CADTH Health Technology Review
The Efficacy and Safety of Biologic Drugs to Treat Severe Asthma
Jason R. Randall, Richard Leigh, Ellen T. Crumley, Sylvia Aponte-Hao, Ngoc Khanh Vu, Karen Martins, Scott Klarenbach
This Rapid Review was conducted by the Alberta Drug and Technology Evaluation Consortium through the Post-Market Drug Evaluation CoLab Network.
Rapid Review
Abbreviations
AEX
asthma exacerbation
BEC
blood eosinophil count
FEV1
forced expiratory volume in 1 second
HRQoL
health-related quality of life
HTA
health technology assessment
RCT
randomized controlled trial
Key Messages
Several biologic drugs have been developed to treat severe asthma, but it is unclear how well they work across different types of asthma.
Comparing the efficacy of biologic drugs for asthma is challenging because of differing definitions of asthma severity and inconsistent application of severity criteria in randomized controlled trials.
The randomized controlled trials and systematic reviews included in this Rapid Review mainly focused on specific severe asthma subtypes (frequently, eosinophilic type 2 asthma). Recruitment and outcome reporting among different asthma subgroups was limited and varied, making it difficult to assess the efficacy of biologic drugs across the specific subgroups of severe asthma.
Determining the efficacy and safety of biologics in the pediatric population is hindered by both the lack of inclusion of children with severe asthma in clinical trials and the lack of outcome reporting specific to this population.
Further synthesis of the existing data is unlikely to provide new insights to further inform the outlined policy questions on biologics in severe asthma.
Introduction and Rationale
Background
Asthma is a spectrum of chronic conditions that exhibit airway inflammation and hyperreactivity.1 Severe asthma affects approximately 5% to 10% of individuals living with asthma. It is characterized by poorly controlled symptoms despite optimal use of front-line treatments such as high-dose inhaled corticosteroids with an adjuvant controller medication and/or systemic corticosteroids.2,3 It is estimated that as many as 250,000 people living in Canada have severe asthma. These individuals account for the majority of the morbidity and mortality related to asthma and incur most of the health care costs associated with treatment and management.4-6 The incremental cost of severe asthma relative to no asthma in Canada is approximately $2,779 per person per year.7
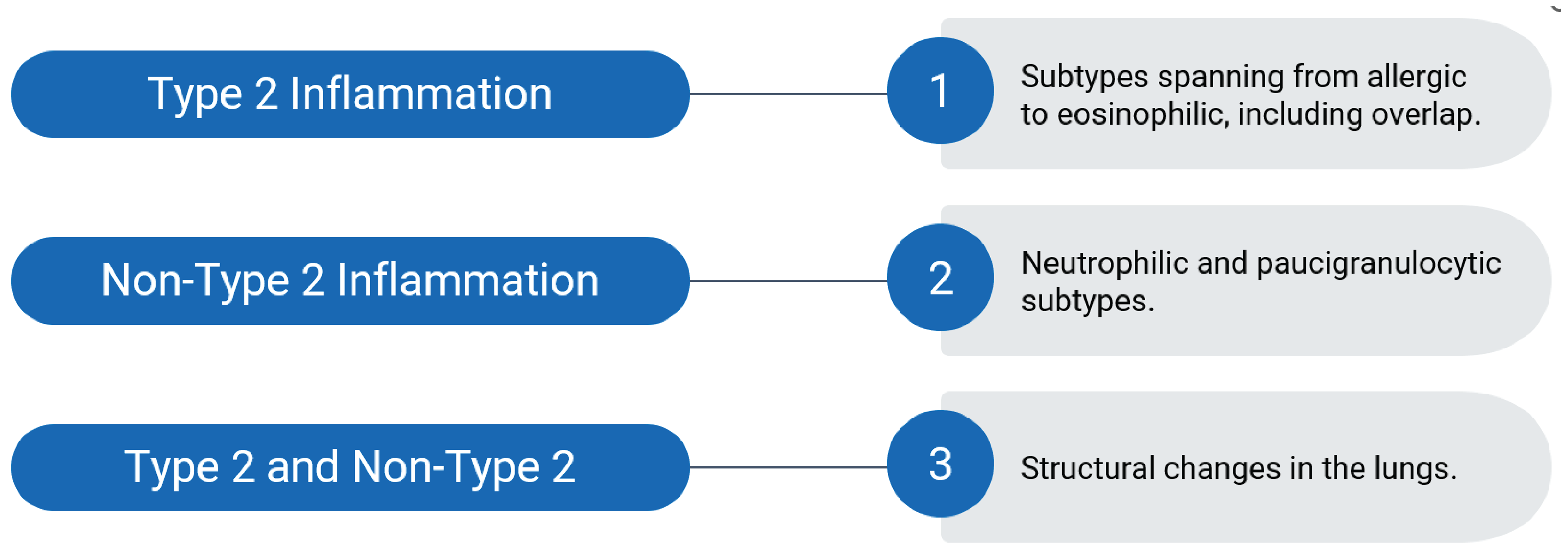
Severe asthma has several typologies (Figure 1), and several biologic drugs have been developed to target inflammation in specific subtypes of severe asthma, namely type 2 eosinophilic or allergic. Type 2 inflammatory asthma is predominately caused by type 2 cytokines and lymphocytes. Subtypes include eosinophilic asthma (characterized by increased eosinophil levels in the airways and blood) and allergic asthma (characterized by elevated immunoglobulin E levels and elevated bronchial responsiveness).8 There is overlap between the subtypes with crosstalk involving cytokine signalling so some patients may have characteristics of both eosinophilic and allergic asthma. Non–type 2 inflammatory asthma is characterized by the absence of type 2 markers with neutrophilic and paucigranulocytic airway inflammation, for which there is evidence suggesting it might respond to benralizumab and tezepelumab.9-11 Additionally, structural changes in the lung, such as fixed airflow obstruction caused by remodelling of the airway wall, can occur in severe asthma with or without the presence of type 2 inflammation; there are no current pharmacological treatments for targeting airway remodelling.12
Policy Issue
In Canada, reimbursement for biologics has occurred for the following drugs and indications: benralizumab and mepolizumab are indicated specifically for severe eosinophilic asthma, dupilumab is indicated for severe asthma with a type 2–eosinophilic subtype, and omalizumab is indicated for allergic asthma (Appendix 1). A Letter of Intent for tezepelumab (indicated for severe asthma) was issued by the pan-Canadian Pharmaceutical Alliance on September 15, 2023. Reslizumab is not currently covered by public drug plans in Canada and therefore was not considered in this review.13,14 Biologics have the potential to offer more effective symptom control for 1 or more subtypes of severe asthma with fewer adverse events compared with oral corticosteroids;13,15 however, there is some evidence of increased adverse events compared with standard care (e.g., inhaled corticosteroids, anticholinergics, and beta agonists).16
The available biologic therapies for severe asthma currently have disparate criteria for use due to the sequential nature of evaluation and listing, and criteria developed based on available information at the time of consideration. The efficacy of biologic drugs along the spectrum of severe asthma is unclear; similarly, the efficacy and safety in children has not been well characterized. Knowledge of the available evidence within and between biologic drugs by patient population and subtypes of severe asthma, and potential subsequent synthesis of available evidence, may inform listing criteria to optimize health and health care system sustainability.
Policy Questions
Is there evidence of comparative efficacy and safety to support harmonization of criteria for use of biologic drugs for patients with severe asthma (compared with current biologic-specific criteria)?
What is the efficacy and safety of each biologic drug by population as defined by specific asthma subtypes (i.e., eosinophilic or allergic with or without specific criteria such as immunoglobulin E levels and eosinophil counts) and age (pediatric: 6 years to 17 years; adult: ≥ 18 years)?
What is the relative efficacy and safety between biologic drugs as defined by specific asthma subtypes and population age?
Objectives
The approach was to conduct the review in 2 parts. Part 1 was a Rapid Review to assess the recent body of evidence available from randomized controlled trials (RCTs) and systematic reviews to determine the feasibility of conducting a more fulsome Health Technology Assessment (HTA).
The aims of the Rapid Review (part 1) were:
to identify and describe the research examining the comparative efficacy and safety of biologics for severe asthma using clinically important outcomes
to characterize the patient populations studied
to determine if further evidence synthesis (systematic review, meta-analysis, indirect treatment comparison) is feasible to address knowledge gaps for specific populations and subgroups with severe asthma.
Part 2 was to be an HTA to provide guidance about the alignment of the drug funding criteria by the public drug plans.
This report presents the findings of the part 1 Rapid Review.
Research Questions
The project identified the literature that addressed the following research questions. It determined whether recent RCTs and systematic reviews addressed these questions, and whether a future systematic review and/or meta-analysis is feasible and needed. Details on the specific interventions and outcomes are included in Table 1.
What is the comparative efficacy of biologic drugs for patients with severe asthma by specific population?
Population defined by severe asthma:
Type 2 asthma
allergic and/or eosinophilic asthma
specific criteria for allergic or eosinophilic asthma (e.g., immunoglobulin E level, bronchial responsiveness, sputum or blood eosinophil count)
Population defined by age:
pediatric (6 years to 17 years); adult (≥ 18 years)
What is the safety of biologic drugs for pediatric populations with severe asthma?
Methods
To inform the conduct of this focused Rapid Review, a review of the existing literature, including RCTs and systematic reviews, was performed. The part 1 study used the CADTH Rapid Review Summary with Critical Appraisal and Peer Review process, with modifications:
The selection of studies and data extraction were conducted by 2 reviewers.
The literature search included additional databases and sources, and the literature search strategy was peer reviewed.
Because it was subsequently decided that part 2 (the HTA) was not required, a decision was made to post the part 1 draft science report for stakeholder feedback.
Literature Search Methods
The literature searches were developed by an experienced librarian with systematic searching experience. A Peer Review of Electronic Search Strategies (PRESS) was performed by a second librarian to optimize the search. Searches were last conducted or updated in May 2023.
The search was restricted to articles published in the past 5 years (2018 onward) and only included those published in English. The search was restricted to RCTs, systematic reviews, meta-analyses, and network meta-analyses conducted using the Ovid interface, and included the following databases and registers: MEDLINE All (1946 to present) via Ovid, Embase (1974 to present) via Ovid, PubMed, Cochrane Database of Systematic Reviews, Cochrane Central Register of Controlled Trials via Wiley Cochrane Library, preprints via EuropePMC.org, ClinicalTrials.gov, WHO ICTRP, Health Canada’s Clinical Trials Database, EU Clinical Trials Register, International Traditional Medicine Clinical Trial Registry, and PROSPERO. The detailed search strategies are presented in Appendix 2.
Criteria | Description |
|---|---|
Population | Adults (≥ 18 years) and children (6 to 17 years) with severe asthma and subtypes of severe asthma (type 2, including eosinophilic and allergic, and non–type 2) |
Interventions |
|
Comparators |
|
Outcomes |
|
Study designs | Randomized controlled trials, systematic reviews, meta-analyses, and network meta-analyses published in 2018 or later |
Subgroup analyses |
|
Selection Criteria and Methods
Study Selection
Two reviewers independently screened titles and abstracts for relevance to the clinical research questions. The full text of potentially relevant articles was retrieved and independently assessed for possible inclusion based on the predetermined selection criteria (Table 1). The 2 reviewers then compared their chosen included and excluded studies; disagreements were discussed until consensus was reached. Both the abstract screening and the full-text screening were pilot tested by 2 reviewers with nonconsensus resolved by third reviewer; clarification of inclusion and exclusion criteria was done as required through pilot testing and calibration.
Exclusion Criteria
Articles were excluded if they did not meet selection criteria outlined in Table 1, were duplicate publications, reported duplicate data on the outcomes of interest, or were published before 2018. Studies that focused on niche subpopulations not identified a priori (e.g., severe asthma with nasal polyps or rhinosinusitis), or study populations of asthma with other conditions (e.g., chronic obstructive pulmonary disorder), were excluded. Post hoc analyses of RCTs were included provided that they added new data relevant to the research and policy questions, and reviewers were confident that the new analysis met the inclusion criteria (e.g., population, intervention, comparator, and outcome [PICO] criteria were clearly met after changes to population via filtering). Systematic reviews, meta-analyses, and network meta-analysis were excluded if they contained data from nonrandomized or observational studies.
Data Extraction and Critical Appraisal
Data Extraction
Information from each article was extracted using a standardized data extraction form. Extracted information encompassed characteristics of the study (year of publication, study design, sample size, and general statistics), trial participants (including characteristics that defined asthma subtype and age groups), inclusion and exclusion criteria, type of intervention(s) or control (including dose, duration, and co-medication), relevant outcomes, and broad results of the clinical efficacy or effectiveness and safety. Specific extracted outcomes included hospitalization, mortality, asthma exacerbations (AEXs), changes in force expiratory volume in 1 second (FEV1), and health-related quality of life (HRQoL). HRQoL was measured using 3 validated questionnaires: the Asthma Control Questionnaire, the Asthma Control Test, and the Asthma Quality of Life Questionnaire.
All data were extracted by 1 reviewer and checked for accuracy by a second independent reviewer. The presence of publications reporting on specific combinations of medications, subgroups, and outcomes was also abstracted. If a recent systematic review or meta-analysis had been conducted for each combination was also captured. Country of origin for each article was not extracted because some studies were conducted across numerous countries to recruit an adequately large sample of participants with severe asthma.
Multiple publications for a unique trial (e.g., supplemental online appendices, companion publications of specific outcomes, or populations from the original study) were handled by extracting the most recently adjudicated data for each outcome specified a priori. Results were presented from the original trial if multiple articles were published based on the same clinical sample and provided unique data relevant to the study question.
Quality Assessment
Risk of bias assessments were conducted on the included RCTs using the second version of the Cochrane Risk of Bias,17 and the systematic reviews using A Measurement Tool to Assess Systematic Reviews second version (AMSTAR 2).18
Data Analysis and Synthesis
Extracted data were summarized heuristically; no meta-analysis or new data analysis was conducted. Statistical significance of results were reported as they were described in the included articles, without attempting any adjustment for multiple comparisons. Outcomes such as HRQoL were generally secondary outcomes in these trials and may be more susceptible to bias from multiple testing. Post hoc analyses reported in the articles are reported in this report without any controlling for potential bias from multiple testing.
Operational definitions for subtypes of severe inflammatory asthma, for which biologics have been developed to target, was determined based on available literature and clinical expert opinion (Table 2).19 Severe inflammatory asthma was characterized as type 2 that was further classified (subtype) based on the presence of eosinophilic and/or allergic markers, or non–type 2. Due to possibility of overlap between type 2 eosinophilic and allergic asthma, characterization by both an eosinophilic and allergic subtype was also included.
Table 2: Operational Definitions for Severe Inflammatory Asthma Subgroups
Criteria | Description |
|---|---|
Severe asthma | Asthma categorized on severity alone, without specifying underlying type(s). Severe asthma is defined as either:
|
Non–type 2 | Asthma without type 2 inflammation or markers of eosinophilic or allergic asthma subtypes. |
Type 2 | Asthma involving type 2 inflammation. Allergic and eosinophilic are nonexclusive subtypes. |
Allergic | Subtype of type 2 asthma identified using immunoglobulin E, and allergen sensitivity as markers. Eosinophilic asthma status is unspecified. |
Eosinophilic | Subtype of type 2 asthma normally identified using blood eosinophil count as the marker. Allergic asthma status is unspecified. |
Nonallergic | Subgroup without allergic markers and eosinophilic asthma status is unspecified. |
Noneosinophilic | Subgroup without eosinophilic markers and allergic asthma status is unspecified. |
Allergic and noneosinophilic | Subgroup with allergic markers but not markers for eosinophilic asthma. |
Eosinophilic and nonallergic | Subgroup with eosinophilic markers but not allergic markers. |
Eosinophilic and allergic | Subgroup with markers for both eosinophilic and allergic asthma. |
Eosinophilic status was determined by blood eosinophil count (BEC) (cells/µL of blood). For this review, the criterion for eosinophilic asthma was set at a BEC of 150 cells/µL or higher at enrolment or a history of BEC 300 cells/µL or higher. The criteria for noneosinophilic asthma was set at a BEC less than 150 cells/µL with no previous history of BEC 300 cells/µL or higher. In some trials, cut-offs of BEC 300 cells/µL or higher and less than 300 cells/µL at enrolment were used to define eosinophilic and noneosinophilic asthma, respectively. Trials investigating tezepelumab also assessed enrolled participants with severe asthma by fractional exhaled nitric oxide levels (trials used several cut-offs methods including less than 25 parts per billion and 25 or more parts per billion, 25 parts per billion to 50 parts per billion, and less than 50 parts per billion and greater than or equal to 50 parts per billion).
Trials were heterogeneous in definition of allergic status, and included thresholds based on immunoglobulin E level, radioallergosorbent test, skin prick test, fluoroenzyme immunoassay, and/or other allergy measures. Given this heterogeneity, we assumed trial-specific criteria used to characterize type 2 allergic asthma were appropriate to define this severe asthma subtype. Although the variation in clinical testing used to establish allergic status was considerable, we relied on these trial-based criteria to define this status in the interest of feasibility. We recognize the variation in the underlying condition across studies resulting from this heterogeneity is a limitation of this Rapid Review but is not a major limitation in the context of assessing the breadth of subgroup analysis in recent publications.
Feasibility of a future meta-analysis or network meta-analysis was determined based on assessment of published literature and availability of data to examine efficacy and safety by specific subgroups with severe asthma.
Summary of Evidence
Quantity of Research Available
Of the 1,014 identified articles, 233 underwent full-text screening. Of these, 47 articles were included in this review that consisted of 26 publications from 13 RCTs9,11,20-43 (2 sets of trials were pooled: MENSA and MUSCA as well as SIROCCO and CALIMA]) and 21 systematic reviews15,16,44-62 (3 systematic reviews without meta-analyses, 8 meta-analyses, 6 network meta-analyses, and 4 indirect treatment comparisons including matching-adjusted indirect comparisons). Details on study selection and included studies are in Appendix 3 and Appendix 4.
Although most data in the included systematic reviews were from RCTs that met the inclusion criteria for this review, some were from trials published before 2018 (e.g., DREAM for mepolizumab). In addition, 1915,16,44-49,51,52,54-62 systematic reviews included in this study contained trials that were outside of the selection criteria (13 included at least 1 trial with moderate to severe asthma16,44-48,54,55,57-59,61,62 and others included trials that administered biologics intravenously or studied other biologics). However, these systematic reviews were included based on the following: more than 75% of the trials included in the systematic review only had participants with severe asthma and it provided relevant data and reported results in a manner that allowed for the abstraction of pertinent information. Appendix 5 shows the RCTs included in the systematic reviews.
Supplemental information: A total of 37 articles were excluded because they contained populations with moderate to severe (versus severe only) asthma, of which a number investigated efficacy and safety of biologic drugs for pediatric populations. These studies are listed in Appendix 6 to facilitate future consideration of nonexclusively severe asthma populations. A list of RCTs of biologics for the treatment of asthma comprising the 13 trials included in this review, relevant trials within included SRs, and additional known major trials (compiled with the assistance of a clinical expert) is found in Appendix 7.
Study Characteristics
Patient Population
The population of interest was individuals identified as living with severe asthma.
There are 2 commonly used definitions of severe asthma: the Global Initiative for Asthma definition and the European Respiratory Society and American Thoracic Society definition, with the latter considered the definitive definition by asthma experts.63,64 These definitions have undergone modifications over the past decade, which introduces the potential for inconsistencies in populations that meet the criteria for severe asthma over time. In general, the trials included in this focused rapid systematic review used the European Respiratory Society and American Thoracic Society definition, which considers a person to have severe asthma if either:
their controlled asthma worsens on tapering of medium- to high-dose inhaled corticosteroid(s) or systemic corticosteroids (or additional biologics)
symptoms remain uncontrolled with the use of high-dose inhaled corticosteroid(s) plus a second controller (and/or systemic corticosteroids).
Uncontrolled asthma is defined as at least 1 of the following: at least 1 AEX requiring hospitalization, intensive care unit stay, or mechanical ventilation in the past year; 2 or more short courses of systemic corticosteroids in the past year; reduced lung functioning (FEV1 < 80% predicted) after appropriate bronchodilator treatment; or an Asthma Control Test score less than 20 or an Asthma Control Questionnaire score of 1.5 or higher.63 Inclusion criteria were frequently poorly described in individual articles. The criteria used to define severe asthma was supplemented by reviewers accessing trial descriptions on clinicaltrials.gov registration records. The inclusion criteria from the registration and/or articles are provided in Table 9.
Randomized Controlled Trials
The number of RCTs by biologic drug and asthma subgroup are presented in Table 3, and the number of participants in these trials by biologic drug and asthma subgroup are presented in Table 4, according to (refer to Appendix 8, Table 10, Table 11, and Table 12 for general information on these RCTs). Characterizing study populations by asthma severity and subtypes was challenging given the changing definitions, evolving understanding of asthma subtypes, and overlap of asthma subtypes. Using available data from included studies, characterization of subtypes was attempted when possible. Trials may have targeted recruitment of a specific subtype and may or may not have reported other information on subtype (e.g., study target population was type 2 eosinophilic asthma, but information on allergic status was or was not reported).
In half the trials, enrolment was open to both adults and children, whereas the other half allowed only adult participants (Table 3). Enrolment of children in the trials was notably limited (Table 4), with a relatively small number of confirmed child participants (229 of a total 7,773 participants; additional children may have been enrolled but not reported).
The largest enrolled asthma subtype was type 2 eosinophilic asthma (Table 4). Trials that targeted patients with this specific subtype of severe asthma investigated the effect of benralizumab (ANDHI, SOLANA) and mepolizumab (MENSA and MUSCA) (Table 9 and Table 10); no data were available on the efficacy of mepolizumab for noneosinophilic patients (Table 13). Although the SIROCCO and CALIMA trial (benralizumab) recruited patients with severe asthma (with no subtype targeted), enrolment was stratified to ensure a large portion of participants had type 2 eosinophilic asthma. RCTs investigating omalizumab targeted enrolment of patients with severe type 2 allergic asthma (EXTRA, NCT01202903, NCT02049294). Although eosinophilic status was reported in some of these trials (Table 14). Trials investigating dupilumab (LIBERTY ASTHMA VENTURE) and tezepelumab (NAVIGATOR, PATHWAY, SOURCE) enrolled patients with severe asthma with no subtype targeted. None of the studies specifically enrolled participants with non–type 2 severe asthma.
Systematic Reviews
Characteristics of the study populations were not well described within the included systematic reviews. Reviews frequently combined trials with varying populations (Table 15) and were classified as type 2 eosinophilic or allergic subtypes. Some systematic reviews did use meta-analysis methods to adjust for differences in populations across the trials.
Table 3: Number of Randomized Controlled Trials by Biologic Drug and Asthma Subgroup
Biologic | N | Patient groups, n | Non–type 2, n | Type 2, n | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
Adult | Children | All type 2 | EOS | Non-EOS | Allergic | Nonallergic | EOS and allergic | |||
4 | 4 | 2 | 2 | 4 | 4 | 2 | 4 | 4 | 4 | |
1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | |
2 | 2 | 1 | 0 | 2 | 2 | 0 | 2 | 2 | 2 | |
3 | 3 | 1 | 0 | 3 | 3 | 3 | 3 | 0 | 3 | |
3 | 3 | 1 | 3 | 3 | 3 | 3 | 3 | 3 | 3 | |
EOS = eosinophilic.
Note: Non–type 2 indicates individuals without markers of either EOS or allergic asthma. “EOS and allergic” indicates individuals with indicators of both EOS and allergic asthma.
Table 4: Number of Participants in Each Randomized Controlled Trial by Biologic Drug and Asthma Subgroup
Trial | N | Patient groups, n | Non–type 2, n | Type 2, n | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
Adult | Children | All type 2 | EOS | Non-EOS | Allergic | Nonallergic | EOS and allergic | |||
Benralizumab | ||||||||||
ANDHI31 | 656 | 656 | 0 | 0 | 656 | 656a | 0 | 352 | 304 | 352 |
1,306 | 1,251 | 55 | 157 | 934 | 728b | 363 | 828 | 478 | 464 | |
1,204 | 1,151 | 53 | 167 | 1,037 | 809b | 395 | 705 | 499 | 477 | |
SOLANA39 | 233 | 233 | 0 | 0 | 233 | 233b | 0 | NR | NR | NR |
Dupilumab | ||||||||||
210 | NR | NR | NR | NR | 89b | 121 | 86 | 124 | NR | |
Mepolizumab | ||||||||||
936 | NR | NR | 0 | 936 | 936a | 0 | 253 | 683 | 253 | |
Omalizumab | ||||||||||
EXTRA30 | 850 | 809 | 39 | 0 | 850 | 414c | 383 | 850 | 0 | 414 |
NCT0120290335 | 608 | 608 | 0 | 0 | 608 | 252b | 337 | 608 | 0 | 252 |
NCT0204929438 | 9 | 9 | 0 | 0 | 9 | NR | NR | 9 | 0 | NR |
Tezepelumab | ||||||||||
1,061 | 979 | 82 | 221 | 820 | 431b | 610 | 680 | 361 | 291 | |
550 | 550 | 0 | 134d | 416 to 468d | 310e | 240 | 296 | 218 | 138d | |
150 | 150 | 0 | NR | NR | 52b | 98 | 59 | 83 | NR | |
EOS = eosinophilic; NR = not reported.
Note: Non–type 2 indicates individuals without indication of either eosinophilic or allergic asthma. The method of determining allergic status varied and was based on immunoglobulin E levels, radioallergosorbent tests, skin prick tests, fluoroenzyme immunoassays, and/or other allergy measures. “EOS and allergic” indicates individuals with indicators of both eosinophilic and allergic asthma. Trial information on clinicaltrials.gov was checked to determine or verify these values. Trial-specific criteria for eosinophilic asthma was determined using blood eosinophil count levels (cells/µL).
aBlood eosinophil of 150 cells/µL or higher at baseline or a history of 300 cells/µL or higher.
bBlood eosinophil of 300 cells/µL or higher.
cBlood eosinophil of 260 cells/µL or higher.
dValues estimated based on 2 of the 4 arms of the PATHWAY study in the pooled analysis by Corren et al.9
eBlood eosinophil of 250 cells/µL or higher.
Interventions and Comparators
Randomized Controlled Trials
In the included trials, the active interventions were benralizumab (4 trials, among which SIROCCO and CALIMA were pooled), dupilumab (1 trial), mepolizumab (2 trials that were pooled), omalizumab (3 trials), and tezepelumab (3 trials) (Table 4, Table 9). In all identified studies, the comparator was a subcutaneous placebo injection that was physically similar to the study drug. In general, “standard-of-care” asthma therapies were allowed in both arms. This is in line with the use of biologic drugs as add-on medications; they are not intended to replace standard asthma therapies (although it is hoped they will reduce the need for oral corticosteroids).
Systematic Reviews
The included systematic reviews compared biologics to placebos. Benralizumab was the most evaluated biologic compared to a placebo (included in 14 SRs), and omalizumab was the least evaluated (included in 4 SRs) (Table 15). Ten of the systematic reviews included a comparative efficacy component — either a network meta-analysis or indirect treatment comparison or matching-adjusted indirect comparison. Mepolizumab (10 systematic reviews), benralizumab (9 systematic reviews), and dupilumab (8 systematic reviews) were evaluated in most of these reviews. Tezepelumab and omalizumab were considered in 3 comparative efficacy reviews each.
Outcome Measures
Randomized Controlled Trials
Main study outcomes are reported in Table 13. AEX was the most common outcome reported (most often as an annualized rate; reported in 11 trials [includes 2 sets of pooled trials]). FEV1 and/or HRQoL outcomes were reported in 12 trials (includes 2 sets of pooled trials). NCT01202903 did not report FEV1, and EXTRA did not report HRQoL. Safety outcomes were less commonly reported (included in 5 studies). Safety outcomes may have been previously reported and were not included in articles identified for this Rapid Review. Hospitalization outcomes were reported in 2 trials, and mortality results were not reported separately in any trial.
Outcomes for subgroups are summarized in Appendix 8 in Tables 14, 16, 17, 18, 19, and 20. Although trials that enrolled individuals with a specific subtype of asthma may have also characterized other subtype characteristics (e.g., enrolled a type 2 eosinophilic population but also characterized allergic status of the population), outcomes were infrequently reported for many specific subgroups (Table 14). Outcomes reported by specific subgroups of asthma are shown in Table 14; outcomes for non–type 2 inflammation were rarely reported (i.e., only 2 of 11), and outcomes by characterization of both eosinophilic status and allergic status were infrequent (5 of 11).
Reporting of trial outcome measures by biologic drug (benralizumab, dupilumab, mepolizumab, and tezepelumab) and type 2 eosinophilic asthma subgroups are presented based on characterization by BEC level (Table 17) and fractional exhaled nitric oxide level (Table 18). Only trials that investigated tezepelumab reported type 2 eosinophilic asthma classified by fractional exhaled nitric oxide levels.
Type 2 allergic asthma subgroups were challenging to assess because a standardized method of characterizing allergic status was not consistently used. Therefore, outcomes for type 2 allergic asthma subtypes are presented in 2 different formats of characterization. Omalizumab eligibility criteria subgroups were reported in Table 19, and other allergic marker subgroups were reported in Table 20). AEX was almost always reported (41 of 47 reported subgroups), and FEV1 and HRQoL were reported for approximately half of extracted 47 subgroup results. No other outcomes were reported for the asthma subgroupings.
Systematic Reviews
Details regarding reported outcomes from the systematic reviews can be found in Appendix 8. Definitions of AEX in the reviews are listed in Table 21. These reviews and meta-analyses reported outcomes on few of the patient subgroups (Table 22) while reporting 20 primary patient population and drug intervention combinations (Table 23). Outcomes were also reported for 23 subgroup and drug intervention combinations (Table 24). Subgroups were stratified primarily by BEC level or fractional exhaled nitric oxide level, by adult and pediatric populations for omalizumab, and by severe asthma type 2 allergic subgroup for tezepelumab. In the primary patient populations, AEX outcomes were consistently reported (95%; 19 of 20 reviews), whereas FEV1 and HRQoL were reported in 13 reviews (65%). Safety outcomes were reported in 11 out of 20 reviews (55%). In the subgroups, AEX outcomes were consistently reported (100%; 23 of 23 subgroups reported), whereas FEV1 (26%; 6 of 23 subgroups reported), HRQoL (13%; 3 of 23 subgroups reported), and safety (9%; 2 of 23 subgroups reported) were reported less frequently.
The identified comparative efficacy reviews (network meta-analyses, indirect treatment comparisons, matching-adjusted indirect comparisons) reported outcomes on 27 primary patient population and drug intervention combinations, as well as 50 subgroup and drug intervention combinations. Eosinophilic subgroups (determined by BEC levels in 34 instances, and fractional exhaled nitric oxide levels in 12 instances) were reported in 46 instances, and allergic subgroups (with unclear cut-offs) were reported in 4 instances (Table 25 and Table 26). In the primary patient population, AEX outcomes were consistently reported (88%; 24 of 27 reviews), whereas FEV1 (44%; 12 instances), HRQoL (30%; 8 of 27 reviews), safety (26%; 7 of 27), and hospitalization (19%; 5 of 27 reviews) outcomes were reported less frequently. Similarly, in the subgroups, AEX outcomes were consistently reported (100%; 50 instances), whereas FEV1 (36%; 18 of 50 subgroups reported) and HRQoL (16%; 8 of 50 subgroups reported) were reported less frequently. All 10 systematic reviews that included a comparative efficacy component reported AEX outcomes in the primary patient population; FEV1 was reported in 5 reviews, HRQoL in 4 reviews, safety in 3 reviews, and hospitalizations in 1 review (Table 27). Half the systematic reviews that included a comparative efficacy component also reported outcomes in a combined 17 subgroups (Table 28). Subgroups were stratified primarily by BEC level (9 subgroups reported) or fractional exhaled nitric oxide level (6 subgroups reported); an allergic subgroup (with unclear cut-offs) and a subgroup based on oral corticosteroid use status were also assessed. All subgroups reported AEX outcomes. FEV1 was reported in 10 subgroups, HRQoL in 8 subgroups, and safety in 1 subgroup; hospitalizations were not reported.
Critical Appraisal
Randomized Controlled Trials
All identified trials had clear study objectives, intervention(s), comparators, and outcomes. Trial registration information was provided, and no significant deviations from the planned studies were noted. However, specific details about the characteristics of enrolled populations were reported inconsistently, and several publications lacked sufficient information about how severe asthma was defined and characterized. In these cases, trial registration information was used to determine enrolment criteria. The variability of the enrolled populations was increased in the included trials because they were conducted during a period when there were shifting standards for the diagnosis of severe asthma.
A Cochrane risk of bias assessment (second version17) was conducted, and the results are shown in Table 5. Our assessment did not identify any high levels of concern for bias. Overall, 4 trials had a low level of concern for bias (ANDHI, NCT02049294, NAVIGATOR, and PATHWAY), and 9 had some level of concern for bias (CALIMA [domains 3 and 5], SIROCCO [domains 3 and 5], SOLANA [domain 1], LIBERTY ASHTMA VENTURE [domain 4], MENSA [domain 5], MUSCA [domain 5], EXTRA [domains 3 and 5], NCT01202903 [domain 3], and SOURCE [domains 4 and 5]). Most of the potential sources of bias were concentrated in a few domains, particularly domain 3 (bias due to missing outcome data), although it was unlikely that the extent of missing data could offset the reported differences in key outcomes, and domain 5 (bias in selection of overall result) that was related to the selection of results based on the number of planned analyses and what was presented in the final publications. The LIBERTY ASTHMA VENTURE and SOURCE trials had levels of some concern within domain 4 (bias in the measurement of outcomes), and the SOLANA trial had some level of concern within domain 1 (bias arising from the randomization process) due to an unclear description of the randomization process in the manuscript. These concerns were unlikely to significantly bias the results in a way that would negate the observed outcomes for the investigated biologics.
Thirteen of the included systematic reviews also conducted Cochrane risk of bias assessments on the included RCTs.15,16,44-46,51,54-56,58,59,61,62 Their findings were similar to our assessment, with the exception of Agache et al. who rated some of the trials (CALIMA, SIROCCO, LIBERTY ASTHMA VENTURE, MENSA, and MUSCA) as having high levels of concern in the domains of attrition, reporting, and/or other bias.15,16,44 However, the rationale for these ratings was unclear.
The various subtypes of severe asthma were not consistently reported. Various studies defined subtypes (such as type 2 eosinophilic or allergic) differently and used different criteria. For example, there were varying thresholds of eosinophil counts to define type 2 eosinophilic asthma (refer to Appendix 8, Table 17 and Table 18). More recent trials focused on patients with severe asthma without restrictions for asthma subtype, while older trials tended to focus on specific asthma subtypes with broader criteria for asthma severity. The internal validity of these trials appears to be acceptable based on our assessments. However, the variation in trial inclusion criteria and protocols limits generalization across trials and outside of the inclusion criteria.
Table 5: Risk of Bias Assessment for Included Randomized Controlled Trials
Biologic | Trial | Risk of biasa | |||||
|---|---|---|---|---|---|---|---|
Domain 1 | Domain 2 | Domain 3 | Domain 4 | Domain 5 | Overall | ||
Benralizumab | ANDHI31 | Low | Low | Low | Low | Low | Low |
Benralizumab | Low | Low | Some | Low | Some | Some | |
Benralizumab | Low | Low | Some | Low | Some | Some | |
Benralizumab | SOLANA39 | Some | Low | Low | Low | Low | Some |
Dupilumab | Low | Low | Low | Some | Some | Some | |
Mepolizumab | Low | Low | Low | Low | Some | Some | |
Mepolizumab | Low | Low | Low | Low | Some | Some | |
Omalizumab | EXTRA30 | Low | Low | Some | Low | Some | Some |
Omalizumab | NCT0120290335 | Low | Low | Some | Low | Low | Some |
Omalizumab | NCT0204929438 | Low | Low | Low | Low | Low | Low |
Tezepelumab | Low | Low | Low | Low | Low | Low | |
Tezepelumab | Low | Low | Low | Low | Low | Low | |
Tezepelumab | Low | Low | Low | Some | Some | Some | |
NR = not reported.
Note: Overall bias was assessed using “'low,” “'some,” and “high” concerns. Information within published articles was cross-referenced to protocols published on clinicaltrials.gov.
aDefinitions of risk of bias domains: Domain 1 = Bias arising from the randomization process. Domain 2 = Bias due to deviations from intended intervention. Domain 3 = Bias due to missing outcome data. Domain 4 = Bias in measurement of outcome. Domain 5 = Bias in selection of overall result.
Systematic Reviews
Similar to individual RCTs, many systematic reviews did not provide a clear description of the included patient populations. In many cases, it was unclear whether the reviews included similar populations. Despite the inclusion and exclusion restrictions applied by the systematic reviews, issues with population variation persisted. Some of the biologics were extensively tested among subgroups of asthma patients, but this occurred without complete characterization, such as type 2 eosinophilic asthma without characterization of allergic status. Despite this issue, biologic drugs were compared with one another in some reviews. Some studies recognized this issue and used sample adjustment methods, such as filtering, matching, and/or weighting, to minimize population differences.
All the included systematic reviews underwent an AMSTAR 2 assessment (refer to Table 29). The framework proposed by Shea et al.18 was used to inform an overall level of confidence (high, moderate, low, critically low) in the results of the systematic reviews based on critical and noncritical domains of weakness. Based on the AMSTAR 2 assessment, the levels of confidence in results of the systematic reviews were considered to be high in 3 reviews,15,16,44 moderate in 2 reviews,52,53 and low or critically low in the remaining 16 reviews. A full description of the AMSTAR 2 assessment is detailed subsequently.
Of the critical domains (AMSTAR 2 items 1, 2, 4, 9, 11, 13, and 15), all the 21 included systematic reviews adequately described their PICO criteria (item 1). However, 13 reviews did not provide sufficient justification for their search strategy, such as language restriction justification (item 4).45-49,51,54,57-62 Although the majority of reviews published their protocols before commencing the review (item 2), 9 reviews did not follow this practice,46,48,49,51,54-56,60,62 which suggests a potential risk of bias due to ad hoc study decisions. In the majority of reviews, a satisfactory approach for assessing the risk of bias was used (item 9). However, 9 did not account for risk of bias when interpreting the results of the review (item 13).47-51,54,59,60,62 The application of meta-analytic methods was appropriate (item 11) with the exception of 1 review51 that employed unsuitable methods (converted rate outcomes into binary outcomes so that odds ratios could be reported). Nine reviews did not report sufficient exploration of potential publication bias (item 15).47-50,55-57,59,62 However, this omission may have been due to the small number of included trials, which prevented this assessment.
In the case of noncritical domains (AMSTAR 2 items 3, 5, 6, 7, 8, 10, 12, 14, and 16), numerous reviews did not meet several of these criteria. None of the authors of the systematic reviews explained their rationale for selecting only RCTs for inclusion (item 3). Although study selection was always performed in duplicate (item 5), data extraction was not described as being performed in duplicate in 10 of the reviews (item 6).46,48,49,51,54-56,58,60,62 Only systematic reviews performed by Agache et al.15,16,44 provided a list of excluded studies and the reasons for their exclusion (item 7). Only 1 study failed to describe the included studies in enough detail (item 8).59 Furthermore, these were the only reviews that assessed the sources of funding for included studies and whether they might introduce bias (item 10). Eight reviews did not assess possible effects of risk of bias on results (item 12).46-51,54,59,60 Heterogeneity observed in the results of the reviews was not sufficiently discussed in 6 reviews.47-50,54,59 In 9 reviews, potential relevant conflicts of interests were not sufficiently detailed to determine whether safeguards against conflicts were taken (item 16).15,16,44,47-51,57
Findings
Our analysis of the included 47 articles indicated that biologics appeared to be effective across important clinical (AEX, FEV1) and patient-reported outcomes (HRQoL) for their current indications with similar outcomes for safety. However, there were gaps in the evidence for each of these drugs among the subgroups of severe asthma (type 2 inflammation further characterized by eosinophilic and allergic markers, and non–type 2 asthma). Assessment of the comparative efficacy of biologic drugs was challenging due to heterogenous definitions of asthma severity and inconsistent application of severity criteria in RCTs, and therefore remains uncertain. Evidence on comparative safety is limited. There was also a lack of evidence on the efficacy and safety of these biologics in severe asthma among children.
Included RCTs enrolled primarily a type 2 inflammatory phenotype patient population (Table 3). Further characterization of this study population by subtype was performed in some studies (e.g., reporting on allergic status in a study that targeted enrolment of a type 2 eosinophilic population), although outcome reporting by asthma subgroups was incomplete (Table 14). Table 30 summarizes the main findings and evidence gaps for the 5 biologics of interest, and Table 31 provides a summary of findings for asthma subgroups (severe asthma, type 2 eosinophilic and/or allergic, and non–type 2).
Mepolizumab and omalizumab had the largest evidence gaps due to trials including only 1 specific asthma subtype. Mepolizumab was only evaluated in type 2 eosinophilic severe asthma; evidence for patients with a type 2 eosinophilic and allergic asthma subtype was also reported (Table 16), but results in a type 2 allergic and noneosinophilic subgroup was not available. Omalizumab was exclusively studied in patients with type 2 allergic severe asthma. Efficacy by eosinophilic status (high or low BEC) was not commonly reported (Table 16).
Eosinophilic status in severe asthma was frequently characterized by BEC levels in both the RCTs and systematic reviews. Although the results generally favoured the intervention across BEC levels, the low BEC subgroups were less likely to be statistically significant. Subgroups for type 2 allergic asthma were regularly reported from trial data in eosinophilic and severe asthma populations, however, the classification of this subtype was less consistent. Few systematic reviews examined this subtype.
In the few trials that enrolled individuals with severe asthma who had a non–type 2 inflammatory phenotype, benralizumab, dupilumab, and tezepelumab were investigated. The trials evaluating benralizumab and tezepelumab reported outcomes in this subtype. These biologics consistently demonstrated a statistically significant improvement in AEX compared to placebo (Table 16). A cut-off of less than 300 BEC was used for benralizumab; however, a cut-off of less than 150 BEC would more clearly identify non–type 2 patients. The direction of this effect was maintained for tezepelumab in a recent re-analysis of the PATHWAY and NAVIGATOR trials9 within a narrow subgroup (N = 96) that more rigorously classified non–type 2 asthma by also including only those with fractional exhaled nitric oxide less than 25 parts per billion (in addition to < 150 BEC and perennial allergies). The reported between-group difference in AEX in this small sample size was not statistically significant.
Among the included RCTs that evaluated the use of biologics in patients with severe asthma, some studies recruited participants younger than 18 years but only a small portion were confirmed as children (n = 229, 3% of the included trial participants). Reporting of outcomes for participants younger than 18 years was infrequent, with only 1 review15 reporting outcomes within this population (pediatric patients with type 2 allergic asthma with omalizumab investigated). A number of studies that evaluated efficacy and safety of biologics in moderate to severe asthma among pediatric populations are listed in Appendix 6 for reference.
Included systematic reviews were consistent with our assessment of the current evidence, with main clinical outcomes and HRQoL generally favouring biologics over placebos (Table 23). Reviews also generally did not identify any risk of serious adverse events, with only 1 review finding a statistically significant risk of adverse events for mepolizumab.16 Assessment of subgroups was more limited in reviews than in published articles on RCTs.
Among the included systematic reviews, 10 reported on comparative efficacy (Table 25). These reviews examined populations that were broadly classified as severe asthma or were based on eosinophilic criteria, without specific characterization of allergic status and limited by a lack of direct comparisons (indirect comparison with attendant limitations). Most comparisons did not reveal significant differences between the included drugs in the targeted patient populations of interest. Although these reviews selected pertinent trials and effectively summarized main study outcomes, they lacked systematic subgroup assessments and often did not fully account for population variations across the trials. In light of these limitations, statistical adjustments were made in some reviews to better compare dissimilar populations (although inconsistencies remained), and some statistically significant differences were found in some of those studies. Benralizumab, mepolizumab, and omalizumab were inferior to tezepelumab and dupilumab in some reviews listed as including trials of type 2 eosinophilic or severe asthma not otherwise. Mepolizumab was superior to benralizumab in HRQoL outcomes and superior to dupilumab in safety outcomes in some reviews of type 2 eosinophilic asthma trials. However, given the underlying heterogeneity across trials, comparative effectiveness between biologics is still uncertain. Subgroup analyses were mostly consistent with overall group results.
Limitations
This was a focused rapid systematic review that searched articles in English that were recently published (from 2018 onward); a more fulsome review may have identified additional studies. Severity of asthma was inconsistently defined. Many trials that studied patients with moderate to severe asthma that were not clearly “severe” asthma were excluded. Handsearching was limited due to the nature of this study; however, PROSPERO and clinical trial registries were checked (including any linked studies listed on the registries). Results of RCTs are reported as simplified positive or negative outcomes with significance noted as a means of simplifying the large volume of complex data, and because of potential variation in effect sizes due to differences in baseline populations. This analysis did not adjust for any potential concerns related to multiple testing or reporting bias due to the substantial number of outcomes that are frequently recorded and published from the included RCTs.
This review was intended to identify and quickly map the available evidence from recent RCTs and systematic reviews. Therefore, an in-depth extraction of specific effect sizes or a meta-analysis or comparative efficacy testing were not performed.
Conclusions and Implications for Decision- or Policy-Making
Conclusions
Recent RCTs and systematic reviews (published in 2018 onward) predominately focused on a limited range of severe asthma subtypes. Children were infrequently included. Outcome reporting for biologic drugs by the subtypes of severe asthma and by age was limited.
In this review, most participants included in RCTs were those with primarily type 2 eosinophilic severe asthma. Biologics indicated for this subtype demonstrated benefit for this patient population (benralizumab, dupilumab, mepolizumab, and tezepelumab) and this benefit may extend to those who also have markers of allergic asthma (type 2 eosinophilic and allergic).
Included systematic reviews that assessed comparative efficacy primarily included trials on the type 2 eosinophilic asthma population. Although conclusions were heterogenous, most found no significant differences among the biologics assessed. Conclusions were limited by population characterization, power, and method (indirect treatment comparison).
Biologics studied in type 2 allergic asthma, other than omalizumab (indicated for this patient population), were limited by variable definition of this subtype. Although there was limited evidence, tezepelumab was shown to be effective in a type 2 allergic severe asthma population defined by the same criteria indicated for omalizumab. Dupilumab was shown to be statistically significantly better for some outcomes compared to omalizumab in an indirect treatment comparison conducted in included systematic reviews in which the dupilumab data were adjusted to match the population from omalizumab trials. However, clinical relevance and validity of this result is uncertain.
There was limited research on the non–type 2 severe asthma population. No trial specifically enrolled individuals with this phenotype. Among a small number of participants with non–type 2 severe asthma, benralizumab and tezepelumab reported positive outcomes (consistently showed a statistically significant reduction in AEXs compared with placebo). However, the benralizumab analysis used a higher than normal BEC level as their cut-off point, which limits clinical interpretation.
There is evidence from subgroup analyses in the PATHWAY and NAVIGATOR studies on tezepelumab that patients with non–type 2 asthma, defined rigorously as those with BEC less than 150 cells/µL, fractional exhaled nitric oxide less than 25 parts per billion, and negative perennial allergy skin tests, may benefit from treatment with tezepelumab. However, data showing efficacy for the other biologic therapies in this subgroup are lacking.
There was insufficient evidence to inform efficacy and safety of biologics in pediatric populations with severe asthma. Full assessment of efficacy and safety would require using subject-specific characteristics (to identify age if not reported) but is likely to be challenging given access to data and the small numbers of children enrolled. Studies on the efficacy and safety of biologics in pediatric populations with moderate to severe asthma have been conducted and could contribute to further evidence synthesis.
Conduct of de novo evidence synthesis would be constrained by incomplete inclusion, characterization, and outcome reporting of study populations by both type 2 allergic and eosinophilic subtypes for each biologic, and small numbers of identified children enrolled in trials. This is unlikely to result in evidence to inform alignment of criteria of biologics in severe asthma.
Overall, biologic drugs are better than placebo across all outcomes for their respective indications. However, comparative efficacy of biologics for these indications is uncertain, and evidence on comparative safety is limited.
Implications for Decision- or Policy-Making
In this part 1 Rapid Review, potential comparative efficacy and safety analysis to answer the proposed research and policy questions is limited by lack of similar eligibility criteria and outcome reporting for all asthma subtypes and patient populations, especially pediatric populations.
Part 2 was to be an HTA to provide guidance concerning the alignment of the drug funding criteria by the public drug plans. Based on the findings of part 1, it is highly unlikely that further evidence synthesis using data from available trials would generate policy-relevant conclusions. As such, CADTH will not proceed with part 2 (the HTA).
References
1.Mayo Clinic. Diseases and conditions. Asthma. 2022; https://www.mayoclinic.org/diseases-conditions/asthma/symptoms-causes/syc-20369653 Accessed 2023 Dec 8.
2.Reihman AE, Holguin F, Sharma S. Management of severe asthma beyond the guidelines. Curr Allergy Asthma Rep. 2020;20(9). PubMed
3.American Academy of Allergy Asthma & Immunology. Severe asthma. 2019; https://www.aaaai.org/tools-for-the-public/conditions-library/asthma/severe-asthma. Accessed 2023 Dec 8.
4.Asthma Canada. Severe asthma. 2022; https://asthma.ca/get-help/severe-asthma/. Accessed 2023 Dec 3.
5.Globe G, Martin M, Schatz M, et al. Symptoms and markers of symptom severity in asthma—content validity of the asthma symptom diary. Health Qual Life Outcomes. 2015;13(1):21. PubMed
6.Ismaila AS, Sayani AP, Marin M, Su Z. Clinical, economic, and humanistic burden of asthma in Canada: a systematic review. BMC Pulm Med. 2013;13(1):70. PubMed
7.Chen W, Safari A, Fitzgerald JM, Sin DD, Tavakoli H, Sadatsafavi M. Economic burden of multimorbidity in patients with severe asthma: a 20-year population-based study. Thorax. 2019;74(12):1113-1119. PubMed
8.Chen M, Shepard K, Yang M, et al. Overlap of allergic, eosinophilic and type 2 inflammatory subtypes in moderate‐to‐severe asthma. Clin Exp Allergy. 2021;51(4):546-555. PubMed
9.Corren J, Menzies-Gow A, Chupp G, et al. Efficacy of tezepelumab in severe, uncontrolled asthma: pooled analysis of PATHWAY and NAVIGATOR studies. Am J Respir Crit Care Med. 2023;04:04.
10.Thomson NC. Novel approaches to the management of noneosinophilic asthma. Ther Adv Respir Dis. 2016;10(3):211-234. PubMed
11.FitzGerald JM, Bleecker ER, Menzies-Gow A, et al. Predictors of enhanced response with benralizumab for patients with severe asthma: pooled analysis of the SIROCCO and CALIMA studies. Lancet Respir Med. 2018;6(1):51-64. PubMed
12.Hsieh A, Assadinia N, Hackett TL. Airway remodeling heterogeneity in asthma and its relationship to disease outcomes. Front Physiol. 2023;14:1113100. PubMed
13.Canonica GW, Blasi F, Paggiaro P, et al. Oral corticosteroid sparing with biologics in severe asthma: a remark of the Severe Asthma Network in Italy (SANI). World Allergy Organ J. 2020;13(10):100464. PubMed
14.pan-Canadian Pharmaceutical Alliance. Cinqair (reslizumab). 2018; https://www.pcpacanada.ca/negotiation/20781. Accessed 2023 Sept 28.
15.Agache I, Rocha C, Beltran J, et al. Efficacy and safety of treatment with biologicals (benralizumab, dupilumab and omalizumab) for severe allergic asthma: A systematic review for the EAACI Guidelines - recommendations on the use of biologicals in severe asthma. Allergy. 2020b;75(5):1043-1057. PubMed
16.Agache I, Beltran J, Akdis C, et al. Efficacy and safety of treatment with biologicals (benralizumab, dupilumab, mepolizumab, omalizumab and reslizumab) for severe eosinophilic asthma. A systematic review for the EAACI Guidelines - recommendations on the use of biologicals in severe asthma. Allergy. 2020a;75(5):1023-1042. PubMed
17.Sterne JAC, Savovic J, Page MJ, et al. RoB 2: a revised tool for assessing risk of bias in randomised trials. BMJ. 2019;366:l4898. PubMed
18.Shea BJ, Reeves BC, Wells G, et al. AMSTAR 2: a critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ. 2017;358:j4008. PubMed
19.Brusselle GG, Koppelman GH. Biologic therapies for severe asthma. N Engl J Med. 2022;386(2):157-171. PubMed
20.Albers FC, Licskai C, Chanez P, et al. Baseline blood eosinophil count as a predictor of treatment response to the licensed dose of mepolizumab in severe eosinophilic asthma. Respir Med. 2019;159:105806. PubMed
21.Bleecker ER, Wechsler ME, FitzGerald JM, et al. Baseline patient factors impact on the clinical efficacy of benralizumab for severe asthma. Eur Respir J. 2018;52(4):10. PubMed
22.Brusselle G, Quirce S, Papi A, et al. Dupilumab efficacy in patients with uncontrolled or oral corticosteroid-dependent allergic and nonallergic asthma. J Allergy Clin Immunol Pract. 2023;11(3):873-884 e811. PubMed
23.Chipps BE, Newbold P, Hirsch I, Trudo F, Goldman M. Benralizumab efficacy by atopy status and serum immunoglobulin E for patients with severe, uncontrolled asthma. Ann Allergy Asthma Immunol. 2018;120(5):504-511.e504. PubMed
24.Corren J, Ambrose CS, Griffiths JM, et al. Efficacy of tezepelumab in patients with evidence of severe allergic asthma: results from the phase 3 NAVIGATOR study. Clin Exp Allergy. 2023;53(4):417-428. PubMed
25.Corren J, Ambrose CS, Salapa K, et al. Efficacy of tezepelumab in patients with severe, uncontrolled asthma and perennial allergy. J Allergy Clin Immunol Pract. 2021;9(12):4334-4342.e4336. PubMed
26.Corren J, Chen S, Callan L, Garcia Gil E. The impact of tezepelumab on hospitalization and emergency department visits in patients with severe uncontrolled asthma: results from the pathway phase 2b trial. Am J Respir Crit Care Med. 2019;199(9).
27.Corren J, Garcia Gil E, Griffiths JM, et al. Tezepelumab improves patient-reported outcomes in patients with severe, uncontrolled asthma in PATHWAY. Ann Allergy Asthma Immunol. 2021;126(2):187-193. PubMed
28.Corren J, Pham TH, Garcia Gil E, et al. Baseline type 2 biomarker levels and response to tezepelumab in severe asthma. Allergy. 2022;77(6):1786-1796. PubMed
29.Domingo C, Maspero JF, Castro M, et al. Dupilumab efficacy in steroid-dependent severe asthma by baseline oral corticosteroid dose. J Allergy Clin Immunol Pract. 2022;10(7):1835-1843. PubMed
30.Hanania NA, Fortis S, Haselkorn T, et al. Omalizumab in asthma with fixed airway obstruction: post hoc analysis of EXTRA. J Allergy Clin Immunol Pract. 2022;10(1):222-228. PubMed
31.Harrison TW, Chanez P, Menzella F, et al. Onset of effect and impact on health-related quality of life, exacerbation rate, lung function, and nasal polyposis symptoms for patients with severe eosinophilic asthma treated with benralizumab (ANDHI): a randomised, controlled, phase 3b trial. Lancet Respir Med. 2021;9(3):260-274. PubMed
32.Humbert M, Albers FC, Bratton DJ, et al. Effect of mepolizumab in severe eosinophilic asthma according to omalizumab eligibility. Respir Med. 2019;154:69-75. PubMed
33.Jackson DJ, Humbert M, Hirsch I, Newbold P, Garcia Gil E. Ability of serum IgE concentration to predict exacerbation risk and benralizumab efficacy for patients with severe eosinophilic asthma. Adv Ther. 2020;37(2):718-729. PubMed
34.Lemiere C, Taille C, Lee JK, et al. Impact of baseline clinical asthma characteristics on the response to mepolizumab: a post hoc meta-analysis of two Phase III trials. Respir Res. 2021;22(1):184. PubMed
35.Li J, Wang C, Liu C, et al. Efficacy predictors of omalizumab in Chinese patients with moderate-to-severe allergic asthma: Findings from a post-hoc analysis of a randomised phase III study. World Allergy Organ J. 2020;13(12):100469. PubMed
36.Menzies-Gow A, Corren J, Bourdin A, et al. Tezepelumab in adults and adolescents with severe, uncontrolled asthma. N Engl J Med. 2021;384(19):1800-1809. PubMed
37.Menzies-Gow A, Wechsler ME, Brightling CE, et al. Long-term safety and efficacy of tezepelumab in people with severe, uncontrolled asthma (DESTINATION): a randomised, placebo-controlled extension study. Lancet Respir Med. 2023;23:23. PubMed
38.Mukherjee M, Kjarsgaard M, Radford K, et al. Omalizumab in patients with severe asthma and persistent sputum eosinophilia. Allergy Asthma Clin Immunol. 2019;15:21. PubMed
39.Panettieri RA, Jr., Welte T, Shenoy KV, et al. Onset of effect, changes in airflow obstruction and lung volume, and health-related quality of life improvements with benralizumab for patients with severe eosinophilic asthma: phase iiib randomized, controlled trial (SOLANA). J Asthma Allergy. 2020;13:115-126. PubMed
40.Prazma CM, Idzko M, Douglass JA, et al. Response to mepolizumab treatment in patients with severe eosinophilic asthma and atopic phenotypes. J Asthma Allergy. 2021;14:675-683. PubMed
41.Rabe KF, Nair P, Brusselle G, et al. Efficacy and safety of dupilumab in glucocorticoid-dependent severe asthma. N Engl J Med. 2018;378(26):2475-2485. PubMed
42.Wardlaw A, Howarth PH, Israel E, et al. Fungal sensitization and its relationship to mepolizumab response in patients with severe eosinophilic asthma. Clin Exp Allergy. 2020;50(7):869-872. PubMed
43.Wechsler ME, Menzies-Gow A, Brightling CE, et al. Evaluation of the oral corticosteroid-sparing effect of tezepelumab in adults with oral corticosteroid-dependent asthma (SOURCE): a randomised, placebo-controlled, phase 3 study. Lancet Respir Med. 2022;10(7):650-660. PubMed
44.Agache I, Song Y, Rocha C, et al. Efficacy and safety of treatment with dupilumab for severe asthma: A systematic review of the EAACI guidelines-Recommendations on the use of biologicals in severe asthma. Allergy. 2020c;75(5):1058-1068. PubMed
45.Akenroye A, Lassiter G, Jackson JW, et al. Comparative efficacy of mepolizumab, benralizumab, and dupilumab in eosinophilic asthma: A Bayesian network meta-analysis. J Allergy Clin Immunol. 2022;150(5):1097-1105.e1012. PubMed
46.Ando K, Fukuda Y, Tanaka A, Sagara H. Comparative efficacy and safety of tezepelumab and other biologics in patients with inadequately controlled asthma according to thresholds of type 2 inflammatory biomarkers: A systematic review and network meta-analysis. Cells. 2022;11(5). PubMed
47.Bateman ED, Khan AH, Xu Y, et al. Pairwise indirect treatment comparison of dupilumab versus other biologics in patients with uncontrolled persistent asthma. Respir Med. 2022;191:105991. PubMed
48.Bourdin A, Husereau D, Molinari N, et al. Matching-adjusted comparison of oral corticosteroid reduction in asthma: systematic review of biologics. Clin Exp Allergy. 2020;50(4):442-452. PubMed
49.Busse W, Chupp G, Nagase H, et al. Anti-IL-5 treatments in patients with severe asthma by blood eosinophil thresholds: Indirect treatment comparison. J Allergy Clin Immunol. 2019;143(1):190-200.e120. PubMed
50.Chagas GCL, Xavier D, Gomes L, Ferri-Guerra J, Oquet REH. Effects of tezepelumab on quality of life of patients with moderate-to-severe, uncontrolled asthma: Systematic review and meta-analysis. Curr Allergy Asthma Rep. 2023;23(6):287-298. PubMed
51.Chen C, Wen T, Wei L. Different IL-5 monoclonal antibody agents in treating severe asthma patients: a systemic review and network meta-analysis of randomized controlled trials (RCTs). Int J Clin Exp Med. 2019;12(6):6512-6519.
52.Henriksen DP, Bodtger U, Sidenius K, et al. Efficacy, adverse events, and inter-drug comparison of mepolizumab and reslizumab anti-IL-5 treatments of severe asthma - a systematic review and meta-analysis. Eur Clin Respir J. 2018;5(1):1536097. PubMed
53.Henriksen DP, Bodtger U, Sidenius K, et al. Efficacy of omalizumab in children, adolescents, and adults with severe allergic asthma: a systematic review, meta-analysis, and call for new trials using current guidelines for assessment of severe asthma. Allergy Asthma Clin Immunol. 2020;16:49. PubMed
54.Lee J, Song J-U, Kim YH. The clinical efficacy of type 2 inflammation-specific agents targeting interleukins in reducing exacerbations in severe asthma: a meta-analysis. Yonsei Med J. 2022;63(6):511-519. PubMed
55.Mahdavian M, Brothers C, Asghari S, Mallay S, Pike J. Impact of benralizumab on asthma control, asthma-related quality of life and lung function in patients with poorly controlled eosinophilic asthma: A systematic review and meta-analysis. Can J Respir Crit Care Sleep Med. 2019;3(2):106-111.
56.Mahdavian M, Mallay SA, Asghari S, Voduc N, Pike JC. Effect of benralizumab on asthma exacerbation rates in patients with severe asthma: Systematic review and meta-analysis. Can J Respir Crit Care Sleep Med. 2020;4(2):133-141.
57.Menzies-Gow A, Steenkamp J, Singh S, et al. Tezepelumab compared with other biologics for the treatment of severe asthma: a systematic review and indirect treatment comparison. J Med Econ. 2022;25(1):679-690. PubMed
58.Nopsopon T, Lassiter G, Chen ML, et al. Comparative efficacy of tezepelumab to mepolizumab, benralizumab, and dupilumab in eosinophilic asthma: A Bayesian network meta-analysis. J Allergy Clin Immunol. 2023;151(3):747-755. PubMed
59.Praetorius K, Henriksen DP, Schmid JM, et al. Indirect comparison of efficacy of dupilumab versus mepolizumab and omalizumab for severe type 2 asthma. ERJ Open Res. 2021;7(3). PubMed
60.Ramonell RP, Iftikhar IH. Effect of anti-IL5, anti-IL5R, anti-IL13 therapy on asthma exacerbations: A network meta-analysis. Lung. 2020;198(1):95-103. PubMed
61.Shaban Abdelgalil M, Ahmed Elrashedy A, Awad AK, et al. Safety and efficacy of tezepelumab vs. placebo in adult patients with severe uncontrolled asthma: a systematic review and meta-analysis. Sci Rep. 2022;12(1):20905. PubMed
62.Zoumot Z, Al Busaidi N, Tashkandi W, et al. Tezepelumab for patients with severe uncontrolled asthma: a systematic review and meta-analysis. J Asthma Allergy. 2022;15:1665-1679. PubMed
63.Chung KF, Wenzel SE, Brozek JL, et al. International ERS/ATS guidelines on definition, evaluation and treatment of severe asthma. Eur Respir J. 2014;43(2):343-373. PubMed
64.Reddel HK, Bacharier LB, Bateman E, et al. Global Initiative for Asthma Strategy 2021: executive summary and rationale for key changes. Am J Respir Crit Care Med. 2022;205(1):17-35. PubMed
Authors and Contributors
Jason R. Randall was involved with conception and design and drafted the original project protocol; screening studies, data extraction, and data analysis; and drafting and revising of the report.
Richard Leigh provided content input to analysis and interpretation of data, key messages, and conclusions and provided revisions on the initial draft and on subsequent revisions for important intellectual content.
Ellen T. Crumley conducted all searches, was the second screener of all results, provided details about how to write up searches, and read the final report and suggested edits.
Sylvia Aponte-Hao contributed to the systematic review, data extraction, and data analysis of the study and reviewed the report.
Ngoc Khanh Vu participated in the development of the study protocol and data collection tools, data collection by extracting information from papers, contributed to the contents of the report, and provided comments for report draft and revisions.
Karen Martins provided substantial contributions to interpretation of study results, including the key messages and conclusion, and contributed to revising the report critically for important intellectual content.
Scott Klarenbach was the senior author and investigator and was involved in the conception, study design, oversight of data acquisition and analysis, critical revision of report including policy implications, and oversight of the project.
Contributors
Content Expert
This individual kindly provided comments on this report:
Karen E. Binkley, HBSc MD FRCPC
Associate Professor
Divisions of Clinical Immunology and Allergy and Clinical Pharmacology, University of Toronto
Acknowledgements
CADTH would like to acknowledge the following individuals:
Christine Perras and David Stock reviewed the drafts and final report.
Emily Farrell provided knowledge mobilization support.
Brandy Appleby provided project management support.
Sarah C. McGill conducted a quality check of the references.
Conflicts of Interest
Jason R. Randall disclosed the following:
Current employment
Real World Evidence Unit, University of Alberta, 2022 to 2024, various drugs and technologies
Ellen T. Crumley disclosed the following:
Payment as advisor or consultant
Liv Agency – Upadacitinib, 2022: Wrote report from recording of live consultancy meeting.
Fusion MD Network – Avelumab, 2022: Attended and wrote report from live consultancy meeting.
Scott Klarenbach disclosed the following:
Research funding or grants
Real World Evidence Consortium (via Bayer) – Outcomes in diabetic kidney disease
Alberta Drug and Technology Evidence Consortium with funding from CADTH – CoLab PMDE Core Network Partner
Real World Evidence Unit and Real World Evidence Consortium (RWEU and RWEC) through the University Hospital Foundation (UHF) (funding to UHF from Roche) – Pathways of care for multiple sclerosis; DMT use in patients with multiple sclerosis
RWEU and RWEC with funding from Allergan – Health care resource use in subjects with migraine; pathways of care post stroke; economic impact of discontinuing or reducing injection frequency of botulinum toxin for the treatment chronic migraine.
RWEU and RWEC with funding from Purdue – Analgesia use in trauma
RWEU and RWEC with funding from GSK and in Partnership with Respiratory Strategic Clinical Network (AB) – Treatment patterns in patients with COPD
RWEU and RWEC with funding from CSL – Immunoglobulin use in AB; treatment patterns in dermatomyositis; incremental cost of SCIg versus IVIg
RWEU and RWEC with funding from Lundbeck – Health care resource use and treatment in depression
RWEU and RWEC with funding from University Hospital Foundation (funding to UHF from NovoNordisk) – Health care resources use in patients with obesity
RWEU and RWEC with funding from UHF (funding from UHF from Jansen) – Health care resource use in patients starting long-acting antipsychotics in schizophrenia
RWEU and RWEC with funding through the University Hospital Foundation (UHF – funding originated from Novartis) – Economic burden of Multiple Sclerosis in Alberta
RWEC funding through Ferring – Budesonide MMX treatment in ulcerative colitis
RWEC funding through IQVIA – Completed a feasibility questionnaire related to data availability for evaluating the cost of cadaver islet cell transplant
RWEC funding through RTI – Completed a feasibility questionnaire related to data availability for evaluating the risk/benefit of a particular drug among those with CKD and cardiovascular morbidity and mortality
RWEU and RWEC funding through Janssen – Evaluating the feasibility of health system data to generate decision-grade real world evidence in Canada – under review
RWEU and RWEC funding through Intuitive – Comparative outcomes between different surgical approaches
Karen Martins disclosed the following:
Member of the Alberta Real World Evidence consortium that conducts investigator-initiated research projects and receives funding from industry.
Richard Leigh disclosed the following:
Speaking engagements
AstraZeneca – Alarmins: 2022–2023
GlaxoSmithKline – Asthma, Precision Medicine: 2022–2023
Sanofi – Asthma, Dupilumab: 2022–2023
Vale – Asthma, inhalers: 2022–2023
Other
Attendee – Advisory board meetings for AstraZeneca, GlaxoSmithKline, and Sanofi
Payment as advisor or consultant
AstraZeneca – Asthma, Alarmins: 2018 to 2023
GlaxoSmithKline – Asthma, precision medicine; biologics: 2018 to 2023
Sanofi – Asthma, Dupilumab: 2019 to 2023
Research funding or grants
AstraZeneca – Asthma, Alarmins: 2018 to 2023
Sanofi – Asthma, Dupilumab: 2019 to 2023
Payment for academic appointments (endowed chairs)
GlaxoSmithKline - Asthma, Precision Medicine; biologics: 2018 to 2023
Received honorariums as advisor from AZ, GSK, and Sanofi. University of Calgary has received funding from AZ, GSK, and Sanofi for clinical trials where Richard Leigh is the Site Principal Investigator. The University of Calgary received an endowment from GSK for a Professorship in Inflammatory Lung Disease – Richard Leigh is the current holder of that Professorship but does not benefit from any personal payments from the Professorship (all funds channelled into Operations).
Karen Binkley disclosed the following:
Speaking engagement and educational lecture
Takeda – Firazyr, Takzhyra
Other – Advisory board member
Takeda – Firazyr, Takzhyra
Biocryst – Orladeo
Payment as advisor or consultant
Medexus – Rupall. Speaker – education lectures on angioedema and urticaria
No other conflicts of interest were declared.
Appendix 1: Approved Indications for Biologics
Note that this appendix has not been copy-edited.
Biologics | Dose | Health Canada indication | CDEC recommendation |
|---|---|---|---|
Benralizumab | 30 mg administered once every 4 weeks for the first 3 doses, and then once every 8 weeks thereafter by SC injection into the thigh, or abdomen. | As an add-on maintenance treatment of adult patients with severe eosinophilic asthma. | As an add-on maintenance treatment for adult patients with severe eosinophilic asthma if the following criteria are met:
|
Dupilumab | Initial dose of 600 mg SC (two 300 mg injections), followed by 300 mg every other week. | As an add-on maintenance treatment in patients aged 6 years and older with severe asthma with a type 2/eosinophilic phenotype or oral corticosteroid–dependent asthma. | For the treatment of severe asthma and with a type 2 or eosinophilic phenotype or oral corticosteroid–dependent asthma if certain conditions are met. |
Mepolizumab | 100 mg administered SC once every 4 weeks. | As add-on maintenance treatment for adults, adolescents, and children (aged 6 years and older) with severe eosinophilic asthma who:
| As an add-on maintenance treatment for adult patients with severe eosinophilic asthma, if the following criteria are met: Initiation Criteria: 1. Patient must have a documented diagnosis of asthma. 2. Patient is inadequately controlled with high-dose inhaled corticosteroids, defined as greater or equal to 500 mcg of fluticasone propionate or equivalent daily, and 1 or more additional asthma controller(s) (e.g., long-acting beta agonists). 3. Patient has 1 of the following: 3.1. blood eosinophil count of ≥ 300 cells/µL AND has experienced 2 or more clinically significant asthma exacerbations in the past 12 months, or 3.2. blood eosinophil count of ≥ 150 cells/µL AND is receiving maintenance treatment with oral corticosteroids. |
Omalizumab | 75 to 375 mg is administered SC every 2 or 4 weeks. Doses of more than 150 mg are divided among more than 1 injection site to limit injections to not more than 150 mg per site | For adult and pediatric patients (6 years of age and above) with moderate to severe persistent asthma who have a positive skin test or in vitro reactivity to a perennial aeroallergen and whose symptoms are inadequately controlled with inhaled corticosteroids. | For adults and adolescents (12 years of age and older) with moderate to severe persistent asthma who have a positive skin test or in vitro reactivity to a perennial aeroallergen, if the following clinical criterion is met: Inability to use, intolerance to, or inadequate response to an inhaled corticosteroid long-acting beta-agonist combination, and at least 1 other reimbursed alternative asthma treatment. |
Tezepelumab | 210 mg SC once every 4 weeks | As an add-on maintenance treatment in adults and adolescents 12 years and older with severe asthma | Add-on maintenance treatment in adults and adolescents 12 years and older with severe asthma, only if: Asthma uncontrolled with high-dose ICS and 1 or more additional asthma controllers. AND Experienced 2 or more clinically significant asthma exacerbations in the past 12 months AND A baseline assessment of asthma symptom control using a validated Asthma Control Questionnaire must be completed before initiation of tezepelumab treatment. |
ICS = inhaled corticosteroids; LABA = long-acting beta agonist; SC = subcutaneous.
Appendix 2: Literature Search Strategy
Note that this appendix has not been copy-edited.
Search Strategies – Final
Updated May 12, 2023
Clinical Trials Registries
Biomed Central. ISRCTN Registry
Searched March 20, 2023, Tezepelumab searched April 13, 2023
Narrowed results to: Condition Category: Respiratory
Xolair
Omalizumab
Nucala
Mepolizumab
Fasenra
Benralizumab
Dupilumab
Dupixent
Searched April 13, 2023
Tezepelumab
Tezspire
Severe asthma
US National Institutes of Health. ClinicalTrials.gov
https://classic.clinicaltrials.gov/ct2/search/advanced
Searched March 20, 2023
(Xolair or omalizumab) and Interventional Studies and severe asthma
(Nucala or mepolizumab) and Interventional Studies and severe asthma
(Fasenra or benralizumab) and Interventional Studies and severe asthma
(Dupilumab or Dupixent) and Interventional Studies and severe asthma
(Tezepelumab or Tezspire) and Interventional Studies and severe asthma
Searched April 13, 2023
EU Clinical Trials Register
https://www.clinicaltrialsregister.eu/ctr-search/search
Searched 20 March 2023, Tezepelumab searched 13 April 2023
(xolair OR omalizumab OR Nucala OR mepolizumab OR Fasenra OR benralizumab OR Dupilumab OR Dupixent) AND severe asthma
(Tezepelumab or Tezspire) AND severe asthma
Searched April 13, 2023
WHO. International Clinical Trials Registry Platform Search Portal (ICTRP)
https://trialsearch.who.int/Default.aspx
Searched April 13, 2023
Narrowed to 2018+
(xolair OR omalizumab) AND severe asthma
(Nucala OR mepolizumab) AND severe asthma
(Fasenra OR benralizumab) AND severe asthma
(Dupilumab OR Dupixent) AND severe asthma
(Tezepelumab or Tezspire) AND severe asthma
PROSPERO: International prospective register of systematic reviews https://www.crd.york.ac.uk/prospero/
Searched 20 March 2023, Tezepelumab searched 13 April 2023
(omalizumab OR xolair OR Nucala OR mepolizumab OR Fasenra OR benralizumab OR Dupilumab OR Dupixent) AND severe asthma AND (Systematic Review OR Meta-Analysis OR Network meta-analysis):RT NOT Animal:DB
(Tezepelumab or Tezspire) AND severe asthma AND (Systematic Review OR Meta-Analysis OR Network meta-analysis):RT NOT Animal:DB
Searched April 13, 2023
MEDLINE
Ovid MEDLINE(R) and Epub Ahead of Print, In-Process, In-Data-Review and Other Non-Indexed Citations and Daily 1946 to May 4, 2023
Searched May 8, 2023
(nucala* or mepolizumab* or bosatria* or SB240563 or SB-240563 or 90Z2UFOE52).ti,ab,ot,rn,hw,nm,kf. 1323
196078-29-2.rn,nm. 0
(Xolair* or omalizumab* or rhuMab-E25 or rhuMabE25 or HSDB 5742 or HSDB5742 or 2P471X1Z11 or UNII2P471X1Z11 or hu 901 or hu901).ti,ab,ot,sh,hw,rn,nm. 3464
exp Omalizumab/ 2308
(“242138 07 4” or “242138074” or 24213807 4 or “242318 074” or 2421380 74).rn,nm. 0
(dupilumab* or dupixent* or regn668 or regn 668 or sar231893 or sar 231893 or 420K487FSG).ti,ab,kf,ot,hw,rn,nm. 2290
(Fasenra* or benralizumab* or BIW 8405 or BIW8405 or medi563 or medi 563 or 71492GE1FX).ti,ab,kf,ot,hw,rn,nm. 719
(tezepelumab* or Tezspire* or amg-157 or amg157 or medi-9929 or medi9929 or medi-19929 or medi19929 or GTPL-8933 or GTPL8933 or RJ1IW3B4QX).ti,ab,kf,ot,hw,nm,rn. 147
or/1-8 6743
exp asthma/ 141601
asthma*.ti,ab,kf. 180248
10 or 11 200291
(severe or eosinophil* or allerg* or type 2 or T2).ti,ab,kf. 1761191
exp Eosinophilia/ 27256
13 or 14 1765364
12 and 15 78179
9 and 16 2752
(Randomized Controlled Trial or Controlled Clinical Trial or Pragmatic Clinical Trial or Clinical Study or Adaptive Clinical Trial or Equivalence Trial).pt. 689435
(Clinical Trial or Clinical Trial, Phase I or Clinical Trial, Phase II or Clinical Trial, Phase III or Clinical Trial, Phase IV or Clinical Trial Protocol).pt. 609848
Multicenter Study.pt. 333420
Clinical Studies as Topic/ 782
exp Clinical Trial/ or exp Clinical Trials as Topic/ or Clinical Trial Protocol/ or Clinical Trial Protocols as Topic/ or exp “Clinical Trial (topic)”/ 1271981
Multicenter Study/ or Multicenter Studies as Topic/ or “Multicenter Study (topic)”/ 352706
Randomization/ 106927
Random Allocation/ 106927
Double-Blind Method/ 175065
Double Blind Procedure/ 0
Double-Blind Studies/ 175065
Single-Blind Method/ 32682
Single Blind Procedure/ 0
Single-Blind Studies/ 32682
Placebos/ 35926
Placebo/ 0
Control Groups/ 1936
Control Group/ 1936
Cross-Over Studies/ or Crossover Procedure/ 55047
(random* or sham or placebo*).ti,ab,hw,kf. 1798183
((singl* or doubl*) adj (blind* or dumm* or mask*)).ti,ab,hw,kf. 266193
((tripl* or trebl*) adj (blind* or dumm* or mask*)).ti,ab,hw,kf. 1582
(control* adj3 (study or studies or trial* or group*)).ti,ab,hw,kf. 1911610
(clinical adj3 (study or studies or trial*)).ti,ab,hw,kf.1422796
(Nonrandom* or non random* or non-random* or quasi-random* or quasirandom*).ti,ab,hw,kf. 54080
(phase adj3 (study or studies or trial*)).ti,ab,hw,kf. 176614
((crossover or cross-over) adj3 (study or studies or trial*)).ti,ab,hw,kf. 76401
((multicent* or multi-cent*) adj3 (study or studies or trial*)).ti,ab,hw,kf. 405419
allocated.ti,ab,hw. 82977
((open label or open-label) adj5 (study or studies or trial*)).ti,ab,hw,kf. 44243
((equivalence or superiority or non-inferiority or noninferiority) adj3 (study or studies or trial*)).ti,ab,hw,kf. 11909
(pragmatic study or pragmatic studies).ti,ab,hw,kf. 596
((pragmatic or practical) adj3 trial*).ti,ab,hw,kf. 7616
((quasiexperimental or quasi-experimental) adj3 (study or studies or trial*)).ti,ab,hw,kf. 11997
trial.ti,kf. 304877
or/18-52 3769161
exp animals/ 26345052
exp animal experimentation/ 10316
exp models animal/ 639361
exp animal experiment/ 10316
nonhuman/ 0
exp vertebrate/ 25603896
or/53-59 26851439
exp humans/ 21226470
exp human experiment/ 0
or/61-62 21226470
60 not 63 5624969
53 not 64 2867628
(systematic review or meta-analysis).pt. 309498
meta-analysis/ or systematic review/ or systematic reviews as topic/ or meta-analysis as topic/ or “meta analysis (topic)”/ or “systematic review (topic)”/ or exp technology assessment, biomedical/ or network meta-analysis/ 347491
((systematic* adj3 (review* or overview*)) or (methodologic* adj3 (review* or overview*))).ti,ab,kf. 313818
((quantitative adj3 (review* or overview* or synthes*)) or (research adj3 (integrati* or overview*))).ti,ab,kf. 15390
((integrative adj3 (review* or overview*)) or (collaborative adj3 (review* or overview*)) or (pool* adj3 analy*)).ti,ab,kf. 38315
(data synthes* or data extraction* or data abstraction*).ti,ab,kf. 39741
(handsearch* or hand search*).ti,ab,kf. 11067
(mantel haenszel or peto or der simonian or dersimonian or fixed effect* or latin square*).ti,ab,kf. 35193
(met analy* or metanaly* or technology assessment* or HTA or HTAs or technology overview* or technology appraisal*).ti,ab,kf. 12007
(meta regression* or metaregression*).ti,ab,kf. 14284
(meta-analy* or metaanaly* or systematic review* or biomedical technology assessment* or bio-medical technology assessment*).mp,hw. 459513
(medline or cochrane or pubmed or medlars or embase or cinahl).ti,ab,hw. 335574
(cochrane or (health adj2 technology assessment) or evidence report).jw. 21358
(comparative adj3 (efficacy or effectiveness)).ti,ab,kf. 17358
(outcomes research or relative effectiveness).ti,ab,kf. 11151
((indirect or indirect treatment or mixed-treatment or bayesian) adj3 comparison*).ti,ab,kf. 4290
(multi* adj3 treatment adj3 comparison*).ti,ab,kf. 291
(mixed adj3 treatment adj3 (meta-analy* or metaanaly*)).ti,ab,kf. 178
umbrella review*.ti,ab,kf. 1420
(multi* adj2 paramet* adj2 evidence adj2 synthesis).ti,ab,kf. 13
(multiparamet* adj2 evidence adj2 synthesis).ti,ab,kf. 18
(multi-paramet* adj2 evidence adj2 synthesis).ti,ab,kf. 11
or/66-87 672747
65 or 88 3298948
17 and 89 1078
limit 90 to (english language and yr=”2018 -Current”) 528
91 not conference abstract.pt. 528
Embase
OVID Embase 1974 to May 12, 2023
Searched May 12, 2023
(nucala* or mepolizumab* or bosatria* or SB240563 or SB-240563 or 90Z2UFOE52).ti,ab,kw,dq. 2533
*mepolizumab/ 1422
*dupilumab/ 3135
(dupilumab* or dupixent* or regn668 or regn 668 or sar231893 or sar 231893).ti,ab,kw,dq. 4338
*benralizumab/ 863
(Fasenra* or benralizumab* or BIW 8405 or BIW8405 or medi563 or medi 563).ti,ab,kw,dq. 1412
*omalizumab/ 4294
(Xolair* or omalizumab* or rhuMab-E25 or rhuMabE25 or HSDB 5742 or HSDB5742 or 2P471X1Z11 or UNII2P471X1Z11 or hu 901 or hu901).ti,ab. 6698
*tezepelumab/ or (tezepelumab* or Tezspire* or amg-157 or amg157 or medi-9929 or medi9929 or medi-19929 or medi19929 or GTPL-8933 or GTPL8933).ti,ab,kf,dq. 294
or/1-9 13479
exp asthma/ 301745
asthma*.ti,ab,kw,dq. 267302
11 or 12 341205
(severe or eosinophil* or allerg* or type 2 or T2).ti,ab,kw,dq. 2583236
exp Eosinophilia/ 66689
exp Eosinophil count/ 21990
or/14-16 2604229
13 and 17 146121
10 and 18 6866
randomized controlled trial/ 783392
randomization/ 99019
controlled clinical study/ 469226
(meta-anal$ or metaanal$).mp. 449740
((systematic$ adj3 review$) or (systematic adj3 overview$)).mp. 566702
or/20-24 1767760
19 and 25 1137
limit 26 to english language 1124
limit 27 to yr=”2018 -Current” 723
28 not conference abstract.pt. 336
Europe PMC
Searched May 1, 2023
((TITLE:”nucala*” OR TITLE:”mepolizumab*” OR TITLE:”bosatria*” OR TITLE:”Xolair*” OR TITLE:”omalizumab*” OR TITLE:”dupilumab*” OR TITLE:”dupixent*” OR TITLE:”Fasenra*” OR TITLE:”benralizumab*” OR TITLE:”Tezepelumab” OR TITLE:”Tezspire”) AND (TITLE:asthma* AND (TITLE:”severe” OR TITLE:”eosinophil*” OR TITLE:”allerg*” OR TITLE:”type 2” OR TITLE:”T2”))) AND (((SRC:MED) NOT (PUB_TYPE:”Review”))) AND (FIRST_PDATE:[2018 TO 2023])
Cochrane Library
Searched March 24, 2023, Tezepelumab searched April 13, 2023
Cochrane Reviews
(nucala* or mepolizumab* or bosatria* or Xolair* or omalizumab* or dupilumab* or dupixent* or Fasenra* or benralizumab*) AND (asthma* AND (severe or eosinophil* or allerg* or type 2 or T2))
Year: 2018 to 2023
Language: English
(Tezepelumab or Tezspire) AND (asthma* AND (severe or eosinophil* or allerg* or type 2 or T2)
Year: 2018 to 2023
Language: English
Cochrane Central Register of Controlled Trials
Issue 2 of 12, February 2023
Year: 2018 to 2023
Language: English
(nucala* or mepolizumab* or bosatria* or Xolair* or omalizumab* or dupilumab* or dupixent* or Fasenra* or benralizumab*) in Title Abstract Keyword AND asthma* in Title Abstract Keyword AND (severe or eosinophil* or allerg* or type 2 or T2) in Title Abstract Keyword NOT post-hoc or posthoc or post hoc in Title Abstract Keyword - (Word variations have been searched)
(Tezepelumab or Tezspire) in Title Abstract Keyword AND asthma* AND (severe or eosinophil* or allerg* or type 2 or T2) in Title Abstract Keyword NOT post-hoc or posthoc or post hoc in Title Abstract Keyword - with Publication Year from 2018 to 2023, with Cochrane Library publication date Between Jan 2018 and Jan 2023, in Trials (Word variations have been searched)
Appendix 3: Selection of Included Studies
Note that this appendix has not been copy-edited.
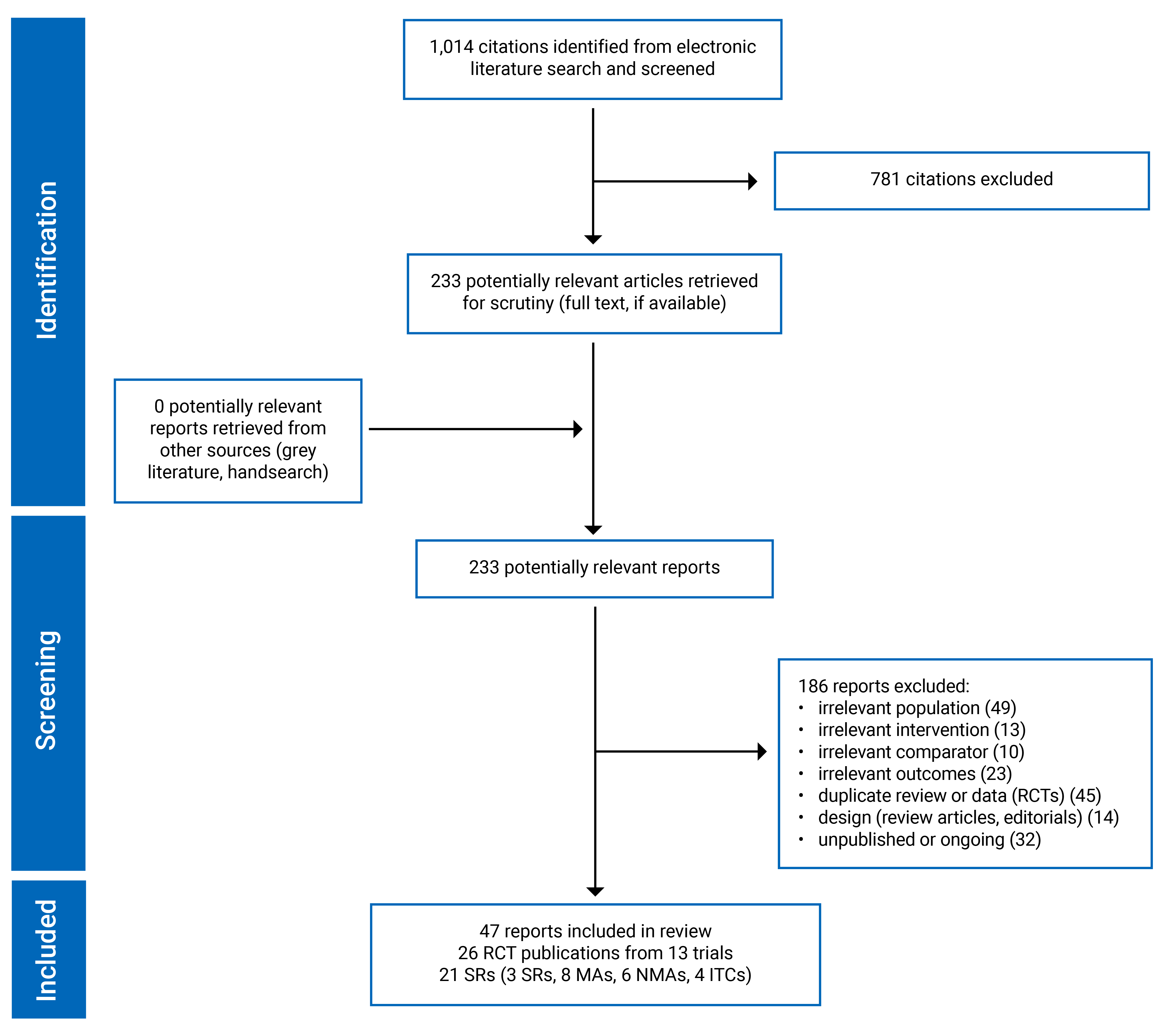
Appendix 4: Included Reports
Note that this appendix has not been copy-edited.
Included RCTs
Albers FC, Licskai C, Chanez P, et al. Baseline blood eosinophil count as a predictor of treatment response to the licensed dose of mepolizumab in severe eosinophilic asthma. Respir Med. 2019;159:105806. PubMed
Bleecker ER, Wechsler ME, FitzGerald JM, et al. Baseline patient factors impact on the clinical efficacy of benralizumab for severe asthma. European Respiratory Journal. 2018;52(4):10. PubMed
Brusselle G, Quirce S, Papi A, et al. Dupilumab efficacy in patients with uncontrolled or oral corticosteroid-dependent allergic and nonallergic asthma. J Allergy Clin Immunol Pract. 2023;11(3):873-884 e811. PubMed
Chipps BE, Newbold P, Hirsch I, Trudo F, Goldman M. Benralizumab efficacy by atopy status and serum immunoglobulin E for patients with severe, uncontrolled asthma. Ann Allergy Asthma Immunol. 2018;120(5):504-511.e504. PubMed
Corren J, Ambrose CS, Griffiths JM, et al. Efficacy of tezepelumab in patients with evidence of severe allergic asthma: Results from the phase 3 NAVIGATOR study. Clin Exp Allergy. 2023;53(4):417-428. PubMed
Corren J, Ambrose CS, Salapa K, et al. Efficacy of tezepelumab in patients with severe, uncontrolled asthma and perennial allergy. J Allergy Clin Immunol Pract. 2021;9(12):4334-4342.e4336. PubMed
Corren J, Chen S, Callan L, Garcia Gil E. The impact of tezepelumab on hospitalization and emergency department visits in patients with severe uncontrolled asthma: results from the pathway phase 2b trial. Am J Resp Crit Care Med. 2019;199(9).
Corren J, Garcia Gil E, Griffiths JM, et al. Tezepelumab improves patient-reported outcomes in patients with severe, uncontrolled asthma in PATHWAY. Ann Allergy Asthma Immunol. 2021;126(2):187-193. PubMed
Corren J, Menzies-Gow A, Chupp G, et al. Efficacy of tezepelumab in severe, uncontrolled asthma: pooled analysis of PATHWAY and NAVIGATOR Studies. Am J Resp Crit Care Med. 2023;04:04.
Corren J, Pham TH, Garcia Gil E, et al. Baseline type 2 biomarker levels and response to tezepelumab in severe asthma. Allergy. 2022;77(6):1786-1796. PubMed
Domingo C, Maspero JF, Castro M, et al. Dupilumab efficacy in steroid-dependent severe asthma by baseline oral corticosteroid dose. J Allergy Clin Immunol Pract. 2022;10(7):1835-1843. PubMed
FitzGerald JM, Bleecker ER, Menzies-Gow A, et al. Predictors of enhanced response with benralizumab for patients with severe asthma: pooled analysis of the SIROCCO and CALIMA studies. Lancet Respir Med. 2018;6(1):51-64. PubMed
Hanania NA, Fortis S, Haselkorn T, et al. Omalizumab in asthma with fixed airway obstruction: post hoc analysis of EXTRA. J Allergy Clin Immunol Pract. 2022;10(1):222-228. PubMed
Harrison TW, Chanez P, Menzella F, et al. Onset of effect and impact on health-related quality of life, exacerbation rate, lung function, and nasal polyposis symptoms for patients with severe eosinophilic asthma treated with benralizumab (ANDHI): a randomised, controlled, phase 3b trial. Lancet Respir Med. 2021;9(3):260-274. PubMed
Humbert M, Albers FC, Bratton DJ, et al. Effect of mepolizumab in severe eosinophilic asthma according to omalizumab eligibility. Respir Med. 2019;154:69-75. PubMed
Jackson DJ, Humbert M, Hirsch I, Newbold P, Garcia Gil E. Ability of serum IgE concentration to predict exacerbation risk and benralizumab efficacy for patients with severe eosinophilic asthma. Adv Ther. 2020;37(2):718-729. PubMed
Lemiere C, Taille C, Lee JK, et al. Impact of baseline clinical asthma characteristics on the response to mepolizumab: a post hoc meta-analysis of two Phase III trials. Respir Res. 2021;22(1):184. PubMed
Li J, Wang C, Liu C, et al. Efficacy predictors of omalizumab in Chinese patients with moderate-to-severe allergic asthma: Findings from a post-hoc analysis of a randomised phase III study. World Allergy Organization Journal. 2020;13(12):100469. PubMed
Menzies-Gow A, Corren J, Bourdin A, et al. Tezepelumab in adults and adolescents with severe, uncontrolled asthma. New Engl J Med. 2021;384(19):1800-1809. PubMed
Menzies-Gow A, Wechsler ME, Brightling CE, et al. Long-term safety and efficacy of tezepelumab in people with severe, uncontrolled asthma (DESTINATION): a randomised, placebo-controlled extension study. Lancet Respir Med. 2023;23:23. PubMed
Mukherjee M, Kjarsgaard M, Radford K, et al. Omalizumab in patients with severe asthma and persistent sputum eosinophilia. Allergy Asthma Clin Immunol. 2019;15:21. PubMed
Panettieri RA, Jr., Welte T, Shenoy KV, et al. Onset of effect, changes in airflow obstruction and lung volume, and health-related quality of life improvements with benralizumab for patients with severe eosinophilic asthma: phase IIIb randomized, controlled trial (SOLANA). J Asthma Allergy. 2020;13:115-126. PubMed
Prazma CM, Idzko M, Douglass JA, et al. Response to mepolizumab treatment in patients with severe eosinophilic asthma and atopic phenotypes. J Asthma Allergy. 2021;14:675-683. PubMed
Rabe KF, Nair P, Brusselle G, et al. Efficacy and safety of dupilumab in glucocorticoid-dependent severe asthma. New Engl J Med. 2018;378(26):2475-2485. PubMed
Wardlaw A, Howarth PH, Israel E, et al. Fungal sensitization and its relationship to mepolizumab response in patients with severe eosinophilic asthma. Clin Exp Allergy. 2020;50(7):869-872. PubMed
Wechsler ME, Menzies-Gow A, Brightling CE, et al. Evaluation of the oral corticosteroid-sparing effect of tezepelumab in adults with oral corticosteroid-dependent asthma (SOURCE): a randomised, placebo-controlled, phase 3 study. Lancet Respir Med. 2022;10(7):650-660. PubMed
Included Systematic Reviews
Agache I, Beltran J, Akdis C, et al. Efficacy and safety of treatment with biologicals (benralizumab, dupilumab, mepolizumab, omalizumab and reslizumab) for severe eosinophilic asthma. A systematic review for the EAACI Guidelines - recommendations on the use of biologicals in severe asthma. Allergy. 2020a;75(5):1023-1042. PubMed
Agache I, Rocha C, Beltran J, et al. Efficacy and safety of treatment with biologicals (benralizumab, dupilumab and omalizumab) for severe allergic asthma: a systematic review for the EAACI Guidelines - recommendations on the use of biologicals in severe asthma. Allergy. 2020b;75(5):1043-1057. PubMed
Agache I, Song Y, Rocha C, et al. Efficacy and safety of treatment with dupilumab for severe asthma: a systematic review of the EAACI guidelines-Recommendations on the use of biologicals in severe asthma. Allergy. 2020c;75(5):1058-1068. PubMed
Akenroye A, Lassiter G, Jackson JW, et al. Comparative efficacy of mepolizumab, benralizumab, and dupilumab in eosinophilic asthma: A Bayesian network meta-analysis. J Allergy Clin Immunol. 2022;150(5):1097-1105.e1012. PubMed
Ando K, Fukuda Y, Tanaka A, Sagara H. comparative efficacy and safety of tezepelumab and other biologics in patients with inadequately controlled asthma according to thresholds of type 2 inflammatory biomarkers: a systematic review and network meta-analysis. Cells. 2022;11(5). PubMed
Bateman ED, Khan AH, Xu Y, et al. Pairwise indirect treatment comparison of dupilumab versus other biologics in patients with uncontrolled persistent asthma. Respir Med. 2022;191:105991. PubMed
Bourdin A, Husereau D, Molinari N, et al. Matching-adjusted comparison of oral corticosteroid reduction in asthma: systematic review of biologics. Clinical & Experimental Allergy. 2020;50(4):442-452. PubMed
Busse W, Chupp G, Nagase H, et al. Anti-IL-5 treatments in patients with severe asthma by blood eosinophil thresholds: Indirect treatment comparison. J Allergy Clin Immunol. 2019;143(1):190-200.e120. PubMed
Chagas GCL, Xavier D, Gomes L, Ferri-Guerra J, Oquet REH. Effects of tezepelumab on quality of life of patients with moderate-to-severe, uncontrolled asthma: systematic review and meta-analysis. Curr Allergy Asthma Rep. 2023;23(6):287-298. PubMed
Chen C, Wen T, Wei L. Different IL-5 monoclonal antibody agents in treating severe asthma patients: a systemic review and network meta-analysis of randomized controlled trials (RCTs). nt J Clin Exp Med. 2019;12(6):6512-6519.
Henriksen DP, Bodtger U, Sidenius K, et al. Efficacy, adverse events, and inter-drug comparison of mepolizumab and reslizumab anti-IL-5 treatments of severe asthma - a systematic review and meta-analysis. Eur Clin Respir J. 2018;5(1):1536097. PubMed
Henriksen DP, Bodtger U, Sidenius K, et al. Efficacy of omalizumab in children, adolescents, and adults with severe allergic asthma: a systematic review, meta-analysis, and call for new trials using current guidelines for assessment of severe asthma. Allergy Asthma Clin Immunol. 2020;16:49. PubMed
Lee J, Song J-U, Kim YH. The clinical efficacy of type 2 inflammation-specific agents targeting interleukins in reducing exacerbations in severe asthma: a meta-analysis. Yonsei Med Jl. 2022;63(6):511-519. PubMed
Mahdavian M, Brothers C, Asghari S, Mallay S, Pike J. Impact of benralizumab on asthma control, asthma-related quality of life and lung function in patients with poorly controlled eosinophilic asthma: A systematic review and meta-analysis. Canadian Journal of Respiratory, Critical Care, and Sleep Medicine. 2019;3(2):106-111.
Mahdavian M, Mallay SA, Asghari S, Voduc N, Pike JC. Effect of benralizumab on asthma exacerbation rates in patients with severe asthma: Systematic review and meta-analysis. Can J Respir Crit Care Sleep Med. 2020;4(2):133-141.
Menzies-Gow A, Steenkamp J, Singh S, et al. Tezepelumab compared with other biologics for the treatment of severe asthma: a systematic review and indirect treatment comparison. J Med Econ. 2022;25(1):679-690. PubMed
Nopsopon T, Lassiter G, Chen ML, et al. Comparative efficacy of tezepelumab to mepolizumab, benralizumab, and dupilumab in eosinophilic asthma: A Bayesian network meta-analysis. J Allergy Clin Immunol. 2023;151(3):747-755. PubMed
Praetorius K, Henriksen DP, Schmid JM, et al. Indirect comparison of efficacy of dupilumab versus mepolizumab and omalizumab for severe type 2 asthma. ERJ Open Res. 2021;7(3). PubMed
Ramonell RP, Iftikhar IH. Effect of anti-IL5, anti-IL5R, anti-IL13 therapy on asthma exacerbations: a network meta-analysis. Lung. 2020;198(1):95-103. PubMed
Shaban Abdelgalil M, Ahmed Elrashedy A, Awad AK, et al. Safety and efficacy of tezepelumab vs. placebo in adult patients with severe uncontrolled asthma: a systematic review and meta-analysis. Sci Rep. 2022;12(1):20905. PubMed
Zoumot Z, Al Busaidi N, Tashkandi W, et al. Tezepelumab for patients with severe uncontrolled asthma: a systematic review and meta-analysis. J Asthma Allergy. 2022;15:1665-1679. PubMed
Appendix 5: Co-Occurrence of Included RCTs
Table 7: Co-Occurrence of Included RCTs in This Review Within the Included Systematic Reviews
Author Year | Included RCTs | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
ANDHI | EXTRA | LIBERY ASTHMA VENTURE | MENSA/ MUSCA | NAVIGATOR | NCT 01202903 | NCT 02049294 | PATHWAY | SIROCCO/ CALIMA | SOLANA | SOURCE | |
Abdelgalil 202261 | NO | NO | NO | NO | YES | NO | NO | YES | NO | NO | NO |
AGACHE 2020a16 | NO | NO | NO | YES | NO | NO | NO | NO | YES | NO | NO |
AGACHE 2020b15 | NO | YES | NO | NO | NO | YES | NO | NO | YES | NO | NO |
AGACHE 2020c44 | NO | NO | YES | NO | NO | NO | NO | NO | NO | NO | NO |
Akenroye 202245 | YES | NO | NO | YES | NO | NO | NO | NO | YES | NO | NO |
Ando 202246 | YES | NO | NO | YES | YES | NO | NO | NO | YES | YES | NO |
Bateman 202247 | NO | YES | NO | YES | NO | NO | NO | NO | YES | NO | NO |
Bourdin 202048 | NO | NO | YES | NO | NO | NO | NO | NO | NO | NO | NO |
Busse 201949 | NO | NO | NO | YES | NO | NO | NO | NO | YES | NO | NO |
Chagas 202350 | NO | NO | NO | NO | YES | NO | NO | YES | NO | NO | YES |
Chen 201951 | NO | NO | NO | YES | NO | NO | NO | NO | YES | NO | NO |
Henriksen 201852 | NO | NO | NO | YES | NO | NO | NO | NO | NO | NO | NO |
Henriksen 202053 | NO | NO | NO | NO | NO | NO | NO | NO | NO | NO | NO |
Lee 202254 | NO | NO | NO | YES | NO | NO | NO | NO | NO | YES | NO |
Mahdavian 201955 | NO | NO | NO | NO | NO | NO | NO | NO | YES | NO | NO |
Mahdavian 202056 | NO | NO | NO | NO | NO | NO | NO | NO | YES | NO | NO |
Menzies-gow 202257 | YES | NO | NO | YES | YES | NO | NO | YES | YES | NO | NO |
Nopsopon 202358 | YES | NO | NO | YES | YES | NO | NO | YES | YES | NO | NO |
Praetorius 202159 | NO | NO | YES | YES | NO | NO | NO | NO | NO | NO | NO |
Ramonell 202060 | NO | NO | YES | YES | NO | NO | NO | NO | YES | NO | NO |
Zoumot 202262 | NO | NO | NO | NO | YES | NO | NO | YES | NO | NO | YES |
Notes: This table has not been copy-edited.
Yes indicates RCT is included in listed review. No indicates RCT is not included in that review.
Appendix 6: Studies Conducted in Moderate to Severe Asthma
Note that this appendix has not been copy-edited.
Systematic Reviews
Ando K, Tanaka A, Sagara H. Comparative efficacy and safety of dupilumab and benralizumab in patients with inadequately controlled asthma: a systematic review. Int J of Mol Sci. 2020;21(3):30. PubMed
Edris A, Lahousse L. Monoclonal antibodies in type 2 asthma: an updated network meta-analysis. Minerva Medica. 2021;112(5):573-581. PubMed
Farne HA, Wilson A, Milan S, Banchoff E, Yang F, Powell CV. Anti-IL-5 therapies for asthma. Cochrane Database Syst Rev. 2022;7:CD010834. PubMed
Fenu G, La Tessa A, Calogero C, Lombardi E. Severe pediatric asthma therapy: omalizumab-a systematic review and meta-analysis of efficacy and safety profile. Front Ped. 2022;10:1033511. PubMed
Fu Z, Xu Y, Cai C. Efficacy and safety of omalizumab in children with moderate-to-severe asthma: a meta-analysis. J Asthma. 2021;58(10):1350-1358. PubMed
Iftikhar IH, Schimmel M, Bender W, Swenson C, Amrol D. Comparative efficacy of anti IL-4, IL-5 and IL-13 drugs for treatment of eosinophilic asthma: a network meta-analysis. Lung. 2018;196(5):517-530. PubMed
Li J, Yang J, Kong L, et al. Efficacy and safety of omalizumab in patients with moderate-to-severe asthma: An analytic comparison of data from randomized controlled trials between Chinese and Caucasians. Asian Pac J Allergy Immunol. 2022;40(3):223-231. PubMed
Liu L, Zhou P, Wang Z, Zhai S, Zhou W. Efficacy and safety of omalizumab for the treatment of severe or poorly controlled allergic diseases in children: a systematic review and meta-analysis. Front Pediatr. 2022;10:851177. PubMed
Liu W, Ma X, Zhou W. Adverse events of benralizumab in moderate to severe eosinophilic asthma: A meta-analysis. Medicine. 2019;98(22):e15868. PubMed
Meng X, Gan J, Liu G, Qin E, Ning H. Efficacy and safety of mepolizumab in patients with severe eosinophilic asthma: A meta-analysis. Int J Clin Exp Med. 2018;11(3):1483-1489.
Pitre T, Jassal T, Angjeli A, et al. A comparison of the effectiveness of biologic therapies for asthma: a systematic review and network meta-analysis. Ann Allergy Asthma Immunol. 2022. PubMed
Tian BP, Zhang GS, Lou J, Zhou HB, Cui W. Efficacy and safety of benralizumab for eosinophilic asthma: a systematic review and meta-analysis of randomized controlled trials. J Asthma. 2018;55(9):956-965. PubMed
Xiong XF, Zhu M, Wu HX, Fan LL, Cheng DY. Efficacy and safety of dupilumab for the treatment of uncontrolled asthma: a meta-analysis of randomized clinical trials. Respiratory Research. 2019;20(1):108. PubMed
Yan K, Balijepalli C, Sharma R, et al. Reslizumab and mepolizumab for moderate-to-severe poorly controlled asthma: an indirect comparison meta-analysis. Immunotherapy. 2019;11(17):1491-1505. PubMed
Zaazouee MS, Alwarraqi AG, Mohammed YA, et al. Dupilumab efficacy and safety in patients with moderate to severe asthma: A systematic review and meta-analysis. Front Pharmacol. 2022;13:992731. PubMed
Randomized Controlled Trials
Bacharier LB, Maspero JF, Katelaris CH, et al. Dupilumab in children with uncontrolled moderate-to-severe asthma. New Engl J Med. 2021;385(24):2230-2240. PubMed
Bansal A, Simpson E, L. Paller ASS, E. C. Blauvelt, A., et al. Conjunctivitis in dupilumab clinical trials for adolescents with atopic dermatitis or asthma. Am J Clin Dermatol. 2021;22(1):101-115. PubMed
Bourdin A, Papi AA, Corren J, et al. Dupilumab is effective in type 2-high asthma patients receiving high-dose inhaled corticosteroids at baseline. Allergy: Eur J Allergy Clin Immunol. 2021;76(1):269-280. PubMed
Busse WW, Humbert M, Haselkorn T, et al. Effect of omalizumab on lung function and eosinophil levels in adolescents with moderate-to-severe allergic asthma. Ann Allergy Asthma Immunol. 2020;124(2):190-196. PubMed
Canonica GW, Bourdin A, Peters AT, et al. Dupilumab demonstrates rapid onset of response across three type 2 inflammatory diseases. J Allergy Clin Immunol Pract. 2022;10(6):1515-1526. PubMed
Castro M, Corren J, Pavord ID, et al. Dupilumab efficacy and safety in moderate-to-severe uncontrolled asthma. N Engl J Med. 2018;378(26):2486-2496. PubMed
Castro M, Rabe KF, Corren J, et al. Dupilumab improves lung function in patients with uncontrolled, moderate-to-severe asthma. Erj Open Research. 2020;6(1). PubMed
Cheng L, Yang T, Ma X, Han Y, Wang Y. Effectiveness and safety studies of omalizumab in children and adolescents with moderate-to-severe asthma. J Pharm Pract. 2021:8971900211038251. PubMed
Corren J, Castro M, Chanez P, et al. Dupilumab improves symptoms, quality of life, and productivity in uncontrolled persistent asthma. Ann Allergy Asthma Immunol. 2019;122(1):41-49.e42. PubMed
Corren J, Castro M, O'Riordan TH, et al. Dupilumab efficacy in patients with uncontrolled, moderate-to-severe allergic asthma. J Allergy Clin Immunol Pract. 2020;8(2):516-526. PubMed
Corren J, Katelaris CH, Castro M, et al. Effect of exacerbation history on clinical response to dupilumab in moderate-to-severe uncontrolled asthma. Eur Resp J. 2021;58(4):10. PubMed
Diver S, Khalfaoui L, Emson C, et al. Effect of tezepelumab on airway inflammatory cells, remodelling, and hyperresponsiveness in patients with moderate-to-severe uncontrolled asthma (CASCADE): a double-blind, randomised, placebo-controlled, phase 2 trial. Lancet Resp Med. 2021;9(11):1299-1312. PubMed
Hanania NA, Castro M, Bateman E, et al. Efficacy of dupilumab in patients with moderate-to-severe asthma and persistent airflow obstruction. Ann Allergy Asthma Immunol. 2023;130(2):206-214.e202. PubMed
Jackson DJ, Bacharier LB, Gergen PJ, et al. Mepolizumab for urban children with exacerbation-prone eosinophilic asthma in the USA (MUPPITS-2): a randomised, double-blind, placebo-controlled, parallel-group trial. Lancet. 2022;400(10351):502-511. PubMed
Rogers L, Holweg CT, Pazwash H et al. Age of asthma onset does not impact the response to omalizumab. Chron Respir Dis. 2023:20(5):14799731231159673. PubMed
Maspero JF, Cardona G, Schonffeldt P, et al. Dupilumab efficacy and safety in Latin American patients with uncontrolled, moderate-to-severe asthma: phase 3 LIBERTY ASTHMA QUEST study. J Asthma. 2022:1-10. PubMed
Maspero JF, Katelaris CH, Busse WW, et al. Dupilumab Efficacy in Uncontrolled, Moderate-to-Severe Asthma with Self-Reported Chronic Rhinosinusitis. J Allergy Clin Immunol Pract. 2020;8(2):527-539.e529. PubMed
Papi A, Corren J, Castro M, et al. Dupilumab reduced impact of severe exacerbations on lung function in patients with moderate-to-severe type 2 asthma. Allergy: Eur J Allergy Clin Immunol. 2023;78(1):233-243. PubMed
Rabe KF, FitzGerald JM, Bateman ED, et al. Dupilumab is effective in patients with moderate-to-severe uncontrolled GINA-defined type 2 asthma irrespective of an allergic asthma phenotype. J Allergy Clin Immunol Pract. 2022;10(11):2916-2924. PubMed
Rhee CK, Park JW, Park HW, Cho YS. Effect of dupilumab in Korean patients with uncontrolled moderate-to-severe asthma: a LIBERTY ASTHMA QUEST Sub-analysis. Allergy Asthma Immunol Res. 2022;14(2):182-195. PubMed
Szefler SJ, Casale TB, Haselkorn T, et al. Treatment benefit with omalizumab in children by indicators of asthma severity. J Allergy Clin Immunol Pract. 2020;8(8):2673-2680.e2673. PubMed
Wechsler ME, Ruddy MK, Pavord ID, et al. Efficacy and safety of itepekimab in patients with moderate-to-severe asthma. New Engl J Med. 2021;385(18):1656-1668. PubMed
Appendix 7: List of Major Trials for Biologics and Trials
Note that this appendix has not been copy-edited.
Table 8: List of Major Trials for Biologics and Trials Included in the Systematic Reviews, Including Out-of-Scope Trials, and Their Broad Inclusion Criteria
Biologic | Trial name | Age | Asthma typology | Extension study | |
|---|---|---|---|---|---|
Severity | Typea | ||||
Benralizumab | ANDHIb, c | Adults | Severe | Eosinophilic | No |
Benralizumab | BORA | Adults and children | Severe | Eosinophilic | Yes |
Benralizumab | CALIMAb, c | Adults and children | Severe | None | No |
Benralizumab | SIROCCOb, c | Adults and children | Severe | None | No |
Benralizumab | SOLANAb | Adults | Severe | Eosinophilic | No |
Benralizumab | ZONDAc | Adults | Severe | Eosinophilic | No |
Dupilumab | DRI12544c | Adults | Moderate to severe | None | No |
Dupilumab | LIBERTY ASTHMA QUESTc | Adults and children | Uncontrolled persistent | None | No |
Dupilumab | LIBERTY ASTHMA VENTUREb, c | Adults and children | Severe | OCS dependent | No |
Dupilumab | Phase IIbc | Adults | Uncontrolled persistent | None | No |
Dupilumab | TRAVERSE | Adults and children | Moderate to severe | None | Yes |
Dupilumab | VOYAGE | Children | Moderate to severe | None | No |
Mepolizumab | DREAMc | Adults and children | Severe | Eosinophilic | No |
Mepolizumab | Haldar 2009c | Adults | Refractory | Eosinophilic | No |
Mepolizumab | MENSAb, c | Adults | Severe | Eosinophilic | No |
Mepolizumab | MUSCAb, c | Adults and children | Severe | Eosinophilic | No |
Mepolizumab | NCT01691508c | Adults and Children | Severe | Eosinophilic | No |
Mepolizumab | NCT02281318c | Adults and Children | Severe | Eosinophilic | No |
Mepolizumab | SIRIUSc | Adults | Severe | Eosinophilic | No |
Omalizumab | 008, 009 and 011c | Adults and children | Moderate to severe | Allergic | No |
Omalizumab | AEROc | Adults | Moderate | Allergic | No |
Omalizumab | ALTO | Adults and children | Moderate to severe | Allergic | No |
Omalizumab | Ayres 2009 c | Adults and children | Moderate to severe | Allergic | No |
Omalizumab | Bardelas 2012c | Adults and children | Inadequately controlled asthma | Allergic | No |
Omalizumab | Bousquet 2011c | Adults and children | Severe | Allergic | No |
Omalizumab | Buhl 2001c | Adults and children | Moderate to severe | Allergic | No |
Omalizumab | Busse 2001c | Adults and children | Severe | Allergic | No |
Omalizumab | EXTRAb, c | Adults | Severe | Allergic | No |
Omalizumab | Hoshino 2012c | Adults | Severe | Allergic | No |
Omalizumab | ICATAc | Children | Persistent | Allergic | No |
Omalizumab | INNOVATEc | Adults and children | Moderate to severe | Allergic | No |
Omalizumab | Holgate 2004c | Adults and children | Severe | Allergic | No |
Omalizumab | Lanier 2009c | Children | Moderate to severe | Allergic | No |
Omalizumab | Massanair 2009c | Adults and children | Moderate to severe | Allergic | No |
Omalizumab | NCT00079937c | Children | Moderate to severe | Allergic | No |
Omalizumab | NCT00264849c | Adults and children | Severe | Allergic | No |
Omalizumab | NCT00454051c | Adult | Severe | Allergic | No |
Omalizumab | NCT01202903b, c | Adult | Moderate to severe/severe | Allergic | No |
Omalizumab | NCT02049294b | Adult | Severe | Allergic | No |
Omalizumab | PROSEc | Children | Moderate to severe | Allergic | No |
Omalizumab | QUALITXc | Adults and children | Severe | Allergic | No |
Omalizumab | Soler 2001c | Adults and children | Moderate to severe | Allergic | No |
Omalizumab | Vignola 2004c | Adults and children | Moderate to severe | Allergic | No |
Tezepelumab | CASCADE | Adults | Moderate to severe | None | No |
Tezepelumab | DESTINATION | Adults and children | Severe | None | Yes |
Tezepelumab | NAVIGATORb, c | Adults and children | Severe | None | No |
Tezepelumab | PATHWAYb, c | Adults | Severe | None | No |
Tezepelumab | SOURCEb, c | Adults | Severe | OCS dependent | No |
OCS = oral corticosteroids.
aAsthma type is the target study population of the trial. “None” indicates that a specific subtype of asthma was not specifically recruited.
bTrial included in randomized controlled trial portion of this report.
cTrial included in 1 or more systematic reviews included in this report.
Appendix 8: Supplementary Tables and Figures
Note that this appendix has not been copy-edited.
Table 9: Inclusion Criteria of the Included RCTs
Intervention | Trial | Asthma enrolment criteria/subtypea | Inclusion criteria |
|---|---|---|---|
Benralizumab | ANDHI31 NCT03170271 | Eosinophilic | A history of physician-diagnosed asthma requiring treatment with medium-to-high dose Inhaled Corticosteroids (ICS) plus asthma controller, for at least 12 months before visit 1. Documented current treatment with high daily doses of ICS plus at least 1 other asthma controller for at least 3 months before visit 1. History of at least 2 asthma exacerbations while on ICS plus another asthma controller that required treatment with systemic corticosteroids (IM, IV, or oral) in the 12 months before visit 1. ACQ6 score ≥ 1.5 at visit 1. Screening pre-bronchodilator (pre-BD) FEV1 of < 80% predicted at visit 2. Excessive variability in lung function by satisfying ≥ 1 of the following criteria: Airway reversibility (FEV1 ≥ 12%) using a short-acting bronchodilator demonstrated at visit 2 or visit 3. Airway reversibility to short-acting bronchodilator (FEV1 ≥ 12%) documented during the 12 months before enrolment visit 1. Daily diurnal peak flow variability of > 10% when averaged more than 7 continuous days during the study run-in period An increase in FEV1 of ≥ 12% and 200 mL after a therapeutic trial of systemic corticosteroid (e.g., OCS), given outside of an asthma exacerbation, documented in the 12 months prior enrolment visit 1. Airway hyperresponsiveness (methacholine: PC20 of < 8 mg/mL, histamine: PD20 of < 7.8 μmol, mannitol: decrease in FEV1 as per the labelled product instructions) documented in the 24 months before randomization visit 4. Peripheral blood eosinophil count either: 300 cells/μL assessed by central laboratory at either visit 1 or visit 2 OR ≥ 150 to < 300 cells/μL assessed by central laboratory at either visit 1 or visit 2, IF ≥ 1 of the following 5 clinical criteria is met: Using maintenance OCS (daily or every other day OCS requirement to maintain asthma control; maximum total daily dose 20 mg prednisone or equivalent) at screening History of nasal polyposis Age of asthma onset ≥ 18 years Three or more documented exacerbations requiring systemic corticosteroid treatment during the 12 months before screening Pre-bronchodilator forced vital capacity < 65% of predicted, as assessed at visit 2 (note that screening pre-BD FEV Inclusion Criterion #6 must still be satisfied) |
Benralizumab | NCT01928771/ NCT01914757 | Severe asthma NOS | Provision of informed consent before any study specific procedures Female and male aged 12 to 75 years, inclusively, at the time of visit 1 History of physician-diagnosed asthma requiring treatment with medium-to-high dose ICS (> 250mcg fluticasone dry powder formulation equivalents total daily dose) and a LABA, for at least 12 months before visit 1. Documented treatment with ICS and LABA for at least 3 months Patients with baseline blood eosinophil counts < 300 cells/ μL and ≥ 300 cells/ μL were recruited at a ratio of approximately 2:1, respectively. |
Benralizumab | SOLANA39 NCT02869438 | Eosinophilic | Documented current treatment with ICS and LABA for at least 30 days before visit 1. The ICS and LABA can be parts of a combination product or given by separate inhalers. The ICS dose must be greater than or equal to 500 mcg/day fluticasone propionate dry powder formulation or equivalent daily. Additional asthma controller medications, e.g., oral corticosteroids, long-acting antimuscarinics (LAMAs), LTRAs, theophylline. are allowed if they have been used for at least 30 days before visit 1. History of at least 2 asthma exacerbations that required treatment with systemic corticosteroids (intramuscular, IV, or oral) in the 12 months before visit 1. For patients receiving corticosteroids as a maintenance therapy, the corticosteroid treatment for the exacerbation is defined as a temporary increase of their maintenance dose. Pre-bronchodilator (pre-BD) FEV1 of < 80% predicted at visit 2 or visit 3 ACQ-6 score ≥ 1.5 at visit 1 Evidence of asthma as documented by airway reversibility (FEV1 ≥ 12% and 200 mL) demonstrated at visit 1, visit 2, or visit 3. For patients entering the body plethysmography substudy, reversibility must be demonstrated at visit 1 or at visit 2 only. Peripheral blood eosinophil count of ≥ 300 cells/μL assessed by central lab at visit 1. Weight of ≥ 40 kg |
Dupilumab | LIBERTY ASTHMA VENTURE22,29,41 NCT02528213 | Severe Asthma NOS | Participants with severe asthma and a well-documented, regular prescribed treatment of maintenance corticosteroids in the 6 months before visit 1 and using a stable OCS dose (i.e., no change of OCS dose) for 4 weeks before visit 1. Participants must be taking 5 to 35 mg/day of prednisone/prednisolone, or the equivalent, at visit 1 and at the randomization visit. In addition, the participants must agree to switch to study-required prednisone/prednisolone as their OCS and use it per protocol for the duration of the study. Existing treatment with high-dose inhaled corticosteroid (ICS; > 500 mcg total daily dose of fluticasone propionate or equivalent) in combination with a second controller (i.e., long-acting beta agonist [LABA], leukotriene receptor antagonist [LTRA]) for at least 3 months with a stable dose of ICS for > = 1 month before visit 1. In addition, participants requiring a third controller for their asthma are considered eligible for this study, and it should also be used for at least 3 months with a stable dose > = 1 month before visit 1. A forced expiratory volume in 1 second (FEV1) < 80% of predicted normal for adults and < = 90% of predicted normal for adolescents at visit 1. Evidence of asthma as documented by either: reversibility of at least 12% and 200 mL in FEV1 after the administration of 200 to 400 mcg (2 to 4 inhalations of albuterol/salbutamol or levalbuterol/levosalbutamol, or of a nebulized solution of albuterol/salbutamol or levalbuterol/levosalbutamol, if considered as a standard office practice) before randomization or documented in the 12 months before visit 1 OR airway hyperresponsiveness (methacholine: provocative concentration that causes a positive reaction [PC20] of < 8 mg/mL) documented in the 12 months before visit 1. Weight > = 30.0 kg |
Mepolizumab | NCT02281318/ NCT01691521 | Eosinophilic | At least 12 years of age at visit 1 and a minimum weight of 45 kg (kg) A well-documented requirement for regular treatment with high-dose inhaled corticosteroid (ICS) in the 12 months before visit 1 with or without maintenance oral corticosteroids Current treatment with an additional controller medication, besides ICS, for at least 3 months or a documented failure in the past 12 months of an additional controller medication for at least 3 successive months Prior documentation of eosinophilic asthma or high likelihood of eosinophilic asthma At visit 1, a pre-bronchodilator FEV1 < 80% (for participants > = 18 years of age), a pre-bronchodilator FEV1 < 90% or FEV1: FVC ratio < 0.8 (for participants 12 to 17 years of age). Previously confirmed history of 2 or more exacerbations requiring treatment with systemic CS |
Omalizumab | EXTRA30 NCT00314574 | Allergic | Have had a history of moderate to severe asthma for at least one year before screening. Have had treatment with a stable regimen of salmeterol 50 mcg twice a day (BID) or formoterol 12 mcg BID for at least 8 weeks before screening Have had treatment with a stable regimen of high-dose inhaled corticosteroids (ICS) for at least 8 weeks before screening Have inadequately controlled asthma Have had at least one asthma exacerbation requiring systemic corticosteroid rescue in the 12 months before the screening visit while receiving treatment with high-dose ICS Have a positive skin test for or a positive, in vitro response to one relevant perennial aeroallergen documented within the 12 months before screening If a patient has not had a positive skin test or in vitro reactivity in the 12 months before screening, the patient must demonstrate a positive response to at least one relevant perennial aeroallergen in a skin or in vitro test before randomization |
Omalizumab | NCT0120290335 | Allergic | Patients who met the following criteria at the time of screening (visit 1) and visit 2 were eligible for inclusion in this study:
|
Omalizumab | NCT0204929438 | Allergic | Patients with confirmed asthma (12% bronchodilator reversibility or PC20 methacholine less than 8 mg/mL), atopy (skin prick test positive to common aeroallergens and elevated serum immunoglobulin E levels), who were symptomatic (ACQ-5 ≥ 1.5) with evidence of sputum eosinophils (> 3%) despite high-dose maintenance corticosteroid therapy. |
Tezepelumab | NCT03347279 | Severe asthma NOS | Age 12 to 80 Documented physician-diagnosed asthma for at least 12 months Participants who have received a physician-prescribed asthma controller medication with medium- or high-dose ICS for at least 12 months. Documented treatment with a total daily dose of either medium or high dose ICS (≥ 500 mcg fluticasone propionate dry powder formulation equivalent total daily dose) for at least 3 months. At least one additional maintenance asthma controller medication is required according to standard practice of care and must be documented for at least 3 months. Morning pre-BD FEV1 < 80% predicted normal (< 90% for participants 12 to 17 yrs.) Evidence of asthma as documented by either: Documented historical reversibility of FEV1 ≥ 12% and ≥ 200 mL in the previous 12 months OR Post-BD (albuterol/salbutamol) reversibility of FEV1 ≥ 12% and ≥ 200 mL during screening. Documented history of at least 2 asthma exacerbation events within 12 months. ACQ-6 score ≥ 1.5 at screening and on day of randomization |
Tezepelumab | NCT02054130 | Severe Asthma NOS | Body mass index between 18 and 40 kg/m2 and weight greater than or equal 40 kg Documented physician-diagnosed asthma – Participants must have received a physician-prescribed asthma controller regimen with medium- or high-dose inhaled corticosteroids (ICS) plus long-acting Beta2 agonist (LABA). If on asthma controller medications in addition to ICS plus LABA, the dose of the other asthma controller medications (leukotriene receptor inhibitors, theophylline, secondary ICS, long-acting antimuscarinics (LAMA), cromones, or maintenance oral prednisone or equivalent up to a maximum of 10 mg daily or 20 mg every other day for the maintenance treatment of asthma) must be stable. Participants must have a documented history of at least 2 asthma exacerbation events OR at least 1 severe asthma exacerbation resulting in hospitalization within the 12 months before first study visit. |
Tezepelumab | NCT03406078 | Severe Asthma NOS | Participants were aged 18 to 80 years with physician-diagnosed asthma, who had been receiving medium-dose inhaled corticosteroids (daily dose of 250 to 500 mcg fluticasone propionate or equivalent) or high-dose inhaled corticosteroids (daily dose of > 500 mcg fluticasone propionate or equivalent) for at least 12 months before screening. Participants who were receiving medium-dose inhaled corticosteroids must have had their dose increased to a high dose for at least 3 months before screening. Participants must have been receiving a long-acting beta 2 agonist with or without additional controller medications for at least 3 months before screening. Participants must have been receiving oral corticosteroids for the treatment of asthma for at least 6 months before screening and must have been taking a stable dose of prednisone or prednisolone 7·5 to 30 mg daily or daily equivalent for at least 1 month before screening. Participants must also have had at least 1 asthma exacerbation (defined as a worsening of asthma symptoms that led to either hospitalization, an emergency department visit that resulted in the use of systemic corticosteroids for ≥ 3 consecutive days, or requirement for systemic corticosteroids for ≥ 3 consecutive days) in the 12 months before screening. Morning pre-bronchodilator FEV1 must have been less than 80% of the predicted normal value at visit 1 (week – 10) or visit 2 (week – 8). Post-bronchodilator FEV1 reversibility of at least 12% and at least 200 mL must have been documented during the 12 months before screening or visit 1 or visit 2. |
ACQ = Asthma Control Questionnaire; BD = bronchodilator; BID = medication taken twice a day; FEV1 = forced expiratory volume in 1 second; FVC = forced vital capacity; GINA = Global Initiative for Asthma; ICS = inhaled corticosteroids; IU = international unit; LABA = long-acting beta agonist; LAMA = long-acting antimuscarinics; LTRA = Leukotriene receptor agonist; OCS = oral corticosteroid; PEF = peak expiratory flow.
aPopulation determined by whether trial required participants to have biomarkers for allergic asthma (allergic), eosinophilic asthma (eosinophilic), or were admitted solely based on having severe asthma (severe asthma).
Table 10: RCT Intervention Characteristics by Biologic, RCT, Enrolled Asthma Subtype, and Patient Subgroup
Intervention | RCT | Asthma subtype enrolled | Patient subgroup | Dosage | Treatment duration |
|---|---|---|---|---|---|
Benralizumab | ANDHI31 NCT03170271 | Eosinophilica | Adults | 30 mg Q4W | 24 weeks |
Benralizumab | NCT01928771/ NCT01914757 | Severe Asthma NOSb | Adults and Children | 30 mg Q4W or Q8W | 48 to 56 weeks |
Benralizumab | SOLANA39 NCT02869438 | Eosinophilica | Adults | 30 mg Q4W | 12 weeks |
Dupilumab | LIBERTY ASTHMA VENTURE22,29,41 NCT02528213 | Severe Asthma NOSb | Adults and Children | 300 mg SC Q2W | 24 weeks |
Mepolizumab | NCT02281318/ NCT01691521 | Eosinophilica | Adults and Children | 100 mg SC Q4W | 24 to 32 weeks |
Omalizumab | EXTRA30 NCT00314574 | Allergicc | Adults and Children | 0.008 mg/kg/IgE Q2W or 0.016 mg/kg/IgE Q4W | 48 weeks |
Omalizumab | NCT0120290335 | Allergicc | Adults | 0.008 mg/kg/IgE Q2W or 0.016 mg/kg/IgE Q4W | 24 weeks |
Omalizumab | NCT0204929438 | Allergicc | Adults | 0.008 mg/kg/IgE Q2W or 0.016 mg/kg/IgE Q4W | 32 weeks |
Tezepelumab | NCT03347279 | Severe Asthma NOSb | Adults and Children | 210 mg SC Q4W | 52 weeks |
Tezepelumab | NCT02054130 | Severe Asthma NOSb | Adults | 70/210 mg SC Q4W or 280 mg SC Q2W | 50 weeks |
Tezepelumab | NCT03406078 | Severe Asthma NOSb | Adults | 210 mg SC Q4W | 48 weeks |
IgE = immunoglobulin E; NOS = not otherwise specified; Q2W = every 2 weeks; Q4W = every 4 weeks; Q8W = every 8 weeks; SC = subcutaneous.
aEosinophilic asthma studies recruited patients based on a minimum eosinophil biomarker level, but may also include patients with concurrent allergic asthma.
bSevere asthma NOS patients recruited based on the severity of asthma without additional requirements for biomarkers of allergic or eosinophilic asthma.
cAllergic asthma studies included patients with a minimum classification of allergic asthma determined by allergic biomarkers, but may also include other subtypes that are not mutually exclusive.
Table 11: Concomitant Medications in RCTs Described in Clinical Trials Registry and/or Publications
Intervention | RCT | Concomitant medications |
|---|---|---|
Benralizumab | ANDHI31 NCT03170271 | ICS plus 1 other controller medication |
Benralizumab | NCT01928771/NCT01914757 | ICS, LABA, with or without OCS and additional controllers |
Benralizumab | SOLANA39 NCT02869438 | ICS and LABA Other asthma controller medications are allowed if they have been used for at least 30 days at time of trial start |
Dupilumab | LIBERTY ASTHMA VENTURE22,29,41 NCT02528213 | OCS, ICS, plus second controller |
Mepolizumab | NCT02281318, NCT01691521 | ICS plus an additional controller, OCS allowed |
Omalizumab | EXTRA30 NCT00314574 | ICS, LABA, permitted to use albuterol as rescue medicine |
Omalizumab | NCT0120290335 | no co-medications were discussed |
Omalizumab | NCT0204929438 | ICS/OCS |
Tezepelumab | NCT03347279 | Participants continued to receive their prescribed controller medications throughout the study. Step-down of oral corticosteroid or inhaled corticosteroids could be done at the discretion of the study physician using the GINA protocol guidance for changes to background asthma medication |
Tezepelumab | NCT02054130 | ICS, LABA, other controller medications allowed if dosage is stable |
Tezepelumab | NCT03406078 | oral corticosteroid Medium- to high-dose ICS LABA, LAMA with or without additional control medications |
GINA = Global Initiative for Asthma; ICS = inhaled corticosteroids; LABA = long-acting beta agonist; LAMA = long-acting antimuscarinics; OCS = oral corticosteroid.
Table 12: RCT-Specific Asthma Exacerbation Definitions From Clinical Trial Registry and/or Publication
Intervention | RCT | Asthma exacerbation definition |
|---|---|---|
Benralizumab | ANDHI31 | An asthma exacerbation was defined as a worsening of asthma that led to any of the following:
|
Benralizumab | An exacerbation was defined as a worsening of asthma that led to 1 of the following: use of systemic corticosteroids (or temporary increase in a stable oral corticosteroid background dosage) for at least 3 days or a single depot-injectable dose of corticosteroid; an asthma-related emergency department or urgent care visit (duration < 24 hour) that required use of systemic corticosteroids; or an asthma-related inpatient hospital admission (duration ≥ 24 hours). | |
Benralizumab | SOLANA39 | Requiring systemic corticosteroid therapy or a temporary increase in maintenance oral corticosteroid dosage within 12 months before enrolment. |
Dupilumab | A severe asthma exacerbation event was defined as a deterioration of asthma during the 24-week treatment period requiring: use of systemic corticosteroids for ≥ 3 days (at least double the dose currently used); and/or hospitalization related to asthma symptoms or emergency room visit because of asthma requiring intervention with a systemic corticosteroid treatment. Annualized event rate was the total number of exacerbations that occurred during the treatment period divided by the total number of participant-years treated. | |
Mepolizumab | Clinically significant exacerbations of asthma are defined as worsening of asthma which required use of systemic corticosteroids (IV or oral steroid like prednisone, for at least 3 days or a single intramuscular corticosteroid dose is required. For maintenance of systemic corticosteroids, at least double the existing maintenance dose for at least 3 days was required) and/or hospitalization and/or emergency department visits. | |
Omalizumab | EXTRA30 | A protocol-defined asthma exacerbation was defined as worsening of asthma symptoms requiring treatment with systemic corticosteroids for 3 or more days; for patients receiving long-term oral corticosteroids, an exacerbation was a 20 mg or more increase in average daily dose of oral prednisone (or a similar dose of another systemic corticosteroid). The rate of protocol-defined asthma exacerbations, normalized by subject-time at risk and computed over the 48-week treatment period in each treatment group. |
Omalizumab | NCT0120290335 | Not specified |
Omalizumab | NCT0204929438 | Not specified |
Tezepelumab | Defined for trial eligibility and end point measures as a worsening of asthma symptoms that led to hospitalization, an emergency department visit that resulted in the use of systemic glucocorticoids for ≥ 3 consecutive days, or the use of systemic glucocorticoids for ≥ 3 consecutive days | |
Tezepelumab | Asthma exacerbation is defined as worsening of asthma that leads to any of the following: use of systemic corticosteroids for at least 3 days, an emergency department visit due to asthma that required systemic corticosteroids, and an inpatient hospitalization due to asthma. The annual annualized exacerbation rate was presented as the total number of exacerbations for the treatment group divided by the total duration of person follow-up. | |
Tezepelumab | Worsening of asthma symptoms that led to either hospitalization, an emergency department visit that resulted in the use of systemic corticosteroids for ≥ 3 consecutive days, or requirement for systemic corticosteroids for ≥ 3 consecutive days |
RCT | Asthma subtype enrolled | Patient subgroup | AEX | FEV1 | HRQoL | Safety | Hospitalization | Mortality |
|---|---|---|---|---|---|---|---|---|
Intervention | ||||||||
Benralizumab | ||||||||
ANDHI31 | Eosinophilic | Adult | ++ | ++ | ACQ ++ | + | NR | NR |
Severe Asthma NOS | Adult and Children | ++ | ++ | ACQ ++, AQLQ ++ | NR | NR | NR | |
SOLANA39 | Eosinophilic | Adult | NR | + | ACQ ++ | + | NR | NR |
Dupilumab | ||||||||
Severe Asthma NOS | Adult and Children | ++ | ++ | ACQ ++ | - | NR | NR | |
Mepolizumab | ||||||||
Eosinophilic | Adult and Children | ++ | ++ | ACQ ++ | NR | NR | NR | |
Omalizumab | ||||||||
EXTRA30 | Allergic | Adult and Children | ++ | ++ | NR | NR | NR | NR |
NCT0120290335 | Allergic | Adult | NR | ++ | ACQ +, AQLQ ++ | NR | NR | NR |
NCT0204929438 | Allergic | Adult | + | + | ACQ + | NR | NR | NR |
Tezepelumab | ||||||||
Severe Asthma NOS | Adult and Children | ++ | ++ | ACQ ++, AQLQ ++ | + | ++ | NR | |
Severe Asthma NOS | Adult | ++ | ++ | ACQ ++, AQLQ ++ | NR | ++ | NR | |
Severe Asthma NOS | Adult | + | ++ | ACQ-6 ++, AQLQ ++ | + | NR | NR | |
ACQ = Asthma Control Questionnaire; ACT = Asthma Control Test; AEX = asthma exacerbation; AQLQ = Asthma Quality of Life Questionnaire; FEV1 = forced expiratory volume in 1 second; HRQoL = Health-related quality of life; NOS = not otherwise specified; NR = not reported.
Note: Asthma enrolment criteria indicates whether a specific type of asthma patients was sampled. + indicates effect favouring treatment, - indicates effect favouring control, = indicates exact equality of outcome, and an additional + or - indicates whether this effect was statistically significant. All RCTs compared biologics as an add-on to standard of care against standard of care plus a placebo.
Table 14: Outcomes Reported for Each Asthma Subgroup
Intervention | RCT | Patient subgroup | Non–Type 2 | Type 2 | ||||
|---|---|---|---|---|---|---|---|---|
EOS/ non-ALL | Non-EOS/ ALL | EOS/ ALL | Eosinophilic NOS | Allergic NOS | ||||
Benralizumab | ANDHI31 | Adults | No | No | No | No | Yes | No |
Benralizumab | Adults and Children | Yes | Yes | Yes | Yes | Yes | Yes | |
Benralizumab | SOLANA39 | Adults | No | Yes | No | Yes | Yes | No |
Dupilumab | Adults and Children | No | No | No | No | Yes | Yes | |
Mepolizumab | Adults and Children | No | Yes | No | Yes | Yes | No | |
Omalizumab | EXTRA30 | Adults and Children | No | No | No | No | No | Yes |
Omalizumab | NCT0120290335 | Adults | No | No | Yes | Yes | No | Yes |
Omalizumab | NCT0204929438 | Adults | No | No | No | No | No | Yes |
Tezepelumab | Adults and Children | Yes | Yes | Yes | Yes | Yes | Yes | |
Tezepelumab | Adults | No | No | No | No | Yes | Yes | |
Tezepelumab | Adults | No | No | No | No | Yes | No | |
ALL = allergic; EOS = eosinophilic; NOS = not otherwise specified.
Note: YES indicates at least 1 outcome reported for that subgroup. NO indicates that no outcomes were reported for that subgroup.
Table 15: Included Systematic Review Summary Table
Author year | Design | PICO populationa | Population | Intervention | # of results | # primary trials | # Patients |
|---|---|---|---|---|---|---|---|
Abdelgalil 202261 | MA | Severe asthmab | Adults | Tezepelumab | 1 | 4 | 1,600 |
Agache, 2020a16 | SR | Severe asthmab | Adults and Children | Benralizumab | 1 | 3 | 2,731 |
Agache, 2020a16 | SR | Severe asthmab | Adults and Children | Dupilumab | 1 | 3 | 2,888 |
Agache, 2020a16 | SR | Severe asthmab | Adults and Children | Mepolizumab | 1 | 3 | 1,262 |
Agache, 2020a16 | SR | Severe asthmab | Adults and Children | Omalizumab | 1 | 5 | 2,127 |
Agache, 2020b15 | SR | Allergic | Adults and Children | Benralizumab | 1 | 3 | 3,208 |
Agache, 2020b15 | SR | Allergic | Adults and Children | Dupilumab | 1 | 1 | 1,083 |
Agache, 2020b15 | SR | Allergic | Adults and Children | Omalizumab | 1 | NR | NR |
Agache, 2020b15 | SR | Allergic | Children | Omalizumab | 1 | NR | NR |
Agache, 2020c44 | SR | Severe asthmab | Adults and Children | Dupilumab | 6 | 3 | 2,888 |
Akenroye 202245 | NMA | Eosinophilic | Adults and Children | B, D, M | 3 | 8 | 7,592 |
Akenroye 202245 | NMA | Eosinophilic | Adults and Children | Benralizumab | 3 | 3 | 3,166 |
Akenroye 202245 | NMA | Eosinophilic | Adults and Children | Dupilumab | 3 | 2 | 2,678 |
Akenroye 202245 | NMA | Eosinophilic | Adults and Children | Mepolizumab | 3 | 3 | 1,748 |
Ando 202246 | NMA | Severe asthmab | Adults and Children | B, D, M, T | 5 | 8 | 4,671 |
Ando 202246 | NMA | Severe asthmab | Adults and Children | Benralizumab | 5 | 4 | 2,574 |
Ando 202246 | NMA | Severe asthmab | Adults and Children | D, T | 4 | 2 | 1,161 |
Ando 202246 | NMA | Severe asthmab | Adults and Children | Dupilumab | 9 | 1 | 633 |
Ando 202246 | NMA | Severe asthmab | Adults and Children | Mepolizumab | 5 | 2 | 936 |
Ando 202246 | NMA | Severe asthmab | Adults and Children | Tezepelumab | 9 | 1 | 528 |
Bateman 202247 | ITC | Severe asthmab | Adults and Children | B, D, M, O | 1 | 12 | 7,550 |
Bateman 202247 | ITC | Severe asthmab | Adults and Children | Benralizumab | 1 | 3 | 2,173 |
Bateman 202247 | ITC | Severe asthmab | Adults and Children | Dupilumab | 1 | 2 | 2,367 |
Bateman 202247 | ITC | Severe asthmab | Adults and Children | Mepolizumab | 1 | 3 | 1,435 |
Bateman 202247 | ITC | Severe asthmab | Adults and Children | Omalizumab | 1 | 4 | 1,575 |
Bourdin 202048 | MAIC | Severe asthmab | Adults and Children | B, D, M | 1 | 3 | 565 |
Bourdin 202048 | MAIC | Severe asthmab | Adults and Children | Benralizumab | 1 | 1 | 220 |
Bourdin 202048 | MAIC | Severe asthmab | Adults and Children | Dupilumab | 1 | 1 | 210 |
Bourdin 202048 | MAIC | Severe asthmab | Adults and Children | Mepolizumab | 1 | 1 | 135 |
Busse 201949 | ITC | Eosinophilic | Adults and Children | B, M | 4 | 4 | 2473 |
Busse 201949 | ITC | Eosinophilic | Adults and Children | Benralizumab | 3 | 2 | 1,537 |
Busse 201949 | ITC | Eosinophilic | Adults and Children | Mepolizumab | 3 | 2 | 936 |
Chagas 202350 | MA | Severe asthmab | Adults and Children | Tezepelumab | 1 | 3 | 1,484 |
Chen 201951 | NMA | Severe asthmab | Adults and Children | B, M | 1 | 8 | 4,049 |
Chen 201951 | NMA | Severe asthmab | Adults and Children | Benralizumab | 1 | 3 | 2,515 |
Chen 201951 | NMA | Severe asthmab | Adults and Children | Mepolizumab | 1 | 5 | 1,534 |
Henriksen 201852 | MA | Eosinophilic | Adults | Mepolizumab | 1 | 8 | 1,244 |
Henriksen 202053 | MA | Allergic | Adults and Children | Omalizumab | 2 | 16 | 3,729 |
Lee 202254 | MA | Severe asthmab | Adults and Children | Benralizumab | 3 | 3 | 1,687 |
Lee 202254 | MA | Severe asthmab | Adults and Children | Dupilumab | 3 | 3 | 2,735 |
Lee 202254 | MA | Severe asthmab | Adults and Children | Mepolizumab | 1 | 5 | 1,822 |
Mahdavian 201955 | MA | Eosinophilic | Adults and Children | Benralizumab | 1 | 4 | 3,081 |
Mahdavian 202056 | MA | Severe asthmab | Adults and Children | Benralizumab | 3 | 3 | 2,730 |
Menzies-Gow 202257 | NMA | Severe asthmab | Adults and Children | B, D, M, O, T | 1 | 16 | NR |
Menzies-Gow 202257 | NMA | Severe asthmab | Adults and Children | B, D, O | 1 | 27 | NR |
Menzies-Gow 202257 | NMA | Severe asthmab | Adults and Children | Benralizumab | 4 | 6 | 6,405 |
Menzies-Gow 202257 | NMA | Severe asthmab | Adults and Children | D, T | 2 | 6 | NR |
Menzies-Gow 202257 | NMA | Severe asthmab | Adults and Children | Dupilumab | 6 | 3 | 2,888 |
Menzies-Gow 202257 | NMA | Severe asthmab | Adults and Children | Mepolizumab | 3 | 3 | 1,262 |
Menzies-Gow 202257 | NMA | Severe asthmab | Adults and Children | Omalizumab | 2 | 18 | 5,080 |
Menzies-Gow 202257 | NMA | Severe asthmab | Adults and Children | Tezepelumab | 6 | 3 | 1,759 |
Nopsopon 202358 | NMA | Eosinophilic | Adults and Children | B, D, M, T | 1 | 10 | 9,201 |
Nopsopon 202358 | NMA | Eosinophilic | Adults and Children | Benralizumab | 1 | 3 | 3,166 |
Nopsopon 202358 | NMA | Eosinophilic | Adults and Children | Dupilumab | 1 | 2 | 2,678 |
Nopsopon 202358 | NMA | Eosinophilic | Adults and Children | Mepolizumab | 1 | 3 | 1,748 |
Nopsopon 202358 | NMA | Eosinophilic | Adults and Children | Tezepelumab | 1 | 2 | 1,609 |
Praetorius 202159 | ITC | Eosinophilic | Adults and Children | D, M | 1 | 7 | NR |
Praetorius 202159 | ITC | Eosinophilic | Adults and Children | D, M, O | 1 | 23 | NR |
Ramonell 202060 | NMA | Eosinophilic | Adults and Children | B, D, M | 1 | 8 | 2,701 |
Ramonell 202060 | NMA | Eosinophilic | Adults and Children | Benralizumab | 1 | 2 | 1,021 |
Ramonell 202060 | NMA | Eosinophilic | Adults and Children | Dupilumab | 1 | 4 | 744 |
Ramonell 202060 | NMA | Eosinophilic | Adults and Children | Mepolizumab | 1 | 2 | 936 |
Zoumot 202262 | MA | Severe asthmab | Adults and Children | Tezepelumab | 12 | 6 | 2,667 |
B = benralizumab; D = dupilumab; ITC = Indirect treatment comparison; M = mepolizumab; MA = meta-analysis; MAIC = matching-adjusted indirect comparison; NMA = network meta-analysis; NR = not reported O = omalizumab; PICO = population, intervention, comparison, outcomes; SR = systematic review; t = tezepelumab
Note: Initials indicate that a comparative effectiveness analysis was performed for those biologics.
aPICO Population is the population of asthma patient targeted for inclusion as described by the publications.
bSevere asthma PICO population indicates no specific characterization or inclusion by asthma subtypes.
Table 16: RCT Outcomes by Asthma Subtype
Intervention and asthma subtype enrolled | Patient subgroup | AEX | FEV1 | HRQoL | Safety | Hospitalization | Mortality | # of Results | Non–type 2 | Type 2 | ||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
EOS/ non-ALL | Non-EOS/ ALL | EOS/ ALL | EOS NOS | ALL NOS | ||||||||||
Intervention | ||||||||||||||
Benralizumab | ||||||||||||||
eosinophilic39 | Adults | NR | + | NR | NR | NR | NR | 8 | No | Yes | No | Yes | Yes | No |
Eosinophilic31 | Adults | + | + | ACQ + | NR | NR | NR | 1 | No | No | No | No | Yes | No |
Eosinophilic39 | Adults | NR | + | ACQ ++ | + | NR | NR | 1 | No | No | No | No | Yes | No |
Eosinophilic31 | Adults | ++ | ++ | ACQ ++ | NR | NR | NR | 3 | No | No | No | No | Yes | No |
Eosinophilic31 | Adults | ++ | ++ | ACQ ++ | + | NR | NR | 1 | No | No | No | No | Yes | No |
Adults and Children | ++ | NR | NR | NR | NR | NR | 6 | No | Yes | No | Yes | No | Yes | |
Adults and Children | + | - | NR | NR | NR | NR | 1 | No | No | No | No | No | No | |
Adults and Children | + | - | ACQ +, AQLQ + | NR | NR | NR | 1 | No | No | Yes | No | No | No | |
Adults and Children | ++ | - | NR | NR | NR | NR | 2 | No | No | Yes | No | No | No | |
Adults and Children | + | + | ACQ + | NR | NR | NR | 1 | No | No | No | No | No | No | |
Adults and Children | ++ | + | NR | NR | NR | NR | 3 | Yes | No | No | No | Yes | No | |
Adults and Children | ++ | + | ACQ +, AQLQ ++ | NR | NR | NR | 1 | Yes | No | No | No | No | No | |
Adults and Children | ++ | ++ | NR | NR | NR | NR | 9 | No | Yes | No | Yes | Yes | Yes | |
Adults and Children | ++ | ++ | ACQ ++ | NR | NR | NR | 2 | No | No | No | No | No | No | |
Adults and Children | ++ | ++ | ACQ ++, AQLQ ++ | NR | NR | NR | 6 | No | Yes | No | Yes | Yes | No | |
Dupilumab | ||||||||||||||
Adults and Children | ++ | + | NR | NR | NR | NR | 1 | No | No | No | No | No | No | |
Adults and Children | ++ | + | ACQ ++, AQLQ++ | NR | NR | NR | 1 | No | No | No | No | No | Yes | |
Adults and Children | ++ | ++ | NR | NR | NR | NR | 5 | No | No | No | No | Yes | No | |
Adults and Children | ++ | ++ | ACQ ++, AQLQ + | NR | NR | NR | 1 | No | No | No | No | No | No | |
Adults and Children | ++ | ++ | ACQ ++ | - | NR | NR | 1 | No | No | No | No | No | No | |
Mepolizumab | ||||||||||||||
Adults and Children | - | NR | ACQ-5 + | NR | NR | NR | 1 | No | Yes | No | No | No | No | |
Adults and Children | + | NR | NR | NR | NR | NR | 1 | No | Yes | No | No | No | No | |
Adults and Children | + | NR | ACQ-5 - | NR | NR | NR | 2 | No | No | No | Yes | No | No | |
Adults and Children | + | NR | ACQ-5 + | NR | NR | NR | 3 | No | Yes | No | Yes | No | No | |
Adults and Children | ++ | NR | NR | NR | NR | NR | 14 | No | Yes | No | Yes | Yes | No | |
Adults and Children | ++ | NR | ACQ-5 + | NR | NR | NR | 3 | No | Yes | No | Yes | No | No | |
Adults and Children | ++ | NR | ACQ-5 ++ | NR | NR | NR | 5 | No | Yes | No | Yes | No | No | |
Adults and Children | NR | NR | ACQ-5 + | NR | NR | NR | 2 | No | No | No | Yes | No | No | |
Adults and Children | NR | NR | NR | NR | NR | NR | 1 | No | No | No | Yes | No | No | |
Adults and Children | + | + | ACQ ++ | NR | NR | NR | 1 | No | No | No | No | Yes | No | |
Adults and Children | ++ | + | ACQ + | NR | NR | NR | 4 | No | Yes | No | Yes | Yes | No | |
Adults and Children | ++ | + | ACQ ++ | NR | NR | NR | 2 | No | No | No | No | Yes | No | |
Adults and Children | ++ | ++ | ACQ + | NR | NR | NR | 1 | No | No | No | Yes | No | No | |
Adults and Children | ++ | ++ | ACQ ++ | NR | NR | NR | 8 | No | Yes | No | No | Yes | No | |
Omalizumab | ||||||||||||||
Allergic35 | Adults | NR | NR | ACQ ++, AQLQ ++ | NR | NR | NR | 1 | No | No | No | No | No | Yes |
Allergic35 | Adults | NR | NR | ACQ +, AQLQ + | NR | NR | NR | 2 | No | No | No | No | No | Yes |
Allergic35 | Adults | NR | ++ | ACQ +, AQLQ ++ | NR | NR | NR | 1 | No | No | No | No | No | Yes |
Allergic35 | Adults | NR | NR | ACQ = , AQLQ - | NR | NR | NR | 1 | No | No | No | No | No | Yes |
Allergic35 | Adults | NR | + | ACQ -, AQLQ + | NR | NR | NR | 1 | No | No | No | Yes | No | No |
Allergic35 | Adults | NR | + | ACQ +, AQLQ + | NR | NR | NR | 1 | No | No | Yes | No | No | No |
Allergic35 | Adults | NR | + | ACQ +, AQLQ ++ | NR | NR | NR | 1 | No | No | Yes | No | No | No |
Allergic38 | Adults | + | + | ACQ + | NR | NR | NR | 1 | No | No | No | No | No | Yes |
Allergic35 | Adults | NR | ++ | AQLQ + | NR | NR | NR | 1 | No | No | No | Yes | No | No |
Allergic30 | Adults and Children | + | + | NR | NR | NR | NR | 2 | No | No | No | No | No | Yes |
Allergic30 | Adults and Children | ++ | + | NR | NR | NR | NR | 1 | No | No | No | No | No | Yes |
Allergic30 | Adults and Children | ++ | ++ | NR | NR | NR | NR | 2 | No | No | No | No | No | Yes |
Tezepelumab | ||||||||||||||
Adults | ++ | NR | NR | NR | NR | NR | 14 | No | No | No | No | Yes | Yes | |
Adults | - | + | ACQ-6 + | NR | NR | NR | 1 | No | No | No | No | No | No | |
Adults | + | ++ | ACQ-6 - | NR | NR | NR | 1 | No | No | No | No | Yes | No | |
Adults | ++ | ++ | NR | NR | NR | NR | 2 | No | No | No | No | No | Yes | |
Adults | ++ | ++ | ACQ-6 + | NR | NR | NR | 2 | No | No | No | No | Yes | No | |
Adults | ++ | ++ | ACQ ++, AQLQ ++ | NR | ++ | NR | 1 | No | No | No | No | No | No | |
Adults | + | ++ | ACQ-6 ++, AQLQ ++ | + | NR | NR | 1 | No | No | No | No | No | No | |
Adults | ++ | ++ | ACQ ++ | ++ | NR | NR | 1 | No | No | No | No | No | No | |
Adults and Children | + | NR | NR | NR | NR | NR | 1 | No | No | No | No | No | No | |
Adults and Children | ++ | NR | NR | NR | NR | NR | 5 | No | No | No | No | No | Yes | |
Adults and Children | NR | - | NR | NR | NR | NR | 2 | No | No | Yes | No | No | No | |
Adults and Children | + | - | NR | NR | NR | NR | 1 | No | No | No | No | No | No | |
Adults and Children | ++ | - | NR | NR | NR | NR | 1 | No | No | No | No | No | No | |
Adults and Children | ++ | + | NR | NR | NR | NR | 1 | Yes | No | No | No | No | No | |
Adults and Children | ++ | + | ACQ ++, AQLQ ++ | NR | NR | NR | 1 | No | No | No | No | No | No | |
Adults and Children | ++ | + | ACQ +, AQLQ + | NR | NR | NR | 2 | No | No | No | No | No | No | |
Adults and Children | NR | ++ | NR | NR | NR | NR | 2 | No | Yes | No | No | No | No | |
Adults and Children | + | ++ | ACQ ++, AQLQ ++ | NR | NR | NR | 1 | No | No | No | No | No | No | |
Adults and Children | ++ | ++ | NR | NR | NR | NR | 9 | Yes | No | No | Yes | Yes | No | |
Adults and Children | ++ | ++ | ACQ ++, AQLQ ++ | NR | NR | NR | 12 | No | No | No | No | Yes | Yes | |
Adults and Children | ++ | ++ | ACQ ++, AQLQ ++ | + | ++ | NR | 1 | No | No | No | No | No | No | |
ACQ = Asthma Control Questionnaire; ACT = Asthma Control Test; AEX = Asthma exacerbation; AQLQ = Asthma Quality of Life Questionnaire; ALL = Allergic asthma; BEC = blood eosinophil count; EOS = Eosinophilic asthma; FEV1 = Forced Expiratory Volume in 1 second; HRQoL = Health-related Quality of Life; NOS = not otherwise specified; NR = not reported.
Note: YES indicates at least 1 outcome reported for that subgroup. NO indicates that no outcomes were reported for that subgroup. + indicates effect favouring treatment, - indicates effect favouring control, = indicates exact equality of outcome, AND an additional + or - indicates whether this effect was statistically significant.
Table 17: RCT Outcomes by BEC Level Characterization
Intervention and asthma subtype enrolled | Patient subgroup | Classification of eosinophilic asthma | AEX | FEV1 | HRQoL | # of Results | Non–type 2 | Type 2 | ||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
EOS/ non-ALL | Non-EOS/ ALL | EOS/ ALL | EOS NOS | ALL NOS | ||||||||
Intervention | ||||||||||||
Benralizumab | ||||||||||||
Adults and Children | BEC < 150 | + | - | NR | 1 | No | No | No | No | No | No | |
Adults and Children | BEC < 300 | + | + | ACQ + | 1 | No | No | No | No | No | No | |
Adults and Children | BEC > = 150 | ++ | ++ | ACQ ++, AQLQ ++ | 1 | No | No | No | No | Yes | No | |
Eosinophilic31 | Adults | BEC > = 150 to < 300 | + | + | ACQ + | 1 | No | No | No | No | Yes | No |
Adults and Children | BEC > = 150 to < 300 | ++ | ++ | NR | 1 | No | No | No | No | Yes | No | |
Eosinophilic31 | Adults | BEC > = 300 | ++ | ++ | ACQ ++ | 1 | No | No | No | No | Yes | No |
Adults and Children | BEC > = 300 | ++ | ++ | ACQ ++, AQLQ ++ | 1 | No | No | No | No | Yes | No | |
Eosinophilic39 | Adults | BEC > = 300 to 449 | NR | + | NR | 1 | No | No | No | No | Yes | No |
Adults and Children | BEC > = 300 to 449 | ++ | + | NR | 1 | No | No | No | No | Yes | No | |
Eosinophilic39 | Adults | BEC > = 450 | NR | + | NR | 1 | No | No | No | No | Yes | No |
Adults and Children | BEC > = 450 | ++ | ++ | ACQ ++, AQLQ ++ | 1 | No | No | No | No | Yes | No | |
Dupilumab | ||||||||||||
Adults and Children | BEC < 150 | ++ | ++ | NR | 1 | No | No | No | No | No | No | |
Adults and Children | BEC < 300 | ++ | + | NR | 1 | No | No | No | No | No | No | |
Adults and Children | BEC > = 150 | ++ | ++ | NR | 1 | No | No | No | No | Yes | No | |
Adults and Children | BEC ≥ 300 | ++ | ++ | NR | 1 | No | No | No | No | Yes | No | |
Mepolizumab | ||||||||||||
Adults and Children | BEC < 150 | ++ | + | ACQ + | 1 | No | No | No | No | Yes | No | |
Adults and Children | BEC > = 150 | ++ | ++ | ACQ ++ | 1 | No | No | No | No | Yes | No | |
Adults and Children | BEC > = 150 to < 300 | + | + | ACQ ++ | 1 | No | No | No | No | Yes | No | |
Adults and Children | BEC > = 300 | ++ | ++ | ACQ ++ | 1 | No | No | No | No | Yes | No | |
Adults and Children | BEC > = 300 to 499 | ++ | + | ACQ ++ | 1 | No | No | No | No | Yes | No | |
Adults and Children | BEC > = 500 | ++ | ++ | ACQ ++ | 1 | No | No | No | No | Yes | No | |
Tezepelumab | ||||||||||||
Adults | BEC < 150 | - | + | ACQ-6 + | 1 | No | No | No | No | No | No | |
Adults | BEC < 150 | ++ | NR | NR | 1 | No | No | No | No | No | No | |
Adults and Children | BEC < 150 | ++ | + | ACQ +, AQLQ + | 1 | No | No | No | No | No | No | |
Adults | BEC < 300 | ++ | NR | NR | 1 | No | No | No | No | No | No | |
Adults and Children | BEC < 300 | ++ | + | ACQ ++, AQLQ ++ | 1 | No | No | No | No | No | No | |
Adults | BEC > = 150 | ++ | NR | NR | 1 | No | No | No | No | Yes | No | |
Adults | BEC > = 150 | ++ | ++ | ACQ-6 + | 1 | No | No | No | No | Yes | No | |
Adults and Children | BEC > = 150 | ++ | ++ | ACQ ++, AQLQ ++ | 1 | No | No | No | No | Yes | No | |
Adults | BEC > = 150 to < 300 | + | ++ | ACQ-6 - | 1 | No | No | No | No | Yes | No | |
Adults and Children | BEC > = 150 to < 300 | ++ | ++ | ACQ ++, AQLQ ++ | 1 | No | No | No | No | Yes | No | |
Adults | BEC > = 300 | ++ | NR | NR | 1 | No | No | No | No | Yes | No | |
Adults | BEC > = 300 | ++ | ++ | ACQ-6 + | 1 | No | No | No | No | Yes | No | |
Adults and Children | BEC > = 300 | ++ | ++ | ACQ ++, AQLQ ++ | 1 | No | No | No | No | Yes | No | |
Adults and Children | BEC > = 300 to 449 | ++ | ++ | ACQ ++, AQLQ ++ | 1 | No | No | No | No | Yes | No | |
Adults and Children | BEC > = 450 | ++ | ++ | ACQ ++, AQLQ ++ | 1 | No | No | No | No | Yes | No | |
ACQ = Asthma Control Questionnaire; ACT = Asthma Control Test; AEX = Asthma exacerbation; AQLQ = Asthma Quality of Life Questionnaire; ALL = Allergic asthma; BEC = blood eosinophil count; EOS = Eosinophilic asthma; FEV1 = Forced Expiratory Volume in 1 second; HRQoL = Health-related Quality of Life; NOS = not otherwise specified; NR = not reported.
Note: YES indicates at least 1 outcome reported for that subgroup. NO indicates that no outcomes were reported for that subgroup. + indicates effect favouring treatment, - indicates effect favouring control, = indicates exact equality of outcome, and an additional + or - indicates whether this effect was statistically significant. No results for hospitalization or mortality outcomes were reported.
Table 18: RCT Outcomes by Fractional Exhaled Nitric Oxide Characterization
Intervention and asthma subtype enrolled | Population | FeNO subgroups | AEX | FEV1 | HRQoL | # of results | Non-type 2 | Type 2 | ||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
EOS/ non-ALL | Non-EOS/ ALL | EOS/ALL | EOS NOS | All NOS | ||||||||
Intervention | ||||||||||||
Tezepelumab | ||||||||||||
Adults | FeNO < 25 ppb | ++ | NR | NR | 1 | No | No | No | No | No | No | |
Adults and Children | FeNO < 25 ppb | ++ | + | ACQ +, AQLQ + | 1 | No | No | No | No | No | No | |
Adults | FeNO < 50 ppb | ++ | NR | NR | 1 | No | No | No | No | No | No | |
Adults | FeNO > = 25 ppb | ++ | NR | NR | 1 | No | No | No | No | Yes | No | |
Adults and Children | FeNO 25 to < 50 ppb | ++ | ++ | ACQ ++, AQLQ ++ | 1 | No | No | No | No | Yes | No | |
Adults | FeNO > = 50 ppb | ++ | NR | NR | 1 | No | No | No | No | Yes | No | |
Adults and Children | FeNO > = 50 ppb | ++ | ++ | ACQ ++, AQLQ ++ | 1 | No | No | No | No | Yes | No | |
Adults and Children | Extension: FeNO < 25 | ++ | NR | NR | 1 | No | No | No | No | No | No | |
Adults and Children | Extension: FeNO > = 25 | ++ | NR | NR | 1 | No | No | No | No | Yes | No | |
ACQ = Asthma Control Questionnaire; ACT = Asthma Control Test; AEX = Asthma exacerbation; AQLQ = Asthma Quality of Life Questionnaire; ALL = Allergic asthma; EOS = Eosinophilic asthma; FeNO = fractional exhaled nitric oxide; FEV1 = Forced Expiratory Volume in 1 second; HRQoL = Health-related Quality of Life; NOS = not otherwise specified; NR = not reported; ppb = parts per billion.
Note: The symbol + indicates effect favouring treatment, - indicates effect favouring control, = indicates exact equality of outcome, AND an additional + or - indicates whether this effect was statistically significant. No results for hospitalization, mortality, or safety outcomes were reported. YES indicates at least 1 outcome reported for that subgroup. NO indicates that no outcomes were reported for that subgroup. FeNO > 25 is used to determine presence of eosinophilic asthma in this table.
Table 19: RCT Outcomes by Omalizumab (Eligibility) Criteria
Asthma subtype enrolled | Population | Omalizumab criteriaa | AEX | FEV1 | HRQoL | # of Results | Non–type 2 | EOS/non-ALL | Non-EOS/ALL | Type 2 High | ||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
EOS/ALL | EOS NOS | ALL NOS | ||||||||||
Intervention | ||||||||||||
Mepolizumab | ||||||||||||
Adults and Children | EU OMA eligible | ++ | + | ACQ + | 1 | No | No | No | Yes | No | No | |
Adults and Children | EU OMA ineligible | ++ | ++ | ACQ ++ | 1 | No | Yes | No | No | No | No | |
Adults and Children | US OMA eligible | ++ | ++ | ACQ + | 1 | No | No | No | Yes | No | No | |
Adults and Children | US OMA ineligible | ++ | ++ | ACQ ++ | 1 | No | Yes | No | No | No | No | |
Tezepelumab | ||||||||||||
Adults | EU OMA eligible | ++ | NR | NR | 1 | No | No | No | No | No | Yes | |
Adults and Children | EU OMA eligible | ++ | NR | NR | 1 | No | No | No | No | No | Yes | |
Adults | EU OMA ineligible | ++ | NR | NR | 1 | No | No | No | No | No | No | |
Adults and Children | EU OMA ineligible | ++ | NR | NR | 1 | No | No | No | No | No | No | |
Adults | US OMA eligible | ++ | NR | NR | 1 | No | No | No | No | No | Yes | |
Adults and Children | US OMA eligible | ++ | NR | NR | 1 | No | No | No | No | No | Yes | |
Adults | US OMA ineligible | ++ | NR | NR | 1 | No | No | No | No | No | No | |
Adults and Children | US OMA ineligible | ++ | NR | NR | 1 | No | No | No | No | No | No | |
ACQ = Asthma Control Questionnaire; ACT = Asthma Control Test; AEX = Asthma exacerbation; AQLQ = Asthma Quality of Life Questionnaire; ALL = Allergic asthma; EOS = Eosinophilic asthma; FEV1 = Forced Expiratory Volume in 1 second; HRQoL = Health-related Quality of Life; NOS = not otherwise specified; NR = not reported; OMA = omalizumab.
Note: The symbol + indicates effect favouring treatment, - indicates effect favouring control, = indicates exact equality of outcome, and an additional + or - indicates whether this effect was statistically significant. YES indicates at least 1 outcome reported for that subgroup. NO indicates that no outcomes were reported for that subgroup.
aOMA eligible means that the group meets the criteria for prescription of omalizumab in the US or EU based on age and a positive skin test or in vitro reactivity to a perennial allergen in inadequately controlled asthma.
Table 20: RCT Outcomes by Recombined Allergy Status
Intervention and asthma subtype enrolled | Population | Allergic/atopica | AEX | FEV1 | HRQoL | # of results | Non–type 2 | Type 2 High | ||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
EOS/ non-ALL | Non-EOS/ ALL | EOS/ ALL | EOS NOS | ALL NOS | ||||||||
Intervention | ||||||||||||
Benralizumab | ||||||||||||
Adults and Children | NO | ++ | NR | NR | 1 | No | No | No | No | No | No | |
Adults and Children | NO | ++ | ++ | NR | 1 | No | Yes | No | No | No | No | |
Eosinophilic39 | Adults | YES | NR | + | NR | 1 | No | No | No | Yes | No | No |
Adults and Children | YES | ++ | NR | NR | 1 | No | No | No | No | No | Yes | |
Adults and Children | YES | ++ | ++ | NR | 2 | No | No | No | No | No | Yes | |
Dupilumab | ||||||||||||
Adults and Children | NO | ++ | ++ | ACQ ++, AQLQ + | 1 | No | No | No | No | No | No | |
Adults and Children | YES | ++ | + | ACQ ++, AQLQ++ | 1 | No | No | No | No | No | Yes | |
Mepolizumab | ||||||||||||
Adults and Children | NO | ++ | NR | NR | 2 | No | Yes | No | No | No | No | |
Adults and Children | NO | ++ | + | ACQ + | 1 | No | Yes | No | No | No | No | |
Adults and Children | YES | + | NR | ACQ-5 + | 1 | No | No | No | Yes | No | No | |
Adults and Children | YES | ++ | NR | NR | 5 | No | No | No | Yes | No | No | |
Adults and Children | YES | ++ | NR | ACQ-5 + | 1 | No | No | No | Yes | No | No | |
Adults and Children | YES | ++ | NR | ACQ-5 ++ | 4 | No | No | No | Yes | No | No | |
Adults and Children | YES | ++ | + | ACQ + | 1 | No | No | No | Yes | No | No | |
Adults and Children | YES | NR | NR | ACQ-5 + | 1 | No | No | No | Yes | No | No | |
Omalizumab | ||||||||||||
Allergic35 | Adults | YES | NR | NR | ACQ ++, AQLQ ++ | 1 | No | No | No | No | No | Yes |
Allergic35 | Adults | YES | NR | NR | ACQ +, AQLQ + | 2 | No | No | No | No | No | Yes |
Allergic35 | Adults | YES | NR | NR | ACQ =, AQLQ - | 1 | No | No | No | No | No | Yes |
Tezepelumab | ||||||||||||
Adults | NO | ++ | ++ | NR | 1 | No | No | No | No | No | No | |
Adults and Children | NO | ++ | ++ | ACQ ++, AQLQ ++ | 2 | No | No | No | No | No | No | |
Adults | YES | ++ | NR | NR | 1 | No | No | No | No | No | Yes | |
Adults | YES | ++ | ++ | NR | 1 | No | No | No | No | No | Yes | |
Adults and Children | YES | ++ | ++ | ACQ ++, AQLQ ++ | 2 | No | No | No | No | No | Yes | |
ACQ = Asthma Control Questionnaire; ACT = Asthma Control Test; AEX = Asthma exacerbation; AQLQ = Asthma Quality of Life Questionnaire; ALL = Allergic asthma; EOS = Eosinophilic asthma; FEV1 = Forced Expiratory Volume in 1 second; HRQoL = Health-related Quality of Life; NOS = not otherwise specified; NR = not reported
Note: The symbol + indicates effect favouring treatment, - indicates effect favouring control, = indicates exact equality of outcome, and an additional + or - indicates whether this effect was statistically significant. YES indicates at least 1 outcome reported for that subgroup. NO indicates that no outcomes were reported for that subgroup.
aAllergic/atopic status was determined by a positive on any test for allergic asthma. Different trials tested for allergic sensitivity using different methods.
Table 21: Asthma Exacerbation Definitions From Systematic Reviews
Author year | Asthma exacerbation definition |
|---|---|
Abdelgalil 202061 | Not specified |
Agache, 2020a16 | Clinically significant asthma exacerbations: episodes of asthma worsening with systemic corticosteroids for 3 or more days, a 2-times increase in the dose of either inhaled corticosteroids or the need for asthma-related emergency treatment. Exacerbation |
Agache, 2020b15 | Clinically significant asthma exacerbation: episodes of asthma worsening requiring treatment with systemic corticosteroids |
Agache, 2020c44 | Severe exacerbation defined as a deterioration of asthma requiring: (a) the use of systemic corticosteroids for ≥ 3 days or (b) hospitalization/emergency room visit because of asthma, requiring systemic corticosteroids |
Akenroye 202245 | Not specified |
Ando 202246 | Not specified |
Bateman 202247 | Definitions listed by study in a table |
Bourdin 202048 | Not specified |
Busse 201949 | Clinically significant exacerbations, defined as an exacerbation requiring treatment with oral/systemic corticosteroids (for patients on maintenance oral corticosteroids, a ≥ 2-fold increase in dose was required) or requiring an emergency department visit or hospital |
Chagas 202350 | Defined as hospitalization, worsening of asthma symptoms that led to either an emergency department visit that resulted in the use of systemic corticosteroids for ≥ 3 consecutive days or use of systemic corticosteroids for ≥ 3 consecutive days |
Chen 201951 | Not specified |
Henriksen 201852 | Not specified |
Henriksen 202053 | Not specified |
Lee 202254 | Asthma exacerbation was defined as treatment with a course of systemic corticosteroids for at least 3 days irrespective of hospitalization |
Mahdavian 201955 | Not specified |
Mahdavian 202056 | Worsening of asthma leading to increase in systemic glucocorticoid dose for ≥ 3 days, emergency department visit due to asthma treated with systemic glucocorticoids additional to the patient's regular maintenance medications, or hospital admission |
Menzies-Gow 202257 | Overall annualized asthma exacerbation rate, including events that did not require hospital/emergency treatment |
Nopsopon 202358 | Clinically significant exacerbations |
Praetorius 202159 | Not specified |
Ramonell 202060 | Clinical asthma exacerbations were defined as a worsening of asthma that resulted in corticosteroid treatment, emergency department or urgent care, or hospitalization |
Zoumot 202262 | Not specified |
Table 22: Systematic Review Patient Subgroups With Reported Outcomes
Intervention | Population | Non–type 2 | Type 2 | ||||
|---|---|---|---|---|---|---|---|
EOS/non-ALL | Non-EOS/ALL | EOS/ALL | EOS NOS | All NOS | |||
Adults and children | No | No | No | No | Yes | Yes | |
Adults and children | No | No | No | No | Yes | Yes | |
Mepolizumab52 | Adults | No | No | No | No | Yes | No |
Adults and children | No | No | No | No | Yes | Yes | |
Adults and children | No | No | No | No | Yes | Yes | |
Omalizumab15 | Children | No | No | No | No | No | Yes |
Tezepelumab61 | Adults | No | No | No | No | No | No |
Adults and children | No | No | No | No | Yes | Yes | |
ALL = allergic asthma; EOS = eosinophilic asthma; NOS = not otherwise specified.
Note: Cells with YES or NO indicate whether any results were reported for that subgroup by biologic drug and population.
Table 23: Systematic Review and Meta-Analysis Main Outcomes
Author, Year | Design | PICO populationa | Popu-lation | AEX | FEV1 | HRQoL | S | # of results | Non–type 2 | Type 2 | ||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
EOS/ non-ALL | Non-EOS/ ALL | EOS/ ALL | EOS NOS | ALL NOS | ||||||||||
Intervention | ||||||||||||||
Benralizumab | ||||||||||||||
Agache 2020a16 | SR | Severe asthmab | Adults and Children | ++ | ++ | AQLQ ++ | - | 1 | No | No | No | No | No | No |
Agache 2020b15 | SR | Allergic | Adults and Children | ++ | + | ACQ-6 ++, AQLQ - | - | 1 | No | No | No | No | No | Yes |
Lee 202254 | MA | Severe asthmab | Adults and Children | ++ | NR | NR | NR | 1 | No | No | No | No | No | No |
Mahdavian 201955 | MA | Eosinophilic | Adults and Children | NR | ++ | ACQ-6 ++, AQLQ ++ | NR | 1 | No | No | No | No | Yes | No |
Mahdavian 202056 | MA | Severe asthmab | Adults and Children | ++ | NR | NR | = | 1 | No | No | No | No | No | No |
Dupilumab | ||||||||||||||
Agache 2020a16 | SR | Severe asthmab | Adults and Children | ++ | ++ | ACQ ++, AQLQ ++ | - | 1 | No | No | No | No | No | No |
Agache 2020b15 | SR | Allergic | Adults and Children | ++ | ++ | ACQ-5 ++ | NR | 1 | No | No | No | No | No | Yes |
Agache 2020c44 | SR | Severe asthmab | Adults and Children | ++ | ++ | ACQ-5: ++, AQLQ: ++ | - | 1 | No | No | No | No | No | No |
Lee 202254 | MA | Severe asthmab | Adults and Children | ++ | NR | NR | NR | 1 | No | No | No | No | No | No |
Mepolizumab | ||||||||||||||
Agache 2020a16 | SR | Severe asthmab | Adults and Children | ++ | ++ | ACQ ++ | - - | 1 | No | No | No | No | No | No |
Henriksen 201852 | MA | Eosinophilic | Adults | ++ | ++ | ACQ ++, AQLQ ++ | ++ | 1 | No | No | No | No | Yes | No |
Lee 202254 | MA | Severe asthmab | Adults and Children | ++ | NR | NR | NR | 1 | No | No | No | No | No | No |
Omalizumab | ||||||||||||||
Agache 2020a16 | SR | Severe asthmab | Adults and Children | ++ | ++ | AQLQ ++ | NR | 1 | No | No | No | No | No | No |
Agache 2020b15 | SR | Allergic | Adults and Children | ++ | ++ | ACQ-6 ++, AQLQ ++ | - | 1 | No | No | No | No | No | Yes |
Tezepelumab | ||||||||||||||
Abdelgalil 202261 | MA | Severe asthmab | Adults | ++ | ++ | ACQ-6 ++, AQLQ12 ++ | ++ | 1 | No | No | No | No | No | No |
Chagas 202350 | MA | Severe asthmab | Adults and Children | ++ | ++ | ACQ ++, AQLQ ++ | ++ | 1 | No | No | No | No | No | No |
Zoumot 202262 | MA | Severe asthmab | Adults and Children | + | NR | NR | NR | 1 | No | No | No | No | No | No |
Zoumot 202262 | MA | Severe asthmab | Adults and Children | ++ | NR | NR | NR | 2 | No | No | No | No | No | No |
Zoumot 202262 | MA | Severe asthmab | Adults and Children | ++ | ++ | ++ | + | 1 | No | No | No | No | No | No |
ACQ = Asthma Control Questionnaire; ACT = Asthma Control Test; AEX = Asthma exacerbation; AQLQ = Asthma Quality of Life Questionnaire; FEV1 = forced expiratory volume in 1 second; HRQoL = Health-related Quality of Life; MA = Meta-analysis; NOS = not otherwise specified; NR = Not reported; PICO = population, intervention, comparison, outcomes; S = safety outcomes; SR = Systematic review.
Note: All analyses compared biologic to a placebo. + indicates effect favouring treatment; - indicates effect favouring control; = indicates exact equality of outcome; an additional + or - indicates whether this effect was statistically significant.
aPICO Population is the population of asthma patient targeted for inclusion as described by the publications.
bSevere asthma PICO population indicates no specific characterization or inclusion by asthma subtypes.
Table 24: Systematic Review and Meta-Analysis Subgroup Outcomes
Author Year | Design | PICO populationa | Population | AEX | FEV1 | HRQoL | S | Subgroups | # of results | Non-type 2 | Type 2 | ||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
EOS/ non-ALL | Non-EOS/ALL | EOS/ALL | EOS NOS | ALL NOS | |||||||||||
Intervention | |||||||||||||||
Benralizumab | |||||||||||||||
Lee 202254 | MA | Severe asthmab | Adults and Children | ++ | NR | NR | NR | BEC < 300 | 1 | No | No | No | No | No | No |
Lee 202254 | MA | Severe asthmab | Adults and Children | ++ | NR | NR | NR | BEC > = 300 | 1 | No | No | No | No | Yes | No |
Mahdavian 202056 | MA | Severe asthmab | Adults and Children | - | NR | NR | NR | low BEC | 1 | No | No | No | No | No | No |
Mahdavian 202056 | MA | Severe asthmab | Adults and Children | ++ | NR | NR | NR | BEC > = 300 or 150 | 1 | No | No | No | No | Yes | No |
Dupilumab | |||||||||||||||
Agache, 2020c44 | SR | Severe asthmab | Adults and Children | ++ | + | NR | NR | FeNO < 25ppb | 1 | No | No | No | No | No | No |
Agache, 2020c44 | SR | Severe asthmab | Adults and Children | ++ | ++ | NR | NR | BEC < 300 | 1 | No | No | No | No | No | No |
Agache, 2020c44 | SR | Severe asthmab | Adults and Children | ++ | ++ | NR | NR | BEC > = 300 | 1 | No | No | No | No | Yes | No |
Agache, 2020c44 | SR | Severe asthmab | Adults and Children | ++ | ++ | NR | NR | FeNO > = 50 ppb | 1 | No | No | No | No | No | No |
Agache, 2020c44 | SR | Severe asthmab | Adults and Children | ++ | ++ | NR | NR | FeNO 25 to < 50 ppb | 1 | No | No | No | No | No | No |
Lee 202254 | MA | Severe asthmab | Adults and Children | ++ | NR | NR | NR | BEC < 300 | 1 | No | No | No | No | No | No |
Lee 202254 | MA | Severe asthmab | Adults and Children | ++ | NR | NR | NR | BEC > = 300 | 1 | No | No | No | No | Yes | No |
Omalizumab | |||||||||||||||
Agache, 2020b15 | SR | Allergic | Children | ++ | NR | AQLQ++ | NR | 6 to 12 years old | 1 | No | No | No | No | No | Yes |
Henriksen 202053 | MA | Allergic | Adults and Children | + | NR | ACT* | ++ | Children | 1 | No | No | No | No | No | Yes |
Henriksen 202053 | MA | Allergic | Adults and Children | ++ | ++ | ACQ ++, AQLQ ++ | + | Adults | 1 | No | No | No | No | No | Yes |
Tezepelumab | |||||||||||||||
Zoumot 202262 | MA | Severe asthmab | Adults and Children | ++ | NR | NR | NR | Allergic/Atopic = YES | 2 | No | No | No | No | No | Yes |
Zoumot 202262 | MA | Severe asthmab | Adults and Children | ++ | NR | NR | NR | Allergic/Atopic = NO | 1 | No | No | No | No | No | No |
Zoumot 202262 | MA | Severe asthmab | Adults and Children | ++ | NR | NR | NR | BEC < 150 | 1 | No | No | No | No | No | No |
Zoumot 202262 | MA | Severe asthmab | Adults and Children | ++ | NR | NR | NR | BEC > = 150 to < 300 | 1 | No | No | No | No | Yes | No |
Zoumot 202262 | MA | Severe asthmab | Adults and Children | ++ | NR | NR | NR | BEC > = 300 to 449 | 1 | No | No | No | No | Yes | No |
Zoumot 202262 | MA | Severe asthmab | Adults and Children | ++ | NR | NR | NR | BEC > = 450 | 1 | No | No | No | No | Yes | No |
Zoumot 202262 | MA | Severe asthmab | Adults and Children | ++ | NR | NR | NR | FeNO < 25ppb | 1 | No | No | No | No | No | No |
Zoumot 202262 | MA | Severe asthmab | Adults and Children | ++ | NR | NR | NR | FeNO > = 25 ppb | 1 | No | No | No | No | No | No |
ACQ = Asthma Control Questionnaire; ACT = Asthma Control Test; ALL = Allergic asthma; AEX = Asthma exacerbation; AQLQ = Asthma Quality of Life Questionnaire; EOS = Eosinophilic asthma; FEV1 = forced expiratory volume in 1 second; HRQoL = Health-related Quality of Life; ITC = Indirect treatment comparison; MA = Meta-analysis; NMA = network meta-analysis; NOS = not otherwise specified; NR = not reported; ppb = parts per billion; PICO = population, intervention, comparison, outcomes; S = safety outcomes; SR = Systematic review;
Note: The symbol + indicates effect favouring treatment, - indicates effect favouring control, = indicates exact equality of outcome, and an additional + or - indicates whether this effect was statistically significant. All analyses compared biologic to a placebo.
aPICO Population is the population of asthma patient targeted for inclusion as described by the publications.
bSevere asthma PICO population indicates no specific characterization or inclusion by asthma subtypes.
Table 25: Comparative Efficacy Reviews Main Outcomes
Author Year | Design | PICO populationa | Population | AEX | FEV1 | HRQoL | S | H | Non–type 2 | Type 2 | ||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
EOS/non-ALL | Non-EOS/ALL | EOS/ALL | EOS NOS | ALL NOS | ||||||||||
Intervention | ||||||||||||||
Benralizumab | ||||||||||||||
Akenroye 202245 | NMA | Eosinophilic | Adults and Children | NR | NR | NR | ++ | NR | No | No | No | No | Yes | No |
Ando 202246 | NMA | Severe asthmab | Adults and Children | ++ | ++ | ACT ++, AQLQ ++ | + | NR | No | No | No | No | No | No |
Bateman 202247 | ITC | Severe asthmab | Adults and Children | ++ | ++ | NR | NR | NR | No | No | No | No | No | No |
Busse 201949 | ITC | Eosinophilic | Adults and Children | ++ | NR | NR | NR | NR | No | No | No | No | Yes | No |
Chen 201951 | NMA | Severe asthmab | Adults and Children | ++ | NR | NR | NR | NR | No | No | No | No | No | No |
Menzies-Gow 202257 | NMA | Severe asthmab | Adults and Children | ++ | NR | NR | NR | + | No | No | No | No | No | No |
Nopsopon 202358 | NMA | Eosinophilic | Adults and Children | ++ | + | ACQ + | NR | NR | No | No | No | No | Yes | No |
Ramonell 202060 | NMA | Eosinophilic | Adults and Children | ++ | NR | NR | NR | NR | No | No | No | No | Yes | No |
Dupilumab | ||||||||||||||
Akenroye 202245 | NMA | Eosinophilic | Adults and Children | NR | NR | NR | = | NR | No | No | No | No | Yes | No |
Ando 202246 | NMA | Severe asthmab | Adults and Children | ++ | ++ | ACT ++, AQLQ ++ | + | NR | No | No | No | No | No | No |
Bateman 202247 | ITC | Severe asthmab | Adults and Children | ++ | ++ | NR | NR | NR | No | No | No | No | No | No |
Menzies-Gow 202257 | NMA | Severe asthmab | Adults and Children | ++ | NR | NR | NR | + | No | No | No | No | No | No |
Nopsopon 202358 | NMA | Eosinophilic | Adults and Children | ++ | ++ | ACQ + | NR | NR | No | No | No | No | Yes | No |
Ramonell 202060 | NMA | Eosinophilic | Adults and Children | ++ | NR | NR | NR | NR | No | No | No | No | Yes | No |
Mepolizumab | ||||||||||||||
Akenroye 202245 | NMA | Eosinophilic | Adults and Children | NR | NR | NR | ++ | NR | No | No | No | No | Yes | No |
Ando 202246 | NMA | Severe asthmab | Adults and Children | ++ | ++ | ACT ++ | + | NR | No | No | No | No | No | No |
Bateman 202247 | ITC | Severe asthmab | Adults and Children | ++ | ++ | NR | NR | NR | No | No | No | No | No | No |
Busse 201949 | ITC | Eosinophilic | Adults and Children | ++ | NR | NR | NR | NR | No | No | No | No | Yes | No |
Chen 201951 | NMA | Severe asthmab | Adults and Children | ++ | NR | NR | NR | NR | No | No | No | No | No | No |
Menzies-Gow 202257 | NMA | Severe asthmab | Adults and Children | ++ | NR | NR | NR | + | No | No | No | No | No | No |
Nopsopon 202358 | NMA | Eosinophilic | Adults and Children | ++ | + | ACQ + | NR | NR | No | No | No | No | Yes | No |
Ramonell 202060 | NMA | Eosinophilic | Adults and Children | ++ | NR | NR | NR | NR | No | No | No | No | Yes | No |
Omalizumab | ||||||||||||||
Bateman 202247 | ITC | Severe asthmab | Adults and Children | ++ | ++ | NR | NR | NR | No | No | No | No | No | No |
Menzies-Gow 202257 | NMA | Severe asthmab | Adults and Children | ++ | NR | NR | NR | + | No | No | No | No | No | No |
Tezepelumab | ||||||||||||||
Ando 202246 | NMA | Severe asthmab | Adults and Children | ++ | ++ | ACT ++, AQLQ ++ | + | NR | No | No | No | No | No | No |
Menzies-Gow 202257 | NMA | Severe asthmab | Adults and Children | ++ | NR | NR | NR | ++ | No | No | No | No | No | No |
Nopsopon 202358 | NMA | Eosinophilic | Adults and Children | ++ | ++ | ACQ ++ | NR | NR | NO | No | No | No | Yes | No |
ACQ = Asthma Control Questionnaire; ACT = Asthma Control Test; AEX = Asthma exacerbation; ALL = Allergic asthma; AQLQ = Asthma Quality of Life Questionnaire; EOS = Eosinophilic asthma; FEV1 = forced expiratory volume in 1 second; H = hospitalizations; HRQoL = Health-related Quality of Life; ITC = Indirect treatment comparison; NMA = network meta-analysis; NOS = not otherwise specified; NR = not reported; PICO = population, intervention, comparison, outcomes; S = safety outcomes.
Note: The symbol + indicates effect favouring treatment, - indicates effect favouring control, = indicates exact equality of outcome, an additional + or - indicates whether this effect was statistically significant. All studies made indirect comparisons through the included placebo control groups.
aPICO Population is the population of asthma patient targeted for inclusion as described by the publications.
bSevere asthma PICO population indicates no specific characterization or inclusion by asthma subtypes.
Table 26: NMA and ITC Subgroup Outcomes
Author Year | Design | Population | PICO populationa | AEX | FEV1 | HRQoL | Subgroups | Non–type 2 | Type 2 | ||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
EOS/ non-ALL | Non-EOS/ALL | EOS/ALL | EOS NOS | ALL NOS | |||||||||
Intervention | |||||||||||||
Benralizumab | |||||||||||||
Menzies-Gow 202257 | NMA | Adults and Children | Severe asthmab | + | NR | NR | Allergic: unclear cut-offs | No | No | No | No | No | Yes |
Ando 202246 | NMA | Adults and Children | Severe asthmab | + | + | NR | BEC < 150 | No | No | No | No | No | No |
Ando 202246 | NMA | Adults and Children | Severe asthmab | ++ | + | NR | BEC < 300 | No | No | No | No | No | No |
Menzies-Gow 202257 | NMA | Adults and Children | Severe asthmab | + | NR | NR | BEC < 300 | No | No | No | No | No | No |
Ando 202246 | NMA | Adults and Children | Severe asthmab | ++ | ++ | AQLQ ++ | BEC ≥ 150 | No | No | No | No | Yes | No |
Busse 201949 | ITC | Adults and Children | Eosinophilic | ++ | NR | NR | BEC ≥ 150 | No | No | No | No | Yes | No |
Akenroye 202245 | NMA | Adults and Children | Eosinophilic | ++ | ++ | NR | BEC ≥ 150 to < 300 | No | No | No | No | Yes | No |
Akenroye 202245 | NMA | Adults and Children | Eosinophilic | ++ | ++ | ACQ ++ | BEC ≥ 300 | No | No | No | No | Yes | No |
Ando 202246 | NMA | Adults and Children | Severe asthmab | ++ | ++ | ACT ++, AQLQ ++ | BEC ≥ 300 | No | No | No | No | Yes | No |
Busse 201949 | ITC | Adults and Children | Eosinophilic | ++ | NR | NR | BEC ≥ 300 | No | No | No | No | Yes | No |
Menzies-Gow 202257 | NMA | Adults and Children | Severe asthmab | ++ | NR | NR | BEC ≥ 300 | No | No | No | No | Yes | No |
Dupilumab | |||||||||||||
Menzies-Gow 202257 | NMA | Adults and Children | Severe asthmab | + | NR | NR | Allergic: unclear cut-offs | No | No | No | No | No | Yes |
Ando 202246 | NMA | Adults and Children | Severe asthmab | + | + | NR | BEC < 150 | No | No | No | No | No | No |
Ando 202246 | NMA | Adults and Children | Severe asthmab | + | + | NR | BEC < 300 | No | No | No | No | No | No |
Menzies-Gow 202257 | NMA | Adults and Children | Severe asthmab | + | NR | NR | BEC < 300 | No | No | No | No | No | No |
Ando 202246 | NMA | Adults and Children | Severe asthmab | ++ | ++ | NR | BEC ≥ 150 | No | No | No | No | Yes | No |
Akenroye 202245 | NMA | Adults and Children | Eosinophilic | ++ | + | NR | BEC ≥ 150 to < 300 | No | No | No | No | Yes | No |
Akenroye 202245 | NMA | Adults and Children | Eosinophilic | ++ | ++ | ACQ ++ | BEC ≥ 300 | No | No | No | No | Yes | No |
Ando 202246 | NMA | Adults and Children | Severe asthmab | ++ | ++ | AQLQ ++ | BEC ≥ 300 | No | No | No | No | Yes | No |
Menzies-Gow 202257 | NMA | Adults and Children | Severe asthmab | ++ | NR | NR | BEC ≥ 300 | No | No | No | No | Yes | No |
Ando 202246 | NMA | Adults and Children | Severe asthmab | + | NR | NR | FeNO < 25 ppb | No | No | No | No | No | No |
Ando 202246 | NMA | Adults and Children | Severe asthmab | ++ | NR | NR | FeNO < 50 ppb | No | No | No | No | No | No |
Ando 202246 | NMA | Adults and Children | Severe asthmab | ++ | NR | NR | FeNO ≥ 25 ppb | No | No | No | No | No | No |
Menzies-Gow 202257 | NMA | Adults and Children | Severe asthmab | + | NR | NR | FeNO ≥ 25 ppb | No | No | No | No | No | No |
Ando 202246 | NMA | Adults and Children | Severe asthmab | ++ | NR | NR | FeNO ≥ 50 ppb | No | No | No | No | No | No |
Menzies-Gow 202257 | NMA | Adults and Children | Severe asthmab | + | NR | NR | FeNO ≥ 50 ppb | No | No | No | No | No | No |
Mepolizumab | |||||||||||||
Menzies-Gow 202257 | NMA | Adults and Children | Severe asthmab | + | NR | NR | Allergic: unclear cut-offs | No | No | No | No | No | Yes |
Ando 202246 | NMA | Adults and Children | Severe asthmab | + | NR | NR | BEC < 150 | No | No | No | No | No | No |
Ando 202246 | NMA | Adults and Children | Severe asthmab | ++ | NR | NR | BEC < 300 | No | No | No | No | No | No |
Ando 202246 | NMA | Adults and Children | Severe asthmab | ++ | NR | NR | BEC ≥ 150 | No | No | No | No | Yes | No |
Busse 201949 | ITC | Adults and Children | Eosinophilic | ++ | NR | NR | BEC ≥ 150 | No | No | No | No | Yes | No |
Akenroye 202245 | NMA | Adults and Children | Eosinophilic | + | + | NR | BEC ≥ 150 to < 300 | No | No | No | No | Yes | No |
Akenroye 202245 | NMA | Adults and Children | Eosinophilic | ++ | ++ | ACQ ++ | BEC ≥ 300 | No | No | No | No | Yes | No |
Ando 202246 | NMA | Adults and Children | Severe asthmab | ++ | NR | NR | BEC ≥ 300 | No | No | No | No | Yes | No |
Busse 201949 | ITC | Adults and Children | Eosinophilic | ++ | NR | NR | BEC ≥ 300 | No | No | No | No | Yes | No |
Menzies-Gow 202257 | NMA | Adults and Children | Severe asthmab | ++ | NR | NR | BEC ≥ 300 | No | No | No | No | Yes | No |
Omalizumab | |||||||||||||
Menzies-Gow 202257 | NMA | Adults and Children | Severe asthmab | ++ | NR | NR | BEC ≥ 300 | No | No | No | No | Yes | No |
Tezepelumab | |||||||||||||
Menzies-Gow 202257 | NMA | Adults and Children | Severe asthmab | + | NR | NR | Allergic: unclear cut-offs | No | No | No | No | No | Yes |
Ando 202246 | NMA | Adults and Children | Severe asthmab | ++ | + | NR | BEC < 150 | No | No | No | No | No | No |
Ando 202246 | NMA | Adults and Children | Severe asthmab | ++ | ++ | NR | BEC < 300 | No | No | No | No | No | No |
Menzies-Gow 202257 | NMA | Adults and Children | Severe asthmab | + | NR | NR | BEC < 300 | No | No | No | No | No | No |
Ando 202246 | NMA | Adults and Children | Severe asthmab | ++ | ++ | AQLQ ++ | BEC ≥ 150 | No | No | No | No | Yes | No |
Ando 202246 | NMA | Adults and Children | Severe asthmab | ++ | ++ | ACT ++, AQLQ ++ | BEC ≥ 300 | No | No | No | No | Yes | No |
Menzies-Gow 202257 | NMA | Adults and Children | Severe asthmab | ++ | NR | NR | BEC ≥ 300 | No | No | No | No | Yes | No |
Ando 202246 | NMA | Adults and Children | Severe asthmab | ++ | NR | NR | FeNO < 25 ppb | No | No | No | No | No | No |
Ando 202246 | NMA | Adults and Children | Severe asthmab | ++ | NR | NR | FeNO < 50 ppb | No | No | No | No | No | No |
Ando 202246 | NMA | Adults and Children | Severe asthmab | ++ | NR | NR | FeNO ≥ 25 ppb | No | No | No | No | No | No |
Menzies-Gow 202257 | NMA | Adults and Children | Severe asthmab | ++ | NR | NR | FeNO ≥ 25 ppb | No | No | No | No | No | No |
Ando 202246 | NMA | Adults and Children | Severe asthmab | ++ | NR | NR | FeNO ≥ 50 ppb | No | No | No | No | No | No |
Menzies-Gow 202257 | NMA | Adults and Children | Severe asthmab | ++ | NR | NR | FeNO ≥ 50 ppb | No | No | No | No | No | No |
ACQ = Asthma Control Questionnaire; ACT = Asthma Control Test; AEX = Asthma exacerbation; ALL = Allergic asthma; AQLQ = Asthma Quality of Life Questionnaire; BEC = blood eosinophil count; EOS = Eosinophilic asthma; FeNO = fractional exhaled nitric oxide; FEV1 = forced expiratory volume in 1 second; HRQoL = Health-related Quality of Life; ITC = Indirect treatment comparison; NMA = network meta-analysis; NOS = Not otherwise specified; NR = Not reported; PICO = population, intervention, comparison, outcomes; ppb = parts per billion.
Note: The symbol + indicates effect favouring treatment, - indicates effect favouring control, = indicates exact equality of outcome, an additional + or - indicates whether this effect was statistically significant. All studies made indirect comparisons through the included placebo control groups.
aPICO Population is the population of asthma patient targeted for inclusion as described by the publications.
bSevere asthma PICO population indicates no specific characterization or inclusion by asthma subtypes.
Table 27: NMA, ITC, and MAIC Comparative Effectiveness Main Outcomes
Author Year | Design | PICO populationa | Intervention | AEX | FEV1 | HRQoL | Safety | Hospitalization |
|---|---|---|---|---|---|---|---|---|
Akenroye 202245 | NMA | Eosinophilic | BENRA, DUPI, MEPO | BENRA, DUPI, MEPO | BENRA, DUPI, MEPO | NR | BENRA, DUPI, MEPO MEPO > DUPI | NR |
Ando 202246 | NMA | Severe asthmab | BENRA, DUPI, MEPO, TEZE | BENRA, DUPI, MEPO, TEZE TEZE > BENRA | BENRA, DUPI, MEPO, TEZE | ACT: BENRA, DUPI, MEPO, TEZE AQLQ: BENRA, DUPI, TEZE | BENRA, DUPI, MEPO, TEZE | NR |
Bateman 202247 | ITC | Severe asthmab | BENRA, DUPI, MEPO, OMA | BENRA, DUPI, MEPO, OMA DUPI > BENRA, MEPO | BENRA, DUPI, MEPO, OMA; DUPI > BENRA | NR | NR | NR |
Bourdin 202048 | MAIC | Severe asthmab | BENRA, DUPI, MEPO | BENRA, DUPI, MEPO | NR | NR | NR | NR |
Busse 201949 | ITC | Eosinophilic | BENRA, MEPO | BENRA, MEPO MEPO > BENRA | NR | ACQ: BENRA, MEPO MEPO > BENRA | NR | NR |
Chen 201951 | NMA | Severe asthmab | BENRA, MEPO | BENRA, MEPO | NR | NR | NR | NR |
Menzies-Gow 202257 | NMA | Severe asthmab | BENRA, DUPI, MEPO, OMA, TEZE | BENRA, DUPI, MEPO, OMA, TEZE | NR | NR | NR | BENRA, DUPI, MEPO, OMA, TEZE |
Nopsopon 202358 | NMA | Eosinophilic | BENRA, DUPI, MEPO, TEZE | BENRA, DUPI, MEPO, TEZE TEZE > BENRA | BENRA, DUPI, MEPO, TEZE | ACQ: BENRA, DUPI, MEPO, TEZE | NR | NR |
Praetorius 202159 | ITC | Eosinophilic | DUPI, MEPO, OMA | DUPI, MEPO, OMA | DUPI, MEPO, OMA; DUPI > MEPO, OMA | ACQ: DUPI, MEPO, OMA AQLQ: DUPI, MEPO, OMA | DUPI, MEPO, OMA | NR |
Ramonell 202060 | NMA | Eosinophilic | BENRA, DUPI, MEPO | BENRA, DUPI, MEPO | NR | NR | NR | NR |
ACQ = Asthma Control Questionnaire; ACT = Asthma Control Test; AEX = Asthma exacerbation; AQLQ = Asthma Quality of Life Questionnaire; BENRA = benralizumab; DUPI = dupilumab; FEV1 = forced expiratory volume in 1 second; H = hospitalization; HRQoL = Health-related Quality of Life; ITC = Indirect treatment comparison; M = mepolizumab; MAIC = Matching-adjusted indirect comparison; NMA = network meta-analysis; NR = Not reported; OMA = omalizumab; PICO = population, intervention, comparison, outcomes; S = safety outcomes; TEZE = tezepelumab.
Note: Biologics tested are indicated by their first initial. If a biologic significantly outperformed 1 or more of the other tested biologics, then the best performing biologic and the statistically inferior biologics are identified using a “>” to mark the superior and inferior biologics (e.g., t > B,O). All studies made indirect comparisons through the included placebo control groups.
aPICO Population is the population of asthma patient targeted for inclusion as described by the papers.
bSevere asthma PICO population indicates no specific characterization or inclusion by asthma subtypes.
Table 28: NMA and ITC Comparative Effectiveness Subgroup Outcomes
Author Year | Design | PICO populationa | Intervention | AEX | FEV1 | HRQoL | S | H | Subgroups | Non–type 2 | Type 2 | ||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
EOS/ non-ALL | Non-EOS/ALL | EOS/ALL | EOS NOS | ALL NOS | |||||||||||
Akenroye 202245 | NMA | Eosinophilic | BENRA, DUPI, MEPO | BENRA, DUPI, MEPO | BENRA, DUPI, MEPO | NR | NR | NR | BEC ≥ 150 to < 300 | No | No | No | No | Yes | No |
Akenroye 202245 | NMA | Eosinophilic | BENRA, DUPI, MEPO | BENRA, DUPI, MEPO | BENRA, DUPI, MEPO | BENRA, DUPI, MEPO | NR | NR | BEC ≥ 300 | No | No | No | No | Yes | No |
Ando 202246 | NMA | Severe asthmab | BENRA, DUPI, MEPO, TEZE | BENRA, DUPI, MEPO, TEZE | BENRA, DUPI, TEZE | NR | NR | NR | BEC < 150 | No | No | No | No | No | No |
Ando 202246 | NMA | Severe asthmab | BENRA, DUPI, MEPO, TEZE | BENRA, DUPI, MEPO, TEZE; MEPO >BENRA | BENRA, DUPI, TEZE | ACT: BENRA, TEZE AQLQ: BENRA, TEZE | NR | NR | BEC ≥ 150 | No | No | No | No | Yes | No |
Ando 202246 | NMA | Severe asthmab | DUPI, TEZE | DUPI, TEZE | NR | NR | NR | NR | FeNO < 25 ppb | No | No | No | No | No | No |
Ando 202246 | NMA | Severe asthmab | DUPI, TEZE | DUPI, TEZE | NR | NR | NR | NR | FeNO < 50 ppb | No | No | No | No | No | No |
Ando 202246 | NMA | Severe asthmab | DUPI, TEZE | DUPI, TEZE | NR | NR | NR | NR | FeNO ≥ 25 ppb | No | No | No | No | Yes | No |
Ando 202246 | NMA | Severe asthmab | DUPI, TEZE | DUPI, TEZE | NR | NR | NR | NR | FeNO ≥ 50 ppb | No | No | No | No | Yes | No |
Ando 202246 | NMA | Severe asthmab | BENRA, DUPI, MEPO, TEZE | BENRA, DUPI, MEPO, TEZE | BENRA, DUPI, TEZE | ACT: BENRA, TEZE | NR | NR | BEC < 300 | NO | NO | NO | NO | NO | NO |
Ando 202246 | NMA | Severe asthmab | BENRA, DUPI, MEPO, TEZE | BENRA, DUPI, MEPO, TEZE; TEZE > BENRA | BENRA, DUPI, TEZE | ACT: BENRA, TEZE AQLQ: BENRA, DUPI, TEZE | NR | NR | BEC ≥ 300 | No | No | No | No | Yes | No |
Busse 201949 | ITC | Eosinophilic | BENRA, MEPO | BENRA, MEPO; MEPO > BENRA | BENRA, MEPO | ACQ: BENRA, MEPO; MEPO > BENRA | NR | NR | BEC ≥ 400 | No | No | No | No | Yes | No |
Busse 201949 | ITC | Eosinophilic | BENRA, MEPO | BENRA, MEPO; MEPO > BENRA | BENRA, MEPO | ACQ: BENRA, MEPO; MEPO >BENRA | NR | NR | BEC ≥ 150 | No | No | No | No | Yes | No |
Busse 201949 | ITC | Eosinophilic | BENRA, MEPO | BENRA, MEPO; MEPO >BENRA | BENRA, MEPO | ACQ: BENRA, MEPO; MEPO >BENRA | NR | NR | BEC ≥ 300 | No | No | No | No | Yes | No |
Menzies-Gow 202257 | NMA | Severe asthmab | BENRA, DUPI, OMA | BENRA, DUPI, OMA | NR | NR | NR | NR | ALL: unclear cut-offs | No | No | No | No | No | Yes |
Menzies-Gow 202257 | NMA | Severe asthmab | DUPI, TEZE | DUPI, TEZE | NR | NR | NR | NR | FeNO ≥ 25 ppb | No | No | No | No | No | No |
Menzies-Gow 202257 | NMA | Severe asthmab | DUPI, TEZE | DUPI, TEZE | NR | NR | NR | NR | FeNO ≥ 50 ppb | No | No | No | No | Yes | No |
Praetorius 202159 | ITC | Eosinophilic | DUPI, MEPO | NR | DUPI, MEPO | ACQ: DUPI, MEPO AQLQ: DUPI, MEPO | MEPO >DUPI | NR | OCS: Yes | No | No | No | No | Yes | No |
ACQ = Asthma Control Questionnaire; ACT = Asthma Control Test; AEX = Asthma exacerbation; ALL = allergic; AQLQ = Asthma Quality of Life Questionnaire; BENRA = benralizumab; BEC = blood eosinophil count; DUPI = dupilumab; EOS = eosinophilic; FeNO = fractional exhaled nitric oxide; FEV1 = forced expiratory volume in 1 second; HRQoL = Health-related Quality of Life; ITC = Indirect treatment comparison; M = mepolizumab; MAIC = Matching-adjusted indirect comparison; NMA = network meta-analysis; NOS = not otherwise specified; NR = Not reported; OMA = omalizumab; OCS = oral corticosteroids; PICO = population, intervention, comparison, outcomes; ppb = parts per billion; TEZE = tezepelumab.
Note: Biologics tested are indicated by their first initial. If a biologic significantly outperformed 1 or more of the other tested biologics, then the best performing biologic and the statistically inferior biologics are identified using a “>” to mark the superior and inferior biologics (e.g., TEZE > BENRA). All studies made indirect comparisons through the included placebo control groups.
aPICO Population is the population of asthma patient targeted for inclusion as described by the publications.
bSevere asthma PICO population indicates no specific characterization or inclusion by asthma subtypes.
Table 29: A Measurement Tool to Assess Systematic Reviews Version 2 (AMSTAR 2): Evaluation of the Included Reviews
Author year | AMSTAR 2 questiona | |||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | 14 | 15 | 16 | |
Abdelgalil 202261 | Yes | Yes | No | No | Yes | Yes | No | Yes | Yes | No | Yes | Yes | Yes | Yes | Yes | Yes |
AGACHE 2020a16 | Yes | Yes | No | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | No |
AGACHE 2020b15 | Yes | Yes | No | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | No |
AGACHE 2020c44 | Yes | Yes | No | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | No |
Akenroye 202245 | Yes | Yes | No | No | Yes | Yes | No | Yes | Yes | No | Yes | Yes | Yes | Yes | Yes | Yes |
Ando 202246 | Yes | No | No | No | Yes | No | No | Yes | Yes | No | Yes | No | Yes | Yes | Yes | Yes |
Bateman 202247 | Yes | Yes | No | No | Yes | Yes | No | Yes | No | No | Yes | No | No | No | No | No |
Bourdin 202048 | Yes | No | No | No | No | No | No | Yes | No | No | N/A | N/A | No | No | No | No |
Busse 201949 | Yes | No | No | No | Yes | No | No | Yes | No | No | Yes | No | No | No | No | No |
Chagas 202350 | Yes | Yes | No | Yes | Yes | Yes | No | Yes | Yes | No | Yes | No | No | No | No | No |
Chen 201951 | Yes | No | No | No | Yes | No | No | Yes | Yes | No | No | No | No | Yes | Yes | No |
Henriksen 201852 | Yes | Yes | No | Yes | Yes | Yes | No | Yes | Yes | No | Yes | Yes | Yes | Yes | Yes | Yes |
Henriksen 202053 | Yes | Yes | No | Yes | Yes | Yes | No | Yes | Yes | No | Yes | Yes | Yes | Yes | Yes | Yes |
Lee 202254 | Yes | No | No | No | Yes | No | No | Yes | Yes | No | Yes | No | No | No | Yes | Yes |
Mahdavian 201955 | Yes | No | No | Yes | Yes | No | No | Yes | Yes | No | Yes | Yes | Yes | Yes | No | Yes |
Mahdavian 202056 | Yes | No | No | Yes | Yes | No | No | Yes | Yes | No | Yes | Yes | Yes | Yes | No | Yes |
Menzies-Gow 202257 | Yes | Yes | No | No | Yes | Yes | No | Yes | Yes | No | Yes | Yes | Yes | Yes | No | No |
Nopsopon 202358 | Yes | Yes | No | No | Yes | No | No | Yes | Yes | No | Yes | Yes | Yes | Yes | Yes | Yes |
Praetorius 202159 | Yes | Yes | No | No | Yes | Yes | No | No | Yes | No | Yes | No | No | No | No | Yes |
Ramonell 202060 | Yes | No | No | No | Yes | No | No | Yes | No | No | Yes | No | No | Yes | Yes | Yes |
Zoumot 202262 | Yes | No | No | No | Yes | No | No | Yes | Yes | No | Yes | Yes | No | Yes | No | Yes |
aAMSTAR 2 questions:
Question 1: Did the research questions and inclusion criteria for the review include the component of PICO (population, intervention, comparison, outcomes)?
Question 2: Did the report of the review contain and explicitly state that the review methods were established before the conduct of the review and did the report justify any significant deviations from the protocol?
Question 3: Did the review authors explain their selection of the study designs for inclusion in the review?
Question 4: Did the review authors use a comprehensive literature search strategy?
Question 5: Did the review authors perform study selection in duplicate?
Question 6: Did the review authors perform data extraction in duplicate?
Question 7: Did the reviews authors provide a list of excluded studies and justify the exclusions?
Question 8: Did the review authors describe the included studies in adequate detail?
Question 9: Did the reviews authors use a satisfactory technique for assessing the risk of bias in individual studies that were included in the review?
Question 10: Did the review authors report on the sources of funding for the studies included in the review?
Question 10: If meta-analysis was performed did the review authors use appropriate methods for statistical combination of results?
Question 12: If meta-analysis was performed, did the review authors assess the potential impact of RoB in individual studies on the results of the meta-analysis or other evidence synthesis?
Question 13: Did the review authors account for RoB in individual studies when interpreting/discussing the results of the review?
Question 14: Did the review authors provide a satisfactory explanation for, and discussion of, any heterogeneity observed in the results of the review?
Question 15: If they performed quantitative synthesis, did the review authors carry out an adequate investigation of publication bias (small study bias) and discuss its likely impact on the results of the review?
Question 16: Did the review authors report any potential sources of conflict of interest, including any funding they received for conducting the review?
Table 30: Summary of Findings and Gaps in Evidence
Biologic | Findings and gaps in evidence |
|---|---|
Benralizumab | Findings: Asthma exacerbations were reduced with benralizumab compared to placebo for a broad asthma population and for eosinophilic and allergic asthma subgroups. FEV1 generally favoured benralizumab but statistical significance was limited to eosinophilic asthma patients. HRQoL outcomes favoured benralizumab but were not consistently significant in noneosinophilic patients. Evidence suggests that benralizumab is safe. |
Gaps in evidence: No outcomes were reported specifically in children. Limited evidence in non–type 2 patients. | |
Dupilumab | Findings: Dupilumab was shown to be superior to placebo for asthma exacerbations, FEV1, and HRQoL outcomes in both eosinophilic and allergic populations. Safety outcomes were similar to placebo. |
Gaps in evidence: No outcomes were reported for specific subgroups: non–type 2, eosinophilic and allergic patients, and patients who were only eosinophilic or allergic, but not both. No outcomes were reported specifically in children. | |
Mepolizumab | Findings: Asthma exacerbations, FEV1, HRQoL, and safety outcomes were significantly better when compared to the placebo group among eosinophilic patients regardless of concurrent allergic asthma status. |
Gaps in evidence: Reporting was limited to patients with eosinophilic markers with or without allergic markers. No evidence was reported for non–type 2 asthma, or allergic-only asthma. No outcomes were reported specifically in children. | |
Omalizumab | Findings: Asthma exacerbations, FEV1, and HRQoL outcomes were superior to placebo for allergic asthma patients. No evidence for increased risk of adverse events reported. Asthma exacerbation and HRQoL outcomes were significantly improved in children. |
Gaps in evidence: No outcomes reported for eosinophilic patients without concurrent allergic markers, or for non–type 2 patients. Outcomes within a pediatric population were obtained from reviews including older studies which may not perfectly align with modern definition of severe asthma. | |
Tezepelumab | Findings: Asthma exacerbations, FEV1, HRQoL were reduced with tezepelumab compared to placebo for a broad asthma population and for both eosinophilic and allergic subgroups. Asthma exacerbations and FEV1 were improved for non–type 2 asthma patients. No evidence for risk of adverse events. Asthma exacerbations and FEV1 were significantly improved in non–type 2, but evidence was limited. |
Gaps in evidence: No outcomes were reported specifically in children. Limited evidence was reported for non–type 2 asthma patients. |
FEV1 = forced expiratory volume in 1 second; HRQoL = Health-related quality of life
Table 31: Summary of Findings by Key Asthma Subgroups
Asthma type | Definition and summary of findings |
|---|---|
Severe asthma | Definition: Asthma categorized on severity alone, without specifying underlying type(s). Severe asthma is defined as: 1) controlled asthma worsens on tapering of medium- to high-dose inhaled corticosteroid(s) or systemic corticosteroids (or additional biologics), or 2) symptoms remain uncontrolled with the use of high-dose inhaled corticosteroid(s) plus a second controller (and/or systemic corticosteroids). |
Findings:
| |
Non–type 2 asthma | Definition: Asthma without Type 2 inflammation or markers of eosinophilic or allergic asthma subtypes |
Findings:
| |
Type 2 eosinophilic asthma | Definition: Subtype of Type 2 asthma normally identified using blood eosinophil count as marker. Allergic asthma status unspecified. |
Findings:
| |
Type 2 allergic asthma | Definition: Subtype of Type 2 asthma identified using immunoglobulin E, and allergen sensitivity as markers. Eosinophilic asthma status unspecified. |
Findings:
| |
Type 2 eosinophilic and allergic asthma | Definition: Subgroup with markers for both eosinophilic and allergic asthma |
Findings:
|
AEX = asthma exacerbation; BEC = blood eosinophil count; FEV1 = forced expiratory volume in 1 second; HRQoL = health-related quality of life.
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up-to-date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third-party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for noncommercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.
Questions or requests for information about this report can be directed to Requests@ CADTH .ca.