CADTH Reimbursement Review
Cenegermin (Oxervate)
Sponsor: Dompé Farmaceutici S.p.A
Therapeutic area: Neurotrophic keratitis
This multi-part report includes:
Clinical Review
Pharmacoeconomic Review
Stakeholder Input
Clinical Review
Abbreviations
AE
adverse event
AMT
amniotic membrane transplantation
CI
confidence interval
ETDRS
Early Treatment Diabetic Retinopathy Study
HRQoL
health-related quality of life
ITT
intention to treat
LS
least squares
MID
minimally important difference
NEI-VFQ-25
National Eye Institute Visual Function Questionnaire-25 items
NK
neurotrophic keratitis
PED
persistent epithelial defect
RCT
randomized controlled trial
rhNGF
recombinant human nerve growth factor
SAE
serious adverse event
SD
standard deviation
SE
standard error
WDAE
withdrawal due to adverse event
Executive Summary
An overview of the submission details for the drug under review is provided in Table 1.
Item | Description |
|---|---|
Drug product | Cenegermin ophthalmic solution (Oxervate), 0.002% (20 mcg/mL), topical eye drops |
Indication | For the treatment of moderate (PED) or severe (corneal ulcer) NK in adults |
Reimbursement request | For the treatment of moderate (PED) or severe (corneal ulcer) NK in adults who have failed conventional nonsurgical treatments |
Health Canada approval status | NOC |
Health Canada review pathway | Priority review |
NOC date | February 8, 2019 |
Sponsor | Dompé Farmaceutici S.p.A |
NK = neurotrophic keratitis; NOC = Notice of Compliance; PED = persistent epithelial defect.
Introduction
Neurotrophic keratitis (NK) is a rare degenerative disorder of the cornea characterized by impaired corneal nerve function with subsequent corneal epitheliopathy. Severity of NK can be categorized as mild (stage 1), moderate (stage 2), or severe (stage 3) based on the extent of corneal involvement, according to the Mackie Classification.1 Moderate and severe NK can profoundly affect patients’ vision and adversely impact their health-related quality of life (HRQoL).2,3 Diagnosis of NK is established from a patient’s medical history, followed by eye examination and testing to assess decreased corneal sensitivity and nerve damage.3,4 The prevalence of NK has been estimated to be less than 5 in 10,000 individuals worldwide, although the condition is most likely underdiagnosed.2 In 2021, approximately 6,100 Canadians were diagnosed with NK, and 2,300 of them had moderate or severe disease.
Management of NK is based on stage and severity of the disease, and the treatment aims to stop the progression of corneal damage and promote epithelial healing. Treatment options for mild NK include removal of the offending agent (e.g., preservative-containing eye drops), if possible, frequent use of preservative-free artificial tears and ointments, autologous serum eye drops, or platelet-rich plasma. Punctal occlusion and treatment of any concomitant lid malposition are also commonly adopted. For moderate NK, treatment options are the same as for mild NK, plus prophylactic topical preservative-free antibiotics, matrix metalloproteinases inhibitors, corneal therapeutic contact lenses, epithelial debridement, tarsorrhaphy, amniotic membrane transplantation (AMT), and conjunctival flaps. For severe NK, additional treatment options can include corneal gluing, synthetic tissue adhesive, corneal neurotization, layered amniotic membrane grafting, and partial or full-thickness corneal transplantation.2-4
Cenegermin is a recombinant human nerve growth factor (rhNGF) for topical ophthalmic use in the treatment of moderate or severe NK. It targets the nerve pathology associated with NK, therefore has the potential to address the healing deficits present in this patient population.3,5 On February 8, 2019, cenegermin was approved by Health Canada for the treatment of moderate or severe NK in adults. The reimbursement request by the sponsor for cenegermin is for the treatment of moderate or severe NK in adults who have failed conventional nonsurgical treatments. Cenegermin is available as topical eye drops, 20 mcg/mL (0.002%). The recommended dose is 1 drop of cenegermin in the conjunctival sac of the affected eye(s) 6 times per day, at 2-hour intervals. Treatment with cenegermin should be continued for 8 weeks.5
The objective of this report is to perform a systematic review of the beneficial and harmful effects of cenegermin (ophthalmic solution, 0.002%, 20 mcg/mL) for the treatment of moderate (persistent epithelial defect [PED]) or severe (corneal ulcer) NK in adults.
Stakeholder Perspectives
The information in this section is a summary of input provided by the patient groups that responded to CADTH’s call for patient input and by clinical experts consulted by CADTH for the purpose of this review.
Patient Input
One patient group, the Canadian Organization for Rare Disorders (CORD), submitted patient input for this review. CORD is a national network that advocates for health policy and a health care system that works for those with rare disorders. The input was based on 15- to 30-minute phone interviews with 12 patients recruited from 3 eye institutes in the US. All respondents had an NK diagnosis and were 24 to 77 years of age (75% > 65 years). Reasons given by respondents for their loss of nerve growth factor included a surface injury to the cornea, prolonged use of contact lenses, eye infections, cataract surgery, or an underlying health condition, such as diabetes. Most patients did not know the stage of severity of their condition. All patients interviewed had experience with cenegermin and completed treatment from 2 weeks to 3 years ago.
All respondents reported experiencing some symptoms before diagnosis, such as blurred, low (peripheral) vision, or (near) loss of vision (in 1 eye). Time to diagnosis ranged from 6 months to 3 years, or more, and most respondents received at least 1 treatment before diagnosis, such as a lubricant or antibiotics. Two patients reported discussing the option of surgery, including AMT to protect the cornea and suturing of the eyelid.
Respondents reported positive experiences with cenegermin, and all respondents completed the 8-week treatment. All respondents reported outcomes favouring cenegermin, although impact and durability varied. Most patients treated 2 to 3 years previously were still benefiting from improved vision and were not experiencing symptoms associated with loss of nerves supporting the cornea. Some patients reported experiencing minor side effects (stinging, pain, headaches, and blurred vision) that went away upon treatment completion. Respondents expressed a desire for an accurate diagnosis at symptom onset, and reported receiving an effective treatment only after long periods of suffering and ineffective or invasive treatments. The input summary suggests that if NK is diagnosed and treated in stage 1, minimal damage and full recovery are usually possible.
Clinician Input
Input From the Clinical Experts Consulted by CADTH
The experts indicated that even though various treatment options are available for patients with moderate or severe NK, not all patients respond to them, and they can become refractory to the current treatments. Some treatment options are associated with complications or cosmetic issues.
In the experts’ opinion, cenegermin has a unique mechanism of action that can cure the disease, not just control symptoms. Cenegermin can be used as a first-line treatment or in combination with the other currently available treatments for NK. This treatment is suitable for patients in any stage of NK. The experts noted that it is not clear which patients would be most likely to benefit from treatment.
In clinical practice, moderate or severe NK can be easily diagnosed; however, it is challenging to identify patients with mild NK because of the subtle clinical examination findings (i.e., no frank epithelial defect) and symptoms at this stage. The diagnosis of NK is typically made by a cornea specialist, after referral from an ophthalmologist or optometrist based on clinical history and examination; in some centres, in vivo confocal microscopy can confirm the diagnosis, but access to this technology is limited to very specialized eye centres. The interpretation of confocal images is also subjective.
The experts stated that treatment response is evaluated using the size of the epithelial defect. Complete resolution (i.e., 0 mm in size) or significant closure (i.e., less than 0.5 mm in size) of the epithelial defect would be clinically meaningful. The experts suggested that during the 8-week treatment period with cenegermin, a patient’s progress needs to be assessed at week 4 and week 8, and again 4 weeks after the completion of the 8-week course. Follow-up time can be tailored, depending on the patient’s response.
The experts indicated that treatment with cenegermin should be discontinued if the patient experiences significant adverse events (AEs), or if the patient is unable to comply with the dosing schedule.
Drug Program Input
In response to Drug Program’s questions regarding access to care from cornea specialists, the clinical expert consulted by CADTH indicated that access to cornea specialists is easier in urban areas. Patients in a rural setting may have difficulty accessing a specialist. One solution to this situation is to have a local general optometrist or ophthalmologist help comanage the patient with a cornea specialist from outside the local area.
For questions related to treatment selection, the clinical expert stated that off-label nonsurgical alternatives are available for patients with moderate or severe NK who have failed certain nonsurgical treatments, which can include preservative-free artificial tears, autologous serum tears, or removal of any offending agents (if possible). If the patients do not respond well to these alternatives within 1 to 2 months of treatment, it would be reasonable to offer them cenegermin as the next step.
Clinical Evidence
Pivotal Studies and Protocol-Selected Studies
Description of Studies
Two phase II, double-blind, randomized controlled trials (RCTs) — NGF02126 (N = 156) and NGF02147 (N = 48) — submitted by the sponsor are included in this systematic review. The objectives of both studies were to evaluate the efficacy and safety of cenegermin eye drops in patients with moderate to severe NK. The studies included adults with a diagnosis of moderate or severe NK. Eligible patients were randomized to receive cenegermin or vehicle therapy for 8 weeks. At the end of the 8-week controlled treatment period, patients in Study NGF0212 entered a 48- or 56-week follow-up period. The duration and treatment during the safety follow-up period was determined by the randomized treatment received and the healing of their PED or corneal ulcer. The follow-up period was 48 weeks (approximately 12 months) for patients who were initially randomized to cenegermin (10 mcg/mL or 20 mcg/mL), regardless of whether or not the patient was completely healed at week 8. The follow-up period was also 48 weeks for patients who were initially randomized to vehicle and who were completely healed at week 8. The follow-up period was 56 weeks for patients who were initially randomized to the vehicle group and who were not completely healed at week 8. These patients were randomly assigned to treatment with cenegermin (10 mcg/mL or 20 mcg/mL) for 8 weeks. In Study NGF0214, patients who completed the 8-week controlled treatment period entered a 24-week follow-up period. In both studies, all patients completely healed at week 8 (including those who received active treatment) were eligible for another course of treatment in the event of recurrence during the follow-up period. The primary efficacy outcome was the proportion of patients that achieved complete corneal healing at week 4 (NGF0212) or week 8 (NGF0214), determined by the central reading centre. Secondary efficacy outcomes included corneal sensitivity, corneal clearing, disease deterioration, and relapse, and the exploratory outcomes included HRQoL. The 10 mcg/mL dose was not approved by Health Canada; therefore, results related to this dose were not included in this review.
In Study NGF0212, the mean age of patients at baseline was 61 years (standard deviation [SD] = 16); 39% of patients were men, 53% had moderate NK, and 47% had severe NK.
In Study NGF0214, the mean age of patients at baseline was 65 years (SD = 14); 30% of patients were men, 69% had moderate NK, and 31% had severe NK.
Efficacy Results
In Study NGF0212, complete healing of the PED or corneal ulcer at week 4, determined by the central reading centre, was achieved in 29 patients (58.0%) in the cenegermin 20 mcg/mL group and 10 patients (19.6%) in the vehicle control group. The difference in the percentage of patients who achieved complete healing at week 4 between the cenegermin 20 mcg/mL group and the vehicle control group was 38.4% (97.06% confidence interval [CI], 18.96% to 57.83%; P < 0.001). Treatment with cenegermin was also related to the higher rate of corneal healing, compared with vehicle therapy, in Study NGF0214. In this study, the proportion of patients who achieved complete corneal healing was 69.6% in the cenegermin-treated group, compared with 29.2% in the vehicle-treated group, at week 8. The between-group difference in corneal healing was 40.4% (95% CI, 14.2 to 66.6; P = 0.006). The clinical experts consulted by CADTH indicated that the differences between cenegermin and vehicle are considered clinically relevant.
For the outcomes of corneal clearing and corneal sensitivity, between-group differences did not reach statistical significance. Corneal clearing was defined as grade 0 on the modified Oxford scale, defined as absence of staining. According to the clinical experts consulted by CADTH, this is a more stringent measure than corneal healing (< 0.5 mm of lesion staining) when assessing treatment effect on NK.
Overall, the potential benefit of cenegermin on HRQoL remains unknown. Differences between cenegermin and vehicle in the overall composite score of the National Eye Institute Visual Function Questionnaire-25 items (NEI-VFQ-25) or the EQ-5D 5-Levels (EQ-5D-5L) health state score were not statistically significant. The relationship between the gains from corneal healing and improvement in a patient’s HRQoL is unclear.
There was no difference between cenegermin and vehicle in reducing the risk of disease deterioration. For patients who had achieved complete corneal healing, 8 weeks of treatment with cenegermin ||| ||| |||||||||| |||| ||||| |||| || ||||||| || ||| || ||||||| |||||, although patients treated with cenegermin ||| |||||| |||| || || |||||||| |||||||| || those treated with vehicle.
Based on the data available, it is unknown whether additional functional improvements could be achieved with longer or repeated courses of cenegermin therapy.
Harms Results
During the 8-week controlled treatment period of NGF0212 and NGF0214, the frequency of AEs was higher in the cenegermin group than in the vehicle group (51.9% versus 38.5% in NGF0212; 91.3% versus 75.0% in NGF0214). Eye-related AEs were more common in both studies (25.0% in the cenegermin group versus 30.8% in the vehicle group in NGF0212; 78.3% in the antioxidant cenegermin group versus 58.3% in the antioxidant vehicle group in NGF0214).
In Study NGF0212, 9 patients (17.3%) in the cenegermin 20 mcg/mL group and 5 patients (9.6%) in the vehicle group experienced a serious AE (SAE), whereas in Study NGF0214, 3 patients (13.0%) in the cenegermin 20 mcg/mL group and 4 patients (16.7%) in the vehicle group experienced an SAE. In Study NGF0212, 9 patients (17.3%) in the cenegermin 20 mcg/mL group and 4 patients (7.7%) in the vehicle control group experienced AEs that led to discontinuation of study treatment, whereas in Study NGF0214, 5 patients (21.7%) in the antioxidant cenegermin 20 mcg/mL group and 7 patients (29.2%) in the antioxidant vehicle group discontinued treatment due to AEs. ||||||| |||||||||||| ||||||||| |||||| |||||| ||| ||||||||| || || |||| ||| |||| ||||||| ||| SAEs and treatment discontinuation in these 2 studies.
One patient in the cenegermin group died during the controlled treatment period in Study NGF0212. The death was not considered to be related to the study drug.
||||||||||||||||| ||| were considered as notable harms in the 2 studies. In NGF0212, notable harms were reported for | |||||||| ||||||| receiving cenegermin 20 mcg/mL and | |||||||| |||||| receiving vehicle during the controlled treatment period; in NGF0214, notable harms were reported for | |||||||| |||||| receiving cenegermin 20 mcg/mL and | |||||||| ||||||| receiving vehicle during the controlled treatment period.
Safety data were analyzed during various treatment periods (controlled, uncontrolled, and follow-up). Significant safety signals were not detected.
Table 2: Summary of Key Results From Studies NGF0212 and NGF0214
Outcomes | NGF0212 | NGF0214 | ||
|---|---|---|---|---|
Cenegermin 20 mcg/mL (N = 52) | Vehicle (N = 52) | Cenegermin 20 mcg/mL (N = 24) | Vehicle (N = 24) | |
Efficacy (ITT analysis set) | ||||
Complete healing achieved (assessed by central reading centre) at week 4, n/N (%) | 29 of 50 (58.0) | 10 of 51 (19.6) | 13 of 23 (56.5) | 9 of 24 (37.5) |
% difference (97.06% CIa for NGF0212, 95% CI for NGF0214) | 38.4 (18.96 to 57.83) | Reference | 19.0 (–9.0 to 47.1) | Reference |
P valueb | < 0.001 | Reference | 0.191 | Reference |
Complete healing achieved (assessed by central reading centre) at week 8, n/N (%) | 37 of 50 (74.0) | 22 of 51 (43.1) | 16 of 23 (69.6) | 7 of 24 (29.2) |
% difference (97.06% CIa for NGF0212, 95% CI for NGF0214) | 30.9 (10.60 to 51.13) | Reference | 40.4 (14.2 to 66.6) | Reference |
P valueb | 0.002 | Reference | 0.006 | Reference |
Complete corneal clearing (assessed by modified Oxford scale) at week 4, n (%) | 8 (19.5) | 3 (7.1) | 3 (13.6) | 1 (4.2) |
% difference (95% CIa) | 12.4 (–2.05 to 26.78) | Reference | 9.5 (–6.9 to 25.9) | Reference |
P valueb | 0.097 | Reference | 0.255 | Reference |
Complete corneal clearing (assessed by modified Oxford scale) at week 8, n (%) | 9 (21.4) | 4 (10.0) | 5 (22.7) | 1 (4.2) |
% difference (95% CIa) | 11.4 (–4.08 to 26.93) | Reference | 18.6 (–0.7 to 37.8) | Reference |
P valueb | 0.157 | Reference | 0.062 | Reference |
Patients experienced deterioration at week 4, n (%) | 1 (2.4) | 2 (4.7) | 2 (10.0) | 1 (5.9) |
% difference (95% CIa) | –2.3 (–23.26 to 18.71) | Reference | 4.1 (–13.1 to 21.4) | Reference |
P valueb | > 0.999 | Reference | 0.647 | Reference |
Patients experienced deterioration at week 8, n (%) | 3 (7.1) | 6 (15.0) | 0 (0) | 2 (13.3) |
% difference (95% CIa) | –7.9 (–29.51 to 13.52) | Reference | –13.3 (–30.5 to 3.9) | Reference |
P valueb | 0.307 | Reference | 0.110 | Reference |
Harms (safety analysis set) | ||||
N | 52 | 52 | 23 | 24 |
AEs, n (%) | 27 (51.9) | 20 (38.5) | 21 (91.3) | 18 (75.0) |
SAEs, n (%) | 9 (17.3) | 5 (9.6) | 3 (13.0) | 4 (16.7) |
WDAE, n (%) | 9 (17.3) | 4 (7.7) | 5 (21.7) | 7 (29.2) |
Deaths, n (%) | 1 (1.9) | 0 | 0 | 0 |
Notable harms, n (%) |||||||||||||||||| ||||||| | | |||||| | | ||||| | | ||||| | | |||||| |
AE = adverse event; CI = confidence interval; ITT = intention to treat; SAE = serious adverse event; WDAE = withdrawal due to adverse event.
Note: In the 2 included studies, for all efficacy outcomes except for the primary outcome, there were no adjustments for multiplicity. In NGF0212, the significance level of the chi-square test was corrected for multiplicity according to the Pocock method, and the 2-sided significance level alpha for statistical tests was 0.0294.
aAsymptotic (Wald) CI.
bP value was from chi-square test.
Critical Appraisal
Studies NGF0212 and NGF0214 were small, phase II, double-blind, vehicle-controlled RCTs. Imbalanced patient characteristics were observed between treatment groups in the 2 studies. In Study NGF0214, patients with moderate NK were more likely to receive vehicle, and patients with severe NK were more likely to receive cenegermin therapy. Although imbalances in baseline characteristics occur in RCTs of treatments for rare diseases despite randomization, the imbalanced characteristics may have an impact on data interpretation and bias the results. In NGF0214, more patients with severe condition (which can be more difficult to treat) received cenegermin therapy; this may bias the results toward the vehicle group. Because of the masking, there is a low risk of performance and detection bias in both studies.
Even though a power calculation was conducted in the 2 studies, there were a lot of withdrawals, resulting in smaller sample sizes at later time points. The dropout rates were high, and withdrawals were imbalanced between groups (in Study NGF0212, more patients in the cenegermin group than in the vehicle group discontinued the treatment due to AEs), which could impact the study results. In both studies, missing post-baseline data were imputed using the last observation carried forward method. Additional sensitivity analyses, using various methods, were conducted to assess the robustness of the primary analysis results. Results of the sensitivity analyses were consistent with those of the primary analysis. Therefore, the results were robust when it comes to the handling of missing data, and the potential for attrition bias is of less concern. Predefined subgroup analyses were rarely conducted in either study to explore the treatment effect of cenegermin in various subgroups, which may be related to the small number of study participants; the findings from these subgroup analyses could be noninformative because of the small sample, lack of power to detect between-group differences, imprecision, and the lack of adjustment for multiplicity.
In the 2 included studies, for all efficacy outcomes except for the primary outcome, there were no adjustments for multiplicity; therefore, no conclusions can be drawn for these outcomes.
A few scales and questionnaires were used in the pivotal studies for the evaluation of treatment effect of cenegermin (e.g., NEI-VFQ-25 and the modified Oxford scale). However, none of these instruments have been validated in patients with NK, therefore it is unclear whether the results are valid, and whether a minimally important difference (MID) can be applied in the NK population.
NK is a chronic disease, and the relapse rate could be high. There is a lack of data on re-treatment with cenegermin, which limits the ability to examine the efficacy and safety of multiple courses of cenegermin.
Conclusions
Two phase II double-blind, vehicle-controlled RCTs (NGF0212 and NGF0214) provided evidence supporting the efficacy and safety of cenegermin eye drops for the treatment of moderate to severe NK in adults. Compared with vehicle therapy, patients who were treated with 8-week cenegermin 20 mcg/mL showed increased corneal healing, and the difference in the proportion of patients achieving complete corneal healing between cenegermin and vehicle therapy was considered statistically and clinically relevant. However, whether treatment with cenegermin is associated with any HRQoL benefit remains unclear. The beneficial effect of cenegermin on improving corneal sensitivity, and reducing disease deterioration or recurrence is unclear, compared with the vehicle therapy.
The incidence of AEs was higher in the cenegermin treatment group than in the vehicle group. The risks of SAEs and treatment discontinuation due to AEs were comparable between treatment groups in both NGF0212 and NGF0214. Patients treated with cenegermin reported more eye-related AEs than those treated with vehicle therapy.
At this stage, there is a lack of evidence to support the longer-term efficacy and safety of re-treatment with cenegermin for patients who relapse. In addition, there is no direct or indirect evidence derived from comparisons of cenegermin and relevant comparators used in clinical practice, such as AMT or tarsorrhaphy.
Introduction
Disease Background
NK is a rare degenerative disorder of the cornea. It is characterized by impaired corneal nerve function, with subsequent corneal epitheliopathy resulting in reduction in reflex tearing and blinking and diminished production of trophic factors, after damage to the ophthalmic branch of the trigeminal nerve. The condition can progress to a PED, stromal thinning, and even corneal perforation.2,3 During this process, nerve growth factor can help promote neuronal sprouting after nerve transection, providing trophic support to neurons after injury, reversing pathologic changes induced by peripheral healing, and regulating blood flow to nerves.3 The severity of NK can be categorized as mild (stage 1), moderate (stage 2), or severe (stage 3) based on the extent of corneal involvement, according to the Mackie Classification.1 Mild NK is the most common presentation of the disease, and is characterized by epithelial changes without a frank epithelial defect. Moderate NK is characterized by an epithelial defect without stromal involvement, and severe NK is defined as an epithelial defect plus stromal involvement, which can range from mild stromal thinning to corneal perforation.2 Moderate and severe NK can profoundly affect the patients’ vision and adversely impact their HRQoL.2,3 The causes of NK include conditions or procedures that can damage the trigeminal nerve, such as ocular causes, systemic conditions, and iatrogenic causes. Common causes of NK are stroke, diabetes, panretinal photocoagulation, herpetic keratitis, surgery (e.g., laser-assisted in situ keratomileusis, keratoplasty, and cataract), contact lens wear, chronic use of topical medications, and use of benzalkonium chloride–containing agents.3
Early diagnosis of NK is essential, but patients with mild NK may go undiagnosed if there are no frank corneal findings; patients are also usually asymptomatic. Patients should be actively screened for NK if they have known risk factors. When NK is diagnosed in the later stages, with the typical corneal findings, vision loss may have become permanent due to corneal scarring or melting. Diagnosis of NK is established based on a patient’s medical history (including concomitant systemic diseases, surgical procedures, physical history, topical medication use, and current symptoms) followed by eye examination and testing to assess decreased corneal sensitivity and nerve damage.3,4
The prevalence of NK has been estimated to be less than 5 in 10,000 individuals worldwide, although the condition is most likely underdiagnosed.2 In 2021, approximately 6,100 Canadians were diagnosed with NK, and 2,300 of them had moderate or severe disease, according to a physician survey.8
Standards of Therapy
Current treatment options can be categorized as medical management, nonsurgical interventions, and surgical interventions. Management of NK is based on stage and severity of the disease, and the treatment aims to stop the progression of corneal damage and promote epithelial healing. More specifically, for mild NK, treatment goals are focused on improving the corneal epithelium and avoiding epithelial breakdown. Treatment at this stage includes removal of the offending agent (e.g., preservative-containing eye drops) if possible, frequent use of preservative-free artificial tears and ointments (which helps to lubricate the ocular surface, reduce biomechanical shear forces, and dilute proinflammatory cytokines in the tear film), autologous serum eye drops, and platelet-rich plasma. Adjunct procedures, such as punctal occlusion, and treatment of any concomitant lid malposition are also commonly adopted. For moderate NK, treatment goals are to promote ocular surface healing, particularly the corneal epithelium, and to prevent any ulcers. Treatment options at this stage are the same as those for mild NK, plus prophylactic topical preservative-free antibiotics, corneal therapeutic contact lenses, epithelial debridement, synthetic tissue adhesive, tarsorrhaphy, AMT, conjunctival flaps, and corneal neurotization. For severe NK, treatments focus on reducing corneal stromal scarring and preventing perforation. At this stage, additional treatment options can include corneal gluing, layered amniotic membrane grafting, and partial or full-thickness corneal transplantation.2-4
According to the clinical experts consulted by CADTH, an ideal treatment for moderate or severe NK would result in complete or near-complete (i.e., < 0.5 mm in size) closure of the epithelial defect and sustained closure of the corneal epithelium without disease relapse. The treatment would be expected to improve visual acuity and the patient’s HRQoL while minimizing drug-related adverse effects and complications. Despite access to a variety of therapeutic options, not all patients respond to the available treatments, and they can become refractory to the current treatment regimens. There is also a need for treatments that do not rely on surgical intervention, which eliminates the associated risks.
Drug
Nerve growth factor is an endogenous protein involved in the differentiation and maintenance of neurons. Cenegermin is an rhNGF produced by Escherichia coli bacteria for topical ophthalmic use in the treatment of moderate or severe NK. As a source of nerve growth factor, cenegermin targets the nerve pathology associated with NK, and therefore has the potential to address the healing deficits present in this patient population.3,5 Cenegermin has not previously been reviewed by CADTH for any indication.
On February 8, 2019, cenegermin ophthalmic solution was approved by Health Canada for the treatment of moderate (PED) or severe (corneal ulcer) NK in adults. The reimbursement request by the sponsor for cenegermin is for the treatment of moderate (PED) or severe (corneal ulcer) NK in adults who have failed conventional nonsurgical treatments.
Cenegermin is available as topical eye drops, 20 mcg/mL (0.002%). The recommended dose is 1 drop of cenegermin in the conjunctival sac of the affected eye(s) 6 times per day at intervals of 2 hours. Treatment with cenegermin should be continued for 8 weeks. Based on the product monograph for cenegermin, infections in the affected eye(s) should be treated and resolved before use of cenegermin. Cenegermin is a growth factor; therefore, it can theoretically affect ocular neoplasms. It is recommended that patients with ocular neoplasms continue to be monitored for cancer progression during and after treatment with cenegermin.5
Stakeholder Perspectives
Patient Group Input
This section was prepared by CADTH staff based on the input provided by patient groups.
One patient group, the Canadian Organization for Rare Disorders (CORD), submitted patient input for this review. CORD is a national network that advocates for health policy and a health care system that works for those with rare disorders. The input was based on 15- to 30-minute phone interviews with 12 patients recruited from 3 eye institutes in the US. All respondents had an NK diagnosis and were 24 to 77 years of age (75% > 65 years). Reasons given by respondents for their loss of nerve growth factor included a surface injury to the cornea, prolonged use of contact lenses, eye infections, cataract surgery, or an underlying health conditions, such as diabetes. Most patients did not know the stage of severity of their condition. All patients interviewed had experience with cenegermin and completed treatment from 2 weeks to 3 years ago.
All respondents reported experiencing some symptoms before diagnosis, such as blurred, low (peripheral) vision, or (near) loss of vision (in 1 eye). Time to diagnosis ranged from 6 months to 3 years or more, and most respondents received at least 1 treatment before diagnosis, such as lubricant or antibiotics. Two patients reported discussing the option of surgery, including AMT to protect the cornea or suturing of the eyelid.
Respondents reported positive experiences with cenegermin, and all respondents completed the 8-week treatment. All respondents reported outcomes favouring cenegermin, although the impact and durability varied from the total resolution of vision, to tearing and blinking problems, some improvement in vision, and stabilization of the eye enough to consider a cornea transplant. Most patients who had the treatment 2 to 3 years ago were still benefiting from improved vision, and were not experiencing symptoms associated with loss of nerves supporting the cornea. Some patients reported experiencing minor side effects (stinging, pain, headaches, and blurred vision) that went away upon treatment completion. Respondents expressed a desire for an accurate diagnosis at symptom onset, and reported receiving an effective treatment only after long periods of suffering and ineffective or invasive treatments. The input summary suggests that if NK is diagnosed and treated in stage 1, minimal damage and full recovery are usually possible. A copy of the patient input is presented in Patient Input.
Clinician Input
Input From Clinical Experts Consulted by CADTH
All CADTH review teams include at least 1 clinical specialist with expertise in the diagnosis and management of the condition for which the drug is indicated. Clinical experts are a critical part of the review team and are involved in all phases of the review process (e.g., providing guidance on the development of the review protocol, assisting in the critical appraisal of clinical evidence, interpreting the clinical relevance of the results, and providing guidance on the potential place in therapy). The following input was provided by 2 clinical specialists with expertise in the diagnosis and management of NK.
Unmet Needs
Even though various treatment options are available for patients with moderate or severe NK, not all patients respond to them, and they can become refractory to current treatments. Certain treatment options, such as surgical interventions, are associated with complications or cosmetic issues. There is a need for treatments that do not rely on surgical intervention, which eliminates the risks associated with surgery.
Place in Therapy
Cenegermin directly stimulates nerve growth in patients with NK, which is a unique mechanism of action compared with any currently available treatments. The clinical experts indicated that, in theory, if there is a lack of nerve growth or damaged nerves leading to NK, and cenegermin can regenerate these nerves and restore their normal function, it may cure the disease, not just control the symptoms. Cenegermin would be suitable for patients who have stopped any offending agents and have failed conservative treatment with preservative-free artificial tears and autologous serum tears, with or without a bandage contact lens. As there is no other drug with this mechanism of action, it can shift the current treatment paradigm if it is offered early in the disease course of NK.
The clinical experts indicated that cenegermin could be used as a first-line treatment or in combination with the current treatments.
Patient Population
The clinical experts indicated that cenegermin is suitable for patients in any stage of NK, although it is not known which patients will benefit most from the treatment. In general, moderate or severe NK can be easily diagnosed by a cornea specialist, based on the patient’s medical history and a clinical examination that shows reduced corneal sensation and breakdown of the corneal epithelium. In vivo confocal microscopy can also be used to directly visualize the abnormal nerves, but access to this technology is limited to very specialized eye centres. Even though patients with mild NK should be considered for treatment with cenegermin, it is challenging to identify these patients in clinical practice because of the subtle clinical examination findings and symptoms at this stage.
Patients without a diagnosis of NK — for example, those showing advanced inflammatory eye disease, severe neovascularization, or corneal scarring — are least suitable for treatment with cenegermin.
Assessing Response to Treatment
In clinical practice, assessment of the size of the epithelial defect using fluorescein staining and cobalt blue filter on slit lamp examination is performed to determine a patient’s response to the treatment. A clinically important response would be complete resolution (i.e., 0 mm in size) or significant closure (i.e., < 0.5 mm in size) of the epithelial defect. The clinical experts suggested that, during the 8-week treatment period for cenegermin, a patient’s progress needs to be assessed every 2 to 4 weeks, depending on the severity of the condition and potential side effects of the treatment, and again 4 weeks after completion of the 8-week course. Follow-up time can be tailored, depending on the patient’s response. If the patient continues to show sustained corneal healing, the appointment intervals can be stretched.
Normalization of corneal sensation and reduction of other NK symptoms are also outcomes of interest to the clinicians.
Discontinuing Treatment
Treatment with cenegermin should be discontinued if significant AEs (such as corneal melting and perforation, microbial keratitis, endophthalmitis, and intolerable eye pain) occur. Treatment should also be stopped if the patient is unable to comply with the dosing schedule.
Prescribing Conditions
Cenegermin can be prescribed by cornea specialists that routinely treat patients with NK. The drug can be administered in both academic and community settings.
Clinician Group Input
No input was provided by clinician groups.
Drug Program Input
The drug programs provide input on each drug being reviewed through CADTH’s reimbursement review processes by identifying issues that may impact the ability to implement a recommendation. The implementation questions and corresponding responses from the clinical experts consulted by CADTH are summarized in Table 3.
Table 3: Summary of Drug Plan Input and Clinical Expert Response
Drug program implementation questions | Clinical expert response |
|---|---|
Specialists experienced in this rare condition (moderate or severe NK) may be limited to urban settings. Staging, monitoring, and follow-up for this home-based therapy could be challenging. | The experts agree that access to cornea specialists is more likely in urban areas, in both academic centres and the community. As long as the patients have access to care from specialists, staging, monitoring, and follow-up would not be an issue with cenegermin. Patients in a rural setting may have difficulty accessing a cornea specialist, which would challenge the diagnosis, monitoring, and follow-up of NK. One solution in this situation is for a local general optometrist or ophthalmologist to comanage the patient with a cornea specialist from outside the local area. |
How will jurisdictions implement the requested indication of “stage 3 (severe) NK patients who have failed nonsurgical treatments” when none of the other nonsurgical alternatives are indicated in this setting? | There are off-label nonsurgical alternatives available for patients with mild or moderate NK who have failed certain nonsurgical treatments. These can include preservative-free artificial tears, autologous serum tears, or removal of any offending agents (if possible). If patients do not respond well to these alternatives within 1 to 2 months of treatment, it would be reasonable to offer them cenegermin in the next step. |
NK = neurotrophic keratitis.
Clinical Evidence
The clinical evidence included in the review of cenegermin is presented the Systematic Review section, which includes pivotal studies provided in the sponsor’s submission to CADTH and Health Canada, as well as studies selected in accordance with an a priori protocol.
Systematic Review (Pivotal and Protocol-Selected Studies)
Objectives
To perform a systematic review of the beneficial and harmful effects of cenegermin (ophthalmic solution, 0.002%) for the treatment of moderate (PED) or severe (corneal ulcer) NK in adults.
Methods
Studies selected for inclusion in the systematic review included pivotal studies provided in the sponsor’s submission to CADTH and Health Canada, as well as those meeting the selection criteria presented in Table 4. Outcomes included in the CADTH review protocol reflect outcomes considered to be important to patients, clinicians, and drug plans.
Table 4: Inclusion Criteria for the Systematic Review
Criteria | Description |
|---|---|
Population | Adult patients with moderate (PED) or severe (corneal ulcer) NK Subgroups:
|
Intervention | Cenegermin ophthalmic solution 0.002% (20 mcg/mL) (instill 1 drop into the affected eye[s] 6 times daily, at 2-hour intervals, for 8 weeks) |
Comparator | Medical management:
Nonsurgical interventional management (e.g., eyelid closure, Botox, punctual plugs, therapeutic corneal contact lenses, tissue adhesives) Surgical interventions (e.g., AMT, tarsorrhaphy, conjunctival flap, corneal transplants, corneal neurotization) |
Outcomes | Efficacy outcomes:
Harms outcomes:
|
Study designs | Published and unpublished phase III and IV RCTs |
AE = adverse event; AMT = amniotic membrane transplant; HRQoL = health-related quality of life; NK = neurotrophic keratitis; PED = persistent epithelial defect; RCT = randomized controlled trial; SAE = serious adverse event; WDAE = withdrawal due to adverse event.
The literature search for clinical studies was performed by an information specialist using a peer-reviewed search strategy, according to the PRESS Peer Review of Electronic Search Strategies tool.9
Published literature was identified by searching the following bibliographic databases: MEDLINE All (1946—) via Ovid and Embase (1974—) via Ovid. All Ovid searches were run simultaneously as a multi-file search. Duplicates were removed using Ovid deduplication for multi-file searches, followed by manual deduplication in Endnote. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. The main search concepts were Oxervate (cenegermin), recombinant human nerve growth factor, and neurotrophic keratitis. The following clinical trials registries were searched: the US National Institutes of Health’s clinical trials.gov, WHO’s International Clinical Trials Registry Platform (ICTRP) search portal, Health Canada’s Clinical Trials Database, and the European Union Clinical Trials Register.
No filters were applied to limit the retrieval by study type. Retrieval was not limited by publication date or by language. Conference abstracts were excluded from the search results. Refer to Appendix 1 for the detailed search strategies.
The initial search was completed on November 22, 2021. Regular alerts updated the search until the meeting of the CADTH Canadian Drug Expert Committee on April 27, 2022.
Grey literature (literature that is not commercially published) was identified by searching relevant websites from the Grey Matters: A Practical Tool for Searching Health-Related Grey Literature tool.10 Included in this search were the websites of regulatory agencies (FDA and European Medicines Agency). Google was used to search for additional internet-based materials. Refer to Appendix 1 for more information on the grey literature search strategy.
Two CADTH clinical reviewers independently selected studies for inclusion in the review based on titles and abstracts, according to the predetermined protocol. Full-text articles of all citations considered potentially relevant by at least 1 reviewer were acquired. Reviewers independently made the final selection of studies to be included in the review, and differences were resolved through discussion.
Findings From the Literature
No studies were identified from the literature search for inclusion in the systematic review (Figure 1). Four reports of 2 studies submitted by the sponsor were included.6,7,11,12 The included studies are summarized in Table 5.
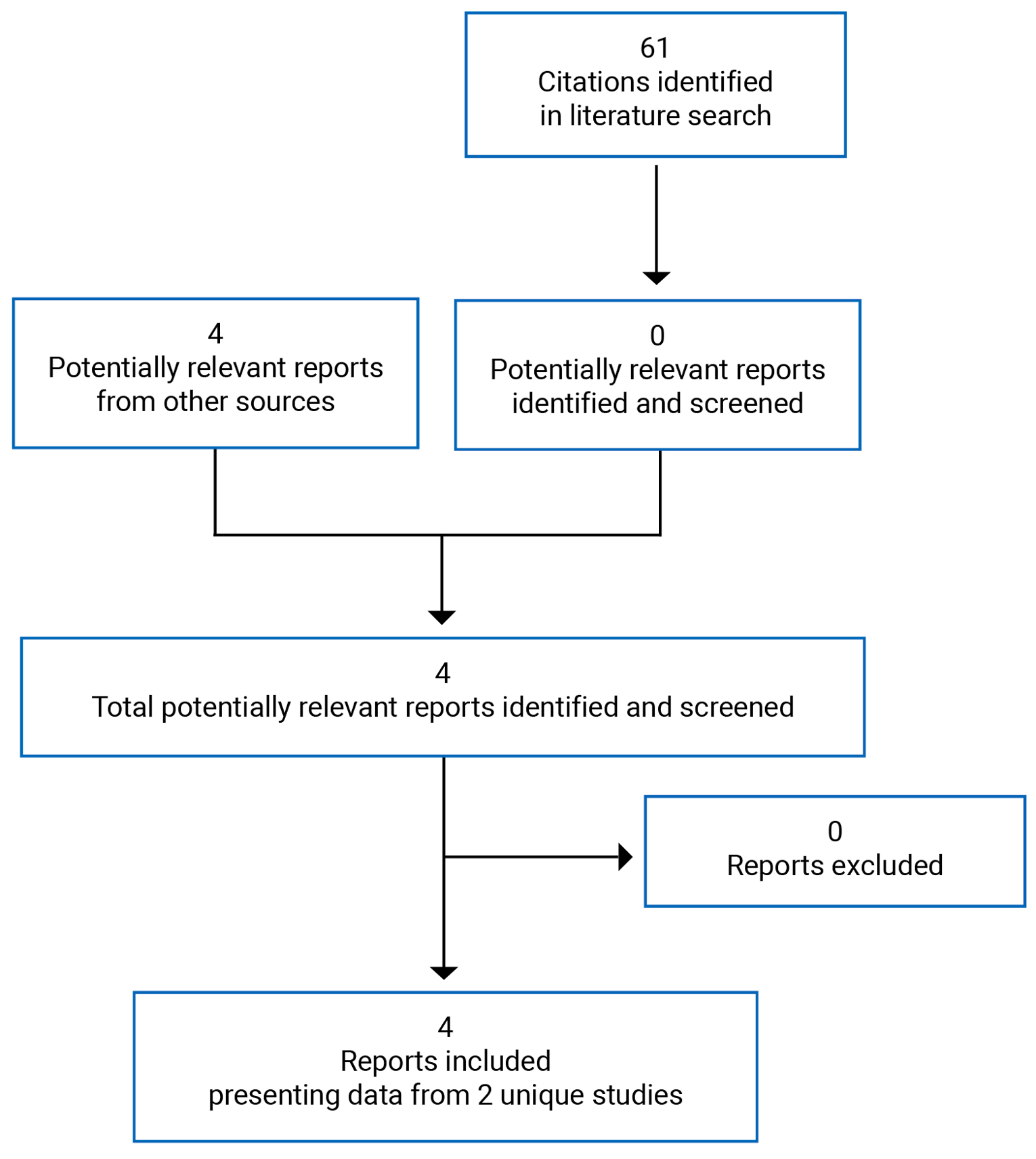
Table 5: Details of Included Studies
Detail | NGF0212 | NGF0214 |
|---|---|---|
Designs and populations | ||
Study design | Phase I/II, DB vehicle-controlled RCT | Phase II, DB vehicle-controlled RCT |
Locations | 6 countries in Europe | 11 sites in the US |
Study period: | January 30, 2013, to July 17, 2015 | May 1, 2015, to August 6, 2016 |
Randomized (N) | 156 | 48 |
Inclusion criteria | Patients 18 years and older with moderate (PED) or severe (corneal ulcer) NK involving only 1 eye (patients with the contralateral eye affected with mild NK could be enrolled) | Patients 18 years and older with moderate (PED) or severe (corneal ulcer) NK involving 1 or 2 eyes |
PED or corneal ulceration of at least 2 weeks’ duration, refractory to 1 or more conventional nonsurgical treatments for NK Evidence of decreased corneal sensitivity within the area of the PED or corneal ulcer and outside the area of the defect in at least 1 corneal quadrant BCDVA score ≤ 75 ETDRS letters in the affected eye No objective clinical evidence of improvement in the PED or corneal ulceration in the 2 weeks before study enrolment | ||
Exclusion criteria | Any active ocular infection or active ocular inflammation not related to NK in the affected eye Any other ocular disease requiring topical ocular treatment in the affected eye during the study treatment period Patients with severe vision loss in the affected eye with no potential for visual improvement in the opinion of the investigator as a result of the study treatment Schirmer test without anesthesia ≤ 3 mm/5 minutes in the affected eye Patients with severe blepharitis and/or severe meibomian gland disease in the affected eye History of any ocular surgery (including laser or refractive surgical procedures) in the affected eye in the 3 months before study enrolment, unless the ocular surgery was considered to be the cause of mild or moderate NK Prior surgical procedure(s) for the treatment of NK (e.g., complete tarsorrhaphy, conjunctival flap) in the affected eye, with the exception of AMT Use of therapeutic contact lenses or contact lens wear for refractive correction during the study treatment periods in the eye with NK Anticipated need for punctual occlusion during the study treatment period Evidence of corneal ulceration involving the posterior third of the corneal stroma, corneal melting, or perforation in the affected eye Presence or history of any ocular or systemic disorder or condition that might have hindered the efficacy of the study treatment or its evaluation Any need for or anticipated change in the dose of systemic medications known to impair the function of the trigeminal nerve | |
Drugs | ||
Intervention | Cenegermin 10 mcg/mL, 1 drop 6 times per day for 8 weeks (0.35 mcg per 35 µL drop) Cenegermin 20 mcg/mL, 1 drop 6 times per day for 8 weeks (0.70 mcg per 35 µL drop) | Antioxidant (L-methionine) cenegermin 20 mcg/mL, 1 drop 6 times per day for 8 weeks (0.70 mcg per 35 µL drop) |
Comparator(s) | Vehicle ophthalmic solution with the same composition as the intervention product but without cenegermin, 1 drop 6 times per day for 8 weeks | Vehicle ophthalmic solution with the same composition as the intervention product, with antioxidant L-methionine but without cenegermin, 1 drop 6 times per day for 8 weeks |
Duration | ||
Phase | ||
DB | 8 weeks | 8 weeks |
Follow-up | 48 or 56 weeks | 24 or 32 weeks |
Outcomes | ||
Primary end point | % of patients achieving complete corneal healing at the week 4 (NGF0212) or week 8 visit (NGF0214), determined by the central reading centre | |
Secondary and Exploratory End Points | Secondary: Controlled treatment period:
Follow-up period
Exploratory:
Safety: AE, SAE, WDAE, death, AEs of special interest | Secondary:
Safety: AE, SAE, WDAE, death, AEs of special interest |
Notes | ||
Publications | Bonini et al. (2018)11 | Pflugfelder et al. (2020)12 |
AMT = amniotic membrane transplantation; BCDVA = best corrected distance visual acuity; DB = double-blind; EQ-5D-5L = EuroQol 5 Dimensions Scale, 5-levels; ETDRS = Early Treatment Diabetic Retinopathy Study; NEI-VFQ-25 = National Eye Institute Visual Functioning Questionnaire-25 items; NK = neurotrophic keratitis; PED = persistent epithelial defect; RCT = randomized controlled trial.
Note: Six additional reports were included (Submission,8 Health Canada Reviewer’s Report,13 FDA Medical Review,14 European Medicines Agency Report,15 Clinical Study Report for NGF0212,6 and Clinical Study Report for NGF02147).
Source: Clinical Study Reports for NGF02126 and NGF0214.7
Description of Studies
Study NGF0212 (N = 156) was a phase I/II, multi-centre, double-blind, vehicle-controlled RCT to evaluate the efficacy and safety of cenegermin for the treatment of moderate or severe NK.6 Eligible patients were randomized (1:1:1), using an Interactive Web Response System, to receive 2-dose regimens (10 mcg/mL or 20 mcg/mL; 1 drop [0.35 μL; 0.35 mcg or 0.70 mcg, respectively], 6 times per day) of cenegermin eye drops or vehicle (with the same composition as the experimental intervention but without cenegermin; 1 drop, 6 times per day) for 8 weeks. During the 8-week double-blind treatment period, the patient, the investigator, all other site staff involved in study assessments and the sponsor’s clinical research personnel were blinded to the treatment allocation. At the end of the 8-week controlled treatment period, patients were defined as completely or noncompletely healed and entered a 48- or 56- week follow-up period. Complete healing was defined as “the greatest diameter of the corneal fluorescein staining in the area of the PED or corneal ulcer, as determined by the reading centre, being less than 0.5 mm.” The follow-up period was 48 weeks (approximately 12 months) for patients who were initially randomized to cenegermin (10 mcg/mL or 20 mcg/mL), regardless of whether the patient was completely healed or not completely healed at week 8. The follow-up period was also 48 weeks for patients who were initially randomized to vehicle and who were completely healed at week 8. The follow-up period was 56 weeks (approximately 14 months) for patients who were initially randomized to vehicle and who were not completely healed at week 8. These patients were randomly assigned to treatment with cenegermin (10 mcg/mL or 20 mcg/mL) for 8 weeks (from week 8 to week 16); this was referred to as the uncontrolled treatment period (Figure 2). At this time, patients who were completely healed could be treated with preservative-free artificial tears, as needed. Those who were not completely healed could receive treatment at the discretion of the investigator. All patients completely healed at week 8 (including those who received active treatment) were eligible for another course of treatment (10 mcg/mL or 20 mcg/mL, depending on the original assignment) in the event of recurrence during the follow-up period. The maximum duration of each patient’s participation in the study was approximately 64 weeks.
The dose of 10 mcg/mL was not approved by Health Canada; therefore, study results of this treatment group were not included in this review.
Figure 2: Study Design of Study NGF0212, Phase II Segment
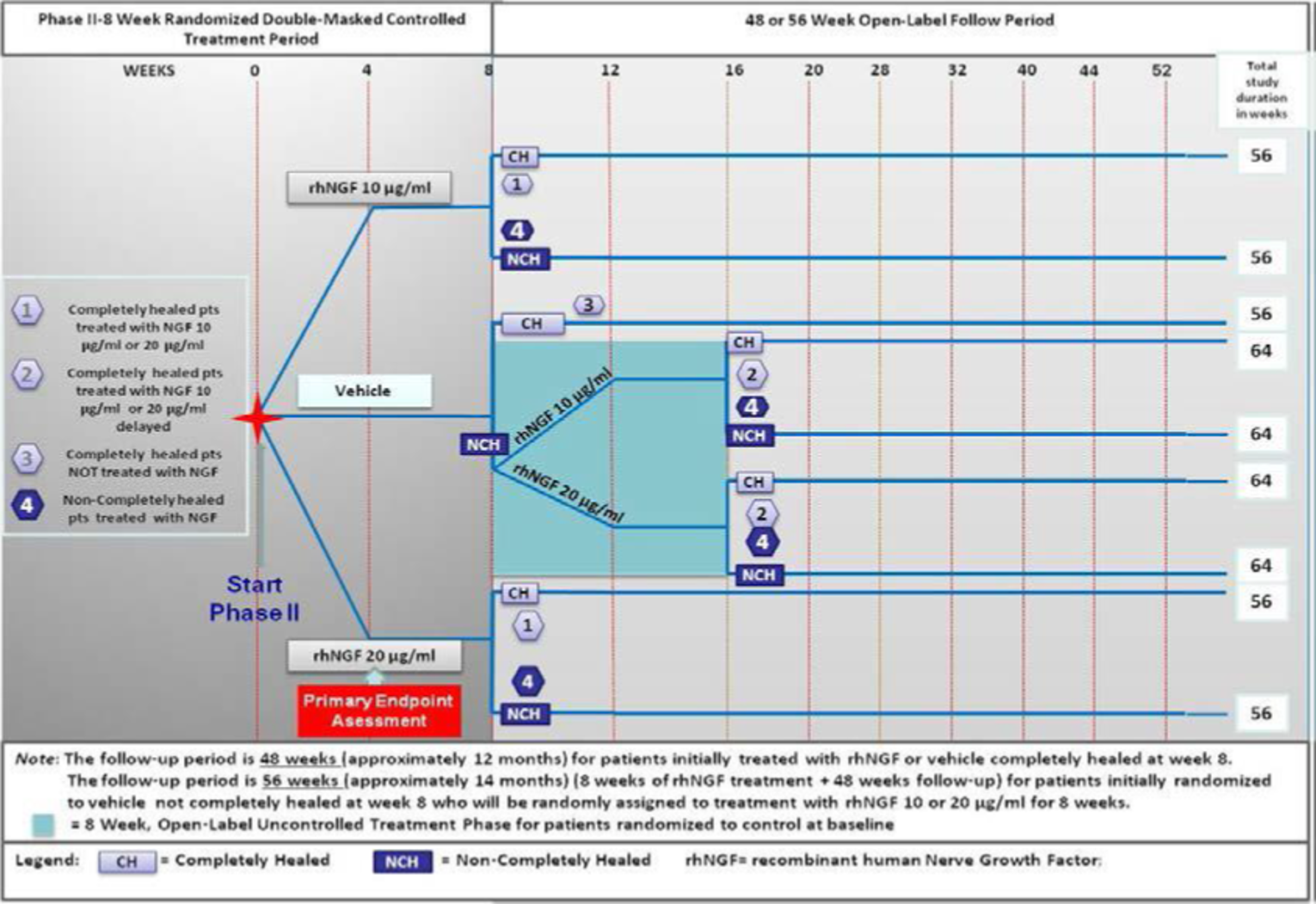
Source: Clinical Study Report for NGF0212.6
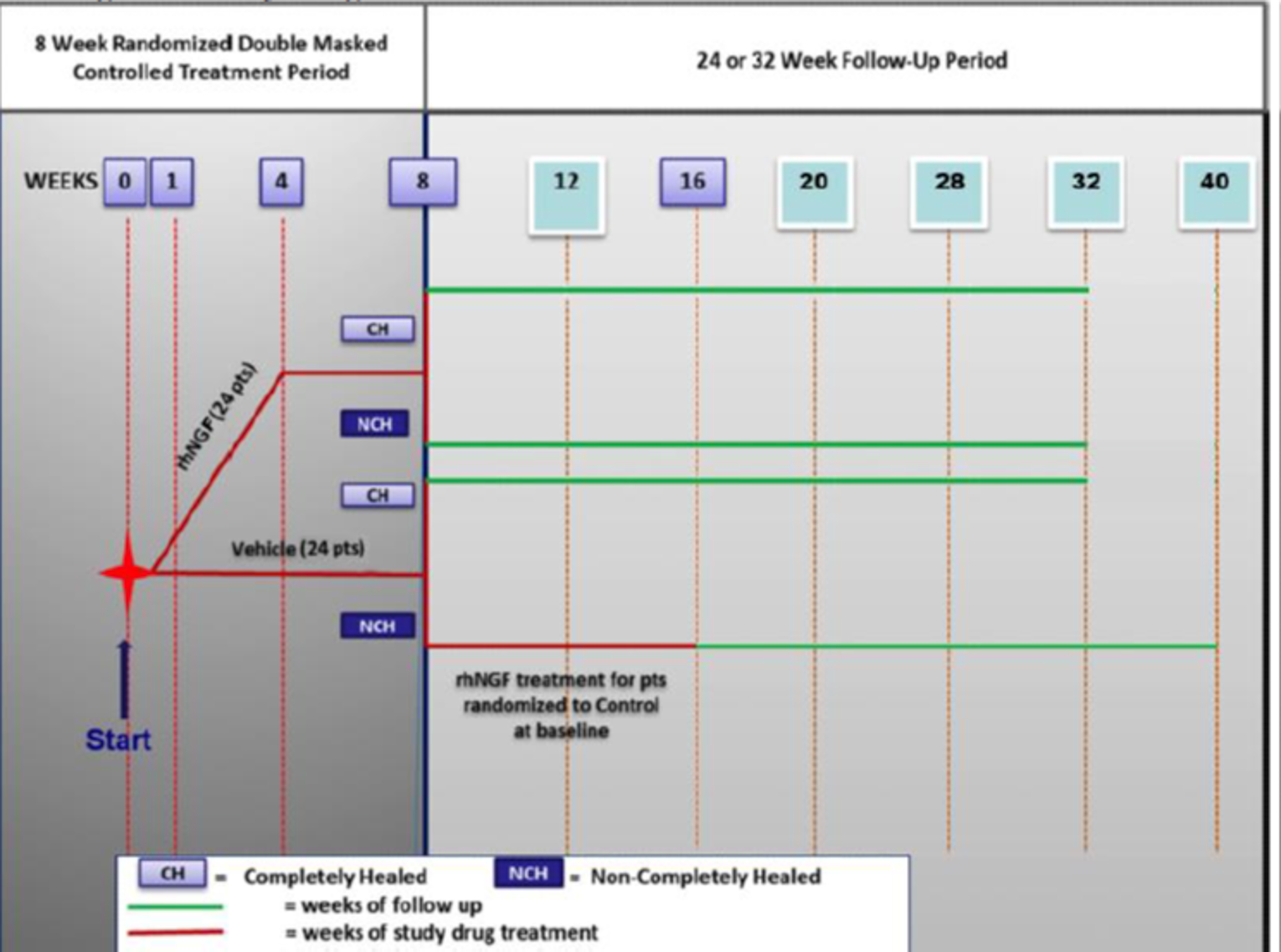
Study NGF0214 (N = 48) was a phase II, multi-centre, double-blind, vehicle-controlled RCT to evaluate the efficacy and safety of antioxidant-containing (L-methionine) cenegermin in patients with moderate to severe NK.7 Eligible patients were randomized (1:1) to receive antioxidant-containing cenegermin 20 mcg/mL (1 drop [35 µL or 0.70 mcg], 6 times per day) or vehicle (with the same composition as the experimental intervention but without cenegermin; 1 drop, 6 times per day) for 8 weeks. During the 8-week controlled treatment period, the patients, investigators, and site staff were blinded to the treatment allocation. At the end of the 8-week controlled treatment period, patients were defined as completely or noncompletely healed, and entered a 24- or 32-week follow-up period. Complete healing was defined in the same way as in Study NGF0212. If not completely healed at week 8, patients initially randomized to the vehicle group during the controlled treatment period were followed for an additional 32 weeks. They were eligible for open-label treatment with cenegermin 20 mcg/mL during the first 8 weeks of the uncontrolled treatment period. Patients not completely healed at week 8 who were randomized to the antioxidant cenegermin group were followed for an additional 24 weeks. They were not eligible for additional antioxidant cenegermin treatment, but could be treated at the discretion of the study investigator with any nonexperimental treatment for NK. Patients completely healed at week 8 of the controlled treatment period, or week 16 in the uncontrolled treatment period, were eligible for 1 additional 8-week course of treatment during the follow-up period or for any nonexperimental NK treatment in the event of a recurrence of moderate or severe NK. They could also receive preservative-free artificial tears at the discretion of the study investigator. The maximum study duration in Study NGF0214 was 40 weeks (approximately 10 months).
Populations
Inclusion and Exclusion Criteria
In both studies, adults (18 years and older) with moderate or severe NK were screened. They were eligible if there was evidence of decreased corneal sensitivity within the area of the PED or corneal ulcer and outside the area of the defect in at least 1 corneal quadrant, with a best corrected distance visual acuity (BCDVA) score of 75 or fewer Early Treatment Diabetic Retinopathy Study (ETDRS) letters, and no objective clinical evidence of improvement in the PED or corneal ulceration in the 2 weeks before study enrolment. In addition, patients in both studies were required to be refractory to 1 or more conventional nonsurgical treatments for NK, such as preservative-free artificial tears, gels or ointments, discontinuation of preserved topical drops and medications that can decrease corneal sensitivity or therapeutic contact lenses. In Study NGF0212, patients with NK involving only 1 eye were eligible, whereas in Study NGF0214, patients with NK involving 1 or both eyes were eligible.
Baseline Characteristics
In both studies, the majority of the patients were female. Most were also not Hispanic, Latino, or Spanish. Patients in Study NGF0212 were slightly younger, on average, than those in Study NGF0214, but had a longer time from initial diagnosis of moderate to severe NK (|||| |||||| |||||| || ||||| ||||||| versus 7.5 to 7.9 months in Study NGF0214). In Study NGF0212, the numbers of patients in each disease stage (2 or 3) were similar in the cenegermin and vehicle arms. However, in Study NGF0214, patients with moderate NK were more likely to receive vehicle and patients with severe NK were more likely to receive cenegermin therapy (Table 6). Patients’ baseline characteristics were analyzed in a safety population in NGF0212, but in an intention-to-treat (ITT) population in NGF0214.
In Study NGF0212, the most commonly used prior medications for NK were topical antibiotics (61.5% in the cenegermin 20 mcg/mL group, 63.5% in the vehicle group), followed by artificial tears, gels, and/or ointments (55.8% in the cenegermin 20 mcg/mL group, 50% in the vehicle group), preservative-free artificial tears, gels, and/or ointments (38.5% in the cenegermin 20 mcg/mL group, 46.2% in the vehicle group), and therapeutic contact lenses (44.2% in the cenegermin 20 mcg/mL group, 21.2% in the vehicle group). In Study NGF0214, commonly used prior treatments for NK were artificial tears (39.1% in the cenegermin 20 mcg/mL group, 33.3% in the vehicle group) and prednisolone acetate (39.1%% in the cenegermin 20 mcg/mL group, 16.7% in the vehicle group).
Table 6: Summary of Baseline Characteristics for Studies NGF0212 and NGF0214
Characteristic | NGF0212 | NGF0214 | ||
|---|---|---|---|---|
Cenegermin 20 mcg/mL (N = 52) | Vehicle (N = 52) | Antioxidant cenegermin 20 mcg/mL (N = 24) | Antioxidant vehicle (N = 24) | |
Age, years, mean (SD) | 62.5 (14.01) | 60.4 (16.78) | 65.9 (13.85) | 64.5 (14.15) |
Gender, n (%) | ||||
Male | 22 (42.3) | 17 (32.7) | 10 (41.7) | 9 (37.5) |
Female | 30 (57.7) | 35 (67.3) | 14 (58.3) | 15 (62.5) |
Ethnicity, n (%) | ||||
Unknown | 1 (1.9) | 6 (11.5) | 4 (16.7) | 4 (16.7) |
Hispanic, Latino, or Spanish | 9 (17.3) | 5 (9.6) | 0 (0.0) | 1 (4.2) |
Not Hispanic, Latino, or Spanish | 42 (80.8) | 41 (78.8) | 20 (83.3) | 19 (79.2) |
Time from initial diagnosis of NK stage 2 (moderate) or stage 3 (severe), months, mean (SD) | 17.50 (32.0) | 15.52 (40.6) | 7.5 (14.51) | 7.9 (8.6) |
Classification of NK, n (%) | ||||
Mild | 0 | 0 | 0 | 0 |
Moderate | 27 (51.9) | 28 (53.8) | 15 (62.5) | 18 (75.0) |
Severe | 25 (48.1) | 24 (46.2) | 9 (37.5) | 6 (25.0) |
Prior treatments, n (%) | ||||
Artificial tears, gels, and/or ointments | 29 (55.8) | 26 (50.0) | | |||||| | | |||||| |
Preservative-free artificial tears, gels, and/or ointments | 20 (38.5) | 24 (46.2) | ||||| | ||||| |
Topical antibiotics | 32 (61.5) | 33 (63.5) | | ||||| | |||| |
Discontinuation of topical medications | 2 (3.8) | 0 | ||||| | ||||| |
Therapeutic contact lens | 23 (44.2) | 11 (21.2) | | ||||| | | |||||| |
Anti-cholinergic agents | 2 (3.8) | 4 (7.7) | ||||| | ||||| |
Autologous serum eye drops | 5 (9.6) | 5 (9.6) | ||||| | ||||| |
Botulinum A toxin injection | 1 (1.9) | 2 (3.8) | ||||| | ||||| |
Cyanoacrylate glue | 0 | 0 | ||||| | ||||| |
Collagenase inhibitors | 0 | 2 (3.8) | ||||| | ||||| |
Tarsorrhaphy | 2 (3.8) | 1 (1.9) | ||||| | ||||| |
Conjunctival flap procedure | 1 (1.9) | 0 | ||||| | ||||| |
AMT | 5 (9.6) | 3 (5.8) | | |||||| | | |||||| |
Other | 20 (38.5) | 28 (53.8) | ||||| | ||||| |
Ganciclovir | NR | NR | | |||||| | |||| |
Moxifloxacin | NR | NR | | |||||| | | |||||| |
Prednisolone acetate | NR | NR | | |||||| | | |||||| |
AMT = amniotic membrane transplantation; NK = neurotrophic keratitis; NR = not reported; SD = standard deviation.
Note: Safety population was used in NGF0212; intention-to-treat population was used in NGF0214.
Interventions
In both studies, upon enrolment in the study, patients were required to discontinue all topical ophthalmic medications and were only allowed to use the study medication provided by the sponsor and topical ophthalmic medications allowed by the study protocol during the course of treatment with cenegermin.
In the phase II segment of NGF0212, enrolled patients were randomized in a 1:1:1 ratio to self-administer topical cenegermin 10 mcg/mL, 20 mcg/mL, or vehicle control, 1 drop 6 times per day. At the end of the 8-week controlled treatment period, patients initially randomized to the vehicle control arm who did not achieve corneal healing at week 8 or deteriorated before 8 weeks were randomly assigned to active study medication (cenegermin 10 mcg/mL or 20 mcg/mL, 1 drop 6 times a day) for an additional 8 weeks. In this study, vehicle control was an ophthalmic solution of the same composition as the experimental intervention, except without cenegermin.
During the controlled treatment period, patients who were receiving systemic medications known to impair the function of the trigeminal nerve (e.g., neuroleptic, antipsychotic, and antihistamine drugs) were advised to continue treatment at a constant level. Patients previously treated with botulinum A toxin injections used to induce pharmacologic blepharoptosis were allowed to enrol, provided the last injection was given at least 90 days before study enrolment. Patients previously treated with AMT could only be enrolled 2 weeks after the membrane had disappeared within the area of the PED or corneal ulcer or at least 6 weeks after their AMT procedure. Patients with punctual occlusion or punctual plugs inserted before the study were advised to maintain the punctual occlusion during the study.
In Study NGF0214, enrolled patients were randomized at baseline in a 1:1 ratio to self-administer either antioxidant cenegermin 20 mcg/mL antioxidant or vehicle, 1 drop (35 μL) 6 times per day. Unlike Study NGF0212, both the experimental intervention and vehicle contained the antioxidant L-methionine. In this study, vehicle control was ophthalmic solution with the same composition as the test product, including the antioxidant L-methionine, but without cenegermin.
During the 8-week controlled treatment phase, any patient, in the opinion of the investigator, considered to be at imminent risk of deterioration of their moderate to severe NK could also be treated with preservative-free topical antibiotics and/or preservative-free topical antiviral eye drops in addition to receiving the randomized intervention 6 times a day. At the end of the controlled treatment period, patients who did not heal during 8-week blinded vehicle treatment were eligible to receive cenegermin in an 8-week open-label treatment period before proceeding to follow-up.
Concomitant use of preservative-free topical antibiotics and/or preservative-free topical antiviral eye drops were allowed in both studies.
In both NGF0212 and NGF0214, in the event that a patient progressed to deterioration of their moderate or severe NK during the 8-week randomized, double-masked, controlled treatment period, the patient’s treatment was unmasked. Patients randomized to either dose of cenegermin were to be discontinued from the study and treated as appropriate at the discretion of the investigator, whereas patients randomized to vehicle control were eligible to initiate treatment with cenegermin, according to their secondary treatment assignment, at the recommendation of the investigator. In the event that a patient progressed to deterioration during treatment with cenegermin during the 8-week uncontrolled treatment period, the patient was to be discontinued from the study.
Outcomes
A list of efficacy end points identified in the CADTH review protocol that were assessed in the clinical trials included in this review are summarized in Table 7. A detailed discussion and critical appraisal of the outcome measures is provided in Appendix 2.
Table 7: Summary of Outcomes of Interest Identified in the CADTH Review Protocol
Outcome measure | NGF0212 | NGF0214 |
|---|---|---|
Corneal healing | Primary/secondary | Primary/secondary |
Corneal sensitivity | Secondary | Secondary |
HRQoL (change in NEI-VFQ-25 scores or EQ-5D-5L scores from baseline) | Exploratory | ||||||||| |
Disease deterioration | Secondary | Secondary |
Use of rescue therapies | Not assessed | |
Need for corneal transplant | Not assessed | |
Disease relapse | Secondary | Secondary |
AE, SAE, WDAE, death, notable harms | Safety | |
AE = adverse event; HRQoL = health-related quality of life; NEI-VFQ-25 = National Eye Institute Visual Function Questionnaire-25 items; SAE = serious adverse event; WDAE = withdrawal due to adverse event.
Corneal Healing
In Study NGF0212, complete corneal healing assessed at week 4 was the primary efficacy end point, whereas in Study NGF0214, complete healing at week 8 was the primary efficacy end point. Corneal healing assessed by local investigator was a secondary efficacy outcome in both Study NGF0212 and Study NGF0214.
In both studies, complete corneal healing was defined as the greatest diameter of the corneal fluorescein staining in the area of the PED or corneal ulcer, as determined by the reading centre, being less than 0.5 mm. Corneal fluorescein staining using the modified Oxford scale was assessed at the slit lamp with a yellow barrier filter and cobalt blue illumination (measured at all visits).
“Corneal clearing” was secondary outcome in the 2 studies. It was defined as grade 0 on the modified Oxford scale, which is an absence of staining. According to the clinical experts consulted by CADTH, this is a more stringent measure than corneal healing (< 0.5 mm of lesion staining) for assessing treatment effect on NK.
Corneal Sensitivity
Corneal sensitivity was a secondary efficacy outcome in both Study NGF0212 and Study NGF0214. This examination was conducted at weeks 4, 6, and 8 in the affected eye(s) in both studies.
Cochet-Bonnet aesthesiometer is a hand-held device that is commonly used for the measurement of sensation, especially tactile. It contains a thin, retractable, nylon monofilament that extends up to 6 cm in length. The length of the device can be adjusted to apply various levels of pressure. The monofilament ranges from 5 mm to 60 mm, and as the length is decreased, the pressure increases from 11 mm/gm to 200 mm/gm. The filament is lightly placed on to the cornea by the clinician, who uses a support that allows manipulation in the x-y-z planes, while the cornea is being viewed through the slit lamp. The patient reports when they can feel the thread touching the ocular surface, and the length of thread at which this occurs is recorded.16,17 In the pivotal trails for Oxervate submission, corneal sensitivity was measured in the affected eye within the area of the PED or corneal ulcer and in each of the 4 quadrants (superior nasal, inferior nasal, superior temporal, and inferior temporal) of the cornea outside the area of the PED or corneal ulcer using a Cochet-Bonnet aesthesiometer before the instillation of any dilating or anesthetic eye drops. Corneal sensitivity is defined as the mean of the 5 measurements. A value of 4 cm or less on Cochet-Bonnet aesthesiometer suggests decreased corneal sensitivity.8
HRQoL
HRQoL was an exploratory outcome in Study NGF0212 and | ||||||||| |||||||| ||||||| || ||||| |||||||| || |||| |||||||| it was measured using the EQ-5D-5L and NEI-VFQ-25, at baseline and at week 8.
NEI-VFQ-25
The NEI-VFQ-25 was assessed by the patient using a self-administered format. This questionnaire was designed to assess HRQoL in patients with visual impairments by representing the patient perspective on the impact of vision problems on functioning. It includes 25 items relevant to 11 vision-related constructs, in addition to a single-item general health component. Responses for each item are converted to a scale from 0 to 100, with 0 representing the worst and 100 representing the best visual functioning. The responses to the 25 vision-related questions are used to generate 11 subscale scores, which are then averaged to produce an overall composite score to be used for analysis. This scale has not been validated in patients with NK. An MID was not established in this patient population.
EQ-5D-5L
The EQ-5D-5L is a generic, self-administered HRQoL measure that consists of 5 dimensions (mobility, self-care, usual activities, pain/discomfort, and anxiety/depression), each of which is measured on a 5-point scale (ranges from 1 = “no problems“ to 5 = “extreme problems”). The 5 dimensions were converted into a Health State Index on a scale of 0 to 1, where scores close to 0 represent a health state of death and a score of 1 represents perfect health. A higher score indicates a more preferred health status. The final EQ-5D-5L question (the “Score for Health Today”) asks respondents to rate their present health status on a vertical 0-to-100 visual analogue scale of 20 cm, with 0 labelled as “worst imaginable health state” and 100 labelled as “best imaginable health state.” The psychometric properties of EQ-5D-5L among patients with NK have not been reported in the literature. An MID for EQ-5D-5L was not established in this patient population.
Disease Deterioration
In both studies, disease deterioration was a secondary efficacy outcome and was measured at weeks 4, 6, and 8. It was defined as an increase in lesion size of at least 1 mm, progression to corneal melting or perforation, decrease in BCDVA by more than 5 ETDRS letters, or onset of infection. Change in lesion size was determined by the central reading centre, which analyzed cornea pictures taken at each visit. Vision was measured at the scheduled study visits using the ETDRS visual acuity chart at 4 m before administration of any eye drops to dilate or anesthetize the eye, or any examination requiring contact with the eye.
Disease Relapse
This was a secondary outcome in the included studies. Disease relapse was defined as new moderate or severe NK lesions that occurred after patients had achieved complete healing of the PED or corneal ulcer.
Time to Relapse
This was a secondary efficacy outcome in the included studies. Time to relapse of PED or corneal ulcer was calculated as date of first relapse visit to date of the 8-week visit.
Safety
AEs, SAEs, withdrawals due to adverse events (WDAEs), and AEs of special interest were recorded in the included studies. In both studies, sight-threatening events were considered AEs of special interest. In Study NGF0212, sight-threatening AEs included AEs that cause a decrease in visual acuity of more than 30 ETDRS letters or more than + 0.6 LogMAR lasting more than 1 hour, AEs that cause a decrease in visual acuity to the level of light perception or worse lasting more than 1 hour, AEs that require surgical intervention to prevent permanent loss of sight, AEs associated with severe intraocular inflammation, and AEs that in the opinion of the investigator may require medical intervention to prevent permanent loss of sight.
Statistical Analysis
Study NGF0212
Based on a conservative estimate of 60% of patients achieving complete healing of the corneal PED or ulcer, compared with 30% in vehicle-treated patients, at 4 weeks, at least 141 evaluable patients (47 per treatment group) were needed in the phase II segment of the study to have 80% power to detect such a difference. Assuming a dropout rate from 10% to 20%, a minimum of 156 patients are expected to be randomized in the phase II segment of the study.
In the primary efficacy analysis, the percentage of patients achieving complete healing of the PED or corneal ulcer at week 4 in the cenegermin 20 mcg/mL group was compared with the percentage in the vehicle control group. The comparison was conducted on data for the phase II segment of the study using a 2 × 2 chi-square test, based on the null hypothesis that there is no association between treatment (cenegermin or vehicle control) and response (complete healing at week 4 [yes/no]). The significance level of the chi-square test for the primary analysis was corrected for multiplicity, according to the Pocock method, and the 2-sided significance level alpha for the statistical tests was 0.0294. In the case of missing data at week 4, the last post-baseline observation before week 4 was carried forward. Pre-specified subgroup analyses based on punctal occlusion status were conduct for corneal healing at any visit from baseline to week 4. Sensitivity analyses based on missing data handling approaches on primary outcome were conducted.
The analyses of the secondary efficacy end points for the phase II segment of the study were split into 2 phases: the 8-week controlled treatment period, and the 12 weeks of follow-up after the controlled treatment period (up to and including the week 20 visit). The number and percentage of patients who achieved complete healing are presented separately by treatment group for each time point specified in the following sections for the phase II segments of the study. The chi-square treatment comparisons described were conducted at the significance level of 0.0294 for the end point of percentage of patients with complete healing, determined by the investigator at week 4. Sensitivity analyses were also conducted for this outcome based on various missing data imputation methods at the significance level of 0.0294. Chi-square tests at a significance level of 0.05 were conducted for the following secondary end points: percentage of patients with complete corneal clearing at other time points, improvement in visual acuity, percentage of patients with improved corneal sensitivity, and percentage of patients with deterioration.
Changes in the NEI-VFQ-25 overall composite score and change in EQ-5D-5L health state score from baseline to week 8 were exploratory end points in Study NGF0212 ||| |||| |||||||| ||||| || |||||| |||||| ||| ||||| |||||||| ||||||||| ||| |||||||| ||||||| ||||||| ||||||||| ||||| || |||||||| |||||||| |||||| ||||| ||||| || ||||| |||||||| ||| ||||||||||| || |||||||| ||||| |||| ||| || ||||||| |||||||||| || |||||| ||| ||||||| |||| |||||||| ||| |||||||||| ||||||| ||||||||| ||||| ||| |||||||||
A Kaplan–Meier analysis of time to onset of deterioration from baseline to week 8 was performed for this outcome.
Study NGF0214
The sample size calculation for Study NGF0214 was based on the assumption of the statistical superiority of antioxidant cenegermin 20 mcg/mL, compared with antioxidant vehicle, and on the preliminary masked data on complete healing from Study NGF0212 after 8 weeks of treatment. The assumption for this target was that 70% of patients in the L-methionine cenegermin 20 mcg/mL group, compared with 30% in the L-methionine vehicle group, would achieve complete healing of the PED at week 8. Thirty-eight patients (19 patients in each treatment arm) were needed to observe, with 80% power, a difference in proportion of 0.40 between treatments for a 1-sided chi-square test. At least 48 patients needed to be randomized to have at least 38 evaluable patients for the statistical analysis.
In the primary efficacy analysis, complete healing at week 8 was analyzed using a 2 × 2 chi-square test with a 2-sided significance level of 0.05 to compare patients receiving 20 mcg/mL cenegermin (with antioxidant) with patients receiving vehicle. No subgroups were defined a priori.
Patients who discontinued before week 4 (and who did not have a post-baseline corneal photograph with fluorescein) were assumed to have been “not completely healed” for the primary efficacy end point if the investigator recorded that the “measurement was not applicable because the greatest dimension of the PED or corneal ulcer evaluated was greater than 1 mm on the slit lamp.” If no post-baseline values were available, no imputation was performed, and the patient was assumed to have a missing “completely healed” end point and was not included in the analysis. All other missing evaluations were imputed using the last observation carried forward method.
A sensitivity analysis was performed on observed cases removing patients who were discontinued from the study before week 4. Two additional sensitivity analyses were planned (patients who were discontinued from the study before a given visit were excluded from the sensitivity analysis of that visit): first, imputing all missing completely healed statuses as failures; and second, using multiple imputation for missing values before study discontinuation.
Secondary efficacy outcomes (e.g., patients with complete corneal healing, improvement in corneal sensitivity, deterioration, and time to relapse) were analyzed using chi-square tests.
In Study NGF0214, for continuous variables, the mean, SD, and 95% CI associated with the mean were reported. For categorical variables, absolute and relative frequencies were reported.
In both studies, in the safety analyses, AEs were grouped into the controlled treatment period, uncontrolled treatment period, and follow-up period, and presented separately for each study period using counts and percentages.
Analysis Populations
In both Study NGF0212 and Study NGF0214, the ITT population was defined as all randomized patients, regardless of when they withdrew from the study. The ITT population was used for all efficacy analyses, including the primary efficacy end point. Patients were summarized according to the treatment to which they were randomized.
The safety population was defined as all randomized patients who received at least 1 dose of study medication. The safety population was used for all safety summaries, by actual treatment received.
Results
Patient Disposition
In Study NGF0212, 156 patients were randomized, with 52 patients randomized to both the cenegermin 20 mcg/mL group and the vehicle group. Sixteen patients (30.8%) in the cenegermin 20 mcg/mL group and 12 patients (23.1%) in the vehicle control group withdrew prematurely from the study. Among them, 13 (25%) in the cenegermin 20 mcg/mL group and 4 (7.7%) in the vehicle control group withdrew on or before week 8. Reasons for withdrawal were provided. Patients treated with cenegermin (56.3%) were more likely to discontinue the study because of AEs, compared with those treated with the vehicle (16.7%). At the end of the follow-up period, 13 patients (25.0%) in the cenegermin 20 mcg/mL group and 15 patients (28.8%) in the vehicle control group completed the 48- or 56-week follow-up periods.
In Study NGF0214, a total of 48 patients were randomized, with 24 patients randomized to both the cenegermin 20 mcg/mL group and the vehicle control group. Thirty-three randomized patients (68.8%) completed the 8-week controlled treatment period: 18 (75.0%) patients in the cenegermin treatment arm and 15 (62.5%) patients in the vehicle arm. Fifteen patients (15 of 48; 31.3%) discontinued early from the controlled treatment period, 6 of whom were in the vehicle group, who entered directly into the uncontrolled treatment period. The remaining 9 patients discontinued the study before week 8. The most common reason for discontinuation was AEs (16.7% patients in the cenegermin 20 mcg/mL group and 12.5% in the vehicle group). At the end of the follow-up period, 13 patients (25.0%) in the cenegermin 20 mcg/mL group and 15 patients (28.8%) in the vehicle control group completed the 24- or 32-week follow-up period.
Details of patient disposition are presented in Table 8.
Disposition | NGF0212 | NGF0214 | |||
|---|---|---|---|---|---|
Cenegermin 20 mcg/mL | Vehicle | Antioxidant cenegermin 20 mcg/mL | Antioxidant vehicle | ||
Screened, N | 186 | 52 | |||
Randomized, n (%) | 156 (83.9) | 48 (92.3) | |||
52 (100) | 52 (100) | 24 (100) | 24 (100) | ||
Completed 8-week controlled treatment period, n (%) | 39 (75) | 48 (92) | 18 (75.0) | 15 (62.5) | |
Vehicle-treated patients entered uncontrolled treatment period and received cenegermin, n (%) | NA | Randomized at week 8: 23 (44.2) 20 mcg/mL: 13 | NA | 13 (54.1) | |
Withdrew from the study, n (%) | 16 (30.8) | 12 (23.1) | NR | NR | |
Discontinued the study during 8-week controlled treatment period, n (%) | 13 (25.0) | 4 (7.7) | 6 (25.0) | 9 (37.5) | |
Reason for discontinuation during controlled period, n (%) | |||||
Adverse events | 9 (56.3) | 2 (16.7) | 4 (16.7) | 3 (12.5) | |
Lack of efficacy | 1 (6.3) | 1 (8.3) | 0 | 0 | |
Lost to follow-up | 0 | 1 (8.3) | 0 | 0 | |
Noncompliance | NR | NR | 0 | 0 | |
Patient death | NR | NR | 0 | 0 | |
Study terminated by sponsor or investigator | NR | NR | 0 | 0 | |
Other | 5 (31.3) | 7 (58.3) | 2 (8.3) | 0 | |
Terminated (entered uncontrolled period) | NR | NR | NR | 6 (25.0) | |
Completed the study to 12-month follow-up, n (%) | 13 (25.0) | 15 (28.8) | 15 (62.5) | 16 (66.7) | |
ITT, N (%) | 52 (100) | 52 (100) | 24 (100) | 24 (100) | |
Safety, N (%) | 52 (100) | 52 (100) | 23 (95.8) | 24 (100) | |
ITT = intention to treat; NA = not applicable; NR = not reported.
Exposure to Study Treatments
|| ||||| |||||||| |||||| ||| |||||||||| ||||||||| |||||| ||| |||| |||||| || |||||||| |||| ||| |||| |||| ||||||| | || || ||||| || ||| |||||||||| || |||||| ||||| ||| |||| ||||||| | || || ||||| || ||| ||||||| ||||||| ||||||||| ||| |||||||||| || |||||| |||||| || |||||||| ||||||| |||||||||||| ||| ||||| |||||||||| || ||||||| |||||| |||| || ||| || |||||||| ||||||| |||||||||||| ||| ||||| |||||||||| || ||||||| |||||| |||| || |||||| |||| || || |||||||| ||||||| |||||||||||| ||| ||||| |||||||||| || |||||||| |||||| |||| || || |||||||| ||||||| |||||||||||| ||| ||||| |||||||||| || |||||||| |||||| |||| || || |||||||| ||||||| |||||||||||| ||| ||||| |||||||||| || |||||||| |||||| |||| || | |||||||| |||||| |||||||||||| ||| ||||| |||||||||| || ||||||||||| ||| ||||||| ||||||| |||||| || |||||||| ||||||| |||||||||||| ||| ||||| |||||||||| || ||||||| |||||| |||| || ||| || |||||||| ||||||| |||||||||||| ||| ||||| |||||||||| || ||||||| |||||| |||| || |||||| |||| || || |||||||| ||||||| |||||||||||| ||| ||||| |||||||||| || |||||||| |||||| |||| || || |||||||| ||||||| |||||||||||| ||| ||||| |||||||||| || |||||||| |||||| |||| || || |||||||| ||||||| |||||||||||| ||| ||||| |||||||||| || |||||||| |||||| |||| || || |||||||| ||||||| |||||||||||| ||| ||||| |||||||||| || ||||||||||| ||||| |||||||| |||||| ||| |||||||||| ||||||||| |||||| ||| |||| |||||| || |||||||| |||| ||| |||| |||| ||||||| | || || ||||| || ||| ||||||||||| |||||||||| || |||||| ||||| ||| |||| |||| ||||||| | || || ||||| || ||| ||||||||||| ||||||| ||||||| |||||||||||| |||||||| ||||||| |||||||||| |||| ||| ||||| ||||| |||||||||| |||||| ||| ||||| ||||||| ||| ||| |||||||||| ||||| ||| ||||| ||||||| ||| ||| ||||||| ||||||
Efficacy
Only efficacy outcomes and analyses of subgroups identified in the review protocol are reported here. Refer to Appendix 2 for detailed efficacy data.
Corneal Healing
Study NGF0212
Complete healing of the PED or corneal ulcer at week 4, as determined by the reading centre, was achieved in 29 patients (58.0%) in the cenegermin 20 mcg/mL group and 10 patients (19.6%) in the vehicle control group. The difference in the percentage of patients who achieved complete healing at week 4 between the cenegermin 20 mcg/mL group and the vehicle control group was 38.4% (97.06% CI, 18.96% to 57.83%) and was statistically significant (P < 0.001).
The findings of the sensitivity analyses (by imputing missing data as failures and by using the multiple imputation method for missing data) were similar to those of the primary efficacy analysis.
Complete healing of the PED or corneal ulcer at week 8, as determined by the reading centre, was achieved in 37 patients (74.0%) in the cenegermin 20 mcg/mL group and 22 patients (43.1%) in the vehicle control group. The difference in the percentage of patients who achieved complete healing at week 8 between the cenegermin 20 mcg/mL group and the vehicle control group was 30.9% (97.06% CI, 10.60% to 51.13%) and was statistically significant (P = 0.002).
Results of complete healing at week 4 or week 8 determined by the investigator were consistent with those assessed by the central reading centre.
||||||| || ||||||||||| |||||||| |||||||| ||||| || |||||||| ||||||||| ||||||||| |||| ||||| |||||||| ||||||| |||||||| || |||||||| |||||||||| ||||||||| |||| |||||||||| ||| ||||||| || |||||| |||||||| ||||||| ||||| |||||||| || ||| |||||||||
Study NGF0214
There was a statistically significant difference in favour of cenegermin between the percentage of patients reaching complete healing at week 8: 69.6% in the cenegermin-treated group versus 29.2% in the vehicle-treated group, mean difference, 40.4% (95% CI, 14.2% to 66.6%; P = 0.006).
There was no statistically significant difference between cenegermin and vehicle in the percentage of patients reaching complete healing at week 4: 56.5% in the cenegermin group versus 37.5% in the vehicle group; between-group difference, 19.0% (95% CI, –9.0% to 47.1%; P = 0.191).
Results of complete healing at week 4 or week 8 determined by the investigator were consistent with those assessed by the central reading centre. Results of primary analysis were supported by preplanned sensitivity analysis, which demonstrated similar results.
Details of results on complete corneal healing are presented in Table 9.
Table 9: Efficacy — Complete Corneal Healing, ITT Population
Efficacy | NGF0212 | NGF0214 | ||
|---|---|---|---|---|
Cenegermin 20 mcg/mL (N = 52) | Vehicle (N = 52) | Antioxidant cenegermin 20 mcg/mL (N = 24) | Antioxidant vehicle (N = 24) | |
Complete healing achieved (assessed by central reading centre) at week 4, n of N (%) | 29 of 50 (58.0) | 10 of 51 (19.6) | 13 of 23 (56.5) | 9 of 24 (37.5) |
% difference (97.06% CIa for NGF0212; 95% CI for NGF0214) | 38.4% (18.96 to 57.83) | Reference | 19.0% (–9.0 to 47.1) | Reference |
P valueb | < 0.001 | Reference | 0.191 | Reference |
Sensitivity analysis: complete healing achieved (assessed by central reading centre) at week 4, n of N (%) | 28 of 52 (53.8) | 10 of 52 (19.2) | NA | |
% difference (97.06% CI for NGF0212; 95% CI for NGF0214) | 34.6% (15.42 to 53.81) | Reference | ||
P value | < 0.001 | Reference | ||
|||||||| ||||||||| |||||||| |||| |||||||| |||||||||| |||||||| ||||||| |||||||| ||||||||| || ||||||| ||||||| ||||||| || |||| || ||| ||| | ||||| |||||| | |||| |||||| | |||||||||| | |
| |||||||||| ||||||| || ||| |||||||| ||| || ||| |||||||| | |||||||||||||| |||||| | ||||||||| | ||
| ||||| | | ||||| | |||
|||||||| ||||||| |||||||| ||||||||| || ||||||||||||| || |||| || ||| ||| | ||||| |||||| | ||||| ||||||| | || |||||| | || |||||| |
| |||||||||| ||||||| ||| ||| |||||||| ||| || ||| |||||||| | ||||||||||||| |||||| | ||||||||| | ||||||||||||| ||||| | ||||||||| |
| |||||| | ||||| | ||||||||| | ||||||| | ||||||||| |
Complete healing achieved (assessed by central reading centre) at week 8, n of N (%) | 37 of 50 (74.0) | 22 of 51 (43.1) | 16 of 23 (69.6) | 7 of 24 (29.2) |
% difference (97.06% CIa for NGF0212; 95% CI for NGF0214) | 30.9% (10.60 to 51.13) | Reference | 40.4% (14.2 to 66.6) | Reference |
P valueb | 0.002 | Reference | 0.006 | Reference |
Sensitivity analysis: complete healing achieved (assessed by central reading centre) at week 8, with site 9 excluded), n of N (%) | 35 of 52 (67.3) | 22 of 52 (42.3) | 14 of 20 (70.0) | 5 of /20 (25.0) |
% difference (97.06% CI for NGF0212; 95% CI for NGF0214) | 25.0% (4.42 to 45.58) | Reference | 45% (17.4 to 72.6) | Reference |
P value | 0.010 | Reference | 0.004 | Reference |
Complete healing achieved (assessed by investigator) at week 8, n of N (%) | 33 of 42 (78.6) | 20 of 38 (52.6) | 15 of 23 (65.2) | 7 of 24 (29.2) |
% difference (97.06% CIa for NGF0212; 95% CI for NGF0214) | 25.9% (3.55 to 48.33) | Reference | 36.1% (9.4 to 62.7) | Reference |
P valueb | 0.014 | Reference | 0.013 | Reference |
CI = confidence interval; ITT = intention to treat; NA = not applicable.
Note: “Complete healing” was defined as the greatest diameter of the corneal fluorescein staining in the area of the PED or corneal ulcer measured at the baseline visit being less than 0.5 mm at the week 4 visit (Study NGF0212) or week 8 visit (Study NGF0214), assessed by the central reading centre evaluating the clinical pictures.
aAsymptotic (Wald) CI.
bP value was from chi-square test. In NGF0212, the significance level for the statistical tests is 0.0294 (adjusted according to Pocock). In NGF0214, the significance level for the statistical tests was 0.05. In the 2 included studies, for all efficacy outcomes except for the primary outcome, there were no adjustments for multiplicity.
Corneal Clearing
Study NGF0212
The difference in the percentage of patients who experienced complete corneal clearing at week 4 between the cenegermin 20 mcg/mL group and the vehicle control group was 12.4% (95% CI, –2.05 to 26.78), but did not reach statistical significance (P = 0.097).
The difference in the percentage of patients who experienced complete corneal clearing at week 8 between the cenegermin 20 mcg/mL group and the vehicle control group was 11.4% (95% CI, –4.08 to 26.93), and was not statistically significant (P = 0.157).
Study NGF0214
At week 4, the percentage of patients with complete corneal clearing measured with modified Oxford scale was 13.6% (3/22) in the cenegermin group versus 4.2% (1/24) in the vehicle group.
At week 8, the percentage of patients with complete corneal clearing measured with modified Oxford scale was 22.7% (5/22) in the cenegermin group versus 4.2% (1/24) in the vehicle group.
Details of results on corneal clearing are presented in Table 10.
Table 10: Efficacy — Complete Corneal Clearing, ITT Population
Efficacy | NGF0212 | NGF0214 | ||
|---|---|---|---|---|
Cenegermin 20 mcg/mL (N = 52) | Vehicle (N = 52) | Cenegermin 20 mcg/mL (N = 24) | Vehicle (N = 24) | |
Complete corneal clearing (assessed by modified Oxford scale) at week 4, n (%) | 8 (19.5) | 3 (7.1) | 3 (13.6) | 1 (4.2) |
Treatment comparison: (cenegermin vs. vehicle; 95% CIa) | 12.4% (–2.05 to 26.78) | Reference | 9.5% (–6.9 to 25.9) | Reference |
P valueb | 0.097 | Reference | 0.255 | Reference |
Complete corneal clearing (assessed by modified Oxford scale) at week 8, n (%) | 9 (21.4) | 4 (10.0) | 5 (22.7) | 1 (4.2) |
Treatment comparison: (cenegermin vs. vehicle; 95% CIa) | 11.4% (–4.08 to 26.93) | Reference | 18.6% (–0.7 to 37.8) | Reference |
P valueb | 0.157 | Reference | 0.062 | Reference |
CI = confidence interval; ITT = intention to treat.
Note: “Complete corneal clear” was defined as grade 0 on the modified Oxford scale (absence of staining).
aAsymptotic (Wald) CI.
bAsymptotic P value based on Pearson statistic from chi-square test.
Corneal Sensitivity
Study NGF0212
There was no significant difference between the cenegermin 20 mcg/mL group and vehicle control group (P = 0.835) in the percentage of patients who achieved an improvement in corneal sensitivity at week 4.
There was no significant difference between the cenegermin 20 mcg/mL group and vehicle control group (P = 0.442) in the percentage of patients who achieved an improvement in corneal sensitivity at week 8.
Study NGF0214
At week 8, adjusted mean (SD) change from baseline in corneal sensitivity was 1.88 (1.40) in the cenegermin 20 mcg/mL group and 1.00 (1.25) in the vehicle group. There was no statistically significant difference between the 2 treatments (P = 0.207).
Details of results of improvement in corneal sensitivity are provided in Table 11.
Table 11: Efficacy — Improvement in Corneal Sensitivity, ITT Population
Efficacy | NGF0212 | NGF0214 | ||
|---|---|---|---|---|
Cenegermin 20 mcg/mL (N = 52) | Vehicle (N = 52) | Antioxidant cenegermin 20 mcg/mL (N = 24) | Antioxidant vehicle (N = 24) | |
Improvement in corneal sensitivity at week 4, n/N (%) | 22/36 (61.1) | 26/41 (63.4) | Baseline, mean (SD): 0.81 |||||| |||| || |||| ||||| |||| |||||| | Baseline, mean (SD): 0.65 |||||| |||| || |||| ||||| |||| |||||| |
% difference, (95% CIa) | –2.3% (–24.01 to 19.40) | Reference | NR | |
P valueb | 0.835 | Reference | ||
Improvement in corneal sensitivity at week 8, n (%) | 29 (76.3) | 26 (68.4) | Baseline, mean (SD): 0.81 |||||| Week 8, mean (SD): 2.91 |||||| |||| | |||||||| |||| |||| ||| || |||| |||| || |||| | Baseline, mean (SD): 0.65 |||||| Week 8, mean (SD): 1.83 |||||| |||| | |||||||| |||| |||| || |||| |||| || |||| |
% difference (95% CIa) | 7.9% (–12.13 to 27.92) | Reference | 0.6 (–0.4 to 1.5) | Reference |
P valueb | 0.442 | Reference | 0.207 | Reference |
CI = confidence interval; ITT = intention to treat; NR = not reported; SD = standard deviation.
Note: A value ≤ 4 cm on Cochet-Bonnet aesthesiometer suggests decreased corneal sensitivity.
aAsymptotic (Wald) CI.
bAsymptotic P value based on Pearson statistic from chi-square test. This analysis was not adjusted for multiple comparisons.
cAnalysis results from an analysis of covariance with treatment as the factor controlling for baseline value, time from diagnosis of NK (months), and baseline value of Schirmer test (mm).
HRQoL
Study NGF0212
The least square (LS) mean change in the NEI-VFQ-25 overall composite score from baseline to week 8 was 4.8 (standard error [SE] = 1.92) in the cenegermin 20 mcg/mL group and 3.2 (SE = 1.94) in the vehicle control group. There was no significant difference in LS mean change from baseline between the cenegermin 20 mcg/mL group and the vehicle control group (|||||||). Note that this was an exploratory outcome in Study NGF0212, and the P value was not adjusted for multiple comparisons.
The LS mean change in EQ-5D-5L health state score from baseline to week 8 was 2.8 (SE = 2.43) in the cenegermin 20 mcg/mL group and 0.2 (SE = 2.45) in the vehicle control group. There was no significant difference in LS mean change from baseline between the cenegermin 20 mcg/mL group and the vehicle control group (|||||||) (Table 12). Note that this was an exploratory outcome in Study NGF0212, and the P value was not adjusted for multiple comparisons.
Study NGF0214
||||||| || ||| ||||||| ||||||||| ||||| || ||||||| ||| |||||||| |||||| ||||| ||||| |||| ||| |||||||| || ||||| ||||||||
Table 12: Efficacy — Health-Related Quality of Life, ITT Population
Efficacy | NGF0212 | |
|---|---|---|
Cenegermin 20 mcg/mL (N = 52) | Vehicle (N = 52) | |
Change in NEI-VFQ-25 overall composite score from baseline to week 8 | ||
LS mean (SE) | 4.8 (1.92) | 3.2 (1.94) |
Mean difference: (LS mean, 95% CI) | |||||||||| ||||| | ||||||||| |
P value | ||||| | ||||||||| |
Change in EQ-5D-5L health state score from baseline to week 8 | ||
LS mean (SE) | 2.8 (2.43) | 0.2 (2.45) |
Mean difference: (LS mean, 95% CI) | ||||||||||| ||||| | ||||||||| |
P value | ||||| | ||||||||| |
CI = confidence interval; EQ-5D-5L = EuroQol 5 Dimension Scale, 5 levels; ITT = intention to treat; LS = least squares; SE = standard error; NEI-VFQ-25 = National Eye Institute Visual Function Questionnaire-25 items.
Note: None of these P values were adjusted for multiple comparison.
Disease Deterioration
Study NGF0212
Among patients with a response available at week 4, 1 of 42 (2%) patients in the cenegermin 20 mcg/mL group and 2 of 43 (5%) patients in the vehicle control group experienced disease deterioration (difference of –2.3% [95% CI, –23.3% to 18.7%] between groups). There was no significant difference in the percentage of patients with deterioration observed at week 4 between the cenegermin 20 mcg/mL group and the vehicle control group (P > 0.999; note that this P value was not adjusted for multiple comparisons). At week 8, 3 of 42 (7%) patients in the cenegermin 20 mcg/mL group and 6 of 40 (15%) patients in the vehicle control group experienced disease deterioration (difference between groups of –7.9% [95% CI, –29.51% to 13.52%]; P = 0.307).
A Kaplan–Meier analysis of time to onset of deterioration from baseline to week 8 (ITT population) was conducted. The median time to onset of deterioration in the 3 treatment groups was not estimable because of the small number of events.
Study NGF0214
From week 1 to week 8, the percentage of patients with deterioration ranged from 0% to 10.0% in the cenegermin 20 mcg/mL group and from 5.9% to 25.0% in the vehicle group. At week 8, the rate of deterioration was 0% in the cenegermin 20 mcg/mL group and 13.3% in the vehicle group.
Details of disease deterioration are provided in Table 13.
Table 13: Efficacy — Deterioration From Baseline, ITT Population
Efficacy | NGF0212 | NGF0214 | ||
|---|---|---|---|---|
Cenegermin 20 mcg/mL (N = 52) | Vehicle (N = 52) | Antioxidant cenegermin 20 mcg/mL (N = 24) | Antioxidant vehicle (N = 24) | |
Patients experienced deterioration at week 4, n of N (%) | 1 of 42 (2.4) | 2 of 43 (4.7) | 2 of 20 (10.0) | 1 of 17 (5.9) |
% difference (95% CIa) | –2.3% (–23.26 to 18.71) | Reference | 4.1% (–13.1 to 21.4) | Reference |
P valueb | > 0.999 | Reference | 0.647 | Reference |
Patients experienced deterioration at week 8, n of N (%) | 3 of 42 (7.1) | 6 of 40 (15.0) | 0 of 18 (0) | 2 of 15 (13.3) |
% difference (95% CIa) | –7.9% (–29.51 to 13.52) | Reference | –13.3% (–30.5 to 3.9) | Reference |
P valueb | 0.307 | Reference | 0.110 | Reference |
CI = confidence interval; ITT = intention to treat.
aExact (Clopper-Pearson) CI.
bAsymptotic P value based on Pearson statistic from chi-square test. The P values were not adjusted for multiple comparisons.
Use of Rescue Therapies
Not assessed in the included studies.
Need for Corneal Transplant
Not assessed in the included studies.
Disease Relapse
Study NGF0212
Time to relapse of PED or corneal ulcer during follow-up for completely healed patients was analyzed. ||| |||| |||| |||| |||||||| ||||||| || ||||||| || ||| || ||||||| ||||| ||| ||||| |||| |||| |||||| || ||| |||||||||| || |||||| ||||| |||||| ||| |||| |||| || ||| ||||||| ||||||| ||||| ||||||
Study NGF0214
In total, 5 patients who were completely healed (5 of 47; 10.6%) experienced a disease relapse and received an additional course of the study treatment: 2 (2 of 23; 8.7%) randomized to cenegermin 20 mcg/mL, and 3 (3 of 24; 12.5%) randomized to initial treatment with vehicle. All patients who were randomized to the vehicle group experienced their relapse treatment after the uncontrolled treatment phase. Range for time to recurrence was 1 to 39 days.
Results of disease recurrence are provided in Table 14.
Table 14: Efficacy — Relapse of PED or Corneal Ulcer During Follow-Up for Completely Healed Patients, ITT Population
Efficacy | Follow-up period | NGF0212 | NGF0214 | ||
|---|---|---|---|---|---|
Cenegermin 20 mcg/mL (N = 65) | Vehicle (N = 29) | Antioxidant cenegermin 20 mcg/mL (N = 24) | Antioxidant vehicle (N = 24) | ||
Patients who achieved complete healing during controlled treatment period with relapse of PED or corneal ulcer during follow-up, n of N (%) | |||||
12 weeks follow-up (week 20/28) | 12 weeks (week 20/28) | 4 of 40 (10) | 0 of 21 (0) | 2 of 23 (8.7) received additional course of cenegermin for relapse | 3 of 24 (12.5) received additional course of cenegermin for relapse |
24 weeks follow-up (week 32/40) | 24 weeks (week 32/40) | 1 of 24 (4.2) | 0 of 18 (0) | ||
36 weeks follow-up (week 44/52) | 36 weeks (week 44/52) | 1 of 16 (6.3) | 0 of 9 (0) | ||
48 weeks follow-up (week 56/64) | 48 weeks (week 56/64) | 0 of 11 (0) | 0 of 8 (0) | ||
Mean time from complete healing to relapse (days), mean (SD) | NA | ||||| ||||||| | |||| |||| |||||||||| | NR | Range = 1 to 39 |
ITT = intention to treat; NA = not applicable; NR = not reported; PED = persistent epithelial defect; SD = standard deviation.
Harms
Only harms identified in the review protocol are reported here. Refer to Table 15 for detailed harms data.
Adverse Events
Study NGF0212
In total, 27 patients (51.9%) in the cenegermin 20 mcg/mL group and 20 patients (38.5%) in the vehicle control group experienced at least 1 AE during the controlled treatment period. Eye disorders were the most frequently reported AEs in both groups: 25.0% in the cenegermin group versus 30.8% in the vehicle group.
During the follow-up period, 17 patients (26.2%) in the cenegermin 20 mcg/mL group and 9 patients (31.0%) in the vehicle control group reported at least 1 AE. The safety profile of cenegermin during this period was similar to that reported during the controlled treatment period.
Study NGF0214
Twenty-one patients (91.3%) receiving antioxidant cenegermin 20 mcg/mL and 18 patients (75.0%) receiving antioxidant vehicle reported at least 1 AE in the controlled treatment period. Eye disorders were the most frequently reported AEs in both groups: 78.3% in the antioxidant cenegermin group versus 58.3% in the antioxidant vehicle group in NGF0214.
A total of 23 (48.9%) patients reported at least 1 AE in the follow-up period: 14 (60.9%) patients randomized to antioxidant cenegermin 20 mcg/mL and 9 (37.5%) randomized to antioxidant vehicle.
Serious Adverse Events
Study NGF0212
Nine patients (17.3%) in the cenegermin 20 mcg/mL group and 5 patients (9.6%) in the vehicle group experienced an SAE during the controlled treatment period. Disease progression was the most frequently reported SAE during the controlled treatment period, occurring in 4 patients (2.6%) overall: 2 in the cenegermin 20 mcg/mL group and 2 in the vehicle control group. Serious AEs of reduced visual acuity and malignant neoplasm progression were each reported in 2 patients (both in the cenegermin group) overall. All other SAEs were reported in 1 patient each.
Six patients in the cenegermin 20 mcg/mL group and 2 patients in the vehicle control group experienced an SAE during the follow-up period.
Study NGF0214
A total of 8 SAEs in 7 (14.9%) patients were reported in the controlled treatment period: 3 (13.0%) in the cenegermin 20 mcg/mL group and 4 (16.7%) in the vehicle group. The reported SAEs included syncope, aqueous humour leakage, corneal thinning, worsening of NK, decreased visual acuity, and ventral hernia.
There were 7 patients (7 of 47; 14.9%) who reported an SAE during the follow-up period; 5 of them were randomized to treatment with cenegermin and 2 were randomized to antioxidant vehicle.
Withdrawals Due to Adverse Events
Study NGF0212
During the controlled treatment period, 9 patients (17.3%) in the cenegermin 20 mcg/mL group and 4 patients (7.7%) in the vehicle control group experienced AEs that led to discontinuation of study treatment. The main reasons related to WDAEs were eye disorders and disease progression.
One patient in the cenegermin 20 mcg/mL group and 1 patient in the vehicle group reported at least 1 AE that led to discontinuation of study treatment during the follow-up period.
Study NGF0214
During the controlled treatment period, 5 patients (21.7%) in the antioxidant cenegermin 20 mcg/mL group and 7 patients (29.2%) in the antioxidant vehicle group discontinued the treatment due to AEs. The main reasons related to WDAEs were eye disorders and disease progression.
Mortality
Study NGF0212
During the controlled treatment period, 1 patient in the cenegermin 20 mcg/mL group died from an SAE of malignant neoplasm progression. The death was not considered to be related to study treatment.
Overall, 6 deaths (||| || |||||||||||| |||||||| ||| ||||||||||| |||||||||| ||||||| |||||||||| ||||||| |||||||| |||||||||| ||||||||||| ||||| ||||||| |||||||| |||||||| |||||||||) were reported during the follow-up period of the study. One patient each in the 20 mcg/mL and vehicle control group died during follow-up. None of the deaths were considered to be related to treatment with the study drug.
Study NGF0214
One death in the antioxidant cenegermin 20 mcg/mL group was reported during the follow-up period. The cause of death was unknown and was not considered to be related to the study drug.
Notable Harms
Study NGF0212
All sight-threatening AEs were considered to be equivalent to an SAE in study NGF0212. Therefore, notable harms |||| |||||||| ||| | |||||||| ||||||| ||||||||| |||||||||| || |||||| ||| | |||||||| |||||| ||||||||| ||||||| |||||| ||| |||||||||| ||||||||| |||||| in this study.
Study NGF0214
|||| ||||||| |||||||| |||||||| || || ||||||| |||||||| || |||||||| ||||||||| |||||||||| ||| | |||||||| ||||||||| |||||||| |||||| ||| |||||||||| ||||||||| |||||||||||| |||||||| ||||||| |||||||| || || ||||||| |||||||| |||||| ||| ||||||||| ||||||||
Table 15: Summary of Harms — Safety Population, Controlled Treatment Period
Harms | NGF0212 | NGF0214 | ||
|---|---|---|---|---|
Cenegermin 20 mcg/mL (N = 52) | Vehicle (N = 52) | Antioxidant cenegermin 20 mcg/mL (N = 23) | Antioxidant vehicle (N = 24) | |
Patients with ≥ 1 AE | ||||
n (%) | 27 (51.9) | 20 (38.5) | 21 (91.3) | 18 (75.0) |
Most common events,a n (%) | ||||
Eye disorders | 13 (25.0) | 16 (30.8) | 18 (78.3) | 14 (58.3) |
Visual acuity reduced | 3 (5.8) | 2 (3.8) | 5 (21.7) | 5 (20.8) |
Eye pain | 5 (9.6) | 4 (7.7) | 7 (30.4) | 2 (8.3) |
Corneal epithelium defect | 0 | 1 (1.9) | 3 (13.0) | 2 (8.3) |
Eye inflammation | 1 (1.9) | 0 | 3 (13.0) | 2 (8.3) |
Lacrimation increased | 0 | 1 (1.9) | 4 (17.4) | 1 (4.2) |
Ocular hyperaemia | 1 (1.9) | 1 (1.9) | 4 (17.4) | 1 (4.2) |
Corneal thinning | NR | NR | 2 (8.7) | 2 (8.3) |
Eye irritation | 0 | 1 (1.9) | 0 | 4 (16.7) |
Ocular discomfort | 0 | 1 (1.9) | 2 (8.7) | 2 (8.3) |
Photophobia | 0 | 1 (1.9) | 2 (8.7) | 2 (8.3) |
Cataract | NR | NR | 3 (13.0) | 0 |
Foreign body sensation in eyes | 0 | 1 (1.9) | 2 (8.7) | 0 |
General disorders and administration site conditions | 2 (3.8) | 7 (13.5) | 4 (17.4) | 6 (25.0) |
Infections and infestations | 7 (13.5) | 2 (3.8) | 4 (17.4) | 2 (8.3) |
Nervous system disorders | 2 (3.8) | 2 (3.8) | 4 (17.4) | 2 (8.3) |
Investigations | < 5% | < 5% | 3 (13.0) | 2 (8.3) |
Gastrointestinal disorders | < 5% | < 5% | 1 (4.3) | 2 (8.3) |
Injury, poisoning and procedural complications | 0 | < 5% | 3 (13.0) | 0 |
Musculoskeletal and connective tissue disorders | NR | NR | 3 (13.0) | 0 |
Skin and subcutaneous tissue disorders | 0 | < 5% | 2 (8.7) | 0 |
Patients with ≥ 1 SAE | ||||
n (%) | 9 (17.3) | 5 (9.6) | 3 (13.0) | 4 (16.7) |
Eye disorders | 2 (3.8) | 3 (5.8) | Syncope 1; Aqueous humour leakage, corneal thinning 1; Worsening of NK 1 | Decreased visual acuity 1; Worsened of NK 2; Ventral hernia 1 |
General disorders and administration site conditions | 2 (3.8) | 2 (3.8) | ||
Neoplasms benign, malignant, and unspecified | 1 (1.9) | 0 | ||
Vascular disorders | 2 (3.8) | 0 | ||
Ear and labyrinth disorders | 1 (1.9) | 0 | ||
Immune system disorders | 1 (1.9) | 0 | ||
Renal and urinary disorders | 1 (1.9) | 0 | ||
Patients who stopped treatment due to AEs | ||||
n (%) | 9 (17.3) | 4 (7.7) | 5 (21.7) | 7 (29.2) |
Eye disorders | 6 (11.5) | 3 (5.8) | 3 (13.0) | 4 (16.7) |
General disorders and administration site conditions | 2 (3.8) | 3 (5.8) | 2 (8.7) | 3 (12.5) |
Cardiac disorders | 1 (1.9) | 0 | 0 | 0 |
Injury, poisoning, and procedural complications | 0 | 0 | 1 (4.3) | 0 |
Immune system disorders | 1 (1.9) | 0 | 0 | 0 |
Investigations | 1 (1.9) | 0 | 0 | 0 |
Neoplasms benign, malignant, and unspecified | 1 (1.9) | 0 | 0 | 0 |
Nervous system disorders | 1 (1.9) | 0 | 0 | 0 |
Deaths | ||||
n (%) | 1 (1.9) | 0 | 0 | 0 |
Notable harms | ||||
||||||||||||||||| ||||||| | ||| | During the study all sight-threatening events were considered equivalent to an SAE in NGF0212 | | |||||| | | |||||||| | |
| |||||| | | ||||| | |||
AE = adverse event; NK = neurotrophic keratitis; NR = not reported; SAE = serious adverse event.
aFrequency > 5%.
Critical Appraisal
Internal Validity
Studies NGF0212 and NGF0214 were small, phase II, double-blind, vehicle-controlled RCTs. In Study NGF0212, appropriate methods were used to randomize patients to treatments and conceal treatment allocation. The method for randomization and allocation concealment in NGF0214 was unclear. In both studies, some relatively large baseline imbalances between groups were observed, for example, sex (42% versus 33% male) and race (98% versus 87% White). There were also some differences in prior treatments across treatment groups. This could suggest selection bias.
In general, patients’ characteristics appear to be similar at baseline between treatment groups. However, imbalanced patient characteristics were observed. In Study NGF0214, patients with moderate NK were more likely to receive vehicle, and patients with severe NK were more likely to receive cenegermin therapy. Although imbalances in baseline characteristics occur in RCTs of treatments for rare diseases despite randomization, the imbalanced characteristics may have an impact on data interpretation and bias the results. In NGF0214, more patients with severe condition (which can be considered more difficult to treat) received cenegermin therapy; this may bias the results in favour of the vehicle group. There was also imbalance in prior NK treatment between treatment groups in the 2 studies; this may affect result interpretation. However, it is unclear to what extent the imbalances in these baseline characteristics influenced the relative treatment effect between cenegermin and vehicle therapy.
Even though a power calculation was conducted in the 2 studies, there were a lot of withdrawals, which resulted in smaller sample sizes at later time points. In NGF0212, 7% to 25% of patients withdrew from the study before the completion of 8-week controlled treatment, and in NGF0214, 25% to 38% of patients withdrew. The dropout rates were high, and withdrawals were imbalanced between groups (more patients in the cenegermin group discontinued treatment due to AEs than in the vehicle group), which could impact the study results. In both studies, missing post-baseline data were imputed using the last observation carried forward method. Additional sensitivity analyses using various methods were conducted to assess the robustness of the primary analysis results. Results of the sensitivity analyses were consistent with those of the primary analysis. Therefore, the results were robust to the handling of missing data, and the potential for attrition bias is of lesser concern. Predefined subgroup analyses were rarely conducted in either study to explore the treatment effect of cenegermin in various subgroups, which may be related to the small number of study participants, and the findings from these subgroup analyses could be noninformative due to the small sample, lack of power to detect between-group differences, imprecision, and lack of adjustment for multiplicity.
In the 2 included studies, for all efficacy outcomes except for the primary outcome, there were no adjustments for multiplicity; therefore, no conclusions can be drawn for these outcomes.
Both studies reported both subjective and objective outcomes. Subjective outcomes can be prone to performance and detection bias; however, patients and all study personnel were blinded to the treatment assignment, so the risk of these biases is low.
A few scales and questionnaires were used in the pivotal studies for the evaluation of treatment effect of cenegermin (e.g., NEI-VFQ-25 and the modified Oxford scale). However, none of these instruments have been validated in patients with NK; therefore, it is unclear whether the results are valid, and whether an MID can be applied in the NK population.
HRQoL is an important clinical outcome for patients with NK, but this was not sufficiently measured; for example, ||| |||||| ||||| ||||| ||||| || | |||||| |||||| ||||| ||||| || ||| |||||||| ||| ||| |||||||| || |||||||. In addition, none of these 2 instrument have been validated in a patient population of NK, and no MID can be found to inform the clinical relevance of the study results.
NK is a chronic disease and recurrence rate could be high. There is a lack of data on re-treatment with cenegermin, so it is difficult to examine the efficacy and safety of multiple courses or maintenance therapy with cenegermin.
External Validity
According to the clinical experts consulted by CADTH, the inclusion criteria for the 2 pivotal studies were generally consistent with clinical practice. Based on the patients’ baseline characteristics, the study populations reflect a typical Canadian population that would receive cenegermin in practice. However, the stringent exclusion criteria can result in a highly selected population, which may not be completely representative of the NK population in Canada and can potentially limit the generalizability of the study results. According to the clinical experts consulted by CADTH, cenegermin can be offered to a broader population, such as those with a history of ocular surgery in the 3 months before cenegermin would be prescribed.
Cenegermin is the first medication that was approved to treat moderate to severe NK, so no active-controlled trial data are available to allow a comparison of relative efficacy and safety between cenegermin and other active treatments in the study population (e.g., AMT or tarsorrhaphy).
With respect to the study duration, the clinical experts indicated that the study duration and follow-up are sufficient to observe the treatment effect and safety profile of cenegermin.
Indirect Evidence
There is no indirect evidence submitted for this review.
A focused literature search for network meta-analyses dealing with Oxervate (cenegermin), recombinant human nerve growth factor, and neurotrophic keratitis was run in MEDLINE All (1946–) via Ovid and in Embase (1974–) via Ovid on November 22, 2021. No limits were applied.
No relevant indirect treatment comparison analyses were identified for this review.
Other Relevant Evidence
There are no other relevant studies submitted for this review.
Discussion
Summary of Available Evidence
Two phase II RCTs (NGF0212, N = 156; NGF0214, N = 48) submitted by the sponsor were included in this systematic review. The objectives of both studies were to evaluate the efficacy and safety of cenegermin eye drops in patients with moderate to severe NK. The studies included adults with a diagnosis of stage 2 or 3 NK. Eligible patients were randomized to receive cenegermin or vehicle therapy for 8 weeks. At the end of the 8-week controlled treatment period, patients in Study NGF0212 entered a 48- or 56-week follow-up period. Duration and treatment during the safety follow-up period were determined based on the randomized treatment received and the healing of PED or corneal ulcer. The follow-up period was 48 weeks (approximately 12 months) for patients who were initially randomized to cenegermin (10 mcg/mL or 20 mcg/mL), regardless of whether or not the patient was completely healed at week 8. The follow-up period was also 48 weeks for patients who were initially randomized to vehicle and who were completely healed at week 8. The follow-up period was 56 weeks for patients who were initially randomized to vehicle and who were not completely healed at week 8. These patients were randomly assigned to treatment with cenegermin (10 mcg/mL or 20 mcg/mL) for 8 weeks. In Study NGF0214, patients who completed the 8-week controlled treatment period entered a 24-week follow-up period. In both studies, all patients completely healed at week 8 (including those receiving active treatment) were eligible for another course of treatment in the event of relapse during the follow-up period.
The primary efficacy outcome was the proportion of patients achieving complete corneal healing at the week 4 (NGF0212) or week 8 (NGF0214) visit, determined by the central reading centre. Secondary efficacy outcomes analyzed in these 2 studies included corneal clearing, corneal sensitivity, disease deterioration, relapse, and HRQoL.
The key limitations of the 2 pivotal studies were imbalances in patients’ baseline characteristics between treatment groups and the potential impact on result interpretation, the small sample size of the studies, the lack of adjustment for multiple comparisons in the analyses for secondary and exploratory outcomes (there is an increased risk of false-positive conclusions, so definite conclusions cannot be drawn for these outcomes), and the lack of efficacy and safety data for the re-treatment of cenegermin in study population. In addition, there is no direct or indirect evidence comparing cenegermin with other therapies available in Canada for moderate to severe NK, such as AMT or tarsorrhaphy.
Interpretation of Results
Efficacy
Outcomes of corneal healing are relevant in clinical trials of NK. They are also identified by the clinicians and patients as important clinical outcomes. NK is a disease related to alterations in corneal nerves, leading to impairment in sensory and trophic function, with consequent breakdown of the corneal epithelium, which affects the health and integrity of the tear film, epithelium, and stroma.18 In theory, as a nerve growth factor, cenegermin has the potential to assist in corneal epithelium recovery and cure the disease.
Corneal healing was defined as the greatest diameter of corneal fluorescein staining in the area of the PED or corneal ulcer, and was assessed by the central reading centre evaluating the clinical pictures. In Study NGF0212, the complete healing of the PED or corneal ulcer at week 4, determined by the central reading centre, was achieved in 29 patients (58.0%) in the cenegermin 20 mcg/mL group and 10 patients (19.6%) in the vehicle control group. The difference in the percentage of patients who achieved complete healing at week 4 between the cenegermin 20 mcg/mL group and the vehicle control group was 38.4% (97.06% CI, 18.96 to 57.83; P < 0.001). Treatment with cenegermin was also related to the higher rate of corneal healing, compared with vehicle therapy, in Study NGF0214. In this study, the proportion of patients achieving complete corneal healing was 69.6% in the cenegermin-treated group versus 29.2% in the vehicle-treated group at week 8; the between-group difference was 40.4% (95% CI, 14.2 to 66.6; P = 0.006). The clinical experts consulted by CADTH indicated that the differences between cenegermin and vehicle are considered clinically relevant.
For the outcomes of corneal clearing and corneal sensitivity, between-group differences did not reach statistical significance. This could be related to the small sample sizes of the 2 pivotal studies and the insufficient power to detect a statistically significant difference between treatment groups in the secondary outcomes. It is a challenge to recruit patients to clinical trials of rare disease. According to the clinical expert consulted by CADTH, complete corneal clearing (grade 0 on the modified Oxford scale) is a more stringent measure than corneal healing (< 0.5 mm of lesion staining); therefore, even though it is an important clinical outcome for NK trials, it may not be the most clinically relevant measurement in practice.
In the included studies, substantial response rates were observed even in the vehicle group. According to the clinical experts consulted by CADTH, if patients were not receiving them before, lubricating eye drops can have an effect. The experts suggested that it would be reasonable to start with preservative-free lubricating eye drops or autologous serum tears, re-evaluate the patient after 1 or 2 months, and if there is no response or progression, then the patient can be offered cenegermin therapy.
Overall, the potential benefit of cenegermin on HRQoL remains unknown. The differences between cenegermin and vehicle in the overall composite score of NEI-VFQ-25 or the EQ-5D-5L health state score was not statistically significant. The relationship between the gains from corneal healing and improvement in patient’s HRQoL was unclear. This may be explained by the nature of the disease. Patients with NK may not experience severe symptoms, especially when decreased corneal sensation presents. Also, none of the HRQoL questionnaires has been validated in patient population of NK, so it is unknown if the scales can accurately reflect the change in corneal condition. Another possible explanation is that if only 1 eye is affected, patients are reliant on the other (healthy) eye, so improvement in the diseased eye might not result in substantial changes to HRQoL. Furthermore, for patients with very severe disease, the epithelial defect may be only 1 aspect of the pathology in the eye. Improvement of the epithelial defect in itself may not substantially impact a patient’s HRQoL.
No difference was found between cenegermin and vehicle in the reduction of risk for disease deterioration, which was defined as an “increase in the lesion size ≥ 1 mm, decrease in BCDVA by more than 5ETDRS letters, progression in lesion depth to corneal melting or perforation, or onset of infection.” For patients who had achieved complete corneal healing, 8 weeks of treatment with cenegermin was not associated with lower risk of recurrence of PED or corneal ulcer, although patients treated with cenegermin had a longer time to NK recurrence than those treated with vehicle. Different factors can influence the risk of disease recurrence, such as a patient’s underlying disease or treatment adherence. Subgroup analyses based on etiology of NK or severity of NK may be useful to explore the treatment effects of cenegermin in different subgroups of patients.
Based on the data available, it is unknown whether additional functional improvements could be achieved with longer or repeated courses of cenegermin therapy.
One implementation issue is that access to cornea specialists can be a challenge for patients living in remote areas. For patients who have no easy access to a cornea specialist, co-management with a cornea specialist and their local optometrist or ophthalmologist would be a solution, with periodic visits to the cornea specialist.
Harms
During the 8-week controlled treatment period of NGF0212 and NGF0214, the frequency of AEs was higher in the cenegermin group than in the vehicle group: 51.9% versus 38.5 in NGF0212; 91.3% versus 75.0% in NGF0214. Patients treated with cenegermin reported more eye pain: 9.6% versus 7.7% in NGF0212; 30.4% versus 8.3% in NGF0214. This is likely due to its potential effect on improving corneal sensation by stimulating regrowth of the nerve in patients with NK. According to input from patient groups, most patients considered these side effects of the treatment to be mild, and they resolved after the treatment was complete.
In the NGF0212 study, 9 patients (17.3%) in the cenegermin 20 mcg/mL group and 5 patients (9.6%) in the vehicle group experienced an SAE, whereas in Study NGF0214, 3 patients (13.0%) in the cenegermin 20 mcg/mL group and 4 patients (16.7%) in the vehicle group experienced an SAE. In Study NGF0212, 9 patients (17.3%) in the cenegermin 20 mcg/mL group and 4 patients (7.7%) in the vehicle control group experienced AEs that led to discontinuation of the study treatment, whereas in Study NGF0214, 5 patients (21.7%) in the antioxidant cenegermin 20 mcg/mL group and 7 patients (29.2%) in the antioxidant vehicle group discontinued the treatment due to AEs. ||||||| |||||||||||| ||||||||| |||||| |||||| ||| ||||||||| || || were the main reasons for SAEs and treatment discontinuation in these 2 studies.
One patient in the cenegermin group died during the controlled treatment period in Study NGF0212. The death was not considered to be related to the study drug.
Notable harms were ||||||||| ||||||||||| ||||||||| || ||| | |||||||, and patients in the cenegermin groups reported more such AEs than those in the vehicle group.
Safety data were analyzed during various treatment periods (controlled and follow-up). Significant safety signals were not detected.
Conclusions
Two phase II, double-blind, vehicle-controlled RCTs (NGF0212 and NGF0214) provided evidence supporting the efficacy and safety of cenegermin eye drops for the treatment of moderate to severe NK in adults. Compared with vehicle therapy, patients who were treated with 8-week cenegermin 20 mcg/mL showed benefits in increased corneal healing, and the difference in the proportion of patients achieving complete corneal healing between cenegermin and vehicle therapy were considered statistically and clinically relevant. However, whether treatment with cenegermin is associated with any HRQoL benefit remains uncertain. The beneficial effect of cenegermin on improving corneal sensitivity and reducing disease deterioration or recurrence is unclear, compared with vehicle therapy.
The incidence of AEs was higher in the cenegermin treatment group than in the vehicle group. The risks of SAEs and treatment discontinuation due to AEs were comparable between treatment groups in both NGF0212 and NGF0214. Patients treated with cenegermin reported more eye-related AEs than those treated with vehicle therapy.
At this stage, there is a lack of evidence to support the longer-term efficacy and safety of re-treatment with cenegermin for patients who relapse. In addition, there is no direct or indirect evidence comparing cenegermin with relevant comparators used in clinical practice, such as AMT or tarsorrhaphy.
References
1.Mackie IA. Neuroparalytic keratitis. In: Fraunfelder F, Roy FH, Meyer SM, eds. Current ocular therapy. Philadelphia (PA): WB Saunders; 1995:452-454.
2.Dohlman TH, Singh RB, Dana R. Advances in the medical management of neurotrophic keratitis. Semin Ophthalmol. 2021;36(4):335-340. PubMed
3.Akpek EK, Afshari N, Ahmad S, et al. An evidence-based approach to the diagnosis and treatment of neurotrophic keratitis. Baltimore (MD): Johns Hopkins Medicine; 2020: https://hopkinscme.cloud-cme.com/assets/hopkinscme/Presentations/28879/28879.pdf Accessed 2022 Jan 25.
4.Dana R, Farid M, Gupta PK, et al. Expert consensus on the identification, diagnosis, and treatment of neurotrophic keratopathy. BMC Ophthalmol. 2021;21(1):327. PubMed
5.Oxervate (cenegermin ophthalmic solution): 0.002% (20 mcg/mL) topical eye drops [product monograph]. Milano (IT): Dompé Farmaceutici S.p.A.; 2019 Feb 8.
6.Clinical Study Report: NGF0212. An 8-week phase I/II, multicenter, randomized, double-masked, vehicle-controlled parallel-group study with a 48-or-56-week follow-up period to evaluate the safety and efficacy of two doses (10 μg/ml and 20 μg/ml) of recombinant human nerve growth factor eye drops solution versus vehicle in patients with stage 2 and 3 of neurotrophic keratitis [internal sponsor’s report]. Milan (IT): Dompé farmaceutici s.p.a.; 2016 Apr 18.
7.Clinical Study Report: NGF0214. An 8-week phase II, multicenter, randomized, double-masked, vehicle controlled, parallel group study with a 24 or 32 week follow-up period to evaluate the efficacy of a formulation containing axti-oxidant of recombinant human nerve growth factor (rhNGF) in 20 μg/ml, eye drops solution versus vehicle containing anti-oxidant in patients with Stage 2 and 3 neurotrophic keratitis [internal sponsor’s report]. Milan (IT): Dompé Farmaceutici S.p.a; 2016 Oct 04.
8.Drug Reimbursement Review sponsor submission: Oxervate (cenegermin ophthalmic solution), 0.002% (20 mcg/mL) topical eye drops preservative-free [internal sponsor’s package]. Oakville (ON): Dompé Farmaceutici S.p.A; 2021 Oct 25.
9.McGowan J, Sampson M, Salzwedel DM, Cogo E, Foerster V, Lefebvre C. PRESS Peer Review of Electronic Search Strategies: 2015 guideline statement. J Clin Epidemiol. 2016;75:40-46. PubMed
10.Grey matters: a practical tool for searching health-related grey literature. Ottawa (ON): CADTH; 2019: https://www.cadth.ca/grey-matters. Accessed 2021 Nov 17.
11.Bonini S, Lambiase A, Rama P, et al. Phase II randomized, double-masked, vehicle-controlled trial of recombinant human nerve growth factor for neurotrophic keratitis. Ophthalmology. 2018;125(9):1332-1343. PubMed
12.Pflugfelder SC, Massaro-Giordano M, Perez VL, et al. Topical recombinant human nerve growth factor (cenegermin) for neurotrophic keratopathy: a multicenter randomized vehicle-controlled pivotal trial. Ophthalmology. 2020;127(1):14-26. PubMed
13.Health Canada reviewer’s report: Oxervate (cenegermin) [internal sponsor’s report]. In: Drug Reimbursement Review sponsor submission: Oxervate (cenegermin ophthalmic solution), 0.002% (20 mcg/mL) topical eye drops preservative-free. Oakville (ON): Dompé Farmaceutici S.p.A; 2021 Oct 25.
14.Center for Drug Evaluation Research. Medical review(s). Oxervate (cenegermin-bkbj) eye drops. Company: Dompé farmaceutici S.p.A. Application No.:761094. Approval date: 08/22/2018 (FDA approval package). Silver Spring (MD): U.S. Food and Drug Administration (FDA); 2018: https://www.accessdata.fda.gov/drugsatfda_docs/nda/2018/761094Orig1s000TOC.cfm. Accessed 2021 Nov 22.
15.Committee for Medicinal Products for Human Use. Assessment report: Oxervate (cenegermin). (European public assessment report). Amsterdam (NL): European Medicines Agency; 2017 May 18: https://www.ema.europa.eu/en/documents/assessment-report/oxervate-epar-public-assessment-report_en.pdf Accessed 2022 Feb 03.
16.Jones LW, Srinivasan S, Ng A, Schulze M. Diagnostic instruments. In: Efron N, ed. Contact lens practice. 3rd ed. Amsterdam (NL): Elsevier Ltd; 2018:327-345.
17.EyeWiki. Corneal esthesiometry. 2022; https://eyewiki.aao.org/Corneal_Esthesiometry. Accessed 2022 Feb 3.
18.Dua HS, Said DG, Messmer EM, et al. Neurotrophic keratopathy. Prog Retin Eye Res. 2018;66:107-131. PubMed
19.Bron AJ, Evans VE, Smith JA. Grading of corneal and conjunctival staining in the context of other dry eye tests. Cornea. 2003;22(7):640-650. PubMed
20.Leonardi A, Dupuis-Deniaud M, Bremond-Gignac D. Clinical efficacy assessment in severe vernal keratoconjunctivitis: preliminary validation of a new penalties-adjusted corneal fluorescein staining score. J Mark Access Health Policy. 2020;8(1):1748492. PubMed
21.Kniestedt C, Stamper RL. Visual acuity and its measurement. Ophthalmol Clin North Am. 2003;16(2):155-170. PubMed
22.Beck RW, Moke PS, Turpin AH, et al. A computerized method of visual acuity testing: adaptation of the early treatment of diabetic retinopathy study testing protocol. Am J Ophthalmol. 2003;135(2):194-205. PubMed
23.Chaikitmongkol V, Nanegrungsunk O, Patikulsila D, Ruamviboonsuk P, Bressler NM. Repeatability and agreement of visual acuity using the ETDRS number chart, Landolt C chart, or ETDRS alphabet chart in eyes with or without sight-threatening diseases. JAMA Ophthalmol. 2018;136(3):286-290. PubMed
24.Beck RW, Maguire MG, Bressler NM, Glassman AR, Lindblad AS, Ferris FL. Visual acuity as an outcome measure in clinical trials of retinal diseases. Ophthalmology. 2007;114(10):1804-1809. PubMed
25.Center for Drug Evaluation and Research. Statistical review(s). Ozurdex (dexamethasone intravitreal implant). Company: Allergan, Inc. Application no.: 022315. Approval date: 6/17/2009 (FDA drug approval package). Rockville (MD): U.S. Food and Drug Administration (FDA); 2009: https://www.accessdata.fda.gov/drugsatfda_docs/nda/2009/022315_ozurdex_toc.cfm. Accessed 2021 Dec 20.
26.Mangione CM, Lee PP, Gutierrez PR, et al. Development of the 25-item National Eye Institute Visual Function Questionnaire. Arch Ophthalmol. 2001;119(7):1050-1058. PubMed
27.Lloyd AJ, Loftus J, Turner M, Lai G, Pleil A. Psychometric validation of the Visual Function Questionnaire-25 in patients with diabetic macular edema. Health Qual Life Outcomes. 2013;11:10. PubMed
28.Marella M, Pesudovs K, Keeffe JE, O’Connor PM, Rees G, Lamoureux EL. The psychometric validity of the NEI VFQ-25 for use in a low-vision population. Invest Ophthalmol Vis Sci. 2010;51(6):2878-2884. PubMed
29.Pesudovs K, Gothwal VK, Wright T, Lamoureux EL. Remediating serious flaws in the National Eye Institute Visual Function Questionnaire. J Cataract Refract Surg. 2010;36(5):718-732. PubMed
30.Thevi T, Abas AL, Stephanie Yen Li C. Comparison between the English and Bahasa Malaysia language versions of the Visual Functioning Questionnaire (VFQ-25) for use in patients with cataracts. BMC Ophthalmol. 2021;21(1):348. PubMed
31.Sivaprasad S, Tschosik E, Kapre A, et al. Reliability and construct validity of the NEI VFQ-25 in a subset of patients with geographic atrophy from the phase 2 Mahalo study. Am J Ophthalmol. 2018;190:1-8. PubMed
32.Naik RK, Gries KS, Rentz AM, Kowalski JW, Revicki DA. Psychometric evaluation of the National Eye Institute Visual Function Questionnaire and Visual Function Questionnaire Utility Index in patients with non-infectious intermediate and posterior uveitis. Qual Life Res. 2013;22(10):2801-2808. PubMed
33.Sugar EA, Burke AE, Venugopal V, et al. Responsiveness of vision-specific and general quality of life metrics to ocular and systemic events in patients with uveitis. Ophthalmology. 2020;127(12):1710-1718. PubMed
34.Burr JM, Cooper D, Ramsay CR, Che Hamzah J, Azuara-Blanco A. Interpretation of change scores for the National Eye Institute Visual Function Questionnaire-25: the minimally important difference. Br J Ophthalmol. 2021;18:18. PubMed
35.Lloyd AJ, Loftus J, Turner M, Lai G, Pleil A. Psychometric validation of the Visual Function Questionnaire-25 in patients with diabetic macular edema. Health Qual Life Outcomes. 2013;11:10. PubMed
36.EuroQol Research Foundation. EQ-5D-5L. About. https://euroqol.org/eq-5d-instruments/eq-5d-5l-about/. Accessed 2022 Jan 4.
37.Tewari HK, Kori V, Sony P, Venkatesh P, Garg S. Snellen chart may be preferable over early treatment diabetic retinopathy study charts for rapid visual acuity assessment. Indian J Ophthalmol. 2006;54(3):214. PubMed
38.Rosenfeld PJ, Brown DM, Heier JS, et al. Ranibizumab for neovascular age-related macular degeneration. N Engl J Med. 2006;355(14):1419-1431. PubMed
39.Brown DM, Kaiser PK, Michels M, et al. Ranibizumab versus verteporfin for neovascular age-related macular degeneration. N Engl J Med. 2006;355(14):1432-1444. PubMed
40.Dong LM, Childs AL, Mangione CM, et al. Health- and vision-related quality of life among patients with choroidal neovascularization secondary to age-related macular degeneration at enrollment in randomized trials of submacular surgery: SST report no. 4. Am J Ophthalmol. 2004;138(1):91-108. PubMed
41.CATT: comparison of age-related macular degeneration treatment trials. ETDRS chart worksheet. Philadelphia (PA): University of Pennsylvania; 2014.
42.Ricci F, Cedrone C, Cerulli L. Standardized measurement of visual acuity. Ophthalmic Epidemiol. 1998;5(1):41-53. PubMed
43.Gangnon RE, Davis MD, Hubbard LD, et al. A severity scale for diabetic macular edema developed from ETDRS data. Invest Ophthalmol Vis Sci. 2008;49(11):5041-5047. PubMed
44.Early Treatment Diabetic Retinopathy Study Research Group. Photocoagulation for diabetic macular edema. Early treatment diabetic retinopathy study report number 1. Arch Ophthalmol. 1985;103(12):1796-1806. PubMed
45.Slakter JS, Stur M. Quality of life in patients with age-related macular degeneration: impact of the condition and benefits of treatment. Surv Ophthalmol. 2005;50(3):263-273. PubMed
46.Joussen AM, Lehmacher W, Hilgers RD, Kirchhof B. Is significant relevant? Validity and patient benefit of randomized controlled clinical trials on age-related macular degeneration. Surv Ophthalmol. 2007;52(3):266-278. PubMed
47.Mangione CM, Berry S, Spritzer K, et al. Identifying the content area for the 51-item National Eye Institute Visual Function Questionnaire: results from focus groups with visually impaired persons. Arch Ophthalmol. 1998;116(2):227-233. PubMed
48.Hazel CA, Petre KL, Armstrong RA, Benson MT, Frost NA. Visual function and subjective quality of life compared in subjects with acquired macular disease. Invest Ophthalmol Vis Sci. 2000;41(6):1309-1315. PubMed
49.Rosser DA, Cousens SN, Murdoch IE, Fitzke FW, Laidlaw DA. How sensitive to clinical change are ETDRS logMAR visual acuity measurements? Invest Ophthalmol Vis Sci. 2003;44(8):3278-3281. PubMed
50.Mangione CM, Lee PP, Pitts J, et al. Psychometric properties of the National Eye Institute Visual Function Questionnaire (NEI-VFQ). Arch Ophthalmol. 1998;116(11):1496-1504. PubMed
51.Dougherty BE, Bullimore MA. Comparison of scoring approaches for the NEI VFQ-25 in low vision. Optom Vis Sci. 2010;87(8):543-548. PubMed
52.Orr P, Rentz AM, Margolis MK, et al. Validation of the National Eye Institute Visual Function Questionnaire-25 (NEI VFQ-25) in age-related macular degeneration. Invest Ophthalmol Vis Sci. 2011;52(6):3354-3359. PubMed
53.Revicki DA, Rentz AM, Harnam N, Thomas VS, Lanzetta P. Reliability and validity of the National Eye Institute Visual Function Questionnaire-25 in patients with age-related macular degeneration. Invest Ophthalmol Vis Sci. 2010;51(2):712-717. PubMed
54.Brooks R. EuroQol: the current state of play. Health Policy. 1996;37(1):53-72. PubMed
55.EuroQol Group. EuroQol--a new facility for the measurement of health-related quality of life. Health Policy. 1990;16(3):199-208. PubMed
56.EuroQol Research Foundation. EQ-5D-5L user guide: basic information on how to use the EQ-5D-5L instrument. 2019: https://euroqol.org/wp-content/uploads/2021/01/EQ-5D-5LUserguide-08-0421.pdf. Accessed 2021 Nov 24.
57.Ameri H, Yousefi M, Yaseri M, Nahvijou A, Arab M, Akbari Sari A. Mapping the cancer-specific QLQ-C30 onto the generic EQ-5D-5L and SF-6D in colorectal cancer patients. Expert rev. 2019;19(1):89-96.
58.Sinnott PL, Joyce VR, Barnett PG. Guidebook: preference measurement in economic analysis. Menlo Park (CA): VA Palo Alto, Health Economics Research Center; 2007: https://www.herc.research.va.gov/files/BOOK_419.pdf. Accessed 2021 Nov 24.
Appendix 1: Literature Search Strategy
Note that this appendix has not been copy-edited.
Clinical Literature Search
Overview
Interface: Ovid
Databases
MEDLINE All (1946-present)
Embase (1974-present)
Note: Subject headings and search fields have been customized for each database. Duplicates between databases were removed in Ovid.
Date of search: November 22, 2021
Alerts: Weekly search updates until project completion
Search filters applied: No filters were applied to limit the retrieval by study type.
Limits
Publication date limit: none
Language limit: none
Conference abstracts: excluded
Syntax | Description |
|---|---|
/ | At the end of a phrase, searches the phrase as a subject heading |
MeSH | Medical Subject Heading |
exp | Explode a subject heading |
* | Before a word, indicates that the marked subject heading is a primary topic; or, after a word, a truncation symbol (wildcard) to retrieve plurals or varying endings |
# | Truncation symbol for one character |
adj# | Requires terms to be adjacent to each other within # number of words (in any order) |
.ti | Title |
.ot | Original title |
.ab | Abstract |
.hw | Heading word; usually includes subject headings and controlled vocabulary |
.kf | Keyword heading word |
.dq | Candidate term word (Embase) |
.pt | Publication type |
.rn | Registry number |
.nm | Name of substance word (MEDLINE) |
medall | Ovid database code: MEDLINE All, 1946 to present, updated daily |
oemezd | Ovid database code; Embase, 1974 to present, updated daily |
Multi-Database Strategy
(cenegermin* or Oxervate* or B6E7K36KT8).ti,ab,kf,ot,hw,nm,rn.
exp Keratitis/
(keratopath* or keratitis*).ti,ab,kf.
(ulcer adj3 cornea*).ti,ab,kf.
(neurotrophic adj3 (epitheliopath* or epitheli* or cornea*)).ti,ab,kf.
or/2-5
(Nerve Growth Factor/ or Nerve Growth Factors/) and recombinant.ti,ab,kf.
(rh-NGF or rhNGF).ti,ab,kf.
(recombinant adj5 ((nerve adj3 growth adj3 factor*) or (astrocyte* adj3 proliferation* adj3 factor*) or (astroglial* adj3 proliferation* adj3 factor*))).ti,ab,kf.
or/7-9
6 and 10
1 or 11
12 use medall
*cenegermin/ or (cenegermin* or Oxervate*).ti,ab,kf,dq.
Neurotrophic keratopathy/
(keratopath* or keratitis*).ti,ab,kf.
(ulcer adj3 cornea*).ti,ab,kf.
(neurotrophic adj3 (epitheliopath* or epitheli* or cornea*)).ti,ab,kf.
or/15-18
Recombinant nerve growth factor/
(rh-NGF or rhNGF).ti,ab,kf,dq.
(recombinant adj5 ((nerve adj3 growth adj3 factor*) or (astrocyte* adj3 proliferation* adj3 factor*) or (astroglial* adj3 proliferation* adj3 factor*))).ti,ab,kf,dq.
or/20-22
19 and 23
14 or 24
25 use oemezd
26 not (conference abstract or conference review).pt.
13 or 27
remove duplicates from 28
Clinical Trials Registries
ClinicalTrials.gov
Produced by the US National Library of Medicine. Targeted search used to capture registered clinical trials.
[Search terms: Oxervate (cenegermin), recombinant human nerve growth factor, neurotrophic keratitis]
WHO ICTRP
International Clinical Trials Registry Platform, produced by the WHO. Targeted search used to capture registered clinical trials.
[Search terms: Oxervate (cenegermin), recombinant human nerve growth factor, neurotrophic keratitis]
Health Canada’s Clinical Trials Database
Produced by Health Canada. Targeted search used to capture registered clinical trials.
[Search terms: Oxervate (cenegermin), recombinant human nerve growth factor, neurotrophic keratitis]
EU Clinical Trials Register
European Union Clinical Trials Register, produced by the European Union. Targeted search used to capture registered clinical trials.
[Search terms: Oxervate (cenegermin), recombinant human nerve growth factor, neurotrophic keratitis]
Grey Literature
Search dates: November 16 to 22, 2021
Keywords: Oxervate (cenegermin), recombinant human nerve growth factor, neurotrophic keratitis
Limits: Publication years: none
Updated: Search updated before the completion of stakeholder feedback period
Relevant websites from the following sections of the CADTH grey literature checklist Grey Matters: A Practical Tool for Searching Health-Related Grey Literature were searched:
Health Technology Assessment Agencies
Health Economics
Clinical Practice Guidelines
Drug and Device Regulatory Approvals
Advisories and Warnings
Drug Class Reviews
Clinical Trials Registries
Databases (free)
Internet Search
Open Access Journals
Appendix 2: Description and Appraisal of Outcome Measures
Note that this appendix has not been copy-edited.
Aim
To describe the following outcome measures and their measurement properties (validity, reliability, responsiveness to change, and MID):
Modified Oxford scale
Best Corrected Visual Acuity (BCVA) measurement with the Early Treatment Diabetic Retinopathy Study (ETDRS) visual acuity chart
National Eye Institute Visual Function Questionnaire-25 items (NEI-VFQ-25)
EQ-5D-5L
Findings
A focused literature search was conducted to identify the psychometric properties and the MID of each of the stated outcome measures. The findings on reliability, validity, responsiveness, and the MID of each outcome measure are summarized in Table 17.
Table 17: Summary of Outcome Measures and Their Measurement Properties
Outcome measure | Type | Conclusions about measurement properties | MID |
|---|---|---|---|
Modified Oxford scale | The original Oxford grading system19 was developed to quantify the amount of epithelial surface damage in patients with dry eye. Following instillation with a dye, the eye is assessed under slit lamp examination and compared with a panel of illustrations representing various degrees of severity of corneal staining. The original grading system consists of 6 grades (absent, minimal, mild, moderate, marked, and severe); the modified version includes 1 additional grade (complete corneal clearing).19,20 | Not assessed in neurotrophic keratitis patients or in patients with eye disorders. | Not assessed in neurotrophic keratitis patients or in patients with eye disorders. |
ETDRS charts | Developed to measure visual acuity. Patients are presented a series of 5 letters of equal difficulty on each line, with standardized spacing between letters and rows. Letters range from 58.18 to 2.92 mm in height, corresponding to Snellen visual acuity fractions of 20/200 to 20/10, respectively. Letter size increases geometrically and equivalently by a factor of 1.2589 (0.1 log unit) per line, moving up the chart (for a total of 14 lines/70 letters).21 | Not assessed in neurotrophic keratitis patients. In patients with and without eye disorders: Reliability: Strong test-retest reliability across patient groups with different levels of visual acuity (< 20/100 to ≥ 20/20): r = 0.70 to 0.95.22,23 For eyes > 20/100, a change in visual acuity of 5 or more letters has a greater than 90% probability of being a real change. For eyes, 20/100, a change of 10 or more letters is required for the same reliability.24 | Not assessed in neurotrophic keratitis patients. In patients with eye disorders: In a review of phase III trials for a treatment for macular edema, the primary efficacy end point was the proportion of patients achieving ≥ 15 points improvement on the ETDRS.25 |
NEI-VFQ-25 | Measures vision-targeted health-related quality of life. Includes 25 items relevant to 11 vision-related constructs, in addition to a single-item general health component. An overall composite score is calculated as the mean of 25 items. Scores for each item and the composite score range from 0 (worst vision functioning) to 100 (best vision functioning).26 | Not assessed in neurotrophic keratitis patients. In patients with eye disorders: Validity: Low to moderate correlations with the ETDRS (r = 0.10 to 0.41) and the EQ-5D-3L VAS (r = 0.16 to 0.43) in patients with diabetic macular edema.27 Moderate correlations with the ETDRS visual acuity for the general vision (r = 0.65) and distance vision (r = 0.66) scores in the worse eye of patients with an eye condition or low vision.26 Improved convergent validity when split into 2 factors (r = 0.59 to 0.84)28,29 or 3 factors (r = 0.42 to 0.74).30 In patients with geographic atrophy: moderate correlations with the MNREAD and the FRI index score for the composite and distance activities scores (r = 0.57 to 0.69).31 Known-groups validity testing identified differences between scores and the mean maximum MNREAD reading speed (≥ 80 vs. < 80 words per minute) and the mean FRI index score (≥ 2.5 vs. < 2.5).31 Reliability: Good internal consistency reliability among patients with eye conditions or low vision (alpha = 0.71 to 0.85).26 Good test-retest reliability in patients with uveitis: ICC > 0.7 for all items except for general vision (ICC = 0.58)32 and in patients with geographic atrophy with ICC values of 0.80, 0.84, and 0.86 for each subscale of near activity, distance activity, and the composite score, respectively.31 Responsiveness: For every 5-letter change in VA there was a corresponding change of 2.70 points (95% CI, 2.12 to 3.29) in patients with uveitis.33 | Not assessed in neurotrophic keratitis patients. In patients with eye disorders; for the composite visual functioning score: 4 to 11 points based on 4 anchor-based methods among patients with PAC or PACG; 5.8 points (median value of 3 anchor-based methods).34 Among patients with macular edema: 3.33 points (SEM-based method); 6.13 points (½ SD-based method).35 |
EQ-5D-5L | Generic preference based HRQoL scale consisting of a VAS with values between 100 (best imaginable health) and 0 (worst imaginable health) as judged by the patient. A composite index score of 5 dimensions: mobility, self-care, usual activities, pain/discomfort, and anxiety/ depression. Five response levels for each dimension ranging from experiencing no problems to extreme problems.36 | Not assessed in neurotrophic keratitis patients or in patients with eye disorders. | Not assessed in neurotrophic keratitis patients or in patients with eye disorders. |
CI = confidence interval; ETDRS = Early Treatment Diabetic Retinopathy Study; FRI = Functional Reading Independence; HRQoL = health-related quality of life; ICC = intraclass correlation coefficient; MID = minimal important difference; MNREAD = Minnesota Low-Vision Reading Test; NEI-VFQ-25 = National Eye Institute Visual Function Questionnaire-25; PAC = Primary Angle Closure; PACG = Primary Angle Closure Glaucoma; SD = standard deviation; SEM = standard error mean; VA = visual acuity; VAS = visual analogue scale
No literature was identified that assessed validity, responsiveness, or reliability in patients with NK. No MID information was identified in populations with NK.
Studies assessing the psychometric properties of the instruments are only summarized if the assessment was done for the English version and in a sample of patients where the majority had an eye disorder.
Modified Oxford Scale
Scoring
The original Oxford Grading Scale, also referred to as the Oxford Grading System, was developed to quantify the amount of epithelial surface damage in patients with dry eye.19 The scale uses a series of simplified illustrative panels of the ocular surface with each panel featuring different densities of dots (which represent appearance of staining with a dye).19 The panels are lettered A to E (with corresponding dot counts) in order of increasing severity of staining. The number of dots increases by 1 log unit between panel A and B and by 0.5 log unit between panels B to E inclusive. The panels are used as a guide to grade the degree of staining seen in the patient.19 The grades are as follows: 0 = absent, I = minimal, II = mild, III = moderate, IV = marked, and V = severe.19 The eye is examined under a slit lamp microscope (using consistent magnification and illumination settings) and a dye is instilled (fluorescein, rose Bengal, and/or lissamine green).19 The examiner raises the patient’s upper eyelid slightly to observe the entire corneal surface.19 The temporal, interpalpebral and nasal conjunctiva are examined as the patient looks nasally and temporally along the horizontal plane, respectively.19 The examiner then compares the overall appearance of ocular staining with the panels to determine the most representative grade.19 The modified Oxford scale is reported to have a 7-point ordinal scale for ocular staining (0, 0.5, 1, 2, 3, 4 and 5) where 0 represents complete corneal clearing.19,20 The NGF0212 and NGF0214 trials used a binary variable: ‘Complete clearing’ and ‘Non-complete clearing;’ where complete clearing, defined as complete absence of staining, was equal to grade 0 on the modified Oxford scale and non-complete clearing was all other non-missing values.6,7
The original Oxford Grading Scale was developed for use in patients with dry eye and its validity, reliability, and responsiveness in patients with NK or other related eye disorders is unknown. As stated in the original article describing the scale, “Because the grading charts used were devised to represent patterns of staining commonly encountered in dry eye, its use is not recommended to quantify staining in other ocular surface disorders.”19 This limitation was also noted in a 2020 study on severe vernal keratoconjunctivitis (VKC) which stated that the pattern of corneal and conjunctival staining differed in patients with VKC than in those with dry eye disease.20
Early Treatment Diabetic Retinopathy Study Charts
Scoring
In the NGF0212 and NGF0214 clinical trials, the best corrected distance visual acuity (BCDVA) was measured at scheduled study visits using the Early Treatment Diabetic Retinopathy Study (ETDRS) letters visual acuity chart at 4 m (13 feet) before the administration of any eye drops.6,7 The ETDRS charts are based on a design by Bailey and Lovie and are commonly used in clinical research.21,37-40 ETDRS charts present a series of 5 letters of equal difficulty on each row with standardized spacing between letters and rows, for a total of 14 lines (70 letters). When 20 or more letters are read correctly at 4 m; the visual acuity letter score is equal to the total number of letters read correctly at 4 m plus 30. If less than 20 letters are read correctly at 4 m, the visual acuity letter score is equal to the total number of letters read correctly at 4 m (number of letters recorded on line 1), plus the total number of letters read correctly at 1 m in the first 6 lines. Therefore, the ETDRS letter score could result in a maximum score of 100.22,41
Charts are used in a standard light box with a background illumination of approximately 150 cd/m2. ETDRS results can be converted to Snellen fractions, another common measure of visual acuity, in which the numerator indicates the distance at which the chart was read, and the denominator the distance at which a person with normal eyesight may discern letters of a particular size. A larger denominator indicates worsening vision. For example, a person with 20/100 vision can read letters at 20 feet that a person with 20/20 vision could read at 100 feet.21,42 ETDRS letters range from 58.18 mm to 2.92 mm in height corresponding to Snellen visual acuity fractions of 20/200 to 20/10 respectively. Further, letter size increases geometrically and equivalently in every line by a factor of 1.2589 (or 0.1 log unit) moving up the chart. Scoring for ETDRS charts is designed to produce a logarithmic score (logMAR) suitable for statistical analysis in which individual letters score 0.02 log units.21
With regards to the relationship between visual acuity measurement and visual function, a loss of 3 or more lines (greater than or equal to 15 letters) on an ETDRS chart corresponds to a doubling of the visual angle and is considered moderate visual loss.43,44 However, visual acuity is only 1 component contributing to overall visual function and the ability to perform everyday visual tasks (e.g., reading, recognizing faces, driving and using the telephone). Overall visual function also depends upon variables such as contrast sensitivity, near vision, colour vision, and sensitivity to glare.45 The various components of visual function will affect the performance of different vision-related tasks by varying degrees. For example, the use of distance acuity to measure the success of treatments for age-related macular degeneration is not optimal given that distance vision is usually 2 ETDRS lines better than reading vision,46 and difficulties with reading is a common complaint among persons with eye disease.47 Rather, contrast sensitivity is a more important contributor to reading performance.46,48
Psychometric Properties
Reliability
Chaikitmongkol et al. (2018)23 examined the repeatability of the ETDRS among 154 adult patients with healthy eyes and eye conditions such as age-related cataract, diabetic macular edema, or age-related macular degeneration. Patients were divided into 4 groups according to their visual acuity (VA) and performed 2 standardized BCVA measurements 30 minutes apart on 3 different Precision Vision ETDRS charts (PV number, Landolt C, and alphabet). Results for the alphabet ETDRS chart (as used in the NGF0212 and NGF0214 trials) showed strong Pearson correlation coefficients;, ranging from 0.93 for those with 20/125 to 20/200 VA to 0.70 for those with 20/20 to 20/25 VA. Similar results were found by Beck et al. (2003)22 in a study examining the test-retest reliability of the ETDRS among 265 patients (mean age: 50 ± 22 years) of which 72% had eye disease. Patients were divided into 3 groups according to their VA values from their initial ETDRS test. Results showed consistently high correlation values between initial and repeat tests across all 3 groups, ranging from 0.86 to 0.95. The study concluded that a change of 10 letters in VA from baseline is likely not related to measurement variability. ETDRS charts may reliably identify changes in visual acuity of 2 lines (10 letters) or more, but not changes of 1 line (5 letters) or less.49 For eyes with acuity better than 20/100, a change in visual acuity of 5 or more letters has a greater than 90% probability of being a real change, while for eyes worse than 20/100, a change of 10 or more letters is required for the same reliability.24
MID
A loss or gain of 3 lines (15 letters) is considered a moderate degree of change and is commonly used as a outcome in clinical trials.46 In a review of phase III trials for a treatment for macular edema, the primary efficacy end point was the proportion of patients achieving at least 15 points improvement on the ETDRS.25
No studies examining the validity or responsiveness of the English version of the NEI-VFQ-25 among patients with eye disorders were identified.
National Eye Institute Visual Function Questionnaire-25
Scoring
The NEI-VFQ was developed to measure vision-targeted HRQoL. The original 51-item questionnaire was developed based on focus groups comprised of persons with a number of common eye conditions (e.g., age-related cataracts, age-related macular degeneration, and diabetic retinopathy).47 The original questionnaire comprises 12 subscales related to general vision, ocular pain, near vision, distance vision, social functioning, mental health, role functioning, dependency, driving, peripheral vision, colour vision, and expectations for future vision. In addition, the questionnaire includes 1 general health subscale.50 A shorter version of the original instrument, the NEI-VFQ-25, was subsequently developed, which retained the multidimensional nature of the original, and is more practical and efficient to administer.26 With the exception of the expectations for future vision, all the constructs listed above were retained in the shortened version, with a reduced number of items within each subscale. Thus, the NEI-VFQ-25 includes 25 items relevant to 11 vision-related constructs, in addition to a single-item general health component. Responses for each item are converted to a 0 to 100 scale, with 0 representing the worst, and 100 the best visual functioning. Items within each construct, or subscale, are averaged to create 12 subscale scores, and averaging of the subscale scores produces the overall composite score. Different scoring approaches for the NEI-VFQ-25 have been proposed.51 Rasch modelling is used to obtain measurements from categorical data. When comparing standard scoring to Rasch analysis and an algorithm to approximate Rasch scores, all methods were highly correlated.51 However, standard scoring is subject to floor and ceiling effects whereby the ability of the least visually able is overestimated and the ability of the most visually able is underestimated.51
Psychometric Properties
Validity
Both versions of the NEI-VFQ were reported to have strong construct validity measures among patients with a wide range of eye conditions26,27 and all but 2 subscale scores (general health and ocular pain) have been shown to be responsive to changes in visual acuity in the better-seeing eye in patients with age-related macular degeneration.52,53 However, some assessments of the psychometric validity of the NEI-VFQ-25 using Rasch scoring and principal component analysis in patients with low vision due to various eye conditions have identified issues with multidimensionality (measurement of more than 1 construct) and poor performance of the subscales.28,29,53 The NEI-VFQ-25 subscales were found to have too few items and were unable to discriminate among the population under measurement who had low visions due to conditions such as retinal diseases, glaucoma, or cataracts and thus were not valid.28,29 Re-engineering the NEI-VFQ-25 into 2 factors (visual functioning and socio-emotional factors) and removing misfit items (e.g., pain around eyes, general health and driving in difficult conditions) improved the psychometric validity of the scale in individuals with low vision with correlation scores ranging from 0.59 to 0.84.28,29 A study by Thevi et al. (2021)30 among patients with cataracts also condensed the items within the NEI-VFQ-25 questionnaire into factors and determined its construct validity. This resulted in 3 main factors: difficulty with activities (9 items), responses to vision (6 items), and general health and vision (3 items). The correlation coefficients for items in each factor ranged from 0.422 to 0.737, indicating that the 3-factor model fits the data well. However, certain items were excluded from the model including driving at night and driving in difficult conditions, accomplishment, limitation of work activities, and pain discomfort. These study results suggest that, among patients with cataracts, the scale would benefit from scale splitting and considering the evidence of multidimensionality, the validity of the single composite score of the NEI-VFQ-25 may be questioned among patients with NK.
In 1 study of patients with diabetic macular edema (DME), convergent validity analysis to examine the relationship between NEI-VFQ-25 scores and other disease-related variables provided mixed results and the NEI-VFQ-25 subscales collectively showed low to moderate correlations with ETDRS visual acuity score for both the study and untreated eyes.35 The Pearson correlation with ETDRS total letters ranged from 0.10 to 0.41 for the study eye with reported values of 0.35 for the near vision subscale and 0.34 for the distance vision subscale.35 Low to moderate correlations were observed between the NEI-VFQ-25 subscales and the EQ-5D-3L Visual Analogue Scale (VAS) ranging from 0.16 for role difficulties to 0.43 for general health; with slightly higher correlations for subscales not related to visual acuity. This suggests that the NEI-VFQ-25 may consider general health measures in addition to vision specific measures. In terms of known group validity, patients who saw more ETDRS letters also scored higher on the NEI-VFQ-25 near and distance subscales as well as on the NEI-VFQ-25 composite. Overall, the authors concluded that despite its documented limitations and the need for an improved instrument, the NEI-VFQ-25 demonstrated a degree of validity to measure HRQoL in patients with DME.35 In a more recent study among patients with geographic atrophy,31 convergent validity was assessed by correlating the NEI-VFQ-25 composite score, near activities, and distance activities with the Minnesota Low-Vision Reading Test (MNRead) binocular reading speed and the Functional Reading Independence (FRI) index score.31 Results indicated moderate correlations with the MNRead with r = 0.61, 0.69, 0.57 and the FRI index score with r = 0.69, 0.73, 0.64 for each of the NEI-VFQ-25 composite score, near activities, and distance activities, respectively. Known-groups validity testing for the baseline mean values of the composite score, near activities, and distance activities identified differences between patients by mean maximum MNRead reading speed (≥ 80 versus < 80 words per minute) and by mean FRI index score (≥ 2.5 versus < 2.5) indicating the ability of the instrument to differentiate between groups.
A study by Mangione et al., (2001)26 among patients across 2 samples (n = 859) with low vision or a chronic eye condition (i.e., age-related cataracts or macular degeneration, diabetic retinopathy, primary open-angle glaucoma, or cytomegalovirus retinitis). Known-group comparisons found significant differences in scores between patients with significant cataract (n = 92) versus a reference group without eye disease (n = 122), indicating the tools ability to detect differences in eye conditions. In terms of convergent validity, an analysis of 597 patients worse eye using Pearson’s correlation coefficient found moderate correlations between ETDRS visual acuity and the NEI-VFQ-25 subscales of general vision, near vision, and distance vision with r = 0.65, 0.68, and 0.66, respectively.
Reliability
Mangione et al., (2001)26 examined the development of the NEI-VFQ-25 questionnaire and found good internal consistency reliability with Cronbach alpha, ranging from 0.71 to 0.85 for each of the subscales. The near vision and distance vision subscales are 3-item subscales on the NEI-VFQ-25; and among the DME population their internal reliability as represented by Cronbach alpha was reported to be good: 0.73 and 0.58 for each subscale, respectively.35 Good internal reliability was also demonstrated for the revised questionnaire created by Thevi et al. (2021)30 which had Cronbach alpha values of 0.904, 0.898, and 0.608 for each of the 3 factors: difficulty with activities, responses to vision problems and general health and vision, respectively.30 Similarly, in a study by Sugar et al. (2020)32 among 224 patients with non-infectious intermediate and posterior uveitis, Cronbach alpha ranged from 0.87 to 0.94 across all multi-item subscales and the overall composite score and in a study among patients with geographic atrophy, an advanced form of age-related macular degeneration, Cronbach alpha for overall composite score was 0.95.31 Good test-retest reliability was noted in the study by Sugar et al.,32 as the intraclass correlation coefficients (ICCs) for each domain were greater than 0.70 except for general vision with an ICC of 0.58 and similar results were noted in the geographic atrophy study with ICC values of 0.80, 0.84, and 0.86 for each domain of near activity, distance activity, and the composite score, respectively.31
Responsiveness
A cohort study examined data measurements collected at 6-month intervals (up to 3 years) from 245 patients enrolled in the Multicenter Uveitis Steroid Treatment (MUST) trial and follow-up study to determine the responsiveness of the instrument.33 Results found that for every 5-letter change in visual acuity there was a corresponding change in the NEI-VFQ-25 of 2.70 points (95% CI, 2.12 to 3.29) with responses to both positive and negative changes in visual acuity. The study concluded that the instrument was more sensitive to changes in visual acuity than the EQ-5D-3L index score and the SF-36 physical component summary.
MID
A retrospective study among 335 adult patients with either Primary Angle Closure (PAC) or Primary Angle Closure Glaucoma (PACG) by Bur et al. (2021)34 estimated the MID for the NEI-VFQ-25. The EQ-5D-3L was used as an anchor and a point-change on the anchor was defined as: none (< 0.065); minimal (0.065 to 0.075), and greater change (> 0.075). Four anchor-based methods were used to examine changes in the NEI-VFQ-25 composite score between baseline and 36 months including: ROC curve and predictive modelling as well as within-group and between-group mean score changes. All 335 patients were included in the ROC curve and predictive modelling analyses with an MID (95% CI) of 5.8 (1.9 to 7.2) and 8.1 (1.7 to 14.8) for each method, respectively. For the mean change methods, 174 patients remained unchanged in their anchor score and only 6 patients had the defined minimal score change between 0.065 to 0.075 and were eligible for the analyses. The MID (95% CI) for the within-group and between-group methods were 10.5 (1.9 to 19.2) and 3.9 (–2.3 to 10.1), respectively. Based on these anchor-based methods, the study concluded an estimated an MID between 4 to 11 points on the NEI-VFQ-25. Estimating the median of 3 of the anchor-based methods (excluding the within-patient method) leads to a MID of 5.8 points.
A psychometric validation study of the NEI-VFQ-25 specifically in patients with DME was conducted in 2013, and 2 distribution-based methods were employed to determine a minimal clinically important difference (MCID) from baseline to week 54.35 Using a 0.5 SD-based approach, the MCID for each NEI-VFQ-25 domain ranged from 8.80 (general vision) to 14.40 (role difficulties) and produced a composite score MCID of 6.13 points. The MCID for the near vision and distance vision subscales were 10.24 and 11.07, respectively. A standard error of measurement (SEM) approach yielded similar MCID estimates from 8.79 (driving) to 14.04 (role difficulties), with a composite score MCID estimate of 3.33 points. This technique lowered the MCID estimates for the near and distance vision subscales, which were reported as 9.17 and 10.19, respectively.
EQ-5D-5L
Scoring
The EQ-5D is a family of HRQoL instruments that may be applied to a wide range of health conditions and treatments.54,55 The first of part of the EQ-5D-5L is a descriptive system that classifies respondents (aged ≥ 12 years) based on the following 5 dimensions: mobility, self-care, usual activities, pain/discomfort, and anxiety/depression. In 2005, updates were made to the original EQ-5D (i.e., the EQ-5D-3L) to create the EQ-5D-5L which includes 5 response levels (as opposed to the original 3 levels) of severity (no problems, slight problems, moderate problems, severe problems, unable to/extreme problems) in each of the dimensions.56 Respondents are asked to choose the level that reflects their health state for each dimension resulting in 3,125 possible health states.57 A scoring function can be used to assign a value to self-reported health states from a set of population-based preference weights.54,55 The second part is a 20 cm visual analogue scale (EQ-VAS) that has end points labelled 0 and 100, with respective anchors of “worst imaginable health state” and “best imaginable health state.” Respondents are asked to rate their health by drawing a line from an anchor box to the point on the EQ-VAS which best represents their health on that day. The EQ-5D index score is generated by applying societal preference weights for the various aforementioned health states.58 Health state index scores less than 0 represent health states that are valued by society as being worse than dead, while scores of 0 and 1.00 are assigned to the health states “dead” and “perfect health,” respectively.
No studies examining the psychometric properties of the English version of the EQ-5D-5L among patients with eye disorders were identified.
Pharmacoeconomic Review
Abbreviations
AMT
amniotic membrane transplantation
BIA
budget impact analysis
CORD
Canadian Organization for Rare Disorders
EMA
European Medicines Agency
HRQoL
health-related quality of life
ICER
incremental cost-effectiveness ratio
NK
neurotrophic keratitis
QALY
quality-adjusted life-year
Executive Summary
The executive summary comprises 2 tables (Table 1 and Table 2) and a conclusion.
Item | Description |
|---|---|
Drug product | Cenegermin ophthalmic solution (Oxervate), 0.002% (20 mcg/mL), topical eye drops |
Submitted price | Cenegermin, 0.002% (20 mcg/mL), ophthalmic solution: $2,111.25 per vial |
Indication | For the treatment of moderate (persistent epithelial defect) or severe (corneal ulcer) NK in adults |
Health Canada approval status | NOC |
Health Canada review pathway | Priority review |
NOC date | NOC received: February 8, 2019 |
Reimbursement request | For the treatment of moderate (persistent epithelial defect) or severe (corneal ulcer) NK in adults who have failed conventional nonsurgical treatments |
Sponsor | Dompé Farmaceutici S.p.A |
Submission history | Previously reviewed: No |
NK = neurotrophic keratitis; NOC = Notice of Compliance.
Table 2: Summary of Economic Evaluation
Component | Description |
|---|---|
Type of economic evaluation | Cost-utility analysis Markov model |
Target population | Adults with moderate to severe NK who have failed conventional nonsurgical treatments |
Treatment | Cenegermin |
Comparators |
|
Perspective | Canadian publicly funded health care payer |
Outcomes | QALYs, LYs |
Time horizon | Lifetime (36 years) |
Key data source | |
Submitted results |
|
Key limitations |
|
CADTH reanalysis results |
|
AMT = amniotic membrane transplantation; EMA = European Medicines Agency; HRQoL = health-related quality of life; ICER = incremental cost-effectiveness ratio; LY = life-year; NK = neurotrophic keratitis; QALY = quality-adjusted life-year; vs. = versus.
Conclusions
Evidence from the 2 pivotal trials (NGF0212 and NGF0214) suggest that use of cenegermin results in more patients achieving corneal healing than a vehicle control in patients with moderate to severe neurotrophic keratitis (NK). No robust comparative data exist for cenegermin versus either amniotic membrane transplantation (AMT) or surgical tarsorrhaphy.
To address limitations with the sponsor’s submitted pharmacoeconomic evaluation, CADTH undertook a reanalysis with the following changes: assumed equivalent clinical efficacies for all 3 treatments, extended the period of clinical follow-up for patients who achieved sustained corneal healing, and reduced the disutility associated with surgical tarsorrhaphy.
Assuming similar clinical effects among the treatments, in the CADTH base case, cenegermin is dominated by AMT (i.e., both treatments provided the same number of quality-adjusted life-years [QALYs], and AMT was $114,597 less costly). When compared with surgical tarsorrhaphy, cenegermin had an incremental cost-effectiveness ratio (ICER) of $1,368,740 per QALY gained (additional QALYs = 0.09; additional costs = $115,898). The incremental QALYs associated with cenegermin relative to surgical tarsorrhaphy were due to the disutility associated with the tarsorrhaphy procedure. A price reduction of 95% is required to achieve cost-effectiveness at a $50,000 per QALY threshold, changing the price of cenegermin from $118,230 to $6,440 per treatment course.
There is a high degree of uncertainty regarding the disutility associated with a surgical tarsorrhaphy. Given the absence of evidence to demonstrate superior clinical efficacy, the additional value of cenegermin is derived from the avoidance of potential discomfort associated with surgical tarsorrhaphy. CADTH notes no disutility is applied to the treatment with cenegermin in the sponsor’s analysis, which is not in line with trial evidence or stakeholder feedback. A scenario analysis that reduced the disutility associated with surgical tarsorrhaphy showed that the ICER of cenegermin, compared with surgical tarsorrhaphy, increased significantly to $23,320,230 per QALY. In this scenario analysis, a price reduction in excess of 97% is required to achieve cost-effectiveness at a $50,000 per QALY threshold compared with surgical tarsorrhaphy.
The results of the cost-effectiveness analysis are driven by the clinical effectiveness of cenegermin relative to surgical comparators (patients achieving sustained corneal healing and likelihood of recurring) and the high cost of cenegermin. Although there is a high degree of uncertainty regarding the potential clinical benefits of cenegermin relative to surgical options, the cost is substantially higher. CADTH notes that if sponsor assumptions pertaining to differential clinical efficacy for each therapy are maintained, using recurrence data from Sacchetti et al. (2022),4 price reductions to achieve cost-effectiveness still exceed 95%.
Stakeholder Input Relevant to the Economic Review
This section is a summary of the feedback received from the patient groups, registered clinicians, and drug plans that participated in the CADTH review process.
CADTH received patient input from the Canadian Organization for Rare Disorders (CORD), a national network for organizations representing patients with rare disorders. CORD interviewed 12 participants from 3 eye institutes in the US who ranged in age from 24 years to 77 years. Patient experience with the disease included irritation on the cornea or inner eyelid, tearing eyes, loss of peripheral vision, blurred and low vision, and near loss of vision in 1 eye. Most respondents were aware of their diagnosis but could not recall the stage of their NK condition. The interviewed patients’ previous experiences with treatment varied from being prescribed lubricant eye drops, antibiotics, and serum eye drops. CORD noted that patients who are undiagnosed may be receiving ineffective treatment or may have been advised to receive a cornea transplant or to have the affected eye sutured shut. Patients noted the importance of an accurate diagnosis at the time of symptom onset, and how that would have reduced long periods of ineffective or invasive treatments. All patients interviewed had been treated with cenegermin from 2 weeks to 3 years ago, and noted positive outcomes with therapy that varied from complete resolution of symptoms, partial restoration of vision, or adequate stabilization to consider a cornea transplant. Patients reported side effects, such as stinging, pain, headaches, and blurred vision, that were resolved upon treatment completion. Patients also noted the simplicity of the initial cornea sensitivity test for screening and its importance given how often NK, a rare disease, is undiagnosed or not recognized by specialists. CORD emphasized that cenegermin is the only treatment specifically for NK, and that it would address the current lack of available, effective treatments.
No registered clinician input was received for this review.
CADTH received drug plan input, noting that earlier, less-progressive stages of NK may be manageable with conventional topical therapies, including preservative-free artificial tears, gels, or ointments. There may also be limitations in staging, monitoring, and follow-up for cenegermin. Given how rare NK is, drug plans also highlighted the difficulties that patients would have in accessing specialists with experience in diagnosis and treatment. Drug plans also noted that none of the other nonsurgical alternatives are indicated in this setting, which creates challenges in implementing the requested indication of stage 3, severe NK patients who have failed nonsurgical treatments. Furthermore, drug plans were concerned about recurrences in approximately 14% to 20% of patients who completed treatment with cenegermin. The dosing regimen of 6 times a day at 2-hour intervals for 8 weeks may also be challenging for patient adherence. Finally, drug plans identified concerns related to the anticipated budget impact of reimbursing cenegermin because it is the only pharmaceutical agent indicated for NK.
The following concerns were addressed in the sponsor’s model:
comparators comprised only of surgical therapies
recurrence was considered in the economic model
cenegermin was the only pharmaceutical agent considered in the budget impact analysis.
CADTH was unable to address the following concerns raised from stakeholder input:
disutility associated with adverse side effects related to cenegermin
potential issues with adherence were not considered in the economic analysis.
Economic Review
The current review is for cenegermin (Oxervate) for adults with moderate to severe NK who have failed conventional nonsurgical treatment.
Economic Evaluation
Summary of Sponsor’s Economic Evaluation
Overview
The sponsor submitted a cost-utility analysis of cenegermin compared with AMT and surgical tarsorrhaphy. The model population comprised adults with moderate to severe NK who failed conventional nonsurgical treatment. This population is a subset of the Health Canada–indicated population, which is adults with moderate to severe NK, regardless of prior nonsurgical treatment attempts. The reimbursement request aligns with the model population.
Cenegermin is self-administered as an ophthalmic solution (eye drop) that contains 20 mcg of cenegermin per mL solution. It is shipped directly to patients in sterile glass vials that contain 1.0 mL of the drug, along with a delivery system kit (i.e., vial adapters, pipettes, and disinfectant wipes). One vial is used per day of treatment. The recommended dosing for cenegermin is 1 drop 6 times per day at 2-hour intervals for 12 hours in the affected eye(s), and treatment continues for 8 weeks. Each vial costs $2,111.25, and a full course of treatment (8 weeks; 56 days) costs $118,230.
The clinical objectives modelled are life-years and QALYs. The reference perspective is the public health care perspective. The time horizon is lifetime, with a maximum age of 100 years, and the discount rate is 1.5%.
Model Structure
The sponsor submitted a Markov state transition cohort model with 7 health states: sustained healing, nonhealing, deteriorated, sustained healing after rescue therapy, nonhealing after rescue therapy, deteriorated after rescue therapy, and death. The model structure is shown in Figure 1 (Appendix 3). The model uses a 4-week cycle length. All patients begin in the baseline health state, from which they can transition to “sustained healing,” “nonhealing,” or “deteriorated” health states or death after treatment initiation. Over time, patients can transition from “sustained healing” to “nonhealing,” and from “nonhealing” to either “sustained healing” or “deteriorated.” From the ‘deteriorated’ health states (both before and after rescue therapy), patients can transition to the respective “nonhealing” health state. Patients can transition to “death” from any health state, the rate of which is assumed to match the general Canadian population.
The model includes 2 definitions of sustained healing: the European Medicines Agency (EMA) definition of the maximum diameter of corneal fluorescent staining is less than 0.5 mm and the FDA definition of the maximum diameter of corneal fluorescent staining is 0 mm. The sponsor’s base-case analysis used the FDA definition. The “deteriorated” health states are defined as corneal fluorescent staining of the maximum diameter for an increase of at least 1 mm, or lesions increased by at least 1 mm, or the previous follow-up best remote correction vision declined by more than 5 Early Treatment Diabetic Retinopathy Study (ETDRS) letters, found corneal dissolution or perforation, or serious corneal infection occurred.
Patients in the “nonhealing” and “deteriorated” health states are eligible for follow-up rescue therapy, and subsequently transition to 1 of the 3 “after rescue therapy” health states. Rescue therapies include a basket of therapies, such as subsequent AMT, surgical tarsorrhaphy, and conjunctival flap or corneal neurotization, and a weighted approach was used for the proportion of patients undergoing each of these procedures. A second course of treatment with cenegermin is not considered. One treatment cycle with rescue therapy is considered, and patients who experience recurrence after rescue therapy are treated with corneal transplantation. Transitions between “sustained healing,” “nonhealing,” and “deteriorated” health states are based on the treatment-specific outcomes applied to the patient cohort.
Model Inputs
The baseline cohort is a population of adults with moderate to severe NK who have failed conventional nonsurgical treatments. The cohort has a starting age of 63.6 years, and the proportion of females is 57.9%, based on the weighted average from the 2 pivotal trials: NGF0212 (REPARO; Bonini et al. [2018]1) and NGF0214 (Pflugfelde et al. [2019]2).
The clinical pathway was informed by clinical trials, literature, and clinical expert opinion via a survey. Patient mortality rates are based on age-based, all-cause mortality in the general Canadian population. The sponsor assumes that there is no additional mortality risk associated with NK or treatment.
Dosing of cenegermin in the model is the same as dosing used in both pivotal trials and that of the reimbursement request. Rates of corneal healing and corneal deterioration at 4 weeks and 8 weeks for cenegermin are based on a pooled analysis from the 2 pivotal trials or from the REPARO trial (NGF0212) alone.1,2 The sponsor reported that the base analysis used the pooled data; however, data from only Study NGF0212 for the 4 weeks and 8 weeks were used for corneal healing parameters. Recurrence rates after cenegermin treatment were obtained from an observational study that followed patients for up to 48 months (9 patients were followed until this time point).3 The sponsor also presents recurrence data for cenegermin that were derived from an observational study by Sacchetti et al. (2002).4
The sponsor conducted a physician survey with 5 Canadian ophthalmologists. The clinical experts completed an Excel-based survey, and weighted averages were calculated to inform the economic model when data from the published literature were not available. Treatment efficacy for both comparator arms was informed by this survey, along with disease recurrence after rescue therapy. Recurrence after primary treatment with AMT was obtained from an observational study of 13 patients treated with AMT and followed for 12 months4; the sponsor assumed that recurrence rates in years 2 to 4 were the same as year 1. Annual recurrence rates of surgical tarsorrhaphy were obtained from published literature, and rates were assumed to be the same over time.5,6
The health utilities of patients at baseline and at the end of the 8 weeks in 3 states (sustained healing, nonhealing, and deteriorated) were derived using a combined analysis of EQ-5D assessments collected in both trials. Changes in utility values for each of the 3 states were also estimated from the EQ-5D pooled analysis. The disutility associated with surgical tarsorrhaphy is a combined disutility of disfigurement and unilateral blindless, and was applied to the first year after surgery. For disutility associated with disfigurement, the sponsor used an estimate from a National Institute for Health and Care Excellence (NICE) review on treating limbal stem cell deficiency after eye burns.7 The value taken from this review represents the disutility for patients with cataracts. Therefore, the sponsor assumes that a patient who undergoes tarsorrhaphy has a decrement in utility equivalent to an individual who develops cataracts. On top of this disutility, the sponsor also assumes an additional disutility associated with unilateral blindness. For this value, the sponsor assumes that the disutility of unilateral blindness equates to a third of the impact of an individual who transitions from perfect sight to bilateral blindness.8
No disutility associated with adverse events after initial treatments or rescue therapies was applied.
The sponsor included direct medical costs associated with health care resource utilization. Surgical interventions included frequencies of pre- and post-operative physician visits, hospitalizations, and outpatient clinic visits, which were obtained from clinical expert opinion. Rates of health care resource utilization for cenegermin were obtained from the pivotal trials. The sponsor assumes that the length of follow-up in the case of sustained healing is 52 weeks, at which point no follow-up costs are included for cenegermin or the comparator groups.
Unit costs of resources were obtained from a number of Canadian sources: physician and outpatient clinic visits from the Ontario Health Insurance Plan Schedule of Benefits for Physician Services9; medication costs were obtained from the Ontario Drug Benefit Formulary10 or publicly available prices; hospitalization costs were obtained from the Canadian Institute for Health Information11; ambulatory or day surgery costs of the surgical interventions were obtained from the Ontario Case Costing Initiative (OCCI)12; and the cost of cenegermin was provided by the sponsor. Costs of adverse events were obtained from Ontario Health Insurance Plan Schedule of Benefits for Physician Services and Ontario Case Costing Initiative when available; when unavailable, the sponsor made assumptions for the cost of the best possible treatment.
Summary of Sponsor’s Economic Evaluation Results
All analyses were run probabilistically (5,000 iterations for the base case and scenario analyses). The deterministic and probabilistic results were similar. The probabilistic findings are presented in the next section.
Base-Case Results
The sponsor’s economic evaluation reports that surgical tarsorrhaphy dominates AMT (i.e., AMT is more costly and provides fewer QALYs than tarsorrhaphy). The sponsor’s economic evaluation shows that cenegermin is more costly (incremental cost = $114,192) and has higher QALYs (incremental QALYs = 0.321) than surgical tarsorrhaphy, with an ICER of $356,096 per QALY. The majority (88%) of the cost of cenegermin is made up of drug acquisition costs ($118,121); the remainder of the costs are direct health care resource use ($13,553). To inform this analysis, the sponsor uses recurrence data from Bruscolini et al. (2021).3 The sponsor also presents results for cenegermin using recurrence data from Sacchetti et al. (2022),4 in which the QALYs derived from cenegermin decrease to 12.11, and total costs increase to $133,926. As this only influences the cenegermin arm, the same results for AMT and tarsorrhaphy, as shown in Table 12 still apply. Therefore, AMT remains dominant, but the ICER for cenegermin, relative to tarsorrhaphy, increases to $1,067,790 per QALY.
Table 3: Summary of the Sponsor’s Economic Evaluation Results
Treatment | Total costs ($) | Total QALYs | Sequential ICER ($ per QALY) |
|---|---|---|---|
Surgical tarsorrhaphy | 17,482 | 12.00 | Reference |
Cenegermin | 131,674 | 12.32 | 356,096 |
AMT | 22,364 | 11.77 | Dominated by surgical tarsorrhaphy |
AMT = amniotic membrane transplantation; ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year.
Source: Sponsor’s pharmacoeconomic submission.13
Sensitivity and Scenario Analysis Results
The sponsor presented scenario analyses that used the EMA corneal healing definition, multiple time horizons (5 years, 10 years, and 25 years), and an analysis using a societal perspective. In sequential analysis, the conclusions of the base-case results did not differ substantially; tarsorrhaphy dominated AMT, and the ICER for cenegermin was slightly lower than that for surgical tarsorrhaphy, at $347,795 per QALY. Analyses of the time horizon showed that the ICER for cenegermin versus tarsorrhaphy increased as the time horizon shortened. One-way sensitivity analyses showed that the results were most sensitive to the rate of sustained healing in the cenegermin group at 8 weeks, compared with surgical tarsorrhaphy, followed by the average age of patients and the discount rate. None of the 1-way analyses presented had a substantial effect on the ICER.
CADTH Appraisal of the Sponsor’s Economic Evaluation
CADTH identified several key limitations to the sponsor’s analysis that have notable implications for the economic analysis:
Limited comparative clinical evidence: Direct evidence for the treatment effect of cenegermin comes from the 2 pivotal trials, in which the comparator was a vehicle control. Evidence comparing cenegermin versus surgical comparators mainly relies on expert opinion. There was 1 comparative study that compared outcomes between cenegermin and AMT, which the sponsor used to estimate NK recurrence rates for both treatments; these results were then used to compare cost-effectiveness between cenegermin and AMT.4 However, this study was observational in design (nonrandomized) and assessed only a small number of patients. Likewise, the study only observed recurrence rates over 12 months, and the sponsor assumes this difference in recurrence is maintained indefinitely. Corneal healing for surgical tarsorrhaphy was assumed, based on expert opinion, and for recurrence rates, the sponsor used data from Cosar et al. (2001).3,5,6 Data for surgical tarsorrhaphy recurrence was therefore incorporated as a naive comparison, and differences between cenegermin and surgical tarsorrhaphy recurrence rates were assumed to be related to treatment effects and not confounding factors. As with AMT, the sponsor assumed that recurrence rates for surgical tarsorrhaphy would be static over time. Clinical expert opinion noted that there was no expectation that the relative probability of recurrence would substantially differ between treatment options. Therefore, the sponsor’s assumption that recurrence rates are higher for surgical interventions, and this difference is maintained indefinitely, is not supported by the evidence presented. The lack of any comparative data for tarsorrhaphy makes any claims of clinical superiority unclear.
Given the limitations of the evidence used to inform comparisons between cenegermin and the 2 surgical comparators, the CADTH analysis assumed that all treatments were equally effective regarding corneal healing, deterioration, and recurrence.
A scenario analysis was conducted on the CADTH base case, maintaining the sponsor’s estimates for corneal healing, deterioration, and recurrence for all interventions obtained from Sacchetti et al. (2022)4 recurrence data.
Disutility of surgical tarsorrhaphy: The sponsor assumed that a –0.21 decrement would be applied the first year after surgical tarsorrhaphy to account for the disutility of disfigurement and unilateral blindness that resulted from the procedure. The disutility associated with disfigurement (–0.14) was sourced from a review conducted by NICE that used cataracts as a proxy. However, NICE reported that the decrement associated with a cataract includes both disutility associated with disfigurement and vision loss. Further, a systematic review on health state utility values associated with unilateral vision loss (i.e., diabetic retinopathy, diabetic macular edema, or age-related macular degeneration) showed that vision loss in your worst seeing eye has minimal impact on overall health-related quality of life (HRQoL).14 Given that the target population, and the population of the pivotal trials, is for patients with NK affecting 1 eye, it is not clear that temporary vision loss after tarsorrhaphy will result in substantial utility loss for these patients. Likewise, according to clinical experts, vision for many patients would be maintained because the procedure would not fully shut the eyelids.
Another study15 by Smith et al. assessed the disutility associated with disfigurement, poor vision, pain, and photosensitivity in 1 eye, and showed that the difference between those with and without disfigurement, pain, and photosensitivity ranged from 0.002 to 0.008, using EQ-5D estimates based on a UK tariff.15 There is a high amount of uncertainty regarding the disutility associated with surgical tarsorrhaphy.
CADTH reduced the disutility of surgical tarsorrhaphy to –0.14, which accounts for the disutility associated with disfigurement and vision loss and eliminates the additional 0.07 decrement that the sponsor included for unilateral blindness. CADTH notes this is not a robust estimate of disutility; therefore, further scenario analyses are warranted. To account for the possibility that the disutility associated with surgical tarsorrhaphy could be as low as 0.008, CADTH conducted a scenario analysis in which a disutility of 0.008 was applied in the first year after the procedure.
Exclusion of re-treatment: The sponsor assumed that re-treatment with cenegermin would not take place if a patient had a recurrence; however, in the pivotal trial, re-treatment with cenegermin was allowed for patients who experienced sustained healing and then recurrence. The clinical experts suggested that they would be inclined to re-treat with cenegermin if a patient experienced improvement during their first treatment course and then deteriorated. Given the submitted cost of cenegermin ($118,230 per 8-week treatment cycle), excluding the option to re-treat with cenegermin likely underestimates the costs because some proportion of patients may be retreated.
Based on the treatment pathway in the pivotal trial and clinical expert opinion, CADTH believes there is the possibility that some patients who achieved sustained healing during their first course of treatment with cenegermin would be considered for a single course of re-treatment if their condition recurs. Because long-term recurrence rates with cenegermin are unclear, if patients are considered for a second treatment with cenegermin, it would result in a considerable increase in the cost per patient (approximately $118,230 per patient) relative to the cost of rescue therapy used in the model (approximately $1,969 per patient). This could not be formally explored in the CADTH reanalysis because of the structure imposed by the sponsor.
Follow-up duration of patients who achieve sustained healing: The sponsor assumed that there would be 52 weeks of follow-up for patients who achieve sustained healing in all 3 comparators. The clinical experts suggested that these patients would likely require lifetime follow-up.
In line with the clinical experts’ opinions, CADTH included the possibility of indefinite follow-up for patients who achieve sustained healing in any of the intervention groups. The same per-cycle cost ($29.21 every 4 weeks) was applied over a lifetime if there was no recurrence or rescue therapy.
Additional limitations were identified but were not considered to be key limitations.
Uncertainty regarding health state utility values: Both clinical trials (NGF0212 and NGF0214) collected patient-reported HRQoL using the EQ-5D questionnaire, EQ-5D visual analogue scale, and the National Eye Institute Visual Functioning Questionnaire-25 items. The change in quality of life from baseline using the EQ-5D |||||||||||||||||||| were in favour of cenegermin; however, it was not statistically significant. The changes from baseline to healing, nonhealing, or deteriorated were applied in the model for the corresponding health states after initial treatment and after rescue therapy. The change from baseline to the nonhealing state demonstrated an increase in HRQoL, despite this state representing no improvement or deterioration of the patients’ condition. The sponsor used a meta-analysis that combined results from the 2 studies15; however, the findings are only available as a conference abstract, so the analysis has not been validated by CADTH. Further, it is unclear whether HRQoL measures taken from patients were based on the EMA or FDA definition of corneal healing, so their appropriateness for use in the base case is unknown.
CADTH notes that despite uncertainty in the health state utilities, the impact on the cost-effectiveness conclusions of cenegermin is limited.
Additionally, the following key assumptions were made by the sponsor and have been appraised by CADTH (refer to Table 4).
Table 4: Key Assumptions of the Submitted Economic Evaluation (Not Noted as Limitations to the Submission)
Sponsor’s key assumption | CADTH comment |
|---|---|
No disutility was applied to patients who experienced AEs after any of the treatments considered or when they deteriorated. | No comparative evidence exists comparing adverse events across treatments, so the impact of this is unknown. It was noted in the patient feedback that there can be some discomfort with cenegermin, but this has not been incorporated into the analysis. |
Only 1 treatment option is considered at a time. | Although it is possible that clinicians will use cenegermin together with a surgical procedure to treat a patient or use AMT together with surgical tarsorrhaphy, there are no data to inform these scenarios. |
One treatment cycle with rescue therapy is considered; if patients experience a recurrence after rescue therapy they are treated with corneal transplantation. | Based on feedback from the CADTH clinical experts, corneal transplantation is only appropriate for a small subset of patients, and not the likely final treatment for many NK patients. A conjunctival flap procedure might be a more appropriate final treatment stage; however, this is included as a rescue therapy. |
All patients adhere to the full treatment course of cenegermin. | Real-world adherence may be different from that within a trial. Nonadherence can lead to full prescriptions being filled but not taken. Therefore, the cost of cenegermin may be unchanged but the efficacy may be decreased. Without data to explore this, the impact of reduced adherence is speculative. It is likely that anything less than full adherence would reduce the cost-effectiveness of cenegermin. |
AE = adverse event; AMT = amniotic membrane transplantation; NK = neurotrophic keratitis.
CADTH Reanalyses of the Economic Evaluation
Base-Case Results
The CADTH base case was derived by making changes in model parameter values and assumptions, in consultation with clinical experts. A summary of the reanalyses that are incorporated in the CADTH base-case reanalysis is presented in Table 5.
Table 5: CADTH Revisions to the Submitted Economic Evaluation
Stepped analysis | Sponsor’s value or assumption | CADTH value or assumption |
|---|---|---|
Correctionsa to sponsor’s base case | ||
1. Use of pooled efficacy data for the cenegermin group | The sponsor intended to use the pooled data from the 2 pivotal trials to inform the base-case analysis, however, used the NGF0212 trial data only. | Used the pooled trial data to inform the 4- and 8-week proportions of patients who achieved corneal healing parameters in the cenegermin group. |
Changes to derive the CADTH base case | ||
1. Treatment efficacy | Assumed different clinical efficacy and recurrence rates for comparator strategies. | Assumed equivalent efficacy for cenegermin and both comparator strategies using pooled efficacy data from pivotal trials. |
2. Length of follow-up in the case of sustained healing | Follow-up with patients who achieve sustained healing for 52 weeks. | Follow-up with patients who achieve sustained healing for their lifetime. |
3. Disutility of surgical tarsorrhaphy | HRQoL decrement of –0.21 for 1 year after surgical tarsorrhaphy. | HRQoL decrement of –0.14 for 1 year after surgical tarsorrhaphy. Scenario analysis conducted that reduced this to –0.008. |
CADTH base case | — | Reanalyses 1, 2, and 3 are used to calculate the CADTH base case. |
HRQoL = health-related quality of life.
aCorrections are minor errors (e.g., transcription errors between report and model, misapplication of distributions or standard errors, probabilistic analyses) that are not identified as limitations.
The CADTH base case resulted in cenegermin being dominated by AMT because both interventions provided the same number of total QALYs and AMT is less costly. Compared with surgical tarsorrhaphy, cenegermin provides an additional 0.09 QALYs, with an incremental cost of $115,897, resulting in an ICER of $1,368,740 per QALY with a 0% probability of being cost-effective at the $50,000 per QALY threshold. The results of the stepped analyses are presented in Table 12 (Appendix 4).
Table 6: Summary of the CADTH Reanalysis Results
Treatment | Total costs ($) | Total QALYs | ICER vs. surgical tarsorrhaphy ($ per QALY) | Sequential ICER ($ per QALY) |
|---|---|---|---|---|
Sponsor-corrected base case | ||||
Surgical tarsorrhaphy | 17,488 | 12.01 | Reference | Reference |
Cenegermin | 131,864 | 12.31 | 380,011 | 380,011 |
AMT | 22,368 | 11.78 | Dominated by surgical tarsorrhaphy | Dominated by surgical tarsorrhaphy |
CADTH base case | ||||
Surgical tarsorrhaphy | 16,165 | 12.42 | NA | Reference |
AMT | 17,466 | 12.51 | 15,125 | 15,665 |
Cenegermin | 132,063 | 12.51 | 1,368,740 | Dominated by AMT |
AMT = amniotic membrane transplantation; ICER = incremental cost-effectiveness ratio; NA = not applicable; QALY = quality-adjusted life-year; vs. = versus.
Scenario Analysis Results
A scenario analysis was conducted using the disutility associated with surgical tarsorrhaphy of –0.008 applied in the first year following procedure. In this scenario analysis, the ICER of cenegermin versus surgical tarsorrhaphy was $23,320,230 (incremental cost = $115,903; incremental QALY = 0.005). Cenegermin remains dominated by AMT because of the lack of clinical benefit of cenegermin assumed in the CADTH base-case analysis (i.e., QALYs gained were equivalent for AMT and cenegermin).
A second scenario analysis maintained the sponsor’s assumptions regarding corneal healing and deterioration for each intervention, but used recurrence data for AMT and cenegermin from Sachetti et al. (2022).4 In this scenario analysis, the ICER of cenegermin versus surgical tarsorrhaphy was $2,498,313 (incremental cost: $116,109; incremental QALY: 0.05). AMT is dominated by surgical tarsorrhaphy in this scenario (i.e., AMT cost more than surgical tarsorrhaphy but provided fewer QALYs).
A scenario analysis investigating price reduction demonstrates that, in the CADTH reanalysis, cenegermin is cost-effective at the $50,000 per QALY threshold, with a price reduction of 95%.
Table 7: CADTH Price Reduction Analyses
Price reduction | Sequential ICER for cenegermin vs. surgical tarsorrhaphy, AMT | |
|---|---|---|
Sponsor-corrected base case using Bruscolini et al. (2022)4 data for cenegermin recurrencea | CADTH reanalysisb | |
No price reduction | $381,277 vs. surgical tarsorrhaphy | $1,368,740 vs. surgical tarsorrhaphy |
10% | $341,320 vs. surgical tarsorrhaphy | $1,229,240 vs. surgical tarsorrhaphy |
20% | $301,363 vs. surgical tarsorrhaphy | $1,089,739 vs. surgical tarsorrhaphy |
30% | $261,407 vs. surgical tarsorrhaphy | $950,239 vs. surgical tarsorrhaphy |
40% | $221,450 vs. surgical tarsorrhaphy | $810,738 vs. surgical tarsorrhaphy |
50% | $181,493 vs. surgical tarsorrhaphy | $671,238 vs. surgical tarsorrhaphy |
60% | $141,537 vs. surgical tarsorrhaphy | $531,738 vs. surgical tarsorrhaphy |
70% | $101,580 vs. surgical tarsorrhaphy | $392,237 vs. surgical tarsorrhaphy |
80% | $61,623 vs. surgical tarsorrhaphy | $252,737 vs. surgical tarsorrhaphy |
90% | $21,667 vs. surgical tarsorrhaphy | $113,237 vs. surgical tarsorrhaphy |
95% | Dominant | $43,490 vs. surgical tarsorrhaphy |
100% | Dominant | Dominant |
AMT = amniotic membrane transplantation; ICERs = incremental cost-effectiveness ratios; vs. = versus.
aIn the sponsor-corrected base case, AMT is dominated by surgical tarsorrhaphy, so only price reductions relative to tarsorrhaphy are presented.
bIn the CADTH reanalysis, AMT dominates cenegermin because of the lack of clinical benefit, so only price reductions relative to tarsorrhaphy are presented.
Overall Conclusions
Evidence from the 2 pivotal trials (NGF0212 and NGF0214) suggests that more patients with moderate to severe NK achieve corneal healing with cenegermin than a vehicle control. No robust comparative data exist for cenegermin versus either AMT or surgical tarsorrhaphy.
To address limitations with the sponsor’s submitted pharmacoeconomic evaluation, CADTH undertook a reanalysis with the following changes: assumed equivalent clinical efficacies for all 3 treatments; extended the period of clinical follow-up for patients who achieved sustained corneal healing; and a reduction in the disutility associated with surgical tarsorrhaphy.
Assuming similar clinical effects among the treatments, in the CADTH base case, cenegermin is dominated by AMT (i.e., both treatments provided the same number of QALYs, but AMT cost $114,597 less). When compared with surgical tarsorrhaphy, cenegermin had an ICER of $1,368,740 per QALY gained (additional QALYs = 0.09; additional costs = $115,898). The incremental QALYs associated with cenegermin relative to surgical tarsorrhaphy are due to the disutility associated with the tarsorrhaphy procedure. A price reduction of 95% is required to achieve cost-effectiveness at the $50,000 per QALY threshold, changing the price of cenegermin from $118,230 to $6,440 per treatment course.
There is a high degree of uncertainty regarding the disutility associated with a surgical tarsorrhaphy. Given the absence of evidence to demonstrate superior clinical efficacy, the additional value of cenegermin is derived from the elimination of potential discomfort associated with surgical tarsorrhaphy. CADTH notes no disutility is applied to treatment with cenegermin in the sponsor’s analysis, which is not in line with trial evidence or stakeholder feedback. A scenario analysis that reduced the disutility associated with surgical tarsorrhaphy showed that the ICER of cenegermin, compared with surgical tarsorrhaphy, increased significantly to $23,320,230 per QALY. In this scenario analysis, a price reduction in excess of 97% is required to achieve cost-effectiveness at the $50,000 per QALY threshold compared with surgical tarsorrhaphy.
The results of the cost-effectiveness analysis are driven by the clinical effectiveness of cenegermin relative to surgical comparators (patients achieving sustained corneal healing and likelihood of recurring) and the high cost of cenegermin. Although there is a high degree of uncertainty regarding potential clinical benefits of cenegermin relative to surgical options, the cost is substantially higher. CADTH notes that if sponsor assumptions pertaining to the differential clinical efficacy for each therapy are maintained, using recurrence data from Sacchetti et al. (2022),4 price reductions required to achieve cost-effectiveness still exceed 95%.
References
1.Pflugfelder SC, Massaro-Giordano M, Perez VL, et al. Topical recombinant human nerve growth factor (cenegermin) for neurotrophic keratopathy: a multicenter randomized vehicle-controlled pivotal trial. Ophthalmology. 2020;127(1):14-26. PubMed
2.Bonini S, Lambiase A, Rama P, et al. Phase II randomized, double-masked, vehicle-controlled trial of recombinant human nerve growth factor for neurotrophic keratitis. Ophthalmology. 2018;125(9):1332-1343. PubMed
3.Bruscolini A, Sacchetti M, Moramarco A, Albanese GM, Cerini A, Lambiase A. The long-term clinical efficacy of recombinant human nerve growth factor in the treatment of neurotrophic keratitis [abstract]. Invest Ophthalmol Vis Sci. 2021;62(8):728.
4.Sacchetti M, Komaiha C, Bruscolini A, et al. Long-term clinical outcome and satisfaction survey in patients with neurotrophic keratopathy after treatment with cenegermin eye drops or amniotic membrane transplantation. Graefes Arch Clin Exp Ophthalmol. 2022;260(3):917-925. PubMed
5.Dana R, Farid M, Gupta PK, et al. Expert consensus on the identification, diagnosis, and treatment of neurotrophic keratopathy. BMC Ophthalmol. 2021;21(1):327. PubMed
6.Cosar CB, Cohen EJ, Rapuano CJ, et al. Tarsorrhaphy: clinical experience from a cornea practice. Cornea. 2001;20(8):787-791. PubMed
7.Holoclar for treating limbal stem cell deficiency after eye burns. (Technology appraisal guidance). London (GB): National Institute for Health and Care Excellence; 2017: https://www.nice.org.uk/guidance/ta467/resources/holoclar-for-treating-limbal-stem-cell-deficiency-after-eye-burns-pdf-82604910595525#:~:text=Holoclar%20is%20recommended%20in%20people,for%20treating%20both%20eyes%20only%3A&text=in%20the%20context%20of%20research,for%20a%20conjunctival%20limbal%20autograft. Accessed 2022 Jan 24.
8.Brown MM, Brown GC, Sharma S, Busbee B. Quality of life associated with visual loss: a time tradeoff utility analysis comparison with medical health states. Ophthalmology. 2003;110(6):1076-1081. PubMed
9.Schedule of benefits for physician services under the Health Insurance Act: effective April 1, 2020. Toronto (ON): Ontario Ministry of Health; 2020.
10.Ontario Ministry of Health, Ontario Ministry of Long-Term Care. Ontario drug benefit formulary/comparative drug index. 2022; https://www.formulary.health.gov.on.ca/formulary/. Accessed 2022 Jan 24.
11.Cost of a standard hospital stay. Ottawa (ON): Canadian Institute for Health Information; 2020: https://yourhealthsystem.cihi.ca/hsp/inbrief?lang=en#!/indicators/015/cost-of-a-standard-hospital-stay-/;mapC1;mapLevel2;/. Accessed 2022 Jan 24.
12.Ontario Case Costing Initiative (OCCI). Toronto (ON): Ontario Health and Long-Term Care; 2017: https://data.ontario.ca/dataset/ontario-case-costing-initiative-occi. Accessed 2022 Jan 24.
13.Pharmacoeconomic evaluation [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Oxervate (cenegermin ophthalmic solution), 0.002% (20 mcg/mL) topical eye drops preservative-free. Oakville (ON): Dompé Farmaceutici S.p.A; 2021 Oct 25.
14.Poku E, Brazier J, Carlton J, Ferreira A. Health state utilities in patients with diabetic retinopathy, diabetic macular oedema and age-related macular degeneration: a systematic review. BMC Ophthalmol. 2013;13:74. PubMed
15.Smith AB, Retzler J, Taylor MJ. Standard gamble to derive utility health states for limbal Stem cell deficiency. Clinicoecon Outcomes Res. 2020;12:535-546. PubMed
16.Oxervate (cenegermin ophthalmic solution): 0.002% (20 mcg/mL) topical eye drops [product monograph]. Milano (IT): Dompé Farmaceutici S.p.A.; 2019 Feb 8.
17.Budget Impact Analysis [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Oxervate (cenegermin ophthalmic solution), 0.002% (20 mcg/mL) topical eye drops preservative-free. Oakville (ON): Dompé Farmaceutici S.p.A; 2021 Oct 25.
18.Sacchetti M, Lambiase A. Diagnosis and management of neurotrophic keratitis. Clin Ophthalmol. 2014;8:571-579. PubMed
19.Sutherland G, Dinh T. Understanding the gap: a pan-Canadian analysis of prescription drug insurance coverage. Ottawa (ON): The Conference Board of Canada; 2017: https://www.conferenceboard.ca/temp/06193ca7-b23c-4583-bfb8-a9cf1c51d244/9326_Understanding-the-Gap__RPT.pdf. Accessed 2022 Jan 24.
20.Statistics Canada. Population estimates on July 1st, by age and sex. Table 17-10-0005-01 (formerly CANSIM 051-0001). 2021; https://www150.statcan.gc.ca/t1/tbl1/en/tv.action?pid=1710000501. Accessed 2022 Jan 24.
Appendix 1: Cost Comparison Table
Note that this appendix has not been copy-edited.
The comparators presented in Table 8 have been deemed to be appropriate based on feedback from clinical expert(s). Comparators may be recommended (appropriate) practice or actual practice. Existing Product Listing Agreements are not reflected in the table and, as such, the table may not represent the actual costs to public drug plans.
Table 8: CADTH Cost Comparison Table for Treatment of Neurotrophic Keratitis
Treatment | Strength / concentration | Form | Price ($)a | Recommended dosageb | Daily cost ($) | 8-week course cost ($) |
|---|---|---|---|---|---|---|
Cenegermin | 20 mcg per mL | 7 × 1 mL multi-dose vial | 14,778.75 | 1 drop 6 times daily (1 vial daily) | 2,111.25 | 118,230 |
Surgical procedures (non-drug interventions) | ||||||
AMT | N/A | N/A | 1,976.00 | N/A | N/A | N/A |
Surgical tarsorrhaphy | N/A | N/A | 778.00 | N/A | N/A | N/A |
AMT = amniotic membrane transplantation; NA = not applicable.
aPrice of cenegermin was submitted by the sponsor and prices of surgical procedures were sourced by the sponsor from the OCCI.12,13
bThe recommended dosages are from the respective product monographs.16
Appendix 2: Submission Quality
Note that this appendix has not been copy-edited.
Description | Yes/No | Comments |
|---|---|---|
Population is relevant, with no critical intervention missing, and no relevant outcome missing | Yes | Considered relevant; however, the modelled population is not the full Health Canada indication. |
Model has been adequately programmed and has sufficient face validity | Yes | Programming errors when switching between pooled analysis and NGF0212 data for cenegermin, otherwise sufficient. |
Model structure is adequate for decision problem | Yes | No comment |
Data incorporation into the model has been done adequately (e.g., parameters for probabilistic analysis) | Yes | No comment |
Parameter and structural uncertainty were adequately assessed; analyses were adequate to inform the decision problem | Yes | No comment |
The submission was well organized and complete; the information was easy to locate (clear and transparent reporting; technical documentation available in enough details) | No | Some information based on conference abstracts; it was unclear how some estimates were derived due to internal calculations not described in the report. CADTH required add-info requests to ascertain some important information. |
Appendix 3: Additional Information on the Submitted Economic Evaluation
Note that this appendix has not been copy-edited.
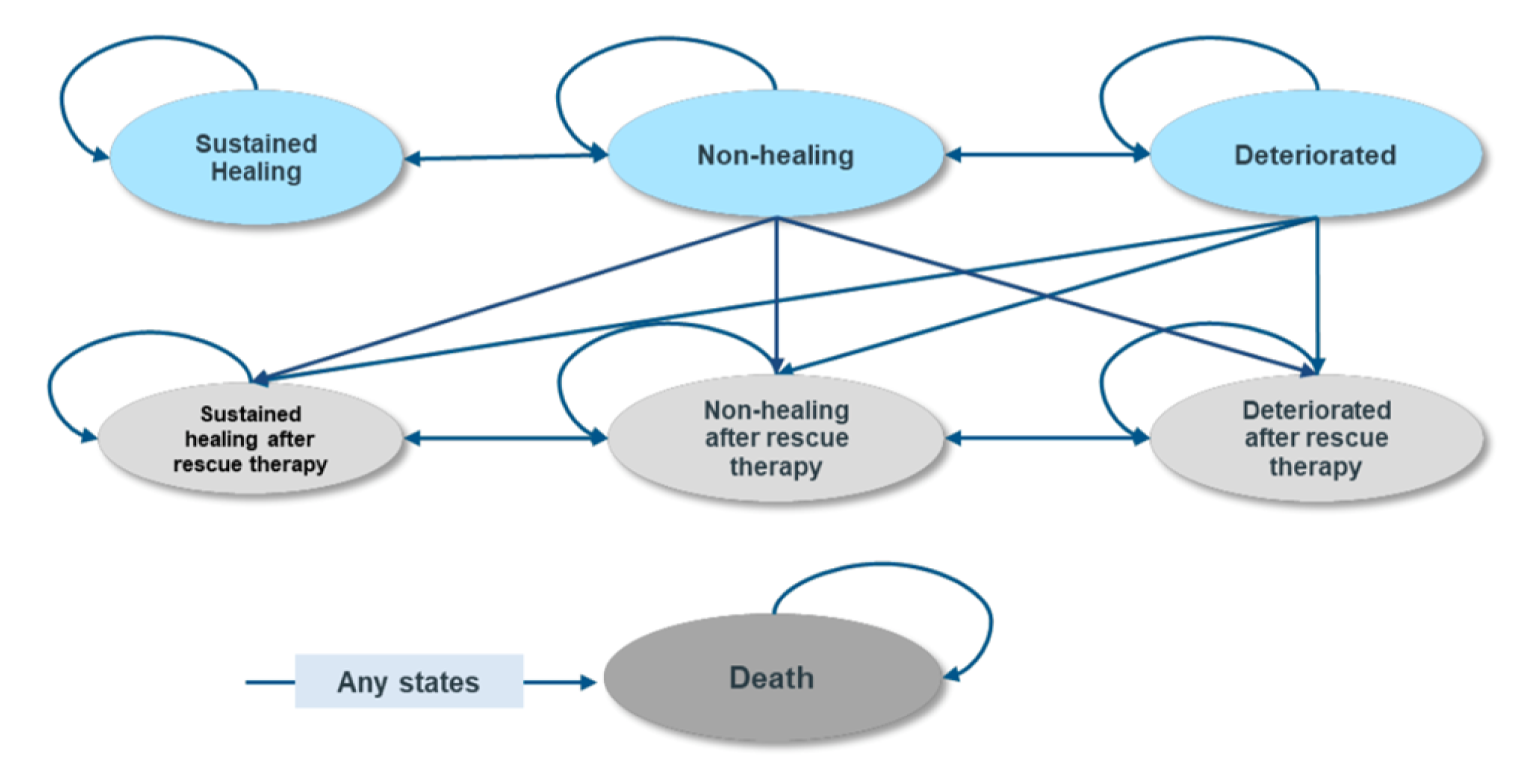
Detailed Results of the Sponsor’s Base Case
Table 10: Disaggregated Summary of Sponsor’s Economic Evaluation Results
Parameter | Cenegermin | Surgical tarsorrhaphy | Amniotic membrane transplantation |
|---|---|---|---|
Discounted life-years | |||
Total | 18.71 | 18.71 | 18.71 |
By health state or data source | |||
Sustained healing | 6.54 | 4.63 | 1.12 |
Nonhealing | 0.13 | 0.13 | 0.15 |
Deteriorated | 0.02 | 0.01 | 0.02 |
Sustained healing after rescue therapy | 1.83 | 2.08 | 2.40 |
Nonhealing after rescue therapy | 2.18 | 2.50 | 2.93 |
Deteriorated after rescue therapy | 8.01 | 9.35 | 12.10 |
Discounted QALYs | |||
Total | 12.32 | 12.00 | 11.77 |
By health state or data source | |||
Sustained healing | 4.69 | 3.32 | 0.80 |
Nonhealing | 0.09 | 0.09 | 0.10 |
Deteriorated | 0.01 | 0.01 | 0.01 |
Sustained healing after rescue therapy | 1.31 | 1.49 | 1.72 |
Nonhealing after rescue therapy | 1.52 | 1.75 | 2.05 |
Deteriorated after rescue therapy | 4.69 | 5.48 | 7.09 |
Disutilities | 0.00 | –0.14 | 0.00 |
Discounted costs ($) | |||
Total | $131,674 | $17,482 | $22,364 |
Drug acquisition | $118,121 | — | — |
Health care resource direct costs | $13,553 | $17,482 | $22,364 |
QALY = quality-adjusted life-year.
Appendix 4: Additional Details on the CADTH Reanalyses and Sensitivity Analyses of the Economic Evaluation
Note that this appendix has not been copy-edited.
Table 11: Disaggregated Summary of CADTH’s Economic Evaluation Results
Parameter | Cenegermin | Surgical tarsorrhaphy | Amniotic membrane transplantation |
|---|---|---|---|
Discounted LYs | |||
Total | 18.71 | 18.71 | 18.71 |
By health state or data source | |||
Sustained healing | 9.08 | 9.08 | 9.10 |
Nonhealing | 0.11 | 0.11 | 0.11 |
Deteriorated | 0.02 | 0.02 | 0.02 |
Sustained healing after rescue therapy | 1.11 | 1.11 | 1.11 |
Nonhealing after rescue therapy | 1.65 | 1.65 | 1.65 |
Deteriorated after rescue therapy | 6.73 | 6.74 | 6.72 |
Discounted QALYs | |||
Total | 12.51 | 12.42 | 12.51 |
By health state or data source | |||
Sustained healing | 6.52 | 6.51 | 6.53 |
Nonhealing | 0.08 | 0.08 | 0.08 |
Deteriorated | 0.01 | 0.01 | 0.01 |
Sustained healing after rescue therapy | 0.80 | 0.80 | 0.80 |
Nonhealing after rescue therapy | 1.15 | 1.15 | 1.15 |
Deteriorated after rescue therapy | 3.95 | 3.95 | 3.94 |
Disutilities | 0.00 | –0.08 | 0.00 |
Discounted costs ($) | |||
Total | $132,063 | $16,165 | $17,466 |
Drug acquisition | $118,121 | — | — |
Health care resource direct costs | $13,941 | $16,165 | $17,466 |
LY= life-year; QALY = quality-adjusted life-year.
Table 12: CADTH Reanalysis Stepped Results
Stepped analysis | Intervention | Total costs ($) | Total QALYs | ICER ($/QALYs) |
|---|---|---|---|---|
Sponsor’s base case | Surgical tarsorrhaphy | $17,482 | 12.00 | Reference |
Cenegermin | $131,674 | 12.32 | $356,096 | |
AMT | $22,364 | 11.77 | Dominated by surgical tarsorrhaphy | |
Corrected sponsor’s base case | Surgical tarsorrhaphy | $17,488 | 12.01 | Reference |
Cenegermin | $131,864 | 12.31 | $380,011 | |
AMT | $22,368 | 11.78 | Dominated by surgical tarsorrhaphy | |
Equivalent efficacy | Surgical tarsorrhaphy | $12,988 | 12.38 | Reference |
AMT | $14,303 | 12.51 | $10,440 | |
Cenegermin | $128,890 | 12.51 | Dominated by AMT | |
Length of follow-up given sustained healing | Surgical tarsorrhaphy | $18,964 | 12.01 | Reference |
Cenegermin | $134,012 | 12.31 | $382,248 | |
AMT | $22,595 | 11.78 | Dominated by surgical tarsorrhaphy | |
Disutility following surgical tarsorrhaphy | Surgical tarsorrhaphy | $17,488 | 12.06 | Reference |
Cenegermin | $131,864 | 12.31 | $449,893 | |
AMT | $22,368 | 11.78 | Dominated by surgical tarsorrhaphy |
Scenario Analyses
CADTH conducted 2 scenario analyses: reducing the disutility associated with surgical tarsorrhaphy from –0.14 to –0.008; maintaining sponsor’s differential efficacy assumptions regarding corneal healing, deterioration, and recurrence, using Sacchetti data for cenegermin recurrence rates.
Table 13: Disaggregated Summary of CADTH’s Scenario Analysis
Stepped analysis | Intervention | Total costs ($) | Total QALYs | ICER ($/QALYs) |
|---|---|---|---|---|
CADTH base case | Surgical tarsorrhaphy | $16,165 | 12.421 | Reference |
AMT | $17,466 | 12.511 | $15,125 | |
Cenegermin | $132,063 | 12.511 | Dominated by AMT | |
Reduced disutility for tarsorrhaphy | Surgical tarsorrhaphy | $16,163 | 12.492 | Reference |
AMT | $17,479 | 12.497 | $261,147 | |
Cenegermin | $132,074 | 12.497 | Dominated by AMT | |
Maintained sponsor’s differential efficacy assumptions regarding corneal healing, deterioration, and recurrence. Used Sacchetti data for cenegermin recurrence rates. | Surgical tarsorrhaphy | $19,242 | 11.984 | Reference |
Cenegermin | $135,351 | 12.031 | $2,498,313 | |
AMT | $22,532 | 11.696 | Dominated by surgical tarsorrhaphy |
Appendix 5: Submitted BIA and CADTH Appraisal
Note that this appendix has not been copy-edited.
Table 14: Summary of Key Take-Aways
Key Take-Aways of the BIA |
|---|
|
Summary of Sponsor’s BIA
The submitted budget impact analysis (BIA) estimated the introduction of cenegermin for the treatment of adult patients with moderate to severe NK who have failed conventional nonsurgical treatment over a 3-year time horizon.17 The analysis took the perspective of Canadian public drug plans using a top-down epidemiological approach and incorporating drug acquisition costs. The target population size was estimated using the prevalence and incidence of NK in Canadian adults, followed by further specifications of population size based on diagnosis rate, the proportion of patients with stage 2 or 3 NK, and the proportion of patients failing nonsurgical therapies. A detailed summary of the sponsor’s methodology for calculating eligible target population is presented in Table 15. The new drug scenario included cenegermin and no relevant nonsurgical treatments (standard care) were identified for the reference case. Key inputs to the BIA are documented in Table 15.
The sponsor’s BIA included the following key assumptions:
Patients receiving cenegermin are removed from analyses in subsequent years due to sponsor assuming re-treatment does not occur
Market shares were estimated through clinician survey
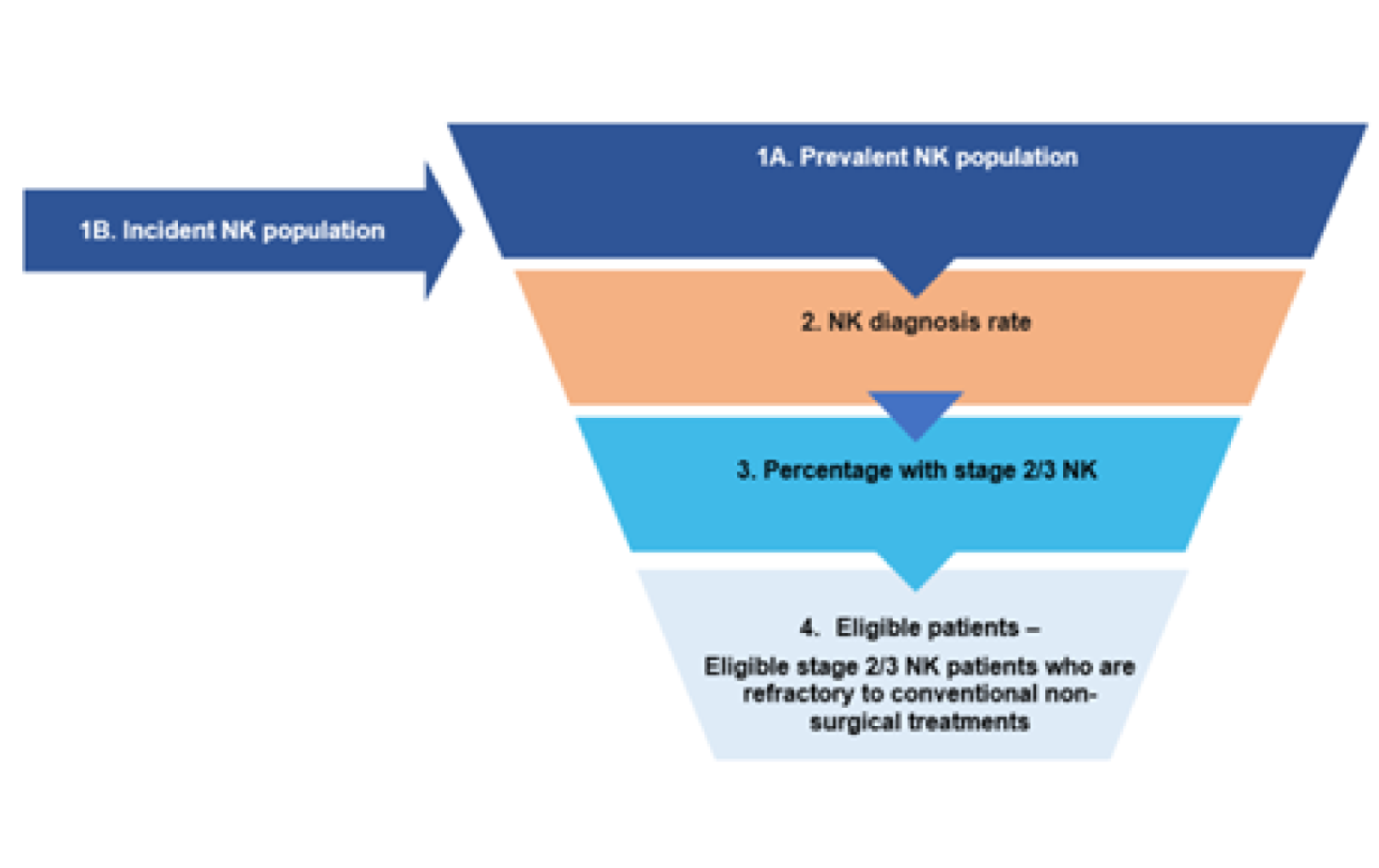
Table 15: Summary of Key Model Parameters
Parameter | Sponsor’s estimate reported as year 1 / year 2 / year 3 if appropriate) |
|---|---|
Target populationa | |
Canadian population (excluding Quebec) | 29,545,581 |
Prevalence of NK per 10,000 (2014)18 | 1.6 |
Incidence of NK per 10,000 (2014) | 0.019 |
Diagnosis rate | 52.50% |
Percentage with stage 2 or 3 NK | 71.00% |
Percentage of patients failed nonsurgical therapies | 59.16% |
Percentage of population covered by public plans | 61.8% |
Market uptake (3 years) | |
Uptake (reference scenario) Cenegermin Standard of Care | 0% / 0% / 0% 100% / 100% / 100% |
Uptake (new drug scenario) Cenegermin Standard of care | 6.00% / 18.79% / 17.10% 94% / 81.21% / 82.9% |
Cost of treatment (per patient) | |
Cost of treatment over 1 year Cenegermin Standard of care | $118,230 $0 |
NK = neurotrophic keratitis.
aPrevalence, incidence, diagnosis rate, percentage with stage 2/3 NK, and percentage failing nonsurgical therapies were parameters derived from the sponsor’s physician survey.17
Summary of the Sponsor’s BIA Results
The sponsor’s estimated budget impact of funding cenegermin for the treatment of adult patients with moderate to severe NK who have failed conventional nonsurgical treatment was $4,729,200 in year 1, $14,069,370 in year 2, and $10,522,470 in year 3, for a 3-year total of $29,321,040.
CADTH Appraisal of the Sponsor’s BIA
CADTH identified several key limitations to the sponsor’s analysis that have notable implications on the results of the BIA:
Market shares for cenegermin are likely underestimated: The sponsor suggests a slow uptake of cenegermin that is expected to decrease by year 3. Given that there are no approved pharmacological therapies available for patients with NK, clinical experts noted that the market shares for cenegermin were likely underestimated. CADTH notes that in the sponsor submitted survey, clinical experts stated that they would recommend cenegermin to 44% to 62% of patients, depending on NK stage. Clinical experts consulted by CADTH also noted that use of the drug may be expanded to stage 1 NK in practice. Both clinician and drug plan inputs indicated that cenegermin could become a new standard of care for treating NK.
As treatment with cenegermin is not chronic, as more people receive cenegermin the smaller the available market size of eligible patients to treat. For example, if 100% of prevalent patients received cenegermin in year 1 then in year 2 only incident cases of NK would be eligible for treatment. Taking this into account, the sponsor estimates that 248 patients will receive cenegermin over 3 years. Over this time, this covers 37% of patients eligible for public reimbursement of cenegermin. This number was felt to be too low and likewise an underestimate from what the sponsor’s conducted clinical survey suggested.
CADTH increased the market shares of cenegermin such that 50% of individuals eligible for public coverage of cenegermin would receive it within 3 years of approval.
Target population is underestimated by excluding those not covered by drug plans: The sponsor assumed that 61.8% of patients would be eligible for public coverage with cenegermin. This is taken from a publication by the Canadian Alliance for Sustainable Health Care.19 However, this assumes that the age distribution of those eligible for cenegermin is the same as the general Canadian population. In the pivotal trial the mean age was 60. Likewise, in the model submitted by the sponsor starting age is 63.6. In the publication from the Canadian Alliance for Sustainable Health Care, 54% of individuals under the age of 65 are cited as being eligible for public coverage.19 Given that public coverage is 100% for patients older than 65 years it is likely that the sponsor has underestimated the proportion of patients eligible for public coverage.
CADTH assumed 50% of patients would be older than 65 years of age, thus receiving 100% public coverage, and 50% would be younger than 65 of whom 54% would receive public coverage. Of note, given the high cost of cenegermin ($118,320) patients might be eligible for public coverage if it poses a financial burden.
As a scenario analysis CADTH increased public coverage to 100%.
Re-treatment is excluded from analyses: The sponsor assumed that no patients would be retreated with cenegermin. Clinicians consulted by CADTH advised that they would continue to follow-up indefinitely with NK patients and likely re-treat patients with cenegermin, should they no longer achieve corneal healing, given they showed an initial response. In some cases, re-treatment may occur in those who are nonhealing but do not deteriorate.
CADTH included a scenario analysis in which 5% of patients would be retreated with cenegermin with the time horizon of the BIA.
Incidence is underestimated: The sponsor assumed that incidence equated to 1.6 patients per 10,000 applied to the Canadian growth rate. There are a few issues with this approach. Firstly, as previously discussed, it would appear the age of eligible patients receiving cenegermin is around the age of 60. Growth rate in this cohort is higher than the average Canadian population.20 Secondly, undiagnosed cases of NK will be diagnosed and cases that are stage 1 will develop into stage 3 over time. The sponsor’s model is static in assuming that undiagnosed cases will remain undiagnosed forever and likewise that stage 1 cases will never develop into stage 2. An increased incidence rate may better account for the growth rate, disease progression, and dynamic population size.
Given the rarity of NK, determining an accurate estimate of incidence over time is challenging. Likewise, establishing an incidence rate that captures those eligible for cenegermin is even more challenging. As a scenario analysis, CADTH increased the incidence rate to 0.19 which represents the number of non-prevalent cases that become eligible for cenegermin over time.
Additional limitations were identified but were not considered to be key limitations. The sponsor has incorrectly stated that the proportion of patients failing nonsurgical therapies was subtracted from stage 2 or 3 patients to calculate the eligible treatment population. The applied calculation in their model multiplies the percentage of those failing by the population with stage 2 or 3 NK, which is correct.
CADTH Reanalyses of the BIA
Table 16: CADTH Revisions to the Submitted Budget Impact Analysis
Stepped analysis | Sponsor’s value or assumption | CADTH value or assumption |
|---|---|---|
Changes to derive the CADTH base case | ||
1. Market shares underestimated (year 1/2/3) | Cenegermin = 6.00% / 18.79% / 17.10% Standard of care = 94.00% / 81.21% / 82.90% | Cenegermin = 6.00% / 18.79% / 25.21% Standard of care = 94.00% / 81.21% / 74.79% |
2. Target population underestimated | 61.8% eligible for public coverage | Patients older than 65 years (50%) receive 100% public coverage, and 54% of patients under 65 (50%) would receive public coverage. Therefore, 77% of patients would be eligible for public coverage. |
CADTH base case | Reanalysis 1 + 2 | |
The results of the CADTH stepwise reanalysis are presented in summary format in Table 17 and a more detailed breakdown is presented in Table 18. Based on the CADTH base case, the budget impact for the reimbursement of cenegermin for the treatment of adult patients with moderate to severe NK who have failed conventional nonsurgical treatment is expected to be $5,911,500 in year 1, $17,498,040 in year 2, and $19,271,490 in year 3. The 3-year total budget impact for cenegermin is $42,681,030. A scenario analysis assessing the budget impact if the price of cenegermin reflected the price in which the ICER would be under the threshold of $50,000 per QALY resulted in a 3-year budget impact of $853,621. A scenario analysis increasing the percentage of the population covered by public plans to 100% led to a 3-year budget impact of $55,331,640. An additional scenario analysis exploring re-treatment in 5% of patients led to a 3-year budget impact of $44,815,082. Lastly, a scenario analysis increasing the incidence rate to 0.19 led to a 3-year budget impact of $47,173,770.
Table 17: Summary of the CADTH Reanalyses of the BIA
Stepped analysis | Three-year total |
|---|---|
Submitted base case | 29,321,040 |
CADTH reanalysis 1 — market shares | 34,286,700 |
CADTH reanalysis 2 — public plans coverage | 36,533,070 |
CADTH base case | 42,681,030 |
BIA = budget impact analysis.
Table 18: Detailed Breakdown of the CADTH Reanalyses of the BIA
Stepped analysis | Scenario | Year 0 (current situation) | Year 1 | Year 2 | Year 3 | Three-year total |
|---|---|---|---|---|---|---|
Submitted base case | Standard of care | $0 | $0 | $0 | $0 | $0 |
Cenegermin | $0 | $4,729,200 | $14,069,370 | $10,522,470 | $29,321,040 | |
Budget impact | $0 | $4,729,200 | $14,069,370 | $10,522,470 | $29,321,040 | |
CADTH base case | Standard of care | $0 | $0 | $0 | $0 | $0 |
Cenegermin | $0 | $5,911,500 | $17,498,040 | $19,271,490 | $42,681,030 | |
Budget impact | $0 | $5,911,500 | $17,498,040 | $19,271,490 | $42,681,030 | |
CADTH scenario analysis: 98% price reduction | Standard of care | $0 | $0 | $0 | $0 | $0 |
Cenegermin | $0 | $118,230 | $349,961 | $385,430 | $853,621 | |
Budget impact | $0 | $118,230 | $349,961 | $385,430 | $853,621 | |
CADTH sensitivity analysis: public plans coverage increased to 100% | Standard of care | $0 | $0 | $0 | $0 | $0 |
Cenegermin | $0 | $7,684,950 | $22,581,930 | $25,064,760 | $55,331,640 | |
Budget impact | $0 | $7,684,950 | $22,581,930 | $25,064,760 | $55,331,640 | |
CADTH sensitivity analysis: re-treatment | Standard of care | $0 | $0 | $0 | $0 | $0 |
Cenegermin | $0 | $6,207,075 | $18,372,942 | $20,235,065 | $44,815,082 | |
Budget impact | $0 | $6,207,075 | $18,372,942 | $20,235,065 | $44,815,082 | |
CADTH sensitivity analysis: increased incidence rate | Standard of care | $0 | $0 | $0 | $0 | $0 |
Cenegermin | $0 | $6,502,650 | $19,271,490 | $21,399,630 | $47,173,770 | |
Budget impact | $0 | $6,502,650 | $19,271,490 | $21,399,630 | $47,173,770 |
BIA = budget impact analysis.
Stakeholder Input
Patient Input
Canadian Organization for Rare Disorders
About the Canadian Organization for Rare Disorders
The Canadian Organization for Rare Disorders (CORD) is Canada’s national network for organizations representing all those with rare disorders. CORD provides a strong common voice to advocate for health policy and a healthcare system that works for those with rare disorders. CORD works with governments, researchers, clinicians and industry to promote research, diagnosis, treatment and services for all rare disorders in Canada.
Website: www.raredisorders.ca
Information Gathering
Recruitment: Participants were recruited through physicians at three eye institutes in the USA: Desai Group (Jamaica, New York), Your Eye Institute (Knightdale, North Carolina), and Price Vision Group (Indianapolis, Indiana). They were approached by the clinic nurse who explained the goal of getting their experience to support a patient submission for access in Canada. The first names and phone numbers of volunteers were passed to CORD, either through phone call, email, or text. CORD called each volunteer individually. Patients were provided with no compensation or any other form of inducement to participate. Upon explaining the purpose and assurance that their comments were anonymous, all consented to the interview. There were no recordings of the interviews; notes were taken during the conversations by the interviewer.
Respondents: There were 12 participants and all completed the entire interview, which lasted from approximately 15 to 30 minutes each. Among the participants, the range in age was 24 to 77 years old with three-fourths over 65 years old and two under 30 years old. All lived in the USA. The younger participants were all employed whereas those over 65 were mostly not working.
There are various reasons why patients experience the loss of nerve growth factor, which is the underlying cause of neurotrophic keratitis (NK), and the participants here represented a cross section of many of these precipitating factors. The two younger patients (24 – 29 years old) thought the source of their condition was physical, surface injury to the cornea in one case and prolonged use of contact lenses (due to the pandemic whereby glasses were challenging with a mask). Several patients said they had gotten an infection in the eye which included various symptoms (e.g., pink eye, abrasion, shingles, dry eye patches). Two respondents said they had had cataract surgery but it is not clear whether this was a trigger for NK. Four respondents indicated they had other conditions which could have been related to NK (diabetes, glaucoma, cardiovascular disease). The remainder said they were not sure of the underlying cause or even whether they had been informed.
Disease Experience
Given the very small number of participants, we will provide some summary information but very importantly individual experiences as well. While NK in the earliest stage may be asymptomatic, all of these respondents reported they had experienced some symptoms prior to diagnosis. Most reported blurred, low (peripheral) vision, or (nearly) loss of vision (in one eye). Some said they had experienced irritation or grittiness on the cornea or inner eyelid. Most had experienced symptoms for six months to three years (or more) prior to diagnosis and treatment.
“My eyesight was getting worse. I couldn’t see any of the letters.”
“Because of the pandemic, I was struggling with wearing glasses with a mask and started wearing my contacts most of the time. My cornea developed these dry patches.”
“I had an infection in my left eye. The doctor prescribed antibiotics but it never went away.”
I had shingles in my eye, probably as the result of a virus, and ended up with extreme damage to the right cornea. My vision was damaged.”
“I was told I wasn’t blinking enough; the nerve was not responsive and as a result the oil didn’t spread around. I needed to remember to blink hard. At 24, I was afraid I would lose sight in that eye forever.”
“I had an infection that led to pink eye and then an abrasion that wouldn’t heal. The doctor prescribed antibiotics but they didn’t help.”
“I have diabetes and glaucoma runs in the family so when I started to lose some vision, the doctor prescribed eye drops which didn’t do all that much. He was planning to do surgery but decided to send me for a second opinion.”
All patients were aware of their diagnosis of neurotrophic keratitis (NK), However, while NK can be categorized into Stages 1, 2, or 3, based on severity, most of the respondents said they had not been told or they did not recall the stage of their NK condition.
For all patients, the risk of losing their eyesight, even in one eye, was very frightening and even traumatic.
“It’s your eyesight. IF you can’t see, you can’t function.”
“I’m all by myself. We moved from Key West to Clearwater [Florida] when my husband was diagnosed with advanced cancer and since had has died, I’m all alone with no family or friends nearby. I have to be able to take care of myself.”
All participants, except one, did not receive the diagnosis of NK from their initial or original “eye doctor” but had been referred to or sought out another ophthalmologist.
The issue seems to be that many ophthalmologists are not aware of NK or how to diagnose it. Howeverm according to the experts that we spoke with, it is quite easy to make an initial diagnosis. With NK, the nerve endings that serve the cornea have died. causing the person to lose feeling on the cornea. Not only does the person fail to blink regularly to keep the eye sufficiently lubricated, but s/he also does not recognize the irritants that routinely fall in the eye and therefore will not blink or clear them away like a person with normal nerve sensations. These go on to cause infections and diminished eyesight.
In fact, as we were told, the initial screening for NK is a simple touch to the cornea with a cotton swab or cotton thread. The person with NK will not blink or pull away because the cornea has no feeling.
“I was unwilling to accept the fact that there was nothing that could be done except maybe surgery. Luckily, I found [the] Eye Institute and met the doctor who said he thought I had NK. He did just this little test of putting a cotton swab on my eye and said he was pretty sure that was what I had. Amazing.”
“I remember my first doctor said he did not think I had NK and prescribed eye drops from blood serum, which cleared up the eye patches about 40%. But two weeks later, they came back.
Experiences With Currently Available Treatments
Most of the respondents had received one or more types of interventions prior to getting a diagnosis of NK. The period of time from onset of symptoms to accurate diagnosis was from 6 months to three years or more. The patients we interviewed were the lucky ones who eventually received an accurate diagnosis of NK and were treated. We did not speak with patients who had not gotten a diagnosis and were potentially still suffering from ineffective treatments or, as bad, interventions that were highly invasive (cornea transplant) or permanently without sight in the affected eye (suturing the eye shut).
Most of these participants recalled being prescribed lubricant or “artificial tear” drops. Most had also been prescribed antibiotics. One patient reported receiving eye drops made from her blood serum.
One patient reported she had had her eye “scraped” by the doctor.
“I would never had let him do it if I had known it would have been as bad as it was.”
Two of the patients said they had discussed the option of surgery, including the possibility of installing an artificial “placenta” to protect the cornea or even to close the eye by suturing the lid.
One older (77-year-old) patient said he had received antivirals but when those didn’t help, the option of surgery was raised.
“The doctor talked about a couple of surgeries that I might need but I can’t recall the exact type he suggested. I just kept asking if there was anything else I could try.”
Another patient (age 71 years) reported that she had been prescribed a number of antibiotics but it never cleared up or stopping the constant “running.”
“I went through a whole gamut of tests and saw so many doctors at the eye institute. But I still couldn’t see out of the eye, only shapes and light. I was told I needed a cornea transplant.”
One patient reported that her physician had made a diagnosis of NK but sent me to another specialist to verify that this was the right diagnosis.
“When the other doctor said it was the right diagnosis, then we talked about another treatment.”
Improved Outcomes
“The good news about neurotrophic keratitis is that it does not have to be a chronic condition. It can be treated and ostensibly “cured.” Even better, it can be easily screened and diagnosed. The bad news is that it is rare so relatively unknown to many physicians, even specialists. Even worse, most patients seemingly endure long periods of suffering, ineffective treatment, or invasive treatments. When asked what they would have liked at the time of symptom onset, most said they would have liked to have gone to a specialist who could have made an accurate diagnosis “right off the top.”
“It would have spared me years of agony and anxiety, especially around losing my eyesight, which is the most important thing.”
“It was so frustrating going to doctor after doctor with no one knowing what was really wrong. Maybe there was nothing different that could have been done but at least I wouldn’t be trying a lot of things that did no good.”
“Given how easy it is test for NK it is important that all doctors are instructed to do this even if it is only a possibility that it is NK.”
“Now that there is a drug treatment, it is even more urgent to test early so people can get treated as soon as possible and don’t lose their eyesight.”
Participant comments reflect strongly the fact that each has had access to an effective treatment but only after a long struggle with ineffective ones.
“I need my eyesight to drive to work and to do my job. So, it was very frustrating when nothing was working.”
“I spent so much time going to different doctors and trying all kinds of things. They were all really nice but couldn’t be sure that anything they were prescribing was going to fix the problem. That was really scary.”
“People should be able to find information about treatments that work but everything I found on line was stuff I already knew and nothing about this new treatment. If I had not found Dr. [X], I would probably have settled for something else and lost my eyesight.”
“A direct line to the right specialist and a direct line to the right treatment.”
“A lot of the treatments are not covered by insurance because they are considered to be “experimental. Some aren’t all that expensive but when you are retired and on a fixed income, it adds up. And especially if they don’t really fix the problem.”
Experience With Drug Under Review
All of the patients interviewed had experience with Oxervate. All had positive outcomes with the therapy, although the impact and durability varied from totally resolving up their vision, tearing, and blinking problems to being able to have some vision and to stabilize the eye enough to consider a cornea transplant. Patients had completed treatment from two weeks to three years ago.
“By the end of treatment, my eye had completely stopped running and I could see out of the eye, not perfectly but well enough to have no limits in what I want to do.”
“I have just finished treatment do don’t know whether it is a permanent fix but the doctor says it was caught at Stage 1 so I should be able to have a complete recovery. I still have to remember to blink and there is still a strip of eye patches but it doesn’t interfere with my vision.”
“I was able to go back to wearing my contacts which is important for my line of work.”
“Before Oxervate, I couldn’t do a natural reflex so I didn’t even notice things that were coming into my eye. Now, no worries.”
“It is like a miracle drug, performing nerve regeneration. I have had no relapse for the past three years.”
“I had a second round because I didn’t get diagnosed until I was pretty advanced. I think the doctor said it was Stage 2 or 3. But since then, my vision seems to be stabilized so I don’t think I will need to do it again.”
“Without Oxervate, I would not be able to live on my own. I would be back to feeling uncertain and helpless going out. I no longer feel depressed and lonely. It really has given me my life back.
Some patients reported experiencing minor side effects (stinging, pain, headaches, blurred vision) that went away when they stopped the eight-week treatment.
All of the patients were able to complete the 8-week course of therapy, despite the onerous schedule of dosing six times a day every two hours.
“I was warned by the doctor that I may experience some pain with the treatment but that was a good thing because it meant the nerve was coming back. It was only about half-way through and totally went away when the treatment was finished.”
“I had it done last year and would recommend Oxervate to anyone who was diagnosed with NK. And, of course, if you have any of these symptoms ask for a test because the doctor may not think of it himself.
In summary, every participant whom we interviewed was positive about the effects of Oxervate in terms of effectiveness in addressing their key symptoms of blurred vision or loss of peripheral vision, running or tearing eyes, and lack of blinking reflex. All reported resolution of symptoms of blurred vision, runny eyes, and inability to protect against foreign matter in the eye. Most who had the treatment two to three years ago were still benefitting from improved vision and none of the symptoms associated with loss of nerves supporting the cornea.
Companion Diagnostic Test
Access to Oxervate is based on a confirmed diagnosis of NK. The initial screening is a cornea sensitivity test that can be performed easily with a cotton swab to the surface of the cornea. Confirmation requires a careful ocular, medical, and surgical history, a thorough examination of the surface of the eye using a biomicroscope with various medical dyes, and a formally assessment of corneal sensitivity.
Anything Else?
Neurotrophic keratitis is a rare condition (< 5 in 10,000) and even more rarely diagnosed because of lack of awareness by patients and healthcare professionals, including specialists. Oxervate is the only treatment specifically for NK. If NK is diagnosed and treated early, in Stage 1, minimal damage and full recovery are usually possible. However, because in the early stage, patients experience minor or no pain and only blurry vision, glitches in vision, floating spots, or other symptoms that could be indicative of other conditions, it is often undiagnosed in the early stage. Moreover, most ophthalmologists are not trained to recognize or suspect NK, which is a rare condition.
Patient Group Conflict of Interest Declaration — Canadian Organization for Rare Disorders
To maintain the objectivity and credibility of the CADTH reimbursement review process, all participants in the drug review processes must disclose any real, potential, or perceived conflicts of interest. This Patient Group Conflict of Interest Declaration is required for participation. Declarations made do not negate or preclude the use of the patient group input. CADTH may contact your group with further questions, as needed.
Did you receive help from outside your patient group to complete this submission? If yes, please detail the help and who provided it.
This submission was completed by the staff and volunteers of CORD.
Did you receive help from outside your patient group to collect or analyze data used in this submission? If yes, please detail the help and who provided it.
Data collection was assisted by referrals from three eye clinics and their expert physicians in the USA. The clinics and physicians had no role in the interviews with the patients but merely provided CORD, with patient informed consent, the first names and phone numbers of these willing to be interviewed.
List any companies or organizations that have provided your group with financial payment over the past two years AND who may have direct or indirect interest in the drug under review.
Table 1: Conflict of Interest Declaration for Canadian Organization for Rare Disorders
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
None | — | — | — | — |
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up-to-date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.