CADTH Reimbursement Review
Elexacaftor-Tezacaftor-Ivacaftor and Ivacaftor (Trikafta)
Sponsor: Vertex Pharmaceuticals (Canada) Incorporated
Therapeutic area: Cystic fibrosis, F508del-CFTR mutation, 6 years and older
This multi-part report includes:
Clinical Review
Pharmacoeconomic Review
Stakeholder Input
Clinical Review
Abbreviations
AE
adverse event
ALT
alanine transaminase
AST
aspartate transaminase
BMI
body mass index
CCFR
Canadian CF Registry
CDEC
CADTH Canadian Drug Expert Committee
CF
cystic fibrosis
CF Canada
Cystic Fibrosis Canada
CFFPR
Cystic Fibrosis Foundation Patient Registry
CFQ-14
Cystic Fibrosis Questionnaire for individuals 14 years of age and older
CFQ-C
Cystic Fibrosis Questionnaire for children 6 to 14 years of age
CFQ-P
Cystic Fibrosis Questionnaire for parents serving as proxies for their child
CFQ-R
Cystic Fibrosis Questionnaire–Revised
CI
confidence interval
ELX
elexacaftor
ELX-TEZ-IVA
elexacaftor-tezacaftor-ivacaftor and ivacaftor
EMA
European Medicines Agency
FEV1
forced expiratory volume in 1 second
F/F
homozygous for F508del mutation in the CFTR gene
F/G
1 F508del mutation and 1 gating mutation in the CFTR gene
F/MF
1 F508del mutation and 1 minimal function mutation in the CFTR gene
F/RF
1 F508del mutation and 1 residual function mutation in the CFTR gene
HR
hazard ratio
HRQoL
health-related quality of life
IQR
interquartile range
ITC
indirect treatment comparison
IVA
ivacaftor
IWRS
interactive web response system
LCI
lung clearance index
LS
least squares
LSMD
least squares mean difference
LUM
lumacaftor
LUM-IVA
lumacaftor-ivacaftor
MID
minimal important difference
MMRM
mixed-effects model for repeated measures
ppFEV1
percent predicted forced expiratory volume in 1 second
OLE
open-label extension
RCT
andomized controlled trial
SAE
serious adverse event
SD
standard deviation
SE
standard error
TEZ
tezacaftor
TEZ-IVA
tezacaftor-ivacaftor and ivacaftor
TSQM
Treatment Satisfaction Questionnaire for Medication
ULN
upper limit of normal
WDAE
withdrawal due to adverse event
Executive Summary
An overview of the submission details for the drug under review is provided in Table 1.
Item | Description |
|---|---|
Drug product | Elexacaftor-tezacaftor-ivacaftor and ivacaftor (Trikafta)
|
Indication | Treatment of cystic fibrosis in patients aged 6 years and older who have at least 1 F508del mutation in the CFTR gene |
Reimbursement request | Initiation criteria
First renewal: In addition to the previously recommended criteria for the 12-and-older population for whom the physician must provide evidence of continued treatment benefit in at least 1 of the predefined criteria (i.e., lung function, pulmonary exacerbations, hospitalizations, body mass index, and the Cystic Fibrosis Questionnaire–Revised) after 6 months of treatment with Trikafta, the sponsor recommends adding a reduction in sweat chloride to the renewal criteria Subsequent renewals annually: The physician must provide evidence of continued treatment benefit with Trikafta for subsequent renewal of reimbursement |
Health Canada approval status | Under review |
Health Canada review pathway | Priority review |
NOC date | Under review |
Sponsor | Vertex Pharmaceuticals (Canada) Incorporated |
CF = cystic fibrosis.
Introduction
Trikafta consists of a fixed-dose combination tablet containing elexacaftor (ELX), tezacaftor (TEZ), and ivacaftor (IVA) co-packaged with a tablet containing ivacaftor (ELX-TEZ-IVA). It is available in 2 dosage strengths:
ELX 50 mg, TEZ 25 mg, and IVA 37.5 mg co-packaged with a tablet containing IVA 75 mg
ELX 100 mg, TEZ 50 mg, and IVA 75 mg co-packaged with a tablet containing IVA 150 mg.
ELX-TEZ-IVA is indicated for the treatment of cystic fibrosis (CF) in patients aged 6 years and older who have at least 1 F508del mutation in the CFTR gene. A deletion of phenylalanine 508 in the first nucleotide binding domain (F508del) is the most common mutation in the CFTR protein that results in CF.1 The Canadian Cystic Fibrosis patient registry reported that 4,344 Canadians were living with CF in 2019. Of these, 87.8% carried at least 1 F508del mutation (47.1% were homozygous and 40.7% were heterozygous).
This is the second submission to CADTH for ELX-TEZ-IVA. CADTH previously reviewed ELX-TEZ-IVA for the treatment of CF in patients aged 12 years and older who have at least 1 F508del mutation in the CFTR gene, the CADTH Canadian Drug Expert Committee (CDEC) recommended that ELX-TEZ-IVA be reimbursed with conditions.2 The sponsor has requested the following reimbursement criteria for the current submission for ELX-TEZ-IVA:
Initiation criteria: Patients aged 6 years and older should have a confirmed diagnosis with CF with at least 1 F508del mutation in the CFTR gene.
First renewal: In addition to the previously recommended criteria for the 12-and-older population whereby the physician must provide evidence of continued treatment benefit in at least 1 of the predefined criteria (i.e., lung function, pulmonary exacerbations, hospitalizations, body mass index [BMI] and Cystic Fibrosis Questionnaire–Revised [CFQ-R]) after 6 months of treatment with ELX-TEZ-IVA, the sponsor recommends adding a reduction in sweat chloride to the renewal criteria.
Subsequent renewals annually: The physician must provide evidence of continued treatment benefit with ELX-TEZ-IVA for subsequent renewal of reimbursement.
Both the initial submission for ELX-TEZ-IVA (12 years and older) and the current submission (6 years and older) were accepted as priority reviews by Health Canada.
The objective of this review was to evaluate the beneficial and harmful effects of ELX-TEZ-IVA at recommended dosages for the treatment of patients aged 6 years and older with cystic fibrosis and who have at least 1 F508del mutation in the CFTR gene.
Stakeholder Perspectives
The information in this section is a summary of input provided by the patient and clinician groups who responded to CADTH’s call for input and from clinical experts consulted by CADTH for the purpose of this review. Complete patient and clinician input received for the current review of ELX-TEZ-IVA is reported in the appendix of this report. The complete input received for the previous CADTH review of ELX-TEZ-IVA is available on the CADTH website (under the Patient Input and Clinician Input sections).
Patient Input
Three patient groups, Cystic Fibrosis Canada (CF Canada), the Canadian Cystic Fibrosis Treatment Society, and CF Get Loud, responded to CADTH’s call for patient input for both the initial CADTH review of ELX-TEZ-IVA (i.e., for patients 12 years of age and older) and for the current review of ELX-TEZ-IVA, which is focused on patients 6 years of age and older.
The patient groups emphasized that CF has a tremendous impact on those living with the condition, their loved ones, and on society. The most significant clinical impact is in the lungs, where patients experience progressive scarring of their airways and a progressive decline in lung function. Patients may suffer from pulmonary exacerbations requiring weeks of hospitalization and IV antibiotics. Malnutrition is another consequence of CF, and those living with the condition are often underweight and may require a feeding tube for supplemental nutrition. Patients may also suffer from CF-related comorbidities, such as CF-related diabetes and CF-related liver disease. In addition to the decline of the physical health of patients with CF, many suffer from the unseen effects of CF. These include, but are not limited to, depression, anxiety, and hopelessness. The mental anguish caused by the ever-present awareness of 1’s mortality cannot be expressed in words and is often not quantified. Parents and caregivers have an overwhelming desire to do something to help their loved ones.
Managing CF requires a demanding treatment routine with regular visits to specialized CF clinics. As the disease progresses, even more time and effort are needed to manage the progressive and debilitating symptoms. The condition has a significant impact on patients’ day-to-day quality of life, affecting life decisions that include education, career, travel, relationships, and family planning.
Patients with CF and their loved ones are seeking treatments that can change the trajectory of the disease and improve both life expectancy and quality of life. Improved outcomes include retaining or increasing lung function, improving digestive health and energy levels, and minimizing symptoms of CF. Patients want to avoid hospital admissions, reduce the need for invasive medical procedures, and minimize the treatment burden of daily therapies. They also wish to avoid the adverse effects of therapies, such as osteoporosis, antimicrobial resistance, and CF-related diabetes or liver dysfunction.
Patient groups emphasized the importance of early and aggressive treatment of CF with a focus on maintaining health and slowing or preventing disease progression. They noted that even those children with CF who appear healthy (e.g., with a percent predicted forced expiratory volume in 1 second [ppFEV1] of 100%) are subjected to an aggressive therapeutic regimen of physiotherapy and antibiotic treatments in addition to special diets and frequent clinic visits. All patient groups stressed that it is important to start treatment with ELX-TEZ-IVA as soon as possible to prevent the irreversible damage that can be caused by CF. The patient groups referenced the initial CADTH recommendation for ELX-TEZ-IVA, noting that they believe the reimbursement conditions are too restrictive, particularly the requirement that patients demonstrate a ppFEV1 of less than 90% to be eligible. The patient groups reported that they believe all patients with at least 1 F508del mutation can benefit from treatment with ELX-TEZ-IVA.
Clinician Input
Input From the Clinical Experts Consulted by CADTH
Similar to the input from the patient groups, the clinical experts consulted by CADTH indicated that there are significant unmet therapeutic needs for patients living with CF. None of the treatments that are currently available can meet the most important goals of therapy, which include prolonging survival, preventing the need for lung transplantation, slowing the decline in lung function over time, or reversing the course of the disease. In addition, the clinical experts noted that the current standard treatments for CF are burdensome for patients and their caregivers.
The clinical experts anticipate that ELX-TEZ-IVA would be used as a preventive therapy with the goal of initiating treatment before a patient develops significant lung disease. The clinical experts noted that ELX-TEZ-IVA could be used in every patient who meets the Health Canada–approved indication, regardless of their current or past treatment regimens. In clinical practice, eligible patients would be identified based on their CFTR genotype; however, no practical method is available to predict who will be most likely to respond to ELX-TEZ-IVA. The patients who are most in need of treatment with ELX-TEZ-IVA include patients with moderate to severe lung disease (e.g., ppFEV1 ≤ 60%), patients whose BMI is less than or equal to 20 kg/m2, patients with frequent pulmonary exacerbations, and those experiencing a rapid decline in forced expiratory volume in 1 second (FEV1). However, it could be argued that all patients, including those with mild lung disease or who are pre-symptomatic, could benefit from treatment when considering the long-term outcomes and the goal of preventing severe outcomes.
The clinical experts noted that the magnitude of improvement with ELX-TEZ-IVA is far greater than with any other currently available treatments for CF (including all other CFTR modulators). ELX-TEZ-IVA would replace earlier CFTR modulators that are significantly less effective (e.g., lumacaftor-ivacaftor (LUM-IVA) [Orkambi] and tezacaftor-ivacaftor and IVA (TEZ-IVA) [Symdeko]) and patients currently receiving those drugs would likely be switched to ELX-TEZ-IVA.
The following end points are routinely assessed in Canadian clinical practice: lung function (e.g., spirometry measures such as forced expiratory volume in 1 second [FEV1]), nutrition and growth (e.g., BMI, BMI z score, and BMI percentile), hospital admissions and outpatient treatments for pulmonary exacerbations, and pulmonary exacerbation frequency per year. The magnitude of improvement in CF outcomes that would be considered clinically significant depends on the baseline status of the patient. After initiating treatment with ELX-TEZ-IVA, those with less-severe or more-advanced disease may show smaller changes from baseline in commonly measured end points, but still experience clinically relevant improvements (e.g., stabilization). For ppFEV1, an improvement of 5% or more would typically be considered clinically meaningful for most patients in Canadian clinical practice. The experts noted that an increase in BMI should only be viewed as a goal of therapy if the patient is malnourished at the time of initiating therapy. Increasing the BMI of a patient who is in the normal range or overweight may pose challenges and should not be viewed as a desirable outcome for evaluating the response to a treatment such as ELX-TEZ-IVA.
Treatment with ELX-TEZ-IVA would most likely be interrupted or discontinued because of adverse events (AEs) or progression to lung transplant. The most likely known AE that would result in discontinuation is development of persistent liver enzyme abnormalities.
The clinical experts noted that prescribing and monitoring of ELX-TEZ-IVA should be done in an adult or pediatric CF clinic.
Clinician Group Input
Three groups of clinicians provided input for the initial CADTH review of ELX-TEZ-IVA (the Canadian Cystic Fibrosis Clinic Directors, CF Canada’s Accelerating Clinical Trials Network, and The Toronto Adult CF Clinic) and 2 groups provided input for the current review (CF Canada’s Accelerating Clinical Trials Network and the Canadian Cystic Fibrosis Clinic Directors/CF Canada Health Care Advisory Council). The input from the clinician groups identified the same unmet medical needs for patients with CF and potential place in therapy for ELX-TEZ-IVA as the clinical experts consulted by CADTH. Similar to the clinical experts consulted by CADTH, the clinician groups noted that the impact of ELX-TEZ-IVA has been dramatic and life-altering for the patients who have received the treatment through Health Canada’s Special Access Programme, compassionate access mechanisms, or clinical trials (including those involving patients who have advanced lung disease).
Drug Program Input
Input was obtained from the drug programs that participate in the CADTH reimbursement review processes. The following were identified as key factors that could affect the implementation of a CADTH recommendation for ELX-TEZ-IVA:
lack of availability of multiple-breath washout testing in most Canadian CF clinics
potential implementation challenges if recommended reimbursement criteria were different for patients aged 6 to 11 years and those 12 years and older.
The clinical experts consulted by CADTH provided advice on the potential implementation issues raised by the drug programs (as discussed in the Drug Program Input section).
Clinical Evidence
Pivotal Studies and Protocol-Selected Studies
Patients Aged 6 to 11 Years
Description of Studies
The evidence identified in the current review of ELX-TEZ-IVA that addressed the expanded patient population (i.e., those between the ages of 6 and 11 years) included: a 24-week, double-blind, placebo-controlled randomized controlled trial (RCT) in patients who were heterozygous for the F508del mutation and who had 1 minimal function mutation in the CFTR gene (F/MF) (Study 116; N = 121) and a 24-week, pivotal, single-arm trial in patients homozygous for the F508del mutation in the CFTR gene (F/F) and patients with F/MF (Study 106B; N = 66). The treatment periods were 24 weeks in Study 116 and Study 106B and both studies included a screening phase (up to 28 days) and a safety follow-up phase (approximately 4 weeks or entry into an open-label extension [OLE] phase study). Study 106B is the second phase of a 2-part study (Part A consisted of a 28-day screening period, a 15-day, single-arm, open-label treatment period, and a 28-day safety follow-up period). Part B was initiated after completion of the internal review of the data in Part A that was used to confirm or adjust the doses to be evaluated in Part B. In accordance with recommended dosage for ELX-TEZ-IVA in Canada, this report focuses on Part B (i.e., Study 106B).
The inclusion and exclusion criteria for the included RCTs were similar except for the CFTR genotypes (i.e., only F/MF in Study 116 and F/F or F/MF in Study 106B) and the thresholds for ppFEV1 (≥ 70% in Study 116 and ≥ 40% in Study 106B) and a score of 2.5 on the lung clearance index (LCI) (≥ 7.5 in Study 116 and not specified for Study 106). Similar to the trials conducted in adult and adolescent patients, patients in Study 116 and 106B were required to have stable CF disease in the opinion of the investigator at the time of screening. The trials excluded patients with a history of colonization with Burkholderia cenocepacia, Burkholderia dolosa, and/or Mycobacterium abscessus. Patients were also considered to be ineligible if they reported an acute upper or lower respiratory infection, pulmonary exacerbation, or changes in therapy (including antibiotics) for pulmonary disease less than 4 weeks before their first dose of the study drug. Patients with a history of solid organ or hematological transplantation were excluded, as were patients with abnormal laboratory values (e.g., hemoglobin < 10 g/dL), abnormal liver function, or abnormal renal function.
The primary end point of Study 116 was absolute change from baseline in LCI2.5; secondary end points were absolute change from baseline in sweat chloride, CFQ-R respiratory domain scores, and CFQ-R non-respiratory domain scores. All efficacy end points in Study 106B were considered secondary objectives; the primary end point was safety and tolerability. The end points included absolute changes from baseline in the following: ppFEV1, LCI2.5, CFQ-R, BMI, BMI z score, weight, weight z score, height, and height z score. In addition, descriptive statistics were provided for pulmonary exacerbations and hospitalization in Study 106B.
Efficacy Results
In Study 116, treatment with ELX-TEZ-IVA was associated with an increase from baseline in ppFEV1 compared with placebo through 24 weeks as measured by a least squares mean difference (LSMD) of 11.0% (95% confidence interval [CI], 6.9 to 15.1). Improvements in ppFEV1 with ELX-TEZ-IVA were observed at the time of the first post-baseline assessment (i.e., day 15) and were higher at all time points throughout the study. In Study 106B, treatment with ELX-TEZ-IVA resulted in a within-group increase in ppFEV1 through 24 weeks (least squares [LS] mean change = 10.2%; 95% CI, 7.9 to 12.6; P < 0.0001). Improvements in ppFEV1 with ELX-TEZ-IVA were observed at the time of the first post-baseline assessment (i.e., day 15) and were greater than baseline at all time points throughout the 24-week treatment period.
In Study 116, treatment with ELX-TEZ-IVA was associated with a reduction in LCI2.5 through 24 weeks compared to placebo (LSMD = −2.26; 95% CI, −2.71 to −1.81; P < 0.0001). Patients in Study 106 demonstrated a within-group reduction in LCI2.5 through 24 weeks (LS mean change = −1.71; 95% CI, −2.11 to −1.30; P < 0.0001). Improvements (reduction) in LCI2.5 with ELX-TEZ-IVA were observed at the time of the first post-baseline assessment (i.e., day 15) and were reduced at all time points throughout both studies.
Pulmonary exacerbations were only captured as AEs in Study 116. The percentage of patients with at least 1 pulmonary exacerbation was greater in the placebo group compared with the ELX-TEZ-IVA group (26.2% versus 1.7%). Pulmonary exacerbations were included as an exploratory end point in Study 106B, in which the annual event rate for overall pulmonary exacerbations was 0.12 events per year. Event rates for pulmonary exacerbations requiring hospitalization and/or IV antibiotic therapy were each 0.03 events per year. There were no statistical comparisons for event rates pre- and post-treatment with ELX-TEZ-IVA.
In Study 116, treatment with ELX-TEZ-IVA was associated with improved health-related quality of life (HRQoL) as measured with the CFQ-R respiratory domain score from baseline compared with placebo through 24 weeks (LSMD = 5.5; 95% CI, 1.0 to 10.0; P = 0.0003). In Study 106B, patients demonstrated an increase from baseline CFQ-R respiratory domain scores through 24 weeks (LS mean absolute change = 7.0; 95% CI, 4.7 to 9.2; P < 0.0001). Changes from baseline in the non-respiratory domains of the CFQ-R were assessed as exploratory end points in Study 106B (but not in Study 116). Scores in non-respiratory domains of the CFQ-R showed a numerical increase from baseline; however, no statistical analyses were conducted.
Absolute change from baseline in sweat chloride through 24 weeks was a secondary end point of Study 116. The ELX-TEZ-IVA group demonstrated statistically significant reductions in sweat chloride compared with the placebo group through 24 weeks (LSMD = −51.2 mmol/L; 95% CI, −55.3 to −47.1). In Study 106B, treatment with ELX-TEZ-IVA resulted in a statistically significant within-group reduction in sweat chloride through 24 weeks. The LS mean absolute change in sweat chloride from baseline through 24 weeks was −60.9 mmol/L (95% CI, −63.7 to −58.2; P < 0.0001).
Harms Results
In Study 116, the overall percentage of patients who experienced 1 or more AEs was greater in the placebo group (93.4%) compared to the ELX-TEZ-IVA group (80.0%). The AEs that were reported in at least 5% of patients in the ELX-TEZ-IVA group and occurred at a frequency 5% or higher than in the placebo group were headache (30.0% versus 19.7%, respectively), rash (10.0% versus 4.9%, respectively), and a positive Staphylococcus test result (6.7% versus 1.6% respectively). Infective pulmonary exacerbations were reported as AEs more commonly in the placebo group compared with the ELX-TEZ-IVA group (26.2% versus 1.7%, respectively). Adverse events were more commonly reported in Study 106B compared with the ELX-TEZ-IVA group of Study 116 (e.g., 1 or more AEs were reported in 98.5% of patients in Study 106B compared with 80.0% in Study 116). In Study 116, 4 patients (6.7%) in the ELX-TEZ-IVA group and 9 patients (14.8%) in the placebo group had 1 or more serious adverse events (SAEs). In Study 106B, a single patient (1.5%) had 3 SAEs (metapneumovirus infection, pneumonia, and rhinovirus infection). In Study 116, a single patient (1.7%) in the ELX-TEZ-IVA group had an AE of a rash that led to study drug discontinuation. No patients in the placebo group discontinued the study drug. In Study 106B, a single patient had an AE of an erythematous rash that led to treatment discontinuation.
Table 2: Summary of Key Results From Pediatric Studies
Analysis | Study 116 | Study 106B (N = 66) | ||
|---|---|---|---|---|
Placebo (N = 61) | ELX-TEZ-IVA (N = 60) | |||
Absolute change in ppFEV1 (%) through week 24 | ||||
Baseline mean (SD) | 87.2 (15.8) | 91.4 (13.8) | 88.8 (17.7) | |
Patients in analysis, n | 59 | 59 | 59 | |
LS mean change (SE) | −1.5 (1.5) | 9.5 (1.5) | 10.2 (1.2) | |
P value within treatment | 0.2977 | < 0.0001 | < 0.0001 | |
LSMD (95% CI) | Reference | 11.0 (6.9, 15.1) | NA | |
P value vs. placebo | Reference | < 0.0001 | NA | |
Absolute change from baseline in LCI2.5 through week 24 | ||||
Baseline mean (SD) | 9.75 (1.95) | 10.26 (2.22) | 9.77 (2.68) | |
Patients in analysis, n | 61 | 60 | 50 | |
LS mean change (SE) | −0.02 (0.16) | −2.29 (0.16) | −1.71 (0.20) | |
P value within treatment | 0.8859 | < 0.0001 | < 0.0001 | |
LSMD (95% CI) | Reference | −2.26 (−2.71 to −1.81) | NA | |
P value vs. placebo | Reference | < 0.0001 | NA | |
Absolute change from baseline CFQ-R respiratory domain through week 24a, b | ||||
Baseline mean (SD) | 82.7 (14.1) | 85.7 (11.7) | 80.3 (15.2) | |
Patients in analysis, n | 61 | 60 | 65 | |
LS mean change (SE) | 0.5 (1.6) | 5.9 (1.6) | 7.0 (1.1) | |
P value within treatment | 0.7693 | 0.0003 | < 0.0001 | |
LSMD (95% CI) | Reference | 5.5 (1.0 to 10.0) | NA | |
P value vs. placebo | Reference | 0.0174 | NA | |
Absolute change from baseline in sweat chloride through week 24a,b | ||||
Baseline mean (SD) | 102.6 (8.6) | 102.8 (10.0) | 102.2 (9.1) | |
Patients in analysis, n | 61 | 60 | 60 | |
LS mean change (SE) | −0.9 (1.5) | −52.1 (1.5) | −60.9 (1.4) | |
P value within treatment | 0.5241 | < 0.0001 | < 0.0001 | |
LSMD (95% CI) | Reference | −51.2 (−55.3 to −47.1) | NA | |
P value vs. placebo | Reference | < 0.0001 | NA | |
Pulmonary exacerbations | ||||
Patients with event, n (%) | 16 (26.2) (AE only) | 1 (1.7) (AE only) | 4 (6.1) | |
Number of events | NA | NA | 4 | |
Event rate per year | NA | NA | 0.12 | |
Pulmonary exacerbations requiring hospitalization | ||||
Patients with event, n (%) | NA | NA | 1 (1.5) | |
Number of events | NA | NA | 1 | |
Event rate per year | NA | NA | 0.03 | |
Pulmonary exacerbations requiring IV antibiotics | ||||
Patients with event, n (%) | NA | NA | 1 (1.5) | |
Number of events | NA | NA | 1 | |
Event rate per year | NA | NA | 0.03 | |
Absolute change in BMI z score at week 24 | ||||
Baseline mean (SD) | NA | NA | −0.16 (0.74) | |
Patients in analysis, n | NA | NA | 33 | |
LS mean (SE) | NA | NA | 0.37 (0.05) | |
95% CI, of LS mean | NA | NA | (0.26 to 0.48) | |
P value | NA | NA | < 0.0001 | |
Absolute change in body weight z score at week 24 | ||||
Baseline mean (SD) | NA | NA | −0.22 (0.76) | |
Patients in analysis, n | NA | NA | 33 | |
LS mean (SE) | NA | NA | 0.25 (0.04) | |
95% CI, of LS mean | NA | NA | (0.16, 0.33) | |
P value | NA | NA | < 0.0001 | |
Summary of adverse events | ||||
At least 1 AE | 57 (93.4) | 48 (80.0) | 65 (98.5) | |
WDAEs | 0 | 1 (1.7) | 1 (1.5) | |
AEs leading to interruption | 0 | 7 (11.7) | 1 (1.5) | |
Grade 3 or 4 AEs | 2 (3.3) | 2 (3.3) | 1 (1.5) | |
SAEs | 9 (14.8) | 4 (6.7) | 1 (1.5) | |
Adverse events of special interest | ||||
Elevated transaminases | 3 (4.9) | 6 (10.0) | 7 (10.6) | |
Discontinuation | 0 | 0 | 0 | |
Interruption | 0 | 0 | 0 | |
Serious events | 0 | 4 (6.7) | 0 | |
Any rash events | 3 (4.9) | 8 (13.3) | 16 (24.2) | |
Discontinuation | 0 | 1 (1.7) | 1 (1.5) | |
Interruption | 0 | 2 (3.3) | 0 | |
Serious events | 0 | 0 | 0 | |
AE = adverse event; BMI = body mass index; CFQ-R = Cystic Fibrosis Questionnaire–Revised; CI = confidence interval; ELX-TEZ-IVA = elexacaftor-tezacaftor-ivacaftor and ivacaftor; F/F = homozygous for F508del mutation in the CFTR gene; F/MF = 1 F508del mutation and 1 minimal function mutation in the CFTR gene; LCI = lung clearance index; LS = least squares; LSMD = least squares mean difference; NA = not applicable; Pex = pulmonary exacerbation; ppFEV1 = percent predicted forced expiratory volume in 1 second; SAE = serious adverse event; SD = standard deviation; SE = standard error; WDAE = withdrawal due to adverse event.
Critical Appraisal
Randomization in Study 116 was performed using an appropriate methodology with adequate allocation concealment (i.e., interactive web response system [IWRS]) and stratification based on relevant prognostic factors (i.e., baseline lung function [LCI2.5 < 10 versus ≥ 10] and baseline weight [< 30 kg versus ≥ 30 kg]). Baseline and demographic characteristics were generally similar across the ELX-TEZ-IVA and placebo groups in Study 116. A higher percentage of patients in the ELX-TEZ-IVA group had a baseline ppFEV1 of greater than 90% (60.0% versus 45.9% for the placebo group) and a lower percentage had a baseline ppFEV1 of less than 70% (6.7% versus 16.4%, respectively). As those with normal lung function (i.e., > 90%) would be less likely to demonstrate short-term improvements in ppFEV1 due to the ceiling effect, this could bias the results for change in ppFEV1 through 24 weeks against ELX-TEZ-IVA.
The study treatments were administered in a double-blind manner in Study 116 and open-label in Study 106. The AE profiles of ELX-TEZ-IVA and the comparators were unlikely to compromise blinding in the study. The exception could be the increased percentage of patients who experienced a rash in the ELX-TEZ-IVA group (13.3% versus 4.9% with placebo); however, this was not expected to seriously affect treatment blinding. Similar to the previously reviewed trials in adults and adolescents, few pediatric patients discontinued either Study 116 (99.2% completion) or Study 106B (97.0% completion). The studies were relatively short in duration, which may in part explain the high percentage of patients who completed. Adherence was reported to be 99% across both Study 116 and Study 106B. In accordance with the study protocols, the use of concomitant medications remained stable throughout the treatment period for all treatment groups. Pulmonary exacerbations in pediatric patients were only evaluated as efficacy end points in the 24-week single-arm trial (Study 106B). The placebo-controlled trial (Study 116) only reported pulmonary exacerbations as AEs. The primary and key secondary end points were analyzed without statistical testing procedures to control the potential for type I error, and the results should therefore be interpreted with caution due to the risk of inflated type I error.
The diagnostic criteria used to screen patients for Study 116 and Study 106 were identical to those used in Study 102, Study 103, and Study 109 for those at least 12 years of age. As noted in the previous CADTH review of ELX-TEZ-IVA, these criteria are consistent with Canadian clinical practice for diagnosing patients with CF who are homozygous for the F508del-CFTR mutation. The Clinical experts consulted by CADTH indicated that the exclusion of patients with a ppFEV1 of less than 70% does not affect the generalizability of Study 116, as these patients are less common in the Canadian pediatric CF population.
Study 106B included outcomes that are considered to be important to patients with CF based on patient group input: respiratory function (i.e., LCI and ppFEV1), nutritional status and growth (e.g., weight, height, and BMI), HRQoL (CFQ-R), and clinical events (e.g., pulmonary exacerbations). The primary efficacy end point in Study 116 (i.e., LCI2.5) differed from that used in the adolescent and adult trials (i.e., ppFEV1). This is reflective of regulatory guidance, which advises that spirometry may not be sensitive enough to detect treatment differences in children with CF. Younger patients with CF may exhibit spirometry values that are within the normal range, but underlying structural deficiencies within the lungs may be detectable using alternative evaluations (e.g., LCI).
The use of placebo as the comparator in Study 116 is appropriate as no other CFTR modulators are currently approved in Canada for use in the treatment of patients with CF aged 6 to 11 years with an F/MF genotype. The absence of a control group in Study 106B limits the ability to interpret the results of the study. In both studies, ELX-TEZ-IVA (or matching placebo in Study 116) was added to the existing therapeutic regimens used by the patients, which is reflective of how ELX-TEZ-IVA would be administered in clinical practice. The clinical experts consulted by CADTH indicated that the background therapies used in Study 116 and 106B were reasonably reflective of the Canadian CF population.
Patients Aged 12 Years and Older
Description of Studies
Four double-blind, phase III RCTs were included in the CADTH systematic review: 1 placebo-controlled trial conducted in patients with the F/MF genotype (Study 102 [N = 405]), 2 active-controlled trials in patients with the F/F genotype (Study 103 [N = 107] and Study 109 [N = 107]), and 1 active-controlled trial in patients who were heterozygous for the F508del mutation and a residual function mutation (F/RF) or who were heterozygous for the F508del mutation and a gating mutation (F/G) (Study 104; N = 259).
The double-blind treatment periods were 24 weeks in duration in Study 102 and Study 109, 8 weeks in Study 104, and 4 weeks in Study 103. Study 103, Study 104, and Study 109 all included a 28-day active-treatment run-in period during which all patients with either an F/F or F/RF genotype received treatment with TEZ-IVA (Study 103, Study 109, and the F/RF subgroup of patients in Study 104) and patients with an F/G genotype received treatment with IVA (F/G subgroup of patients in Study 104). Patients were subsequently randomized to receive ELX-TEZ-IVA or to remain on the active treatment administered during the run-in period. All the studies included a screening phase (up to 28 days) and a safety follow-up phase (approximately 4 weeks or entry into an OLE phase study).
The inclusion and exclusion criteria for the included RCTs were similar except for the CFTR genotypes (i.e., F/MF, F/F, F/G, or F/RF). Patients were required to have stable CF disease in the opinion of the investigator and a ppFEV1 of between 40% and 90% at the time of screening. The trials excluded patients with a history of colonization with Burkholderia cenocepacia, Burkholderia dolosa, and/or Mycobacterium abscessus. Patients were also ineligible if they reported an acute upper or lower respiratory infection, pulmonary exacerbation, or changes in therapy (including antibiotics) for pulmonary disease less than 4 weeks before the first dose of the study drug. Patients with a history of solid organ or hematological transplantation were excluded, as were patients with abnormal laboratory values (e.g., hemoglobin < 10 g/dL) abnormal liver function, or abnormal renal function.
Efficacy Results
Patients With F/MF Genotype (Study 102): Treatment with ELX-TEZ-IVA was associated with a statistically significant absolute increase from baseline in ppFEV1 compared with placebo at 4 weeks (LSMD = 13.8%; 95% CI, 12.1 to 15.4; P < 0.0001) and 24 weeks (LSMD = 14.3%; 95% CI, 12.7 to 15.8; P < 0.0001). Improvements in ppFEV1 with ELX-TEZ-IVA were observed at the time of the first post-baseline assessment (i.e., day 15) and were higher at all time points throughout the study. Results for change from baseline in ppFEV1 were generally consistent across all subgroup analyses, including those based on age (12 to < 18 years or ≥ 18 years) and ppFEV1 at screening (< 70% or ≥ 70%). The sponsor conducted an additional post hoc subgroup analysis for the subset of patients with a ppFEV1 below 40% at baseline (16 of 203 [7.9%] in the placebo group and 18 of 200 [9.0%] in the ELX-TEZ-IVA group), in which the absolute difference in ppFEV1 with ELX-TEZ-IVA versus placebo was 15.2% (95% CI, 7.3 to 23.1) at 4 weeks and 18.4% (95% CI, 11.5 to 25.3) at 24 weeks.
Treatment with ELX-TEZ-IVA was associated with a lower rate of pulmonary exacerbations compared with placebo (rate ratio = 0.37; 95% CI, 0.25 to 0.55). Similarly, treatment with ELX-TEZ-IVA was associated with lower rates of pulmonary exacerbations requiring hospitalization (rate ratio = 0.29; 95% CI, 0.14 to 0.61) and pulmonary exacerbations requiring IV antibiotic therapy (rate ratio = 0.22; 95% CI, 0.11 to 0.43). Hazard ratios (HRs) favoured ELX-TEZ-IVA over placebo for time to first pulmonary exacerbation (HR = 0.34; 95% CI, 0.22 to 0.52), time to first pulmonary exacerbation requiring hospitalization (HR = 0.25; 95% CI, 0.11 to 0.58), and time to first pulmonary exacerbation requiring IV antibiotics (HR = 0.19; 95% CI, 0.09 to 0.39).
Treatment with ELX-TEZ-IVA was associated with a statistically significant improvement in BMI at 24 weeks compared with placebo (LSMD = 1.04 kg/m2; 95% CI, 0.85 to 1.23; P < 0.0001). In patients less than 20 years of age (n = 145), those treated with ELX-TEZ-IVA demonstrated improvements in BMI z scores compared with placebo (LSMD = 0.30; 95% CI, 0.17 to 0.43). Similarly, the ELX-TEZ-IVA group demonstrated greater improvement in body weight at 24 weeks compared with the placebo group (LSMD = 2.9 kg; 95% CI, 2.3 to 3.4).
Treatment with ELX-TEZ-IVA was associated with a statistically significant and clinically meaningful improvement in CFQ-R respiratory domain scores from baseline compared with placebo through 24 weeks (LSMD = 20.2; 95% CI, 17.5 to 23.0).
The ELX-TEZ-IVA group demonstrated statistically significant reductions in sweat chloride compared with the placebo group at 4 weeks (LSMD = −41.2 mmol/L; 95% CI, −44.0 to −38.5) and 24 weeks (LSMD = −41.8; 95% CI, −44.4 to −39.3).
The Treatment Satisfaction Questionnaire for Medication (TSQM) was included as an exploratory end point for patients between the ages of 12 and 17 years. The difference in change from baseline favoured ELX-TEZ-IVA compared with placebo in the domains for global satisfaction (LSMD = 11.9; 95% CI, 1.8 to 22.0) and effectiveness (LSMD = 14.4; 95% CI, 3.5 to 25.4). The TSQM was not included as an end point in Study 109.
Patients With F/F Genotype (Study 103 and Study 109): In Study 103, treatment with ELX-TEZ-IVA was associated with a statistically significant and clinically meaningful increase from baseline in ppFEV1 compared with TEZ-IVA at 4 weeks (LSMD = 10.0%; 95% CI, 7.4 to 12.6; P < 0.0001). Improvements in ppFEV1 with ELX-TEZ-IVA were observed at the time of the first post-baseline assessment (i.e., day 15) and were higher at all time points throughout the study. The results for change from baseline in ppFEV1 were generally consistent across all subgroup analyses. A post hoc subgroup analysis from Study 103 suggested that the magnitude of the observed treatment effect (LS mean = 7.8%; 95% CI, 4.8 to 10.8) for CFTR modulator–experienced patients is less than that for CFTR-modulator–naive patients (LS mean = 13.2%; 95% CI, 8.5 to 17.9). In Study 109, treatment with ELX-TEZ-IVA was associated with a statistically significant absolute increase from baseline in ppFEV1 compared with TEZ-IVA through 24 weeks (LSMD = 10.2%; 95% CI, 8.2 to 12.1; P < 0.0001).
Pulmonary exacerbations were only captured as AEs in Study 103 and Study 109. The percentage of patients with 1 or more pulmonary exacerbations was greater in the TEZ-IVA group compared with the ELX-TEZ-IVA group in both studies.
Compared with TEZ-IVA, treatment with ELX-TEZ-IVA was associated with improvements in BMI at 4 weeks in Study 103 (LSMD = 0.60 kg/m2; 95% CI, 0.41 to 0.79) and body weight at 4 weeks (LSMD = 1.6 kg; 95% CI, 1.0 to 2.1). Changes from baseline in BMI and body weight were not investigated in Study 109.
Treatment with ELX-TEZ-IVA was associated with a statistically significant and clinically meaningful improvement in CFQ-R respiratory domain scores from baseline compared with TEZ-IVA at 4 weeks in Study 103 (LSMD = 17.4; 95% CI, 11.8 to 23.0) and through 24 weeks in Study 109 (LSMD = 15.9; 95% CI, 11.7 to 20.1).
The ELX-TEZ-IVA group experienced statistically significant reductions in sweat chloride compared with the TEZ-IVA group at 4 weeks (LSMD = −45.1 mmol/L; 95% CI, −50.1 to −40.1) in Study 103 and through 24 weeks in Study 109 (LSMD = −42.8; 95% CI, −46.2 to −39.3; P < 0.0001).
The TSQM was included as an exploratory end point in Study 103 for patients between the ages of 12 and 17 years. The ELX-TEZ-IVA group demonstrated improvements compared with the TEZ-IVA group in the domains for global satisfaction (LSMD = 11.9; 95% CI, 1.8 to 22.0) and effectiveness (LSMD = 14.4; 95% CI, 3.5 to 25.4). The TSQM was not included as an end point in Study 109.
Patients With F/G and F/RF Genotypes (Study 104): Treatment with ELX-TEZ-IVA was associated with a statistically significant within-group improvement in ppFEV1 through 8 weeks (LS mean change = 3.7%; 95% CI, 2.8 to 4.6; P < 0.0001). Treatment with ELX-TEZ-IVA was associated with a statistically significant improvement in ppFEV1 compared to the control group (LSMD = 3.5%; 95% CI, 2.2 to 4.7; P < 0.0001). Subgroup analyses based on the comparator group (patient genotype) demonstrated absolute improvements in ppFEV1 with ELX-TEZ-IVA versus IVA (LSMD = 5.8; 95% CI, 3.5 to 8.0) and versus TEZ-IVA (LSMD = 2.0; 95% CI, 0.5 to 3.4).
Pulmonary exacerbations were only captured as AEs. Compared with the pooled control group (TEZ-IVA and IVA), fewer ELX-TEZ-IVA-treated patients reported 1 or more pulmonary exacerbations (10.3% versus 2.3%, respectively).
Mean BMI increased in both the pooled control group (LS mean = 0.16 kg/m2; standard error [SE] = 0.06) and the ELX-TEZ-IVA group (LS mean = 0.28 kg/m2; SE = 0.06]) with no statistically significant difference between the groups (LSMD = 0.13 kg/m2; 95% CI, −0.03 to 0.29).
The ELX-TEZ-IVA group experienced a statistically significant increase in CFQ-R respiratory domain scores from baseline (LS mean within-group change = 10.3; 95% CI, 8.0 to 12.7; P < 0.0001). Treatment with ELX-TEZ-IVA also resulted in an increase in CFQ-R respiratory domain scores compared to the pooled TEZ-IVA and IVA control groups (LSMD = 8.7; 95% CI, 5.3 to 12.1; P < 0.0001). Subgroup analyses demonstrated similar effect sizes for ELX-TEZ-IVA compared with IVA in patients with an F/G genotype (LSMD = 8.9; 95% CI, 3.8 to 14.0; P = 0.0008) and for ELX-TEZ-IVA compared with TEZ-IVA in patients with an F/RF genotype (LSMD = 8.5; 95% CI, 4.0 to 13.1; P = 0.0003). No statistical analyses were performed for changes from baseline in the non-respiratory domains of the CFQ-R.
The ELX-TEZ-IVA group demonstrated a statistically significant decrease in sweat chloride from baseline (LS mean = −22.3 mmol/L; 95% CI, −24.5 to −20.2; P < 0.0001). Treatment with ELX-TEZ-IVA also resulted in a decrease in sweat chloride from baseline compared to the pooled control group (LSMD = −23.1 mmol/L; 95% CI, −26.1 to −20.1; P < 0.0001).
Harms Results
Patients With F/MF Genotype (Study 102): The overall percentage of patients who experienced 1 or more AEs was 96.0% in the placebo group and 93.1% in the ELX-TEZ-IVA group. The percentage of patients who experienced 1 or more SAEs was 20.9% in the placebo group and 13.9% in the ELX-TEZ-IVA group. Pulmonary exacerbations were the most reported SAE and were more frequent in the placebo group compared with the ELX-TEZ-IVA group (16.4% versus 5.4%, respectively). Few other SAEs were reported for more than 1 patient in each treatment group. Two withdrawals due to adverse events (WDAEs) were reported in the ELX-TEZ-IVA group (1.0%) and none were reported in the placebo group. The reasons for discontinuation from the ELX-TEZ-IVA group included portal hypertension (0.5.%) and rash (0.5%).
Patients With F/F Genotype (Study 103 and 109): The overall percentages of patients who experienced 1 or more AEs in Study 103 and Study 109 were 63.5% and 88.5% in the TEZ-IVA groups, respectively, compared with 58.2% and 92.0% in the ELX-TEZ-IVA groups, respectively. The percentage of patients who experienced 1 or more SAEs was 15.9% in the TEZ-IVA group compared with 5.7% in the ELX-TEZ-IVA group of Study 109. The difference between the groups was due to a greater percentage of patients in the TEZ-IVA group experiencing a pulmonary exacerbation compared with the ELX-TEZ-IVA group (11.4% versus 1.1, respectively). Serious AEs were rare in the 4-week Study 103 and reported for only 1 patient in the TEZ-IVA group (pulmonary exacerbation) and 2 patients in the ELX-TEZ-IVA group (pulmonary exacerbation and rash) (1.9% versus 3.6%, respectively). No WDAEs were reported in either the TEZ-IVA or ELX-TEZ-IVA groups in Study 103. In Study 109, WDAEs were reported for 2 patients (2.3%) in the TEZ-IVA group (compulsive disorder and psychotic disorder) and 1 patient (1.1%) in the ELX-TEZ-IVA group (anxiety and depression).
Patients With F/G and F/RF Genotypes (Study 104): The overall percentage of patients who experienced 1 or more AEs was 66.7% in the ELX-TEZ-IVA group and 65.9% in the control group. The percentage of patients who experienced 1 or more SAEs was 8.7% in the control group compared with 3.8% in the ELX-TEZ-IVA group. The difference between the groups was due to a greater percentage of patients in the control group experiencing a pulmonary exacerbation that was classified as an SAE compared with the ELXTEZ-IVA group (5.6% versus 1.5%, respectively). There were 2 WDAEs in the control group (1.6%; pulmonary exacerbation, and anxiety and depression) and 1 in the ELX-TEZ-IVA group (0.8%; elevated alanine transaminase [ALT] and aspartate transaminase [AST] levels).
Table 3: Summary of Key Results From Studies in Adolescent and Adult Patients
Result | Study 102 (F/MF) 24 weeks | Study 103 (F/F) 4 weeks | Study 109 (F/F) 24 weeks | Study 104 (F/G and F/RF) 8 weeks | |||||
|---|---|---|---|---|---|---|---|---|---|
Placebo (N = 203) | ELX-TEZ-IVA (N = 200) | TEZ-IVA (N = 52) | ELX-TEZ-IVA (N = 55) | TEZ-IVA (N = 88) | ELX-TEZ-IVA (N = 87) | Control (N = 126) | ELX-TEZ-IVA (N = 132) | ||
Absolute change in ppFEV1 (%) | |||||||||
Baseline, mean (SD) | 61.3 (15.5) | 61.6 (15.0) | 60.2 (14.4) | 61.6 (15.4) | 64.2 (15.1) | 63.0 (16.7) | 68.1 (16.4) | 67.1 (15.7) | |
LS mean change (SE) | −0.4 (0.5) | 13.9 (0.6) | 0.4 (0.9) | 10.4 (0.9) | 1.0 (0.7) | 11.2 (0.7) | 0.2 (0.5) | 3.7 (0.5) | |
LSMD (95% CI) | 14.3 (12.7 to 15.8) | 10.0 (7.4 to 12.6) | 10.2 (8.2 to 12.1) | 3.5 (2.2 to 4.7) | |||||
P value | < 0.0001a | < 0.0001a | < 0.0001b | < 0.0001b | |||||
Absolute change in CFQ-R (respiratory domain) | |||||||||
Baseline, mean (SD) | 70.0 (17.8) | 68.3 (16.9) | 72.6 (17.9) | 70.6 (16.2) | 73.1 (17.6) | 71.2 (19.6) | 77.3 (15.8) | 76.5 (16.6) | |
LS mean change (SE) | −2.7 (1.0) | 17.5 (1.0) | −1.4 (2.0) | 16.0 (2.0) | 1.2 (1.5) | 17.1 (1.5) | 1.6 (1.2) | 10.3 (1.2) | |
LSMD (95% CI) | 20.2 (17.5 to 23.0) | 17.4 (11.8 to 23.0) | 15.9 (11.7 to 20.1) | 8.7 (5.3 to 12.1) | |||||
P value | < 0.0001b | < 0.0001 | < 0.0001a | < 0.0001 | |||||
Absolute change in BMI (kg/m2) | |||||||||
Baseline, mean (SD) | 21.31 (3.14) | 21.49 (3.07) | 21.88 (4.12) | 21.75 (3.19) | 21.92 (3.89) | 21.17 (3.43) | 24.05 (4.71) | 24.07 (4.72) | |
LSM change (SE) | 0.09 (0.07) | 1.13 (0.07) | −0.07 (0.07) | 0.53 (0.07) | 0.15 (0.13) | 1.59 (0.13) | 0.16 (0.06) | 0.28 (0.06) | |
LSMD (95% CI) | 1.04 (0.85 to 1.23) | 0.60 (0.41 to 0.79) | 1.44 (1.07 to 1.82) | 0.13 (−0.03 to 0.29) | |||||
P value | < 0.0001b | < 0.0001 | < 0.0001 | NA | |||||
Absolute change in SwCl (mmol/L) | |||||||||
Baseline, mean (SD) | 102.9 (9.8) | 102.3 (11.9) | 90.0 (12.3) | 91.4 (11.0) | 89.8 (11.7) | 89.0 (12.2) | 56.4 (25.5) | 59.5 (27.0) | |
LS mean change (SE) | −0.4 (0.9) | −42.2 (0.9) | 1.7 (1.8) | −43.4 (1.7) | −3.4 (1.2) | −46.2 (1.3) | 0.7 (1.1) | −22.3 (1.1) | |
LSMD (95% CI) | −41.8 (−44.4 to −39.3) | −45.1 (−50.1 to −40.1) | −42.8 (−46.2 to −39.3) | −23.1 (−26.1 to −20.1) | |||||
P value | < 0.0001b | < 0.0001b | < 0.0001 | < 0.0001 | |||||
Pulmonary exacerbations | |||||||||
Patients with event, n (%) | 76 (37.4) | 31 (15.5) | NA | NA | NA | ||||
Event rate per year | 0.98 | 0.37 | |||||||
Rate ratio (95% CI) | 0.37 (0.25 to 0.55) | ||||||||
P value | < 0.0001 | ||||||||
Pulmonary exacerbations requiring hospitalization | |||||||||
Patients with event, n (%) | 27 (13.3) | 7 (3.5) | NA | NA | NA | ||||
Event rate per year | 0.24 | 0.07 | |||||||
Rate ratio (95% CI) | 0.29 (0.14 to 0.61) | ||||||||
P value | < 0.0001 | ||||||||
Pulmonary exacerbations requiring IV antibiotics | |||||||||
Patients with event, n (%) | 42 (20.7) | 9 (4.5) | NA | NA | NA | ||||
Event rate per year | 0.36 | 0.08 | |||||||
Rate ratio (95% CI) | 0.22 (0.11 to 0.43) | ||||||||
P value | < 0.0001 | ||||||||
Time to first pulmonary exacerbation | |||||||||
Hazard ratio (95% CI) | 0.34 (0.22 to 0.52) | NA | NA | NA | |||||
P value | < 0.0001 | ||||||||
Time to first pulmonary exacerbation requiring hospitalization | |||||||||
Hazard ratio (95% CI) | 0.25 (0.11 to 0.58) | NA | NA | NA | |||||
P value | 0.0011 | ||||||||
Time to first pulmonary exacerbation requiring IV antibiotics | |||||||||
Hazard ratio (95% CI) | 0.19 (0.09 to 0.39) | NA | NA | NA | |||||
P value | < 0.0001 | ||||||||
Summary of adverse events | |||||||||
At least 1 AE | 193 (96.0) | 188 (93.1) | 33 (63.5) | 32 (58.2) | 81 (92.0) | 77 (88.5) | 83 (65.9) | 88 (66.7) | |
WDAEs | 0 | 2 (1.0) | 0 | 0 | 2 (2.3) | 1 (1.1) | 2 (1.6) | 1 (0.8) | |
Interruption due to AEs | 10 (5.0) | 19 (9.4) | 0 | 0 | 1 (1.1) | 2 (2.3) | 3 (2.4) | 5 (3.8) | |
Grade 3 or 4 AEs | 15 (7.5) | 19 (9.4) | 1 (1.9) | 0 | 7 (8.0) | 7 (8.0) | 4 (3.2) | 5 (3.8) | |
SAEs | 42 (20.9) | 28 (13.9) | 1 (1.9) | 2 (3.6) | 14 (15.9) | 5 (5.7) | 11 (8.7) | 5 (3.8) | |
Most common adverse events | |||||||||
Infective PEx of CF | 95 (47.3) | 44 (21.8) | 6 (11.5) | 1 (1.8) | 36 (40.9) | 10 (11.5) | 13 (10.3) | 3 (2.3) | |
Sputum increased | 39 (19.4) | 40 (19.8) | 3 (5.8) | 3 (5.5) | 16 (18.2) | 10 (11.5) | 8 (6.3) | 6 (4.5) | |
Headache | 30 (14.9) | 35 (17.3) | 4 (7.7) | 3 (5.5) | 18 (20.5) | 25 (28.7) | 19 (15.1) | 11 (8.3) | |
Cough | 77 (38.3) | 34 (16.8) | 4 (7.7) | 8 (14.5) | 23 (26.1) | 11 (12.6) | 18 (14.3) | 3 (2.3) | |
Adverse events of special interest | |||||||||
Elevated transaminases | 8 (4.0) | 22 (10.9) | 1 (1.9) | 2 (3.6) | 1 (1.1) | 6 (6.9) | 1 (0.8) | 8 (6.1) | |
Discontinuation | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 1 (0.8) | |
Interruption | 3 (1.5) | 2 (1.0) | 0 | 0 | 0 | 2 (2.3) | 1 (0.8) | 0 | |
Serious events | 1 (0.5) | 0 | 0 | 0 | 0 | 1 (1.1) | 0 | 0 | |
Any rash events | 13 (6.5) | 22 (10.9) | 2 (3.8) | 2 (3.6) | 2 (2.3) | 11 (12.6) | 5 (4.0) | 4 (3.0) | |
Discontinuation | 0 | 1 (0.5) | 0 | 0 | 0 | 0 | 0 | 0 | |
Interruption | 1 (0.5) | 4 (2.0) | 0 | 0 | 0 | 1 (1.1) | 1 (0.8) | 1 (0.8) | |
Serious events | 1 (0.5) | 3 (1.5) | 0 | 1 (1.8) | 0 | 0 | 0 | 0 | |
AE = adverse event; BMI = body mass index; CF = cystic fibrosis; CFQ-R = Cystic Fibrosis Questionnaire–Revised; CI = confidence interval; ELX-TEZ-IVA = elexacaftor/tezacaftor-ivacaftor and ivacaftor; F/F = homozygous for F508del mutation in the CFTR gene; F/G = 1 F508del mutation and 1 gating mutation in the CFTR gene; F/MF = 1 F508del mutation and 1 minimal function mutation in the CFTR gene; F/RF = 1 F508del mutation and 1 residual function mutation in the CFTR gene; LS = least squares; LSMD = least squares mean difference; NA = not applicable; PEx = pulmonary exacerbation; ppFEV1 = percent predicted forced expiratory volume in 1 second; SAE = serious adverse event; SD = standard deviation; SE = standard error; SwCl = sweat chloride; TEZ-IVA = tezacaftor-ivacaftor and ivacaftor; URTI = upper respiratory tract infection; WDAE = withdrawal due to adverse event.
aPre-specified primary end point.
bPre-specified key secondary end point.
Source: Clinical Study Reports5-8 and additional information provided by sponsor.9
Critical Appraisal
Randomization was stratified based on relevant prognostic factors (i.e., age, sex, baseline ppFEV1, and prior CFTR-modulator use [in Study 104]).5,6,10,11 Baseline and demographic characteristics were generally well balanced across the treatment groups in each of the included studies. Study treatments were administered in a double-blind manner, with all groups issued the same number of tablets each day. The AE profile of ELX-TEZ-IVA and the comparators was unlikely to compromise blinding in any of the included trials. Few patients discontinued the trials (the completion rate ranged from 96.8% to 100%), although the studies were relatively short in duration, which may partly explain the high percentage of patients who completed.5,6,10,11 Adherence with the study treatments was reported to be greater than 99% across all treatment groups in the included trials.5,6,10,11 In accordance with the study protocols, the use of concomitant medications remained stable throughout the treatment period for all treatment groups. The only exceptions were the lower usage rates of some antibiotics for pulmonary exacerbations in the ELX-TEZ-IVA group relative to the placebo group in Study 102 (this difference was attributable to the efficacy of ELX-TEZ-IVA for reducing pulmonary exacerbations relative to placebo). The primary and key secondary end points were analyzed with statistical testing procedures that controlled the type I error rate, and all end points within the statistical testing hierarchies were statistically significant.
The diagnostic criteria used in Study 103 and Study 109 were consistent with Canadian clinical practice for identifying patients with CF who are homozygous for the F508del-CFTR mutation. The gating and residual function mutations that were used to select patients for inclusion in Study 104 were consistent with the approved indications for TEZ-IVA and IVA in Canada.7,12,13 Because there were no widely accepted criteria for defining minimal function mutations in the CFTR gene, identification of patients with minimal function mutations in Study 102 relied on a novel approach designed by the sponsor (i.e., in vitro response to TEZ, IVA, or TEZ-IVA).5 The clinical experts consulted by CADTH noted that terms “residual function” and “minimal function” are not currently used in Canadian clinical practice. Because patients with CF with more-severe lung disease (e.g., ppFEV1 < 40% at screening) or a normal ppFEV1 at screening (≥ 90%) were excluded from the studies,5,6,10,11 the results of the included studies are applicable primarily to patients with moderate (FEV1 of 40% to 69%) to mild (FEV1 of 70% to 89%) lung disease. As patients with advanced lung disease are an important subgroup with a high level of unmet medical need, CADTH supplemented this review with additional evidence from observational studies to address this important gap in the RCT evidence.
Study 103, Study 104, and Study 109 included an open-label, 4-week, active-treatment period with TEZ-IVA or IVA before randomization. As such, these trials were essentially investigating switching to ELX-TEZ-IVA from either TEZ-IVA or IVA compared with remaining on TEZ-IVA for patients with an F/F or F/RF genotype or remaining on IVA for patients with an F/G genotype. As TEZ-IVA is not widely reimbursed in Canada, the switching design limits the generalizability of the studies directly to the Canadian setting. To address this potential gap in the evidence, the sponsor supplied CADTH with indirect comparisons to provide an estimate of ELX-TEZ-IVA versus placebo for those with an F/F or F/RF genotype.
Indirect Comparisons
Patients Aged 6 to 11 Years
Description of Studies
The sponsor conducted a single indirect comparison for patients ages 6 to 11 with an F/F genotype to derive relative estimates of clinical efficacy for ELX-TEZ-IVA versus LUM-IVA; ELX-TEZ-IVA versus placebo; and ELX-TEZ-IVA versus TEZ-IVA. TEZ-IVA is not currently approved by Health Canada or reimbursed by the Canadian public drug programs for use in patients aged 6 to 11 years. To conduct the primary indirect comparisons, the sponsor extracted 24-week individual-level patient data for those with an F/F genotype from the following studies: ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||VVVVVVVVVVVV. Additional sensitivity analyses were performed using 8-week data.
Efficacy Results
The sponsor reported the following indirect estimates of effect for ELX-TEZ-IVA compared with placebo for absolute change from baseline through 24 weeks: |||||||||||||||||||||||||||||||||||||||| for ppFEV1; |||||||||||||||||||||||||||||||||||||||| for LCI2.5; |||||||||||||||||||||||||||||||||||||||| for BMI z score; and |||||||||||||||||||||||||||||||||||||||| for the CFQ-R respiratory domain. The sponsor reported the following indirect estimates of effect for ELX-TEZ-IVA compared with LUM-IVA for absolute change from baseline through 24 weeks: ||||||||||||||||||||||||||||| for ppFEV1; |||||||||||||||||||||||||||||||||||||||| for LCI2.5; |||||||||||||||||||||||||||||||||||||||| for BMI z score; and |||||||||||||||||||||||||||||||||||||||| for the CFQ-R respiratory domain.
Harms Results
The indirect comparison filed by the sponsor did not include any comparisons for AEs.
Critical Appraisal: The primary limitation of the indirect treatment comparison (ITC) was the difference in study design across the included studies ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||VVVVVVVVVVVV.
Patients Aged 12 Years and Older
Description of Studies
The sponsor conducted indirect comparisons to derive relative estimates of the clinical efficacy for ELX-TEZ-IVA compared to local standard of care in the F/F, F/RF and F/G populations, given the absence of RCTs. Although head-to-head trials were conducted for ELX-TEZ-IVA versus TEZ-IVA (for patients with F/F or F/RF genotypes) and IVA (for patients with an F/G genotype), the sponsor conducted indirect comparisons to derive estimates of effect for ELX-TEZ-IVA versus LUM-IVA for patients with an F/F genotype and ELX-TEZ-IVA versus placebo for those an F/F, F/G, or F/RF genotype. A literature search conducted by CADTH did not identify any additional published indirect comparisons that included the patients, interventions, and outcomes identified in the protocol for CADTH’s review of ELX-TEZ-IVA.
All the sponsor’s indirect comparisons were conducted using the Bucher method for continuous end points. The sponsor stated that the Bucher method was considered the most appropriate approach for these indirect comparisons because of the 4-week active-treatment run-in periods in the ELX-TEZ-IVA trials. As the studies for TEZ-IVA, LUM-IVA, and IVA all enrolled patients who were naive to CFTR-modulator treatment, the baselines were not considered sufficiently comparable to the ELX-TEZ-IVA studies to conduct a meta-analysis of individual patient data.
Efficacy Results
For patients with an F/F genotype, indirect comparisons were performed for ELX-TEZ-IVA versus placebo and ELX-TEZ-IVA versus LUM-IVA. The direct evidence for ELX-TEZ-IVA versus TEZ-IVA was from Study 104 (the direct estimate for TEZ-IVA versus placebo) was from the EVOLVE trial, and the direct estimate for LUM-IVA versus placebo was derived from a meta-analysis of the TRAFFIC and TRANSPORT trials. The sponsor reported the following indirect estimates of effect for ELX-TEZ-IVA compared with placebo for absolute change from baseline through 24 weeks: |||||||||||||||||||||||||||||||||||| for ppFEV1; |||||||||||||||||||||||||||||||||||| for BMI; and |||||||||||||||||||||||||||||||||||| for the CFQ-R respiratory domain.
For patients with an F/G genotype, indirect comparisons were performed for ELX-TEZ-IVA versus placebo. The direct evidence for ELX-TEZ-IVA versus IVA was derived from a subgroup analysis of Study 104 and the estimates for IVA versus placebo were derived from a meta-analysis of subgroup data from 3 studies (STRIVE, KONNECTION, and KONDUCT). The sponsor reported the following indirect estimates of effect for ELX-TEZ-IVA compared with placebo for absolute change from baseline through 8 weeks: |||||||||||||||||||||||||||||||||||| for ppFEV1; |||||||||||||||||||||||||||||||||||| for BMI; and |||||||||||||||||||||||||||||||||||| for the CFQ-R respiratory domain.
For patients with an F/RF genotype, indirect comparisons were performed for ELX-TEZ-IVA versus placebo. The direct evidence for ELX-TEZ-IVA versus TEZ-IVA was derived from a subgroup analysis of Study 104 and the estimates for TEZ-IVA versus placebo were from the EXPAND trial. The sponsor reported the following indirect estimates of effect for ELX-TEZ-IVA compared with placebo for absolute change from baseline through 8 weeks: |||||||||||||||||||||||||||||||||||| for ppFEV1; |||||||||||||||||||||||||||||||||||| for BMI; and |||||||||||||||||||||||||||||||||||| for the CFQ-R respiratory domain.
Harms Results
The indirect comparison filed by the sponsor did not include any comparisons for AEs.
Critical Appraisal
The primary limitation of the indirect comparisons was the difference in study design across the included studies. The ELX-TEZ-IVA studies (i.e., Study 104 and Study 109) included an open-label, 4-week, active-treatment period with TEZ-IVA or IVA before randomization. As none of the other trials used in the indirect comparisons had a similar run-in period, the study designs, baseline values, and the end-point values for the common comparator were different. As both the ELX-TEZ-IVA and the comparator groups of Study 104 and Study 109 received 4 weeks of treatment with a CFTR-modulator, the direction of any potential bias associated with the run-in period is uncertain.
Other Relevant Evidence
CADTH also reviewed additional studies that did not meet the eligibility criteria of the systematic review but may address important gaps in the evidence from the pivotal and supportive RCTs. These included 2 long-term extension-phase studies (Study 107 and Study 105), 2 indirect comparisons submitted by the sponsor, 2 observational studies that evaluated the use of ELX-TEZ-IVA in patients with advanced lung disease, 1 study that modelled the potential impact of ELX-TEZ-IVA on CF-related morbidity and mortality, and 3 observational studies that included a subset of patients with normal lung function at the time of initiating treatment with ELX-TEZ-IVA.
Long-Term Extension Studies
Patients Aged 6 to 11 Years
Study 107 is an ongoing, multi-centre, OLE study that enrolled patients who completed Study 106 (children with CF who are 6 years of age and older with either an F/F genotype or F/MF genotype). Two participants discontinued the study drug before week 24 of Study 106 and did not enter Study 107. Interim results were reported after all patients (n = 64) had completed the 24-week visit.
Efficacy Results
Treatment resulted in improvements in all measures consistent with Study 106. Compared to baseline values of Study 106, ELX-TEX-IVA treatment improved ppFEV1 (9.5%; SE = 1.3), sweat chloride concentration (−64.7 mmol/L; SE = 1.7), CFQ-R respiratory domain score (12.9 points; SE = 1.2), BMI (1.27 kg/m2; SE = 0.15), BMI z score (0.34; SE = 0.06), and LCI2.5 (−1.91; SE = 0.18) at the extension study week 24 interim analysis. Overall, in the 24-week pivotal study and through the week 24 interim analysis of the OLE study, 5 children (7.6%) had protocol-defined pulmonary exacerbations, with an observed annual rate of pulmonary exacerbations of 0.07. There were no CF-related hospitalizations in either the pivotal study or through the week 24 interim analysis of the OLE study.
Harms Results
Most patients (79.7%) reported AEs that were either mild (51.6%) or moderate (28.1%) in severity. The most common AEs were upper respiratory tract infections (14.1%), headaches (10.9%), and vomiting (10.9%). There were no discontinuations through the week 24 interim analysis.
Critical Appraisal
Study 107 is an extension of Study 106 that had been critically appraised earlier. The findings from this interim analysis were retrieved from a poster presentation at the North American Cystic Fibrosis Conference. As no further details were provided by the sponsor, CADTH could not fully critically appraise this study at the time of this review.14 Two patients discontinued the study drug before week 24 and did not enter the OLE study but no explanation for their withdrawal was provided. Issues with the generalizability of these data are the same as for the parent double-blind study.
Patients Aged 12 Years and Older
Study 105 is an ongoing, open-label, uncontrolled trial that enrolled patients who had completed Study 102 or 103 (patients with either an F/MF or an F/F genotype). Interim results were reported for 24 weeks of follow-up for Study 102 patients and 36 weeks for Study 103 patients (data cut-off of October 2019).15 Results from the week 96 interim analysis were presented at the North American Cystic Fibrosis Conference.16 A total of 506 patients were enrolled in the extension study (n = 400 for Study 102 and n = 107 for Study 102) and 42 participants prematurely discontinued treatment before the week 96 visit. Reasons for discontinuing include AEs (n = 8), pregnancy (n = 6), refusal of further dosing (n = 9), commercial drug availability (n = 12), and other reasons (n = 7).
Efficacy Results
Among patients previously enrolled in Study 102, the absolute change from baseline to week 24 in ppFEV1 was similar for patients who switched from placebo to ELX-TEZ-IVA (14.9%; 95% CI, 13.5 to 16.3) and for those who remained on ELX-TEZ-IVA (14.3%; 95% CI, 12.9% to 15.7%) during the extension study. Patients previously enrolled in Study 103 reported an absolute change from baseline to week 36 in ppFEV1 of 12.8% (95% CI, 10.1 to 15.4) and 11.9% (95% CI, 9.3 to 14.5) during the extension study, for patients previously treated with TEZ-IVA and ELX-TEZ-IVA, respectively.
During treatment with ELX-TEZ-IVA, the annual event rate for pulmonary exacerbations was 0.27 (95% CI, 0.19 to 0.39) for those previously treated with placebo and 0.32 (95% CI, 0.24 to 0.44) for those previously treated with ELX-TEZ-IVA in Study 102, and 0.30 (95% CI, 0.20 to 0.45) for those previously enrolled in Study 103.
The LS mean change from baseline to week 24 for the CFQ-R respiratory domain was 19.2 (95% CI, 16.7 to 21.7) for those switched from placebo to ELX-TEZ-IVA (Study 102), and 20.1 (95% CI, 17.6 to 22.6) for those who received ongoing ELX-TEZ-IVA treatment. The LS mean change was 13.8 (95% CI, 8.9 to 18.8) and 14.3 (95% CI, 9.5 to 19.2), respectively, for patients from Study 103 who were switched from TEZ-IVA to ELX-TEZ-IVA and those treated with ELX-TEZ-IVA in both study periods.
The absolute change in BMI from baseline to week 24 (Study 102) or week 36 (Study 103) ranged from an LS mean of 1.2 kg/m2 to 1.3 kg/m2. The change from baseline in BMI z scores was reported for patients who were 20 years of age or younger at the start of the parent studies. The point estimate for the LS mean change from baseline in z scores ranged from 0.30 to 0.43 across the different treatment populations.
Among patients previously enrolled in Study 102, the absolute change from week 24 to week 96 in the ppFEV1 was similar for patients who switched from placebo to ELX-TEZ-IVA (absolute change = 15.2%; 95% CI, 13.6 to 16.7) and for those who remained on ELX-TEZ-IVA (absolute change = 14.3%; 95% CI, 12.7 to 15.8) during the extension study. Patients previously enrolled in Study 103 reported an absolute change from week 4 to week 96 in the ppFEV1 of 12.4% (95% CI, 9.6 to 15.1) and 11.5% (95% CI, 8.8 to 14.2) during the extension study for patients previously treated with TEZ-IVA and ELX-TEZ-IVA, respectively.
The estimated mean pulmonary exacerbation rate per 48 weeks for participants with F/MF genotypes was 0.21 (95% CI, 0.17 to 0.26) for the week 96 interim analysis compared with 0.98 in the placebo group of the F/MF parent study. The estimated mean pulmonary exacerbation rate per 48 weeks for participants with the F/F genotype was 0.21 (95% CI, 0.14 to 0.30) for the week 96 interim analysis. Because part of this OLE study overlapped with the COVID-19 pandemic, restrictions on social interactions likely contributed to reductions in pulmonary exacerbations for patients with CF.
For patients previously enrolled in Study 102, the absolute change from week 24 to extension-period week 96 in the CFQ-R respiratory domain was 20.1 points (95% CI, 17.5 to 22.6) for those switched from placebo to ELX-TEZ-IVA, and 21.7 points (95% CI, 19.1 to 24.1) for those who received ongoing ELX-TEZ-IVA treatment. The absolute change was 15.6 points (95% CI, 11.0 to 20.1) and 18.0 points (95% CI, 13.6 to 22.5) for patients from Study 103 who were switched from TEZ-IVA to ELX-TEZ-IVA and those treated with ELX-TEZ-IVA, respectively, in both study periods. The absolute change in BMI from week 24 (Study 102) or week 4 (Study 103) to week 96 ranged from 1.3 kg/m2 to 1.9 kg/m2. The absolute change in sweat chloride concentration from week 24 (study 102) or week 4 (study 103) to week 96 ranged from −45.8 mmol/L to −49.7 mmol/L in patients previously enrolled in Study 102 or 103.
Harms Results
Most patients (93%) reported 1 or more AEs during the extension study. The most reported AEs were infective pulmonary exacerbation of CF (25%), cough (23%), oropharyngeal pain (15%) and nasopharyngitis (14%). Seven patients (1.4%) stopped treatment due to AEs and 80 patients (16%) experienced 1 or more SAEs.
Most patients (98%) reported 1 or more AEs during the extension study (586 events per 100 person-years). The most reported events were infective pulmonary exacerbations of CF (38%), coughing (36%), oropharyngeal pain (26%), headaches (25%) and nasopharyngitis (23%). Eleven patients (2.2%) stopped treatment due to AEs, 126 patients (25%) experienced an SAE, and grade 3 or 4 AEs were reported by 84 (17%).
Critical Appraisal
Study 105 is an ongoing, uncontrolled, open-label trial that enrolled patients who had completed Study 102 or Study 103. As this was an unblinded study, patients’ expectations of treatment may have biased the reporting of subjective outcomes, such as respiratory symptoms (as measured by the CFQ-R) or harms. Extension studies are often limited by selection bias, as only patients who are tolerant to treatment and complete the parent studies are eligible to enrol. For Study 105, the risk of selection bias may be low, given that only 7 patients (1.4%) out of the 513 randomized in the parent studies were not enrolled or treated in the extension study. During the first 24 weeks of follow-up, discontinuation of treatment was also low (9 patients, 1.8%). However, the frequency of missing data was higher than others for some outcomes. Issues with the generalizability of these data are the same as for the parent double-blind studies. The findings from the week 96 OLE interim analysis were retrieved from a poster presentation at the North American Cystic Fibrosis Conference and no further details were provided by the sponsor.
Observational Studies in Patients With Advanced Lung Disease
Two observational studies provided short-term data on the efficacy and safety of ELX-TEZ-IVA in patients with CF who had advanced pulmonary disease (ppFEV1 < 40% or under evaluation for lung transplantation). All patients had at least 1 F508del-CFTR mutation.
Irish Cohort (Adults)
A retrospective chart review by O’Shea et al. (2021)17 reported data for 14 patients who were followed for a mean duration of 4.9 months after starting ELX-TEZ-IVA. The mean age of patients was 34.4 years (range = 19 to 46). Statistically significant improvements were reported for mean ppFEV1, which increased from 27% (standard deviation [SD] = 7.3) at baseline to 36% (SD = 16.5) after a mean follow-up of 26 days; mean BMI, which increased from 20.7 kg/m2 (SD = 3.6) to 22.1 kg/m2 (SD = 3.4); and mean sweat chloride, which decreased from 105 mmol/L (SD = 15) to 54 mmol/L (SD = 23) after an average of 62 days of follow-up. The rate of infective pulmonary exacerbations requiring hospitalization was 0.28 events per month (SD = 0.17) in the 12 months before ELX-TEZ-IVA, and 0.04 events per month (SD = 0.07) during the 4.9-month follow-up period (P < 0.001).
French Cohort (Adolescents and Adults)
A prospective cohort study by Burgel et al. (2021)18 reported data for 245 patients who were followed for a median of 84 days after initiating treatment with ELX-TEZ-IVA. The median age of patients treated was 31 years (interquartile range [IQR] = 24 to 38), of which 17 (7%) were adolescents. The mean change from baseline in ppFEV1 was 15.1% (95% CI, 13.8 to 16.4) and the change from baseline in weight was 4.2 kg (95% CI, 3.9 to 4.6), based on pooled data from 1- and 3-month assessments. The authors reported statistically significant reductions in the percentage of patients receiving long-term oxygen (43% at baseline versus 23% at 3 months), noninvasive ventilation (28% at baseline versus 20% at 3 months); and enteral tube feeding (18% at baseline versus 10% at 3 months). Data were missing for 31% of patients at the 3-month visits, with no imputation in the analyses. Prior to the initiation of ELX-TEZ-IVA, 16 patients were waiting for a lung transplant and 37 were under consideration for inclusion as transplant candidates in the next 3 months (a total of 53 patients; 22%). At the end of follow-up, 5 patients (2%) were on the transplant list or being considered for transplant, 2 patients (0.8%) had received a transplant, and 1 patient had died while waiting for a transplant (0.4%).
Critical Appraisal
The 2 observational studies provided descriptive data on the effects of ELX-TEZ-IVA in patients with CF with advanced lung disease. The short-term results showed acute increases in ppFEV1 and weight that were comparable to those observed in the clinical trials; but these should be interpreted with caution given the limitations of the open-label, uncontrolled, observational study designs, and the small sample size (N = 14) for the Irish cohort. Both studies had a limited follow-up duration, and the monitoring and reporting of patient outcomes were affected by the COVID-19 pandemic and lockdown measures. The large amount of missing data for some outcomes makes it challenging to interpret and generalize the results of these studies.
Observational Studies in Patients With Normal Lung Function
Interim Analysis From HELIO Study
HELIO is an ongoing multi-centre, prospective, observational study conducted in the US to evaluate the clinical effectiveness of ELX-TEZ-IVA in a real-world setting (N = approximately 200). The study will compare data from a 12-month period before initiating treatment with ELX-TEZ-IVA with data after 16 months of treatment with ELX-TEZ-IVA. At the time of the interim analysis, data were available from ||||||||| patients with a ppFEV1 of greater than 90% at the time of enrolment. The sponsor reported that this subgroup of patients had a mean baseline ppFEV1 of ||||||||| before starting treatment and a mean ppFEV1 of ||||||||| after an average of ||||||||| months of treatment. No interim data were reported for change from baseline in BMI and BMI z scores, pulmonary exacerbations, pulmonary exacerbations requiring IV antibiotics, or pulmonary exacerbations requiring hospitalization, although these were pre-specified end points in the HELIO study.
US Cystic Fibrosis Foundation Patient Registry
The sponsor provided an unpublished analysis from the US Cystic Fibrosis Foundation Patient Registry (CFFPR). Individuals who met the following criteria were included in the analysis: a CFFPR record of initiating treatment with ELX-TEZ-IVA between October 21, 2019, and December 31, 2019; at least 12 years of age on the date of initiating treatment with ELX-TEZ-IVA; an F/MF or F/F genotype; a ppFEV1 assessment available both within 90 days before and any time after ELX-TEZ-IVA initiation through March 15, 2020 (cut-off date); and a final ppFEV1 measurement before ELX-TEZ-IVA initiation (baseline) of greater than 90%. There were |||||| patients with the F/MF genotype and |||||| patients with the F/F genotype who met the inclusion criteria. The mean ages of patients in the F/MF and F/F subgroups were |||||| and |||||| years, respectively. Among patients with the F/F genotype |||||| patients (||||||) had been exposed to a CFTR modulator prior to initiation of ELX-TEZ-IVA. Among patients with the F/MF genotype |||||| (||||||) had been exposed to a CFTR modulator prior to ELX-TEZ-IVA initiation. The mean baseline ppFEV1 values for patients in the F/MF and F/F subgroups were |||||| and ||||||, respectively. The mean changes in ppFEV1 from baseline in the F/MF and F/F subgroup of patients with a baseline ppFEV1 of greater than 90% were |||||| and ||||||, respectively. Similar to the HELIO study, no statistical analyses were reported and no other end points were specified.
PROMISE Study
The PROMISE study is an ongoing, prospective, observational study to understand the effects of ELX-TEZ-IVA in clinical use in the US. The study is sponsored by the Cystic Fibrosis Foundation, and programmatic funding was provided by the National Institutes of Health. Patients were included if they met the following criteria: participants were 12 years of age or older, they had at least 1 copy of the F508del mutation, and they had the intent to initiate ELX-TEZ-IVA by the participant’s physician. Due to restrictions during the pandemic, the time frame to complete the pre-planned 6-month assessment was extended, and results were reported. Additional 18- and 30-month study visits are planned. The average age of patients in the interim dataset meeting the inclusion and exclusion criteria (N = 487) was 25.1 years. Almost half the patients were F508del homozygous (48.5%), and 26.7% (n = 130) of patients had a baseline ppFEV1 of less than 65%, and 40.2% (n = 196) had a baseline ppFEV1 of 90% or greater. For patients who completed the 6-month visit (n = 356) and for the subgroup of patients with a ppFEV1 of less than 90% (n = 148), the mean changes in ppFEV1 from baseline were 9.8 points and 6.5 points, respectively. The mean changes in sweat chloride concentration from baseline for patients who completed the 6-month visit (n = 383) and for the subgroup of patients with a ppFEV1 of greater than 90% (n = 158), were −41.7 mmol/L and −39.7 mmol/L, respectively. The mean changes in CFQ-R respiratory domain scores for patients who completed the 6-month visit (n = 302) and for the subgroup of patients with a ppFEV1 of greater than 90% (n = 120), were 20.4 points and 15.7 points, respectively. The mean changes in BMI for adult patients who completed the 6-month visit (n = 326) and for the subgroup of patients with a ppFEV1 of greater than 90% (n = 76), were 1.2 kg/m2 and 0.8 kg/m2, respectively. The mean changes in BMI z scores for pediatric patients who completed the 6-month visit (n = 139) and for the subgroup of patients with a ppFEV1 of greater than 90% (n = 93), were 0.3 and 0.3, respectively.
Simulation Study for Morbidity and Mortality
Stanojevic et al. (2020)19 used a microsimulation model to estimate the impact of treatment with ELX-TEZ-IVA in eligible patients in Canada. The model forecast an increase in median survival and a reduction in pulmonary exacerbations with the introduction of ELX-TEZ-IVA. The outcomes from these simulations are contingent on the validity of several assumptions that were required to build the model and extrapolate the impacts out to 10 years. There is uncertainty in the extrapolation of short-term effects of ELX-TEZ-IVA in a subset of patients with CF to the broader population in the longer term, and in the generalizability of observational data for IVA on the rate of decline in ppFEV1 to patients treated with ELX-TEZ-IVA. Moreover, the model likely overestimates the proportion of patients with CF who may receive ELX-TEZ-IVA and the impact of treatment on pulmonary exacerbations.
Conclusions
For patients 6 to 11 years of age, a 24-week, double-blind, placebo-controlled RCT (Study 116; N = 121) and a pivotal, single-arm, open-label trial (Study 106B; N = 66) demonstrated that treatment with ELX-TEZ-IVA resulted in clinically meaningful improvements in lung function (increase in ppFEV1), nutritional status (increase in BMI z scores), and HRQoL (increase in CFQ-R respiratory domain scores) and CF biomarkers (reduction in sweat chloride). In addition, AE data suggested that ELX-TEZ-IVA reduced the occurrence of pulmonary exacerbations in pediatric patients. The clinical studies for ELX-TEZ-IVA were limited to patients with an F/MF (Study 116 and Study 106B) or F/F genotype. As Study 106B was a single-arm trial, the sponsor conducted an indirect comparison to derive estimates for the comparative efficacy of ELX-TEZ-IVA versus placebo, LUM-IVA, and TEZ-IVA. No clinical studies were conducted on ELX-TEZ-IVA in pediatric patients with F/RF or F/G genotypes; however, the clinical experts noted that ELX-TEZ-IVA would result in clinically meaningful improvements for these patients, based on the evidence reported for ELX-TEZ-IVA in adult patients with F/RF and F/G genotypes and the results in pediatric studies of patients with F/F and F/MF genotypes. This is consistent with the input from patient and clinician groups who have indicated all patients with at least 1 F508del mutation are likely to benefit from treatment with ELX-TEZ-IVA.
For patients 12 years and older, a 24-week, placebo-controlled RCT (Study 102; N = 403) conducted in patients with an F/MF genotype demonstrated that, compared with placebo, 24 weeks of treatment with ELX-TEZ-IVA was associated with statistically significant and clinically meaningful improvements in lung function (increase in ppFEV1), nutritional status (increase in BMI), HRQoL (increase in CFQ-R respiratory domain scores), CF biomarkers (reduction in sweat chloride), and a reduced rate of pulmonary exacerbations, including events that required IV antibiotics and/or hospitalization to manage. Three additional double-blind, active-controlled RCTs compared switching to ELX-TEZ-IVA after 4 weeks of treatment with either TEZ-IVA or IVA with remaining on those other CFTR modulators. Study 103 (N = 107; 4 weeks) and Study 109 (N = 175; 24 weeks), which were conducted in patients with an F/F genotype, demonstrated that treatment with ELX-TEZ-IVA was associated with statistically significant and clinically meaningful improvements in ppFEV1 and CFQ-R compared with remaining on TEZ-IVA. Study 104 (N = 258; 8 weeks) demonstrated that switching to ELX-TEZ-IVA was associated with statistically significant and clinically meaningful improvements in ppFEV1 compared with remaining on IVA in patients with an F/G genotype and a modest improvement compared with remaining on TEZ-IVA for patients with an F/RF genotype. Patients with advanced lung disease were largely excluded from the phase III RCTs; however, post hoc subgroup analyses and data from 2 short-term observational studies suggest that treatment with ELX-TEZ-IVA resulted in clinically meaningful improvements in lung function in these patients.
Patients with normal lung function (i.e., ppFEV1 > 90%) were considered an important subgroup for the current review of ELX-TEZ-IVA. Approximately half of the pediatric patients in Study 106B and Study 116 had a baseline ppFEV1 of greater than 90%. For those 12 years and older, in addition to the previously reviewed HELIO and CFFPR data, the current review included subgroup data for patients with a baseline ppFEV1 of greater than 90% from a new observational study in adolescent and adults (PROMISE). Although limited by open-label administration and the lack of a control group, the data from PROMISE suggest that patients aged 12 and older with a ppFEV1 of greater 90% at the time of initiating treatment with ELX-TEZ-IVA experienced meaningful improvements in ppFEV1, BMI, and CFQ-R scores.
ELX-TEZ-IVA was well tolerated in the target patient populations (i.e., 6 years of age or older with at least 1 F508del mutation). Serious AEs and WDAEs were rare in the included studies. The product monograph notes that elevated transaminases have been observed in patients treated with ELX-TEZ-IVA and recommends that ALT and AST be assessed before initiating treatment with ELX-TEZ-IVA, every 3 months during the first year of treatment, and annually thereafter. The clinical experts consulted by CADTH noted that the recommendations for monitoring ELX-TEZ-IVA treatment were not anticipated to result in a substantial increase in the number of the clinic visits for patients with CF (particularly after the first year of initiating the treatment).
Introduction
Disease Background
Cystic fibrosis, an autosomal recessive condition, is the most common fatal genetic disease affecting children and young adults in Canada. It is caused by mutations in the CFTR gene, which is located on chromosome 7. The CFTR gene encodes a chloride channel that regulates ion and fluid transport across cell membranes. When the CFTR protein is dysfunctional, secretions become tenacious and sticky, resulting in pathology in multiple organs, including the lungs, large and small intestines, pancreatic and bile ducts, and the vas deferens. The F508del mutation is the most common mutation that results in CF.1 The Canadian Cystic Fibrosis Registry reported that 4,344 Canadians were living with CF in 2019. Of these, 87.8% of patients carried at least 1 F508del mutation (47.1% were homozygous and 40.7% were heterozygous).1
More than 2,090 variants of CFTR proteins have been identified among patients with CF.1 The variants have been classified as impaired biosynthesis (class I), defective protein maturation and accelerated degradation (class II), defective regulation of CFTR at the plasma membrane (class III), defective chloride conductance (class IV), diminished CFTR transcription (class V), and accelerated turnover at the cell surface (class VI).20 Variants within classes I to III are associated with severe CF as they are considered non-functional, while CFTR variants in classes IV to VI may retain CFTR function.20,21 The F508del mutation is typically associated with a class II CFTR mutation and is a severe mutation resulting in significant loss of function of the CFTR protein. A F508del defect causes CFTR misfolding and most of the protein is removed before it can reach the cell membrane. In addition, F508del-CFTR proteins present a defect in channel gating, are unstable, and experience rapid turnover at the cell membrane.22,23 Genotyping for mutations in the CFTR gene is performed routinely on almost all patients with CF in Canada and is also part of the newborn screening process.1
Cystic fibrosis results in airway obstruction, chronic endobronchial infection, and inflammation, which ultimately lead to destruction of lung tissue through development of bronchiectasis and loss of lung function.24 Although chronic pulmonary therapies instituted early in the disease have reduced the decline in lung function over time, patients who are homozygous for the F508del mutation will develop chronic infection with Pseudomonas and progressive bronchiectasis and airway obstruction. In a cohort of approximately 1,000 healthy young children with CF who did not have Pseudomonas infection at enrolment, there was a greater annual decline in FEV1 over the following 4 years in those who were homozygous for the F508del mutation.25 Chronic endobronchial infection of the airways with bacterial pathogens, such as Pseudomonas aeruginosa (reported in 38% of Canadian patients with CF in 2019)1 is associated with a more rapid loss of lung function.26 Acute or chronic endobronchial infections result in further destruction of lung tissue and is associated with respiratory morbidity. Lung disease accounts for the vast majority (> 80%) of death in patients with CF.1,27
Pulmonary exacerbations are associated with lung function decline and mortality, and may require treatment with IV antibiotics and hospitalization. The Cystic Fibrosis Foundation has reported that approximately a third of patients with CF will have 1 or more pulmonary exacerbations per year requiring IV antibiotics.28
Maintenance of pulmonary function (FEV1) and fewer respiratory exacerbations are associated with increased survival.29 Pulmonary management of CF therefore aims to clear the airways of secretions and treat lung pathogens to minimize inflammation.
Patients who are homozygous or heterozygous for the F508del mutation typically have pancreatic, gastrointestinal, and nutritional disease as well as progressive pulmonary damage. Gastrointestinal and pancreatic involvement results in pancreatic exocrine insufficiency in most individuals with CF, causing malabsorption of fats and fat-soluble vitamins, which leads to malnutrition. Maintaining adequate nutrition is associated with improved clinical outcome and longevity for patients with CF.30 Virtually all of these people will be pancreatic insufficient and need to take life-long pancreatic enzyme replacements with every meal as well as fat-soluble vitamin therapy. With increasing age, these patients will develop CF-related diabetes and require therapy with insulin. In 2019, CF-related diabetes was reported in 22.0% of Patients in Canada with CF (33.5% of adults and 3.3% of children).1
The median age of survival in Canada for a child born with CF in 2019 is estimated to be 53.4 years.1 The Canadian Cystic Fibrosis Registry has reported in increase in the median age of death for patients with CF in Canada since the year 2000.1 In 2019 the median age of death was 42.1 years compared with 27.7 years in 2000, 35.1 years in 2013, and 38.9 years in 2016.1,31,32 There is a clear unmet need for better CF therapies, as discussed in the Patient Group Input and Clinician Input sections.
Standards of Therapy
The goals of CF therapy include preservation of lung function by minimizing pulmonary infection and inflammation; restoration of baseline pulmonary function, symptoms, and level of inflammation after acute respiratory exacerbations; and maintenance of adequate nutrition. The choice of a therapeutic regimen for CF depends on organ involvement. The severity of lung function impairment and the presence of bacterial pathogens are deterministic factors when selecting chronic pulmonary therapy.
Treatments that are approved and/or available can be broadly classified as either therapies used to manage symptoms, complications, and comorbidities of CF or therapies to correct underlying defects in the CFTR protein, known as CFTR modulators.
Management of Symptoms, Complications, and Comorbidities
Respiratory treatments consist of physiotherapy and pharmacologic agents such as inhaled antibiotics (e.g., tobramycin, aztreonam, or colistin), anti-inflammatory agents, or mucolytics (e.g., hypertonic saline and/or dornase alfa).33 Nutritional treatments consist of high-calorie and high-fat diets and pancreatic enzyme replacement for those with pancreatic insufficiency.27,33 Pulmonary exacerbations are treated with oral or IV antibiotics.34 These treatments do not halt, but only slow, the decline in lung function and the progression of disease.
CFTR Modulators
CFTR modulators are a class of medications that aim to correct the underlying defects of the CFTR protein. The CFTR modulators that are currently marketed in Canada or other jurisdictions are classified as potentiators and correctors. Potentiators function by increasing the channel-open probability of the CFTR protein at the cell surface. Ivacaftor is a CFTR potentiator. Correctors function by improving the conformational stability of F508del-CFTR protein, resulting in an increased expression of the F508del-CFTR protein at the cell surface. Lumacaftor, TEZ, and ELX are CFTR correctors.
Table 6 provides a summary of the CFTR modulators currently marketed or under review in Canada, the CFTR mutations and age ranges for which they been approved by Health Canada, and the reimbursement status within the public drug programs. The currently available CFTR modulators are not approved for use in all patients with at least 1 F508del mutation. The approved indications currently cover those who are homozygous for F508del mutations (Orkambi and Symdeko), heterozygous for the 508del mutation, and who also have 1 of the following mutations: residual function mutation (Symdeko) or a gating mutation (Kalydeco). A subset of individuals who are heterozygous for the F508del mutation will therefore not be covered by the existing indications. In addition, the clinical benefit of some of the existing treatments (e.g., Orkambi) has been described as modest, leaving an unmet medical need for treatments with the potential to offer greater treatment effects and benefits.35 In 2019, CF Canada reported that 658 individuals (216 children and 442 adults) were receiving treatment with CFTR modulators, with 146 receiving Kalydeco, 368 receiving Orkambi, and 186 receiving Symdeko.1
Drug
Trikafta consists of a fixed-dose combination tablet available as ELX, TEZ, and IVA co-packaged with a tablet containing IVA (ELX-TEZ-IVA). It is available in 2 dosage strengths:
ELX 50 mg, TEZ 25 mg, and IVA 37.5 mg co-packaged with a tablet containing IVA 75 mg
ELX 100 mg, TEZ 50 mg, and IVA 75 mg co-packaged with a tablet containing IVA 150 mg.
ELX-TEZ-IVA is indicated for the treatment of CF in patients aged 6 years and older who have at least 1 F508del mutation in the CFTR gene. The sponsor has requested the following reimbursement criteria for ELX-TEZ-IVA:
Initiation criteria: Patients and aged 6 years and older must have a confirmed diagnosis with CF with at least 1 F508del mutation in the CFTR gene.
First renewal: In addition to the previously recommended criteria for the 12-and-older population whereby the physician must provide evidence of continued treatment benefit in 1 or more of the predefined criteria (i.e., lung function, pulmonary exacerbations, hospitalizations, BMI and CFQ-R) after 6 months of treatment with Trikafta, the sponsor recommends adding reduction in sweat chloride the to the renewal criteria.
Subsequent renewals annually: The physician must provide evidence of continued treatment benefit with Trikafta for subsequent renewal of reimbursement.
Mechanism of Action
ELX-TEZ-IVA is the third treatment specifically indicated for the treatment of patients with CF who have F508del mutation(s) in the CFTR gene. This mutation is believed to be associated with misfolding of the CFTR protein, which results in a lower quantity of CFTR expression at the cell surface. In addition to the reduced quantity of the protein, the mutation results in a CFTR protein that is less stable and has defective channel gating compared with wild-type CFTR. Treatment with ELX-TEZ-IVA results in an increased quantity and improved function of the F508del-CFTR protein at the cell surface, through the following mechanisms35-37:
ELX and TEZ improve the conformational stability of F508del-CFTR protein, resulting in an increased expression of the F508del-CFTR protein at the cell surface.
IVA increases the channel-open probability of the CFTR protein at the cell surface.
Recommended Dosage
The recommended dosage of ELX-TEZ-IVA for patients aged 6 to less than 12 years who weigh less than 30 kg is a combination of 2 tablets in the morning (each containing ELX 50 mg, TEZ 25 mg, and IVA 37.5 mg) and 1 standalone tablet (containing IVA 75 mg) taken in the evening. For those aged 6 to less than 12 years who weigh 30 kg or more and those 12 years and older, the recommended dosage is 2 combination tablets in the morning (each containing ELX 100 mg, TEZ 50 mg, and IVA 75 mg) and 1 standalone tablet (containing IVA 150 mg) taken in the evening (Table 4). Both tablets are administered orally (swallowed whole) and should be taken approximately 12 hours apart with fat-containing food. Table 5 provides a summary of the recommended dosage adjustments for patients with hepatic insufficiency or those receiving concomitant treatment with moderate CYP3A inhibitors (e.g., fluconazole, or erythromycin) or strong CYP3A inhibitors (e.g., ketoconazole, itraconazole, posaconazole, voriconazole, telithromycin, and clarithromycin).
Age (weight) | Morning dose (2 tablets) | Evening dose (1 tablet) |
|---|---|---|
6 to < 12 years (< 30 kg) | Elexacaftor 50 mg, tezacaftor 25 mg, and ivacaftor 37.5 mg | Ivacaftor 75 mg |
6 to < 12 years (≥ 30 kg) | Elexacaftor 100 mg, tezacaftor 50 mg, and ivacaftor 75 mg | Ivacaftor 150 mg |
≥ 12 years | Elexacaftor 100 mg, tezacaftor 50 mg, and ivacaftor 75 mg | Ivacaftor 150 mg |
Source: Product monograph.36
Table 5: Recommended Dosage Adjustments
Condition | Classification | Dosage adjustment |
|---|---|---|
Hepatic insufficiency | Mild (Child-Pugh Class A) | No dosage adjustments |
Moderate (Child-Pugh Class B) | Use not recommendeda | |
Severe (Child-Pugh Class C) | Should not be used | |
CYP3A Inhibitors | Moderate CYP3A Inhibitors | Morning: 2 ELX-TEZ-IVA tablets (day 1); 1 IVA tablet (day 2) Evening: no dose |
Strong CYP3A Inhibitors | Morning: 2 ELX-TEZ-IVA tablets (twice weekly; 3 to 4 days apart) Evening: no dose |
ELX-TEZ-IVA = elexacaftor-tezacaftor-ivacaftor and ivacaftor; IVA = ivacaftor.
aTreatment of patients with moderate hepatic impairment should only be considered when there is a clear medical need and the benefits are expected to outweigh the risks. If used, ELX-TEZ-IVA should be used with caution at a reduced dosage, as follows: 2 ELX-TEZ-IVA tablets alternating with 1 elexacaftor-tezacaftor-ivacaftor tablet taken in the morning, on alternating days. The evening dose of the ivacaftor tablet should not be taken.
Previous CADTH Reviews
This is the second submission to CADTH for ELX-TEZ-IVA. CADTH previously reviewed ELX-TEZ-IVA for the treatment of CF in patients aged 12 years and older who have at least 1 F508del mutation in the CFTR gene; CDEC recommended that ELX-TEZ-IVA be reimbursed with conditions.2
CADTH has previously reviewed IVA alone for the following indications: patients 6 years of age and older who have 1 of the following mutations in the CFTR gene: G551D, G1244E, G1349D, G178R, G551S, S1251N, S1255P, S549N, S549R, or G970R; and patients 18 years of age and older who have an R117H mutation in the CFTR gene.38-40 For each of these indications, CDEC recommended that IVA be reimbursed with conditions. LUM-IVA was previously reviewed for the treatment of CF in patients who are homozygous for the F508del mutation in the CFTR gene and received do-not-reimburse recommendations in 2016 and 2018.41,42 CADTH was unable to recommend reimbursement for TEZ-IVA as the manufacturer did not file a submission.43
Stakeholder Perspectives
Patient Group Input
This section was prepared by CADTH staff based on the input provided by patient groups.
Three patient groups, CF Canada, the Canadian Cystic Fibrosis Treatment Society, and CF Get Loud, responded to CADTH’s call for patient input for both the initial CADTH review of ELX-TEZ-IVA (i.e., for patients 12 years and older) and for the current review of ELX-TEZ-IVA, which is focused on patients 6 years and older.
Information from CF Canada was based on a survey of patients and caregivers that was conducted for the previous CADTH review of ELX-TEZ-IVA, Cystic Fibrosis Registry Annual Data Reports, press releases, news stories, and government submissions, as well as information gathered through social media campaigns, posts from individuals, and traditional media sources. In addition, CF Canada cites information that was presented at the 2021 North American Cystic Fibrosis Conference. For its initial submission to CADTH, CF Get Loud gathered information from a letter campaign that received 11,364 letters from Canadians, a town hall with CF experts and leaders, and from 20 Canadians who are currently receiving treatment ELX-TEZ-IVA. For the current submission, CF Get Loud gathered information from interviews with parents of children living with CF. Canadian CF Treatment Society gathered information through discussions with parents and caregivers of young patients with CF, advocates and physicians located in Canada.
The patient groups emphasized that CF has tremendous impact on those living with the condition, their loved ones, and on society. The most significant clinical impact is in the lungs, where patients experience progressive scarring of their airways and a progressive decline in lung function. Patients may suffer from pulmonary exacerbations requiring weeks of hospitalization and IV antibiotics. Malnutrition is another consequence of CF, and those living with the condition are often underweight and may require a feeding tube for supplemental nutrition. Patients may also suffer from CF-related comorbidities, such as CF-related diabetes and CF-related liver disease. In addition to the decline of the physical health of patients with CF, many suffer from the unseen effects of CF. These include, but are not limited to, depression, anxiety, and hopelessness. The mental anguish caused by the ever-present awareness of 1’s mortality cannot be expressed in words and can be difficult to quantify. Parents and caregivers often have an overwhelming desire to do something to help their loved ones.
Table 6: Key Characteristics of CFTR Modulators
Characteristics | Trikafta (ELX-TEZ-IVA and IVA) | Orkambi (LUM-IVA) | Symdeko (TEZ-IVA and IVA) | Kalydeco (IVA) |
|---|---|---|---|---|
Mechanism of action | CFTR potentiator (IVA) and correctors (ELX/TEZ) | CFTR potentiator (IVA) and corrector (LUM) | CFTR potentiator (IVA) and corrector (TEZ) | CFTR potentiator |
Indicationa | Patients aged ≥ 6 years who have at least 1 F508del mutation in the CFTR gene | Patients aged ≥ 2 years of age who are homozygous for the F508del mutation in the CFTR gene | Patients aged ≥ 12 years who are homozygous for the F508del mutation or who are heterozygous for the F508del mutation and have 1 of the following CFTR mutations: P67L, D110H, R117C, L206W, R352Q, A455E, D579G, 711 + 3A→G, S945L, S977F, R1070W, D1152H, 2789 + 5G→A, 3272 to 26A→G, and 3849 + 10kbC→T | Tablets: Patients ≥ 6 years and weighing ≥ 25 kg with 1 of the following CFTR mutations: G551D, G1244E, G1349D, G178R, G551S, S1251N, S1255P, S549N or S549R Tablets: Patients aged ≥ 18 years with an R117H CFTR mutation Granules: Children ≥ 12 months and weighing 7 kg to < 25 kg with 1 of the following CFTR mutations: G551D, G1244E, G1349D, G178R, G551S, S1251N, S1255P, S549N, or S549R |
Route of administration | Oral tablets | Oral tablets and granules | Oral tablets | Oral tablets and granules |
Recommended dosage | 6 to < 12 years (weighing < 30 kg) Morning: ELX 100 mg, TEZ 50 mg, and IVA 75 mg Evening: IVA 75 mg 6 to < 12 years (weighing ≥ 30 kg) or ≥ 12 years Morning: ELX 200 mg, and TEZ 100 mg, and IVA 150 mg Evening: IVA 150 mg | Tablets:
Granules:
| Morning: TEZ 100 mg and IVA150 mg Evening: IVA 150 mg | Tablets: IVA 150 mg q.12.h. Granules:
|
Serious adverse effects or safety issues | Product monographs of each of the products include a warning about the risk of elevated transaminases (ALT and AST), and monitoring of liver function is recommended before initiating treatment every 3 months during the first year of treatment and annually thereafter.{, 2018 Dec 11 #89;, 2019 Jan 25 #92;, 2020 Aug 21 #95;, 2021 Jul 26 #98} Product monograph recommends that ELX-TEZ-IVA not be used in patients in patients with severe hepatic impairment; dosage-reduction scenarios are provided in the product monographs for IVA, TEZ-IVA, and LUM-IVA.{, 2021 Jul 26 #98} | |||
CADTH reviews | Aged ≥ 12 years: Reimbursement with conditions2 | Non-submission43 | ||
ALT = alanine transaminase; AST = aspartate transaminase; ELX = elexacaftor; ELX-TEZ-IVA = elexacaftor-tezacaftor-ivacaftor; IVA = ivacaftor; LUM = lumacaftor; LUM-IVA = lumacaftor-ivacaftor; q.12.h. = every 12 hours; TEZ = tezacaftor; TEZ-IVA = tezacaftor-ivacaftor and ivacaftor.
aHealth Canada–approved indications.
Source: Product monographs for Trikafta,{, 2021 Jul 26 #98} Orkambi,{, 2018 Dec 11 #89} Symdeko,{, 2020 Aug 21 #95} and Kalydeco.{, 2019 Jan 25 #92}.
Managing CF requires a demanding treatment routine with regular visits to specialized CF clinics. As the disease progresses, even more time and effort are needed to manage the progressive and debilitating symptoms. The condition has a significant impact on day-to-day quality of life, affecting life decisions that include education, careers, travel, relationships, and family planning.
Patients with CF and their loved ones are seeking treatments that can change the trajectory of the disease and improve both life expectancy and quality of life. Improved outcomes include retaining or increasing lung function, improving digestive health and energy levels, and minimizing symptoms of CF. Patients want to avoid hospital admissions, reduce the need for invasive medical procedures, and minimize the treatment burden of daily therapies. They also wish to avoid the adverse effects of therapies, such as osteoporosis, antimicrobial resistance, and CF-related diabetes or liver dysfunction.
Patient groups emphasized the importance of early and aggressive treatment of CF with a focus on maintaining health and slowing or preventing disease progression. They noted that even those children with CF who appear healthy (e.g., a ppFEV1 of 100%) are subjected to an aggressive therapeutic regimen of physiotherapy and antibiotic treatments in addition to special diets and frequent clinic visits. All patient groups stressed that it is important to start treatment with ELX-TEZ-IVA as soon as possible to prevent the irreversible damage caused by CF. The patient groups referenced the initial CADTH recommendation for ELX-TEZ-IVA, noting that they believe the reimbursement policies are too restrictive, particularly the requirement that patients demonstrate a ppFEV1 of less than 90% to be eligible. The patient groups stated that they believe all patients with at least 1 F508del mutation can benefit from treatment with ELX-TEZ-IVA.
Complete patient input received for the current review of ELX-TEZ-IVA is reported in the appendix of this report. The complete input received for the previous CADTH review if ELX-TEZ-IVA is available on the CADTH website and discussed in the Patient Input section).
Clinician Input
Input From Clinical Experts Consulted by CADTH
All CADTH review teams include at least 1 clinical specialist with expertise regarding the diagnosis and management of the condition for which the drug is indicated. Clinical experts are a critical part of the review team and are involved in all phases of the review process (e.g., providing guidance on the development of the review protocol; assisting in the critical appraisal of clinical evidence; interpreting the clinical relevance of the results; and providing guidance on the potential place in therapy). In addition, as part of the ELX-TEZ-IVA review, CADTH convened panels of clinical experts from across Canada to characterize unmet therapeutic needs, assist in identifying and communicating situations where there are gaps in the evidence that could be addressed through the collection of additional data, promote the early identification of potential implementation challenges, gain further insight into the clinical management of patients living with a condition, and explore the potential place in therapy of the drug (e.g., potential reimbursement conditions).
Unmet Needs
Patients living with CF have significant unmet therapeutic needs. None of the treatments currently available can effectively achieve the most important goals of therapy: prolong survival, prevent the need for lung transplantation, prevent an accelerated decline in lung function over time, or reverse the course of the disease. In addition, the current standard treatments are burdensome for patients and their caregivers. Patients may not respond or may stop responding over time to the currently available treatments.
Place in Therapy
As a CFTR modulator, ELX-TEZ-IVA functions by increasing the amount of CFTR protein at the cell surface (ELX and TEZ) and by improving the transport of chloride through the CFTR protein (IVA). The mechanism of action for ELX-TEZ-IVA is attractive because it acts directly on the CFTR protein to address the defects responsible for the CF phenotype. ELX-TEZ-IVA would be added to existing treatments such as physiotherapy, mucolytics, anti-infectives, and anti-inflammatory treatments (such as azithromycin). The clinical experts noted that ELX-TEZ-IVA would replace earlier CFTR modulators (e.g., Orkambi and Symdeko) that are significantly less effective, and patients currently receiving those drugs would likely be switched to ELX-TEZ-IVA if they meet eligibility and age criteria.
It is anticipated that ELX-TEZ-IVA would be used as a preventive therapy with the goal of initiating treatment before the patient develops significant lung disease. The current treatment paradigm would be significantly altered if ELX-TEZ-IVA can successfully prevent or delay progression to end organ disease (e.g., lung transplant).
Patient Population
The diagnosis of CF is not challenging in routine clinical practice. As all provinces and territories have instituted CF screening for newborns, most people with CF are now identified as newborns and have a confirmed diagnosis by 1 month of age (on average). Sweat chloride testing is available and reliably used to confirm the screening test. The provinces and territories have slightly different testing algorithms and CFTR-mutation screening panels; however, all provinces and territories have effective processes. Almost 100% of newly diagnosed infants would have both CFTR mutations identified. Infants who are not identified via newborn screening (i.e., false negatives), are usually diagnosed before 1 year of age after the development of clinical symptoms of CF. There are clear diagnostic guidelines and little variability in expert opinion. Misdiagnosis and underdiagnosis of CF is exceedingly rare in Canadian clinical practice.
Every patient who meets the Health Canada–approved indication could be eligible for ELX-TEZ-IVA, regardless of their current or past treatment regimens. From a medical perspective, there is no rationale for a patient to demonstrate an inadequate or loss of response to prior therapies before initiating treatment with ELX-TEZ-IVA. It would be reasonable to require patients to complete important standard CF therapies at the same time as receiving treatment with ELX-TEZ-IVA. In clinical practice, eligible patients would be identified based on their CFTR genotype; however, there is no practical method that could be used to predict who will be most likely to respond to ELX-TEZ-IVA.
Applicability of Existing Reimbursement Criteria to Pediatrics
The CADTH recommendation for patients 12 years of age and older includes an initiation criterion that patients are required to have a ppFEV1 of less than or equal to 90% to be eligible for reimbursement. The included trials demonstrated that pediatric patients with a ppFEV1 of greater than 90% experienced clinically meaningful improvements in lung function. Input from patient groups, clinician groups, and the clinical experts consulted by CADTH noted that patients should be eligible for treatment with ELX-TEZ-IVA irrespective of their baseline lung function. There was consensus that those with normal lung function should not be excluded from reimbursement.
Regarding the baseline measurements that must be completed before initiating treatment with ELX-TEZ-IVA, the clinical experts noted the frequency of pulmonary exacerbations can be quite low in pediatric patients and that 12 months would be a more appropriate time frame for evaluation. The nutritional end points (i.e., weight, height, and BMI) are typically measured using z scores and/or BMI percentiles for pediatric patients. The clinical experts noted that CFQ-R scores are typically only collected when conducting research, and not in clinical practice for pediatric patients. As such, this criterion could be challenging to implement in pediatric clinical practice. It would require additional resources for CF clinics to administer the CFQ-R instrument, document the responses, and track changes in scores over time. Differences in record-keeping across Canada (e.g., paper and/or electronic health record systems) were noted as an additional challenge when including CFQ-R assessments in the reimbursement criteria for ELX-TEZ-IVA in pediatric patients.
Table 7: CADTH-Recommended Reimbursement Conditions for ELX-TEZ-IVA in Patients at Least 12 Years of Age
Reimbursement Conditions |
|---|
Initiation |
1. Confirmed diagnosis of CF with at least 1 F508del mutation in the CFTR gene |
2. Aged 12 years and older |
3. ppFEV1 ≤ 90% |
#4.# The following measurements must be completed before initiating treatment with ELX-TEZ-IVA:
|
5. Patients should be optimized with best supportive care for their CF at the time of initiation |
6. The maximum duration of initial reimbursement is for 6 months |
Renewal |
#7.# For the first renewal, the physician must provide at least 1 of the following to demonstrate benefit after 6 months of treatment with ELX-TEZ-IVA:
|
8. The physician must provide evidence of continuing benefit from treatment with ELX-TEZ-IVA for subsequent renewal of reimbursement; subsequent renewals should be assessed annually |
Discontinuation |
9. Patient has undergone lung transplantation |
Prescribing |
10. Prescribing of ELX-TEZ-IVA and monitoring of treatment response should be limited to CF specialists |
11. ELX-TEZ-IVA should not be reimbursed in combination with other CFTR modulators |
BMI = body mass index; CF = cystic fibrosis; CFQ-R = Cystic Fibrosis Questionnaire–Revised; ELX-TEZ-IVA = elexacaftor-tezacaftor-ivacaftor and ivacaftor; FEV1 = forced expiratory volume in 1 second; ppFEV1 = percent predicted forced expiratory volume in 1 second; TEZ-IVA = tezacaftor-ivacaftor and ivacaftor.
Assessing Response to Treatment
The magnitude of improvement in CF outcomes that would be considered clinically significant depends on the baseline status of the patient. The following end points are routinely assessed in Canadian clinical practice: FEV1, nutrition and growth (e.g., BMI, BMI z score, or BMI percentile), hospital admissions and outpatient treatments for pulmonary exacerbations, and pulmonary exacerbation frequency per year. The initial review of ELX-TEZ-IVA noted that CF-related quality-of-life scales can be applied in clinical practice; however, these are not routinely applied in the pediatric setting. Each of these end points are discussed below with reflections on the applicability of the existing CADTH criteria to the expanded patient population.
Spirometry
The CADTH recommendation for patients 12 years or age and older included a criterion that those who demonstrate an improvement of 5% or greater in ppFEV1 relative to baseline should be eligible for initial renewal of reimbursement. The clinical experts noted that there would be a ceiling effect for those with normal lung function, and demonstrating an improvement of 5% or greater in ppFEV1 would be more challenging for these patients. It was noted that the stabilization of lung function (e.g., absence of a decline) or slowing the decline in ppFEV1 is also clinically important and could be considered as evidence that the patient is benefiting from ELX-TEZ-IVA.
BMI and BMI Z Scores
The CADTH recommendation for patients ages 12 years and older included the following as a potential renewal criterion for ELX-TEZ-IVA: no decline in BMI at 6 months compared with the baseline BMI assessment. The pediatric clinical experts noted that BMI z scores and/or BMI percentiles are typically used in clinical practice for pediatric patients with CF and that the existing criterion could be applicable if modified accordingly. However, the pediatric experts suggested that the criterion could be adjusted to provide flexibility within the standard error (SE) of the BMI z score measurement and that 6 months may not be sufficient time to accurately assess the response to treatment. The clinical experts noted that assessment of BMI at 12 months would be more appropriate. The longer time was suggested to account for events that could temporarily reduce BMI (e.g., increased physical activity in summer months and growth spurts). It was strongly noted that discontinuation of ELX-TEZ-IVA in such patients would not be clinically appropriate.
Pulmonary Exacerbations
The CADTH recommendation for patients aged 12 years and older included the following as a potential renewal criterion for ELX-TEZ-IVA: a decrease in the total number of days for which the patient received treatment with oral and/or IV antibiotics for pulmonary exacerbations compared with the 6-month period before initiating treatment or a decrease in the total number of pulmonary exacerbations requiring oral and/or IV antibiotics compared with the 6-month period before initiating treatment. Pulmonary exacerbations were less frequent in the studies that enrolled patients 6 to 11 years of age (e.g., 0.12 events per year in Study 106B) compared with the trials in adults and adolescents (e.g., 0.98 and 0.37 events per year in the placebo and ELX-TEZ-IVA groups, respectively, in Study 102). The clinical experts consulted by CADTH indicated that this is reflective of clinical practice, where these events are less common in children with relatively normal lung function. The clinical experts suggested that this renewal criterion would be reasonable for the use of ELX-TEZ-IVA in some pediatric patients, but that patients who have not experienced a pulmonary exacerbation or those with a very low annual rate of pulmonary exacerbations would also benefit from treatment. In particular, the experts noted that a large subset of pediatric patients have not required antibiotic treatment in the year preceding the CADTH review, which is usual and likely due to the exceptional isolation and infection control that patients with CF and their families have adopted in response to the ongoing COVID-19 pandemic. Similar to the criterion for BMI, it was noted that 12 months would be a more appropriate time frame for evaluating changes in pulmonary exacerbations.
Quality of Life
The CADTH recommendation for patients ages 12 years and older included the following as a potential renewal criterion for ELX-TEZ-IVA: improvement by 4 points or more in the CFQ-R respiratory domain scale. As noted previously, implementation of the CFQ-R instrument in pediatric clinical practice would require additional resources for the CF clinics to administer the CFQ-R instrument, document the responses, and track changes in scores over time.
Sweat Chloride
The previous CADTH recommendation did not include sweat chloride testing as an initiation or renewal condition for ELX-TEZ-IVA. The sponsor has requested that “reduction in sweat chloride” be included as a reimbursement condition for ELX-TEZ-IVA in the current review. The pediatric clinical experts agreed with the prior input from the review of ELX-TEZ-IVA in patients aged 12 years and older, noting that sweat chloride testing should be not used to evaluate the response to ELX-TEZ-IVA for the purposes of drug reimbursement because it is not clearly predictive of clinically important outcomes and only reflects the mechanism of action of CFTR modulators such as ELX-TEZ-IVA. It was noted that poor adherence to the treatment regimen over a short period of time could influence sweat chloride results. In its comments on the draft CADTH report, the sponsor noted that sweat chloride testing has been included in the CF Canada Canadian Clinical Consensus Guideline for Initiation, Monitoring and Discontinuation of CFTR Modulator Therapies for Patients with Cystic Fibrosis, which recommend monitoring the reduction in sweat chloride for patients 6 years and older at baseline, the 3-month visit, and the 12-month visit after initiating treatment with a CFTR modulator (Appendix 1).
Discontinuing Treatment
The CADTH recommendation for patients 12 years of age and older stated that reimbursement should be discontinued in patients who have undergone lung transplantation. It was noted that, unlike the adolescent and adult CF population, lung transplants rare in those 6 to 11 years of age. Given the expected benefit of ELX-TEZ-IVA on nutrition and growth end points in the younger age group, it was anticipated that clinicians would consider ELX-TEZ-IVA for patients in this age group even post–lung transplant if it were not contraindicated due to medication interactions.
Prescribing Conditions
As with the previous review of ELX-TEZ-IVA, the only appropriate setting for initiation and monitoring of treatment with ELX-TEZ-IVA remains an adult or pediatric CF clinic. This treatment will typically be initiated and monitored in the outpatient clinic setting by a CF physician and the associated multidisciplinary team (e.g., specialists in respirology, infectious diseases, and gastroenterology). The experts noted that the drug may also be initiated in hospital. It would not be appropriate that a non-specialty setting or physician prescribe and monitor treatment with ELX-TEZ-IVA.
Clinician Group Input
This section was prepared by CADTH staff based on the input provided by clinician groups.
Three groups of clinicians provided input for the initial CADTH review of ELX-TEZ-IVA (the Canadian Cystic Fibrosis Clinic Directors, CF Canada’s Accelerating Clinical Trials Network, and The Toronto Adult CF Clinic) and 2 groups provided input for the current review (Cystic Fibrosis Canada’s Accelerating Clinical Trials Network and the Canadian Cystic Fibrosis Clinic Directors/CF Canada Health Care Advisory Council). Complete clinician input received for the current review of ELX-TEZ-IVA is reported in an appendix to this report. The complete input and feedback received for the previous CADTH review if ELX-TEZ-IVA is available on the CADTH website in the Clinician Input and Stakeholder Feedback sections). The input from the clinician groups identified the same unmet medical needs for patients with CF and potential place in therapy for ELX-TEZ-IVA as the clinical experts consulted by CADTH. Similar to the clinical experts consulted by CADTH, the clinician groups noted that the impact of ELX-TEZ-IVA has been dramatic and life-altering for the patients who have received the treatment. The groups emphasized that patients should be eligible for treatment with ELX-TEZ-IVA irrespective of their baseline lung function. There was consensus that those with normal lung function should not be excluded from reimbursement.
Drug Program Input
The drug programs provide input on each drug being reviewed through CADTH’s reimbursement review processes by identifying issues that may affect their ability to implement a recommendation. The implementation questions and corresponding responses from the clinical experts consulted by CADTH are summarized in Table 8.
Table 8: Summary of Drug Plan Input and Clinical Expert Response
Drug program implementation questions | Clinical expert response |
|---|---|
Implementation issues from the review of ELX-TEZ-IVA in patients 6 years of age and older | |
Can the clinical experts confirm that multiple-breath washout tests are only available at specialty clinics at children’s hospitals and not available at all pulmonary function testing clinics? | This measurement is not currently used in routine Canadian clinical practice. |
Unlike the pivotal trials for patients aged 12 years and older, patients with a ppFEV1 ≥ 90% were eligible for the trials conducted in patients aged 6 to 11 years. The drug programs have noted that a discrepancy in recommended reimbursement criteria for the 2 patient populations (those aged 6 to 11 years and those 12 years and older) would be challenging for the drug programs to operationalize. Is there evidence to suggest that these patients would benefit from treatment with ELX-TEZ-IVA? | The pediatric trials enrolled patients with a FEV1 > 70% (|||||| and 46% of patients had ppFEV1 > 90% in Study 116 and Study 106B, respectively). These trials demonstrated meaningful improvements in LCI, ppFEV1, BMI z score, and CFQ-R. Therefore, ELX-TEZ-IVA has been shown to have clinical benefit for pediatric patients with a ppFEV1 > 90%. For those 12 years and older, the PROMISE study suggested that patients with a ppFEV1 > 90% at the time of initiating treatment with ELX-TEZ-IVA experienced improvements in ppFEV1 (absolute change of 6.52%; 95% CI, 5.18 to 7.86); BMI (absolute change of 0.82 kg/m2; 95% CI, 0.50 to 1.13); and CFQ-R (absolute change of 15.66; 95% CI, 12.80 to 18.52). |
Prior implementation issues from the review of ELX-TEZ-IVA in patients 12 years of age and older | |
Should prescribing be limited to physicians with expertise in the management of CF? | The only setting appropriate for assessment of patients for this treatment, initiation of treatment, and monitoring of treatment is an adult or pediatric CF clinic. |
What clinical outcome measures should be used to assess therapeutic response to treatment with ELX-TEZ-IVA? | The following end points have been suggested for adult patients:
|
What magnitude of improvement would be clinically significant for ppFEV1? What would be the appropriate intervals for evaluating response to treatment? | For typical patients in Canadian practice, an improvement in ppFEV1 of greater than or equal to 5% would typically be considered clinically meaningful. However, the magnitude of improvement in ppFEV1 that would be considered clinically significant depends on the baseline status of the patient. Those with a very low ppFEV1 may see smaller improvements from baseline, but even stabilization in such patients can be clinically important. FEV1 is routinely assessed in the target population and the experts noted that evaluations could be performed 3 to 4 times per year. |
What magnitude of improvement would be clinically significant for BMI? What would be the appropriate intervals for evaluating response to treatment based on BMI? | Increases in BMI should only be viewed as a marker of improvement in patients who are malnourished. (i.e., BMI < 20). For those patients, the goal of therapy is to increase BMI into the normal range. |
Should therapeutic response be assessed using different criteria for patients who are naive to CFTR-modulator therapy compared with those who are switching from a different CFTR modulator to ELX-TEZ-IVA? | The magnitude of improvement with ELX-TEZ-IVA is far greater than any other currently available treatments for CF (including all other CFTR modulators). ELX-TEZ-IVA would replace earlier CFTR modulators (e.g., Orkambi and Symdeko) that are significantly less effective and patients currently receiving those drugs would likely be switched to ELX-TEZ-IVA. |
The product monograph indicates that patients with severe hepatic impairment should not be treated with ELX-TEZ-IVA. Would these recommendations be followed in clinical practice? | Clinicians may attempt to treat those with severe hepatic impairment using ELX-TEZ-IVA at a reduced dosage, as opposed to using the reduced dosages of the alternative CFTR modulators, which are unlikely to provide the same level of clinical benefit. It was noted that therapeutic trials should be considered for all patients when the potential for benefit exceeds the risk. |
Patients with a ppFEV1 of less than 40% at screening were excluded from the pivotal and supportive phase III trials. Is there evidence to suggest that these patients would benefit from treatment with ELX-TEZ-IVA? | Subgroup data from Study 102 and 2 observational studies included in the CADTH review provided short-term data on the efficacy and safety of ELX-TEZ-IVA in patients with CF who had advanced pulmonary disease. These studies suggested that treatment with ELX-TEZ-IVA resulted in a clinically meaningful improvement in ppFEV1 for patients who had a baseline ppFEV1 of less than 40%. The clinical experts consulted by CADTH, the clinician groups who provided input, and the patient groups that provided input have all noted anecdotal evidence, based on clinical experience, that ELX-TEZ-IVA is beneficial for those with advanced lung disease. |
Patients with a ppFEV1 of greater than 90% at screening were excluded from the pivotal and supportive phase III trials. Is there evidence to suggest that these patients would benefit from treatment with ELX-TEZ-IVA? | These patients may benefit from treatment with ELX-TEZ-IVA. However, prioritization should be for those patients with more significant disease burden. |
What clinical criteria could be used to identify patients with rapidly progressive disease? | There are no currently accepted definitions for patients with rapidly progressive disease. |
What clinical criteria could be used to determine if patients are nonresponders to treatment with ELX-TEZ-IVA (i.e., potential discontinuation criteria)? | Based on the available evidence, nonresponders to ELX-TEZ-IVA are likely to be rare. The primary reasons for discontinuing treatment are likely to be related to adverse events (e.g., abnormal liver function tests, rash, or excessive weight gain). |
BMI = body mass index; CF = cystic fibrosis; CI = confidence interval; ELX-TEZ-IVA = elexacaftor-tezacaftor-ivacaftor and ivacaftor; FEV1 = forced expiratory volume in 1 second; ppFEV1 = percent predicted forced expiratory volume in 1 second.
Clinical Evidence
The clinical evidence included in the review of ELX-TEZ-IVA is presented in 3 sections. The first section, the systematic review, includes pivotal studies provided in the sponsor’s submission to CADTH and Health Canada, as well as those studies that were selected according to an a priori protocol. The second section includes indirect evidence from the sponsor and indirect evidence selected from the literature that met the selection criteria specified in the review. The third section includes sponsor-submitted long-term extension studies and additional relevant studies that were considered to address important gaps in the evidence included in the systematic review.
Systematic Review (Pivotal and Protocol-Selected Studies)
Objectives
To perform a systematic review of the beneficial and harmful effects of ELX 100 mg, TEZ 50 mg, and IVA 75 mg taken each morning and 150 mg of IVA taken each evening for the treatment of patients aged 6 years and older with CF who have at least 1 F508del mutation in the CFTR gene.
Methods
Studies selected for inclusion in the systematic review included pivotal studies provided in the sponsor’s submission to CADTH and Health Canada, as well as those meeting the selection criteria presented in Table 9. Outcomes included in the CADTH review protocol reflect outcomes considered to be important to patients, clinicians, and drug plans.
Table 9: Inclusion Criteria for the Systematic Review
Criteria | Description |
|---|---|
Population | Patients aged 6 years and older with CF and who have at least 1 F508del mutation in the CFTR gene. Subgroups:
|
Intervention |
|
Comparators |
|
Outcomesa | Efficacy outcomes:
Harms outcomes:
|
Study designs | Published and unpublished phase III and IV randomized controlled trials |
CF = cystic fibrosis; ELX = elexacaftor; FEV1 = forced expiratory volume in 1 second; F/F = homozygous for F508del mutation; F/G = 1 F508del mutation and 1 gating mutation in the CFTR gene; F/MF = 1 F508del mutation and 1 minimal function mutation in the CFTR gene; F/RF = 1 F508del mutation and 1 residual function mutation in the CFTR gene; IVA = ivacaftor; LUM-IVA = lumacaftor-ivacaftor; TEZ = tezacaftor; TEZ-IVA = tezacaftor-ivacaftor and ivacaftor.
aOutcomes included in the CADTH review protocol reflect outcomes considered to be important to patients, clinicians, and the drug programs.
Source: Clinical Study Reports.3-8
The literature search for clinical studies was performed by an information specialist using a peer-reviewed search strategy according to the PRESS Peer Review of Electronic Search Strategies checklist (https://www.cadth.ca/resources/finding-evidence/press).45 Published literature was identified by searching the following bibliographic databases: MEDLINE All (1946‒) via Ovid and Embase (1974‒) via Ovid. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. The main search concept was Trikafta (elexacaftor-tezacaftor-ivacaftor). Clinical trials registries searched included the US National Institutes of Health’s clinicaltrials.gov, the WHO’s International Clinical Trials Registry Platform (ICTRP) search portal, Health Canada’s Clinical Trials Database, and the European Union Clinical Trials Register.
No filters were applied to limit the retrieval by study type. Retrieval was not limited by publication date or by language. Conference abstracts were excluded from the search results. Appendix 1 provides detailed search strategies.
The initial search was completed on February 22, 2021. Regular alerts updated the search until the CDEC meeting on June 16, 2021.
Grey literature (literature that is not commercially published) was identified by searching relevant websites from the Grey Matters: A Practical Tool For Searching Health-Related Grey Literature checklist (https://www.cadth.ca/grey-matters).46 Included in this search were the websites of regulatory agencies (FDA and European Medicines Agency [EMA]). Google was used to search for additional internet-based materials. See Appendix 1 for more information on the grey literature search strategy.
These searches were supplemented by reviewing bibliographies of key papers and through contacts with appropriate experts. In addition, the manufacturer of the drug was contacted for information regarding unpublished studies.
Two CADTH clinical reviewers independently selected studies for inclusion in the review based on titles and abstracts, according to the predetermined protocol. Full-text articles of all citations considered potentially relevant by at least 1 reviewer were acquired. Reviewers independently made the final selection of studies to be included in the review, and differences were resolved through discussion.
Findings From the Literature
A total of 6 studies were identified for inclusion in the systematic review (Figure 1). The included studies are summarized in Table 10 and Table 11. A list of excluded studies is presented in Appendix 2.
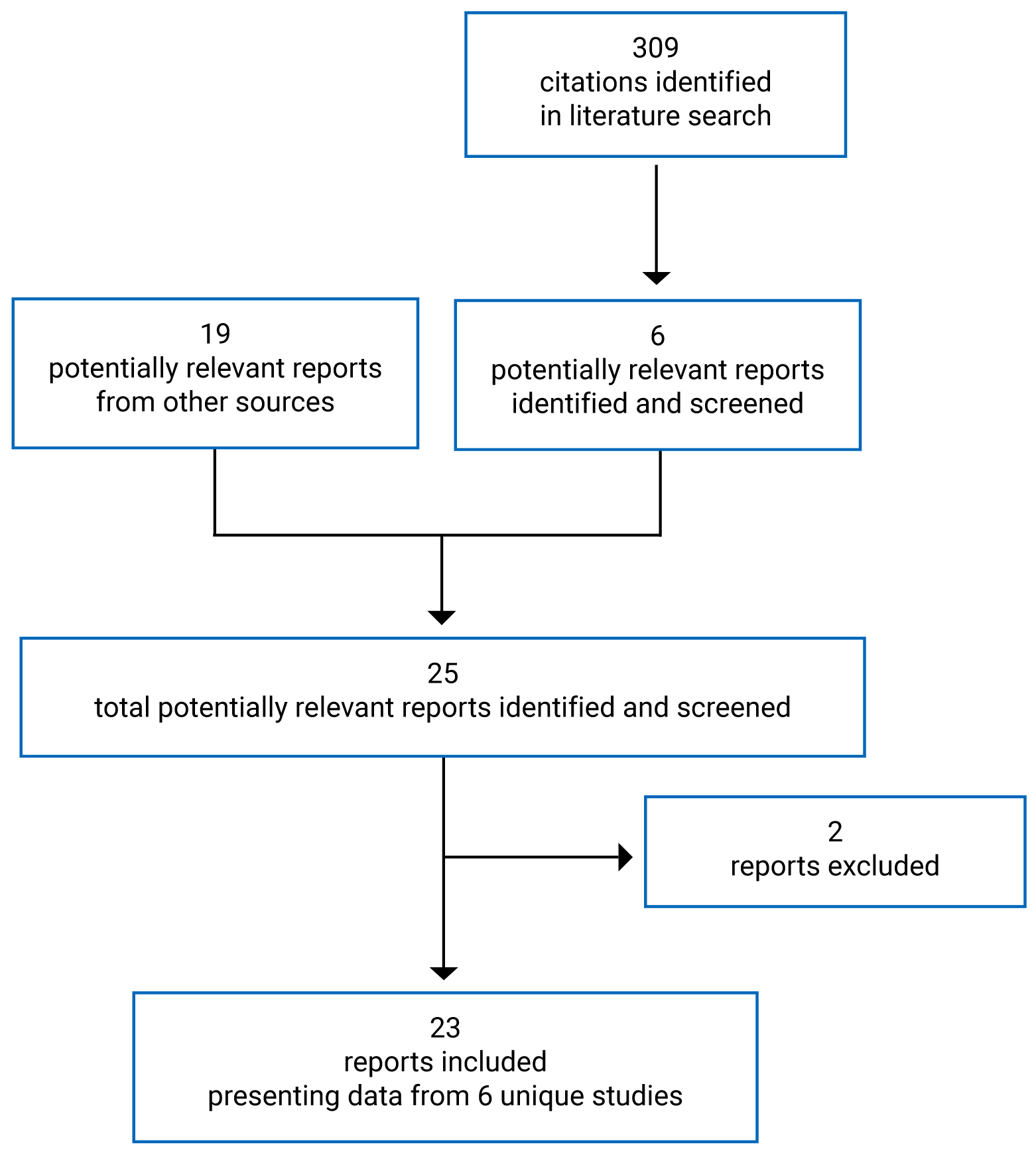
Table 10: Details of Included Studies for Pediatric Patients
Detail | Study 106; AURORA (F/F and F/MF) | Study 116; GALILEO (F/MF) |
|---|---|---|
Designs and populations | ||
Study design | Phase III, open-label, single-arm trial with 2 parts: Part A: 15-day, open-label study to evaluate pharmacokinetics, safety, and tolerability Part B: 24-week, open-label study to evaluate efficacy, pharmacokinetics, safety, and tolerability | Phase IIIb, randomized, double-blind, placebo-controlled, parallel-group, multi-centre |
Locations | Part A: 6 sites in the US Part B: 21 sites in the US, Australia, Canada, UK, and Ireland | 34 sites in Australia, Canada, Israel, Switzerland, the UK, Denmark, France, Germany, the Netherlands, and Spain |
Patient enrolment dates | Part A Study initiation: October 2, 2018 Study completion: January 16, 2019 Part B Study initiation: August 5, 2019 Study completion: August 7, 2020 | Study initiation: June 19, 2020 Study completion: May 17, 2021 |
Randomized (N) | Part A: 16 Part B: 66 | 121
|
Inclusion criteria |
|
|
Exclusion criteria |
| |
Drugs | ||
Intervention | Part A: ELX 100 mg, TEZ 50 mg, and IVA 75 mg (every morning) plus IVA 75 mg (every evening) Part B:
| < 30 kg: ELX 100 mg, TEZ 50 mg, and IVA 75 mg (every morning) plus IVA 75 mg (every evening) ≥ 30 kg: ELX 200 mg, TEZ 100 mg, and IVA 150 mg (every morning) plus IVA 75 mg (every evening) |
Comparator(s) | None | Placebo |
Duration | ||
Phase | ||
Run-in | Part A: 28 days Part B: 28 days | 28 days |
Treatment | Part A: 15 days (open-label) Part B: 24 weeks (open-label) | 24 weeks (double-blind) |
Follow-up | Part A: 28 days Part B: 28 days or entry into OLE | 28 days or entry into OLE |
Outcomes | ||
Primary end point | Part A: Pharmacokinetic parameters of ELX-TEZ-IVA Part B: Safety and tolerability | Absolute change in LCI2.5 from baseline through week 24 |
Secondary and exploratory end points | Part A:
Part B
|
|
Notes | ||
Publications | Zemanick et al. (2021)47 Clinicaltrials.gov48 | Clinicaltrials.gov49 |
ALP = alkaline phosphatase; ALT = alanine transaminase; AST = aspartate transaminase; BMI = body mass index; CF = cystic fibrosis; CFQ-R = Cystic Fibrosis Questionnaire–Revised; ELX = elexacaftor; ELX-TEZ-IVA = elexacaftor-tezacaftor-ivacaftor and ivacaftor; F/F = homozygous for F508del mutations in the CFTR gene; F/MF = 1 F508del mutation and 1 minimal function mutation in the CFTR gene; GFR = glomerular filtration rate; GGT = gamma-glutamyl transferase; IVA = ivacaftor; LCI = lung clearance index; OLE = open-label extension; ppFEV1 = percent predicted forced expiratory volume in 1 second; SwCl = sweat chloride; TEZ = tezacaftor; ULN = upper limit of normal.
Note: Seven additional reports were included: Clinical Study Reports,3,4 European Public Assessment Report,50 Common Technical Document,51 the Sponsor’s Clinical Summary,52 and clinicaltrials.gov.4849
Source: Clinical Study Reports.3,4
Table 11: Details of Included Studies for Adolescent and Adult Patients
Characteristics | Study 102 (F/MF) | Study 103 (F/F) | Study 104 (F/RF, F/G) | Study 109 (F/F) |
|---|---|---|---|---|
Designs and populations | ||||
Study design | Phase III, double-blind, parallel-group, placebo-controlled RCT | Phase III, double-blind, parallel-arm, active-controlled superiority, RCT | Phase III, double-blind, parallel-arm, active-controlled, superiority, RCT | Phase IIIb, double-blind, parallel-arm, active-controlled, RCT |
Locations | 110 sites; 13 countries: Australia, Austria, Belgium, Canada, Czech Republic, France, Germany, Greece, Italy, the Netherlands, Sweden, UK, US | 44 sites; 4 countries: Belgium, the Netherlands, the UK, US | 96 sites; 11 countries: Australia, Belgium, Canada, France, Germany, Ireland, Italy, Spain, the Netherlands, UK, US | 35 sites; 4 countries: UK, Germany, Belgium, Australia |
Patient enrolment dates | First patient enrolled: June 15, 2018 Last study visit: April 14, 2019 | First patient enrolled: August 2018 Last study visit: December 28, 2018 | First patient enrolled: August 28, 2019 Last study visit: June 12, 2020 | First patient enrolled: October 3, 2019 Last study visit: July 24, 2020 |
Randomized (N) | 405
| 107
| 259
| 107
|
Inclusion criteria |
|
|
|
|
Exclusion criteria |
| |||
Drugs | ||||
Intervention | ELX 200 mg, TEZ 100 mg, and IVA 150 mg (every morning) plus IVA 150 (every evening) | |||
Comparator(s) | Placebo | TEZ 100 mg and IVA 150 mg (every morning) plus IVA 150 (every evening) | TEZ 100 mg and IVA 150 mg (every morning) plus IVA 150 (every evening) IVA 150 mg (every morning) plus IVA 150 (every evening) | TEZ 100 mg and IVA 150 mg (every morning) plus IVA 150 mg (every evening) |
Duration | ||||
Phase | ||||
Screening | 28 days | 28 days | 28 days | 28 days |
Run-in | Not applicable | 28 days | 28 days | 28 days |
Double-blind | 24 weeks | 4 weeks | 8 weeks | 8 weeks |
Follow-up | 28 days (or enter OLE) | 28 days (or enter OLE) | 28 days (or enter OLE) | 28 days (or enter OLE) |
Outcomes | ||||
Primary end point |
|
|
|
|
Secondary and exploratory end points |
|
|
|
|
Notes | ||||
Publications | Clinicaltrials.gov58 | Clinicaltrials.gov11 | ||
ALP = alkaline phosphatase; ALT = alanine transaminase; AST = aspartate transaminase; BMI = body mass index; CF = cystic fibrosis; CFQ-R = Cystic Fibrosis Questionnaire–Revised; ELX = elexacaftor; ELX-TEZ-IVA = elexacaftor-tezacaftor-ivacaftor and ivacaftor; F/F = homozygous for F508del mutations in the CFTR gene; F/RF = 1 F508del mutation and 1 residual function mutation in the CFTR gene; F/MF = 1 F508del mutation and 1 minimal function mutation in the CFTR gene; F/G = 1 F508del mutation and 1 gating mutation in the CFTR gene; GFR = glomerular filtration rate; GGT = gamma-glutamyl transferase; IVA = ivacaftor; OLE = open-label extension; PEx = pulmonary exacerbation; ppFEV1 = percent predicted forced expiratory volume in 1 second; RCT = randomized controlled trial; RD = respiratory domain; RF = residual function mutation in the CFTR gene; SwCl = sweat chloride; TEZ = tezacaftor; TEZ-IVA = tezacaftor-ivacaftor and ivacaftor; TSQM = Treatment Satisfaction Questionnaire for Medication; ULN = upper limit of normal.
Note: Eight additional reports were included: Clinical Study Reports,5,6,10,11 FDA Multi-Discipline Review,35 European Public Assessment Report,59 Common Technical Document,51 and the Sponsor’s Clinical Summary.60
Source: Clinical Study Reports.5,6,10,11
Description of Studies
Table 12 provides an overview of the studies that were summarized and appraised by CADTH for the current review of ELX-TEZ-IVA. Four double-blind, phase III, RCTs were included in the CADTH systematic review: 1 placebo-controlled trial conducted in patients who were heterozygous for the F508del mutation and who had 1 minimal function mutation (Study 102); 2 active-controlled trials in patients who were homozygous for the F508del mutation (Study 103 and Study 109); and 1 active-controlled trial in patients who were heterozygous for the F508del mutation and a residual function mutation or a gating mutation (Study 104).
CADTH also reviewed additional studies that did not meet the eligibility criteria of the systematic review but may address important gaps in the evidence from the pivotal and supportive RCTs. These included 1 long-term extension-phase study (Study 105),15 1 indirect comparison filed by the sponsor,52 2 observational studies that evaluated the use of ELX-TEZ-IVA in patients with advanced lung disease,17,18 and 1 study that modelled the potential impact of ELX-TEZ-IVA on morbidity and mortality.19
Population | Study ID or author | Design | Duration | Status |
|---|---|---|---|---|
Studies included in systematic review | ||||
6 to 11 years; F/MF | Study 1164 | Phase III, DB, placebo-controlled RCT | 24 weeks | Complete |
6 to 11 years; F/MF, F/F | Study 106B3 | Pivotal, phase III, single-arm trial | 24 weeks | Complete |
≥ 12 years; F/MF | Study 1025 | Pivotal, phase III, DB, placebo-controlled RCT | 24 weeks | Complete |
≥ 12 years; F/F | Study 1036 | Pivotal, phase III, DB, active-controlled RCT | 4 weeks | Complete |
Study 10910 | Phase III, DB, active-controlled RCT | 24 weeks | Complete | |
≥ 12 years; F/RF, F/G | Study 10411 | Phase III, DB, active-controlled RCT | 8 weeks | Complete |
Long-term extension studies | ||||
6 to 11 years; F/MF, F/F | Study 10761 | Extension study of Study 106B | Up to 96 weeks | Ongoing |
≥ 12 years; F/F, F/MF | Study 10515 | Extension study of Studies 102 and 103 | Up to 96 weeks | Ongoing |
Indirect comparisons | ||||
6 to 11 years; F/F | Sponsor’s indirect comparison52 | MMRM model with individual patient data | 8 to 24 weeks | NA |
≥ 12 years; F/F, F/G, F/RF | Sponsor’s indirect comparison62 | Bucher method indirect comparisons | 8 to 24 weeks | NA |
Studies in patients with advanced lung disease | ||||
≥ 12 years; F/F, F/MF | O’Shea et al. (2020)17 | Retrospective observational study | Approximately 5 months | Complete |
≥ 12 years; F/F, F/othera | Burgel et al. (2020)18 | Prospective observational study | Approximately 3 months | Complete |
Studies that included a subset of patients with normal lung function | ||||
≥ 12 years; F/F, F/MF, F/G or F/other | PROMISE63 | Prospective observational study | 24 weeks | Complete |
≥ 12 years; F/MF, or F/uncharacterized | HELIO | Prospective observational study | NR | Ongoing |
≥ 12 years; F/F, F/MF | US CFFPR | Prospective observational study | NR | Ongoing |
Study modelling impact on morbidity and mortality | ||||
≥ 12 years; F/otherb | Stanojevic et al. (2020)19 | Microsimulation transition model using Canadian CF Registry data | Up to 2030 | NA |
DB = double-blind; F/F = homozygous for F508del mutations in the CFTR gene; F/G = 1 F508del mutation and 1 gating mutation in the CFTR gene; F/MF = 1 F508del mutation and 1 minimal function mutation in the CFTR gene; F/other = 1 F508del mutation and 1 other mutation; F/RF = 1 F508del mutation and 1 residual function mutation in the CFTR gene; F/uncharacterized = 1 F508del mutation and 1 uncharacterized mutation; NA = not applicable; NR = not reported; RCT = randomized controlled trial.
aGenotypes for patients who were heterozygous for the F508del mutation were not reported by Burgel et al. (2020).
bThe microsimulation was conducted based on patients with at least 1 F508del mutation with no separate analyses based on the genotype of patients.
Patients Aged 6 to 11 Years
Placebo-Controlled Trial (Study 116; F/MF Genotype)
Study 116 was a phase III, multinational, parallel-group, placebo-controlled, randomized trial conducted to investigate the efficacy and safety of ELX-TEZ-IVA in patients with CF who are heterozygous for the F508del mutation and who have a minimal function mutation (F/MF). Study 116 was conducted at 34 sites in Australia, Canada, Israel, Switzerland, the UK, Denmark, France, Germany, the Netherlands, and Spain. There were 3 sites in Canada ||||||. As shown in Figure 2, Study 116 consisted of a 28-day screening period, a 24-week double-blind treatment period, and a 28-day follow-up period. Patients who completed the 24-week treatment period could enrol in the OLE study (VX20 to 445 to 119) or enter the 28-day safety follow-up period. Eligible patients were randomized (1:1) to receive ELX-TEZ-IVA or a matching placebo. Those weighing less than 30 kg received ELX 100 mg, TEZ 50 mg, and IVA 75 mg every morning plus IVA 75 mg every evening and those weighing 30 kg or more received ELX 200 mg, TEZ 100 mg, and IVA 150 mg every morning plus IVA 150 mg every evening. Randomization was conducted using an IWRS and stratified by the screening visit values for LCI2.5 (< 10 versus ≥ 10) and body weight (< 30 kg versus ≥ 30 kg).4
Figure 2: Schematic of the Design of Study 116
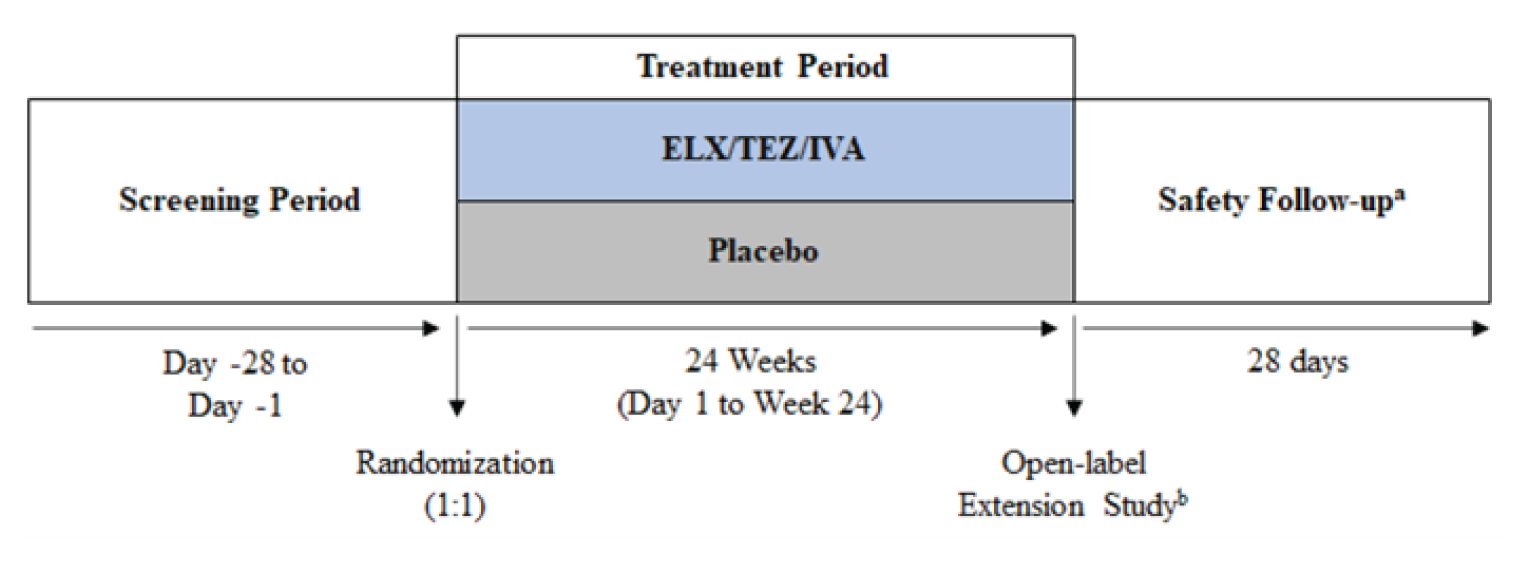
ELX/TEZ/IVA = elexacaftor-tezacaftor-ivacaftor and ivacaftor.
Source: Clinical Study Report.4
Single-Arm Trial (Study 106; F/F or F/MF Genotype)
Study 106 was a phase III, 2-part, multi-centre study evaluating the pharmacokinetics, safety, and tolerability of ELX-TEZ-IVA patients 6 to 11 years of age with an F/F or an F/MF genotype. Study 106 was conducted at 21 sites in the US, Australia, Canada, the UK, and Ireland. There were 2 sites in Canada ||||||||||||. As shown in Figure 3 and Figure 4, Study 106 included 2 parts (A and B). Part A consisted of a 28-day screening period, a 15-day, single-arm, open-label treatment period, and a 28-day safety follow-up period. Part B was initiated after completion of the internal review of the data in Part A that were used to confirm or adjust the doses to be evaluated in Part B. Similar to Part A, Part B of Study 106 included a 28-day screening period, which was followed by a 24-week single-arm, open-label treatment period. Those who completed the Part B treatment period and were not permanently discontinued were offered the opportunity to enrol in an optional OLE study (VX19 to 445 to 107).
Figure 3: Schematic of the Design of Study 106 Part A
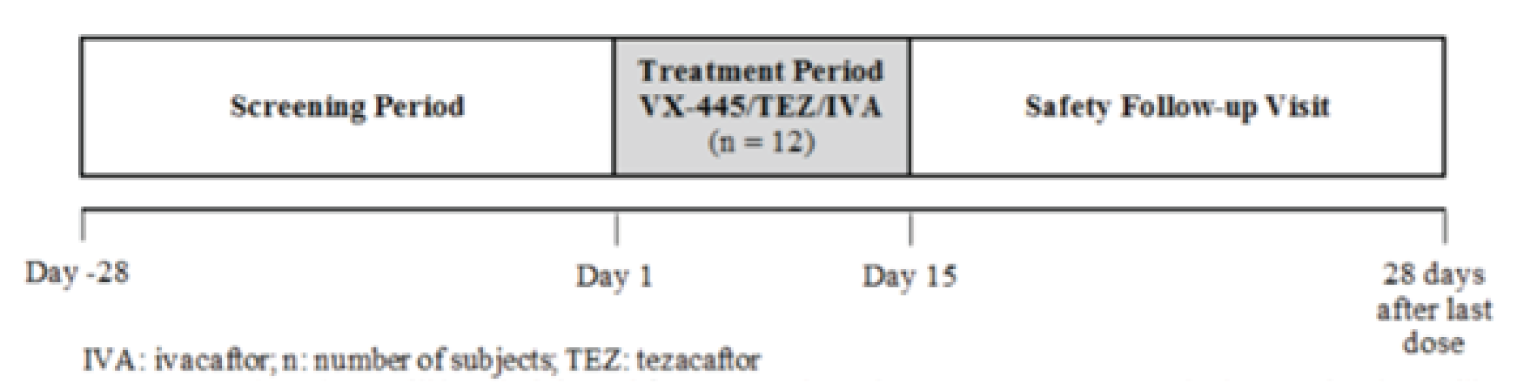
IVA = ivacaftor; VX-445/TEZ/IVA = elexacaftor-tezacaftor-ivacaftor and ivacaftor; TEZ = tezacaftor.
Source: Clinical Study Report.3
Figure 4: Schematic of the Design of Study 106 Part B
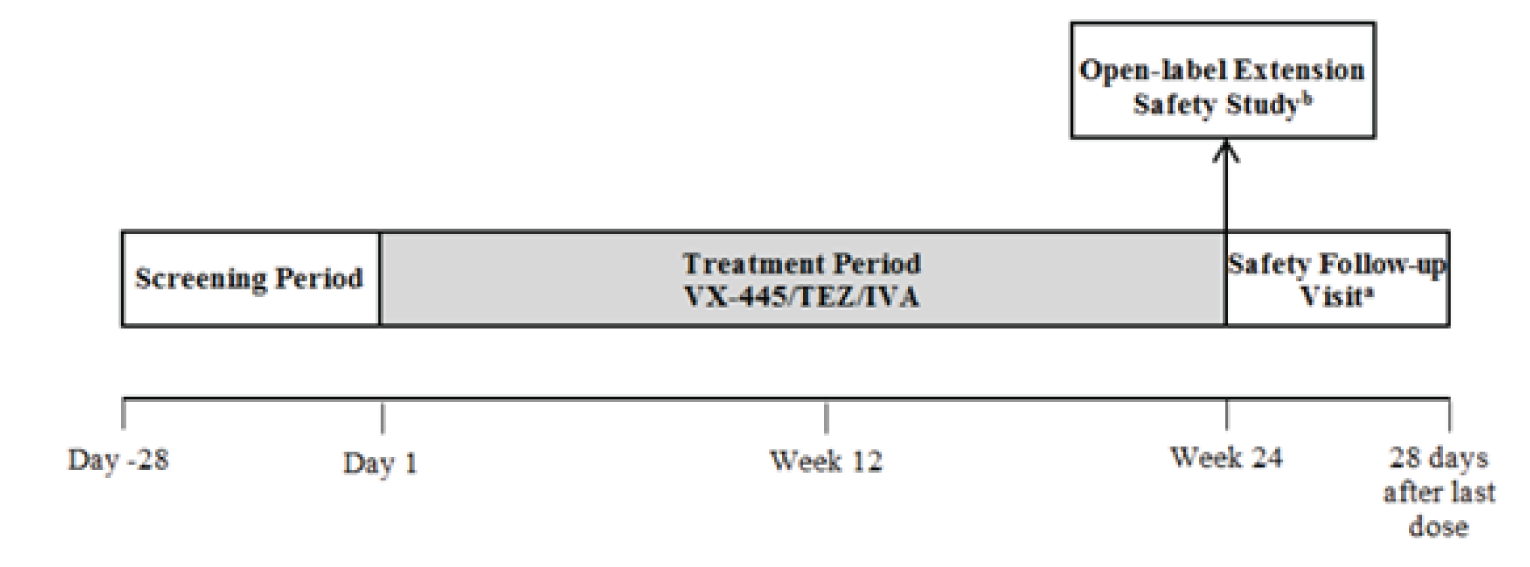
VX-445/TEZ/IVA = elexacaftor-tezacaftor-ivacaftor and ivacaftor.
Source: Clinical Study Report.3
Patients Aged 12 Years and Older
Patients With F/MF Genotype
Study 102 was a pivotal, phase III, multinational, parallel-group, placebo-controlled, randomized trial conducted to investigate the efficacy and safety of ELX-TEZ-IVA in patients with CF who are heterozygous for the F508del mutation and who have a minimal function mutation. Study 102 was conducted at 110 sites in 13 countries, including 6 sites in Canada (n = 24). As shown in Figure 5, Study 102 consisted of a 28-day screening period, a 24-week double-blind treatment period, and a 28-day follow-up period. Patients who completed the 24-week treatment period could enrol in the OLE (Study 105) or enter the 28-day safety follow-up period. Eligible patients were randomized (1:1) to receive ELX-TEZ-IVA (ELX 200 mg, TEZ 100 mg, and IVA 150 mg every morning plus IVA 150 mg every evening) or a matching placebo. Randomization was conducted using an IWRS and stratified by ppFEV1 at screening (< 70% or ≥ 70%), age at screening (less than 18 years or ≥ 18 years of age), and sex (male or female).
An interim efficacy analysis was planned after 140 or more patients completed the week 4 visit and 100 or more patients completed the week 12 visit. The interim analysis was performed by an external independent biostatistician who was not involved in the conduct of Study 102. The results of the interim analysis were reviewed by the independent data monitoring committee. If the committee declared that Study 102 had crossed the pre-specified efficacy boundary, then the study could be unblinded by a limited team from the sponsor for the purposes of preparing a regulatory submission. Those who were unblinded were not to be involved in or influence the conduct of the remaining part of Study 102. All patients (and their parents, caregivers, or companions), site personnel (including the investigator, the site monitor, and the study team), and members of the sponsor’s study team remained blinded until the final database lock.
Figure 5: Schematic of the Design of Study 102
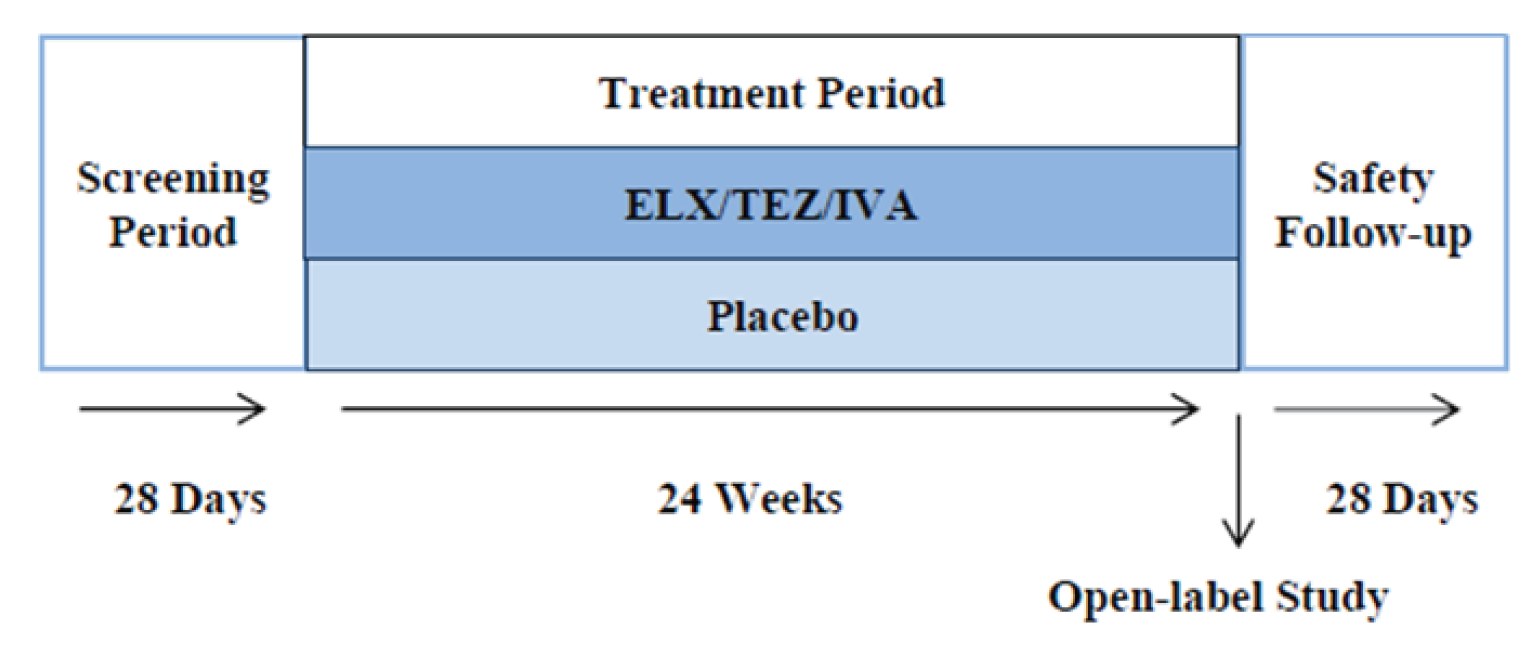
ELX/TEZ/IVA = elexacaftor-tezacaftor-ivacaftor and ivacaftor.
Source: Common Technical Document, section 2.7.3.64
Patients With F/F Genotype
Study 103 was a pivotal, phase III, multinational, parallel-group, active-controlled, randomized trial conducted to investigate the efficacy and safety of ELX-TEZ-IVA in patients with CF who are homozygous for the F508del mutation (F/F). The trial was conducted at 44 sites in 4 countries (Belgium, the Netherlands, the UK, and the US). As shown in Figure 6, Study 103 consisted of a 28-day screening period, a 28-day open-label run-in period during which all patients received TEZ 100 mg and IVA 150 mg once daily in the morning and IVA 150 mg once daily in the evening, a 4-week double-blind treatment period, and a 28-day follow-up period. Patients who completed the 4-week treatment period could enrol in the OLE (Study 105) or enter the 28-day safety follow-up period. Eligible patients were randomized (1:1) to receive ELX-TEZ-IVA (ELX 200 mg, TEZ 100 mg, and IVA 150 mg every morning plus IVA 150 mg every evening) or to continue with TEZ 100 mg once daily and IVA 150 mg every 12 hours. As the morning dose of ELX-TEZ-IVA is administered as 2 tablets (each containing ELX 100 mg, TEZ 50 mg, and IVA 75 mg), patients randomized to the TEZ-IVA group also received a matching placebo tablet for the morning dosage to maintain blinding (i.e., both groups administered 2 tablets in the morning and 1 in the evening). Randomization was conducted using an IWRS and stratified by ppFEV1 at screening (< 70% or ≥ 70%) and age at screening (less than 18 years or ≥ 18 years of age).
Figure 6: Schematic of the Design of Study 103
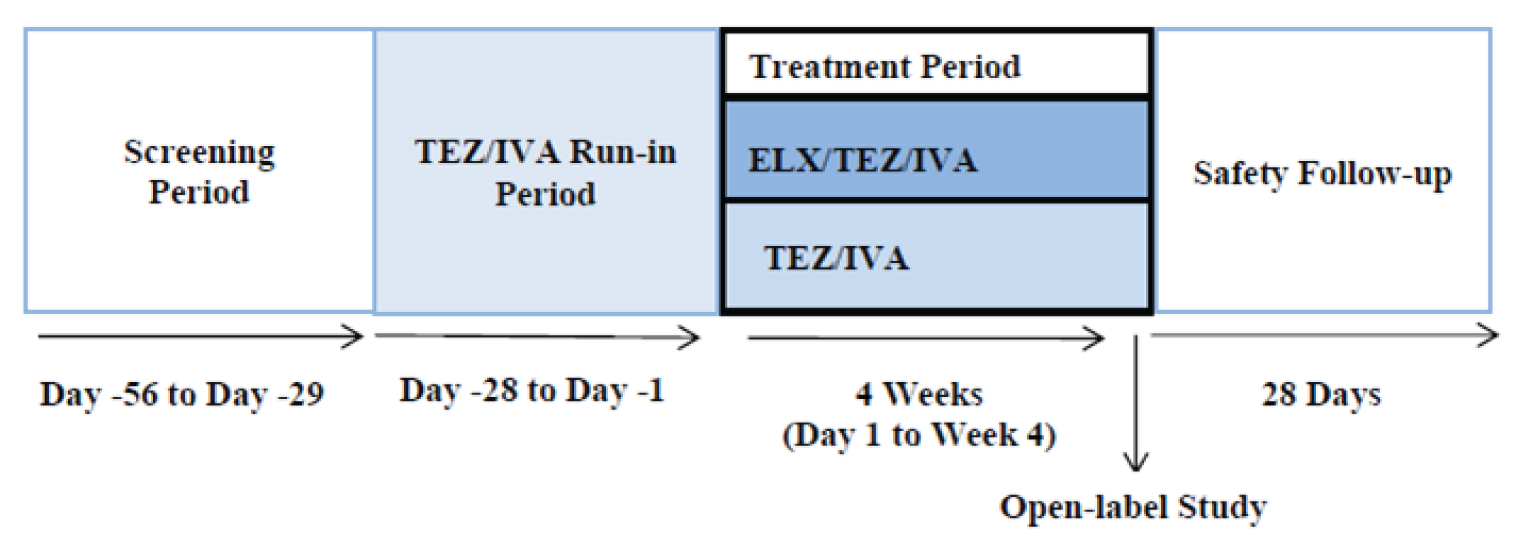
ELX/TEZ/IVA = elexacaftor-tezacaftor-ivacaftor and ivacaftor; TEZ/IVA = tezacaftor-ivacaftor.
Source: Common Technical Document section 2.7.3.64
Study 109 was a phase IIIb, multinational, parallel-group, active-controlled, randomized trial conducted to investigate the efficacy and safety of ELX-TEZ-IVA in patients with CF who are homozygous for the F508del mutation (F/F). The trial was conducted at 35 sites in 4 countries (the UK, Germany, Belgium, and Australia).10 As shown in Figure 7, Study 109 consisted of a 28-day screening period, a 28-day open-label run-in period during which all patients received TEZ 100 mg once daily and IVA 150 mg every 12 hours (TEZ-IVA), a 24-week double-blind treatment period, and a 28-day follow-up period.10 Patients who completed the 24-week treatment period could enrol in the OLE study (NCT04362761)65 or enter the 28-day safety follow-up period. Eligible patients were randomized (1:1) to receive ELX-TEZ-IVA (ELX 200 mg, TEZ 100 mg, and IVA 150 mg every morning plus IVA 150 mg every evening) or to continue with TEZ-IVA.10 As the morning dose of ELX-TEZ-IVA is administered as 2 tablets (each containing ELX 100 mg, TEZ 50 mg, and IVA 75 mg), patients randomized to the TEZ-IVA group also received a matching placebo tablet for the morning dose to maintain blinding (i.e., both groups administered 2 tablets in the morning and 1 in the evening).10 Randomization was stratified by ppFEV1 and ppFEV1 category (i.e., < 70 versus ≥ 70) at day −14 of the TEZ-IVA run-in period; age at screening (< 18 versus ≥ 18 years of age), and whether the patient was receiving CFTR-modulator treatment at screening (yes versus no).10
Figure 7: Schematic of the Design of Study 109
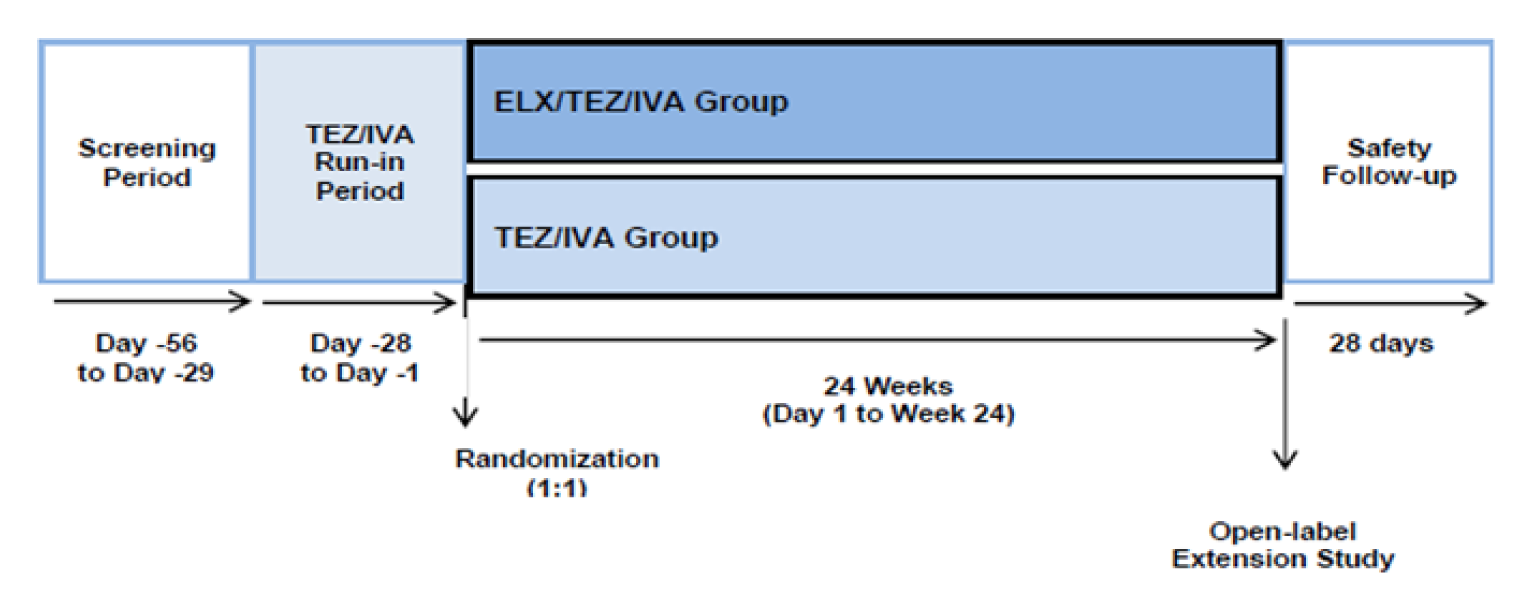
ELX/TEZ/IVA = elexacaftor-tezacaftor-ivacaftor and ivacaftor; TEZ/IVA = tezacaftor-ivacaftor.
Source: Sponsor’s Clinical Summary.60
Patients With F/RF or F/G Genotype
Study 104 was a phase III, multinational, parallel-group, active-controlled, randomized trial conducted to investigate the efficacy and safety of ELX-TEZ-IVA in patients with CF who are heterozygous for the F508del mutation and a gating mutation (F/G) or a residual function mutation (F/RF).11 This study was conducted at 96 sites in 11 countries (Australia, Belgium, Canada, France, Germany, Ireland, Italy, Spain, the Netherlands, the UK, and the US).11 As shown in Figure 8, Study 104 consisted of a 28-day screening period, a 28-day open-label run-in period during which all patients with an F/RF genotype received TEZ 100 mg once daily and IVA 150 mg every 12 hours (TEZ-IVA) and those with an F/G genotype received IVA 150 mg every 12 hours, with a 4-week double-blind treatment period, and a 28-day follow-up period.11 Patients who completed the 4-week treatment period could enrol in the OLE study (VX18 to 445 to 110)66 or enter the 28-day safety follow-up period. Eligible patients were randomized (1:1) to receive ELX-TEZ-IVA (ELX 200 mg, TEZ 100 mg, and IVA 150 mg every morning plus IVA 150 mg every evening) or to the control group, whose members would continue with TEZ-IVA or IVA as per their genotype.11 As the morning dose of ELX-TEZ-IVA is administered as 2 tablets (each containing ELX 100 mg, TEZ 50 mg, and IVA 75 mg), patients randomized to the control group (TEZ-IVA or IVA) also received a matching placebo tablet for the morning dose to maintain blinding (i.e., both groups administered 2 tablets in the morning and 1 in the evening). Randomization was conducted using an IWRS and stratified by comparator group (IVA versus TEZ-IVA), ppFEV1 at the day −14 visit, and sweat chloride at the day −14 visit.11
Figure 8: Schematic of the Design of Study 104
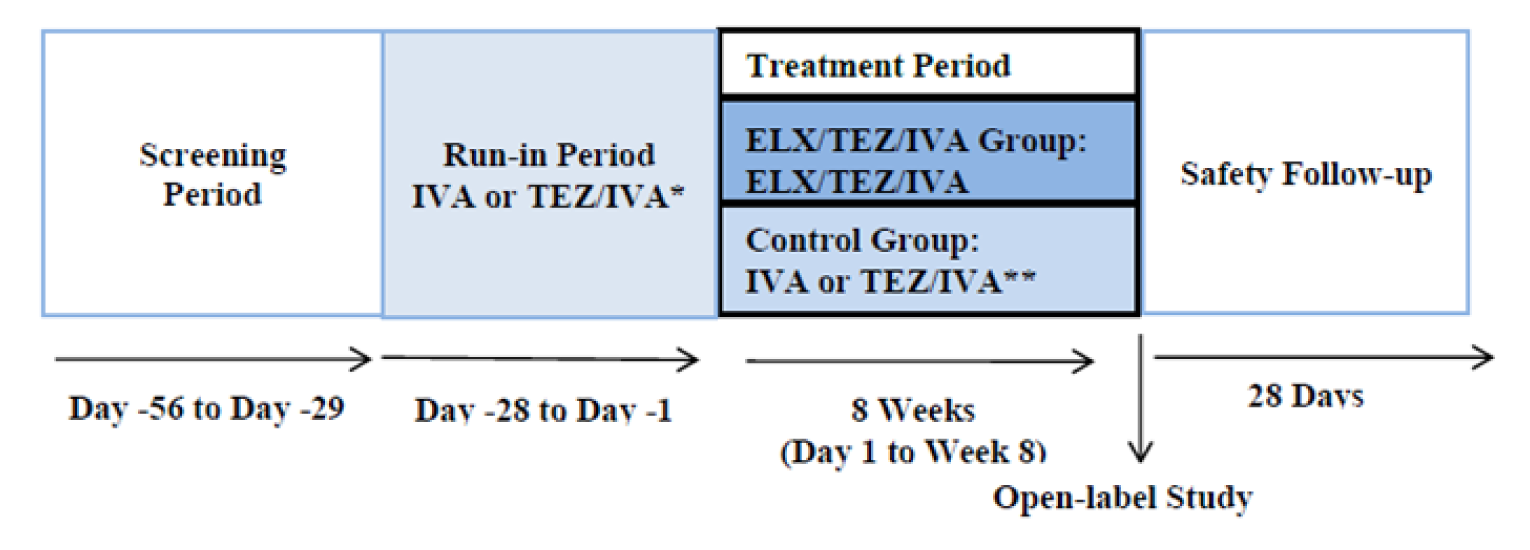
ELX/TEZ/IVA = elexacaftor-tezacaftor-ivacaftor and ivacaftor; IVA = ivacaftor; TEZ/IVA = tezacaftor-ivacaftor.
Source: Common Technical Document, section 2.7.3.64
Populations
Inclusion and Exclusion Criteria
Patients Aged 6 to 11 Years
Placebo-Controlled Trial (Study 116; F/MF Genotype): Patients aged 6 through 11 years (inclusive) were eligible for inclusion in Study 116 if they were heterozygous for F508del and a minimal function mutation in the CFTR gene and had a confirmed diagnosis of CF (determined by the investigator). Details regarding classification of minimal function mutations are described in the section for Study 102. Patients were required to weigh 15 kg or more, have stable CF disease in the opinion of the investigator, a ppFEV1 of 70% or greater, and an LCI2.5 result of 7.5 or greater at the time of screening. The trial excluded patients with a history of colonization with Burkholderia cenocepacia, Burkholderia dolosa, and/or Mycobacterium abscessus. Patients were also considered ineligible if they reported an acute upper or lower respiratory infection, pulmonary exacerbation, or changes in therapy (including antibiotics) for pulmonary disease within 28 days before their first dose of TEZ-IVA in the run-in period. Patients with a history of solid organ or hematological transplantation were excluded, as were patients with abnormal laboratory values (e.g., hemoglobin < 10 g/dL), abnormal liver function, or abnormal renal function.4
Single-Arm Trial (Study 106; F/F or F/MF Genotype): Patients aged 6 through 11 years (inclusive) were eligible for inclusion in Study 106 if they were homozygous for the F508del mutation (F/F) or heterozygous for F508del and an minimal function mutation in the CFTR gene and had a confirmed diagnosis of CF (determined by the investigator). Details regarding classification of minimal function mutations are described in the following section for Study 102. Patients were required to weigh 15 kg or more, have stable CF disease in the opinion of the investigator, and a ppFEV1 of 40 or greater at the time of screening. The trial excluded patients with a history of colonization with Burkholderia cenocepacia, Burkholderia dolosa, and/or Mycobacterium abscessus. Patients were also considered to be ineligible if they reported an acute upper or lower respiratory infection, pulmonary exacerbation, or changes in therapy (including antibiotics) for pulmonary disease within 28 days before first dose of TEZ-IVA in the run-in period. Patients with a history of solid organ or hematological transplantation were excluded, as were patients with abnormal laboratory values (e.g., hemoglobin < 10 g/dL), abnormal liver function, or abnormal renal function.3
Patients Aged 12 Years and Older
Patients With F/MF Genotype (Study 102): Patients aged 12 years and older were eligible for inclusion in Study 102 if they were heterozygous for F508del with a minimal function mutation in the CFTR gene and a confirmed diagnosis of CF (determined by the investigator).34 To be considered minimal function, the mutation was required to meet at least 1 of the following criteria:
biologic plausibility of no translated CFTR protein (i.e., the genetic sequence predicts the complete absence of CFTR protein)
in vitro testing that supports lack of responsiveness to TEZ, IVA, or TEZ-IVA, and evidence of clinical severity on a population basis.5
The mutations that were classified as minimal function based on in vitro testing met the following criteria in the sponsor’s in vitro experiments: baseline chloride transport of less than 10% of wild-type CFTR and an increase in chloride transport of less than 10% over baseline following the addition of TEZ, IVA, or TEZ-IVA in the assay. Clinical severity on a population basis was determining using The Clinical and Functional Translation of CFTR (CFTR2)67 patient registry. Patients with these mutations on 1 allele and F508del on the other allele exhibited evidence of clinical severity as defined as an average sweat chloride level of greater than 86 mmol/L and the prevalence of pancreatic insufficiency greater than 50%.5 A complete list of minimal function mutations is provided in Table 13.
Patients were also required to have stable CF disease in the opinion of the investigator and a ppFEV1 of between 40% and 90% at the time of screening.5 The trials excluded patients with a history of colonization with Burkholderia cenocepacia, Burkholderia dolosa, and/or Mycobacterium abscessus. Patients were also considered ineligible if they reported an acute upper or lower respiratory infection, pulmonary exacerbation, or changes in therapy (including antibiotics) for pulmonary disease within 4 weeks before their first dose of the study drug.34 Patients with a history of solid organ or hematological transplantation were excluded, as were patients with abnormal laboratory values (e.g., hemoglobin < 10 g/dL), abnormal liver function, or abnormal renal function.34
Table 13: Minimal Function Mutations in Study 102
Criteria | Mutations | ||||
|---|---|---|---|---|---|
Truncation mutations
| Q2X | L218X | Q525X | R792X | E1104X |
S4X | Q220X | G542X | E822X | W1145X | |
W19X | Y275X | G550X | W882X | R1158X | |
G27X | C276X | Q552X | W846X | R1162X | |
Q39X | Q290X | R553X | Y849X | S1196X | |
W57X | G330X | E585X | R851X | W1204X | |
E60X | W401X | G673X | Q890X | L1254X | |
R75X | Q414X | Q685X | S912X | S1255X | |
L88X | S434X | R709X | Y913X | W1282X | |
E92X | S466X | K710X | Q1042X | Q1313X | |
Q98X | S489X | Q715X | W1089X | Q1330X | |
Y122X | Q493X | L732X | Y1092X | E1371X | |
E193X | W496X | R764X | W1098X | Q1382X | |
W216X | C524X | R785X | R1102X | Q1411X | |
Splice mutations
| 185 + 1G-->T | 711 + 1G-->T | 1525 to 1G-->A | 1812 to 1G-->A | 3120 + 1G-->A |
296 + 1G-->A | 711 + 5G-->A | 1898 + 1G-->C | 1898 + 1G-->A | 3121 to 2A-->G | |
296 + 1-->GT | 712 to 1G-->T | 1717 to 8G-->A | 2622 + 1G-->A | 3121 to 1G-->A | |
405 + 1G-->A | 1248 + 1G-->A | 1717 to 1G-->A | 2790 to 1G-->C | 3500 to 2A-->G | |
405 + 3A-->C | 1249 to 1G-->A | 1811 + 1G-->C | 3040G-->C (G970R) | 3600 + 2insT | |
406 to 1G-->A | 1341 + 1G-->A | 1811 + 1.6kbA-->G | 3850 to 1G-->A | 4005 + 1G-->A | |
621 + 1G-->T | 1525 to 2A-->G | 1811 + 1643G-->T | 3120G-->A | 4374 + 1G-->T | |
Small (≤ 3 nucleotides) insertion/deletion frameshift mutations
| 182delT | 1078delT | 1677delTA | 2711delT | 3737delA |
306insA | 1119delA | 1782delA | 2732insA | 3791delC | |
306delTAGA | 1138insG | 1824delA | 2869insG | 3821delT | |
365 to 366insT | 1154insTC | 1833delT | 2896insAG | 3876delA | |
394delTT | 1161delC | 2043delG | 2942insT | 3878delG | |
442delA | 1213delT | 2143delT | 2957delT | 3905insT | |
444delA | 1259insA | 2183AA→G | 3007delG | 4016insT | |
457TAT→G | 1288insTA | 2184delA | 3028delA | 4021dupT | |
541delC | 1343delG | 2184insA | 3171delC | 4022insT | |
574delA | 1471delA | 2307insA | 3171insC | 4040delA | |
663delT | 1497delGG | 2347delG | 3271delGG | 4279insA | |
849delG | 1548delG | 2585delT | 3349insT | 4326delTC | |
935delA | 1609delCA | 2594delGT | 3659delC | ||
Non-small (> 3 nucleotide) insertion/deletion frameshift mutations
| CFTRdele1 | CFTR50kbdel | CFTRdele17a-18 | 602del14 | 2372del8 |
CFTRdele2 | CFTRdup6b-10 | CFTRdele19 | 852del22 | 2721del11 | |
CFTRdele2,3 | CFTRdele11 | CFTRdele19 to 21 | 991del5 | 2991del32 | |
CFTRdele2 to 4 | CFTRdele13,14a | CFTRdele21 | 1461ins4 | 3121977_3499 + 248del2515 | |
CFTRdele3 to 10,14b-16 | CFTRdele14b-17b | CFTRdele22 to 24 | 1924del7 | 3667ins4 | |
CFTRdele4 to 7 | CFTRdele16 to 17b | CFTRdele22,23 | 2055del9→A | 4010del4 | |
CFTRdele4 to 11 | CFTRdele17a,17b | 124del23bp | 2105 to 2117 del13insAGAAA | 4209TGTT-->AA | |
Class II, III, IV mutations not responsive to TEZ, IVA, or TEZ-IVA
| A46Db | I507del | R560T | Y569Db | L1077Pb |
G85E | V520F | R560S | L1065P | M1101K | |
R347P | A559Tb | A561E | R1066C | N1303K | |
L467Pb | — | — | — | — | |
IVA = ivacaftor; PI = pancreatic insufficiency; SwCl = sweat chloride; TEZ = tezacaftor; TEZ-IVA = tezacaftor-ivacaftor and ivacaftor.
Source: Clinical Study Report.5
Patients With F/F Genotype: Patients aged 12 years and older were eligible for inclusion in Study 103 and Study 109 if they were homozygous for the F508del mutation in the CFTR gene and had a confirmed diagnosis of CF (determined by the investigator). Patients were also required to have stable CF disease in the opinion of the investigator and a ppFEV1 of between 40% and 90% at the time of screening.6,10 The trial excluded patients with a history of colonization with Burkholderia cenocepacia, Burkholderia dolosa, and/or Mycobacterium abscessus.6,10 Patients were also considered ineligible if they reported an acute upper or lower respiratory infection, pulmonary exacerbation, or changes in therapy (including antibiotics) for pulmonary disease within 28 days before their first dose of TEZ-IVA in the run-in period.6,10 Patients with a history of solid organ or hematological transplantation were excluded, as were patients with abnormal laboratory values (e.g., hemoglobin < 10 g/dL), abnormal liver function, or abnormal renal function.6,10
Patients With F/G and F/RF Genotypes: Patients aged 12 years and older were eligible for inclusion in Study 104 if they were heterozygous for the F508del mutation and either a gating mutation (F/G) or a residual function mutation (F/RF) in a jurisdiction where regulatory authorities had approved treatment with IVA and/or TEZ-IVA for their genotype and age group.11 Table 14 provides a summary of the gating mutations and residual function mutations.
Patients must have a confirmed diagnosis of CF with have stable disease (both determined based on the opinion of the investigator) and a ppFEV1 of between 40% and 90% at the time of screening.11 The trial excluded patients with a history of colonization with Burkholderia cenocepacia, Burkholderia dolosa, and/or Mycobacterium abscessus.11 Patients were also considered ineligible if they reported an acute upper or lower respiratory infection, pulmonary exacerbation, or changes in therapy (including antibiotics) for pulmonary disease within 28 days before their first dose of TEZ-IVA in the run-in period.11 Patients with a history of solid organ or hematological transplantation were excluded, as were patients with abnormal laboratory values (e.g., hemoglobin < 10 g/dL), abnormal liver function, or abnormal renal function.11
Table 14: Gating and Residual Function Mutations in Study 104
Category | Mutations | ||
|---|---|---|---|
Gating mutations in the CFTR gene | R117H | G551D | G1244E |
G178R | G551S | S1251N | |
S549N | G1069R | S1255P | |
S549R | R1070Q | G1349D | |
Residual function mutations in the CFTR gene | 711 + 3A > G | R117C | S977F |
2789 + 5G > A | E193K | F1052V | |
3272 to 26A > G | L206W | K1060T | |
3849 + 10kbC > T | R347H | A1067T | |
E56K | R352Q | R1070W | |
P67L | A455E | F1074L | |
R74W | D579G | D1152H | |
D110E | E831X | D1270N | |
D110H | S945L | ||
Source: Clinical Study Report.11
Baseline and Demographic Characteristics
Patients Aged 6 to 11 Years
Placebo-Controlled Trial (Study 116; F/MF Genotype): The baseline and demographic characteristics in Study 116 were generally similar across the ELX-TEZ-IVA and placebo groups. Compared with the placebo group, a higher percentage of patients in the ELX-TEZ-IVA group had a baseline ppFEV1 > 90% |||||||||||||||||||||||| and lower proportion had baseline ppFEV1 < 70% ||||||||||||||||||||||||. A greater proportion of patients in the ELX-TEX-IVA group reporting prior usage of inhaled antibiotics compared with the placebo group |||||||||||||||||||||||| and a higher percentage of those in the placebo group reported prior use of a bronchodilator ||||||||||||||||||||||||||||||.4
Single-Arm Trial (Study 106; F/F or F/MF Genotype): The baseline and demographic characteristics in Study 106 are similar to those in Study 116, with the exception of the CFTR genotype. Study 106 enrolled patients with F/F or F/MF genotypes and Study 116 was limited to those with an F/MF genotype.3
Table 15: Summary of Baseline and Demographic Characteristics in Pediatric Studies
Characteristics | Study 116 | Study 106 | ||
|---|---|---|---|---|
Placebo (N = 61) | ELX-TEZ-IVA (N = 60) | Part A (N = 16) | Part B (N = 66) | |
CFTR genotype group, n (%) | ||||
F/F | NA | NA | 7 (43.8) | 29 (43.9) |
F/MF | 61 (100) | 60 (100) | 9 (56.3) | 37 (56.1) |
Sex, n (%) | ||||
Male | 26 (42.6) | 25 (41.7) | 5 (31.3) | 27 (40.9) |
Female | 35 (57.4) | 35 (58.3) | 11 (68.8) | 39 (59.1) |
Child-bearing potential, n (%) | ||||
Yes | 17 (48.6) | 19 (54.3) | 2 (18.2) | 39 (100.0) |
No | 18 (51.4) | 16 (45.7) | 9 (81.8) | 0 |
Age at baseline (years) | ||||
Mean (SD) | 9.2 (1.7) | 9.1 (1.8) | 9.0 (2.0) | 9.3 (1.9) |
Median | 9.1 (6.3 to 11.7) | 8.9 (6.1 to 12.0) | 8.9 (6.1 to 12.1) | 9.6 (6.1 to 12.1) |
Race, n (%) | ||||
White | 42 (68.9) | 45 (75.0) | 16 (100.0) | 58 (87.9) |
Black or African-American | 0 | 1 (1.7) | 0 | 0 |
Asian | 0 | 1 (1.7) | 0 | 1 (1.5) |
American Indian or Alaska Native | 0 | 1 (1.7) | 0 | 0 |
Not collected per local regulations | 18 (29.5) | 11 (18.3) | 0 | 8 (12.1) |
Other | 1 (1.6) | 0 | 0 | 0 |
Multiracial | 0 | 1 (1.7) | 0 | 0 |
Ethnicity, n (%) | ||||
Hispanic or Latino | 0 | 1 (1.7) | 0 | 0 |
Not Hispanic or Latino | 42 (68.9) | 48 (80.0) | 16 (100.0) | 58 (87.9) |
Not collected per local regulations | 19 (31.1) | 11 (18.3) | 0 | 8(12.1) |
Weight (kg) | ||||
Mean (SD) | 29.8 (8.6) | 29.1 (7.6) | 29.3 (6.7) | 30.0 (7.7) |
Median (range) | 27.3 (18.2 to 59.8) | 27.1 (16.2 to 51.5) | 28.5 (18.1 to 42.8) | 29.0 (18.1 to 53.6) |
Weight-for-age z score | ||||
Mean (SD) | −0.29 (0.96) | −0.27 (0.99) | −0.05 (0.61) | −0.22 (0.76) |
Median (range) | −0.32 (−3.42 to 1.95) | −0.29 (−2.46 to 1.52) | −0.14 (−1.13 to 1.37) | −0.23 (−2.45 to 1.34) |
Height (cm) | ||||
Mean (SD) | 134.6 (13.3) | 132.3 (11.7) | 133.0 (9.9) | 134.1 (12.3) |
Median (range) | 133.5 (99.7 to 163.3) | 131.1 (109.4 to 159.4) | 134.2 (110.6 to 150.1) | 136.0 (111.8 to 162.3) |
Height-for-age z score | ||||
Mean (SD) | 0.01 (1.26) | −0.17 (1.02) | 0.14 (1.17) | −0.11 (0.98) |
Median (range) | 0.14 (−6.36 to 2.19) | −0.16 (−2.55 to 1.90) | 0.19 (−2.01 to 2.63) | −0.05 (−2.42 to 2.09) |
BMI (kg/m2) | ||||
Mean (SD) | 16.11 (2.32) | 16.33 (1.84) | 16.35 (2.13) | 16.39 (1.69) |
Median (range) | 15.65 (13.04 to 27.86) | 15.87 (13.54 to 21.91) | 15.68 (13.34 to 20.36) | 16.25 (13.36 to 20.94) |
BMI-for-age z score | ||||
Mean (SD) | −0.39 (0.92) | −0.17 (0.85) | −0.16 (0.75) | −0.16 (0.74) |
Median (range) | −0.33 (−2.57 to 2.14) | −0.16 (−1.88 to 1.59) | −0.31 (−1.92 to 1.11) | −0.20 (−2.16 to 1.13) |
LCI2.5 at screening, n (%) | ||||
< 10 | 35 (57.4) | 34 (56.7) | NR | NR |
≥ 10 | 26 (42.6) | 26 (43.3) | NR | NR |
Weight (kg) at screening, n (%) | ||||
< 30 | 38 (62.3) | 39 (65.0) | NR | 36 (54.5) |
≥ 30 | 23 (37.7) | 21 (35.0) | NR | 30 (45.5) |
< 25 kg | NR | NR | 4 (25.0) | NR |
≥ 25 to < 40 kg | NR | NR | 11 (68.8) | NR |
≥ 40 kg | NR | NR | 1 (6.3) | NR |
LCI2.5 at baseline | ||||
Mean (SD) | 9.75 (1.95) | 10.26 (2.22) | NR | 9.77 (2.68) |
Median (range) | 9.14 (6.91 to 15.75) | 9.71 (7.13 to 18.36) | NR | 9.21 (6.86 to 20.14) |
Sweat chloride (mmol/L) at baseline | ||||
Mean (SD) | 102.6 (8.6) | 102.8 (10.0) | 104.1 (10.6) | 102.2 (9.1) |
Median (range) | 104.0 (83.5 to 123.0) | 103.5 (77.0 to 123.5) | 107.5 (83.5 to 115.0) | 101.5 (75.5 to 122.0) |
ppFEV1 category at baseline, n (%) | ||||
< 70 | 10 (16.4) | 4 (6.7) | 2 (12.5) | 10 (15.2) |
≥ 70 to ≤ 90 | 23 (37.7) | 20 (33.3) | 8 (50.0) | 22 (33.3) |
> 90 | 28 (45.9) | 36 (60.0) | 6 (37.5) | 30 (45.5) |
Missing | 0 | 0 | 0 | 4 (6.1) |
ppFEV1 at baseline | ||||
Mean (SD) | 87.2 (15.8) | 91.4 (13.8) | 85.1 (16.1) | 88.8 (17.7) |
Median (range) | 89.6 (55.8 to 119.6) | 93.0 (44.6 to 121.8) | 84.8 (46.4 to 111.7) | 89.3 (39.0 to 127.1) |
CFQ-R respiratory domain score (child’s version) at baseline | ||||
Mean (SD) | 82.7 (14.1) | 85.7 (11.7) | NA | 80.3 (15.2) |
Median (range) | 83.3 (50.0 to 100.0) | 83.3 (50.0 to 100.0) | NA | 83.3 (33.3 to 100.0) |
Prior use of CFTR modulator, n (%) | ||||
Yes | 0 | 0 | NR | 14 (21.2) |
No | 61 (100) | 60 (100) | NR | 52 (78.8) |
Prior use of dornase alfa,a n (%) | ||||
Yes | 41 (67.2) | 42 (70.0) | NR | 54 (81.8) |
No | 20 (32.8) | 18 (30.0) | NR | 12 (18.2) |
Prior use of azithromycin,a n (%) | ||||
Yes | 9 (14.8) | 11 (18.3) | NR | 19 (28.8) |
No | 52 (85.2) | 49 (81.7) | NR | 47 (71.2) |
Prior use of inhaled antibiotic,a n (%) | ||||
Yes | 8 (13.1) | 15 (25.0) | NR | 8 (12.1) |
No | 53 (86.9) | 45 (75.0) | NR | 58 (87.9) |
Prior use of any bronchodilator,a n (%) | ||||
Yes | 46 (75.4) | 38 (63.3) | NR | 61 (92.4) |
No | 15 (24.6) | 22 (36.7) | NR | 5 (7.6) |
Prior use of any inhaled bronchodilator,a n (%) | ||||
Yes | 46 (75.4) | 38 (63.3) | NR | 61 (92.4) |
No | 15 (24.6) | 22 (36.7) | NR | 5 (7.6) |
Prior use of any inhaled hypertonic saline,a n (%) | ||||
Yes | 46 (75.4) | 46 (76.7) | NR | 52 (78.8) |
No | 15 (24.6) | 14 (23.3) | NR | 14 (21.2) |
Prior use of any inhaled corticosteroids,a n (%) | ||||
Yes | 18 (29.5) | 15 (25.0) | NR | 38 (57.6) |
No | 43 (70.5) | 45 (75.0) | NR | NR |
Infection with Pseudomonas aeruginosa within 2 years before screening, n (%) | ||||
Positive | NR | NR | NR | 26 (39.4) |
Negative | NR | NR | NR | 40 (60.6) |
BMI = body mass index; CFQ-R = Cystic Fibrosis Questionnaire–Revised; ELX-TEZ-IVA = elexacaftor-tezacaftor-ivacaftor and ivacaftor; F/F = homozygous for F508del mutation in the CFTR gene; F/MF = 1 F508del mutation and 1 minimal function mutation in the CFTR gene; LCI = lung clearance index; ppFEV1 = percent predicted forced expiratory volume in 1 second; SD = standard deviation.
aIncluded medications administered during the 56 days before the first dose of study drug in the treatment period.
Source: Clinical Study Report.3,4
Patients Aged 12 Years and Older
Patients With F/MF Genotype: The baseline and demographic characteristics in Study 102 were similar across the ELX-TEZ-IVA and placebo groups, with the exception of a higher percentage of patients in the ELX-TEZ-IVA group reporting prior use of inhaled hypertonic saline compared with the placebo group (73.5% versus 62.6%, respectively) and a higher percentage of those in the ELX-TEZ-IVA group reported to have an infection with Pseudomonas aeruginosa within 2 years of screening (75.0% versus 70.0%, respectively).5 Body mass index z scores were calculated for patients less than 20 years of age at screening (mean = −0.40 [SD = 0.98] and −0.37 [SD = 0.79] in the placebo and ELX-TEZ-IVA groups, respectively).5
Patients With F/F Genotype: The baseline and demographic characteristics in Study 103 were generally similar across the ELX-TEZ-IVA and TEZ-IVA groups except for the prior use of CF medications and recent infection with Pseudomonas aeruginosa. A greater percentage of patients in the ELX-TEZ-IVA group of Study 103 reported prior use of azithromycin compared with the TEZ-IVA group (60.0% versus 48.1%, respectively), inhaled antibiotics (63.6% versus 53.8), bronchodilator (98.2% versus 90.4%), and inhaled corticosteroids (65.5% versus 53.8%).6 Conversely, prior use of inhaled hypertonic saline was greater in the TEZ-IVA group compared with the ELX-TEZ-IVA group (78.8% versus 69.1%, respectively).6 A greater percentage of patients in ELX-TEZ-IVA group were reported to have an infection with P. aeruginosa within 2 years of screening (70.9% versus 59.6%, respectively).6
The baseline and demographic characteristics in Study 109 were similar across the ELX-TEZ-IVA and TEZ-IVA groups with the exception that a greater percentage of patients in the TEZ-IVA group reported prior use of dornase alfa compared with the ELX-TEX-IVA group (81.8% versus 71.3%, respectively) and inhaled hypertonic saline (64.8% versus 58.6%).
Patients With F/G and F/RF Genotypes: Study 104 enrolled patients with either an F/G or an F/RF genotype. The percentages of patients with an F/RF genotype were 64.3% and 62.1% in the placebo and ELX-TEZ-IVA groups, respectively, and the percentages with an F/G genotype were 35.7% and 37.9% in the placebo and ELX-TEZ-IVA groups, respectively.11 As shown in Table 16, data for TEZ-IVA and IVA groups are pooled into a single “control” group. The ELX-TEZ-IVA and control groups were well balanced for all baseline and demographic characteristics, with the exception of a greater percentage of patients with prior usage of inhaled antibiotics in the placebo group compared with the ELX-TEZ-IVA group (44.4% versus 37.1%, respectively.)11
Table 16: Summary of Baseline and Demographic Characteristics in Adolescent and Adult Patients
Characteristics, n (%) | Study 102 (F/MF) | Study 103 (F/F) | Study 109 (F/F) | Study 104 (F/G and F/RF) | ||||
|---|---|---|---|---|---|---|---|---|
Placebo (N = 203) | ELX-TEZ-IVA (N = 200) | TEZ-IVA (N = 52) | ELX-TEZ-IVA (N = 55) | TEZ-IVA (N = 52) | ELX-TEZ-IVA (N = 55) | Control (N = 126) | ELX-TEZ-IVA (N = 132) | |
Sex, n (%) | ||||||||
Male | 105 (51.7) | 104 (52.0) | 24 (46.2) | 24 (43.6) | 43 (48.9) | 44 (50.6) | 65 (51.6) | 65 (49.2) |
Female | 98 (48.3) | 96 (48.0) | 28 (53.8) | 31 (56.4) | 45 (51.1) | 43 (49.4) | 61 (48.4) | 67 (50.8) |
Child-bearing potential, n (%) | ||||||||
Yes | 96 (98.0) | 94 (97.9) | 24 (85.7) | 28 (90.3) | 44 (97.8) | 42 (97.7) | 48 (78.7) | 50 (74.6) |
No | 2 (2.0) | 2 (2.1) | 4 (14.3) | 3 (9.7) | 1 (2.2) | 1 (2.3) | 13 (21.3) | 17 (25.4) |
Age at baseline (years) | ||||||||
Mean (SD) | 26.8 (11.3) | 25.6 (9.7) | 27.9 (10.8) | 28.8 (11.5) | 27.8 (11.0) | 27.9 (11.8) | 37.6 (14.3) | 37.7 (14.7) |
Median (range) | 25.0 (12.3 to 64.0) | 24.4 (12.1 to 59.9) | 27.6 (12.4 to 60.5) | 27.4 (12.7 to 54.1) | 27.8 (12.7 to 51.5) | 25.9 (12.2 to 58.7) | 37.9 (13.4 to 72.7) | 37.2 (12.3 to 69.8) |
≥ 12 to < 18 years | 60 (29.6) | 56 (28.0) | 14 (26.9) | 16 (29.1) | 27 (30.7) | 25 (28.7) | 9 (7.1) | 15 (11.4) |
≥ 18 years | 143 (70.4) | 144 (72.0) | 38 (73.1) | 39 (70.9) | 61 (69.3) | 62 (71.3) | 117 (92.9) | 117 (88.6) |
Hispanic or Latino, n (%) | ||||||||
Yes | 12 (5.9) | 4 (2.0) | 3 (5.8) | 2 (3.6) | 2 (2.3) | 1 (1.1) | 4 (3.2) | 5 (3.8) |
No | 175 (86.2) | 187 (93.5) | 49 (94.2) | 52 (94.5) | 83 (94.3) | 85 (97.7) | 114 (90.5) | 117 (88.6) |
Not collecteda | 16 (7.9) | 9 (4.5) | 0 | 1 (1.8) | 3 (3.4) | 1 (1.1) | 8 (6.3) | 10 (7.6) |
Race, n (%) | ||||||||
White | 184 (90.6) | 186 (93.0) | 52 (100.0) | 54 (98.2) | 88 (100.0) | 85 (97.7) | 111 (88.1) | 122 (92.4) |
African-American | 2 (1.0) | 4 (2.0) | 0 | 0 | 0 | 0 | 2 (1.6) | 0 |
Asian | 1 (0.5) | 0 | 0 | 0 | 0 | 3 (3.4) | 0 | 0 |
American Indian | 1 (0.5) | 0 | 0 | 0 | 0 | 0 | 1 (0.8) | 0 |
Other | 1 (0.5) | 2 (1.0) | 0 | 0 | 0 | 0 | 4 (3.2) | 1 (0.8) |
Not collecteda | 16 (7.9) | 9 (4.5) | 0 | 1 (1.8) | 0 | 0 | 9 (7.1) | 9 (6.8) |
Geographic region, n (%) | ||||||||
North America | 120 (59.1) | 118 (59.0) | 33 (63.5) | 34 (61.8) | 0 | 0 | 48 (38.1) | 49 (37.1) |
Europe/Australia | 83 (40.9) | 82 (41.0) | 19 (36.5) | 21 (38.2) | 88 (100) | 87 (100) | NA | NA |
Europe | NA | NA | NA | NA | NA | NA | 64 (50.8) | 70 (53.0) |
Australia | NA | NA | NA | NA | NA | NA | 14 (11.1) | 13 (9.8) |
Weight (kg) | ||||||||
Mean (SD) | 58.3 (12.7) | 59.8 (12.9) | 59.8 (14.8) | 59.9 (12.7) | 61.6 (14.5) | 58.8 (12.1) | 69.6 (17.4) | 69.5 (16.6) |
Median (range) | 58.0 (31.3 to 105.2) | 58.0 (29.0 to 108.0) | 55.0 (36.0 to 100.0) | 59.0 (36.0 to 91.2) | 60.5 (34.0 to 111.0) | 58.0 (32.0 to 83.0) | 67.0 (41.0 to 133.0) | 67.4 (37.0 to 125.2) |
BMI (kg/m2) | ||||||||
Mean (SD) | 21.31 (3.14) | 21.49 (3.07) | 21.88 (4.12) | 21.75 (3.19) | 21.92 (3.89) | 21.17 (3.43) | 24.05 (4.71) | 24.07 (4.72) |
Median (range) | 20.80 (14.42 to 33.80) | 21.36 (15.01 to 30.86) | 20.75 (15.61 to 34.60) | 21.35 (16.00 to 28.44) | 21.28 (15.52 to 39.33) | 21.22 (13.84 to 35.56) | 23.07 (16.51 to 41.62) | 23.15 (15.81 to 44.36) |
ppFEV1 category at screening, n (%) | ||||||||
< 70% | 128 (63.1) | 133 (66.5) | 36 (69.2) | 37 (67.3) | 53 (60.2) | 55 (63.2) | 67 (53.2) | 74 (56.1) |
≥ 70% | 74 (36.5) | 67 (33.5) | 16 (30.8) | 18 (32.7) | 35 (39.8) | 32 (36.8) | 59 (46.8) | 58 (43.9) |
Missing | 1 (0.5) | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
ppFEV1 category at baseline, n (%) | ||||||||
< 40 | 16 (7.9) | 18 (9.0) | 4 (7.7) | 6 (10.9) | 2 (2.3) | 6 (6.9) | 2 (1.6) | 2 (1.5) |
≥ 40 to < 70 | 120 (59.1) | 114 (57.0) | 34 (65.4) | 31 (56.4) | 52 (59.1) | 50 (57.5) | 63 (50.0) | 70 (53.0) |
≥ 70 to ≤ 90 | 62 (30.5) | 66 (33.0) | 14 (26.9) | 18 (32.7) | 29 (33.0) | 26 (29.9) | 52 (41.3) | 53 (40.2) |
> 90 | 5 (2.5) | 2 (1.0) | 0 | 0 | 5 (5.7) | 5 (5.7) | 9 (7.1) | 7 (5.3) |
ppFEV1 at baseline (%) | ||||||||
Mean (SD) | 61.3 (15.5) | 61.6 (15.0) | 60.2 (14.4) | 61.6 (15.4) | 64.2 (15.1) | 63.0 (16.7) | 68.1 (16.4) | 67.1 (15.7) |
Median (range) | 60.9 (32.3 to 93.7) | 61.6 (33.8 to 97.1) | 58.4 (35.0 to 89.0) | 61.0 (35.0 to 87.4) | 66.1 (35.4 to 94.4) | 62.1 (31.9 to 102.7) | 68.6 (31.1 to 104.1) | 68.3 (29.7 to 113.5) |
Sweat chloride (mmol/L) | ||||||||
Mean (SD) | 102.9 (9.8) | 102.3 (11.9) | 90.0 (12.3) | 91.4 (11.0) | 89.8 (11.7) | 89.0 (12.2) | 56.4 (25.5) | 59.5 (27.0) |
Median (range) | 104.0 (68.5 to 137.0) | 103.0 (22.5 to 156.0) | 90.8 (60.5 to 112.0) | 92.8 (67.0 to 114.0) | 92.3 (47.5 to 113.0) | 89.0 (51.0 to 116.0) | 54.0 (10.0 to 109.5) | 56.8 (10.0 to 116.5) |
CFQ-R (respiratory domain) | ||||||||
Mean (SD) | 70.0 (17.8) | 68.3 (16.9) | 72.6 (17.9) | 70.6 (16.2) | 73.1 (17.6) | 71.2 (19.6) | 77.3 (15.8) | 76.5 (16.6) |
Median (range) | 72.2 (16.7 to 100.0) | 72.2 (16.7 to 100.0) | 72.2 (27.8 to 100.0) | 72.2 (22.2 to 94.4) | 77.8 (27.8 to 100.0) | 72.2 (11.1 to 100.0) | 77.8 (11.1 to 100.0) | 77.8 (0.0 to 100.0) |
CFTR-modulator use at screening, n (%) | ||||||||
Yes | 0 | 0 | 34 (65.4) | 32 (58.2) | 39 (44.3) | 39 (44.8) | 59 (46.8) | 64 (48.5) |
No | 203 (100) | 200 (100) | 18 (34.6) | 23 (41.8) | 49 (55.7) | 48 (55.2) | 67 (53.2) | 68 (51.5) |
Prior use of dornase alfa, n (%) | ||||||||
Yes | 164 (80.8) | 162 (81.0) | 48 (92.3) | 51 (92.7) | 72 (81.8) | 62 (71.3) | 66 (52.4) | 69 (52.3) |
No | 39 (19.2) | 38 (19.0) | 4 (7.7) | 4 (7.3) | 16 (18.2) | 25 (28.7) | 60 (47.6) | 63 (47.7) |
Prior use of azithromycin, n (%) | ||||||||
Yes | 114 (56.2) | 110 (55.0) | 25 (48.1) | 33 (60.0) | 44 (50.0) | 49 (56.3) | 57 (45.2) | 57 (43.2) |
No | 89 (43.8) | 90 (45.0) | 27 (51.9) | 22 (40.0) | 44 (50.0) | 38 (43.7) | 69 (54.8) | 75 (56.8) |
Prior use of inhaled antibiotic, n (%) | ||||||||
Yes | 132 (65.0) | 118 (59.0) | 28 (53.8) | 35 (63.6) | 57 (64.8) | 51 (58.6) | 56 (44.4) | 49 (37.1) |
No | 71 (35.0) | 82 (41.0) | 24 (46.2) | 20 (36.4) | 31 (35.2) | 36 (41.4) | 70 (55.6) | 83 (62.9) |
Prior use of any bronchodilator, n (%) | ||||||||
Yes | 191 (94.1) | 187 (93.5) | 47 (90.4) | 54 (98.2) | 80 (90.9) | 75 (86.2) | 111 (88.1) | 113 (85.6) |
No | 12 (5.9) | 13 (6.5) | 5 (9.6) | 1 (1.8) | 8 (9.1) | 12 (13.8) | 15 (11.9) | 19 (14.4) |
Prior use of any inhaled corticosteroids, n (%) | ||||||||
Yes | 119 (58.6) | 120 (60.0) | 28 (53.8) | 36 (65.5) | 58 (65.9) | 56 (64.4) | NR | NR |
No | 84 (41.4) | 80 (40.0) | 24 (46.2) | 19 (34.5) | 30 (34.1) | 31 (35.6) | NR | NR |
Prior use of any inhaled hypertonic saline, n (%) | ||||||||
Yes | 127 (62.6) | 147 (73.5) | 41 (78.8) | 38 (69.1) | 52 (59.1) | 53 (60.9) | 54 (42.9) | 57 (43.2) |
No | 76 (37.4) | 53 (26.5) | 11 (21.2) | 17 (30.9) | 36 (40.9) | 34 (39.1) | 72 (57.1) | 75 (56.8) |
Pseudomonas aeruginosa infection within 2 years of screening, n (%) | ||||||||
Positive | 142 (70.0) | 150 (75.0) | 31 (59.6) | 39 (70.9) | 58 (65.9) | 59 (67.8) | 74 (58.7) | 79 (59.8) |
Negative | 61 (30.0) | 50 (25.0) | 21 (40.4) | 16 (29.1) | 30 (34.1) | 28 (32.2) | 52 (41.3) | 53 (40.2) |
BMI = body mass index; CFQ-R = Cystic Fibrosis Questionnaire–Revised; ELX-TEZ-IVA = elexacaftor-tezacaftor-ivacaftor and ivacaftor; F/F = homozygous for F508del mutation in the CFTR gene; F/G = 1 F508del mutation and 1 gating mutation in the CFTR gene; F/MF = 1 F508del mutation and 1 minimal function mutation in the CFTR gene; F/RF = 1 F508del mutation and 1 residual function mutation in the CFTR gene; NA = not applicable; NR = not reported; ppFEV1 = percent predicted forced expiratory volume in 1 second; SD = standard deviation; TEZ-IVA = tezacaftor-ivacaftor and ivacaftor.
aNot collected in accordance with local regulations.
Source: Clinical Study Reports5,6,10,11 and additional information provided by the sponsor.9,68
Interventions
Study Drugs
Patients Aged 6 to 11 Years
Placebo-Controlled Trial (Study 116; F/MF Genotype): Randomized patients received either ELX-TEZ-IVA or matching placebo tablets taken every morning and evening. Those weighing less than 30 kg received ELX 100 mg, TEZ 50 mg, and IVA 75 mg every morning plus IVA 75 mg every evening and those weighing 30 kg or more received ELX 200 mg, TEZ 100 mg, and IVA 150 mg every morning plus IVA 150 mg every evening. The placebo tablets were identical in appearance to either the ELX-TEZ-IVA and IVA tablets.4
Single-Arm Trial (Study 106; F/F or F/MF Genotype): All patients in Part A received ELX 200 mg, TEZ 100 mg, and IVA 150 mg every morning plus IVA 150 mg every evening. In Part B, those weighing less than 30 kg received ELX 100 mg, TEZ 50 mg, and IVA 75 mg every morning plus IVA 75 mg every evening and those weighing 30 kg or more received ELX 200 mg, TEZ 100 mg, and IVA 150 mg every morning plus IVA 150 mg every evening.3
Patients Aged 12 Years and Older
Patients With F/MF Genotype: Study 102 did not include a run-in period. Randomized patients received either ELX-TEZ-IVA (2 tablets for a total dose of ELX 200 mg, TEZ 100 mg, and IVA 150 mg every morning and 1 tablet of IVA 150 mg every evening) or matching placebo tablets taken every morning and evening. The placebo tablets were identical in appearance to either the ELX-TEZ-IVA and IVA tablets.
Patients With F/F Genotype: Patients in Study 103 and Study 109 underwent a 28-day open-label run-in period during which they received treatment with open-label TEZ 100 mg and IVA 150 mg once daily in the morning and IVA 150 mg once daily in the evening. Randomized patients received either ELX-TEZ-IVA (2 tablets for a total dose of ELX 200 mg, TEZ 100 mg, and IVA 150 mg every morning and 1 tablet of IVA 150 mg every evening) or continued with TEZ-IVA. As the morning dose of ELX-TEZ-IVA is administered as 2 tablets (each containing ELX 100 mg, TEZ 50 mg, and IVA 75 mg), patients randomized to the TEZ-IVA group also received 2 matching placebo tablets for the morning dose and those in the ELX-TEZ-IVA group received 1 matching placebo tablet to maintain blinding (i.e., both groups received 3 tablets in the morning and 1 in the evening). The placebo and active tablets were identical in appearance.
Patients With F/G and F/RF Genotypes: Patients in Study 104 underwent a 28-day open-label run-in period during which all patients with an F/RF genotype received TEZ 100 mg and IVA 150 mg once daily in the morning and IVA 150 mg once daily in the evening and those with an F/G genotype received IVA 150 mg every 12 hours. Randomized patients received either ELX-TEZ-IVA (2 tablets for a total dose of ELX 200 mg, TEZ 100 mg, and IVA 150 mg every morning and 1 tablet with IVA 150 mg every evening) or to the control group, whose members would continue with TEZ-IVA or IVA for those with F/RF and F/G genotypes, respectively.11 As the morning dose of ELX-TEZ-IVA is administered as 2 tablets (each containing ELX 100 mg, TEZ 50 mg, and IVA 75 mg), patients randomized to the control groups (TEZ-IVA or IVA) were also given 2 matching placebo tablets for the morning dose to maintain blinding and those in the ELX-TEZ-IVA group received 1 matching placebo tablet (i.e., both groups received 3 tablets in the morning and 1 in the evening). The placebo and active tablets were identical in appearance.
Table 17: Dosage Regimens for the Study Drugs
Study | Intervention | Comparator |
|---|---|---|
Pediatric studies | ||
Study 116 (F/MF) | Morning: 2 ELX-TEZ-IVA tablets + 1 placebo tablet Evening: 1 IVA tablet | Morning: 2 placebo tablets Evening: 1 placebo tablet |
Study 106 (F/F or F/MF) | Morning: 2 ELX-TEZ-IVA tablets Evening: 1 IVA tablet | NA |
Adolescent and adult studies | ||
Study 102 (F/MF) | Morning: 2 ELX-TEZ-IVA tablets Evening: 1 IVA tablet | Morning: 2 placebo tablets Evening: 1 placebo tablet |
Study 103 (F/F) | Morning: 2 ELX-TEZ-IVA tablets + 1 placebo tablet Evening: 1 IVA tablet | Morning: 1 TEZ-IVA tablet + 2 placebo tablets Evening: 1 IVA tablet |
Study 109 (F/F) | Morning: 2 ELX-TEZ-IVA tablets + 1 placebo tablet Evening: 1 IVA tablet | Morning: 1 TEZ-IVA tablet + 2 placebo tablets Evening: 1 IVA tablet |
Study 104 (F/G or F/RF) | Morning: 2 ELX-TEZ-IVA tablets + 1 placebo tablet Evening: 1 IVA tablet | F/G Group Morning: 1 IVA tablet + 2 placebo tablets Evening: 1 IVA tablet F/RF Group Morning: 1 TEZ-IVA tablet + 2 placebo tablets Evening: 1 IVA tablet |
ELX-TEZ-IVA = elexacaftor-tezacaftor-ivacaftor and ivacaftor; IVA = ivacaftor; F/F = homozygous for F508del mutation in the CFTR gene; F/G = 1 F508del mutation and 1 gating mutation in the CFTR gene; F/MF = 1 F508del mutation and 1 minimal function mutation in the CFTR gene; F/RF = 1 F508del mutation and 1 residual function mutation in the CFTR gene; NA = not applicable; TEZ-IVA = tezacaftor-ivacaftor and ivacaftor.
Source: Clinical Study Reports.3-6,10,11
Dose Modifications and Interruptions
The study protocols stated that no dose modifications for toxicity were permitted in the trials; however, dose interruptions were permitted for patients who met pre-specified criteria related to liver function tests and rash. For the liver function tests, administration of the study treatments was to be interrupted immediately if the patient met any of the following criteria: ALT or aspartate transaminase (AST) greater than 8 times the upper limit of normal (ULN); ALT or AST greater than 5 times the ULN for more than 2 weeks; and ALT or AST greater than 3 times the ULN, in association with total bilirubin greater than 2 times ULN and/or clinical jaundice. The potential causes of the elevated liver function tests were to be investigated and treatment was to be discontinued if subsequent ALT or AST values confirmed the initial elevations (i.e., exceeded the thresholds for treatment interruption) and no convincing alternative etiology was identified (e.g., acetaminophen use, viral hepatitis, or alcohol ingestion). If an alternative, reversible cause of elevated transaminases was identified, the study treatment could be resumed once the patient’s transaminase levels returned to baseline or to no greater than 2 times the ULN (whichever was greater). Treatment was also to be interrupted for patients who developed a generalized rash that was a grade 3 or higher AE or an SAE.
Concomitant Medications
Study participants were to remain on a stable CF treatment regimen from 28 days before the start of the run-in period through to completion of the study. Stable CF treatment regimen was defined as the current treatment regimen for CF that the patient had been receiving. Guidelines for stable treatment regimens for CF are as follows:
Those using inhaled tobramycin or other chronically inhaled antibiotics should remain on the regimen throughout the study.
Those who cycle onto and off of an inhaled antibiotic should continue on their prior schedule. The timing of the first dose of the study drug on the day 1 visit should be synchronized as closely as possible (e.g., not more than ± 3 days) to the first day in the cycle onto the inhaled antibiotic.
Those who alternate between 2 different inhaled antibiotics should remain on the same cycling schedule during the study. The timing of the first dose of study drug on the day 1 visit should be synchronized as closely as possible (e.g., not more than ± 3 days) to the first day in the cycle onto 1 of the inhaled antibiotics.
Outcomes
A list of efficacy end points identified in the CADTH review protocol that were assessed in the clinical trials included in this review is provided in Table 18. These end points are further summarized in the following section. A detailed description and appraisal of the outcome measures is provided in Appendix 4.
Table 18: Summary of Outcomes of Interest Identified in the CADTH Review Protocol
End point | Time point | Adolescents and adults | Pediatrics | ||||
|---|---|---|---|---|---|---|---|
Study 102 | Study 103 | Study 104 | Study 109 | Study 116 | Study 106B | ||
Spirometry | |||||||
Absolute change in ppFEV1 | At week 4 | Primary (global) Key secondary (Europe) | Primary | NA | NA | NA | NA |
Through 8 weeks | NA | NA | Primary (within-group) Key secondary (vs. control) | NA | NA | NA | |
Through week 24 | Primary (Europe) Key secondary (Europe) | NA | NA | Key secondary | Other | Other | |
Absolute change in LCI2.5 | Through week 24 | NA | NA | NA | NA | Primary | Other |
Pulmonary exacerbations | |||||||
Number of PEx | Through week 24 | Key secondary | NA | NA | NA | NA | Other |
Number of PEx requiring hospitalization | Through week 24 | Other | NA | NA | NA | NA | Other |
Number of PEx requiring IV antibiotics | Through week 24 | Other | NA | NA | NA | NA | Other |
Number of PEx requiring IV antibiotics or hospitalization | Through week 24 | Other | NA | NA | NA | NA | Other |
Time to first PEx | Through week 24 | Other | NA | NA | NA | NA | NA |
Time to first hospitalization for PEx | Through week 24 | Other | NA | NA | NA | NA | NA |
Time to first IV antibiotics for PEx | Through week 24 | Other | NA | NA | NA | NA | NA |
Duration of PEx | Through week 24 | Other | NA | NA | NA | NA | Other |
Duration of hospitalization for PEx | Through week 24 | Other | NA | NA | NA | NA | Other |
Duration of IV antibiotics for PEx | Through week 24 | Other | NA | NA | NA | NA | Other |
Duration of hospitalization or IV antibiotics for PEx | Through week 24 | Other | NA | NA | NA | NA | Other |
Body composition | |||||||
Absolute change in BMI | At 4 weeks | NA | Other | NA | NA | NA | NA |
At 8 weeks | NA | NA | Other | NA | NA | NA | |
At 24 weeks | Key secondary | NA | NA | NA | NA | Other | |
Absolute change in BMI z score | At 24 weeks | Other | NA | NA | NA | NA | Other |
Absolute change in weight | At 4 weeks | NA | Other | NA | NA | NA | NA |
At 24 weeks | Other | NA | NA | NA | NA | Other | |
Absolute change in weight z score | At 24 weeks | NA | NA | NA | NA | NA | Other |
Absolute change in height | At 24 weeks | NA | NA | NA | NA | NA | Other |
Absolute change in height z score | At 24 weeks | NA | NA | NA | NA | NA | Other |
Sweat chloride | |||||||
Absolute change in sweat chloride | At 4 weeks | Key secondary | Key secondary | NA | NA | NA | NA |
Through 8 weeks | NA | NA | Key secondary (within-group and vs. control) | NA | NA | NA | |
Through week 24 | Key secondary | NA | NA | Other | Other | Other | |
Patient-reported outcomes | |||||||
Absolute change in CFQ-R (RD) | At 4 weeks | Key secondary | Key secondary | NA | NA | NA | NA |
Through 8 weeks | NA | NA | Other (within-group and vs. control) | NA | NA | NA | |
Through week 24 | Key secondary | NA | NA | Primary | Other | Other | |
Absolute change in CFQ-R (non-RD) | At 4 weeks | NA | Other | NA | NA | NA | NA |
Through 8 weeks | NA | NA | Other | NA | NA | NA | |
Through week 24 | Other | NA | NA | NA | Other | Other | |
Absolute change in TSQM | At 4 weeks | NA | Other | NA | NA | NA | NA |
At 24 weeks | Other | NA | NA | NA | NA | NA | |
Hospitalizations | |||||||
Planned hospitalizations | Through week 24 | Other | NA | NA | NA | NA | Other |
Unplanned hospitalizations | Through week 24 | Other | NA | NA | NA | NA | Other |
Duration of planned hospitalizations | Through week 24 | Other | NA | NA | NA | NA | Other |
Duration of unplanned hospitalizations | Through week 24 | Other | NA | NA | NA | NA | Other |
BMI = body mass index; CFQ-R = Cystic Fibrosis Questionnaire–Revised; LCI = lung clearance index; NA = not applicable; PEx = pulmonary exacerbation; ppFEV1 = percent predicted forced expiratory volume in 1 second; ; RD = respiratory domain; TSQM = Treatment Satisfaction Questionnaire for Medication.
Percent Predicted FEV1
Percent predicted FEV1 (in L) was calculated using the ratio of FEV1 to the predicted FEV1. The predicted FEV1 was calculated using the equations of the Global Lung Function Initiative.5,69 Absolute change from baseline was calculated as post-baseline value minus baseline value. Absolute change from baseline in ppFEV1 was the primary end point of 3 of the included studies:
Study 102 (versus placebo): evaluated at 4 weeks and through 24 weeks in the global European protocols
Study 103 (versus TEZ-IVA): evaluated at 4 weeks
Study 104 (within-group change for ELX-TEZ-IVA): evaluated through 8 weeks.5,6,11
Due to the onset of the COVID-19 pandemic, patients in Study 104, Study 116, and Study 106B could be provided with spirometry devices to perform in-home assessments of lung function (as clinic visits were not occurring). As noted in the Statistical Analysis section, sensitivity analyses were performed to investigate the impact of including and excluding the in-home spirometry measurements.
At the time of this review, a literature search did not identify an accepted MID for absolute change from baseline in ppFEV1 for patients with CF. The clinical experts consulted by CADTH noted that an absolute improvement of 5% is typically considered to be meaningful for acute changes in ppFEV1; however, it was noted that even stabilization of ppFEV1 can be meaningful for patients, particularly those who are at risk of rapid decline. Both the clinical experts consulted by CADTH and the clinician groups who provided input into this review noted that slowing the decline in lung function is considered to be more important than short-term increases.
Lung Clearance Index
The LCI is a multiple-breath washout test that estimates the number of lung-volume turnovers required to clear the lung of an inert gas.70 The test is sensitive to changes in the small airways, and may be able to detect pulmonary disease in patients with normal FEV1.71,72 The LCI assessments were derived from multiple-breath washout testing using nitrogen gas. Absolute change from baseline in LCI2.5, the number of lung turnovers required to reduce the end tidal nitrogen concentration to 2.5% of the starting value, was the primary end point of Study 116 and secondary end point in Study 106B. The baseline and post-baseline assessments of LCI were performed pre-bronchodilator and before dosing of the study medications.3,4
Pulmonary Exacerbations
Pulmonary exacerbations were evaluated as an efficacy end point in Study 102 and Study 106B. Pulmonary exacerbations were defined as a change in antibiotic therapy (IV, inhaled, or oral) for any 4 or more of the following signs or symptoms: change in sputum; new or increased hemoptysis; increased cough; increased dyspnea; malaise, fatigue, or lethargy; temperature above 38°C; anorexia or weight loss; sinus pain or tenderness; change in sinus discharge; change in physical examination of the chest; decrease in lung function by at least 10% (based on spirometry); or radiographic changes indicative of pulmonary infection. Changes in antibiotic therapy for sinopulmonary signs and/or symptoms were determined and documented by the study investigator at each study visit.5
Several of the criteria for sinopulmonary signs and symptoms were assessed by the investigator alone (including a temperature above 38°C, anorexia or weight loss, sinus pain or tenderness, change in physical examination of chest, decrease in pulmonary function by 10% (based on spirometry), and radiographic changes indicative of pulmonary infection). Changes in sputum; new or increased hemoptysis; increased coughing; increased dyspnea, malaise, fatigue, or lethargy; and change in sinus discharge were independently assessed by the investigator, or together with patient descriptions evaluated and reported by the investigator. There does not appear to have been an independent adjudication of pulmonary exacerbation events.
The following end points related to exacerbations were evaluated in Study 102:
rate of pulmonary exacerbations
rate of pulmonary exacerbations requiring hospitalization
rate of pulmonary exacerbations requiring IV antibiotics
rate of pulmonary exacerbations requiring IV antibiotics or hospitalization
time to first pulmonary exacerbation
time to first hospitalization for pulmonary exacerbation
time to first IV antibiotic therapy for pulmonary exacerbation
time to first pulmonary exacerbation requiring IV antibiotics or hospitalization
duration of pulmonary exacerbations
duration of hospitalization for pulmonary exacerbation
duration of IV antibiotic therapy for pulmonary exacerbation
duration of IV antibiotic therapy or hospitalization for pulmonary exacerbation.
Only descriptive statistics were reported for Study 106B for the number and duration of pulmonary exacerbations, pulmonary exacerbations requiring hospitalization, pulmonary exacerbations requiring IV antibiotics, and pulmonary exacerbations requiring IV antibiotics or hospitalization.3
Body Mass Index, Body Weight, and Height
Three of the included studies for patients aged 12 years and older evaluated changes from baseline in BMI (Studies 102, 103, and 104).5,6,11 Analysis used BMI-for-age z scores for patients 12 to 20 years of age in Study 102.5 Absolute change from baseline in BMI at 24 weeks was a key secondary end point of Study 102.5 Studies 103 and 104 included absolute change from baseline at 4 and 8 weeks, respectively, as an additional efficacy end point.6,11
For the studies of patients aged 6 to 11 years, Study 106B evaluated absolute change from baseline in BMI, BMI z scores, weight, weight z scores, height, and height z scores at 24 years.3
Cystic Fibrosis Questionnaire–Revised
The CFQ-R is a disease-specific HRQoL instrument designed for patients with CF that is available in age-appropriate versions for children aged 6 to 13 years (CFQ-C), parents who serve as a proxy for their child (CFQ-P), and individuals 14 years of age and older (CFQ-14).73 For children aged 6 to 11 years, the CFQ-C is interviewer-administered, and for 12- and 13-year-olds, it is self-administered.74 The number of items and domains vary between versions; the CFQ-C includes 35 items within 8 domains, the parent version has 44 items and 11 domains, and the adolescent and adult version has 50 items within 12 domains (Figure 28).73,74 The domains in the adolescent and adult version an HRQoL module including physical functioning, vitality, emotional functioning, social or school functioning, role functioning, body image, eating problems, and treatment burden; a symptoms module that includes respiratory symptoms, digestive symptoms, and weight; and a health perception module. A 4-point Likert scale is used to measure frequency (always, often, sometimes, or never), intensity (a great deal, somewhat, a little, or not at all), and true-false scales (very true, somewhat true, somewhat false, or very false). Items within domains are summed and standardized. Individual domain scores range from 0 to 100, with higher scores indicating better HRQoL.73 The scales are designed to measure symptoms and functioning during the 2-week period before administration of the questionnaire.75 A difference of at least 4 points in the respiratory domain score of the CFQ-R is commonly cited as the minimal important difference (MID) for patients with CF.76
The absolute change from baseline in the CFQ-R respiratory domain score was the primary end point of Study 109 and a pre-specified key secondary end point in Study 102 (through 4 and 24 weeks, respectively) and Study 103 (through 4 weeks).5,6,10,11 Absolute change from baseline in the non-respiratory domain scores were included as other efficacy end points in Study 102 (through 24 weeks), Study 103 (at 4 weeks), Study 104 (through 8 weeks), Study 116 (through 24 weeks), and Study 106B (through 24 weeks).3-6,11 Due to the COVID-19 pandemic, some patients in Study 104, Study 109, Study 116, and Study 106B were provided with the CFQ-R to perform in-home assessments. As noted in the Statistical Analysis section, sensitivity analyses were performed to investigate the impact of including and excluding in-home evaluations of the CFQ-R.
Treatment Satisfaction Questionnaire for Medication
The TSQM is an instrument used to assess a patient’s satisfaction with the study medication and includes 4 domains: effectiveness, side effects, convenience, and global satisfaction.5,6 The TSQM consists of 14 items in 4 domains: effectiveness (items 1, 2, 3), side effects (items 4, 5, 6, 7, 8), convenience (items 9, 10, 11), and global satisfaction (items 12, 13, 14).5 A 5- or 7-point Likert scale is used to score the domains, and each domain score ranges from 0 (least satisfied) to 100 (most satisfied).5,77 The TSQM was included as an additional efficacy end point in Study 102 (evaluated through 24 weeks) and Study 103 (evaluated at 4 weeks).5,6 The sponsor reported that patients between the ages of 12 and 17 years completed the TSQM to meet European regulatory commitments.5,6
Sweat Chloride
Sweat chloride samples were obtained from patients using an approved collection device. At each time point, 2 samples were collected, 1 from each of the patient’s arms, and sent to a central laboratory for analysis.5 All of the included studies evaluated absolute change from baseline in sweat chloride. Absolute change from baseline in sweat chloride was a key secondary end point in Study 102 (evaluated at 4 weeks and through 24 weeks), Study 103 (evaluated at 4 weeks), and Study 104 (evaluated as the within-group change for the ELX-TEZ-IVA group through 8 weeks). Absolute change from baseline in sweat chloride through 24 weeks was an additional efficacy end point in Study 116 and Study 106B.3,4
Hospitalizations
Study 102 and Study 106B included the frequency and duration of planned and unplanned CF hospitalizations as additional end points.
Planned hospitalizations for CF (i.e., antibiotic therapy) were assumed to be for pre-planned IV antibiotic therapy or for pre-planned treatment of CF-related clinical issues or events. Patients who received IV antibiotics for the treatment of an acute pulmonary exacerbation were not included in this category of planned hospitalization.
Unplanned hospitalizations for CF were those due to reasons other than protocol-defined acute pulmonary exacerbations, including non–protocol-defined pulmonary exacerbations or other CF-related reasons (e.g., pancreatitis or distal intestinal obstruction syndrome).
It is important to note that neither the planned nor the unplanned hospitalization end points included hospitalizations due to protocol-defined pulmonary exacerbations.68 Pulmonary exacerbations requiring hospitalization were evaluated separately (as reported in the section on pulmonary exacerbations).
Adverse Events
Adverse events were defined as any untoward medical occurrence in a patient during the study, including newly occurring events or worsening of pre-existing conditions (e.g., increased in its severity or frequency). An AE was considered serious if it met any of the following descriptions or outcomes: fatal; life-threatening; inpatient hospitalization or prolongation of hospitalization; persistent or significant disability/incapacity, congenital anomaly or birth defect; or an important medical event that jeopardized the patient or required medical or surgical intervention to prevent 1 of the outcomes.
Statistical Analysis
Power Calculations
Patients Aged 6 to 11 Years
Placebo-Controlled Trial (Study 116; F/MF Genotype): In Study 116, the power calculation was based on |||||||||||||||||||||||| dropout rate in both the ELX-TEZ-IVA and placebo groups. Assuming a within-group SD in LCI2.5 of 1.5, a treatment difference of −1.0 between ELX-TEZ-IVA and placebo, and a sample size of 49 patients in each group completing the double-blind treatment phase, the study had an approximately 90% power for the LCI2.5 hypothesis testing, based on a 2-sided, 2-sample t-test at a significance level of 0.05.4
Single-Arm Trial (Study 106B; F/F or F/MF Genotype): In Study 106B, the sponsor planned to enrol 56 patients and assumed that approximately 45 patients would complete the 24-week treatment phase. Incidence of AEs was a safety end point. The study would have at least a 90% chance of observing an AE in at least 1 patient if the true incidence rate was 5%, and a greater than 95% chance of observing an AE in at least 1 patient if the true incidence rate was 10%. The probabilities were calculated by assuming a binomial distribution for the number of AEs using the safety analysis set.3
Patients Aged 12 Years and Older
Patients With F/MF Genotype: In Study 102, the power calculation was based on 180 patients and a 10% dropout rate in both the ELX-TEZ-IVA and placebo groups for the final analysis, and 70 patients and a 5% dropout rate in both groups for the interim analysis. Assuming a within-group SD of 7%, the trial was estimated to have 98% and 99% powers at the interim and final analyses, respectively, to detect a treatment difference of 5% in the primary end point (absolute change from baseline in ppFEV1 at 4 weeks) across the ELX-TEZ-IVA and placebo groups, with 2-sided alphas of 0.044 (interim analysis) and 0.01 (final analysis).
Patients With F/F Genotype: In Study 103, the power calculation was based on 100 patients and a 5% dropout rate at 4 weeks. For the primary end point of absolute change in ppFEV1 from baseline at 4 weeks, assuming a within-group SD of 7%, this trial was estimated to have an approximately 93% power to detect a difference of 5.0% for the primary end point, with a 2-sided alpha of 0.05.
In Study 109, the power calculation was based on 158 patients and a 10% dropout rate through 24 weeks. For the primary end point of absolute change in CFQ-R respiratory domain score from baseline through 24 weeks, assuming a dropout rate of 10% and a within-group SD of 18 points, a sample size of 158 patients was estimated to have approximately 90% power to detect a difference of 10 points for the primary end point, with a 2-sided alpha of 0.05. For the key secondary end point of absolute change in ppFEV1 from baseline through 24 weeks, assuming a dropout rate of 10% and a within-group SD of 7%, a sample size of 158 patients was estimated to have an approximately 98% power to detect a treatment difference of 5%, with a 2-sided alpha of 0.05.
Patients With F/G or F/RF Genotype: In Study 104, the power calculation was based on 125 patients in the ELX-TEZ-IVA group and a 10% dropout rate after 8 weeks. For the primary efficacy end point of absolute change in ppFEV1 from baseline through 8 weeks for the ELX-TEZ-IVA group, assuming a within-group SD of 7.0%, the trial was estimated to have a greater than 99% power to detect a within-group difference of 3.0% (1 sample t-test at a 2-sided significance level of 0.05).
Primary Outcomes
In Study 102, Study 103, and Study 104, absolute changes from baseline in ppFEV1 were calculated using a mixed-effects model for repeated measures (MMRM) approach. The models for Study 102 and Study 103 included treatment group, visit, and treatment-by-visit interaction as fixed effects, with continuous baseline ppFEV1, age at screening (< 18 versus ≥ 18 years of age), and sex (male versus female) as covariates. The model for Study 104 included treatment group, visit, and treatment-by-visit interaction as fixed effects, with continuous baseline ppFEV1, continuous baseline sweat chloride, and comparator group (i.e., IVA or TEZ-IVA) as covariates. Missing post-baseline values were not imputed for efficacy analyses conducted using the MMRM approach (i.e., data were assumed to be missing at random). Sensitivity analyses using multiple imputation were performed to assess the robustness of the primary analyses.
Two statistical analysis protocols were used in Study 102: a “global” protocol that absolute change in ppFEV1 from baseline at 4 weeks as the primary end point and a European protocol that specified absolute change in ppFEV1 from baseline through week 24 as the primary end point.5 The analysis conducted “at 4 weeks” used the 4-week evaluation as the end point, and the analysis that was conducted “through 24 weeks” used an average of weeks 4, 8, 12, 16, and 24. The sponsor noted that this was due to regulatory requirements in different jurisdictions (i.e., European regulators requested that the primary end point be evaluated through 24 weeks).5 As a result, the statistical testing order of the primary and first key secondary end points was reversed in the 2 protocols (i.e., the primary end point in the global protocol was the first key secondary end point in the European protocol and vice versa).5
Secondary and Other Efficacy End Points
The statistical evaluation of the continuous key and other secondary end points (e.g., ppFEV1, BMI, CFQ-R, weight, and TSQM) was conducted using an MMRM similar to the evaluation used for the primary analysis, but with the addition of the baseline value for the end point of interest as a covariate. For the number of pulmonary exacerbations in Study 102 (overall and those requiring IV antibiotics or hospitalization), the comparison between the ELX-TEZ-IVA and comparator (i.e., placebo) groups was conducted using regression analyses for a negative binomial distribution with sex, baseline age group (< 18 versus ≥ 18 years), and baseline ppFEV1 severity at screening (< 70% versus ≥ 70%) as covariates. Time to first pulmonary exacerbation (any exacerbation and those requiring IV antibiotics or hospitalization) was analyzed using a Cox regression. The sponsor’s model included a main effect for treatment, with covariates for sex, baseline age group (< 18 versus ≥ 18 years), and ppFEV1 severity at screening (< 70% versus ≥ 70%).
Subgroup Analyses
The CADTH review protocol identified 4 subgroups of interest: severity of disease (based on baseline FEV1), CFTR genotype (F/F, F/MF, F/G, F/RF), prior therapy with CFTR modulator(s), and patient age. The different subgroups that were investigated in the included clinical studies are described in the following section.
Patients Aged 6 to 11 Years
Placebo-Controlled Trial (Study 116; F/MF Genotype): No pre-specified or post hoc subgroup analyses were reported for Study 116.
Single-Arm Trial (Study 106; F/F or F/MF Genotype): In Study 106B, ad hoc subgroup analyses by genotype subgroup were reported by the sponsor for ppFEV1, sweat chloride, CFQ-R respiratory domain score, and LCI2.5. The subgroup analyses were conducted using an MMRM similar to that used in the primary analysis. No adjustment of multiplicity was made in the subgroup analyses.3
Patients Aged 12 Years and Older
Patients With F/MF Genotype: In Study 102, the following pre-planned subgroup analyses were conducted for the primary end point (i.e., absolute change in ppFEV1): age at screening (< 18 years or ≥ 18 years); ppFEV1 at baseline (< 70% or ≥ 70%); sex (male or female); geographic region (North America or Europe/Australia); prior use of inhaled antibiotic (yes or no); prior use of dornase alfa (yes or no); prior use of inhaled bronchodilator (yes or no); prior use of inhaled hypertonic saline (yes or no); prior use of inhaled corticosteroids (yes or no); prior use of azithromycin (yes or no); and infection with Pseudomonas aeruginosa within 2 years of the screening visit (positive or negative).5 An additional post hoc subgroup analysis was performed for the subset of patients with a ppFEV1 below 40% at baseline. The subgroup analyses were conducted using an MMRM similar to that used in the primary analysis. There was no adjustment of multiplicity in the subgroup analyses.
Patients With F/F Genotype: In Study 103, the following pre-planned subgroup analyses were conducted for the primary end point (i.e., absolute change in ppFEV1): age at screening (< 18 years or ≥ 18 years); ppFEV1 at baseline (< 70% or ≥ 70%); sex (male or female); geographic region (North America or Europe); prior use of inhaled antibiotic (yes or no); prior use of dornase alfa (yes or no); prior use of inhaled bronchodilator (yes or no); prior use of inhaled hypertonic saline (yes or no); prior use of inhaled corticosteroids (yes or no); prior use of azithromycin (yes or no); and infection with Pseudomonas aeruginosa within 2 years of the screening visit (positive or negative).6 An additional post hoc subgroup analysis was performed based on prior exposure to CFTR modulators (treatment-naive or treatment-experienced). In Study 109, the following pre-planned subgroup analyses were conducted for the primary end point (i.e., absolute change in the respiratory domain of the CFQ-R): age at screening (< 18 years or ≥ 18 years); ppFEV1 at baseline (< 70% or ≥ 70%); sex (male or female); and CFTR modulator use at screening (yes or no).10 For both studies, the subgroup analyses were conducted using an MMRM similar to that used in the primary analysis. There was no adjustment of multiplicity in the subgroup analyses.
Patients With F/G or F/RF Genotype: In Study 104, the following pre-planned subgroup analyses were conducted: age at screening (< 18 years or ≥ 18 years); ppFEV1 at baseline (< 70% or ≥ 70%); sex (male or female); geographic region (North America or Europe and Australia); and comparator group (TEZ-IVA comparator or IVA comparator).11 The subgroup analyses were conducted using an MMRM similar to that used in the primary analysis. There was no adjustment of multiplicity in the subgroup analyses.
Multiplicity Adjustment
Patients Aged 6 to 11 Years
Placebo-Controlled Trial (Study 116; F/MF Genotype): No adjustments were made for multiple comparisons.4
Single-Arm Trial (Study 106; F/F or F/MF Genotype): No adjustments were made for multiple comparisons.3
Patients Aged 12 Years and Older
Patients With F/MF Genotype: Study 102 included 2 study protocols: a global protocol and a European protocol. The timing and methods for evaluating the primary end point differed between the 2 protocols. In the global protocol, a Lan and DeMets alpha-spending function was applied to control the overall type I error rate of 0.05 for the primary end point during the interim analysis and the final analysis such that an alpha of 0.01 would be preserved for the final analysis. The actual alpha at the interim analysis was determined by the number of patients included in the analysis and, because all patients had been on treatment for at least 4 weeks at the time of the analysis, the primary end point of absolute change in ppFEV1 at 4 weeks was tested at an alpha of 0.05 during the interim analysis. The interim analysis was therefore the primary analysis for Study 102. For the European protocol, the primary end point of absolute change in ppFEV1 through 24 weeks was tested at an alpha of 0.05.
The key secondary end points in Study 102 were tested at an alpha of 0.05 only if the primary end point was statistically significant. A hierarchical testing procedure was used to control the type I error rate and for a test to be considered statistically significant all previous tests within the hierarchy must be statistically significant at the 0.05 level. The testing order for the key secondary end points was:
absolute change in ppFEV1 from baseline through 24 weeks (global protocol) or at 4 weeks (European protocol)
number of pulmonary exacerbations through 24 weeks
absolute change in sweat chloride from baseline through 24 weeks
absolute change in CFQ-R RD from baseline through 24 weeks
absolute change in BMI from baseline at 24 weeks
absolute change in sweat chloride from baseline at 4 weeks
absolute change in CFQ-R respiratory domain from baseline at 4 weeks.5
Patients With F/F Genotype: In Study 103, the key secondary end points were formally tested at an alpha of 0.05 only if the primary end point was statistically significant. A hierarchical testing procedure was used to control the type I error rate for the multiple key secondary end points tested at an alpha of 0.05. For a test to be considered statistically significant, the previous test within the hierarchy must be statistically significant at the 0.05 level. The testing order of the key secondary end points was:
absolute change in sweat chloride from baseline at 4 weeks
absolute change in CFQ-R RD score from baseline at 4 weeks.6
In Study 109, a hierarchical fixed-sequence testing procedure was used to first test the primary end point and then the key secondary end point to control the overall family-wise type I error at a 2-sided alpha of 0.05. The key secondary end point was tested only after the primary end point was determined to be statistically significant.10
Patients With F/G or F/RF Genotype: In Study 104, the key secondary end points were formally tested at an alpha of 0.05 only if the primary end point was statistically significant. A hierarchical testing procedure was used to control the overall type I error rate at an alpha of 0.05 for the primary and key secondary end points tested. For a test to be considered statistically significant within the testing hierarchy, all previous tests within the hierarchy must be statistically significant at the 0.05 level. The testing order of the key secondary end points was:
absolute change in sweat chloride from baseline through 8 weeks within the ELX-TEZ-IVA group
absolute change in ppFEV1 from baseline through 8 weeks for the ELX-TEZ-IVA group compared to the control group
absolute change in sweat chloride from baseline through 8 weeks for the ELX-TEZ-IVA group compared to the control group.11
Data Imputation Methods
The MMRM analyses performed in all the included studies assumed that data were missing at random, and no imputation of missing data was performed. As shown in Table 19, sensitivity analyses were performed using multiple imputation to assess the impact of missing data. Missing values were imputed starting from the first visit with missing values, for which all subsequent visits were also missing. Intermediate missing data (i.e., missing values that fell between 2 non-missing values) were assumed to be missing at random and therefore were not imputed.5,6,10,11
Table 19: Statistical Analysis of Efficacy End Points
End point | Statistical model | Adjustment factors | Sensitivity analyses |
|---|---|---|---|
Study 116 | |||
Absolute change in LCI2.5, ppFEV1, SwCl, and CFQ-R (RD) | MMRM | LCI2.5 at baseline (continuous) Body weight at screening (< 30 vs. ≥ 30 kg) | Not applicable |
Study 106B | |||
Absolute change ppFEV1 | MMRM | ppFEV1 at baseline (continuous) CFTR genotype group (F/F or F/MF) | MMRM (multiple imputation) MMRM (pooled clinic and home-assessed spirometry)a MMRM (clinic-assessed in extended analysis visit windows)b |
Absolute change in SwCl | MMRM | SwCl at baseline (continuous) CFTR genotype group (F/F or F/MF) | MMRM (clinic-assessed in extended analysis visit windows)b |
Absolute change in CFQ-R (RD) | MMRM | CFQ-R (RD) child’s version at baseline (continuous) CFTR genotype group (F/F or F/MF) | MMRM (pooled clinic and home-assessed)c |
Number of PEx, PEx requiring IV antibiotics and/or hospitalization | Descriptive statistics (annualized event rate) | Not applicable | Not applicable |
Study 102 | |||
Absolute change ppFEV1 | MMRM | Sex (male vs. female) Age at screening (< 18 or ≥ 18 years) ppFEV1 at baseline (continuous) | MMRM (multiple imputation) |
Absolute change in: SwCl, BMI, CFQ-R, body weight | MMRM | Sex (male vs. female) Age at screening (< 18 or ≥ 18 years) ppFEV1 (continuous) | Not applicable |
BMI z score | MMRM | Sex (male vs. female) ppFEV1 at baseline (continuous) | |
Number of PEx, PEx requiring IV antibiotics and/or hospitalization | NBR | Sex (male vs. female) Age at screening (< 18 or ≥ 18 years) ppFEV1 at baseline (continuous) | |
Time to first: PEx, PEx requiring IV antibiotics and/or hospitalization | Cox regression | Sex (male vs.. female) Age at screening (< 18 or ≥ 18 years) ppFEV1 at baseline (continuous) | |
Study 103 | |||
Absolute change ppFEV1 | MMRM | Sex (male vs. female) age at screening (< 18 or ≥ 18 years) ppFEV1 at baseline (continuous) | MMRM (multiple imputation) |
Absolute change in: SwCl, BMI, CFQ-R, TSQM, and body weight | MMRM | Sex (male vs. female) Age at screening (< 18 or ≥ 18 years) ppFEV1 at baseline (continuous) | Not applicable |
Study 104 | |||
Absolute change ppFEV1 | MMRM | ppFEV1 at baseline (continuous) SwCl at baseline (continuous) Comparator group (IVA or TEZ-IVA) | MMRM (multiple imputation) MMRM (pooled clinic and home-assessed spirometry)a |
Absolute change SwCl | MMRM | ppFEV1 at baseline (continuous) SwCl at baseline (continuous) Comparator group (IVA or TEZ-IVA) | MMRM any SwCl values < 10 mmol/L were considered missing |
Absolute change in CFQ-R (RD) | MMRM | ppFEV1 at baseline (continuous) SwCl at baseline (continuous) Comparator group (IVA or TEZ-IVA) | MMRM (only data assessed in clinic)d |
Study 109 | |||
Absolute change in CFQ-R (RD) | MMRM | Age at screening (< 18 or ≥ 18 years) CFTR-modulator use at screening (yes or no) ppFEV1 at baseline (continuous) | MMRM (multiple imputation) MMRM (only data assessed in clinic)d |
Absolute change in: SwCl and ppFEV1 | MMRM | Age at screening (< 18 or ≥ 18 years) CFTR-modulator use at screening (yes or no) ppFEV1 at baseline (continuous) | MMRM (multiple imputation) |
BMI = body mass index; CFQ-R = Cystic Fibrosis Questionnaire–Revised; F/F = homozygous for F508del mutation in the CFTR gene; F/MF = 1 F508del mutation and 1 minimal function mutation in the CFTR gene; IVA = ivacaftor; LCI = lung clearance index; MMRM = mixed-effects model for repeated measures; NBR = negative binomial regression; PEx = pulmonary exacerbation; ppFEV1 = percent predicted forced expiratory volume in 1 second; RD = respiratory domain; SwCl = sweat chloride; TEZ-IVA = tezacaftor-ivacaftor and ivacaftor; TSQM = Treatment Satisfaction Questionnaire for Medication.
aPrimary analysis was conducted with clinic spirometry data only. Due to the COVID-19 pandemic, home-assessed spirometry (i.e., spirometry assessed independently by the patients at home) was permitted. An additional analysis that included pooled clinic and home-assessed spirometry was performed.
bAll clinic-assessed spirometry data were collected through completion of study participation using the extended analysis visit windows (i.e., including data from unscheduled visits conducted after week 24 to capture safety laboratory testing missed due to the COVID-19 pandemic).
cDue to the COVID-19 pandemic, CFQ-R was permitted to be performed at home. The main analysis included only clinic-assessed measurements and a sensitivity analysis was performed using pooled CFQ-R data assessed at the clinic and at home.
dDue to the COVID-19 pandemic, CFQ-R was permitted to be performed at home. The main analysis included pooled CFQ-R data assessed at the clinic and at home and an additional analysis was performed that included only the CFQ-R data that were assessed at the clinic.
Source: Clinical Study Reports.3-6,10,11
Analysis Populations
The analysis sets that were used to evaluate the safety and efficacy end point in the included studies are summarized in Table 20.
Study | Dataset | Description |
|---|---|---|
Study 116 | All subjects set | All randomized patients or received at least 1 dose of the study drug; used for individual patient data listings and disposition summary |
Full analysis set | All randomized patients who carry the intended CFTR allele mutations and received at least 1 dose of study drug; used for all final efficacy analyses | |
Safety set | All patients who received at least 1 dose of the study drug; used for safety analyses | |
Study 106 | All subjects set | All patients who were enrolled or received at least 1 dose of the study drug; used for individual patient data listings and disposition summary |
Full analysis set | All patients who were enrolled or received at least 1 dose of the study drug; used for individual patient data listings and disposition summary | |
Safety set | All patients who received at least 1 dose of the study drug; used for safety analyses | |
Study 102 | All subjects set | All randomized patients or received at least 1 dose of the study drug; used for individual patient data listings and disposition summary |
Full analysis set | All randomized patients who carry the intended CFTR allele mutations and received at least 1 dose of the study drug; used for all final efficacy analyses | |
Interim full analysis set | Patients in the full analysis set whose scheduled week 4 visit was on or before the data cut-off (contains the same patients as the full analysis set); used for the interim efficacy analyses | |
Safety set | All patients who received at least 1 dose of the study drug; used for safety analyses | |
Study 103 Study 104 Study 109 | All subjects set | All randomized patients or received at least 1 dose of study drug; used for individual patient data listings and disposition summary |
Full analysis set | All randomized patients who carry the intended CFTR allele mutations and received at least 1 dose of study drug; used for all efficacy analyses | |
Safety set (run-in) | All patients who received at least 1 dose of run-in period drug (i.e., TEZ-IVA or IVA); used for safety analyses in the run-in period | |
Safety set (treatment period) | All patients who received at least 1 dose of study drug; used for safety analyses in the treatment period |
IVA = ivacaftor; TEZ-IVA = tezacaftor-ivacaftor and ivacaftor.
Source: Clinical Study Reports.3-6,10,11
Results
Patient Disposition
Patients Aged 6 to 11 Years
Placebo-Controlled Trial (Study 116; F/MF Genotype)
In Study 116, a total of 140 patients were screened for inclusion and 121 patients were randomized (13.6% failed to the meet the eligibility criteria). Sixty-one patients were randomized to the placebo group and 60 to the ELX-TEZ-IVA group. The full analysis set included all randomized patients. All the patients in the placebo group and 98.3% of those in the ELX-TEZ-IVA group completed the study, for an overall completion rate of 99.2%. Adverse events were cited as the reason for discontinuation for the 1 patient who discontinued the study treatment. All of the patients who completed the study elected to continue in the OLE phase.4
Table 21: Patient Disposition in Study 116
Disposition, n (%) | Placebo | ELX-TEZ-IVA | Total |
|---|---|---|---|
All subjects set | 61 | 60 | 121 |
Randomized | 61 | 60 | 121 |
Safety set | 61 | 60 | 121 |
Full analysis set | 61 | 60 | 121 |
Completed treatment | 61 (100.0) | 59 (98.3) | 120 (99.2) |
Discontinued treatment | 0 | 1 (1.7) | 1 (0.8) |
AE | 0 | 1 (1.7) | 1 (0.8) |
Completed study | 61 (100.0) | 59 (98.3) | 120 (99.2) |
Discontinued study | 0 | 1 (1.7) | 1 (0.8) |
AE | 0 | 1 (1.7) | 1 (0.8) |
Entered open-label extension | 61 (100.0) | 59 (98.3) | 120 (99.2) |
AE = adverse event; ELX-TEZ-IVA = elexacaftor-tezacaftor-ivacaftor and ivacaftor.
Source: Clinical Study Report.4
Single-Arm Trial (Study 106; F/F or F/MF Genotype)
In part A of Study 106, a total of 16 patients were screened for inclusion and all patients were enrolled. All of the patients in Part A completed the study and the full analysis set included all patients. In Part B, a total of 69 patients were screened for inclusion, 66 patients were enrolled (4.3% failed to the meet the eligibility criteria), and 97.0% of patients completed the study. One patient discontinued to due AEs and another due to concerns regarding the COVID-19 pandemic. All of the patients who completed the study elected to continue in the OLE phase.3
Table 22: Patient Disposition in Study 106
Disposition, n (%) | ELX-TEZ-IVA |
|---|---|
Part A | |
All subjects set | 16 |
Full analysis set | 16 |
Safety set | 16 |
Completed treatment | 16 (100.0) |
Prematurely discontinued treatment | 0 |
Completed study | 16 (100.0) |
Part B | |
All subjects set | 66 |
Full analysis set | 66 |
Safety set | 66 |
Completed treatment | 64 (97.0) |
Prematurely discontinued treatment | 2 (3.0) |
AE | 1 (1.5) |
Othera | 1 (1.5) |
Completed study | 64 (97.0) |
Prematurely discontinued the study | 2 (3.0) |
AE | 1 (1.5) |
Withdrawal of consent (not due to AE) | 1 (1.5) |
Rollover to the extension study | 64 (97.0) |
Prematurely discontinued the study | 0 |
AE = adverse event; ELX-TEZ-IVA = elexacaftor-tezacaftor-ivacaftor and ivacaftor.
aThe patient did not want to leave home due to the COVID-19 pandemic and switched to a commercially available drug.
Source: Clinical Study Report.3
Patients Aged 12 Years and Older
Patient disposition is summarized in Table 23 for Study 102 (the study that did not include a run-in period) and in Table 24 and Table 25 for Study 103, Study 104, and Study 109 (the studies with a run-in period).
Patients With F/MF Genotype
In Study 102, a total of 438 patients were screened for inclusion and 405 patients were randomized (7.5% failed to the meet the eligibility criteria)9 — 204 patients to the placebo group and 201 to the ELX-TEZ-IVA group. One patient in each group was randomized but never received the study drug; therefore, a total of 403 patients were included in the full analysis set for the interim and final analyses. All the patients in the placebo group and 98.5% of those in the ELX-TEZ-IVA group completed the study, for an overall completion rate of 99.3%. Reasons for discontinuation included AEs (n = 2) and pregnancy (n = 1). All of the patients who completed the study elected to continue in the OLE phase.5
Table 23: Patient Disposition in a Study Without a Run-in Period (Study 102)
Disposition, n (%) | Placebo | ELX-TEZ-IVA |
|---|---|---|
All subjects set | 204 | 201 |
Interim full analysis set | 203 | 200 |
Full analysis set | 203 | 200 |
Safety set | 201 | 202 |
Randomized | 204 | 201 |
Randomized but not dosed | 1 | 1 |
Completed treatment | 203 (100) | 197 (98.5) |
Prematurely discontinued treatment | 0 | 3 (1.5) |
AE | 0 | 2 (1.0) |
Patient refused further dosing | 0 | 0 |
Death | 0 | 0 |
Pregnancy (self or partner) | 0 | 1 (0.5) |
Completed study | 203 (100) | 197 (98.5) |
Prematurely discontinued the study | 0 | 3 (1.5) |
Adverse event | 0 | 1 (0.5) |
Withdrawal of consent (not AE) | 0 | 1 (0.5) |
Death | 0 | 0 |
Other | 0 | 1 (0.5) |
Rolled over to open-label study | 203 (100) | 197 (98.5) |
AE = adverse event; ELX-TEZ-IVA = elexacaftor-tezacaftor-ivacaftor and ivacaftor.
Source: Clinical Study Report.5
Patients With F/F Genotype
In Study 103, a total of 118 patients were screened for inclusion and 113 were enrolled in the 28-day TEZ-IVA run-in period (4.2% failed to the meet the eligibility criteria). A total of 108 patients were randomized — 56 to the ELX-TEZ-IVA group and 52 to the TEZ-IVA group. One patient in the ELX-TEZ-IVA group was randomized but never received the study drug, leaving 107 patients in the full analysis set. All of the patients in both the ELX-TEZ-IVA and TEZ-IVA groups completed the study, for an overall completion rate of 100%, and all of the patients elected to continue in the OLE phase.6
In Study 109, a total of 180 patients were screened for inclusion and 176 were enrolled in the 28-day TEZ-IVA run-in period (2.2% failed to the meet the eligibility criteria). One patient was excluded from the trial during the run-in period due to a pulmonary exacerbation. This patient was randomized to the ELX-TEZ-IVA group but discontinued before the first dose of study treatments in the double-blind phase. Therefore, 176 patients were randomized — 88 to the ELX-TEZ-IVA group and 88 to the TEZ-IVA group — but only 175 patients were included in the full analysis set. The proportions of patient who completed the study were 98.9% and 97.7% in the ELX-TEZ-IVA and TEZ-IVA groups, respectively. Two patients withdrew from TEZ-IVA group due to AEs and 1 patient withdrew from the ELX-TEZ-IVA group due to AEs. All of the patients who completed the study elected to enrol in the OLE phase.10
Patients With F/G or F/RF Genotypes
A total of 300 patients were screened for inclusion in Study 104, and 29 (9.7%) failed to the meet the eligibility criteria for the study. A total of 271 patients were enrolled in the 28-day run-in phase, during which they received treatment with TEZ-IVA or IVA for those with F/RF and F/G mutations, respectively. Ten patients (3.7%) withdrew during the run-in phase. The reasons for discontinuation included AEs (n = 2; 0.7%); refusal to undergo further dosing (n = 1; 0.4%); failure to meet the eligibility criteria for Study 104 (n = 1; 0.4%). The sponsor reported that, of the 6 patients who discontinued for “other” reasons (as shown in Table 24), 5 withdrew due to the onset of the COVID-19 pandemic and 1 for reasons that were related to the eligibility of the study. A total of 259 patients were randomized (133 in the ELX-TEZ-IVA group and 126 in the TEZ-IVA or IVA group — referred to as the control group). A single patient in the ELX-TEZ-IVA group discontinued before the first dose of the study treatments in the double-blind phase; the full analysis set therefore included 258 patients. The proportions of patient who completed the study were 99.2% and 96.8% in the ELX-TEZ-IVA and control groups, respectively. Two patients withdrew from the control group due to AEs and 1 patient withdrew from the ELX-TEZ-IVA group due to AEs. With the exception of 1 patient in each of the treatment groups, all the patients who completed the study elected to enrol in the OLE study.
Table 24: Patient Disposition Within the Run-in Periods (Study 103, Study 104, and Study 109)
Disposition, n (%) | Study 103 (F/F) | Study 109 (F/F) | Study 104 (F/G and F/RF) |
|---|---|---|---|
TEZ-IVA | TEZ-IVA | TEZ-IVA or IVA | |
All subjects set | 113 | 176 | 271 |
Safety set (run-in period) | 113 | 176 | 271 |
Discontinued treatment | 6 (5.3) | 1 (0.6) | 10 (3.7) |
Adverse event | 5 (4.4) | 0 | 2 (0.7) |
Refused further dosing | 1 (0.9) | 0 | 1 (0.4) |
Eligibility criteria not met | 0 | 1 (0.6) | 1 (0.4) |
Other | 0 | 0 | 6 (2.2) |
Discontinued study | 6 (5.3) | 1 (0.6) | 12 (4.4) |
Adverse event | 4 (3.5) | 1 (0.6) | 3 (1.1) |
Consent withdrawn | 2 (1.8) | 0 | 2 (0.7) |
Other | 0 | 0 | 7 (2.6) |
Exposure to Study Treatments
Patients Aged 6 to 11 Years
Study Treatments
Patient exposure to the study drugs is summarized in Table 25. The median treatment duration was 24 weeks in Study 116, 14.9 days in Study 106 Part A, and 23.8 weeks in Study 106 Part B. Adherence to the study treatments, which was evaluated by counting the number of study drugs at each visit, was reported to be 100% in both Study 116 and Study 106B.3,4
Table 25: Patient Disposition Within the Treatment Periods (Study 103, Study 104, and Study 109)
Disposition, n (%) | Study 103 (F/F) | Study 109 (F/F) | Study 104 (F/G and F/RF) | |||
|---|---|---|---|---|---|---|
TEZ-IVA | ELX-TEZ-IVA | TEZ-IVA | ELX-TEZ-IVA | TEZ-IVA or IVA | ELX-TEZ-IVA | |
Full analysis set | 52 | 55 | 88 | 87 | 126 | 132 |
Safety set (treatment period) | 52 | 55 | 88 | 87 | 126 | 132 |
Randomized | 52 | 56 | 88 | 88 | 126 | 133 |
Randomized but not dosed | 0 | 1 | 0 | 1 | 0 | 1 |
Completed treatment | 52 (100.0) | 55 (100.0) | 86 (97.7) | 86 (98.9) | 122 (96.8) | 131 (99.2) |
Discontinued study | 0 | 0 | 2 (2.3) | 1 (1.1) | 4 (3.2) | 1 (0.8) |
Adverse event | 0 | 0 | 2 (2.3) | 1 (1.1) | 2 (1.6) | 1 (0.8) |
Physician decision | 0 | 0 | 0 | 0 | 1 (0.8) | 0 |
Other | 0 | 0 | 0 | 0 | 1 (0.8) | 0 |
Completed study | 52 (100.0) | 55 (100.0) | 86 (97.7) | 86 (98.9) | 122 (96.8) | 131 (99.2) |
Entered open-label study | 52 (100.0) | 55 (100.0) | 86 (97.7) | 86 (98.9) | 121 (96.0) | 130 (98.5) |
ELX-TEZ-IVA = elexacaftor-tezacaftor-ivacaftor and ivacaftor; F/F = homozygous for F508del mutations in the CFTR gene; F/G = 1 F508del mutation and 1 gating mutation in the CFTR gene; F/RF = 1 F508del mutation and 1 residual function mutation in the CFTR gene; IVA = ivacaftor; TEZ-IVA = tezacaftor-ivacaftor and ivacaftor.
Source: Clinical Study Reports.6,10,11
Concomitant Therapies
Prior and concomitant medications that were used by 20% or more of patients in the included studies are summarized in Table 26. The most commonly used concomitant medications included mucolytics (inhaled sodium chloride and dornase alfa), bronchodilators (fluticasone and salbutamol), antibiotics (azithromycin), pancreatic enzymes (pancreatin and pancrelipase), vitamin supplements, proton-pump inhibitors (omeprazole and lansoprazole), and bile acid (ursodeoxycholic acid).3,4
Table 26: Summary of Exposure to Study Drugs in Pediatric Patients
Exposure | Study 116 | Study 106 | ||
|---|---|---|---|---|
Placebo (N = 61) | ELX-TEZ-IVA (N = 60) | Part A (N = 16) | Part B (N = 66) | |
Total exposure | ||||
Patient weeks | 1,466.9 | 1,421.7 | 34.1 | 1570.4 |
Exposure duration (weeks unless otherwise noted) | ||||
Mean (SD) | 24.0 (0.4) | 23.7 (3.0) | 14.9 days (0.68) | 23.8 (3.0) |
Median (range) | 24.0 (23.1 to 25.0) | 24.0 (1.0 to 25.0) | 15.0 days (14 to 16) | 24.1 (0.1 to 24.9) |
ELX-TEZ-IVA = elexacaftor-tezacaftor-ivacaftor and ivacaftor; SD = standard deviation.
Source: Clinical Study Reports.3,4
Patients Aged 12 Years and Older
Study Treatments
Patient exposure to the study drugs is summarized in Table 27. The median treatment duration was 24 weeks in Study 102 and Study 109, 4 weeks in Study 103, and 8 weeks in Study 104.5,6,10,11 Adherence with the study treatments, which was evaluated by counting the number of study drugs at each visit, was reported to be 99.2% in Study 102, 100% in Study 103, 99.8% in Study 109, and 99.6% in Study 104.5,6,10,11
Table 27: Concomitant Medications Used by at Least 20% of Pediatric Patients
Preferred name (%) | Study 116 | Study 106 | |
|---|---|---|---|
Placebo (N = 61) | ELX-TEZ-IVA (N = 60) | Part B (N = 66) | |
≥ 1 medication | 61 (100.0) | 60 (100.0) | 66 (100.0) |
Pancreatin | 53 (86.9) | 52 (86.7) | 46 (69.7) |
Sodium chloride | 54 (88.5) | 51 (85.0) | 57 (86.4) |
Dornase alfa | 40 (65.6) | 43 (71.7) | 55 (83.3) |
Salbutamol | 45 (73.8) | 36 (60.0) | 53 (80.3) |
Ursodeoxycholic acid | 15 (24.6) | 21 (35.0) | NR |
Paracetamol | 18 (29.5) | 12 (20.0) | 17 (25.8) |
Omeprazole | 16 (26.2) | 12 (20.0) | 16 (24.2) |
Vitamin D (not otherwise specified) | 17 (27.9) | 11 (18.3) | NR |
Retinol | 14 (23.0) | 11 (18.3) | NR |
Fluticasone propionate | NR | NR | 23 (34.8) |
Multi-vitamina | NR | NR | 20 (30.3) |
Salbutamol sulphate | NR | NR | 14 (21.2) |
Lansoprazole | NR | NR | NR |
Azithromycin | NR | NR | 20 (30.3) |
Colecalciferol | NR | NR | NR |
Pancrelipase | NR | NR | 19 (28.8) |
Fluticasone | NR | NR | NR |
Sodium bicarbonate or sodium chloride | NR | NR | NR |
Ibuprofen | NR | NR | 20 (30.3) |
Macrogol 3350 | NR | NR | 18 (27.3) |
Vitamins (not otherwise specified) | NR | NR | 14 (21.2) |
ELX-TEZ-IVA = elexacaftor-tezacaftor-ivacaftor and ivacaftor.
aAscorbic acid, betacarotene, biotin, calcium pantothenate, colecalciferol, cyanocobalamin, folic acid, nicotinamide, phytomenadione, pyridoxine hydrochloride, retinolpalmitate, riboflavin, thiamine mononitrate, tocopherol, and zinc ascorbate.
Concomitant Therapies
Prior and concomitant medications that were used by at least 20% of patients in the included studies are summarized in Table 28. The most commonly used concomitant medications included mucolytics (inhaled sodium chloride and dornase alfa), bronchodilators (fluticasone propionate, salmeterol xinafoate, and salbutamol), antibiotics (ciprofloxacin, sulfamethoxazole-trimethoprim, azithromycin, tobramycin, aztreonam lysine, and colistimethate sodium), pancreatic enzymes (pancreatin and pancrelipase), vitamin supplementals (tocopherol and cholecalciferol), a proton-pump inhibitor (omeprazole); and bile acid (ursodeoxycholic acid).5,6,10,11
Table 28: Summary of Exposure to the Study Drugs in Adolescent and Adult Patients
Exposure | Study 102 (F/MF) | Study 103 (F/F) | Study 109 (F/F) | Study 104 (F/G and F/RF) | ||||
|---|---|---|---|---|---|---|---|---|
Placebo (N = 201) | ELX-TEZ-IVA (N = 202) | TEZ-IVA (N = 52) | ELX-TEZ-IVA (N = 55) | TEZ-IVA (N = 88) | ELX-TEZ-IVA (N = 87) | Control (N = 126) | ELX-TEZ-IVA (N = 132) | |
Total exposure | ||||||||
Patient weeks | 4,758.7 | 4,761.3 | 204.7 | 221.3 | 2,074.1 | 2,062.7 | 993.4 | 1,050.4 |
Exposure duration (weeks) | ||||||||
Mean (SD) | 23.7 (2.39) | 23.6 (2.62) | 3.9 (0.42) | 4.0 (0.37) | 23.6 (2.2) | 23.7 (1.9) | 7.9 (0.9) | 8.0 (0.7) |
Median (range) | 24.0 (0.3 to 25.1) | 24.0 (1.0 to 25.1) | 4.0 (3.1 to 4.7) | 4.0 (3.3 to 4.9) | 24.0 (7.3 to 24.9) | 24.0 (6.7 to 24.7) | 8.0 (1.3 to 9.1) | 8.0 (0.6 to 9.0) |
ELX-TEZ-IVA = elexacaftor-tezacaftor-ivacaftor and ivacaftor; F/F = homozygous for F508del mutations in the CFTR gene; F/G = 1 F508del mutation and 1 gating mutation in the CFTR gene; F/MF = 1 F508del mutation and 1 minimal function mutation in the CFTR gene; F/RF = 1 F508del mutation and 1 residual function mutation in the CFTR gene; SD = standard deviation; TEZ-IVA = tezacaftor-ivacaftor and ivacaftor.
Source: Clinical Study Reports.5,6,10,11
Patients With F/MF Genotype
A larger percentage of patients in the ELX-TEZ-IVA group were using inhaled sodium chloride compared with the placebo group (81.5% versus 74.9%).5 Three antibiotics were more commonly used in the placebo group compared with the ELX-TEZ-IVA group: tobramycin (55.7% versus 39.0%), ciprofloxacin (35.0% versus 16.0%), and trimethoprim-sulfamethoxazole (26.1 versus 17.0%).5
Patients With F/F Genotype
Study 103 and Study 109 had the smallest sample sizes of the 4 included studies and the greatest number of imbalances in the use of concomitant medications across the treatment groups.6,10 In Study 103, a greater percentage of patients in the ELX-TEZ-IVA group compared with the TEZ-IVA group received treatment with salbutamol (65.5% versus 59.6, respectively), azithromycin (58.2% versus 46.2%), ursodeoxycholic acid (27.3% versus 19.2%), and fluticasone propionate–salmeterol xinafoate (25.5% versus 17.3%).6 A greater percentage of patients in the TEZ-IVA group compared with the ELX-TEZ-IVA group received treatment with inhaled sodium chloride (82.7% versus 74.5% for the ELX-TEZ-IVA, respectively), fluticasone propionate (34.6% versus 29.1%), and omeprazole (28.8% versus 18.2%).6 In Study 109, a greater percentage of patients in the ELX-TEZ-IVA group compared with the TEZ-IVA group received treatment with aztreonam lysine (25.3% versus 18.2%, respectively) and colistimethate sodium (41.4% versus 31.8%). A greater percentage of patients in the TEZ-IVA group compared with the ELX-TEZ-IVA group received treatment with dornase alfa (81.8% versus 71.3%, respectively), tobramycin (40.9% and 29.9%), cholecalciferol (31.8% versus 25.3%), and ciprofloxacin (33.0% versus 17.2%).10
Patients With F/G or F/RF Genotypes
The prior and concomitant medications used in Study 104 were well balanced across the ELX-TEZ-IVA and the control group.11 The percentage of patients using some concomitant medications was considerably lower in Study 104 compared with the other included trials. These included dornase alfa (52.7% in Study 104 versus 81.6% in Study 102, 92.5% in Study 103, and 76.6% in Study 109), inhaled sodium chloride (51.9% in Study 104 versus 78.2% in Study 102, 78.5% in Study 103, and 75.4% in Study 109), and pancreatin (51.9% in Study 104 versus 63.5% in Study 102, 65.4% in Study 103, and 93.7% in Study 109).5,6,10,11
Table 29: Concomitant Medications Used by at Least 20% of Adolescent and Adult Patients
Concomitant medication, n (%) | Study 102 (F/MF) | Study 103 (F/F) | Study 109 (F/F) | Study 104 (F/G and F/RF) | ||||
|---|---|---|---|---|---|---|---|---|
Placebo (N = 203) | ELX-TEZ-IVA (N = 200) | TEZ-IVA (N = 52) | ELX-TEZ-IVA (N = 55) | TEZ-IVA (N = 88) | ELX-TEZ-IVA (N = 87) | Control (N = 126) | ELX-TEZ-IVA (N = 132) | |
≥ 1 medication | 203 (100.0) | 200 (100.0) | 52 (100.0) | 55 (100.0) | 88 (100.0) | 87 (100.0) | 126 (100.0) | 132 (100.0) |
Dornase alfa | 165 (81.3) | 164 (82.0) | 48 (92.3) | 51 (92.7) | 72 (81.8) | 62 (71.3) | 66 (52.4) | 70 (53.0) |
Sodium chloride | 152 (74.9) | 163 (81.5) | 43 (82.7) | 41 (74.5) | 67 (76.1) | 65 (74.7) | 66 (52.4) | 68 (51.5) |
Salbutamol | 154 (75.9) | 152 (76.0) | 31 (59.6) | 36 (65.5) | 57 (64.8) | 57 (65.5) | 72 (57.1) | 80 (60.6) |
Pancreatin | 130 (64.0) | 126 (63.0) | 33 (63.5) | 37 (67.3) | 84 (95.5) | 80 (92.0) | 51 (40.5) | 49 (37.1) |
Azithromycin | 118 (58.1) | 111 (55.5) | 24 (46.2) | 32 (58.2) | 47 (53.4) | 48 (55.2) | 58 (46.0) | 57 (43.2) |
Tobramycin | 113 (55.7) | 78 (39.0) | 17 (32.7) | 15 (27.3) | 36 (40.9) | 26 (29.9) | — | — |
Colecalciferol | 87 (42.9) | 89 (44.5) | 19 (36.5) | 20 (36.4) | 28 (31.8) | 22 (25.3) | 38 (30.2) | 44 (33.3) |
Pancrelipase | 62 (30.5) | 62 (31.0) | 16 (30.8) | 15 (27.3) | — | — | — | — |
Ibuprofen | 58 (28.6) | 62 (31.0) | — | — | 16 (18.2) | 22 (25.3) | — | — |
Aztreonam lysine | 63 (31.0) | 56 (28.0) | 13 (25.0) | 12 (21.8) | — | — | — | — |
Acetaminophen | 58 (28.6) | 58 (29.0) | — | — | 31 (35.2) | 27 (31.0) | — | — |
Ciprofloxacin | 71 (35.0) | 32 (16.0) | — | — | 29 (33.0) | 15 (17.2) | — | — |
Ursodeoxycholic acid | 43 (21.2) | 56 (28.0) | 10 (19.2) | 15 (27.3) | 27 (30.7) | 28 (32.2) | — | — |
Fluticasone, salmeterol xinafoate | 51 (25.1) | 42 (21.0) | 9 (17.3) | 14 (25.5) | 18 (20.5) | 20 (23.0) | — | — |
Fluticasone | 45 (22.2) | 46 (23.0) | 18 (34.6) | 16 (29.1) | - | - | — | — |
Omeprazole | 47 (23.2) | 44 (22.0) | 15 (28.8) | 10 (18.2) | 24 (27.3) | 26 (29.9) | — | — |
Sulfamethoxazole; trimethoprim | 53 (26.1) | 34 (17.0) | — | — | — | — | — | — |
Salbutamol sulphate | 44 (21.7) | 38 (19.0) | — | — | — | — | — | — |
Tocopherol | — | — | — | — | 21 (23.9) | 20 (23.0) | — | — |
Colistimethate sodium | — | — | — | — | 28 (31.8) | 36 (41.4) | — | — |
ELX-TEZ-IVA = elexacaftor-tezacaftor-ivacaftor and ivacaftor; F/F = homozygous for F508del mutations in the CFTR gene; F/G = 1 F508del mutation and 1 gating mutation in the CFTR gene; F/MF = 1 F508del mutation and 1 minimal function mutation in the CFTR gene; F/RF = 1 F508del mutation and 1 residual function mutation in the CFTR gene; TEZ-IVA = tezacaftor-ivacaftor and ivacaftor.
Efficacy
Only those efficacy outcomes and analyses of subgroups identified in the review protocol are reported here. Appendix 3 provides detailed efficacy data.
Forced Expiratory Volume in 1 Second
Patients Aged 6 to 11 Years
Placebo-Controlled Trial (Study 116; F/MF Genotype): In Study 116, treatment with ELX-TEZ-IVA was associated with a statistically significant increase from baseline in ppFEV1 compared with placebo through 24 weeks (LSMD = 11.0%; 95% CI, 6.9 to 15.1). As shown in Figure 9, improvements in ppFEV1 with ELX-TEZ-IVA were observed at the time of the first post-baseline assessment (i.e., day 15) and were higher at all time points throughout the study.4 The sponsor provided updated data to CADTH demonstrating post hoc subgroup analyses for patients with a ppFEV1 90% or less and greater than 90% of baseline. As shown in Table 103, the increase from baseline in ppFEV1 was |||||||||||||||||||||||||||||||||||||||||| for those with a ppFEV1 90% or less at baseline and |||||||||||||||||||||||||||||||||||||||||||||||||||||| for those with a ppFEV1 greater than 90% at baseline.78
Single-Arm Trial (Study 106; F/F or F/MF Genotype): In Study 106 Part B, treatment with ELX-TEZ-IVA resulted in a statistically significant within-group increase in ppFEV1 through 24 weeks (LS mean change = 10.2%; 95% CI, 7.9 to 12.6; P < 0.0001). As shown in Figure 9, improvements in ppFEV1 with ELX-TEZ-IVA were observed at the time of the first post-baseline assessment (i.e., day 15) and were greater than baseline at all time points throughout the 24-week treatment period. A sensitivity analysis was performed using the multiple imputation method to assess for impacts, and the results were consistent with the primary analysis (LS mean change = 9.9; 95% CI, 7.9 to 11.9; P < 0.0001). An additional pre-specified sensitivity analysis that included home-based spirometry was permitted due to the COVID-19 pandemic; results were also similar to the primary analysis (LS mean change = 10.7; 95% CI, 8.3 to 13.0; P < 0.0001).3
Figure 9: Absolute Change From Baseline in ppFEV1 in Study 116 and Study 106B
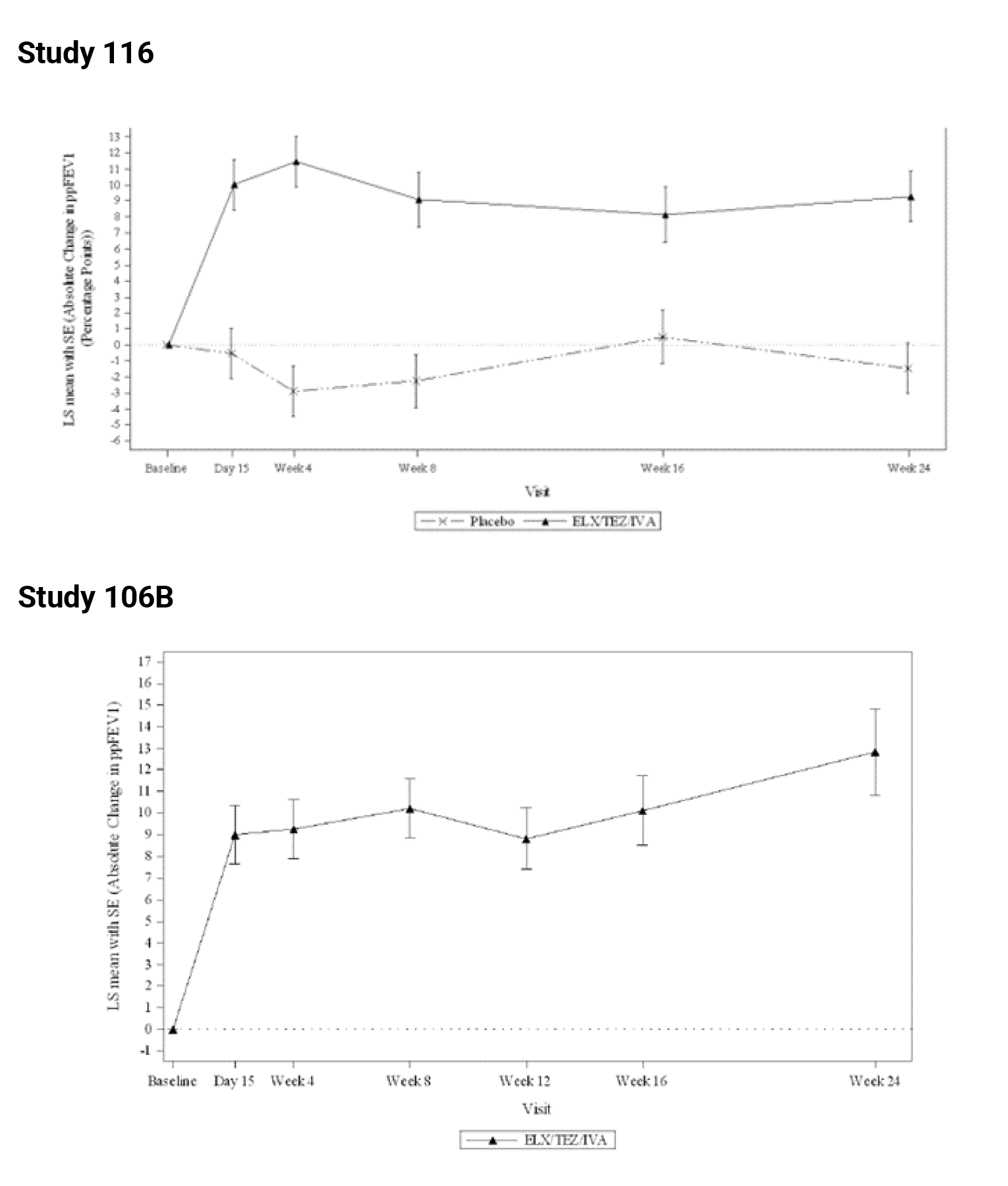
ELX/TEZ/IVA = elexacaftor-tezacaftor-ivacaftor and ivacaftor; LS = least squares; ppFEV1 = percent predicted forced expiratory volume in 1 second; SE = standard error.
Patients Aged 12 Years and Older
Patients With F/MF Genotype: Treatment with ELX-TEZ-IVA was associated with a statistically significant increase from baseline in ppFEV1 compared with placebo at 4 weeks (13.8%; 95% CI, 12.1 to 15.4; P < 0.0001) and 24 weeks (14.3%; 95% CI, 12.7 to 15.8; P < 0.0001). As shown in Figure 10, improvements in ppFEV1 with ELX-TEZ-IVA were observed at the time of the first post-baseline assessment (i.e., day 15) and were higher at all time points throughout the study. Results of the sensitivity analyses using MMRM with multiple imputation were consistent with the result of the primary analysis (Table 30).5
Table 30: Absolute Change From Baseline to Week 24 in ppFEV1 in Pediatric Studies
Analysis | Study 116 | Study 106B (N = 66) | |
|---|---|---|---|
Placebo (N = 61) | ELX-TEZ-IVA (N = 60) | ||
Baseline mean (SD) | 87.2 (15.8) | 91.4 (13.8) | 88.8 (17.7) |
Patients in analysis | 59 | 59 | 59 |
LS mean change (SE) | −1.5 (1.5) | 9.5 (1.5) | 10.2 (1.2) |
P value within treatment | 0.2977 | < 0.0001 | < 0.0001 |
LSMD (95% CI) | Reference | 11.0 (6.9 to 15.1) | NA |
P value vs. placebo | Reference | < 0.0001 | NA |
CI = confidence interval; ELX-TEZ-IVA = elexacaftor-tezacaftor-ivacaftor and ivacaftor; LSMD = least squares mean difference; NA = not applicable; ppFEV1 = percent predicted forced expiratory volume in 1 second; SD = standard deviation; SE = standard error.
Source: Clinical Study Reports.3,4
Results for change from baseline in ppFEV1 were generally consistent across all subgroup analyses, including those based on age (12 to < 18 years or ≥ 18 years) and ppFEV1 at screening (< 70% or ≥ 70%) (Table 104).5 The sponsor conducted an additional post hoc subgroup analysis for the subset of patients with a ppFEV1 below 40% at baseline (16 of 203 [7.9%] in the placebo group and 18 of 200 [9.0%] in the ELX-TEZ-IVA group). Treatment with ELX-TEZ-IVA was associated with an improvement in absolute change in ppFEV1 at 4 weeks (LSMD = 15.2%; 95% CI, 7.3 to 23.1) and through 24 weeks (LSMD = ||||||||||||||||||||||||||||||||||||).5 Complete details regarding these subgroup analyses in patients with advanced lung disease are provided in Table 105.
Figure 10: Absolute Change From Baseline in ppFEV1 in F/MF Genotype
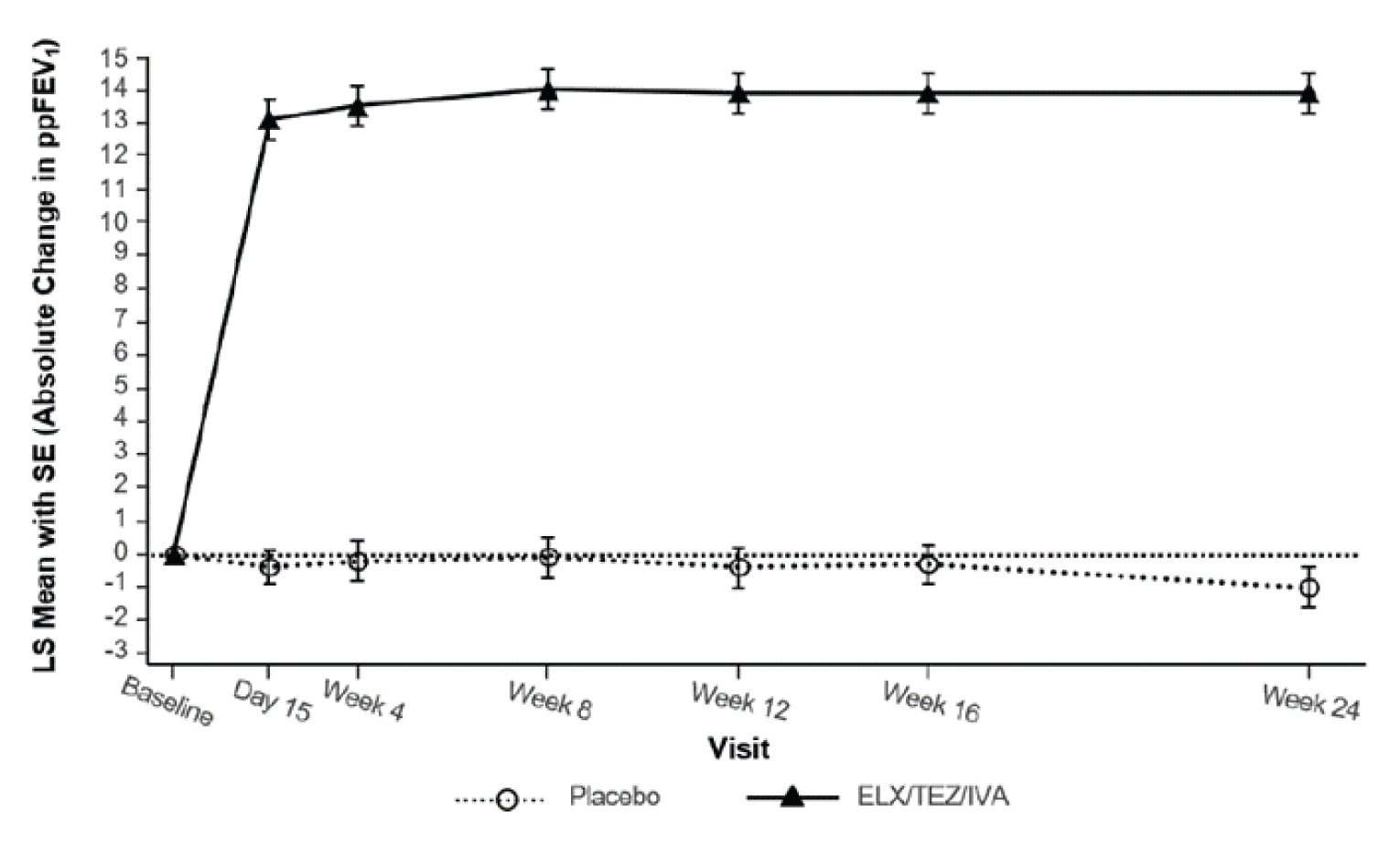
LS = least squares; ELX/TEZ/IVA = elexacaftor-tezacaftor-ivacaftor and ivacaftor; ppFEV1 = percent predicted forced expiratory volume in 1 second; SE = standard error.
Source: Product monograph.36
Patients With F/F Genotype: Absolute change from baseline in ppFEV1 at 4 weeks was the primary end point of Study 103. Treatment with ELX-TEZ-IVA was associated with a statistically significant increase from baseline in ppFEV1 compared with TEZ-IVA at 4 weeks (10.0%; 95% CI, 7.4 to 12.6; P < 0.0001) (Table 31).5 As shown in Figure 11, improvements in ppFEV1 with ELX-TEZ-IVA were observed at the time of the first post-baseline assessment (i.e., day 15) and were higher at all time points throughout the study.5 Results of the sensitivity analyses using an MMRM with multiple imputation were consistent with the result of the primary analysis (LSMD = 9.3%; 95% CI, 6.8 to 11.7).5 The results for change from baseline in ppFEV1 were generally consistent across all subgroup analyses; however, the confidence intervals for the analyses of subgroups with small sample sizes, such as those for patients aged 12 to 18 years, were wide (Table 106).5 The EMA reported the results of an additional post hoc subgroup analysis from Study 103 (CFTR modulator–naive [n = 41] versus treatment-experienced [n = 66]). The observed treatment effect was 7.8% (95% CI, 4.8 to 10.8) for CFTR modulator–experienced patients and 13.2% (95% CI, 8.5 to 17.9) for CFTR modulator–naive patients.59,79
Absolute change from baseline in ppFEV1 through 24 weeks was a pre-specified key secondary end point of Study 109. Treatment with ELX-TEZ-IVA was associated with a statistically significant absolute increase from baseline in ppFEV1 compared with TEZ-IVA through 24 weeks (LSMD = 10.2%; 95% CI, 8.2 to 12.1; P < 0.0001) (Table 31).10 Results of the sensitivity analyses using a MMRM with multiple imputation were consistent with the result of the primary analysis (LSMD = 10.1%; 95% CI, 8.2 to 11.9).10 Subgroup analyses were not conducted for change from baseline in ppFEV1 in Study 109.10
Table 31: Change from Baseline in ppFEV1 in F/MF Genotype in Study 102
Analysis | Placebo (N = 203) | ELX-TEZ-IVA (N = 200) |
|---|---|---|
Absolute change from baseline at 4 weeksa | ||
Baseline mean (SD) | 61.3 (15.5) | 61.6 (15.0) |
LS mean change (SE) | −0.2 (0.6) | 13.6 (0.6) |
Patients in analysis | 188 | 185 |
LSMD (95% CI) | 13.8 (12.1 to 15.4) | |
P value (vs. placebo) | < 0.0001b | |
Absolute change from baseline at 4 weeks (multiple imputation)a | ||
Baseline mean (SD) | 61.3 (15.5) | 61.6 (15.0) |
LS mean change (SE) | −0.2 (0.6) | 13.6 (0.6) |
Patients in analysis | 203 | 200 |
LSMD (95% CI) | 13.8 (12.2 to 15.5) | |
P value (vs. placebo) | < 0.0001 | |
Absolute change from baseline through 24 weeksc | ||
Baseline mean (SD) | 61.3 (15.5) | 61.6 (15.0) |
LS mean change (SE) | −0.4 (0.5) | 13.9 (0.6) |
Patients in analysis | 203 | 196 |
LSMD (95% CI) | 14.3 (12.7 to 15.8) | |
P value (vs. placebo) | < 0.0001d | |
Absolute change from baseline through 24 weeks (multiple imputation)c | ||
Baseline mean (SD) | 61.3 (15.5) | 61.6 (15.0) |
LS mean change (SE) | −0.4 (0.5) | 13.8 (0.5) |
Patients in analysis | 203 | 200 |
LSMD (95% CI) | 14.3 (12.8 to 15.8) | |
P value (vs. placebo) | < 0.0001 | |
CI = confidence interval; ELX-TEZ-IVA = elexacaftor-tezacaftor-ivacaftor and ivacaftor; F/MF = 1 F508del mutation and 1 minimal function mutation in the CFTR gene; LS = least squares; LSMD = least squares mean difference; MMRM = mixed-effects model for repeated measures; ppFEV1 = percent predicted forced expiratory volume in 1 second; SD = standard deviation; SE = standard error.
aThe MMRM included data from the day 15 and week 4 visits, with treatment, visit, and treatment-by-visit interaction as fixed effects and baseline ppFEV1, age group at screening (< 18, ≥ 18 years of age), and sex (male, female) as covariates. For the multiple imputation sensitivity analysis, the same MMRM as the primary analysis was used, including all the data up to week 4. Missing ppFEV1 assessments were imputed only for visits for which all subsequent visits through week 4 were also missing (i.e., missing values that fall between 2 non-missing ones were not imputed).
bPre-specified primary end point.
cThe MMRM included final data from all available visits, with treatment, visit, and treatment-by-visit interaction as fixed effects and baseline ppFEV1, age group at screening (< 18, ≥ 18 years of age), and sex (male, female) as covariates. However, the day 15 visit was not included in the estimation of the average treatment effect through week 24. For the multiple imputation sensitivity analysis, the same MMRM as the primary analysis was used. Missing ppFEV1 assessments were imputed only for visits for which all subsequent visits through week 24 were also missing (i.e., missing values that fall between 2 non-missing values were not imputed).
dPre-specified key secondary end point.
Source: Clinical Study Report.5
Figure 11: Absolute Change from Baseline in ppFEV1 in F/F Genotype
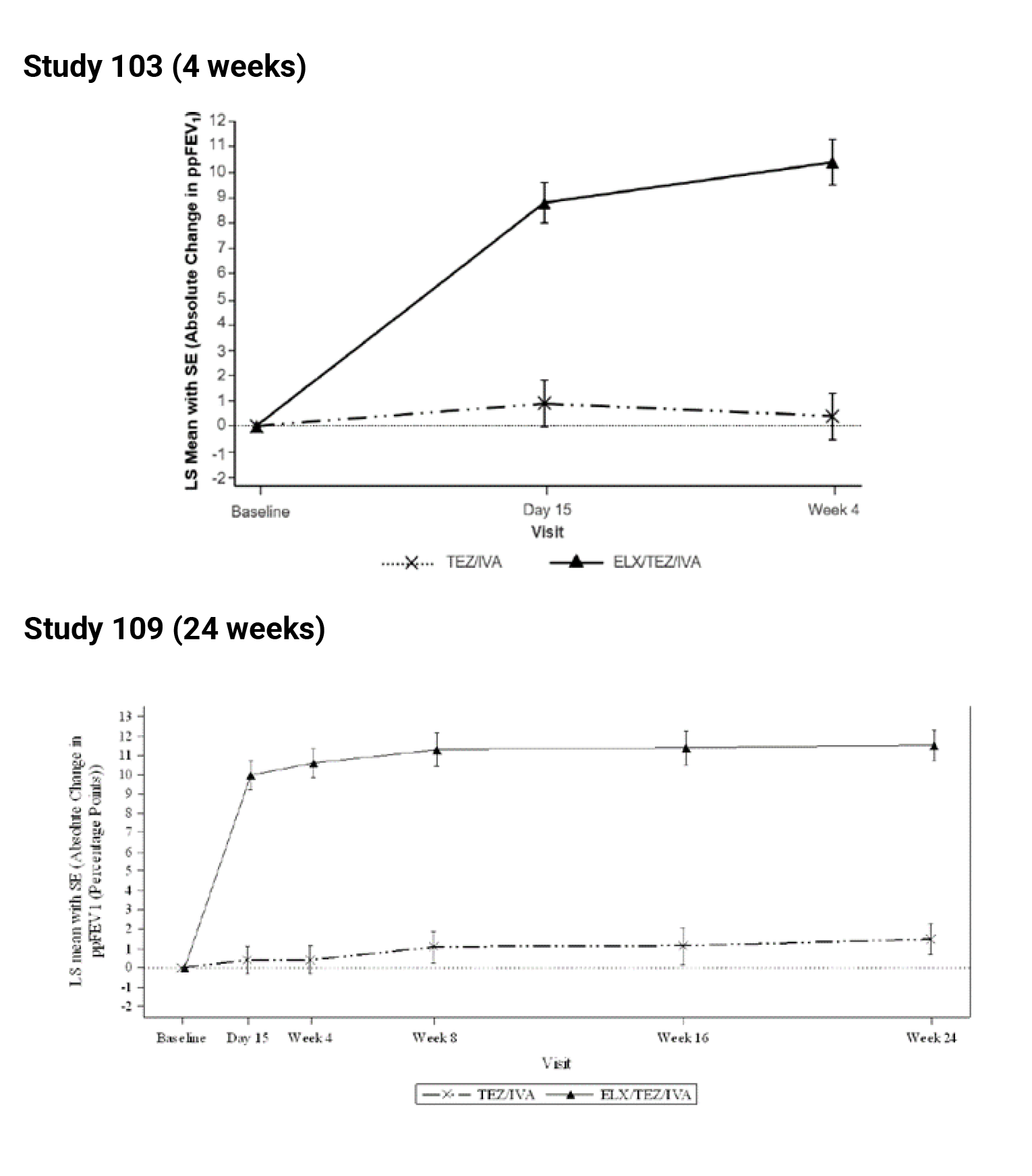
ELX/TEZ/IVA = elexacaftor-tezacaftor-ivacaftor and ivacaftor; LS = least squares; ppFEV1 = percent predicted forced expiratory volume in 1 second; SE = standard error; TEZ-IVA = tezacaftor-ivacaftor and ivacaftor.
Patients With F/G and F/RF Genotypes: The primary end point of Study 104 was absolute change baseline in ppFEV1 through 8 weeks for the ELX-TEZ-IVA group (i.e., within-group change from baseline).11 Treatment with ELX-TEZ-IVA was associated with a statistically significant improvement in ppFEV1 through 8 weeks (LS mean change: 3.7%; 95% CI, 2.8 to 4.6; P < 0.0001) (Table 32).11 Results of the sensitivity analyses using an MMRM with multiple imputation were consistent with the result of the primary analysis. An additional pre-specified analysis was performed that included spirometry assessed independently by the patients at home (due to the COVID-19 pandemic), and the results were similar to the primary analysis (LSMD = 3.8; 95% CI, 2.9 to 4.7).11
Absolute change from baseline in ppFEV1 through 8 weeks in the ELX-TEZ-IVA group compared to the control group was a pre-specified key secondary end point of Study 104.11 Treatment with ELX-TEZ-IVA was associated with a statistically significant improvement in ppFEV1 compared to the control group (LSMD = 3.5%; 95% CI, 2.2 to 4.7; P < 0.0001) (Table 32).11 Similar results were obtained with a sensitivity analyses using an MMRM with multiple imputation (LSMD = 3.6%; 95% CI, 2.3 to 4.8; P < 0.0001).11
Subgroup analyses based on the comparator group (i.e., patient genotype) demonstrated improvements in ppFEV1 through 8 weeks with ELX-TEZ-IVA versus IVA (LSMD = 5.8; 95% CI, 3.5 to 8.0) and a smaller effect versus TEZ-IVA (LSMD = 2.0; 95% CI, 0.5 to 3.4).
Table 32: Change from Baseline in ppFEV1 in F/F Genotype
Analysis | Study 103 (F/F) at 4 weeks | Study 109 (F/F) through 24 weeks | ||
|---|---|---|---|---|
TEZ-IVA (N = 52) | ELX-TEZ-IVA (N = 55) | TEZ-IVA (N = 88) | ELX-TEZ-IVA (N = 87) | |
Absolute change from baseline at 4 weeksa or 24 weeksb | ||||
Baseline mean (SD) | 60.2 (14.4) | 61.6 (15.4) | 64.2 (15.1) | 63.0 (16.7) |
LS mean change (SE) | 0.4 (0.9) | 10.4 (0.9) | 1.0 (0.7) | 11.2 (0.7) |
Patients in analysis | 49 | 53 | 87 | 86 |
LSMD (95% CI) | 10.0 (7.4 to 12.6) | 10.2 (8.2 to 12.1) | ||
P value (vs. TEZ-IVA) | < 0.0001c | < 0.0001d | ||
Absolute change from baseline at 4 weeksa or 24 weeks (multiple imputation)b | ||||
Baseline mean (SD) | 60.2 (14.4) | 61.6 (15.4) | 64.2 (15.1) | 63.0 (16.7) |
LS mean change (SE) | 0.6 (0.9) | 9.9 (0.9) | 1.3 (0.6) | 11.3 (0.7) |
Patients in analysis | 52 | 55 | 88 | 87 |
LSMD (95% CI) | 9.3 (6.8 to 11.7) | 10.1 (8.2 to 11.9) | ||
P value (vs. TEZ-IVA) | < 0.0001 | < 0.0001 | ||
CI = confidence interval; ELX-TEZ-IVA = elexacaftor-tezacaftor-ivacaftor and ivacaftor; F/F = homozygous for F508del mutations in the CFTR gene; LS = least squares; LSMD = least squares mean difference; MMRM = mixed-effects model for repeated measures; ppFEV1 = percent predicted forced expiratory volume in 1 second; SD = standard deviation; SE = standard error; TEZ-IVA = tezacaftor-ivacaftor and ivacaftor.
aThe MMRM included data from all available visits, with treatment, visit, and treatment-by-visit interaction as fixed effects and baseline ppFEV1 and age group at the screening visit (< 18, ≥ 18 years of age) as covariates. For the multiple imputation sensitivity analysis, the same MMRM as the primary analysis was used, including all the data up to week 4. Missing ppFEV1 assessments were imputed only for visits for which all subsequent visits through week 4 were also missing (i.e., missing values that fall between 2 non-missing values were not imputed).
bThe MMRM included data collected in clinic from all available visits up to week 24 with treatment, visit, and treatment by visit as fixed effects; baseline ppFEV1, age group at screening (≥ 12 to < 18 vs. ≥ 18 years), and CFTR-modulator use at screening (yes vs. no) were covariates.
cPre-specified primary end point.
dPre-specified key secondary end point.
Source: Clinical Study Reports.6,10
Table 33: Absolute Change From Baseline in ppFEV1 in F/G or F/RF Genotypes Through 8 Weeksa
Analysis | Study 104 (F/G or F/RF) | Study 104 (F/G) | Study 104 (F/RF) | |||
|---|---|---|---|---|---|---|
Control (N = 126) | ELX-TEZ-IVA (N = 132) | IVA (N = 45) | ELX-TEZ-IVA (N = 50) | TEZ-IVA (N = 81) | ELX-TEZ-IVA (N = 82) | |
Baseline mean (SD) | 68.1 (16.4) | 67.1 (15.7) | 68.1 (16.6) | 66.0 (14.8) | 68.1 (16.4) | 67.8 (16.3) |
Patients in analysis | 114 | 115 | 42 | 42 | 72 | 73 |
LS mean change (SE) | 0.2 (0.5) | 3.7 (0.5) | 0.1 (0.9) | 5.8 (0.8) | 0.5 (0.5) | 2.5 (0.5) |
LS MD (95% CI) | 3.5 (2.2 to 4.7) | 5.8 (3.5 to 8.0) | 2.0 (0.5 to 3.4) | |||
P value (vs. control) | < 0.0001b | < 0.0001 | 0.0093 | |||
CI = confidence interval; ELX-TEZ-IVA = elexacaftor-tezacaftor-ivacaftor and ivacaftor; F/G = 1 F508del mutation and 1 gating mutation in the CFTR gene; F/RF = 1 F508del mutation and 1 residual function mutation in the CFTR gene; LS = least squares; LSMD = least squares mean difference; MMRM = mixed-effects model for repeated measures; ppFEV1 = percent predicted forced expiratory volume in 1 second; SD = standard deviation; SE = standard error.
aPre-specified key secondary end point.
bA similar MMRM method as for the primary analysis was applied to each subgroup category, with treatment, visit, and treatment by visit as fixed effects and baseline ppFEV1 and baseline SwCl as covariates.
Table 34: Absolute Change From Baseline Through Week 24 in LCI2.5 in Pediatric Studies
Analysis | Study 116 | Study 106 Part B | |
|---|---|---|---|
Placebo (N = 61) | ELX-TEZ-IVA (N = 60) | ELX-TEZ-IVA (N = 66) | |
Baseline mean (SD) | 9.75 (1.95) | 10.26 (2.22) | 9.77 (2.68) |
Patients in analysis | 61 | 60 | 50 |
LS mean change (SE) | −0.02 (0.16) | −2.29 (0.16) | −1.71 (0.20) |
P value within treatment | 0.8859 | < 0.0001 | < 0.0001 |
LSMD (95% CI) | Reference | −2.26 (−2.71 to −1.81) | NA |
P value vs. placebo | Reference | < 0.0001 | NA |
CI = confidence interval; ELX-TEZ-IVA = elexacaftor-tezacaftor-ivacaftor and ivacaftor; LS least squares; LSMD = least squares mean difference; SD = standard deviation; SE = standard error.
Source: Clinical Study Reports.3,4
Figure 12: Absolute Change from Baseline in ppFEV1 in F/G or F/R Genotypes
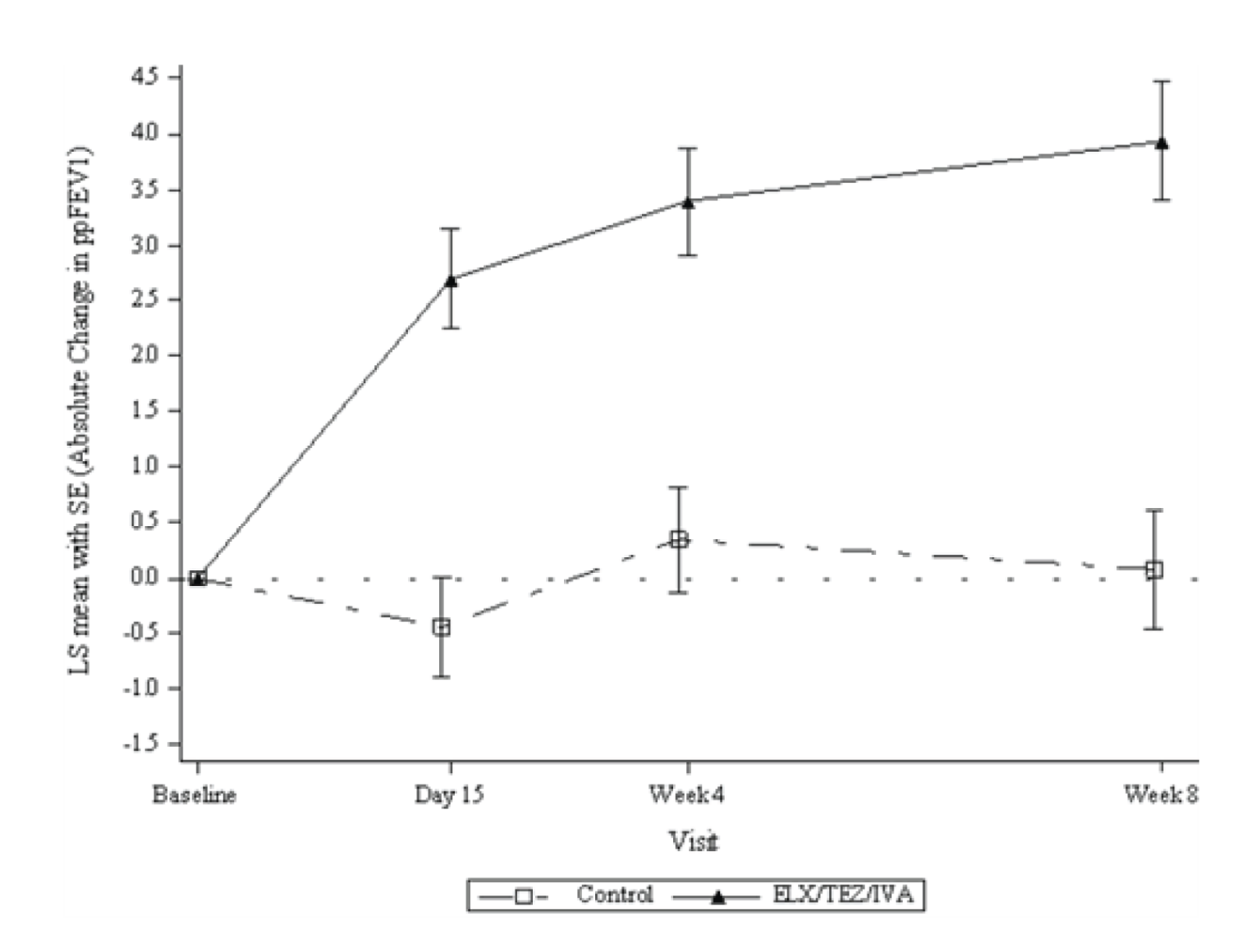
ELX/TEZ/IVA = elexacaftor-tezacaftor-ivacaftor and ivacaftor; LS = least squares; ppFEV1 = percent predicted forced expiratory volume in 1 second; SE = standard error.
Source: Clinical Study Report.11
Lung Clearance Index
Patients Aged 6 to 11 Years
Placebo-Controlled Trial (Study 116; F/MF Genotype): Treatment with ELX-TEZ-IVA was associated with a statistically significant reduction in LCI2.5 through 24 weeks compared to placebo (LSMD = −2.26; 95% CI, −2.71 to −1.81; P < 0.0001). As shown in Figure 13, improvements in LCI2.5 with ELX-TEZ-IVA were observed at the time of the first post-baseline assessment (i.e., day 15) and were reduced at all time points throughout the study.4
Single-Arm Trial (Study 106; F/F or F/MF Genotype): Patients in Study 106 demonstrated a statistically significant within-group reduction in LCI2.5 through 24 weeks (LS mean change = −1.71; 95% CI, −2.11 to −1.30; P < 0.0001). As shown in Figure 13, improvements in LCI2.5 with ELX-TEZ-IVA were observed at the time of the first post-baseline assessment (i.e., day 15) and were reduced at all time points throughout the study.3
Figure 13: Absolute Change from Baseline in LCI2.5
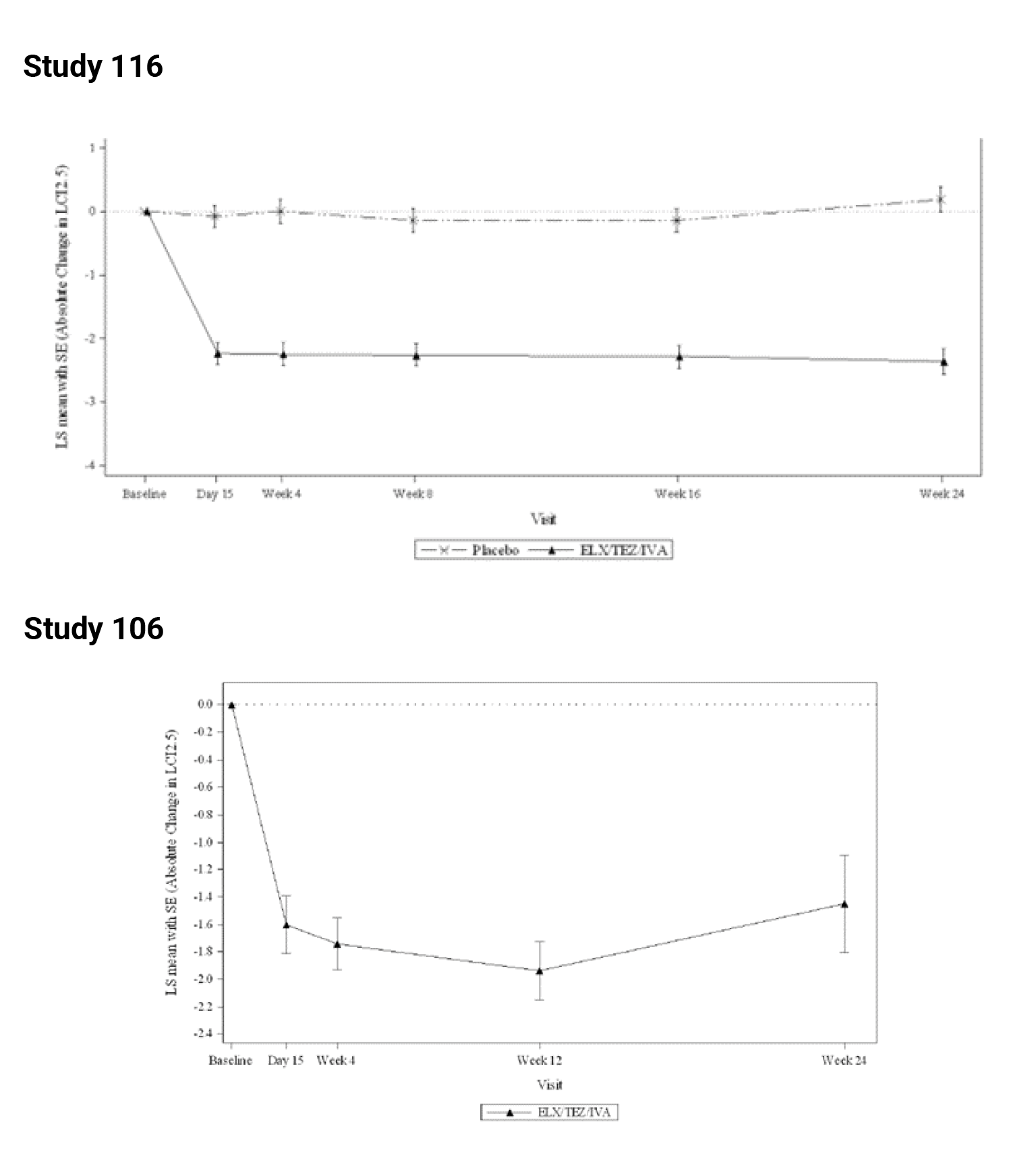
ELX/TEZ/IVA = elexacaftor-tezacaftor-ivacaftor and ivacaftor; LCI = lung clearance index; LS = least squares; SE = standard error.
Pulmonary Exacerbations
Patients Aged 6 to 11 Years
Placebo-Controlled Trial (Study 116; F/MF Genotype): Pulmonary exacerbations were only captured as AEs in Study 116. Compared with the placebo group, fewer ELX-TEZ-IVA–treated patients reported 1 or more pulmonary exacerbations (26.2% versus 1.7%, respectively).
Single-Arm Trial (Study 106; F/F or F/MF Genotype): The annual event rate for overall pulmonary exacerbations was 0.12. Event rates for pulmonary exacerbations requiring hospitalization and/or IV antibiotic therapy were each 0.03 per year.
Patients Aged 12 Years and Older
Patients With F/MF Genotype: In Study 102, treatment with ELX-TEZ-IVA was associated with a lower rate of the pulmonary exacerbations compared with placebo (rate ratio = 0.37; 95% CI, 0.25 to 0.55).5 Similarly, treatment with ELX-TEZ-IVA was associated with lower rates of pulmonary exacerbations requiring hospitalization (0.29; 95% CI, 0.14 to 0.61) and pulmonary exacerbations requiring IV antibiotic therapy (0.22; 95% CI, 0.11 to 0.43) (Table 35).5
Table 35: Summary of Pulmonary Exacerbations in Pediatric Study (Full Analysis Set, Part B)
PEx analyses | Study 106 Part B (ELX-TEZ-IVA) (N = 66) |
|---|---|
Total number of days (years) of the PEx analysis perioda | 11,060 (32.9) |
PEx overall | |
Number of subjects with events, n (%) | 4 (6.1) |
Number of events | 4 |
Observed event rate per year | 0.12 |
PEx requiring hospitalization | |
Number of subjects with events, n (%) | 1 (1.5) |
Number of events | 1 |
Observed event rate per year | 0.03 |
PEx requiring IV antibiotic therapy | |
Number of subjects with events, n (%) | 1 (1.5) |
Number of events | 1 |
Observed event rate per year | 0.03 |
PEx requiring hospitalization or IV antibiotic therapy | |
Number of subjects with events, n (%) | 1 (1.5) |
Number of events | 1 |
Observed event rate per year | 0.03 |
ELX-TEZ-IVA = elexacaftor-tezacaftor-ivacaftor and ivacaftor; PEx = pulmonary exacerbation.
aTotal number of days = sum of the individual duration (actual number of days) of the PEx analysis period across all subjects. Total number of years = total number of days / 336. Observed event rate per year = total number of events × 336 / total number of days of the PEx analysis period. The event rate was calculated based on 336 days (48 weeks) in a year.
Source: Clinical Study Reports.3
Data for time to first pulmonary exacerbation are summarized in Table 36. Hazard ratios favoured ELX-TEZ-IVA compared with placebo for time to first pulmonary exacerbation (HR = 0.34; 95% CI, 0.22 to 0.52), time to first pulmonary exacerbation requiring hospitalization (HR = 0.25; 95% CI, 0.11 to 0.58), time to first pulmonary exacerbation requiring IV antibiotics (HR = 0.19; 95% CI, 0.09 to 0.3) and time to first pulmonary exacerbation requiring hospitalization or IV antibiotics (HR = 0.19; 95% CI, 0.09 to 0.39).5 For all end points related to pulmonary exacerbations, the results demonstrated statistically significant differences in favour of ELX-TEZ-IVA.
Table 36: Risk of Pulmonary Exacerbations in F/MF Genotype in Study 102
Pulmonary exacerbations | Placebo (N = 203) | ELX-TEZ-IVA (N = 200) |
|---|---|---|
Any pulmonary exacerbationa | ||
Patients with events, n (%) | 76 (37.4) | 31 (15.5) |
Number of events | 113 | 41 |
Event rate per year | 0.98 | 0.37 |
Rate ratio (95% CI) | 0.37 (0.25 to 0.55) | |
P value | < 0.0001b | |
Pulmonary exacerbations requiring hospitalizationa | ||
Patients with events, n (%) | 27 (13.3) | 7 (3.5) |
Number of events | 32 | 9 |
Event rate per year | 0.24 | 0.07 |
Rate ratio (95% CI) | 0.29 (0.14 to 0.61) | |
P value | 0.0010 | |
Pulmonary exacerbations requiring IV antibioticsa | ||
Patients with events, n (%) | 42 (20.7) | 9 (4.5) |
Number of events | 51 | 11 |
Event rate per year | 0.36 | 0.08 |
Rate ratio (95% CI) | 0.22 (0.11 to 0.43) | |
P values | < 0.0001 | |
Pulmonary exacerbations requiring hospitalization or IV antibioticsa | ||
Patients with events, n (%) | 42 (20.7) | 9 (4.5) |
Number of events | 52 | 11 |
Event rate per year | 0.37 | 0.08 |
Rate ratio (95% CI) | 0.22 (0.11 to 0.42) | |
P value | < 0.0001 | |
CI = confidence interval; ELX-TEZ-IVA = elexacaftor-tezacaftor-ivacaftor and ivacaftor; F/MF = 1 F508del mutation and 1 minimal function mutation in the CFTR gene.
aTreatment comparison was carried out using a negative binomial regression model with treatment as a fixed effect; baseline ppFEV1, age at screening (< 18 vs. ≥ 18 years of age), and sex (male vs. female) as covariates; and the logarithm of the patient-specific pulmonary exacerbation analysis period duration in years as the offset. The event rate was calculated based on 336 days (48 weeks) in a year. As the negative binomial regression model did not converge for pulmonary exacerbations requiring hospitalization, a Poisson model with the same structure was used.
bPre-specified key secondary end point.
Source: Clinical Study Report.5
Table 37 provides a summary of the annualized duration of pulmonary exacerbations in Study 102 for the placebo and ELX-TEZ-IVA groups. Compared with placebo, treatment with ELX-TEZ-IVA was associated with a reduced duration of pulmonary exacerbations (mean = 24.9 days [SD = 44.7] versus 6.3 days [SD = 16.9]; P < 0.0001), pulmonary exacerbations requiring hospitalization (mean = 9.9 [SD = 30.7] versus 1.6 [SD = 9.1]; P = 0.0002), pulmonary exacerbations requiring IV antibiotics (mean = 14.3 years [SD = 35.0] versus 1.9 years [SD = 9.5]; P < 0.0001), and pulmonary exacerbations requiring IV antibiotics or hospitalization (mean = 14.5 [SD = 35.3] versus 1.9 [SD = 9.5]; P < 0.0001).
Table 37: Time to First Pulmonary Exacerbation in F/MF Genotype in Study 102
Pulmonary exacerbations | Placebo (N = 203) | ELX-TEZ-IVA (N = 200) |
|---|---|---|
Time to first PExa | ||
Patients with events, n (%) | 76 (37.4) | 31 (15.5) |
Hazard ratio, (95% CI) | 0.34 (0.22 to 0.52) | |
P value | < 0.0001 | |
Probability of event-free survival 24 weeks (95% CI) | 0.629 (0.558 to 0.692) | 0.842 (0.783 to 0.886) |
P value from log rank test | < 0.0001 | |
Time to first PEx requiring hospitalizationa | ||
Patients with events, n (%) | 27 (13.3) | 7 (3.5) |
Hazard ratio (95% CI) | 0.25 (0.11 to 0.58) | |
P value vs. placebo | 0.0011 | |
Probability of event-free survival 24 weeks (95% CI) | 0.867 (0.812 to 0.907) | 0.965 (0.927 to 0.983) |
P value from log rank test | 0.0004 | |
Time to first PEx requiring IV antibioticsa | ||
Patients with events, n (%) | 42 (20.7) | 9 (4.5) |
Hazard ratio (95% CI) | 0.19 (0.09 to 0.39) | |
P value vs. placebo | < 0.0001 | |
Probability of event-free survival 24 weeks (95% CI) | 0.793 (0.731 to 0.843) | 0.955 (0.915 to 0.976) |
P value vs. placebo | < 0.0001 | |
Time to first PEx requiring hospitalization or IV antibioticsa | ||
Patients with events, n (%) | 42 (20.7) | 9 (4.5) |
Hazard ratio (95% CI) | 0.19 (0.09 to 0.39) | |
P value vs. placebo | < 0.0001 | |
Probability of event-free survival 24 weeks (95% CI) | 0.793 (0.731 to 0.843) | 0.955 (0.915 to 0.976) |
P value vs. placebo | < 0.0001 | |
CI = confidence interval; ELX-TEZ-IVA = elexacaftor-tezacaftor-ivacaftor and ivacaftor; F/MF = 1 F508del mutation and 1 minimal function mutation in the CFTR gene; PEx = pulmonary exacerbation.
aHazard ratios and P values were calculated using Cox proportional hazard regression, with time to first PEx or censoring as the time, treatment as factor, and baseline ppFEV1, age at screening (< 18 vs. ≥ 18 years of age) and sex (male vs. female) as covariates. Probability of event-free survival was estimated using Kaplan–Meier methods.
Source: Clinical Study Report.5
Figure 14: Time to First Pulmonary Exacerbation in F/MF Genotype
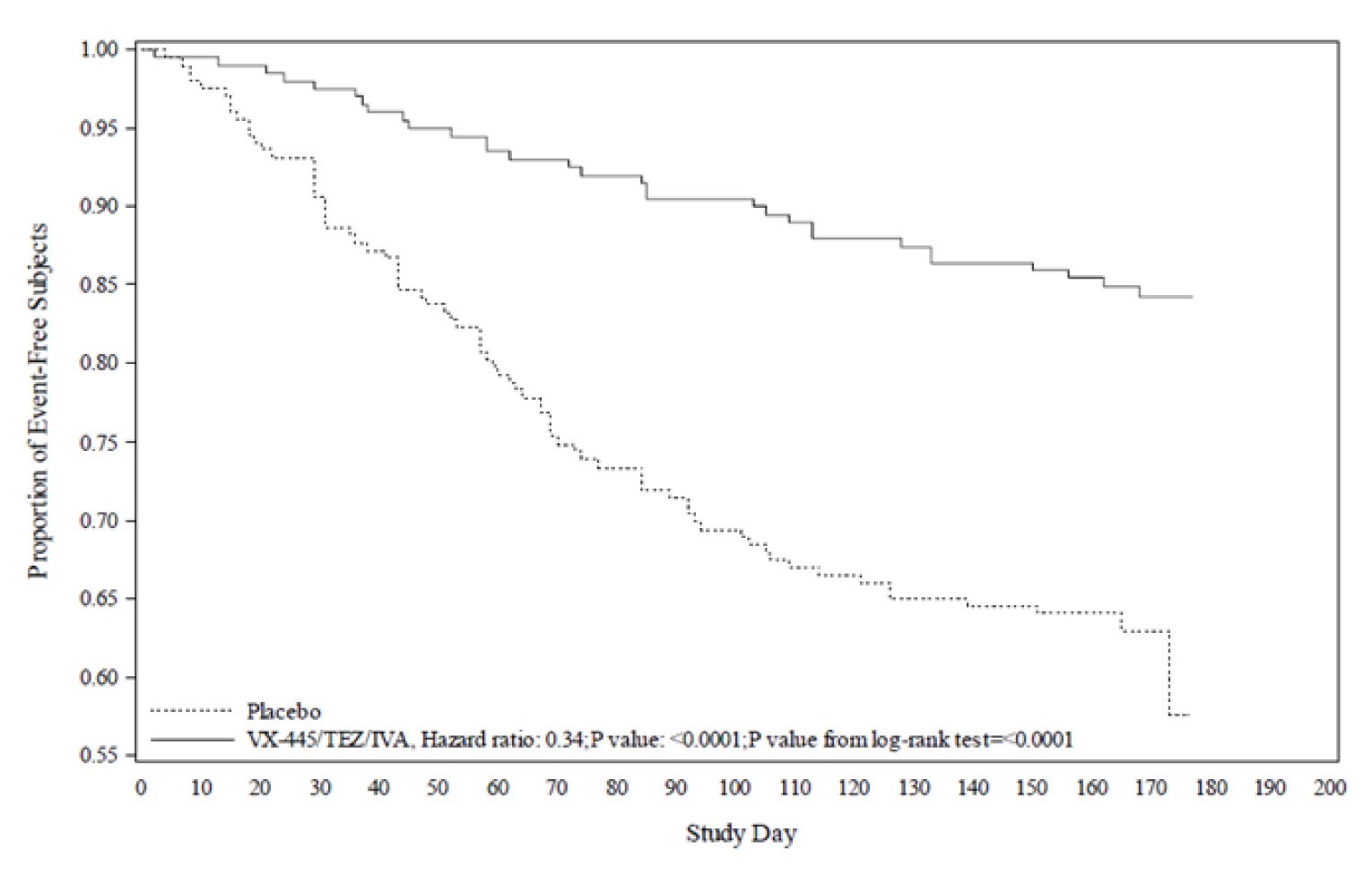
VX-445/TEZ/IVA = elexacaftor-tezacaftor-ivacaftor and ivacaftor.
Source: Clinical Study Report.5
Table 38: Duration of Pulmonary Exacerbations in F/MF Genotype in Study 102
Pulmonary exacerbations | Placebo (N = 203) | ELX-TEZ-IVA (N = 200) | |
|---|---|---|---|
Annualized duration of PExa | |||
Mean (SD) | 24.9 (44.7) | 6.3 (16.9) | |
Median (range) | 0.0 (0.0 to 248.0) | 0.0 (0.0 to 90.9) | |
P value vs. placebo | < 0.0001 | ||
Annualized duration of PEx requiring hospitalizationa | |||
Mean (SD) | 9.9 (30.7) | 1.6 (9.1) | |
Median | 0.0 (0.0 to 214.7) | 0.0 (0.0 to 80.0) | |
P value vs. placebo | 0.0002 | ||
Annualized duration of PEx requiring IV antibioticsa | |||
Mean (SD) | 14.3 (35.0) | 1.9 (9.5) | |
Median | 0.0 (0.0 to 214.7) | 0.0 (0.0 to 80.0) | |
P value vs. placebo | < 0.0001 | ||
Annualized duration of PEx requiring IV antibiotics or hospitalizationa | |||
Mean (SD) | 14.5 (35.3) | 1.9 (9.5) | |
Median | 0.0 (0.0 to 214.7) | 0.0 (0.0 to 80.0) | |
P value vs. placebo | < 0.0001 | ||
ELX-TEZ-IVA = elexacaftor-tezacaftor-ivacaftor and ivacaftor; F/MF = 1 F508del mutation and 1 minimal function mutation in the CFTR gene; PEx = pulmonary exacerbation; SD = standard deviation .
aAnnualized duration = total number of days with the corresponding event × 336 / total duration of the PEx analysis period in days; for analysis purposes, 1 year is defined as 48 weeks or 336 days. P values were based on a stratified ppFEV1 group at screening (< 70 vs. ≥ 70), age group at screening (≥ 12 to < 18 vs. ≥ 18 years), and sex (male vs. female) using a Wilcoxon rank sum test.
Source: Clinical Study Report.5
Patients With F/F Genotype: Pulmonary exacerbations were only captured as AEs in Study 103 and Study 109.6,10 The percentage of patients with 1 or more pulmonary exacerbations was greater in the TEZ-IVA group compared with the ELX-TEZ-IVA group in both Study 103 (11.5% versus 1.8%, respectively) and Study 109 (40.9% versus 11.5%, respectively).6,10
Patients With F/G and F/RF Genotypes: Pulmonary exacerbations were only captured as AEs in Study 104.11 Compared with the control group, fewer ELX-TEZ-IVA-treated patients reported 1 or more pulmonary exacerbations (10.3% versus 2.3%, respectively).11
Body Mass Index, Body Weight, and Height
Patients Aged 6 to 11 Years
Placebo-Controlled Trial (Study 116; F/MF Genotype): Change from baseline BMI, body weight, and height were not reported for Study 116.
Single-Arm Trial (Study 106; F/F or F/MF Genotype): In Study 106 Part B, patients demonstrated statistically significant within-group increases from baseline in BMI (LS mean change = 1.02 kg/m2; 95% CI, 0.76 to 1.28; P < 0.0001), BMI z score (LS mean change = 0.37; 95% CI, 0.26 to 0.48; P < 0.0001), body weight (kg) (LS mean change = 3.0 kg; 95% CI, 2.5 to 3.5; P < 0.0001), weight z score (LS mean change = 0.25; 95% CI, 0.16 to 0.33; P < 0.0001), height (LS mean change = 2.3 cm; 95% CI, 1.9 to 2.7; P < 0.0001) and height z score (LS mean change = −0.05; 95% CI, −0.12 to 0.01; P = 0.1057).3
Patients Aged 12 Years and Older
Patients With F/MF Genotype: Study 102 included change from baseline in BMI at 24 weeks as a key secondary end point. Change from baseline in BMI z scores (for patients younger than 20 years of age) and change from baseline in body weight at 24 weeks were pre-specified non-key secondary end points.5 Treatment with ELX-TEZ-IVA was associated with a statistically significant improvement in BMI at 24 weeks compared with placebo (LSMD = 1.04 kg/m2; 95% CI, 0.85 to 1.23; P < 0.0001) (Table 39).5 In patients younger than 20 years of age (n = 145), those treated with ELX-TEZ-IVA demonstrated improvements in BMI z score compared with placebo (LSMD = 0.30; 95% CI, 0.17 to 0.43).5 Similarly, the ELX-TEZ-IVA group demonstrated greater improvement in body weight at 24 weeks compared with the placebo group (LSMD = 2.9 kg; 95% CI, 2.3 to 3.4).5
Patients With F/F Genotype: Study 103 included absolute change from baseline in BMI and body weight as exploratory end points (Table 39). Compared with TEZ-IVA, treatment with ELX-TEZ-IVA was associated with improvements in BMI at 4 weeks (LSMD = 0.60 kg/m2; 95% CI, 0.41 to 0.79) and body weight at 4 weeks (LSMD = 1.6 kg; 95% CI, 1.0 to 2.1).6 Change from baseline in BMI and body weight were not pre-specified end points for Study 109 or reported in the Clinical Study Report; however, post hoc analyses for these end points were conducted and included in the sponsor’s ITC.
Patients With F/G and F/RF Genotypes: Study 104 included absolute change from baseline in BMI at 8 weeks as an additional end point with no statistical analysis performed.11 At 8 weeks mean BMI had increased in both the control group (LS mean = 0.16 kg/m2; SE = 0.06) and the ELX-TEZ-IVA group (LS mean = 0.28 kg/m2; SE = 0.06) (LSMD = 0.13 kg/m2; 95% CI, −0.03 to 0.29).11
Table 39: Change From Baseline in Body Mass Index, Body Weight, and Height
Analysis | Study 106 Part B ELX-TEZ-IVA (N = 66) | |||||
|---|---|---|---|---|---|---|
BMI | BMI z score | Weight (kg) | Weight z score | Height (cm) | Height z score | |
Baseline mean (SD) | 16.39 (1.69) | −0.16 (0.74) | 30.0 (7.7) | −0.22 (0.76) | 134.1 (12.3) | −0.11 (0.98) |
Patients in analysis | 33 | 33 | 33 | 33 | 33 | 33 |
LS mean (SE)a | 1.02 (0.13) | 0.37 (0.05) | 3.0 (0.2) | 0.25 (0.04) | 2.3 (0.2) | −0.05 (0.03) |
95% CI, of LS mean | (0.76 to 1.28) | (0.26 to 0.48) | (2.5 to 3.5) | (0.16 to 0.33) | (1.9 to 2.7) | (−0.12 to 0.01) |
P value | < 0.0001 | < 0.0001 | < 0.0001 | < 0.0001 | < 0.0001 | 0.1057 |
BMI = body mass index; CI = confidence interval; ELX-TEZ-IVA = elexacaftor-tezacaftor-ivacaftor and ivacaftor; F/F = homozygous for F508del mutation in the CFTR gene; F/MF = 1 F508del mutation and 1 minimal function mutation in the CFTR gene; LS = least squares; SD = standard deviation; SE = standard error.
aThe mixed-effects model for repeated measures included data from all available visits up to week 24, with visit as a fixed effect and baseline value of the relevant growth parameter (BMI, weight, height, or associated z score) and genotype group (F/F or F/MF) as covariates. A Kenward-Roger approximation was used for denominator degrees of freedom. An unstructured covariance structure was used to model the within-subject errors.
Source: Clinical Study Reports.3
Table 40: Change from Baseline in BMI, BMI Z Scores, and Body Weight
Analysis | Study 102 (F/MF) at 24 weeks | Study 103 (F/F) at 4 weeks | Study 104 (F/G and F/RF) at 8 weeks | |||
|---|---|---|---|---|---|---|
Placebo (N = 203) | ELX-TEZ-IVA (N = 200) | TEZ-IVA (N = 52) | ELX-TEZ-IVA (N = 55) | Control (N = 126) | ELX-TEZ-IVA (N = 132) | |
Absolute change from baseline in BMI (kg/m2) at 24 weeks,a 4 weeks,a and 8 weeksc | ||||||
N (all patients) | 203 | 200 | 52 | 55 | 126 | 132 |
Baseline mean (SD) | 21.31 (3.14) | 21.49 (3.07) | 21.88 (4.12) | 21.75 (3.19) | 24.05 (4.71) | 24.07 (4.72) |
LS mean change (SE) | 0.09 (0.07) | 1.13 (0.07) | −0.07 (0.07) | 0.53 (0.07) | 0.16 (0.06) | 0.28 (0.06) |
Patients in analysis | 202 | 198 | 52 | 55 | 107 | 110 |
LSMD (95% CI) | 1.04 (0.85 to 1.23) | 0.60 (0.41 to 0.79) | 0.13 (−0.03 to 0.29) | |||
P value | < 0.0001d | < 0.0001 | NA | |||
Absolute change from baseline in BMI z score at 24 weeksa | ||||||
N (patients < 20 years) | 74 | 71 | NA | NA | ||
Baseline mean (SD) | −0.40 (0.98) | −0.37 (0.79) | ||||
LS mean change (SE) | 0.04 (0.05) | 0.34 (0.05) | ||||
Patients in analysis | 68 | 64 | ||||
LSMD (95% CI) | 0.30 (0.17 to 0.43) | |||||
P value | < 0.0001e | |||||
Absolute change from baseline in body weight (kg) at 24 weeksa and 4 weeksa | ||||||
N (all patients) | 203 | 200 | 52 | 55 | NA | |
Baseline mean (SD) | 58.3 (12.7) | 59.8 (12.9) | 59.8 (14.8) | 59.9 (12.7) | ||
LS mean change (SE) | 0.5 (0.2) | 3.4 (0.2) | −0.1 (0.2) | 1.5 (0.2) | ||
Patients in analysis | 202 | 198 | 52 | 55 | ||
LSMD (95% CI) | 2.9 (2.3 to 3.4) | 1.6 (1.0 to 2.1) | ||||
P value | < 0.0001 | < 0.0001 | ||||
BMI = body mass index; CI = confidence interval; ELX-TEZ-IVA = elexacaftor-tezacaftor-ivacaftor and ivacaftor; F/F = homozygous for F508del mutation in the CFTR gene; F/G = 1 F508del mutation and 1 gating mutation in the CFTR gene; F/MF = 1 F508del mutation and 1 minimal function mutation in the CFTR gene; F/RF = 1 F508del mutation and 1 residual function mutation in the CFTR gene; LS = least squares; IVA = ivacaftor; LSMD = least squares mean difference; MMRM = mixed-effects model for repeated measures; NA = not applicable; SD = standard deviation; SE = standard error; TEZ-IVA = tezacaftor-ivacaftor and ivacaftor.
aThe MMRM included final data from all available visits, with treatment, visit, and treatment-by-visit interaction as fixed effects and baseline ppFEV1, age group at screening (< 18, ≥ 18 years of age) and sex (male, female) as covariates.
cThe MMRM included data from all available visits up to week 8, with treatment, visit, and treatment × visit as fixed effects and baseline ppFEV1, baseline sweat chloride, and comparator group (IVA comparator group vs. TEZ-IVA comparator group) as covariates.
dPre-specified key secondary end point.
ePre-specified other secondary end point.
Source: Clinical Study Report.5,6
Cystic Fibrosis Questionnaire–Revised (Respiratory Domain)
Patients Aged 6 to 11 Years
Placebo-Controlled Trial (Study 116; F/MF Genotype): Treatment with ELX-TEZ-IVA was associated with a statistically significant improvement in CFQ-R respiratory domain scores from baseline compared with placebo through 24 weeks (LSMD = 5.5; 95% CI, 1.0 to 10.0; P = 0.0003).4
Single-Arm Trial (Study 106; F/F or F/MF Genotype): In Study 106 Part B, patients demonstrated a statistically significant within-group increase from baseline CFQ-R respiratory domain scores through 24 weeks (LS mean absolute change = 7.0; 95% CI, 4.7 to 9.2; P < 0.0001).3
Patients With F/MF Genotype: Study 102 included 2 key secondary end points related to absolute change from baseline in CFQ-R respiratory domain scores. Change from baseline through 24 weeks was the fourth key secondary end point, and change from baseline at 4 weeks was the seventh and final key secondary end point. Treatment with ELX-TEZ-IVA was associated with a statistically significant improvement in CFQ-R respiratory domain scores from baseline compared with placebo through 24 weeks (LSMD = 20.2; 95% CI, 17.5 to 23.0) and at week 4 (LSMD = 20.1; 95% CI, 16.9 to 23.2) (Table 41).
Patients With F/F Genotype: Study 103 included absolute change from baseline in CFQ-R respiratory domain scores at 4 weeks as a key secondary end point. Treatment with ELX-TEZ-IVA was associated with a statistically significant improvement in CFQ-R respiratory domain scores from baseline compared with TEZ-IVA at 4 weeks (LSMD = 17.4; 95% CI, 11.8 to 23.0) (Table 41).
Study 109 included absolute change from baseline in CFQ-R respiratory domain scores through 24 weeks as the primary end point. Treatment with ELX-TEZ-IVA was associated with a statistically significant improvement in CFQ-R respiratory domain scores from baseline compared with TEZ-IVA through 24 weeks (LSMD = 15.9; 95% CI, 11.7 to 20.1) (Table 41).10
Table 41: Change from Baseline in CFQ-R (Respiratory Domain) in Pediatric Studies
Analysis | Study 116 | Study 106 Part B | |
|---|---|---|---|
Placebo (N = 61) | ELX-TEZ-IVA (N = 60) | ELX-TEZ-IVA (N = 66) | |
Absolute change through week 24a,b | |||
Baseline mean (SD) | 82.7 (14.1) | 85.7 (11.7) | 80.3 (15.2) |
Patients in analysis | 61 | 60 | 65 |
LS mean change (SE) | 0.5 (1.6) | 5.9 (1.6) | 7.0 (1.1) |
P value within treatment | 0.7693 | 0.0003 | < 0.0001 |
LSMD (95% CI) | Reference | 5.5 (1.0 to 10.0) | NA |
P value vs. placebo | Reference | 0.0174 | NA |
CFQ-R = Cystic Fibrosis Questionnaire–Revised; CI = confidence interval; ELX-TEZ-IVA = elexacaftor-tezacaftor-ivacaftor and ivacaftor; F/F = homozygous for F508del mutation in the CFTR gene; F/MF = 1 F508del mutation and 1 minimal function mutation in the CFTR gene; LS = least squares; LSMD = least squares mean difference; MMRM = mixed-effects model for repeated measures; ppFEV1 = percent predicted forced expiratory volume in 1 second; SD = standard deviation; SE = standard error.
aThe MMRM included data from all available visits, with treatment, visit, and treatment-by-visit interaction as fixed effects and baseline LCI2.5 and weight at screening (< 30 kg vs. ≥ 30 kg) as covariates. A Kenward-Roger approximation was used for denominator degrees of freedom. An unstructured covariance structure was used to model the within-subject errors.
bThe MMRM included clinic-assessed data from all available visits, with visit as a fixed effect and baseline CFQ-R respiratory domain scores and genotype group (F/F or F/MF) as covariates. A Kenward-Roger approximation was used for denominator degrees of freedom. An unstructured covariance structure was used to model the within-subject errors.
Source: Clinical Study Reports.3,4
Patients With F/G and F/RF Genotypes: In Study 104, the ELX-TEZ-IVA group demonstrated a statistically significant increase in CFQ-R respiratory domain scores from baseline through 8 weeks (LS mean within-group = 10.3 points; 95% CI, 8.0 to 12.7; P < 0.0001). Treatment with ELX-TEZ-IVA also resulted in an increase in CFQ-R respiratory domain scores through 8 weeks compared to the control group (LSMD = 8.7; 95% CI, 5.3 to 12.1; P < 0.0001). As shown in Table 42, subgroup analyses demonstrated similar effect sizes for ELX-TEZ-IVA compared with IVA in patients with an F/G genotype (LSMD = 8.9; 95% CI, 3.8 to 14.0; P = 0.0008) and for ELX-TEZ-IVA compared with TEZ-IVA in patients with an F/RF genotype (LSMD = 8.5; 95% CI, 4.0 to 13.1; P = 0.0003).
Table 42: Change From Baseline in CFQ-R Respiratory Domain Scores for Patients With F/MF and F/F Genotypes
CFQ-R respiratory domain | Study 102 (F/MF) through 24 weeksa | Study 103 (F/F) at 4 weeksa | Study 109 (F/F) through 24 weeksb | |||
|---|---|---|---|---|---|---|
Placebo (n = 203) | ELX-TEZ-IVA (n = 200) | TEZ-IVA (N = 52) | ELX-TEZ-IVA (N = 55) | TEZ-IVA (N = 88) | ELX-TEZ-IVA (N = 87) | |
Absolute change from baseline in CFQ-R respiratory domain scores at 24 weeks and 4 weeks | ||||||
Baseline mean (SD) | 70.0 (17.8) | 68.3 (16.9) | 72.6 (17.9) | 70.6 (16.2) | 73.1 (17.6) | 71.2 (19.6) |
LS mean change (SE) | −2.7 (1.0) | 17.5 (1.0) | −1.4 (2.0) | 16.0 (2.0) | 1.2 (1.5) | 17.1 (1.5) |
Patients in analysis | 203 | 200 | 52 | 55 | 88 | 87 |
LSMD (95% CI) | 20.2 (17.5 to 23.0) | 17.4 (11.8 to 23.0) | 15.9 (11.7 to 20.1) | |||
P value | < 0.0001c | < 0.0001 | < 0.0001d | |||
CFQ-R = Cystic Fibrosis Questionnaire–Revised; CI = confidence interval; ELX-TEZ-IVA = elexacaftor-tezacaftor-ivacaftor and ivacaftor; F/F = homozygous for F508del mutation in the CFTR gene; F/G = 1 F508del mutation and 1 gating mutation in the CFTR gene; F/MF = 1 F508del mutation and 1 minimal function mutation in the CFTR gene; F/RF = 1 F508del mutation and 1 residual function mutation in the CFTR gene; LS = least squares; LSMD = least squares mean difference; MMRM = mixed-effects model for repeated measures; SD = standard deviation; SE = standard error; TEZ-IVA = tezacaftor-ivacaftor and ivacaftor.
aThe MMRM included final data from all available visits, with treatment, visit, and treatment-by-visit interaction as fixed effects and baseline ppFEV1, age group at screening (< 18, ≥ 18 years of age) and sex (male, female) as covariates.
bThe MMRM included CFQ-R respirator domain data collected in clinics and at home from all available visits up to week 24 with treatment, visit, and treatment by visit as fixed effects; baseline ppFEV1, age group at screening (≥ 12 to < 18 vs. ≥ 18 years), and CFTR modulator use at screening (yes vs. no) as covariates.
cPre-specified key secondary end point.
dPre-specified primary end point.
Source: Clinical Study Reports.5,6,10
Cystic Fibrosis Questionnaire–Revised (Non-Respiratory Domains)
Patients Aged 6 to 11 Years
Placebo-Controlled Trial (Study 116; F/MF Genotype): Non-respiratory domains of the CFQ-R were not reported in Study 116.
Single-Arm Trial (Study 106; F/F or F/MF Genotype): Changes from baseline in the non-respiratory domains of the CFQ-R were assessed as exploratory end points in Study 106 Part B. As shown in Table 43, the scores showed a numerical increase from baseline; however, no statistical analyses were conducted.3
Table 43: Change From Baseline in CFQ-R Respiratory Domain Scores for Patients With F/G and F/RF Genotypes
CFQ-R respiratory domain | Study 104 (F/G or F/RF) | Study 104 (F/RF subgroup) | Study 104 (F/G subgroup) | |||
|---|---|---|---|---|---|---|
Control (N = 126) | ELX-TEZ-IVA (N = 132) | TEZ-IVA (N = 81) | ELX-TEZ-IVA (N = 82) | IVA (N = 45) | ELX-TEZ-IVA (N = 50) | |
Absolute change from baseline in CFQ-R respiratory domain scores at 8 weeks | ||||||
Baseline mean (SD) | 77.3 (15.8) | 76.5 (16.6) | 78.1 (14.7) | 76.7 (16.9) | 75.8 (17.6) | 76.3 (16.4) |
LS mean change (SE) | 1.6 (1.2) | 10.3 (1.2) | 1.9 (1.6) | 10.4 (1.6) | 1.3 (1.9) | 10.2 (1.8) |
Patients in analysis | 126 | 130 | 81 | 81 | 45 | 49 |
LSMD (95% CI) | 8.7 (5.3 to 12.1) | 8.5 (4.0 to 13.1) | 8.9 (3.8 to 14.0) | |||
P value (vs. comparator) | < 0.0001 | 0.0003 | 0.0008 | |||
CI = confidence interval; ELX-TEZ-IVA = elexacaftor-tezacaftor-ivacaftor and ivacaftor; F/G = 1 F508del mutation and 1 gating mutation in the CFTR gene; F/RF = 1 F508del mutation and 1 residual function mutation in the CFTR gene; LS = least squares; LSMD = least squares mean difference; SD = standard deviation; SE = standard error; TEZ-IVA = tezacaftor-ivacaftor and ivacaftor.
aThe mixed-effects model for repeated measures included data from all available visits up to week 8, with treatment, visit, and treatment by visit as fixed effects and baseline ppFEV1, baseline sweat chloride, and comparator group (IVA or TEZ-IVA comparator group) as covariates.
Source: Clinical Study Report.11
Patients Aged 12 Years and Older
Patients With F/MF Genotype: Changes from baseline in the non-respiratory domains of the CFQ-R were assessed as exploratory end points in Study 102. As shown in Table 46, the change from baseline in the ELX-TEZ-IVA treatment group was greater than in the placebo group for the following CFQ-R domains: physical functioning, vitality, emotional state, body image, eating disturbances, treatment burden, health perceptions, weight, role limitations, and social limitations (i.e., all domains with the exception of digestion).
Patients With F/F Genotype: Changes from baseline in the non-respiratory domains of the CFQ-R were assessed as exploratory end points in Study 103.6 The change from baseline in the ELX-TEZ-IVA treatment group was greater than in the placebo group for the following CFQ-R domains: physical functioning, vitality, eating disturbances, health perceptions, weight, role limitations, and social limitations (Table 44).6 Changes from baseline in the non-respiratory domains of the CFQ-R were not assessed in Study 109.
Patients With F/G and F/RF Genotypes: No statistical analyses were performed for changes from baseline in the non-respiratory domains of the CFQ-R in Study 104 (descriptive statistics are summarized in Table 44).
Table 44: Change From Baseline in CFQ-R Non-Respiratory Domain Scores
CFQ-R domains | Study 106 Part B ELX-TEZ-IVA | |
|---|---|---|
Child’s version | Parent and caregiver version | |
Physical functioning | ||
Baseline mean (SD) | 84.5 (16.4) | 88.9 (13.5) |
Average change (SD) | 2.2 (13.2) | 4.5 (11.9) |
Patients in analysis | 65 | 66 |
Vitality | ||
Baseline mean (SD) | NA | 74.3 (13.0) |
Average change (SD) | 2.1 (11.8) | |
Patients in analysis | 66 | |
Emotional state | ||
Baseline mean (SD) | 78.3 (13.6) | 86.8 (10.7) |
Average change (SD) | 1.7 (11.9) | 1.4 (9.1) |
Patients in analysis | 65 | 66 |
School | ||
Baseline mean (SD) | NA | 80.7 (18.4) |
Average change (SD) | 3.9 (14.4) | |
Patients in analysis | 66 | |
Body image | ||
Baseline mean (SD) | 87.7 (18.0) | 80.5 (23.7) |
Average change (SD) | 3.1 (11.9) | 1.6 (13.9) |
Patients in analysis | 65 | 66 |
Eating disturbances | ||
Baseline mean (SD) | 85.8 (19.4) | 79.3 (23.8) |
Average change (SD) | 2.3 (14.3) | 3.4 (18.4) |
Patients in analysis | 65 | 66 |
Treatment burden | ||
Baseline mean (SD) | 75.6 (21.7) | 59.0 (23.5) |
Average change (SD) | 2.5 (20.6) | 3.9 (18.0) |
Patients in analysis | 65 | 66 |
Health perceptions | ||
Baseline mean (SD) | NA | 78.8 (15.9) |
Average change (SD) | 6.3 (14.2) | |
Patients in analysis | 66 | |
Weight | ||
Baseline mean (SD) | NA | 59.0 (33.7) |
Average change (SD) | 13.5 (26.5) | |
Patients in analysis | 65 | |
Digestion | ||
Baseline mean (SD) | 77.4 (26.4) | 73.7 (20.6) |
Average change (SD) | 4.3 (23.9) | 8.0 (14.8) |
Patients in analysis | 65 | 66 |
Social | ||
Baseline mean (SD) | 69.0 (14.7) | NA |
Average change (SD) | 1.9 (14.8) | |
Patients in analysis | 65 | |
ELX-TEZ-IVA = elexacaftor-tezacaftor-ivacaftor and ivacaftor; NA = not applicable; SD = standard deviation.
Source: Clinical Study Report.3
Sweat Chloride
Patients Aged 6 to 11 Years
Placebo-Controlled Trial (Study 116; F/MF Genotype): Absolute change from baseline in sweat chloride through 24 weeks was a secondary end point of Study 116. The ELX-TEZ-IVA group demonstrated statistically significant reductions in sweat chloride compared with the placebo group through 24 weeks (LSMD = −51.2 mmol/L; 95% CI, −55.3 to −47.1) (Table 45).4
Single-Arm Trial (Study 106; F/F or F/MF Genotype): In Study 106 Part B, treatment with ELX-TEZ-IVA resulted in a statistically significant within-group reduction in sweat chloride through 24 weeks. The LS mean absolute change in sweat chloride from baseline through 24 weeks was −60.9 mmol/L (95% CI, −63.7 to −58.2; P < 0.0001).3
Table 45: Change from Baseline in CFQ-R Non-Respiratory Domain Scores
CFQ-R domains | Study 102 (F/MF) through 24 weeksa | Study 103 (F/F) at 4 weeksa | Study 104 (F/G or F/RF) through 8 weeksb | |||
|---|---|---|---|---|---|---|
Placebo (n = 203) | ELX-TEZ-IVA (n = 200) | TEZ-IVA (N = 52) | ELX-TEZ-IVA (N = 55) | Control (N = 126) | ELX-TEZ-IVA (N = 132) | |
Physical functioning | ||||||
Baseline mean (SD) | 76.4 (21.6) | 76.5 (21.7) | 76.3 (24.5) | 75.2 (24.0) | 76.5 (21.7) | 77.2 (20.6) |
LS mean change (SE) | −3.3 (0.9) | 9.2 (0.9) | −1.9 (1.9) | 9.9 (1.9) | 0.2 (1.0) | 4.4 (1.0) |
Patients in analysis | 203 | 200 | 52 | 55 | 126 | 130 |
LSMD (95% CI) | 12.5 (9.9 to 15.0) | 11.8 (6.5 to 17.0) | 4.2 (1.4 to 7.0) | |||
P value (vs. comparator) | < 0.0001c | < 0.0001c | NA | |||
Vitality | ||||||
Baseline mean (SD) | 63.8 (18.3) | 62.8 (17.1) | 60.6 (19.9) | 61.4 (17.6) | 65.0 (18.9) | 66.0 (18.8) |
LS mean change (SE) | −5.3 (1.0) | 7.9 (1.0) | −3.6 (2.4) | 8.9 (2.3) | −0.4 (1.3) | 4.6 (1.3) |
Patients in analysis | 179 | 185 | 44 | 49 | 122 | 123 |
LSMD (95% CI) | 13.1 (10.5 to 15.8) | 12.5 (6.0 to 19.0) | 5.0 (1.5 to 8.5) | |||
P value | < 0.0001c | 0.0002c | NA | |||
Emotional state | ||||||
Baseline mean (SD) | 80.2 (16.7) | 82.0 (16.0) | 80.3 (17.8) | 82.1 (14.7) | 78.9 (18.4) | 82.3 (16.3) |
LS mean change (SE) | −0.9 (0.7) | 2.5 (0.7) | 1.1 (1.2) | 2.9 (1.1) | −0.6 (0.9) | 1.0 (0.8) |
Patients in analysis | 203 | 200 | 52 | 55 | 126 | 130 |
LSMD (95% CI) | 3.4 (1.5 to 5.2) | 1.8 (−1.4 to 5.1) | 1.6 (−0.8 to 4.0) | |||
P value | 0.0004c | 0.2727 | NA | |||
Body image | ||||||
Baseline mean (SD) | 77.2 (23.5) | 78.8 (22.1) | 86.1 (21.9) | 80.0 (20.7) | 81.1 (21.0) | 84.0 (20.0) |
LS mean change (SE) | 0.4 (1.0) | 4.2 (1.0) | −0.2 (1.5) | 2.2 (1.5) | 0.6 (1.0) | 0.5 (1.0) |
Patients in analysis | 203 | 200 | 52 | 55 | 126 | 130 |
LSMD (95% CI) | 3.8 (1.2 to 6.5) | 2.4 (−1.7 to 6.6) | −0.1 (−3.0 to 2.7) | |||
P value | 0.0048c | 0.2496 | NA | |||
Eating disturbances | ||||||
Baseline mean (SD) | 89.1 (17.5) | 90.0 (17.9) | 90.0 (16.8) | 89.1 (19.8) | 92.1 (15.8) | 89.8 (19.1) |
LS mean change (SE) | −2.4 (0.8) | 2.5 (0.8) | −0.4 (2.0) | 6.4 (1.9) | −1.2 (1.0) | 1.5 (1.0) |
Patients in analysis | 203 | 200 | 52 | 55 | 126 | 130 |
LSMD (95% CI) | 4.9 (2.6 to 7.1) | 6.8 (1.3 to 12.4) | 2.7 (−0.1 to 5.4) | |||
P value | < 0.0001 | 0.0155 | NA | |||
Treatment burden | ||||||
Baseline mean (SD) | 61.4 (20.2) | 59.2 (19.2) | 58.5 (21.5) | 59.4 (20.4) | 65.8 (21.3) | 69.0 (21.7) |
LS mean change (SE) | −2.0 (0.8) | 4.9 (0.8) | 0.3 (1.9) | 3.7 (1.9) | 2.4 (1.1) | 4.4 (1.1) |
Patients in analysis | 203 | 200 | 52 | 55 | 126 | 130 |
LSMD (95% CI) | 6.8 (4.5 to 9.2) | 3.4 (−2.0 to 8.7) | 1.9 (−1.0 to 4.9) | |||
P value | < 0.0001c | 0.2153 | ||||
Health perceptions | ||||||
Baseline mean (SD) | 64.2 (20.1) | 63.5 (20.5) | 61.6 (23.2) | 63.5 (20.3) | 68.0 (20.6) | 69.3 (19.6) |
LS mean change (SE) | −4.4 (1.1) | 12.6 (1.1) | −0.5 (2.2) | 9.0 (2.0) | −0.9 (1.2) | 5.1 (1.2) |
Patients in analysis | 179 | 185 | 44 | 49 | 122 | 123 |
LSMD (95% CI) | 17.0 (14.1 to 20.0) | 9.5 (3.6 to 15.4) | 6.0 (2.7 to 9.4) | |||
P value | < 0.0001c | 0.0018c | NA | |||
Weight | ||||||
Baseline mean (SD) | 74.1 (31.7) | 74.4 (31.0) | 81.8 (28.3) | 78.2 (33.0) | 89.1 (23.6) | 88.8 (24.3) |
LS mean change (SE) | 0.1 (1.7) | 13.2 (1.7) | −5.0 (3.2) | 7.5 (2.9) | 1.8 (1.5) | 2.0 (1.5) |
Patients in analysis | 179 | 185 | 44 | 49 | 122 | 123 |
LSMD (95% CI) | 13.1 (8.3 to 17.9) | 12.5 (4.1 to 20.9) | 0.2 (−3.9 to 4.3) | |||
P value | < 0.0001c | 0.0041c | NA | |||
Digestion | ||||||
Baseline mean (SD) | 83.4 (16.9) | 83.1 (18.1) | 80.3 (22.7) | 83.0 (18.5) | 85.8 (14.1) | 85.7 (17.8) |
LS mean change (SE) | −0.4 (0.9) | 2.1 (0.9) | 0.2 (2.2) | 1.1 (2.1) | −1.2 (1.2) | −1.4 (1.2) |
Patients in analysis | 203 | 200 | 52 | 55 | 126 | 130 |
LSMD (95% CI) | 2.5 (−0.1 to 5.1) | 0.9 (−5.1 to 6.9) | −0.3 (−3.6 to 3.0) | |||
P value | 0.0594 | 0.7634 | NA | |||
Role limitations | ||||||
Baseline mean (SD) | 83.3 (15.2) | 81.7 (17.5) | 79.0 (17.2) | 80.4 (19.9) | 84.2 (16.7) | 87.3 (17.4) |
LS mean change (SE) | −2.4 (0.8) | 4.4 (0.8) | 0.8 (1.8) | 6.8 (1.7) | 0.4 (1.2) | 0.7 (1.1) |
Patients in analysis | 179 | 185 | 44 | 49 | 122 | 123 |
LSMD (95% CI) | 6.8 (4.6 to 9.1) | 6.0 (1.1 to 10.9) | 0.3 (−2.9 to 3.5) | |||
P value | < 0.0001c | 0.0167c | NA | |||
Social limitations | ||||||
Baseline mean (SD) | 68.8 (17.9) | 70.5 (17.0) | 73.5 (16.3) | 67.9 (17.7) | 67.4 (20.3) | 69.7 (19.9) |
LS mean change (SE) | −1.3 (0.8) | 4.6 (0.8) | 1.5 (1.5) | 6.9 (1.5) | −2.0 (1.2) | 0.6 (1.2) |
Patients in analysis | 203 | 200 | 52 | 55 | 126 | 130 |
LSMD (95% CI) | 5.9 (3.7 to 8.0) | 5.4 (1.2 to 9.6) | 2.6 (−0.8 to 6.0) | |||
P value | < 0.0001c | 0.0131c | NA | |||
CI = confidence interval; ELX-TEZ-IVA = elexacaftor-tezacaftor-ivacaftor and ivacaftor; F/F = homozygous for F508del mutation in the CFTR gene; F/G = 1 F508del mutation and 1 gating mutation in the CFTR gene; F/MF = 1 F508del mutation and 1 minimal function mutation in the CFTR gene; F/RF = 1 F508del mutation and 1 residual function mutation in the CFTR gene; LS = least squares; LSMD = least squares mean difference; MMRM = mixed-effects model for repeated measures; NA = not applicable; SD = standard deviation; SE = standard error; TEZ-IVA = tezacaftor-ivacaftor and ivacaftor.
aThe MMRM included final data from all available visits, with treatment, visit, and treatment-by-visit interaction as fixed effects and baseline ppFEV1, age group at screening (< 1 8, ≥ 18 years of age) and sex (male, female) as covariates.
bThe MMRM included data from all available visits up to week 8, with treatment, visit, and treatment × visit as fixed effects and baseline ppFEV1, baseline sweat chloride and comparator group (IVA comparator group vs. TEZ-IVA comparator group) as covariates.
cNo adjustment for multiplicity was performed; all P values are therefore considered nominal.
Patients Aged 12 Years and Older
Patients With F/MF Genotype: Absolute change from baseline in sweat chloride at 4 weeks and 24 weeks were key secondary end points of Study 102. The ELX-TEZ-IVA group demonstrated statistically significant reductions in sweat chloride compared with the placebo group at 4 weeks (LSMD = −41.2 mmol/L; 95% CI, −44.0 to −38.5) and 24 weeks (LSMD = −41.8 mmol/L; 95% CI, −44.4 to −39.3) (Table 46).5
Table 46: Change From Baseline in Sweat Chloride in Pediatric Studies
Analysis | Study 116 | Study 106 Part B | |
|---|---|---|---|
Placebo (N = 61) | ELX-TEZ-IVA (N = 60) | ELX-TEZ-IVA (N = 66) | |
Baseline mean (SD) | 102.6 (8.6) | 102.8 (10.0) | 102.2 (9.1) |
Patients in analysis | 61 | 60 | 60 |
LS mean change (SE) | −0.9 (1.5) | −52.1 (1.5) | −60.9 (1.4) |
P value within treatment | 0.5241 | < 0.0001 | < 0.0001 |
LSMD (95% CI) | Reference | −51.2 (−55.3 to −47.1) | NA |
P value vs. placebo | Reference | < 0.0001 | NA |
CI = confidence interval; ELX-TEZ-IVA = elexacaftor-tezacaftor-ivacaftor and ivacaftor; LS = least squares; LSMD = least squares mean difference; NA = not applicable; SD = standard deviation; SE = standard error.
Source: Clinical Study Reports.3,4
Patients With F/F Genotype: Absolute change from baseline in sweat chloride at 4 weeks and through 24 weeks were key secondary end points of Study 103 and 109, respectively. The ELX-TEZ-IVA group demonstrated statistically significant reductions in sweat chloride compared with the TEZ-IVA group at 4 weeks (LSMD = −45.1 mmol/L; 95% CI, −50.1 to −40.1) in Study 103 and through 24 weeks in Study 109 (LSMD = −42.8; 95% CI, −46.2 to −39.3; P < 0.0001) (Table 47).6,10
Table 47: Change From Baseline in Sweat Chloride in Adolescent and Adult Patients With F/MF Genotype
Analysis | Placebo (N = 203) | ELX-TEZ-IVA (N = 200) |
|---|---|---|
Absolute change from baseline in sweat chloride at 4 weeks (mmol/L)a | ||
Baseline mean (SD) | 102.9 (9.8) | 102.3 (11.9) |
LS mean change (SE) | 0.1 (1.0) | −41.2 (1.0) |
Patients in analysis | 196 | 193 |
LSMD (95% CI) | −41.2 (−44.0 to −38.5) | |
P value (vs. placebo) | < 0.0001b | |
Absolute change from baseline in sweat chloride through 24 weeks (mmol/L)a | ||
Baseline mean (SD) | 102.9 (9.8) | 102.3 (11.9) |
LS mean change (SE) | −0.4 (0.9) | −42.2 (0.9) |
Patients in analysis | 201 | 199 |
LSMD (95% CI) | −41.8 (−44.4 to −39.3) | |
P value (vs. placebo) | < 0.0001b | |
CI = confidence interval; ELX-TEZ-IVA = elexacaftor-tezacaftor-ivacaftor and ivacaftor; F/MF = 1 F508del mutation and 1 minimal function mutation in the CFTR gene; LS = least squares; LSMD = least squares mean difference; MMRM = mixed-effects model for repeated measures; SD = standard deviation; SE = standard error.
aThe MMRM included final data from all available visits, with treatment, visit, and treatment-by-visit interaction as fixed effects and baseline ppFEV1, age group at screening (< 18, ≥ 18 years of age) and sex (male, female) as covariates.
bPre-specified key secondary end point.
Source: Clinical Study Report.5
Patients With F/G and F/RF Genotypes: Absolute change from baseline in sweat chloride through 8 weeks within the ELX-TEZ-IVA group and compared with the control were key secondary end points of Study 104. The ELX-TEZ-IVA group demonstrated a statistically significant decrease in sweat chloride from baseline through 8 weeks (LS mean = −22.3 mmol/L; 95% CI, = −24.5 to −20.2; P < 0.0001) (Table 48). Treatment with ELX-TEZ-IVA also resulted in a decrease in sweat chloride from baseline through 8 weeks compared to the control group (LSMD = −23.1 mmol/L; 95% CI, −26.1 to −20.1); P < 0.0001).11
Table 48: Change from Baseline in Sweat Chloride in Adolescents and Adults With F/F Genotype
Analysis | Study 103 (F/F) at 4 weeksa | Study 109 (F/F) through 24 weeksb | ||
|---|---|---|---|---|
TEZ-IVA (N = 52) | ELX-TEZ-IVA (N = 55) | TEZ-IVA (N = 88) | ELX-TEZ-IVA (N = 87) | |
Baseline mean (SD) | 90.0 (12.3) | 91.4 (11.0) | 89.8 (11.7) | 89.0 (12.2) |
LS mean change (SE) | 1.7 (1.8) | −43.4 (1.7) | −3.4 (1.2) | −46.2 (1.3) |
Patients in analysis | 48 | 54 | 88 | 87 |
LSMD (95% CI) | −45.1 (−50.1 to −40.1) | −42.8 (−46.2 to −39.3) | ||
P value (vs. TEZ-IVA) | < 0.0001c | < 0.0001 | ||
CI = confidence interval; ELX-TEZ-IVA = elexacaftor-tezacaftor-ivacaftor and ivacaftor; F/F = homozygous for F508del mutation in the CFTR gene; LS = least squares; LSMD = least squares mean difference; MMRM = mixed-effects model for repeated measures; SD = standard deviation; SE = standard error; TEZ-IVA = tezacaftor-ivacaftor and ivacaftor.
aThe MMRM included final data from all available visits, with treatment, visit, and treatment-by-visit interaction as fixed effects and baseline ppFEV1, age group at screening (< 18, ≥ 18 years of age) and sex (male, female) as covariates.
bThe MMRM included data from all available visits up to week 24 with treatment, visit, and treatment by visit as fixed effects; baseline ppFEV1, age group at screening (≥ 12 to < 18 vs. ≥ 18 years), and CFTR-modulator use at screening (yes vs. no) as covariates.
cPre-specified key secondary end point.
Source: Clinical Study Report.6,10
Treatment Satisfaction Questionnaire for Medication
The TSQM was included as an exploratory end point in Study 102 and Study 103 for patients between the ages of 12 and 17 years.
Patients With F/MF Genotype: As shown in Table 49, the ELX-TEZ-IVA group in Study 102 demonstrated improvements compared with the placebo group in the domains for global satisfaction (LSMD = 24.2; 95% CI, 13.6 to 34.9), side effects (LSMD = −4.6; 95% CI, −8.5 to −0.7), and effectiveness (LSMD = 23.2; 95% CI, 13.8 to 32.7).5
Patients With F/F Genotype: In Study 103, the ELX-TEZ-IVA group demonstrated improvements compared with the TEZ-IVA group in the domains for global satisfaction (LSMD = 11.9; 95% CI, 1.8 to 22.0) and effectiveness (LSMD = 14.4; 95% CI, 3.5 to 25.4) (Table 49).6 The TSQM was not included as an end point in Study 109.10
Patients With F/G and F/RF Genotypes: The TSQM was not included as an end point in Study 104.11
Table 49: Change from Baseline in Sweat Chloride in F/G and F/RF Genotypes
Analysis | Patients with F/G or F/RF | Study 104 (F/RF subgroup) | Study 104 (F/G subgroup) | |||
|---|---|---|---|---|---|---|
Control (N = 126) | ELX-TEZ-IVA (N = 132) | TEZ-IVA (N = 81) | ELX-TEZ-IVA (N = 82) | IVA (N = 45) | ELX-TEZ-IVA (N = 50) | |
Absolute change from baseline in sweat chloride at 8 weeks | ||||||
Baseline mean (SD) | 56.4 (25.5) | 59.5 (27.0) | 61.4 (27.3) | 64.7 (27.9) | 47.6 (19.1) | 50.9 (23.3) |
Patients in analysis | 119 | 120 | 75 | 77 | 44 | 43 |
LS mean change (SE) | 0.7 (1.1) | −22.3 (1.1) | 1.7 (1.3) | −23.1 (1.3) | −1.8 (2.0) | −21.8 (2.0) |
LSMD (95% CI) | −23.1 (−26.1 to −20.1) | −24.8 (−28.4 to −21.2) | −20.0 (−25.4 to −14.6) | |||
P value vs. control | < 0.0001 | < 0.0001 | < 0.0001 | |||
CI = confidence interval; ELX-TEZ-IVA = elexacaftor-tezacaftor-ivacaftor and ivacaftor; F/G = 1 F508del mutation and 1 gating mutation in the CFTR gene; F/RF = 1 F508del mutation and 1 residual function mutation in the CFTR gene; IVA = ivacaftor; LS = least squares; LSMD = least squares mean difference; SD = standard deviation; SE = standard error; TEZ-IVA = tezacaftor-ivacaftor and ivacaftor.
Note: The MMRM included data from all available visits up to week 8, with treatment, visit, and treatment by visit as fixed effects and baseline ppFEV1, baseline sweat chloride, and comparator group (IVA or TEZ-IVA comparator group) as covariates.
Source: Clinical Study Report.11
Hospitalizations
Patients Aged 6 to 11 Years
Placebo-Controlled Trial (Study 116; F/MF Genotype): Hospitalizations were not reported in Study 116.
Single-Arm Trial (Study 106; F/F or F/MF Genotype): The annual event rates for planned and unplanned CF-related hospitalizations were each 0 per year.3
Patients Aged 12 Years and Older
Patients With F/MF Genotype: Table 50 provides a summary of the data for planned and unplanned hospitalizations for CF that were reported during Study 102. Nine events of planned hospitalization for CF were reported for 7 patients (3.4%) in the placebo group compared with 1 event (0.5%) in the ELX-TEZ-IVA group (P = 0.0677). The mean annualized duration of planned hospitalizations for CF was lower in the ELX-TEZ-IVA group compared with the placebo group was 0.1 days (SD = 1.4) versus 1.0 days (SD = 7.4). There were 21 unplanned hospitalization events in the placebo group (17 patients [8.4%]) and 15 events in the ELX-TEZ-IVA group (13 patients [6.5%]). There was no statistically significant difference in the rate of unplanned hospitalizations for CF between the placebo and ELX-TEZ-IVA groups (rate ratio = 0.80; 95% CI, 0.38 to 1.70; P = 0.5592). There was no statistically significant difference between the ELX-TEZ-IVA and placebo groups for the mean annualized durations of unplanned hospitalizations for CF (1.0 days [SD = 4.7] versus 3.0 days [SD = 12.6]; P = 0.5724, respectively).5
Table 50: Absolute Change From Baseline in TSQM in F/MF and F/F Genotypes
Analysis | Study 102 (F/MF) through 24 weeksa | Study 103 (F/F) at 4 weeksb | ||
|---|---|---|---|---|
Placebo (N = 60) | ELX-TEZ-IVA (N = 56) | TEZ-IVA (N = 14) | ELX-TEZ-IVA (N = 16) | |
Global satisfaction | ||||
Baseline mean (SD) | 76.6 (16.4) | 72.1 (21.2) | 87.2 (8.9) | 78.1 (23.4) |
LS mean change (SE) | −8.9 (3.7) | 15.3 (3.9) | −1.0 (3.6) | 11.0 (3.4) |
Patients in analysis | 56 | 52 | 14 | 16 |
LSMD (95% CI) | 24.2 (13.6 to 34.9) | 11.9 (1.8 to 22.0) | ||
P value | < 0.0001c | 0.0222c | ||
Convenience | ||||
Baseline mean (SD) | 75.0 (16.4) | 72.9 (21.0) | 85.9 (10.5) | 82.6 (15.3) |
LS mean change (SE) | 6.6 (3.0) | 13.9 (3.1) | 1.7 (3.7) | 6.3 (3.5) |
Patients in analysis | 56 | 52 | 14 | 16 |
LSMD (95% CI) | 7.3 (−1.2 to 15.7) | 4.6 (−5.9 to 15.1) | ||
P value | 0.0914 | 0.3794 | ||
Side effects | ||||
Baseline mean (SD) | 98.7 (5.7) | 99.9 (0.9) | 99.1 (3.3) | 96.5 (8.8) |
LS mean change (SE) | −0.1 (1.3) | −4.7 (1.4) | 0.0 (2.5) | −3.5 (2.3) |
Patients in analysis | 57 | 52 | 14 | 16 |
LSMD (95% CI) | −4.6 (−8.5 to −0.7) | −3.4 (−10.4 to 3.6) | ||
P value | 0.0198c | 0.3255 | ||
Effectiveness | ||||
Baseline mean (SD) | 67.8 (20.9) | 68.9 (15.9) | 75.0 (12.3) | 71.5 (17.6) |
LS mean change (SE) | v9.5 (3.3) | 13.7 (3.4) | −0.9 (3.9) | 13.6 (3.6) |
Patients in analysis | 59 | 53 | 14 | 16 |
LSMD (95% CI) | 23.2 (13.8 to 32.7) | 14.4 (3.5 to 25.4) | ||
P value | < 0.0001c | 0.0116c | ||
CI = confidence interval; ELX-TEZ-IVA = elexacaftor-tezacaftor-ivacaftor and ivacaftor; F/F = homozygous for F508del mutation in the CFTR gene; F/MF = 1 F508del mutation and 1 minimal function mutation in the CFTR gene; LS = least squares; LSMD = least squares mean difference; SD = standard deviation; SE = standard error; TEZ-IVA = tezacaftor-ivacaftor and ivacaftor; TSQM = Treatment Satisfaction Questionnaire for Medication.
aAnalysis of covariance included data from week 24, with treatment as a fixed effect and baseline ppFEV1 and sex (male vs. female) as covariates.
bAnalysis of covariance included data from week 4, with treatment as a fixed effect and continuous baseline ppFEV1 as a covariate.
cNo adjustment for multiplicity was performed; therefore, all P values are considered nominal.
Source: Clinical Study Reports.5,6
Table 51: Cystic Fibrosis-Related Hospitalizations in Patients with F/MF Genotype
Analysis | Placebo (N = 203) | ELX-TEZ-IVA (N = 200) |
|---|---|---|
Total number of days (years) | 34,187 (101.7) | 33,453 (99.6) |
Planned hospitalizations for CF | ||
Number of patients with events, n (%) | 7 (3.4) | 1 (0.5) |
Number of events | 9 | 1 |
Estimated event rate per yeara | NA | NA |
Rate ratio, 95% CI, | NA | |
P value vs. placebo | 0.0677 | |
Unplanned hospitalizations for CF | ||
Number of patients with events, n (%) | 17 (8.4) | 13 (6.5) |
Number of events | 21 | 15 |
Estimated event rate per yearb | 0.19 | 0.15 |
Rate ratio, 95% CI | 0.80 (0.38 to 1.70) | |
P value vs. placebo | 0.5592 | |
Annualized duration of planned hospitalizations for CF | ||
Mean (SD) | 1.0 (7.4) | 0.1 (1.4) |
Median (range) | 0.0 (0.0 to 91.6) | 0.0 (0.0 to 19.9) |
P value vs. placeboc | 0.0218 | |
Annualized duration of unplanned hospitalizations for CF | ||
Mean (SD) | 3.0 (12.6) | 1.0 (4.7) |
Median (range) | 0.0 (0.0 to 81.1) | 0.0 (0.0 to 40.2) |
P value vs. placeboc | 0.5724 | |
CF = cystic fibrosis; CI = confidence interval; ELX-TEZ-IVA = elexacaftor-tezacaftor-ivacaftor and ivacaftor; F/MF = 1 F508del mutation and 1 minimal function mutation in the CFTR gene; NA = not applicable; SD = standard deviation.
aIf fewer than 5 events occurred in either treatment group, no model-based estimates were produced and the P value was based on a Fisher exact test.
bAnalysis is based on negative binomial regression model: count = treatment + baseline ppFEV1 + age group at screening (≥ 12 to < 18 vs. ≥ 18 years) + sex (male vs. female), with log (duration of the analysis period in years) as offset.
cP values were based on a Wilcoxon rank sum test stratified by ppFEV1 group at screening (< 70% vs. ≥ 70%), age group at screening (≥ 12 to < 18 vs. ≥ 18 years), sex (male vs. female). No adjustment for multiplicity was performed;, all P values are therefore considered nominal.
Source: Clinical Study Report.5
Patients With F/F Genotype: Hospitalizations were only captured in the safety evaluations in Study 103 and Study 109.6,10
Patients With F/G and F/RF Genotypes: Hospitalizations were only captured in the safety evaluation of Study 104.11
Harms
Only those harms identified in the review protocol are reported here.
Table 52: Summary of Harms in Pediatric Patients
Adverse events, n (%) | Study 116 | Study 106 | ||
|---|---|---|---|---|
Placebo (N = 61) | ELX-TEZ-IVA (N = 60) | Part A (N = 16) | Part B (N = 66) | |
1 or more adverse events | 57 (93.4) | 48 (80.0) | 12 (75.0) | 65 (98.5) |
Withdrawal due to adverse events | 0 | 1 (1.7) | 0 | 1 (1.5) |
Adverse events leading to interruption | 0 | 7 (11.7) | 1 (6.3) | 1 (1.5) |
Grade 3 or 4 adverse events | 2 (3.3) | 2 (3.3) | 1 (6.3) | 1 (1.5) |
Serious adverse events | 9 (14.8) | 4 (6.7) | 0 | 1 (1.5) |
ELX-TEZ-IVA = elexacaftor-tezacaftor-ivacaftor and ivacaftor.
Source: Clinical Study Reports.3,4
Adverse Events
Patients Aged 6 to 11 Years
Placebo-Controlled Trial (Study 116; F/MF Genotype): Table 53 provides a summary of the most frequently reported AEs in the included pediatric studies (i.e., those occurring in 5% or more of patients in 1 of the treatment groups). In Study 116, the overall percentage of patients who experienced 1 or more AE was greater in the placebo group (93.4%) compared to the ELX-TEZ-IVA group (80.0%). Adverse events that were reported in 5% or more of patients in the ELX-TEZ-IVA group and occurred at a frequency that was 5% or greater than that of the placebo group included headache (30.0% versus 19.7%), rash (10.0% versus 4.9%), and a positive Staphylococcus test result ||||||||||||||||||||||||. Infective pulmonary exacerbations were reported as AEs more commonly in the placebo group compared with the ELX-TEZ-IVA group (26.2% versus 1.7%). The following other events were more commonly reported in the placebo group: cough (42.6% versus 23.3%), abdominal pain (27.9% versus 8.3%), oropharyngeal pain (19.7% versus 5.0%), nausea (||||||||||||||||||||||||), fatigue (||||||||||||||||||), FEV decreased (||||||||||||||||||), and nasal polyps (||||||||||||||||||).4
Single-Arm Trial (Study 106; F/F or F/MF Genotype): Adverse events were more commonly reported in Study 106 Part B compared with the ELX-TEZ-IVA group of Study 116 (e.g., 1 or more AE was reported in 98.5% of patients in Study 106 compared with 80.0% in Study 116).
Table 53: Summary of Harms in Adolescent and Adult Patients
Adverse events, n (%) | Study 102 (F/MF) | Study 103 (F/F) | Study 109 (F/F) | Study 104 (F/G and F/RF) | ||||
|---|---|---|---|---|---|---|---|---|
Placebo (N = 201) | ELX-TEZ-IVA (N = 202) | TEZ-IVA (N = 52) | ELX-TEZ-IVA (N = 55) | TEZ-IVA (N = 88) | ELX-TEZ-IVA (N = 87) | Control (N = 126) | ELX-TEZ-IVA (N = 132) | |
1 or more AEs | 193 (96.0) | 188 (93.1) | 33 (63.5) | 32 (58.2) | 81 (92.0) | 77 (88.5) | 83 (65.9) | 88 (66.7) |
WDAEs | 0 | 2 (1.0) | 0 | 0 | 2 (2.3) | 1 (1.1) | 2 (1.6) | 1 (0.8) |
AEs leading to interruption | 10 (5.0) | 19 (9.4) | 0 | 0 | 1 (1.1) | 2 (2.3) | 3 (2.4) | 5 (3.8) |
Grade 3 or 4 AEs | 15 (7.5) | 19 (9.4) | 1 (1.9) | 0 | 7 (8.0) | 7 (8.0) | 4 (3.2) | 5 (3.8) |
SAEs | 42 (20.9) | 28 (13.9) | 1 (1.9) | 2 (3.6) | 14 (15.9) | 5 (5.7) | 11 (8.7) | 5 (3.8) |
AE = adverse event; ELX-TEZ-IVA = elexacaftor-tezacaftor-ivacaftor and ivacaftor; F/F = homozygous for F508del mutation in the CFTR gene; F/G = 1 F508del mutation and 1 gating mutation in the CFTR gene; F/MF = 1 F508del mutation and 1 minimal function mutation in the CFTR gene; F/RF = 1 F508del mutation and 1 residual function mutation in the CFTR gene; SAE = serious adverse event; TEZ-IVA = tezacaftor-ivacaftor and ivacaftor; WDAE = withdrawal due to adverse event.
Source: Clinical Study Reports.5,6,10,11
Patients Aged 12 Years and Older
Table 54 provides a summary of the most frequently reported AEs in the included studies (i.e., those occurring in 5% or more of patients in 1 of the treatment groups).
Patients With F/MF Genotype: In Study 102, the overall percentage of patients who experienced 1 or more AEs was similar between the placebo group (96.0%) and the ELX-TEZ-IVA group (93.1%). Infective pulmonary exacerbations were the most reported AEs in both the placebo and ELX-TEZ-IVA groups. Consistent with efficacy data, there were fewer patients with pulmonary exacerbations reported as AEs in the ELX-TEZ-IVA group compared with the group (47.3% versus 21.8%). Adverse events that were reported in at least 5% of patients in the ELX-TEZ-IVA group and occurred at a frequency at least 5% higher than that of the placebo group were: diarrhea (12.9% versus 7.0%), increased ALT increased (9.9% versus 3.5%), increased AST (9.4% versus 2.0%), rhinorrhea (8.4% versus 3.0%), and influenza (6.9% versus 1.5%).5
Patients With F/F Genotype: In Study 103, the overall percentage of patients who experienced 1 or more AEs was 63.5% in the TEZ-IVA group and 58.2% in the ELX-TEZ-IVA group. Infective pulmonary exacerbations of CF were the most reported AEs in the TEZ-IVA group and these events occurred at a higher frequency in comparison with the ELX-TEZ-IVA group (11.5% versus 1.8%). Adverse events that were reported in 5% or more of patients in the ELX-TEZ-IVA group and occurred at a frequency at least 5% higher than that of the TEZ-IVA group were: cough (14.5% versus 7.7%), oropharyngeal pain (7.3% versus 0%), and respiration abnormal (5.5% versus 0%).6
In Study 109, the overall percentage of patients who experienced 1 or more AEs was 92.0% in the TEZ-IVA group compared with 88.5% in the ELX-TEZ-IVA group. Infective pulmonary exacerbations of CF were the most reported AEs in the TEZ-IVA group and these events occurred at a higher frequency in comparison with the ELX-TEZ-IVA group (40.9% versus 11.5%). Adverse events that were reported in 5% or more of patients in the ELX-TEZ-IVA group and occurred at a frequency at least 5% higher than that of the TEZ-IVA group were: headache (28.7% versus 20.5%), increased ALT (6.9% versus 1.1%), increased AST (5.7% versus 0%), nasal congestion (6.9% versus 0%), rash (8.0% versus 0%), and productive cough (9.2% versus 3.4%).10
Patients With F/G and F/RF Genotypes: In Study 104, the overall percentages of patients who experienced 1 or more AEs were 66.7% in the ELX-TEZ-IVA group and 65.9% in the control group.11 Adverse events that were reported in at least 5% of patients in the ELX-TEZ-IVA group and occurred at a frequency at least 5% higher than that of the control group were increased ALT (6.1% versus 0%) and increased AST (6.1% versus 0%).11
Table 54: Adverse Events Occurring in at Least 5% of Pediatric Patients
Adverse events, n (%) | Study 116 | Study 106 Part B (N = 66) | |
|---|---|---|---|
Placebo (N = 61) | ELX-TEZ-IVA (N = 60) | ||
1 or more adverse events | 57 (93.4) | 48 (80.0) | 65 (98.5) |
Headache | 12 (19.7) | 18 (30.0) | 16 (24.2) |
Cough | 26 (42.6) | 14 (23.3) | 28 (42.4) |
Nasopharyngitis | 9 (14.8) | 7 (11.7) | NR |
Productive cough | 6 (9.8) | 7 (11.7) | NR |
Rhinorrhea | 7 (11.5) | 7 (11.7) | 8 (12.1) |
Rash | 3 (4.9) | 6 (10.0) | 8 (12.1) |
Abdominal pain | 17 (27.9) | 5 (8.3) | 8 (12.1) |
Increased ALT | 3 (4.9) | 5 (8.3) | 7 (10.6) |
Abdominal pain upper | 5 (8.2) | 4 (6.7) | 5 (7.6) |
Diarrhea | 6 (9.8) | 4 (6.7) | 7 (10.6) |
Pruritus | 0 | 4 (6.7) | NR |
Staphylococcus test positive | 1 (1.6) | 4 (6.7) | NR |
Increase AST | 1 (1.6) | 3 (5.0) | NR |
Nasal congestion | 3 (4.9) | 3 (5.0) | 10 (15.2) |
Oropharyngeal pain | 12 (19.7) | 3 (5.0) | 12 (18.2) |
Rhinitis | 5 (8.2) | 3 (5.0) | NR |
Steatorrhea | 0 | 3 (5.0) | NR |
URTI | 5 (8.2) | 3 (5.0) | 11 (16.7) |
Viral URTI | NR | NR | 8 (12.1) |
Vomiting | 4 (6.6) | 3 (5.0) | 7 (10.6) |
Arthralgia | 4 (6.6) | 1 (1.7) | NR |
Bacterial test positive | 4 (6.6) | 1 (1.7) | NR |
Infective PEx of CF | 16 (26.2) | 1 (1.7) | NR |
Nausea | 5 (8.2) | 1 (1.7) | NR |
Fatigue | 5 (8.2) | 0 | 5 (7.6) |
Decreased FEV | 4 (6.6) | 0 | NR |
Nasal polyps | 5 (8.2) | 0 | NR |
Pyrexia | NR | NR | 14 (21.2) |
Influenza | NR | NR | 7 (10.6) |
Productive cough | NR | NR | 5 (7.6) |
Constipation | NR | NR | 4 (6.1) |
Ear infection | NR | NR | 4 (6.1) |
ALT = alanine transaminase; AST = aspartate transaminase; CF = cystic fibrosis; ELX-TEZ-IVA = elexacaftor-tezacaftor-ivacaftor and ivacaftor; FEV = forced expiratory volume; NR = not reported; PEx = pulmonary exacerbation; URTI = upper respiratory tract infection.
Source: Clinical Study Reports.3,4
Serious Adverse Events
Patients Aged 6 to 11 Years
In Study 116, a total of 4 patients (6.7%) in the ELX-TEZ-IVA group and 9 patients (14.8%) in the placebo group had 1 or more SAEs. No SAE occurred in more than 1 patient in the ELX-TEZ-IVA group. Three patients (4.9%) in the placebo group had an SAE of infective pulmonary exacerbations of CF. In Study 106, no patients had SAEs in Part A and 1 patient (1.5%) had 3 SAEs (metapneumovirus infection, pneumonia, and rhinovirus infection) in Part B. All 3 events were considered to be moderate in severity and did not lead to study treatment discontinuation or interruption.3
Patients Aged 12 Years and Older
Table 55 provides a summary of the SAEs that were reported in the included adolescent and adult studies.
Patients With F/MF Genotype: In Study 102, the percentage of patients who experienced 1 or more SAEs was 20.9% in the placebo group compared with 13.9% in the ELX-TEZ-IVA group.5 The most commonly reported SAE in either treatment group was infective pulmonary exacerbation of CF. There were more pulmonary exacerbation SAEs in the placebo group compared with the ELX-TEZ-IVA group (16.4% versus 5.4%). Few other SAEs were reported for more than 1 patient in each treatment group.5
Patients With F/F Genotype: In Study 103, SAEs were rare and reported for only 1 patient in the TEZ-IVA group (pulmonary exacerbation) and 2 patients in the ELX-TEZ-IVA group (pulmonary exacerbation and rash) (1.9% and 3.6%, respectively).6 In Study 109, the percentages of patients who experienced 1 or more SAEs were 15.9% in the TEZ-IVA group and 5.7% in the ELX-TEZ-IVA group. The difference between the groups was due to a greater proportion of patients in the TEZ-IVA group who experienced a pulmonary exacerbation that was classified as an SAE compared with the ELX-TEZ-IVA group (11.4% versus 1.1). No other SAEs were reported for more than 1 patient in each treatment group.10
Patients With F/G and F/RF Genotypes: In Study 104, the percentage of patients who experienced 1 or more SAEs was 8.7% in the control group compared with 3.8% in the ELX-TEZ-IVA group.11 The difference between the groups was due to a greater percentage of patients in the control group who experienced a pulmonary exacerbation that was classified as an SAE compared with the ELX-TEZ-IVA group (5.6% versus 1.5%). There were no other SAEs that were reported for more than 1 patient in each treatment group.11
Table 55: Adverse Events Occurring in at Least 5% of Adolescent and Adult Patients
Adverse events | Study 102 (F/MF) | Study 103 (F/F) | Study 109 (F/F) | Study 104 (F/G and F/RF) | ||||
|---|---|---|---|---|---|---|---|---|
Placebo (N = 201) | ELX-TEZ-IVA (N = 202) | TEZ-IVA (N = 52) | ELX-TEZ-IVA (N = 55) | TEZ-IVA (N = 88) | ELX-TEZ-IVA (N = 87) | Control (N = 126) | ELX-TEZ-IVA (N = 132) | |
1 or more AEs | 193 (96.0) | 188 (93.1) | 33 (63.5) | 32 (58.2) | 81 (92.0) | 77 (88.5) | 83 (65.9) | 88 (66.7) |
Infective PEx of CF | 95 (47.3) | 44 (21.8) | 6 (11.5) | 1 (1.8) | 36 (40.9) | 10 (11.5) | 13 (10.3) | 3 (2.3) |
Increased sputum | 39 (19.4) | 40 (19.8) | 3 (5.8) | 3 (5.5) | 16 (18.2) | 10 (11.5) | 8 (6.3) | 6 (4.5) |
Headache | 30 (14.9) | 35 (17.3) | 4 (7.7) | 3 (5.5) | 18 (20.5) | 25 (28.7) | 19 (15.1) | 11 (8.3) |
Cough | 77 (38.3) | 34 (16.8) | 4 (7.7) | 8 (14.5) | 23 (26.1) | 11 (12.6) | 18 (14.3) | 3 (2.3) |
Diarrhea | 14 (7.0) | 26 (12.9) | 3 (5.8) | 2 (3.6) | 7 (8.0) | 8 (9.2) | 8 (6.3) | 5 (3.8) |
URTI | 22 (10.9) | 24 (11.9) | 2 (3.8) | 4 (7.3) | 5 (5.7) | 9 (10.3) | — | — |
Nasopharyngitis | 26 (12.9) | 22 (10.9) | 2 (3.8) | 4 (7.3) | 13 (14.8) | 17 (19.5) | — | — |
Abdominal pain | 12 (6.0) | 20 (9.9) | 1 (1.9) | 3 (5.5) | 7 (8.0) | 4 (4.6) | 2 (1.6) | 7 (5.3) |
Increased ALT | 7 (3.5) | 20 (9.9) | — | — | 1 (1.1) | 6 (6.9) | 0 | 8 (6.1) |
Oropharyngeal pain | 25 (12.4) | 20 (9.9) | 0 | 4 (7.3) | 7 (8.0) | 11 (12.6) | - | - |
Increased AST | 4 (2.0) | 19 (9.4) | — | — | 0 | 5 (5.7) | 0 | 8 (6.1) |
Increased blood CPK | 9 (4.5) | 19 (9.4) | — | — | — | — | — | — |
Nasal congestion | 15 (7.5) | 19 (9.4) | 1 (1.9) | 3 (5.5) | 0 | 6 (6.9) | — | — |
Rash | 9 (4.5) | 18 (8.9) | — | — | 0 | 7 (8.0) | — | — |
Pyrexia | 19 (9.5) | 17 (8.4) | — | — | — | — | — | — |
Rhinorrhea | 6 (3.0) | 17 (8.4) | — | — | — | — | — | — |
Nausea | 14 (7.0) | 16 (7.9) | 3 (5.8) | 1 (1.8) | — | — | 9 (7.1) | 2 (1.5) |
Rhinitis | 11 (5.5) | 15 (7.4) | — | — | — | — | — | — |
Influenza | 3 (1.5) | 14 (6.9) | — | — | — | — | — | — |
Productive cough | 16 (8.0) | 12 (5.9) | — | — | 3 (3.4) | 8 (9.2) | — | — |
Vomiting | 10 (5.0) | 12 (5.9) | — | — | - | - | — | — |
Hemoptysis | 28 (13.9) | 11 (5.4) | 5 (9.6) | 2 (3.6) | 6 (6.8) | 3 (3.4) | — | — |
Sinusitis | 8 (4.0) | 11 (5.4) | — | — | — | — | — | — |
Increased blood bilirubin | 2 (1.0) | 10 (5.0) | — | — | — | — | — | — |
Fatigue | 20 (10.0) | 9 (4.5) | 2 (3.8) | 3 (5.5) | - | - | — | — |
Constipation | 12 (6.0) | 6 (3.0) | — | — | - | - | — | — |
Bacterial test positive | 10 (5.0) | 5 (2.5) | — | — | 5 (5.7) | 1 (1.1) | — | — |
Dyspnea | 13 (6.5) | 5 (2.5) | — | — | — | — | — | — |
Respiration abnormal | — | — | 0 | 3 (5.5) | — | — | — | — |
AE = adverse event; ALT = alanine transaminase; AST = aspartate transaminase; CF = cystic fibrosis; CPK = creatine phosphokinase; ELX-TEZ-IVA = elexacaftor-tezacaftor-ivacaftor and ivacaftor; F/F = homozygous for F508del mutation in the CFTR gene; F/G = 1 F508del mutation and 1 gating mutation in the CFTR gene; F/MF = 1 F508del mutation and 1 minimal function mutation in the CFTR gene; F/RF = 1 F508del mutation and 1 residual function mutation in the CFTR gene; PEx = pulmonary exacerbation; TEZ-IVA = tezacaftor-ivacaftor and ivacaftor; URTI = upper respiratory tract infection.
Table 56: Serious Adverse Events
Serious adverse events, n (%) | Study 102 (F/MF) | Study 103 (F/F) | Study 109 (F/F) | Study 104 (F/G and F/RF) | ||||
|---|---|---|---|---|---|---|---|---|
Placebo (N = 201) | ELX-TEZ-IVA (N = 202) | TEZ-IVA (N = 52) | ELX-TEZ-IVA (N = 55) | TEZ-IVA (N = 88) | ELX-TEZ-IVA (N = 87) | Control (N = 126) | ELX-TEZ-IVA (N = 132) | |
1 or more serious adverse event | 42 (20.9) | 28 (13.9) | 1 (1.9) | 2 (3.6) | 14 (15.9) | 5 (5.7) | 11 (8.7) | 5 (3.8) |
Blood and lymphatic system disorders | 0 | 0 | 0 | 0 | 0 | 1 (1.1) | 0 | 0 |
Thrombocytopenia | 0 | 0 | 0 | 0 | 0 | 1 (1.1) | 0 | 0 |
Infections and infestations | 36 (17.9) | 13 (6.4) | 1 (1.9) | 1 (1.8) | 10 (11.4) | 1 (1.1) | 8 (6.3) | 2 (1.5) |
Infective PEx of CF | 33 (16.4) | 11 (5.4) | 1 (1.9) | 1 (1.8) | 9 (10.2) | 1 (1.1) | 7 (5.6) | 2 (1.5) |
Influenza | 0 | 3 (1.5) | 0 | 0 | 0 | 0 | 0 | 0 |
Genital herpes simplex | 0 | 1 (0.5) | 0 | 0 | 0 | 0 | 0 | 0 |
Oral herpes | 0 | 1 (0.5) | 0 | 0 | 0 | 0 | 0 | 0 |
Atypical mycobacterial LRTI | 1 (0.5) | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
Coccidioidomycosis | 1 (0.5) | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
Lung infection | 1 (0.5) | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
Pneumonia | 1 (0.5) | 0 | 0 | 0 | 0 | 0 | 1 (0.8) | 0 |
Viral sinusitis | 1 (0.5) | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
LRTI | 0 | 0 | 0 | 0 | 1 (1.1) | 0 | 0 | 0 |
Cellulitis | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 1 (0.8) |
Ear and labyrinth disorders | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 1 (0.8) |
Tinnitus | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 1 (0.8) |
Respiratory, thoracic, and mediastinal disorders | 6 (3.0) | 4 (2.0) | 0 | 0 | 1 (1.1) | 0 | 1 (0.8) | 1 (0.8) |
Hemoptysis | 3 (1.5) | 2 (1.0) | 0 | 0 | 1 (1.1) | 0 | 1 (0.8) | 1 (0.8) |
Diaphragmatic paralysis | 0 | 1 (0.5) | 0 | 0 | 0 | 0 | 0 | 0 |
Nasal polyps | 0 | 1 (0.5) | 0 | 0 | 0 | 0 | 0 | 0 |
Painful respiration | 1 (0.5) | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
Pleuritic pain | 1 (0.5) | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
Pneumothorax spontaneous | 1 (0.5) | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
Investigations | 0 | 0 | 0 | 0 | 0 | 1 (1.1) | 0 | 0 |
Increased ALT | 0 | 0 | 0 | 0 | 0 | 1 (1.1) | 0 | 0 |
Endocrine disorders | 0 | 0 | 0 | 0 | 0 | 0 | 1 (0.8) | 0 |
Hyperparathyroidism primary | 0 | 0 | 0 | 0 | 0 | 0 | 1 (0.8) | 0 |
Gastrointestinal disorders | 1 (0.5) | 3 (1.5) | 0 | 0 | 1 (1.1) | 0 | 0 | 0 |
Upper abdominal pain | 0 | 1 (0.5) | 0 | 0 | 0 | 0 | 0 | 0 |
Distal intestinal obstruction syndrome | 0 | 1 (0.5) | 0 | 0 | 1 (1.1) | 0 | 0 | 0 |
Small intestinal obstruction | 1 (0.5) | 1 (0.5) | 0 | 0 | 0 | 0 | 0 | 0 |
Hepatobiliary disorders | 1 (0.5) | 3 (1.5) | 0 | 0 | 0 | 0 | 0 | 1 (0.8) |
Cholangitis | 0 | 1 (0.5) | 0 | 0 | 0 | 0 | 0 | 0 |
Gallbladder enlargement | 0 | 1 (0.5) | 0 | 0 | 0 | 0 | 0 | 0 |
Portal hypertension | 0 | 1 (0.5) | 0 | 0 | 0 | 0 | 0 | 0 |
Hypertransaminasemia | 1 (0.5) | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
Cholecystitis | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 1 (0.8) |
Skin, subcutaneous tissue disorders | 2 (1.0) | 3 (1.5) | 0 | 1 (1.8) | 0 | 0 | 0 | 0 |
Rash | 1 (0.5) | 2 (1.0) | 0 | 1 (1.8) | 0 | 0 | 0 | 0 |
Rash pruritic | 0 | 1 (0.5) | 0 | 0 | 0 | 0 | 0 | 0 |
Hypersensitivity vasculitis | 1 (0.5) | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
Injury, poisoning and procedural complications | 0 | 2 (1.0) | 0 | 0 | 0 | 0 | 0 | 0 |
Post-procedural hemorrhage | 0 | 1 (0.5) | 0 | 0 | 0 | 0 | 0 | 0 |
Upper limb fracture | 0 | 1 (0.5) | 0 | 0 | 0 | 0 | 0 | 0 |
Musculoskeletal and connective tissue disorders | 1 (0.5) | 2 (1.0) | 0 | 0 | 0 | 0 | 0 | 0 |
Musculoskeletal chest pain | 0 | 1 (0.5) | 0 | 0 | 0 | 0 | 0 | 0 |
Rhabdomyolysis | 0 | 1 (0.5) | 0 | 0 | 0 | 0 | 0 | 0 |
Back pain | 1 (0.5) | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
Nervous system disorders | 1 (0.5) | 2 (1.0) | 0 | 0 | 0 | 0 | 0 | 0 |
Axonal neuropathy | 0 | 1 (0.5) | 0 | 0 | 0 | 0 | 0 | 0 |
Mental impairment | 0 | 1 (0.5) | 0 | 0 | 0 | 0 | 0 | 0 |
Neuroglycopenia | 1 (0.5) | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
General disorders and administration-site conditions | 1 (0.5) | 1 (0.5) | 0 | 0 | 0 | 0 | 0 | 0 |
Adverse drug reaction | 0 | 1 (0.5) | 0 | 0 | 0 | 0 | 0 | 0 |
Medical device site inflammation | 1 (0.5) | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
Metabolism and nutrition disorders | 1 (0.5) | 0 | 0 | 0 | 0 | 1 (1.1) | 0 | 0 |
Hypoglycemia | 1 (0.5) | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
Type 3 diabetes mellitus | 0 | 0 | 0 | 0 | 0 | 1 (1.1) | 0 | 0 |
Psychiatric disorders | 1 (0.5) | 0 | 0 | 0 | 3 (3.4) | 1 (1.1) | 0 | 0 |
Depression | 1 (0.5) | 0 | 0 | 0 | 0 | 1 (1.1) | 1 (0.8) | 0 |
Suicidal ideation | 1 (0.5) | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
Anxiety | 0 | 0 | 0 | 0 | 1 (1.1) | 1 (1.1) | 1 (0.8) | 0 |
Insomnia | 0 | 0 | 0 | 0 | 1 (1.1) | 0 | 0 | 0 |
Obsessive-compulsive disorder | 0 | 0 | 0 | 0 | 1 (1.1) | 0 | 0 | 0 |
Psychotic disorder | 0 | 0 | 0 | 0 | 1 (1.1) | 0 | 0 | 0 |
Renal and urinary disorders | 2 (1.0) | 0 | 0 | 0 | 0 | 1 (1.1) | 0 | 0 |
Acute kidney injury | 1 (0.5) | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
Renal colic | 1 (0.5) | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
Nephrolithiasis | 0 | 0 | 0 | 0 | 0 | 1 (1.1) | 0 | 0 |
Cardiac disorders | 0 | 0 | 0 | 0 | 1 (1.1) | 0 | 0 | 0 |
Extrasystoles | 0 | 0 | 0 | 0 | 1 (1.1) | 0 | 0 | 0 |
ALT = alanine transaminase; CF = cystic fibrosis; ELX-TEZ-IVA = elexacaftor-tezacaftor-ivacaftor and ivacaftor; F/F = homozygous for F508del mutation in the CFTR gene; F/G = 1 F508del mutation and 1 gating mutation in the CFTR gene; F/MF = 1 F508del mutation and 1 minimal function mutation in the CFTR gene; F/RF = 1 F508del mutation and 1 residual function mutation in the CFTR gene; LRTI = lower respiratory tract infection; PEx = pulmonary exacerbation; TEZ-IVA = tezacaftor-ivacaftor and ivacaftor.
Withdrawals Due to Adverse Events
Patients Aged 6 to 11 Years
In Study 116, a single patient (1.7%) in the ELX-TEZ-IVA group had an AE of rash that led to study drug discontinuation. The event was assessed as severe and possibly related to the study drug. The study drug was withdrawn and the event resolved. No subjects in the placebo group discontinued the study drug. In Study 106, no patients had AEs that led to discontinuation of the study drug and 1 patient (1.5%) in Part B had an AE of rash erythematous that led to treatment discontinuation. The event was assessed by the investigator as moderate in severity and related to the study drug. The study drug was withdrawn, a single dose of cetirizine was administered, and the event resolved the next day.3,4
Patients Aged 12 Years and Older
Patients With F/MF Genotype: In Study 102, there were 2 WDAEs reported in the ELX-TEZ-IVA group (1.0%) and none in the placebo group. The reasons for discontinuation from the ELX-TEZ-IVA group included portal hypertension (0.5.%) and rash (0.5%).
Patients With F/F Genotype: No WDAEs were reported in either the TEZ-IVA or ELX-TEZ-IVA groups in Study 103. In Study 109, 2 patients (2.3%) withdrew from the TEZ-IVA group and 1 patient (1.1%) withdrew from the ELX-TEZ-IVA group as result of AEs. The AEs that resulted in withdrawal from TEZ-IVA group included obsessive-compulsive disorder (1.1%) and psychotic disorder (1.1%). The AEs that resulted in withdrawal from ELX-TEZ-IVA group included anxiety and depression (1 patient [1.1%] with both events).
Patients With F/G and F/RF Genotypes: In Study 104, there were 2 WDAEs from the control group (1.6%) and 1 in the ELX-TEZ-IVA group (0.8%). The AEs that resulted in withdrawal from the control group included infective pulmonary exacerbation (0.8%) and anxiety and depression (1 patient [0.8%] with both events). The AEs that resulted in withdrawal from ELX-TEZ-IVA group included 1 patient with elevated ALT and AST levels.
Table 57: Withdrawals Due to Adverse Events
Events, n (%) | Study 102 (F/MF) | Study 103 (F/F) | Study 109 (F/F) | Study 104 (F/G and F/RF) | ||||
|---|---|---|---|---|---|---|---|---|
Placebo (N = 203) | ELX-TEZ-IVA (N = 200) | TEZ-IVA (N = 52) | ELX-TEZ-IVA (N = 55) | TEZ-IVA (N = 88) | ELX-TEZ-IVA (N = 87) | Control (N = 126) | ELX-TEZ-IVA (N = 132) | |
Any WDAE | 0 | 2 (1.0) | 0 | 0 | 2 (2.3) | 1 (1.1) | 2 (1.6) | 1 (0.8) |
Infections and infestations | 0 | 0 | 0 | 0 | 0 | 0 | 1 (0.8) | 0 |
Infective PEx of CF | 0 | 0 | 0 | 0 | 0 | 0 | 1 (0.8) | 0 |
Hepatobiliary disorders | 0 | 1 (0.5) | 0 | 0 | 0 | 0 | 0 | 0 |
Portal hypertension | 0 | 1 (0.5) | 0 | 0 | 0 | 0 | 0 | 0 |
Skin and subcutaneous tissue disorders | 0 | 1 (0.5) | 0 | 0 | 0 | 0 | 0 | 0 |
Rash | 0 | 1 (0.5) | 0 | 0 | 0 | 0 | 0 | 0 |
Investigations | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 1 (0.8) |
Increased ALT | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 1 (0.8) |
Increased AST | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 1 (0.8) |
Psychiatric disorders | 0 | 0 | 0 | 0 | 2 (2.3) | 1 (1.1) | 1 (0.8) | 0 |
Anxiety | 0 | 0 | 0 | 0 | 0 | 1 (1.1) | 1 (0.8) | 0 |
Depression | 0 | 0 | 0 | 0 | 0 | 1 (1.1) | 1 (0.8) | 0 |
OCD | 0 | 0 | 0 | 0 | 1 (1.1) | 0 | 0 | 0 |
Psychotic disorder | 0 | 0 | 0 | 0 | 1 (1.1) | 0 | 0 | 0 |
ALT = alanine transaminase; AST = aspartate transaminase; CF = cystic fibrosis; ELX-TEZ-IVA = elexacaftor-tezacaftor-ivacaftor and ivacaftor; F/F = homozygous for F508del mutation in the CFTR gene; F/G = 1 F508del mutation and 1 gating mutation in the CFTR gene; F/MF = 1 F508del mutation and 1 minimal function mutation in the CFTR gene; F/RF = 1 F508del mutation and 1 residual function mutation in the CFTR gene; OCD = obsessive-compulsive disorder; PEx = pulmonary exacerbation; TEZ-IVA = tezacaftor-ivacaftor and ivacaftor.
Interruptions Due to Adverse Events
Patients Aged 6 to 11 Years
In Study 116, a total of 7 patients (11.7%) in the ELX-TEZ-IVA group interrupted the study drug due to an AE. The AEs that led to treatment interruption that occurred in 2 or more patients were increased ALT and AST levels. No patients in the placebo group had AEs that led to treatment interruption. In Study 106, 1 patient (6.3%) in Part A had an AE of maculopapular rash that led to treatment interruption and 1 patient (1.5%) in Part B had AEs of diarrhea, vomiting, and pyrexia that led to treatment interruption.3,4
Patients Aged 12 Years and Older
Patients With F/MF Genotype: In Study 102, AEs leading to treatment interruption were reported for 10 patients (5.0%) in the placebo group and 19 patients (9.4) in the ELX-TEZ-IVA group.
Patients With F/F Genotype: There were no treatment interruptions due to AEs reported in either the TEZ-IVA or ELX-TEZ-IVA groups in Study 103. In Study 109, treatment interruptions due to AEs were reported for 1 patient (1.1%) in the TEZ-IVA group and 2 patients (2.3%) in the ELX-TEZ-IVA group.
Patients With F/G and F/RF Genotypes: In Study 104, AEs leading to treatment interruption were reported for 3 patients (2.4%) in the control group and 5 patients (3.8%) in the ELX-TEZ-IVA group.
Mortality
No deaths were reported in any of the included studies.5,6,10,11
Notable Harms
The sponsor identified elevated transaminase events and rash events as AEs of special interest in its analysis of safety data from the included studies.5,6,10,11 In consultation with clinical experts, CADTH has also included ophthalmological AEs as additional AEs of interest for this review.
Elevated Transaminase Adverse Events
Elevated transaminase events included any of the following: abnormal ALT, increased ALT, abnormal AST, increased AST, abnormal hepatic enzyme, increased hepatic enzyme, hypertransaminasemia, abnormal liver function test, increased liver function test, abnormal transaminases, and increased transaminases.5
Patients Aged 6 to 11 Years
Table 58 summarizes the elevated transaminase AEs in the pediatric studies. In Study 116, 6 patients (10.0%) in the ELX-TEZ-IVA group and 3 patients (4.9%) in the placebo group had at least 1 elevated transaminase event. All events were mild or moderate in severity. |||||| patients |||||| in the ELX-TEZ-IVA group interrupted the study drug due to elevated transaminase events. No subjects discontinued the study drug due to elevated transaminase events. In Study 106, a single patient (6.3%) in Part A with a history of increased liver function tests had a nonserious AE of increased transaminases 1 day after the last dose of study drug treatment. In Part B, 7 patients (10.6%) had elevated transaminase events. All of the events were mild or moderate in severity. None of the events were serious or led to treatment discontinuation or interruption.3,4
Table 58: Treatment Interruptions Due to Adverse Events
Events, n (%) | Study 102 (F/MF) | Study 103 (F/F) | Study 109 (F/F) | Study 104 (F/G and F/RF) | ||||
|---|---|---|---|---|---|---|---|---|
Placebo (N = 203) | ELX-TEZ-IVA (N = 200) | TEZ-IVA (N = 52) | ELX-TEZ-IVA (N = 55) | TEZ-IVA (N = 88) | ELX-TEZ-IVA (N = 87) | Control (N = 126) | ELX-TEZ-IVA (N = 132) | |
Any AEs leading to treatment interruption | 10 (5.0) | 19 (9.4) | 0 | 0 | 1 (1.1) | 2 (2.3) | 3 (2.4) | 5 (3.8) |
Skin and subcutaneous tissue disorders | 2 (1.0) | 4 (2.0) | 0 | 0 | 0 | 1 (1.1) | 1 (0.8) | 2 (1.5) |
Rash | 1 (0.5) | 3 (1.5) | 0 | 0 | 0 | 0 | 0 | 0 |
Pruritus | 0 | 1 (0.5) | 0 | 0 | 0 | 0 | 0 | 1 (0.8) |
Rash pruritic | 0 | 1 (0.5) | 0 | 0 | 0 | 0 | 0 | 0 |
Hypersensitivity vasculitis | 1 (0.5) | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
Rash macular | 0 | 0 | 0 | 0 | 0 | 1 (1.1) | 0 | 1 (0.8) |
Urticaria | 0 | 0 | 0 | 0 | 0 | 0 | 1 (0.8) | 0 |
Investigations | 3 (1.5) | 4 (2.0) | 0 | 0 | 1 (1.1) | 2 (2.3) | 1 (0.8) | 1 (0.8) |
Increased ALT | 2 (1.0) | 2 (1.0) | 0 | 0 | 0 | 2 (2.3) | 0 | 0 |
Increased AST | 1 (0.5) | 1 (0.5) | 0 | 0 | 0 | 1 (1.1) | 0 | 0 |
Increased conjugated bilirubin | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 1 (0.8) |
Increased blood bilirubin | 0 | 1 (0.5) | 0 | 0 | 1 (1.1) | 0 | 0 | 1 (0.8) |
Increased blood CPK | 0 | 1 (0.5) | 0 | 0 | 0 | 0 | 0 | 0 |
Increased blood creatinine | 1 (0.5) | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
Increased blood LDH | 0 | 0 | 0 | 0 | 0 | 1 (1.1) | 0 | 0 |
Increased CRP | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 1 (0.8) |
Increased liver function test | 0 | 0 | 0 | 0 | 0 | 0 | 1 (0.8) | 0 |
Infections and infestations | 1 (0.5) | 5 (2.5) | 0 | 0 | 0 | 0 | 0 | 0 |
Infective PEx of CF | 1 (0.5) | 2 (1.0) | 0 | 0 | 0 | 0 | 0 | 0 |
Influenza | 0 | 2 (1.0) | 0 | 0 | 0 | 0 | 0 | 0 |
Genital herpes simplex | 0 | 1 (0.5) | 0 | 0 | 0 | 0 | 0 | 0 |
Oral herpes | 0 | 1 (0.5) | 0 | 0 | 0 | 0 | 0 | 0 |
Musculoskeletal and connective tissue disorders | 1 (0.5) | 2 (1.0) | 0 | 0 | 0 | 0 | 0 | 0 |
Rhabdomyolysis | 0 | 2 (1.0) | 0 | 0 | 0 | 0 | 0 | 0 |
Back pain | 1 (0.5) | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
Blood and lymphatic system disorders | 0 | 0 | 0 | 0 | 0 | 1 (1.1) | 0 | 0 |
Thrombocytopenia | 0 | 0 | 0 | 0 | 0 | 1 (1.1) | 0 | 0 |
Ear and labyrinth disorders | 1 (0.5) | 0 | 0 | 0 | 0 | 0 | 0 | 1 (0.8) |
Tinnitus | 1 (0.5) | 0 | 0 | 0 | 0 | 0 | 0 | 1 (0.8) |
Gastrointestinal disorders | 0 | 2 (1.0) | 0 | 0 | 0 | 0 | 1 (0.8) | 1 (0.8) |
DIOS | 0 | 1 (0.5) | 0 | 0 | 0 | 0 | 0 | 0 |
Gastritis | 0 | 1 (0.5) | 0 | 0 | 0 | 0 | 1 (0.8) | 0 |
Small intestinal obstruction | 0 | 1 (0.5) | 0 | 0 | 0 | 0 | 0 | 0 |
Tongue ulceration | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 1 (0.8) |
Hepatobiliary disorders | 2 (1.0) | 2 (1.0) | 0 | 0 | 0 | 0 | 0 | 0 |
Cholangitis | 0 | 1 (0.5) | 0 | 0 | 0 | 0 | 0 | 0 |
Gallbladder enlargement | 0 | 1 (0.5) | 0 | 0 | 0 | 0 | 0 | 0 |
Hepatocellular injury | 1 (0.5) | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
Hypertransaminasemia | 1 (0.5) | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
Psychiatric disorders | 1 (0.5) | 1 (0.5) | 0 | 0 | 0 | 0 | 0 | 0 |
Emotional distress | 0 | 1 (0.5) | 0 | 0 | 0 | 0 | 0 | 0 |
Depression | 1 (0.5) | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
Intentional self-injury | 1 (0.5) | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
Suicidal ideation | 1 (0.5) | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
Respiratory, thoracic, and mediastinal disorders | 0 | 1 (0.5) | 0 | 0 | 0 | 0 | 0 | 0 |
Hemoptysis | 0 | 1 (0.5) | 0 | 0 | 0 | 0 | 0 | 0 |
AE = adverse event; ALT = alanine transaminase; AST = aspartate transaminase; CF = cystic fibrosis; CPK = creatine phosphokinase; CRP = C-reactive protein; DIOS = distal intestinal obstruction syndrome; ELX-TEZ-IVA = elexacaftor-tezacaftor-ivacaftor and ivacaftor; F/F = homozygous for F508del mutation in the CFTR gene; F/G = 1 F508del mutation and 1 gating mutation in the CFTR gene; F/MF = 1 F508del mutation and 1 minimal function mutation in the CFTR gene; F/RF = 1 F508del mutation and 1 residual function mutation in the CFTR gene; LDH = lactate dehydrogenase; PEx = pulmonary exacerbation; TEZ-IVA = tezacaftor-ivacaftor and ivacaftor.
Patients Aged 12 Years and Older
Patients With F/MF Genotype: In Study 102, 1 or more elevated transaminase events were reported for 10.9% of patients in the ELX-TEZ-IVA group compared with 4.0% in the placebo group.5 The majority of events were mild or moderate in severity. None of the events were considered serious in the ELX-TEZ-IVA group (1 serious event was reported in the placebo group). Events leading to treatment interruption were reported for 2 patients (1.0%) in the ELX-TEZ-IVA group and 3 patients (1.5%) in the placebo group. No events led to discontinuation of the study drug during the double-blind treatment period (1 patient in the ELX-TEZ-IVA who had their treatment interrupted eventually discontinued from the OLE without resuming treatment).5 The median time to onset of first elevated transaminase event was 57.0 days (range = 1 to 176) in the ELX-TEZ-IVA group and 58.0 days (range = 1 to 169) in the placebo group. The median duration of elevated transaminase events was 17.0 days (range = 4 to 153) in the ELX-TEZ-IVA group and 17.0 days (range = 5 to 52) in the placebo group.5 Additional relevant hepatic AEs were reported for 1.5% of patients in the ELX-TEZ-IVA group (hepatic cirrhosis, hepatocellular injury, and portal hypertension) and 0.5% in the placebo group (hepatocellular injury). None of the events in the ELX-TEZ-IVA group were considered serious.5
Patients With F/F Genotype: In Study 103, 1 or more elevated transaminase events were reported for 3.6% of patients in the ELX-TEZ-IVA group compared with 1.9% in the TEZ-IVA group.6 All of the events were mild in severity and none resulted in the interruption or discontinuation of the study drug. The median time to onset of first elevated transaminase event was 8.0 days (range = 1 to 15) in the ELX-TEZ-IVA group and the 1 event in the TEZ-IVA group occurred at day 30.6 The median duration of elevated transaminase events was 22.0 days (range = 15 to 29) in the ELX-TEZ-IVA group and the duration was not reported for the single event in the TEZ-IVA group.6
In Study 109, 1 or more elevated transaminase events were reported for 6.9% of patients in the ELX-TEZ-IVA group compared with 1.1% in the TEZ-IVA group. One patient in the ELX-TEZ-IVA group had an event that was considered serious (the single event in the TEZ-IVA was not serious). Events leading to treatment interruption were reported for 2 patients (2.3%) in the ELX-TEZ-IVA group and none in the TEZ-IVA group.10 No events led to discontinuation of the study drug during the double-blind treatment period. The median time to onset of first elevated transaminase event was 67.0 days (range = 12 to 169 days) in the ELX-TEZ-IVA group and the patient with events in the TEZ-IVA group was first reported at day 1. The median duration of elevated transaminase events was 16.5 days (range = 3 to 52) in the ELX-TEZ-IVA group and 25.0 (range = 7 to 43) in the TEZ-IVA group.10
Patients With F/G and F/RF Genotypes: In Study 104, 1 or more elevated transaminase events were reported for 6.1% of patients in the ELX-TEZ-IVA group compared with 0.8% in the control group.11 All of the events were mild or moderate in severity. One patient in the ELX-TEZ-IVA group discontinued the study drug because of elevated transaminases (ALT > 8 × ULN and AST > 5 × ULN). No patients in the control group discontinued the study drug due to transaminase elevations.11 No transaminase elevation events resulted in treatment interruption in the ELX-TEZ-IVA group and 1 event (0.8%) led to interruption in the control group. The median time to onset of first elevated transaminase event was 19.0 days (range = 4 to 29) in the ELX-TEZ-IVA group and the 1 event in the control group was reported at day 1. The median duration of elevated transaminase events was 19.0 days (range = 4 to 29) in the ELX-TEZ-IVA group and the 1 event in the control group had a duration of 16 days.11
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||||||||| | |
|---|---|---|---|
|||||||||||||||||||||||| | |||||||||||||||||||||||| | ||
|||||||||||||||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| |
|||||||||||||||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| | |||
|||||||||||||||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| |
|||||||||||||||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| |
ALT = alanine transaminase; AST = aspartate transaminase; ELX-TEZ-IVA = elexacaftor-tezacaftor-ivacaftor and ivacaftor; F/F = homozygous for F508del mutation in the CFTR gene; F/MF = 1 F508del mutation and 1 minimal function mutation in the CFTR gene; max. = maximum; TEZ-IVA = tezacaftor-ivacaftor and ivacaftor.
Note: Redacted rows have been deleted.
Source: Clinical Study Reports.3,4
Rash Adverse Events
Rash events were defined as any 1 of 48 different AEs, including rash, urticaria, dermatitis, and erythema.5
Patients Aged 6 to 11 Years
Table 60 summarizes the rash AEs in the pediatric studies. In Study 116, 8 patients (13.3%) in the ELX-TEZ-IVA group and 3 patients (4.9%) in the placebo group had a least 1 rash event. The majority of events were mild or moderate in severity. A single patient (1.7%) in the ELX-TEZ-IVA group had a rash event that led to treatment discontinuation. Two patients (3.3%) in the ELX-TEZ-IVA group interrupted the study drug due to rash events; both successfully resumed the study drug without recurrence of rash. No subjects in the placebo group had rash events that led to treatment discontinuation or interruption. In Study 106 Part A, 5 patients (31.3%) had a total of 6 rash events. All events were mild in severity. One patient had an AE of maculopapular rash that led to study drug interruption. In Part B, 16 patients (24.2%) subjects had at least 1 rash event. All rash events were mild or moderate in severity. One patient had a rash event that led to treatment discontinuation.3,4
Table 60: Elevated Transaminase Adverse Events in Adolescent and Adult Patients
Elevated transaminase adverse events, n (%) | Study 102 (F/MF) | Study 103 (F/F) | Study 109 (F/F) | Study 104 (F/G and F/RF) | ||||
|---|---|---|---|---|---|---|---|---|
Placebo (N = 203) | ELX-TEZ-IVA (N = 200) | TEZ-IVA (N = 52) | ELX-TEZ-IVA (N = 55) | TEZ-IVA (N = 88) | ELX-TEZ-IVA (N = 87) | Control (N = 126) | ELX-TEZ-IVA (N = 132) | |
Any events | 8 (4.0) | 22 (10.9) | 1 (1.9) | 2 (3.6) | 1 (1.1) | 6 (6.9) | 1 (0.8) | 8 (6.1) |
ALT increased | 7 (3.5) | 20 (9.9) | 0 | 1 (1.8) | 1 (1.1) | 6 (6.9) | 0 | 8 (6.1) |
AST increased | 4 (2.0) | 19 (9.4) | 1(1.9) | 1 (1.8) | 0 | 5 (5.7) | 0 | 8 (6.1) |
Hypertransaminasemia | 1 (0.5) | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
Increased transaminases | 0 | 0 | 0 | 1 (1.8) | 0 | 0 | 0 | 0 |
Increased liver function test | 0 | 0 | 0 | 0 | 0 | 0 | 1 (0.8) | 0 |
Events by maximum severity | ||||||||
Mild | 4 (2.0) | 12 (5.9) | (1.9) | 2 (3.6) | 1 (1.1) | 2 (2.3) | 1 (0.8) | 5 (3.8) |
Moderate | 4 (2.0) | 8 (4.0) | 0 | 0 | 0 | 4 (4.6) | 0 | 2 (1.5) |
Severe | 0 | 2 (1.0) | 0 | 0 | 0 | 0 | 0 | 1 (0.8) |
Life-threatening | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
Missing | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
Events leading to discontinuation | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 1 (0.8) |
Events leading to interruption | 3 (1.5) | 2 (1.0) | 0 | 0 | 0 | 2 (2.3) | 1 (0.8) | 0 |
Serious events | 1 (0.5) | 0 | 0 | 0 | 0 | 1 (1.1) | 0 | 0 |
Events leading to death | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
ALT = alanine transaminase; AST = aspartate transaminase; ELX-TEZ-IVA = elexacaftor-tezacaftor-ivacaftor and ivacaftor; F/F = homozygous for F508del mutation in the CFTR gene; F/G = 1 F508del mutation and 1 gating mutation in the CFTR gene; F/MF = 1 F508del mutation and 1 minimal function mutation in the CFTR gene; F/RF = 1 F508del mutation and 1 residual function mutation in the CFTR gene; TEZ-IVA = tezacaftor-ivacaftor and ivacaftor.
Table 61: Rash Adverse Events in Pediatric Patients
Rash adverse events, n (%) | Study 116 | Study 106 Part B (N = 66) | |
|---|---|---|---|
Placebo (N = 61) | ELX-TEZ-IVA (N = 60) | ||
Any rash events, n (%) | 3 (4.9) | 8 (13.3) | 16 (24.2) |
Rash | 3 (4.9) | 6 (10.0) | 8 (12.1) |
Maculopapular rash | 0 | 2 (3.3) | 2 (3.0) |
Erythematous rash | 0 | 0 | 3 (4.5) |
Papular rash | 0 | 0 | 2 (3.0) |
Skin exfoliation | 0 | 0 | 1 (1.5) |
Urticaria | 0 | 0 | 1 (1.5) |
Events by maximum severity | |||
Mild | 3 (4.9) | 3 (5.0) | 13 (19.7) |
Moderate | 0 | 3 (5.0) | 3 (4.5) |
Severe | 0 | 2 (3.3) | 0 |
Life-threatening | 0 | 0 | 0 |
Missing | 0 | 1 (1.7) | 0 |
Events leading to discontinuation | 0 | 1 (1.7) | 1 (1.5) |
Events leading to interruption | 0 | 2 (3.3) | 0 |
Serious events | 0 | 0 | 0 |
ELX-TEZ-IVA = elexacaftor-tezacaftor-ivacaftor and ivacaftor.
Patients Aged 12 Years and Older
Patients With F/MF Genotype: In Study 102, 1 or more rash AEs were reported for 10.9% of patients in the ELX-TEZ-IVA group compared with 6.5% in the placebo group.5 The majority of events were mild or moderate in severity; 3 patients (1.5%) in the ELX-TEZ-IVA group had events that were considered serious (rash [n = 2] and rash pruritic [n = 1]) and 1 patient (0.5%) had a serious rash event in the placebo group. Events leading to treatment interruption were reported for 4 patients (2.0%) in the ELX-TEZ-IVA group and 1 patient (0.5%) in the placebo group.5 One patient in the ELX-TEZ-IVA group and no patients in the placebo group discontinued the treatment due to a rash AE. The median time to onset of first rash event was 13.5 days (range = 5 to 157) in the ELX-TEZ-IVA group and 27.0 days (range = 1 to 157) in the placebo group. The median duration of rash events was 7.0 days (range = 1 to 92) in the ELX-TEZ-IVA group and 8.0 days (range = 2 to 61) in the placebo group.5
Patients With F/F Genotype: In Study 103, 1 or more rash AEs were reported for 3.6% of patients in the ELX-TEZ-IVA group compared with 3.8% in the TEZ-IVA group. One event in the ELX-TEZ-IVA group was considered serious and none were reported in the TEZ-IVA group. No rash events led to study drug interruption or discontinuation.6 The median time to onset of the first rash event was 10.5 days (range = 10 to 11) in the ELX-TEZ-IVA group and 20.5 days (range = 14 to 27) in the TEZ-IVA group. The median duration of rash events was 7.0 days (range = 1 to 13) in the ELX-TEZ-IVA group and was not reported for the TEZ-IVA group.6
In Study 109, 1 or more rash AEs were reported for 12.6% of patients in the ELX-TEZ-IVA group compared with 2.3% in the TEZ-IVA group. All the events were mild or moderate in severity. Events leading to treatment interruption were reported for 1 patient (1.1%) in the ELX-TEZ-IVA group and none were reported in the TEZ-IVA group.10 No events led to discontinuation of the study drugs during the double-blind treatment period. The median time to onset of first rash adverse event was 42.5 days (range = 2 to 138 days) in the ELX-TEZ-IVA group and 31.5 (range = 8 to 55) in the TEZ-IVA group. The median duration of elevated transaminase events was 10.0 days (range = 1 to 135) in the ELX-TEZ-IVA group and 2.0 (range = 1 to 3) in the TEZ-IVA group.10
Patients With F/G and F/RF Genotypes: In Study 104, 1 or more rash AEs were reported for 3.0% of patients in the ELX-TEZ-IVA group compared with 4.0% in the control group. All the events were mild or moderate in severity. Events leading to treatment interruption were reported for 1 patient (0.8%) in the ELX-TEZ-IVA group and 1 patient (0.8%) in the TEZ-IVA group. No events led to discontinuation of the study treatments. The median time to onset of the first rash event was 27.5 days (range = 10 to 38) in the ELX-TEZ-IVA group and 13.0 days (range = 5 to 47) in the TEZ-IVA group. The median duration of rash events was 5.5 days (range = 3 to 10) in the ELX-TEZ-IVA group and 10.0 days (range = 3 to 51) in the TEZ-IVA group.5
Table 62: Rash Adverse Events in Adolescent and Adult Patients
Rash adverse events, n (%) | Study 102 (F/MF) | Study 103 (F/F) | Study 109 (F/F) | Study 104 (F/G and F/RF) | ||||
|---|---|---|---|---|---|---|---|---|
Placebo (N = 203) | ELX-TEZ-IVA (N = 200) | TEZ-IVA (N = 52) | ELX-TEZ-IVA (N = 55) | TEZ-IVA (N = 88) | ELX-TEZ-IVA (N = 87) | Control (N = 126) | ELX-TEZ-IVA (N = 132) | |
Any rash events | 13 (6.5) | 22 (10.9) | 2 (3.8) | 2 (3.6) | 2 (2.3) | 11 (12.6) | 5 (4.0) | 4 (3.0) |
Dermatitis allergic | 0 | 1 (0.5) | 0 | 0 | 0 | 0 | 0 | 0 |
Drug hypersensitivity | 1 (0.5) | 0 | 0 | 0 | 0 | 1 (1.1) | 0 | 0 |
Rash | 9 (4.5) | 18 (8.9) | 2 (3.8) | 2 (3.6) | 0 | 7 (8.0) | 2 (1.6) | 2 (1.5) |
Erythematous rash | 1 (0.5) | 0 | 0 | 0 | 0 | 1 (1.1) | 0 | 0 |
Generalized rash | 0 | 2 (1.0) | 0 | 0 | 0 | 0 | 0 | 0 |
Macular rash | 0 | 1 (0.5) | 0 | 0 | 0 | 1 (1.1) | 1 (0.8) | 1 (0.8) |
Pruritic rash | 0 | 1 (0.5) | 0 | 0 | 0 | 0 | 0 | 1 (0.8) |
Urticaria | 3 (1.5) | 1 (0.5) | 0 | 0 | 2 (2.3) | 0 | 1 (0.8) | 0 |
Perioral dermatitis | 0 | 0 | 0 | 0 | 0 | 1 (1.1) | 0 | 0 |
Pustular rash | 0 | 0 | 0 | 0 | 0 | 0 | 1 (0.8) | 0 |
Events by maximum severity | ||||||||
Mild | 10 (5.0) | 17 (8.4) | 2 (3.8) | 2 (3.6) | 2 (2.3) | 8 (9.2) | 4 (3.2) | 2 (1.5) |
Moderate | 3 (1.5) | 4 (2.0) | 0 | 0 | 0 | 3 (3.4) | 1 (0.8) | 2 (1.5) |
Severe | 0 | 1 (0.5) | 0 | 0 | 0 | 0 | 0 | 0 |
Life-threatening | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
Missing | NR | NR | 0 | 0 | 0 | 0 | 0 | 0 |
Events leading to discontinuation | 0 | 1 (0.5) | 0 | 0 | 0 | 0 | 0 | 0 |
Events leading to interruption | 1 (0.5) | 4 (2.0) | 0 | 0 | 0 | 1 (1.1) | 1 (0.8) | 1 (0.8) |
Serious events | 1 (0.5) | 3 (1.5) | 0 | 1 (1.8) | 0 | 0 | 0 | 0 |
Events leading to death | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
ELX-TEZ-IVA = elexacaftor-tezacaftor-ivacaftor and ivacaftor; F/F = homozygous for F508del mutation in the CFTR gene; F/G = 1 F508del mutation and 1 gating mutation in the CFTR gene; F/MF = 1 F508del mutation and 1 minimal function mutation in the CFTR gene; F/RF = 1 F508del mutation and 1 residual function mutation in the CFTR gene; NR = not reported; TEZ-IVA = tezacaftor-ivacaftor and ivacaftor.
Ophthalmological Adverse Events
Patients Aged 6 to 11 Years
No patients in Study 116 or Study 106 had AEs of cataracts or lens opacity.3,4
Patients Aged 12 Years and Older
Patients With F/MF Genotype: In Study 102, ophthalmologic exams were performed at screening and at the week 24 study visit for patients younger than 18 years of age. Treatment-emergent cataracts were reported for 1 patient in both the ELX-TEZ-IVA and placebo groups (0.5% in both groups). Both events were mild in severity and did not require treatment or lead to interruption or discontinuation of the study drug.5
Patients With F/F Genotype: Ophthalmologic exams were performed for patients younger than 18 years of age at screening in both Study 103 and Study 109. Follow-up examinations were not required during the double-blind treatment periods of either study (only during the safety follow-up or enrolment in the OLE study).6,10 There were no treatment-emergent cataracts in Study 103.35 In Study 109, a single patient in both the ELX-TEZ-IVA and TEZ-IVA groups (1.1%) had AEs of cataracts. The events were mild in severity and did not require treatment.10
Patients With F/G and F/RF Genotypes: In Study 104, ophthalmologic exams were performed for patients younger than 18 years of age at screening and at the safety follow-up visit (i.e., no examinations took place during the double-blind treatment period). No treatment-emergent cataracts were reported in Study 104.
Critical Appraisal
Patients Aged 6 to 11 Years
Internal Validity
Randomization in Study 116 was performed using an appropriate methodology with adequate allocation concealment (i.e., an IWRS) and stratification based on relevant prognostic factors (i.e., baseline lung function [LCI2.5 < 10 versus ≥ 10] and baseline weight [< 30 kg versus ≥ 30 kg]). Baseline and demographic characteristics were generally well balanced across the ELX-TEZ-IVA and placebo groups in Study 116. A higher percentage of patients in the ELX-TEZ-IVA group had a baseline ppFEV1 of greater than 90% (|||||||||||||||||||||) and a lower proportion had a baseline ppFEV1 of less than 70% (||||||||||||||||||). As those with normal lung function (i.e., > 90%) would be less likely to demonstrate short-term improvements in ppFEV1 due to the ceiling effect, this could potentially bias the results for change in ppFEV1 through 24 weeks against ELX-TEZ-IVA. A greater proportion of patients in the ELX-TEZ-IIVA group reported prior use of inhaled antibiotics compared with the placebo group (||||||||||||||||||||||||). As has been noted in previous CADTH reviews of CFTR modulators, it is unclear if greater use of antibiotics at baseline would be correlated with an increased risk of an exacerbation (e.g., the antibiotics are provided to those who are at the greatest risk) or a decreased risk of an exacerbation (e.g., the concomitant use of antibiotics provides a protective effect that would lower the risk). The clinical experts consulted by CADTH indicated that there did not appear to be any differences across the treatment groups that would be clinically relevant.
The study treatments were administered in a double-blind manner in Study 116 and open-label in Study 106. Patients in both the ELX-TEZ-IVA and placebo groups in Study 116 were issued the same number of tablets each day (2 tablets in the morning and 1 in the evening). The ELX-TEZ-IVA and IVA tablets were identical in appearance to the comparator tablets (i.e., placebo and TEZ-IVA). The AE profile of ELX-TEZ-IVA and the comparators was unlikely to compromise blinding in the study. The only exceptions could be the increased percentage of patients who experienced a rash in the ELX-TEZ-IVA group, although this affected only a minority of patients (13.3% versus 4.9% in the comparator groups). The clinical experts noted that experience in practice has shown that adult patients treated with ELX-TEZ-IVA may exhibit an increase in productive cough shortly after initiating therapy, which could lead to some inference of treatment allocation in the study. The proportion of patients reporting a productive cough difference in Study 116 was similar in the ELX-TEZ-IVA and placebo groups of Study 116 (||||||||||||||||||||||||). Overall, the clinical experts consulted by CADTH indicated that the differences in AEs were unlikely to lead to unblinding in the trial.
Similar to the previously reviewed trials in adults and adolescents, few pediatric patients discontinued either Study 116 (99.2% completion) or Study 106 (100% completion for Part A and 97.0% completion for Part B). The studies were relatively short in duration, which may in part explain the high percentage of patients who completed. The full analysis sets included nearly all randomized patients.
Adherence to the study treatments was evaluated by counting the number of study drugs at each visit and was reported to be 99% across both Study 116 and Study 106. In accordance with the study protocols, the use of concomitant medications remained stable throughout the treatment period for all treatment groups.
There are no globally accepted definitions for pulmonary exacerbations in patients with CF. The definitions used in the included studies were considered to be appropriate by regulatory authorities and the clinical experts consulted by CADTH. There was no independent adjudication of pulmonary exacerbation events. Pulmonary exacerbations in pediatric patients were only evaluated as efficacy end points in the 24-week single-arm trial (Study 106B). The placebo-controlled trial (Study 116) only reported pulmonary exacerbations as AEs. In response to an inquiry from CADTH regarding why pulmonary exacerbations were not included as an efficacy end point, the sponsor reported that a treatment effect may have been difficult to detect in Study 116 given the relative rareness of these events in younger patients relative to older patients. The differences in pulmonary exacerbations reported as AEs in the placebo and ELX-TEZ-IVA groups (1.7% versus 26.2%, respectively) were considered clinically relevant by the experts consulted by CADTH.
Statistical power calculations were reported for both Study 106 and Study 116 and a sufficient number of patients were enrolled and completed both of the studies. The MMRM analyses for the primary evaluations assumed data were missing at random, which may not be a valid assumption. However, the amount of missing data in the trials was low.
Because the secondary end points were analyzed without statistical testing procedures to control the type I error rate, the results should be interpreted with caution due to the risk of inflated type I error.
External Validity
A greater proportion of the populations in Study 116 and Study 106 were female (57.9% and 59.1%, respectively), which is not reflective of the Canadian CF population, of which a majority of patients are male (53.4%); Canadian registry data have indicated that female patients with CF tend to have poorer long-term survival compared with males,1 but this is unlikely to affect the generalizability of the results of Study 116 and Study 106B, which were short-term trials (i.e., 24 weeks) conducted in children (as previously noted by the EMA in its review of LUM-IVA).80 Similar to the studies conducted in those 12 years of age and older, the majority of patients 6 to 11 years of age who were included in the studies were White and from North America. The clinical experts consulted by CADTH indicated that the study populations were similar to the target population in Canada.
The diagnostic criteria used to screen patients for Study 116 and Study 106 were identical to those used in Study 102, Study 103, and Study 109 for those 12 years of age and older. As noted in the previous CADTH review of ELX-TEZ-IVA, these criteria are consistent with Canadian clinical practice for diagnosing patients with CF who are homozygous for the F508del-CFTR mutation. As noted for the trials in adolescent and adult patients, the term “minimal function” is not currently used in Canadian clinical practice.
Enrolment in Study 116 was limited to patients with a ppFEV1 of 70% or greater at screening; it was therefore more restrictive than the 40% threshold that was used in Study 106B and in the included trials for those 12 years and older (i.e., Study 102, Study 103, Study 104, and Study 109). The ppFEV1 threshold for inclusion in Study 116 of 70% or greater is identical to those of the phase III pediatric studies that were conducted for other combinations of CFTR modulators (i.e., Study 109 for LUM-IVA and Study 115 for TEZ-IVA).81,82
Clinical experts consulted by CADTH indicated that the exclusion of patients with a ppFEV1 of less than 70% does not affect the generalizability of Study 116, as these patients are uncommon in the Canadian pediatric CF population. Data from the Canadian Cystic Fibrosis Registry (2019) indicate that 58.9% of Canadian children with CF (ages 6 to 17 years) have normal lung function (i.e., ppFEV1 ≥ 90%).1 The median ppFEV1 of 91.7% and 89.3% in Studies 116 and 106B, respectively, is similar to the median ppFEV1 reported for pediatric patients with CF in Canada (93.4% in 2019).
Both Study 116 and Study 106B specified that patients were required to have an LCI2.5 of at least 7.5 to be eligible. As this measurement is not currently used in routine Canadian clinical practice, the generalizability of the inclusion criteria based on this specific threshold is uncertain. However, the clinical experts consulted by CADTH suggested that, overall, and based on other baseline characteristics, the study population is reflective of Canadian pediatric patients with CF.
Study 106B also included a range of outcomes that are important to patients with CF based on patient group input: respiratory function (i.e., LCI and ppFEV1), nutritional status and growth (e.g., weight, height, and BMI), health-related quality of life (CFQ-R), and clinical events (e.g., pulmonary exacerbations). The primary efficacy end point in Study 116 (LCI2.5) differed from that used in the trials of adolescents and adult trials (ppFEV1). This is reflective of regulatory guidance, which notes that spirometry may not be sensitive enough to detect treatment differences in children with cystic fibrosis. Younger patients with CF may demonstrate spirometry values that are within the normal range, but there may be underlying structural deficiencies within the lungs that can be detected using alternative evaluations (e.g., LCI).71,80 Although LCI is used as an end point in clinical studies, it is not routinely used in Canadian clinical practice and the clinical relevance of differences in this end point have not be characterized.80,83 The clinical experts consulted by CADTH indicated that LCI is not reliably correlated with FEV1. A literature review conducted by CADTH found that variable correlation was observed between FEV1 and LCI in children (Appendix 5).
Pulmonary exacerbations were only reported as AEs in Study 116. The clinical experts consulted by CADTH noted that the proportion of patients who reported 1 or more pulmonary exacerbations in the placebo group (26.2%) over the 24-week study period was a reasonable reflection of the rates that would be anticipated in Canada for pediatric patients with CF who are not receiving treatment with a CFTR modulator.
In Study 116, the placebo group demonstrated an LS mean decrease in ppFEV1 of 1.5%. Data from the Canadian Cystic Fibrosis Registry (2013) suggested that, because patients with CF undergo a decline in lung function of 0.2% per year between the ages of 6 and 11 years,31 the decrease of 1.5% at 24 weeks reported for the placebo group of Study 116 may not be reflective of Canadian patients. The clinical experts consulted by CADTH suggested that this would not be reflective of the decline expected in Canadian patients and could be due to challenges performing the FEV1 measurement in a younger patient population. The limitations of spirometry testing in younger children with relatively normal lung function have been documented by regulatory authorities71 and were an important consideration in sponsor’s decision to use LCI2.5 as the primary end point in the clinical development programs for CFTR modulators in pediatric patients.83
Similar to the ELX-TEZ-IVA trials in patients 12 years and older, Study 116 and Study 106B excluded patients with a history of colonization with Burkholderia cenocepacia, Burkholderia dolosa, and/or Mycobacterium abscessus. CF Canada reports that a small minority of patients in Canada were reported to have colonization with Burkholder species (3.7% in 2019), with only 12.3% of those cases reported in children.1 The clinical experts consulted by CADTH noted that the exclusion of such patients does not significantly reduce the generalizability of the study results.
The proportion of patients in Study 106B who were positive for Pseudomonas aeruginosa was 39%, which is close to the rate reported in the overall Canadian CF population (37% in 2016), but greater than the 20% infection rate reported for children aged 6 to 10 years in the 2019 CF Canada registry. This information was not captured for Study 116. The clinical experts consulted by CADTH noted that the rate of P. aeruginosa infection in Study 106B likely exceeds the rate in Canadian pediatric patients with CF, which may be due to the aggressive treatment pursued in Canada to eradicate P. aeruginosa infection once detected.
Similar to the phase III studies for CFTR modulators, including those for ELX-TEZ-IVA patients aged 12 years and older, Study 116 and Study 106B excluded patients who had a respiratory infection, pulmonary exacerbation, or changes in their therapy for pulmonary disease within 4 weeks before the first dose of study drug. According to the previous CADTH review of ELX-TEZ-IVA,84 the clinical experts consulted by CADTH noted that the exclusion of these patients is unlikely to limit the generalizability of the results to the broader population of patients with CF.
The use of placebo as a comparator in Study 116 is appropriate as no other CFTR modulators are currently approved in Canada for use in the treatment of patients with CF aged 6 to 11 and an F/MF genotype. The absence of a control group in Study 106B limits the ability to interpret the results of the study.
In both studies, ELX-TEZ-IVA (or matching placebo in Study 116) was added to the existing therapeutic regimens used by the patients, which is reflective of how ELX-TEZ-IVA would be administered in clinical practice. The clinical experts consulted by CADTH indicated that the background therapies used in Study 116 and Study 106B were reasonably reflective of the Canadian CF population. The exceptions were dornase alfa (used by 68.6% and 81.8% in Study 116 and 106B, respectively), which exceeded expected use in Canada (approximately 35% of children in 2019)1; and inhaled antibiotics (used by 19.0% and 12.1% in Study 116 and 106B, respectively) which is lower than the anticipated use in Canada (e.g., approximately 60% of children with CF used inhaled tobramycin in 2019).1 The clinical experts noted that this difference is unlikely to limit the generalizability of the study results.
The 24-week study treatment periods were sufficient for observing treatment differences in the primary end points of Study 116; however, the duration was too short to determine whether treatment with ELX-TEZ-IVA has the potential to modify the course of disease for patients with CF. In addition, the clinical experts consulted by CADTH suggested that 24 weeks is not likely enough time to observe meaningful changes in BMI, particularly in a younger patient population that is relatively healthy.
Patients in Study 116 and Study 106B received extensive contact with health professionals over the 28-week study periods (i.e., 7 clinic visits and 2 or 3 phone contacts). This level of contact is not reflective of routine care for patients with CF and relatively stable disease.
Table 63: Assessment of Generalizability of Evidence from Pediatric Studies
Domain | Factor | Evidence | CADTH's assessment of generalizability |
|---|---|---|---|
Population | Age | The included trials enrolled patients between the ages of 6 and 11 years. | This is reflective of the expanded indication under review by CADTH. |
Severity of disease | Patients with CF and moderate or severe lung disease (e.g., ppFEV1 < 70% at screening) were excluded from Study 116. | Th clinical experts consulted by CADTH indicated that the exclusion of patients with a ppFEV1 of less than 70% does not affect the generalizability of Study 116, as these patients are uncommon in the Canadian pediatric CF population. | |
Burkholderia cepacia complex | The studies excluded patients with a history of colonization with B. cenocepacia, B. dolosa, and/or Mycobacterium abscessus. | The clinical experts consulted by CADTH noted that the exclusion of such patients does not significantly lower the generalizability of the study results, given that these patients represent a small minority of those who could be eligible for ELX-TEZ-IVA and that the clinical management of such patients is more complex and variable. | |
Race | The study populations comprised almost exclusively White patients. | This is reflective of most patients with CF in Canada, although the percentage is slightly higher than the percentage reported for the overall CF population in Canada (93.2% in 2019). | |
Intervention | ELX-TEZ-IVA | All the included studies investigated the use of ELX-TEZ-IVA at the dosage recommended in the product monograph. | This is reflective of how ELX-TEZ-IVA would be used in clinical practice. |
Concomitant medications | Concomitant medications for CF are reported in Table 26 for the pediatric clinical studies. | Concomitant medications were generally consistent with those used in Canadian clinical practice, except for dornase alfa and inhaled antibiotics. | |
Comparator | Placebo | Placebo was the comparator in Study 116. | The use of placebo as the comparator in Study 116 is appropriate as there are no drugs currently approved for use in the treatment of patients with CF aged 6 to 11 with CF an F/MF genotype. |
Outcomes | Lung clearance index | The primary efficacy end point in Study 116 was change from baseline in LCI2.5. | Although LCI is used as an end point in clinical studies, it is not routinely used in Canadian clinical practice and the clinical relevance of differences in this end point has not been characterized. |
ppFEV1 | ppFEV1 was included as a secondary end point in the pediatric clinical studies. | ppFEV1 declined by 1.5% over the 24-week study period in the placebo group. This likely exceeds the rate of decline that would be anticipated in a typical Canadian patients with CF between 6 and 11 years of age. | |
Pulmonary exacerbations | Pulmonary exacerbations were only reported as adverse events in Study 116. | The clinical experts consulted by CADTH noted that the proportion of patients who reported 1 or more pulmonary exacerbations in the placebo group (26.2%) over the 24-week study period was a reasonable reflection of the rates that would be anticipated in Canada for pediatric patients with CF who are not receiving treatment with a CFTR modulator. | |
Setting | Clinics | The included RCTs were conducted at specialized CF clinics. | This is consistent with Canadian clinical practice where patients are managed in specialized CF clinics. |
Locations and Canadian sites | Most patients in Study 104 were from Europe and Study 109 was conducted exclusively in Europe and Australia. | The clinical experts consulted by CADTH noted that the results from the studies in Europe and Australia would likely be generalizable to the Canadian setting. | |
Contact with health care professionals | Patients in Studies 116 and 106B received extensive contact with health professionals over the 28-week study periods (i.e., 7 clinic visits and 2 or 3 phone contacts). This level of contact is not reflective of routine care for patients with CF and relatively stable disease. | This level of contact is not reflective of routine care for patients with CF with relatively stable disease. Patients with stable disease would typically been seen 4 times per year (reduced to 3 times per year during the COVID-19 pandemic). |
CF = cystic fibrosis; F/MF = 1 F508del mutation and 1 minimal function mutation in the CFTR gene; LCI = lung clearance index; ppFEV1 = percent predicted forced expiratory volume in 1 second; RCT = randomized controlled trial.
Patients Aged 12 Years and Older
Internal Validity
Randomization was performed using an appropriate methodology with adequate allocation concealment (i.e., interactive web response system) and stratification based on relevant prognostic factors (i.e., age, sex, baseline ppFEV1, and [in Study 104] prior CFTR-modulator usage).5,6,10,11 Baseline and demographic characteristics were generally well balanced across the treatments of each of the studies. The only exceptions were differences between some CF therapies at baseline and infection with Pseudomonas aeruginosa within 2 years of screening. In Study 102 and 103, a greater percentage of patients in ELX-TEZ-IVA group were reported to have infection with P. aeruginosa within 2 years of screening compared with the comparator groups (75.0% versus 70.0% and 70.9% versus 59.6% in Study 102 and Study 103, respectively).5,6 The clinical experts consulted by CADTH noted that this difference is unlikely to be clinically relevant. Similarly, the reviewers for the EMA and FDA concluded that the demographic and baseline characteristics were balanced between the treatment groups of Study 102 and Study 103.35,59
The percentage of patients using inhaled hypertonic saline relative to the comparator groups was greater in the ELX-TEZ-IVA group in Study 102 (73.5% versus 62.6%, respectively) but lower in the ELX-TEZ-IVA group in Study 103 (78.8% versus 69.1%, respectively).5,6 In Study 104, a greater percentage of patients in the TEZ-IVA group relative to the comparator groups reported prior use of dornase alfa (81.8% versus 71.3%, respectively) and inhaled hypertonic saline (64.8% versus 58.6%, respectively).11 It is possible that the treatment groups could be favoured with greater use in the respiratory end points, but these patients may have had more-severe disease that required additional treatment, and any potential impact of these imbalances is uncertain. The clinical experts consulted by CADTH noted that the differences are unlikely to be clinically relevant. Differences were also noted in Study 103 and Study 104 regarding baseline use of antibiotics in the treatment of CF. Greater proportions of patients in the ELX-TEZ-IVA group of Study 103 compared with the TEZ-IVA group reported using azithromycin (60.0% versus 48.1%, respectively) and inhaled antibiotics (63.6% versus 53.8, respectively).6 Conversely, fewer ELX-TEZ-IVA–treated patients reported prior use of inhaled antibiotics compared with those in the placebo group (44.4% versus 37.1%, respectively).6 As has been noted in previous CADTH reviews of CFTR modulators, it is unclear if greater use of antibiotics at baseline would be correlated with an increased risk of an exacerbation (e.g., when the antibiotics are provided to those who are at the greatest risk) or a decreased risk of an exacerbation (e.g., when the concomitant use of antibiotics provides a protective effect that would lower the risk).83 Reviewers for the FDA noted that the handling of concomitant and prohibited medications was reasonable in the pivotal trials.35
Study treatments were administered in a double-blind manner, with all groups issued the same number of tablets each day (3 tablets in Study 102 and 4 tablets in Study 103, Study 104, and Study 109).5,6,10,11 The ELX-TEZ-IVA and IVA tablets were identical in appearance to the comparator tablets (i.e., placebo and TEZ-IVA). The AE profile of ELX-TEZ-IVA and the comparators was unlikely to compromise blinding in the study. The only exceptions could be the increased percentage of patients who experienced a rash in the ELX-TEZ-IVA groups of the 2 24-week trials, although this only affected a minority of patients (8.9% versus 4.5% for the comparator group, in Study 103 and 8.0% versus 0%, respectively, in Study 109).6,11 The clinical experts consulted by CADTH noted that these events were unlikely to lead to unblinding. Reviewers for the FDA noted that the methods for blinding in the pivotal trials were acceptable.35
Patient disposition was thoroughly documented and well reported by the sponsor in its application to CADTH. Few patients discontinued the trials (the completion rate ranged from 96.8% to 100%), although the studies were relatively short in duration, which may in part explain the high percentage of patients who completed.5,6,10,11 The full analysis sets included nearly all randomized patients. Reviewers for the EMA noted that the amount of missing data in the pivotal studies was minimal and not a concern.59
Adherence to the study treatments was evaluated by counting the number of study drugs at each visit and was reported to be greater than 99% across all treatment groups in Study 102, Study 103, Study 104, and Study 109.5,6,10,11 In accordance with the study protocols, the use of concomitant medications remained stable throughout the treatment period for all treatment groups. The only exceptions were the lower use of some antibiotics for pulmonary exacerbations in the ELX-TEZ-IVA group relative to the placebo group in Study 102.5 Reviewers for the EMA noted that this difference was a consequence of the efficacy of ELX-TEZ-IVA for reducing pulmonary exacerbations relative to placebo.59
There are no globally accepted definitions for pulmonary exacerbations in patients with CF. The definitions used in the included studies were considered to be appropriate by regulatory authorities and the clinical experts consulted by CADTH.35,59 There was no independent adjudication of pulmonary exacerbation events. As shown in Table 3, when evaluated as an efficacy end point, fewer patients in Study 102 met the criteria for a pulmonary exacerbation compared to the number of events reported as AEs (e.g., 37% versus 47% in the placebo group).5 Pulmonary exacerbations were only evaluated as efficacy end points in the 24-week placebo-controlled trial (Study 102).5 In response to an inquiry from CADTH, the sponsor reported that pulmonary exacerbations were not included in the active-controlled trials because the studies would not have the power to detect a difference in pulmonary exacerbations between ELX-TEZ-IVA and the active comparators.68 As both TEZ-IVA and IVA have been shown to reduce the frequency of pulmonary exacerbations in previous placebo-controlled trials with patients who have F/F, F/RF, or F/G genotypes, the sponsor noted that a prohibitively large number of patients would be required to sufficiently power the studies to detect a statistically significant reduction in pulmonary exacerbations.68
Statistical power calculations were reported for all of the included studies and a sufficient number of patients were enrolled and completed the studies.5,6,10,11 The number of withdrawals from the trials was well below the 5% or 10% proportion assumed in the sponsor’s statistical power calculations. The MMRM analyses for the primary evaluations assumed data were missing at random, which may not be a valid assumption. However, the amount of missing data in the trials was low and sensitivity analyses using multiple imputation were supportive of the primary analyses. Similarly, reviewers for the FDA and EMA noted that the amount of missing data was low in the pivotal trials and did not raise any concerns regarding the statistical approaches used by the sponsor.35,59
The primary end point in Study 102 was the absolute change from baseline in ppFEV1 to 4 weeks in the global protocol through 24 weeks in the European protocol.5 The rationale for this difference in protocols was due to guidance from the EMA on the clinical development of drugs for the treatment of CF which states that ppFEV1 should be evaluated after 24 weeks of treatment.85 As the global protocol involved the use of an interim analysis at 4 weeks, the sponsor included a multiplicity adjustment in the statistical analysis plan to control the overall type I error rate at 0.05 for the primary end point (using a Lan and DeMets alpha-spending function).5 The key secondary end points of all of the included studies were tested using a hierarchical approach to control the overall type I error rate at 0.05. All end points within the statistical testing hierarchies were statistically significant. Subgroup analyses and exploratory end points (e.g., TSQM, CFQ-R non-respiratory domains, and hospitalizations) were tested with adjustment for multiple comparisons, and all P values are considered nominal.
Study 103, Study 104, and Study 109 all included a 4-week run-in period during which patients received open-label treatment with TEZ-IVA (for those with F/F or F/RF genotypes) or IVA (for those with F/G genotypes).6,10,11 Reviewers for the EMA noted that the duration of the run-in period may have been too short to allow patients who were naive to CFTR-modulator therapy to fully realize the benefits of initiating therapy with TEZ-IVA or IVA at the time of the baseline assessment.59 As such, the treatment effects for ELX-TEZ-IVA may be overestimated in the overall study populations. As a result, the EMA requested that the results for the post hoc subgroup analysis of CFTR modulator–naive and –experienced patients be included in the summary of product characteristics for ELX-TEZ-IVA.59,86
External Validity
The diagnostic criteria used in the screening process for Study 103 and Study 109 were consistent with Canadian clinical practice for identifying patients with CF who are homozygous for the F508del-CFTR mutation. The gating and residual function mutations that were used to select patients for inclusion in Study 104 were consistent with the approved indications for TEZ-IVA and IVA in Canada.3,11,12 There were no widely accepted criteria for defining minimal function mutations in the CFTR gene; therefore, the identification of patients with minimal function mutations in Study 102 relied on a novel approach designed by the sponsor.5 Eligible mutations were identified as having 1 or more of the following characteristics: a genetic sequence that predicts no translated CFTR protein, mutations that lack in vitro responsiveness to TEZ, IVA, or TEZ-IVA, and evidence of clinical severity on a population level (average sweat chloride > 86 mmol/L, and a > 50% prevalence of pancreatic insufficiency).5 The majority of patients enrolled in Study 102 (314 of 403; 78%) had mutations that met the first criterion (i.e., no CFTR protein).59 Overall, the criteria used by the sponsor to identify patients with minimal function mutations in the CFTR gene were considered acceptable by the FDA reviewers.35 The clinical experts consulted by CADTH noted that terms “residual function” and “minimal function” are not currently used in Canadian clinical practice and that patients are not currently differentiated based on the presence of “residual function” or “minimal function” mutations.
Patients with CF with more-severe lung disease (e.g., ppFEV1 < 40%) or a normal ppFEV1 (≥ 90%) at screening were excluded from the studies.5,6,10,11 The results of the included studies are therefore primarily applicable to patients with moderate (i.e., a FEV1 of 40% to 69%) to mild (i.e., an FEV1 of 70% to 89%) lung disease. This is identical to the phase III trials conducted by the sponsor for other approved combination CFTR modulators (LUM-IVA and TEZ-IVA).87-93 The sponsor reported that this population was selected because it was considered to be the patient group most likely to show an improvement in lung function in a clinical trial based on its experience with other therapies targeting CF lung disease.64 These screening criteria resulted in trial populations for which the proportion of patients with mild lung disease was generally similar to the adult CF population in Canada (approximately 27% of patients had mild lung disease in 2019)1 in Study 102 (31.8%), Study 103 (29.9%), and Study 109 (31.4%), although the proportion of patients with mild disease was greater in Study 104 (40.7%).5,6,10,11 The proportion of patients with moderate lung disease in the included studies ranged from 51.6% in Study 104 to 60.7% in Study 103, which is greater than the proportions reported within the overall adult CF population in Canada (approximately 38% in 2019).1 A small minority of patients with a ppFEV1 of less than 40% at baseline were enrolled in the included studies (range = 1.6% in Study 104 to 9.3% in Study 103).5,6,10,11 These patients with lower lung function would have satisfied the study inclusion criteria in the screening phase, then have demonstrated a ppFEV1 of below 40% at their baseline evaluation. An ad hoc subgroup analysis in Study 102 provided some efficacy data for this small subgroup of patients and suggested that ELX-TEZ-IVA resulted in meaningful improvements relative to placebo.5 CADTH considered the results of additional clinical studies conducted to evaluate the use of ELX-TEZ-IVA in patients with CF who are having advanced lung disease, as discussed in the Patients With Advanced Lung Disease section).17,18
A majority of the participants were from North America in Study 102 (59%) and Study 103 (63%); however, the majority (51.9%) were from Europe in Study 104 (with 37.6% from North America), and Study 109 was conducted exclusively in Europe and Australia.5,6,10,11 The clinical experts consulted noted that the results from the studies in Europe and Australia would likely be generalizable to the Canadian setting. The included RCTs were conducted at specialized CF clinics.5,6,10,11 The clinical experts consulted by CADTH and the clinician groups who provided input indicated that this is consistent with Canadian clinical practice, where patients are managed in specialized CF clinics.
The study populations comprised almost exclusively White patients (e.g., 99% in Study 103 and Study 109),5,6,10,11 which is reflective of the majority of patients with CF in Canada, although the percentage is slightly higher than the proportion reported for the overall CF population in Canada (93.2% in 2019).1 Both Study 102 and Study 104 reported at least 90% of patients were White, but each had a large proportion of patients for whom these data were not collected in accordance with local regulations (6.2% and 7.0%, respectively).5,11
The Cystic Fibrosis Foundation clinical practice guidelines recommend that adult women and men (≥ 20 years of age) maintain a BMI at or above 22 kg/m2 and 23 kg/m2, respectively. Mean baseline BMI was similar in Study 102, Study 103, and Study 109 (range = 21.40 kg/m2 to 21.81 kg/m2)5,6,10; which is slightly below the estimated national median BMI for adult patients with CF (22.7 kg/m2) in Canada.1 In contrast, the mean baseline BMI was greater in Study 104 at 24.06 kg/m2 (23.33 kg/m2and 24.49 kg/m2for those with F/G and F/RF genotypes, respectively).11
The included studies excluded patients with a history of colonization with Burkholderia cenocepacia, B. dolosa, and/or Mycobacterium abscessus.5,6,10,11 The Canadian Cystic Fibrosis Registry indicated that 3.7% of patients with CF in Canada (87.7% of whom were adults) were infected with species belonging to the Burkholderia cepacia complex in 2019.1 The clinical experts consulted by CADTH noted that the exclusion of such patients does not significantly lower the generalizability of the study results, given that these patients represent a small minority of those who could be eligible for ELX-TEZ-IVA, and that the clinical management of such patients is more complex and variable than those without Burkholderia cepacia infection.
The proportion of patients in the included studies who were positive for Pseudomonas aeruginosa ranged from 59.3% in study 104 to 72.5% in Study 102 which appears to be greater than what would be expected in the Canadian CF population. Canadian-specific data for P. aeruginosa infection rates are not available for a mixed population of adults and adolescents (i.e., those 12 years and older); however, 2019 data are available for the overall Canadian CF population who had not received a lung transplant (38.3%; 1,173 [78.9%] of whom were adults). This suggests that approximately 50% of Canadian adults (1,173 of 2,366) living with CF who had not undergone a lung transplant were positive for P. aeruginosa in 2019. Subgroup analyses demonstrated similar results with ELX-TEZ-IVA in patients with and without P. aeruginosa in the 2 years before screening.
The included studies excluded patients who had a respiratory infection, pulmonary exacerbation, or changes in their therapy for pulmonary disease within 4 weeks before the first dose of study drug. This is identical to the exclusion criteria that were used in the pivotal trials for the other CFTR modulators that are currently approved. The clinical experts consulted by CADTH noted that the exclusion of these patients is unlikely to limit the generalizability of the results to the broader patient population with CF.
The use of placebo as the comparator in Study 102 was considered to be appropriate by the FDA and the EMA.35,59 This study was conducted in patients who were heterozygous for the F508del mutation and had a minimal function mutation in the CFTR gene; a patient population that is not addressed by any of the indications for the approved CFTR modulators. For patients who were homozygous for the F508del mutation (Study 103 and Study 109), TEZ-IVA (Symdeko) was an appropriate comparator as this drug is currently approved in Canada for the treatment of these patients (although it has not been reviewed by CADTH and is not currently reimbursed by the participating drug programs).3,43 Study 104 included 2 subpopulations of patients with CF (i.e., F/RF and F/G) and used different active comparators for each population: TEZ-IVA for those with the F/RF genotype and IVA for those who with the F/G genotype. These are appropriate comparators for these populations as both products are currently approved in Canada for use in these populations.3,12
All the included studies investigated the use of ELX-TEZ-IVA at the dosage recommended in the product monograph: ELX 200 mg, TEZ 100 mg, and IVA 150 mg in the morning (administered as 2 oral tablets) and IVA 150 mg in the evening (administered in a single oral tablet). In Study 103, Study 104, and Study 109, TEZ-IVA was administered at the dosage recommended in the Canadian product monograph (i.e., TEZ 100 mg and IVA 150 mg in the morning and IVA 150 mg in the evening).3 Similarly, in Study 104, patients with the F/G genotype in the control group received the dosage of IVA that is recommended in the Canadian product monograph for adults and adolescents (i.e., a single 150 mg tablet every 12 hours).12 Due to the need to ensure that the treatment groups received the same number of tablets, patients in Study 103, Study 104, and Study 109 underwent a more complicated dosage regimen than would be required for typical administration of ELX-TEZ-IVA.6,10,11 In clinical practice, patients using the typical recommended dosage of ELX-TEZ-IVA would take 2 tablets in the morning and 1 in the evening (i.e., 3 tablets per day). In contrast, patients in Study 103, Study 104, and Study 109 would take 3 tablets in the morning and 1 tablet in the afternoon (i.e., 4 tablets per day).6,10,11 Nevertheless, as noted previously, adherence to study treatment regimens was high throughout the run-in and double-blind treatment periods.
Three of the ELX-TEZ-IVA studies (i.e., Study 103, Study 104, and Study 109) included an open-label, 4-week, active-treatment period with TEZ-IVA or IVA before randomization. As such, these trials were essentially investigating switching to ELX-TEZ-IVA from either TEZ-IVA or IVA compared with remaining on TEZ-IVA for patients with an F/F or F/RF genotype or remaining on IVA for patients with an F/G genotype. As TEZ-IVA is not widely reimbursed in Canada, the switching design limits the generalizability of the studies directly to the Canadian setting. To address this potential gap in the evidence, the sponsor filed indirect comparisons with CADTH to provide an estimate of the effectiveness of ELX-TEZ-IVA versus placebo for those with an F/F or F/RF genotype.
All studies compared the addition of the study treatments to ongoing standard CF-management therapies, which is reflective of how ELX-TEZ-IVA and other CFTR modulators would be administered in clinical practice. In general, the background therapies that were reported at baseline in the included studies were consistent with those used in Canadian clinical practice, except for dornase alfa. The proportion of adult patients using dornase alfa in Canadian clinical practice was reported to be approximately 50% in 2019. This is similar to the percentage using dornase alfa in Study 104 (52.9%),11 but much lower than the percentages in Study 102 (80.9%), Study 103 (92.5%), and Study 109 (76.6%).5,6,10
Similar to the pivotal trials for LUM-IVA87 and TEZ-IVA,90,91 patients in the included studies for ELX-TEZ-IVA were permitted to use inhaled hypertonic saline during the trials. Inhaled hypertonic saline is commonly used in Canadian clinical practice; therefore, this feature improves the generalizability of the studies compared with the pivotal IVA studies (i.e., STRIVE, ENVISION, and KONNECTION),94-96 in which patients were required to discontinue use of hypertonic saline. As CDEC previously noted, the exclusion of concomitant inhaled hypertonic saline was an important limitation of the IVA clinical.38,39
All the included studies evaluated absolute change from baseline in ppFEV1 as a primary and/or secondary end point; however, the timing of evaluation and placement with the statistical testing hierarchy differed across the trials (Table 18). Spirometry measurements were standardized and performed according to the American Thoracic Society Guidelines (e.g., pre-bronchodilator and before dosing).97,98 Study 102 evaluated the impact of ELX-TEZ-IVA on a range of different outcomes that are important in the management of CF. These included respiratory function (i.e., ppFEV1), nutritional status and growth (e.g., weight and BMI), HRQoL (CFQ-R), and clinical events (e.g., pulmonary exacerbations). The other studies included fewer end points (as summarized in Table 18); however, reviewers for the FDA noted that the end points in Study 103 were acceptable for a CF-development program and acceptable for a 4-week clinical trial.35 As noted in the input from clinician groups, the end points in the clinical trials largely aligned with those that are evaluated in routine clinical practice.
The 4-, 8-, and 24-week treatment periods used in the included studies were sufficient for observing treatment differences in the primary and secondary end points; however, the duration was insufficient to determine whether treatment with ELX-TEZ-IVA has the potential to modify the course of disease for patients with CF with 1 or more F508del-CFTR mutations. Reviewers for the EMA also noted that important efficacy parameters such as exacerbations and BMI cannot be reliably measured in a study with a duration of 4 weeks (i.e., the duration of Study 103) and considered the extension data from Study 105 to be an acceptable source of longer-term efficacy data.59 CADTH supplemented this review with data from Study 105 (as noted in the long term Extension Studies section)15 as well as the sponsor’s simulation study used to estimate the impact of CFTR-modulator treatment on morbidity and mortality. (This is discussed in the Simulation Study for Morbidity and Mortality section).19
As with the pivotal trials conducted for IVA, LUM-IVA, and TEZ-IVA, patients with CF who had received a lung transplant (or any organ or hematological transplant) were excluded from the ELX-TEZ-IVA studies.5,6,10,11 According to the CF Canada registry, 7.8% of the Canadian CF population had received a lung transplant as of 20191; this is a relatively large subpopulation of patients who were not studied in the clinical trials. The clinician groups who provided input noted there is a lack of evidence regarding whether ELX-TEZ-IVA would benefit patients with CF who have had a lung transplant. The experts consulted by CADTH noted that ELX-TEZ-IVA would not likely be initiated in patients who have undergone a lung transplant. For those who have undergone a liver transplant, ELX-TEZ-IVA could be initiated as the drug may improve the patient’s lung function. Post-liver transplant patients would likely receive additional monitoring for potential toxicity with a lower threshold for interrupting or discontinuing the drug (due to the potential risk of hepatic adverse events with ELX-TEZ-IVA).
As is common in clinical trial settings, patients enrolled in the included RCTs received extensive contact with health professionals over the study periods (e.g., 7 clinic visits and 1 phone contact over a 6-month period in Study 102).5,6,10,11 This level of contact is not reflective of routine care for patients with CF with relatively stable disease. The clinical experts consulted by CADTH and the clinician groups who provided input noted that patients with CF are typically seen once every 3 months (although the frequency of visits has been lower in some cases due to the COVID-19 pandemic). The experts consulted by CADTH noted that the level of contact in the clinical trials is typical for CF studies and would not affect the generalizability of the results to the target population in Canada.
Adherence to study treatment regimens was high throughout the treatment periods of all studies (i.e., > 99%). The clinical experts consulted by CADTH noted that the level of adherence observed in the included studies is not reflective of typical adherence in Canada for adults and adolescents with CF, where adherence with treatments, including orally administered treatments, is considerably lower.66
Indirect Evidence
Objectives and Methods for the Summary of Indirect Evidence
Patients Aged 6 to 11 Years
The sponsor’s objective for the indirect comparisons were to derive relative estimates of clinical efficacy for ELX-TEZ-IVA compared to local standard of care in the F/F population, given the absence of direct comparisons.52
Patients Aged 12 Years and Older
The sponsor’s objective for the indirect comparisons were to derive relative estimates of clinical efficacy for ELX-TEZ-IVA compared to local standard of care in the F/F, F/RF and F/G populations, given the absence of RCTs.62 Although head-to-head trials were conducted for ELX-TEZ-IVA versus TEZ-IVA (for patients with F/F or F/RF genotypes) and IVA (for patients with an F/G genotype), the sponsor conducted indirect comparisons to derive estimates of effect for:
ELX-TEZ-IVA versus LUM-IVA (for jurisdictions that only reimburse LUM-IVA for patients with an F/F genotype and not TEZ-IVA)
ELX-TEZ-IVA versus placebo (for jurisdictions that do not reimburse an CFTR modulators for the genotype of interest).
Description of Indirect Comparisons
As shown in Table 64, the sponsor conducted indirect comparisons investigating the comparative efficacy of ELX-TEZ-IVA versus other CFTR modulators and placebo for patients aged 12 years and older with F/F, F/G, and F/RF genotypes. For patients aged 6 to 11 years, the sponsor conducted an indirect comparison investigating the comparative efficacy of ELX-TEZ-IVA versus other CFTR modulators and placebo for patients with an F/F genotypes.52
Table 64: Assessment of Generalizability of Evidence from Adolescent and Adult Studies
Domain | Factor | Evidence | CADTH's assessment of generalizability |
|---|---|---|---|
Population | Age | The included trials enrolled patients who were at least 12 years of age at screening. | This is reflective of the indication under review by CADTH. |
Severity of disease | Patients with CF and more-severe lung disease (e.g., ppFEV1 < 40% at screening) or a normal ppFEV1 at screening (≥ 90%) were excluded from the RCTs. | The results of the included studies are primarily applicable to patients with moderate (i.e., ppFEV1 of 40% to 69%) to mild (i.e., ppFEV1 of 70% to 89%) lung disease. An ad hoc subgroup analysis in Study 102 provided some efficacy data for a small subgroup of patients with ppFEV1 and suggested that ELX-TEZ-IVA resulted in clinically meaningful improvements relative placebo. | |
Post-transplant | Patients with CF who had received a lung transplant (or any organ or hematological transplant) were excluded from the ELX-TEZ-IVA studies. | The experts consulted by CADTH noted that ELXTEZ-IVA would not likely be initiated in patients who have undergone a lung transplant. ELX-TEZ-IVA could be initiated in patients who have undergone a liver transplant (as the drug may improve their lung function). Post-liver transplant patients would likely receive additional monitoring for potential toxicity with a lower threshold for interrupting or discontinuing the drug. | |
Burkholderia cepacia complex | The studies excluded patients with a history of colonization with B. cenocepacia, B. dolosa, and/or Mycobacterium abscessus. | The clinical experts consulted by CADTH noted that the exclusion of such patients does not significantly lower the generalizability of the study results, given that these patients represent a small minority of those who could be eligible for ELX-TEZ-IVA and that the clinical management of such patients is more complex and variable. | |
Race | The study populations comprised almost exclusively White patients. | This is reflective of most patients with CF in Canada, although the percentage is slightly higher than the percentage reported for the overall CF population in Canada (93.2% in 2019). | |
Intervention | ELX-TEZ-IVA | All the included studies investigated the use of ELX-TEZ-IVA at the dosage recommended in the product monograph. | In clinical practice, patients using the typical recommended dosage of ELX-TEZ-IVA would take 2 tablets in the morning and 1 in the evening (i.e., 3 tablets per day). In contrast, patients in Study 103, Study 104, and Study 109 would take 3 tablets in the morning and 1 tablet in the afternoon (i.e., 4 tablets per day). |
Concomitant medications | Concomitant medications for CF are reported in for the included studies. | Concomitant medications were generally consistent with those used in Canadian clinical practice except for dornase alfa (estimated to be used by approximately 50% of adults). This is similar to the percentage using dornase alfa in Study 104, but lower than the percentages in Study 102, Study 109, and Study 109. | |
Comparator | Placebo | Placebo was the comparator in Study 102. | The use of placebo as the comparator in Study 102 is appropriate as no drugs are currently approved for use in the treatment of patients with CF who have an F/MF genotype. |
TEZ-IVA | TEZ-IVA was the comparator in Study 103, Study 109, and in Study 104 for the subset of patients with an F/RF genotype. | TEZ-IVA was an appropriate comparator in these studies as this drug is currently approved in Canada for the treatment of patients with CF and an F/F or F/RF genotype (although it has not been reviewed by CADTH and is not currently reimbursed by the participating drug programs). | |
IVA | IVA was the comparator for the subset of patients in Study 104 with an F/G genotype. | IVA was an appropriate comparator in Study 104 for patients with an F/G genotype as this drug is currently approved in Canada for the treatment of patients with CF and gating mutations (including those who are heterozygous for the F058del mutation). | |
Outcomes | Hospitalizations | Planned and unplanned hospitalizations for CF did not include events that were due to protocol-defined pulmonary exacerbations. | Pulmonary exacerbations are the most common reason for CF-related hospitalizations in Canada; therefore, the exclusion of these events limits the generalizability of the planned and unplanned hospitalization end points. Those end points should be interpreted in conjunction with the data for pulmonary exacerbations that required hospitalization. |
Setting | Clinics | The included RCTs were conducted at specialized CF clinics. | This is consistent with Canadian clinical practice, where patients are managed in specialized CF clinics. |
Locations and Canadian sites | Most patients in Study 104 were from Europe and Study 109 was conducted exclusively in Europe and Australia. | The clinical experts consulted noted that the results from the studies in Europe and Australia would likely be generalizable to the Canadian setting. | |
Contact with health care professionals | Patients enrolled in the included RCTs received extensive contact with health professionals over the study periods (e.g., 7 clinic visits and 1 phone contact in Study 102). | This level of contact is not reflective of routine care for patients with CF with relatively stable disease. Patients with stable disease would typically been seen 4 times per year (reduced to 3 times per year during the COVID-19 pandemic). |
CF = cystic fibrosis; ELX-TEZ-IVA = elexacaftor-tezacaftor-ivacaftor and ivacaftor; F/F = homozygous for F508del mutation in the CFTR gene; F/G = 1 F508del mutation and 1 gating mutation in the CFTR gene; F/MF = 1 F508del mutation and 1 minimal function mutation in the CFTR gene; F/RF = 1 F508del mutation and 1 residual function mutation in the CFTR gene; IVA = ivacaftor; ppFEV1 = percent predicted forced expiratory volume in 1 second; RCT = randomized controlled trial; TEZ-IVA = tezacaftor-ivacaftor and ivacaftor.
Table 65: Study Selection Criteria and Methods for Indirect Treatment Comparisons
Characteristics | ITCs for patients 12 years age and older | ITC for patients with F/F 6 to 11 years of age | ||
|---|---|---|---|---|
ITC for patients with F/F | ITC for patients with F/G | ITC for patients with F/RF | ||
Population | Patients with ≥ 12 years of age with F/F genotype | Patients with CF ≥ 12 years of age with F/G genotype | Patients with CF ≥ 12 years of age with F/RF genotype | Patients with CF 6 to 11 years of age with F/F genotype |
Intervention | ELX 200 mg, TEZ 100 mg, and IVA 150 mg (every morning) plus IVA 150 mg (every evening) | ELX 200 mg, TEZ 100 mg, and IVA 150 mg (every morning) plus IVA 150 mg (every evening) | ||
Comparator |
|
|
|
|
Outcome |
|
|
|
|
Study design |
|
|
|
|
Publication characteristics | Not reported | Not reported | Not reported | Not reported |
Exclusion criteria | Not reported | Not reported | Not reported | Not reported |
Databases searched | Not reported | Not reported | Not reported | Not reported |
Selection process | Not reported | Not reported | Not reported | Not reported |
Data extraction process | Not reported | Not reported | Not reported | Not reported |
Quality assessment | Not reported | Not reported | Not reported | Not reported |
BMI = body mass index; CFQ-R = Cystic Fibrosis Questionnaire–Revised; CFTR = cystic fibrosis transmembrane conductance regulator; ELX-TEZ-IVA = elexacaftor-tezacaftor-ivacaftor and ivacaftor; F/F = homozygous for F508del mutations in the CFTR gene; F/G = 1 F508del mutation and 1 gating mutation in the CFTR gene; F/RF = 1 F508del mutation and 1 residual function mutation in the CFTR gene; ITC = indirect treatment comparison; IVA = ivacaftor; LUM-IVA = lumacaftor-ivacaftor; ppFEV1 = percent predicted forced expiratory volume in 1 second; q.12.h. = every 12 hours; RCT = randomized controlled trial; RD = respiratory domain; SwCl = sweat chloride; TEZ-IVA = tezacaftor-ivacaftor and ivacaftor.
Source: Sponsor’s indirect treatment comparisons.52,62
Indirect Treatment Comparison for Patients Aged 6 to 11 Years With F/F Genotype
Study Selection Methods
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||. A systematic literature search and review was not undertaken by the sponsor to identify studies for inclusion. The sponsor reported that, because Vertex Pharmaceuticals is the only manufacturer with relevant CFTR modulators and conducted all the relevant phase III trials, a systematic literature review was unlikely to retrieve any additional relevant evidence.52 CADTH did not identify any additional studies that would have met the inclusion criteria but were not included in the ITC.
Indirect Treatment Comparison Analysis Methods
The ITCs for ELX-TEZ-IVA versus LUM-IVA, TEZ-IVA, and placebo as well as LUM-IVA and TEZ-IVA versus placebo were conducted using an MMRM meta-analysis approach using individual patient-level data from patients with the F/F genotype in the relevant treatment groups from each of the included trials. The sponsor reported that an MMRM meta-analysis approach was the most appropriate methodology for the following factors:
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||The relevant comparisons for the CADTH review are ELX-TEZ-IVA versus LUM-IVA or IVA (as TEZ-IVA is not approved for use in patients aged 6 to 11 years in Canada. |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Results for Indirect Treatment Comparison Analysis
Included Studies
The evidence network for the studies of patients who have an F/F genotype is shown in Figure 16. Indirect comparisons were performed for ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Figure 15: Indirect Comparison Network for F/F Genotype for Pediatric Studies

Figure was redacted.
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Study Characteristics
Table 66 provides a summary of the characteristics of the studies that were included in the indirect comparison for patients with an F/F genotype. |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Table 66: Indirect Comparisons in Patients Aged 6 to 11 Years With F/F Genotype
Within-group estimates (study) | End pointa |
|---|---|
|
|
BMI = body mass index; CFQ-R = Cystic Fibrosis Questionnaire–Revised; ELX-TEZ-IVA = elexacaftor-tezacaftor-ivacaftor and ivacaftor; LUM-IVA = lumacaftor-ivacaftor; ppFEV1 = percent predicted forced expiratory volume in 1 second; TEZ-IVA = tezacaftor-ivacaftor and ivacaftor.
aAnalyses for TEZ-IVA were conducted at 8 weeks.
Source: Sponsor’s indirect treatment comparison.52
Baseline Characteristics
As shown in Table 67, the baseline and demographic characteristics were generally similar across the studies that were included in the F/F indirect comparisons. For the comparisons of interest for this review (i.e., ELX-TEZ-IVA versus LUM-IVA or placebo), baseline ppFEV1, LCI2.5, weight-for-age z scores, and BMI-for-age z scores were similar across the treatment groups, with the exception of BMI z scores, which were greater in the TEZ-IVA 661 to 113 Part B study 0.39 (SD = 0.90) compared with the other trials (range = −0.09 [SD = 0.86] to 0.09 [SD = 0.96]). Baseline CFQ-R respiratory domain scores were lower for the placebo (77.1) and LUM-IVA groups (78.5) compared with the ELX-TEZ-IVA and TEZ-IVA groups (81.8 and 83.2, respectively).
Table 67: Study Characteristics Patients Aged 6 to 11 Years With F/F Genotype
Characteristics | ELX-TEZ-IVA | LUM-IVA | TEZ-IVA | ||
|---|---|---|---|---|---|
Study 106B | 809 to 109 | 809 to 011B | 661 to 113B | 661 to 115a | |
Study design | Single-arm, open-label | Double-blind RCT | Single-arm, open-label | Single-arm, open-label | Double-blind RCT |
Study population |
|
|
|
|
|
Treatment groups |
|
|
|
|
|
CFTR washout requirements | ≥ 28 days before day 1 visit | ≥ 30 days before screening visit | ≥ 30 days before screening visit | ≥ 30 days before day 1 visit (≥ 28 for LUM-IVA) | ≥ 28 days before day 1 visit |
Treatment duration | 24 weeks | 24 weeks | 24 weeks | 24 weeks | 8 weeks |
Baseline ppFEV1 inclusion criteria | ≥ 40% (GLI) | ≥ 70% (Wang equation) | ≥ 40% (Wang equation) | ≥ 40% (GLI) | ≥ 70% (GLI) |
Sample size |
|
|
|
|
|
Primary efficacy end point | NA | Absolute change from baseline in LCI2.5 through week 24 | NA | NA | Absolute change from baseline in LCI2.5 through week 8 |
Other efficacy end points included in this indirect treatment comparison |
|
|
|
|
|
BMI = body mass index; CFQ-R = Cystic Fibrosis Questionnaire–Revised; ELX-TEZ-IVA = elexacaftor-tezacaftor-ivacaftor and ivacaftor; F/F = homozygous for F508del mutation in the CFTR gene; F/MF = 1 F508del mutation and 1 minimal function mutation in the CFTR gene; F/RF = 1 F508del mutation and 1 residual function mutation in the CFTR gene; GLI = Global Lung Function Initiative; IVA = ivacaftor; LCI = lung clearance index; LUM-IVA = lumacaftor-ivacaftor; PEx = pulmonary exacerbations; ppFEV1 = percent predicted forced expiratory volume in 1 second; RD = respiratory domain; SwCl = sweat chloride; TEZ-IVA = tezacaftor-ivacaftor and ivacaftor.
aSensitivity analysis only.
Source: Sponsor’s indirect treatment comparison.52
Indirect Comparison Results
Table 68 provides a summary of the results for the indirect comparisons for studies conducted in patients with an F/F genotype. ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Critical Appraisal
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Table 68: Baseline Characteristics in Patients Aged 6 to 11 Years With F/F Genotype
Characteristics | ELX-TEZ-IVA in Study 106B (N = 29) | Placebo in Study 809 to 109 (N = 101) | LUM-IVA in Study 809 to 109 and Study 809 to 011 Part B pooled (N = 160) | TEZ-IVA in Study 661 to 113 Part B (N = 61) | TEZ-IVA in Study 661 to 115 (N = 42) | TEZ-IVA in Study 661 to 113 Part B and Study 661 to 115 pooled (N = 103) |
|---|---|---|---|---|---|---|
Sex, n (%) | ||||||
Male | 12 (41.4) | 43 (42.6) | 66 (41.3) | 31 (50.8) | 20 (47.6) | 51 (49.5) |
Female | 17 (58.6) | 58 (57.4) | 94 (58.8) | 30 (49.2) | 22 (52.4) | 52 (50.5) |
Age at screening (years) | ||||||
Mean (SD) | 8.3 (1.9) | 8.9 (1.6) | 8.8 (1.6) | 8.0 (1.8) | 8.5 (1.6) | 8.2 (1.7) |
Median | 8.0 | 9.0 | 9.0 | 8.0 | 9.0 | 8.0 |
Mean ppFEV1 (SD) | 87.3 (18.3) | 88.6 (11.1) | 87.5 (13.6) | 91.2 (12.4) | NA | 88.7 (12.9) |
Mean LCI2.5 | 10.26 (3.36) | 10.26 (2.24) | 10.25 (2.42) | NA | 9.84 (2.17) | NA |
Mean weight z score (SD) | −0.23 (0.59) | −0.21 (0.76) | −0.14 (0.90) | 0.18 (0.94) | NA | −0.04 (0.90) |
Mean BMI z score (SD) | −0.10 (0.61) | −0.14 (0.88) | −0.09 (0.86) | 0.39 (0.90) | NA | 0.09 (0.96) |
Mean CFQ-R RD (SD) | 81.8 (12.0) | 77.1 (15.5) | 78.5 (14.4) | 81.7 (13.9) | NA | 83.2 (12.5) |
BMI = body mass index; CFQ-R (RD) = Cystic Fibrosis Questionnaire–Revised respiratory domain; ELX-TEZ-IVA = elexacaftor-tezacaftor-ivacaftor and ivacaftor; F/F = homozygous for F508del mutation in the CFTR gene; LCI = lung clearance index; LUM-IVA = lumacaftor-ivacaftor; NA = not applicable; pFEV1 = percent predicted forced expiratory volume in 1 second; SD = standard deviation; TEZ-IVA = tezacaftor-ivacaftor and ivacaftor.
Source: Sponsor’s indirect treatment comparison.52
|||||||||||||||||||||||||||| | |||||||||||||||||||||||||||| | |||||||||||||||||||||||||||| | |||||||||||||||||||||||||||| | |||||||||||||||||||||||||||| |
|---|---|---|---|---|
|||||||||||||||||||||||||||| | ||||
|||||||||||||||||||||||||||| | |||||||||||||||||||||||||||| | |||||||||||||||||||||||||||| | |||||||||||||||||||||||||||| | |||||||||||||||||||||||||||| |
|||||||||||||||||||||||||||| | |||||||||||||||||||||||||||| | |||||||||||||||||||||||||||| | |||||||||||||||||||||||||||| | |||||||||||||||||||||||||||| |
|||||||||||||||||||||||||||| | ||||
|||||||||||||||||||||||||||| | |||||||||||||||||||||||||||| | |||||||||||||||||||||||||||| | |||||||||||||||||||||||||||| | |||||||||||||||||||||||||||| |
|||||||||||||||||||||||||||| | |||||||||||||||||||||||||||| | |||||||||||||||||||||||||||| | |||||||||||||||||||||||||||| | |||||||||||||||||||||||||||| |
BMI = body mass index; CFQ-R = Cystic Fibrosis Questionnaire–Revised; CI = confidence interval; ELX-TEZ-IVA = elexacaftor-tezacaftor-ivacaftor and ivacaftor; F/F = homozygous for F508del mutation in the CFTR gene; LUM-IVA = lumacaftor-ivacaftor; ppFEV1 = percent predicted forced expiratory volume in 1 second; SwCl = sweat chloride; TEZ-IVA = tezacaftor-ivacaftor and ivacaftor.
Note: Redacted rows have been deleted.
Source: Sponsor’s indirect treatment comparison.52
Table 70: Summary of Pulmonary Exacerbations Reported in F/F Genotype
Pulmonary exacerbations | ELX-TEZ-IVA Study 106B (N = 29) | Placebo Study 809 to 109 (N = 101) | LUM-IVA Study 809 to 109 (N = 103) |
|---|---|---|---|
Total number of days (years) of the PEx analysis period | 4,909 (14.6) | 16,736 (49.8) | 16,789 (50.0) |
Pulmonary exacerbations | |||
Patients with events | 0 | 15 | 20 |
Total number of events | 0 | 18 | 24 |
Observed event rate per year | 0.00 | 0.36 | 0.48 |
Pulmonary exacerbations requiring hospitalization | |||
Patients with events | 0 | 5 | 8 |
Total number of events | 0 | 6 | 8 |
Observed event rate per year | 0.00 | 0.12 | 0.16 |
Pulmonary exacerbations requiring IV antibiotic therapy | |||
Patients with events | 0 | 5 | 7 |
Total number of events | 0 | 6 | 7 |
Observed event rate per year | 0.00 | 0.12 | 0.14 |
ELX-TEZ-IVA = elexacaftor-tezacaftor-ivacaftor and ivacaftor; F/F = homozygous for F508del mutation in the CFTR gene; LUM-IVA = lumacaftor-ivacaftor.
Table 71: CADTH Assessment of Homogeneity for the ITC for the F/F Genotype
Characteristics | Description and handling of potential effect modifiers |
|---|---|
Disease severity | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |
Treatment history | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |
Clinical trial eligibility criteria | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |
Dosing of comparators | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |
Definitions of end points | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |
Timing of end-point evaluation or trial duration | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |
Withdrawal frequency | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |
Clinical trial setting | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |
Study design | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |
ELX-TEZ-IVA = elexacaftor-tezacaftor-ivacaftor and ivacaftor; F/F = homozygous for F508del mutation in the CFTR gene; ITC = indirect treatment comparison; LUM-IVA = lumacaftor/ivacaftor; MMRM = mixed-effects model for repeated measures; ppFEV1 = percent predicted forced expiratory volume in 1 second; SwCl = sweat chloride; TEZ-IVA = tezacaftor-ivacaftor and ivacaftor.
Indirect Treatment Comparison for Patients 12 Years and Older With F/F Genotype
Study Selection Methods
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||. Whether a systematic literature search and review was undertaken by the sponsor to identify studies for inclusion was not reported; however, CADTH did not identify any additional studies that would have met the inclusion criteria but were not included in the ITC.
Indirect Treatment Comparison Analysis Methods
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Table 72: Indirect Comparisons in Patients 12 Years and Older With F/F Genotype
Indirect estimate | Direct estimates (study) | End points |
|---|---|---|
ELX-TEZ-IVA vs. placebo |
|
|
ELX-TEZ-IVA vs. LUM-IVA |
|
BMI = body mass index; CFQ-R = Cystic Fibrosis Questionnaire–Revised; ELX-TEZ-IVA = elexacaftor-tezacaftor-ivacaftor and ivacaftor; F/F = homozygous for F508del mutation in the CFTR gene; LUM-IVA = lumacaftor-ivacaftor; ppFEV1 = percent predicted forced expiratory volume in 1 second; SwCl = sweat chloride; TEZ-IVA = tezacaftor-ivacaftor and ivacaftor.
Source: Sponsor’s indirect treatment comparison.62
Results for Indirect Treatment Comparison Analysis
Included Studies
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Figure 16: Indirect Comparison Network for F/F Genotype

Note: Figure was redacted at the request of the sponsor.
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Study Characteristics
Table 73 provides a summary of the characteristics of the studies that were included in the indirect comparison of patients with an F/F genotype. |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Table 73: Study Characteristics for Patients 12 Years and Older With F/F Genotype
Characteristics | Study 109 | EVOLVE | TRAFFIC/TRANSPORT |
|---|---|---|---|
Study population | Patients with F/F genotype and ≥ 12 years of age | ||
Run-in period | 4 weeks with TEZ-IVA | None | None |
Treatment period | 24 weeks | 24 weeks | 24 weeks |
Treatment groups | ELX-TEZ-IVA TEZ-IVA | TEZ-IVA Placebo | LUM-IVA (2 different dosing groups) Placebo |
ppFEV1 inclusion criteria at screening | 40% to 90% | 40% to 90% | 40% to 90% |
Schedule of assessments | Day 1, day 15, week 4, every 4 weeks thereafter | Day 1, day 15, week 4, every 4 weeks thereafter | Day 1, day 3, day 15, week 4, every 4 weeks thereafter |
Sample size | ELX-TEZ-IVA: 87 TEZ-IVA: 88 | TEZ-IVA: 248 Placebo: 256 | LUM-IVA: 369 Placebo: 371 |
Primary efficacy end point | Absolute change in CFQ-R respiratory domain score from baseline through 24 weeks | Absolute change from baseline in ppFEV1 through 24 weeks | Absolute change from baseline in ppFEV1 at 24 weeks (as assessed by the average absolute change at weeks 16 and 24) |
Other efficacy end points | SwCl, ppFEV1, BMI, weight-for-age z score, CFQ-R | SwCl, PEx, BMI, weight-for-age z score, CFQ-R | PEx, BMI, weight-for-age z score, CFQ-R |
BMI = body mass index; CFQ-R = Cystic Fibrosis Questionnaire–Revised; ELX-TEZ-IVA = elexacaftor-tezacaftor-ivacaftor and ivacaftor; F/F = homozygous for F508del mutation in the CFTR gene; LUM-IVA = lumacaftor/ivacaftor; PEx = pulmonary exacerbations; ppFEV1 = percent predicted forced expiratory volume in 1 second; SD = standard deviation; SwCl = sweat chloride; TEZ-IVA = tezacaftor-ivacaftor and ivacaftor.
Source: Sponsor’s indirect treatment comparison.62
Baseline Characteristics
As shown in Table 74, the mean ppFEV1 values in Study 109 were 64.2% and 63.0% in the TEZ-IVA and ELX-TEZ-IVA groups, respectively, compared with 59.6% and 58.8%, respectively, in the placebo and TEZ-IVA groups of EVOLVE, and 59.5% and 59.8%, respectively, in the placebo and LUM-IVA groups of the pooled TRAFFIC/TRANSPORT studies. The proportion of male and female patients in each study was similar. The median age of patients was lowest in the TRAFFIC/TRANSPORT studies (23.0 and 24.0 years in the placebo and LUM-IVA groups, respectively) and highest in the TEZ-IVA group of Study 109 (27.7 years). The EVOLVE study had a lower proportion of adolescent patients compared with Study 109 and TRAFFIC/TRANSPORT. Sweat chloride levels were lower in Study 109 (89.8 mmol/L and 89.0 mmol/L in the TEZ-IVA and ELX-TEZ-IVA groups, respectively) compared with those in the EVOLVE trial (100.5 mmol/L and 101.3 mmol/L in the placebo and TEZ-IVA groups, respectively). Mean BMI was similar across the included studies.
Table 74: Baseline Characteristics for Patients 12 Years and Older With F/F Genotype
Characteristics | Study 109 | EVOLVE | TRAFFIC/TRANSPORT | ||||
|---|---|---|---|---|---|---|---|
TEZ-IVA (N = 88) | ELX-TEZ-IVA (N = 87) | Placebo (N = 256) | TEZ-IVA (N = 248) | Placebo (N = 371) | LUM-IVA (N = 369) | ||
Sex, n (%) | Male | 43 (48.9) | 44 (50.6) | 131 (51.2) | 127 (51.2) | 190 (51.2) | 187 (50.7) |
Female | 45 (51.1) | 43 (49.4) | 125 (48.8) | 121 (48.8) | 181 (48.8) | 182 (49.3) | |
Age at screening, years | Mean (SD) | 27.6 (11.0) | 27.8 (11.8) | 25.7 (9.5) | 26.9 (11.2) | 25.3 (10.4) | 25.2 (9.6) |
Median | 27.7 | 25.7 | 25.0 | 25.0 | 23.0 | 24.0 | |
Age group at screening, n (%) | ≥ 12 to < 18 | 27 (30.7) | 25 (28.7) | 58 (22.7) | 58 (23.4) | 98 (26.4) | 98 (26.6) |
≥ 18 | 61 (69.3) | 62 (71.3) | 198 (77.3) | 190 (76.6) | 273 (73.6) | 271 (73.4) | |
ppFEV1 | Mean (SD) | 64.2 (15.1) | 63.0 (16.7) | 59.6 (15.0) | 58.8 (14.0) | 59.5 (13.2) | 59.8 (13.6) |
BMI (kg/m2) | Mean (SD) | 21.92 (3.89) | 21.17 (3.43) | 21.12 (2.88) | 20.96 (2.95) | 21.02 (2.92) | 21.50 (3.03) |
SwCl (mmol/L) | Mean (SD) | 89.8 (11.7) | 89.0 (12.2) | 100.5 (10.2) | 101.3 (10.9) | NA | NA |
CFQ-R (RD) score | Mean (SD) | 73.1 (17.6) | 71.2 (19.6) | 69.9 (16.6) | 70.1 (16.8) | 68.8 (17.3) | 68.3 (18.0) |
BMI = body mass index; CFQ-R (RD) = Cystic Fibrosis Questionnaire–Revised; ELX-TEZ-IVA = elexacaftor-tezacaftor-ivacaftor and ivacaftor; F/F = homozygous for F508del mutation in the CFTR gene; LUM-IVA = lumacaftor-ivacaftor; NA = not applicable; ppFEV1 = percent predicted forced expiratory volume in 1 second; RD = respiratory domain; SD = standard deviation; SwCl = sweat chloride; TEZ-IVA = tezacaftor-ivacaftor and ivacaftor.
Source: Sponsor’s indirect treatment comparison.62
Indirect Comparison Results
Table 74 provides a summary of the results for the direct and indirect comparisons for studies conducted in patients with an F/F genotype. The sponsor reported the following indirect estimates of effect for ELX-TEZ-IVA compared with placebo: |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Indirect estimates of effect for ELX-TEZ-IVA compared with placebo are provided for each of the CFQ-R domains. |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Table 75: Results of Direct and Indirect Comparison for F/F Genotype
End point | Direct estimate ELX-TEZ-IVA vs. TEZ-IVA LSMD (95% CI), P value | ||||||||||||||||||||||||||||||||||| | |
|---|---|---|---|
|||||||||||| | |||||||||||| | ||
Absolute change in ppFEV1 from baseline through 24 weeks | 10.2 (8.2 to 12.1), < 0.0001 | |||||||||||| | |||||||||||| |
Absolute change in sweat chloride from baseline through 24 weeks | −42.9 (−46.3 to −39.5), < 0.0001 | |||||||||||| | |||||||||||| |
Absolute change in BMI (kg/m2) from baseline at 24 weeks | 1.44 (1.07 to 1.82), < 0.0001 | |||||||||||| | |||||||||||| |
Absolute change in weight-for-age z score from baseline at 24 weeks | 0.40 (0.31 to 0.49), < 0.0001 | |||||||||||| | |||||||||||| |
Absolute change from baseline through 24 weeks in CFQ-R domain score | |||||||||||| | |||||||||||| | |
Respiratory symptoms | 16.0 (11.9 to 20.1), < 0.0001 | |||||||||||| | |||||||||||| |
Physical functioning | 8.2 (4.4 to 12.0), < 0.0001 | |||||||||||| | |||||||||||| |
Vitality | 7.2 (2.3 to 12.2), 0.0047 | |||||||||||| | |||||||||||| |
Emotional functioning | 3.8 (0.4 to 7.2), 0.0274 | |||||||||||| | |||||||||||| |
Body image | 2.9 (−0.9 to 6.7), 0.1383 | |||||||||||| | |||||||||||| |
Eating problems | 4.1 (0.5 to 7.7), 0.0268 | |||||||||||| | |||||||||||| |
Treatment burden | 5.8 (2.1 to 9.6), 0.0023 | |||||||||||| | |||||||||||| |
Health perceptions | 9.3 (4.6 to 14.0), 0.0001 | |||||||||||| | |||||||||||| |
Weight | 9.9 (3.7 to 16.2), 0.0020 | |||||||||||| | |||||||||||| |
Digestive symptoms | 0.8 (−3.0 to 4.7), 0.6640 | |||||||||||| | |||||||||||| |
Role functioning | 6.6 (2.3 to 10.9), 0.0030 | |||||||||||| | |||||||||||| |
Social functioning | 5.4 (1.4 to 9.3), 0.0077 | |||||||||||| | |||||||||||| |
BMI = body mass index; CFQ-R = Cystic Fibrosis Questionnaire–Revised; CI = confidence interval; ELX-TEZ-IVA = elexacaftor-tezacaftor-ivacaftor and ivacaftor; ; F/F = homozygous for F508del mutation in the CFTR gene; LSMD = least squares mean difference; LUM-IVA = lumacaftor-ivacaftor; ppFEV1 = percent predicted forced expiratory volume in 1 second; SwCl = sweat chloride; TEZ-IVA = tezacaftor-ivacaftor and ivacaftor.
Source: Sponsor’s indirect treatment comparison.62
Critical Appraisal
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Table 76: CADTH Assessment of Homogeneity of the ITC for the F/F Genotype
Characteristics | Description and handling of potential effect modifiers |
|---|---|
Disease severity | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |
Treatment history | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |
Clinical trial eligibility criteria | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |
Dosing of comparators | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |
Response in the common comparator (i.e., placebo) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |
Definitions of end points | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |
Timing of end point evaluation or trial duration | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |
Withdrawal frequency | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |
Clinical trial setting | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |
Study design | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |
ELX-TEZ-IVA = elexacaftor-tezacaftor-ivacaftor and ivacaftor; F/F = homozygous for F508del mutation in the CFTR gene; ITC = indirect treatment comparison; LUM-IVA = lumacaftor/ivacaftor; MMRM = mixed-effects model for repeated measures; ppFEV1 = percent predicted forced expiratory volume in 1 second; SwCl = sweat chloride; TEZ-IVA = tezacaftor-ivacaftor and ivacaftor.
Indirect Treatment Comparison for Patients 12 Years and Older With F/G Genotype
Study Selection Methods
The criteria used by the sponsor to select studies for study inclusion in the ITC in patients with the F/G genotype were as follows:
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||.It was not reported if a systematic literature search and review was undertaken by the sponsor to identify studies for inclusion; however, CADTH did not identify any additional studies that would have met the inclusion criteria but were not included in the ITC.
ITC Analysis Methods
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Table 77: Indirect Comparisons for Patients 12 Years and Older With F/G Genotype
Indirect estimate | Direct estimates (study) | End points |
|---|---|---|
ELX-TEZ-IVA vs. placebo | ELX-TEZ-IVA vs. TEZ-IVA (subgroup data from Study 104) plus IVA vs. placebo (meta-analysis of STRIVE, KONNECTION, and KONDUCT) | ppFEV1 (through 8 weeks) CFQ-R (through 8 weeks) SwCl (through 8 weeks) BMI (at 8 weeks) Weight-for-age z score (at 8 weeks) |
BMI = body mass index; CFQ-R = Cystic Fibrosis Questionnaire–Revised; ELX-TEZ-IVA = elexacaftor-tezacaftor-ivacaftor and ivacaftor; F/G = 1 F508del mutation and 1 gating mutation in the CFTR gene; ppFEV1 = percent predicted forced expiratory volume in 1 second; SwCl = sweat chloride; TEZ-IVA = tezacaftor-ivacaftor and ivacaftor.
Source: Sponsor’s indirect treatment comparison.62
Results of the Indirect Treatment Comparison Analysis
Included Studies
The evidence network for the studies with patients who have an F/G genotype is shown in Figure 17. An indirect comparison was performed for ELX-TEZ-IVA versus placebo. ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Figure 17: Indirect Comparison Network for Patients 12 Years and Older With F/G Genotype

Note: Figure was redacted at the request of the sponsor.
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Study Characteristics
Table 73 ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Table 78: Study Characteristics for Patients 12 Years and Older With F/G Genotype
Characteristics | Study 104 (subset of F/G) | STRIVE (subset of F/G551D) | KONNECTION (subset of F/non-G551D) | KONDUCT (subset of F/R117H) |
|---|---|---|---|---|
Study population | Patients with F/G (including F/R117H) or F/RF genotypes and ≥ 12 years of age | Patients with ≥ 1 G551D gating mutation and ≥ 12 years of age | Patients with ≥ 1 non-G551D gating mutation and ≥ 6 years of age | Patients with ≥ 1 R117H mutation and ≥ 6 years of age |
Design | DB, active-controlled, parallel-group RCT | DB, active-controlled, parallel-group RCT | DB placebo-controlled, crossover RCT | DB, active-controlled, parallel-group RCT |
Active run-in period | 4 weeks with TEZ-IVA or IVA | None | None | None |
Treatment period | 8 weeks | 48 weeks | 8 weeks | 24 weeks |
Treatment groups | ELX-TEZ-IVA TEZ-IVA (F/RF) IVA (F/G) | IVA Placebo | IVA Placebo | IVA Placebo |
ppFEV1 inclusion criteria at screening | 40% to 90% | 40% to 90% | ≥ 40% | 40% to 90% for patients ≥ 12 years |
Schedule of assessments | Day 1, day 15, week 4, week 8 | Day 1, day 15, week 8, every 4 weeks thereafter | Day 1, week 2, week 4, week 8 of each treatment period | Day 1, week 2, week 4, week 8, week 16, week 24 |
Sample size | |||||||||||||||||||||||||||||||||||| | |||||||||||||||||||||||||||||||||||| | |||||||||||||||||||||||||||||||||||| | |||||||||||||||||||||||||||||||||||| |
Subset of patients included in ITC | |||||||||||||||||||||||||||||||||||| | |||||||||||||||||||||||||||||||||||| | |||||||||||||||||||||||||||||||||||| | |||||||||||||||||||||||||||||||||||| |
Primary efficacy end point | Absolute change in ppFEV1 from baseline through 8 weeks | Absolute change in ppFEV1 from baseline through 24 weeks | Absolute change in ppFEV1 from baseline through 8 weeks | Absolute change in ppFEV1 from baseline through 24 weeks |
Other end points | BMI, CFQ-R, SwCl, weight | BMI, CFQ-R, PEx, SwCl, weight | BMI, CFQ-R, PEx SwCl, weight | BMI, CFQ-R, PEx SwCl, weight |
BMI = body mass index; CFQ-R = Cystic Fibrosis Questionnaire–Revised; DB = double-blind; ELX-TEZ-IVA = elexacaftor-tezacaftor-ivacaftor and ivacaftor; F/G = 1 F508del mutation and 1 gating mutation in the CFTR gene; F/R117H = 1 F508del mutation and 1 R117H mutation in the CFTR gene; F/RF = 1 F508del mutation and 1 residual function mutation in the CFTR gene; IVA = ivacaftor; ITC = indirect treatment comparison; LUM-IVA = lumacaftor/ivacaftor; PEx = pulmonary exacerbations; ppFEV1 = percent predicted forced expiratory volume in 1 second; RCT = randomized controlled trial; SD = standard deviation; SwCl = sweat chloride; TEZ-IVA = tezacaftor-ivacaftor and ivacaftor.
Source: Sponsor’s indirect treatment comparison.62
Baseline Characteristics
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Indirect Comparison Results
Table 79 |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Table 79: Baseline Characteristics for Patients 12 Years and Older With F/G Genotype
Characteristics | Study 104 subset of F/G | |||||||||||||||||||||||||||||||||||| | |||
|---|---|---|---|---|---|
IVA (N = 45) | ELX-TEZ-IVA (N = 50) | |||||||||||||||| | |||||||||||||||| | ||
Sex, n (%) | Male | 28 (62.2) | 28 (56.0) | |||||||||||||||| | |||||||||||||||| |
Female | 17 (37.8) | 22 (44.0) | |||||||||||||||| | |||||||||||||||| | |
Age at screening (years) | Mean (SD) | 30.7 (11.2) | 33.4 (13.8) | |||||||||||||||| | |||||||||||||||| |
Median | 29.0 | 32.7 | |||||||||||||||| | |||||||||||||||| | |
Age group at screening, n (%) | ≥ 12 to < 18 | 6 (13.3) | 8 (16.0) | |||||||||||||||| | |||||||||||||||| |
≥ 18 | 39 (86.7) | 42 (84.0) | |||||||||||||||| | |||||||||||||||| | |
ppFEV1 | Mean (SD) | 68.1 (16.6) | 66.0 (14.8) | |||||||||||||||| | |||||||||||||||| |
BMI (kg/m2) | Mean (SD) | 22.91 (3.39) | 23.71 (3.76) | |||||||||||||||| | |||||||||||||||| |
SwCl (mmol/L) | Mean (SD) | 47.6 (19.1) | 50.9 (23.3) | |||||||||||||||| | |||||||||||||||| |
CFQ-R RD score | Mean (SD) | 75.8 (17.6) | 76.3 (16.4) | |||||||||||||||| | |||||||||||||||| |
BMI = body mass index; CFQ-R (RD) = Cystic Fibrosis Questionnaire–Revised respiratory domain; ELX-TEZ-IVA = elexacaftor-tezacaftor-ivacaftor and ivacaftor; F/G = 1 F508del mutation and 1 gating mutation in the CFTR gene; F/R117H = 1 F508del mutation and 1 R117H mutation in the CFTR gene; IVA = ivacaftor; ppFEV1 = percent predicted forced expiratory volume in 1 second; SD = standard deviation; SwCl = sweat chloride.
Note: Redacted columns have been deleted.
Source: Sponsor’s indirect treatment comparison.62
Critical Appraisal
Table 80 ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Table 80: Results of Direct and Indirect Comparison for Patients 12 Years and Older With F/G Genotype
End point | Direct estimate ELX-TEZ-IVA vs. IVA LSMD (95% CI), P value | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| | |
|---|---|---|---|
|||||||||||||||| | |||||||||||||||| | ||
Absolute change in ppFEV1 from baseline through 8 weeks | 5.7 (3.5 to 7.9) < 0.0001 | |||||||||||||||| | |||||||||||||||| |
Absolute change in SwCl from baseline through 8 weeks | −20.9 (−27.7 to −14.1) < 0.0001 | |||||||||||||||| | |||||||||||||||| |
Absolute change in BMI (kg/m2) from baseline at 8 weeks | 0.16 (−0.10 to 0.42) 0.2142 | |||||||||||||||| | |||||||||||||||| |
Absolute change in weight-for-age z scored from baseline at 8 weeks | 0.01 (−0.06 to 0.08) 0.7765 | |||||||||||||||| | |||||||||||||||| |
Absolute change from baseline through 8 weeks in CFQ-R domain score | — | |||||||||||||||| | |||||||||||||||| |
Respiratory symptoms | 8.8 (3.7 to 13.9) 0.0010 | |||||||||||||||| | |||||||||||||||| |
Physical functioning | 5.3 (0.8 to 9.7) 0.0205 | |||||||||||||||| | |||||||||||||||| |
Vitality | 1.1 (−4.1 to 6.2) 0.6792 | |||||||||||||||| | |||||||||||||||| |
Emotional functioning | 2.1 (−1.6 to 5.8) 0.2659 | |||||||||||||||| | |||||||||||||||| |
Body image | −3.0 (−7.9 to 2.0) 0.2383 | |||||||||||||||| | |||||||||||||||| |
Eating problems | −1.3 (−5.2 to 2.6) 0.4976 | |||||||||||||||| | |||||||||||||||| |
Treatment burden | 2.3 (−2.1 to 6.6) 0.3075 | |||||||||||||||| | |||||||||||||||| |
Health perceptions | 4.8 (−0.1 to 9.7) 0.0568 | |||||||||||||||| | |||||||||||||||| |
Weight | −3.5 (−10.3 to 3.3) 0.3106 | |||||||||||||||| | |||||||||||||||| |
Digestive symptoms | 3.0 (−1.5 to 7.6) 0.1881 | |||||||||||||||| | |||||||||||||||| |
Role functioning | 0.8 (−5.3 to 6.9) 0.7878 | |||||||||||||||| | |||||||||||||||| |
Social functioning | 2.8 (−2.6 to 8.1) 0.3064 | |||||||||||||||| | |||||||||||||||| |
BMI = body mass index; CFQ-R = Cystic Fibrosis Questionnaire–Revised; CI = confidence interval; ELX-TEZ-IVA = elexacaftor-tezacaftor-ivacaftor and ivacaftor; F/G = 1 F508del mutation and 1 gating mutation in the CFTR gene; IVA = ivacaftor; LSMD = least squares mean difference; ppFEV1 = percent predicted forced expiratory volume in 1 second; SwCl = sweat chloride.
Source: Sponsor’s indirect treatment comparison.62
Table 81: CADTH Assessment of Homogeneity of the ITC for the F/G Genotype
Characteristics | Description and handling of potential effect modifiers |
|---|---|
Disease severity | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |
Treatment history | Patients in Study 104 underwent open-label treatment with IVA or TEZ-IVA (for those with F/G and F/RF genotypes, respectively) for 4 weeks before initiating treatment with the randomized study drugs (i.e., none of the patients were naive to CFTR-modulator therapy at the time of baseline measurements). |
Clinical trial eligibility criteria | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |
Dosing of comparators | The study drugs were used in accordance with recommendations in the Canadian product monographs for ELX-TEZ-IVA and ivacaftor. |
Response in the common comparator (i.e., placebo) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |
Definitions of end points | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |
Timing of end point evaluation or trial duration | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |
Withdrawal frequency | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |
Clinical trial setting | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |
Study design | As shown in Table 77, there were differences in the following aspects of the studies: ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |
CF = cystic fibrosis; CFQ-R = Cystic Fibrosis Questionnaire–Revised; ELX-TEZ-IVA = elexacaftor-tezacaftor-ivacaftor and ivacaftor; F/G = 1 F508del mutation and 1 gating mutation in the CFTR gene; F/R117H = 1 F508del mutation and 1 R117H mutation in the CFTR gene; F/RF = 1 F508del mutation and 1 residual function mutation in the CFTR gene; ITC = indirect treatment comparison; IVA = ivacaftor; MMRM = mixed-effects model for repeated measures; ppFEV1 = percent predicted forced expiratory volume in 1 second; RCT = randomized controlled trial; RD = respiratory domain; SD = standard deviation; SwCl = sweat chloride; TEZ-IVA = tezacaftor-ivacaftor and ivacaftor.
Indirect Treatment Comparison for Patients 12 Years and Older With F/RF Genotype
Study Selection Methods
The criteria used by the sponsor to select studies for study inclusion in the ITC in patients with the F/RF genotype were as follows:
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||. It was not reported if a systematic literature search and review was undertaken by the sponsor to identify studies for inclusion; however, CADTH did not identify any additional studies that would have met the inclusion criteria but were not included in the ITC.
Indirect Treatment Comparison Analysis Methods
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Results of Indirect Treatment Comparison Analysis
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Figure 18: Indirect Comparison Network for F/RF Genotype

Figure was redacted.
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Study Characteristics
Table 82 |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Table 82: Indirect Comparisons for Patients 12 Years and Older With F/RF Genotype
Indirect estimate | Direct estimates (study) | End points |
|---|---|---|
ELX-TEZ-IVA vs. placebo | ELX-TEZ-IVA vs. TEZ-IVA (subgroup data from Study 104) plus TEZ-IVA vs. placebo (EXPAND) | ppFEV1 (through 8 weeks) CFQ-R (through 8 weeks) SwCl (through 8 weeks) BMI (at 8 weeks) Weight-for-age z score (at 8 weeks) |
BMI = body mass index; CFQ-R = Cystic Fibrosis Questionnaire–Revised; CFTR = cystic fibrosis transmembrane conductance regulator; ELX-TEZ-IVA = elexacaftor-tezacaftor-ivacaftor and ivacaftor; F/RF = 1 F508del mutation and 1 residual function mutation in the CFTR gene; SwCl = sweat chloride; TEZ-IVA = tezacaftor-ivacaftor and ivacaftor.
Source: Sponsor’s indirect treatment comparison.62
Table 83: Study Characteristics for Patients 12 Years and Older With F/RF Genotype
Characteristics | Study 104 | EXPAND |
|---|---|---|
Study population | Patients with F/G (incl. F/R117H) or F/RF genotypes and ≥ 12 years of age | Patients with F/RF genotypes and ≥ 12 years of age |
Design | Double-blind, active-controlled, parallel-group RCT | Double-blind, placebo-controlled, crossover RCT |
Active run-in period | 4 weeks with TEZ-IVA or IVA | None |
Treatment period | 8 weeks | 8 weeks |
Treatment groups | ELX-TEZ-IVA TEZ-IVA (F/RF) IVA (F/G) | TEZ-IVA IVA Placebo |
ppFEV1 inclusion criteria at screening | 40% to 90% | 40% to 90% |
Schedule of assessments | Day 1, day 15, week 4, week 8 | Day 1, day 15, week 4, week 8, week 12 of each treatment period |
Sample size | |||||||||||||||||||||||||||||||||| | |||||||||||||||||||||||||||||||||| |
Subset of patients included in F/RF ITC | |||||||||||||||||||||||||||||||||| | |||||||||||||||||||||||||||||||||| |
Primary efficacy end point | Absolute change in ppFEV1 from baseline through 8 weeks | Absolute change in ppFEV1 from baseline through average of week 4 and week 8 measurements |
Other end points | BMI, CFQ-R, SwCl, body weight (Did not include PEx as an efficacy end point) | BMI, CFQ-R, PEx, SwCl, body weight |
BMI = body mass index; CFQ-R = Cystic Fibrosis Questionnaire–Revised; ELX-TEZ-IVA = elexacaftor-tezacaftor-ivacaftor and ivacaftor; F/G = 1 F508del mutation and 1 gating mutation in the CFTR gene; F/RF = 1 F508del mutation and 1 residual function mutation in the CFTR gene; F/R117H = one F508del mutation and one R117H mutation in the CFTR gene; ITC = indirect treatment comparison; IVA = ivacaftor; PEx = pulmonary exacerbation; ppFEV1 = percent predicted forced expiratory volume in 1 second; RCT = randomized controlled trial; SwCl = sweat chloride; TEZ-IVA = tezacaftor-ivacaftor and ivacaftor.
Source: Sponsor’s indirect treatment comparison.62
Baseline Characteristics
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Indirect Comparison Results
Table 84 ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Table 84: Baseline Characteristics for Patients 12 Years and Older With F/RF Genotype
Characteristics | Study 104 | |||||||||||||||||| | |||
|---|---|---|---|---|---|
TEZ-IVA (N = 81) | ELX-TEZ-IVA (N = 82) | |||||||||||| | |||||||||||| | ||
Sex, n (%) | Male | 37 (45.7) | 37 (45.1) | |||||||||||| | |||||||||||| |
Female | 44 (54.3) | 45 (54.9) | |||||||||||| | |||||||||||| | |
Age at screening (years) | Mean (SD) | 41.3 (14.4) | 40.1 (14.7) | |||||||||||| | |||||||||||| |
Median | 42.0 | 40.3 | |||||||||||| | |||||||||||| | |
Age group at screening, n (%) | 12 to < 18 | 3 (3.7) | 7 (8.5) | |||||||||||| | |||||||||||| |
≥ 18 | 78 (96.3) | 75 (91.5) | |||||||||||| | |||||||||||| | |
ppFEV1 | Mean (SD) | 68.1 (16.4) | 67.8 (16.3) | |||||||||||| | |||||||||||| |
BMI (kg/m2) | Mean (SD) | 24.68 (5.22) | 24.29 (5.23) | |||||||||||| | |||||||||||| |
SwCl (mmol/L) | Mean (SD) | 61.4 (27.3) | 64.7 (27.9) | |||||||||||| | |||||||||||| |
CFQ-R (RD) score | Mean (SD) | 78.1 (14.7) | 76.7 (16.9) | |||||||||||| | |||||||||||| |
BMI = body mass index; CFQ-R (RD) = Cystic Fibrosis Questionnaire–Revised respiratory domain; ELX-TEZ-IVA = elexacaftor-tezacaftor-ivacaftor and ivacaftor; F/RF = 1 F508del mutation and 1 residual function mutation in the CFTR gene; ppFEV1 = percent predicted forced expiratory volume in 1 second; SD = standard deviation; SwCl = sweat chloride; TEZ-IVA = tezacaftor-ivacaftor and ivacaftor.
Source: Sponsor’s indirect treatment comparison.62
Critical Appraisal for Indirect Treatment Comparison Analysis
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
As noted in Table 85, there are important differences in the baseline and end point values across Study 104 and the |||||||||||||||||||||||||| due to the 4 weeks of active treatment that patients in Study 104 received before randomization.
Table 85: Results of Direct and Indirect Comparison for Patients 12 Years and Older With F/RF Genotype
End point | Direct estimate ELX-TEZ-IVA vs. TEZ-IVA LSMD (95% CI), P value | |||||||||||||||||||||||||||||||||||||||||||||||||||| | |
|---|---|---|---|
|||||||||||||||||||||||||| | |||||||||||||||||||||||||| | ||
Absolute change in ppFEV1 from baseline through 8 weeks | 1.9 (0.5 to 3.4) 0.0104 | |||||||||||||||||||||||||| | |||||||||||||||||||||||||| |
Absolute change in SwCl from baseline through 8 weeks | −24.1 (−27.6 to −20.5) < 0.0001 | |||||||||||||||||||||||||| | |||||||||||||||||||||||||| |
Absolute change in BMI (kg/m2) from baseline at 8 weeks | 0.13 (−0.08 to 0.33) 0.2245 | |||||||||||||||||||||||||| | |||||||||||||||||||||||||| |
Absolute change in weight-for-age z score from baseline at 8 weeks | 0.03 (−0.02 to 0.08) 0.2253 | |||||||||||||||||||||||||| | |||||||||||||||||||||||||| |
Absolute change from baseline through 8 weeks in CFQ-R domain score | — | |||||||||||||||||||||||||| | |||||||||||||||||||||||||| |
Respiratory symptoms | 8.8 (4.3 to 13.4) 0.0002 | |||||||||||||||||||||||||| | |||||||||||||||||||||||||| |
Physical functioning | 3.6 (−0.1 to 7.3) 0.0569 | |||||||||||||||||||||||||| | |||||||||||||||||||||||||| |
Vitality | 7.0 (2.3 to11.8) 0.0042 | |||||||||||||||||||||||||| | |||||||||||||||||||||||||| |
Emotional functioning | 1.2 (−1.9 to 4.4) 0.4367 | |||||||||||||||||||||||||| | |||||||||||||||||||||||||| |
Body image | 1.2 (−2.2 to 4.7) 0.4813 | |||||||||||||||||||||||||| | |||||||||||||||||||||||||| |
Eating problems | 4.8 (1.0 to 8.5) 0.0128 | |||||||||||||||||||||||||| | |||||||||||||||||||||||||| |
Treatment burden | 1.5 (−2.5 to 5.6) 0.4546 | |||||||||||||||||||||||||| | |||||||||||||||||||||||||| |
Health perceptions | 6.8 (2.3 to 11.2) 0.0031 | |||||||||||||||||||||||||| | |||||||||||||||||||||||||| |
Weight | 2.5 (−2.7 to 7.7) 0.3500 | |||||||||||||||||||||||||| | |||||||||||||||||||||||||| |
Digestive symptoms | −2.3 (−6.9 to 2.2) 0.3090 | |||||||||||||||||||||||||| | |||||||||||||||||||||||||| |
Role functioning | 0.0 (−3.7 to 3.7) 0.9973 | |||||||||||||||||||||||||| | |||||||||||||||||||||||||| |
Social functioning | 2.4 (−2.0 to 6.8) 0.2858 | |||||||||||||||||||||||||| | |||||||||||||||||||||||||| |
BMI = body mass index; CFQ-R = Cystic Fibrosis Questionnaire–Revised; CI = confidence interval; ELX-TEZ-IVA = elexacaftor-tezacaftor-ivacaftor and ivacaftor; F/RF = 1 F508del mutation and 1 residual function mutation in the CFTR gene; LSMD = least squares mean difference; ppFEV1 = percent predicted forced expiratory volume in 1 second; SwCl = sweat chloride; TEZ-IVA = tezacaftor-ivacaftor and ivacaftor.
Source: Sponsor’s indirect treatment comparison.62
Summary of Indirect Treatment Comparisons
Patients Aged 6 to 11 Years
The sponsor conducted |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| differences in baseline characteristics.
Patients Aged 12 Years and Older
The sponsor conducted ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
For patients with an F/F genotype, ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
For patients with an F/G genotype, ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
For patients with an F/RF genotype, ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
The primary limitation of the ITCs was the difference in study design across the included studies. The ELX-TEZ-IVA studies (i.e., Study 104 and Study 109) included the open-label, 4-week, active-treatment period with TEZ-IVA or IVA before randomization. |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| As both the ELX-TEZ-IVA and the comparator groups of Study 104 and Study 109 received 4 weeks of treatment with a CFTR modulator, ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Other Relevant Evidence
This section includes a summary of the long-term extension study included in the sponsor’s submission to CADTH and additional relevant studies that were considered to address important gaps in the evidence included in the systematic review. Additional information is required on the longer-term efficacy and safety of ELX-TEZ-IVA, and in patients with an FEV1 of less than 40%, who were excluded from the RCTs. Data from extension Study 105,15,101 and from 2 observational studies in patients with advanced lung disease, have therefore been summarized.17,18 Because the longer-term impacts of ELX-TEZ-IVA on CF-related morbidity and mortality are unknown, the modelling study by Stanojevic et al. (2020)19 has been appraised in this section.
Long-Term Extension Studies
Patients Aged 6 to 11 Years
This section includes data from Study 107, an ongoing, multi-centre, OLE study submitted by the sponsor to CADTH. This study was designed to evaluate the long-term safety and efficacy of ELX-TEZ-IVA in children with CF who are 6 years of age and older and are either homozygous for F508del-CFTR (F/F genotype) or heterozygous for F508del-CFTR and a minimal function mutation (F/MF genotypes).
Methods
Study 107 is an ongoing, open-label, uncontrolled trial that enrolled patients with CF aged 6 years and older who are homozygous or heterozygous for the F508del mutation, and who completed Study 106. A total of 64 patients were enrolled, with safety and efficacy data reported for 64 patients who received at least 1 dose of the study drug. The results are summarized for the interim analysis that was conducted after all patients had reached the 24-week visit.
Populations
All patients who completed study drug treatment in Study 106 or completed study visits up to the last scheduled visit in Study 106 were eligible for Study 107. Two participants discontinued the study drug before week 24 of Study 106 and did not enter the OLE study. A total of 64 children entered the OLE study from the 24-week pivotal study and received 1 or more doses of ELX-TEZ-IVA in the OLE study; patient demographics and clinical characteristics at baseline are shown in Table 86. The majority of patients were female (60.9%), with a mean age of 9.3 years (SD = 1.8). At baseline, the mean BMI was 16.32 (SD = 1.66) and ppFEV1 was 88.3 (SD = 17.6).
Table 86: Assessment of Homogeneity of the ITC for the F/RF Genotype
Characteristics | Description and handling of potential effect modifiers |
|---|---|
Disease severity | Age: Median age at screening was greater in Study 104 (42.0 and 40.3 years in the TEZ-IVA and ELX-TEZ-IVA groups, respectively) and |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| ppFEV1: Study 104 had a higher mean ppFEV1 at baseline (68.1% and 67.8% in the TEZ-IVA and ELX-TEZ-IVA groups, respectively) compared with those in the |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| SwCl: Baseline sweat chloride levels were lower in Study 104 (61.4 mmol/L and 64.7 mmol/L in the TEZ-IVA and ELX-TEZ-IVA groups, respectively) compared with the |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| CFQ-R: Baseline CFQ-R respiratory domain scores were greater in Study 104 (78.1 and 76.7 in the placebo and TEZ-IVA groups, respectively) compared with the |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |
Treatment history | Patients in Study 104 underwent open-label treatment with IVA or TEZ-IVA (for those with F/G and F/RF genotypes respectively) for 4 weeks before initiating treatment with the randomized study drugs (i.e., none of the patients were naive to CFTR-modulator therapy at the time of baseline measurements). |
Clinical trial eligibility criteria | The inclusion criteria differed across the 2 studies with respect to CFTR genotypes. Study 104 enrolled patients with F/G (including F/R117H) or an F/RF genotype. |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |
Response in the common comparator (i.e., TEZ-IVA) | Due to the different designs of Study 104 and the ||||||||||||||||||||||||||, there are important differences in the change from baseline within the TEZ-IVA groups that were included in the indirect comparisons:
|
Dosing of comparators | Both ELX-TEZ-IVA and TEZ-IVA were administered in accordance with recommendations in the Canadian product monographs.3,36 However, patients in the TEZ-IVA group of Study 104 would have received this drug for a total of 12 weeks (i.e., 4 weeks in the run-in period and then 8 weeks in the double-blind phase) compared with only ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||. |
Definitions of end points | The end points included in the ITC were similarly defined and evaluated for each of the included studies. |
Timing of end point evaluation or trial duration | Both Study 104 and |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |
Withdrawal frequency | There were few withdrawals from each of the trials included in the ITC analysis. |
Clinical trial setting | Both Study 104 and |||||||||||||||||||||||||| were phase III RCTs conducted at specialized CF clinics. |
Study design | Study 104 and |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| in Study 104 where all patients received treatment with TEZ-IVA before randomization. |
CF = cystic fibrosis; CFQ-R = Cystic Fibrosis Questionnaire–Revised; ELX-TEZ-IVA = elexacaftor-tezacaftor-ivacaftor and ivacaftor; F/G = 1 F508del mutation and 1 gating mutation in the CFTR gene; F/R117H = 1 F508del mutation and 1 R117H mutation in the CFTR gene; F/RF = 1 F508del mutation and 1 residual function mutation in the CFTR gene; ITC = indirect treatment comparison; IVA = ivacaftor; MMRM = mixed-effects model for repeated measures; ppFEV1 = percent predicted forced expiratory volume in 1 second; RCT = randomized controlled trial; SwCl = sweat chloride; TEZ-IVA = tezacaftor-ivacaftor and ivacaftor.
Intervention
All patients received weight-based dosing (Part A): Patients with a weight less than 30 kg at day 1 received 50% of the adult dose of ELX-TEZ-IVA (ELX 100 mg once daily, TEZ 50 mg once daily, and IVA 75 mg every 12 hours). Patients with a weight greater than or equal to 30 kg at OLE day 1 or at any 2 consecutive study visits during the treatment period received the adult dose of ELX-TEZ-IVA (ELX 200 mg once daily, TEZ 100 mg once daily, and IVA 150 mg every 12 hours).
Outcomes
The primary end point is safety and tolerability, as assessed by AEs, clinical laboratory values, electrocardiography, vital signs, pulse oximetry, and ophthalmologic examinations. Secondary end points include absolute changes in ppFEV1, sweat chloride concentrations, CFQ-R respiratory domain scores, BMI and BMI z scores, and LCI2.5. The numbers of pulmonary exacerbations and CF-related hospitalizations were also assessed as secondary end points.
Statistical Analysis
Safety data were summarized using descriptive statistics. An MMRM was used to analyze changes from baseline in ppFEV1, sweat chloride concentration, CFQ–R respiratory domain scores, BMI and BMI z scores, and LCI2.5. These analyses were similar to the analyses performed in the 24-week pivotal study. Analysis of the number of pulmonary exacerbations and CF-related hospitalizations were based on summary statistics.
Patient Disposition
Of the 66 patients included in Study 106, only 2 participants discontinued the study drug before week 24 and did not enter the OLE study.
Efficacy
Table 87 provides a summary of the change from baseline in ppFEV1, sweat chloride, CFQ-R respiratory domain, BMI, BMI z score and weight after 24 weeks of the extension period. Treatment with ELX-TEZ-IVA resulted in improvements in all measures consistent with the pivotal study. Overall, in the 24-week pivotal study and through the week 24 interim analysis of the OLE study, 5 children (7.6%) had protocol-defined pulmonary exacerbations, for an observed annual rate of pulmonary exacerbations of 0.07. In comparison, the annual rate was 0.12 in Study 106. There were no CF-related hospitalizations in either the pivotal study or through the week 24 interim analysis of the OLE.
Table 87: Baseline and Demographic Characteristics for Study 107
Baseline characteristicsa | ELX-TEZ-IVA (N = 64) |
|---|---|
Sex, n (%) | |
Male | 25 (39.1) |
Female | 39 (60.9) |
Age at baseline (years) | |
Age, mean (SD) | 9.3 (1.8) |
Weight at baseline (kg) | |
Weight < 30 kg, n (%) | 35 (54.7) |
Genotype groups, n (%) | |
F/F | 28 (43.8) |
F/MF | 36 (56.3) |
Clinical characteristics at baselinea | |
ppFEV1, mean (SD), percentage points | 88.3 (17.6) |
SwCl concentration, mean (SD), mmol/L | 102.2 (9.2) |
CFQ-R respiratory domain score, mean (SD), points | 79.8 (15.2) |
BMI, mean (SD), kg/m2 | 16.32 (1.66) |
BMI z score, mean (SD) | −0.19 (0.73) |
LCI2.5, mean (SD) | 9.87 (2.68) |
BMI = body mass index; CFQ–R = Cystic Fibrosis Questionnaire–Revised; ELX-TEZ-IVA = elexacaftor-tezacaftor-ivacaftor and ivacaftor; F/F = homozygous for F508del mutation in the CFTR gene; F/MF = 1 F508del mutation and 1 minimal function mutation in the CFTR gene; LCI2.5 = lung clearance index; ppFEV1 = percent predicted forced expiratory volume in 1 second; SD = standard deviation; SwCl = sweat chloride.
aBaseline is defined as the pivotal study (Study 445 to 106) baseline.
Source: Ratjen et al. (2021).14
Subgroup Analysis of Secondary End Points
An ad hoc subgroup analysis of absolute change in ppFEV1 and sweat chloride concentration was conducted (Table 88). Consistent with the pivotal study, the decrease in the LS mean sweat chloride concentration was greater in the F/F genotype group (−73.3 [SE = 2.0]) compared with the F/MF group (−58.8 [SE = 2.6]) from baseline at extended week 24 of the OLE study.
Table 88: Summary of Efficacy Outcomes
End points | Study 106 (N = 66) through week 24 | Study 107 (N = 64) week 24 interim analysis |
|---|---|---|
ppFEV1, LS mean (SE), percentage points | 10.2 (1.2) | 9.5 (1.3) |
Sweat chloride concentration, LS mean (SE), mmol/L | −60.9 (1.4) | −64.7 (1.7) |
CFQ–R respiratory domain score, LS mean (SE), points | 7.0 (1.1) | 12.9 (1.2) |
BMI, LS mean (SE), kg/m2 | 1.02 (0.13) | 1.27 (0.15) |
BMI z score, LS mean (SE) | 0.37 (0.05) | 0.34 (0.06) |
LCI2.5, LS mean (SE) | −1.71 (0.20) | −1.91 (0.18) |
BMI = body mass index; CFQ-R = Cystic Fibrosis Questionnaire–Revised; LCI2.5 = lung clearance index; LS = least squares; ppFEV1 = percent predicted forced expiratory volume in 1 second; SE = standard error.
Harms
Most patients (79.7%) had AEs in the OLE study through the week 24 interim analysis, which were either mild (51.6%) or moderate (28.1%) in severity for all (Table 89). The most common AEs (≥ 10%) were upper respiratory tract infections (14.1%), headaches (10.9%), and vomiting (10.9%). Two patients (3.1%) had serious AEs (exposure-adjusted event rate = 3.83 per 100 person-years): 1 patient had a serious AE of idiopathic intracranial hypertension that led to study drug interruption (the study drug was resumed after symptoms improved) and the other pediatric patient had a serious AE of an anaphylactic reaction due to accidental peanut exposure that resolved on the same day. Three patients (4.7%) had ALT and/or AST levels of more than 3 times the ULN, with 1 patient having ALT and/or AST levels greater than 5 times the ULN. No patients had an ALT and/or AST level greater than 3 time the ULN with bilirubin levels more than twice the ULN. The exposure-adjusted event rate for AEs of elevated transaminase levels was 17.23 per 100 person-years compared with 31.84 per 100 person-years in the pivotal study. The exposure-adjusted event rate for rash events was 9.57 per 100 person-years compared with 60.79 per 100 person-years in the pivotal study. There were no notable safety findings in other clinical or laboratory assessments. There were no discontinuations through the week 24 interim analysis.
Table 89: Subgroup Analysis of Secondary End Points
End points | Study 106 through week 24 | Study 107 week 24 interim analysis | ||
|---|---|---|---|---|
F/F (N = 29) | F/MF (N = 37) | F/F (N = 28) | F/MF (N = 36) | |
ppFEV1 | ||||
Baseline, mean (SD) | 87.3 (18.3) | 89.8 (17.5) | — | — |
Absolute change, LS mean (SE) | 11.2 (2.0) | 9.1 (1.4) | 12.2 (2.1) | 7.0 (1.4) |
SwCl | ||||
Baseline, mean (SD) | 99.3 (10.8) | 104.4 (7.2) | — | — |
Absolute change, LS mean (SE) | −70.4 (2.4) | −55.1 (1.9) | −73.3 (2.0) | −58.8 (2.6) |
F/F = homozygous for F508del mutation in the CFTR gene; F/MF = 1 F508del mutation and 1 minimal function mutation in the CFTR gene; ppFEV1 = percent predicted forced expiratory volume in 1 second; LS = least squares; SD = standard deviation; SE = standard error; SwCl = sweat chloride.
Source: Ratjen et al. (2021).14
Critical Appraisal
Internal Validity: Study 107 is an extension of Study 106, which was critically appraised earlier. Two patients discontinued the study drug before week 24 and did not enter the OLE study, but no explanation for the withdrawals was provided. The findings from this interim analysis were retrieved from a poster presentation at the North American Cystic Fibrosis Conference and no further details were provided by the sponsor.14 The limited details of the study precluded a full critical appraisal.
External Validity: Issues with the generalizability of these data are the same as for the parent double-blind study. The Critical Appraisal section of the systemic review provides a discussion on the external validity of Study 106.
Patients Aged 12 Years and Older
This section includes data from Study 105, an ongoing, OLE study submitted by the sponsor to CADTH.15,101 This study provides data on the longer-term safety and efficacy of ELX-TEZ-IVA in patients with CF (12 years and older) with either the F/F or F/MF genotype. The extension-phase studies for patients who were enrolled in Study 104 (i.e., Study 110) and Study 109 (i.e., Study 113) are currently ongoing and no data were available at the time of CADTH’s review.
Methods
Study 105 is an ongoing, open-label uncontrolled trial that enrolled patients with CF aged 12 years and older, who are homozygous or heterozygous for the F508del mutation and who completed Study 102 or 103 (i.e., patients with either an F/MF or an F/F genotype). A total of 507 patients were enrolled, with safety and efficacy data reported for 506 patients who received at least 1 dose of the study drug. The results are summarized for the pre-specified second interim analysis that was conducted after all patients had reached the 24-week visit (data cut-off date of October 2019).15 The planned treatment duration is 96 weeks, plus a 4-week safety follow-up period.
Populations
All patients who completed Study 102 or Study 103 were eligible for Study 105. This included patients who had their treatment interrupted in the double-blind parent study but completed the last study visit. Inclusion and exclusion criteria for Study 102 and Study 103 are provided in the Pivotal Studies section of this report.
The demographics of patients included in Study 105 are provided in Table 90, with a breakdown according to parent study and prior treatment received. The baseline data reported reflects the baseline measurement in the parent study. In the overall population of Study 105, half the patients were male, with a mean age of 26.7 years (SD = 10.7). Most patients were White (94%) and from North America (60%). The mean BMI was 21.5 kg/m2 (SD = 3.2) and the mean ppFEV1 was 61.2 (SD = 15.1).
Other prior medications included dornase alfa (84%), azithromycin (55%), inhaled antibiotics (62%), bronchodilators (94%), inhaled hypertonic saline (70%), and inhaled corticosteroids (61%). Overall, 71% of patients had an infection with Pseudomonas aeruginosa in the 2 years before screening for the parent study.
End points | Study 106 (N = 66) Mean exposure = 23.8 weeks | Study 107 week 24 interim analysis (N = 64) Mean exposure = 39.2 weeks | ||
|---|---|---|---|---|
Patients (%) | Events per 100 PYs | Patients (%) | Events per 100 PYs | |
Patients with a TEAE and total TEAEs | 65 (98.5) | 987.04 | 51 (79.7) | 315.83 |
Upper respiratory tract infection | 11 (16.7) | 40.52 | 9 (14.1) | 17.23 |
Headache | 16 (24.2) | 55.00 | 7 (10.9) | 19.14 |
Vomiting | 7 (10.6) | 28.95 | 7 (10.9) | 17.23 |
Cough | 28 (42.4) | 121.57 | 6 (9.4) | 13.40 |
Rhinorrhea | 8 (12.1) | 26.05 | 5 (7.8) | 9.57 |
Increased ALT | 7 (10.6) | 26.05 | 5 (7.8) | 11.48 |
Pyrexia | 14 (21.2) | 55.00 | 4 (6.3) | 11.48 |
Abdominal pain | 8 (12.1) | 26.05 | 4 (6.3) | 7.66 |
Nasal congestion | 10 (15.2) | 40.52 | 3 (4.7) | 5.74 |
Diarrhea | 7 (10.6) | 23.16 | 3 (4.7) | 5.74 |
Oropharyngeal pain | 12 (18.2) | 40.52 | 1 (1.6) | 1.91 |
Rash | 8 (12.1) | 28.95 | 1 (1.6) | 1.91 |
Viral upper respiratory tract infection | 8 (12.1) | 23.16 | 1 (1.6) | 3.83 |
Influenza | 7 (10.6) | 23.16 | 0 | 0 |
TEAE = treatment-emergent adverse events; ALT = alanine transaminase; PY = person-years.
Source: Ratjen et al. (2021).14
Intervention
All patients received open-label ELX 200 mg, TEZ 100 mg, and IVA 150 mg every morning and IVA 150 mg every evening (or the same dosage as previously received in Study 102 or Study 103). Patients could continue a stable regimen of supportive treatments for CF. This included chronic administration of prednisone or prednisolone (maximum 10 mg/day) or 60 mg/day for up to 5 days.
The study drug was interrupted or stopped if the patient met pre-specified criteria for elevated liver function enzymes or bilirubin, or if they reported a generalized rash of grade 3 or higher or had a rash-related SAE.
Outcomes
The primary objective of Study 105 was to examine the safety and tolerability of ELX-TEZ-IVA, with longer-term efficacy as a secondary objective of the trial. Outcomes reported included the absolute change from baseline in the ppFEV1, absolute change from baseline in sweat chloride, number of pulmonary exacerbations, time to first pulmonary exacerbation, absolute change from baseline in BMI, BMI z score, body weight, and absolute change from baseline in CFQ-R respiratory domain scores.
Pulmonary exacerbations were defined using the same criteria as in Study 102 (a change in antibiotic therapy [IV, inhaled, or oral] for any 4 or more of the following signs or symptoms: change in sputum; new or increased hemoptysis; increased cough; increased dyspnea; malaise, fatigue, or lethargy; temperature above 38°C; anorexia or weight loss; sinus pain or tenderness; change in sinus discharge; change in physical examination of the chest; decrease in lung function by at least 10% (based on spirometry); or radiographic changes indicative of pulmonary infection). Changes in antibiotic therapy for sinopulmonary signs and/or symptoms were determined and documented by the study investigator at each study visit.
Statistical Analysis
Efficacy and safety data were based on the full analysis set, which included all patients who received at least 1 dose of ELX-TEZ-IVA in Study 105. The baseline value for efficacy outcomes was the most recent non-missing value collected before the first dose of ELX-TEZ-IVA in the parent study, whereas for safety outcomes, the baseline value was the most recent measurement before the first dose of ELX-TEZ-IVA in either the parent study or Study 105.
The change from baseline outcomes were analyzed using MMRM methods for each individual parent study and included covariates for treatment (as randomized in the parent study), visit, treatment × visit interaction, parent-study baseline ppFEV1, age group at screening of the parent study (< 18 years versus ≥ 18 years). The analysis of data from Study 102 also included a covariate for sex (male versus female).
A negative binomial regression model was used to analyze the number of pulmonary exacerbations for each parent study separately, starting from the first dose of ELX-TEZ-IVA in either the parent or the extension study. The model included covariates for the parent-study baseline ppFEV1 and age group at screening of the parent study (≥ 12 to < 18 versus ≥ 18 years) with log (duration of cumulative ELX-TEZ-IVA efficacy period in years) as an offset. The analysis of Study 102 data also included a covariate for sex (male versus female).
Time to first pulmonary exacerbation was analyzed based on the number of days from the start of ELX-TEZ-IVA in either the parent or extension study until the first pulmonary exacerbation. Patients without an event were censored at the cumulative treatment efficacy period end date. Kaplan–Meier methods were used to present the cumulative exacerbation-free survival rate.
There was no a priori hypothesis tested and no adjustment for multiple statistical testing, or imputation for missing data.
Patient Disposition
Of the 405 patients randomized to Study 102, a total of 400 (99%) entered the extension study and 399 received at least 1 dose of ELX-TEZ-IVA. Seven patients (1.8%) discontinued treatment before 24 weeks due to AEs (4 patients), patient refusal (1 patient), loss to follow-up (1 patient) and pregnancy (1 patient) (Table 91).
Among patients previously randomized in Study 103 (N = 108), 105 enrolled and were treated in Study 105 (97%). Two patients (1.9%) stopped treatment before the 24-week visit (both due to AEs), and 5 patients had stopped treatment before the week 48 visit (3 patients due to AEs and 2 patients due to pregnancy). Overall, 46% of patients previously enrolled in Study 103 and none from Study 102 had completed the week 48 visit in Study 105 at the interim analysis cut-off date.
Results from the week 96 interim analysis were presented at the North American Cystic Fibrosis Conference.16 A total of 506 patients were enrolled in the extension study, as shown in Figure 19 (n = 400 from Study 102 and n = 107 from Study 102) and 42 participants prematurely discontinued treatment before the week 96 visit. Reasons for discontinuing include AEs (n = 8), pregnancy (n = 6), refused further dosing (n = 9), commercial drug availability (n = 12), and other reasons (n = 7).
Table 91: Patient Demographics for Study 105 (Full Analysis Set)
Baseline characteristica | Parent Study 102 | Parent Study 103 | Study 105 | ||
|---|---|---|---|---|---|
Prior placebo (N = 203) | Prior ELX-TEZ-IVA (N = 196) | Prior TEZ-IVA (N = 52) | Prior ELX-TEZ-IVA (N = 55) | Any ELX-TEZ-IVA (N = 506) | |
Sex, n (%) | |||||
Male | 105 (51.7) | 102 (52.0) | 24 (46.2) | 24 (43.6) | 255 (50.4) |
Female | 98 (48.3) | 94 (48.0) | 28 (53.8) | 31 (56.4) | 251 (49.6) |
Age at baseline (years) | |||||
Mean (SD) | 26.8 (11.3) | 25.7 (9.7) | 27.9 (10.8) | 28.8 (11.5) | 26.7 (10.7) |
Median (range) | 25.0 (12.3 to 64.0) | 24.4 (12.1 to 59.9) | 27.6 (12.4 to 60.5) | 27.4 (12.7 to 54.1) | 25.1 (12.1 to 64.0) |
≥ 12 to < 18 years | 60 (29.6) | 55 (28.1) | 14 (26.9) | 16 (29.1) | 145 (28.7) |
≥ 18 years | 143 (70.4) | 141 (71.9) | 38 (73.1) | 39 (70.9) | 361 (71.3) |
Race, n (%) | |||||
White | 184 (90.6) | 183 (93.4) | 52 (100.0) | 54 (98.2) | 473 (93.5) |
African-American | 2 (1.0) | 4 (2.0) | 0 | 0 | 6 (1.2) |
Asian | 1 (0.5) | 0 | 0 | 0 | 1 (0.2) |
American Indian | 1 (0.5) | 0 | 0 | 0 | 1 (0.2) |
Other | 1 (0.5) | 2 (1.0) | 0 | 0 | 3 (0.6) |
Not collectedb | 16 (7.9) | 8 (4.1) | 0 | 1 (1.8) | 25 (4.9) |
Hispanic or Latino, n (%) | |||||
Yes | 12 (5.9) | 4 (2.0) | 3 (5.8) | 2 (3.6) | 21 (4.2) |
No | 175 (86.2) | 184 (93.9) | 49 (94.2) | 52 (94.5) | 460 (90.9) |
Not collected b | 16 (7.9) | 8 (4.1) | 0 | 1 (1.8) | 25 (4.9) |
Geographic region, n (%) | |||||
North America | 120 (59.1) | 117 (59.7) | 33 (63.5) | 34 (61.8) | 304 (60.1) |
Europe/Australia | 83 (40.9) | 79 (40.3) | 19 (36.5) | 21 (38.2) | 202 (39.9) |
Weight (kg) | |||||
Mean (SD) | 58.3 (12.7) | 60.0 (12.9) | 59.8 (14.8) | 59.9 (12.7) | 59.3 (13.0) |
Median (range) | 58.0 (31.3 to 105.2) | 58.0 (29.0 to 108.0) | 55.0 (36.0 to 100.0) | 59.0 (36.0 to 91.2) | 58.0 (29.0 to 108.0) |
BMI (kg/m2) | |||||
Mean (SD) | 21.3 (3.14) | 21.5 (3.08) | 21.9 (4.12) | 21.8 (3.19) | 21.5 (3.23) |
Median (range) | 20.8 (14.4 to 33.8) | 21.4 (15.0 to 30.9) | 20.8 (15.6 to 34.6) | 21.4 (16.0 to 28.4) | 21.1 (14.4 to 34.6) |
ppFEV1 category at baseline, n (%) | |||||
< 40 | 16 (7.9) | 18 (9.2) | 4 (7.7) | 6 (10.9) | 44 (8.7) |
≥ 40 to < 70 | 120 (59.1) | 112 (57.1) | 34 (65.4) | 31 (56.4) | 297 (58.7) |
≥ 70 to ≤ 90 | 62 (30.5) | 65 (33.2) | 14 (26.9) | 18 (32.7) | 159 (31.4) |
> 90 | 5 (2.5) | 1 (0.5) | 0 | 0 | 6 (1.2) |
ppFEV1 at baseline | |||||
Mean (SD) | 61.3 (15.5) | 61.4 (14.9) | 60.2 (14.4) | 61.6 (15.4) | 61.2 (15.1) |
Median (range) | 60.9 (32.3 to 93.7) | 61.4 (33.8 to 97.1) | 58.4 (35.0 to 89.0) | 61.0 (35.0 to 87.4) | 60.9 (32.3 to 97.1) |
Sweat chloride (mmol/L) at baseline | |||||
Mean (SD) | 102.9 (9.8) | 102.4 (11.9) | 90.0 (12.3) | 91.4 (11.0) | 100.1 (12.0) |
Median (range) | 104.0 (68.5 to 137.0) | 103.0 (22.5 to 156.0) | 90.8 (60.5 to 112.0) | 92.8 (67.0 to 114.0) | 102.0 (22.5 to 156.0) |
CFQ-R respiratory domain at baseline | |||||
Mean (SD) | 70.0 (17.8) | 68.2 (16.8) | 72.6 (17.9) | 70.6 (16.2) | 69.6 (17.2) |
Median (range) | 72.2 (16.7 to 100.0) | 72.2 (16.7 to 100.0) | 72.2 (27.8 to 100.0) | 72.2 (22.2 to 100.0) | 72.2 (16.7 to 100.0) |
Medication use at screening, n (%) | |||||
CFTR modulator | NR | NR | NR | NR | NR |
Dornase alfa | 164 (80.8) | 161 (82.1) | 48 (92.3) | 51 (92.7) | 424 (83.8) |
Azithromycin | 114 (56.2) | 109 (55.6) | 25 (48.1) | 33 (60.0) | 281 (55.5) |
Inhaled antibiotic | 132 (65.0) | 116 (59.2) | 28 (53.8) | 35 (63.6) | 311 (61.5) |
Bronchodilator | 192 (94.6) | 184 (93.9) | 47 (90.4) | 54 (98.2) | 477 (94.3) |
Inhaled corticosteroids | 122 (60.1) | 120 (61.2) | 28 (53.8) | 36 (65.5) | 306 (60.5) |
Hypertonic saline | 129 (63.5) | 145 (74.0) | 42 (80.8) | 38 (69.1) | 354 (70.0) |
Pseudomonas aeruginosa infection within 2 years of screening, n (%) | |||||
Positive | 142 (70.0) | 147 (75.0) | 31 (59.6) | 39 (70.9) | 359 (70.9) |
Negative | 61 (30.0) | 49 (25.0) | 21 (40.4) | 16 (29.1) | 147 (29.1) |
BMI = body mass index; CFQ-R = Cystic Fibrosis Questionnaire–Revised; ELX/TEV/IVA = elexacaftor-tezacaftor-ivacaftor and ivacaftor; ppFEV1 = percent predicted forced expiratory volume in 1 second; NR = not reported; SD = standard deviation; TEZ-IVA = tezacaftor-ivacaftor and ivacaftor.
aBaseline of parent study (i.e., Study 102 or Study 103).
bNot collected in accordance with local regulations.
Source: Clinical Study Report.15
Figure 19: Patient Disposition in Open-Label Extension Study 105 — Week 96
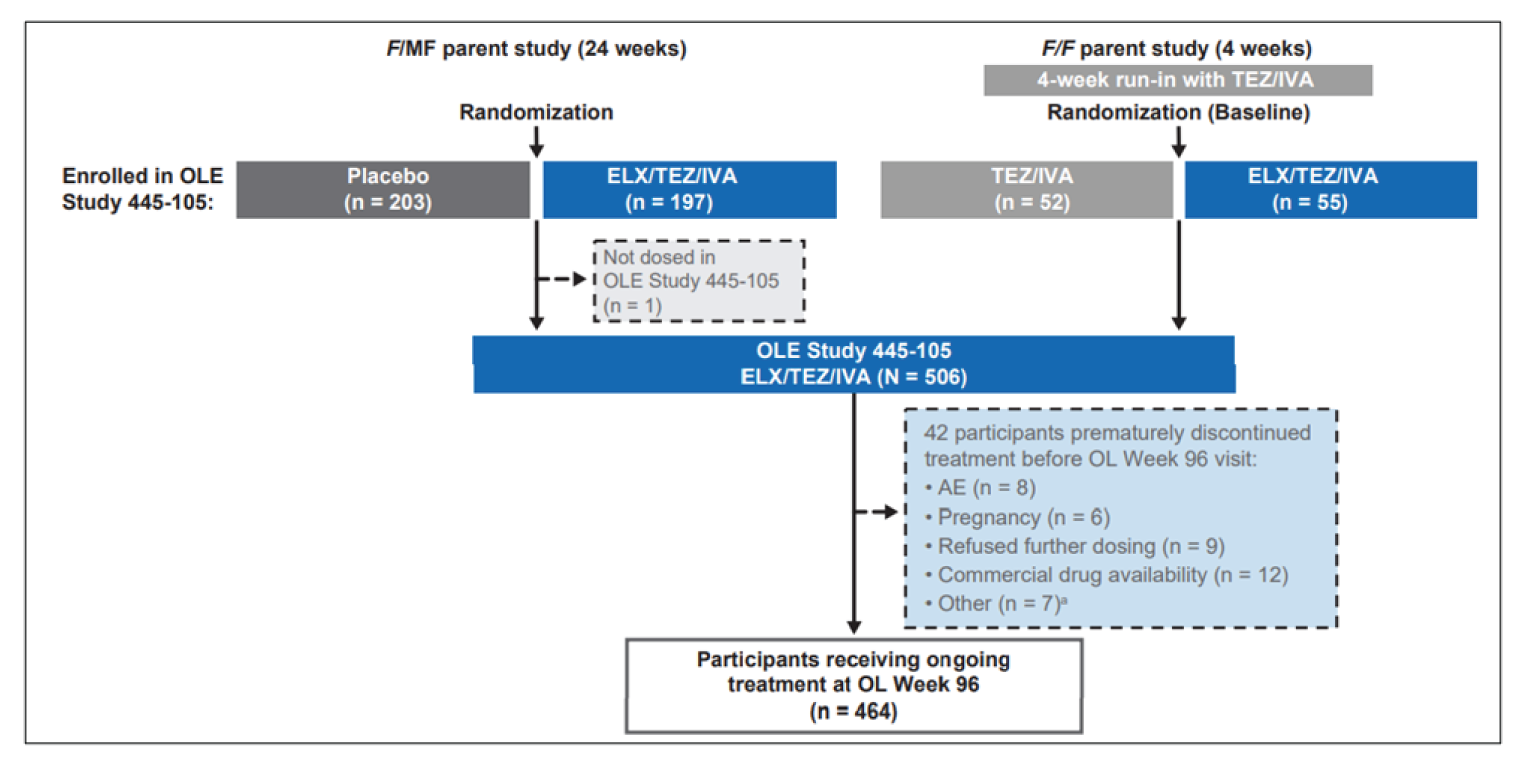
AE = adverse event; ELX-TEZ-IVA = elexacaftor-tezacaftor-ivacaftor and ivacaftor; F/F = homozygous for F508del mutation in the CFTR gene; F/MF = 1 F508del mutation and 1 minimal function mutation in the CFTR gene; OL = open-label; OLE = open-label extension; TEZ-IVA = tezacaftor-ivacaftor and ivacaftor.
Source: Daines et al. (2021).16
Exposure to Study Treatments
During Study 105, the total duration of exposure to ELX-TEZ-IVA was 392 person-years, with a mean exposure of 37.2 weeks (SD 8.9), and median of 36.5 weeks (range 1.4 to 55.4 weeks) (N = 506). The cumulative exposure to ELX-TEZ-IVA for the parent studies and Study 105 was 497 person-years, with a mean treatment duration of 46.7 weeks (SD = 13.3) and median duration of 49.0 weeks (range 1.0 to 69.1 weeks) (N = 510). At the interim analysis, 45% of patients had been treated for longer than 24 weeks but less than 48 weeks, and 53% of patients had been treated for longer than 48 weeks but less than 72 weeks.
Efficacy
Table 92 provides a summary of the change from baseline in ppFEV1, sweat chloride, CFQ-R respiratory domain, BMI, BMI z score and weight after 96 weeks of the extension period for those patients who enrolled from Study 102 and Study 103. Between 2% and 7% of patients were excluded or missing from the interim analyses (number of patients with missing BMI z score data were not reported).
Among patients previously enrolled in Study 102, the absolute change from week 24 to week 96 in the ppFEV1 was similar for patients who switched from placebo to ELX-TEZ-IVA (absolute change = 15.2%; 95% CI, 13.6 to 16.7) and for those who remained on ELX-TEZ-IVA (absolute change = 14.3%; 95% CI, 12.7 to 15.8) during the extension study. Patients previously enrolled in Study 103 reported an absolute change from week 4 to week 96 in the ppFEV1 of 12.4% (95% CI, 9.6 to 15.1) and 11.5% (95% CI, 8.8 to 14.2) during the extension study, for patients previously treated with TEZ-IVA and ELX-TEZ-IVA, respectively.
For patients previously enrolled in Study 102, the absolute change from week 24 to extension-period week 96 in the CFQ-R respiratory domain was 20.1 points (95% CI, 17.5 to 22.6) for those switched from placebo to ELX-TEZ-IVA, and 21.7 points (95% CI, 19.1 to 24.1) for those who received ongoing ELX-TEZ-IVA treatment. The absolute change was 15.6 points (95% CI, 11.0 to 20.1) and 18.0 points (95% CI, 13.6 to 22.5) for patients from Study 103 who were switched from TEZ-IVA to ELX-TEZ-IVA, respectively, and those treated with ELX-TEZ-IVA in both study periods (Table 92).
The absolute change in BMI from week 24 (Study 102) or week 4 (Study 103) to week 96 ranged from 1.3 kg/m2 to 1.9 kg/m2.
The absolute change in sweat chloride concentration from week 24 (study 102) or week 4 (study 103) to week 96 ranged from −45.8 mmol/L to −49.7 mmol/L in patients previously enrolled in Study 102 or 103 (Table 92).
Table 92: Patient Disposition of Study 105
Disposition, n (%) | Prior placebo Study 102 | Prior ELX-TEZ-IVA Study 102 | Prior TEZ-IVA Study 103 | Prior ELX-TEZ-IVA Study 103 | Any ELX-TEZ-IVA Study 105 |
|---|---|---|---|---|---|
Enrolled, N | 203 | 197 | 52 | 55 | 507 |
Completed 24-week visit, N (%) | 200 (98.5) | 192 (98) | 51 (98.1) | 54 (98.2) | 497 (98.2) |
Discontinued treatment before week 24 visit, n (%) | 3 (1.5) | 4 (2.0) | 1 (1.9) | 1 (1.8) | 9 (1.8) |
Adverse events | 2 (1.0) | 2 (1.0) | 1 (1.9) | 1 (1.8) | 6 (1.2) |
Patient refusal | 0 | 1 (0.5) | 0 | 0 | 1 (0.2) |
Lost to follow-up | 1 (0.5) | 0 | 0 | 0 | 1 (0.2) |
Pregnancy (self or partner) | 0 | 1 (0.5) | 0 | 0 | 1 (0.2) |
Completed week 48 visit, N (%) | 0 | 0 | 24 (46.2) | 25 (45.5) | 49 (9.7) |
Discontinued treatment before week 48 visit, n (%) | 4 (2.0) | 4 (2.0) | 3 (5.8) | 2 (3.6) | 13 (2.6) |
Adverse events | 2 (1.0) | 2 (1.0) | 2 (3.8) | 1 (1.8) | 7 (1.4) |
Patient refusal | 1 (0.5) | 1 (0.5) | 0 | 0 | 2 (0.4) |
Lost to follow-up | 1 (0.5) | 0 | 0 | 0 | 1 (0.2) |
Pregnancy (self or partner) | 0 | 1 (0.5) | 1 (1.9) | 1 (1.8) | 3 (0.6) |
Full analysis set | 203 | 196 | 52 | 55 | 506a |
Safety set | 201 | 198 | 52 | 55 | 506 a |
ELX-TEZ-IVA = elexacaftor-tezacaftor-ivacaftor and ivacaftor; TEZ-IVA = tezacaftor-ivacaftor and ivacaftor.
aOne patient was enrolled in Study 105 but never received a dose of ELX-TEZ-IVA and was excluded from the full analysis and safety sets.
Source: Clinical Study Report.15
During treatment with ELX-TEZ-IVA, the annual event rate for pulmonary exacerbations and time to first pulmonary exacerbation were similar across the patient populations analyzed (Table 93). The annual pulmonary exacerbation event rates were 0.27 (95% CI, 0.19 to 0.39) and 0.32 (95% CI, 0.24 to 0.44) for those previously enrolled in Study 102 and 0.30 (95% CI, 0.20 to 0.45) for those previously enrolled in Study 103. The event-free survival probabilities were approximately 0.85 at 24 weeks and 0.73 at 36 weeks. The estimated mean pulmonary exacerbation rate per 48 weeks for participants with F/MF genotypes was 0.21 (95% CI, 0.17 to 0.26) for the week 96 interim analysis compared with 0.98 in the placebo group of the F/MF parent study. The estimated mean pulmonary exacerbation rate per 48 weeks for participants with the F/F genotype was 0.21 (95% CI, 0.14 to 0.30) for the week 96 interim analysis. Because part of this OLE study overlapped with the COVID-19 pandemic, restrictions on social interactions likely contributed to reductions in pulmonary exacerbation for patients with CF.
Table 93: Summary of Efficacy Outcomes for Study 105 (Week 96 — Open-Label Extension)
Outcome | F/MF genotypes Study 105 (week 96) | F/F genotypes Study 105 (week 96) | ||
|---|---|---|---|---|
Placebo to ELX-TEZ-IVA (N = 203) | ELX-TEZ-IVA to ELX-TEZ-IVA (N = 196) | TEZ-IVA to ELX-TEZ-IVA (N = 52) | ELX-TEZ-IVA to ELX-TEZ-IVA (N = 55) | |
Absolute change in ppFEV1 (95% CI), percentage points a | 15.2 (13.6 to 16.7) | 14.3 (12.7 to 15.8) | 12.4 (9.6 to 15.1) | 11.5 (8.8 to 14.2) |
Absolute change in SwCl concentration (95% CI), mmol/L | −48.6 (−51.3 to −45.8) | −45.8 (−48.5 to −43.0) | −48.3 (−53.7 to −42.8) | −49.7 (−55.0 to −44.4) |
Absolute change in CFQ-R respiratory domain score (95%CI), points b | 20.1 (17.5 to 22.6) | 21.7 (19.1 to 24.1) | 15.6 (11.0 to 20.1) | 18.0 (13.6 to 22.5) |
Absolute change in BMI (95% CI), kg/m2 c | 1.87 (1.61 to 2.13) | 1.58 (1.32 to 1.84) | 1.28 (0.80 to 1.76) | 1.50 (1.03 to 1.96) |
Estimated mean PEx event rate per 48 weeks (95% CI) | 0.21 (0.17 to 0.26) | 0.21 (0.14 to 0.30) | ||
BMI = body mass index; CFQ-R = Cystic Fibrosis Questionnaire–Revised; CFTR = cystic fibrosis transmembrane conductance regulator; CI = confidence interval; ELX-TEZ-IVA = elexacaftor-tezacaftor-ivacaftor and ivacaftor; F/F = homozygous for F508del mutation in the CFTR gene; F/MF = 1 F508del mutation and 1 minimal function mutation in the CFTR gene; PEx = pulmonary exacerbation; ppFEV1 = percent predicted forced expiratory volume in 1 second; SwCl = sweat chloride; TEZ-IVA = tezacaftor-ivacaftor and ivacaftor.
aData analyzed using the baseline from the parent study. The mixed-effects model for repeated measures with covariates for treatment (as randomized in parent study), visit, treatment × visit interaction, parent-study baseline ppFEV1, and age group at screening of the parent study (< 18 years vs. ≥ 18 years). Analysis of data from Study 102 also included a covariate for sex (male vs. female).
bFor patients previously enrolled in Study 103 the change from baseline in sweat chloride and CFQ-R respiratory domain were reported for the 24-week visit of the extension study.
cBMI z score was analyzed for patients 20 years of age and younger from the start of the parent study.
Source: Daines et al., (2021).16
Table 94: Summary of Pulmonary Exacerbations Outcomes for Study 105 (Full Analysis Set)
Analysis | Study 105 (week 24) | Study 105 (week 36) | |
|---|---|---|---|
Placebo in Study 102 N = 203 | ELX-TEZ-IVA in Study 102 N = 196 | TEZ-IVA or ELX-TEZ-IVA in Study 103 N = 107 | |
Cumulative number of pulmonary exacerbationsa | |||
Total number of years of the cumulative treatment period | 145.7 | 241.0 | 111.1 |
Number of patients included in analysis (%) | 203 (99.5) | 200 (99.5) | 107 (99) |
Number of patients with events (%) | 35 (17.2) | 55 (27.5) | 27 (25.2) |
Number of events | 44 | 84 | 33 |
Estimated event rate per year (95% CI)b | 0.27 (0.19 to 0.39) | 0.32 (0.24 to 0.44) | 0.30 (0.20 to 0.45) |
Time to first pulmonary exacerbation | |||
Number of patients included in analysis (%)a | 203 (99.5) | 200 (99.5) | 107 (99) |
Number of patients with events (%) | 35 (17.2) | 55 (27.5) | 27 (25.2) |
Probability of event-free survival at 24 weeks, KM estimate (95% CI) | 0.85 (0.79 to 0.89) | 0.84 (0.79 to 0.89) | 0.85 (0.77 to 0.91) |
Probability of event-free survival at 24 weeks, KM estimate (95% CI) | NA | 0.73 (0.66 to 0.79) | 0.74 (0.65 to 0.82) |
CI = confidence interval; ELX-TEZ-IVA = elexacaftor-tezacaftor-ivacaftor and ivacaftor; TEZ-IVA = tezacaftor-ivacaftor and ivacaftor.
aPulmonary exacerbations event rate was calculated as the total number of events multiplied by 336 days, divided by the total number of days from the first dose of ELX-TEZ-IVA in the parent or extension study (1 year = 336 days). The analysis included 405 patients enrolled in Study 102 and 108 patients enrolled in Study 103.
bNegative binomial model that includes covariates for parent study baseline ppFEV1 and age group at screening of the parent study (≥ 12 to < 18 vs. ≥ 18 years) with log(duration of cumulative ELX-TEZ-IVA efficacy period in years) as an offset. Analysis of Study 102 data also included a covariate for sex (male vs. female).
Source: Clinical Study Report.15
Harms
Most patients (98%) reported 1 or more AEs during the extension study (586 events per 100 person-years). The most reported events were infective pulmonary exacerbation of CF (38%), cough (36%), oropharyngeal pain (26%), headache (25%) and nasopharyngitis (23%). Eleven patients (2.2%) stopped treatment due to AEs, 126 patients (25%) experienced an SAE, and grade 3 or 4 AEs were reported by 84 (17%). There was 1 death during the study due to an AE of accidental oxycodone toxicity that was considered unrelated to the study drug. Sixty-five patients (13%) reported an elevated transaminase event; treatment was interrupted for 17 patients as a result, and 4 discontinued the study drug. Levels of ALT and/or AST more than 3 times, 5 times, and 8 times the ULN were reported in 50 (9.9%), 25 (4.9%), and 9 (1.8%) participants, respectively. Rash events were reported by 74 patients (15%). One rash event was classified as an SAE that resolved after treatment was discontinued.
Table 95: Summary of Harms in Study 105
Harms | F/MF parent study | F/F Study 105 (week 96) ELX-TEZ-IVA (N = 506) n (%) | |
|---|---|---|---|
Placebo (N = 201) n (%) | ELX-TEZ-IVA (N = 202) n (%) | ||
Mean exposure | 23.7 weeks | 23.6 weeks | 105.7 weeks |
All AEs | 193 (96.0) | 188 (93.1) | 498 (98.4) |
Serious AEs | 42 (20.9) | 28 (13.9) | 126 (24.9) |
Related serious AEs | 2 (1.0) | 6 (3.0) | 15 (3.0) |
AEs leading to discontinuation | 0 | 2 (1.0) | 11 (2.2) |
AEs leading to interruption | 10 (5.0) | 19 (9.4) | 44 (8.7) |
AEs by maximum severity | |||
Mild | 53 (26.4) | 67 (33.2) | 118 (23.3) |
Moderate | 125 (62.2) | 102 (50.5) | 296 (58.5) |
Severe | 14 (7.0) | 19 (9.4) | 81 (16.0) |
Life-threatening | 1 (0.5) | 0 | 3 (0.6) |
AEs by strongest relationship | |||
Not related | 83 (41.3) | 53 (26.2) | 144 (28.5) |
Unlikely related | 58 (28.9) | 39 (19.3) | 131 (25.9) |
Possibly related | 46 (22.9) | 86 (42.6) | 198 (39.1) |
Related | 6 (3.0) | 10 (5.0) | 25 (4.9) |
Most common AEs (> 15%) | |||
Infective PEx of CF | 95 (47.3) | 44 (21.8) | 191 (37.7) |
Cough | 77 (38.3) | 34 (16.8) | 183 (36.2) |
Oropharyngeal pain | 25 (12.4) | 20 (9.9) | 132 (26.1) |
Headache | 30 (14.9) | 35 (17.3) | 124 (24.5) |
Nasopharyngitis | 26 (12.9) | 22 (10.9) | 114 (22.5) |
Sputum increased | 39 (19.4) | 40 (19.8) | 100 (19.8) |
Upper respiratory tract infection | 22 (10.9) | 24 (11.9) | 99 (19.6) |
Pyrexia | 19 (9.5) | 17 (8.4) | 95 (18.8) |
Nasal congestion | 15 (7.5) | 19 (9.4) | 81 (16.0) |
Fatigue | 20 (10.0) | 9 (4.5) | 80 (15.8) |
AE = adverse event; CF = cystic fibrosis; ELX-TEZ-IVA = elexacaftor-tezacaftor-ivacaftor and ivacaftor; ; F/F = homozygous for F508del mutation in the CFTR gene; F/MF = 1 F508del mutation and 1 minimal function mutation in the CFTR gene; NR = not reported; PEx = pulmonary exacerbation.
aReported in 10% of patients.
bReported in at least 2 patients.
Source: Daines et al. (2021).16
Critical Appraisal
Internal Validity: Study 105 is an ongoing, uncontrolled, open-label trial that enrolled patients with CF (aged 12 years and older) who had at least 1 F508del mutation and who had completed Study 102 or Study 103. As this was an unblinded study, patient’s expectations of treatment could potentially have biased the reporting of subjective outcomes, such as respiratory symptoms (as measured by the CFQ-R), or harms. Extension studies are often limited by selection bias, as only patients who are tolerant to treatment and complete the parent studies are eligible to enrol. For Study 105, the risk of selection bias may be low, given that only 7 patients (1.4%) out of the 513 randomized in the parent studies were not enrolled or treated in the extension study. During the first 24 weeks of follow-up, discontinuation of treatment was also low (9 patients, 1.8%), however the frequency of missing data was higher for some outcomes relative to others. The change from baseline in ppFEV1 and sweat chloride analyses were missing for 6% to 9% of patients at 24 weeks, compared to 2% to 4% with missing data for the change in CFQ-R respiratory domain, BMI, and body weight. The extent of missing data for the change in BMI z scores was unclear. For the efficacy outcomes there was no imputation for missing data, and the MMRM model assumed that data are missing at random, which may not be a valid assumption; however, the extent of missing data was less than 10%.
Data on pulmonary exacerbations were based on a standard definition; however, events were not adjudicated by an independent committee. Because interpretation of the exacerbation rate is difficult given the lack of a comparator group, it is not possible to differentiate the treatment effects of ELX-TEZ-IVA from other factors, such as seasonality, that may affect exacerbations.
The findings from the week 96 OLE interim analysis were retrieved from a poster presentation at the North American Cystic Fibrosis Conference and no further details were provided by the sponsor.
External Validity: Issues with the generalizability of these data are the same as for the parent double-blind studies. The Critical Appraisal section of the systematic review discusses the external validity of Study 102 and Study 103.
Observational Studies in Patients With Advanced Lung Disease
Two observational studies in patients with advanced pulmonary disease were identified in the literature search conducted by CADTH. The retrospective chart review by O’Shea et al. (2021) included 14 patients who received ELX-TEZ-IVA through a managed care program in Ireland.17 The prospective observational cohort study conducted by Burgel et al. (2021) reported data for 245 patients who received ELX-TEZ-IVA through an early-access program in France.18
Description and Appraisal of Irish Cohort Study
Methods
O’Shea et al. (2021)17 reported on a retrospective chart review conducted at the Irish National Referral Centre for Adult CF based in an academic health centre in Dublin, Ireland. Through a managed access program, patients who were homozygous for F508del or heterozygous for F508del with a second minimal function CFTR mutation were eligible to receive ELX-TEZ-IVA if they had severe lung disease (defined as FEV1 < 40% predicted) or were on an active lung transplantation list.
Populations
A total of 14 adult patients were initiated on ELX-TEZ-IVA between December 2019 and July 2020. The study included 9 women and 5 men with severe lung disease, 2 of whom were on the transplant list. The mean age of patients was 34.4 years (range = 19 to 46). Eight patients (57%) were homozygous for the F508del mutation and had previously received CFTR-modulatory therapy. The other 6 patients were heterozygous for the F508del mutation. All patients were pancreatic-insufficient. Other comorbidities included CF-related diabetes (9 patients) and CF-related liver disease (6 patients), including 1 patient who required dose reduction of ELX-TEZ-IVA due to Child-Pugh Score B liver disease. In the year before initiating ELX-TEZ-IVA, the patients had a median of 3 hospitalizations (IQR = 2.0 to 4.3) and required a median total of 77 days of IV treatment (IQR = 43.5 to 137.5). Mean ppFEV1, BMI, and sweat chloride levels at baseline are shown in Table 96.
Interventions
All patients received open-label ELX-TEZ-IVA (dose not specified).
Outcomes
Outcomes of interest included the change from baseline in ppFEV1, BMI, and sweat chloride levels, the number of infective pulmonary exacerbations, days spend on IV antibiotics, and the presence of CF comorbidities (i.e., CF-related diabetes or liver disease).
Statistical Analysis
A paired t-test was used to analyze the change in ppFEV1, BMI, and sweat chloride levels, with a 2-sided P value of less than 0.05 considered statistically significant. The most recent outcome measurement before the start of ELX-TEZ-IVA was used as the baseline values. The frequency of pulmonary exacerbations was analyzed as the number of events per month, compared with the monthly frequency of events in the year before starting therapy. A chi-square test was used to analyze categorical variables.
Exposure to Study Treatments
Patients were followed for a mean of 4.9 months (SD = 1.9; range 1 to 8 months) after starting ELX-TEZ-IVA.
Efficacy
The rate of infective pulmonary exacerbations requiring hospitalization was 0.28 events per month (SD = 0.17) in the 12 months before ELX-TEZ-IVA, and 0.04 events per month (SD = 0.07) during the 4.9-month follow-up period (P < 0.001) (N = 7).
The mean ppFEV1 improved from 27% (SD = 7.3) at baseline to 36% (SD = 16.5) after a mean follow-up of 26 days (N = 14) (Table 96). The mean BMI increased from 20.7 kg/m2 (SD = 3.6) to 22.1 kg/m2 (SD = 3.4) (N = 14), and the mean sweat chloride fell from 105 mmol/L (SD = 15) to 54 mmol/L (SD = 23) (N = 11) after an average of 62 days of follow-up.
Harms
The most common treatment-related AEs are summarized in Table 96. These events included gastrointestinal symptoms (10%), localized cutaneous rash (7%), myalgia (5%) and increased bilirubin 3 or more times the ULN (5%). No patients permanently stopped treatment due to AEs, but 14 patients (6%) had treatment interrupted during the follow-up period reported (median = 84 days; IQR = 70 to 104). Rash was the most common reason for temporary discontinuation of ELX-TEZ-IVA. No patients had their therapy interrupted due to increases in liver enzymes, bilirubin, or creatine phosphokinase levels.
Table 96: Summary of Efficacy Outcomes — Irish Cohort Study
Outcome | N | Baseline | End point | P valuea | Follow-up time, days, mean (SD) |
|---|---|---|---|---|---|
ppFEV1, %, mean (SD) | 14 | 27.3 (7.3) | 36.3 (16.5) | < 0.0001 | 26.4 (4.2) |
BMI, kg/m2, mean (SD) | 14 | 20.7 (3.6) | 22.1 (3.4) | < 0.0001 | 62 (35) |
Sweat chloride, mmol/L, mean (SD) | 11 | 104.9 (15.0) | 53.6 (23.3) | < 0.0001 | 64 (84) |
BMI = body mass index; ppFEV1 = percent predicted forced expiratory volume in 1 second; SD = standard deviation.
aPaired t-test.
Source: O’Shea et al. (2021).17
Harms
One patient experienced an SAE and required hospitalization for distal intestinal obstruction syndrome. One other patient required treatment interruption due to an acute kidney injury that was considered unrelated to the ELX-TEZ-IVA. No other AEs were reported by O’Shea et al. (2021).17
Critical Appraisal
O’Shea et al. (2021) provides descriptive data for 14 patients with advanced lung disease who were treated with open-label ELX-TEZ-IVA. The mean follow-up time was limited (less than 5 months) and variable, with the change in ppFEV1 and BMI reported after an average of 1 to 2 months. Exacerbation data appear to be available only for 7 of the 14 patients, and the accuracy and completeness of these data are uncertain. Due to the retrospective design, the study relied on data already collected, which may be missing or inaccurate. Moreover, monitoring and reporting of patient outcomes may have been affected by the COVID-19 pandemic and lockdown measures. Some of the differences observed in the frequency of exacerbations may be attributable to seasonal variation and, considering the short follow-up time, these data should be interpreted with caution. The generalizability of the findings may be limited given that they were based on a limited sample of patients from a single centre in Ireland and may be subject to selection bias. In addition, the study was published as a letter to the editor and has not undergone peer review.
Description and Appraisal of French Cohort Study
Methods
The objective of the prospective cohort study by Burgel et al. (2021) was to evaluate the real-world efficacy and safety of ELX-TEZ-IVA in patients with CF and advanced pulmonary disease.18 The study, conducted by the French CF Reference Center Network, included patients from all 47 CF centres in France who received ELX-TEZ-IVA through an early-access program.
Populations
Starting in December 2019, patients with CF were eligible to receive ELX-TEZ-IVA through an early-access program if they were 12 years or older, had a least 1 F508del mutation, and had advanced respiratory disease (defined as a ppFEV1 < 40%), or were under evaluation for lung transplantation. All patients who received ELX-TEZ-IVA in France between December 2020 and August 2021 were included in the study (N = 245).
The median age of patients treated was 31 years (IQR = 24 to 38), of which 17 were adolescents (7%) (Table 95). Most patients were male (55%) and heterozygous for the F508del mutation (59%). The median baseline ppFEV1 was 29% (IQR = 24% to 34%). Most patients were pancreatic-insufficient (96%), 43% had CF-related diabetes, and 6% had cirrhosis or portal hypertension. The patients had received a median 43 days of IV antibiotics (IQR = 24 to 70) and spent 7 days in hospital (IQR = 0 to 29) in the past 12 months.
Most patients were not receiving a CFTR modulator at the start of the study (186 patients, 76%). Of these patients, 41 had previously received LUM-IVA or IVA but had stopped treatment due to AEs (30 patients), lack of effectiveness (10 patients) or other reasons (1 patient). At the start of the study, 59 patients (24%) were switched from another CFTR modulator to ELX-TEZ-IVA (55 from LUM-IVA, 3 from TEZ-IVA, and 1 from IVA). The patients enrolled were receiving the following other CF therapies at baseline: azithromycin (70%); inhaled antibiotics (76%); dornase alfa (54%); inhaled hypertonic saline (19%); inhaled corticosteroids (50%); oral corticosteroids (11%); long-term oxygen therapy (44%); noninvasive ventilation (29%); and enteral tube feeding (18%).
Figure 20: Baseline Characteristics — French Cohort Study
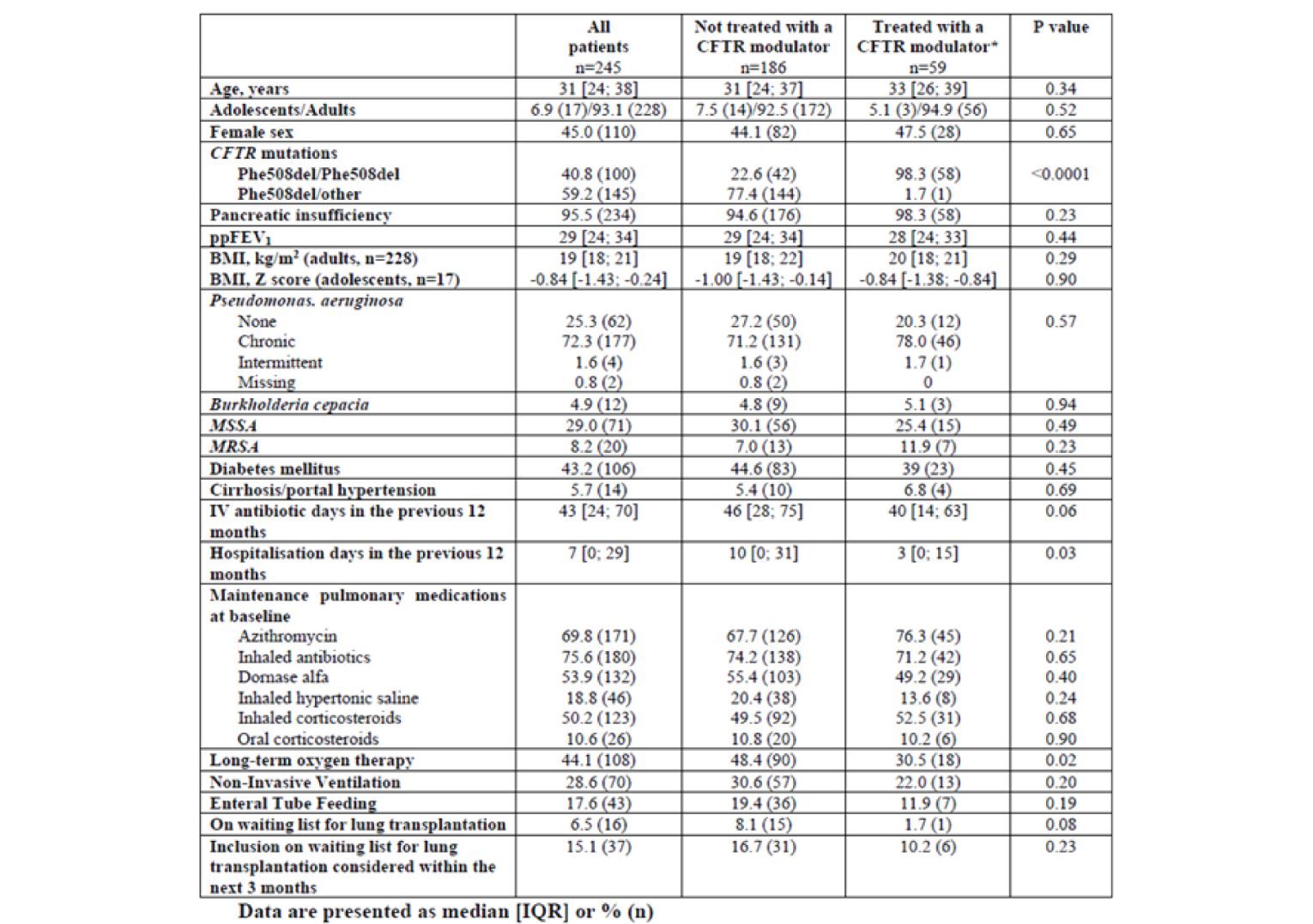
BMI = body mass index; MRSA = methicillin-susceptible Staphylococcus aureus; MSSA = methicillin-susceptible S. aureus; ppFEV1 = percent predicted forced expiratory volume in 1 second.
*lumacaftor-ivacaftor, n=55 patients; tezacaftor-ivacaftor, n=3 patients; ivacaftor, n=1 patient.
Source: Reproduced from Burgel et al. (2021).18
Interventions
Patients received open-label ELX 200 mg plus TEZ 100 mg once daily, and IVA 150 mg twice daily unless dose modifications were required according to the manufacturer’s recommendations.
Outcomes
Key outcomes were lung transplantation and death, as well as underlying treatment requirements (i.e., oxygen and enteral tube feeding). Change in lung function (ppFEV1) and weight (kg) were compared between patients who were and were not receiving another CFTR modulator before starting ELX-TEZ-IVA. Comparisons were also completed for patients who were and were not on long-term oxygen or noninvasive ventilation before initiation, and for patients with a ppFEV1 increase above and below the median response for the cohort.
Comparisons were made on the mean number of lung transplantations per year in 2020 versus 2018 to 2019 for all patients with CF in France (approximately 7,500 patients in 2019). Re-transplantations were not included in the counts. The number of deaths without transplantation for 2020 was compared to data from 2015 to 2018. Historical data were obtained from the French CF Registry (deaths) and the Agence de la Biomédecine Registry (transplants), and 2020 data were supplied by the French CF and transplant centres.
Data on patient characteristics were collected at baseline and subsequent visits from the CF centres. Treatment-related AEs documented by the referral physicians were collected from patients’ charts. Scheduled visits were planned at baseline and 1, 3, 6, and 12 months after initiating therapy.
Statistical Analysis
Available data were reported descriptively with between-group comparisons analyzed using a chi-square test or t-test. The change from baseline in ppFEV1 and weight were analyzed using a Wilcoxon paired test. The McNemar paired test was used to analyze the proportion of patients treated with long-term oxygen, noninvasive ventilation, or enteral tube feeding at baseline and at 1 and 3 months post-initiation. Statistical significance was determined based on a P value of less than 0.05. No a priori hypotheses were defined and there was no imputation for missing data.
Due to the COVID-19 pandemic and the disruption in scheduled clinic visits, some patients were missing the 1- or 3-month follow-up visits. The authors therefore pooled data for the 2 time points and analyzed the results using the best available data (median observation time 73 days; IQR = 32 to 88 days). No details were provided on how the pooled analysis was conducted.
Patient Disposition
A total of 245 patients were included in the study. At the interim analysis cut-off date (September 7, 2020), 7 patients had not had a follow-up visit and 2 patients had received a lung transplant shortly after initiation and were excluded from the analysis. Outcome data were therefore reported for 236 patients (96%).
Exposure to Study Treatments
Most patients received the standard dose of ELX-TEZ-IVA (94%), but 15 patients had doses reduced due to drug interactions (10 patients), pre-existing liver disease (3 patients), or other reasons (2 patients). At the interim data analysis cut-off, the median follow-up time was 84 days (range = 16 to 209; IQR = 70 to 104) after the start of ELX-TEZ-IVA.
Efficacy
For the overall cohort, the change from baseline data for ppFEV1 and weight were reported based on pooled 1- and 3-month end-point data. The change from baseline in the ppFEV1 was 15.1% (95% CI, 13.8 to 16.4; P < 0.0001; N = 232) and weight was 4.2 kg (95% CI, 3.9 to 4.6; P < 0.0001; N = 236). The change in ppFEV1 and weight for the subgroup of patients who were switched from another CFTR modulator to ELX-TEZ-IVA and those who were not receiving a CFTR modulator at the start of ELX-TEZ-IVA therapy are summarized in Figure 21.
Figure 21: Change in ppFEV1 and Weight — French Cohort Study
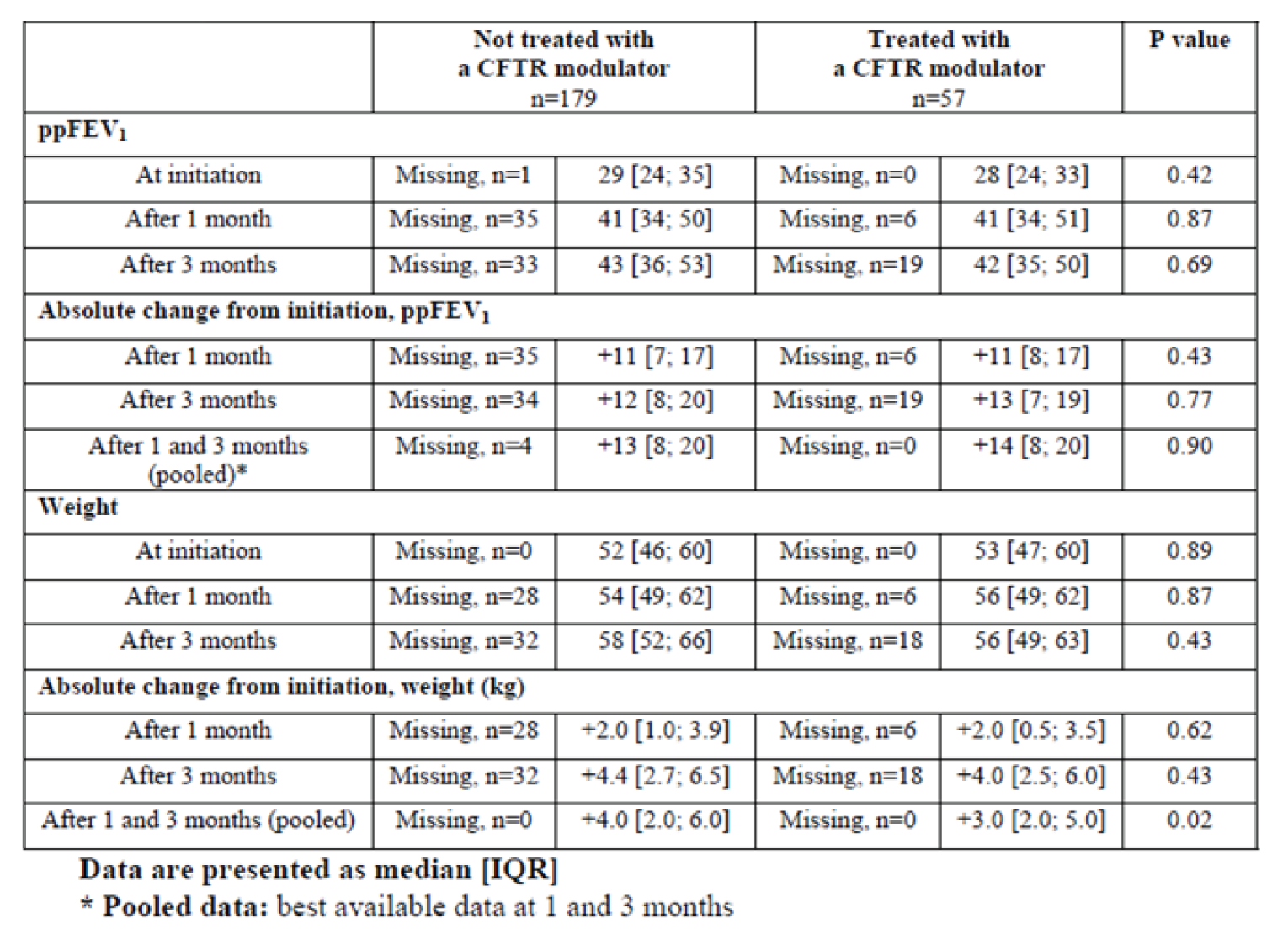
ppFEV1 = percent predicted forced expiratory volume in 1 second.
Source: Reproduced from Burgel et al. (2021).18
Prior to the start of ELX-TEZ-IVA therapy, 43% and 28% of patients were receiving long-term oxygen or noninvasive ventilation, respectively (data are missing for 4% of patients). At the 1-month visit, 31% and 24% of patients were on oxygen or noninvasive ventilation (missing data for 18% of patients) and at the 3-month visit 23% and 20% remained on oxygen or noninvasive ventilation (missing data for 32% of patients) (P < 0.001 for comparisons versus baseline).
At the start of therapy, 18% of patients were receiving enteral tube feeding, with 12% and 10% on enteral feeding at the 1- and 3-months visits (P < 0.01 versus baseline). Data were missing for 6%, 18%, and 31% of patients at baseline and the 1-month and 3-month visits, respectively.
Prior to initiation of ELX-TEZ-IVA, 16 patients were waiting for a lung transplant and 37 were under consideration for inclusion as transplant candidates in the next 3 months (for a total of 53 patients; 22%). At the end of follow-up, 5 patients (2%) were on the transplant list or being considered for transplant, 2 patients had received a transplant (0.8%), and 1 had patient died while waiting for transplant (0.4%).
Among all patients with CF in France, 33 patients received a lung transplant in 2020 (33 of 265 patients; 12.5%) compared with 72 patients in 2018 and 80 patients in 2019 (overall, 152 of 735 patients; 21%) (Fischer exact test P = 0.002). In 2020, 16 patients with CF died without transplant, compared to an average of 20 patients per year for 2015 to 2018. Sixteen of 33 patients who received a transplant and 10 of 16 who died in 2020 were eligible to receive ELX-TEZ-IVA (i.e., had at least 1 F508del mutation); however only 3 patients had received ELX-TEZ-IVA.
No data were reported on the use of IV antibiotics to treat pulmonary exacerbations.
Table 97: Adverse Events Potentially Attributable to Treatment — French Cohort Study
Adverse event | n (%) |
|---|---|
Localized cutaneous rash | 17 (7.2) |
Generalized cutaneous rash | 9 (3.8) |
Gastrointestinal symptoms | 24 (10.2) |
Myalgia | 11 (4.7) |
Headache | 10 (4.2) |
Elevated alanine aminotransferase ≥ 3 x ULN | 6 (2.5) |
Elevated aspartate aminotransferase ≥ 3 x ULN | 2 (0.8) |
Increase bilirubin ≥ 3 x ULN | 11 (4.7) |
Creatine phosphokinase ≥ 3 x ULN | 8 (3.4) |
ULN = upper limit of normal.
Note: Total N = 236.
Source: Burgel et al. (2021).18
Critical Appraisal
Internal Validity: Burgel et al. (2021)18 provides descriptive data on 245 patients in France with CF and advanced lung disease who were treated with ELX-TEZ-IVA. The prospective, uncontrolled cohort study included all patients who received ELX-TEZ-IVA through an early-access program (from all 47 CF centres in France). However, not all patients who were potentially eligible for ELX-TEZ-IVA received treatment. The authors estimated that approximately 78% of eligible patients with advanced lung disease who had 1 or more F508del mutation were included in the study. As no information was provided on the patients who did not receive ELX-TEZ-IVA, it is difficult to evaluate the potential for selection bias or whether the patients included in the study are representative of the larger population of patients with advanced pulmonary disease.
Although the study was prospective in design, there were no details on how outcome data were captured, and the planned visit schedule was disrupted due to the COVID-19 pandemic. The 1- and 3-month outcome data were missing for 14% to 32% of patients, with no imputation for missing data. Although the authors attempted to address the missing data for ppFEV1 and weight by pooling the “best available data,” the methods used were not clearly stated. Selecting the “best” result could potentially bias the results if a “better” 1-month result was selected for inclusion in the analysis in patients who were showing a decline in pulmonary function at 3 months. Due to the extent of missing data on the need for oxygen, noninvasive ventilation or enteral tube feeding (18% to 32%), it is difficult to interpret the results of these outcomes.
There were no a priori hypotheses and no adjustment for multiplicity for the outcomes tested. Between-group comparisons were conducted based on a chi-square test or t-test, with no adjustment for potential confounders. The observed reduction in lung transplants in patients with CF was potentially confounded by the disruption to the health care system caused by the COVID-19 pandemic and the availability of donor organs. Burgel et al. (2021) reported that the overall number of lung transplants was 26% lower in 2020. No details were provided on the patient characteristics and other factors that may have affected the transplant rates, and the crude estimate of the change in the number of transplants should therefore be interpreted with caution.
The follow-up time was limited (median = 84 days) and the authors stated the treatment duration was insufficient to determine the impact on IV antibiotic use. Limited data were reported on AEs during treatment.
External Validity: The clinical experts consulted by CADTH noted the study populations are similar to patients with CF in Canada who have severe illness and that the outcomes assessed were clinically relevant.
Simulation Study for Morbidity and Mortality
The objective of the study by Stanojevic et al. (2020)19 was to estimate the potential impact of ELX-TEZ-IVA on morbidity and mortality of patients with CF, including the impact of delayed access to therapy, using a microsimulation model.
Model Structure and Inputs
The model included 4 transition states: mild (ppFEV1 > 70%); moderate (ppFEV1 = 40% to 70%); severe lung function (ppFEV1 < 40%); and transplant. It also included states for lost to follow-up and death. Based on the transition probabilities, patients could randomly move through the states until either lost to follow-up, death, or transplant.
Individual patient history data from the Canadian CF Registry (CCFR) were used to populate the model. The CCFR includes patients with CF who are followed by 1 of 42 CF clinics in Canada and who have provided consent to participate in the registry (> 99%). All patients who were alive in 2018 were included as the initial population, with their age and pulmonary function state in 2018 used as the baseline.
Transition probabilities were calculated using a logistic regression model based on CCFR data from 2017 to 2018. CCFR data from 2017 were also used to determine the baseline rate of pulmonary exacerbations (i.e., IV antibiotic administered in the hospital or at home) for patients with mild, moderate, and severe lung function status (0.09, 0.09 and 2.2 events per year, respectively).
Based on incidence rates from the CCFR, the model assumed 130 patients would be newly diagnosed per year, distributed across the age spectrum as follows: 0 to 1 years, 69%; 1 to 2 years, 15%; 2 to 18 years, 9%; and 18 to 40 years, 6%. The model assumed that children under 6 years of age would have mild pulmonary disease, and that 2.5% of patients aged 20 to 60 years would be lost to follow-up per year (no loss to follow-up for those less than 20 years of age).
All patients 12 years or older who had 1 or more F508del mutation were assumed to receive treatment with ELX-TEZ-IVA. Based on data from Study 102,53 the model assumed patients would show a mean acute increase of 13.8% (SD = 8.6) in the absolute ppFEV1. The model also included a 63% reduction in the rate of pulmonary exacerbations (i.e., 0.055 events per year for patients in the mild state, 0.055 events per year in the moderate state, and 1.35 events per year for the severe state). Observational data for IVA was used to predict the rate of lung function decline in patients treated with triple therapy (rate of decline reduced by an average of 50%; SD = 5%).102 The rate of death or transplant was the same for treated and untreated patients.
The population was simulated from 2019 to 2030 for scenarios that assumed there were no new therapies (baseline analysis) and if ELX-TEZ-IVA was introduced in 2021 or 2025. Ten replications of each scenario were performed, and the results were averaged. The Kaplan–Meier survival curves and median survival were estimated based on individuals’ vital status in 5-year blocks (i.e., the median age of survival between 2021 and 2025, or 2026 and 2030). The analysis was run using R software (MicSim package).
Results
The initial population included 4,440 patients who had a reported pulmonary function values in 2017 or 2018 (children less than 6 years of age were assumed to be in the healthy state). Of these patients, 62% had mild, 23% had moderate, and 9% had severe lung function values. The baseline model, which assumed no new therapies were introduced, estimated the CF population would increase to 5,415 patients (SD = 15) by 2030 and have a similar distribution of lung function states as the initial population (mild, 59%; moderate, 22%; severe, 8%). In the simulation in which eligible patients received ELX-TEZ-IVA starting in 2021, the total CF population increased to 5,497 patients (SD = 10) in 2030. The distribution of patients with mild, moderate, and severe lung function was 69%, 19%, and 4%, respectively. If ELX-TEZ-IVA was introduced in 2025, the model estimated there would be 5,450 patients (SD = 15) with CF in 2030, and 66%, 20%, and 6% would have mild, moderate, and severe lung function, respectively.
Figure 22 depicts a projected survival curve for each scenario in 2030. The estimated median age of survival for the initial population was 57.6 years (95% CI, 52.2 to 62.3), and for the baseline scenario (no new treatments) it was 58.4 years (95% CI, 56.9 to 59.8) 2030. If ELX-TEZ-IVA was introduced in 2021, the estimated median age of survival was 67.5 years (95% CI, 66.7 to 68.4), and if ELX-TEZ-IVA was introduced in 2025, the median age of survival was estimated at 63.1 years (95% CI, 62.4 to 63.9) in 2030. The simulated difference in median age of survival was 9.2 years (95% CI, 7.5 to 10.8) and 3.3 years (95% CI, 1.7 to 5.0) if ELX-TEZ-IVA was introduced in 2021 or 2025 respectively, compared with the baseline scenario.
The simulations projected that the total number of pulmonary exacerbations requiring hospitalization or home IV antibiotics would be reduced if all eligible patients received treatment with ELX-TEZ-IVA starting in 2021 (early) or 2025 (delayed) compared with baseline. The early-introduction scenario predicted 1,700 (SD = 14) exacerbations in 2030, and the delayed introduction of ELX-TEZ-IVA led to a prediction of 1,957 exacerbations (SD = 25). In comparison, the baseline scenario predicted 2,310 exacerbations (SD = 37) in 2030. Cumulatively, the model predicted 25,370 exacerbations (SD = 177) between 2,019 and 2,030 in the baseline scenario, with 2,141 fewer events (95% CI, 2043 to 2239) in the delayed scenario, and 4,135 (95% CI, 4,042 to 4,226) fewer events in the early-adoption scenario for ELX-TEZ-IVA.
The model projected there would be 146 fewer transplants by 2030 if ELX-TEZ-IVA was introduced in 2021, and 98 fewer transplants if introduced in 2025.
Figure 22: Microsimulation of Projected Median Survival in 2030
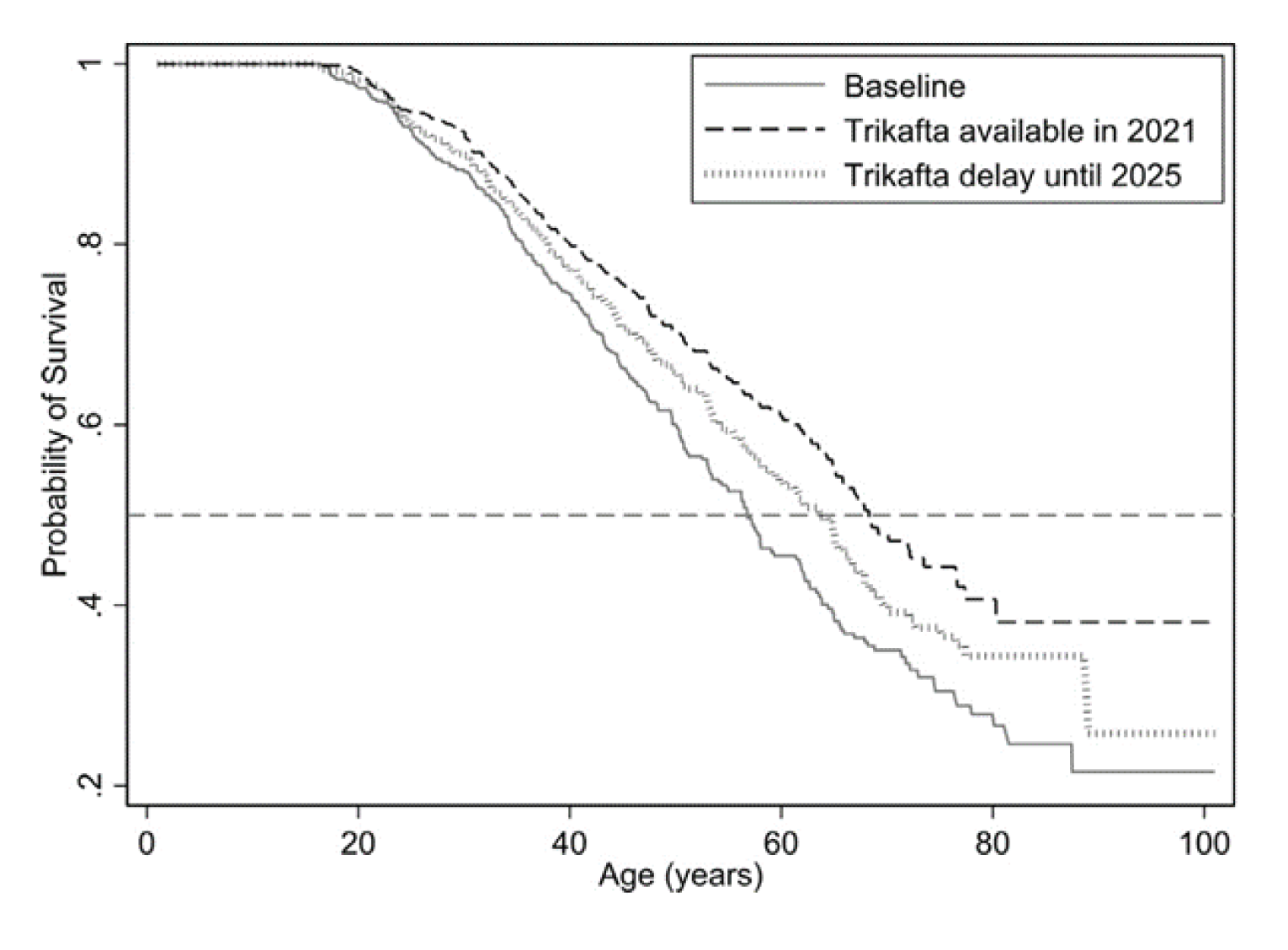
Note: Comparison of the projected median age of survival in 2030 from a single simulation in the baseline scenario (no new therapies or treatments, current transition rates), if ELX/TEZ/IVA are introduced in 2021 (“early”), and if ELX/TEZ/IVA is delayed until 2025 (“delayed”).
Source: Reprinted from Journal of Cystic Fibrosis, 20(2), Stanojevic S, Vukovojac K, Sykes J, Ratjen F, Tullis E, Stephenson AL, Projecting the impact of delayed access to elexacaftor-tezacaftor-ivacaftor for people with Cystic Fibrosis, pg.P243 to 249, 2021, with permission from Elsevier.19
Critical Appraisal
Stanojevic et al. (2020)19 used a microsimulation model to estimate the impact of treatment with ELX-TEZ-IVA in eligible patients in Canada. Individual-level patient data from the CCFR were used to inform the transition probabilities, exacerbation, and incidence rates and to model the initial population. Use of Canadian data improves the applicability to the current decision problem. In addition, the CCFR has internal checks and validation steps in the electronic data-capture system and quarterly audits to verify and validate the data, which improves the accuracy and completeness of the observational data.
The key issue with the simulation study is the number of assumptions required to build the model and extrapolate the impacts out to 10 years. The major assumptions that impart uncertainty are:
The effects of ELX-TEZ-IVA on ppFEV1 and exacerbations were informed by Study 102, which was 24 weeks in duration. Currently 48 weeks of data from an uncontrolled extension study are available to determine if the observed effects persist over the longer term.
The model assumes that all patients treated with ELX-TEZ-IVA experience an acute increase in ppFEV1, regardless of their genotype, baseline ppFEV1, or prior exposure to CFTR modulators. The mean 13.8% acute increase in ppFEV1 used to populate the model was based Study 102, which enrolled a specific subset of patients with CF (i.e., F/MF mutation; CFTR modulator treatment–naive; and a ppFEV1 ≥ 40 and ≤ 90). It is unclear if the acute effects observed apply to patients who were excluded from this trial. Variation in the acute treatment effects was observed across the other ELX-TEZ-IVA trials, which enrolled treatment-experienced patients with different genotypes. These studies reported between-group differences ranging from 3.5% to 10.2% in absolute change in ppFEV1. Moreover, because none of the trials included patients with normal ppFEV1, it is unclear if the acute change in ppFEV1 observed with treatment of ELX-TEZ-IVA is applicable to this population.
The model assumes a 50% reduction in decline in ppFEV1 over time compared with patients not receiving a CFTR modulator, based on US and UK longer-term observational studies with IVA. Currently, no information is available on the impact of ELX-TEZ-IVA on ppFEV1 over time, and the background rate of decline in ppFEV1 in the CF population is uncertain. It is unclear if the results of US and UK observational data are representative of the population that receives ELX-TEZ-IVA.
The model assumed a 63% reduction in pulmonary exacerbations for patients treated with ELX-TEZ-IVA based on 24 weeks of data from Study 102. There are issues with the extrapolation of short-term data from a subset of patients with CF to the entire modelled population in the longer term. It also appears that, because the modelled reduction in pulmonary exacerbations was in addition to the impacts of changes in ppFEV1 on pulmonary exacerbations, the effect on exacerbations may be overestimated.
The model assumes all patients 12 years or older with at least 1 F508del mutation will receive treatment for the duration of the simulation. This likely overestimates the number of patients who will be treated, as it does not consider patients with contraindications to treatment, or discontinuation of therapy due to adverse effects or other reasons. The model makes no allowances for nonadherence to treatment and its impact on treatment effects.
No sensitivity analyses were conducted to estimate the impact of various assumptions on the simulation results.
Stanojevic et al. (2020)19 also listed other limitations of the model, including the decision to base the definition of disease states on pulmonary function, which is not the only predictor of disease severity or mortality, and the assumption that the incidence of CF would remain stable despite the possibility that incidence may decline over time due to the implementation of pre-natal screening for CF.
Synopsis of Real-World Analyses Conducted on the Effectiveness of ELX-TEZ-IVA in Patients With a Pre-Treatment ppFEV1 of Greater Than 90%
Background
The efficacy and safety of ELX-TEZ-IVA among patients aged 12 years and older with CF have been studied in the pivotal phase III Study 102 and Study 103 clinical trials. One of the key inclusion criteria in the phase III clinical trials is patients with a ppFEV1 value between 40% and 90%. Clinical efficacy of ELX-TEZ-IVA among patients with a pre-treatment ppFEV1 of greater than 90% is unknown. Vertex conducted 2 separate descriptive analyses of the effectiveness of ELX-TEZ-IVA among patients with a ppFEV1 of greater than 90% in the real-world setting. Analysis and the corresponding results are described in the following section.
Interim Analysis of a Subgroup of Patients With a ppFEV1 of Greater Than 90% in the HELIO Real-World Study
Methods: HELIO is an ongoing multi-centre, prospective, observational study of the clinical effectiveness of ELX-TEZ-IVA in a real-world US setting. The study is sponsored by Vertex Pharmaceuticals and no drug was supplied for the study. All study data, including clinical characteristics (age and genotype) and ppFEV1 values based on in-clinic spirometry, were extracted from patient electronic medical records. An interim analysis of data between the time of approval of ELX-TEZ-IVA (October 21, 2019) and the interim cut-off date (December 11, 2020) was conducted.
Figure 23: Schematic of the Design of the HELIO Study
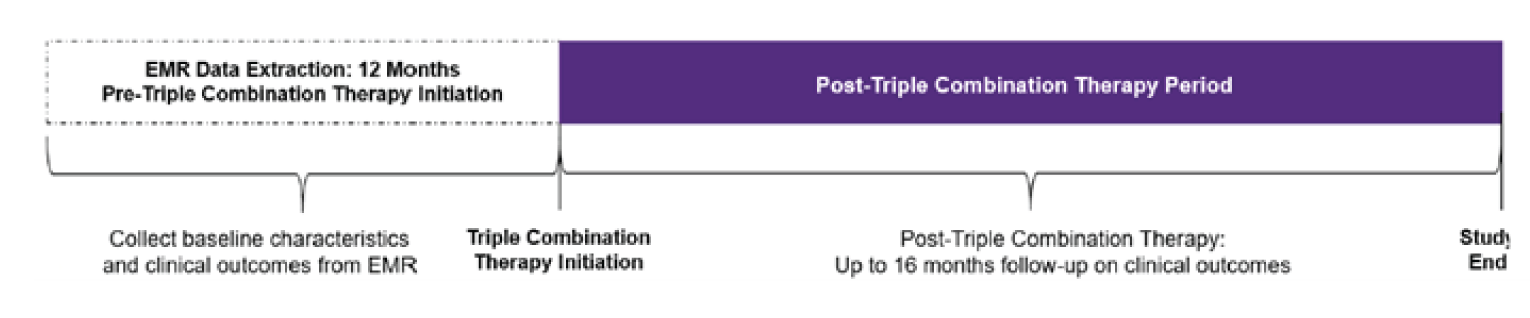
EMR = electronic medical record.
Source: Sponsor’s clinical summary.{, 2021 Jan 21 #101}
Population: Patients were included if they met the following criteria:
a diagnosis of CF for those 12 years of age and older who have an F508del-CFTR mutation on 1 allele and either a minimal function CFTR allele (F/MF) or a mutation that has not been characterized as either F508del, minimal function, residual function, or gating on the second allele (F/uncharacterized)
a prescription for ELX-TEZ-IVA
Twelve months or longer of medical history information before ELX-TEZ-IVA initiation
at least 6 months of data following initial prescription of ELX-TEZ-IVA.
Patients were excluded if they had enrolled in an interventional clinical trial or if they were exposed to investigational agents VX-445 (elexacaftor) or VX-659 within 12 months before initiation of ELX-TEZ-IVA. Patients with an F/MF genotype included in this analysis had 1 of the 991 minimal function mutations.
Baseline characteristics for the interim analysis of the HELIO study are reported in Table 97. The average age of patients in the interim dataset meeting the inclusion and exclusion criteria (N = 100) was 25.3 years. The majority of patients had an F/MF genotype (88.0%), while the remaining 12% of patients had 1 F508del allele and a second mutation that was uncharacterized (excluding patients with F/F, F/G, and F/RF genotypes who were eligible for treatment with a different CFTR modulator). The sponsor reported that 13.4% (n = 13) of patients had a baseline ppFEV1 of less than 40%, and 22.7% (n = 22) had a baseline ppFEV1 of 90% or greater.
Intervention: All patients received open-label ELX-TEZ-IVA.
Outcomes: Means and SD for age, pre-ELX-TEZ-IVA ppFEV1 (baseline ppFEV1), post-ELX-TEZ-IVA ppFEV1, and absolute change from baseline in ppFEV1 measures were estimated descriptively. Baseline ppFEV1 was defined as the last ppFEV1 measure on or before the first dose of ELX-TEZ-IVA. A post–ELX-TEZ-IVA ppFEV1 measure was defined as the average of all ppFEV1 measures that were available between the day after the first dose of ELX-TEZ-IVA up to the interim cut-off date. Last, a subgroup analysis of these measures in patients with a baseline ppFEV1 of greater than 90% was conducted.
Efficacy: Among patients who had a baseline ppFEV1 measure and 1 or more ppFEV1 measures in the post–ELX-TEZ-IVA period (n = 73), the mean change in ppFEV1 from baseline through the post-ELX-TEZ-IVA period was 9.5 points. In patients with baseline ppFEV1 of greater than 90% ||||||||||||| , the corresponding mean change in ppFEV1 through the post–ELX-TEZ-IVA period was ||||||||||||| (Table 98).
Table 98: Summary of the HELIO Study
Criteria | Description |
|---|---|
Population | Key inclusion criteria:
Key exclusion criteria:
|
End points | The following end points were described through the pre- and post-ELX-TEZ-IVA period using data collected from the patient’s EMR:
|
Data analysis |
|
BMI = body mass index; CF = cystic fibrosis; ELX-TEZ-IVA = elexacaftor-tezacaftor-ivacaftor and ivacaftor; EMR = electronic medical record; interim analysis = interim analysis; MF = minimal function; OGTT = oral glucose tolerate test; PEx = pulmonary exacerbations; ppFEV1 = percent predicted forced expiratory volume in 1 second.
Table 99: Baseline Characteristics for HELIO Interim Analyses
Characteristics | Interim full analysis set (N = 100) | ||||||||||||||||||||||||||||||||||||||| |
|---|---|---|
Sex, n (%) Male Female | 51 (51.0) 49 (49.0) | |||||||||||||||||||||||||||||||| |
Baseline age, years, mean (SD) ≥ 12 to < 18 ≥ 18 | 25.3 (12.8) 35 (35.0) 65 (65.0) | |||||||||||||||||||||||||||||||| |
Baseline ppFEV1, mean (SD) < 40 ≥ 40 to < 70 ≥ 70 to < 90 ≥ 90 | 71.0 (22.7) 13 (13.4) 27 (27.8) 35 (36.1) 22 (22.7) | |||||||||||||||||||||||||||||||| |
Genotype, n (%) F/MF F/other | 88 (88.0) 12 (12.0) | |||||||||||||||||||||||||||||||| |
Baseline weight, kg, mean (SD) | 59.1 (16.1) | |||||||||||||||||||||||||||||||| |
Baseline height, cm, mean (SD) | 163.7 (10.7) | |||||||||||||||||||||||||||||||| |
Baseline BMI, kg/m2, mean (SD) | 21.83 (4.34) | |||||||||||||||||||||||||||||||| |
Medical history, n (%) Distal ileal obstruction syndrome CF-related diabetes CF liver disease Chronic kidney disease | 1 (1.0) 11 (11.0) 4 (4.0) 2 (2.0) | |||||||||||||||||||||||||||||||| |
BMI = body mass index; CF = cystic fibrosis; F/MF = 1 F508del mutation and 1 minimal function mutation in the CFTR gene; F/other = 1 F508del mutation and 1 other mutation in the CFTR gene; ppFEV1 = percent predicted forced expiratory volume in 1 second; SD = standard deviation
Source: Sponsor’s clinical summary.{, 2021 Jan 21 #101}
||||||||||||||||||||||||||||||||||||||| | ||||||||||||||||||||||||||||||||||||||| |
|---|---|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| | |
||||||||||||| | ||||||||||||| |
||||||||||||| | ||||||||||||| |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| | |
||||||||||||| | ||||||||||||| |
||||||||||||| | ||||||||||||| |
Note: Redacted rows have been deleted.
Source: Sponsor’s clinical summary.{, 2021 Jan 21 #101}
Analysis of Patients With a ppFEV1 Of Greater Than 90% in US Cystic Fibrosis Foundation Patient Registry Real-World Data
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
||||||||||||| | ||||||||||||| | |
|---|---|---|
||||||||||||| | ||||||||||||| | |
||||||||||||| | ||||||||||||| | ||||||||||||| |
||||||||||||| | ||||||||||||| | ||||||||||||| |
Note: Redacted rows have been deleted.
Source: Sponsor’s clinical summary.{, 2021 Jan 21 #101}
Sponsor’s Conclusions: Results from 2 separate analyses of real-world data show that ELX-TEZ-IVA treatment is associated with clinically meaningful improvements in ppFEV1 in a subset of patients with a pre-treatment ppFEV1 of greater than 90%. The magnitude of treatment effects in the F/MF group were similar in both studies. The magnitude of treatment effect was lower in the F/F subgroup of patients relative to the corresponding effect size in the F/MF subgroup. This could be because of the high rate of previous exposure to CFTR modulators before initiation of ELX-TEZ-IVA in the F/F group.
Limitations Identified by the Sponsor: These findings are based on observational studies using data that were not collected for research purposes. The lack of a comparator group in these studies makes causal interpretation of these results impossible. Some of the data in these real-world studies were collected during the COVID-19 period. The impact of the COVID-19 pandemic on the measurements or missing data were not evaluated.
Interim Analysis of a Subgroup of Patients With a ppFEV1 of Greater Than 90% in the PROMISE Real-World Study
Methods: The PROMISE study is an ongoing, prospective observational study of the effects of ELX-TEZ-IVA in clinical use in the US. The study is sponsored by the Cystic Fibrosis Foundation, and programmatic funding was provided by the National Institutes of Health. Participants enrolled and completed a baseline study visit before initiating ELX-TEZ-IVA. Three subsequent visits occurred 1, 3, and 6 months after initiating therapy. A core set of clinical assessments was conducted in all participants at each visit: spirometry, sweat chloride (not at the third visit), height, weight, and completion of the respiratory domain of the CFQ-R. Due to restrictions during the pandemic, the allowable time frame to complete the 6-month visit was extended, and results are reported in this study. Additional 18- and 30-month study visits are planned.
Population: Patients were included if they met the following criteria:
12 years of age or older
at least 1 copy of F508del
the intent to initiate ELX-TEZ-IVA by the participant’s physician.
Key exclusion criteria included use of ELX-TEZ-IVA within 180 days of baseline, new chronic therapy initiation or treatment for nontuberculous mycobacterial infection within 28 days of baseline, and initiation of acute antibiotics or systemic corticosteroids within 14 days of baseline.
Table 102: Summary of the PROMISE Study
Criteria | Description |
|---|---|
Population | Key inclusion criteria:
Key exclusion criteria:
|
End points |
|
Data analysis |
|
BMI = body mass index; CF = cystic fibrosis; CFQ-R = Cystic Fibrosis Questionnaire–Revised; ELX-TEZ-IVA = elexacaftor-tezacaftor-ivacaftor and ivacaftor; ppFEV1 = percent predicted forced expiratory volume in 1 second.
Source: Nichols et al. (2021).63
Baseline characteristics for the interim analysis of the PROMISE study are reported in Table 97. The average age of patients in the interim dataset meeting the inclusion and exclusion criteria (N = 487) was 25.1 years. The majority of patients were F508del homozygous (48.5%), and 26.7% (n = 130) of patients had a baseline ppFEV1 of less than 65%, and 40.2% (n = 196) had a baseline ppFEV1 of 90% or greater.
Table 103: Baseline Characteristics for PROMISE Interim Analyses
Characteristics | Interim full analysis set (N = 487) | Subgroup with baseline ppFEV1 > 90% (n = 196) |
|---|---|---|
Sex at birth, n (%) | ||
Male | 241 (49.5) | NA |
Female | 246 (50.5) | NA |
Age, years, mean (SD) | 25.1 (10.7) | NA |
Baseline ppFEV1, mean (SD) | 80.5 (22.7) | 102.3 (8.2) |
< 65, n (%) | 130 (26.7) | 0 |
65 to 90, n (%) | 161 (33.1) | 0 |
> 90, n (%) | 196 (40.2) | 196 (100) |
Genotype, n (%) | ||
F508del homozygous | 236 (48.5) | NA |
F508del heterozygous (minimal functiona) | 195 (40.0) | NA |
F508del heterozygous (G551D) | 35 (7.2) | NA |
F508del heterozygous (other) | 21 (4.3) | NA |
Baseline weight, kg, mean (SD) | 65.6 (13.6) | NA |
Baseline BMI adults | ||
n | 326 | 93 |
kg/m2 mean (SD) | 23.1 (4.0) | 24.3 (3.6) |
Baseline BMI z score for pediatric patients | ||
n | 159 | 103 |
mean (SD) | 0.2 (0.9) | 0.3 (0.8) |
BMI = body mass index; ppFEV1 = percent predicted forced expiratory volume in one second; SD = standard deviation.
aMF = minimal function mutation defined by the VX-445 to 102 study eligibility list.
Source: Nichols et al. (2021).63
Intervention: All patients received ELX-TEZ-IVA.
Outcomes: Improvements from baseline to 6 months occurred in all outcome measures in the overall study population
Efficacy: For patients who completed the 6-month visit (n = 356), the mean change in ppFEV1 from baseline was 9.8 points. In the subgroup of patients with a ppFEV1 of greater than 90% (n = 196), the corresponding mean change was 6.5 points (Table 93). The mean changes in sweat chloride concentration from baseline for patients who completed the 6-month visit (n = 383) and for the subgroup of patients with a ppFEV1 of greater than 90% (n = 158) were −41.7 mmol/L and −39.7 mmol/L respectively. The mean changes in CFQ-R respiratory domain scores for patients who completed the 6-month visit (n = 302) and for the subgroup of patients with a ppFEV1 of greater than 90% (n = 120), were 20.4 points and 15.7 points respectively. The mean changes in BMI for adult patients who completed the 6-month visit (n = 326) and for the subgroup of patients with a ppFEV1 of greater than 90% (n = 76), were 1.2 kg/m2 and 0.8 kg/m2, respectively. The mean changes in BMI z scores for pediatric patients who completed the 6-month visit (n = 139) and for the subgroup of patients with a ppFEV1 of greater than 90% (n = 93), were 0.3 and 0.3 respectively.
Table 104: Outcomes for all Patients and Subgroups With a ppFEV1 of Greater Than 90% in PROMISE
End point | Time point | Total population (N = 487) | Subgroup with ppFEV1 > 90% (n = 196) |
|---|---|---|---|
ppFEV1 | Baseline (n = 487), mean (SD) | 80.5 (22.7) | 102.3 (8.2) |
At 6-month visit (n = 356), mean (SD) | 90.9 (21.5) | 108.2 (9.8) | |
Absolute change from baseline to 6-month visit, change (95% CI) | 9.76 (8.76 to 10.76) | 6.52 (5.18 to 7.86) | |
Sweat chloride | Baseline (n = 462), mean (SD) | 88.0 (18.4) | 87.9 (19.7) |
At 6-month visit (n = 383), mean (SD) | 45.7 (21.2) | 46.1 (23.5) | |
Change from baseline to 6-month visit, change (95% CI) | −41.70 (−43.80 to −39.60) | −39.72 (−43.15 to −36.29) | |
CFQ-R (respiratory domain) | Baseline (n = 410), mean (SD) | 70.3 (18.2) | 77.4 (16.2) |
At 6-month visit (n = 302), mean (SD) | 90.5 (11.3) | 92.6 (9.7) | |
Change from baseline to 6-month visit, change (95% CI) | 20.39 (18.28 to 22.50) | 15.66 (12.80 to 18.52) | |
BMI (adults) | Baseline (n = 326), mean (SD) | 23.1 (4.0) | 24.3 (3.6) |
At 6-month visit (n = 268), mean (SD) | 24.5 (4.6) | 25.1 (3.9) | |
Change from baseline to 6-month visit, change (95% CI) | 1.24 (1.05 to 1.44) | 0.82 (0.50 to 1.13) | |
BMI z score (pediatrics) | Baseline (n = 159), mean (SD) | 0.2 (0.9) | 0.3 (0.8) |
At 6-month visit (n = 139), mean (SD) | 0.5 (0.8) | 0.5 (0.8) | |
Change from baseline to 6-month visit, change (95% CI) | 0.30 (0.22 to 0.37) | 0.25 (0.17 to 0.33) |
BMI = body mass index; CFQ-R = Cystic Fibrosis Questionnaire–Revised; CI = confidence interval; ppFEV1 = percent predicted forced expiratory volume in 1 second.
Discussion
Summary of Available Evidence
The evidence for the review of ELX-TEZ-IVA in patients 6 years of age and older was derived from a systematic literature review of pivotal and phase III studies supplemented with additional studies to address important gaps in the RCT evidence. CADTH previously reviewed ELX-TEZ-IVA for treatment of CF in patients aged 12 years and older who have at least 1 F508del mutation in the CFTR gene. Following the completion of CADTH’s review, the Health Canada–approved indication was subsequently expanded to include patients 6 years of age and older. The current CADTH review is for the full Health Canada–approved indication (i.e., evidence for the originally reviewed population and new expanded population has been included).
Patients Aged 6 to 11 Years
The current CADTH review focused on the new evidence available for ELX-TEZ-IVA for use in patients 6 years and older. The included studies for patients aged 6 to 11 years consisted of a pivotal, open-label, single-arm trial (Study 106B) and a double-blind, placebo-controlled RCT (Study 116). As reflected in the Canadian product monograph, these studies used a lower dosage of ELX-TEZ-IVA for patients weighing less than 30 kg (i.e., ELX 100 mg, TEZ 50 mg, and IVA 75 mg in the morning and IVA 75 mg in the evening). Those weighing 30 kg or more received the same dosage as is currently recommended for patients 12 years and older (i.e., ELX 200 mg, TEZ 100 mg, and IVA 150 mg in the morning and 150 mg IVA in the evening). The additional evidence identified in the current review of ELX-TEZ-IVA that addressed the expanded patient population (i.e., those between the ages of 6 and 11 years of age) included a 24-week, double-blind, placebo-controlled RCT in patients with the F/MF genotype (Study 116; N = 121),4 a 24-week, pivotal, single-arm trial in patients with the F/F and F/MF genotypes (Study 106B; N = 66),3 and an indirect comparison submitted by the sponsor for patients with the F/F genotype.52
Patients Aged 12 Years and Older
The evidence from the initial CADTH review of ELX-TEZ-IVA in patients 12 years of age and older included 4 double-blind, phase III, RCTs: a 24-week, placebo-controlled trial conducted in patients with the F/MF genotype (Study 102 [N = 405]), an active-controlled trial in patients with the F/F genotype (one 4 weeks in duration [Study 103; N = 107] and the other 24 weeks in duration [Study 109; N = 107]), and an active-controlled trial in patients with the F/RF or F/G genotypes (Study 104; N = 259). The evidence from these studies was supplemented with 24-week data from 1 long-term extension-phase study (Study 105), 1 indirect comparison submitted by the sponsor,62 2 observational studies that evaluated the use of ELX-TEZ-IVA in patients with advanced lung disease,17,18 1 study that modelled the potential impact of ELX-TEZ-IVA on CF-related morbidity and mortality,19 and interim reports from 2 observational studies that included a subset of patients who had normal lung function (i.e., ppFEV1 > 90%) at the time of initiating treatment with ELX-TEZ-IVA (HELIO [n = 15] and US CFFPR [N = 765]).103 For patients aged 12 years and older, the current review included updated 96-week data from Study 105 and an additional observational study that included a subset of patients with a ppFEV1 of greater than 90% at the time of initiating treatment with ELX-TEZ-IVA (PROMISE [n = 196]).63
Study 102 evaluated a range of outcomes that are important in the management of CF, including respiratory function (i.e., ppFEV1), nutritional status and growth (e.g., body weight and BMI), symptoms (CFQ-R respiratory domain), and clinical events (e.g., pulmonary exacerbations). The other studies included fewer outcomes and no other studies evaluated pulmonary exacerbations as efficacy end points. In general, the end points that were in the clinical trials largely align with those that are evaluated in routine Canadian clinical practice.
The inclusion and exclusion criteria for the included RCTs that were conducted in patients at least 12 years of age were similar except for the CFTR genotypes (i.e., F/MF, F/F, F/G or F/RF). Study 103, Study 104, and Study 109 all included a 28-day active-treatment run-in period during which all patients with either an F/F or F/RF genotype received TEZ-IVA (Study 103, Study 109, and the F/RF subset of patients in Study 104) and patients with an F/G genotype received IVA (the F/G subset of patients in Study 104). Patients were subsequently randomized to receive ELX-TEZ-IVA or remain on the active treatment administered during the run-in period. Patients were also required to have stable CF disease in the opinion of the investigator and a ppFEV1 of between 40% and 90% at the time of screening for all the RCTs conducted in those at least 12 years of age.
Patients with advanced lung disease (i.e., ppFEV1 < 40%) were an important subgroup for this review, as they may represent those in the greatest need of additional intervention. Limited data were available for these patients from an ad hoc subgroup analysis in Study 102; however, CADTH conducted additional literature searches to identify other clinical studies conducted to evaluate the use of ELX-TEZ-IVA in patients with CF who are having advanced lung disease.
All the studies excluded patients who were infected with some Burkholderia cepacia complex species (i.e., B. cenocepacia and B. dolosa). These patients represent 3.7% of overall the patient population with CF in Canada1; however, the clinical experts consulted by CADTH noted that the exclusion of such patients does not substantially reduce the generalizability of the study results. This is similar to previous commentary from the Cystic Fibrosis Foundation in US in its publication on the considerations for the use of another CFTR modulator (LUM-IVA), which suggests there is no basis to conclude that patients with CF and these infections would not benefit from treatment and that such patients may derive the greatest benefit from treatment due to their increased risk for accelerated disease progression and mortality.104
The CF Canada registry reports that 7.8% of the Canadian CF population had received a lung transplant as of 2019 and that the estimated median time of survival for patients with CF who receive a lung transparent is 10.6 years post-transplant.1 Similar to the clinical development programs for the other approved CFTR modulators,87,90,91,95,96 patients who had received a lung transplant (or any organ or hematological transplant) were excluded from the ELX-TEZ-IVA clinical trials. Recommendations from the Institute for Clinical and Economic Review noted that, although patients who have had a liver transplant were excluded from the clinical trials, they should not be excluded from coverage as clinical expert input indicated that these patients would be likely to benefit from ELX-TEZ-IVA.105 The clinician groups who provided input noted there is a lack of evidence regarding whether or not ELX-TEZ-IVA would benefit patients with CF who have had a lung transplant. The experts consulted by CADTH noted that ELXTEZ-IVA would not likely be initiated in patients who have undergone a lung transplant. For those who have undergone a liver transplant, ELX-TEZ-IVA could be initiated as the drug may improve the patient’s lung function. Post–liver transplant patients would likely receive additional monitoring for potential toxicity with a lower threshold for interrupting or discontinuing the drug (due to the potential risk of hepatic adverse events with ELX-TEZ-IVA). The sponsor noted in its commentary on the draft CADTH reports that the safety and efficacy of ELX-TEZ-IVA was not evaluated in transplanted patients in the clinical trial program. However, the sponsor stated that ELX-TEZ-IVA has been shown to improve multiple clinical outcomes, including nutritional outcomes, and could potentially benefit patients who had had received lung or liver transplants as CF is multisystemic in nature and continues to progress after organ transplant. The sponsor stated that some clinicians in the US have been treating post-transplant patients with strict monitoring protocols to limit possible drug-drug interactions and that outcomes suggest that ELX-TEZ-IVA could be used in these patients. However, the sponsor noted that the only available data at the time of CADTH’s review are case reports with small sample sizes.106-109
Interpretation of Results
Efficacy
Patients Aged 6 to 11 Years
ELX-TEZ-IVA was associated with a statistically significant improvement in LCI2.5 compared with placebo after 24 weeks of treatment (absolute reduction = −2.26; 95% CI, −2.71 to −1.81].4 The LCI is not currently used in Canadian clinical practice to evaluate lung function in patients with CF, but has been recommended for use as an end point in clinical trials conducted in younger patients.71 This is because spirometry may not be sensitive enough to detect treatment differences in patients who have relatively normal lung function but may still have underlying structural abnormalities in the lungs. Previous CADTH reviews of CFTR modulators in pediatric patients noted that the sponsor indicated that LCI is correlated with FEV1 in its ability to measure airway disease, which has been validated as an end point. CADTH’s review of the literature found the correlation between LCI and FEV1 varied across studies, an observation that was supported by the clinical experts consulted by CADTH. In their review of LUM-IVA, Health Canada reviewers noted that the sponsor cited a workshop hosted by the EMA on end points in CF clinical trials as the source for the −1 improvement being clinically relevant, although that particular report indicates that an MID for this end point has not been established. In its comments on the draft CADTH report, the sponsor provided additional commentary on the relevance of the change in LCI observed in Study 106B and Study 116. The sponsor noted that a review by Perrem et al. (2018) reported that a relative change of 15% between visits is likely outside the intrinsic variability of the multiple-breath washout test and physiologically relevant (a threshold that was exceeded in Study 116 [a placebo-adjusted relative decrease of 22%] and Study 106B [a relative decrease of 17%]).110 The sponsor also noted that the within-group improvement of −1.71 in Study 106B and the placebo-adjusted improvement of −2.26 in Study 116 could be considered clinically relevant as they are greater than the annual rate of deterioration in LCI2.5 seen in patients 6 through 11 years of age ( + 0.21 units/year) who were naive to CFTR-modulator treatment as assessed in a longitudinal study.111 Overall, the clinical experts consulted by CADTH indicated that LCI is not currently used in Canadian practice and that there is no consensus in the Canadian clinical community regarding the magnitude of improvement in LCI2.5 that would be considered clinically relevant.
As with the studies conducted in adolescent and adult patients, treatment with ELX-TEZ-IVA resulted in a statistically significant and clinically important improvement in ppFEV1 after 24 weeks of treatment compared with placebo in Study 116 (LSMD = 11.0%; 95% CI, 6.9 to 15.1). Analyses of change from baseline in ppFEV1 in Study 116 were not adjusted for multiplicity and should be interpreted accordingly. Although the patients in Study 116 had a greater baseline ppFEV1 (87.2% and 91.4% in the placebo and ELX-TEZ-IVA groups, respectively) compared with the placebo-controlled trial in adolescents and adults (61.3% and 61.6% in the placebo and ELX-TEZ-IVA groups of Study 102, respectively), the absolute improvement from baseline in ppFEV1 was similar in the 2 patient populations (absolute improvements of 11.0% in Study 116 and 14.3% in Study 102). The indirect comparison demonstrated that ELX-TEZ-IVA was associated with clinically meaningful improvements in ppFEV1 through 24 weeks compared with placebo (13.9%; 95% CI, 10.2 to 17.6), LUM-IVA (11.5%; 95% CI, 7.9 to 15.1), and TEZ-IVA (10.0%; 95% CI, 6.0 to 13.9).
Study 106B demonstrated within-group improvements from baseline in all nutritional end points (BMI, BMI-for-age z score, weight, weight-for-age z score, and height) except for height-for-age z score. It is challenging to interpret these results in the absence of a control group, given that the trial involved extensive contact with health professionals in the clinical trial setting and no nutritional end points were included in the placebo-controlled Study 116. However, the clinical experts consulted by CADTH noted that the changes in BMI z scores in Study 106B and the indirect comparison were much greater than would be anticipated for patients who had not received a CFTR modulator and should be considered clinically relevant.
Pulmonary exacerbations were included as an exploratory end point in Study 106B (with no statistical analyses performed to examine change from baseline in annual exacerbation rate) and were only captured as AEs in Study 116. In response to an inquiry from CADTH regarding why pulmonary exacerbations were not included as an efficacy end point, the sponsor reported that a treatment effect may be difficult to detect in Study 116 given the relative rareness of these events in younger patients relative to older patients. In Study 116 the proportion of patients who experienced 1 or more pulmonary exacerbations during the double-blind treatment phase was numerically lower in the ELX-TEZ-IVA group compared with the placebo group (1.7% versus 26.2%, respectively), although no statistical analyses were performed and no standard definitions for pulmonary exacerbations were recorded as AEs. Acknowledging the limitations of excluding pulmonary exacerbations as an efficacy end point in Study 116, the clinical experts consulted by CADTH suggested that the difference between the placebo and ELX-TEZ-IVA groups in pulmonary exacerbations reported as AEs is likely clinically important for pediatric patients.
Treatment with ELX-TEZ-IVA was associated with a statistically significant difference in CFQ-R respiratory domain scores after 24 weeks compared with placebo (LSMD = 5.5; 95% CI, 1.0 to 10.0). The MID for the CFQ-R respiratory domain is typically cited to be 4.0 points, a threshold that was exceeded in both Study 116 (versus placebo) and Study 106B (within-group), although the estimates of effect were imprecise, as shown by the wide CIs. The clinical experts consulted by CADTH considered the results clinically relevant.
The clinical studies for ELX-TEZ-IVA were limited to patients with an F/MF (Study 116 and Study 106B) or F/F genotype (Study 106B). No clinical studies were conducted with ELX-TEZ-IVA in pediatric patients with F/RF or F/G genotypes; however, the clinical experts noted that ELX-TEZ-IVA would result in clinically meaningful improvements for these patients, based on the evidence reported for ELX-TEZ-IVA in adult patients with F/RF and F/G genotypes and the results in F/F and F/MF pediatric studies. This is consistent with the input from patient and clinician groups, who indicated all patients with at least 1 F508del mutation are likely to benefit from treatment with ELX-TEZ-IVA.
Patients With Normal Lung Function
The CADTH recommendation for patients aged 12 years and older included an initiation criterion that patients were required to have a ppFEV1 of no more than 90% to be eligible for reimbursement. These patients were excluded from the phase III trials conducted in adolescents and adults, and data were limited to subgroups from open-label, uncontrolled, interim analyses from the HELIO and CFFPR observational studies that reported on a single end point (i.e., change from baseline in ppFEV1) with no statistical analyses (HELIO [n = 15]; and data from the CFFPR [N = 765]). As such, patients with normal lung function (i.e., ppFEV1 > 90%) were considered an important subgroup for the current review of ELX-TEZ-IVA. In addition to the previously reviewed HELIO and CFFPR data, the current review included subgroup data for patients with a baseline ppFEV1 of greater than 90% from a new observational study in adolescent and adults (PROMISE). Although limited by open-label administration and the lack of a control group, the data from PROMISE suggested that patients aged 12 and older with a ppFEV1 of greater than 90% at the time of initiating treatment with ELX-TEZ-IVA experienced improvements in ppFEV1 (absolute change of 6.52%; 95% CI, 5.18 to 7.86); BMI (absolute change of 0.82 kg/m2; 95% CI, 0.50 to 1.13); and CFQ-R (absolute change of 15.66; 95% CI, 12.80 to 18.52). In addition, approximately half of the pediatric patients in Study 106B and Study 116 had a baseline ppFEV1 of greater than 90%. The included pediatric trials demonstrated that these patients experienced improvements in lung function, BMI z score, quality of life, and pulmonary exacerbations (although only evaluated as AEs) that are clinically meaningful.
Patients Aged 12 Years and Older
Potential improvements in lung function can be evaluated based on short-term changes from baseline (e.g., absolute change from baseline in ppFEV1) or long-term changes evaluating the impact of an intervention on the CF disease course. The data included in this review of ELX-TEZ-IVA include short-term changes as evaluated in the pivotal and supportive clinical trials, and longer-term changes as assessed in the longer-term extension-phase study and modelled in the sponsor’s microsimulation study. When considering lung function measurements in a chronic condition such as CF, the clinical experts consulted by CADTH indicated that the ability of CFTR-modulator treatments such as ELX-TEZ-IVA to result in long-term changes is generally considered to be more clinically relevant than acute changes in ppFEV1. Similar statements have been made by regulatory authorities (Health Canada and the EMA),112 and health technology assessment agencies (National Institute for Health and Care Excellence and the Australian Pharmaceutical Benefits Advisory Committee) in prior reviews of CFTR modulators.113,114
With respect to the data from the short-term studies (i.e., 4 to 24 weeks), it is important to note the active-treatment run-in period in 3 of the 4 RCTs makes it challenging to compare the results across the different genotypes. All patients included in Study 103, Study 104, and Study 109 were receiving treatment with a CFTR modulator at baseline (IVA for those with an F/G genotype or TEZ-IVA for those with an F/F or F/RF genotype). In addition, a subset of patients in Study 104 were receiving treatment with a CFTR modulator at the time of screening. As such, the absolute improvements in ppFEV1 within the ELX-TEZ-IVA groups are likely lower than would be anticipated in patients who are naive to CFTR-modulator therapy.
While no published information on the MID in absolute change in ppFEV1 in CF was identified by CADTH, the clinical experts consulted by CADTH noted that CF specialists would generally consider an absolute improvement in ppFEV1 of at least 5% to be clinically relevant. In patients with an F/MF genotype, ELX-TEZ-IVA was associated with a statistically significant and clinically meaningful absolute improvement in ppFEV1 compared with placebo (LSMD = 13.8%; 95% CI, 12.1 to 15.4). Similar results were reported for placebo-treated patients who were crossed over to ELX-TEZ-IVA in Study 105, which demonstrated an absolute increase from baseline in ppFEV1 of 14.9% (95% CI, 13.5 to 16.3) at 24 weeks. In patients with an F/F genotype, switching to ELX-TEZ-IVA after 24 weeks of open-label treatment with TEZ-IVA was associated with statistically significant and clinically meaningful absolute improvements in ppFEV1 compared with remaining on TEZ-IVA (LSMD = 10.0%; 95% CI, 7.4 to 12.6 in Study 103 and 10.2%; 95% CI, 8.2 to 12.1 in Study 109). When compared with patients with an F/G genotype remaining on IVA and patients with an F/RF genotype remaining on TEZ-IVA, the absolute improvements observed after switching to ELX-TEZ-IVA were more modest (LSMD = 5.8% [95% CI, 3.5 to 8.0] and 2.0% [95% CI, 0.5 to 3.4], respectively).
The magnitude of the treatment effect reported for patients with F/MF and F/F genotypes is similar to the 10.6% to 12.5% improvement in ppFEV1 at 24 weeks that was observed with IVA monotherapy compared to placebo in the treatment of patients with CF with gating mutations (STRIVE, ENVISION, and KONNECTION)94-96 and exceeds the improvements in the pivotal trials for LUM-IVA (TRAFFIC [2.6%] and TRANSPORT [3.0%]),87 TEZ-IVA (EVOLVE [4.0%] and EXPAND [6.8%]),92,93 and IVA for patients with the R117H mutation (KONDUCT; 5.0% improvement).99 Using these placebo-controlled trials of TEZ-IVA, LUM-IVA, and IVA, the sponsor conducted indirect comparisons to estimate the placebo-adjusted response for ELX-TEZ-IVA for patients with F/F, F/G, and F/RF genotypes. For all 3 genotypes, the indirect estimates of effect for ELX-TEZ-IVA compared with placebo (14.1%; 95% CI, 11.9 to 16.2 for F/F genotypes, 15.1%; 95% CI, 12.1 to 18.0 for F/G genotypes, and 8.7%; 95% CI, 6.8 to 10.5 for F/RF genotypes) were considered clinically relevant by the experts consulted by CADTH.
Patients with a ppFEV1 below 40% at screening were excluded from the RCTs; however, a small number of patients (range = 1.6% in Study 104 to 9.3% in Study 103) satisfied the screening requirements, but had a ppFEV1 that fell below 40% between the run-in period and study baseline.5,6,10,11 These patients with lower lung function would have satisfied the study inclusion criteria in the screening phase, then have demonstrated a ppFEV1 of less than 40% at their baseline evaluation. A post hoc subgroup analysis in Study 102 provided some efficacy data for this important subgroup of patients and suggested that ELX-TEZ-IVA improves lung function relative to placebo (mean absolute improvement in ppFEV1 of ||||||||||||| ||||||||||||| weeks).5 This increase in ppFEV1 was considered clinically meaningful by the experts consulted by CADTH. The input received from clinician groups also noted that patients with a ppFEV1 of less than 40% who have received ELX-TEZ-IVA in Canadian CF clinics (through the Special Access Programme or compassionate access) have demonstrated clinically meaningful improvements to the treatment. Similar results were reported in the prospective cohort study conducted by Burgel et al. (2021), who evaluated the real-world efficacy and safety of ELX-TEZ-IVA in patients with CF and a ppFEV1 of less than 40%.18 This study included patients from all 47 CF centres in France who received open-label ELX-TEZ-IVA through an early-access program (N = 245). Pooled data following 1 to 3 months of treatment demonstrated a clinically meaningful absolute improvement from baseline in ppFEV1 of 15.1% (95% CI, 13.8 to 16.4). The retrospective chart review by O’Shea et al. (2021) included 14 patients with advanced lung disease who received ELX-TEZ-IVA through a managed care program in Ireland.17 Patients were followed for a mean of 4.9 months (SD = 1.9) after starting ELX-TEZ-IVA. The authors reported that mean ppFEV1 improved from 27% (SD = 7.3) at baseline to 36% (SD = 16.5) after approximately 4 weeks of treatment (P < 0.0001).
Burgel et al. (2021) reported reductions in the proportion of patients receiving long-term oxygen (43% at baseline versus 23% at 3 months), noninvasive ventilation (28% at baseline versus 20% at 3 months); and enteral tube feeding (18% at baseline versus 10% at 3 months) that were statistically significant; however, the results were limited by a large amount of missing data due to the onset of the COVID-19 pandemic during the study period. Burgel et al. (2021) also reported that, before initiation of ELX-TEZ-IVA, 16 patients were waiting for a lung transplant and 37 were under consideration for inclusion as transplant candidates within the next 3 months (n = 53 patients; 22%). At the end of the follow-up period, there was a reduction in the number of patients on the transplant list or being considered for transplant (5 patients). As only 2 patients had received a transplant (0.8%) and 1 patient had died while awaiting a transplant (0.4%); the reduction appears to be attributable to an improvement in the condition of these patients. The clinical experts consulted by CADTH, the clinician groups who provided input, and the patient group input received by CADTH also noted that ELX-TEZ-IVA has been shown to be beneficial for patients whose lung function has deteriorated to the extent where they have been referred to the lung transplant waiting list, with many improving to the point where they no longer required transplantation.
Patients with normal lung function (i.e., ppFEV1 > 90%) were also excluded from the included studies.5,6,10,11 As with those who have severe lung disease, these patients were excluded from the pivotal and supportive phase III trials as they were considered less likely to be able to show an improvement in lung function in a short-term clinical trial.64 The clinical experts consulted by CADTH and the clinician groups who provided input noted that patients who have a ppFEV1 of greater than 90% often show early signs of CF lung disease (e.g., bronchiectasis, mucus plugging, or early mild declines in the FEV1), and could potentially benefit from treatment with ELX-TEZ-IVA. The potential for ELX-TEZ-IVA to reduce the frequency of pulmonary exacerbations was noted as an important potential benefit for those with normal lung function. At the time of CADTH’s review, clinical trials have not been conducted to investigate the benefit of ELX-TEZ-IVA in patients with normal lung function.
The ability of an intervention to result in long-term changes in lung function is a more accurate reflection of CF treatment goals and is considered to be a more clinically relevant end point compared with acute changes in ppFEV1.112-114 The included RCTs were too short to draw conclusions regarding whether or not treatment with ELX-TEZ-IVA would reduce the slope of decline in ppFEV1. Stanojevic et al. (2020)19 used a microsimulation model to estimate the impact of treatment with ELX-TEZ-IVA in eligible patients in Canada. The model forecast an increase in median survival and a reduction in pulmonary exacerbations with the introduction of ELX-TEZ-IVA. The outcomes from these simulations are contingent on the validity of several assumptions that were required to build the model and extrapolate the impacts out to 10 years. There is uncertainty in the extrapolation of short-term effects of ELX-TEZ-IVA in a subset of patients with CF to the broader population in the longer-term, and in the generalizability of observational data with IVA on the rate of decline in ppFEV1 in patients treated with ELX-TEZ-IVA. Moreover, the model likely overestimates the proportion of patients with CF who may receive ELX-TEZ-IVA and the impact of treatment on pulmonary exacerbations.
As pulmonary exacerbations are currently the most common reason for hospitalization of patients with CF,31 these events were identified as an outcome of interest by the patient groups who provided input on this review. Pulmonary exacerbations are clinically significant events for patients with CF and are correlated with increased mortality, greater decline in lung function, reduced quality of life, and increased health costs.115-119 In addition, it has been estimated that many patients with CF experience a permanent reduction in lung function following an exacerbation (i.e., their lung function will not recovery to the level it was before the exacerbation). In a large sample of patients with CF (N = 8,479), Sanders et al. (2010) estimated that 25% of patients with CF who experienced a pulmonary exacerbation failed to recover to their baseline FEV1.120 A similar observation has been made in an analysis in pediatric patients with CF, with 23% of patients failing to recover to their baseline FEV1 after being treated with IV antibiotics for a pulmonary exacerbation.121
Treatment with ELX-TEZ-IVA was associated with a statistically significant reduction in the risk of pulmonary exacerbations, including those requiring hospitalization and IV antibiotic therapy, in the 24-week placebo-controlled trial (Study 102). Throughout the extension phase (Study 105), the rate of pulmonary exacerbations that was observed in the double-blind treatment phase appeared to be maintained for patients receiving ELX-TEZ-IVA (0.37 and 0.32 events per person-year at 24 and 48 weeks of follow-up, respectively). In addition, patients who crossed over from placebo to ELX-TEZ-IVA in Study 105 experienced a lower rate of pulmonary exacerbations compared with the rate during the double-blind phase (0.98 versus 0.27 events per person-year at 24 weeks of follow-up).5,15 The clinical experts consulted by CADTH and regulatory reviewers (FDA and EMA) noted that the reduction in pulmonary exacerbations in Study 102 is clinically meaningful.35,59 In patients with advanced lung disease, the retrospective chart review by O’Shea et al. (2021) observed a reduced rate of pulmonary exacerbations requiring hospitalization (0.28 events per month in the 12 months before ELX-TEZ-IVA versus and 0.04 events per month during the 4.9 month follow-up period based on data from 7 patients [P < 0.001]). This reduction would be considered clinically important based on the input from the clinical experts consulted by CADTH.
Pulmonary exacerbations were only reported as AEs in Study 103, Study 104, and Study 109.6,10,11 In response to an inquiry from CADTH regarding why pulmonary exacerbations were not included as efficacy end points in these trials, the sponsor reported that the active-controlled trials would not have sufficient statistical power to detect a difference in pulmonary exacerbations between ELX-TEZ-IVA and the active comparators.68 As both TEZ-IVA and IVA have been shown to reduce the frequency of pulmonary exacerbations in previous placebo-controlled trials with patients who have F/F, F/RF, or F/G genotypes, the sponsor noted that a prohibitively large number of patients would be required to give the studies sufficient power to detect a reduction in pulmonary exacerbations.68 While it is acknowledged that a study designed to evaluate the effects of a treatment on exacerbations would likely require a sizable patient population and a duration of at least 12 months, particularly if an active-treatment comparator was used, it is not clear that such a study with these features would not be feasible. In all 3 of the active-controlled studies, the proportions of patients who experienced 1 or more pulmonary exacerbations during the double-blind treatment phases were numerically lower in the ELX-TEZ-IVA group compared with the comparator groups, although no statistical analyses were performed and no standard definitions for pulmonary exacerbations were recorded as AEs.6,10,11
There are no globally accepted definitions for pulmonary exacerbations in patients with CF. The definitions used in Study 102 were considered to be appropriate by regulatory authorities and the clinical experts consulted by CADTH.35,59 The clinical experts consulted by CADTH noted there would be some variation in routine clinical practice in the threshold for diagnosing and treating pulmonary exacerbations across different CF clinics and/or physicians. This was also evident in Study 102, in which fewer patients met the criteria for a pulmonary exacerbation when evaluated as an efficacy end point compared to the number of exacerbations reported as AEs (e.g., 37% versus 47% in the placebo group).5 Although there are no standard definitions currently used in Canadian clinical practice, the clinical experts consulted by CADTH noted that the number of exacerbation events experienced by patients with CF is currently tracked in CF clinics.
Given that CFTR modulators are systemic treatments, the pivotal studies for ELX-TEZ-IVA included end points such as BMI and body weight to evaluate the effect of treatment on the nutritional status of patients with CF. Treatment with ELX-TEZ-IVA was associated with statistically significant improvements in BMI compared with placebo at 24 weeks in those with an F/MF genotype and compared with TEZ-IVA at 4 weeks in those with an F/F genotype (LSMD = 1.04 kg/m2; 95% CI, 0.85 to 1.23; and 0.60 kg/m2; 95% CI, 0.41 to 0.79, respectively). The clinical experts consulted by CADTH noted that the improvements in BMI with ELX-TEZ-IVA are clinically meaningful. Similarly, reviewers for the EMA noted that the improvements observed in Study 102 after 24 weeks of treatment with ELX-TEZ-IVA are clinically relevant.59 Reviewers for the FDA considered the improvements in BMI that were reported in Study 103 to be clinically relevant; however, the EMA considered the 4-week duration the study to be too short to evaluate the potential benefits of CFTR-modulator treatment on an end point such as BMI.59 As such, the extension-phase data from Study 105 were considered by the EMA and noted as supportive of a clinical benefit for patients with an F/F genotype.59 The 24-week interim analysis from Study 105 suggested that patients with an F/F genotype who received ELX-TEZ-IVA for a minimum of 24 weeks experienced similar within-group improvements from baseline compared with those in Study 102.15 In 14 patients with advanced lung disease, the retrospective chart review by O’Shea et al. (2021) reported that the mean BMI increased from 20.7 kg/m2 (SD = 3.6) to 22.1 kg/m2 (SD = 3.4) after approximately 2 months of treatment with ELX-TEZ-IVA.
As stated in the patient group input, CF has a major impact on the quality of life of patients and their caregivers. Treatment with ELX-TEZ-IVA demonstrated statistically significant and clinically meaningful improvements in HRQoL (i.e., CFQ-R) in each of the included studies. The magnitude of improvement in the CFQ-R respiratory domain scores with ELX-TEZ-IVA was 20.2 (95% CI, 17.5 to 23.0) at 24 weeks compared with placebo for patients with an F/MF genotype. In the trials in which patients switched to ELX-TEZ-IVA, the improvements in the CFQ-R respiratory domain scores were 15.9 (95% CI, 11.7 to 20.1) at 24 weeks compared with remaining on TEZ-IVA in patients with an F/F genotype, 8.9 (95% CI, 3.8 to 14.0) at 8 weeks compared with remaining on IVA in patients with an F/G genotype, and 8.5 (95% CI, 4.0 to 13.1) at 8 weeks compared with remaining on TEZ-IVA in patients with an F/RF genotype. The MID for the CFQ-R respiratory domain is typically cited to be 4.0 points, a threshold that was exceeded in all the included trials. The clinical experts consulted by CADTH and reviewers for the FDA and EMA considered the results to be clinically relevant.35,59
The CADTH review did not identify any RCTs that specifically addressed the use of ELX-TEZ-IVA in patients with prior failure or intolerance to another CFTR modulator. The clinical experts consulted by CADTH noted that prior failure or intolerance to a CFTR modulator should not preclude a patient from receiving a trial with ELX-TEZ-IVA.
The patient input received by CADTH emphasized that the therapeutic regimen for patients with CF requires considerable time each day and is demanding both physically and mentally for those living with CF and their caregivers. Patients have expressed interest in therapeutic options that could help alleviate their existing treatment burden. Treatment with ELX-TEZ-IVA was shown to reduce the need for IV antibiotics in Study 102; however, all the included studies investigated the addition of ELX-TEZ-IVA to ongoing therapies being used by eligible patients. Concomitant therapies were to remain stable throughout the trial to avoid confounding the study results (except for antibiotics for the treatment of pulmonary of exacerbations). A large RCT is currently being planned to investigate the discontinuation of some concomitant CF therapies (hypertonic saline and dornase alfa) after stabilization with ELX-TEZ-IVA (SIMPLIFY; N = 800).122,123 The clinical experts consulted by CADTH and the clinician groups who provided input all noted that ELX-TEZ-IVA should be used as an add-on therapy.
Harms
ELX-TEZ-IVA was well tolerated in the target patient populations (i.e., at least 6 years of age with at least 1 F508del mutation). There have been no updates to the warnings and precautions section of ELX-TEZ-IVA product monograph since the previous CADTH review.
Serious AEs and withdrawals due to AEs were rare in the included studies. The clinical experts consulted by CADTH noted that intolerance to ELX-TEZ-IVA has been rare in clinical practice with adolescents and adults. The clinical experts consulted by CADTH noted that patients who experience significant AEs following initial treatment with ELX-TEZ-IVA would not likely be completely discontinued from treatment; rather, treatment with ELX-TEZ-IVA would likely be interrupted and the patient would be rechallenged with the drug following resolution of the event(s). This is consistent with the input received from the 3 clinician groups, who noted that discontinuation of therapy should be considered in patients who have clinically significant adverse effects that persist and recur after stopping and re-initiating therapy. It is currently unclear if the lower dosage form (i.e., ELX 50 mg, TEZ 25 mg, and IVA 37.5 mg plus IVA 75 mg) would be useful in clinical practice for adults who demonstrate intolerance to the higher dosage.
Similar to the development programs for the other CFTR modulators (IVA, LUM-IVA, and TEZ-IVA), patients with abnormal liver function were excluded from the phase III ELX-TEZ-IVA trials. The clinical experts consulted by CADTH noted that most patients who could be eligible for ELX-TEZ-IVA would not have hepatic impairment. The product monograph recommends that the dosage of ELX-TEZ-IVA should be adjusted in patients with moderate hepatic impairment and that the drug should not be used in patients with severe hepatic impairment.36 These recommendations are more restrictive than those in the product monographs for IVA, LUM-IVA, or TEZ-IVA,12,36,44 all of which provide dosage-reduction scenarios for patients with CF who have severe hepatic impairment. The clinical experts consulted by CADTH suggested that clinicians may attempt to treat patients with severe hepatic impairment using ELX-TEZ-IVA at a reduced dosage, as opposed to using the reduced dosages of the alternative CFTR modulators, which are unlikely to provide the same level of clinical benefit.
The product monograph notes that elevated transaminases have been observed in patients treated with ELX-TEZ-IVA and recommends that ALT and AST levels be assessed before initiating treatment with ELX-TEZ-IVA, every 3 months during the first year of treatment, and annually thereafter.36 The clinical experts consulted by CADTH noted that the recommendations for monitoring would likely be followed by the clinical community. The clinical experts consulted by CADTH and the clinician groups who provided input noted that patients with CF are typically seen once every 3 months (although the frequency has declined in some cases due to the COVID-19 pandemic). As such, the recommended monitoring regimen for ELX-TEZ-IVA was not anticipated to result in a substantial increase in the number of the clinic visits for patients with CF, particularly after the first year of initiating the treatment.
Similar to IVA, LUM-IVA, and TEZ-IVA, the product monograph for ELX-TEZ-IVA notes that cases of noncongenital cataracts without an impact on vision have been reported in pediatric patients who were treated with IVA-containing regimens.3,12,36,44 The product monograph states that the patients who experienced these events had other risk factors (e.g., corticosteroid use or exposure to radiation); however, a possible risk attributable to treatment with IVA cannot be excluded. As such, it is recommended that pediatric patients initiating treatment with ELX-TEZ-IVA receive baseline and follow-up ophthalmological examinations.36 The clinical experts consulted by CADTH noted that children with CF currently have an ophthalmological examination before starting treatment with a CFTR modulator and are monitored on an ongoing basis thereafter.
The sponsor’s indirect comparisons did not investigate the comparative safety of ELX-TEZ-IVA versus IVA, LUM-IVA, or TEZ-IVA.52,62 The clinical trials included in this review demonstrated that ELX-TEZ-IVA does not appear to be associated with the respiratory AEs (e.g., dyspnea and abnormal respiration) that were reported in the pivotal trials of LUM-IVA.41,42,44,83,124
Other Considerations
The sponsor is currently conducting phase III trials investigating the safety, tolerability, and pharmacokinetics of ELX-TEZ-IVA in patients aged 2 to 5 years.125 This is similar to the clinical development programs for LUM-IVA and TEZ-IVA. In Canada, the initial Health Canada approval of LUM-IVA was granted in 2016 for patients aged 12 years and older and subsequently expanded to patients aged 6 to 11 years in 2017 and then to patients aged 2 to 5 in 2018.126 The FDA extended the approval of ELX-TEZ-IVA to include an 177 additional mutations in the CFTR gene that have shown to be responsive to ELX-TEZ-IVA based on data from in vitro assays.10,37
Conclusions
For patients aged 6 to 11 years, a 24-week, double-blind, placebo-controlled RCT (Study 116; N = 121) and a pivotal, single-arm, open-label trial (Study 106B; N = 66) demonstrated that treatment with ELX-TEZ-IVA resulted in clinically meaningful improvements in lung function (increase in ppFEV1), nutritional status (increase in BMI z score), HRQoL (increase in CFQ-R respiratory domain scores) and CF biomarkers (reduction in sweat chloride). In addition, AE data suggested that ELX-TEZ-IVA reduced the occurrence of pulmonary exacerbations in pediatric patients. The clinical studies for ELX-TEZ-IVA were limited to patients with an F/MF (Study 116 and Study 106B) or F/F genotype. As Study 106B was a single-arm trial, the sponsor conducted an indirect comparison to derive estimates for the comparative efficacy of ELX-TEZ-IVA versus placebo, LUM/IVA, and TEZ/IVA. No clinical studies have been conducted with ELX-TEZ-IVA in pediatric patients with F/RF or F/G genotypes; however, the clinical experts noted that ELX-TEZ-IVA would result in clinically meaningful improvements for these patients, based on the evidence reported for ELX-TEZ-IVA in adult patients with F/RF and F/G genotypes and the results in F/F and F/MF pediatric studies. This is consistent with the input from patient and clinician groups who have indicated all patients with at least 1 F508del mutation are likely to benefit from treatment with ELX-TEZ-IVA.
For patients 12 years and older, a 24-week, placebo-controlled RCT (Study 102; N = 403) conducted in patients with an F/MF genotype demonstrated that, compared with placebo, 24 weeks of treatment with ELX-TEZ-IVA was associated with statistically significant and clinically meaningful improvements in lung function (increase in ppFEV1), nutritional status (increase in BMI), HRQoL (increase in CFQ-R respiratory domain scores), CF biomarkers (reduction in sweat chloride), and a reduced rate of pulmonary exacerbations, including events that required IV antibiotics and/or hospitalization to manage. Three additional double-blind, active-controlled RCTs investigated switching to ELX-TEZ-IVA after 4 weeks of treatment with either TEZ-IVA or IVA compared with remaining on those other CFTR modulators. Study 103 (N = 107; 4 weeks) and Study 109 (N = 175; 24 weeks), which were conducted in patients with an F/F genotype, demonstrated that treatment with ELX-TEZ-IVA was associated with statistically significant and clinically meaningful improvements in ppFEV1 and CFQ-R compared with remaining on TEZ-IVA. Study 104 (N = 258; 8 weeks) demonstrated that switching to ELX-TEZ-IVA was associated with statistically significant and clinically meaningful improvements in ppFEV1 compared with remaining on IVA in patients with an F/G genotype treatment, and a modest improvement compared with remaining on TEZ-IVA for patients with an F/RF genotype. Patients with advanced lung disease were largely excluded from the phase III RCTs; however, post hoc subgroup analyses and data from 2 short-term observational studies suggest that treatment with ELX-TEZ-IVA resulted in clinically meaningful improvements in lung function in these patients.
Patients with normal lung function (i.e., ppFEV1 > 90%) were considered an important subgroup for the current review of ELX-TEZ-IVA. Approximately half of the pediatric patients in Study 106B and Study 116 also had a baseline ppFEV1 of greater than 90%. For those 12 years and older, in addition to the previously reviewed HELIO and CFFPR data, the current review included subgroup data for patients with a baseline ppFEV1 of greater than 90% from a new observational study in adolescents and adults (PROMISE). Although limited by open-label administration and the lack of a control group, the data from PROMISE suggested that patients aged 12 years and older with a ppFEV1 of greater than 90% at the time of initiating treatment with ELX-TEZ-IVA experienced meaningful improvements in ppFEV1, BMI, and CFQ-R.
ELX-TEZ-IVA was well tolerated in the target patient populations (i.e., 6 years of age and older with at least 1 F508del mutation). Serious AEs and withdrawals due to AEs were rare in the included studies. The product monograph notes that elevated transaminases have been observed in patients treated with ELX-TEZ-IVA, and it recommends that ALT and AST be assessed before initiating treatment with ELX-TEZ-IVA, every 3 months during the first year of treatment, and annually thereafter. The clinical experts consulted by CADTH noted that the recommendations for monitoring with ELX-TEZ-IVA were not anticipated to result in a substantial increase in the number of the clinic visits for patients with CF (particularly after the first year of initiating the treatment).
References
1.The Canadian Cystic Fibrosis registry: 2019 annual data report. Toronto (ON): Cystic Fibrosis Canada; 2020: https://www.cysticfibrosis.ca/registry/2019AnnualDataReport.pdf. Accessed 2021 Dec 1.
2.CADTH Canadian Drug Expert Committee (CDEC) final recommendation: elexacaftor / tezacaftor / ivacaftor and ivacaftor (Trikafta - Vertex Pharmaceuticals [Canada] Incorporated). Ottawa (ON): CADTH; 2021 Sept 16: https://cadth.ca/sites/default/files/DRR/2021/SR0673%20Trikafta%20-%20CADTH%20Final%20Rec%20Revised.pdf. Accessed 2021 Dec 7.
3.Clinical Study Report: VX18-445-106. A phase 3 study evaluating the pharmacokinetics, safety, and tolerability of VX-445/TEZ/IVA triple combination therapy in cystic fibrosis subjects 6 through 11 years of age [internal sponsor's report]. Boston (MA): Vertex Pharmaceuticals Incorporated; 2020 Nov 11.
4.Clinical Study Report: VX19-445-116. A phase 3b, randomized, placebo-controlled study evaluating the efficacy and safety of elexacaftor/tezacaftor/ivacaftor in cystic fibrosis subjects 6 through 11 years of age who are heterozygous for the F508del mutation and a minimal function mutation (F/MF) [internal sponsor's report]. Boston (MA): Vertex Pharmaceuticals Incorporated; 2021 Aug 27.
5.Clinical Study Report: study 102. A phase 3, randomized, double-blind, controlled study evaluating the efficacy and safety of VX-445 combination therapy in subjects with cystic fibrosis who are heterozygous for the F508del mutation and a minimal function mutation (F/MF) [internal sponsor's report]. Toronto (ON): Vertex Pharmaceuticals Incorporated; 2019 Jul 2.
6.Clinical Study Report: study 103. A phase 3, randomized, double-blind, controlled study evaluating the efficacy and safety of VX-445 combination therapy in subjects with cystic fibrosis who are homozygous for the F508del mutation (F/F) [internal sponsor's report]. Toronto (ON): Vertex Pharmaceuticals Incorporated; 2019 Jun 18.
7.Clinical Study Report: study 104. A phase 3, randomized, double-blind, controlled study evaluating the efficacy and safety of elexacaftor combination therapy in subjects with cystic fibrosis who are heterozygous for the F508del mutation and a gating or residual function mutation (F/G and F/RF genotypes) [internal sponsor's report]. Toronto (ON): Vertex Pharmaceuticals Incorporated; 2020 Aug 28.
8.Clinical Study Report: study 109. A phase 3b, randomized, double-blind, controlled study evaluating the efficacy and safety of elexacaftor/tezacaftor/ivacaftor in cystic fibrosis subjects, homozygous for F508del [internal sponsor's report]. Toronto (ON): Vertex Pharmaceuticals Incorporated; 2020 Oct 16.
9.Vertex response to March 10, 2021 request for additional information regarding Trikafta CADTH review [internal additional sponsor's information]. Toronto (ON): Vertex Pharmaceuticals (Canada) Incorporated; 2021 Mar 22.
10.Vertex Pharmaceuticals Incorporated. Vertex announces FDA approvals of TRIKAFTA® (elexacaftor/tezacaftor/ivacaftor and ivacaftor), SYMDEKO® (tezacaftor/ivacaftor and ivacaftor) and KALYDECO® (ivacaftor) for use in people with CF with certain rare mutations. 2020; https://news.vrtx.com/press-release/vertex-announces-fda-approvals-trikaftar-elexacaftortezacaftorivacaftor-and-ivacaftor. Accessed 2021 Dec 1.
11.Vertex Pharmaceuticals Incorporated. NCT04105972: A study evaluating the efficacy and safety of VX-445/tezacaftor/ivacaftor in cystic fibrosis subjects, homozygous for F508del. ClinicalTrials.gov. Bethesda (MD): U.S. National Library of Medicine; 2020: https://clinicaltrials.gov/ct2/show/NCT04105972. Accessed 2021 Dec 1.
12.Kalydeco®: ivacaftor tablets 150 mg, ivacaftor granules 50 mg per packet, 75 mg per packet [product monograph]. Toronto (ON): Vertex Pharmaceuticals (Canada) Incorporated; 2019 Jan 25: https://pdf.hres.ca/dpd_pm/00049400.PDF. Accessed 2021 Dec 1.
13.Symdeko®, tezacaftor/ivacaftor tablets and ivacaftor tablets, tezacaftor 100 mg/ivacaftor 150 mg tablets and ivacaftor 150 mg tablets, oral [product monograph]. Toronto (ON): Vertex Pharmaceuticals (Canada) Incorporated; 2020 Aug 21: https://pdf.hres.ca/dpd_pm/00058025.PDF. Accessed 2021 Dec 1.
14.Ratjen F EH, Gaffin JM, McColley SA, Roesch E. Elexacaftor/ Tezacaftor/ Ivacaftor in Children 6 Years of Age and Older With Cystic Fibrosis and at Least One F508del Allele: Interim Results From a Phase 3, Open-Label Extension Study (VX19-445-107), Poster 562. Paper presented at: North American Cystic Fibrosis Conference (virtual), 2-5 November 2021.
15.Clinical Study Report: study 105. A phase 3, open-label study evaluating the long-term safety and efficacy of VX-445 combination therapy in subjects with cystic fibrosis who are homozygous or heterozygous for the F508del mutation) [internal sponsor's report]. Toronto (ON): Vertex Pharmaceuticals Incorporated; 2020 Mar 20.
16.Daines CL, Tullis E, Costa S, et al. Long-Term Safety and Efficacy of Elexacaftor/ Tezacaftor/ Ivacaftor in People With Cystic Fibrosis and at Least One F508del Allele: 96-Week Interim Results From an Open-Label Extension Study. Poster 681. Paper presented at: 35th Annual North American Cystic Fibrosis Conference (virtual) 2021.
17.O'Shea KM, O'Carroll OM, Carroll C, et al. The efficacy of elexacaftor/tezacaftor/ivacaftor in patients with cystic fibrosis and advanced lung disease. Eur Respir J. 2020;05:05.
18.Burgel PR, Durieu I, Chiron R, et al. Rapid improvement after starting elexacaftor-tezacaftor-ivacaftor in patients with cystic fibrosis and advanced pulmonary disease. Am J Respir Crit Care Med. 2021;18:18. PubMed
19.Stanojevic S, Vukovojac K, Sykes J, Ratjen F, Tullis E, Stephenson AL. Projecting the impact of delayed access to elexacaftor/tezacaftor/ivacaftor for people with cystic fibrosis. J Cyst Fibros. 2020;05:05.
20.Rowe SM, Miller S, Sorscher EJ. Cystic fibrosis. N Engl J Med. 2005;352(19):1992-2001. PubMed
21.Veit G, Avramescu RG, Chiang AN, et al. From CFTR biology toward combinatorial pharmacotherapy: expanded classification of cystic fibrosis mutations. Mol Biol Cell. 2016;27(3):424-433. PubMed
22.Lukacs GL, Verkman AS. CFTR: folding, misfolding and correcting the DeltaF508 conformational defect. Trends Mol Med. 2012;18(2):81-91. PubMed
23.Okiyoneda T, Barriere H, Bagdany M, et al. Peripheral protein quality control removes unfolded CFTR from the plasma membrane. Science. 2010;329(5993):805-810. PubMed
24.Flume PA, O'Sullivan BP, Robinson KA, et al. Cystic fibrosis pulmonary guidelines: chronic medications for maintenance of lung health. Am J Respir Crit Care Med. 2007;176(10):957-969. PubMed
25.Cogen J, Emerson J, Sanders DB, et al. Risk factors for lung function decline in a large cohort of young cystic fibrosis patients. Pediatr Pulmonol. 2015;50(8):763-770. PubMed
26.Emerson J, Rosenfeld M, McNamara S, Ramsey B, Gibson RL. Pseudomonas aeruginosa and other predictors of mortality and morbidity in young children with cystic fibrosis. Pediatr Pulmonol. 2002;34(2):91-100. PubMed
27.Canadian consensus statement on aerosolized antibiotic use in cystic fibrosis. Toronto (ON): Cystic Fibrosis Canada; 2020: https://www.cysticfibrosis.ca/uploads/About%20Us/CFC005%20AEROSOLIZED%20ANTIBIOTIC%20_englishFinal.pdf. Accessed 2021 Dec 1.
28.Cystic Fibrosis Foundation patient registry 2019 annual data report. Bethesda (MD): Cystic Fibrosis Foundation; 2020: https://www.cff.org/Research/Researcher-Resources/Patient-Registry/2019-Patient-Registry-Annual-Data-Report/. Accessed 2021 Dec 1.
29.Liou TG, Adler FR, Fitzsimmons SC, Cahill BC, Hibbs JR, Marshall BC. Predictive 5-year survivorship model of cystic fibrosis. Am J Epidemiol. 2001;153(4):345-352. PubMed
30.Corey M, McLaughlin FJ, Williams M, Levison H. A comparison of survival, growth, and pulmonary function in patients with cystic fibrosis in Boston and Toronto. J Clin Epidemiol. 1988;41(6):583-591. PubMed
31.The Canadian Cystic Fibrosis registry: 2013 annual report. Toronto (ON): Cystic Fibrosis Canada; 2015: https://www.cysticfibrosis.ca/uploads/cf%20care/Canadian-CF-Registry-2013-FINAL.pdf. Accessed 2021 Dec 1.
32.The Canadian Cystic Fibrosis registry: 2016 annual data report. Toronto (ON): Cystic Fibrosis Canada; 2017: https://www.cysticfibrosis.ca/registry/2016AnnualDataReport.pdf. Accessed 2021 Dec 8.
33.Mogayzel PJ, Jr., Naureckas ET, Robinson KA, et al. Cystic fibrosis pulmonary guidelines. Chronic medications for maintenance of lung health. Am J Respir Crit Care Med. 2013;187(7):680-689. PubMed
34.Flume PA, Mogayzel PJ, Jr., Robinson KA, et al. Cystic fibrosis pulmonary guidelines: treatment of pulmonary exacerbations. Am J Respir Crit Care Med. 2009;180(9):802-808. PubMed
35.Center for Drug Evaluation and Research. Multi-Disciplinary Review. Trikafta (elexacaftor, tezacaftor and ivacaftor tablets; ivacaftor tablets). Company: Vertex Pharmaceuticals Incorporated. Application No.: 212273. Approval date: 10/21/2019 (FDA approval package). Rockville (MD): U.S. Food and Drug Administration (FDA); 2019: https://www.accessdata.fda.gov/drugsatfda_docs/nda/2019/212273Orig1s000MultidisciplineR.pdf. Accessed 2021 Dec 1.
36.Trikafta®: elexacaftor tezacaftor/ivacaftor tablets and ivacaftor tablets, oral 100 mg/50 mg/75 mg and 150 mg [product monograph]. Toronto (ON): Vertex Pharmaceuticals (Canada) Incorporated; 2020 Nov 11.
37.Center for Drug Evaluation and Research. Label. Trikafta (elexacaftor, tezacaftor and ivacaftor tablets; ivacaftor tablets). Company: Vertex Pharmaceuticals Incorporated. Application No.: 212273. Approval date: 10/21/2019 (FDA approval package). Rockville (MD): U.S. Food and Drug Administration (FDA); 2020: https://www.accessdata.fda.gov/drugsatfda_docs/label/2019/212273s000lbl.pdf. Accessed 2021 Dec 1.
38.CADTH Canadian Drug Expert Committee (CDEC) final recommendation: ivacaftor (Kalydeco - Vertex Pharmaceuticals [Canada] Incorporated). Ottawa (ON): CADTH; 2013 Mar 22: https://www.cadth.ca/sites/default/files/cdr/complete/cdr_complete_Kalydeco_March-25-13_e.pdf. Accessed 2021 Dec 1.
39.CADTH Canadian Drug Expert Committee (CDEC) final recommendation: ivacaftor (Kalydeco - Vertex Pharmaceuticals [Canada] Incorporated). Ottawa (ON): CADTH; 2014 Dec 19: https://www.cadth.ca/sites/default/files/cdr/complete/cdr_complete_SR0379_Kalydeco_Dec-23-14.pdf. Accessed 2021 Dec 1.
40.CADTH Canadian Drug Expert Committee (CDEC) final recommendation: ivacaftor (Kalydeco - Vertex Pharmaceuticals [Canada] Incorporated). Ottawa (ON): CADTH; 2015 Nov 19: https://www.cadth.ca/sites/default/files/cdr/complete/SR0430_complete_Kalydeco_R117H_Nov-23-15_e.pdf. Accessed 2021 Dec 1.
41.CADTH Canadian Drug Expert Committee (CDEC) final recommendation: lumacaftor/ivacaftor (Orkambi - Vertex Pharmaceuticals [Canada] Incorporated). Ottawa (ON): CADTH; 2016 Oct 26: https://www.cadth.ca/sites/default/files/cdr/complete/SR0471_complete_Orkambi-Oct-28-16.pdf. Accessed 2021 Dec 1.
42.CADTH Canadian Drug Expert Committee (CDEC) final recommendation: lumacaftor/ivacaftor (Orkambi - Vertex Pharmaceuticals [Canada] Incorporated). Ottawa (ON): CADTH; 2018 Sep 26: https://www.cadth.ca/sites/default/files/cdr/complete/SR0559%20Orkambi%20-%20CDEC%20Final%20Recommendation%20October%204%2C%202018.pdf. Accessed 2021 Dec 1.
43.CADTH reimbursement review status: tezacaftor/ivacaftor. 2019; https://www.cadth.ca/tezacaftorivacaftor. Accessed 2021 Dec 1.
44.Orkambi®, lumacaftor/ivacaftor tablets 100 mg/125 mg and 200 mg/125 mg, lumacaftor/ivacaftor granules 100 mg/125 mg and 150 mg/188 mg [product monograph]. Toronto (ON): Vertex Pharmaceuticals (Canada) Incorporated; 2018 Dec 11: https://pdf.hres.ca/dpd_pm/00048664.PDF. Accessed 2021 Dec 1.
45.McGowan J, Sampson M, Salzwedel DM, Cogo E, Foerster V, Lefebvre C. PRESS Peer Review of Electronic Search Strategies: 2015 guideline statement. J Clin Epidemiol. 2016;75:40-46. PubMed
46.Grey matters: a practical tool for searching health-related grey literature. Ottawa (ON): CADTH; 2019: https://www.cadth.ca/grey-matters. Accessed 2021 Dec 1.
47.Zemanick ET, Taylor-Cousar JL, Davies J, et al. A Phase 3 Open-Label Study of Elexacaftor/Tezacaftor/Ivacaftor in Children 6 through 11 Years of Age with Cystic Fibrosis and at Least One F508del Allele. Am J Respir Crit Care Med. 2021;203(12):1522-1532. PubMed
48.Vertex Pharmaceuticals Incorporated. NCT03691779: Evaluation of VX 445/TEZ/IVA in Cystic Fibrosis Subjects 6 Through 11 Years of Age. ClinicalTrials.gov. Bethesda (MD): U.S. National Library of Medicine; 2021: https://clinicaltrials.gov/ct2/show/NCT03691779. Accessed 2021 Dec 7.
49.Vertex Pharmaceuticals Incorporated. NCT04353817: A study evaluating efficacy and safety of elexacaftor/tezacaftor/ivacaftor in subjects 6 through 11 years of age with cystic fibrosis and F/MF genotypes. ClinicalTrials.gov. Bethesda (MD): U.S. National Library of Medicine; 2020: https://clinicaltrials.gov/ct2/show/NCT04353817. Accessed 2021 Dec 1.
50.Committee for Medicinal Products for Human Use. Assessment report variation: Kaftrio (ivacaftor/tezacaftor/elexacaftor). (European public assessment report). Amsterdam (NL): European Medicines Agency; 2021: https://www.ema.europa.eu/en/documents/variation-report/kaftrio-h-c-005269-x-0008-g-epar-public-assessment-report-variation_en.pdf. Accessed 2022 Jan 28.
51.Common technical document 2.7.3 summary of clinical efficacy [internal sponsor's package]. Toronto (ON): Vertex Pharmaceuticals Incorporated; 2021 Jan 22.
52.Drug Reimbursement Review sponsor submission: Trikafta, oral elexacaftor 50 mg / tezacaftor 25 mg / ivacaftor 37.5 mg and ivacaftor 75 mg; elexacaftor 100 mg / tezacaftor 50 mg / ivacaftor 75 mg and ivacaftor 150 mg; [internal sponsor's package]. Toronto (ON): Vertex Pharmaceuticals (Canada) Incorporated; 2021 Nov 5.
53.Middleton PG, Mall MA, Dřevínek P, et al. Elexacaftor-tezacaftor-ivacaftor for cystic fibrosis with a single Phe508del allele. N Engl J Med. 2019;381(19):1809-1819. PubMed
54.Vertex Pharmaceuticals Incorporated. NCT03525444: A phase 3 study of VX-445 combination therapy in subjects with cystic fibrosis heterozygous for the F508del mutation and a minimal function mutation (F/MF). ClinicalTrials.gov. Bethesda (MD): U.S. National Library of Medicine; 2020: https://clinicaltrials.gov/ct2/show/NCT03525444. Accessed 2020 Dec 20.
55.Heijerman HGM, McKone EF, Downey DG, et al. Efficacy and safety of the elexacaftor plus tezacaftor plus ivacaftor combination regimen in people with cystic fibrosis homozygous for the F508del mutation: a double-blind, randomised, phase 3 trial. Lancet. 2019;394(10212):1940-1948. PubMed
56.Department of error. Lancet. 2020;395(10238):1694.
57.Vertex Pharmaceuticals Incorporated. NCT03525548: A study of VX-445 combination therapy in CF subjects homozygous for F508del (F/F). ClinicalTrials.gov. Bethesda (MD): U.S. National Library of Medicine; 2020: https://clinicaltrials.gov/ct2/show/NCT03525548. Accessed 2021 Dec 1.
58.Vertex Pharmaceuticals Incorporated. NCT04058353: A phase 3 study of VX-445 combination therapy in cystic fibrosis (CF) subjects heterozygous for F508del and a gating or residual function mutation (F/G and F/RF genotypes). ClinicalTrials.gov. Bethesda (MD): U.S. National Library of Medicine; 2020: https://clinicaltrials.gov/ct2/show/NCT04058353. Accessed 2021 Dec 1.
59.Committee for Medicinal Products for Human Use. Assessment report: Kaftrio (ivacaftor/tezacaftor/elexacaftor). (European public assessment report). Amsterdam (NL): European Medicines Agency; 2020: https://www.ema.europa.eu/en/documents/assessment-report/kaftrio-epar-public-assessment-report_en.pdf. Accessed 2021 Dec 1.
60.Clinical value of triple combination therapy (elexacaftor/tezacaftor/ivacaftor & ivacaftor) for the treatment of cystic fibrosis in patients 12 years of age and older who have at least one F508 deletion mutation in the CFTR gene [internal sponsor's report]. Toronto (ON): Vertex Pharmaceuticals (Canada); 2021 Jan.
61.Vertex Pharmaceuticals Incorporated. NCT04183790: Evaluation of Long-term Safety and Efficacy of VX-445 Combination Therapy in Subjects With Cystic Fibrosis Who Are 6 Years of Age and Older. ClinicalTrials.gov. Bethesda (MD): U.S. National Library of Medicine; 2021: https://clinicaltrials.gov/ct2/show/NCT04183790 Accessed 2021 Dec 7.
62.Drug Reimbursement Review sponsor submission: Trikafta, elexacaftor 100 mg, TEZacaftor 50 mg/ivacaftor 75 mg tablets and ivacaftor 150 mg tablets; elexacaftor 50 mg, TEZacaftor 25 mg/ivacaftor 37.5 mg tablets and ivacaftor 75 mg tablets oral [internal sponsor's package]. Toronto (ON): Vertex Pharmaceuticals (Canada) Incorporated; 2021 Jan 21.
63.Nichols DP, Paynter AC, Heltshe SL, et al. Clinical Effectiveness of Elexacaftor/Tezacftor/Ivacaftor in People with Cystic Fibrosis. Am J Respir Crit Care Med. 2021;16:16.
64.Vertex Pharmaceuticals Incorporated. NCT04545515: A study evaluating the long-term safety and efficacy of elexacaftor/tezacaftor/ivacaftor in cystic fibrosis (CF) subjects 6 years and older and F/MF genotypes. ClinicalTrials.gov. Bethesda (MD): U.S. National Library of Medicine; 2020: https://clinicaltrials.gov/ct2/show/NCT04545515. Accessed 2021 Dec 1.
65.Vertex Pharmaceuticals Incorporated. NCT04362761: A study evaluating the long-term safety of elexacaftor combination therapy. ClinicalTrials.gov. Bethesda (MD): U.S. National Library of Medicine; 2021: https://clinicaltrials.gov/ct2/show/NCT04362761. Accessed 2021 Mar 25.
66.Vertex Pharmaceuticals Incorporated. NCT04058366: Study evaluating the long-term safety and efficacy of VX-445 combination therapy. ClinicalTrials.gov. Bethesda (MD): U.S. National Library of Medicine; 2021: https://clinicaltrials.gov/ct2/show/NCT04058366. Accessed 2021 March 25.
67.US CF Foundation, Johns Hopkins University, The Hospital for Sick Children. The Clinical and Functional TRanslation of CFTR (CFTR2). 2011; http://cftr2.org. Accessed 2021 Mar 2.
68.Vertex response to March 15, 2021 request for additional information regarding Trikafta CADTH review [internal additional sponsor's information]. Toronto (ON): Vertex Pharmaceuticals (Canada) Incorporated; 2021 Mar 23.
69.Quanjer PH, Stanojevic S, Cole TJ, et al. Multi-ethnic reference values for spirometry for the 3-95-yr age range: the global lung function 2012 equations. Eur Respir J. 2012;40(6):1324-1343. PubMed
70.Subbarao P, Milla C, Aurora P, et al. Multiple-Breath Washout as a Lung Function Test in Cystic Fibrosis. A Cystic Fibrosis Foundation Workshop Report. Ann Am Thorac Soc. 2015;12(6):932-939. PubMed
71.Report of the workshop on end points for cystic fibrosis clinical trials. London (GB): European Medicines Agency; 2012: https://www.ema.europa.eu/docs/en_GB/document_library/Report/2012/12/WC500136159.pdf. Accessed 2021 Dec 8.
72.Kent L, Reix P, Innes JA, et al. Lung clearance index: evidence for use in clinical trials in cystic fibrosis. J Cyst Fibros. 2014;13(2):123-138. PubMed
73.Quittner AL, Sawicki GS, McMullen A, et al. Erratum to: psychometric evaluation of the Cystic Fibrosis Questionnaire-Revised in a national, US sample. Qual Life Res. 2012;21(7):1279-1290. PubMed
74.Tluczek A, Becker T, Grieve A, et al. Health-related quality of life in children and adolescents with cystic fibrosis: convergent validity with parent-reports and objective measures of pulmonary health. J Dev Behav Pediatr. 2013;34(4):252-261. PubMed
75.Henry B, Aussage P, Grosskopf C, Goehrs JM. Development of the Cystic Fibrosis Questionnaire (CFQ) for assessing quality of life in pediatric and adult patients. Qual Life Res. 2003;12(1):63-76. PubMed
76.Quittner AL, Modi AC, Wainwright C, Otto K, Kirihara J, Montgomery AB. Determination of the minimal clinically important difference scores for the Cystic Fibrosis Questionnaire-Revised respiratory symptom scale in two populations of patients with cystic fibrosis and chronic Pseudomonas aeruginosa airway infection. Chest. 2009;135(6):1610-1618. PubMed
77.Regnault A, Balp MM, Kulich K, Viala-Danten M. Validation of the treatment satisfaction questionnaire for medication in patients with cystic fibrosis. J Cyst Fibros. 2012;11(6):494-501. PubMed
78.Vertex response to April 19, 2022 request for additional information regarding Trikafta CADTH review [internal additional sponsor's information]. Toronto (ON): Vertex Pharmaceuticals (Canada) Incorporated; 2022 April 22.
79.Summary of product characteristics: Kaftrio 75 mg/50 mg/100 mg film-coated tablets. Amsterdam (NL): European Medicines Agency; 2020: https://www.ema.europa.eu/documents/product-information/kaftrio-epar-product-information_en.pdf. Accessed 2021 Dec 1.
80.Committee for Medicinal Products for Human Use. Assessment report variation: Orkambi (ivacaftor/lumacaftor). (European public assessment report). Amsterdam (NL): European Medicines Agency; 2017: https://www.ema.europa.eu/en/documents/variation-report/orkambi-epar-assessment-report-variation_en.pdf. Accessed 2021 Dec 7.
81.Vertex Pharmaceuticals Incorporated. NCT03559062: A Study to Evaluate Efficacy and Safety of TEZ/IVA in Subjects Aged 6 Through 11 Years With Cystic Fibrosis. ClinicalTrials.gov. Bethesda (MD): U.S. National Library of Medicine; 2020: https://clinicaltrials.gov/ct2/show/NCT03559062. Accessed 2021 Dec 7.
82.Vertex Pharmaceuticals Incorporated. NCT02514473: A Study to Evaluate the Efficacy and Safety of Lumacaftor in Combination With Ivacaftor in Subjects With CF, Homozygous for the F508del-CFTR Mutation. ClinicalTrials.gov. Bethesda (MD): U.S. National Library of Medicine; 2017: https://clinicaltrials.gov/ct2/show/NCT02514473 Accessed 2021 Dec 8.
83.CADTH Common Drug Review Clinical Review Report: lumacaftor/ivacaftor (Orkambi - Vertex Pharmaceuticals [Canada] Incorporated). Ottawa (ON): CADTH; 2018 Oct: https://www.cadth.ca/sites/default/files/cdr/clinical/SR0559_Orkambi_CL_Report.pdf. Accessed 2021 Dec 1.
84.CADTH Reimbursement Review Clinical and Pharmacoeconomic Review Report: elexacaftor-tezacaftor ivacaftor and ivacaftor (Trikafta - Vertex Pharmaceuticals [Canada] Incorporated). Ottawa (ON): CADTH; 2021: https://www.cadth.ca/sites/default/files/DRR/2021/SR0673-combined-report.pdf. Accessed 2021 Dec 7.
85.Committee for Medicinal Products for Human Use. Guideline on the clinical development of medicinal products for the treatment of cystic fibrosis. Amsterdam (NL): European Medicines Agency; 2009: https://www.ema.europa.eu/en/documents/scientific-guideline/guideline-clinical-development-medicinal-products-treatment-cystic-fibrosis-first-version_en.pdf. Accessed 2021 Dec 1.
86.Phuan PW, Haggie PM, Tan JA, et al. CFTR modulator therapy for cystic fibrosis caused by the rare c.3700A>G mutation. J Cyst Fibros. 2020;14:14. PubMed
87.Wainwright CE, Elborn JS, Ramsey BW, et al. Lumacaftor–ivacaftor in patients with cystic fibrosis homozygous for Phe508del CFTR. N Engl J Med. 2015;373(3):220-231. PubMed
88.Vertex Pharmaceuticals Incorporated. NCT01807923: A study of lumacaftor in combination with ivacaftor in cystic fibrosis subjects aged 12 years and older who are homozygous for the F508del-CFTR mutation (TRAFFIC). ClinicalTrials.gov. Bethesda (MD): U.S. National Library of Medicine; 2015: https://clinicaltrials.gov/ct2/show/NCT01807923. Accessed 2021 Dec 1.
89.Vertex Pharmaceuticals Incorporated. NCT01807949: A study of lumacaftor in combination with ivacaftor in cystic fibrosis subjects aged 12 years and older who are homozygous for the F508del-CFTR mutation (TRANSPORT). ClinicalTrials.gov. Bethesda (MD): U.S. National Library of Medicine; 2016: https://clinicaltrials.gov/ct2/show/NCT01807949. Accessed 2021 Dec 1.
90.Vertex Pharmaceuticals Incorporated. NCT02392234: A phase 3 study to evaluate the efficacy and safety of ivacaftor and VX-661 in combination with ivacaftor in subjects aged 12 years and older with cystic fibrosis, heterozygous for the F508del-cystic fibrosis transmembrane conductance regulator (CFTR) mutation. ClinicalTrials.gov. Bethesda (MD): U.S. National Library of Medicine; 2018: https://clinicaltrials.gov/ct2/show/NCT02392234. Accessed 2021 Dec 1.
91.Vertex Pharmaceuticals Incorporated. NCT02412111: A phase 3 study of tezacaftor (VX-661) in combination with ivacaftor (VX-770) in subjects aged 12 years and older with cystic fibrosis (CF), who have one F508del-CFTR mutation and a second mutation that has been demonstrated to be clinically responsive to ivacaftor. ClinicalTrials.gov. Bethesda (MD): U.S. National Library of Medicine; 2019: https://clinicaltrials.gov/ct2/show/NCT02412111. Accessed 2021 Dec 1.
92.Taylor-Cousar JL, Munck A, McKone EF, et al. Tezacaftor-ivacaftor in patients with cystic fibrosis homozygous for Phe508del. N Engl J Med. 2017;377(21):2013-2023. PubMed
93.Rowe SM, Daines C, Ringshausen FC, et al. Tezacaftor-ivacaftor in residual-function heterozygotes with cystic fibrosis. N Engl J Med. 2017;377(21):2024-2035. PubMed
94.Vertex Pharmaceuticals Incorporated. NCT01614470: Study of ivacaftor in subjects with cystic fibrosis (CF) who have a non-G551D CF transmembrane conductance regulator (CFTR) gating mutation (KONNECTION). ClinicalTrials.gov. Bethesda (MD): U.S. National Library of Medicine; 2014: https://clinicaltrials.gov/ct2/show/NCT01614470. Accessed 2021 Dec 1.
95.Ramsey BW, Davies J, McElvaney NG, et al. A CFTR potentiator in patients with cystic fibrosis and the G551D mutation. N Engl J Med. 2011;365(18):1663-1672. PubMed
96.Davies JC, Wainwright CE, Canny GJ, et al. Efficacy and safety of ivacaftor in patients aged 6 to 11 years with cystic fibrosis with a G551D mutation. Am J Respir Crit Care Med. 2013;187(11):1219-1225. PubMed
97.Miller MR, Crapo R, Hankinson J, et al. General considerations for lung function testing. Eur Respir J. 2005;26(1):153-161. PubMed
98.Miller MR, Hankinson J, Brusasco V, et al. Standardisation of spirometry. Eur Respir J. 2005;26(2):319-338. PubMed
99.Moss RB, Flume PA, Elborn JS, et al. Efficacy and safety of ivacaftor in patients with cystic fibrosis who have an Arg117His-CFTR mutation: a double-blind, randomised controlled trial. Lancet Respir Med. 2015;3(7):524-533. PubMed
100.De Boeck K, Munck A, Walker S, et al. Efficacy and safety of ivacaftor in patients with cystic fibrosis and a non-G551D gating mutation. J Cyst Fibros. 2014;13(6):674-680. PubMed
101.Griese M, Costa S, Linnemann RW, et al. Safety and efficacy of elexacaftor/tezacaftor/ivacaftor for 24 weeks or longer in people with cystic fibrosis and one or more F508del alleles: interim results of an open-label phase 3 clinical trial. Am J Respir Crit Care Med. 2021;203(3):381-385. PubMed
102.Volkova N, Moy K, Evans J, et al. Disease progression in patients with cystic fibrosis treated with ivacaftor: data from national US and UK registries. J Cyst Fibros. 2020;19(1):68-79. PubMed
103.Synopsis of Real-world Analyses Conducted on the Effectiveness of ELX/TEZ/IVA in Patients with Pre-treatment ppFEV1 > 90 [internal additional sponsor's information]. Toronto (ON): Vertex Pharmaceuticals (Canada) Incorporated; 2021 Jul 30.
104.Considerations for the use of lumacaftor and ivacaftor fixed dose combination oral tablets (Orkambi™) for the management of persons with cystic fibrosis and two F508del CFTR mutations. Bethesda (MD): Cystic Fibrosis Foundation; 2015: https://www.cff.org/PDF-Archive/Orkambi-Whitepaper/. Accessed 2021 Mar 16.
105.Modulator treatments for cystic fibrosis: final policy recommendations. Boston (MA): Institute for Clinical and Economic Review; 2020: http://icerorg.wpengine.com/wp-content/uploads/2020/08/ICER_CF_Policy_Recs_092320.pdf. Accessed 2021 Dec 1.
106.Jakharia K, Doligalski C, Lobo L, Coakley R. Impact of Trikafta on lung function in a cystic fibrosis transplant patient. Chest. 2020;158(4):A2378.
107.Ragan HH, Autry E, Bomersback T. The use of elexacaftor/tezacaftor/ivacaftor in patients with cystic fibrosis post-liver transplantation [abstract 788]. Paper presented at: 34th Annual North American Cystic Fibrosis Conference. 2020 Oct 7-23; Virtual experience.
108.Turowski J, Lehr C, Valapour M, Dasenbrook E. Impact of elexacaftor/tezacaftor/ivacaftor on tacrolimus trough levels in individuals at least 3 years post-lung transplant [abstract 787]. Paper presented at: 34th Annual North American Cystic Fibrosis Conference. 2020 Oct 7-23; Virtual experience.
109.Fitzgerald L, Jia S. Initiating elexacaftor/tezacaftor/ivacaftor in post-lung transplant CF patients [abstract 792]. Paper presented at: 34th Annual North American Cystic Fibrosis Conference. 2020 Oct 7-23; Virtual experience.
110.Perrem L, Rayment JH, Ratjen F. The lung clearance index as a monitoring tool in cystic fibrosis: ready for the clinic? Curr Opin Pulm Med. 2018;24(6):579-585. PubMed
111.Frauchiger BS, Binggeli S, Yammine S, et al. Longitudinal course of clinical lung clearance index in children with cystic fibrosis. Eur Respir J. 2021;58(1). PubMed
112.Committee for Medicinal Products for Human Use. Assessment report: Orkambi (ivacaftor/lumacaftor). (European public assessment report). Amsterdam (NL): European Medicines Agency; 2016: https://www.ema.europa.eu/en/documents/assessment-report/orkambi-epar-public-assessment-report_en.pdf. Accessed 2021 Dec 1.
113.National Institute for Health and Care Excellence. Lumacaftor–ivacaftor for treating cystic fibrosis homozygous for the F508del mutation. (Technology appraisal guidance TA398) 2016; https://www.nice.org.uk/guidance/ta398/resources/lumacaftorivacaftor-for-treating-cystic-fibrosis-homozygous-for-the-f508del-mutation-pdf82602916891333. Accessed 2021 Mar 16.
114.Public summary document: lumacaftor and ivacaftor: tablet containing lumacaftor 200 mg with ivacaftor 125 mg Orkambi®. Canberra (AU): Pharmaceutical Benefit Advisory Committee; 2017: https://www.pbs.gov.au/industry/listing/elements/pbac-meetings/psd/2017-07/files/lumacaftor-ivacaftor-psd-july-2017.pdf. Accessed 2021 Apr 9.
115.Bhatt JM. Treatment of pulmonary exacerbations in cystic fibrosis. Eur Respir Rev. 2013;22(129):205-216. PubMed
116.de Boer K, Vandemheen KL, Tullis E, et al. Exacerbation frequency and clinical outcomes in adult patients with cystic fibrosis. Thorax. 2011;66(8):680-685. PubMed
117.Solem CT, Vera-Llonch M, Liu S, Botteman M, Castiglione B. Impact of pulmonary exacerbations and lung function on generic health-related quality of life in patients with cystic fibrosis. Health Qual Life Outcomes. 2016;14:63. PubMed
118.Waters V, Atenafu EG, Salazar JG, et al. Chronic Stenotrophomonas maltophilia infection and exacerbation outcomes in cystic fibrosis. J Cyst Fibros. 2012;11(1):8-13. PubMed
119.Waters V, Stanojevic S, Atenafu EG, et al. Effect of pulmonary exacerbations on long-term lung function decline in cystic fibrosis. Eur Respir J. 2012;40(1):61-66. PubMed
120.Sanders DB, Bittner RC, Rosenfeld M, Hoffman LR, Redding GJ, Goss CH. Failure to recover to baseline pulmonary function after cystic fibrosis pulmonary exacerbation. Am J Respir Crit Care Med. 2010;182(5):627-632. PubMed
121.Sanders DB, Hoffman LR, Emerson J, et al. Return of FEV1 after pulmonary exacerbation in children with cystic fibrosis. Pediatr Pulmonol. 2010;45(2):127-134. PubMed
122.Mayer-Hamblett N, Nichols DP, Odem-Davis K, et al. Evaluating the impact of stopping chronic therapies after modulator drug therapy in cystic fibrosis: the SIMPLIFY study design. Ann Am Thorac Soc. 2021. PubMed
123.Nichols D. NCT04378153: Impact of discontinuing chronic therapies in people with cystic fibrosis on highly effective CFTR modulator therapy (SIMPLIFY). ClinicalTrials.gov. Bethesda (MD): U.S. National Library of Medicine; 2020: https://clinicaltrials.gov/ct2/show/NCT04378153. Accessed 2021 Feb 23.
124.CADTH Common Drug Review Clinical Review Report: lumacaftor/ivacaftor (Orkambi - Vertex Pharmaceuticals [Canada] Incorporated). Ottawa (ON): CADTH; 2016 Jan 26: https://www.cadth.ca/sites/default/files/cdr/clinical/SR0471_Orkambi_CL_Report.pdf. Accessed 2021 Dec 1.
125.Vertex Pharmaceuticals Incorporated. NCT04537793: Evaluation of ELX/TEZ/IVA in Cystic Fibrosis (CF) Subjects 2 Through 5 Years. ClinicalTrials.gov. Bethesda (MD): U.S. National Library of Medicine; 2020: https://clinicaltrials.gov/ct2/show/NCT04537793. Accessed 2021 Dec 1.
126.Health Canada. Notice of Compliance (NOC) for Orkambi. 2020; https://health-products.canada.ca/noc-ac/index-eng.jsp. Accessed 2021 Dec 1.
127.Davies JC, Moskowitz SM, Brown C, et al. VX-659-tezacaftor-ivacaftor in patients with cystic fibrosis and one or two Phe508del alleles. N Engl J Med. 2018;379(17):1599-1611. PubMed
128.Keating D, Marigowda G, Burr L, et al. VX-445-tezacaftor-ivacaftor in patients with cystic fibrosis and one or two Phe508del alleles. N Engl J Med. 2018;379(17):1612-1620. PubMed
129.Bhatia R, Kaye M, Roberti-Miller A. Longitudinal assessment of exercise capacity and quality of life outcome measures in cystic fibrosis: a year-long prospective pilot study. J Eval Clin Pract. 2020;26(1):236-241. PubMed
130.Issues in the design of clinical trials of aerosolized antimicrobials for the treatment of cystic fibrosis. Day 2: efficacy end points for clinical trials of aerolised antimicrobials. Silver Spring (MD): U.S. Food and Drug Administration; 2010: https://www.fda.gov/downloads/Drugs/NewsEvents/UCM231055.pdf. Accessed 2021 Mar 24.
131.Robinson PD, Latzin P, Verbanck S, et al. Consensus statement for inert gas washout measurement using multiple- and single- breath tests. Eur Respir J. 2013;41(3):507-522. PubMed
132.Hatziagorou E, Avramidou V, Kirvassilis F, Tsanakas J. Use of lung clearance index to assess the response to intravenous treatment in cystic fibrosis. Hippokratia. 2015;19(1):47-52. PubMed
133.Welsh L, Nesci C, Tran H, Tomai M, Ranganathan S. Lung clearance index during hospital admission in school-age children with cystic fibrosis. J Cyst Fibros. 2014;13(6):687-691. PubMed
134.Vermeulen F, Proesmans M, Boon M, Havermans T, De Boeck K. Lung clearance index predicts pulmonary exacerbations in young patients with cystic fibrosis. Thorax. 2014;69(1):39-45. PubMed
135.Stanojevic S, Davis SD, Retsch-Bogart G, et al. Progression of Lung Disease in Preschool Patients with Cystic Fibrosis. Am J Respir Crit Care Med. 2017;195(9):1216-1225. PubMed
136.Oude Engberink E, Ratjen F, Davis SD, Retsch-Bogart G, Amin R, Stanojevic S. Inter-test reproducibility of the lung clearance index measured by multiple breath washout. Eur Respir J. 2017;50(4). PubMed
137.Poncin W, Singer F, Aubriot AS, Lebecque P. Agreement between multiple-breath nitrogen washout systems in children and adults. J Cyst Fibros. 2017;16(2):258-266. PubMed
138.Grosse-Onnebrink J, Mellies U, Olivier M, Werner C, Stehling F. Chest physiotherapy can affect the lung clearance index in cystic fibrosis patients. Pediatr Pulmonol. 2017;52(5):625-631. PubMed
139.Quittner AL, Buu A, Messer MA, Modi AC, Watrous M. Development and validation of The Cystic Fibrosis Questionnaire in the United States: a health-related quality-of-life measure for cystic fibrosis. Chest. 2005;128(4):2347-2354. PubMed
140.Modi AC, Lim CS, Driscoll KA, Piazza-Waggoner C, Quittner AL, Wooldridge J. Changes in pediatric health-related quality of life in cystic fibrosis after IV antibiotic treatment for pulmonary exacerbations. J Clin Psychol Med Settings. 2010;17(1):49-55. PubMed
Appendix 1: Summary of Cystic Fibrosis Canada Guidelines
Note that this appendix has not been copy-edited.
Indications for Starting CFTR-Modulator Therapy
All Canadians with a confirmed diagnosis of cystic fibrosis should have access to Health Canada approved CFTR modulators based on their variants in CFTR.
The diagnosis of CF requires:
Clinical symptoms/features or a positive newborn screen and either
Two disease-causing CFTR variants; Or
Sweat chloride concentration >60 mmol/L (On 2 occasions if only one CFTR variant known).
To be eligible for CFTR-modulator therapy, the following will apply:
1. Mutation: F508del/Any CFTR variant or gating variant/Any CFTR variant or R117H/Any CFTR variant
These genotype recommendations are based on phase III clinical trials showing substantial clinical improvement with CFTR modulators and Health Canada approval.
2. Age: as approved by Health Canada
CFTR modulators should be initiated at the YOUNGEST age possible with the goal of attenuating disease progression and improving clinical status. Data suggest that early introduction can reverse disease progression, such as restoring pancreatic function. There is NO data to support withholding CFTR modulators until significant clinical symptoms have developed or a drop in lung function occurs.
3. Lung function: No minimum or maximum FEV1
In Canada, due to improvements in care, early-stage lung disease is increasingly being seen in adolescents and adults with CF as defined by conventional spirometry measurement. This will become common with the availability of highly effective modulator therapy. However, FEV1 is not a useful marker in mild lung disease, in part, due to its relatively insensitivity to detection of early small airways destruction. This is illustrated, when patients with CF with no abnormality in lung function underwent chest CT imaging. Despite a normal FEV1 there was evidence of significant structural lung disease. Additionally, several trials have shown that in patients with normal lung function (ppFEV1 > 90%) the addition of a CFTR modulator caused further significant gains in ppFEV1, illustrating improvement to be made in mild CF lung disease. The most recent data showed in children aged 6-11 years with an average ppFEV1: 89% of whom 45% had ppFEV1 > 90%, the addition of ELX-TEZ-IVA produced an increase in ppFEV1 of 10%. Consequently, no upper limit of lung function should be required for eligibility as further significant gains in respiratory health can be made in patients with CF with mild lung disease.
Patients with lung function that is low (ppFEV1 < 40%) or are awaiting lung transplantation also improve on treatment to the point where many no longer need transplantation. Consequently, no lower limit of lung function should be required for eligibility.
4. Pancreatic status: Pancreatic sufficient and insufficient
Pancreatic status does not affect eligibility. The majority of patients with CF are pancreatic-insufficient but some patients are not. Early introduction of CFTR-modulator therapy has the potential to restore pancreatic function or delay onset of pancreatic insufficiency. In patients with pancreatic sufficiency, CFTR modulators will likely preserve pancreatic function.
Health Care Advisory Council Guidelines for Prescribing a CFTR Modulator
Figure 24 summarizes the various different Health Canada approved CFTR modulators. The recommended CFTR variant, age of initiation and duration for each modulator is provided.
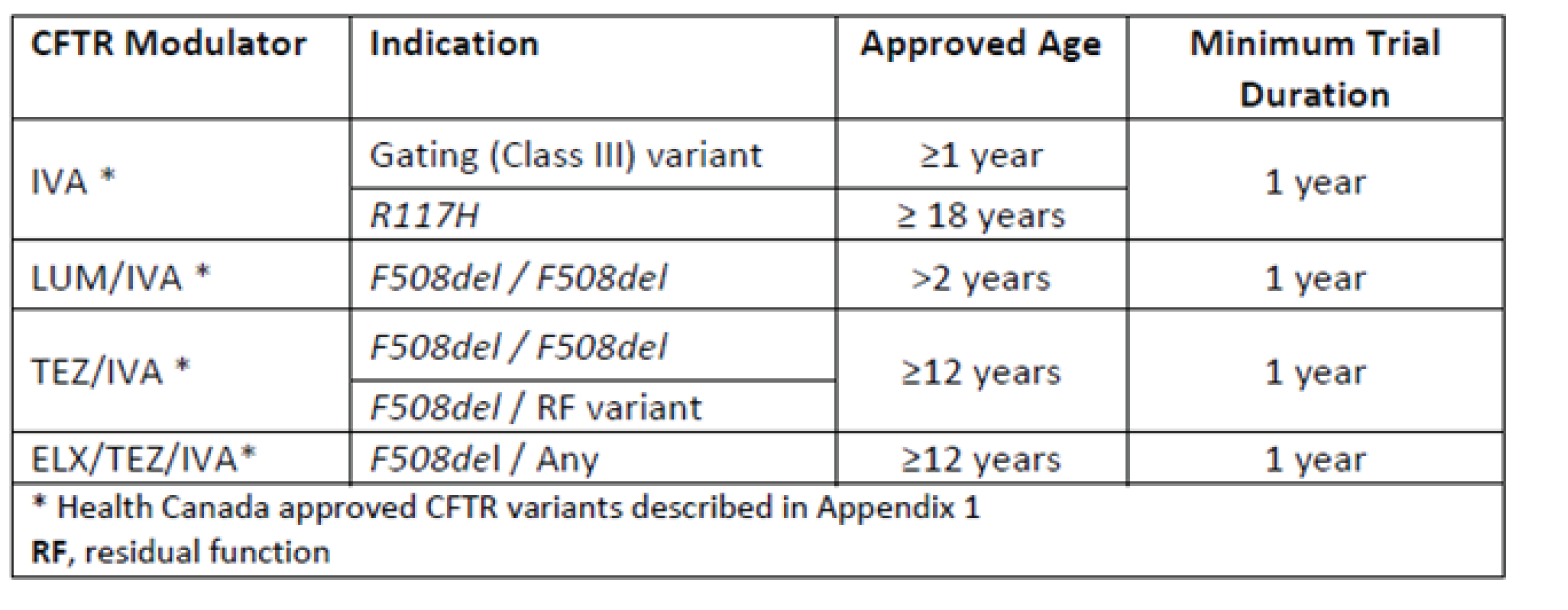
Pre-Modulator Assessment
If a patient has not had a confirmatory sweat test and/or CF genotyping this should be undertaken. Baseline clinical assessments required are illustrated in Figure 25 and Figure 26. These should be obtained when the patient is clinically stable.
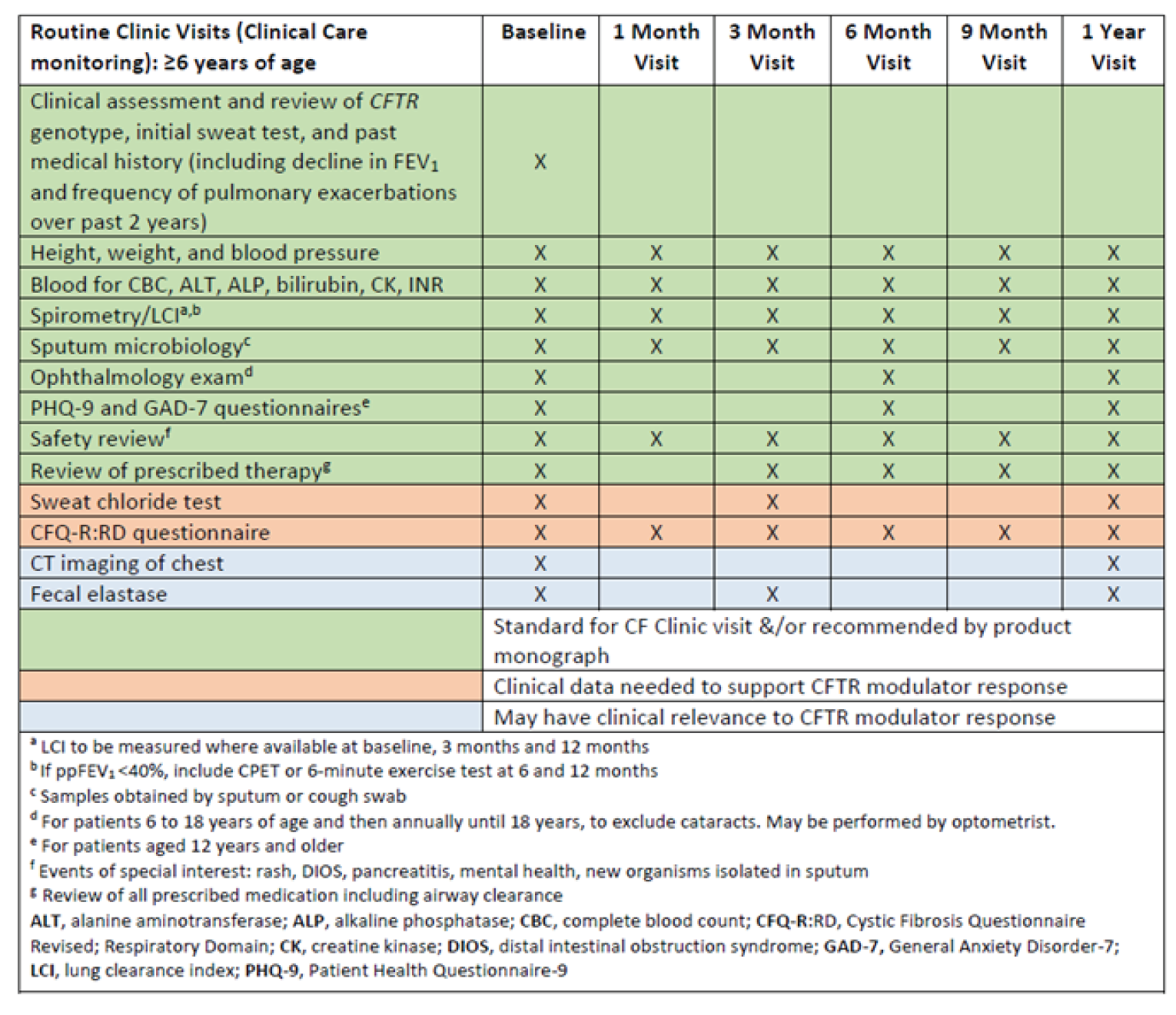
Figure 26: Schedule for Baseline Evaluation and Monitoring of Patients Under 6 Years Who Commence on CFTR Modulators
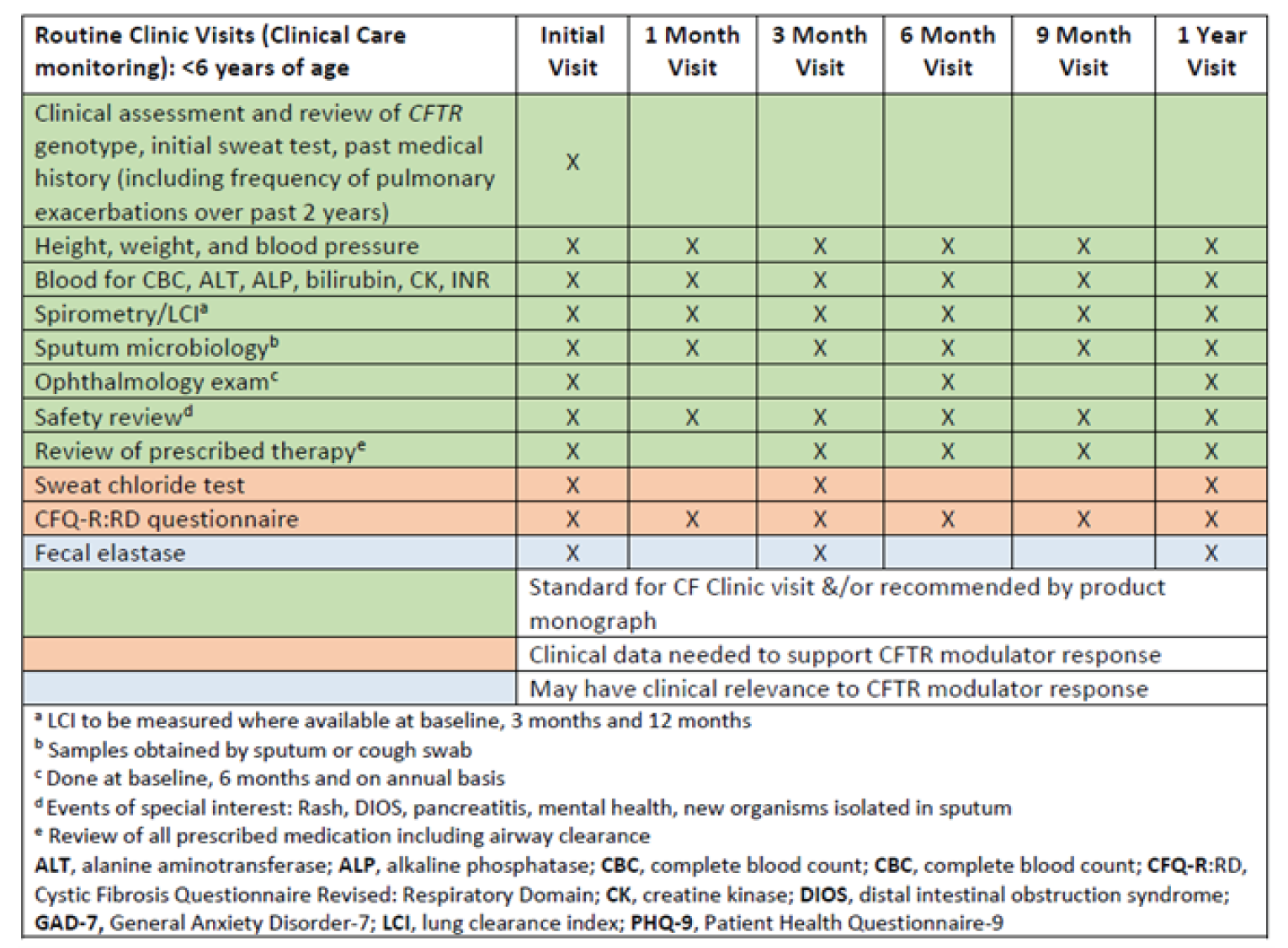
Response to Therapy
Clinical trials for CFTR modulators have reported improvements in lung function and weight and reduced pulmonary exacerbations requiring antibiotics. As CFTR modulators are systemic medications, they impact CFTR function in the sweat glands as measured by the concentration of chloride in sweat. Although this does not have direct clinical significance at an individual level other than reducing risk of dehydration or heat stroke, it is a biomarker of the effect of CFTR modulators and trials have shown modulator use is associated with a reduction in sweat chloride.
Longer-term follow-up studies have evaluated the impact of CFTR modulators on FEV1 rate of decline. These studies have shown an improvement in lung function trajectory with a slowing in the rate of FEV1 decline compared to patients not on CFTR modulators. However, patients STILL have a decline in FEV1 over time DESPITE the impact of CFTR modulators. Patients with CF have bronchiectasis with chronic infection and irreversible structural lung damage which will impact FEV1 recovery and trajectory. As life expectancy improves for patients with CF it is expected that FEV1 will still decline year to year due to the natural aging of the patient even in the presence of CFTR modulators.
Modelling and real-life experience with CFTR-modulator introduction have shown significant reduction in disease severity and improvement in clinical parameters in patients with significant disease burden. In addition, patients report an impact on respiratory symptoms, sleep quality, general well-being and physical self-esteem, and a reduced treatment burden. Patients reported renewed and unexpected physical strength, leading to greater self-confidence, autonomy and long-term planning, after treatment initiation.
Consideration should be given to CF-related comorbidities. Although not reported in clinical studies, patients may experience improvement in CF issues such as sinus disease, pancreatitis and CF-related diabetes with the introduction of CFTR modulators.
Data has suggested that there may be responders and nonresponders to CFTR-modulator therapy. In order to identify responders, the recommendation is to evaluate CFTR-modulator therapy for a MINIMUM duration of 1 year. This duration is needed to accurately assess reductions in pulmonary exacerbations, provide adequate lung function data to determine improvement and stabilization of FEV1 over time and monitor improvement in nutrition.
Meaningful clinical responses to be monitored include:
Improvement in lung function as measured by FEV1 or lung clearance index (LCI) (where available) obtained at a time of clinical stability
Reduction in the number of pulmonary exacerbations
Stabilization of lung function over time (i.e., attenuation of the usual decline in lung function)
Reduction or stabilization of respiratory symptoms
Improvement in nutritional status
Improvement in quality-of-life scores
Reduction in sweat chloride
Concurrent Treatment
At the present time, all patients commenced on a CFTR modulator should continue with current treatments as directed by their CF clinic (e.g., pancreatic enzymes, mucolytics, inhaled antibiotics, bronchodilators, anti-inflammatory agents). They should continue to be monitored quarterly as per CF standards of care. Ongoing clinical studies will determine if any CF treatments can be discontinued once patients are on CFTR-modulator therapy. The schedule of clinical assessment and monitoring is outlined in Figure 25 and Figure 26.
Treatment Response
It is expected that responders will have at:
3 months:
Absolute improvement in ppFEV1 of >5%, measured at time of clinical stability; OR
A decrease in sweat chloride by 20% or 20 mmol/L from baseline; OR
Improvement in respiratory symptoms (as measured by CFQ-R: Respiratory Domain) > 4 points.
12 months:
No adverse events or medication safety issues, and one or more of:
Reduction in pulmonary exacerbations (IV or oral antibiotic treatment) by 20%; OR
Stabilization of lung function rate of decline above baseline; OR
Improvement in nutritional status with normalization of growth and nutrition; OR
Radiological improvement or stability in Chest CT scan.
Figure 27 is a summary of changes in expected outcomes for responders to different CFTR modulators
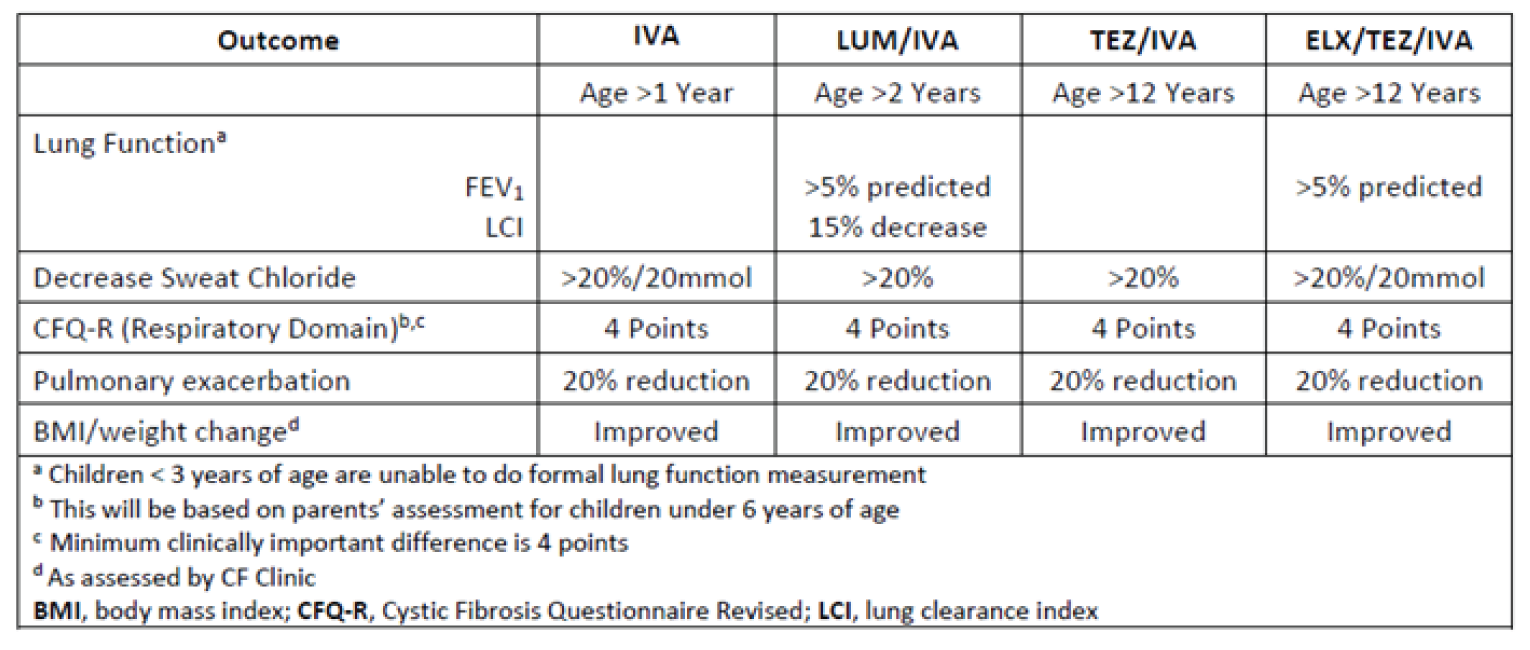
Monitoring
Comprehensive monitoring of patients who are commenced on CFTR modulators is detailed in tables 2a and 2b. Clinics should aim to follow this schedule in order to demonstrate response to therapy.
Side Effects
After initiation of CFTR modulators, it is important to focus on safety outcomes and monitor for potential adverse effects (Table 4). A systematic review of safety outcomes reported in real-world studies of the 4 market-available CFTR modulators has recently been published and is an excellent source of reference, but there are limited reports of longer-term real-world experience, especially with ELX-TEZ-IVA. Therefore, vigilant post-market monitoring for both expected and unexpected adverse effects is warranted.
Safety issues of note are:
i) Liver enzymes and/or bilirubin
Elevated transaminases have been observed in patients on CFTR modulators. Isolated elevation in bilirubin can also be seen in some cases. This can occur at any time during treatment even if the modulator has been previously well tolerated. Rarely does this result in the need to interrupt therapy, reduce the dose, or discontinue the modulator. Elevated transaminases and bilirubin will need to be reviewed to further determine the need to interrupt therapy, reduce the dose, or discontinue the modulator (Table 5). It is recommended that liver enzymes should be monitored every 3 months in the first year and then annually. For individuals with moderate or severe CF-related liver disease, recommendations for dosage adjustments are available. Worsening of liver function has been observed in patients with pre-existing cirrhosis and portal hypertension who have started CFTR modulators.
ii) Rash or hypersensitivity reactions
Rash is relatively common following initiation of CFTR modulators and has been reported in real-world studies for each of IVA, LUM-IVA, and TEZ-IVA. Rare cases of delayed hypersensitivity reactions have also been reported. Few individuals required interruption or discontinuation of therapy for rash or hypersensitivity reactions. Similar occurrence was seen in clinical trials, with cases of rash being reported for all 4 CFTR modulators, and serious rash or discontinuation due to rash being reported for ELX-TEZ-IVA and LUM-IVA. The incidence of rash events appears to be higher in female patients with CF, particularly those on hormonal contraceptives, and more frequent on ELX-TEZ-IVA, but the mechanism behind this is unclear.
iii) Drop in FEV1 and respiratory symptoms
Of the available CFTR modulators, LUM-IVA has had the highest reported respiratory-related side effects. Chest tightness, dyspnea, increased sputum, and declines in ppFEV1 were among the most common respiratory symptoms and tended to occur within the first few days after initiation. Bronchodilators were beneficial in mitigating symptoms of chest tightness, wheeze, and increased work of breathing in some individuals. Improvement in or resolution of symptoms occurred within 1–4 weeks following initiation, but symptoms and/or ppFEV1 below baseline could persist beyond this and some patients may require a dose reduction or discontinuation altogether to achieve resolution.
iv) GI-related adverse effects
Symptoms of abdominal pain, nausea, and vomiting have been reported in the real-world studies, but rarely prompted discontinuation of therapy. Concerns have been raised about the potential for distal intestinal obstruction syndrome (DIOS) following initiation of highly effective CFTR modulators. Therefore, patients with chronic constipation and/or other risk factors for DIOS should be closely monitored following initiation.
v) Blood pressure elevation
Elevations in blood pressure were reported in the phase III clinical trials for LUM-IVA and ELX-TEZ-IVA. For ELX-TEZ-IVA, 4% of treated subjects had systolic blood pressure >140 mm Hg and 10 mm Hg increase from baseline on at least 2 occasions. Similarly, 1% had diastolic blood pressure >90 mm Hg and 5 mm Hg increase from baseline on at least 2 occasions. The mechanism by which CFTR modulators may cause blood pressure elevations remains unclear.
vi) Creatinine kinase
Creatinine kinase elevations have been reported in clinical trials for all 4 CFTR modulators. Clinical context of elevations is important, as CK levels fluctuate significantly with exercise and physical activity, especially if intensive, and may take a few days to normalize thereafter. Although the clinical relevance of CK elevations is unclear, some cases may be serious enough to warrant interruption or discontinuation of therapy.
vii) Mental health
Cases of negative impacts on mental health (e.g., depression, anxiety) have been reported for all 4 market-available CFTR modulators, even in individuals without a prior history of mental health concerns, raising a signal for a potential association with CFTR modulators. Although a causal relationship has not been established and a mechanism is not clear, it is an important potential outcome to be mindful of. In addition, there are significant drug-drug interactions with LUM-IVA and antidepressant medications.
viii) Cataracts
Cases of noncongenital lens opacities have been reported in pediatric patients treated with IVA-containing regimens. Although other risk factors were present in some cases (such as corticosteroid use, exposure to radiation), a possible risk attributable to treatment with IVA cannot be excluded. Baseline and follow-up ophthalmological examinations are recommended in pediatric patients initiating treatment with CFTR modulators to be done at baseline, 6 months and on annual basis until age 18.
Drug-Drug Interactions
It is important to assess for drug-drug interactions when starting or stopping medications in an individual on a CFTR modulator or when transitioning from different CFTR modulators. IVA, TEZ, and ELX are substrates of cytochrome P450 (CYP) enzyme CYP3A. Therefore, strong and moderate inhibitors (e.g., azole antifungals) of CYP3A can increase exposure to IVA, TEZ, and ELX, while inducers (e.g., rifampin) can decrease serum levels. Recommendations are available for how to dose-adjust modulators when taken concomitantly with moderate or strong CYP3A inhibitors, but concomitant use with inducers should be avoided. It is important to note that foods and herbal products can also affect CYP3A (food or drinks containing grapefruit can inhibit CYP3A in the gastrointestinal tract, while the herbal product St. John’s wort induces CYP3A).
CFTR modulators have also been associated with inhibition or induction of enzymes. IVA and one of its metabolites weakly inhibit CYP3A and P-glycoprotein (P-gp), and potentially CYP2C9. Because of the potential impact on CYP3A and CYP2C9, the international normalized ratio should be closely monitored in individuals on warfarin who are starting or stopping a CFTR modulator. Alternatively, LUM is an inducer of CYP3A and UDP-glucuronosyltransferase (UGT) enzymes, and may increase metabolism of concomitant medications that are substrates of these enzymes (e.g., hormonal contraceptives, azole antifungals, select immunosuppressants and psychotropic medications).
Special considerations for patients receiving IVA, LUM-IVA, TEZ-IVA CFTR Modulators
Health Canada approved ELX-TEZ-IVA in June 2021 for CFTR variants F508del/Any in patients 12 years and older. In the near future this age limit will likely be reduced to >6 years of age. A small number of children will remain on either LUM-IVA or IVA. Data has shown that ELX-TEZ-IVA has superiority over TEZ-IVA in patients with 2 copies of F508del. In a study comparing patients F508del/MF or gating variant who were randomized to either continue taking TEZ-IVA or IVA or switched to ELX-TEZ-IVA a modest incremental improvement in FEV1 was observed, with significant gains in CFQ-R-Resp domain and further reduction in sweat chloride levels. All patients on IVA, LUM-IVA or TEZ-IVA, should have the opportunity to transition to the triple therapy combination, ELX-TEZ-IVA.
Pregnancy and CFTR Modulators
CFTR modulators may increase fertility in women with CF due to improvement in clinical status and to their impact on the mucus in the cervix and uterus and so it is important for women on CFTR modulators to use birth control to prevent unplanned pregnancies. The clinical trials of CFTR modulators excluded women who were not using effective contraception, so the effect of these drugs on a developing human fetus is unknown. Animal studies of the individual drugs IVA, LUM, TEZ and ELX CFTR indicate no impact on organogenesis at normal human doses. Real-world experience is limited but case reports and an international survey have demonstrated that CFTR modulators appear to be well tolerated during pregnancy. As discontinuation of CFTR modulators has been associated with significant decline in clinical status, the risks/benefits of CFTR therapy during pregnancy must be discussed, ideally before pregnancy. CFTR modulators are expressed in breast milk. As CFTR modulators have been associated with cataracts in children, it would be advisable that infants born to mothers taking CFTR modulators have ophthalmologic examination.
Patients With CF Who Have Received a Lung Transplantation
Lung transplant is a treatment option for people with CF with end-stage lung disease. While CFTR modulators would not be expected to directly improve lung graft function, they have potential to alleviate extrapulmonary manifestations of CF such as chronic rhinosinusitis and gastrointestinal disease. Of note, paranasal sinuses may act as a reservoir for pathogens following transplantation, therefore treatment of chronic rhinosinusitis with CFTR modulators may reduce respiratory infectious complications after lung transplantation.
With the introduction of ELX-TEZ-IVA, evidence is emerging of its use after lung transplant. Drug-drug interaction between CFTR modulators and immunosuppressants, such as calcineurin inhibitors, should be expected. In addition, liver injury secondary to use of CFTR modulators may complicate management of a lung transplant recipient prescribed antimicrobials and immune suppressing medications associated with hepatoxicity. The general recommendations on response to CFTR-modulator therapy following initiation would not be applicable to the lung transplant population. It is recommended that a CF specialist be involved in the initiation of CFTR modulators and subsequent monitoring of a patient with CF who has undergone lung transplant and commenced on a CFTR modulator.
Discontinuation
Discontinuation (or dose reduction) of CFTR-modulator therapy should be considered in patients who have clinically significant adverse effects that persist or recur despite a decrease in dose (if appropriate) and/or stopping and rechallenge. Examples of these reactions may include:
Elevation of transaminases (Table 5) beyond the higher range of fluctuations observed in patients with CF (>8X ULN) or 3XULN of transaminases and bilirubin (> 2 x ULN)
Allergic reactions to treatment and failed desensitization challenges
However, the risk-benefit of discontinuing treatment should be considered on a case-by-case basis depending on the severity of the adverse event and risk of stopping treatment. Therapy should be discontinued in patients who, as assessed by the CF team, do not meet criteria for response to the CFTR modulator or are non-adherent to the CFTR modulator. This decision to discontinue therapy should be done after clinical stability, any confounding comorbidities have been assessed and nonadherence issues have been addressed.
How to Start CFTR Modulators
Given the large number of patients who will qualify for CFTR modulators, initiation will at first impose challenges on individual CF clinics. How this will be undertaken will be determined by individual CF centres based on the number of eligible patients, clinic resources and provincial availability. For patients who have had a significant adverse reaction to a CFTR modulator and a rechallenge is deemed appropriate, or if initiation at a reduced dose and titrating to full-dose is preferred, potential protocols are summarized in the systematic review performed by Dagenais et al.
Summary
The approval of CFTR modulators by Health Canada is a milestone in CF care and is the first time that a CF treatment has targeted the basic defect and not the consequences of the disease. Real-world evidence suggests that CFTR modulators will slow the progression of disease and reduce mortality. All patients who are eligible should be started on therapy as soon as possible to prevent lung disease progression and comorbidities.
Patients should be started on an age-appropriate, CFTR variant-specific modulator with a recommended duration of at least 1 year. Response to therapy and safety should be monitored. If response to therapy is seen, then patients will continue indefinitely on the CFTR-modulator therapy and standard of care treatment. Follow-up will be determined by their CF clinic. Discontinuation of modulator therapy should be performed in patients with significant side effects or those who are deemed nonresponders after 1 year of therapy. Efficacy data should be collected as part of the Canadian Cystic Fibrosis Registry or as part of a prospective study.
Appendix 2: Literature Search Strategy
Note that this appendix has not been copy-edited.
Clinical Literature Search
Overview
Interface: Ovid
Databases:
MEDLINE All (1946–)
Embase (1974–)
Note: Subject headings and search fields have been customized for each database. Duplicates between databases were removed in Ovid.
Date of Search: February 22, 2021
Alerts: Bi-weekly search updates until project completion
Study Types: No search filters were applied
Limits:
No date or language limits were used
Conference abstracts: excluded
Syntax | Description |
|---|---|
/ | At the end of a phrase, searches the phrase as a subject heading |
MeSH | Medical Subject Heading |
exp | Explode a subject heading |
* | Before a word, indicates that the marked subject heading is a primary topic; or, after a word, a truncation symbol (wildcard) to retrieve plurals or varying endings |
adj# | Requires terms to be adjacent to each other within # number of words (in any order) |
.ti | Title |
.ot | Original title |
.ab | Abstract |
.hw | Heading word; usually includes subject headings and controlled vocabulary |
.kf | Author keyword heading word (MEDLINE) |
.kw | Author keyword (Embase) |
.dq | Candidate term word (Embase) |
.pt | Publication type |
.mp | Mapped term |
.rn | Registry number |
.nm | Name of substance word (MEDLINE) |
.yr | Publication year |
medall | Ovid database code: MEDLINE All, 1946 to present, updated daily |
oemezd | Ovid database code; Embase, 1974 to present, updated daily |
Multi-Database Strategy
Search Strategy
(trikafta* or kaftrio* or (ELX adj2 TEZ adj2 IVA) or (elexacaftor adj2 tezacaftor adj2 ivacaftor)).ti,ab,kf,ot,hw,rn,nm.
(ivacaftor* or kalydeco* or symdeko* or symkevi* or VX770 or VX-770 or Y740ILL1Z).ti,ab,kf,ot,hw,rn,nm.
(elexacaftor* or VX-445* or VX445 or WHO 11180 or WHO11180 or RN67GMB0V).ti,ab,kf,ot,hw,rn,nm.
(tezacaftor* or symdeko* or symkevi* or VX661 or VX-661 or RW88Y506K).ti,ab,kf,ot,hw,rn,nm.
2 and 3 and 4
1 or 5
(((triple or tri) adj3 (combination* or combo or therap*)) or ETI).ti,ab,kf.
Cystic Fibrosis/ or ((cystic adj2 fibrosis) or mucoviscidos* or fibrocystic or F508del).ti,ab,kf.
7 and 8
6 or 9
10 use medall
*elexacaftor plus ivacaftor plus tezacaftor/
(trikafta* or kaftrio* or (ELX adj2 TEZ adj2 IVA) or (elexacaftor adj2 tezacaftor adj2 ivacaftor)).ti,ab,kw,dq.
12 or 13
*ivacaftor/ or *ivacaftor plus tezacaftor/
(ivacaftor* or kalydeco* or symdeko* or symkevi* or VX770 or VX-770).ti,ab,kw,dq.
15 or 16
*elexacaftor/
(elexacaftor* or VX-445* or VX445 or WHO 11180 or WHO11180 or RRN67GMB0V0).ti,ab,kw,dq.
18 or 19
*tezacaftor/ or *ivacaftor plus tezacaftor/
(tezacaftor* or symdeko* or symkevi* or VX661 or VX-661 or 8RW88Y506K).ti,ab,kw,dq.
21 or 22
17 and 20 and 23
14 or 24
(((triple or tri) adj3 (combination* or combo or therap*)) or ETI).ti,ab,kf,dq.
Cystic Fibrosis/ or ((cystic adj2 fibrosis) or mucoviscidos* or fibrocystic or F508del).ti,ab,kw,dq.
26 and 27
25 or 28
(conference review or conference abstract).pt.
29 not 30
31 use oemezd
11 or 32
remove duplicates from 33
Clinical Trial Registries
ClinicalTrials.gov
Produced by the US National Library of Medicine. Targeted search used to capture registered clinical trials.
[Search -- Studies with results trikafta or kaftrio or vx-445 or elexacaftor]
WHO ICTRP
International Clinical Trials Registry Platform, produced by the World Health Organization. Targeted search used to capture registered clinical trials.
[Search terms -- trikafta or kaftrio or vx-445 or elexacaftor]
Health Canada’s Clinical Trials Database
Produced by Health Canada. Targeted search used to capture registered clinical trials.
[Search terms -- trikafta or kaftrio or vx-445 or elexacaftor]
EU Clinical Trials
Register European Union Clinical Trials Register, produced by the European Union. Targeted search used to capture registered clinical trials.
[Search terms -- trikafta or kaftrio or vx-445 or elexacaftor]
Grey Literature
Search dates: February 8–16, 2021
Keywords: trikafta, kaftrio, vx-445, elexacaftor, ELX-TEZ-IVA, cystic fibrosis
Limits: None
Updated: Search updated prior to the completion of stakeholder feedback period
Relevant websites from the following sections of the CADTH grey literature checklist Grey Matters: A Practical Tool For Searching Health-Related Grey Literature (https://www.cadth.ca/grey-matters) were searched:
Health Technology Assessment Agencies
Health Economics
Clinical Practice Guidelines
Drug and Device Regulatory Approvals
Advisories and Warnings
Drug Class Reviews
Clinical Trials Registries
Databases (free)
Health Statistics
Internet Search
Appendix 3: Excluded Studies
Note that this appendix has not been copy-edited.
Reference | Reason for exclusion |
|---|---|
Davies JC, Moskowitz SM, Brown C, et al. VX-659-tezacaftor-ivacaftor in patients with cystic fibrosis and one or two Phe508del alleles. N Engl J Med. 2018;379(17):1599-1611.127 | Intervention (not ELX-TEZ-IVA) |
Keating D, Marigowda G, Burr L, et al. VX-445-tezacaftor-ivacaftor in patients with cystic fibrosis and one or two Phe508del alleles. N Engl J Med. 2018;379(17):1612-1620.128 | Study design (phase II) |
ELX-TEZ-IVA = elexacaftor-tezacaftor-ivacaftor and ivacaftor.
Appendix 4: Detailed Outcome Data
Note that this appendix has not been copy-edited.
||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||
|---|---|---|---|---|---|---|
||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | |||
||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| |
||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | |
||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| |
||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | |
||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| |
||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | |
||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| |
||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | |
CI = confidence interval; ELX-TEZ-IVA = elexacaftor-tezacaftor-ivacaftor and ivacaftor; LS = least squares; LSMD = least squares mean difference; n = number of patients in subgroup analysis; ppFEV1 = percent predicted forced expiratory volume in 1 second; SE = standard error.
Source: Sponsor provided additional information.78
||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | |||
|---|---|---|---|---|---|---|
||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | |||
||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| |
||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | |
||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| |
||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | |
CI = confidence interval; ELX-TEZ-IVA = elexacaftor-tezacaftor-ivacaftor and ivacaftor; LS = least squares; LSMD = least squares mean difference; n = number of patients in subgroup analysis; ppFEV1 = percent predicted forced expiratory volume in 1 second; SE = standard error.
MMRM analyses for the subgroups were similar to those performed for the primary analyses.
Source: Clinical Study Report.5
Table 109: Subgroup Analyses for Absolute Change from Baseline in ppFEV1 for Patients with Baseline ppFEV1 < 40% (Study 102)
Subgroups | Study 102 (M/F) | ||
|---|---|---|---|
Placebo (N = 16) | ELX-TEZ-IVA (N = 18) | ||
At 4 weeks | Baseline mean (SD) | 37.5 (2.1) | 37.0 (1.7) |
LS mean (SE) | 0.8 (2.8) | 16.0 (2.6) | |
Patients in analysis | 16 | 17 | |
LSMD (95% CI) | 15.2 (7.3 to 23.1) | ||
P value | < 0.0001 | ||
||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| |
||||||||||||| | ||||||||||||| | ||||||||||||| | |
||||||||||||| | ||||||||||||| | ||||||||||||| | |
||||||||||||| | ||||||||||||| | ||
||||||||||||| | ||||||||||||| | ||
CI = confidence interval; ELX-TEZ-IVA = elexacaftor-tezacaftor-ivacaftor and ivacaftor; F/MF = one F508del mutation and one minimal function mutation in the CFTR gene; LSMD = least squares mean difference; LS = least squares; ppFEV1 = percent predicted forced expiratory volume in one second; SD = standard deviation; SE = standard error.
MMRM analyses for the subgroups were similar to those performed for the primary analyses.
Source: Clinical Study Report.5
||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | |||
|---|---|---|---|---|---|---|
||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | |||
||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| |
||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | |
||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| |
||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | |
CI = confidence interval; ELX-TEZ-IVA = elexacaftor-tezacaftor-ivacaftor and ivacaftor; LS = least squares; LSMD = least squares mean difference; n = number of patients in subgroup analysis; ppFEV1 = percent predicted forced expiratory volume in 1 second; SE = standard error; TEZ-IVA = tezacaftor-ivacaftor and ivacaftor.
MMRM analyses for the subgroups were similar to those performed for the primary analyses.
Source: Clinical Study Report.6
Appendix 5: Description and Appraisal of Outcome Measures
Note that this appendix has not been copy-edited.
Aim
To describe the following outcome measures and review their measurement properties (validity, reliability, responsiveness to change, and MID):
FEV1 (primary outcome in Study 102, 103 and 104; key secondary outcome in Study 109)
LCI (primary outcome in Study 116 and secondary outcome in Study 106B)
CFQ-R respiratory symptom domain (primary outcome in Study 109, key secondary outcome in Study 102 and 103, other outcome in Study 104)
Findings
Table 111: Summary of Outcome Measures and Their Measurement Properties
Outcome Measure | Type | Conclusions About Measurement Properties | MID |
|---|---|---|---|
FEV1 | Pulmonary function test (maximal amount of air forcefully exhaled in one second) | FEV1 has been shown to relate to morbidity, disease progression, and mortality in CF, and thus is a meaningful surrogate marker for survival. FEV1 is highly dependent on patient cooperation and effort to perform test and can only be used on children old enough to comprehend and follow the instructions given. It has a ceiling effect for patients with mild lung impairment. | Not defined |
LCI | Pulmonary function test (the number of lung-volume turnovers required to clear the lung of an inert gas) | LCI has shown discriminant validity for known groups however it is not known if LCI is predictive of longer-term changes in health status. Variable correlation was observed between FEV1 and LCI in children. Measurements using different LCI systems are not interchangeable and further testing standardization is required. Limited longitudinal data are available to understand how LCI changes by age, sex or ethnic group. | Not defined |
CFQ-R Respiratory Symptom Domain | Respiratory symptom scale of a disease-specific HRQoL instrument | Validity: Showed strong discriminant validity between sick versus well patients with CF, and acceptable convergent validity. Assessment of construct validity showed moderate correlation with FEV1 and weak correlation with the number of exacerbations. Reliability: Internal consistency reliability and test-retest reliability was acceptable. Responsiveness: Limited assessment of responsiveness reported in the literature. | Anchor-based: Stable CF: 4.0 points76; Exacerbation of CF: 8.5 pointst76 Distribution-based: |
CF = cystic fibrosis; CFQ-R = Cystic Fibrosis Questionnaire–Revised; FEV1 = forced expiratory volume in one second; HRQoL = health-related quality of life; MID = minimal important difference.
Forced Expiratory Volume in 1 Second
FEV1 is the maximal amount of air forcefully exhaled in one second, expressed in litres.98 The measured volume is converted to a percentage of predicted normal value, which is adjusted based on age, sex, and body composition.98 FEV1 is used to establish the severity of lung disease (normal or mild pulmonary dysfunction, > 70% predicted; moderate dysfunction, 40% to 69% predicted; and severe dysfunction, < 40% predicted), tracking changes in lung function over time, and in evaluating the effectiveness of therapeutic interventions in cystic fibrosis (CF).85,98
FEV1 is a commonly used end point for clinical trials of obstructive lung diseases including CF130 and is the preferred end point in the EMA guidance document on the development of therapeutic drugs for CF, based on the fact that the main pulmonary defect in CF is obstructive.85 FEV1 has been shown to relate to morbidity, disease progression, and mortality in CF, making it a meaningful surrogate marker for survival.85,130,71
However, there are limitations with the use of FEV1 for patients with CF:
The manoeuvre required to assess FEV1 is highly dependent on patient cooperation and effort:
The test (spirometry) should be repeated at least 3 times to ensure reproducibility98
Spirometry can only be used on children old enough to comprehend and follow the instructions given (6 years old or more), and only on patients who are able to understand and follow instructions85,130
FEV1 can generally only be underestimated. The only exception in which FEV1 can be overestimated is in individuals with some diseases where a softer exhalation can reduce the spasm or collapse of lung tissue, thereby artificially elevating the measure
FEV1 is unable to detect early lung damage or early bronchiectasis in patients with CF.71
There are limited data on the magnitude of change in FEV1 that is clinically meaningful. The short-term variability in FEV1 is unclear for patients with CF.71
There are no established MID for FEV1 in patients with CF.71 Bhatia, Kaye and Roberti-Miller129 estimated the MID for the ppFEV1 based on data from 12 patients with moderate to severe CF who were followed for 1 year. They reported an MID of 7.1%, that was calculated using distribution-based methods (i.e., half the SD at baseline). However, the authors of this study stated this estimate was preliminary and required validation.129
FEV1 improvement has a ceiling effect for patients with mild lung impairment.130
FEV1 decline is only meaningful over time and is subject to seasonal and environmental effects.130
The EMA suggests a study duration of 6 months for the demonstration of efficacy on respiratory function (based on repeated measurements of FEV1) with a 12-month follow-up for safety.85
CF is a multi-organ disease and FEV1 only measures lung health.130
Lung Clearance Index
The lung clearance index (LCI) is a measure of overall lung ventilation inhomogeneity.70 This multiple-breath washout test estimates the number of lung-volume turnovers required to clear the lung of an inert gas. The test is sensitive to changes in the small airways, and may be able to detect pulmonary disease in patients with normal FEV1.71,72 Several commercial and research-specific multiple-breath washout devices have been developed. These devices include a patient interface (i.e., face mask), flow meter, gas analyzer or mass spectrometer (to analyze gas concentrations), and a gas delivery system.131
Software is required to analyze the results, and quality assurance testing is needed to ensure the performance of the test was satisfactory (i.e., within-session reproducibility).131 The test may use an extrinsic inert gas, such as sulphur hexafluoride or helium, or an intrinsic gas, such as nitrogen. During the wash-in phase for an extrinsic gas test, the patient inhales the test gas until the delivered gas concentrations and the exhaled concentration are equal. In the washout phase the patient inhales room air and continues normal tidal breathing until the exhalation concentration of the gas falls to 1/40th (LCI2.5) or 1/20th (LCI5) of the wash-in concentration. For the test using nitrogen, there is no wash-in phase as the concentration of nitrogen is normally at 80%. During the washout phase the patient inhales 100% oxygen until nitrogen levels fall to 1/40th or 1/20th of initial values. As ventilation worsens, the number of tidal breaths and expired volumes required to clear the gas increases, thus higher LCI values indicate greater ventilation inhomogeneity. The LCI is calculated as the mean of 2 or 3 tests that meet acceptable performance standards (e.g., functional residual capacity values within 10%). In 2012 the European Respiratory Society (ERS) and the American Thoracic Society (ATS) published a guidelines for washout equipment specifications, test performance and analysis, and outlined essential principles of multiple-breath washout testing.131
Kent et al. conducted a review of the evidence for the use of LCI in clinical trials in patients with CF.72 These studies were conducted predominantly in children, and most were cross-sectional studies that were completed prior to the ERS/ATS guidelines for LCI testing were published. LCI was able to discriminate between patients with CF and healthy individuals in 22 of 23 studies reviewed. Variable correlation was observed between FEV1 and LCI among 10 studies in children, and moderate to strong correlation was found between LCI and various structural abnormalities observed in high resolution computed tomography (Spearman correlation coefficient range 0.31 to 0.77; 5 studies).72 LCI detected treatment effects after 4 weeks of inhaled dornase alpha or hypertonic saline, and after a course of IV antibiotics in patients with an exacerbation or colonized with Pseudomonas aeruginosa.72,132 In contrast, another study found no statistically significant difference in LCI at admission and at discharge among 27 school-aged children hospitalized to receive IV antibiotics for a pulmonary exacerbation of CF.133
In a single-centre study by Vermeulen et al.,134 LCI z scores were negatively correlated with FEV1 z scores (Spearman correlation coefficient r = -0.642) and CRQ-R respiratory score (r = -0.431) in children aged 5 to 20 years with CF (N = 63, mean LCI 10.8 [SD 3.1] Exhalyzer D nitrogen device).134 Of the 53 patients with a normal FEV1, 42 (79%) had an abnormal LCI (defined as a z score >2). Time to first pulmonary exacerbation (defined as change in respiratory status that was treated with IV antibiotics) decreased with worsening LCI quartiles (log rank test P < 0.001), FEV1 z score quartiles (P = 0.002) and CFQ-R respiratory quartiles (P = 0.001) over the 1 year follow-up.134 Another study that examined the change in lung function over one year in healthy preschool children (N = 78) and those with CF (N = 78) found that ppFEV1 and LCI were able to discriminate between groups.135 LCI also showed an increase over time (i.e., worsening) in patients with CF compared to stable LCI in healthy age-matched children.135
Kent et al. reported inter-test repeatability in children with CF, and found variability of 0.96 units of LCI (coefficient of repeatability), and 2.6% to 9.2% (coefficient of variation) for tests performed 1.5 hours to 12 weeks apart (patient demographics not reported).72 Oude Engberink et al. evaluated the inter-test reproducibility of the LCI in healthy preschool children and children with stable CF who were aged 2.5 years to 6 years. Repeated measures of LCI were obtained using the Exhalzyder D device, 1 to 3 months apart over one year, and inter-visit reproducibility was calculated using several methods (Table 108). The authors stated that interpretation of the LCI in terms of an absolute change was prone to bias, as a key assumption for Bland-Altman limits of agreement or coefficient of repeatability, was not met. Use of the results of these tests, which suggested a 1-unit change in healthy children would be clinically meaningful, would lead to an over-estimation of clinically relevant changes in patients with higher LCI values.136The authors concluded that repeated measures of the LCI should be interpreted as a percentage change, and ±15% represents physiologically relevant change that is greater than biologic variability of the test.136
Table 112: Inter-Test Reproducibility of the LCI in Preschool Children
Analysis | Healthy | Stable CF |
|---|---|---|
N | 71 | 77 |
Median LCI (range) at baseline | 7.1 (6.1, 8.1) | 8.9 (6.4, 16.2) |
Measures of reproducibility for LCI | ||
Absolute mean difference | –0.03 | –0.05 |
Percentage change (95% limits) | –0.14 (–15, 15) | 1.27 (–25, 27) |
Percent coefficient of variation | 4.3% | 7.7% |
ICC | 0.4 | 0.7 |
Bland-Altman limits of agreementa | –1.1 to 1.1 | –2.9 to 2.8 |
Coefficient of repeatabilitya | 0.9 | 2.0 |
CF = cystic fibrosis; ICC = intraclass correlation coefficient; LCI = lung clearance index.
aTest assumes the within-patient standard deviation is proportional to the magnitude of the measurement, which was not met for the LCI in healthy children or those with cystic fibrosis.
Source: Oude Engberink et al.136
Poncin et al.137 found that the agreement between 2 commercial nitrogen multiple-breath washout devices was poor, with the Exhalyer D measuring higher LCI values than the EasyOne Pro device, in adults and children with CF (N = 104) and those without CF (N = 101). The difference was deemed to be clinically relevant as it exceed the anticipated magnitude of the between-test variability (10%).137 Thus there may be issues with comparing LCI results between clinical trials.
The feasibility of the LCI was estimated from the percentage of patients who could successfully complete 1 to 3 LCI tests within a session. Based on data from 19 patient groups (infants to adults), 24% to 100% of patients were able to successfully complete the LCI test.72 Grosse-Onnebrink et al. found that chest physiotherapy can have a short-term impact on LCI, potentially biasing results, and therefore the timing of physiotherapy in relation to LCI should be considered in clinical trials.138
Limitations:
Measurements using different inert gases, devices or analytical software are not interchangeable and thus normative data from one system cannot be used for other devices.70 Standardization of procedures is required in order to compare results between studies.131
The MCID has not been defined. Limited longitudinal data are available to understand how ventilation inhomogeneity indices change during normal lung development, by age, sex or ethnic group.70,131 These data are required to define whether an intervention exceeds the intrinsic variability of the test.71
It is unclear if improvement in LCI is predictive of longer-term changes in health status, such as the change in FEV1 or frequency of exacerbations.70
Several procedural specific issues require further evaluation. Some examples include defining the optimal washout cut-off value (i.e., 1/40th or 1/20th of initial gas concentration), the number of repeated tests required to ensure accurate results, and impact of sedation on breathing pattern and LCI in infants or young children.131
The test has less potential for use in trials in patients with advanced lung disease due to the long measurement times and greater variability.
Cystic Fibrosis Questionnaire–Revised
The CFQ-R is a disease-specific HRQoL instrument designed for patients with CF, comprised of age-appropriate versions for children aged six to 3 (CFQ-C), their parents (who serve as a proxy for their child; CFQ-P), and individuals ≥ 14 years of age (CFQ-14).73 For children 6 to 11, the CFQ-C is interviewer-administered, and for 12 and 13 year-olds, it is self-administered.74 The number of items and domains vary between versions with the child version including 35 items within 8 domains, the parent version has 44 items and 11 domains, and the adolescent and adult version has 50 items within 12 domain (Figure 28).73,74 The domains included in the adolescent and adult version are as follows: HRQoL module including physical functioning, vitality, emotional functioning, social or school functioning, role functioning, body image, eating problems, treatment burden; symptoms module that includes respiratory symptoms, digestive symptoms, and weight; and a health perception module. A 4-point Likert scale is used to measure frequency (always, often, sometimes, never), intensity (a great deal, somewhat, a little, not at all) and true-false scales (very true, somewhat true, somewhat false, very false). Items within domains are summed and standardized. Individual domain scores range from 0 to 100, with higher scores indicating better HRQoL.73 The scales are designed to measure symptoms and functioning during the 2-week period prior to administration of the questionnaire.75
In Study 102, 103, 104, and 109, patients aged 12 and 13 years completed the CFQ-C and their parents completed the CFQ-P questionnaire. All patients who were 14 years and older completed the CFQ-14 version. The survey was provided in the patient’s native language, if a validated translation was available, otherwise the patient did not complete the questionnaire.
Figure 28: CFQ-R Scales and Exemplar Items
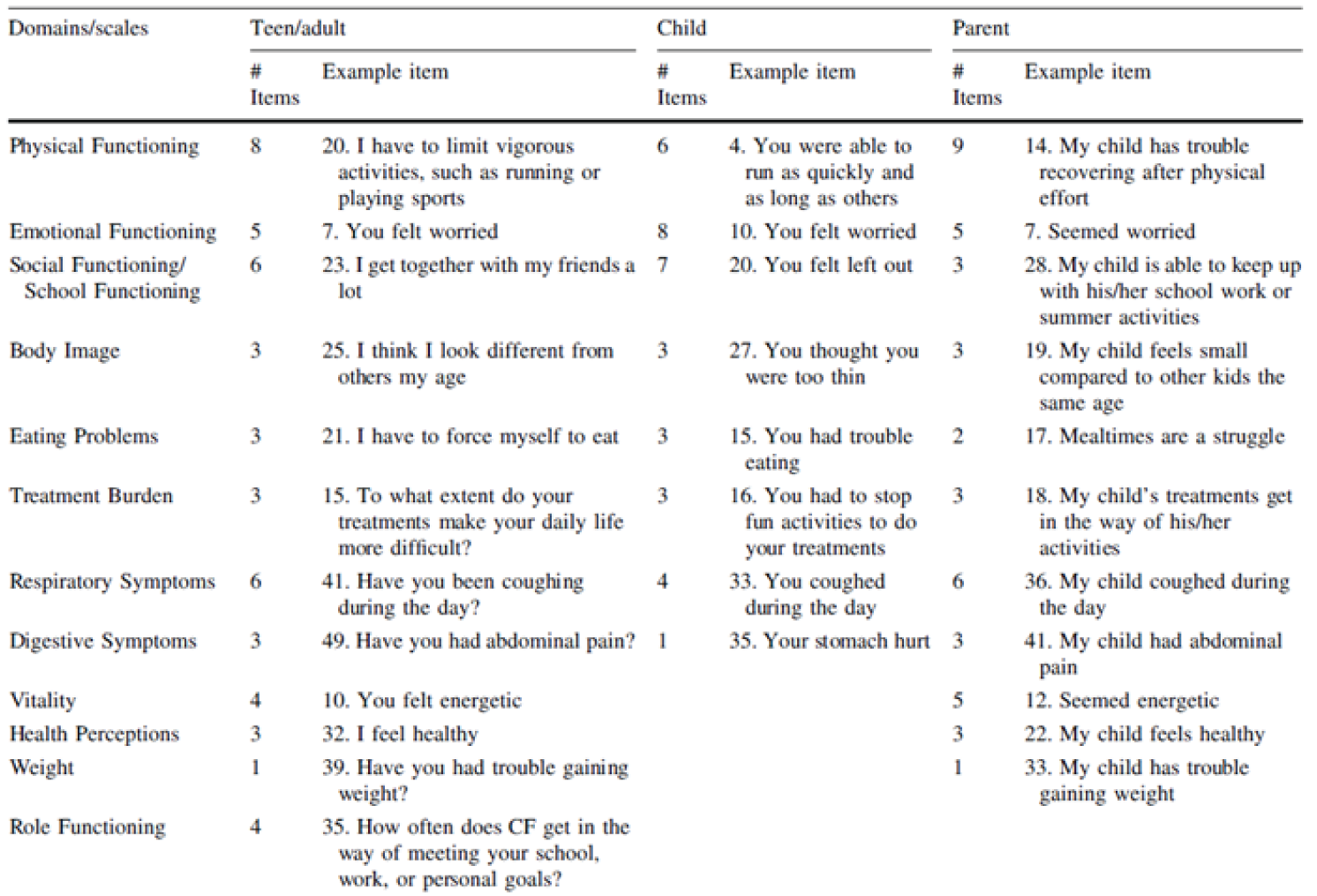
Source: Reprinted by permission from Springer Nature: Springer Nature Quality of Life Research. Erratum to: Psychometric evaluation of the Cystic Fibrosis Questionnaire–Revised in a national, US sample. Quittner AL, Sawicki GS, McMullen A, et al. (2021).73
Several studies have evaluated the validity and reliability of the CFQ-R questionnaire.73 and its original version.74,75,139,140 Quittner et al. (2012)73 examined the psychometric properties of the CFQ-R using data from the Epidemiologic Study of Cystic Fibrosis, a national US multi-centre longitudinal cohort study containing CFQ-R and health outcomes data from 7,330 patients aged 6 to 70 years, plus data from 2,728 parents for the CFQ-P. Quittner et al. (2012)73 reported adequate internal consistency (Cronbach alpha ≥ 0.70) for most domains and scales on each of the 3 versions, with lower reliability (< 0.6) found for treatment burden, social functioning, or school functioning. For the respiratory symptom domain, the Cronbach alpha reported was 0.87, 0.69, 0.82 for the CRQ-14, CFQ-C, and CFQ-P, respectively.73
Discriminant validity was demonstrated as CFQ-R scores were consistently lower for patients who were sick, compared with those who were well for all 3 versions of the instrument.73 If a patient’s clinical encounter form included any documentation of “sickness” within 21 days of the CFQ-R completion date, the patient was considered sick. For the respiratory domain specifically, the effect size for the difference in mean scores for sick versus well patients with CF ranged from –0.59 to –0.95 across the 3 versions.73
Discriminant validity was also assessed by testing the ability of the CFQ-R scales to differentiate between groups of patients with increasing severity of disease based on ppFEV1. It was hypothesized that most CFQ-R scales (except for digestion) would vary by lung function. For all 3 versions of the questionnaire, statistically significant differences in scores were detected between disease severity stages for most CFQ-R domains. Scores for the digestion domain showed no difference across the pulmonary function disease stages.73 For children, however, this analysis had limitations, because this population had less variability in disease severity as few school-age children had a FEV1 < 70% predicted.73
Construct validity: There was fair-to-moderate correlations between CFQ-R scales and health outcomes, including ppFEV1 (correlation range, 0.25 to 0.51), number of pulmonary exacerbations treated with IV antibiotics (range: −0.23 to −0.35), and BMI (range: 0.22 to 0.44).73 The strongest correlations were demonstrated for the physical functioning and respiratory domains with ppFEV1 (range: 0.33 to 0.51 and 0.32 to 0.42, respectively) and for the weight scale and BMI (range: 0.42 and 0.44 on the CFQ-P and CFQ-14, respectively). The respiratory domain showed weak correlation with the number of exacerbations (range: --0.24 to -0.29).73 Overall, the correlations were lower for the CFQ-C and CFQ-P than the CFQ-14.
Quittner et al. (2012)73 also reported fair-to-moderate agreement between the child and parent versions on all scales of the CFQ-R (intraclass correlation coefficient range: 0.26 to 0.56); however, stronger agreement was found on domains that measured more observable signs and symptoms, such as physical functioning (r = 0.46), eating problems (r = 0.56), and respiratory symptoms (r = 0.55).73 Tluczek et al. (2013)74 examined parent-child concordance in CFQ (original version) domains for children aged 8 years to 13 years and adolescents aged 14 years to 18 years (total N = 92 pairs). Five of the domains of the CFQ-C instrument were similar to the parent-reported CFQ-14, with children reporting better HRQoL than parents for the digestive symptoms and body image domains.74 Male children reported worse HRQoL on emotional functioning that their parents. Adolescents rated HRQoL higher than their parents on weight, body image, digestive symptoms, eating disturbance, physical and emotional functioning, treatment burden, and respiratory symptoms.74 Many of the differences were driven by male adolescents.74
Quittner et al. (2005)73 showed the CFQ-14 (original 44 item version) correlated well with the SF-36 based on data from 212 adolescents and adults with CF with mild to severe pulmonary disease. Correlations were strong (range: 0.57 to 0.84) between similar dimensions of the CFQ-14 and SF-36 (physical, health perceptions and general health, vitality, role/role physical, emotional functioning, and mental health, and social) and weak to moderate (range: 0.19 to 0.42) between scales not expected to be related (digestion and role scales of the CFQ and general health and mental health scales of the SF-36). Test-retest reliability was also assessed on a subset of 21 patients with stable disease. With repeat administration over 14 days the intraclass correlation coefficients ranged from 0.45 (social domain) to 0.90 (respiratory symptoms), with 7 of 12 domains showing intraclass correlations that exceeded the generally accepted threshold of 0.7 for reliability.139 In the initial development of the CFQ instrument, Henry et al. (2003)75 reported test-retest reliability was acceptable for the CFQ-14 respiratory domain (ICC 0.88) but not for the CFQ-C respiratory domain (ICC 0.48) when tests were repeated approximately 8 days apart in 22 adolescents or adults, and 22 children with stable CF.
Limited data were identified that evaluated the responsiveness of the CFQ (original version) domains. Henry et al. (2003)75 reported large effect size (0.63 to 1.17) for the respiratory symptom and physical functioning domains of the CFQ-14 and CFQ-C in 24 adolescents or adults, and 17 children who showed clinical improvement after antibiotic treatment for an exacerbation. The effect size for other domains were moderate to weak.75
The MID was estimated for the CFQ-R respiratory symptom scale in 2 study populations: one with patients with stable CF and chronic P. aeruginosa airway infection (N = 140); the other with patients with exacerbation of CF and chronic P. aeruginosa airway infection (N = 84).76 Both anchor-based and distribution-based methods were used. The anchor-based methods used a Global Rating of Change Questionnaire that assessed patients’ perceptions of the change in their respiratory symptoms. The MID for patients with stable disease was estimated to be 4.0 points, and for patients with exacerbation, 8.5 points.76 The MID values based on distribution methods (0.5 SD of mean change in scores or 1 SE of the mean for baseline scores) showed similar results for the stable patients (MID 6.2 and 6.1) and those with an exacerbation (9.6 and 10.1).76 Another study estimated the MID for the CFQ-R respiratory scale based on longitudinal data from 12 patients with CF with moderate to severe pulmonary disease who were followed for 1 year. Using distribution-based methods, the MID estimates ranged from 6.0 to 8.4 points (mean 7.3) in this pilot study.129
The main limitations of the CFQ-R are ceiling effects for certain scales (notably the eating and weight scale for the CFQ-14, eating, digestion, and body image for CFQ-C; and eating, weight, body image, and school functioning for CFQ-P), potential difficulty for patients to understand some of the items (e.g., CFQ-R respiratory, item “trouble breathing”), and concerns that a patient may not be able to distinguish between some of the response items on the scale (e.g., response choices such as “somewhat” versus “a little”).73,130
Pharmacoeconomic Review
Abbreviations
BIA
budget impact analysis
BSC
best supportive care
CF
cystic fibrosis
CF Canada
Cystic Fibrosis Canada
ELX-TEZ-IVA
elexacaftor-tezacaftor-ivacaftor and ivacaftor
F/F
homozygous for F508del mutation in the CFTR gene
F/G
1 F508del mutation and 1 gating mutation in the CFTR gene
F/MF
1 F508del mutation and 1 minimal function mutation in the CFTR gene
F/RF
1 F508del mutation and 1 residual function mutation in the CFTR gene
ICER
incremental cost-effectiveness ratio
IVA
ivacaftor
LUM-IVA
lumacaftor-ivacaftor
ppFEV1
percent predicted forced expiratory volume in 1 second
QALY
quality-adjusted life-year
TEZ
tezacaftor-ivacaftor
Executive Summary
The executive summary comprises 2 tables (Table 1 and Table 2) and a conclusion.
Item | Description |
|---|---|
Drug product | Elexacaftor-tezacaftor-Ivacaftor (Trikafta) — elexacaftor 100 m, tezacaftor 50 mg, and ivacaftor 75 mg combination tablet and ivacaftor 150 mg (tablet) or elexacaftor 50 mg, tezacaftor 25 mg, and ivacaftor 37.5 mg combination tablet and ivacaftor 75 mg tablet |
Submitted price | Elexacaftor-tezacaftor-ivacaftor (Trikafta) — elexacaftor 100 m, tezacaftor 50 mg, and ivacaftor 75 mg combination tablet or elexacaftor 50 mg, tezacaftor 25 mg, and ivacaftor 37.5 mg combination tablet and ivacaftor 75 mg tablet: $840 per daily dose |
Indication | Proposed: for the treatment of cystic fibrosis in patients aged 6 years and older who have at least 1 F508del mutation in the CFTR gene |
Health Canada approval status | Pre-NOC |
Health Canada review pathway | Priority review |
NOC date | Anticipated: April 20, 2022 |
Reimbursement request | As per indication |
Sponsor | Vertex Pharmaceuticals (Canada) Incorporated |
Submission history | Previously reviewed: Yes Elexacaftor-tezacaftor-ivacaftor (combination tablet) and ivacaftor Indication: Cystic fibrosis, F508del-CFTR mutation in patients aged 12 years and older Recommendation date: September 16, 2021 Recommendation: List with criteria and conditions, including a substantial reduction in price |
NOC = Notice of Compliance.
Table 2: Summary of Economic Evaluation
Component | Description |
|---|---|
Type of economic evaluation | Cost-utility analysis Microsimulation |
Target population | Patients with CF aged 6 years and older who have at least 1 F508del mutation in the CFTR gene, represented by the following 4 genotypes considered in separate analyses:
|
Treatment | ELX-TEZ-IVA with BSC |
Comparators |
|
Perspective | Canadian publicly funded health care payer |
Outcomes | QALYs, life-years |
Time horizon | Lifetime (approximately 92 years) |
Key data source |
|
Submitted results |
|
Key limitations |
|
CADTH reanalysis results | CADTH conducted a reanalysis that included: the removal of an additional benefit of ELX-TEZ-IVA, LUM-IVA, and IVA on the long-term rate of decline in ppFEV1 and pulmonary exacerbations; the removal of dynamic pricing; the inclusion of health care–related costs for patients on CFTR modulators in the period for which they achieved survival benefits compared to BSC; the removal of an adjustment to drug acquisition costs by patient compliance; the equating of hospital and pharmacotherapy costs; and the removal of a treatment-specific utility increment for patients on ELX-TEZ-IVA.
ELX-TEZ-IVA was not cost-effective at a willingness-to-pay threshold of $50,000 per QALY in any scenario conducted by CADTH. A price reduction in excess of 90% for ELX-TEZ-IVA is required for all 4 genotypes for ELX-TEZ-IVA to be considered cost-effective at a willingness-to-pay threshold of $50,000 per QALY in comparison with BSC. The key scenario assessing the cost-effectiveness of ELX-TEZ-IVA in the full Health Canada population resulted in ICERs ranging from $1,129,990 to $1,868,095 per QALY compared to BSC; ELX-TEZ-IVA is not cost-effective at the submitted price. |
BSC = best supportive care; CF = cystic fibrosis; -TEZ-IVA = elexacaftor-tezacaftor-ivacaftor and ivacaftor; F/F = homozygous for F508del mutation in the CFTR gene; F/G = 1 F508del mutation and 1 gating mutation in the CFTR gene; F/MF = 1 F508del mutation and 1 minimal function mutation in the CFTR gene; F/RF = 1 F508del mutation and 1 residual function mutation in the CFTR gene; ICER = incremental cost-effectiveness ratio; IVA = ivacaftor; LUM-IVA = lumacaftor-ivacaftor; ppFEV1 = percent predicted forced expiratory volume in 1 second; QALY = quality-adjusted life-year.
Conclusions
The clinical evidence submitted by the sponsor demonstrated that elexacaftor-tezacaftor-ivacaftor and ivacaftor (ELX-TEZ-IVA) led to statistically and clinically significant improvements in acute percent predicted forced expiratory volume in 1 second (ppFEV1) and weight-for-age z scores when compared with relevant comparators in patients aged 6 to 11 whose genotypes were homozygous for the F508del mutation in the CFTR gene (F/F) or who had 1 F508del mutation and 1 minimal function mutation in the CFTR gene (F/MF). There were no clinical studies conducted with ELX-TEZ-IVA in pediatric patients with 1 F508del mutation and 1 residual function mutation in the CFTR gene (F/RF) or 1 F508del mutation and 1 gating mutation in the CFTR gene (F/G) genotypes; however, the clinical experts noted that ELX-TEZ-IVA would result in clinically meaningful improvements for these patients, based on the evidence reported for ELX-TEZ-IVA in adult patients with the F/RF and F/G genotypes and the results of studies of pediatric patients with the F/F and F/MF genotypes. Results were similar in patients aged 12 years and older with regard to acute change in ppFEV1 in all genotypes, and evidence from 1 trial in the F/F subgroup indicated ELX-TEZ-IVA reduced the rate of pulmonary exacerbations in comparison with placebo. However, these conclusions were based on short-term studies (maximum of 96 weeks) and there was no evidence on the long-term impact of ELX-TEZ-IVA on the rate of decline of ppFEV1 or pulmonary exacerbation rates beyond the trial period for any genotype or age group.
CADTH identified several major limitations with the submitted economic evaluation; the following were addressed in reanalyses: the removal of an additional benefit of CFTR modulators on the long-term rate of decline in ppFEV1 and pulmonary exacerbations; the removal of dynamic pricing of CFTR modulators; the inclusion of costs for ELX-TEZ-IVA in the period for which it achieved a survival benefit in comparison with best supportive care (BSC); the removal of an adjustment to drug acquisition costs by patient compliance; and the removal of a treatment-specific utility increment for patients on ELX-TEZ-IVA. In comparison with BSC, the CADTH base-case analysis resulted in an incremental cost-effectiveness ratio (ICER) of $1,434,435 per quality-adjusted life-year (QALY) in the F/F genotype; $1,653,605 per QALY in the F/MF genotype; $2,437,481 per QALY in the F/RF genotype; and $1,531,443 per QALY in the F/G genotype. For the F/F genotype, a pairwise ICER of $680,560 per QALY was estimated compared to lumacaftor-ivacaftor (LUM-IVA). For the F/G genotype, a pairwise ICER of $622,381 per QALY was estimated in comparison with ivacaftor (IVA) monotherapy. Results of the CADTH reanalysis were aligned with the sponsor’s, in that ELX-TEZ-IVA was not cost-effective in any of the genotype subgroups at conventionally acceptable ICER thresholds.
The key drivers in the analyses are drug acquisition costs and assumptions in the long term benefits with ELX-TEZ-IVA, which were uncertain. Treatment with ELX-TEZ-IVA was not cost-effective at a willingness-to-pay threshold of $50,000 per QALY in any scenario conducted by CADTH. A price reduction in excess of 90% for ELX-TEZ-IVA is required for all 4 genotypes for ELX-TEZ-IVA to be considered cost-effective at a willingness-to-pay threshold of $50,000 per QALY in comparison with BSC. Results of the key scenario analysis assessing the cost-effectiveness of ELX-TEZ-IVA in the full Health Canada–indicated population were similar to those from the CADTH base case, with ICERs ranging from $1,129,990 to $1,868,095 per QALY compared to BSC.
Stakeholder Input Relevant to the Economic Review
This section is a summary of the feedback received from the patient groups, registered clinicians, and drug plans that participated in the CADTH review process.
CADTH received 1 submission from Cystic Fibrosis Canada (CF Canada) as part of the call for patient input. Information was gathered via a survey of Canadian patients and caregivers, notified through email, social media, or postings at cystic fibrosis (CF) clinics. Patient input noted how burdensome CF can be, on both patients living with the disease and their caregivers. Many patients currently only receive treatment for the management of symptoms, which includes treatments, such as IV infusions, that are associated with negative side effects and significant time commitments to administer. The input noted that, while other CFTR modulators are reimbursed in Canada, their availability is still limited and a significant proportion of the CF population remains unable to access treatment. Some patients had experience with the various available CFTR available such as IVA, LUM-IVA, and the drug under review. More than half of patients who had received ELX-TEZ-IVA experienced significant improvements in their condition with limited side effects.
Clinician group input was received from CF Canada’s Accelerating Clinical Trials Network Executive Committee and Canadian Cystic Fibrosis Clinic Directors. Clinicians noted that standard of care includes antibiotics, mucolytics, bronchodilators, pancreatic enzymes, and vitamins. Of the CFTR modulators available, IVA monotherapy is only indicated in approximately 4% of CF cases that have the genetic “gating” mutation for which this drug has been shown to be effective. Two therapies have been developed for patients with the F/F genotype, but of the 2, only LUM-IVA is available in Canada, and eligibility criteria are restrictive. The clinicians indicated that ELX-TEZ-IVA would be a highly impactful treatment, and, given that its indication includes patients who have only 1 copy of the F508del mutation in addition to those with 2 copies, that it could affect nearly 90% of CF patients in Canada and it would become the standard of care in the indicated population over existing CFTR modulators and supportive therapy. Clinicians noted that patients aged 6 to 11 years with the F/MF genotype have the greatest unmet need due to severe clinical manifestations and the fact that no CFTR therapies are currently indicated for these patients. Clinicians noted that ELX-TEZ-IVA leads to substantial improvements in lung function and quality of life, and represents a breakthrough compared to other funded therapies. If approved, this drug is expected to replace other comparators and become first-line therapy.
Drug plan input noted a discrepancy between enrolment criteria for patients aged 6 to 11 years compared to those older than 12 years, in that the clinical trials for those aged 6 to 11 years included patients with a ppFEV1 of greater than 90%. Plans suggested that all eligible patients will switch from other CFTR modulators to ELX-TEZ-IVA. The drug plans noted that ELX-TEZ-IVA has undergone negotiations with the pan-Canadian Pharmaceutical Alliance.
Two of these concerns were addressed in the sponsor’s model:
The choice of comparators in the sponsor's model aligned with clinician and patient input.
All patients were assumed to receive standard of care, consisting of antibiotics, mucolytics, and pancreatic enzymes.
In addition, CADTH addressed some of these concerns by increasing the market uptake of ELX-TEZ-IVA in the budget impact, in line with clinician and drug plan input.
CADTH was unable to address the concern raised in stakeholder input that its analyses are based on publicly available prices and do not incorporate the presence of confidential, negotiated prices.
Economic Review
The current review is for ELX-TEZ-IVA for the treatment of CF in patients aged 6 years and older who have at least 1 F508del mutation in the CFTR gene.
Economic Evaluation
Summary of Sponsor’s Economic Evaluation
Overview
The sponsor submitted a cost-utility analysis assessing ELX-TEZ-IVA in combination with BSC for the treatment of CF in patients 6 to 11 years of age who have at least 1 F508del mutation in the CFTR gene, represented by the F/F, F/M, FF/RF, and F/G (inclusive of R117H) genotypes.
The sponsor compared the submitted drug regimen with BSC alone in all 4 subgroups, as well as with LUM-IVA in the F/F subgroup and IVA monotherapy in the subgroup of patients with a F/G genotype.1 The modelled population is aligned with a subset of the Health Canada indication and funding request, which had not been previously submitted to CADTH, specifically patients 6 to 11 years of age. CADTH has previously reviewed ELX-TEZ-IVA for the treatment of CF in patients aged 12 years and older who have at least 1 F508del mutation in the CFTR gene.2 CADTH focused its review for this submission on the population aged 6 to 11, but also considered the sponsor’s scenario analysis, which included all patients 6 years of age and older.
The recommended dose of ELX-TEZ-IVA is 2 tablets of ELX 100 mg, TEZ 50 mg, and IVA 75 mg taken in the morning and 1 tablet of IVA 150 mg taken in the evening, approximately 12 hours apart, with fat-containing food.3 Both the triple-combination tablet and IVA 150 mg tablet cost $280.00 per tablet, for a daily cost of treatment of $840.00 and an annual cost of $306,810 per patient. Treatment with BSC alone consisted of recommended medications (such as mucolytics, inhaled and oral antibiotics, inhaled hypertonic saline, nutritional supplements, enteral tube feeding, pancreatic enzymes, antifungal agents, and corticosteroids) and physiotherapy. The daily per-patient cost associated with IVA monotherapy was $840.00, or an annual cost of $306,810, based on its list price. The daily per-patient cost associated with LUM-IVA was $682.14, or an annual cost of $249,153, based on its list price. All patients on CFTR-modulator therapies also received BSC. The costs associated with ELX-TEZ-IVA and IVA monotherapy were adjusted for compliance in the sponsor’s submission.
The clinical outcomes predicted by the model were QALYs and life-years. The economic analysis was undertaken over a lifetime time horizon of approximately 92 years from the perspective of the public health care payer. Discounting at 1.5% per annum was applied to both costs and outcomes.1
Model Structure
The sponsor conducted a patient-level simulation model (i.e., a microsimulation), with a typical patient profile for each genotype informed by various CFTR-modulator trials. The patient profile was run through the model to project a patient’s CF disease progression and associated life expectancy, costs, and utilities (Figure 1). In the sponsor’s base case, the average patient profile was run 250 times, and the expected costs and clinical effects of ELX-TEZ-IVA, BSC, LUM-IVA (for the F/F genotype only), and IVA monotherapy (for the F/G genotype only) were calculated. This process was repeated 100 times for each genotype. During each cycle for a given patient profile, the hypothetical average patient was at risk of various clinical events associated with costs, mortality, and utility values. At the beginning of each cycle, the model would calculate a patient’s mortality risk based on a Cox proportional hazards model, which linked survival in CF patients to several risk factors.4 The following characteristics were included in the calculation of mortality risk: age, sex, ppFEV1, annual number of pulmonary exacerbations, prior respiratory infection status, CF-related diabetes, weight-for-age z scores, and pancreatic sufficiency status. Age, ppFEV1, pulmonary exacerbation rate, and weight-for-age z scores were updated with each cycle a patient remained alive, while the remaining characteristics remained static. If a patient remained alive, the model also tracked treatment discontinuation and lung transplant eligibility and occurrence. Treatment with a CFTR modulator was assumed to affect disease progression and mortality through effects relating to ppFEV1, weight-for-age z scores, and pulmonary exacerbation rates. During each cycle, patients would accrue life-years and QALYs, whereas costs were applied at the end of each run of 250 patients for efficiency gains.
Model Inputs
The baseline age-specific risk of death in the model was derived from a cohort study of the Canadian CF Registry by Stephenson et al.5 The Kaplan–Meier data from this study were digitized and extrapolated using parametric survival analysis to generate a mortality risk for the lifetime time horizon, with the Gompertz curve selected as the best fitting option. This baseline hazard was then adjusted using a Cox proportional hazards model developed by Liou et al.,4 which accounted for the patient characteristics listed in the Model Structure section. The hazard of mortality in the model was assumed to be no lower than that of the general population of Canada.
The characteristics informing the mortality risk in the model were based on an average patient profile generated primarily from pooled mean baseline characteristics of CFTR-modulator trials, and were specific to each genotype. The trials informing the baseline characteristics of age, sex, ppFEV1 and weight-for-age z score included the trials for LUM-IVA, tezacaftor-ivacaftor (TEZ-IVA), and IVA monotherapy, in addition to the trials for ELX-TEZ-IVA, to create a larger sample size. For the homozygous F/F genotype, data from Study 011 Part B and Study 109 (both of which involved LUM-IVA) were used, in addition to data for the subset of F/F patients from Study 113 and Study 115 (TEZ-IVA) and Study 106 (ELX-TEZ-IVA).6-10 Patients in Study 106, Study 113, and Study 115 may have had a prior history of CFTR-modulator use but were required to undergo a 28-day washout period before screening, their baseline characteristics were therefore considered by the sponsor to be reflective of a CFTR modulator–naive population. Studies 106 and Study 116 (both ELX-TEZ-IVA) were used to inform the baseline characteristics in the F/MF population.8,11 The heterozygous F/RF population’s baseline characteristics were informed by Study 113 and Study 115,9,10 while the ENVISION, KONNECTION, and KONDUCT trials (all IVA monotherapy), informed the F/G population.12-14 The baseline rate of pulmonary exacerbations requiring IV antibiotics and/or hospitalization was derived from Whiting et al.15 The rate of CF-related diabetes at baseline was based on a study of the CF Canada patient registry,16 and a patient’s status was assumed to not change over the entire time horizon.
Table 3: Baseline Characteristics Key Data Sources
Genotype | Source |
|---|---|
F/F | Study 011 Part B and Study 1096,7 Subset of F/F patients from Study 106, Study 113, and Study 1158-10 |
F/MF | |
F/RF | |
F/G, inclusive of R117H |
F/F = homozygous for F508del mutation in the CFTR gene; F/G = 1 F508del mutation and 1 gating mutation in the CFTR gene; F/MF = 1 F508del mutation and 1 minimal function mutation in the CFTR gene; F/RF = 1 F508del mutation and 1 residual function mutation in the CFTR gene.
As noted previously, ppFEV1, the annual number of pulmonary exacerbations, and weight-for-age z scores could be affected by treatment, and were updated every cycle, along with age. All other characteristics remained constant from baseline. The treatment effects of CFTR modulators considered in the model were derived from the relevant phase III studies and open-label extension studies. As the assignment of baseline mortality hazards in the model was based on a CFTR modulator–naive population, the analysis required placebo-adjusted estimates of clinical efficacy for CFTR modulators. An indirect treatment comparison was performed using individual-level patient data from relevant phase III randomized-controlled trials. |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Patients on BSC alone were expected to not experience any acute increases in ppFEV1 or weight-for-age z score, and were assumed to experience a long-term decline in ppFEV1 in line with a study by Leung et al.18 The same rate of decline was applied to all genotypes, except the F/RF genotype, as it is typically associated with a milder form of disease and therefore a slower rate of decline. The reduction in rate of decline for patients receiving CFTR modulators in comparison with BSC was not available from the ITC, the sponsor’s trials assessing ELX-TEZ-IVA, or other clinical trials. Based on registry-matched analyses, the reduction in rate of ppFEV1 decline for patients aged 6 to 11 years receiving LUM-IVA and IVA was assumed to be the same as that calculated for patients older than 12 years on each of these medications.1 Data from Study 105 showed that patients receiving ELX-TEZ-IVA were assumed to experience a 96-week “maintenance period” during which their ppFEV1 did not decline at all after initial treatment.19 Following this maintenance period, their lung function was assumed to decline, but at a rate of only 20% of the decline associated with BSC, based on registry data specific to TEZ-IVA and other assumptions. Patients on IVA and LUM-IVA were assumed to experience 47.1% and 42% reductions in their rate of ppFEV1 decline compared to BSC based on retrospective, observational studies.20,21
The baseline rate of occurrence of pulmonary exacerbations each cycle was based on the patient’s ppFEV1 and age, according to a formula derived by Goss et al.22 and was not genotype-specific. This rate was applied as derived by Goss et al. to all patients in the sponsor’s base-case analysis, which assessed patients 6 years of age and older, regardless of treatment received. Once patients turned 12 years old, the rate of pulmonary exacerbations for patients on CFTR modulators, including ELX-TEZ-IVA, was adjusted by a rate ratio derived by the sponsor. This also applied to the scenario analysis for patients aged 12 years and older. This was based on an assumed additional treatment impact on pulmonary exacerbations beyond those explained by the improvements in ppFEV1 in CFTR modulator–treated patients captured in the Goss et al., formula. The sponsor attempted to calibrate the pulmonary exacerbation rate ratio for patients on a CFTR modulator observed in the trials with that of a patient receiving BSC alone to account for the potential double counting of the benefit due to the superior ppFEV1 observed with CFTR modulators. This was done for rates over a 2-year period and assumed to apply to the entirety of the time horizon.
The sponsor’s model also accounted for treatment discontinuation and compliance. Discontinuation rates for the model period corresponding to the trial duration period were obtained from the relevant phase III trials, whereas open-label extension studies were used to inform a “post-acute” phase of the model up to an additional 96 weeks in length, after which no patients discontinued treatment in the model.23-26 If a patient discontinued a CFTR, they no longer received the impact of treatment on lung function decline or pulmonary exacerbation rate, but did maintain their acute increase in ppFEV1 and weight-for-age z score. The sponsor also used compliance rates from the trials to inform treatment costs in the acute period (first 24 weeks), which were genotype-specific, and observational data from use of LUM-IVA to inform a compliance rate beyond the trial period. Compliance was assumed to have no impact on treatment efficacy, and only affected the costs associated with CFTR modulators. The rate of lung transplantation was derived by the sponsor, and a separate mortality risk for patients following a lung transplant was applied based on a study in the literature.27 Neither were genotype-specific. The sponsor assumed that 11.3% of patients with a ppFEV1 under 30% would receive a lung transplant. Adverse events in the model were based on the relevant phase III trials for the respective genotypes and CFTR modulators.
Costs considered in the model included those associated with drug acquisition, monitoring, disease management, pharmacotherapy, diagnostic, pulmonary exacerbations, adverse events, and lung transplantation. The cost of ELX-TEZ-IVA was submitted by the sponsor, whereas the prices of comparator drugs were obtained from the Ontario Exceptional Access Program formulary.28 For CFTR modulators, including ELX-TEZ-IVA, the sponsor employed a dynamic pricing approach, whereby the introduction of a first generic into the market after loss of patent exclusivity would lead to a 25% reduction in the prices of all drugs, followed by a second generic entry further reducing their prices by 50%. These assumptions were based on a pan-Canadian Pharmaceutical Alliance office framework for pricing expectations upon generic entry.29 Additional costs associated with CFTR-modulator use included monitoring costs consisting of liver function tests and ophthalmologist visits, according to their product monographs, with the costs obtained from the Ontario Schedule of Benefits.30,31
Routine medical care associated with CF, consisting of clinician visits, hospitalizations, infection prevention, and management of comorbidities, was also included in the model. Such costs were applied in the model by disease severity, defined based on ppFEV1 thresholds, and further divided into costs related to pulmonary exacerbations and non-pulmonary exacerbations. A sponsor-commissioned burden-of-illness study, consisting of a chart review, was used to inform the health care resource use associated with the routine disease-management costs,1 and was further supplemented by data from the 2014 CF Canada patient registry.1 Costs related to physician and laboratory services were obtained from the Ontario Schedule of Benefits, while hospitalization costs were derived from a study by Skolnik et al.32 The sponsor further adjusted the disease-management costs specific to inpatient visits and pharmacotherapy for patients on CFTR modulators, based on studies in the literature that indicated a reduction in CF-related inpatient admissions and outpatient IV and antibiotic use.33,34 As a result, differential annual inpatient costs and annual pharmacotherapy costs were estimated for patients on BSC alone and those on CFTR modulators. The sponsor also excluded disease-management costs for patients on CFTR modulators after a similar patient on BSC had died in a given simulation, while only incurring costs for CFTR-modulator therapy for the remainder of the time horizon. Lung transplantation costs were obtained from Alberta Health Services, with follow-up costs obtained from the literature.35,36 The cost of each adverse event was assumed to be equal to the cost of a single assessment by a general practitioner.30
In the absence of utilities based on a generic instrument (e.g., the EQ-5D), the sponsor used an equation developed by Solem et al. that included ppFEV1 and pulmonary exacerbations as predictors of an EQ-5D index utility score. For this calculation, each pulmonary exacerbation was assumed to last 21.7 days, based on the TRAFFIC and TRANSPORT trials.37 The sponsor also included a treatment-specific utility increment for patients receiving ELX-TEZ-IVA, as it was felt that the equation by Solem et al. did not capture the impact of treatment on non-respiratory outcomes. This was not applied to patients receiving other CFTR modulators. The utility for a patient post-lung transplant was obtained from a study by Whiting et al.15 No disutilities related to adverse events were included in the model, as they were assumed to have minimal impact on patient quality of life.
Summary of Sponsor’s Economic Evaluation Results
All analyses were run probabilistically, with 250 average patients individually simulated for 100 iterations for the base-case and scenario analyses. The deterministic and probabilistic results were similar. The probabilistic findings are presented in the following section. The sponsor’s base case is based on publicly available list prices for comparators.
Base-Case Results
The sponsor presented its results by genotype. For the F/F genotype, ELX-TEZ-IVA was associated with $2,792,413 in incremental costs and 8.63 incremental QALYs when compared with LUM-IVA, for an ICER of $323,602 per QALY. Compared to BSC, ELX-TEZ-IVA was associated with $6,662,694 in incremental costs and 14.76 incremental QALYs, for an ICER of $451,377 per QALY. In the F/MF genotype, ELX-TEZ-IVA was associated with $6,689,307 in incremental costs and 14.66 incremental QALYs when compared with BSC, for an ICER of $456,394 per QALY. In the F/RF genotype, fewer incremental costs ($6,678,270) and fewer incremental QALYs (10.27) were observed with ELX-TEZ-IVA, for an ICER of $650,475 per QALY compared with BSC. For the F/G genotype, ELX-TEZ-IVA was associated with an ICER of $437,639 and $238,159 per QALY, for the comparison with BSC and IVA monotherapy.
The sponsor also presented a weighted ICER for all genotypes combined, weighted by their prevalence and by comparator market share. The overall weighted ICER was $456,044 per QALY in comparison with the relevant standard of care.
Table 4: Summary of the Sponsor’s Economic Evaluation Results by Genotype
Drug | Total costs ($) | Incremental costs ($) | Total LYs | Incremental LYs | Total QALYs | Incremental QALYs | ICER ($ per QALY) |
|---|---|---|---|---|---|---|---|
Homozygous for F508del-CFTR (F/F) | |||||||
BSC | 880,221 | Reference | 26.09 | Reference | 24.03 | Reference | Reference |
ELX-TEZ-IVA | 7,542,916 | 6,662,694 | 39.64 | 13.55 | 38.79 | 14.76 | 451,377 |
LUM-IVA | 4,750,503 | Reference | 32.48 | Reference | 30.16 | Reference | Reference |
ELX-TEZ-IVA | 7,542,916 | 2,792,413 | 39.64 | 7.16 | 38.79 | 8.63 | 323,602 |
Heterozygous for F508del-CFTR (F/MF) | |||||||
BSC | 877,546 | Reference | 26.11 | Reference | 24.06 | Reference | Reference |
ELX-TEZ-IVA | 7,566,854 | 6,689,307 | 39.53 | 13.42 | 38.72 | 14.66 | 456,394 |
Heterozygous for F508del-CFTR (F/RF) | |||||||
BSC | 758,996 | Reference | 29.85 | Reference | 27.68 | Reference | Reference |
ELX-TEZ-IVA | 7,437,266 | 6,678,270 | 38.74 | 8.89 | 37.95 | 10.27 | 650,475 |
Heterozygous for F508del-CFTR (F/G) | |||||||
BSC | 986,009 | Reference | 25.96 | Reference | 23.83 | Reference | Reference |
ELX-TEZ-IVA | 7,541,447 | 6,555,438 | 39.62 | 13.66 | 38.81 | 14.98 | 437,639 |
IVA | 6,362,340 | Reference | 36.37 | Reference | 33.86 | Reference | Reference |
ELX-TEZ-IVA | 7,541,447 | 1,179,107 | 39.62 | 3.25 | 38.81 | 4.95 | 238,159 |
BSC = best supportive care; ELX-TEZ-IVA = elexacaftor-tezacaftor-ivacaftor and ivacaftor; F/F = homozygous for F508del mutation in the CFTR gene; F/G = 1 F508del mutation and 1 gating mutation in the CFTR gene; F/MF = 1 F508del mutation and 1 minimal function mutation in the CFTR gene; F/RF = 1 F508del mutation and 1 residual function mutation in the CFTR gene; ICER = incremental cost-effectiveness ratio; IVA = ivacaftor; LUM-IVA = lumacaftor-ivacaftor; LY = life-year; QALY = quality-adjusted life-year.
Source: Sponsor’s pharmacoeconomic submission.1
Sensitivity and Scenario Analysis Results
The sponsor conducted a main scenario analysis in the full indicated population for ELX-TEZ-IVA, consisting of all patients with CF aged 6 years and older who have at least 1 F508del mutation in the CFTR gene. The weighted ICER resulting from this scenario was $407,601 per QALY, with incremental costs and QALYs of $4,825,052 and 11.84, respectively. The sponsor conducted several other scenarios to examine the impact of discounting and static pricing on the results in those aged 6 to 11 years. The scenario with the largest impact was that which assumed static pricing for all drugs, instead of the sponsor’s base-case assumption of dynamic pricing resulting in price reductions for CFTR-modulator therapies at the end of patent exclusivity. This scenario resulted in a weighted ICER of $717,206 per QALY.
CADTH Appraisal of the Sponsor’s Economic Evaluation
CADTH identified several key limitations to the sponsor’s analysis that have notable implications on the economic analysis:
Long-term impact of treatment with ELX-TEZ-IVA, LUM-IVA, or IVA on ppFEV1 rate of decline is uncertain: In addition to an acute increase in ppFEV1 from treatment with a CFTR modulator, the sponsor assumed that treatment with ELX-TEZ-IVA would result in a 96-week “maintenance period” following this acute increase, based on data from Study 105.19 This assumption was deemed reasonable by clinical experts. However, the sponsor also assumed that treatment with a CFTR modulator would slow the long-term rate of decline of ppFEV1 when compared with the rate of decline of patients not receiving disease-modifying treatment. In the absence of available data for ELX-TEZ-IVA in support of this assumption, the sponsor assumed that evidence from TEZ-IVA studies would be applicable, given its 2 components are part of the ELX-TEZ-IVA formulation. Due to the absence of data specific to ELX-TEZ-IVA in support of a slowing of the rate of lung function decline, this assumption is highly uncertain. Additionally, the relative reduction in the rate of decline in ppFEV1 with TEZ-IVA used to inform the value for ELX-TEZ-IVA was based on a retrospective analysis and may not have accounted for all confounders, as the analysis could only adjust for variables captured in the registry used to conduct the analysis. Additionally, the analysis was based on only 96 weeks of data, yet the reduction in rate of decline was applied to the entire model time horizon after the 96-week maintenance period, meaning there is no long-term evidence in support of this assumption for TEZ-IVA, let alone ELX-TEZ-IVA. The sponsor’s model was not flexible enough to change this relative rate reduction over time. Overall, these issues lead to uncertainty surrounding the benefit of ELX-TEZ-IVA on long-term ppFEV1, leading to a potential overestimate of the total QALYs and a potential underestimate of the costs associated with ELX-TEZ-IVA in the sponsor’s base case.
CADTH removed the long-term relative reduction in the rate of ppFEV1 decline for all CFTR modulators after 96 weeks in the CADTH base case.
Assumption of an impact of CFTR-modulator therapy on pulmonary exacerbation rates beyond its impact mediated by improvements in ppFEV1 is highly uncertain: The sponsor used a relationship identified in the literature to determine the baseline pulmonary exacerbation rate according to ppFEV1 and age. The sponsor determined that its model initially produced an overestimate of the rate of pulmonary exacerbations with ELX-TEZ-IVA using this relationship alone when compared with BSC with respect to the relative risk of pulmonary exacerbations from the pivotal trial, Study 102. The sponsor calibrated the first 2 years of pulmonary exacerbation rates in the model with the values from the trial to determine an additional relative reduction in pulmonary exacerbations with ELX-TEZ-IVA beyond its impact mediated by changes in ppFEV1. This rate ratio was only applied to the population aged 12 years and older due to a lack of data in the subgroup of patients 6 to 11 years of age. While the clinical experts consulted by CADTH acknowledged this assumption was plausible, it is uncertain how long this additional benefit would be observed. The sponsor assumed this additional impact on pulmonary exacerbations would be applicable for the entire modelled time horizon, starting from when a patient reached 12 years of age, despite having data for only up to 48 weeks. This potentially underestimates the number of pulmonary exacerbations and overestimates total QALYs and underestimates costs of ELX-TEZ-IVA.
CADTH removed the additional reduction in pulmonary exacerbations beyond the impact mediated by ppFEV1 in the CADTH base case for all CFTR modulators for the population aged 12 and older in the period for which there was no observed data.
Dynamic pricing for CFTR-modulator therapies is uncertain and underestimates drug acquisition costs with ELX-TEZ-IVA: The sponsor’s submitted base case employed a dynamic pricing approach for ELX-TEZ-IVA. Following the loss of patent exclusivity, generics were assumed to be introduced, leading to a 25% reduction in the price of ELX-TEZ-IVA with the first generic, followed by a 50% reduction in price with the introduction of a second generic after 18 and 19 years in the model time horizon, respectively. Similar assumptions were included for IVA and LUM-IVA. While price reductions arising from the availability of generic entrants is possible, there is tremendous uncertainty as to if and when price reductions for ELX-TEZ-IVA would occur. Patents are frequently extended (i.e., evergreened), leading to uncertainty with the exact timing of entry of a generic, and there is no guaranteed number of generic entries in the market. CADTH guidance states that full costs for ELX-TEZ-IVA at its submitted price for the entire time horizon should be accounted for. In the sponsor’s base case, dynamic pricing reduces the total drug acquisition costs associated with the CFTR modulators, biasing results in their favour.
CADTH disabled the dynamic pricing function in the CADTH reanalysis.
Compliance-adjusted drug costs underestimate the total costs associated with ELX-TEZ-IVA and other CFTR modulators: The sponsor adjusted the price of the CFTR modulators by the assumed compliance rate (93%) in the “post-acute” period of the model (i.e., the period for which there was no observed data), with the assumption that savings would be incurred by the health care system based on a lack of compliance. There is limited evidence to support the real-world compliance rate and the sponsor did not adjust treatment efficacy in the model to align accordingly. Additionally, because the drugs would be dispensed regardless of whether the patients were compliant, the public health care payer would bear the full costs of drug acquisition. This adjustment resulted in an underestimate of the drug acquisition costs associated with CFTR modulators, biasing results in their favour in comparison with BSC.
CADTH’s reanalysis assumed patients were 100% compliant to ensure all drug acquisition costs were accounted for.
Exclusion of health care costs in the period over which there is a gain in survival leads to an underestimation of the costs associated with ELX-TEZ-IVA: The sponsor failed to consider costs associated with CF care for patients on CFTR modulators after a similar patient on BSC had died, i.e., only considering CFTR-modulator therapy costs for the remainder of the time horizon. This assumption was made based on the sponsor asserting that accounting for the costs borne by the health care system for the additional period of survival associated with ELX-TEZ-IVA does not align with how society values treatment. This exclusion of costs incurred by the health care system does not reflect the perspective of the public health care payer. This assumption led to an underestimate of the total costs associated with ELX-TEZ-IVA.
CADTH included all costs relevant to the public health care payer in the additional survival period for patients on ELX-TEZ-IVA and IVA in the CADTH base case.
Impact of ELX-TEZ-IVA on health care resource use beyond its impact mediated through improving lung function is uncertain. Health-state costs in the sponsor’s submitted model were primarily based on ppFEV1, with greater costs for patients with a worse ppFEV1. The sponsor included costs associated with inpatient and outpatient hospitalizations, routine antibiotics, and diagnostics. The sponsor further adjusted the disease-management costs specific to inpatient hospital visits and pharmacotherapy for patients on CFTR modulators, based on studies in the literature that indicated a reduction in CF-related inpatient admissions and outpatient IV and antibiotic use.33,34 As a result, differential annual inpatient costs and annual pharmacotherapy costs were estimated for patients on BSC alone and those on CFTR modulators. Upon review of the sponsor’s sources for the reductions in costs associated with inpatient hospital visits and pharmacotherapy, CADTH noted that the studies cited by the sponsor were observational before-and-after studies, assessing the impact of CFTR-modulator use on relevant costs. These studies did not indicate whether they controlled for patient ppFEV1, or any other factors for that matter. As a result, it is difficult to determine whether the magnitude of difference in costs before and after CFTR-modulator use observed in these studies was due to ppFEV1, which was already factored into the sponsor’s submitted model via treatment efficacy, or another factor as asserted by the sponsor. The sponsor’s approach likely underestimated the inpatient hospital visit and outpatient antibiotic-use costs associated with CFTR-modulator use, biasing results in favour of ELX-TEZ-IVA.
CADTH assumed inpatient hospital costs and annual pharmacotherapy costs were the same for all patients in the model with a similar ppFEV1, regardless of whether they were receiving a CFTR modulator.
Treatment-specific utility increment for patients on ELX-TEZ-IVA leads to potential overestimation of total benefit. The sponsor based the utility values in the submitted model on an equation by Solem et al.37 that determines a utility based on the EQ-5D according to a patient’s ppFEV1 and whether they experienced a pulmonary exacerbation. The sponsor included an additional utility increment for patients on ELX-TEZ-IVA based on an analysis comparing the utility scores, according to the 8-dimension Cystic Fibrosis Questionnaire–Revised of patients on ELX-TEZ-IVA versus those on placebo in the relevant ELX-TEZ-IVA trials, adjusting for ppFEV1. This analysis revealed a difference in utility score for patients on ELX-TEZ-IVA in comparison with BSC that was not explained by ppFEV1. The sponsor’s analysis comparing Cystic Fibrosis Questionnaire–Revised scores from the trials did not account for pulmonary exacerbation rates, which were already included in the sponsor’s utility estimate, meaning the difference observed in the sponsor’s analysis may be explained by pulmonary exacerbations. It is difficult to know what proportion of the difference in utility scores from the trial is attributable to pulmonary exacerbations, although pulmonary exacerbations were accounted for in Solem et al. equation. The sponsor should have explicitly modelled other events it assumed contribute to quality of life not captured by Solem et al. to allow for greater transparency with respect to what contributes to the quality of life estimates and to what extent. The inclusion of a treatment-specific utility increment for patients on ELX-TEZ-IVA potentially leads to double counting of utility gains, likely biasing results in favour of ELX-TEZ-IVA.
CADTH removed the treatment-specific utility increment with ELX-TEZ-IVA in the CADTH base-case analysis.
Survival benefit with ELX-TEZ-IVA is overestimated and model estimate of median survival does not meet face validity: The outputs of the sponsor’s model indicate the median age of death for patients on ELX-TEZ-IVA is between 81.8 and 83.5 years depending on the genotype. In addition, the comparison to BSC resulted in nearly 30 undiscounted, incremental life-years-gained for ELX-TEZ-IVA in some genotypes. This result is highly unlikely or, at the very least, highly uncertain given the limitations of the long-term efficacy of ELX-TEZ-IVA and other CFTR modulators. The clinical experts consulted by CADTH for this review indicated that the sponsor’s base-case results overestimated the survival benefit of ELX-TEZ-IVA based on the evidence currently available. In addition to an overestimate of the magnitude of survival benefit with ELX-TEZ-IVA, the median age of death for patients on ELX-TEZ-IVA did not meet face validity. For example, the survival results for the F/F genotype in particular suggested a superior survival outcome for CF patients on ELX-TEZ-IVA compared with the general population. The sponsor’s model predicted that 4.4% of CF patients would still be alive at age 100, which is greater than the 3.5% observed in the general Canadian population (data from Statistics Canada from 2017 to 2019).38 These results do not meet face validity; the clinical experts consulted by CADTH reported that they did not expect the effects of ELX-TEZ-IVA would result in superior survival for CF patients than that of the general population.
While CADTH was unable to directly modify the survival assumptions for ELX-TEZ-IVA, the base-case changes in treatment efficacy corresponded to survival results in the CADTH base case that more accurately reflected clinical expert opinion.
Model lacked transparency and its programming prevented CADTH from fully exploring the associated uncertainties: The sponsor’s submitted model was programmed with limited transparency, with many inputs and outputs being the result of Visual Basic for Applications coding rather than formula-based operations. CADTH was unable to fully explore the uncertainty with parameters in the model, although results of the deterministic stepwise analysis met face validity.
CADTH was unable to address this limitation in reanalysis.
Additionally, several key assumptions were made by the sponsor and have been appraised by CADTH (Table 5).
Table 5: Key Assumptions of the Submitted Economic Evaluation (Not Noted as Limitations to the Submission)
Sponsor’s key assumption | CADTH comment |
|---|---|
Mortality with CF is assumed to be no lower than that of the general population. | Appropriate. |
Pancreatic insufficiency, prior respiratory infection, and CF-related diabetes status were assumed to remain unchanged from baseline over time. | Appropriate. |
Patients experience an acute change in weight-for-age z score, which is assumed to be maintained throughout their lifetime. | Uncertain. Once younger patients transition to adulthood the value of a weight-for-age z score increase would likely be diminished or at least uncertain, according to clinical experts. |
Data on the acute increase in ppFEV1 from the aged 12-and-older population were assumed to be applicable to the aged 6-to-11 population in the F/G and F/RF subgroups. | Appropriate, according to clinical experts. |
Treatment with ELX-TEZ-IVA would result in a 96-week “maintenance period” following this acute increase. | Appropriate, according to clinical experts. |
CF = cystic fibrosis; F/G = 1 F508del mutation and 1 gating mutation in the CFTR gene; F/RF = 1 F508del mutation and 1 residual function mutation in the CFTR gene; ppFEV1 = percent predicted forced expiratory volume in 1 second.
CADTH Reanalyses of the Economic Evaluation
Base-Case Results
The CADTH base case was derived by making changes in model parameter values and assumptions, in consultation with clinical experts. CADTH undertook a stepped analysis, incorporating each change detailed in Table 6 into the sponsor’s model to highlight the impact of each change. Each genotype is presented separately. The summary results of the CADTH reanalyses for the F/F genotype are presented in Table 7. The results for the F/MF, F/RF and F/G genotypes are presented in Appendix 4.
Table 6: CADTH Revisions to the Submitted Economic Evaluation
Stepped analysis | Sponsor’s value or assumption | CADTH value or assumption |
|---|---|---|
Changes to derive the CADTH base case | ||
1. Reduction in rate of ppFEV1 decline compared with BSC (after 96 weeks) | 80% for ELX-TEZ-IVA 47.1% for IVA 42% for LUM-IVA | No reduction in rate of decline of ppFEV1 |
2. Pulmonary exacerbation rate ratio with CFTR modulators compared to BSC | ELX-TEZ-IVA: 0.31 IVA: 0.72 LUM-IVA: 0.46 | 1.0 for all CFTR modulators |
3. Dynamic pricing of CFTR modulators | 25% price reduction after 18 years for ELX-TEZ-IVA, 10 years for LUM-IVA, and 8 years for IVA 50% price reduction after 19 years for ELX-TEZ-IVA, 11 years for LUM-IVA, and 9 years for IVA | No price reduction over entire time horizon |
4. Patient compliance rate in post-acute period | 93% | 100% |
5. Disease-management costs in period of survival benefit while on ELX-TEZ-IVA | Not included | Included |
6. Impact of ELX-TEZ-IVA on hospital and inpatient visit costs beyond impact on lung function | Annual inpatient costs BSC
CFTR modulator
Annual pharmacotherapy costs BSC
CFTR modulator
| Annual inpatient costs All comparators
Annual pharmacotherapy costs All comparators
|
7. Treatment-specific utility associated with ELX-TEZ-IVA | Included additional utility increment of 0.08 while on ELX-TEZ-IVA | No utility increment for ELX-TEZ-IVA use |
CADTH base case | Reanalysis 1 + 2 + 3 + 4 + 5 + 6 + 7 | |
BSC = best supportive care; ELX-TEZ-IVA = elexacaftor-tezacaftor-ivacaftor and ivacaftor; IVA = ivacaftor; LUM-IVA = lumacaftor-ivacaftor; ppFEV1 = percent predicted forced expiratory volume in 1 second.
For the F/F genotype, ELX-TEZ-IVA was associated with incremental costs of $4,043,775 and 5.94 QALYs when compared with LUM-IVA, for an ICER of $680,560 per QALY. Compared to BSC, ELX-TEZ-IVA was associated with incremental costs of $9,961,485 and 6.94 QALYs, for an ICER of $1,434,435 per QALY. In the heterozygous F/MF genotype, $9,684,715 in incremental costs and 5.86 incremental QALYs were observed for ELX-TEZ-IVA compared to BSC, for an ICER of $1,653,605 per QALY. In the heterozygous F/RF genotype, $10,174,150 in incremental costs and 4.17 incremental QALYs were observed for ELX-TEZ-IVA compared to BSC, for an ICER of $2,437,481 per QALY. And for the F/G genotype, ELX-TEZ-IVA was associated with an ICER of $1,531,443 when compared with BSC, and $622,381 when compared with IVA. The comparisons to LUM-IVA and IVA are based on publicly available prices. The full results of the CADTH base case are presented in Table 8 and examples of disaggregate results for all genotypes are available in Appendix 4.
The sponsor’s model also produced an overall ICER, weighted for each genotype and the relative market shares of the available comparators (in F/F, 98% BSC and 2% LUM-IVA; in F/G, 33% BSC and 67% IVA; all others, 100% BSC). The weighted ICER was $1,531,196 per QALY. The change to the sponsor’s base case that had the greatest impact on the results was the removal of dynamic pricing due to the introduction of generic options, emphasizing the impact of drug acquisition costs as a key driver of the model. The next most impactful change was that in which the reduction in rate of long-term ppFEV1 decline for CFTR modulators in comparison with BSC was removed.
Table 7: Summary of the Stepped Analysis of the CADTH Reanalysis Results — F/F Genotype (Deterministic)
Stepped analysis | Drug | Total costs ($) | Total QALYs | ICER ($ per QALY) |
|---|---|---|---|---|
Sponsor’s base case | BSCa | 964,725 | 24.2 | Reference |
ELX-TEZ-IVA | 7,589,601 | 39.9 | 422,519 | |
LUM-IVA | 4,747,123 | 29.7 | Reference | |
ELX-TEZ-IVA | 7,589,601 | 39.9 | 280,029 | |
CADTH reanalysis 1 – ppFEV1 decline | BSCa | 964,725 | 24.2 | Reference |
ELX-TEZ-IVA | 6,879,391 | 34.4 | 577,823 | |
LUM-IVA | 4,462,549 | 26.4 | Reference | |
ELX-TEZ-IVA | 6,879,391 | 34.4 | 302,622 | |
CADTH reanalysis 2 – pulmonary exacerbation rate ratio | BSCa | 964,725 | 24.2 | Reference |
ELX-TEZ-IVA | 7,597,453 | 39.6 | 430,334 | |
LUM-IVA | 4,778,502 | 29.0 | Reference | |
ELX-TEZ-IVA | 7,597,453 | 39.6 | 265,242 | |
CADTH reanalysis 3 – dynamic pricing | BSCa | 964,725 | 24.2 | Reference |
ELX-TEZ-IVA | 11,493,087 | 39.9 | 671,474 | |
LUM-IVA | 7,071,570 | 29.7 | Reference | |
ELX-TEZ-IVA | 11,493,087 | 39.9 | 435,589 | |
CADTH reanalysis 4 – compliance in post-acute phase | BSCa | 964,725 | 24.2 | Reference |
ELX-TEZ-IVA | 8,128,517 | 39.9 | 456,890 | |
LUM-IVA | 5,062,844 | 29.7 | Reference | |
ELX-TEZ-IVA | 8,128,517 | 39.9 | 302,017 | |
CADTH reanalysis 5 – survival costs included | BSCa | 964,725 | 24.2 | Reference |
ELX-TEZ-IVA | 7,726,321 | 39.9 | 431,239 | |
LUM-IVA | 4,872,496 | 29.7 | Reference | |
ELX-TEZ-IVA | 7,726,321 | 39.9 | 281,147 | |
CADTH reanalysis 6 – hospital costs | BSCa | 964,725 | 24.2 | Reference |
ELX-TEZ-IVA | 7,721,235 | 39.9 | 430,914 | |
LUM-IVA | 4,879,463 | 29.7 | Reference | |
ELX-TEZ-IVA | 7,721,235 | 39.9 | 279,959 | |
CADTH reanalysis 7 – treatment-specific utility | BSCa | 964,725 | 24.2 | Reference |
ELX-TEZ-IVA | 7,589,601 | 37.8 | 487,599 | |
LUM-IVA | 4,747,123 | 29.7 | Reference | |
ELX-TEZ-IVA | 7,589,601 | 37.8 | 352,756 | |
CADTH base case (1 + 2 + 3 + 4 + 5 + 6 + 7) (probabilistic) | BSCa | 880,221 | 24.0 | Reference |
ELX-TEZ-IVA | 10,841,706 | 31.0 | 1,434,435 | |
LUM-IVA | 6,797,931 | 25.0 | Reference | |
ELX-TEZ-IVA | 10,841,706 | 31.0 | 680,560 |
BSC = best supportive care; ELX-TEZ-IVA = elexacaftor-tezacaftor-ivacaftor and ivacaftor; F/F = homozygous for F508del mutation in the CFTR gene; ICER = incremental cost-effectiveness ratio; LUM-IVA = lumacaftor-ivacaftor;QALY = quality-adjusted life-year.
Table 8: Summary of the CADTH Base-Case Results by Genotype
Drug | Total costs ($) | Incremental costs ($) | Total QALYs | Incremental QALYs | ICER ($ per QALY) |
|---|---|---|---|---|---|
Homozygous for F508del-CFTR (F/F) | |||||
BSC | 880,221 | Reference | 24.0 | Reference | Reference |
ELX-TEZ-IVA | 10,841,706 | 9,961,485 | 31.0 | 6.9 | 1,434,435 |
LUM-IVA | 6,797,931 | Reference | 25.0 | Reference | Reference |
ELX-TEZ-IVA | 10,841,706 | 4,043,775 | 31.0 | 5.9 | 680,560 |
Heterozygous for F508del-CFTR (F/MF) | |||||
BSC | 877,546 | Reference | 24.1 | Reference | Reference |
ELX-TEZ-IVA | 10,562,262 | 9,684,715 | 29.9 | 5.9 | 1,653,605 |
Heterozygous for F508del-CFTR (F/RF) | |||||
BSC | 758,996 | Reference | 27.7 | Reference | Reference |
ELX-TEZ-IVA | 10,933,146 | 10,174,150 | 31.9 | 4.2 | 2,437,481 |
Heterozygous for F508del-CFTR (F/G) | |||||
BSC | 986,009 | Reference | 23.8 | Reference | Reference |
ELX-TEZ-IVA | 10,630,705 | 9,644,696 | 30.1 | 6.3 | 1,531,443 |
IVA | 9,782,785 | Reference | 28.8 | Reference | Reference |
ELX-TEZ-IVA | 10,630,705 | 847,920 | 30.1 | 1.4 | 622,381 |
BSC = best supportive care; ELX-TEZ-IVA = elexacaftor-tezacaftor-ivacaftor and ivacaftor; F/F = homozygous for F508del mutation in the CFTR gene; F/G = 1 F508del mutation and 1 gating mutation in the CFTR gene; F/MF = 1 F508del mutation and 1 minimal function mutation in the CFTR gene; F/RF = 1 F508del mutation and 1 residual function mutation in the CFTR gene; ICER = incremental cost-effectiveness ratio; IVA = ivacaftor; LUM-IVA = lumacaftor-ivacaftor; QALY = quality-adjusted life-year.
Source: Sponsor’s pharmacoeconomic submission.1
Scenario Analysis Results
Price-reduction analyses were conducted using the sponsor and CADTH base cases, assuming proportional price reductions for ELX-TEZ-IVA (Table 9) for the summary of price reductions. Appendix 4 provides full price-reduction analyses for all genotypes, including results for the entire population combined and weighted by prevalence and market shares, and in comparison with LUM-IVA for the F/F genotype and IVA for the F/G genotype. Using the CADTH base case, a price reduction in excess of 90% is required for ELX-TEZ-IVA to be cost-effective at a willingness-to-pay threshold of $50,000 per QALY in comparison with BSC for all genotypes. The price reduction required varies by genotype but is smallest for the F/F genotype and is greatest for the F/MF genotype.
Table 9: CADTH Price-Reduction Analyses
Analysis | ICERs for ELX-TEZ-IVA vs. BSC ($ per QALY) | |
|---|---|---|
Price reduction | Sponsor base case | CADTH reanalysis |
Homozygous for F508del-CFTR (F/F) | ||
No price reduction | 451,377 | 1,434,435 |
90% | 2,238 | 138,287 |
95% | Dominant | 64,365 |
99% | Dominant | 5,228 |
Heterozygous for F508del-CFTR (F/MF) | ||
No price reduction | 456,394 | 1,653,605 |
90% | 2,815 | 170,366 |
95% | Dominant | 82,030 |
99% | Dominant | 11,362 |
Heterozygous for F508del-CFTR (F/RF) | ||
No price reduction | 650,475 | 2,437,481 |
90% | 13,521 | 208,718 |
95% | Dominant | 91,356 |
99% | Dominant | Dominant |
Heterozygous for F508del-CFTR (F/G) | ||
No price reduction | 437,639 | 1,531,443 |
90% | Dominant | 149,509 |
95% | Dominant | 71,710 |
99% | Dominant | 9,471 |
BSC = best supportive care; ELX-TEZ-IVA = elexacaftor-tezacaftor-ivacaftor and ivacaftor; F/F = homozygous for F508del mutation in the CFTR gene; F/G = 1 F508del mutation and 1 gating mutation in the CFTR gene; F/MF = 1 F508del mutation and 1 minimal function mutation in the CFTR gene; F/RF = 1 F508del mutation and 1 residual function mutation in the CFTR gene; ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year.
CADTH also undertook a series of scenario analyses to determine the impact of alternative assumptions on the cost-effectiveness of ELX-TEZ-IVA. These included:
Assessing the cost-effectiveness of ELX-TEZ-IVA in the entire Health Canada population (i.e., all patients greater than 6 years of age), not just those aged 6 to 11.
A reduction in pulmonary exacerbations observed with ELX-TEZ-IVA, LUM-IVA, and IVA based on observed trial data was assumed to apply in the period for which there was no available data for the entire time horizon, according to the sponsor’s base-case assumption.
The rates of ppFEV1 decline with ELX-TEZ-IVA, LUM-IVA, and IVA were 80.0%, 42.0%, and 47.1% slower, respectively, in comparison with BSC, according to the sponsor’s base-case assumption.
Treatment-specific utility increment from benefits beyond improvements in lung function and pulmonary exacerbations for patients on ELX-TEZ-IVA were included, according to the sponsor’s base-case assumption.
The results of CADTH scenario analyses are available in Table 10 for the F/F genotype and Appendix 4 for the F/MF, F/RF and F/G genotypes. The key scenario assessing the cost-effectiveness of ELX-TEZ-IVA in the full Health Canada population resulted in ICERs ranging from $1,129,990 to $1,868,095 per QALY compared to BSC, and an overall weighted ICER of $1,136,142 per QALY. These results for the full population are similar to those observed in the previous review of ELX-TEZ-IVA in patients aged 12 and older only, with ICERs in excess of $1 million observed for all genotypes compared to BSC.2
Among the other scenarios highlighting the impact of assuming additional benefit with ELX-TEZ-IVA despite a lack of supporting evidence, none produced an ICER below $878,073 per QALY when compared to BSC. These scenario analyses are again driven by the high drug acquisition costs with ELX-TEZ-IVA that offset the estimated QALY gains.
Table 10: Summary of the CADTH Scenario Analyses — F/F Genotype
Scenario analysis | Drug | Total costs ($) | Total QALYs | ICER ($ per QALYs) |
|---|---|---|---|---|
1. Entire Health Canada populationa | BSC | 1,321,324 | 20.27 | Reference |
ELX-TEZ-IVA | 9,376,702 | 27.40 | 1,129,990 | |
LUM-IVA | 6,016,382 | 21.41 | Reference | |
ELX-TEZ-IVA | 9,376,702 | 27.40 | 560,841 | |
2. Long-term reduction in pulmonary exacerbations included for CFTR modulators | BSC | 964,725 | 24.2 | Reference |
ELX-TEZ-IVA | 11,112,535 | 32.3 | 1,251,228 | |
LUM-IVA | 7,071,221 | 26.4 | Reference | |
ELX-TEZ-IVA | 11,112,535 | 32.3 | 689,583 | |
3. Slower rate of decline in ppFEV1 | BSC | 964,725 | 24.2 | Reference |
ELX-TEZ-IVA | 12,657,560 | 37.5 | 878,073 | |
LUM-IVA | 7,817,789 | 29.0 | Reference | |
ELX-TEZ-IVA | 12,657,560 | 37.5 | 567,291 | |
4. Inclusion of treatment-specific utility increment for patients on ELX-TEZ-IVA | BSC | 964,725 | 24.2 | Reference |
ELX-TEZ-IVA | 10,869,281 | 33.0 | 1,129,225 | |
LUM-IVA | 6,883,525 | 25.1 | Reference | |
ELX-TEZ-IVA | 10,869,281 | 33.0 | 505,890 |
BSC = best supportive care; ELX-TEZ-IVA = elexacaftor-tezacaftor-ivacaftor and ivacaftor; F/F = homozygous for F508del mutation in the CFTR gene; ICER = incremental cost-effectiveness ratio; LUM-IVA = lumacaftor-ivacaftor; ppFEV1 = percent predicted forced expiratory volume in 1 second; QALY = quality-adjusted life-year.
aThis scenario was run probabilistically, while the other scenarios were run deterministically.
Issues for Consideration
CADTH previously reviewed ELX-TEZ-IVA for the treatment of CF in patients aged 12 years and older who have at least 1 F508del-CFTR mutation.2 The submitted price in that review was the same, with a daily cost of $840, or $280 per tablet. The committee recommended reimbursement of ELX-TEZ-IVA with conditions, including a price reduction of 90%. Results from the current review of ELX-TEZ-IVA were similar, indicating that this drug is not cost-effective at the submitted price and would require a significant price reduction.
CADTH reviewed LUM-IVA in 2018 for the treatment of CF in patients aged 6 and older who are homozygous for the F508del mutation. Based on a lack of clinical evidence, the committee recommended not reimbursing LUM-IVA in this population.39 CADTH also reviewed IVA monotherapy in 2015 for the treatment of CF in patients with the R117H gating mutation. The committee recommended reimbursement of IVA with conditions, including a substantial reduction in price as the drug was not considered cost-effective at the submitted price.40
Overall Conclusions
The clinical evidence submitted by the sponsor demonstrated that ELX-TEZ-IVA led to statistically and clinically significant improvements in acute ppFEV1 and weight-for-age z scores when compared with relevant comparators in patients aged 6 to 11 years with the F/F and F/MF genotypes. There were no clinical studies conducted with ELX-TEZ-IVA in pediatric patients with the F/RF or F/G genotypes; however, the clinical experts noted that ELX-TEZ-IVA would result in clinically meaningful improvements for these patients, based on the evidence reported for ELX-TEZ-IVA in adult patients with F/RF and F/G genotypes and the results in F/F and F/MF pediatric studies. Results were similar in patients aged 12 year and older with regard to acute change in ppFEV1 in all genotypes, and evidence from 1 trial in the F/F subgroup indicated ELX-TEZ-IVA reduced the rate of pulmonary exacerbations in comparison with placebo. However, these conclusions were based on short-term studies (maximum of 96 weeks) and there was no evidence on the long-term impact of ELX-TEZ-IVA on the rate of decline of ppFEV1, or pulmonary exacerbation rates beyond the trial period for any genotype or age group.
Beyond a lack of evidence on the long-term benefits of ELX-TEZ-IVA, CADTH identified several additional major limitations with the submitted economic evaluation. The sponsor included several assumptions around drug costs and health care resource use, including dynamic drug pricing due to generic entry, adjusting drug costs for patient compliance, adjustment of hospital and pharmacotherapy costs, and the exclusion of disease-management costs for the period for which ELX-TEZ-IVA was associated with a survival benefit. These assumptions led to an underestimate of the total drug acquisition and health care costs associated with ELX-TEZ-IVA. The sponsor also included a treatment-specific utility increment to account for the impact of treatment with ELX-TEZ-IVA beyond its impact mediated by ppFEV1 and pulmonary exacerbations, but the estimate by the sponsor likely leads to double counting of benefits already incorporated in the model.
Several of these limitations were addressed in the CADTH base-case reanalysis. Changes to the model included: removal of an additional benefit of CFTR modulators on the long-term rate of decline in ppFEV1 and pulmonary exacerbations beyond those mediated by ppFEV1; the removal of dynamic pricing of CFTR modulators; the inclusion of costs for ELX-TEZ-IVA in the period for which it achieved a survival benefit in comparison with BSC; the removal of an adjustment to drug acquisition costs by patient compliance; the removal of an adjustment to hospital and pharmacotherapy costs; and the removal of a treatment-specific utility increment for patients on ELX-TEZ-IVA. In comparison with BSC, the CADTH base-case analysis resulted in an ICER of $1,434,435 per QALY in the F/F genotype; $1,653,605 per QALY in the F/MF genotype; $2,437,481 per QALY in the F/RF genotype; and $1,531,443 per QALY in the F/G genotype. For the F/F genotype, a pairwise ICER of $680,560 per QALY was estimated compared to LUM-IVA. For the F/G genotype, a pairwise ICER of $622,381 per QALY was estimated in comparison with IVA monotherapy. Results of the CADTH reanalysis were aligned with the sponsor’s, in that ELX-TEZ-IVA is not cost-effective in any of the genotype subgroups at conventionally acceptable ICER thresholds.
The key drivers in the analysis were the acquisition costs of CFTR modulators, as well assumptions related to the long-term benefits associated with ELX-TEZ-IVA, which were uncertain. ELX-TEZ-IVA was not cost-effective at a willingness-to-pay threshold of $50,000 per QALY in any scenario conducted by CADTH, including scenarios in which CADTH reincorporated the additional long-term benefits of reducing the rate of decline of ppFEV1, additional benefits on rates of pulmonary exacerbations, or the on-treatment utility increment with ELX-TEZ-IVA. The price reduction required for ELX-TEZ-IVA to be considered cost-effective at a willingness-to-pay threshold of $50,000 per QALY ranges from 90% to greater than 95%, depending on the comparator and genotype considered. These results are aligned with the findings of the previous CADTH review of ELX-TEZ-IVA, which suggested a price reduction in excess of 90% was required when considering a patient population 12 years of age and older. When CADTH conducted a scenario analysis that considered the entire population aged 6 years and older, results and conclusions were aligned with those from the 6-to-11 and 12-and-older age groups analyzed separately.
References
1.Pharmacoeconomic evaluation [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Trikafta (triple combination therapy [elexacaftor/tezacaftor/ivacaftor & ivacaftor]) tablets, oral 100 mg/50 mg/75 mg and 150 mg. Toronto (ON): Vertex Pharmaceuticals (Canada) Incorporated; 2021 Jan 22.
2.CADTH. CADTH Reimbursement Recommendation elexacaftor-tezacaftor-ivacaftor and ivacaftor (Trikafta). 2021; https://www.cadth.ca/sites/default/files/DRR/2021/SR0673%20Trikafta%20-%20CADTH%20Final%20Rec%20Revised.pdf. Accessed Jan 21, 2022.
3.Trikafta®, 100 mg elexacaftor, 50 mg tezacaftor, 75 mg ivacaftor (combination tablet) and 150 mg ivacaftor [product monograph]. Toronto (ON): Vertex Pharmaceuticals (Canada) Incorporated; 2020 Nov 11.
4.Liou TG, Adler FR, Fitzsimmons SC, Cahill BC, Hibbs JR, Marshall BC. Predictive 5-year survivorship model of cystic fibrosis. Am J Epidemiol. 2001;153(4):345-352. PubMed
5.Stephenson AL, Tom M, Berthiaume Y, et al. A contemporary survival analysis of individuals with cystic fibrosis: a cohort study. Eur Respir J. 2015;45(3):670-679. PubMed
6.Milla C, Ratjen F, Marigowda G, Liu F, Waltz D. Lumacaftor/ivacaftor in patients aged 6-11 years with cystic fibrosis and homozygous for F508del-CFTR. Am J Respir Crit Care Med. 2017;195(7):912-920. PubMed
7.Ratjen F, Hug C, Marigowda G, Tian S, Huang X. Efficacy and safety of lumacaftor and ivacaftor in patients aged 6-11 years with cystic fibrosis homozygous for F508del-CFTR: a randomised, placebo-controlled phase 3 trial. Lancet Respir Med. 2017;5(7):557-567. PubMed
8.Zemanick E, Taylor-Cousar JL, Davies J, Gibson R, Mall M. A phase 3 open-abel study of ELX/TEZ/IVA in children 6 through 11 years of age with CF and at least one F508del allele. Am J Respir Crit Care Med. 2021.
9.Walker S, Flume PA, McNamara J, Solomon M, Chilvers MA. A phase 3 study of tezacaftor in combination with ivacaftor in children aged 6 through 11 years with cystic fibrosis. Journal of cystic fibrosis: official journal of the European Cystic Fibrosis Society. 2019;18(5):708-713.
10.Davies J, Sermet-Gaudelus I, Naehrlich L, Harris R, Campbell D. A phase 3, double-blind, parallel-group study to evaluate the efficacy and safety of tezacaftor in combination with ivacaftor in participants 6 through 11 years of age with cystic fibrosis homozygous for F508del or heterozygous for the F508del-CFTR mutation and a residual function mutation. Journal of cystic fibrosis: official journal of the European Cystic Fibrosis Society. 2021;20(1):68-77.
11.Incorporated VP. A Phase 3b, Randomized, Placebo-controlled Study Evaluating the Efficacy and Safety of Elexacaftor/Tezacaftor/Ivacaftor in Cystic Fibrosis Subjects 6 Through 11 Years of Age Who Are Heterozygous for the F508del Mutation and a Minimal Function Mutation (F/MF). Clinical Study Report (Study VX19-445-116; version 1.0). 2021.
12.Davies JC, Wainwright CE, Canny GJ, et al. Efficacy and safety of ivacaftor in patients aged 6 to 11 years with cystic fibrosis with a G551D mutation. Am J Respir Crit Care Med. 2013;187(11):1219-1225. PubMed
13.De Boeck K, Munck A, Walker S, et al. Efficacy and safety of ivacaftor in patients with cystic fibrosis and a non-G551D gating mutation. J Cyst Fibros. 2014;13(6):674-680. PubMed
14.Moss R, Flume PA, Elborn JS, Cooke J, Rowe S. Efficacy and safety of ivacaftor in patients with cystic fibrosis who have an Arg117His-CFTR mutation: a double-blind, randomised controlled trial. Lancet Respir Med. 2015;3(7):524-533. PubMed
15.Whiting P, Al M, Burgers L, et al. Ivacaftor for the treatment of patients with cystic fibrosis and the G551D mutation: a systematic review and cost-effectiveness analysis. Health Technol Assess. 2014;18(18):1-106. PubMed
16.Canada CF. The Canadian cystic fibrosis patient registry 2018 annual data report. Toronto, Ontario2019.
17.Barry P, Mall M, Alvarez A, Colombo C, de Winter-de Groot K. Triple Therapy for Cystic Fibrosis Phe508del-Gating and -Residual Function Genotypes. NEJM. 2021;385(9):815-825. PubMed
18.Leung GJ, Cho TJ, Kovesi T, Hamid JS, Radhakrishnan D. Variation in lung function and nutritional decline in cystic fibrosis by genotype: an analysis of the Canadian cystic fibrosis registry. J Cyst Fibros. 2020;19(2):255-261. PubMed
19.Griese M, Costa S, Linnemann R, Mall M, McKone EF. Safety and Efficacy of Elexacaftor/Tezacaftor/Ivacaftor for≥ 24 Weeks in People With CF and≥ 1 F508del Allele: Interim Results of an Open-Label Phase Three Clinical Trial. Am J Respir Crit Care Med. 2020.
20.Konstan MW, McKone EF, Moss R, Marigowda G, Tian S. Assessment of safety and efficacy of long-term treatment with combination lumacaftor and ivacaftor therapy in patients with cystic fibrosis homozygous for the F508del-CFTR mutation (PROGRESS): a phase 3, extension study. Lancet Respir Med. 2017;5(2):107-118. PubMed
21.Sawicki G, McKone EF, Pasta D, Millar S, Wagener J. Sustained Benefit from ivacaftor demonstrated by combining clinical trial and cystic fibrosis patient registry data. Am J Respir Crit Care Med. 2015;192(7):836-842. PubMed
22.Goss CH, Burns JL. Exacerbations in cystic fibrosis. 1: Epidemiology and pathogenesis. Thorax. 2007;62(4):360-367. PubMed
23.Clinical Study Report: study 102. A phase 3, randomized, double-blind, controlled study evaluating the efficacy and safety of VX-445 combination therapy in subjects with cystic fibrosis who are heterozygous for the F508del mutation and a minimal function mutation (F/MF) [internal sponsor's report]. Toronto (ON): Vertex Pharmaceuticals Incorporated; 2019 Jul 2.
24.Clinical Study Report: study 103. A phase 3, randomized, double-blind, controlled study evaluating the efficacy and safety of VX-445 combination therapy in subjects with cystic fibrosis who are homozygous for the F508del mutation (F/F) [internal sponsor's report]. Toronto (ON): Vertex Pharmaceuticals Incorporated; 2019 Jun 18.
25.Clinical Study Report: study 104. A phase 3, randomized, double-blind, controlled study evaluating the efficacy and safety of elexacaftor combination therapy in subjects with cystic fibrosis who are heterozygous for the F508del mutation and a gating or residual function mutation (F/G and F/RF Genotypes) [internal sponsor's report]. Toronto (ON): Vertex Pharmaceuticals Incorporated; 2020 Aug 21.
26.Clinical Study Report: study 109. A phase 3b, randomized, double-blind, controlled study evaluating the efficacy and safety of elexacaftor/tezacaftor/ivacaftor in cystic fibrosis subjects, homozygous for F508del [internal sponsor's report]. Toronto (ON): Vertex Pharmaceuticals Incorporated; 2020 Oct 16.
27.Stephenson AL, Sykes J, Berthiaume Y, et al. Clinical and demographic factors associated with post-lung transplantation survival in individuals with cystic fibrosis. J Heart Lung Transplant. 2015;34(9):1139-1145. PubMed
28.Exceptional Access Program (EAP). Toronto (ON): Ontario Ministry of Health, Ontario Ministry of Long-Term Care; 2021: https://www.health.gov.on.ca/en/pro/programs/drugs/odbf/odbf_except_access.aspx. Accessed 2021 Apr 22.
29.Government of Saskatchewan Drug Plan and Extended Benefits Branch. Pan-Canadian generics. Pan-Canadian tiered pricing framework. 2014: http://formulary.drugplan.health.gov.sk.ca/PanCanadianGenerics. Accessed 2021 Apr 22.
30.Schedule of benefits for physician services under the Health Insurance Act: effective April 1, 2020. Toronto (ON): Ontario Ministry of Health; 2020: https://www.health.gov.on.ca/en/pro/programs/ohip/sob/physserv/sob_master20200306.pdf. Accessed 2021 Apr 22.
31.Schedule of benefits for laboratory services: effective July 1, 2020. Toronto (ON): Ontario Ministry of Health; 2020: https://www.health.gov.on.ca/en/pro/programs/ohip/sob/lab/lab_mn2020.pdf. Accessed 1800 Jan 1.
32.Skolnik K, Ronksley P, Pendharkar S, Wick J, Quon B. Hospitalization-related costs for canadian cystic fibrosis patients. Pedatr Pulmonol. 2018;53(S2):S148-S456.
33.Feng LB, Grosse SD, Green RF, Fink AK, Sawicki GS. Precision medicine in action: the impact of ivacaftor on cystic fibrosis-related hospitalizations. Health Aff (Millwood). 2018;37(5):773-779. PubMed
34.Hassan M, Bonafede M, Limone B, Hodgkins P, Suthoff E, Sawicki G. 28 Reduction in pulmonary exacerbations (PEx) after initiation of ivacaftor: a retrospective cohort study among patients with cystic fibrosis (CF) treated in real-world settings. J Cyst Fibros. 2016;15.
35.Government of Alberta. Alberta Interactive Health Data Application. Average cost of lung transplant procedure in 2017/2018. 2019; http://www.ahw.gov.ab.ca/IHDA_Retrieval/. Accessed 2021 Apr 22.
36.Vasiliadis H-M, Collet J-P, Penrod JR, Ferraro P, Poirier C. A cost-effectiveness and cost-utility study of lung transplantation. J Heart Lung Transplant. 2005;24(9):1275-1283. PubMed
37.Solem CT, Vera-Llonch M, Tai M, O’Callaghan L. Pulmonary exacerbations, lung dysfunction, and Eq-5d measures in adolescents and adults with cystic fibrosis and homozygous for the F508del-Cftr mutation. Value Health. 2016;19(3):A116-A117.
38.Table: 13-10-0114-01. Life expectancy and other elements of the life table, Canada, all provinces except Prince Edward Island. Ottawa (ON): Statistics Canada; 2020: https://www150.statcan.gc.ca/t1/tbl1/en/tv.action?pid=1310011401. Accessed 1800 Mth Dd.
39.CADTH. CADTH Canadian Drug Expert Committee Recommendation LUM/IVA. 2018; https://www.cadth.ca/sites/default/files/cdr/complete/SR0559%20Orkambi%20-%20CDEC%20Final%20Recommendation%20October%204%2C%202018.pdf. Accessed Jan 21, 2022.
40.CADTH. CADTH Canadian Drug Expert Committee Final Recommendation Ivacaftor. 2015; https://www.cadth.ca/sites/default/files/cdr/complete/SR0430_complete_Kalydeco_R117H_Nov-23-15_e.pdf. Accessed Jan 21, 2022.
41.Kalydeco®, Ivacaftor tablets150 mg, Ivacaftor granules 50 mg per packet, 75 mg per packet [product monograph]. Toronto, Ontario: Vertex Pharmaceuticals (Canada) Incorporated; 2019: https://pdf.hres.ca/dpd_pm/00049400.PDF.
42.Incorporated vP. Orkambi product monograph. 2017; https://pdf.hres.ca/dpd_pm/00041660.PDF. Accessed Dec 17, 2021.
43.Table: 17-10-0057-01 Projected population, by projection scenario, age and sex, as of July 1 (x 1,000). Ottawa (ON: Statistics Canada; 2022: https://www150.statcan.gc.ca/t1/tbl1/en/tv.action?pid=1710005701. Accessed 1800 Jan 1.
Appendix 1: Cost-Comparison Table
Note that this appendix has not been copy-edited.
The comparators presented in the following table have been deemed to be appropriate based on feedback from clinical expert(s) and drug plans. Comparators may be recommended (appropriate) practice or actual practice. Existing product listing agreements are not reflected in the table and, as such, the table may not represent the actual costs to public drug plans.
Table 11: CADTH Cost-Comparison Table of CFTR-Modulator Therapies for Cystic Fibrosis
Treatment | Strength | Form | Price ($) | Recommended dosagea | Daily cost ($) | Annual cost ($) |
|---|---|---|---|---|---|---|
Elexacaftor- tezacaftor-ivacaftor (Trikafta) | 100 mg/ 50 mg/ 75 mg 50 mg/ 25 mg/ 37.5 mg | Tablet | 280.0000a | Two tablets in the morning | 560.00 | 204,540 |
Ivacaftor | 150 mg 75 mg | Tablet | 280.0000a | 150 mg in evening at least 12 hours apart from elexacaftor- tezacaftor-ivacaftor dose | 280.00 | 102,270 |
Regimen cost | 840.00 | 306,810 | ||||
CFTR-modulator therapies | ||||||
Ivacaftor (Kalydeco) | 150 mg | Tablet | 420.0000 | 150 mg twice daily | 840.00 | 306,810 |
Lumacaftor- ivacaftor (Orkambi) | 100 mg/ 125 mg | Tablet | 170.5357 | 200/250 mg twice daily | 682.14 | 249,153 |
Note: All prices are from the Ontario Exceptional Access Program formulary (accessed December 2021),28 unless otherwise indicated, and do not include dispensing fees. Annual costs are based on 365.25 days per year.
aRecommended dosages are from the respective product monographs.3,41,42
bSponsor submitted price.1
Appendix 2: Submission Quality
Note that this appendix has not been copy-edited.
Description | Yes/No | Comments |
|---|---|---|
Population is relevant, with no critical intervention missing, and no relevant outcome missing | Yes | No comment |
Model has been adequately programmed and has sufficient face validity | No | Model lacks transparency with regards to programming, leading to some issues with some scenario analyses |
Model structure is adequate for decision problem | Yes | No comment |
Data incorporation into the model has been done adequately (e.g., parameters for probabilistic analysis) | No | Deterministic results change when running the model probabilistically, which is unexpected and difficult to validate due to the lack of transparency |
Parameter and structural uncertainty were adequately assessed; analyses were adequate to inform the decision problem | Yes | No comment |
The submission was well organized and complete; the information was easy to locate (clear and transparent reporting; technical documentation available in enough details) | Yes | No comment |
Appendix 3: Additional Information on the Submitted Economic Evaluation
Note that this appendix has not been copy-edited.
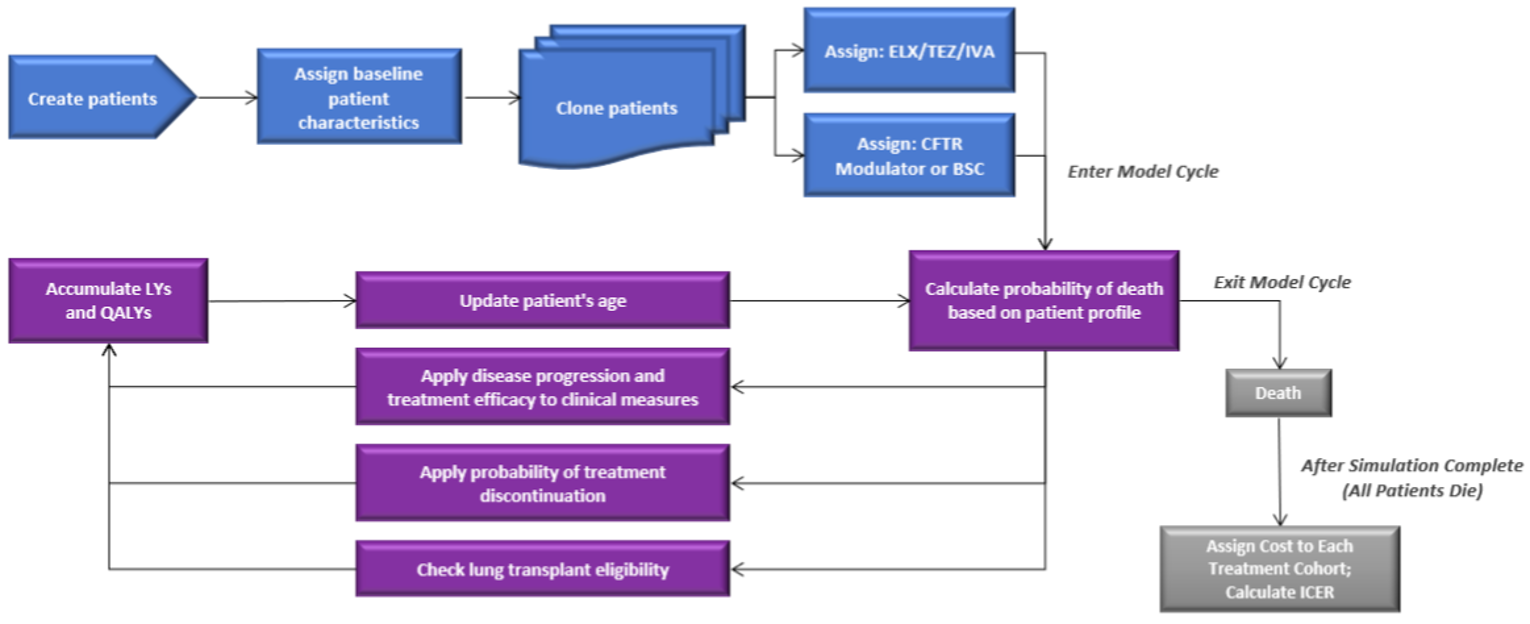
Appendix 4: Additional Details on the CADTH Reanalyses and Sensitivity Analyses of the Economic Evaluation
Note that this appendix has not been copy-edited.
Detailed Results of CADTH Base Case
Table 13: Disaggregated Summary of CADTH’s Economic Evaluation Results — F/F Genotype
Parameter | ELX-TEZ-IVA | LUM-IVA | Incremental | ELX-TEZ-IVA | BSC | Incremental |
|---|---|---|---|---|---|---|
Discounted LYs | ||||||
Total | 33.26 | 27.13 | 6.12 | 33.26 | 26.09 | 7.17 |
Discounted QALYs | ||||||
Total | 30.98 | 25.04 | 5.94 | 30.98 | 24.03 | 6.94 |
Discounted costs | ||||||
Total | $10,841,706 | $6,797,931 | $4,043,775 | $10,841,706 | $880,221 | $9,961,485 |
Drug acquisition | $10,017,041 | $5,928,879 | $4,088,162 | $10,017,041 | $0 | $10,017,041 |
Non-PEx–related disease-management costs | $500,805 | $432,980 | $67,825 | $500,805 | $419,324 | $81,481 |
PEx-related costs | $320,289 | $433,214 | -$112,925 | $320,289 | $457,812 | -$137,522 |
Lung transplant costs | $290 | $590 | -$342 | $290 | $652 | -$362 |
Adverse event cost | $3,056 | $2,070 | $986 | $3,056 | $2,434 | $622 |
Monitoring Cost | $225 | $197 | $27 | $225 | $0 | $225 |
ICER ($/QALY) | 680,560 | 1,434,435 | ||||
BSC = best supportive care; ELX = elexacaftor; ICER = incremental cost-effectiveness ratio; IVA = ivacaftor; LY = life-year; PEx = pulmonary exacerbations; QALY = quality-adjusted life-year; TEZ = tezacaftor.
Table 14: Disaggregated Summary of CADTH’s Economic Evaluation Results — F/MF Genotype
Parameter | ELX-TEZ-IVA | BSC | Incremental |
|---|---|---|---|
Discounted LYs | |||
Total | 32.14 | 26.11 | 6.03 |
Discounted QALYs | |||
Total | 29.92 | 24.06 | 5.86 |
Discounted costs | |||
Total | $10,562,262 | $877,546 | $9,684,715 |
Drug acquisition | $9,728,512 | $0 | $9,728,512 |
Non-PEx–related disease-management costs | $486,691 | $419,063 | $67,627 |
PEx-related costs | $342,676 | $455,404 | −$112,728 |
Lung transplant costs | $245 | $641 | −$396 |
Adverse event cost | $3,916 | $2,438 | $1,478 |
Monitoring cost | $223 | $0 | $223 |
ICER ($ per QALY) | 1,653,605 | ||
BSC = best supportive care; ELX = elexacaftor; ICER = incremental cost-effectiveness ratio; IVA = ivacaftor; LY = life-year; PEx = pulmonary exacerbations; QALY = quality-adjusted life-year; TEZ = tezacaftor.
Table 15: Disaggregated Summary of CADTH’s Economic Evaluation Results — F/RF Genotype
Parameter | ELX-TEZ-IVA | BSC | Incremental |
|---|---|---|---|
Discounted LYs | |||
Total | 34.08 | 29.85 | 4.22 |
Discounted QALYs | |||
Total | 31.85 | 27.68 | 4.17 |
Discounted costs | |||
Total | $10,933,146 | $758,996 | $10,174,150 |
Drug acquisition | $10,254,499 | $0 | $10,254,499 |
Non-PEx–related disease-management costs | $487,391 | $447,676 | $39,715 |
PEx-related costs | $187,190 | $308,301 | −$121,111 |
Lung transplant costs | $0 | $4 | −$4 |
Adverse event cost | $3,840 | $3,014 | $826 |
Monitoring cost | $226 | $0 | $226 |
ICER ($ per QALY) | 2,437,481 | ||
BSC = best supportive care; ELX = elexacaftor; ICER = incremental cost-effectiveness ratio; IVA = ivacaftor; LY = life-year; PEx = pulmonary exacerbations; QALY = quality-adjusted life-year; TEZ = tezacaftor.
Table 16: Disaggregated Summary of CADTH’s Economic Evaluation Results — F/Gating Genotype
Parameter | ELX-TEZ-IVA | IVA | Incremental | ELX-TEZ-IVA | BSC | Incremental |
|---|---|---|---|---|---|---|
Discounted LYs | ||||||
Total | 32.42 | 31.15 | 1.26 | 32.42 | 25.96 | 6.45 |
Discounted QALYs | ||||||
Total | 30.13 | 28.77 | 1.36 | 30.13 | 23.83 | 6.30 |
Discounted costs | ||||||
Total | $10,630,705 | $9,782,785 | $847,920 | $10,630,705 | $986,009 | $9,644,696 |
Drug acquisition | $9,749,220 | $8,840,577 | $908,644 | $9,749,220 | $0 | $9,749,220 |
Non-PEx–related disease-management costs | $496,678 | $490,490 | $6,188 | $496,678 | $432,287 | $64,390 |
PEx-related costs | $380,507 | $448,702 | −$68,194 | $380,507 | $550,239 | −$169,732 |
Lung transplant costs | $420 | $743 | −$373 | $420 | $1,071 | −$651 |
Adverse event cost | $3,657 | $2,055 | $1,602 | $3,657 | $2,412 | $1,245 |
Monitoring cost | $222 | $219 | $3 | $222 | $0 | $222 |
ICER ($ per QALY) | 622,381 | — | ||||
BSC = best supportive care; ELX = elexacaftor; ICER = incremental cost-effectiveness ratio; IVA = ivacaftor; LY = life-year; QALY = quality-adjusted life-year; PEx = pulmonary exacerbations; TEZ = tezacaftor.
Table 17: Summary of the Stepped Analysis of the CADTH Reanalysis Results — F/MF Genotype (Deterministic)
Stepped analysis | Drug | Total costs ($) | Total QALYs | ICER ($/QALYs) |
|---|---|---|---|---|
Sponsor’s base case | BSCa | 981,560 | 24.3 | Ref. |
ELX-TEZ-IVA | 7,658,936 | 39.9 | 428,334 | |
CADTH reanalysis 1 – ppFEV1 decline | BSCa | 981,560 | 24.3 | Ref. |
ELX-TEZ-IVA | 6,838,303 | 33.6 | 632,730 | |
CADTH reanalysis 2 – pulmonary exacerbations | BSCa | 981,560 | 24.3 | Ref. |
ELX-TEZ-IVA | 7,642,678 | 39.3 | 444,103 | |
CADTH reanalysis 3 – dynamic pricing | BSCa | 981,560 | 24.3 | Ref. |
ELX-TEZ-IVA | 11,582,906 | 39.9 | 680,045 | |
CADTH reanalysis 4 – compliance | BSCa | 981,560 | 24.3 | Ref. |
ELX-TEZ-IVA | 8,201,530 | 39.9 | 463,140 | |
CADTH reanalysis 5 – survival costs | BSCa | 981,560 | 24.3 | Ref. |
ELX-TEZ-IVA | 7,806,879 | 39.9 | 437,824 | |
CADTH reanalysis 6 – hospital costs | BSCa | 981,560 | 24.3 | Ref. |
ELX-TEZ-IVA | 7,795,353 | 39.9 | 437,084 | |
CADTH reanalysis 7 – treatment-specific utility | BSCa | 981,560 | 24.3 | Ref. |
ELX-TEZ-IVA | 7,658,936 | 37.7 | 498,018 | |
CADTH base case (1 + 2 + 3 + 4 + 5 + 6 + 7) (probabilistic) | BSCa | 877,546 | 24.1 | Ref. |
ELX-TEZ-IVA | 10,562,262 | 29.9 | 1,653,605 |
BSC = best supportive care; ELX = elexacaftor; ICER = incremental cost-effectiveness ratio; IVA = ivacaftor; QALY = quality-adjusted life-year; TEZ = tezacaftor; Ref = reference.
Table 18: Summary of the Stepped Analysis of the CADTH Reanalysis Results — F/RF Genotype (Deterministic)
Stepped analysis | Drug | Total costs ($) | Total QALYs | ICER ($/QALYs) |
|---|---|---|---|---|
Sponsor’s base case | BSCa | 857,471 | 27.6 | Ref. |
ELX-TEZ-IVA | 7,455,693 | 38.8 | 590,066 | |
CADTH reanalysis 1 – ppFEV1 decline | BSCa | 857,471 | 27.6 | Ref. |
ELX-TEZ-IVA | 7,041,896 | 35.7 | 769,726 | |
CADTH reanalysis 2 – pulmonary exacerbations | BSCa | 857,471 | 27.6 | Ref. |
ELX-TEZ-IVA | 7,405,692 | 38.1 | 623,394 | |
CADTH reanalysis 3 – dynamic pricing | BSCa | 857,471 | 27.6 | Ref. |
ELX-TEZ-IVA | 11,211,136 | 38.8 | 925,907 | |
CADTH reanalysis 4 – compliance | BSCa | 857,471 | 27.6 | Ref. |
ELX-TEZ-IVA | 7,982,670 | 38.8 | 637,192 | |
CADTH reanalysis 5 – survival costs | BSCa | 857,471 | 27.6 | Ref. |
ELX-TEZ-IVA | 7,545,032 | 38.8 | 598,055 | |
CADTH reanalysis 6 – hospital costs | BSCa | 857,471 | 27.6 | Ref. |
ELX-TEZ-IVA | 7,604,083 | 38.8 | 603,336 | |
CADTH reanalysis 7 – treatment-specific utility | BSCa | 857,471 | 27.6 | Ref. |
ELX-TEZ-IVA | 7,455,693 | 36.8 | 721,109 | |
CADTH base case (1 + 2 + 3 + 4 + 5 + 6 + 7 + 8) (probabilistic) | BSCa | 758,996 | 27.7 | Ref. |
ELX-TEZ-IVA | 10,933,146 | 31.9 | 2,437,481 |
BSC = best supportive care; ELX = elexacaftor; ICER = incremental cost-effectiveness ratio; IVA = ivacaftor; QALY = quality-adjusted life-year; TEZ = tezacaftor; Ref = reference.
Table 19: Summary of the Stepped Analysis of the CADTH Reanalysis Results – F/Gating Genotype (Deterministic)
Stepped analysis | Drug | Total costs ($) | Total QALYs | ICER ($/QALYs) |
|---|---|---|---|---|
Sponsor’s base case | BSCa | 1,130,392 | 23.9 | Ref. |
ELX-TEZ-IVA | 7,571,466 | 39.5 | 412,948 | |
IVA | 6,449,503 | 33.6 | Ref. | |
ELX-TEZ-IVA | 7,571,466 | 39.5 | 188,801 | |
CADTH reanalysis 1 – ppFEV1 decline | BSCa | 1,130,392 | 23.9 | Ref. |
ELX-TEZ-IVA | 6,832,477 | 33.6 | 589,534 | |
IVA | 5,934,341 | 29.0 | Ref. | |
ELX-TEZ-IVA | 6,832,477 | 33.6 | 196,841 | |
CADTH reanalysis 2 – pulmonary exacerbations | BSCa | 1,130,392 | 23.9 | Ref. |
ELX-TEZ-IVA | 7,594,910 | 39.1 | 426,561 | |
IVA | 6,466,714 | 33.2 | Ref. | |
ELX-TEZ-IVA | 7,594,910 | 39.1 | 193,102 | |
CADTH reanalysis 3 – dynamic pricing | BSCa | 1,130,392 | 23.9 | Ref. |
ELX-TEZ-IVA | 11,434,473 | 39.5 | 660,611 | |
IVA | 10,102,752 | 33.6 | Ref. | |
ELX-TEZ-IVA | 11,434,473 | 39.5 | 224,099 | |
CADTH reanalysis 4 – compliance | BSCa | 1,130,392 | 23.9 | Ref. |
ELX-TEZ-IVA | 8,106,221 | 39.5 | 447,232 | |
IVA | 6,877,528 | 33.6 | Ref. | |
ELX-TEZ-IVA | 8,106,221 | 39.5 | 206,762 | |
CADTH reanalysis 5 – survival costs | BSCa | 1,130,392 | 23.9 | Ref. |
ELX-TEZ-IVA | 7,731,824 | 39.5 | 423,229 | |
IVA | 6,694,530 | 33.6 | Ref. | |
ELX-TEZ-IVA | 7,731,824 | 39.5 | 174,553 | |
CADTH reanalysis 6 – hospital costs | BSCa | 1,130,392 | 23.9 | Ref. |
ELX-TEZ-IVA | 7,708,585 | 39.5 | 421,739 | |
IVA | 6,586,938 | 33.6 | Ref. | |
ELX-TEZ-IVA | 7,731,824 | 39.5 | 188,748 | |
CADTH reanalysis 7 – treatment-specific utility | BSCa | 1,130,392 | 23.9 | Ref. |
ELX-TEZ-IVA | 7,571,466 | 37.3 | 481,244 | |
IVA | 6,449,503 | 33.6 | Ref. | |
ELX-TEZ-IVA | 7,571,466 | 37.3 | 300,876 | |
CADTH base case (1 + 2 + 3 + 4 + 5 + 6 + 7 + 8) (probabilistic) | BSCa | 986,009 | 23.8 | Ref. |
ELX-TEZ-IVA | 10,630,705 | 30.1 | 1,531,443 | |
IVA | 9,782,785 | 28.8 | Ref. | |
ELX-TEZ-IVA | 10,630,705 | 30.1 | 622,381 |
BSC = best supportive care; ELX = elexacaftor; ICER = incremental cost-effectiveness ratio; IVA = ivacaftor; QALY = quality-adjusted life-year; TEZ = tezacaftor; Ref = reference.
Scenario Analyses
Table 20: CADTH Price-Reduction Analyses — F/F Genotype
Analysis | ICERs for ELX-TEZ-IVA vs. LUM-IVA ($/QALY) | ICERs for ELX-TEZ-IVA vs. BSC ($/QALY) | ||
|---|---|---|---|---|
Price reduction | Sponsor base case | CADTH reanalysis | Sponsor base case | CADTH reanalysis |
No price reduction | 323,602 | 680,560 | 451,377 | 1,434,435 |
20% | 135,763 | 340,476 | 329,123 | 1,173,197 |
40% | Dominant | Dominant | 235,727 | 877,508 |
60% | Dominant | Dominant | 142,332 | 581,820 |
80% | Dominant | Dominant | 48,936 | 286,132 |
90% | Dominant | Dominant | 2,238 | 138,287 |
95% | Dominant | Dominant | Dominant | 64,365 |
99% | Dominant | Dominant | Dominant | 5,228 |
BSC = best supportive care; ELX = elexacaftor; ICER = incremental cost-effectiveness ratio; IVA = ivacaftor; QALY = quality-adjusted life-year; TEZ = tezacaftor; vs. = versus.
Table 21: CADTH Price-Reduction Analyses — F/MF Genotype
Analysis | ICERs for ELX-TEZ-IVA vs. BSC ($/QALY) | |
|---|---|---|
Price reduction | Sponsor base case | CADTH reanalysis |
No price reduction | 456,394 | 1,653,605 |
20% | 333,774 | 1,407,060 |
40% | 239,214 | 1,053,718 |
60% | 144,655 | 700,377 |
80% | 50,095 | 347,036 |
90% | 2,815 | 170,366 |
95% | Dominant | 82,030 |
99% | Dominant | 11,362 |
BSC = best supportive care; ELX = elexacaftor; ICER = incremental cost-effectiveness ratio; IVA = ivacaftor; QALY = quality-adjusted life-year; TEZ = tezacaftor; vs. = versus.
Table 22: CADTH Price-Reduction Analyses — F/RF Genotype
Analysis | ICERs for ELX-TEZ-IVA vs. BSC ($/QALY) | |
|---|---|---|
Price reduction | Sponsor base case | CADTH reanalysis |
No price reduction | 650,475 | 2,437,481 |
20% | 461,945 | 1,851,790 |
40% | 333,824 | 1,382,341 |
60% | 205,703 | 912,892 |
80% | 77,582 | 443,443 |
90% | 13,521 | 208,718 |
95% | Dominant | 91,356 |
99% | Dominant | Dominant |
BSC = best supportive care; ELX = elexacaftor; ICER = incremental cost-effectiveness ratio; IVA = ivacaftor; QALY = quality-adjusted life-year; TEZ = tezacaftor; vs. = versus.
Table 23: CADTH Price-Reduction Analyses — F/Gating Genotype
Analysis | ICERs for ELX-TEZ-IVA v. IVA ($/QALY) | ICERs for ELX-TEZ-IVA vs. BSC ($/QALY) | ||
|---|---|---|---|---|
Price reduction | Sponsor base case | CADTH reanalysis | Sponsor base case | CADTH reanalysis |
No price reduction | 238,159 | 622,381 | 437,639 | 1,531,443 |
20% | Dominant | Dominant | 319,772 | 1,238,693 |
40% | Dominant | Dominant | 226,595 | 927,497 |
60% | Dominant | Dominant | 133,419 | 616,302 |
80% | Dominant | Dominant | 40,243 | 305,107 |
90% | Dominant | Dominant | Dominant | 149,509 |
95% | Dominant | Dominant | Dominant | 71,710 |
99% | Dominant | Dominant | Dominant | 9,471 |
BSC = best supportive care; ELX = elexacaftor; ICER = incremental cost-effectiveness ratio; IVA = ivacaftor; QALY = quality-adjusted life-year; TEZ = tezacaftor; vs. = versus.
Table 24: CADTH Price-Reduction Analyses — Weighted Analysis, All Genotypes Combined
Analysis | ICERs for ELX-TEZ-IVA vs. standard of care ($/QALY) | |
|---|---|---|
Price reduction | Sponsor base case | CADTH reanalysis |
No price reduction | 456,044 | 1,531,196 |
20% | 325,119 | 1,237,266 |
40% | 225,296 | 898,280 |
60% | 125,473 | 559,295 |
80% | 25,650 | 220,309 |
90% | Dominant | 50,816 |
95% | Dominant | Dominant |
99% | Dominant | Dominant |
ELX = elexacaftor; ICER = incremental cost-effectiveness ratio; IVA = ivacaftor; QALY = quality-adjusted life-year; TEZ = tezacaftor; vs. = versus.
Table 25: Summary of the CADTH Scenario Analyses — F/MF Genotype
Scenario analysis | Drug | Total costs ($) | Total QALYs | ICER ($/QALYs) |
|---|---|---|---|---|
1. Entire Health Canada populationa | BSC | 1,297,036 | 20.27 | Ref. |
ELX-TEZ-IVA | 9,253,877 | 27.16 | 1,155,851 | |
2. Long-term reduction in pulmonary exacerbations included for CFTR modulators | BSC | 981,560 | 24.3 | Ref. |
ELX-TEZ-IVA | 10,950,031 | 31.4 | 1,397,896 | |
3. Slower rate of decline in ppFEV1 | BSC | 981,560 | 24.3 | Ref. |
ELX-TEZ-IVA | 12,712,041 | 37.1 | 914,096 | |
4. Inclusion of treatment-specific utility increment for patients on ELX-TEZ-IVA | BSC | 981,560 | 24.3 | Ref. |
ELX-TEZ-IVA | 10,634,494 | 31.8 | 1,289,660 |
BSC = best supportive care; ELX = elexacaftor; ICER = incremental cost-effectiveness ratio; IVA = ivacaftor; QALY = quality-adjusted life-year; TEZ = tezacaftor; Ref = reference.
aThis scenario was run probabilistically, while the other scenarios were run deterministically.
Table 26: Summary of the CADTH Scenario Analyses — F/RF Genotype
Scenario analysis | Drug | Total costs ($) | Total QALYs | ICER ($/QALYs) |
|---|---|---|---|---|
1. Entire Health Canada populationa | BSC | 1,199,209 | 20.72 | Ref. |
ELX-TEZ-IVA | 8,353,824 | 24.55 | 1,868,095 | |
2. Long-term reduction in pulmonary exacerbations included for CFTR modulators | BSC | 857,471 | 27.6 | Ref. |
ELX-TEZ-IVA | 11,386,270 | 33.5 | 1,787,631 | |
3. Slower rate of decline in ppFEV1 | BSC | 857,471 | 27.6 | Ref. |
ELX-TEZ-IVA | 12,159,279 | 36.1 | 1,331,234 | |
4. Inclusion of treatment-specific utility increment for patients on ELX-TEZ-IVA | BSC | 857,471 | 27.6 | Ref. |
ELX-TEZ-IVA | 11,019,030 | 34.0 | 1,580,811 |
BSC = best supportive care; ELX = elexacaftor; ICER = incremental cost-effectiveness ratio; IVA = ivacaftor; QALY = quality-adjusted life-year; TEZ = tezacaftor; Ref = reference.
aThis scenario was run probabilistically, while the other scenarios were run deterministically.
Table 27: Summary of the CADTH Scenario Analyses — F/Gating Genotype
Scenario analysis | Drug | Total costs ($) | Total QALYs | ICER ($/QALYs) |
|---|---|---|---|---|
1. Entire Health Canada populationa | BSC | 1,183,267 | 19.99 | Ref. |
ELX-TEZ-IVA | 9,020,190 | 26.79 | 1,151,193 | |
IVA | 8,186,629 | 23.85 | Ref. | |
ELX-TEZ-IVA | 9,020,190 | 26.79 | 282,937 | |
2. Long-term reduction in pulmonary exacerbations included for CFTR modulators | BSC | 1,130,392 | 23.9 | Ref. |
ELX-TEZ-IVA | 10,969,060 | 31.4 | 1,310,132 | |
IVA | 9,954,142 | 29.0 | Ref. | |
ELX-TEZ-IVA | 10,969,060 | 31.4 | 422,840 | |
3. Slower rate of decline in ppFEV1 | BSC | 1,130,392 | 23.9 | Ref. |
ELX-TEZ-IVA | 12,655,803 | 36.8 | 890,145 | |
IVA | 11,246,165 | 33.2 | Ref. | |
ELX-TEZ-IVA | 12,655,803 | 36.8 | 387,764 | |
4. Inclusion of treatment-specific utility increment for patients on ELX-TEZ-IVA | BSC | 1,130,392 | 23.9 | Ref. |
ELX-TEZ-IVA | 10,887,978 | 32.3 | 1,165,506 | |
IVA | 9,901,114 | 28.5 | Ref. | |
ELX-TEZ-IVA | 10,887,978 | 32.3 | 261,235 |
BSC = best supportive care; ELX = elexacaftor; ICER = incremental cost-effectiveness ratio; IVA = ivacaftor; QALY = quality-adjusted life-year; TEZ = tezacaftor; Ref = reference.
aThis scenario was run probabilistically, while the other scenarios were run deterministically.
Appendix 5: Submitted Budget Impact Analysis and CADTH Appraisal
Note that this appendix has not been copy-edited.
Table 28: Summary of Key Take-Aways
Key take-aways of the Budget Impact Analysis |
|---|
|
Summary of Sponsor’s Budget Impact Analysis
The sponsor submitted an epidemiology-based budget impact analysis (BIA), assessing the expected budgetary impact of the reimbursement of ELX-TEZ-IVA for the treatment of CF in patients who are 6 to 11 years of age with at least 1 F508del-CFTR mutation. The analysis was conducted over a 3-year time horizon, from 2022 to 2024, with 2021 as the base year. The perspective taken was that of Canadian public drug payers, with only drug acquisition costs included. The BIA considered a reference scenario in which only LUM-IVA (for F/F patients) and IVA monotherapy (for F/gating patients) were available. The new drug scenario included ELX-TEZ-IVA, LUM-IVA, and IVA monotherapy. All patients were assumed to receive background BSC and, as such, these costs were excluded. The sponsor’s estimate of market size is primarily based on data generated from the CF Canada patient registry, and further reduced based on the proportion of patients covered by provincial formularies, Figure 2. Key inputs to the BIA are documented in Table 29.
The sponsor also made the following key assumptions:
All patients with CF are captured in the Canadian CF patient registry.
65% of indicated patients would be covered by provincial drug programs, and the other 35% would have private insurance coverage.
The market uptake of ELX-TEZ-IVA would be ||%, ||%, and ||% in Years 1 through 3, respectively.
The compliance rate for CFTR modulators was assumed to be 93%.
Genotype-specific subpopulations grow at the same rate as the general CF population.
No drug mark-up or dispensing fees were considered in the base-case analysis.
Figure 2: Sponsor’s Estimation of the Size of the Eligible Population

This figure has been redacted at the request of the sponsor.
Source: Sponsor’s budget impact submission.43
Table 29: Summary of Key Model Parameters
Parameter | Sponsor’s estimate (reported as Year 1 / Year 2 / Year 3 if appropriate) |
|---|---|
Target population | |
Number of patients eligible for drug under review | 263 / 267 / 271 |
Market Uptake (3 years) for Ontario | |
Uptake (reference scenario) LUM-IVA IVA BSC alone | ||% / ||% / ||% ||% / ||% / ||% ||% / ||% / ||% |
Uptake (new drug scenario) ELX-TEZ-IVA LUM-IVA IVA BSC | ||% / ||% / ||% ||% / ||% / ||% ||% / ||% / ||% ||% / ||% / ||% |
Cost of treatment (per patient) | |
Cost of treatment annually, adjusted for 93% compliance ELX-TEZ-IVA LUM-IVA IVA Best supportive care | $285,333 $231,712 $285,333 $0 |
ELX = elexacaftor; IVZ = ivacaftor; LUM = lumacaftor; TEZ = tezacaftor.
Summary of the Sponsor’s Budget Impact Analysis Results
Results of the sponsor’s base case estimates that the incremental budget impact associated with the reimbursement of ELX-TEZ-IVA for the treatment of CF in patients who are 6 to 11 years of age with at least 1 F508del-CFTR mutation would be $56,639,388 in Year 1, $61,392,782 in Year 2, and $63,721,433 in Year 3, for a cumulative 3-year budget impact of $181,753,603.
The sponsor conducted several sensitivity analyses assessing the impact of alternative assumptions related to compliance rates, predicted utilization rates of ELX-TEZ-IVA and IVA, as well as increasing the size of the eligible patient population. All had a significant impact on results, with the greatest impact observed for the scenario in which market uptake was increased by 10%, resulting in a 3-year budget impact of $200,426,205. Another scenario that had a large effect on the results was when compliance was assumed to be 100%, resulting in a 3-year budget impact of $195,433,982.
CADTH Appraisal of the Sponsor’s Budget Impact Analysis
CADTH identified several key limitations to the sponsor’s analysis that have notable implications on the results of the BIA:
Anticipated uptake of ELX-TEZ-IVA is underestimated: The sponsor assumed that the uptake of ELX-TEZ-IVA in the new drug scenario for all genotypes would be ||% in the first year, ||% in the second year, and ||% in the third. The clinical experts consulted by CADTH for this review considered these estimates to be underestimated, and that between 90% and 100% of patients eligible for ELX-TEZ-IVA would be prescribed ELX-TEZ-IVA. The sponsor’s assumed market uptake underestimated the total costs associated with the uptake of ELX-TEZ-IVA in the sponsor’s base case, leading to an underestimate of the total budget impact associated with ELX-TEZ-IVA.
CADTH assumed 95% market uptake for ELX-TEZ-IVA in all 3 years of the BIA.
Compliance-adjusted drug costs underestimate the total costs associated with the uptake of ELX-TEZ-IVA to public drug plans: In their base case, the sponsor adjusted the price of ELX-TEZ-IVA by the assumed compliance rate (93%), with the assumption that savings would be incurred by public drug plans due to patients not being 100% compliant. There is limited evidence to support the real-world compliance rate with ELX-TEZ-IVA; thus, the sponsor used compliance data from LUM-IVA.1 Additionally, the full complement of ELX-TEZ-IVA would be dispensed, regardless of whether the patient was compliant, thus resulting in the full costs of treatment being incurred by the public drug payer. This underestimated the total costs associated with ELX-TEZ-IVA and its total budget impact.
CADTH assumed patients were 100% compliant in reanalyses, in alignment with the CADTH pharmacoeconomic base case.
Estimated proportion of patients with public coverage for CFTR-modulator therapy is uncertain: The sponsor assumed 65% of the population indicated for ELX-TEZ-IVA would have public coverage, thus reducing the total eligible population size by 35%. The evidence cited by the sponsor for this assumption was internal data not available to CADTH, and uncertainty remains as to the proportion of the indicated population who would be covered by public drug plans. There is uncertainty in the proportion of patients with public versus private insurance. If more than 65% of the population would be covered, the anticipated budget impact associated with ELX-TEZ-IVA would be higher. If fewer are covered, the anticipated budget impact would be lower.
CADTH assumed 65% coverage in the base-case analysis, and tested scenarios of 50% coverage and 100% coverage.
CADTH Reanalyses of the Budget Impact Analysis
Based on the identified limitations, CADTH’s base-case analysis included changes to the anticipated market share of ELX-TEZ-IVA in all 3 years and to the patient compliance rate.
Table 30: CADTH Revisions to the Submitted Budget Impact Analysis
Stepped analysis | Sponsor’s value or assumption | CADTH value or assumption |
|---|---|---|
Corrections to sponsor’s base case | ||
None | — | — |
Changes to derive the CADTH base case | ||
1. Market share of ELX-TEZ-IVA | ||% / ||% / ||% | 95% / 95% / 95% |
2. Patient compliance | 93% | 100% |
CADTH base case | Reanalysis 1 + 2 | |
ELX = elexacaftor; IVZ = ivacaftor; TEZ = tezacaftor.
The results of the CADTH stepwise reanalysis are presented in summary format in Table 31 and a more detailed breakdown is presented in Table 32. Based on the CADTH base case, the budget impact of the reimbursement of ELX-TEZ-IVA for the treatment of CF in patients who are 6 to 11 years of age with at least 1 F508del-CFTR mutation is expected to be $75,400,782 in year 1, $75,841,648 in year 2, and $76,845,222 in year 3, with a 3-year total of $228,087,652. Scenario analyses were conducted around the proportion of patients expected to have public drug coverage. The 3-year budget impact totals for these analyses were $175,452,040 and $350,904,080 when 50% and 100% of patients were assumed to have public coverage, respectively.
The previous CADTH review of ELX-TEZ-IVA in patients greater than 12 years old estimated a budget impact of $1,279,931,452. As the budget impact submitted for this review is specifically for the population between 6 and 11 years of age, the 3-year budget impact for the reimbursement of ELX-TEZ-IVA for patients 6 years of age and older is expected to be $1,508,019,104.
Table 31: Summary of the CADTH Reanalyses of the Budget Impact Analysis
Stepped analysis | Three-year total |
|---|---|
Submitted base case | $181,753,603 |
CADTH reanalysis 1 – market share | $212,121,516 |
CADTH reanalysis 2 – compliance | $195,433,982 |
CADTH base case | $228,087,652 |
BIA = budget impact analysis.
Table 32: Detailed Breakdown of the CADTH Reanalyses of the Budget Impact Analysis
Stepped analysis | Scenario | Year 0 (current situation) | Year 1 | Year 2 | Year 3 | Three-year total |
|---|---|---|---|---|---|---|
Submitted base case | Reference | $2,005,072 | $2,038,767 | $2,073,028 | $2,107,866 | $6,219,662 |
New drug | $2,005,072 | $58,678,156 | $63,465,811 | $65,829,300 | $187,973,266 | |
Budget impact | $0 | $56,639,388 | $61,392,782 | $63,721,433 | $181,753,603 | |
CADTH base case | Reference | $2,155,991 | $2,192,223 | $2,229,063 | $2,266,523 | $6,687,809 |
New drug | $2,155,991 | $77,593,005 | $78,070,711 | $79,111,745 | $234,775,461 | |
Budget impact | $0 | $75,400,782 | $75,841,648 | $76,845,222 | $228,087,652 | |
CADTH scenario analysis 1: 50% public coverage | Reference | $1,658,455 | $1,686,325 | $1,714,664 | $1,743,479 | $5,144,468 |
New drug | $1,658,455 | $59,686,927 | $60,054,393 | $60,855,188 | $180,596,508 | |
Budget impact | $0 | $58,000,601 | $58,339,729 | $59,111,709 | $175,452,040 | |
CADTH scenario analysis 2: 100% coverage | Reference | $3,316,910 | $3,372,651 | $3,429,328 | $3,486,958 | $10,288,937 |
New drug | $3,316,910 | $119,373,854 | $120,108,787 | $121,710,376 | $361,193,016 | |
Budget impact | $0 | $116,001,203 | $116,679,458 | $118,223,418 | $350,904,080 | |
CADTH scenario analysis 3: 90% price reduction from PE report | Reference | $2,155,991 | $2,192,223 | $2,229,063 | $2,266,523 | $6,687,809 |
New drug | $2,155,991 | $8,726,491 | $8,046,894 | $7,911,174 | $24,684,559 | |
Budget impact | $0 | $6,534,268 | $5,817,830 | $5,644,652 | $17,996,750 |
BIA = budget impact analysis; PE = pharmacoeconomic.
Stakeholder Input
Patient Input
Cystic Fibrosis Canada
About Cystic Fibrosis Canada
Since being founded by parents in 1960, Cystic Fibrosis Canada has grown into a leading organization with a central role engaging people living with cystic fibrosis, parents and caregivers, volunteers, researchers and healthcare professionals, government and donors. We have advanced research and care that has quadrupled life expectancy. We work together to change lives through treatment, research, information and support. Despite our progress we are not yet done. Half of the people with cystic fibrosis who died over the past three years were younger than 34. A child born with cystic fibrosis in 2019 has only a 50% chance of living to 54. We will keep pushing, keep going further until all people with cystic fibrosis experience — and enjoy everything life has to offer.
Cystic Fibrosis Canada funds basic, discovery science and clinical research, and has helped establish core facilities across the country. We provide financial support to the forty-one multi-disciplinary cystic fibrosis clinics that see nearly all Canadians living with cystic fibrosis and maintain close relationships with the clinical and research communities. We have invested over $261M in research and clinical care support. The close relationships with the research, clinical and patient communities gives us an excellent understanding the disease. We are the most respected and trusted source for information on cystic fibrosis in Canada and provide an information and resource service to the community that includes publishing a comprehensive resource compendium for the community. In addition, we maintain close relationships with our sister organizations around the world, which allow for the rapid sharing of information and adoption of best practices. We launched in 2018 the Cystic Fibrosis Canada Accelerating Clinical Trials (CF CanACT) network that now includes 10 of the 41 cystic fibrosis clinics serving over 60% of Canadians with cystic fibrosis. CF CanACT also works closely with our international partners to conduct protocol reviews, share Data Safety Monitoring Boards, and help speed clinical trial progress.
Cystic Fibrosis Canada manages the Canadian Cystic Fibrosis Registry (the Registry). The Registry contains the clinical information on nearly all Canadians with cystic fibrosis, living or deceased, with data going back to the 1970’s. The Registry publishes an annual report that describes the current status of the cystic fibrosis population in Canada and national trends over time. The data in the Registry is also used by investigators in Canada and around the world to better understand the disease and the impact of therapeutic efforts as well as to propose improvements to care.
We work closely with our patient community to advocate to improve their health and well-being. In 2020, Cystic Fibrosis Canada’s National Advocacy Network consisted of over 200 well-trained advocates and a basket of tools to help them in their efforts. We’ve been able to help the cystic fibrosis community by amplifying their voices through coordinated efforts that have addressed both national and regional priorities.
Cystic Fibrosis Canada’s contributions have led to significant improvements care and quality of life for people living with cystic fibrosis. As a result, Canada has one of the highest median ages of survival in the world.
Cystic Fibrosis Canada is pleased to provide patient group input to CADTH’s consideration of Trikafta for the treatment of cystic fibrosis (CF) in patients aged 6 years and older who have at least one F508del mutation in the cystic fibrosis transmembrane conductance regulator (CFTR) gene. We appreciate the consideration CADTH gave to our submission on the 12+ population and to our response and our clinicians and researchers' responses to the draft criteria. CF clinicians and researchers share this sentiment. Collectively, we look forward to providing CADTH with a suite of submissions for the 6+ population in Canada to help guide CDEC’s deliberations to ensure the broadest access possible for this life-changing therapy.
Information Gathering
Cystic Fibrosis Canada gathered information for this submission through many channels, including a cross-Canada survey of patients and caregivers in January 2021. We reference Cystic Fibrosis Canada’s publications, including the 2019 Canadian CF Registry Annual Data Report, press releases, news stories, government submissions, as well as information gathered through social media campaigns, posts from individuals and traditional media sources.
We cite scientific literature, clinical trial data and other published studies on Trikafta and its impact on health outcomes, as well as a Cystic Fibrosis Canada funded study published in the fall of 20201 that projects the impact on the Canadian cystic fibrosis population of access to Trikafta. Where appropriate (in descriptions of the general impact of cystic fibrosis on life for example) we have used information gathered for our recently submitted CADTH and INESSS submissions, as well as those from the submissions of CF clinicians and researchers.
We reference findings that were recently presented at the 2021 North American Cystic Fibrosis Conference2.
Patients and caregivers were invited through postings at cystic fibrosis clinics, through direct email, Facebook, and other social media channels, to participate in a survey conducted from January 18 until January 25, 2021. In total,1,455 people responded to our survey. According to their residence, all respondents live in Canada. The percentages provided below refer to the percentage of individuals who responded to a given question in the survey.
Thirty-one percent of all respondents were adults living with cystic fibrosis, 17% a spouse or caregiver of an adult living with cystic fibrosis, 12% parents of one or more children with cystic fibrosis between the ages of 12-17 years, and 20% were parents of one or more children with cystic fibrosis aged 11 years or younger. Twenty percent of the respondents did not belong to any of these categories and were excluded from further analyses.
At the time of the survey, of the 422 adults with cystic fibrosis who responded, 12% were taking Trikafta through Health Canada’s Special Access Program (SAP), 7% received it through a clinical trial and all but one adult was still accessing it.
As reported by responding caregivers, 5% of children 11 years of age or younger accessed Trikafta as part of a clinical trial, fewer than one percent received the drug through the Special Access Program, and 3.5% of respondents in this age group tried to access Trikafta through the SAP but were unsuccessful. Of the remaining participants, the caregivers of 79% of those 11 years of age or younger noted that their children were indicated for Trikafta, while 5% of caregivers for this cohort stated that their children were not indicated for Trikafta.
Disease Experience
Cystic fibrosis is the most common fatal genetic disease affecting children and young adults in Canada. There is no cure. It is a complex disease caused by mutations in the gene for the Cystic Fibrosis Transmembrane Conductance Regulator (CFTR). There are over 2,090 known mutations. Cystic fibrosis has a tremendous impact on the people who live with it, their loved ones, and on society. Every week in Canada, two people are diagnosed with cystic fibrosis, one of them through newborn screening. Every week in Canada, one person with cystic fibrosis will die.
Cystic fibrosis causes various effects on the body, but mainly affects the digestive system and lungs. The clinical progression of cystic fibrosis can vary greatly from person to person, even with the same mutations. The most significant clinical impact is in the lungs, where patients have difficulty in clearing secretions, which in combination, with aberrant inflammation leads to persistent infections with cycles of inflammation that are ineffective in clearing infections. This leads to progressive scarring of the airways and a progressive and sometimes rapid decline in lung function. Pulmonary/ infection/ cardiovascular complications cause eighty percent of cystic fibrosis fatalities.3
Patients may suffer from pulmonary exacerbations (PEx, flares of lung disease) requiring weeks of treatment with antibiotics and often requiring hospitalization and I.V. antibiotics. PEx cause rapid decline of lung function and more rapid disease progression and are associated with a greater risk of death4. Other consequences of having cystic fibrosis include malnutrition and very low BMI, and cystic fibrosis-related comorbidities like cystic fibrosis-related diabetes (CFRD) and cystic fibrosis-related liver disease.
Thanks to significant progress in treatment and care, most children with cystic fibrosis will reach adulthood. The estimated median survival of Canadians with cystic fibrosis in 2019 was 54 years of age.3 There were no deaths amongst 6-11 year olds in 2019.
As the disease advances more time and effort are needed to manage the progressive and debilitating symptoms. Children with cystic fibrosis may need to quit school or go part-time, adults with cystic fibrosis may need to leave the work force or undertake part-time work, as may caregivers of children and adults with cystic fibrosis.
Our four year old grandson has missed out in so much of his life that he deserves more childhood instead of all the time the medications and therapies take away. – Grandparent of a child with CF
Growing up, I spent a lot of my life trying to show everyone that I was tough and that I could handle CF because I didn’t want their worry or their pity. I have to live my life knowing that it’s most likely going to be shorter than my parents’ lives. Shorter than my younger brother’s life. No one should have to live like that. Now that I’m an adult living with CF, the realities of the disease are catching up to me. My health is worse than it’s ever been before. Not having enough breath to do the things I want to do on a daily basis is incredibly frustrating. I want to have enough breath to run up the stairs. To hike down to the dock and go fishing with my dad. To clean the house. CF is slowly stealing my life from me. I have dreams. I want to get married and not break my husband’s heart when CF stops mine. – Adult with CF
I have experienced many health crises related to cystic fibrosis leaving me with no other option but to consider a double- lung transplant. In 2011 my lung function reached an all-time low sitting at 26 percent and my family and I were faced with the difficult reality of having to make a decision. At this point I was so exhausted I couldn’t even perform basic tasks. – Adult with CF
I struggled to keep up with work and university and had to spend up to 2 hours a day on exhausting, never ending, treatments. For 20 years I had about 3 hospital admissions a year. This meant I had over 60 hospital admissions, equaling more than 3 years of my life in hospital. – Adult with CF
When two of my children were first diagnosed, the doctor told me I’d never go back to work again. It is a full-time job keeping my children healthy. From helping with their physio to clear mucus, frequent CF clinic visits, hospital stays, and on top of that ensuring our third child does not feel left out as a healthy child. – Parent of a child with CF
My 11 year old daughter spends in excess of 26 hours a week trying to stay healthy. The fight against CF is all encompassing for the family. It requires giving up 2 to 7 hours every day for her therapies. The physical therapies take a toll on my and my wife’s bodies. We both have repetitive strain injuries and arthritis in our hands, wrists and shoulder. This commitment requires scheduling all meals and everyone’s activities around her therapies. We restrict our social activities to prevent passing on colds and flus. Each day that a control for cystic fibrosis is not available to her is a day that her lungs are deteriorating. All the treatments that she has access to only try to mitigate her existing health problems, none address the root cause. Without the availability of drugs that fix the basic defect in cystic fibrosis, our daughter and others like her will lose their valiant fight as they pass away while gasping for air. – Parent of a child with CF
I lost three friends in three months, while they waited for a lung transplant. It’s not right to bury your friends all under the age of 25. I’ve been to more funerals than weddings in my life. – Adult with cystic fibrosis
Moreover, research has shown that patients with chronic diseases (defined as a condition that persists for longer than three months) can often have anxiety and depression. It is estimated that up to one third of individuals with a serious medical condition will experience depression. Depression is one of the most common complications of chronic illness like cystic fibrosis, and it also affects caregivers5.
On April 1st, 2011 my son and daughter were both diagnosed with Cystic Fibrosis. It remains the most devastating news I have ever received. My 9-year-old son has already spend in total over 6 months of his life in the hospital. Each time he is away from school, his friends, his extra-curricular activities, his bed, his family. He is stuck in a hospital room attached to cords and tubes. He’s not allowed to leave his room due to infection control. It’s complete isolation. Being away from home for 2 weeks at a time affects the whole family. My daughter has developed separation anxiety. – Parent of a child with CF
She had a really rough first four or five years. Constantly sick, in and out of the hospital, had trouble gaining weight … it’s a lot of she just ‘can’t breathe.’ She can’t breathe in, and she can’t breathe out a full amount of breath. In the last two years, she’s become a different person because of this disease. In March, she tried to take her life because she said, living with cystic fibrosis is not living it’s surviving the life she doesn’t want to live. – Parent of a child with CF
Experiences With Currently Available Treatments
There are hundreds of therapies that aid in symptom management of cystic fibrosis in the categories of: antibiotics, supplemental vitamins, aerosol bronchodilators, mucolytics and pancreatic enzymes, anti-inflammatories, and steroids. Most cystic fibrosis patients take pancreatic enzymes, multi-vitamins and nutritional supplements to maintain normal growth. Cystic fibrosis patients work tirelessly every day to improve the clearance of secretions from their lungs. This is done by performing airway clearance techniques at least twice a day for about 30-60 minutes per session. Inhaled medications are used to open the airways while inhaled antibiotic treatments are used to control infections. The total time spent on maintaining lung health is well over two hours each day. Patients frequently have periods of infection and acute inflammation called exacerbations that require a hospital stay of at least two weeks and that frequently last four weeks. The steroids that are used to reduce the inflammation and help patients recover from the exacerbation ultimately damage organs in the long run, contributing to the development of cystic fibrosis related diabetes (CFRD) in 35.2% of all Canadian cystic fibrosis adults.
Many of the other drugs that patients need to take on a regular basis also have negative side-effects. Antibiotics can cause kidney damage and total lifetime dose must be controlled; others permanently stain the teeth. Chronic use of antibiotics leads to resistance and, as patients age, a need to try multiple antibiotics to find one that works. Because patients are on so many drugs, drug to drug interactions become difficult to manage and can interfere with optimum therapy. Since therapy starts at the age of diagnosis, this process begins at an early age for many, often two to three weeks old thanks to newborn screening for cystic fibrosis, now provided right across Canada. Newborn screening was put in place so that treatment can begin as early as possible, to help slow the progression of the symptoms of the disease.
Right now my child cannot access any modulators, and preventative therapies currently are not taking away the progression of her disease. Quality of life is hugely impacted and lessened, having no modulator to improve her overall health and help her body be protected from other illnesses. – Parent of a child with CF
Hospitalizations interfere with school, and jobs, for both adult patients and the parents of children with cystic fibrosis. In 2019, there were 1,952 hospitalizations recorded which added up to almost 25,246 days spent in hospital (nearly 70 years total). This does not include visits to the out-patient cystic fibrosis clinics. A total of 4,316 (99.4%) individuals with cystic fibrosis visited a cystic fibrosis clinic at least once in 2019 with 3,367 (77.5%) having three or more clinic visits. Twenty-one percent of cystic fibrosis patients travel more than 250 km one-way to their cystic fibrosis clinic to receive routine care, with the concomitant interruptions on day-to-day life. At home, individuals with cystic fibrosis had 842 courses of home IV therapy adding up to over 15,530 days on home IV antibiotics3.
In terms of time, money and overall health, the burden of care on those who live with cystic fibrosis, their caregivers and society is tremendous. Over the course of a year, people with cystic fibrosis can take tens of thousands of symptom management medicines and supplements. Together inhaled and physio chest therapies can take between 2-4 hours a day, every day of the year.
Long-term use of powerful antibiotics to fight chronic, persistent infection ultimately leads to anti-microbial resistance. Patients describe the fear of running out of options.
I am running out of options due to antibiotic resistance & low lung functions, so this is a possible treatment when without it, I have no other option. – Adult with cystic fibrosis
I am running out of options due to antibiotic resistance … I hope [Trikafta] comes quickly, as I am sick but not sick enough for SAP, which is very hard to cope mentally that I am suffering with no options, and my health is deteriorating, but I’m not dying enough to get it yet, so I am concerned about the damage to my lungs while I wait that could have been avoided when Trikafta exists. – Adult with cystic fibrosis.
Eventually the ongoing cycles of infection and inflammation destroy the lungs. Lung transplantation is the last recourse for people with end-stage cystic fibrosis. Between 1988 and 2019 eight hundred and eighty-four individuals with cystic fibrosis had received one or more lung transplants, with three hundred eighty-five post-transplant reported deaths, or 499 survivors. Fifty percent of today’s lung transplant recipients are expected to live over 10 years3.
A summary of the day in the life of one cystic fibrosis patient with advanced disease, during the evaluation period pre-transplant:
A typical day at home: 6:00-7:30 AM: intravenous (IV) antibiotics (2x40 mins). They connect with my picc-line. It's rather tedious because of the many steps of the procedure: disinfect, flush with saline, connect the antibiotic, wait 40 minutes, flush with saline again, connect the next antibiotic, wait 40 minutes... etc. Very often, my Mum, Dad or sister will do this for me while I sleep in, so I can catch a bit more sleep. 8:00-9:00 AM: wake-up routine; asthma meds, inhaled antibiotics and enzymes, pep-mask physiotherapy, wash all the nebulizers, prep any meds that need to be reconstituted. 9:00-10:00 AM: breakfast; meal routine: check blood sugar, take insulin, have breakfast, morning pills (the usuals + check calendar for the ones on a variable schedule), Scandishake, after-breakfast meds, if any (check calendar). 1:00-2:00 PM: lunch; repeat meal routine; 2:00-4:00 PM: IV antibiotics (3x40 mins), (concurrent) 3:00-3:10 PM: inhaled antibiotics. 4:00-5:00 PM: exercise.
6:00-7:00 PM: supper; repeat meal routine. 8:00-9:00 PM: clapping physiotherapy. 9:00-9:30 PM: bedtime routine; asthma meds, inhaled antibiotic, bedtime meds (check calendar). 10:00-11:30 PM: IV medications (2x40 mins) Fairly often, my Mum, Dad or sister will do this one for me too so I can go to bed a bit earlier. Juggling the timing of everything is a bit of a headache, mostly because I need to space out eating with physiotherapy (doing physio or exercise tends to give me coughing fits, which makes me throw up if I've eaten too recently). On most days I've also got a limited amount of energy, so I've got to manage my activities to make sure I don't crash before the end of the day. Other regular tasks include: keeping medical appointments (1/week or more); preparing pills in advance (it saves time at meals); speaking with my pharmacist 2- 3 x a week to order meds, arrange delivery...and…staying on top of insurance reimbursements (3-4 hours / month or so). – Adult with cystic fibrosis6
Experience With Currently Available CFTR Modulators
Trikafta is the first, third generation CFTR modulator. All modulators are tailored for specific CFTR mutations. The first-generation modulator, Kalydeco, is now broadly available in Canada, but it took years for it to be so. Kalydeco treats about 4 percent of people living with cystic fibrosis. Orkambi and Symdeko are both second-generation modulators and could benefit as many as 50% of Canadians with cystic fibrosis. Orkambi recently became available in several Canadian jurisdictions, but access is extremely limited. Symdeko is only available through some private drug plans. The drug has not been reviewed by CADTH.
Clinical benefits gained from Kalydeco are similar but more modest than those from Trikafta. Although the patient populations served are distinct, patients on Kalydeco with a F508del mutation are likely to benefit from Trikafta. On average, clinical benefit gained from Orkambi or Symdeko are substantially more modest than those from Trikafta and more patients reported intolerable side effects with Orkambi in particular, however individual responses were highly variable, and some patients report having benefited greatly from one, or another of the earlier modulators. Any Canadian on or eligible for, Orkambi or Symdeko is likely to benefit substantially from Trikafta.
[Trikafta is] clinically shown to work better than Orkambi- which my child is on. - Parent of a child with CF
Being on Orkambi increased my energy and overall improved my symptoms and it was great. I am thankful that I got to take Orkambi and stabilize my health. It was able to stabilize my health and I felt great. But it did not alleviate as many symptoms as Trikafta. When I started Trikafta it was life changing. It not only alleviated 99% of all mucus in my lungs. It increased my lung function significantly. Being on trikafta gave me a chance at living a life without an imminent need for a lung transplant. It has allowed me to put my cystic fibrosis on the back burner and it not be the only focus in my life. My cf is more of an inconvenience than a death sentence now that j am taking Trikafta. For me the obvious choice is that Trikafta works significantly better than Orkambi for my body. – Person living with CF
This individual provided a detailed description of their experience on Orkambi, then Symdeko and finally with Trikafta. Their experience with Trikafta is presented under the Place in Therapy section.
I had the privilege of accessing Orkambi in 2016, Symdeko in 2018 and, as a recipient of compassionate access, Trikafta in 2020. … I began taking Orkambi in 2016 and shortly thereafter my declining health stabilized. My lung function (FEV1) remained stable for 1.5 years, I had significantly more energy and I gained a much needed 25 lbs in 4 months, which helped me finally reach a more normal, healthy weight class for my height and age. Orkambi slowed my rapid decline but I was still seeing losses and I knew that there was a next generation medication in the pipeline called Symdeko, as I had participated in a 30-day study for that one years before. When Symdeko was approved by Health Canada I was able to again access it within only a few months on my group benefit plan. Symdeko increased my FEV1 slightly for a time and the side effect of severe acid reflux I experienced while on Orkambi was resolved with Symdeko. Unfortunately, my CF lung disease, though progression was slowed, was severe at this point and I had several complications in 2019 which led to testing to initiate the lung transplant process. - Person living with CF
Together, all prior generation CFTR modulators could only help up to 54% of Canadians with cystic fibrosis based purely on genetic background. It comes as no surprise that in our January 2021 survey, 79% of respondents answered “yes” when asked if they think that there is a gap, or unmet need, in current therapies that they believe Trikafta will alleviate. Trikafta alone could help up to 90% of Canadians with cystic fibrosis.
Unmet needs include the fact that right now my child cannot access any modulators, and preventative therapies currently are not taking away the progression of her disease. Quality of life is hugely impacted and lessened, having no modulator to improve her overall health and help her body be protected from other illnesses. – Parent of a child with CF
Trikafta targets the root cause of cystic fibrosis and helps break the cycle of infection and deteriorating lung function. Our son calls this drug a 'dream come true.' We are forever grateful to the CF community for their efforts in making this day a reality. While this is an exciting day, we look forward to the day when every Canadian who needs Trikafta can access it. – Parent of a child with CF
[Trikafta is] proactive rather than reactive - preserve lung function and health. – Parent of a child with CF [Trikafta] would be a preferred modulator, as others may have adverse side effects. – Parent of a child with CF
Caregiver Impact: Current Therapies
Spouses or caregivers of an adult living with cystic fibrosis accounted for 34% of caregiver respondents to our January 2021 survey, 25% were parents of one or more children with cystic fibrosis between the ages of 12-17 years, and 41% were parents of one or more children with cystic fibrosis aged 11 years or younger.
Of the 384 caregivers who responded and care for children with at least one F508del mutation, at the time of our January survey, 87% had not sought access to Trikafta. Five percent care for children who tried to access Trikafta through the Special Access Program but were unsuccessful, and 2% care for children who had access through a clinical trial but no longer do.
All of these people care for Canadians following current standard of care (SOC).
Current standard of care focuses on maintaining health and preventing progression. This is why children, who appear healthy and may have over 100% predicted FEV1 are nonetheless subjected to an aggressive regimen of physiotherapy and antibiotic treatments in addition to special diets and frequent (quarterly or more) clinic visits. Despite this aggressive early treatment, all patients will ultimately progress. This also explains why it is so vital to start children on Trikafta as soon as possible: to slow the progression of the disease and the irreversible damage it does to the body.
People with cystic fibrosis may take over a hundred different pills a day, along with an hour more of chest physiotherapy, and preparation and inhalation of aerosolized drugs, and injection of others, like insulin or i.v. antibiotics. Virtually all currently accessible therapies treat individual symptoms or individual organs. All people with cystic fibrosis take these symptom management drugs to survive. Their caregivers help them manage these medicines as well as their chest physiotherapy, not to mention countless other things that many Canadians with cystic fibrosis can’t do because of their disease.
Our survey findings indicate that the burden on caregivers of individuals with cystic fibrosis on SOC in terms of time and energy is significant. Of the caregivers of adults, 40% spend 10 hours or less per week on caregiving activities, but 33% spend between 11-20 hours per week and another 27% spend more than 20 hours per week on caregiving activities. Of the caregivers of children only 17% spend less than 10 hours per week, 53% spend 11-20 hours, 17% spend 21-30 hours and another 12% spend over 30 hours weekly on disease management.
While it might seem counter-intuitive that caregivers spend more time caring for children who are in general far healthier than adults, the reality is that care is complex and parents carry the full burden of caregiving, whereas patients typically transition gradually to adult care by increasingly adopting responsibility for their own care. While access to Trikafta will not eliminate standard of care, it can reduce the time and energy required in delivering SOC.
The combined total burden of care on both patients and caregivers to simply follow SOC to stabilize health as much as possible is that of at least a part-time job for most families, and for some families, equivalent to a full-time job, for each patient. For multi-patient households, the burden is multiplied. It should come as no surprise when one parent of multi-patient households typically leaves the work force to care for the children.
Amongst caregivers of children with cystic fibrosis, 60% of reporting caregivers had to take time off work, 12% had to leave full-time work for part-time work, 13% had to quit work altogether and 2% had to take time off school or leave school altogether.
I have had to quit my job and go on social assistance when I was a single mother. Now I am married but I still miss work due to my child's condition. – Parent of a child with CF
My husband has missed work, I’ve missed opportunities for work, hospitalization and treatments make it impossible to plan and meet obligations sometimes. – Parent of a child with CF
My wife quit her job and became a stay-at-home Mom when our daughter was born – Parent of a child with CF
I am a single mother, I can’t quit my full-time job - if I could, I would to care for my daughter. Instead I juggle hospital stays and remote working while she is in hospital or off sick. – Parent of a child with CF
I have just been fired from 10 years of employment with no notice or severance as my performance suffered too much due to caregiver burn out. – Parent of a child with CF
More than two thirds (72%) of reporting caregivers said that caregiving had a negative impact on their mental health while 11% felt that it had a positive effect. Parents and caregivers have an overwhelming desire to do something to help their loved ones. The observation of one parent suggests that caregiving may help counter the negative impact the diagnosis has on mental health. Just over half – 55% – of caregivers said caregiving had a positive impact on their relationship with the recipient. Seventeen percent felt it had a negative impact.
I have had mental health problems watching my child fall ill. – Parent of a child with CF
When asked about what their child taking Trikafta could mean for them personally, caregivers said:
If my child received this drug, I believe it could improve her health so much so that we would feel comfortable having our lives return to a more normal social state. Such as in having her enroll in school and outside activities and travel, and allow my return to my career. Our family life and social life would greatly improve and benefit in our overall mental health. The stress of having to protect her health has completely altered our lifestyle, it keeps us from living a full life, we live an isolated life in protecting our childs health without any modulators, a decline in health is very real concern and it affects us greatly in our quality of life. – Parent of a child with CF
I hope that my child would experience the benefits of a better mental health, better physical health. It would bring relief to us as
We hope for access to Trikafta...no matter the age or current health status. I truly believe by accessing Trikafta, not only will my childs health be greatly improved both physically and mentally. But it would allow our child and our family to become happier and much more fulfilled in life and much better contributing members of society. Our child would benefit by having a much more carefree childhood and experience all the fun things a child should instead of being held back and isolated from doing things due to her health, so her overall wellness would be an amazing improvement. We could more easily see a future and a healthy long life for our child like her peers instead of fearing the fatal disease that cripples our family. Our caregiving duties and stress would be greatly reduced to much more manageable levels without the constant fear and worry of the future of our childs health. Our mental health overall would benefit from this as well. I as the full-time caregiver, could return to my career that I had to leave when our child was diagnosed. Not only that, but by accessing these drugs, the health care system wouldn't be so burdened by the constant need for medical intervention and hospital stays to help and deal with the progression of the disease. – Parent of a child with CF
Improved Outcomes
Trikafta is the first, third-generation CFTR modulator. It has the potential to treat up to 90% of Canadians with cystic fibrosis and represents the single biggest advancement in treating cystic fibrosis in the history of the disease. It’s been proven to significantly improve health outcomes. The remarkable impact the drug has had on what has been an inevitably fatal disease has led to intense media interest. The Washington Post named it number one of nineteen good things that happened in 20197. In 2021, almost 500 media stories were written about the drug in Canada, as was outlined in CF Canada’s October 26 submission to INESSS regarding the access criteria it recommended for Trikafta.
Canadian research released in August 2020 predicts that rapid access to Trikafta could result in extraordinary health benefits by 2030, including 15% fewer deaths, 60% fewer people living with severe lung disease and an increased estimated median age of survival for a child born with cystic fibrosis of 9.2 years1. Understandably, expectations amongst the cystic fibrosis community are high, but also down to earth. Patients often simply want, and hope for, ‘normalcy’, and now that more people in Canada can access Trikafta, that sense of normalcy feels within reach for many.
My hope is that with access to Tikafta, my child will gain weight and lung function. Hopefully, he might be able to 'live' as other 10 year olds do- including partaking in activities that other 10 year olds do. Currently, he is a prisoner to his disease as he is restricted around his daily therapies which take time, knowledge and dedication. He is very embarrassed and aware that he requires extra support/therapy that other kids do not- even something as simple as taking enzymes at lunch time. He is very self conscious of this and he has voiced that he tries not to cough and refrain from going to the bathroom as he doesn't like to draw attention to himself in the classroom. As a mother, I only want the best for my child and to see him live a happy and healthy life. My hope is that Trikafta will be able to take him one step closer to that dream and maybe one day, his CF will be a controlled condition- not something he fights on a daily basis. – Parent of a child with CF
I am a 29 year old male living with cystic fibrosis, I truly believe this drug will finally change me to the point where I can finally think of myself as "normal" or "healthy" i've never known what its like to feel like a normal healthy person. I feel alienated in my own body. Living with Cystic Fibrosis is not easy. Growing up as a young boy in elementary school I went to school every day thinking I was different than every other kid there, and not different in a good way. I truly believe this drug can help me have a sense of normalcy. – Adult with cystic fibrosis
From popping pills and puffing in salt water to lunch breaks spent forcing myself to cough and strategically planning my grocery shopping trips... Living with cystic fibrosis means constantly trying to balance being normal and being chronically ill. It's more than just taking medication. I have to make choices all day, every day to make my health a priority, while still finding time to enjoy an evening out and taking snapchat selfies.
Unless you or a loved one has lived with it, what most people don't realize about cystic fibrosis, or any chronic illness, is that there's much more to it than just taking medications. Being sick is practically a full-time job and affects nearly every aspect of your life. Everything from simple tasks like grocery shopping, to making huge life decisions like what career field I wanted to go into have been influenced by my health.
Every day for me is a "sick day" because every day comes with an hour and a half to two hours’ worth of inhaled medications and airway clearance, five hours of being hooked up to a feeding tube, over two dozen pills and vitamins, another two dozen digestive enzymes and over 50 units of insulin. But the truth is... that's a "good" sick day.
Some days I have more than that because as I like to call it, I'm "sick sick". When I'm fighting a virus or infection, which I was during this day, I spend at least 4 hours a day actively hooked up to IV therapy through a mediport that's permanently embedded in my chest wall. I double my respiratory therapy and I add in various other medicines as needed like nasal sprays/rinses, pain and nausea management medications. Or I get put on steroids, which mean doubling my hydration to avoid my digestive system from developing an obstruction. Those weeks are when CF rears its ugly side and wreak havoc on my daily life.
All in all though, I'm fortunate enough to be able to keep an active, normal lifestyle on top of managing my health. That hasn't always been true, I've struggled more in the past and it won't always be true in the future. Cystic fibrosis is a progressive disease and it will get worse as I get older. There's no way to sugar coat that. But there is a way to be thankful for the beautiful life I have now and live each day to the fullest, being the best person, patient and advocate for cystic fibrosis that I can be!
Please note, not every person living with cystic fibrosis will take these same medications or make these same decisions. Each person, even each day, can look different. But this is my story and I hope you all enjoy hearing it! - Adult with CF
I am overcome with the personal stories and clinical improvements in lung function that people have on trikafta. My daughter is 8, her last PFTs came in at 55%. I truly believe that trikafta would give us time between illnesses, time to work and be a part of our community, time to enjoy life and get breaks for mental health stability. Every time she gets a cold now, without a modulator, she requires increased medications and therapies. Trikafta will reduce the amount of time she is isolated (and me!). No other modulators will help her, she has 1 D508 and a class 1 mutation 711+1G>T. This is our hope. – Parent of a child with CF
Patients long for the ability to breathe unencumbered, to live without fear that normal activities will cause further damage. They also want to be able to contribute to society. Parents and caregivers hope for better, healthier lives for their loved ones.
Access to Trikafta would change our world completely, my son would be able to achieve and pursue his goals and dreams, countless medical appointments and other medications would be reduced, family productivity now and in the future with go up exponentially, all of a sudden you would have thousands of individuals and their families who could focus on careers, businesses the overall long-term economic benefit would be tremendous. – Parent of a child with CF
My daughter would have fewer hospitalizations, more time being a kid. She would live a MUCH longer life. Have hopes and dreams. Less stress and less worry about dying. Be a normal 11 year old. Go to school, play with friends. I would get to be a mom. I wouldn't have to be a nurse and doctor and advocate. I could be the mom I always wanted to be. – Parent of a child with CF
As described above, cystic fibrosis is a highly heterogeneous disease, with many possible symptoms. Clinical progress is highly variable, even amongst individuals with the same CFTR mutations. Individual patients may be more dramatically impacted by different symptoms, all of which can have a negative impact on survival.
Even though my daughter is far below the minimum age at this time, to have the promise of Trikafta to look forward to would be an amazing thing- knowing that she would have the chance to save her health from the earliest possible time and live as normal a life as her sisters. To not have to worry about the likelihood of multiple hospitalizations every year, or having to wait for and endure a lung transplant, or develop further CF-related complications would be an incredible relief. – Parent of a child with CF
Many patients struggle with maintaining their weight, (a concern given that a low body mass index (BMI) correlates with poor post-transplant outcomes and correlates negatively with survival in general) and believe Trikafta will help achieve a healthier BMI. – CF clinician
Cystic fibrosis is a relentlessly progressive disease. Young patients with mild disease may live nearly normal lives because the progressive damage that is occurring to their organs has not yet manifested in ways that can be seen without clinical measures. Many patients and their clinicians see Trikafta’s potential to slow the progression of the disease or prevent co-morbidities from developing in the first place as the most important potential benefit.
Having access to Trikafta would give me the opportunity to strive toward my goal of becoming a doctor and helping others the way I have been helped throughout my life. I would be able to have children and live a relatively normal life without having the extreme physical and mental challenges that cystic fibrosis causes. [Without] Trikafta, there is no guarantee I will live past 25 years old as it is very unpredictable. Currently, my lung function is high but Trikafta is a medicine that works best in preventing damage. I need to have access to it before the damage becomes irreversible. – Adult with cystic fibrosis
I hope it will slow the progression of my disease so that I have the ability to live more comfortably in the moment without being in constant state of distress over what my future holds.– Adult with cystic fibrosis
My daughter is 3. Access to Trikafta at a young age could mean fewer hospitalizations, fewer medications, less lung deterioration or slower deterioration. It literally could mean that she could get pregnant when older, have a family, work full time and have a future that includes planning for retirement not early death. LIFE CHANGING both physically and mentally for us all. – Parent of a child with CF
Even individuals currently on a CFTR modulator anticipate seeing a benefit from switching to Trikafta.
I am currently on Orkambi and although it has helped me greatly, I believe Trikafta will help me more now that I am beginning to plateau on Orkambi. – Adult with cystic fibrosis
Prior to its approval by Health Canada the anticipation for this drug was exceptionally high.
I grew up hoping for something like this. It is a daily struggle right now to live, especially knowing that there is medicine that could help me. It is a special kind of hell. – Adult with cystic fibrosis
Experience With Drug Under Review
Some public programs in Canada started reimbursing Trikafta as soon as September 2021. As of November 2021, some private drug and all public programs in Canada had committed to covering Trikafta for those who meet the eligibility criteria. Unfortunately, eligibility criteria are not uniform across payers or jurisdictions, in part because CADTH’s recommendation for coverage for those 12 years old and over placed a controversial upper limit on lung function. With one exception, no other jurisdiction worldwide has placed such a restriction on access. The Health Canada indication is currently limited to those who are 12 years of age or older who have at least one copy of the F508del mutation.
As a result of the relatively recent public reimbursement of Trikafta, most patients with experience with the drug accessed it through either clinical trials or through the Special Access Program (SAP). Fifty-seven respondents to our January 2021 survey had experience with Trikafta. Sixteen were part of a clinical trial on Trikafta and continued to access Trikafta, whereas forty-one received access to Trikafta through the SAP. These are two distinct populations. The clinical trials recruited patients with mild to moderate disease (FEV1 between 40%-90% predicted normal), whereas the SAP grants compassionate access to patients with advanced disease, (FEV1 is invariably below 40%. We are unaware of a lower limit). Fifty-three of the above respondents offered descriptions of their experience with Trikafta8: forty-six (87%) found their experience with Trikafta to be very positive, six (11%) found it to be positive. One respondent (2%) indicated a neutral experience. There were no negative or very negative experiences reported.
Of the 57 total respondents with experience with Trikafta 53 offered detailed descriptions of their experience. Figure 1 shows the percentage of the 53 respondents who felt Trikafta improved various clinical parameters, but importantly also reveals the impressions of patients beyond what was measured clinically. For example, 72% believe that Trikafta decreased the rate of progression of symptoms. Three other subjective parameters support the very positive impact that Trikafta had on quality of life: 75% of respondents felt they had more energy, secretion clearance improved for 67% and just over 50% believe Trikafta improved both sleep (51%), and mental health (52%).
Lung function has increased by over 10%. No side effects have been experienced. - Parent of a child with CF My son has had a 180 degree turn around in his health. We are so very blessed. - Parent of child with CF Amazing improvements in weight, energy and lung function – Parent of child with CF
Total game changer. Weight gain, hasn’t been sick at all since starting trikafta about a year ago – Parent of a child with CF
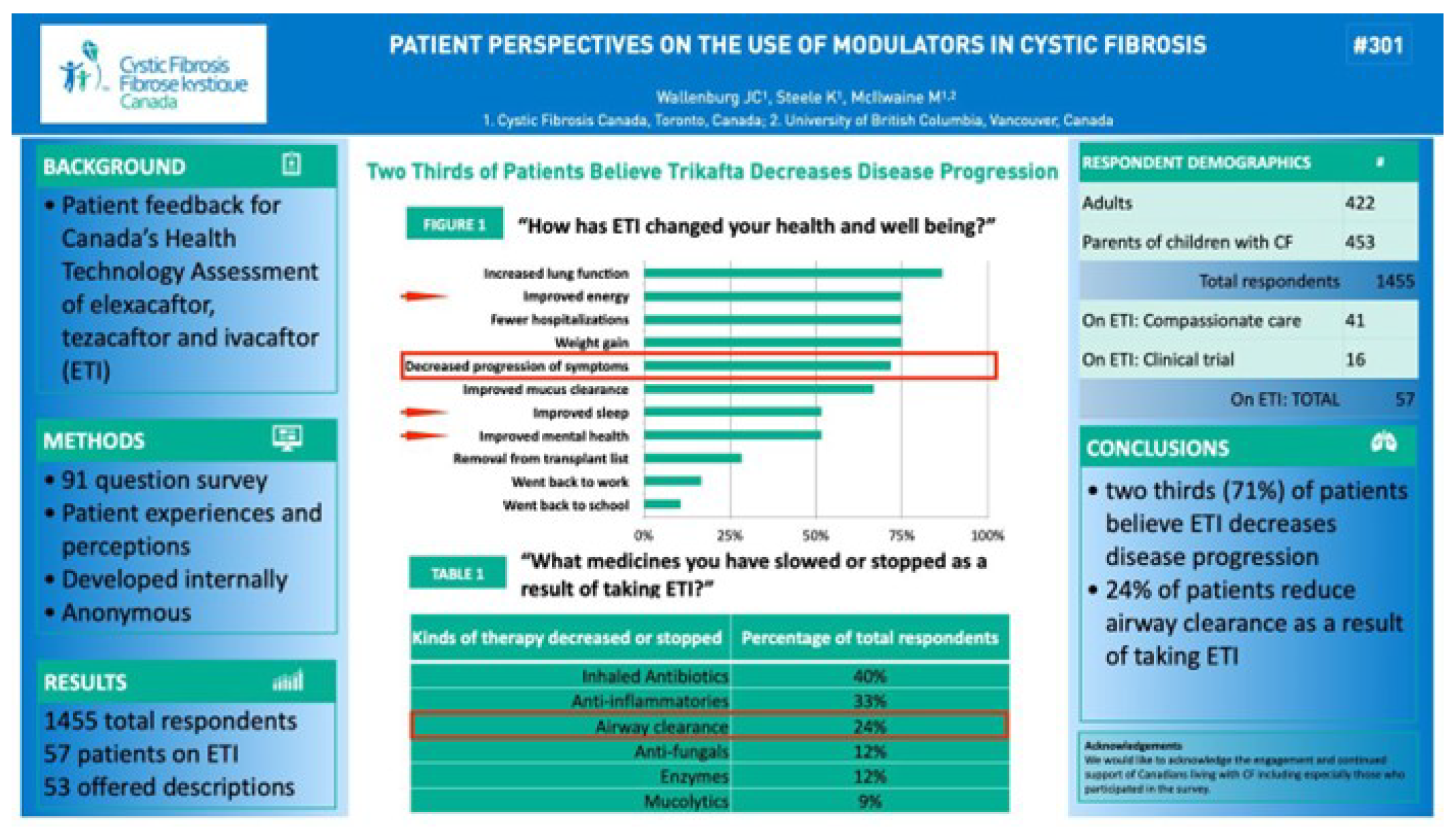
Of the clinically measurable parameters, patients reported that Trikafta improved lung function better than other therapies for 84% of the respondents, and improved nutrition for 68%. Eighty percent noted fewer pulmonary exacerbations (PEx). Nine adults under evaluation for transplants were removed from the list. Side effects were reported in 51% of respondents and included headache (22%), rash (12%), upper respiratory tract symptoms (URTI) (9%), elevated liver enzymes (6%), abdominal pain (10%) and nausea (3%). Respondents also reported on the acceptability of side effects. Headache, URTI and rash were deemed acceptable whereas elevated liver enzymes, abdominal pain and nausea were not.
People with cystic fibrosis have a very heavy treatment burden. To what extent does the improvement in quality of life that Trikafta brings lead to changes in the treatment burden? Significantly, 60% of respondents described slowing or stopping therapies as a result of taking Trikafta (see table in Figure 1). Five of the six therapies listed in the table in Figure 1 could reasonably be reduced because of improved clinical symptoms. For example, a reduction in infections and /or PEx could readily lead to a reduction in antibiotic use or anti-inflammatories, and similar arguments can be made for anti-fungals, pancreatic enzymes and mucolytics. This is consistent with the results of the clinical trials, and in time should be confirmed with Registry data for the population at large.
However, there is no reason for reducing airway clearance therapy, except personal choice, and 24% of respondents admitted to slowing or stopping airway clearance therapy. Standard of care calls for all patients, including children with healthy appearing lungs and non-productive coughs, to performance airway clearance therapy at least twice daily. Adult patients typically have positive feedback that coughing is productive – they produce and expel contaminated sputum. It might seem reasonable to patients whose sputum production is significantly reduced after starting on Trikafta, to also reduce airway clearance. This is not recommended but may be a natural outcome from dramatically improved quality of life after a very heavy life-long treatment burden.
See under the Treatment Goals section for the detailed description of this individual’s experience on Orkambi, then Symdeko. Here, their experience with Trikafta is presented.
I had the privilege of accessing Orkambi in 2016, Symdeko in 2018 … Unfortunately, my CF lung disease, though progression was slowed, was severe at this point and I had several complications in 2019 which led to testing to initiate the lung transplant process.
Fortunately, before that process was complete, I was approved for compassionate access to Trikafta in summer 2020. I did not have too high of expectations as I knew how my body did and did not respond to both Orkambi and Symdeko. My expectations were far too low! Trikafta began working within hours of my first dose and the mucous that lined my lungs was purged. Within a couple weeks, I did not need full-time supplemental oxygen, except for cardio exercise and my energy levels were higher than they have been in 10-15 years. I could take a deep breath and laugh without a coughing fit, something I had been unable to do for nearly a decade! I was finally able to participate in my life again instead of watching my family from the sidelines, something I truly believed would not be possible unless I received the gift of life, a double lung transplant. I still have severe CF lung disease as Trikafta cannot repair my scarred lungs and this is why it is so important that this medication be accessible before permanent irreversible damage has occurred so that Canadian children may not have to bear the burden of disease and trauma I have experienced. I can only imagine what my life would be like right now if Trikafta had been available to me when I was a young child. Since summer 2020, my lung function (FEV1) has increased by over 10 points and continues to slowly increase even 18 months later, which is not supposed to happen with a progressive disease like CF, but does because of Trikafta. In addition to that, before Trikafta, I typically was hospitalized every ±120 days for a minimum of three weeks at a time, for IV antibiotics and therapies to combat the chronic bacteria that live in my lungs. This need for acute care remained the case for much of my time on the previous modulators, Orkambi and Symdeko although my quality of life did improve and my lung function remained stable. I had been taking Trikafta for over 550 days before I needed a two-week hospital admission and this is a huge demonstrable improvement in need for acute care. However, looking beyond the numbers, I now have hope for the future for myself and our family. I am no longer wholly dependent on my spouse for my daily needs and I have confidence that I can carry out my daily tasks and not require days to recover from the exertion of completing them. I can tackle my basic needs like my airway clearing physio, household chores, groceries and still have energy for activities with my family and these are things I am forever grateful for.– Adult living with CF
For the past 30 years, my parents have prayed and hoped for a drug that could cure CF. Trikafta is the closest thing we have ever seen. It is, truly, a miracle drug. I am one of the incredibly lucky few chosen to take part in the drug trial while it was being tested. My health improved dramatically, and almost overnight. When I began the trial, my CF lung function indicator, FEV, was around 75%. It had been decreasing 1-2% every year for the last 10 years. Within 2 weeks my FEV was back up to 89%. Two weeks later I was at 94%. My mother cried when I told her. Those were numbers I hadn’t seen in more than a decade. In addition to measurable FEV numbers, my stamina was way higher. I am an avid mountain hunter and I didn’t get winded nearly as quickly as usual. My digestive system became less volatile. My energy levels were up, my appetite increased dramatically. And, perhaps the most shocking thing of all, I gained weight! From when I started the drug to today, I am up 20 pounds. That is mind-blowing. My doctors actually had to tell me to decrease the amount of high fat foods I was eating. Those were words I never thought I would hear in my wildest imagination. – Adult with cystic fibrosis
Twenty percent of respondents to our January 2021 survey were parents of one or more children with cystic fibrosis aged 11 years or younger. As reported by responding caregivers, 5.8% of children 11 years of age or younger accessed Trikafta as part of a clinical trial, and none received the drug through the Special Access Program. Given that Trikafta is not yet available for sale in Canada, the 11 children with cystic fibrosis aged 6-11 years who gained access through clinical trials are the only group with lived experience with the drug for whom we have data. Their experience is included above. Of the 11 children who participated in trials and whose parents responded to the survey, nine felt the experience was very positive, and two that it was positive. There were no neutral, negative or very negative responses. When asked to explain their responses, they described the following changes in their child’s health:
My son has had a 180 degree turn around in his health. We are so very blessed. – Parent of a child with CF
My son has never enjoyed better health than he has since accessing this drug. His chronic intestinal issues have cleared up (within days) and he had the longest period in his life without antibiotics. He’s gained weight and height at a rapid rate. He looks healthy. – Parent of a child with CF
My son very healthy – Parent of a child with CF
Amazing improvements in weight, energy and lung function – Parent of a child with CF We have seen some improvement in PFTs – Parent of a child with CF
Total game changer. Weight gain, hasn’t been sick at all since starting trikafta about a year ago – Parent of a child with CF Their growth and health has been excellent. – Parent of a child with CF
Lung function has increased by over 10%. No side effects have been experienced. – Parent of a child with CF
It’s like she doesn’t have CF anymore. She doesn’t cough, she doesn’t produce mucous, she is full of energy, she has an appetite and gains weight normally, she sleeps better, the list goes on! – Parent of a child with CF
Most parents felt that headache or nasal congestion were acceptable side-effects, whereas high liver enzymes and cataracts were not. Not surprisingly all parents felt Trikafta was easier to take than other CF medications, especially when compared to nebulized symptom management medications. In addition, as one parent described it: “it’s a struggle to have my child take [other medications] as he saw no benefit. With Trikafta he saw the benefit immediately and since then I have never had to fight or force him to take any of his medications.” Table 1 shows the responses when parents were asked “How has Trikafta changed your child's health and well- being?”. The question allowed parents to choose all answers that apply.
Table 1: How Has Trikafta Changed Your Child's Health and Well-Being?
Answer Choices | Responses | |
|---|---|---|
Increased lung function | 83.33% | 10 |
Weight gain | 75.00% | 9 |
Improved energy | 58.33% | 7 |
Slowing or stopping progression of symptoms | 50.00% | 6 |
Fewer hospitalizations | 50.00% | 6 |
Improved mucus clearance | 41.67% | 5 |
Improved mental health | 25.00% | 3 |
Went back to school | 25.00% | 3 |
Improved sleep | 16.67% | 2 |
This group of patients is of importance because cystic fibrosis is a progressive disease and this age group is generally in better health than older cohorts. This is reflected in data available for this category in the Registry. Of the individuals with spirometry records in the Registry (99% of individuals with CF over 12 yrs have a documented ppFEV1, 91% of individuals aged 6-11 have at least one documented ppFEV1) 73% of children aged 6-11 have a ppFEV1 >90% predicted, whereas only 27% of patients 12 and older test at >90% predicted (Stephanie Cheng, Director, Registry, Cystic Fibrosis Canada, personal communication). Disease progression is evident when looking at the median ppFEV1 vs. age of individuals with cystic fibrosis. There is a steady, rapid decline in lung function from the earliest recorded spirometry measures through a patients’ early twenties (figure 173).
There are few published studies that have looked at the 6-11 year old cohort specifically, however Zemanick et.al. evaluated the safety and efficacy of Trikafta in younger patients in a 24-week phase 3 open-label study in children 6 through 11 years of age with cystic fibrosis and at least one F508del CFTR allele. Their results show that the safety and efficacy of Trikafta in the children studied are consistent with those reported in adults and adolescents with cystic fibrosis, supporting the use of Trikafta in this younger patient population. Their results demonstrate that “the safety and efficacy of ELX/TEZ/IVA in these children are consistent with those reported in adults and adolescents with cystic fibrosis, supporting use of ELX/TEZ/IVA in this younger patient population.”9
Reflective of the generally better health of the 6-11 yr old cohort, subjects in Zemanick et.al. study had substantially higher baseline ppFEV1 (~89%) than seen in the phase 3 studies in the 12 yr and older cohort (~62%). Baseline quality of life as measured by CFQ- R respiratory domain scores were also substantially higher. Despite the higher baselines, treatment with Trikafta led to significant improvements in both ppFEV1 (10.2%) and CFQ-R respiratory domain scores (7 points), consistent with results from other CFTR modulator studies.
The recently published interim results from the Phase 3 open-label extension of the above trial confirmed the initials observations that Trikafta was generally safe and well tolerated. In addition, the “clinically meaningful improvements in lung function, respiratory symptoms, systemic CFTR activity, and nutritional parameters observed in the pivotal study were maintained through week 24 of the OLE study”2 confirming that Trikafta provides durable benefit in 6-11 year old subjects.
Importantly, the mean ppFEV1 baseline score for 6-11 year olds was 88.3%, very close to the upper limit of the inclusion criteria for the pivotal phase 3 study of Trikafta in patients 12+. CADTH’s controversial recommendation to limit access to Trikafta to patients whose baseline ppFEV1 is ≤90% seems anchored in the suggestion that no evidence exists to support its benefit to patients whose baseline ppFEV1 90%. It is clear from the data of the Zemanick et.al. and Ratjen et.al. publications cited above, that Trikafta provides significant clinical benefit to all patients regardless of initial status.
This is also reflected in the feedback from caregivers.
There are no words to describe the improvement in my mental health. My anxiety attacks have stopped. I can sleep through the night. I actually have time for myself. Watching my sons health improve and seeing him be able to function and have the potential to become a productive member of society rather than live a bed ridden sick life has been the miracle I had always prayed for. – Parent of a child with CF
His own outlook has dramatically improved and he looks forward to waking up, going to school and going to work. He has a second chance at life that he does not take for granted! Trikafta has blessed our family in so many ways and we are forever grateful – Parent of a child with CF
This medication is a life changer. I feel so fortunate that my son has access but I worry about when the trial is over. We need this medicine in Canada. – Parent of a child with CF
I’m hopeful that Trikafta will have a long term positive results for my daughter’s health.– Parent of a child with CF
Benefits to healthier patients with baseline spirometry greater than 90% was also confirmed in the findings of the PROMISE study, a post-approval, real-world, observational study to understand the effects of Trikafta in clinical use in the USA10. Nichols et.al. found substantial improvements across a range of clinical outcomes, including for a large subset of 196 patients whose baseline ppFEV1 was at or above 90% that saw a clinically significant mean improvement of 6.5% as well as improvements in CFQ-R of over 15 points, and an increase in mean BMI of +0.82.
The lived experiences of Canadians who have recently gained access to Trikafta or have a prolonged experience with it are consistent with the results observed in the clinical trials, the open-label extension studies and the post-approval real-world observational studies. In all cases, and regardless of baseline spirometry measures, patients see significant benefits.
I no longer want to celebrate the day that I was born. The day I truly want to celebrate is my Trikafta birthday. This is the first day that I have a sense of a future. Blowing out the candles on my cake on my first anniversary of Trikafta was so incredible, and I had the breath to blow out every single candle. My real birthday was counting down until death, and my Trikafta birthday is about counting up. And it’s about life. – Adult with CF
My son has never enjoyed better health than he has since accessing this drug. His chronic intestinal issues have cleared up (within days) and he had the longest period in his life without antibiotics. He’s gained weight and height at a rapid rate. He looks healthy. – Parent of a child with CF
It’s like she doesn’t have CF anymore. She doesn’t cough, she doesn’t produce mucous, she is full of energy, she has an appetite and gains weight normally, she sleeps better, the list goes on! – Parent of a child with CF
Companion Diagnostic Test
Trikafta is currently indicated only for patients having at least one F508del mutation. As of December 2021, there are over 2100 known mutations of the CFTR gene, according to the Cystic Fibrosis Mutation Database (CFTR1). Fortunately, in Canada, genetic mutations have been identified and recorded in the Registry for 99% of all living Canadians with cystic fibrosis who were seen in a cystic fibrosis clinic in 2019 so patients eligible for Trikafta are readily identifiable.
Mutations of CFTR are generally classified according to structural functional defects into one of more mutation classes, ranging from I to VI11. F508del is classically considered a class II mutation as are many other, often rare, mutations and the possibility that Trikafta may be effective for other mutations is an area of active investigation. Preclinical model systems played a critical role in the development of CFTR modulators and have the potential to support the use of modulator therapies in new populations12. The US Food and Drug Administration (FDA) has in fact accepted the concept that positive drug responses in a laboratory system using Fisher Rat Thyroid (FRT) cells may be used as a surrogate for clinical efficacy and has used in-vitro data derived from that system to extend the label of Kalydeco, Symdeko and Trikafta to include multiple rare mutations13.
While it is not currently possible to determine who will benefit from Trikafta in advance of administering the drug, a number of studies are underway to identify in-vitro assays with the potential to predict clinical response to CFTR modulators at an individual level14.
Cystic Fibrosis Canada has partnered with the Hospital for Sick Children and Genome Canada on a project to develop predictive tools that will help clinicians determine the right medicine for the right patient15. In addition, trials are underway in Europe to use rectal organoids to test in vitro a patient’s response to drugs16.
In summary, the entire Canadian population of patients eligible for Trikafta are already identified for the clinicians that will ultimately prescribe the drug. Canada’s CF clinicians have the Canadian Clinical Consensus Guideline for Initiation, Monitoring and Discontinuation of CFTR Modulator Therapies for Patients with Cystic Fibrosis in place to help them manage access to modulators, including Trikafta. The Canadian Cystic Fibrosis Registry will continue to track all patients on the drug allowing for post-approval analyses of Trikafta’s benefits and limitations and laboratory tools that will predict whether a patient is expected to benefit from a drug are under development and should be available soon.
Anything Else?
CADTH’s recommendation with respect to the use of Trikafta for Canadians aged 12 and over living with cystic fibrosis was largely sound but included an ill-advised ceiling on eligibility limiting access to patients with a baseline ppFEV1 of ≤90%. This decision was based not on evidence but on the absence of it. As cited above, ample evidence now exists supporting the use of Trikafta in all populations approved by Health Canada.
Furthermore, Cystic Fibrosis Canada’s key recommendations are that:
CADTH recommend that Canada’s public drug programs fund Trikafta for those who are 6+ without any upper limit on lung function start criteria.
CADTH work with Canada’s public drug programs to empower CF clinicians to guide prescribing and renewal activities, as governed by the Canadian Clinical Consensus Guideline for Initiation, Monitoring and Discontinuation of CFTR Modulator Therapies for Patients with Cystic Fibrosis.
CADTH recommend that in-vitro testing be accepted by Canada’s public payers as effective tools for identifying rare mutations that will benefit from CFTR modulators as soon as correlation with clinical outcomes have been confirmed.
Patient Group Conflict of Interest Declaration — Cystic Fibrosis Canada
Did you receive help from outside your patient group to complete this submission? If yes, please detail the help and who provided it.
Cystic Fibrosis Canada prepared this submission.
Did you receive help from outside your patient group to collect or analyze data used in this submission? If yes, please detail the help and who provided it.
No.
List any companies or organizations that have provided your group with financial payment over the past 2 years AND who may have direct or indirect interest in the drug under review.
Table 2: Conflict of Interest Declaration for Cystic Fibrosis Canada
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
AbbVie | — | — | — | X |
Horizon Pharmaceuticals | — | — | X | — |
Mylan Pharmaceuticals ULC | — | — | — | X |
Vertex Pharmaceuticals Canada | — | — | — | X |
AstraZeneca Canada Inc | X | — | — | — |
Bayer Canada Inc | X | — | — | — |
Gilead Sciences Inc | — | — | — | X |
Merck Frost Canada Inc | — | — | X | — |
I hereby certify that I have the authority to disclose all relevant information with respect to any matter involving this patient group with a company, organization, or entity that may place this patient group in a real, potential, or perceived conflict of interest situation.
Patient Group: Cystic Fibrosis Canada
Date: December 16, 2021
References
Stanojevic, S. et al. Projecting the impact of delayed access to elexacaftor/tezacaftor/ivacaftor for people with Cystic Fibrosis. J. Cyst. Fibros. 109, 1521 (2020).
Ratjen, F. et al. 562: Elexacaftor/tezacaftor/ivacaftor in children aged 6 and older with cystic fibrosis and at least 1 F508del allele: Interim results from a Phase 3 open-label extension study. J Cyst Fibros 20, S265 (2021).
The 2019 Annual Data Report of the Canadian Cystic Fibrosis Registry. https://www.cysticfibrosis.ca/ registry/2019AnnualDataReport.pdf (2020).
Stanford, G. E., Dave, K. & Simmonds, N. J. Pulmonary exacerbations in adults with cystic fibrosis - a grown-up issue in a changing CF landscape. Chest 159, 93–102 (2021).
Quittner, A. L. et al. International Committee on Mental Health in Cystic Fibrosis: Cystic Fibrosis Foundation and European Cystic Fibrosis Society consensus statements for screening and …. Thorax (2016).
Wallenburg, M. Typical day at home. Typical day at home https://marikasmotorcyclediaries.wordpress.com/2014/02/19/typical-day- at-home/ (2014).
Editorial Board. Opinion: 19 good things that happened in 2019. Washington Post (2017).
Wallenburg, J., Steele, K. & McIlwaine., M. 301: Patient perspectives on the use of modulators in cystic fibrosis. J. Cyst. Fibros. 20, S145 (2021).
Zemanick, E. T. et al. A Phase 3 Open-Label Study of Elexacaftor/Tezacaftor/Ivacaftor in Children 6 through 11 Years of Age with Cystic Fibrosis and at Least One F508del Allele. Am. J. Resp. Crit. Care 203, 1522–1532 (2021).
Nichols, D. P. et al. Clinical Effectiveness of Elexacaftor/Tezacftor/Ivacaftor in People with Cystic Fibrosis. Am. J. Resp. Crit. Care (2021) doi:10.1164/rccm.202108-1986oc.
Veit, G. et al. From CFTR biology toward combinatorial pharmacotherapy: expanded classification of cystic fibrosis mutations.Molecular biology of the cell 27, 424–433 (2016).
Clancy, J. P. et al. CFTR modulator theratyping: Current status, gaps and future directions. J Cyst Fibros 18, 22–34 (2019).
Goor, F. V., Yu, H., Burton, B. & Hoffman, B. J. Effect of ivacaftor on CFTR forms with missense mutations associated with defects in protein processing or function. J. Cyst. Fibros. 13, 29–36 (2014).
Dumas, M.-P., Xia, S., Bear, C. E. & Ratjen, F. Perspectives on the translation of in-vitro studies to precision medicine in Cystic Fibrosis. Ebiomedicine 73, 103660 (2021).
Eckford, P. D. W. et al. The CF Canada-Sick Kids Program in individual CF therapy: A resource for the advancement of personalized medicine in CF. J. Cyst. Fibros. 18, 35–43 (2019).
Mourik, P. van et al. Rationale and design of the HIT-CF organoid study: stratifying cystic fibrosis patients based on intestinal organoid response to different CFTR-modulators. Transl. Medicine Commun. 5, 9 (2020).
CF Get Loud
Overview
Thank you for the opportunity to give feedback on the most recent indication for Trikafta: the treatment of cystic fibrosis (CF) in patients aged 6 years and older who have at least one F508del mutation in the cystic fibrosis transmembrane conductance regulator (CFTR) gene.
The CF Get Loud community members are CF families fighting for the future of CF families in Canada. We are passionate volunteers that have a common goal - to save the lives of CF patients. The Executive Members of the CF Get Loud team have all narrowly escaped succumbing to the harsh reality of our terminal illness. All three were born in the 1980’s during a time when CF was known as a childhood disease because many patients were never given the opportunity to reach adulthood. We have experienced much of the full spectrum of trauma that this disease has to deliver and lived to tell about it. We wholeheartedly understand the decades of hardship that CF children will endure and it is our deepest desire to change this.
In 1989, the researchers at the Hospital for Sick Children in Toronto, Canada isolated the gene that causes CF. At that time, our community was told to ‘hold on a little longer’ because a cure would be coming soon. So we fought, spending our lives battling this disease and many of us lost the battle. It seemed that no matter how strong we were, no matter how many times we proved that we are warriors, CF proved it was stronger. We waited for the ‘miracle medications’ that our doctors promised were on the horizon. No one could predict that it would take until October 2019 for this life-saving medication called Trikafta to be released to the CF patient population in the US. In 2020, after a long advocacy battle, some patients in Canada were fortunate enough to begin taking Trikafta. For many of us, including this Executive Team, the medicine nearly came too late. Like a parachute opening at the last moment, Trikafta arrived just in time to slow our descent. Unfortunately, this arrival came decades after severe irreversible damage to our bodies had already been done. This cruel routine of getting sicker while waiting for a second chance must end immediately.
We are now fighting for the next generation of CF kids – ages 6 and up. It’s a very personal fight for us because in these kids, we see our past. We see the childhood that was stripped away. We see the heartbroken parent holding on to the hope that they will not outlive their own children. In these children we see the opportunity for them to unleash their full potential, free from the burden of this merciless disease, to give them a fresh start and a way to ‘right’ the past that we as adults cannot undo. It’s within this generation’s lifetime that we will see CF will go from a terminal disease to a manageable illness if access to modern medicine is granted from birth. In this submission we need you, Canada’s healthcare decision makers, to understand why we cannot let these children continue to suffer when the future of modern medicine is already here. This community needs unrestricted access to Trikafta.
The Long Battle for Trikafta
This is now the third time we have had the opportunity to express our views on the indications for this medication, so we will forgo the structured format used in previous submissions and speak from the heart.
At this stage we must assume that you are aware of what CF is and what a medication like Trikafta means for the thousands of Canadian families that have had the misfortune of facing a CF diagnosis. However, in the unlikely event that you are not, we will summarize it succinctly: CF kills 100% of the time. Its ruthlessness knows no measure. To add insult to injury, every patient’s condition is different, regardless of mutation combination. This means that our CF population of around 4400 Canadians is extremely diverse in symptom manifestation and severity. In spite of this diversity, the 90% of us that can benefit from Trikafta have one thing in common; our lives can be changed completely due to this life-saving medication.
We find ourselves writing another iteration of what we have been using our waning breaths to communicate for the better part of two years: that this drug will absolutely change the lives of 4,000 Canadians living with CF and by extension, another 40,000 Canadians that are impacted on a daily basis by those living with CF. Those of us with this disease often use the phrase, “living with CF” because the alternative, “dying from CF” is not an option for us or our families. From a very young age, we learn that there is no option but to fight to survive, thus becoming “CF warriors”.
In September of 2021, you released your final recommendation on Trikafta. Since then, all the provinces and territories have made it available through their public plans. Unfortunately, this has been a very hollow victory. We are thankful to witness our Canadian brothers and sisters get access to this miracle drug but are very much aware of the many roadblocks that remain. The majority of these are because of your final recommendations released this past September. Private insurance companies continue to deny access to Canadians. Public access paths have put families in the impossible financial position of having to pay exorbitant deductibles in order to access this medication. Left with no choice in an already difficult situation, families are left dealing with renewed hope while enduring compounding stress in other areas of life. We are asking that you give our community hope by extending access to those CFers 6 years and older, free of stipulations or exclusions.
As things stand, even with limited publicly funded access, there are already plenty of obstacles. The assessment on the benefits of this medication lies solely and exclusively with the medical care teams who are our experts in the subject matter. Just as it is not up to the patients on whether they can access a drug, the decision to access life- saving medication should remain with the appropriate medical professionals and should not be up to a bureaucratic and pharmacoeconomic panel to decide. Our community feels betrayed as our elected officials and other governing entities have failed to understand the magnitude and scope of this disease. It has been 786 days since Trikafta became available in the US. Frustratingly, Canadians have only gained access to this same drug as recently as a month ago through publicly funded means. Your recommendation has played a significant role in this equation and we ask that you give it the importance and careful deliberation it warrants. CF can’t wait. CF does not wait. You have a chance to prevent the unnecessary suffering that CF families are destined to endure by recommending access with no restrictions for anyone 6 years and older that can benefit from this breakthrough medication.
The VOICES of CF Families Across Canada
CF Get Loud interviewed mothers across Canada and the word HOPE was stated again and again. Hope has been a motivator for patients and caregivers throughout the history of this devastating disease. It helps these families persevere but hope is not a strategy. We need an action plan to give these children back their childhoods.
Camille Gillcash-Sposito and 5-year-old Finn)
“Trikafta is Hope. Our son is 5 years old and currently "healthy". But despite the 2+ hours of physiotherapy we do daily as prevention, exercise and excessive nutritional planning and brainstorming trying to maintain his weight (currently in the bottom 3% for his age), we are already starting to see signs of progression.”
“We don’t want to have to think about the very real possibility that we will outlive our Son.”
How will Trikafta change your child’s future?
“Trikafta is Hope. Our son is 5 years old and currently "healthy". But despite the 2+ hours of physiotherapy we do daily as prevention, exercise and excessive nutritional planning and brainstorming trying to maintain his weight (currently in the bottom 3% for his age), we are already starting to see signs of progression.” It shows itself as increased daily coughing, despite not being sick. Low desire to eat, making it difficult to maintain weight and grow. Anxiety and resistance to his necessities of life, especially his therapy. It is hope that he can have a normal childhood without the "extras". It is hope that this fatal genetic disease will not define who he is. We don’t want to have to think about the very real possibility that we will outlive our son.”
How will Trikafta change you (the caregiver’s) future?
Trikafta will allow us to not live in constant fear of what exposures might land Finn in the hospital. Not having to think about things in the context of consequences. "If we play in these Autumn leaves, will he be exposed to bacteria and fungus that will cause him to get a lung infection and end up in the hospital?" Telling him constantly we can't do things because of the potential health consequences of them. We don’t want to have to think about the very real possibility that we will outlive our son.
How soon do you want your child to have access to Trikafta?
We would like to have Trikafta for Finn as soon as possible. We think that preventative medicine is a much better approach for so many different reasons. Number 1 reason is why would you want someone's health to decline enough, before you will allow them access to something that can prevent decline? To me, this is a form of cruelty that we wouldn't bestow upon our pets, and yet we put qualifying criteria on a medication so that a child's health has to deteriorate far enough before they are provided treatment. I can't fathom how this is considered an ethical approach to medicine.
What were your initial thoughts/feelings when you first heard of Trikafta?
We were ecstatic to see the progress of gene modulating drugs. When Finn was first diagnosed in 2016, there were currently no modulators that he would qualify for based on his specific genetic mutations. Trikafta is the first drug developed for him and up to 90% of other CFers. It is such a wondrous feeling knowing that development and progression on drugs for CF patients continues to advance and is expanding in its efficacy to more patients. It gives us hope that someday soon, there may be a cure for ALL patients living with CF.
How does CF impact your child’s life?
Currently, Finnegan has been resisting his therapy. He sees his 2 year old little sister being able to play when he needs to sit at the table to do his breathing exercises. He is acutely aware of precautions necessary to keep him safe. He understands why he needs to take his enzymes, why wearing a mask is important, washing hands and doing therapy. He has had many tests performed from blood work, CT scan, x rays and routine throat swabs. He has a lot of anxiety with most of these and some of it he has gotten used to, but others it seems traumatizing for him. He used to talk about getting his throat swab at clinic as soon as he found out we were going. The entire 1-2 hour drive to sick kids would be him crying and getting upset thinking about it. He has since overcome this fear, but many of the other tests he gets on a regular basis are similar experiences for him.
Have you spoken to your child’s care team about Trikafta?
Briefly when it was first approved by Health Canada. But because he is way too young for current approval, we haven't discussed anything at length yet. We are hoping that we can have the opportunity to begin treatment sooner rather than later, before irreversible lung damage begins, and Finnegan's quality of life begins to deteriorate. We know that it isn't a matter of IF, but a matter of WHEN his lung function begins to decline.
Melanie Morin-Pelletier and 12-year-old CF son
“I don’t think I will ever recover from the trauma of almost losing my newborn son to CF. My son has had gastric issues since birth as well as issues with his liver and pancreas. Despite his “normal” lung function, nothing about his life or my life with CF feels normal.”
How will Trikafta change your child’s future?
Trikafta will stop the progression of the disease in my son's lungs and help with his gastric, pancreatic and liver issues. He is about to start high school and Trikafta would mean not spending as much time in hospital and not spending as many hours every day doing treatments. Trikafta means being able to attend college or university, choosing the future that you want and becoming a productive citizen.
What were your initial thoughts/feelings when you first heard of Trikafta?
I was very hopeful when I started seeing the research results showing that Trikafta had such a positive impact on CFers quality of life (regardless of lung function numbers), on lungs and gastric issues, and that it meant adding decades to a CFer’s life.
When was the first time that you felt CF impacted your child’s life? What was their lung function?
My son was born with meconium ileus and required bowel surgeries when he was 4 days old and 5 weeks old. I don’t think I will ever recover from the trauma of almost losing my newborn son to CF. My son has had gastric issues since birth as well as issues with his liver and pancreas. Despite his “normal” lung function, nothing about his life or my life with CF feels “normal”. Five months after my son was born, I was diagnosed with CF as an adult. My lung function is also considered “normal”, although there is obviously serious damage in my lungs. Last year, I spent an entire week in the hospital coughing up mouthfuls of blood multiple times a day for 7 days straight. My PFTs [pulmonary function test] don’t tell that story. Because PFTs only tell a tiny part of the Cystic Fibrosis story.
How does CF impact your child’s life?
He hates having to do hours of breathing treatments every day and it does have an impact on his activities and him being a kid. Every time he wants to eat something he must come and see me or call me so we can evaluate the amount of fat in the food and take the required number of enzymes. He needs to take about 20 pills every day and carry them around everywhere he goes. He’s had to miss many birthday parties and other kid’s activities in his life because we have to be extra careful not to be in contact with anyone who could potentially be sick. What people have been through during the current pandemic -all the extra measures and being partially confined- reflect his life since he was born.
Have you spoken to your child’s care team about Trikafta?
Yes. They are very supportive. But they feel that with the current lung function criteria, it would be a waste of time to apply to the provincial program. We already know that our insurance company will decline him as they have told us that it is not covered by my employer. Since we have private insurance, even if they don’t cover Trikafta, we will not be allowed to apply through OHIP+.
Does your child know of Trikafta?
Yes, he was incredibly happy and hopeful when he heard years ago the impact that Trikafta has on CFers. Like us, he feels let down by this system that tells him that his life is not worth the price of the drug. Why else would the CADTH put this 90% criteria for lung function when evidence shows that Trikafta improves lung function for patients with greater than 90% lung function? Saving money should never be more important than saving lives.
“I wish my mom and dad didn’t have to worry. I wish they didn’t have to always do fundraisers for a cure. My wish would be to be more normal.”
How will Trikafta change your child’s future?
Until Trikafta, the future for my kids has been so uncertain. Seeing so many families struggle and lose loved ones to this disease has been heart wrenching. Trikafta would give us hope for the future.
Trikafta would make the endless treatments, meds, and trips to the children’s hospital (4 hours away) multiple times a year, worthwhile. It would make our efforts to keep them healthy this long, not in vain.
How will Trikafta change you (the caregiver’s) future?
The fear of their lives being shortened or more challenging than they should be keeps us up at night. So many people have worked so hard for so long to make this dream a reality for the 4500 Canadians living with CF. This drug would absolve fears and give us hope for a beautiful life for our kids. CF only takes. The only family vacation we have ever been on was a wish trip. My husband and I use our vacation to stay home when they are sick, take them to a clinic, or for testing, and it would be lovely to use vacation for vacation!
When was the first time that you felt CF impacted your child’s life? What was their lung function?
Keira cultured pseudomonas when she was 4 and it was before she could have her FEV1 measured. It was the first time I realized that this was going to be a real battle for the whole family. For our son, it was when his BMI was dropping and affecting his lung function. He had a g-tube placed and that was another eye opener. This is a club that nobody wants to be part of, but with Trikafta, the battle is changing.
How does CF impact your child’s life?
As they get older and as they learn the ways in which they are different from other kids, the impacts are getting bigger. When they were little, CF life was just “their normal”. Now they are starting to build resentments and feel sadness. It’s almost like grief when they see how simple others this age have things. Something as simple as a class trip or sleepover required so many extra steps. As they get older, they know what the numbers mean and it’s just so much pressure to stay healthy and do all the things needed to stay healthy.
Does your child know of Trikafta?
A few words from Keira (age 11):
“I feel like Trikafta is going to change my life by increasing my lung function so I can take less meds and stop doing treatments at sleepovers.
I would hope for less trips to Ottawa and more family vacations.
My wish with Trikafta is that less people will call me skinny, and comment on the food I have to eat to stay healthy.
I wish my mom and dad didn’t have to worry. I wish they didn’t have to always do fundraisers for a cure. My wish would be to be more normal.”
Renee Berdan and 7-year-old Greta
“It can be hard to have hope when we’ve lived through such trauma, but Trikafta changes that. It gives us hope for her future and that she can give a long, full life.”
We have a 7-year-old CF daughter named Greta and an 8-year-old healthy son named Lennan. We also had a third child named Ander that passed away unexpectedly from CF related complications shortly after he was born 4.5 years ago. The trauma of losing a child in that way, combined with the daily challenges and difficulties of fighting the same disease in a living child, is incredibly difficult.
One of the things we have had to face, especially since burying one child from CF already and facing the reality and severity of this disease, is that one day we would likely have to say goodbye to our beautiful girl too. It can be hard to have hope when we’ve lived through such trauma, but Trikafta changes that. It gives us hope for her future and that she can give a long, full life. If she can start this medication before the inevitable damage settles into her lungs, it exponentially increases her chances of a long, bright future.
Greta is one of the brightest 7 year olds I’ve ever met. I know I’m biased because I’m her mom, but so many people she meets comment on what a light she has inside her. It’s not just me. She is a gift, and has the potential to impact the world. Let’s give her the opportunity to share her light for as long as possible.
Rebecca Reiter and 9-year-old Emma
“CF gave me the advantage of being stronger in life but it takes a lot of time and I have to do some stuff that the other kids don't have to do and sometimes I can't go to things to stay healthy. It has made me a responsible person. I also try to make sure I make the best of each day.”
How will Trikafta change your child’s future?
Emma: It will change my future by giving me the opportunity of doing stuff that I've never really got the chance to do because I've been too busy with CF.
Rebecca (Mom): Trikafta will change my child's future, even saying those words is powerful in itself! She is a creative, hard-working and joyful girl and I want her to experience achieving her goals and dreams and establish a fulfilling life with nothing holding her back.
How will Trikafta change you (the caregiver’s) future?
Rebecca (Mom): Trikafta will literally help Emma breath, and give me a long awaited breath/sigh of relief. CF doesn't get a day off, and while we are happy and live each day to the fullest, there is always a worry of infection, lung decline or rounds of medication in the background. There is a weight on a caretaker's shoulders that can be lifted with Trikafta. I would increase my hours as a teacher too!
How soon do you want your child to have access to Trikafta?
Emma: I want to have access to Trikafta now because I think it’s going to change my life and I'm really excited for it. Rebecca (Mom): As a mother, I want to protect my daughter’s health and Trikafta can do this. Trikafta can prevent further decline. We need it now!
What were your initial thoughts/feelings when you first heard of Trikafta?
Rebecca (Mom): Tears of hope streamed down my face. Emma has a rare mutation and other modulators won't work for her. Trikafta is a dream come true.
How does CF impact your life as a patient?
Emma: CF gave me the advantage of being stronger in life but it takes a lot of time and I have to do some stuff that the other kids don't have to do and sometimes I can't go to things to stay healthy. It has made me a responsible person. I also try to make sure I make the best of each day.
Danielle Weil and 3-year-old Emme:
“We now have hope that Emme will be able to live a normal, healthy life and that her twin sister Erin and now her younger sister Clare will never have to have that conversation with us to prepare them for losing their sister.”
“They [the doctors] flat out said that this was "the one" that they have been waiting for since the discovery of the CF gene.”
“She won't remember the fight to get Trikafta here but we will make sure that she can look back at what everyone went through to get it to Canada for kids and adults like her, living with CF.”
How will Trikafta change your child’s future?
To us, Trikafta is the hope that Emme will HAVE a future. With a median age of survival of 52 for children born when Emme was, we have had to accept that Emme may not live a full and healthy life. We have had to prepare, since she was 12 days old, that a conversation will one day take place with her twin sister to tell her that she will outlive Emme and be left without her twin. Not only would she lose her sister, but she would have to watch as Emme's health inevitably declines as she herself remains healthy and we as her parents would have to watch and help her deal with survivors' guilt. Trikafta has already changed everything for us in that regard - we now have hope that Emme will be able to live a normal, healthy life and that her twin sister Erin and now her younger sister Clare will never have to have that conversation with us to prepare them for losing their sister.
How will Trikafta change you (the caregiver’s) future?
I believe that Trikafta will not necessarily reduce our workload as caregivers, but will reduce the burden of the unknown. We had less than 48 hours after Emme was born to enjoy our time as parents to healthy babies before her complications were made apparent, and the stress of that and her subsequent diagnosis has never left. With Trikafta, we can know that her health is not riding on our efforts alone and we hopefully will not have to get to the point where our efforts are not enough. The physical toll of physiotherapy as well as the mental toll of keeping track of medications, schedules, constant doctors appointments and tests, listening and analyzing every cough or sniffle, preparing for all of the 'what ifs', figuring out how we will pay for all of the out of pocket expenses, etc. Trikafta will not take it all away, but it will definitely lighten the load.
When was the first time that you felt CF impacted your child’s life? What was their lung function?
I think we have felt the impact of CF for Emme since we began her daily treatments at about 2 months of age. With the unique situation she is in being a twin, she has grown up side by side with her sister who does not have CF and while they are used to the routine of medications and treatments, it has always been a glaring difference between the two. Where Erin is free to run around and play during treatment time, Emme is restricted by her mask or need to sit in her assigned positions during physiotherapy. She cannot simply start eating a meal when everyone sits around the table, but has to wait until her enzymes are prepared and given to her (usually with a reminder from her sister, who recognizes that Emme gets something different before eating and has now started asking for them herself).
Have you spoken to your child’s care team about Trikafta?
We have discussed modulators in the past, at which time her clinician made it clear that they were waiting for Trikafta not only because they wanted to make sure there would be no potential issue with changing from one modulator to another, but also because the results coming out of Trikafta were above and beyond anything that they were seeing with the earlier generations of modulators. They flat out said that this was "the one" that they have been waiting for since the discovery of the CF gene, and at her very young age the results were worth waiting for. Now that it's here, I think as we hear more about the 6-11 application and Emme gets closer to qualifying based on her age, they are going to be starting the ball rolling to get her onto it as soon as possible
Does your child know of Trikafta?
Emme does not understand the gravity of Trikafta, but we have made sure to document the journey of all of our advocates and CF Canada's fight so that she can see in the future how incredible this has all been. We have made sure to have a tangible, participatory celebration with each success such as a small sushi dinner party (one of her personal favourite meals), making celebratory cupcakes, having T-shirts made, etc. as well as participating in videos and such with pictures, colouring pages, etc. She won't remember the fight to get Trikafta here but we will make sure that she can look back at what everyone went through to get it to Canada for kids and adults like her, living with CF.
Marilyn Snarr and 5-year-old Jack
“For the first time in Jack’s life we allowed ourselves to start dreaming of his future. A future that we were too afraid to think about before. Learning about Trikafta gave us so much hope and excitement for Jack’s future.”
How will Trikafta change your child’s future?
Trikafta will change Jack’s future by giving him a future he may have never known. When we were told that Jack has Cystic Fibrosis we had no idea what that would mean for his future. Would he live 40 years? 20 years? Maybe less? The thought of losing Jack and the thought of Jack not getting to experience a long and happy life was awful. Trikafta gives us hope that Jack will get to experience that long and happy life that we worried he wouldn’t get to experience. Trikafta means that Jack can dream the biggest dreams for his life and not feel limited by Cystic Fibrosis. It gives Jack the future that we feared he wouldn’t get to have.
How will Trikafta change you (the caregiver’s) future?
Jack’s CF diagnosis was devastating for our entire family. The amount of worry that we have experienced in Jack’s short life has been more than we could have imagined. That worry can be a heavy weight to carry for a parent. Trikafta gives us hope for a brighter future for Jack. Our worries about Jack going to school or participating in activities are replaced by excitement about everything he will get to do. Having Jack on Trikafta would remove a huge amount of worry that we experience as caregivers.
How soon do you want your child to have access to Trikafta?
Our hope is that Jack can access Trikafta as soon as he turns 6 years old in January. We have read about the tremendous benefits that CF patients have already experienced since starting Trikafta and are excited for Jack to begin his journey. We know that CF is progressive so it is important that we start Jack on Trikafta as soon as possible.
What were your initial thoughts/feelings when you first heard of Trikafta?
We can remember reading about Kalydeco and Orkambi shortly after Jack was born.
While those medications were not giving the same results as Trikafta we were so excited about the possibility that they held. That a medication could treat the underlying cause of Cystic Fibrosis. We heard rumours of the medications in the pipeline and that they could be game changers for CF. Nothing prepared us for just how amazing the results were. We started reading stories of the amazing results CF patients were experiencing on Trikafta. For the first time in Jack’s life we allowed ourselves to start dreaming of his future. A future that we were too afraid to think about before. Learning about Trikafta gave us so much hope and excitement for Jack’s future.
When was the first time that you felt CF impacted your child’s life? What was their lung function?
When I think of CF impacting Jack’s life the first thing that comes to mind are his clinic visits. His visits have become easier over time but for the first few years, going to the clinic was very stressful for Jack. He was scared of being in the clinic, scared of getting an x-ray, scared of getting blood drawn, scared for the whole experience. Jack didn’t have a choice in any of this. We understand the importance of clinic visits and would always try to make them as positive as possible but that was not easy to watch as a parent. Jack’s fear of the clinic carried into many other fears. Fear of the dentist, the eye doctor, anything that he related to the CF clinic. That really impacted the first few years of his life as he had a really hard time trusting medical professionals.
How does CF impact your child’s life?
As Jack approaches his sixth birthday he has started to ask more questions about his Cystic Fibrosis. He asks questions like; why do I have Cystic Fibrosis? Why don’t you have Cystic Fibrosis? Will my Cystic Fibrosis go away? We can see Jack trying to put the pieces of the puzzle together and it can be difficult at times. We would never want Jack to feel ashamed of his CF or to feel different about it. We tell Jack that he is just like all of his friends. He can still have fun, still go to school, still play the sports he loves. We explain that we just need to do a few extra things to make sure that he stays healthy and that his future is bright.
Does your child know of Trikafta?
Yes, we have spoken to Jack about Trikafta and the amazing effects that people have been experiencing. Jack is excited about the idea of a medication helping people who live with Cystic Fibrosis. He is excited about keeping his lungs healthy so that he can keep doing all of the things that he loves. Our whole family shares in the excitement for Trikafta and what it will mean for Jack’s life.
Sheralin Spring and 5-year-old Wyatt
“When I first heard about Trikafta it gave me the first feelings of hope since Wyatt was diagnosed”
“ When we first found out his diagnosis, there was a feeling of ‘will I have to bury my child one day?’ It is an awful thought to have and the hope of Trikafta and a more normal life, we find ourselves not worrying about that anymore.”
How will Trikafta change your child’s future?
Trikafta would mean we wouldn’t have to worry so much about Wyatt’s future. Instead of planning for hospital stays and sick days, we can start planning for what sports he is going to play, what he wants to be when he is older, etc. Trikafta would mean that his future wouldn’t be so uncertain.
How will Trikafta change you (the caregiver’s) future?
Trikafta would allow me, as Wyatt’s caregiver, to worry less about his health and instead just simply worry about the same things any parent does. It would mean not having to save for hospital admissions, when my husband would have to miss work to help take care of Wyatt and the other kids. It would mean not having to answer those hard questions like “mom, Wyatt won’t ever die from CF will he?”. It would also mean I could plan for a career without the uncertainty of sick days and hospital admissions that can become very frequent with CF.
How soon do you want your child to have access to Trikafta?
Wyatt turns 6 in January and it would be the absolute best birthday present for him to get access to Trikafta while he is 6 years old.
What were your initial thoughts/feelings when you first heard of Trikafta?
When I first heard about Trikafta it gave me the first feelings of hope since Wyatt was diagnosed. Even the idea that there was a medication out there that could impact his life so positively brought us such relief. As we have heard many stories of success and good health in adults with CF taking Trikafta, it has just solidified our hope for Wyatt’s future once he can take Trikafta. When we first found out his diagnosis, there was a feeling of “will I have to bury my child one day?” It is an awful thought to have and the hope of Trikafta and a more normal life, we find ourselves not worrying about that anymore.
When was the first time that you felt CF impacted your child’s life? What was their lung function?
Shortly after diagnosis, at just 3 weeks old, Wyatt got his first lung infection and it resulted in a collapsed lung. It was that moment when we realized the severity of cystic fibrosis and the impact it would have on his life. Wyatt is not old enough for an accurate lung function test yet.
How does CF impact your child’s life?
At just 5 years old, Wyatt is already beginning to ask why he has CF. He does not understand why he has it, but his siblings do not. We are lucky that he is very compliant with his daily therapy, but there are times when he does not want to come inside from playing outdoors to do his therapy, or stop doing what he is doing. With Trikafta, he would have so much more time to spend just being a kid.
Catherine Trail and 5-year-old Susanna
“We tried to explain that CF wasn’t a punishment for behaviour; it was just the way she was born. Then she looked me right in the eyes and told me that she wished she had never been born. She expressed that her life was hard and that it wasn’t fair that no one else in the house had this disease. ”
How soon do you want your child to have access to Trikafta?
I want my child to have access to a gene modulator as soon as possible. I don’t want these drugs to be treated as a last resort after significant lung damage has already occurred. We don’t wait until tumours metastasize to a certain size before we treat them. We treat them right away. My daughter has been well, relatively speaking, in that her lung function is over 100%. But, at 5 years old, she already works so hard to maintain that. She gets up at 5:30am to complete an hour of nebs and lung physiotherapy before she can go to school. She is woken up in the middle of the night for oral antibiotics. She comes home from school instead of going to the playground with her friends because we also need to do nebs and physio before dinner and bed. Her life is restricted in a way that other kids’ lives are not. She doesn’t want to have sleepovers because she doesn’t want her friends at school to know that she is different. Even her own grandparents have never taken her for an overnight because they don’t feel comfortable managing her physio and medications. Although we do our best to keep things as “normal” as possible, she does make sacrifices. Everyone in this house does because her disease affects everyone. Gene modulators can’t come soon enough. Easing her treatment burden, lessening her reliance on drugs and antibiotics, keeping her out of the hospital — all of these things would help her have a more “normal” childhood like she deserves.
How does CF impact your child’s life?
The first time my daughter really understood the concept of cystic fibrosis was right around her fourth birthday after a particularly hard time getting her to comply with physio and breathing exercises. In one instant, it seemed to dawn on her that no one else in the family had CF — not her parents, and not her little sister. I will never forget how inconsolable she was as she asked us, through tears, why she had been born “bad” while her sister had been born “good”. We tried to explain that CF was not a punishment—she didn’t do anything to deserve this disease. Still, for the next two weeks, she was particularly well mannered and kind. At some point she asked why she still had CF since she had been so good. Again, we tried to explain that CF wasn’t a punishment for behaviour; it was just the way she was born. Then she looked me right in the eyes and told me that she wished she had never been born. She expressed that her life was hard and that it wasn’t fair that no one else in the house had this disease. At 4 years old, I don’t know how much she understood about what she was saying. But it felt like someone stabbed me in the heart. And I looked at her and tried to picture her at 10, and then 15, and then 20. Will a part of her still think she has done something to deserve this? What will her mental health be like? How do I make any of this easier for her?
Janire Ascanio and 5-year-old Luca
“ Kids need preventative treatment not only palliative or reactive treatments.”
How will Trikafta change your child’s future?
I truly believe that my kid will have a better chance to grow old and experience quality of life. Trikafta will bring that opportunity to live a life not only to live a disease.
How will Trikafta change you (the caregiver’s) future?
It would mean less time in hospital, more time to spend doing family stuff, having better sleep, a balance on mental health and financial relief.
How soon do you want your child to have access to Trikafta?
As soon as possible is approved for his age. Kids need preventative treatment not only palliative or reactive treatments.
What were your initial thoughts/feelings when you first heard of Trikafta?
Hope and a better future for my child. Strength and courage for me to keep him as healthy as possible for that day when he receives the first pill.
When was the first time that you felt CF impacted your child’s life? What was their lung function?
When he was 1 year old, his team agreed that he needed to go for sinus surgery. That time I knew CF was taking control, hearing doctors saying he is too young for this but it is the only option. I felt that CF was progressing quicker than my expectation as a parent.
How does CF impact your child’s life?
There are no options when it’s time for physio, when a yucky medicine needs to be swallowed, when there is need of a hospitalization, when we have to spend half a day in medical appointments. We have to do it and put aside whatever fun stuff he wants to do instead.
Janna McKenzie and 7-year-old Hudson
“Hudson smiles more than any kid I know. He is so positive despite being aware of the cruel truths of his condition. Recently I helplessly overheard as he listened to an ad that popped up on YouTube promoting organ donorship. It featured Matt, a paramedic with CF who almost died at 23 before receiving a double lung transplant. Hudson now says he needs Trikafta so that he won't die when he is 23.”
An open letter from Hudson’s family
CADTH, please let me express my gratitude for the opportunity to submit my family's testimony in respect to the importance of a positive recommendation for Trikafta for the 6-11 year olds. Respectfully, you have the power to change the grim trajectory of Cystic Fibrosis in our, 7-year-old son, Hudson’s life. I hold the utmost confidence that you will make the right decision, to recommend funding of Trikafta based on the guidelines outlined by the CF doctors and clinicians, for Hudson and all other children like him.
I'll start by telling you that Hudson could be considered one of the 'lucky' ones. Lucky that he was chosen to be part of the drug trial for the CFTR modulator, Orkambi, starting just as he turned 3. Lucky that following the conclusion of the study my private insurer continues coverage of this medication.
To say Orkambi has worked wonders for him would be a gross understatement. Would you believe that Orkambi has given Hudson a working pancreas?!? That's right, one of his organs, that had previously been non-functioning, is now working. Earlier on we battled to keep up the weight of a baby in clear discomfort, who never slept, wanting to feed almost continuously only to pass what he ate too frequently in oily, foul-smelling stools. As an infant, his fecal elastase numbers were considered unrecordable, with a reading of 11 ug/g. Severe pancreatic insufficiency is <100 ug/g. Recent testing showed his fecal elastase is now 261 ug/g with the normal range being greater than 200 ug/g. His doctors have taken him off his digestive enzymes and special access vitamins. Today Hudson is a strapping, young lad at 99th centile for height and weight.
This result is not indicative of what was seen in the adult study population, once damage to the pancreas had already occurred, but is proof of the immense potential that early access to CFTR modulators could hold. Among other benefits, what a gift it would be, to give a child with CF improved pancreatic function. Simple digestion in children with CF is not something to be taken for granted with ongoing challenges ranging from oily stools, abdominal pain, constipation/blockages requiring surgery, and some being so malnourished they have no option but to undergo feeding tube placement surgeries, with all their risks and burdensome maintenance. It also stands to reason that increased pancreatic function would substantially reduce their likelihood of developing CF related diabetes, with all its risks, needles and again burdensome blood sugar maintenance requirements.
Now, don't get me wrong, CF has thrown Hudson more knocks than is fair for any 7 year old, which I might add he handles with grace. Lung infections/health are why Hudson needs access to Trikafta now.
Without fail or complaint, every single day, Hudson takes his medications and does two sessions of inhaled meds and physio. Despite this dedication, he has already had bouts with some of the bacteria that are particularly scary and dangerous for people with CF including Allergic Bronchopulmonary Aspergillosis (ABPA), Methicillin-resistant Staphylococcus Aureus (MRSA), and Pseudomonas Aeruginosa. We have already seen Hudson's lung function (FEV1) dip into the mid-70s during an exacerbation. I shiver to extrapolate when the continuation of this rate of decline will result in a required lung transplant.
Hudson has had multiple surgeries (bronchoscopy/PICC line insertion) under general anaesthetic and counts his days when in-patient by the number of 'sleeps', typically in the double digits. Following his last procedure, the surgeon described the condition of his lungs, in a way which will stick with me for some time, as having 'giant' mucous plugs.
Analysis of samples following that procedure showed that he was growing a type of mould in his lungs called Aspergillus. Blood samples confirmed that he was having a strong allergic reaction to it (ABPA) causing his deterioration and which can lead to permanent lung damage. His treatment for this included a course of high-dose steroids that frighteningly would lower his immunity during a respiratory pandemic.
Our fight against the MRSA superbug involved an intensive 28-day at-home eradication protocol with oral and nebulized antibiotics, and topical/environmental decontamination. We disinfected everything daily, including our poor boy. His battle with Pseudomonas Aeruginosa added 2 hours of inhaled treatments for 28 days to his already heavy treatment schedule. Both infections have been associated with a faster decline in lung function.
Hudson smiles more than any kid I know. He is so positive despite being aware of the cruel truths of his condition. Recently I helplessly overheard as he listened to an ad that popped up on YouTube promoting organ donorship. It featured Matt, a paramedic with CF who almost died at 23 before receiving a double lung transplant. Hudson now says he needs Trikafta so that he won't die when he is 23.
I’d like to share a quote from the memoir, “Salt in My Soul: An Unfinished Life”, by Mallory Smith, who, after a lifelong battle with CF, passed away in 2017 at the age of 25. “Our genes dictate the endpoint; our choices, environment, and chance dictate how fast we get there and the rockiness of the descent.” We, Hudson especially, work our butts off every day to keep him as healthy as possible but desperately need access to the life-changing medication, Trikafta, to steady his descent. Please give Hudson and others like him this chance. — The McKenzie Family — Janna, Josh, Hudson & Victoria
This is just a small sample of the CF voices from across Canada.
CF Get Loud would like to publicly thank these families for sharing their vulnerable CF experiences. We have shared 11 families in this submission and we are actively working with thousands of families across Canada every day to advocate for a better future.
We will keep fighting in honour of the past, present and future Canadians with cystic fibrosis. We ask that CADTH recommend full reimbursement for Trikafta ages 6 and older without any genetic discrimination or required health decline. Allow our cystic fibrosis clinicians to prescribe the best medication for the healthiest long-term outcomes of the patients.
Patient Group Conflict of Interest Declaration — CF Get Loud
Our group has compiled data from advocacy initiatives held since January of 2020 and participated in by the Canadian CF community. No additional help outside our patient group was received to complete this submission. Our group did not receive any help to collect or analyse the data used in this submission. Our group has not had any financial payment from any company or organization since our inception. We are a patient and family volunteer group.
Table 3: Conflict of Interest Declaration for CF Get Loud
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
N/A | — | — | — | — |
I hereby certify that I have the authority to disclose all relevant information with respect to any matter involving this patient group with a company, organization, or entity that may place this patient group in a real, potential, or perceived conflict of interest situation.
Patient Group: CF Get Loud
Date: December 16, 2021
Canadian Cystic Fibrosis Treatment Society
About the Canadian Cystic Fibrosis Treatment Society
The Canadian Cystic Fibrosis Treatment Society was incorporated as a Non-for-Profit Organization in 2014. Its singular mandate is to advocate for individuals with cystic fibrosis (CF) that require access to medications and medical procedures that save and improve lives.
In carrying out this mandate we challenge, where necessary, private insurance companies, pharmaceutical companies, government and its agencies or quasi-judicial agencies, health charities and hospitals and the health care system. Our challenge to each of these entities is to rise to the occasion and ensure that no one with cystic fibrosis is left without the medical treatment that they require and that their physician has prescribed for them.
We carry out this advocacy in the boardroom and have, when necessary, also worked with patients and law firms to advance a patient’s interest in the court room.
The organization was founded by Chris MacLeod who has cystic fibrosis and was in need of the life sustaining medication Kalydeco in 2012. He was on 4 liters of oxygen a minute and had spent weeks on end at St. Michaels Hospital in Toronto with limited to no meaningful response to intravenous antibiotic treatment. He was recommended for Kalydeco by his treating physician. Kalydeco had not yet been submitted to Health Canada. He was permitted compassionate use by the manufacturer, but the medication was not allowed in through the Special Access Program.
He realized that there was no one who advocated for individuals with CF in situations such as the one he found himself in. He pulled together a team and secured access for himself to Kalydeco. However, it was clear that an organization needed to be established to advocate for individuals with CF when they needed treatment and access to such treatment was denied. The Canadian CF Treatment Society is housed at his law firm, Cambridge LLP. It is through the support of his firm, his law partners and the volunteer members of the Board of Directors that the work of the Treatment Society can proceed.
Our website is www.cfadvocacynow.com
Information Gathering
The information in this submission has been gathered by discussions with parents and caregivers of young patients with cystic fibrosis, advocates and physicians located in Canada.
The Canadian Cystic Fibrosis Treatment Society has received dozens of emails from parents requesting access to Trikafta for their children ages 6-11.
Disease Experience
Individuals are born with cystic fibrosis. CF causes various effects on the body, but mainly affects the digestive system and lungs. The degree of cystic fibrosis severity differs from person to person, however, the persistence and ongoing infection in the lungs, with destruction of lungs and loss of lung function, will eventually lead to death in the majority of people with CF.
The lungs are often infected, attacking the organ relentlessly until the patient simply cannot get sufficient oxygen to sustain life. The damage to the lungs is too great to recover and either a lung transplant is required, or they expire.
Patients’ bodies must constantly be fending off infections, which requires significant energy that can be provided by medicines such as Trikafta. Patients don’t have the physical resources because you can’t digest the food to fight infection and the infection is constantly and continuously attacking the lungs.
Parents and caregivers must constantly be monitoring their younger children’s symptoms and treatments – whether they be physiotherapy, nebulizer treatments or intake of medicines. Young patients are often admitted to the hospital with severe lung infections. Thanks to therapies though, children can live somewhat normal lifestyles. They must, however, undergo daily treatments in order to control the mucus buildup in their lungs.
Experiences With Currently Available Treatments
Medicines that are the most effective for patients with CF on the Canadian market are gene modulator therapies. They also significantly simplify the lives of CF patients and their caregivers. For younger patients and their caregivers, this can be experienced in the context of school. A significant burden is lifted for children, parents, and teachers, as youth can more actively participate in school and do not have to be pulled aside for inhaled therapies or physical therapy. Parents and teachers are also offered more peace of mind, since the medicines help stabilize the condition.
There are currently four gene modulator therapies available in this country, two of them in which children ages 6-11 could qualify for. Gene modulators normalize the genetic defect in cystic fibrosis and there appear to be virtually no side effects. Each drug addresses a different gene type.
Kalydeco, an oral medicine with fat-containing food, helps the protein made by the cystic fibrosis transmembrane conductance regulator (CFTR) gene function better. This results in improved lung function and other aspects of cystic fibrosis such as increasing weight. As of now, children aged 6 years or older who have one of nine CFTR gene mutations are eligible for the medicine. Although these may seem like multiple mutations, overall, only 4% of cystic fibrosis patients in Canada (including adults) are eligible for Kalydeco.
Patients who have access to Kalydeco have experienced significant improvements in their quality of life. However, as mentioned above, due to limiting criteria, very few Canadians and even fewer youth currently have access to this therapy.
Orkambi is a disease modifying drug that can improve lung function, reduce the number of pulmonary exacerbations, and can improve the nutritional status of some people who have two copies of the most common mutation of cystic fibrosis: F508del. Orkambi treats up to 50% of Canadians living with cystic fibrosis. However, due to negative recommendations from both CADTH and INESSS, and restrictive criteria set forth by a few Canadian provinces, Cystic Fibrosis Canada reported that only 1 patient in Canada has had access to the medicine.
Improved Outcomes
A treating physician and the patient must ultimately decide the best treatment regime for a given patient.
Research suggests that Trikafta may slow or prevent the progression of CF. When started at an early age, this has potential to avoid or delay the most common complications of CF before they start. Furthermore, the triple-combination therapy has proven to be an extremely positive alternative for patients who do not respond well to other modulators. It is estimated that this breakthrough medicine could be effective for 90% of CF patients, regardless of their lung capacity.
Highly effective CFTR modulators, such as Trikafta, are known to have a transformative effect on the health and well-being of many people with CF. But these therapies do not reverse established damage to lungs and other organs. This is one of the reasons it is important to start on Trikafta at a young age. Research suggests that beginning treatment with a modulator early could help slow or even prevent the irreversible progression of cystic fibrosis, dramatically altering the course of disease over time.
It is vital that we provide as many opportunities as possible for youth to be able to strive and live long and productive lives with Trikafta.
Experience With Drug Under Review
Canadian CF patients who have spoken with the society have described Trikafta as nothing short of game-changing and revolutionary. It is the difference between living a full life, participating in society, contributing to the economy, and improving the life and outcomes of others. With younger patients gaining access to Trikafta, we are setting them up for a brighter future, and longer and better life expectancy. Access to this life-changing medicine at an early age is absolutely critical.
Companion Diagnostic Test
N/A
Anything Else?
N/A
Patient Group Conflict of Interest Declaration — Canadian Cystic Fibrosis Treatment Society
To maintain the objectivity and credibility of the CADTH reimbursement review process, all participants in the drug review processes must disclose any real, potential, or perceived conflicts of interest. This Patient Group Conflict of Interest Declaration is required for participation. Declarations made do not negate or preclude the use of the patient group input. CADTH may contact your group with further questions, as needed.
Did you receive help from outside your patient group to complete this submission? If yes, please detail the help and who provided it.
No
Did you receive help from outside your patient group to collect or analyze data used in this submission? If yes, please detail the help and who provided it.
No
List any companies or organizations that have provided your group with financial payment over the past 2 years AND who may have direct or indirect interest in the drug under review.
Table 4: Conflict of Interest Declaration for the Canadian Cystic Fibrosis Treatment Society
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
N/A | — | — | — | — |
I hereby certify that I have the authority to disclose all relevant information with respect to any matter involving this patient group with a company, organization, or entity that may place this patient group in a real, potential, or perceived conflict of interest situation.
Patient Group: Canadian Cystic Fibrosis Treatment Society
Date: January 2022
Clinician Input
Cystic Fibrosis Canada’s Accelerating Clinical Trials Network Executive Committee
About the Cystic Fibrosis Canada’s Accelerating Clinical Trials Network Executive Committee
The Physicians who are submitting this proposal are Executive Committee members of Cystic Fibrosis Canada’s Accelerating Clinical Trials Network (CF CanACT). CF CanACT operates under the auspices of Cystic Fibrosis Canada and its purpose is to conduct world class clinical trials in Cystic Fibrosis (CF) in Canada. This is integral to bringing new therapeutics and better care to CF patients in Canada. All CF CanACT sites are affiliated with one or more of the 41 multi-disciplinary CF clinics that provide care to nearly all Canadians with CF. The Physicians represent 10 Cystic Fibrosis Clinics across Canada that provide care to 60% of the CF population. In addition, these Physicians represent the leading clinical researchers in CF in Canada. https://cysticfibrosis.ca/our-programs/clinical-trials-network
Information Gathering
Information supporting this submission was gathered by the following means:
Cystic Fibrosis Canada’s Data Registry which contains aggregate clinical information on nearly all people living with CF in Canada.
Outcomes of patients who have participated in clinical trials within the network, especially CFTR modulator trials.
Publications from the scientific literature.
Personal experience of the CF physicians treating patients with CF.
Current Treatments
Cystic Fibrosis (CF) is the most commonly inherited genetic condition in Canada affecting over 4,300 Canadians, with an incidence of approximately 1 in 3,600 live births. CF is a progressive, degenerative multi-system disease that mainly affects the lungs and digestive system. In the lungs, where the effects are most devastating, a build-up of thick mucus causes severe respiratory problems. Mucus also builds up in the pancreas and digestive tract, making it difficult to digest and absorb nutrients from food. Consequently, the mainstay of treatment is prevention of lung disease and ensuring good nutrition and growth.
Historically, patients would die in early childhood. Newborn screening has allowed the natural history of the disease to be modified and reduce the decline in lung function with the earlier administration of new and improved treatments. This has translated into increased patient survival. Despite this advance, death for CF patients still occurs in early to mid adulthood with the median age of death reported at 42 years (2019), compared to 33 (2018) and 27 years (2000) respectively.
Currently in Canada, there are 4344 people living with CF. Of those, 566 are children aged 6-11. Within this age group, there are 504 children who carry the mutations for which Trikafta is effective. Annually, these children attend outpatient clinics 3 - 4 times per year. Overall, owing to the quality of care received, children in this age range with CF are clinically quite well. Median lung function is in the normal range (98.03%) and nutrition is good (median BMI percentile 45.98). However, they still experience pulmonary exacerbations (flare ups of lung disease). In 2019 in this age group there were 103 pulmonary exacerbations requiring intravenous antibiotics of which 84 required hospitalization.
Current therapy in CF (prior to the age of CFTR modulator medications) focuses on the management and prevention of the long-term complications of the disease (eg. malnutrition, chronic infection, lung function decline etc.) with an aim to slow disease progression. This paradigm of preventing sequelae is the cornerstone of modern CF care.
Historically, children with CF died in early childhood of malnutrition. The introduction of aggressive nutritional supplementation and pancreatic enzyme replacement therapy was the first great advance in the care of people with CF and allowed survival into later childhood and early adulthood. Modern CF treatment focuses on optimising growth and maintaining adequate nutrition. Due to pancreatic insufficiency, the majority of patients require pancreatic enzyme supplementation in addition to fat soluble vitamin supplementation. This promotes good nutrition and is critically linked to overall health and survival.
As survival improves, the main cause of morbidity and mortality in people with CF is lung damage due to a vicious cycle of retained mucus, infection, inflammation and lung destruction. Breaking this cycle of retained mucus and lung destruction is the mainstay of modern pulmonary CF care. This is achieved by regular daily chest physiotherapy, inhaled mucolytics (e.g. hypertonic saline, Pulmozyme™) and either acute or chronic suppressive inhaled antibiotic therapy (e.g. TOBI™, Cayston™, others). This strategy aims to slow the evolving lung damage and the resultant decline in lung function that ultimately lead to respiratory failure and death. While these treatments are effective, they can only slow this decline.
Given the multisystem impact of CF, complications arise as the patient ages and so all patients have regular screening for complications in various organ systems. Specifically, CF-related diabetes is very prevalent with up to 33% adult patients needing to use insulin. Liver disease is common and, if medical management is unsuccessful, leads to liver transplantation. Additionally, patients are at risk of early development of osteoporosis. Issues with fertility are common with most men being infertile and women sub-fertile. There is an increased risk of cancer particularly bowel cancer as well as inflammatory bowel disease and celiac disease. All of these conditions are routinely screened for in clinic and are part of the preventative paradigm in CF care.
CF care is holistic and emotional wellness is now a significant problem within this patient group. Data has shown that over 30% of patients and/or caregivers are currently suffering from either anxiety or depression. This has become a high priority in this patient group and is the focus of a national incentive. Proactive screening for mental health complications and timely referral to mental health practitioners is now integrated into CF care.
Newborn screening is the epitome of preventative care in CF. Since 2018, all babies born in Canada are screened for CF at birth. This accounts for 2/3rd of the 160 annual CF diagnoses. The aim of newborn screening and the time-consuming CF treatment regime is to alter the natural history, control symptoms and reduce morbidity associated with recurrent pulmonary exacerbations and hospitalisations. However, all of these therapies address downstream consequences of the genetic defect in CF. There is no cure. Approved medications aim at altering and slowing the trajectory of lung function decline. Ultimately, when respiratory failure occurs, lung transplantation is the only option to try to extend life expectancy and improve quality of life.
CFTR modulators have been developed to tackle the underlying defect of CF. Although not a cure, these medications restore the function of the CFTR protein, a chloride and bicarbonate channel, at the cell surface. CFTR modulators are tailored to work to correct specific mutations and are an example of precision (personalized) medicine. Correction of CFTR protein function at an early age is congruent with the overall preventative paradigm of CF treatment – early correction will hopefully prevent disease progression and irreversible damage.
The first CFTR modulator commercially available was ivacaftor (IVA), which was approved in by Health Canada in 2012. It is effective in patients who have “gating” mutations, which is only 4% of Canadians with CF. It is an extremely effective medication, which provides substantial clinical benefits of increasing lung function, reducing hospitalizations and improving nutritional status, and real-world evidence of improving survival and decreasing need for lung transplant. It is currently funded both at a 3rd party and provincial level.
For patients with 2 copies of the most common CF mutation, F508del (~50% of Canadians with CF), lumacaftor/ivacaftor (LUM/IVA; Orkambi™) and tezacaftor/ivacaftor (TEZ/IVA; Symdeko™) have been developed. Despite Health Canada approval, only Orkambi™ is available provincially and only under very restrictive access criteria in Alberta, Saskatchewan and Ontario, and through Quebec’s ‘patient d’exception’ programme. Consequently only 12% of Canadian CF patients receive these, mostly through participation in clinical trials or 3rd party payers.
Recently, elexacaftor/tezacaftor/ivacaftor (ELX/TEZ/IVA; Trikafta™) has been approved by Health Canada for people with CF aged 12 years and older. In vitro, this medication effectively recovers CFTR function in cells with one or two copies of the F508del mutation. This medication is also extremely effective clinically in people with CF with one or two copies of F508del over 12 years of age and in those age 6-11 (see detailed description below). For this section, it is important to note that the inclusion criterion include people with one copy of F508del in the targeted population. Previous generations of CFTR modulator medications were only indicated for people with gating mutations (Kalydeco™), or two copies of F508del. This group (one or two copies of F508del) includes ~90% of Canadians with CF, so this represents a significant expansion of the population that is genetically eligible for this class of medications.
Reference
Cystic Fibrosis Canada. (2020). The Canadian Cystic Fibrosis Registry 2019 Annual Data Report. Toronto, Canada: Cystic Fibrosis Canada.
Treatment Goals
As highlighted in the Current Treatments section, an ideal treatment in CF would fully address the basic molecular defect in CF and restore normal chloride transport on the cell surface. If applied at an early enough age, complete and early correction of CFTR function would prevent the multisystem downstream effects that are ultimately fatal for people living with CF. Research continues to develop tools to completely correct CFTR function (this may be gene therapy, or perfected small molecule interventions). Elexacaftor/tezacaftor/ivacaftor is the first “third generation” CFTR modulator. In vitro, this medication provides the greatest restoration of CFTR function observed to date.
Clinically important outcomes in CF have been established over the years in many clinical trials. These include:
Improves and/or stabilizes lung function
Prevents and/or reduces pulmonary exacerbations
Improves and/or stabilizes nutrition and growth
Minimizes and/or reverses other multisystem complications of CF disease
Improves emotional wellness
Improves quality of life
Allows attendance at school, university and work with minimal disruption
Reduces burden of care and number of therapies needed to maintain health
Alters the disease trajectory
As the overall population of people with CF becomes healthier with improved treatment, it is important to realise that the efficacy outcomes used in previous trials may not be applicable to ongoing drug trials. Lung function may be normal at baseline in a young child - the treatment goal in that population is to prevent longitudinal disease progression, and an acute response in the outcomes above (eg. improvement in FEV1, improvement in nutrition etc) may be blunted due to increased baseline. The earlier we commence treatment on modulators, the greater the chance of keeping this population healthier. This paradigm of disease prevention is consistent with the overall treatment approach to CF outlined in the Current Treatments section.
Treatment Gaps (Unmet Needs)
Considering the treatment goals in the previous section, please describe goals (needs) that are not being met by currently available treatments.
Current treatments such as inhaled antibiotics and mucus thinning agents target downstream consequences of CF lung disease (e.g. infection, thick, dehydrated mucus) and therefore do not treat the root cause or reverse the course of disease. These treatments require nebulization and therefore are extremely time-consuming to administer (2-3 hours per day). Thus, they adversely impact quality of life and school productivity at a critical time of childhood development. This demanding treatment regimen also influences medication adherence and mental health.
Response to currently available, second generation, CFTR modulator therapies (LUM/IVA, TEZ/IVA) for F508del homozygous patients is variable and most patients continue to experience lung disease progression. Furthermore, there are significant side effects related to the use of LUM/IVA (e.g. chest tightness, blood pressure elevation) and numerous drug-drug interactions.
Current treatments do not reverse extra-pulmonary manifestations of CF including sinusitis, exocrine pancreatic insufficiency, diabetes, liver disease, and bowel manifestations.
Which patients have the greatest unmet need for an intervention such as the drug under review?
Patients aged 6-11 years with a single copy of F508del paired with another CF mutation (i.e. F508del heterozygous) that is not a gating or residual function mutation have the greatest unmet need as there are currently no approved CFTR modulator therapies available to them. In patients with a single copy of F508del and a “minimal function” mutation, clinical manifestations are severe and the drug under review is considered a breakthrough as it leads to substantial improvements in lung function and respiratory-related quality of life and markedly reduces exacerbations and hospitalizations.
Patients with two copies of F508del (i.e. F508del homozygous) also have substantial unmet need as only a minority (~12%) have been able to access LUM/IVA or TEZ/IVA due to the lack of public reimbursement in most provinces. Furthermore, in the minority of patients who have been able to access these therapies, response is variable and side effects can be considerable. The drug in this present review, leads to tremendous improvements beyond the effects related to LUM/IVA and TEZ/IVA and has fewer side effects and drug-drug interactions than LUM/IVA.
Children between 6-11 years old often have lung disease that can be underestimated with outcome measures typically used in adolescents and adults with CF such as forced expiratory volume in 1 second (FEV1). Imaging studies involving CT and MRI demonstrate structural and functional abnormalities, respectively, within the first few years of life despite “normal” lung function based on FEV1 and therefore lung disease progresses in a silent manner. Despite “normal” lung function based on FEV1, there are a number of indicators of active disease and treatment burden in this age group. Based on a study involving the U.S. CF Foundation registry characterizing disease burden in CF children between the ages of 6-11 years, the hospitalization event rate was 0.5 per year, pulmonary exacerbation event rate was 0.4 per year, 96% had at least one positive respiratory culture with growth of a microorganism, 63% had at least one CF-related complication (pancreatic, hepatobiliary, pulmonary, gastrointestinal, psychological), and 16% required a gastrostomy tube for supplemental feeding due to poor nutritional outcomes (1). Currently available treatments do not reverse the course of disease or prevent end-organ damage.
Due to ceiling effects in the outcomes measure, FEV1 is relatively insensitive to improvements in lung function in patients with early lung disease (FEV1 > 90% predicted). Nonetheless, improvements in this group still have been observed in response to ELX/TEZ/IVA. A group of 196 CF patients 12 years and older who have a normal lung function (FEV1> 90%) showed an improvement in lung function with an increase in FEV1 of 6.5% at 6 months post commencement of treatment. Respiratory quality of life score based on the CFQ-R Resp domain increased by 15.7 points, sweat chloride levels decreased by 39.7 mmol/L and BMI increased by 0.82 kg/m2 (2).
The drug under review will address these unmet needs by treating the underlying CFTR defect. Prompt diagnosis in combination with effective treatment starting early in life improves clinical outcomes and can prevent disease sequelae including bronchiectasis, impaired growth, and pancreatic insufficiency.
References
Bresnick K, Arteaga-Solis E, Millar SJ, Laird G, LeCamus C. Burden of cystic fibrosis in children <12 years of age prior to the introduction of CFTR modulator therapies. BMJ Open Respir Res. 2021 Dec;8(1):e000998. doi: 10.1136/bmjresp-2021-000998. PMID: 34857524.
Nichols DP, Paynter AC, Heltshe SL, Donaldson SH, Frederick CA, Freedman SD et al. Clinical Effectiveness of Elexacaftor/Tezacftor/Ivacaftor in People with Cystic Fibrosis. AJRCCM Article in Press. Published November 16, 2021 as 10.1164/rccm.202108-1986OC.
Place in Therapy
How would the drug under review fit into the current treatment paradigm?
Triple combination modulator therapy (ELX/TEZ/IVA) addresses the underlying disease process in cystic fibrosis (CF) and is added on to current standard of care for CF as a first-line therapy for those patients with the appropriate CF mutations (genotype). This CFTR modulator therapy is specifically targeted to each patients’ genotype.
The current treatment paradigm for CF divides therapies into those that address the basic defect (CFTR modulators) and those that treat the consequences of the defect (for example: inhaled antibiotics, inhaled mucolytics, bronchodilators, anti-inflammatory drugs, physiotherapy).
Phase 3 trials in patients 6 years and older have demonstrated that the addition of ELX/TEZ/IVA to standard of care results in significant improvements in clinically important outcomes of lung function, pulmonary exacerbations, weight and QOL (1,2,3). Consensus guidelines and Standard of Care guidelines already include CFTR modulator therapies (4, 5), but they have not been recommended to replace prior therapies such as inhaled antibiotics that treat consequences of the defect because end-organ damage has already occurred and therefore these treatments remain necessary. Future research will determine if some of these other standard of care therapies can be safely removed for patients on ELX/TEZ/IVA and whether introduction of ELX/TEZ/IVA earlier in life will prevent the need for inhaled antibiotics, inhaled mucolytics, and other standard of care treatments.
ELX/TEZ/IVA is not the first therapy that addresses the underlying defect in CF, but rather it is an improvement on existing CFTR modulator therapies. This therapy would replace other CFTR modulators that are currently available. When compared to the Health Canada-approved CFTR modulator (TEZ/IVA), Phase 3 trials have demonstrated greater efficacy of ELX/TEZ/IVA (2). ELX/TEZ/IVA is also indicated for a broader CF population as has been shown to be effective in all patients who have at least one F508del mutation (1,5). In this sense it is, for F508del heterozygote CF patients, a first-line therapy that addresses the underlying defect in CF.
References
Middleton, P.G.; Mall, M.A.; Drevinek, P.; Lands, L.C.; McKone, E.F.; Polineni, D.; Ramsey, B.W.; Taylour-Cousar, J.L.; Tullis, E.; Vermeulen, F.; et al. Elexacaftor-tezacaftor-ivacaftor for cystic fibrosis with a single Phe508del allele. N. Eng. J. Med. 2019, 381, 1809–1819, doi:10.1056/NEJMoa1908639.
Heijerman, H.G.; McKone, E.F.; Downey, D.G.; Van Braeckel, E.; Rowe, S.M.; Tullis, E.; Mall, M.A.; Welter, J.J.; Ramsey, B.W.; McKee, C.M.; et al. Efficacy and safety of the elexacaftor plus tezacaftor plus ivacaftor combination regimen in people with cystic fibrosis homozygous for the F508del mutation: A double-blind, randomised, phase 3 trial. Lancet 2019, 394, 1940–1948, doi:10.1016/S0140-6736(19)32597-8.
Zemanick, Taylor-Cousar, Davies, et al. A Phase 3 Open-Label Study of Elexacaftor/Tezacaftor/Ivacaftor in Children 6 through 11 Years of Age with Cystic Fibrosis and at Least One F508del Allele. Am J Respir Crit Care Med Vol 203, Iss 12, pp 1522–1532, Jun 15, 2021
Ren CL, Morgan RL, Oermann C, Resnick HE, Brady C, et al. Cystic fibrosis pulmonary guidelines: use of cystic fibrosis transmembrane conductance regulator modulator therapy in patients with cystic fibrosis. Ann Am Thorac Soc 2018;15:271–280.
Canadian clinical consensus guideline for initiation of monitoring and discontinuation of CFTE modulator therapies for patients with cystic fibrosis. Cystic Fibrosis Standard of Care documents 2021, https://www.cysticfibrosis.ca/uploads/CFC%20Modulator%20Guidelines_RevisedOct62021%20(003)
Please indicate whether or not it would be appropriate to recommend that patients try other treatments before initiating treatment with the drug under review. Please provide a rationale from your perspective.
Patients starting CFTR modulator therapy should already be receiving standard of care treatments as indicated for the extent and characteristics of their disease (e.g. chest physiotherapy for airway clearance, mucolytics, inhaled antibiotics for chronic airway infection, anti-inflammatory therapies, bronchodilators, pancreatic enzymes, fat soluble vitamins, insulin). ELX/TEZ/IVA should be added to this therapy regardless of treatment response to standard of care as it is the only therapy that targets the defect in CFTR. For patients with at least one copy of F508del currently on IVA, TEZ/IVA or LUM/IVA, it is beneficial to switch to ELX/TEZ/IVA.
How would this drug affect the sequencing of therapies for the target condition?
There would be no difference in the sequence of pulmonary therapies however, the addition of ELX/TEZ/IVA would hopefully delay disease progression, especially if commenced early in life and thus delay the need for other therapies including lung transplant. There may be the potential that treatment with ELX/TEZ/IVA will result in improvements in clinical status so that other standard of care therapy will no longer be required.
Which patients would be best suited for treatment with the drug under review?
Phase 3 trials demonstrated similar treatment effect in a broad age range (between 6-11 years of age, between 12-17 years of age and over age 18 years of age) and in patients with either relatively mild disease or in those with established disease and low lung function (FEV1 below and above 70% predicted). There were no subgroups that did not respond (age, gender, country, presence of Pseudomonas, therapies) (1,2). A recent study has also demonstrated benefit in patients with advanced CF lung disease (3). A Phase 3 study in children 6 to 11 years of age (4) has shown a similar improvement in lung function, quality of life and body-mass index for age than older age groups.
CF is a life-long, progressive disease and the chronic lung infection, inflammation and recurrent pulmonary exacerbations lead to progressive decline in lung function. Fifty percent of the decline in lung function can be attributed to pulmonary exacerbations (5) and so reduction in frequency of exacerbations is an important goal of therapy. The Canadian CF Registry shows that the steepest rate of decline in lung function occurs in the adolescent CF population in patients on current standard of care and thus starting CFTR modulator therapy as early as possible may prevent this from occurring (6). Early treatment with highly-effective CFTR modulators is expected to reduce this decline in lung function and improve quality of life in CF patients over their lifespan.
Figure 3: Median FEV1Ppercent vs. Age of Cystic Fibrosis Individuals (5-year Moving Window), 2000 and 2019*
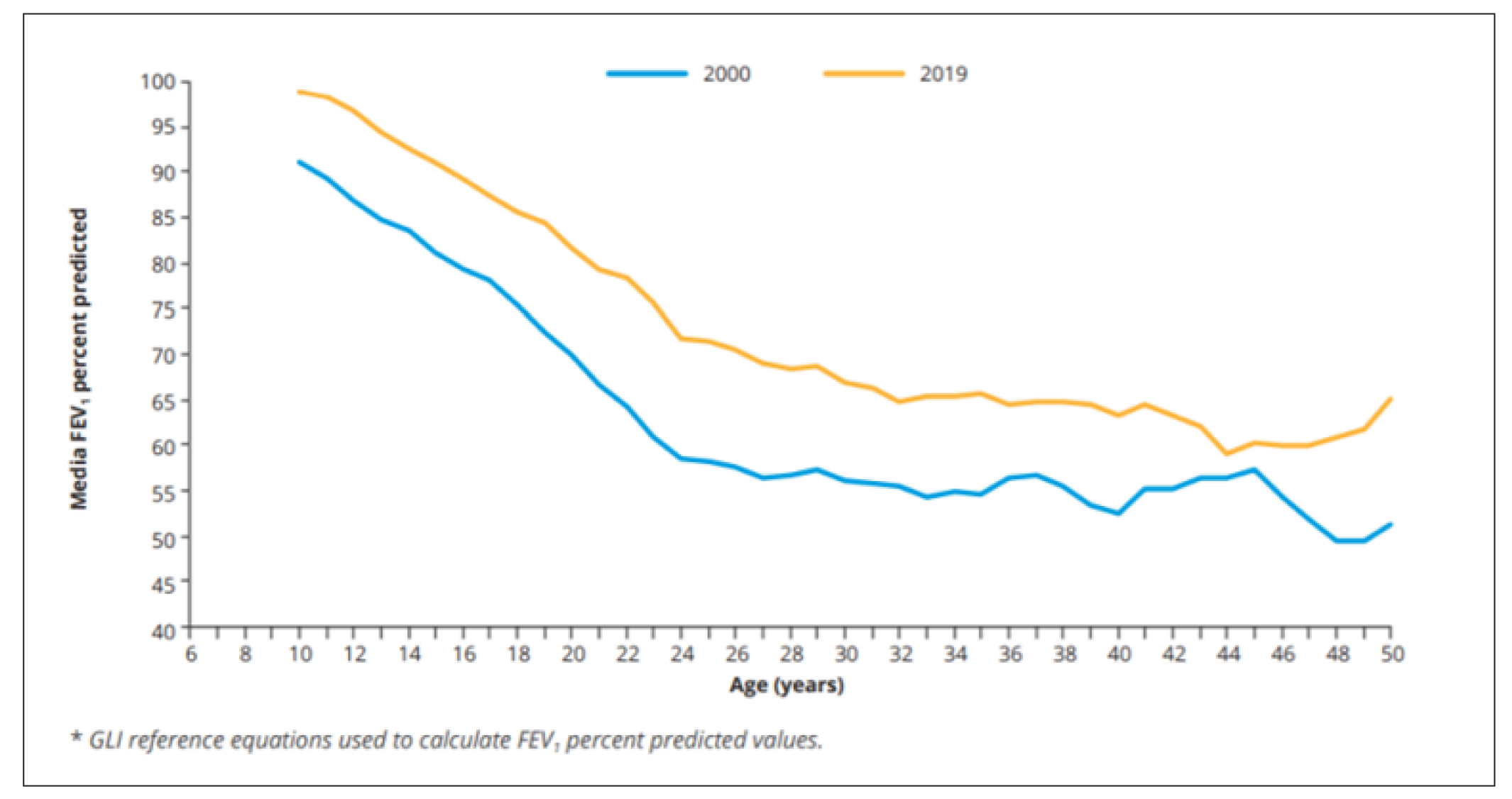
References
Middleton, P.G.; Mall, M.A.; Drevinek, P.; Lands, L.C.; McKone, E.F.; Polineni, D.; Ramsey, B.W.; Taylour-Cousar, J.L.; Tullis, E.; Vermeulen, F.; et al. Elexacaftor-tezacaftor-ivacaftor for cystic fibrosis with a single Phe508del allele. N. Eng. J. Med. 2019, 381, 1809–1819, doi:10.1056/NEJMoa1908639.
Heijerman, H.G.; McKone, E.F.; Downey, D.G.; Van Braeckel, E.; Rowe, S.M.; Tullis, E.; Mall, M.A.; Welter, J.J.; Ramsey, B.W.; McKee, C.M.; et al. Efficacy and safety of the elexacaftor plus tezacaftor plus ivacaftor combination regimen in people with cystic fibrosis homozygous for the F508del mutation: A double-blind, randomised, phase 3 trial. Lancet 2019, 394, 1940–1948, doi:10.1016/S0140-6736(19)32597-8.
O'Shea KM, O'Carroll OM, Carroll C, Grogan B, Connolly A, O'Shaughnessy L, Nicholson T, Gallagher CG, McKone EF. The efficacy of Elexacaftor/Tezacaftor/Ivacaftor in patients with cystic fibrosis and advanced lung disease. Eur Respir J 2020. doi: 10.1183/13993003.03079-2020. Epub ahead of print. PMID: 33154033.
Nichols DP, Paynter AC, Heltshe SL, Donaldson SH, Frederick CA, Freedman SD et al. Clinical Effectiveness of Elexacaftor/Tezacftor/Ivacaftor in People with Cystic Fibrosis. AJRCCM Article in Press. Published November 16, 2021 as 10.1164/rccm.202108-1986OC
Waters V, Stanojevic S, Atenafu EG, Lu A, Yau Y, Tullis E and Ratjen F. Effect of pulmonary exacerbations on long-term lung function decline in cystic fibrosis. Eur Respir J 2012;40:61-6.
Cystic Fibrosis Canada. (2020). The Canadian Cystic Fibrosis Registry 2019 Annual Data Report. Toronto, Canada: Cystic Fibrosis Canada.
How would patients best suited for treatment with the drug under review be identified?
Potential candidates must have cystic fibrosis, i.e. typical symptoms, or a positive newborn screen test and either possessing two disease-causing Cystic Fibrosis Transmembrane Conductance Regulator (CFTR) mutations or have a sweat chloride >60 mmol/L (when not on CFTR modulator therapy)(1). To be eligible for ELX/TEZ/IVA, the individual with CF must have at least one F508del mutation. All potential recipients need to have documented genetic testing demonstrating two CFTR mutations, of which at least one is F508del.
Genetic testing and sweat chloride testing should be performed at accredited CF clinics, of which there are 41 across Canada, giving wide access to diagnostic testing. Newborn screening, which is responsible for identifying 66% of new diagnoses, has been in place in certain regions of Canada for over a decade, but for a shorter time in other regions. As such, current CF patients are a mix of those diagnosed by newborn screening and those diagnosed because of symptomatic presentation. Some patients present at a later age either due to missed diagnosis or milder symptoms. Such late diagnoses are expected to be less frequent over time because of newborn screening.
The mechanism of action of the drug is to increase the function of F508del mutant CFTR, specifically the F508del mutation, but potentially others as well. Mutant CFTR results in loss of lung function, malnutrition, elevated sweat chloride values, and male infertility, as the most common symptoms. Ultimately it is loss of lung function that accounts for the majority of premature deaths.
Given that there are many patients with lung function (spirometry, typically Forced Expiratory Volume in one-second (FEV1)) that is low (<40%) waiting for lung transplantation who have improved on this treatment to the point that they no longer need transplantation, there should be no lower limit of lung function to be eligible. Given that 1) lung function is often normal despite progression of structural lung damage, and that this damage begins early in life despite newborn screening, 2) that this drug results in fewer pulmonary exacerbations (acute worsening of symptoms requiring antibiotics) that contribute to progressive lung damage (in 12 years and older the rate of exacerbation was decreased by 63%, in 6-11 year olds incidence was lower than previously reported in those on dual modulator therapy), 3) the baseline lung function (FEV1) in the study of the drug in patients 6-11 year old with at least one copy of F508del was 88% predicted and there was an absolute increase of 10.2% in percent predicted FEV1 after 24 weeks (2) and in the real-world experience with this drug in those 12 years of age and older with at least one copy of F508del with a baseline function >90% FEV1 (mean 102%) there was an absolute increase of 6.5% after 6 months, there should also be no upper limit of lung function for eligibility. Additional information from the study of 6-11 year olds demonstrated significant improvements in the lung clearance index. The lung clearance index is a recently developed measure that reflects ventilation inhomogeneity cause by lung damage. In this study, the baseline value was mildly elevated (9.77, upper limit of normal 8) and decreased by 1.71, close to the upper limit of normal. This again supports providing access to this drug for all CF patients 6-11 years of age with at least one copy of F508del.
References
Villanueva G, Marceniuk G, Murphy MS, Walshaw M, Cosulich R; Guideline Committee. Diagnosis and management of cystic fibrosis: Summary of NICE guidance. BMJ. 2017 Oct 26;359:j4574. doi: 10.1136/bmj.j4574.
Zemanick ET, Taylor-Cousar JLL, Davies J, Gibson RL, Mall MA, McKone EFM, et al. A Phase 3 Open-Label Study of Elexacaftor/Tezacaftor/Ivacaftor in Children 6 through 11 Years of Age with Cystic Fibrosis and at Least One F508del Allele.
Which patients would be least suitable for treatment with the drug under review?
As demonstrated in studies of CF infants diagnosed by newborn screening, structural lung damage begins early in life (1). As such, there is “silent” or pre-symptomatic disease. All cystic fibrosis patients with at least one F508del mutation should be eligible. Drug-drug interactions may require that certain other medications be changed or the dosage be changed, but these are few and used infrequently in the CF population. The only contraindication to treatment is in patients with severe liver disease (Child Pugh Class C).
Those patients who have undergone lung transplantation will not receive lung function benefits. However, their sinus disease, which can be debilitating, is expected to improve with ELX/TEV/IVA (2). Improving sinus disease can diminish the risk of developing chronic rejection post-lung transplantation, so ELX/TEV/IVA should be considered in those lung transplant recipients with significant sinus disease. Their sweat chloride values will also improve, thus avoiding episodes of severe dehydration that can occur.
References
Sly PD, Gangell CL, Chen L, Ware RS, Ranganathan S, Mott LS, Murray CP, Stick SM; AREST CF Investigators. Risk factors for bronchiectasis in children with cystic fibrosis. N Engl J Med 2013 May 23;368(21):1963-70. doi: 10.1056/NEJMoa1301725. PMID: 23692169.
DiMango E, Overdevest J, Keating C, Francis SF, Dansky D, Gudis D. Effect of highly effective modulator treatment on sinonasal symptoms in cystic fibrosis. J Cyst Fibros. 2020 Jul 18:S1569-1993(20)30794-3. doi: 10.1016/j.jcf.2020.07.002. Epub ahead of print. PMID: 32694034.
Is it possible to identify those patients who are most likely to exhibit a response to treatment with the drug under review?
The clinical trials have demonstrated that those patients with at least one F508del mutation, regardless of the second mutation, respond to this therapy, as noted by improvements in lung function, weight, and reduced pulmonary exacerbations requiring antibiotics. In the 6-11 year old population, lung function (FEV1) improved by an absolute 10.2% even though baseline lung function was 88% of predicted. In real-world experience with the drug in those 12 years of age and older, with baseline function >90% (102%) there was an absolute increase of 6.2% after 6 months. As CFTR modulators are systemic medications, they impact CFTR function in the sweat glands as measured by the concentration of chloride in sweat (sweat chloride). This does have clinical significance as it reduces the risk for dehydration and heat stroke, and it is a biomarker of the effect of CFTR modulator at the biochemical level. In the trial of this drug on 6-11 year old patients, the sweat chloride fell below the diagnostic threshold in 80% of participants with the F508del/minimal function mutations and in 100% in the F508del homozygous participants. Changes in sweat chloride are generally predictive of lung function changes at a population (but not an individual) level (1). The drug has already been approved in those 12 years and older with at least one copy of Fdel508 with lung function<40%. Therefore, any patient with at least one copy of F508del should be considered as likely to respond to this drug.
Reference
Fidler MC, Beusmans J, Panorchan P, Van Goor F. Correlation of sweat chloride and percent predicted FEV1 in cystic fibrosis patients treated with ivacaftor. J Cyst Fibros. 2017 Jan;16(1):41-44. doi: 10.1016/j.jcf.2016.10.002. Epub 2016 Oct 20. PMID: 27773592.
What outcomes are used to determine whether a patient is responding to treatment in clinical practice?
The outcomes of interest are those measured regularly at the quarterly CF clinic visits as part of standard of care. At each clinic visit, patients have spirometry to measure lung function, have their weight and height measured, and provide a sputum sample for culture. Assessment by the CF physician would review their respiratory and other CF symptoms and determine the presence of pulmonary exacerbations at or between clinic visits. Thus, additional visits or testing is not required to assess response to therapy with CFTR modulators. Quality of life questionnaires (e.g. CFQ-R for respiratory symptoms and SNOT-22 for sinus disease) can also be employed.
What would be considered a clinically meaningful response to treatment?
Meaningful clinical responses include:
Improvement in lung function (FEV1)
Stabilization of lung function over time (i.e. prevention of the usual decline in lung function)
Improvements in the lung clearance index (LCI)
Reduction in the number of pulmonary exacerbations
Reduction or stabilization of respiratory symptoms
Improvement in nutritional status
As the treatment goal of this progressive disease is to slow decline in lung function and reduce mortality, the most important outcomes are 1, 2 and 3.
How often should treatment response be assessed?
Treatment response time intervals depend on the outcome measure used. For outcome measures 1,2, 3, 5 and 6, assessments should be performed in the first 3 months of therapy, then every 3 to 6 months in the first year of treatment, and on a yearly basis subsequently. Pulmonary exacerbations should be assessed on a yearly basis.
What factors should be considered when deciding to discontinue treatment?
Discontinuation of therapy should be considered in patients who have clinically significant adverse effects that persist and recur after stopping and re-initiating therapy.
Examples of these reactions include (but are not limited to):
Elevation of liver function tests beyond the higher range of fluctuations observed in CF patients
Allergic reactions to treatment
However, the risk-benefit of discontinuing treatment should be considered on a case-by-case basis depending on the severity of the adverse event and risk of stopping treatment.
What settings are appropriate for treatment with the drug under review?
Treatment should be limited to CF patients attending the cystic fibrosis clinics accredited by CF Canada.
For non-oncology drugs, is a specialist required to diagnose, treat, and monitor patients who might receive the drug under review?
Drug should be prescribed and monitored by a CF Clinic Physician.
Conflict of Interest Declarations for the CF CanACT Executive Committee
To maintain the objectivity and credibility of the CADTH drug review programs, all participants in the drug review processes must disclose any real, potential, or perceived conflicts of interest. This conflict of interest declaration is required for participation. Declarations made do not negate or preclude the use of the clinician group input. CADTH may contact your group with further questions, as needed. Please see the Procedures for CADTH Drug Reimbursement Reviews (under the Place in Therapy section) for further details.
Did you receive help from outside your clinician group to complete this submission? If yes, please detail the help and who provided it.
Yes, we required data from the CF Canada Registry specific to 6-11 year olds.
Did you receive help from outside your clinician group to collect or analyze any information used in this submission? If yes, please detail the help and who provided it.
Yes, we required data from the CF Canada Registry specific to 6-11 year olds.
List any companies or organizations that have provided your group with financial payment over the past two years AND who may have direct or indirect interest in the drug under review. Please note that this is required for each clinician who contributed to the input — please add more tables as needed (copy and paste). It is preferred for all declarations to be included in a single document.
Declaration for Clinician 1
Name: Brad Quon
Position: Medical Lead, CF CanACT; Adult CF Physician, St. Paul’s Hospital; Associate Professor of Medicine, University of British Columbia
Date: 07-12-2021
Table 5: COI Declaration for the CF CanACT Executive Committee — Clinician 1
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
Vertex | — | X | — | — |
Declaration for Clinician 2
Name: Felix Ratjen
Position: Division Head, Respiratory Medicine, SickKids
Date: 6-12-2021
Table 6: COI Declaration for the CF CanACT Executive Committee — Clinician 2
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
No COI | — | — | — | — |
Declaration for Clinician 3
Name: Larry Lands
Position: Professor of Pediatrics, McGill University
Date: 07-12-2021
Table 7: COI Declaration for the CF CanACT Executive Committee — Clinician 3
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
Vertex | — | X | — | — |
Declaration for Clinician 4
Name: Jonathan Rayment
Position: Respirologist, BC Children’s Hospital, Clinical Assistant Professor, Pediatrics, University of British Columbia.
Date: 6-12-2021
Table 8: COI Declaration for the CF CanACT Executive Committee — Clinician 4
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
Polarean LLC | X | — | — | — |
Vertex | — | — | — | X |
Declaration for Clinician 5
Name: Patrick Daigneault
Position: Pediatric Respirologist and Cystic Fibrosis Clinic Director – Centre Mère-Enfant du CHU de Québec
Date: 6-12-2021
Table 9: COI Declaration for the CF CanACT Executive Committee — Clinician 5
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
No COI | — | — | — | — |
Canadian Cystic Fibrosis Clinic Directors and CF Canada Healthcare Advisory Council
About the Canadian Cystic Fibrosis Clinic Directors and CF Canada Healthcare Advisory Council
There are 41 cystic fibrosis clinics in Canada, delivering multi-disciplinary specialty care to people with cystic fibrosis. Each clinic has a physician who serves as the medical director of the clinic, in addition to clinic staff physicians. Clinic directors and cystic fibrosis clinic staff physicians have special training, expertise, and experience in delivering medical care and support to people with cystic fibrosis.
In addition, CF clinicians are represented within the CF Healthcare advisory council, which develops CF care policy and guidelines to support the CF clinic directors and community. This submission has been written by the authors on behalf of all the Canadian CF Clinic directors.
Information Gathering
The information included in this submission was gathered in several ways:
Personal experience gained by working with and delivering medical services to people with cystic fibrosis.
Personal experience treating people with cystic fibrosis who received elexacaftor/tezacaftor/ivacaftor and ivacaftor, either during participation in clinical trials, through the Health Canada Special Access Program, and/or since the Health Canada marketing authorization for persons ages 12 years and older.
Review of the medical and scientific literature, including clinical trial results.
The Cystic Fibrosis Canada Canadian Cystic Fibrosis Registry, a collection of patient data and other information regarding CF care and outcomes.
The Canadian Clinical Consensus Guideline for Initiation, Monitoring and Discontinuation of CFTR Modulator Therapies for Patients with Cystic Fibrosis
Current Treatments
Cystic fibrosis (CF) is a fatal, progressive genetic disease that affects approximately 4,300 Canadians, with an incidence of approximately 1/3,600 live births. In 2019 there were 116 new cases diagnosed in Canada, with 76 of those diagnosed through provincial newborn screening programs.1 It is a lifelong, chronic, degenerative disease that affects multiple organ systems, most importantly the lungs and the digestive system.
Of the 4,344 individuals living with CF, 580 (14%) were children in the 6 –11 year age group according to the Canadian Cystic Fibrosis Registry.2
People living with cystic fibrosis are prescribed a multitude of treatments, including high-calorie high-fat high-protein diets, medications, and airway clearance treatments. Because it has been shown that the physiological manifestations of CF start very early in life, even in asymptomatic patients and before many tests will show significant changes, many of these treatments start at the time of diagnosis (including in infancy) and continue every day throughout life. There are several classes of medications commonly used in CF, including acute and chronic antibiotic therapies, mucolytics, bronchodilators, pancreatic enzymes, fat soluble vitamin supplementation, insulin for people with cystic fibrosis related diabetes, and ursodiol for liver disease. Physiotherapy (airway clearance) treatments are prescribed once to several times a day. Most people with cystic fibrosis spend at least 2 hours a day on treatments, and this time commitment increases as the severity of the disease increases.
Cystic fibrosis transmembrane regulator (CFTR) modulators are revolutionary treatments in CF care. Non-modulator treatments are aimed at targeting symptoms, treating exacerbations, and slowing the progression of what is a life-long, degenerative, and fatal disease. CFTR modulators are the first commercially available therapies that are targeted at correcting the defect in CF by improving the production and function of the abnormal CFTR protein. Although none of the modulators are a cure for CF, the improvement in CFTR production and function does help to alleviate symptoms, improve clinical parameters such as lung function, body mass index, pulmonary exacerbations, and sweat chloride measurements, and have been shown to have a positive effect on quality of life in people with CF (pwCF). The second-generation modulators had a modest but important clinical effect, but the response to the third-generation modulator, elexacaftor-tezacaftor-ivacaftor (ELX-TEZ-IVA) is substantially greater and more comparable to the response of pwCF with eligible mutations to ivacaftor.
The first- and second-generation CFTR modulator medications ivacaftor, lumacaftor-ivacaftor, and tezacaftor-ivacaftor, were the first commercially available treatments to treat the underlying disease mechanism: a poorly produced and/or malfunctioning CFTR protein. Ivacaftor is currently approved for pwCF ages 4 months and up who have one or two of a small number of CFTR mutations, representing only about 4% of Canadians with CF. Alone, ivacaftor is not effective in pwCF who have two copies of the most common F508del mutation3 or who carry one F508del and another mutation not responsive to ivacaftor. Lumacaftor-ivacaftor (Orkambi) is currently indicated in Canada for pwCF ages 2 years and older who are homozygous for the F508del mutation. However, the response to lumacaftor-ivacaftor in clinical trials was more modest that those seen with elexacaftor-tezacaftor-ivacaftor.4,5. Tezacaftor-ivacaftor (Symdeko) is currently only approved for persons ages 12 years and older who are homozygous for F508 del or who are heterozygous for F508del and a small group of other mutations. Due to cost and reimbursement issues, many pwCF who are eligible have not been able to access this medication and off label use in the 6-11 year age group has been negligible.2 The response to tezacaftor-ivacaftor in clinical trials is significantly more modest than that to ELX-TEZ-IVA. Although the true cost to payers of these medications has been confidential, based on the list price there is no cost advantage to prescribing lumacaftor-ivacaftor or tezacaftor-ivacaftor to pwCF who are eligible for ELX-TEZ-IVA.
Due to cost and reimbursement policies, many pwCF eligible for lumacaftor-ivacaftor have not been able to access the medication. There are currently 504 children ages 6-11 in the Canadian Cystic Fibrosis Registry who have at least one F508del mutation and so might be eligible for therapy with ELX-TEZ-IVA. In 2019, 16 were listed as having received ivacaftor, 45 received ivacaftor-lumacaftor, and <5 had received ivacaftor-tezacaftor. Thus, most children ages 6-11 with CF were not being treated with the available CFTR modulators.2
Since ELX-TEZ-IVA received the initial market authorization, access to the medication is limited by type of insurance and province of residence. Some provinces and some private insurers did not restrict reimbursement to pwCF with a percent predicted FEV1 (ppFEV1) of <90%, while others followed the CADTH recommendations. In the provinces that did not restrict reimbursement, roll out of the medication for pwCF with treatable mutations has been steady. In more restrictive provinces and for pwCF with more restrictive private insurance plans, access has been reduced. This particularly affects younger pwCF who are more likely to have a ppFEV1 >90%, despite already have detectable CF lung disease. The Canadian Clinical Consensus Guideline for use of CFTR modulator therapies in pwCF provides comprehensive recommendations for criteria for initiation, monitoring, and response for children aged 6 years and older. Within this guideline, the recommendation is that all patients with eligible mutations aged 6 years and older should have the opportunity to be treated with ELX-TEZ-IVA irrespective of lung function.
ELX-TEZ-IVA was available for patients ages 12 and older with very severe lung disease via a special access program prior to the initial Health Canada approval. However, since Health Canada issued the Notice of Compliance for the 12 years and older age group, there has only been a small program for severely ill patients who are in gaps where there is not public nor private payment coverage. This program is managed by Vertex Pharmaceuticals and is designed to provide medication to a very limited group of patients for a short duration.
In addition to these treatments, the recommendations for CF care include routine medical visits to the cystic fibrosis clinic every three months. Additional visits may be required due to illness or for closer follow up of progressing symptoms, severe disease, or pre- and post-transplant care. Hospitalizations and home intravenous treatments may be required for acute respiratory infections or other complications of cystic fibrosis, such as distal intestinal obstructive syndrome. According to the 2019 Cystic Fibrosis Registry report, Canadians with CF had over 18,900 clinic visits that year and logged 25,200 hospital days and 15,500 home IV treatment days.1 In the 6-11 year age group, 64 children had at least 1 hospitalization in 2019 for pulmonary exacerbation (down from 84/year in 2015 and 2017). In addition, there were 19 courses of home IV antibiotics in this age cohort.2
Lung transplant is a treatment for end-stage CF pulmonary disease. It comes with risk factors and additional treatment burden and does not address CF disease in other organ systems. The median length of survival after lung transplant reported in the 2019 Registry report was 10.6 years, so it is not a cure, and the direct cost of medical care involved in lung transplant is around $1,000,000. Lung transplantation is only offered at four centres in Canada, and relocating to one of these centres (Toronto, Montreal, Edmonton, or Vancouver) is required during parts of the transplant process.
Treatment Goals
Life is challenging for a child with CF. They start on the daily routine at diagnosis: physiotherapy, enzyme supplementation with almost everything they eat, have to follow a special diet, sit through prolonged nebulizer treatments, and submit to other therapies and medications have an impact on their daily functioning. Frequent medical appointments and hospital admissions mean time away from school and family, disrupting family, social, and school relationships. For the 6–11-year age group, an ideal treatment would be one that decreased the daily intrusion of the disease into their life and the impact of CF on the usual activities of childhood.
It would be easy to take and not burdensome or time consuming. It would be easy for care givers and older children to take to help make adherence easier. It would be easy to integrate with the important normal activities of childhood, such as family life, education, peer relationships, extracurricular activities, development, and play. The treatment would not cause them to stick out as different from their peers.
Reduction of treatment burden is a major goal for pwCF, their families/caregivers, and their medical teams. An ideal treatment would decrease the burden on families of children with CF, as parents are the main caregivers providing the extra nutrition, physiotherapy, medication regimens, and medical visits needed, and would allow adults with CF to remain independent longer. By delaying the progression of the disease and the disability associated with moderate and severe lung disease, it would allow people with CF to remain in school, to pursue creative endeavors, and to engage in other activities that benefit society. It would help alleviate other non-direct medical costs, such as parental lost days of work related to CF care and illness.
It would improve the quality and duration of life. It would decrease the amount of time spent in the health care system, including time for specialty clinic visits, sick visits, and hospitalizations. It would delay disease progression. It would decrease the development of co-morbidities of the disease (CF diabetes, osteoporosis, poor growth, delayed puberty). It would eliminate or delay the need for double lung transplant.
It would allow people with CF to plan more confidently for careers, relationships, and having a family.
The risks of the treatment would be minor compared to the benefits. Care givers and older children would feel comfortable that the treatment is safe and effective.
People with CF and caregivers of children with CF have been shown to have increased incidence of anxiety and depression with a prevalence of around 30%. An important treatment goal is to address the effects of the disease on mental health. A treatment should also be accessible, reducing the potential for uncertainty and stress related to obtaining, paying for, and continuing the treatment.
An ideal treatment would also be cost effective and available to all persons with the disease who could benefit from it, regardless of insurance status, province of residence, or other restrictive criteria not associated with potential for response.
It is not easy being an adolescent or an adult with CF, either. Those ages 12 and up also have similar goals: decreasing the burden of treatment, improving and preserving lung function, reducing symptoms, minimizing the effect of the disease on many aspects of their daily lives, functioning as productive members of society, and delaying the progression of the disease that leads to the need for lung transplant and/or death at a young age.
Treatment Gaps (Unmet Needs)
Considering the treatment goals in the previous section, please describe goals (needs) that are not being met by currently available treatments.
Most of the currently available treatments only treat the symptoms and complications of CF and attempt to slow down the eventual fatal progression of the disease.
While ivacaftor is a highly effective CFTR modulator, it is effective for only about 4% of Canadians with CF and is not effective for CF patients who are homozygous for F508del or who carry one F508del mutation and a mutation that is not treatable by ivacaftor. These patients make up approximately 88% of people with CF.
The only currently approved modulator for pwCF ages 6-11 years is lumacaftor-ivacaftor. While it has shown positive effects on respiratory function, body mass index, and quality of life measures, the effects are modest4 and cost-effectiveness concerns have led to barriers to access for many. Only 45 Canadian children ages 6-11 were treated with it in 2019.2 Tezacaftor-ivacaftor is not approved by Health Canada for the 6-11 year age group and in the 12 years and older group the effect has not been as substantial as that shown by highly effective modulators.5,6
For pwCF ages 12 years and older, follow up studies7 and real-life clinical experience in other countries and in Canadian provinces where reimbursement of ELX-TEZ-IVA is not limited by the FEV1 criteria have shown that a positive therapeutic response to the medication is not limited only to persons with a ppFEV1 of <90%. In the PROMISE study, subjects with an FEV1 > 90% showed significant improvements in ppFEV1, sweat chloride measurement, CFQ-R Respiratory domain score, and BMI. Although the authors state that due to the study design, caution is needed in making conclusions on ppFEV1 change based on baseline FEV1, there are significant changes in several secondary outcomes.
Despite the impact CF newborn screening has on altering the natural history of children with CF, these patients still have lung disease and other manifestations of CF from early in life even when pulmonary function measurements are relatively preserved, and these changes are progressive, cumulative, and ultimately lead to death. Restricted reimbursement has led to a lack of access for Canadians with CF who could reasonably benefit from this medication. This is continuing to have an important and long-lasting effect on these persons.
Development of progressive, non-reversible lung disease and antibiotic resistance in bacteria involved in acute and chronic lung infections due to repeated antibiotic exposure make treatment of infection more challenging with time.
Adherence to treatment and simplifying treatment burden is a major concern for people with CF and for CF clinicians. Burden of care is high and increases with age and the severity of the disease. A recent study by the James Lind Alliance Priority Setting Partnership (JLA PSP) in cystic fibrosis surveyed people with CF, parents of children with CF, and health care workers to determine perceived priorities for CF research. Important themes than emerged were that the lived experience of treatment burden in CF is high, that it extends beyond just the time taken to perform routine daily treatments, and that the impact on daily life varies. Adherence to the more burdensome treatments, such as nebulized antibiotics and airway clearance, are often the first to be missed. Of the subset of people with CF who answered questions regarding work and education, “87% felt that their treatments get in the way of their job or career and 77% (168/217) in the way of their education. Two thirds (67%) reported that their treatments get in the way of family relationships, relationship with a partner (69%), and relationships with friends (75%). An impact of treatments on socialising and on sports and hobbies was reported by 81% and 80%, respectively.”8 Treatments need to be able to be easily integrated into daily life, to not form a barrier that limits participation in important activities during childhood, such as school, family life, peer relationships, sports, hobbies, and play.
Other treatments to treat the molecular basis of the disease, such as gene therapy, have been under development for years but have not yet progressed beyond the research stage.
The development of a highly effective CFTR modifier such as elexacaftor/tezacaftor/ivacaftor fills a niche in CF care that is not currently occupied by another equally effective treatment.
There will remain approximately 10% of people with CF in Canada who have CFTR mutations that do not respond to any of the current CFTR modulator therapies. Research continues to find a treatment for this group.
Which patients have the greatest unmet need for an intervention such as the drug under review?
ELX-TEZ-IVA has the potential to treat approximately 90% of Canadians with cystic fibrosis.
Currently, children below the age of 12 years do not have access to ELX-TEZ-IVA. While many medications are prescribed “off-label” in pediatrics, the cost of ELX-TEZ-IVA makes this impracticable. Children in this age group already show sequelae of CF disease, and optimizing treatment is essential to limit the effects of the disease and slow disease progression.
Although children ages 6-11 years who are homozygous for F508del (2 copies) are eligible for lumacaftor/ivacaftor, the high cost and lack of payment coverage means that most patients do not have access to this medication, and it is less effective in clinical trials than ELX-TEZ-IVA. To quote a parent “Why have an iPhone 6 when the iPhone 12 is available?”
Another group in need are persons ages 12 and up with an FEV1>90% predicted. These pwCF have symptoms and sequelae of the disease, experience a high treatment burden and high disease impact on their daily life, and can suffer from pulmonary exacerbations, poor weight gain, and other morbidities associated with cystic fibrosis, despite having relatively preserved lung function testing results. Currently, unequal access to ELX-TEZ-IVA has been stressful for pwCF who are unable to qualify for coverage due to their lung function and province of residence or public vs. private insurance status. There has been uncertainty regarding whether access will be available, a lack of mobility within Canada for fear of losing coverage by moving to another province or changing jobs, and some “survivor guilt” in those who have access but know that others do not.
Place in Therapy
How would the drug under review fit into the current treatment paradigm? Is there a mechanism of action that would complement other available treatments, and would it be added to other treatments?
Currently, ELX-TEZ-IVA is added on to existing therapies. There are studies underway, particularly in the US, where this medication is widely available and reimbursed and is part of the regular treatment guidelines, to look at the effect decreasing the number or intensity of other CF treatments in people taking ELX-TEZ-IVA. This would be a real paradigm shift in the treatment of CF.
More recently the Canadian guidelines recommend that ELX-TEZ-IVA be added on to existing therapies for a duration of one year to start, at which point response to therapy will be evaluated and recorded as part of the national CANimpact study.
The impact on lung transplantation in CF has been impressive. Centres are reporting that patients on the lung transplant list and under evaluation for transplant are improving on ELX-TEZ-IVA to the extent that they no longer currently need lung transplant. This is having a major positive impact.
While ELX-TEZ-IVA is not the first CFTR modulator developed, it is so far the most effective for most persons with CF, including for pwCF ages 6 and up, and expands the number of people who will be eligible for treatment with a modulator, according to clinical trial results. As mentioned in previous sections, it does address the underlying disease process: decreased production and lack of function of the defective CFTR protein.
A Canadian group used a microsimulation transition model to estimate the effect of the introduction of ELX-TEZ-IVA on the Canadian CF population. In this model, the number of persons with severe lung disease decreased by 60%, the number of pulmonary exacerbations decreased by 19%, and the number of lung transplants decreased by 146 during the period 2021-2030 if the medication is introduced by 2021. Decreasing the need for acute treatments and lung transplant would be a shift in the role of these treatments in the disease.9
Please indicate whether or not it would be appropriate to recommend that patients try other treatments before initiating treatment with the drug under review. Please provide a rationale from your perspective.
Persons with CF in Canada will have already been prescribed the standard treatments, whether or not they initiate treatment with ELX-TEZ-IVA, under the current treatment recommendations. They would continue the current treatments aimed at controlling symptoms and disease progression.
Because the cost of ELX-TEZ-IVA is similar to less effective CFTR modulators, there is no advantage to starting one of them prior to starting ELX-TEZ-IVA. If coverage and reimbursement criteria for ivacaftor/tezacaftor and ivacaftor/lumacaftor remains the same, these will also not be financially viable options for most Canadian CF patients.
How would this drug affect the sequencing of therapies for the target condition?
The sequence of therapies will not change if the new therapy fails. If the person’s condition changes or further information suggests that the medication may then be effective, it could be tried again, with careful monitoring for effectiveness.
Which patients would be best suited for treatment with the drug under review?
Because the effects of this medication depend on the CFTR genotype, it has currently been found effective in persons with at least one copy of the F508del mutation. Health Canada approval has been requested for persons 6 years of age and older, and studies have included people with all severities of lung disease with no FEV1 cap. In the Phase 3 study of ELX-TEZ-IVA in children ages 6-11, 45.5% of participants had a ppFEV1 90% at baseline and the study showed a significant mean absolute change from baseline of 10.2 percentage points, a significant result despite the population in this study starting with a higher FEV1 that the population chosen for the adolescent/adult studies.5
Because CF is a chronic, progressive, and eventually fatal disease, all patients with CF who are eligible for this therapy are at need of the intervention. Limiting it to pwCF with an arbitrary lung function threshold does not address the progressive nature of the disease at an earlier stage, where the progression to severe disease and disability could be prevented or delayed.
Many of the clinical studies in persons ages 12 and older only included persons with lung function measured by ppFEV1 of between 40-90%. While this design was important for clinical trials, further clinical experience and research results have found that the medication was useful in patients with FEV1 < 40%.7 In patients with FEV1 > 90%, there are often early signs of CF lung disease present, such as bronchiectasis, mucus plugging, or early mild declines in FEV1% predicted that could benefit from therapy with ELX-TEZ-IVA. Fortunately, reimbursement was recommended for this group.
How would patients best suited for treatment with the drug under review be identified?
As the Canadian Cystic Fibrosis clinic system is well established and covers almost all persons with CF in Canada, patients best suited for this medication would be identified by their CF care provider based on the genotype of their CFTR mutations and other clinical factors. The criteria for diagnosing CF are well established and standardized, and the appropriate tests are available at CF clinics.
CFTR genotype is performed as part of the diagnostic standards for persons with CF (with consent) and is available to the practitioner prescribing the medication.
Because CF is a genetic, progressive chronic disease, manifestations of the disease start in early life. Treatment with this potentially disease altering medication should not be held until persons become more symptomatic or until lung function deteriorates below an arbitrary threshold.
The recent Canadian guidelines clearly define patients who should be treated with a CFTR modulator.
Which patients would be least suitable for treatment with the drug under review?
Any patient who does not have a CFTR mutation genotype that would respond to the medication, or persons with a known allergy, a medical or other contraindication (such as severe liver disease), or other adverse reaction to this or a similar medication as described in the product monograph or Canadian guidelines.
Is it possible to identify those patients who are most likely to exhibit a response to treatment with the drug under review?
Patients would be identified by their CF clinic care provider based on having an eligible CFTR genotype and no contraindications to this therapy.
What outcomes are used to determine whether a patient is responding to treatment in clinical practice?
Spearheaded by the Health Advisory Group at Cystic Fibrosis Canada, a group of Canadian CF clinicians have developed standardized guidelines for all patients starting on CFTR modulator treatment and for assessing response.10 In addition to the regular clinic visits every three months, an additional visit has been recommended 1 month after starting therapy with ELX-TEZ-IVA to assess the initial response to therapy, to screen for side effects, and to address patient concerns. At follow up visits, outcomes measured include a history and physical exam, pulmonary function testing (including ppFEV1), measurement of height/weight and calculation of BMI, laboratory tests to follow parameters associated with potential side effects (liver enzymes, creatine kinase), sputum microbiology, quality of life questionnaires and mental health screening, and a review of prescribed therapies. Fecal elastase and sweat chloride levels will be monitored at intervals. Regular follow up with a yearly ophthalmological examination is also recommended. Optional examinations include a follow up chest CT.
These outcomes align with those identified in the clinical trials and with normal standard care of patients with CF.
What would be considered a clinically meaningful response to treatment?
The improvements that have been measured in most clinical trials include pulmonary function testing, pulmonary exacerbations and antibiotic use, weight and nutritional status, and quality of life. In clinical practice, patients have reported feeling better, having fewer symptoms such as cough or shortness of breath, having less difficulty maintaining a healthy weight, missing less work or school due to hospitalization for pulmonary exacerbations, and stabilization of the disease. Increased attention to quality-of-life measures and screening measures to detect mental health issues have led to these aspects also being included as measures of response to treatment clinically.
These treatment responses include some quantifiable measures (pulmonary function, BMI) that should not vary across physicians. Whether a pwCF is admitted to hospital or treated as an outpatient for a pulmonary exacerbation may be physician, centre, or location dependent and may also be affected by other factors. However, the effect of the medication on disease stability should not vary greatly by physician. Quality of life measures and patient reported symptoms should also not be practitioner dependent.
Criteria for determining response to therapy has been clearly identified by the Canadian Guideline, including recommendations for dose interruption and discontinuation.
How often should treatment response be assessed?
Because of the routine clinic visits at three-month intervals, treatment response is assessed frequently. An additional visit at 1 month after initiating therapy was added as noted above.
The Canadian Guideline for longitudinal assessment of treatment response has been developed and disseminated to CF clinics, and a national, multi-centre study will be evaluating the response to ELX-TEZ-IVA in Canadian real-world use.
On a population basis, the Canadian CF Registry will be used to track changes in factors such as hospitalization, lung function decline, mortality, and lung transplant.
What factors should be considered when deciding to discontinue treatment?
As with any treatment, discontinuation should be considered if a severe side effect, allergy, or other adverse event occurs. With this medication, the development of signs of worsening liver disease or other significant side effects may require stopping treatment. The Canadian guidelines provide recommendation for dose reduction or discontinuation.
What settings are appropriate for treatment with the drug under review?
This treatment should be prescribed by CF practitioners at an accredited Cystic Fibrosis clinic. It is a twice daily, oral treatment, so it will be taken as an outpatient as part of the person’s standard routine.
For non-oncology drugs, is a specialist required to diagnose, treat, and monitor patients who might receive the drug under review?
Almost all patients with cystic fibrosis in Canada are followed at accredited Cystic Fibrosis clinics, which are staffed by professionals who have the training and experience in diagnosing, treating, and monitoring persons with CF who would be treated with this medication.
Additional Information
The cystic fibrosis clinic is one place where we see how the quantitative data and research results translate into significant impacts on the lives of our patients with CF.
The median percent predicted FEV1 (ppFEV1) of children ages 6-11 in the Canadian CF Data Registry in 2019 was 98.0%, but about 28% had a ppFEV1 <90% (161 out of the 563 with at least 1 ppFEV1 measurement). Out of the 580 patients in the registry in this age group, 64 had at least one hospitalization for a pulmonary exacerbation. This number was decreased from previous years, with a range of 76-84 children with at least one hospitalization in each year from 2015-2018 and a total of 96-133 hospitalizations in total for this age group during the same period. In addition, there were 19 courses of home IV antibiotics in this age group. Median BMI percentile for ages 6-11 in the Registry was 45.98% in 2019,2 while in the general population the median should be closer to 50%.
Most 6–11-year-old children are thinking about other things than their FEV1 or BMI. The classical developmental task at age 6-11 is to develop competence and in the Eriksonian model this stage is designated as Industry vs. Inferiority.11 Children are becoming aware of their abilities and are developing self-confidence. Participation in school, extracurricular, and family activities are key. Peer relationships and comparing themselves to others are also important. Having a chronic disease can affect this crucial stage of development in ways that can have long lasting effects, just as the physical manifestations of CF have ongoing sequelae.
We know that pulmonary and GI manifestations of CF are present prenatally and throughout infancy and childhood, including before there is any measurable signal in FEV1.12,13 We also know that children with better lung function, later chronic colonization with P. aeruginosa, and better nutritional status when young usually do better in the long run, with slower decline in lung function and disease progression.
An improvement in lung function and improved nutritional status can correspond to improved performance in sports and not getting picked last for the team. For children, it can also mean not having to be excused in the middle of class to have a bowel movement and not being embarrassed to use a public washroom for fear of being teased about the foul-smelling gas associated with CF. Improved nutritional status does not just mean an improved BMI but can also lead to improvements in resting energy expenditure, GI microbiome, and fat and fat-free mass, potentially translating into more muscle strength, less anxiety about maintaining the current high calorie, high fat, high protein CF diet, and less reliance on supplemental nutrition.14
Periods of picky eating or fussiness, routine for many children, take on a dark implication for caregivers of children with CF. The stakes are higher. For a child, wondering if they can eat a classmate’s birthday cupcake when they don’t have a spare enzyme pill can lead to either sticking out as different if they don’t or risking the gastrointestinal consequences of an accident if they do. Every meal or snack is a reminder of the disease.
In the clinic, we see how a chronic cough can interfere with sleep and the resulting fatigue interferes with learning at school. It can be disruptive to daily activities and during the pandemic baseline CF respiratory symptoms have led to concern and additional investigations.
These concerns may not seem major, but they are part of the everyday unceasing impact of CF on a child’s life.
A hospitalization can mean two missed weeks of school, falling behind in class, missing a dance recital, and the child having to explain to friends where they were and why. We also know that lung function does not always recover to baseline after a pulmonary exacerbation, so decreasing the number of exacerbations should help preserve lung function.15 Changes to the lung microbiome after treatment with ELX-TEZ-IVA may lead to fewer pulmonary exacerbations, better lung health, and decreased burden of troublesome classic CF associated microorganisms.16
Children become aware of what having CF means in the long term and start to hear of others who are ill or have died of CF, leading to fear and uncertainty.
Parental missed days of work for appointments and hospitalizations can affect the family’s financial security and lead to increased parental and child stress.
The effect of ELX-TEZ-IVA on quality of life of pwCF and caregivers has been meaningful and important.17
While there are models for evaluating the effect of a medication on direct health care costs, the cost-benefit of a healthier childhood is harder to calculate but is nevertheless very important.
There are also ethical questions to consider in reviewing medications for rare diseases, and the usual parameters such as standard figures per QALY (quality adjusted life year) may not be applicable for this group.18 Also, the lack of reimbursement for some pwCF with ppFEV1 raises questions of equity within the health care system, especially when evidence and clinical experience is now supporting a clinical response in those with ppFEV1 >90%.
Adolescents and adults with CF also have important, restrictive impacts on their life due to the disease. It impacts many aspects of their daily lives: the time to do treatments can impact school, extracurricular activities, family life, friendships, relationships, and employment. Adolescence is another crucial period of development, where the individual is forming their identity and establishing their aspirations and values. Having CF affects this strongly. Hospitalizations for pulmonary exacerbations, growth and physical maturation issues, nutritional demands, and fear of having a significantly shortened life span affect planning for the future. For adults, developing a future, partnerships, parenting, and career decisions, and taking a place as a productive member of society are also affected by the disease. Does an adolescent plan to go to university and become a health economist, or will that pwCF run out of time and not be able to complete a degree and put it to use? Highly effective CFTR modulator therapies aren’t a cure for CF, but when they are used early and effectively may decrease the burden and progression of CF and help modify the effect of having the disease during these crucial life stages.
When we meet with the parents of a baby newly diagnosed through newborn screening, they ask us if there is hope. They know that CF is a progressive, fatal disease. With the arrival of the highly effective CFTR modulators, we have been able to pass on the hope that, with treatment, the burden of CF will be less than previously and their child’s daily life and future less clouded by the disease. For adults living with CF, it means being able to plan for a future that didn’t previously seem likely and to continue to contribute. For CF clinicians and care teams, it holds out the promise of being able to help our patients reach their goals and spend less time on treatments, procedures and hospitalizations.
There has not been a completed randomized, double blinded, placebo-controlled trial of ELX-TEZ-IVA in the 6 -11-year age group. Due to availability of a CFTR modulator for this age group (lumacaftor-ivacaftor), using a placebo-controlled design for this group was reasoned to be unethical.5 Based on the results of previous trials in other age groups and the strength of the signal, the study design was adequate to show the advantages of ELX-TEZ-IVA compared to the baseline in study participants. There is currently a randomized, placebo-controlled trial underway in the 6—11 year age group for persons heterozygous for the F508del mutation and a minimal function mutation, as there is no commercially available CFTR modulator for this cohort.
References
Cystic Fibrosis Canada. (2020). The Canadian Cystic Fibrosis Registry 2019 Annual Data Report. Toronto, Canada: Cystic Fibrosis Canada.
Unpublished data obtained from the Canadian Cystic Fibrosis Registry. Data inquiry December 2021.
Flume PA, Liou TG, Borowitz DS, et al. Ivacaftor in subjects with cystic fibrosis who are homozygous for the F508del-CFTR mutation. Chest. 2012;142(3):718-724. doi:10.1378/chest.11-2672.
Milla CE, Ratjen F, Marigowda G, Liu F, Waltz D, Rosenfeld M; VX13-809-011 Part B Investigator Group *. Lumacaftor/Ivacaftor in Patients Aged 6-11 Years with Cystic Fibrosis and Homozygous for F508del-CFTR. Am J Respir Crit Care Med. 2017 Apr 1;195(7):912-920. doi: 10.1164/rccm.201608-1754OC.
Zemanick ET, Taylor-Cousar JL, Davies J, et al. A Phase 3 Open-Label Study of Elexacaftor/Tezacaftor/Ivacaftor in Children 6 through 11 Years of Age with Cystic Fibrosis and at Least One F508del Allele. Am J Respir Crit Care Med. 2021 Jun 15;203(12):1522-1532. doi: 10.1164/rccm.202102-0509OC
Flume PA, Biner RF, Downey DG, et al.; VX14-661-110 study group. Long-term safety and efficacy of tezacaftor-ivacaftor in individuals with cystic fibrosis aged 12 years or older who are homozygous or heterozygous for Phe508del CFTR (EXTEND): an open-label extension study. Lancet Respir Med. 2021 Jul;9(7):733-746. doi: 10.1016/S2213-2600(20)30510-5.
Nichols DP, Paynter AC, Heltshe SL, et al for the PROMISE Study Group. Clinical effectiveness of Elexacaftor/Tezacaftor/Ivacaftor in people with cystic fibrosis. Am J Respir Crit Care Med. 2021, article in press, doi: 10.1164/rccm.202108-1986OC
Davies G, Rowbotham NJ, Smith S, Elliot ZC, Gathercole K, Rayner O, et al. Characterising burden of treatment in cystic fibrosis to identify priority areas for clinical trials. J Cyst Fibros 2020;19(3):499–502.
Stanojevic S, et al. Projecting the impact of delayed access to elexacaftor/tezacaftor/ivacaftor for people with Cystic Fibrosis. J Cyst Fibros, article in press, published online August 23, 2020. DOI:https://doi.org/10.1016/j.jcf.2020.07.017
The Canadian Clinical Consensus Guideline for Initiation, Monitoring and Discontinuation of CFTR Modulator Therapies for Patients with Cystic Fibrosis. July 2021: https://www.cysticfibrosis.ca/uploads/CFC%20Modulator%20Guidelines_RevisedOct62021%20(003).pdf
Erikson, Erik H. (Erik Homburger), 1902-1994. The Erik Erikson Reader. New York :W.W. Norton, 2000.
Grasemann, H and Ratjen F, Early lung disease in cystic fibrosis. Lancet Resp Med, 2013;1(2):148-157. doi.org/10.1016/S2213-2600(13)70026-2.
Kelly, T., Buxbaum, J. Gastrointestinal Manifestations of Cystic Fibrosis. Dig Dis Sci 60, 1903–1913 (2015). https://doi.org/10.1007/s10620-015-3546-7
Bass R, Brownell JN, Stallings VA. The Impact of Highly Effective CFTR Modulators on Growth and Nutrition Status. Nutrients. 2021;13(9):2907. doi:10.3390/nu13092907
Sanders, D.B., Bittner, R.C., Rosenfeld, M., Redding, G.J. and Goss, C.H. (2011), Pulmonary exacerbations are associated with subsequent FEV1 decline in both adults and children with cystic fibrosis. Pediatr. Pulmonol., 46: 393-400. https://doi.org/10.1002/ppul.21374
Sosinski LM, Mar L.M. Sosinski, C.M. H, K.A. Neugebauer et al., A restructuring of microbiome niche space is associated with Elexacaftor-Tezacaftor-Ivacaftor therapy in the cystic fibrosis lung, Journal of Cystic Fibrosis, https://doi.org/10.1016/j.jcf.2021.11.003 (article in press).
Van Brunt, K., et al. Impact of treatment with elexacaftor/tezacaftor/ivacaftor and ivacaftor in people with cystic fibrosis and caregivers in the United States: A qualitative study.(abstract) Journal of Cystic Fibrosis 20 (2021): S137-S138.
Zimmermann BM, Eichinger J, Baumgartner MR. A systematic review of moral reasons on orphan drug reimbursement. Orphanet J Rare Dis. 2021;16(1):292. Published 2021 Jun 30. doi:10.1186/s13023-021-01925-
Conflict of Interest Declarations for the Canadian Cystic Fibrosis Clinic Directors and CF Canada Healthcare Advisory Council
To maintain the objectivity and credibility of the CADTH drug review programs, all participants in the drug review processes must disclose any real, potential, or perceived conflicts of interest. This conflict of interest declaration is required for participation. Declarations made do not negate or preclude the use of the clinician group input. CADTH may contact your group with further questions, as needed. Please see the Procedures for CADTH Drug Reimbursement Reviews (under the Place in Therapy section) for further details.
Did you receive help from outside your clinician group to complete this submission? If yes, please detail the help and who provided it.
Particularly, no assistance was received from any pharmaceutical company.
Did you receive help from outside your clinician group to collect or analyze any information used in this submission? If yes, please detail the help and who provided it.
We requested some unpublished data from the Cystic Fibrosis Canada Canadian Cystic Fibrosis Patient Registry that is used in this submission.
List any companies or organizations that have provided your group with financial payment over the past two years AND who may have direct or indirect interest in the drug under review. Please note that this is required for each clinician who contributed to the input — please add more tables as needed (copy and paste). It is preferred for all declarations to be included in a single document.
Declaration for Clinician 1
Name: Dr. Zofia Zysman-Colman, MDCM
Position: Pediatric respiratory medicine, Cystic Fibrosis Clinic, attending physician, CHU Sainte-Justine, Montreal, QC
Date: 15-12-2021
Table 10: COI Declaration for Canadian Cystic Fibrosis Clinic Directors and CF Canada Healthcare Advisory Council — Clinician 1
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
Vertex (Speaker’s fee) | X | — | — | — |
Declaration for Clinician 2
Name: Dr. Dimas Mateos-Corral, MD
Position: Clinical Associate Professor, CF Clinic Director, IWK Health Centre, Halifax, Nova Scotia
Date: 14-12-2021
Table 11: COI Declaration for Canadian Cystic Fibrosis Clinic Directors and CF Canada Healthcare Advisory Council — Clinician 2
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
Vertex Pharmaceuticals | — | X | — | — |
Declaration for Clinician 3
Name: Dr. Mark Chilvers, MRCPCH, MD, BSc, MBChB
Position: Clinical Associate Professor, CF Clinic Director, BC Children’s Hospital, Vancouver, BC. Chair of CF Canada Healthcare Advisory Council
Date: 14-12-2021
Table 12: COI Declaration for Canadian Cystic Fibrosis Clinic Directors and CF Canada Healthcare Advisory Council — Clinician 3
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
Vertex Pharmaceuticals | — | — | X | — |
Declaration for Clinician 4
Name: Dr. Martha L. McKinney, MD MPH FRCPC
Position: Clinical Lecturer, Department of Pediatrics, CF Clinic Physician, University of Alberta/Stollery Children’s Hospital, Edmonton, AB
Date: 15-12-2021
Table 13: COI Declaration for Canadian Cystic Fibrosis Clinic Directors and CF Canada Healthcare Advisory Council — Clinician 4
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
Vertex Pharmaceuticals | X | — | — | — |
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up-to-date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
Redactions: Confidential information in this document may be redacted at the request of the sponsor in accordance with the CADTH Drug Reimbursement Review Confidentiality Guidelines
Stakeholder Input: The views expressed in each submission are those of the submitting organization or individual; not necessarily the views of CADTH or of other organizations. As such, they are independent of CADTH and do not necessarily represent or reflect the view of CADTH. No endorsement by CADTH is intended or should be inferred. By filing with CADTH, the submitting organization or individual agrees to the full disclosure of the information. CADTH does not edit the content of the submissions.
CADTH does use reasonable care to prevent disclosure of personal information in posted material; however, it is ultimately the submitter’s responsibility to ensure no identifying personal information or personal health information is included in the submission. The name of the submitting organization or individual and all conflict of interest information are included in the submission; however, the name of the author, including the name of an individual patient or caregiver submitting the patient input, are not posted.
Accessibility: CADTH is committed to treating people with disabilities in a way that respects their dignity and independence, supports them in accessing material in a timely manner, and provides a robust feedback process to support continuous improvement. All materials prepared by CADTH are available in an accessible format. Where materials provided to CADTH by a submitting organization or individual are not available in an accessible format, CADTH will provide a summary document upon request. More details on CADTH’s accessibility policies can be found here.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.