CADTH Reimbursement Review
Pegvaliase (Palynziq)
Sponsor: BioMarin Pharmaceutical (Canada Inc.)
Therapeutic area: Phenylketonuria
This multi-part report includes:
Clinical Review
Pharmacoeconomic Review
Stakeholder Input
Clinical Review
Abbreviations
ACMG
American College of Medical Genetics and Genomics
ADHD
attention-deficit/hyperactivity disorder
ADHD-RS-IV
Attention Deficit Hyperactivity Disorder Response Scale (investigator-rated)
AE
adverse event
AESI
adverse event of special interest
BMI
body mass index
BRIEF
Behavior Rating Inventory of Executive Function
CanPKU
Canadian PKU and Allied Disorders
CGI-S
Clinical Global Impression Severity
CI
confidence interval
FAAN
Food Allergy and Anaphylaxis Network
HAE
hypersensitivity adverse event
HRQoL
health-related quality of life
ITT
intention-to-treat
LNAA
large neutral amino acid
LSM
least squares mean
MedDRA
Medical Dictionary for Regulatory Affairs
MID
minimal important difference
mITT
modified intention-to-treat
MMRM
mixed model for repeated measures
MNT
medical nutritional therapy
NIAID
National Institute of Allergy and Infectious Diseases
PAH
phenylalanine hydroxylase
Phe
phenylalanine
PKU
phenylketonuria
PKUDOS
Phenylketonuria Demographics, Outcome, and Safety
PKU POMS
Phenylketonuria-Specific Profile of Mood States
POMS
Profile of Mood States
PSM
propensity score matching
RDT
randomized discontinuation trial
SAE
serious adverse event
SD
standard deviation
SGA
Subject Global Assessment
TMD
total mood dysfunction
Executive Summary
An overview of the submission details for the drug under review is provided in Table 1.
Item | Description |
|---|---|
Drug product | Pegvaliase (Palynziq), pre-filled syringes: 2.5 mg/0.5 mL (5 mg/mL), 10 mg/0.5 mL (20 mg/mL), 20 mg/mL, solution for subcutaneous injection |
Indication | Palynziq (pegvaliase injection) is indicated to reduce blood phenylalanine concentrations in patients with phenylketonuria aged 16 years and older who have inadequate blood phenylalanine control (blood phenylalanine levels greater than 600 µmol/L) despite dietary management |
Reimbursement request | For the treatment of patients with phenylketonuria aged 16 years and older who have inadequate blood phenylalanine control (blood phenylalanine levels greater than 600 μmol/L) despite prior treatment with sapropterin |
Health Canada approval status | NOC |
Health Canada review pathway | Standard |
NOC date | March 30, 2022 |
Sponsor | BioMarin Pharmaceutical (Canada) Inc. |
NOC = Notice of Compliance.
Source: CADTH review submission1 and draft product monograph2 for pegvaliase.
Introduction
Phenylketonuria (PKU) is a monogenic autosomal recessive disorder and 1 of the most common inborn errors of metabolism.3 Patients with PKU have mutations in both alleles of the PAH gene encoding phenylalanine hydroxylase (PAH), an enzyme that catalyzes the conversion of phenylalanine (Phe) to tyrosine using tetrahydrobiopterin as a cofactor.3 A wide variety of PAH gene mutations give rise to variations in clinical phenotype and disease severity.3,4 Deficiency of PAH leads to uncontrolled blood Phe, which then crosses the blood-brain barrier, where it has neurotoxic effects.3,4 Phenylketonuria is universally identified via newborn screening programs in Canada; uncontrolled Phe levels in untreated PKU during early childhood profoundly impair brain function and development.5 In adolescents and adults, uncontrolled Phe levels are associated with behavioural and psychiatric problems (inattentiveness and mood dysfunction, often collectively referred to as “executive dysfunction”).6 Symptoms of PKU, in conjunction with treatments, negatively affect the health-related quality of life (HRQoL) of patients with respect to employment, social relationships, and mental health.7
Phenylketonuria is rare, with an incidence of approximately 1 in 12,000 to 1 in 15,000 live births in Canada (equivalent to approximately 300 new cases per year). According to the sponsor, approximately 3,133 patients are living with PKU in Canada at present, of whom approximately ||||| are being managed and approximately ||| are 16 years of age or older and currently being treated with sapropterin.1 PKU is diagnosed shortly after birth by newborn screening using biochemical and genetic tests. Physicians specializing in genetics and metabolic diseases are required to diagnose, treat, and monitor patients with PKU at hospital-based genetic or metabolic clinics that have support from dietitians trained in PKU management.
According to clinical experts consulted by CADTH for this review, the current cornerstone of PKU treatment is lifelong dietary control of Phe intake to curb blood Phe levels. This is principally accomplished by providing Phe-free foods and metabolic formulas with a small amount of “complete” Phe-containing protein allowed on top, sometimes collectively referred to as medical nutritional therapy (MNT). Adherence of adult patients with PKU to MNT is extremely challenging because low-protein medical food is very unpleasant to taste and smell. Other than dietary restriction, the only other approved medication is sapropterin, a cofactor of the deficient PAH enzyme in PKU. Approximately 25% of patients with milder PKU have a biochemically detectable response to sapropterin.8
Pegvaliase is a recombinant Phe ammonia lyase enzyme that converts Phe to ammonia and trans-cinnamic acid. The Health Canada indication for pegvaliase is “Palynziq (pegvaliase injection) is indicated to reduce blood phenylalanine concentrations in patients with phenylketonuria (PKU) aged 16 years and older who have inadequate blood phenylalanine control (blood phenylalanine levels greater than 600 micromol/L) despite dietary management.” Pegvaliase is supplied as a solution (2.5 mg/0.5 mL [5 mg/mL], 10 mg/0.5 mL [20 mg/mL], 20 mg/mL) in pre-filled syringes. Pegvaliase is self-administered at a titrated maintenance dose (following induction and titration) required to achieve a blood Phe level of 600 µmol/L or lower by subcutaneous injection. The objective of this report was to perform a systematic review of the beneficial and harmful effects of pegvaliase (self-administered subcutaneous injection, titrated to a maintenance dose required to achieve blood Phe levels of 600 μmol/L or lower; maximum dose 60 mg daily) for the treatment of patients with PKU aged 16 years and older who have inadequate blood Phe control (blood Phe levels greater than 600 μmol/L) on existing management.
Stakeholder Perspectives
The information in this section is a summary of input provided by the patient groups who responded to CADTH’s call for patient input and from clinical experts consulted by CADTH for the purpose of this review.
Patient Input
One submission, from the Canadian PKU and Allied Disorders (CanPKU) association, was received for this review. Between November 30, 2021, and December 25, 2021, CanPKU conducted online surveys of 68 patients with PKU (46 patients in Canada and 14 in the US) and telephone interviews with 5 patients experienced with pegvaliase (1 patient in Canada and 4 in the US). Respondents described how PKU symptoms and the PKU protein-restricted diet had affected their physical and mental health, employment, and social relationships. Almost all respondents (≥ 95%) had experience with low-protein medical foods and formulas and 65% had experience with Kuvan (sapropterin), while only 21% had experience with pegvaliase. Respondents described barriers to existing therapies, including poor taste, lack of satiety, inconvenient preparation and administration, high cost, and limited availability.
The vast majority (≥ 85%) of respondents identified Phe control, reducing PKU symptoms, limiting long-term disease consequences, improving neurocognitive function, managing diet, reducing burden of treatment, improving HRQoL, and increasing natural protein intake as key outcomes of interest. Respondents experienced with pegvaliase reported that the drug limited long-term disease consequences; controlled Phe levels; reduced PKU symptoms; and had tolerable side effects, such as injection-site reactions, joint pain, and skin reactions.
Clinician Input
Input From Clinical Experts Consulted by CADTH
Two clinical specialists with expertise in the diagnosis and management of pediatric and adult patients with PKU who have inadequate Phe control provided input for this review. The clinical experts stated that currently available therapies (MNT with or without sapropterin) can in theory successfully meet treatment goals by decreasing Phe levels and preventing the neuropsychological complications of PKU. However, because adherence to MNT is generally low, MNT is not effective in most patients and only a small proportion of patients with milder PKU will respond to sapropterin. Pegvaliase would be used as last-line treatment following MNT and, if appropriate, sapropterin. Pegvaliase may shift the treatment paradigm for some adult patients with PKU by allowing liberalization of diets while maintaining Phe control.
The 2 clinical experts consulted by CADTH for this review differed on the subset of patients with PKU who would benefit most from pegvaliase. One expert reported that patients with high and uncontrolled Phe are most in need of an intervention to improve metabolic control that will lead to a decrease in their Phe levels and improved Phe tolerance. The clinical expert could not rule out the possibility that patients who are poorly compliant with MNT could become more compliant to therapies (including pegvaliase) over time as Phe levels decrease and their focus improves. The second clinical expert stated that patients with PKU who are highly compliant with MNT and other therapies and have the most severe forms of PKU would be the most suitable for treatment with pegvaliase. These patients are generally able to achieve Phe levels within the control range but have the most unpalatable diets and experience large deviations in Phe levels. These patients can be identified by assessing compliance with MNT and other therapy (using mean Phe values) and PKU severity (using PAH genotyping, variability in Phe levels, and/or degree of restriction of complete protein intake). This clinical expert indicated that patients who are noncompliant with therapy would be the least suitable for treatment with pegvaliase.
The clinical experts agreed that complete protein tolerance (or Phe tolerance) and blood Phe levels are the most convenient tests to assess response to treatment and are most often used in clinical trials. Clinically meaningful responses to treatment would be, in order of importance, increased complete protein tolerance (or Phe tolerance) and protein intake to levels in the general population, improvement in HRQoL, and improvement in psychological metrics (neurocognitive performance, mood, attention, and working memory). According to the clinical experts, high blood Phe levels can be used to show that pegvaliase treatment is ineffective, and stability of Phe levels with the treatment range can demonstrate improvements in protein tolerance in patients with low Phe who liberalize their diets to include natural foods. Patients who cannot maintain acceptable Phe levels (or whose levels are not monitored) with MNT and pegvaliase are noncompliant and should be discontinued from treatment, as should patients who experience significant adverse reactions.
Clinician Group Input
A group of 3 physicians who care for adult patients with PKU in Canada provided input for this review. Although the clinician group echoed the challenges in adhering to the PKU diet and the limited proportion of patients who can benefit from sapropterin, views contrasting with those of the clinical experts consulted by CADTH were presented on: the connection between blood Phe levels and neurologic symptoms, diet liberalization, and associated impacts on HRQoL in adult patients with PKU, which the clinician group reported were tightly and reversibly linked; the importance of Phe control as a treatment goal and marker of treatment response in and of itself; the patient subset most suitable for pegvaliase treatment, which the clinician group described as patients noncompliant with dietary restrictions who cannot benefit from sapropterin and therefore have poor or no Phe control; the patient subset least suitable for pegvaliase treatment, which the clinician group identified as patients able to maintain Phe levels within a target range on MNT with or without sapropterin; and the risks of Phe levels below 30 µmol/L resulting from overtreatment with pegvaliase in patients who do not comply with Phe monitoring, which the clinician group described as a potential concern. According to the clinician group, pegvaliase would be offered as last-line treatment for adult patients with PKU who have elevated Phe levels and neuropsychiatric symptoms and are able to self-administer the injection.
Drug Program Input
The Formulary Working Group identified the following jurisdictional implementation issues: relevant comparators, considerations for initiation of therapy, considerations for continuation or renewal of therapy, considerations for discontinuation of therapy, considerations for prescribing of therapy, generalizability, care provision, and system and economic issues. The clinical experts consulted by CADTH for this review weighed evidence from the included study and other clinical considerations to provide responses to the CADTH Provincial Advisory Group’s drug program implementation questions. Table 4 provides more details.
Clinical Evidence
Pivotal Studies and Protocol-Selected Studies
Description of Studies
PRISM-2 was a phase III, 4-part, 4-arm, double-blind, placebo-controlled randomized discontinuation trial (RDT) with an extension period of open-label treatment (N = 215).9-16 The major feeder study for the PRISM-2 trial was the PRISM-1 trial,16,17 a phase III, open-label study to assess the safety and tolerability of 2 pegvaliase dosage regimens (20 mg or 40 mg once daily; details are provided in the Other Relevant Evidence section). The main eligibility criteria for feeder studies were patients with PKU aged 16 years or older with blood Phe levels of greater than 600 µmol/L who were able to maintain a consistent diet. Dietary Phe control and adherence to MNT was not a requirement for participation in the feeder studies or the PRISM-2 trial. Following enrolment and screening at 29 centres in the US, patients either entered into part 1 (open-label Phe assessment) or directly into part 4 (open-label extension). In part 1, patients were randomized in a 1:1 ratio to receive open-label pegvaliase (20 mg or 40 mg once daily, vial and syringe) for up to 13 weeks; blood Phe levels were measured every 2 weeks. Patients who achieved a mean blood Phe reduction of 20% or greater from treatment-naive baseline and who were able to maintain their randomized pegvaliase dose were eligible for inclusion in the part 2 (RDT) modified intention-to-treat (mITT) set, while those who did not achieve this degree of Phe reduction or were unable to maintain their randomized pegvaliase dose due to adverse events (AEs) transitioned directly to part 4 (the open-label extension). In part 2, patients in each dose group (20 mg or 40 mg once daily, vial and syringe) were randomized 2:1 to either continue receiving their assigned dose of pegvaliase or to receive a matching-administration placebo over 8 weeks of double-blind treatment. In part 3, patients who completed part 2 received open-label pegvaliase (dose as assigned in part 1) in 2 formats (vial and syringe or pre-filled syringe) for 6 weeks and pharmacokinetics and pharmacodynamics were compared. Part 4 was an open-label extension in which patients received open-label pegvaliase (up to 60 mg once daily, pre-filled syringe) for up to 274 weeks. Only data for part 2 of the PRISM-2 RDT are described in the Systematic Review section of this report.
The primary objective of the PRISM-2 study was to evaluate the efficacy of pegvaliase in decreasing blood Phe levels by observing changes from part 2 baseline to part 2, week 8 in patients previously exposed to pegvaliase who received either pegvaliase (20 or 40 mg/day) or a matching-administration placebo in the RDT. Secondary objectives (all hierarchically tested) included comparing changes in the Attention Deficit Hyperactivity Disorder Response Scale (investigator-rated) (ADHD-RS-IV) inattention subscale scores (among participants with drug-naive baseline scores > 9 as well as all participants), Phenylketonuria-Specific Profile of Mood States (PKU POMS) (self-rated) confusion subscale scores and total mood dysfunction (TMD) scores, and Profile of Mood States (POMS) (self-rated) TMD scores from part 2 baseline to part 2, week 8 among patients previously exposed to pegvaliase who were randomized to receive either pegvaliase (20 mg/day or 40 mg/day) or a matching placebo in the RDT.
Almost all patients in the PRISM-2 trial were White (98.1%) and almost all were adults aged 18 years or older (94.9%); the average age was approximately 30 years. According to the clinical experts consulted by CADTH for this review, baseline blood Phe, mood and inattention symptoms, and protein intake in the PRISM-2 study population were as expected for adult patients with PKU with poor or no Phe control and limited adherence to MNT.
Efficacy Results
Key efficacy results of part 2 of the PRISM-2RDT are summarized in Table 2. A poolability assessment of the 2 placebo groups (20 mg/day and 40 mg/day) indicated that the magnitude of blood Phe increase from part 2 baseline to part 2, week 8 differed between the 2 placebo groups; the primary and secondary efficacy analyses were therefore conducted by comparing the pooled active group (patients who continued on their assigned dose of pegvaliase from part 1 in the part 2 RDT) versus the 20 mg/day placebo group and the 40 mg/day placebo group separately. At part 2, week 8 and in the mITT set, the least squares mean (LSM) change in blood Phe level from part 2 baseline was 26.50 µmol/L (95% confidence interval [CI], −68.26 to 121.26) in the pooled active group, 949.75 µmol/L (95% CI, 760.38 to 1,139.11) in the 20 mg/day placebo group, and 664.77 µmol/L (95% CI, 465.45 to 864.10) in the 40 mg/day placebo group. The difference in LSM change from baseline comparing the pooled active group to the 20 mg/day placebo group was −923.25 µmol/L (95% CI, −1,135.04 to −711.46; P < 0.0001). The difference in LSM change from baseline between the pooled active group and the 40 mg/day placebo group was −638.27 µmol/L (95% CI, −858.97 to −417.57; P < 0.0001). A cumulative distribution function analysis showed that at part 2, week 8 in the pooled active group, ||||| of patients had blood Phe of 120 µmol/L or lower while approximately ||| ||||||| had blood Phe between 600 µmol/L and 1,200 µmol/L, and approximately ||| ||||||| had blood Phe of 1,200 µmol/L or greater. By contrast, no patients in the placebo groups had blood Phe of 120 µmol/L or lower, while approximately ||| ||||||| had blood Phe between 600 µmol/L and 1,200 µmol/L, and approximately ||||| |||||||| had blood Phe of 1,200 µmol/L or greater.
No statistically significant differences were observed between treatment groups in ADHD-RS-IV inattention subscale scores among participants with drug-naive baseline scores of greater than 9, and further statistical testing for other neurocognitive or neuropsychiatric symptoms (ADHD-RS-IV inattention subscale scores among all participants, PKU POMS [self-rated] confusion subscale scores, PKU POMS [self-rated] TMD scores, and POMS [self-rated] TMD scores) was halted due to the hierarchical testing procedure. Changes in protein intake and HRQoL were not evaluated in part 2 of the PRISM-2 trial.
Harms Results
Key harms results of part 2 of the PRISM-2 RDT are summarized in Table 2. AEs were reported for the pooled active group (patients who continued to receive either 20 mg/day or 40 mg/day pegvaliase during the RDT) and the pooled placebo group (patients who received either 20 mg/day or 40 mg/day pegvaliase in part 1 and then switched to placebo during the RDT), as well as, in some cases, individual dose groups. In part 2 of the PRISM-2 trial, 83.3% of patients receiving active pegvaliase and 93.1% of patients receiving placebo experienced AEs. Common AEs in both the pooled active and pooled placebo groups were arthralgia (13.6% of those in the pooled active group and 10.3% of those in the pooled placebo group), headache (pooled active = 12.1% and pooled placebo = 24.1%), fatigue (pooled active = 10.6% and pooled placebo = 10.3%), anxiety (pooled active = 10.6% and pooled placebo = 6.9%), and injection-site bruising (pooled active = 4.5% and pooled placebo = 10.3%). Serious AEs (SAEs) occurred in 2 patients (3.0%) receiving active pegvaliase and 1 patient (3.4%) receiving placebo. AEs leading to dose reduction or interruption occurred in 1 patient (1.5%) receiving pegvaliase and 1 patient (3.4%) receiving placebo. No patients in part 2 of the PRISM-2 trial had AEs leading to discontinuation of the study drug. No deaths occurred during part 2 of the PRISM-2 trial.
Several study protocol-defined AEs of special interest (AESIs) occurred more frequently in patients receiving active pegvaliase than in those receiving placebo. These included hypersensitivity AEs (HAEs) (pooled active = 39.4% and pooled placebo = 13.8%), generalized skin reactions lasting 14 days or more (pooled active = 10.6% and pooled placebo = 0%), and injection-site skin reactions lasting 14 days or more (pooled active = 7.6% and pooled placebo = 3.4%). Arthralgia and injection-site reactions occurred at similar frequencies in patients receiving active pegvaliase (arthralgia = 13.6% and injection-site reaction = 24.2%) and in those receiving placebo (arthralgia = 10.3% and injection-site reaction = 24.1%). Among notable harms identified for this review, those occurring more frequently in patients receiving active pegvaliase than in those receiving placebo were rash (pooled active = 7.6% and pooled placebo = 3.4%), urticaria (pooled active = |||| and pooled placebo = ||), pruritis (pooled active = 7.6% and pooled placebo = 3.4%), injection-site pruritis (pooled active = |||| and pooled placebo = ||), diarrhea (pooled active = |||| and pooled placebo = ||), injection-site erythema (pooled active = |||| and pooled placebo = ||), and erythema (pooled active = |||| and pooled placebo = ||). No anaphylaxis events or systemic hypersensitivity reactions occurred during part 2 of the PRISM-2 trial.
Table 2: Summary of Key Results From PRISM-2 Part 2 RDT
Result | Active (pegvaliase) | Placebo | Pooled active n = 58 mITT n = 66 safety | Pooled placebo n = 28 mITT n = 29 safety | ||
|---|---|---|---|---|---|---|
20 mg/day n = 29 mITT n = 34 safety | 40 mg/day n = 29 mITT n = 32 safety | 20 mg/day n = 14 mITT n = 15 safety | 40 mg/day n = 14 mITT n = 14 safety | |||
Change from part 2 baseline to part 2, week 8 in blood Phe, µmol/L (mITT) | ||||||
Part 2 baseline Mean (SD) | NA | NA | 563.9 (504.62) | 508.2 (363.68) | 503.9 (520.28) | NA |
Part 2 week 8 Mean (SD) | NA | NA | 1,509.0 (372.64) | 1,164.4 (343.32) | 559.2 (569.47) | NA |
Mean (SD) change from part 2 baseline | NA | NA | 996.4 (555.00) | 599.0 (507.40) | 18.6 (279.43) | NA |
LSM change from part 2 baseline (95% CI) | NA | NA | 949.75 (760.38 to 1,139.11) | 664.77 (465.45 to 864.10) | 26.50 (−68.26 to 121.26) | NA |
Difference in LSM (95% CI) | NA | NA | Pooled active vs. 20 mg/day placebo: −923.25 (−1,135.04 to −711.46) Pooled active vs. 40 mg/day placebo: −638.27 (−858.97 to −417.57) | NA | ||
P valuea | NA | NA | Pooled active vs. 20 mg/day placebo: < 0.0001 Pooled active vs. 40 mg/day placebo: < 0.0001 | NA | ||
Harms, n (%) (safety population) | ||||||
AEs | || |||||| | || |||||| | || |||||| | || |||||| | 55 (83.3) | 27 (93.1) |
SAEs | ||||||| | | ||||| | | ||||| | ||||||| | 2 (3.0) | 1 (3.4) |
WDAEs | 0 | 0 | 0 | 0 | 0 | 0 |
Deaths | P | 0 | 0 | 0 | 0 | 0 |
AESIs, n (%) (safety population) | ||||||
Anaphylaxis (NIAID-FAAN criteria) | 0 | 0 | 0 | 0 | 0 | 0 |
Anaphylaxis (Brown’s severe criteria) | 0 | 0 | 0 | 0 | 0 | 0 |
Hypersensitivity AEs | || |||||| | || |||||| | | |||||| | | |||||| | 26 (39.4) | 4 (13.8) |
Generalized skin reaction ≥ 14 days in duration | | |||||| | | ||||| | ||||||| | ||||||| | 7 (10.6) | 0 |
Injection-site skin reaction ≥ 14 days in duration | | ||||| | | ||||| | ||||||| | | ||||| | 5 (7.6) | 1 (3.4) |
Arthralgia | | |||||| | | ||||| | | ||||| | | |||||| | 9 (13.6) | 3 (10.3) |
Injection-site reaction | | |||||| | | |||||| | | |||||| | | |||||| | 16 (24.2) | 7 (24.1) |
Notable harms, n (%) (safety population) | ||||||
Acute systemic hypersensitivity reactions (anaphylaxis) | ||||||
Syncope | NR | NR | NR | NR | ||||||| | ||||||| |
Hypotension | NR | NR | NR | NR | ||||||| | ||||||| |
Hypoxia | NR | NR | NR | NR | ||||||| | ||||||| |
Dyspnea | NR | NR | NR | NR | ||||||| | ||||||| |
Wheezing | NR | NR | NR | NR | ||||||| | ||||||| |
Chest discomfort/ tightness | NR | NR | NR | NR | ||||||| | ||||||| |
Tachycardia | NR | NR | NR | NR | ||||||| | ||||||| |
Angioedema | NR | NR | NR | NR | ||||||| | ||||||| |
Flushing | NR | NR | NR | NR | ||||||| | ||||||| |
Rash | NR | NR | NR | NR | 5 (7.6) | 1 (3.4) |
Urticaria | NR | NR | NR | NR | | ||||| | ||||||| |
Pruritus | NR | NR | NR | NR | 5 (7.6) | 1 (3.4) |
Injection-site pruritus | NR | NR | NR | NR | | ||||| | ||||||| |
Vomiting | NR | NR | NR | NR | | ||||| | | ||||| |
Nausea | NR | NR | NR | NR | | ||||| | | ||||| |
Diarrhea | NR | NR | NR | NR | | ||||| | ||||||| |
Other systemic hypersensitivity reactions | ||||||
Severe angioedema | NR | NR | NR | NR | ||||||| | ||||||| |
Severe serum sickness | NR | NR | NR | NR | ||||||| | ||||||| |
Injection-site reactions | NR | NR | NR | NR | 5 (7.6) | 2 (6.9) |
Injection-site induration | NR | NR | NR | NR | | ||||| | ||||||| |
Injection-site pain | NR | NR | NR | NR | | ||||| | | ||||| |
Injection-site swelling | NR | NR | NR | NR | | ||||| | | ||||| |
Injection-site erythema | NR | NR | NR | NR | | ||||| | ||||||| |
Arthralgia | 7 (20.6) | 2 (6.3) | 1 (6.7) | 2 (14.3) | 9 (13.6) | 3 (10.3) |
Lymphadenopathy | NR | NR | NR | NR | | ||||| | | ||||| |
Cough | NR | NR | NR | NR | 0 | 2 (6.9) |
Headache | NR | NR | NR | NR | 8 (12.1) | 7 (24.1) |
Abdominal pain | NR | NR | NR | NR | | ||||| | ||||||| |
Abdominal pain upper | NR | NR | NR | NR | | ||||| | | ||||| |
Alopecia | NR | NR | NR | NR | 2 (3.0) | 3 (10.3) |
Erythema | NR | NR | NR | NR | | ||||| | ||||||| |
Myalgia | NR | NR | NR | NR | | ||||| | | ||||| |
AE = adverse event; AESI = adverse event of special interest; CI = confidence interval; FAAN = Food Allergy and Anaphylaxis Network; LSM = least squares mean; mITT = modified intention-to-treat; NA = not applicable; NIAID = National Institute of Allergy and Infectious Diseases; NR = not reported; Phe = phenylalanine; RDT = randomized discontinuation trial; SAE = severe adverse event; SD = standard deviation; WDAE = withdrawal due to adverse event.
aP value based on a mixed model for repeated measures with study drug (pegvaliase or placebo), visit, and drug-by-visit interaction as factors adjusting for baseline blood Phe concentration. P values for comparisons between the pooled active group and each of the placebo groups were adjusted for multiple testing using a Hochberg procedure.
Source: PRISM-2 Clinical Study Report.9
Critical Appraisal
A major limitation of part 2 of the PRISM-2 RDT was the small size of the study and associated uncertainty. In addition, internal validity concerns included bias inherent to the RDT design (recruitment of a population of patients who did not discontinue treatment in feeder studies or part 1 of the PRISM-2 trial due to AEs or patient preference, who were able to achieve target dose in feeder studies, and who achieved a ≥ 20% decrease in blood Phe during part 1 of the PRISM-2 trial), baseline imbalances between treatment groups in gender, body mass index (BMI), mean blood Phe level, protein intake, and inattention and mood symptoms, uncertainty regarding the measurement properties or minimal important differences (MIDs) of any of the efficacy outcomes used in the study (and associated uncertainty regarding the connection between changes in blood Phe at part 2, week 8 and other outcomes, including inattention and mood symptoms, protein tolerance, diet liberalization, and HRQoL), and uncertainty in adherence to pegvaliase and consistency in dietary protein intake, both of which were self-reported.
There was some uncertainty regarding the target population of adult patients with PKU most appropriate for pegvaliase and the degree of generalizability of the PRISM-2 part 2 RDT results to this population. The study recruited patients with uncontrolled Phe who were willing and able to self-administer pegvaliase. Changes in blood Phe observed in the study would not be generalizable to patients with good Phe control, although the clinical experts consulted by CADTH for this review noted that these patients would be likely to benefit from treatment. The primary analysis of blood Phe may also not be generalizable to the general population of adult patients with PKU, which, according to the clinical experts, includes many patients who will not comply with any therapy, including pegvaliase. The specific relevance of pegvaliase-induced changes in blood Phe levels in the PRISM-2 RDT, measured at 1 or a few time points (e.g., week 4 and week 8 of the part 2 RDT), to improvements in dietary protein tolerance, neurocognitive and neuropsychiatric symptoms, and HRQoL, was uncertain. According to the clinical experts consulted by CADTH for this review, blood Phe measurements are highly variable in patients with PKU and the point estimate of Phe control associated with pegvaliase treatment at part 2, week 8 of the PRISM-2 trial provided no randomized trial evidence on duration or consistency of Phe control in patients.
Indirect Comparisons
No indirect evidence was identified for this review.
Other Relevant Evidence
PRISM-1 Trial
The PRISM-1 trial was a phase III, open-label, randomized, multi-centre study of the safety and tolerability of pegvaliase among drug-naive patients with PKU (N = 261).16,17 Of the 215 patients participating in the PRISM-2 trial, 203 (94.4%) entered from PRISM-1, making it the major feeder study for PRISM-2. PRISM-1 is briefly summarized in this section to provide context for the patient population enrolled in PRISM-2, as well as to contribute additional safety data. The primary objective of PRISM-1 was to characterize the safety and tolerability of induction, titration, and maintenance dosing in pegvaliase-naive patients with PKU who self-administered pegvaliase up to 20 mg/day or 40 mg/day. Patients with PKU aged 16 years or older were eligible to participate if they had blood Phe levels of greater than 600 µmol/L and had not been previously exposed to pegvaliase. Patients were randomized 1:1 to receive up to 20 mg/day or 40 mg/day pegvaliase for up to 36 weeks. Both randomized dose groups experienced reductions from baseline blood Phe levels. The mean blood Phe concentration at baseline was 1,232.7 µmol/L (standard deviation [SD] = 386.36) in the intention-to-treat (ITT) set and the mean reduction from baseline was ||||| |||||||| µmol/L at week 28 (n = 133) and ||||| |||||||| µmol/L at week 36 (n = 80). Almost all patients (99.6%) experienced AEs, most commonly arthralgia (65.1%), injection-site reactions (56.7%), injection-site erythema (45.2%), headache (31.4%), rash (25.7%), injection-site pruritis (24.9%), and injection-site pain (21.5%). SAEs occurred in 10.0% of patients; the most common SAE was anaphylaxis (3.1%). Anaphylaxis as defined by criteria established by the National Institute of Allergy and Infectious Diseases (NIAID) and the Food Allergy and Anaphylaxis Network (FAAN) occurred in 6.9% of patients and anaphylaxis as defined by NIAID-FAAN criteria meeting Brown’s severe criteria occurred in 1.5% of patients. Most patients (88.1%) experienced HAEs, including arthralgia (65.1%), generalized skin reaction lasting 14 days or more (22.6%), injection-site reactions (86.2%), injection-site skin reactions lasting 14 days or more (26.4%), serum sickness (3.1%), and angioedema (35.6%).
PRISM-2 Trial
Evidence from the non-RDT portions of the PRISM-2 trial,9-16 including the part 4 open-label extension (N = 215), is briefly summarized in this section to provide insight into the long-term safety of pegvaliase treatment (including dosages of no more than 60 mg/day in the part 4 open-label extension). In the PRISM-2 trial, patients were treated with open-label pegvaliase in part 1 (20 mg/day or 40 mg/day, up to 13 weeks), part 3 (20 mg/day or 40 mg/day, 6 weeks), and part 4 (up to 60 mg/day, up to 274 weeks). In all parts of the study, self-reported adherence to pegvaliase was high with good exposure. Table 20 provides detailed harms data for PRISM-2 part 1, part 3, and part 4, and the overall study. In the overall PRISM-2 study, ||||| of patients receiving open-label pegvaliase experienced AEs and ||||| of patients experienced SAEs, the majority of which occurred during the open-label extension. No deaths occurred in the overall PRISM-2 study. Approximately |||| ||||||| of patients experienced AEs leading to pegvaliase dose reduction or interruption but only |||| of patients experienced AEs leading to pegvaliase discontinuation. Most patients ||||||| experienced HAEs. Approximately ||||| |||||||| of patients ||||||| experienced injection-site reactions, approximately ||| |||||| ||||||| experienced arthralgia, and nearly |||| |||||| each) experienced generalized skin reactions lasting 14 days or more and injection-site skin reactions lasting 14 days or more. Anaphylaxis reactions occurred in |||| of patients, acute systemic hypersensitivity reactions occurred in |||| of patients, and angioedema occurred in |||| of patients.
PRISM-3 Trial
PRISM-3 was an exploratory phase III substudy to evaluate executive function in adults with PKU participating in the PRISM-2 trial (N = 9).18 Although the study addressed outcomes (executive function and self-perception) that were not evaluated in the PRISM-2 trial, interpretation was limited by the small sample size.
Comparative Evidence With Sapropterin and MNT
Zori et al. (2019)19 conducted a retrospective observational cohort study of adolescent and adult patients with PKU receiving pegvaliase with or without MNT, sapropterin plus MNT, or MNT alone. A cohort of patients who received pegvaliase plus MNT in the phase II 165 to 205 trial or phase III PRISM studies (PRISM-1 and PRISM-2) were compared using a propensity score matching (PSM) approach with a historical control of patients who received sapropterin plus MNT or MNT alone who participated in the Phenylketonuria Demographics, Outcome, and Safety (PKUDOS) registry.20 The outcomes evaluated in the study included change in blood Phe and natural protein intake after 1 and 2 years of treatment. Greater decreases in blood Phe levels and increases in protein intake from natural food were observed for patients treated with pegvaliase compared with patients receiving sapropterin plus MNT or MNT alone. However, because of numerous limitations in study design involving comparisons with a historical control cohort, potential bias due to the nonrandomized study design and PSM approach, and statistical limitations (exploratory analysis only), no clear conclusions could be drawn about the comparative effectiveness of pegvaliase, sapropterin plus MNT, and MNT alone.
Conclusions
Data from the PRISM-2 RDT suggested that continued self-administration of pegvaliase injections led to statistically significant and potentially clinically meaningful differences in blood Phe levels after 8 weeks compared with withdrawal of pegvaliase and injection of placebo. Low blood Phe (≤ 120 µmol/L) was observed in approximately half of patients receiving active pegvaliase. Durability and consistency of Phe control were not evaluated in the PRISM-2 RDT. Furthermore, the benefit in reducing blood Phe levels may have been overestimated relative to the general population of adult patients with PKU due to the enriched design of the RDT, which selected for patients more likely to adhere to and respond to pegvaliase. Despite significant differences in Phe at week 8 in patients receiving pegvaliase and placebo, no differences in inattention or mood symptoms were observed. Other outcomes important to patients, including HRQoL and protein tolerance, were not assessed in the PRISM-2 RDT. Efficacy data from nonrandomized studies, including the PRISM-2 open-label extension and an observational study comparing pegvaliase with sapropterin plus MNT and MNT alone, was limited by potential bias and/or confounding. The safety profile of pegvaliase, established through the phase III PRISM trials, including the open-label extension of PRISM-2, pointed to HAEs, arthralgia, injection-site reactions, generalized skin reactions lasting for 14 days or more, and generalized injection skin reactions lasting for 14 days of more as common side effects. Anaphylaxis and angioedema were less common but clinically important side effects. Other limitations of the available evidence included an unclear relationship between the magnitude of changes in blood Phe at a single time point (in the PRISM-2 RDT) and changes in other outcomes of importance to patients with PKU, as well as uncertainty regarding the target population of patients with PKU most appropriate for pegvaliase. The observed changes in blood Phe in the PRISM-2 RDT were aligned with 1 of the outcomes identified as important by patients with PKU, and there is clearly an unmet need for additional efficacious treatments for PKU with higher uptake and adherence rates compared with MNT.
Introduction
Disease Background
Phenylketonuria is a monogenic autosomal recessive disorder and 1 of the most common inborn errors of metabolism.3 Patients with PKU have mutations in both alleles of the PAH gene, which encodes an enzyme that catalyzes the conversion of Phe to tyrosine using tetrahydrobiopterin as a cofactor.3 A wide variety of PAH mutations give rise to variations in clinical phenotype and disease severity.3,4 A deficiency of PAH leads to uncontrolled blood Phe, which then crosses the blood-brain barrier, where it has neurotoxic effects.3,4 According to the clinical experts consulted by CADTH for this review, the subset of “brittle” patients who experience large fluctuations in Phe levels despite compliance with diet and some degree of Phe control is of particular concern. Phenylketonuria is universally identified via newborn screening programs in Canada; uncontrolled Phe levels in untreated PKU during early childhood profoundly impair brain function and development.5 In adolescents and adults, uncontrolled Phe levels are associated with behavioural and psychiatric problems (inattentiveness and mood dysfunction, often collectively referred to as “executive dysfunction”).6 Symptoms of PKU, in conjunction with treatments, negatively affect patient HRQoL with respect to employment, social relationships, and mental health.7
The disorder is rare, with an incidence of approximately 1 in 12,000 to 1 in 15,000 live births in Canada (equivalent to approximately 300 new cases per year). Applying the 1-in-15,000 figure to Canada’s 2018 population produces a rough estimate of 2,472 Canadian patients with PKU,21 of whom approximately 2,000 would be aged 16 years or older.22 According to the sponsor, approximately 3,133 patients with PKU are living in Canada at present, approximately ||||| of whom are being managed and ||| are aged 16 years or older and currently being treated with sapropterin1; the sources of these estimates were not clear.
According to the clinical experts consulted by CADTH for this review, PKU is diagnosed shortly after birth by newborn screening using biochemical and genetic tests. Physicians specializing in genetics and metabolic diseases are required to diagnose, treat, and monitor patients with PKU at hospital-based genetic or metabolic clinics that have support from dietitians trained in PKU management.
Standards of Therapy
According to the clinical experts consulted by CADTH for this review, the current cornerstone of PKU treatment is lifelong dietary control of Phe intake to curb blood Phe levels. This is principally accomplished by providing Phe-free foods and metabolic formulas (generated from protein hydrolysate), with a small amount of “complete” Phe-containing protein allowed on top. The combination of dietary restriction and Phe-free medical foods is sometimes collectively referred to as MNT. Some Phe must be provided because it is an essential amino acid. American College of Medical Genetics and Genomics (ACMG) guidelines state that the goal of treatment is to maintain Phe levels of 120 µmol/L to 360 µmol/L.23 European guidelines state that the primary goal of treatment is normal neurocognitive and psychosocial functioning through maintaining Phe concentrations between 120 µmol/L and 360 µmol/L up to the age of 12 years and up to 600 µmol/L thereafter.24 Patients are monitored via blood sampling (either venous or dried blood spots) on a regular interval. Other than dietary restriction, the only other approved medication is sapropterin, a cofactor of the deficient PAH enzyme in PKU. Sapropterin coverage varies by province, and approximately 25% of patients with PKU have a biochemically detectable response (usually defined as a 30% drop in blood Phe on an equivalent Phe load) to sapropterin.8 Large neutral amino acid (LNAA) supplements are used to control neurologic symptoms in a tiny fraction of patients with PKU, primarily those who cannot control Phe levels through diet.
The clinical experts emphasized that current treatments work around the presence of disease but do not modify the underlying mechanisms and do not target PKU symptoms specifically, only Phe levels. The relationship between Phe levels and other outcomes is extremely clear for infants, young children, and pregnant women. Infants with unrestricted Phe have profound mental handicaps, and high Phe during pregnancy can cause birth defects. The relationship between Phe levels and symptoms is more tenuous in older age groups, and restricting adolescents and adults to the same Phe range (120 µmol/L to 360 µmol/L) used for children is a relatively recent innovation. Formerly restricted patients with poor Phe control have variable neurocognitive features as adults, and this group includes those who appear to have no symptoms and do not control their Phe for this reason. The temporal association between high Phe levels and complications is so weak that patients cannot truly sense elevation in Phe, nor does decreasing Phe rapidly alter any consequences of PKU.
The PKU treatment paradigm is based on evidence that long-term Phe elevation in early childhood profoundly affects brain function and development. The major goal of treatment in patients 16 years and older is to preserve mental capacity, usually collectively considered as executive function. Secondary goals are improvement of HRQoL through the reduction of symptoms such as inattentiveness, clouded cognition, anxiety, and depression as well as improving the ability to maintain employment and relationships. An ideal treatment would normalize Phe levels and eliminate these risks without the use of dietary restriction, which is cumbersome, requires modification based on Phe levels, and itself negatively affects HRQoL.
Drug
Key characteristics of pegvaliase are shown in Table 3. Pegvaliase is administered at a titrated maintenance dose (following induction and titration) required to achieve blood Phe levels of 600 µmol/L or lower by self-administered subcutaneous injection. The drug is not approved for use in Canada for other indications and has not been previously reviewed by CADTH. The mechanism of action of pegvaliase is replacement of the deficient PAH enzyme in patients with PKU with a polyethylene glycolylated recombinant Phe ammonia lyase enzyme that converts Phe to ammonia and trans-cinnamic acid.
Pegvaliase underwent a standard review process by Health Canada and received a Notice of Compliance on March 30, 2022. The proposed Health Canada indication for pegvaliase is: “Palynziq (pegvaliase injection) is indicated to reduce blood phenylalanine concentrations in patients with phenylketonuria (PKU) aged 16 years and older who have inadequate blood phenylalanine control (blood phenylalanine levels greater than 600 micromol/L) despite dietary management.” The FDA indication is: “Palynziq is a phenylalanine-metabolizing enzyme indicated to reduce blood phenylalanine concentrations in adult patients with phenylketonuria who have uncontrolled blood phenylalanine concentrations greater than 600 micromol/L on existing management.”25 The European Medicines Agency indication is: “Palynziq is indicated for the treatment of patients with phenylketonuria (PKU) aged 16 years and older who have inadequate blood phenylalanine control (blood phenylalanine levels greater than 600 micromol/L) despite prior management with available treatment options.”26 The sponsor’s reimbursement request is: “For the treatment of patients with PKU aged 16 years and older who have inadequate blood Phe control (blood Phe levels greater than 600 μmol/L) despite prior treatment with sapropterin.” This funding request differs from the proposed Health Canada indication by requiring prior treatment with sapropterin as a prerequisite for initiation of pegvaliase treatment. The sponsor clarified that nonresponse to sapropterin was not considered a condition for initiation of pegvaliase in its funding request.
Table 3: Key Characteristics of Pegvaliase, Sapropterin, and Medical Nutritional Therapy
Characteristic | Pegvaliase | Sapropterin | MNT |
|---|---|---|---|
Mechanism of action | Enzyme substitution therapy with a PEGylated recombinant Phe ammonia lyase enzyme that converts Phe to ammonia and trans-cinnamic acid | Enzyme cofactor that can stabilize residual PAH enzymes, improve the oxidative metabolism of Phe, and decrease Phe levels in some patients | Dietary restriction to avoid Phe-containing natural foods plus supplementation with Phe-free medical foods |
Indicationa | Palynziq (pegvaliase injection) is indicated to reduce blood Phe concentrations in patients with PKU 16 years and older who have inadequate blood Phe control (blood phenylalanine levels greater than 600 µmol/L) despite dietary management | In conjunction with a Phe-restricted diet to reduce blood Phe levels in patients with HPA due to tetrahydrobiopterin-responsive phenylketonuria | NA |
Route of administration | Subcutaneous injection | Oral | Oral |
Recommended dosage | Titrated to a maintenance dose required to achieve blood Phe level 600 μmol/L or lower; maximum dosage of 60 mg daily | 10 mg/kg to 20 mg/kg once daily | NA |
Serious adverse effects or safety issues | Systemic hypersensitivity reactions including anaphylaxis | NA | NA |
Other | NA | Response depends on presence of residual PAH activity, which can be predicted to some extent based on genotyping | NA |
HPA = hyperphenylalaninemia; NA = not applicable; PAH = phenylalanine hydroxylase; PEG = polyethylene glycol; Phe = phenylalanine.
aHealth Canada–approved or proposed indication.
Source: CADTH review submission,1 draft product monograph for pegvaliase,2 and product monograph for sapropterin.27
Stakeholder Perspectives
Patient Group Input
This section was prepared by CADTH staff based on the input provided by patient groups. The original patient group submission can be found in the Stakeholder Input section.
One submission, from CanPKU, was received for this review. Between November 30, 2021, and December 25, 2021, CanPKU conducted online surveys of 68 patients with PKU (46 in Canada and 14 in the US) and telephone interviews with 5 patients experienced with pegvaliase (1 in Canada and 4 in the US). Respondents explained how PKU symptoms and the PKU protein-restricted diet had affected their physical and mental health, employment, and social relationships. Almost all respondents (≥ 95%) had experience with low-protein medical foods and formulas, 65% had experience with Kuvan, and only 21% had experience with pegvaliase. Respondents described barriers to existing therapies, including poor taste, lack of satiety, inconvenient preparation and administration, high cost, and limited availability.
The vast majority (≥ 85%) of respondents identified Phe control, reducing PKU symptoms, limiting long-term disease consequences, improving neurocognitive function, managing diet, reducing burden of treatment, improving HRQoL, and increasing natural protein intake as key outcomes of interest. Respondents experienced with pegvaliase reported that the drug limited long-term disease consequences, controlled Phe levels, reduced PKU symptoms, and had tolerable side effects, such as injection-site reactions, joint pain, and skin reactions.
Clinician Input
Input From Clinical Experts Consulted by CADTH
All CADTH review teams include at least 1 clinical specialist with expertise in the diagnosis and management of the condition for which the drug is indicated. Clinical experts are a critical part of the review team and are involved in all phases of the review process (e.g., providing guidance on the development of the review protocol, assisting in the critical appraisal of clinical evidence, interpreting the clinical relevance of the results, and providing guidance on the potential place in therapy). The following input was provided by 2 clinical specialists with expertise in the diagnosis and management pediatric and adult patients with PKU who have inadequate Phe control.
Unmet Needs
According to the clinical experts consulted by CADTH for this review, all goals of treatment could potentially be met by available therapies (MNT with or without sapropterin). Delivery of MNT can prevent severe neuropsychological complications when supplied immediately once PKU diagnosis is established in infancy. However, because adherence of adolescent and adult patients with PKU to therapy is extremely challenging, treatment is not effective in most patients. Medical food is very unpleasant to taste and smell and, while it is available, coverage varies by province. This creates many barriers to its daily use, including enjoyment of food and socialization, especially through shared meals. Adults with PKU who were diagnosed early and treated continuously experience higher rates of comorbidities than the general population, including anxiety, depression, hyperactivity and inattentiveness, deficits in executive function, and social isolation; these factors may be due in part to the severely restrictive PKU diet.
Place in Therapy
The clinical experts stated that pegvaliase has a distinct mechanism of action through the direct elimination of circulating Phe. This allows it to complement dietary restriction. The rationale for pegvaliase complementing sapropterin is minimal, as sapropterin has a comparatively weak mechanism of action and is only effective in patients with the mildest PKU. Pegvaliase does not address the underlying disease process (loss of PAH activity) directly, but bypasses it. Pegvaliase is not a first-line treatment, and the sponsor is not seeking approval or reimbursement for younger children and infants. Patients cannot be “intolerant” to dietary restriction of Phe in the classical sense nor can dietary restriction be “contraindicated.” However, poor compliance severely limits the impact of dietary restriction in adults with PKU. Pegvaliase may shift the treatment paradigm for some adult patients with PKU by allowing liberalization of diet while maintaining Phe control.
According to the clinical experts consulted by CADTH, all patients are prescribed dietary restriction, while the use of sapropterin depends on the PAH genotype of the patient and provincial rules for sapropterin reimbursement. The use of pegvaliase should be properly viewed as a potentially more palatable choice for decreasing Phe levels. Recommending that patients try other forms of treatment to achieve Phe control before pegvaliase is equivalent to instructing them to adhere to the PKU diet. Making this a criterion for initiation of therapy could result in pegvaliase access only for patients who are medically noncompliant.
Patient Population
The 2 clinical experts consulted by CADTH for this review had different opinions regarding the subset of patients with PKU who would benefit most from pegvaliase. One clinical expert stated that patients with high and uncontrolled Phe are most in need of an intervention to improve metabolic control that will lead to a decrease in their Phe levels and improved Phe tolerance. The clinical expert could not rule out the possibility that patients who are poorly compliant with MNT could become more compliant to therapies (including pegvaliase) over time as Phe levels decrease and their focus improves. A second clinical expert described the target group of patients with PKU most in need of intervention as those who have an established track record of high compliance with diet and other therapies and who have the most severe forms of PKU. Patients who are able to follow dietary restrictions are the most likely to regularly inject themselves with pegvaliase and follow the instructions for its use. These patients are generally able to achieve PKU levels within the control range but have the most unpalatable diets and experience large deviations in Phe levels even with good control. They would therefore receive the largest benefit in improved access to complete protein and stabilization of Phe.
The clinical experts stated that patients most suitable for pegvaliase therapy can be identified by assessing patient compliance with diet and other therapies (as measured by mean Phe values over a period of approximately 12 months as well as adherence to a monthly monitoring schedule). Severity can be determined by PAH genotyping, assessing variability in Phe levels, and/or by degree of restriction of complete protein intake; the latter 2 can only be applied to patients generally in the Phe control range.
According to the clinical experts, there are few diagnostic issues for PKU, which is identified universally in Canada by screening newborns, and there is minimal potential for misdiagnosis. A tiny number of patients may have non–PAH-associated hyper-Phe syndromes (e.g., disorders of biopterin metabolism) but most are correctly identified through the existing diagnostic algorithm, which includes biochemical and genetic tests. It may be necessary to screen for disorders of biopterin metabolism in patients who have not been genotyped or where genotyping did not identify biallelic variants in PAH, as the optimal medication for pterin synthetic disorders is sapropterin, not pegvaliase.
The clinical experts emphasized that patients who are noncompliant with therapy (including diet) are the least suitable for treatment with pegvaliase. Noncompliance is an major problem in the PKU population. Noncompliant patients will receive no benefit from pegvaliase, and, if they are noncompliant with administration instructions, the medication could cause harm. Likelihood of response to pegvaliase treatment is probably a poor criterion for patient selection, and the use of this criterion for sapropterin has been a serious problem for providers. Few patients who do not respond to pegvaliase with reduction in Phe have been identified. Indeed, patients who are noncompliant (and least suitable for treatment) will appear to have the best response to a single dose of pegvaliase.
In their feedback to CADTH on this clinical review report, the sponsor noted that both patients with uncontrolled and controlled Phe with differing degrees of MNT compliance would be appropriate for pegvaliase treatment and emphasized that MNT compliance was not an eligibility criterion for the initiation of pegvaliase in the pivotal trial.
Assessing Response to Treatment
The clinical experts agreed that complete protein tolerance (or Phe tolerance) and blood Phe levels are the most convenient tests to assess response to treatment and are most often used in clinical trials. After starting on pegvaliase, some patients with PKU will show decreases in their Phe levels, which will allow for diet modification and increase in complete protein tolerance. Patients who are compliant with their diets and who switch to pegvaliase would not be expected to show improvements in Phe levels if these are already optimal, limiting the utility of Phe levels as an outcome. However, the clinical experts noted that Phe levels may drop below the treatment’s recommended range if dietary Phe intake is not adjusted. In addition, patients who manage to completely switch to pegvaliase and do not require dietary restriction will show no further improvement in Phe levels.
According to the clinical experts, clinically meaningful responses to treatment would be, in order of importance: increased complete protein tolerance (or Phe tolerance) and protein intake to levels comparable with those of the general population, improvement in HRQoL, and improvement in psychological metrics (neurocognitive performance, mood, attention, and working memory). The clinical experts stated that blood Phe levels can be used to show that pegvaliase treatment is ineffective. Patients who cannot maintain acceptable Phe levels (or whose levels are not monitored) within the treatment’s recommended range with dietary restriction and pegvaliase are noncompliant and should be discontinued from treatment.
The clinical experts noted that patients would be monitored annually (by reviewing Phe values on a monthly schedule and by an annual review of protein tolerance), but that response evaluation would be performed at a shorter interval (perhaps 4 months) as patients will need to adjust their diets based on Phe levels. Improvement in complete protein tolerance would not be expected to be observed after stabilization on pegvaliase but should be maintained.
Discontinuing Treatment
According to the clinical experts consulted by CADTH for this review, high Phe levels or significant adverse reactions indicate an absence of clinical benefit of pegvaliase.
Prescribing Conditions
The clinical experts stated that pegvaliase should be administered by specialized centres with expertise in the complex management of patients with PKU. These are usually hospital-based genetic or metabolic clinics that have support from dietitians trained in PKU management. In jurisdictions where it has been approved (e.g., the US), pegvaliase is subject to monitoring in an outpatient setting during initial administration and titration of doses. Centres also must be certified to administer the drug. Similar rules would probably have to be put in place in Canada.
According to the clinical experts, specialists in genetics and metabolic diseases are the appropriate physicians to diagnose, treat, and monitor patients with PKU. In some limited cases involving patients who are geographically dispersed, part of this role (e.g., monitoring of adverse reactions) could be assumed by a family physician with remote oversight. Telehealth communication is already used to manage and follow remotely located patients, and the same tools could be used to monitor patients treated with pegvaliase (including those performing self-injections at home).
Diagnosis of PKU is typically established via newborn screening programs and confirmed with biochemical and genetic tests during the neonatal period. Apart from identifying disorders of biopterin metabolism, additional diagnostic testing for PKU as a requirement for pegvaliase would be an unnecessary burden as there is no realistic possibility that a physician and their patient would seek this medication or diagnosis.
Clinician Group Input
This section was prepared by CADTH staff based on the input provided by clinician groups. The original clinician group submission can be found in the Stakeholder Input section.
A group of 3 physicians specialized in treating metabolic disorders who care for adult patients with PKU in Canada provided input for this review. Although the clinician group echoed the challenges in adhering to the PKU diet and the limited proportion of patients who can benefit from sapropterin, contrasting views were presented on: the connection between blood Phe levels and neurologic symptoms, diet liberalization, and associated impacts on HRQoL in adult patients with PKU, which the clinician group described as tightly and reversibly linked; the importance of Phe control as a treatment goal and marker of treatment response in and of itself; the patient subset most suitable for pegvaliase treatment, which the clinician group identified as patients noncompliant with dietary restrictions who cannot benefit from sapropterin and therefore have poor or no Phe control; the patient subset least suitable for pegvaliase treatment, which the clinician group described as patients able to maintain Phe levels within target range on MNT with or without sapropterin; and the risks of Phe levels below 30 µmol/L resulting from overtreatment with pegvaliase in patients who do not comply with Phe monitoring, which the clinician group reported was a potential concern. According to the clinician group, pegvaliase would be offered as last-line treatment to adult patients with PKU who have elevated Phe levels and neuropsychiatric symptoms and who are able to self-administer the injections.
Drug Program Input
The drug programs provide input on each drug being reviewed through CADTH’s reimbursement review processes by identifying issues that may affect their ability to implement a recommendation. The implementation questions and corresponding responses from the clinical experts consulted by CADTH are summarized in Table 4.
Table 4: Summary of Drug Plan Input and Clinical Expert Response
Implementation issues | Clinical experts’ response |
|---|---|
Relevant comparators | |
A comparator was not included in the submitted trials; the sponsor stated that placebo was the appropriate comparator, noting that a significant proportion of patients does not respond to sapropterin (e.g., challenges with long-term adherence to a Phe-restricted diet and PAH deficiency). There is a retrospective comparison of long-term treatment effectiveness of pegvaliase vs. sapropterin plus diet and diet alone (Zori et al. [2019]); this was not a head-to-head study. It compared the effectiveness of long-term pegvaliase treatment to standard care (i.e., sapropterin plus diet or diet alone) among adults with PKU 18 years and older with blood Phe levels above 600 µmol/L. Normalization of blood Phe levels (defined as ≤ 120 µmol/L) was achieved in 45% of patients receiving pegvaliase and in none of those receiving sapropterin plus diet. After 2 years of follow-up, 68% of patients on pegvaliase vs. 20% of those on sapropterin plus diet achieved European Union guideline–recommended Phe levels of 600 µmol/L or lower; 65% of patients on pegvaliase vs. 8% on sapropterin plus diet achieved the US guideline–recommended level of 360 µmol/L. There are limitations associated with this study, including nonrandomized patient populations and confounding baseline factors. What is the appropriate comparator for pegvaliase (sapropterin plus diet vs. placebo)? | The appropriate comparator for pegvaliase is dietary restriction. “Placebo” is not the most appropriate comparator because all patients are prescribed dietary restriction (although many are not compliant) and the clinical experts viewed this diet as medical food (equivalent to medication). The clinical experts agreed that some patients are not responsive to sapropterin. |
Sapropterin is the only medication available in Canada for the treatment of PKU in conjunction with a Phe-restricted diet. Access to sapropterin is restricted in some jurisdictions through special authorization (e.g., New Brunswick), limited use (e.g., NIHB) or through exceptional access/drug status program (e.g., Ontario and Saskatchewan). Sapropterin was reviewed by CDEC (October 26, 2016) and received a positive recommendation (BH4-responsive PKU). Not all jurisdictions may have sapropterin listed, which would be a consideration if existing management is sapropterin plus diet. | For CDEC consideration. |
Considerations for initiation of therapy | |
Newborn screening for PKU is standard in Canada; diagnosed infants are started immediately on treatment to prevent long-term neurologic damage. Blood Phe is controlled over the life course to reduce the risk of serious outcomes associated with PKU. Initiation criteria for sapropterin (CDEC recommendation) in the aforementioned jurisdictions, in general, state that baseline blood Phe levels should be > 360 µmol/L despite compliance with a low-protein diet (require at least 2 levels during 3- to- 6-month time frame). In the PRISM-1 study (a phase III, multi-centre, open-label trial that randomized pegvaliase-naive patients to receive 1 of 2 regimens of pegvaliase), patients with a blood Phe concentration above 600 µmol/L for at least 6 months before the study were eligible. Given the sponsor’s reimbursement request, would pegvaliase be accessed when patients have baseline blood Phe levels above 600 µmol/L for at least 6 months, despite adherence with treatment of sapropterin plus Phe-restricted diet? What would be required as confirmation of Phe concentration above 600 µmol/L (e.g., 1 measurement in the last 30 days before treatment initiation)? The ACMG guidelines state that the goal of treatment is to maintain Phe concentrations in a range of 120 µmol/L to 360 µmol/L. European guidelines state that the primary goal of treatment is normal neurocognitive and psychosocial functioning through maintaining phenylalanine concentrations between 120 µmol/L and 360 µmol/L up to the age of 12 years and to no more than 600 µmol/L thereafter. There are no Canadian guidelines; however, the Canadian management of PKU is generally more aligned with the ACMG treatment guidelines (sponsor’s clinical summary). How would patients with blood Phe levels between 360 µmol/L and 600 µmol/L be managed depending on the current Canadian standard of practice and the patient’s clinical picture? | No patient in otherwise good health can be adherent to a properly designed Phe-restricted diet and have Phe levels above 600 µmol/L for 6 months. This is physiologically impossible and Phe levels of all patients with PKU can theoretically be controlled with a proper diet. A compliant patient on diet with or without sapropterin would have Phe levels of 600 µmol/L or less; those that have higher levels are noncompliant. Nevertheless, most adult patients with PKU will not be able to meet treatment goals and attain Phe levels of 600 µmol/Lor lower due to limited compliance. Applying a greater than 600 µmol/L Phe threshold for pegvaliase initiation would punish compliant patients and reward those who will not comply with any therapy. This criterion would mean that patients with Phe levels within the recommended range who are compliant and will benefit from treatment would not be eligible. The experts noted that it would be less expensive and more effective on a national basis to allow the medication to be used for compliant patients. According to the clinical experts, Phe monitoring is typically done monthly for adults. An average of values (at least 4) over a 6-month period would be required to produce a realistic vision of Phe control. Single Phe values are too variable. Canadian centres use the US guidelines (recommended Phe range for all ages 120 µmol/L to 360 µmol/L). Maintaining this control is difficult for older patients, and efforts are ongoing to compare the US and European guidelines. |
The reimbursement request is for patients 16 years and older. What about those who are younger than 16 years of age? | The clinical experts were not aware of robust studies of pegvaliase in this age group; however, they noted that there is no clear reason to think it could not be effective. |
Can the clinical experts provide some guidance into how pegvaliase will be managed during pregnancy (unplanned and planned)? | The product monograph advises against use in pregnant women. One published anecdotal report suggests that use of pegvaliase during pregnancy is potentially dangerous due to low Phe levels that have can compromise fetal growth. In general, Phe control in women with PKU during pregnancy must be liberalized to prevent periods of very low Phe levels. |
Would it be possible to clarify “existing management” (e.g., sapropterin plus restricted diet vs. restricted diet) before accessing pegvaliase? With the reimbursement request, it looks like pegvaliase is second line (first line perhaps being sapropterin). What is the place in therapy for pegvaliase (medication-naive vs. medication-experienced)? | Sapropterin has entirely different mechanisms of action. Pegvaliase works regardless of PAH genotype, while responsiveness to sapropterin is genotype-dependent based on residual enzyme activity. Restricting the use of pegvaliase to patients previously been treated with sapropterin may lead to unnecessary use of sapropterin in patients whose PAH genotypes indicate they will not benefit from this treatment. |
Discontinuation of pegvaliase decreased after the first 6 months of treatment (50 participants discontinued in the first 6 months and an additional 50 participants discontinued for the duration of the study). Forty patients (15.3%) discontinued due to AEs; the most common AEs leading to discontinuation were anaphylaxis, arthralgia, injection-site reactions, and generalized rash. For patients who have experienced anaphylaxis while on treatment with pegvaliase, can re-treatment be considered? Would patients who experienced other AEs that led to discontinuation be eligible for re-treatment? If so, is there a time frame by which this request should be made? For patients who are planning for pregnancy, at what point would they be eligible for re-treatment? | Pegvaliase desensitization has been described anecdotally in published studies but re-treatment would likely be contraindicated for patients who experience anaphylaxis. Patients who experience other (non-anaphylaxis) AEs may be re-treated but re-treatment and its time frame would depend on the nature and severity of the reaction. Pregnant women should be able to restart pegvaliase immediately after giving birth. The risk for lactating mothers appears to be low. |
Currently, sapropterin is the only medication available for the treatment of PKU. Although the inclusion criteria in the trials for sapropterin and pegvaliase may not be similar, should we consider alignment with the elements of the reimbursement criteria (e.g., requirement of blood Phe levels, requirement for Phe-restricted diet, managed by a specialist in metabolic and/or biochemical diseases) for sapropterin? | Medical foods are also available for the treatment of PKU. Alignment with the sapropterin guidelines may be problematic for patients and clinicians. Sapropterin and pegvaliase use should be based on responsiveness and compliance, not on Phe levels pre-treatment. |
Considerations for continuation or renewal of therapy | |
There is a need for regular monitoring of Phe levels (once a month, until maintenance dose is established). Is there a fasting and postprandial requirement? Once the maintenance dose is established, periodic blood Phe monitoring is recommended to assess control in blood Phe levels. Are blood Phe levels easily accessible within the jurisdictions (e.g., Life Labs)? | Clinicians do not generally insist on timing of levels to meals because the diurnal fluctuation of Phe is unpredictable. Blood Phe levels are easily monitored by a home-dried blood spot, which is provided by the clinic and covered by plans. |
Currently, sapropterin is the only medication available for the treatment of PKU. For pegvaliase, should alignment with elements of the reimbursement criteria for renewal of sapropterin be considered? What would be the percentage decrease in blood Phe levels given the patient’s pre-treatment level on existing therapy given a dose and treatment duration? How would a therapeutic response be defined in the context of pegvaliase? | Response to treatment would likely be a poor criterion to consider, and the use of this criterion for sapropterin has been problematic for providers. Few patients who do not respond to pegvaliase with reduction in Phe levels have been identified. Indeed, patients who are noncompliant (and least suitable for treatment) will appear to have the best response to a single dose of pegvaliase. A therapeutic response should be defined by increased natural protein tolerance. |
Considerations for discontinuation of therapy | |
What parameters would be considered when describing loss of response, or absence of clinical benefit with pegvaliase in this population? For example, parameters such as blood Phe concentration (which appears to be related to dose, treatment duration and individual immune response), lack of normalization of diet, patient’s HRQoL, patient’s cognitive function, and tolerability. According to the draft product monograph, time to response, which is achieving blood Phe levels of 600 µmol/L or lower, varies among patients. The draft product monograph advises discontinuing pegvaliase in patients who have not achieved an adequate response after 48 weeks of continuous treatment with the maximum dosage of 60 mg once per day. How is an inadequate response defined? The physician may decide, with the patient, to continue pegvaliase treatment in those patients who show other beneficial effects (e.g., ability to increase protein intake from intact food or improvement of neurocognitive symptoms). | High Phe levels or significant adverse reactions indicate loss of response to or absence of clinical benefit from pegvaliase, most commonly due to poor compliance with administration of the medication. A period of 48 weeks is far too long to continue the medication with no evidence of benefit. Most often a 16-week period (induction, titration, and part of maintenance) would be sufficient to establish suitability of treatment. The ability to increase protein intake should be a criterion for defining therapeutic response. |
Is there any guidance on treatment interruptions with regard to dose recommendations based on the when the last dose of pegvaliase was administered (restart previous dose or restart with induction and titration schedule)? | In most cases, restarting the previous dose would be acceptable. |
Considerations for prescribing of therapy | |
The draft product monograph provides recommended induction, titration, and maintenance dosing. For patients who do not have a trained observer to accompany them for at least 1 hour following each injection during induction and titration, would they continue receiving injections at the clinic? Clinic visits may incur travel expense (induction: fixed dose; titration: uncertain duration dependent on patient’s tolerability). Depending on the blood Phe levels achieved, is there a possibility for the patient to administer pegvaliase less than once daily during maintenance (e.g., twice weekly, 4 times weekly)? | Although in-clinic observation can be associated with additional expenses, there must be a trained observer present. In practice the drug could be titrated to the desired effect. Low Phe values are not safe for patients (at least for those treated with diet with or without sapropterin). Reducing the schedule for patients with low values therefore appears to be practical. Low Phe may be less of a concern for patients on pegvaliase who have less restricted complete protein intake, as they have regular access to a source of dietary Phe. |
Would patients be able to easily access specialists who manage patients with PKU such as physicians and dieticians with expertise in metabolic disorders? | Access to physicians might be challenging for patients who do not live in metropolitan centres. However, because of the COVID-19 pandemic, telehealth clinic visits have increased in use and most clinics are organized in a virtual format. This would allow access to specialists and dietitians for patients with PKU being treated with pegvaliase. |
Are there any clinical situations in which the combination treatment of sapropterin and pegvaliase would be appropriate? Also, the draft product monograph states that 2 patients receiving concomitant injections of medroxyprogesterone acetate suspension containing PEG experienced hypersensitivity reactions. Are there implementation considerations regarding possible recommendations for this population? | There is no particularly good rationale for using both medications simultaneously. Although medroxyprogesterone acetate formulations can contain PEG, it remains unclear whether the hypersensitivity reactions in these 2 patients could have been a coincidence. Depo-Provera is widely used by adult women with PKU because it is effective birth control. Clinics, observers, and patients should be especially vigilant for signs of hypersensitivity reactions for patients using Depo-Provera. |
Generalizability | |
Patients younger than 16 years of age were excluded from the trial. | For CDEC consideration. |
The sponsor estimates that ||| patients with PKU out of an estimated |||| patients nationally 16 years and older are being managed. What proportion of these patients are currently being treated with sapropterin? What number of patients are not controlled on sapropterin plus diet? This would inform number of patients that may switch to pegvaliase. | Less than 10% of adult patients with PKU are estimated to be on sapropterin (and dietary restriction) because of limited availability. The clinical experts noted that compassionate access is being slowly discontinued. Among patients 16 years or older, approximately 90% of those on sapropterin and diet would not have controlled Phe (generally defined as 120 µmol/L to 360 µmol/L). |
Care provision | |
The medication may be started in a hospital setting, while maintenance therapy could be provided in a community setting. Considerations may include that the patient is able to communicate issues associated with AEs, is able to self-inject, has a trained observer to accompany them for at least 1 hour after each administration for at least the first 6 months of treatment, and have access to emergency services. | For CDEC consideration. |
Pegvaliase is stored refrigerated (2°C to 8°C) but may be stored in its sealed tray at room temperature (20°C to 25°C) for up to 30 days with protection from sources of heat. After removal from refrigeration, the product must not be returned to the refrigerator. How will it be dispensed taking the requirement for a cooling storage container into consideration? | The drug used for treatment in clinic could be stored in a cooled container if convenient. Pegvaliase for at home use would be dispensed and remain at room temperature. |
Pre-medication is recommended before each dose administered during induction and titration. Due to the potential for an acute systemic hypersensitivity reaction, monitoring and managing may be needed in the hospital setting. | For CDEC consideration. |
System and economic issues | |
Existing patients may be switched to pegvaliase as indicated in the reimbursement request; however, what about new patients who are not currently managed with sapropterin plus diet? Does the anticipated budget impact only take into consideration the shift from sapropterin plus diet? | All patients are prescribed dietary restriction. Sapropterin prescription should not be considered here. Conditioning prescription of pegvaliase on previous trial of sapropterin will only lead to unnecessary costs. |
Costs include drug acquisition and administration costs, Phe-restricted diet and formula costs, test and medical visit costs, pre-medication costs, and adverse event costs. What about loss of productivity costs dependent on patient’s health state and costs related to patient comorbidities? | These could be considered benefits rather than costs if treatment leads to improved health state. Loss of productivity related to adverse reactions to pegvaliase would in most cases be a minor consideration. |
Sapropterin has successfully gone through price negotiations (concluded with a February 13, 2020, letter of intent | For CDEC consideration. |
ACMG = American College of Medical Genetics and Genomics; AE = adverse event; BH4 = tetrahydrobiopterin; CDEC = CADTH Canadian Drug Expert Committee; HRQoL = health-related quality of life; NIHB = non-insured health benefit; PAH = phenylalanine hydroxylase; PEG = polyethylene glycol; Phe = phenylalanine; PKU = phenylketonuria.
Clinical Evidence
The clinical evidence included in the review of pegvaliase is presented in 2 sections. The first section, the systematic review, includes pivotal studies provided in the sponsor’s submission to CADTH and Health Canada, as well as those studies that were selected according to an a priori protocol. No indirect evidence was submitted by the sponsor or identified from the literature that met the selection criteria specified in the review. The second section includes sponsor-submitted long-term extension studies and additional relevant studies that were considered to address important gaps in the evidence included in the systematic review.
Systematic Review (Pivotal and Protocol-Selected Studies)
Objectives
To perform a systematic review of the beneficial and harmful effects of pegvaliase (self-administered subcutaneous injection, titrated to a maintenance dose required to achieve a blood Phe level of 600 μmol/L or lower; maximum dose 60 mg daily) for the treatment of patients with PKU aged 16 years and older who have inadequate blood Phe control (blood Phe levels greater than 600 μmol/L) on existing management.
Methods
Studies selected for inclusion in the systematic review will include pivotal studies provided in the sponsor’s submission to CADTH and Health Canada, as well as those meeting the selection criteria presented in Table 5. Outcomes included in the CADTH review protocol reflect those considered to be important to patients, clinicians, and drug plans.
The systematic review protocol presented was established before the granting of a Notice of Compliance from Health Canada.
Table 5: Inclusion Criteria for the Systematic Review
Criteria | Description |
|---|---|
Patient population | Adult patients (age ≥ 16 years) with PKU who have inadequate blood Phe control (blood Phe levels greater than 600 μmol/L) on existing management. Subgroups
|
Intervention | Pegvaliase (self-administered subcutaneous injection, titrated to a maintenance dose required to achieve blood Phe level of 600 μmol/L or lower; maximum dose 60 mg daily) |
Comparators |
|
Outcomes | Efficacy outcomes
Harms outcomes
|
Study design | Published and unpublished phase III and IV randomized controlled trials |
HRQoL = health-related quality of life; MNT = medical nutritional therapy; Phe = phenylalanine; PKU = phenylketonuria.
The literature search for clinical studies was performed by an information specialist using a peer-reviewed search strategy according to the PRESS Peer Review of Electronic Search Strategies checklist.28
Published literature was identified by searching the following bibliographic databases: MEDLINE All (1946—) via Ovid and Embase (1974—) via Ovid. All Ovid searches were run simultaneously as a multi-file search. Duplicates were removed using Ovid deduplication for multi-file searches, followed by manual deduplication in EndNote. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. The main search concept was pegvaliase. Clinical trials registries searched included the US National Institutes of Health’s clinicaltrials.gov, WHO’s International Clinical Trials Registry Platform search portal, Health Canada’s Clinical Trials Database, and the European Union Clinical Trials Register.
No filters were applied to limit the retrieval by study type. Retrieval was not limited by publication date or by language. Conference abstracts were excluded from the search results. Appendix 1 provides the detailed search strategies.
The initial search was completed on February 3, 2022. Regular alerts updated the search until the meeting of the CADTH Canadian Drug Expert Committee on May 16, 2022.
Grey literature (literature that is not commercially published) was identified by searching relevant websites from the Grey Matters: A Practical Tool For Searching Health-Related Grey Literature checklist.29 Included in this search were the websites of regulatory agencies (FDA and European Medicines Agency). Google was used to search for additional internet-based materials. Appendix 1 provides more information on the grey literature search strategy.
A focused literature search for network meta-analyses dealing with PKU was run in MEDLINE All (1946–) on February 2, 2022. No limits were applied to the search.
These searches were supplemented by reviewing bibliographies of key papers and through contacts with appropriate experts. Two CADTH clinical reviewers independently selected studies for inclusion in the review based on titles and abstracts, according to the pre-determined protocol. Full-text articles of all citations considered potentially relevant by at least 1 reviewer were acquired. Reviewers independently made the final selection of studies to be included in the review, and differences were resolved through discussion.
Findings From the Literature
Eight reports9-16 of a single study were identified from the literature for inclusion in the systematic review (Figure 1). The included study is summarized in Table 6.
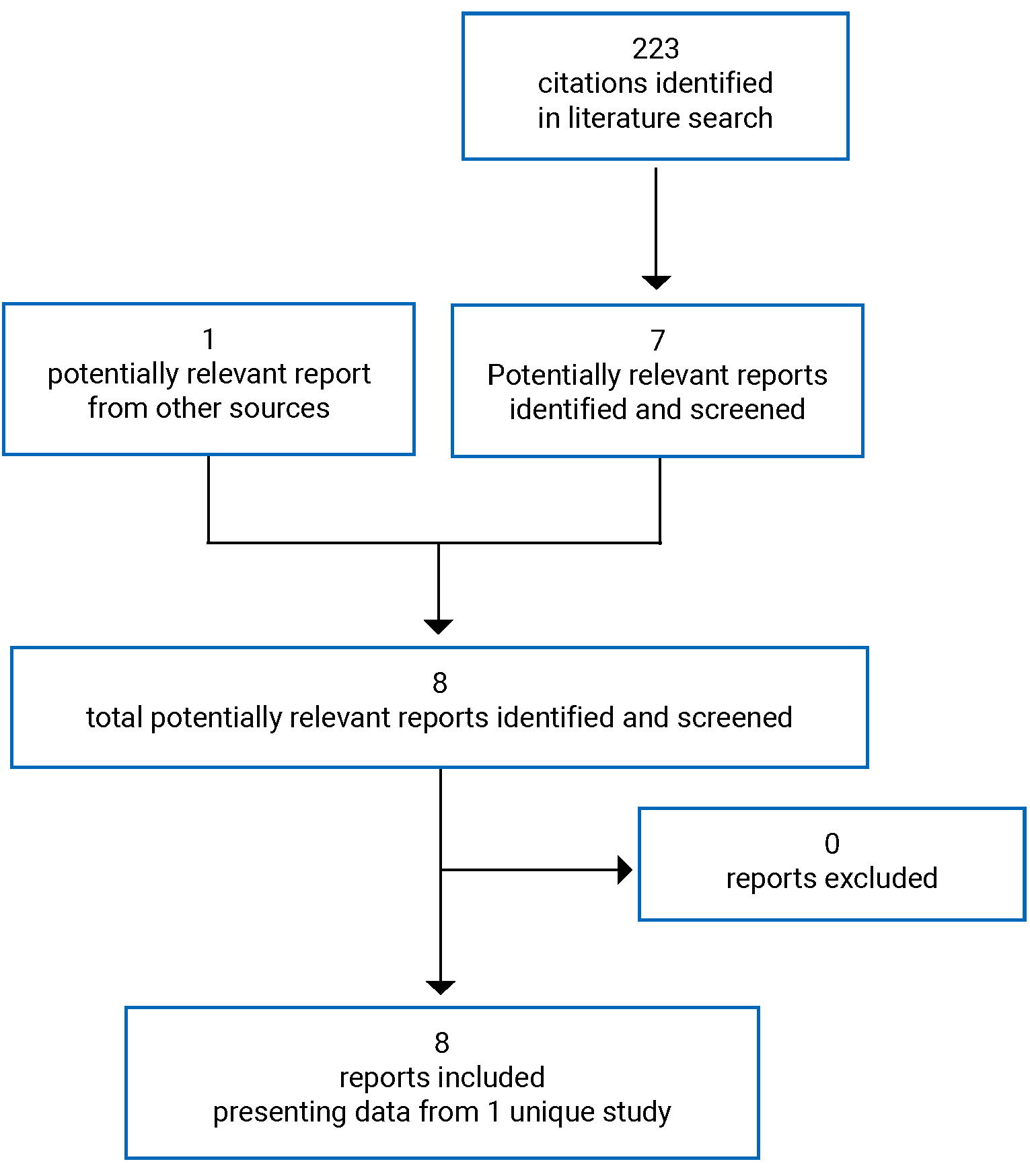
Table 6: Details of the PRISM-2 Study
Detail | PRISM-2 |
|---|---|
Designs and populations | |
Study design | 4-part, 4-arm, double-blind, placebo-controlled RDT with open-label extension |
Locations | 29 study centres in the US |
Patient enrolment dates | July 29, 2013, to not reported |
Data cut-off date | February 5, 2019 |
Randomized (N) | 215 |
Inclusion criteria |
|
Exclusion criteria |
|
Drugs | |
Interventions |
|
Comparator |
|
Duration | |
Phase | |
Part 1 | Screening and open-label blood Phe assessment (n = 164) |
3 to 13 weeks | |
Part 2 | Double-blind, placebo-controlled RDT (n = 95) |
8 weeks | |
Part 3 | Pharmacokinetic and/or pharmacodynamic comparability assessment (n = 89) |
6 weeks | |
Part 4 | Open-label extension (n = 202) |
Up to 274 weeks | |
Outcomes | |
Primary end point | Change in blood Phe concentration from part 2 baseline to part 2, week 8 |
Secondary, tertiary, and exploratory end points | Secondary:
Tertiary:
Exploratory:
|
Notes | |
Publications | Aryal et al. (2021)10 Bilder et al. (2021)11 Qi et al. (2021)15 Larimore et al. (2019)14 Gupta et al. (2018)12 Harding et al. (2018)13 Thomas et al. (2018)16 |
ADHD = attention-deficit/hyperactivity disorder; ADHD-RS-IV = Attention Deficit Hyperactivity Disorder Rating Scale (investigator-rated); AE = adverse event; MNT = medical nutritional therapy; PEG = polyethylene glycol; Phe = phenylalanine; PKU = phenylketonuria; PKUDOS = Phenylketonuria Demographics, Outcome, and Safety; POMS = Profile of Mood States; PKU DOS = Phenylketonuria-Specific Profile of Mood States; RDT = randomized discontinuation trial; TMD = total mood disturbance; ULN = upper limit of normal.
Note: One additional report was included (PRISM-2 Clinical Study Report).
Source: PRISM-2 Clinical Study Report.9
Description of Studies
PRISM-2 was a phase III, 4-part, 4-arm, double-blind placebo-controlled RDT with an extension period of open-label treatment (N = 215).9-16 The study was funded by the sponsor. The major feeder study for the PRISM-2 trial was the PRISM-1 trial,16,17 a phase III, open-label study to assess the safety and tolerability of 2 pegvaliase dosage regimens (20 mg or 40 mg once daily; Other Relevant Evidence section), while a small number of patients were enrolled from phase II studies (PAL-00330 and 165 to 20531). The main eligibility criteria for all 3 feeder studies were patients with PKU aged 16 years or older with blood Phe levels of greater than 600 µmol/L (at screening and the prior 6 month average based on available data) who were able to maintain a consistent diet. Dietary Phe control and adherence to MNT were not requirements for participation in feeder studies. For entry into the PRISM-2 trial, patients with PKU aged 16 to 70 years had to have completed a pegvaliase feeder study, have a stable pegvaliase dose regimen for 2 weeks or longer before screening, be able to comprehend and complete or answer prompts for the ADHD-RS-IV, PKU POMS, and POMS, and have a competent observer available for injections. Patients using other investigational products or medications to treat PKU (e.g., LNAAs, sapropterin) were excluded.
A summary of the design of the PRISM-2 study is shown in Figure 2. Following enrolment and screening at 29 centres in the US, patients either first entered part 1 (open-label Phe assessment) or were directly enrolled in part 4 (open-label extension) if they were unable to achieve the target pegvaliase dose (20 mg/day or 40 mg/day) in the feeder study or due to closure of enrolment in part 2 after target enrolment was met. In part 1, patients were randomized 1:1 to receive open-label pegvaliase (20 mg or 40 mg once daily, vial and syringe) for up to 13 weeks; blood Phe levels were measured every 2 weeks. Randomization to 2 different dosages was based on the design of the PRISM-1 study (fixed maintenance dosages of 20 mg/day and 40 mg/day), which, unlike prior phase II studies in which the maintenance dose was titrated in individual patients to achieve a Phe level of 600 µmol/L or lower, was meant to support licensure of pegvaliase. The rationale for randomization to 20 mg/day and 40 mg/day, rather than selection of a single fixed maintenance dosage, was not stated. Patients who achieved a mean blood Phe reduction of 20% or greater (based on 2 consecutive assessments) from treatment-naive baseline and were able to maintain their randomized pegvaliase dose were eligible for part 2 (RDT), while those who did not achieve this degree of Phe reduction or were unable to maintain their randomized pegvaliase dose due to AEs transitioned directly to part 4 (open-label extension). In part 2, patients in each dosage group (20 mg or 40 mg once daily, vial and syringe) were randomized 2:1 to either continue receiving their assigned dosage of pegvaliase or to receive a matching-administration placebo over 8 weeks of double-blind treatment. Participants, investigators, site personnel, and the sponsor were blind to treatment allocation until all randomized participants in part 2 had completed or discontinued the RDT. Randomization was stratified by mean blood Phe level over the last 2 measurements (600 µmol/L or lower versus greater than 600 µmol/L) and ADHD-RS-IV inattention subscale score at PRISM-1 treatment-naive baseline (≤ 12 versus > 12 or missing). In part 3, patients who completed part 2 received open-label pegvaliase (dosage as assigned in part 1) in 2 formats (vial and syringe or pre-filled syringe) for 6 weeks and pharmacokinetics and pharmacodynamics were compared. Part 4 was an open-label extension in which patients received open-label pegvaliase (up to 60 mg once daily, pre-filled syringe) for up to 274 weeks. Only data for the part 2 RDT of the PRISM-2 study are described in the Systematic Review section of this report; the Other Relevant Evidence section provides non-comparative evidence from parts 1, 3, and 4. The data cut-off was February 5, 2019.
The primary objective of the PRISM-2 study was to evaluate the efficacy of pegvaliase in decreasing blood Phe levels by observing changes from part 2 baseline to part 2, week 8 in patients previously exposed to pegvaliase who received either pegvaliase (20 or 40 mg/day) or a matching-administration placebo in the RDT. Secondary objectives (all hierarchically tested) included comparing changes in ADHD-RS-IV inattention subscale scores (among participants with drug-naive baseline scores > 9 as well as all participants), PKU POMS (self-rated) confusion subscale scores, PKU POMS (self-rated) TMD scores, and POMS (self-rated) TMD scores from part 2 baseline to part 2, week 8 among patients previously exposed to pegvaliase who were randomized to receive either pegvaliase (20 mg/day or 40 mg/day) or a matching placebo in the RDT. Tertiary objectives in part 2 included change from part 2 baseline in protein intake from medical food and intact food at each scheduled visit, discontinuations from part 2 due to neuropsychiatric AEs, and change from part 2 baseline in various neurocognitive and neuropsychiatric parameters at each scheduled visit in part 2. Exploratory objectives analyzed in other parts of the study included studying the long-term efficacy of pegvaliase via changes in blood Phe levels, ADHD-RS-IV, PKU POMS, and POMS total scores and subscale scores, and protein intake medical food and intact food.
Figure 2: PRISM-2 Study Design
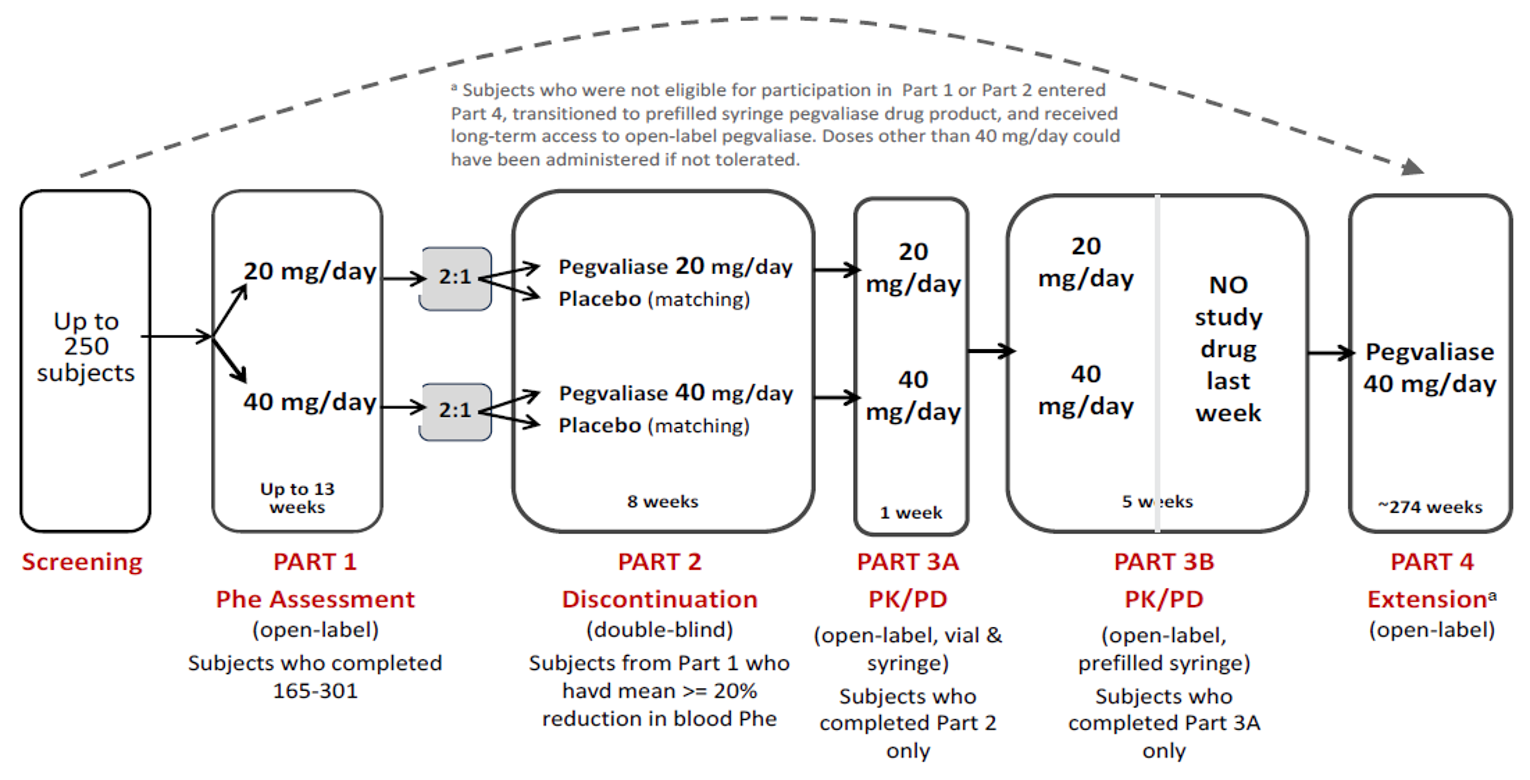
165 to 301 = PRISM-1; PD = pharmacodynamics; Phe = phenylalanine; PK = pharmacokinetics.
aDuring part 4, open-label pegvaliase could have been administered at dosages of up to 60 mg/day.
Source: PRISM-2 Clinical Study Report.9
Populations
Inclusion and Exclusion Criteria
Key inclusion and exclusion criteria for the PRISM-2 study are summarized in Table 6. Adolescent and adult patients with PKU (aged 16 to 70 years) were eligible if they had completed a prior pegvaliase study (PRISM-116,17 or phase II studies PAL-00330 and 165 to 20531; all feeder studies required blood Phe above 600 µmol/L at naive baseline), had a stable pegvaliase dose regimen for 2 weeks or longer, were able to maintain a consistent diet, were able to comprehend and complete or answer prompts for the ADHD-RS-IV, PKU POMS, and POMS, had a competent observer available for injections, and had stable doses of medications for ADHD, depression, anxiety, or other psychiatric disorders for 8 weeks or longer before enrolment. Patients using other investigational products or medications to treat PKU (e.g., LNAAs, sapropterin) were excluded, as were those using injectable drugs containing polyethylene glycol, including medroxyprogesterone.
Baseline Characteristics
The baseline demographic and disease characteristics of participants in the PRISM-2 study (from the drug-naive feeder study as well as PRISM-2 part 2) are shown in Table 7. The mean age for all participants was 29.22 years (SD = 8.74). Only 11 participants (5.1%) were adolescents aged 16 or 17 years. In both placebo groups of the RDT, 42.9% of participants were female compared with 53.4% of participants in the pooled active group. Nearly all participants (98.1%) were White, while 1 participant (0.5%) was American Indian or Alaska Native and 2 participants (0.9%) were Black/African-American. The mean weight and BMI in the 20 mg/day placebo group were 94.0 kg (SD = 27.17) and 32.6 kg/m2 (SD = 7.75), respectively, compared with 73.1 kg (SD = 16.49) and 25.6 kg/m2 (SD = 4.37), respectively, in the 40 mg/day placebo group, and 78.6 kg (SD = 21.55) and 27.8 kg/m2 (SD = 6.85), respectively, in the pooled active group.
Mean blood Phe levels at drug-naive baseline were 1,459.1 µmol/L (SD = 354.71) in the 20 mg/day placebo group, 1,108.9 µmol/L (SD = 266.84) in the 40 mg/day placebo group, and 1,318.0 µmol/L (SD = 351.09) in the pooled active group. Mean blood Phe levels at PRISM-2 part 2 baseline were 563.9 µmol/L (SD = 504.62) in the 20 mg/day placebo group, 508.2 µmol/L (SD = 363.68) in the 40 mg/day placebo group, and 563.9 µmol/L (SD = 504.62) in the pooled active group. Mean daily protein intake from intact food at drug-naive baseline was 46.5 g (SD = 40.48) in the 20 mg/day placebo group, 35.2 g (SD = 21.02) in the 40 mg/day placebo group, and 42.6 g (SD = 25.39) in the pooled active group. Mean daily protein intakes from intact food at PRISM-2 part 2 baseline were 38.1 g (SD = 26.42) in the 20 mg/day placebo group, 39.4 g (SD = 22.69) in the 40 mg/day placebo group, and 49.0 g (SD = 23.84) in the pooled active group. Mean daily protein amounts from medical food at drug-naive baseline were 21.2 g (SD = 25.4) in the 20 mg/day placebo group, 29.8 g (SD = 25.79) in the 40 mg/day placebo group, and |||| ||||||| g in the pooled active group. No participants in the 20 mg/day placebo group, ||||| of participants in the 40 mg/day placebo group, and ||||| of participants in the pooled active group had restricted protein intake, defined as obtaining more than 75% of dietary protein from medical food. Imbalances at drug-naive baseline and at part 2 baseline between the pooled active group and 1 or more placebo groups were present to varying degrees in neurocognitive or neuropsychiatric symptoms (ADHD-RS-IV inattention subscale scores among all participants with baseline scores ≥ 9 and among all participants, PKU POMS confusion subscale scores, PKU POMS TMD scores, and POMS TMD scores).
Although rates of prior sapropterin use were not reported in the PRISM-2 study, 224 of 261 patients (85.8%) enrolled in PRISM-1 (the major feeder study for PRISM-2) were questioned and 196 (87.5%) reported prior sapropterin use.
Table 7: Summary of Drug-Naive Baseline and Part 2 Baseline Demographic and Disease Characteristics in the PRISM-2 Study
Characteristic | All participants (N = 215) | mITT population | ||
|---|---|---|---|---|
Placebo 20 mg/day (n = 14) | Placebo 40 mg/day (n = 14) | Pooled active (n = 58) | ||
Age at naive baseline, years | ||||
Mean (SD) | 29.22 (8.74) | 30.50 (10.96) | 30.00 (10.22) | 29.66 (8.38) |
Median (range) | 28.00 (16.00 to 55.00) | 27.50 (19.00 to 51.00) | 25.50 (18.00 to 50.00) | 29.00 (16.00 to 50.00) |
16 to < 18, n (%)a | 11 (5.1) | 0 | 0 | 3 (5.2) |
18 to < 66, n (%) | 204 (94.9) | 14 (100.0) | 14 (100.0) | 55 (94.8) |
Sex at naive baseline, n (%) | ||||
Female | 105 (48.8) | 6 (42.9) | 6 (42.9) | 31 (53.4) |
Male | 110 (51.2) | 8 (57.1) | 8 (57.1) | 27 (46.6) |
Race at naive baseline, n (%) | ||||
White | 211 (98.1) | 13 (92.9) | 14 (100.0) | 58 (100.0) |
American Indian or Alaska Native | 1 (0.5) | 0 | 0 | 0 |
Black/African-American | 2 (0.9) | 1 (7.1) | 0 | 0 |
Weight at naive baseline,b kg | ||||
N | 214 | 14 | 13 | 58 |
Mean (SD) | 79.3 (21.15) | 94.0 (27.17) | 73.1 (16.49) | 78.6 (21.55) |
Median (range) | 75.1 (41.5 to 143.0) | 87.9 (47.4 to 143.0) | 67.7 (51.8 to 108.4) | 73.1 (42.0 to 135.9) |
Body mass index at naive baseline,b kg/m2 | ||||
n | 214 | 14 | 13 | 58 |
Mean (SD) | 27.9 (6.66) | 32.6 (7.75) | 25.6 (4.37) | 27.8 (6.85) |
Median (range) | 26.9 (17.1 to 46.7) | 33.6 (19.2 to 45.4) | 24.2 (18.3 to 33.0) | 26.8 (17.2 to 46.3) |
Blood Phe concentration at naive baseline, µmol/L | ||||
Mean (SD) | 1,225.6 (378.98) | 1,459.1 (354.71) | 1,108.9 (266.84) | 1,318.0 (351.09) |
Median (range) | 1,196.0 (285.0,c to 2,229.0) | 1,504.5 (76.1 to 2,116.0) | 1,064.5 (695.0 to 1,549.0) | 1,291.0 (713.0 to 2,143.0) |
Blood Phe concentration at part 2 baseline, µmol/L | ||||
Mean (SD) | NA | 563.9 (504.62) | 508.2 (363.68) | 563.9 (504.62) |
Median (range) | NA | NR | NR | NRs |
ADHD-RS-IV inattention subscale score at naive baseline for participants with score > 9 | ||||
n | |||||||| | |||||||| | |||||||| | |||||||| |
Mean (SD) | |||| |||||| | |||| |||||| | |||| |||||| | |||| |||||| |
Median (range) | |||| |||||| ||||| | |||| |||| ||| | |||| |||| ||| | |||| |||| ||| |
ADHD-RS-IV inattention subscale score at part 2 baseline for participants with score > 9 | ||||
n | |||||||| | |||||||| | |||||||| | |||||||| |
Mean (SD) | |||||||| | ||| |||||| | ||| |||||| | ||| |||||| |
Median (range) | |||||||| | ||| ||| ||| | ||| ||| ||| | ||| ||| ||| |
ADHD-RS-IV inattention subscale score at naive baselined | ||||
n | |||||||| | |||||||| | |||||||| | |||||||| |
Mean (SD) | ||| |||||| | |||| |||||| | ||| |||||| | |||| |||||| |
Median (range) | ||| ||||| ||||| | ||| ||||| ||||| | ||| ||||| ||||| | |||| ||||| ||||| |
ADHD-RS-IV inattention subscale score at part 2 baselined | ||||
n | |||||||| | |||||||| | |||||||| | |||||||| |
Mean (SD) | |||||||| | ||| |||||| | ||| |||||| | ||| |||||| |
Median (range) | |||||||| | ||| ||| ||| | ||| ||| ||| | ||| ||| ||| |
POMS TMD score at naive baseline (self-rated)d | ||||
n | |||||||| | |||||||| | |||||||| | |||||||| |
Mean (SD) | |||| ||||||| | |||| ||||||| | |||| ||||||| | |||| ||||||| |
Median (range) | |||| ||||||| |||||| | |||| ||||||| ||||| | |||| |||||| ||||| | |||| ||||||| |||||| |
POMS TMD score at part 2 baseline (self-rated) | ||||
n | |||||||| | |||||||| | |||||||| | |||||||| |
Mean (SD) | |||||||| | |||| ||||||| | |||| ||||||| | |||| ||||||| |
Median (range) | |||||||| | |||| ||||| ||| | |||| ||||| ||| | ||| ||||| |||| |
PKU POMS TMD (self-rated) score at naive baselined | ||||
n | |||||||| | |||||||| | |||||||| | |||||||| |
Mean (SD) | |||| ||||||| | |||| ||||||| | ||| |||||| | |||| ||||||| |
Median (range) | |||| |||||| ||||| | |||| |||||| ||||| | ||| |||||| ||||| | |||| |||||| ||||| |
PKU POMS TMD (self-rated) score at part 2 baseline | ||||
n | |||||||| | |||||||| | |||||||| | |||||||| |
Mean (SD) | |||||||| | ||| ||||||| | ||| |||||| | ||| ||||||| |
Median (range) | |||||||| | |||| |||| ||| | ||| |||| ||| | ||| ||||| ||| |
PKU POMS confusion subscale score at naive baselined | ||||
N | |||||||| | |||||||| | |||||||| | |||||||| |
Mean (SD) | ||| |||||| | ||| |||||| | ||| |||||| | ||| |||||| |
Median (range) | ||| ||||| ||||| | ||| ||||| |||| | ||| ||||| |||| | ||| ||||| ||||| |
PKU POMS confusion subscale score at part 2 baseline | ||||
n | |||||||| | |||||||| | |||||||| | |||||||| |
Mean (SD) | |||||||| | ||| |||||| | ||| |||||| | ||| |||||| |
Median (range) | |||||||| | ||| ||| || | ||| ||| || | ||| ||| || |
Daily protein from intact food at naive baseline,e g | ||||
n | 196 | 12 | 14 | 48 |
Mean (SD) | 38.4 (27.96) | 46.5 (40.48) | 35.2 (21.02) | 42.6 (25.39) |
Median (range) | 29.1 (3.6 to 155.3) | 28.6 (16.9 to 155.3) | 31.0 (9.6 to 64.9) | 40.5 (4.2 to 121.5) |
Daily protein from intact food at part 2 baseline, g | ||||
Mean (SD) | NA | 38.1 (26.42) | 39.4 (22.69) | 49.0 (23.84) |
Median (range) | NA | 25.2 (NR) | 36.1 (NR) | 43.0 (NR) |
Daily protein from medical food at naive baseline, g | ||||
n | 196 | 12 | 14 | 48 |
Mean (SD) | 27.9 (29.08) | 21.2 (25.4) | 29.8 (25.79) | 20.9 (26.34) |
Median (range) | 20.0 (0.0 to 120.0) | 10.0 (0.0 to 66.7) | 27.5 (0.0 to 73.2) | 0.5 (0.0 to 91.2) |
Protein intake at naive baseline | ||||
Restricted protein intake,f n (%) | 36 (16.7) | 0 | 2 (14.3) | | |||||| |
ADHD-RS-IV = Attention Deficit Hyperactivity Disorder Rating Scale (investigator-rated); mITT = modified intention-to-treat; NR = not reported; Phe = phenylalanine; PKU POMS = Phenylketonuria-Specific Profile of Mood States; POMS = Profile of Mood States; SD = standard deviation; TMD = total mood disturbance.
aUnder amendment 1 (January 10, 2014) of the study protocol, participants 16 years of age and older were eligible.
bOne participant in the 40 mg/day placebo group did not have weight and height measured at baseline in PRISM-1.
cOne participant had a naive baseline Phe level of 600 µmol/L or lower, which was different from the blood Phe level assessed at the time of screening that met the eligibility criterion for entry into the study.
dThe ADHD-RS-IV hyperactivity-impulsivity subscale and POMS tools were not used in PRISM-1 until the first protocol amendment; only participants who had baseline assessments were included. Possible scores for the ADHD-RS-IV inattention and hyperactivity-impulsivity subscales ranged from 0 to 27, with higher scores indicative of more severe symptoms. Possible scores for the POMS TMD ranged from −32 to 200, scores for the PKU POMS TMD ranged from −12 to 58, and scores for the PKU POMS confusion subscale ranged from 0 to 11, with higher scores indicative of more severe symptoms. Neurocognitive and neuropsychiatric tools were not administered in phase II feeder studies.
eThe daily recommended allowance for total protein for adults in the general population is 0.75 g/kg. For an 80 kg individual, approximately 60 g of daily protein is recommended.
fParticipants were considered to be on restricted protein intake if more than 75% of total daily protein intake was from medical food. Total daily protein intake was the sum of daily protein intake from medical food and daily protein intake from intact food.
Source: PRISM-2 Clinical Study Report.9
Interventions
During part 1, patients were randomized 1:1 to receive open-label pegvaliase (20 mg or 40 mg once daily, vial and syringe) for up to 13 weeks. In part 2, patients in each dose group (20 mg or 40 mg once daily, vial and syringe) were randomized 2:1 to either continue receiving their assigned dose of pegvaliase or to receive a matching placebo over 8 weeks of double-blind treatment. In part 3, patients who completed part 2 received open-label pegvaliase (dosage as assigned in part 1) in 2 formats (vial and syringe or pre-filled syringe) for 6 weeks and their pharmacokinetics and pharmacodynamics were compared. Part 4 was an open-label extension in which patients received open-label pegvaliase (up to 60 mg once daily, pre-filled syringe) for up to 274 weeks.
All pegvaliase injections were self-administered. Induction and titration to 20 mg/day or 40 mg/day was accomplished in the feeder studies for PRISM-2 (PRISM-1 or phase II studies PAL-003 and 165 to 205). For PRISM-2 part 2 (RDT), either pegvaliase or matching-administration placebo (a dextran solution of similar appearance and consistency) was provided in similarly labelled vials. Training on drug storage, self-injection (vial and syringe as well as pre-filled syringe), identification of AEs, and use of epinephrine was provided both in feeder studies and as a condition for participation in PRISM-2. Participants were given 2 epinephrine injectors at the beginning of the study and were instructed to always carry 1 injector with them. An observer was required for self-injections performed for 1 week after re-introduction of the study drug following an interruption of 4 days or longer. Moreover, during pegvaliase titration or dose increases (part 4) as well as during re-introduction of the study drug, patients received mandatory pre-medication with H1 and H2 blockers with or without nonsteroidal anti-inflammatory drugs or antipyretics (e.g., acetaminophen) before pegvaliase injections for 1 week.
The only PKU-related cointervention of relevance in PRISM-2 was dietary protein intake from intact and medical food (including MNT). Participants were asked to maintain daily protein intake from natural food and medical food through the duration of this study as changes in these parameters could confound efficacy assessments. A dietitian managed patient protein intake for the duration of the study. Throughout the study, all participants were instructed to take 500 mg of a tyrosine supplement 3 times per day with meals.
The study drug could be dose-reduced, interrupted, or permanently discontinued for patients who had HAEs (the Outcomes section provides details). For HAEs of grade 3 or higher related to study drug (and grade 4 HAEs irrespective of relationship to study drug) that were suspected by the investigator and sponsor medical monitor to meet Brown’s criteria for severe,32 the study drug could be permanently discontinued. For grade 3 HAEs related to the study drug that were not suspected to meet Brown’s criteria for severe, grade 3 HAEs not related to the study drug, and HAEs of grade 2 or lower, pegvaliase administration could be dose-reduced or interrupted. Dosages could be reduced from 60 mg/day to 40 mg/day (part 4 only), from 40 mg/day to 20 mg/day, from 20 mg/day to 10 mg/day, or from 10 mg/day to 5 mg/day. Once HAEs other than anaphylaxis improved to grade 1 or were resolved, dosing could be returned to the level administered before the onset of the AE. Suspected anaphylaxis was assessed in clinics, including laboratory evaluations. Following resolution of an anaphylaxis event, dosing could be resumed following the described incremental dose-reduction rules, or with further reduction. Table 8 lists the rules for dosing changes in response to HAEs in the PRISM-2 study.
Outcomes
A list of efficacy end points identified in the CADTH review protocol that were assessed in the clinical trials included in this review is provided in Table 9. These end points are further summarized in the following section. A detailed discussion and critical appraisal of the outcome measures is provided in Appendix 2.
Table 8: Dosing Changes in Response to HAEs in the PRISM-2 Study
CTCAE gradea | Related to study drug | Action with study drug | Individual stopping criteriad | Hypersensitivity reaction visit assessmente | ||
|---|---|---|---|---|---|---|
Maintainedb | Reducedc | Interruptedc | ||||
1 | Yes or No | Yes | (Yes) Optional | (Yes) Optional | NA | Investigator discretion |
2 | Yes or No | Yes | (Yes) Optional | (Yes) Optional | NA | Investigator discretion |
3 | No | Yes | (Yes) Optional | (Yes) Optional | NA | Investigator discretion |
3 | Yes | Yes | (Yes) Optional | (Yes) Optional | NA | Yes (if within 24 hours of onset) |
3d | Yes | NA | NA | NA | Yes Consult with sponsor medical monitor | Yes (if within 24 hours of onset) |
4d | Yes or No | NA | NA | NA | Yes Consult with sponsor medical monitor | Yes (if within 24 hours of onset) |
CTCAE = Common Terminology Criteria for Adverse Events, version 4.03; HAE = hypersensitivity adverse event; NA = not applicable.
aCTCAE grade determination was performed by the investigator either via telephone or clinic visit.
bThe investigator instructed the participant to maintain the pegvaliase dose at the time of adverse event onset until improvement to grade 1 or resolution (according to the investigator assessment in the clinic or via telephone).
cThe pegvaliase dose could have been reduced or interrupted if necessary as determined by the investigator. The investigator should have consulted with the sponsor’s medical monitor before performing dose reductions during PRISM-2 Part 2.
dIf a participant had an HAE of grade 3 or higher that was related to the study drug and was suspected to meet Brown’s criteria for severe in the judgment of the investigator and the sponsor’s medical monitor, the participant could have been permanently discontinued from study drug.
eIf the investigator determined that an HAE of grader 3 or higher was related to administration of pegvaliase, the participant was asked to return to the clinic within 24 hours of event onset for evaluation, including laboratory tests (chemistry, hematology, urinalysis, antidrug immunoglobulin E, antidrug- polyethylene glycol immunoglobulin E [sampling performed > 8 hours after event onset and before the next dose of study drug], urine albumin to creatinine ratio, urinary N-methyl histamine, high-sensitivity C-reactive protein, complement component, complement component 4, tryptase, and urinary N-methylhistamine).
Source: PRISM-2 Clinical Study Report.9
Table 9: Summary of Outcomes of Interest Identified in the CADTH Review Protocol
Outcome measure | PRISM-2 |
|---|---|
Change from part 2 baseline in protein intake from medical food and intact food at each scheduled visit in part 2 | Tertiary |
Change in blood Phe concentration from part 2 baseline to part 2 week 8 | Primary |
Change in ADHD-RS-IV Inattention subscale scorea from part 2 baseline to part 2, week 8 among participants with baseline scores > 9 in PRISM-1 (Study 165 to 301) | Secondary |
Change in ADHD-RS-IV Inattention subscale scorea from part 2 baseline to part 2, week 8 among all participants | Secondary |
Change in PKU POMS (self-rated) confusion subscale scoreb from part 2 baseline to part 2, week 8 | Secondary |
Change in PKU POMS (self-rated) TMD scorec from part 2 baseline to part 2, week 8 | Secondary |
Change in POMS (self-rated) TMD scored from part 2 baseline to part 2, week 8 | Secondary |
Discontinuation from part 2 due to neuropsychiatric AEs | Tertiary |
Change from part 2 baseline in ADHD-RS-IV total scoree and ADHD-RS-IV hyperactivity-impulsivity subscale scoresa at each scheduled visit in part 2 | Tertiary |
Change from part 2 baseline in POMS (observer-rated) TMD scored and tension, depression, anger, fatigue, confusion, and vigour subscale scoresf at each scheduled visit in part 2 | Tertiary |
Change from part 2 baseline in POMS (self-rated) tension, depression, anger, fatigue, confusion, and vigour subscale scoresf at each scheduled visit in part 2 | Tertiary |
Change from part 2 baseline in PKU POMS anxiety, depression, anger, activity, and tiredness subscale scoresg at each scheduled visit in part 2 | Tertiary |
AEs, SAEs, WDAEs, deaths | Safety |
AESIs (anaphylaxis, angioedema, hypersensitivity AEs, injection-site reactions, injection-site skin reactions ≥ 14 days in duration, generalized skin reactions ≥ 14 days in duration, arthralgia, serum sickness) | Safety |
Notable harms: acute systemic hypersensitivity reactions (anaphylaxis) manifested by syncope, hypotension, hypoxia, dyspnea, wheezing, chest discomfort and/or tightness, tachycardia, angioedema (swelling of face, lips, eyes, and tongue), flushing, rash, urticaria, pruritus, and gastrointestinal symptoms (e.g., vomiting, nausea, and diarrhea); other systemic hypersensitivity reactions (e.g., severe angioedema, severe serum sickness); injection-site reactions; arthralgia, lymphadenopathy; cough; headache; abdominal pain; alopecia; erythema; and myalgia | Safety |
ADHD-RS-IV = Attention Deficit Hyperactivity Disorder Rating Scale (investigator-rated); AE = adverse event; AESI = adverse event of special interest; Phe = phenylalanine; PKU POMS = Phenylketonuria-Specific Profile of Mood States; POMS, Profile of Mood States; SAE = serious adverse event; TMD = total mood disturbance; WDAE = withdrawal due to adverse event.
aScores for ADHD-RS-IV subscales, including the Inattention subscale, range from 0 to 27, with higher scores indicative of a greater degree of impairment.
bScores for the PKU POMS confusion subscale range from 0 to 11, with higher scores indicative of a greater degree of impairment.
cScores for PKU POMS TMD range from −12 to 58, with higher scores indicative of a greater degree of impairment.
dScores for POMS TMD range from −32 to 200, with higher scores indicative of a greater degree of impairment.
eADHD-RS-IV total score ranges from 0 to 54, with higher scores indicative of a greater degree of impairment.
fScores for POMS subscales depend on the number of items (tension, 0 to 28; depression, 0 to 60; anger, 0 to 48; fatigue, 0 to 28; confusion, 0 to 28; and vigour, 0 to 32). Higher scores are indicative of a greater degree of impairment.
gScores for PKU POMS subscales depend on the number of items (anxiety, 0 to 16; depression, 0 to 16; anger, 0 to 12; activity, 0 to 12; and tiredness, 0 to 12). Higher scores are indicative of a greater degree of impairment.
Source: PRISM-2 Clinical Study Report.9
All primary and secondary efficacy outcomes in PRISM-2 were assessed in part 2 (RDT). The primary outcome was change in blood Phe level from part 2 baseline to part 2, week 8. Changes in inattention and mood symptoms from part 2 baseline to part 2, week 8 were assessed as secondary hierarchically tested outcomes; these included ADHD-RS-IV33 inattention subscale scores (among participants with drug-naive baseline scores > 9 and among all participants), PKU POMS34 confusion subscale scores, PKU POMS TMD scores, and POMS1 TMD scores. Among secondary outcomes, the ADHD-RS-IV is investigator-rated while the PKU POMS and POMS are patient-reported. Tertiary efficacy outcomes planned to be evaluated in part 2 but not controlled for multiplicity were change in protein intake from medical food and intact food from part 2 baseline at each scheduled visit (weeks 1, 4, and 8), discontinuations due to neuropsychiatric AEs, and changes from part 2 baseline at each scheduled visit in various inattention and mood symptoms (ADHD-RS-IV total score, ADHD-RS-IV hyperactivity-impulsivity subscale score, POMS [observer-rated] TMD score and subscale scores, POMS [self-rated] subscale scores, and PKU POMS subscale scores). Protein intake was measured using 3-day patient-completed diet diaries that were reviewed at clinic visits by study dietitians.
A detailed discussion and critical appraisal of efficacy outcomes used in the PRISM-2 study is provided in Appendix 2. Aside from 1 study demonstrating acceptable internal consistency reliability of the PKU POMS,34 no studies of the measurement properties of any of the efficacy outcomes used in the PRISM-2 study among adult patients with PKU were identified. According to the clinical experts consulted by CADTH for this review, blood Phe level is broadly understood to mechanistically drive the symptoms of PKU, has been associated with neurocognitive and neuropsychiatric symptoms in some studies, and is often used in clinical trials due to convenience. However, the clinical experts stated that the magnitude of blood Phe decreases as well as the duration and consistency of metabolic control required for adult patients with PKU to achieve improvements in other outcomes (such as dietary Phe tolerance, neurocognitive and neuropsychiatric symptoms, and HRQoL) is not known at present.
Harms outcomes included treatment-emergent AEs, SAEs, AEs requiring dose interruption or dose reduction, withdrawals due to AEs, and AESIs. The following were considered AESIs: anaphylaxis, angioedema, HAEs, injection-site reactions, injection-site skin reactions lasting for 14 days or more, generalized skin reactions lasting 14 days or more, arthralgia, and serum sickness. Hypersensitivity AEs, including anaphylaxis and angioedema, were identified using a broad algorithmic Standardized Medical Dictionary for Regulatory Activities (MedDRA) Query (SMQ) for anaphylactic reactions along with a modified version of the SMQ for hypersensitivity that included additional preferred terms. Anaphylaxis was defined by NIAID-FAAN criteria35 and Brown’s severe criteria.32 AEs that began or worsened on or after the start of protocol therapy until 30 days after the last dose of study drug were captured. AEs were defined as any untoward medical occurrence and were coded according to MedDRA version 18.036 and graded according to version 4.03 of the National Cancer Institute Common Terminology Criteria for Adverse Events.37
Statistical Analysis
Statistical analysis of efficacy outcomes in the PRISM-2 study is summarized in Table 10. No interim analyses were planned or conducted. The primary efficacy analysis was conducted after all participants had completed or discontinued part 2 (RDT).
Determination of Sample Size
For part 2 (RDT), the planned sample size (approximately 72 participants; 48 in the active groups and 24 in placebo groups) would provide 97% power to detect a statistically significant difference in the change in blood Phe from part 2 baseline to part 2, week 8 between the pooled active group and the pooled placebo group with a 2-sided type I error rate of 0.05. The assumptions in this power calculation were that, by part 2, week 8, participants in the pooled active group would maintain mean blood Phe levels of no more than 700 µmol/L with a common SD of 400 µmol/L, and participants in the pooled placebo group would have increased mean blood Phe levels to 1,100 µmol/L or greater, with a common SD of 400 µmol/L.
This planned sample size (N = 72) would provide approximately 70% power to detect a statistically significant difference in change from part 2 baseline to part 2, week 8 in ADHD-RS-IV inattention subscale scores (among participants with drug-naive baseline scores > 9 and among all participants) between the pooled active group and the placebo group using the sequential procedure for multiplicity adjustment within the secondary end points described in the following section. The assumptions in this power calculation were (i) a mean difference between the pooled active group and pooled placebo group among participants with a drug-naive baseline ADHD-RS-IV inattention subscale score above 9 of 5 (SD = 5.5) and (ii) 50% of participants in the mITT population had a drug-naive baseline ADHD-RS-IV inattention subscale score above 9. No power calculations for other secondary outcomes were provided.
Poolability Assessment
To test for potential differences between the 2 placebo groups (20 mg/day and 40 mg/day), change in blood Phe from part 2 baseline to part 2, week 8 was compared by a mixed model for repeated measures (MMRM) analysis with placebo group, visit, and group-by-visit interaction as factors, adjusting for baseline blood Phe level. If P was less than or equal to 0.1, the primary efficacy analysis was to be performed for the pooled active group versus the 20 mg/day placebo group and the 40 mg/day placebo group separately. No poolability assessment was performed for the 20 mg/day and 40 mg/day active pegvaliase treatment groups because it was assumed that there would be no carryover effects for these patients in part 2 (as opposed to patients randomized to receive placebo in part 2, in which carryover effects may differ based on the pegvaliase dose in part 1).
Control of type I Error
Type I error was controlled using a hierarchical testing strategy. Between the primary and secondary efficacy outcomes in part 2, and within the secondary outcomes, a sequential hypothesis testing procedures was used for multiplicity adjustment. The primary outcome (change in blood Phe level from part 2 baseline to part 2, week 8) was tested first, followed by change from part 2 baseline to part 2, week 8 in ADHD-RS-IV inattention subscale score among participants with drug-naive baseline scores above 9, change from part 2 baseline to part 2, week 8 in ADHD-RS-IV inattention subscale score among all participants, change from part 2 baseline to part 2, week 8 in PKU POMS confusion subscale score, change from part 2 baseline to part 2, week 8 in PKU POMS TMD score, and change from part 2 baseline to part 2, week 8 in POMS TMD score. Tertiary efficacy outcomes were not included in the hierarchical testing strategy and were not adjusted for multiplicity.
If poolability was not confirmed and the primary efficacy analysis was to be performed for the pooled active group versus the 20 mg/day and 40 mg/day placebo groups separately, the Hochberg method was used to adjust for multiple comparisons.
Analysis Methods
In the primary efficacy analysis, change in blood Phe concentration from part 2 baseline to part 2, week 8 was compared for the mITT set between the pooled active group versus the 20 mg/day placebo group and between the pooled active group versus the 40 mg/day placebo group using the MMRM method with the study drug group (pegvaliase, placebo), visit, and drug-by-visit interaction as factors adjusting for baseline blood Phe and without imputation for missing blood Phe concentrations. Analysis using MMRM was conducted under a missing-at-random assumption. The study was considered positive if both comparisons resulted in a P value of less than 0.05 or a comparison of either the 40 mg/day placebo group or 20 mg/day placebo group versus the pooled active group resulted in a P value of less than 0.025 favouring the pooled active group. In addition, a responder analysis using a cumulative distribution function approach was conducted, and descriptive and summary statistics were prepared.
Analyses of secondary efficacy outcomes were conducted according to the primary MMRM analysis adjusted for the appropriate baseline variable.
Sensitivity Analyses
Sensitivity analyses were conducted for the primary efficacy analysis of Phe levels as well as for secondary analyses of inattention and mood symptoms. Sensitivity analyses included MMRM in the mITT set, with replacement of missing values by multiple imputation and last observation carried forward imputation, MMRM analysis in the ITT set without imputation, and MMRM analysis in the per-protocol set without imputation. An additional sensitivity analysis was conducted by comparing individual dose groups (20 mg/day or 40 mg/day; MMRM, mITT set, no imputation). To assess the impact of protein intake on the primary efficacy outcome (blood Phe), an analysis of covariance model was used to evaluate change in blood Phe levels with study drug group (pegvaliase, placebo), baseline blood Phe, and change from baseline in protein intake from intact food at week 8 of part 2 in the model.
Subgroup Analyses
To explore the uniformity of the effect of study drug, analyses were performed to determine the potential interaction of subgroups with study drug using the MMRM method of the primary analysis with an additional subgroup covariate-by treatment interaction. The following groups were tested separately: baseline blood Phe categories at part 2 baseline visit (≤ 50% reduction versus > 50% from drug-naive baseline using the mean of 2 consecutive blood Phe measurements), baseline ADHD-RS-IV inattention subscale categories (≤ 9 versus > 9) for POMS-related secondary efficacy end points; sex (female versus male), BMI (< 25 kg/m2, ≥ 25 kg/m2, < 30 kg/m2, ≥ 30 kg kg/m2), and immunogenicity.
Table 10: Statistical Analysis of Efficacy End Points in PRISM-2
End point | Position in statistical hierarchy | Statistical model | Adjustment factors | Handling of missing data | Sensitivity analyses |
|---|---|---|---|---|---|
Part 2 | |||||
Change in blood Phe concentration from part 2 baseline to part 2, week 8 | 1 (2-sided alpha = 0.05 for both comparisons of the pooled active group vs. the 20 mg/day placebo group and the pooled active group vs. the 40 mg/day placebo group, or 2-sided alpha = 0.025 for either of these 2 comparisons) |
| Study drug group, visit, and drug-by-visit interaction as factors adjusting for baseline Phe | MAR assumption |
|
Change in ADHD-RS-IV inattention subscale score from part 2 baseline to part 2, week 8 among participants with baseline scores > 9 in PRISM-1 (Study 165 to 301) | 2 (alpha according to primary analysis of Phe levels) |
| According to primary analysis of Phe levels but adjusting for baseline ADHD-RS-IV inattention subscale score | According to primary analysis of Phe levels | According to primary analysis of Phe levels |
Change in ADHD-RS-IV inattention subscale score from part 2 baseline to part 2, week 8 among all participants | 3 (alpha according to primary analysis of Phe levels) |
| According to primary analysis of Phe levels but adjusting for baseline ADHD-RS-IV inattention subscale score | According to primary analysis of Phe levels | According to primary analysis of Phe levels |
Change in PKU POMS (self-rated) confusion subscale score from part 2 baseline to part 2, week 8 | 4 (alpha according to primary analysis of Phe levels) |
| According to primary analysis of Phe levels but adjusting for baseline PKU POMS (self-rated) confusion subscale score | According to primary analysis of Phe levels | According to primary analysis of Phe levels |
Change in PKU POMS (self-rated) TMD score from part 2 baseline to part 2, week 8 | 5 (alpha according to primary analysis of Phe levels) |
| According to primary analysis of Phe levels but adjusting for baseline PKU POMS (self-rated) TMD score | According to primary analysis of Phe levels | According to primary analysis of Phe levels |
Change in POMS (self-rated) TMD score from part 2 baseline to part 2, week 8 | 6 (alpha according to primary analysis of Phe levels) |
| According to primary analysis of Phe levels but adjusting for baseline POMS (Self-Rated) TMD score | According to primary analysis of Phe levels | According to primary analysis of Phe levels |
Change from part 2 baseline in protein intake from medical food and intact food at each scheduled visit in part 2 | Not included | Descriptive and summary statistics | NA | NA | NA |
Discontinuation from part 2 due to neuropsychiatric AEs | Not included | Descriptive and summary statistics | NA | NA | NA |
Change from part 2 baseline in ADHD-RS-IV total score and ADHD-RS-IV hyperactivity-impulsivity subscale scores at each scheduled visit in part 2 | Not included | Descriptive and summary statistics | NA | NA | NA |
Change from part 2 baseline in POMS (observer-rated) TMD and tension, depression, anger, fatigue, confusion, and vigour subscale scores at each scheduled visit in part 2 | Not included | Descriptive and summary statistics | NA | NA | NA |
Change from part 2 baseline in POMS (self-rated) tension, depression, anger, fatigue, confusion, and vigour subscale scores at each scheduled visit in part 2 | Not included | Descriptive and summary statistics | NA | NA | NA |
Change from part 2 baseline in PKU POMS anxiety, depression, anger, activity, and tiredness subscale scores at each scheduled visit in part 2 | Not included | Descriptive and summary statistics | NA | NA | NA |
Safety (AEs, SAEs, WDAEs, mortality, notable harms) | Not included | Descriptive and summary statistics | None | NA | None |
ADHD-RS-IV = Attention Deficit Hyperactivity Disorder Rating Scale (investigator-rated); AE = adverse event; ANCOVA = analysis of covariance; CDF = cumulative distribution function; ITT = intention-to-treat; LOCF = last observation carried forward; LSM = least squares mean; MAR = missing at random; mITT = modified intention-to-treat; MMRM = mixed model for repeated measures; NA = not applicable; Phe = phenylalanine; PKU POMS = Phenylketonuria-Specific Profile of Mood States; POMS = Profile of Mood States; PP = per-protocol; SAE = serious adverse event; TMD = total mood disturbance; vs. = versus; WDAE = withdrawal due to adverse event.
Source: PRISM-2 Clinical Study Report.9
Analysis Populations
The ITT set was defined as all participants randomized to PRISM-2 part 2. The mITT set consisted of all participants who reached the randomized pegvaliase dose of 20 mg/day or 40 mg/day and were randomized into part 2 with a mean blood Phe reduction of 20% or greater (using the last 2 consecutive blood Phe assessments of part 1) from drug-naive baseline. The distinction between the ITT and the mITT sets occurred because some participants had already enrolled in part 2 when the blood Phe reduction criterion (≥ 20%) for inclusion in the mITT set was established by protocol amendment. The per-protocol set consisted of all subjects in the mITT set who were compliant with the study protocol and had no major protocol violations that were considered to have affected efficacy. The safety population consisted of all participants who enrolled into the study and all participants who enrolled into each study part for analysis by study part.
Results
Patient Disposition
Overall patient disposition in the PRISM-2 study is shown in Figure 3 and Table 11. A total of 215 participants were enrolled in the PRISM-2 study; numbers of patients screened and reasons for screen failure were not provided. Almost all patients (n = 203, 94.4%) had previously completed the PRISM-1 study. Fifty-one patients (23.7%) entered PRISM-2 Part 4 (open-label extension) directly, 33 (15.3%) because they did not achieve target pegvaliase dose in PRISM-1 and 18 (8.4%) because enrolment in part 2 was closed. Of the 164 patients participating in part 1, 12 (7.3%) discontinued the study early, while 57 (34.8%) transitioned directly to part 4 (open-label extension) due to failure to meet the blood Phe reduction criterion of 20% or greater for entry in part 2 imposed in protocol amendment 2 (n = 39; 23.7%), closure of part 2 enrolment (n = 9; 5.5%), or other reasons that were not stated (n = 9; 5.5%). The remaining 95 patients proceeded to part 2 (RDT), of whom 86 met the blood Phe reduction criterion of 20% or greater and made up the mITT set. Only 1 patient (1.1%) discontinued the study early during part 2. Of the 95 participants in part 2, 89 proceeded to part 3 (pharmacokinetic and/or pharmacodynamic analysis), while 5 (5.3%) transitioned directly to part 4 (open-label extension) due to AEs or other reasons that were not stated. Of the 202 patients in part 4 who received open-label pegvaliase, 30 (14.9%) discontinued the study early.
Figure 3: PRISM-2 Study Disposition
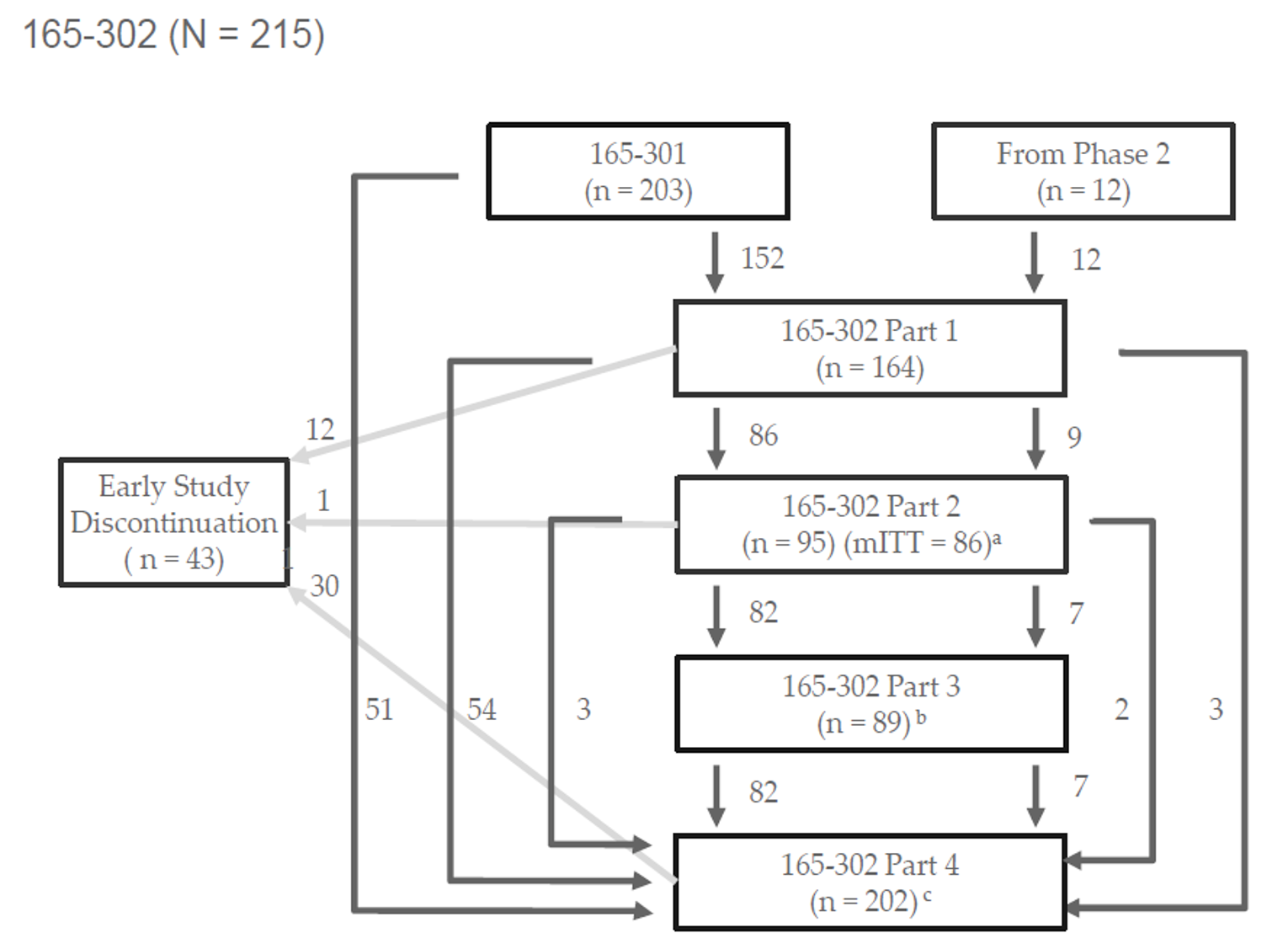
165 to 301 = PRISM-1; 165 to 302 = PRISM-2; mITT = modified intention-to-treat.
aParticipants were not included in the primary efficacy analysis (mITT) if they did not have a mean blood Phe reduction of 20% or greater (using the last 2 consecutive blood Phe assessments of part 1) from baseline levels as established by amendment 2. Some participants had already enrolled in part 2 when this criterion for inclusion in the mITT was implemented.
bOnly participants enrolled under amendment 2 were considered for the pharmacokinetic and pharmacodynamic analyses; 58 of the 89 participants who entered part 3 were enrolled under amendment 2 and were included for the pharmacokinetic and/or pharmacodynamic analyses.
cA total of 51 participants entered part 4 directly from PRISM-1 because they did not achieve target dose in PRISM 1 (n = 33) or were affected by closure of enrolment into part 2 (n = 18) after the target enrolment had been met. Another 57 participants entered directly from part 1 because they did not meet the blood Phe reduction criterion to qualify for entry into part 2 (n = 39), due to closure of enrolment in part 2 (n = 9), or for other reasons as instructed by the sponsor (n = 9).
Source: PRISM-2 Clinical Study Report.9
The ITT set of PRISM-2 part 2 (RDT) consisted of all 95 patients enrolled in part 2 who were randomized to 1 of the 4 dose groups of pegvaliase or matching placebo (both 20 mg/day or 40 mg/day). All 95 patients received the study drug as determined by randomized allocation and were included in the safety population. The mITT set consisted of the subset of patients in the ITT (n = 86; 90.5%) who met the blood Phe reduction criterion of 20% or greater during part 1. The per-protocol set consisted of the subset of patients in the mITT (n = 80; 84.2%) who were compliant with the study protocol and had no major protocol violations that were considered to have affected the efficacy analyses.
Table 11: Disposition of Participants in PRISM-2
Patient disposition | Participants from PRISM-1 (165 to 301) | Participants from phase II studies (PAL-003, 165 to 205) | Total |
|---|---|---|---|
Entered PRISM-2 (165 to 302), Na | 203 | 12 | 215 |
Treated in PRISM-2 (165 to 302), n (%) | 203 (100.0) | 12 (100.0) | 215 (100.0) |
Entered PRISM-2 (165 to 302) part 1, n (%) | 152 (74.9) | 12 (100.0) | 164 (76.3) |
Progressed from part 1 to part 2, n (%) | 86 (42.4) | 9 (75.0) | 95 (44.2) |
Progressed from part 1 to part 4, n (%) | 54 (26.6) | 3 (25.0) | 57 (26.5) |
Did not achieve blood Phe reduction of ≥ 20% by end of part 1, n (%) | NR | NR | 38 (17.7) |
Enrolment into part 2 closed, n (%) | NR | NR | 10 (4.7) |
Other, n (%) | NR | NR | 9 (4.2) |
Discontinued study during part 1, n (%) | 12 (5.9) | 0 | 12 (5.6) |
Discontinued study drug during part 1, n (%) | 12 (5.9) | 0 | 12 (5.6) |
Entered PRISM-2 (165 to 302) part 2, n (%)b | 86 (42.4) | 9 (75.0) | 95 (44.2) |
Progressed from part 2 to part 3, n (%) | 82 (40.4) | 7 (58.3) | 89 (41.4) |
Progressed from part 2 to part 4, n (%)c | 3 (1.5) | 2 (16.7) | 5 (2.3) |
Discontinued study drug during part 2, n (%)d | 1 (0.5) | 0 | 1 (0.5) |
Discontinued study drug during part 2, n (%)d | 1 (0.5) | 0 | 1 (0.5) |
Entered PRISM-2 (165 to 302) part 3, n (%) | 82 (40.4) | 7 (58.3) | 89 (41.4) |
Progressed from part 3 to part 4, n (%) | 82 (40.4) | 7 (58.3) | 89 (41.4) |
Discontinued study during part 3, n (%) | 0 | 0 | 0 |
Discontinued study drug during part 3, n (%) | 0 | 0 | 0 |
Entered PRISM-2 (165 to 302) part 4, n (%)e | 190 (93.6) | 12 (100.0) | 202 (94.0) |
Entered part 4 from PRISM-1 (165 to 301)f | 51 (25.1) | 0 | 51 (23.7) |
Did not achieve target dose in PRISM-1 (165 to 301) | NR | NR | 33 (15.3) |
Enrolment into part 2 closed | NR | NR | 18 (18.4) |
Completed part 4 | 161 (79.3) | 11 (91.7) | 172 (80.0) |
Discontinued study during part 4g | 29 (14.3) | 1 (8.3) | 30 (14.0) |
Discontinued study drug during part 4a | 33 (16.3) | 1 (8.3) | 34 (15.8) |
Analysis populations (part 2), n (%) | |||
Screened | NR | NR | NR |
Intention to treata | NR | NR | 95 (100.0) |
Modified intention-to-treat | NR | NR | 86 (90.5) |
Per-protocol | NR | NR | 80 (84.2) |
Safety | NR | NR | 95 (100.0) |
NR = not reported; Phe = phenylalanine.
aUsed as the denominator to calculate percentages.
bSome participants may have been enrolled in part 2 before the blood Phe eligibility criterion having been established with amendment 2. Participants were not included in the primary efficacy analysis (modified intention-to-treat) if they did not have a mean blood Phe reduction of 20% or greater (using the last 2 consecutive blood Phe assessments of part 1) from baseline levels.
cParticipants who were unable to complete part 2 due to an adverse event transitioned directly into part 4. One participant transitioned from part 2 to part 4 and did not perform part 3 assessments; the reason for moving from part 2 directly to part 4 was not due to an adverse event.
dOne participant who completed the week 8 visit of part 2 and then withdrew consent (due to participant decision) was considered to have discontinued early from the study because they did not subsequently enter part 3 or part 4.
eParticipants who did not meet the part 2 eligibility criterion, were unable to complete part 1 due to an adverse event, did not complete PRISM-1 (165 to 301) with a dose of 20 mg/day or 40 mg/day, or could not maintain a dose of 20 mg/day or 40 mg/day during part 1 were to transition directly into part 4.
fParticipants enrolled into part 4 directly from PRISM-1 (Study 165 to 301) because of the early closure of Study 165 to 301 by the sponsor.
gOne participant withdrew from the study due to an investigator’s decision. However, the participant was captured in the list of participants who were withdrawn from the study due to an adverse event.
Source: PRISM-2 Clinical Study Report.9
Patient disposition for the PRISM-2 part 2 RDT by randomized study drug assignment is shown in Table 12. Four of 58 patients (6.9%) randomized to receive active pegvaliase and 1 of 28 patients (3.6%) randomized to receive placebo during part 2 transitioned directly to part 4 (open-label extension) due to AEs. Only 1 patient in the 40 mg/day active placebo group discontinued the study during part 2.
Important protocol deviations during the overall PRISM-2 study and during PRISM-2 part 2 are summarized in Table 13. The denominators for important protocol deviations and their occurrence by randomized treatment group were not provided. The most common important protocol deviation was self-reported departure from protein intake instructions outlined in the study protocol (n = 18 patients, representing 18.9% of the ITT). The degree of deviation from baseline protein intake required for classification as an important protocol deviation was not stated.
Table 12: Disposition of Participants by Randomized Study Drug Assignment in PRISM-2 Part 2 (mITT)
Disposition category | Active (pegvaliase) | Placebo | ||
|---|---|---|---|---|
20 mg/day active | 40 mg/day active | 20 mg/day placebo | 40 mg/day placebo | |
Entered PRISM-2 (165 to 302) part 2, Na | 29 | 29 | 14 | 14 |
Participants from PRISM-1 (165 to 301), n (%) | 26 (89.7) | 24 (82.8) | 13 (92.9) | 14 (100.0) |
Participants from phase II studies (PAL-003, 165 to 205), n (%) | 3 (10.3) | 5 (17.2) | 1 (7.1) | 0 |
Progressed from part 2 to part 3 | 28 (96.6) | 25 (86.2) | 14 (100.0) | 13 (92.9) |
Progressed from part 2 to part 4 (due to AEs)b | 1 (3.4) | 3 (10.3) | 0 | 1 (7.1) |
Discontinued study drug during part 2 | 0 | 1 (3.4) | 0 | 0 |
Discontinued study during part 2 | 0 | 1 (3.4) | 0 | 0 |
AE = adverse event; mITT = modified intention-to-treat.
aUsed as the denominator to calculate percentages.
bParticipants who were unable to complete part 2 due to an AE transitioned directly into part 4. One participant transitioned from part 2 to part 4 and did not perform part 3 assessments; the move from part 2 directly to part 4 was not due to an AE.
Source: PRISM-2 Clinical Study Report.9
Table 13: Important Protocol Deviations in PRISM-2
Protocol deviation category | N |
|---|---|
Participants with ≥ 1 important protocol deviation during the study | |
Received more than 2 doses of study drug < 12 hours apart on the same calendar day with total dosage > 60 mg/daya | 15 |
Administered the wrong study drug presentation during part 3b | 3 |
Participants with ≥ 1 important protocol deviation during part 2 | |
Missing study drug workbook in part 2 | 2 |
1 or more secondary end point assessments were not performed for week 1 of part 2 (or were performed outside of the protocol-defined visit window) | 6 |
1 or more secondary end point assessments were not performed for week 8 of part 2 (or were performed outside of the protocol-defined visit window)c | 8 |
Received incorrect study drug during part 2d | 2 |
Deviated from the protein intake instructions outlined in the protocol during part 2 | 18 |
Initiated or changed psychiatric or sleep medication in part 2e | 3 |
aA total of 78 participants received 2 doses on the same calendar day, with 1,214 dose records (out of 211,101 total records) reporting 2 doses administered within 1 calendar day. Of these 78 participants, 31 were identified by a clinical review of the data as having had 2 doses less than 12 hours apart, with a total of 49 such dose events. In the clinical review of the data, none of these dose events were associated with a clinically important adverse event.
bThree participants) received at least 1 dose of pre-filled syringe drug presentation rather than vial-and-syringe drug presentation during week 1 of part 3A due to site error.
cParticipants who did not perform the last visit of part 2 (day 56) within the protocol-defined visit window (day 49 to day 56) affected the poolability testing for the primary and secondary efficacy analyses and were to be reported as major protocol deviations. Five additional participants in the pooled active group and 3 additional participants in the pooled placebo group performed the last assessment of week 8 on day 57 (i.e., 1 day after the protocol-defined visit window and before dosing in part 3).
dTwo participants were dispensed the incorrect study drug during part 2 due to pharmacy error. One participant was dispensed an unblinded vial of the study drug (active), and another participant was dispensed a blinded vial of the study drug that did not match the study drug assigned by the interactive web response system. The study blind was not considered to have been broken due to the incorrect drug having been dispensed. Both participants were included in the primary and secondary efficacy analyses.
eThree participants had changes to their medication during part 2, which were reported as major protocol deviations. The changes to medications were not reported until after the participants had completed part 2.
Source: PRISM-2 Clinical Study Report.9
Exposure to Study Treatments
Treatment exposure in the PRISM-2 study is summarized in Table 14. Adherence to pegvaliase treatment was self-reported by patients using workbooks and checked by study staff by counting used and unused vials and syringes. The mean daily dose received was similar to that planned in the allocated treatment group across all groups. The mean study drug use rate (defined as the total amount of study drug taken during part 2 divided by the planned dose) was 96.3% in the pooled active group and 97.6% in the pooled placebo group. Nearly all participants had study drug use rates of 80% or greater in part 2.
Table 14: Treatment Exposure in PRISM-2 Part 2 (Safety Population)
Treatment exposure | Active (pegvaliase) | Placeboa | Pooled active (n = 66) | Pooled placebo (n = 29)a | ||
|---|---|---|---|---|---|---|
20 mg/day active (n = 34) | 40 mg/day active (n = 32) | 20 mg/day placebo (n = 15) | 40 mg/day placebo (n = 14) | |||
Daily dose received, mg | ||||||
Mean (SD) | |||| |||||| | |||| |||||| | |||| |||||| | |||| |||||| | |||| ||||||| | |||| |||||| |
Median (range) | |||| |||| ||| | |||| |||| ||| | |||| |||| ||| | |||| |||| ||| | |||| |||| ||| | |||| |||| ||| |
Duration of exposure, days | ||||||
Mean (SD) | 56.0 (1.57) | 52.7 (9.56) | 55.9 (0.26) | 54.1 (7.52) | 54.4 (6.91) | 55.0 (5.21) |
Median (range) | 56.0 (54 to 64) | 56.0 (21 to 57) | 56.0 (56 to 56) | 56.0 (28 to 57) | 56.0 (21 to 64) | 56.0 (28 to 57) |
Study drug use rate,b % | ||||||
Mean (SD) | |||| |||||| | |||| |||||| | |||| |||||| | |||| |||||| | |||| |||||| | |||| |||||| |
Median (range) | |||| |||| |||| | |||| |||| |||| | ||||| |||| |||| | |||| |||| |||| | |||| |||| |||| | ||||| |||| |||| |
Study drug use ≥ 80% | ||||||
n (%) | || |||||| | || |||||| | || ||||||| | || ||||||| | || |||||| | || ||||||| |
Total duration of exposurec | ||||||
Person-years | 5.2 | 4.6 | 2.3 | 2.1 | 9.8 | 4.4 |
SD = standard deviation.
aFor placebo groups, the dose was for amount of placebo received.
bThe study drug use rate was calculated as the total amount of study drug taken during part 2 divided by the planned dose (number of days in part 2 multiplied by the randomized dose level). For participants randomized to receive placebo, the study drug usage rate was calculated as the number of days with a nonmissing dose divided by the duration of part 2. Study drug use rate was based on the intention-to-treat population.
cExposure duration was calculated as last exposure date: first exposure date + 1. If a participant had no exposure data for more than 28 consecutive days, this missing exposure period was subtracted from the duration.
Source: PRISM-2 Clinical Study Report.9
Adherence to consistent dietary intake of protein from medical food and intact food was self-reported by patients using 3-day diet diaries that were reviewed at clinic visits by dietitians. A consistent diet was defined as 1 in which changes in intact food protein and medical food protein intake were less than 10% from baseline. Additional counselling by the dietitian was provided for patients who self-reported changes in intact food protein or medical food protein intake of 10% of greater. For patients who self-reported changes from baseline of 25% or greater in intake of intact food protein or medical food protein, the dietitian counselled resumption of the baseline diet; if changes of 25% or greater persisted at the next study visit (after 4 weeks), the sponsor’s medical monitor was contacted to discuss further actions related to nonadherence with diet. The proportions of patients who self-reported changes from study baseline and part 2 baseline in protein intake of 10% or greater and 25% or greater during part 2 were not stated.
Efficacy
Only those efficacy outcomes and analyses of subgroups identified in the review protocol are reported in the following section. Appendix 3 provides detailed efficacy data (sensitivity and subgroup analyses of the primary outcome, change in blood Phe level from part 2 baseline to part 2, week 8).
Change From Part 2 Baseline in Protein Intake From Medical Food and Intact Food at Each Scheduled Visit in Part 2
Changes in protein tolerance were not directly addressed in PRISM-2 part 2. Participants were instructed to maintain a consistent level of protein intake during part 2 to ensure that changes in blood Phe concentrations were attributable to the study drug rather than to changes in protein intake.
Mean daily protein intake from intact food during PRISM-2 part 2 is shown in Table 15. At part 2 baseline, mean daily protein intake over the prior 3 days from intact food was 38.1 g (SD = 26.42) in the 20 mg/day placebo group, 39.4 g (SD = 22.69) in the 40 mg/day placebo group, and 49.0 g (SD = 23.84) in the pooled active group. At part 2, week 8, mean daily protein intake over the prior 3 days from intact food was |||| ||||||| g in the 20 mg/day placebo group, |||| ||||||| g in the 40 mg/day placebo group, and |||| ||||||| g in the pooled active group.
Table 15: Mean Daily Protein Intake From Intact Food at PRISM-2 Part 2 Baseline and Part 2 Week 8 (mITT)
Characteristic | All participants (N = 215) | mITT set | ||
|---|---|---|---|---|
Placebo 20 mg/day (n = 14) | Placebo 40 mg/day (n = 14) | Pooled active (n = 58) | ||
Daily protein from intact food at part 2 baseline; g | ||||
Mean (SD) | NA | 38.1 (26.42) | 39.4 (22.69) | 49.0 (23.84) |
Median (range) | NA | 25.2 (NR) | 36.1 (NR) | 43.0 (NR) |
Daily protein from intact food at part 2, week 8; g | ||||
Mean (SD) | NA | |||| ||||||| | |||| ||||||| | |||| ||||||| |
Median (range) | NA | |||| |||| | |||| |||| | |||| |||| |
mITT = modified intention-to-treat; NA = not applicable; NR = not reported; SD = standard deviation.
Source: PRISM-2 Clinical Study Report.9
Health-Related Quality of Life
HRQoL was not evaluated as an outcome in the PRISM-2 study.
Change in Blood Phe Concentration From Part 2 Baseline to Part 2, Week 8
The results of an MMRM analysis of changes in blood Phe levels from part 2 baseline to part 2, week 8 of the PRISM-2 study are shown in Table 16, Figure 4, and Figure 5. Poolability of the 2 placebo groups (20 mg/day and 40 mg/day), as assessed by MMRM analysis, indicated a difference (P = 0.0424, pre-specified significance level of 0.1) in the magnitude of blood Phe increase from part 2 baseline to part 2, week 8 between the 2 placebo groups. The primary and secondary efficacy analyses were therefore conducted by comparing the pooled active group versus the 20 mg/day placebo group and the 40 mg/day placebo group separately.
At part 2, week 8, the LSM change in blood Phe level from part 2 baseline was 26.50 µmol/L (95% CI, −68.26 to 121.26) in the pooled active group, 949.75 µmol/L (95% CI, 760.38 to 1,139.11) in the 20 mg/day placebo group, and 664.77 µmol/L (95% CI, 465.45 to 864.10) in the 40 mg/day placebo group. The difference in LSM change from baseline between the pooled active group and the 20 mg/day placebo group was −923.25 µmol/L (95% CI, −1,135.04 to −711.46; P < 0.0001). The difference in LSM change from baseline between the pooled active group and the 40 mg/day placebo group was −638.27 µmol/L (95% CI, −858.97 to −417.57; P < 0.0001).
Sensitivity analyses imputing missing data and in other analysis sets (ITT and per-protocol), as well as an analysis of covariance model adjusting for changes in protein intake, were consistent with the primary efficacy analysis results (Appendix 3). To test for potential subgroup covariates by treatment interactions, MMRM analysis with baseline blood Phe (≤ 50% versus > 50% reduction from drug-naive baseline using the mean of 2 consecutive measurements) as a covariate was performed and produced results similar to those of the primary analysis (Appendix 3).
Table 16: MMRM of Change From Part 2 Baseline in Blood Phe Concentration (µmol/L) at Part 2, Week 8 (mITT)
Part 2 randomized study drug group | n | Part 2 baseline mean (SD), µmol/L | Part 2 week 8 mean (SD), µmol/L | Mean (SD) change from Part 2 baseline, µmol/L | LSM change from Part 2 baseline (95% CI), µmol/L | Difference in LSM (95% CI), µmol/L | P valuea |
|---|---|---|---|---|---|---|---|
Pooled active | 58 | 503.9 (520.28) | 559.2 (569.47) | 18.6 (279.43) | 26.50 (−68.26 to 121.26) | Reference | Reference |
20 mg/day placebo | 14 | 563.9 (504.62) | 1,509.0 (372.64) | 996.4 (555.00) | 949.75 (760.38 to 1,139.11) | −923.25 (−1,135.04 to −711.46) | < 0.0001 |
40 mg/day placebo | 14 | 508.2 (363.68) | 1,164.4 (343.32) | 599.0 (507.40) | 664.77 (465.45 to 864.10) | −638.27 (−858.97 to −417.57) | < 0.0001 |
CI = confidence interval; LSM = least squares mean; mITT = modified intention-to-treat; Phe = phenylalanine; SD = standard deviation.
aP value based on a mixed model for repeated measures with the study drug (pegvaliase or placebo), visit, and drug-by-visit interaction as factors adjusting for baseline blood Phe concentration. P values for comparisons between the pooled active group and each of the placebo groups were adjusted for multiple testing using a Hochberg procedure.
Source: PRISM-2 Clinical Study Report.9
Figure 4: Least Squares Mean (SE) Change From Baseline in Blood Phe Concentration (µmol/L) to Week 8 of Part 2 (mITT)
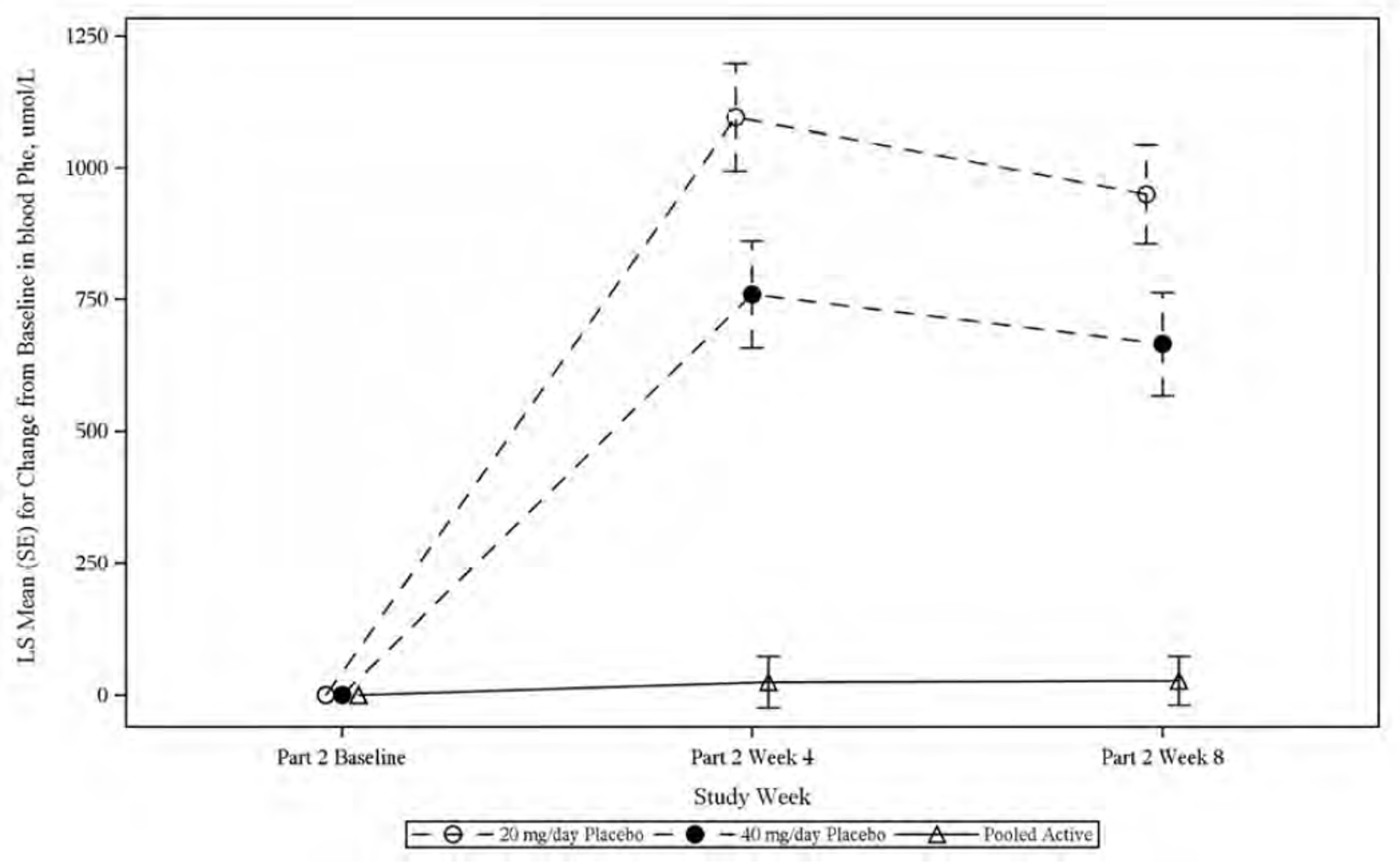
LS = least squares; mITT = modified intention-to-treat; Phe = phenylalanine; SE = standard error of the mean.
Source: PRISM-2 Clinical Study Report.9
Figure 5: Mean (SE) Observed Blood Phe Concentration From Drug-Naive Baseline Through PRISM-2 Part 2 (mITT)
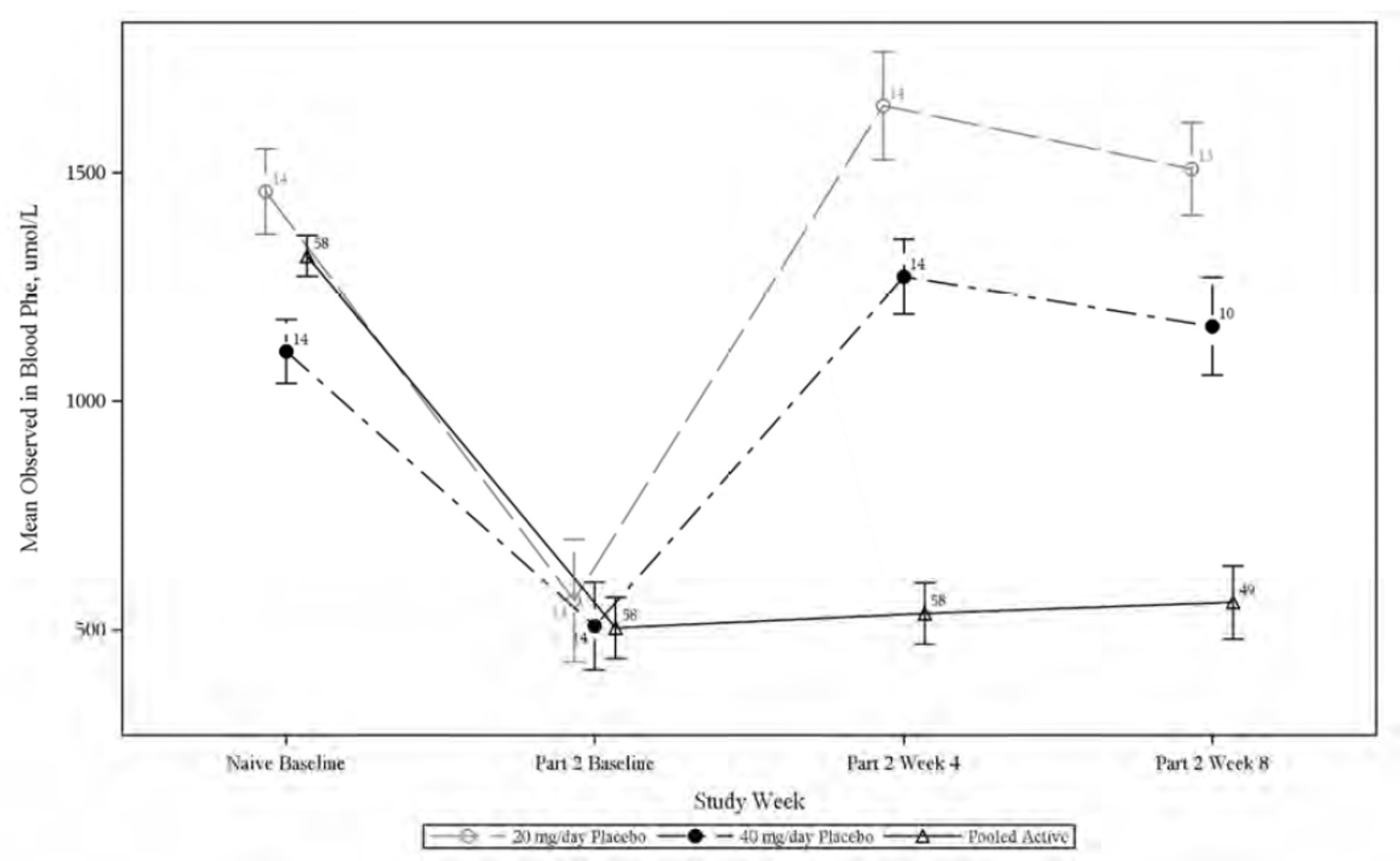
mITT = modified intention-to-treat; Phe = phenylalanine; SE = standard error of the mean.
Note: Numbers indicate sample size.
Source: PRISM-2 Clinical Study Report.9
Descriptive statistics for the percentage of participants in part 2 who met blood Phe reduction thresholds at part 2, week 8 are shown in Table 17. In the pooled active group, ||||| of patients sustained the previously achieved reductions of 20% of greater in blood Phe required for inclusion in the mITT at part 2, week 8 compared with |||| of patients in the 20 mg/day placebo group and ||||| of patients in the 40 mg/day placebo group. In the pooled active group, || patients ||||||| had blood Phe levels of 120 µmol/L or lower at part 2, week 8 while only ||| patients |||||| had blood Phe between 120 µmol/L and 360 µmol/L. The remaining || patients ||||||| had blood Phe levels of less than 600 µmol/L.
Table 17: Percentage of Participants Who Met Blood Phe Reduction Thresholds at Week 8 of Part 2 (mITT)
Percentage of participants | Placebo | Pooled active (n = 58) | |
|---|---|---|---|
20 mg/day placebo (n = 14) | 40 mg/day placebo (n = 14) | ||
Percentage of participants (n) with ≥ 20% blood Phe reduction using last 2 blood Phe measures | |||| ||| | ||||| ||| | 83.7% (41) |
Percentage of participants (n) with blood Phe reduction ≤ 600 µmol/L | || ||| | ||||| ||| | 51.0% (25) |
Percentage of participants (n) with blood Phe reduction ≤ 360 µmol/L | || ||| | || ||| | 51.0% (25) |
Percentage of participants (n) with blood Phe reduction ≤ 120 µmol/L | || ||| | || ||| | 46.9% (23) |
mITT = modified intention-to-treat; Phe = phenylalanine.
Source: PRISM-2 Clinical Study Report.9
A cumulative distribution function analysis of blood Phe levels at part 2, week 8 is shown in Figure 6. In the pooled active group, approximately |||| of patients had blood Phe levels of 120 µmol/L or lower while approximately ||| ||||||| had blood Phe between 600 µmol/L and 1,200 µmol/L and approximately ||| ||||||| had blood Phe of 1,200 µmol/L or greater. By contrast, in the placebo groups, no patients had blood Phe of 120 µmol/L or lower, while approximately ||| ||||||| had blood Phe between 600 µmol/L and 1,200 µmol/L and approximately ||||| |||||||| had blood Phe of 1,200 µmol/L or greater.
Figure 6: CDF Plot of Blood Phe Concentration at Part 2, Week 8 (mITT With Available Data) — Redacted

Figure redacted at the sponsor's request.
Source: PRISM-2 Clinical Study Report.9
Change in Neurocognitive and Neuropsychiatric Symptoms From Part 2 Baseline to Part 2, Week 8
The results of an MMRM analysis of changes in neurocognitive and neuropsychiatric symptoms (ADHD-RS-IV inattention subscale score among participants with PRISM-1 baseline score > 9 and among all participants, PKU POMS confusion subscale score, PKU POMS TMD score, and POMS TMD score) from part 2 baseline to part 2, week 8 of the PRISM-2 study are shown in Table 18, Figure 7, and Figure 8. No clear differences were observed between treatment groups. Because of the hierarchical testing procedure, P values in Table 18 following the nonsignificant results of testing for differences in ADHD-RS-IV inattention subscale scores among participants with a PRISM-1 baseline score of greater than 9 (P = 0.0591 and P = 0.2447) were considered descriptive.
Table 18: MMRM of Change From Part 2 Baseline in Neurocognitive and Neuropsychiatric Symptom Scores at Part 2, Week 8 (mITT)
Neurocognitive/ neuropsychiatric symptom scale | na | Part 2 baseline mean (SD) | Part 2 week 8 mean (SD) | Mean (SD) change from part 2 baseline | LSM change from part 2 baseline (95% CI) | Difference in LSM (95% CI)b | P valuec |
|---|---|---|---|---|---|---|---|
ADHD-RS-IV inattention subscale score (participants with PRISM-1 baseline score of > 9), part 2 | |||||||
Pooled active | 26 | 7.5 (5.29) | 9.9 (4.97) | 2.5 (4.69) | 3.05 (1.10 to 5.00) | Reference | Reference |
20 mg/day placebo | 5 | 8.0 (3.94) | 7.8 (3.69) | −0.5 (2.52) | −1.62 (−6.07 to 2.83) | 4.67 (−0.19 to 9.53) | 0.0591 |
40 mg/day placebo | 6 | 4.7 (4.50) | 5.5 (2.65) | −1.0 (3.56) | 0.28 (−4.05 to 4.61) | 2.77 (−1.99 to 7.52) | 0.2447 |
ADHD-RS-IV inattention subscale score, part 2 | |||||||
Pooled active | 58 | 5.9 (5.54) | 6.8 (5.98) | 0.8 (4.62) | 1.24 (0.03 to 2.45) | Reference | Reference |
20 mg/day placebo | 14 | 5.0 (4.26) | 6.0 (4.58) | 1.2 (3.00) | 0.74 (1.52 to 3.01) | 0.50 (−2.07 to 3.06) | 0.7007d |
40 mg/day placebo | 14 | 2.9 (3.68) | 3.2 (2.86) | −0.4 (3.44) | −0.40 (−2.93 to 2.12) | 1.64 (−1.16 to 4.45) | 0.2469d |
PKU POMS confusion subscale score, part 2 | |||||||
Pooled active | 58 | 2.2 (2.04) | 2.4 (2.46) | 0.3 (2.46) | 0.59 (−0.08 to 1.27) | Reference | Reference |
20 mg/day placebo | 14 | 2.1 (1.49) | 3.3 (2.72) | 1.4 (2.47) | 1.42 (0.14 to 2.70) | −0.82 (−2.28 to 0.63) | 0.2612d |
40 mg/day placebo | 14 | 1.2 (1.53) | 2.0 (2.00) | 0.5 (2.22) | 0.60 (−0.81 to 2.01) | −0.00 (−1.57 to 1.56) | 0.9969d |
PKU POMS TMD, part 2 | |||||||
Pooled active | 58 | 8.0 (13.24) | 9.1 (14.43) | 1.8 (12.01) | 2.07 (−1.28 to 5.42) | Reference | Reference |
20 mg/day placebo | 14 | 8.6 (10.84) | 12.4 (11.32) | 4.3 (11.96) | 5.16 (−1.24 to 11.56) | −3.09 (−10.31 to 4.13) | 0.3968d |
40 mg/day placebo | 14 | 5.0 (8.56) | 6.8 (12.97) | 0.0 (14.08) | 2.00 (−4.90 to 8.89) | 0.08 (−7.59 to 7.75) | 0.9844d |
POMS TMD (self-rated), part 2 | |||||||
Pooled active | 58 | 19.9 (35.41) | 23.0 (33.06) | 6.0 (29.84) | 6.05 (−1.52 to 13.62) | Reference | Reference |
20 mg/day placebo | 14 | 18.1 (28.26) | 24.6 (27.69) | 7.3 (26.23) | 8.11 (−6.29 to 22.50) | −2.06 (−18.32 to 14.20) | 0.8017d |
40 mg/day placebo | 14 | 13.3 (21.63) | 13.8 (26.39) | −1.7 (29.34) | 0.62 (−14.98 to 16.22) | 5.43 (−11.92 to 22.77) | 0.5349d |
ADHD-RS-IV = Attention Deficit Hyperactivity Disorder Rating Scale (investigator-rated); CI = confidence interval; LSM = least squares mean; mITT = modified intention-to-treat; MMRM = mixed model for repeated measures; PKU POMS = Phenylketonuria-Specific Profile of Mood States; POMS = Profile of Mood States; SD = standard deviation; TMD = total mood disturbance.
aSome participants did not have part 2 neurocognitive and neuropsychiatric assessment data collected. The ADHD-RS-IV inattention subscale, PKU POMS, and POMS tools were not performed in PRISM-1 until a protocol amendment; only participants who had baseline assessments were included. Participants who were included in the mITT population from a phase II study were not included because neurocognitive and neuropsychiatric tools were not administered in the phase II studies.
bNegative values indicate a decline in symptom score (toward improvement) while positive values indicate an increase in symptom score (toward decline).
cP values were adjusted for multiple comparisons among primary and secondary outcomes using a hierarchical step-down procedure. P values for comparisons between the pooled active group and each of the placebo groups were adjusted for multiple testing using a Hochberg procedure.
dStatistical testing for these end points followed a prior failed end point in the testing hierarchy and therefore these P values should be interpreted descriptively.
Source: PRISM-2 Clinical Study Report.9
Figure 7: Least Squares Mean (SE) Change From Baseline in ADHD-RS-IV Inattention Subscale Score for Participants With Baseline Score Above 9 to Week 8 of Part 2 (mITT) — Redacted

Figure redacted at the sponsor's request.
Source: PRISM-2 Clinical Study Report.9
Figure 8: Least Squares Mean (SE) Change From Baseline in ADHD-RS-IV Inattention Subscale Score to Week 8 of Part 2 (mITT) — Redacted

Figure redacted at the sponsor's request.
Source: PRISM-2 Clinical Study Report.9
Discontinuation From Part 2 Due to Neuropsychiatric Adverse Events
One participant receiving 40 mg/day pegvaliase was unblinded during part 2 due to a SAE of grade 3 anxiety. The participant discontinued part 2 and moved into part 4 and continued the study drug.
Other Tertiary Efficacy Outcomes
Analyses of other tertiary efficacy outcomes (change from part 2 baseline in ADHD-RS-IV total score, ADHD-RS-IV hyperactivity-impulsivity subscale scores, POMS [observer-rated] TMD and subscale scores, POMS [self-rated] subscale scores, and PKU POMS subscale scores at each scheduled visit in part 2) were not performed given the nonsignificant results of the secondary analysis of inattention and mood symptoms.
Harms
Only those harms identified in the review protocol are reported in the following section. Table 19 provides detailed harms data from PRISM-2 part 2.
Adverse Events
In PRISM-2 part 2, 83.3% of patients receiving active pegvaliase and 93.1% of patients receiving placebo experienced AEs. Common AEs in both the pooled active and pooled placebo groups were arthralgia (13.6% in the pooled active group and 10.3% in the pooled placebo group), headache (pooled active = 12.1% and pooled placebo = 24.1%), fatigue (pooled active = 10.6% and pooled placebo = 10.3%), anxiety (pooled active = 10.6% and pooled placebo = 6.9%), and injection-site bruising (pooled active = 4.5% and pooled placebo = 10.3%).
Serious AEs
In PRISM-2 part 2, SAEs occurred in 2 patients (3.0%) receiving active pegvaliase and 1 patient (3.4%) receiving placebo.
AEs Leading to Dose Reduction or Interruption
In PRISM-2 part 2, AEs leading to a dose reduction or interruption occurred in 1 patient (1.5%) receiving pegvaliase and 1 patient (3.4%) receiving placebo.
Withdrawals Due to AEs
No patients in PRISM-2 part 2 had AEs leading to discontinuation of study drug.
Mortality
No deaths occurred during PRISM-2 part 2.
Notable Harms
In PRISM-2 part 2, several study protocol–defined AESIs occurred more frequently in patients receiving active pegvaliase than in those receiving placebo. These included HAEs (39.4% of pooled active patients and 13.8% of pooled placebo patients), generalized skin reactions lasting 14 days or more (pooled active = 10.6% and pooled placebo = 0%), and injection-site skin reactions lasting 14 days or more (pooled active = 7.6% and pooled placebo = 3.4%). Arthralgia and injection-site reactions occurred at similar frequencies in patients receiving active pegvaliase (arthralgia = 13.6%; injection-site reactions = 24.2%) and in those receiving placebo (arthralgia = 10.3%; injection-site reactions = 24.1%).
Among notable harms identified for this review, those occurring more frequently in patients receiving active pegvaliase than in those receiving placebo were rash (pooled active = 7.6% and pooled placebo = 3.4%), urticaria (pooled active = |||| and pooled placebo = ||), pruritis (pooled active = 7.6% and pooled placebo = 3.4%), injection-site pruritis (pooled active = |||| and pooled placebo = ||), diarrhea (pooled active = |||| and pooled placebo = ||), injection-site erythema (pooled active = |||| and pooled placebo = ||), and erythema (pooled active = |||| and pooled placebo = ||).
No anaphylaxis events or systemic hypersensitivity reactions occurred during PRISM-2 part 2.
Table 19: Summary of Harms in PRISM-2 Part 2 (Safety Population)
Harm | Active (pegvaliase) | Placebo | Pooled active (n = 66) | Pooled placebo (n = 29) | ||
|---|---|---|---|---|---|---|
20 mg/day (n = 34) | 40 mg/day (n = 32) | 20 mg/day (n = 15) | 40 mg/day (n = 14) | |||
Patients with ≥ 1 AE | ||||||
n (%) | || |||||| | || |||||| | || |||||| | || |||||| | 55 (83.3) | 27 (93.1) |
Common AEs, n (%)a | ||||||
Arthralgia | | |||||| | | ||||| | | ||||| | | |||||| | 9 (13.6) | 3 (10.3) |
Headache | NR | NR | NR | NR | 8 (12.1) | 7 (24.1) |
Upper respiratory tract infection | NR | NR | NR | NR | 1 (1.5) | 5 (17.2) |
Injection-site bruising | NR | NR | NR | NR | 3 (4.5) | 3 (10.3) |
Fatigue | NR | NR | NR | NR | 7 (10.6) | 3 (10.3) |
Anxiety | NR | NR | NR | NR | 7 (10.6) | 2 (6.9) |
Alopecia | NR | NR | NR | NR | 2 (3.0) | 3 (10.3) |
Patients with ≥ 1 SAE | ||||||
n (%) | |||||| | | ||||| | | ||||| | |||||| | 2 (3.0) | 1 (3.4) |
Common SAEs, n (%)b | ||||||
Grade 3 depression | 0 | 1 (3.1) | 0 | 0 | 1 (1.5) | 0 |
Grade 3 anxiety | 0 | 1 (3.1) | 0 | 0 | 1 (1.5) | 0 |
Grade 1 increased blood creatine phosphokinase | 0 | 0 | 1 (6.7) | 0 | 0 | 1 (3.4) |
Patients with ≥ 1 AE causing dose reduction or interruption | ||||||
n (%) | 0 | 1 (3.1) | 1 (6.7) | 0 | 1 (1.5) | 1 (3.4) |
Patients with ≥ 1 AE causing study drug discontinuation | ||||||
n (%) | 0 | 0 | 0 | 0 | 0 | 0 |
Patients with ≥ 1 AE causing study discontinuation | ||||||
n (%) | 0 | 0 | 0 | 0 | 0 | 0 |
Deaths | ||||||
n (%) | 0 | 0 | 0 | 0 | 0 | 0 |
AESIs, n (%) | ||||||
Anaphylaxis (NIAID-FAAN criteria) | 0 | 0 | 0 | 0 | 0 | 0 |
Anaphylaxis (Brown’s severe criteria) | 0 | 0 | 0 | 0 | 0 | 0 |
Hypersensitivity AEs | || |||||| | || |||||| | | |||||| | | |||||| | 26 (39.4) | 4 (13.8) |
Generalized skin reaction ≥ 14 days in duration | | |||||| | | ||||| | |||||| | |||||| | 7 (10.6) | 0 |
Injection-site skin reaction ≥ 14 days in duration | | ||||| | | ||||| | ||||||| | | ||||| | 5 (7.6) | 1 (3.4) |
Arthralgia | | |||||| | | ||||| | | ||||| | | |||||| | 9 (13.6) | 3 (10.3) |
Injection-site reaction | | |||||| | | |||||| | | |||||| | | |||||| | 16 (24.2) | 7 (24.1) |
Notable harms, n (%) | ||||||
Acute systemic hypersensitivity reactions (anaphylaxis) | ||||||
Syncope | NR | NR | NR | NR | |||||| | |||||| |
Hypotension | NR | NR | NR | NR | |||||| | |||||| |
Hypoxia | NR | NR | NR | NR | |||||| | |||||| |
Dyspnea | NR | NR | NR | NR | |||||| | |||||| |
Wheezing | NR | NR | NR | NR | |||||| | |||||| |
Chest discomfort and/or tightness | NR | NR | NR | NR | |||||| | |||||| |
Tachycardia | NR | NR | NR | NR | |||||| | |||||| |
Angioedema | NR | NR | NR | NR | |||||| | |||||| |
Flushing | NR | NR | NR | NR | |||||| | |||||| |
Rash | NR | NR | NR | NR | 5 (7.6) | 1 (3.4) |
Urticaria | NR | NR | NR | NR | | ||||| | |||||| |
Pruritus | NR | NR | NR | NR | 5 (7.6) | 1 (3.4) |
Injection-site pruritus | NR | NR | NR | NR | | ||||| | |||||| |
Vomiting | NR | NR | NR | NR | | ||||| | | ||||| |
Nausea | NR | NR | NR | NR | || ||||| | | ||||| |
Diarrhea | NR | NR | NR | NR | | ||||| | |||||| |
Other systemic hypersensitivity reactions | ||||||
Severe angioedema | NR | NR | NR | NR | |||||| | |||||| |
Severe serum sickness | NR | NR | NR | NR | |||||| | |||||| |
Injection-site reactions | NR | NR | NR | NR | 5 (7.6) | 2 (6.9) |
Injection-site induration | NR | NR | NR | NR | | ||||| | |||||| |
Injection-site pain | NR | NR | NR | NR | | ||||| | | ||||| |
Injection-site swelling | NR | NR | NR | NR | | ||||| | | ||||| |
Injection-site erythema | NR | NR | NR | NR | | ||||| | |||||| |
Arthralgia | 7 (20.6) | 2 (6.3) | 1 (6.7) | 2 (14.3) | 9 (13.6) | 3 (10.3) |
Lymphadenopathy | NR | NR | NR | NR | | ||||| | | ||||| |
Cough | NR | NR | NR | NR | 0 | 2 (6.9) |
Headache | NR | NR | NR | NR | 8 (12.1) | 7 (24.1) |
Abdominal pain | NR | NR | NR | NR | | ||||| | |||||| |
Abdominal pain upper | NR | NR | NR | NR | | ||||| | | ||||| |
Alopecia | NR | NR | NR | NR | 2 (3.0) | 3 (10.3) |
Erythema | NR | NR | NR | NR | | ||||| | |||||| |
Myalgia | NR | NR | NR | NR | | ||||| | | ||||| |
AE = adverse event; AESI = adverse event of special interest; FAAN = Food Allergy and Anaphylaxis Network; NIAID = National Institute of Allergy and Infectious Diseases; NR = not reported; SAE = serious adverse event.
Note: Treatment-emergent AEs reported in this table were defined as any untoward medical occurrence occurring after administration of the first dose of study drug and within 30 days of the last dose of study drug. AEs were coded using version 18.0 of the Medical Dictionary for Regulatory Affairs and graded according to version 4.03 of the National Cancer Institute’s Common Terminology Criteria for Adverse Events.
aAdverse events with a frequency of 10% or greater overall in the overall study and a frequency of 10% or greater in the pooled active or pooled placebo study group during part 2 are reported.
bAll SAEs occurring during part 2 are reported.
Source: PRISM-2 Clinical Study Report.9
Critical Appraisal
Internal Validity
PRISM-29-16 was a phase III, 4-part, 4-arm, double-blind, placebo-controlled RDT with an extension period of open-label treatment conducted in adolescent and adult patients with PKU who completed a prior pegvaliase study (N = 215). Only evidence from the part 2 RDT (ITT n = 95; mITT n = 86) is included in the Systematic Review section of this report. The relatively small size of the PRISM-2 study was expected due to the rarity of PKU. According to the sponsor, the RDT design of the study was selected because of its efficiency in demonstrating therapeutic efficacy in a small study population, due to concerns of unblinding resulting from HAEs over a longer treatment period, and to minimize long-term exposure to placebo for ethical reasons. However, the RDT design has limitations in its ability to estimate the magnitude of absolute treatment effects and harms in the overall population of adult patients with PKU.
The RDT design of PRISM-2 part 2 was associated with an unavoidable but notable risk of bias. Losses to follow-up in PRISM-2 part 2 were minimal: only 1 patient discontinued part 2 early. However, participants in the major feeder trial, PRISM-1, were pre-screened for their ability to maintain a consistent diet as an eligibility criterion. Ability to maintain a consistent diet was also applied as an eligibility criterion for PRISM-2. Only patients who completed a feeder study were eligible, and those who discontinued feeder studies early due to AEs, noncompliance, or patient and/or physician decision were not included. For example, only 203 of 261 participants in PRISM-1 entered PRISM-2, while the remaining 58 patients (22.2%) did not. Upon entry into PRISM-2, patients who did not achieve the target dosage (20 mg/day or 40 mg/day) in PRISM-1 (33 of 203; 16.3%) transitioned directly to part 4 (open-label extension). Of the 164 patients who entered PRISM-2 part 1, 12 (7.3%) discontinued the study early due to AEs or patient and/or physician decision, while 39 (23.8%) did not meet the blood Phe reduction criterion of 20% or greater for the part 2 mITT set. The clinical expert agreed that the PRISM-2 RDT population was enriched for patients who would be more likely to tolerate and adhere to pegvaliase and therefore would be more likely to respond to treatment than the general adult PKU population with blood Phe levels above 600 µmol/L.
Randomization in PRISM-2 part 2 appeared generally successful in balancing baseline demographic and disease characteristics between study groups. However, because of the small number of participants and the fact that the 2 placebo groups could not be pooled for efficacy analyses, some baseline imbalances between groups were present and of potential prognostic significance. In PRISM-2 part 2, 53.4% of patients in the pooled active group were female compared with 42.9% of participants in the placebo groups. According to the clinical experts consulted by CADTH for this review, gender is a factor in compliance with PKU treatment, with women having higher rates of adherence. In the 20 mg/day placebo group, the mean BMI was 32.6 (SD = 7.75) kg/m2. According to the clinical experts consulted by CADTH for this review, BMI is associated with diet and Phe control in adult patients with PKU. There were also baseline imbalances (in drug-naive, part 2, or both baselines) of varying degrees between the pooled active group and 1 or both placebo groups in blood Phe level, mood and inattention symptoms evaluated as secondary outcomes, and protein intake from medical food and intact food. According to the clinical experts consulted by CADTH for this review, these imbalances would not limit interpretation of the study results.
The psychometric properties of the outcomes evaluated in primary and secondary efficacy analyses in PRISM-2 (blood Phe level, ADHD-RS-IV inattention subscale score, PKU POMS confusion subscale score, PKU POMS TMD, POMS TMD) have not been studied in adult patients with PKU apart from a study demonstrating acceptable internal consistency reliability of the PKU POMS.34 No information on MIDs for any of the outcomes evaluated was available. According to the clinical experts consulted by CADTH for this review, blood Phe can be used to show that PKU treatment is ineffective, while consistent decreases in Phe levels during treatment can potentially indicate treatment effects in conjunction with improvements in protein tolerance, inattention and mood symptoms, and HRQoL. However, input from a group of 3 clinicians challenged this assessment and emphasized the importance of Phe control as a treatment goal and marker of treatment response in and of itself. All clinicians agreed that blood Phe levels mechanistically drive PKU symptoms. However, according to the clinical experts consulted by CADTH for this review, the magnitude of blood Phe decreases, as well as the duration and consistency of metabolic control required for adult patients with PKU to achieve improvements in other outcomes (such as dietary Phe tolerance, neurocognitive and neuropsychiatric symptoms, and HRQoL), is not known at present. However, the clinical experts emphasized that diet liberalization enabled by Phe control is the goal of PKU treatment and they expected that sustained decreased Phe levels induced by treatment with pegvaliase of sufficient magnitude, consistency and duration could in theory lead to improvements in neurocognitive and neuropsychiatric symptoms, protein tolerance, and HRQoL.
Several statistical issues should be considered when interpreting the results of the PRISM-2 study. Statistical tests were appropriate, and multiplicity was controlled using a hierarchical testing strategy. Some data were missing for the primary efficacy analysis of change in Phe levels from part 2 baseline to part 2 week 8 (15 of 86 patients in the mITT population; 17.4%). Missing data were not replaced in the primary efficacy analysis, but were accounted for under a missing-at-random assumption, which was further evaluated in sensitivity analyses using a variety of imputation techniques (multiple imputation and last observation carried forward), all of which showed similar results. The potential for heterogeneity among the 4 dose groups in the RDT (20 mg/day and 40 mg/day active pegvaliase and placebo) complicated interpretation of results. Heterogeneity between the placebo groups was accounted for by separate testing; however, heterogeneity between the pegvaliase groups was not addressed as it was assumed that there were no carryover effects in either group. This assumption was not formally evaluated. Although evidence was limited for secondary efficacy outcomes (inattention and mood symptoms) identified as important to patients, the clinical experts consulted by CADTH for this review agreed that differences in neurocognitive and neuropsychiatric function were unlikely to be detectable over the 8-week period of the PRISM-2 RDT using the available instruments because of the relatively short duration and high variability in the symptoms of adult patients with established PKU. No efficacy analyses of pre-specified subgroups were planned and the impact of baseline blood Phe levels on the primary outcome was evaluated only by testing for potential baseline blood Phe (≤ 50% versus > 50% reduction from drug-naive baseline) treatment interactions in MMRM analysis. This analysis was exploratory, not specifically powered to evaluate individual strata, and not adjusted for multiplicity.
Another major concern in the PRISM-2 study was adherence to pegvaliase and to consistent protein intake, both of which were patient-reported (although pegvaliase adherence was also confirmed by vial counting). Despite high self-reported adherence to pegvaliase injections that was confirmed by collection and counting of empty drug vials and syringes, a clear dichotomy was observed in the blood Phe levels of patients randomized to continue receiving active pegvaliase in part 2: roughly half of participants had Phe levels of 120 µmol/L or lower, while the other half had either poor Phe control (Phe levels of 600 µmol/L to 1,200 µmol/L; approximately 1-quarter) or no Phe control (Phe levels of 1,200 µmol/L or greater). With the high treatment-compliance rates reported in the pivotal trial, the clinical experts consulted by CADTH were unable to provide an explanation for the relatively high proportion of patients who did not achieve normalization of blood Phe levels (defined as 120 µmol/L or lower) in the pooled active group. Based on the kinetics of blood Phe following a single pegvaliase injection,38 the clinical experts stated that the most plausible reason for this pattern could be low compliance to pegvaliase in the pooled active group. Uncertainty in adherence to the study protocol for study drug administration limited interpretation of the relationship between pegvaliase administration and changes in blood Phe levels in the RDT. Also of potential concern was adherence to diet and maintenance of stable protein intake; patients who self-reported deviations from baseline protein intake from medical food and intact food faced escalating pressure from study dietitians to self-report compliant values. Changes in protein intake, if they were imbalanced by study group and especially considering the small sample size of the individual placebo groups, could have confounded the primary efficacy analysis of blood Phe levels either in favour of or against pegvaliase.
External Validity
According to the clinical experts consulted by CADTH for this review, the demographic and disease characteristics of patients enrolled in the PRISM-2 study were reflective of the Canadian population of adolescent and adult patients with PKU they would see in their clinical practice. Similarly, the clinical experts expected that the study eligibility criteria would result in recruitment of a patient population reflective of Canadian practice, albeit a cross-section more likely to tolerate and adhere to pegvaliase than the general PKU population (as discussed earlier in the Internal Validity section). The clinical experts confirmed that eligibility criteria related to neurocognitive and linguistic capacity and concurrent conditions would eliminate only a small proportion of patients with PKU who would not be good candidates for pegvaliase. The clinical experts stated that, although nearly all patients in the PRISM-2 study were White (98.1%) and 18 years of age or older (94.9%), and despite the enrichment of the study population for treatment-compliant patients who were able to tolerate pegvaliase, the study results would be generalizable to most adult and adolescent patients with PKU, including adolescent patients (aged 16 and 17 years), pegvaliase-naive patients, and patients with good or limited Phe control who are compliant with MNT.
Planned dosing of pegvaliase in the PRISM-2 study was aligned with Health Canada–approved dosing. Although adherence to the dosing regimen was assessed by counting empty drug vials and unused syringes, because of the self-reported nature of reporting adherence to treatment (i.e., injections were not monitored) some level of uncertainty remains around the actual dosing received by the study participants. As the PRISM-2 study population was enriched for pegvaliase tolerance, compliance, and responsiveness, and was poorly or not adherent to therapy, this could limit generalizability of the primary analysis of blood Phe levels to all adult patients with PKU. According to the clinical experts consulted by CADTH, the general population of adult patients with PKU would probably be less compliant than the trial population, and therefore mean reductions in blood Phe level would likely be smaller in real-world clinical practice than those observed in the PRISM-2 study.
There was substantial disagreement in the input received by CADTH from clinical experts and clinician groups on the target population of patients with PKU most and least appropriate for pegvaliase treatment. The overall goal of the phase III PRISM studies was to evaluate the efficacy of pegvaliase in adult patients with PKU with poorly controlled blood Phe (above 600 µmol/L). One clinical expert consulted by CADTH for this review stated that that patients compliant with MNT, who would generally have Phe levels above 600 µmol/L, would be the most suitable candidates for pegvaliase; by contrast, another clinical expert as well as clinician group input suggested that patients noncompliant with dietary restriction who cannot benefit from sapropterin and therefore have poor or no Phe control (Phe above 600 µmol/L) would be the targeted population. Nevertheless, the clinical experts agreed that the results of the study would be generalizable to patients with some or good Phe control (600 µmol/L or lower) who are compliant with MNT. In this group of patients, pegvaliase treatment could permit liberalization of diets while maintaining Phe control.
Several of the outcomes in PRISM-2 part 2 (blood Phe levels, inattention and mood symptoms) were identified as clinically important by patients and clinicians alike. The specific relevance of pegvaliase-induced changes in blood Phe levels in the PRISM-2 RDT, measured at 1 or a few time points, to improvements in dietary protein tolerance, neurocognitive and neuropsychiatric symptoms, and HRQoL, was uncertain. According to the clinical experts consulted by CADTH for this review, the duration of follow-up in the part 2 RDT was adequate for point estimation of the impact of pegvaliase discontinuation on blood Phe level but potentially insufficient for assessment of inattention and mood symptoms in patients with PKU.
Patients in the PRISM-2 study were likely followed up more frequently by clinicians and dietitians than the average adult Canadian PKU patient. According to clinical experts consulted by CADTH for this review, a large proportion of adult patients with PKU are averse to monitoring and tend to exhibit weak treatment compliance. Patients in PRISM-2 may also have received better training on pegvaliase injections than would be expected in Canadian practice. However, the clinical experts consulted by CADTH for this review did not anticipate that these factors would limit generalizability of the study findings.
Pegvaliase dosing in the PRISM-2 RDT (20 mg/day or 40 mg/day pegvaliase) differed from the Health Canada–recommended induction, titration, and maintenance dosing (maximum 60 mg/day) in terms of the maximum possible dose. Part 2 of the PRISM-2 trial had a relatively short duration of 8 weeks, and potentially longer titration periods could establish the precise maintenance doses required for individual patients with PKU to maintain blood Phe levels within a safe window while permitting liberalization of diet. However, the clinical experts consulted by CADTH for this review did not expect that these factors would limit generalizability of the study findings.
One important generalizability concern in the PRISM-2 study was that, given the acknowledged high variability between measurements of Phe levels in individual adult patients with PKU, a statistically significant decrease in mean blood Phe at a single time point (week 8 of the PRISM-2 part 2 RDT) provided limited evidence to substantiate sustained decreases in blood Phe levels of sufficient magnitude to realize improvements in PKU patient inattention and mood symptoms, HRQoL, and protein intake. At week 8 of the PRISM-2 part 2 RDT, there was no direct evidence to support changes in any important end points (inattention and mood symptoms, HRQoL, or protein intake) beyond Phe level. Placebo-controlled longitudinal analyses of per-patient blood Phe control over time, and correlations with improvements in protein tolerance and neurocognitive and/or neuropsychiatric symptoms, were not reported in PRISM-2. The clinical experts consulted by CADTH for this review acknowledged that, given the high variation in the blood Phe measurements of patients with PKU and potential changes over time in pegvaliase adherence, the point estimate of Phe control at part 2 week 8 of PRISM-2 provided no randomized trial evidence on duration or consistency of Phe control.
Indirect Evidence
No indirect evidence was identified for this review.
Other Relevant Evidence
This section includes submitted long-term extension studies and additional relevant studies included in the sponsor’s submission to CADTH that were considered to address important gaps in the evidence included in the systematic review.
PRISM-1 Trial
The PRISM-1 trial was a phase III, open-label, randomized, multi-centre study to assess the safety and tolerability of pegvaliase among drug-naive patients with PKU (N = 261).16,17 The PRISM-1 trial was the major feeder study for the PRISM-2 trial. As 203 of 215 (94.4%) of patients participating in the PRISM-2 trial entered from PRISM-1 trial, the study is briefly summarized here to provide context for the patient population enrolled in the PRISM-2 trial, as well as to contribute additional safety data. The primary objective of the PRISM-1 trial was to characterize the safety and tolerability of induction, titration, and maintenance dosing in pegvaliase-naive patients with PKU who self-administered pegvaliase up to 20 mg/day or 40 mg/day. Patients with PKU aged 16 years or older were eligible to participate if they had blood Phe levels above 600 µmol/L and had not been previously exposed to pegvaliase. Patients were randomized 1:1 to receive up to 20 mg/day or 40 mg/day pegvaliase for up to 36 weeks. Both randomized dose groups experienced reductions from baseline blood Phe levels. The mean blood Phe concentration at baseline was 1,232.7 µmol/L (SD = 386.36) in the ITT set and the mean reduction from baseline was ||||| |||||||| µmol/L at week 28 (n = 133) and ||||| |||||||| µmol/L at week 36 (n = 80). Almost all patients (99.6%) experienced AEs, most commonly arthralgia (65.1%), injection-site reactions (56.7%), injection-site erythema (45.2%), headaches (31.4%), rash (25.7%), injection-site pruritis (24.9%), and injection-site pain (21.5%). Serious AEs occurred in 10.0% of patients; the most common SAE was anaphylaxis (3.1%). Anaphylaxis according to the NIAID-FAAN criteria occurred in 6.9% of patients and anaphylaxis as defined by NIAID-FAAN criteria meeting Brown’s severe criteria occurred in 1.5% of patients. Most patients (88.1%) experienced HAEs, including arthralgia (65.1%), generalized skin reactions lasting 14 days or more (22.6%), injection-site reactions (86.2%), injection-site skin reactions lasting 14 days or more (26.4%), serum sickness (3.1%), and angioedema (35.6%).
PRISM-2 Trial
Evidence from part 1, part 3, and part 4 of the PRISM-2 trial,9-16 including the part 4 open-label extension, is briefly summarized here to provide insight into the long-term safety and efficacy of pegvaliase treatment (including doses up to 60 mg/day in the part 4 open-label extension). The Systematic Review section includes an overall description of the PRISM-2 study (N = 215).
Safety
In the PRISM-2 trial, patients were treated with open-label pegvaliase in part 1 (20 mg/day or 40 mg/day, up to 13 weeks), part 3 (20 mg/day or 40 mg/day, 6 weeks), and part 4 (up to 60 mg/day, up to 274 weeks). In all parts of the study, self-reported adherence to pegvaliase was high with good exposure. Table 20 lists detailed harms data in PRISM-2 part 1, part 3, part 4, and the overall study. In the overall PRISM-2 study, ||||| of patients receiving open-label pegvaliase experienced AEs and ||||| of patients experienced SAEs, the majority of which occurred during the open-label extension. No deaths occurred in the overall PRISM-2 study. Approximately |||| ||||||| of patients experienced AEs leading to pegvaliase dose reduction or interruption but only |||| of patients experienced AEs leading to pegvaliase discontinuation. Most patients ||||||| experienced HAEs. Approximately ||||| |||||||| of patients ||||||| experienced injection-site reactions, approximately ||| |||||| ||||||| experience arthralgia, and nearly |||| |||||| ||||| experienced generalized skin reactions lasting 14 days or more and injection-site skin reactions lasting 14 days or more. Anaphylaxis reactions occurred in |||| of patients, acute systemic hypersensitivity reactions occurred in |||| of patients, and angioedema occurred in |||| of patients.
Table 20: Summary of Harms in PRISM-2 Part 1, Part 3, and Part 4 (Safety Population)
Harms | Part 1 (n = 164) | Part 3 (n = 60)a | Part 4 (n = 202) | Overall (N = 215)b |
|---|---|---|---|---|
Patients with ≥ 1 AE | ||||
n (%) | ||| |||||| | || |||||| | ||| |||||| | ||| |||||| |
Patients with ≥ 1 SAEc | ||||
n (%) | | ||||| | | ||||| | || |||||| | || |||||| |
Patients with ≥ 1 AE causing dose reduction or interruption | ||||
n (%) | | ||||| | | ||||| | || |||||| | ||| |||||| |
Patients with ≥ 1 AE causing study drug discontinuation | ||||
n (%) | | ||||| | |||| | | |||||| | || |||||| |
Patients with ≥ 1 AE causing study discontinuation | ||||
n (%) | | ||||| | |||| | | ||||| | | ||||| |
Deaths | ||||
n (%) | 0 | 0 | 0 | 0 |
AESIs, n (%) | ||||
Anaphylaxis (NIAID-FAAN criteria) | | ||||| | |||| | || ||||| | || ||||| |
Anaphylaxis (Brown’s severe criteria) | |||| | |||| | |||| | |||| |
Acute systemic hypersensitivity reaction (confirmed by external expert)e | NR | NR | | ||||| | | ||||| |
Severe acute systemic hypersensitivity reaction (confirmed by external expert)e | NR | NR | |||| | |||| |
Anaphylaxis (FDA criteriae) | NR | NR | || ||||| | || ||||| |
Angioedemae,f | NR | NR | | ||||| | | ||||| |
Hypersensitivity AEs | || |||||| | || |||||| | ||| |||||| | ||| |||||| |
Generalized skin reaction ≥ 14 days in duration | | ||||| | | ||||| | || |||||| | || |||||| |
Injection-site skin reaction ≥ 14 days in duration | || ||||| | | ||||| | || |||||| | || |||||| |
Arthralgiag | || |||||| | | |||||| | ||| |||||| | ||| |||||| |
Injection-site reaction | || |||||| | || |||||| | ||| |||||| | ||| |||||| |
AE = adverse event; AESI = adverse event of special interest; FAAN = Food Allergy and Anaphylaxis Network; NIAID = National Institute of Allergy and Infectious Diseases; NR = not reported; SAE = serious adverse event.
Note: Treatment-emergent AEs reported in this table were defined as any untoward medical occurrence occurring after administration of the first dose of study drug and within 30 days of the last dose of study drug. Adverse events were coded using version 18.0 of the Medical Dictionary for Regulatory Affairs, and graded according to version 4.03 of the National Cancer Institute’s Common Terminology Criteria for Adverse Events.
aThe part 3 safety population included only the 60 participants who enrolled in part 3 after amendment 2 and qualified for inclusion in pharmacokinetic assessments with 2 different drug presentations. Safety data from the remaining 29 participants in part 3 of the study before amendment 2 is not included in this separate part 3 summary but the data were captured as part of the overall PRISM-2 safety totals.
bThe analysis population is all participants who entered PRISM-2.
cAdditional AEs (8 events in 4 participants) were upgraded by the sponsor to SAEs and were not factored into the incidence reported in summary tables.
dOne participant withdrew from the study due to an investigator’s decision but was captured in the list of participants who were withdrawn due to an AE.
eData were assessed for part 4 and overall only.
fBased on sponsor’s clinical adjudication of angioedema. The change in search strategy and definition was applied for part 4 and overall data only.
gBased on a broad standard Medical Dictionary for Regulatory Affairs query of selected preferred terms that also included arthralgia, back pain, musculoskeletal pain, pain in extremity, and neck pain. The change in search strategy and definition was applied for part 4 and overall data only.
Source: PRISM-2 Clinical Study Report.9
Efficacy
Among patients who remained on open-label pegvaliase during PRISM-2 part 4, within 24 months, ||| of participants achieved a blood Phe level of 600 μmol/L or lower, ||| of participants achieved blood Phe of 360 μmol/L or lower, and ||| (increasing to ||| after 48 months of treatment) achieved blood Phe of 120 μmol/L or lower.1 These figures were based on point measurements (i.e., patients had to meet these Phe thresholds once only to be counted). Among patients who remained on open-label pegvaliase during PRISM-2 part 4, long-term (48 months) assessment of neurocognitive and neuropsychiatric symptoms showed improvements in inattention and mood symptoms that were correlated with blood Phe reduction.1 Among patients who remained on open-label pegvaliase during PRISM-2 part 4, protein intake from natural protein (and therefore dietary Phe) increased from a mean of 1,700.2 (SD = 1,194.4) mg dietary Phe at baseline to 2,123.2 mg (SD = 1,302.2) at 1 year and 2,679.7 mg (SD = 1,285.7) at 2 years.1 At month 48, mean daily protein intake increased by 7.1 g (SD = 32.2) from baseline levels, with an overall increase in natural protein and decrease in protein from medical food.1
Critical Appraisal
According to the clinical experts consulted by CADTH for this review, long-term trends over time in blood Phe levels, inattention and mood symptoms, and protein intake in PRISM-2 part 4 may be partially attributed to selection bias: patients who remained on treatment were potentially more treatment-compliant, may have had lesser degrees of inattention and mood symptoms, and may have had better protein tolerance than those who discontinued from open-label treatment. The long-term efficacy evidence from PRISM-2 part 4 was noncomparative and nonrandomized. In addition, longitudinal analyses of per-patient Phe control were not reported.
PRISM-3 Trial
The PRISM-3 trial was an exploratory phase III substudy to evaluate executive function in adults with PKU participating in PRISM-2 (N = 9).18 The study is briefly summarized here because it addressed outcomes (executive function and self-perception) that were not evaluated in PRISM-2. Although targeted enrolment was approximately 100 patients, only 9 were enrolled in PRISM-3 by the closure of enrolment in PRISM-2 part 2 (RDT). The reasons for the low enrolment were unclear as all adult participants in PRISM-2 (age 18 to 70 years) were eligible for PRISM-3. Patients participated in the PRISM-3 substudy for up to 63 weeks. The primary outcome was executive function assessed using a selected set of 3 tasks from the Cambridge Neuropsychological Test Automated Battery tool: rapid visual processing, spatial working memory, and stop-signal task. Patient self-perception of their current state was measured using a Subject Global Assessment (SGA) questionnaire consisting of 7 questions about current state perception of attention, energy level, tiredness, confusion, sadness, anger, and tension over the previous 7 days. The SGA and the Cambridge Neuropsychological Test Automated Battery tasks were administered at PRISM-2 part 2 baseline and part 2, week 8. At part 2 week 8, patients receiving active pegvaliase (n = 6) had numeric improvements compared with patients receiving placebo (n = 3) in rapid visual processing mean response latency (mean change = 24.23 ms versus −18.03 ms), spatial working memory between errors 4 to 8 Boxes (mean change = −4.2 versus 3.0), and stop-signal task reaction time (mean change = 8.42 ms versus 58.93 ms). No differences in SGA questionnaire responses were observed between patients treated with pegvaliase and those treated with placebo.
Comparative Evidence With Sapropterin and MNT
One additional retrospective observational cohort study by Zori et al. (2019)19 did not meet the selection criteria for inclusion in the systematic review but is summarized here because it was designed to generate comparative evidence of the efficacy of pegvaliase plus MNT, sapropterin plus MNT, and MNT in adolescent and adult patients with PKU.19 The results of this study were used to inform the transitions between health states in the sponsor’s economic model (CADTH Pharmacoeconomic Report).
Methods
Zori et al. conducted a retrospective observational cohort study of adult patients with PKU receiving pegvaliase with or without MNT, sapropterin plus MNT, or MNT alone. A cohort of patients who received pegvaliase plus MNT in the phase II 165 to 205 trial or phase III PRISM studies (PRISM-1 and PRISM-2) were compared using a PSM approach with a historical control of patients who received sapropterin plus MNT or MNT alone and participated in the PKUDOS registry.20 The outcomes evaluated in the study included change in blood Phe and natural protein intake after 1 and 2 years of treatment. The source studies (pegvaliase trials and the PKUDOS registry) took place in the US.
Populations
Patient data from participants in pegvaliase clinical trials and matched historical cohorts selected by PSM from the PKUDOS registry were used to select the study cohort. Pegvaliase patients were those who were originally enrolled in the parent studies 165 to 205 (24 patients) and the phase III PRISM studies (261 patients) and participated in extension studies (PAL-003 and PRISM-2 part 4).1 Inclusion criteria for the pegvaliase cohort included adolescents or adult patients with PKU (age ≥ 16 years) with a baseline Phe greater than 600 µmol/L who received induction, titration, and maintenance dosing of pegvaliase (5 mg to 60 mg daily self-administered injection). Patients included in the sapropterin plus MNT and MNT-alone groups were identified from the PKUDOS registry.20 This registry is a phase IV voluntary observational study of patients with PKU who are or have been treated with sapropterin, or who intend to take sapropterin within 90 days of registry enrolment, with data (from 2007 onwards) on 1,867 patients at the time of the study by Zori et al. Patients in the sapropterin plus MNT group included those in the PKUDOS registry who intended to initiate sapropterin within 90 days, had 1 or more pre-treatment blood Phe value measurements, baseline blood Phe (last available measurement before initiating sapropterin) greater than 600 µmol/L, were 18 years or older at sapropterin initiation, and available information on sapropterin dosing (5 mg to 20 mg daily). Although patients in the PKUDOS registry were not required nor monitored for dietary restriction, the product monograph for sapropterin27 states that sapropterin is indicated in conjunction with a Phe-restricted diet to reduce blood Phe levels. This group is referred to as sapropterin plus MNT. Patients in the MNT-alone group included those in the PKUDOS registry who received a Phe-restricted diet alone who had previously received sapropterin before enrolling in the registry or who discontinued sapropterin, had baseline blood Phe (last available measurement before initiating sapropterin) greater than 600 µmol/L, and who were 18 years or age or older.
Propensity scores for PSM were estimated using logistic regression with probability of treatment as the outcome (pegvaliase, sapropterin plus MNT, or MNT alone). Baseline blood Phe concentration, age, and gender were included in the PSM model. A propensity score including baseline dietary Phe was considered in a sensitivity analysis due to smaller sample size. Patients in the sapropterin plus MNT or MNT-alone groups were randomly ordered according to propensity score and then sequentially matched (1:1) using the nearest neighbour method) to a pegvaliase patient. Of the 1,867 patients who participated in the PKUDOS registry, 221 intended to initiate sapropterin; 64 met the inclusion criteria and were propensity-score matched to 1 of the 285 patients who received pegvaliase. A total of 557 patients had previously received sapropterin, of whom 125 who were on MNT alone met the inclusion criteria and were propensity score matched to 1 of the 285 patients who received pegvaliase.
As the PKUDOS registry (N = 1,867; 52.8% female; mean age of 16 years [SD = 13]; mean blood Phe of 585 µmol/L [SD = 407]; mean baseline daily natural protein intake of 20 g [SD = 21] included patients of all ages, the mean age was lower for this group than for the pegvaliase-treated patients, who were adults only (N = 285; 50.2% female; mean age of 29 years [SD = 9]; mean blood Phe of 1,227 µmol/L [SD = 379]; mean baseline natural protein intake of 38 g [SD = 28]). Baseline blood Phe was the last available measurement before starting pegvaliase or sapropterin; for the MNT-alone group, baseline blood Phe was the measurement closest to the enrolment date within 90 days in case sapropterin was discontinued before enrolment or the value closest to the discontinuation date within 90 days of discontinuation if sapropterin was discontinued after enrolment. Because the propensity score was calculated based on age, sex, and baseline blood Phe concentration, the groups were well balanced with respect to these characteristics. Sixty-four patients who received pegvaliase (59.4% female; mean age of 32 years [SD = 9]; mean blood Phe of 1,172 µmol/L [SD = 329], mean baseline natural protein intake of 33 g [SD = 19]) were matched to 64 patients who received sapropterin plus MNT [57.8% female; mean age of 33 years [SD = 10]; mean blood Phe of 1,176 µmol/L [SD = 383]; mean baseline natural protein intake of 36 g [SD = 31]). A total of 125 patients who received pegvaliase (44.8% female; mean age of 30 years [SD = 8]; mean blood Phe of 1,085 µmol/L [SD = 294]; mean baseline natural protein intake of 34 g [SD = 24]) were matched to 125 patients who received MNT alone (44.8% female; mean age of 31 years [SD = 11]; mean blood Phe of 1,089 µmol/L [SD = 302]; mean baseline natural protein intake of 25 g [SD = 19]). Baseline mean daily natural protein intake was roughly similar across groups.
Interventions
Patients in the pegvaliase group received daily self-administered subcutaneous injections (5 mg to 60 mg). Patients who were in the pegvaliase trials were instructed to maintain consistent protein intake from natural foods and MNT during the trial unless Phe decreased to less than 30 µmol/L. Dietary control of Phe and adherence to MNT were not requirements for entering the pegvaliase trials. Patients in the sapropterin plus MNT group received 5 mg to 20 mg sapropterin orally, and would have been encourage to consume a low Phe diet (MNT) according to prescribing information in the sapropterin product monograph.27 Patients in the MNT alone cohort did not receive pegvaliase or sapropterin. As both historical cohorts were derived from the PKUDOS registry, participants did not receive any specific trial-related interventions such as study visits, questionnaires, education or bloodwork, or any specific dietary interventions.
Outcomes
Outcomes were based on available data from the PKUDOS registry patients (and matched pegvaliase patients) who had at least 1 measurement of Phe levels after treatment for 1 or 2 years. Outcomes included: mean blood Phe concentration at 1 and 2 years; change in blood Phe from baseline; percentages of patients achieving blood Phe of 600 µmol/L or lower, 60 µmol/L or lower, and 120 µmol/L or lower; percentages of patients achieving reductions of 20% or greater, 30% or greater, or 50% or greater from baseline in blood Phe; and natural intact protein (g/day). Reduction in blood Phe was calculated as: baseline blood Phe minus the year 1 or year 2 blood Phe value divided by baseline blood Phe. Follow-up blood Phe concentrations at 1 and 2 years were the levels recorded within 365 days ± 45 days or 730 days ± 90 days. If there was more than 1 value for blood Phe, the median was used.
For patients in the sapropterin plus diet and diet-alone groups, natural intact protein (g/day) was defined as total protein intake minus medical food protein intake. For patients receiving pegvaliase, natural intact protein (g/day) was defined as average dietary protein intake from intact food.
Statistical Analysis
To evaluate differences in blood Phe reductions between treatment groups in the patients with PKU and uncontrolled Phe (blood Phe above 600 μmol/L), mean change in blood Phe reduction from baseline was modelled with treatment as the primary factor and propensity score as the secondary factor. There was no formal statistical hypothesis testing or power calculations, and the results were presented as descriptive analyses with no control of type I error.
Patient Disposition
Although there were 1,867 patients in the PKUDOS registry, only 64 patients receiving sapropterin plus MNT and 125 patients receiving MNT alone were matched to patients receiving pegvaliase. Follow-up data were available for only a subset of these patients. At year 1, data were available for 43 pegvaliase patients and 25 sapropterin plus MNT patients of the 64 matched pairs, and for 87 pegvaliase patients and 51 MNT-alone patients of the 125 matched pairs. At year 2 follow-up data were available for 40 pegvaliase patients and 25 sapropterin plus MNT patients (of 64 matched pairs), and 80 pegvaliase patients and 42 MNT-alone patients (of the 125 matched pairs). There was a far higher rate of missing data for Phe levels among patients from the PKUDOS registry, particularly those in the MNT-alone group.
Exposure to Study Treatments
Adherence to pegvaliase in the phase III PRISM trials was self-reported as very high, leading to good exposure. No information was provided on adherence for the patients receiving sapropterin plus MNT or MNT alone participating in the PKUDOS registry.
Efficacy
Overall, a greater number of patients in the pegvaliase groups achieved lower blood Phe levels compared with the other groups. Among the 43 patients in the pegvaliase group matched to the sapropterin plus MNT group with data available, mean Phe decreased from 1,180 µmol/L (SD = 317) to 505 µmol/L (SD = 509) at 1 year. For the 25 patients in the sapropterin plus MNT group with data available, mean Phe decreased from 1,075 µmol/L (SD = 419) to 807 µmol/L (SD = 389). The LSM difference between Phe levels in the pegvaliase and sapropterin plus MNT groups was −399.4 µmol/L (95% CI, −660.2 to −138.7) at 1 year. At year 2, mean blood Phe levels decreased from a baseline of 1,195 µmol/L (SD = 323) to 427 µmol/L (SD = 527) (n = 40 pegvaliase patients) and from a baseline of 1,060 µmol/L (SD = 337) to 891 µmol/L (SD = 381) (n = 25 sapropterin plus MNT group) with an LSM difference between groups of −647.6 µmol/L (95% CI, −910.0 to −385.3).
For the 87 patients in the pegvaliase group matched to MNT alone group with data available, mean Phe decreased from 1,089 µmol/L (SD = 289) to 473 µmol/L (SD = 451) at 1 year. For the 51 patients in the MNT-alone group with data available, mean blood Phe levels decreased from 1,037 µmol/L (SD = 271) to 1,022 µmol/L (SD = 322) at 1 year. The LSM difference between the pegvaliase and MNT-alone groups was −567.8 µmol/L (95% CI, −708.3 to −427.4) at 1 year. At year 2, mean blood Phe levels decreased from baseline of 1,107 µmol/L (SD = 293) to 302 µmol/L (SD = 392) (n = 80 pegvaliase patients) and from a baseline of 1,051 µmol/L (SD = 302) to 965 µmol/L (SD = 359) (n = 42 MNT alone patients) with an LSM difference between groups of −670.9 µmol/L (95% CI, −824.1 to −517.7).
Higher proportions of patients in the pegvaliase group achieved Phe reductions at various thresholds compared with matched patients receiving sapropterin plus MNT or MNT alone. In addition, patients in the pegvaliase group had increased natural protein intake from baseline at follow-up compared with matched patients receiving sapropterin plus MNT or MNT alone. However, little data on protein intake were available for some groups at follow-up, particularly in the sapropterin plus MNT group (4 patients at 1 year and 7 patients at 2 years). Data for the 4-factor PSM cohort (including baseline dietary Phe) analysis demonstrated similar findings in terms of reduction in blood Phe and increased protein intake.
Harms
Comparisons of harms between patients receiving pegvaliase in the phase III PRISM trials and patients receiving sapropterin plus MNT or MNT alone participating in the PKUDOS registry were uninformative. AE were not actively solicited in the PKUDOS registry.20
Critical Appraisal
Internal Validity
The study by Zori et al. was a post hoc exploratory analysis of patients participating in phase III clinical trials of pegvaliase compared with a historic control of patients participating in the PKUDOS registry who received sapropterin plus MNT or MNT alone. Due to the nonrandomized design, there was the potential for confounding of treatment-effect estimates by known and unknown confounders or by natural fluctuations over the course of PKU that cannot be adjusted for by the PSM analysis.
A major limitation associated with assessing the results of any analyses from a registry is the potential for data to be incomplete. In addition, data are not verified (at the source) as they would be in the context of a clinical trial. Although there were 1,867 patients in the PKUDOS registry, few patients receiving MNT alone and sapropterin plus MNT could be matched to patients receiving pegvaliase; follow-up data were collected for only a subset of these participants at 1 and 2 years. There are many potential sources of bias that could affect measurements of blood Phe levels that were not measured as part of the PKUDOS registry and would therefore be missing from the information used for PSM in the study by Zori et al. Because the PSM was based on baseline blood Phe, age, and gender, the groups were well balanced for these factors. However, many factors that may have affected levels of blood Phe were not included in the PSM approach, including but not limited to: PAH genotype, PKU severity, race or ethnicity, education, socioeconomic status, insurance status, measured Phe tolerance, other medical conditions, mental health conditions, neuropsychological deficits, dietary intervention or education, rationale for prescribing sapropterin, type and dose of MNT, BMI, drug dosing, compliance or adherence, or differences in clinical approach. These factors were not captured and their impact on blood Phe measurements in different groups could not be accounted for in the current analysis.
The relatively rigorous conditions of a clinical trial (mandated bloodwork, follow-up visits, and dietary reminders and interventions) imply monitoring and clinical care that are fundamentally distinct from those of a voluntary observational registry under real-world conditions. These different conditions may have affected blood Phe in the study by Zori et al. For example, variability in blood Phe data could be due to differences in analytical measurements between centres and inconsistency in the number of blood Phe measurements acquired per patient. In the PKUDOS registry, assessments were based on current medical practice at each separate study centre, and variability in sample methods differed by site.20 Patients in the PKUDOS registry were not required nor followed to ensure adherence to MNT; no information about patient adherence with sapropterin or MNT was reported. Information about MNT intake was not described.20 Diet and MNT intake may have varied between the pegvaliase, sapropterin plus MNT, and MNT-alone groups. Potential differences in these factors and their effects on blood Phe limit interpretation of the findings of the study by Zori et al.
The limitations of blood Phe as a study outcome are discussed in the main report. Point observations of blood Phe levels was measured at year 1 and 2 in the study by Zori et al. and could have been affected by numerous factors, mostly adherence to therapy, including diet and MNT. Although the number of blood Phe values used for the outcome was not stated, this was probably a very low number of observations for comparison purposes. As information on diet or MNT was not captured in the PKUDOS registry, and patients were not required to follow any dietary restrictions nor track protein intake, dietary Phe, or MNT, these factors may have affected single blood Phe level measurements, limiting the conclusions that can be drawn about the relative impacts of pegvaliase, sapropterin plus MNT, or MNT alone on blood Phe.
Only a small number of patients were included in the analysis set for efficacy outcomes. The analysis was not pre-specified and lacked control for type I error, and all results are therefore exploratory. There was a lack of planned hypothesis testing (and lack of sample-size considerations related to hypothesis testing). Time effects may have affected the study outcome as the historical control took place in a different time frame. These statistical limitations affect the conclusions that can be drawn from the study.
External Validity
The retrospective observational cohort study design with a historical control makes it difficult to generalize beyond the population of the study by Zori et al. Selection of small numbers of patients from the PKUDOS registry who had blood Phe greater than 600 µmol/L limits generalizability to patients with similar features. However, the clinical experts consulted by CADTH for this review stated that, in Canada, patients would not continue on sapropterin if they maintained high blood Phe levels. The patient population derived from the PKUDOS registry had either recently initiated sapropterin or had discontinued sapropterin; these groups may not be representative of the general population of patients with PKU. Changes in the natural history of the disease, dietary interventions, education or availability or uptake of MNT may have been affected by the use of historic control data.
Discussion
Summary of Available Evidence
One phase III, 4-part, 4-arm, double-blind placebo-controlled RDT with an extension period of open-label treatment (PRISM-2,9-16 N = 215 adolescent and adult patients with PKU) contributed evidence to this report. In addition, the PRISM-1 trial,16,17 a phase III, open-label, randomized, multi-centre study to assess the safety and tolerability of pegvaliase among drug-naive patients with PKU (N = 261), contributed additional evidence related to the safety of pegvaliase, and the PRISM-3 trial, an exploratory phase III substudy to evaluate executive function in adults with PKU participating in PRISM-2 (N = 9),18 addressed outcomes (executive function and self-perception) that were not evaluated in the PRISM-2 trial. Finally, an observational retrospective cohort study by Zori et al.19 was intended to assess the comparative efficacy of pegvaliase, sapropterin plus MNT, and MNT alone in adult patients with PKU.
The pivotal PRISM-2 study provided the only randomized controlled trial evidence of pegvaliase against an appropriate comparator (placebo with or without MNT) for this review. According to the clinical experts consulted by CADTH for this review, the baseline characteristics of the PRISM-2 study population were broadly representative of adolescent and adult patients with PKU who would be candidates for pegvaliase. Almost all patients were White adults 18 years or age or older; the average age was approximately 30 years. According to the clinical experts, baseline blood Phe, mood and inattention symptoms, and protein intake in the PRISM-2 study were as expected for adult patients with PKU with poor or no Phe control and limited adherence to MNT. However, the experts acknowledged that the PRISM-2 study population was enriched for patients (those who did not discontinue treatment in feeder studies or PRISM-2 part 1 due to AEs or patient preference, who were able to achieve target dose in feeder studies, and who achieved a decrease in blood Phe of 20% or greater during PRISM-2 part 1). The major limitations of the PRISM-2 RDT were uncertainty in adherence to pegvaliase and to dietary protein intake, both of which were self-reported, and unclear relevance of pegvaliase-induced decreases in blood Phe of the reported magnitude at a single time point (week 8) to consistency and durability of long-term Phe control, improved inattention and mood symptoms, improved protein tolerance and diet liberalization, and improved HRQoL.
Interpretation of Results
Efficacy
The PRISM-2 RDT did not address several key outcomes that were identified by clinical experts consulted by CADTH for this review as the goal of treatment in adult patients with PKU (improved protein tolerance and HRQoL). These outcomes were also identified as important by patients. The clinical experts consulted by CADTH for this review stated that blood Phe levels can be used to show that pegvaliase treatment is ineffective, and in patients with low Phe who liberalize their diets to include natural foods, stability of Phe levels with the treatment range can demonstrate improvements in protein tolerance. A clinician group had contrasting views and viewed blood Phe as an important marker of treatment response. However, all clinicians agreed that blood Phe is an acceptable surrogate measure that is widely used in clinical trials for reasons of convenience, and is well established to mechanistically drive the symptoms of PKU.
Withdrawal of pegvaliase from patients in the placebo groups of the PRISM-2 RDT led to increases in blood Phe at part 2, week 8 (the difference in LSM change from baseline between the pooled active group and the 20 mg/day placebo group was −923.25 µmol/L, and the difference between the pooled active group and the 40 mg/day placebo group was −638.27 µmol/L). This difference was statistically and clinically meaningful, according to the clinical experts consulted by CADTH for this review, and was driven by the approximately half of patients in the pooled active group with very low Phe (≤ 120 µmol/L). The clinical experts indicated that the very low Phe levels in the subset of patients (roughly half) whom they speculated were taking pegvaliase injections had the potential to lead to improvements in other important outcomes, such as inattention and mood symptoms, HRQoL, and protein tolerance. However, the clinical experts acknowledged that no MID is known for the degree of reduction of blood Phe and its duration that would lead to improvements in other outcomes. In addition, the questionable accuracy of self-reported adherence data for pegvaliase and protein intake (which could be a major confounder of changes in blood Phe levels) was an important source of uncertainty in the primary analysis of Phe levels. In PRISM-2, blood Phe levels were studied at only a single time point in the primary efficacy analysis, and there was no randomized controlled trial evidence regarding the durability and consistency in Phe control associated with pegvaliase.
The clinical experts consulted by CADTH for this review acknowledged that, outside of a trial setting, compliance with pegvaliase would likely be lower among adult patients with PKU and blood Phe levels above 600 µmol/L than that observed in the PRISM-2 RDT. The proportion of patients in a real-world clinical setting who would comply with pegvaliase injections, and the resulting degree of Phe control that would be achieved in the overall adult PKU population, was uncertain.
Despite drastic decreases in blood Phe at part 2, week 8 in pegvaliase-treated patients compared with placebo-treated patients, no statistically significant differences were observed in ADHD-RS-IV inattention subscale scores among participants with a drug-naive score of 9 or greater, and further conclusions could not be drawn for other measures of inattention and mood symptoms (ADHD-RS-IV inattention subscale among all participants, PKU POMS confusion subscale, PKU POMS TMD, or POMS TMD) due to halting of the testing procedure. According to the clinical experts consulted by CADTH for this review, this was not surprising given the relatively short observation period and challenges in measuring inattention and mood symptoms in adult patients with PKU with established disease, who can experience differing degrees of neuropsychiatric and neurocognitive deficits irrespective of blood Phe level.
There was disagreement in the input received by CADTH from clinical experts and clinician groups on the target population of patients with PKU most and least appropriate for pegvaliase treatment (patients with good compliance to MNT and blood Phe of 600 µmol/L or less versus patients with uncontrolled blood Phe of greater than 600 µmol/L who are poorly compliant with MNT). The subgroup of patients with PKU for whom the findings of the PRISM-2 RDT in terms of blood Phe control are most relevant was uncertain. Presumably these would be patients with uncontrolled Phe and poor compliance with diet who are nevertheless willing and able to adhere to pegvaliase injections. This may represent a niche population, as the clinical experts consulted by CADTH for this review expected that adherence to MNT and pegvaliase would be correlated in many patients. Because of the enrichment design of the PRISM-2 RDT, the magnitudes of treatment effects (blood Phe decreases) may be overestimated for a large proportion of adult patients with PKU who would be less compliant and less able to tolerate pegvaliase. Long-term trends in adherence to pegvaliase and evaluation of patients who achieved durable Phe control was not evaluated in the PRISM-2 RDT. Nevertheless, the clinical experts agreed that the findings of the PRISM-2 RDT (reduced blood Phe following pegvaliase injection in adult patients with uncontrolled Phe at baseline) could be generalized to patients who are compliant with diet and have some degree of Phe control.
Analyses of long-term open-label pegvaliase treatment in PRISM-2 part 4 (open-label extension) were suggestive of continued Phe control over time in some patients. However, the absence of a comparison group, attrition bias, and lack of per-patient longitudinal Phe data limited interpretation of long-term efficacy. Analysis of executive function in the PRISM-3 substudy was limited by a small sample size (N = 9). Because of numerous limitations in the study design involving comparisons with a historical control cohort from the PKUDOS registry, potential bias due to the nonrandomized study design and PSM approach, missing data, and statistical limitations (exploratory analysis only), no clear conclusions could be drawn concerning the comparative effectiveness of pegvaliase, sapropterin plus MNT, and MNT based on the observational retrospective cohort study by Zori et al.
Harms
The phase III PRISM studies, including PRISM-1 and PRISM-2 with its open-label extension, provide a consistent picture of the safety profile of pegvaliase injections. Safety data from the placebo-controlled RDT (PRISM-2 part 2) over a treatment period of 8 weeks suggested that HAEs, generalized skin reactions lasting 14 days or more, injection-site skin reactions lasting 14 days or more, rash, urticaria, pruritis, and erythema were potentially associated with pegvaliase rather than placebo injections. During longer-term open-label treatment with pegvaliase in the PRISM-2 study (in which it was not possible to separate the impacts of pegvaliase and the self-injection procedure), HAEs, arthralgia, and injection-site reactions occurred in |||| patients, while generalized skin reactions lasting 14 days or more and injection-site skin reactions lasting 14 days or more occurred in |||||| |||| of patients. Anaphylaxis occurred in |||| of patients and angioedema occurred in |||| of patients. Pegvaliase received a black-box warning from the FDA due to the risk of anaphylaxis.
Because treatment adherence in the PRISM-2 trial was self-reported and these data were potentially flawed, according to the clinical experts consulted for this review (based on high adherence but lack of Phe control in approximately half of patients), AE rates may have been underestimated in the study. In addition, patients with PKU participating in the PRISM-2 study took mandatory pre-medication during re-introduction of study drug, and were likely medically followed more frequently and received additional training on AE detection and management compared with the general population of adult PKU population. According to the clinical experts consulted by CADTH for this review, these factors would not be major impediments to generalizing the safety profile of pegvaliase in the PRISM-2 study to real-world clinical practice.
Conclusions
Data from the PRISM-2 RDT suggest that continued self-administration of pegvaliase injections led to statistically significant and potentially clinically meaningful differences in blood Phe levels after 8 weeks compared with withdrawal of pegvaliase and injection of placebo. Low blood Phe (≤ 120 µmol/L) was observed in approximately half of patients receiving active pegvaliase. Durability and consistency of Phe control were not evaluated in the PRISM-2 RDT. Furthermore, the estimated benefit in reducing blood Phe levels may have been overestimated relative to the general population of adult patients with PKU due to the enriched design of the RDT, which selected for patients more likely to adhere and respond to pegvaliase. Despite significant differences in Phe at week 8 in patients receiving pegvaliase and placebo, no conclusions could be drawn regarding differences in inattention or mood symptoms resulting from continued treatment with pegvaliase. Other outcomes important to patients, including HRQoL and protein tolerance, were not assessed in the PRISM-2 RDT. Efficacy data from nonrandomized studies, including the PRISM-2 open-label extension and an observational study comparing pegvaliase with sapropterin plus MNT and MNT alone, was limited by potential bias and/or confounding. The safety profile of pegvaliase, established through the phase III PRISM trial, including the open-label extension of PRISM-2, pointed to HAEs, arthralgia, injection-site reactions, generalized skin reactions lasting 14 days or more, and generalized injection skin reactions lasting 14 days or more as common side effects. Anaphylaxis and angioedema were less common but clinically important serious adverse effects. Other limitations of the available evidence included an unclear relationship between the magnitude of changes in blood Phe at a single time point (in the PRISM-2 RDT) and changes in other outcomes of importance to patients with PKU, as well as uncertainty regarding the target population of patients with PKU most appropriate for pegvaliase. The observed changes in blood Phe in the PRISM-2 RDT were aligned with 1 of the outcomes identified as important by patients with PKU, and there is clearly an unmet need for additional efficacious treatments for PKU with higher uptake and adherence rates compared with MNT.
References
1.Drug Reimbursement Review sponsor submission: Palynziq (pegvaliase injection), 2.5 mg/0.5 ml (5 mg/ml), 10 mg/0.5 ml (20 mg/ml), 20 mg/ml, solution for injection in a prefilled syringe [internal sponsor's package]. Woodridge (ON): Biomarin Pharmaceutical (Canada) Inc.; 2021 Dec 22.
2.PALYNZIQ® (pegvaliase injection): solution 2.5 mg/0.5 ml (5 mg/ml), 10 mg/0.5 ml (20 mg/ml), 20 mg/1.0 ml (20 mg/ml) subcutaneous injection [product monograph]. Toronto (ON): BioMarin Pharmaceutical (Canada) Inc.; 2022 Mar 30.
3.Blau N, van Spronsen FJ, Levy HL. Phenylketonuria. Lancet. 2010;376(9750):1417-1427. PubMed
4.van Spronsen FJ, Blau N, Harding C, Burlina A, Longo N, Bosch AM. Phenylketonuria. Nat Rev Dis Prim. 2021;7(1):36. PubMed
5.Surtees R, Blau N. The neurochemistry of phenylketonuria. Eur J Pediatr. 2000;159 Suppl 2:S109-113. PubMed
6.Trefz F, Maillot F, Motzfeldt K, Schwarz M. Adult phenylketonuria outcome and management. Mol Genet Metab. 2011;104 Suppl:S26-30. PubMed
7.Simon E, Schwarz M, Roos J, et al. Evaluation of quality of life and description of the sociodemographic state in adolescent and young adult patients with phenylketonuria (PKU). Health Qual Life Outcomes. 2008;6:25. PubMed
8.Burton BK, Grange DK, Milanowski A, et al. The response of patients with phenylketonuria and elevated serum phenylalanine to treatment with oral sapropterin dihydrochloride (6R-tetrahydrobiopterin): a phase II, multicentre, open-label, screening study. J Inherit Metab Dis. 2007;30(5):700-707. PubMed
9.Clinical Study Report: 165-302. A four-part, phase 3, randomized, double-blind, placebo-controlled, four-arm, discontinuation study to evaluate the efficacy and safety of subcutaneous injections of BMN 165 self administered by adults with phenylketonuria [internal sponsor's report]. Novato (CA): BioMarin Pharmaceutical Inc.; 2019 Oct 9.
10.Aryal M, Lau K, Boyer R, et al. Achieving efficacy in subjects with sustained pegvaliase-neutralizing antibody responses. Mol Genet Metab. 2021;134(3):235-242. PubMed
11.Bilder DA, Arnold GL, Dimmock D, et al. Improved attention linked to sustained phenylalanine reduction in adults with early-treated phenylketonuria. Am J Med Genet A. 2022;188(3):768-778. PubMed
12.Gupta S, Lau K, Harding CO, et al. Association of immune response with efficacy and safety outcomes in adults with phenylketonuria administered pegvaliase in phase 3 clinical trials. EBioMedicine. 2018;37:366-373. PubMed
13.Harding CO, Amato RS, Stuy M, et al. Pegvaliase for the treatment of phenylketonuria: A pivotal, double-blind randomized discontinuation Phase 3 clinical trial. Mol Genet Metab. 2018;124(1):20-26. PubMed
14.Larimore K, Nguyen T, Badillo B, et al. Depletion of interfering IgG and IgM is critical to determine the role of IgE in pegvaliase-associated hypersensitivity. J Immunol Methods. 2019;468:20-28. PubMed
15.Qi Y, Patel G, Henshaw J, et al. Pharmacokinetic, pharmacodynamic, and immunogenic rationale for optimal dosing of pegvaliase, a PEGylated bacterial enzyme, in adult patients with phenylketonuria. Clin Transl Sci. 2021;14(5):1894-1905. PubMed
16.Thomas J, Levy H, Amato S, et al. Pegvaliase for the treatment of phenylketonuria: Results of a long-term phase 3 clinical trial program (PRISM). Mol Genet Metab. 2018;124(1):27-38. PubMed
17.Clinical Study Report: 165-301. A phase 3, open-label, randomized, multi-center study to assess the safety and tolerability of an induction, titration, and maintenance dose regimen of BMN 165 self-administered by adults with phenylketonuria not previously treated with BMN 165 [internal sponsor's report]. Novato (CA): Biomarin Pharmaceutical Inc.; 2017 Mar 17.
18.Clinical Study Report: 165-303. A phase 3 substudy to evaluate executive function in adults with phenylketonuria who are participating in the phase 3 study, 165-302 [internal sponsor's report]. Novato (CA): BioMarin Pharmaceutical Inc.; 2018 Jun 19.
19.Zori R, Ahring K, Burton B, et al. Long-term comparative effectiveness of pegvaliase versus standard of care comparators in adults with phenylketonuria. Mol Genet Metab. 2019;128(1-2):92-101. PubMed
20.Longo N, Arnold GL, Pridjian G, et al. Long-term safety and efficacy of sapropterin: the PKUDOS registry experience. Mol Genet Metab. 2015;114(4):557-563. PubMed
21.Hillert A, Anikster Y, Belanger-Quintana A, et al. The genetic landscape and epidemiology of phenylketonuria. Am J Hum Genet. 2020;107(2):234-250. PubMed
22.Statistics Canada. Population and demography statistics. 2022; https://statcan.gc.ca/en/subjects-start/population_and_demography. Accessed 2022 Mar 5.
23.Vockley J, Andersson HC, Antshel KM, et al. Phenylalanine hydroxylase deficiency: diagnosis and management guideline. Genet Med. 2014;16(2):188-200. PubMed
24.van Wegberg AMJ, MacDonald A, Ahring K, et al. The complete European guidelines on phenylketonuria: diagnosis and treatment. Orphanet J Rare Dis. 2017;12(1):162. PubMed
25.U. S. Food and Drug Administration (FDA). Drug Approval Package: PALYNZIQ (pegvaliase-pqpz). 2018; https://www.accessdata.fda.gov/drugsatfda_docs/nda/2018/761079Orig1s000TOC.cfm. Accessed 2022 Mar 5.
26.European Public Assessment Report (EPAR): Palynziq (pegvaliase). Amsterdam (NL): European Medicines Agency; 2019: https://www.ema.europa.eu/en/medicines/human/EPAR/palynziq. Accessed 2022 Mar 5.
27.Kuvan® (sapropterin dihydrochloride): 100 mg tablets [product monograph]. Toronto (ON): BioMarin Pharmaceutical (Canada) Inc.; 2016 Oct 14: https://pdf.hres.ca/dpd_pm/00036799.PDF. Accessed 2022 Mar 5.
28.McGowan J, Sampson M, Salzwedel DM, Cogo E, Foerster V, Lefebvre C. PRESS Peer Review of Electronic Search Strategies: 2015 guideline statement. J Clin Epidemiol. 2016;75:40-46. PubMed
29.Grey matters: a practical tool for searching health-related grey literature. Ottawa (ON): CADTH; 2019: https://www.cadth.ca/grey-matters. Accessed 2022 Jan 19.
30.Longo N, Zori R, Wasserstein MP, et al. Long-term safety and efficacy of pegvaliase for the treatment of phenylketonuria in adults: combined phase 2 outcomes through PAL-003 extension study. Orphanet J Rare Dis. 2018;13(1):108. PubMed
31.Burton BK, Longo N, Vockley J, et al. Pegvaliase for the treatment of phenylketonuria: Results of the phase 2 dose-finding studies with long-term follow-up. Mol Genet Metab. 2020;130(4):239-246. PubMed
32.Brown SG. Clinical features and severity grading of anaphylaxis. J Allergy Clin Immunol. 2004;114(2):371-376. PubMed
33.Wyrwich KW, Auguste P, Yu R, et al. Evaluation of neuropsychiatric function in phenylketonuria: psychometric properties of the ADHD Rating Scale-IV and Adult ADHD Self-Report Scale inattention subscale in phenylketonuria. Value Health. 2015;18(4):404-412. PubMed
34.Bacci ED, Wyrwich KW, Gries KS, et al. An adaptation of the Profile of Mood States for use in adults with phenylketonuria. Journal of Inborn Errors of Metabolism and Screening. 2016;4:2326409816669373.
35.Loprinzi Brauer CE, Motosue MS, Li JT, et al. Prospective validation of the NIAID/FAAN criteria for emergency department diagnosis of anaphylaxis. J Allergy Clin Immunol Pract. 2016;4(6):1220-1226. PubMed
36.International Council for Harmonisation of Technical Requirements for Pharmaceuticals for Human Use (ICH). Medical Dictionary for Regulatory Activities (MedDRA) version 21.1. 2018; https://www.meddra.org. Accessed 2022 Jan 1.
37.National Cancer Institute (NCI). Common Terminology Criteria for Adverse Events (CTCAE) version 4.03. 2010; https://ctep.cancer.gov/protocoldevelopment/electronic_applications/ctc.htm. Accessed 2022 Jan 1.
38.Longo N, Harding CO, Burton BK, et al. Single-dose, subcutaneous recombinant phenylalanine ammonia lyase conjugated with polyethylene glycol in adult patients with phenylketonuria: an open-label, multicentre, phase 1 dose-escalation trial. Lancet. 2014;384(9937):37-44. PubMed
39.Cleary M, Trefz F, Muntau AC, et al. Fluctuations in phenylalanine concentrations in phenylketonuria: a review of possible relationships with outcomes. Mol Genet Metab. 2013;110(4):418-423. PubMed
40.Hood A, Grange DK, Christ SE, Steiner R, White DA. Variability in phenylalanine control predicts IQ and executive abilities in children with phenylketonuria. Mol Genet Metab. 2014;111(4):445-451. PubMed
41.Hood A, Antenor-Dorsey JA, Rutlin J, et al. Prolonged exposure to high and variable phenylalanine levels over the lifetime predicts brain white matter integrity in children with phenylketonuria. Mol Genet Metab. 2015;114(1):19-24. PubMed
42.Viau KS, Wengreen HJ, Ernst SL, Cantor NL, Furtado LV, Longo N. Correlation of age-specific phenylalanine levels with intellectual outcome in patients with phenylketonuria. J Inherit Metab Dis. 2011;34(4):963-971. PubMed
Appendix 1: Literature Search Strategy
Note that this appendix has not been copy-edited.
Clinical Literature Search
Overview
Interface: Ovid
Databases:
MEDLINE All (1946–)
Embase (1974–)
Note: Subject headings and search fields have been customized for each database. Duplicates between databases were removed in Ovid.
Date of search: February 3, 2022
Alerts: Bi-weekly search updates until project completion
Search filters applied: No filters were applied to limit the retrieval by study type.
Limits:
No date or language limits were used
Conference abstracts: excluded
Syntax | Description |
|---|---|
/ | At the end of a phrase, searches the phrase as a subject heading |
ad | MeSH subheading for administration and dosage |
tu | MeSH subheading for therapeutic use |
exp | Explode a subject heading |
* | Before a word, indicates that the marked subject heading is a primary topic; or, after a word, a truncation symbol (wildcard) to retrieve plurals or varying endings |
adj# | Requires terms to be adjacent to each other within # number of words (in any order) |
.ti | Title |
.ot | Original title |
.ab | Abstract |
.hw | Heading word; usually includes subject headings and controlled vocabulary |
.kf | Keyword heading word |
“ “ | Searches the text between quotation marks as an exact term/phrase |
? | Truncation symbol for one or no characters only |
.dq | Candidate term word (Embase) |
.pt | Publication type |
.rn | Registry number |
.nm | Name of substance word (MEDLINE) |
medall | Ovid database code: MEDLINE All, 1946 to present, updated daily |
oemezd | Ovid database code; Embase, 1974 to present, updated daily |
Multi-Database Strategy
Phenylalanine Ammonia-Lyase/ad, tu
(palynziq* or pegvaliase* or BMN165 or BMN 165 or PEGPAL or PEG-PAL or rAvPAL* or phenylase or N6UAH27EUV).ti,ab,kf,ot,hw,rn,nm.
((pegylated or recombinant) adj4 phenylalanine ammonia lyase).ti,ab,kf,ot,hw,rn,nm.
1 or 2 or 3
Enzyme Replacement Therapy/ or (enzyme adj3 (replac* or substitut*) adj2 (treat* or therap*)).ti,ab,kf.
exp Phenylketonurias/ or (Phenylketonuria* or PKU or “261600” or McKusick 26160 or ((phenylalanine hydroxylase or PAH or Tetrahydrobiopterin or BH4 or Dihydropteridine reductase or DHPR) adj2 deficien*) or hyperphenylalanin?emia* or HPA or Folling* disease or Foelling* disease).ti,ab,kf.
5 and 6
4 or 7
8 use medall
*pegvaliase/
(palynziq* or pegvaliase* or BMN165 or BMN 165 or PEGPAL or PEG-PAL or rAvPAL* or phenylase).ti,ab,kf,dq.
((pegylated or recombinant) adj4 phenylalanine ammonia lyase).ti,ab,kf,dq.
10 or 11 or 12
enzyme replacement/ or (enzyme adj3 (replac* or substitut*) adj2 (treat* or therap*)).ti,ab,kf,dq.
Phenylketonuria/ or (Phenylketonuria* or PKU or “261600” or McKusick 26160 or ((phenylalanine hydroxylase or PAH or Tetrahydrobiopterin or BH4 or Dihydropteridine reductase or DHPR) adj2 deficien*) or hyperphenylalanin?emia* or HPA or Folling* disease or Foelling* disease).ti,ab,kf,dq.
14 and 15
13 or 16
17 not (conference abstract or conference review).pt.
18 use oemezd
9 or 19
remove duplicates from 20
Clinical Trials Registries
ClinicalTrials.gov
Produced by the US National Library of Medicine. Targeted search used to capture registered clinical trials.
[Search — palynziq OR pegvaliase OR BMN165 OR “BMN 165” OR PEGPAL OR “PEG-PAL” OR rAvPAL OR ravpalpeg]
WHO ICTRP
International Clinical Trials Registry Platform, produced by the WHO. Targeted search used to capture registered clinical trials.
[Search terms — palynziq OR pegvaliase OR BMN165 OR “BMN 165” OR PEGPAL OR “PEG-PAL” OR rAvPAL OR ravpalpeg]
Health Canada’s Clinical Trials Database
Produced by Health Canada. Targeted search used to capture registered clinical trials.
[Search terms — palynziq, pegvaliase, BMN165, BMN 165, PEGPAL, PEG-PAL, rAvPAL, ravpalpeg]
EU Clinical Trials Register
European Union Clinical Trials Register, produced by the European Union. Targeted search used to capture registered clinical trials.
[Search terms — palynziq OR pegvaliase OR BMN165 OR “BMN 165” OR PEGPAL OR “PEG-PAL” OR rAvPAL OR ravpalpeg]
Grey Literature
Search dates: January 17, 2021 – February 3, 2022
Keywords: palynziq*, pegvaliase*, BMN165, BMN 165, PEGPAL, PEG-PAL, rAvPAL*
Limits: None
Updated: Search updated before the completion of stakeholder feedback period
Relevant websites from the following sections of the CADTH grey literature checklist Grey Matters: A Practical Tool for Searching Health-Related Grey Literature were searched:
Health Technology Assessment Agencies
Health Economics
Clinical Practice Guidelines
Drug and Device Regulatory Approvals
Advisories and Warnings
Drug Class Reviews
Clinical Trials Registries
Databases (free)
Internet Search
Appendix 2: Description and Appraisal of Outcome Measures
Note that this appendix has not been copy-edited.
Aim
To describe the outcome measures summarized in Table 22, and review their measurement properties including validity, reliability, responsiveness to change, and the MID.
Table 22: Outcome Measures Included in PRISM-2 Part 2
Outcome measure | Type |
|---|---|
Blood Phe concentration | Primary |
ADHD-RS-IV | Secondary, tertiary |
PKU POMS | Secondary |
POMS | Secondary, tertiary |
Dietary protein intake | Tertiary |
ADHD-RS-IV = Attention Deficit Hyperactivity Disorder Rating Scale (Investigator-Rated); Phe = phenylalanine; PKU POMS = PKU-Specific Profile of Mood States; POMS = Profile of Mood States.
Source: PRISM-2 Clinical Study Report.9
Findings
The validity, reliability, responsiveness, and the MID of each outcome measure is summarized and evaluated in Table 23.
Table 23: Summary of Outcome Measures and Their Measurement Properties
Outcome measure | Type | Conclusions about measurement properties | MID |
|---|---|---|---|
Blood Phe concentration | Deleterious effects on neurocognition, intelligence, and executive functioning are associated with high blood and brain concentrations of Phe in patients with PKU. The purpose of dietary Phe restriction is to lower blood and brain Phe levels; thus, reducing the risk of damage to the brain.39 | No studies regarding the psychometric properties of blood Phe concentration in adult patients with PKU were found. | Unknown |
POMS | A 65-item, self-administered questionnaire that assesses mood through 7 domains: tension-anxiety, depression-dejection, anger-hostility, vigour-activity, fatigue-inertia, confusion-bewilderment, friendliness. Each item is rated on a 5-point Likert scale (0 = not at all; 1 = a little; 2 = moderately; 3 = quite a bit; 4 = extremely).34 In the PRISM-2 study, the recall period used was the last 1 week. The POMS TMD score is calculated by adding subscale scores and then subtracting vigour-activity. POMS TMD scores range from −32 to 200.9 | No studies regarding the psychometric properties of POMS (TMD or subscale scores) in adult patients with PKU were found. | Unknown |
PKU POMS | A 20-item self-administered modified questionnaire specific for PKU that assesses 6 mood domains: anxiety, depression, anger, activity, tiredness, confusion. Each item is rated on a 5-point Likert scale (0 = not at all; 1 = a little; 2 = moderately; 3 = quite a bit; 4 = extremely).34 In the PRISM-2 study, the recall period used was the last 1 week. Scores for the confusion subscale range from 0 to 11. The PKU POMS TMD score is calculated by adding subscale scores and then subtracting vigour-activity PKU POMS TMD scores range from −12 to 58.9 | Validity: For convergent validity, the Pearson correlation between a version of the ADHD-RS-IV that was modified for use in adults and activity, anxiety, confusion, tiredness, anger, and depression domains were −0.04, 0.33, 0.60, 0.28, 0.31, and 0.15, respectively.34m Reliability: For internal consistency reliability, the Cronbach alpha ranged from 0.75 to 0.87.34 Responsiveness: For responsiveness, the Pearson correlation between ADHD-RS-IV and activity, anxiety, confusion, tiredness, anger, and depression domains were −0.40, 0.43, 0.52, 0.34, 0.32, and 0.21, respectively.34 | Unknown |
Dietary protein intake | To control blood Phe levels, patients with PKU reduce their intake of natural protein and instead consume specially formulated medical foods representing protein sources that are free of Phe. Dietary Phe intake is mainly determined by blood Phe level. One of the goals of therapy for patients with PKU is to improve dietary Phe tolerance. An improvement in Phe tolerance is defined as an increase in dietary Phe intake while maintaining blood Phe levels at the recommended range, thereby increasing natural protein intake.23 | No studies regarding the psychometric properties of dietary protein intake in adult patients with PKU were found. | Unknown |
ADHD-RS-IV total score | An 18-item, clinician-administered scale assessing the severity of inattention and hyperactivity-impulsivity symptoms. It consists of 2 subscales (inattention and hyperactivity-impulsivity) and a total score. Each item is rated on a 4-point Likert scale (0 = never or rarely; 1 = sometimes; 2 = often; 3 = very often). The recall period is the past month. Subscale scores range from 0 to 27.33 The total score ranges from 0 to 54.9 | Studies of psychometric properties were identified only for the ADHD-RS-IV inattention subscale in children. Note that the summary provided is derived from a study that included roughly equal numbers of children and adults with PKU, and descriptions of ADHD-RS-IV relate to children with PKU, not adults. Validity: For construct validity, the ADHD-RS-IV inattention subscale was able to discriminate between known groups using the CGI-S scale at baseline (P < 0.05). For convergent validity, the ADHD-RS-IV inattention subscale was moderately correlated with the CGI-S scale (Spearman correlation ≥ 0.56) and strongly correlated with the BRIEF Working Memory subscale (Pearson correlation ≥ 0.76).33 Reliability: For test-retest reliability, the intraclass correlation coefficient was 0.87 between baseline and week 4 in the stable placebo-arm sample. For internal consistency reliability, the Cronbach alpha was 0.93.33 Responsiveness: For responsiveness, the correlation (Spearman r ≥ 0.20) in change scores between the ADHD-RS-IV inattention subscale and CGI-S scale did not meet the threshold for establishing responsiveness (r ≥ 0.30). The correlation (Pearson r ≥ 0.43) in change scores between the ADHD-RS-IV inattention subscale and BRIEF and BRIEF-Adult Version Working Memory subscales was moderate. The change scores in ADHD-RS-IV inattention subscale in patients who experienced a change in disease status according to the BRIEF Working Memory subscale were not statistically different (P = 0.149).33 | Unknown |
ADHD-RS-IV = Attention Deficit Hyperactivity Disorder Rating Scale (Investigator-Rated); CGI-S = Clinical Global Impression Severity; MID = minimal important difference; Phe = phenylalanine; PKU = phenylketonuria; PKU POMS = Phenylketonuria-Specific Profile of Mood States; POMS = Profile of Mood States.
Blood Phe Concentration
It is well known that deleterious effects on neurocognition, intelligence, and executive functioning are associated with high blood and brain concentrations of Phe in patients diagnosed with PKU.39 The purpose of dietary Phe restriction is to lower blood and brain Phe levels; thus, reducing the risk of damage to the brain.
There is speculation that fluctuations in Phe levels are of potential significance in their relation to intelligence and neurocognition; however, there remains no current definition regarding Phe fluctuations, and these have been measured in many different ways (e.g., SD, regression analysis of Phe concentrations, standard error of the estimate, and mean and its accompanying SD of index dietary control [IDC] measured by 6-month mean Phe values).39 In the review by Cleary et al.39 it was noted that a number of studies have reported that the highest concentrations of Phe were reported in the morning in patients with PKU (children and adults) when observing diurnal variation of blood Phe levels. Other studies summarized in this review have also reported that there may be up to 400% variation in day-to-day blood Phe levels in adults with well-controlled PKU, that blood Phe levels fluctuate to a larger extent in patients with PKU when compared to their healthy counterparts, that blood Phe concentrations increase with age while there is uncertainty surrounding whether fluctuations decrease with age, and that fluctuations may be influenced by PAH genotype, rates of growth, dietary adherence, diet, and illness.39
With regard to the impact of blood Phe fluctuations on the brain, Cleary et al.39 reported that healthy individuals have approximately equal concentrations of blood and brain Phe, while increases in Phe concentrations in the blood is higher than increases in the brain in patients with PKU. In addition, they noted that peaks of Phe levels last longer, are not as steep, and occur later in the brain when compared to blood in these patients.39 There is conflicting evidence regarding the effects of Phe fluctuations on neurocognition and other measures of brain activity in patients with PKU, with some studies showing correlations between Phe fluctuations and deficits in executive functioning, cognition, and intelligence while others finding no associations.39 Hood et al.40 reported that Phe variability was a better predictor of cognitive performance when compared to the various other aforementioned indices of Phe control, along with being a better predictor of executive functioning in children aged 5 years and older when compared to patients under 5 years of age. Hood et al.41 retrospectively analyzed microstructural white matter integrity using mean diffusivity from diffusion tensor imaging and various Phe indices to measure blood Phe concentrations in early and continuously treated children with PKU to determine if prolonged exposure to both high and variable levels of blood Phe correlated with white matter compromise. The authors reported that microstructural white matter integrity compromise was correlated with mean Phe, the IDC, mean exposure, and the SD of exposure, indicating that high and variable blood Phe concentrations were predictors of white matter compromise in children with PKU.41 Viau et al.42 suggested that there was an association between measures of intelligence and the quality of metabolic blood Phe control during certain developmental periods in a study of mostly children with PKU. Perceptual reasoning appeared to be strongly associated with proper blood Phe control during ages 0 to 6 and 7 to 12 years, with specific areas of verbal comprehension being affected by increases of blood Phe levels in children aged 0 to 6 years.42 However, the evidence obtained by Viau et al.42 was not supportive that blood Phe level variability was a good predictor of intelligence. That being said, all of these results indicate that continual blood Phe concentrations should be monitored and controlled in childhood and that this should continue throughout the life of patients with PKU.39-41
According to the ACMG, relaxation of Phe control can lead to the development of neurocognitive deficits and psychiatric symptoms, which can ultimately have an impact on quality of life. Hence, ACMG recommends that blood Phe levels be monitored and controlled throughout the life of a patient with PKU.23 For patients with early-treated PKU who have discontinued therapy, ACMG recommends that treatment be reinitiated to lower blood Phe levels because this group of patients may see benefit, including improvement in neuropsychological symptoms. For patients with untreated or late-treated PKU, ACMG recommends that treatment be offered to lower blood Phe levels because this group of patients may still see benefit, including improvement in behaviour and psychiatric symptoms.23 However, the magnitude of decrease in blood Phe levels as well as the duration and consistency of metabolic control required to see improvements in outcomes, such as Phe tolerance, neurocognitive and neuropsychiatric symptoms, and HRQoL, are not known. Further, studies determining the psychometric properties, including the MID, of blood Phe concentration in the adult PKU population, were not found.
Profile of Mood States (POMS)
The original POMS is a 65-item, self-administered questionnaire that assesses a patient’s transient and variable mood states. Six mood domains are evaluated: tension-anxiety (9 items), depression-dejection (15 items), anger-hostility (12 items), vigour-activity (8 items), fatigue-inertia (7 items), and confusion-bewilderment (7 items). The friendliness domain (7 items) was later determined by the original POMS developers to be too weak to be scored, resulting in a 58-item POMS. The full list of items can be found in the POMS user manual. Each item is rated on a 5-point Likert scale (0 = not at all; 1 = a little; 2 = moderately; 3 = quite a bit; and 4 = extremely). The POMS has been widely used in different therapeutic areas and as a result, the instrument has been modified a number of times, including the removal of, addition of, and changes in the items and domains, to adapt the questionnaire for its use in a targeted patient population or for a specific culture.34
Extensive validation studies have not been conducted for any version of the POMS.34 No studies regarding the psychometric properties of the POMS in adults with PKU were found.
PKU-Specific Profile of Mood States (PKU POMS)
Bacci et al.34 adapted the original POMS to better assess relevant mood states in adult patients with PKU. Qualitative and quantitative assessments were conducted to determine the comprehensibility, acceptability, relevance, and the performance of each item and domain in the PKU population. The result was the development of the PKU POMS, a 20-item, self-administered questionnaire that assesses 6 renamed mood domains (items): anxiety (panicky, uneasy, nervous, anxious), depression (unhappy, sad, discouraged, lonely), anger (angry, grouchy, annoyed), activity (lively, active, energetic), tiredness (worn out, exhausted, sluggish), and confusion (confused, unable to concentrate, forgetful). Each item is rated on a 5-point Likert scale (0 = not at all; 1 = a little; 2 = moderately; 3 = quite a bit; and 4 = extremely).34
Psychometric Properties of the PKU POMS
Bacci et al.34 used the PKU POMS to ascertain its validity, reliability, and responsiveness in adult patients with PKU from an open-label study (PRISM-1) who were undergoing treatment with pegvaliase and completed the POMS on day 1. Any correlations with plasma Phe were exploratory because according to the authors, it was uncertain if a change in plasma Phe would correspond to a change in mood states.
Validity
For convergent validity, each domain of the PKU POMS was compared to ADHD-RS-IV (modified version with adult prompts) and plasma Phe values using Pearson correlations (n = 114). The Pearson correlation between ADHD-RS-IV (adult version) and activity, anxiety, confusion, tiredness, anger, and depression domains were −0.04, 0.33, 0.60, 0.28, 0.31, and 0.15, respectively. The correlation between ADHD-RS-IV (adult version) and anxiety, confusion, and anger domains were statistically significant (P < 0.05). The Pearson correlation between plasma Phe and all 6 domains ranged from 0 to 0.17, none of which were statistically significant.
Reliability
For internal consistency reliability, the Cronbach alpha ranged from 0.75 to 0.87, indicating each domain measured the same construct.
Responsiveness
For responsiveness, the change scores between day 1 and end of study for each PKU POMS domain was compared to the ADHD-RS-IV (adult version) and plasma Phe using Pearson correlation. The Pearson correlation between ADHD-RS-IV (adult version) and activity, anxiety, confusion, tiredness, anger, and depression domains were –0.40, 0.43, 0.52, 0.34, 0.32, and 0.21, respectively (n = 65). The correlation between ADHD-RS-IV (adult version) and activity, anxiety, confusion, tiredness, and anger domains were statistically significant (P < 0.05). The Pearson correlation between plasma Phe and activity, anxiety, confusion, tiredness, anger, and depression domains were –0.25, 0.34, 0.47, 0.15, 0.26, and 0.32, respectively (n = 52). The correlation between plasma Phe values and anxiety, confusion, and depression domains were statistically significant (P < 0.05).
Clinical Relevance
Studies determining the minimally MID for adults with PKU on the PKU POMS were not found.
Dietary Protein Intake
Dietary therapy with the restriction of dietary Phe intake is defined as the reduced intake of natural protein that is replaced with a protein source that is free of Phe to lower blood Phe levels. The recommended daily dietary intake of Phe, tyrosine, and protein for patients with PKU can be found in the ACMG practice guidelines for PKU.23 Dietary Phe intake is determined by blood Phe levels but it can also be influenced by various factors including residual PAH activity, age, rate of growth, and responsiveness to pharmacological therapy. Reduced intake of natural protein can lead to an inadequate consumption of protein, nutrients, and calories that are necessary for maintenance of health and growth. Hence, modified low-protein foods and medical foods, which are a mixture of amino acids and free of Phe, are medically necessary to meet daily nutritional requirements in patients with PKU on dietary therapy. However, medical foods may not always contain an appropriate amount of nutrients because nutritional requirements can vary depending on a patient’s unique needs at different stages of life and in the presence of comorbidities. For patients who are able to maintain metabolic control with respect to blood Phe levels using dietary therapy alone, the benefits of adding on a pharmacologic agent would be an improvement in Phe tolerance, liberalization of diet, and enhanced HRQoL. An improvement in Phe tolerance is defined as an increase in dietary Phe intake while maintaining Phe control, thereby increasing natural protein intake.23 However, studies determining the psychometric properties, including the MID, of Phe tolerance and natural protein intake in adult patients with PKU were not found.
Attention Deficit Hyperactivity Disorder Rating Scale (Investigator-Rated) (ADHD-RS IV)
The ADHD-RS-IV is based on the fourth edition of the Diagnostic and Statistical Manual of Mental Disorders criteria used to assess ADHD symptoms in children and is completed by a parent or guardian.33 The full scale comprises 18 items that are separated into 2 subscales: an Inattention subscale and a Hyperactivity/Impulsivity subscale. Each of the subscales is composed of 9 items that assesses the frequency of ADHD symptoms, with each item rated on a 4-point Likert frequency scale (0 = never or rarely; 1 = sometimes; 2 = often; and 3 = very often).33 The recall period is 1 month. A higher score corresponds with worse severity of ADHD. This scale has been observed to be valid and reliable in patients with ADHD.33 In the Inattention subscale, scores range from 0 to 27, with greater inattentive severity measured with higher scores.33
The investigators in the PRISM-2 study9 modified the original ADHD-RS-IV to use a shorter recall period (duration not specifically described) as well as adult prompts.
Studies of the psychometric properties for the ADHD-RS-IV inattention subscale in children were identified and summarized in the following section.
Psychometric Properties of the ADHD-RS-IV Inattention Subscale
Wyrwich et al.33 used the 9-item inattention subscale in both ADHD-RS-IV and Adult ADHD Self-Report Scale to ascertain its validity, reliability, and responsiveness in child (n = 86) and adult (n = 120) patients, respectively, with PKU from a randomized controlled trial (Study PKU-016) who were undergoing treatment with sapropterin. For the purposes of this review, only the psychometric properties of the ADHD-RS-IV inattention subscale in children have been summarized.
Validity
For construct validity, the ADHD-RS-IV inattention subscale was able to discriminate between known groups using the Clinical Global Impression Severity (CGI-S) scale at baseline (P < 0.05). For convergent validity, the ADHD-RS-IV inattention subscale was compared to the CGI-S scale and the Behaviour Rating Inventory of Executive Function (BRIEF) Working Memory subscale using Spearman and Pearson correlations, respectively. At baseline, the ADHD-RS-IV inattention subscale was moderately correlated with the CGI-S scale (r ≥ 0.56) and strongly correlated with the BRIEF Working Memory subscale (r ≥ 0.76).
Reliability
For test-retest reliability, the intraclass correlation coefficient was 0.87 between baseline and week 4 in the stable placebo-arm sample (n = 25). For internal consistency reliability, the Cronbach alpha was 0.93 at baseline. Since the intraclass correlation coefficient and Cronbach alpha were greater than or equal to 0.60 and 0.70, respectively, the ADHD-RS-IV inattention subscale demonstrated acceptable agreement between test and retest scores and each of its items were measuring the same construct.
Responsiveness
For responsiveness, the change scores between baseline and week 13 for ADHD-RS-IV inattention subscale was compared to the CGI-S scale and BRIEF and BRIEF-Adult Version Working Memory subscales using Spearman and Pearson correlations, respectively. The correlation (r ≥ 0.20) in change scores between the ADHD-RS-IV inattention subscale and CGI-S scale did not meet the pre-specified threshold for establishing responsiveness (r ≥ 0.30) but was statistically significant (P < 0.01). The correlation (r ≥ 0.43) in change scores between the ADHD-RS-IV inattention subscale and BRIEF and BRIEF-Adult Version Working Memory subscales was moderate and statistically significant (P < 0.001), indicating the inattention subscale was able to detect change in subjects known to have changed in this neurocognitive outcome. However, the change scores in ADHD-RS-IV inattention subscale for patients who experienced a change in disease status between baseline and week 13 were not statistically different (P = 0.149). Disease status was categorized by using the clinically significant threshold of t score ≥ 65 on the BRIEF Working Memory subscale, with higher scores indicating greater severity in this neurocognitive function.
Clinical Relevance
Studies determining the MID for adult patients with PKU using the ADHD-RS-IV inattention subscale were not found.
Appendix 3: Detailed Outcome Data
Note that this appendix has not been copy-edited.
Table 24: Sensitivity Analyses of Change From Part 2 Baseline in Blood Phe Concentration (µmol/L) at Part 2, Week 8
Sensitivity analysis | n | LSM change from part 2 baseline (95% CI) | Difference in LSM (95% CI) | P valuea |
|---|---|---|---|---|
MMRM with multiple imputation, mITT set | ||||
Pooled active | 58 | ||||| |||||||| ||||||| | ||||||| |||||||||| |||||||| | ||||||| |
20 mg/day placebo | 14 | |||||| |||||||| |||||||| | ||
Pooled active | 58 | ||||| |||||||| ||||||| | ||||||| ||||||||| |||||||| | ||||||| |
40 mg/day placebo | 14 | |||||| |||||||| ||||||| | ||
MMRM with LOCF imputation, mITT set | ||||
Pooled active | 58 | ||||| |||||||| ||||||| | ||||||| |||||||||| |||||||| | ||||||| |
20 mg/day placebo | 14 | |||||| |||||||| |||||||| | ||
Pooled active | 58 | ||||| |||||||| ||||||| | ||||||| ||||||||| |||||||| | ||||||| |
40 mg/day placebo | 14 | |||||| |||||||| ||||||| | ||
MMRM, ITT set | ||||
Pooled active | 66 | ||||| |||||||| ||||||| | ||||||| |||||||||| |||||||| | ||||||| |
20 mg/day placebo | 15 | |||||| |||||||| |||||||| | ||
Pooled active | 66 | ||||| |||||||| ||||||| | ||||||| ||||||||| |||||||| | ||||||| |
40 mg/day placebo | 14 | |||||| |||||||| ||||||| | ||
MMRM, PP set | ||||
Pooled active | 54 | ||||| |||||||| ||||||| | ||||||| |||||||||| |||||||| | ||||||| |
20 mg/day placebo | 12 | |||||| |||||||| |||||||| | ||
Pooled active | 54 | ||||| |||||||| ||||||| | ||||||| ||||||||| |||||||| | ||||||| |
40 mg/day placebo | 14 | |||||| |||||||| ||||||| | ||
CI = confidence interval; ITT = intention-to-treat; LOCF = last observation carried forward; LSM = least squares mean; mITT = modified intention-to-treat; MMRM = mixed model repeated measures; Phe = phenylalanine; PP = per-protocol; SD = standard deviation.
aP value based on MMRM with study drug (pegvaliase or placebo), visit, and study drug-by-visit interaction as factors adjusting for baseline blood Phe concentration.
Source: PRISM-2 Clinical Study Report.9
Table 25: ANCOVA Model of Change From Part 2 Baseline in Blood Phe Concentration (µmol/L) Adjusted by Change From Baseline Daily Intact Protein Intake at Part 2, Week 8 (mITT)
Change from baseline blood Phe level | Placebo 20 mg/day (n = 14) | Placebo 40 mg/day (n = 14) | Pooled active (n = 58) |
|---|---|---|---|
Part 2, week 4 | |||
n | |||| | |||| | |||| |
LSM (SE)a | |||||| |||||||| | ||||| |||||||| | |||| ||||||| |
Part 2, week 8 | |||
n | |||| | |||| | |||| |
LSM (SE)a | ||||| |||||||| | ||||| |||||||| | |||| ||||||| |
ANCOVA = analysis of covariance; LSM = least squares mean; mITT = modified intention-to-treat; Phe = phenylalanine; SE = standard error.
aFrom ANCOVA model with change from baseline as the response variable and treatment, change from baseline protein intake, and baseline blood Phe concentration as factors.
Source: PRISM-2 Clinical Study Report.9
Table 26: MMRM Analysis of Change From Part 2 Baseline in Blood Phe Concentration (µmol/L) With Interaction of Baseline Phe Categories at Part 2, Week 8 (mITT)
Treatment | n | Part 2 baseline Mean (SD) | Part 2 week 8 Mean (SD) | Change from baseline at part 2, week 8 | Difference in LSMs (95% CI)a (Active vs. placebo) | P valuea | |
|---|---|---|---|---|---|---|---|
Mean (SD) | LSM (95% CI)a | ||||||
Pooled Active | 58 | 503.9 (520.28) | 559.2 (569.47) | 18.6 (279.43) | ||||| |||||||| ||||||| | ||||||| ||||||||| |||||||| | < 0.0001 |
Pooled Placebo | 28 | 536.1 (432.54) | |||||| |||||||| | ||||| |||||||| | |||||| |||||||| ||||||| | ||
Pooled Active | 58 | 503.9 (520.28) | 559.2 (569.47) | 18.6 (279.43) | ||||| |||||||| ||||||| | ||||||| |||||||||| |||||||| | < 0.0001 |
20 mg/day Placebo | 14 | 563.9 (504.62) | 1,509.0 (372.64) | 996.4 (555.00) | |||||| |||||||| |||||||| | ||
Pooled Active | 58 | 503.9 (520.28) | 559.2 (569.47) | 18.6 (279.43) | ||||| |||||||| ||||||| | ||||||| ||||||||| |||||||| | < 0.0001 |
40 mg/day Placebo | 14 | 508.2 (363.68) | 1,164.4 (343.32) | 599.0 (507.40) | |||||| |||||||| ||||||| | ||
20 mg/day Active | 29 | 596.8 (582.75) | 553.0 (582.39) | −65.9 (192.02) | ||||| ||||||||| ||||||| | ||||||| |||||||||| |||||||| | < 0.0001 |
20 mg/day Placebo | 14 | 563.9 (504.62) | 1,509.0 (372.64) | 996.4 (555.0) | |||||| |||||||| |||||||| | ||
40 mg/day Active | 29 | 410.9 (439.95) | 566.3 (567.47) | 114.1 (332.40) | |||||| |||||||| ||||||| | ||||||| ||||||||| |||||||| | < 0.0001 |
40 mg/day Placebo | 14 | 508.2 (363.68) | 1,164.4 (343.32) | 599.0 (507.40) | |||||| |||||||| ||||||| | ||
CI = confidence interval; LSM = least squares mean; mITT = modified intention-to-treat; MMRM = mixed model repeated measures; Phe = phenylalanine; SD = standard deviation.
aP value from MMRM model with change from baseline in Phe as the response variable, and treatment, visit, baseline Phe category, and treatment-by-visit, treatment-by-baseline Phe category, and treatment-by-visit-by-baseline Phe category interactions. Baseline Phe categories were ≤ 50% Phe reduction from naive baseline and > 50% Phe reduction from naive baseline using mean of last 2 consecutive Phe measurements in part 1.
Source: PRISM-2 Clinical Study Report.9
Pharmacoeconomic Review
Abbreviations
BIA
budget impact analysis
HRQoL
health-related quality of life
ICER
incremental cost-effectiveness ratio
MNT
medical nutrition therapy
Phe
phenylalanine
PKU
phenylketonuria
PKUDOS
Phenylketonuria Demographic, Outcomes, and Safety Registry
PSM
propensity score matching
QALY
quality-adjusted life-year
TTO
time trade-off
WTP
willingness to pay
Executive Summary
The executive summary comprises 2 tables (Table 1 and Table 2) and a conclusion.
Item | Description |
|---|---|
Drug product | Pegvaliase (Palynziq), solution for injection |
Submitted price | Pegvaliase: 2.5 mg/0.5 mL pre-filled syringe: $405.00 10 mg/0.5 mL pre-filled syringe: $405.00 20 mg/0.5 mL pre-filled syringe: $405.00 |
Indication | To reduce blood phenylalanine concentrations in patients with phenylketonuria aged 16 years and older who have inadequate blood phenylalanine control (blood phenylalanine levels greater than 600 µmol/L) despite dietary management |
Health Canada approval status | NOC |
Health Canada review pathway | Standard |
NOC date | March 30, 2022 |
Reimbursement request | For the treatment of patients with phenylketonuria aged 16 years and older who have inadequate blood phenylalanine control (blood phenylalanine levels greater than 600 µmol/L) despite prior treatment with sapropterin |
Sponsor | BioMarin Pharmaceutical (Canada) Inc. |
Submission history | Previously reviewed: No |
NOC = Notice of Compliance.
Table 2: Summary of Economic Evaluation
Component | Description |
|---|---|
Type of economic evaluation | Cost-utility analysis Markov model |
Target population | Patients with PKU aged 16 years and older with uncontrolled blood phenylalanine levels on existing management |
Treatment | Pegvaliase, 5 mg to 60 mg daily plus MNT |
Comparators |
|
Perspective | Canadian publicly funded health care payer |
Outcomes | QALYs, life-years |
Time horizon | Lifetime (84 years) |
Key data source | PRISM clinical trials, propensity score matching study |
Submitted results | Compared to MNT alone: ICER = $501,486 per QALY ($6,515,338 incremental costs and 12.99 incremental QALYs) Compared to sapropterin plus MNT: ICER = dominant ($738,722 savings and 15.71 incremental QALYs) |
Key limitations |
|
CADTH reanalysis results |
|
ICER = incremental cost-effectiveness ratio; MNT = medical nutrition therapy; Phe = phenylalanine; PKU = phenylketonuria; QALY = quality-adjusted life-year.
Conclusions
Data from the PRISM-2 trial suggest that continued self-administration of pegvaliase injections led to statistically significant and potentially clinically meaningful decreases in blood phenylalanine (Phe) levels after 8 weeks compared with withdrawal of pegvaliase and injection of placebo. These changes aligned with 1 of the outcomes identified as important by patients with phenylketonuria (PKU). A observational propensity score matching (PSM) study by Zori et al. (2019) comparing pegvaliase to sapropterin plus medical nutrition therapy (MNT) and MNT alone had numerous limitations in study design involving comparison with a historical control cohort, potential bias due to the nonrandomized study design and PSM approach, and statistical limitations (exploratory analysis only). Furthermore, derived transition probabilities appeared unreliable and lacked face validity. Ultimately, no clear conclusions could be drawn concerning the comparative effectiveness of pegvaliase, sapropterin plus MNT, and MNT alone.
Due to both the absence of robust comparative evidence and the inappropriateness of the model structure, CADTH was unable to derive a base-case analysis. Instead, an exploratory reanalysis was conducted that adjusted health-state utility values to be more in line with those measured in other chronic conditions in Canada, increased pegvaliase syringe use in maintenance years, lowered MNT adherence in patients using sapropterin and pegvaliase, and adjusted patient starting age to better reflect the diverse ages of patients with PKU in Canada. Due to the Health Canada indication and to differing mechanisms of action leading to a broader patient population as candidates for pegvaliase rather than sapropterin, CADTH considered the comparison of pegvaliase to MNT alone to be the most relevant.
In this exploratory analysis, the incremental cost-effectiveness ratio (ICER) associated with pegvaliase plus MNT was $1,923,797 per quality-adjusted life-year (QALY) when compared to MNT alone. A price reduction of at least 99% for pegvaliase would be required to achieve an ICER below $50,000 per QALY compared to MNT. However, estimates of cost-effectiveness for pegvaliase relative to comparators are highly uncertain. As such, the price reductions likely underestimate the true reduction needed to ensure cost-effectiveness.
CADTH was unable to adjust for major limitations, including the lack of direct comparative clinical data, uncertain and implausible transition probabilities informing comparative efficacy, the model’s structural reliance on blood Phe level to predict health-related quality of life (HRQoL), the lack of adherence as a predictor of blood Phe level, the absence of modelling discontinuation rates for ineffective treatments, and the potential inappropriateness of the reimbursement request.
Stakeholder Input Relevant to the Economic Review
This section is a summary of the feedback received from the patient groups, registered clinicians, and drug plans that participated in the CADTH review process.
CADTH received 1 patient group submission from the Canadian PKU and Allied Disorders association for the review of pegvaliase. Input was based on an online patient survey run in late 2021 that received responses from 68 people, 46 of whom were from Canada. Patients described their PKU as causing difficulties maintaining employment; fitting in socially due to events based around food; mood and mental health difficulties leading to isolation; and financial strain (48% of respondents living in Canada indicated that they needed financial assistance due to costs associated with PKU and its treatment). On a scale of 1 to 5, with 5 being “strongly agree” and 1 “strongly disagree” that they are compliant with their low-protein diet, the average rating was 3.3 (patients on pegvaliase excluded). Patients emphasized cost and lack of available low-protein foods, time required to plan and prepare foods, lack of satiety, poor taste and smell, social pressure to eat with others, inexact protein and Phe values on commercial products, and mental exhaustion due to the effort required to track food intake as barriers to compliance. Synthetic formulas were reported to cause stomach issues, migraines, embarrassment (i.e., drinking them in public), difficulties remaining at a healthy weight due to high calorie formulations, and bad breath. Patients who responded to sapropterin reported better ability to function and lower Phe levels; however, the number of daily pills required, barriers to access, and the lack of improvement in dietary restrictions were reported as negatives. Thirteen Americans and 1 Canadian patient were using pegvaliase, and 13 of these 14 rated their quality of life as “better” or “much better” than before, reporting liberalization of their diet, absence of “brain fog,” improved focus at work, improved anxiety, and improved social experiences.
One group of 3 metabolic physicians who care for adults with PKU in Montreal, Toronto, and Vancouver supplied input. These clinicians emphasized that, in adulthood, elevated Phe levels manifest as often reversible cognitive, neurologic, and psychiatric symptoms that can result in headaches, tremors, short-term memory loss, difficulty focusing, anxiety, and depression. The physicians noted that dietary restrictions are cumbersome and unpalatable, and that adherence to them requires planning and motivation, both of which are impaired by elevated Phe levels, and many patients are unable to adhere to these restrictions. While sapropterin is accessible in some jurisdictions, the clinicians estimated that 70% to 80% of patients with PKU would not respond to sapropterin due to the extent of their mutation, and these patients require the most significant protein restriction due to the severity of their PKU. The clinicians indicated that dietary treatment, with or without sapropterin depending on PAH mutation and response, should be tried before pegvaliase. Patients who are unable to adhere to dietary treatment and/or have an insufficient response to sapropterin, and therefore have persistently elevated blood Phe levels causing neuropsychiatric symptoms, were deemed most likely to benefit most from pegvaliase; however, this opinion differed from that of the clinical experts consulted by CADTH, who indicated that patients who are adherent to MNT are most likely to be adherent to pegvaliase and are therefore most likely to benefit. The ability to liberalize dietary restrictions while maintaining target blood Phe levels were seen as important outcomes for patient quality of life.
Drug plan input noted patients must be capable of self-injection of pegvaliase, and that the pegvaliase product monograph states that an observer must be present during, and for at least 1 hour after, each injection for the first 6 months of therapy. The observer must be able to recognize the signs and symptoms of an acute systemic hypersensitivity reaction, administer epinephrine, and call for emergency medical support if required; additional clinic visits may be required for patients without access to such an observer. Drug plan input also noted that sapropterin has successfully gone through price negotiations. Two of these concerns were addressed in the sponsor’s model:
Quality of life was linked to blood Phe level. Patients at higher Phe levels required more psychiatric and nurse practitioner visits compared with those at lower levels.
Pegvaliase introduction was associated with training cost.
In addition, CADTH addressed 2 of these concerns by assuming that MNT adherence is also difficult for patients on sapropterin and pegvaliase, and by adjusting utility values to be more in line with psychological symptoms. CADTH was unable to address the following concerns raised from stakeholder input:
the direct association between MNT adherence, blood Phe level, and quality of life.
lack of response to sapropterin would lead to its discontinuation.
Economic Review
The current review is for pegvaliase (Palynziq) for patients with PKU aged 16 and older with uncontrolled Phe levels despite dietary management.
Economic Evaluation
Summary of Sponsor’s Economic Evaluation
Overview
Pegvaliase is indicated to reduce blood Phe concentrations in patients with PKU aged 16 years and older who have inadequate blood Phe control (blood Phe levels greater than 600 µmol/L) despite dietary management.1 This differs from the reimbursement request, which is for the treatment of patients with PKU aged 16 years and older who have inadequate blood Phe control (blood Phe levels greater than 600 µmol/L) despite prior treatment with sapropterin.2 Pegvaliase is administered by subcutaneous injection, with an initial dose of 2.5 mg weekly for 4 weeks. The dose should then be escalated gradually based on tolerability, with a suggested titration of 2.5 mg twice weekly for 1 week, 10 mg weekly for 1 week, 10 mg twice weekly for 1 week, 10 mg 4 times weekly for 1 week, then 10 mg daily for 1 week. Maintenance dosing begins at 20 mg daily for 12 to 24 weeks and may be increased to 40 mg (2 injections) daily for 16 weeks, and then to the maximum dose of 60 mg (3 injections) daily, individualized to achieve blood Phe levels of 600 µmol/L or lower. The sponsor has submitted pegvaliase at a price of $405.00 per pre-filled syringe containing 2.5 mg, 10 mg, or 20 mg of pegvaliase.3 At this price, the cost per patient of the titration year ranges from $130,205 (assuming the slowest recommended titration to 20 mg daily) to $260,615 (assuming the fastest recommend titration to 60 mg daily), while that of maintenance years thereafter ranges from $147,825 (20 mg daily) to $443,475 (60 mg daily).
The sponsor submitted 2 cost-utility analyses to compare the cost-effectiveness of pegvaliase plus MNT to sapropterin plus MNT, and pegvaliase plus MNT to MNT alone in patients with blood Phe levels greater than 600 µmol/L.3 In the absence of direct evidence, a PSM study4 was used to retrospectively compare data from the pegvaliase clinical trials5-7 against the Phenylketonuria Demographics, Outcomes, and Safety (PKUDOS) registry, a US-based voluntary patient registry run by the sponsor to monitor the safety of Kuvan (sapropterin), which is also a sponsor product.8 As pegvaliase patients were matched to individual patient-level data from the PKUDOS registry for each of sapropterin plus MNT and MNT alone (the latter in patients who had received sapropterin before registry enrolment or who discontinued sapropterin), pegvaliase inputs and results differ between the 2 analyses.
The sponsor adopted a lifetime time horizon (84 years), with the analysis conducted from the perspective of a publicly funded health care payer. Future costs and benefits were discounted at a rate of 1.5% per year, and the model cycle length was 1 year.
Model Structure
The sponsor’s model consisted of a Markov model with 6 health states based on blood Phe levels: uncontrolled classical PKU (blood Phe ≥ 1,200 μmol/L); uncontrolled PKU (blood Phe 600 μmol/L to 1,200 μmol/L); insufficiently controlled PKU (blood Phe 360 μmol/L to 600 μmol/L); controlled PKU (blood Phe 120 μmol/L to 360 μmol/L); normal Phe level (< 120 μmol/L); and death (Figure 1 in Appendix 3). Based on expert opinion, patients entered the model in an uncontrolled state, with 74% of patients entering the model with blood Phe between 600 μmol/L and 1,200 µmol/L, and the remaining 26% with blood Phe of 1,200 µmol/L or greater. Patients could then transition from 1 of these Phe level health states to another every year (cycle) for the remainder of their lives.
Model Inputs
Patients entered the model at 16 years of age, the age patients are eligible for treatment with pegvaliase,1 with a mean body weight of 77.2 kg.5 Patients remained on their assigned treatment for the rest of their lives; discontinuation was not considered in the model.
Efficacy in the model was implemented through transition probabilities between blood Phe level health states. For the first 4 cycles, patients transitioned through the various health states in probabilities derived from the sponsor’s submitted propensity score study,4 and patients were then assumed to have the same transition probabilities as the fourth cycle for the remainder of their lives (Table 9). Transition probabilities for pegvaliase differed depending on which comparator was being assessed, due to the matching of individual patient-level data. Mortality was based on Statistics Canada estimates of age-matched mortality rates; PKU was therefore assumed to have no effect on mortality.9
Health-state utility values were derived from a time trade-off (TTO) study performed on a sample of the general adult population in Sweden and the Netherlands10 as follows: blood Phe 1,200 μmol/L or greater was assumed to be equivalent to severe symptoms while on diet restriction and medical food (utility weight = 0.171); blood Phe between 600 μmol/L and 1,200 μmol/L was equivalent to moderate symptoms on diet restriction and medical food (utility weight = 0.514); blood Phe between 360 μmol/L and 600 μmol/L was equivalent to having no symptoms and a partly restricted diet with medical food (utility weight = 0.695); blood Phe between 120 μmol/L and 360 μmol/L was equivalent to having no symptoms and a partly restricted diet without medical food (utility weight = 0.739); and blood Phe less than 120 μmol/L was equivalent to having no symptoms and no dietary restrictions (utility weight = 0.807).
Adverse events (AEs) were derived from patients on the 40 mg/day dosage of pegvaliase in the PRISM-301 trial5 and included those with a grade 3 or higher severity and with an incidence of at least 3%. Only immune-system disorders (including anaphylaxis) were included and were applied as 1-time events in the first model cycle (disutility decrement = 0.02). AEs were not assumed to occur for patients using sapropterin or MNT.
Treatment costs included drug acquisition costs for pegvaliase at the submitted price,3 with patients undergoing titration according to the minimum length of time between dose escalations outlined in the product monograph,1 such that 1.4% of patients reached a maintenance dose of 5 mg daily, 11.1% at 10 mg daily, 19.4% at 20 mg daily, 50% at 40 mg daily, and 18.1% at 60 mg daily, based on the sponsor’s internal estimates (methodology not provided). After the first year, patients were assumed to use an average of ||| syringes daily, based on a cross-sectional analysis of daily syringe use of patients in the clinical trials whose pegvaliase dose had not increased for at least 12 months. Sapropterin acquisition costs were based on the Ontario Drug Benefit Formulary Exceptional Access Program list price,11 assuming a dose of 19 mg/kg/day, or 15 daily tablets. The cost of fully restricted MNT, including supplementation of 0.8 g/kg of medical formula and assuming that 40% of 2,250 kcal/day would come from low-protein foods, was estimated to be $11,175 per patient per year, based on prices in the SickKids Specialty Food Shop as a proxy for prices across Canada.12 Patients receiving MNT alone were assumed to require 100% of the cost of dietary supplementation, while those on sapropterin were assumed to need 75% of the cost. Patients on pegvaliase were assumed to need 53.2% of the cost of MNT in the first year, and 23.9% in subsequent years. Additionally, treatment cost was modified by compliance, with patients on MNT alone assumed to be 20% adherent to their diet; while patients using sapropterin were assumed to be 92% adherent to sapropterin, with no adherence-related reduction in MNT costs, and patients using pegvaliase were assumed to be 81% adherent to pegvaliase, with no adherence-related reduction in MNT costs.
Other costs within the model included those for blood tests and dietician, specialist, and primary care visits based on blood Phe level, as well as the cost of initial injection training and nurse supervision for the first pegvaliase dose, and costs for auto-injectable epinephrine units, antihistamines, antipyretics, and the treatment of immune-system AEs for patients using pegvaliase.
Summary of Sponsor’s Economic Evaluation Results
The sponsor submitted probabilistic analyses for pegvaliase plus MNT compared to sapropterin plus MNT and pegvaliase plus MNT compared to MNT alone. Deterministic and probabilistic results were similar. The sponsor’s analyses, which are presented in the following section, were based on 5,000 iterations. More detailed results are presented in Appendix 3.
Base-Case Results
The sponsor’s base-case results for both pegvaliase plus MNT compared to MNT alone and pegvaliase plus MNT compared to sapropterin plus MNT are listed in Table 3. When compared to MNT, pegvaliase plus MNT was associated with an additional 12.992 QALYs at an additional cost of $6,515,338, for an ICER of $501,486 per QALY gained, with 0% of iterations being cost-effective at a willingness to pay (WTP) threshold of $50,000 per QALY. When compared to sapropterin plus MNT, pegvaliase plus MNT was associated with 15.713 additional QALYs and savings of $738,722, making pegvaliase dominant over sapropterin (more effective and less costly), with 96% of iterations being cost-effective at a WTP threshold of $50,000 per QALY.
Table 3: Summary of the Sponsor’s Economic Evaluation Results
Drug | Total costs ($) | Incremental costs ($) | Total QALYs | Incremental QALYs | ICER vs. sapropterin ($ per QALY) |
|---|---|---|---|---|---|
Pegvaliase plus dietary restriction compared to dietary restriction alone | |||||
MNT alone | 141,700 | Reference | 14.322 | Reference | Reference |
Pegvaliase plus MNT | 6,657,039 | 6,515,338 | 27.314 | 12.992 | 501,486 |
Pegvaliase plus dietary restriction compared to sapropterin plus dietary restriction | |||||
Sapropterin plus MNT | 7,395,111 | Reference | 10.961 | Reference | Reference |
Pegvaliase plus MNT | 6,656,389 | −738,722 | 26.674 | 15.713 | Pegvaliase dominant |
ICER = incremental cost-effectiveness ratio; MNT = medical nutrition therapy; QALY = quality-adjusted life-year.
Source: Sponsor’s pharmacoeconomic submission.3
Sensitivity and Scenario Analysis Results
The sponsor conducted a series of sensitivity analyses varying individual utility weights, dietary usage, health care resource use, and proportion of patients starting in the 1,200 µmol/L Phe level state by 25% of their base-case mean value. None of these analyses had a substantial impact on the results. The sponsor also conducted 2 scenario analyses that used internally conducted Delphi panel-elicited utilities (not specified) in place of those derived from the TTO study. Both of these scenarios reported fewer incremental QALYs gained with the use of pegvaliase plus MNT compared with the sponsor’s base case, with pegvaliase plus MNT remaining dominant over sapropterin plus MNT, while the ICER for pegvaliase plus MNT compared to MNT alone ranged from $642,882 to $986,488 per QALY gained.
CADTH Appraisal of the Sponsor’s Economic Evaluation
CADTH identified several key limitations to the sponsor’s analysis that have notable implications on the economic analysis:
Comparative clinical efficacy is highly uncertain and lacks face validity: Direct evidence comparing pegvaliase plus MNT to sapropterin plus MNT or MNT alone was not available. Comparative clinical efficacy in the sponsor’s model (i.e., the transition probabilities between health states) was derived using a PSM approach from a retrospective cohort study. This study compared patients using pegvaliase plus MNT in the phase II 165-205 trial or phase III PRISM trials with a historical control of patients participating in the voluntary PKUDOS registry who received MNT alone, and sapropterin with MNT.4 As a result of numerous limitations in the study design (the PSM approach, internal and external validity, lack of adherence information, and statistical limitations), the ability to draw clear conclusions concerning the comparative effectiveness of pegvaliase plus MNT, sapropterin plus MNT, or MNT alone using this study is limited (refer to CADTH Clinical Report, Comparative Evidence with Sapropterin and MNT).
For the PSM approach, patients in the MNT-alone group had previously received and discontinued sapropterin, while those in the sapropterin plus MNT group were newly initiating sapropterin. Transition probabilities for pegvaliase differed depending on which comparator was being assessed due to the matching of individual patient-level data between the available trial patients and those in the PKUDOS registry. These differences in matched patients, the prevalence of missing Phe level data (particularly in the MNT-alone group), the absence of adherence data for PKUDOS registry patients, and potentially the difference in previous treatment experience between cohorts, lead to unintuitive results when comparing analyses; the sponsor’s model makes it appear that sapropterin plus MNT leads to the accrual of fewer QALYs than MNT alone, which is not consistent with previous reviews of sapropterin.13
In addition to uncertainty in comparative efficacy among treatment groups, the transition probabilities of the model lack reliability and face validity even within treatments (Table 9). For example, a pegvaliase patient with a blood Phe of 1,200 µmol/L or greater in year 4 had a 100% chance of remaining in the uncontrolled state for the remainder of their life when the comparator was sapropterin, yet a patient in the same health state also receiving pegvaliase had a 61% chance of improving in future years when the comparator was MNT alone. Similarly, a pegvaliase patient entering the model with a blood Phe level of 1,200 µmol/L or greater had a higher chance of normalizing their Phe level within a year than did a patient entering the model with a Phe level between 600 µmol/L and 1,200 µmol/L when the comparator is sapropterin, which the clinical experts consulted by CADTH indicated was not clinically plausible. Differences such as these have large impacts on the predicted QALYs associated with all included treatments, and therefore decrease the certainty in the model’s ability to predict either the absolute or relative efficacy of treatment with pegvaliase.
CADTH was unable to adjust for this limitation in reanalyses. As such, CADTH was unable to derive a base-case analysis and instead conducted an exploratory reanalysis. Consequently, all modelled cost-effectiveness results are highly uncertain.
The model structure does not adequately capture the health condition: Health states in the sponsor’s model are entirely driven by blood Phe level, such that in a given cycle, patients with low blood Phe experience a high quality of life, while those with high blood Phe experience a lower quality of life. According to the clinical experts consulted by CADTH, it is difficult for patients to estimate their relative blood Phe level based on their current or recent symptom levels; this suggests that individual blood Phe measurements are not predictive of longer-term trends in patients’ HRQoL. Additionally, adherence to therapy was not related to blood Phe level in the model; however, in clinical practice, patients who are adherent to MNT and/or to pegvaliase will attain control of their blood Phe levels, while those who are not adherent to therapy are less likely to attain control. The clinical experts stated that patients who are not adherent to MNT are more likely to have blood Phe levels above 600 µmol/L and would therefore be eligible for pegvaliase under the Health Canada indication1; however, patients who are not adherent to MNT may also be less likely to be adherent to pegvaliase and therefore less likely to benefit from it than patients who can be adherent and well controlled with MNT alone.
The model structure also does not consider discontinuation; once modelled patients are assigned to a treatment, they continue that treatment for the remainder of their lives, regardless of clinical response, AEs, adherence, or patient preference. This is not consistent with clinical trial data; not all sapropterin or pegvaliase patients remained on therapy for the duration of the study period within their respective trials. Additionally, patients whose blood Phe level does not improve during a 6-month trial of sapropterin due to intolerance, lack of adherence, or lack of response are unlikely to continue sapropterin. The costs associated with sapropterin in the model are therefore severely overestimated and it is unclear what effect this would have on relative efficacy as reported in Zori et al., given the limitations of the analysis method. Similarly, should pegvaliase be reimbursed, it is unlikely that patients who are unable to achieve satisfactory improvements in blood Phe levels due to intolerance or lack of adherence will remain on pegvaliase, reducing its cost but also the potential for further quality-of-life benefits.
CADTH was unable to adjust for this limitation in exploratory reanalyses. Uncertainty in the actual impact of individual blood Phe measures on quality of life, the absence of adherence having an effect on blood Phe and quality of life, and the absence of discontinuation, greatly increase the uncertainty in the modelled results.
The health-state utility values lack face validity: The sponsor based the utility values for each blood Phe–based health state on a pre-publication version of a TTO utility study conducted in the Swedish and Dutch general populations on the symptoms and dietary restrictions of PKU (as described earlier in the Model Inputs section).10 However, the sponsor assumed that patients in the below-120 µmol/L blood Phe level health state have a utility equivalent to having no symptoms, dietary restrictions, or medical food, while those in the 120 µmol/L to 360 µmol/L and 360 µmol/L to 600 µmol/L health states have partly restricted diets without and with medical food, respectively. Further, the sponsor assumed those with a Phe level above 600 µmol/L are on a fully restricted diet with medical food and assumed to have moderate (600 µmol/L to 1,200 µmol/L) or severe (≥ 1,200 µmol/L) symptoms. These assumptions do not accurately reflect the models’ assumptions around reduced adherence to dietary restrictions in the MNT group (20% adherence), nor the reduced requirement for MNT dietary restrictions in the pegvaliase group (23% of the full diet). If patients are assumed to only be 20% adherent to their dietary restrictions in the MNT group, then they are not experiencing the full quality-of-life decrease that would be expected for patients who are adherent to fully restrictive MNT, as estimated in the TTO study. Likewise, if patients on pegvaliase in the below-120 µmol/L health state still require 23% of a fully restrictive MNT, then they are not enjoying the full quality of life associated with a fully unrestricted diet as reported in the TTO study.
Additionally, the TTO methodology is associated with a number of limitations that may distort or exaggerate health states as estimated by the public, compared to HRQoL as measured in patients.14 The utility scores reported in Olofsson et al. (2021) for symptoms and dietary restrictions related to PKU appear implausible when compared to utility-score norms reported for a variety of chronic conditions by Statistics Canada.15 For example, a utility score of 0.171 for severe PKU symptoms requiring dietary restriction and medical food is substantially lower than utility score norms reported for mood disorders (0.643), effects of a stroke (0.581), and Alzheimer disease or other dementia (0.374), while a score of 0.807 for asymptomatic PKU with no dietary restriction is only somewhat lower that of the general Canadian population (0.863).15 Given this discrepancy, the sponsor’s base-case utility scores overestimate the quality-of-life gain associated with normalizing blood Phe levels. The clinical experts consulted by CADTH indicated that adults living with uncontrolled PKU would not have a health-state utility value worse than that of Alzheimer disease, and instead considered patients with a mood disorder to be more appropriate proxies for uncontrolled PKU, with health states representing increasing levels of blood Phe control associated with increasing utility.
In the exploratory reanalysis informed by clinical expert opinion, CADTH assumed patients with blood Phe above 1,200 µmol/L would have a utility value similar to patients with a mood disorder (0.643), while those with blood Phe below 120 µmol/L would have a utility value only slightly lower (−0.010, assumption) than that of the general population of Canada (0.863). The other health states representing levels of Phe control of less than 120 µmol/L and greater than or equal to 1,200 µmol/L were assumed to have utilities that increased linearly.
The requested reimbursement population is not clinically appropriate: In the reimbursement request, the sponsor has altered the population of interest from the indication’s phrasing of “inadequate blood Phe control despite dietary management” to “inadequate blood Phe control despite prior treatment with sapropterin.” However, sapropterin is not reimbursed in all jurisdictions, and treatment with pegvaliase may therefore also be inaccessible in those jurisdictions. Additionally, sapropterin is only effective in patients with milder forms of PKU associated with specific PAH mutations; according to the clinical experts consulted by CADTH, treatment with sapropterin is ineffective in patients with more severe forms of the PAH mutation and the possibility of response can be predicted based on genotype in some patients. As such, treatment with sapropterin in these patients would not be considered in clinical practice and the subgroups of adult patients with PKU who would be candidates for pegvaliase would be broader than those of sapropterin. Finally, by including a pegvaliase group that included but did not require patients with previous exposure to sapropterin,7 a sapropterin group whose previous exposure to sapropterin was unreported, and an MNT group who had previously discontinued sapropterin,4 the sponsor did not compare groups representing the reimbursement request population in either analysis.
CADTH was unable to adjust for this limitation in its exploratory reanalysis. Requiring patients to have failed a trial of sapropterin before being able to access pegvaliase may inappropriately increase sapropterin use for patients in whom treatment with sapropterin is likely to be futile. Given the Health Canada indication, CADTH considered the comparison of pegvaliase plus MNT to MNT alone to be the most relevant.
Pegvaliase maintenance dosing is underestimated: The sponsor estimated that patients from year 2 onward would use an average of ||| syringes daily based on the “real-world” number of syringes used daily by patients whose dose had not gone up for at least 1 year in a cross-sectional analysis of clinical trial patients.3 The sponsor then applied the 81% adherence rate from the trial on top of this “real-world” daily syringe use to derive its modelled input of 1.06 syringes daily. However, if the sponsor’s usage data represents actual syringe use by trial patients as presented, then adherence has already been accounted for in the data and applying an additional adherence rate artificially deflates the cost of pegvaliase. In contrast, if the dose distribution for PRISM patients as reported at a mean duration of treatment of 18.5 months is used to estimate a weighted-average mean daily syringe use of 1.74,16 and the adherence rate of 81% reported in the same publication is then applied, then the average daily syringe use would be 1.41 syringes per patient per day.
In the exploratory reanalysis, CADTH used an average daily pegvaliase syringe use in the maintenance phase of 1.74 and applied an 81% adherence rate.
Adherence to dietary therapy is overestimated for some comparators: The sponsor’s model assumes that patients on MNT alone would ideally receive a fully supplemented diet, accruing 100% of the estimated cost of formulas and low-Phe specialty foods needed for such supplementation. However, patients using MNT alone were assumed to only be 20% adherent on average, accruing only 20% of the cost of dietary supplementation. The clinical experts consulted by CADTH considered this a reasonable estimate. The sponsor’s model then assumes that patients receiving sapropterin require only 75% of a fully supplemented diet, while those receiving pegvaliase require 53% of a fully supplemented diet in the first year, and 24% per year thereafter, without further consideration for MNT adherence in these patients. The clinical experts consulted by CADTH did not consider it reasonable to assume that patients on sapropterin or pegvaliase would be fully adherent to their reduced requirement for MNT (dietary liberalization). Instead, the clinical expert estimated that patients using sapropterin or pegvaliase would not use more than 40% of a fully restricted diet if patients on MNT alone were using 20%.
CADTH assumed in its exploratory reanalysis that patients using sapropterin would only accrue 40% of the cost of the full dietary supplementation estimate, while those using pegvaliase would accrue 40% in the first year, and 24% each year thereafter.
Patient age at model entry is inappropriately modelled: The sponsor’s model assumes all patients will begin therapy at 16 years of age, the youngest age for which pegvaliase is indicated. However, patients with PKU in Canada have a wide range of ages. Even if pegvaliase becomes and remains the standard of care for adult patients with PKU, it will be several decades before the mean age at which patients start pegvaliase would approach 16 years. In contrast, the mean age of participants in the PRISM-2 study was 29 years (standard deviation = 8.74), with a range of 16 to 55 years.16 While this parameter has little impact on the ICER, due to the lack of treatment discontinuation in the model, it remains a key limitation that would have a profound impact on results were discontinuation modelled appropriately.
CADTH reanalyses incorporated a gamma distribution for patient age with a mean of 29 years, a standard deviation of 8.74, and a minimum and maximum of 16 and 55 years, respectively, consistent with patients in the PRISM-2 study. All analyses incorporating this change in age and time horizon also included a formula correction when calculating the probability of a patient being in any given health state after year 5 to ensure the model did not return DIV/0 errors.
Additionally, the following key assumptions made by the sponsor have been appraised by CADTH (Table 4).
Table 4: Key Assumptions of the Submitted Economic Evaluation (Not Noted as Limitations to the Submission)
Sponsor’s key assumption | CADTH comment |
|---|---|
Resource use in managed patients (i.e., blood and medical visits). | Acceptable. The sponsor’s model assumes that patients with uncontrolled PKU will have 4 blood tests annually, while those under better control will have monthly tests. Patients with uncontrolled PKU will have more psychiatric and nurse practitioner visits than those with better control, while those with uncontrolled or insufficiently controlled PKU will have more dietician and specialist visits than those who are either uncontrolled or controlled. These costs are not significant drivers within the model, nor do they appear unreasonable. |
Patients with PKU have the same risk of mortality and thus the same lifespan as the general population of Canada. | Acceptable. Patients with PKU are more likely to have attention deficits as well as mental health symptoms that may affect mortality. However, as the sponsor’s model assumes patients both accrue treatment costs as well as benefits for the duration of their lives, altering mortality has little impact on the resulting incremental cost-effectiveness ratio. |
Anaphylaxis and/or immune reactions only occur in first cycle. | Uncertain. Modelled patients are assumed to only experience immune-related adverse events related to pegvaliase in the first year of use. However, the pegvaliase product monograph includes warnings and recommendations that epinephrine auto-injectors should be prescribed and carried by patients for the full length of treatment with pegvaliase. The costs related to auto-injectors do not have a large impact on the model; however, the continuing potential for immune reactions that could lead to adverse health outcomes or discontinuation may affect cost-effectiveness. |
PKU = phenylketonuria.
CADTH Reanalyses of the Economic Evaluation
Base-Case Results
CADTH could not derive a base-case reanalysis due to limitations in the comparative clinical evidence, the structure of the model, and uncertainty in the health-utility values. Instead, CADTH conducted a series of reanalyses exploring areas of uncertainty in the sponsor’s model, where possible, and combined them into a merged exploratory reanalysis.
Table 5: CADTH Revisions to the Submitted Economic Evaluation
Stepped analysis | Sponsor’s value or assumption | CADTH value or assumption |
|---|---|---|
Correctionsa to sponsor’s base case | ||
None | — | — |
Changes to derive the CADTH base case | ||
1. Utilities — mood disorder as proxy | < 120 µmol/L: 0.807 120 µmol/L to 360 µmol/L: 0.739 360 µmol/L to 600 µmol/L: 0.695 600 µmol/L to 1,200 µmol/L: 0.514 > 1,200 µmol/L: 0.171 | < 120 µmol/L: 0.853 120 µmol/L to 360 µmol/L: 0.801 360 µmol/L to 600 µmol/L: 0.748 600 µmol/L to 1,200 µmol/L: 0.696 > 1,200 µmol/L: 0.643 |
2. Pegvaliase maintenance therapy | ||| syringes per day × 81% adherence = ||| syringes per day | 1.76 syringes per day × 81% adherence = 1.4 syringes per day |
3. Medical nutrition therapy usage | Diet alone: 20% Sapropterin: 75% Pegvaliase: 53% year 1, 24% thereafter | Diet alone: 20% Sapropterin: 40% Pegvaliase: 40% year 1, 24% thereafter |
4. Patient age | Mean: 16 years, not varied probabilistically | Mean: 28 years; SD = 8.74 years; gamma distribution: minimum 16 years, maximum 55 years |
CADTH combined exploratory analysis | Reanalyses 1 + 2 + 3 + 4 | |
SD = standard deviation.
aCorrections are minor errors (e.g., transcription errors between report and model, misapplication of distributions, or standard errors in probabilistic analyses) that are not identified as limitations.
Due to limitations in the clinical evidence, CADTH was unable to derive a base-case reanalysis. In the combined exploratory analysis, when compared to MNT alone, the use of pegvaliase plus MNT was associated with $7,665,703 in incremental costs and 3.98 incremental QALYs, for an ICER of $1,923,797 per QALY; 0% of iterations would be considered cost-effective at a WTP threshold of $50,000 per QALY. When compared to sapropterin plus MNT, pegvaliase plus MNT was associated with $1,447,045 in incremental costs and 3.88 incremental QALYs, for an ICER of $373,320 per QALY, with 12% of iterations being cost-effective at a WTP threshold of $50,000 per QALY. Due to the factors that could not be addressed, including the lack of robust comparative clinical data, the flawed model structure, absence of discontinuation, and the clinical appropriateness of the reimbursement request, estimates of cost-effectiveness for pegvaliase relative to its comparators are highly uncertain. Although price-reduction scenarios were conducted (refer to Appendix 4, Table 14), the estimated price reductions likely underestimate the true reduction needed to ensure cost-effectiveness.
Table 6: Summary of the Stepped Analysis of the CADTH Reanalysis Results
Stepped analysis | Drug | Total costs ($) | Total QALYs | ICER ($ per QALY) |
|---|---|---|---|---|
Pegvaliase plus MNT vs. MNT alone | ||||
Sponsor’s base case, probabilistic | MNT alone | 141,700 | 14.32 | Reference |
Pegvaliase plus MNT | 6,657,039 | 27.31 | 501,486 | |
Sponsor’s base case, deterministic | MNT alone | 141,727 | 14.31 | Reference |
Pegvaliase plus MNT | 6,655,574 | 27.30 | 501,112 | |
CADTH reanalysis 1: mood disorder as utility proxy | MNT alone | 141,727 | 18.18 | Reference |
Pegvaliase plus MNT | 6,655,574 | 28.36 | 640,059 | |
CADTH reanalysis 2: maintenance therapy | MNT alone | 141,727 | 14.31 | Reference |
Pegvaliase plus MNT | 8,781,852 | 27.30 | 664,688 | |
CADTH reanalysis 3: MNT usage | MNT alone | 141,727 | 14.31 | Reference |
Pegvaliase plus MNT | 6,654,595 | 27.30 | 501,037 | |
CADTH reanalysis 4: patient age | MNT alone | 125,735 | 12.71 | Reference |
Pegvaliase plus MNT | 5,910,374 | 24.21 | 503,087 | |
CADTH exploratory analysis (1 to 4), probabilistic | MNT alone | 122,827 | 24.08 | Reference |
Pegvaliase plus MNT | 7,606,267 | 27.97 | 1,925,916 | |
CADTH exploratory analysis (1 to 4), deterministic | MNT alone | 125,735 | 24.63 | Reference |
Pegvaliase plus MNT | 7,791,438 | 28.92 | 1,923,797 | |
Pegvaliase plus MNT vs. sapropterin plus MNT | ||||
Sponsor’s base case, probabilistic | Sapropterin plus MNT | 7,395,111 | 10.96 | Reference |
Pegvaliase plus MNT | 6,656,389 | 26.67 | Dominant | |
Sponsor’s base case, deterministic | Sapropterin plus MNT | 7,308,290 | 10.95 | Reference |
Pegvaliase plus MNT | 6,654,918 | 26.66 | Dominant | |
CADTH reanalysis 1: mood disorder as utility proxy | Sapropterin plus MNT | 7,308,290 | 27.28 | Reference |
Pegvaliase plus MNT | 6,654,918 | 31.74 | Dominant | |
CADTH Reanalysis 2: syringe use | Sapropterin plus MNT | 7,308,290 | 10.95 | Reference |
Pegvaliase plus MNT | 8,781,196 | 26.66 | 93,716 | |
CADTH Reanalysis 3: MNT use | Sapropterin plus MNT | 7,145,899 | 10.95 | Reference |
Pegvaliase plus MNT | 6,653,939 | 26.66 | Dominant | |
CADTH Reanalysis 4: patient age | Sapropterin plus MNT | 6,488,019 | 10.12 | Reference |
Pegvaliase plus MNT | 5,909,817 | 23.62 | Dominant | |
CADTH exploratory analysis (1 to 4), probabilistic | Sapropterin plus MNT | 6,264,932 | 23.73 | Reference |
Pegvaliase plus MNT | 7,605,740 | 27.49 | 356,868 | |
CADTH exploratory analysis (1 to 4), deterministic | Sapropterin plus MNT | 6,343,836 | 24.26 | Reference |
Pegvaliase plus MNT | 7,790,882 | 28.14 | 373,320 | |
ICER = incremental cost-effectiveness ratio; MNT = medical nutrition therapy; QALY = quality-adjusted life-year.
Note: Results of all steps are presented deterministically. Reanalyses incorporating a change in patient age also included a correction to the formula for calculating proportion of patients in each health state per year to avoid DIV/0 errors in years after the time horizon was exceeded.
Issues for Consideration
The price of sapropterin is likely lower than estimated in the model: The reimbursement review of sapropterin by CADTH indicated that a substantial price reduction from $33 per 100 mg tablet would be required for sapropterin plus MNT to be considered cost-effective compared to MNT alone.17 The pan-Canadian Pricing Alliance negotiation process for Kuvan (sapropterin) successfully concluded with a letter of intent.18 It is therefore likely that the actual prices paid by public plans for sapropterin are lower than the publicly available list price of $33 per tablet. As such, all ICERs estimating the cost-effectiveness of pegvaliase compared to sapropterin are underestimated.
Overall Conclusions
Data from the PRISM-2 trial suggest that continued self-administration of pegvaliase injections led to statistically significant and potentially clinically meaningful decreases in blood Phe levels after 8 weeks compared with withdrawal of pegvaliase and injection of placebo. These changes were aligned with 1 of the outcomes identified as important by patients with PKU. The observational PSM study by Zori et al. comparing pegvaliase to sapropterin plus MNT and MNT alone had numerous limitations in study design involving comparison with a historical control cohort, potential bias due to the nonrandomized study design and PSM approach, and statistical limitations (exploratory analysis only). Furthermore, derived transition probabilities appeared unreliable and lacked face validity. Ultimately, no clear conclusions could be drawn concerning the comparative effectiveness of pegvaliase, sapropterin plus MNT, and MNT alone.
Due to both the absence of robust comparative evidence and the inappropriateness of the model structure, CADTH was unable to derive a base-case analysis. Instead, an exploratory reanalysis was conducted that adjusted health-state utility values to be more in line with those measured in other chronic conditions in Canada, increased pegvaliase syringe use in maintenance years, lowered MNT adherence in patients using sapropterin and pegvaliase, and adjusted patient starting age to better reflect the diverse ages of patients with PKU in Canada. Due to the Health Canada indication and to differing mechanisms of action leading to a broader patient population being candidates for pegvaliase than sapropterin, CADTH considered the comparison of pegvaliase to MNT alone to be the most relevant.
In this exploratory analysis, the ICER associated with pegvaliase plus MNT was $1,923,797 per QALY when compared to MNT alone. A price reduction of a least a 99% for pegvaliase would be required to achieve an ICER below $50,000 per QALY compared to MHT. However, estimates of cost-effectiveness for pegvaliase relative to comparators are highly uncertain. As such, the price reductions likely underestimate the true reduction needed to ensure cost-effectiveness.
CADTH was unable to adjust for major limitations, including the lack of direct comparative clinical data, uncertain and implausible transition probabilities informing comparative efficacy, the model’s structural reliance on blood Phe level to predict HRQoL, the lack of adherence as a predictor of blood Phe level, the absence of modelling discontinuation rates for ineffective treatments, and the potential inappropriateness of the reimbursement request.
References
1.PALYNZIQ® (pegvaliase injection): solution 2.5 mg/0.5 ml (5 mg/ml), 10 mg/0.5 ml (20 mg/ml), 20 mg/1.0 ml (20 mg/ml) subcutaneous injection [product monograph]. Toronto (ON): BioMarin Pharmaceutical (Canada) Inc.; 2022 Mar 30.
2.Drug Reimbursement Review sponsor submission: Palynziq (pegvaliase injection), 2.5 mg/0.5 ml (5 mg/ml), 10 mg/0.5 ml (20 mg/ml), 20 mg/ml, solution for injection in a prefilled syringe [internal sponsor's package]. Woodridge (ON): Biomarin Pharmaceutical (Canada) Inc.; 2021 Dec 22.
3.Pharmacoeconomic evaluation [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Palynziq (pegvaliase injection), 2.5 mg/0.5 ml (5 mg/ml), 10 mg/0.5 ml (20 mg/ml), 20 mg/ml, solution for injection in a prefilled syringe. Woodridge (ON): Biomarin Pharmaceutical (Canada) Inc.; 2021 Dec 22.
4.Zori R, Ahring K, Burton B, et al. Long-term comparative effectiveness of pegvaliase versus standard of care comparators in adults with phenylketonuria. Mol Genet Metab. 2019;128(1-2):92-101. PubMed
5.Clinical Study Report: 165-301. A phase 3, open-label, randomized, multi-center study to assess the safety and tolerability of an induction, titration, and maintenance dose regimen of BMN 165 self-administered by adults with phenylketonuria not previously treated with BMN 165 [internal sponsor's report]. Novato (CA): Biomarin Pharmaceutical Inc.; 2017 Mar 17.
6.Clinical Study Report: 165-303. A phase 3 substudy to evaluate executive function in adults with phenylketonuria who are participating in the phase 3 study, 165-302 [internal sponsor's report]. Novato (CA): BioMarin Pharmaceutical Inc.; 2018 Jun 19.
7.Clinical Study Report: 165-302. A four-part, phase 3, randomized, double-blind, placebo-controlled, four-arm, discontinuation study to evaluate the efficacy and safety of subcutaneous injections of BMN 165 self administered by adults with phenylketonuria [internal sponsor's report]. Novato (CA): BioMarin Pharmaceutical Inc.; 2019 Oct 9.
8.BioMarin Pharmaceutical. NCT00778206: PKUDOS: Phenylketonuria (PKU) Demographic, Outcomes, and Safety Registry (PKUDOS). ClinicalTrials.gov. Bethesda (MD): U.S. National Library of Medicine; 2022: https://clinicaltrials.gov/ct2/show/NCT00778206. Accessed 2022 Feb 16.
9.Table: 13-10-0114-01. Life expectancy and other elements of the life table, Canada, all provinces except Prince Edward Island. Ottawa (ON): Statistics Canada; 2022: https://www150.statcan.gc.ca/t1/tbl1/en/tv.action?pid=1310011401. Accessed 2022 Feb 18.
10.Olofsson S, Gralen K, Hoxer C, Okhuoya P, Persson U. The impact on quality of life of diet restrictions and disease symptoms associated with phenylketonuria: a time trade-off and discrete choice experiment study. Eur J Health Econ. 2021. PubMed
11.Exceptional Access Program (EAP). Toronto (ON): Ontario Ministry of Health; Ontario Ministry of Long-Term Care; 2021: https://www.health.gov.on.ca/en/pro/programs/drugs/odbf/odbf_except_access.aspx. Accessed 2022 Feb 18.
12.The Hospital for Sick Children (SickKids). Specialty Food Shop. 2022; https://www.specialtyfoodshop.ca/. Accessed 2022 Feb 17.
13.Common Drug Review pharmacoeconomic review report: Sapropterin dihydrochloride (Kuvan) in conjunction with a phenylalanine (Phe)-restricted diet to reduce blood Phe levels in patients with hyperphenylalaninemia (HPA) due to tetrahydrobiopterin-(BH4)-responsive phenylketonuria (PKU). Ottawa (ON): CADTH; 2017 Sep: https://www.cadth.ca/sites/default/files/cdr/pharmacoeconomic/SR0472_Kuvan_PE_Report_e.pdf. Accessed 2022 Mar 30.
14.Lugner AK, Krabbe PFM. An overview of the time trade-off method: concept, foundation, and the evaluation of distorting factors in putting a value on health. Expert Rev Pharmacoecon Outcomes Res. 2020;20(4):331-342. PubMed
15.Guertin JR, Humphries B, Feeny D, Tarride JE. Health Utilities Index Mark 3 scores for major chronic conditions: population norms for Canada based on the 2013 and 2014 Canadian Community Health Survey. Ottawa (ON): Statistics Canada; 2018: https://www150.statcan.gc.ca/n1/pub/82-003-x/2018011/article/00001-eng.htm. Accessed 2022 Mar 14.
16.Thomas J, Levy H, Amato S, et al. Pegvaliase for the treatment of phenylketonuria: Results of a long-term phase 3 clinical trial program (PRISM). Mol Genet Metab. 2018;124(1):27-38. PubMed
17.CADTH Canadian Drug Expert Committee (CDEC) final recommendation: Kuvan (BioMarin Pharmaceuticals Canada Inc.). Ottawa (ON): CADTH; 2016 Oct 26: https://www.cadth.ca/sites/default/files/cdr/complete/SR0472_complete_Kuvan-Oct-28-16.pdf. Accessed 2021 Mar 29.
18.pan-Canadian Pharmaceutical Alliance. Kuvan (sapropterin dihydrochloride). 2020; https://www.pcpacanada.ca/negotiation/20957. Accessed 2022 Mar 28.
19.Saskatchewan Drug Plan: search formulary. 2022; https://formulary.drugplan.ehealthsask.ca/SearchFormulary. Accessed 2022 Oct 20.
20.Canadian PKU and Allied Disorders Inc. Canada PKU coverage report card – April 2016. 2016; https://canpku.org/resources/Documents/Advocacy/2016-Canada-PKU-Coverage-Report-Card.pdf. Accessed 2022 Feb 18.
21.Table: 17-10-0005-01. Population estimates on July 1st, by age and sex. Ottawa (ON): Statistics Canada; 2022: https://www150.statcan.gc.ca/t1/tbl1/en/tv.action?pid=1710000501. Accessed 2022 Feb 18.
22.Indigenous Services Canada. Non-Insured Health Benefits program: First Nations and Inuit Health Branch: Annual report 2019 to 2020. Ottawa (ON): Government of Canada; 2021: https://www.sac-isc.gc.ca/eng/1624462613080/1624462663098. Accessed 2022 Feb 18.
23.Levy HL, Milanowski A, Chakrapani A, et al. Efficacy of sapropterin dihydrochloride (tetrahydrobiopterin, 6R-BH4) for reduction of phenylalanine concentration in patients with phenylketonuria: a phase III randomised placebo-controlled study. Lancet. 2007;370(9586):504-510. PubMed
24.Budget Impact Analysis [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Palynziq (pegvaliase injection), 2.5 mg/0.5 ml (5 mg/ml), 10 mg/0.5 ml (20 mg/ml), 20 mg/ml, solution for injection in a prefilled syringe. Woodridge (ON): Biomarin Pharmaceutical (Canada) Inc.; 2021 Dec 22.
25.Sutherland G, Dinh T. Understanding the gap: a pan-Canadian analysis of prescription drug insurance coverage. Ottawa (ON): The Conference Board of Canada; 2017: https://www.conferenceboard.ca/temp/92eab14b-ea12-4d9b-9ffd-e18cb7cdda9e/9326_Understanding-the-Gap__RPT.pdf. Accessed 2022 Mar 24.
Appendix 1: Cost Comparison Table
Note that this appendix has not been copy-edited.
The comparators presented in the following table have been deemed to be appropriate based on feedback from clinical experts. Comparators may be recommended (appropriate) practice or actual practice. Existing product listing agreements are not reflected in the table and as such, the table may not represent the actual costs to public drug plans.
Table 7: CADTH Cost Comparison Table for PKU
Treatment | Strength/ concentration | Form | Price | Recommended dosage | Daily cost | Annual cost |
|---|---|---|---|---|---|---|
Pegvaliase (Palynziq) | 2.5 mg/0.5 mL 10 mg/0.5 mL 20 mg/1 mL | Pre-filled syringe | 405.0000a | 2.5 mg once per week for 4 weeks, then titrated to the daily maintenance dose required to achieve blood phenylalanine level ≤ 600 µmol/L; maximum of 60 mg dailyb | Titration phase: 57.86 to 1,215.00 Maintenance: 405.00 to 1,215.00 | Titration year: 130,410 to 261,630c Maintenance years: 147,825 to 443,475 |
Sapropterin (Kuvan) | 100 mg 100 mg 500 mg | Tablet Sachet Sachet | 33.0000de 33.0000e 165.0000e | Initial: 10 mg/kg once daily. Once responsiveness to has been established, dose may be adjusted within a range of 5 to 20 mg/kg daily. | 132.00 to 495.00f | 48,180 to 180,675f |
PKU = phenylketonuria.
Note: Prices do not include markups or dispensing fees.
aSponsor’s submitted price.3
bAfter a 4-week induction of 2.5 mg once weekly, titration should continue as follows, with dose increasing once weekly: 2.5 mg twice weekly, then 10 mg once weekly, then 10 mg twice weekly, then 10 mg 4 times weekly, then 10 mg daily. Maintenance therapy should begin at 20 mg daily for 12 to 24 weeks and can then be increased to 40 mg (two 20 mg injections) daily for 16 or more weeks, with a maximum dose of 60 mg (three 20 mg injections) daily.1
cLower figure assumes titration up to 20 mg daily, higher figure assumes titration up to 60 mg daily with 12 weeks between the 20 mg and 40 mg daily doses, and 16 weeks between the 40 mg and 60 mg daily doses, the fastest titration recommended in the product monograph. Assumes 365 days in a year.
dOntario Drug Benefit Exceptional Access Program list price (accessed January 2022).11
eSaskatchewan Formulary list price.19
fAssumes a patient who weighs 75 kg.
Appendix 2: Submission Quality
Note that this appendix has not been copy-edited.
Description | Yes/no | Comments |
|---|---|---|
Population is relevant, with no critical intervention missing, and no relevant outcome missing | No | The reimbursement request of requiring a trial of sapropterin is not clinically appropriate, as the likelihood of sapropterin response can be predicted by PAH mutation type in some patients. |
Model has been adequately programmed and has sufficient face validity | No | There are large differences in the health-state utilities, and the plausibility and lack of reliability in the transition probabilities do not meet face validity. |
Model structure is adequate for decision problem | No | The lack of discontinuation in the model does not allow for the assessment of the decision problem in a clinically or economically relevant way. |
Data incorporation into the model has been done adequately (e.g., parameters for probabilistic analysis) | Yes | — |
Parameter and structural uncertainty were adequately assessed; analyses were adequate to inform the decision problem | No | Refer to comments above. |
The submission was well organized and complete; the information was easy to locate (clear and transparent reporting; technical documentation available in enough details) | No | Key background information, including data from the sponsor’s patient support program, was not submitted. Adherence was not discussed in the submitted report but is a substantial driver of the model. |
Appendix 3: Additional Information on the Submitted Economic Evaluation
Note that this appendix has not been copy-edited.
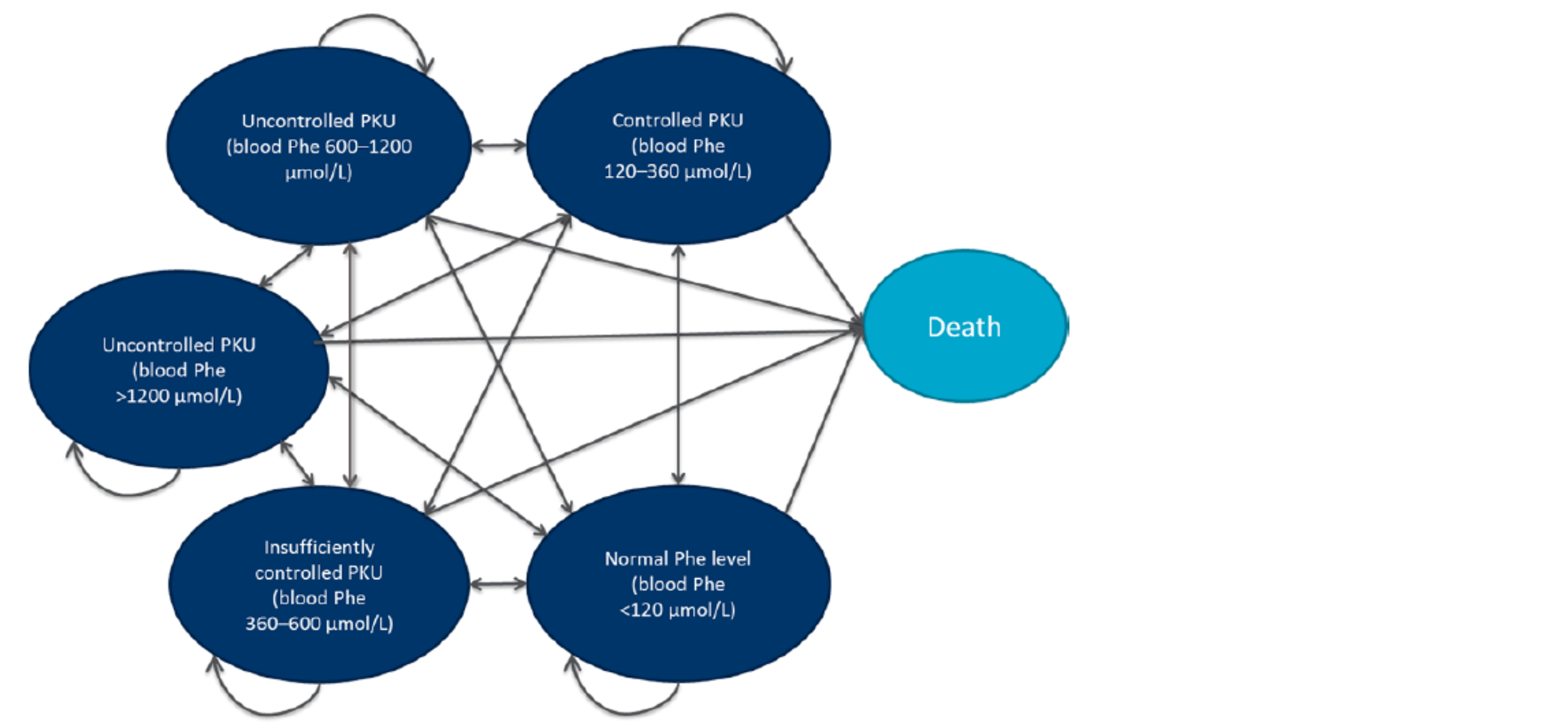
Phe = phenylalanine; PKU = phenylketonuria.
Source: Sponsor’s submitted Pharmacoeconomic Report, Figure 11.3
Table 9: Transition Probabilities Between Health States in Sponsor’s Economic Model
Blood Phe | Pegvaliase plus diet | Diet alone | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
µmol/L | < 120 | 120 to 360 | 360 to 600 | 600 to 1200 | > 1,200 | < 120 | 120 to 360 | 360 to 600 | 600 to 1200 | > 1,200 |
Year 1 | ||||||||||
600 to 1200 | ||||| | ||||| | ||||| | ||||| | ||||| | ||||| | ||||| | ||||| | ||||| | ||||| |
> 1,200 | ||||| | ||||| | ||||| | ||||| | ||||| | ||||| | ||||| | ||||| | ||||| | ||||| |
Year 2 | ||||||||||
< 120 | ||||| | ||||| | ||||| | ||||| | ||||| | ||||| | ||||| | ||||| | ||||| | ||||| |
120 to 360 | ||||| | ||||| | ||||| | ||||| | ||||| | ||||| | ||||| | ||||| | ||||| | ||||| |
360 to 600 | ||||| | ||||| | ||||| | ||||| | ||||| | ||||| | ||||| | ||||| | ||||| | ||||| |
600 to 1,200 | ||||| | ||||| | ||||| | ||||| | ||||| | ||||| | ||||| | ||||| | ||||| | ||||| |
> 1,200 | ||||| | ||||| | ||||| | ||||| | ||||| | ||||| | ||||| | ||||| | ||||| | ||||| |
Year 3 | ||||||||||
< 120 | ||||| | ||||| | ||||| | ||||| | ||||| | ||||| | ||||| | ||||| | ||||| | ||||| |
120 to 360 | ||||| | ||||| | ||||| | ||||| | ||||| | ||||| | ||||| | ||||| | ||||| | ||||| |
360 to 600 | ||||| | ||||| | ||||| | ||||| | ||||| | ||||| | ||||| | ||||| | ||||| | ||||| |
600 to 1,200 | ||||| | ||||| | ||||| | ||||| | ||||| | ||||| | ||||| | ||||| | ||||| | ||||| |
> 1,200 | ||||| | ||||| | ||||| | ||||| | ||||| | ||||| | ||||| | ||||| | ||||| | ||||| |
Year 4+ | ||||||||||
< 120 | ||||| | ||||| | ||||| | ||||| | ||||| | ||||| | ||||| | ||||| | ||||| | ||||| |
120 to 360 | ||||| | ||||| | ||||| | ||||| | ||||| | ||||| | ||||| | ||||| | ||||| | ||||| |
360 to 600 | ||||| | ||||| | ||||| | ||||| | ||||| | ||||| | ||||| | ||||| | ||||| | ||||| |
600 to 1,200 | ||||| | ||||| | ||||| | ||||| | ||||| | ||||| | ||||| | ||||| | ||||| | ||||| |
> 1,200 | ||||| | ||||| | ||||| | ||||| | ||||| | ||||| | ||||| | ||||| | ||||| | ||||| |
µmol/L | Pegvaliase plus diet | Sapropterin plus diet | ||||||||
< 120 | 120 to 360 | 360 to 600 | 600 to 1200 | > 1,200 | < 120 | 120 to 360 | 360 to 600 | 600 to 1200 | > 1,200 | |
Year 1 | ||||||||||
600 to 1200 | ||||| | ||||| | ||||| | ||||| | ||||| | ||||| | ||||| | ||||| | ||||| | ||||| |
> 1,200 | ||||| | ||||| | ||||| | ||||| | ||||| | ||||| | ||||| | ||||| | ||||| | ||||| |
Year 2 | ||||||||||
< 120 | ||||| | ||||| | ||||| | ||||| | ||||| | ||||| | ||||| | ||||| | ||||| | ||||| |
120 to 360 | ||||| | ||||| | ||||| | ||||| | ||||| | ||||| | ||||| | ||||| | ||||| | ||||| |
360 to 600 | ||||| | ||||| | ||||| | ||||| | ||||| | ||||| | ||||| | ||||| | ||||| | ||||| |
600 to 1,200 | ||||| | ||||| | ||||| | ||||| | ||||| | ||||| | ||||| | ||||| | ||||| | ||||| |
> 1,200 | ||||| | ||||| | ||||| | ||||| | ||||| | ||||| | ||||| | ||||| | ||||| | ||||| |
Year 3 | ||||||||||
< 120 | ||||| | ||||| | ||||| | ||||| | ||||| | ||||| | ||||| | ||||| | ||||| | ||||| |
120 to 360 | ||||| | ||||| | ||||| | ||||| | ||||| | ||||| | ||||| | ||||| | ||||| | ||||| |
360 to 600 | ||||| | ||||| | ||||| | ||||| | ||||| | ||||| | ||||| | ||||| | ||||| | ||||| |
600 to 1,200 | ||||| | ||||| | ||||| | ||||| | ||||| | ||||| | ||||| | ||||| | ||||| | ||||| |
> 1,200 | ||||| | ||||| | ||||| | ||||| | ||||| | ||||| | ||||| | ||||| | ||||| | ||||| |
Year 4+ | ||||||||||
< 120 | ||||| | ||||| | ||||| | ||||| | ||||| | ||||| | ||||| | ||||| | ||||| | ||||| |
120 to 360 | ||||| | ||||| | ||||| | ||||| | ||||| | ||||| | ||||| | ||||| | ||||| | ||||| |
360 to 600 | ||||| | ||||| | ||||| | ||||| | ||||| | ||||| | ||||| | ||||| | ||||| | ||||| |
600 to 1,200 | ||||| | ||||| | ||||| | ||||| | ||||| | ||||| | ||||| | ||||| | ||||| | ||||| |
> 1,200 | ||||| | ||||| | ||||| | ||||| | ||||| | ||||| | ||||| | ||||| | ||||| | ||||| |
Phe = phenylalanine.
Source: Sponsor’s pharmacoeconomic submission,3 based on Zori et al.4 Starting health states are presented in rows, while states being transitioned into are presented in columns.
Detailed Results of the Sponsor’s Base Case
Table 10: Disaggregated Summary of Sponsor’s Probabilistic Economic Evaluation Results — Pegvaliase Plus Phe-Restricted Diet Versus Phe-Restricted Diet Alone
Parameter | Pegvaliase | Phe-restricted diet | Incremental |
|---|---|---|---|
Discounted LYs | |||
Total | 41.337 | 41.337 | 0.000 |
Phe ≥ 1,200 µmol/L | 4.597 | 22.179 | −17.582 |
Phe 600 to 1,200 µmol/L | 7.210 | 15.476 | −8.266 |
Phe 360 to 600 µmol/L | 4.936 | 3.606 | 1.330 |
Phe 120 to 360 µmol/L | 6.847 | 0.076 | 6.771 |
Phe < 120 µmol/L | 17.747 | 0.000 | 17.747 |
Discounted QALYs | |||
Total | 27.314 | 14.322 | 12.992 |
Phe ≥ 1,200 µmol/L | 0.787 | 3.797 | −3.010 |
Phe 600 to 1,200 µmol/L | 3.709 | 7.960 | −4.252 |
Phe 360 to 600 µmol/L | 3.433 | 2.508 | 0.925 |
Phe 120 to 360 µmol/L | 5.062 | 0.056 | 5.005 |
Phe < 120 µmol/L | 14.324 | 0.000 | 14.324 |
Discounted costs ($) | |||
Total costs | 6,657,039 | 141,700 | 6,515,338 |
Treatment costs | 6,507,526 | 0 | 6,508,526 |
Phe-restricted diet costs | 111,887 | 92,763 | 19,124 |
Premedication costs | 11,406 | 0 | 11,406 |
Resource use costs | 26,147 | 48,938 | 22,791 |
Adverse event costs | 74 | 0 | 74 |
ICER ($/QALY) | 501,486 | ||
ICER = incremental cost-effectiveness ratio; LY = life-year; Phe = phenylalanine; QALY = quality-adjusted life-year.
Table 11: Disaggregated Summary of Sponsor’s Probabilistic Economic Evaluation Results — Pegvaliase Plus Phe-Restricted Diet Versus Sapropterin Plus Phe-Restricted Diet
Parameter | Pegvaliase plus Phe-restricted diet | Sapropterin plus Phe-restricted diet | Incremental |
|---|---|---|---|
Discounted LYs | |||
Total | 41.337 | 41.337 | 0.000 |
Phe ≥ 1,200 µmol/L | 5.464 | 31.774 | –26.310 |
Phe 600 to 1,200 µmol/L | 5.174 | 6.410 | –1.236 |
Phe 360 to 600 µmol/L | 12.857 | 2.449 | 10.408 |
Phe 120 to 360 µmol/L | 3.914 | 0.704 | 3.210 |
Phe < 120 µmol/L | 13.928 | 0.000 | 13.928 |
Discounted QALYs | |||
Total | 26.674 | 10.961 | 15.713 |
Phe ≥ 1,200 µmol/L | 0.935 | 5.440 | –4.505 |
Phe 600 to 1,200 µmol/L | 2.661 | 3.297 | –0.636 |
Phe 360 to 600 µmol/L | 8.942 | 1.703 | 7.239 |
Phe 120 to 360 µmol/L | 2.893 | 0.520 | 2.373 |
Phe < 120 µmol/L | 11.242 | 0.000 | 11.242 |
Discounted costs ($) | |||
Total costs | 6,656,389 | 7,395,111 | 738,722 |
Treatment costs | 6,507,526 | 6,992,953 | 485,427 |
Phe-restricted diet costs | 111,887 | 348,110 | 236,223 |
Premedication costs | 9,284 | 0 | 9,284 |
Resource use costs | 27,619 | 54,048 | 26,429 |
Adverse event costs | 74 | 0 | 74 |
ICER ($/QALY) | Pegvaliase plus Phe-diet is dominant (–47,013) | ||
ICER = incremental cost-effectiveness ratio; LY = life-year; Phe = phenylalanine; QALY = quality-adjusted life-year.
Appendix 4: Additional Details on the CADTH Reanalyses and Sensitivity Analyses of the Economic Evaluation
Note that this appendix has not been copy-edited.
Detailed Results of CADTH Base Case
Table 12: Disaggregated Summary of CADTH’s Probabilistic Combined Reanalysis Results — Pegvaliase Plus Phe-Restricted Diet Versus Phe-Restricted Diet Alone
Parameter | Pegvaliase | Phe-restricted diet | Incremental |
|---|---|---|---|
Discounted LYs | |||
Total | 35.805 | 35.805 | 0.000 |
Phe ≥ 1,200 µmol/L | 3.961 | 19.118 | −15.157 |
Phe 600 to 1,200 µmol/L | 6.295 | 13.504 | −7.209 |
Phe 360 to 600 µmol/L | 4.247 | 3.108 | 1.139 |
Phe 120 to 360 µmol/L | 5.930 | 0.076 | 5.853 |
Phe < 120 µmol/L | 15.373 | 0.000 | 15.373 |
Discounted QALYs | |||
Total | 27.971 | 24.083 | 3.888 |
Phe ≥ 1,200 µmol/L | 2.549 | 12.304 | −9.755 |
Phe 600 to 1,200 µmol/L | 4.381 | 9.397 | −5.016 |
Phe 360 to 600 µmol/L | 3.172 | 2.321 | 0.851 |
Phe 120 to 360 µmol/L | 4.750 | 0.061 | 4.689 |
Phe < 120 µmol/L | 13.120 | 0.000 | 13.120 |
Discounted costs ($) | |||
Total costs | 6,657,039 | 141,700 | 6,515,338 |
Treatment costs | 7,477,149 | 0 | 7,477,149 |
Phe-restricted diet costs | 96,480 | 80,461 | 16,019 |
Premedication costs | 9,890 | 0 | 9,890 |
Resource use costs | 22,675 | 42,366 | −19,691 |
Adverse event costs | 74 | 0 | 74 |
ICER ($/QALY) | 1,924,916 | ||
ICER = incremental cost-effectiveness ratio; LY = life-year; Phe = phenylalanine; QALY = quality-adjusted life-year.
Table 13: Disaggregated Summary of CADTH’s Probabilistic Combined Reanalysis Results — Pegvaliase Plus Phe-Restricted Diet Versus Sapropterin Plus Phe-Restricted Diet
Parameter | Pegvaliase plus Phe-restricted diet | Sapropterin plus Phe-restricted diet | Incremental |
|---|---|---|---|
Discounted LYs | |||
Total | 35.805 | 35.805 | 0.000 |
Phe ≥ 1,200 µmol/L | 4.734 | 26.354 | −21.620 |
Phe 600 to 1,200 µmol/L | 4.609 | 6.334 | −1.725 |
Phe 360 to 600 µmol/L | 10.966 | 2.421 | 8.546 |
Phe 120 to 360 µmol/L | 3.392 | 0.696 | 2.696 |
Phe < 120 µmol/L | 12.103 | 0.000 | 12.103 |
Discounted QALYs | |||
Total | 27.492 | 23.734 | 3.757 |
Phe ≥ 1,200 µmol/L | 3.047 | 16.961 | −13.914 |
Phe 600 to 1,200 µmol/L | 3.207 | 4.407 | −1.200 |
Phe 360 to 600 µmol/L | 8.192 | 1.808 | 6.383 |
Phe 120 to 360 µmol/L | 2.717 | 0.558 | 2.160 |
Phe < 120 µmol/L | 10.329 | 0.000 | 10.329 |
Discounted costs ($) | |||
Total costs | 7,605,740 | 6,264,932 | 1,340,808 |
Treatment costs | 7,477,149 | 6,057,905 | 1,419,243 |
Phe-restricted diet costs | 96,480 | 160,934 | −64,454 |
Premedication costs | 8,056 | 0 | 8,056 |
Resource use costs | 23,981 | 46,093 | −22,112 |
Adverse event costs | 74 | 0 | 74 |
ICER ($/QALY) | 356,868 | ||
ICER = incremental cost-effectiveness ratio; LY = life-year; Phe = phenylalanine; QALY = quality-adjusted life-year.
Price-Reduction Analyses
In the sponsor’s base-case analysis, when compared to dietary restriction alone, the price of pegvaliase would need to be reduced by 88.6% to be considered cost-effective at a WTP threshold of $50,000 per QALY, while pegvaliase plus MNT was dominant over sapropterin plus MNT.
When considering CADTH’s combined exploratory reanalyses, the price of pegvaliase would need to be reduced by 99% to be considered cost-effective at a willingness to pay of $50,000 per QALY when comparing it to diet alone, or by 16% when compared to sapropterin plus diet (Table 14).
Due to limitations in the analyses which could not be mitigated, estimates of cost-effectiveness for pegvaliase relative to it comparators are highly uncertain, and resultant estimates of a recommended price reduction likely underestimate the true reduction needed to ensure cost-effectiveness.
Table 14: CADTH Price-Reduction Analyses
Analysis | ICERs for pegvaliase + diet vs. comparator | |
|---|---|---|
Price reduction | Sponsor base case | CADTH combined reanalysis |
Pegvaliase + MNT vs. MNT alone | ||
No price reduction | 501,486 | 1,924,753 |
10% | 450,515 | 1,735,297 |
20% | 399,545 | 1,545,842 |
30% | 348,576 | 1,356,386 |
40% | 297,606 | 1,166,930 |
50% | 246,637 | 977,474 |
60% | 195,667 | 788,019 |
70% | 144,697 | 598,563 |
80% | 93,728 | 409,107 |
90% | 42,759 | 219,651 |
Pegvaliase + MNT vs. sapropterin + MNT | ||
No price reduction | Dominant | 356,788 |
10% | Dominant | 160,775 |
20% | Dominant | Dominant |
30% | Dominant | Dominant |
40% | Dominant | Dominant |
50% | Dominant | Dominant |
60% | Dominant | Dominant |
70% | Dominant | Dominant |
80% | Dominant | Dominant |
90% | Dominant | Dominant |
ICER = incremental cost-effectiveness ratio; MNT = medical nutrition therapy.
Appendix 5: Submitted Budget Impact Analysis and CADTH Appraisal
Note that this appendix has not been copy-edited.
Table 15: Summary of Key Take-Aways
Key take-aways of the BIA |
|---|
|
Summary of Sponsor’s Budget Impact Analysis
In the submitted budget impact analysis (BIA), the sponsor assessed the introduction of pegvaliase for the treatment of patients with PKU aged 16 years or older who have blood Phe levels ≥ 600 µmol/mL, despite prior treatment with sapropterin. The BIA was undertaken from the perspective of a Canadian public drug plan payer, over a 3-year time horizon (Q2 2022 to Q1 2025) using a registry-based approach (the BioMarin RareConnections™ registry).
The sponsor included drug acquisition costs and costs for dietary supplementation (low-Phe foods and supplements) for patients on MNT alone or sapropterin and MNT, in jurisdictions which reimburse them. Data for the model were obtained from various sources including: the sponsor’s Patient Support Program data, a dosing analysis conducted by the sponsor, Ontario Drug Benefit Exceptional Access Program list prices,11 SickKids Specialty Food Shop prices,12 a jurisdictional reimbursement report card from CanPKU,20 Statistics Canada,21 the NIHB annual report,22 and the scientific literature.23 Key inputs to the BIA are documented in Table 17.
Key assumptions of the sponsor’s BIA:
Dietary supplementation costs are funded by jurisdictional drug plans.
Patients are 100% adherent to all treatments.
Patients using pegvaliase do not incur dietary supplementation costs.
Patients who have not tried sapropterin will not receive pegvaliase regardless of PAH mutation type.
Patients in the sponsor’s Patient Support Program represent all patients eligible for pegvaliase.
Table 16: Summary of Key Model Parameters
Parameter | Sponsor’s estimate (reported as Year 1/Year 2/Year 3 if appropriate) |
|---|---|
Target population | |
Number of in-clinic patients with PKU ≥ 16 years who have been treated with sapropterin by base year | |||a |
Proportion of sapropterin responders who have Phe ≥ 600 µmol/L after sapropterin | ||%b |
Proportion of patients who have Phe ≥ 600 µmol/L after sapropterin | 46.3%c |
Public plan coverage eligibility | 40.7% to 100% depending on jurisdictiond |
Annual growth rate | −0.3% to 1.6% depending on jurisdictione |
Market uptake (reference scenario, 3 years) | |
Sapropterin + MNT | ||||% / ||||% / ||||%f |
MNT alone | ||||% / ||||% / ||||%g |
Market uptake (new drug scenario, 3 years) | |
Pegvaliase + MNT | ||% / ||% / ||%h |
Sapropterin + MNT | ||% / ||% / ||% |
MNT alone | ||% / ||% / ||% |
Cost of treatment (per patient per year) | |
Pegvaliase Sapropterin Diet | $||||||| (||| syringes daily) $180,799 (15 tablets daily) $10,144 in Alberta, Saskatchewan, Ontario, NIHB $3,600 in Prince Edward Island $3,000 in British Columbia $550 in New Brunswick, Nova Scotia $0 in Manitoba, Newfoundland and Labrador |
MNT = medical nutrition therapy; NIHB = Non-Insured Health Benefits; Phe = phenylalanine; PKU = phenylketonuria; SK = Saskatchewan.
aCited as Patient Support Program, data on file. BioMarin Pharmaceuticals Inc. December 3, 2021.24
bCited as Expert Data on File by the sponsor.24
cLevy et al. 2007.23
dFrom Sutherland and Dinh (2017).25 Ontario’s coverage eligibility was used as a proxy for Alberta, New Brunswick and Nova Scotia.
eProjected by inflating each jurisdiction’s annual population growth. Number of NIHB patients was estimated using a ratio between the NIHB-eligible population and the 2021 Canadian population.24
fThe proportion of patients who respond to sapropterin and have blood Phe ≥ 600 µmol/L post-sapropterin (||%) by the proportion who have blood Phe ≥ 600 µmol/L post-sapropterin (46.3%).
gThe remaining patients who did not respond to sapropterin (100% to 21.6%).
hSponsor’s internal forecast, with 25% coming from sapropterin patients and 75% from MNT alone.
Summary of the Sponsor’s BIA Results
Results of the sponsor’s base case suggested that the reimbursement of pegvaliase for the treatment of patients aged 16 years and older with PKU who have blood Phe levels above 600 µmol/L, despite treatment with sapropterin, was associated with an incremental cost of $4,213,286 in year 1, $5,949,928 in year 2, and $7,716,640 in year 3, for a 3-year incremental budget impact of $17,879,853.
CADTH Appraisal of the Sponsor’s BIA
CADTH identified several key limitations to the sponsor’s analysis that have notable implications on the results of the BIA:
Population size is uncertain and does not represent the Health Canada indication: The sponsor estimated the population who would be eligible for treatment with pegvaliase by including all patients that enrolled in their RareConnections program since inception who were older than 16 years of age, and further refined it to include only those whose blood Phe was ≥ 600 µmol/L after sapropterin. According to the sponsor, enrolment in the program included patients who met jurisdictional reimbursement criteria or an-Canadian Pricing Alliance letter of intent reimbursement criteria in jurisdictions currently negotiating product listing agreements, as well as patients with private insurance coverage. As such, patients who do not meet public funding criteria for sapropterin reimbursement and do not have private insurance are not included, nor, presumably, are patients for whom sapropterin was not considered a treatment option. Therefore, the modelled population does not represent the full population indicated by Health Canada (i.e., patients who have blood phenylalanine levels greater than 600 µmol/l despite dietary management). According to the clinical experts consulted by CADTH, reimbursement of sapropterin is currently changing as patients transition from patient support programs to stricter jurisdictional criteria, potentially decreasing the eligible population. Additionally, should pegvaliase be reimbursed, the clinical experts consulted by CADTH considered it possible that some adult patients previously lost to follow-up due to inability to follow MNT restrictions and lack of response to or suitability for sapropterin, may once again seek out medical assistance to access pegvaliase.
CADTH was unable to account for this limitation in reanalyses. The magnitude and net direction of these uncertainties in the eligible population are unclear.
Pegvaliase dosing was inappropriately modelled: The sponsor’s model assumed that all patients receiving pegvaliase would require ||| syringes per day, as assumed in maintenance years in the sponsor’s base-case cost-utility analysis. However, in the first year of reimbursement, nearly all patients on pegvaliase would be initiating therapy and titrating their dose upward until reaching their optimal dose. These patients would then continue onto maintenance therapy, while new patients would begin their titration in years 2 and 3, as applicable. In line with CADTH’s appraisal of the submitted CUA analysis, CADTH assumed that 1.74 syringes would be required in maintenance years, and that adherence rates would apply.
CADTH assumed all patients in the first year would accrue the mean cost of a titration year as estimated in the CUA model. In the second and third years, new patients would accrue titration costs, while the rest would accrue maintenance year costs at a rate of 1.74 syringes per day. All patients were also assumed to be 83% adherence to therapy with pegvaliase, thus the average daily syringe use in maintenance years was 1.4 syringes per patients daily.
Sapropterin dosing did not incorporate adherence: Unlike the CUA model, the sponsor did not consider adherence to sapropterin. Like for pegvaliase, and for consistency with the CUA, CADTH incorporated adherence to therapy into the BIA model.
CADTH assumed the same adherence rate for sapropterin as was used in the CUA (92%).
Dietary costs may not be funded under jurisdictional drug plans and were inappropriately modelled: The sponsor’s model included the cost of MNT for patients on MNT alone or on sapropterin plus MNT, but unlike in the CUA analysis, did not include costs related to MNT for patients receiving pegvaliase. This biases the sponsor’s BIA result in favour of pegvaliase due to the exclusion of a cost that will still be accrued by patients who receive pegvaliase. Additionally, while the CUA accounted for low adherence rates associated with MNT, the BIA did not, thus all MNT and sapropterin patients accrued the full cost of MNT therapy up to the maximum reimbursed within each jurisdiction. Finally, sponsors’ base-case analyses are conducted from the perspective of Canadian drug plan programs, but it is unclear whether MNT is funded through drug plan budgets or through alternate public funding programs.
CADTH removed the cost of MNT therapy from the CADTH base-case reanalysis. A scenario was conducted where MNT was reintroduced, however the less strict MNT requirements (dietary liberalization) and adherence rates used in the CADTH CUA reanalyses were also incorporated.
Market share uptake uncertain: The sponsor assumed that pegvaliase would capture 25% of the eligible market share in the first year of its reimbursement, rising to 45% by year 3 based on internal forecasts and clinical expert opinion. The clinical experts consulted by CADTH believed that given constraints likely to be placed on patient access, and patient and clinician hesitancy, 45% may be an overestimate by year 3.
CADTH conducted a scenario analysis assuming pegvaliase would capture 20%, 25%, and 30% of the eligible market in years 1, 2, and 3, respectively. This scenario should be considered exploratory.
CADTH Reanalyses of the BIA
CADTH revised the sponsor’s submitted analysis by incorporating dosing from the CADTH combined reanalysis of the CUA for pegvaliase including adherence, incorporating adherence into sapropterin use, and removing the cost of MNT from the drug plan payer perspective of the base-case analysis (Table 17).
Table 17: CADTH Revisions to the Submitted BIA
Stepped analysis | Sponsor’s value or assumption | CADTH value or assumption |
|---|---|---|
Corrections to sponsor’s base case | ||
None | — | — |
Changes to derive the CADTH base case | ||
Pegvaliase dosing | ||| syringes per day, maintenance therapy assumed in all years | Dosing as done in the CADTH CUA reanalysis with weighted-average titration year for patients in their first year of therapy, followed by 1.74 daily syringes in maintenance years, all subject to an 81% adherence rate |
Sapropterin dosing | 100% adherence | 92% adherence rate as in CUA |
NMT costs | MNT and sapropterin + NMT incur full cost of reimbursed dietary supplementation. No NMT costs associated with patients using pegvaliase | MNT costs removed from the base case |
CADTH base case | 1 + 2 + 3 | |
CUA = cost-utility analysis; MNT = medical nutrition therapy.
The results of the CADTH step-wise reanalysis are presented in summary format in Table 18 and a more detailed breakdown is presented in Table 19. Applying these changes resulted in a 3-year budget impact of $18,734,806.
Table 18: Summary of the CADTH Reanalyses of the BIA
Stepped analysis | 3-year total |
|---|---|
Submitted base case | $17,879,853 |
CADTH reanalysis 1: Pegvaliase dosing and adherence | $17,516,726 |
CADTH reanalysis 2: Sapropterin adherence | $18,338,037 |
CADTH reanalysis 3: MNT costs removed | $18,639,750 |
CADTH base case (1 through 3) | $18,734,806 |
MNT = medical nutrition therapy.
CADTH also conducted additional scenario analyses (Table 19), including reintroducing the cost of MNT but under the dietary liberalization and adherence rates assumed in the CADTH combined exploratory reanalysis of the CUA up to the maximum reimbursement limit within each jurisdiction, and a scenario assuming pegvaliase would only reach 20%, 25% and 30% uptake of the eligible market share in years 1 through 3, respectively.
Table 19: Detailed Breakdown of the CADTH Reanalyses of the BIA
Stepped analysis | Scenario | Year 0 (current situation) | Year 1 | Year 2 | Year 3 | 3-year total |
|---|---|---|---|---|---|---|
Submitted base case | Reference | $5,336,727 | $5,381,717 | $5,427,202 | $5,473,189 | $16,282,108 |
New drug | $5,336,727 | $9,595,002 | $11,377,130 | $13,189,830 | $34,161,962 | |
Budget impact | $0 | $4,213,286 | $5,949,928 | $7,716,640 | $17,879,853 | |
CADTH base case | Reference | $4,254,389 | $4,291,060 | $4,328,140 | $4,365,635 | $12,984,836 |
New drug | $4,254,389 | $7,937,104 | $10,829,582 | $12,952,956 | $31,719,642 | |
Budget impact | $0 | $3,646,043 | $6,501,441 | $8,587,322 | $18,734,806 | |
CADTH scenario analysis A: NMT with adherence | Reference | $4,471,424 | $4,509,931 | $4,548,867 | $4,588,239 | $13,647,037 |
New drug | $4,471,424 | $8,184,266 | $11,049,019 | $13,186,069 | $32,419,353 | |
Budget impact | $0 | $3,674,335 | $6,500,151 | $8,597,830 | $18,772,316 | |
CADTH scenario analysis B: lower pegvaliase uptake | Reference | $4,254,389 | $4,291,060 | $4,328,140 | $4,365,635 | $12,984,836 |
New drug | $4,254,389 | $7,207,895 | $9,087,988 | $10,181,487 | $26,477,369 | |
Budget impact | $0 | $2,916,835 | $4,759,847 | $5,815,852 | $13,492,534 |
MNT = medical nutrition therapy.
Stakeholder Input
Patient Group Input
Canadian PKU and Allied Disorders
About Canadian PKU and Allied Disorders
Canadian PKU and Allied Disorders (CanPKU) is a non-profit association of members, first organized in the spring of 2008 and based in Toronto, Ontario. We are dedicated to providing accurate news, information and support to families and professionals dealing with phenylketonuria (PKU) and similar, rare, inherited metabolic disorders. Our mission is to improve the lives of people with PKU and allied disorders and the lives of their families.
Information Gathering
Online patient surveys were conducted in English and French between November 30 and December 25, 2021. The survey asked questions about the impact of PKU on the lives of patients as well as the effect of current treatments. Questions were also directed specifically to patients with Palynziq treatment experience. Potential respondents were identified through the CanPKU mailing list as well as international partner organizations. Messages were also posted on PKU and Palynziq-themed social media groups.
A total of 68 people completed the patient survey, 61 in English and 7 in French. Of these respondents, 46 are from Canada (representing 9 provinces: Alberta, British Columbia, Manitoba, New Brunswick, Newfoundland and Labrador, Nova Scotia, Ontario, Quebec and Saskatchewan), 14 are from the United States, 2 are from France, 1 is from Algeria and 5 didn’t provide their location.
Disease Experience
All 68 respondents have been diagnosed with PKU. 63 respondents were diagnosed through newborn screening, 1 was diagnosed at ten months of age, 1 was diagnosed at one year of age, 1 at twenty-one months, 1 at two years and 1 person’s answer was unclear.
PKU Lived Experience
The manufacturer’s submission will have documented the many physical and psychological/psychiatric symptoms of PKU. We would like to use this section to present patient quotes about how these symptoms affect PKU patients in their day-to-day life.
“I often find it difficult to convey the enormity of the lived experience of PKU and the low-protein diet to an unaffected layperson, and so with a working knowledge of the neurology and biochemistry of neurotoxic Phe levels, I tend to use the alcoholic’s analogy: Imagine yourself to be a recovering alcoholic who honestly wants to right his/her life, but all of the doctors, specialists, and dieticians you consult for help inform you that you cannot fully quit alcohol cold-turkey, but in fact you must manage and maintain a very low intake of it throughout the rest of your life. Not only that, but minute amounts of alcohol are found in almost everything you will eat, and it’s up to you to determine when and where to ingest those minute amounts. Sometimes you may dine out with friends only to ingest more alcohol than you thought, because you were never privy to the recipe. Everyone you know or interact with will be having this alcohol, you will be expected to as well, but you’ll have to explain to everyone why you have to have less, and your social plans will be hampered by it – at worst, you will be ostracized and excluded. If you mismanage your dietary intake of alcohol, you’ll feel worse at first. Often times the negative effects begin hours after ingesting too much alcohol and increase insidiously. In the long run you won’t even know when you’ve slipped over that cliff into neurotoxic oblivion. Substitute ‘protein’ for ‘alcohol’, and you’re just beginning to understand what classical PKUer’s are up against. The low-protein diet has always been a Band-Aid solution treatment, not the end-all-be-all.”
Employment
“PKUers often describe the difficulty of holding down a job. I can’t count the number of jobs I have walked away from over the last twenty-five years. This was due to an intolerable level of stress and anxiety that would build up over time and it would plague me. Eventually, and adding in the PKU fog, I would reach breaking point. The smallest thing sets me off and I would be off out the door, without warning. I have walked away from many jobs that I’ve loved over the years, and some great colleagues/friends too. Some of those jobs I have been exceptionally good at doing, and I’ve always known I had the potential to make them into a decent career. But I couldn’t help repeating the same patterns of behaviour over and over. Consequently, I self-sabotaged many good opportunities over the years because I was binging on food. This led to me losing all faith in myself and my abilities when hitting rock bottom.”
Social Relations and Isolation
“One of the reasons I struggle with social and emotional relationships is so many social events are based around eating and drinking.”
“It's like you never quite fit in and you can’t tell why. You can't eat what your friends and family does, your medication and metabolic formula isn't viewed as importantly as diabetes, and people don’t understand how difficult our symptoms can be, even when we manage our diet properly.”
“Because I find myself going underground when I struggle, I drop out of communication with people; many friendships over the years have been lost through lack of contact, not wanting to go out, or even not wanting to be around people.”
« Être une personne PCU, ça nous rend très retiré socialement. On ne peut aller dans les restaurants, dans des souper de famille, durant les rassemblements, personne ne pense à ce que nous ayons quelque chose à manger, certains évitent de nous inviter ne sachant pas quoi faire avec notre alimentation… certains ne comprennent pas les enjeux énergétiques reliés à tout ça. » (“Being a PKU person makes us very withdrawn socially. We can't go to restaurants, family dinners, or take part in gatherings. Nobody thinks that we have something to eat, some even avoid inviting us, not knowing what to do with our diet… People do not understand the energy issues related to all this.”)
Protein-Restricted Diet
All diagnosed PKU patients are familiar with the protein-restricted PKU diet, which is medically prescribed and overseen. The word diet can understate the severity of the disorder. It is a therapy of medical necessity. Until Palynziq, strict restrictions on the intake of all forms of natural protein was a part of almost all PKU treatment plans. The restriction on natural protein intake is proxy for restricting the intake of the amino acid phenylalanine (Phe) which is an integral part of natural protein. However, PKU patients frequently have difficulty complying with this approach to therapy
When asked if they agree with the statement “I am compliant with the low-protein PKU diet,” on a scale of 1 (strongly disagree) to 5 (strongly agree), the average rating was 3.3 (n=51). Patients on Palynziq are not included in these results because they are supposed to maintain a normal diet.
Table 1: Compliance with a Low-Protein PKU Diet
Rating | Responses |
|---|---|
1 | 13.73% (7) |
2 | 9.80% (5) |
3 | 29.41% (15) |
4 | 27.45% (14) |
5 | 19.61% (10) |
Asked about the barriers to compliance with the low-protein diet, respondents cited:
the cost and lack of availability of low-protein foods,
the time required to plan and prepare low-protein meals,
hunger and a lack of satiety from low-protein foods,
the poor taste of many low-protein foods,
the social pressure to eat with friends and colleagues,
inexact protein values on commercial products,
absence of phenylalanine levels on commercial products, and
the mental exhaustion of constantly tracking food intake.
Experiences With Currently Available Treatments
All 68 respondents provided information about the PKU treatments that they have received. Large majorities of respondents have treatment experience with PKU special low-protein foods (96%) and PKU formulas (94%). A majority of respondents also have experience with Kuvan (65%). Treatment experience with Palynziq (21%) and large neutral amino acids (12%) were much less common.
Table 2: PKU Treatments Received
Treatments Received | n |
|---|---|
PKU special low-protein foods | 65 |
PKU amino acid formulas | 64 |
Kuvan | 44 |
Palynziq | 14 |
Large neutral amino acids | 8 |
PKU Amino Acid Formulas – Synthetic Protein
Poor taste and inconvenience were the most commonly cited problems with PKU formulas, though people noted that flavours have improved over time. Respondents also noted that changing formulas is difficult which causes problems when certain brands become unavailable.
Comments about PKU amino acid formulas:
“The acids in formula have caused stomach issues, and extreme bad breath.”
“Formula - tastes horrible and smells worse. I always felt embarrassed to drink it in public, but medical guidelines are to drink it throughout the day. It is inconvenient as you always need access to water and a container to make it in. Even premade ones need to be refrigerated to contain the taste and smell.”
« Les formules ne sont pas adaptées pour moi. Trop sucrée= migraines à la fin de la journée. Trop peu sucrée= pas de motivation à prendre et sous forme d’acides aminés= trop acide et je régurgite immédiatement. » (“The formulas are not suitable for me. Some are too sweet which gives me headaches at the end of the day. Others are not sweet enough, so I have no motivation to take them. The ones in the amino acid form are too acidic and I regurgitate them immediately.")
PKU Special Low-Protein, Low-Phenylalanine Foods
Poor taste, high cost and lack of availability were the most commonly cited problems with PKU special low-protein, low-phenylalanine foods. However, people noted that the quality of these foods has improved over time.
Comments about PKU special low-protein foods:
“The experience following a low protein diet plus a medical PKU formula has been nothing less than daunting. The challenges faced every single day are nothing short of disheartening. The person that is so used to having whatever they want to eat wherever they go, has no idea what it’s like to have this burden every single solitary day.”
“On the diet, you’re constantly hungry, constantly trying to find something in your protein range.”
“It is extremely difficult to live with such a restricted diet, the medical foods taste terrible and don’t have the healthiest ingredients, and the formula we have to drink multiple times a day is even more terrible tasting and difficult to consume.”
Kuvan (sapropterin)
The most common problem with Kuvan is that many people fail to respond to it. Respondents also complained about the large number of pills (20+) that have to be consumed daily, as dosage depends on body weight However, continuing Kuvan users were generally pleased with its benefits.
Comments about Kuvan:
“Without [Kuvan], I would not be able to function near the capacity I do now.”
“As a teenager, I was tested on Kuvan and was unresponsive, which was devastating to me.”
“Kuvan has helped me achieve generally lower levels than my baseline, but has not allowed me to increase my protein intake. Sometimes it feels like a hassle to take so many pills because it doesn’t allow me to eat more protein, because my diet is the same, but it is helping my blood levels so I continue to take it.”
Symptom Management with Current Therapies
When asked if they agree with the statement “My current therapies are able to manage my PKU symptoms,” on a scale of 1 (strongly disagree) to 5 (strongly agree), the average rating was exactly 3.0 (n=54) suggesting that the benefits of current therapies are real but also limited. Patients currently on Palynziq are not included in these results.
Table 3: Management of PKU Symptoms with Current Therapies
Rating | Responses |
|---|---|
1 | 18.52% (10) |
2 | 9.23% (5) |
3 | 38.88% (21) |
4 | 20.37% (11) |
5 | 13.96% (7) |
Unmet Treatment Needs
When asked if they had unmet treatment needs in their day-to-day lives, patient comments included:
“I want to eat normally and not have to track everything so closely.”
“Although I think we’re incredibly fortunate to have access to what we have, at the same time, it is incredibly limiting and the mental health impacts are a significant concern.”
“I would appreciate more assistance with my mental health and how it is intertwined with my PKU. There are no therapists who specialize in our population.”
“I feel hungry all the time and even with my treatments, I feel bad.”
“Formula is unbearable in taste and alternatives, when available, are just as disheartening.”
Barriers to Treatment
The most commonly cite barriers to treatment were the cost of treatment (42%, n=59) and lack of availability in Canada (41%). These were followed by lack of distribution for treatment products (24%) and travel distance to access treatment (17%).
Comments include:
“Only have access to KUVAN via yearly application and is not prescribed to me regularly. Causes stress that I might not receive my medication someday.”
“Not much low protein foods in the grocery store.”
48% of Canadian respondents said that they needed financial assistance due to costs associated with PKU or its treatment.
Improved Outcomes
Respondents were asked to evaluate the importance of different outcomes for their treatment on a scale of 1 (not important) to 5 (very important). Every outcome received a score of 4.65 or higher. However, limiting long-term disease consequences and improving quality of life were ranked as the most important outcomes.
Table 4: Importance of Outcomes Related to Treatment
Importance of outcome | 1 - not important | 2 | 3 | 4 | 5 – very important | Average |
|---|---|---|---|---|---|---|
Controlling Phe levels | 0.00% 0 | 1.47% 1 | 4.41% 3 | 5.88% 4 | 88.24% 60 | 4.81 68 |
Reducing PKU symptoms | 2.94% 2 | 1.47% 1 | 5.88% 4 | 4.41% 3 | 85.29% 58 | 4.65 68 |
Limiting long-term disease consequences | 0.00% 0 | 0.00% 0 | 1.47% 1 | 4.41% 3 | 94.12% 64 | 4.93 68 |
Improving neurocognitive function | 1.47% 1 | 0.00% 0 | 5.88% 4 | 5.88% 4 | 86.78% 59 | 4.76 68 |
Managing diet | 0.00% 0 | 0.00% 0 | 5.88% 4 | 8.82% 6 | 85.29% 58 | 4.79 68 |
Reducing burden of treatment | 0.00% 0 | 1.47% 1 | 7.35% 5 | 5.88% 4 | 85.29% 58 | 4.75 68 |
Improving quality of life | 0.00% 0 | 0.00% 0 | 4.41% 3 | 2.94% 2 | 92.65% 63 | 4.88 68 |
Comments include:
“It would be nice to have your entire life NOT revolve around low pro food prep, cooking, managing formula, diet, bloodwork, etc...a NORMAL life, not a life where you come home from working full time to controlling your PKU full time when you're not working.”
“These are all extremely important! We need opportunities to these treatments to live a full life and be a part of society in a healthy way.”
“My ultimate goal is to be able to manage a healthy lifestyle.”
85% of respondents (n=68) also said that they would like to increase their natural protein intake. Several respondents discussed the health problems that can come from their limited intake of natural protein:
“So many PKU foods are carb based and metabolic formulas are typically high in sugar and calories.”
“Increasing natural protein would help me feel satiated and be able to eat healthy and filling foods that aren’t overly processed. PKU specialty food products are highly processed by nature.”
“I would like to improve the quality of my food but I don't have the allowance.”
“I would love to be able to lose some weight which is hard on a diet full of carbs. I would rather fill up on meat and veggies than carbs and veggies.”
Several women noted that they wanted treatments that could keep their Phe levels healthy during conception and pregnancy to prevent birth defects and because they could not tolerate PKU formulas while pregnant.
Experience With Drug Under Review
14 respondents have treatment experience with Palynziq. 13 are from the United States and 1 is from Canada. 5 respondents agreed to participate in telephone interviews with staff members to discuss their treatment experience.
4 respondents have been treated with Palynziq for more than 5 years, 3 have been treated for 2-5 years, 5 for 1-2 years, 1 for 6-12 months and 1 for less than 6 months.
All 14 respondents are still receiving Palynziq.
Quality of Life
Respondents were asked to rate the change to their quality of life on Palynziq compared to other treatments on a scale of 1 (much worse) to 5 (much better). Respondents feel that Palynziq has improved their quality of life in every category. Indeed, every category had an average ranking of 4.43 or higher. The greatest benefit was to limit long-term disease consequences, controlling Phe levels and reducing PKU symptoms.
Table 5: Change in Quality of Life on Palynziq
Change to quality of life on Palynziq | 1 – much worse | 2 | 3 | 4 | 5 – much better | Average |
|---|---|---|---|---|---|---|
Controlling Phe levels | 0.00% 0 | 0.00% 0 | 7.14% 1 | 14.29% 2 | 78.57% 11 | 4.71 14 |
Reducing PKU symptoms | 0.00% 0 | 0.00% 0 | 7.14% 1 | 14.29% 2 | 78.57% 11 | 4.71 14 |
Limiting long-term disease consequences | 0.00% 0 | 0.00% 0 | 0.00% 0 | 21.43% 3 | 64.29% 9 | 4.75 12 |
Improving neurocognitive function | 0.00% 0 | 0.00% 0 | 7.14% 1 | 21.43% 3 | 71.43% 10 | 4.64 14 |
Managing diet | 0.00% 0 | 0.00% 0 | 14.29% 2 | 21.43% 3 | 64.29% 9 | 4.50 14 |
Reducing burden of treatment | 7.14% 1 | 0.00% 0 | 0.00% 0 | 28.57% 4 | 64.29% 9 | 4.43 14 |
Improving quality of life | 0.00% 0 | 0.00% 0 | 7.14% 1 | 14.29% 2 | 64.29% 9 | 4.67 12 |
Comments include:
“Palynziq is nothing short of a miracle for me. It is so much more than just liberalizing my diet - it literally makes my life easier multiple times per day. It makes me realize just how much PKU impacted my life in ways I didn’t realize.”
“My life is completely changed, for the better, because of Palynziq. I have NO brain fog, less depression, feel a part of my life, and don't feel isolated.”
“My PKU symptoms have basically vanished. I’m just more of a normal person. I have more good days than bad days mentally. My focus at work is so much better.”
“All of these aspects have improved almost 10-fold and has allowed me to live a much better life.”
“Palynziq has completely transformed my life. Even when I was on-diet for PKU, I still experienced many of the symptoms such as anxiety, brain fog, skin problems, and socializing problems. Palynziq has helped reduce all of that and it feels like a weight lifted off my shoulders.”
In interviews, several respondents also talked about how Palynziq had given them a clarity of thought that they didn’t even know was possible. Until they were treated with Palynziq, elevated Phe levels had been clouding their mind for so long that they didn’t realize that it was possible to function without this brain fog.
Side Effects
Side effects from Palynziq were reported by all respondents. Injection site reactions (86%, n=14), joint pain (79%) and skin reactions (71%) were the most commonly reported side effects.
When patients were asked how much they could tolerate the side effects associated with Palynziq on a scale of 1 (completely intolerable) to 10 (completely tolerable), the average score was 8.9 with no ranking lower than a 6. While Palynziq side effects are common, they appear to be manageable, often with the aid of other medications.
Companion Diagnostic Test
n/a
Anything Else?
Patient Recommendation
When patients were asked if they would recommend Palynziq to other patients for treatment of PKU, 13 respondents (93%) said that they would and 1 said that they would not. The one negative respondent said that they wanted maybe to be an option, but cited the side effects, insurance problems and confusion caused by the changes to their treatment regime as the reason for their lack of recommendation.
Other respondents commented:
“Palynziq is the first and only treatment that I have ever received for my lifelong inherited medical condition, and I wouldn’t trade in that experience for the world.”
“[Palynziq] has given me a new lease of life with exponentially better quality of life.”
“[Palynziq] is the first and only treatment for my inborn error of metabolism that has effectively stabilized my Phe levels and measurably improved my quality of life - the only one.”
“I'm still waiting to fully respond but my levels are going down and it hasn't been a year.”
“I have nothing but positive things to say. Palynziq had been an incredible life changer and I would go through all of my reactions again to get it. Honestly, it will be an amazing disservice to the Canadian population if this is not approved.”
“I have been able to open up my diet making me feel more comfortable at social events where food is major part of the happening. It has also allowed me to be more effective at work with a clear mind and focus.”
“My positives far outweigh any negatives for me. It is nothing short of a miracle. For me, Palynziq has essentially been a cure for PKU. I responded quickly and at a low dose, and I have had minimal side effects. I hope every patient with PKU has the ability to try Palynziq if they want to.”
Patient Group Conflict of Interest Declaration
To maintain the objectivity and credibility of the CADTH reimbursement review process, all participants in the drug review processes must disclose any real, potential, or perceived conflicts of interest. This Patient Group Conflict of Interest Declaration is required for participation. Declarations made do not negate or preclude the use of the patient group input. CADTH may contact your group with further questions, as needed.
Did you receive help from outside your patient group to complete this submission? If yes, please detail the help and who provided it.
Adam Waiser, an independent consultant, prepared the submission with the assistance and oversight of CanPKU officers.
Did you receive help from outside your patient group to collect or analyze data used in this submission? If yes, please detail the help and who provided it.
Adam Waiser, an independent consultant, created the patient survey, conducted patient interviews and analyzed the data with the assistance and oversight of CanPKU officers.
List any companies or organizations that have provided your group with financial payment over the past 2 years AND who may have direct or indirect interest in the drug under review.
Table 6: Financial Disclosure for Canadian PKU and Allied Disorders
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
BioMarin | — | — | — | X |
Clinician Group Input
Metabolic Physicians Caring for Adults with PKU
About Metabolic Physicians Caring for Adults with PKU
We are three metabolic physicians (geneticists with expertise in metabolic disease) that care primarily for adults with phenylketonuria (PKU) in academic centers across Canada (Montreal, Toronto, and Vancouver). Together we care for over 275 adults with PKU.
Information Gathering
We reviewed the currently published literature on pegvaliase from PubMed including published clinical trial data and international clinical practice guideline recommendations. Working in the field for several years, we have also gathered knowledge during attendance at international conferences on inherited metabolic disease and spoken to metabolic physician colleagues and dietitians who prescribe this medication currently in other jurisdictions.
Current Treatments
The amino acid phenylalanine (Phe) is neurotoxic. Individuals with PKU have dysfunctional phenylalanine hydroxylase enzymes and are unable to metabolize Phe which results in accumulation within the central nervous symptom resulting in significant cognitive impairment and psychiatric manifestations among other physical symptoms.
In childhood, prolonged exposure to elevated Phe results in intellectual disability and seizures. With early diagnosis and ongoing treatment, cognitive disability is completely preventable. For this reason, PKU is the prototypical disease for newborn screening and has been screened for in this country since the 60s.
In adulthood, elevated Phe manifests as, often reversible, cognitive, neurological, and psychiatric symptoms. For many adult individuals with PKU, elevated phenylalanine levels result in headaches, tremor, short-term memory loss, difficulty focusing, and word finding difficulties. Psychiatric manifestations including anxiety and depression also appear to be worsened by elevated Phe. These manifestations often have significant implications for individuals with PKU and, as a result, often impacts individuals’ ability to complete educational requirements, keep up with work demands and/or adhere to dietary treatment (see below).
As a result, it is well established that individuals with PKU require lifelong treatment to normalize their phenylalanine levels. Revealed the goal for serum plasma phenylalanine control in adults (a proxy measurement of CNS phenylalanine] is not well-defined. Many adults appear to remain symptom-free when plasma Phe levels are kept below 600 µmol/L; however it is clear that some individuals with PKU require a more significant restriction [less than 360 µmol/L] to avoid many of the symptoms listed above.
The mainstay of treatment is in dietary modification to decrease the amount of Phe consumed; to do this, patients significantly restrict their natural protein intake and supplement their diet proteins with Phe-free medical formula. For most patients, natural protein restriction requires individuals to adhere to a diet completely different from family members, friends, colleagues, and peers who are unaffected. As an example, the protein content of regular breads or pastas (among many other foods which we do not typically think of as being high protein) often dictates individuals choose a lower protein alternative. This, together with the requirement to consume medical formulas which are often unpalatable and cumbersome to prepare makes adhering to the treatment extremely challenging, particularly in adulthood. Adherence to the strict dietary control typically requires meal planning and motivation, both of which are impaired by elevated Phe levels.
Some patients with PKU have benefited from Health Canada approved sapropterin [treatment Kuvan] which is currently available in some Canadian jurisdictions. This is an oral preparation that acts by a chaperone-like mechanism and increases activity of endogenous phenylalanine hydroxylase; sapropterin often allows with an amenable phenylalanine hydroxylase variants to reduce their protein restriction and maintain phenylalanine levels within the target treatment range. Not every patient responds to this treatment. It is often the more mildly affected patients who respond best as their phenylalanine hydroxylase variants do not impair enzyme activity as significantly. Unfortunately, this means more severely affected patients continue to require strict dietary modifications and are often unsuccessful in meeting treatment goals.
Treatment Goals
Normalization of phenylalanine levels improves cognitive and psychiatric symptoms which in turn will facilitate individuals’ ability to meet educational and vocational goals (REF). Pegvaliase often allows patients to near completely normalize their diet and maintain goal phe levels. This will result in improved quality of life for patients allowing them to consume more typical meals together with family members, friends, colleagues, and peers.
Treatment Gaps (Unmet Needs)
Considering the treatment goals, please describe goals (needs) that are not being met by currently available treatments.
Many patients are unable to adhere to the strict dietary requirements that are the mainstay of treatment for individuals with PKU. Seventy - eighty percent (70-80%) of individuals with PKU are not amenable to treatment with sapropterin.
Which patients have the greatest unmet need for an intervention such as the drug under review?
A subpopulation of Individuals with PKU who are unable to adhere to prescribed dietary treatment and/or do not have a sufficient response to sapropterin and therefore have persistently elevated plasma Phe causing neuropsychiatric symptoms would benefit most from pegvaliase. Typically, patients that are not amenable to sapropterin treatment have more severe disease and require a more significant protein restriction in order to maintain target plasma Phe levels.
If individuals were able to tolerate and self-administer pegvaliase, it would allow patients to liberalize their restricted diet and to maintain therapeutic levels of plasma Phe and result in improved quality of life and functioning.
Place in Therapy
How would the drug under review fit into the current treatment paradigm?
Pegvaliase uses a different mechanism of action than currently available treatments for PKU: pegvaliase acts to break down Phe into ammonia and trans-cinnamic acid. Pegvaliase may be used in combination with dietary treatment, but diet treatment can often be liberalized as the medication is titrated. The medication also reduces plasma, and therefore cerebral, phenylalanine. Pegvaliase is intended to be used in individuals who are unable to meet target phenylalanine levels with diet treatment alone and would be the last-line of treatment possibility for adults with PKU.
Please indicate whether or not it would be appropriate to recommend that patients try other treatments before initiating treatment with the drug under review. Please provide a rationale from your perspective.
Dietary treatment, with or without sapropterin (depending on patient response, as discussed above), would be tried before initiating treatment with pegvaliase.
How would this drug affect the sequencing of therapies for the target condition?
This would be an additional therapy. If individuals do not respond to pegvaliase, the only current option is to return to diet therapy with or without sapropterin.
Which patients would be best suited for treatment with the drug under review?
Patients with PKU who are unable to achieve therapeutic Phe concentration with therapies currently available in their jurisdiction.
How would patients best suited for treatment with the drug under review be identified?
Individuals who are followed by metabolic physicians who have Phe levels above therapeutic range whilst attempting to follow treatment.
Which patients would be least suitable for treatment with the drug under review?
Individuals who are able to maintain Phe levels within target range with diet therapy (with or without sapropterin). Individuals unable to self-administer the pegvaliase injection. Individuals who are unable to self-monitor and have an observer monitor them for hypersensitivity reactions. Individuals unable or unwilling to monitor for treatment responsiveness or overtreatment (phenylalanine deficiency).
Is it possible to identify those patients who are most likely to exhibit a response to treatment with the drug under review?
It is not possible to make this prediction.
What outcomes are used to determine whether a patient is responding to treatment in clinical practice?
Reduction in phenylalanine levels and/or increased natural protein (or phenylalanine) tolerance. This was the primary outcome for phase 3 clinical trial (Harding et al., 2018). Neuropsychiatric outcomes are challenging to quantify precisely in individual patients.
What would be considered a clinically meaningful response to treatment?
Reduction in plasma Phe levels to a range for which the individual demonstrates an improvement in symptoms; for some adults this is less than 600 µmol/L for others it is less than 360 µmol/L. Liberalization of diet should also be considered a response to treatment if it results in improved quality of life and mental health.
How often should treatment response be assessed?
It is currently recommended that individuals with PKU have plasma Phe measured on a monthly basis either with venous sampling or postage of a blood spot card from capillary blood sampling.
What factors should be considered when deciding to discontinue treatment?
Treatment should be discontinued if adverse events occur that cannot be tolerated, treated with medication, or amenable to adjustment in medication dose (or titration protocol) or if patients do not show efficacy (above) within 1 year of initiating pegvaliase.
What settings are appropriate for treatment with the drug under review?
Care is provided as an out-patient in subspeciality inherited metabolic diseases clinics.
For non-oncology drugs, is a specialist required to diagnose, treat, and monitor patients who might receive the drug under review?
Yes. All patients under treatment for PKU are followed at large centers with expertise in metabolic medicine (metabolic geneticist) with specialized metabolic dietitians.
Additional Information
There are a relatively small number of inherited metabolic disease clinics across Canada and even fewer that specialize in care of adult patients. Patient education and close supervision is required to initiate and titrate pegvaliase, this together with patient the increased monitoring (medical and dietary) that would be required at a metabolic center would place a significant demand on already resource poor metabolics clinics. Provision for training and funding additional personnel for this purpose will be required.
Conflict of Interest Declarations
To maintain the objectivity and credibility of the CADTH drug review programs, all participants in the drug review processes must disclose any real, potential, or perceived conflicts of interest. This conflict of interest declaration is required for participation.
Declarations made do not negate or preclude the use of the clinician group input. CADTH may contact your group with further questions, as needed. Please see the Procedures for CADTH Drug Reimbursement Reviews (section 6.3) for further details.
Did you receive help from outside your clinician group to complete this submission? If yes, please detail the help and who provided it.
No. Only the physicians listed below created and reviewed this document.
Did you receive help from outside your clinician group to collect or analyze any information used in this submission? If yes, please detail the help and who provided it.
No.
List any companies or organizations that have provided your group with financial payment over the past two years AND who may have direct or indirect interest in the drug under review. Please note that this is required for each clinician who contributed to the input.
Declaration for Clinician 1
Name: Graeme AM Nimmo
Position: Clinical and Metabolic Geneticist, Assistant Professor of Medicine, University of Toronto
Date: 25-11-2021
Table 7: Conflict of Interest Declaration for Metabolic Physician 1
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
BioMarin | — | — | — | X |
Above I am disclosing the donation to the University Health Network Foundation in the form of an unrestricted educational grant from BioMarin to support patient and education of other care providers in this clinic. This does not contribute to my salary. I have not received personal support from BioMarin.
Declaration for Clinician 2
Name: Anna Lehman
Position: Medical Director, Adult Metabolic Diseases Clinic, Vancouver General Hospital and Associate Professor or Medical Genetics, University of British Columbia
Date: 25 Dec 2021
Table 8: Conflict of Interest Declaration for Metabolic Physician 2
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
Biomarin | — | X | — | — |
Declaration for Clinician 3
Name: Alan O’Brien
Position: Clinical and metabolic geneticist, Medical genetics clinic, Centre Hospitalier de l’Université de Montréal (CHUM), Montréal, QC; Assistant clinical professor, Université de Montréal.
Date: 28-12-2021
Table 9: Conflict of Interest Declaration for Metabolic Physician 3
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
Nothing to declare | — | — | — | — |
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up-to-date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
Redactions: Confidential information in this document may be redacted at the request of the sponsor in accordance with the CADTH Drug Reimbursement Review Confidentiality Guidelines.
Stakeholder Input: The views expressed in each submission are those of the submitting organization or individual; not necessarily the views of CADTH or of other organizations. As such, they are independent of CADTH and do not necessarily represent or reflect the view of CADTH. No endorsement by CADTH is intended or should be inferred. By filing with CADTH, the submitting organization or individual agrees to the full disclosure of the information. CADTH does not edit the content of the submissions.
CADTH does use reasonable care to prevent disclosure of personal information in posted material; however, it is ultimately the submitter’s responsibility to ensure no identifying personal information or personal health information is included in the submission. The name of the submitting organization or individual and all conflict of interest information are included in the submission; however, the name of the author, including the name of an individual patient or caregiver submitting the patient input, are not posted.
Accessibility: CADTH is committed to treating people with disabilities in a way that respects their dignity and independence, supports them in accessing material in a timely manner, and provides a robust feedback process to support continuous improvement. All materials prepared by CADTH are available in an accessible format. Where materials provided to CADTH by a submitting organization or individual are not available in an accessible format, CADTH will provide a summary document upon request. More details on CADTH’s accessibility policies can be found here.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.