomized design, the recalculations do not completely mitigate the heterogeneity associated with differences between induction responders in treat-through versus re-randomized trials. The clinical expert consulted by CADTH noted that the maintenance recalculations do not sufficiently address whether and how the half-life of the initial therapies that patients receive during induction influences response during maintenance. Even with the sponsor’s adjustment, if patients received a biologic therapy with a long half-life during induction and were re-randomized to maintenance, the placebo rate in that re-randomized group would be higher than if patients received a shorter-acting therapy during induction. CADTH considered that the ITC results used in the sponsor’s model may have underestimated the uncertainty in treatment effects, since ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||. CADTH was unable to assess the concerns identified in this limitation because the sponsor’s model did not have an option to explore the NMA results using random-effects models. Although differences between biologic therapies may exist, the available evidence provides limited guidance on the magnitude and direction of those differences.
CADTH performed a reanalysis by assuming equal clinical efficacy among biologic therapies, including ozanimod. Since CT efficacy was represented by the placebo arms of the clinical trials included in the NMA, it remained unchanged. In accordance with the clinical expert consulted by CADTH, the difference in the length of induction periods across treatments is clinically meaningful and aligned with clinical practice. As such, the CADTH reanalysis refrained from assuming equal induction periods across treatments.
CADTH also conducted a scenario analysis assuming numerical differences in clinical efficacy between ozanimod and its biologic comparators, informed by the sponsor’s NMA.
Probability of serious infection in the biologic-experienced population has confounding: The sponsor-commissioned ITC reported that all treatments had low event rates across safety outcomes. Due to the low event numbers, the ITC did not have sufficient data to assess relative treatment safety between comparators; for each included comparator, the model comprised risk inputs for AEs derived from the number of patients with each event among the biologic-naive and biologic-experienced groups of the induction and maintenance phases of efficacy trials. The vedolizumab trial was the only 1 to report disaggregated AE rates for the naive and experienced subgroups, while the trials for every other biologic reported AE rates relevant to either the biologic-naive or mixed populations. When consolidating this evidence, the sponsor applied mixed AE rates and, when otherwise unavailable, biologic-naive AE rates, to the biologic-experienced population. This was done for every biologic comparator, including ozanimod, with the exception of vedolizumab IV and SC. Although applying the rate of AEs in the mixed and biologic-naive populations to the biologic-experienced population likely underestimates the costs and overestimates the QALYs expected in this population across treatments, applying subgroup-specific AE rates only to some treatments biases the cost-effectiveness results against those therapies. The clinical expert consulted by CADTH noted that this practice created an unjustifiably high probability of serious infection for vedolizumab in the biologic-experienced population which, paradoxically, is regarded to be among the biologic therapies with more advantageous safety profiles. The clinical expert also remarked that disease activity is the leading predictor of serious infection and, as such, biologic-experienced patients, who tend to have more severe disease, are more likely to experience AEs a priori. Thus, it cannot be ascertained whether the probability of serious infection is due to treatment alone, given that the severity of disease activity and the corresponding subgroup-specific AE rate are unequally distributed between biologic therapies.
CADTH conducted a reanalysis assuming that the rate of serious infections did not differ between comparators.
CADTH also conducted a scenario analysis assuming numerical differences in the risk of AEs between ozanimod and its comparators, informed by the rates reported in the respective trials. CADTH applied the rates for serious infection reported in the mixed population of the efficacy trials to the biologic-experienced analysis of every biologic therapy, including vedolizumab IV and SC.
Utility values used by the sponsor lack reporting quality: The sponsor’s base case used utility data for non-surgical health states from a publication by Woehl et al. (2008).9 Other utility values for the response without remission, remission, and active UC health states based on 5-level EQ-5D (EQ-5D-5L) data were collected in TRUE NORTH and, hence, could have been used instead. More recent sources of utility data for this population were not considered by the sponsor. Among them, Vaizey et al. (2014)17 report utility values that lie between those of Woehl et al. and those collected in TRUE NORTH.18 The utility value for active moderate to severe disease in Woehl et al. (0.41) is considerably lower than Vaizey et al. (0.71),17 Swinburn et al. (0.68),1,19 and the TRUE NORTH pivotal trial (0.73).1 Although the utility values from Woehl et al. were previously used in the submissions to CADTH for tofacitinib, vedolizumab, and adalimumab for UC,20-22 the reliability of these estimates was critiqued in these previous reviews. Moreover, considering the inherent difficulty of assessing the methodological quality of a study that is only available as an abstract, it is insufficient to cite consistency with other appraisals as the reason for choosing the Woehl et al. data over other available sources. CADTH acknowledges that the values based on the pivotal trial may overestimate utility due to its re-randomized design, whereby only patients with UC who had achieved a response in the induction phase were permitted to continue into maintenance for assessment of health-related quality of life.
The CADTH base case used the utility values from Swinburn et al. (2012), as provided by the sponsor in the submitted model.
Inconsistencies in the application of dose escalation: The sponsor assumed that 30% of patients receiving adalimumab, golimumab, infliximab, tofacitinib, or ustekinumab would be prescribed escalated doses during the maintenance phase. The clinical expert consulted by CADTH indicated that within the Canadian standard of practice, dose escalation may be performed upon disease flare or nonresponse and, rarely, if a patient is stable and responding well to treatment. Clinical practice guidelines suggest that, in some instances, patients who have previously experienced anti-TNF failure may benefit from a higher maintenance dose.23 Hence, it may be reasonable that an escalated dose was modelled for a proportion of biologic-naive and biologic-experienced patients in the maintenance phase. The sponsor relied on expert opinion, real-world sources, and a previous National Institute for Health and Care Excellence (NICE) submission (TA633)24 to assign the proportion of patients who received either a normal or escalated dose of biologics in the maintenance phase. However, according to the clinical expert consulted by CADTH, a dose–response relationship exists, as patients who receive an escalated dose are more likely to achieve clinical response and remission relative to patients receiving the Health Canada–approved dosing schedule. It is thus important that the proportion of patients receiving an escalated dose within the economic model be consistent with the dose mix studied within the included clinical trials that informed the model’s comparative efficacy data. While the approach of relying on expert opinion to inform the proportion of patients prescribed escalated doses may potentially be more reflective of clinical practice, the clinical efficacy data were not adjusted accordingly. Whereas the sponsor’s model assumed a singular dose mix of 30% on escalated doses across biologic therapies, the NMA results leveraged for the model incorporated data from sensitivity analyses that pooled the doses of the same active drug with the same method of administration across trials that had different proportions of patients on normal and escalated dose regimens. As such, 2 doses of the same drug were treated as the same treatment in the NMA, with events and the number of patients achieving response and remission pooled together as a single treatment. This limitation is concerning, given that the dose-mix regimen used in the model is unlikely to be reflective of the NMA inputs that informed the relative efficacy of treatments.
The CADTH base case set the proportion of patients receiving an escalated dose to 0 across biologic therapies.
Distribution of the basket of concomitant therapies for primary biologic therapies was clinically unjustified: The model assumes that 19.90% of patients prescribed any biologics, and upward of 31.69% of patients prescribed tofacitinib, would also receive prednisolone throughout the maintenance phase. The clinical expert consulted by CADTH remarked that while the practice of concomitant therapy varies widely according to individual patient needs, current Canadian clinical guidelines25 indicate that steroids should be tapered off by the time patients enter the maintenance phase of a biologic therapy. The clinical expert did not discount that a gap may exist between clinical guidelines and clinical practice, even if the persistent use of steroids during treatment maintenance would be considered poor disease management. CADTH considered that the sponsor’s distribution of the basket of concomitant therapies, which is informed by the 2016 Royal College of Physicians (UK) national audit,26 should reasonably align with current clinical practice. As such, CADTH considered this assumption to be acceptable, albeit an over-simplification that is likely to overestimate the use of concomitant CT across biologic therapies. The sponsor also assumed that patients receiving tofacitinib would not be prescribed azathioprine and, alternatively, that a greater proportion of them would be prescribed the remainder of concomitant therapies. While the clinical expert agreed that azathioprine is not recommended for patients who receive tofacitinib, current clinical practice does not suggest that these patients are more likely to be prescribed other concomitant therapies as substitutes. The clinical expert also noted that vedolizumab is usually prescribed as a monotherapy, while patients on anti-TNFs tend to be prescribed conventional immunosuppressants in addition to the anti-TNF.
CADTH conducted a reanalysis by increasing the proportion of patients who receive tofacitinib and vedolizumab as monotherapy. The CADTH base case also increased the proportion of patients on anti-TNFs who are prescribed conventional immunosuppressants by 10%.
Resource use not reflective of clinical practice: The sponsor declared that the frequency of use of all health resources relevant to disease management, including regular outpatient visits, blood tests, endoscopy, and inpatient care without colectomy, were aligned with the health care resource use presented in the cost-effectiveness model developed by Tsai et al. (2008),14 which reported annual resource use for each of the model’s health states estimated by a UK gastroenterologist panel. Recent CADTH and NICE submissions20,24,27 for the treatment of moderately to severely active UC in the indicated biologic-naive and biologic-experienced populations are aligned with the Tsai et al. estimates of health state–specific resource use. While the sponsor explicitly claimed that the disease management resource use data inputted in the model were aligned with Tsai et al. and, specifically, with NICE submission TA633,24 the model’s resource use relevant to consultant visits and blood tests was downwardly adjusted. The clinical expert consulted by CADTH advised that the disease management resource use relevant to Canadian practice could not be assumed to be lower than that reported in Tsai et al. Indeed, the clinical expert noted that, given the uncertainty regarding the long-term safety profiles of the biologic drugs currently prescribed to treat moderate to severe UC, disease management resource use estimates should be conservative and aligned with published evidence.
CADTH conducted a reanalysis by inputting the health state–specific per-patient annual resource use of consultant visits and blood tests as per the Tsai et al. (2008) estimates.
Treatment effect is assumed to be constant: The model is underpinned by a key efficacy assumption that treatment effect, and the corresponding loss of response, is constant throughout the maintenance phase and over the lifetime time horizon. The sponsor explained that this assumption is required due to the lack of interim response and remission data from the maintenance clinical trials, as well as the lack of longer-term follow-up, to inform how the absolute and relative loss of response varies over time. Although this is a significant limitation of the model, as it potentially overestimates treatment efficacy across treatments, CADTH accepts the sponsor’s approach and agrees with the assumption of a constant risk over time. The sponsor conducted a scenario analysis to illustrate the possible impact of the declining loss of response risk, which assumed a 1-off 25% reduction in the loss of response after the first 2 years of treatment across therapies, which is based on the clinical advice leveraged for the ustekinumab NICE submission.24 The clinical expert consulted by CADTH noted that, given the potential for biologic-exposed patients with moderate to severe UC to develop anti-drug antibodies, it would be reasonable to assume an increasing risk in the first year followed by a relatively constant loss of response after that. This was also suggested by Ferrante et al. (2008),28 who reported a longer follow-up in 81 patients with refractory UC treated with infliximab. However, it should be noted that data regarding loss of response are sparse, and current clinical practice suggests that the risk may well be different across biologic drugs as well as between patients with varying degrees of disease severity.
CADTH conducted scenario analyses that assumed a non-constant risk, whereby a 1-time 30% reduction in treatment efficacy from the start of year 2 was applied to all treatments.
Inclusion of a comparator that is not currently publicly reimbursed: The sponsor’s model included ustekinumab as a currently reimbursed treatment for moderately to severely active UC. The negotiation process with the pan-Canadian Pharmaceutical Alliance (pCPA) for ustekinumab concluded on July 28, 2021, without agreement. Hence, the therapy is not currently reimbursed for this indication by the Canadian publicly funded health care payer, whose perspective guides this economic evaluation. While patients may access ustekinumab through private payers as well as through out-of-pocket payments, these are beyond the scope of the present review, as CADTH’s focus is the public health care payer.
CADTH conducted a reanalysis that excluded ustekinumab from the list of comparators.
Model lacks transparency: The economic model submitted by the sponsor lacked transparency, as it included numerous hidden sheets, columns, and rows, rendering it difficult to track inputs and outputs throughout. The coding of the model was highly inefficient, as simple calculations were spread over multiple sheets. By way of illustration, there was duplication of key efficacy parameters across sheets, contributing to a lack of clarity as to which parameters should be edited to implement changes.
CADTH was unable to address this limitation.
Additionally, the following key assumptions were made by the sponsor and appraised by CADTH (Table 5).
Table 5: Key Assumptions of the Submitted Economic Evaluation
Sponsor’s key assumption | CADTH comment |
|---|---|
Patients losing treatment response were assumed to discontinue treatment. Discontinuation due to reasons other than loss of response and AEs was not modelled. | Acceptable as a simplifying assumption. |
Patients undergoing revision surgery were assumed to achieve remission after the surgery and to not have any surgery-related complications. | Acceptable as a simplifying assumption. However, the relapsing-remitting nature of the disease is not accurately captured after revision surgery. |
The cycle length of 2 weeks is comparatively shorter than that used in the submission to CADTH for tofacitinib (i.e., 8 weeks) and the submission to CADTH for vedolizumab (i.e., 10 weeks and 1 year for the induction and maintenance phases, respectively). | Acceptable. By accommodating varying regimens of UC treatment and allowing the inclusion of induction periods of different lengths, the 2-week cycle length may capture treatment-related costs more accurately. |
Resource use for disease management and treatment monitoring and surgery-related inputs were assumed to be similar across all populations included in the model. | This is uncertain, although acceptable as a simplifying assumption. |
Patients were assumed to remain on any specified escalated dose regimens for the entire duration of the treatment. | According to the clinical expert consulted by CADTH, the proportion of patients with moderately to severely active UC who are prescribed dose de-escalation during the maintenance phase is marginal and, thus, deemed unlikely to significantly impact expected costs in the model. |
AE = adverse event; UC = ulcerative colitis.
CADTH Reanalyses of the Economic Evaluation
Base-Case Results
CADTH’s reanalysis addressed several limitations within the economic model. The CADTH base case was derived by making changes in model parameter values and assumptions, in consultation with clinical expert feedback. The following changes were applied: excluding ustekinumab as a comparator, assuming the clinical efficacy of all biologic treatments to be equal to ozanimod’s, applying alternate utility values for non-surgical health states, assuming the proportion of patients receiving an escalated dose to be 0% across biologic therapies, adjusting the proportion of patients receiving concomitant CT across biologic therapies to reflect Canadian clinical practice, aligning disease management resource use to published literature, and assuming the probability of serious infection and treatment discontinuation due to AEs is equal across therapies. It should be noted that although CADTH’s base case assumes equal clinical efficacy and safety across therapies, it does not assume equal treatment induction periods, as these are clinically meaningful and in accordance with Canadian clinical practice. Thus, though narrower, marginal differences in QALYs remained.
Table 6 details each change made to derive the CADTH revised base case, which was conducted in a stepwise approach to highlight the impact of each change. The summary of results from the stepped reanalysis is presented in Table 20 and Table 21.
Regarding the biologic-naive population, the results of the CADTH reanalysis were similar to the sponsor’s base case in that the same 2 therapies, CT and tofacitinib, remained on the CEF (Table 7). Regarding the biologic-experienced population, while the sponsor’s base case suggested that CT, infliximab biosimilar, and tofacitinib were on the CEF, results from the CADTH reanalysis suggest instead that 4 therapies remain on the CEF: CT, infliximab biosimilar, tofacitinib, and golimumab (Table 8). All other biologic therapies were either strictly dominated or subject to extended dominance. Ozanimod was strictly dominated by infliximab biosimilar in both the biologic-naive and -experienced populations. The probability that ozanimod is cost-effective at a willingness-to-pay threshold of $50,000 per QALY for either population was 0%.
A detailed breakdown of the disaggregated results is available in Table 22, Table 23, Table 24, and Table 25.
Table 6: CADTH Revisions to the Submitted Economic Evaluation
Stepped analysis | Sponsor’s value or assumption | CADTH value or assumption |
|---|---|---|
Corrections to the sponsor’s base case | ||
None. | — | — |
Changes to derive the CADTH base case | ||
1. Comparators | Included ustekinumab. | Excluded ustekinumab. |
2. Comparative efficacy | Probabilities of response and remission derived from the NMA that indicated numerical effect differences between biologic therapies (Table 11, Table 12, Table 13, and Table 14, Appendix 3). | Clinical efficacy of all biologic treatments assumed to be equal to ozanimod. |
3. Comparative safety | Risk inputs for AEs derived from the number of patients with each event among biologic-naive and -experienced groups from efficacy trials for each comparator (Table 15 and Table 16, Appendix 3). | Per-cycle probability of serious infection and per-cycle probability of treatment discontinuation due to AEs of all therapies assumed to be equal to ozanimod. |
4. Utility values |
|
|
5. Dose escalation | 30% | 0% |
6. Concomitant CT | Distribution of concomitant CT informed by the 2016 Royal College of Physicians (UK) national audit. | Proportion of patients on concomitant CT adjusted to reflect Canadian clinical practice (Table 19, Appendix 4). |
7. Resource use | Consultant visits:
Blood tests:
| Consultant visits:
Blood tests:
|
CADTH base case, biologic-naive | Combined revisions 1 + 2 + 3 + 4 + 5 + 6 + 7 | |
CADTH base case, biologic-experienced | Combined revisions 1 + 2 + 3 + 4 + 5 + 6 + 7 | |
AE = adverse event; CT = conventional therapy; NMA = network meta-analysis; UC = ulcerative colitis.
Table 7: Summary of the CADTH Reanalysis Results (Probabilistic), Biologic-Naive
Drug | Total costs | Total QALYs | Sequential ICER |
|---|---|---|---|
Conventional therapy | $161,741 | 16.241 | Reference |
Tofacitinib | $164,818 | 16.275 | $89,428 |
Dominated treatments | |||
Ozanimod | $163,849 | 16.250 | Strictly dominated by infliximab biosimilar |
ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year.
Note: Only non-dominated treatments are presented. Strictly dominated ozanimod is presented as the drug under review.
Table 8: Summary of the CADTH Reanalysis Results (Probabilistic), Biologic-Experienced
Drug | Total costs | Total QALYs | Sequential ICER |
|---|---|---|---|
Conventional therapy | $97,414 | 16.432 | Reference |
Infliximab biosimilar | $99,360 | 16.451 | $101,345 |
Tofacitinib | $99,555 | 16.452 | $278,848 |
Golimumab | $99,756 | 16.452 | $1,260,486 |
Dominated treatments | |||
Ozanimod | $99,446 | 16.444 | Strictly dominated by infliximab biosimilar |
ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year.
Note: Only non-dominated treatments are presented. Strictly dominated ozanimod is presented as the drug under review.
Scenario Analysis Results
CADTH undertook price reduction analyses based on the sponsor’s and CADTH’s base case. Based on the CADTH base case of the sponsor-submitted model, a price reduction of 73% would be necessary to achieve cost-effectiveness at a willingness-to-pay threshold of $50,000 per QALY in the biologic-naive population (Table 28), while a price reduction of 66% would be required in the biologic-experienced population (Table 29). As the CADTH base case assumes equal comparative efficacy and safety across treatments, CADTH also considered price reductions based on the submitted price for ozanimod and the publicly accessible list prices of all other biologics (Table 9, Appendix 1), which indicated that a price reduction of 43% during the first year, and 51% thereafter, would be required for ozanimod to be no more costly than adalimumab biosimilar, which is the least costly biologic therapy for moderately to severely active UC.
CADTH undertook a series of exploratory analyses to determine the impact of alternative assumptions on the cost-effectiveness of ozanimod, which are outlined as follows:
assumed numerical differences in clinical efficacy and safety between ozanimod and its comparators
assumed a non-constant loss of response risk whereby a 1-time 30% reduction in treatment efficacy from the start of year 2 was applied to all treatments; this scenario was conducted concomitantly with scenario 1
The results of these analyses are presented in Table 30 and Table 31. Ozanimod remained dominated in all scenarios.
Issues for Consideration
According to the clinical expert consulted by CADTH, ozanimod is unlikely to be prescribed for patients with moderate to severe UC with sinus bradycardia, first- or second-degree atrioventricular block, or a history of myocardial infarction or heart failure, as other biologic therapy options would be more suitable for these patient subgroups. Moreover, since concomitant use of heart rate–lowering drugs during ozanimod initiation may be associated with severe bradycardia and heart block, prescribing clinicians would also need to take drug-drug interactions into account, which is not currently the case for most biologic therapies. These factors will likely impact prescribing behaviours among clinicians and may limit the candidate population that could be prescribed ozanimod relative to other biologic therapies with more advantageous safety profiles.
Ozanimod may be self-administered and is the only other oral, small-molecule biologic drug in the current therapeutic space. This ease of administration was noted as an important outcome for patients and clinical expert feedback in their respective inputs.
The modelled price of biologic therapies is based on publicly accessible list prices and does not reflect existing confidential pricing that has been negotiated by public plans. When existing confidential discounts on biologic therapies are considered, greater price reductions than those referenced in this report would be required to achieve cost-effectiveness.
Overall Conclusions
Based on an appraisal of the TRUE NORTH trial, the CADTH clinical reviewers found that ozanimod was efficacious in inducing and maintaining clinical remission and clinical response, as well as in achieving mucosal healing, durable clinical response, and histologic remission when compared with placebo in patients with moderately to severely active UC. However, CADTH noted that the generalizability of the trial data to the Canadian setting was limited due to the re-randomization study design and the option for enrolment into an open-label trial during the maintenance period. Since there are no trials comparing ozanimod with the advanced therapies of interest (i.e., biologics and small-molecule drugs), comparisons among treatments were based on the sponsor-commissioned NMA. The CADTH Clinical Review determined that the applicability of the ITC is impacted by the heterogeneity of the study designs and patient populations across trials; the impact of this on the results of the NMA could not be assessed. An additional published ITC was identified, although similar limitations were noted in terms of the heterogeneity of the study design and patient populations. CADTH concluded there is a high degree of uncertainty with respect to the comparative clinical efficacy and safety of ozanimod versus advanced treatments for moderate to severe UC.
In its base case, CADTH attempted to address the limitations identified with the economic analysis submitted by the sponsor by making the following changes in model parameter values and assumptions, in consultation with clinical experts: excluding ustekinumab as a comparator; assuming the clinical efficacy and safety of all biologic treatments (note that biologic refers to anti-TNF therapies and small-molecule drugs) to be equal to ozanimod’s; applying alternate utility values for non-surgical health states; assuming the proportion of patients receiving an escalated dose to be 0% across biologic therapies; adjusting the proportion of patients receiving concomitant CT across biologic therapies to reflect Canadian clinical practice; and aligning disease management resource use to published literature. However, these reanalyses need to be considered in the context of the submitted model, as concerns regarding the transparency and validity of the model output were noted.
The results from the CADTH base case were similar to the sponsor’s base case in that ozanimod was not among the optimal treatments (i.e., not on the CEF) in either population (biologic-naive or biologic-experienced). Ozanimod was strictly dominated (more costly and less effective) when compared with infliximab biosimilar in both the biologic-naive and biologic-experienced populations. A price reduction of between 43% and 73% is necessary for ozanimod to be considered an optimal therapy at a $50,000 per QALY willingness-to-pay threshold, depending on the patient population and comparative data assumptions.
References
1.Bristol Myers Squibb. Cost-utility analysis of ZEPOSIA® (ozanimod) for the treatment of moderate-to-severe ulcerative colitis in Canada. Quebec (QC): Bristol Myers Squibb;2022.
2.Scott FL, Clemons B, Brooks J, et al. Ozanimod (RPC1063) is a potent sphingosine-1-phosphate receptor-1 (S1P1) and receptor-5 (S1P5) agonist with autoimmune disease-modifying activity. Br J Pharmacol. 2016;173(11):1778-1792. PubMed
3.Celgene Inc. PRODUCT MONOGRAPH INCLUDING PATIENT MEDICATION INFORMATION PR ZEPOSIA®ozanimod, capsules, 0.23 mg, 0.46 mg and 0.92 mg, oral, Sphingosine 1-phosphate receptor modulator. Quebec (QC): Celgene Inc., a Bristol Myers Squibb company; January 15 2021.
4.Sandborn WJ, Feagan BG, D’Haens G, et al. Ozanimod as Induction and Maintenance Therapy for Ulcerative Colitis. N Engl J Med. 2021;385(14):1280-1291. PubMed
5.Bristol Myers Squibb. Ozanimod (ZEPOSIA®) for the Treatment of Moderate-to-Severe Ulcerative Colitis, Technical Report: Systematic Literature Review and Network Meta-Analysis of Clinical Evidence. Quebec, Canada: Bristol Myers Squibb;2021.
6.Targownik LE, Singh H, Nugent Z, Bernstein CN. The epidemiology of colectomy in ulcerative colitis: results from a population-based cohort. Am J Gastroenterol. 2012;107(8):1228-1235. PubMed
7.Causey MW, Stoddard D, Johnson EK, et al. Laparoscopy impacts outcomes favorably following colectomy for ulcerative colitis: a critical analysis of the ACS-NSQIP database. Surg Endosc. 2013;27(2):603-609. PubMed
8.Suzuki H, Ogawa H, Shibata C, et al. The long-term clinical course of pouchitis after total proctocolectomy and IPAA for ulcerative colitis. Dis Colon Rectum. 2012;55(3):330-336. PubMed
9.Woehl A, Hawthorne AB, Morgan CL, Punekar Y, McEwan P. Pg113 the Epidemiology and Health Care Resource Use in Patients with Crohn’s Disease: A Population Based Uk Study. Value Health. 2007;10(6).
10.Arseneau KO, Sultan S, Provenzale DT, et al. Do patient preferences influence decisions on treatment for patients with steroid-refractory ulcerative colitis? Clin Gastroenterol Hepatol. 2006;4(9):1135-1142. PubMed
11.Ara R, Brazier J. Populating an Economic Model with Health State Utility Values: Moving toward Better Practice. Value Health. 2010;13(5). PubMed
12.Life expectancy and other elements of the complete life table, three-year estimates, Canada, all provinces except Prince Edward Island. Ottawa (ON): Statistics Canada; 2020.
13.Jess T, Gamborg M, Munkholm P, Sorensen TI. Overall and cause-specific mortality in ulcerative colitis: meta-analysis of population-based inception cohort studies. Am J Gastroenterol. 2007;102(3):609-617. PubMed
14.Tsai HH, Punekar YS, Morris J, Fortun P. A model of the long-term cost effectiveness of scheduled maintenance treatment with infliximab for moderate-to-severe ulcerative colitis. Aliment Pharmacol Ther. 2008;28(10):1230-1239. PubMed
15.Fausel R, Afzali A. Biologics in the management of ulcerative colitis - comparative safety and efficacy of TNF-alpha antagonists. Ther Clin Risk Manag. 2015;11:63-73. PubMed
16.Kopylov U, Seidman E. Predicting durable response or resistance to antitumor necrosis factor therapy in inflammatory bowel disease. Therap Adv Gastroenterol. 2016;9(4):513-526. PubMed
17.Vaizey CJ, Gibson PR, Black CM, et al. Disease status, patient quality of life and healthcare resource use for ulcerative colitis in the UK: an observational study. Frontline Gastroenterol. 2014;5(3):183-189. PubMed
18.Sandborn WJ, Feagan BG, Hanauer S, et al. Long-Term Efficacy and Safety of Ozanimod in Moderately to Severely Active Ulcerative Colitis: Results From the Open-Label Extension of the Randomized, Phase 2 TOUCHSTONE Study. J Crohns Colitis. 2021;15(7):1120-1129. PubMed
19.Swinburn P, Elwick H, Bean K, Curry A, Patel S, Bodger K. PTU-127: The impact of surgery on health related quality of life in ulcerative colitis. Gut. 2012;61(A237-A.).
20.CADTH COMMON DRUG REVIEW Pharmacoeconomic Review Report TOFACITINIB (XELJANZ). Ottawa (ON): CADTH; 2019: https://www.cadth.ca/sites/default/files/cdr/pharmacoeconomic/sr0572-xeljanz-pharmacoeconomic-report.pdf. Accessed 2022 May 2.
21.CADTH COMMON DRUG REVIEW Pharmacoeconomic Review Report VEDOLIZUMAB (ENTYVIO SC). Ottawa (ON): CADTH; 2020: https://www.cadth.ca/sites/default/files/cdr/pharmacoeconomic/sr0635-entyvio-pharmacoeconomic-review-report.pdf. Accessed 2022 May 2.
22.CADTH COMMON DRUG REVIEW Pharmacoeconomic Review Report ADALIMUMAB (HUMIRA). Ottawa (ON): CADTH; 2016: https://www.cadth.ca/sites/default/files/cdr/pharmacoeconomic/SR0450_Humira_UC_PE_Report.pdf. Accessed 2022 May 2.
23.Bansback N, Tsuchiya A, Brazier J, Anis A. Canadian valuation of EQ-5D health states: preliminary value set and considerations for future valuation studies. PLoS One. 2012;7(2):e31115. PubMed
24.Ustekinumab for treating moderately to severely active ulcerative colitis. London (UK): National Institute for Health and Care Excellence 2020.
25.Bressler B, Marshall JK, Bernstein CN, et al. Clinical practice guidelines for the medical management of nonhospitalized ulcerative colitis: the Toronto consensus. Gastroenterology. 2015;148(5):1035-1058 e1033. PubMed
26.National clinical audit of biological therapies. UK inflammatory bowel disease (IBD) audit - Annual report London (UK): Royal College of Physicians; 2016.
27.CADTH COMMON DRUG REVIEW Pharmacoeconomic Review Report USTEKINUMAB (STELARA/STELARA IV). Ottawa (ON): CADTH; 2020: https://www.cadth.ca/sites/default/files/cdr/pharmacoeconomic/sr0627-stelara-pharmacoeconomic-review-report.pdf. Accessed 2022 May 2.
28.Ferrante M, Vermeire S, Fidder H, et al. Long-term outcome after infliximab for refractory ulcerative colitis. J Crohns Colitis. 2008;2(3):219-225. PubMed
29.Bristol Myers Squibb. Budget Impact Analysis of ZEPOSIA® (Ozanimod) in Patients with Moderate-to-Severe Active Ulcerative Colitis (UC) Pan-Canadian Analysis (Adapted from Global BIM Report). Quebec (QC): Bristol Myers Squibb;2021.
30.Annual Demographic Estimates: Canada, Provinces and Territories. Ottawa (ON): Statistics Canada; 2020: https://www150.statcan.gc.ca/n1/pub/91-215-x/91-215-x2020001-eng.htm. Accessed 2022 May 02.
31.National precription drug utilization information system - Plan information document. Ottawa (ON): Canadian Institute for Health Information; 2021.
32.Harbord M, Annese V, Vavricka SR, et al. The First European Evidence-based Consensus on Extra-intestinal Manifestations in Inflammatory Bowel Disease. J Crohns Colitis. 2016;10(3):239-254. PubMed
Appendix 1: Cost Comparison Table
Note that this appendix has not been copy-edited.
The comparators presented in the following table have been deemed to be appropriate by clinical experts. Comparators may be recommended (appropriate) practice, versus actual practice. Comparators are not restricted to drugs but may be devices or procedures. Costs are sponsor list prices, unless otherwise specified. Existing Product Listing Agreements are not reflected in the table and as such may not represent the actual costs to public drug plans.
Table 9: CADTH Cost Comparison Table for Severe to Moderate Active UC
Drug/ comparator | Strength | Dosage form | Price ($) | Recommended dosage | Average cost per month ($) | Average cost per year ($) |
|---|---|---|---|---|---|---|
Ozanimod (Zeposia) | 0.25 mg 0.5 mg 1 mg | Cap | $68.4929a $68.4929a $68.4932b | 0.25 mg daily on days 1-4, 0.5 daily on days 5-7, then 1 mg daily thereafterc | Year 1: $2,083.34 Thereafter: $2,083.34 | Year 1: $25,000 Thereafter: $25,000 |
Comparators — Biologics | ||||||
Adalimumab (Humira) | 40 mg/0.8 mL | Prefilled syringe or auto-injector for SC injection | $769.9700 | 160 mg at week 0, 80 mg at week 2, then 40 mg every other week thereafterd | Year 1: $1,924.93 Thereafter: $1,668.27 | Year 1: $23,099 Thereafter: $20,019 |
Adalimumab (Hulio) | 40 mg/0.8 mL | Prefilled syringe or auto-injector for SC injection | $471.2700e | 160 mg at week 0, 80 mg at week 2, then 40 mg every other week thereafterf | Year 1: $1,178.18 Thereafter: $1,021.09 | Year 1: $14,138 Thereafter: $12,253 |
Golimumab (Simponi) | 50 mg/0.5 mL 100 mg/1 mL | Prefilled syringe or auto-injector for SC injection | $1,555.1700g $1,557.0000g | 200 mg at week 0, 100 mg at week 2, then 50 mg every 4 weeks thereafterh | Year 1: $1944.42 Thereafter: $1,684.77 | Year 1: $23,333 Thereafter: $20,217 |
Infliximab (Inflectra) | 100 mg | Vial for IV infusion | $525.0000 | 5 mg/kg at week 0, 2, and 6, then every 8 weeks thereafteri | Year 1: $1,400.00 Thereafter: $1,225.00 | Year 1: $16,800 Thereafter: $14,700 |
Infliximab (Remicade) | 100 mg | Vial for IV infusion | $977.0000g | 5 mg/kg at week 0, 2, and 6, then every 8 weeks thereafterj | Year 1: $2,605.33 Thereafter: $2,279.67 | Year 1: $31,264 Thereafter: $27,356 |
Infliximab (Renflexis) | 100 mg | Vial for IV infusion | $493.0000 | 5 mg/kg at week 0, 2, and 6, then every 8 weeks thereafterk | Year 1: $1,314.67 Thereafter: $1,150.33 | Year 1: $15,776 Thereafter: $13,804 |
Tofacitinib (Xeljanz) | 5 mg 10 mg | Tab | $23.9589 $42.3436l | 10 mg twice daily for at least 8 weeks, then 5 mg twice daily thereafterm | Year 1: $1,625.10 Thereafter: $1,453.51 | Year 1: $19,501 Thereafter: $17,442 |
Ustekinumab (Stelara) | 130 mg/26.0 mL 90 mg/1.0 mL | Vial for IV infusion Prefilled Syringe for SC injection | $2,079.8400n $4,593.1400n | 6 mg/kg IV at week 0, then 90 mg SC every 8 weeks thereaftern | Year 1: $2,816.53 Thereafter: $2,679.33 | Year 1: $33,798 Thereafter: $32,152 |
Vedolizumab (Entyvio) (IV) | 300 mg | Vial for IV infusion | $3,291.0000g | 300 mg at week 0, 2, 6, then every 8 weeks thereaftero | Year 1: $2,194.00 Thereafter: $1,919.75 | Year 1: $26,328 Thereafter: $23,037 |
Vedolizumab (Entyvio) (SC) | 108 mg/0.68 mL | Prefilled syringe or pen for SC injection | $822.5000p | Following 300 mg IV infusions at weeks 0 and 2, 108 mg SC injection is administered every 2 weeks as maintenance only (from week 4 onward)o | Year 1: $2,193.50 Thereafter: $1,782.08 | Year 1: $26,322 Thereafter: $21,385 |
Comparators — Aminosalicylates | ||||||
5-ASA (Asacol, Asacol 800) | 400 mg 800 mg | Tab | $0.5597 $1.1358 | Active: 2 to 8 tabs daily in divided doses Maint: 4 tabs daily in divided dosesq | $34.05 to $136.19 | $409 to $1,634 |
5-ASA (Mesasal) | 500 mg | Ent. Tab | $0.6559 | Active: 1.5 to 3 g tabs daily in divided doses Maint: 1.5 g daily in divided dosesr | $59.85 to $119.70 | $718 to $1,436 |
5-ASA (Mezavant) | 1.2 g | Delayed ER-Tab | $1.7284 | Active: 2 to 4 tabs once daily Maint: 2 tabs dailys | $105.14 to $210.29 | $1,262 to $2,523 |
5-ASA (Pentasa) | 500 mg 1,000 mg | ER-Tab | $0.5881 $1.1761 | 0.5 to 1 g 4 times daily (2 g daily dose)t | $71.55 to $143.09 | $859 to $1,717 |
1g | Supp | $1.9962 | 1 g dailyt | $60.72 | $729 | |
1g/100mL 4g/100mL | Enema Enema | $4.4790 $6.0400 | 1 to 4 g daily | $136.24 to $183.72 | $1,635 to $2,205 | |
5-ASA (Salofalk) | 500 mg | Ent.Tab | $0.6445 | Active: 3 g to 4 g daily in divided dosesu Maint: 1.5 to 3 g per day in divided dosesu | $117.62 to $156.83 | $1,411 to $1,882 |
500 mg 1,000 mg | Supp Supp | $1.5314 $2.2495 | 1 to 1.5 g/dayd | $68.42 to $115.00 | $821 to $1,380 | |
4 g/60 g | Rect Susp | $8.1360 | Active: 4 g nightly Maint: 2 g nightly or 4 g every 2 nights | $247.47 $123.74 | $2,970 $1,485 | |
Olsalazine (Dipentum) | 250 mg | Cap | $0.5330 | Active: 1 g to 3 g daily in divided dosesl Maint: 1 g daily in divided dosesl | Year 1: 64.85 to 194.55 Thereafter: $64.85 | Year 1: $778 to $2,335 Thereafter: $778 |
Sulfasalazine (Salazopyrin, generics) | 500 mg | Tab | $0.1804 | Active: 1 g to 2 g 3 to 4 times dailyu Maint: 1 g 2 to 3 times dailyu | Year 1: $32.92 to $65.85 Thereafter: $21.95 to $32.92 | Year 1: $395 to $790 Thereafter: $263 to $395 |
Comparators — Corticosteroids | ||||||
Betamethasone enema (Betnesol) | 5 mg/100mL | Enema | $11.8214 | 5 mg nightlyl | $359.57 | $4,315 |
Budesonide (Entocort) | 3 mg | Cap | $1.8653g | 3 mg 3 times per day up to 8 weeks, followed by 6 mg daily for up to 3 monthsl | $54.48 | $654 |
Hydrocortisone enema (Cortenema) (Cortifoam) | 100 mg/60 mL | Enema | $8.2541 | 60 mL nightly or every other night | $125.53 to $251.06 | $1,506 to $3,013 |
15 g/pack (14 doses) | Rect. Aerosol | $117.8800 | One dose nightly or every other nightl | $117.88 to $235.80 | $1,415 to $2,830 | |
Hydrocortisone (Solu-cortef) | 100 mg 250 mg | Vial | $4.1500g $7.2000g | 100 mg to 500 mg IV daily to induce remission; then switch to other agentl | $126.25 to $438.00 | $1,515 to $5,256 |
Prednisone (generic) | 1 mg 5 mg 50 mg | Tab | $0.1095g $0.0220 $0.1735 | 40 mg to 60 mg daily to induce remission; then lower dosel | $5.42 to $8.08 | $64 to $79, or lower |
Comparators — Immunomodulators | ||||||
Azathioprine (generic) | 50 mg | Tab | $0.2405 | up to 2.5 mg/kg dailyl | $29.26 | $351 |
Azathioprine (Imuran) | 50 mg | Tab | $1.0927 | $132.95 | $1,595 | |
Mercaptopurine (Purinethol and generic) | 50 mg | Tab | $2.8610 | 1.5 to 2.5 mg/kg dailyl | $261.07 to $348.09 | $3,133 to $4,177 |
Methotrexate (generic) | 2.5 mg 10 mg | Tab | $0.6325 $2.7000g | 10 to 25 mg weeklyl | $11.70 to $28.88 | $140 to $347 |
cap = capsule; ent = enteric; er = extended release; maint = maintenance; sol inj = solution for injection; supp = suppository; tab = tablet.
aBased on price submitted by sponsor for a multiple strength starter pack consisting of the dose escalated capsules of treatment for days 1 through 7.
bBased on price submitted by sponsor for 28 units.
cReports dose of ozanimod hydrochloride (HCl); a 0.25 mg, 0.5 mg, and 1 mg of ozanimod HCl equivalents to 0.23 mg, 0,46, and 0.92 mg of ozanimod, respectively.
dHealth Canada Drug Database.
ePrice obtained from Ontario Drug Benefit Formulary.
fProduct monograph Adalimumab (Hulio).
gPrice obtained from Saskatchewan Drug Benefit (August 2019).
hProduct monograph Simponi golimumab injection.
iProduct monograph infliximab (Inflectra).
jProduct monograph infliximab (Remicade).
kProduct monograph infliximab (Renflexis).
lXeljanz CADTH CDR Pharmacoeconomic Report.
mProduct Monograph Tofacitinib (Xeljanz).
nBased on sponsor’s submission.
oProduct Monograph Vedolizumab (Entyvio).
pPrice obtained from Ontario Exceptional Access Program.
q5-ASA Asacol.
r5-ASA Mesasal.
s5-ASA Mezavant.
t5-ASA Pentasa.
uRxTx.
Source: Ontario Drug Benefit / Comparative Drug Index (effective from August 2019) unless otherwise noted, Annual period assumes 52 weeks, 365 days.
Appendix 2: Submission Quality
Note that this appendix has not been copy-edited.
Description | Yes/No | Comments |
|---|---|---|
Population is relevant, with no critical intervention missing, and no relevant outcome missing | No | The model includes a comparator that is not currently reimbursed by the public health care payer, whose perspective guides the economic evaluation and budget impact analysis. |
Model has been adequately programmed and has sufficient face validity | No | See CADTH Appraisal for limitations with model programming and validity of the model. |
Model structure is adequate for decision problem | Yes | The model structure is acceptable. However, the relapsing-remitting nature of the disease is not accurately captured post-revision surgery. |
Data incorporation into the model has been done adequately (e.g., parameters for probabilistic analysis) | Yes | No comment. |
Parameter and structural uncertainty were adequately assessed; analyses were adequate to inform the decision problem | Yes | No comment. |
The submission was well organized and complete; the information was easy to locate (clear and transparent reporting; technical documentation available in enough details) | Yes | The reporting in the pharmacoeconomic and budget impact submissions is clear and consistent with the respective Excel models. Technical documentation regarding the sponsor-commissioned NMA reported the comparative efficacy findings in detail. |
Appendix 3: Additional Information on the Submitted Economic Evaluation
Note that this appendix has not been copy-edited.
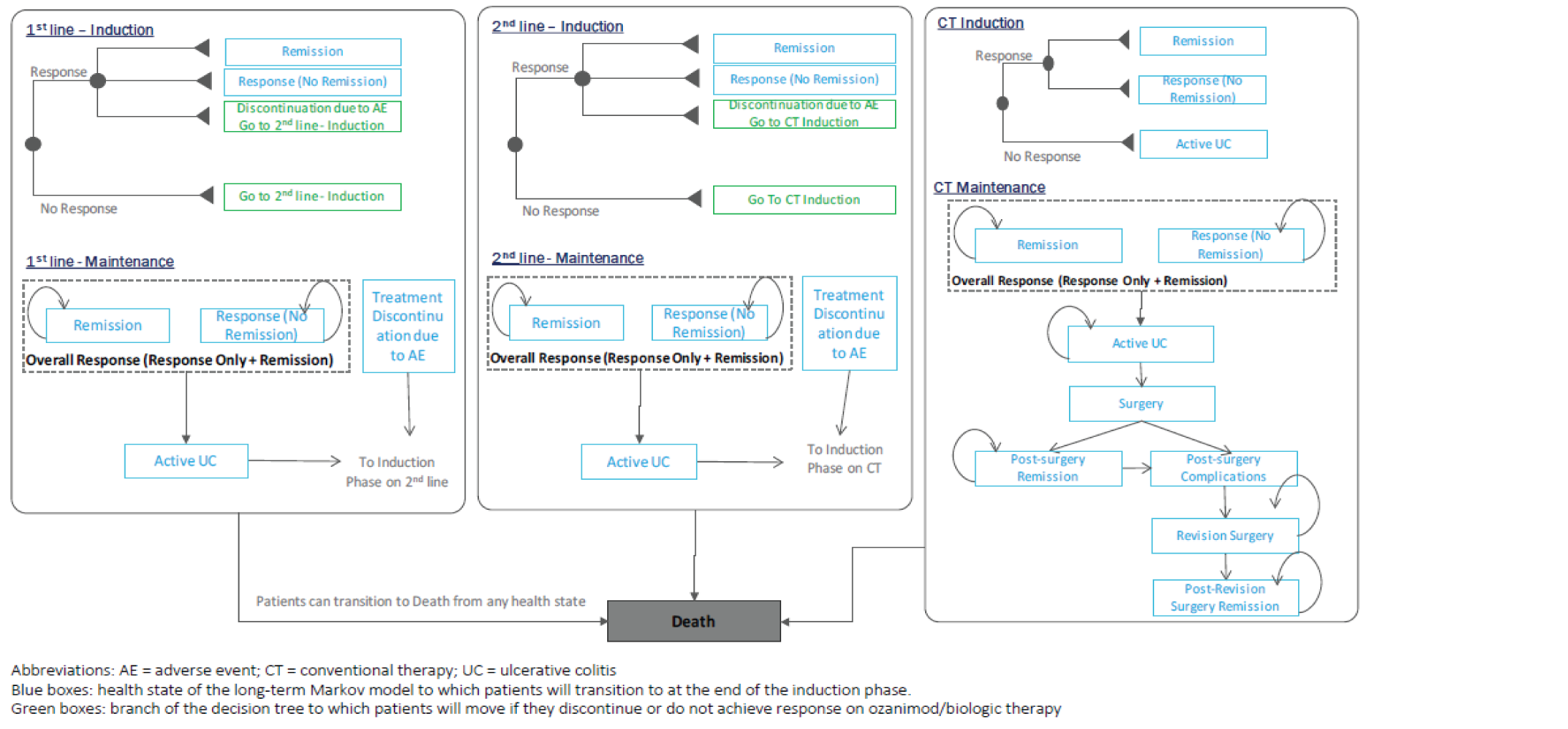
Detailed Results of the Sponsor’s Base Case
Sponsor’s Base-Case Model Inputs
Table 11: Base-Case Efficacy Inputs, Induction Phase
Drug | Biologic-naive | Biologic-experienced | ||||
|---|---|---|---|---|---|---|
No response | Response | Remission | No response | Response | Remission | |
Ozanimod | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
Adalimumab (brand/bio) | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
Golimumab | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
Infliximab (brand/bio) | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
Tofacitinib | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
Ustekinumab | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
Vedolizumab (IV) | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
Vedolizumab (SC) | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
Conventional Therapy | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
No response = no response, no remission; response = response, no remission; remission = response and remissions; IV = intravenous, SC = subcutaneous.
Table 12: Base-Case Efficacy Inputs, Maintenance Phase
Drug | Biologic-naive | Biologic-experienced | ||||
|---|---|---|---|---|---|---|
No response | Response | Remission | No response | Response | Remission | |
Ozanimod | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
Adalimumab (brand/bio) | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
Golimumab | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
Infliximab (brand/bio) | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
Tofacitinib | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
Ustekinumab | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
Vedolizumab (IV) | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
Vedolizumab (SC) | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
Conventional Therapy | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
No response = no response, no remission; Response = response, no remission; Remission = response and remissions; IV = intravenous, SC = subcutaneous
Table 13: Base-Case Efficacy Inputs for Subsequent Treatment, Induction Phase
Drug | Biologic-naive | Biologic-experienced | ||||
|---|---|---|---|---|---|---|
No Response | Response | Remission | No Response | Response | Remission | |
Ozanimod | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
Adalimumab (brand/bio) | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
Golimumab | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
Infliximab (brand/bio) | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
Tofacitinib | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
Ustekinumab | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
Vedolizumab (IV) | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
Vedolizumab (SC) | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
Conventional Therapy | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
No response = no response, no remission; Response = response, no remission; Remission = response and remissions; IV = intravenous, SC = subcutaneous
Table 14: Base-Case Efficacy Inputs for Subsequent Treatment, Maintenance Phase
Drug | Biologic-naive | Biologic-experienced | ||||
|---|---|---|---|---|---|---|
No response | Response | Remission | No response | Response | Remission | |
Ozanimod | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
Adalimumab (brand/bio) | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
Golimumab | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
Infliximab (brand/bio) | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
Tofacitinib | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
Ustekinumab | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
Vedolizumab (IV) | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
Vedolizumab (SC) | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
Conventional Therapy | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
No response = no response, no remission; response = response, no remission; remission = response and remissions; SC = subcutaneous
Table 15: Base-Case Per-Cycle Probability of Treatment-Related Serious Infections
Drug | Biologic-naive | Biologic-experienced | ||
|---|---|---|---|---|
Induction | Maintenance | Induction | Maintenance | |
Ozanimod | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
Adalimumab (brand/bio) | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
Golimumab | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
Infliximab (brand/bio) | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
Tofacitinib | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
Ustekinumab | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
Vedolizumab (IV) | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
Vedolizumab (SC) | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
Conventional therapy | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
SC = subcutaneous
Table 16: Percentage of Patients Discontinuing Treatment Due to Adverse Events (Per Cycle)
Drug | Ind. | Mnt. | Sub. Ind. | Sub. Mnt. | Ind. | Mntn. | Sub. Ind. | Sub. Mnt. |
|---|---|---|---|---|---|---|---|---|
Ozanimod | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
Adalimumab (brand/bio) | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
Golimumab | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
Infliximab (brand/bio) | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
Tofacitinib | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
Ustekinumab | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
Vedolizumab (IV) | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
Vedolizumab (SC) | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
Conventional Therapy | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
Ind. = induction; Mnt. = maintenance; Sub. = subsequent treatment; SC = subcutaneous.
Sponsor’s Complete Base-Case Results
Table 17: Sponsor’s Economic Evaluation Results, Biologic-Naive Population
Drug | Total Costs | Total QALYs | Sequential ICER ($/QALY) |
|---|---|---|---|
Conventional therapy | $130,017.91 | 12.039 | Reference |
Adalimumab Biosimilar | $142,039.22 | 12.159 | Extendedly dominated |
Infliximab Biosimilar | $150,707.31 | 12.268 | Extendedly dominated |
Adalimumab | $150,723.70 | 12.159 | Strictly dominated |
Ozanimod | $151,715.60 | 12.225 | Strictly dominated |
Golimumab | $156,986.16 | 12.302 | Extendedly dominated |
Vedolizumab (SC) | $165,193.11 | 12.564 | Extendedly dominated |
Ustekinumab | $171,147.19 | 12.288 | Strictly dominated |
Infliximab | $171,562.61 | 12.268 | Strictly dominated |
Tofacitinib | $172,338.57 | 12.692 | $64,809.23 |
Vedolizumab (IV) | $174,062.14 | 12.506 | Strictly dominated |
CEF = cost-effectiveness frontier; QALY = quality-adjusted life-year; CT = conventional therapy; SC = subcutaneous.
Note: The submitted analysis is based on the publicly available prices of the comparator treatments.
Source: Sponsor’s pharmacoeconomic submission.1
Table 18: Sponsor’s Economic Evaluation Results, Biologic-Experienced Population
Drug | Total costs | Total QALYs | Sequential ICER ($/QALY) |
|---|---|---|---|
Conventional therapy | $131,217.95 | 11.913 | Reference |
Adalimumab biosimilar | $139,126.69 | 11.976 | Extendedly dominated |
Adalimumab | $144,669.39 | 11.976 | Strictly dominated |
Ozanimod | $150,516.73 | 12.123 | Extendedly dominated |
Infliximab biosimilar | $151,407.60 | 12.206 | $68,903.53 |
Vedolizumab (SC) | $154,254.03 | 12.217 | Extendedly dominated |
Vedolizumab (IV) | $155,765.81 | 12.124 | Strictly dominated |
Ustekinumab | $156,242.45 | 12.038 | Strictly dominated |
Tofacitinib | $157,453.73 | 12.282 | $79,494.99 |
Golimumab | $157,685.51 | 12.240 | Strictly dominated |
Infliximab | $171,817.89 | 12.206 | Strictly dominated |
CEF = cost-effectiveness frontier; QALY = quality-adjusted life-year; CT = conventional therapy; SC = subcutaneous.
Note: The submitted analysis is based on the publicly available prices of the comparator treatments.
Source: Sponsor’s pharmacoeconomic submission.1
Appendix 4: Additional Details on the CADTH Reanalyses and Sensitivity Analyses of the Economic Evaluation
Note that this appendix has not been copy-edited.
Detailed Inputs of CADTH Base Case
Table 19: Distribution of the Basket of Concomitant CT per Primary Biologic Therapy
Treatment | MES | OLS | SUL | PRED | HYD | AZA | 6MP | MTX | BUD | None |
|---|---|---|---|---|---|---|---|---|---|---|
Sponsor’s base-case inputs | ||||||||||
Ozanimod | 11.77% | 11.77% | 11.77% | 19.90% | 0.60% | 37.20% | 1.00% | 2.50% | 3.50% | 0.00% |
Tofacitinib/ustekinumab | 18.74% | 18.74% | 18.74% | 31.69% | 0.96% | 0.00% | 1.59% | 3.98% | 5.57% | 0.00% |
Other biologics | 11.77% | 11.77% | 11.77% | 19.90% | 0.60% | 37.20% | 1.00% | 2.50% | 3.50% | 0.00% |
CADTH’s base-case inputs | ||||||||||
Ozanimod | 11.77% | 11.77% | 11.77% | 19.90% | 0.60% | 37.20% | 1.00% | 2.50% | 3.50% | 0.00% |
Adalimumab (brand/bio) | 11.06% | 11.06% | 11.06% | 19.19% | 0.00% | 40.97% | 1.10% | 2.75% | 2.81% | 0.00% |
Golimumab | 11.06% | 11.06% | 11.06% | 19.19% | 0.00% | 40.97% | 1.10% | 2.75% | 2.81% | 0.00% |
Infliximab (brand/bio) | 11.06% | 11.06% | 11.06% | 19.19% | 0.00% | 40.97% | 1.10% | 2.75% | 2.81% | 0.00% |
Tofacitinib | 11.77% | 11.77% | 11.77% | 19.90% | 0.60% | 0.00% | 1.00% | 2.50% | 3.49% | 37.20% |
Ustekinumab | 11.77% | 11.77% | 11.77% | 19.90% | 0.60% | 0.00% | 0.00% | 0.00% | 3.49% | 40.70% |
Vedolizumab (IV/SC) | 11.77% | 11.77% | 11.77% | 19.90% | 0.60% | 0.00% | 0.00% | 0.00% | 3.49% | 40.70% |
MES = mesalazine; OLS = olsalazine; SUL = sulfasalazine; PRED = prednisolone; HYD = hydrocortisone; AZA = azathioprine; 6MP = 6-mercaptopurine; MTX = methotrexate; BUD = budesonide, none = no concomitant CT; bio = biosimilar; SC = subcutaneous.
Detailed Results of CADTH Base Case
Table 20: Summary of the Stepped Analysis of the CADTH Reanalysis Results (Deterministic), Biologic-Naive
Stepped analysis | Drug | Total costs ($) | Total QALYs | Sequential ICER ($/QALYs) |
|---|---|---|---|---|
Sponsor’s base case | Conventional Therapy | $130,018 | 12.039 | Reference |
Tofacitinib | $172,339 | 12.692 | $64,809 | |
CADTH reanalysis 1: Comparators | Conventional Therapy | $130,295 | 12.113 | Reference |
Tofacitinib | $171,315 | 12.735 | $65,905 | |
CADTH reanalysis 2: Comparative efficacy | Conventional Therapy | $130,295 | 12.113 | Reference |
Adalimumab Biosimilar | $143,809 | 12.281 | $80,102 | |
Tofacitinib | $154,914 | 12.371 | $123,529 | |
CADTH reanalysis 3: Comparative safety | Conventional Therapy | $126,030 | 12.122 | Reference |
Tofacitinib | $165,579 | 12.705 | $67,756 | |
CADTH reanalysis 4: Utility values | Conventional Therapy | $130,295 | 18.545 | Reference |
Tofacitinib | $171,315 | 18.886 | $120,326 | |
CADTH reanalysis 5: Dose escalation | Conventional Therapy | $130,295 | 12.113 | Reference |
Tofacitinib | $162,080 | 12.735 | $51,068 | |
CADTH reanalysis 6: Concomitant CT | Conventional Therapy | $130,295 | 12.113 | Reference |
Tofacitinib | $170,668 | 12.735 | $64,866 | |
CADTH reanalysis 7: Resource use | Conventional Therapy | $137,165 | 12.113 | Reference |
Tofacitinib | $177,929 | 12.735 | $65,495 | |
CADTH base case: 1 + 2 + 3 + 4 + 5 + 6 + 7 | Conventional Therapy | $132,899 | 18.554 | Reference |
Adalimumab Biosimilar | $144,386 | 18.657 | $111,310 | |
Tofacitinib | $152,009 | 18.684 | $278,203 | |
Golimumab | $154,135 | 18.690 | $348,559 |
ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year.
Table 21: Summary of the Stepped Analysis of the CADTH Reanalysis Results (Deterministic), Biologic-Experienced
Stepped analysis | Drug | Total costs ($) | Total QALYs | Sequential ICER ($/QALYs) |
|---|---|---|---|---|
Sponsor’s base case | Conventional Therapy | $131,218 | 11.913 | Reference |
Infliximab Biosimilar | $151,408 | 12.206 | $68,904 | |
Tofacitinib | $157,454 | 12.282 | $79,495 | |
CADTH reanalysis 1: Comparators | Conventional Therapy | $131,499 | 11.987 | Reference |
Infliximab Biosimilar | $151,372 | 12.270 | $70,171 | |
Tofacitinib | $156,973 | 12.338 | $82,376 | |
CADTH reanalysis 2: Comparative efficacy | Conventional Therapy | $131,499 | 11.987 | Reference |
Adalimumab Biosimilar | $143,400 | 12.179 | $62,144 | |
Tofacitinib | $153,093 | 12.253 | $130,109 | |
CADTH reanalysis 3: Comparative safety | Conventional Therapy | $127,166 | 11.995 | Reference |
Infliximab Biosimilar | $148,111 | 12.311 | $66,323 | |
Tofacitinib | $152,064 | 12.331 | $192,863 | |
CADTH reanalysis 4: Utility values | Conventional Therapy | $131,499 | 18.478 | Reference |
Infliximab Biosimilar | $151,372 | 18.629 | $131,868 | |
Tofacitinib | $156,973 | 18.666 | $153,890 | |
CADTH reanalysis 5: Dose escalation | Conventional Therapy | $131,499 | 11.987 | Reference |
Tofacitinib | $151,767 | 12.338 | $57,709 | |
CADTH reanalysis 6: Concomitant CT | Conventional Therapy | $131,499 | 11.987 | Reference |
Infliximab Biosimilar | $151,316 | 12.270 | $69,977 | |
Tofacitinib | $156,586 | 12.338 | $77,492 | |
CADTH reanalysis 7: Resource use | Conventional Therapy | $138,406 | 11.987 | Reference |
Infliximab Biosimilar | $158,184 | 12.270 | $69,836 | |
Tofacitinib | $163,761 | 12.338 | $82,020 | |
CADTH base case: 1 + 2 + 3 + 4 + 5 + 6 + 7 | Conventional Therapy | $134,073 | 18.486 | Reference |
Adalimumab Biosimilar | $144,066 | 18.598 | $89,783 | |
Tofacitinib | $150,853 | 18.621 | $292,568 | |
Golimumab | $152,585 | 18.626 | $353,480 |
ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year.
Table 22: Disaggregated Costs in the CADTH Reanalysis, Biologic-Naive
Drug | Drug Acqt. | Drug Admin. | Tx. Mntrg. | Disease Mgmt. | AE | Con. CT | Surgery | Total |
|---|---|---|---|---|---|---|---|---|
Ozanimod | $57,859 | $430 | $1,636 | $99,892 | $1,352 | $946 | $1,733 | $163,849 |
Adalimumab | $57,509 | $433 | $1,623 | $99,934 | $1,351 | $934 | $1,734 | $163,519 |
Adalimumab Biosimilar | $56,749 | $433 | $1,623 | $99,934 | $1,351 | $934 | $1,734 | $162,758 |
Golimumab | $58,036 | $432 | $1,625 | $99,806 | $1,351 | $952 | $1,732 | $163,934 |
Infliximab | $59,313 | $615 | $1,628 | $99,818 | $1,352 | $952 | $1,732 | $165,408 |
Infliximab Biosimilar | $57,468 | $616 | $1,628 | $99,818 | $1,352 | $952 | $1,732 | $163,565 |
Tofacitinib | $59,129 | $430 | $1,680 | $99,502 | $1,352 | $997 | $1,728 | $164,818 |
Vedolizumab (IV) | $59,256 | $661 | $1,622 | $99,634 | $1,351 | $971 | $1,730 | $165,224 |
Vedolizumab (SC) | $59,614 | $477 | $1,622 | $99,570 | $1,351 | $980 | $1,729 | $165,344 |
Conventional Therapy | $55,666 | $430 | $1,613 | $100,056 | $1,352 | $889 | $1,736 | $161,741 |
Acqt. = acquisition; Admin. = administration; Tx = treatment; Mgmt. = management; AE = adverse event; Con. = concomitant: CT = conventional therapy; SC = subcutaneous.
Table 23: Disaggregated QALYs Gained in the CADTH Reanalysis, Biologic-Naive
Drug | Active UC | Response (no remission) | Remission | Post-surgery | Total |
|---|---|---|---|---|---|
Ozanimod | 12.156 | 0.357 | 1.339 | 2.401 | 16.250 |
Adalimumab | 12.160 | 0.355 | 1.334 | 2.403 | 16.248 |
Adalimumab biosimilar | 12.160 | 0.355 | 1.334 | 2.403 | 16.248 |
Golimumab | 12.140 | 0.362 | 1.358 | 2.400 | 16.256 |
Infliximab | 12.143 | 0.361 | 1.354 | 2.400 | 16.255 |
Infliximab biosimilar | 12.143 | 0.361 | 1.354 | 2.400 | 16.255 |
Tofacitinib | 12.099 | 0.359 | 1.427 | 2.393 | 16.275 |
Vedolizumab (IV) | 12.117 | 0.359 | 1.399 | 2.396 | 16.267 |
Vedolizumab (SC) | 12.107 | 0.358 | 1.414 | 2.395 | 16.271 |
Conventional therapy | 12.179 | 0.350 | 1.310 | 2.405 | 16.241 |
QALY = quality-adjusted life-year; SC = subcutaneous; UC = ulcerative colitis.
Table 24: Disaggregated Costs in the CADTH Reanalysis, Biologic-Experienced
Drug | Drug Acqt. | Drug Admin. | Tx. Mntrg. | Disease Mgmt. | AE | Con. CT | Surgery | Total |
|---|---|---|---|---|---|---|---|---|
Ozanimod | $19,544 | $0 | $1,565 | $75,426 | $1,241 | $56 | $1,614 | $99,446 |
Adalimumab | $18,714 | $2 | $1,551 | $75,564 | $1,239 | $29 | $1,616 | $98,714 |
Adalimumab Biosimilar | $18,170 | $2 | $1,551 | $75,564 | $1,239 | $29 | $1,616 | $98,171 |
Golimumab | $19,987 | $3 | $1,554 | $75,293 | $1,239 | $69 | $1,612 | $99,756 |
Infliximab | $21,396 | $205 | $1,557 | $75,303 | $1,240 | $68 | $1,612 | $101,381 |
Infliximab Biosimilar | $19,375 | $204 | $1,557 | $75,304 | $1,240 | $68 | $1,612 | $99,360 |
Tofacitinib | $19,755 | $0 | $1,589 | $75,289 | $1,240 | $70 | $1,612 | $99,555 |
Vedolizumab (IV) | $19,592 | $140 | $1,548 | $75,424 | $1,239 | $45 | $1,614 | $99,602 |
Vedolizumab (SC) | $20,171 | $48 | $1,549 | $75,321 | $1,239 | $60 | $1,612 | $100,001 |
Conventional Therapy | $17,388 | $0 | $1,541 | $75,628 | $1,241 | $0 | $1,616 | $97,414 |
Acqt. = acquisition; Admin. = administration; Tx = treatment; Mgmt. = management; AE = adverse event; Con. = concomitant: CT = conventional therapy; SC = subcutaneous.
Table 25: Disaggregated QALYs Gained in the CADTH Reanalysis, Biologic-Experienced
Drug | Active UC | Response, no remission | Remission | Post-surgery | Total |
|---|---|---|---|---|---|
Ozanimod | 14.633 | 0.157 | 0.118 | 1.539 | 16.444 |
Adalimumab | 14.651 | 0.148 | 0.098 | 1.543 | 16.436 |
Adalimumab Biosimilar | 14.651 | 0.148 | 0.098 | 1.543 | 16.436 |
Golimumab | 14.610 | 0.162 | 0.147 | 1.537 | 16.452 |
Infliximab | 14.613 | 0.161 | 0.144 | 1.537 | 16.451 |
Infliximab Biosimilar | 14.613 | 0.161 | 0.144 | 1.537 | 16.451 |
Tofacitinib | 14.611 | 0.162 | 0.146 | 1.536 | 16.452 |
Vedolizumab (IV) | 14.629 | 0.155 | 0.125 | 1.540 | 16.445 |
Vedolizumab (SC) | 14.613 | 0.154 | 0.150 | 1.537 | 16.451 |
Conventional Therapy | 14.662 | 0.145 | 0.085 | 1.544 | 16.432 |
UC = ulcerative colitis; IV = intravenous; SC = subcutaneous.
Table 26: Probabilistic Cost-Effectiveness Sequential Analysis From the CADTH Reanalysis, Biologic-Naive
Drug | Cost | QALYs | Incremental Cost | Incremental QALYs | ICER |
|---|---|---|---|---|---|
Conventional therapy | $161,741 | 16.241 | Reference | Reference | Reference |
Adalimumab biosimilar | $162,758 | 16.248 | — | — | Extendedly dominated by a combination of conventional therapy and tofacitinib |
Adalimumab | $163,519 | 16.248 | — | — | Strictly dominated by adalimumab biosimilar |
Infliximab biosimilar | $163,565 | 16.255 | — | — | Extendedly dominated by a combination of conventional therapy and tofacitinib |
Ozanimod | $163,849 | 16.250 | — | — | Strictly dominated by infliximab biosimilar |
Golimumab | $163,934 | 16.256 | — | — | Extendedly dominated by a combination of conventional therapy and tofacitinib |
Tofacitinib | $164,818 | 16.275 | $3,077 | 0.034 | $89,428 |
Vedolizumab (IV) | $165,224 | 16.267 | — | — | Strictly dominated by tofacitinib |
Vedolizumab (SC) | $165,344 | 16.271 | — | — | Strictly dominated by tofacitinib |
Infliximab | $165,408 | 16.255 | — | — | Strictly dominated by golimumab, tofacitinib, vedolizumab (IV), vedolizumab (SC) |
ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year; SC = subcutaneous.
Table 27: Probabilistic Cost-Effectiveness Sequential Analysis From the CADTH Reanalysis, Biologic-Experienced
Drug | Cost | QALYs | Incremental Cost | Incremental QALYs | ICER |
|---|---|---|---|---|---|
Conventional Therapy | $97,414 | 16.432 | Reference | Reference | Reference |
Adalimumab Biosimilar | $98,171 | 16.436 | — | — | Extendedly dominated by a combination of Conventional Therapy and Infliximab Biosimilar |
Adalimumab | $98,714 | 16.436 | — | — | Strictly dominated by Adalimumab Biosimilar |
Infliximab Biosimilar | $99,360 | 16.451 | $1,946 | 0.019 | $101,345 |
Ozanimod | $99,446 | 16.444 | — | — | Strictly dominated by Infliximab Biosimilar |
Tofacitinib | $99,555 | 16.452 | $195 | 0.001 | $278,848 |
Vedolizumab (IV) | $99,602 | 16.445 | — | — | Strictly dominated by Infliximab Biosimilar, Tofacitinib |
Golimumab | $99,756 | 16.452 | $201 | 0.000 | $1,260,486 |
Vedolizumab (SC) | $100,001 | 16.451 | — | — | Strictly dominated by Golimumab, Infliximab Biosimilar, Tofacitinib |
Infliximab | $101,381 | 16.451 | — | — | Strictly dominated by Golimumab, Tofacitinib |
ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year; IV = intravenous; SC = subcutaneous.
Scenario Analyses
Table 28: CADTH Price Reduction Analyses, Biologic-Naive
Price reduction | Sponsor base-case ICER ($/QALY) | CADTH base-case ICER ($/QALY) |
|---|---|---|
Ozanimod submitted price | WTP < $64,810: CT WTP ≥ $64,810: Tofacitinib | WTP < $111,287: CT $111,287 < WTP < $277,869: Adalimumab Bio. $277,869 < WTP < $352,972: Tofacitinib WTP ≥ $352,972: Golimumab |
10% 20% 30% 40% 50% | WTP < $65,911: CT WTP ≥ $65,911: Tofacitinib | |
55% | WTP < $48,734: CT $48,734 < WTP < $72,910: Ozanimod WTP ≥ $72,910: Tofacitinib | |
60% | WTP < $42,343: CT $42,343 < WTP < $75,514: Ozanimod WTP ≥ $75,514: Tofacitinib | |
70% | WTP < $29,563: CT WTP ≥ $80,721: Tofacitinib $29,563 < WTP < $80,721: Ozanimod | WTP < $56,238: CT $56,238 < WTP < $398,019: Ozanimod WTP ≥ $398,019: Golimumab |
73% | WTP < $25,729: CT $25,729 < WTP < $82,284: Ozanimod WTP ≥ $82,284: Tofacitinib | WTP < $49,119: CT $49,119 < WTP < $415,444: Ozanimod WTP ≥ $415,444: Golimumab |
ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year; CT = conventional therapy; Bio. = biosimilar; WTP = willingness-to-pay threshold.
Notes: Only non-dominated strategies are presented.
The term WTP has been used to denote that if a value is above, below or between the values stated, then the treatment stated is the optimal treatment based on that WTP value or range.
Table 29: CADTH Price Reduction Analyses, Biologic-Experienced
Price reduction | Sponsor base-case ICER ($/QALY) | CADTH base case ICER ($/QALY) |
|---|---|---|
Ozanimod submitted price | WTP < $68,904: CT $68,904 < WTP < $79,495: Infliximab Bio. WTP ≥ $79,495: Tofacitinib | WTP < $89,756: CT $89,756 < WTP < $293,431: Adalimumab Bio. $293,431 < WTP < $352,970: Tofacitinib WTP ≥ $352,970: Golimumab |
10% 20% | WTP < $70,154: CT $70,154 < WTP < $82,410: Infliximab Bio. WTP ≥ $82,410: Tofacitinib | |
30% | WTP < $63,419: CT $63,419 < WTP < $84,454: Ozanimod WTP ≥ $84,454: Tofacitinib | |
40% | WTP < $53,140: CT $53,140 < WTP < $97,916: Ozanimod WTP ≥ $97,916: Tofacitinib | |
44% | WTP < $49,029: CT $49,029 < WTP < $103,300: Ozanimod WTP ≥ $103,300: Tofacitinib | |
50% | WTP < $42,862: CT $42,862 < WTP < $111,377: Ozanimod WTP ≥ $111,377: Tofacitinib | WTP < $80,707: CT $80,707 < WTP < $291,030: Ozanimod $291,030 < WTP < $352,970: Tofacitinib WTP ≥ $352,970: Golimumab |
60% | WTP < $32,584: CT $32,584 < WTP < $124,839: Ozanimod WTP ≥ $124,839: Tofacitinib | WTP < $61,445: CT $61,445 < WTP < $362,074: Ozanimod WTP ≥ $362,074: Golimumab |
66% | WTP < $26,417: CT $26,417 < WTP < $132,919: Ozanimod WTP ≥ $132,919: Tofacitinib | WTP < $49,888: CT $49,888 < WTP < $399,189: Ozanimod WTP ≥ $399,189: Golimumab |
ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year; CT = conventional therapy; Bio. = biosimilar; WTP = willingness-to-pay threshold.
Notes: Only non-dominated strategies are presented.
The term WTP has been used to denote that if a value is above, below or between the values stated, then the treatment stated is the optimal treatment based on that WTP value or range.
Table 30: Summary of Scenario Analyses Conducted on CADTH Base Case, Biologic-Naive
Scenario analysis | Drug | Total costs ($) | Total QALYs | Sequential ICER ($/QALY) |
|---|---|---|---|---|
CADTH base case | Conventional therapy | $161,741 | 16.241 | Reference |
Tofacitinib | $164,818 | 16.275 | $89,428 | |
1. Differential clinical efficacy and safety | Conventional therapy | $167,446 | 14.946 | Reference |
Tofacitinib | $167,714 | 14.949 | $88,190 | |
2. One-time 30% reduction in clinical efficacy from year 2 | Conventional therapy | $153,344 | 16.285 | Reference |
Tofacitinib | $160,741 | 16.364 | $93,204 |
ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year.
Table 31: Summary of Scenario Analyses Conducted on CADTH Base Case, Biologic-Experienced
Scenario analysis | Drug | Total costs ($) | Total QALYs | Sequential ICER ($/QALY) |
|---|---|---|---|---|
CADTH base case | Conventional therapy | $97,414 | 16.432 | Reference |
Infliximab biosimilar | $99,360 | 16.451 | $101,345 | |
Tofacitinib | $99,555 | 16.452 | $278,848 | |
Golimumab | $99,756 | 16.452 | $1,260,486 | |
1. Differential clinical efficacy and safety | Conventional therapy | $144,004 | 20.438 | Reference |
Tofacitinib | $152,098 | 20.516 | $105,001 | |
2. One-time 30% reduction in clinical efficacy from year 2 | Conventional therapy | $172,517 | 21.213 | Reference |
Tofacitinib | $172,636 | 21.214 | $99,379 |
ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year.
Appendix 5: Submitted BIA and CADTH Appraisal
Note that this appendix has not been copy-edited.
Table 32: Summary of Key Take-Aways
Key take-aways of the BIA |
|---|
|
Summary of Sponsor’s BIA
The sponsor sought to determine the incremental budget impact of reimbursing ozanimod in patients with moderately to severely active UC from the perspective of Canada, which includes all participating public drug plans within the territory (except for Quebec), as well as the Non-Insured Benefits Program (NIHB). The sponsor estimated the budget impact analysis (BIA) via an incremental comparison of 2 scenarios: one that considers costs associated with currently available therapies used to treat patients with moderate to severe UC (i.e., reference scenario), and a second one that considers costs in a world where ozanimod is reimbursed for the same population (i.e., new scenario). The costs associated with the cohort of eligible patients were forecasted over a 3-year time horizon for both scenarios.29 The size of the eligible population of patients treated for moderate to severe UC covered by public drug programs in the baseline “year zero” of the model (i.e., July 2022 to June 2023) was estimated using a funnel approach based on demographic and epidemiological sources informing the incidence and prevalence of UC in Canada, as well as the population growth rate.30 The number of patients expected to receive each therapy in each year of the BIA model derived from the sponsor’s available data on annual market shares.29 Key inputs to the BIA are documented in Table 33.
Key model assumptions:
Eligible patients were assumed to remain on a given treatment for a full year. As such, treatment discontinuation and switching due to treatment-emergent AEs or loss of response are assumed to be captured in the model by variations in market share for each year.
The model includes neither overall nor UC-specific mortality, given the limited time horizon and lack of mortality data.
The introduction of ozanimod into the market is assumed to have no impact on UC incidence and diagnosis rate.
The analysis does not consider extended induction dosing.
The expenditures associated with disease management (i.e., disease monitoring) are excluded from the BIA. The sponsor assumed that these would be similar for each comparator under both the current and future market mix scenarios.
The model omits the cost of surgery due to the relatively short time horizon and low rate of surgery for UC.
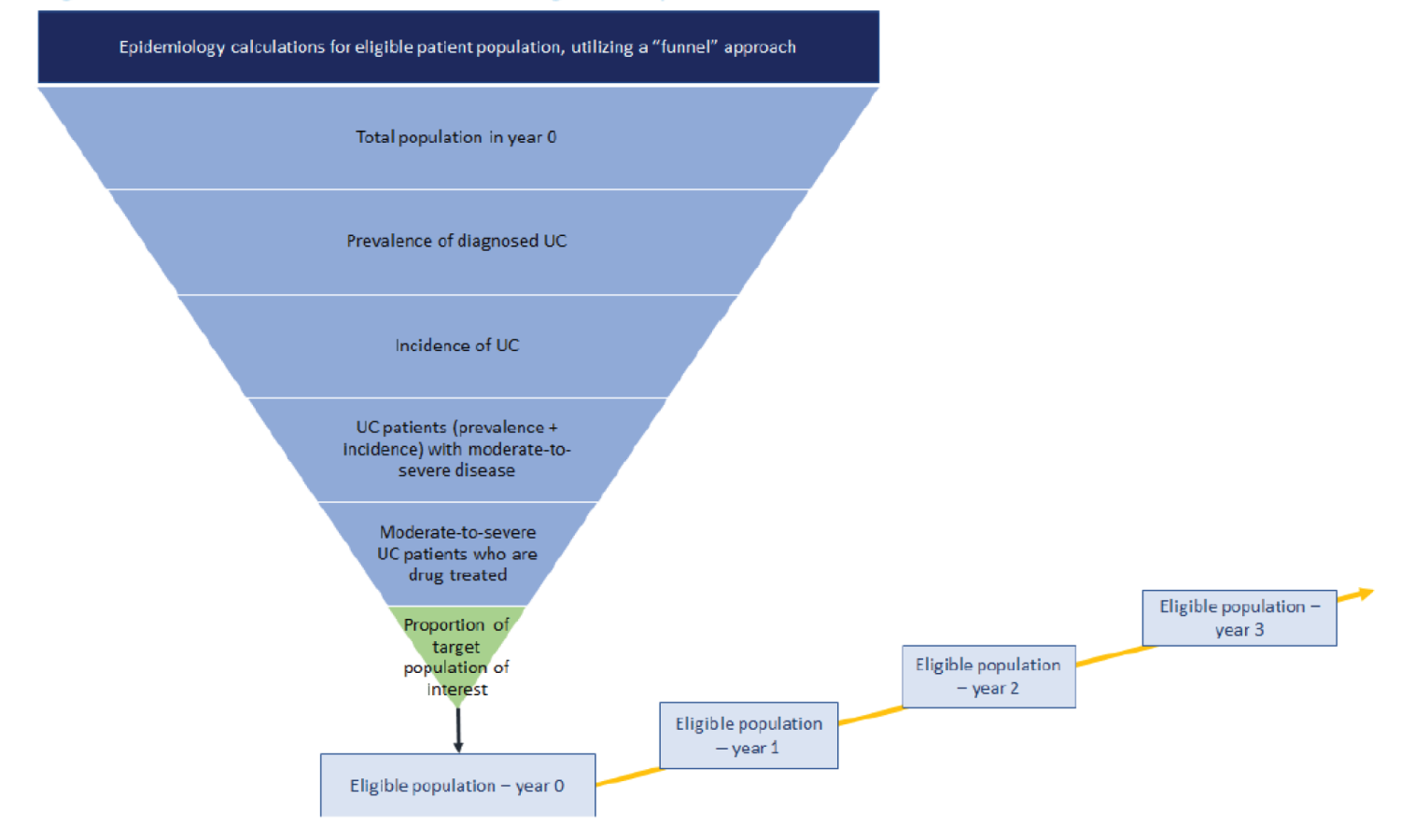
Table 33: Summary of Key Model Parameters
Parameter | Sponsor’s estimate (year 1 / year 2 / year 3) | |
|---|---|---|
Target population | ||
Methodology used to calculate population size | Funnel approach | |
Prevalence of diagnosed UC | 0.34% | Refer to Figure 2. |
Incidence of UC per 100,000 | 10.8 | |
% of UC patients with moderate to severe disease | 35.00% | |
% of moderate to severe UC patients who are drug-treated | 90.00% | |
% of drug-treated moderate to severe UC patients who are biologic-naive | 60.00% | |
% of drug-treated moderate to severe UC patients who are biologic-experienced | 40.00% | |
Annual growth rate, treatment eligible population (%) | 0.48% | |
Number of patients eligible for drug under review | Biologic-naive population: 22,304 / 24,827 / 27,427 Biologic-experienced population: 14,869 / 16,551 / 18,284 | |
Market uptake (3 years) | ||
Uptake (reference scenario) – Biologic-naïve: Adalimumab Adalimumab biosimilar Golimumab Infliximab Infliximab biosimilar — Renflexis Tofacitinib Ustekinumab Vedolizumab (IV) Vedolizumab (SC) Conventional Therapy Infliximab biosimilar – Inflectra | 19.69% / 14.52% / 16.01% 6.02% / 6.84% / 5.89% 0.90% / 0.97% / 0.89% 25.41% / 22.32% / 23.11% 1.77% / 2.30% / 2.44% 1.95% / 2.36% / 2.64% 15.98% / 19.56% / 18.62% 22.44% / 23.30% / 24.41% 0.00% / 0.00% / 0.00% 0.00% / 0.00% / 0.00% 5.84% / 7.83% / 5.99% | |
Uptake (reference scenario) – Biologic-experienced: Adalimumab Adalimumab biosimilar Golimumab Infliximab Infliximab biosimilar — Renflexis Tofacitinib Ustekinumab Vedolizumab (IV) Vedolizumab (SC) Conventional Therapy Infliximab biosimilar – Inflectra | 6.45% / 3.97% / 4.64% 6.02% / 6.61% / 6.78% 1.57% / 1.43% / 1.28% 8.95% / 7.32% / 8.20% 3.33% / 3.30% / 3.18% 7.23% / 7.52% / 8.77% 40.96% / 43.51% / 42.29% 19.63% / 17.51% / 15.92% 0.00% / 0.00% / 0.00% 0.00% / 0.00% / 0.00% 5.86% / 8.83% / 8.94% | |
Uptake (new drug scenario) – Biologic-naïve: Ozanimod Adalimumab Adalimumab biosimilar Golimumab Infliximab Infliximab biosimilar — Renflexis Tofacitinib Ustekinumab Vedolizumab (IV) Vedolizumab (SC) Conventional Therapy Infliximab biosimilar – Inflectra | 2.46% / 5.76% / 6.00% 14.16% / 15.09% / 12.26% 6.67% / 5.55% / 6.54% 0.95% / 0.84% / 0.90% 21.77% / 21.77% / 19.01% 2.25% / 2.30% / 2.89% 2.30% / 2.48% / 2.93% 19.08% / 17.55% / 20.29% 22.73% / 23.00% / 22.14% 0.00% / 0.00% / 0.00% 0.00% / 0.00% / 0.00% 7.63% / 5.65% / 7.03% | |
Uptake (new drug scenario) – Biologic-experienced: Ozanimod Adalimumab Adalimumab biosimilar Golimumab Infliximab Infliximab biosimilar — Renflexis Tofacitinib Ustekinumab Vedolizumab (IV) Vedolizumab (SC) Conventional Therapy Infliximab biosimilar – Inflectra | 3.62% / 12.57% / 15.07% 3.83% / 4.06% / 2.95% 6.37% / 5.93% / 5.66% 1.37% / 1.12% / 1.09% 7.05% / 7.17% / 5.80% 3.18% / 2.78% / 3.30% 7.25% / 7.67% / 7.43% 41.93% / 36.98% / 36.35% 16.88% / 13.92% / 14.39% 0.00% / 0.00% / 0.00% 0.00% / 0.00% / 0.00% 8.51% / 7.82% / 7.97% | |
Cost of treatment (per patient)a | ||
Annual cost of treatment (Year 1): Ozanimod Adalimumab Adalimumab biosimilar Golimumab Infliximab Infliximab biosimilar – Renflexis Tofacitinib Ustekinumab Vedolizumab (IV) Infliximab biosimilar – Inflectra | $27,069.05 $27,107.77 $16,153.93 $32,548.74 $36,556.20 $18,378.97 $21,430.01 $36,572.16 $28,091.07 $19,752.72 | |
Annual cost of treatment (Year 2+): Ozanimod Adalimumab Adalimumab biosimilar Golimumab Infliximab Infliximab biosimilar – Renflexis Tofacitinib Ustekinumab Vedolizumab (IV) Infliximab biosimilar – Inflectra | $27,085.08 $23,531.93 $14,034.27 $28,615.93 $27,993.63 $14,082.20 $19,206.89 $32,598.02 $23,582.24 $15,133.55 | |
SC = subcutaneous.
aThe annual costs of treatment in the BIA for all comparators are higher than reported in the cost tables. While the cost tables represent the acquisition cost per dose of treatment, the sponsor’s costs in the BIA model include a wholesale mark-up (0.34% of acquisition cost) and a pharmacy mark-up (7.37% of acquisition cost) as per the National Prescription Drug Utilization Information.31
Summary of the Sponsor’s BIA Results
The sponsor’s BIA estimates that 3,625 biologic-naive patients with UC will be treated with ozanimod in the first 3 years of public reimbursement. The incremental expenditures associated with ozanimod’s reimbursement in this population were estimated to be $1,028,004 in year 1, $2,397,081 in year 2, and $3,106,607 in year 3, for a combined 3-year budget impact of $6,531,692 (0.26%). As it regards the biologic-experienced patient population, the sponsor’s BIA estimates that 5,374 patients will be treated with ozanimod in the first 3 years of public reimbursement. The incremental expenditures associated with ozanimod’s reimbursement in the biologic-experienced population were estimated to be $432,079 in year 1, $1,925,073 in year 2, and $2,935,081 in year 3, for a combined 3-year budget impact of $5,292,233 (0.31%).
CADTH Appraisal of the Sponsor’s BIA
CADTH identified several key limitations to the sponsor’s analysis that have notable implications on the results of the BIA:
Inclusion of a comparator that is not currently publicly reimbursed: The sponsor’s BIA model includes ustekinumab as a currently reimbursed treatment for moderate to severe UC. Ustekinumab’s negotiation process with the pan-Canadian Pharmaceutical Alliance concluded on July 28, 2021, without agreement. Hence, the therapy is not currently reimbursed for this indication by the Canadian publicly funded health care payer, whose perspective guides both the economic evaluation and the BIA. While patients may access ustekinumab through private payers, as well as through out-of-pocket payments, these are out of scope as CADTH’s focus is the public health care payer.
CADTH conducted reanalysis by excluding ustekinumab from the list of publicly reimbursed treatment options.
Exclusion of costs associated with concomitant CT: The sponsor excluded costs relevant to the practice of concomitant CT for biologic therapies from the BIA model. The use of concomitant CT for the treatment of moderate to severe UC when co-administered with a primary biologic agent is widely acknowledged in Canadian clinical guidelines and practice. Moreover, the proportion of patients who are prescribed concomitant therapy is not negligible and, in fact, relevant to include in the BIA considering that the basket and distribution of concomitant CT varies substantially across biologic therapies.
CADTH conducted reanalysis by including costs associated with concomitant CT. Both the costs and patient distributions are aligned to those applied by CADTH in the reanalysis of the sponsor’s pharmacoeconomic model.
There is uncertainty in the projected market share of ozanimod: The clinical expert indicated that it would be reasonable to expect ozanimod to capture more biologic-experienced patients, relative to biologic-naive patients, during its first year of introduction. This could be expected as prior biologic-failure patients may seek out a biologic therapy with a novel mechanism of action and be encouraged by the prospect of ozanimod. However, the clinical expert also noted that since evidence from the pivotal trial demonstrates that ozanimod is not significantly effective as an induction therapy for biologic-experienced moderate to severe UC patients, the sponsor’s market projections for years 2 and 3 are overly optimistic.
CADTH conducted reanalysis by applying relatively more conservative market shares for ozanimod in the biologic-experienced population for years 2 and 3, which are assumed to be slightly higher than the sponsor’s projected market share in the biologic-naive population for the same years (6.18% and 6.60%, respectively).
There is uncertainty in the projected capture rates of ozanimod: Sponsor assumed that ozanimod would proportionally displace market share from all treatments. According to the clinical expert consulted by CADTH, ozanimod would likely capture greater market from currently available first-line biologic therapies for UC patients tending toward moderate disease severity. Hence, it would be reasonable to expect ozanimod to equally displace the market share of vedolizumab and adalimumab as these are commonly prescribed first-line biologics for the indicated population.
CADTH was not able to address this limitation as it was not possible to conduct reanalysis by assuming that ozanimod displaces the market share of vedolizumab and adalimumab in the model.
There is uncertainty in the projected candidate population that would be prescribed ozanimod: The sponsor does not make any revisions to ozanimod’s market share despite clinical trial evidence demonstrating its increased risk of sinus bradycardia, which is not present for other biologic therapies. Although cardiovascular involvement rarely occurs in UC patients, cardiovascular disease incidence among them is modestly higher than that in the general population.32 The clinical expert consulted by CADTH noted that ozanimod would likely not be prescribed for moderate to severe UC patients with sinus bradycardia, first- or second-degree atrioventricular block, or a history of myocardial infarction or heart failure, as other biologic therapy options would be more suitable for these patient subgroups. The clinical expert also remarked that since concomitant use of heart rate–lowering drugs during ozanimod initiation may be associated with severe bradycardia and heart block, prescribing clinicians would also need to take drug-drug interactions into account, which is not currently the case for most biologic therapies. It would, thus, be reasonable to assume that the candidate population that could be prescribed ozanimod is relatively limited when compared with other biologic therapies with more advantageous safety profiles.
CADTH could not ascertain the size of the candidate population with a history of cardiac conditions, for whom ozanimod would not be the preferred biologic therapy option. Though no reanalysis was undertaken to address this limitation, CADTH considers that the sponsor’s expectation regarding ozanimod’s market share is slightly overestimated as a result.
CADTH Reanalyses of the BIA
Table 34: CADTH Revisions to the Submitted Budget Impact Analysis
Stepped analysis | Sponsor’s value or assumption | CADTH value or assumption |
|---|---|---|
Corrections to sponsor’s base case | ||
None. | — | — |
Changes to derive the CADTH base case | ||
1. Treatment options | Ustekinumab included. | Ustekinumab excluded.a |
2. Concomitant CT | Costs relevant to concomitant CT for biologic therapies excluded. | Costs associated with concomitant CT were included in the BIA. Distribution of patients receiving concomitant CT across biologic therapies aligned to that applied by CADTH in the reanalysis of the CUA model (Table 19, Appendix 4). |
3. Market share of ozanimod in the biologic-experienced population |
Year 2: 12.57% Year 3: 15.07% | Year 1: 3.62% Year 2: 6.18% Year 3: 6.60% |
CADTH base case, biologic-naive | Combined revisions 1 + 2 | |
CADTH base case, biologic-experienced | Combined revisions 1 + 2 + 3 | |
CT = conventional therapy; BIA = budget impact analysis.
aCADTH removed ustekinumab, as well as the patient population receiving ustekinumab from this analysis. Based on market share data obtained from IQVIA, the sponsor assumed that 15.98% (biologic-naive) and 40.96% (biologic-experienced) of the patient population would receive ustekinumab in year zero (i.e., current situation). As ustekinumab is not currently publicly funded, these patients would be receiving the drug privately. CADTH also undertook a scenario analysis (Scenario 2), in which the proportion of patients that would receive ustekinumab is redistributed across therapies.
The results of the CADTH stepwise reanalyses are presented in summary format in Table 35. Based on the CADTH base case, the budget impact associated with ozanimod’s reimbursement in the indicated target population is expected to be $13,066,443 in year 1, $27,131,379 in year 2, and $34,040,229 in year 3, with a 3-year total of $74,238,052.
Table 35: Summary of the CADTH Reanalyses of the BIA, Mixed Population
Stepped analysis | Three-year total |
|---|---|
Submitted base case | $11,823,925 |
Biologic-naive population | $6,531,692 |
Biologic-experienced population | $5,292,233 |
CADTH reanalysis 1 | $111,513,514 |
Biologic-naive population | $30,578,695 |
Biologic-experienced population | $80,934,818 |
CADTH reanalysis 2 | $13,025,618 |
Biologic-naive population | $6,971,878 |
Biologic-experienced population | $6,053,740 |
CADTH reanalysis 3 | $9,196,042 |
Biologic-naive population | $6,531,692 |
Biologic-experienced population | $2,664,350 |
CADTH base case | $74,238,052 |
Biologic-naive population | $31,450,890 |
Biologic-experienced population | $42,787,162 |
BIA = budget impact analysis. Submitted analysis is based on the publicly available prices of the comparator treatments.
CADTH conducted additional scenario analyses to address remaining uncertainty, using the CADTH base case. Results for the mixed population (biologic-naive and biologic-experienced) are provided in Table 36.
Assuming 30% of patients receiving adalimumab, golimumab, infliximab, and tofacitinib would be prescribed escalated doses during the maintenance phase.
Assuming the market share of ustekinumab is redistributed proportionally across therapies.
Assuming a 73% price reduction in the biologic-naive and biologic-experienced populations.
Assuming a 66% price reduction in the biologic-naive and biologic-experienced populations.
Assuming a 43% price reduction during the first year, and 51% thereafter, in both populations.
Table 36: Detailed Breakdown of the CADTH Reanalyses of the BIA, Mixed Population
Stepped analysis | Scenario | Year 0 (current situation) | Year 1 | Year 2 | Year 3 | Three-year total |
|---|---|---|---|---|---|---|
Submitted base case | Reference | $1,011,120,015 | $953,065,191 | $1,063,751,223 | $1,166,789,250 | $4,194,725,679 |
New drug | $1,011,120,015 | $954,525,274 | $1,068,073,377 | $1,172,830,938 | $4,206,549,604 | |
Budget impact | $0 | $1,460,083 | $4,322,154 | $6,041,688 | $11,823,925 | |
CADTH base case | Reference | $706,151,193 | $610,241,369 | $696,788,170 | $731,007,608 | $2,744,188,341 |
New drug | $706,151,193 | $623,307,812 | $723,919,550 | $765,047,838 | $2,818,426,393 | |
Budget impact | $0 | $13,066,443 | $27,131,379 | $34,040,229 | $74,238,052 | |
CADTH scenario analysis 1: Escalated dose | Reference | $850,158,363 | $780,149,444 | $890,063,079 | $933,957,910 | $3,454,328,796 |
New drug | $850,158,363 | $788,457,999 | $905,824,539 | $955,450,966 | $3,499,891,866 | |
Budget impact | $0 | $8,308,554 | $15,761,461 | $21,493,055 | $45,563,070 | |
CADTH scenario analysis 2: Ustekinumab’s market share redistributed | Reference | $946,464,063 | $854,441,749 | $960,512,441 | $1,037,727,754 | $3,799,146,007 |
New drug | $946,464,063 | $862,765,912 | $986,811,565 | $1,074,218,866 | $3,870,260,407 | |
Budget impact | $0 | $8,324,163 | $26,299,124 | $36,491,112 | $71,114,400 | |
CADTH scenario analysis 3: 73% price reduction | Reference | $706,151,193 | $610,241,369 | $696,788,170 | $731,007,608 | $2,744,188,341 |
New drug | $706,151,193 | $601,929,102 | $675,665,579 | $708,919,447 | $2,692,665,321 | |
Budget impact | $0 | –$8,312,267 | –$21,122,592 | –$22,088,161 | –$51,523,020 | |
CADTH scenario analysis 4: 66% price reduction | Reference | $706,151,193 | $610,241,369 | $696,788,170 | $731,007,608 | $2,744,188,341 |
New drug | $706,151,193 | $603,979,115 | $680,292,672 | $714,301,622 | $2,704,724,602 | |
Budget impact | $0 | –$6,262,254 | –$16,495,499 | –$16,705,987 | –$39,463,739 | |
CADTH scenario analysis 5: 43% price reduction in year 1 and 51% thereafter | Reference | $706,151,193 | $610,241,369 | $696,788,170 | $731,007,608 | $2,744,188,341 |
New drug | $706,151,193 | $610,714,873 | $690,207,871 | $725,834,853 | $2,732,908,790 | |
Budget impact | $0 | $473,504 | -$6,580,299 | –$5,172,756 | –$11,279,551 |
BIA = budget impact analysis. Submitted analysis is based on the publicly available prices of the comparator treatments.
Stakeholder Input
Patient Input
Crohn’s and Colitis Canada
About Crohn’s and Colitis Canada
Crohn’s and Colitis Canada is the only national, volunteer-based health charity focused on finding the cures for Crohn’s disease and ulcerative colitis, the two main forms of inflammatory bowel disease (IBD) and improving the lives of children and adults affected by these diseases. https://crohnsandcolitis.ca/
Crohn’s and Colitis Canada is one of the top health charity funders of Crohn’s and colitis research in the world, investing over $135 million in research since our founding in 1974. The organization also delivers on its promise through patient programs, advocacy and awareness. We help improve the quality of lives today by:
Sharing accurate and reliable information on treatments, research and issues related to life with Crohn’s and colitis through website, print materials, webinars and live events;
Increasing public washroom access through the GoHere program;
Raising awareness about these Canadian diseases with bilingual public communication;
Offering kids with Crohn’s or colitis camp experience; and
Providing a peer support program to newly diagnosed people.
Crohn’s and Colitis Canada is comprised of approximately 65,000 supporters including volunteers, donors or individuals interested in engaging with the organization. There is no paid membership. Crohn’s and Colitis Canada is governed by a national volunteer Board of Directors. The organization has a network of volunteer-led Chapters in 46 communities across the country, offering information, events, fundraising opportunities and encouragement. There are thousands of volunteers from coast-to-coast supporting Crohn’s and Colitis Canada’s mission.
Information Gathering
Information summarized in this section was compiled from a variety of sources. Information was drawn from Crohn’s and Colitis Canada (CCC) published reports, including the 2018 “Impact of Inflammatory Bowel Disease (IBD) in Canada Report”, a survey conducted in late 2017-early 2018 to better understand the priority needs and concerns of IBD patients and their caregivers (over 3,500 respondents), a survey deployed in late 2021 specifically on therapeutics and ozanimod (442 respondents), and a phone interview of one patient who participated in the Zeposia clinical trial conducted in Canada.
Disease Experience
Ulcerative colitis (UC) is a life-long, episodic, autoimmune disease that primarily affects the large intestine. UC can be diagnosed in all age groups, but most diagnoses are amongst youth, young adults (16 – 30 years) and seniors. The majority of Canadians living with UC are working-age Canadians. UC symptoms include unpredictable urgent bowel movements, bloody diarrhea, bloating, abdominal pain and fatigue. UC unfortunately affects every aspect of a person’s life from family, friends and work activities. Due to unpredictable urgency of bowel movements, accidents are not uncommon, especially when a patient is experiencing a flare. Patients often hide their disease from work colleagues, friends and even relatives because of the perceived stigma of the condition being a “poop” disease. Unable to predict when their next flare will occur and how to control their flare, isolation, stress and anxiety are companions to the patient’s disease journey. In extreme cases, patients have thought of suicide because of their inability to control/cope with the impacts of UC on their personal and social lives, as well as consequences in their career or school. Dating, sex and safe pregnancies (for females) are also common concerns amongst people with UC. Chronic fatigue and anemia are also consequences of UC.
A primary concern for UC patients is the unpredictability, urgency and frequency of bowel movements, especially during active disease (flare). Even during times of remission, people with UC feel that they can’t be too far away from the bathroom. Blood in the stool and abdominal pain were noted as important aspects of the disease, however bathroom access dominated concerns since it changed people’s lifestyle. As one surveyee stated, “when you have to go to the washroom 20 times a day, it impacts everything you do.” Another says, “When the disease takes control of your body, you feel very tired. When my large bowel is affected, I get bloody diarrhea quick and practically live in the bathroom. It plays havoc with my head; I can’t sleep, and I get headaches and other problems as a result.”
People living with UC must limit their activities. The disease makes it challenging to work. “You simply can’t lead a normal life of working and going to the office.” For others, “UC hampered my ability to earn a living.” Because of the stigma associated with these diseases, it is difficult for an individual to disclose their condition.
Experiences With Currently Available Treatments
Canadians have one of the highest rates of prevalence of ulcerative colitis, however, when compared with other Western countries, there are fewer treatment options available for people with moderate to severe forms of colitis. Once diagnosed, patients are often prescribed first line treatments that include anti-inflammatory class of drugs (5-ASA, mesalamine) together with corticosteroids used to control flares. For those who are unresponsive or develop a moderate to severe form of IBD, second line treatments usually consist of immune-modulators/immunosuppressants, sometimes together with corticosteroids and biologics. These classes of medication work to reduce inflammation by suppressing the immune system.
These drugs often work well for those experiencing mild to moderate levels of colitis, but often fail in maintaining remission for those experiencing severe forms. For some patients, these treatments keep their condition in remission for long periods of time at early stages of their disease, and for others using aminosalicylates or immunosuppressants the treatments did not change their symptoms and overall condition.
Most patients do not report experiencing side effects in taking aminosalicylates. Some patients report liver problems arise from taking immunosuppressants (azathiopurine). The majority of patients do report numerous side effects from steroid use. Most common cited effects included mood swings (easily angered or high anxiety), moon face, and weight gain. One interviewee mentioned that Predisone use, with 16 pills a day, made him feel better by 60% but never ended bloody stools. It also led to the development of cataracts in both eyes. The negative impact of steroid use over the long term, including increased mortality and morbidity, is well documented in scientific literature.
For the patients who provided these testimonials, initially these treatments would help to relieve some symptoms, but it did not control their symptoms, including the constant and urgent use of the washrooms. Furthermore, none of those surveyed achieved and maintained remission indefinitely.
People experiencing severe forms of colitis may be prescribed biologics that inhibit the inflammatory pathway.
One surveyee stated that because of the protocol from his private insurer, he had to go through first line available therapies before he could get access to the biologic drug that worked for him. It took him three years to go through this process also taking a toll on his mental well-being and disease progression.
Improved Outcomes
Patients seek any treatments that can mitigate these symptoms to protect a patient’s ability to work productively, attend school and social events, and even basic daily necessities like leaving the house to run errands or have the energy to maintain a household or raise children. Quality of life could be greatly improved in UC patients if their flares are brought into remission.
Experience With Drug Under Review
The below feedback is based on a survey that Crohn’s and Colitis Canada conducted in November 2021 and a phone interview with one patient who gained access to Zeposia by participating in a clinical trial and is still being treated with Zeposia.
Of the 442 survey respondents, 7 were prescribed Zeposia. All 7 respondents and the phone interviewee had access to Zeposia via the clinical trial.
Prior to being prescribed Zeposia, respondents indicated that their UC was active and that they had been prescribed a series of drugs, including steroids to manage their disease. Half of the respondents had been prescribed at least one biologic. Unmanaged symptoms included chronic pain and frequent unpredictable bowel movements. Consequences of the unmanaged flares were fatigue, anxiety and depression, inability to work or attend school, anemia, and a general feeling of a lack of control over their lives. When asked which of the symptoms were most important in managing their disease, all respondents indicated pain/discomfort and anxiety.
Benefits: Of the seven survey respondents, one experienced ongoing side effects of Zeposia and discontinued the trial. A second respondent indicated that they did not notice any significant benefit with Zeposia. The below summary of benefits is based on the five survey respondents and the one phone interviewee. Benefits included ease of use, improved symptoms and quality of life with a general sense of feeling healthier and happier. They were able to resume work or school, socialize more and even travel. As one person noted “Zeposia gave my life back. From being in chronic pain, feeling constantly tired from my bloody diarrhea, and feeling depressed…I am healed…my ulcers are gone…no more injections [for biologics]…I just take a pill….I used to take 21 pills a day to try to manage my disease…I now take 8 pills a day.”
Disadvantages: Half of the respondents indicated that the Zeposia capsules were difficult to swallow.
Side Effects: Four of the eight UC patients experienced no side effects of Zeposia. A fifth respondent also reported no side effects but this patient also reported no noticeable benefits of Zeposia. One respondent reported multiple side effects (headache, serious infection, joint pain, nasopharyngitis) and discontinued using Zeposia. One reported high blood pressure but remained on Zeposia because of the noticeable difference on his/her symptoms and quality of life. We did not ask how his/her high blood pressure was managed.
Companion Diagnostic Test
Fecal calprotectin is a biomarker for inflammation in the gut. As all participants gained access to Zeposia via a clinical trial and fecal calprotectin testing was part of the trial protocol, none had barriers to accessing the test. However, some noted challenges with the travel time / distance of the clinic or lab.
Anything Else?
No.
Conflict of Interest Declaration — Crohn’s and Colitis Canada
To maintain the objectivity and credibility of the CADTH reimbursement review process, all participants in the drug review processes must disclose any real, potential, or perceived conflicts of interest. This Patient Group Conflict of Interest Declaration is required for participation. Declarations made do not negate or preclude the use of the patient group input. CADTH may contact your group with further questions, as needed.
Did you receive help from outside your patient group to complete this submission?
No.
Did you receive help from outside your patient group to collect or analyze data used in this submission?
No.
List any companies or organizations that have provided your group with financial payment over the past 2 years AND who may have direct or indirect interest in the drug under review.
Table 1: Financial Disclosures for Crohn’s and Colitis Canada
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
Bristol Myers Squibb | — | — | — | X |
Gastrointestinal Society
About the Gastrointestinal Society
As the Canadian leader in providing trusted, evidence-based information on all areas of the gastrointestinal tract, the GI (Gastrointestinal) Society is committed to improving the lives of people with GI and liver conditions, supporting research, advocating for appropriate patient access to health care, and promoting gastrointestinal and liver health.
Canadian healthcare professionals request more than 600,000 of our BadGut® Basics patient information pamphlets each year, and tens of thousands of Canadians benefit from our important quarterly publication, the Inside Tract® | Du coeur au ventreMD newsletter. GI Society support group meetings offer a wealth of information for those newly diagnosed with a gastrointestinal disorder, as well as those who have lived with a condition for years.
The GI Society is a national charity formed in 2008 on the groundwork of its partner organization, the Canadian Society of Intestinal Research (CSIR), which was founded in Vancouver in 1976. We receive national and international attention, simply because we have earned the respect of both the gastrointestinal medical community and Canadians who battle GI and liver issues daily. During 2021, our English (www.badgut.org) and French (www.mauxdeventre.org) websites had 6.7 million page views by 5.8 million unique users. This is increasing year over year.
All our programs and services focus on providing Canadians with trusted, commercial-free, medically-sound information on gut and liver diseases and disorders in both official languages. Our BadGut® lectures (currently on hiatus due to the pandemic), quarterly Inside Tract® newsletter, pamphlets, and educational videos arm Canadians with the information they require to better understand and manage their specific needs. We also work closely with healthcare professionals and governments at all levels toward system-wide improvements in care and treatment.
Information Gathering
The information we used to complete this questionnaire was obtained primarily through questionnaires:
2015 survey on biologics and biosimilars (then called subsequent entry biologics) completed by 423 Canadians (English: 317 and French: 106) with inflammatory bowel disease (IBD), including Crohn’s disease and ulcerative colitis,
2018 survey on the unmet need in IBD completed by 432 Canadians with IBD,
2020 survey completed by 579 respondents regarding the unmet needs of IBD, and
2020 survey on biosimilars with 145 respondents, most of whom had IBD.
We also had contact with patients affected by IBD through one-to-one conversations at our BadGut® Lectures; a patient roundtable; recent phone/email/social media interactions with individuals who have IBD; and stories submitted over time by patients.
Disease Experience
Ulcerative colitis can arise at any age, commonly occurring in young people. There is an increased risk for those who have a family member with the condition. Currently, Canada has among the highest prevalence and incidence yet reported in the world, with approximately 120,000 diagnosed individuals.
Diarrhea, rectal bleeding, and abdominal pain are common symptoms. Inflammation decreases the intestine’s absorptive surfaces, triggering watery stools that can lead to fecal urgency and poor control of bowel function. Low red blood cell count (anemia) can result from blood loss due to ulcerations in the intestine and from general malnutrition due to the debilitating effects of the disease.
Some patients have extra-intestinal manifestations, including fever, inflammation of the eyes or joints (arthritis), ulcers of the mouth or skin, tender and inflamed nodules on the shins, and numerous other conditions. Anxiety and stress are major factors.
Ulcerative colitis often has a profound effect on an individual’s life – physically, emotionally, and socially, both at home and at school or in the workplace. It is particularly difficult for children and young adults since it often affects a person’s sense of self.
More than anything, patients have told us that sustained remission/treatment response is more important than relieving any one symptom. As a chronic disease, it is never just one flare that dominates the impact of the disease, but the constant concern that there will be future flares, possibly worse than the last, and at unpredictable times, which can disastrously disrupt patients’ lives.
The following quotes are from individuals describing what it feels like during a flare of IBD (including ulcerative colitis), and what their biggest concern is, from our most recent survey, in their own words:
“Your gut aches and burns and there is often blood in the toilet. You lose your appetite and weight, unhealthily! My biggest concern is I'm going to run out of meds to help!”
“It’s like I can’t control anything, I feel weak and can barely get up. My biggest concern is usually when I see blood and determining at what point to go to the ER.”
“The pain is worse than childbirth...and I have 3 kids...1 labour without drugs.”
“Worst flu symptoms, fatigue, lethargy, like swallowing glass and chili and then having constipation and diarrhea at the same time. Gut cramps and hunger cramps at the same time. Want to die. Biggest concern is needing a toilet at all times with zero minutes waiting time.”
“It feels like my guts are in a vise. The nausea can be so bad I can't move or even vomit and the diarrhea is so painful I'll be literally screaming in the bathroom.”
“The worst part is fear of irreversible permanent damage that will affect your day-to-day life forever.”
“It is so exhausting and feels like it will never end. You start to question if you can still live the life you planned. And no-one gives you a break.”
“A flare can come out of nowhere and completely disrupt your life. Pain can sometimes be so bad that it keeps you in bed. You mostly spend life either asleep or on the toilet. My biggest concern during a flare is being able to keep up with my responsibilities (work, school, social, etc.).”
“It feels like your body is betraying you. You can’t plan anything in advance because you don’t know how your body will feel on a day to day basis.”
It’s one thing to read a list of common symptoms or data on how this disease affects patients, but it is the individual stories of these patients, as summarized above, which astound us and motivate us to support patients’ need for more diversity in effective treatments. In addition, treatments should improve quality of life, not cause more symptoms, pain, frustration, or hardship.
Experiences With Currently Available Treatments
The treatment of ulcerative colitis is multi-faceted; it includes managing the symptoms and consequences of the disease along with therapies targeted to reduce the underlying inflammation. Typically, a patient starts on one type of treatment and, if there is inadequate response, then switches to another type.
5-ASA helps to settle acute inflammation and, for some patients, keeps the inflammation inactive when taken on a long-term basis (maintenance). To reduce inflammation in moderate to severe cases, corticosteroids can help. For topical relief in the colon, corticosteroids are available in rectal formulations. These are inconvenient therapies that make it difficult for patients to keep a normal routine, even though they offer relief for those with mild to moderate disease. Also, if a patient has significant diarrhea, then the rectal medications may be difficult to hold in place for sufficient time to be effective. Immunosuppressive agents reduce dependence on steroids and help patients who have steroid-resistant disease, but it could take up to six months or more of therapy to see results. A newer medication, a Janus kinase (JAK) inhibitor, typically works faster than the other immunosuppressive medications and is in oral form, but many recent health risks have arisen.
Biologics treat ulcerative colitis when, initially used medications fail to relieve symptoms. There are a variety of mechanisms through which they work. However, these also do not work for all patients, and sometimes an individual will experience remission upon beginning biologic therapy but might find that it stops working after some time.
While there are a few options available, patients still have a lot of difficulty obtaining remission or adequate symptom relief. In one of our most surveys, we asked patients if the currently available medications are adequate to control their disease. Only 24% of those with IBD thought that the available medications are adequate. Conversely, 56% found them to be only somewhat adequate and 20% not adequate. Patients are still suffering, and they need new and effective options to achieve mucosal healing and reduce the debilitating symptoms of ulcerative colitis.
Improved Outcomes
Patients affected by ulcerative colitis need access to medications that work. Inadequate access to medication results in preventable patient suffering (e.g., continual, debilitating disease symptoms; secondary illnesses such as depression and anxiety disorders; and loss of family/social interactions). It also leads to unnecessary usage of healthcare resources (e.g., hospital stays, surgeries, diagnostic procedures, other medications) and a ripple effect of financial burden on the government and taxpayers (e.g., through inability to work, long-term disability claims, biologic-related debt, and even bankruptcy).
When the patient receives the right medication at the right time and for the right duration – as determined between physician and patient – these individuals can live full, rewarding lives as productive, valuable citizens who participate in the workforce and community. However, since patients respond differently to various medications, and in some cases stop responding to medications after using them for some time, it is important to have a variety of options available.
Experience With Drug Under Review
We haven’t spoken with contacts who have used this medication to treat ulcerative colitis. However, we know that patients want more options, particularly those in pill form, such as Zeposia®. While biologic medications are very effective, the injections or infusions required are a lot of work and effort, particularly for those with a chronic disease. Therefore, having more options to try before being prescribed a biologic is helpful for many patients.
Companion Diagnostic Test
Not applicable.
Anything Else?
No.
Conflict of Interest Declaration — Gastrointestinal Society
Did you receive help from outside your patient group to complete this submission?
No.
Did you receive help from outside your patient group to collect or analyze data used in this submission?
No.
List any companies or organizations that have provided your group with financial payment over the past two years AND who may have direct or indirect interest in the drug under review.
Table 2: Conflict of Interest Declaration for the Gastrointestinal Society
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
Bristol Myers Squibb in 2021 | — | — | X | — |
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up-to-date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
Redactions: Confidential information in this document may be redacted at the request of the sponsor in accordance with the CADTH Drug Reimbursement Review Confidentiality Guidelines
Stakeholder Input: The views expressed in each submission are those of the submitting organization or individual; not necessarily the views of CADTH or of other organizations. As such, they are independent of CADTH and do not necessarily represent or reflect the view of CADTH. No endorsement by CADTH is intended or should be inferred. By filing with CADTH, the submitting organization or individual agrees to the full disclosure of the information. CADTH does not edit the content of the submissions.
CADTH does use reasonable care to prevent disclosure of personal information in posted material; however, it is ultimately the submitter’s responsibility to ensure no identifying personal information or personal health information is included in the submission. The name of the submitting organization or individual and all conflict of interest information are included in the submission; however, the name of the author, including the name of an individual patient or caregiver submitting the patient input, are not posted.
Accessibility: CADTH is committed to treating people with disabilities in a way that respects their dignity and independence, supports them in accessing material in a timely manner, and provides a robust feedback process to support continuous improvement. All materials prepared by CADTH are available in an accessible format. Where materials provided to CADTH by a submitting organization or individual are not available in an accessible format, CADTH will provide a summary document upon request. More details on CADTH’s accessibility policies can be found here.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.