Drugs, Health Technologies, Health Systems
Systematic Review
Overview of Systematic Reviews of ICIs in NSCLC With EGFR, ALK, ROS1, and RET Actionable Driver Mutations
Authors: Shariq Najeeb, Said Yousef Abdelrazeq, Shannon E. Kelly, Xiaoqin Wang, Becky Skidmore, Nazmun Nahar, Melissa Brouwers, George A. Wells
This Systematic Review was conducted by the POst-Market Drug Evaluation Team (PODET) through the Post-Market Drug Evaluation (PMDE) CoLab Network.
PROSPERO Registration Number: CRD42024490981
Key Messages
The effectiveness and safety of immune checkpoint inhibitor (ICI) monotherapy in patients with previously treated advanced or metastatic non–small cell lung cancer with EGFR, ALK, ROS1, or RET actionable driver mutations or chromosomal rearrangements is currently uncertain.
We assessed the efficacy and safety of ICIs in patients with this condition whose disease did not respond well to previous chemotherapy.
We reviewed 13 systematic reviews of randomized controlled trials (RCTs). The quality assessment of these reviews revealed critical methodological flaws.
All 13 systematic reviews focused on survival and progression-free survival (PFS) for patients with non–small cell lung cancer and EGFR gene mutations. The systematic reviews generally considered the same set of 4 clinical trials and did not report on other outcomes or patient groups, except for 1 review that looked at patients with different levels of anti-PD-L1 expression.
We found no evidence on the efficacy and safety of ICIs in patients with ALK, ROS1, or RET mutations.
Overall, the systematic reviews concluded that using ICIs alone, as a second-line therapy or beyond, does not significantly improve overall survival (OS) and PFS compared to chemotherapy in patients with non–small cell lung cancer with EGFR gene mutations.
No conclusions can be made regarding the benefits of ICIs in patients with EGFR mutations based on histology or high antiprogrammed death-ligand 1 antibody expression levels.
The safety of ICIs in patients with EGFR, ALK, ROS1, or RET actionable driver mutations could not be assessed because of the lack of evidence provided in the included systematic reviews.
Abbreviations
AMSTAR 2
A MeaSurement Tool to Assess systematic Reviews 2
CDA-AMC
Canada’s Drug Agency
ICI
immune checkpoint inhibitor
MA
meta-analysis
NMA
network meta-analysis
NRS
nonrandomized study
NSCLC
non–small cell lung cancer
OS
overall survival
PD-L1
programmed death-ligand 1
PFS
progression-free survival
PICO
participants, intervention, controls, outcomes
RCT
randomized controlled trial
SR
systematic review
Introduction and Rationale
Background
Lung cancer is the most frequently diagnosed cancer in Canada and the leading cause of cancer-related deaths in both males and females. In 2021, it was projected that there would be more than 29,600 new diagnoses, accounting for 12.5% of all new cancer cases in males and 13.3% of all new cancer cases in females.1 Additionally, lung cancer was expected to lead to 21,000 deaths, representing 24.2% of all cancer-related deaths in males and 25.8% of all cancer-related deaths in females.1 The adjusted 5-year net survival estimate in Canada for all forms of lung cancers is 22%1 and, in the US, the anticipated 5-year survival for patients with non–small cell lung cancer (NSCLC) is approximately 25%, and for patients with stage IV disease, the anticipated 5-year survival rate is 7%.2 Smoking is an established risk factor for developing lung cancer, accounting for more than 72% of newly diagnosed cases in Canada.1,3 NSCLC is broadly categorized into 2 subtypes: squamous cell carcinoma and nonsquamous cell carcinoma.4 Squamous cell NSCLC, formerly known as epidermoid carcinoma, typically originates in the larger central airways of the lungs and is strongly associated with a history of smoking.5 It often presents with symptoms such as coughing, chest pain, and coughing up blood, and is frequently diagnosed at an earlier stage compared to other types of NSCLC. On the other hand, nonsquamous NSCLC, including adenocarcinoma and large cell carcinoma, generally occurs peripherally and may present more commonly with symptoms related to peripheral lesions, such as chest pain or pleural effusion, in addition to cough and dyspnea.6
Early diagnosis improves the prognosis of the disease and its responsiveness to therapy. Diagnosis is based on histology and symptom presentation.3,7 Patients may experience worsening coughs, chest pain, hemoptysis, malaise, weight loss, dyspnea, and/or hoarseness at clinical presentation or upon chest imaging.1,3 In advanced or metastatic disease, patients experience additional symptom burdens such as troubled breathing, chronic cough and chest pain, pain in bone or spine, yellowing of the skin or eyes, weakness or numbness of arms or legs, fatigue and unexplained weight loss, depression, insomnia, and pain.8,9 Staging at diagnosis is key in determining disease prognosis and facilitates treatment selection.3,9 Late diagnosis is a significant contributing factor to early mortality and is challenging for disease management in real-world practice. More than 50% of NSCLC diagnoses in Canada are made at stage IV with only about 23% of cases diagnosed at early stage I.1
The expression of genomic oncogenic driver mutations in tumours is known to be a root factor for oncogenesis in some tumours. In recent years, several pharmacological therapies have been developed to target these mutated, malfunctioning genes. Predictive drivers identified in recent years include EGFR, ROS1, KRAS, ALK, BRAF, and others. These discoveries greatly influenced treatment strategies that, in practice, improved patient quality of life and increased OS for patients.9-11 Prevalence estimates from studies show that about 1% to 2% of NSCLC cases are RET fusion-positive,12 1% are ROS1 fusion-positive,13 17% have activating mutations in the EGFR gene,14 and 5% have an ALK rearrangement.15,16
Drugs targeting EGFR, ROS1, NTRK, ALK, and RET mutations in advanced or metastatic NSCLC have been recommended for reimbursement by Canada’s Drug Agency (CDA-AMC) and funded by the provinces, they are now available in the Canadian public health care system. Conversely, drugs for BRAF V600, KRAS G12C, and MET exon 14 skipping mutations are available on the Canadian market but were not recommended for reimbursement or funded by the provinces. These latter drugs are only available to patients who are covered by private insurance or who are willing to spend the cost out of pocket. These drugs and their associated biomarkers are not a consideration for postmarket CDA-AMC systematic reviews such as the present report, which focuses on policy-relevant health interventions.
ICI drugs such as nivolumab, atezolizumab, and nivolumab are also available to treat NSCLC. They harness the immune system to fight cancer by targeting proteins (PD-1, PD-L1, CTLA-4) that act as checkpoints, allowing T-cells to recognize and destroy cancer cells more effectively.17 The ICI drugs approved for the treatment of NSCLC in Canada are presented in Table 1. ICI drugs such as nivolumab, pembrolizumab, and atezolizumab were originally introduced into practice in patients with previously treated advanced or metastatic NSCLC. Practice has evolved as the evidence base has developed. ICIs are now more widely used as a first-line therapy in these patients.18 Systemic pharmacotherapies such as ICIs can be given to patients who have either locally advanced disease that is confined to the chest area and nearby lymph nodes but is not amenable to surgery, or those who have metastatic disease that has spread to other organs. Systemic therapies can also be given in the adjuvant setting after surgery to reduce the risk of recurrence, and in the neoadjuvant setting before surgery to reduce tumour size.
Evidence has shown that tumours bearing specific mutations and managed with therapies targeting these mutations at the biochemical level will respond well to treatment. As such, it is widely recommended to first treat tumours bearing actionable mutations with these targeted therapies. Another key finding is that ICI drugs exhibit much smaller antitumour activity in cancers with these identified mutations than in their unmutated counterparts.19-21 Consequently, Health Canada product monographs22-24 and CDA-AMC algorithms recommend use of ICIs only after prior use of a targeted therapy and a course of platinum-based chemotherapy.25-27 This has been translated into CDA-AMC provisional funding algorithms for ALK, EGFR, and RET aberrations in NSCLC.25-27 While clinical guidelines recommend using ICIs after targeted therapy and chemotherapy, uncertainties persist regarding their benefits in later lines of therapy and compared with alternative chemotherapy. In NSCLC, PD-L1 levels may predict response to ICI drugs, but similar uncertainties persist.28 Addressing this issue will involve assessing ICI effectiveness and safety in advanced NSCLC, considering specific driver mutations (i.e., EGFR, ALK, RET, and ROS1), and evaluating their place in the treatment sequence.
Policy Issue
Currently, ICI monotherapy with atezolizumab, nivolumab, or pembrolizumab is indicated for advanced or metastatic NSCLC, regardless of mutational status, following prior chemotherapy. Currently, publications (including systematic reviews [SRs]29 on this topic) provide no overall consensus on the use of ICIs in the second-line setting or beyond resulting in any substantial benefits to patients with mutated NSCLC, nor is there consensus on how they compare with single-drug nonplatinum chemotherapies, which is a classical option in this setting. Therefore, this review aims to provide a critical overview of the published SRs that compare the efficacy and safety of ICI monotherapy to other chemotherapeutic drugs in patients with advanced or metastatic NSCLC with specific mutations or chromosomal rearrangements (i.e., EGFR, ALK, RET, ROS1) who have experienced previous chemotherapy.
Table 1: ICI Drugs for Advanced or Metastatic NSCLC Currently Reimbursed in Canada
Drug (trade name, manufacturer) | Presentation (ATC code) | Approved use |
|---|---|---|
Pembrolizumab22 (Keytruda, Merck) | Solution for infusion 100 mg/4 mL vial (L01FF02) | First-line monotherapy for metastatic NSCLC in adults with PD-L1 expression (TPS ≥ 1%), excluding those with EGFR or ALK genomic aberrations, and those ineligible for surgery or definitive chemoradiation. Treatment of adults with metastatic squamous NSCLC in combination with carboplatin and either paclitaxel or nab-paclitaxel, without prior systemic chemotherapy treatment for metastatic NSCLC. Monotherapy for metastatic NSCLC in adults whose tumours express PD-L1 (TPS ≥ 1%) and have disease progression on or after platinum-containing chemotherapy. Patients with EGFR or ALK genomic tumour aberrations should have received authorized therapy for these aberrations before receiving Keytruda. |
Nivolumab23 (Opdivo, Bristol Myers Squibb) | IV Infusion, 10 mg nivolumab /mL 40 mg and 100 mg single-use vials (L01FF01) | Locally advanced or NSCLC with progression after platinum-based chemotherapy. Patients with EGFR or ALK genomic tumour aberrations should experience disease progression on a therapy targeting these aberrations before starting Opdivo. |
Atezolizumab24 (Tecentriq, Roche) | Solution for infusion, 60 mg per mL; 840 mg and 1,200 mg single-use vial (L01FF05) | As adjuvant treatment following complete resection and no progression after platinum-based adjuvant chemotherapy for adults with stage II to IIIA* NSCLC, whose tumours have PD-L1 expression on ≥ 50% of tumour cells. As first-line monotherapy for metastatic NSCLC in adults with high PD-L1 expression (PD-L1 stained ≥ 50% of tumour cells or PD-L1 stained tumour-infiltrating immune cells, covering ≥ 10% of the tumour area), determined by a validated test, and without EGFR or ALK genomic tumour aberrations. For the treatment of adult patients with locally advanced or metastatic NSCLC with progression on or after platinum-based chemotherapy. Patients with NSCLC with EGFR or ALK genomic tumour aberrations should have disease progression on a therapy for these aberrations before receiving Tecentriq. |
ATC = Anatomical Therapeutic Chemical; NSCLC = non–small cell lung carcinoma; PD-L1 = programmed death-ligand 1; TPS = Tumor Proportion Score.
Policy Questions
How should ICI monotherapies after chemotherapy be funded in patients with advanced/metastatic NSCLC harbouring actionable driver mutations (i.e., ALK, EGFR, ROS1, or RET genomic aberrations)?
Should all chemotherapy options be exhausted before funding immuno-oncology monotherapy?
Purpose
To assess the efficacy and safety of ICI treatments as second-line or subsequent monotherapies in patients with NSCLC harbouring actionable driver mutations (e.g., ALK, EGFR, ROS1, or RET genomic aberrations), in comparison to traditional chemotherapeutic agents and optimal supportive care.
Research Questions
What is the evidence for the clinical efficacy of atezolizumab, nivolumab, and pembrolizumab monotherapy in patients with advanced or metastatic NSCLC with EGFR, ALK, RET, or ROS1 actionable driver mutations that have progressed on prior chemotherapy compared with patients who receive single-drug nonplatinum chemotherapy?
What is the evidence for the safety of atezolizumab, nivolumab, and pembrolizumab monotherapy in patients with advanced or metastatic NSCLC with EGFR, ALK, RET, or ROS1 actionable driver mutations that have progressed on prior chemotherapy compared with patients who receive single-drug nonplatinum chemotherapy?
What is the evidence around how the clinical efficacy of atezolizumab, nivolumab, and pembrolizumab may vary by the actionable driver mutations of interest?
Opportunities for Feedback
Interested parties were given the opportunity to comment on the proposed project protocol that informed this report and were invited to provide feedback on the draft report.
Protocol Development
The protocol and review followed guidance from the Cochrane Handbook for Systematic Reviews of Interventions30 and the Preferred Reporting Items for Overviews of Reviews (PRIOR) checklist.31-33 The protocol was written a priori, followed throughout the review process, and registered in advance through the PROSPERO International Prospective Register of Systematic Reviews (registration number: CRD42024490981). There are no deviations from the protocol to report.
Clinical Review
Preliminary literature assessment revealed that several SRs answering the research questions had been published. Consequently, the research questions were addressed using an overview of SRs.
Literature Search Methods
An experienced medical information specialist developed and tested the search strategies through an iterative process in consultation with the review team. Another senior information specialist peer-reviewed the MEDLINE strategy before execution using the Peer Review of Electronic Search Strategies (PRESS) Checklist.34
Using the multifile option and deduplication tool available on the Ovid platform, we searched Ovid MEDLINE ALL, Embase Classic+Embase, and the Cochrane Database of Systematic Reviews.
The strategies utilized a combination of controlled vocabulary (e.g., “Carcinoma, Non-Small-Cell Lung,” “Neoplasm Metastasis,” “Antineoplastic Agents, Immunological”) and keywords (e.g., “NSCLC,” “metastatic,” “atezolizumab”). We applied a systematic review filter to the MEDLINE and Embase searches. We adjusted vocabulary and syntax as necessary across the databases. There were no language restrictions, but we limited results to the publication years 2013 to the present. Where applicable, we removed animal-only, conference abstracts, opinion pieces, and other irrelevant publication types. We downloaded and deduplicated the records using EndNote version 9.3.3 (Clarivate Analytics). The complete literature search strategy is presented in Appendix 1.
Searches were executed on January 26, 2024 and updated monthly until April 24, 2024.
Selection Criteria
The selection criteria employed in this overview is presented in presented in Table 2. Protocols, conference abstracts, non-English records, and nonsystematic reviews were excluded.
Criteria | Description |
|---|---|
Population | Adults with advanced or metastatic NSCLCa with RET fusion, ALK rearrangement, ROS1 mutation, or EGFR mutation that is considered actionable by targeted therapy who have been previously treated with platinum-based chemotherapy.b Subgroups PD-L1 expression:
|
Intervention | Atezolizumab, nivolumab, or pembrolizumab as monotherapy |
Comparators | Docetaxel, gemcitabine, or pemetrexed as monotherapy, or best supportive carec |
Outcomes | At least one of:
|
Study designs | Systematic reviews of RCTs and/or NRSsf |
NRS = nonrandomized study; NSCLC = non–small cell lung cancer; OS = overall survival; PD-L1 = programmed cell death-ligand 1; PFS = progression-free survival; RCT = randomized controlled trial.
aThis refers to individuals with locally advanced NSCLC who are not candidates for surgical resection or definitive chemoradiation or who have metastatic NSCLC.
bActionable driver mutations will be considered separately.
cInclusion of best supportive care as defined by study authors. This comparator expanded consideration to patients who may have no current chemotherapy options remaining.
dThis outcome focused on change in total score. Additional subscale domains were considered when total scores were not reported.
eGrade 3 or 4, or adverse events requiring emergency department visit or hospitalization.
fSRs of, or including, NRSs were considered for populations or outcomes of interest only when no RCT evidence was available.
Population
The population of interest was adults with advanced or metastatic NSCLC with RET fusion, ALK rearrangement, ROS1 mutation, or EGFR mutation that is considered actionable by targeted therapy who have been previously treated with platinum-based chemotherapy. We also considered subgroups within the study populations with levels of PD-L1 expression as follows: less than 1%, 1% and higher, 50% and higher, or unknown levels. If a review included a mixed population, only data pertaining to the populations of interest were considered.
Intervention and Comparators
The interventions of interest were atezolizumab, nivolumab, or pembrolizumab as monotherapy. Eligible comparators were docetaxel, gemcitabine, or pemetrexed as monotherapy or best supportive care. We did not limit the inclusion of interventions or comparators based on dose, dosing intervals, or duration of treatment.
Outcomes Definition
The efficacy outcomes of interest were OS, PFS, objective response rate, and quality of life or health-related quality of life.
The safety outcomes were the total number of adverse events (AEs), immune-mediated AEs, infusion-related AEs, serious adverse events (SAEs), withdrawals due to AEs, and mortality. Immune-mediated AEs commonly attributed to ICI drugs are immune-mediated pneumonitis, colitis, hepatitis, endocrinopathies, skin AEs, and cardiac disorders. Infusion-related AEs were considered based on author-reported AEs occurring minutes to hours after drug infusion, including broadly described reactions and/or anaphylaxis. Graded AEs as reported by study authors (grade 3 or grade 4) or any AE requiring an emergency department visit or hospitalization were considered SAEs.
During full-text review, records were excluded when outcomes of interest were not reported.
Study Designs
SRs of RCTs were eligible for inclusion. Reviews of, or including, nonrandomized studies (NRSs) were considered only when there was no RCT evidence available for a population or outcome of interest.
Study Selection Process
The study selection process was documented according to guidance from PRISMA.35 Before the screening process, a pilot screening exercise on 2 included SRs was conducted. Two reviewers screened the studies independently, and all records deemed potentially relevant were obtained in full-text format. Any disagreements were discussed with or adjudicated by a third reviewer. The reviewers were not blinded to study authors or the centre of publication before study selection. Study screening and assessment of eligibility were facilitated and standardized using DistillerSR software. The study selection process was presented using the PRISMA flow chart.
Data Extraction
A standardized data extraction form was developed and reviewed by CDA-AMC and a content expert. One reviewer extracted data and the extraction was audited by a second reviewer. Pilot data extraction was conducted on 2 of the included SRs, and data extraction forms were optimized before use.
From each SR, the following data were extracted:
bibliographic information (first author, year, citation)
review eligibility criteria
search details (dates and limitations)
synthesis approach (i.e., descriptive, meta-analysis [MA])
included studies (study design, type, and counts)
patients included
patient characteristics, including relevant mutations, any prognostic factors at baseline (e.g., treatment history, prior use of ICI drug as either targeted or adjuvant therapy, number of previous therapies, stage at diagnosis, smoking history and status at diagnosis, Eastern Cooperative Oncology Group [ECOG] performance status)
interventions (doses, intervals, duration)
controls (doses, intervals, duration)
efficacy outcomes
safety outcomes
synthesized results as reported, including the descriptive or pooled summary effects of each comparison for each outcome if the MA was conducted (including associated measures of variation or precision if applicable)
results from the RCT-level risk-of-bias assessment
authors’ conclusions pertinent to outcomes of interest
funding sources and author declarations.
Additional data to inform the SR quality assessment were also extracted (e.g., reported methods, rationale for review inclusions, or limitations). Where other out-of-scope study data were reported in a review, only data for our population, intervention, comparator, and outcomes of interest were extracted. Efficacy and safety outcomes were extracted for populations with mutations of interest and for subgroups of these populations reporting PD-L1 expression levels (categorized as less than 1%, 1% and higher, 50% and higher, and unknown or unreported) if such data were provided in each SR.
Data from RCTs included by the SRs were prioritized. Information was only considered from NRSs where available and when a unique population or outcome not covered by the RCTs was reported.
Additionally, the overlap of the primary studies in the included SRs (i.e., multiple SRs of the same primary studies) was considered. Any important nuances and/or discrepancies in the outcomes or results reported were descriptively summarized.
Quality Assessment
We used A MeaSurement Tool to Assess Systematic Reviews 2 (AMSTAR 2)36 to assess the methodological quality of the included SRs. AMSTAR 2 can be applied to SRs including RCTs or NRSs. The following elements of the included SRs were assessed: description of the PICO (participants, intervention, controls, outcomes), protocol, and review methodology; rationale behind selecting study design, search strategy, duplication of the data extraction, and study selection process; list of excluded studies; quality and discussion of the risk-of-bias assessment; funding of the selected studies and MA; explanation of the heterogeneity; publication bias assessment; and any conflict of interests with the authors of the reviews and funding sources.
One reviewer completed the assessment, and the results were audited by a second reviewer. Any disagreements were resolved by discussion. An overall rating was assessed for each review considering AMSTAR 2 guidance for rating overall confidence in the results of the review.36 A rating of High indicates that the SR provides an accurate and comprehensive summary of the results of the available studies that address the research questions; Moderate indicates that the SR has more than 1 weakness but no critical flaws; Low indicates that the SR has 1 critical flaw and possibly other identified weaknesses; and Critical indicates that the SR has more than 1 critical flaw and should not be relied on to provide an accurate and comprehensive summary of the evidence informing the research questions. For the purposes of these ratings, critical flaws were not having registered a protocol before commencement of the review, inadequate literature search, lack of justification for excluded studies, and lack of a risk-of-bias assessment for studies included in the review. The strengths and limitations for each included review were summarized alongside the overall ratings assessed.
For an SR involving a network meta-analysis (NMA), the confidence of the results is dependent not only on the SR methods, which can be assessed with the AMSTAR 2, but also on the analytic complexities in estimating specific pairwise effects in the NMA and the assumptions of goodness of fit of the model, homogeneity, and consistency, which also need to be assessed.37
No de novo risk-of-bias assessments were conducted for the primary studies included in each review. We summarized the author-assessed results for any reported risk-of-bias assessment of the eligible RCTs or NRSs included in each SR and summarized the reported strengths and limitations. We additionally considered any discrepancies or deficiencies in the risk-of-bias assessments reported by the authors of the included SRs.
Data Analyses and Synthesis
A descriptive summary of the characteristics of the included reviews was completed. For each population of interest (RET gene fusion, ALK gene rearrangement, ROS1 mutation, or EGFR gene mutation), results for each efficacy and safety outcome of interest were summarized and synthesized narratively based on the author-reported findings across the SRs. Results are also presented for any reported quantitative syntheses for all outcomes of interest, including all relative or absolute effects. For pairwise MA this includes the model (fixed effects or random-effects model), the meta-analytic estimates (such as the hazard ratio [HR] effect estimate and confidence interval [CI]) and measure of heterogeneity (I2). For NMA, this includes the probabilistic approach (Bayesian), the network meta-analytic estimates based on direct and indirect evidence (such as HR) and mean difference effect estimates and credible interval [CrI]) and ranking methods such as the surface under the cumulative ranking curve (SUCRA) for a treatment, which is a Bayesian summary of the ranking of multiple competing treatments, which can be interpreted as the estimated proportion of treatments worse than the treatment of interest. No new quantitative syntheses were planned (e.g., MA of individual or aggregate study results). Data for each actionable driver mutation were considered separately when summarizing the quantitative results extracted from the included SRs.
Summary of Evidence
Quantity of Research Available
A total of 1,101 records were identified in the literature search. Following screening titles and abstracts, 1,025 records were excluded, and 60 potentially relevant records were retrieved for full-text review. Of these, 47 were excluded for various reasons (Appendix 4, Table 16); and 13 records reporting 13 unique SRs met the inclusion criteria (Figure 1). Details on the included SRs are provided in Table 3.
Summary of Study Characteristics
The study characteristics for the 13 included SRs are summarized in Table 3.
Study and Patient Characteristics
Description of SRs
Of the 13 eligible SRs,38-50 10 included an MA38-46,50 and 3 included an NMA.47,48,49 All included SRs reported RCTs with eligible populations. None of the SRs reported any eligible NRSs including patients of interest.
Broadly, the number of individual RCTs included in the SRs ranged between 3 RCTs and 31 RCTs; however, only a small proportion (i.e., between 2 and 4 RCTs per included SR)51-54 included patients with NSCLC with the mutations of interest. The characteristics of the 4 relevant RCTs reporting patients of interest are described in Appendix 3, Table 12.
While the overall number of patients with NSCLC included in the RCTs considered in the SRs was large (range, 1,903 to 9,983), the number of patients with 1 of the eligible mutations was small (range, 146 to 272) or not reported at all.38-50
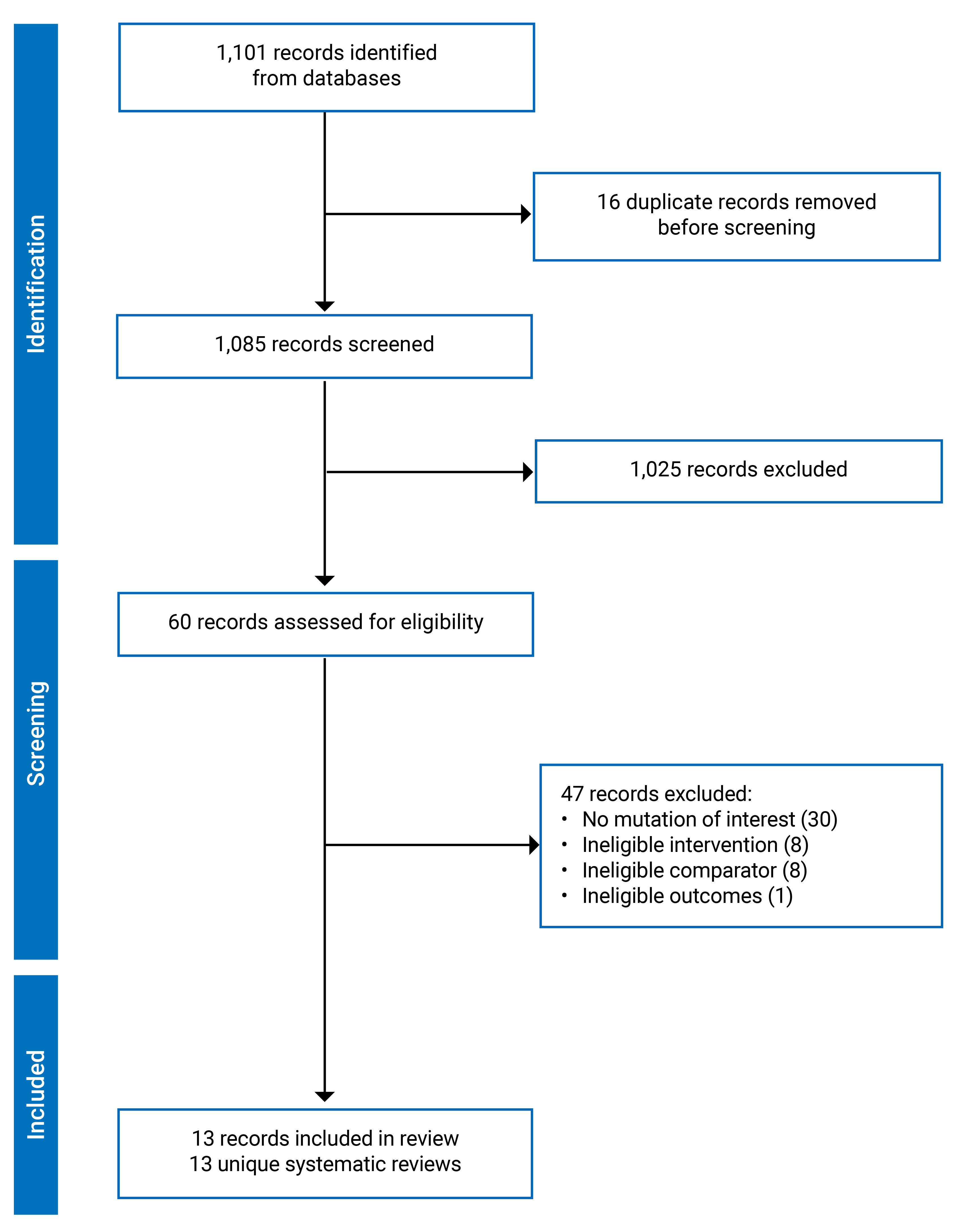
Table 3: Characteristics of Included SRs
SR | Number of primary studies and review method | Patients, mutation type, age, and sex in primary studies | Previous treatment and line of current treatment in the population of interest | Drug comparisona | Outcomes (number of RCTs informing the PICO) |
|---|---|---|---|---|---|
Wang (2016)38 | 9 RCTs, MA | Overall: 3,032 Age: NR Sex: NR EGFR-positive: NR Age: NR Sex: NR | Previous treatment: standard chemotherapy Line: NR | ICI (nivolumab or pembrolizumab) vs. docetaxelb | OS (2) |
Lee (2017)39 | 3 RCTs, MA | Overall: 1,903 Age: NR Sex: NR EGFR-positive: 186 Age: NR Sex: NR | Previous treatment: not specified Line: NR | ICI (atezolizumab or nivolumab or pembrolizumab) vs. docetaxelb | OS (3) |
Sheng (2017)40 | 14 RCTs, MA | Overall: 2,475 Age: median, 62 years to 63 years Sex: NR EGFR-positive: 168 Age: NR Sex: NR | Previous treatment: not specified Line: NR | ICI (nivolumab or pembrolizumab) vs. docetaxelc | OS (2) PFS (2) |
Huang (2018)41 | 7 RCTs, MA | Overall: 3,871 Age (< 65 years): 53% to 58%; 1 study, n/a Sex: (male): NR Sex (female): 24% to 93% EGFR-positive: 272 Age: NR Sex: NR | Previous treatment: not specified Line: second- and third-line | ICI (atezolizumab or nivolumab or pembrolizumab) vs. docetaxelb | OS (4) |
Jiang (2018)42 | 5 RCTs, MA | Overall: 3,025 Age: 61 years to 64 years Sex (female): NR Sex (male): 1,850 (61.16%) EGFR-positive: NR Age: 61 years to 64 years Sex: NR ALK-positive: NRd Age: NR Sex: NR | Previous treatment: not specified Line: second line and beyond | ICI (atezolizumab or nivolumab or pembrolizumab) vs. docetaxelc ICI (nivolumab or pembrolizumab) vs. docetaxelc | OS (3) PFS (2) |
Abdel-Rahman (2018)43 d | 5 RCTs, MA | Overall: 3,013 Age: NR Sex: NR EGFR-positive: NR Age: NR Sex: NR | Previous treatment: platinum-based doublets Treatment history: NR Line: NR | ICI (atezolizumab or nivolumab or pembrolizumab) vs. docetaxelb | OS (4) |
Liu (2018)44 | 5 RCTs, MA | Overall: 2,910 Age: NR Sex (female): NR Sex (male): 53% to 82% EGFR-positive: 146 Age: NR Sex: NR | Previous treatment: not specified Line: second and third lines | ICI (atezolizumab or nivolumab or pembrolizumab) vs. docetaxelb | OS (3) |
Khan (2018)45 d | 7 RCTs, MA | Overall: 3,867 Age: NR Sex: NR EGFR-positive: NR Age: NR Sex: NR | Previous treatment: not specified Line: second and third lines | ICI (atezolizumab or nivolumab or pembrolizumab) vs. docetaxelc | OS (3) PFS (2) |
Lee (2018)46 | 5 RCTs, MA | Overall: 3,025 Age (≥ 65 years): 1,302 (43%) Sex (female): NR Sex (male): 1,425 (47.1%) EGFR-positive: 271 Age: NR Sex: NR | Previous treatment: not specified Line: second line and beyond | ICI (atezolizumab or nivolumab or pembrolizumab) vs. docetaxelb | OS (4) |
Almutairi (2019)47 d | 5 RCTs, NMA | Overall: 3,024 Age: NR Sex: NR EGFR-positive: NR Age: NR Sex: NR | Previous treatment: not specified Line: second and third lines | Comparisons:e
| OS (NR) PFS (NR) |
Cavanna (2019)48 | 4 RCTs, MA 4 RCTs, NMA | Overall: 2,753 Age: NR Sex: NR EGFR-positive: 272 Age: NR Sex: NR | Previous treatment: TKI therapy Line: second and third lines | Comparisons:e
| OS (4) |
Vickers (2019)49 | 31 RCTs,f NMA | Overall: 9,983 Age: NR Sex: NR EGFR-positive: NR Age: NR Sex: NR | Previous treatment: Not specified Line: second line | Comparisons:e
| OS (NR) PFS (NR) |
An (2021)50 | 12 RCTs, MA | Overall: 7,442 Age: NR Sex: NR EGFR-positive: NR Age: NR Sex: NR | Previous treatment: not specified Line: second line and beyond | ICI (atezolizumab or nivolumab or pembrolizumab) vs. docetaxelb ICI (nivolumab or pembrolizumab) vs. docetaxelb | OS (3) PFS (2) |
ICI = immune checkpoint inhibitor; MA = meta-analysis; NMA = network meta-analysis; NR = not reported; OS = overall survival; PICO = participants, intervention, controls, outcomes; PFS = progression-free survival; RCT = randomized control trial; SR = systematic review; TKI = tyrosine kinase inhibitor; vs. = versus.
aThe listed drug comparisons all align with the prespecified interventions and comparators outlined in the PICO framework.
bFixed effects model.
cRandom effects model.
dThe primary studies described data regarding ALK, but none of them stratified OS or PFS data based on ALK status.
eIn the NMA, pairwise comparisons between any drug and any comparator in the evidence network are available. Here, we focus only on pairwise comparisons involving the interventions and comparators of interest.
fNMA of several RCTs, but it was not possible to ascertain which RCTs were used for the analyses.
gBest supportive care is not defined or described.
hUsing the random effect model for significant (P < 0.05) results were given for nivolumab vs. docetaxel (75 mg/m2 every 3 weeks) per subgroup.
Characteristics of Patients Included in the SRs
The gender and age of the patients were inconsistently reported.40-42,46 The SRs broadly included RCTs reporting patients with a mean age of 60 years or older. The proportion of male patients in the included RCTs ranged from 47.1% to 82.0%.41,42,44,46 In 1 SR, patients with NSCLC were categorized by patients’ lung cancer histology (i.e., nonsquamous or squamous) and further by their PD-L1 expression levels.49 This review provided the proportions of participants who were Asian and not Asian in each group (range 0.8% Asian to 21.0% Asian), and the proportion of patients who were Asian was used as a study-level covariate to investigate statistical model fit by authors. The study did not investigate outcomes within this subgroup of patients.
Characteristics of Patients With NSCLC and Mutations of Interest
The 13 SRs included RCTs that reported on patients who were positive for EGFR mutations. Of these, 3 SRs noted small proportions of patients who were positive for ALK rearrangement (range 0% to 4%), and no additional details for these patients are reported.43,45,47 None of the SRs included RCTs that reported patients with NSCLC with a ROS1 mutation or RET fusion.38-50
The SR-reported characteristics for the patients in the included RCTs who had NSCLC and EGFR mutations were very limited or nonexistent.38-50 The total number of patients who were EGFR-positive in the included RCTs was reported by 4 SRs (range 168 patients to 272 patients).39-41,46 None of the included SRs reported any sex or age information for these patients.38-50
All 13 included SRs described the patients with EGFR mutations as being pretreated in some way;38-50 very few reported details about the drugs used in the treatment history.38-42,44-47,49,50 For example, the treatment characteristics defining the included RCT patient populations may have differentiated these studies as investigating treatments that were either first-line or not first-line, but the details of the previous treatments received were not reported.50 One SR considered patients previously treated with tyrosine kinase inhibitors (TKIs).48 In 1 SR, the treatment history of 2 of the 4 included RCTs was reported to be platinum-based chemotherapy, but the treatment history for the patients in the remaining trials was not reported.43 Included RCTs in 1 SR recruited patients treated with second-line ICI monotherapy; however, no details on the first line of therapy were given.49 In 3 SRs, outcomes of ICI monotherapies as second-line or unspecified subsequent lines were analyzed.42,46,50 Both second- and third-line ICI monotherapies were included in 5 SRs.41,44,45,47,48 In 4 SRs, the patients were described as previously treated, but the previous treatment details were not provided.38-40,43
One NMA reported the proportion of patients who were identified as Asian in subgroups of participants with EGFR-positive status based on histology (squamous/nonsquamous) and PD-L1 thresholds of ≥ 5% or < 5% (range 0.8% Asian to 18.8% Asian).
Interventions
The SRs considered at least 1 of the interventions of interest. All 13 SRs examined nivolumab,38-50 12 SRs examined pembrolizumab,38-48,50 and 10 SRs examined atezolizumab.39,41-48,50 In all SRs, the interventions included were monotherapy.38-50
Eleven SRs pooled the ICI interventions to consider the class effect.38-46,48,50 Among these, 8 SRs considered the class effect of nivolumab, pembrolizumab, or atezolizumab;39,41-46,50 3 SRs considered the class effect for nivolumab or pembrolizumab;38,40,42 and 1 SR with NMA considered both the class effect of nivolumab, pembrolizumab, or atezolizumab and the effect of each intervention individually.48 One SR considered only the individual effects of nivolumab, pembrolizumab, or atezolizumab,47 and 1 considered nivolumab only in various dosing regimens.49
Comparators
All included SRs included RCTs that compared ICI therapy to docetaxel.38-50 One SR also considered RCT data comparing nivolumab to both pemetrexed and best supportive care (for which no definition was provided).49 This was the only review to state the dose for the comparator (docetaxel) — frequent low dose, 60 mg/kg, 75 mg/kg, and 100 mg/kg, and pemetrexed at 500 mg/m2.49 No other comparator details were reported. Three SRs involved evidence networks for conducting NMA, in which case all pairwise comparisons of the drugs in the network are considered based on direct and indirect evidence.38-50
Efficacy Outcomes
The included SRs focused on summarizing 2 outcomes of interest in the RCTs: OS and PFS.38-50 All outcomes are for patients with NSCLC with the EGFR mutation, and no other efficacy outcomes for the population of interest were reported. OS was reported in all 13 SRs, but the range of RCTs used for the outcome data (3 RCTs to 4 RCTs) was only mentioned in 11 SRs.38-46,48,50 PFS was included in 4 SRs from 2 RCTs.40,42,45,50 In 2 SRs, the RCTs used for PFS outcomes were not clear.47,49
Safety Outcomes
None of the SRs reported any of the safety outcomes of interest for the included RCTs of ICI monotherapy for patients with NSCLC with EGFR mutations.38-50
Important Subgroups
While many of the SRs considered patients’ PD-L1 expression status, only 1 review reported results for any outcomes of interest in patients with EGFR-positive NSCLC. In the review, an NMA model was used to compare the efficacy of nivolumab (3 mg/kg) with docetaxel, best supportive care, and pemetrexed in patients with EGFR-positive nonsquamous or squamous NSCLC with PD-L1 expression of < 5% or ≥ 5%.49 No other subgroups of interests were identified across the SRs.
Overlap of RCTs in the SRs
The overlap of the RCTs included in the SRs reporting efficacy outcomes of interest is detailed in Table 13 and Table 14 (Appendix 2). A total of 4 unique RCTs51-54 including patients with NSCLC and a mutation of interest were identified from the trials included in the SRs. All 4 compared an ICI monotherapy to docetaxel. The CheckMate05751 trial assessed nivolumab, the Keynote-01054 trial assessed pembrolizumab, and the OAK53 and POPLAR trials assessed atezolizumab.
OS for nivolumab from the CheckMate05751 trial was considered in 10 SRs,38-44,46,48,50 for pembrolizumab from the Keynote-01054 trial in 9 SRs,38,40-50 and for atezolizumab from the OAK53 trial in 5 SRs41,43-46,48,49 and from the POPLAR52 trial in 8 SRs.39,41,43,45-49
Fewer RCTs reported PFS. The CheckMate05751 and OAK53 trials both reported PFS for nivolumab and atezolizumab and were considered by 3 SRs,40,42,50
The RCTs informing the analyses in 2 SRs45,47 and 1 NMA,49 were not reported. Therefore, RCT overlap assessment was not possible. No safety outcomes specific to the population of interest were assessed in any SR, and so overlap assessment was not feasible.38-50
Data Analysis and Synthesis
Efficacy: OS
The results of the pairwise MA and NMA for OS for ICI monotherapy compared to docetaxel in patients with NSCLC with EGFR mutations are described in the following paragraphs. A detailed summary of these results is presented in Table 4.
Meta-Analysis
In the pairwise MAs for OS, the different ICI monotherapies were combined and considered as a single class of ICI drugs and compared to docetaxel. No dose was provided for any of the drugs assessed.
ICI (Nivolumab, Pembrolizumab) Monotherapy Versus Docetaxel
Two SRs compared nivolumab or pembrolizumab monotherapy as an ICI drug class to docetaxel.38,40 Both SR considered the same 2 RCTs (CheckMate 057, Keynote 010) and each found no statistically significant difference for OS (HR = 1.05; 95% CI, 0.69 to 1.59).
SR | Included RCTs | Comparisona,b (n) | Result |
|---|---|---|---|
MA | |||
ICI (nivolumab, pembrolizumab) monotherapy vs. docetaxel | |||
Wang (2016)38 | CheckMate 057, Keynote 010 | ICI vs. docetaxel (n = NR)c | HR = 1.05 95% CI, 0.69 to 1.59 I2 = 0% |
Sheng (2017)40 | CheckMate 057, Keynote 010 | ICI vs. docetaxel (n = 168)d | HR = 1.05, 95% CI, 0.69 to 1.59 I2 = NR |
ICI (atezolizumab, nivolumab, pembrolizumab) monotherapy vs. docetaxel | |||
Abdel-Rahman (2018)43 | CheckMate 057, Keynote 010, POPLAR, OAK | ICI vs. docetaxel (n = NR)c | HR = 1.11 95% CI, 0.80 to 1.53 I2 = 0% |
Lee (2018)46 | CheckMate 057, Keynote 010, POPLAR, OAK | ICI vs. docetaxel (n = 271)c | HR = 1.11 95% CI, 0.80 to 1.53 I2 = 0% |
Cavanna (2019)48 | CheckMate 057, Keynote 010, POPLAR, OAK | ICI vs. docetaxel (n = 272)d | HR = 1.12 95% CI, 0.85 to 1.38 I2 = NR |
Huang (2018)41 | CheckMate 057, Keynote 010, POPLAR, OAK | ICI vs. docetaxel (n = 272)c | HR = 1.12 95% CI, 0.80 to 1.53 I2 = 0% |
Liu (2018)44 | CheckMate 057, Keynote 010, OAK | ICI vs. docetaxel (n = 253)c | HR = 1.11 95% CI, 0.80 to 1.55 I2 = 0% |
An (2021)50 | CheckMate 057, Keynote 010, OAK | ICI vs. docetaxel (n = NR)c | HR = 1.12 95% CI, 0.80 to 1.56 I2 = 0% |
Lee (2017)39 | CheckMate 057, Keynote 010, POPLAR | ICI vs. docetaxel (n = 186)c | HR = 1.05 95% CI, 0.70 to 1.55 I2 = 0.80% |
Jiang (2018)42 | CheckMate 057, Keynote 010, OAK | ICI vs. docetaxel (n = NR)d | HR = 1.12 95% CI, 0.80 to 1.56 I2 = 0% |
Khan (2018)45 | NR | ICI vs. docetaxel (n = NR)d | HR = 1.14 95% CI, 0.85 to 1.53 I2 = NR |
NMA | |||
Almutairi (2019)47 | RCTs in the evidence network for NMA CheckMate 057, Keynote 010, POPLAR, OAK | Atezolizumab vs. docetaxel (n = NR)c | HR = 1.25 95% CrI, 0.71 to 2.18 |
Nivolumab vs. docetaxel (n = NR)c | HR = 1.18 95% CrI, 0.69 to 1.99 | ||
Pembrolizumab vs. docetaxel (n = NR)c | HR = 0.87 95% CrI, 0.45 to 1.70 | ||
Cavanna (2019)48 | RCTs in the evidence network for NMA CheckMate 057, Keynote 010, POPLAR, OAK | Atezolizumab vs. nivolumab vs. pembrolizumab vs. docetaxel (n = 272)c | SUCRA-treatment ranking:e
|
CI = confidence interval; CrI = credible interval; HR = hazard ratio; I2 = I-square statistic; ICI = immune checkpoint inhibitor; MA = meta-analysis; NMA = network meta-analysis; NR = not reported; OS = overall survival; RCT = randomized control trial; SR = systematic review; SUCRA = surface under the cumulative ranking; vs. = versus.
aIntervention doses were not reported in any of the SRs.
bTwo or more ICI are considered 1 class and compared with docetaxel.
cFixed effects model.
dRandom-effects model.
eCrIs not reported.
ICI (Atezolizumab, Nivolumab, Pembrolizumab) Monotherapy Versus Docetaxel
Nine SRs compared atezolizumab, nivolumab, or pembrolizumab monotherapy as an ICI drug class to docetaxel.43 Four of these SRs considered the same 4 RCTs (CheckMate 057, Keynote 010, POPLAR, OAK) and each found no significant difference for OS (e.g., HR = 1.11; 95% CI, 0.80 to 1.53).43,46,48 Not including the POPLAR RCT, 3 SRs considered the same 3 RCTs (CheckMate 057, Keynote 010, OAK) and also found similar results of no significant difference for OS (e.g., HR = 1.12; 95% CI, 0.80 to 1.56).39,42,50 An SR including the RCTs CheckMate 057, Keynote 010, and POPLAR found no statistically significant difference for OS (HR = 1.05; 95% CI, 0.70 to 1.55),39 while another SR arrived at a different conclusion without identifying the included RCTs (HR = 1.14; 95% CI, 0.85 to 1.53).45
Network Meta-Analysis
In 2 NMAs, individual ICI drugs were compared to docetaxel as the reference node. None of the NMAs reporting OS considered best supportive care or pemetrexed. No dose was provided for any of the drugs assessed.
Individual ICI Monotherapies Versus Docetaxel
In 1 SR/NMA that used a Bayesian model, results indicated no statistically significant OS benefit for patients with EGFR-mutated NSCLC taking atezolizumab (HR = 1.25; 95% credible interval [CrI], 0.71 to 2.18), nivolumab (HR = 1.18; 95% CrI, 0.69 to 1.99) or pembrolizumab (HR = 0.87; 95% CrI, 0.45 to 1.70) when compared to docetaxel.47
A second NMA reported SUCRA treatment rankings for OS and found that docetaxel ranked higher than the other treatments (60.0%) — followed by pembrolizumab (48.0%), atezolizumab (46.0%), and nivolumab (45.6%) — in patients with NSCLC with EGFR mutations. The hazard ratios were not reported.48
Efficacy: PFS
The results for PFS for ICI monotherapy compared to docetaxel in patients with NSCLC with EGFR mutations are described in the following paragraphs. A detailed summary of these results is presented in Table 5.
Meta-Analysis
In the pairwise MAs for PFS, the different ICI monotherapies were combined and considered as a single class of ICI drugs in 4 SRs.40,42,45,50 No dose was provided for any of the drugs assessed.
ICI (Nivolumab, Pembrolizumab) Monotherapies Versus Docetaxel
Three SRs compared nivolumab or pembrolizumab monotherapy as an ICI drug class to docetaxel.40,42,50 All 3 SRs considered the same 2 RCTs (CheckMate 057, Keynote 010), and each found that these ICI drugs were inferior to docetaxel in improving PFS (e.g., HR =1.57; 95% CI, 1.06 to 2.32).
ICI (Atezolizumab, Nivolumab, Pembrolizumab) Monotherapies Versus Docetaxel
One SR compared atezolizumab, nivolumab, or pembrolizumab as an ICI drug class to docetaxel.45 This SR did not identify the included RCTs and found that these ICI drugs were inferior to docetaxel in improving PFS (HR = 1.57; 95% CI, 1.07 to 2.31).45
Network Meta-Analysis
Individual ICI Monotherapies Versus Docetaxel
In 1 SR, an NMA model was used to compare ICI drugs nivolumab and pembrolizumab individually to docetaxel as the reference node.47 Results for nivolumab (HR = 1.46; 95% CrI, 0.90 to 2.36) and pembrolizumab (HR = 1.79; 95% CrI, 0.94 to 3.41) showed no statistically significant improvement in PFS when compared individually to docetaxel.47 Furthermore, using SUCRA, docetaxel ranked higher (SUCRA = 89%) than both the individual drugs in improving PFS.47
Table 5: Results by SR for PFS
SR | Included RCTs | Comparisons (n) | Result HR, 95% CI/CrI, I2 |
|---|---|---|---|
MA | |||
ICI (nivolumab, pembrolizumab) monotherapies vs. docetaxel | |||
An (2021)50 | Checkmate 057, Keynote 010 | ICI vs. docetaxel (n = NR)a,b | HR = 1.57 95% CI, 1.06 to 2.32 I2 = 0% |
Sheng (2017)40 | Checkmate 057, Keynote 010 | ICI vs. docetaxel (n = 168)b,c | HR = 1.57 95% CI, 1.07 to 2.31 I2 = NR |
Jiang (2018)42 | Checkmate 057, Keynote 010 | ICI vs. docetaxel (n = NR)b,c | HR = 1.57 95% CI, 1.07 to 2.31 I2 = 0% |
ICI (atezolizumab, nivolumab, pembrolizumab) monotherapies vs. docetaxel | |||
Khan (2018)45 | NR | Atezolizumab, nivolumab, pembrolizumab vs. docetaxel (n = NR)b,c,d | HR = 1.57 95% CI, 1.07 to 2.31 I2 = NR |
NMA | |||
Almutairi (2019)47 | RCTs in the evidence network for NMA CheckMate 057, Keynote 010 | Nivolumab vs. docetaxel (n = NR)a,e | HR = 1.46 95% CrI, 0.90 to 2.36 |
Pembrolizumab vs docetaxel (n = NR)a,e | HR = 1.79 95% CrI, 0.94 to 3.41 | ||
CI = confidence interval; CrI = credible interval; HR = hazard ratio; ICI = immune checkpoint inhibitor; I2 = I-square statistic; MA = meta-analysis; NMA = network meta-analysis; NR = not reported; PFS = progression-free survival; RCT = randomized control trial; SR = systematic review; vs. = versus.
aFixed effects model.
bTwo or more ICI were pooled as 1 class and compared with docetaxel.
cRandom effects model.
dThe RCTs included in the analysis were not specified.
eDocetaxel ranked higher than both nivolumab and pembrolizumab (SUCRA for docetaxel: 89%).
Important Subgroups
One SR used an NMA model to assess subgroups based on PD-L1 expression level in several included RCTs of ICI used to treat squamous and nonsquamous NSCLC with EGFR mutations.49 PD-L1 subgroups were categorized based on expression levels of less than 5% and 5% or more.49 In the NMA for OS, nivolumab (3 mg/kg) was compared with best supportive care, various doses of docetaxel, and 500 mg/m2 pemetrexed. For PFS, nivolumab (3 mg/kg) was compared with various doses of docetaxel and 500 mg/m2 pemetrexed.
OS With PD-L1 Expression Levels of Less Than 5% and 5% or More
Nonsquamous NSCLC
Results for OS in the subgroup of patients with nonsquamous NSCLC are provided in Table 6. In patients with nonsquamous NSCLC with EGFR mutations, regardless of the PD-L1 expression levels, nivolumab was more effective in improving OS when compared to best supportive care for PD-L1 less than 5% and PD-L1 5% or more.49 Among patients with PD-L1 less than 5%, there was no significant improvement in OS observed with nivolumab compared to docetaxel at frequent low dose, 60 mg/kg, 75 mg/kg, or 100 mg/kg.49 However, in patients with PD-L1 of 5% or more, nivolumab was more effective than docetaxel at frequent low doses, 60 mg/kg, 75 mg/kg, or 100 mg/kg.49 Similarly, compared to 500 mg/m2 pemetrexed, nivolumab was more effective in patients with PD-L1 of 5% or more but not in patients with PD-L1 of less than 5%.49
Squamous NSCLC
Results for OS in the subgroup of patients with squamous NSCLC are provided in Table 7. In patients with squamous NSCLC with EGFR mutations, regardless of the PD-L1 expression levels (PD-L1 < 5% or PD-L1 ≥ 5%), nivolumab was more effective in improving OS than best supportive care.49 When compared to frequent low doses of docetaxel, 60 mg/kg or 75 m/kg nivolumab was more effective regardless of the PD-L1 levels.49 However, there was no significant difference between nivolumab and 100 mg/kg docetaxel.49
Table 6: Subgroup Results for OS for Patients With Nonsquamous NSCLC
SR | Included RCTs | Comparison | PD-L1 expression | Result |
|---|---|---|---|---|
Mean OS timea | MD, 95% CrI (months) | |||
Vickers (2019)49 | RCTs included in the NMAb | Nivolumab 3 mg/kg vs. best supportive care | PD-L1 < 5% | MD = 8.6 95% CrI, 3.5 to 13.9 |
PD-L1 ≥ 5% | MD = 20.0 95% CrI, 11.8 to 31.2 | |||
Nivolumab 3 mg/kg vs. docetaxel frequent low dose | PD-L1 < 5% | MD = 3.3 95% CrI, −0.5 to 7.9 | ||
PD-L1 ≥ 5% | MD = 14.8 95% CrI, 7.1 to 25.8 | |||
Nivolumab 3 mg/kg vs. docetaxel 60 mg/kg every 3 weeks | PD-L1 < 5% | MD = 2.4 95% CrI, −1.4 to 6.9 | ||
PD-L1 ≥ 5% | MD = 13.8 95% CrI, 6.3 to 24.8 | |||
Nivolumab 3 mg/kg vs. docetaxel 75 mg/kg every 3 weeks | PD-L1 < 5% | MD = 1.5 95% CrI, −1.9 to 5.9 | ||
PD-L1 ≥ 5% | MD = 12.9 95% CrI, 5.6 to 23.8 | |||
Nivolumab 3 mg/kg vs. docetaxel 100 mg/kg every 3 weeks | PD-L1 < 5% | MD = 0.4 95% CrI, −4.3 to 5.4 | ||
PD-L1 ≥ 5% | MD = 11.7 95% CrI, 4.1 to 23.0 | |||
Nivolumab 3 mg/kg vs. pemetrexed 500 mg/m2 | PD-L1 < 5% | MD = −0.6 95% CrI, −5.3 to 4 | ||
PD-L1 ≥ 5% | MD = 10.8 95% CrI, 3.1 to 21.9 | |||
Probability of survivalc | HR, 95% CrId,e | |||
Vickers (2019)49 | RCTs included in the NMAb | Nivolumab 3 mg/kg vs. docetaxel 75 mg/kg every 3 weeks | PD-L1 < 5% | NR |
PD-L1 ≥ 5% | HR = 12.5 95% CrI, 4.8 to 23.9 | |||
CrI = credible interval; HR = hazard ratio; MD = mean difference; NMA = network meta-analysis; NR = not reported; NSCLC = non–small cell lung carcinoma; OS = overall survival; PD-L1 = programmed death-ligand 1; RCT = randomized control trial; SR = systematic review; vs. = versus.
aMean survival time is the area under the probability of survival curve with a horizon of 60 years.
bThirty-one RCTs were identified in the overall evidence network for the NMA, but unspecified RCTs were identified for the subgroup analysis for patients with EGFR-positive NSCLC.
cTime to event (i.e., death or progression) — random-effects model.
dA random-effects model represented results with a significant (P < 0.05) benefit over single-agent docetaxel (75 mg/m2).
eHR > 1 indicates greater probability of OS for nivolumab.
Table 7: Subgroup Results for OS for Patients With Squamous NSCLC
SR | Included RCTs | Comparison | PD-L1 expression | Result |
|---|---|---|---|---|
Mean OS timea | MD, 95% CrI (months) | |||
Vickers (2019)49 | RCTs included in the NMAb | Nivolumab 3 mg/kg vs. best supportive care | PD-L1 < 5% | MD = 11.8 95% CrI, 6.1 to 19.1 |
PD-L1 ≥ 5% | MD = 14.2 95% CrI, 7.0 to 24.4 | |||
Nivolumab 3 mg/kg vs. docetaxel frequent low dose | PD-L1 < 5% | MD = 7.1 95% CrI, 2.1 to 14.1 | ||
PD-L1 ≥ 5% | MD = 9.5 95% CrI, 3.0 to 19.5 | |||
Nivolumab 3 mg/kg vs. docetaxel 60 mg/kg every 3 weeks | PD-L1 < 5% | MD = 6.3 95% CrI, 1.4 to 13.1 | ||
PD-L1 ≥ 5% | MD = 8.7 95% CrI, 2.3 to 18.7 | |||
Nivolumab 3 mg/kg vs. docetaxel 75 mg/kg every 3 weeks | PD-L1 < 5% | MD = 5.5 95% CrI, 0.7 to 12.4 | ||
PD-L1 ≥ 5% | MD = 8.0 95% CrI, 1.6 to 17.8 | |||
Nivolumab 3 mg/kg vs. docetaxel 100 mg/kg every 3 weeks | PD-L1 < 5% | MD = 4.5 95% CrI, −1.1 to 11.7 | ||
PD-L1 ≥ 5% | MD = 7.0 95% CrI, 0.0 to 17.0 | |||
Nivolumab 3 mg/kg vs. pemetrexed 500 mg/m2 | PD-L1 < 5% | MD = 9.2 95% CrI, 4.0 to 16.5 | ||
PD-L1 ≥ 5% | MD = 11.6 95% CrI, 4.7 to 21.9 | |||
Probability of survivalc | HR, 95% CrId,e | |||
Vickers (2019)49 | RCTs included in the NMAb | Nivolumab 3 mg/kg vs. docetaxel, 75 mg/kg every 3 weeks | PD-L1 < 5% | HR = 5.7 95% CrI, 0.6 to 13.1 |
PD-L1 ≥ 5% | HR = 7.9 95% CrI, 1.4 to 18.1 | |||
CrI = credible interval; HR = hazard ratio; MD = mean difference; NMA = network meta-analysis; NSCLC = non–small cell lung carcinoma; OS = overall survival; PD-L1 = programmed death-ligand 1; RCT = randomized control trial; SR = systematic review; vs. = versus.
aMean survival time is the area under the probability of survival curve with a horizon of 60 years.
bThirty-one RCTs were identified in the overall evidence network for the NMA, but unspecified RCTs were identified for the subgroup analysis for patients with EGFR-positive NSCLC.
cTime to event (i.e., death or progression) — random-effects model.
dRandom-effects model represented results with a significant (P < 0.05) benefit over single-agent docetaxel (75 mg/m2).
eHR > 1 indicates greater probability of OS for nivolumab.
PFS With PD-L1 Expression Levels of Less Than 5% and 5% or More
Nonsquamous NSCLC
Results for PFS in the subgroup of patients with nonsquamous NSCLC are provided in Table 8. In patients with nonsquamous NSCLC with EGFR mutation and PD-L1 of 5% or more, nivolumab was more effective in improving PFS when compared to docetaxel at 60 mg/kg, 75 mg/kg, or 100 mg/kg.49 However, no significant differences were observed among patients with nonsquamous NSCLC, EGFR mutation, and PD-L less than 5% when nivolumab was compared with docetaxel at 60 mg/kg, 75 mg/kg, or 100 mg/kg.49 Similarly, when compared to pemetrexed, nivolumab was more effective in improving PFS with PD-L1 of 5% or more but not with PD-L less than 5%.49
Table 8: Subgroup Results for PFS for Patients With Nonsquamous NSCLC
SR | Included RCTs | Comparison | PD-L1 expression | Result |
|---|---|---|---|---|
Mean PFS timea | MD, 95% CrI (months) | |||
Vickers (2019)49 | RCTs included in the NMAb | Nivolumab 3 mg/kg vs. docetaxel 60 mg/kg every 3 weeks | PD-L1 < 5% | MD = −0.6 95% CrI, −2.7 to 1.8 |
PD-L1 ≥ 5% | MD = 5.1 95% CrI, 1.9 to 8.7 | |||
Nivolumab 3 mg/kg vs. docetaxel 75 mg/kg every 3 weeks | PD-L1 < 5% | MD = −0.7 95% CrI, −1.9 to 1.1 | ||
PD-L1 > 5% | MD = 5.0 95% CrI, 2.2 to 8.2 | |||
Nivolumab 3 mg/kg vs. docetaxel 100 mg/kg every 3 weeks | PD-L1 < 5% | MD = −0.7 95% CrI, −2.3 to 1.3 | ||
PD-L1 > 5% | MD = 5.0 95% CrI, 2.1 to 8.3 | |||
Nivolumab 3 mg/kg vs. pemetrexed 500 mg/m2 | PD-L1 < 5% | MD = −1.1 95% CrI, −3.3 to 1.1 | ||
PD-L1 ≥ 5% | MD = 4.6 95% CrI, 1.2 to 8.1 | |||
Probability of survivalc | HR, 95% CrId,e | |||
Vickers, 201949 | RCTs included in the NMAb | Nivolumab 3 mg/kg vs. docetaxel 75 mg/kg every 3 weeks | PD-L1 < 5% | NR |
PD-L1 ≥ 5% | HR = 4.4 95% CrI, 0.8 to 7.6 | |||
CrI = credible interval; HR = hazard ratio; MD = mean difference; NMA = network meta-analysis; NR = not reported; NSCLC = non–small cell lung carcinoma; PD-L1 = programmed death-ligand 1; PFS = progression-free survival; RCT = randomized control trial; SR = systematic review; vs. = versus.
aMean survival time is the area under the probability of survival curve with a horizon of 60 years.
bThirty RCTs were identified in the overall evidence network for the NMA, but unspecified RCTs were identified for the subgroup analysis for patients with EGFR-positive NSCLC.
cTime to event (i.e., death or progression) — random-effects model.
dA random-effects model represented results with a significant (P < 0.05) benefit over single-agent docetaxel (75 mg/m2).
eHR > 1 indicates greater probability of PFS for nivolumab.
Squamous NSCLC
Results for PFS in the subgroup of patients with squamous NSCLC are provided in Table 9. In patients with squamous NSCLC with EGFR mutation and PD-L1 of 5% or more, nivolumab was more effective in improving PFS when compared to docetaxel at 60 mg/kg, 75 mg/kg, or 100 mg/kg.49 However, no significant differences were observed among patients with squamous NSCLC, EGFR mutation, and PD-L1 less than 5% when nivolumab was compared with docetaxel at 60 mg/kg, 75 mg/kg, or 100 mg/kg.49 Similarly, when compared to pemetrexed, nivolumab was more effective in improving PFS with PD-L1 of 5% or more but not with PD-L1 less than 5%.49
Table 9: Subgroup Results for PFS for Patients With Squamous NSCLC
SR | Included RCTs | Comparison | PD-L1 expression | Result |
|---|---|---|---|---|
Mean PFS timea | MD, 95% CrI (months) | |||
Vickers (2019)49 | RCTs included in the NMAb | Nivolumab 3 mg/kg vs. docetaxel 60 mg/kg every 3 weeks | PD-L1 < 5% | MD = 2.8 95% CrI, −0.4 to 6.3 |
PD-L1 ≥ 5% | MD = 5.7 95% CrI, 1.7 to 10.5 | |||
Nivolumab 3 mg/kg vs. docetaxel 75 mg/kg every 3 weeks | PD-L1 < 5% | MD = 2.6 95% CrI, 0.0 to 5.8 | ||
PD-L1 ≥ 5% | MD = 5.7 95% CrI, 1.8 to 10.1 | |||
Nivolumab 3 mg/kg vs. docetaxel 100 mg/kg every 3 weeks | PD-L1 < 5% | MD = 2.6 95% CrI, −0.1 to 6.1 | ||
PD-L1 ≥ 5% | MD = 5.6 95% CrI, 1.6 to 10.1 | |||
Nivolumab 3 mg/kg vs. pemetrexed 500 mg/m2 | PD-L1 < 5% | MD = 4.3 95% CrI, 0.6 to 8.0 | ||
PD-L1 ≥ 5% | MD = 7.2 95% CrI, 2.7 to 12.1 | |||
Probability of survivalc | HR, 95% CrId,e | |||
Vickers (2019)49 | RCTs included in the NMAb | Nivolumab 3 mg/kg vs docetaxel 75 mg/kg every 3 weeks | PD-L1 < 5% | HR = 2.7 95% CrI, 0.1 to 6.2 |
PD-L1 ≥ 5% | HR = 5.4 95% CrI, 1.6 to 9.6 | |||
CrI = credible interval; HR = hazard ratio; MD = mean difference; NMA = network meta-analysis; NSCLC = non–small cell lung carcinoma; PD-L1 = programmed death-ligand 1; PFS = progression-free survival; RCT = randomized control trial; SR = systematic review; vs. = versus.
aMean survival time is the area under the probability of survival curve with a horizon of 60 years.
bThirty RCTs were identified in the overall evidence network for the NMA, but unspecified RCTs were identified for the subgroup analysis for patients with EGFR-positive NSCLC.
cTime to event (i.e., death or progression) — random-effects model.
dIn this SR, for the random-effects model, only results with a significant (P < 0.05) benefit over single-agent docetaxel (75 mg/m2) were reported.
eHR > 1 indicates greater probability of PFS for nivolumab.
Safety: All Outcomes
Although some of the included SRs assessed safety outcomes,38,40,42,44,45,47,50 none considered or reported AEs and SAEs specific to patients with NSCLC and any of the gene mutations of interest for this review. It is unclear if any of the RCTs included in the SRs report safety outcomes stratified for patients with NSCLC with the EGFR gene mutation.
Summary of Authors’ Critical Appraisal
Ten SRs assessed the risk-of-bias for the RCTs included in the review and, of these, 7 reported results for the assessments. Three SRs did not report any critical appraisal.38,39,48
Risk-of-bias results overall and across domains generally assessed the RCTs included by the SRs to be at low risk of bias for most domains assessed. However, lack of blinding of participants and personnel (performance bias) and outcome status (detection bias) was a common limitation noted in 7 SRs for the included RCTs (ratings were high or unclear for associated risk of bias).
Summary of Publication Bias Assessment
Six SRs considered publication bias across the included RCTs. No substantial publication bias was reported.40-42,44,46,50
Summary of Authors’ Conclusions
Overall conclusions relevant to patients with EGFR-positive NSCLC, by SR, are summarized in Table 15 (Appendix 3). Of the 13 SRs included, 9 reported conclusions relevant to patients with NSCLC with EGFR gene mutations for either OS (n = 8)38-41,44,46,48,50 or PFS (n = 1).42
Author conclusions for OS, which were consistent across all reviews, were that ICI therapy did not result in OS benefits for patients with NSCLC with EGFR gene mutations, even when OS benefits were seen in broader populations or other subpopulations.38-41,44,46,48,50
In a single SR reporting conclusions based on PFS, the authors deduced that ICI therapy did not result in any benefits for PFS in patients with NSCLC with EGFR gene mutations.42
Summary of Critical Appraisal of SRs
The quality assessment of the 13 included SRs, conducted with AMSTAR 2, is presented in Table 10. All SRs were assessed to be critically low in methodological quality because of at least 2 critical flaws (range 2 critical flaws to 3 critical flaws) related to not having registered a protocol before the commencement of the reviews, inadequacy of the literature search, a lack of justification for RCTs excluded, and/or a lack of a risk-of-bias assessment for studies included in the review. The reporting quality of the methods and results varied greatly and impacted the ratings for each item assessed using AMSTAR 2. According to guidance from AMSTAR 2, more than 1 critical flaw in an SR indicates that the review should not be relied on to provide an accurate and comprehensive summary of the available studies.
All included SRs had a clearly defined PICO.38-50 Only 1 SR had its protocol registered before the commencement of the review process. However, this SR was assessed to have a deviation from the protocol that was not justified (omission of a planned outcome: objective response rate).49 None of the authors of the included SRs justified their selection of the study designs (RCTs) for inclusion.38-50 Some details regarding the search strategy were provided in 10 out of the 13 included SRs, but none of them included a comprehensive summary of methods applied or reported searching references from the bibliographies of the included RCTs.38,39,41,42,44-46,48-50 Three SRs did not report any details of the search methodology.40,43,47
In 6 reviews, the study selection was carried out in duplicate by 2 reviewers40,42,45-47,49 while the remaining SRs did not include any details about the selection process.38,39,43,48,50 Data extraction in duplicate was described in 8 reviews.38,41,44,46-49 A list of excluded studies was provided by 1 SR.43
In 12 SRs, the included RCTs and the populations within were described in the text or an associated table of characteristics. However, the data reported were not comprehensive or sufficient.38-44,46-50 In fact, the included trials were described in sufficient detail in only 1 SR.45 In 7 SRs, the mutations within the populations were not described in detail.38,43,44,46,48-50
The risk of bias was not assessed in all SRs, and in several SRs, the results from the assessment were not presented fulsomely or at all. In none of the included SRs was the information regarding the funding of the primary studies extracted or reported.38-50
In 10 SRs, results were combined for MA using appropriate methods.38,40-46,49,50 However, in 1 study, heterogeneity was not considered for pooling of results,40 and in 2 SRs, no clear justification was provided for the pooling of results.47,48 The impact of any potential biases on the MA was not considered in 10 SRs,38-41,43-49 and the overall impact of any biases across the included trials was discussed in only 2 SRs.42,43 The majority of the included SRs reported low or negligible heterogeneity related to the reported outcomes, and in those that did report significant heterogeneity, the potential causes were discussed.38,39,41-46,48-50 Publication bias analysis was conducted, and its potential impact on the outcomes was discussed in 6 SRs.40-42,44,46,50 In the remaining studies, either the publication bias analysis was not conducted or its results or impact were not reported.38,39,43,45,47-49 The potential conflicts of interest and sources of funding were declared in all but 1 SR.38-46,48-50 AMSTAR 2 is not intended to comprehensively assess the quality of NMA, so only the relevant SR features were assessed.
Table 10: Critical Appraisal of Included SRs Using AMSTAR 2
SR | AMSTAR 2 — Item number | Rating | |||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
1 | 2a | 3 | 4a | 5 | 6 | 7a | 8a | 9a | 10 | 11 | 12 | 13 | 14 | 15 | 16 | ||
Wang (2016)38 | Y | N | N | PY | N | Y | N | PYb | N | N | Y | N | N | Y | N | Y | Criticalc (3 items) |
Lee (2017)39 | Y | N | N | PY | N | Y | N | PY | N | N | Y | N | N | Y | N | Y | Criticalc (3 items) |
Sheng (2017)40 | Y | N | N | N | Y | N | N | PY | PY | N | N | N | N | N | Y | Y | Criticalc (3 items) |
Huang (2018)41 | Y | N | N | PY | N | Y | N | PY | N | N | Y | N | N | Y | Y | Y | Criticalc (3 items) |
Jiang (2018)42 | Y | N | N | PY | Y | N | N | PY | Y | N | Y | Y | Y | Y | Y | Y | Criticalc (2 items) |
Abdel-Rahman (2018)43 | Y | N | N | N | N | N | Y | PYb | Y | N | Y | N | Y | Y | N | Y | Criticalc (2 items) |
Liu (2018)44 | Y | N | N | PY | N | Y | N | PYd | Y | N | Y | N | N | Y | Y | Y | Criticalc (2 items) |
Khan (2018)45 b | Y | N | N | PY | Y | N | N | Y | Y | N | Y | N | N | Y | N | Y | Criticalc (2 items) |
Lee (2018)46 | Y | N | N | PY | Y | Y | N | PYb | N | N | Y | N | N | Y | Y | Y | Criticalc (3 items) |
Almutairi (2019)47 | Y | N | N | N | Y | Y | N | PY | PY | N | N | N | N | N | N | N | Criticalc (3 items) |
Cavanna (2019)48 | Y | N | N | PY | N | Y | N | PYb | N | N | N | N | N | Y | N | Y | Criticalc (3 items) |
Vickers (2019)49 | Y | PYb | N | PY | Y | N | N | Nb | N | N | Y | N | N | Y | N | Y | Criticalc (3 items) |
An (2021)50 | Y | N | N | PY | N | Y | N | PY | Y | N | Y | Y | N | Y | Y | Y | Criticalc (2 items) |
N = no; PY = partial yes; SR = systematic review; Y = yes.
aItem designated as a potentially critical flaw.
bMutations were not adequately described.
cThe SR was rated to be of critically low methodological quality because of more than 1 critical flaw and possibly other potential weaknesses. The SR should not be relied on to provide an accurate and comprehensive summary of the available studies.
dThe SR was registered in PROSPERO.
Three SRs involved an NMA.38-46,48-50 The critical appraisal of their SR methods using AMSTAR 2 found that the SRs were of critically low methodological quality because of more than 1 critical flaw and possibly other potential weaknesses. For an SR involving an NMA, the confidence of the results is dependent not only on the SR methods using AMSTAR 2 but also on whether the analytic complexities in estimating specific pairwise effects in the NMA were assessed — in particular, the assumptions of goodness of fit of the model, homogeneity, and consistency. The summaries of these assessments are provided in Table 11. One SR did not report whether any of these assumptions were assessed.38-46,48-50 A second SR did not report on the goodness of fit of the models, briefly reported on homogeneity, and indicated that consistency could not be assessed because the evidence network did not have any closed loops, which was needed for the of assessment of consistency.38-46,48-50The third SR conducted an in-depth evaluation of all 3 assumptions and reported specific statistics for each assumption by outcome.38-46,48-50 Of the 3 SRs, it provided the most robust assessment of the NMA assumptions. However, as for the AMSTAR 2 assessment of these 3 SRs, the assessment of the assumptions reported did not alter the conclusion that these SRs should not be relied on to provide an accurate and comprehensive summary of the available studies.
Table 11: Assessment of Critical Assumptions for NMA
SR | Goodness of fit | Homogeneity | Consistency |
|---|---|---|---|
Almutairi (2019)47 | NR | NR | NR |
Cavanna (2019)48 | NR | Assessed I2 | NC |
Vickers (2019)49 | Assessed deviance information criterion | Assessed I2 | Assessed node splitting |
I2 = I-square statistic; NC = not calculable; NMA = network meta-analysis; NR = nor reported; SR = systematic review.
Discussion
Summary of Evidence
The aim of this overview of SRs was two-fold: to determine the efficacy of atezolizumab, nivolumab, or pembrolizumab monotherapy in patients with advanced or metastatic NSCLC with EGFR, ROS1, RET, or ALK actionable driver mutations who have been previously treated with platinum chemotherapy, and to establish whether their use is safe for patients.
The project scope was informed by engaging with clinical experts and decision-makers to better understand the considerations for treatment with these ICI drugs and the potential health system impacts. A total of 13 publications met the final inclusion criteria and reported findings from up to 4 RCTs on the use of atezolizumab, nivolumab, or pembrolizumab monotherapy or docetaxel. Of these, 1 review reported additional comparators and used an NMA model to estimate the comparative indirect effects of nivolumab to pemetrexed and best supportive care. All included reviews considered RCTs involving patients with EGFR-positive NSCLC. A small proportion of patients in some of the RCTs included in the SRs has ALK-positive NSCLC; however, no data for patients with ALK-positive NSCLC were reported. None of the SRs of RCTs included patients with an RET or ROS1 mutation. All RCTs of patients with EGFR-positive NSCLC included in the SRs were published between 2015 and 2017. This is not surprising given the relatively stable treatment landscape over the time period covered by the reviews, but we cannot rule out that RCT data for this population or others of interest have been published since August 2020 (the date of the most recent SR search).
Efficacy outcomes were limited to OS and PFS, and none explicitly reported details of the interventions (e.g., dosing regimen, duration of treatment, dosing interval). There was little data to inform the interpretation of the study results based on the context of the clinical trial. It would have been informative to consider how long patients were followed, what other anticancer treatments may have been administered, and what the rates of switching treatment were. None of the reviews reported safety outcomes specific to patients with EGFR, ROS1, RET, and ALK actionable driver mutations.
Patients in all studies were eligible to receive ICI drugs in the RCTs included in the reviews if they had a history of previous treatment. However, the reviews did not provide details about which medications were considered in the patients from the included RCTs. These details are likely reported in the eligibility criteria of the primary studies. No patient characteristics were reported for the individuals with EGFR gene mutations from the RCTs considered in the reviews. Only 4 reviews reported characteristics for broader groups of patients with NSCLC with and without actionable driver mutations. In these patients, mean age broadly ranged from 60 years to 65 years, and the proportion of male patients ranged from 47% to 85%. One review considered the histology of patients with EGFR-positive NSCLC (squamous versus nonsquamous) combined with PD-L1 levels. A careful, comprehensive examination of patient characteristics in context with the study design is necessary to understand the extent to which the findings are limited by differences in the study populations (i.e., because of baseline patient characteristics). It is unclear whether patients in the included studies are likely to be broadly generalizable to the current Canadian setting.
The methodological quality of the SRs as assessed using AMSTAR 2 varied, and appraisal was limited by insufficient reporting of many items and/or lack of rationale to support decisions made at the review level. This made it difficult to assess the methodological rigour. At least half of the included reviews could be considered of relatively poor quality because they did not report or address fundamental methodological components, including comprehensive details about the search strategy, the selection process, and characteristics of the included RCTs and patients, or because they did not assess the risk of bias.
In 6 SRs that did assess risk of bias for the included RCTs, lack of blinding was an overall limitation. The SRs provided insufficient detail for the individual RCTs considered to permit sufficient understanding of how these biases could have impacted study findings, if at all.
Interpretation of Clinical Results
Benefits of ICI Monotherapy in Patients With NSCLC With Actionable Driver Mutations
Based on the results of this overview, there is overall evidence that ICI monotherapy does not offer any significant benefit in improving OS and PFS over conventional chemotherapy when used for the treatment of NSCLC with EGFR mutation following another treatment. However, there is insufficient evidence to evaluate or account for prior therapies.38-50 While all the reviews were assessed to have reporting limitations, which may have influenced methodological quality, there is consistency of findings across the included reviews for OS.
One NMA reported that a subgroup of patients with nonsquamous NSCLC, EGFR mutation, or PD-L1 expression levels of 5% or more benefited from nivolumab monotherapy more than those with PD-L1 expression levels of less than 5%.49 However, as the previous treatment regimens could not be determined and the quantity of evidence available in the network was unclear, these results should be interpreted with caution. The RCTs included in the SRs were broadly assessed to be at low risk of bias for most domains. However, lack of blinding was a limitation noted universally, so detection and performance bias cannot be ruled out. Although 1 SR did report the proportions of participants who were Asian and not Asian included in their analyses,49 the majority of the SRs included in this overview did not report the sex, age distribution, ethnicity, or any other characteristics of patients with NSCLC with EGFR mutations, which made it difficult to assess how ICI monotherapy might perform across different demographic groups.38-48,50 Data for other populations of interest were not reported, except to note that very small proportions of participants in the included trials (under 5%) had ALK mutations. None of the RCTs included in any of the SRs considered ROS1 or RET mutations, so the efficacy of ICI drugs in these patient groups remains unclear.
Safety of ICI Monotherapy in Patients With NSCLC With Actionable Driver Mutations
Adverse and severe adverse effects associated with atezolizumab, nivolumab, and pembrolizumab were not assessed for the populations of patients with EGFR-positive NSCLC in the included SRs, so no conclusions can be made regarding the safety of these ICI drugs in patients with NSCLC with EGFR gene mutations. Data for other populations of interest were not reported, except to note that small proportions of participants in the included trials (under 5%) had ALK mutations. None of the RCTs included in any of the SRs considered ROS1 or RET gene mutations, so the efficacy of ICI drugs in these patient groups also remains unclear. Harms commonly documented with ICI drugs include fatigue, skin rash, diarrhea or constipation, nausea, vomiting, decreased appetite, cough, shortness of breath, fever, chills, body aches, joint or muscle pain, and changes in liver function.55 Additionally, rare but serious side effects such as immune-related AEs, including pneumonitis, colitis, hepatitis, or thyroid disorders, may occur. Patients receiving ICI drug therapy require close monitoring by health care providers to detect and manage side effects promptly.56
Strengths and Limitations of the Overview
Strengths
We designed, implemented, and conducted an overview of SRs following the best practices outlined in the Cochrane Handbook of SRs of Interventions. The literature search was continuously updated to include the most recent reviews published up to April 24, 2024. We located a number of reviews, each with varying scope and methodology, that broadly converged on similar conclusions, which adds to the robustness of this overview of reviews.
Limitations
The main limitations of this review are the lack of identified clinical evidence for any patients with ALK-positive, RET-positive, or ROS1-positive NSCLC, the methodological quality of the included SRs, and the lack of clinical evidence to inform any conclusions about the safety of the interventions in any population of interest. Interpretation of the reported clinical evidence was limited by the reporting quality of the SRs. This overview did not capture RCTs published since the last search date of the included SRs (August 18, 2020), and evidence from observational studies was not considered.30 Only 2 clinical efficacy outcomes were reported. It is not clear if data for other outcomes of interest, including harms, may be available for patients with actionable driver mutations from the primary study publications or other published records. This overview relied on RCT data reported by the included SRs, which was insufficient to answer our research questions fulsomely. Data extracted from the SRs and the included RCTs were not cross-checked for accuracy or missing information against the primary study publications, except where discrepancies were found.
Conclusions and Implications for Policy-Making
What Is the Evidence for the Clinical Efficacy of Atezolizumab, Nivolumab, and Pembrolizumab Monotherapy in Previously Treated Patients With Advanced or Metastatic NSCLC With Actionable Driver Mutations?
To determine the efficacy of the use of atezolizumab, nivolumab, and pembrolizumab monotherapy in previously treated patients with advanced or metastatic NSCLC with EGFR, ROS1, RET, or ALK actionable driver mutations, an overview of SRs was undertaken. Thirteen reviews were included in this review. We conclude, based on efficacy data from up to 4 RCTs for OS and 2 RCTs for PFS included in the SRs that, as a class, ICI monotherapy does not provide significant improvements in OS and PFS relative to chemotherapy in patients with EGFR-positive NSCLC who have received previous treatment. Because of the limited granularity in the population data presented, we are unable to make any conclusions specific to patients in this group that may have received platinum-based chemotherapy as a first-line treatment. No evidence was identified for similar patients with NSCLC with ROS1 or RET mutations or ALK rearrangement.
Findings from 1 systematic review suggest that histology and PD-L1 expression could be used to inform the selection of EGFR-positive NSCLC patients who may experience a beneficial response to ICI monotherapy in second-line settings. However, these findings should be interpreted with caution until they can be confirmed in additional high-quality research studies for this population or others. All the SRs included in this overview did not provide information on the demographics or health status of previously treated patients with NSCLC with EGFR mutations, making it unfeasible to recommend ICI drugs in any specific age, sex, or other groups within this population. PD-L1 expression and histology may be indicators of potential response to ICI drugs in the second-line setting or beyond for patients with EGFR-mutated NSCLC. However, no evidence for pembrolizumab or atezolizumab is available in the RCTs included by the SRs to permit assessment of the consistency of the evidence for the available treatments.
The results from all included SRs should be interpreted with caution because of significant methodological and reporting flaws. Additionally, the findings regarding clinical efficacy in populations with EGFR mutations may not accurately and comprehensively represent the data available from the individual RCTs.
What Is the Evidence for the Safety of Atezolizumab, Nivolumab, and Pembrolizumab Monotherapy in Previously Treated Patients With Advanced or Metastatic NSCLC With Actionable Driver Mutations?
None of the included SRs in our overview of reviews specifically examined the relative adverse effects and safety profile of ICI monotherapies in patients with EGFR-mutated NSCLC or any of the other mutations of interest. This is likely attributable to reporting limitations of the RCTs, which did not stratify the reported safety data by mutation status for the patients noted to have EGFR- or ALK-mutated NSCLC. As a result, it is challenging to determine the overall safety of the individual ICI monotherapies or as a class in the patient population covered in this overview of reviews. There is no expectation that the toxicity profile would differ for atezolizumab, nivolumab, and pembrolizumab, and it is reasonable to expect that the safety overall would be similar to first- and second-line use and to that of populations with unmutated tumours. SRs of higher quality, RCTs, or observational studies focusing on analyzing the safety of ICI monotherapy in patients with EGFR-, ROS1-, RET-, or ALK-mutated NSCLC are needed to ascertain the overall safety of ICI monotherapy drugs in these patients.
References
1.Canadian cancer statistics. Toronto (ON): Canadian Cancer Statistics Advisory Committee; 2021: https://cdn.cancer.ca/-/media/files/research/cancer-statistics/2021-statistics/2021-pdf-en-final.pdf. Accessed 2022 Jan 5.
2.Cancer.Net American Society of Clinical Oncology (ASCO). Lung cancer - non-small cell: statistics. 2021; https://www.cancer.net/cancer-types/lung-cancer-non-small-cell/statistics. Accessed 2022 Jan 12.
3.National Cancer Institute. Non-small cell lung cancer treatment (PDQ®) – health professional version. 2021; https://www.cancer.gov/types/lung/hp/non-small-cell-lung-treatment-pdq. Accessed 2021 Dec 4.
4.Yakut T, Schulten H-J, Demir A, et al. Assessment of molecular events in squamous and non-squamous cell lung carcinoma. Lung Cancer. 2006;54(3):293-301. PubMed
5.Socinski MA, Obasaju C, Gandara D, et al. Clinicopathologic features of advanced squamous NSCLC. J Thorac Oncol. 2016;11(9):1411-1422. PubMed
6.Bansal P, Osman D, Gan GN, Simon GR, Boumber Y. Recent advances in targetable therapeutics in metastatic non-squamous NSCLC. Front Oncol. 2016;6:195170. PubMed
7.Lung Cancer Canada. Lung cancer staging in Canada. 2020; https://www.lungcancercanada.ca/Lung-Cancer/Staging.aspx. Accessed 2021 Dec 4.
8.Iyer S, Roughley A, Rider A, Taylor-Stokes G. The symptom burden of non-small cell lung cancer in the USA: a real-world cross-sectional study. Support Care Cancer. 2014;22(1):181-187. PubMed
9.National Comprehensive Cancer Network (NCCN). Non-small cell lung cancer. NCCN Clinical Practice Guidelines in Oncology. 2021; https://www.nccn.org/guidelines/guidelines-detail?category=1&id=1450. Accessed 2021 Dec 4.
10.Planchard D, Popat S, Kerr K, et al. Metastatic non-small cell lung cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Lugano (CH): European Society for Medical Oncology; 2020: https://www.esmo.org/content/download/347819/6934778/1/ESMO-CPG-mNSCLC-15SEPT2020.pdf. Accessed 2021 Dec 4.
11.Ellis PM, Vella ET, Ung YC. Systemic treatment for patients with advanced non-small cell lung cancer. (Guideline 7-10, version 3). Toronto (ON): Cancer Care Ontario; 2016: https://www.cancercareontario.ca/en/guidelines-advice/types-of-cancer/31811. Accessed 2021 Dec 4.
12.Cascetta P, Sforza V, Manzo A, et al. RET inhibitors in non-small-cell lung cancer. Cancers (Basel). 2021;13(17):01.
13.Davies KD, Le AT, Theodoro MF, et al. Identifying and targeting ROS1 gene fusions in non-small cell lung cancer. Clin Cancer Res. 2012;18(17):4570–4579. PubMed
14.Kris MG, Johnson BE, Berry LD, et al. Using multiplexed assays of oncogenic drivers in lung cancers to select targeted drugs. JAMA. 2014;311(19):1998-2006. PubMed
15.Kwak EL, Bang YJ, Camidge DR, et al. Anaplastic lymphoma kinase inhibition in non-small-cell lung cancer. N Engl J Med. 2010;363(18):1693-1703. PubMed
16.Shaw AT, Solomon BJ, Besse B, et al. ALK Resistance Mutations and Efficacy of Lorlatinib in Advanced Anaplastic Lymphoma Kinase-Positive Non–Small-Cell Lung Cancer. J Clin Oncol. 2019;37(16):1370-1379. PubMed
17.Dempke WCM, Fenchel K, Uciechowski P, Dale SP. Second-and third-generation drugs for immuno-oncology treatment—the more the better? Eur J Cancer. 2017;74:55-72. PubMed
18.Jaiyesimi IA, Leighl NB, Ismaila N, et al. Therapy for Stage IV Non–Small Cell Lung Cancer Without Driver Alterations: ASCO Living Guideline, Version 2023.3. J Clin Oncol. 2024.
19.Dantoing E, Piton N, Salaün M, Thiberville L, Guisier F. Anti-PD1/PD-L1 Immunotherapy for Non-Small Cell Lung Cancer with Actionable Oncogenic Driver Mutations. Int J Mol Sci. 2021;22(12):6288. PubMed
20.Mazieres J, Drilon A, Lusque A, et al. Immune checkpoint inhibitors for patients with advanced lung cancer and oncogenic driver alterations: results from the IMMUNOTARGET registry. Ann Oncol. 2019;30(8):1321–1328. PubMed
21.Luciani A, Ghidini A, Borgonovo K, Parati MC, Petrelli F. Outcome of non-small-cell lung cancer with driven mutations treated with anti-PD-(L)1 agents: A systematic review. Tumori. 2022;3008916221122601. PubMed
22.Keytruda (pembrolizumab): solution for infusion 100 mg/4 mL vial [product monograph]. Kirkland (QC): Merck Canada Inc.; 2024 Aug 7: https://pdf.hres.ca/dpd_pm/00071768.PDF. Accessed 2024 Jan 9.
23.Opdivo (nivolumab): Intravenous Infusion, 10 mg nivolumab /mL 40 mg and 100 mg single-use vials [product monograph]. Saint-Laurent (QC): Bristol-Myers Squibb Canada; 2024 Jun 28: https://pdf.hres.ca/dpd_pm/00070041.PDF. Accessed 2024 Jan 9.
24.Tecentriq (atezolizumab): concentrate for solution for infusion, 60 mg/mL 1200 mg/20 mL and 840 mg/14 mL single use vials for intravenous infusion [product monograph]. . Mississauga (ON): Hoffmann-La Roche Ltd.; 2024 Mar 13: https://pdf.hres.ca/dpd_pm/00071423.PDF. Accessed 2024 Jan 9.
25.Provisional Funding Algorithm. Indication: Anaplastic Lymphoma Kinase–Positive Non–Small Cell Lung Cancer. (CADTH Reimbursement Review). Ottawa (ON): CADTH; 2022: https://www.cadth.ca/sites/default/files/pdf/PH0009-ALK%2BNSCLC-Algorithm.pdf. Accessed 2023 Aug 16.
26.Provisional Funding Algorithm. Indication: Advanced or Metastatic Non–Small Cell Lung Cancer with activating epidermal growth factor receptor mutations. (CADTH Reimbursement Review). Ottawa (ON): CADTH; 2023: https://www.cadth.ca/sites/default/files/DRR/2023/PH0028-NSCLC-EGFR.pdf. Accessed 2023 Aug 16.
27.Provisional Funding Algorithm. Indication: RET fusion-positive Non–Small Cell Lung Cancer. (CADTH Reimbursement Review). Ottawa (ON): CADTH; 2023: https://www.cadth.ca/sites/default/files/DRR/2023/PH0026-Implementation-Advice-Report-Algorithm-RET-Positive-NSCLC.pdf. Accessed 2023 Aug 16.
28.Passiglia F, Bronte G, Bazan V, et al. PD-L1 expression as predictive biomarker in patients with NSCLC: a pooled analysis. Oncotarget. 2016;7(15):19738. PubMed
29.Luciani A, Ghidini A, Borgonovo K, Parati MC, Petrelli F. Outcome of non-small-cell lung cancer with driven mutations treated with anti-PD-(L)1 agents: A systematic review. Tumori. 2023;109(5):442-449. PubMed
30.Higgins JPT, Thomas J, Chandler J, et al. Cochrane Handbook for Systematic Reviews of Interventions version 6.4 (updated August 2023). Cochrane; 2023: www.training.cochrane.org/handbook. Accessed 2021 Dec 4.
31.Pollock M, Fernandes RM, Pieper D, et al. Preferred Reporting Items for Overviews of Reviews (PRIOR): a protocol for development of a reporting guideline for overviews of reviews of healthcare interventions. Syst Rev. 2019;8(1):335. PubMed
32.Gates M, Gates A, Pieper D, et al. Reporting guideline for overviews of reviews of healthcare interventions: development of the PRIOR statement. BMJ. 2022;378:e070849. PubMed
33.Moher D, Shamseer L, Clarke M, et al. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst Rev. 2015;4:1-9. PubMed
34.McGowan J, Sampson M, Salzwedel DM, Cogo E, Foerster V, Lefebvre C. PRESS Peer Review of Electronic Search Strategies: 2015 Guideline Statement. J Clin Epidemiol. 2016;75:40-46. PubMed
35.Moher D, Altman DG, Liberati A, Tetzlaff J. PRISMA statement. Epidemiology. 2011;22(1):128. PubMed
36.Shea BJ, Reeves BC, Wells G, et al. AMSTAR 2: a critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ. 2017;358:j4008. PubMed
37.Donegan S, Williamson P, D'Alessandro U, Tudur Smith C. Assessing key assumptions of network meta-analysis: a review of methods. Res Synth Methods. 2013;4(4):291-323. PubMed
38.Wang C, Yu X, Wang W. A meta-analysis of efficacy and safety of antibodies targeting PD-1/PD-L1 in treatment of advanced nonsmall cell lung cancer. Medicine (Baltimore). 2016;95(52):e5539. PubMed
39.Lee CK, Man J, Lord S, et al. Checkpoint Inhibitors in Metastatic EGFR-Mutated Non-Small Cell Lung Cancer-A Meta-Analysis. J Thorac Oncol. 2017;12(2):403-407. PubMed
40.Sheng Z, Zhu X, Sun Y, Zhang Y. The efficacy of anti-PD-1/PD-L1 therapy and its comparison with EGFR-TKIs for advanced non-small-cell lung cancer. Oncotarget. 2017;8(34):57826-57835. PubMed
41.Huang Q, Zhang H, Hai J, et al. Impact of PD-L1 expression, driver mutations and clinical characteristics on survival after anti-PD-1/PD-L1 immunotherapy versus chemotherapy in non-small-cell lung cancer: A meta-analysis of randomized trials. Oncoimmunology. 2018;7(12):e1396403. PubMed
42.Jiang Q, Xie M, He M, Yan F, Zhang X, Yu S. Anti-PD-1/PD-L1 antibodies versus docetaxel in patients with previously treated non-small-cell lung cancer. Oncotarget. 2018;9(7):7672-7683. PubMed
43.Abdel-Rahman O. Smoking and EGFR status may predict outcomes of advanced NSCLC treated with PD-(L)1 inhibitors beyond first line: A meta-analysis. Clin Respir J. 2018;12(5):1809-1819. PubMed
44.Liu J, Zhong Y, Peng S, Zhou X, Gan X. Efficacy and safety of PD1/PDL1 blockades versus docetaxel in patients with pretreated advanced non-small-cell lung cancer: a meta-analysis. Onco Targets Ther. 2018;11:8623-8632. PubMed
45.Khan M, Lin J, Liao G, et al. Comparative analysis of immune checkpoint inhibitors and chemotherapy in the treatment of advanced non-small cell lung cancer: A meta-analysis of randomized controlled trials. Medicine (Baltimore). 2018;97(33):e11936. PubMed
46.Lee CK, Man J, Lord S, et al. Clinical and Molecular Characteristics Associated With Survival Among Patients Treated With Checkpoint Inhibitors for Advanced Non-Small Cell Lung Carcinoma: A Systematic Review and Meta-analysis. JAMA Oncol. 2018;4(2):210-216. PubMed
47.Almutairi AR, Alkhatib N, Martin J, et al. Comparative efficacy and safety of immunotherapies targeting the PD-1/PD-L1 pathway for previously treated advanced non-small cell lung cancer: A Bayesian network meta-analysis. Crit Rev Oncol Hematol. 2019;142:16-25. PubMed
48.Cavanna L, Citterio C, Orlandi E. Immune checkpoint inhibitors in EGFR-mutation positive TKI-treated patients with advanced non-small-cell lung cancer network meta-analysis. Oncotarget. 2019;10(2):209-215. PubMed
49.Vickers AD, Winfree KB, Cuyun Carter G, et al. Relative efficacy of interventions in the treatment of second-line non-small cell lung cancer: a systematic review and network meta-analysis. BMC Cancer. 2019;19(1):353. PubMed
50.An R, Zhao F, Wang L, Shan J, Wang X. Predictive effect of molecular and clinical characteristics for the OS and PFS efficacy of anti-PD-1/PD-L1 immunotherapy in patients with NSCLC: a meta-analysis and systematic review. BMJ Open. 2021;11(12):e047663.
51.Borghaei H, Paz-Ares L, Horn L, et al. Nivolumab versus Docetaxel in Advanced Nonsquamous Non-Small-Cell Lung Cancer. N Engl J Med. 2015;373(17):1627-1639. PubMed
52.Fehrenbacher L, Spira A, Ballinger M, et al. Atezolizumab versus docetaxel for patients with previously treated non-small-cell lung cancer (POPLAR): a multicentre, open-label, phase 2 randomised controlled trial. Lancet. 2016;387(10030):1837-1846. PubMed
53.Rittmeyer A, Barlesi F, Waterkamp D, et al. Atezolizumab versus docetaxel in patients with previously treated non-small-cell lung cancer (OAK): a phase 3, open-label, multicentre randomised controlled trial. Lancet. 2017;389(10066):255-265. PubMed
54.Herbst RS, Baas P, Kim DW, et al. Pembrolizumab versus docetaxel for previously treated, PD-L1-positive, advanced non-small-cell lung cancer (KEYNOTE-010): a randomised controlled trial. Lancet. 2016;387(10027):1540-1550. PubMed
55.Santini FC, Rizvi H, Plodkowski AJ, et al. Safety and efficacy of re-treating with immunotherapy after immune-related adverse events in patients with NSCLC. Cancer Immunol Res. 2018;6(9):1093-1099. PubMed
56.Hu Y-B, Zhang Q, Li H-J, et al. Evaluation of rare but severe immune related adverse effects in PD-1 and PD-L1 inhibitors in non-small cell lung cancer: a meta-analysis. Transl Lung Cancer Res. 2017;6(Suppl 1):S8. PubMed
Authors and Contributors
Shariq Najeeb contributed by screening studies; extracting data; analyzing and interpreting results, figures, and tables; verifying and assessing quality; and drafting and revising the report.
Said Yousef Abdelrazeq contributed by screening studies; extracting data; analyzing and interpreting results, figures, and tables; verifying and assessing quality; and drafting and revising the report.
Shannon E. Kelly contributed to the conceptualization and design of the approach, provided research oversight, and contributed to the interpretation of results and drafting and finalizing the report.
Xiaoqin Wang contributing by screening of the studies; extracting data; proof-reading; and verifying and assessing quality.
Nazmun Nahar contributed by drafting tables and assisting with referencing of the report.
Melissa Brouwers contributed to the conceptualization and design of the approach and provided final approval to this version of the report.
George A. Wells acted as the principal investigator by developing and leading the approach and by contributing to the validation of the results, interpretation of the results, drafting, and finalizing the report.
Research Information Science
Becky Skidmore designed and executed the literature search strategy, monitored search alerts, prepared the search methods section and appendix, and provided final approval to the version of the report.
Contributors
We thank Kaitryn Campbell, MLIS, MSc (Hamilton, ON) for peer-reviewing the MEDLINE search strategy.
Conflicts of Interest
George A. Wells disclosed the following:
VBI Vaccines Inc. (2020–current): Coronavirus Vaccine. Data Safety Monitoring Board – Member.
Thermedical (2021–current): Ablation system and catheter needle. Design and analysis advice for preparation of FDA Submission.
VBI Vaccines Inc. (2020–current): Coronavirus Vaccine. Design and Analysis Advice for preparation of FDA Submission.
No other conflicts of interest were declared.
Appendix 1: Literature Search Strategy
Please note that this appendix has not been copy-edited.
NSCLC – Immunotherapy
Final Strategy
2024 Jan 26
Last Update: 2024 Apr 24
Ovid Multifile
Database: Embase Classic+Embase < 1947 to 2024 April 23 > , Ovid MEDLINE(R) ALL < 1946 to April 23, 2024 > , EBM Reviews - Cochrane Database of Systematic Reviews < 2005 to April 17, 2024 >
Search Strategy:
Carcinoma, Non-Small-Cell Lung/ (154252)
(Squamous Cell Carcinoma/ or Adenocarcinoma/ or Large Cell Carcinoma/) and exp Lung Neoplasms/ (83483)
((neoplas* or cancer* or tumo?r* or carcinoma* or malignan* or oncolog* or h?emangioma* or blastoma* or carcinosarcoma* or carcino-sarcoma* or leuk?emia* or lymphoma* or melanoma* or mesenchymoma* or sarcoma* or thymoma* or granuloma*) adj3 ((non-small-cell or nonsmall-cell or large-cell or squamous-cell or epidermoid* or planocellular or plano-cellular) adj3 (lung or lungs or pneumo* or bronch* or pulmon*or pleuropulmon* or pleuro-pulmon*))).tw,kw,kf. (255204)
((adenocancer* or adenoma* or adenocarcinoma* or adeno-carcinoma*) adj3 (lung or lungs or pneumo* or bronch* or pulmon* or pleuropulmon* or pleuro-pulmon*)).tw,kw,kf. (89960)
(NSCLC or NSCLCs).tw,kw,kf. (183616)
or/1-5 [NSCLC] (409414)
exp Neoplasm Metastasis/ (1095139)
Neoplasm Recurrence, Local/ (198219)
(meta adj sta*).tw,kw,kf. (1751)
(metastas* or metastatic* or recur* or secondar* or relaps* or advanc* or inoperab* or disseminat* or spread or migration? or lethal* or incurable or noncurable or non-curable or uncurable or progressive or terminal or invasiv* or aggressiv*).tw,kw,kf. (12463012)
(late? adj2 stage?).tw,kw,kf. (188459)
((stage? or grade? or type?) adj2 (3a* or 3b* or 3c* or III* or 4a* or 4b* or 4c* or IV*)).tw,kw,kf. (545350)
(“stage 3” or “stage 4” or met or mets or N1 or N2? or N3? or pN1? or pN2? or pN3?).tw,kw,kf. (1468368)
or/7-13 [ADVANCED/METASTATIC CANCER] (14133430)
6 and 14 [NSCLC - ADVANCED/METASTATIC] (254024)
(atezolizumab* or “mpdl 3280” or mpdl3280 or “mpdl 3280a” or mpdl3280a or “rg 7446” or rg744 or “ro 5541267” or ro5541267 or tecentriq$2 or tecntriq$2 or anti-PDL1 or anti-PD-L1 or 0INE2SFD9E or 52CMI0WC3Y or 1380723-44-3).tw,kw,kf,rn. (31709)
Nivolumab/ (47234)
(nivolumab* or “ba 1104” or ba1104 or “bms 936558” or bms936558 or “cmab 819” or cmab819 or HSDB 8256 or L01XC17 or “ly 01015” or ly01015 or “mdx 1106” or mdx1106 or “ono 4538” or ono4538 or opdivo$2 or “pbp 2101” or pbp2101 or xdivane$2 or 31YO63LBSN or 946414-94-4).tw,kw,kf,rn. (53862)
(pembrolizumab* or “bcd 201” or bcd201 or keytruda$2 or lambrolizumab$2 or “mk 3475” or mk3475 or “pbp 2102” or pbp2102 or “sch 900475” or sch900475 or xtrudane$2 or DPT0O3T46P or HSDB 8257 or L01XC18 or 1374853-91-4).tw,kw,kf. (31871)
Antineoplastic Agents, Immunological/ (15243)
((antineoplastic? or anti-neoplastic?) adj2 (monoclonal antibod* or mono-clonal antibod* or monoclonal anti-bod* or mono-clonal anti-bod* or MAB or MABs)).tw,kw,kf. (62)
Immune Checkpoint Inhibitors/ (41206)
((immune checkpoint or CTLA-4 or Cytotoxic T-Lymphocyte-Associated Protein 4 or PD-1 or PD-1-PD-L1 or PD-L1 or Programmed Cell Death Protein 1 or Programmed Death-Ligand 1) adj3 (inhibition or inhibitor? or blocker? or blockade?)).tw,kw,kf. (118479)
((ICI or ICIs) adj5 immun*).tw,kw,kf. (30282)
or/16-24 [DRUGS OF INTEREST, DRUG CLASS] (186759)
15 and 25 [ADVANCED/METASTATIC NSCLC - DRUGS/DRUG CLASS OF INTEREST] (27135)
exp Animals/ not Humans/ (17781750)
26 not 27 [ANIMAL-ONLY REMOVED] (25777)
(address or autobiography or bibliography or biography or dictionary or directory or editorial or “expression of concern” or festschrift or historical article or interactive tutorial or lecture or legal case or legislation or news or newspaper article or patient education handout or personal narrative or portrait or video-audio media or webcast or (letter not (letter and randomized controlled trial))).pt. (4742130)
28 not 29 [OPINION PIECES, PUBLICATION TYPES NOT OF INTEREST REMOVED] (25221)
Systematic Review.pt. (268117)
exp Systematic Reviews as Topic/ (47785)
Meta Analysis.pt. (199401)
exp Meta-Analysis as Topic/ (85250)
(meta-analy* or metanaly* or metaanaly* or met analy* or integrative research or integrative review* or integrative overview* or research integration or research overview* or collaborative review*).tw,kw,kf. (715293)
(systematic review* or systematic overview* or evidence-based review* or evidence-based overview* or (evidence adj3 (review* or overview*)) or evidence map* or meta-review* or meta-overview* or meta-synthes* or mapping review? or rapid review* or “review of reviews” or scoping review? or umbrella review? or technology assessment* or HTA or HTAs).tw,kw,kf. (926991)
exp Technology Assessment, Biomedical/ (30305)
(cochrane or health technology assessment or evidence report or systematic reviews).jw. (70476)
Network Meta-Analysis/ (14873)
(network adj (MA or MAs)).tw,kw,kf. (55)
(NMA or NMAs or MTC or MTCs or MAIC or MAICs).tw,kw,kf. (26556)
indirect* compar*.tw,kw,kf. (9267)
(indirect treatment* adj1 compar*).tw,kw,kf. (1864)
(mixed treatment* adj1 compar*).tw,kw,kf. (1601)
(multiple treatment* adj1 compar*).tw,kw,kf. (579)
(multi-treatment* adj1 compar*).tw,kw,kf. (16)
simultaneous* compar*.tw,kw,kf. (3087)
mixed comparison?.tw,kw,kf. (174)
or/31-48 [SR FILTER] (1411289)
30 and 49 [ADVANCED/METASTATIC NSCLC - DRUGS/DRUG CLASS OF INTEREST - SRs] (1716)
limit 50 to yr=”2013-current” [DATE LIMIT APPLIED] (1706)
51 use medall [MEDLINE RECORDS] (558)
exp non small cell lung cancer/ (241315)
((neoplas* or cancer* or tumo?r* or carcinoma* or malignan* or oncolog* or h?emangioma* or blastoma* or carcinosarcoma* or carcino-sarcoma* or leuk?emia* or lymphoma* or melanoma* or mesenchymoma* or sarcoma* or thymoma* or granuloma*) adj3 ((non-small-cell or nonsmall-cell or large-cell or squamous-cell or epidermoid* or planocellular or plano-cellular) adj3 (lung or lungs or pneumo* or bronch* or pulmon*or pleuropulmon* or pleuro-pulmon*))).tw,kw,kf. (255204)
((adenocancer* or adenoma* or adenocarcinoma* or adeno-carcinoma*) adj3 (lung or lungs or pneumo* or bronch* or pulmon* or pleuropulmon* or pleuro-pulmon*)).tw,kw,kf. (89960)
(NSCLC or NSCLCs).tw,kw,kf. (183616)
or/53-56 [NSCLC] (390475)
exp lung metastasis/ (70505)
metastasis/ (495014)
micrometastasis/ (8423)
tumor recurrence/ (74982)
(meta adj sta*).tw,kw,kf. (1751)
(metastas* or metastatic* or recur* or secondar* or relaps* or advanc* or inoperab* or disseminat* or spread or migration? O r lethal* or incurable or noncurable or non-curable or uncurable or progressive or terminal or invasiv* or aggressiv*).tw,kw,kf. (12463012)
(late? adj2 stage?).tw,kw,kf. (188459)
((stage? or grade? or type?) adj2 (3a* or 3b* or 3c* or III* or 4a* or 4b* or 4c* or IV*)).tw,kw,kf. (545350)
(“stage 3” or “stage 4” or met or mets or N1 or N2? or N3? or pN1? or pN2? or pN3?).tw,kw,kf. (1468368)
or/58-66 [ADVANCED/METASTATIC CANCER] (14025151)
57 and 67 [NSCLC - ADVANCED/METASTATIC] (238266)
atezolizumab/ (17334)
(atezolizumab* or “mpdl 3280” or mpdl3280 or “mpdl 3280a” or mpdl3280a or “rg 7446” or rg744 or “ro 5541267” or ro5541267 or tecentriq$2 or tecntriq$2 or anti-PDL1 or anti-PD-L1 or 0INE2SFD9E or 52CMI0WC3Y or 1380723-44-3).tw,kw,kf,rn. (31709)
nivolumab/ (47234)
(nivolumab* or “ba 1104” or ba1104 or “bms 936558” or bms936558 or “cmab 819” or cmab819 or HSDB 8256 or L01XC17 or “ly 01015” or ly01015 or “mdx 1106” or mdx1106 or “ono 4538” or ono4538 or opdivo$2 or “pbp 2101” or pbp2101 or xdivane$2 or 31YO63LBSN or 946414-94-4).tw,kw,kf,rn. (53862)
pembrolizumab/ (41310)
(pembrolizumab* or “bcd 201” or bcd201 or keytruda$2 or lambrolizumab$2 or “mk 3475” or mk3475 or “pbp 2102” or pbp2102 or “sch 900475” or sch900475 or xtrudane$2 or DPT0O3T46P or HSDB 8257 or L01XC18 or 1374853-91-4).tw,kw,kf. (31871)
immunological antineoplastic agent/ (15243)
antineoplastic monoclonal antibody/ (3192)
((antineoplastic? or anti-neoplastic?) adj2 (monoclonal antibod* or mono-clonal antibod* or monoclonal anti-bod* or mono-clonal anti-bod* or MAB or MABs)).tw,kw,kf. (62)
immune checkpoint inhibitor/ (41530)
((immune checkpoint or CTLA-4 or Cytotoxic T-Lymphocyte-Associated Protein 4 or PD-1 or PD-1-PD-L1 or PD-L1 or Programmed Cell Death Protein 1 or Programmed Death-Ligand 1) adj3 (inhibition or inhibitor? or blocker? or blockade?)).tw,kw,kf. (118479)
((ICI or ICIs) adj5 immun*).tw,kw,kf. (30282)
or/69-80 [DRUGS OF INTEREST, DRUG CLASS] (193071)
68 and 81 [ADVANCED/METASTATIC NSCLC - DRUGS/DRUG CLASS OF INTEREST] (27455)
(exp animal/ or exp animal model/ or exp animal experiment/ or nonhuman/ or exp vertebrate/) not (exp human/ or exp human experiment/) (13434292)
82 not 83 [ANIMAL-ONLY REMOVED] (27113)
editorial.pt. (1492539)
84 not 85 [OPINION PIECES, PUBLICATION TYPES NOT OF INTEREST REMOVED] (26912)
“systematic review”/ (722201)
“systematic review (topic)”/ (34669)
meta analysis/ (512787)
“meta analysis (topic)”/ (55639)
(meta-analy* or metanaly* or metaanaly* or met analy* or integrative research or integrative review* or integrative overview* or research integration or research overview* or collaborative review*).tw,kw,kf. (715293)
(systematic review* or systematic overview* or evidence-based review* or evidence-based overview* or (evidence adj3 (review* or overview*)) or evidence map* or meta-review* or meta-overview* or meta-synthes* or mapping review? or rapid review* or “review of reviews” or scoping review? or umbrella review? or technology assessment* or HTA or HTAs).tw,kw,kf. (926991)
exp biomedical technology assessment/ (30305)
(cochrane or health technology assessment or evidence report or systematic reviews).jw. (70476)
network meta-analysis/ (14873)
(network adj (MA or MAs)).tw,kw,kf. (55)
(NMA or NMAs or MTC or MTCs or MAIC or MAICs).tw,kw,kf. (26556)
indirect* compar*.tw,kw,kf. (9267)
(indirect treatment* adj1 compar*).tw,kw,kf. (1864)
(mixed treatment* adj1 compar*).tw,kw,kf. (1601)
(multiple treatment* adj1 compar*).tw,kw,kf. (579)
(multi-treatment* adj1 compar*).tw,kw,kf. (16)
simultaneous* compar*.tw,kw,kf. (3087)
mixed comparison?.tw,kw,kf. (174)
or/87-104 [SR FILTER] (1532431)
86 and 105 [ADVANCED/METASTATIC NSCLC - DRUGS/DRUG CLASS OF INTEREST - SRs] (2059)
conference abstract.pt. (5118750)
106 not 107 [CONFERENCE ABSTRACTS REMOVED] (1600)
limit 108 to yr=”2013-current” [DATE LIMIT APPLIED] (1590)
109 use emczd [EMBASE RECORDS] (1026)
((neoplas* or cancer* or tumo?r* or carcinoma* or malignan* or oncolog* or h?emangioma* or blastoma* or carcinosarcoma* or carcino-sarcoma* or leuk?emia* or lymphoma* or melanoma* or mesenchymoma* or sarcoma* or thymoma* or granuloma*) adj3 ((non-small-cell or nonsmall-cell or large-cell or squamous-cell or epidermoid* or planocellular or plano-cellular) adj3 (lung or lungs or pneumo* or bronch* or pulmon*or pleuropulmon* or pleuro-pulmon*))).ti,ab,kw. (249854)
((adenocancer* or adenoma* or adenocarcinoma* or adeno-carcinoma*) adj3 (lung or lungs or pneumo* or bronch* or pulmon* or pleuropulmon* or pleuro-pulmon*)).ti,ab,kw. (88832)
(NSCLC or NSCLCs).ti,ab,kw. (182264)
or/111-113 [NSCLC] (343224)
(meta adj sta*).ti,ab,kw. (1731)
(metastas* or metastatic* or recur* or secondar* or relaps* or advanc* or inoperab* or disseminat* or spread or migration? or lethal* or incurable or noncurable or non-curable or uncurable or progressive or terminal or invasiv* or aggressiv*).ti,ab,kw. (12411069)
(late? adj2 stage?).ti,ab,kw. (187804)
((stage? or grade? or type?) adj2 (3a* or 3b* or 3c* or III* or 4a* or 4b* or 4c* or IV*)).ti,ab,kw. (541727)
(“stage 3” or “stage 4” or met or mets or N1 or N2? or N3? or pN1? or pN2? or pN3?).ti,ab,kw. (1461134)
or/115-119 [ADVANCED/METASTATIC CANCER] (13874954)
114 and 120 [NSCLC - ADVANCED/METASTATIC] (216389)
(atezolizumab* or “mpdl 3280” or mpdl3280 or “mpdl 3280a” or mpdl3280a or “rg 7446” or rg744 or “ro 5541267” or ro5541267 or tecentriq$2 or tecntriq$2 or anti-PDL1 or anti-PD-L1 or 0INE2SFD9E or 52CMI0WC3Y or 1380723-44-3).ti,ab,kw. (20925)
(nivolumab* or “ba 1104” or ba1104 or “bms 936558” or bms936558 or “cmab 819” or cmab819 or HSDB 8256 or L01XC17 or “ly 01015” or ly01015 or “mdx 1106” or mdx1106 or “ono 4538” or ono4538 or opdivo$2 or “pbp 2101” or pbp2101 or xdivane$2 or 31YO63LBSN or 946414-94-4).ti,ab,kw. (31806)
(pembrolizumab* or “bcd 201” or bcd201 or keytruda$2 or lambrolizumab$2 or “mk 3475” or mk3475 or “pbp 2102” or pbp2102 or “sch 900475” or sch900475 or xtrudane$2 or DPT0O3T46P or HSDB 8257 or L01XC18 or 1374853-91-4).ti,ab,kw. (30734)
((antineoplastic? or anti-neoplastic?) adj2 (monoclonal antibod* or mono-clonal antibod* or monoclonal anti-bod* or mono-clonal anti-bod* or MAB or MABs)).ti,ab,kw. (60)
((immune checkpoint or CTLA-4 or Cytotoxic T-Lymphocyte-Associated Protein 4 or PD-1 or PD-1-PD-L1 or PD-L1 or Programmed Cell Death Protein 1 or Programmed Death-Ligand 1) adj3 (inhibition or inhibitor? or blocker? or blockade?)).ti,ab,kw. (112818)
((ICI or ICIs) adj5 immun*).ti,ab,kw. (29826)
or/122-127 [DRUGS OF INTEREST, DRUG CLASS] (152247)
121 and 128 [ADVANCED/METASTATIC NSCLC - DRUGS/DRUG CLASS OF INTEREST] (21726)
limit 129 to yr=”2013-current” (21693)
130 use coch [CDSR RECORDS] (3)
52 or 110 or 131 [ALL DATABASES] (1587)
(2024012* or 2024013* or 202402* or 202403* or 202404*).dt. (416908)
52 and 133 [MEDLINE RECORDS - UPDATE PERIOD] (29)
(2024012* or 2024013* or 202402* or 202403* or 202404*).dc. (643921)
110 and 135 [EMBASE RECORDS - UPDATE PERIOD] (51)
(2024012* or 2024013* or 202402* or 202403* or 202404*).up. (1640026)
131 and 137 [CDSR RECORDS - UPDATE PERIOD] (0)
134 or 136 or 138 [ALL DATABASES - UPDATE PERIOD] (80)
remove duplicates from 139 (55) [TOTAL UNIQUE RECORDS – UPDATE PERIOD]
140 use medall [MEDLINE UNIQUE RECORDS - UPDATE PERIOD] (28)
140 use emczd [EMBASE UNIQUE RECORDS - UPDATE PERIOD] (27)
Appendix 2: Assessment of Included Study Overlap Across Included SRs
Note that this appendix has not been copy-edited.
Table 12: General Characteristics of Primary Studies as Reported in the Included SRs
Characteristicsa | RCT (author and trial name) | |||
|---|---|---|---|---|
Borghaei et al. (CHECKMATE-057) | Herbst et al. | Rittmeyer et al. | Fehrenbacher et al. (POPLAR) | |
Clinical trial no. | NCT01673867 | NCT01905657 | NCT02008227 | NCT01903993 |
Total number of patients analyzed (N) | 582 | 1,034 | 850 | 287 |
Included mutations of interest | EGFR, ALKb | EGFR, ALKb | EGFR, ALKb | EGFR, ALKb |
Intervention (n) | Nivolumab (292) | Pembrolizumab (691) | Atezolizumab (425) | Atezolizumab (144) |
Comparator (n) | Docetaxel (290) | Docetaxel (343) | Docetaxel (425) | Docetaxel (143) |
Outcomes of interest assessed for population with relevant mutationb | OS, PFS | OS, PFS | OS | OS |
Overall findings in population of interestc | No significant difference in OS and PFS between intervention and comparator in patients with NSCLC with EGFR mutations. | No significant difference in OS and PFS between intervention and comparator in patients with NSCLC with EGFR mutations. | No significant difference in OS between intervention and comparator in patients with NSCLC with EGFR mutations. PFS not reported. | No significant difference in OS between intervention and comparator in patients with NSCLC with EGFR mutations. PFS not reported. |
NSCLC = non–small cell lung cancer; OS = overall survival; PFS = progression-free survival; RCT = randomized controlled trial; SR = systematic reviews.
aThis table was adapted from data shared in 2 included SRs.47,50
bPatients with NSCLC with these mutations were documented in the study population; however, outcomes were only reported for patients with EGFR-positive NSCLC.
cAll findings are based on results reported for patients with EGFR-positive NSCLC.
Table 13: Overlap of RCTs in the SRs — OS
SR, | Number of RCTs Included in the SRs that report the outcome in population of interest | RCTs included in the SR (author, study) | |||
|---|---|---|---|---|---|
Borghaei et al., | Herbst et al., | Rittmeyer at al., | Fehrenbacher et al., | ||
Wang (2016)38 | 2 | x | x | NI | NI |
Lee (2017)39 | 3 | x | x | NI | x |
Sheng (2017)40 | 2 | x | x | NI | NI |
Huang (2018)41 | 4 | x | x | x | x |
Jiang (2018)42 | 3 | x | x | x | NI |
Abdel-Rahman (2018)43 | 4 | x | x | x | x |
Liu (2018)44 | 3 | x | x | x | NI |
Khan (2018)45 | 3 | Unspecified | |||
Lee (2018)46 | 4 | x | NI | x | x |
Almutairi (2019)47 | 4a | Unspecified | |||
Cavanna (2019)48 | 4a | x | x | x | x |
Vickers (2019)49 | (31)b | Unspecified | |||
An (2021)50 | 3 | x | x | x | NI |
Number of times studies cited in overlapsc | 10 | 9 | 7 | 5 | |
NI = not included; NR = not reported; RCT = randomized controlled trial; SR = systematic review.
aRCTs considered in the evidence network for the network meta-analysis.
bThirty-one RCTs identified in the overall evidence network for the network meta-analysis but unspecified RCTs identified for the subgroup analysis for patients with EGFR-positive NSCLC.
cThe unspecified RCTs in 3 SRs are not included in the overall overlap.
Table 14: Overlap of RCTs in the SRs — PFS
SR, | Number of RCTs included in the SRs that report the outcome in population of interest | RCTs included in the systematic review (author, study) | |||
|---|---|---|---|---|---|
Borghaei et al., | Herbst et al., | Rittmeyer at al., | Fehrenbacher et al., | ||
Wang (2016)38 | NI | NI | NI | NI | NI |
Lee (2017)39 | NI | NI | NI | NI | NI |
Sheng (2017)40 | 2 | x | x | NI | NI |
Huang (2018)41 | NI | NI | NI | NI | NI |
Jiang (2018)42 | 2 | x | x | NI | NI |
Abdel-Rahman (2018)43 | NI | NI | NI | NI | NI |
Liu (2018)44 | NI | NI | NI | NI | NI |
Khan (2018)45 | 2 | Unspecified | NI | NI | |
Lee (2018)46 | NI | NI | NI | NI | NI |
Almutairi (2019)47 | 2a | Unspecified | NI | NI | |
Cavanna (2019)48 | NI | NI | NI | NI | NI |
Vickers (2019)49 | (31)b | Unspecified | NI | NI | |
An (2021)50 | 2 | x | x | NI | NI |
Number of times studies cited in overlapsc | 3 | 3 | 0 | 0 | |
NI = not included; NR = not reported; PFS = progression-free survival; RCT = randomized controlled trial; SR = systematic review.
aRCTs considered in the evidence network for the network meta-analysis.
bThirty-one RCTs were identified in the overall evidence network for the network meta-analysis, but unspecified RCTs were identified for the subgroup analysis for patients with EGFR-positive NSCLC.
cThe unspecified RCTs in 3 SRs are not included in the overall overlap.
Appendix 3: Characteristics of the Included SRs
Table 15: Search Databases, Inclusion and Exclusion Criteria, Mutation and PD-L1 Levels, Conclusion, and Funding Source of the Included Studies
First author (publication year) | Search databases Date of search Publication years of included primary studies | Inclusion criteria | Mutation, PD-L1 levels | Exclusion criteria | Funding source | Authors’ conclusion |
|---|---|---|---|---|---|---|
Wang (2016)38 | ScienceDirect, and Web of Science. 20 May 2016 2015 to 2016 | Studies evaluated anti-PD-1/PD-L1 agents for patients with NSCLC with or without a report of PD-L1 expression level. Studies included 1 or all the following: ORR, OS, and PFS. | EGFR positive NR | Letters, editorials, expert opinions, case reports, duplicate publications, and reviews. | None | The results showed a significant improvement in OS of patients with NSCLC with wild-type EGFR; nevertheless, the same results were not observed in patients with NSCLC with mutant EGFR. |
Lee (2017)39 | MEDLINE, Embase, PubMed, and the Cochrane Central Register of Controlled Trials databases 01 Jan.1996 to 01 July 2016 2015 to 2016 | Randomized trials that compared immune checkpoint inhibitors against chemotherapy in the second-line setting. | EGFR positive NR | NR | None | In EGFR-mutant advanced NSCLC, immune checkpoint inhibitors do not improve OS over that with docetaxel. |
Sheng (2017)40 | Cochrane Controlled Trial Register, Embase, MEDLINE, Science Citation Index NR 2015 to 2016 | RCTs met the following criteria: (1) They dealt only with patients with previously treated advanced NSCLC. (2) They enrolled patients treated with anti-PD-1/PD-L1 therapy or EGFR TKIs.(3) Acceptable comparator was docetaxel. (4) They could provide data about AE, RR, OS, and PFS. (5) These studies are prospective. | EGFR positive NR | NR | None | The HRs in this analysis of OS favoured anti-PD-1/PD-L1 therapy across most prespecified subpopulation; the exceptions were the subpopulation who lived in “the rest-of-the world geographic region,” those with age more than 75 years, those with central nervous system metastases, those who had never smoked, and those with EGFR mutation. |
Huang (2018)41 | PubMed, Web of Knowledge, and Central databases 31 December 2016 2015 to 2017 | All eligible studies were randomized trials that compared the survival of anti-PD-1/PD-L1 immunotherapy against chemotherapy in adult patients with advanced NSCLC. | EGFR positive NR | NR | NIHR Imperial Biomedical Research Centre, NIHR, and Action Against Cancer | “Patients with a … EGFR wild-type tumour have improved survival benefit from immunotherapy compared with … EGFR mutant NSCLC, respectively.” |
Jiang (2018)42 | PubMed, Embase, and Cochrane Library 01 April 2017 2015 to 2017 | The inclusion criteria were: (1) RCT; (2) patients with advanced or metastatic NSCLC after failure of previous treatments; (3) anti-PD-1/PD-L1 antibodies treatment as compared with chemotherapy; (4) published in English; (5) reported OR rate, toxicity data, or at least one form of survival data. | EGFR positive NR | NR | Funding: Grants from the General Research Program of Zhejiang Provincial Department of Health | For patients with NSCLC with EGFR mutations, anti-PD-1/PD-L1 therapy was an unfavourable factor of PFS. |
Abdel-Rahman (2018)43 d | PubMed 01 February 2017 2015 to 2017 | Patients with histologically diagnosed pretreated advanced NSCLC. Interventions: The 3 PD-1/PD-L1 inhibitors (nivolumab, pembrolizumab, and atezolizumab) vs docetaxel. Outcomes: Impact of different clinical/biological factors including histology, age, smoking, ECOG PS, CNS metastasis, PD-L1 status, EGFR status, KRAS status, and ALK status in prediction of outcomes of pretreated advanced NSCLC patients treated with PD-1/PD-L1 inhibitors. | EGFR positive NR | NR | None | No conclusion on mutation of interest. |
Liu (2018)44 | PubMed, Embase, and the Cochrane Library 27 December 2017 2015 to 2017 | RCTs, a comparison with docetaxel, at least one efficacy outcome and one safety outcome reported, and the full text being available. | EGFR positive NR | Letters, expert opinions, case reports, reviews, articles without available data, and duplicate publications. | Major Project of Jiangxi Natural Science Foundation, and the National Natural Science Foundation of China | Patients with NSCLC with wild-type EGFR or smoking history showed improved OS in the PD-1/PD-L1 group compared to that of the control group receiving docetaxel monotherapy; however, no such effect was seen for patients with NSCLC with EGFR mutations and a no-smoking history. |
Khan (2018)45 d | PubMed, Cochrane Library, and Web of Science 01 December 2017 2015 to 2017 | RCTs comparing the anti-PD1/PD-L1 therapies with chemotherapy in advanced NSCLC. Also provided data of OS, PFS, and AEs to analyze the efficacy and safety of | EGFR positive NR | Any RCT with incomplete data was excluded. | National Natural Science Foundation Of China and Guangzhou Key Medical Discipline Construction Project | No conclusion on mutation of interest. |
Lee (2018)46 | MEDLINE, Embase, PubMed, and the Cochrane Central Register of Controlled Trials. For abstracts- American Society of Clinical Oncology, the European Society for Medical Oncology, and the World Conference on Lung Cancer. 30 January 2017 2015 to 2017 | RCTs that compared IOs with docetaxel in the second-line setting compared to docetaxel to assess OS. | EGFR positive NR | NR | None | Checkpoint inhibitors, compared with docetaxel, are associated with significantly prolong OS in second-line therapy in NSCLC. The finding of no OS benefit for patients with NSCLC with EGFR-mutant tumours suggests that checkpoint inhibitors should be considered only after other effective therapies have been exhausted. |
Almutairi (2019)47 | MEDLINE/PubMed, Cochrane Library, and Embase, US FDA websites, and the European Medicines Agency. 01 June 2018 NR | Phase II/III RCTs that assessed the efficacy and/or safety of FDA-approved IOs that target PD-1 (nivolumab, pembrolizumab) and its ligand PD-L1 (atezolizumab) in previously treated advanced NSCLC, including updates for these trials. | EGFR positive NR | Studies on pediatric populations or comparing alternate treatment doses of the same product. | None | No clear conclusion on mutation of interest. |
Cavanna (2019)48 | MEDLINE, PubMed, clinicaltrials.gov, American Society of Clinical Oncology NR 2015 to 2017 | Phase II and III RCTs of different second- and third-line IOs for NSCLC previously treated with TKIs, with available EGFR mutations. | EGFR positive NR | NR | NR | Results suggest that patients with NSCLC with EGFR mutations previously treated with TKIs show better OS when treated with docetaxel in comparison to checkpoint inhibitors treatment. |
Vickers (2019)49 | MEDLINE, PubMed, Embase, Biosciences Information Service, Cochrane Library, Abstracts - scientific meetings, American Society of Clinical Oncology, the European Society of Medical Oncology, International Association for the Study of Lung Cancer. 01 September 2015 NR | Phase II and III RCTs in adult patients with locally advanced or metastatic NSCLC and whose disease had progressed after first-line chemotherapy. Intervention of interest (nivolumab pembrolizumab). Comparator of interest (docetaxel, and Best supportive care). | EGFR positive PD-L1 < 5% PD-L1 ≥ 5% | NR | Eli Lilly and Company | No clear conclusion on mutation of interest. |
An (2021)50 | PubMed, Embase, Cochrane Library, clinicaltrial.gov, China National Knowledge Infrastructure, WanFang database, VIP database (China Science and Technology Journal Database) and China Biology Medicine disc), 18 August 2020 2015 to 2017 | (1) Prospective RCTs; (2) evaluate the clinical efficacy of anti-PD-1/PD-L1 immunotherapy and chemotherapy in patients with NSCLC; (3) the study must report the OS, PFS, ORR and AEs (4) the HRs and risk ratios (RRs) with 95% CIs for OS and PFS and data including age, sex, histology, smoking status, PD-L1 expressing status, ECOG PS, EGFR, and KRAS mutation status can be drawn out from the text. | EGFR positive NR | (1) Retrospective or prospective observational cohort studies; (2) phase I trials; (3) reviews, meta-analysis, letters, case reports, conference abstracts, expert opinions, cell and animal experiments; (4) duplicate publications; (5) studies with insufficient data; (6) patients have inconsistent baselines. | Zhejiang Medical Health Science and Technology Planning Project | EGFR might be a potential predictor for the therapeutic effect of anti PD-1/PD-L1 immunotherapy in specific patients with NSCLC. |
AE = adverse event; CNKI = China National Knowledge Infrastructure; CNS = central nervous system; ECOG PS = Eastern Cooperative Oncology Group performance score; HRs = hazard ratios; MA = meta-analysis; RCT = randomized control trial; NA = not available; NIHR = National Institutes of Health Research; NR = not reported; ORR = objective response rate; OS = overall survival; PD-L1 = programmed death-ligand 1; PFS = progression-free survival; QA = quality appraisal; RR = response rate; RRs = risk ratios; SR = systematic review.
Note: This table has not been copy-edited.
Appendix 4: Excluded Records
Please note that this appendix has not been copy-edited.
Table 16: List of Excluded Studies With Reason for Exclusion
Number | Citation |
|---|---|
No mutation of interest (n = 30) | |
1 | Olivares-Hernandez A, Gonzalez Del Portillo E, Tamayo-Velasco A, Alvaro, Figuero-Perez, Luis, Zhilina-Zhilina, Svetlana, Fonseca-Sanchez, Emilio, Miramontes-Gonzalez, Jose Pablo. Immune checkpoint inhibitors in non–small cell lung cancer: from current perspectives to future treatments-a systematic review. Ann Transl Med. 2023;11:354 |
2 | Chen, Mo, Wei, Lingyun, Wang, Qin, Xie, Jingyuan, Xu, Ke, Lv, Tangfeng, Song, Yong, Zhan, Ping. Efficacy of different therapies for brain metastases of non–small cell lung cancer: a systematic review and meta-analysis. Transl lung Cancer Res. 2023;12:689 to 706 |
3 | Wu, Changjin, Li, Wentan, Tao, Hongyu, Zhang, Xiyan, Xin, Yu, Song, Ruomeng, Wang, Kaige, Zuo, Ling, Cai, Yuanyi, Wu, Huazhang, Hui, Wen. Cost-effectiveness of first-line immunotherapy for advanced non–small cell lung cancer with different PD-L1 expression levels: A comprehensive overview. Crit Rev Oncol Hematol. 2024;193:104195 |
4 | Shimizu, Takashi, Inoue, Eisuke, Ohkuma, Ryotaro, Kobayashi, Shinichi, Tsunoda, Takuya, Wada, Satoshi. Soluble PD-L1 changes in advanced non–small cell lung cancer patients treated with PD-1 inhibitors: an individual patient data meta-analysis. Front Immunol. 2023;14:1308381 |
5 | Nuccio, Antonio, Viscardi, Giuseppe, Salomone, Fabio, Servetto, Alberto, Venanzi, Francesco Maria, Riva, Silvia Teresa, Oresti, Sara, Ogliari, Francesca Rita, Vigano, Mariagrazia, Bulotta, Alessandra, Cameron, Robert, Esposito, Alessandra, Hines, Jacobi, Bianco, Roberto, Reni, Michele, Cascone, Tina, Garassino, Marina Chiara, Torri, Valter, Veronesi, Giulia, Cinquini, Michela, Ferrara, Roberto. Systematic review and meta-analysis of immune checkpoint inhibitors as single agent or in combination with chemotherapy in early-stage non–small cell lung cancer: Impact of clinicopathological factors and indirect comparison between treatment strategies. Eur J Cancer. 2023;195:113404 |
6 | Chen, Wei, Chen, Jiayi, Zhang, Lin, Cheng, Sheng, Yu, Junxian. Network meta-analysis of first-line immune checkpoint inhibitor therapy in advanced non-squamous non–small cell lung cancer patients with PD-L1 expression > = 50. BMC Cancer. 2023;23:791 |
7 | Hu, Yue, Liu, Shan, Wang, Lixing, Liu, Yu, Zhang, Duohan, Zhao, Yinlong. Treatment-free survival after discontinuation of immune checkpoint inhibitors in mNSCLC: a systematic review and meta-analysis. Frontiers Immunol. 2023;14:1202822 |
8 | Li, Yan, Liang, Xueyan, Li, Huijuan, Chen, Xiaoyu. Efficacy and safety of immune checkpoint inhibitors for advanced non–small cell lung cancer with or without PD-L1 selection: A systematic review and network meta-analysis. Chinese Med J. 2023;136:2156 to 2165 |
9 | Xu, Z., Liang, J., Fu, R., Yang, L., Xin Chen, Y., Ren, W., Lu, Y., Qiu, X., Gu, Q. Effect of PD-L1 Expression for the PD-1/L1 Inhibitors on Non–small cell lung cancer: A Meta-analysis Based on Randomized Controlled Trials. Clin Oncol. 2023;35:640 to 651 |
10 | Zhang, Chengkai, Zhou, Wenjianlong, Zhang, Dainan, Ma, Shunchang, Wang, Xi, Jia, Wang, Guan, Xiudong, Qian, Ke. Treatments for brain metastases from EGFR/ALK-negative/unselected NSCLC: A network meta-analysis. Open Med. 2023;18:20220574 |
11 | Yang, Fang, Wang, Yucai, Tang, Lin, Mansfield, Aaron Scott, Adjei, Alex A., Leventakos, Konstantinos, Duma, Narjust, Wei, Jia, Wang, Lifeng, Liu, Baorui, Molina, Julian R. Efficacy of immune checkpoint inhibitors in non–small cell lung cancer: A systematic review and meta-analysis. Front Oncol. 2022;12:955440 |
12 | Kim, Jinchul, Ha, Hyerim, Park, Jisun, Cho, Jinhyun, Lim, Joo Han, Lee, Moon Hee. Association of Smoking Status with Efficacy of First-line Immune Checkpoint Inhibitors in Advanced Non–small cell lung cancers: A Systematic Review and Meta-analysis. J Cancer. 2022;13:364 to 372 |
13 | Peng, Siyu, Ying, Ariel Fangting, Tai, Bee Choo, Soo, Ross Andrew. A meta-analysis on immune checkpoint inhibitor efficacy for advanced non–small cell lung cancer between East Asians vs. non-East Asians. Transl Lung Cancer Res. 2020;9:1124 to 1137 |
14 | Landre, Thierry, Justeau, Gregoire, Assie, Jean-Baptiste, Chouahnia, Kader, Davoine, Claire, Taleb, Cherifa, Chouaid, Christos, Duchemann, Boris. Anti-PD-(L)1 for KRAS-mutant advanced non-small-cell lung cancers: a meta-analysis of randomized-controlled trials. Cancer Immunol Immunother. 2022;71:719 to 726 |
15 | Di Federico, Alessandro, De Giglio, Andrea, Nuvola, Giacomo, Deiana, Chiara, Conci, Nicole, Gelsomino, Francesco, Ardizzoni, Andrea. PD-(L)1 inhibitors as single-agent or in combination with chemotherapy for advanced, PD-L1-high non–small cell lung cancer: a meta-analysis. Future Oncol. 2021;17:4415 to 4424 |
16 | Zheng, Yuhui, Yao, Meihong, Yang, Yinghong. Higher Tumor Mutation Burden Was a Predictor for Better Outcome for NSCLC Patients Treated with PD-1 Antibodies: A Systematic Review and Meta-analysis. SLAS Technol. 2021;26:605 to 614 |
17 | Hu, Caihong, Liang, Zhengbo, Lai, Ping, Wang, Xiaofang, Zhao, Changming. Efficacy of atezolizumab to treat non-small-cell lung cancer: a meta-analysis based on randomized clinical trials. Die Pharmazie. 2021;76:215 to 219 |
18 | Nan, Zhang, Guoqing, Wang, Xiaoxu, Yu, Yin, Mi, Xin, He, Xue, Li, Rong, Wang. The Predictive Efficacy of Tumor Mutation Burden (TMB) on Nonsmall Cell Lung Cancer Treated by Immune Checkpoint Inhibitors: A Systematic Review and Meta-Analysis. BioMed Res Int. 2021;2021:1780860 |
19 | Connock, Martin, Armoiry, Xavier, Tsertsvadze, Alexander, Melendez-Torres, G. J., Royle, Pamela, Andronis, Lazaros, Clarke, Aileen. Comparative survival benefit of currently licensed second or third line treatments for epidermal growth factor receptor (EGFR) and anaplastic lymphoma kinase (ALK) negative advanced or metastatic non–small cell lung cancer: a systematic review and secondary analysis of trials. BMC Cancer. 2019;19:392 |
20 | Silvinato, Antonio, Floriano, Idevaldo, Bernardo, Wanderley Marques. Advanced non–small cell lung cancer - Treatment with Pembrolizumab. AMB Rev Assoc Med Bras. 2019;65:1423 to 1432 |
21 | Armoiry, Xavier, Tsertsvadze, Alexander, Connock, Martin, Royle, Pamela, Melendez-Torres, G. J., Souquet, Pierre-Jean, Clarke, Aileen. Comparative efficacy and safety of licensed treatments for previously treated non–small cell lung cancer: A systematic review and network meta-analysis. PloS One. 2018;13:e0199575 |
22 | Crequit, Perrine, Chaimani, Anna, Yavchitz, Amelie, Attiche, Nassima, Cadranel, Jacques, Trinquart, Ludovic, Ravaud, Philippe. Comparative efficacy and safety of second-line treatments for advanced non–small cell lung cancer with wild-type or unknown status for epidermal growth factor receptor: a systematic review and network meta-analysis. BMC Med. 2017;15:193 |
23 | Kim, Jung Han, Kim, Hyeong Su, Kim, Bum Jun. Prognostic value of KRAS mutation in advanced non-small-cell lung cancer treated with immune checkpoint inhibitors: A meta-analysis and review. Oncotarget. 2017;8:48248 to 48252 |
24 | Li, Jie, He, Qi, Yu, Xiu, Khan, Khalid, Weng, Xuanwen, Guan, Minjie. Complete response associated with immune checkpoint inhibitors in advanced non-small-cell lung cancer: a meta-analysis of nine randomized controlled trials. Cancer Manage Res. 2019;11:1623 to 1629 |
25 | Chen, Shuo, Hu, Bin, Li, Hui. A meta-analysis of nivolumab for the treatment of advanced non-small-cell lung cancer. OncoTargets Therap. 2018;11:7691 to 7697 |
26 | Wu, Di, Duan, Chongyang, Wu, Fenfang, Chen, Liyong, Chen, Size. Which treatment is preferred for advanced non-small-cell lung cancer with wild-type epidermal growth factor receptor in second-line therapy? A meta-analysis comparing immune checkpoint inhibitor, tyrosine kinase inhibitor and chemotherapy. Oncotarget. 2017;8:66491 to 66503 |
27 | Huang, Jiaxing, Zhang, Yaxiong, Sheng, Jin, Zhang, Hongyu, Fang, Wenfeng, Zhan, Jianhua, Zhou, Ting, Chen, Ying, Liu, Lin, Zhang, Li. The efficacy and safety of nivolumab in previously treated advanced non-small-cell lung cancer: a meta-analysis of prospective clinical trials. OncoTargets Therap. 2016;9:5867 to 5874 |
28 | Chen, L., Zhao, P., Cao, K., Jin, L., Xu, R., Tang, X. Efficacy and safety of immune checkpoint inhibitors in the treatment of non–small cell lung cancer: A meta-analysis. J Mind Behav. 2018;38:780 to 791 |
29 | Wan, Q., Yang, Y., Li, Y. L. Efficacy and safety of PD-1 antibody/PD-L1 antibody vs. docetaxel in non-small-cell lung cancer: a Meta-analysis. Chinese J New Drugs. 2018;27:229 to 235 |
30 | Zhang, Tongtong, Li, Shuluan, Chang, Jianhua, Qin, Yan, Li, Chao. Impact of BMI on the survival outcomes of non–small cell lung cancer patients treated with immune checkpoint inhibitors: a meta-analysis. BMC Cancer. 2023;23:1023 |
Ineligible outcome (n = 1) | |
1 | Yu, Dahui, Yuan, Chong, Zhang, Hedan, Chu, Wenyan. The association of efficacy with PD-1/PD-L1 inhibition and tumour mutational burden in advanced nonsmall cell lung cancer: A PRISMA-guided literature review and meta-analysis. Medicine. 2022;101:e29676 |
Ineligible intervention(s) (n = 8) | |
2 | Wang, Zhen, Zhou, Fang, Xu, Shan, Wang, Kang, Ding, Huan. The efficacy and safety of immune checkpoint inhibitors for patients with EGFR-mutated non–small cell lung cancer who progressed on EGFR tyrosine-kinase inhibitor therapy: A systematic review and network meta-analysis. Cancer Med. 2023;12:18516 to 18530 |
3 | Daei Sorkhabi, Amin, ZareDini, Mahta, Fazlollahi, Asra, Sarkesh, Aila, Naseri, Amirreza, Mousavi, Seyed Ehsan, Nejadghaderi, Seyed Aria, Sullman, Mark J. M., Kolahi, Ali-Asghar, Safiri, Saeid. The safety and efficacy of tislelizumab, alone or in combination with chemotherapy, for the treatment of non–small cell lung cancer: a systematic review of clinical trials. BMC PulmMed. 2023;23:495 |
4 | Luciani, Andrea, Ghidini, Antonio, Borgonovo, Karen, Parati, Maria Chiara, Petrelli, Fausto. Outcome of non-small-cell lung cancer with driven mutations treated with anti-PD-(L)1 agents: A systematic review. Tumori. 2023;109:442 to 449 |
5 | Chen, Jiarui, Liu, Xingyu, Zhang, Junhong, Huang, Zhao, Zeng, Wei, Hu, Jing, Chen, Gang, Gong, Yan, Liu, Yu, Xie, Conghua. Frontline anti-PD-1/PD-L1 vs. bevacizumab in advanced non-small-cell lung cancer: a network meta-analysis. Future Oncol. 2022; 18:1651 to 1664 |
6 | Ba, He, Liu, Lei, Peng, Qiang, Chen, Jie, Zhu, Yao-Dong. The relationship between blood-based tumour mutation burden level and efficacy of PD-1/PD-L1 inhibitors in advanced non–small cell lung cancer: a systematic review and meta-analysis. BMC Cancer. 2021;21:1220 |
7 | Liu, Lihui, Bai, Hua, Seery, Samuel, Li, Sini, Wang, Chao, Xue, Pei, Zhao, Jie, Wang, Jie. Efficacy and safety of treatment modalities across EGFR selected/unselected populations with non–small cell lung cancer and brain metastases: A systematic review and Bayesian network meta-analysis. Lung Cancer. 2021;158:74 to 84 |
8 | Wei, Y., Du, Q., Peng, X., Jin, J., Guo, H., Li, Y., Li, Q. Effects of Clinicopathological Characteristics on the Survival of Patients Treated with PD-1/PD-L1 Inhibitor Monotherapy or Combination Therapy for Advanced Cancer: A Systemic Review and Meta-Analysis. J Immunol Res. 2020;2020:5269787 |
9 | Chen, J., Lu, W., Chen, M., Cai, Z., Zhan, P., Liu, X., Zhu, S., Ye, M., Lv, T., Lv, J., Song, Y., Wang, D. Efficacy of immunotherapy in patients with oncogene-driven non-small-cell lung cancer: a systematic review and meta-analysis. Ther Adv Med Oncol. 2024;16 |
Ineligible comparator(s) (n = 8) | |
10 | Guaitoli, Giorgia, Tiseo, Marcello, Di Maio, Massimo, Friboulet, Luc, Facchinetti, Francesco. Immune checkpoint inhibitors in oncogene-addicted non–small cell lung cancer: a systematic review and meta-analysis. Transl Lung Cancer Res. 2021;10:2890 to 2916 |
11 | Sun, Si, Liu, Chang, Duan, Chunyan, Yu, Songxia, Zhang, Qiao, Xu, Nana, Yu, Bo, Wu, Xianghua, Wang, Jialei, Hu, Xingjiang, Yu, Hui. Efficacy and safety of immune checkpoint inhibitors in post-TKI NSCLC patients harboring EGFR mutations. J Cancer Res Clin Oncol. 2023;149:2937 to 2949 |
12 | Hu, Dahai, Pang, Xijiao, Luo, Ji, Zhou, Jiaxin, Wang, Nan, Tang, Hui, Wang, Liang, Zhao, Xiaoxu. The correlation between the influencing factors and efficacy of immune checkpoint inhibitor therapy: an umbrella meta-analysis of randomized controlled trials. Ann Med. 2023;55:2215543 |
13 | Yu, Yunfang, Zeng, Dongqiang, Ou, Qiyun, Liu, Shengbo, Li, Anlin, Chen, Yongjian, Lin, Dagui, Gao, Quanlong, Zhou, Haiyu, Liao, Wangjun, Yao, Herui. Association of Survival and Immune-Related Biomarkers With Immunotherapy in Patients With Non–small cell lung cancer: A Meta-analysis and Individual Patient-Level Analysis. JAMA Netw Open. 2019;2:e196879 |
14 | Wang, Shuai, Hao, Jiatao, Wang, Hao, Fang, Yong, Tan, Lijie. Efficacy and safety of immune checkpoint inhibitors in non–small cell lung cancer. Oncoimmunology. 2018;7:e1457600 |
15 | Akers, K. G., Oskar, S., Zhao, B., Frederickson, A. M., Arunachalam, A. Clinical Outcomes of PD-1/PD-L1 Inhibitors Among Patients With Advanced or Metastatic Non–small cell lung cancer With BRAF, ERBB2/HER2, MET, or RET Alterations: A Systematic Literature Review. J Immunotherap. 2023 |
16 | Liu, Wenjie, Huo, Gengwei, Chen, Peng. Efficacy of Atezolizumab for Advanced Non–small cell lung cancer Based on Clinical and Molecular Features: A Meta-Analysis. Front Immunol. 2022;13:909027 |
17 | Ma, X., Zhang, Y., Wang, S., Yu, J. Predictive value of tumour mutation burden (TMB) with targeted next-generation sequencing in immunocheckpoint inhibitors for non–small cell lung cancer (NSCLC). J Cancer. 2020;12:584 to 594 |
ISSN: 2563-6596
This work was conducted by the POst-Market Drug Evaluation Team (PODET) through the Post-Market Drug Evaluation (PMDE) CoLab Network. It was supported by Canada’s Drug Agency (CDA-AMC) and its Post-Market Drug Evaluation Program through funding provided by Health Canada.
CDA-AMC is a pan-Canadian health organization. Created and funded by Canada’s federal, provincial, and territorial governments, we’re responsible for driving better coordination, alignment, and public value within Canada’s drug and health technology landscape. We provide Canada’s health system leaders with independent evidence and advice so they can make informed drug, health technology, and health system decisions, and we collaborate with national and international partners to enhance our collective impact.
CoLab is a pan-Canadian network of experts in applied research, scientific methods, and data analysis. CoLab members work with the Post-Market Drug Evaluation Program to produce credible and timely evidence on postmarket drug safety and effectiveness.
Disclaimer: CDA-AMC has taken care to ensure that the information in this document was accurate, complete, and up to date when it was published, but does not make any guarantee to that effect. Your use of this information is subject to this disclaimer and the Terms of Use at cda-amc.ca.
The information in this document is made available for informational and educational purposes only and should not be used as a substitute for professional medical advice, the application of clinical judgment in respect of the care of a particular patient, or other professional judgments in any decision-making process. You assume full responsibility for the use of the information and rely on it at your own risk.
CDA-AMC does not endorse any information, drugs, therapies, treatments, products, processes, or services. The views and opinions of third parties published in this document do not necessarily reflect those of CDA-AMC. The copyright and other intellectual property rights in this document are owned by the Canadian Agency for Drugs and Technologies in Heath (operating as CDA-AMC) and its licensors.
This document is the property of PODET. CDA-AMC has a nonexclusive, limited, royalty-free, worldwide, nontransferable, fully paid-up, and irrevocable license to use the report in support of its objects, mission, and reasonable operational requirements.