CADTH Reimbursement Review
Fostamatinib (Tavalisse)
Sponsor: Medison Pharma Canada Inc.
Therapeutic area: Chronic immune thrombocytopenia
This multi-part report includes:
Clinical Review
Pharmacoeconomic Review
Stakeholder Input
Clinical Review
Abbreviations
AE
adverse event
ALT
alanine transaminase
AST
aspartate transaminase
CI
confidence interval
CrI
credible interval
HRQoL
health-related quality of life
IBLS
immune thrombocytopenia bleeding scale
ITC
indirect treatment comparison
ITP
immune thrombocytopenia
ITT
intention to treat
IVIG
intravenous immunoglobulin
LOCF
last observation carried forward
NMA
network meta-analysis
OR
odds ratio
PDSA
Platelet Disorder Support Association
RCT
randomized controlled trial
RD
risk difference
SAE
serious adverse event
SD
standard deviation
SF-36
Short Form (36) Health Survey
TPO-RA
thrombopoietin receptor agonist
Executive Summary
An overview of the submission details for the drug under review is provided in Table 1.
Item | Description |
|---|---|
Drug product | Fostamatinib (Tavalisse), 100 mg or 150 mg tablet, oral |
Indication | Health Canada indication: for the treatment of thrombocytopenia in adult patients with chronic ITP who have had an insufficient response to other treatments |
Reimbursement request | For the treatment of thrombocytopenia in adult patients with ITP who have had an insufficient response to a TPO-RA in jurisdictions where TPO-RA reimbursement is available, or after failure of corticosteroids and other earlier-line treatments in jurisdictions where TPO-RA reimbursement is not available |
Health Canada approval status | NOC |
Health Canada review pathway | Priority review |
NOC date | November 19, 2020 |
Sponsor | Medison Pharma Canada Inc. |
ITP = immune thrombocytopenia; NOC = Notice of Compliance; TPO-RA = thrombopoietin receptor agonist.
Introduction
Immune thrombocytopenia (ITP) is an autoimmune disease characterized by low platelet counts and increased bleeding risk.1 Primary ITP is not triggered by a specific condition or event, while secondary ITP is caused by or associated with another condition. Chronic ITP lasts 12 months or more after the initial diagnosis while persistent ITP lasts 3 to 12 months after initial diagnosis. A 2010 narrative review of international studies suggested that the incidence of ITP among adults is approximately 3.3 per 100,000 per year while the prevalence is 10 per 100,000. Patients with ITP may experience bleeding (mild, severe, or critical) and fatigue, and have a reduced health-related quality of life (HRQoL) due to the disease and its treatment. Treatment is generally indicated when the platelet count is low (e.g., < 20,000/µL or 30,000/µL) and/or if the patient is experiencing bleeding.1 The main goals of therapy in ITP are to prevent severe or critical bleeding, reduce or eliminate patients’ symptoms, minimize adverse effects from treatments, and ultimately improve patient HRQoL.2 Recommended treatments that target platelet levels above 20,000/µL to 30,000/µL appear to reduce the risk of major bleeding.2,3 Corticosteroids or IV immunoglobulin (IVIG) are recommended by guidelines as first-line therapy.2,3 Patients may not respond to these treatments or relapse. In such patients, several subsequent-line treatments are available, such as a splenectomy; rituximab; thrombopoietin receptor agonists (TPO-RAs) such as romiplostim and eltrombopag; fostamatinib; or immunosuppressants.2,3 The optimal sequence of second- and subsequent-line therapies is often unclear due to a lack of comparative efficacy and safety data, patient heterogeneity, and access and/or reimbursement issues.2,3 Not all patients respond to treatment with second- or third-line treatment options. Patients can also become refractory to treatment options or relapse after achieving remission.2,3 Chronic ITP is therefore characterized by a chronic relapsing course and multiple lines of therapy over time.
Fostamatinib is indicated for the treatment of chronic ITP in adult patients who have had an insufficient response to other treatments.4 It reduces destruction of platelets via inhibition of spleen tyrosine kinase.4 Fostamatinib is initiated at a dosage of 100 mg twice daily and is taken orally.4 If the platelet count has not increased to at least 50,000/µL after 4 weeks, then the dosage can be increased to 150 mg twice daily.4 Fostamatinib underwent an expedited review at Health Canada.
The objective of this report was to perform a systematic review of the beneficial and harmful effects of fostamatinib for the treatment of thrombocytopenia in adult patients with chronic ITP who have had an insufficient response to other treatments.
Stakeholder Perspectives
This section summarizes input provided by the patient groups who responded to CADTH’s call for patient input and from clinical experts consulted by CADTH for the purpose of this review.
Patient Input
One patient group submission, prepared by the Platelet Disorder Support Association (PDSA), was received for this review. How the data were collected to inform the submission was not described; however, patient experiences with fostamatinib were gathered from the PDSA’s Facebook group. The patient input submission suggested that patients with ITP are fearful of life-threatening bleeding, face physical and emotional consequences from their disease (e.g., fatigue, anxiety, and depression), and restrict their activities because of their disease. The submission also suggested that ITP and its treatment interfere with daily life and negatively affect HRQoL. Patients are often more concerned with managing symptoms and improving HRQoL than with platelet counts. Myriad treatment options are available to manage ITP, and it is difficult to predict who will respond to a particular treatment and who will develop resistance to a treatment over time. In addition, patients may not be able to afford or access available options. It is therefore important that patients have options available in case they do not respond to a therapy, the therapy stops working, or they experience bleeding.
Clinician Input
Input From Clinical Experts Consulted by CADTH
The clinical experts consulted by CADTH suggested that standard first-line therapy for ITP includes corticosteroids, and IVIG is often added when an immediate increase in platelets is required, although the effect of IVIG is often transient. The experts noted that a significant proportion of patients will not respond to steroids and, of those that do, many will relapse once steroids are tapered. At this point, a splenectomy is the traditional second-line therapy if the patient is a suitable candidate. More recently, rituximab has emerged as an alternative second-line therapy. If both a splenectomy and rituximab have failed (or are contraindicated), a large number of third-line therapies are available, including immunosuppressant medications such as azathioprine or cyclophosphamide, or TPO-RAs such as eltrombopag or romiplostim. There is little evidence to guide the selection of second- or third-line therapy, and decisions depend on both local reimbursement considerations and patient-specific factors.
The clinical experts consulted by CADTH stated that treatment goals are to reduce bleeding and prolong life. Increasing the platelet count is generally considered to be a reasonable surrogate for both goals. Improving HRQoL is also an important goal.
The clinical experts emphasized that not all patients respond to available therapies, and even if remission is achieved, long-term remission is not guaranteed. The clinical experts noted how accessibility to appropriate second- and third-line therapies can be a challenge, as not all options are reimbursed in each province or because reimbursement criteria differ across provinces. Administration of existing therapies can also be a challenge and there are adverse effects with existing treatments. Therapies with demonstrated efficacy, convenience of administration, and a low risk of adverse effects would therefore fill an unmet need for treatment of ITP.
The clinical experts stated that contemporary ITP guidelines suggest that, in general, a splenectomy or rituximab can be considered as second-line therapy. Several third-line options are available; however, the comparative efficacy of these agents is unclear. It can therefore be difficult to determine the best treatment option for a particular patient, and there is often no single clearly defined treatment pathway. Decisions end up being driven largely by access. It is challenging to identify the optimal place for fostamatinib in a therapeutic algorithm. The clinical experts noted that rituximab or a splenectomy are reasonable second-line choices (TPO-RAs may also be considered second-line choices in some patients). The safety profile of fostamatinib and the fact that it is administered orally suggest it may be considered a reasonable third-line therapy rather than reserved for patients who have failed or do not have access to TPO-RAs, as has been proposed by the sponsor. However, regardless of where it sits in the therapeutic algorithm, it would be advantageous for clinicians if fostamatinib was available as a treatment option for specific patients. The clinical experts noted that the ITP population is heterogenous, and the available data and current understanding of ITP pathophysiology make it impossible to determine who will respond best to fostamatinib and who are most susceptible to adverse effects.
Bleeding is an important outcome in the treatment of ITP, and ultimately any treatment should reduce the occurrence of clinically important bleeding while improving HRQoL. In practice, clinicians rely on platelet response, which is assumed to reduce the risk of clinically relevant bleeding and, as a secondary benefit, reduce the need for rescue therapy. In general, an increase in platelet count can be seen as early as 2 weeks into treatment with fostamatinib, although some patients may not respond until week 12. If a response is observed, clinicians would likely continue to use the treatment long-term with monthly monitoring. A sustained response would generally be considered a platelet count of 30,000/µL to 50,000/µL for the duration of a treatment cycle (e.g., 24 weeks). If a response has not been seen by approximately 24 weeks, most clinicians would likely consider the treatment to have failed and would discontinue it. If there are issues related to safety or tolerability, treatment would generally be discontinued earlier, particularly if it is affecting a patient’s HRQoL.
Clinician Group Input
A group of 19 Canadian hematologists submitted input on fostamatinib. The clinician group submission echoed the opinions of the expert panel. The clinician group submission suggested that fostamatinib would be likely used after first-line therapy as second-line or subsequent-line therapy. The clinician group submission reported that fostamatinib would be used as a single drug after first-line therapy has failed. Fostamatinib was described as an alternative to other second- and subsequent-line therapies and should be considered before a splenectomy, immunosuppressive drugs, and rituximab and its biosimilars, and should be used at a line of therapy similar to that of maintenance treatments such as TPO-RAs. The clinician group submission stated that patients earlier in their ITP disease course may respond better to fostamatinib. Using it as a second-line treatment may therefore offer advantages, such as limiting exposure to complications or toxicities from other drugs. However, the greatest need is still in patients who have relapsed multiple times despite treatment.
Drug Program Input
Drug programs asked whether concomitant therapy (e.g., corticosteroids or danazol) is required with fostamatinib as some patients from relevant clinical trials used concomitant therapy. The clinical experts noted that concomitant therapy is likely not necessary to continue and could often be discontinued if and when it is considered unnecessary. Drug programs also asked how the time to response for fostamatinib compares to other available treatments. The clinical experts reported that fostamatinib has a similar time to response as TPO-RAs and is faster than rituximab. The drug programs inquired about the threshold for initiating treatment in cases of ITP and the clinical experts clarified that the usual threshold is less than 30,000/µL. The drug programs also asked if fostamatinib should only be reimbursed for people with ITP for more than 3 years based on subgroup analyses in relevant clinical trials. The clinical experts noted that trials were likely underpowered to detect a response in subgroups and indicated that it would not be appropriate to exclude patients from reimbursement based on a duration of ITP of less than 3 years. Drug programs asked if public payers should only fund fostamatinib after the patient has failed all second-line therapies (splenectomy, rituximab, and TPO-RAs). The clinical experts suggested that, given the lack of comparative evidence among treatment options, it is challenging to put fostamatinib in front of established second-line therapies such as rituximab or a splenectomy (unless there are specific contraindications), and that it may be more reasonable to position fostamatinib at a level of treatment similar to that of TPO-RAs. The drug program asked what a typical treatment course of fostamatinib would be and the clinical experts suggested that, because it has not been used extensively in practice to date, there is no recognized typical course of treatment. The drug programs also asked if, based on adverse event (AE) data from the relevant clinical trials, fostamatinib can be considered to be poorly tolerated. The clinical experts stated that, because the placebo group in the trials also experienced high rates of AEs, they cannot say that fostamatinib is poorly tolerated.
Clinical Evidence
Pivotal Studies and Protocol-Selected Studies
Description of Studies
Two identically designed 24-week double-blind randomized controlled trials (RCTs), FIT1 (N = 76)5 and FIT2 (N = 74),6 evaluated the efficacy and safety of fostamatinib versus placebo in patients with primary ITP for more than 3 months who had received at least 1 previous ITP treatment and had a baseline platelet count below 30,000/µL in at least 3 counts in the preceding 3 months. The FIT1 trial was conducted in Australia, Canada, 4 countries in Europe (Denmark, Hungary, Italy, the Netherlands), the UK, and the US, while the FIT2 trial was conducted in 8 countries in Europe (Austria, Bulgaria, Czech Republic, Germany, Norway, Poland, Romania, Spain). In the FIT1 trial, 51 patients were randomized to fostamatinib and 25 to placebo, while in the FIT2 trial, 50 patients were randomized to fostamatinib and 24 to placebo. The primary efficacy end point in both trials was achievement of stable platelet response, defined as a platelet count of least 50,000/µL at 4 of the last 6 study visits between weeks 14 and 24. These trials also measured the use of rescue therapy, bleeding-related serious adverse events (SAEs), and HRQoL (via the Short Form [36] Health Survey [SF-36]), along with harms.
In the FIT1 trial, the mean age was 57 years (standard deviation [SD] = 18) in the fostamatinib group and 53 years (SD = 16) in the placebo group. In the fostamatinib group, 59% of patients were female compared to 68% in the placebo group. The mean duration of ITP was 13 years (SD = 14) in the fostamatinib group versus 9 years (SD = 10) in the placebo group. Patients in the fostamatinib group had used a median of 5 prior ITP treatments (range = 1 to 10) while patients in the placebo group had used a median of 3 (range = 1 to 9). More patients in the placebo group had used steroids (100%) and TPO-RAs (60%) compared to the fostamatinib group (90% for steroids and 51% for TPO-RAs). In the FIT1 and FIT2 trials, the rate of concomitant steroid use was higher in the placebo group (56% in the FIT1 trial and 63% in the FIT2 trial) compared to the fostamatinib group (37% in the FIT1 trial and 44% in the FIT2 trial). In the FIT1 trial, the rates of prior splenectomy were similar (40%) in both groups. In the FIT2 trial, the mean age was 49 years (SD = 15) in the fostamatinib group and 50 years (SD = 17) in the placebo group. In the fostamatinib group, 62% of the patients were female compared to 54% in the placebo group. The mean duration of ITP was 12 years (SD = 13) in the fostamatinib group versus 11 years (SD = 8) in the placebo group. Patients in both groups had used a median of 3 previous ITP treatments (range = 1 to 10). The rate of previous individual ITP medication use was similar between groups. The rates of a prior splenectomy was higher in the placebo group (38% versus 28% in the fostamatinib group).
Efficacy Results
In the FIT1 trial, 18% of patients in the fostamatinib group experienced a stable platelet response compared to 0% in the placebo group (risk difference [RD] = 18%; 95% confidence interval [CI], 7.2 to 28; P = 0.026). In the FIT2 trial, 18% of patients in the fostamatinib group experienced a stable platelet response compared to 4% in the placebo group (RD = 14%; 95% CI, 0.5 to 27; P = 0.15), a difference that was not statistically significant.
In the FIT1 trial, 31% of patients in the fostamatinib group required rescue therapy before week 10 compared to 44% of patients in the placebo group. After week 10, rescue therapy was required for 14% of patients in the fostamatinib group compared to 28% of the placebo group. In the FIT2 trial, 18% of patients in the fostamatinib group required rescue therapy before week 10 compared to 29% of patients in the placebo group. After week 10, only 2% of patients in the fostamatinib group required rescue therapy compared to 21% in the placebo group. In the FIT1 trial, ||||| of patients in the fostamatinib group experienced a bleeding-related SAE compared to |||||| in the placebo group. In the FIT2 trial, ||||| of patients in the fostamatinib group experienced a bleeding-related SAE compared to ||||| in the placebo group. No statistical testing was applied to these outcomes.
For the quality-of-life outcome, no differences in SF-36 scores were evident between the fostamatinib and placebo groups at any time point in the FIT1 trial. At week 24, there was |||||||||| providing SF-36 data in the placebo group and ||||| patients in the fostamatinib group. In the FIT2 trials, no differences in SF-36 scores were evident between the fostamatinib and placebo groups at week 12 or week 24. At week 24 in the FIT2 trial, there were ||||||||||| providing SF-36 data in the placebo group and ||||| patients in the fostamatinib group. The effect of fostamatinib on HRQoL is unclear from the FIT1 and the FIT2 trials.
Both the FIT1 and FIT2 trials conducted subgroup analyses for the primary efficacy end point. In the FIT1 trial, among patients with prior TPO-RA treatment, 15% of the fostamatinib group experienced a stable platelet response compared to 0% of the placebo group (RD = 15%; 95% CI, 1.5 to 29). Among patients without prior TPO-RA treatment, 20% of the fostamatinib group experienced a stable platelet response compared to 0% of the placebo group (RD = 20%; 95% CI, 4.3 to 36). In the FIT2 trial, among patients with prior TPO-RA treatment, 15% of the fostamatinib group experienced a stable platelet response compared to 0% of the placebo group (RD = 15%; 95% CI, −0.6 to 31). Among patients without prior TPO-RA treatment, 20% of the fostamatinib group experienced a stable platelet response compared to 7% of the placebo group (RD = 13%; 95% CI, −6.8 to 33). In the FIT1 trial, among patients with a prior splenectomy, 15% of the fostamatinib group experienced a stable platelet response compared to 0% of the placebo group (RD = 15%; 95% CI, −0.6 to 31). Among patients without a prior splenectomy, 19% of the fostamatinib group experienced a stable platelet response compared to 0% of the placebo group (RD = 19%; 95% CI, 5.4 to 33). In the FIT2 trial, among patients with prior splenectomy, 21% of the fostamatinib group experienced a stable platelet response compared to 0% of the placebo group (RD = 21%; 95% CI, −0.1 to 43). Among patients without prior splenectomy, 17% of the fostamatinib group experienced stable platelet response compared to 7% of the placebo group (RD = 10%; 95% CI, −7.5 to 28).
The following outcomes identified in the protocol were not reported in either the FIT1 or FIT2 trial: duration of response, symptoms, hospitalizations, or emergency room visits.
Harms Results
In the FIT1 trial, among patients in the fostamatinib group, the most common AEs (≥ 5%) were diarrhea (41%), nausea (29%), increased alanine transaminase (ALT) (18%), increased aspartate transaminase (AST) (16%), headache (14%), dizziness (18%), epistaxis (18%), fatigue (12%), and hypertension (26%). The most common AEs in the placebo group were diarrhea (16%), headache (24%), dizziness (16%), epistaxis (16%), and dyspnea (12%). In the FIT2 trial, the most common AEs in the fostamatinib group were diarrhea (18%), epistaxis (12%), and hypertension (14%). The most common AEs in the placebo group were diarrhea (13%), nausea (13%), headache (13%), hypertension (13%), and thrombocytopenia (13%).
In the FIT1 trial, 16% of patients in the fostamatinib group had at least a single SAE (febrile neutropenia, immune thrombocytopenic purpura, thrombocytopenia, retinal tear, diarrhea, pneumonia, syncope, vaginal hemorrhage, or epistaxis) compared to 20% in the placebo group (anemia, congestive cardiac failure, gastrointestinal hemorrhage, menorrhagia, chronic obstructive pulmonary disease, epistaxis). In the FIT2 trial, 10% of patients in the fostamatinib group had at least a single SAE (epistaxis, bronchitis, contusion, decreased platelet count, plasma cell myeloma, transient ischemic attack, or hypertensive crisis) compared to 26% in the placebo group (thrombocytopenia, menorrhagia, muscle rupture, infection, or petechiae). In the FIT1 trial, 16% of patients in the fostamatinib group withdrew due to any AE (abdominal pain, diarrhea, neutropenia, thrombocytopenia, increased ALT, chest pain, pneumonia, or syncope) compared to 8% in the placebo group (abdominal discomfort or epistaxis). In the FIT2 trial, 4% of patients in the fostamatinib group withdrew due to any AE compared to 9% in the placebo group. In the fostamatinib group, 1 patient (2%) withdrew due to plasma cell myeloma and 1 due to headache. In the placebo group, 1 patient (4%) withdrew due to diarrhea and 1 due to hypertension. One patient in the FIT1 trial died in the placebo group due to sepsis. In the FIT2 trial, a single patient died in the fostamatinib group due to plasma cell myeloma.
In the FIT1 trial, |||||| of patients in the fostamatinib group experienced an infection compared to |||||| in the placebo group. In the FIT2 trial, |||||| of patients in the fostamatinib group and |||||| of patients in the placebo group experienced an infection. In both the FIT1 and FIT2 trials, ||||| of patients in the fostamatinib group experienced neutropenia compared to ||||| in the placebo group. In the FIT1 trial, |||||| of patients in the fostamatinib group experienced elevated liver transaminase levels compared to ||||| in the placebo group. In the FIT2 trial, ||||| of patients in the fostamatinib group experienced elevated liver transaminase levels compared to ||||| in the placebo group.
Table 2: Summary of Key Results from Pivotal and Protocol-Selected Studies
Result | FIT1 | FIT2 | ||
|---|---|---|---|---|
Fostamatinib (N = 51) | Placebo (N = 25) | Fostamatinib (N = 50) | Placebo (N = 24) | |
Stable platelet response (≥ 50,000/µL) at 4 of 6 visits between weeks 14 and 24a | ||||
n (%) | 9 (18) | 0 (0) | 9 (18) | 1 (4) |
Risk difference (95% CI) | 18 (7.2 to 28.1) | 14 (0.5 to 27.1) | ||
P value | 0.026 | 0.15 | ||
Mean IBLS score across 24 weeksb | ||||
Number of patients contributing to the analysis | 51 | 25 | 50 | 24 |
Mean IBLS over 24 weeks (SD) | 0.13 (0.12) | 0.14 (0.10) | 0.04 (0.08) | 0.06 (0.07) |
Difference in means (95% CI) | −0.01 (−0.1 to 0.0) | −0.01 (−0.05 to 0.02) | ||
P value | 0.66 | 0.49 | ||
Mean WHO bleeding scale score across 24 weeksb | ||||
Number of patients contributing to the analysis | 51 | 25 | 50 | 24 |
Mean score over 24 weeks (SD) | 0.61 (0.66) | 0.46 (0.56) | 0.26 (0.38) | 0.38 (0.47) |
Difference in means (95% CI) | 0.15 (−0.2 to 0.5) | −0.12 (−0.32 to 0.09) | ||
P value | 0.34 | 0.25 | ||
Use of rescue therapy after week 10 | ||||
n (%) | 7 (14) | 7 (28) | 1 (2) | 5 (21) |
Risk difference (95% CI) | NR | NR | ||
P value | NR | NR | ||
Bleeding-related SAEs | ||||
n (%) | 2 (4) | 3 (12) | 2 (4) | 2 (8) |
Risk difference (95% CI) | NR | NR | ||
P value | NR | NR | ||
Harms, n (%) | ||||
AEs | 49 (96) | 19 (76) | 36 (71) | 18 (78) |
SAEs | 8 (16) | 5 (20) | 5 (10) | 6 (26) |
WDAEs | 8 (16) | 2 (8) | 2 (4) | 2 (9) |
Death | 0 (0) | 1 (4) | 1 (2) | 0 |
Notable harms | ||||
Infection, n (%) | |||||| | |||||| | |||||| | |||||| |
Neutropenia, n (%) | |||||| | |||||| | |||||| | |||||| |
Transaminase elevation, n (%) | |||||| | |||||| | |||||| | |||||| |
Hypertension, n (%) | |||||| | |||||| | |||||| | |||||| |
Nausea, n (%) | |||||| | |||||| | |||||| | |||||| |
Diarrhea, n (%) | |||||| | |||||| | |||||| | |||||| |
AE = adverse event; CI = confidence interval; IBLS = immune thrombocytopenia bleeding scale; SAE = serious adverse event; SD = standard deviation; WDAE = withdrawal due to adverse event.
aIntention-to-treat population, 2-sided Fisher exact test with a significance level of 0.05.
bIntention-to-treat population, 2-sided, 2-sample t-test.
Source: FIT1 Clinical Study Report5 and FIT2 Clinical Study Report.6
Critical Appraisal
The FIT1 and FIT2 trials were at an overall low risk of bias, although there were some concerns regarding selective outcome reporting (sensitivity analyses and subgroup analyses were not pre-specified) and a potential for unblinding due to high dropout rates due to a lack of response. In both the FIT1 and FIT2 trials, the fostamatinib and placebo groups were generally balanced in baseline characteristics, although some baseline imbalances in each trial may have introduced bias. For example, there were differences in the rates of specific previous ITP treatments used in the FIT1 trials and differences in the rate of prior splenectomy in the FIT2 trial, as well as higher concomitant steroid use in the placebo group in both trials. The rate of study discontinuation was high in both the FIT1 and FIT2 trials and was imbalanced between study groups in both trials, primarily due to discontinuation from the trials because of a lack of treatment response. Because patients discontinuing due to a lack of response were treated as nonresponders and an intention-to-treat (ITT) approach to the analysis was used, the high discontinuation rate did not appear to bias the primary outcome. However, for the SF-36 outcome, the high study-discontinuation rate meant limited data were available at week 24 (e.g., 1 patient in the placebo group at week 24 in the FIT1 trial, and 2 patients in the placebo group at week 24 in the FIT2 trial). It was therefore not possible to draw any meaningful conclusions from the SF-36 data at week 24 due to the limited amount of data from study discontinuations. Given the small number of patients in each subgroup and low event rates, there was likely insufficient power to detect any differences between treatments in these subgroups. This is reflected by wide CIs in the RD.
The small number of patients and low event rates for certain outcomes (ITP bleeding scale [IBLS] and WHO bleeding scale scores, bleeding-related SAEs, and the use of rescue therapy) make it challenging to draw conclusions about any difference between treatment groups for these secondary end points. These outcomes may also have been biased by imbalances in concomitant steroid use. Neither the FIT1 nor the FIT2 trial were powered for secondary end points and there was no adjustment for multiplicity for secondary end points; these outcomes should therefore be interpreted with caution.
Clinical experts indicated that the population of the FIT1 and FIT2 trials are broadly comparable to the population of patients with ITP in Canada, and the results of these trials are therefore likely generalizable to the Canadian population. The long duration of ITP and multiple previous treatments among patients in the FIT2 trial mirrors what is commonly seen among patients with ITP in clinical practice in Canada. However, the clinical experts did note generalizability concerns with the FIT1 and FIT2 trials in some Canadian contexts, as patients in both trials were predominantly White. The experts also noted that, because patients with secondary ITP were excluded from the FIT1 and FIT2 trials, findings may not be generalizable to those with secondary ITP. Further, the specific types of previous treatments used in the FIT1 and FIT2 trials differ from those commonly seen at a similar point in ITP treatment in Canada. The clinical experts pointed out that, based on the duration of ITP for patients in the FIT1 and FIT2 trials, a greater portion of chronic ITP patients in Canada would have had a prior splenectomy. Moreover, the extent of previous rituximab use in the FIT1 trial is higher than what would be seen in Canada at a similar stage of treatment. In terms of outcome assessment in the FIT1 and FIT2 trials, the clinical experts noted that bleeding outcomes are likely the most important in practice, but that treatment response is most commonly measured by platelet counts.
The FIT1 and FIT2 trials provided limited data on clinically important outcomes such as HRQoL, rescue therapy, and bleeding events. The clinical experts do not use the IBLS and WHO bleeding scale in practice, and the relevance of the bleeding outcome scales used in the trials is unclear. Further, the event rates for the post hoc bleeding-related SAE outcome made it challenging for the clinical experts to comment on the relevance or meaningfulness of these findings. The clinical experts found that the lower rate of rescue therapy use among patients treated with fostamatinib compared to placebo in the FIT1 and FIT2 trials could be meaningful, but they also noted the relatively low event rates. Similarly, given the small numbers and low event rates in the subgroup analyses, the clinical experts could not draw meaningful conclusions about whether any subgroup differences were likely to exist (e.g., based on a prior splenectomy or TPO-RA treatment). Another challenge with both the FIT1 and FIT2 trials is that the comparator is placebo. In chronic ITP, if the platelet count is below 20,000/µL, as it was at baseline for patients in both trials, the clinical experts (and clinical practice guidelines) indicated that treatment would be warranted. Placebo may therefore not be an appropriate comparator for fostamatinib. Indeed, the FIT1 and FIT2 trials do not address the comparative efficacy of fostamatinib against other second- or third-line ITP treatments.
Indirect Comparisons
Description of Studies
Two indirect treatment comparison (ITC) studies were reviewed. The Wojciechowski et al.7 study was a systematic review and ITC comparing fostamatinib to 3 TPO-RAs (avatrombopag, eltrombopag, and romiplostim) among patients with chronic ITP who had inadequate response to previous therapy. The sponsor also submitted a systematic review and ITC8 in which fostamatinib was compared to rituximab among patients with chronic or persistent ITP.
In the Wojciechowski study, the authors conducted a network meta-analysis (NMA) using a Bayesian framework, Markov chain Monte Carlo method, and fixed-effects model. The authors assessed consistency using a modified Bucher approach and used trace plots to assess convergence. They assessed the following outcomes: durable platelet response, need for rescue therapy, and WHO bleeding events, all up to 24 weeks. No sensitivity analyses were conducted. The authors reported outcomes as odds ratios (ORs) with 95% credible intervals (CrIs). Seven phase III, double-blind RCTs were included and contributed data on various clinical outcomes for the ITC: 2 trials for avatrombopag, 1 for eltrombopag, 2 for romiplostim, and 2 for fostamatinib. Six of the trials were placebo-controlled, and 1 compared avatrombopag with eltrombopag. In this ITC, the number of patients ranged from 12 to 135 in active treatment arms, the length of follow-up ranged from 24 to 36 weeks, and the median duration of disease ranged from 1.6 to 10.8 years. The median ages and median platelet counts at baseline ranged from 41 to 57 years and 14 × 109/L to 24 × 109/L, respectively. The number of previous treatments and concomitant ITP therapy varied across trials as well. The definitions of durable response were relatively similar for all the treatments to allow for comparisons, although the definitions were different in the FIT 1 and FIT 2 trials (4 of 6 visits over weeks 14 to 24) compared with the other trials (at least 6 of the last 8 weeks of treatment). To compare bleeding events among all treatments, it was assumed that WHO grade 2 to grade 4 bleeds were equivalent to grade 2 to grade 5 bleeds reported in NCT00102336 and moderate to severe bleeds reported in the FIT1 and FIT2 studies.
In the sponsor-submitted ITC, a random-effects model was used; there was no assessment of consistency and convergence was assessed via the Gelman-Rubin statistic. One outcome, overall platelet response, was assessed in this ITC and reported as ORs, which represent the relative likelihood of achieving a platelet response when receiving 1 therapy compared against another therapy. The results were presented using the posterior median treatment effects and 95% CrIs). The authors performed a sensitivity analysis using different definitions of platelet response and doses of rituximab. Six RCTs were included and contributed evidence. Authors of the ITC indicated that the inclusion of fostamatinib in the treatment paradigms aims to address patients with the greatest unmet need. Patients who are successfully treated with a splenectomy or TPO-RAs are unlikely to require additional treatment with a new intervention. To address the patients with the greatest unmet need, fostamatinib focuses on patients who do not have access to long-term, effective therapy options, including those who receive short courses of rituximab and those on a watch-and-rescue regimen. In the trials included in the ITC, the number of enrolled patients ranged from 57 to 138. The trial duration ranged from 4 weeks to 78 weeks. Three doses of rituximab were evaluated: 2 or 4 once-weekly 375 mg/m2 doses, 2 once-weekly doses of 750 mg/m2, or 4 once-weekly doses of 100 mg/m2. The definition of platelet response varied across the included trials.
Efficacy Results
In the Wojciechowski study, based on evidence from 6 studies, the results of the NMA suggested that no treatment was favoured when fostamatinib was compared with various TPO-RAs for durable platelet response. Data on reduction in the use of concomitant ITP therapies were not available for fostamatinib. Based on 6 studies, the NMA suggested that no treatment was favoured when fostamatinib was compared with TPO-RAs for need for rescue therapy. Results from 7 studies suggested that no treatment was favoured when fostamatinib was compared with TOP-RAs for the incidence of any bleeding events. Further, based on 6 studies, the NMA suggested that no treatment was favoured when fostamatinib was compared with TPO-RAs for the incidence of WHO grade 2 to grade 4 bleeding events.
In the sponsor-submitted ITC, results demonstrated that fostamatinib was favoured compared to placebo for the outcome of overall platelet response (OR = 4.85; 95% CrI, 1.86 to 14.45). Fostamatinib was also favoured when compared to rituximab for the outcome of overall platelet response (OR = 4.93; 95% CrI, 1.44 to 18.93).
Harms Results
Only the Wojciechowski study assessed AEs. Based on the results from 5 studies, the NMA suggested that no treatment was favoured when fostamatinib was compared with TPO-RAs for the incidence of any AEs.
Critical Appraisal
The Wojciechowski ITC did not discuss how any potential biases in the trials could have an impact on data analyses in the ITC and the possible solutions. For example, it did not discuss whether sensitivity analyses were conducted to assess the impact of studies with poor quality. Multiple clinical outcomes, including the incidence of AEs, were evaluated in this study, which allows for a comprehensive evaluation of the clinical benefits and risks of the study drugs. Definitions of these outcomes were similar across the trials. Trial characteristics and patients’ baseline characteristics in the studies included in the systematic review and ITC were reported. Potential sources of heterogeneity with respect to the baseline characteristics, such as disease duration (which ranged from 1.6 to 10.8 years), number of previous treatments, and concomitant ITP medication, were identified based on these data. This difference in patient baseline characteristics may vary the response between groups and may not allow groups to be comparable. The analysis of efficacy and safety data presented was limited by the size of the evidence base. Due to the small evidence base and potential heterogeneity across all studies, the results of this analysis are largely noninformative due to imprecision and bias.
Only overall platelet response was evaluated in the sponsor-submitted ITC. It is unclear whether treatment with fostamatinib would be useful in improving clinical outcomes, such as reduction in subsequent bleeding events and the need for rescue therapy, and improvement in patients’ HRQoL. Potential sources of heterogeneity with respect to the baseline characteristics were identified in this ITC. During the feasibility analysis period, several potential treatment-effect modifiers, such as baseline demographic characteristics, medical history (e.g., time since ITP diagnosis, prior treatment for ITP, and concomitant medications), were identified by the sponsor. However, the clinical experts consulted by the sponsor indicated that none of these patient characteristics could be considered treatment-effect modifiers in the study population (patients with chronic and persistent ITP who can receive fostamatinib or rituximab) due to a lack of evidence. Other patient characteristics in the study population could be treatment-effect modifiers that were not measured. Heterogeneity across the included trials therefore needs to be further assessed and adjusted. Rituximab was the only comparator in this ITC, and its study results can only be generalized to patients with persistent or chronic ITP who did not receive prior TPO-RAs therapy or had not undergone a splenectomy. Indeed, the lack of comparators was a major limitation of both the sponsor-submitted and the Wojciechowski ITCs.
Other Relevant Evidence
Description of Studies
The FIT3 trial was considered other relevant evidence.9 This was an open-label extension study of the FIT1 and FIT2 trials to examine the efficacy and safety of long-term fostamatinib among patients with chronic or persistent ITP at 54 sites in 16 countries (Canada, the US, Australia, the European Union, and the UK). The trial consisted of monthly visits for 18 months, then every-other-month visits for a maximum of 5 years of treatment. A total of 123 patients from the FIT1 and FIT2 trials completing the week 24 evaluation or withdrawing early (starting at week 12) due to a lack of response were eligible for this trial. All patients received open-label fostamatinib. Patients were assigned to 1 of 2 treatment groups, responders and nonresponders, depending on their response in the FIT1 or FIT2 trial. The responders group (last platelet count ≥ 50,000/µL) initiated open-label fostamatinib treatment using the dosage and regimen (150 mg twice a day or 100 mg twice a day) that achieved a stable platelet count in the previous study, whereas the nonresponders group (last platelet count < 50,000/µL) initiated their treatment with 100 mg twice a day during the trial (Figure 5). At month 1, the dosage for patients with a platelet count of less than 50,000/µL and tolerating the study drug well was increased to 150 mg twice a day. However, the dosage of fostamatinib was reduced to as low as 100 mg once a day if any dose-limiting AEs were observed among patients. The primary efficacy outcome was achievement of a platelet response by 12 weeks and maintenance for 12 months. A stable platelet response was a platelet count of at least 50,000/μL at 4 or more of 6 biweekly visits during weeks 14 to 24 or, for patients initiating fostamatinib in the extension phase, at least 1 platelet count of 50,000/μL or greater in the first 3 months followed by platelet counts of at least 50,000/μL at the subsequent 2 of 3 monthly visits without the use of rescue medication. The primary efficacy outcome had 2 versions. For version 1, efficacy was assessed among patients who were on active treatment in either the FIT1 or FIT2 trial, in the current extension study, or in both a FIT trial and the extension trial. For version 2, efficacy was assessed among patients assigned to placebo in either of the prior FIT1 or FIT2 trials. The secondary efficacy outcomes were reported as the duration of platelet response among patients and the response among patients with a reduction in the dose of concomitant ITP medication while maintaining an adequate platelet count. For the safety measurement, the outcomes assessed and summarized in the report were: the frequency and severity of bleeding according to the IBLS and WHO bleeding scale; change from baseline in liver function, blood pressure, and neutrophil count; and the incidence and severity of gastrointestinal effects, infection, and overall AEs. In the FIT3 trial, 60% of patients were female, the median age was 52 years (SD = 16), and patients were predominantly White (92%). A total of 59 patients were from the FIT1 trial and 64 patients were from the FIT2 trial.
A post hoc analysis of the FIT1, FIT2, and FIT3 trials by Boccia et al. (2020) was also considered relevant evidence. Authors compared the platelet response rate (≥ 50,000/µL and ≥ 30,000/µL at any visit, without receiving rescue therapy within 4 weeks) in patients who received fostamatinib as second-line therapy to those who had received fostamatinib as third- or later-line therapy for chronic ITP. A total of 145 patients were included, 32 receiving fostamatinib (median age of 50 years, 59% female) and 113 as later-line treatment (median age of 54 years, 60% female).
Efficacy Results
For the primary efficacy outcome (version 1) in the FIT3 trial, 19 patients (15.4%) had a platelet response within 12 weeks of taking fostamatinib and maintained a stable platelet response for at least 12 months after achieving the initial response (95% CI, 9.6 to 23.1). For the primary efficacy outcome (version 2), among 44 patients who were treated with placebo in the FIT1 or FIT2 trial and fostamatinib in the FIT3 trial, 10 (22.7%) were responders, while 34 (77.3%) remained nonresponders in both prior trials and in the FIT3 trial.
In the post hoc analysis by Boccia et al., 25 patients (78%) receiving fostamatinib as second-line therapy achieved a platelet response of a least 50,000/µL compared to 54 patients (48%) on later-line therapy. The authors reported that the response decreased with each additional line of prior therapy.
Harms Results
Most patients (80%) experienced at least 1 AE during the treatment phase of the FIT3 trial. The most frequently reported AEs were diarrhea (29%), hypertension (18%), petechiae (15%), epistaxis (15%), headache (12%), upper respiratory tract infection (11%), dizziness (11%), contusion (10%), nausea (9%), vomiting (9%), fatigue (8%), cough (8%), and thrombocytopenia (8%). Serious AEs with were reported for 28% of patients, with thrombocytopenia being the most frequently reported among 7% patients. A total of 18 patients (15%) withdrew from the trial due to an AE and 4 people (3%) died.
In the post hoc analysis by Boccia et al., the authors reported that AE rates were 72% for second-line therapy and 94% for later-line therapy. The most common AEs were hypertension (31% in the second line versus 19% in the later line), diarrhea (25% versus 39%, respectively), upper respiratory tract infections (16% versus 11% respectively), and elevated liver transaminase levels (26% versus 16%, respectively).
Critical Appraisal
The main limitation of the FIT3 trial is the open-label design and the lack of a comparator group. The open-label design may influence the perception of improvement by patients and clinicians, potentially affecting the reporting of harms and efficacy measures. Additionally, there was a potential for survival and selection bias as the other 13 patients who discontinued the prior studies due to AEs were excluded. This could result in a greater enrolment of patients who were better able to tolerate fostamatinib and possibly fewer AEs being reported. The FIT3 trial also saw a high rate of discontinuation (76.4%) during the open-label phase. The limitations with the study design make it challenging to interpret the results and form conclusions on long-term efficacy and safety.
As participants in the FIT3 trial were predominantly White (92%), the results may not be generalizable to other racial groups commonly seen at some centres in Canada. The experts also noted that patients with secondary ITP were excluded from the FIT3 trial, and trial findings therefore may not be generalizable to those with secondary ITP. The clinical experts also noted that the co-interventions (i.e., concomitant ITP medication) used in the FIT3 trial, as with the FIT1 and FIT2 trials, reflect real-world practice in Canada. Similar to the FIT1 and FIT2 trials, the FIT3 trial provided limited data on clinically important outcomes such as quality of life, rescue therapy, and bleeding events.
Internal and external validity concerns from the FIT1, FIT2, and FIT3 trials apply to the post hoc analysis by Boccia et al., which was subject to concerns related to selective outcome reporting. The analysis was not pre-planned, and the outcome used differs from those in the FIT1 and FIT2 trials as response to therapy was based on the platelet count at a single visit. Patients in the different treatment groups were not randomized and there was no adjustment for confounding. As such, concerns related to selection bias and bias due to confounding reduce the certainty in these results.
Conclusions
Management of chronic ITP is challenging as patients frequently relapse or are refractory to treatments and therefore often cycle through multiple ITP treatments. Treatment is complicated by a lack of evidence on comparative efficacy and safety of second- and subsequent-line treatment options, access issues, and safety and/or tolerability of available options. In 2 double-blind RCTs, fostamatinib, which is an ITP treatment with a novel mechanism of action, led to a modest improvement in platelet count response compared to placebo among patients with heavily pre-treated, primary, chronic ITP. There were limited or no data on outcomes important to patients such as bleeding rates, symptoms, and quality of life. The impact of fostamatinib on these outcomes therefore remains unclear. Subgroup analyses (based, for example, on previous lines of therapy) were not able to provide insight into which patient groups are most likely to respond to treatment. It is also difficult to draw conclusions about the comparative efficacy of fostamatinib versus other ITP treatments. Two ITC studies were included in this review, suggesting that fostamatinib may be comparable to TPO-RAs and had favourable efficacy to rituximab in terms of platelet count response. However, these studies have important limitations, and it is challenging to draw firm conclusions about comparative efficacy based on their results. In the FIT1 and FIT2 trials, fostamatinib appeared to lead to a higher rate of adverse effects, such as diarrhea, nausea, hypertension, and elevated liver transaminase compared to placebo, while the FIT3 trial did not identify any long-term safety concerns beyond these adverse effects. Overall, this review suggests that fostamatinib is another potential treatment option for patients with chronic, heavily pre-treated primary ITP. The drug leads to a platelet count response in a modest proportion of patients and is generally well tolerated compared to placebo, although its comparative efficacy and safety versus other ITP treatments, and its effect on patient-important clinical outcomes, remain unclear.
Introduction
Disease Background
Immune thrombocytopenia is a “primary” or “secondary” autoimmune disorder characterized by low platelet counts and increased bleeding risk.1 It is thought to be caused by antibodies directed against platelet antigens, leading to increased platelet destruction.1 Primary ITP is not triggered by a specific condition or event while secondary ITP is caused by or associated with another condition, such as chronic lymphocytic leukemia, systemic lupus erythematous, antiphospholipid syndrome, among others.1 Primary ITP accounts for approximately 80% of cases.10 It is also defined based on the duration, with acute or newly diagnosed ITP referring to the first 3 months after diagnosis, persistent ITP referring to 3 to 12 months after diagnosis, and chronic ITP referring to more than 12 months after diagnosis.1 Little contemporary data are available on the incidence and prevalence of ITP in Canada. A 2010 narrative review of international studies suggested that the incidence of ITP among adults is approximately 3.3 per 100,000 per year, while the prevalence is 10 per 100,000, both of which increase with increasing age.11 An American study using data from 2010 to 2016 suggested that the annual incidence of ITP in the US was 6.1 per 100,000 persons.12 The rate of fatal hemorrhage among patients with ITP was been estimated to be between 0.016 and 0.039 cases per patient-year, and this rate increases with age.13 The predicted 5-year mortality rate for patients 60 years of age and older was 48% in a study of 1,817 patients with ITP.13 Further, the authors of this study estimated that a 30-year-old woman with ITP would lose 15 quality-adjusted life-years from her life expectancy.13
Patients with ITP may be asymptomatic, although patients can experience bleeding and other symptoms.14 Bleeding can be mild; for example, patients may experience petechiae, purpura, or nosebleeds.14 In cases of intracranial hemorrhage or gastrointestinal bleeding, it can be more severe or critical.1 Indeed, severe or critical bleeding is a major concern among patients with ITP. Predictors of critical bleeding include platelet count (< 10,000/µL or < 20,000/µL), previous bleeding, and chronic ITP (> 12 months in duration). Patients with ITP also commonly experience fatigue.15 Patients with ITP have a reduced quality of life, resulting from fatigue, bleeding, and ITP treatments.16
Because ITP is considered a diagnosis of exclusion, the diagnostic evaluation primarily concerns excluding other possible causes of low platelet count and/or finding potential conditions leading to low platelet counts (i.e., secondary ITP).1 In addition, because ITP is an isolated thrombocytopenia, patients with the disease do not have anemia or leukopenia.1 Diagnosis involves taking a history (questioning regarding bleeding and symptoms), physical examination, and laboratory testing (e.g., a complete blood count and peripheral blood smear).1 Clinical experts suggested that initial diagnosis and management may be carried out by internal medicine clinicians, while patients with chronic ITP will generally be managed by hematologists.
Standards of Therapy
The need for treatment to increase platelet counts among patients with ITP is based on assessments of bleeding (site, acuity, and severity), platelet count, bleeding risk factors, and previous treatments. Treatment to increase platelet count is generally recommended if the platelet count is below 20,000/µL to 30,000/µL and/or if the patient is experiencing bleeding. Patients with severe or critical bleeding are recommended to receive urgent treatment to stop bleeding and raise platelet counts.
The main goals of therapy in ITP are to prevent severe or critical bleeding, reduce or eliminate patients’ symptoms, minimize adverse effects from treatments, and ultimately improve patient quality of life.2 Treatments are recommended to increase platelet levels to above 20,000/µL to 30,000/µL, which appears to reduce the risk of major bleeding.2,3 American and International guidelines recommend that, for initial treatment of newly diagnosed ITP, corticosteroids (for 2 weeks then tapered) or IVIG (for 1 to 5 days) be used as first-line therapy. Anti-D immune globulin is another alternative in patients with bleeding or at high risk of bleeding.2,3 Long-term corticosteroid treatment is generally not a recommended treatment option as the harms outweigh the benefits.2
After corticosteroids or IVIG are stopped, many patients (one-third of patients in the first year and up to 80% within 5 years) experience a relapse in their condition in the form of reduced platelet counts and/or symptoms.2 Once patients have relapsed, the sequence of subsequent treatments is less clear.2,3 Multiple second- and third-line treatments are available for ITP; however, there is a lack of comparative efficacy data to provide evidence on a clear sequential treatment pathway. Possible treatment options include a splenectomy; rituximab; TPO-RAs such as romiplostim or eltrombopag; fostamatinib; and immunosuppressants (e.g., azathioprine and cyclophosphamide). The International Consensus Report on the Investigation and Management of Primary ITP highlights these treatment options in subsequent-line treatment of ITP but does not identify a preferred pathway among them.2 These guidelines state that the recommended option is generally based on available resources and patient preferences. The guidelines further note that “robust” evidence supports the use of TPO-RAs, rituximab, and fostamatinib in subsequent-line treatment of ITP. The American Society of Hematology guidelines for ITP suggest rituximab, a splenectomy, or TPO-RAs as second-line treatment options.3 They state that the decision is based on patient preferences and other patient-specific factors (age and comorbidities), as well as access (cost and availability). These guidelines also acknowledge the low certainty of the evidence on comparative efficacy and state that individualization of therapy and shared decision-making (based on these factors) are important in identifying the appropriate subsequent-line ITP treatment.
In the Canadian context, the choice of subsequent-line treatment depends on patient-specific factors (e.g., increased susceptibility to adverse effects of a treatment, contraindications, preferences) as well as access (i.e., whether a treatment is listed on a provincial drug formulary and/or whether the patient meets the criteria for reimbursement). Consequently, some options may not be available or appropriate to all patients. Further, some patients may not be surgical candidates and splenectomy carries risks such as infection. Rituximab has been shown to be effective in achieving a platelet response but has a risk of fatal infusion reactions, hepatitis B reactivation, and progressive multifocal leukoencephalopathy, among other harms.2 Indeed, many of the second- and third-line treatment options carry risks of important harms. For example, TPO-RAs increase the risk of bone marrow reticulin fibrosis and arterial and venous thrombosis.2 Options also differ in terms of their administration. For example, rituximab is given as an infusion at a clinic or hospital over several weeks, while eltrombopag is a daily continuous oral medication that cannot be taken within several hours of calcium. Overall, the potential chance of achieving platelet response must be considered against the potential harms of the different agents and administration factors, as well as access issues.3
The clinical experts consulted by CADTH emphasized that not all patients respond to treatment with second- or third-line treatment options. Further, patients become refractory to treatment options or relapse after achieving remission. Chronic ITP is therefore characterized by a chronic relapsing course and multiple lines of therapy over time.
Drug
Fostamatinib is indicated for the treatment of chronic ITP in adult patients who have had an insufficient response to other treatments.4 Fostamatinib treatment should be initiated and remain under the supervision of a physician who is experienced in the treatment of hematological diseases.4 Fostamatinib reduces the destruction of platelets via inhibition of spleen tyrosine kinase.4 Fostamatinib is initiated at a dosage of 100 mg twice daily and is taken orally. If the platelet count has not increased to at least 50,000/µL after 4 weeks, then the dosage can be increased to 150 mg twice daily.4 Fostamatinib underwent an expedited review at Health Canada. The sponsor is requesting reimbursement for fostamatinib for the treatment of thrombocytopenia in adult patients with ITP who have had an insufficient response to a TPO-RA in jurisdictions where TPO-RA reimbursement is available, or after failure of corticosteroids and other earlier-line treatments in jurisdictions where TPO-RA reimbursement is not available.
Fostamatinib is contraindicated in patients who are hypersensitive to the drug or any ingredient in the formulation, and is also contraindicated in pregnancy.4 The product monograph carries warnings for bone remodelling, stating that fostamatinib targets pathways involved in bone metabolism.4 The monograph notes that the effects of fostamatinib on bone remodelling are unclear; however, there are potential risks in those with actively growing bones (e.g., children and young adults), and patients with osteoporosis or fractures should be closely monitored. Hypertension has been reported among patients treated with fostamatinib.4 Patients with hypertension may be more susceptible to hypertensive effects, and blood pressure should be closely monitored.4 Other warnings in the monograph include heart rate and conduction abnormalities, gastrointestinal side effects (particularly diarrhea), neutropenia, elevated transaminases, and infections.4
Table 3: Key Characteristics of Fostamatinib, Rituximab, Eltrombopag, and Romiplostim
Characteristic | Fostamatinib | Rituximab | Eltrombopag | Romiplostim |
|---|---|---|---|---|
Mechanism of action | Reduces destruction of platelets via inhibition of spleen tyrosine kinase | Depletion of CD20 antigens | Stimulates platelet production by initiating a signalling cascade at thrombopoietin receptors | |
Indicationa | For the treatment of thrombocytopenia in adult patients with chronic ITP who have had an insufficient response to other treatments | No indication for the treatment of ITP | For treatment of chronic ITP to increase platelet counts in adult and pediatric patients 1 year of age and older who have had an insufficient response to corticosteroids or immunoglobulins | To increase the platelet levels in adults patients with ITP who are nonsplenectomized and have had an inadequate response or are intolerant to corticosteroids and/or immunoglobulins; or who are splenectomized and have had an inadequate response to splenectomy |
Route of administration | Oral | IV | Oral | Subcutaneous |
Recommended dosage | Initiate at a dosage of 100 mg taken orally twice daily; after 4 weeks, if platelet count has not increased to at least 50 × 109/L, increase dosage to 150 mg twice daily | 375 mg/m2 once a week for 5 weeks or 100 mg once a week for 4 weeks | Initial dosage is 25 mg once daily (then adjusted, if necessary, based on platelet counts) | Initial dosage is 1 mcg/kg based on actual body weight once weekly, then adjusted based on platelet count |
Serious adverse effects or safety Issues | Contraindicated in patients who are hypersensitive to the drug or any ingredient in the formulation and during pregnancy; should be used with caution in patients with hypertension | Serious adverse effects include infusion reactions, progressive multifocal leukoencephalopathy, tumour lysis syndrome, hepatitis B reactivation, infections; contraindicated in people with type 1 hypersensitivity reactions or anaphylactic reactions to murine proteins, Chinese hamster ovary cell proteins or any component of the product, and patients who have had progressive multifocal leukoencephalopathy | Contraindicated in patients with severe hepatic impairment or those who are hypersensitive to the product or any of its excipients; should be used with caution in chronic hepatitis C patients with cirrhosis | Contraindicated in patients who are hypersensitive to drug or any ingredient in the formulation; should not be used in patients with myelodysplastic syndromes; recurrence of thrombocytopenia below pre-treatment levels and serious life-threatening or fatal bleeding after discontinuation have been reported |
ITP = immune thrombocytopenia.
aHealth Canada–approved indication.
Source: Product monographs4,17-19 and Lucchini et al. (2019).20
Stakeholder Perspectives
Patient Group Input
This section was prepared by CADTH staff based on the input provided by patient groups.
One patient group submission, authored by the PDSA, was received for this review. The PDSA, founded in 1998, is a US-based international nonprofit organization and a registered nonprofit corporation in Canada. Its members are dedicated to enhancing the lives of patients with ITP and other platelet disorders through advocacy, education, research, and support. The PDSA has 635 Canadian adults and children in its database and has 7 support groups, including chapters in London, Niagara, Toronto, Waterloo, Ottawa, and Vancouver. The PDSA has received funding from argenx, Amgen, Dova/Sobi, Novartis, UCB, CSL Behring, Principa, Pfizer, Sanofi, Momenta, and Rigel. The association did not receive help from outside the patient group to prepare its submission. The submission includes patient comments from the PDSA Facebook page gathered from the US and Canada between 2018 and present — these comments were from people who had taken fostamatinib and therefore pertain only to the section on patient experiences with fostamatinib. The submission did not describe how the rest of the input was gathered.
Disease Experience
Immune thrombocytopenia is unpredictable and affects both the patient and their entire family. Patient quality of life is affected in multiple ways. Patients are fearful about the risk of life-threatening bleeding but also face physical and emotional consequences, such as fatigue, anxiety, depression, pain, and sleep disturbances. These symptoms are often more concerning to patients than platelet counts. Patients with ITP may restrict or avoid activities (e.g., travelling or participating in sports), and require frequent monitoring, which, along with symptoms, interferes with their daily activities. The disease can also make treatment, including medical procedures and surgery, more complex. These factors further lead to anxiety, fear, and depression.
Experience With Treatment
Several therapies are available for treatment of ITP, and each have different risk-benefit profiles and limitations. Multiple therapies can also be used at once. Prednisone can increase platelet counts but is recommended for short-term use due to the risk of side effects with longer-term use. Both IVIG and anti-D immune globulin are short-term treatment options that can be used as rescue therapy to increase platelet counts but are not suitable for long-term therapy. Treatments aimed at producing long-term increases in platelet counts include rituximab, splenectomy, TPO-RAs, and fostamatinib. However, not all patients will respond to these therapies, and side effects are a concern. Patients therefore often cycle through different options to find a therapy that will be tolerated and raise platelet counts.
The PDSA identified a selection of Facebook posts among people with lived experience of fostamatinib treatment from 2018 to present. Patients that commented had generally tried other therapies. Patients commenting suggested that fostamatinib was effective in increasing platelet counts, with some noting that it took approximately 2 weeks to increase platelet counts. Some patients who had been on fostamatinib long-term (16 months to 2 years) stated that they continued to have a platelet count response. Some patients commented that they had not experienced adverse effects, while others noted adverse but manageable effects, such as diarrhea, elevated blood pressure, or stomach upset.
Improved Outcomes
It is difficult to predict who will respond to a particular treatment and who will develop resistance to a treatment over time. Further, patients may not be able to afford or access available options. It is therefore important that patients have options available in case they do not respond to a therapy, the therapy stops working, or they experience bleeding. Patients prefer treatments that do not affect their daily lives and patients find it easier to take a pill than to go to a hospital or clinic to receive treatment. Patients also prefer a treatment that has minimal side effects and a durable response. Patients experience anxiety from possible bleeding, as well as nose bleeds, mouth blisters, and fatigue, and want a therapy that means they will not live in fear of when their next bleed will be. An ITP therapy should improve quality of life, not reduce it.
Clinician Input
Input From Clinical Experts Consulted by CADTH
All CADTH review teams include at least 1 clinical specialist with expertise in the diagnosis and management of the condition for which the drug is indicated. Clinical experts are a critical part of the review team and are involved in all phases of the review process (e.g., providing guidance on the development of the review protocol; assisting in the critical appraisal of clinical evidence; interpreting the clinical relevance of the results; and providing guidance on the potential place in therapy). In addition, as part of the fostamatinib review, a panel of 4 clinical experts from across Canada was convened to characterize unmet therapeutic needs, assist in identifying and communicating situations where there are gaps in the evidence that could be addressed through the collection of additional data, promote the early identification of potential implementation challenges, gain further insight into the clinical management of patients living with a condition, and explore the potential place in therapy of the drug (e.g., potential reimbursement conditions). A summary of this panel discussion follows.
Current Treatments
Standard first-line therapy for ITP includes corticosteroids, and IVIG (or, in rhesus disease–positive patients, rhesus-immune globulin) is often added when an immediate increase in platelets is required, although its effect is often transient. A significant proportion of patients will not respond to steroids and, of those that do, many will relapse once steroids are tapered. At this point, traditional second-line therapy is a splenectomy if the patients is a suitable candidate. More recently, rituximab has emerged as an alternative second-line therapy. If both a splenectomy and rituximab have failed (or are contraindicated), a large number of third-line therapies are available, including immunosuppressant medications such as azathioprine or cyclophosphamide, or TPO-RAs such as eltrombopag or romiplostim. There is little evidence to guide the selection of third-line therapy, and decisions depend on local reimbursement considerations as patient-specific factors.
Treatment Goals
Broad clinician treatment goals are to reduce bleeding and prolong life. Increasing the platelet count is generally considered to be a reasonable surrogate for those 2 goals. Improving quality of life is also an important goal but must be balanced against the inconvenience and side effects of the treatments used (e.g., fatigue, cognition, mood, interference with daily life, and frequent hospital visits), which many clinicians may overlook in their focus on the patient’s platelet count.
Unmet Needs
The current treatment paradigm for ITP poses myriad challenges. Not all patients respond to available therapies, and even if remission is achieved, long-term remission is not guaranteed. Durable remission for ITP remains a challenge. Further, while corticosteroids and IVIG are generally accessible to patients, accessibility to appropriate second- and third-line therapies can be a challenge. This is because not all options are reimbursed in each province or because reimbursement criteria differ across provinces. For example, in Ontario patients must fail 2 or more therapies after steroids and IVIG before being eligible for TPO-RAs, meaning that these agents are not available to many patients until later in the treatment pathway. Administration of existing therapies can also be a challenge, for example, when there is a need to travel to a hospital or clinic for administration of rituximab. Adhering to oral TPO-RA dosing regimens can also be difficult as the drugs must be administered on an empty stomach. There are also adverse effects with existing treatments — a splenectomy carries short-term perioperative risks as well as longer-term risks of thrombosis and infections with encapsulated bacteria, while rituximab increases susceptibility to hepatitis B reactivation and increases vulnerability to opportunistic infections. The availability of therapies with demonstrated efficacy, convenience of administration, and a low risk of adverse effects would therefore fill an unmet need for treatment of ITP.
Place in Therapy
Contemporary ITP guidelines suggest that, in general, a splenectomy or rituximab can be considered second-line therapy. Several third-line options are available; however, the comparative efficacy of these drugs is unclear, it can be difficult to know what the best treatment option is for a particular patient, and there is often no single clearly defined treatment pathway. Decisions end up being driven largely by access. Given the lack of comparative efficacy data, the influence of patient-specific factors on decisions, and the current reimbursement landscape, it is challenging to identify the optimal place in the therapeutic algorithm for fostamatinib, which is a novel spleen tyrosine kinase inhibitor recently approved for the treatment of ITP. The clinical experts consulted by CADTH noted that rituximab or a splenectomy are reasonable second-line choices (TPO-RAs may also be considered second-line choices in some patients). The safety profile of fostamatinib and the fact that it is administered orally suggest it may be considered a reasonable third-line therapy rather than reserved for patients who have failed or do not have access to TPO-RAs, as has been proposed by the sponsor. However, regardless of where it sits in the therapeutic algorithm, it would be advantageous for clinicians to have fostamatinib as an additional treatment option for specific patients.
Patient Population
Subgroup analysis of data from randomized controlled trials (RCTs) suggests that patients who have failed fewer prior ITP treatments may respond to fostamatinib better than those who have been more heavily pre-treated. As these data are prone to selection bias, the clinical experts stated that they would not base their treatment decisions on this finding and noted that it would be helpful to have an additional treatment option even in patients who had failed many previous therapies. The ITP population is heterogenous, and the available data and current understanding of ITP pathophysiology make it impossible to determine which specific patients will respond best and who are most susceptible to adverse effects. However, the panel agreed that having fostamatinib as an option for patients would be desirable, regardless of where patients are in their disease course.
Assessing Response to Treatment
Bleeding is an important outcome in the treatment of ITP, and ultimately any treatment should reduce the occurrence of clinically important bleeding while improving quality of life. In practice, clinicians rely on platelet response, which is assumed to reduce the risk of clinically relevant bleeding and, as a secondary benefit, reduce the need for rescue therapy. No quality-of-life scales that are particular to ITP are used in practice. In general, an increase in platelet count can be seen as early as 2 weeks into treatment with fostamatinib, although some patients may not respond until week 12. If a response is observed, clinicians would likely continue to use the treatment long-term with monthly monitoring. A sustained response would generally be considered a platelet count of 30,000/µL to 50 000/µL for the duration of a treatment cycle (e.g., 24 weeks). If a response has not been seen by approximately 24 weeks, clinicians would generally consider that the treatment has not worked and would discontinue it. If there are issues related to safety or tolerability, treatment would generally be discontinued earlier, particularly if it is affecting a patient’s quality of life.
Prescribing Conditions
Clinicians practising general internal medicine frequently prescribe corticosteroids for the initial management of ITP. However, patients requiring second-line treatment are often referred to a hematologist. Patients with ITP for many years who have tried multiple therapies are often seen by multiple hematologists. While hematologists usually take responsibility for selecting treatment for ITP, primary care physicians may share responsibility for monitoring AEs.
Clinician Group Input
This section was prepared by CADTH staff based on input provided by clinician groups.
A group of 19 Canadian hematologists submitted input on fostamatinib. This group included clinicians from Alberta, Ontario, Nova Scotia, British Columbia, Quebec, and Newfoundland, and was informed by a literature review, current clinical practice guidelines, and clinical practice. The report also incorporated data from a survey conducted in July 2021 among 5 physicians based in the US with experience prescribing fostamatinib. The survey was conducted by Blue Ribbon Project Inc. and commissioned by Accelera Canada in partnership with Advocacy Solutions.
Current Treatments
The clinician group submission echoes the opinions of the expert panel. The clinician group noted that patients with ITP can have a wide range of clinical manifestations (from asymptomatic with low platelet counts to severe or life-threatening bleeding). Further, patients can follow a variable disease course, with sometimes long periods of stability and intermittent episodes of bleeding. Variability and unpredictability can be challenging and lead to a poor quality of life for patients as well as health-system impacts. Similar to the expert panel, the clinician group noted that many different treatment options are available, but patients often have relapses or do not respond to particular agents. Corticosteroids and/or IVIG are first-line options; however, there is a lack of data to guide the correct order or sequence of second- and subsequent-line therapies. In addition, the treatment paradigm differs across provinces in Canada due to differences in access and reimbursement policies.
Treatment Goals
Treatment goals highlighted by the clinician group align with what was reported by the clinical experts: patients want to alleviate symptoms, improve quality of life, and reduce the impact of ITP on their daily lives, in addition to reducing the risk of serious bleeding. Patients are also concerned about the side effects of medications and the costs of treatments. Clinician goals align with these patient goals, but clinicians also often focus on increasing platelet counts and minimizing health-system impacts. Finding an optimal treatment option that is tailored to the individual requires discussion with patients.
Unmet Needs
The clinician group submission echoed that of the clinical experts. The clinician group suggested that no treatments available to date have been shown to address key outcomes of interest for patients and patient goals of care, such as improvements in energy levels or mental health. The clinician group suggested that most treatments may actually worsen fatigue and mental stress. The submission suggested that there is a need for treatments that are better tolerated and that lead to better adherence, which can be a challenge in ITP. The clinician group stated that the patients with the greatest unmet need are those with severe refractory diseases who have failed first-line therapies and subsequent lines of therapy. The group added that having a drug that is given orally may improve adherence due its ease of administration.
Place in Therapy
The clinician group stated that fostamatinib is the first drug to target phagocytosis of platelets and therefore has a novel mechanism of action. The group suggested that fostamatinib would be likely be used after first-line therapy as second-line or subsequent-line therapy. The clinician group submission reported that fostamatinib would provide an alternative to other second- and subsequent-line therapies and should be considered before a splenectomy, immunosuppressive drugs, and rituximab and its biosimilars, and be comparable to maintenance treatments such as the TPO-RAs.
Patient Population
The clinician group submission stated that patients early in their ITP disease course may respond better to fostamatinib. Using it as a second-line therapy may offer advantages such as limiting exposure to complications or toxicities from other drugs. However, the greatest need is still in patients who have relapsed multiple times despite treatment.
Assessing Response to Treatment
The clinician group suggested that, in practice, platelet count and lack of rescue therapy were appropriate ways to assess response. The submission suggested that achieving the goals of the patient, clinician, and health care system would represent a clinically meaningful response. The clinician group stated that most effective response would be a prolonged life through the reduction of the risk of life-threatening bleeding. The submission from the clinician group suggested that an ITP treatment would be discontinued if there is disease progression (drop in platelets or increased bleeding), the patient develops side effects, or there is a need for rescue therapy.
Prescribing Conditions
The clinician group suggested that fostamatinib can be used in the outpatient setting (in hospital clinic) as well as in the emergency room and in hospitalized patients.
Drug Program Input
The drug programs provide input on each drug being reviewed through CADTH’s reimbursement review processes by identifying issues that may affect their ability to implement a recommendation. The implementation questions and corresponding responses from the clinical experts consulted by CADTH are summarized in Table 4.
Table 4: Summary of Drug Plan Input and Clinical Expert Response
Drug program implementation questions | Clinical expert response |
|---|---|
Relevant comparators | |
Fostamatinib was compared to placebo in the FIT1 and FIT 2 multi-centre, randomized, double-blind studies.
If fostamatinib is used, will these patients also require concomitant therapy with chronic low-dose glucocorticoids, azathioprine, or danazol? | It is likely unnecessary to continue concomitant medications and patients would generally be motivated to stop other drugs if they are not necessary. |
In some jurisdictions, to obtain public funding for the relevant comparator, eltrombopag (Revolade), the patient must have previously used rituximab. Some clinicians in these jurisdictions have stated that they are reluctant to start patients with a low platelet count on rituximab and would prefer to start therapy with eltrombopag because eltrombopag’s onset of action is greater than that of rituximab. How does the onset of action of fostamatinib compare to that of other comparator therapies? | The onset of action for fostamatinib is comparable to those of TPO-RAs, although it is likely faster than rituximab. |
Considerations for initiation of therapy | |
Some guidelines recommending the start of second-line therapy at a platelet count of < 20,000/µL. Is it reasonable to reserve fostamatinib for patients with platelet counts < 20,000/µL or < 30,000/µL according to the inclusion criteria of the clinical trials? | The usual threshold for starting therapy is < 30,000/µL. While guidelines sometimes state that treatment should be started when a platelet count is < 20,000/µL to 30,000/µL, most still use a count of < 30,000/µL and, for the sake of consistency, it would be less confusing to have the same threshold for starting fostamatinib. |
In the subgroup analysis of the pooled data from FIT1 and FIT2 trials, it appears that patients who had ITP for < 3 years did not respond to fostamatinib. Should these patients be eligible for public funding of this therapy? | While patients with ITP for < 3 years did not have a statistically significant response to treatment with fostamatinib, this likely reflects the fact that the study was not powered to show a difference in individual subgroups (wide confidence intervals were noted) and excluding this subgroup from treatment with fostamatinib would not be appropriate. |
Prior therapies required for eligibility in both the FIT1 and FIT2 trials:
In both the FIT1 and FIT2 trials, the median number of unique prior ITP therapies is 3. What is fostamatinib’s place in therapy relative to other second-line therapies (splenectomy, rituximab, and TPO-RAs)? Should public payers fund fostamatinib after the patient has failed all second-line therapies (splenectomy, rituximab, and TPO-RAs)? | Treatment decisions in Canada are strongly influenced by the availability of reimbursement. Given the lack of comparative evidence among treatment options, it is challenging to put fostamatinib in front of established second-line therapies such as rituximab or a splenectomy (unless there are specific contraindications). It may be more reasonable to position fostamatinib at a level of treatment similar to that of TPO-RAs. |
Considerations for continuation or renewal of therapy | |
Two different bleeding scales were used during the study (the WHO scale and IBLS), even though the clinical meaningfulness of neither scale was validated, particularly with respect to incremental changes. What monitoring parameters would be used in clinical practice to determine if fostamatinib is safe and effective (e.g., what platelet counts would be targeted)? | Platelet count is the main parameter that is monitored. |
Considerations for discontinuation of therapy | |
The clinical trials were 6 months long. If a patient responds to fostamatinib, would they be continued on therapy indefinitely or will they be tapered off after several years (e.g., 2 to 3 years) and assessed for remission? | Because fostamatinib has not yet been widely used, it is too early to know what the best treatment course is. |
Care provision issues | |
Non-infectious diarrhea events occurred in 30% of patients receiving therapy, and the study protocol recommended loperamide to treat diarrhea. For those with experience using fostamatinib, what percentage of treated patients develop diarrhea and is this consistent with the clinical trials? Given most side effects were experienced in “double digits,” is fostamatinib considered a drug that is poorly tolerated? | Fostamatinib cannot be considered to be poorly tolerated based on these data as placebo also saw high rates (“double digits”) of some adverse effects. In practice, patients will have different values and preferences related to tolerating adverse effects. |
IBLS = immune thrombocytopenia bleeding scale; ITP = immune thrombocytopenia; IVIG = IV immunoglobulin; TPO-RA = thrombopoietin receptor agonist.
Clinical Evidence
The clinical evidence included in the review of fostamatinib is presented in 3 sections. The first section, the systematic review, includes pivotal studies provided in the sponsor’s submission to CADTH and Health Canada, as well as those studies that were selected according to an a priori protocol. The second section includes indirect evidence from the sponsor and indirect evidence selected from the literature that met the selection criteria specified in the review. The third section includes sponsor-submitted long-term extension studies and additional relevant studies that were considered to address important gaps in the evidence included in the systematic review.
Systematic Review (Pivotal and Protocol-Selected Studies)
Objectives
To perform a systematic review of the beneficial and harmful effects of fostamatinib for the treatment of thrombocytopenia in adult patients with of chronic ITP who have had an insufficient response to other treatments.
Methods
Studies selected for inclusion in the systematic review included pivotal studies provided in the sponsor’s submission to CADTH and Health Canada, as well as those meeting the selection criteria presented in Table 5. Outcomes included in the CADTH review protocol reflect outcomes considered to be important to patients, clinicians, and drug plans.
Table 5: Inclusion Criteria for the Systematic Review
Criteria | Description |
|---|---|
Patient population | Adult patients with chronic ITP who have had insufficient response to other treatments Subgroups: Number and class of prior therapies used |
Intervention | Fostamatinib 100 mg or 150 mg twice daily taken orally |
Comparators | A combination of 1 or more of the following:
|
Outcomes | Efficacy outcomes:
Harms outcomes: AEs, SAEs, WDAEs, mortality Notable harms: infection, hypertension, bone remodelling, neutropenia, elevated liver enzymes, nausea, abdominal pain, dizziness, diarrhea |
Study design | Published and unpublished phase III and IV RCTs |
AE = adverse event; ITP = chronic immune thrombocytopenia; IVIG = IV immunoglobulin; RCT = randomized controlled trial; SAE = serious adverse event; WDAE = withdrawal due to adverse event.
The literature search for clinical studies was performed by an information specialist using a peer-reviewed search strategy according to the PRESS Peer Review of Electronic Search Strategies checklist.21
Published literature was identified by searching the following bibliographic databases: MEDLINE All (1946—) via Ovid and Embase (1974—) via Ovid. All Ovid searches were run simultaneously as a multi-file search. Duplicates were removed using Ovid deduplication for multi-file searches, followed by manual deduplication in EndNote. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. The main search concept was fostamatinib. Clinical trials registries searched included the US National Institutes of Health’s clinicaltrials. gov, the WHO International Clinical Trials Registry Platform (ICTRP) search portal, Health Canada’s Clinical Trials Database, and the European Union Clinical Trials Register.
No filters were applied to limit retrieval by study type. Retrieval was not limited by publication date or by language. Conference abstracts were excluded from the search results. Appendix 1 provides detailed search strategies.
The initial search was completed on August 20, 2021. Regular alerts updated the search until the meeting of the CADTH Canadian Drug Expert Committee on December 15, 2021.
Grey literature (literature that is not commercially published) was identified by searching relevant websites from the Grey Matters: A Practical Tool For Searching Health-Related Grey Literature checklist.22 Included in this search were the websites of regulatory agencies (US FDA and European Medicines Agency). Google was used to search for additional internet-based materials. Appendix 1 provides more information on the grey literature search strategy.
Two CADTH clinical reviewers independently selected studies for inclusion in the review based on titles and abstracts, according to the predetermined protocol. Full-text articles of all citations considered potentially relevant by at least 1 reviewer were acquired. Reviewers independently made the final selection of studies to be included in the review, and differences were resolved through discussion.
In addition to the indirect evidence provided by the sponsor, additional indirect evidence that includes the patients, interventions, comparators, and outcomes specified in Table 5 was summarized and critically appraised, if considered relevant by CADTH. A focused literature search for NMAs dealing with immune thrombocytopenia was run in MEDLINE All (1946–) on August 20, 2021. No limits were applied to the search.
Findings from the Literature
Two studies5,6 were identified from the literature for inclusion in the systematic review (Figure 1). The included studies are summarized in Table 6. A list of excluded studies is presented in Appendix 2.
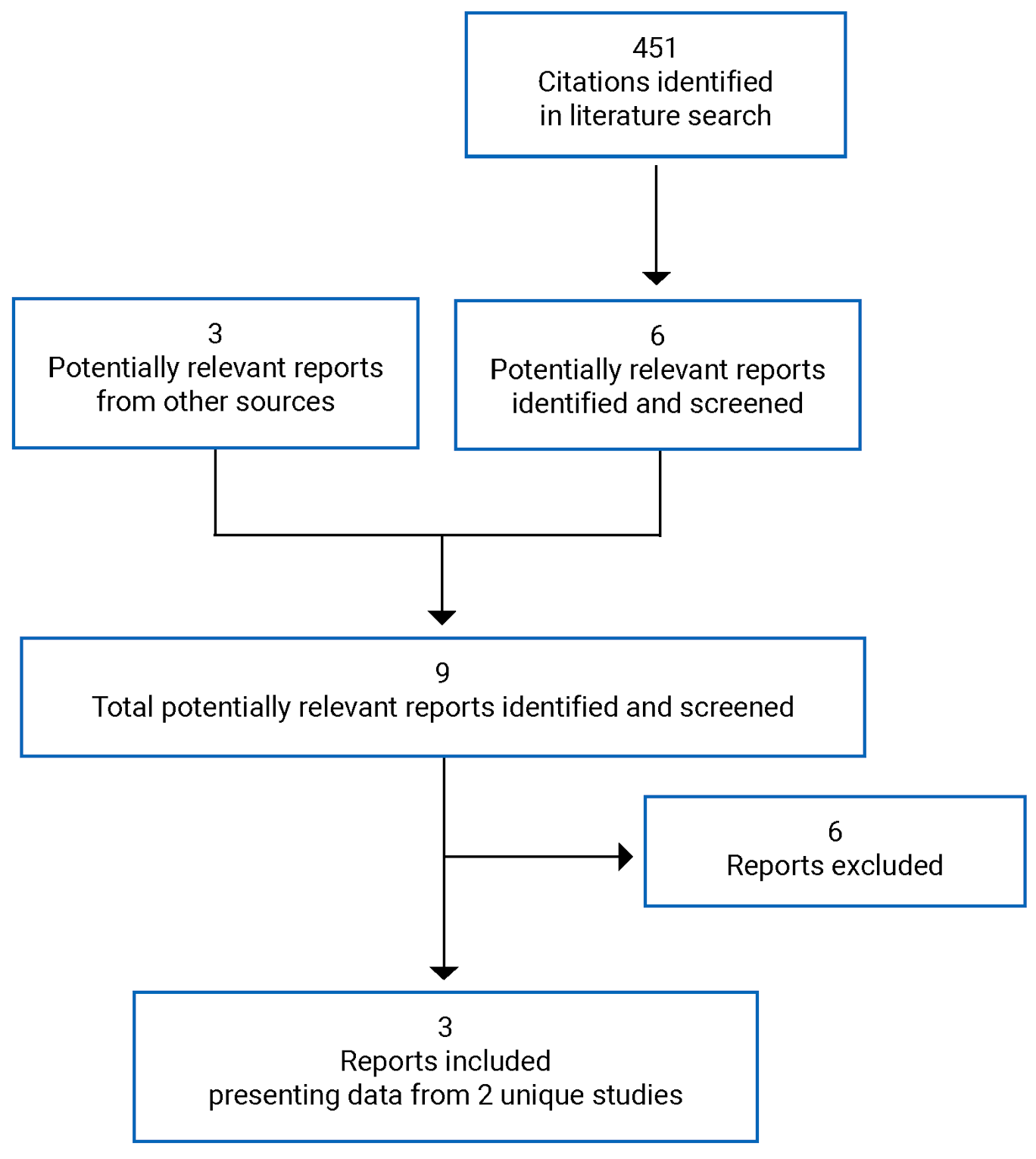
Table 6: Details of Included Studies
Study detail | FIT1 | FIT2 |
|---|---|---|
Designs and populations | ||
Study design | Double-blind RCT | Double-blind RCT |
Locations | Australia, Canada, Denmark, Hungary, Italy, the Netherlands, the UK, and the US | Europe (Austria, Bulgaria, Czech Republic, Germany, Norway, Poland, Romania, Spain) |
Patient enrolment dates | July 14, 2014, to April 21, 2016 | January 9, 2015, to August 31, 2016 |
Randomized (N) | 76 | 74 |
Inclusion criteria | ≥ 18 years of age, diagnosis of ITP for > 3 months; platelet count averaged < 30,000/µL from at least 3 counts in the preceding 3 months; have received ≥ 1 typical regimen for ITP (e.g., TPO-RA, corticosteroids with or without splenectomy, IVIG); concurrent treatment consisting of glucocorticoids, azathioprine, or danazol for 14 days before baseline (any other agents for ITP must have been discontinued during washout); female patients must have been postmenopausal or surgically sterile or not pregnant or lactating and agreed to use birth control throughout study | |
Exclusion criteria | Secondary ITP; autoimmune hemolytic anemia; history of active clinically significant disorder that could affect conduct of study or pharmacokinetics of study drug; any major cardiovascular event within 6 months before randomization; uncontrolled hypertension (SBP ≥ 140 mm Hg or DBP ≥ 90 mm Hg); history of coagulopathy; bleeding assessment score of grade 2 by IBLS at any site; laboratory abnormalities; significant infection at time of screening and/or baseline; acute GI symptoms at time of screening and/or baseline; received blood products within 2 weeks before randomization (except IVIG or anti-D immunoglobin G); any major surgery within 28 days before randomization | |
Drugs | ||
Intervention | Fostamatinib 100 mg twice daily, increased to 150 mg twice daily at or after 4 weeks if platelet count < 50,000/µLa | |
Comparator(s) | Placeboa | |
Duration | ||
Phase | ||
Run-in | 1 to 4 weeks | |
Double-blind | 24 weeks | |
Follow-up | 2 weeks | |
Outcomes | ||
Primary end point | Achievement of stable platelet response by week 24, defined as a platelet count of ≥ 50,000/µL on at least 4 of the last 6 scheduled visits between weeks 14 and 24 | |
Secondary and exploratory end points | Secondary:
Exploratory:
| |
Publications | Bussel (2018)23 | Bussel (2018)23 |
DBP = diastolic blood pressure; ITP = immune thrombocytopenia; GI = gastrointestinal; IBLS = immune thrombocytopenia bleeding scale; IVIG = IV immunoglobulin; RCT = randomized controlled trial; SAE = serious adverse event; SBP = systolic blood pressure; SF-36 = Short Form (36) Health Survey; TPO-RA = thrombopoietin receptor agonist.
aAllowed concomitant therapies were glucocorticoids (< 20 mg equivalent prednisone per day), azathioprine, or danazol.
Source: FIT1 Clinical Study Report,5 FIT2 Clinical Study Report,6 and Bussel (2018).23
Description of Studies
Two studies met the inclusion criteria. The FIT15 (N = 76) and FIT26 (N = 74) trials were identically designed double-blind RCTs. Both studies were funded by Rigel Pharmaceuticals Inc. The FIT1 trial was conducted in Australia, Canada (3 sites), Europe, the UK, and the US from July 2014 to April 2016, while the FIT2 trial was conducted in Europe from January 2015 to August 2016. Both trials evaluated the efficacy and safety of fostamatinib compared to placebo among patients with persistent, chronic ITP. Randomization occurred in a 2:1 ratio of fostamatinib to placebo and was stratified by platelet count (< or ≥ 15,000/μL) and a previous splenectomy (yes or no). Before patients were randomized, there was a washout period during which all other ITP therapies were discontinued. The washout period differed according to the specific drug, ranging from 7 days for IVIG to 8 weeks for an alkylating drug. Patients were allowed to continue on corticosteroids (at doses < 20 mg of prednisone equivalent per day), azathioprine, and danazol. In the FIT1 trial, 117 patients were screened and 41 failed screening (3 withdrew consent, 10 failed inclusion criteria, 30 failed exclusion criteria, and 3 failed for other reasons). In the FIT2 trial, 107 patients were screened and 33 failed screening (1 withdrew consent, 15 failed inclusion criteria, 19 failed exclusion criteria, 1 patient was pregnant, and 2 failed for other reasons). In the FIT1 trial, 51 patients were randomized to receive fostamatinib and 25 were randomized to receive placebo, while in the FIT2 trial, 50 patients were randomized to fostamatinib and 24 were randomized to placebo.
Populations
Inclusion and Exclusion Criteria
Both the FIT1 and FIT2 trials enrolled patients 18 years of age and older who had a diagnosis of ITP for at least 3 months and who had received at least 1 previous treatment for ITP. Patients in both trials had to have an average platelet count of less than 30,000/µL from 3 qualifying counts in the previous 3 months, and at least 2 of these counts had to be from the screening period (the 30 days leading up to baseline). Female patients had to be postmenopausal, be surgically sterile, or agree to use an acceptable method of birth control throughout the study. Concurrent treatment for ITP (other than corticosteroids at doses < 20 mg of prednisone equivalent per day, azathioprine, and danazol) was not allowed. Because patients in both trials must have had no known etiology for ITP, those with secondary ITP were excluded. Patients were also excluded if they had a cardiovascular event in the 6 months before randomization, uncontrolled or poorly controlled hypertension (blood pressure ≥ 140/90 mm Hg), surgery in the previous 28 days, any blood products in the 2 weeks before randomization, an infection at screening or baseline, an IBLS score of grade 2, a history of coagulopathy, or an active clinically significant disorder that could affect the pharmacokinetics of fostamatinib.
Baseline Characteristics
In the FIT1 trial, patients in the fostamatinib group were older than the placebo group (a mean age of 57 years versus 53 years), while the proportion of females was lower in the fostamatinib group compared to the placebo group (59% versus 68%, respectively). The patients were predominantly White (86% in fostamatinib group and 84% in placebo) in both FIT1 trial groups. The majority of patients had chronic ITP in both groups, although the proportion was higher in the fostamatinib group compared to the placebo group (94% versus 88%, respectively). Patients in the fostamatinib group had a longer duration of ITP (a mean of 13 years versus 9 years in the placebo group) and had received more previous ITP treatments (a median of 5 compared to 3 in the placebo group). The rate of a previous splenectomy was similar in both groups (39% in fostamatinib and 40% in placebo). Most of the patients had received steroids previously — the proportion was higher in the placebo group compared to the fostamatinib group (100% in placebo versus 90% in fostamatinib). Other common previous treatments included rituximab (51% in fostamatinib versus 44% in placebo), TPO-RAs (51% versus 60%, respectively), and immunoglobulins (65% versus 68%, respectively). The baseline platelet count was higher in the placebo group (a mean of 16,936/µL) compared to the fostamatinib group (a mean of 16,215/µL).
In the FIT2 trial, the baseline age was similar in both groups (a mean of 49 years in the fostamatinib group versus 50 years in the placebo group) while there were more females in the fostamatinib group (62% versus 54% in the placebo group). All patients were White in both groups. Most patients in the FIT2 trial had chronic ITP (94% in fostamatinib group and 96% in placebo group). The duration of ITP was similar between groups (a mean of 12 years in the fostamatinib group and 11 years in the placebo group) while the median number of prior treatments was 3 in both groups. The rate of a previous splenectomy was higher in the placebo group (38%) compared to the fostamatinib group (28%). Most patients had received steroids previously (96% in fostamatinib and 92% in placebo), while other common treatments included TPO-RAs (40% in fostamatinib versus 42% in placebo), immunoglobulins (65% versus 68%, respectively), and azathioprine (34% versus 38%, respectively). The baseline platelet count was higher in the placebo group (a mean of 17,333/µL) compared to fostamatinib (a mean of 15,860/µL).
Patients in the FIT1 trial were older on average than those in the FIT2 trial. Across both trials, most patients were White. The duration of ITP, rate of a previous splenectomy, and use of prior ITP treatments was similar between the FIT1 and FIT2 trials.
Table 7: Summary of Baseline Characteristics (Intention-to-Treat Population)
Characteristic | FIT1 | FIT 2 | ||
|---|---|---|---|---|
Fostamatinib N = 51 | Placebo N = 25 | Fostamatinib N = 50 | Placebo N = 24 | |
Age | ||||
Mean (SD) | 57 (18) | 53 (16) | 49 (15) | 50 (17) |
Median (range) | 57 (20 to 88) | 57 (26 to 77) | 50 (21 to 82) | 50 (20 to 78) |
Sex, n (%) | ||||
Female | 30 (59) | 17 (68) | 31 (62) | 13 (54) |
Male | 21 (41) | 8 (32) | 19 (38) | 11 (46) |
Race, n (%) | ||||
White | 44 (86) | 21 (84) | 50 (100) | 24 (100) |
Asian | 3 (6) | 2 (8) | 0 | 0 |
Black or African-American | 2 (4) | 2 (8) | 0 | 0 |
Other | 2 (4) | 0 | 0 | 0 |
Height, cm | ||||
Mean (SD) | 166 (11) | 169 (11) | 171 (10) | 169 (11) |
Median (range) | 165 (143 to 188) | 168 (148 to 194) | 170 (156 to 190) | 169 (152 to 186) |
Weight, kg | ||||
Mean (SD) | 79 (25) | 86 (29) | 80 (17) | 82 (17) |
Median (range) | 71 (47 to 163) | 82 (58 to 204) | 79 (49 to 124) | 85 (45 to 107) |
ITP, n (%) | ||||
Persistent | 3 (6) | 3 (12) | 3 (6) | 1 (4) |
Chronic | 48 (94) | 22 (88) | 47 (94) | 23 (96) |
Duration of ITP, years | ||||
Mean (SD) | 13 (14) | 8.9 (10) | 12 (13) | 11 (8) |
Median (range) | 7.5 (0.6 to 53) | 5.5 (0.4 to 45) | 9 (0.3 to 50) | 11 (0.9 to 29) |
Most recent platelet count before screening, /µL | ||||
Mean (SD) | 16,215 (10,439) | 16,936 (9,686) | 15,860 (8,647) | 17,333 (10,285) |
Median (range) | 17,000 (0 to 34,000) | 17,000 (2,000 to 35,000) | 13,500 (0 to 34,000) | 21,000 (1,000 to 35,000) |
Previous splenectomy, n (%) | ||||
Yes | 20 (39) | 10 (40) | 14 (28) | 9 (38) |
No | 31 (61) | 15 (60) | 36 (72) | 15 (62) |
Prior unique ITP treatments, median (range) | 5.0 (1 to 10) | 3.0 (1 to 9) | 3.0 (1 to 10) | 3.0 (1 to 10) |
Previous ITP treatment, n (%) | ||||
Steroid | 46 (90) | 25 (100) | 48 (96) | 22 (92) |
Rituximab | 26 (51) | 11 (44) | 8 (16) | 3 (13) |
TPO-RA | 26 (51) | 15 (60) | 20 (40) | 10 (42) |
Cyclophosphamide | 3 (6) | 2 (8) | 5 (10) | 4 (17) |
Danazol | 7 (14) | 4 (16) | 13 (26) | 5 (21) |
Dapsone | 10 (20) | 3 (12) | NR | NR |
Immunoglobulins | 33 (65) | 17 (68) | 19 (38) | 10 (42) |
Azathioprine | 14 (28) | 9 (36) | 17 (34) | 9 (38) |
Cyclosporine | 6 (12) | 0 (0) | 8 (16) | 4 (17) |
Mycophenolate | 12 (24) | 8 (32) | 2 (4) | 0 (0) |
Concomitant treatment, n (%) | ||||
Danazol | 1 (2) | 0 | 1 (2) | 0 |
Platelets | 2 (4) | 1 (4) | 0 | 1 (4) |
Steroid | 19 (37) | 14 (56) | 22 (44) | 15 (63) |
Immunoglobulins | 15 (29) | 7 (28) | 6 (12) | 6 (25) |
ITP = immune thrombocytopenia; SD = standard deviation; TPO-RA = thrombopoietin receptor agonist.
Source: FIT1 Clinical Study Report5 and FIT2 Clinical Study Report.6
Interventions
In both the FIT1 and FIT2 trials, patients randomized to the fostamatinib group received an initial dosage of fostamatinib 100 mg twice daily. Patients in the placebo group took matching placebo. Fostamatinib and matched placebo were taken orally and self-administered. If the platelet count was greater than 50,000/µL, patients remained on the 100 mg twice daily dosage (or matching placebo). If the platelet count was less than 50,000/µL at or after week 4, the dosage of fostamatinib was increased to 150 mg twice daily (or matching placebo) if the patients were tolerating the study drug. The dosage was reduced to fostamatinib 100 mg once daily if patients experienced dose-limiting adverse effects. Patients in both arms were allowed to receive concomitant corticosteroids (equivalent to < 20 mg of prednisone equivalent per day), danazol, or azathioprine. New ITP treatments could not be started, with the exception of rescue therapy. Rescue therapy was permitted for patients with a platelet count below 50,000/µL who were at immediate risk of bleeding or with clinically significant bleeding or wet purpura, or with a platelet count below 50,000/µL and requiring urgent surgery. Rescue therapy could include IVIG, anti-D, or IV methylprednisolone. Beginning at week 12, if the platelet count was less than 50,000/µL (or in the absence of an increase of at least 20,000/µL among patients with a platelet count of less than 15,000/µL at baseline), patients were considered nonresponders and could discontinue participation in the study. Patients could also withdraw from the study if they received rescue therapy after week 10.
Outcomes
A list of efficacy end points identified in the CADTH review protocol that were assessed in the clinical trials included in this review is provided in Table 8. These end points are also summarized in the following section. A detailed discussion and critical appraisal of the outcome measures are provided in Appendix 3.
Table 8: Summary of Outcomes of Interest Identified in the CADTH Review Protocol
Outcome measure | FIT1 | FIT2 |
|---|---|---|
Achievement of stable platelet response (platelet count of ≥ 50,000/µL at 4 or more of the last 6 scheduled visits between week 14 and week 24) | Primary | Primary |
Achievement of platelet response at week 12 | Secondary | Secondary |
Achievement of platelet response at week 24 | Secondary | Secondary |
Achievement of platelet count ≥ 30,000/µL at week 12 among patients with baseline platelet count < 15,000/µL | Secondary | Secondary |
Achievement of platelet count ≥ 30,000/µL at week 24 among patients with baseline platelet count < 15,000/µL | Secondary | Secondary |
Frequency and severity of bleeding according to IBLS over 24 weeks | Secondary | Secondary |
Frequency and severity of bleeding according to WHO bleeding scale over 24 weeks | Secondary | Secondary |
SF-36 (quality of life) | Secondary | Secondary |
Use of rescue therapy | Exploratory | Exploratory |
Onset of platelet effect in responders | Exploratory | Exploratory |
Bleeding-related SAEs | Exploratory | Exploratory |
IBLS = immune thrombocytopenia bleeding scale; SAE = serious adverse effects; SF-36 = Short Form (36) Health Survey.
Source: FIT1 Clinical Study Report5 and FIT2 Clinical Study Report.6
The primary outcome for both the FIT1 and FIT2 trials was the achievement of a stable platelet response, which was defined as a platelet count of at least 50,000/µL on at least 4 of the last 6 scheduled visits between week 14 and week 24. Secondary efficacy outcomes included achievement of a platelet response (≥ 50,000/µL) at week 12, achievement of a platelet response (≥ 50,000/µL) at week 24, achievement of a platelet count of least 30,000/µL at week 12 among patients with a baseline platelet count of less than 15,000/µL, and achievement of a platelet count of 30,000/µL of greater at week 24 among patients with a baseline platelet count of at less than 15,000/µL. Platelet count was assessed at baseline and every 2 weeks thereafter (± 3 days). Platelet counts were performed by local laboratories affiliated with the clinical sites enrolling patients.
Another secondary outcome was the frequency and severity of bleeding according to the IBLS and the WHO bleeding scale over 24 weeks. This was reported as the mean of IBLS and WHO assessments over 24 weeks per group. Bleeding assessments were performed at baseline and every 2 weeks throughout the study. The IBLS scale assesses bleeding at 9 anatomic sites over the previous week and is rated from 0 (no bleeding) to 2 (marked bleeding). The WHO bleeding scale measures severity of bleeding from 0 (no bleeding) to 4 (debilitating blood loss). Bleeding scale assessments were performed by a physician, a doctor of osteopathic medicine, a physician’s assistant, or a nurse practitioner, and were performed by the same assessor for each patient at all study visits, whenever possible. Another secondary outcome was quality of life, as measured by the SF-36 questionnaire, which is a health survey consisting of 36 questions from 8 HRQoL domains. The SF-36 was completed by patients on their own at baseline, week 4, week 12, and week 24. For exploratory post hoc analyses, the investigators measured the onset of platelet effect in responders, use of rescue therapy, and bleeding-related serious adverse effects. The investigators also conducted exploratory analyses of subgroups according to age (< 57 years or ≥ 57 years), sex, prior experience with TPO-RA, a prior splenectomy, and baseline platelet counts (< 15,000/µL or ≥ 15,000/µL).
The clinical study reports for the FIT 1 and FIT2 trials state that all efficacy and safety measures were standard (i.e., they were widely used and generally recognized as reliable, accurate, and relevant). Contract research organizations were responsible for study conduct, data management, and statistical analysis. An electronic case report form was used to record data, which was completed by study staff. A safety contract research organization set up the safety database and was responsible for data entry, coding, and preparation of safety reports.
Treatment-emergent adverse events were either new or detectable exacerbations of pre-existing conditions. The AE reporting period began with the first dose of study and ended with the final study visit. Serious adverse events were any untoward medical occurrences that resulted in death, were life-threatening, required inpatient hospitalization, or resulted in significant disability or incapacity. Investigators assessed the occurrence of AEs and SAEs at all evaluation time points during the study. When AE or SAEs were volunteered by patients, discovered by staff during questions, or detected by physical exams or laboratory tests, the AEs were recorded in a case report form and coded using the Medical Dictionary for Regulatory Activities.
Statistical Analysis
The primary efficacy outcome for the FIT1 and FIT2 trials was a stable platelet response as defined previously. Patients who discontinued treatment before week 24 because of a lack of efficacy or an AE, or who received rescue treatment after 10 weeks, were considered nonresponders. The proportion of patients achieving a stable platelet response in each treatment group was calculated for the ITT population. The authors reported the RD and 95% CI around the RD based on the normal approximation. The null hypothesis was that there was no difference in the proportion of responders for the fostamatinib group compared to placebo. The investigators used a 2-sided Fisher exact test to test the null hypothesis, with a significance level of 0.05. The sample size was calculated to provide a 90% power for the primary efficacy outcome, using a 2:1 ratio for fostamatinib: placebo, and assuming the proportion of responders in the fostamatinib group would be 0.4 and the proportion of responders in the placebo group would be 0.05. The required sample size was 75 patients. The last observation carried forward (LOCF) method was used to impute missing data for the primary outcome. The LOCF was used to impute missing platelet counts for patients who withdrew from the study early (due to reasons other than lack of efficacy, use of rescue therapy, or an AE; patients withdrawing for those reasons were deemed nonresponders). In the FIT2 trial, the investigators also used multiple imputation as a sensitivity analysis of the primary outcome when there were missing platelet count data. This analysis was stated to be pre-planned in the Clinical Study Report for FIT2; however, no information on the methods for this analysis were identified in the Clinical Study Report nor protocol. In the results section of the FIT2 Clinical Study Report, the investigators stated that missing platelet counts were imputed using the SAS MINANALYZE procedure, and reported proportions were the average of 10,000 iterations.
Secondary efficacy outcomes involving platelet counts were analyzed the same way as the primary outcome (including data imputation using LOCF). For the IBLS and WHO bleeding scale data, the mean of the assessment scores was calculated across the 24-week treatment period. The investigators used a 2-sided, 2-sample t-test to evaluate the difference in means. Descriptive statistics were used to describe rescue therapy use and bleeding-related SAEs; however, no statistical test was used to evaluate differences between treatment groups. Exploratory subgroup analyses for the primary outcome involved calculating the proportion achieving the primary efficacy end point in each treatment group within the subgroup, calculating an RD, and reporting a 95% CI, around the RD. No statistical test was performed to evaluate differences between treatment arms in different subgroups.
For AEs, the investigators reported the number and proportion of patients with at least 1 AE during the double-blind treatment period.
Analysis Populations
In the FIT1 and FIT2 trials, the ITT population included all randomized patients. The ITT population was used for analysis of all efficacy analyses and patients were analyzed according to their randomized treatment assignment. The per-protocol population was all patients with no major protocol violations (those not receiving any study treatment, not receiving correct study treatment, or failing to meet eligibility criteria). All outcomes analyzed in the per-protocol population were according to patients’ randomized treatment assignment. The safety population was all randomized patients who received any amount of study drug, and patients were analyzed according to the treatment they received.
Results
Patient Disposition
In the FIT1 trial, 117 patients were screened, and 76 patients (65%) were randomized — 51 to fostamatinib and 25 to placebo. A total of 39 patients (76%) in the fostamatinib group discontinued the study early, while 24 patients (96%) in the placebo group discontinued early. In the FIT2 trial, 107 patients were screened and 74 (69%) were randomized — 50 to fostamatinib and 24 to placebo. A total of 37 patients (74%) in the fostamatinib group discontinued from the study early, while 22 patients (92%) in placebo group discontinued early. Reasons for discontinuation from the FIT1 and FIT2 trials are listed in Table 9. In the FIT1 trial, 55% of patients in the fostamatinib group discontinued early due to a lack of response compared to 88% in the placebo group. In the FIT2 trial, 66% of patients in the fostamatinib group discontinued early due to a lack of response compared to 79% in the placebo group.
Disposition | FIT1 | FIT2 | ||
|---|---|---|---|---|
Fostamatinib | Placebo | Fostamatinib | Placebo | |
Screened, N | 117 | 107 | ||
Randomized, N | 51 | 25 | 50 | 24 |
Discontinued from study early, N | 39 | 24 | 37 | 22 |
Reason for discontinuation, N (%) | ||||
Lack of response (at week 12 or later) | 28 (55) | 22 (88) | 33 (66) | 19 (79) |
Adverse event meeting study-discontinuation criteria | 4 (8) | 1 (4) | 0 | 2 (8) |
Other adverse event | 3 (6) | 1 (4) | 2 (4) | 0 |
Patient decision | 1 (2) | 0 | 1 (2) | 1 (4) |
Patient noncompliant | 1 (2) | 0 | 0 | 0 |
Lost to follow-up | 1 (2) | 0 | 0 | 0 |
Investigator discretion | 1 (2) | 0 | 1 (2) | 0 |
ITT, N | 51 | 25 | 50 | 24 |
PP, N | 51 | 25 | 49 | 23 |
Safety, N | 51 | 25 | 51 | 23 |
ITT = intention to treat; PP = per protocol.
Source: FIT1 Clinical Study Report5 and FIT2 Clinical Study Report.6
Exposure to Study Treatments
In the FIT1 trial, the mean duration of exposure was 99 days (SD = 46) for fostamatinib and 94 days (SD = 30) for placebo. The mean overall compliance (actual number of tablets taken divided by total number expected to be taken) was 93% in the fostamatinib group and 96% in the placebo group. In the fostamatinib group, 2% of patients received concomitant danazol, 4% received concomitant platelets, 37% received concomitant steroids, and 29% received concomitant immunoglobulins. In the placebo group, 56% of patients received concomitant steroids, 4% of patients received concomitant platelets, and 28% of patients received concomitant immunoglobulins. Use of rescue therapy is reported as an efficacy outcome.
In the FIT2 trial, the mean duration of exposure was 112 days (SD = 41) in the fostamatinib group and 88 days (SD = 36) in the placebo group. The mean overall compliance was 99% in the fostamatinib group and 98% in the placebo group. In the fostamatinib group, 2% of patients received concomitant danazol, 44% received concomitant steroids, and 12% received concomitant immunoglobulins. In the placebo group, 4% of patients took concomitant platelets, 63% of patients received concomitant steroids, and 25% of patients received concomitant immunoglobulins. Use of rescue therapy is reported as an efficacy outcome.
Efficacy
Only those efficacy outcomes and analyses of subgroups identified in the review protocol are reported here; Appendix 3 provides detailed efficacy data. Pooled outcome data for the FIT1 and FIT2 trial were reported in a single publication.23 These data are also presented in Appendix 3. The following outcomes identified as important in the review protocol were not measured in the FIT1 trial nor the FIT2 trial: emergency room visits, hospitalizations, treatment-free remission, and symptoms.
Stable Platelet Response
In the FIT1 trial, 18% of patients in the fostamatinib group experienced a stable platelet response compared to 0% in the placebo group (RD = 18%; 95% CI, 7.2 to 28; P = 0.026).
In the FIT2 trial, 18% of patients in the fostamatinib group experienced a stable platelet response compared to 4% in the placebo group (RD = 14%; 95% CI, 0.5 to 27; P = 0.15).
Platelet Count of 50,000/µL or Greater
In the FIT1 trial, 22% of patients in the fostamatinib group achieved a platelet count of at least 50,000/µL at week 12 compared to 0% in the placebo group (RD = 22%; 95% CI, 10 to 33; P = 0.013). At week 24, 16% of patients in the fostamatinib group achieved a platelet count of at least 50,000/µL compared to 0% in the placebo group (RD = 16%; 95% CI, 5.7 to 26; P = 0.047).
In the FIT2 trial, 24% of patients in the fostamatinib group achieved a platelet count of at least 50,000/µL at week 12 compared to 13% in the placebo group (RD = 12%; 95% CI, −6.3 to 29; P = 0.36). At week 24, 16% of patients in the fostamatinib group achieved a platelet count of at least 50,000/µL compared to 4% in the placebo group (RD = 12%; 95% CI, −1.1 to 25; P = 0.26).
Platelet Count of 30,000/µL or Greater and 20,000/µL or Greater Above Baseline in Patients With a Low Baseline Platelet Count (Less Than 15,000/µL)
In the FIT1 trial, 16% of patients with a low baseline platelet count in the fostamatinib group achieved a platelet count of at least 30,000/µL and at least 20,000/µL above baseline at week 12 compared to 0% in the placebo group (RD = 16%; 95% CI, 1.6 to 30; P = 0.28). At week 24, 16% of patients with a low baseline platelet count in the fostamatinib group achieved a platelet count of 30,000/µL or greater and 20,000/µL or greater above baseline compared to 0% in the placebo group (RD = 16%; 95% CI, 1.6 to 30; P = 0.28).
In the FIT2 trial, 27% of patients with a low baseline platelet count in the fostamatinib group achieved a platelet count of 30,000/µL or greater and 20,000/μL or greater above baseline at week 12 compared to 11% in the placebo group (RD = 16%; 95% CI, −12 to 44; P = 0.64). At week 24, 14% of patients with a low baseline platelet count in the fostamatinib group achieved a platelet count of 30,000/µL or greater and 20,000/μL or greater above baseline compared to 0% in the placebo group (RD = 14%; 95% CI, −0.7 to 28; P = 0.54).
Bleeding Assessments
In the FIT1 trial, the mean IBLS score across 24 weeks was 0.13 (SD = 0.12) in the fostamatinib group and 0.14 (SD = 0.10) in the placebo group (difference in means = −0.01; 95% CI, −0.1 to 0.0; P = 0.66). The mean WHO bleeding scale score across 24 weeks in the fostamatinib group was 0.61 (SD = 0.66) compared to 0.46 (SD = 0.56) in the placebo group (difference in means = 0.15; 95% CI, −0.2 to 0.5; P = 0.34).
In the FIT2 trial, the mean IBLS score across 24 weeks was 0.04 (SD = 0.08) in the fostamatinib group and 0.06 (SD = 0.07) in the placebo group (difference in means = −0.01; 95% CI, −0.05 to 0.02; P = 0.49). The mean WHO bleeding scale score across 24 weeks in the fostamatinib group was 0.26 (SD = 0.38) compared to 0.38 (SD = 0.47) in the placebo group (difference in means = −0.12; 95%−CI, −0.32 to 0.09; P = 0.25).
Use of Rescue Therapy
In the FIT1 trial, 31% of patients in the fostamatinib group required rescue therapy before week 10 compared to 44% of patients in the placebo group. After week 10, 14% of patients in the fostamatinib group required rescue therapy compared to 28% in the placebo group.
In the FIT2 trial, 18% of patients in the fostamatinib group required rescue therapy before week 10 compared to 29% of patients in the placebo group. After week 10, 2% of patients in the fostamatinib group required rescue therapy compared to 21% in the placebo group.
Bleeding-Related Serious Adverse Events
In the FIT1 trial, ||| of patients in the fostamatinib group experienced a bleeding-related SAE compared to ||| in the placebo group. In the FIT2 trial, ||| of patients in the fostamatinib group experienced a bleeding-related SAE compared to ||| in the placebo group.
Short Form (36) Health Survey
In the FIT1 trial, there were no differences in SF-36 scores between the fostamatinib and placebo groups at any time point. At week 24, there was ||||||||| providing SF-36 data in the placebo group and |||| patients in the fostamatinib group.
In the FIT2 trial, there were no differences in SF-36 scores between the fostamatinib and placebo groups at week 12 or week 24; however, at week 4 the mean change from baseline in the fostamatinib group for bodily pain was |||| compared to |||| in the placebo group (difference in mean change from baseline = ||||||||||||). At week 4 the mean change from baseline for general health (difference in mean change from baseline = ||||||||||||) and physical health (difference in mean change from baseline = |||||||||||) was also greater in the fostamatinib group compared to placebo. At week 24 in the FIT2 trial, there were |||||||||||| providing SF-36 data in the placebo group and |||| patients in the fostamatinib group.
Time to Response Among Responders
In the FIT1 trial, the mean time to a platelet count of 50,000/µL or greater among responders was 39 days (range = 15 to 73 days; median not reported). In the FIT2 trial, the mean time to a platelet count of 50,000/µL or greater among responders was 22 days (median = 15 days; range = 12 to 56 days).
Table 10: Primary and Secondary Efficacy Outcomes (Intention-to-Treat Population)
Efficacy outcome | FIT1 | FIT2 | |||
|---|---|---|---|---|---|
Fostamatinib (N = 51) | Placebo (N = 25) | Fostamatinib (N = 50) | Placebo (N = 24) | ||
Primary outcome; stable platelet response (≥ 50,000/µL) on 4 of 6 visits between weeks 14 and 24a | |||||
n (%) | 9 (18) | 0 (0) | 9 (18) | 1 (4) | |
Risk difference (95% CI) | 18 (7.2 to 28.1) | 14 (0.5 to 27.1) | |||
P value | 0.0261 | 0.1519 | |||
Primary outcome: stable platelet response (≥ 50,000/µL) on 4 of 6 visits between weeks 14 and 24 (sensitivity analysis using multiple imputation for missing platelet counts)b | |||||
n (%) | NR | NR | 18%c | 4%c | |
Risk difference (95% CI) | NR | 14 (0.16 to 27) | |||
P value | NR | 0.047 | |||
Secondary outcome; platelet count ≥ 50,000/µL at week 12a | |||||
Platelet count ≥ 50,000/µL at week 12a | |||||
n (%) | 11 (22) | 0 (0) | 12 (24) | 3 (13) | |
Risk difference (95% CI) | 22 (10 to 33) | 12 (−6.3 to 29) | |||
P value | 0.013 | 0.36 | |||
Platelet count ≥ 50,000/µL at week 24a | |||||
n (%) | 8 (16) | 0 (0) | 8 (16) | 1 (4) | |
Risk difference (95% CI) | 16 (5.7 to 26) | 12 (−1.1 to 25) | |||
P value | 0.047 | 0.26 | |||
Platelet count ≥ 30,000/µL and ≥ 20,000/µL above baseline in patients with low baseline platelet count < 15,000/µL at week 12a | |||||
n (%) | 4 (16) | 0 (0) | 6 (27) | 1 (11) | |
Risk difference (95% CI) | 16 (1.6 to 30) | 16 (−12 to 44) | |||
P value | 0.28 | 0.64 | |||
Platelet count ≥ 30,000/µL and ≥ 20,000/µL above baseline in patients with low baseline platelet count < 15,000/µL at week 24a | |||||
n (%) | 4 (16) | 0 (0) | 3 (14) | 0 | |
Risk difference (95% CI) | 16 (1.6 to 30) | 14 (−0.7 to 28) | |||
P value | 0.28 | 0.54 | |||
Mean IBLS score across 24 weeksd | |||||
Mean IBLS score over 24 weeks (SD) | 0.13 (0.12) | 0.14 (0.10) | 0.04 (0.08) | 0.06 (0.07) | |
Difference in means (95% CI) | −0.01 (−0.1 to 0.0) | −0.01 (−0.05 to 0.02) | |||
P value | 0.66 | 0.49 | |||
Mean WHO bleeding score across 24 weeksd | |||||
Mean score over 24 weeks (SD) | 0.61 (0.66) | 0.46 (0.56) | 0.26 (0.38) | 0.38 (0.47) | |
Difference in means (95% CI) | 0.15 (−0.2 to 0.5) | −0.12 (−0.32 to 0.09) | |||
P value | 0.34 | 0.25 | |||
Use of rescue therapy before week 10 | |||||
n (%) | 16 (31) | 11 (44) | 9 (18) | 7 (29) | |
Risk difference (95% CI) | NR | NR | |||
P value | NR | NR | |||
Use of rescue therapy after week 10 | |||||
n (%) | 7 (14) | 7 (28) | 1 (2) | 5 (21) | |
Risk difference (95% CI) | NR | NR | |||
P value | NR | NR | |||
Bleeding-related SAEs | |||||
n (%) | ||||| | |||||| | ||||| | ||||| | |
Risk difference (95% CI) | NR | NR | |||
P value | NR | NR | |||
CI = confidence interval; NR = not reported; SD = standard deviation.
aIntention-to-treat population, 2-sided Fisher exact test with a significance level of 0.05.
bIntention-to-treat population; P value is from a Fisher exact test, testing for an RD between treatments. Missing platelet count values were imputed using multiple imputation methods. An SAS MIANALYZE procedure was used to combine estimates across imputations. Reported percentages and P values are based on the average of 10,000 iterations.
cOnly proportion provided.
dIntention-to-treat population, 2-sided, 2-sample t-test.
Source: FIT1 Clinical Study Report5 and FIT2 Clinical Study Report.6
Subgroup Analysis
Both the FIT1 and FIT2 trials conducted subgroup analyses for the primary efficacy end point. Results are presented in Table 11.
In the FIT1 trial, among patients with prior experience with TPO-RA treatment, 15.4% of patients in the fostamatinib group experienced a stable platelet response compared to 0% in the placebo group (RD = 15.4%; 95% CI, 1.5 to 29.3). Among patients without prior experience with TPO-RA treatment, 20% of patients in the fostamatinib group experienced a stable platelet response compared to 0% in the placebo group (RD = 20%; 95% CI, 4.3 to 35.7). In the FIT2 trial, among patients with prior experience with TPO-RA treatment, 15% of patients in the fostamatinib group experienced a stable platelet response compared to 0% in the placebo group (RD = 15%; 95% CI, −0.6 to 30.6). Among patients without prior experience with TPO-RA treatment, 20% of patients in the fostamatinib group experienced a stable platelet response compared to 7% in the placebo group (RD = 12.9%; 95% CI, −6.8 to 32.5).
In the FIT1 trial, among patients with a prior splenectomy, 15% of patients in the fostamatinib group experienced a stable platelet response compared to 0% in the placebo group (RD = 15%; 95% CI, −0.6 to 30.6). Among patients without a prior splenectomy, 19.4% of patients in the fostamatinib group experienced a stable platelet response compared to 0% in the placebo group (RD = 19.4%; 95% CI, 5.4 to 33.3). In the FIT2 trial, among patients with a prior splenectomy, 21.4% of patients in the fostamatinib group experienced a stable platelet response compared to 0% in the placebo group (RD = 21.4%; 95% CI, −0.1 to 42.9). Among patients without a prior splenectomy, 16.7% of patients in the fostamatinib group experienced a stable platelet response compared to 6.7% in the placebo group (RD = 10%; 95% CI, −7.5 to 27.5).
Table 11: Subgroup Analyses for Primary Efficacy Outcome (Intention-to-Treat Population)
Outcome | FIT1 | FIT2 | ||
|---|---|---|---|---|
Fostamatinib | Placebo | Fostamatinib | Placebo | |
Stable platelet response (≥ 50,000/µL) on 4 of 6 visits between weeks 14 and 24 in patients with prior TPO-RAa | N = 26 | N = 15 | N = 20 | N = 10 |
n (%) | 4 (15) | 0 (0) | 3 (15) | 0 |
Risk difference (95% CI) | 15 (1.5 to 29.3) | 15 (−0.6 to 31) | ||
P value | NR | NR | ||
Stable platelet response (≥ 50,000/µL) on 4 of 6 visits between weeks 14 and 24 in patients with no prior TPO-RAa | N = 25 | N = 10 | N = 30 | N = 14 |
n (%) | 5 (20) | 0 (0) | 6 (20) | 1 (7) |
Risk difference (95% CI) | 20 (4.3 to 36) | 13 (−6.8 to 33) | ||
P value | NR | NR | ||
Stable platelet response (≥ 50,000/µL) on 4 of 6 visits between weeks 14 and 24 in patients with a prior splenectomya | N = 20 | N = 10 | N = 14 | N = 9 |
n (%) | 3 (15) | 0 (0) | 3 (21) | 0 |
Risk difference (95% CI) | 15 (−0.6 to 31) | 21 (−0.1 to 43) | ||
P value | NR | NR | ||
Stable platelet response (≥ 50,000/µL) on 4 of 6 visits between weeks 14 and 24 in patients with no prior splenectomya | N = 31 | N = 15 | N = 36 | N = 15 |
n (%) | 6 (19) | 0 (0) | 6 (17) | 1 (7) |
Risk difference (95% CI) | 19 (5.4 to 33) | 10 (−7.5 to 28) | ||
P value | NR | NR | ||
CI = confidence interval; NR = not reported; TPO-RA = thrombopoietin receptor agonist.
aIntention-to-treat population, no statistical test performed.
Source: FIT1 Clinical Study Report5 and FIT2 Clinical Study Report.6
Subgroup analyses of the stable platelet response rate (primary efficacy end point) based on data pooled from the 2 studies support the consistency of the efficacy of fostamatinib across subpopulations based on disease-related characteristics (baseline platelet count, prior splenectomy, previous use of a TPO-RA, and previous use of rituximab) and demographics (age or sex). Patients who had ITP for less than 3 years did not respond to fostamatinib as well as those who had ITP for more than 3 years; however, these results could have been affected by the small number of patients who had ITP for less than 3 years. Results appear in Figure 2.
Figure 2: Subgroup Analyses for the Primary Efficacy Outcome of Stable Platelet Response at Week 24 Pooled From FIT1 and FIT2
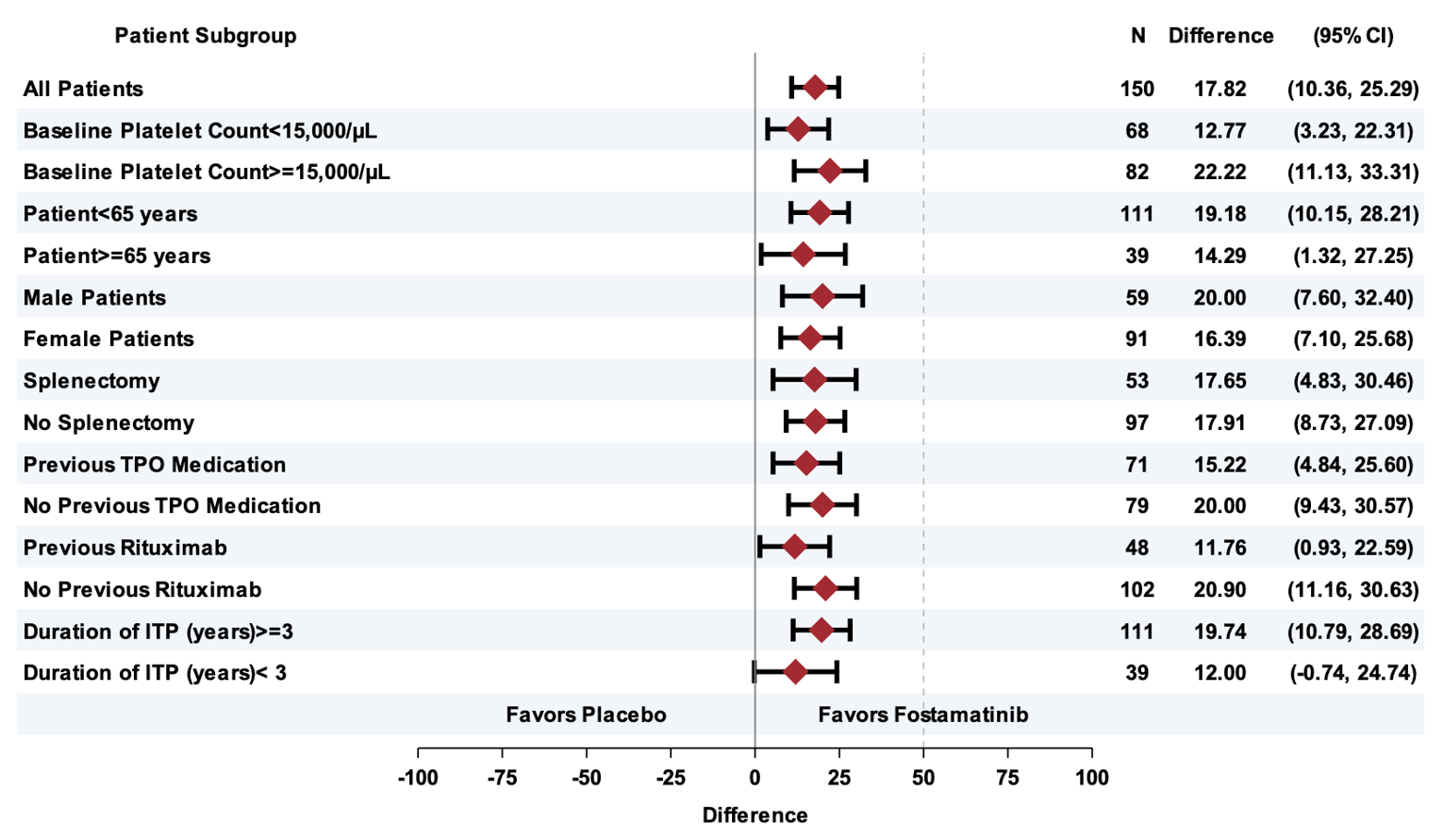
CI = confidence interval; ITP = immune thrombocytopenia; TPO = thrombopoietin.
Source: Tavalisse Drug Reimbursement Review submission.24
Harms
Only those harms identified in the review protocol are reported. Table 12 provides detailed harms data.
Adverse Events
In the FIT1 trial, 96% of patients in the fostamatinib group experienced an AE compared to 76% of patients in the placebo group. In the fostamatinib group, the most common AEs were diarrhea (41%), nausea (29%), increased ALT (18%), increased AST (16%), headache (14%), dizziness (18%), epistaxis (18%), fatigue (12%), and hypertension (26%). The most common AEs in the placebo group were diarrhea (16%), headache (24%), dizziness (16%), epistaxis (16%), and dyspnea (12%).
In the FIT2 trial, 71% of patients in the fostamatinib group experienced an AE compared to 78% in the placebo group. The most common AEs in the fostamatinib group were diarrhea (18%), epistaxis (12%), and hypertension (14%). The most common AEs in the placebo group were diarrhea (13%), nausea (13%), headache (13%), hypertension (13%), and thrombocytopenia (13%).
Serious Adverse Events
In the FIT1 trial, 16% of patients in the fostamatinib group had at least 1 SAE compared to 20% in the placebo group. In the fostamatinib group, 1 patient (2%) experienced febrile neutropenia, 1 patient experienced immune thrombocytopenic purpura, 1 patient a retinal tear, 1 patient diarrhea, 1 patient pneumonia, 1 patient syncope, 1 patient vaginal hemorrhage, and 1 patient epistaxis. In the placebo group, 1 patient (4%) experienced anemia, 1 patient cardiac congestive failure, 1 patient gastrointestinal hemorrhage, 1 patient sepsis, 1 patient menorrhagia, 1 patient chronic obstructive pulmonary disease, and 1 patient epistaxis.
In the FIT2 trial, 10% of patients in the fostamatinib group had at least 1 SAE compared to 26% in the placebo group. In the fostamatinib group, 1 patient (2%) had epistaxis, 1 patient had bronchitis, 1 had a contusion, 1 a platelet count decrease, 1 plasma cell myeloma, 1 a transient ischemic attack, and 1 a hypertensive crisis. In the placebo group, 3 patients (13%) had thrombocytopenia, 1 menorrhagia, 1 a muscle rupture, 1 an infection, and 1 petechiae.
Withdrawals Due to Adverse Events
In the FIT1 trial, 16% of patients in the fostamatinib group withdrew due to any AE compared to 8% in the placebo group. In the fostamatinib group, 1 patient (2%) withdrew due to abdominal pain, 1 due to diarrhea, 1 due to neutropenia, 1 due to thrombocytopenia, 1 due to increased ALT, 1 due to chest pain, 1 due to pneumonia, and 1 due to syncope. In the placebo group, 1 patient (4%) withdrew due to abdominal discomfort and 1 due to epistaxis.
In the FIT2 trial, 4% of patients in the fostamatinib group withdrew due to any AE compared to 9% in the placebo group. In the fostamatinib group, 1 patient (2%) withdrew due to plasma cell myeloma and 1 due to headache. In the placebo group, 1 patient (4%) withdrew due to diarrhea and 1 due to hypertension.
Mortality
In the FIT1 trial, 1 patient died in the placebo group due to sepsis. In the FIT2 trial, 1 patient died in the fostamatinib group due to plasma cell myeloma.
Notable Harms
In the FIT1 trial, ||||| of patients in the fostamatinib group experienced an infection compared to ||| in the placebo group. In the FIT2 trial, ||||| of patients in the fostamatinib group and ||| of patients in the placebo group experienced an infection. In both the FIT1 and FIT2 trials, |||| of patients in the fostamatinib group experienced neutropenia compared to |||| in the placebo group. In the FIT1 trial, ||||| of patients in the fostamatinib group experienced elevated liver transaminase levels compared to |||| in the placebo group. In the FIT2 trial, |||| of patients in the fostamatinib group experienced elevated liver transaminase levels compared to |||| in the placebo group.
Harms | FIT1 Fostamatinib N = 51 | FIT1 Placebo N = 25 | FIT2 Fostamatinib N = 51 | FIT2 Placebo N = 23 |
|---|---|---|---|---|
Number of patients with any AE, n (%) | 49 (96) | 19 (76) | 36 (71) | 18 (78) |
Most common events,a n (%) | ||||
Diarrhea | 21 (41) | 4 (16) | 9 (18) | 3 (13) |
Nausea | 15 (29) | 1 (4) | 4 (8) | 3 (13) |
Constipation | 3 (6) | 1 (4) | NA | NA |
Abdominal pain | 3 (6) | 0 | NA | NA |
Flatulence | 3 (6) | 0 | NA | NA |
Vomiting | 2 (4) | 2 (8) | NA | NA |
Rectal hemorrhage | 0 | 2 (8) | NA | NA |
Increased ALT | 9 (18) | 0 | NA | NA |
Increased AST | 8 (16) | 0 | NA | NA |
Increased blood pressure | 3 (6) | 1 (4) | NA | NA |
Headache | 7 (14) | 6 (24) | 3 (6) | 3 (13) |
Dizziness | 9 (18) | 4 (16) | NA | NA |
Dysgeusia | 4 (8) | 0 | NA | NA |
Epistaxis | 9 (18) | 4 (16) | 6 (12) | 1 (4) |
Dyspnea | 3 (6) | 3 (12) | NA | NA |
Oropharyngeal pain | 1 (2) | 2 (8) | NA | NA |
URTI | 5 (10) | 1 (4) | NA | NA |
UTI | 3 (6) | 0 | NA | NA |
Fatigue | 6 (12) | 1 (4) | NA | NA |
Pyrexia | 2 (4) | 2 (8) | NA | NA |
Chest pain | 4 (8) | 1 (4) | NA | NA |
Hypertension | 13 (26) | 1 (4) | 7 (14) | 3 (13) |
Rash | 4 (8) | 0 | 3 (6) | 1 (4) |
Musculoskeletal pain | 0 | 2 (8) | NA | NA |
Anemia | 2 (4) | 2 (8) | NA | NA |
Contusion | 3 (6) | 0 | 3 (6) | 0 |
Thrombocytopenia | NA | NA | 0 | 3 (13) |
Hematoma | NA | NA | 1 (2) | 2 (9) |
Bronchitis | NA | NA | 3 (6) | 0 |
Petechiae | NA | NA | 2 (4) | 2 (9) |
Number of patients with at least 1 serious AE | ||||
n (%) | 8 (16) | 5 (20) | 5 (10) | 6 (26) |
Most common events,b n (%) | ||||
Anemia | 0 | 1 (4) | NA | NA |
Febrile neutropenia | 1 (2) | 0 | NA | NA |
Immune thrombocytopenic purpura | 1 (2) | 0 | NA | NA |
Thrombocytopenia | 1 (2) | 0 | 0 | 3 (13) |
Cardiac failure — congestive | 0 | 1 (4) | NA | NA |
Retinal tear | 1 (2) | 0 | NA | NA |
Diarrhea | 1 (2) | 0 | NA | NA |
Gastrointestinal hemorrhage | 0 | 1 (4) | NA | NA |
Pneumonia | 1 (2) | 0 | NA | NA |
Sepsis | 0 | 1 (4) | NA | NA |
Syncope | 1 (2) | 0 | NA | NA |
Menorrhagia | 0 | 1 (4) | 0 | 1 (4) |
Vaginal hemorrhage | 1 (2) | 0 | NA | NA |
COPD | 0 | 1 (4) | NA | NA |
Epistaxis | 1 (2) | 1 (4) | 1 (2) | 0 |
Bronchitis | NA | NA | 1 (2) | 0 |
Contusion | NA | NA | 1 (2) | 0 |
Muscle rupture | NA | NA | 0 | 1 (4) |
Infection | NA | NA | 0 | 1 (4) |
Decreased platelet count | NA | NA | 1 (2) | 0 |
Plasma cell myeloma | NA | NA | 1 (2) | 0 |
TIA | NA | NA | 1 (2) | 0 |
Petechiae | NA | NA | 0 | 1 (4) |
Hypertensive crisis | NA | NA | 1 (2) | 0 |
Number of patients with any AE leading to study drug withdrawal | ||||
n (%) | 8 (16) | 2 (8) | 2 (4) | 2 (9) |
Most common events,b n (%) | ||||
Abdominal discomfort | 0 | 1 (4) | NA | NA |
Abdominal pain | 1 (2) | 0 | NA | NA |
Diarrhea | 1 (2) | 0 | 0 | 1 (4) |
Neutropenia | 1 (2) | 0 | NA | NA |
Thrombocytopenia | 1 (2) | 0 | NA | NA |
Increased ALT | 1 (2) | 0 | NA | NA |
Epistaxis | 0 | 1 (4) | NA | NA |
Chest pain | 1 (2) | 0 | NA | NA |
Pneumonia | 1 (2) | 0 | NA | NA |
Syncope | 1 (2) | 0 | NA | NA |
Hypertension | NA | NA | 0 | 1 (4) |
Plasma cell myeloma | NA | NA | 1 (2) | 0 |
Headache | NA | NA | 1 (2) | 0 |
Number of patients with any AE leading to death | ||||
n (%) | 0 (0) | 1 (4) | 1 (2) | 0 |
Sepsis, n (%) | 0 | 1 (4) | NA | NA |
Plasma cell myeloma, n (%) | NA | NA | 1 (2) | 0 |
Number of patients with a notable harm | ||||
Infection, n (%) | |||||| | |||||| | |||||| | |||||| |
Neutropenia, n (%) | |||||| | |||||| | |||||| | |||||| |
Elevated transaminase level, n (%) | |||||| | |||||| | |||||| | |||||| |
AE = adverse event; ALT = alanine transaminase; AST = aspartate transaminase; COPD = chronic obstructive pulmonary disease; NA = not applicable; TIA = transient ischemic attack; URTI = upper respiratory tract infection; UTI = urinary tract infection.
aFrequency greater than 5%.
bFrequency greater than 2%.
Source: FIT1 Clinical Study Report,5 and FIT2 Clinical Study Report.6
Critical Appraisal
Internal Validity
Both the FIT1 and FIT2 trials were double-blind and, according to the clinical study reports, the unblinding procedure was not used during the studies; however, unblinding for patients and clinicians may have been possible as a platelet response in patients receiving placebo would not likely be observed. There was high adherence to the study treatments in both groups. Overall, the FIT1 and FIT2 trials were at low risk of bias due to protocol deviations from intended interventions. In the FIT1 and FIT2 trials, outcome data were available for nearly all participants randomized for the primary outcome; bias from missing outcome data for the primary outcome was therefore unlikely. However, there were missing outcome data for the HRQoL outcome. The measurement of outcomes in the FIT1 and FIT2 trials was the same in both groups. Outcome assessors were not aware of the intervention received by patients and, even if they were aware, it would be unlikely to influence assessment of platelet counts. The FIT1 and FIT2 trials were therefore at low risk of bias for measurement of outcomes. In the FIT1 trial, data were reported according to a pre-specified analysis plan, and post hoc analyses were acknowledged as such and described in the methods, with the exception of subgroup analyses that were not described in the methods or protocol. In the FIT2 trial, data were generally reported according to a pre-specified plan; however, a sensitivity analysis involving multiple imputation for the primary outcome was reported in the results. This analysis was claimed to be pre-specified, although there was no description in the methods section of the clinical study report or protocol. Similar to the FIT2 trial, subgroup analyses were not described in the methods or protocol, creating some concerns in the FIT1 and FIT2 trials related to selective outcome reporting.
In both the FIT1 and FIT2 trials, treatment groups were generally balanced in terms of baseline characteristics such as platelet count, rate of previous splenectomy, and age, although some imbalances existed. In the FIT1 trial, there was a higher proportion of females in the placebo group (68%) compared to the fostamatinib group (59%), while in the FIT2 trial the proportion of females was higher in the fostamatinib group (62% versus 54% in placebo). In the FIT1 trial, the fostamatinib group had a slightly longer duration of ITP on average (a mean of 13 years versus 9 years in the placebo group) and had used a greater number of previous ITP therapies (a median of 5 versus 3 in placebo group) compared to placebo, although this was likely not of major prognostic importance as both groups had longstanding ITP and were heavily pre-treated. There were also possible imbalances in the rates of specific treatments used in the FIT1 trial — for example, the rate of prior steroid use was higher in the placebo group versus fostamatinib (100% versus 90%, respectively), along with the rate of prior TPO-RA use (60% in placebo versus 51% in fostamatinib). In the FIT2 trial, the rate of prior splenectomy was higher in the placebo group (38%) compared to the fostamatinib group (28%). Subgroup analyses did not reveal differences in the response rate based on prior use of TPO-RAs or a splenectomy. However, these analyses were likely underpowered, and it is possible that baseline imbalances in prior treatments used may have introduced bias. Further, in both the FIT1 and FIT2 trials, the rate of concomitant steroid use was higher in the placebo group compared to the fostamatinib group, and rescue therapy use was higher in the placebo group as well. This may have introduced bias against the fostamatinib treatment group. The rate of study discontinuation was high in both the FIT1 and FIT2 trials and was imbalanced between study groups in both trials. The most common reason for discontinuation was a lack of treatment response after week 12 (e.g., 55% in the fostamatinib group and 88% in the placebo group of the FIT1 trial). In both groups, these patients were deemed to be nonresponders. However, for the SF-36 outcome, the high study-discontinuation rate meant limited data were available at week 24 (e.g., 1 patient in the placebo group at week 24 in the FIT1 trials, and 2 patients in the placebo group at week 24 in the FIT2 trial). Differences in the SF-36 outcome favoured fostamatinib at week 4; however, the differences were not likely clinically meaningful as they occurred so early in the trial, and it was not possible to draw any meaningful conclusions from the SF-36 data at week 24 due the limited amount of data from study discontinuations.
Imputation of the LOCF was used in both the FIT1 and FIT2 trials for missing platelet count data. Platelet count data were imputed for 3 patients in the fostamatinib group (all deemed to be nonresponders) in the FIT1 trial. In the FIT2 trial, data were imputed for 2 patients (1 responder and 1 nonresponder) in the fostamatinib group and 1 patient in the placebo group (deemed a nonresponder). The 1 patient in the fostamatinib group deemed a responder had a baseline platelet count of 5,000/µL. The count rose to 84,000/µL at week 12, 99,000/µL at week 14, and 101,000/µL at week 16, after which point no platelet counts were available. The effect of using the LOCF for imputation in the FIT and FIT2 trials therefore did not appear to have a major impact on the outcomes.
Subgroup analyses were not pre-specified or adjusted for multiplicity. Given the small number of patients in each subgroup and low event rates, there was likely insufficient power to detect any differences between treatment groups in these subgroups. This is reflected by wide CIs in the RD. The small number of patients and low event rates for certain outcomes (bleeding-related SAEs and use of rescue therapy) make it challenging to draw conclusions surrounding any difference between treatment arms for these secondary end points. As mentioned previously, the high study-discontinuation rate meant there was a large amount of missing data for the SF-36 outcome, making it impossible to draw conclusions about differences between treatment groups for this outcome. Because neither the FIT1 trial nor the FIT2 trial were powered for secondary end points and there was no adjustment for multiplicity for secondary end points, these outcomes should be interpreted with caution.
External Validity
The clinical experts consulted by CADTH indicated that the population of the FIT1 and FIT2 trials are broadly comparable to the population of patients with ITP in Canada, and the results of these trials are likely generalizable in Canada. The long duration of ITP and multiple previous treatments among patients in the FIT2 trial mirrors what is commonly seen in patients with ITP in clinical practice in Canada. However, the clinical experts did note some generalizability concerns with the FIT1 and FIT2 trials. First, because the FIT1 and FIT2 participants were predominantly White, the results from these trials may not be generalizable to other racial groups commonly seen at some centres in Canada (although the experts noted that the role of race and/or ethnicity in treatment response was not clear). The experts also noted that, because patients with secondary ITP were excluded from the FIT1 and FIT2 trials, the trial findings may not be generalizable to those with secondary ITP. Further, the specific types of previous treatments used in the FIT1 and FIT2 trials differ from those commonly seen at a similar point in ITP treatment in Canada. The clinical experts pointed out that, based on the duration of ITP for patients in the FIT1 and FIT2 trials, a higher portion of chronic ITP patients in Canada would have had a prior splenectomy. Moreover, the extent of previous use of rituximab in the FIT1 trial is higher than what would be seen in Canada at a similar stage of treatment. Nevertheless, the high median number of previous therapies used over the course of ITP reflects what would be seen in Canadian practice. The clinical experts also noted that the co-interventions (i.e., concomitant ITP medication use) during the FIT1 and FIT2 trials are also reflective of real-world practice in Canada, as steroids would commonly be continued while a patient is initiated on a new long-term treatment strategy such as fostamatinib.
In terms of outcome assessment in the FIT1 and FIT2 trials, the clinical experts noted that, while bleeding outcomes are likely the most important in practice, treatment response is most commonly assessed by measuring platelet counts. The experts also stated that having serial platelet measurements at weeks 14 to 24 is reflective of how patients would be followed in clinical practice. The approach used to assess platelets in the FIT1 and FIT2 trials is therefore generalizable. However, the experts found the definition for response to therapy in the FIT1 and FIT2 trials to be overly strict, stating that achieving a platelet count exceeding 30,000/µL would be considered a response in practice, particularly if a patient is asymptomatic. As a result, the primary outcome definition used in the FIT1 and FIT2 trials may not be reflective of how response to therapy is assessed in routine practice.
The FIT1 and FIT2 trials provided limited data on clinically important outcomes such as quality of life, rescue therapy, and bleeding events. The clinical experts do not use the IBLS and WHO bleeding scales in practice, and the relevance of the bleeding outcome scales used in the FIT1 and FIT2 trials is unclear. Further, the event rates for the post hoc bleeding-related SAE outcome made it challenging for the clinical experts to comment on the relevance or meaningfulness of these findings. The clinical experts found that the lower rate of rescue therapy use among patients treated with fostamatinib compared to placebo in the FIT1 and FIT2 trials could be meaningful, but they also noted the relatively low event rates.
Another challenge with both the FIT1 and FIT2 trials is that the comparator is placebo. In chronic ITP, if a platelet count is below 20,000/µL, as it was at baseline for patients in both trials, the clinical experts (and clinical practice guidelines) indicate that treatment would be warranted. Placebo therefore may not be an appropriate comparator for fostamatinib. Indeed, the FIT1 and FIT2 trials do not address the comparative efficacy of fostamatinib against other second- or third-line ITP treatments. However, the clinical experts suggested that the response rate seen in the FIT1 trial and FIT2 with fostamatinib among heavily pre-treated patients is meaningful for those who have taken several prior therapies and have a long duration of ITP.
Indirect Evidence
Objectives and Methods for the Summary of Indirect Evidence
As there was no direct evidence comparing fostamatinib to other active therapies for the treatment of chronic ITP in adult patients who have had an insufficient response to other treatments, a review of indirect evidence was undertaken. In addition to reviewing the sponsor’s submission, CADTH conducted a literature search to identify potentially relevant ITCs in patients with ITP. A focused literature search for ITCs and NMAs dealing with ITP was run in MEDLINE All (1946–) on August 20, 2021. No limits were applied to the search. Titles, abstracts, and full-text articles were screened for inclusion by 1 reviewer based on the population, intervention, comparator, and outcome criteria outlined in Table 5.
One sponsor-submitted ITC was included in this review.8 One relevant ITC by Wojciechowski et al. was identified in the literature search.7
Description of Indirect Comparisons
Both the sponsor-submitted ITC and the Wojciechowski study included a systematic review of the literature and an ITC that compared the current pharmaceutical treatments with each other for chronic ITP. In the sponsor-submitted ITC, fostamatinib was compared to rituximab. In the Wojciechowski study, fostamatinib was compared to 3 TPO-RAs: avatrombopag, eltrombopag, and romiplostim.
Methods of the Sponsor-Submitted Indirect Treatment Comparison
Objectives
The objective of the sponsor-submitted report for patients with chronic ITP was to conduct a systematic review and, if possible, an ITC to evaluate the relative efficacy and safety of fostamatinib versus other treatments currently available in Canada and Europe for this population. Chronic ITP was defined as ITP with a duration of at least 12 months.
Study Selection Methods
A literature systematic review was performed in 2019 and updated in 2021 to identify all relevant clinical evidence to inform the NMA of fostamatinib in patients with chronic ITP. Multiple databases were searched. The inclusion and exclusion criteria used for study selection to inform the NMA are presented in Table 13. Study selection and data extraction were conducted by 2 reviewers independently. The quality of the included studies was not assessed.
Methods of the Indirect Treatment Comparison by Wojciechowski et al.
Objectives
The objective of this report was to conduct an ITC to evaluate the relative efficacy and safety of avatrombopag, relative to eltrombopag, romiplostim, and fostamatinib, for patients with chronic ITP who were not responding adequately to corticosteroids. Chronic ITP was defined as ITP with a duration of at least 12 months.
Study Selection Methods
A systematic literature search was conducted to identify RCTs and observational studies involving adult patients with chronic ITP. Multiple databases were searched to identify clinical trials that evaluated the efficacy and safety of drug therapies for chronic ITP. By definition, chronic ITP is required to have a duration of at least 12 months; however, some included trials may have been designed and conducted before the current definition of chronic ITP was developed; and patients with a shorter disease duration, e.g., at least 6 months, may have been recruited. Such studies were deemed eligible for this analysis if all other inclusion criteria for the NMA were met, and the average duration of the disease was at least 12 months.
Inclusion and exclusion criteria for the clinical studies for the 2 systematic reviews are presented in Table 13.
Table 13: Study Selection Criteria and Methods for Indirect Treatment Comparisons
Selection criteria | Sponsor-submitted ITC | Wojciechowski et al. (2021) |
|---|---|---|
Population | Adult patients with chronic or persistent ITP | Adult patients (≥ 18 years of age) with chronic ITP who had inadequate response to previous therapy |
Intervention and/or comparators |
|
|
Outcome |
|
|
Study design |
|
|
Exclusion criteria |
|
|
Databases searched | MEDLINE, PubMed, Embase, Cochrane Database of Systematic Reviews (Reviews and Protocol), and CENTRAL | Embase, MEDLINE, CENTRAL, and the Cochrane Database of Systematic Reviews |
Selection process | Two reviewers independently screened articles | Not specified; the authors indicated that the study was performed in line with the PRISMA guidelines |
Data extraction process | Two reviewers independently extracted data; a third expert was called in to decide in case of discrepancy | Not specified; the study was performed in line with the PRISMA guidelines |
Quality assessment | Not performed | A tool based on guidance for undertaking reviews in health care from CRD |
AE = adverse event; CRD = Centre for Reviews and Dissemination; EMA = European Medicines Agency; HRQoL = health-related quality of life; ITC = indirect treatment comparison; ITP = immune thrombocytopenia; PRISMA = Preferred Reporting Items for Systematic Review and Meta-Analyses; RCT = randomized controlled trial; SAE = serious adverse event.
Source: Sponsor-submitted indirect treatment comparison8 and Wojciechowski et al. (2021).7
Analysis Methods of the Sponsor-Submitted Indirect Treatment Comparison
In the feasibility assessment of this study, the following patient baseline characteristics were considered potential treatment-effect modifiers in patients receiving fostamatinib or rituximab:
age
gender
ethnicity
time since ITP diagnosis
prior TPO-RAs treatment
prior rituximab treatment
baseline platelet count
concomitant medications
prior splenectomy.
The clinical experts consulted by the sponsor indicated that none of these pre-specified patient characteristics could be considered reliable treatment-effect modifiers in the study population due to a lack of evidence.
In the analyses, the probabilities of platelet response were modelled using a logit link function. A random-effects model within the Bayesian framework was selected. In this model, prior distributions for the parameters were specified. Where sufficient sample data were available, conventional reference prior distributions were used:
Trial-specific baseline:

Treatment effects relative to reference treatment:

Between-study SD of treatment effects:

In the case of insufficient sample data in a network, the prior for τ2 proposed by Ren et al.25 was used, which was a truncated prior (a lognormal [−2.56, 1.742]). The truncation was based on the judgment that the hazard ratio divided by the OR in 1 study would be no more than 10 times greater than in another. In the case of 0 events, a continuity correction was applied by adding 1 to the denominator and 0.5 to the numerator.
For all outcomes, a burn-in of 70,000 iterations of a Markov chain was used, with a further 50,000 iterations retained to estimate parameters using 1 chain and thinning every 5 iterations.
The model fit was examined by comparing the total residual deviance to the total number of data points included in the analysis and deviance information criterion. The results showed that the model fit the data well, with a total residual deviance of 12.66 being close to the number of data points (13) included in the analysis. Overall platelet response was assessed in this ITC and reported as the OR, which represents the relative likelihood of achieving a platelet response when comparing 1 received therapy against another. The results were presented using the posterior median treatment effects (95% Cr). The estimated between-study SD, τ, for each analysis was also presented. Values below 0.05 were considered to indicate low heterogeneity. Values between 0.05 and 0.5 were considered to indicate moderate heterogeneity. Values between 0.5 and 1.0 were considered to indicate high heterogeneity. Values above 1.0 were considered to indicate extremely high heterogeneity.
Three analyses were performed in this ITC:
Analysis 1 used a definition of overall platelet response from each study publication and included the results from all included publications. In this analysis, the outcome of interest in the FIT1 and FIT2 trials was more than 1 platelet count of 50,000/µL or greater during weeks 0 to 12, while the outcome of interest was a platelet count exceeding 30,000/µL in other included trials.
Analysis 2 used alternative definitions of overall platelet response for the FIT1 and FIT2 trials, defined as a platelet count greater than 30,000/µL by week 4 of treatment, and including the results from all 4 rituximab publications. In this analysis, the outcome of interest was a platelet count of exceeding 30,000/µL at the study end.
Analysis 3 involved a comparison to the Ghanima study (2015) only, using the same definition for outcomes as analysis 2 (a platelet count greater than 30,000/µL by week 4 of treatment). In this analysis, the outcome of interest was a platelet count of greater than 30,000/µL at the study end.
All analyses in this study were conducted using the software package WinBUGS and R.
Indirect Treatment Comparison Analysis Methods in Wojciechowski et al.
The NMA was conducted within a Bayesian framework, and a Markov chain Monte Carlo method was implemented in WinBUGS with vague prior distributions for model parameters. Noninformative prior distributions were used for the model’s nuisance parameters, treatment-effect parameters (normal distributions with a mean of 0 and a variance of 104), and heterogeneity parameters (uniform distribution between 0 and 5 for between-trial SD) for the Bayesian analysis.
Fixed-effects and random-effects models were fitted to the data, with model fit based on the deviance information criterion. In this study, the fixed-effects model was preferred when fewer estimable parameters were evaluated. Three chains were run for each analysis, with either 25,000 or 50,000 burn-in iterations for the fixed-effects and random-effects models, respectively, followed by 25,000 iterations. Trace plots were generated to assess convergence. The consistency of the results within closed loops of the network was tested using a modified Bucher approach.
Outcomes were presented as ORs or incidence rate ratios with corresponding 95% CrIs. The significant and imbalanced discontinuation introduced a high risk of bias. To adjust for this imbalance due to discontinuation, the NMA was conducted using estimated incidence rate ratios for the need for rescue therapy and the incidence of any bleeding events, WHO grade 2 to 4 bleeding events, and any AEs.
Table 14: Indirect Treatment Comparison Analysis Methods
Methods | Sponsor-submitted ITC | Wojciechowski et al. |
|---|---|---|
ITC methods | Bayesian approach | Bayesian approach |
Priors | Conventional reference prior distributions were adopted if there were sufficient sample data; otherwise, a truncated prior was used | Vague priors were set for model parameters |
Assessment of model fit | Total residual deviance: 12.66 (close to the number of data points included in the analysis, which was 13) Between-study standard deviation: 0.22 DIC | DIC (results not reported) |
Assessment of consistency | Not assessed | Modified Bucher approach |
Assessment of convergence | Convergence to the target posterior distributions was assessed using the Gelman-Rubin statistic, for 2 chains with different initial values | Trace plots were generated |
Outcomes | Platelet response | This study was not used to inform the pharmacoeconomic analysis for the submission |
Follow-up time points | 24 to 78 weeks | Up to 24 weeks |
Construction of nodes | NR | NR |
Sensitivity analyses | Yes, using alternative definitions of overall platelet response for the FIT-1 and FIT-2 trials, and focusing on focusing on specific doses of rituximab | NA |
Subgroup analysis | NA | NA |
Methods for pairwise meta-analysis | NA | NA |
DIC = deviance information criterion; ITC = indirect treatment comparison; NA = not available; NR = not reported.
Source: Sponsor-submitted indirect treatment comparison8 and Wojciechowski et al.7
Results of Indirect Treatment Comparisons
Summary of Included Studies
Sponsor-Submitted Indirect Treatment Comparison
From the literature systematic review, 3,233 studies were identified, and among them, a total of 31 studies were evaluated in a feasibility assessment to determine if it was possible to conduct an ITC in the study population. Six RCTs were included and contributed evidence on overall platelet response for the ITC. Authors of the ITC indicated fostamatinib was included in the treatment paradigms to address patients with the greatest unmet need. Patients who were successfully treated with a splenectomy or TPO-RAs were unlikely to require additional treatment with a new intervention. To address the patients with the greatest unmet need, fostamatinib focused on those patients who did not have access to long-term effective therapy options, such as those who received short courses of rituximab and those on a watch-and-rescue regimen.
In the trials included in ITC, the number of enrolled patients ranged from 57 to 138. The trial duration ranged from 4 weeks to 78 weeks. Three doses of rituximab were evaluated: 2 or 4 once-weekly 375 mg/m2 doses, 2 once-weekly 750 mg/m2 doses, or 4 once-weekly 100 mg/m2 doses (Figure 3). The definition of platelet response varied across the included trials.
Figure 3 presents the network of evidence for overall platelet response in patients with chronic or persistent ITP in the sponsor-submitted ITC.
Figure 3: Network of Evidence for Platelet Response
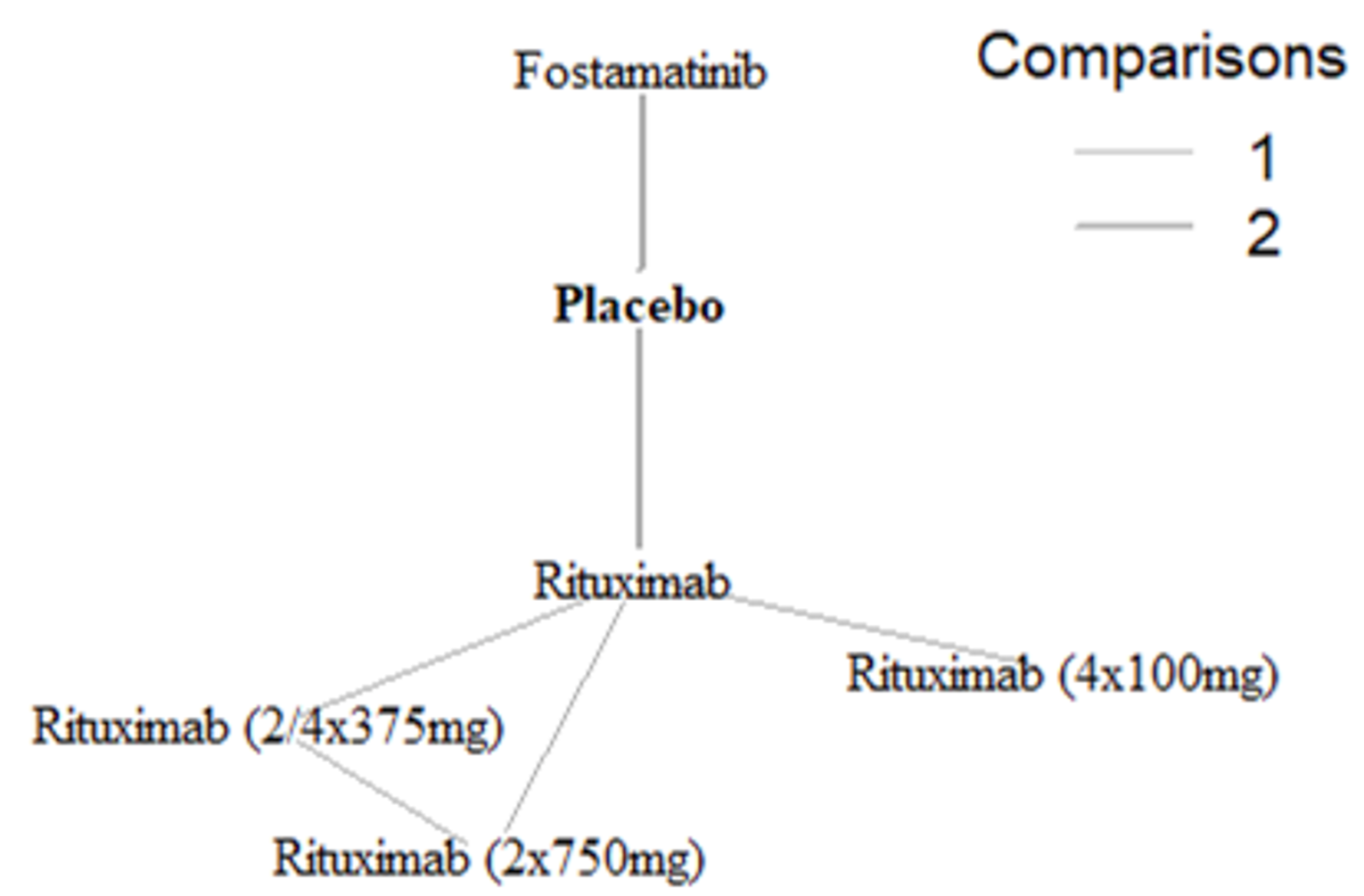
Source: Sponsor-submitted indirect treatment comparison.8
Table 15: Summary of Trials Included in the Sponsor-Submitted ITC
Study | Study design | Treatment 1 | Treatment 2 | Treatment 3 |
|---|---|---|---|---|
FIT1 | Randomized (2:1), multi-centre, double-blind, placebo-controlled trial | Placebo | Fostamatinib | NA |
FIT2 | Randomized (2:1), multi-centre, double-blind, placebo-controlled trial | Placebo | Fostamatinib | NA |
Arnold (2012) | Randomized, concealed, blinded, placebo-controlled trial | Placebo | Rituximab | NA |
Ghanima (2015) | Multi-centre, randomized, double-masked, placebo-controlled trial (NCT00344149) | Placebo | Rituximab | NA |
Zwaginga (2015) | Multi-centre randomized open-label phase II trial on 3 rituximab dosing schemes in immune thrombocytopenia patients | Rituximab | Rituximab (2/4 × 375 mg) | Rituximab (2 × 750 mg) |
Zaja (2012) | Results of updated single-institution experience with rituximab salvage therapy in adults with ITP | Rituximab | Rituximab (4 × 100 mg) | NA |
ITC = indirect treatment comparison; NA = not applicable.
Source: Sponsor-submitted ITC.8
The heterogeneity of the included RCTs was assessed to determine whether an NMA would have been possible. When comparing patient baseline characteristics, the average age was considered homogenous across all studies and ranged for most trials between 40 and 57 years. The average duration of ITP was heterogenous in the included studies. The baseline platelet counts were similar across trials (Table 16).
Table 16: Baseline Characteristics of Included Trials in the Sponsor-Submitted ITC
Study characteristic | FIT1 (N = 76) | FIT2 (N = 74) | Arnold (2012) (N = 60) | Ghanima (2015) (N = 109) | Zwaginga (2015) (N = 138) | Zaja (2012) (N = 57) | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
Placebo (N = 25) | Fostamatinib (N = 51) | Placebo (N = 24) | Fostamatinib (N = 50) | Placebo (N = 27) | Rituximab (N = 33) | Placebo (N = 54) | Rituximab (N = 55) | Rituximab (N = 46) | Rituximab (2/4x 375mg) (N = 43) | Rituximab (2× 750mg) (N = 49) | Rituximab (n-32) | Rituximab (4x 100mg) (N = 25) | |
Study duration | 24 weeks | 24 weeks | 24 weeks | 78 weeks | 24 weeks | 52 weeks | |||||||
Age, median (range), years | 57 (26 to 77) | 57 (20 to 88) | 50 (20 to 78) | 50 (21 to 82) | 40 (31 to 59) | 40 (30 to 59) | 46 (28 to 60) | 46 (27 to 61) | 56 (18 to 77) | 51 (18 to 80) | 53 (17 to 82) | 51 (16 to 80) | 43 (14 to 74) |
Female, n (%) | 17 (68) | 47 (62) | 13 (54) | 31 (62) | 16 (59.3) | 19 (57.6) | 39 (72) | 40 (73) | (59) | (53) | (55) | NR | NR |
Ethnicity, Caucasian n (%) | 21 (84) | 65 (86) | 24 (100) | 50 (100) | NR | NR | NR | NR | NR | NR | NR | 32 (100) | 25 (100) |
ITP duration, median (range), months | 66 (4.8 to 540) | 90 (7.2 to 636) | 129.6 (10.8 to 349.2) | 105.6 (3.6 to 602.4) | 8 (1 to 40) | 3 (1 to 47) | 11.5 (3.2 to 48.6) | 8.5 (1.8 to 66.3) | 11.7 (0.2 to 212) | 21.8 (0.5 to 324) | 14.1 (0.8 to 377) | 31 (3 to 264) | 24 (2 to 324) |
Baseline platelet count 109/L, median (range)/μ | 17 | 17 | 22 | 13 | 14 (10 to 23) | 15 (4 to 23) | 21 (9 to 29) | 16 (6 to 27) | 14 (3 to 36) | 19 (2 to 38) | 15 (1 to 30) | 18 | 32 |
Number of prior therapies | Median (range): 5.0 (1 to 10) | Median (range): 3.0 (1 to 9) | Median (range): 3.0 (1 to 10) | Median (range): 3.0 (1 to 13) | NR | NR | NR | NR | NR | NR | NR | 1, n (%): 32 (100) 2, n (%): 14 (44) 3, n (%): 1 (3) | 1, n (%): 25 (100) 2, n (%): 12 (48) 3, n (%): 3 (12) |
ITC = indirect treatment comparison; ITP = immune thrombocytopenia.
Source: Sponsor-submitted ITC.8
Wojciechowski Study
A total of 1,822 publications were identified from the literature search, and among them, 64 studies were evaluated in a feasibility assessment to determine if it was possible to conduct an ITC in the study population. Seven phase III, double-blind RCTs were included and contributed evidence on various clinical outcomes to the ITC (Table 17): 2 for avatrombopag, 1 for eltrombopag, 2 for romiplostim, and 2 for fostamatinib. Six of them were placebo-controlled trials, and 1 was designed to compared avatrombopag versus eltrombopag.
Figure 4 presents the network of evidence for overall platelet response in patients with chronic or persistent ITP in the Wojciechowski ITC.
Figure 4: Network of Evidence in the Wojciechowski Study
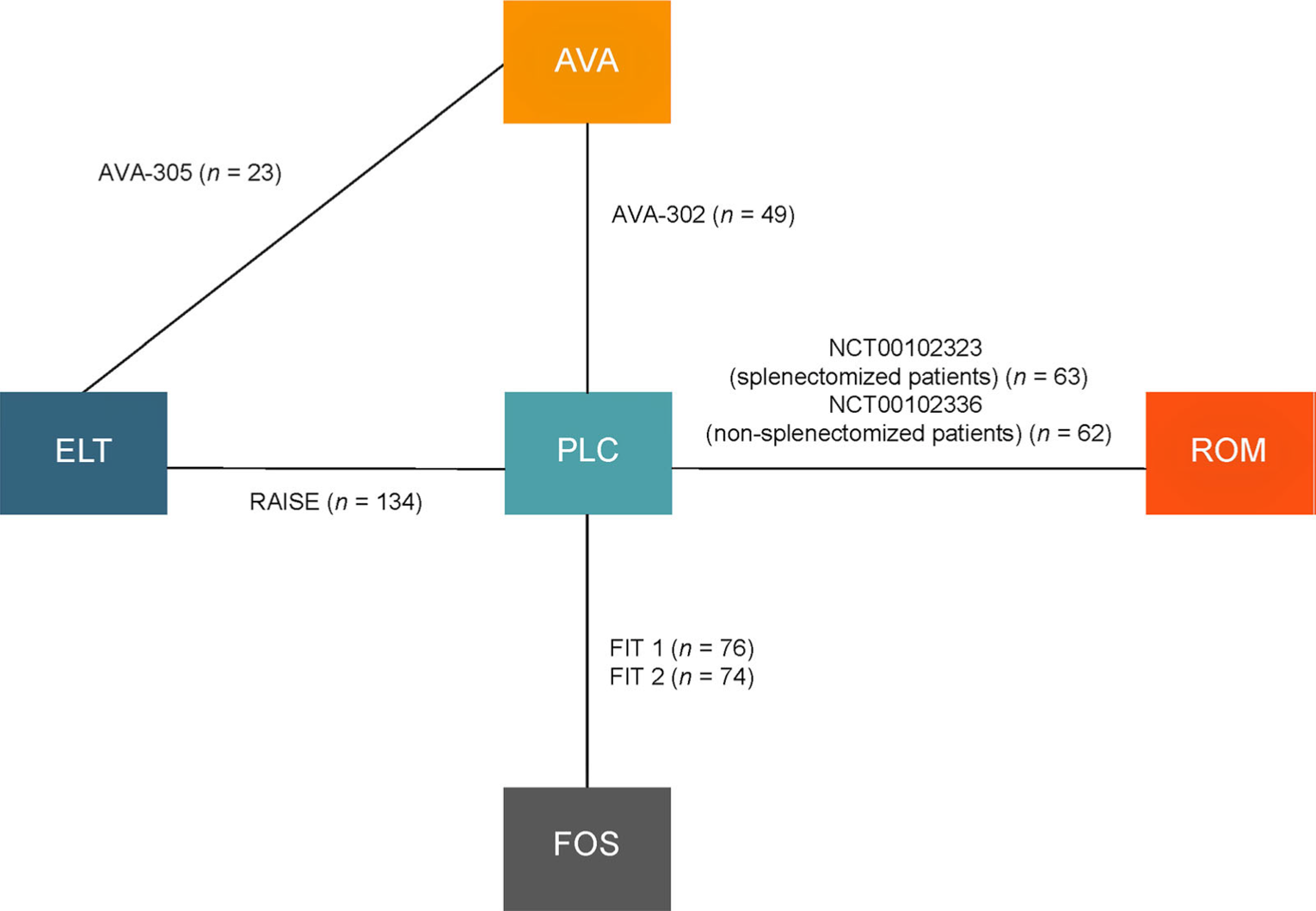
AVA = avatrombopag; ELT = eltrombopag; FOS = fostamatinib; PLC = placebo; ROM = romiplostim.
Source: Wojciechowski et al.7 This work is licensed under the Creative Commons Attribution 4.0 International (CC BY-NC 4.0) Licence. Full text available at https://creativecommons.org/licenses/by-nc/4.0/.
Table 17: Summary of Trials Included in Wojciechowski ITC
Study | Study design | Treatment 1 | Treatment 2 | Primary outcome |
|---|---|---|---|---|
AVA-302 | Phase III, multi-centre, double-blind, RCT, 35 centres in multiple countries | AVA | Placebo | Number of weeks with PC ≥ 50 × 109/L during 6-month treatment period |
AVA-305 | Phase III, multi-centre, double-blind, RCT, 72 centres in 10 countries | AVA | ELT | Change from baseline in local PC for the 6-month treatment period |
RAISE | Phase III, multi-centre, double-blind, RCT, 75 centres in 23 countries | ELT | Placebo | Percentage of responders |
NCT00102323 (splenectomized patients) | Phase III, multi-centre, double-blind RCT, 35 sites in the US and Europe | ROM | Placebo | Durable platelet response during the last 8 weeks of treatment and other platelet response parameters |
NCT00102336 (nonsplenectomized patients) | ROM | Placebo | ||
FIT1 | Phase III, multi-centre, double-blind RCT | FOS | Placebo | Stable response (response on ≥ 4 of the last 6 visits between weeks 14 and 24) |
FIT2 | FOS | Placebo |
AVA = avatrombopag; ELT = eltrombopag; FOS = fostamatinib; PC = platelet count; RCT = randomized controlled trial; ROM = romiplostim.
Source: Wojciechowski et al.7
In this ITC, the number of patients (12 to 135 in active treatment arms), length of follow-up (24 to 36 weeks), and median duration of disease (1.6 to 10.8 years) varied across the trials. The median age and median platelet count at baseline ranged from 41 to 57 years and 14 × 109/L to 24 × 109/L, respectively. The number of previous treatments and concomitant ITP therapy also varied across trials (Table 18).
Table 18: Baseline Characteristics of Included Trials in the Wojciechowski ITC
Study | Treatment (n) | Median age, years (range) | Median duration of ITP, | Median platelet count, | ≥ 3 previous treatments, | Concomitant ITP therapy, |
|---|---|---|---|---|---|---|
AVA-302 | AVA (32) | 46.4 (14.2)a | NR | 14.1 (8.6)a | 19 (60)a | 15 (46.9) |
PLC (17) | 41.2 (14.7)a | NR | 12.7 (7.8)a | 9 (53) | 7 (41.2) | |
AVA-305 | AVA (12) | 50.8 (23.0)a | NR | 8.5 (3.0 to 27.5) | NR | 2 (16.7)a |
ELT (11) | 45.4 (20.1)a | NR | 15.0 (9.0 to 29.5) | NR | 1 (9.1)a | |
RAISE | ELT (135) | 47.0 (34 to 56) | NR | 16 (8 to 22) | 75 (56) | 63 (47) |
PLC (62) | 52.5 (43 to 63) | NR | 16 (9 to 24) | 32 (52) | 31 (50) | |
NCT00102323 (splenectomized patients) | ROM (42) | 51 (27 to 88) | 7.75 (0.6 to 44.8) | 14 (3 to 29) | 39 (93) | 12 (29) |
PLC (21) | 56 (26 to 72) | 8.50 (1.1 to 31.4) | 15 (2 to 28) | 20 (95) | 6 (29) | |
NCT00102336 (nonsplenectomized patients) | ROM (41) | 52 (21 to 80) | 2.20 (0.1 to 31.6) | 19 (2 to 29) | 15 (37) | 11 (27) |
PLC (21) | 46 (23 to 88) | 1.60 (0.1 to 16.2) | 19 (5 to 31) | 5 (24) | 10 (48) | |
FIT1 | FOS (51) | 57 (20 to 88) | 7.5 (0.6 to 53.0) | 16.20 (1 to 51) | 3.0 (1 to 9)b | NR |
PLC (25) | 57 (26 to 77) | 5.5 (0.4 to 45.0) | 15.84 (1 to 48) | 5.0 (1 to 10)b | NR | |
FIT2 | FOS (50) | 50 (21 to 82) | 8.8 (0.3 to 50.2) | 15.90 (1 to 33) | 3.0 (1 to 13)b | NR |
PLC (24) | 50 (20 to 78) | 10.8 (0.9 to 29.1) | 23.96 (1 to 156) | 3.0 (1 to 10)b | NR |
AVA = avatrombopag; ELT = eltrombopag; FOS = fostamatinib; NR = not reported; PLC = placebo; ROM = romiplostim.
aMean (standard deviation).
bPrior unique treatments for ITP, median (range)
Source: Wojciechowski et al.7
Data were available allowing a comparison of the following outcomes for all treatments: durable platelet response, need for rescue treatment, and WHO grade 2 to 4 bleeding events. Data for reduction in the use of concomitant ITP therapies were not available for fostamatinib. The definitions of durable response were relatively similar for all the treatments to allow for comparisons, although the definition was different in the FIT1 and FIT2 trials (4 of 6 visits over weeks 14 to 24) compared with the other trials (at least 6 of the last 8 weeks of treatment). To compare bleeding events among all treatments, it was assumed that WHO grade 2 to 4 bleeds were equivalent to grade 2 to 5 bleeds reported in NCT00102336 and moderate to severe bleeds reported in the FIT1 and FIT2 studies.
Results
Sponsor-Submitted Indirect Treatment Comparison
Overall platelet response: The definition of overall platelet response varied across studies included in the ITC. A series of analyses was performed using different definitions of platelet response. Results of analyses 1, 2, and 3 are presented in Table 19. The difference between fostamatinib and rituximab was statistically significant in analysis 1 only.
Table 19: Overall Response (95% CrI) for Fostamatinib Versus Other Treatments for Overall Platelet Response in the Sponsor-Submitted Indirect Treatment Comparison
Comparison between FOS and comparators | Overall platelet response | ||
|---|---|---|---|
Analysis 1 (based on 6 RCTs) | Analysis 2 (based on 6 RCTs) | Analysis 3 (based on 3 RCTs) | |
FOS vs. RIT | 4.93 (1.44 to 18.93) | 3.96 (0.96 to 20.49) | 0.33 (0.05 to 2.03) |
RIT (2 or 4 × 375 mg) vs. FOS | 0.16 (0.03 to 0.79) | 0.20 (0.03 to 1.13) | NA |
RIT (4 × 100 mg) vs. FOS | 0.11 (0.02 to 0.62) | 0.14 (0.02 to 0.96) | NA |
RIT (2 × 750 mg) vs. FOS | 0.18 (0.03 to 0.86) | 0,22 (0.03 to 1.25) | NA |
FOS vs. placebo | 4.85 (1.86 to 14.45) | 3.90 (1.21 to 16.22) | 3.96 (1.20 to 16.89) |
CrI = credible interval; FOS = fostamatinib; NA = not available; RIT = rituximab; vs. = versus.
Note: Statistically significant results are shown in bold. Treatment effects greater than 1 favoured the intervention (on the left in column 1). Analysis 1: definitions of OR from each study publication were used and including the results from all 6 publications. Analysis 2: alternative definition of OR for FIT1 and FIT2, defined as a platelet count greater than 30,000/µL by week 4 of treatment, were used, and including the results from all 4 rituximab publications. Analysis 3: compared to Ghanima et al. population only, using the same definition of outcome (platelet count greater than 30,000/µL by week 4 of treatment).
Source: Sponsor-submitted indirect treatment comparison.8
Wojciechowski Study
Durable platelet response: Based on evidence from 6 studies, there was no difference between fostamatinib and various TPO-RAs in durable platelet response.
Reduction in use of concomitant ITP medication: Data for reduction in the use of concomitant ITP therapies were not available for fostamatinib.
Need for rescue therapy: Based on 6 studies, there was no difference between fostamatinib and TPO-RAs in the need for rescue therapy.
Incidence of any bleeding events: Based on results from 7 studies, there was no difference between fostamatinib and TOP-RAs in the incidence of any bleeding events.
Incidence of WHO grade 2 to 4 bleeding events: Based on 6 studies, there was no difference between fostamatinib and TPO-RAs in the incidence of WHO grade 2 to 4 bleeding events.
Any adverse event: Based on the results from 5 studies, there was no difference between fostamatinib and TPO-RAs in the incidence of any AEs.
Details of the results are presented in Table 20.
Table 20: Odds Ratio or Incidence Rate Ratio for Fostamatinib Versus Other Treatments for Efficacy and Safety Outcomes in the Wojciechowski Study
Comparison between FOS and other treatments | Durable platelet response OR (95% CrI) | Reduction in use of concomitant ITP drug | Need for rescue therapy IRR (95% CrI) | Incidence of any bleeding events IRR (95% CrI) | Incidence of WHO grade 2 to 4 bleeding events IRR (95% CrI) | Any adverse events IRR (95% CrI) |
|---|---|---|---|---|---|---|
vs. AVA | 0.11 (0 to 8.04) | NA | 0.51 (0.09 to 2.72) | 1.46 (0.59 to 3.59) | 0.76 (0.14 to 4.12) | 1.10 (0.55 to 2.17) |
vs. ELT | 0.77 (0.09 to 14.59) | NA | 0.81 (0.37 to 1.80) | 0.56 (0.28 to 1.10) | 0.57 (0.20 to 1.59) | 0.70 (0.43 to 1.15) |
vs. ROM | 0.24 (0.01 to 5.58) | NA | 1.07 (0.47 to 2.44) | 0.55 (0.26 to 1.20) | 0.87 (0.26 to 2.88) | 0.69 (0.40 to 1.20) |
vs. placebo | 10.94 (2.13 to 181.70) | NA | 0.37 (0.21 to 0.65) | 0.50 (0.27 to 0.91) | 0.38 (0.15 to 0.96) | 0.69 (0.47 to 1.02) |
AVA = avatrombopag; CrI = credible interval; ELT = eltrombopag; FOS = fostamatinib; IRR = incidence rate ratio; OR = odds ratio; NA = not available; ROM = romiplostim.
Note: Fixed-effects models were adopted. Results are shown in bold when fostamatinib was favoured vs. the comparator.
Source: Wojciechowski et al.7
Critical Appraisal of the Sponsor-Submitted Indirect Treatment Comparison and Wojciechowski Study
In both ITCs, the analysis of efficacy and safety data presented was limited by the size of the evidence base.
Sponsor-Submitted Indirect Treatment Comparison
In this ITC, studies were identified and selected using a systematic review approach. For example, multiple databases were searched, and 2 independent reviewers selected the studies based on specific inclusion and exclusion criteria and performed data extraction. Quality assessment of the included studies was not performed.
One outcome (overall platelet response) was evaluated in this study. Because there is no clear evidence of a direct correlation between the degree of thrombocytopenia and bleeding symptoms, it is unclear whether treatment with fostamatinib would be useful in improving clinical outcomes such as reduction in subsequent bleeding events and the need for rescue therapy, and improvement in patient HRQoL.
Trial characteristics and patient baseline characteristics of the studies included in the systematic review and ITC were reported. Based on the data presented, potential sources of heterogeneity with respect to the baseline characteristics were identified, such as disease duration (ranging from 24 to 78 weeks) and definition of overall platelet response. During the feasibility analysis period, several potential treatment-effect modifiers were identified by the sponsor, such as baseline demographic characteristics, medical history (e.g., time since ITP diagnosis, prior treatment for ITP, and concomitant medications). However, the clinical experts consulted by the sponsor indicated that none of these patient characteristics could be considered treatment-effect modifiers in the study population (patients with chronic and persistent ITP who can receive treatment of fostamatinib or rituximab) due to a lack of evidence. According to the clinical experts consulted by CADTH, these are all important treatment-effect modifiers, as are other patient characteristics in the study population, such as cycles and doses of prior corticosteroid therapy, previous lines of therapy, and severity of previous bleeding events. However, such data were not provided in the ITC, and heterogeneity across the included trials needs to be further assessed and adjusted.
Because the definition of platelet response varied across included trials, sensitivity analyses based on different definitions of this outcome were performed. Results of these analyses were consistent and favoured fostamatinib, showing that treatment with fostamatinib was associated with a higher probability of achieving an overall platelet response compared with rituximab, although the difference was statistically significant only when the definition of overall platelet response from each study was used.
A narrower patient group was the interest of this ITC. The authors assumed that patients who were successfully treated with a splenectomy or TPO-RAs were unlikely to require additional treatment with a new intervention, and they stated that the target population of this study was patients who did not have access to long-term effective therapy options, such as those who received short courses of rituximab and those on a watch-and-rescue regimen. Rituximab was therefore the only comparator in this ITC, and its study results can be generalized only to patients with persistent or chronic ITP who did not receive prior TPO-RA therapy or had not undergone a splenectomy. The absence of other comparators is a key limitation of this ITC.
Wojciechowski Study
In this ITC, studies were identified and selected according to pre-specified inclusion and exclusion criteria. Multiple databases were searched. The authors stated that the study was conducted in line with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines, which suggested that the standard practice of minimizing the bias of selecting studies for inclusion had been used. Quality assessment of the included studies was performed using a validated tool. However, there was no discussion of how any potential biases in the trials could affect data analyses in the ITC and possible solutions (e.g., whether sensitivity analyses were conducted to assess the impact of studies with poor quality). Multiple clinical outcomes, including the incidence of AEs, were evaluated in this study, which allows for a comprehensive evaluation of the clinical benefits and risks of the study drugs. Definitions of these outcomes were similar across the trials.
Trial characteristics and patient’s baseline characteristics of the studies included in the systematic review and ITC were reported. Potential sources of heterogeneity with respect to the baseline characteristics were identified based on these data, such as disease duration (ranging from 1.6 to 10.8 years), number of previous treatments, and concomitant ITP medication. This difference in patient’s baseline characteristics may vary the response between groups and may not allow groups to be comparable.
The analysis of efficacy and safety data presented was limited by the size of the evidence base. Due to the small evidence base and low incidence of SAEs across all studies, the results of this analysis are largely noninformative. This is particularly true when looking at comparative safety issues, especially for inclusion in economic models and comparative efficacy studies, resulting in imprecision due to small effect sizes and large CrIs.
Summary
Based on the results of the sponsor-submitted ITC, fostamatinib was favoured over rituximab in achieving overall platelet response in patients with persistent or chronic ITP. However, this study has a number of limitations that affect internal and external validity, such the inability to comprehensively assess clinical heterogeneities across the included studies and their impact on the study results, the inability to explore the relative treatment effect of fostamatinib in various subgroups, and the lack of other important efficacy and safety data for the ITP treatments of interest. In addition, the comparative efficacy and safety of fostamatinib to other active ITP therapies, such as TPO-RAs, was unknown for the study population due to a lack of evidence.
Based on the findings from the Wojciechowski ITC, which evaluated the relative efficacy and safety of currently available active treatments for patients with chronic ITP who did not have adequate response to corticosteroids, it remains uncertain if there was a significant difference between fostamatinib and TPO-RAs in achieving durable platelet response, reducing the need for rescue therapy, and decreasing bleeding and other AEs. The applicability of this ITC is affected by the limited size of the evidence base and heterogeneity in patient populations across trials. Overall, the results of this analysis must be interpreted with caution.
Other Relevant Evidence
This section includes an open-label extension study and 2 additional relevant studies included in the sponsor’s submission to CADTH that were considered to address important gaps in the evidence included in the systematic review.
Long-Term Extension Studies
One open-label extension study (FIT3) has been summarized to provide additional evidence regarding the long-term safety and efficacy of fostamatinib 150 mg twice daily if the platelet count was less than 50,000/µL and the study drug was well tolerated or reduced to a dose as low as fostamatinib 100 mg once daily if dose-limiting AEs (as defined by the protocol for patients with persistent or chronic ITP) were observed. Data for this summary were presented in the Clinical Study Report dated October 15, 2014, with a data cut-off for the final report of June 01, 2020.9
Methods
The FIT3 (C788 to 049) trial was a multi-centre, phase III, open-label extension study conducted at 54 sites in 16 countries (Canada, the US, Australia, the European Union, and the UK). The primary objective was the assessment of the long-term safety of fostamatinib among patients with persistent or chronic ITP. The secondary objectives were the establishment of the long-term efficacy of the drug as well as the assessment of the pharmacokinetics profile.
The trial consisted of 18 monthly visits followed by every-other-month visits for a maximum of 5 years of treatment or until the drug was commercially available for all patients, whichever occurred first. A total of 123 patients from the FIT1 (C788 to 047) and FIT2 (C788 to 048) trials who completed the week 24 evaluation or withdrew early (starting at week 12) due to a lack of response were included in this trial. Patients were blinded to their respective treatment assignment, either active or placebo, in the FIT1 or FIT2 studies.
During the FIT3 trial, all patients received open-label fostamatinib. Moreover, patients could continue to receive concomitant ITP medications that were allowed in the FIT1 and FIT2 studies or could receive a reduced dose of the concomitant medications in case their platelet count was stable at 50,000/µL or greater. Patients were allocated into 2 treatment groups, responders and nonresponders, depending on their response in the previous FIT1 or FIT2 studies. The responders group (last platelet count ≥ 50,000/µL) initiated open-label fostamatinib treatment using the same dosage and regimen (150 mg twice a day or 100 mg twice a day) that achieved a stable platelet count in the previous study, whereas the nonresponders group (last platelet count < 50,000/µL) initiated their treatment with 100 mg twice a day during the trial (Figure 5). At month 1, the dosage for patients showcasing a platelet count of less than 50,000/µL and tolerating the study drug well was increased to 150 mg twice a day. The dosage of fostamatinib was reduced to as low as 100 mg once daily if any dose-limiting AEs were observed among patients.
Figure 5: Initial Treatment Allocation
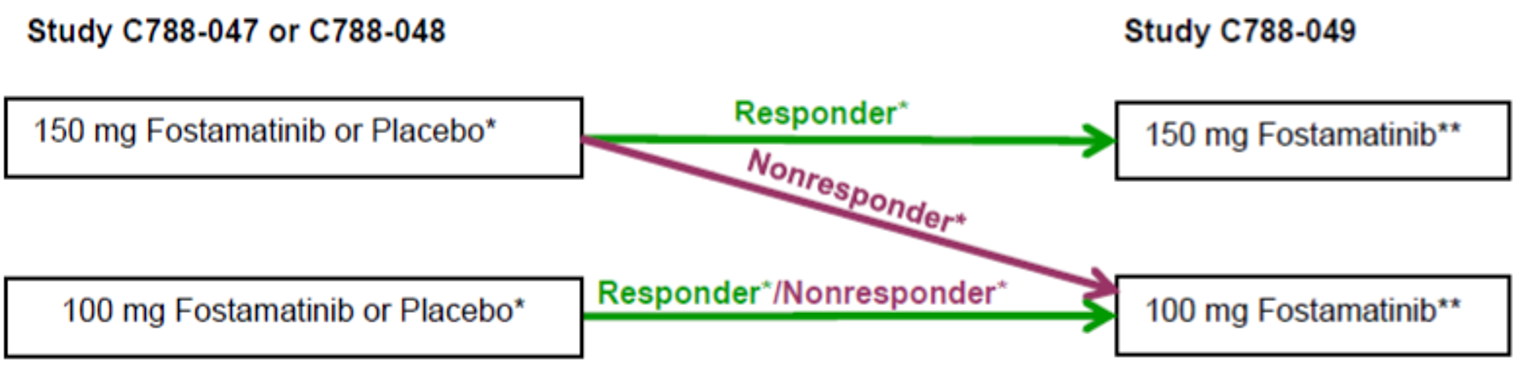
Note: Doses were administered twice a day unless the dose was reduced to once a day.
* Treatment assignment and dose from the previous study.
** At month 1, patients receiving fostamatinib 100 mg twice a day had the dose escalated to fostamatinib 150 mg twice a day if the platelet count was less than 50,000/µL and fostamatinib was well tolerated.
Source: Clinical Study Report for FIT3.9
After 12 weeks (3 months) of treatment, as well as 4 or more weeks at a dosage of 150 mg twice a day, patients whose platelet count was consistently less than 50,000/µL were required to withdraw from the trial.
Populations
Patients were eligible to participate in the FIT3 study if they met the following inclusion criteria:
They were able to give written informed consent.
They completed the week 24 evaluation of FIT1 or FIT2 studies or withdrew early (starting at week 12) due to a lack of response, with up to 7 days between the last day of treatment in previous study and initial dosing in FIT3.
They were male or female, aged at least 18 years.
Female patients were either postmenopausal for at least 1 year or surgically sterile; in the case of childbearing potential, they were not pregnant or lactating and using birth control method during the whole study period and for 30 days after the last dose.
They had the ability to understand the nature of the study and associated hazards, as well as to communicate effectively with the investigator regarding these issues.
Patients were not eligible to participate in the FIT3 study if they met any of the following exclusion criteria:
They had withdrawn from the FIT1 or FIT2 study before week 12 or for any reason except lack of response.
They had poorly controlled hypertension (persistent or repeated systolic ≥ 140 mm Hg or diastolic ≥ 90 mm Hg) during FIT1 or FIT2, irrespective of the receival of anti-hypertensive treatment.
They had laboratory abnormalities during enrolment, such as a neutrophil count of less than 1000/µL, a leukocyte count of less than 2000/µL, a lymphocyte count below 750/µL, hemoglobin below 10 g/dL, or transaminase levels (ALT or AST) above 1.5 × the upper limit of normal, bilirubin > 1.5 × the upper limit of normal, or an estimated glomerular filtration rate below 30 mL/minute.
They had significant infection, acute infection such as influenza, or some known inflammatory process.
They had received any blood or blood products within 2 weeks before their enrolment. (Exceptions could be IVIG or IV anti-D immunoglobulin, if used as rescue therapy.)
Patient baseline characteristics are summarized in Table 21. Among patients enrolled in the FIT3 trial, the mean age was 51.8 years (SD = 15.9), more than half of the patients were female (60.2%), and the mean body mass index was 28.37 kg/m2 (SD = 7.66).
Table 21: Baseline Characteristics of FIT3 – Treated Population
Characteristics | Fostamatinib (N = 123) |
|---|---|
Demographics | |
Age (years), mean (SD) | 51.8 (15.9) |
Female, n (%) | 74 (60.2) |
Body mass index (kg/m2), mean (SD) | 28.37 (7.66) |
Race, n (%) | NA |
White | 113 (91.9) |
Black | 4 (3.3) |
Asian | 4 (3.3) |
Other | 2 (1.6) |
Ethnicity, n (%) | NA |
Not Hispanic or Latino | 121 (98.4) |
Hispanic or Latino | 2 (1.6) |
NA = not applicable; SD = standard deviation.
Source: Clinical Study Report for FIT3.9
Interventions
During the trial, all patients received open-label fostamatinib, which was self-administered twice a day by mouth, once in the morning and once in the evening, for up to 5 years or until the drug became commercially available for all patients, whichever happened first. In cases of reduced doses due to AEs, the drug had to be taken in the morning. In the event of a missing dose, patients were advised to take the next dose and not to take 2 doses simultaneously.
The initial treatment allocation is shown in Figure 5 . Patients were assigned to 1 of 2 groups of treatments, responders and nonresponders, depending on their response in the previous FIT1 or FIT2 studies. The responders group (last platelet count ≥ 50,000/µL) initiated open-label fostamatinib treatment with the same dosage and regimen (150 mg twice a day or 100 mg twice a day) that achieved a stable platelet count in the previous study, whereas the nonresponders (last platelet count < 50,000/µL) initiated their treatment with 100 mg twice a day during the trial. At month 1, the dosage for patients showing a platelet count of less than 50,000/µL and tolerating the study drug well was increased to 150 mg twice a day. The dosage of fostamatinib was reduced to as low as 100 mg once daily if any dose-limiting AEs were observed among patients.
During the trial patients were allowed to continue any concomitant medications and/or treatments for ITP therapies that were allowed in the FIT1 and FIT2 studies. Allowed concomitant medications and/or treatments for ITP therapies were glucocorticoids at a dosage of up to 20 mg of prednisone, danazol, or azathioprine daily. For patients who demonstrated a stable platelet count of 50,000/µL or greater, tapering of the dose of their concomitant medication was considered. No new treatments for ITP were allowed except as rescue medication. Because it was an open-label extension, all patients, investigators, and staff members were aware of the treatment received, which was fostamatinib. However, each patient remained blinded to their assignment group from the previous FIT1 and FIT2 studies during trial.
Outcomes
The primary objective of the FIT3 trial was the assessment of the long-term safety of fostamatinib among patients with persistent or chronic ITP. The secondary objectives were the establishment of the long-term efficacy of the drug as well as the assessment of the pharmacokinetic profile. The primary efficacy outcome of fostamatinib were summarized in this report by the platelet counts and the requirement of dose adjustment. Stable platelet response was a platelet count of 50,000/μL or greater at 4 or more of 6 biweekly visits during weeks 14 to 24 or, for patients initiating fostamatinib in the extension phase, at least 1 platelet count of at least 50,000/μL in the first 3 months of fostamatinib treatment followed by platelet counts of at least 50,000/μL at the subsequent 2 of 3 monthly visits without use of rescue medication. The primary efficacy outcome had 2 versions. For version 1, efficacy was assessed among patients who were on active treatment in either the FIT1 or FIT2 studies, in the current extension study, or in both. For version 2, efficacy was assessed among patients assigned to placebo in either of the prior FIT1 or FIT2 studies. The secondary efficacy outcomes were reported as the duration of platelet response among patients and the response (yes or no) among patients with a reduction in the dose of concomitant ITP medication while maintaining an adequate platelet count. For the safety measurement, the outcomes assessed and summarized in the report were the frequency and severity of bleeding according to the IBLS and WHO bleeding scales; change from baseline in liver function, blood pressure, and neutrophil count; the incidence and severity of gastrointestinal effects (diarrhea, nausea, vomiting, and abdominal pain), infection, and overall AEs. For the pharmacokinetic end point summary, the profile of R406 (the active metabolite of fostamatinib), was determined, including maximum plasma concentration, area under the curve, and time to maximum plasma concentration in a subset of patients.
Statistical Analysis
Sample size was calculated using the patients’ numbers in the prior FIT1 and FIT2 studies and their eligibility and willingness to participate in the FIT3 trial. The efficacy and safety analyses were performed among the treated population, including all enrolled and treated patients in this trial. The primary efficacy measurement was calculation of a platelet count at every study visit. The primary efficacy end point was analyzed in 2 versions.
Version 1 included the assessment of efficacy among all patients while they were on active treatment in 1 of the prior FIT1 or FIT2 studies, in the present FIT3 extension study, or in both. For this version, the achievement and maintenance of a stable platelet count was defined as achievement of a platelet count of 50,000/μL or greater within 12 weeks of beginning active treatment; and achievement of a sustained stable platelet response, defined as no 2 visits, at least 4 weeks apart, with a platelet count below 50,000/μL and no intervening visit with a platelet count of 50,000/μL or greater unrelated to rescue therapy, within a period of 12 months following initial achievement of the target platelet count.
Version 2 was the assessment of a within-patient, between-study comparison of fostamatinib and placebo among patients assigned to placebo in either of the prior FIT1 or FIT2 studies. For this version the achievement and maintenance of a stable platelet count was defined as achievement of a platelet count of 50,000/μL or greater within 12 weeks of beginning treatment (placebo treatment in the prior FIT1 or FIT2 study and fostamatinib treatment in the FIT3 extension study); and achievement of a sustained stable platelet response, defined as no 2 visits, at least 4 weeks apart, with a platelet count below 50,000/μL and no intervening visit with a platelet count of 50,000/μL or greater, unrelated to rescue therapy, within a period of 12 weeks following initial achievement of the target platelet count.
For the assessment of secondary efficacy outcome, the Kaplan–Meier method was used to analyze the duration of platelet response. Descriptive statistics were used to perform and summarize additional platelet counts analyses.
For the safety analysis, coding of AEs according to the Medical Dictionary for Regulatory Activities version 18.1 was used. Descriptive statistics were presented by visit for the actual values and the changes from baseline for vital signs and quantitative laboratory tests. The mean of the IBLS scores across visits during the treatment period was also summarized using descriptive statistics.
Patient Disposition
Patient disposition is summarized in Table 22. A total of 124 patients out of 150 from the prior FIT1 and FIT2 studies were screened for the FIT3 trial. Of those 124 individuals, 1 failed screening and 123 patients were enrolled. Among these 123 patients in the treated population, 44 were randomized to placebo and 79 to fostamatinib in their previous study (FIT1 or FIT2). Among the 123 patients, 94 (76.4%) withdrew from the study prematurely. The most common reason for patient withdrawal (accounting for 35.9% of all patients) during this trial was a lack of platelet response after week 12 or later. Other reasons for withdrawal included patient’s own decision for 11 patients (8.9%), development of AEs related to the trial for 11 (8.9%), other AEs for 10 (8.1%), lack of a platelet response before week 12 for 9 (7.3%), sponsor’s decision for 6 (4.9%), noncompliance for 2 (1.6%), and investigator’s discretion for 1 (0.8%) patient for being nonresponsive to fostamatinib.
Table 22: Patient Disposition in the FIT3 Study
Study detail | Fostamatinib, 150 mg or 100 mg |
|---|---|
Screened, n | 124 |
Rollover from Study C788 to 047 (FIT1), n (%) | 59 (48.0) |
Rollover from Study C788 to 048 (FIT2), n (%) | 64 (52.0) |
Completed the open-label study, n (%) | 29 (23.6) |
Discontinued from the open-label study, n (%) | 94 (76.4) |
Reason for discontinuation, n (%) | |
Lack of response after week 12 or later | 44 (35.8) |
Patient’s decision | 11 (8.9) |
Developing study related AE | 11 (8.9) |
Other AEs | 10 (8.1) |
Lack of response before week 12 | 9 (7.3) |
Sponsor’s decision | 6 (4.9) |
Noncompliance and no adherence to study responsibilities | 2 (1.6) |
Investigator’s discretion | 1 (0.8) |
AE = adverse event.
Source: Clinical Study Report for FIT3.9
Exposure to Study Treatments
The mean duration of exposure to fostamatinib was 598.7 days (SD = 607.2) and the median duration of exposure to fostamatinib was 180.0 (range = 28 to 1,773) days.
Some therapeutic treatments were allowed as rescue therapy for patients experiencing platelet counts of less than 50,000/µL. The rescue therapy was administered to the patients in the following situations:
a platelet count of less than 50,000/µL and at immediate risk of bleeding or with clinically significant bleeding or wet purpura
a platelet count of less than 50,000/µL and requiring urgent or emergent surgery.
For the FIT3 trial, the allowed therapeutic regimens included:
IVIG: up to 1 g/kg × 1 to 3 days, or
IV anti-D immunoglobin G: up to 50 to 75 mcg/kg × 1 to 2 days, or
IV methylprednisolone up to 1 g/day for 1 to 3 days or oral dexamethasone up to 40 mg/day for 1 to 2 days or oral prednisone up to 1 mg/kg/day for 1 to 3 days.
Treatment compliance was calculated as the ratio of the total number of actual doses divided by the total number of expected doses during the treatment period in the FIT3 trial. The mean overall compliance was 104.79% (SD = 29.52) for fostamatinib, the mean overall compliance was 99.5%, and the median (number of missed doses) was 1.0 (range = 0 to 803).
Efficacy
Efficacy results are summarized in Table 23. For the primary efficacy outcome (version 1), 19 patients (15.4%) had a platelet response within 12 weeks of taking fostamatinib and maintained a stable platelet response for at least 12 months after achieving the initial response (95% CI, 9.6% to 23.1%). For the primary efficacy outcome (version 2), among 44 patients who were treated with placebo in the FIT1 or FIT2 trials and fostamatinib in the FIT3 trial, 10 (22.7%) were responders, while 34 (77.3%) remained nonresponders in both the prior trials and the FIT3 trial.
For the secondary efficacy outcome, 13 of the 19 primary efficacy responders (version 1) who were treated with fostamatinib in 1 of the prior studies, the minimum and maximum duration of response was 427 days and 1,661 days, respectively. In 6 of the 19 responders who received placebo in 1 of the prior studies (version 1), the minimum and maximum duration of response was 1,340 days and 1,743 days, respectively. In 10 of the 19 responders who got placebo in 1 of the prior studies (version 2), the minimum and maximum duration of response was 194 days and 1,743 days, respectively.
Table 23: Efficacy Outcomes of FIT3 Study – Treated Population
Outcomes | Fostamatinib (N = 123) |
|---|---|
Primary efficacy end point version 1 | |
Achievement by 12 weeks and maintenance for 12 months of a stable platelet response | |
Yes, n (%) | 19 (15.4) |
No, n (%) | 104 (84.6) |
95% CI, for % yes | 9.6 to 23.1 |
Primary efficacy end point version 2 | |
Responders: patients treated with placebo in prior studies | |
Responders in the prior study and FIT3 trial, n (%) | 1 (2.3) |
Responders in the prior study but nonresponder in FIT3 trial, n (%) | 0 |
Nonresponders in the prior study but responder in FIT3 trial, n (%) | 9 (20.5) |
Nonresponders in the prior study and FIT3 trial, n (%) | 34 (77.3) |
Total responders in the FIT3 trial, n (%) | 10 (22.7) |
Total nonresponders in the FIT3 trial, n (%) | 34 (77.3) |
Secondary efficacy end point | |
Duration of platelet response based on platelet count and rescue medication (days) | |
Patients with any platelet responsea | |
n | 57 |
Kaplan–Meier estimated median | 127.0 |
95% CI, for true median | 71.0 to 483.0 |
Minimum to maximum | 8 to > 1,743 |
All FIT3 primary efficacy end point version 1 respondersb | |
n | 19 |
Kaplan–Meier estimated median | > 1,743 |
95% CI, for true median | NE to NE |
Minimum–Maximum | 427 to > 1,743 |
Fostamatinib receiving patients in prior studies who were FIT3 primary efficacy end point version 1 respondersb | |
n | 13 |
Kaplan–Meier estimated median | > 1,661 |
95% CI, for true median | NE to NE |
Minimum to maximum | 427 to > 1,661 |
Placebo patients in prior studies who were FIT3 primary efficacy end point version 1 respondersb | |
n | 6 |
Kaplan–Meier Estimated Median | > 1,743 |
95% CI, for true median | NE to NE |
Minimum to maximum | 1,340 to > 1,743 |
Placebo patients in prior studies who were FIT3 primary efficacy end point version 2 respondersc | |
N | 10 |
Kaplan–Meier estimated median | > 1,743 |
95% CI, for true median | NE to NE |
Minimum to maximum | 194 to > 1,743 |
CI = confidence interval; NE = not estimable.
aAchievement of a platelet count of at least 50,000/µL unrelated to rescue therapy by 12 weeks following active treatment.
bAchievement by 12 weeks and maintenance for 12 months of a stable platelet response.
cAchievement by 12 weeks and maintenance for 12 weeks of a stable platelet response.
Source: Clinical Study Report of FIT3.9
Harms
Safety results are summarized in Table 24. Most patients (79.7%) experienced at least 1 AE during the treatment phase of the FIT3 trial. The most frequently reported AEs were diarrhea (29.3%), hypertension (17.9%), petechiae (15.4%), epistaxis (15.4%), headache (12.2%), upper respiratory tract infection (11.4%), dizziness (10.6%), contusion (9.8%), nausea (8.9%), vomiting (8.9%), fatigue (8.1%), cough (8.1%), and thrombocytopenia (8.1%). Serious AEs with were reported for 27.6% of patients, with thrombocytopenia being the most frequently reported among 6.5% patients.
During the FIT3 trial, a total of 18 patients (14.6%) withdrew from the trial due to an AE, with diarrhea being the most commonly reported AE among 4.1% patients, followed by neutropenia and increased hepatic enzyme among 1.6% patients. Four people (3.3%) died, 1 each due to the following AEs: endocarditis bacterial, pneumonia, sepsis, and cardio-respiratory arrest.
Table 24: Safety Outcomes of FIT3 Study (Treated Population)
Outcome | Fostamatinib (N = 123) |
|---|---|
Patients with ≥ 1 AE, n (%) | 98 (79.7) |
Any AE,a n (%) | NA |
Diarrhea | 36 (29.3) |
Hypertension | 22 (17.9) |
Petechiae | 19 (15.4) |
Epistaxis | 19 (15.4) |
Headache | 15 (12.2) |
URTI | 14 (11.4) |
Dizziness | 13 (10.6) |
Contusion | 12 (9.8) |
Nausea | 11 (8.9) |
Vomiting | 11 (8.9) |
Fatigue | 10 (8.1) |
Cough | 10 (8.1) |
Thrombocytopenia | 10 (8.1) |
Nasopharyngitis | 9 (7.3) |
Arthralgia | 8 (6.5) |
Edema peripheral | 7 (5.7) |
Myalgia | 7 (5.7) |
Rash | 7 (5.7) |
Pyrexia | 7 (5.7) |
Patients with ≥ 1 SAE, n (%) | 34 (27.6) |
Any SAE,b n (%) | NA |
Thrombocytopenia | 8 (6.5) |
Epistaxis | 3 (2.4) |
Sepsis | 2 (1.6) |
Gastrointestinal hemorrhage | 2 (1.6) |
Transaminases increased | 2 (1.6) |
Patients with any WDAEs, n (%) | 18 (14.6) |
Diarrhea | 5 (4.1) |
Neutropenia | 2 (1.6) |
Hepatic enzyme increased | 2 (1.6) |
Blood bilirubin increased | 1 (0.8) |
Transaminases increased | 1 (0.8) |
Blood pressure increased | 1 (0.8) |
Platelet count increased | 1 (0.8) |
Abdominal pain upper | 1 (0.8) |
Thrombocytopenia | 1 (0.8) |
Tachycardia | 1 (0.8) |
Peroneal nerve palsy | 1 (0.8) |
Rash | 1 (0.8) |
Patients with any AE leading to death, n (%) | 4 (3.3) |
Endocarditis bacterial | 1 (0.8) |
Pneumonia | 1 (0.8) |
Sepsis | 1 (0.8) |
Cardio-respiratory arrest | 1 (0.8) |
Patients with notable harms, n (%) | NA |
Infection | 48 (39.0) |
AE = adverse event; NA = not applicable; SAE = serious adverse event; URTI = upper respiratory tract infection; WDAE = withdrawal due to adverse event.
aFrequency 5% or greater.
bFrequency 2% or greater.
Source: Clinical Study Report for FIT3.9
Critical Appraisal
Internal Validity
The open-label extension study had several limitations imposed by the overall design. First, the lack of a randomized comparison group to provide context and control for potential confounders and the open-label design may influence the perception of improvement by patients and clinicians, which could affect the reporting of harms. As part of the eligibility criteria for the open-label extension, patients had to complete 1 of the prior studies, potentially allowing for selection bias. From the total population that completed the FIT1 and FIT2 studies (n = 150), a total of 124 (82.7%) enrolled in the open-label extension. There was no clear explanation for half on those 26 patients (17.3%) not enrolling in the FIT3 trial. Additionally, there was a potential for survival bias as the other 13 patients who discontinued the prior studies due to AEs were excluded (7 in the fostamatinib group and 2 in the placebo group in the FIT1 trial, and 2 in the fostamatinib group and 2 in the placebo group in the FIT2 trial). This could result in a greater enrolment of patients who were better able to tolerate fostamatinib and possibly fewer AEs being reported. Any lack of follow-up after discontinuing FIT3 could mean that important long-term safety data are also missing. The high rate of discontinuations (76.4%) during the open-label phase was mostly due to a lack of response, with the most common reasons being a lack of platelet response at week 12 or later (35.8%), patient decision (8.9%), development of a study-specific AE (8.9%), and other AEs (8.1%). The limitations with the study design make it challenging to interpret the results and form conclusions with certainty.
External Validity
Because the patients who took part in the FIT3 were originally from the parent studies and the eligibility criteria remained the same, it is reasonable to expect that the same limitations to generalizability are relevant to the open-label extension. For example, because the participants were predominantly White (91.9%), the results from these trials may not be generalizable to other racial groups commonly seen at some centres in Canada (although the experts noted that the role of race and/or ethnicity in treatment response was not clear). The experts also noted that patients with secondary ITP were excluded from the FIT3 trial, and trial findings may therefore not be generalizable to those with secondary ITP. Moreover, the experts found the definition for response to therapy in the FIT3 trials, as in the FIT1 and FIT2 trials, to be overly strict, and they stated that achieving a platelet count of at least 30,000/µL would be considered a response in practice, particularly if a patient is asymptomatic. The primary outcome definition used in the FIT3 trial therefore may not be reflective of how response to therapy is assessed in routine practice. The clinical experts also noted that the co-interventions (i.e., concomitant ITP medication) used in the FIT3 trial, as in the FIT1 and FIT2 trials, are also reflective of real-world practice in Canada, as steroids would commonly be continued while a patient is initiated on a new long-term treatment strategy such as fostamatinib.
As with the FIT1 and FIT2 trials, the FIT3 trial provided limited data on clinically important outcomes such as quality of life, rescue therapy, and bleeding events. Because the clinical experts do not use the IBLS and WHO bleeding scales in practice, the relevance of the bleeding outcome scales used in the FIT3 trial is unclear. Further, the event rates for the post hoc bleeding-related SAE outcome made it challenging for the clinical experts to comment on the relevance or meaningfulness of these findings.
Post Hoc Analyses of the FIT1, FIT2, and FIT3 Trials
In a post hoc analysis conducted by Boccia et al. (2020),26 the efficacy of fostamatinib was assessed earlier in the ITP disease course by including patients from the FIT1, FIT2, and FIT3 studies. The data cut-off date for this post hoc analysis was December 2019. For the evaluation process, patient subgroups were compared by line of therapy (second-line versus third- or later-line) and the chronic ITP progression stage (persistent versus early or late stage of disease). The proportions of patients achieving a platelet response of 50,000/µL or greater and 30,000/µL or greater, without any rescue therapy within 4 weeks, were assessed. A total of 145 patients were assessed in this study, 32 receiving fostamatinib as second-line treatment (median age of 50; 59% female), and 113 as other-line treatment (median age of 54; 60% female). The response rates were observed to be higher in the second-line therapy group (78% using fostamatinib) compared with the third or later lines of therapy (48%), presenting fostamatinib as more effective as second-line therapy for chronic ITP patients. The safety results were similar for patients in both therapy lines.26 The authors reported that AE rates were 72% for second-line therapy and 94% for later-line therapy. The most common AEs were hypertension (31% in second-line versus 19% in later-line therapy), diarrhea (25% versus 39%, respectively), upper respiratory tract infections (16% versus 11%, respectively), and elevated liver transaminase (26% versus 16%, respectively). Considering the limitations of the post hoc analysis, the results from this study should be interpreted with caution. As this study included patients from the FIT1, FIT2 and FIT3 studies, the corresponding internal and external validity considerations would be applicable to this post hoc analysis as well. In addition, lack of randomization or stratification for lines of therapies before fostamatinib treatment and the small number of patients in the second-line therapy group compared to the third- and other-line of therapy may potentially lead to bias. The differences in the 2 groups in terms of time since ITP diagnosis, stages of ITP progression, baseline platelet counts, and prior ITP medications used may have affected the efficacy of fostamatinib in those groups differently.
In another post hoc analysis conducted by Cooper et al. (2021),27 thrombotic risk was assessed while patients were on long-term treatment with fostamatinib. A total of 146 patients from the FIT1, FIT2, and FIT3 trials were included in this study, with up to 5 years of treatment and a data cut-off date of December 2019.23,28 Although the investigators claimed an effective and long-term treatment for ITP with a low incidence of thromboembolic events among patients, the results should be interpreted with caution considering the post hoc nature of the trial and the prospect of associated bias.
Discussion
Summary of Available Evidence
The FIT1 (N = 76) and FIT2 (N = 74) trials were identically designed 24-week double-blind RCTs that evaluated the efficacy and safety of fostamatinib versus placebo in patients with primary ITP for longer than 3 months who had received at least 1 previous ITP treatment and had a baseline platelet count below 30,000/µL. In the FIT1 trial, 51 patients were randomized to fostamatinib and 25 to placebo, while in the FIT2 trial, 50 patients were randomized to fostamatinib and 24 to placebo. The primary efficacy end point in both trials was achievement of a stable platelet response, defined as a platelet count of 50,000/µL or greater at 4 of the last 6 study visits between weeks 14 and 24.
Two ITCs were reviewed. The Wojciechowski study was a systematic review and ITC comparing fostamatinib to 3 TPO-RAs (avatrombopag, eltrombopag, and romiplostim) among patients with chronic ITP who had inadequate response to previous therapy. Seven phase III, double-blind RCTs were included and contributed data on various efficacy and harms outcomes to the ITC. The authors assessed the following outcomes: durable platelet response, need for rescue therapy, and WHO bleeding events, all up to 24 weeks. The sponsor also submitted a systematic review and ITC in which fostamatinib was compared to rituximab among patients with chronic or persistent ITP. Six RCTs were included and contributed evidence. A single outcome, overall platelet response, was assessed in this ITC.
One additional study, FIT3, was considered as other relevant evidence. This was an open-label extension study of FIT1 and FIT2 to examine the efficacy and safety of long-term fostamatinib among people with chronic or persistent ITP. A total of 59 patients from FIT1 and 64 patients from FIT2 who completed the week 24 evaluation or withdrew early (starting at week 12) due to a lack of response were eligible for this trial. All patients received open-label fostamatinib. The primary efficacy outcome was achievement of a platelet response by 12 weeks and maintenance for 12 months. A stable platelet response was a platelet count of 50,000/μL or greater at 4 or more of 6 biweekly visits during weeks 14 to 24 or, for patients initiating fostamatinib in the extension phase, a platelet count of at least 50,000/μL in the first 3 months followed by platelet counts of at least 50,000/μL at the subsequent 2 of 3 monthly visits without use of rescue medication. In the FIT3 trial, 60% of patients were female, the mean age was 52 years (SD = 16), and patients were predominantly White (92%).
A post hoc analysis of the FIT1, FIT2, and FIT3 trials was conducted by Boccia et al.26 and was also considered relevant. Patient subgroups were compared by line of therapy for fostamatinib (second-line versus third- or later-line) and the chronic ITP progression stage (persistent versus early or late stage of disease). A total of 145 patients were assessed in this study, 32 receiving fostamatinib as second-line treatment and 113 as other-line treatment.
Interpretation of Results
Efficacy
The results of the FIT1 and FIT2 trials suggest that fostamatinib leads to a modestly higher rate of stable treatment response (approximately 18%) compared to placebo (0 to 4%) in a group of heavily pre-treated patients with primary, chronic ITP. While the use of rescue therapy and rate of bleeding-related SAEs were lower in the fostamatinib groups compared to placebo, the event rates for these outcomes were low and the trials were not powered to detect differences in these outcomes. Further, due to the high discontinuation rate in the FIT1 and FIT2 trials, limited data were available on quality of life (measured by the SF-36), and it was impossible to determine whether there were any differences between fostamatinib and placebo. Subgroup analyses suggested that there were no differences in platelet response for people treated with a prior splenectomy or TPO-RAs versus those who were not so treated, but these analyses were not pre-specified and were likely underpowered (with wide CIs and low event rates). The clinical experts consulted by CADTH noted that it would be challenging to base treatment decisions on, or draw meaningful conclusions from, the subgroup analyses. Overall, the clinical experts emphasized that another treatment option that produces a modest improvement in platelet response would be helpful in clinical practice, given that patients are often refractory to multiple treatments.
In the FIT3 trial, long-term platelet response (≥ 12 months) was observed in 15% of patients who responded in the FIT1 and FIT2 trials, and 23% of patients of patients receiving placebo in the FIT1 and FIT2 trials but starting fostamatinib in FIT3. These results suggest that a portion of patients will achieve long-term platelet responses; however, there was no comparator group in this extension study, it was open-label, and there was a potential for selection bias. The FIT1 and FIT2 trials were conducted in a primarily White population, and patients with secondary ITP were excluded. In addition, the rates of prior treatments (e.g., rituximab and a splenectomy) may not reflect Canadian practice, creating generalizability concerns in the Canadian context.
The clinical experts noted a lack of comparative efficacy data for second- and third-line ITP treatments, including with fostamatinib. Two ITCs provided evidence on comparative efficacy. Wojciechowski et al. reported that no treatment was favoured when fostamatinib was compared to TPO-RAs among patients who did not achieve an adequate response to corticosteroids in terms of platelet response rates and reduction in bleeding event outcomes, and it remains uncertain if there was a significant difference for fostamatinib compared to TPO-RAs in achieving a durable platelet response. There were important limitations in this ITC due to the small size of the evidence base and heterogeneity in patient populations across included trials. The sponsor also submitted an ITC that suggested that fostamatinib was superior to rituximab in achieving an overall platelet response among patients with persistent or chronic ITP. This ITC also was not able assess clinical heterogeneities across eligible studies or their impact on study results. Moreover, the study only assessed platelet response and had a potential for selective reporting. Due to limited comparators and important methodological limitations, the ITCs provide limited additional insight into comparative efficacy of fostamatinib compared to other second- or subsequent-line ITP therapies.
The lack of comparative efficacy and safety data, as well as uncertainty around the optimal treatment pathway in second- and subsequent-line treatment of ITP, is reflected in guidelines for ITP.2,3 These guidelines highlight the low certainty of evidence regarding ITP treatment options, making it difficult to weigh options against each another. Guidelines therefore acknowledge that individualization of therapy and shared decision-making are important in the treatment of ITP and should incorporate the duration of ITP, comorbidities, age of the patient, access to medications (cost and availability), and patient preferences.3 This consideration was echoed by clinical experts, who noted that it was challenging to compare fostamatinib to other second- or subsequent-line ITP treatment options but that the modest efficacy with respect to platelet count response meant it represented another treatment option among heavily pre-treated patients who are in need of options for managing ITP.
Clinical experts and patients highlighted how reducing bleeding risk and improving symptoms and quality of life are particularly important in chronic ITP, considering how these factors negatively affect patients. The patient group highlighted how symptom and quality-of-life improvement is likely more important to patients compared with platelet counts. Clinicians and patients also reported that an ideal ITP treatment should be convenient and easy to administer for a patient. Unfortunately, the available evidence provided limited insight on outcomes important to patients and clinicians as the eligible and relevant trials (and ITCs) focused primarily on platelet counts. Some outcomes important to patients, such as bleeding and quality of life, were secondary or post hoc outcomes with low event rates and/or limited outcome data, and it was not possible to draw conclusions about fostamatinib’s effect on these outcomes. While fostamatinib is an oral medication, convenience and adherence were not compared in any of the relevant evidence and as such the extent to which fostamatinib leads to improvements in these measures compared to existing treatments is unclear. Platelet response is the main way that clinicians assess treatment response in clinical practice. The clinical experts noted that platelet response is expected to correlate with reduced bleeding risk; however, they acknowledged that available evidence with fostamatinib provides limited insight regarding its effect on quality of life, symptoms, and bleeding outcomes (bearing in mind that there are limited data on such outcomes for most ITP treatments).
Harms
In the FIT1, FIT2, and FIT3 trials, fostamatinib was generally well tolerated. The most common AEs were diarrhea, nausea, elevated liver transaminase levels, and hypertension. The rate of infections in the FIT1 trial was higher in the fostamatinib group (|||) compared to placebo (|||), which was mainly attributed to upper respiratory tract infections and urinary tract infections. The rate of SAEs was similar between groups in the FIT1 trial, while in the FIT2 trial the placebo group had a higher rate of SAEs (26% versus 10% in fostamatinib group). The rate of withdrawals due to AEs was higher in the fostamatinib group compared to placebo in the FIT1 trial (16% versus 8%, respectively), and the rate of withdrawals due to AEs in both groups was similar in the FIT2 trial. The FIT3 trial did not identify any long-term safety concerns with fostamatinib, although there was no comparator group in this study. The clinical experts did not highlight any major concerns regarding the safety of fostamatinib, noting that gastrointestinal adverse effects, hypertension, and elevated transaminase levels were consistent with what is known about fostamatinib. They noted that hypertension would be important to monitor in patients treated with fostamatinib. The clinician group input stated that fostamatinib is considered to have a favourable side-effect profile in the context of ITP treatment. The FIT1, FIT2, and FIT3 trials did not provide insight on the comparative safety of fostamatinib versus other second- or subsequent-line therapies for ITP. The Wojciechowski ITC found no statistically significant differences between fostamatinib and TPO-RAs in the incidence of any AEs; however, this ITC had important limitations. The data on the safety and tolerability of fostamatinib compared to other ITP treatments are therefore limited.
Conclusions
Management of chronic ITP is challenging as patients frequently relapse or are refractory to treatments, and patients often cycle through multiple ITP treatments. Treatment is complicated by a lack of evidence on comparative efficacy and the safety of second- and subsequent-line treatment options, access issues, and the safety and tolerability of available options. In 2 double-blind RCTs, fostamatinib, which is an ITP treatment with a novel mechanism of action, led to a modest improvement in platelet count responses compared to placebo among patients with chronic, heavily pre-treated primary ITP. There were little or no data on outcomes important to patients, such as bleeding rates, symptoms, and quality of life, and the impact of fostamatinib on these outcomes remains unclear. Subgroup analyses (e.g., based on previous lines of therapy) were not able to provide insight into which patient groups are the most likely to respond to treatment. It is also difficult to draw conclusions about the comparative efficacy of fostamatinib versus other ITP treatments. Both ITC studies included in this review suggest that fostamatinib may be comparable to TPO-RAs and have a favourable efficacy comparable to that of rituximab in terms of platelet count response. However, there were important limitations in these studies, and it is challenging to draw firm conclusions about comparative efficacy based on these studies. In the FIT1 and FIT2 trials, fostamatinib appeared to lead to a higher rate of adverse effects such as diarrhea, nausea, hypertension, and elevated liver transaminase levels, compared to placebo, while the FIT3 trial did not identify any long-term safety concerns beyond these adverse effects. Overall, this review suggests that fostamatinib is another potential treatment option for patients with chronic, heavily pre-treated primary ITP. The drug leads to a platelet count response in a modest proportion of patients and is generally well tolerated compared to placebo, although its comparative efficacy and safety versus other ITP treatments, and its effect on outcomes important to patients, remain unclear.
References
1.Arnold DM, Leung LKL, Tirnauer JS. Immune thrombocytopenia (ITP) in adults: clinical manifestations and diagnosis. In: Post TW, ed. UpToDate. Waltham (MA): UpToDate; 2021: www.uptodate.com. Accessed 2021 Oct 20.
2.Provan D, Arnold D, Bussel J, et al. Updated international consensus report on the investigation and management of primary immune thrombocytopenia. Blood Adv. 2019;3(22). PubMed
3.Neunert C, Terrell D, Arnold D, et al. American Society of Hematology 2019 guidelines for immune thrombocytopenia. Blood Adv. 2019;3(23). PubMed
4.Tavalisse (fostamatinib): 100 mg and 150 mg tablet (as as fostamatinib disodium hexahydrate), oral [product monograph]. Toronto (ON): Medison Pharma Canada Inc.; 2020 Nov 17.
5.Clinical Study Report: C-935788-047. A phase 3, multicenter, randomized, double-blind, placebo-controlled study of fostamatinib disodium in the treatment of persistent/chronic immune thrombocytopenic purpura [internal sponsor's report]. San Francisco (CA): Rigel Pharmaceuticals, Inc.; 2017 Mar 3.
6.Clinical Study Report: C-935788-048. A phase 3, multicenter, randomized, double-blind, placebo-controlled study of fostamatinib disodium in the treatment of persistent/chronic immune thrombocytopenic purpura [internal sponsor's report]. San Francisco (CA): Rigel Pharmaceuticals, Inc.; 2017 Mar 28.
7.Wojciechowski P, Wilson K, Nazir J, et al. Efficacy and Safety of Avatrombopag in Patients with Chronic Immune Thrombocytopenia: A Systematic Literature Review and Network Meta-Analysis. Adv Ther. 2021;38(6):3113-3128. PubMed
8.Network meta-analysis to evaluate the clinical efficacy of treatments in idiopathic thrombocytopenic purpura (ITP) [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Tavalisse (fostamatinib), 100 mg and 150 mg tablet, oral. Toronto (ON): Medison Pharma Canada Inc.; 2021 Jul 12.
9.Clinical Study Report: C-935788-049. A phase 3 open-label extension study of fostamatinib disodium in the treatment of persistent/chronic immune thrombocytopenic purpura [internal sponsor's report]. San Francisco (CA): Rigel Pharmaceuticals, Inc.; 2021 Feb 23.
10.Samson M, Fraser W, Lebowitz D. Treatments for Primary Immune Thrombocytopenia: A Review. Cureus. 2019;11(10):e5849. PubMed
11.Terrell D, Beebe L, Vesely S, Neas B, Segal J, George J. The incidence of immune thrombocytopenic purpura in children and adults: A critical review of published reports. Am J Hematol. 2010;85(3). PubMed
12.Weycker D, Hanau A, Hatfield M, et al. Primary immune thrombocytopenia in US clinical practice: incidence and healthcare burden in first 12 months following diagnosis. J Med Econ. 2020;23(2). PubMed
13.Cohen Y, Djulbegovic B, Shamai-Lubovitz O, Mozes B. The bleeding risk and natural history of idiopathic thrombocytopenic purpura in patients with persistent low platelet counts. Arch Intern Med. 2000;160(11). PubMed
14.Swinkels M, Rijkers M, Voorberg J, Vidarsson G, Leebeek FWG, Gerard Jansen AJ. Emerging Concepts in Immune Thrombocytopenia. Front Immunol. 2018;9:880. PubMed
15.Cooper N, Kruse A, Kruse C, et al. Immune thrombocytopenia (ITP) World Impact Survey (iWISh): Patient and physician perceptions of diagnosis, signs and symptoms, and treatment. Am J Hematol. 2021;96(2). PubMed
16.Nazaryan H, Liu Y, Sirotich E, Duncan J, Nazy I, Arnold D. Second-Line Therapy for Immune Thrombocytopenia: Real-World Experience in Canada. Can J Gen Intern Med. 2020;15(4):28-35.
17.Revolade (eltrombopag): 12.5 mg, 25 mg, 50 mg and 75 mg eltrombopag (as eltrombopag olamine) tablets, [product monograph]. Dorval (QC): Novartis Pharmaceuticals Canada Inc.; 2017 May 11: https://pdf.hres.ca/dpd_pm/00039266.PDF. Accessed 2021 Oct 20.
18.Nplate (romiplostim for injection): lyophilized powder for solution 250 mcg/0.5 mL and 500 mcg/1 mL [product monograph]. Mississauga (ON): Amgen Canada Inc.; 2021 Aug 04: https://pdf.hres.ca/dpd_pm/00062536.PDF. Accessed 2021 Oct 20.
19.Rituxan (rituximab): 10 mg/mL intravenous infusion [product monograph]. Mississauga (ON): Hoffmann-La Roche Ltd.; 2021 Jan 28: https://www.rochecanada.com/PMs/Rituxan/RituxanIV_PM_E.pdf. Accessed 2021 Oct 20.
20.Lucchini E, Zaja F, Bussel J. Rituximab in the treatment of immune thrombocytopenia: what is the role of this agent in 2019? Haematologica. 2019;104(6):1124-1135. PubMed
21.McGowan J, Sampson M, Salzwedel DM, Cogo E, Foerster V, Lefebvre C. PRESS Peer Review of Electronic Search Strategies: 2015 guideline statement. J Clin Epidemiol. 2016;75:40-46. PubMed
22.Grey matters: a practical tool for searching health-related grey literature. Ottawa (ON): CADTH; 2019: https://www.cadth.ca/grey-matters. Accessed 2021 Aug 8.
23.Bussel J, Arnold DM, Grossbard E, et al. Fostamatinib for the treatment of adult persistent and chronic immune thrombocytopenia: Results of two phase 3, randomized, placebo-controlled trials. Am J Hematol. 2018;93(7):921-930. PubMed
24.Drug Reimbursement Review sponsor submission: Tavalisse (fostamatinib), 100 mg and 150 mg tablet, oral [internal sponsor's package]. Toronto (ON): Medison Pharma Canada Inc.; 2021 Jul 22.
25.Ren S, Oakley JE, Stevens JW. Incorporating Genuine Prior Information about Between-Study Heterogeneity in Random Effects Pairwise and Network Meta-analyses. Med Decis Making. 2018;38(4):531-542. PubMed
26.Boccia R, Cooper N, Ghanima W, et al. Fostamatinib is an effective second-line therapy in patients with immune thrombocytopenia. Br J Haematol. 2020;190(6):933-938. PubMed
27.Cooper N, Altomare I, Thomas MR, et al. Assessment of thrombotic risk during long-term treatment of immune thrombocytopenia with fostamatinib. Ther Adv Hematol. 2021;12:20406207211010875. PubMed
28.Bussel JB, Arnold DM, Boxer MA, et al. Long-term fostamatinib treatment of adults with immune thrombocytopenia during the phase 3 clinical trial program. Am J Hematol. 2019;94(5):546-553. PubMed
29.Yang R, Lin L, Yao H, Ji O, Shen Q. Therapeutic options for adult patients with previously treated immune thrombocytopenia - a systematic review and network meta-analysis. Hematol. 2019;24(1):290-299. PubMed
30.Page LK, Psaila B, Provan D, et al. The immune thrombocytopenic purpura (ITP) bleeding score: assessment of bleeding in patients with ITP. Br J Haematol. 2007;138(2):245-248. PubMed
31.Fogarty PF, Tarantino MD, Brainsky A, Signorovitch J, Grotzinger KM. Selective validation of the WHO Bleeding Scale in patients with chronic immune thrombocytopenia. Curr Med Res Opin. 2012;28(1):79-87. PubMed
32.Signorovitch J, Brainsky A, Grotzinger KM. Validation of the FACIT-fatigue subscale, selected items from FACT-thrombocytopenia, and the SF-36v2 in patients with chronic immune thrombocytopenia. Qual Life Res. 2011;20(10):1737-1744. PubMed
33.Miller AB, Hoogstraten B, Staquet M, Winkler A. Reporting results of cancer treatment. Cancer. 1981;47(1):207-214. PubMed
34.Ware J, Kosinski M, Bjorner JB, Turner-Bowker DM, Gandek B, Maruish ME. Determining important differences in scores. User's manual for the SF-36v2 health survey. 2nd ed. Lincoln (RI): Quality Metric Inc; 2007.
35.Leung YY, Ho K, Zhu T, Tam L-S, Kun E, Li E. Testing scaling assumptions, reliability and validity of medical outcomes study short-form 36 health survey in psoriatic arthritis. Rheumatology (Oxford). 2010;49:1495-1501. PubMed
Appendix 1: Literature Search Strategy
Note that this appendix has not been copy-edited.
Clinical Literature Search
Overview
Interface: Ovid
Databases:
MEDLINE All (1946-present)
Embase (1974-present)
Note: Subject headings and search fields have been customized for each database. Duplicates between databases were removed in Ovid.
Date of search: August 20, 2021
Alerts: Biweekly search updates until project completion
Search filters applied: No filters were applied to limit the retrieval by study type.
Limits:
Conference abstracts: excluded
Syntax | Description |
|---|---|
/ | At the end of a phrase, searches the phrase as a subject heading |
MeSH | Medical Subject Heading |
* | Before a word, indicates that the marked subject heading is a primary topic; or, after a word, a truncation symbol (wildcard) to retrieve plurals or varying endings |
.ti | Title |
.ot | Original title |
.ab | Abstract |
.hw | Heading word; usually includes subject headings and controlled vocabulary |
.kf | Author keyword heading word (MEDLINE) |
.kw | Author keyword (Embase) |
.dq | Candidate term word (Embase) |
.pt | Publication type |
.rn | Registry number |
.nm | Name of substance word (MEDLINE) |
medall | Ovid database code: MEDLINE All, 1946 to present, updated daily |
oemezd | Ovid database code; Embase, 1974 to present, updated daily |
Multi-Database Strategy
(fostamatinib* or Tavalisse* or Tavlesse* or R935788 or R-935788 or R788 or R-788 or SQ8A3S5101 or 86EEZ49YVB or X9417132K8 or R 406 or R406 or R950091 or R 950091 or NSC-745942 or NSC745942 or R-935788 or R935788 or tamatinib fosdium).ti,ab,kf,ot,hw,nm,rn.
1 use medall
*fostamatinib/ or (fostamatinib* or Tavalisse* or Tavlesse* or R935788 or R-935788 or R788 or R-788 or R 406 or R406 or R950091 or R 950091 or NSC-745942 or NSC745942 or R-935788 or R935788 or tamatinib fosdium).ti,ab,kw,dq.
3 use oemezd
(conference review or conference abstract).pt.
4 not 5
2 or 6
remove duplicates from 7
Clinical Trials Registries
ClinicalTrials.gov
Produced by the US National Library of Medicine. Targeted search used to capture registered clinical trials.
[Search -- Studies with results | fostamatinib or Tavalisse or Tavlesse | immune thrombocytopenia OR ITP ]
WHO ICTRP
International Clinical Trials Registry Platform, produced by the World Health Organization. Targeted search used to capture registered clinical trials.
[Search terms -- fostamatinib or Tavalisse or Tavlesse | immune thrombocytopenia OR ITP]
Health Canada’s Clinical Trials Database
Produced by Health Canada. Targeted search used to capture registered clinical trials.
[Search terms -- fostamatinib or Tavalisse or Tavlesse | immune thrombocytopenia OR ITP]
EU Clinical Trials Register
European Union Clinical Trials Register, produced by the European Union. Targeted search used to capture registered clinical trials.
[Search terms -- fostamatinib or Tavalisse or Tavlesse | immune thrombocytopenia OR ITP]
Grey Literature
Search dates: August 10-16, 2021
Keywords: fostamatinib, Tavalisse, Tavlesse, ITP, immune thrombocytopenia
Limits: none
Updated: Search updated prior to the meeting of the CADTH Canadian Drug Expert Committee (CDEC)
Relevant websites from the following sections of the CADTH grey literature checklist Grey Matters: A Practical Tool for Searching Health-Related Grey Literature were searched:
Health Technology Assessment Agencies
Health Economics
Clinical Practice Guidelines
Drug and Device Regulatory Approvals
Advisories and Warnings
Drug Class Reviews
Clinical Trials Registries
Databases (free)
Health Statistics
Internet Search
Open Access Journals.
Appendix 2: Excluded Studies
Note that this appendix has not been copy-edited.
Reference | Reason for exclusion |
|---|---|
Cooper (2021)27 | Study design |
Wojciechowski (2021)7 | Review article |
Boccia (2020)26 | Study design |
Bussel (2019)28 | Study design |
Yang (2019)29 | Review article |
FIT3 Clinical Study Report9 | Study design |
Appendix 3: Description and Appraisal of Outcome Measures
Note that this appendix has not been copy-edited.
Aim
To describe the following outcome measures and review their measurement properties (validity, reliability, responsiveness to change, and MID):
ITP bleeding scale (IBLS)
World Health Organization (WHO) bleeding scale
Short Form (36) Health Survey Version 2 (SF-36v2)
Findings
Table 27: Summary of Outcome Measures and Their Measurement Properties
Outcome measure | Type | Conclusions about measurement properties | MID |
|---|---|---|---|
ITP bleeding scale (IBLS) | IBLS is comprised of 11 anatomical site-specific bleeding grades from 0 (none) to 2 (marked bleeding). | Reliability: 92% of the sites were graded identically, demonstrating a good inter-observer reliability. The values for Kappa statistics were – 0.71 for skin (Hx), 0.66 for skin (PE), 0.52 for oral (Hx), 0.46 for oral (PE), 0.58 for epistaxis, and 0.78 for GYN.30 Interquartile ranges (IQRs) were from - 0.8% to + 1.3% with ICCs 0.63, and from - 4.7% to + 3.4% with ICCs 0.77 for the IBLS in the RAISE and EXTEND studies, respectively.31 Validity: While assessing the construct validity by determining inter-instrument correlations (item-to-item and item-to-domain correlations) between the WHO bleeding scale and the IBLS, a positive correlation was observed between the WHO bleeding scale and the IBLS, showing a similar association between platelet counts and severity of bleeding. However, the IBLS demonstrated more capability in capturing more details about bleeding than the WHO bleeding scale. Responsiveness: Moderate responsiveness; effect size, standardized response and responsiveness statistic were 0.719, 0.741 and 0.640 in RAISE, and 0.560, 0.561 and 0.506 in EXTEND studies. | None identified |
WHO bleeding scale | The WHO bleeding scale is an instrument used to classify bleeding among ITP patients on a 5-point scale. The scale grading follows as: 0 (no bleeding), 1 (petechiae), 2 (mild blood loss), 3 (gross blood loss), and 4 (debilitating blood loss). | Reliability: The interquartile ranges (IQRs) were from - 0.8% to + 1.3% with ICCs 0.75, and from - 4.7% to + 3.4% with ICCs 0.70 for the WHO bleeding scale in the RAISE and EXTEND studies. Validity: While assessing the construct validity by determining inter-instrument correlations (item-to-item and item-to-domain correlations) between the WHO bleeding scale and the IBLS and between the WHO bleeding scale and platelet counts, and by describing the relationship between the scale and clinical outcomes, a positive correlation was observed between the WHO bleeding scale and IBLS, showing a similar association between platelet counts and severity of bleeding. Moreover, during known group comparison assessment, significant associations (p<0.05) were observed between the WHO bleeding scale and many clinical outcomes. Responsiveness: Moderate responsiveness; effect size, standardized response and responsiveness statistic were 0.714, 0.745 and 0.560 in RAISE, and 0.622, 0.487 and 0.588 in EXTEND studies. | Ranged from 0.33 to 0.40 |
SF-36 Health Survey Version 2 | The SF-36 consists of 8 sub-domains. The SF-36 provides 2 component summaries, PCS and MCS. The 8 sub-domains are each measured on a scale of zero to 100, with an increase in score indicating improvement in health status. | Reliability and Validity: SF-36 item-to-domain score correlations >0.20, and Cronbach alpha values for SF-36v2 domains ≥0.75, for all items and if each item was deleted from scale. ICCs for test–retest reliability evaluation in clinically stable patients were >0.7 in both RAISE and EXTEND studies. Construct validity was supported by moderate to strong score correlations. SF-36v2 had been reported to be less responsive compared to the disease-specific measures of fatigue based on the ability to capture change.32 | None identified |
GYN = gynecological; IQRs = The interquartile ranges; MID = minimal important difference.
ITP Bleeding Scale
The IBLS is an assessment method for objective quantification of bleeding symptoms among ITP patients. IBLS is comprised of 11 anatomical site-specific bleeding grades from 0 (none) to 2 (marked bleeding) and is assessed by history over the previous week (Hx) for all, and by physical examination (PE) for 2 of these sites. The sites are – skin (PE), oral (PE), skin (Hx), oral (Hx), epistaxis, gastrointestinal (GI), urinary (U), gynecological (GYN), pulmonary, intracranial hemorrhage, subconjunctival hemorrhage.
In a pilot study conducted between 2004 to 2005 among 65 ITP patients, IBLS had been used to analyze the correlation of platelet variables with bleeding. In this study, 92% of the sites were graded identically, demonstrating a good inter-observer reliability. The values for Kappa statistics were – 0.71 for skin (Hx), 0.66 for skin (PE), 0.52 for oral (Hx), 0.46 for oral (PE), 0.58 for epistaxis, and 0.78 for GYN.30 In addition to this study, IBLS had been evaluated in 2 long-term, phase III clinical trials named RAISE and EXTEND, where participants were chronic ITP patients taking eltrombopag. In these studies, the clinical investigator assessed the blooding grade based on verbal responses and physical examination.31
Intraclass correlation coefficients for test–retest reliability were calculated using 2 consecutive bleeding grades corresponding to the nearest platelet counts for each patient. The interquartile ranges (IQRs) were from - 0.8% to + 1.3% with ICCs 0.63, and from - 4.7% to + 3.4% with ICCs 0.77 for the IBLS in the RAISE and EXTEND studies, respectively.
Construct validity was assessed by determining inter-instrument correlations (item-to-item and item-to-domain correlations) between the WHO bleeding scale and the IBLS. The relationship between the WHO bleeding scale and the IBLS had been described by comparing mean WHO grades with mean IBLS summary scores at baseline, as well as by assessing the associations between scores on each patient-reported outcome instrument and platelet counts at baseline and last on-treatment. In addition, WHO grades were cross-classified with item-level responses for the IBLS items to demonstrate the relationship between the 2 scales. A positive correlation was observed between the WHO bleeding scale and the IBLS, showing a similar association between platelet counts and severity of bleeding. However, the IBLS demonstrated more capability in capturing more details about bleeding than the WHO bleeding scale.
The responsiveness was assessed by calculating the differences in grades from baseline to last-on-treatment evaluation among patients with a platelet count response. The responsiveness among patients were computed using 3 indices: effect size = D/SD0 , standardized response mean = D/ SD*, and responsiveness statistic = D/SD# . Here D denotes the mean score change of interest (i.e., mean change from baseline among patients with platelet count response), SD0 denotes the SD of scores at baseline, SD* is the SD of D, and SD# is the SD of D among patients with no response to treatment. However, the responsiveness measures assessed in the study demonstrated a statistical property of the bleeding scales in the population under study and could not be used as a description of how patients responded to therapy in the RAISE and EXTEND studies. In the RAISE study containing 129 patients, the responsiveness scores comprising the effect size, standardized response and responsiveness statistic were 0.719, 0.741 and 0.640, respectively, whereas in the EXTEND study among 71 patients, the effect size, standardized response and responsiveness statistic were 0.560, 0.561 and 0.506, respectively, showcasing moderate responsiveness for the IBLS in both studies.31
The MID was not assessed for IBLS among ITP patients in any study.
WHO Bleeding Scale
The WHO bleeding scale is an instrument used to classify bleeding among ITP patients on a 5-point scale. The scale grading follows as: 0 (no bleeding), 1 (petechiae), 2 (mild blood loss), 3 (gross blood loss), and 4 (debilitating blood loss).31 Originally developed for bleeding assessment among cancer patients,33 the performance of WHO bleeding scale had been evaluated among chronic ITP patients taking eltrombopag in 2 long-term, phase III clinical trials, RAISE and EXTEND studies.31
Intraclass correlation coefficient for test–retest reliability were calculated using 2 consecutive bleeding grades corresponding to the nearest platelet counts for each patient. The interquartile ranges (IQRs) were from - 0.8% to + 1.3% with ICCs 0.75, and from - 4.7% to + 3.4% with ICCs 0.70 for the WHO bleeding scale in the RAISE and EXTEND studies, respectively.
Construct validity was assessed in 2 ways - by determining inter-instrument correlations (item-to-item and item-to-domain correlations) between the WHO bleeding scale and the IBLS and between the WHO bleeding scale and platelet counts, and by describing the relationship between the scale and clinical outcomes. A positive correlation was observed between the WHO bleeding scale and IBLS, showing a similar association between platelet counts and severity of bleeding while assessing inter-instrument correlations. Moreover, during known group comparison assessment, significant associations (p<0.05) were observed between the WHO bleeding scale and many clinical outcomes.
The responsiveness was assessed by calculating the differences in grades from baseline to last-on-treatment evaluation among patients with a platelet count response. The responsiveness among patients were computed using 3 indices: effect size = D/SD0, standardized response mean = D/ SD*, and responsiveness statistic = D/SD#. Here D denotes the mean score change of interest (i.e., mean change from baseline among patients with platelet count response), SD0 denotes the SD of scores at baseline, SD* is the SD of D, and SD# is the SD of D among patients with no response to treatment. However, the responsiveness measures assessed in the study demonstrated a statistical property of the bleeding scales in the population under study and could not be used as a description of how patients responded to therapy in the RAISE and EXTEND studies. In the RAISE study containing 129 patients, the effect size, standardized response and responsiveness statistic were 0.714, 0.745 and 0.560, respectively, indicating moderate responsiveness. In the EXTEND study among 71 patients, the effect size, standardized response and responsiveness statistic were 0.622, 0.487 and 0.588, respectively, showcasing moderate responsiveness for 2 responsiveness indices, and just below the 0.50 threshold for moderate responsiveness for 1 index.
The estimated MID for the WHO bleeding scale ranged from 0.33 to 0.40.31
Short Form (36) Health Survey
SF-36 is a generic health assessment questionnaire that has been used in clinical trials to study the impact of chronic disease on HRQoL. SF-36 consists of 8 domains: physical functioning, role physical, bodily pain, general health, vitality, social functioning, role emotional, and mental health. SF-36 also provides 2 component summaries: the physical component summary (SF-36 PCS) and the mental component summary (SF-36 MCS), which are created by aggregating the 8 domains. The SF-36 PCS, SF-36 MCS and 8 domains are each measured on a scale of 0 to 100, with an increase in score indicating improvement in health status. In general use of SF-36, a change of 2 to 4 points in each domain or 2 to 3 points in each component summary indicates a clinically meaningful improvement as determined by the patient.34 The summary scales are scored using norm-based methods, with regression weights and constants derived from the general US population. Both the PCS and MCS scales are transformed to have a mean of 50 and an SD of 10 in the general US population. Therefore, all scores above/below 50 are considered above/below average for the general US population.35
The validity, reliability, and responsiveness of SF-36v2 had been assessed in 2 clinical trials, RAISE and EXTEND studies, prescribing eltrombopag to patients previously treated for chronic ITP. RAISE was a 6-month, phase III, randomized, double-blind, placebo-controlled study with 197 ITP patients, whereas EXTEND was an open-label extension study containing 154 patients. In the RAISE study, SF-36v2 PCS and MCS mean scores were below but within 1 SD of the US population standardized mean, as well as the mean scores for the 7 out of 8 domains. Sufficient and acceptable internal consistency had been reported, demonstrating all SF-36 item-to-domain score correlations >0.20, and Cronbach alpha values for SF-36v2 domains ≥0.75, for all items and if each item was deleted from scale, in both RAISE and EXTEND studies. More specifically, Cronbach alpha values for SF-36v2 were between 0.75 and 0.94 at baseline and between 0.83 and 0.95 at the last assessment in RAISE, and between 0.78 and 0.94 at baseline and between 0.79 and 0.96 at the last assessment in EXTEND.
ICCs for test–retest reliability evaluation in clinically stable patients were >0.7 in both RAISE and EXTEND studies. In RAISE, this value was applicable for physical function, general health, and vitality domains (n = 50–55), and in EXTEND for all domains of SF-36, except bodily pain and emotional role (n = 126–132). Here the calculation of ICC for clinically stable patients were based on assessments from 2 consecutive pair of visits when platelet counts for each patient were considered most similar (mean of 42 days for RAISE and 39–43 days in EXTEND). However, no absolute degree of similarity had been imposed between studied pair of visits. During sensitivity analyses, ICCs were calculated using a subgroup of patients with ≤15% change in platelet counts between 2 consecutive visits (mean of 49–52 days for RAISE and 45–50 days in EXTEND). For sensitivity analysis, ICCs in clinically stable patients were ≥0.72 for all domains and summary measures of SF-36-v2, except social function and emotional role.
Construct validity of SF-36v2 was assessed by testing hypotheses about relationships with other instruments and with clinical outcomes, and was supported by moderate to strong score correlations between scores at baseline, and between the change scores of the PRO measures in both studies. While evaluating the longitudinal construct validity of measures by stratifying patients into responders or nonresponders and comparing the change score on each measure between groups based on magnitude of effect, a statistically significant difference between responders and nonresponders was observed for SF-36v2. Regarding the responsiveness, SF-36v2 had been reported to be less responsive compared to the disease-specific measures of fatigue based on the ability to capture change.32
No MID had been assessed for SF-36v2 among ITP patients.
Pharmacoeconomic Review
Abbreviations
BIA
budget impact analysis
HRQoL
health-related quality of life
ICER
incremental cost-effectiveness ratio
ICH
intracranial hemorrhage
ITP
immune thrombocytopenia
IVIG
intravenous immunoglobulin
NMA
network meta-analysis
OR
odd ratio
PDSA
Platelet Disorder Support Association
QALY
quality-adjusted life-year
TPO-RA
thrombopoietin receptor agonist
TTO
time trade-off
Executive Summary
The executive summary comprises 2 tables (Table 1 and Table 2) and a conclusion.
Item | Description |
|---|---|
Drug product | Fostamatinib (Tavalisse), oral tablet |
Submitted price | Fostamatinib: |
Indication | For the treatment of thrombocytopenia in adult patients with chronic ITP who have had an insufficient response to other treatments |
Health Canada approval status | NOC |
Health Canada review pathway | Priority review |
NOC date | November 19, 2020 |
Reimbursement request | For the treatment of thrombocytopenia in adult patients with ITP who have had an insufficient response to a TPO-RA in jurisdictions where TPO-RA reimbursement is available, or after failure of corticosteroids and other earlier-line treatments in jurisdictions where TPO-RA reimbursement is not available |
Sponsor | Medison Pharma Canada Inc. |
Submission history | Previously reviewed: No |
ITP = immune thrombocytopenia; NOC = Notice of Compliance; TPO-RA = thrombopoietin receptor agonist.
Table 2: Summary of Economic Evaluation
Component | Description |
|---|---|
Type of economic evaluation | Cost-utility analysis Markov model |
Target population | Health Canada–indicated population: adult patients with chronic ITP (> 12 months) who are either resistant or refractory to previous lines of treatment Reimbursement requested population: adult patients with chronic ITP (> 12 months) who have had an insufficient response to a TPO-RA in jurisdictions where TPO-RA reimbursement is available, or after failure of corticosteroids and other earlier-line treatments in jurisdictions where TPO-RA reimbursement is not available |
Treatment | Fostamatinib |
Comparators | Rituximab Watch and rescue |
Perspective | Canadian publicly funded health care payer |
Outcomes | QALYs, LYs |
Time horizon | Lifetime (59 years) |
Key data source | FIT1 trial, FIT2 trial, FIT 3 trial, and an NMA |
Submitted results | Health Canada–indicated population:
Reimbursement requested population:
|
Key limitations |
|
CADTH reanalysis results |
|
ICER = incremental cost-effectiveness ratio; ITP = immune thrombocytopenia; LY = life-year; NMA = network meta-analysis; QALY = quality-adjusted life-year; TPO-RA = thrombopoietin receptor agonist.
Conclusions
The CADTH clinical review found fostamatinib led to a modest improvement in platelet count response compared to placebo among patients with chronic immune thrombocytopenia (ITP). Fostamatinib was generally well tolerated compared to placebo, but its effect on clinical outcomes important to patients such as bleeding rates, symptoms, and quality of life remains unclear. The sponsor-submitted indirect treatment comparison found fostamatinib was favoured over rituximab in achieving overall platelet response, but this study had a number of limitations that affected internal and external validity. Additionally, the comparative efficacy and safety of fostamatinib to other active ITP therapies, such as thrombopoietin receptor agonists (TPO-RAs), was not explored. Given the absence of evidence, the comparative efficacy and safety of fostamatinib versus other relevant ITP treatments, and effect on clinical outcomes important to patients, remain unclear.
CADTH undertook reanalyses to address limitations with the sponsor’s submission. These reanalyses included: assuming that the extrapolation of transition probabilities is based on the number of individuals at risk; altering the rate of rescue medication usage; and revising blood platelet health state utilities. Additionally, the reanalyses corrected a number of coding and modelling errors, primarily related to the way that probabilities were translated across difference cycle lengths (e.g., weekly probabilities into 4-week cycles).
CADTH was unable to estimate an ICER for the Health Canada indication for fostamatinib, as the economic model did not reflect this indication and was missing relevant comparators (i.e., TPO-RAs, long-term steroids, and immunosuppressant drugs). For the sponsor’s reimbursement request, the CADTH base-case sequential analysis found fostamatinib was more effective and more costly than watch and rescue (incremental quality-adjusted life-years [QALYs]: 0.77, incremental cost: $164,368), and had an incremental cost-effectiveness ratio (ICER) of $212,783 per QALY. Compared to watch and rescue, rituximab was dominated (i.e., had higher costs and lower effectiveness). The probability that fostamatinib was cost-effective at a $50,000 willingness-to-pay threshold was less than 0.01%. Probabilistic results were hampered by how the sponsor propagated parameter uncertainty throughout the model. A price reduction of 60.2% for fostamatinib is needed to achieve an ICER of $50,000 per QALY in the requested reimbursement population.
The 2 main drivers of the model findings include the acquisition costs of fostamatinib, and the risk of rescue events and subsequent need for rescue therapy in both the fostamatinib and watch-and-rescue strategies. The latter risk is informed by limited data from the FIT trials, increasing the uncertainty in the economic findings.
Stakeholder Input Relevant to the Economic Review
This section is a summary of feedback received from the patient groups, registered clinicians, and drug plans that participated in the CADTH review process.
CADTH received 1 patient input submission from the Platelet Disorder Support Association (PDSA) for this review. Patient comments from 2018 to present were collected from the PDSA Facebook page and appear to include primarily international patients. Patients comments included in the submission noted increasing platelet counts while using fostamatinib, reduced steroid use, manageable side effects such as elevated blood pressure and chronic diarrhea, and a better individual response than the patients had experienced on previous therapies, which included steroids, IV immunoglobulin (IVIG), rituximab, a splenectomy, and TPO-RAs. The PDSA noted that ITP affects the overall health-related quality of life (HRQoL) of patients and their families, with a constant risk of life-threatening bleeding, elevated levels of fatigue, anxiety, depression, physical pain, sleep disturbances, and feelings of isolation and inadequacy due to activity restrictions. The PDSA also noted that patients often do not have a choice of treatment as they may not respond well to some therapies and may be unable to afford others, that fostamatinib is a daily pill that is easier to use than injections or infusions requiring travel to a clinic or hospital, and that an adequate preventive therapy might avoid expenses associated with ITP such as potential hospitalizations, life-support, treatments such as IVIG, and the long-term effects of steroid use.
One joint clinician input submission, commissioned by Accelera Canada in partnership with Advocacy Solutions, was received. Nineteen Canadian hematologists participated in the submission, which noted that the treatment paradigm for ITP is not uniform across Canada, due to differential access to therapies, and that most treatments are not approved by Health Canada but are required by public plans to access Health Canada–approved treatments. The clinician submission indicated fostamatinib should be used as a second or subsequent line of therapy after corticosteroids and before a splenectomy, immunosuppressant drugs, or rituximab, and be comparable to maintenance treatments such as TPO-RAs. Patients are expected to respond better to fostamatinib earlier in their treatment course.
Drug plan input noted that, in some jurisdictions, a patient must have previously used rituximab to access a TPO-RA; the sponsor’s reimbursement request has placed rituximab after TPO-RAs in its proposed treatment paradigm. The plans also noted that evidence for fostamatinib appears to have similar issues to those of eltrombopag, which was not recommended by the CADTH Common Drug Expert Committee due to concerns with the primary outcome of its trials, a lack of comparative evidence to other available treatments, and a lack of cost-effectiveness. Additionally, the plans expressed uncertainty about the assumed market uptake of fostamatinib in the budget impact analysis (BIA), as well as the cost of rituximab given the availability of biosimilar products.
Two of these concerns were addressed in the sponsor’s model:
Based on data from the FIT trials, differential adverse-event rates are accounted for.
HRQoL is captured in the model.
In addition, CADTH conducted scenario analyses in the BIA exploring uncertainty in the proportion of patients who would qualify for fostamatinib, the expected market uptake of fostamatinib, and the price of rituximab and blood products.
CADTH was unable to address the following concerns raised from stakeholder input:
The treatment order assumed by the sponsor, in which fostamatinib is used after TPO-RAs or in place of TPO-RAs in jurisdictions that do not fund them, rather than in an earlier line of therapy.
The lack of direct clinical evidence comparing fostamatinib to active treatments in use for chronic ITP in Canada.
As multiple comparators were missing, the cost-effectiveness of fostamatinib as a second-line therapy could not be evaluated.
Economic Review
The current review is for fostamatinib (Tavalisse) for adult patients with chronic ITP (> 12 months), who are either resistant or refractory to previous lines of treatment.
Economic Evaluation
Summary of Sponsor’s Economic Evaluation
Overview
The sponsor submitted a cost-utility analysis of fostamatinib compared to rituximab and a treatment of watch and rescue in adult patients with chronic ITP (> 12 months), who are either resistant or refractory to previous lines of treatment.1 The modelled population resembled the Canadian ITP population and matched the reimbursement request, but does not align with the Health Canada indication as several comparators were missing.2 Two subgroup analyses were conducted depending on whether a patient had received treatment with TPO-RAs. A cost-utility analysis was taken from the perspective of the Canadian publicly funded health care system.
Fostamatinib is available as 100 mg or 150 mg tablets in bottles of 60 tablets. The recommended dosage of fostamatinib is 100 mg twice daily,2 and if after 4 weeks platelet counts do not increase to at least 50,000/μL the dosage is increased to 150 mg twice daily. As treatment is continued, it should target the lowest dose of fostamatinib required to achieve a platelet count of 50,000/μL. According to clinical experts consulted by CADTH, the majority of patients receive a dosage of rituximab at 375 mg/m2 administered weekly for 4 weeks, while a minority received 100 mg administered weekly for 4 weeks. Watch and rescue consisted of monitoring patients who are not receiving therapy and administering rescue medication when platelet counts drop below unsafe thresholds, or during bleed events. Rescue medication could consist of IVIG, IV methylprednisolone, platelet transfusion, oral dexamethasone, or oral prednisolone.
The analysis assumed no administration costs for fostamatinib as it was administered orally. Administration costs for rituximab consisted of inpatient IV infusion costs. Administration costs were considered for rescue medication that was administered via infusion. The total drug acquisition costs per 28-day model cycle for fostamatinib was $5,600 for those receiving 200 mg daily and $8,400 for those receiving 300 mg daily. The total drug acquisition costs for rituximab during the first 28-day model cycle was $9,504 for those receiving doses of 375 mg/m2 and $1,188 for those receiving 100 mg. There were no drug acquisition costs for rituximab beyond the first cycle. The drug acquisition costs for rescue therapies included $4,657 for IVIG, $41 for methylprednisolone, $101 for platelet transfusion, $7 for oral dexamethasone, and $2 for oral prednisolone. The probability of receiving each specific rescue medication depended on platelet counts and the treatment received, with individuals being able to receive more than 1 drug per rescue event. Wastage was considered in the economic evaluation.
The clinical outcomes modelled included QALYs, life-years, incidence of severe disability from intracranial hemorrhage (ICH), and adverse events. The economic evaluation used a discount rate of 1.5% per year for both costs and health outcomes.
Model Structure
A cohort state transition (Markov) model was developed with health states that capture the chronic nature of treatment-resistant ITP. Most health states were defined by the surrogate outcome of platelet count, which was linked in the model to the frequency of bleeding events and the need for rescue medication. The model aims to capture the clinical benefit through an increase in platelet count, which arises from effective disease control and results in reduced morbidity and mortality. The health states of the model therefore capture a patient’s differing levels of platelet counts, as well as the long-term sequelae resulting from severe bleed events. The model has 4 mutually exclusive health states: “nonresponse” (platelet count < 30,000/µL of blood), “partial response” (platelet count between 30,000/µL and 50,000/µL of blood), “response” (platelet count > 50,000/µL of blood) and “death”; patients can transition between any of the non-dead states. All patients who enter the model are assumed to be in the nonresponse health state. The full model structure with all possible transitions is presented in Figure 1.
The model has several key assumptions. In the model, patients could have a lack of response to treatment, which is defined as having a blood platelet count of less than 30,000/µL. Patients who respond to treatment transition into either the response or partial response health states; transition probabilities are informed by the FIT clinical trials and the results of a network meta-analysis (NMA). The model captures the number of bleed events (outpatient bleeds and severe bleeds resulting in inpatient care) and rescue events within each health state to determine the differences in costs, mortality, and quality of life. The model assumes the 28-day cycle length is sufficiently short if it is less than the shortest period in which 2 bleed events could realistically occur, while still being sufficiently long to capture the length of rescue treatment. A patient can therefore only have 1 bleed event per cycle and 1 rescue event. The model assumes all patients have a platelet count–dependent risk of an ICH and patients who experience an ICH will consequently have a severe disability (a modified Rankin scale score of 4 or 5) for the remaining cycles. The model assumes all patients have a risk of death, including a risk of death from severe bleed events and non–disease-specific factors. A half-cycle correction is applied to both costs and health outcomes to account for the fact that events do not occur precisely at the beginning or the end of each cycle, and instead could occur at any point during the cycle.
Model Inputs
The model structure, clinical parameters, and model assumptions were informed by the FIT1,3 FIT2,4 and FIT35 clinical trials. The FIT1 and FIT2 trials were 24-week phase III multi-centre, randomized, double-blind placebo studies in which participants were assigned to treatment with fostamatinib or a placebo watch-and-rescue group. The fostamatinib group was given 100 mg twice a day, with the option to increase to 150 mg twice a day after 4 weeks, depending on platelet count. In this economic analysis, the sponsor used efficacy data for the placebo group of the FIT trials to inform the first 4 weeks of the watch-and-rescue strategy. As data from the FIT1 and FIT2 trials were only available for up to 24 weeks, further efficacy data from the FIT3 trial was used up to 60 months. The FIT3 trial was a phase III, multi-centre, single-arm, open-label study clinical trial examining the long-term effects of fostamatinib. Individuals enrolled who had platelet counts of at least 50,000/μL started treatment with the same dosage and regimen as the randomized studies, or 100 mg twice a day for individuals who were nonresponders in the FIT1 and FIT2 trials. As the FIT trials were conducted worldwide, the baseline patient characteristics were sourced from Canadian-specific values for generalizability to the target population. The population in the economic model was 57% female and 43% male, and patients entered the model at an average age of 41, based on the mean age of patients with ITP observed in the McMaster ITP registry (2020).6 Canadian population-level mortality estimates were inflated using disease-specific mortality hazard ratios accounting for post-stroke disability, hemorrhaging, and infection. Hazard ratios were dependent on platelet counts.
Health-related quality of life was sourced from the literature and assigned based on platelet counts and severe disability. In the reference case, the economic model also assigned a disutility for caregivers of patients who experienced severe disability after an ICH. Utility values sourced from the literature were adjusted to the baseline age of 41 years using methods outlined in Ara and Brazier.7 Utility values associated with platelet counts were sourced from Szende et al.,8 a UK study that estimated health-utility values associated with ITP using time trade-off (TTO) methods. Disutility due to disability after ICH for patients and caregivers was sourced from Dewilde et al.,9 a study in Belgium that used the EQ-5D 3-Levels questionnaire to elicit health-utility values. Health-disutility values for severe bleed events and adverse events were sourced from published literature, which used a mix of TTO, EQ-5D, and standard gamble elicitation methods.7,10-14 Health-disutility values for severe bleed events were calculated by subtracting the baseline utility for ICH from the utility post–severe bleed event. The rate of adverse events for patients receiving fostamatinib or watch and rescue were sourced from the FIT trials.15 The rate of adverse events for patients receiving rituximab was sourced from Ghanima et al.16
The model considered the following cost components: drug treatment cost, costs of rescue treatment, cost of pre-surgical prophylaxis, health-state costs based on clinical events and routine resource use, and adverse-event costs. All costs assumed a 2020 cost year with costs sourced from before 2020 inflated using the consumer price index.17 Drug acquisition costs were sourced from provincial formularies and health care databases, and calculated using Canadian dosing regimens.18,19 The cost of wastage for rituximab was incorporated, and dosing was based on the body surface area of the average member of the Canadian population. Administrative costs for rituximab were sourced from Tam et al.20 and based on the average length of infusions.21 Fostamatinib was assumed to have no administrative costs as it was administered orally. Rescue medication dosing was sourced from guidelines and the literature,22,23 while unit costs were obtained from the literature and provincial formularies.19,24,25 Administrative costs for rescue medications were considered. The rates of rescue medication in the FIT trials were used to inform usage rates in the economic analysis. Bleed-event rates were obtained from the literature and costs were sourced from schedules of benefits, administrative databases, and the literature.18,26-28 For ICH, routine resource use rates were obtained from key opinion leaders, varying both by platelet count and model cycle. Resource unit costs for hematologist consultations, blood tests, and biochemistry were sourced from national cost databases. Costs associated with severe disability due to ICH were obtained from Goeree et al.29 Other adverse-event costs were sourced from Bussel et al.15 and Ghanima et al.16
An NMA was conducted to provide an indirect treatment comparison between fostamatinib and rituximab through a common comparator of placebo (watch and rescue). The results of the NMA are summarized and presented as odds ratios (ORs). Specifically, the ORs of rituximab (375 mg/m2) versus fostamatinib, rituximab (100 mg) versus fostamatinib, and placebo versus fostamatinib are generated by the NMA. The observed transition probabilities for patients receiving fostamatinib in the FIT trials are used as the reference transitions and then the ORs from the NMA are applied to these probabilities for both rituximab and watch and rescue. Specifically, the ORs are applied to the probabilities of achieving either a partial or full platelet response, as ORs computed within the NMA are based on a definition of response of the achievement of a platelet count of at least 30,000/μL. The probability of nonresponse is calculated as 1 minus the probabilities of achieving either a partial or full platelet response. The transition matrices for both rituximab and watch and rescue, computed using the ORs provided by the NMA, are applied in the appropriate cycles in the Markov trace. The model assumes that these ORs are time-invariant and are applied in the same fashion each cycle.
Summary of Sponsor’s Economic Evaluation Results
Base-Case Results
The sponsor’s base-case analysis was run probabilistically for 5,000 iterations. Fostamatinib was found to have the highest expected cost ($1,084,675) and the highest QALY gain (14.977). Rituximab was found to be more costly and less effective than watch and rescue and was therefore dominated. Compared to watch and rescue, the ICER for fostamatinib is $149,029 per QALY gained. The probability that fostamatinib was cost-effective at a willingness-to-pay threshold of $50,000 per QALY is 1.08%.
Table 3: Summary of the Sponsor’s Economic Evaluation Results
Drug | Total costs ($) | Total QALYs | Sequential ICER ($ per QALY) |
|---|---|---|---|
Watch and rescue | 953,563 | 14.098 | Reference |
Rituximab | 961,498 | 14.089 | Dominateda |
Fostamatinib | 1,084,675 | 14.977 | 149,029 |
ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year.
aDominated refers to a treatment having a higher total cost and lower total QALYs when compared to the previous less-costly treatment.
Source: Sponsor’s pharmacoeconomic submission.1
Sensitivity and Scenario Analysis Results
Seven scenario analyses were conducted to evaluate the impact of adjusting key parameter values or assumptions. These scenarios modified the discount rates, reduced the time horizon, used inputs from the FIT trials stratified by whether patients had received TPO-RA therapy, and varied how the NMA results were implemented and the source for the rate of the bleed events. When restricting the FIT trials to patients who had not previously received TPO-RA therapy, the ICER for fostamatinib compared to watch and rescue was $133,171 per QALY gained. When restricting the FIT trials to patients who had received TPO-RA therapy, the ICER was $145,978 per QALY gained when comparing fostamatinib to watch and rescue. In all scenarios, except for varying the implementation of NMA results, rituximab was dominated by watch and rescue.
CADTH Appraisal of the Sponsor’s Economic Evaluation
CADTH identified several key limitations to the sponsor’s analysis that have notable implications on the economic analysis:
Missing comparators: Based on feedback from clinical experts consulted for this review, relevant comparators were excluded by the sponsor, specifically TPO-RAs, long-term steroids, and immunosuppressant agents. Additionally, the clinical experts consulted by CADTH did not agree that watch and rescue was an appropriate therapy at this late stage of therapy, and would instead prescribe an immunosuppressant drug the patient had not previously tried.
CADTH was unable to address this limitation in reanalyses. As such, the cost-effectiveness of fostamatinib relative to these other comparators is unknown.
Unknown cost-effectiveness for the Health Canada indication: The modelled population aligned with the reimbursement request of adult patients with ITP who had an insufficient response to a TPO-RA in jurisdictions where TPO-RA reimbursement is available, or after failure of corticosteroids and other earlier-line treatments in jurisdictions where TPO-RA reimbursement is not available. This does not reflect the Health Canada indication of adult patients with ITP who have had insufficient response to previous treatments, as later lines of therapy beyond first-line corticosteroids use vary; patients could therefore have an insufficient response to therapies other than TPO-RAs, making various treatments relevant comparators. To evaluate the full indication, additional comparators need to be included, and the cost-effectiveness of fostamatinib for the Health Canada indication is unknown.
Additionally, input received from clinicians indicated that the preferred place in therapy for fostamatinib would be as early as the second line. Should fostamatinib be reimbursed as second-line therapy, the appropriate comparators would include rituximab, TPO-RAs, immunosuppressant drugs, and a splenectomy.
CADTH was unable to address this limitation in its reanalysis.
Uncertainty when extrapolating the duration of treatment response: Due to the limited follow-up of the FIT1 and FIT2 trials for treatment response, the probability of remaining in a state with a platelet count of greater than 50,000/μL after 24 weeks in the model was estimated using data from 13 responders in the FIT3 trial. An exponential distribution was fit to the maximum follow-up time (1,661 days) as less than 50% of the 13 responders had experienced an event. This model parameter was fixed in the sponsor’s submission, and alternative distribution fits were not provided.
CADTH was able to partially address this limitation. CADTH conducted a scenario analysis using the sponsor’s exponential distribution fit to the mid-point between the minimum and maximum follow-up, which was 721 days. CADTH also conducted a scenario analysis by fitting an exponential distribution to the observed values for overall responders in FIT3 at the end of follow-up (65% of responders remained responders at 28 months). CADTH also conducted a scenario analysis by fitting an exponential distribution on the 24-month percentage of the 13 responders still responding (77% at 24 months for blood platelet counts > 30,000/μL). Given the lack of alternative parametric models, CADTH was unable to fully address the uncertainty surrounding the duration of treatment response for responders.
Uncertainty when extrapolating platelet response data: Beyond the clinical trial follow-up period (24 weeks), the probability of transitioning from a platelet count of between 30,000/μL and 50,000/μL to fewer than 30,000/μL was based on a weighted average of the transition probabilities for weeks 1 to 4, weeks 5 to 12, and weeks 13 to 24. It is unclear if this is appropriate, as the sponsor modelled a time effect and the 3 time points had unique transition probabilities. Additionally, the sponsor’s weighted average assumed that 60% of the data available to inform transition probabilities beyond week 24 was sourced from only 20 of the 102 patients in the fostamatinib arm of the FIT1 and FIT2 trials. Of those 20 patients, only 5 experienced a transition to a different blood platelet count state during that period.
To address this limitation, CADTH modified the base case by informing the transition probabilities beyond the trial follow-up period (24 weeks) using data from the transitions observed from week 1 to week 24 weighted by the number of days at risk. While this approach does not consider a time treatment effect for fostamatinib, it ensures that more patient data from the FIT trials are used to inform transition probabilities. Additionally, CADTH conducted a scenario analysis in which the transition probabilities for model cycle 6 and onward are equal to those in model cycles 4 to 5.
Utilities incorrectly sourced from a variety of methods: The sponsor’s economic model uses utility estimates from the literature that were derived from a variety of elicitation techniques. The primary utility estimate of HRQoL associated with platelet count was sourced using an unvalidated TTO method. CADTH guidelines recommend the use of an indirect method, such as the EQ-5D, healthy utility index, or Short Form Six-Dimensions Health Utility Survey, based on a generic classification system.30 The disutility due to disability after ICH, severe bleeds, and adverse events were elicited from TTO, ED-5D, and standard gamble elicitation methods. The sponsor did not attempt to crosswalk its values into a single measure. Given this limitation, the utility estimates, and consequently the QALY estimates, are likely to be imprecise and unreliable.
CADTH sourced utility estimates from a study that relied on an indirect elicitation method (EQ-5D) to estimate health utilities across a range of platelet counts among patients with ITP.31 The CADTH base case was modified to include these utilities, which were derived using a weighted average of the reported platelet counts to represent the model’s platelet count health states. The utilities used were 0.81, 0.82, and 0.815 for the health state associated with blood platelet counts of fewer than 30,000/μL, 30,000/μL to 50,000/ μL, and greater than 50,000/μL, respectively.
Inappropriate use of a constant benefit for fostamatinib compared to watch and rescue and rituximab over the lifetime model time horizon: Clinical experts consulted by CADTH indicated that the response rate for fostamatinib is unlikely to be constant over time (i.e., likely to decrease). The sponsor’s model assumes that the relative benefit of fostamatinib over watch and rescue will be the same at year 10 as it is in year 1. This assumption is likely generating a lower ICER for fostamatinib compared to watch and rescue.
CADTH explored this limitation by conducting 2 scenario analyses that limited the time horizon of the cost-effectiveness model to 5 years (the duration of the FIT3 trial) and 10 years.
Possibly overestimated rate of rescue medication use: In the sponsor’s submission, the rate of rescue medication among responders (blood platelet counts > 50,000/μL) treated with watch and rescue is 7 times higher than for those who are receiving rituximab or fostamatinib (0.603 events per model cycle compared to 0.072). This value was estimated from a small subgroup of individuals from the FIT1 and FIT2 trials. Clinicians consulted by CADTH indicated that this value was unlikely to represent typical clinical practice.
To address this limitation, CADTH modified the base-case analysis so that the rate of rescue medication is conditional on response status as opposed to response status and treatment. Additionally, CADTH created a scenario analysis in which the risk of rescue medication in the watch-and-rescue group is equal to 1.70 times the risk in the rituximab or fostamatinib treatments groups. This number represents the overall increase in the rate of rescue medication usage from those who received placebo compared to fostamatinib in the FIT1 and FIT2 trials.
Limitations associated with indirect evidence: The NMA used by the sponsor did not differentiate between levels of platelet response. Instead, an outcome of overall platelet response was used, and the sponsor’s NMA did not estimate a platelet count–specific OR. Further, the sponsor applied its pooled estimate so that the relative benefit of fostamatinib was the same for all blood platelet count states. This is likely to generate more optimistic estimates of fostamatinib as the largest treatment benefit is seen in partial platelet response, and by lumping the treatment effects of partial and full responses, the treatment effect of full response may be artificially inflated.
CADTH was unable to fully address this limitation. CADTH conducted a scenario analysis using a different analysis from the NMA (i.e., analysis 3) that generated more conservative estimates of the benefit of fostamatinib.
Failure of parameter uncertainty to accurately reflect uncertainty around the ICER: Incorporation of parameter uncertainty did not follow CADTH guidelines, as the sponsor did not source uncertainty estimates for most of the parameters. Instead, 98% of model parameters used an arbitrary standard error of 20% of the mean. This is also the case for model inputs for which the sponsor had generated standard errors, such as the OR from the NMA the sponsor conducted. Additionally, uncertainty in the remaining key model parameters were improperly implemented, which reduced uncertainty in the modelled results. For example, the uncertainty surrounding the transition probabilities is modelled using a Dirichlet distribution, with the input being the hypothetical modelled cohort (e.g., 1,000 patients) multiplied by the transition probability. As the hypothetical population increases, the uncertainty is reduced in the transition matrices. Given this uncertainty, it is unclear whether cost-effectiveness outcomes are underestimated or overestimated; however, improper incorporation of uncertainty biases the cost-effectiveness outcomes.
CADTH was unable to address this limitation in its reanalysis.
Use of surrogate outcomes: The health states in the model obtained from the FIT trials are defined by blood platelet counts, which are surrogate outcomes for survival and HRQoL. While the clinical experts consulted by CADTH indicated that these were appropriate proxies for effective disease control, this introduces additional uncertainty to the sponsor’s model in how effective disease control translates to estimates of life-years and QALYs.
CADTH was unable to address this limitation in its reanalysis.
Additionally, the following key assumptions were made by the sponsor and have been appraised by CADTH (Table 4).
Table 4: Key Assumptions of the Submitted Economic Evaluation Not Noted as Limitations to the Submission
Sponsor’s key assumption | CADTH comment |
|---|---|
The sponsor assumed proportional odds in the NMA. | This assumption is likely inappropriate. Treatment effects on platelet response were modelled in the NMA in the form of proportional (time-independent) odds ratios. However, some degree of time dependency in these treatment-specific odds ratios can be expected over the model time horizon. |
The Markov assumption was imposed in the sponsor’s decision-analytic model. | The Markov assumption is not appropriate in this economic evaluation, as under the Markov assumption there is no memory of the number of times individuals have been nonresponders. It is likely that an individual who is a nonrespondent multiple times is at a lower risk of response compared to an individual who has been a nonresponder only once. An individual-level simulation approach or implementation of tunnel states in the Markov model would have been more appropriate to account for this. |
The sponsor assumed the rate of rescue events in need of medication is time-dependent. | This assumption is likely inappropriate, as the rates of rescue events requiring medication have the potential to vary over time. As patients progress through different time points, their rates of rescue events in need of medication are likely to increase or decrease, depending on the state they are in. |
Compliance was assumed to be 100% for fostamatinib and rituximab. | This assumption is inappropriate as clinicians consulted by CADTH indicated this is an overestimate of compliance. In addition, fostamatinib compliance in the FIT1 and FIT2 trials were 93% and 99%, respectively. |
Only 1 bleed event occurs per 28-day period. | This assumption is appropriate, as clinicians consulted by CADTH indicated that, while not impossible, patients were not likely to experience many severe bleeding events during the 28-day model cycle. |
NMA = network meta-analysis.
CADTH Reanalyses of the Economic Evaluation
Base-Case Results
The CADTH base case was derived by making changes in model parameter values and assumptions, in consultation with clinical experts (Table 5).
Table 5: CADTH Revisions to the Submitted Economic Evaluation
Stepped analysis | Sponsor’s value or assumption | CADTH value or assumption | |
|---|---|---|---|
Corrections to sponsor’s base case | |||
The probability sourced from repeated events was implemented incorrectly: in the sponsors model the rate of rescue medication was assumed to be equal to the number of events divided by the total number of weeks at risk multiplied by the number of weeks in a model cycle; CADTH modified these rates to be equal to the probability of incurring an event for the duration of the model cycle | |||
Changes to derive the CADTH base case | |||
1. Rate of rescue medication | Based on platelet response status and treatment received | Based solely on platelet response status | |
2. Extrapolation of transition matrices | Weighted average of transition probabilities for cycle 1, cycles 2 and 3, and cycles 4 through 6; weights were based on the number of cycles, so 19% of patients in the fostamatinib arm of the FIT trials provided 50% of the data for projections of transition matrices | Weighted average of transition probabilities for cycle 1, cycles 2 and 3, and cycles 4 through 6; weights were based on the number of patient cycles at risk for each cycles’ transition probability matrix | |
3. Utility values by blood platelet level | Sourced from the literature using a non-validated TTO elicitation method | Sourced from the literature using EQ-5D values | |
CADTH base case | Combined revisions 1 + 2 + 3 | ||
CADTH’s base-case results are presented in Table 7 and stepped reanalysis in Table 6. Disaggregated results of the CADTH reanalysis are presented in Table 12. In CADTH’s base case, fostamatinib was associated with the highest total discounted costs ($924,745) and QALYs (15.32) over the lifetime horizon. The ICER comparing fostamatinib to watch and rescue was $212,783 per QALY. Rituximab was dominated (i.e., had higher costs and fewer QALYs) than the watch-and-rescue strategy. The probability that fostamatinib was cost-effective at a willingness-to-pay threshold of $50,000 per QALY was less than 0.01%. The percentages of QALYs generated within the 5-year trial period for FIT3 were 24.1%, 23.8%, and 24.0% for the watch-and-rescue, fostamatinib, and rituximab strategies, respectively.
Table 6: Summary of the Stepped Analysis of the CADTH Reanalysis Results
Analysis element | Drug | Total costs ($) | Total QALYs | Sequential ICER |
|---|---|---|---|---|
Sponsors base case | Watch and rescue | 953,563 | 14.098 | Reference |
Fostamatinib | 1,084,675 | 14.977 | 149,029 | |
Rituximab | 961,498 | 14.089 | Dominateda | |
Sponsors corrected base case | Watch and rescue | 855,397 | 14.33 | Reference |
Fostamatinib | 996,186 | 15.19 | 164,305 | |
Rituximab | 863,532 | 14.32 | Dominateda | |
1. Rate of rescue medication | Watch and rescue | 761,915 | 14.19 | Reference |
Fostamatinib | 927,824 | 15.02 | 200,837 | |
Rituximab | 771,384 | 14.18 | Dominateda | |
2. Extrapolation of transition matrices | Watch and rescue | 854,865 | 14.28 | Reference |
Fostamatinib | 993,910 | 15.14 | 161,728 | |
Rituximab | 863,009 | 14.28 | Dominateda | |
3. Utility values by blood platelet level | Watch and rescue | 854,126 | 14.68 | Reference |
Fostamatinib | 994,482 | 15.48 | 174,559 | |
Rituximab | 862,283 | 14.67 | Dominateda | |
CADTH base case 1 + 2 + 3 | Watch and rescue | 760,376 | 14.55 | Reference |
Fostamatinib | 924,745 | 15.32 | 212,783 | |
Rituximab | 769,885 | 14.54 | Dominateda |
ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year.
aDominated indicates that a treatment is more costly and less effective (fewer QALYs) than the reference.
Table 7: Summary of the CADTH Reanalysis Results
Drug | Total costs ($) | Total QALYs | ICER vs. watch and rescue ($ per QALY) | Sequential ICER |
|---|---|---|---|---|
Sponsor-corrected base case | ||||
Watch and rescue | 855,397 | 14.33 | Reference | Reference |
Fostamatinib | 996,186 | 15.19 | 164,305 | 164,305 |
Rituximab | 863,532 | 14.32 | Dominateda | Dominateda |
CADTH base case | ||||
Watch and rescue | 760,376 | 14.55 | Reference | Reference |
Fostamatinib | 924,745 | 15.32 | 212,783 | 212,783 |
Rituximab | 769,885 | 14.54 | Dominateda | Dominateda |
ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-years; vs. = versus.
aDominated refers to a treatment having a higher total cost and fewer total QALYs when compared to the previous less-costly treatment.
Scenario Analysis Results
CADTH conducted price-reduction analyses using the corrected sponsor’s base case and CADTH base case (Table 8). The price-reduction scenarios varied the price of fostamatinib. A price reduction of 42% was required to achieve an ICER of $50,000 per QALY for the sponsor’s base case. A price reduction of 60.2% was required to achieve an ICER of $50,000 per QALY for the CADTH base case.
Table 8: CADTH Price-Reduction Analyses
Percentage costs | ICERs for fostamatinib vs. | |
|---|---|---|
Price reduction | Sponsor base case | CADTH reanalysis |
No price reduction | 149,029 | 212,783 |
10% | 125,285 | 185,712 |
20% | 101,410 | 158,640 |
30% | 77,535 | 131,569 |
40% | 53,659 | 104,498 |
50% | 29,784 | 77,426 |
60% | 5,909 | 50,355 |
70% | Watch and rescue dominated | 23,283 |
ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year.
Additionally, CADTH conducted scenario analyses varying how transition probabilities were projected beyond the trial follow-up period, the NMA analysis used, the duration of response, and how the risk of rescue medication was implemented. The largest impact on cost-effectiveness estimates was made by the rate of rescue events. Detailed results of the scenario analyses are provided in Table 13. Two exploratory scenarios were conducted by modifying the CADTH base case so that the transition probabilities for fostamatinib were informed from the patients in the FIT1 and FIT2 trials depending on whether an individual had previously received TPO-RA therapy. These exploratory scenarios were limited by the sample size of the FIT1 and FIT2 trials, the assumptions made for transition probabilities when no transitions were observed, and the fact that the NMA’s resulting OR used to model effectiveness was not stratified by whether TPO-RA therapy was previously received.
Overall Conclusions
The CADTH clinical review found fostamatinib led to a modest improvement in platelet count response compared to placebo among patients with chronic ITP. Fostamatinib was generally well tolerated compared to placebo, but its effect on clinical outcomes important to patients, such as bleeding rates, symptoms, and quality of life, remains unclear. The sponsor-submitted indirect treatment comparison found fostamatinib was favoured over rituximab in achieving overall platelet response, but this study had a number of limitations that affected internal and external validity. Additionally, the comparative efficacy and safety of fostamatinib to other active ITP therapies, such as TPO-RAs, was not explored. Given the absence of evidence, the comparative efficacy and safety of fostamatinib versus other relevant ITP treatments, and effect on patient-important clinical outcomes, remain unclear.
CADTH undertook reanalyses to address limitations with the sponsor’s submission. These reanalyses included assuming that the extrapolation of transition probabilities is based on the number of individuals at risk; altering the rate of rescue medication usage; and revising blood platelet health-state utilities. Additionally, the reanalyses corrected a number of coding and modelling errors, primarily related to the way that probabilities were translated across difference cycle lengths (e.g., weekly probabilities into 4-week cycles).
CADTH was unable to estimate an ICER for the Health Canada indication of fostamatinib, as the economic model did not reflect this indication and was missing relevant comparators (i.e., TPO-RAs, long-term steroids, and immunosuppressant drugs). For the sponsor’s reimbursement request, the CADTH base-case sequential analysis found fostamatinib was more effective and more costly than watch and rescue (incremental QALYs: 0.77; incremental cost: $164,368) and had an ICER of $212,783 per QALY. Compared to watch and rescue, rituximab was dominated (i.e., had higher costs and lower effectiveness). The probability that fostamatinib was cost-effective at a $50,000 willingness-to-pay threshold was less than 0.01%. Probabilistic results were hampered by how the sponsor propagated parameter uncertainty throughout the model. A price reduction of 60.2% for fostamatinib is needed to achieve an ICER of $50,000 per QALY in the requested reimbursement population.
The 2 main drivers of the model findings include the acquisition costs of fostamatinib, and the risk of rescue events and subsequent need for rescue therapy in both the fostamatinib and watch-and-rescue strategies. The latter risk is informed by limited data from the FIT trials, increasing the uncertainty in the economic findings.
References
1.Pharmacoeconomic evaluation [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Tavalisse (fostamatinib), 100 mg and 150 mg tablet, oral. Toronto (ON): Medison Pharma Canada Inc.; 2021 Jul 22.
2.Tavalisse (fostamatinib): 100 mg and 150 mg tablet (as as fostamatinib disodium hexahydrate), oral [product monograph]. Toronto (ON): Medison Pharma Canada Inc.; 2020 Nov 17.
3.Rigel Pharmaceuticals. NCT02076412: A efficacy and safety study of fostamatinib in the treatment of persistent/chronic immune thrombocytopenic purpura (ITP) (FIT). ClinicalTrials.gov. Bethesda (MD): U.S. National Library of Medicine; 2019: https://clinicaltrials.gov/ct2/show/results/NCT02076412. Accessed 2021 Oct 12.
4.Rigel Pharmaceuticals. NCT02076399: A efficacy and safety study of R935788 in the treatment of persistent/chronic immune thrombocytopenic purpura (ITP) (FIT2). ClinicalTrials.gov. Bethesda (MD): U.S. National Library of Medicine; 2019: https://clinicaltrials.gov/ct2/show/NCT02076399. Accessed 2021 Oct 12.
5.Bussel JB, Arnold DM, Boxer MA, et al. Long-term fostamatinib treatment of adults with immune thrombocytopenia during the phase 3 clinical trial program. Am J Hematol. 2019;94(5):546-553. PubMed
6.Nazaryan H, Liu Y, Sirotich E, Duncan J, Nazy I, Arnold D. Second-Line Therapy for Immune Thrombocytopenia: Real-World Experience in Canada. Can J Gen Intern. 2020;14:28-35.
7.Ara R, Brazier JE. Populating an economic model with health state utility values: moving toward better practice. Value Health. 2010;13(5):509-518. PubMed
8.Szende A, Brazier J, Schaefer C, Deuson R, Isitt JJ, Vyas P. Measurement of utility values in the UK for health states related to immune thrombocytopenic purpura. Curr Med Res Opin. 2010;26(8):1893-1903. PubMed
9.Dewilde S, Annemans L, Lloyd A, et al. The combined impact of dependency on caregivers, disability, and coping strategy on quality of life after ischemic stroke. Health Qual Life Outcomes. 2019;17(1):31. PubMed
10.Iskedjian M, Tinmouth AT, Arnold DM, Deuson R, Isitt JJ, Mikhael J. Elicitation of utility scores in Canada for immune thrombocytopenia treated with romiplostim or watch and rescue. J Med Econ. 2012;15(2):313-331. PubMed
11.Sullivan PW, Valuck R, Saseen J, MacFall HM. A comparison of the direct costs and cost effectiveness of serotonin reuptake inhibitors and associated adverse drug reactions. CNS Drugs. 2004;18(13):911-932. PubMed
12.Zhang L, Guo X, Zhang J, et al. Health-related quality of life among adults with and without hypertension: A population-based survey using EQ-5D in Shandong, China. Sci Rep. 2017;7(1):14960. PubMed
13.Beusterien KM, Davies J, Leach M, et al. Population preference values for treatment outcomes in chronic lymphocytic leukaemia: a cross-sectional utility study. Health Qual Life Outcomes. 2010;8:50. PubMed
14.Xu R, Insinga RP, Golden W, Hu XH. EuroQol (EQ-5D) health utility scores for patients with migraine. Qual Life Res. 2011;20(4):601-608. PubMed
15.Bussel J, Arnold DM, Grossbard E, et al. Fostamatinib for the treatment of adult persistent and chronic immune thrombocytopenia: Results of two phase 3, randomized, placebo-controlled trials. Am J Hematol. 2018;93(7):921-930. PubMed
16.Ghanima W, Khelif A, Waage A, et al. Rituximab as second-line treatment for adult immune thrombocytopenia (the RITP trial): a multicentre, randomised, double-blind, placebo-controlled trial. Lancet. 2015;385(9978):1653-1661. PubMed
17.Table 18-10-0005-01. Consumer Price Index, annual average, not seasonally adjusted. Ottawa (ON): Statistics Canada; 2021: https://www150.statcan.gc.ca/t1/tbl1/en/tv.action?pid=1810000501. Accessed 2021 Oct 12.
18.Ontario Case Costing Initiative (OCCI). Toronto (ON): Ontario Health and Long-Term Care; 2017: https://data.ontario.ca/dataset/ontario-case-costing-initiative-occi. Accessed 2021 Oct 12.
19.Ontario Ministry of Health, Ontario Ministry of Long-Term Care. Ontario drug benefit formulary/comparative drug index. 2021; https://www.formulary.health.gov.on.ca/formulary/. Accessed 2021 Oct 12.
20.Tam VC, Ko YJ, Mittmann N, et al. Cost-effectiveness of systemic therapies for metastatic pancreatic cancer. Curr Oncol. 2013;20(2):e90-e106. PubMed
21.Versus Arthritis. What is rituximab and how is it used? 2021; https://www.versusarthritis.org/about-arthritis/treatments/drugs/rituximab/. Accessed 2021 Oct 12.
22.Almizraq RJ, Branch, D.R. Efficacy and mechanism of intravenous immunoglobulin treatment for immune thrombocytopenia in adults. Ann Blood. 2021;6.
23.McCrae K. Immune thrombocytopenia: no longer 'idiopathic'. Cleve Clin J Med. 2011;78(6):358-373. PubMed
24.Hill-Strathy M, Pinkerton PH, Thompson TA, et al. Evaluating the appropriateness of platelet transfusions compared with evidence-based platelet guidelines: An audit of platelet transfusions at 57 hospitals. Transfusion. 2021;61(1):57-71. PubMed
25.Blackhouse G, Gaebel K, Xie F, et al. Cost-utility of Intravenous Immunoglobulin (IVIG) compared with corticosteroids for the treatment of Chronic Inflammatory Demyelinating Polyneuropathy (CIDP) in Canada. Cost Eff Resour Alloc. 2010;8:14. PubMed
26.Gernsheimer TB, George JN, Aledort LM, et al. Evaluation of bleeding and thrombotic events during long-term use of romiplostim in patients with chronic immune thrombocytopenia (ITP). J Thromb Haemost. 2010;8(6):1372-1382. PubMed
27.Allen R, Bryden P, Grotzinger KM, Stapelkamp C, Woods B. Cost-Effectiveness of Eltrombopag versus Romiplostim for the Treatment of Chronic Immune Thrombocytopenia in England and Wales. Value Health. 2016;19(5):614-622. PubMed
28.Singh SM, Micieli A, Wijeysundera HC. Economic evaluation of percutaneous left atrial appendage occlusion, dabigatran, and warfarin for stroke prevention in patients with nonvalvular atrial fibrillation. Circulation. 2013;127(24):2414-2423. PubMed
29.Goeree R, Blackhouse, G., Petrovic, R., Salama, S. Cost of stroke in Canada: a 1-year prospective study. J Med Econ. 2005;8:147-167.
30.Guidelines for the economic evaluation of health technologies: Canada. 4th ed. Ottawa (ON): CADTH; 2017: https://www.cadth.ca/dv/guidelines-economic-evaluation-health-technologies-canada-4th-edition. Accessed 2021 Oct 12.
31.Snyder CF, Mathias SD, Cella D, Isitt JJ, Wu AW, Young J. Health-related quality of life of immune thrombocytopenic purpura patients: results from a web-based survey. Curr Med Res Opin. 2008;24(10):2767-2776. PubMed
32.Exceptional Access Program (EAP). Toronto (ON): Ontario Ministry of Health; Ontario Ministry of Long-Term Care; 2021: https://www.health.gov.on.ca/en/pro/programs/drugs/odbf/odbf_except_access.aspx. Accessed 2021 Oct 12.
33.DeltaPA. Ottawa (ON): IQVIA; 2021: https://www.iqvia.com/. Accessed 2021 Oct 12.
34.Provan D, Arnold DM, Bussel JB, et al. Updated international consensus report on the investigation and management of primary immune thrombocytopenia. Blood Adv. 2019;3(22):3780-3817. PubMed
35.Table: 17-10-0005-01 Population estimates on July 1st, by age and sex. Ottawa (ON): Statistics Canada; 2021: https://www150.statcan.gc.ca/t1/tbl1/en/tv.action?pid=1710000501. Accessed 2021 Oct 4.
36.Feudjo-Tepie MA, Robinson NJ, Bennett D. Prevalence of diagnosed chronic immune thrombocytopenic purpura in the US: analysis of a large US claim database: a rebuttal. J Thromb Haemost. 2008;6(4):711-712; author reply 713. PubMed
37.Budget Impact Analysis [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Tavalisse (fostamatinib), 100 mg and 150 mg tablet, oral. Toronto (ON): Medison Pharma Canada Inc.; 2021 Jul 22.
38.Ghanima W, Cooper N, Rodeghiero F, Godeau B, Bussel JB. Thrombopoietin receptor agonists: ten years later. Haematologica. 2019;104(6):1112-1123. PubMed
39.Patel VL, Mahevas M, Lee SY, et al. Outcomes 5 years after response to rituximab therapy in children and adults with immune thrombocytopenia. Blood. 2012;119(25):5989-5995. PubMed
40.Common technical document 2.7.4 summary of clinical safety: Tavalisse [internal sponsor's report]. Rigel Pharmaceuticals Inc.; 2019 Aug.
41.Arnold D, Clare R, Salib M, et al. The McMaster ITP registry: assessing the prevalence, clinical and laboratory features of immune thrombocytopenia [conference paper]. 56th Annual Meeting of the American Society of Hematology Conference; 2014; San Francisco (CA).
42.Saskatchewan Drug Plan: search formulary. 2021; https://formulary.drugplan.ehealthsask.ca/SearchFormulary. Accessed 2021 Oct 12.
43.BloodBrief: an update on IVIG and SCIG. Ottawa (ON): Canadian Blood Services; 2017: https://www.blood.ca/sites/default/files/BloodBrief-IVIG-SCIG-Overview-Aug-2017.pdf. Accessed 2021 Oct 17.
44.Bank of Canada. Inflation calculator. 2021; https://www.bankofcanada.ca/rates/related/inflation-calculator/. Accessed 2021 Oct 12.
Appendix 1: Cost-Comparison Table
Note that this appendix has not been copy-edited.
The comparators presented in the following table have been deemed to be appropriate based on feedback from clinical expert(s). Comparators may be recommended (appropriate) practice or actual practice. Existing Product Listing Agreements are not reflected in the table and as such, the table may not represent the actual costs to public drug plans.
Table 9: CADTH Cost-Comparison Table for Treatment-Resistant Chronic ITP
Treatment | Strength / concentration | Form | Price | Recommended dosage | Daily cost ($) | Course or annual cost ($) |
|---|---|---|---|---|---|---|
Fostamatinib (Tavalisse) | 100 mg 150 mg | Tablet | 80.8700a 121.3050a | Initially 100 mg twice daily. After 4 weeks, increase to 150 mg twice daily if platelet count has not reached at least 50 × 109/L | 161.74 to 242.61 | 59,035 to 88,553 |
TPO-RAs | ||||||
Eltrombopag (Revolade) | 25 mg 50 mg | Tablet | 65.0000b 130.0000b | Initially 50 mg once daily (25 mg in Asian patients). After 2 weeks, increase dose by 25 mg if platelet count < 50 × 109/L, up to a maximum of 75 mg daily. Reduce dose when platelet count is above 200 × 109/L | 65.00 to 195.00 | 23,725 to 71,175c |
Romiplostim (Nplate) | 250 mcg/0.5 mL 500 mcg/1 mL | Vial of lyophilized powder for solution | 1,021.7900b 2,043.6000b | 1 mcg/kg SC weekly, adjusting by increments of 1 mcg/kg until platelet count ≥ 50 × 109/L; do not exceed 10 mcg/kg | 145.97 initially, up to 437.91 | 53,279 initially, up to 159,837 |
CD20 Inhibitor (off-label) | ||||||
Rituximab (Rituxan, Truxima, Riximyo, Ruxience) | 10 mg/mL | 10 mL 50 mL Single use vials | 297.0000 1,485.0000 | 375 mg/m2 IV once per week for 4 weeksd | NA | Cost per 4-week course: 8,316 |
100 mg IV once per week for 4 weeksd | NA | Cost per 4-week course: 1,188 | ||||
Immunosuppressants (off-label) | ||||||
Azathioprine (generic) | 50 mg | Tablet | 0.2405 | 1 to 2 mg/kg daily, maximum 150 mg/dayd | 0.48 to 0.72 | 176 to 263 |
Cyclosporin A (Neoral, generic) | 10 mg 25 mg 50 mg 100 mg | Tablet | 0.6700 0.9952 1.9400 3.8815 | 5 mg/kg/day for 6 days, then 2.5 to 3 mg/kg/dayd | Initial: 15.53 Then: 7.76 to 9.70 | 2,881 to 3,577 |
100 mg/mL | Oral solution | 5.4030 | Initial: 21.61 Then: 10.81 to 12.97 | 4,009 to 4,785 | ||
Cyclophosphamide (Procytox) | 25 mg 50 mg | Tablet | 0.3545 0.4773 | 1 to 2 mg/kg daily for at least 16 weeksd | 0.83 to 1.43 | 304 to 523 |
200 mg 500 mg 1,000 mg 2,000 mg | Vial for injection 20mg/mL | 74.23e 93.14e 168.8300e 310.6000e | 0.3 to 1 g/m2 IV every 2 to 4 weeks for one to 3 dosesd | NA | Per course: 167 to 932 | |
Danazol (Cyclomen) | 50 mg 100 mg 200 mg | Capsule | 1.0212 1.5156 2.4220 | 200 mg 2 to 4 times dailyd | 4.84 to 9.69 | 1,768 to 3,536 |
Dapsone (generic) | 100 mg | Tablet | 0.7031 | 100 mg per dayd | 0.70 | 257 |
Myco-phenolate mofetil (generic) | 250 mg 500 mg | Capsule | 0.3712 0.7423 | 1.5 to 2 g/day for at least 12 weeksd | 2.23 to 2.97 | 813 to 1,084 |
Vincristine (generic) | 1 mg/mL | Solution for injection | 30.6000 | 6 mg total at 1 to 2 mg per weekly infusiond | NA | Per course: 184 |
Vinblastine (generic) | 10 mg/ 10 mL | Solution for injection | 185.6300e | 30 mg total at 10 mg per weekly infusiond | NA | Per course: 557 |
IV = IV; SC = subcutaneous; TPO-RA = thrombopoietin receptor agonist.
Note: Costs do not include administration, markup, or dispensing fees, but do include wastage where applicable. Patients are assumed to have a body weight of 80 kg and a body surface area of 1.8m2. Prices are from the Ontario Drug Benefit Formulary (Accessed August 2021) unless otherwise indicated.19
aSponsor’s submitted price.1
bOntario Drug Benefit Exceptional Access Program price (accessed August 2021),32) and wholesale price from IQVIA Delta PA (accessed August 2021).33
cMaximum annual cost would only be reached if patients never reach a platelet count over 200 × 109/L.
dOff-label use, dosing from the 2019 Updated international consensus on investigation and management of primary immune thrombocytopenia, including supplemental information.34
eIQVIA Delta PA wholesale pricing (Accessed August 2021).33
Appendix 2: Submission Quality
Note that this appendix has not been copy-edited.
Description | Yes/No | Comments |
|---|---|---|
Population is relevant, with no critical intervention missing, and no relevant outcome missing | No | The sponsor’s submission does not reflect the Health Canada indication and is missing comparators deemed relevant by clinicians consulted by CADTH. |
Model has been adequately programmed and has sufficient face validity | Yes | No comment. |
Model structure is adequate for decision problem | Yes | No comment. |
Data incorporation into the model has been done adequately (e.g., parameters for probabilistic analysis) | Yes | No comment. |
Parameter and structural uncertainty were adequately assessed; analyses were adequate to inform the decision problem | No | Parameter uncertainty was arbitrarily assigned for the majority of model inputs to 20% of the estimate’s value. For key model inputs, parameter uncertainty was incorrectly modelled. In particular, it was not modelled as a function of the sample underlying the model parameter but of the size of the hypothetical population. |
The submission was well organized and complete; the information was easy to locate (clear and transparent reporting; technical documentation available in enough details) | No | The submission is missing sections. Section 1.4 Review of economic evidence only contains a copy of the corresponding section from the CADTH Guidelines but no content. |
Appendix 3: Additional Information on the Submitted Economic Evaluation
Note that this appendix has not been copy-edited.
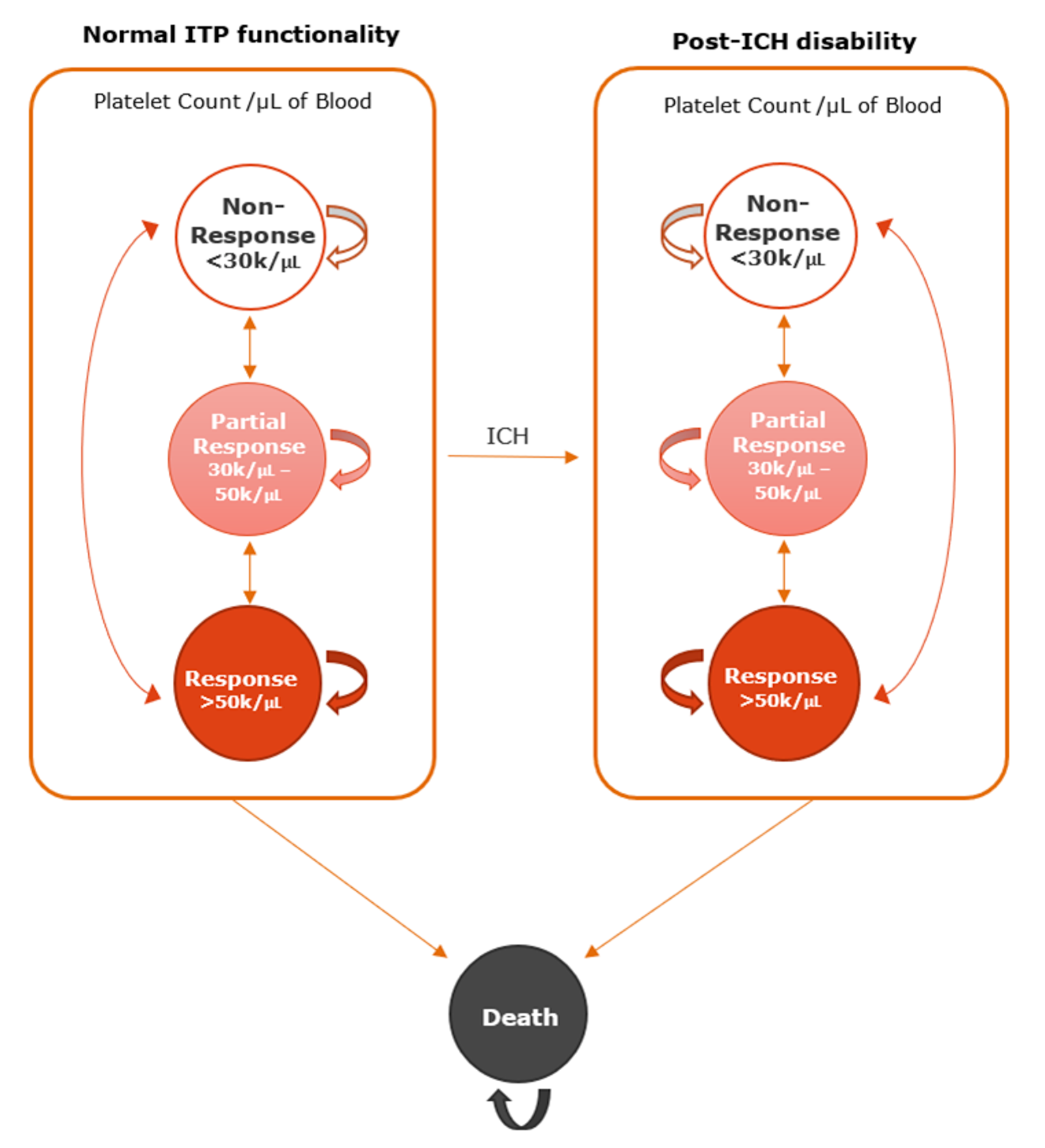
Detailed Results of the Sponsor’s Base Case
Table 11: Disaggregated Results from the Sponsor’s Base Case
Treatment | Component | Value | Incremental (vs. reference) |
|---|---|---|---|
Discounted LYs | |||
Watch and rescue | Nonresponse < 30,000/µL | 15.78 | Ref. |
Partial response 30,000/µL to 50,000/µL | 2.98 | Ref. | |
Response > 50,000/µL | 1.49 | Ref. | |
Severe disability post-ICH < 30,000/µL | 2.58 | Ref. | |
Severe disability post-ICH > 50,000/µL | 0.16 | Ref. | |
Severe disability post-ICH 30,000/µ to 50,000/µL | 0.19 | Ref. | |
Total | 23.17 | Ref. | |
Rituximab | Nonresponse < 30,000/µL | 15.81 | 0.03 |
Partial response 30,000/µL to 50,000/µL | 2.95 | −0.03 | |
Response > 50,000/µL | 1.49 | −0.01 | |
Severe disability post-ICH < 30,000/µL | 2.58 | 0.00 | |
Severe disability post-ICH > 50,000/µL | 0.16 | 0.00 | |
Severe disability post-ICH 30,000/µL to 50,000/µL | 0.19 | 0.00 | |
Total | 23.17 | 0.00 | |
Fostamatinib | Nonresponse < 30,000/µL | 14.56 | −1.22 |
Partial response 30,000/µL to 50,000/µL | 2.83 | −0.15 | |
Response > 50,000/µL | 3.51 | 2.01 | |
Severe disability post-ICH < 30,000/µL | 2.29 | −0.29 | |
Severe disability post-ICH > 50,000/µL | 0.15 | −0.01 | |
Severe disability post-ICH 30,000/µL to 50,000/µL | 0.17 | −0.02 | |
Total | 23.49 | 0.32 | |
Discounted QALYs | |||
Watch and rescue | Nonresponse < 30,000/µL | 10.78 | Ref. |
Partial response 30,000/µL to 50,000/µL | 2.25 | Ref. | |
Response > 50,000/µL | 1.21 | Ref. | |
Severe disability post-ICH < 30,000/µL | 0.15 | Ref. | |
Severe disability post-ICH > 50,000/µL | 0.02 | Ref. | |
Severe disability post-ICH 30,000/µL to 50,000/µL | 0.02 | Ref. | |
Total | 14.43 | Ref. | |
Rituximab | Nonresponse < 30,000/µL | 10.80 | 0.02 |
Partial response 30,000/µL to 50,000/µL | 2.23 | −0.03 | |
Response > 50,000/µL | 1.20 | −0.01 | |
Severe disability post-ICH < 30,000/µL | 0.15 | 0.00 | |
Severe disability post-ICH > 50,000/µL | 0.02 | 0.00 | |
Severe disability post-ICH 30,000/µL to 50,000/µL | 0.02 | 0.00 | |
Total | 14.42 | −0.01 | |
Fostamatinib | Nonresponse < 30,000/µL | 9.88 | −0.89 |
Partial response 30,000/µL to 50,000/µL | 2.14 | −0.12 | |
Response > 50,000/µL | 2.89 | 1.68 | |
Severe disability post-ICH < 30,000/µL | 0.13 | −0.02 | |
Severe disability post-ICH > 50,000/µL | 0.02 | 0.00 | |
Severe disability post-ICH 30,000/µL to 50,000/µL | 0.02 | 0.00 | |
Total | 15.08 | 0.65 | |
Discounted costs ($) | |||
Watch and rescue | Adverse-event costs | 510 | Ref. |
Cost of pre-surgical prophylaxis | 32,743 | Ref. | |
Cost of rescue treatment | 672,589 | Ref. | |
Health-state cost | 146,971 | Ref. | |
Treatment cost | 0 | Ref. | |
Total costs | 852,814 | Ref. | |
Rituximab | Adverse-event costs | 509 | −1 |
Cost of pre-surgical prophylaxis | 32,774 | 31 | |
Cost of rescue treatment | 671,664 | -−926 | |
Health-state cost | 147,196 | 224 | |
Treatment cost | 8,197 | 8,197 | |
Total costs | 860,340 | 7,526 | |
Fostamatinib | Adverse-event costs | 647 | 137 |
Cost of pre-surgical prophylaxis | 31,149 | −1,594 | |
Cost of rescue treatment | 630,708 | −41,881 | |
Health-state cost | 136,107 | −10,865 | |
Treatment cost | 173,876 | 173,876 | |
Total costs | 972,487 | 119,673 | |
ICER vs. reference ($) | |||
Watch and rescue | Ref. | ||
Rituximab | Dominateda | ||
Fostamatinib | 149,029 | ||
ICER = incremental cost-effectiveness Ratio; QALY = quality-adjusted life-year, LY = life-year; Ref. = reference.
aDominated indicates that a treatment is more costly and less effective (lower QALYs) than the reference.
Appendix 4: Additional Details on the CADTH Reanalyses and Sensitivity Analyses of the Economic Evaluation
Note that this appendix has not been copy-edited.
Table 12: Disaggregated Summary of CADTH’s Economic Evaluation Results
Treatment | Component | Value | Incremental (vs. reference) |
|---|---|---|---|
Discounted LYs | |||
Watch and rescue | Nonresponse < 30,000/µL | 15.68 | Ref. |
Partial response 30,000/µL to 50,000/µL | 3.85 | Ref. | |
Response > 50,000/µL | 0.64 | Ref. | |
Severe disability post-ICH < 30,000/µL | 2.68 | Ref. | |
Severe disability post-ICH > 50,000/µL | 0.06 | Ref. | |
Severe disability post-ICH 30,000/µL to 50,000/µL | 0.16 | Ref. | |
Total | 23.07 | Ref. | |
Rituximab | Nonresponse < 30,000/µL | 15.72 | 0.04 |
Partial response 30,000/µL to 50,000/µL | 3.80 | −0.05 | |
Response > 50,000/µL | 0.64 | 0.00 | |
Severe disability post-ICH < 30,000/µL | 2.69 | 0.00 | |
Severe disability post-ICH > 50,000/µL | 0.06 | 0.00 | |
Severe disability post-ICH 30,000/µL to 50,000/µL | 0.16 | 0.00 | |
Total | 23.07 | 0.00 | |
Fostamatinib | Nonresponse < 30,000/µL | 14.09 | −1.60 |
Partial response 30,000/µL to 50,000/µL | 3.60 | −0.25 | |
Response > 50,000/µL | 3.33 | 2.70 | |
Severe disability post-ICH < 30,000/µL | 2.29 | −0.39 | |
Severe disability post-ICH > 50,000/µL | 0.06 | 0.00 | |
Severe disability post-ICH 30,000/µL to 50,000/µL | 0.14 | −0.02 | |
Total | 23.51 | 0.44 | |
Discounted QALYs | |||
Watch and rescue | Nonresponse < 30,000/µL | 10.80 | Ref. |
Partial response 30,000/µL to 50,000/µL | 2.97 | Ref. | |
Response > 50,000/µL | 0.50 | Ref. | |
Severe disability post-ICH < 30,000/µL | 0.24 | Ref. | |
Severe disability post-ICH > 50,000/µL | 0.01 | Ref. | |
Severe disability post-ICH 30,000/µL to 50,000/µL | 0.03 | Ref. | |
Total | 14.55 | Ref. | |
Rituximab | Nonresponse < 30,000/µL | 10.83 | 0.03 |
Partial response 30,000/µL to 50,000/µL | 2.93 | −0.04 | |
Response > 50,000/µL | 0.51 | 0.00 | |
Severe disability post-ICH < 30,000/µL | 0.24 | 0.00 | |
Severe disability post-ICH > 50,000/µL | 0.01 | 0.00 | |
Severe disability post-ICH 30,000/µL to 50,000/µL | 0.03 | 0.00 | |
Total | 14.54 | −0.01 | |
Fostamatinib | Nonresponse < 30,000/µL | 9.63 | −1.17 |
Partial response 30,000/µL to 50,000/µL | 2.76 | −0.20 | |
Response > 50,000/µL | 2.69 | 2.19 | |
Severe disability post-ICH < 30,000/µL | 0.20 | −0.04 | |
Severe disability post-ICH > 50,000/µL | 0.01 | 0.00 | |
Severe disability post-ICH 30,000/µL to 50,000/µL | 0.02 | 0.00 | |
Total | 15.32 | 0.77 | |
Discounted costs ($) | |||
Watch and rescue | Adverse-event costs | 506 | Ref. |
Cost of pre-surgical prophylaxis | 32,701 | Ref. | |
Cost of rescue treatment | 579,010 | Ref. | |
Health-state cost | 148,160 | Ref. | |
Treatment cost | 0 | Ref. | |
Total Costs | 760,376 | Ref. | |
Rituximab | Adverse-event costs | 505 | −1 |
Cost of pre-surgical prophylaxis | 32,739 | 38 | |
Cost of rescue treatment | 579,690 | 679 | |
Health-state cost | 148,406 | 246 | |
Treatment cost | 8,546 | 8,546 | |
Total Costs | 769,885 | 9,509 | |
Fostamatinib | Adverse-event costs | 684 | 178 |
Cost of pre-surgical prophylaxis | 30,541 | −2,160 | |
Cost of rescue treatment | 551,206 | −27,804 | |
Health-state cost | 133,895 | −14,265 | |
Treatment cost | 208,419 | 208,419 | |
Total costs | 924,745 | 164,369 | |
ICER vs. reference ($ per QALY) | |||
Watch and rescue | Ref. | ||
Rituximab | Dominateda | ||
Fostamatinib | 212,783 | ||
ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year; LY = life-year; Ref. = reference.
aDominated indicates that a treatment is more costly and less effective (lower QALYs) than the reference.
Scenario Analyses
Table 13: Summary of Scenario Analyses Results
Study details | Drug | Total costs ($) | Total QALYs | Sequential ICER ($/QALY) |
|---|---|---|---|---|
CADTH base case | Watch and rescue | 760,376 | 14.55 | Ref. |
Fostamatinib | 924,745 | 15.32 | 212,783 | |
Rituximab | 769,885 | 14.54 | Dominateda | |
Scenario 1: Transition probabilities for cycles 6+ equal to those of cycles 4 to 5. | Watch and rescue | 818,114 | 13.86 | Ref. |
Fostamatinib | 971,713 | 14.67 | 191,008 | |
Rituximab | 827,110 | 13.86 | Dominateda | |
Scenario 2: Risk of rescue medication in the watch-and-rescue group is equal to 1.70x the risk in the rituximab or fostamatinib treatments groups. | Watch and rescue | 1,085,961.0 | 14.691 | Ref. |
Fostamatinib | 1,198,902.6 | 15.494 | $140,559 | |
Rituximab | 1,092,428.2 | 14.682 | Dominateda | |
Scenario 3: Using results from NMA analysis 3 | Watch and rescue | 758,125 | 14.54 | Ref. |
Fostamatinib | 924,226 | 15.32 | 214,975 | |
Rituximab | 767,665 | 14.53 | Dominateda | |
Scenario 4: Duration of treatment response equal to the mid-point of minimum and max follow-up observed in FIT 3 trial | Watch and rescue | 760,482 | 14.54 | Ref. |
Fostamatinib | 879,016 | 15.07 | 224,845 | |
Rituximab | 769,993 | 14.53 | Dominateda | |
Scenario 5: Duration of treatment fit to the observed values for overall responders in FIT 3 at the end of follow-up (65% of responders remaining responders at 28 months). | Watch and rescue | 759,358 | 14.54 | Ref. |
Fostamatinib | 895,863 | 15.15 | 221,427 | |
Rituximab | 768,898 | 14.53 | Dominateda | |
Scenario 6: Duration of treatment response equal to percentage of responders at 24 months (the 24-month percentage of the 13 responders still responding [77% for those with > 30,000/μL blood platelet counts]). | Watch and rescue | 759,629 | 14.53 | Ref. |
Fostamatinib | 889,889 | 15.12 | 219,059 | |
Rituximab | 769,129 | 14.52 | Dominateda | |
Scenario 7: Model time horizon set to 5 years (duration of FIT 3 trial). | Watch and rescue | 155,690 | 3.51 | Ref. |
Fostamatinib | 234,796 | 3.66 | 559,341 | |
Rituximab | 165,328 | 3.51 | Dominateda | |
Scenario 8: Model time horizon set to 10 years. | Watch and rescue | 294,939 | 6.45 | Ref. |
Fostamatinib | 410,593 | 6.73 | 415,221 | |
Rituximab | 304,462 | 6.44 | Dominateda | |
Scenario 9: Transition probabilities for fostamatinib informed by FIT1 and FIT2 data for individuals who did not receive TPO-RA therapy. | Watch and rescue | 773,545 | 14.49 | Ref. |
Fostamatinib | 915,040 | 15.19 | 202,340 | |
Rituximab | 782,481 | 14.49 | Dominateda | |
Scenario 10: Transition probabilities for fostamatinib were informed by individuals in FIT1 and FIT2 who received TPO-RA therapy. | Watch and rescue | 812,020 | 13.94 | Ref. |
Fostamatinib | 1,051,189 | 15.10 | 206,554 | |
Rituximab | 820,673 | 13.94 | Dominateda |
ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-years, Ref. = reference.
aDominated indicates that a treatment is more costly and less effective (lower QALYs) than the reference.
Appendix 5: Submitted BIA and CADTH Appraisal
Note that this appendix has not been copy-edited.
Table 14: Summary of Key Takeaways
Key Takeaways of the BIA |
|---|
|
Summary of Sponsor’s BIA
In the submitted base-case BIA, the sponsor assessed the introduction of fostamatinib for the treatment of adult patients with chronic ITP who have insufficient response to TPO-RAs in jurisdictions where TPO-RA reimbursement is available, or after failure of corticosteroids and other earlier-line treatments in jurisdictions where TPO-RA reimbursement is unavailable. The BIA was undertaken from the perspective of a Canadian public payer over a 3-year time horizon (2022 to 2024), using an epidemiological approach that was heavily influenced by TPO-RA claims data. The sponsor included drug acquisition costs. Data for the model were obtained from various sources including Statistics Canada, the published literature, ODB Formulary list prices, IQVIA Pharmastat data, and the sponsor’s internal data. Key inputs to the BIA are documented in Table 16.
Key assumptions to the BIA included:
In jurisdictions that do not fund TPO-RAs, patients were assumed to become eligible for fostamatinib or rituximab therapy in the same proportion as patients became eligible for TPO-RAs in jurisdictions that fund them.
Immunosuppressant agents other than rituximab are not used at late lines of therapy (i.e., where patients might be eligible for TPO-RAs).
Table 15: Summary of Key Model Parameters
Parameter | Sponsor’s estimate (reported as year 1 / year 2 / year 3 if appropriate) |
|---|---|
Target population | |
Adult population of jurisdiction Prevalence of chronic ITP Proportion of chronic ITP population with public coverage Proportion of patients treated with TPO-RA in reimbursing jurisdictions Ontario Saskatchewan Proportion of patients ‘eligible’ for TPO-RA with no access (other jurisdictions) Proportion of patients in TPO-RA reimbursing jurisdictions who do not respond | Varies by jurisdictiona 23.6 per 100,000b 56.3% / 55.6% / 55.0%c Estimated from projected TPO-RA salesd 7.8% / 8.2% / 8.6% 14.4% / 17.1% / 19.8% 11.1% / 12.7% / 14.2%e 50%f |
Number of patients eligible for drug under review | 253 / 282 / 312 |
Market Uptake Reference Scenario (3 years) | |
Rituximab Proportion assigned to rituximab requiring treatment or re-treatment each year Watch and wait | 50% / 50% / 50%g 74.5%h 50% / 50% / 50%g |
Market Uptake New Drug Scenario (3 years) | |
Uptake (new drug scenario) Fostamatinib Rituximab Proportion assigned to rituximab requiring treatment or re-treatment each year Watch and wait | |||||||||||||||||||| | ||||||||||||||||||| | 74.5%h |||||||||||||||||||| |
Cost of treatment (per patient over one year) | |
Fostamatinib Rituximab Eltrombopag Romiplostim Watch and rescue alone Watch and rescue with fostamatinib or rituximab | $76,450i $5,346j $47,450k $53,279k $29,781l $16,305l |
ITP = immune thrombocytopenia; TPO-RA = thrombopoietin receptor agonist.
aBased on Statistics Canada populations estimates,35 extrapolated with Excel linear projection tool.
bDiagnosed prevalence of chronic ITP in adults from 2008 US claims data.36
cBased on IQVIA Pharmastat TPO-RA public-private split of sales data trend, 2016 to 2020.37
dNumber of TPO-RA patients treated in Ontario and Saskatchewan was calculated by dividing the annual sales data for eltrombopag and romiplostim by the average annual cost per patient (assuming 50 mg daily for eltrombopag, 3 mcg/kg/weekly for a 70 kg patient for romiplostim). Proportion of patients treated with a TPO-RA was calculated by dividing the estimated number of TPO-RA patients in reimbursing jurisdictions by the total number of ITP patients estimated through prevalence data.37
eThe mean of the proportion of ITP patients treated with a TPO-RA in Ontario and Saskatchewan was used to determine fostamatinib eligibility in jurisdictions which do not fund TPO-RAs.37
fAbsence of durable platelet count response, as reported in a 2019 review article.38
gAssumption.
hProportion requiring an additional treatment the following year, based on long-term cure rate of 25.5% from the literature.39
iAssumes median dose of 259 mg daily from FIT1/FIT2.40
jAssumes half of patients receive 100 mg weekly for 4 weeks, and remainder receive 375 mg/m2 for 4 weeks (718 mg per dose), source uncited.37
kAssumes 50 mg daily for eltrombopag and 3 mcg/kg/weekly for a 70 kg patient for romiplostim.
lWatch and rescue includes IV immunoglobulin, IV methylprednisone, platelet transfusions, oral prednisone, and/or dexamethasone at a frequency of 0.398 every 28 days when no preventive therapy is used, and 0.218 every 28 days when used with fostamatinib or rituximab.
Summary of the Sponsor’s BIA Results
Results of the sponsor’s base case suggest that the incremental budget impact associated with the reimbursement of fostamatinib after TPO-RA failure or where TPO-RAs are not reimbursed would be $2,564,931 in Year 1, $6,684,057 in Year 2, and $10,547,537 in Year 3, for a 3-year budgetary increase of $19,796,525, excluding dispensing fees and markups. The sponsor conducted a series of sensitivity analyses varying the prevalence of ITP, the response rate of TPO-RAs, the doses of fostamatinib and rituximab, the proportion of rituximab versus watch-and-rescue use, the long-term durability of rituximab response, and the market uptake of fostamatinib. The 3-year results of all sensitivity analyses ranged from $14,705,582 to $23,334,299.
CADTH Appraisal of the Sponsor’s BIA
CADTH identified several key limitations to the sponsor’s analysis that have notable implications on the results of the BIA:
Population is not consistent with the Health Canada indication: Fostamatinib is indicated for the treatment of chronic ITP in adult patients who have had an insufficient response to other treatments, a place in therapy consistent with clinician group input submitted for this review that indicated fostamatinib would be appropriate as a second-line therapy after corticosteroids. In contrast, the sponsor’s reimbursement request is for patients who have failed to sufficiently respond to a TPO-RA in jurisdictions that reimburse TPO-RAs as an alternative to late/last line treatment, or after patients fail to respond to corticosteroids and other earlier-line treatments in jurisdictions which do not reimburse TPO-RAs.
CADTH was unable to adjust for this limitation in reanalyses. The budgetary impact of reimbursing fostamatinib for the full population indicated by Health Canada is unknown but would be substantially higher than estimated in the sponsor’s base case.
Assumption that jurisdictions will use reimbursement criteria from other jurisdictions is inappropriate: In estimating the population who would be eligible for fostamatinib in jurisdictions which do not fund TPO-RA therapy, the sponsor assumed such jurisdictions will fund fostamatinib only if patients would have been eligible for a TPO-RA under the requirements set by other jurisdictions that do fund them. The assumption that 1 jurisdiction will follow funding requirements set by another jurisdiction for a separate class of medications is inappropriate.
CADTH was unable to adjust for this limitation in reanalyses. Should jurisdictions who do not reimburse TPO-RAs choose to reimburse fostamatinib under different eligibility criteria than those used for TPO-RAs in jurisdictions that reimburse them, the budget impact is unknown.
Population size is uncertain: The sponsor estimated the number of patients who would be eligible for a TPO-RA by estimating the total number of patients with chronic ITP using epidemiological data, and then using projected IQVIA Pharmastat total costs per year paid for TPO-RAs divided by the average estimated cost per year of the TPO-RAs to estimate the number of patients. The number of patients estimated to use TPO-RAs was then divided by the number of patients with chronic ITP to determine the proportion of patients who would be eligible for fostamatinib. This method is highly uncertain and requires assumptions around average dosing and use, consistent costs, access, and total patient numbers. The sponsor’s method resulted in an estimate of 9% of chronic ITP patients using a TPO-RA in 2021 (7% in Ontario, 12% in Saskatchewan), rising to 14% in 2024. However, according to the McMaster ITP registry,41 between 2010 and 2014 20.5% of ITP patients had received a TPO-RA.
CADTH exploratory reanalyses assumed that 20.5% of chronic ITP patients received a TPO-RA if their jurisdiction reimbursed them or would have been eligible for fostamatinib if their jurisdiction did not reimburse TPO-RAs in 2021, increasing by 1% per year of the time horizon.
Inappropriate comparators: The sponsor has assumed that patients who have failed TPO-RAs or who do not have access to them would instead receive either rituximab or no preventive therapy (watch and rescue). However, according to the clinical experts consulted by CADTH, rituximab is often used before TPO-RAs and is 1 of the therapies that patients may fail to adequately respond to to access TPO-RA therapy.32,42 Patients who had already had an inadequate response to rituximab would not receive it again after or instead of a TPO-RA. The clinical experts consulted by CADTH did not agree that watch and rescue was an appropriate therapy at this late stage of therapy, but would instead prescribe an immunosuppressant agent the patient had not previously tried. Additionally, input received from clinicians indicated that the preferred place in therapy for fostamatinib would be as early as second line; should fostamatinib be reimbursed as second-line therapy, the appropriate comparators would include rituximab, immunosuppressant agents, and splenectomy.
CADTH was unable to account for this limitation in reanalyses.
Proportion of claims paid by public plans uncertain: The sponsor’s analysis estimates the proportion of fostamatinib and rituximab claims which would be publicly funded by using the cost of TPO-RAs derived from 2016 to 2019 IQVIA Pharmastat that are publicly funded in Ontario, Quebec, and Saskatchewan divided by the total cost of TPO-RAs (public and private) in those jurisdictions. As stated above, this assumes that fostamatinib will be publicly funded in all jurisdictions in a manner consistent with TPO-RAs in Ontario and Saskatchewan. Uncertainty is further increased by assuming that costs paid by public and private plans can be used as a proxy for the number of patients reimbursed publicly and privately, despite the cost per unit being systematically higher for private payers in the same dataset.
CADTH was unable to account for the uncertainty in the assumption that fostamatinib will be publicly reimbursed at a proportion similar to that of TPO-RAs in jurisdictions which fund them, however CADTH exploratory reanalyses did incorporate the proportion of claims that were public versus private rather than the proportion of costs in estimating the proportion of patients who could be expected to be publicly reimbursed.
Fostamatinib discontinuation rates were not accounted for: The sponsor’s model assumed that patients who received fostamatinib would remain on therapy for the duration of the 3-year time horizon. However, 55% of patients receiving fostamatinib in the FIT1 trial discontinued due to lack of response.3 In clinical practice, these patients are likely to discontinue fostamatinib and begin therapy with another agent.
CADTH exploratory reanalyses assumed 55% of patients initiating fostamatinib each year would discontinue it by the following year, ceasing to accrue fostamatinib acquisition costs thereafter. Discontinuing patients were assumed to continue on watch and rescue instead. CADTH was unable to incorporate switching to subsequent active therapies into this analysis.
Rescue therapy needs are uncertain: The sponsor’s model originally included rescue event resource use for the watch-and-rescue group, while rescue events for the fostamatinib and rituximab groups were added upon request from CADTH. The number of these events estimated per cycle were based on blended data from a small group of individuals in the FIT1 and FIT2 trials.3,4 The rate of rescue therapy use among responders (> 50,000/μL blood platelet counts) treated with watch and rescue was 7x higher than for those who were receiving rituximab or fostamatinib (0.603 events per model cycle compared to 0.072). The clinical experts consulted by CADTH indicated that this value was unlikely to represent typical clinical practice. To address this limitation in the CADTH base case for the cost-utility analysis model, the rate of rescue therapy was made conditional on response status as opposed to response status and treatment arm.
In a scenario analysis, CADTH weighted the probability of receiving rescue therapy each cycle by the number of life-years spent in each health state for each treatment group.
Market uptake of fostamatinib is uncertain: The sponsor assumed that of eligible patients, | % would use fostamatinib in the first year of its reimbursement, ||||||% in Year 2 and ||||% in Year 3, |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||. The clinical experts consulted by CADTH, as well as input from the drug plans, found these estimates to be highly uncertain given the perceived lack of other adequate options at the therapeutic line the sponsor has requested for reimbursement, and the reimbursement limitations imposed for other therapies.
CADTH’s exploratory reanalyses assumed fostamatinib captured 30% of the eligible patient population in Year 1, rising to 50% and 65% in Years 2 and 3, respectively.
Comparator costs are uncertain: The sponsor used publicly available list prices for pharmaceutical agents (rituximab, steroids) and costs derived from the literature to estimate the cost of blood products required for rescue events. It is likely that due to confidential price negotiations, jurisdictions are paying substantially less for these products than estimated, although the extent to which the included costs are overestimated is unknown. A 2017 report by Canadian Blood Services43 reported figures leading to an estimated cost of IVIG of $62.39 per gram which, when inflated to 2021 prices,44 reduced the estimated cost per administration of IVIG from $5,623 to $5,200. Additionally, the clinical experts consulted by CADTH indicated that the 375 mg per week for 4 weeks dose of rituximab is used more frequently in Canada than assumed by the sponsor.
CADTH’s exploratory reanalyses reduced the cost of IVIG administration to be consistent with costs derived from a Canadian Blood Services report. Additional scenario analyses were conducted halving the acquisition cost of rituximab or assuming that rituximab would be used at its 375 mg/m2 dose 90% of the time.
CADTH Reanalyses of the BIA
Due to the extent of limitations in the sponsor’s model, CADTH was unable to estimate a base case for the BIA. Instead, CADTH conducted a combined exploratory reanalysis by increasing the proportion of patients who would meet TPO-RA reimbursement criteria, deriving the proportion of patients eligible for TPO-RAs from claims data rather than cost data, assuming patients not responding to fostamatinib discontinue by the following year, and increasing the assumed market uptake of fostamatinib in patients deemed eligible for it. See Table 16.
Table 16: CADTH Revisions to the Submitted Budget Impact Analysis
Stepped analysis | Sponsor’s value or assumption | CADTH value or assumption |
|---|---|---|
Corrections to sponsor’s base case | ||
None. | — | — |
Changes to derive the CADTH exploratory reanalysis | ||
1. Proportion eligible for TPO-RA therapy | 11% / 13% / 14% | 22.5% / 23.5% / 24.5% |
2. Proportion publicly funded | 56% / 56% / 55% | 63% / 63% / 62% |
3. Fostamatinib discontinuation | No discontinuation | 55% of patients starting fostamatinib are assumed to discontinue the following year and switch to watch and rescue |
4. Reduced cost of IVIG | Annual cost IVIG: $5,623 | Annual cost IVIG: $5,200 |
5. Market uptake of fostamatinib | |||| / |||| / |||| | 30% / 50% / 65% |
CADTH combined exploratory analysis | 1 through 5 | |
IVIG = IV immunoglobulin; TPO-RA = thrombopoietin receptor agonist.
The results of the CADTH step-wise exploratory reanalysis are presented in summary format in Table 17 and a more detailed breakdown is presented in CADTH also conducted additional scenarios around the combined exploratory reanalysis (Table 18) including halving the cost of rituximab paid by plans, assuming 90% of rituximab patients are using the 375 mg/m2 regimen, matching the need for rescue therapy to the method used in the CADTH base-case economic evaluation (see main body of report), and assuming a 60.2% price reduction for fostamatinib, consistent with the CADTH Price Reduction Analysis for the Economic Evaluation (see Table 8). Applying these changes resulted in a 3-year budget impact of $47,021,389.
Table 17: Summary of the CADTH Reanalyses of the BIA
Stepped analysis | Three-year total |
|---|---|
Submitted base case | $19,796,525 |
CADTH reanalysis 1: Proportion eligible for TPO-RA therapy | $50,414,362 |
CADTH reanalysis 2: Proportion publicly funded | $19,806,683 |
CADTH reanalysis 3: Fostamatinib discontinuation | $15,787,646 |
CADTH reanalysis 4: Reduced IVIG cost | $19,941,943 |
CADTH reanalysis 5: higher fostamatinib uptake | $28,390,313 |
CADTH combined exploratory reanalysis: 1 through 5 | $47,021,389 |
IVIG = IV immunoglobulin; TPO-RA = thrombopoietin receptor agonist.
Table 18: Detailed Breakdown of the CADTH Reanalyses of the BIA
Stepped analysis | Scenario | Year 0 (current situation) | Year 1 | Year 2 | Year 3 | Three-year total |
|---|---|---|---|---|---|---|
Submitted base case | Reference | $5,482,476 | $6,321,120 | $7,059,627 | $7,798,134 | $26,661,358 |
New drug | $5,482,476 | $8,886,051 | $13,743,684 | $18,345,671 | $46,457,883 | |
Budget impact | $0 | $2,564,931 | $6,684,057 | $10,547,537 | $19,796,525 | |
CADTH combined exploratory analysis | Reference | $14,156,806 | $14,657,488 | $15,233,274 | $15,809,059 | $45,699,821 |
New drug | $14,156,806 | $26,552,672 | $29,753,591 | $36,414,947 | $92,721,210 | |
Budget impact | $0 | $11,895,184 | $14,520,317 | $20,605,888 | $47,021,389 | |
CADTH scenario analysis 1: rituximab cost halved | Reference | $13,593,742 | $14,074,510 | $14,627,395 | $15,180,279 | $43,882,184 |
New drug | $13,593,742 | $26,144,588 | $29,450,651 | $36,194,874 | $91,790,113 | |
Budget impact | $0 | $12,070,077 | $14,823,256 | $21,014,595 | $47,907,929 | |
CADTH scenario analysis 2: 90% use higher rituximab dose | Reference | $14,857,508 | $15,382,972 | $15,987,256 | $16,591,540 | $47,961,769 |
New drug | $14,857,508 | $27,060,511 | $30,130,582 | $36,688,815 | $93,879,908 | |
Budget impact | $0 | $11,677,539 | $14,143,326 | $20,097,275 | $45,918,139 | |
CADTH scenario analysis 3: watch-and-rescue events matched to CADTH CUA | Reference | $12,106,183 | $12,534,342 | $13,026,724 | $13,519,106 | $39,080,172 |
New drug | $12,106,183 | $24,310,989 | $26,967,336 | $33,405,414 | $84,683,739 | |
Budget impact | $0 | $11,776,648 | $13,940,612 | $19,886,308 | $45,603,567 | |
CADTH scenario analysis 4: 60.2% fostamatinib PR | Reference | $14,156,806 | $14,657,488 | $15,233,274 | $15,809,059 | $45,699,821 |
New drug | $14,156,806 | $18,468,702 | $20,197,224 | $22,779,586 | $61,445,512 | |
Budget impact | $0 | $3,811,213 | $4,963,950 | $6,970,528 | $15,745,691 |
BIA = budget impact analysis; CUA = cost-utility analysis; PR = price reduction.
Stakeholder Input
Patient Group Input
Platelet Disorder Support Association
About the Platelet Disorder Support Association
The Platelet Disorder Support Association (PDSA) is dedicated to enhancing the lives of patients with immune thrombocytopenia (ITP) and other platelet disorders through advocacy, education, research and support. Founded in 1998, PDSA is a U.S. based non- profit with an international reach, and we are registered as a non-profit corporation in Canada.
We have on average 70,000 unique visitors to our website per month (www.pdsa.org). In 2020, Canada was one of the top three countries providing unique visitors to the PDSA website. We have 16,414 contacts in our data base (13,461 adults and children; 2,953 physicians) from 130 countries. In Canada alone, we have 635 adults and children in our data base, and 115 physicians. We have 59 support groups throughout the US, Canada, and New Zealand. In Canada specifically, we have seven support groups including in the London, Niagara, Toronto, Waterloo, Ottawa and Vancouver regions. We also have a full time Research Program Manager, Jennifer DiRaimo, MS, CCGC, who is Canadian and works remotely from London Ontario. PDSA has a Canadian board member, Dr. Donnie Arnold, from McMaster University in Hamilton.
PDSA holds a Canadian Regional Meeting for patients/caregivers annually, when conditions permit for an in-person event outside of a pandemic. During our annual three-day patient conference, we host a separate Canadian ITP meeting with two of our medical advisors, Donald Arnold, M.D. from McMaster University in Hamilton, Ontario and John Semple, PhD who recently left St. Michaels hospital in Toronto, Ontario to accept a prestigious academic position at Lund University in Sweden. We are frequently invited to speak about the patient experience at Canadian events. This year, PDSA has been invited to speak at the National ITP Advisory Board Meeting in May (2021), sponsored by Novartis Canada.
Information gathering
The following patient comments were collected from the PDSA Facebook page. Due to access issues to this drug, to collect enough meaningful experiences for you we had to go back as far as 2018-present. The following (see below) represent people from across the U.S. and Canada and are from adult patients only:
“Im on Tavalisse for the last 2 years and haven’t had any adverse side effects. The good thing is that my platelets are … 160-210K. Never had these numbers. Before I went through every medication/protocol possible and my platelets were 10K or below.”
“Excited to see platelets at 63000! Highest in year since diagnosed. On tavalisse and 10 mg steroids. I normally stay 20-30000. Been on rituximab and Promacta and now tavalisse which none have keep my platelets up.”
“Promacta stopped being effective after many years for me dropping to 2k, Tavalisse has kept me above 70K …”
“it keeps me around 150,000 – 200,000… I’ve been on Tavalisse for 2 years.” “With Tavalisse I am between 55,000-204,000”
“16 months on Tavalisse, platelets were 467 yesterday”
“For me, mine went up to over 200,000 after a week. Not sure what experience others have had but I’ve never been below 200,000 since I started taking it.”
“I had an immediate response within a week also going into the 200s.. I’ve had an upset stomach here and there but nothing major.” “Tavalisse … holding me steady and rising, 188k. Yesterday, I got to kick off 2020 with a bang! 500k for the first count of the year !!!” “Yes. Platelets shot up for me and I am also doing Nplate. 13 to 39 to 59 last week. I am usually below 20 for years on Nplate.”
“I’ve been on Tavalisse for almost 2 years (Nplate and Promacta didn’t work for me). A game changer for me! I did come with side effects – elevated blood pressure and chronic diarrhea but both are managed. My numbers have been 80-350K, much better than 20K or lower where they sat for a year.”
“Game changer for me. It gave me my life back – no steroids. The side effects are manageable and so much better than with any of the other drugs I took.”
“I started (Tavalisse) in August. Currently at 127K – tapered off of prednisone 4 weeks ago. This is the longest period of time that counts have remained stable.. have tried it all!”
“I began taking this at the end of November and it seems to work platelets stay between 89-149K last week 113K. I take 100mg twice a day.”
“Wish this was in Canada since nothing else works platelets have been under 5K for months.” “You guys!!! After 2 weeks on Tavalisse, my patelets are at 189 thousand!!!”
“I’m on the lowest dose, every other day, no side effects except a rare upset stomach and last count was 370. I was diagnosed 12 years ago. Have tried prednisone, ivig, Promacta, Rituxan, dexamethasone, splenectomy, … and Tavalisse has been the only one I can tolerate and that has worked long term.”
“If you all can get on tavalisse, do it! No side effects for me (yet). It’s been 3 weeks. Can you say 320? I’ve done promacta and n- plate with terrible side effects. This stuff works.”
“So far so good! Took about 2 1/2 weeks to kick in”
“I’ve been doing Tavalisse for about 3 months and I am doing great on 300mg my counts have been remaining at 400K since last week.”
“Ok, Canadians. My doctor said I probably wouldn't be able to get it unless my spleen is removed.”
Disease experience
Having a bleeding disorder impacts not only the individual, but their entire family. Patients with ITP face a complex set of challenges. Due to the heterogeneity of ITP’s pathophysiology and disease course, living with ITP can be difficult and unpredictable despite several available therapies with different mechanisms of action.
The multifaceted burden of living with ITP impacts the overall health-related quality of life (HRQoL) of patients and their families. Aside from the constant risk for serious life-threatening bleeding, patients experience both physical and emotional consequences living with their disease on a daily basis. ITP is associated with elevated levels of fatigue, anxiety, depression, physical pain for some, and sleep disturbances despite having good support systems in place. The levels of fatigue, anxiety, pain, and depression reported within the ITP registry participants exceeds what is reported in the general population. For many ITP patients, these symptoms are front and center among their concerns, rather than the clinical measures of platelet counts.
Guilt and disappointment over limited abilities and restricted activities due to a low platelet count likely further contribute to the negative emotional burden on ITP patients. The symptoms that accompany the disease and the constant monitoring of platelet counts interfere with daily activities also lead to anxiety, fear, depression, and embarrassment over unexplained bruises or blood blisters, isolation, inadequacy, and frustration with a patients’ inability to control their body and their health. To minimize bleeding risks, patients with ITP need to routinely weight the risks associated with their daily activities, and sometimes forgo travelling or participating in sporting or social events. ITP presents an additional layer of complexity for patients who require a specialized medical procedure or surgery, or become pregnant, or find themselves in the care of a specialist health care provider in an emergency situation who might not be current in their knowledge about ITP. Fatigue associated with ITP is often debilitating.
Together, this demonstrates the multifaceted effect ITP has on overall QoL.
ITP does not have to go into remission for a patient’s quality of life to improve – to have an increase in a platelet count where it elevates the risk for bleeding and improves fatigue is always the goal. While it may seem like ITP is a simple ‘benign’ disease on the surface, nothing could be farther from the truth. There are many complexities associated with ITP regarding disease etiology, risks, treatment responses, and heterogeneity in clinical symptoms.
Experiences with Currently Available Treatments
There are many treatments for ITP. They all have different risks, benefits, and limitations. Not to mention, many have a high burden of toxicity. Hematologists may use several treatments at once to increase their success rate. This is common due to the impact ITP has on the immune system.
Prednisone — Prednisone is a synthetic medicine (i.e., corticosteroid) similar to cortisone, a natural substance produced in the body’s adrenal glands. It is used in the treatment of ITP because it has been shown to increase the platelet count while it is being taken. However, the effects are short term, while the side-effects are often long- term. In the past, ITP patients were forced to ensure steroids on a daily basis putting their health at risk. As a result, the revised updated 2019 professional American Society of Hematology (ASH) ITP guidelines suggest using steroids for no longer than 6 weeks, and that if the platelet count is still low, to consider an alternative therapy such as a TPO-RA (such as Revolade® or Nplate®).
Possible side effects: Prednisone is generally only given for a few weeks at a time because it can have serious side effects with long-term use. And even when it is given for a short time, side effects include irritability, stomach upsets, sleep disturbances, increased appetite, weight gain, puffy cheeks, frequent urination, sugar in the urine, loss of bone density, cataracts, or acne.
Intravenous gamma globulin (IVIg) — IVIg is a liquid concentrate of antibodies purified from the plasma (the liquid portion of the blood that doesn’t contain red blood cells) of healthy blood donors.
Possible side effects: Some patients treated with IVIg experience nausea and vomiting, headaches or fever and rarely, aseptic meningitis, abnormal blood clots or kidney failure. This is an expensive short term therapy solution as often after a week or so the platelet count will drop. It is designed to be a ‘rescue’ therapy similar to corticosteroids for patients with ITP.
Anti-Rho(D) immune globulin (WinRho SDF®, Rhophylac®) — Anti-D is also a liquid concentrate of antibodies derived from healthy human plasma. However, this medicine is targeted against the Rh factor* on red blood cells. It is thought that anti-D binds to red blood cells to such an extent that the spleen is fully occupied eliminating red blood cells and does not have much opportunity to remove the antibody-coated platelets. Like IVIg, the response is usually rapid but temporary. It also is designed to be a ‘rescue’ therapy similar to corticosteroids for patients with ITP, and can only be utilized by Rh+ patients, and those who have not had a previous serious serum reaction to IVIG.
Possible side effects: Temporary side effects from anti-D include fever, headache, chills, nausea and vomiting, anemia, and rarely, kidney failure.
Monoclonal antibodies — Rituximab (Rituxan®) is a monoclonal antibody approved by the FDA in November 1997 for treatment of lymphoma, a type of cancer. It is increasingly being used to treat ITP. It reduces the number of B cells. After rituximab treatment, the body can take up to a year to replace the eliminated B cells and have the immune system and antibody production back in full working order.
Possible side effects: Side effects that developed following 7% of infusions included headaches, chills, fever, and body aches. For patients with hypersensitivity to blood products there is a remote risk of anaphylaxis (shock response). A very small number of patients may experience severe anemia, which requires immediate medical attention. This is very rare. This therapy is used to elevate the platelet count more ‘long-term’ however for some ITP patients do not respond, or their platelet count drops after a few months. Some ITP patients have reported longer-term success.
Platelet growth factors (such as Revolade® or Nplate® ) — Platelet growth factors or thrombopoietin (TPO) receptor agonists are a class of treatments for ITP that stimulate the bone marrow to produce more platelets.
Possible side effects: Side-effects are not common, however those that have been reported include joint and muscle pain, dizziness, insomnia, indigestion, and ‘pins and needles’ sensations. Potential exists for patients to develop reticulum (fibrous growths) in the bone marrow however this is ultra-rare. The platelet count to drop below the pre-treatment count if the treatment is discontinued.
Splenectomy - A splenectomy is the surgical removal of the spleen. The spleen acts like a large lymph node, helping to maintain a healthy immune system and cleaning the blood of foreign matter. In ITP, the antibody-coated platelets are often removed from circulation by the spleen. Thus, if the spleen is removed, the platelets will remain in the blood stream. However, a significant proportion (30-40%) of ITP patients will not see a change in their platelet count after having their spleen removed.
Possible side effects: The immediate complication rate from surgery is about 10%, require even more time in the hospital, although estimates vary. The fatality rate from the surgery is about 1% (1 in every 100 people) for an open splenectomy and much less for a laproscopic procedure. Since the spleen is responsible for making antibodies, filtering the blood, and removing bacteria, those without a spleen have an impaired immune system, difficulties recovering from pneumonia, meningitis, Hib flu, sepsis, hospital- based infections, malaria and other parasitic diseases, babesiosis (a tick-borne disease) and gram-negative bacterial diseases from animal bites. People who have had a splenectomy have more microparticles in their blood, giving them an increased risk of dementia and heart attacks from blood clots. They are also more prone to blood vessel complications. This surgical procedure results in taking up limited surgical space, occupying a limited hospital bed, and requires ongoing medications while putting the patient at risk for complications requiring even more time off work/school, and death.
Fostamatinib - A new approach to treating ITP is the use of a spleen tyrosine kinase (SYK) inhibitor. The agent fostamatinib disodium hexahydrate (TAVALISSE®) may slow the destruction of antibody-coated platelets in people with chronic ITP by specifically targeting SYK. Spleen tyrosine kinase (SYK) is part of a network of proteins (found in certain cells of the immune system) that triggers platelet destruction.
Possible side effects: Adverse reactions reported included high blood pressure, elevated liver enzymes, diarrhea, and a decrease in white blood cell counts. Common less serious side effects include nausea, rash, dizziness, tiredness, respiratory infection, chest pain, and stomach (abdomen) pain.
Improved Outcomes
Patients often do not have a choice. They may not respond well (or at all) to other therapies or be able to afford other options. There is no way to predict who will respond to a certain treatment, and who will not. It is also not clear who will develop a resistance to a particular drug over time, and who will not. Patients need options available to them to switch if their current therapy is no longer worker, and their bleeding is not under control, or they are at risk to have a critical bleed.
Ideally, patients want therapies that do not impact their schedule and daily life since they often already miss a lot of work due to their multiple appointments and fatigue. It is much easier and more convenient to take a daily pill then go into the hospital or clinic for a weekly injection or to have a six-hour infusion like IVIG. Time off work and parking are expenses. Patients also want something that has little to no side effects and aren’t willing to feel terrible all of the time like they do on steroids, highlighting the need for therapies to improve quality of life, not further reduce. Patients want a therapy that lasts longer than a week. They don’t want to live when and where the next bleed will be. Fear and anxiety of nose bleeds that can last for hours, mouth blisters, bruises all over their body, and debilitating fatigue. ITP is a rare disease. Even rarer are those that require therapy on a daily basis. It perhaps is more cost-effective to treat ITP and cover the cost of the drugs those that need it require, than to deal with the long-term costs of hospitalizations, life- support if an ICH or other life-threatening bleeding occurs, and the cost on society if ITP patients are unable to work and require disability because they cannot attend work regularly. The cost of IVIG weekly is very high. The cost of treating steroid related long term health concerns is perhaps even greater. It’s time to treat ITP patients with humanity and cover drugs that treat with minimal side effects and last. Prevention is key with ITP.
Experience With Drug Under Review
Currently, access to Fostamatinib in Canada is only through private insurance or self-pay. Fostamatinib is not an up-front therapy for ITP patients, so often this drug is accessed by patients who have tried multiple therapies in past and their platelet count continues to be low, and they continue to be at risk for critical bleeding. For many ITP patients who have not had a response to Rituximab or a TPO agent, Fostamatinib may be there only hope. Fostamatinib is taken daily orally, so it is easier and more convenient to use than other medications compared to other treatments requiring patients to come into the clinic or doctor’s office for a weekly injection, taking high dose steroids that cause mood issues and physical side effects, or having a splenectomy where a major organ is removed not always addressing the low platelet count and then leaving the individual unable to fight of various infections without a spleen. These scenarios are recommended against, in the new updated ASH (2019) guidelines.
Anything Else?
While there are a number of treatments for ITP, for many with ITP these current therapies do not work. Patients often cycle on and off various therapies in the hopes that the treatment will raise the platelet count. For the small number of ITP patients requiring this therapy, what would be the downside in covering the cost for them when this drug may save their live? ITP patients refractory to steroids and other ITP therapies are at high for critical bleeding. The side- effects that could happen as a result of taking this drug can be successfully managed (such as elevated blood pressure). The trade-off seems simple – treat the side effects because you cannot bring back an ITP patient who has died.
Conflict of Interest Declaration for the Platelet Disorder Support Association
To maintain the objectivity and credibility of the CADTH CDR and pCODR programs, all participants in the drug review processes must disclose any real, potential, or perceived conflicts of interest. This Patient Group Conflict of Interest Declaration is required for participation. Declarations made do not negate or preclude the use of the patient group input. CADTH may contact your group with further questions, as needed.
Did you receive help from outside your patient group to complete this submission? If yes, please detail the help and who provided it.
No
Did you receive help from outside your patient group to collect or analyze data used in this submission? If yes, please detail the help and who provided it.
No
List any companies or organizations that have provided your group with financial payment over the past two years AND who may have direct or indirect interest in the drug under review.
PDSA has received funding from the following pharma companies: Argenx, Amgen, Dova/Sobi, Novartis, UCB, CSL Behring, Principia, Pfizer, Sanofi, Momenta, Rigel.
Novartis and Amgen currently have ITP drugs in Canada.
Table 1: Conflict of Interest Declaration for Platelet Disorder Support Association
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
Amgen | — | — | — | X |
Novartis | — | — | — | X |
Rigel | — | — | — | X |
Argenx | — | — | — | — |
Dova/Sobi | — | — | — | — |
UCB | — | — | — | — |
CSL Behring | — | — | — | — |
Principia | — | — | — | — |
Pfizer | — | — | — | — |
Sanofi | — | — | — | — |
Momenta | — | — | — | — |
Rigel | — | — | — | — |
Clinician Group Input
Hematology
About Hematology
This submission represents the collective perspectives of 19 Canadian hematologists who collaborated to produce a thoughtful and compelling submission on the therapy under review: Fostamatinib (Tavalisse). The goal is to help inform the expert committee’s deliberative process for the condition, Chronic Immune Thrombocytopenia (‘ITP’), in need of an additional therapeutic for patients diagnosed with relapsed ITP.
Hematologists are medical doctors who specialize in the management of blood and blood related disorders. These disorders include malignant and non-malignant hematological disorders, including rare blood diseases such as (ITP).
The clinicians who collaborated to provide meaningful and relevant input are as follows:
Dr. Nicole Laferriere, Dr. Sudeep Shivakumar, Dr. Anna Nikonova, Dr. LM Larratt, Dr. Colin Yee, Dr. Vinai Bhagirath, Dr. Matthew Kang, Dr. Philip George Kuruvilla, Dr. Mark Blostein, Dr. Alejandro Lazo-Langner, Dr. Zachary Liederman, Dr. Christine M. Cserti-Gazdewich, Dr. Lakshman Vasanthamohan, Dr. Yulia Lin, Dr. Hayley Merkeley, Dr. Kuljit Grewal, Dr. Siraj Mithoowani, Dr. Sadiya Kukaswadia.
Each clinician’s Conflict of Interest declaration is included and appears at the end of this submission.
Information Gathering
To ensure the valuable clinician perspective was captured and provided for the therapy under review, Accelera Canada in partnership with Advocacy Solutions commissioned the services of Blue Ribbon Project Inc. to assist with the coordination and preparation of the joint clinician input submission. Blue Ribbon Project reached out to six U.S.-based hematologists having clinical experience prescribing the therapy under review, five of whom were prepared to complete an online clinician survey (prepared by Blue Ribbon Project Inc.), whose results would help inform the submission. The survey was sent for completion on July 13, 2021 and closed on July 23rd, 2021. The data was analyzed and incorporated into the submission on July 25th, 2021, at which point the submission was sent to 198 clinicians across Canada on July 28th, 2021 – August 9, 2021, for their review and input.
Information was also gathered from a review of the literature and guided by current clinical practice guidelines provided by the American Society of Hematology updated in 2019 as well as the International Consensus Report issued in 2019. The information was incorporated into the submission as observed in and supported by clinical practice.
Current treatments
Describe the current treatment paradigm for the disease
ITP is a non-malignant autoimmune disease where the patients’ own immune systems attack their own platelets with associated impaired platelet production leading to a reduction in platelet counts (low platelets called thrombocytopenia). The incidence is estimated to be 2 to 5 in 100,000 persons per year and a prevalence of 10 to 24 per 100,000 persons. These individuals have a variety of clinical manifestation from being asymptomatic with incidental low platelet counts to more severe bleeding and even life-threatening internal haemorrhage. The natural history of patients with ITP can vary from long periods of stability to intermittent episodes of severe bleeding requiring numerous interventions. This variability and uncertainty in disease course can be very unsettling to patients and impact their lives and challenging for the healthcare system. Patients with ITP live with the unpredictable nature of the fluctuations that are inherent to this disease resulting in poor quality of life, anxiety, depression, frequent laboratory investigations and numerous clinical visits. Healthcare systems struggle with the potential of these patients having sudden relapses requiring emergency visits, hospitalizations, interventions for bleeding complications, and the search for treatment options.
ITP treatment options are varied and described below. However, there are ITP patients who despite current available therapies will continue to have relapses in their disease and live with the complications of bleeding and infections related to these treatments. Ultimately, patients with severe and refractory ITP are at four times higher risk of mortality than the general population. Newer and more efficacious treatments are urgently required for this vulnerable patient population.
The current treatment paradigm of ITP in the Canadian context is non-uniform across the provinces given differential access to therapies and may differ between individual clinicians. Most Canadian physicians treating patients with ITP rely on clinical guidelines, our colleagues, and various specialty conferences to name a few sources. The clinical guidelines include the American Society of Hematology updated in 2019 and the International Consensus Report in 2019. These are often challenging to follow due to limitations in access to treatment options in Canada compared to the sequence or options that are recommended in the guidelines. Further, most treatment options are not Health Canada indicated for the treatment of ITP but are required in order to gain access to Health Canada approved treatments by provincial funding bodies. The following is a general discussion that may be possible in the Canadian context:
Typically, patients with ITP are monitored and not treated unless they are symptomatic (bleeding) or have severe thrombocytopenia (e.g. platelets < 30 consistently).
First line treatment options include corticosteroids such as prednisone or dexamethasone. In general, the type of corticosteroid may be selected on a case-by-case basis between the physician and patient taking into account patient preferences, comorbidities, ability to adhere to a tapering regimen, and desire to achieve a quicker response. Responses may take up to several days to a few weeks in some cases. If a more rapid response is required, then often intravenous immunoglobulin (IVIg) is given.
Note: None of these first line treatments are Health Canada approved for the treatment of ITP. Furthermore, they may have variable efficacy and the majority of patients with ITP will relapse and require second and subsequent lines of therapies. These treatments do not modify the underlying disease and act to treat immediate thrombocytopenia, symptoms, and hope to reduce or prevent bleeding.
Second or subsequent lines of therapies include a myriad of options where clinical data is lacking to help guide the correct order or sequencing of treatments. Treatments include surgery – splenectomy or medical therapies – immunosuppressive agents (azathioprine, cyclophosphamide, cyclosporine, mycophenolate, danazol, etc), monoclonal antibodies such as rituximab and its biosimilars, thrombopoietin receptor agonists (TPO- RAs) romiplostim or eltrombopag, and now novel therapies such as the oral Syk inhibitor, fostamatinib. Of these, only the two TPO-RAs romiplostim and eltrombopag and the oral Syk inhibitor, fostamatinib, are Health Canada approved for the treatment of ITP. The clinical guidelines suggest the use of TPO-RAs, rituximab and fostamatinib, typically in second line. However, in the Canadian context, this is not possible unless patients have private insurance coverage. As an example, in Ontario, the Exceptional Access Program, will only cover a TPO- RA when a patient has undergone first line therapy, a splenectomy, and failed two other second line therapies (all not Health Canada approved) before funding a TPO-RA (which is Health Canada approved).
Note: Currently, only two TPO-RAs, romiplostim and eltrombopag, and the oral Syk inhibitor, fostamatinib, are Health Canada approved for the treatment of ITP. Although a splenectomy may alter the natural history of ITP in the majority of patients, it is associated with surgical and anaesthetic complications, risks of major overwhelming sepsis that is greatly reduced (but not eliminated) by current vaccinations, and risks of clotting (thrombosis). Most of these therapies do not change the natural history of ITP and often are required for a period of time to treat symptoms. Thus most of these treatments are used for a finite period of time. The TPO-RAs and Syk inhibitor fostamatinib are considered maintenance therapies that are used for an indefinite period of time.
Treatment goals
What are the most important goals that an ideal treatment would address?
The goals of treatment may be different depending upon whose perspective you are attempting to capture: patient vs treating physician.
The patient wishes to prolong life by reducing the risk of life-threatening bleeding. Goals also include a cross section of health-related factors that impact their quality of life from reducing fatigue, reduced cognitive function, anxiety, and depression. Some patients want to reduce the impact the disease has on their families, friends, and caregivers who attend clinic visits, furnish transportation, supply mental and social support, and who are also called upon for emergencies. Most of these patients also want to reduce the number of laboratory tests they do, the number of clinic visits they attend, and the time away from their personal and family lives. Patients on treatments are very concerned about side effects, the need for on-going monitoring, and the effects sustained on them and their families. Unfortunately, most treatments including rescue therapies with steroids and IVIg have significant effects on patients. Steroids lead to mood swings, irritability, agitation, insomnia, acid reflux, poor diabetic control, and increased risks of infections just to name a few. IVIg requires a significant amount of time during a day or two and may need to be repeated. There are numerous patients who cannot afford the time away from work or time away from caring for their dependents. Although there are numerous treatment options listed above, other than the concern of the treatment not working or side effects, is the tremendous weight and burden of cost. Patients who do not have private insurance often worry about the financial burden they can incur with these treatments that impact themselves and their families.
The treating physician goals are somewhat complementary to those listed above but have other unique features. The goal certainly is to prolong life by reducing the risk of life-threatening bleeding. To be able to accomplish this, the goal is to increase platelet counts to “safe” ranges that may differ for day-to-day activities, perioperatively, and during pregnancy if applicable. The goals to improve all of the health-related quality of life parameters noted above by patients is also tempered by the goal to choose treatments that may be in the best interest of the patient. Certain drugs may exacerbate an underlying condition (such as steroids with diabetes), or interact with other medications (such as azathioprine with allopurinol), or be time sensitive (such as avoiding rituximab prior to COVID vaccinations), or be contraindicated (such as splenectomy in a non- surgical candidate). Further, physician goals are to try to minimize costs to the patient and to the healthcare system (such as indiscriminate use of IVIg for weekly maintenance of ITP). Often this requires a discussion with patients to find the best available therapies that are uniquely tailored for that individual and working in conjunction with pharmacists, drug access facilitators, provincial funding bodies, private insurance, hospital drug and therapeutic committees, local MPPs, and industry.
The U.S. clinician survey results highlighted the treating physician goals as the following:
“..to reduce the severity of treatment-induced symptoms, minimize adverse events, improve health related quality of life and minimize monitoring” such that it complements and aligns with the goals of an ideal treatment setting for the patient. Appearing below are the replies to Q10 from the online survey furnished by US clinicians who have experience with the therapy under review (Figure 1).
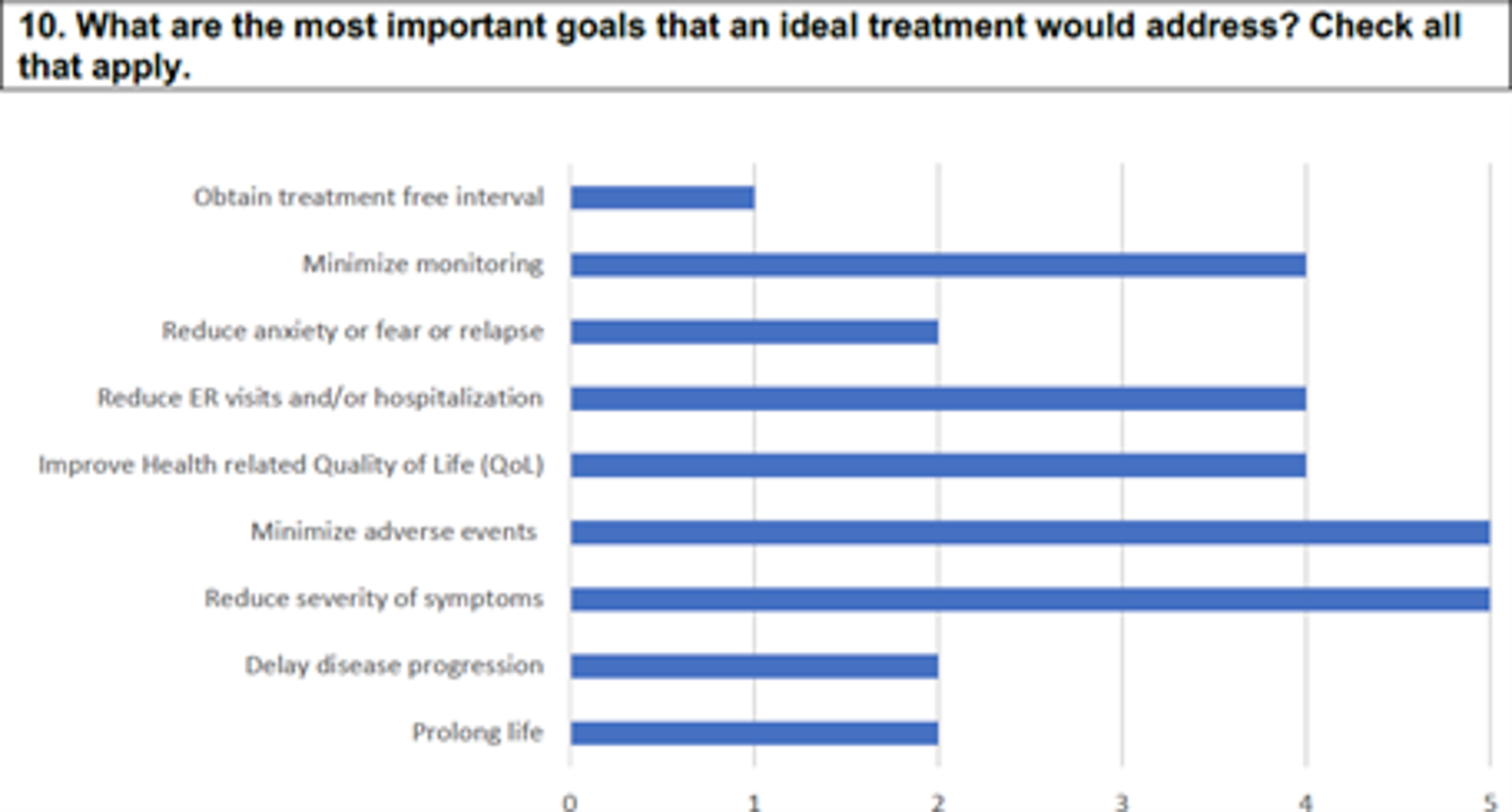
Treatment gaps (unmet needs)
Considering the treatment goals in Section 4, please describe goals (needs) that are not being met by currently available treatments.
Unfortunately, ITP is a rare non-malignant hematologic condition that is very heterogenous in its presentation. Although it is not a malignancy, it is not so “benign” as it sounds as noted previously. Severe refractory ITP patients have a four-fold increase in mortality and numerous others suffer from increased risks of bleeding and infection. Thus, the unmet goals include the following:
Not all patients respond to available treatments. Although there is a myriad of treatment options, unfortunately, most adult patients with ITP have a chronic relapsing and remitting course requiring multiple lines of therapy.
Patients become refractory to current treatment options. Some patients are either refractory to one or more treatments and others relapse at some time after the initial treatment response. In either case, these patients with this roller coaster natural history may lead to multiple emergency room visits, clinic visits, hospitalizations, and lab tests. Even in maintenance treatment options, patients may become refractory.
Currently, there is no true cure for ITP. Although a splenectomy may alter the natural history of the disease in some cases and be considered a “cure”, it is only for a subset of ITP patients.
No treatments are available to address key outcomes. In terms of patient goals of care, one aspect that is not well studied and managed is ITP associated fatigue and effect on mental health. Although most treatments proposed by treating physicians is to treat their platelet count and reduce bleeding these often do not address a patient’s fatigue and mental health. Further, most treatments may contribute to worsening of their fatigue and mental stress.
Treatments are needed that are better tolerated. As mentioned, there are a myriad of ITP treatment options but all are associated with side effects and often do not address key outcomes for patients such as their fatigue and mental health. Most of the treatment options are not even Health Canada approved for ITP. Most of the treatment options suppress the immune system that is significant in a patient population with a significant chronic disease diagnosed with other comorbidities.
Treatments are needed to improve compliance. Due to the aforementioned concerns and side effects, patient adherence to medications can be challenging. From a treating physician perspective, the goal may be to improve platelet counts to reduce the risk of bleeding, but patients may not view this benefit over the side effects and burden of the medication (cost, access, travel, etc). Oral therapies are typically better adhered to than non-oral therapies. This also leads to the argument for a better formulation of medications that help with improving patient compliance.
Some of the online survey open-ended replies provided by our U.S. colleagues included:
“Proceeding to the therapy under review could potentially avoid a splenectomy, especially in younger patients, safe therapy in patients with prior history of blood clots. Could alter the natural history of disease.”
“Tavalisse brings a unique combination of an oral targeted therapy with a good durability and favorable side effect profile and consequently minimizing clinic trips/visits and avoiding injections or surgery.”
Which patients have the greatest unmet need for an intervention such as the drug under review?
In adults with ITP, the greatest unmet need is for those with severe refractory disease. This population includes patients who have tried first line therapies, had a splenectomy, and tried other lines of therapy. Often, multiple lines of treatment failure are predictive of reduced response to other available therapies and four-fold risk in mortality. These patients often have significant burden of disease with personal stress, anxiety, depression and impact on their families. Often, we call these patients multiply relapsed/refractory ITP patients because they would have gone through at least 2 to 10 lines of therapy.
For the multiply relapsed/refractory ITP patients, they are at their wits’ end and often the treating physician is at his/her wits’ end. These patients have a huge impact on the healthcare system in terms of requiring numerous treatments, emergency room visits, hospitalizations, clinic visits and laboratory tests.
The drug under review, fostamatinib, would address the unmet need in this patient population as it would provide a drug with a novel mechanism of action, a Syk inhibitor, that may work in patients where other treatments didn’t work. Like TPO-RAs, fostamatinib, is considered a maintenance therapy that may reduce the significant roller coast platelet counts. Furthermore, this drug is given orally and may improve compliance compared to some non-oral agents for it has ease of administration in the comfort of a patient’s home with little to no supervision.
Place in therapy
How would the drug under review fit into the current treatment paradigm?
In ITP, platelet destruction is mediated by (spleen tyrosine kinase) Syk-dependent phagocytosis of FcγR-bound platelets. Further, Syk also plays a role in antibody formation. Fostamatinib is an oral Syk inhibitor that is a competitive inhibitor of the Syk catalyst domain and leads to impaired Fc receptor signalling & theoretically B-cell signalling thereby mitigating the mechanistic effect of ITP. Given its novel mechanism of action compared to all previous ITP treatments, it can be used as a single agent in those who have failed another ITP treatment and theoretically may be combined with other ITP treatments to provide a synergistic effect.
No, the drug under review is not the first treatment approved that will address the underlying disease process. All other drugs are trying to address the underlying disease process whether it is to mitigate the antibody-mediated destruction of platelets (such as prednisone, IVIg, splenectomy, etc.) or to increase platelet production (TPO-RAs). However, it is the first drug that targets the important Syk-dependent phagocytosis of platelets.
The drug under review would likely be used as a single agent after first-line therapy. Specifically, fostamatinib would be used in 2nd or subsequent line therapies as monotherapy.
Yes, the drug under review will likely cause a shift in the current treatment paradigm. It would provide an alternative to the above mentioned second and subsequent line therapies such as splenectomy, immunosuppressive agents, rituximab and its biosimilars, and TPO-RAs. Ideally, it should be considered before splenectomy, immunosuppressive agents, rituximab and its biosimilars and be comparable to maintenance treatments such as the TPO-RAs.
Open ended replies furnished in the online survey by U.S. based clinicians reinforce this recommendation:
“I prefer to use it as a second line agent or in lieu of splenectomy or after failure of TPO mimetics. If history of prior thrombosis, it is my preferred drug in second line.”
“Tavalisse could reasonably be one of the main 2nd line choices of treatment (after initial therapy with corticosteroids). My experience has been to use this medication rather than romiplostim, rituximab, or splenectomy in the 2nd line.”
Please indicate whether or not it would be appropriate to recommend that patients try other treatments before initiating treatment with the drug under review. Please provide a rationale from your perspective.
As mentioned above, the drug under review would likely be used as a single agent after first-line therapy. First-line therapy should remain as corticosteroids such as prednisone or dexamethasone and in some cases where a rapid response is required IVIg should be given.
However, for second and subsequent line therapies, it should be considered before splenectomy, immunosuppressive agents, rituximab and its biosimilars and be comparable to maintenance treatments such as the TPO-RAs.
Additional open-ended replies were captured by our colleagues in the U.S. through the clinician online survey and are kindly provided: “The lack of thrombotic risk and marrow fibrosis, makes this the ideal second line agent in my view.”
“It would be appropriate to consider other therapies such as splenectomy and rituximab, but there are multiple advantages of Tavalisse as an oral targeted therapy with good durability and favorable side effect profile that make it clinically attractive.”
How would this drug affect the sequencing of therapies for the target condition?
In ITP, first-line therapy should remain as corticosteroids such as prednisone or dexamethasone and in some cases where a rapid response is required IVIg should be given.
The drug under review should be used in second and subsequent line therapies before splenectomy, immunosuppressive agents, rituximab and its biosimilars and be comparable to maintenance treatments such as the TPO-RAs.
If after the therapy has failed, then consider splenectomy, immunosuppressive agents, rituximab and its biosimilars. This would not be a significant departure to the typical sequencing of therapies.
Typically, in ITP, patients are not treated with the same drug in a subsequent line of therapy.
Which patients would be best suited for treatment with the drug under review?
It is likely that ITP patients earlier in their disease course will respond better to fostamatinib. Thus, utilizing it in 2nd line likely has the advantages of better and more robust response and limiting exposure to the complications and toxicities of other lines of therapy such as splenectomy, immunosuppressive agents, rituximab and its biosimilars.
As discussed before, the patients who are multiply relapsed/refractory are the most in need of an intervention. However, to reduce patients from becoming multiply treated with options that are not Health Canada approved, has numerous toxicities, and overall, not highly effective would also have the benefit of treating ITP patients earlier with this novel agent.
The drug under review, fostamatinib, does have adverse effects such as diarrhea, hypertension, nausea, dizziness, and elevated ALT. It would be a case-by-case discussion with patients, assessing their comorbid conditions, and balancing these potential side effects.
How would patients best suited for treatment with the drug under review be identified?
ITP patients are managed predominantly by Hematologists, internists, and family physicians. With relapsed disease, these patients are referred to Hematologists and so are identified in Hematology clinics. In relapsed disease, patients may end up in the Emergency rooms or be admitted to hospital where they are also referred to Hematologists. ITP patients with relapsed disease are best suited for fostamatinib and are identified when they are referred or followed by a Hematologist.
Relapsed ITP includes a drop in platelets (<30), clinical bleeding, or both. This condition may be challenging to diagnose in routine clinical practice initially as ITP is a diagnosis of exclusion. However, for relapsed disease, it is not difficult. These would be patients who have responded to ITP treatment(s) and as such the treatment response is diagnostic of ITP itself. It is these relapsed patients who would be candidates for the drug under review and who would most likely benefit from this treatment.
For relapsed ITP, the diagnosis is relatively easy as their platelets drop to less than 30. Platelet counts are done on a standard CBC that is available in all labs.
It is possible that ITP can be misdiagnosed. However, as mentioned above, relapsed ITP is relatively easy to diagnose given the diagnostic utility of having prior evidence of response to ITP treatment. It is possible that ITP can be underdiagnosed as low platelets in some patients may be attributed to another disorder even in the relapsed setting. For example: An ITP patient is admitted with a viral infection and the drop in platelets is attributed to a viral infection rather than a relapse in ITP.
Yes, asymptomatic patients with relapsed ITP (i.e., having platelets < 30) should be treated. The current American Society of Hematology 2019 guidelines provides support for this.
According to our U.S. colleagues, in addition to lab tests, ITP patients may also be identified through clinician examination (Survey Q5) (Figure 2).

Which patients would be least suitable for treatment with the drug under review?
ITP patients who have or likely will have unmanageable or debilitating side effects listed (diarrhea, hypertension, nausea, dizziness, and ALT increase) would be least suitable for the therapy under review.
Is it possible to identify those patients who are most likely to exhibit a response to treatment with the drug under review?
Currently, we are not aware of predictive factors for treatment with fostamatinib other than earlier use in ITP as it is likely to increase response rates.
What outcomes are used to determine whether a patient is responding to treatment in clinical practice?
In ITP, patients are monitored regularly with bloodwork (CBC that includes their platelet counts), clinically in a healthcare setting (clinics, hospital), and lack of “rescue” therapy are ways to assess good outcomes of therapy.
U.S. based clinicians’ perspectives aligned well with the Canadian point of view as per the data appearing below. In Question 12, clinicians identified the following outcomes used in clinical practice to determine if a patient is responding to the therapy under review (Figure 3).
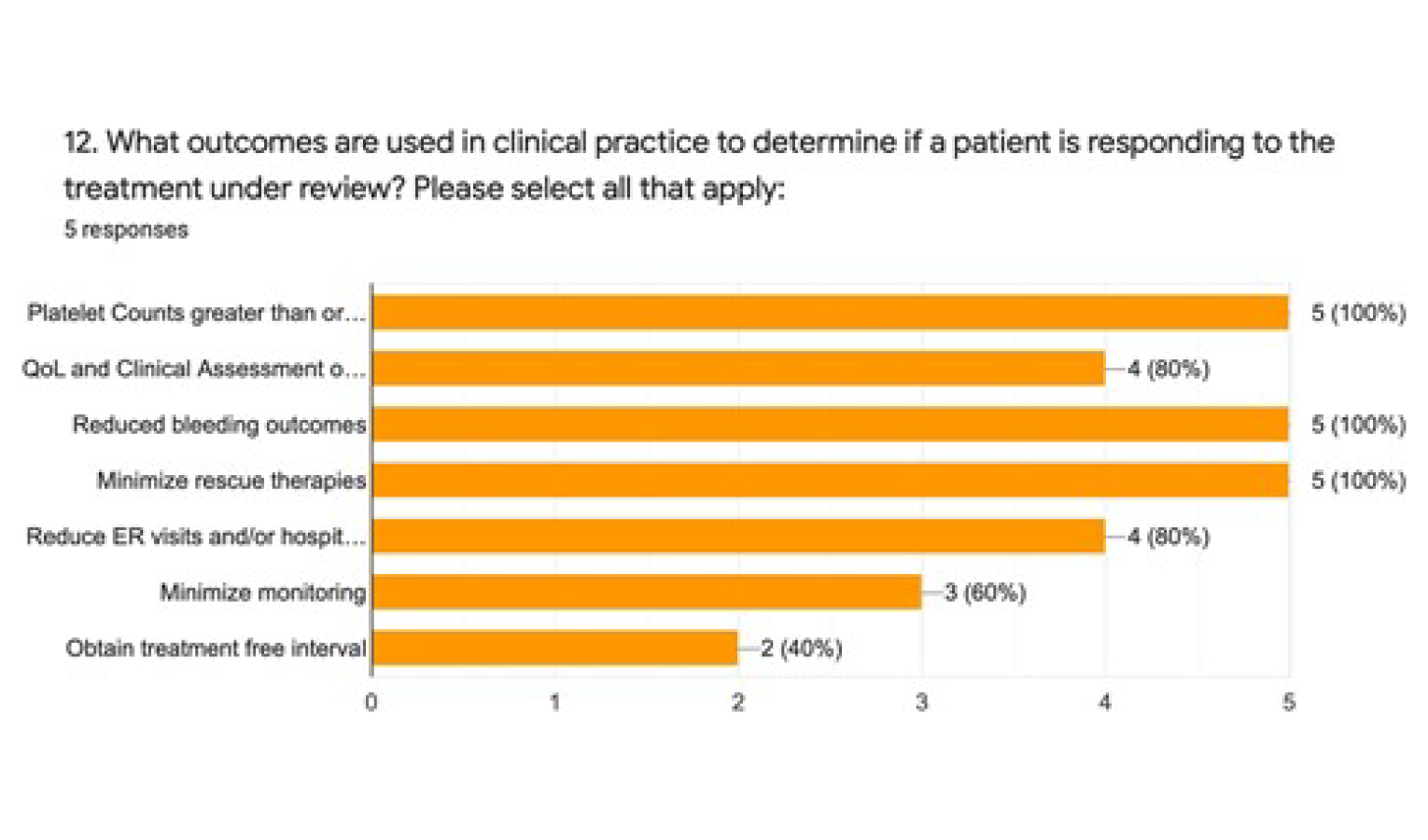
100% of U.S. based clinicians selected the following top three (3) outcomes:
Minimize rescue therapies
Reduce bleeding outcomes
Platelet counts greater than or equal to 30
What would be considered a clinically meaningful response to treatment?
A clinically meaningful response would be the totality of achieving the goals desired by the patient, physician, and healthcare system. As discussed previously, most of these goals are complementary and, in this context, would also be considered clinically meaningful. The most evident response is to prolong life by reducing the risk of life-threatening bleeding. To achieve this, it requires an increase in platelet counts to “safe” ranges that may differ for day-to-day activities, perioperatively, and during pregnancy if applicable. These would be major “milestones”. However, clinically meaningful must take into consideration the health-related quality of life parameters noted above by patients and an ability to maintain these parameters (Figure 4).
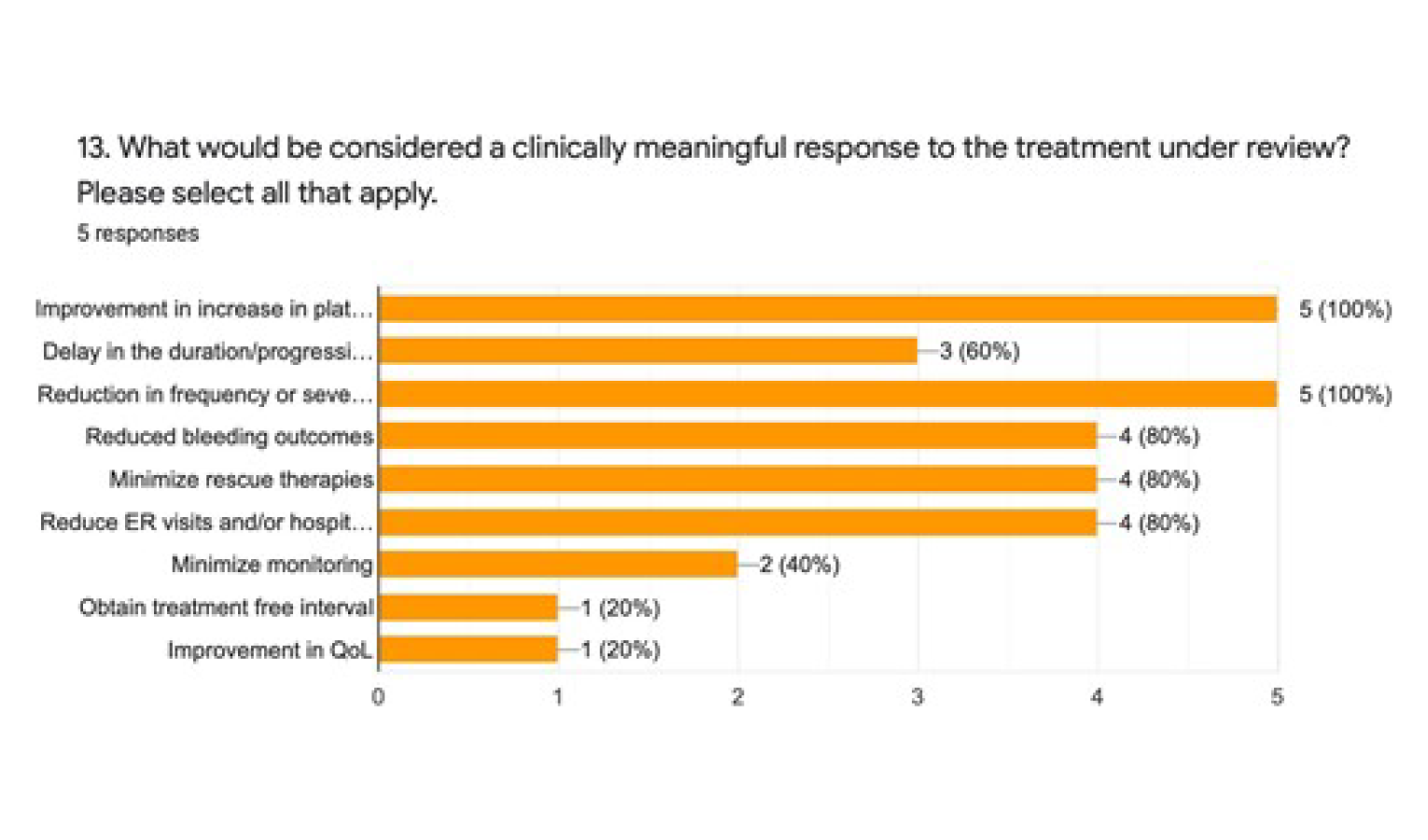
In the clinician survey that was sent to our U.S. based colleagues, 100% of the respondents selected the following as clinically meaningful responses to the drug under review (Q13):
Improvement in increase in platelet count (greater than or equal to 30)
Reduction in frequency in or severity of disease-related symptoms (i.e., fatigue, excessive bruising, and bleeding)
How often should treatment response be assessed?
ITP patients are heterogeneous in clinical presentation and treatment response. Typically, in adult outpatients with ITP, they will require weekly bloodwork and/or assessments that can gradually be reduced in frequency depending on response. There is no specific guideline for how often to assess based on platelet levels.
What factors should be considered when deciding to discontinue treatment?
ITP treatments are often discontinued if there is disease progression (worsening drop in platelets, increased bleeding), develop adverse side effects, or require “rescue” treatments.
The U.S. Clinicians concurred as per the data captured in Figure 5.
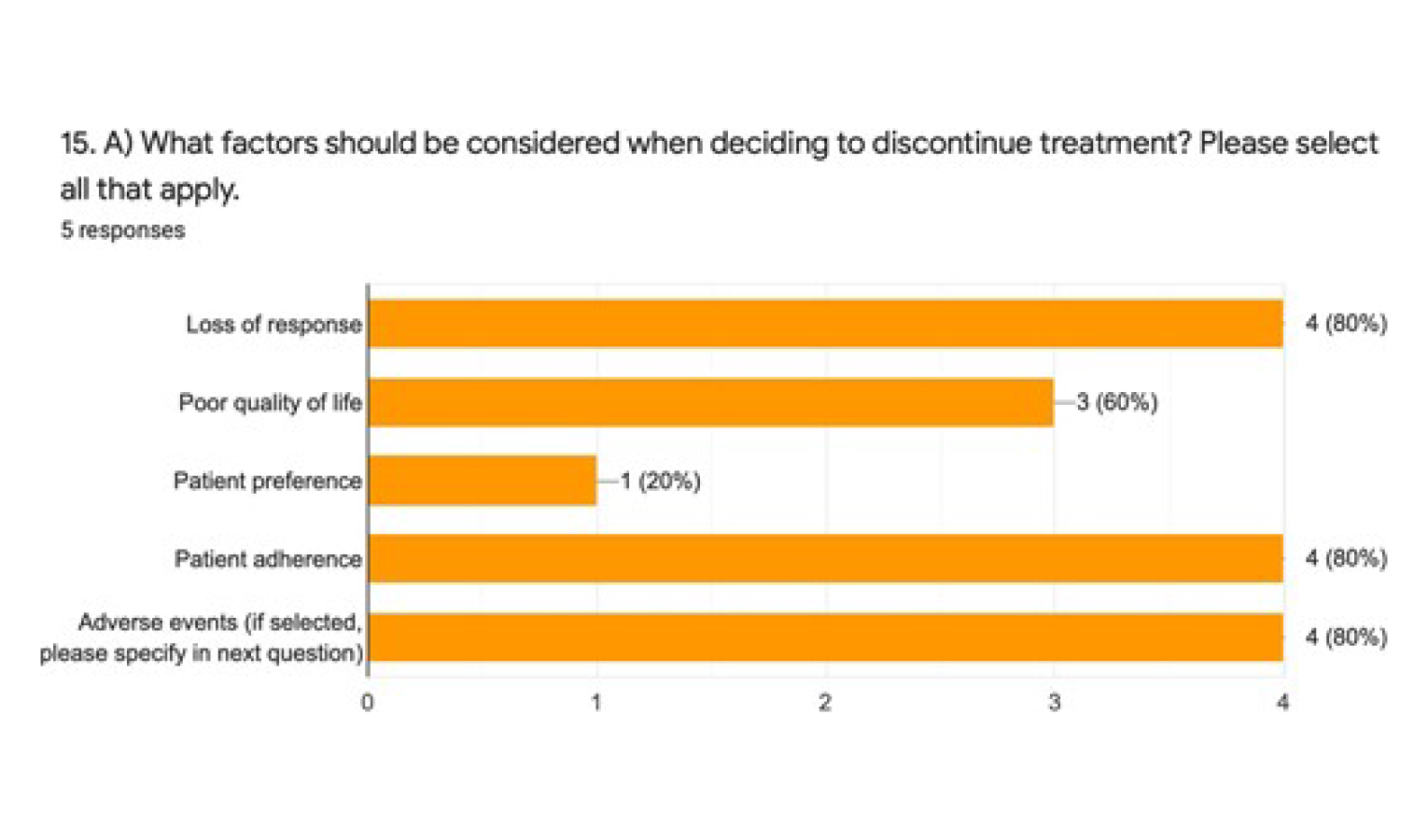
It is important to note that the patient’s preferences and values should also be taken into consideration when deciding to discontinue a therapy as reflected in the survey results above.
What settings are appropriate for treatment with the drug under review?
The drug under review can be appropriate in the outpatient setting (patients seen in clinic) and in the emergency room & hospitalized patients (if failing other treatments fostamatinib may give a median response of approximately 15 days). The therapy has the added benefit and convenience of oral administration, thereby providing the patient with ease in administration and a reduction in a burden to the healthcare system.
For non-oncology drugs, is a specialist required to diagnose, treat, and monitor patients who might receive the drug under review?
Typically, as discussed above ITP patients with relapsed disease are referred to a Hematologist for diagnosis, treatment, and monitoring.
Additional information
Is there any additional information you feel is pertinent to this review?
The drug under review is an active agent that works best when used early in the course of the disease trajectory. It can spare patients from an invasive surgery, such as a splenectomy and the associated immune suppression. The therapy is an oral agent which is easily administered in the comfort of a patient’s home, minimizing clinic visits and potential hospitalizations. It is well tolerated, prevents the destruction of platelets efficiently in the spleen, and maintains stable platelet counts. It is deemed to have a good side effect profile whose safety data has been deemed acceptable. Patients have the option of taking the therapy with food or fasting which is considered a convenience. To date, there have been no reports of severe/fatal liver toxicities.
If publicly funded, Fostamatinib would be an extremely important second line therapeutic option for ITP patients who have progressed on first line and who might be spared from an invasive surgical procedure such as splenectomy and the resulting immunosuppression.
Collectively, we strongly support and urge that a positive funding recommendation be issued for Fostamatinib for the second line treatment of thrombocytopenia in adult patients with chronic immune thrombocytopenia who have had an insufficient response to other treatments. We maintain it aligns well with the identified need for a new, more effective, quickly, and easily administered, less toxic treatment option that is capable of maintaining a good quality of life with a longer progression free survival. It provides a clinically meaningful improvement in quality of life in addition to fewer adverse events and a preferred toxicity profile. It should be the new standard of care for the ITP patient population in second line therapy.
Conflict of Interest Declarations for Hematology
To maintain the objectivity and credibility of the CADTH drug review programs, all participants in the drug review processes must disclose any real, potential, or perceived conflicts of interest. This conflict of interest declaration is required for participation.
Declarations made do not negate or preclude the use of the clinician group input. CADTH may contact your group with further questions, as needed. Please see the Procedures for CADTH Drug Reimbursement Reviews (section 6.3) for further details.
Did you receive help from outside your clinician group to complete this submission? If yes, please detail the help and who provided it.
Yes. Accelera Canada in partnership with Advocacy Solutions commissioned the services of Filomena Servidio-Italiano from Blue Ribbon Project Inc. to assist with the planning, coordination and facilitation of this joint clinician input submission, its data analysis and assistance preparing this submission.
Did you receive help from outside your clinician group to collect or analyze any information used in this submission? If yes, please detail the help and who provided it.
Yes, Accelera Canada in partnership with Advocacy Solutions commissioned the services of Filomena Servidio-Italiano from Blue Ribbon Project Inc. to assist with the planning, coordination and facilitation of this joint clinician input submission, its data analysis and assistance preparing this submission.
List any companies or organizations that have provided your group with financial payment over the past two years AND who may have direct or indirect interest in the drug under review. Please note that this is required for each clinician that contributed to the input — please add more tables as needed (copy and paste). It is preferred for all declarations to be included in a single document.
Declaration for Clinician 1
Name: Cyrus C. Hsia
Position: Hematologist, London, Ontario
Date: 19-07-2021
Table 2: Declaration for Hematology Clinician 1
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
Amgen | X | — | — | — |
Novartis | X | — | — | — |
Medison | X | — | — | — |
Sobi | X | — | — | — |
Declaration for Clinician 2
Name: Matthew Kang
Position: Hematologist, Burlington, Ontario
Date: 28-07-2021
Table 3: Declaration for Hematology Clinician 2
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
Amgen | X | — | — | — |
Bristol-Myers Squibb | X | — | — | — |
Gilead/Kite | X | — | — | — |
Janssen | — | — | X | — |
Medison | X | — | — | — |
Novartis | X | — | — | — |
Declaration for Clinician 3
Name: Lakshman Vasanthamohan
Position: Hematologist, Lakeridge Health, Oshawa, ON
Date: 29-07-2021
Table 4: Declaration for Hematology Clinician 3
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
No COI | — | — | — | — |
Declaration for Clinician 4
Name: Sudeep Shivakumar
Position: Hematologist, Hlifax, Nova Scotia
Date: 30-Jul-2021
Table 5: Declaration for Hematology Clinician 4
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
Sobi | X | — | — | — |
Declaration for Clinician 5
Name: Philip George Kuruvilla
Position: Medical Oncologist
Date: 30/7/2021
Table 6: Declaration for Hematology Clinician 5
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
Amgen | X | — | — | — |
Novartis | X | — | — | — |
Medison | X | — | — | — |
Declaration for Clinician 6
Name: Mark Blostein
Position: Associate Professor of Medicine
Date: 31-07-2021
Table 7: Declaration for Hematology Clinician 6
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
Amgen | X | — | — | — |
Novartis | X | — | — | — |
Pfizer | X | — | — | — |
Servier | X | — | — | — |
Bayer | X | — | — | — |
Declaration for Clinician 7
Name: Hayley Merkeley
Position: Hematologist, Vancouver, BC
Date: 2-08-2021
Table 8: Declaration for Hematology Clinician 7
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
Amgen | X | — | — | — |
Medison | X | — | — | — |
Shire/Takeda | X | — | — | — |
Celgene/BMS | — | — | — | — |
Novartis educational grant | — | — | X | — |
Declaration for Clinician 8
Name: Alejandro Lazo-Langner
Position: Chair/Chief, Hematology, Western University
Date: 02-08-2021
Table 9: Declaration for Hematology Clinician 8
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
No COI | — | — | — | — |
Declaration for Clinician 9
Name: Kuljit Grewal
Position: Hematologist, Associate Professor, Memorial University of Newfoundland
Date: 03-08-2021
Table 10: Declaration for Hematology Clinician 9
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
Amgen | X | — | — | — |
Novartis | X | — | — | — |
Declaration for Clinician 10
Name: Colin Yee
Position: Hematologist, Kitchener, Ontario
Date: 03-08-2021
Table 11: Declaration for Hematology Clinician 10
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
No COI | — | — | — | — |
Declaration for Clinician 11
Name: Nicole Laferriere
Position: Hematologist, Thunder Bay, Ontario (TBRHSC)
Date: 03-08-2021
Table 12: Declaration for Hematology Clinician 11
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
AMGEN Canada | X | — | — | — |
Astellas Pharma | X | — | — | — |
Gilead | X | — | — | — |
Abbvie Corporation | X | — | — | — |
Janssen Ortho | X | — | — | — |
TEVA | X | — | — | — |
Novartis Pharmaceuticals | X | — | — | — |
Sanofi | X | — | — | — |
ROCHE | X | — | — | — |
Bristol Myers Squibb | X | — | — | — |
Takeda | X | — | — | — |
LEO Pharma | X | — | — | — |
Declaration for Clinician 12
Name: Zachary Liederman
Position: Hematologist, Toronto, Ontario
Date: 03-08-2021
Table 13: Declaration for Hematology Clinician 12
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
Sobi | X | — | — | — |
Declaration for Clinician 13
Name: Yulia Lin
Position: Hematology, Transfusion Medicine Specialist, Sunnybrook Health Sciences Centre
Date: 03-August-2021
Table 14: Declaration for Hematology Clinician 13
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
No COI | — | — | — | — |
Declaration for Clinician 14
Name: Siraj Mithoowani
Position: Hematologist, Hamilton, Ontairo
Date: 05-08-2021
Table 15: Declaration for Hematology Clinician 14
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
Leo Pharma | X | — | — | — |
Declaration for Clinician 15
Name: Vinai Bhagirath
Position: Assistant Professor, McMaster University
Date: 06/08/2021
Table 16: Declaration for Hematology Clinician 15
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
Pfizer | X | — | — | — |
Bayer | X | — | — | — |
Declaration for Clinician 16
Name: Christine M. Cserti-Gazdewich
Position: Transfusion Medicine Specialist & Clinical Hematologist
Date: 06-08-2021
Table 17: Declaration for Hematology Clinician 16
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
No COI | — | — | — | — |
Declaration for Clinician 17
Name: Loree Larratt
Position: Professor Emeritus University of Alberta
Date: August 8, 2021
Table 18: Declaration for Hematology Clinician 17
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
Tavalisse | X | — | — | — |
Declaration for Clinician 18
Name: Anna Nikonova
Position: Hematologist, Assistant Professor McGill University, MUHC, Montreal, QC
Date: 09-08-2021
Table 19: Declaration for Hematology Clinician 18
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
Janssen | X | — | — | — |
Celgene | X | — | — | — |
Declaration for Clinician 19
Name: Sadiya Kukaswadia
Position: MD, FRCPC
Date: August 9, 2021
Table 20: Declaration for Hematology Clinician 19
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
No COI | — | — | — | — |
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up-to-date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
Redactions: Confidential information in this document may be redacted at the request of the sponsor in accordance with the CADTH Drug Reimbursement Review Confidentiality Guidelines
Stakeholder Input: The views expressed in each submission are those of the submitting organization or individual; not necessarily the views of CADTH or of other organizations. As such, they are independent of CADTH and do not necessarily represent or reflect the view of CADTH. No endorsement by CADTH is intended or should be inferred. By filing with CADTH, the submitting organization or individual agrees to the full disclosure of the information. CADTH does not edit the content of the submissions.
CADTH does use reasonable care to prevent disclosure of personal information in posted material; however, it is ultimately the submitter’s responsibility to ensure no identifying personal information or personal health information is included in the submission. The name of the submitting organization or individual and all conflict of interest information are included in the submission; however, the name of the author, including the name of an individual patient or caregiver submitting the patient input, are not posted.
Accessibility: CADTH is committed to treating people with disabilities in a way that respects their dignity and independence, supports them in accessing material in a timely manner, and provides a robust feedback process to support continuous improvement. All materials prepared by CADTH are available in an accessible format. Where materials provided to CADTH by a submitting organization or individual are not available in an accessible format, CADTH will provide a summary document upon request. More details on CADTH’s accessibility policies can be found here.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.